
Notes
Article history
The research reported in this issue of the journal was funded by the HTA programme as project number 12/151/03. The contractual start date was in August 2013. The draft report began editorial review in August 2014 and was accepted for publication in March 2015. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HTA editors and publisher have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
Pamela Enderby undertakes advisory work for the Royal College of Speech and Language Therapists.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2016. This work was produced by Baxter et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Introduction
Stuttering is a complex disorder that may encompass social and emotional elements. It may comprise overt stuttering behaviours that may be apparent to a listener (such as the repetition of the beginning sound of a word or blocking in which a word appears to get stuck while being articulated). Stuttering also may encompass covert behaviours that may be undetectable to a listener, such as avoidance of particular words or situations. Despite many years of research, there is no certainty regarding the cause of stuttering, although differences in brain structure and functioning in people who stutter have been identified. Over time, those who stutter often develop a salient fear of speaking that becomes a deep-rooted obstacle impeding a person’s social and vocational opportunities. 1
Treatments for stuttering (which is more often known as stammering in the UK) have been available for children and adults since the 1950s. These treatments have encompassed diverse techniques from the use of carbon dioxide, or pharmacological interventions, to those that are behaviourally based. Recent interventions have begun to place a growing emphasis on negative cognitions and related anxiety with regard to stuttering in adults, and on related temperament issues in children and young people. Although many treatments exist, there remains little agreement as to which should be used and when. 2 In children, there is also a lack of consensus regarding when an intervention should begin as there is the complication of a high percentage of young children described as having transient stuttering recovering spontaneously. 3
In young children, treatment may involve combinations of indirect approaches that aim to modify the environment via parents and thereby have an impact on fluency, attitudes, feelings, fears and language, or direct approaches that involve working with the child to change individual speech behaviours. The use of indirect rather than direct approaches distinguishes treatment for stuttering in young children from those used for older children and adult interventions. Historically, there have been two broad philosophies within the field, with a distinction between stuttering modification approaches (stutter more fluently), which aim to reduce avoidance behaviours and negative attitudes and thereby modify stuttering episodes, and fluency-shaping approaches (speak more fluently), which teach new and controlled speech production patterns. These more fluent patterns are learned in formal practice sessions before gradually being generalised to normal conversational settings with these interventions seeking to achieve complete fluency for the people who stutter. These approaches to intervention may have become less defined in current practice, with interventions commonly drawing on a range of influences.
A number of new approaches for treating stuttering have become available in recent years, including the Lidcombe Program (LP), the McGuire Program, the Camperdown Program and also the use of cognitive–behavioural therapy (CBT) based approaches. These interventions may be offered by a growing range of private providers in addition to interventions available via state-funded therapy services. A range of criticisms of these interventions for people who stutter have been voiced. Fluency-shaping approaches have been criticised for leading to unnatural sounding speech with difficulty implementing the techniques in certain situations, and methods that aim to modify stuttering episodes have been criticised for offering only short-term benefit. Both of these approaches have been criticised as offering limited effectiveness owing to the propensity for relapse among people who have completed programmes. 1 In addition to these programmes, the use of mechanical delayed auditory feedback (DAF) devices has been reported to have some success in reducing stuttering. However, there are concerns that these positive outcomes may occur predominantly when reading aloud, rather than in normal conversational interactions. 4
Although there has been a considerable growth in the range of interventions available to people who stutter, it has been highlighted that there is a need for greater use of evidence-based approaches. 3 A recent review of interventions for adults who stutter concluded that, although there was some evidence that fluency-shaping approaches may have the most robust outcomes, no single treatment is able to achieve successful outcomes with all participants. 5 Much of the review evidence to date has evaluated only behavioural programmes, which may be because they tend to have objective measures of effectiveness (i.e. reduction in overt stuttering episodes). There has been less examination of treatments that use outcome measures other than stuttering frequency. Primary research using a broader range of outcome measures is likely to use non-controlled study designs and, thus, be excluded from many systematic reviews.
The growing range of available treatment options for children and adults who stutter presents a challenge for clinicians, service managers and commissioners who need to have access to the best available treatment evidence to guide them in providing the most appropriate interventions. 2 Core outcomes for stuttering have not been established and there is considerable debate within the field regarding what a ‘good’ outcome from intervention should be. Proponents of fluency-shaping approaches use measures such as the number of stutters occurring per sentence, or the percentage of words spoken fluently. However, there are increasing calls to consider the outcome from the perspective of the person who stutters, with use of measures of self-perception, satisfaction with the intervention and well-being. These approaches consider effectiveness in terms of psychological change rather than solely greater spoken fluency.
Research questions
Specific aims of the study were:
-
To systematically identify, appraise and synthesise international evidence on the clinical effectiveness of non-pharmacological interventions to treat stuttering in pre-school children, school aged children, adolescents and adults.
-
To determine how applicable this evidence might be to the UK context, including identifying perceptions of staff and people who stutter regarding potential obstacles to successful outcomes following intervention.
The objective was to present a synthesis which outlines international evidence on interventions for stuttering including recommendations regarding which are most likely to be effective and produce a broad and long-term impact.
The review addressed the following research questions:
-
What are the effects of non-pharmacological interventions for developmental stuttering on communication and/or the well-being of children, adolescents and adults who stutter?
-
What are the factors that may enhance or militate against successful outcomes following intervention?
The patient group
The patient group considered in this review is people who have a stutter (and/or clutter) of developmental origin. The patient group included any age.
The intervention
The interventions defined in this review were any interventions that have the stated purpose of having beneficial outcomes for people who stutter.
Comparator
Interventions that have any comparator group of participants, or those interventions that have no comparator, were included.
Outcomes
The outcomes of interest were any outcomes that were considered to be of benefit for people who stutter in enhancing their communicative interactions or well-being.
How this study has changed from protocol
The study was completed with two very minor changes to the protocol. First, the original protocol had stated that we would exclude support group interventions. Although we found no studies that met our inclusion criteria and reported this type of intervention in isolation, we found literature that included this element as part of a programme of intervention. The patient and public members of our steering group also emphasised the potentially important role of support groups for people who stutter; therefore, this exclusion criterion was removed from the protocol. The second change related to consideration of outcomes that were eligible for inclusion. The original protocol placed no exclusions on the types of outcome that would be considered in the review. However, during the identification phase we identified a small quantity of literature carried out in laboratory conditions that reported stuttering behaviours only when reading aloud, with no measure of spoken interaction. As these data did not relate to functional speech (speech for the purposes of communication) we clarified the inclusion criteria for the review as being studies reporting beneficial outcome for communicative interaction or well-being.
Chapter 2 Methods
A number of reviews of interventions for specific populations or a specific type of intervention have been carried out in the field of stuttering; however, a broad-based systematic review across all forms of intervention for adults and children was needed. We adopted a review method that was able to combine multiple data types to produce a broad evidence synthesis. We believe that this approach was required to best examine the international evidence on interventions and ascertain whether or not, and how, these interventions would be best applied in a UK context in order to inform future guidelines and the implementation of effective treatments in the NHS.
Development of the review protocol
A review protocol was developed prior to beginning the study. The protocol outlined the research questions and detailed methods for carrying out the review in line with guidance from the Centre for Reviews and Dissemination. 6 The protocol encompassed methods for identifying research evidence; the method for selecting studies; the method of data extraction; the process of assessing the methodological rigour of included studies; and synthesis methods. The protocol was registered with the PROSPERO database number CRD42013004861.
Involvement of patients and the public
People who stutter, a charity for stuttering and also health professionals working in the field were involved in development of the review protocol. The advisory group for the project also had representation from these groups in order to provide advice regarding potential sources of data during the searching phase of the work and later in the process in order to assist the team in understanding and interpreting the review findings. The representation on the advisory group of patient and public members was also valuable in terms of identifying avenues for dissemination and translating the key messages of the work for a lay audience.
Identification of studies
Search strategies
A systematic and comprehensive literature search of key health, medical and linguistic databases was undertaken in August 2013 to February 2014. The searching process aimed to identify studies that reported the clinical effectiveness of interventions for people who stutter and also studies that reported the views and perceptions of people who stutter and staff regarding interventions. Searching was carried out for both reviews in parallel, with allocation to either effectiveness or qualitative reviews at the point of identification and selection of studies for potential inclusion. The search process was recorded in detail with lists of databases searched, date search run, limits applied, number of hits and duplication as per PRISMA guidelines. 7 The search strategy is presented in Appendix 1.
The search involved combining terms for the population (stuttering) with terms for the interventions of interest, that is, non-pharmacological interventions. This highly sensitive search strategy (i.e. not using terms for comparators, outcomes or study design) was possible because scoping searches retrieved relatively small and manageable numbers of citations. The aim of the strategy was to identify all studies on non-pharmacological interventions for stuttering.
The search strategy was developed by the information specialist on the team (Anna Cantrell) who undertook electronic searching using iterative methods to create a database of citations using Reference Manager version 12 (Thomson ResearchSoft, San Francisco, CA, USA). The search followed a process whereby search terms were developed initially from scrutinising relevant review articles, followed by scrutinising retrieved papers to inform further searching.
The first main project search was run on MEDLINE (via Ovid) and PsycINFO (via Ovid) in August 2013. Following minor amendments to the search terms, a further iteration of the search was then conducted on a larger range of databases in October to November 2013. Topic experts and clinicians in the field were consulted for additional search terms and for suggestions of additional relevant studies or interventions at regular advisory group meetings and at a clinician workshop session.
In addition to standard electronic database searching, later in the project (February 2014) citation searching was undertaken for all included qualitative citations and searches were conducted for additional papers by the first authors of all included qualitative studies. In order to ensure that the most up-to-date literature was not missed, we also conducted hand screening of journals in April 2014 to identify any work published since the main searches had been carried out. The journals that we searched by hand were International Journal of Language & Communication Disorders; Journal of Speech and Hearing Research; Journal of Communication Disorders; Asia Pacific Journal of Speech Language and Hearing; Clinical Linguistics and Phonetics; Journal of Fluency Disorders; and International Journal of Speech-Language Pathology.
Sources searched
The following electronic databases were searched for published and unpublished research evidence from 1990 onwards.
First search iteration
-
MEDLINE (via OvidSP).
-
PsycINFO (via OvidSP).
Second search iteration
-
EMBASE (via OvidSP).
-
Cumulative Index to Nursing and Allied Health Literature (EBSCOhost).
-
The Cochrane Library (Wiley) including the Cochrane Systematic Reviews Database, Cochrane Controlled Trials Register, Database of Abstracts of Reviews of Effects, Health Technology Assessment and NHS Economic Evaluation Database databases.
-
Applied Social Sciences Index and Abstracts (ProQuest).
-
Linguistics and Language Behavior Abstracts LLBA (ProQuest).
-
Science Citation Index (Web of Science).
-
Social Science Citation Index (Web of Science).
-
Conference Proceedings Citation Index – Science (Web of Science).
-
Sociological Abstracts (ProQuest).
-
Evidence for Policy and Practice Information and Co-ordinating Centre databases.
All citations were imported into Reference Manager and duplicates deleted prior to scrutiny by members of the team.
Search restrictions
Searches were limited by date (1990 to present) as the advent of new programmes may have led to changed practice and the review was aiming to synthesise the most up-to-date evidence. This date criterion was set as it marked a major change in interventions for stuttering associated with publication of the first papers reporting the Lidcombe Approach, with the field from this date forward addressing the need for more public evidence for effectiveness. The review thus encompassed nearly 25 years of research.
The searches did not set an English-language restriction. Although we intended that the review would be predominantly limited to work published in English to ensure that papers were relevant to the UK context, we aimed to search for and include any additional key international papers.
Inclusion and exclusion criteria
Population
-
The population eligible for inclusion was a person who stutters of any age. This included those with overt stuttering behaviours such as repetition of syllables or blocking, those with covert behaviours such as word avoidance and also those diagnosed with any other disorder of developmental fluency such as cluttering.
-
The review excluded people with a fluency disorder which had been acquired rather than developmental, such as non-fluency associated with an identified neurological impairment (such as head injury, stroke or Parkinson’s disease).
-
We included studies whose participants were described as being clutterers. Although cluttering is considered a distinct disorder from stuttering, it is recognised in the field that it may be challenging to differentially diagnose, and can also co-occur with stuttering. Therefore, we took the decision to search for and include any literature meeting our criteria, which examined interventions for this population. However, this work would be highlighted in the results as a separate population group.
-
The review excluded papers reporting interventions for children who have been defined as having normal non-fluency by the authors of the source study.
-
The qualitative review considered studies reporting the views and perceptions of interventions for stuttering. The population was people who stutter, their relatives, friends or significant others, together with the views of staff delivering interventions.
Interventions
-
The review included any intervention that had the stated aim of being of benefit to people who stutter. This could be by either reducing the frequency of occurrence of behaviours (overt and/or covert), or by aiming to address communication and/or social restrictions.
-
Non-pharmacological interventions were included.
-
Interventions delivered in any setting by any agent were included. This encompassed treatments provided as part of state-funded health service provision, those offered by private providers and interventions delivered by charitable or voluntary organisations.
-
The review excluded interventions that are pharmacological.
-
The review excluded interventions that do not have the stated aim of improving fluency outcomes, for example general relaxation or massage sessions, or the provision of information about stuttering.
Comparators
-
Studies with any comparator including an alternative intervention, no intervention or usual practice were eligible for inclusion. This included studies that compared pharmacological to non-pharmacological intervention.
-
Studies comparing pharmacological intervention to no intervention were excluded.
Outcomes
-
Any outcome relating to a positive effect on the communication or emotional well-being of people who stutter was included.
-
Relevant outcome measures included test scores on a standardised assessment such as frequency of non-fluent words; patient self-report of covert stuttering; patient experience; report of frequency of stuttering from a significant other such as a teacher or employer; and patient or staff views and perceptions of obstacles to intervention effectiveness.
-
Outcomes related to reading aloud only, rather than any measure of communicative interaction were excluded.
Study design
-
The review included designs which may be termed randomised controlled trials (RCTs), randomised cross-over trials, cluster randomised trials, quasi-experimental studies, cohort studies, before-and-after/longitudinal studies, case–control studies and non-survey cross-sectional studies.
-
Case reports (a single participant), case series (defined as reporting data from two or three participants) and survey (questionnaire) study designs were excluded.
-
The qualitative review examined studies that reported the views of people who stutter or staff perceptions. Any qualitative method was eligible for inclusion (such as interviews and focus groups). Non-qualitative data collection methods such as questionnaire/survey designs were excluded.
Other inclusion/exclusion criteria
-
The review included studies from any Organisation for Economic Co-operation and Development (OECD) country, thus studies from non-OECD countries were excluded.
-
Studies published in English and key studies published in other languages were included. Studies published in languages other than English without an English abstract were excluded. Studies published in languages other than English which had English abstracts were considered; however, only those considered to be key studies that may add significantly to the review (based on the information in the abstract) were eligible for translation and inclusion.
-
Grey literature (unpublished evaluations) from the UK was eligible for inclusion.
Selection of papers
Citations retrieved via the searching process were uploaded to a Reference Manager database. This database of study titles and abstracts was independently screened by two reviewers and disputes resolved by consulting other team members. This screening process entailed the systematic coding of each citation according to its content. Codes were applied to each paper based on a categorisation developed by the team from previous systematic review work. The coding included categorising papers falling outside of the inclusion criteria (e.g. excluded population, excluded design, excluded intervention) and citations potentially relevant to the clinical effectiveness review and those potentially relevant to the qualitative review.
Full-paper copies of all citations coded as potentially relevant were then retrieved for systematic screening. Papers excluded at this full paper screening stage were recorded and detail regarding the reason for exclusion was provided.
Data extraction strategy
Studies that meet the inclusion criteria following the selection process above were read in detail and data extracted. An extraction form was developed using the previous expertise of the review team, to ensure consistency in data retrieved from each study. The data extraction form recorded authors, date, study design, study aim, study population, comparator (if any) and details of the intervention (including who provided the intervention, type of intervention and dosage). Three members of the research team carried out the data extraction. Data for each individual study were extracted by one reviewer and in order to ensure rigour, each extraction was checked against the paper by a second member of the team.
Quality appraisal strategy
Quality assessment is a key aspect of systematic reviews in order to ensure that poorly designed studies are not given too much weight, so as not to bias the conclusions of a review. As the review included a wide range of study designs, this had an impact on the tool that we selected. Quality assessment of the clinical effectiveness studies was based on the Cochrane criteria for judging risk of bias. 8 This evaluation method classifies studies in terms of sources of potential bias within studies: selection bias, performance bias, attrition bias, detection bias and reporting bias. As the assessment tool used within this approach is designed for randomised controlled study designs, we adapted the criteria to make them suitable for use across wider study designs, including observational as well as experimental designs. We anticipated that using controlled designs would be challenging for this literature (particularly owing to the ethical issue of withholding treatment).
Therefore, we aimed to use an appraisal tool that would provide a detailed examination of quality elements across the literature, which would enable the study conclusions to go beyond reporting that higher-quality controlled research designs were needed. In order to focus our evaluation, we also identified aspects within the risk of bias criteria that related particularly to the stuttering literature. These included the use of in-clinic versus real-life situation speech data and the process of collecting and evaluating the speech sample data (Table 1).
| Potential risk of bias | Bias present? | Detail of concerns |
|---|---|---|
| 1. Selection bias Method used to generate the allocation sequence, method used to conceal the allocation sequence, characteristics of participant group/s Consider: sample size (> or < 10), recruitment process, any issues with participants |
Yes/no/unclear | |
| 2. Performance bias Measures used to blind participants and personnel and outcome assessors, presence of other potential threats to validity Consider: blinding of assessment of speech data, any other concerns |
Yes/no/unclear | |
| 3. Attrition bias Incomplete outcome data, high level of withdrawals from the study |
Yes/no/unclear | |
| 4. Detection bias Accuracy of measurement of outcomes, length of follow-up Consider: clinic vs. outside clinic measures, process of collection of speech data |
Yes/no/unclear | |
| 5. Reporting bias Selective reporting, accuracy of reporting Consider: use of descriptive vs. inferential statistics, pooling of data vs. individual reporting |
Yes/no/unclear |
The summarising of quality appraisal scoring within and across clinical effectiveness studies is a source of debate in the field of systematic reviews, with the calculation of overall scores for each study discouraged. 8 Following assessment of the study against each criterion, we considered the overall categorisation of studies as having either higher risk of bias or lower risk of bias. ‘Higher-risk’ studies were those assessed as having bias such that it is likely to affect the interpretation of the results and ‘lower-risk’ studies were those for which bias is unlikely to have affected the results. The final categorisation was influenced by an aggregate approach (how many areas were of concern), but also by considering whether or not the study contained any particular potential bias that jeopardised the whole study findings. Thus, although the number of ‘yes’ responses was used as an indicator of a higher/lower bias rating of quality, it formed only part of the overall rating decision. In order to produce an inclusive review, no quality requirements were set for inclusion; however, the risk of bias was fully considered and detailed in reporting the results of the review. It is important to note that we deliberately used the comparative categorisation of higher/lower to provide an indication of stronger or weaker studies across the literature included in this review. However, a ‘lower’-risk study should not be assumed to be ‘low risk’ (to be outlined in Chapter 3, Quality of the evidence available) as few studies used comparator groups and even fewer used full randomisation; therefore, even the better-quality papers in the review may be subject to bias. See Appendix 2 for detail of the rating for each included study.
Assessment of quality for the qualitative papers was carried out using an 8-item tool adapted from the Critical Appraisal Skills Programme tool for qualitative studies (Table 2). 9 The quality scoring for each study is presented in tabular form across each of the eight items (see Appendix 3). We also present a narrative summary of the issues arising from quality assessment across the set of included papers, with categorising of studies by the research team as having either higher risk (for which weaknesses in reporting or carrying out a study could affect the reliable interpretation of the conclusions) versus lower risk of bias.
| Quality item | Assessment |
|---|---|
| 1. Was there a clear statement of the aim of the research? | Yes/no |
| 2. Is a qualitative methodology appropriate to address the aims of the research? | Yes/no |
| 3. Was the recruitment strategy appropriate to the aims of the research? | Yes/no/unclear |
| 4. Were the data collected in a way that addressed the research issue? | Yes/no/unclear |
| 5. Has the relationship between researcher and participant been adequately considered? | Yes/no |
| 6. Have ethical issues been taken into account? | Yes/no/unclear |
| 7. Was the data analysis sufficiently rigorous? | Yes/no |
| 8. Is there a clear statement of findings? | Yes/no |
Data analysis and synthesis strategy
Effectiveness studies
Data were synthesised in a form appropriate to the data type. It was proposed that meta-analysis calculating summary statistics would be used if heterogeneity permitted, with use of graphs, frequency distributions and forest plots. It was anticipated that subgroups including age of participants, learning disability, intervention content and delivery agent would be examined if numbers permitted. However, the heterogeneity of the included work precluded summarising the studies via meta-analysis.
Clinical effectiveness review findings were reported using narrative synthesis methods. We tabulated characteristics of the included studies and examined outcomes by typologies, outcome measurement, intervention dosage and length of follow-up. Relationships between studies and outcomes within these typologies were scrutinised.
Qualitative studies
Qualitative data were synthesised using thematic synthesis methods10 in order to develop an overview of recurring perceptions of potential obstacles to successful outcomes within the data. This method comprises familiarisation with each paper and coding of the finding sections (which constitute the ‘data’ for the synthesis), according to key concepts within the findings. Although some data may directly address the research question, sometimes information such as barriers and facilitators to implementation has to be inferred from the findings, as the original study may not have been designed to have the same focus as the review question. 10
Metasynthesis
The third element of the review comprised an overarching synthesis of the clinical effectiveness and qualitative elements, to describe how the results of each section of evidence may contribute to our understanding of implementation and outcomes for stuttering interventions. The aim was to produce a ‘state of the art’ review11 that would provide information for researchers, policy-makers and practitioners. New methods to review and synthesise different types of data have been suggested, including the use of grouping data by subquestions (one for qualitative studies and one for quantitative studies) and the use of a synthesis matrix to compare features of interventions with barriers and facilitators reported by intervention participants. 12,13 The use of both qualitative and quantitative data in a single review has been recommended as having the potential to shed light on negative trial results, to identify social factors, as a means of examining issues of implementation, and potentially having a key role in assisting in the interpretation of significance and applicability for practitioners and service planners. 14
We had planned to metasynthesise findings from the two reviews via a tabular comparison of intervention outcomes and views and perceptions. However, the body of literature contained only limited data reporting perceptions of intervention and only one mixed-methods study examining both outcomes and views. In place of a tabular metasynthesis we have therefore combined the clinical effectiveness and qualitative review findings by developing a conceptual framework. This framework draws on logic model methods to metasynthesise the intervention typologies and content of interventions, with potential barriers and facilitators to intended outcomes from the qualitative review. 15 It also details outcome measures reported in the clinical effectiveness literature, together with factors influencing longer-term impact and types of impact from the qualitative studies. This method of synthesis using a logic model approach aims to assist in the communication and understanding of the complex pathway between interventions and long-term outcomes for people who stutter.
Chapter 3 Results of the effectiveness review
Quantity of the evidence available
The initial electronic database searches identified 4578 citations following deduplication. From this database of citations, 215 potentially relevant papers were retrieved for further scrutiny. Detailed examination of these articles resulted in 109 papers that met the inclusion criteria for the review of clinical effectiveness. Two further papers relating to the review of effectiveness were identified from additional searching strategies (hand-searching of journals). Six further papers were identified from scrutinising reference lists or hand-searching (all qualitative). One paper used a mixed-methods design and, therefore, contributed to both reviews. Figure 1 provides a detailed illustration of the process of study selection.
FIGURE 1.
The process of study selection and exclusion.

Type of evidence available
Study design
Table 3 details the included effectiveness papers categorised by study design. We have provided a definition of each category in order to ensure clarity. The reporting of study design used by authors encompassed a variety of terminology, with terms in some instances not accurately representing the true design. Fourteen papers16–29 reported studies with a comparator, of these four17,18,24,25 randomly allocated participants to each arm of the study, six16,19–23 allocated participants using quasi-randomisation methods (such as consecutive randomising) and one29 was a controlled before-and-after study with no allocation. Of these 14 papers, three reported data from the same study16,20,21 with the greatest proportion of included empirical work using a before-and-after design (pre- to post measure).
| Design | Study |
|---|---|
| RCT, quasi-RCT, controlled before and after (participants in more than one study arm) (14) | Craig et al. 1996 (quasi-RCT),16 Cream et al. 2010,17 De Veer et al. 2009,18 Franklin et al. 2008 (quasi-RCT),19 Hancock and Craig 1998 (quasi-RCT),20 Hancock et al. 1998 (quasi-RCT),21 Harris et al. 2002 (quasi-RCT),22 Hewat et al. 2006 (quasi-RCT),23 Jones et al. 2005,24 Jones et al. 2008,25 Lattermann et al. 2008,26 Lewis et al. 2008,27 Menzies et al. 2008,28 Onslow et al. 199429 (controlled before and after) |
| Before and after (reported pre-intervention and post-intervention data with no comparator group) (86) | Amster and Klein 2007,30 Andrews et al. 2012,31 Baumeister et al. 2003,32 Beilby et al. 2012,33 Berkowitz et al. 1994,34 Block et al. 1996,35 Block et al. 2004,36 Block et al. 2005,37 Block et al. 2006,38 Blomgren et al. 2005,39 Blood 1995,40 Boberg and Kully 1994,41 Bonelli et al. 2000,42 Bray and James 2009,43 Bray and Kehle 1998,44 Carey et al. 2010,45 Cocomazzo et al. 2012,46 Craig et al. 2002,47 Cream et al. 2009,48 Druce and Debney 1997,49 Elliott et al. 1998,50 Femrell et al. 2012,51 Foundas et al. 2013,52 Franken et al. 1992,53 Franken et al. 2005,54 Gagnon and Ladouceur 1992,55 Gallop and Runyan 2012,56 Hancock and Craig 2002,57 Harrison et al. 2004,58 Hasbrouck 1992,59 Hudock and Kalinowski 2014,60 Huinck et al. 2006,61 Ingham et al. 2013,62 Ingham et al. 2001,63 Iverach et al. 2009,64 Jones et al. 2000,65 Kaya and Alladin 2012,66 Kaya 2011,67 Kingston et al. 2003,68 Koushik et al. 2009,69 Laiho and Klippi 2007,70 Langevin and Boberg 1993,71 Langevin and Boberg 1996,72 Langevin et al. 2006,73 Langevin et al. 2010,74 Lawson et al. 1993,75 Leahy and Collins 1991,76 Lincoln et al. 1996,77 Lutz 2009,78 Mallard 1998,79 Millard et al. 2008,80 Millard et al. 2009,81 Miller and Guitar 2009,82 Nilsen and Ramberg 1999,83 O’Brian et al. 2003,84 O’Brian et al. 2008,85 O’Brian et al. 2013,86 O’Donnell et al. 2008,87 Onslow et al. 1990,88 Onslow et al. 1992,89 Onslow et al. 1996,90 Pape-Neumann 2004,91 Pollard et al. 2009,92 Reddy et al. 2010,93 Riley and Ingham 2000,94 Rosenberger et al. 2007,95 Rousseau et al. 2007,96 Ryan and Van Kirk 1995,97 Sicotte et al. 2003,98 Smits-Bandstra and Yovetich 2003,99 Stewart 1996,100 Stidham et al. 2006,101 Stuart et al. 2004,102 Stuart et al. 2006,103 Trajkovski et al. 2011,104 Van Borsel et al. 2003,105 von Gudenberg 2006,106 von Gudenberg et al. 2006,107 Wagaman et al. 1993,108 Wagaman et al. 1995,109 Ward 1992,110 Wille 1999,111 Wilson et al. 2004,112 Woods et al. 2002,113 Yairi and Ambrose 1992,114 Yaruss et al. 2006115 |
| Mixed methods (used both quantitative and qualitative methods of data collection) (1) | Irani et al. 2012116 |
| Cross-sectional (data from a single time point only) (11) | Allen 2011,117 Antipova et al. 2008,118 Armson and Stuart 1998,119 Armson and Kiefte 2008,120 Armson et al. 2006,4 Koushik et al. 2011,121 Lincoln and Onslow 1997 (follow-up data only),122 Onslow et al. 2002,123 Ratynska et al. 2012,124 Unger et al. 2012,125 Zimmerman et al. 1997126 |
Although 26 studies carried out outcome assessment immediately following the intervention,4,19,22,26,34,35,42,43,48,52,54,60,65,67–69,83,93,111,118–120,123–126 there were 51 papers reporting follow-up periods of 12 months or more16,20,21,25,27–29,37,38,40,41,45–47,49,51,56,57,59,61,63,66,69,71–74,77,79–82,84,90,91,96,97,100,103,104,106–110,112,114–117,122 (Table 4).
| Length of follow-up | Study |
|---|---|
| Immediate (26) | Antipova et al. 2008,118 Armson and Stuart 1998,119 Armson and Kiefte 2008,120 Armson et al. 2006,4 Berkowitz et al. 1994,34 Block et al. 1996,35 Bonelli et al. 2000,42 Bray and James 2009,43 Cream et al. 2009,48 Foundas et al. 2013,52 Franken et al. 2005,54 Franklin et al. 2008,19 Harris et al. 2002,22 Hudock and Kalinowski 2014,60 Jones et al. 2000,65 Kaya 2011,67 Kingston et al. 2003,68 Koushik et al. 2011,69 Lattermann et al. 2008,26 Nilsen and Ramberg 1999,83 Onslow et al. 2002,123 Ratynska et al. 2012,124 Reddy et al. 2010,93 Unger et al. 2012,125 Wille 1999,111 Zimmerman et al. 1997126 |
| ≤ 4 weeks (4) | De Veer et al. 2009,18 Harrison et al. 2004,58 Lawson et al. 1993,75 Onslow et al. 199289 |
| 1–2 months (6) | Baumeister et al. 2003,32 Bray and Kehle 1998,44 Riley and Ingham 2000,94 Smits-Bandstra and Yovetich 2003,99 Stidham et al. 2006,101 Woods et al. 2002113 |
| 3–4 months (8) | Amster and Klein 2007,30 Beilby et al. 2012,33 Block et al. 2004,36 Lutz 2009,78 O’Donnell et al. 2008,87 Pollard et al. 2009,92 Stuart et al. 2004,102 Van Borsel et al. 2003105 |
| 5–6 months (9) | Blomgren et al. 2005,39 Cream et al. 2010,17 Franken et al. 1992,53 Gagnon and Ladouceur 1992,55 Hewat et al. 2006,23 Iverach et al. 2009,64 Leahy and Collins 1991,76 O’Brian et al. 2008,85 Sicotte et al. 200398 |
| 9 months (8) | Andrews et al. 2012,31 Elliott et al. 1998,50 Ingham et al. 2013,62 Jones 2005,24 Laiho and Klippi 2007,70 O’Brian et al. 2013,86 Onslow et al. 1990,88 Rosenberger et al. 200795 |
| 12–18 months (26) | Allen 2011,117 Blood 1995,40 Carey et al. 2010,45 Cocomazzo et al. 2012,46 Craig et al. 1996,16 Druce and Debney 1997,49 Hancock and Craig 1998,20 Hancock et al. 1998,21 Kaya and Alladin 2012,66 Langevin and Boberg 1993,71 Langevin and Boberg 1996,72 Lewis et al. 2008,27 Mallard 1998,79 Menzies et al. 2008,28 Millard et al. 2008,80 Millard et al. 2009,81 Miller and Guitar 2009,82 O’Brian et al. 2003,84 Onslow et al. 1994,29 Ryan and Van Kirk 1995,97 Stuart et al. 2006,103 Trajkovski et al. 2011,104 von Gudenberg 2006,106 Wagaman et al. 1993,108 Ward 1992,110 Wilson et al. 2004112 |
| 2 years (12) | Boberg and Kully 1994,41 Craig et al. 2002,47 Femrell et al. 2012,51 Hancock and Craig 2002,57 Huinck et al. 2006,61 Ingham et al. 2001,63 Langevin et al. 2006,73 Lincoln et al. 1996,77 Pape-Neumann 2004,91 Rousseau et al. 2007,96 Stewart 1996,100 Yairi and Ambrose 1992114 |
| 3 years (3) | Hasbrouck 1992,59 Onslow et al. 1996,90 Yaruss et al. 2006115 |
| Up to 5 years (6) | Block et al. 2005,37 Block et al. 2006,38 Gallop and Runyan 2012,56 Langevin et al. 2010,74 von Gudenberg et al. 2006,107 Wagaman et al. 1995109 |
| > 5 years (4) | Lincoln and Onslow 1997,122 Irani et al. 2012,116 Jones et al. 2008,25 Koushik et al. 200969 |
Country of origin
A categorisation of included studies by country of origin is presented in Table 5. The greatest proportion of work was reported by authors based in Australia (39 papers), followed by the USA (26 papers). Eight papers were from the UK.
| Country of origin | Study |
|---|---|
| Australia (39) | Andrews et al. 2012,31 Beilby et al. 2012,33 Block et al. 1996,35 Block et al. 2004,36 Block et al. 2005,37 Block et al. 2006,38 Bonelli et al. 2000,42 Carey et al. 2010,45 Cocomazzo et al. 2012,46 Craig et al. 1996,16 Craig et al. 2002,47 Cream et al. 2009,48 Cream et al. 2010,17 Druce and Debney 1997,49 Franklin et al. 2008,19 Hancock and Craig 1998,20 Hancock and Craig 2002,57 Hancock et al. 1998,21 Harris et al. 2002,22 Harrison et al. 2004,58 Hewat et al. 2006,23 Iverach et al. 2009,64 Jones et al. 2000,65 Lewis et al. 2008,27 Lincoln et al. 1996,77 Lincoln and Onslow 1997,122 Menzies et al. 2008,28 O’Brian et al. 2003,84 O’Brian et al. 2008,85 O’Brian et al. 2013,86 Onslow et al. 1994,29 Onslow et al. 1990,88 Onslow et al. 1992,89 Onslow et al. 1996,90 Onslow et al. 2002,123 Rousseau et al. 2007,96 Trajkovski et al. 2011,104 Wilson et al. 2004,112 Woods et al. 2002113 |
| USA (26) | Amster and Klein 2007,30 Berkowitz et al. 1994,34 Blomgren et al. 2005,39 Blood 1995,40 Boberg and Kully 1994,41 Elliott et al. 1998,50 Foundas et al. 2013,52 Gallop and Runyan 2012,56 Hasbrouck 1992,59 Hudock and Kalinowski 2014,60 Ingham et al. 2013,62 Ingham et al. 2001,63 Irani et al. 2012,116 Mallard 1998,79 Miller and Guitar 2009,82 Pollard et al. 2009,92 Riley and Ingham 2000,94 Ryan and Van Kirk 1995,97 Stidham et al. 2006,101 Stuart et al. 2004,102 Stuart et al. 2006,103 Wagaman et al. 1993,108 Wagaman et al. 1995,109 Yairi and Ambrose 1992,114 Yaruss et al. 2006,115 Zimmerman et al. 1997126 |
| Canada (11) | Armson and Stuart 1998,119 Armson and Kiefte 2008,120 Armson et al. 2006,4 Gagnon and Ladouceur 1992,55 Koushik et al. 2009,69 Langevin and Boberg 1993,71 Langevin and Boberg 1996,72 Langevin et al. 2010,74 O’Donnell et al. 2008,87 Sicotte et al. 2003,98 Smits-Bandstra and Yovetich 200399 |
| Germany (9) | Baumeister et al. 2003,32 Lattermann et al. 2008,26 Lutz 2009,78 Pape-Neumann 2004,91 Rosenberger et al. 2007,95 Unger et al. 2012,125 von Gudenberg 2006,106 von Gudenberg et al. 2006,107 Wille 1999111 |
| UK (8) | Allen 2011,117 Bray and James 2009,43 Bray and Kehle 1998,44 Lawson et al. 1993,75 Millard et al. 2008,80 Millard et al. 2009,81 Stewart 1996,100 Ward 1992110 |
| The Netherlands (4) | De Veer et al. 2009,18 Franken et al. 1992,53 Franken et al. 2005,54 Huinck et al. 200661 |
| Sweden (2) | Femrell et al. 2012,51 Nilsen and Ramberg 199983 |
| Turkey (2) | Kaya and Alladin 2012,66 Kaya 201167 |
| New Zealand (2) | Antipova et al. 2008,118 Jones et al. 200524 |
| Finland (1) | Laiho and Klippi 200770 |
| Ireland (1) | Leahy and Collins 199176 |
| India (1) | Reddy et al. 201093 |
| Poland (1) | Ratynska et al. 2012124 |
| Belgium (1) | Van Borsel et al. 2003105 |
| Across countries (4) | Jones et al. 2008,25 Kingston et al. 2003,68 Koushik et al. 2011,121 Langevin et al. 200673 |
Intervention dosage
We endeavoured to identify from author report how many hours of intervention were provided in the included studies (Table 6). Papers varied considerably with regard to the level of detail provided and, therefore, the table below may not be completely accurate in representing intervention dosage, but is based on information we could glean. It can be seen that a sizeable proportion of the papers varied the number of hours of intervention according to individual need. This makes comparing effectiveness by dosage unfeasible. It can also be seen from the table that the contact time ranged from fewer than 10 hours to more than 75 hours, again making the drawing of comparisons between different interventions on the basis of dosage problematic. The interventions that had shorter contact times tended to be those which were based on the use of technology (such as DAF systems). The interventions with longer contact time (perhaps unsurprisingly) tended to be those with multiple elements.
| Intervention detail | Studies |
|---|---|
| Hours varied by individual participant. The range or mean is detailed if provided by authors (27) | Femrell et al. 201251 (9–46 visits), Franken et al. 200554 (mean 11.5 sessions), Gagnon and Ladouceur 1992,55 Ingham et al. 2013,62 Ingham et al. 2001,63 Jones et al. 2000,65 Jones et al. 2005,24 Jones et al. 2008,25 Kingston et al. 2003,68 Koushik et al. 200969 (6–10 visits), Koushik et al. 2011121 Lattermann et al. 200826 (average 13 sessions), Lewis et al. 200827 (mean 49 consultations), Lincoln and Onslow, 1997122 (mean 10.5 sessions), Lincoln et al. 199677 (median 12 sessions), Miller and Guitar 200982 (mean 19.8 sessions), O’Brian et al. 200384 (range 13–29 hours), O’Brian et al. 201386 (median 11 visits), O’Donnell et al. 2008,87 Onslow et al. 199429 (median 10.5 hours), Pape-Neumann 2004,91 Rousseau et al. 2007,96 Wagaman et al. 1993,108 Wagaman et al. 1995109 (average 10 sessions), Wilson et al. 2004112 (range 3–26 consultations), Woods et al. 2002,113 Yaruss et al. 2006115 |
| Individual < 10 hours (19) | Antipova et al. 2008,118 Block et al. 2006,39 Bray and Kehle 1998,44 Carey et al. 2010,45 Cream et al. 2009,48 Elliott et al. 1998,50 Foundas et al. 2013,52 Franklin et al. 2008,19 Gallop and Runyan 2012,56 Hudock and Kalinowski 2014,60 Millard et al. 2008,80 Millard et al. 2009,81 O’Brian et al. 2008,85 Pollard et al. 2009,92 Stuart et al. 2004,102 Stuart et al. 2006,103 Unger et al. 2012,125 Van Borsel et al. 2003,105 Zimmerman et al. 1997126 |
| Unclear (16) | Allen 2011,117 Andrews et al. 2012,31 Armson and Stuart 1998,119 Armson et al. 2006,4 Armson and Kiefte 2008,120 Bonelli et al. 2000,42 Bray and James 2009,43 Hewat et al. 2006,23 Langevin and Boberg 1996,72 Leahy and Collins 199176 Onslow et al. 1990,88 Onslow et al. 2002,123 Ratynska et al. 2012,124 Trajkovski et al. 2011,104 Wille 1999,111 Yairi and Ambrose 1992114 |
| Individual + group 30–75 hours (11) | Block et al. 2005,37 Block et al. 2006,38 Blomgren et al. 2005,39 Craig et al. 1996,16 Cream et al. 2010,17 Hancock et al. 1998,21 Irani et al. 2012,116 Iverach et al. 2009,64 Langevin and Boberg 1993,71 Lawson et al. 1993,75 Menzies et al. 200828 |
| Individual + group > 75 hours (9) | Boberg and Kully 1994,41 Huinck et al. 2006,61 Langevin et al. 2006,73 Langevin et al. 2010,74 Nilsen and Ramberg 1999,83 Onslow et al. 1992,89 Onslow et al. 1996,90 Rosenberger et al. 2007,95 Stewart 1996100 |
| Individual 20–50 hours (8) | Block et al. 2004,36 Cocomazzo et al. 2012,46 De Veer et al. 2009,18 Reddy et al. 2010,93 Riley and Ingham 2000,94 Sicotte et al. 2003,98 Stidham et al. 2006,101 Ward 1992110 |
| Individual 10–19 hours (6) | Beilby et al. 2012,33 Harris et al. 2002,22 Harrison et al. 2004,58 Kaya and Alladin 2012,66 Kaya 2011,67 Ryan and Van Kirk 199597 |
| Individual > 75 hours (4) | Blood 1995,40 Franken et al. 1992,53 von Gudenberg 2006,106 von Gudenberg et al. 2006107 |
| Child group + parent group 10–19 hours (3) | Craig et al. 2002,47 Hancock and Craig 2002,57 Hancock and Craig 199820 |
| Child group + parent group 20–50 hours (3) | Druce and Debney 199749 (six sessions of 5 hours each for parents and children during a 1-week intensive course), Mallard 199879 (2-week intensive), Smits-Bandstra and Yovetich 200399 (3-week semi-intensive) |
| Individual + parent group (2) | Berkowitz et al. 199434 (8 hours for parents, not clear for children), Laiho and Klippi 200770 (at least 30 hours) |
| Individual + group 10–20 hours contact time (2) | Amster and Klein 2007,30 Hasbrouck 199259 |
| Parent group (1) | Lutz 200978 (12 hours) |
| Reported by length of treatment time only (1) | Baumeister et al. 200332 (3 weeks) |
Intervention provider
In terms of the person delivering the intervention, 51 studies reported that clinicians provided the therapy. In all except three cases these clinicians were speech and language pathologists/therapists (two interventions were delivered by clinical psychologists and one jointly by a therapist and psychologist). Fifty papers16–36,51–54,56–60,65–72,79,82–90,100–102 were unclear with regards to who delivered the sessions; it was presumed that in most cases this was the author/s. Eleven studies reported that student clinicians had been used to provide therapy, with supervision by qualified staff.
Number and type of studies excluded
As can be seen from Figure 1, a large number of citations were excluded at initial screening of title and abstract. Many of these retrieved citations were excluded as not relating to stuttering. A large number of these had been retrieved by our searches as they included reference to fluency (e.g. reading fluency, fluency of movement). In addition, the term ‘clutter’ resulted in papers relating to untidiness in the home. In addition, we found reference to a number of medical conditions not related to communication which include the term ‘stutter’. Other factors that underpinned large numbers of exclusions were papers consisting of general discussion rather than reporting data; articles relating to diagnosis and causation; and studies reporting the development or discussion of outcome measures.
Appendix 4 lists the studies initially identified as being potentially relevant but which were subsequently excluded at full-paper stage. The rationale for the exclusion of each is provided.
Quality of the evidence available
Quality assessment of the included papers using the tool previously described resulted in 35 studies16,17,20–28,33,37–39,45,46,54,57,58,61,64,65,69,72–74,82,86,92,96,97,104,108,113 being categorised as being at lower risk of bias and 77 studies4,21,29–32,34–36,40–44,47–53,55,56,59,60,62,63,66–68,70,71,75–81,83–85,87–91,93–95,98–103,105–107,109–112,114–126 were categorised as being at higher risk of bias. Note our earlier discussion regarding the use of higher/lower categorisation rather than high/low. Few studies used controlled designs and, of these, the allocation process was frequently carried out by pseudo rather than completely randomised procedures. The areas which tended to distinguish studies rated as having higher potential for bias were (1) having samples of fewer than 10 participants; (2) reporting data by individual rather than pooling findings; (3) using only descriptive statistics [means and standard deviation (SDs)]; (4) failing to blind assessors to the time point of data collection; (5) limited length of speech data samples; and (6) concerns regarding the process of data collection. See Appendix 2 for details of the completed assessment for each study. In many of the smaller before-and-after studies (and some of those with larger samples) the process of selection of individuals whose data would be reported was unclear. It seemed likely (and was sometimes mentioned) that interventions had been delivered to larger numbers of people who stutter with only a sample of these being presented. The possibility that those recruited and reported may differ from those who were not recruited and reported must be considered a potential significant source of bias in interpretation of the data for these studies (see Quality of the evidence available).
Population
Table 7 presents the included studies categorised by the type of participants. As can be seen, the greatest number of studies reported findings from interventions carried out with adults who stutter, followed by school age and then pre-school children. Nine studies delivered interventions to mixed age groups of participants.
| Participant type | Study |
|---|---|
| Pre-school (including children and parents) (15) | Bonelli et al. 2000,42 Femrell et al. 2012,51 Franken et al. 2005,54 Harrison et al. 2004,58 Jones et al. 2005,24 Kingston et al. 2003,68 Lewis et al. 2008,27 Millard et al. 2008,80 Millard et al. 2009,81 Miller and Guitar 2009,82 Onslow et al. 1994,29 Onslow et al. 1990,88 Trajkovski et al. 2011,104 Yairi and Ambrose 1992,114 Yaruss et al. 2006115 |
| Parents only (1) | Lutz 200978 |
| Predominantly school age (greatest proportion of participants aged 4–11 years) (26) | Andrews et al. 2012,31 Berkowitz et al. 1994,34 Bray and Kehle 1998,44 Druce and Debney 1997,49 Elliott et al. 1998,50 Gagnon and Ladouceur 1992,55 Harris et al. 2002,22 Jones et al. 2008,25 Jones et al. 2000,65 Koushik et al. 2009,69 Koushik et al. 2011,121 Laiho and Klippi 2007,70 Lattermann et al. 2008,26 Lincoln et al. 1996,77 Lincoln and Onslow 1997,122 Mallard 1998,79 O’Brian et al. 2013,86 Onslow et al. 2002,123 Riley and Ingham 2000,94 Rousseau et al. 2007,96 Smits-Bandstra and Yovetich 2003,99 von Gudenberg 2006,106 Wagaman et al. 1993,108 Wagaman et al. 1995,109 Wilson et al. 2004,112 Woods et al. 2002113 |
| School age and adolescents (8) | Baumeister et al. 2003;32 Block et al. 2004,36 Craig et al. 1996,16 Hancock et al. 1998,21 Rosenberger et al. 2007,95 Ryan and Van Kirk 1995,97 Sicotte et al. 2003,98 Wille 1999111 |
| Adolescents (aged > 11 years) (5) | Craig et al. 2002,47 Hancock and Craig 2002,57 Hancock and Craig 1998,20 Lawson et al. 1993,75 Nilsen and Ramberg 199983 |
| Adults (47) | Allen 2011,117 Amster and Klein 2007,30 Antipova et al. 2008,118 Armson and Stuart 1998,119 Armson and Kiefte 2008,120 Armson et al. 2006,4 Beilby et al. 2012,33 Block et al. 1996,35 Block et al. 2005,37 Block et al. 2006,38 Blomgren et al. 2005,39 Blood 1995,40 Bray and James 2009,43 Carey et al. 2010,45 Cocomazzo et al. 2012,46 Cream et al. 2009,48 Cream et al. 2010,17 De Veer et al. 2009,18 Foundas et al. 2013,52 Franken et al. 1992,53 Franklin et al. 2008,19 Hasbrouck 1992,59 Hudock and Kalinowski 2014,60 Huinck et al. 2006,61 Ingham et al. 2013,62 Ingham et al. 2001,63 Irani et al. 2012,116 Iverach et al. 2009,64 Kaya and Alladin 2012,66 Kaya 2011,67 Langevin and Boberg 1993,71 Langevin and Boberg 1996,72 Langevin et al. 2010,74 Langevin et al. 2006,73 Leahy and Collins 1991,76 Menzies et al. 2008,28 O’Brian et al. 2003,84 O’Brian et al. 2008,85 O’Donnell et al. 2008,87 Onslow et al. 1996,90 Pollard et al. 2009,92 Reddy et al. 2010,93 Stewart 1996,100 Stidham et al. 2006,101 Unger et al. 2012,125 Van Borsel et al. 2003,105 Zimmerman et al. 1997126 |
| Mixed age (9) | Boberg and Kully 1994,41 Gallop and Runyan 2012,56 Hewat et al. 2006,23 Onslow et al. 1992,89 Pape-Neumann 2004,91 Ratynska et al. 2012,124 Stuart et al. 2004,102 Stuart et al. 2006,103 von Gudenberg et al. 2006107 |
| Unclear (1) | Ward 1992110 |
Cluttering
As outlined earlier, we took the decision to search for and include any work that examined interventions for people who clutter – a related speech fluency difficulty. We found only one paper which met our inclusion criteria and identified some of the participants as people who clutter. 72
Assessment of clinical effectiveness analysed by intervention type
We grouped the effectiveness papers according to the content of the intervention. The literature we identified used a variety of terms to describe the intervention reported (e.g. ‘speak more fluently’ vs. ‘stutter more fluently’, ‘indirect’ vs. ‘direct’, ‘speech restructuring’ treatment vs. ‘speech modification’ therapy). In order to avoid potential confusion between different authors’ use of terminology, we adopted the classification below which endeavours to categorise the approaches taken within the included studies. The categorisation consists of seven typologies: (1) feedback and technology interventions which aim to change auditory feedback systems (22 papers4,17,35,36,43,44,48,52,56,60,87,92,101–103,105,118–120,124–126); (2) cognitive interventions which aim to lead to psychological change (six papers18,30,66,67,76,93); (3) behavioural modification interventions which aim to change child or parental behaviour, or the behaviour of an adult who stutters (29 papers19,22–27,29,42,51,58,65,68,69,77–82,86,88,96,112,113,115,121–123); (4) speech motor interventions (18 papers31,37,38,45,46,49,53,62–64,84,85,89,90,104,106,107,114) which aim to impact on the mechanisms of speech production such as the respiratory, laryngeal or articulatory systems; (5) speech motor combined with cognitive interventions (18 papers32–34,39,41,61,70–75,83,95,99,100,110,116); (6) multiple component interventions (11 papers40,47,50,55,57,59,91,98,108,109,117); and (7) studies which compared interventions to each other (eight papers16,20,21,28,54,94,97,111).
Feedback and technology interventions
Twenty-two papers were included that described the effectiveness of a range of a technologies aiming to reduce the frequency or severity of stuttering in speech (Table 8). The earliest of these papers was published in 1996, and the most recent in 2014, with 13 of the papers from North America (see Table 8). The greatest proportion of the technologies described were devices that alter the way that a person who stutters hears their own speech [altered auditory feedback (AAF)] by changing the frequency [frequency altered feedback (FAF)] and/or by introducing a delay before the speech is heard (DAF). All but one of the included studies52 either compared stuttering level while using a device with stuttering level with no use of the device, or compared fluency level using different device settings. The other paper52 compared use of a device in people who stutter with use by non-stuttering speakers. All but one of the papers92 in this group was rated as being at higher risk of bias. The papers described the use of AAF under a variety of conditions including reading, monologue and conversation (either in person or via the telephone).
| Study detail | Design | Risk of bias | Country | Population |
|---|---|---|---|---|
| Antipova et al. 2008118 | Cross-sectional | Higher | New Zealand | Adults, n = 8 |
| Armson and Stuart 1998119 | Cross-sectional | Higher | Canada | Adults, n = 12 |
| Armson et al. 20064 | Cross-sectional | Higher | Canada | Adults, n = 13 |
| Armson and Kiefte 2008120 | Cross-sectional | Higher | Canada | Adults, n = 31 |
| Block et al. 200436 | Before and after | Higher | Australia | Aged 10–16 years, n = 12 |
| Block et al. 199635 | Before and after | Higher | Australia | Adults, n = 18 |
| Bray and James 200943 | Before and after | Higher | UK | Adults, n = 5 |
| Bray and Kehle 199844 | Before and after | Higher | UK | Aged 8–13 years, n = 4 |
| Cream et al. 200948 | Before and after | Higher | Australia | Adults, n = 12 |
| Cream et al. 201017 | RCT | Lower | Australia | Adults, n = 89 |
| Foundas et al. 201352 | Before and after | Higher | USA | Adults, n = 24 |
| Gallop and Runyan 201256 | Before and after | Higher | USA | Adults, n = 11 |
| Hudock and Kalinowski 201460 | Before and after | Higher | USA | Adults, n = 9 |
| O’Donnell et al. 200887 | Before and after | Higher | Canada | Adults, n = 7 |
| Pollard et al. 200992 | Before and after | Lower | USA | Adults, n = 11 |
| Ratynska et al. 2012124 | Cross-sectional | Higher | Poland | Mixed, n = 335 |
| Stidham et al. 2006101 | Before and after | Higher | USA | Adults, n = 10 |
| Stuart et al. 2004102 | Before and after | Higher | USA | Adolescents and adults, n = 7 |
| Stuart et al. 2006103 | Before and after | Higher | USA | Adolescents and adults, n = 9 |
| Unger et al. 2012125 | Cross-sectional | Higher | Germany | Adults, n = 30 |
| Van Borsel et al. 2003105 | Before and after | Higher | Belgium | Adults, n = 9 |
| Zimmerman et al. 1997126 | Cross-sectional | Higher | USA | Adults, n = 9 |
This type of intervention alters the auditory feedback process in people who stutter with the aim of reducing the proportion of stuttered speech. Although the precise area of change and way that these interventions act to reduce stuttering is debated, it has been proposed that they may activate a ‘mirror neural system’ to link perception with production or, alternatively, that they have an impact on timing processes that control speaking rate. In the following synthesis we have detailed only the findings relating to conversational interaction (or monologue if no conversational measure was available). Many of the papers contained further detailed data regarding outcomes in terms of reading aloud. 4,17,35,36,48,52,56,60,87,92,102,103,105,118–120,124–126
Use of the SpeechEasy device (Janus Development Group, Inc., NC, USA) was reported in six papers. 4,52,56,87,92,120 These studies explored the use of the technology in laboratory, clinical and naturalistic contexts and examined follow-up for periods up to 59 months. Sample sizes ranged from seven to 31 individuals with no studies using a control group design. Five out of the six papers were assessed as being at higher risk of bias, with only one92 judged to have a lower risk of bias.
All studies reported some degree of effectiveness for this intervention. Armson et al. 4 found stuttering was significantly reduced having the device in place versus no device (p = 0.01) with a small effect size (ES) of 0.108. However, there was considerable individual variation in responses, with the suggestion that those having lower initial stuttering had better outcomes. A second paper by Armson and Kiefte120 also reported significant decreases in stuttering rate with SpeechEasy compared with stuttering rate without SpeechEasy for all but two of 31 participants (p < 0.001, ES 0.724). The mean stuttering frequency pre-device was 16.4 and with device the mean was 2.3, an average reduction during monologue of 60.7%. Participant self-rating of stuttering severity also improved during the device condition (from 5.95 to 3.29; p = 0.028, ES 0.658). The paper examined whether or not stuttering reduction was at the expense of reduction in speech naturalness or rate and concluded that participants had a slower than normal rate both with and without the device. Naturalness ratings increased to just below normal levels with the device. The Foundas et al. 52 paper echoes these findings, with a significant reduction in stuttering frequency with the SpeechEasy device in place and activated versus in place but not producing DAF or FAF (p = 0.014, a 36.7% reduction). The paper examined the effect of different device settings and concluded that the setting preferred by the participants was more effective than the default setting. In contrast to the findings above, individuals with more severe stuttering at baseline had a greater benefit.
Three papers examined longer-term outcomes of SpeechEasy intervention. 56,87,92 One56 followed up device users following initial fitting. Eight of the 11 participants were still using the device at a mean of 37 months’ follow-up. The study found that level of dysfluency (for the seven participants that data were available for) was not significantly different at long-term follow-up than it had been at first fitting (p = 943). However, there was significant variation with three having increased fluency, one was unchanged and three had worsened fluency since initial fitting. Analysis of data for all 11 people who stutter (those who continued to use the device and those who did not) found that all had significantly improved levels of fluency from before they were fitted with SpeechEasy to the current time point (p = 0.017). The authors suggested that this indicates carry over effect from the device even when use discontinues. However, an alternative interpretation may question the long-term value of using the device in that continued users did not differ from non-users. In support of this, the study reports that at time of follow-up there was no difference in fluency whether the device was worn or not worn (p = 0.92).
The second paper reporting longer-term follow-up data92 similarly casts some doubt on the long-term clinical effectiveness of SpeechEasy and this paper was judged to be at lower risk of bias. This study examining beyond-clinic data found a positive effect on the percentage of syllables that are stuttered in the shorter term following fitting (p = 0.02); however, no significant effect on the percentage of syllables that are stuttered at 4-month follow-up (p = 0.090). Self-report scores on the Stuttering Severity Index (SSI) and Overall Assessment of the Speaker’s Experience of Stuttering Questionnaire (OASES) showed no difference pre- to post intervention; however, the Perceptions of Stuttering Inventory (PSI) scores had significantly improved (p < 0.05). Only 4 out of the 11 participants had purchased the device, eight reported they disliked the irritating background noise and five that they disliked being unable to hear self/others. Six reported that using the device had increased their confidence in speaking and six reported that they had an overall increase in fluency using it.
The O’Donnell et al. 87 paper includes beyond-clinic measures using data obtained via the telephone. This study followed participants at regular intervals for 16 weeks after fitting and included speech data and participant self-report. Use of the device varied from 2 hours per day to 15 hours per day. Stuttering reduced for all participants at the baseline evaluation point (by 75.5–97.9%); however, there was considerable variation in outcome between participants at the final follow-up. Four stuttered less with the device than those without it and three stuttered less without the device than those with it. Five of the seven stuttered more at follow-up than they had at baseline with the device in use (although all had reduced levels of stuttering when not using the device than they had previously). Analysis of the beyond-clinic telephone recordings indicated positive outcomes for five participants, with mean reduction in stuttering ranging from 20% to 94.4% when conversing with the experimenter while having the device in place, compared with not using it. On self-report measures, six participants described reduced struggle or avoidance behaviour with five participants identifying substantial benefit.
Six papers reported the use of other feedback devices combining DAF and FAF. All were considered to be at higher risk of bias. 35,103,104,118,124,125 Antipova et al. 118 used The Pocket Speech Lab (Casa Futura Technologies, CO, USA) with eight participants and found all reduced the percentage of words stuttered using the device by an average of 3–4%. The paper details individual response under eight different AAF conditions with a significant difference between these and the no-device condition (p = 0.049) in terms of the percentage of syllables that are stuttered. The authors report a trend for those with more severe stuttering to have a greater reduction; however, they highlighted the significant individual variability in response. Unger et al. 125 found a significant reduction in SSI severity rating (p = 0.000) for 30 participants using the VA 601i Fluency Enhancer (VoiceAmp Ltd , Middlesex, UK) or the SmallTalk devices (Casa Futura Technologies, CO, USA). Individual variability in outcome was also emphasised in this study. The Digital Speech Aid (Digital Recordings – Advanced R & D, Nova Scotia, NS, Canada) was evaluated in a study with a larger sample of 335 individuals. 124 Statistically significant improvement in the number of dysfluent syllables was observed using the device than non-use (p < 0.005). In dialogue, the odds ratio (OR) of exhibiting dysfluency without the device was 0.58 and with the device in use was 0.18. Although moderate or considerable improvement was found for 84.5% of participants, deterioration or lack of improvement was found for 15.5%.
Use of the Edinburgh Masker (Casa Futura Technologies, Boulder, CO, USA) in both clinic and home settings was evaluated by Block et al. 35 Results for the 18 participants showed a decrease in the percentage of syllables that are stuttered for all across all conditions (conversation with experimenter: 2.1% reduction of syllables that are stuttered, conversation familiar person: 2.6% reduction of syllables that are stuttered, telephone: 2.8% reduction of syllables that are stuttered). The authors reported that an analysis of variance (ANOVA) was performed which indicated a significant reduction in stuttering; however, the details of this are not provided. Some individual differences in response are described (eight participants increased stuttering on at least one task) and although speaking rate was found to be unaffected, speech naturalness appeared to be reduced using the device (p < 0.01).
Companion papers103,104 report 4-month and 12-month follow-up data from intervention using a self-contained in-the-ear prosthetic fluency device providing both FAF and DAF. The earlier paper103 describes three experiments using the equipment. The proportion of stuttered syllables was significantly reduced for the seven participants in experiment 1 when they used the device during monologue (p = 0.011, a 67% reduction of syllables that are stuttered). Similarly, for eight participants in experiment 2 there was a significant reduction in proportion of stuttered syllables (p = 0.0028). The third experiment focused on evaluating speech naturalness and found that speech while using the device was rated as more natural sounding than without (p < 0.0001), although scores were below that for normal speakers. The follow-up paper similarly outlines three experiments. The first found that initial reductions in stuttered syllables reported at initial fitting with the device in place compared with no device were repeated at 12 months (p < 0.0001), with a 75% reduction in percentage of syllables that are stuttered using the device during monologue. Experiment 2 details significantly improved PSI scores at 12 months compared with scores prior to receiving the device. Participants were asked to self-report current levels and recall previous, but this means the reliability of these data must be questioned. Experiment 3 examines speech naturalness and found an increased naturalness rating at 12 months compared with 4 months and that speech while using the device was rated as more natural than without (although as with the earlier paper was less natural than normal speakers).
Three papers focused on the use of AAF devices to reduce stuttering during use of the telephone. 44,60,126 The most recent paper60 examined the effectiveness of different combinations of DAF and FAF during scripted telephone conversations. Although this study could be perceived to be using a reading aloud only outcome and, therefore, falls within the exclusion criteria, the script was considered to be similar to notes that a person who stutters may make in everyday life when making a telephone call and so the study offered more functional outcomes. Stuttering frequencies in both AAF conditions for all nine participants were significantly lower than the non-altered feedback condition (p < 0.0001, an average of a 65% reduction). These findings are similar to an earlier paper126 which reported a reduction in stuttering frequency of 55–60% using AAF during scripted telephone conversations (p = 0.004) with a positive effect for all nine participants. Bray and James44 support the clinical effectiveness of using an AAF device when making telephone calls. The Telephone Assistive Device (VoiceAmp Ltd, Middlesex, UK) evaluated in this study reduced stuttering frequency for four out of five participants (group mean 8.28% pre-device and mean 4.82 using device). The authors suggested some improvement in self-reported feelings and attitude following use of the device, but there are limited data to support this.
One paper reported the use of FAF only,119 and another the use of DAF only. 105 Amson and Stuart119 found that although some improvement to reading using FAF was observed, there was no significant effect on the number of stuttering events during monologue, with 10 out of the 12 participants showing no benefit. Use of DAF over 3 months105 was found to significantly reduce the percentage of stuttered words (when using the device compared with not using it) for non-functional speech tasks and picture description (p = 0.050); however, not significantly for conversation (p = 0.066). Levels of stuttering without the device in place were significantly reduced from baseline levels for all but conversation (p = 0.0666). Overall levels of stuttering when using the device from baseline to 3-month follow-up had not significantly changed. Self-report perception of fluency (using median scores on the summary table provided) was that fluency using DAF was better than fluency without DAF for four out of nine participants (unchanged for four, worse for one).
Other types of technology evaluated in the literature were bone conduction stimulation and electromyography (EMG). Stidham et al. 101 reported the use of bone conduction stimulation with DAF which participants used for at least 4 hours a day for 4 weeks. Although baseline to immediate post provision of the device indicated a significant reduction in stuttering (p < 0.001), the effect had faded at 2- and 6-week follow-up. Of the nine participants, slightly more than half reported that their speech had improved using the device (56%) and 66% rated it as helpful to some degree. However, the headband element of the device was described as being uncomfortable and obtrusive.
Two papers examined the use of EMG feedback. One of these16 compared EMG with two other interventions and will be outlined in detail later (see Papers comparing interventions). In summary, this study found that for 6 out of the 10 children taking part, EMG reduced stuttering to less than 1% of syllables that are stuttered immediately post intervention, with four children remaining at this level at 1-year follow-up. The other paper36 used EMG with 12 children and adolescents daily over a 5-day period. There was a reduction of mean 36.7% in stuttering after treatment (pre-mean 4.9% of syllables are stuttered to post mean 4.4% of syllables are stuttered), however it was noted that rate of speech post intervention was only around half that of a non-stuttering population. One participant had a worse percentage of syllables that are stuttered following intervention.
The final papers included in this categorisation of feedback and technology interventions were three papers outlining the use video self-modelling (VSM) (participant viewing of videos of themselves which had been edited to remove stuttering). The self-modelling intervention tested by Bray and Kehle44 was carried out on seven occasions over 6 weeks. Results are reported descriptively by the four individual participants, with mean number of stuttered words ranging from 5.9 to 9.1 at baseline and 0.3 to 3.2 at the 8-week follow-up. A more recent paper48 evaluated the viewing of edited videos daily over a 1-month period. This study investigated the potential use of this intervention with people who stutter who had received previous interventions but had relapsed. Results indicated a significant reduction of 5.4% of syllables that are stuttered (p < 0.0001) post intervention, an ES of 1.1. Self-reported rating of severity also was significantly reduced (p < 0.0001, ES 1.4), with no significant adverse effect on speech naturalness found. A second paper from this research team17 evaluated VSM as part of the maintenance programme following a smooth speech/prolonged speech (PS) intervention. The study (which was judged as at lower risk of bias) compared standard maintenance with VSM over a 4-week post-intervention period. It found that there was no significant difference between standard maintenance and VSM outcomes in terms of percentage of syllables that are stuttered (p = 0.92), self-rated anxiety (p = 0.12) or avoidance (p = 0.69); however, self-reported rating of typical and worst severity were better in the VSM group (p = 0.062 and p = 0.012). Participants in this group rated their satisfaction with fluency as greater (p = 0.043) and quality-of-life scores were higher (p = 0.027).
Cognitive interventions
This category of interventions may have content that includes reduction of tension, anxiety, fear, shame or stress; or a greater acceptance or feeling of control over stuttering; improved self-esteem; or more positive perceptions of own communication and desensitisation to the stutter. The interventions aim to effect change in psychological or psychosocial processes in people who stutter. This type of intervention may be used alone or to support, optimise or prepare for other interventions and may traditionally have been delivered by counsellors or psychologists. However, it is increasingly being perceived as part of a speech and language pathologist’s role, particularly in the UK. The anticipated outcomes may be direct speech gains, psychological well-being gains that lead to improved speech, or alternatively gains which do not aim to change the frequency or severity of the stutter but instead relate to living successfully with stuttering.
Six papers were identified within this intervention typology. There was one paper published in the early 1990s,76 with other articles published 2002–12. 18,30,66,67,93 The work originated from a broad range of countries (Ireland, Australia, the Netherlands, India, Turkey) and all were judged to be at higher risk of bias (Table 9).
| Study details | Design | Risk of bias | Country | Population |
|---|---|---|---|---|
| Amster and Klein 200730 | Before and after | Higher | USA | Adults, n = 8 |
| De Veer et al. 200918 | RCT | Higher | The Netherlands | Adults, n = 37 |
| Kaya and Alladin 201266 | Before and after | Higher | Turkey | Adults, n = 59 |
| Kaya 201167 | Before and after | Higher | Turkey | Adults, n = 93 |
| Leahy and Collins 199176 | Before and after | Higher | Ireland | Adults, n = 5 |
| Reddy et al. 201093 | Before and after | Higher | India | Adults, n = 5 |
Two papers evaluated CBT. 30,93 Reddy et al. 93 presented the study findings as a series of five descriptive case reports only. The article outlines that SSI scores improved between pre and post assessment. It presents a formula for calculating percentage of therapy change but fails to include these data. Reportedly, three clients had clinically significant improvement in anxiety symptoms and dysfunctional cognitions and there was some benefit in self-reported quality of life, but details of this are very limited. An intervention reported by Amster and Klein30 was described as having CBT as the main focus; however, also included stuttering modification treatment for the final 8 out of 12 sessions. The study found a significant decrease (p = 0.035, ES 1.80) in participant self-rating of perfectionism during the early weeks of the treatment to mid-point, which was maintained at 15-week follow-up (no pre- to post data provided). Participants reported improved communication attitudes at the end of the programme and at follow-up (p = 0.017). Speech fluency scores using SSI were mean 24.38 at baseline, mean 11.75 post treatment and mean 13.75 at follow-up (ES 0.74 pre-treatment to mid-treatment and ES 0.51 mid-treatment to post treatment).
Leahy and Collins76 based a 10-session group intervention on personal construct psychology (PCP). Changes in SSI are reported by individual and range from 3 to 31 pre-intervention and from 0 to 10 post intervention for the five participants. However, this evaluation of PCP has a significant flaw as the clients received concurrent individual fluency therapy.
A paper by Kaya and Alladin66 and another by Kaya67 describe the use of hypnosis alone and hypnosis combined with diaphragmatic exercise for people who stutter. Rating of fluency pre and post intervention showed a significant effect (p < 0.000) with informal patient report in the later paper stating that all but four participants were ‘doing well’. Although these papers have reasonably large sample sizes (93 and 59, respectively) the rating scale used for evaluating fluency has considerable limitations.
The Mindfulness-Based Stress Reduction programme as a potential intervention for stuttering was examined by De Veer et al. 18 Although this is one of few studies identified that used a controlled design, the recruitment and allocation process together with only self-report measures resulted in a rating of higher potential for bias. The authors found a significant difference post intervention between intervention and control groups in measures of stress (p < 0.001), anxiety about speech situations (p < 0.01), self-efficacy trust (p < 0.01), locus of control (p < 0.001), coping (p < 0.05) and attitude towards speech situations (p < 0.01). Average ESs were found for self-efficacy beliefs, coping and attitude towards speech situations (d = 0.55, 0.62 and 0.48, respectively). ESs were large for stress, anxiety and locus of control (d = 1.16, 1.07 and 0.76, respectively). There was some maintenance of these positive outcomes at the 4-week follow-up.
Behaviour modification
The greatest number of papers identified that related to a single intervention was the LP. This intervention is based on operant conditioning principles with the content focusing on training parents to provide feedback (verbal contingencies) for stuttered speech and stutter-free speech. The precise mechanism of change whereby verbal contingencies lead to a reduction in frequency of stuttering is unclear and may include neural reorganisation, motoric alterations or changing system demands. In the LP, thresholds of percentage of syllables stuttered and stuttering severity determines progress from the first to the second stage of the intervention.
Twenty-two papers considered aspects of the programme including effectiveness in the short and longer term, predictors of treatment time, predictors of responsiveness, applicability in different countries and components of intervention delivery such as telehealth. 22,24–27,29,42,51,58,65,68,69,77,82,86,88,96,112,113,121–123 These papers compared intervention with no intervention and originate predominantly from Australia. An additional paper54 compared the LP with Demands and Capacities intervention and is therefore considered in detail in the section on papers comparing programmes. This intervention type, as well as having the largest number of papers, also tended to be where the quality was higher with 12 papers assessed as being at lower risk of bias (Table 10).
| Study details | Design | Risk of bias | Country | Population |
|---|---|---|---|---|
| Bonelli et al. 200042 | Before and after | Higher | Australia | Pre-school, n = 9 |
| Femrell et al. 201251 | Before and after | Higher | Sweden | Pre-school, n = 10 |
| Harris et al. 200222 | Quasi-RCT | Lower | Australia | Children – age unclear, n = 23 |
| Harrison et al. 200458 | Before and after | Lower | Australia | Pre-school, n = 38 |
| Jones et al. 200065 | Before and after | Lower | Australia | Pre-school, n = 216 |
| Jones et al. 200524 | RCT | Lower | New Zealand | Pre-school, n = 54 |
| Jones et al. 200825 | RCT | Lower | Australia/New Zealand/USA | School age, n = 28 |
| Kingston et al. 200368 | Before and after | Higher | UK | Pre-school, n = 78 |
| Koushik et al. 200969 | Before and after | Lower | Canada | School age, n = 11 |
| Koushik et al. 2011121 | Cross-sectional (retrospective case note analysis) | Higher | USA | Pre-school, n = 134 |
| Lattermann et al. 200826 | Quasi-RCT | Lower | Germany | Pre-school, n = 45 |
| Lewis et al. 200827 | RCT | Lower | Australia | Pre-school, n = 18 |
| Lincoln and Onslow 1997122 | Cross-sectional (follow-up data only) | Higher | Australia | School age, n = 43 |
| Lincoln et al. 199677 | Before and after | Higher | Australia | School age, n = 11 |
| Miller and Guitar 200982 | Cross-sectional (long-term outcomes data only) | Lower | USA | Pre-school, n = 15 |
| O’Brian et al. 201386 | Before and after | Lower | Australia | Pre-school, n = 57 |
| Onslow et al. 199429 | Controlled before and after | Higher | Australia | Pre-school, n = 11 |
| Onslow et al. 199088 | Before and after | Higher | Australia | Pre-school, n = 4 |
| Onslow et al. 2002123 | Cross-sectional | Higher | Australia | School age, n = 8 |
| Rousseau et al. 200796 | Before and after | Lower | Australia | Children – unspecified age, n = 29 |
| Wilson et al. 2004112 | Before and after | Higher | Australia | Pre-school and school age, n = 5 |
| Woods et al. 2002113 | Before and after | Lower | Australia | Pre-school and school age, n = 8 |
Behaviour modification programmes such as the LP are used largely with pre-school children. It is important to note that studies evaluating interventions in this population face the challenge of demonstrating not only if the intervention achieves change, but also need to fully consider the possibility of spontaneous remission of stuttering in participants. Although there is some variation in reported rates of spontaneous improvement, the figure is generally recognised as being in the region of 80% of children. 114 The recovery figures relate to a general population but precise figures for spontaneous improvement in clinical populations are currently unknown. The length of time since onset is believed to be a significant influencing factor in whether or not development stuttering resolves. In order to demonstrate clear evidence of effectiveness in populations of young children, interventions need to demonstrate not only evidence of effectiveness but change beyond a level of 80% recovery.
Of the 11 papers focusing primarily on clinical effectiveness of the LP, four reported early data from the 1990s. 29,77,88,123 These studies found positive effects on the percentage of syllables that are stuttered for small groups of participants, and indicated benefits (achievement of < 1.5% of syllables are stuttered) continuing to 12-month follow-up. One of these papers highlighted ethical issues with control group designs for this population. 29 The seven more recent articles were published between 2000 and 2012 and confirm the effectiveness of the LP using larger groups and stronger study designs. Harris et al. 22 found a significant mean reduction in the percentage of syllables that are stuttered of 39% (p < 0.001) pre- to post intervention in the nine children in the LP intervention group. This compared with a reduction of 16% for nine of the children who had not received the intervention and an increase of 6–54% of syllables that are stuttered in four other children in the control group. Owing to the control group design, this paper was able to demonstrate a greater improvement than spontaneous remission alone (although randomisation was quasi- rather than fully randomised).
The papers by Jones et al. 24,25 present data from a RCT with immediate, 12-month and up to 5-year follow-up. The first paper reported a reduction of 2.3% of syllables that are stuttered at 9 months and the second paper reported that 16 out of 19 participants who had completed the intervention and could be contacted had 0–1.1% of syllables that are stuttered at 5-year follow-up. Three participants had relapsed to pre-intervention levels; however, the reduction between pre-intervention and follow-up remained significant (p < 0.0001). Parental satisfaction was high and none of the children had received treatment other than the LP. Of the few participants in the control group who could be contacted, five out of the eight were reported to have recovered spontaneously.
Four papers published between 2008 and 2012 add further strength to the evidence of effectiveness of the LP. Lattermann et al. 26 evaluated use of the programme in Germany using a randomised design and a sample of 46 children. The intervention group decreased the percentage of syllables that are stuttered by 6.9% at home measurement compared with the comparator waiting list group reduction of 1.6% of syllables that are stuttered at 16 weeks post intervention. The in-clinic measures showed a similar reduction of 6.8% of syllables that are stuttered for the intervention group compared with 3.6% of syllables that are stuttered in the comparator group at 16 weeks post intervention, with a significant effect (p = 0.003 home and p = 0.025 clinic). The reduction in the percentage of syllables that are stuttered was not at the expense of a reduction in rate of speech.
Femrell et al. 51 reported outcomes at 2 years following intervention with the LP in Sweden. Eight out of the 10 participants completed the programme with a significant reduction in the mean percentage of syllables that are stuttered from 7.6% to 0.1%, a large ES of d = 2.9. The two dropouts withdrew early as parents were satisfied with the benefits achieved. Parents had been offered the choice of receiving the LP or an alternative intervention – all had chosen the LP. Koushik et al. 69 investigated use of the programme with older children (aged 6–10 years). Mean percentage of syllables that are stuttered at baseline was 9.2% and 1.9% of syllables are stuttered at follow-up, with no adverse effect on speech rate.
O’Brian et al. 84 explored the use of the LP in community clinics, rather than specialist centres. The study found a mean parental rating of severity at baseline of 5.2 and at 9-month follow-up parental rating of severity was mean 2.1. At 9 months, the mean percentage of syllables that are stuttered was 1.7% (no baseline provided) with a range of 0.1% to 13% of syllables stuttered and 47% of the children had a percentage of syllables that are stuttered below 1%. Some individual variation was highlighted, with 6 out of the 37 completing stage 1 reportedly having high severity ratings of 5–7. In addition to clinical effectiveness, this paper examined factors contributing to outcome. It reported that the clinician having a high level of specialist training was important in achieving optimal outcomes and that more severe stuttering was associated with longer intervention duration and higher dosage.
Nine further papers relating to the LP consider implementation issues and predictors of outcomes. Miller and Guitar82 replicated findings of effectiveness (an 86% reduction in stuttering severity measured by SSI p < 0.001, ES 3.7) reported in other papers when the programme was delivered by less experienced but specifically trained clinicians assisted by student clinicians. Children with more severe stuttering pre-intervention (≥ 5% of syllables stuttered) required a longer treatment time. Pre-treatment severity also predicted number of clinic sessions received in the Koushik et al. 121 and Rousseau et al. 96 studies. In Koushik et al. ,69 there was no association between sex, age or onset to treatment time and outcome; however, there was a seemingly counter-intuitive association between more frequent attendance and longer treatment time. Two further papers65,68 echoed the association between severity and time needed for treatment (OR 3.5 for more severe stutter to take longer to treat; p < 0.001). Eleven sessions was the typical length of treatment to complete stage 1. Although the earlier paper65 found a lack of association between onset to treatment time and outcome, Kingston et al. 68 (which combined data with the Jones et al. 65 study) detected an association between children stuttering for longer before treatment and reduced treatment time (OR 0.52).
Papers by Woods et al. ,113 Onslow et al. 123 and Bonelli et al. 42 explored the outcomes and impact of the LP. The first of these113 reported no evidence of an adverse effect on child behaviour, child mental health or parent–child relationship over the course of intervention for eight children and their mothers. The second42 found a positive effect on maternal speech rate following the programme for nine mothers (who had taken part in earlier studies). Onslow et al. 123 concluded that there was no evidence of an adverse impact on speech timing or language function in eight children (two of whom were in the Bonelli study42 and six in earlier studies77,122). Harrison et al. 58 aimed to evaluate which components of the LP may be the more important factors underpinning outcome. The authors evaluated (1) 4 weeks of parental requests to self-correct (verbal contingencies) compared with 4 weeks with no parental correction and (2) 4 weeks of parents completing severity ratings compared with 4 weeks of no rating. They concluded that parental verbal contingencies were likely to be the active element rather than completion of rating checklists.
The final two papers examining the LP investigated the potential for delivery of the programme via telehealth. Lewis et al. 27 concluded that telehealth delivery was effective (73% reduction in stuttering compared with a no intervention group; p = 0.02); however, required additional clinician input (costing around three times more than the standard version). A later paper112 in a small study with high dropout rates confirmed the clinical effectiveness but need for greater number of consultations for telehealth delivery of the programme.
Other interventions that we categorised as behaviour modification focused on changing behaviours within the family, predominantly parent behaviour and parent–child interaction. Four papers were identified which evaluated these interventions in children, all of which were rated as being at higher risk of bias. 78–81 As with the LP, they were primarily targeted at pre-school children and, thus, need to consider spontaneous recovery within their assessment of outcomes. Two additional papers in this category evaluated behaviour modification programmes with adults (Table 11). 21,23
| Study detail | Design | Risk of bias | Country | Population |
|---|---|---|---|---|
| Franklin et al. 200819 | Quasi-RCT | Higher | Australia | Adults, n = 60 |
| Hewat et al. 200623 | Quasi-RCT | Lower | Australia | Adolescents and adults, n = 30 |
| Lutz 200978 | Before and after | Higher | Germany | Parents, n = 11 |
| Mallard 199879 | Before and after | Higher | USA | School age, n = 28 |
| Millard et al. 200880 | Before and after | Higher | UK | Pre-school, n = 6 |
| Millard et al. 200981 | Before and after | Higher | UK | Pre-school, n = 10 |
| Yaruss et al. 2006115 | Before and after | Higher | USA | Pre-school, n = 17 |
Two papers from the UK by Millard80,81 evaluated parent–child interaction therapy. This intervention combines helping parents to manage their child’s stuttering through parent-identified interaction targets (such as reducing their rate of speech or complexity of language), with family strategies to develop confidence. In the earlier paper,80 which report data by individual participant, six children were followed up for a 12-month period. Three of these had reduced their stuttering severity on a 0–7 scale from 2, 3 and 5 to zero (normal speech), one had reduced from 2 to 1, one was unchanged and one reportedly did not reduce with this intervention, but reduced from 5 to 2 with a period of direct intervention. The later study81 aimed to use a randomised design but was forced to remove this comparator condition mid-way through. Data are reported by individual participant using cumulative sum control charts. Of the six children in the intervention group, four reportedly showed systematic reductions in stuttering frequency from baseline to follow-up at 12 months, which may be attributable to the intervention. One out of the four control group children showed a systematic reduction. From chart data, parental ratings of child fluency and confidence in managing stuttering appeared to increase.
Yaruss et al. 115 report a family-focused treatment targeting parent communication modification and parent and child understanding and acceptance of stuttering. Following the training there was a significant reduction in the 17 children’s dysfluencies (p < 0.001) as rated by the clinician. Parental rating scale data also indicated improved fluency and overall satisfaction with the treatment. The parent education component was rated as the most helpful element. Eleven of the children were discharged from therapy without requiring direct child intervention. Another study examining parent understanding and acceptance was reported by Lutz. 78 This weaker-quality paper reported that following a weekend parent workshop, 92% of participants rated themselves as having changed their attitude towards stuttering.
The Rustin programme was evaluated by Mallard. 79 This is a family-oriented intervention which includes a range of elements encompassing speech skills, transfer skills and social skills, which is delivered via children groups and parent groups. The therapy emphasises that families need to find the most appropriate intervention methods for them, with assistance from the clinician. The children in this study were school aged (5–12 years) rather than pre-school aged and the paper reports that 23 out of the 28 families (82%) did not receive any further intervention following the programme. The authors noted that the areas of the programme rated as most important by parents ‘had nothing to do with speech modification’, and instead were ‘letting the child take responsibility’, ‘family discussion’ and ‘listening’.
Although all the above interventions are used with children, an additional intervention that we categorised as behaviour modification is used with adults who stutter. Self-imposed time-out treatment is, like the LP, based on an operant conditioning approach. This intervention was evaluated in two papers that met our inclusion criteria, one rated as lower and one as higher risk of bias. This treatment involves participants learning to modify their behaviour by pausing for a moment after a stuttering episode. Hewat et al. 23 found individual diversity in response to the intervention. The mean reduction in the percentage of syllables that are stuttered from pre-treatment to post stage 1 was 53.6%. More than half (from figure total 13 of 22 [sic]) the participants reduced their stuttering frequency by more than 50%. Six participants reduced by 50–60%, three participants by 60–70% and four had an 80–90% reduction (numbers are approximate as taken from figure). Speech naturalness was judged as being poorer than non-stutterers post intervention but compared favourably with people who had completed PS treatment. Participants reported general satisfaction with the intervention.
The second paper assessing time-out19 found a significant reduction in the percentage of syllables that are stuttered between baseline and post treatment (mean 5.8% vs. 3.9% syllables stuttered; p < 0.007). A control group increased their stuttering in same time frame (from baseline 4.9% to 6.4% syllables stuttered; p < 0.007). There was no adverse effect on speech rate, with the intervention group increasing syllables per minute (SPM) post intervention. There was evidence of an association between stuttering severity and outcome (more severe responded better), and amount of previous therapy and outcome (more previous therapy responded better).
Speech motor interventions
Eighteen papers evaluated interventions that we classified in our typology as speech motor interventions. 31,37,38,45,46,49,53,62–64,84,85,89,90,104,106,107,114 The content of these interventions is focused on the mechanisms of speech production (breathing, vocal fold vibration, articulation of sounds) with reduction in the severity or frequency of stuttering achieved by altering speech motor patterns. People who stutter may be taught to change their speech pattern, for example by prolonging sounds, reducing speech rate or making articulation more soft or smooth. These interventions are referred to variously in the literature as ‘behavioural treatments’, ‘talk more fluently approaches’, ‘speech restructuring’ and ‘fluency shaping’. In order to be clear within our typology, we have labelled them as ‘speech motor’ rather than ‘speech behaviour’, in order to avoid confusion between these therapies and interventions targeting parent–child behaviour. These interventions typically include a clinician modelling the desired pattern and teaching the participant to use it. As the approach entails changing a participant’s usual pattern of speech, an important aspect to consider when evaluating speech motor interventions is not only the degree to which the therapy reduces the frequency or severity of stuttering, but also whether the speech produced using the changed motor pattern is acceptable to the speaker (and listeners) or whether it sounds slow and unnatural.
Although these interventions were given various labels, the largest group were described as consisting of teaching PS. This included the Camperdown Program, which is based on control of stuttering using PS. Seven papers from a team at the University of Sydney, NSW, Australia, and La Trobe University, VA, Australia, outline results from evaluation of PS treatment. These papers were published between 1992 and 2012, with four (mostly older papers) graded as being at higher risk of bias,84,85,89,90 and three graded as being at lower risk of bias. 38,46,47 Table 12 shows a summary of these studies.
| Study detail | Design | Risk of bias | Country | Population |
|---|---|---|---|---|
| Andrews et al. 201231 | Before and after | Higher | Australia | School age, n = 10 |
| Block et al. 200537 | Before and after | Lower | Australia | Adults, n = 80 |
| Block et al. 200638 | Before and after | Lower | Australia | Adults, n = 80 |
| Carey et al. 201045 | Before and after | Lower | Australia | Adults, n = 40 |
| Cocomazzo et al. 201246 | Before and after | Lower | Australia | Adults, n = 12 |
| Druce and Debney 199749 | Before and after | Lower | Australia | School age, n = 15 |
| Franken et al. 199253 | Before and after | Higher | The Netherlands | Adults, n = 32 |
| Ingham et al. 201362 | Before and after | Higher | USA | Adults, n = 30 |
| Ingham et al. 200163 | Before and after | Higher | USA | Adults, n = 5 |
| Iverach et al. 200964 | Before and after | Lower | Australia | Adults, n = 64 |
| O’Brian et al. 200384 | Before and after | Higher | Australia | Adults, n = 30 |
| O’Brian et al. 200885 | Before and after | Higher | Australia | Adults, n = 10 |
| Onslow et al. 199289 | Before and after | Higher | Australia | Adolescents and adults, n = 14 |
| Onslow et al. 199690 | Before and after | Higher | Australia | Adults, n = 18 |
| Trajkovski et al. 2011104 | Before and after | Lower | Australia | Pre-school, n = 17 |
| von Gudenberg 2006106 | Before and after | Higher | Germany | Unclear, n = unclear |
| von Gudenberg et al. 2006107 | Before and after | Higher | Germany | School age, n = 32 |
| Yairi and Ambrose 1992114 | Before and after | Higher | USA | Pre-school, n = 27 |
The lower-quality papers reported improvement in the percentage of syllables that are stuttered following intervention and at up to 12-month follow-up. O’Brian et al. 84 for example found pre-treatment mean 7.9% of syllables stuttered reduced to 0.4% of syllables stuttered at 12-months maintenance and Onslow et al. 90 found the percentage of syllables that are stuttered generally at, or near, zero for 9 out of the 12 clients (the other three scored > 1%), and a mean 82% reduction in stuttering frequency from baseline to immediate follow-up and 74% reduction at 6 months. 85 Evaluation of mean naturalness scores indicated that post intervention there was no significant impact on naturalness;89,90 however, one paper noted that people who stutter could be distinguished from non-stuttering speakers (mean 4.5 vs. matched control participants mean 3.6; p = 0.025) although the difference was less than one naturalness scale value. 84 Speech rate also did not appear to be adversely affected, for example all participants increased speech rate with the group mean increasing from 184 SPM to 228 SPM. 85
The three papers judged as being at lower risk of bias, similarly reported positive effects of PS intervention. Block et al. 38 reported a pre-treatment mean percentage of syllables that are stuttered of 4.9% (SD 4.4%). Levels of stuttering reduced to a mean of 0.9% (SD 1.4%) of syllables stuttered immediately post treatment and 1.5% (SD 2.2%) of syllables stuttered at 3-month follow-up. At 12 months, the mean percentage of syllables that are stuttered was 2.6% (significant difference from baseline; p = 0.04) and at 3.5–5 years, during a surprise telephone call, the mean percentage of syllables that are stuttered was 1.6%. Carey et al. 45 echoed positive outcomes using a telehealth delivery and conventional delivery of the Camperdown Program. Cocomazzo et al. 46 used supervised student clinicians to deliver the intervention and found that similar outcomes could be achieved to that obtained by qualified clinicians (pre-treatment percentage of syllables that are stuttered 5.7%, immediate post treatment 1.0% of syllables stuttered, 12-month follow-up 2.4% of syllables stuttered, ES 0.61–0.75). Speech naturalness scores echoed the earlier work38 in finding that participants who completed the treatment had scores averaging one scale point below (less natural) than non-stuttering speakers. Variation in effect on naturalness was described by Cocomazzo et al. 46
Block et al. 38 examined possible predictors of successful outcomes and concluded that only baseline stuttering severity and short-term response to intervention predicted longer-term outcomes. Age, sex, perceived locus of control, attitude to communication or previous treatment did not predict long-term outcome. The authors highlighted that 46% of variance between participants at long-term follow-up was unaccounted for.
Another paper that evaluated speech motor programmes in adults examined a smooth speech intensive treatment. 37 The study found the reduction of the percentage of syllables that are stuttered following treatment was statistically significant (pre-treatment 5.4% of syllables stuttered and post treatment 1.8% of syllables stuttered, large ES 0.86) and at 3.5- to 5-year follow-up the mean stuttering rate was 1.6% of syllables stuttered. A paper from the Netherlands53 found an improvement from 27.7% of syllables stuttered pre-intervention to 5.8% of syllables stuttered post intervention and change from baseline but considerable relapse to 16.3% of syllables stuttered at 6-month follow-up. There was no impact on speech rate and some positive effect on rating of speech distortion; however, dynamics/prosody rating was no nearer to non-stuttering speakers post intervention than it has been before the therapy. Iverach et al. 64 examined whether or not the presence of a mental health disorder had an impact on outcomes following speech motor intervention. The authors found that stuttering frequency and situation avoidance were significantly worse for participants who had a mental health disorder.
Two papers by Ingham et al. 62,63 judged to be at higher risk of bias examined the use of Modified Phonation Intervals. Ingham et al. 63 described five adults as achieving stutter-free and natural sounding speech immediately and at 12-month follow-up after completing the intervention. The later paper62 focused on examining brain activity as a potential predictor of outcome following modified phonation intervals or PS intervention, and reports some positive outcome data (a pre-treatment mean of 7.1% of syllables stuttered and end of treatment mean percentage of syllables that are stuttered of 1.0%).
Speech motor interventions are not only used with adolescent and adult populations but also with children. von Gudenberg106 and von Gudenberg et al. 107 evaluated Kasseler Stuttering Therapy, Yairi and Ambrose114 describe slow speech therapy outcomes and Druce et al. 49 describe their intervention as most closely approximating the Gradual Increase in Length and Complexity of an Utterance (GILCU) model. This was the only paper evaluating speech motor interventions with children that was rated as being of lower risk of bias49 but all papers reported positive outcomes. The von Gudenberg et al. 107 paper from Germany found large ESs for their treatment comparing baseline to 1-year follow-up (d = 0.96 for 9- to 13-year-olds, and d = 0.88 for 14- to 19-year-olds). The other paper evaluating the Kassel smooth speech and PS treatment106 reported no adverse effect on speech naturalness or speech rate and improved self-perception of their speech among participants. Druce et al. 49 also reported positive outcomes. From pre-intervention to after the intensive week intervention the mean percentage of syllables that are stuttered for the group decreased by 7.6% to 1.75% (p = 0.0015).
The Yairi and Ambrose paper114 differs from the others in the group by using a natural history approach to compare pre-school children who received an intervention with no-intervention controls, rather than evaluating the clinical effectiveness of a specific intervention. The study highlights the importance of considering natural recovery in this population, as it found that although the intervention group reduced their level of stuttering, there was no significant difference between this group and untreated children over time. Both had a downwards trend in dysfluency and there was no significant difference between them (p = 0.4).
The final papers in this group examined interventions for pre-school and school-aged children termed syllable timed speech (STS). The paper judged at lower risk of bias104 evaluated STS and reported a mean stuttering reduction of 96% in beyond-clinic conversations from pre-treatment 6% of syllables that are stuttered to 12-month follow-up 0.2% of syllables that are stuttered (large ES 1.8). In another evaluation of STS, Andrews et al. 31 found the group mean percentage of syllables that are stuttered reduced from 14.4% at baseline to 6.7% at follow-up (p = 0.015, medium ES 0.7). Data on self-reported severity, situation avoidance and quality of life confirmed these positive outcomes, but the authors noted considerable individual variation in response to the intervention.
Speech motor combined with cognitive elements
As mentioned above (see Cognitive interventions), cognitive interventions may be used as an intervention type in isolation, or alternatively may form part of a programme. Eighteen papers reported interventions that combined speech motor therapy with elements of cognitive interventions (Table 13). In contrast with the cognitive interventions only category, in which all papers were considered to be at higher risk of bias, one-third of these papers combining cognitive with speech motor elements were judged to be at lower risk of bias.
| Study design | Design | Risk of bias | Country | Population |
|---|---|---|---|---|
| Baumeister et al. 200332 | Before and after | Higher | Germany | School age and adolescents, n = 37 |
| Beilby et al. 201233 | Before and after | Lower | Australia | Adults, n = 20 |
| Berkowitz et al. 199434 | Before and after | Higher | USA | School age, n = 8 |
| Blomgren et al. 200539 | Before and after | Lower | USA | Adults, n = 19 |
| Boberg and Kully 199441 | Before and after | Higher | USA | Adolescents and adults, n = 49 |
| Huinck et al. 200661 | Before and after | Lower | The Netherlands | Adults, n = 25 |
| Irani et al. 2012116 | Mixed methods | Higher | USA | Adults, n = 7 |
| Laiho and Klippi 200770 | Before and after | Higher | Finland | School age, n = 21 |
| Langevin and Boberg 199371 | Before and after | Higher | Canada | Adults, n = 10 |
| Langevin and Boberg 199672 | Before and after | Lower | Canada | Adults, n = 4 |
| Langevin et al. 200673 | Before and after | Lower | Canada and the Netherlands | Adults, n = 25 |
| Langevin et al. 201074 | Before and after | Lower | Canada | Adults, n = 17 |
| Lawson et al. 199375 | Before and after | Higher | UK | Adolescents, n = 15 and 19 |
| Nilsen and Ramberg 199983 | Before and after | Higher | Sweden | Adolescents, n = 13 |
| Rosenberger et al. 200795 | Before and after | Higher | Germany | School-age children and adolescents, n = 19 and 15 |
| Smits-Bandstra and Yovetich 200399 | Before and after | Higher | Canada | School age, n = 3 |
| Stewart 1996100 | Before and after | Higher | UK | Adults, n = 12 |
| Ward 1992110 | Before and after | Higher | UK | Unclear, n = 4 |
The Comprehensive Stuttering Program (CSP) for adolescents and adults was evaluated in six papers,41,61,71–74 with all but one of these from a research team in Canada. This intervention incorporates speech motor techniques with cognitive strategies to have an impact on emotional and attitudinal aspects in addition to speech fluency. Of the three papers published in the 1990s,41,71,72 only the later paper72 was rated as being at lower risk of bias. All papers reported a substantial reduction in client percentage of syllables that are stuttered following intervention. The later paper72 reported that four participants improved stuttering by 55–99% following the CSP, mean percentage of syllables that are stuttered at baseline was 61.3% and 12.5% at immediate follow-up. Langevin and Boberg (1993)71 reported a pre-treatment mean of 15.3% of syllables that are stuttered during a telephone call, 0.8% post treatment, and 2.4% of syllables that are stuttered at a 12- to 14-month follow-up telephone call. Boberg and Kully41 found pre- to immediate post-treatment mean percentage of syllables that are stuttered decreased from 19.59% to 1.29% for the adult group and 14.32% to 1.75% for the adolescent group. As with the Langevin and Boberg paper,71 this study indicated some fading of effect, as percentage of syllables that are stuttered had increased from 1.29% immediately post intervention to 4.27% at 4 months and 6.03% at 12 months for the adult group, and from 1.75% immediately post treatment to 3.65% at 4 months and 3.89% at 12 months for the adolescent group. The authors found no adverse effect on speech fluency following the CSP, with the mean SPM increasing from 126.5 pre-treatment to 140.7 post treatment. The Langevin and Boberg71 paper is interesting in that it reported data for people who exhibit cluttering in addition to stuttering, as a separate group to people who stutter. They noted that adults who clutter respond more poorly to intervention.
The three more-recent papers all had stronger designs and were judged to be at lower risk of bias. One paper reports long-term outcomes in Canada,74 another considers predictors of outcomes in the Netherlands61 and the third compares the findings across Canadian and Dutch populations. 73 Langevin et al. 74 present 5-year follow-up data from 18 adults following treatment with CSP (including some participants that were reported in the 1993 and 2006 studies). Since the earlier study,72 eight individuals had attended refresher sessions and 10 had not. Pre-intervention mean percentage of syllables that are stuttered was 15.86% and immediate post-intervention percentage of syllables that are stuttered was 0.90% (pre- to post intervention; p < 0.001, ES d = –2.07), with 1-year follow-up mean of 3.59% of syllables that are stuttered. At subsequent yearly time points, the percentage of syllables that are stuttered remained reasonably stable (4.38%, 3.81%, 3.76%, 4.98%) with pre-intervention to 5-year follow-up reduction significantly different (p = 0.02, ES d = –1.16). Other measures [S24, Self-Efficacy Scaling by Adult Stutterers (SESAS), PSI] also indicated self-report benefits for participants at 2 years post intervention and SPM increased following treatment. Langevin et al. 73 compared data sets from Canada and the Netherlands, with ESs of d = 0.52 (Dutch), d = 0.86 Canada and d = 0.69 (pooled). For the Dutch group, 71% were categorised as maintaining clinically significant reductions at 2 years, and 86% in the Canadian group. Both groups of participants had mean naturalness ratings that were within the range of mean ratings reported for non-stutterers (range 2.3–3.6).
Individual variation in patterns reported in studies of the CSP was investigated by Huinck et al. 61 They found that those with the most severe stutter pre-intervention had the most immediate gain, but tended to be more likely to regress. Severity of stuttering did not predict severity of negative emotions, with people having more negative emotions tending to rate their stutter as worse than it actually was.
In three papers39,70,75 authors described their intervention for adults only or adolescents and adults as being based on stuttering modification techniques used by Van Riper. 127 The Successful Stuttering Management Program includes confrontation of stuttering (targeting attitudes and perceptions), stuttering modification techniques (prolongation, cancellation and pull outs) and maintenance. Blomgren et al. ,39 in a study judged to be at lower risk of bias, found statistically significant improvements at 6 months post treatment on client-reported perceptions (the Avoidance and Expectancy subscales of the PSI; p < 0.001) and two specific affective functioning measures (the Psychic and Somatic Anxiety subscales of the Multicomponent Anxiety Inventory IV (MCAI-IV); p = 0.078 and 0.036, respectively). However, statistically significant reductions were not evident on objective measures of dysfluency for the adult participants (during monologue, mean 17.8% pre-intervention to 11.8% post intervention, and 13.8% at 6 months post intervention). Another intervention drawing on Van Riper’s methods127 for therapy with adults was outlined in Lawson et al. 75 This method was described as combining block modification, avoidance reduction and elements of PCP. The study found positive changes in avoidance on PSI but no change in percentage of syllables that are stuttered, struggle or expectancy. The positive effect on avoidance was unchanged at 1-month follow-up.
Laiho and Klippi70 evaluated an intervention drawing on Van Riper’s methods127 with children and adolescents. The intervention had a positive effect on stuttering severity (a reduction in percentage of syllables that are stuttered) for 14 out of the 21 participants (mean percentage of syllables that are stuttered pre-intervention was 4.45% and post intervention was 2.7%: a 38% improvement; p = 0.001). The amount of avoidance behaviour also reduced for 13 participants (p = 0.001) and positive feedback was received from participants. Rosenberger et al. 95 combined stuttering modification with social interaction activities and awareness tasks for children who stutter. Positive effects were found for stuttering rate (p < 0.001) and anxiety (p < 0.025).
Other papers reporting outcomes from programmes for children which combined speech motor and cognitive elements include Berkowitz et al. ,34 Smits-Bandura and Yovetich99 and Baumeister et al. 32 The Smits-Bandura and Yovetich99 programme achieved some reduction in behavioural and attitudinal stuttering symptoms; however, it was reported that 90% of the participants required further therapy after 2 months. Berkowitz et al. 34 outlined findings following intervention with the Cooper Personalised Fluency Control Therapy Program. Although there appeared to be some benefit, the results are reported as scores on individual tests and general description only. Baumeister et al. 32 found a significant reduction in stutter frequency following an intensive summer camp encompassing speech, cognitive and social elements. The data are limited by analysis of different groups of participants at different time points, but indicates a reduction from 22.2% of syllables that are stuttered to 9.5% of syllables that are stuttered (ES 1.29).
Other papers reporting outcomes for adults from speech motor and cognitive interventions include Nilsen and Ramberg,83 Ward,110 Stewart100 and Irani et al. 116 All were rated as being at higher risk of bias. Irani116 is notable as the only study we identified that used a mixed-methods study design. The paper has therefore been included in both the review of effectiveness and the qualitative review. The intervention combined cognitive and speech motor elements including CBT in an intensive programme. The percentage of syllables that are stuttered pre-intervention to post intervention during conversation was significantly improved with a large ES of 1.12. S24 scores (ES 1.19) and locus of control of behaviour (LCB) assessment (ES 0.75) also indicated benefits pre- to post intervention. Participants were interviewed at a follow-up interval of between 2 and 6 years post intervention, with improvement compared with baseline sustained (ES 1.25–1.97; p < 0.07). However, the table of participants details that three out of the seven participants received more than one course of intervention.
Ward110 evaluated semi-intensive fluency therapy (SIFT), which is described as similar to CSP but with identification, prolongation and transfer phases. Pre-intervention percentage of syllables that are stuttered for the group during conversation was 10.2% and post-intervention percentage of syllables that are stuttered was 3.3%. Stewart100 examined attitude change during therapy and maintenance. At baseline, the mean percentage of words stuttered was 30.6% (SD 28.28%). After attitude change sessions, the percentage of words stuttered group mean was 30.7% (SD 34.5%). After 1 year, the group mean was 12.6% (SD 25.78%) and after 2 years the group mean was 19.7% (SD 18.9%). The author noted that the specific attitude-change sessions did not seem to result in significant changes, but change was apparent in most of the attitude measures following the technique sessions. During transfer and maintenance, the group maintained speech gains but a small number of participants had poor maintenance. A paper from Sweden83 used independent listener and therapist ratings of change. Overall, 12 out of the 13 participants were rated as having improved on at least one aspect measured. The most recently published paper in this final group of studies is Allen,117 a paper from the UK, which examined e-mail as a component of a speech modification and counselling intervention. The limited evaluation data outline that out of the 16 clients who used e-mail as part of therapy, 11 were discharged (two owing to non-response) and five clients remained on the caseload.
The final paper in this group assessed the effectiveness of Acceptance and Commitment Therapy (ACT). 33 The intervention was carried out weekly over 8 weeks and included mindfulness skills in the programme. Although this study used a before-and-after design with no comparator group and a large number of self-report measures, it included speech data and exhibited rigor in collection and analysis of data and, therefore, was rated as comparatively at lower risk of bias. Results from this study showed statistically significant gains across all measures from pre- to post treatment and at 3-month follow-up. Percentage stuttered syllables reduced from pre-intervention mean 6.42% to post-intervention mean 1.39% and mean 1.77% at follow-up (p < 0.001). Psychological measures such as OASES also improved significantly post intervention and at follow-up (p < 0.001).
Multiple elements
Eleven papers described interventions that included multiple components across our typology of interventions, or were papers that evaluated a range of interventions (Table 14).
| Study | Design | Risk of bias | Country | Population |
|---|---|---|---|---|
| Allen 2011117 | Cross-sectional | Higher | UK | Adults, n = 16 |
| Blood 199540 | Before and after | Higher | USA | Adults, n = 4 |
| Craig et al. 200247 | Before and after | Higher | Australia | Adolescents, n = 6 |
| Elliott et al. 199850 | Before and after | Higher | USA | School age, n = 5 |
| Gagnon and Ladouceur 199255 | Before and after | Higher | Canada | School age, n = 4 and 4 |
| Hancock and Craig 200257 | Before and after | Lower | Australia | Adolescents, n = 12 |
| Hasbrouck 199259 | Before and after | Higher | USA | Adults, n = 117 |
| Pape-Neumann 200491 | Before and after | Higher | Germany | Adults, n = 100 |
| Sicotte et al. 200398 | Before and after | Higher | Canada | School age, n = 6 |
| Wagaman et al. 1993108 | Before and after | Higher | USA | School age, n = 8 |
| Wagaman et al. 1995109 | Before and after | Higher | USA | Adolescents, n = 7 |
Three treatment programmes included EMG feedback, one for children and two for adolescent clients. Hancock and Craig57 and Craig et al. 47 examined a retreatment programme for adolescents who were experiencing difficulty maintaining fluency following intervention. The therapy included EMG, smooth speech, relaxation, cognitive and self-management components. The follow-up level of percentage of syllables that are stuttered at 12 months was no different for the retreatment intervention compared with the initial intervention. However, the retreatment intervention resulted in significantly lower percentage of syllables that are stuttered at 2-year follow-up than the initial intervention 2-year follow-up. The SPM scores were also significantly better for retreatment at 2-year follow-up than initial treatment 2-year follow-up. Narrative in the Craig et al. 47 paper describes individual difference in response, with two participants showing immediate improvement after the relapse programme; however, they had relapsed to > 5% of syllables that are stuttered at 2-year follow-up. Two other participants reportedly improved quickly and gains were maintained (‘well below 5% of syllables that are stuttered’) at 2 years. The final two participants reportedly improved more slowly but at 2 years remained ‘well below’ 5% of syllables that are stuttered. Hasbrouk59 also described a treatment programme including EMG combined with airflow training, relaxation and desensitisation used with adult military service personnel. The mean number of stutters for the 151 participants reduced from 5.34% to 0.18% with all reaching the criterion level of < 1% stuttered words. The author noted that the programme was less effective for those with more severe stuttering at baseline.
The intervention reported by Blood40 involved motor speech changes assisted by a biofeedback computer program together with POWER, a relapse management prevention approach targeting self-efficacy and cognitive–behaviour modification. At the end of phase 1, all participants had reduced stuttering to the criterion level of < 3% of syllables that are stuttered. Two increased percentage of syllables that are stuttered to > 3% during the second and third phases; however, did not relapse to pre-treatment levels. The feeling and thinking scales all showed positive changes, which were maintained at 6 and 12 months.
Four other papers included regulation of airflow in the intervention components. These papers from North America report intervention with 5- to 11-year-old children. The interventions included regulated breathing, awareness training, social support, easy speech and relaxation. Positive outcomes following intervention were reported for the majority of participants across the studies. Elliott et al. 50 found four out of the five children reduced stuttering to < 3% stuttered words, Gagnon and Ladouceur55 described a similar reduction with gains retained at 6-month follow-up. Wagaman et al. 108 reported that all eight children reduced the proportion of stuttered words to < 3% and that parents rated the intervention as acceptable. A paper reporting longer follow-up data from this study109 found that for five out of seven participants, the follow-up mean percentage of syllables that are stuttered at 3- to 5-year follow-up was lower than at 1-year follow-up. For the other two participants, the mean percentage of syllables that are stuttered had increased from 1-year follow-up level but the score remained well below their pre-intervention stuttering levels.
Pape-Neumann91 evaluated interventions which were chosen by clinicians rather than examining a particular therapy type. For any intervention delivered to children, data indicated a reduction in stuttering frequency of ES 0.63 post intervention. For adolescents and adults, the ES across any intervention was 0.77. A positive impact on avoidance of communication, attitude towards communication, self-judgement of stuttering in social situations and everyday life was also recorded across the therapies. Sicotte et al. 98 examined the feasibility and application of telemedicine across an unspecified typical therapy for six children and adults who stutter. Data are limited but all participants improved fluency with some benefits retained at the 6-month follow-up.
Papers comparing interventions
Our final typology contains papers that had the purpose of directly comparing interventions with each other. We identified eight papers that compared interventions with one another (rather than having no comparator, or comparing an intervention with no intervention). These papers were generally of reasonable quality, with only two considered to be at higher risk of bias (Table 15).
| Study | Design | Risk of bias | Country | Population |
|---|---|---|---|---|
| Craig et al. 199616 | Quasi-RCT | Lower | Australia | Children and adolescents, n = 97 |
| Franken et al. 200554 | Before and after | Lower | The Netherlands | Pre-school, n = 23 |
| Hancock et al. 199821 | Cross-sectional (further analysis of RCT data) | Lower | Australia | Children and adolescents, n = 77 |
| Hancock and Craig 199820 | Cross-sectional (further analysis of RCT data) | Lower | Australia | Adolescents, n = 97 |
| Menzies et al. 200828 | RCT | Lower | Australia | Adults, n = 30 |
| Riley and Ingham 200094 | Before and after | Higher | USA | School age, n = 12 |
| Ryan and Van Kirk 199597 | Before and after | Lower | USA | School age and adolescents, n = 24 |
| Wille 1999111 | Before and after | Higher | Germany | School age and adolescents, n = 14 |
Franken et al. ,54 in a paper judged as being at lower risk of bias, compared the LP with Demands and Capacities Model (DCM) treatment for pre-school children. For the LP, the mean stuttering frequency within an audio-recorded sample decreased from 7.2% (SD 2.0%) at baseline to 3.7% (SD 2.1%) post intervention. For the DCM treatment, the means decreased from 7.9% (SD 7.1%) at baseline to 3.1% (SD 2.1%) post intervention. Stuttering severity was rated on a scale by clinician and parent with a significant effect from pre-intervention to post intervention (p < 0.01) for both interventions with no significant difference between them (p > 0.10).
Menzies et al. ,28 in another higher-quality study, compared speech motor intervention alone with speech motor combined with CBT. Post-treatment percentage of syllables that are stuttered at follow-up was around half that at baseline. The authors found no difference in percentage of syllables that are stuttered between the two groups, with the additional CBT treatment having no additional impact on the stuttering reduction than speech restructuring treatment alone. Although not affecting speech outcome, the group who received the CBT showed greater improvement on measures of anxiety and avoidance.
Bioresonance therapy was compared with standard speech therapy in a study from Germany. 111 The groups received one therapy for 10 sessions and then swapped to the other therapy for the second 10 sessions. There was some improvement in fluency during the first 4 months of therapy, but no further improvement in the second therapy phase for which intervention programmes changed. Data were limited and there was considerable variation in individual response to the intervention, meaning that was not possible to conclude whether or not bioresonance therapy was more effective.
The method of gradually increasing length and complexity of utterances was compared with DAF by Ryan and Van Kirk. 97 The study found that, although both interventions achieved a significant reduction in the percentage of syllables that are stuttered (p < 0.01), the GILCU programme was slightly superior in terms of generalisation of fluency. Riley and Ingham94 compared the effect of speech motor training (SMT) (emphasis on speech motor skills) with extended length of utterance (ELU) intervention (response-contingent feedback without direct SMT), specifically on vowel duration measures and stuttering frequency. Across both interventions there was a median decrease in the percentage of syllables that are stuttered of 3.19% (41% reduction), with 37% reduction for SMT and 64% reduction for ELU (the ELU intervention had a significantly greater effect; p = 0.04).
The Craig et al. 16 study mentioned earlier (see Feedback and technology interventions) compared EMG with intensive smooth speech and home-based speech for children and adolescents. All the therapies included reward and response contingencies, overcorrection, transfer, maintenance and self-monitoring. The study found that the percentage of syllables that are stuttered was significantly reduced baseline to post intervention and at 3-month and 12-month follow-up. The three treatments were found to be equally effective (p = 0). Two further papers20,21 examined longer-term outcomes and possible predictors of relapse following these interventions. At 4- to 6-year follow-up there continued to be no significant difference between the interventions in terms of effectiveness. An association was suggested between having a more severe stutter pre-intervention and being less anxious immediately post therapy, with having a higher level of stuttering in the long term.
Summary of effectiveness evidence
The review of intervention effectiveness found a substantial body of work (112 papers), which we divided into a typology of seven categories. Across the set of papers, the predominant finding was a report of some degree of positive outcome for people who stutter resulting from these interventions. Although the potential for reporting bias must be a consideration, the overall conclusion from examining this literature is that a diverse range of intervention types have some evidence of clinical effectiveness underpinning their use for people who stutter.
However, it is important to note that the literature has considerable variation in quality, with around three-quarters of the studies rated as being at higher risk of bias. The set of papers generally reported small numbers of participants, with few using designs with comparator groups. It is important to note that our criterion of higher versus lower quality is comparative across the set of papers, with only a small proportion of the literature using the highest quality controlled designs and very few achieving the ‘gold standard’ of full randomisation. Therefore, as a whole, there is little that could be considered to be at very low risk of bias. However, results from the higher-quality studies did not seem to be contradictory to those with greater potential risk of bias. In addition, on a positive note, the body of work does contain a sizeable number of studies with lengthy follow-up periods. Twenty-five papers had a follow-up period of 2 years or more, providing evidence that, although some fading of effect was likely, positive outcomes could persist in the longer term. The only group of interventions for which effects were of more short-term duration was the feedback and technology group, which seemed to offer people who stutter a more immediate gain in fluency to be used in particular situations of difficulty, such as talking on the telephone.
Measurement of effectiveness
The most significant challenge in comparing clinical effectiveness between different studies and interventions is the vast range of outcome measures used to evaluate change following an intervention. Outcomes measured include those relating to the frequency or severity of stuttering (number or percentage of words stuttered, number or percentage of syllables stuttered, rating of stuttering severity, number of stuttering events), perceived self-efficacy/control/esteem, anxiety/stress/depression level, self-perceptions of or attitude to speech/stutter, perception of self/others as being a stutterer, avoidance of words/situations, parent verbal interaction, rate of speech and perceived naturalness. The literature used three main strategies to evaluate the effect on these outcomes: first, by comparing percentage change pre-intervention to post intervention; second, by reporting level of frequency at baseline and again post intervention, and then using statistical means to examine the difference; and third, by descriptively comparing the severity level or need for further intervention pre- to post intervention.
Much of the literature reports the percentage of reduction in stuttered speech pre- to post intervention (e.g. baseline and follow-up assessment of percentage of syllables or words that are stuttered). However, these ‘degree of change’ measures have a significant limitation in that baseline stuttering severity will influence how substantial any positive change can be. An examination of baseline levels of stuttering among participants across studies reveals a high level of variation in the fluency of participants prior to the intervention, between studies and, importantly, within a study. For example, Lincoln et al. 77 reported a baseline mean among participants ranging from 5% of syllables that are stuttered to 18.9% of syllables that are stuttered, whereas Langevin and Boberg71 found a baseline stuttering rate ranging from 3.6% of syllables that are stuttered to 9.4% of syllables that are stuttered. Participants in the Rousseau et al. 96 study appeared to have a low baseline of 3% of syllables that are stuttered. Many studies highlighted that there was considerable individual variation in outcome31,38,52 with some linking this to baseline level of severity (e.g. O’Brian et al. 86).
Although caution is thus required when comparing reports of positive percentage reductions pre- to post intervention between papers with participants who have differing baseline stuttering levels, analysis of reduction of the percentage of syllables that are stuttered within each intervention typology reveals evidence of reduction across intervention approaches. Within the ‘feedback and technology’ group, authors reported percentage reductions in syllables stuttered of between 3% and 87%. In the ‘behaviour modification’ typology, percentage reductions in syllables stuttered ranged from 69% of syllables that are stuttered to 97% for the LP and 53% for the one paper23 reporting this measure using other interventions. In the ‘speech motor’ group, reductions in percentage of syllables that are stuttered were reported varying from 22% to 96%. For ‘speech motor plus cognitive’, the one paper70 using this measure found a 38% reduction in percentage of syllables that are stuttered. Among the ‘multiple components’ group, reductions of 52% and 89% were described and a 36.5% and 63.5% improvement in a comparison paper evaluating ELU and SMT interventions, respectively.
In addition to the requirement to consider baseline stuttering levels when evaluating these papers, it is also important to consider the impact of any change for the person who stutters. This requires consideration of not only change but clinical (or personal) impact of the improvement. It has been proposed that in order to be clinically significant, an intervention should result in a 50% reduction in stuttering. 93 Examining the set of papers (all 111 included studies) reporting percentage change in syllables stuttered with this criterion reveals that six out of the eight ‘feedback and technology’ group, all five of the Lidcombe papers, one non-LP behaviour modification paper, five of the six ‘speech motor’ papers and both of the multiple component interventions reached this level, again confirming that a range of intervention approaches identified could result in clinically significant improvement.
The second method for evaluating change was to report the level of stuttering frequency at baseline and again post intervention. These papers reported effectiveness in terms of p-values or ESs rather than percentage change. 24,30–32,37,48,51,73,74,82,91,104,106,116 In the ‘feedback and technology’ group, an ES of 0.14 was reported for stuttering (during monologue only) in one paper,119 and an ES of 1.1 for reduction of stuttering frequency in another48 and statistically significant changes were reported in nine papers. 4,35,52,56,92,118,120,124,125 In the ‘cognitive’ group, an ES of 0.74 for reduction in stuttering was found in one study30 and three papers reported statistically significant differences. 18,30,66 In the behaviour modification group ESs of 2.9, 2.3 and 2.3 are described,24,51,82 and eight papers provided evidence of statistically significant effects. 22,24–26,51,53,82,84 Speech motor and speech motor plus cognitive approach papers reported ESs of 0.70, 0.86, 1.80, 0.96, 0.88, 1.29, 1.12, 6.86 and 14.9630–32,37,73,74,104,106,116 and seven reported statistically significant effects. 32,39,70,73–75,95 One multiple component paper reported an ES of 0.6391 and three comparison papers described significant effects for each of the interventions they evaluated. 16,54,97 This set of findings thus supports the conclusion that a range of interventions may be effective for people who stutter. As with the percentage change evaluations described above, statistical significance may differ from clinical (or personal) significance and mask individual variation in outcomes. Statistical significance is also heavily dependent on sample size as very small effects can be statistically significant with a large sample, while relatively large effects may not be statistically significant with a smaller sample.
The third approach to evaluating outcomes considered level of stuttering before and again after an intervention, or whether or not further intervention was required. Although there is some debate regarding what is a ‘good outcome’ in terms of the level of stuttering following an intervention, many studies use a ≤ 3% of syllables that are stuttered level as being an acceptable degree of dysfluency and thus may be a target for interventions to achieve. 55 Four papers66,67,76,93 in the ‘cognitive’ group used severity scales to evaluate difference (two a scale developed by the author66,67 and two the SSI76,93), these studies found positive outcomes. The papers reporting the LP often included data from severity rating scales and the programme uses threshold levels of percentage of syllables that are stuttered in order for participants to move through the intervention stages. Four non-LP ‘behaviour modification’ papers78,80,81,115 reported positive outcomes in terms of parent report, stuttering severity or need for further therapy post intervention. Five ‘speech motor’ papers38,46,84,85,90 report reduced levels of percentage of syllables that are stuttered post therapy (to 0.9%, 1.6%, 1%, 0.4%, near 0%), three41,71,72 ‘speech motor plus cognitive’ (to 1.29%, 0.53%, 0.1–3.8%), six40,50,55,59,108,109 multiple component papers (to < 3% in four papers,40,50,55,108 < 2% in two papers59,109). These papers further confirm that using this approach to measuring effectiveness, there is evidence of positive outcomes for people who stutter across a range of intervention approaches.
Although stuttering frequency or severity measures were the most frequent outcome data reported, a smaller number of papers considered wider effects on the person who stutters or self-rated perceptions of stuttering. One feedback and technology paper92 used PSI scores and found that the significant effect of the technology immediately post fitting was not maintained at follow-up. The ‘cognitive’ interventions group (as may be expected) tended to use a wider range of measures to evaluate efficacy. They indicated that the intervention could have an impact on not only stuttered speech but also self-perceptions and attitudes. De Veer et al. ,18 for example, reported large ESs on anxiety and locus of control. In the ‘speech motor and cognitive category’, Lawson et al. 75 found change in PSI scores with reduction in avoidance the greatest area of change.
Dose–response outcomes
We endeavoured to examine the included literature to explore whether or not the number of hours of intervention could be linked to outcomes for people who stutter. The heterogeneity in measures used and variation in time points assessed made this type of analysis problematic; however, in order to explore this potential relationship we tabulated papers that included statistical analysis (p-values or ESs; Table 16). It can be seen that not only did different measures preclude drawing robust conclusions regarding a relationship, but also there was a substantial body of literature which reported that intervention hours varied between individuals receiving the same intervention. Interventions varied from only a few hours (mostly technology and feedback) to > 75 hours. If interventions included residential components, time was estimated as being more than ‘working day hours’ as many reported including evening social activities. However, for these studies, potentially all waking hours could be considered intervention hours making the estimate of ‘more than 75 hours’ potentially considerably below that actually received.
| Time | Study |
|---|---|
| Reported by length of treatment time only | Baumeister et al. 2003 (3 weeks):32 reduction 22.2% to 9.5%, ES 1.29 |
| Individual < 10 hours | Cream et al. 2009:48 ES 1.1 reduction in stuttering frequency. Mean percentage of syllables stuttered was 7.7% pre-intervention and 2.3% post intervention Franklin et al. 2008:19 post-treatment intervention group mean percentage of syllables stuttered was 3.9% (range 0.5–25.6%, SD 5.6%). Control group 6.4% (range 0.5–20.7%, SD 5.1%) Gallop and Runyan 2012:56 comparison of pre-fitting of device with current use or non-use of the device significant decrease in stuttering [F(1,6) = 17.44; p = 0.006] Pollard et al. 2009:92 statistically significant effect of SpeechEasy immediately post fitting compared with baseline [PSI score t(16) = 3.13; p = 0.014]. Effect not maintained at follow-up. No other pre- to post assessments reached significance (p > 0.05 for SSI and OASES) Stuart et al. 2004:102 statistically significant main effect of device [F(1,6) = 13.2, Huynh–Felt p = 0.011]. The proportion of stuttered syllables was reduced by approximately 90% during reading and 67% during monologue Unger et al. 2012:125 statistically significant main effect in the occurrence of stuttered syllables between the control (no device) and active DAF/FAF conditions [F(1.76, 51.08) = 4.89; p = 0.014] Van Borsel et al. 2003:105 conversation with an examiner significantly improved z-value = –1.051; p = 0.293 Zimmerman et al. 1997:126 significant main effect of the AAF condition [F(2,8) = 13.56; p = 0.0004, ŵ2 = 0.48] |
| Individual 10–19 hours | Harris et al. 2002:22 treatment group improved significantly more than the control group (F = 5.02; p < 0.05). The intervention group therefore improved twice as much as controls Kaya 2011:67 baseline stuttering rank judged as 3.06 (SD 1.33) scale units, after intervention 8.06 (SD 1.08) scale units. Mean difference –4.99 (SD 1.63) scale units. Pre and post measurements statistically significant (p < 0.000) |
| Individual 20–50 hours | De Veer et al. 2009:18 ES average for self-efficacy beliefs, coping and attitude towards speech situations (d = 0.55, 0.62 and 0.48, respectively). ES large for stress, anxiety and locus of control (d = 1.16, 1.07 and 0.76, respectively) Riley and Ingham 2000:94 63.5% reduction (p < 0.04). Difference between SMT and ELU intervention significant (p = 0.04) |
| Individual more than 75 hours | von Gudenberg et al. 2006107 after 1 year: 9- to 13-year-olds show an effect of d = 0.96, and 14- to 19-year-olds of d = 0.88. All ESs are large |
| Individual + group 10–20 hours contact time | Amster and Klein 2007:30 d = 0.74 (pre- to mid-treatment) and d = 0.51 |
| Individual + group 30–75 hours | Block et al. 2006:38 percentage of syllables stuttered pre-treatment was 5.4% and immediately post treatment was 1.8%. Large ES 0.86. The mean 3.5- to 5-year follow-up stuttering rate was 1.6% of syllables that are stuttered Craig et al. 1996:16 significant differences between control group and all treatment groups across all contexts (p < 0.001). Pre-treatment scores differed significantly from immediate post treatment (p < 0.001) Cream et al. 2010:17 there was an apparent difference between groups for the primary outcome of percentage of syllables that are stuttered at assessment 4. However, when adjusted for percentage of syllables that are stuttered at assessments 1 and 2, this difference was not statistically significant (mean difference: 0.06%, 95% CI –1.3% to 1.4%; p = 0.92) Irani et al. 2012:116 percentage of syllables stuttered pre- to post conversation was ES 1.12, 95% CI –0.07 to 2.17. Pre-intervention to time of interview was 1.97, 95% CI 0.59 to 3.09 Lawson et al. 1993:75 avoidance scores before the course significantly higher than after [F(1,42) = 13.99; p < 0.001]. Significant overall improvement on the PSI for all areas although avoidance greatest change. Struggle [F(3,122) = 3.03; p < 0.05], avoidance [F(3,122) = 14.02; p < 0.001], expectancy [F(3,122) = 4.80; p < 0.01] |
| Individual + group > 75 hours | Huinck et al. 2006:61 percentage of syllables that are stuttered pre- to post mean difference was 9.17 (SE 1.655; p < 0.0001), pre-intervention to follow-up was 3.09 (SE 0.913; p < 0.001), pre-intervention to follow-up was 3.79 (SE 0.866; p < 0.0001) Langevin et al. 2006:73 ES at 2 years was 6.86 in the Canadian group. ES at 2 years was 7.62 in the Dutch group Langevin et al. 2010:74 pre-intervention mean percentage of syllables stuttered was 15.86%, immediate post-intervention mean percentage of syllables stuttered was 0.9% and 5-year follow-up mean percentage of syllables stuttered was 4.98%. Pre- to post intervention was significant p < 0.001 (large ES –14.96), pre-5-year follow-up p = 0.002 (large ES –11.49) Rosenberger et al. 2007:95 reduction of stutter rate (p < 0.001) for T1, T2, and T3 |
| Individual + parent group | No studies |
| Child group + parent group 10–20 hours | Hancock and Craig 1998:20 significant difference (p < 0.001) pre- to post initial intervention for percentage of syllables that are stuttered at immediate post intervention, 3 months post intervention, 12 months post intervention and 2 years post intervention |
| Child group + parent group 20–50 hours | Druce and Debney 1997:49 (6.5 hours for parents and 1 week intensive for children). From pre-intervention to after the intensive week, the mean percentage of syllables stuttered for the group decreased by 7.6% to 1.75% with a SE of 0.54, change in the percentage of syllables that are stuttered with treatment statistically significant (95% CI –11.7 to –3.5; p = 0.0015) |
| Parent group | No studies |
| Unclear | Andrews et al. 2012:31 ES = 0.7 Armson and Stuart 1998:119 significant difference only for number of stuttering events during monologue; p = 0.10, ES 0.14. Not significant: number of syllables (p = 0.41, ES 0), or per cent stuttering (p = 0.46, ES 0) Trajkovski et al. 2011:104 ES = 1.8 |
| Hours varied by individual participant | Femrell et al. 2012:51 (9–46 visits) significant [t(7) = 4.3; p < 0.01] decrease in mean percentage of syllables that are stuttered before and after treatment [7.6% (SD 4.9%) vs. 0.1% (SD 0.2%), respectively] with large ES (d = 2.9) an average reduction of 97.8% after stage 2 Franken et al. 2005:54 (mean 11.5 sessions) the means decreased from 7.2% (SD 2.0%) to 3.7% (SD 2.1%). For DCM treatment, the means decreased from 7.9% (SD 7.1%) to 3.1% (SD 2.1%) Jones et al. 2005:24 ES 2.3% of syllables stuttered (95% CI 0.8% to 3.9%; p = 0.003) Jones et al. 2008:25 mean difference 55.5% of syllables that are stuttered (p < 0.0001), an 80% reduction in stuttering frequency Koushik et al. 2009:69 (6–10 visits) mean percentage of syllables stuttered baseline = 9.2% (SD 7.8%) and 1.9% (SD 1.3%), range 0.2–3.8%. At follow-up, significant difference (p = 0.0002) Lattermann et al. 2008:26 (average 13 sessions), F(1,41) = 10.300; p = 0.003, partial η2 = 0.201, the improvement in the treatment group significantly more than control group Lewis et al. 2008:27 (mean 49 consultations) estimated to be a 73% decrease in stuttering (95% CI 25% to 90%; p = 0.02) Miller and Guitar 2009:82 (mean 19.8 sessions) significant pre- to post change; p < 0.001, ES 2.3 Pape-Neumann 2004:91 stutter frequency ES = 0.63, naturalness of speech ES = 0.60, speech rate ES = 0.37. ES for avoidance of communication, attitude towards communication, self-judgement of stuttering in social situations and impact on all day life all = 1.70 Rousseau et al. 2007:96 percentage of syllables that are stuttered scores significant reduction (p < 0.0001) Yaruss et al. 2006:115 baseline mean stuttering frequency 16.4% (SD 6.6%), after treatment 3.2% (SD 2.0%). Significant reduction (z-value = 3.517; p < 0.001) |
Conclusions regarding any dose–response relationship are therefore limited owing to challenges extracting accurate information from studies and issues of differing outcome measurement. Interestingly, there was little discussion regarding how the contact hours had been determined for interventions with pre-designed schedules. Papers relating to the LP reported that individuals with more severe stuttering tended to require a greater number of contact hours and those with greater time since onset tended to require more sessions. There was no clear evidence that increasing contact hours for all participants led to more positive outcomes. Dose–response relationships seemed to be associated with characteristics of the people who stutter rather than the type and dosage of intervention.
Long-term effects
Fifty-one papers reported data at follow-up of 1 year or more following intervention. 16,20,21,25,27–29,37,38,40,41,45–47,49,51,56,57,59,61,63,66,69,71–74,77,79–82,84,90,91,96,97,100,103,104,106–110,112,114–117,122 The feedback and technology group, perhaps unsurprisingly owing to the nature of the interventions, tended to report immediate follow-up, with the effect of this technology demonstrated as a ‘quick fix’ method to reduce the percentage of syllables stuttered. Studies predominantly reported effects in laboratory rather than everyday settings; however, there was evidence to demonstrate its value in situations such as using the telephone. The other typologies provide evidence of long-term benefits (e.g. one study73 reports 71–86% of participants maintained gains) although there is evidence of fading of effect for many studies and substantial individual variation in the degree of preservation of effect. One study38 described that 46% of variance in effect at long-term follow-up between participants could not be accounted for.
Having considered the range of outcomes measured and examined evidence of positive outcomes across intervention approaches, a key question resulting from the review is that if these diverse types of intervention can all be effective then what is it about interventions that achieve change, what is the active ingredient that may be common across these differing programmes? Having analysed the intervention typologies and the outcomes, we then turned to the qualitative findings to seek further understanding of how these interventions may lead to their intended outcomes and whether or not the individual variation in outcomes reported may be explained by this literature.
Chapter 4 Results of the review of perceptions of people who stutter and staff providing service
The qualitative review used the same systematic review process of searching, selection, extraction and synthesis as the review of clinical effectiveness; however, this review differed in terms of inclusion/exclusion criteria and the method of synthesis as outlined in Chapter 2. Papers were quality appraised using the Critical Appraisal Skills Programme tool outlined earlier. 9 The research question for the qualitative review was: what are the factors that may enhance or mitigate against successful outcomes for people who stutter following intervention? It included data from individuals who have completed an intervention for stuttering in which papers reported views and perceptions regarding potential obstacles to them achieving successful outcomes following intervention. This included people who stutter, their parents, carers, partners and staff providing interventions.
As outlined in the Chapter 2, qualitative data were synthesised using thematic synthesis methods to develop an overview of recurring perceptions within the data. This method comprises familiarisation with each paper and coding of the finding sections. We analysed the themes to identify perceptions of interventions by type and then to examine data across the lifespan. In this section we will report the recurring themes relating to view of interventions, first by population subgroup (children, adolescents, adults, older adults) and then describe data outlining perceptions of stuttering across the lifespan.
Quantity of the research available
From an initial 4578 citations, 4363 were rejected on inspection of title/abstract. Twenty citations were deemed relevant to the second research question and, of these, six were excluded on reading the full paper (n = 14). A second search produced a further eight citations of which one was unable to be sourced (n = 7). The reference lists of all included papers were scrutinised for further relevant citations. Thirty-eight citations were identified as potential inclusions, of which six were deemed relevant on further inspection. Of these, five were included on reading the full paper. See Figure 1 for an illustration of the process of selection of papers. The total number of qualitative papers included in the review of views and perceptions was 25. One mixed-methods paper also contributed data to this element of the review, giving a total of 26 included studies. In three cases, two papers reported findings from the same study, giving 23 unique studies. A list of exclusions following the reading of full papers is presented in Appendix 4.
Type of research available
Study design
All but one of the included studies used semistructured interviews to collect data. 128–151 Two studies used repeated interviews,139,140 one included telephone as well as face-to-face interviews139 and one study used only web conferencing technology to collect interview data. 116 One study supplemented interviews with questionnaires,128 two studies added focus groups131,136 and a further study used only focus groups. 152 Eleven studies described a phenomenological approach to analysis,116,129,134,135,138,139,142,148–151 and two used Grounded Theory. 146,147 Seven studies reported using Thematic Analysis,116,128,137,140,142,143,152 one Framework Analysis136 and one Content Analysis. 144 A further three did not report a specific method of analysis, although two of these described stages representing a thematic approach. 132,133,141
All included studies examined lived experiences and coping strategies of being a person who stutters or a spouse/mother/parent of a person who stutters. One study focused on reflections of childhood experiences of stuttering by adults who stutter. 141 One study focused on ethnicity and another on the client/therapist relationship. 137,143 Five studies assessed views following therapy or self-help conference,116,136,139,140,145 two of these explored parental views about the LP139,140 and two explored adult experiences of PS therapy. 134,135 One study reported adolescent perceptions of a range of therapies including an intensive week-long course in PS, an intensive week-long course in Smooth Speech, individual PS therapy and the Camperdown approach. 141 One study assessed the experience of late recovery from stuttering. 128
Population
Of the included papers, four were published in the UK,131,136,140,150 11 in the USA,116,128,137,138,142,146–149,151 three in Canada,130,132,133 six in Australia129,134,135,139,141,152 and two in South Africa. 133,143 Populations in all but one study were adults (one assessed the views of adolescents and young adults who stuttered). 141 Of these, two studies included parents (one included mothers only) of children who stutter139,140 and two assessed the views of spouses129,130 (one included both fluent and dysfluent partners129) of people who stutter. One study focused on the interaction between stuttering and ethnicity, with a sample of African American males. 137 No papers described participants as being clutterers.
Quality of included papers
All included papers were quality assessed using the tool described in Chapter 2. Appendix 4 details the completed assessment for each paper. Of the 26 included studies, 18 were assessed as being at lower risk of bias and eight studies were assessed as being at higher risk due predominantly to a lack of reporting of elements (Table 17). See Table 17 for a summary of the papers.
| Author, country | Sample | Data collection method | Population | Focus of research | Data analysis methods as reported |
|---|---|---|---|---|---|
| Anderson and Felsenfeld 2003,128 USA | n = 6 | Interviews | Adults | Experiences of late recovery from stuttering | Thematic analysis |
| Beilby et al. 2013,129 Australia | n = 20 (10 dyads) | Mixed methods: interviews, questionnaires | Dyads (adults who stutter and their current life partner) | Impact of stuttering on adults who stutter and their partners | Phenomenology |
| Boberg and Boberg 1990,130 Canada | n = 15 | Interviews | Wives of people who stutter | How spouses are affected by their spouse’s stuttering | Not reported |
| Bricker-Katz et al. 2010,152 Australia | n = 11 | Focus groups | Adults > 55 years | Perceptions of people who stutter of limitations to activity and participation | Thematic analysis |
| Butler 2013,131 UK | n = 38 | Focus groups (self-help meetings) and interviews | Adults | Perspectives of people who stutter on their speech dysfluency and responses to their speech dysfluency | Grounded theory |
| Corcoran and Stewart 1995,132 Canada Corcoran and Stewart 1998,133 Canada |
n = 7 n = 7 |
Interviews | Adults | Experiences of adults who stutter | Immersion and crystallisation in the data to identify what is meaningful |
| Cream et al. 2003,134 Australia Cream et al. 2004,135 Australia |
n = 10 n = 10 |
Interviews | Adults | Experiences of adults who stutter | Phenomenology Line-by-line, holistic and selective thematic analysis |
| Crichton-Smith 2002,136 UK | n = 14 | Interviews | Adults who have/have not received therapy | The communicative experiences and coping strategies of adults who stutter | Framework analysis |
| Daniels et al. 2006,137 USA | n = 10 | Interviews | African American men who stutter | How African American men who stutter view communication, identity and life choices | Thematic analysis |
| Daniels et al. 2012,138 USA | n = 21 | Interviews and focus groups | Adults who stutter | Primary and secondary school experiences of adults who stutter | Phenomenology |
| Goodhue et al. 2010,139 Australia/ New Zealand | n = 16 | Repeat face-to-face and telephone interviews (nine with each participant) | Mothers of children who stutter | Mothers’ experiences of implementing the LP with their child | Phenomenology and thematic analysis |
| Hayhow 2009,140 UK | n = 16 (14 children) | Repeat face-to-face interviews (interviews repeated once with six participants) | Parents of children who stutter | Parents’ experiences of implementing the LP with their child | Thematic analysis and use of NVivo version 10 (QSR International Pty Ltd, Melbourne, VIC, Australia) |
| Hearne et al. 2008,141 Australia | n = 13 | Focus groups and interviews | Adolescents and young adults who stutter | Experience of stuttering and therapy for stuttering during the adolescent years. Reasons for reticence in seeking out therapy | Not described as a particular analysis method. The steps described include familiarisation and categorisation of themes |
| Hughes et al. 2011,142 USA | n = 7 | Interviews | Adults who stutter | Exploration of family experience of people who stutter related to their interactions with family members, speech therapy and stuttering management | Phenomenology and thematic analysis |
| Irani et al. 2012,116 USA | n = 7 | Interviews via web-conferencing technology | Adults who stutter | To gain a deeper understanding of clients’ perceptions of an Intensive Stuttering Clinic for Adolescents and Adults programme and measure long-term treatment outcomes | Phenomenology and thematic analysis |
| Kathard et al. 2004,143 South Africa | n = 7 | Biographical interviews | Adults who stutter | To explore processes shaping self-identity formation and the actions of people who stutter | Cross-case and thematic analysis |
| Klompas and Ross 2004,144 South Africa | n = 16 | Interviews | Adults who stutter | Life experiences of a group of South African adults who stutter and the impact of stuttering on their quality of life | Content analysis |
| Plexico et al. 2005,145 USA | n = 7 | Interviews | Adults who stutter | Understanding of how adults have been able to successfully manage their stuttering | Phenomenology and thematic analysis |
| Plexico et al. 2009,146 and Plexico et al. 2009147 (companion papers), USA | n = 9 n = 9 |
Interviews | Adults who stutter | To identify patterns of coping responses by adults responding to the stress resulting from the threat of stuttering To develop a model of coping and a better understanding of the complexities within the coping responses of people who stutter |
Grounded theory |
| Plexico et al. 2010,148 USA | n = 28 | Interviews | Adults who stutter | The underlying factors that contribute to a successful or unsuccessful therapeutic interaction between clients and their clinicians | Phenomenology |
| Plexico and Burrus 2012,149 USA | n = 12 | Interviews | Parents of children who stutter | To describe in detail the underlying factors that may be relevant to being a parent of a child who stutters | Phenomenology |
| Stewart and Richardson 2004,150 UK | n = 8 | Interviews | Adults who stutter | Experiences of adults who have completed a course of therapy for stuttering | Phenomenology |
| Trichon and Tetnowski 2011,151 USA | n = 12 | Interviews | Adults who stutter | To understand the lived experience of individuals who attended a self-help conference(s) for people who stutter from the perspective of a person who stutters | Phenomenology |
Data relating to views of interventions
We analysed studies according to the type of interventions described (if possible) to differentiate experiences. This allowed us to map qualitative and quantitative findings for later metasynthesis across the two reviews. We also categorised papers that reported views of interventions by population, to identify therapeutic experiences that might contrast or overlap between children who stutter and adults who stutter. For each population we examined potential barriers and facilitators to outcomes following therapy, together with factors that may be influential on the longer-term impact of interventions.
Views about interventions aimed at children
Eleven of the included papers provided data about experiences and views following childhood interventions for developmental stuttering;116,128,129,131–135,138,141,142 however, none of these studies included participants that were children at the time of the research. Nine papers included retrospective data relating to childhood experiences in adult samples. 128,132,136–138,142–145 Three further papers described parental experiences of supporting their children through therapy. 139,140,149 Two papers139,140 evaluated parental experiences of implementing the LP, which was developed specifically for early stuttering intervention. The programme comprises parental training to give appropriate and timely feedback to the child on stuttering instances. The treatment mechanism is reinforcement of non-stuttered speech through parental praise, which needs to outweigh reminders not to stutter by at least five instances to one. 123
Potential barriers and facilitators to positive outcomes from therapy for children
Barriers and facilitators identified related to accessing therapy, therapy techniques, therapist–client relationships, parental expectations and perceptions about their own involvement, children’s experiences, and perceived effectiveness.
Accessing therapy
Issues of access included reported difficulty in attending appointments at a clinic and accessing therapy during childhood. For children engaged in the LP, weekly clinic visits were described by some parents as being burdensome. One suggested way of overcoming this was to provide a combination of clinic visits and distance therapy. 140 Although retrospective data highlighted a general lack of suitable speech therapy during childhood, there was evidence from the studies of changing approaches to childhood therapy, with more activity within schools in relation to treating speech impairments. In one paper,138 it was suggested that an important aspect for children was for them to know who they can speak to in school to access support. In another paper,141 an adolescent participant spoke retrospectively of receiving positive support at school, because his teacher had experienced stuttering. This teacher not only exhibited experiential awareness, but he also provided advice about finding assistance.
Therapy techniques
Aspects of childhood speech therapy that were reported as having been unhelpful in hindsight included an undue focus on behavioural techniques, ignoring the emotional aspect of treatment and a lack of attention to the individuality of each pupil. 132,138 Specific strategies advised by therapists during childhood such as avoidance were, in retrospect, identified by people who stutter as not being beneficial for long-term recovery, with some taught techniques having to be unlearned later. Some approaches which were viewed as being unhelpful had also been recommended to family members who had tried to assist the child. Unhelpful approaches could lead to frustration that could, in turn, demotivate the client to continue with therapy. 142
Therapist–client relationship
The relationship between therapist and client was reportedly an important aspect of a positive therapy experience. However, in one study,132 some therapists were perceived as not having wanted to become involved in the treatment process. The suggestion of having access to a life counsellor to provide emotional and practical support to cope with life stages, in addition to sessions with a speech therapist, was viewed positively. 142 In another study it was suggested that school teachers should receive training in the current guidelines so that they can better support pupils who stutter. 138
Parental expectations and perceptions about their own involvement
Two papers provide detailed descriptions of parental expectations and perceptions of the LP. 139,140 All but one mother in the first study reported that they had expected that the LP would deliver improvements in speech quickly and that their child would be ‘fixed.’139 The mothers described in this paper,139 and one mother in the second study,140 reportedly did not expect to have to deliver the therapy themselves, nor did they anticipate the sustained effort and commitment required. Authors of the first paper139 described low expectations of outcome among participants (based on perceptions of the programme being comprised with only relatively simple methods); however, these initially low expectations had been surpassed in reality. Parents were described as expressing surprise at how little commenting on speech was encouraged on the programme, apart from during ‘talk time’, how much stuttered speech was allowed to continue, and how the children were encouraged to discover strategies for themselves. 140
Hayhow140 described some parents being very enthusiastic about the LP, whereas others appeared to have no strong positive or negative feelings. One parent was sceptical about it prior to registering, but she voiced satisfaction once she perceived that the programme could achieve benefit. Other parents were described as wondering why they had not thought of the positive reinforcement aspect themselves prior to joining the programme. Mothers reportedly found the programme easy to carry out in theory but sometimes reported difficulty remaining focused, especially when speech improved. 139 There were concerns voiced about the responsibility of correctly implementing the treatment with their child, which created feelings of anxiety and pressure, as well as feelings of failure when therapy was unsuccessful. 139,140 However, other parents reported positive feelings in that they could assist in their child’s therapy rather than leave it all to professionals. 140
There was also a reported lack of understanding about the long-term aims of the LP and where their progress was heading. A suggested solution to this was for documentation to be provided for parents at the beginning of therapy to advise them about what to expect and the timing of incremental steps of the LP, as well as having something that could inform their partner. However, one participant stated that the benefits of this approach depend on the individual’s learning style. 139 For some mothers, documentation about the LP and a support group was suggested as a way of sharing experiences and gaining contact with other parents who were implementing the LP. 139,140
One paper describing perceptions of other (unspecified) interventions found that some parents whose children received therapy arranged through the school system reported feeling dissatisfied. 150 In particular, they reported feeling uninformed and uninvolved in their child’s therapy. There was also a perception that group therapy was not satisfactory as it did not address individual needs. Some of the techniques that parents were advised to carry out by therapists could be perceived as frustrating and unrealistic in terms of time required and the way that techniques produced unnatural sounding speech.
Children’s experiences
Two papers139,149 reported parental perceptions regarding their children’s experiences during therapy. A further two studies132,138 outlined adult memories of experiences from their own childhood. In the first paper,139 which examined the LP, more than half of the mothers reported that the children enjoyed the programme, both in therapy sessions and at home, and that the children were instrumental in reminding their mothers about therapy and about receiving rewards. Praise from the mother was cited as a positive factor; however, in contrast, other children reportedly did not like consistently hearing feedback on their speech and in some cases mothers reported sensitivity and annoyance at hearing the word ‘smooth’. In order to address this issue, other terms had been introduced, such as ‘great talking’. In the other study, which included data relating to children’s experiences, some parents reported that they did not think that the therapy they had undertaken had been suited to their child’s needs. 140
Studies examining adult reflection on past childhood experiences of therapy reported general dissatisfaction. This may be due to the relatively undeveloped nature of therapeutic services historically compared with current provision. Participants in two papers reported that the speech therapy that they had received as a child during their school years generally focused on behavioural techniques and did not acknowledge the emotional impact of stuttering. 132,138 Participants reported that more discussion about such aspects of stuttering and perhaps a support group would have been appreciated. One participant commented that for young children, methods that incorporate relaxation and cognitive restructuring would be useful. Encouragement to practise talking at a young age was also mentioned as important. 138
Perceived effectiveness
Goodhue et al. 139 found that most mothers who were enrolled on the LP perceived that it was effective in reducing stuttering. Only one mother reportedly questioned the effectiveness, as her child had not shown consistent progression over the 6 months of therapy. Parents in another study (that did not specify which particular programmes children had received) reported variability in perceptions of effectiveness. Some parents could see improvement while others perceived that the therapy was unhelpful. 150
Parents reported that increased quality time with their child was a major benefit of the LP, particularly in the early stage. 139,140 It was not specifically the amount of time spent but the exclusive time together that was reported to enhance the bond between child and parent. 139 In addition, parents gained skills in managing stuttering as well as in parenting generally. Other benefits included raised awareness for the child about their speech fluency and an ability later in the process to adapt therapy at home according to the needs of their child. 139,140 The children’s confidence was also reported to increase, particularly when stuttering was reduced. Increased confidence was manifested in being more willing to try new things and being less shy. In addition, being able to speak more fluently at home increased confidence to do so with other people. 139
Retrospective accounts of therapy received showed varied views of effectiveness. A participant in one study128 attributed recovery at least in part to therapy received as a child, while in other studies there was evidence that childhood therapy was not perceived as being helpful. 132,141,143 Techniques suggested in one paper to enhance young children in increasing their fluency included relaxation, cognitive restructuring and generally encouraging talking. 138
Obstacles to long-term impact: maintenance in the ‘real world’
In addition to examining perceptions of interventions that had been received, the qualitative studies considered factors that may influence whether or not short-term gains were maintained in the longer term, to achieve a long-term impact. The factors identified that could be influential in achieving longer-term benefit were parental experiences, perceived family support and perceived support from the school.
Parental experiences
Although the techniques of the LP were reported to be easy to understand and implement in theory, in practice mothers reported difficulty keeping up the momentum in the face of setbacks, such as relapse. 140 They reported having insufficient time to carry out the objectives regularly because they were busy, often fitting in treatment around work and caring for siblings. Caring for siblings meant that concentration on treatment was often disrupted so that even a 10-minute dedicated time slot with the child who stutters was difficult to achieve. Forgetting to praise their child all the time, especially when stuttering showed signs of improvement, was also an issue. 139
Reported solutions to these barriers included using a previously established routine such as ‘story time’ as a time to implement structured conversations and breakfast/walking to school as a time to implement unstructured conversations. To overcome forgetting to implement treatment, visual reminders around the house for the child and mother were suggested, such as the promise of a toy reward that sits on top of the fridge or obtaining a star on a pin board when the child has achieved a set goal. Regular clinic sessions and telephone calls from the therapist also served as reminders to mothers. With regard to caring for siblings, it was reported that having a family member such as the father or grandparent around to take the sibling to a different room, or to involve the sibling in an activity or with toys, or to carry out conversations while a younger sibling was asleep was useful during conversation sessions. Success with these strategies depended on the sibling’s personality, developmental stage and mood. 139
Some mothers expressed concern that treatment was being carried out properly by them, with confidence in their own ability to implement therapy fluctuating according to the severity of the child’s stuttering. Although a mother’s confidence improved with their child’s improved fluency, conversely it waned when fluency deteriorated. Signs of improved speech motivated mothers to carry on with the therapy, whereas when speech deteriorated mothers felt lost for solutions. 139 In addition, some parents experienced difficulty taking a firm lead in the process, resulting in therapy being conducted on the child’s terms. 140 Hayhow140 speculated that positive progress influenced the parent’s ability to persist with treatment. The author also suggested that sessions could be arranged without the child present to allow the therapist to explore progress with the parents.
Some parents held beliefs about stuttering that were at odds with the underpinning theories of the LP. Difficulty in implementing some of the procedures was reported by parents that had initially been ambivalent about the programme. 140 Some parents described a reluctance to discuss stuttering at home owing to feelings of discomfort and embarrassment for the child, a perceived lack of knowledge about the subject and the perception that nothing could be done and that there was no clear end point. When speech therapy was discussed in the family, it was often instigated by the attendance at speech therapy sessions, which made parents feel more comfortable about discussing the subject.
A consistent theme across parental samples was the reported need for support to help them cope with having a child who stutters and/or with the commitment required to support therapy. 139,149 Such support was usually sought from significant others, such as partners or mothers, or from friends. Mothers were reported to provide emotional support while friends gave advice. Although support could be obtained through a formal group, one parent stated that on arrival it frightened her to meet with parents of teenage children who had been attending therapy for years. 150
Perceived family support
Retrospective accounts highlighted the desire for parental support for children’s emotional experiences so that they could discuss feelings openly in a caring environment, or for family members who could act as role models in the area of stuttering. For example, one participant found meaningful support from his brother who also stuttered. 142 However, another participant reported that speech therapy was arranged for her brother but not for herself until a relative of the family suggested to her mother that therapy might be useful. 132
There were cases reported of silence within families in respect to stuttering, perhaps due to an inability to confront the emotional implications of dysfluency. 132,142 However, as children, participants often perceived pressure from family members to be fluent, perhaps due to reactions from family members that indicated that stuttering was unacceptable. One participant reported retrospectively that as a child he felt he could not stutter in front of his mother, because she was the one taking him to therapy sessions and discussing his progress with the therapist. 142 When family-based discussion did take place, there was evidence that it tended to be at the surface level, which included practical aspects but not the underlying nature of stuttering and therapy. Practical support reported from family members related to finding a therapist, providing transport to and from therapy sessions and paying for stuttering therapy. 142 Well-meaning attempts by family members to intervene with stuttering behaviour such as asking the child to slow their speech or concentrate on breathing were in retrospect reported as not beneficial and/or frustrating. 142
Perceived support from the school
Initial progress with the aims of the LP could be disrupted by changing circumstances such as experiences at school. 140 There were mixed views in one study about educating school children generally about stuttering to try and improve understanding and reduce the extent of teasing and bullying that can take place. Although this suggestion was received positively by some, for others there was a perception that being educated about stuttering was not the same as experiencing stuttering and, therefore, would make little difference. Written information might be ignored by their peers and in some cases children who stuttered were not keen to let others know about their ‘problem’. 141
Views about interventions aimed at adolescents
Three included papers provided evidence relating to therapy for stuttering during adolescence. 128,132,141 Compared with the extent of available evidence about childhood and adult therapy, evidence about adolescent therapy was limited.
One participant in the Anderson and Felsenfield study128 attributed their recovery from stuttering as partly to therapy received during childhood, but also to taking public speaking courses during adolescence. Another interviewee132 reported starting to receive therapy in grade 8, although there was dissatisfaction that therapy focused on techniques without addressing psychological issues. Only one study reported on perceptions about therapy experiences in the adolescent age group. 141
Potential barriers and facilitators to outcomes
As with the interventions for children, reported barriers to successful intervention for adolescents were accessing therapy, therapy techniques and therapist–client relationship. An additional theme of acceptability of therapy was identified for the adolescent group.
Accessing therapy
Adolescents who participated in one study141 identified a number of factors that might hinder the initiation of therapy in adolescence. There was a reported lack of awareness about what stuttering is or whether or not they did in fact ‘stutter’. Participants did not tend to know other people who stuttered and one participant reported not feeling able to read about stuttering through embarrassment should someone see the book. With a lack of outlets to discuss their stuttering due to silence and lack of awareness, one participant reported not mentioning his stuttering and stated that he may have been in denial himself. Another participant reflected that they thought stuttering was an emotional problem and another that they did not have a label for what they were experiencing. These participants could not identify the need to seek help to reduce dysfluency; however, identifying with an adult who has experienced stuttering could be beneficial. One participant recalled such a teacher who encouraged her to seek help.
Another issue that was reported in the study with adolescents was a desire not to feel different and having therapy would mean admitting difference, particularly within the family. 141 However, when the decision to attend therapy was made, it was reported to be important that it was their own decision. To have attended for intervention at an earlier stage in life was regarded as inappropriate in their case, as they did not feel ready to take this step, nor did they want to be dictated to by parents.
Therapy techniques
Adolescents in the Hearne et al. study141 found transfer tasks particularly useful during the therapy process. These include undertaking tasks outside the centre, such as in shops, where questions were asked in the real world.
Therapist–client relationship
A suggestion made by adolescents about therapy was to swap clinicians so that participants could experience talking to a range of people. 141
Acceptability of therapy
One study focused on the adolescent age group following experiences with a range of intensive group and non-intensive individual therapies including Smooth Speech, PS and the Camperdown Program. 141 Participants realised the benefits of therapy but did not enjoy some aspects of the process. Hearne et al. 141 found that adolescents overwhelmingly reported having a preference for group therapy for several reasons. First, there were benefits from attending group sessions with other adolescents because they tended to have similar interests, such as sport. Second, it was also reported to be beneficial to attend with other people who stuttered as they could learn from each other and see that they were not alone in having problems with fluency. Third, being with other people who stutter in this setting made it feel easier to speak out loud, even if the stutterer was not familiar with the therapeutic technique. The minority of participants in this study that preferred individual therapy felt that one-to-one sessions should come first until the participant gained some confidence and then attend group therapy, which would be helpful in making comparisons of progress within the group.
There was positive feedback from attending an intensive 1-week therapy course, as this meant that techniques could be reinforced each day and there was little time to forget. Attending therapy once every 2 weeks was regarded as less acceptable, because the gap between meant that techniques could easily be forgotten. Evidence suggests that, although evaluations of specific therapies for the adolescent age group have not been published recently, views of adolescent therapy highlight the importance of addressing social and psychosocial needs at this stage of life. 141
Obstacles to long-term impact
Maintenance in the ‘real world’
Adolescents in one study141 identified the challenge of maintaining techniques for stuttering once regular therapy visits were finished. There was a distinct difference between the environment at clinics, which were reported to feel supportive, and the ‘real world’, which was less predictable. Some participants reported relapses following the end of regular visits. Relapses were associated with lack of practise due to forgetting, being busy (e.g. having other competing commitments such as sport) or feeling self-conscious about using a technique. Speaking with family and friends was reported to feel more comfortable and, therefore, did not require fluency techniques. Some participants admitted that they ‘couldn’t be bothered’ to practise or that they ‘got lazy.’ For this age group, practising speech could easily slip down the list of priorities. It was suggested by participants that the maintenance aspect of therapy needed to be worked on in the weeks following the sessions. More follow-ups were suggested during this time, perhaps once a month. 141
Perceived support
For adolescents, there was a reported lack of awareness about stuttering in significant people around them, such as parents, teachers, friends and classmates. 141 Coupled with their own lack of awareness about stuttering, it was reported to be difficult to express what they felt or explain what was happening to others. As for childhood recollections, adolescents in this study reported experiencing silence within the family regarding stuttering as well as ineffective intervention by teachers at school. There was also one report of having been spoken to by parents as if stuttering was their own fault. 141 In these cases, attending therapy was not deemed to be well supported by significant others.
Educating peers about stuttering was a concept that generated mixed views. Some thought this might reduce teasing, while others thought that even if their peers were more aware, they would still not know what it was like experientially to stutter. Others did not necessarily want to admit that they had a stutter and so were not keen on the idea of providing peers with literature about the topic, although another participant held the view that educating his parents in this way would have been helpful.
Although it was important for all but one adolescent participating in this study to make decisions about therapy attendance on their own, support from the family, when given in a positive way, was acknowledged as helpful. For example, one mother made the telephone calls necessary to arrange therapy. Families were also reported to give support by reminding participants to practise techniques.
Views about interventions aimed at adults
Nineteen of the included papers reported on studies that focused on the adult experience of stuttering and therapy. 116,128–137,143–148,150,151 Of these, three explored experiences of PS therapy,132–135 one116 evaluated a 15-day residential intensive programme and another focused on the implications of group therapy. 150 The remaining studies included some data about specific therapies and strategies although the study did not focus on any intervention in particular.
One study151 included attendees of a self-help conference and another study136 compared a group that had received therapy and one that had not. Plexico et al. 148 assessed characteristics of speech therapists from the attendee perspective, and Boberg and Boberg130 interviewed wives of stutterers. Two studies focused on ethnicity and its interaction with stuttering. 138,143
Potential barriers and facilitators to outcomes
As with the children and adolescent reports, themes relating to barriers and facilitators to adult therapy included accessing therapy, therapy techniques, therapist–client relationship, perceived effectiveness and acceptability of therapy.
Accessing therapy
As already described (see Perceived support), the need for therapy was often identified by a partner. 128,129 Certain life events may also motivate change, such as getting married and having to make a speech, or having children. 130 Awareness about the availability of therapy was reported to increase the perception that something could be done to help. For one participant, this knowledge of the ability to change became an important part of life and motivation for attending therapy. 147 Adults who stutter reported that they were willing, once motivated, to travel large distances if necessary to obtain therapy. In one case, a participant was willing to travel from the USA to the UK, even though therapy was eventually provided closer to home. 147
Therapy techniques
Using PS techniques slowed down speech so that participants spoke more fluently; however, this was reported to feel as if the people who stutter was ‘passing themselves off’ as someone who is fluent, which felt to some extent fraudulent. This feeling led to anxiety that they would be caught out if they stuttered. 134 Fear of difficult speaking situations was reported to dispose people who stutter towards escape mechanisms rather than facing their stuttering. One of the most feared situations for people who stutter is speaking on the telephone. Two ways of addressing this fear were desensitisation for this situation116 and disclosure about stuttering at the beginning of the call. 144 Once fear diminished, these mechanisms could be replaced with approach methods that involved challenging the self, taking risks and problem solving. Facing difficult situations also began a process by which participants reported that they could almost forget that they stuttered in the sense that they no longer felt consumed by stuttering and its consequences. 147
Within the literature were reports of people who stutter using techniques and strategies that they perceived would assist their fluency, or their ability to cope in uncomfortable situations. According to Corcoran and Stewart,133 people who stutter are trying to protect themselves from harmful consequences that could arise from stuttering. Stuttering was reported as posing a threat to a positive self-identity131 and held the risk of being discredited by others, so that ways of preventing stuttering by any means were attempted. 131,134 Strategies included avoidance of situations or particular words133 or by using physical techniques to exert some control over breathing. 131 Strategies were sometimes suggested by the lay community or by therapists, or they were invented by the people who stutter. People who stutter reported that they used self-therapy outside the therapeutic environment. Self-disclosure was used frequently with the consequence of a reduction in fear for both the people who stutter and the listener. Disclosing to the listener eliminated surprise for them and allowed the person who stutters a sense of freedom in not feeling the need to use avoidance behaviours. 145
There were reports of epiphany moments when people who stutter suddenly gained an insight into what was happening for them, combined with an understanding of stuttering itself. 132,144,150 One participant reported that once they had removed the fear of speaking through talking to others and understanding more, fluency improved. However, positive changes in self-identity and confidence could lead to reactions from partners who were used to less assertion in the relationship. 132 Heightened awareness and accountability for speech goals was also reported to enhance fluency and this was important whether people who stutter were carrying out formal therapy or self-directed techniques. 146
In included studies, participants referred to enrolling onto drama and elocution classes as well as consulting psychotherapists and hypnotism specialists,144 counsellors145 or joining self-help groups in order to try and control their stuttering. 135
Therapist–client relationship
A reported influence on the acceptability of therapy was the attitude of the therapist and the relationship between client and therapist. 132,136,142,144,148 Participants identified the most helpful and unhelpful aspects of therapists who deliver interventions to people who stutter. Client-centred therapists were described as most helpful as they customised programmes to meet individual needs (e.g. techniques such as fluency shaping or speech modification techniques may be more or less suitable to different people). Effective therapists were reported to be professional, passionate, committed and confident. They understand and believe in the therapeutic process and the ability of those who stutter to change. They actively listen to the people who stutter and are patient, non-judgemental and caring. This builds feelings of confidence, acceptance, understanding and trust, which motivates attendance at therapy sessions. Irani et al. 116 reported that attendees’ experiences and perceived benefits from an intensive therapy course were positively or negatively affected by the therapists’ responses and demeanour. For Daniels et al. ,138 effective therapists also took into account sociocultural aspects of the experience of people who stutter.
However, there were reports within the literature of therapists who gave the impression that they did not want to work with people who stutter. 132 Ineffective therapists were associated with a lack of understanding about the stuttering experience and a lack of patience, as if they were only ‘attending to earn their pay cheque’. They focused on isolated skills and activities regardless of their effectiveness instead of taking the person and their needs and preferences into account. This could reportedly leave a person who stutters feeling misunderstood, inadequate, shameful and discouraged. Judgemental attitudes were quoted as leaving one person who stutters feeling as if they were ‘under the microscope’. There were reports of therapists blaming or chastising people who stutter for dysfluencies that the person who stuttered perceived were out of their own control. In addition, there was a reported lack of understanding about how taught techniques might transfer into the real world, so that people who stutter felt embarrassed when they practised them in social situations. 148
Experiences with ineffective clinicians were reported to result in people who stutter feeling negative towards the therapeutic process with emotions of frustration, anger, embarrassment and guilt. Such therapists were reported to be ineffective in conveying a sense of acceptance, understanding and trust so that a therapeutic alliance was not fostered. For the people who stutter, this decreased their motivation to attend therapy sessions and practise fluency techniques, regarding their therapy experiences as a waste of money. 148
Effectiveness of therapy
It was reported that the frequency and severity of stuttering tended to decrease following PS therapy, but stuttering did not cease. 133 When control of stuttering occurred using PS, it was associated with a rise in self-esteem and confidence. 134,135 In an evaluation of a 15-day residential intensive programme, various strategies such as easy onsets, PS and pull-outs were taught that were perceived as helpful. Counselling strategies (CBT was a component of the programme) allowed a positive attitude to be adopted that impacted on the participant’s ability to manage stuttering and confront feared situations through desensitisation. Transferring skills to the ‘real world’ was also reported to be advantageous. The authors report that completing these activities contributed to participant perceptions that the treatment was effective. 116
In one study150 group therapy was reported as effective, with change only occurring when they had joined the group. One participant found group therapy more effective than individual sessions, improving his confidence and self-esteem. Similarly, other participants reported changes in their life including employment and social activities, based on increased confidence. Another participant became more fluent because he felt so comfortable with the group. Desensitisation was reported to be effective, allowing participants to overcome their fears. However, in this study, relaxation, rate control and focusing on the content of utterances were also reported to be effective by different people who stutter, with individuals reporting different experiences. 136,150 There was no consensus between participants about which technique generally was the most beneficial. For this reason, the authors of one paper emphasise the importance for individuals to design their own ‘toolbox’ of strategies. 140 Strategies were also reported to change according to different situations, for example the workplace environment demanded more attention to speech than being at home. 116,136
One interesting finding was that more stuttering was reported by people who stutter when they perceived that they were under pressure not to stutter. When the therapy/therapist did not make this demand, stuttering was reported to decrease. 116 Similarly, Plexico et al. 145 reported that people who stutter felt better when they stopped trying to hide their stutter, so that effective therapy was in part a process of accepting the stutter.
Increasing the knowledge of those who stutter about stuttering was reported to have a positive effect on confidence which, in turn, raised the ability to be able to take action and put behavioural interventions into place. There was a reported shift from an emotional response to stuttering to a cognitive response. Emotions were regarded as unreliable compared with cognitive aspects of stuttering that were perceived as more stable and, therefore, easier to control. 147
Attending speech therapy sessions reportedly ‘opened up’ the opportunity to talk about stuttering and to gain some control over it. 136 In the outside world, therapy encouraged people who stutter to take risks and take responsibility for their speech by adopting a positive attitude. 145 Attendance at a self-help conference was reported to enhance self-disclosure and discussion about stuttering outside the conference environment. 151
Therapy also allowed adults who stutter to meet with other people who stutter. 130,136 Couples met other couples who were in a similar situation and discussed experiences. Speaking about stuttering at therapy could also improve communication channels between couples, particularly where stuttering had not been openly discussed previously. 130 Therapy in particular was reported to encourage interaction between people who stutter,116,150 as was attendance at a self-help conference. 151
Although there were reports of support from significant others such as partners, Boberg and Boberg130 found that suggestions from family members and partners about how to deal with stuttering might be ignored. However, similar advice made by a therapist was taken on board by participants, perhaps because the therapist is regarded as more knowledgeable on the topic of stuttering.
Acceptability of therapy
Prolonged speech techniques were described as sounding unnatural to the people who stutter and listeners and as removing the variability, spontaneity and passion in normal speech. Use of PS could result in the participant feeling even more ‘different’ following therapy than they did previously, making it less acceptable in some ‘real-world’ situations. There was the reported perception that speaking more slowly than people who do not stutter created a difference that was of limited acceptability, particularly for younger adults. Using a less pronounced form of PS brought an increased risk of stuttering and associated anxiety with being discredited while trying to appear fluent. PS was described as being burdensome as it requires work on two levels – the content of the conversation as well as the technique of speech. This effort could sometimes be reported as overwhelming. 134 In addition, there was a reported skills gap in that PS required training to use it effectively and participants expressed frustration when this training was not available. 134
Evaluation of a 15-day residential intensive programme highlighted the importance of being with other people who stutter. This allowed shared experiences as well as the feeling that participants were not alone with their problem. The intensity of the programme was compared with 1-hour sessions by one participant in a positive light, because more time could be spent working on techniques. 116
Participants of group therapy assessed by Stewart and Richardson150 reported that meeting other people who stutter and sharing experiences reduced their feelings of isolation. Some participants reported that they had made lasting friendships from the group sessions. However, there were reports that the group situation was ‘artificial’ compared with outside, with a suggestion that therapy should include independent ideas, even if they are not useful for all the group members. Another participant reported a lack of attention to psychological approaches. 150 Generally, participants reported that the setting within which therapy is delivered is important to improve fluency. Settings that are relaxed and non-judgemental are more likely to result in improvement. 146
There were reports in a South African study of the unhelpfulness of therapy in the majority of participants from one study. 144 Therapy was also perceived as boring by some and techniques were reported to be difficult to carry out in real-life situations. Strategies that were perceived by most participants to be less difficult as well as helpful included the Easy Relaxed Approach and the Easy Relaxed Approach Smooth Movement, shortening sentences, changing words or phrases, utilising airflow, interjections or filler sounds, light contacts, advertising and deep breathing, although airflow, deep breathing and rehearsing were reported as more difficult by three participants. 144
Obstacles to long-term impact: maintenance in the ‘real world’
In one study,150 a suggestion was made to follow-up group therapy sessions with booster sessions, advanced sessions or day courses to allow participants to take their techniques further. This may assist participants who are not able to remember the tools for maintenance following therapy. 150 Similarly, an evaluation of an intensive therapy course identified the benefits of follow-up to reinforce the learning that has been carried out. 116
Learning and maintaining techniques to control stuttering was reported to require extraordinary amounts of effort and energy. 135,136 This effort was required owing to the constant need to remain aware and attentive while in speaking situations to prevent ‘falling off the fluency wagon’. 128 People who stutter reported feeling responsible for such fluency lapses because of their lack of dedication to practising taught techniques and tendency to revert to habitual speaking patterns. 136
People who stutter reported feeling less in control over situations in which there was more than one other person present, such as social events, as this decreased predictability and reliability about how and when they might be able to respond to varied interactions. 135,147 Conversely, with one person present there was usually some degree of shared understanding of the situation for the people who stutter. 134 Fear and anxiety were reported to have a detrimental effect on carrying out behavioural techniques. 147 For example, speaking from a less knowledgeable position or a less socially validated role increased dysfluency. 131 Once a person who stutters felt more comfortable with themselves and fear diminished, techniques became easier. One participant remarked that no matter what technique was used to improve fluency, having self-confidence (which had to be worked at) was important to maintaining the behaviour and remaining in the situation. 147
When stuttering occurred during a period of relative fluency, it was reported to have the potential to evoke early memories of being discredited or laughed at, creating anxiety and more dysfluency. The authors describe this as being trapped in a loop of responding to the reactions of others. 134
Techniques were often reported as not being used in a consistent way following therapy. People who stutter reported choosing when and where to use them, depending on their audience. For example, there may not be a perceived need when among family or friends. 144 There was a reported tendency to practise techniques in situations that were less threatening, such as alone or with one other person. This meant that speaking in situations in which more than one person was present (described by the authors as ‘riding the four-way-rocker’) continued to instil feelings of loss of control. 135
Another factor that had an impact on maintenance was having previous success with a technique. Success was reported to improve confidence in continuing to use that technique. 147 However, the absence of practise in, for example making small talk, telling jokes, using irony and generally conversing in different situations over many years, meant that adults who stutter were still working on these aspects of speech as well as on their fluency. There was also a reported fading of motivation as techniques became habitual following therapy without any further increase in fluency. 134
Perceived support
Adults who stutter describe experiencing support from their therapist, when there was a positive client–therapist alliance, their partners and from other people who stutter through group therapy or friendships. 132,150 One participant reported being transformed from a state of confusion about their stuttering to a better understanding by talking to a fellow person who stutters. 132 People who stutter reported that isolation could be reduced by seeking out informational, emotional and protective support, and protective support acted as a buffer for people who stutter from discrediting by others. Therapy provided informational as well as technical support to modify stuttering, while family and friends were likely to provide emotional and protective support. To provide emotional and protective support required a neutral or empathic non-judgemental attitude towards stuttering. 147 Life partnerships were not always reported to be based on honesty about stuttering, leaving the people who stutter feeling isolated in an environment of silence. 130
Conversely, if partners and other significant people were supportive and accepting, people who stutter reported this as crucial to their recovery. Two participants reported that their partners were instrumental in encouraging them to attend therapy sessions. 128,129 Spouses were also reported as potentially supportive with regard to emotional issues and practising techniques. However, although spousal involvement in therapeutic efforts was regarded as mainly positive, reducing the spouse’s feelings of being peripheral to the process, it could be difficult for them to attend therapy owing to work or child care commitments. In addition, in some relationships, the presence of a spouse could be distracting rather than helpful for the people who stutter or could hinder progress towards independence. 130
Other support systems identified in the included studies were professional counselling, support groups, mentors and the church. 145,147 One reported motivator for change was meeting successful people who stutter. Counselling was reported to be helpful in the transitional process to eliminate negative attitudes. 145
Interventions aimed at older adults
One included study152 focused on stuttering experiences in older adults, although no specific therapy was assessed. Many of the issues for older adults will be shared with adults in general, so this section only comments on the impact of older adulthood on stuttering intervention.
Potential barriers and facilitators to outcomes
Perceived effectiveness of therapy
Older adults in the Bricker-Katz et al. 152 study had managed their stuttering in different ways over the years, either through taught strategies such as smooth speech or their own adaptations. For example, stopping and taking a deep breath was described as a self-directed technique and one participant used writing to communicate when the words would not come through speech. Some participants reported that they had tried a range of therapies but felt ‘let down’ as they did not offer the ‘magic bullet’ that was hoped for.
Acceptability of therapy
Although group therapy was acknowledged as a useful way of delivering therapy later in the process, this group preferred individual sessions to begin with. This would allow work to be carried out on ‘deep seated things’ in privacy and build confidence before joining group sessions. It was important that the therapist was experienced and knowledgeable about stuttering in older people and that the person who stutters feels understood by them. 152
Obstacles to long-term impact: maintenance in the ‘real world’
Similar to adults who stutter, older adults found implementing taught techniques challenging in the real world as strategies to improve fluency hindered spontaneity. The ongoing work required by people who stutter to maintain fluency had been off-putting and there was a sense that older participants would only continue seeking the ‘magic bullet’ if there was a guarantee of success without complexity or undue time commitment. According to Bricker-Katz et al. ,152 stuttering was managed in much the same way by older adults as when they were younger, but changes to health status in later years may affect the ability to maintain the cognitive and physical effort required to achieve fluency. In some ways, the impact of stuttering was reduced, because more allowance was made for older people in terms of communication proficiency because, for example, many older adults are known to manage impairments resulting from strokes.
Perceived support
Older adults in this study had similar fear-based issues that needed to be reduced to build confidence. Self-disclosing their stuttering to others was reported to be useful in easing communication, thus reducing fear. Support from others who understood their stuttering was also important.
Stuttering across the lifespan
From the 26 included papers, there was evidence to suggest that people who stutter are impacted by life stages in relation to how they address their stuttering. 116,128–152 To some extent, the way that stuttering is addressed is influenced by interactions with other people in day-to-day situations. It is also influenced by growing maturity and acceptance of ones self as a stutterer.
Childhood: stuttering as ‘mysterious and uncontrollable’
Evidence from included studies showed that the majority of participants reflected on their school years as the most difficult period. 129 There were reports of teasing or bullying from other children as well as a lack of understanding by teachers144,147,152 and general negative reactions. 136 As a child, stuttering was regarded as ‘mysterious and uncontrollable’. 147
Teachers might speak to parents about potential treatments, leaving the child out of the discussion. 141 For one mother of a young child receiving therapy, starting school was reported to have a negative impact on progress. 140 For children from ethnic minority backgrounds, the feeling of being ‘other’ was increased owing to the combined effects of ethnicity and stuttering. 137 The lack of a suitable role model was reported to be a barrier to being able to negotiate life as a child stutterer. 142 During school years, reading aloud in front of the class could be a particular source of distress that was reported to distract from learning. 138,141,143 There was a reported anguish regarding being accepted and, therefore, behaviour would be adjusted to fit into the mainstream environment. 138
In one study,152 older participants reflected on the missed opportunity for treatment when they were young children, comparing this situation to current practice. This might have helped people who stutter to develop coping strategies much earlier in life. In one study, people who stutter reported that their parents did not know what to do about their stuttering when they were young and speech therapists were not available through school. 132 However, there were also reports of a lack of interest in attending therapy as a child. 147
People who stutter also reflected on how their stuttering was addressed by the family, with mixed findings. Some adults reflected on their childhood as a positive experience and cited ways that parents had been supportive. 138,142 Although some parents were reported to be supportive of their child and instrumental in arranging and transporting their child to speech therapy sessions, others reported an atmosphere of silence and denial about stuttering, perhaps due to a lack of information. 132,143,145 Even well-intentioned parents did not always behave in ways that were practically or emotionally helpful to the child. 131,132 Parents reported not knowing whether or not the stuttering was abnormal or serious enough to address, especially when the child was young. It was hoped that the child would ‘grow out of it’ and only when this was clearly not going to happen would parents seek help. 149
Experiences of speech therapy during childhood were also varied. There were accounts in the studies of therapy addressing practical issues with practical solutions, while the emotional side of stuttering was not explored. 132
Adolescence: getting ‘sick of stuttering’
Children reaching adolescence following therapy might have improved their fluency, but still reported feeling isolated or ‘hollow inside’, understanding themselves to be different. 145 Stuttering could remain a predominating feature of the self-concept at this age. 147 Adolescence is a stage during which one is entering college education or employment as well as developing relationships and socialising becomes important. 131,138 Situations that involved communicating with a number of listeners were reported to be particularly challenging;146 therefore, expectations about fluency changed with life events such as work, social events and relationships. 131,141 Often it was such changes that created an impetus for seeking therapy as well as the idea that it was up to themselves to make the change. 147
Conversely, some participants felt that adolescence was not an optimum time to start attending therapy, particularly if they were being told to do so by parents. Young people would be more likely to attend when they felt ready and could arrange appointments themselves. 141 One participant reported not feeling mature enough to be able to open up to a therapist at this age. 116 Another study highlighted a general lack of motivation to work with their speech at this stage of life. 147
Strategies learned as a child, such as avoidance of situations that required speaking in front of others or to strangers, sometimes continued through adolescence, creating a limited environment for personal and professional growth. 133 For participants entering the world of employment, speaking on the telephone and giving presentations were activities most reported to be feared. 134 In one study, 50% of participants did not regard stuttering as a barrier to finding work, but for four participants stuttering was regarded as a barrier because communication was an important part of their chosen career. 144
Prolonged speech was evaluated in three papers. 133–135 One of the issues for young people was the perceived unnaturalness of speech following PS therapy, as speech is slowed down. One participant discussed the conflict he experienced between this type of speech and his usual passionate personality. 134
Adulthood: stuttering as ‘a hindrance’
From included studies, there was a sense that people who stutter gradually gained a sense of self as they matured and that this incorporated being a stutterer. There was acceptance of the fact that they would probably not be rid of stuttering but would continue to manage it through life. 129,145 Participants reported that as adults they understood more about stuttering and also more about themselves. Feeling easier in one’s skin allowed therapy to become easier to carry out. One participant reported that stuttering had been a lesson in how to deal with adversity. 147 However, there was also a reported sense of pressure to overcompensate for stuttering through a range of achievements such as having a nicer car or obtaining a good degree at university. 138,144 For people who stutter and are from an ethnic background, this pressure was reported to be magnified. 137 Having a stutter in the workplace increased perceptions of people who stutter that clients would think they were not knowledgeable. 143 There was a continued fear of using the telephone and speaking up in the presence of others. 146 Significant events, such as starting a new career, meeting a partner, getting married or having children could be the impetus to attend therapy which had not been present before. 134,141,147 Support and involvement from partners was a significant influence on the success, or otherwise, of therapy. 130
The slow speech effects of PS were perceived as no longer such an issue once participants reached ≥ 50 years, as by this time listeners would be more confident in what is being said. 134 Attending National Stuttering Association conferences was reported by people who stutter to ease embarrassment about discussing their stuttering. 151
Late adulthood: a ‘certain degree of acceptance’
The theme of acceptance was notable in the narratives of older adult participants; however, acceptance was not necessarily related to improved speech, but also to a shift in attitude. There were reports from some of less fear of the negative evaluations of others, becoming less self-conscious and expecting less effectiveness from attempts to treat stuttering as the years progressed. Participants also reported that the perceptions of others might also be less fearful because ageing is commonly associated with other health issues that could affect speech, such as a stroke. There was still hope expressed by some that speech therapy might unlock new insights well into later life. 152
There was also less of an impact if they were no longer part of a workforce,152 a stage of life that, for some younger participants, included carrying out dreaded activities as well as the effort required in attempting to project a professional and knowledgeable image to others. 134,136 For older adults who were still working, the impact of this remained; some participants found stuttering more difficult to cope with as they grew older owing to having less emotional energy to deal with stressful situations.
Summary of qualitative evidence
The review of qualitative papers found a limited body of work (26 papers) focusing on retrospective perceptions of adults or adolescents who stutter, or parents of children who stutter. We did not find any studies eligible for inclusion that examined perceptions of children regarding interventions being received. We also did not find any literature meeting our criteria that reported the views of staff delivering the interventions. The literature had variation in quality predominantly owing to elements being not reported; however, around two-thirds were judged as being of a higher standard.
The literature provides insight into the barriers and facilitators that may enhance or mitigate positive outcomes from stuttering interventions. Table 18 provides a summary table of these factors operating at an individual level, factors relating to the intervention, and interpersonal and social elements.
| Domain | Focus | Barriers | Facilitators |
|---|---|---|---|
| Individual (person who stutters or parent of person who stutters) | Emotional | Fear elicited by negative situations Anxiety/apprehension about current/future communication Threat to self-identity Avoidance of situations Denial of stuttering |
Attending to emotional, psychological and knowledge-based needs Breaking out of the cycle of fear – epiphany Leads to increased confidence and acceptance |
| Informational | Lack of knowledge Lack of skills |
Raising awareness in schools Information from therapist Shared experiences with other people who stutter |
|
| Practical | Extent of effort/commitment Lack of time Forgetting to practise |
Adopting strategies such as integrating practise into daily routines, visual reminders, asking for practical support | |
| Interventions | Approaches to therapy | Limited to techniques only One-size-fits-all approach Unrealistic aims Difficult to implement in ‘real world’ |
Encompass emotional/psychological/social Tailored to clients needs Accessible aims Incorporates ‘real-world’ practice |
| Maintenance | Practise not reinforced Long periods without therapy |
Strategies to reinforce practise Intensive courses Regular follow-up sessions |
|
| Interpersonal/social | Therapist characteristics | Lacking knowledge Lacking patience Blaming |
Client-centred approach |
| External support | Lack of knowledge ‘Silencing’ stuttering Non-acceptance of dysfluency Teasing/bullying/socially discrediting |
Involving parents, teachers, partners and peers in therapeutic process Meeting other people who stutter and their parents/partners Raising public awareness |
In the individual domain, that is the person who stutters or parent delivering the intervention, barriers to implementation and potential facilitators to overcome or prevent barriers were reported at the emotional, informational and practical levels. At the emotional level, previous negative experiences could lead to fear and anxiety of situations in which verbal communication was required. Fear and anxiety were temporarily relieved by avoiding such situations and/or by attempting to deny stuttering as a part of one’s self. Therefore, to facilitate effective implementation of therapies, it was reported that emotional challenges require attention before practical strategies to reduce stuttering are introduced. At the informational level, lack of information and skills to deal with stuttering were reported as barriers that could be overcome through greater awareness in schools for both pupils and parents. This would also reduce feelings of isolation for the child who stutters. Effective therapists also helped people who stutter to improve their knowledge and skills, and frequent contact with other people who stutter increased learning through shared experiences. At the practical level, the continued effort required was hampered by perceived lack of time as well as forgetting to practise. Strategies to overcome these barriers were suggested in the literature and were mainly centred round integrating practise into everyday routines so that it became less of an effort to remember and implement. Other suggestions include designing a self-reminder system and requesting support from others.
Reported barriers in the intervention domain included the tendency to focus on single techniques without paying attention to the emotional, psychological and practical needs of the person who stutters as described in Views about interventions aimed at adults. There was evidence from the literature that individually tailored therapies were more acceptable, as people who stutter have a broad range of early experiences, arriving at therapy with a diverse range of skills and challenges. Some therapies were also reported to be difficult to implement in the ‘real world’ compared with the therapeutic environment. Efforts to incorporate therapeutic practices into everyday situations, such as shopping trips, were therefore valued. Maintaining strategies to reduce dysfluency was reported to be challenging, particularly where long periods of time elapsed between sessions. Intensive engagement with therapy such as a residential course allowed people who stutter the continuity of therapy over a period of time. Regular follow-ups were suggested as a way of reinforcing therapeutic aims once initial sessions were completed.
Some interpersonal/social barriers that were perceived as unhelpful were reported in therapeutic relationships. For example, when a therapist lacks knowledge or is not interested in stuttering or in the emotional needs of the people who stutter. There were histories of negative experiences with therapists that had an impact on the motivation of the people who stutter to continue therapy. From the literature, a client-centred approach addressed these issues, creating an environment of shared learning. Similarly, interactions with family, peers, friends and figures of authority at school and work could have an impact on the feelings of competence in social and formal situations for people who stutter. The literature suggested that silence or blame around stuttering had been a common experience that isolated people who stutter, further emphasising the feeling of difference and stigma. This was likely owing to a lack of awareness among family members and school/work peers. Increased exposure to people who stutter and their families’ stories was reported to help reduce these feelings. Similarly, raised public awareness and knowledge about stuttering experiences create an environment in which the phenomenon becomes less mysterious, encouraging people around people who stutter to understand and provide support for therapy.
Chapter 5 Integrating the findings: metasynthesis of effectiveness and qualitative studies
In this section we will draw the two review elements together in an overarching synthesis. We present a conceptual model that has been developed by combining data from the review of intervention effectiveness, together with findings from the review of qualitative literature (Figure 2). The model illustrates elements of the complex pathway from interventions to long-term impact for people who stutter, identifying links in the chain of reasoning underpinning assumptions regarding how and why an intervention may achieve positive outcomes. The model details intervention types, intervention content, outcome and factors influencing outcomes along the pathway from intervention to long-term impact.
FIGURE 2.
Summary diagram detailing elements of the pathway between interventions and outcomes.
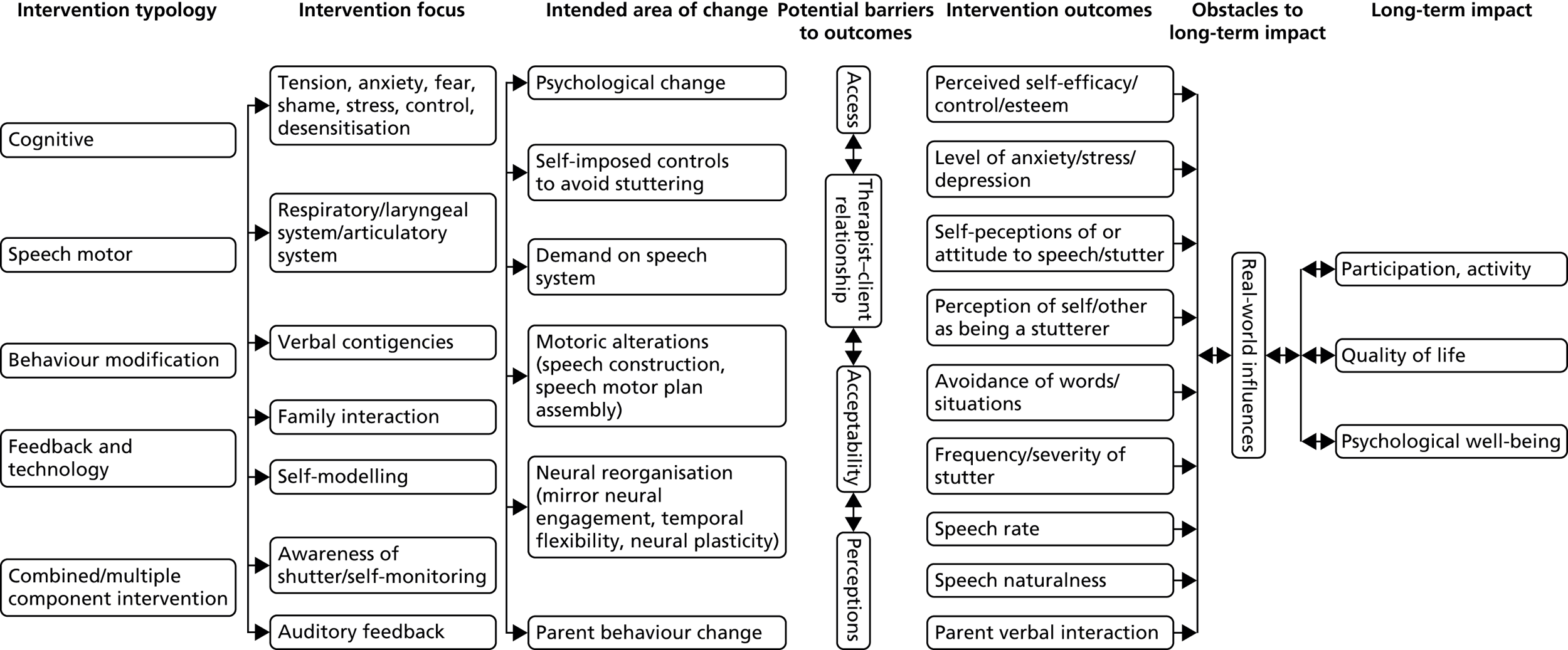
In the protocol we had planned to carry out a metasynthesis of the two review elements by tabulating and comparing data across intervention and qualitative papers. However, this method of metasynthesis was not possible as we identified only one paper that used a mixed-methods design to report both elements of an intervention and views of participants. 116 The qualitative literature also tended to describe general perceptions of interventions without identifying them, rather than exploring views of specific interventions that we could compare and contrast with the clinical effectiveness findings.
The construction of the conceptual diagram draws on logic modelling techniques15 that aim to set out the mechanisms whereby an intervention may lead to its intended impact. Figure 2 is read from left to right, with individual elements of the model drawn from the literature that we included in this review and have been described in Chapters 3 and 4. It should be noted that the arrows in the diagram do not represent a cause–effect relationship between factors, but instead indicate where associations can be made and the flow of if X then Y reasoning. The evidence base also currently does not permit individual elements to be conclusively linked to successive elements in the pathway, for example the precise mechanism whereby parental contingencies lead to improvement in children’s fluency is currently unclear.
The first column summarises the typology of interventions that we identified and described in Chapter 3, categories of intervention which we termed feedback and technology, cognitive, speech motor, combined interventions and other interventions. The second column outlines the content of these different types of interventions. The third column indicates the presumed mechanisms outlined by authors in the included literature that may be the ‘active ingredient’ in why an intervention effects a change on a person who stutters. The literature is currently unclear regarding how exactly interventions produce positive outcomes; therefore, in Figure 2 individual interventions have not been linked to these effects and, instead, the model indicates that the group of interventions may be associated with these areas of change.
The fourth column draws on the qualitative literature detailed in Chapter 4, to identify elements that may act as barriers or facilitators to the interventions having a positive outcome in the short term (during or immediately following an intervention). The fifth column details the outcomes that were measured and reported in the effectiveness literature that we scrutinised. Although the frequency/severity of the observed stuttering behaviour was the most commonly measured outcome, it can be seen how wide ranging the outcomes were that studies used to evaluate an intervention. This column illustrates how establishing what a ‘good outcome’ following an intervention should be is challenging. The relationship between individual elements in this column is also complex, as the frequency/severity of stuttering may be a direct outcome, but also an indirect effect of changes in other outcomes and in turn may influence other elements. This outcome is therefore indicated as a bi-directional arrow.
The sixth column again draws on the qualitative literature to highlight the elements that were described by parents and people who stutter who could impact on longer-term positive outcomes. The real-world influences which were described may be significant in helping to explain the individual variation in outcomes reported in the intervention studies. The qualitative review also highlighted that different real-world factors impacted at different stages of the life course.
The final column details the long-term aims for people who stutter, to achieve participation and engagement in activities of life, quality of life and psychological wellbeing. Figure 2 highlights the complexity of the pathway from the first column interventions to this end point.
Chapter 6 Discussion and conclusions
This wide-ranging review of the literature on interventions for people who stutter identified a sizeable body of work and included 138 papers in the evidence synthesis. The review classified around one-third of the included work as being at lower risk of bias, providing stronger evidence that these health technologies are able to produce positive outcomes. The review found evidence of clinical effectiveness for a range of intervention types, with most intervention studies able to demonstrate a positive effect for at least some participants.
However, the individual variability in response was significant, with little evidence that any intervention would be successful for all who received it. In the generally positive reporting of study findings, there was, in many cases, a sizeable number who did not achieve benefit and in the lower-quality studies the potential for participants reported to differ from those not recruited and/or reported cannot be ruled out. In relation to interventions for children who stutter, the natural recovery rate remains an issue, with research unable to conclusively differentiate those who will spontaneously recover from those who will have long-term stuttering requiring intervention.
The comparison of stuttering interventions with each other is adversely affected by variation in systems of measurement and variation in intervention contact hours. There is little available research that compares the clinical effectiveness of different interventions and thus a very limited pool of evidence for clinicians and people who stutter to draw on in selecting an optimal intervention. Currently, core outcomes for stuttering have not been established and studies that we identified used a range of outcomes including clinician-measured counts, independent listener counts and rating by the people who stutter. The challenge in establishing what a ‘good outcome’ following intervention should be is a key issue for the field. Although a sizeable body of studies included in this review reported clinical effectiveness in terms of percentage reduction in dysfluency, it is debatable how significant a reduction of, for example, 2–3 syllables per 100 syllables might be for the everyday functioning of a person who stutters, or indeed whether or not this reduction in overt stuttering level was the issue of most concern for the people who stutter. Although there is some evidence of increasing involvement of people who stutter in the determination of outcomes, the field remains dominated by measures of overt stuttering behaviours, in particular the percentage of syllables that are stuttered. The qualitative literature highlights the different views of people who stutter regarding their stutter and their differing needs at different stages of life, with a reduction in overt stuttering only being one aspect. Further understanding regarding how, and to what degree, intervention outcomes relate to the everyday lives of people who stutter is needed. Only a small number of papers (all relating to the LP) considered whether or not interventions could have a potential adverse impact. 113,128 Studies describing speech motor interventions often considered the effect on speech naturalness, but rating was often carried out by an independent listener, with few including rating or perceptions from the people who stutter. The qualitative literature included descriptions of people who stutter engaging in an ongoing process of weighing up the decision of whether or not to use taught techniques to reduce the stutter at the expense of sounding ‘different’.
This systematic review did not include consideration of the economical aspects of these health technologies. If questions regarding the cost-effectiveness of interventions for stuttering are to be investigated, further understanding of the short- and long-term outcomes is needed. The conceptual model we developed which summarises the pathway from interventions to impacts highlights both the complexity of outcome measurement and the need for greater understanding regarding how and why these interventions may lead to positive effects.
Analysis of the robustness of the results and limitations
The review findings are based on data from a substantial number of published studies and consider both quantitative and qualitative evidence. The work included a range of study designs encompassing both controlled and non-comparator studies. However, the body of work reporting single and multiple case studies was excluded, together with surveys. Although case studies are able to potentially contribute useful data, their inherent propensity for bias and the availability of a large volume of higher-quality designs underpinned our decision to exclude them from this review.
The body of work that we included encompassed both studies that we categorised as being at higher risk of bias and those at lower risk. Around two-thirds were considered to be at higher risk of bias. We considered whether or not to use quality criteria as a basis for rejection, but this would have precluded analysis and reporting of a large quantity of literature. Few of the studies used controlled designs and of these, the allocation process was frequently carried out by pseudo- rather than completely randomised procedures. In total, there were 14 randomised controlled designs in the set of studies. The quality of the evidence available was limited by many studies having small sample sizes, reporting data by individual rather than pooling findings and failing to blind assessors to the time point of data collection. In many of the smaller before-and-after studies (and some of those with larger samples) the process of selection of individuals whose data would be reported was unclear. It seemed likely (and was sometimes mentioned) that interventions had been delivered to larger numbers of people who stutter with only a sample of these being presented. The possibility that those recruited and reported may differ from those who were not must be considered a potential significant source of bias in interpretation of the data for these studies.
We had intended to carry out a meta-analysis of the clinical effectiveness data, but the heterogeneous nature of the literature and variability in outcome reporting meant that we completed a narrative synthesis. The lack of mixed-methods designs and qualitative papers that described specific interventions precluded our planned metasynthesis approach, which juxtaposes quantitative and qualitative results. Instead we used the two sets of data to develop a conceptual model that sets out components of the pathway from interventions to impacts and which we believe provides a useful tool to aid understanding the results of the review.
Implications for health care
The review indicates that a variety of interventions can produce positive outcomes for people who stutter. The evidence does not permit recommendation of programmes that are more effective compared with those that are less effective – all intervention types seemed able to lead to benefit for some participants. The heterogeneity in outcomes measures and interventions meant that we were only able to compare intervention efficacy at a narrative level. The wide range in outcomes reported by the intervention studies suggests a lack of consensus between researchers and clinicians about what are the critical outcomes following therapy, with the qualitative literature also highlighting variation in what outcomes may be most important to individual patients. We were unable to demonstrate any clear dose–response relationship, meaning that, currently, interventions with many hours of contact did not seem to offer substantially different outcomes to those with fewer. The qualitative literature provides some insight into factors that are perceived to facilitate successful outcomes (see Table 18), which include ensuring that interventions encompass emotional/psychological/social aspects, incorporating ‘real-world’ elements, having follow-up sessions and interacting with other people who stutter.
The clinical effectiveness evidence highlights the individual variation in responses across all intervention typologies and different methods/doses of delivery. The qualitative evidence suggests a need for individual choice in selecting a programme that best meets a person’s needs, with variation in outcome potentially linked to factors at the level of the individual, the intervention and interpersonal/social factors.
Recommendations for research
-
Although finding a substantial number of studies, the literature tended to be limited in breadth, with the majority of papers reporting before-and-after evaluations of a particular intervention using a small number of participants. Therefore, the field has a good body of small-sample baseline follow-up investigations suggesting that alternative study designs are required in the future, such as research comparing interventions. Around two-thirds of the intervention studies were classified as being at potential higher risk of bias with more robust study designs needed. Development of research in the area would be enhanced by greater collaboration between different teams. Recruitment of larger samples of participants would be easier across multiple research teams, particularly in order to establish more homogenous groups for study. The comparison of interventions with each other similarly requires greater collaboration between different teams.
-
There seems to be a research gap around aspects of process evaluation such as intervention fidelity, practitioner specific effects, acceptability and feasibility. We noted that the relationship between dosage and response was unclear, with programmes providing little or no rationale for pre-defined contact hours. Not much of the literature included consideration of resource and training implications of interventions – information that is needed in order to inform commissioning as well as clinical decisions.
-
Although the literature currently has a tendency for focusing on demonstrating that a particular intervention is effective, the evidence base suggests a need, instead, to explain how and why therapy works and, in particular, a need to further investigate individual variation in response. The use of more mixed-method research could help to address these evidence gaps by exploring in-depth participant experiences and factors underpinning outcomes.
-
The measurement of outcomes in the field is a considerable obstacle to the evaluation of clinical effectiveness. Although different studies continue to use varied measures of stuttering, comparison between them remains challenging. Although measures of overt stuttering behaviours continue to dominate evaluation, the establishment of core outcomes that are of importance and relevance to people who stutter seems to be an urgent priority. Here, again, greater collaboration between different research teams is needed in order to learn more about the impact on subgroups of participants and optimal measures of change.
-
A gap in the qualitative literature concerns the views of children receiving therapy. Although the issues relating to young people taking part in research are not insubstantial, a reliance on retrospective recall of adults regarding their childhood means that views will inevitably be of historic approaches and potentially affected by later experiences.
-
Another recommendation for future studies concerns the recruitment of less heterogeneous participants. Although it is recognised that investigators have a limited pool to recruit from, many studies had variation in baseline characteristics of participants, which adds to the challenge of investigating why and for whom interventions are most successful. Factors such as severity of stuttering and length of onset have been suggested as being influential in outcomes. It would be useful for future studies to recruit with limited variance on these variables in order to explore other elements of individual variability. Demonstration of the efficacy of paediatric interventions continues to be impacted by uncertainty regarding spontaneous recovery. Investigation of response by particular subgroups may add additional insight to this area.
-
An issue for research in the area was highlighted by the qualitative literature. An element described as facilitating successful outcomes for people who stutter was a client-centred approach and an individually tailored intervention. This is at odds with some of the programmes evaluated in the included literature, which offer a carefully structured and planned product. If ‘real-world’ interventions in clinical practice are bespoke and tailored for each individual client drawing on a variety of approaches and techniques, research should ensure that studies that are able to contribute evidence that is applicable to practice.
-
We were able to identify only one study that specifically reported participants who were cluttering. Research on interventions for this disorder seems to be very underdeveloped.
-
A further gap concerns the lack of qualitative studies regarding professional views and experiences of interventions.
Acknowledgements
We wish to express our thanks to the members of our advisory group for their valuable expertise and input: Dr Sharon Millard, Mr Norbert Lieckfeldt (British Stammering Association), Dr Luke Boorman and Mr Richard Seals. Thank you also to Rebekka Niepelt for assisting with translation of papers.
Contributions of authors
Susan Baxter (research fellow) was principal investigator, responsible for study management and led the review of effectiveness and metasynthesis.
Maxine Johnson (research fellow) led the review of qualitative evidence and contributed to the metasynthesis.
Lindsay Blank (research fellow) contributed as a senior reviewer to all elements of the review.
Anna Cantrell (information specialist) developed the search strategy and led the searching and identification of literature.
Shelagh Brumfitt (Emeritus Professor of speech and language therapy education) provided topic expertise in the field of stuttering.
Pamela Enderby (Professor of community rehabilitation) provided expertise in research methods and translation of findings for professionals and patients.
Elizabeth Goyder (Professor of public health) acted as senior methodologist.
Publications
Baxter S, Johnson M, Blank L, Cantrell A, Brumfitt S, Enderby P, et al. The state of the art in non-pharmacological interventions for developmental stuttering. Part 1: systematic review of effectiveness. Int J Lang Commun Disord 2015;50:676–718.
Johnson M, Baxter S, Blank L, Cantrell A, Brumfitt S, Enderby P, et al. The state of the art in non-pharmacological interventions for developmental stuttering. Part 2: qualitative evidence synthesis of views and experiences [published online ahead of print June 30 2015]. Int J Lang Commun Disord 2015.
Data sharing statement
This is an evidence synthesis and the data are largely described in the report. Further information can be obtained from the corresponding author.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HTA programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HTA programme or the Department of Health.
References
- Saltuklaroglu T, Kalinowski J, Robbins M, Crawcour S, Bowers A. Comparisons of stuttering frequency during and after speech initiation in unaltered feedback, altered auditory feedback and choral speech conditions. Int J Lang Commun Disord 2009;44:1000-17. http://dx.doi.org/10.1080/13682820802546951.
- Herder C, Howard C, Nye C, Vanryckeghem M. Effectiveness of behavioural stuttering treatment: a systematic review and meta-analysis. Contemp Issues Commun Sci Disord 2006;33:61-73.
- Sidavi A, Fabus A. A review of stuttering intervention approaches for preschool-age and elementary school-age children. Contemp Issues Commun Sci Disord 2010;37:14-26.
- Armson J, Kiefte M, Mason J, De CD. The effect of SpeechEasy on stuttering frequency in laboratory conditions. J Fluency Disord 2006;31:137-52. http://dx.doi.org/10.1016/j.jfludis.2006.04.004.
- Blomgren M. Stuttering treatment for adults: an update on contemporary approaches. Semin Speech Lang 2010;31:272-82. http://dx.doi.org/10.1055/s-0030-1265760.
- Systematic Reviews: CRD’s Guidance for Undertaking Systematic Reviews in Healthcare. University of York, York: Centre for Reviews and Dissemination; 2009.
- Moher D, Liberati A, Tetzlaff J, Altmann D. Prisma Group . Preferred reporting items for systematic reviews and meta-analyses: the PRISMA guidelines. BMJ 2009;339:332-6. http://dx.doi.org/10.1136/bmj.b2535.
- Cochrane Collaboration . Cochrane Handbook for Systematic Reviews of Interventions, Cochrane Collaboration 2011. www.cochrane-handbook.org (accessed 4 September 2012).
- Critical Appraisal Skills Programme . CASP Qualitative Checklist 2013. http://media.wix.com/ugd/dded87_951541699e9edc71ce66c9bac4734c69.pdf (accessed 4 September 2012).
- Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol 2008;8. http://dx.doi.org/10.1186/1471-2288-8-45.
- Grant M, Booth A. A typology of reviews: an analysis of 14 review types and associated methodologies. Health Info Libr J 2009;26:91-108. http://dx.doi.org/10.1111/j.1471-1842.2009.00848.x.
- Oliver S, Harden A, Rees R, Shepherd J, Brunton G, Garcia J, et al. An emerging framework for including different types of evidence in systematic reviews for public policy. Evaluation 2005;11:428-46. http://dx.doi.org/10.1177/1356389005059383.
- Thomas J, Harden A, Oakley A, Oliver S, Sutcliffe K, Rees R, et al. Integrating qualitative research with trials in systematic reviews. BMJ 2004;328:1010-12. http://dx.doi.org/10.1136/bmj.328.7446.1010.
- Dixon-Woods M, Fitzpatrick R, Roberts K. Including qualitative research in systematic reviews: opportunities and problems. J Eval Clin Pract 2001;7:125-33. http://dx.doi.org/10.1046/j.1365-2753.2001.00257.x.
- Weiss C. Theory-based evaluation: past, present and future. New Dir Eval 2007;76:68-81.
- Craig A, Hancock K, Chang E, McCready C, Shepley A, McCaul A, et al. A controlled clinical trial for stuttering in persons aged 9 to 14 years. J Speech Hear Res 1996;39:808-26. http://dx.doi.org/10.1044/jshr.3904.808.
- Cream A, O’Brian S, Jones M, Block S, Harrison E, Lincoln M, et al. Randomized controlled trial of video self-modeling following speech restructuring treatment for stuttering. J Speech Lang Hear Res 2010;53:887-97. http://dx.doi.org/10.1044/1092-4388(2009/09-0080).
- De Veer S, Brouwers A, Evers W, Tomic W. A pilot study of the psychological impact of the mindfulness-based stress reduction program on persons who stutter. Eur Psychotherapy 2009;9:39-56.
- Franklin DE, Taylor CL, Hennessey NW, Beilby JM. Investigating factors related to the effects of time-out on stuttering in adults. Int J Lang Commun Disord 2008;43:283-99. http://dx.doi.org/10.1080/13682820701449893.
- Hancock K, Craig A. Predictors of stuttering relapse one year following treatment for children aged 9 to 14 years. J Fluency Disord 1998;23:31-48. http://dx.doi.org/10.1016/S0094-730X(97)00028-4.
- Hancock K, Craig A, McCready C, McCaul A, Costello D, Campbell K, et al. Two- to six-year controlled-trial stuttering outcomes for children and adolescents. J Speech Lang Hear Res 1998;41:1242-52. http://dx.doi.org/10.1044/jslhr.4106.1242.
- Harris V, Onslow M, Packman A, Harrison E, Menzies R. An experimental investigation of the impact of 24 the Lidcombe Program on early stuttering. J Fluency Disord 2002;27:203-13. http://dx.doi.org/10.1016/S0094-730X(02)00127-4.
- Hewat S, Onslow M, Packman A, O’Brian S. A phase II clinical trial of self-imposed time-out treatment for stuttering in adults and adolescents. Disabil Rehabil 2006;15:33-42. http://dx.doi.org/10.1080/09638280500165245.
- Jones M, Onslow M, Packman A, Williams S, Ormond T, Schwarz I, et al. Randomised controlled trial of the Lidcombe programme of early stuttering intervention. BMJ 2005;24. http://dx.doi.org/10.1136/bmj.38520.451840.E0.
- Jones M, Onslow M, Packman A, O’Brian S, Hearne A, Williams S, et al. Extended follow-up of a randomized controlled trial of the Lidcombe Program of Early Stuttering Intervention. Int J Lang Commun Disord 2008;43:649-61. http://dx.doi.org/10.1080/13682820801895599.
- Lattermann C, Euler HA, Neumann K. A randomized control trial to investigate the impact of the Lidcombe Program on early stuttering in German-speaking preschoolers. J Fluency Disord 2008;33:52-65. http://dx.doi.org/10.1016/j.jfludis.2007.12.002.
- Lewis C, Packman A, Onslow M, Simpson JM, Jones M. A phase II trial of telehealth delivery of the Lidcombe Program of early stuttering intervention. Am J Speech Lang Pathol 2008;17:139-49. http://dx.doi.org/10.1044/1058-0360(2008/014).
- Menzies RG, O’Brian S, Onslow M, Packman A, St Clave T, Block S. An experimental clinical trial of a cognitive–behavior therapy package for chronic stuttering. J Speech Lang Hear Res 2008;51:1451-64. http://dx.doi.org/10.1044/1092-4388(2008/07-0070).
- Onslow M, Andrews C, Lincoln M. A control/experimental trial of an operant treatment for early stuttering. J Speech Lang Hear Res 1994;37:1244-59. http://dx.doi.org/10.1044/jshr.3706.1244.
- Amster BJ, Klein ER. Perfectionism in people who stutter: preliminary findings using a modified cognitive-behavioral treatment approach. Behav Cogn Psychother 2007;36:35-40. http://dx.doi.org/10.1017/S1352465807003967.
- Andrews C, O’Brian S, Harrison E, Onslow M, Packman A, Menzies R. Syllable-timed speech treatment for school-age children who stutter: a phase I trial. Lang Speech Hear Serv Sch 2012;43:359-69. http://dx.doi.org/10.1044/0161-1461(2012/11-0038).
- Baumeister H, Caspar F, Herziger F. Treatment outcome study of the stuttering therapy summer camp 2000 for children and adolescents. Psychother Psychosom Med Psychol 2003;53:455-63.
- Beilby JM, Byrnes ML, Yaruss JS. Acceptance and commitment therapy for adults who stutter: psychosocial adjustment and speech fluency. J Fluency Disord 2012;37:289-99. http://dx.doi.org/10.1016/j.jfludis.2012.05.003.
- Berkowitz M, Cook H, Haughey MJ. A non-traditional fluency program developed for the public school setting. Lang Speech Hear Serv Sch 1994;25:94-9. http://dx.doi.org/10.1044/0161-1461.2502.94.
- Block S, Ingham RJ, Bench RJ. The effects of the Edinburgh Masker on stuttering. Aust J Hum Commun Disord 1996;24:11-8. http://dx.doi.org/10.3109/asl2.1996.24.issue-1.02.
- Block S, Onslow M, Roberts R, White S. Control of stuttering with EMG feedback. Adv Sp Lang Pathol 2004;6:100-6. http://dx.doi.org/10.1080/14417040410001708521.
- Block S, Onslow M, Packman A, Gray B, Dacakis G. Treatment of chronic stuttering: outcomes from a student training clinic. Int J Lang Commun Disord 2005;40:455-66. http://dx.doi.org/10.1080/03093640500088161.
- Block S, Onslow M, Packman A, Dacakis G. Connecting stuttering management and measurement: IV. Predictors of outcome for a behavioural treatment for stuttering. Int J Lang Commun Disord 2006;41:395-406. http://dx.doi.org/10.1080/13682820600623853.
- Blomgren M, Roy N, Callister T, Merrill RM. Intensive stuttering modification therapy: a multidimensional assessment of treatment outcomes. J Speech Lang Hear Res 2005;48:509-23. http://dx.doi.org/10.1044/1092-4388(2005/035).
- Blood GW. A behavioral–cognitive therapy program for adults who stutter: computers and counseling. J Comm Disord 1995;28:165-80. http://dx.doi.org/10.1016/0021-9924(95)00008-2.
- Boberg E, Kully D. Long-term results of an intensive treatment program for adults and adolescents who stutter. J Speech Lang Hear Res 1994;37:1050-9. http://dx.doi.org/10.1044/jshr.3705.1050.
- Bonelli P, Dixon M, Ratner NB, Onslow M. Child and parent speech and language following the Lidcombe Programme of early stuttering intervention. Clin Ling Phonetics 2000;14:427-46. http://dx.doi.org/10.1080/026992000415868.
- Bray M, James S. An evaluation of a telephone assistive device (TAD) for people who stutter. Int J Speech Lang Pathol 2009;11:54-60. http://dx.doi.org/10.1080/17549500802596263.
- Bray MA, Kehle TJ. Self-modeling as an intervention for stuttering. School Psychol Rev 1998;27:587-98.
- Carey B, O’Brian S, Onslow M, Block S, Jones M, Packman A. Randomized controlled non-inferiority trial of a telehealth treatment for chronic stuttering: the Camperdown Program. Int J Lang Commun Disord 2010;45:108-20. http://dx.doi.org/10.3109/13682820902763944.
- Cocomazzo N, Block S, Carey B, O’Brian S, Onslow M, Packman A, et al. Camperdown Program for adults who stutter: a student training clinic phase I trial. Int J Lang Commun Disord 2012;47:365-72. http://dx.doi.org/10.1111/j.1460-6984.2012.00150.x.
- Craig A, Hancock K, Cobbin D. Managing adolescents who relapse following treatment for stuttering. Asia Pacific J Speech Lang Hear 2002;7:79-91. http://dx.doi.org/10.1179/136132802805576490.
- Cream A, O’Brian S, Onslow M, Packman A, Menzies R. Self-modelling as a relapse intervention following speech-restructuring treatment for stuttering. Int J Lang Commun Disord 2009;44:587-99. http://dx.doi.org/10.1080/13682820802256973.
- Druce T, Debney S. Evaluation of an intensive treatment program for stuttering in young children. J Fluency Disord 1997;22:169-86. http://dx.doi.org/10.1016/S0094-730X(97)00005-3.
- Elliott AJ, Miltenberger RG, Rapp J, Long ES, McDonald R. Brief application of simplified habit reversal to treat stuttering in children. J Behav Ther Experiment Psychiatry 1998;29:289-302. http://dx.doi.org/10.1016/S0005-7916(98)00034-2.
- Femrell L, Avall M, Lindstrom E. Two-year follow-up of the Lidcombe Program in ten Swedish-speaking children. Folia Phoniatr Logop 2012;64:248-53. http://dx.doi.org/10.1159/000342149.
- Foundas AL, Mock JR, Corey DM, Golob EJ, Conture EG. The SpeechEasy device in stuttering and nonstuttering adults: fluency effects while speaking and reading. Brain Lang 2013;126:141-50. http://dx.doi.org/10.1016/j.bandl.2013.04.004.
- Franken MC, Boves L, Peters HF, Webster RL. Perceptual evaluation of the speech before and after fluency shaping stuttering therapy. J Fluency Disord 1992;17:223-41. http://dx.doi.org/10.1016/0094-730X(92)90035-O.
- Franken MC, Kielstra-Van der Schalk CJ, Boelens H. Experimental treatment of early stuttering: a preliminary study. J Fluency Disord 2005;30:189-99. http://dx.doi.org/10.1016/j.jfludis.2005.05.002.
- Gagnon M, Ladouceur R. Behavioral treatment of child stutterers: replication and extension. Behav Ther 1992;23:113-29. http://dx.doi.org/10.1016/S0005-7894(05)80312-0.
- Gallop RF, Runyan CM. Long-term effectiveness of the SpeechEasy fluency-enhancement device. J Fluency Disord 2012;37:334-43. http://dx.doi.org/10.1016/j.jfludis.2012.07.001.
- Hancock K, Craig A. The effectiveness of re-treatment for adolescents who stutter. Asia Pacific J Speech Lang Hearing 2002;7:138-56. http://dx.doi.org/10.1179/136132802805576391.
- Harrison E, Onslow M, Menzies R. Dismantling the Lidcombe Program of early stuttering intervention: verbal contingencies for stuttering and clinical measurement. Int J Lang Commun Disord 2004;39:257-67. http://dx.doi.org/10.1080/13682820310001644551.
- Hasbrouck JM. FAMC Intensive Stuttering Treatment Program: ten years of implementation. Mil Med 1992;157:244-7.
- Hudock D, Kalinowski J. Stuttering inhibition via altered auditory feedback during scripted telephone conversations. Int J Lang Commun Disord 2014;49:139-47. http://dx.doi.org/10.1111/1460-6984.12053.
- Huinck WJ, Langevin M, Kully D, Graamans K, Peters HF, Hulstijn W. The relationship between pre-treatment clinical profile and treatment outcome in an integrated stuttering program. J Fluency Disord 2006;31:43-6. http://dx.doi.org/10.1016/j.jfludis.2005.12.001.
- Ingham RJ, Wang Y, Ingham JC, Bothe AK, Grafton ST. Regional brain activity change predicts responsiveness to treatment for stuttering in adults. Brain Lang 2013;127:510-19. http://dx.doi.org/10.1016/j.bandl.2013.10.007.
- Ingham RJ, Kilgo M, Ingham JC, Moglia R, Belknap H, Sanchez T. Evaluation of a stuttering treatment based on reduction of short phonation intervals. J Speech Lang Hear Res 2001;44:1229-44. http://dx.doi.org/10.1044/1092-4388(2001/096).
- Iverach L, Jones M, O’Brian S, Block S, Lincoln M, Harrison E, et al. The relationship between mental health disorders and treatment outcomes among adults who stutter. J Fluency Disord 2009;34:29-43. http://dx.doi.org/10.1016/j.jfludis.2009.02.002.
- Jones M, Onslow M, Harrison E, Packman A. Treating stuttering in young children: predicting treatment time in the Lidcombe Program. J Speech Lang Hear Res 2000;43:1440-50. http://dx.doi.org/10.1044/jslhr.4306.1440.
- Kaya Y, Alladin A. Hypnotically assisted diaphragmatic exercises in the treatment of stuttering: a preliminary investigation. Int J Clin Experiment Hypnosis 2012;60:175-20. http://dx.doi.org/10.1080/00207144.2012.648063.
- Kaya Y. The effect of regulator and stiffener exercises for speaking mechanics on the stuttering education and therapy. Energy Educ Sci Tech Part B 2011;3:253-68.
- Kingston M, Huber A, Onslow M, Jones M, Packman A. Predicting treatment time with the Lidcombe Program: replication and meta-analysis. Int J Lang Commun Disord 2003;38:165-77. http://dx.doi.org/10.1080/1368282031000062882.
- Koushik S, Shenker R, Onslow M. Follow-up of 6–10-year-old stuttering children after Lidcombe program treatment: a phase I trial. J Fluency Disord 2009;34:279-90. http://dx.doi.org/10.1016/j.jfludis.2009.11.001.
- Laiho A, Klippi A. Long- and short-term results of children’s and adolescents’ therapy courses for stuttering. Int J Lang Commun Disord 2007;42:367-82. http://dx.doi.org/10.1080/13682820600939028.
- Langevin M, Boberg E. Results of an intensive stuttering therapy program. J Speech-Lang Path Audiol 1993;17:158-66.
- Langevin M, Boberg E. Results of intensive stuttering therapy with adults who clutter and stutter. J Fluency Disord 1996;21:315-27. http://dx.doi.org/10.1016/S0094-730X(96)00034-4.
- Langevin M, Huinck WJ, Kully D, Peters HF, Lomheim H, Tellers M. A cross-cultural, long-term outcome evaluation of the ISTAR Comprehensive Stuttering Program across Dutch and Canadian adults who stutter. J Fluency Disord 2006;31:229-56. http://dx.doi.org/10.1016/j.jfludis.2006.06.001.
- Langevin M, Kully D, Teshima S, Hagler P, Narasimha Prasad NG. Five-year longitudinal treatment outcomes of the ISTAR Comprehensive Stuttering Program. J Fluency Disord 2010;35:123-40. http://dx.doi.org/10.1016/j.jfludis.2010.04.002.
- Lawson R, Pring T, Fawcus M. The effects of short courses in modifying the attitudes of adult and adolescent stutterers to communication. Eur J Disord Commun 1993;28:299-308. http://dx.doi.org/10.3109/13682829309060042.
- Leahy MM, Collins G. Therapy for stuttering: experimenting with experimenting. Irish J Psychol Med 1991;8:37-9.
- Lincoln M, Onslow M, Lewis C, Wilson L. A clinical trial of an operant treatment for school-age children who stutter. Am J Speech Lang Pathol 1996;5:73-85. http://dx.doi.org/10.1044/1058-0360.0502.73.
- Lutz C. The Hamburg Workshop for Parents of Stuttering Children (HAWESK). Forum Logopadie 2009;23:6-14.
- Mallard AR. Using problem-solving procedures in family management of stuttering. J Fluency Disord 1998;23:127-35. http://dx.doi.org/10.1016/S0094-730X(97)00047-8.
- Millard SK, Nicholas A, Cook FM. Is parent–child interaction therapy effective in reducing stuttering?. J Speech Lang Hear Res 2008;51:636-50. http://dx.doi.org/10.1044/1092-4388(2008/046).
- Millard SK, Edwards S, Cook FM. Parent–child interaction therapy: adding to the evidence. Int J Speech Lang Pathol 2009;11:61-76. http://dx.doi.org/10.1080/17549500802603895.
- Miller B, Guitar B. Long-term outcome of the Lidcombe Program for early stuttering intervention. Am J Speech Lang Pathol 2009;18:42-9. http://dx.doi.org/10.1044/1058-0360(2008/06-0069).
- Nilsen CH, Ramberg C. Evaluation of a Scandinavian intensive program for stuttering in adolescence. Logoped Phoniatr Vocol 1999;24:66-75. http://dx.doi.org/10.1080/140154399435138.
- O’Brian S, Onslow M, Cream A, Packman A. The Camperdown Program: outcomes of a new prolonged-speech treatment model. J Speech Lang Hear Res 2003;46:933-46. http://dx.doi.org/10.1044/1092-4388(2003/073).
- O’Brian S, Packman A, Onslow M. Telehealth delivery of the Camperdown Program for adults who stutter: a phase I trial. J Speech Lang Hear Res 2008;51:184-95. http://dx.doi.org/10.1044/1092-4388(2008/014).
- O’Brian S, Iverach L, Jones M, Onslow M, Packman A, Menzies R. Effectiveness of the Lidcombe Program for early stuttering in Australian community clinics. Int J Speech Lang Pathol 2013;15:593-60. http://dx.doi.org/10.3109/17549507.2013.783112.
- O’Donnell JJ, Armson J, Kiefte M. The effectiveness of SpeechEasy during situations of daily living. J Fluency Disord 2008;33:99-119. http://dx.doi.org/10.1016/j.jfludis.2008.02.001.
- Onslow M, Costa L, Rue S. Direct early intervention with stuttering: some preliminary data. J Speech Hear Disord 1990;55:405-16. http://dx.doi.org/10.1044/jshd.5503.405.
- Onslow M, Hayes B, Hutchins L, Newman D. Speech naturalness and prolonged-speech treatments for stuttering: further variables and data. J Speech Lang Hear Res 1992;35:274-82. http://dx.doi.org/10.1044/jshr.3502.274.
- Onslow M, Costa L, Andrews C, Harrison E, Packman A. Speech outcomes of a prolonged-speech treatment for stuttering. J Speech Lang Hear Res 1996;39:734-49. http://dx.doi.org/10.1044/jshr.3904.734.
- Pape-Neumann J. Results of the test-phase of PEVOS, program for the evaluation of stuttering therapy. Forum Logopadie 2004;18:18-22.
- Pollard R, Ellis JB, Finan D, Ramig PR. Effects of the SpeechEasy on objective and perceived aspects of stuttering: a 6-month, phase I clinical trial in naturalistic environments. J Speech Lang Hear Res 2009;52:516-33. http://dx.doi.org/10.1044/1092-4388(2008/07-0204).
- Reddy RP, Sharma MP, Shivashankar N. Cognitive behavior therapy for stuttering: a case series. Indian J Psychol Med 2010;32:49-53. http://dx.doi.org/10.4103/0253-7176.70533.
- Riley GD, Ingham JC. Acoustic duration changes associated with two types of treatment for children who stutter. J Speech Lang Hear Res 2000;43:965-78. http://dx.doi.org/10.1044/jslhr.4304.965.
- Rosenberger S, Schulet K, Metten C. Intensive stuttering therapy Susanne Rosenberger – first results of an evaluation study. Forum Logopadie 2007;21:20-5.
- Rousseau I, Packman A, Onslow M, Harrison E, Jones M. An investigation of language and phonological development and the responsiveness of preschool age children to the Lidcombe Program. J Commun Disord 2007;40:382-97. http://dx.doi.org/10.1016/j.jcomdis.2006.10.002.
- Ryan BP, Van Kirk RB. Programmed stuttering treatment for children: comparison of two establishment programs through transfer, maintenance, and follow-up. J Speech Hear Res 1995;38:61-75. http://dx.doi.org/10.1044/jshr.3801.61.
- Sicotte C, Lehoux P, Fortier-Blanc J, Leblanc Y. Feasibility and outcome evaluation of a telemedicine application in speech-language pathology. J Telemed Telecare 2003;9:253-8. http://dx.doi.org/10.1258/135763303769211256.
- Smits-Bandstra SM, Yovetich WS. Treatment effectiveness for school age children who stutter. J Speech-Lang Pathol Audiol 2003;27:125-33.
- Stewart T. A further application of the Fishbein and Ajzen model to therapy for adult stammerers. Eur J Disord Commun 1996;31:445-64. http://dx.doi.org/10.3109/13682829609031331.
- Stidham KR, Olson L, Hillbratt M, Sinopoli T. A new antistuttering device: treatment of stuttering using bone conduction stimulation with delayed temporal feedback. Laryngoscope 2006;116:1951-5. http://dx.doi.org/10.1097/01.mlg.0000236079.52499.0b.
- Stuart A, Kalinowski J, Rastatter M, Saltuklaroglu T, Dayalu V. Investigations of the impact of altered auditory feedback in-the-ear devices on the speech of people who stutter: initial fitting and 4-month follow-up. Int J Lang Commun Disord 2004;39:93-113. http://dx.doi.org/10.1080/13682820310001616976.
- Stuart A, Kalinowski J, Saltuklaroglu T, Guntupalli VK. Investigations of the impact of altered auditory feedback in-the-ear devices on the speech of people who stutter: one-year follow-up. Disabil Rehabil 2006;30:757-65. http://dx.doi.org/10.1080/09638280500386635.
- Trajkovski N, Andrews C, Onslow M, O’Brian S, Packman A, Menzies R. A phase II trial of the Westmead Program: syllable-timed speech treatment for pre-school children who stutter. Int J Speech Lang Path 2011;13:500-9. http://dx.doi.org/10.3109/17549507.2011.578660.
- Van Borsel J, Reunes G, Van den Bergh N. Delayed auditory feedback in the treatment of stuttering: clients as consumers. Int J Lang Commun Disord 2003;38:119-29. http://dx.doi.org/10.1080/1368282021000042902.
- von Gudenberg AW. Kassel stuttering therapy: evaluation of a computer aided therapy. Forum Logopadie 2006;20:6-11.
- von Gudenberg AW, Neumann K, Euler HA. The Kassel Stuttering Therapy fills the gap of therapy options for older children. Forum Logopadie 2006;20:24-9.
- Wagaman JR, Miltenberger RG, Arndorfer RE. Analysis of a simplified treatment for stuttering in children. J Appl Behav Anal 1993;26:53-61. http://dx.doi.org/10.1901/jaba.1993.26-53.
- Wagaman JR, Miltenberger RG, Woods D. Long-term follow-up of a behavioral treatment for stuttering in children. J Appl Behav Anal 1995;28:233-4. http://dx.doi.org/10.1901/jaba.1995.28-233.
- Ward D. Outlining semi-intensive fluency therapy. J Fluency Disord 1992;17:243-55. http://dx.doi.org/10.1016/0094-730X(92)90036-P.
- Wille A. Bioresonance therapy (biophysical information therapy) in stuttering children. Forsch Komplement Med 1999;6:50-2. http://dx.doi.org/10.1159/000057134.
- Wilson L, Onslow M, Lincoln M. Telehealth adaptation of the Lidcombe Program of early stuttering intervention: five case studies. Am J Speech Lang Pathol 2004;13:81-93. http://dx.doi.org/10.1044/1058-0360(2004/009).
- Woods S, Shearsby J, Onslow M, Burnham D. Psychological impact of the Lidcombe Program of early stuttering intervention. Int J Lang Commun Disord 2002;37:31-40. http://dx.doi.org/10.1080/13682820110096670.
- Yairi E, Ambrose N. A longitudinal study of stuttering in children: a preliminary report. J Speech Hear Res 1992;35:755-60. http://dx.doi.org/10.1044/jshr.3504.755.
- Yaruss JS, Coleman C, Hammer D. Treating preschool children who stutter: description and preliminary evaluation of a family-focused treatment approach. Lang Speech Hear Serv Sch 2006;37:118-36. http://dx.doi.org/10.1044/0161-1461(2006/014).
- Irani F, Gabel R, Daniels D, Hughes S. The long term effectiveness of intensive stuttering therapy: a mixed methods study. J Fluency Disord 2012;37:164-78. http://dx.doi.org/10.1016/j.jfludis.2012.04.002.
- Allen CR. The use of email as a component of adult stammering therapy: a preliminary report. J Telemed Telecare 2011;17:163-7. http://dx.doi.org/10.1258/jtt.2010.100114.
- Antipova EA, Purdy SC, Blakeley M, Williams S. Effects of altered auditory feedback (AAF) on stuttering frequency during monologue speech production. J Fluency Disord 2008;33:274-90. http://dx.doi.org/10.1016/j.jfludis.2008.09.002.
- Armson J, Stuart A. Effect of extended exposure to frequency-altered feedback on stuttering during reading and monologue. J Speech Lang Hear Res 1998;41:479-90. http://dx.doi.org/10.1044/jslhr.4103.479.
- Armson J, Kiefte M. The effect of SpeechEasy on stuttering frequency, speech rate, and speech naturalness. J Fluency Disord 2008;33:120-34. http://dx.doi.org/10.1016/j.jfludis.2008.04.002.
- Koushik S, Hewat S, Shenker RC, Jones M, Onslow M. North-American Lidcombe Program file audit: replication and meta-analysis. Int J Speech Lang Path 2011;13:301-7. http://dx.doi.org/10.3109/17549507.2011.538434.
- Lincoln MA, Onslow M. Long-term outcome of early intervention for stuttering. Am J Speech Lang Pathol 1997;6:51-8. http://dx.doi.org/10.1044/1058-0360.0601.51.
- Onslow M, Stocker S, Packman A, McLeod S. Speech timing in children after the Lidcombe Program of early stuttering intervention. Clin Ling Phon 2002;16:21-33. http://dx.doi.org/10.1080/02699200110092577.
- Ratynska J, Szkielkowska A, Markowska R, Kurkowski M, Mularzuk M, Skarzynski H. Immediate speech fluency improvement after application of the Digital Speech Aid in stuttering patients. Med Sci Monit 2012;18:CR9-12. http://dx.doi.org/10.12659/MSM.882191.
- Unger JP, Gluck CW, Cholewa J. Immediate effects of AAF devices on the characteristics of stuttering: a clinical analysis. J Fluency Disord 2012;37:122-34. http://dx.doi.org/10.1016/j.jfludis.2012.02.001.
- Zimmerman S, Kalinowski J, Stuart A, Rastatter M. Effect of altered auditory feedback on people who stutter during scripted telephone conversations. J Speech Lang Hear Res 1997;40:1130-44. http://dx.doi.org/10.1044/jslhr.4005.1130.
- Van Riper C. The Treatment of Stuttering. Englewood Cliffs, NJ: Prentice-Hall; 1973.
- Anderson TK, Felsenfeld S. A thematic analysis of late recovery from stuttering. Am J Speech Lang Pathol 2003;12:243-53. http://dx.doi.org/10.1044/1058-0360(2003/070).
- Beilby JM, Byrnes ML, Meagher EL, Yaruss JS. The impact of stuttering on adults who stutter and their partners. J Fluency Disord 2013;38:14-29. http://dx.doi.org/10.1016/j.jfludis.2012.12.001.
- Boberg J, Boberg E. The other side of the block. J Fluency Disord 1990;15:61-75. http://dx.doi.org/10.1016/0094-730X(90)90033-O.
- Butler C. Identity and stammering: negotiating hesitation, side-stepping repetition, and sometimes avoiding deviation. Sociol Health Illn 2013;35:1113-27. http://dx.doi.org/10.1111/1467-9566.12025.
- Corcoran JA, Stewart MA. Therapeutic experiences of people who stutter. J Speech Lang Path Audiol 1995;19:89-96.
- Corcoran JA, Stewart M. Stories of stuttering: a qualitative analysis of interview narratives. J Fluency Disord 1998;23:247-64. http://dx.doi.org/10.1016/S0094-730X(98)00020-5.
- Cream A, Onslow M, Packman A, Llewellyn G. Protection from harm: the experience of adults after therapy with prolonged-speech. Int J Lang Commun Disord 2003;38:379-95. http://dx.doi.org/10.1080/13682820310001598166.
- Cream A, Packman A, Llewellyn G. The playground rocker: a metaphor for communication after treatment for adults who stutter. Adv Speech Lang Pathol 2004;6:182-7. http://dx.doi.org/10.1080/14417040412331283048.
- Crichton-Smith I. Communicating in the real world: accounts from people who stammer. J Fluency Disord 2002;27:333-52. http://dx.doi.org/10.1016/S0094-730X(02)00161-4.
- Daniels DE, Hagstrom F, Gabel RM. A qualitative study of how African American men who stutter attribute meaning to identity and life choices. J Fluency Disord 2006;31:200-15. http://dx.doi.org/10.1016/j.jfludis.2006.05.002.
- Daniels DE, Gabel RM, Hughes S. Recounting the K-12 school experiences of adults who stutter: a qualitative analysis. J Fluency Disord 2012;37:71-82. http://dx.doi.org/10.1016/j.jfludis.2011.12.001.
- Goodhue R, Onslow M, Quine S, O’Brian S, Hearne A. The Lidcombe Program of early stuttering intervention: mothers’ experiences. J Fluency Disord 2010;35:70-84. http://dx.doi.org/10.1016/j.jfludis.2010.02.002.
- Hayhow R. Parents’ experiences of the Lidcombe Program of early stuttering intervention. Int J Speech Lang Pathol 2009;11:20-5. http://dx.doi.org/10.1080/17549500802571704.
- Hearne A, Packman A, Onslow M, Quine S. Stuttering and its treatment in adolescence: the perceptions of people who stutter. J Fluency Disord 2008;33:81-98. http://dx.doi.org/10.1016/j.jfludis.2008.01.001.
- Hughes CD, Gabel RM, Goberman AM, Hughes S. Family experiences of people who stutter. Can J Speech-Lang Pathol Audiol 2011;35:45-5.
- Kathard H, Pillay M, Samuel M, Reddy V. Genesis of self-identity as disorder: life histories of people who stutter. S Afr J Commun Disord 2004;51:4-14.
- Klompas M, Ross E. Life experiences of people who stutter, and the perceived impact of stuttering on quality of life: personal accounts of South African individuals. J Fluency Disord 2004;29:275-30. http://dx.doi.org/10.1016/j.jfludis.2004.10.001.
- Plexico L, Manning WH, Dilollo A. A phenomenological understanding of successful stuttering management. J Fluency Disord 2005;30:1-22. http://dx.doi.org/10.1016/j.jfludis.2004.12.001.
- Plexico LW, Manning WH, Levitt H. Coping responses by adults who stutter: part I. Protecting the self. J Fluency Disord 2009;34:87-107. http://dx.doi.org/10.1016/j.jfludis.2009.06.001.
- Plexico L, Manning WH, Levitt H. Coping responses by adults who stutter: part II. Approaching the problem and achieving agency. J Fluency Disord 2009;34:108-26. http://dx.doi.org/10.1016/j.jfludis.2009.06.003.
- Plexico L, Manning W, Dilollo A. Client perceptions of effective and ineffective therapeutic alliances during treatment for stuttering. J Fluency Disord 2010;35:333-54. http://dx.doi.org/10.1016/j.jfludis.2010.07.001.
- Plexico LW, Burrus E. Coping with a child who stutters: a phenomenological analysis. J Fluency Disord 2012;37:275-88. http://dx.doi.org/10.1016/j.jfludis.2012.06.002.
- Stewart T, Richardson G. A qualitative study of therapeutic effect from a user’s perspective. J Fluency Disord 2004;29:95-108. http://dx.doi.org/10.1016/j.jfludis.2003.11.001.
- Trichon M, Tetnowski J. Self-help conferences for people who stutter: a qualitative investigation. J Fluency Disord 2011;36:290-5. http://dx.doi.org/10.1016/j.jfludis.2011.06.001.
- Bricker-Katz G, Lincoln M, McCabe P. Older people who stutter: barriers to communication and perceptions of treatment need. Int J Lang Commun Disord 2010;45:15-30. http://dx.doi.org/10.3109/13682820802627314.
Appendix 1 Search strategy
Ovid MEDLINE
Date of search: search conducted from 1990 to August 2013.
-
Stuttering/
-
stutter$.tw.
-
stammer$.tw.
-
clutter$.tw.
-
(fluency adj2 disorder$).tw.
-
non-fluen$.tw.
-
dysfluen$.tw.
-
(syllable adj2 (repet$ or repeat$)).tw.
-
(word adj2 (repet$ or repeat$ or block$ or avoid$)).tw.
-
or/1-9
-
language therapy/ or speech therapy/
-
((speech or language) adj2 therap$).tw.
-
Family Therapy/
-
((famil$ or parent$ or child$) adj4 (treatment$ or therap$ or intervention$ or program$ or group$ or counsel$)).tw.
-
(indirect adj2 (approach$ or treatment$ or therap$ or intervention$ or program$)).tw.
-
demands-capacity model$.tw.
-
response$ contingenc$ approach$.tw.
-
exp Behavior Therapy/
-
(behavio?r adj2 (therap$ or modification or conditioning)).tw.
-
(conditioning adj therap$).tw.
-
Conditioning, Operant/
-
(operant adj2 conditioning$).tw.
-
(instrumental adj2 learning$).tw.
-
lidcombe.tw.
-
(cognitive adj2 restruct$).tw.
-
(manag$ or modification).tw.
-
Cognitive Therapy/
-
(cognitive behavio?r therap$ or cbt).tw.
-
ssmp.tw.
-
“successful stuttering management program$”.tw.
-
“voluntary stuttering”.tw.
-
“iowa approach”.tw.
-
pseudostutter$.tw.
-
desensiti?$.tw.
-
(fluen$ adj2 shap$).tw.
-
(speech adj2 restructur$).tw.
-
(gradual increase adj6 utterance).tw.
-
gilcu.tw.
-
“extended length utterance program$”.tw.
-
elu.tw.
-
((language or speech) adj2 training$).tw.
-
((metronome or rhythm) adj conditioned speech).tw.
-
(speech adj2 (prolong$ or smooth$ or slow$)).tw.
-
stretch$ syllable$.tw.
-
control$ rate$.tw.
-
“intensive smooth speech”.tw.
-
iss.tw.
-
“home based smooth speech”.tw.
-
hss.tw.
-
“speech motor training”.tw.
-
((breath$ or airflow or (air adj1 flow)) adj2 regulat$).tw.
-
(self model adj2 fluent speech).tw.
-
shadowing.tw.
-
Electromyography/
-
(“electromyograph$ feedback” or emg).tw.
-
(“excessive muscular tension technique$” or eng).tw.
-
(feedback adj2 (system or app$)).tw.
-
auditory feedback.tw.
-
(“masking auditory feedback” or maf).tw.
-
(“delayed auditory feedback” or daf).tw.
-
“frequency altered feedback”.tw.
-
(“altered auditory feedback” or aaf).tw.
-
speecheasy.tw.
-
prolong$.tw.
-
“monterey fluency program$”.tw.
-
token economy/
-
“token economy”.tw.
-
(token adj2 (system$ or reinforcement$)).tw.
-
“synergistic stuttering therap$”.tw.
-
“comprehensive stuttering program$”.tw.
-
“intensive treatment program$”.tw.
-
“fluency plus program$”.tw.
-
(“intensive stuttering clinic$” or uuisc).tw.
-
“fluency rules program$”.tw.
-
support group$.tw.
-
Self-Help Groups/
-
self help group$.tw.
-
exp Acupuncture Therapy/
-
acupuncture.tw.
-
“camperdown program$”.tw.
-
“american institute for stuttering program$”.tw.
-
“precision fluency shaping program$”.tw.
-
11 or 12 or 13 or 14 or 15 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38 or 40 or 41 or 43 or 45 or 46 or 47 or 48 or 49 or 50 or 51 or 53 or 54 or 55 or 56 or 57 or 58 or 59 or 60 or 61 or 62 or 63 or 64 or 65 or 66 or 67 or 68 or 69 or 70 or 71 or 72 or 73 or 74 or 75 or 76 or 77 or 78 or 79 or 80 or 81 or 82
-
11 or 12 or 13 or 14 or 15 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38 or 40 or 41 or 43 or 45 or 46 or 47 or 48 or 49 or 50 or 51 or 53 or 54 or 55 or 56 or 57 or 58 or 59 or 60 or 61 or 62 or 63 or 64 or 66 or 67 or 68 or 70 or 71 or 74 or 75 or 76 or 77 or 78 or 79 or 80 or 82
-
10 and 83
-
10 and 83
-
10 and 84
-
limit 85 to yr=“1990 -Current”
The Cochrane Library
Date of search: January 1990 to August 2013.
#1 MeSH descriptor: [Stuttering] explode all trees
#2 stutter*:ti,ab,kw (Word variations have been searched)
#3 stammer*:ti,ab,kw (Word variations have been searched)
#4 cluttering:ti,ab,kw (Word variations have been searched)
#5 fluency disorder*:ti,ab,kw (Word variations have been searched)
#6 disorder* fluency:ti,ab,kw (Word variations have been searched)
#7 non-fluen*:ti,ab,kw (Word variations have been searched)
#8 dysfluen* or disfluen*:ti,ab,kw (Word variations have been searched)
#9 syllable (repet* or repeat*):ti,ab,kw (Word variations have been searched)
#10 word (repet* or repeat* or block* or avoid*):ti,ab,kw (Word variations have been searched)
#11 #1 or #2 or #3 or #4 or #5 or #6 or #7 or #8 or #9 or #10
#12 MeSH descriptor: [Language Therapy] explode all trees
#13 MeSH descriptor: [Speech Therapy] explode all trees
#14 (speech or langauge) therap*:ti,ab,kw (Word variations have been searched)
#15 MeSH descriptor: [Family Therapy] explode all trees
#16 ((famil* or parent* or child*) and (treatment* or therap* or intervention* or program* or group* or counsel*)):ti,ab,kw (Word variations have been searched)
#17 indirect (approach* or treatment* or therap* or intervention* or program*):ti,ab,kw (Word variations have been searched)
#18 demands-capacity model*:ti,ab,kw (Word variations have been searched)
#19 response* contingenc* approach*:ti,ab,kw (Word variations have been searched)
#20 MeSH descriptor: [Behavior Therapy] explode all trees
#21 ((behaviour or behavior) and (therap* or modification or conditioning)):ti,ab,kw (Word variations have been searched)
#22 conditioning therap*:ti,ab,kw (Word variations have been searched)
#23 MeSH descriptor: [Conditioning, Operant] explode all trees
#24 operant conditioning*:ti,ab,kw (Word variations have been searched)
#25 instrumental learning*:ti,ab,kw (Word variations have been searched)
#26 lidcombe:ti,ab,kw (Word variations have been searched)
#27 cognitive restruct*:ti,ab,kw (Word variations have been searched)
#28 manag* or modification:ti,ab,kw (Word variations have been searched)
#29 MeSH descriptor: [Cognitive Therapy] explode all trees
#30 cognitive (behavior or behaviour) therap*:ti,ab,kw (Word variations have been searched)
#31 cbt:ti,ab,kw (Word variations have been searched)
#32 ssmp:ti,ab,kw (Word variations have been searched)
#33 “successful stuttering management program*”:ti,ab,kw (Word variations have been searched)
#34 “voluntary stuttering”:ti,ab,kw (Word variations have been searched)
#35 “iowa approach”:ti,ab,kw (Word variations have been searched)
#36 pseudostutter*:ti,ab,kw (Word variations have been searched)
#37 desensiti*:ti,ab,kw (Word variations have been searched)
#38 fluen* shap*:ti,ab,kw (Word variations have been searched)
#39 speech restructur*:ti,ab,kw (Word variations have been searched)
#40 gradual increase utterance:ti,ab,kw (Word variations have been searched)
#41 gilcu:ti,ab,kw (Word variations have been searched)
#42 “extended length utterance program*”:ti,ab,kw (Word variations have been searched)
#43 elu:ti,ab,kw (Word variations have been searched)
#44 (language or speech) training*:ti,ab,kw (Word variations have been searched)
#45 (metronome or rhythm) conditioned speech:ti,ab,kw (Word variations have been searched)
#46 speech (prolong* or smooth* or slow*):ti,ab,kw (Word variations have been searched)
#47 stretch* syllable*:ti,ab,kw (Word variations have been searched)
#48 control* rate*:ti,ab,kw (Word variations have been searched)
#49 “intensive smooth speech”:ti,ab,kw (Word variations have been searched)
#50 iss:ti,ab,kw (Word variations have been searched)
#51 “home based smooth speech”:ti,ab,kw (Word variations have been searched)
#52 hss:ti,ab,kw (Word variations have been searched)
#53 “speech motor training”:ti,ab,kw (Word variations have been searched)
#54 “speech motor training”:ti,ab,kw (Word variations have been searched)
#55 (breath* or airflow) regulat*:ti,ab,kw (Word variations have been searched)
#56 air flow regulat*:ti,ab,kw (Word variations have been searched)
#57 self model fluent speech:ti,ab,kw (Word variations have been searched)
#58 shadowing:ti,ab,kw (Word variations have been searched)
#59 MeSH descriptor: [Electromyography] explode all trees
#60 “electromyograph* feedback”:ti,ab,kw (Word variations have been searched)
#61 emg:ti,ab,kw (Word variations have been searched)
#62 “excessive muscular tension technique*”:ti,ab,kw (Word variations have been searched)
#63 eng:ti,ab,kw (Word variations have been searched)
#64 feedback (system or app*):ti,ab,kw (Word variations have been searched)
#65 auditory feedback:ti,ab,kw (Word variations have been searched)
#66 “masking auditory feedback”:ti,ab,kw (Word variations have been searched)
#67 “delayed auditory feedback”:ti,ab,kw (Word variations have been searched)
#68 “frequency altered feedback”:ti,ab,kw (Word variations have been searched)
#69 “altered auditory feedback”:ti,ab,kw (Word variations have been searched)
#70 maf or daf or aaf:ti,ab,kw (Word variations have been searched)
#71 speecheasy:ti,ab,kw (Word variations have been searched)
#72 prolong*:ti,ab,kw (Word variations have been searched)
#73 “monterey fluency program*”:ti,ab,kw (Word variations have been searched)
#74 MeSH descriptor: [Token Economy] explode all trees
#75 “token economy”:ti,ab,kw (Word variations have been searched)
#76 token (system* or reinforcement*):ti,ab,kw (Word variations have been searched)
#77 “synergistic stuttering therap*”:ti,ab,kw (Word variations have been searched)
#78 “comprehensive stuttering program*”:ti,ab,kw (Word variations have been searched)
#79 “intensive treatment program*”:ti,ab,kw (Word variations have been searched)
#80 “fluency plus program*”:ti,ab,kw (Word variations have been searched)
#81 “intensive stuttering clinic*”:ti,ab,kw (Word variations have been searched)
#82 uuisc:ti,ab,kw (Word variations have been searched)
#83 “fluency rules program*”:ti,ab,kw (Word variations have been searched)
#84 support group*:ti,ab,kw (Word variations have been searched)
#85 MeSH descriptor: [Self-Help Groups] explode all trees
#86 self help group*:ti,ab,kw (Word variations have been searched)
#87 MeSH descriptor: [Acupuncture Therapy] explode all trees
#88 acupuncture:ti,ab,kw (Word variations have been searched)
#89 “camperdown program*”:ti,ab,kw (Word variations have been searched)
#90 “american institute for stuttering program*”:ti,ab,kw (Word variations have been searched)
#91 “precision fluency shaping program*”:ti,ab,kw (Word variations have been searched)
#92 #12 or #13 or #14 or #15 or #16 or #17 or #19 or #20 or #21 or #22 or #23 or #24 or #25 or #26 or #27 or #28 or #29 or #30 or #31 or #32 or #37 or #38 or #39 or #43 or #44 or #45 or #46 or #47 or #48 or #49 or #50 or #51 or #52 or #53 or #54 or #55 or #56 or #57 or #58 or #59 or #60 or #61 or #63 or #64 or #65 or #67 or #69 or #70 or #71 or #72 or #74 or #75 or #76 or #79 or #84 or #85 or #86 or #87 or #88 or #89
#93 #11 and #92
#90 limit 87 to (humans and yr=“1990 -Current”)
#91 limit 85 to yr=“1990 -Current”
Appendix 2 Quality appraisal of intervention studies
| Study | Risk of bias yes/no/unclear | ||||||
|---|---|---|---|---|---|---|---|
| 1. Selection bias: method used to generate the allocation sequence, method used to conceal the allocation sequence, presence of control, characteristics of participants at baseline, ± 10 sample | 2. Performance bias: method used to blind participants and personnel and outcome assessors, presence of other potential threats to validity. Collection and assessment of speech sample | 3. Attrition bias: incomplete outcome data, high level of withdrawals from the study. High dropout rate (> 15%) | 4. Detection bias: accuracy of measurement of outcomes, length of follow-up. Reliable tool used, adequate speech sample, outside laboratory recording, immediate vs. longer-term follow-up | 5. Reporting bias: selective reporting, accuracy of reporting, use of inferential vs. descriptive statistics, pooled or individual reporting | Overall risk of bias. Lower/higher | Detail of concerns | |
| Allen 2011117 | Yes | Yes | No | Yes | Yes | Higher | Small sample. Unclear research questions and recruitment justification. Poor reporting |
| Amster and Klein 200730 | Yes | Yes | No | Yes | No | Higher | Small sample. No control. Volunteered sample |
| Andrews et al. 201231 | Yes | Yes | Yes | No | No | Higher | Small sample. No control. Volunteered sample |
| Antipova et al. 2008118 | Yes | Yes | No | Yes | No | Higher | Small sample. No control. Volunteered sample |
| Armson and Stuart 1998119 | Yes | Yes | No | Yes | No | Higher | Small sample. Experimental design with no follow-up. Single session tests. Kappa scoring methods not described reliability/results |
| Armson et al. 20064 | Yes | Yes | No | Yes | No | Higher | Small sample. Experimental design with no follow-up |
| Armson and Kiefte 2008120 | Yes | Yes | No | Yes | No | Higher | Mid-sized sample. Experimental design with no follow-up. First 31 people taken into study |
| Baumeister et al. 200332 | Yes | Yes | Yes | No | No | Higher | Large sample, but no control group. Participants showed different severity of disorder that influenced results. Some participants dropped out or were not assessed at baseline |
| Beilby et al. 201233 | No | Unclear | No | No | No | Lower | Unclear if raters were blinded to time point, 3-month follow-up |
| Berkowitz et al. 199434 | Yes | Yes | No | No | No | Higher | Very small sample. No control. No blinding in assessment, self-reports used |
| Block et al. 200436 | No | No | No | Yes | Yes | Higher | Sample (n = 19). 5-minute conversation, 5-minute reading. Unclear who recorded away from clinic. Basic results for post-treatment periods, 3-month follow-up, limited analysis |
| Block et al. 200537 | No | No | No | No | No | Lower | Large sample. Self-report inventory used at 3.5-year follow-up with 87% of sample response rate. Unclear length of speech sample |
| Block et al. 200638 | No | No | No | No | No | Lower | Same study as 2005 paper37 with further examination of variables |
| Block et al. 199635 | No | No | No | Yes | No | Higher | Larger sample. No dropout. Immediate measurement during intervention. Experimental setting, 5-minute samples |
| Blomgren et al. 200539 | Yes | Unclear | No | No | No | Lower | Sample (n = 12). Some use of self-reported outcome measures post study. 4-minute speech sample, unclear if rater blinded, 6-month follow-up |
| Blood 199540 | Yes | Yes | No | Yes | Yes | Higher | Extremely small sample. Flawed recruitment. Use of self-reported outcomes |
| Boberg and Kully 199441 | No | Unclear | No | Yes | Yes | Higher | Sample (n = 42). No control. Telephone call sample 2 minutes. Unclear if raters blind to time point, percentage change reported |
| Bonelli et al. 200042 | Yes | No | No | No | Yes | Higher | Sample (n = 9) selected from earlier study, no pooling of data reported by individual only |
| Bray and James 200943 | Yes | Yes | No | Yes | Yes | Higher | Small sample. Use of self-reported outcomes |
| Bray and Kehle 199844 | Yes | Yes | No | Yes | Yes | Higher | Small sample of volunteers (n = 4). Content of speech sample and listener varied between individuals and time, descriptive data by individual only |
| Carey et al. 201045 | No | No | No | No | No | Lower | n = 20 per trial arm, with 7.5% loss to follow-up, 12-month follow-up, 10-minute recording via telephone, blinded assessment |
| Cocomazzo et al. 201246 | No | No | Yes | Unclear | No | Lower | n = 12 participants and dropouts, blinded rating, beyond clinic recordings made by participant but asked to make only one. 12-month follow-up |
| Craig et al. 199616 | No | No | No | Yes | No | Lower | Larger sample. Raters blinded. 12-month follow-up, 5-minute speech samples |
| Craig et al. 200247 | Yes | Yes | No | Yes | No | Higher | Small sample (n = 6) selected from previous study. 2-year follow-up, descriptive data for individuals only, home measure potential for bias |
| Cream et al. 200948 | Yes | No | Yes | Yes | No | Higher | Sample (n = 10), 5-minute recordings. Use of some self-reported outcomes. Two dropouts in small sample, blinded assessor, immediate post assessment |
| Cream et al. 201017 | No | No | No | No | No | Lower | Randomised sample with acceptable dropout rate, blinded assessment, 6-month follow-up |
| De Veer et al. 200918 | Yes | Yes | No | Yes | No | Higher | Selection of potential participants by researchers. No detail of randomisation. No measure of fluency, self-report measures only |
| Druce et al. 199749 | Yes | No | No | Yes | No | Lower | Sample (n = 15) with adequate follow-up, 2-minute speech sample, raters blinded |
| Elliott et al. 199850 | Yes | Yes | No | No | Yes | Higher | Small sample (n = 5). 5-minute conversation sample, reported by individuals, limited analysis |
| Femrell et al. 201251 | Yes | Yes | Yes | Yes | No | Higher | Sample (n = 10 with n = 2 loss to follow-up), 10-minute conversation, assessed by clinician, not blinded |
| Foundas et al. 201352 | No | Unclear | No | Unclear | No | Higher | Sample (n = 24, n = 10 control) with control and experimental conditions. Immediate outcomes, length of sample not reported. Unclear whether or not blinded |
| Franken et al. 199253 | No | No | No | Yes | No | Higher | Fair sized sample (n = 32) 6-month follow-up. Rating scale used. Blinded assessment. Control normal speakers, 5-minute recordings. Purpose to compare normal to post intervention rather than evaluate interventions per se |
| Franken et al. 200554 | No | No | Yes | Yes | No | Lower | Small sample randomised to one of two arms. Loss to follow-up. Recordings made by parents. Blinded assessors |
| Franklin et al. 200819 | No | Yes | No | Unclear | No | Higher | Larger sample, but participants were not randomised to each condition. Assessment carried out by authors. Not blinded. Immediate follow-up. Sample 1500 syllables |
| Gagnon and Ladouceur 199255 | Yes | Unclear | No | Unclear | Yes | Higher | Small samples used in separate studies. Data presented by individual, lack of clarity regarding data collection and evaluation |
| Gallop and Runyan 201256 | Yes | Unclear | Unclear | Yes | Yes | Higher | Sample (n = 11). No control. No explanation of recruitment criteria. 15-minute telephone samples, not reported if blinded, informal follow-up |
| Hancock and Craig 199820 | Yes | No | No | No | No | Lower | Larger sample (n = 77). 12-month follow-up. Pseudorandomisation, 5-minute speech sample, in clinic at distance via telephone |
| Hancock et al. 199821 | Yes | No | No | No | No | Lower | Same study as Hancock and Craig 1998.20 This paper reports some different outcomes |
| Hancock and Craig 200257 | Yes | No | No | Yes | No | Lower | Sample (n = 12) selected from earlier study. 5-minute only speech sample |
| Harris et al. 200222 | No | No | Yes | No | No | Lower | Small study. (n = 29), 6 dropped out (21%) |
| Harrison et al. 200458 | No | No | Yes | No | No | Lower | (n = 46), 8 dropped out |
| Hasbrouck 199259 | Unclear | Yes | No | No | Unclear | Higher | Larger sample. No control. No blinding. Very sparse details given about recruitment, attrition, analysis |
| Hewat et al. 200623 | No | No | Yes | Yes | No | Lower | n = 30 recruited, dropout varied from 27% to 40% at different stages of the study. In-clinic recording and participant selected recording. Rating blinded |
| Hudock and Kalinowski 201460 | Unclear | No | No | Yes | Yes | Higher | Small study (n = 9). No detail of recruitment. Scripted telephone conversations. Immediate measurement |
| Huinck et al. 200661 | Unclear | No | No | No | No | Lower | Sample (n = 25). No details given about recruitment methods |
| Ingham et al. 201362 | Yes | Unclear | Yes | Yes | No | Higher | Volunteer participants, 9 out of 21 did not complete. 3-minute monologue, 3-minute conversation. Study purpose to compare normal to people who stutter; however, contains before and after data. No detail of whether or not raters blinded. Immediate follow-up, in-clinic rating |
| Ingham et al. 200163 | Yes | No | No | Yes | No | Higher | Small sample (n = 5). Use of some self-reported measures. Participants submitted own recording for beyond-clinic measure. Not detailed whether or not raters blinded, data reported by participant |
| Irani et al. 2012116 | No | Unclear | No | Yes | No | Higher | Mixed-methods study. Some self reported measures. Use of inferential statistics, small sample (n = 7) little detail of speech sample analysis |
| Iverach et al. 200964 | No | No | No | Yes | No | Lower | Larger sample (n = 64). Use of some self-reported measures |
| Jones et al. 200065 | No | No | No | No | No | Lower | Large sample (n = 261 children, 4% dropout rate, all explained) |
| Jones et al. 200524 | No | No | No | No | No | Lower | Larger sample (n = 54 children, 13% dropout rate, all explained) |
| Jones et al. 200825 | No | No | Yes | No | No | Lower | This is a 5-year follow-up of the earlier study.24 31% of the original treatment group could not be recontacted and 68% of the control group |
| Kaya and Alladin 201266 | Yes | No | No | Yes | No | Higher | No comparator group. No detail regarding how stuttering occurrences defined. Immediate assessment at final session |
| Kaya 201167 | Yes | Yes | No | Yes | No | Higher | Assessment via 2-minute speech sample only, rating scale measure used very limited |
| Kingston et al. 200368 | No | Yes | No | Yes | No | Higher | Larger sample (n = 78 children). Assessment was carried out by the clinician/researcher with no blinding. Purpose of paper to examine associations (predict treatment time) rather than outcomes |
| Koushik et al. 200969 | No | No | No | No | Yes | Lower | Sample (n = 12 children), 1 dropped out |
| Koushik et al. 2011121 | Unclear | Unclear | No | Unclear | No | Higher | Pooled data from five clinical sites. Larger sample (n = 134 in final analysis). Retrospective file audit. Purpose of study to examine associations rather than evaluate outcomes |
| Laiho and Klippi 200770 | No | Yes | No | Yes | No | Higher | Sample (n = 21). No control. Assessment via video by author, parent-report data for beyond clinic data. Follow-up data only parent report |
| Langevin and Boberg 199371 | Yes | No | Yes | No | No | Higher | Small sample, high dropout rate (n = 21 participants, 11 dropped out) data reported by individual |
| Langevin and Boberg 199672 | Yes | No | Yes | No | No | Lower | n = 25 in one group, n = 16 in other. 2-year follow-up, some loss to follow-up. 2/3-minute samples of speech in clinic and via telephone. Raters probably blinded |
| Langevin et al. 200673 | No | No | No | No | No | Lower | n = 18 participants. No control. Small loss to follow-up |
| Langevin et al. 201074 | Yes | No | Yes | No | No | Lower | 5-year follow-up of earlier study |
| Lattermann et al. 200826 | No | No | No | No | No | Lower | Sample (n = 46). Blinded rating |
| Lawson et al. 199375 | No | No | No | Yes | No | Higher | Self-report measures only used, 1-month follow-up, some dropout |
| Leahy and Collins 199176 | Yes | Yes | No | Yes | Yes | Higher | No comparator group. Small sample size (n = 5). Measures taken by student clinician carrying out intervention. Longer follow-up only for two participants. Reporting by individual only |
| Lewis et al. 200827 | No | No | No | No | No | Lower | Small sample (n = 8 in intervention group, n = 10 in control group) |
| Lincoln et al. 199677 | No | No | No | Yes | Yes | Higher | Sample (n = 11). High dropout of potential participants (n = 22 recruited). Some pooled data. Some reporting of individuals only, 12-month follow-up, parent-recorded speech data |
| Lincoln and Onslow 1997122 | No | Yes | Yes | Yes | Yes | Higher | Long-term outcomes of earlier studies. Large initial dropout of potential participants. Parents collected speech sample, parent report questionnaire, descriptive data |
| Lutz 200978 | Yes | Yes | No | Yes | No | Higher | Findings from a workshop for parents using before-and-after questionnaires |
| Mallard 199879 | No | Yes | No | Yes | Yes | Higher | Only measure of success was ‘is child in S&L therapy 1 year after intervention?’. No control group, limited analysis |
| Menzies et al. 200828 | No | No | No | No | No | Lower | Smaller sample (n = 32), 2 dropped out, 16 in each condition |
| Millard et al. 200880 | No | No | Yes | No | No | Higher | Small sample (n = 9) high dropout rate (30%). Blinded rating. In-clinic assessment, 12-month follow-up, data by individual only |
| Millard et al. 200981 | No | No | Yes | No | Yes | Higher | Small sample (n = 10). High dropout rate Parent-recorded video data. Control group for initial allocation but removed part way, no pooled data descriptive statistics only |
| Miller and Guitar 200982 | No | No | No | No | No | Lower | Long-term follow-up, many participants at minimum level. Only 2 dropouts out of 15, limited speech sample |
| Nilsen and Ramberg 199983 | No | No | No | Yes | No | Higher | 2 dropouts out of 13. Use of some scales with limited scoring and analysis, data reported by individual |
| O’Brian et al. 200384 | No | No | No | Yes | Yes | Higher | 5 dropouts out of 30. Reasonable sample. No comparator. Participant-selected recordings. Limited statistical analysis |
| O’Brian et al. 200885 | No | No | Yes | No | Yes | Higher | 16 out of 30 completed. Descriptive analysis |
| O’Brian et al. 201386 | No | No | No | No | No | Lower | No control |
| O’Donnell et al. 200887 | Yes | No | No | No | Yes | Higher | Small sample (n = 7). n = 5 from previous study who had shown most benefit. Data reported by individual participant |
| Onslow et al. 199429 | Unclear | No | Yes | Yes | No | Higher | High withdrawal for control and intervention. No detail of allocation. Audio recordings made by parents. Descriptive statistics |
| Onslow et al. 199088 | Yes | Yes | No | No | Yes | Higher | No comparator group. Sample (n = 4). Presentation of findings via figures only. No grouping of data |
| Onslow et al. 199289 | Unclear | No | No | No | No | Higher | Focuses on speech naturalness data only comparing people who stutter and non-stutterers. No control group. Immediate follow-up. Recruitment process unclear |
| Onslow et al. 199690 | Unclear | No | Yes | No | No | Higher | Data reported for only 18 out of 32 recruited |
| Onslow et al. 2002123 | Yes | No | No | No | Yes | Higher | Small sample (n = 8), 6 of whom in previous studies. For two participants, parent-only recordings. Descriptive data presented by individual only. Purpose of paper to evaluate one aspect of intervention outcome |
| Pape-Neumann 200491 | Yes | Yes | Yes | Yes | Yes | Higher | This is a pilot study which presents data from a range of interventions |
| Pollard et al. 200992 | No | Yes | No | Yes | No | Lower | Sample (n = 11). No dropout. Samples collected at non-laboratory locations. Non-blinded scoring. Immediate outcomes |
| Ratynska et al. 2012124 | Yes | Yes | No | Unclear | No | Higher | Large sample found other treatment ineffective. No dropout. No blinding of assessment. Incomplete description of data collection |
| Reddy et al. 201093 | Unclear | Unclear | No | Unclear | Unclear | Higher | Small sample (n = 5). Limited reporting of findings beyond description of cases |
| Riley and Ingham 200094 | Unclear | Unclear | No | Unclear | Yes | Higher | Sample (n = 12). Pseudorandomisation. No blinding of assessors. Unclear beyond clinic data collection. Unclear whether 12 or 6 participants being reported. No reporting of control group outcomes |
| Rosenberger et al. 200795 | Yes | Yes | Yes | No | No | Higher | Two groups were compared that have an uneven number of participants. Some dropout. Limited blinding and speech measures |
| Rousseau et al. 200796 | No | Yes | No | No | No | Lower | Reasonable sample large proportion of parent-recorded samples. No analysis of dropouts |
| Ryan and Van Kirk 199597 | No | Yes | Yes | No | No | Lower | Reasonable sample (n = 24, n = 20 completed all elements). Pseudorandomisation. No blinding of speech evaluation |
| Sicotte et al. 200398 | Yes | Yes | No | Yes | No | Higher | Sample (n = 6). Rating scales only. Purpose of study evaluate intervention fidelity rather than outcomes |
| Smits-Bandstra and Yovetich 200399 | Yes | Unclear | No | Yes | No | Higher | Small groups. Each time point presented separately in table form, limited discussion of trends over time. Six participants had received other intervention immediately prior. 3-minute sample, assume no blinding, limited statistical analysis |
| Stewart 1996100 | No | Yes | No | Yes | No | Higher | Reasonable sample (n = 15). No blinding of assessment. 3-minute conversation. Limited analysis of speech behaviour data. No outside clinic measure. Reasonable follow-up |
| Stidham et al. 2006101 | Yes | Yes | No | No | No | Higher | Volunteers recruited. Small sample (n = 9). Immediate follow-up. No blinding as assessment. In-laboratory evaluation |
| Stuart et al. 2004102 | Unclear | Yes | No | No | No | Higher | No detail of recruitment. Non-blinded assessment. In-laboratory evaluation. Limited speech sample |
| Stuart et al. 2006103 | Unclear | Yes (for some elements) | No | Yes | No | Higher | No detail of recruitment. No blinding of assessment for first studies. Limited speech sample (300 syllables). Reasonable follow-up. In-clinic assessment |
| Trajkovski et al. 2011104 | No | No | Yes | Yes | No | Lower | 8 out of 17 completed. Data provided for dropouts. Limited pooled data. Parent-collected recordings |
| Unger et al. 2012125 | Yes | Yes | No | Yes | No | Higher | Volunteer participants. Reasonable sample. In-clinic only. Immediate follow-up. No blinding of assessment 2 × 5-minute monologues |
| Van Borsel et al. 2003105 | Yes | Yes | No | No | No | Higher | Volunteer participants. In-clinic data. No blinding of recordings. Small sample (n = 9) |
| von Gudenberg 2006106 | Yes | Yes | Yes | Yes | Yes | Higher | No clear description of any measurement. Participants or methods used. More a evaluation of collected data up to now |
| von Gudenberg et al. 2006107 | Yes | Yes | Yes | Yes | Yes | Higher | Detailed description of the therapy reasons why this therapy may be effective and a good approach for young adults. However, presented results are outcomes with no clear description of methodology and limited analysis |
| Wagaman et al. 1993108 | Yes | No | No | No | No | Lower | Follow-up data only |
| Wagaman et al. 1995109 | Yes | No | No | Yes | No | Higher | Small sample. No long-term follow-up |
| Ward 1992110 | Yes | Yes | No | Unclear | No | Higher | No long-term outcomes. Reports pilot study findings only. Small sample |
| Wille 1999111 | Yes | Yes | Yes | Yes | Yes | Higher | No clear description of method. Data collection. Data analyses. No reference to other literature |
| Wilson et al. 2004112 | No | Yes | Yes | No | Yes | Higher | Small sample. Dropouts and lack of data |
| Woods et al. 2002113 | Yes | No | No | No | No | Lower | Small sample (n = 8). 1-month follow-up. No speech data. Study focuses on cognitive and language assessments |
| Yairi and Ambrose 1992114 | No | Unclear | Yes | No | No | Higher | Reasonable sample (n = 27). 2-year follow-up. Speech sample small (around 500 words). 6 dropout, unclear whether or not speech assessors blinded. In-clinic data |
| Yaruss et al. 2006115 | No | Yes | No | Yes | No | Higher | Sample (n = 17). Speech rated by clinician. Follow-up to 2 years with no dropout. At least 200-word sample. Unclear how collected. Limited analysis |
| Zimmerman et al. 1997126 | No | Unclear | No | Yes | No | Higher | Small sample (n = 9). No long-term follow-up. Scripted conversations. Unclear if rater blinded |
Appendix 3 Quality appraisal of qualitative studies
| Study | 1. Was there a clear statement of the aim of the research? | 2. Is a qualitative methodology appropriate to address the aims of the research? | 3. Was the recruitment strategy appropriate to the aims of the research? | 4. Were data collected in a way that addressed the research issue? | 5. Has the relationship between researcher and participant been adequately considered? | 6. Have ethical issues been taken into account? | 7. Were the data analysis sufficiently rigorous? | 8. Is there a clear statement of findings? | Overall lower/higher risk of bias; detail of concerns |
|---|---|---|---|---|---|---|---|---|---|
| Anderson and Felsenfeld 2003128 | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Lower |
| Beilby et al. 2013129 | Yes | Yes | Unclear | Yes | Yes | Yes | Unclear | Yes | Higher; recruitment and data analysis unclear |
| Boberg and Boberg 1990130 | Yes | Yes | Unclear | Yes | No | No | Not reported | Yes, | Higher; detail of data missing |
| Bricker-Katz et al. 2010152 | Yes | Yes | Yes | Yes | Partial | Partial | Yes | Yes | Higher; detail missing |
| Butler 2013131 | Yes | Yes | Yes | Yes | Partial | Yes | Yes | Yes | Lower |
| Corcoran and Stewart 1995132 | Yes | Yes | No | Yes | Yes | No | Unclear | Yes | Higher; lack of detail, unclear recruitment |
| Corcoran and Stewart 1998133 | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Lower |
| Cream et al. 2003134 | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Lower |
| Cream et al. 2004135 | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Lower |
| Crichton-Smith 2002136 | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Lower |
| Daniels et al. 2012138 | Yes | Yes | Yes | Yes | Yes | Partial | Yes | Yes | Lower |
| Daniels et al. 2006137 | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Lower |
| Goodhue et al. 2010139 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Lower |
| Hayhow 2009140 | Yes | Yes | Partial | Yes | Partial | Unclear | Yes | Yes | Higher; lack of detail |
| Hearne et al. 2008141 | Yes | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Lower |
| Hughes et al. 2011142 | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Lower |
| Irani et al. 2012116 | Yes | Yes | Yes | Yes | Yes | Partial | Yes | Yes | Lower |
| Kathard et al. 2004143 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Lower |
| Klompas and Ross 2004144 | Yes | Yes | Yes | Yes | No | Yes | No | Yes | Higher; lack of detail and superficial analysis |
| Plexico et al. 2005145 | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Lower |
| Plexico et al. 2009146 | Yes | Yes | Partial | Yes | Yes | No | Yes | Yes | Lower |
| Plexico et al. 2009147 | Yes | Yes | Partial | Yes | Yes | No | Yes | Yes | Higher |
| Plexico et al. 2010148 | Yes | Yes | Partial | Yes | Yes | No | Yes | Yes | Lower |
| Plexico and Burrus 2012149 | Yes | Yes | Partial | Yes | Yes | No | Yes | Yes | Lower |
| Stewart and Richardson 2004150 | Yes | Yes | Yes | Yes | Partial | No | Yes | Yes | Lower |
| Trichon and Tetnowski 2011151 | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Higher; detail missing |
Appendix 4 Studies excluded at full paper review
| Authors, date | Reason |
|---|---|
| Armson J, Foote S, Witt C, Kalinowski J, Stuart A. Effect of frequency altered feedback and audience size on stuttering. Eur J Disord Commun 1997;32:359–66 | Laboratory investigation of FAF during reading aloud |
| Bajaj A, Hodson B, Westby C. Communicative ability conceptions among children who stutter and their fluent peers: a qualitative exploration. J Fluency Disord 2005;30:41–64 | Alludes to outcomes of therapy, that children use therapy terms to describe their speech but nothing directly relevant |
| Blood GW. A behavioral–cognitive therapy program for adults who stutter: computers and counseling. J Commun Disord 1995;28:165–80 | Case series, three participants |
| Bothe AK, Finn P, Bramlett RE. Pseudoscience and the SpeechEasy: Reply to Kalinowski, Saltuklaroglu, Stuart, and Guntupalli. Am J Speech Lang Pathol 2007;16:77–83 | Letter to editor reply to critique of previous paper |
| Butcher C, McFadden D, Quinn B, Ryan BP. The effects of language training on stuttering in young children, without and with contingency management. J Dev Phys Disabil 2003;15:255–80 | Design: case series |
| Cai S, Beal DS, Ghosh SS, Tiede MK, Guenther FH, Perkell JS. Weak responses to auditory feedback perturbation during articulation in persons who stutter: evidence for abnormal auditory-motor transformation. PLOS ONE 2012;7:e41830 | No intervention, relates to diagnosis |
| Carey B, O’Brian S, Onslow M, Packman A, Menzies R. Webcam delivery of the Camperdown Program for adolescents who stutter: a phase I trial. Lang Speech Hear Serv Sch 2012;43:370–80 | Three participants |
| Carr SM, O’Brian S, Hewat S, Onslow M, Packman A, Menzies R. Investigating parent delivery of the Lidcombe Program. Internat J Speech Lang Pathol 2011;13:308–16 | Describes fidelity of intervention. May be relevant for qualitative review? |
| Craig AR, Calver P. Following up on treated stutterers: studies of perceptions of fluency and job status. J Speech Hear Res 1991;34:279–84 | Survey data |
| Craig AR, Kearns M. Results of a traditional acupuncture intervention for stuttering. J Speech Hear Res 1995;38:572–8 | Two case studies |
| Dayalu VN, Saltuklaroglu T, Kalinowski J, Stuart A, Rastatter MP. Producing the vowel /a/ prior to speaking inhibits stuttering in adults in the English language. Neurosci Lett 2001;306:111–15 | Laboratory assessment of vowel insertion during reading aloud |
| de Vries U. ‘Loudly-slowly-intelligibly’: One phase of the therapy for children who stutter. Vierteljahresschrift fur Heilpadagogik und ihre Nachbargebiete 1990;6:60–72 | Book chapter, general discussion |
| de Vries U. ‘Loudly-slowly-intelligibly’: One phase of the therapy for children who stutter. Vierteljahresschrift fur Heilpadagogik und ihre Nachbargebiete 1990;6:60–72 | General description of intervention only |
| Eichstadt A, Watt N, Girson J. Evaluation of the efficacy of a stutter modification program with particular reference to two new measures of secondary behaviors and control of stuttering. J Fluency Disord 1998;23:231–46 | Non OECD country |
| Foundas AL, Bollich AM, Feldman J, Corey DM, Hurley M, Lemen LC, et al. Aberrant auditory processing and atypical planum temporale in developmental stuttering. Neurology 2004;63:1640–6 | Laboratory assessment of DAF during reading aloud |
| Freeman K, Armson J. Extent and stability of stuttering reduction during choral reading. J Speech Lang Pathol Audiol 1998;22:188–202 | Examines choral speech producing temporary reduction during experiment |
| Fry JP, Botterill WM, Pring TR. The effect of an intensive group therapy program for young adults who stutter: a single subject study. Int J Speech Lang Pathol 2009;11:12–19 | Data for three participants |
| Gabel RM, Colcord RD, Petrosino L. A study of the self-talk of adults who do and do not stutter. Percept Mot Skills 2001;92:835–42 | No intervention |
| Green T. The effects of stuttering upon psycho-social adjustment and personality characteristics. Logoped Phoniatr Vocol 1997;22:25–38 | Not qualitative or clinical effectiveness study |
| Guntupalli VK, Nanjundeswaran C, Kalinowski J, Dayalu VN. Past speech therapy experiences of individuals exploring a new stuttering treatment. Percept Mot Skills 2011;112:975–80 | Survey |
| Hayasaka K. Factors related to persistence and improvement of stuttering in children. Scandinavian J Logoped Phoniatr 1993;18:65–72 | Examines links with improvement but outcome data not possible to identify from reporting |
| Hearne A, Packman A, Onslow M, O’Brian S. Developing treatment for adolescents who stutter: a phase I trial of the Camperdown Program. Lang Speech Hear Serv Sch 2008;39:487–97 | Case series, three participants |
| Helgadottir FD, Menzies RG, Onslow M, Packman A, O’Brian S. Online CBT II: a phase I trial of a standalone, online CBT treatment program for social anxiety in stuttering. Behav Change 2009;26:254–70 | Design |
| Hudock D, Dayalu VN, Saltuklaroglu T, Stuart A, Zhang J, Kalinowski J. Stuttering inhibition via visual feedback at normal and fast speech rates. Int J Lang Commun Disord 2011;46:169–78 | Emphasis on evaluating if visual speech feedback adversely impacts on speech rate |
| Ingham RJ, Moglia RA, Frank P, Ingham JC, Cordes AK. Experimental investigation of the effects of frequency-altered auditory feedback on the speech of adults who stutter. J Speech Lang Hear Res 1997;40:361–72 | Case series |
| Ingham RJ, Kilgo M, Ingham JC, Moglia R, Moglia R, Belknap H, et al. Evaluation of a stuttering treatment based on reduction of short phonation intervals J Speech Lang Hear Res 2001;6:1229–44 | Case series, three participants |
| Ingham RJ, Sato W, Finn P, Belknap H. The modification of speech naturalness during rhythmic stimulation treatment of stuttering. J Speech Lang Hear Res 2001;44:841–52 | Duplicate paper |
| Ingham RJ, Warner A, Byrd A, Cotton J. Speech effort measurement and stuttering: investigating the chorus reading effect. J Speech Lang Hear Res 2006;49:660–70 | Compares effect of chorus reading on speech effort in stutterers vs. normal speakers |
| Ingham RJ, Bothe AK, Jang E, Yates L, Cotton J, Seybold I. Measurement of speech effort during fluency-inducing conditions in adults who do and do not stutter. J Speech Lang Hear Res 2009;52:1286–301 | Compares self-rated speech effort in stutterers vs. normal speakers |
| Iverach L, Jones M, O’Brian S, Block S, Lincoln M, Harrison E, et al. The relationship between mental health disorders and treatment outcomes among adults who stutter. J Fluency Disord 2009;34:29–43 | Minor correction to previous paper only |
| Kalinowski J, Stuart A. Stuttering amelioration at various auditory feedback delays and speech rates. Eur J Disord Commun 1996;31:259–69 | Laboratory assessment of DAF during reading aloud |
| Kalinowski J, Stuart A, Rastatter MP, Snyder G, Dayalu V. Inducement of fluent speech in persons who stutter via visual choral speech. Neurosci Lett 2000;281:198–200 | Laboratory assessment of visual coral speech during memorised reading aloud |
| Kalinowski J, Armson J, Roland-Mieszkowski M, Stuart A, Gracco VL. Effects of alterations in auditory feedback and speech rate on stuttering frequency. Lang Speech 1993;36:1–16 | Examines elements of auditory feedback |
| Kalinowski J, Stuart A, Rastatter MP, Snyder G, Dayalu V. Inducement of fluent speech in persons who stutter via visual choral speech. Neurosci Lett 2000;281:198–200 | Letter, no data |
| Kalinowski J, Dayalu VN, Saltuklaroglu T. Cautionary notes on interpreting the efficacy of treatment programs for children who stutter. Int J Lang Commun Disord 2002;37:359–61 | Letter, no data |
| Kalinowski J, Stuart A, Wamsley L, Rastatter MP. Effects of monitoring condition and frequency-altered feedback on stuttering frequency. J Speech Lang Hear Res 1999;42:1347–54 | Examines types of auditory feedback |
| Kathard H. Sharing stories: life history narratives in stuttering research. Int J Lang Commun Disord 2001;36(Suppl. 7):52–7 | Discusses life history research, mentions need to engage with feelings and significance of stuttering in life but no data of direct relevance |
| Kiefte M, Armson J. Dissecting choral speech: properties of the accompanist critical to stuttering reduction. J Commun Disord 2008;41:33–48 | Compares choral speech with AAF when reading |
| Kuniszyk-Jozkowiak W, Smolka E, Adamczyk B. Effect of acoustical, visual and tactilr echo on speech fluency of stutterers. Folia Phoniatr Logop 1996;44:193–200 | Explores different types of auditory feedback |
| Langevin M, Packman A, Onslow M. Parent perceptions of the impact of stuttering on their preschoolers and themselves. J Commun Disord 2010;43:407–23 | Impact of stuttering on parents, no data regarding interventions. |
| Lincoln M, Packman A, Onslow M, Jones M. An experimental investigation of the effect of altered auditory feedback on the conversational speech of adults who stutter. J Speech Lang Hear Res 2010;53:1122–31 | Explores DAF in different conditions |
| Macleod J, Kalinowski J, Stuart A, Armson J. Effect of single and combined altered auditory feedback on stuttering frequency at two speech rates. J Commun Disord 1995;28:217–28 | Explores types of DAF |
| Metten C, Bosshardt HG, Jones M, Eisenhuth J, Block S, Carey B, et al. Dual tasking and stuttering: from the laboratory to the clinic. Disabil Rehabil 2011;33:933–44 | Laboratory testing prior to case series with three participants |
| Miltenberger RG, Wagaman JR, Arndorfer RE. Simplified treatment and long term follow-up for stuttering in adults: a study of two cases. J Behav Ther Experiment Psychiatry 1996;27:181–8 | Two case studies |
| Nakao A, Tanaka N, Coleman C. My personal experience with speech therapy for stuttering at the Stuttering Center of Western Pennsylvania. Acta Medica Okayama 2001;55:193–5 | Letter to the editor, no data |
| Neiman GS, Rubin RB. Changes in communication apprehension, satisfaction, and competence in foreign dialect and stuttering clients. J Commun Disord 1991;24:353–66 | Fewer than 50% of stuttering participants |
| Nejati V, Pouretemad HR, Bahrami H. Attention training in rehabilitation of children with developmental stuttering. NeuroRehabilitation 2013;32:297–303 | Non OECD (Islamic republic of Iran) |
| Nicholas A, Millard SK. The case for early intervention with pre-school dysfluent children. Int J Lang Commun Disord 1998;33(Suppl. 1):374–7 | Conference abstract only |
| O’Brian S, Onslow M. Clinical management of stuttering in children and adults. BMJ 2011;342:d3742 | General overview |
| Onslow M, O’Brian S, Harrison E. The Lidcombe Programme of early stuttering intervention: methods and issues. Eur J Disord Commun 1997;32:231–50 | General discussion |
| Onslow M, Packman A, Stocker S, van Doorn J, Siegel GM. Control of children’s stuttering with response-contingent time-out: behavioral, perceptual, and acoustic data. J Speech Lang Hear Res 1997;40:121–33 | General discussion of the LP |
| Onslow M, Ratner NB, Packman A. Changes in linguistic variables during operant, laboratory control of stuttering in children. Clin Linguist Phon 2001;15:651–62 | Two case studies |
| Onslow M, O’Brian S, Harrison E. The Lidcombe Programme: maverick or not? Eur J Disord Commun 1997;32:261–6 | Three case studies |
| Packman A, Onslow M. Investigating optimal intervention intensity with the Lidcombe Program of early stuttering intervention. Int J Speech Lang Pathol 2012;14:467–70 | Overview of the LP evidence |
| Paden EP, Ambrose NG, Yairi E. Phonological progress during the first 2 years of stuttering. J Speech Lang Hear Res 2002;45:256–67 | Examines phonological development in stuttering children |
| Petrunik M. Stutterers’ adaptations to non-avoidance therapy: primary/secondary deviance theory as a professional treatment ideology. Social Problems 1980;31:125–38 | Published prior to cut-off date |
| Ramig PR. High reported spontaneous stuttering recovery rates: fact or fiction? Lang Speech Hear Serv Sch 1993;24:156–60 | Survey |
| Rami MK, Diederich E. Effect of reading with reversed speech on frequency of stuttering in adults. Percept Mot Skills 2005;100:387–93 | Examines reading with reversed speech |
| Saltuklaroglu T, Dayalu VN, Kalinowski J, Stuart A, Rastatter MP. Say it with me: stuttering inhibited. J Clin Experiment Neuropsychol 2004;26:161–8 | Examines visual speech/choral speech |
| Saltuklaroglu T, Kalinowski J, Robbins M, Crawcour S, Bowers A. Comparisons of stuttering frequency during and after speech initiation in unaltered feedback, altered auditory feedback and choral speech conditions. Int J Lang Commun Disord 2009;44:1000–17 | Examines nature of stuttering |
| Saltuklaroglu T, Kalinowski J, Robbins M, Crawcour S, Bowers A. Comparisons of stuttering frequency during and after speech initiation in unaltered feedback, altered auditory feedback and choral speech conditions. Int J Lang Commun Disord 2009;44:1000–17 | Compares different types of DAF |
| Sassi FC, de Andrade CR. Acoustic analyses of speech naturalness: a comparison between two therapeutic approaches. Profono 2004;16:31–8 | Non OECD country (Brazil) |
| Simon AM. Intensive Therapy Course for Adults who Stutter. World Congress on Fluency Disorders; Research, Treatment and Self-Help in Fluency Disorders–New Horizon. Philadelphia, PA: International Fluency Association; 1997 | Survey (conference abstract) |
| Snyder GJ, Blanchet P, Waddell D, Ivy LJ. Effects of digital vibrotactile speech feedback on overt stuttering frequency. Percept Mot Skills 2009;108:271–80 | Examines laboratory use of visual speech feedback |
| Snyder GJ, Hough MS, Blanchet P, Ivy LJ, Waddell D. The effects of self-generated synchronous and asynchronous visual speech feedback on overt stuttering frequency. J Commun Disord 2009;42:235–44 | Examines use of self-generated visual feedback on overt stuttering during reading aloud |
| Sparks G, Grant DE, Millay K, Walker-Batson D, Hynan LS. The effect of fast speech rate on stuttering frequency during delayed auditory feedback. J Fluency Disord 2002;27:187–200 | Examines effect of different rates of speech using DAF |
| St Louis KO, Myers FL, Cassidy LJ, Michael AJ, Penrod SM, Litton BA, et al. Efficacy of delayed auditory feedback for treating cluttering: two case studies. J Fluency Disord 1996;29:305–14 | Two case studies |
| St Louis KO, Myers FL, Faragasso K, Townsend PS, Gallaher AJ. Perceptual aspects of cluttered speech. J Fluency Disord 2004;29:213–35 | Explores listener judgement of fluency in cluttering |
| Stewart T, Brosh H. The use of drawings in the management of adults who stammer. J Fluency Disord 1997;22:35–50 | Case study of two participants |
| Story RS, Alfonso PJ, Harris KS. Pre- and posttreatment comparison of the kinematics of the fluent speech of persons who stutter. J Speech Hear Res 1996;39:991–1005 | Case series, three participants |
| Stuart A, Kalinowski J. The perception of speech naturalness of post-therapeutic and altered auditory feedback speech of adults with mild and severe stuttering. Folia Phoniatr Logoped 2004;56:347–57 | Describes nature of speech naturalness no intervention |
| Stuart A, Frazier CL, Kalinowski J, Vos PW. The effect of frequency altered feedback on stuttering duration and type. J Speech Lang Hear Res 2008;51:889–97 | Duplicate paper |
| Stuart A, Kalinowski J, Rastatter MP. Effect of monaural and binaural altered auditory feedback on stuttering frequency. J Acoustic Soc Am 1997;101:3806–9 | Examination of DAF frequency alterations during reading |
| Stuart A, Kalinowski J, Rastatter MP. Effect of monaural and binaural altered auditory feedback on stuttering frequency. J Acoustic Soc Am 1997;101:3806–9 | Examines use of a passive resonator during reading a passage |
| Stuart A, Frazier CL, Kalinowski J, Vos PW. The effect of frequency altered feedback on stuttering duration and type. J Speech Lang Hear Res 2008;51:889–97 | Examines links between FAF and stuttering type |
| Stuart A, Kalinowski J, Armson J, Stenstrom R, Jones K. Fluency effect of frequency alterations of plus/minus one-half and one-quarter octave shifts in auditory feedback of people who stutter. J Speech Hear Res 1996;39:396–401 | Examines types of DAF |
| Swift MC, O’Brian S, Hewat S, Onslow M, Packman A, Menzies R. Investigating parent delivery of the Lidcombe Program. Int J Speech Lang Pathol 2011;13:308–16 | Case series, three participants |
| Teshima S, Langevin M, Hagler P, Kully D. Post-treatment speech naturalness of comprehensive stuttering program clients and differences in ratings among listener groups. J Fluency Disord 2010;35:44–58 | Participants are non-stutterers, no intervention |
| Trajkovski N, Andrews C, Onslow M, Packman A, O’Brian S, Menzies R. Using syllable-timed speech to treat preschool children who stutter: a multiple baseline experiment. J Fluency Disord 2009;34:1–10 | Case series, three participants |
| Waddell DE, Goggans PM, Snyder GJ. Novel tactile feedback to reduce overt stuttering. Neuroreport 2012;23:727–30 | Laboratory examination of tactile feedback during reading of a passage |
| Webber MJ, Packman A, Onslow M. Effects of self-modelling on stuttering. Int J Lang Commun Disord 2004;39:509–22 | Case series, three participants |
| Sandrieser P. Mini-KIDS – a concept for direct treatment of early childhood stuttering. Forum Logopadie 2003;17:6–13 | Description only, no data |
| Natke U. Reduction of stuttering frequency using frequency-shifted and delayed auditory feedback. Folia Phoniatr Logopaed 2000;52:151–9 | Evaluation of reading aloud under laboratory conditions |
Appendix 5 Extraction tables clinical effectiveness studies
| Details of study | Methods | Outcome measures | Main results | Limitations/comments |
|---|---|---|---|---|
| Allen 2011117 Country: UK Study design: cross-sectional Data collection method: record of e-mail content Aim: to evaluate e-mail as a component of a therapy programme Detail of participants (number, any reported demographics): 16 clients aged 19–52 years, 14 male and two female Severity of their overt and covert stuttering ranged from mild to severe |
Therapeutic intervention was based on individual presentation, blending speech modification techniques and counselling support in both face-to-face appointments and e-mail exchanges. E-mail served two functions: administrative and therapeutic. Number of hours: e-mail time Delivered by who? Clinician Control: none Length of follow-up: none Response and/or attrition rate: two clients did not complete the intervention |
Number of e-mails sent Content of e-mails Outcome of therapy |
A total of 472 e-mail messages were exchanged with the group, of which 328 (69%) were primarily administrative, in arranging face-to-face appointments. The other 144 e-mail messages (31%) were primarily therapeutic, in monitoring ongoing treatment goals or offering problem-solving guidance. Often e-mail messages contained both administrative and therapeutic elements. Of the 16 clients who used e-mail as part of therapy, 11 were discharged (two owing to non-response). Five clients remained on the caseload. The paper describes a range of benefits but these have no data underpinning them | |
| Amster and Klein 200730 Country: UK Study design: before and after Data collection method: questionnaire/assessment evaluations Aim: to determine if a modified CBT approach alone and combined with stuttering modification could help reduce perfectionist tendencies and stuttering behaviours. Detail of participants (number, any reported demographics): eight participants, five male and three female, aged 27–56 years (mean 44 years, SD 9.9 years) |
Modified CBT with and without stuttering modification therapy. Hours: treatment consisted of six individual 1-hour sessions and six 90-minute group sessions with the authors serving as clinicians. At week four, stuttering modification was introduced and reviewed in both individual and group sessions Delivered by: authors (clinicians) Control: none Length of follow-up: 15 weeks compared at pre-treatment, mid-treatment (3 weeks), after 6 weeks of treatment and at 15-week follow-up, after treatment was withdrawn Response and/or attrition rate: all participants attended all 12 sessions during the 6-week time frame |
Burns Perfectionism Scale, SSI, Modified Erikson Communication Attitude Scale | From pre-treatment to post-treatment stuttering severity and perfectionism significantly decreased. Participants related that they did not care as much about making mistakes when they spoke. They reported that their fears about stuttering reduced and that they were no longer striving to speak perfectly. At pre-treatment, all participants met criteria for stuttering on the SSI-3 ranging from very mild to very severe. Pairwise comparisons as measured by the Wilcoxon signed-rank test reflected statistically significant improvements in participants’ speech fluency from pre-treatment to mid-treatment (when CBT was the sole treatment). Participants significantly decreased stuttering (z-value = −2.3; p = 0.021). SSI-3 scores for people who stutter at pre-treatment were mean 24.38, SD 9.01; and at mid-point, SSI-3 scores were mean 16.88, SD 11.11. At post treatment, SSI-3 scores were mean 11.75, SD 8.79; and at follow-up, SSI-3 scores were mean 13.75 and SD 8.63. ESs using Cohen’s d were 0.74 (pre-treatment to mid-treatment) and 0.51 (mid-treatment to post treatment). At pre-treatment, all participants performed within the perfectionist range on both current (mean 9.75; SD 5.1) and child recollection (mean 9.75; SD 8.5) formats. Participants decreased an average of 13 points on the Burns Perfectionism Scale (a 40-point scale). The Wilcoxon signed-rank test indicated that perfectionism scores for people who stutter at pre-treatment (mean 9.75, SD 5.06) significantly decreased by mid-treatment (mean = −2.38, SD 8.09), z-value = −2.1; p = 0.035. The ES using Cohen’s d was 1.80. From mid-point to end of treatment when stuttering modification was introduced, perfectionism continued to decline, but not significantly (z-value = −1.7; p > 0.05). Perfectionism continued to decline after treatment was withdrawn (z-value = −2.2; p = 0.027). Post treatment, participants had significantly more positive attitudes about communication (pre-treatment mean 19.00, SD 3.46, mid-treatment mean 17.00, SD 5.15 and post-treatment mean 12.38, SD 4.95). Attitudes did not significantly change by the mid-point of the treatment, but by the end of the 6-week programme, participants showed a significant improvement in their attitude towards speaking as they found it easier to talk with others, were more confident about their speaking ability and less nervous or embarrassed to talk (pre-treatment to post-treatment z-value = −2.38; p = 0.017). This was maintained at follow-up (mean 12.13, SD 6.33) | |
| Andrews et al. 201231 Country: Australia Study design: before and after Data collection method: parent rating Aim: to determine the outcomes of a simple STS treatment for school-age children who stutter Detail of participants (number, any reported demographics): 10 participants, eight male and two female, aged 6–12 years (mean 8.8 years) Seven participants had received previous LP treatment of varying duration and with variable success |
STS treatment involved training the children and their parents to use STS at near-normal speech rates. The technique was practised in the clinic and at home with the parents during everyday conversations. The only additional procedures being prompts to use the speech pattern and reinforcement for using it. The treatment was delivered by a parent and was supervised by a SLP. Treatment was provided in two stages. The aim of stage 1 was to instate a low level of stuttering with STS; the aim of stage 2 was to maintain this low level of stuttering for the long term Hours: unclear Delivered by: unclear Control: none Length of follow-up: 9 months. Assessment 1 occurred within 2 weeks before the start of treatment; assessment 2 occurred 9 months after the start of treatment Response and/or attrition rate: one child withdrew from treatment before assessment 2 |
Percentage of syllables that are stuttered Parent severity rating using the 10-point LP scale Participant self-reports of stuttering severity, avoidance, speech satisfaction and quality of life |
9 months after commencing treatment, stuttering had decreased by > 50% for half of the children, with two children attaining 81% and 87% reduction. Intention-to-treat analysis showed a clinically and statistically significant reduction in stuttering for the group even when a withdrawn participant was included. These results were mostly confirmed by self-reported stuttering severity ratings and were supported by improved situation avoidance and quality-of-life scores. There was considerable individual variation in response to the treatment. The group mean percentage of syllables that are stuttered at assessment 1 was 14.4% (SD 16.5%) and at assessment 2 was 6.7% (SD 6.8%). This difference was significant, t(9) = 2.99; p = 0.015. Medium Cohen d ES was 0.7. Half of the children reduced their stuttering by > 50%, with two children attaining 81% and 87% reduction. Three children attained reductions in the 30–50% range. Two children showed no reduction. The group mean for self-reported stuttering severity at assessment 1 was 5.4 (SD 1.4) and at assessment 2 was 2.8 (SD 1.1). This difference was significant, t(9) = 4.85; p = 0.00089. 8 out of the 10 children reported reduced avoidance of speaking situations at assessment 2, with a reduction in self-rating of avoidance of speaking situations from 14.7 at baseline to 11.7 at 9 months. This difference was significant, t(9) = 2.87; p = 0.018. All children except participant 9 were reportedly more satisfied with their speech at assessment 2. The group mean of self-rating of avoidance of speaking situations decreased from 6.0 to 2.7. This difference was significant, t(9) = 5.14; p < 0.001. Quality-of-life scores improved for all but one of the children (participant 3). The mean dropped from 54 at assessment 1 to 40 at assessment 2. This difference was significant, t(9) = 3.37; p < 0.005 | |
| Antipova et al. 2008118 Country: New Zealand Study design: cross-sectional Data collection method: speech samples from DVD recording Aim: to investigate the immediate effects of eight AAF parameters on stuttering frequency during monologue speech production on two occasions Detail of participants (number, any reported demographics): eight participants aged 16–55 years (mean 35 years, SD 12.95 years) |
The Pocket Speech Lab (Casa FuturaTechnologies®, Boulder, CO, USA) was used to produce auditory feedback alterations Six types of combined DAF and FAF and two types of DAF alone were tested Hours: 3 × 90-minute sessions – an introductory session and two testing sessions Delivered by: not reported Control: no AAF compared with eight AAF conditions Length of follow-up: immediate Response and/or attrition rate: none |
Stuttering frequency. Lidcombe Behavioural Data Language to identify stuttering moments |
The present study found that AAF is an effective means to reduce stuttering frequency during monologue speech production. All eight AAF experimental conditions reduced stuttering frequency; however, there was substantial variability in the stuttering reduction effect across experimental conditions and across participants. The type of speech task had no significant effect on stuttering frequency (t = 1.77, degrees of freedom = 7; p = 0.119). The reduction of stuttering frequency varied across individuals from 23% to 97% during the first testing session and from 3% to 88% during the second one. There was also instability in stuttering reduction across the two testing sessions. On average, a 75 milliseconds time delay on its own and a combination of the 75 milliseconds time delay and a half octave downwards frequency shift were found to be more effective than other combinations of AAF parameters that were investigated | |
| Armson and Stuart 1998119 Country: Canada Study design: cross-sectional Data collection method: recorded speech Aim: to examine the effect of FAF Detail of participants (number, any reported demographics): 12 participants, 10 male and two female, age range 20–50 years, mean 35 years. Four currently receiving treatment others had received in past between 1 month and 15 years previously. Rated by the authors as five mild, six moderate and one severe. Six no previous experience of AAF, two had used Edinburgh masker, one DAF and five briefly used in previous study |
Recruited via a local clinic and self-help group Each individual recorded for 5 minutes without FAF then 10 minutes with FAF then 5 minutes without FAF Number of hours: N/A Delivered by who? FAF device Control: none Length of follow-up: none Response and/or attrition rate: N/A |
Stuttering episodes Syllables produced % stuttering Speech rate |
FAF effective for some participants during reading only. Significant difference when using FAF for total number of syllables produced increased, number of stuttering episodes decreased and per cent stuttering decreased for reading. Number stuttering events p < 0.001, ES 0.62, number syllables p = 0.0071, ES 0.39, per cent stuttering p = 0.0056, ES 0.41. 10 of the 12 participants showed no positive effect on stuttering frequency of FAF during monologue. Significant difference only for number of stuttering events during monologue; p = 0.1, ES 0.14. Not significant number syllables p = 0.41, ES 0.00; or per cent stuttering p = 0.46, ES 0.00. Considerable variation between participants. Three showed large reduction in stuttering during FAF returning to baseline following FAF. Six showed initial large reduction in stuttering, which faded during the intervention and the final three experienced little effect of the intervention | |
| Armson et al. 20064 Country: Canada Study design: cross-sectional Data collection method: one of two graduate students in speech-language pathology counted stuttering episodes for each sample Aim: to evaluate the effect of SpeechEasy Detail of participants (number, any reported demographics): 13 adults |
SpeechEasy Stuttering frequencies in two baseline conditions were compared with stuttering frequencies with the device fitted according to the manufacturer’s protocol. For each of the four conditions – the two baseline and two experimental conditions – participants produced speech in three contexts: oral reading, monologue and conversation Each participant was fitted with a programmable SpeechEasy Basic behind-the-ear unit. The behind-the-ear model is an external device that is worn behind the pinna and connects to a mould that fits in the ear canal SpeechEasy software permits manipulation of settings for three variables: FAF, DAF and volume Control: none Length of follow-up: N/A Response and/or attrition rate: none |
Stuttering episodes Percentage of syllables that are stuttered |
Relative to the initial baseline condition stuttering was reduced by 74%, 36% and 49% for reading, monologue and conversation, respectively, in the second baseline. In comparison, stuttering was reduced by 42%, 30% and 36%, respectively, with the device in place, but before participants were instructed to deliberately prolong vowels. Raw stuttering frequencies and differences across participants, task and condition were evaluated. There were highly significant differences for participant (F12,124 = 32.4; p < 0.001), speech task (F2,124 = 6.6; p < 0.002) and condition (F3,124 = 25.54; p < 0.001). Although mean stuttering levels increased in the post-device condition relative to levels in the device conditions, they failed to reach pre-device levels, suggesting some degree of treatment carryover effect | |
| Armson and Kiefte 2008120 Country: Canada Study design: cross-sectional Data collection method: data were collected during the course of an otherwise routine initial dispensing session with a client to demonstrate the product Aim: to measure the effects of SpeechEasy Detail of participants (number, any reported demographics): 31 adults, 20 male and 11 female, aged 18–51 years, (mean 27.7 years) With one exception, all participants had received or were currently receiving some form of behavioural therapy. An additional 30 adult volunteers were recruited to evaluate speech naturalness of samples collected from the participants who stutter |
SpeechEasy device Speech measures were compared for samples obtained with and without the device in place in a dispensing setting. Settings for three variables can be programmed in the device: volume, DAF and FAF For each of the two conditions, participants produced speech in two contexts: reading and monologue. For the reading task, participants read aloud two 300-syllable passages taken from Grade 8 and 9 social studies and science texts – a different passage for each condition. For the monologue task, participants were asked to talk continuously for 3 minutes about a topic of their choice. If they hesitated or paused noticeably, they were prompted by the SLP Control: none Length of follow-up: immediate Response and/or attrition rate: none |
Participant self-rating of stuttering severity Stuttering frequency Speech rate Speech naturalness |
Mean stuttering frequencies were reduced by 79% and 61% for the device compared with the control conditions on reading and monologue tasks, respectively. Means for stuttering frequency in the no device condition were 16.4 and 15.8 stuttering events per 100 syllables for the reading and monologue tasks, respectively (medians: 11.3 and 10.0 stuttering events, respectively) while, for the device condition, means were 2.3 and 5.9 stuttering events per 100 syllables for reading and monologue tasks, respectively (medians: 1.3 and 4.0 stuttering events, respectively). Average reduction in stuttering frequency for all participants during the reading task was 78.8% (SD 28.8%), while average reduction in stuttering across conditions for all participants during the monologue task was 60.7% (SD 35.5%). Mean severity self-ratings decreased by 3.5 points for oral reading and 2.7 points for monologue on a 9-point scale. Despite dramatic reductions in stuttering frequency, mean global speech rates in the device condition increased by only 8% in the reading task and 15% for the monologue task, and were well below normal. Furthermore, complete elimination of stuttering was not associated with normalised speech rates. Nevertheless, mean ratings of speech naturalness improved markedly in the device compared with the control condition and at 3.3 and 3.2 for reading and monologue, respectively, were only slightly outside the normal range | |
| Baumeister et al. 200332 Country: Germany Study design: before and after Data collection method: four assessment points – baseline (T1); pre-treatment (T2); post treatment (T3); follow-up (T4) Aim: to evaluate the therapy concept of an intensive stutter camp and to estimate if this concept is transferable to current practical work Detail of participants (number, any reported demographics): 37 participants, 33 male, 4 female; with different severity of stuttering (mean 21.1%); age: 9–19 years |
Stuttering summer camp. 70 direct therapy sessions. Indirect therapy sessions (social networking, short therapeutic interventions), (not quantified) Number of hours: 3 weeks (for children under 12 years, just 2 weeks) Delivered by who? Clinician Control: none Length of follow-up: 2 months Response and/or attrition rate: 12 participants did not complete the baseline because of local difficulties; 20 participants did not complete the follow-up because of local difficulties, most of the participants who completed the follow-up were participants who showed a severe stuttering at baseline or pre-treatment assessment |
Frequency of stuttering Speech rate Naturalness of speaking Non-verbal naturalness Attitude towards communication Avoidance of stuttering Influence of social situations and influence of mood |
Significant reduction of stutter frequency between T2 and T3 (d = 1.87) and T3 and T4 (d = 1.43). Speech rate (measured by words per minutes in performances of tasks for stutter frequency): general improvement of speech rate between T2 and T3 (d = –0.65 to 0.79) and T3 and T4 (d = –1.41 to 1.75); some of the ESs were significant; however, results are influenced by missing participants to different assessment points. Some participants showed significant slower performances in reading tasks. Naturalness of speaking and non-verbal naturalness: significant improvement in naturalness of speaking (T2 and T3: d = 1.20 to 1.31; T3 and T4: d = 1.41) and significant improvement in non-verbal naturalness (T2 and T3: d = 0.94 to 1.13; T3 and T4: d = 1.11). Attitude towards communication: significant positive improvement about attitudes from each assessment point to the next one. Avoidance of stuttering: significant positive self-evaluation improvement (T2 and T3: d = 0.82 to 1.03; T3 and T4: d = –0.36) between T3 and T4 no significant improvement. Influence of social situations and influence of mood: significant improvement of influence of social situations (T2 and T3: d = 0.71 to 0.74; T3 and T4: d = –0.25) but no improvement of influence of mood (T2 and T3: d = 0.26 to 0.30; T3 and T4: d = –0.40) | Results were analysed in different steps as not all participants could be included for every analyses (in general), one group T2 and T3 analyses, another group just T3 and T4 analyses |
| Beilby et al. 201233 Country: Australia Study design: before and after Data collection method: unclear Aim: to assess the effectiveness of an ACT group intervention programme for adults who stutter Detail of participants (number, any reported demographics): 20 participants, 10 male and 10 female (mean age = 28.75 years; SD 11.07 years; range = 19–65 years) |
Integrated ACT programme The programme consisted of 2-hour therapeutic sessions conducted weekly for eight consecutive weeks. It was an integrated programme designed to improve (1) psychosocial functioning, (2) readiness for therapy and change, (3) utilisation of mindfulness skills and psychological flexibility and (4) frequency of stuttering Hours: 2 hours for 8 weeks Delivered by? Unclear Control: none Length of follow-up: 3 months post treatment Response and/or attrition rate: none |
Stuttered speech frequency Overall assessment of speaker’s experience of stuttering Modified stages of change questionnaire Mindful scales |
Results from this study showed statistically significant gains across all measures of interest from pre-treatment to post treatment and continuing on to 3-month follow-up. Prior to the commencement of the ACT intervention programme, half (50%) of adults with a stutter/stutter demonstrated a stutter frequency rating of < 5% of syllables that are stuttered with the remaining 50% demonstrating stuttered frequency rating of > 5% of syllables that are stuttered. The repeated measures ANOVA indicated that frequency of the stuttered speech was reduced and maintained significantly over time. At the post-treatment time point, three participants (15%) were assessed with stuttered frequency ratings ranging from 3% to 3.5%, with the remaining participants 85% demonstrating stuttered frequency ratings of < 2% of syllables that are stuttered. At the follow-up treatment time point, two participants (10%) were assessed with a stutter frequency rating ranging from 4% to 4.5%, with the remaining participants (90%) demonstrating stuttered frequency ratings of < 2% of syllables that are stuttered | |
| Berkowitz et al. 199434 Country: USA Study design: before and after Data collection method: assessment scales, views of parents Aim: to evaluate a fluency programme delivered in a school setting Detail of participants (number, any reported demographics): eight participants, six male and two female, age range 5 years 11 months to 13 years 8 months |
Cooper Personalized Fluency Control Therapy Program used with children – emphasis on attitudes and control. Phase 1 assessment of attitudes and behaviour, phase 2 identification of behaviours and attitude, phase 3 changing behaviours (modifying and controlling speech and concomitant behaviours, e.g. gentle air stream adjusting volume, changing intonation), and phase 4 transfer and maintenance. Parent programme included focus on attitudes, issues and beliefs and change in behaviour. Considerable amount of time on attitudinal issues before changing behaviours Number of hours: 1.5 hours once per week after school children’s group, 2 hours once a week evening for parents over 1 month Delivered by who? Authors Control: none Length of follow-up: immediate Response and/or attrition rate: not reported |
SSI Cooper Personalized Fluency Control Therapy Revised Parent perceptions |
Results given as scores on the different measures pre and post intervention only rather than any descriptive or inferential statistics. Positive change in attitude towards stuttering. Reduction in verbal and non-verbal behaviours associated with stuttering for all students on SSI. Parents reported a greater level of knowledge and awareness, and acceptance and attitudes towards stuttering | |
| Block et al. 200436 Country: Australia Study design: before and after Data collection method: observer speech rating Aim: to replicate previous studies on EMG biofeedback using larger sample Detail of participants (number, any reported demographics): 12 participants aged 10–16 years (mean age 13 years). None had received biofeedback treatment, six had received PS treatment |
EMG intervention. Each day, participants were randomly assigned to one of two groups of six participants. One group received the EMG procedures and the other group engaged in speaking activities, in and out of the clinic setting. The groups alternated between EMG biofeedback and the generalisation activities throughout the day, and each group received an equal amount of time with each. Participants kept a speech diary and parents joined activities for last hour of the day. Sweets were given as rewards for EMG session Number of hours: 6 hours per day over five consecutive days. The EMG treatment comprised 10, 45-minute, sessions. Homework assignments each evening. Delivered by who? Two clinicians and two students Control: none Length of follow-up: three time points: immediate post treatment, after 1 week and 3 months later Response and/or attrition rate: none |
Percentage of syllables that are stuttered SPM |
Mean percentage of syllables that are stuttered in conversation at home, 1 week pre-treatment and 1 day pre-treatment were 7.1% and 7.6% respectively. Mean percentage of syllables that are stuttered in conversation at home 1 week post treatment and 3 months post treatment were 4.9% and 4.4% respectively. Pooling pre-treatment and post-treatment measures, these data constitute a reduction of 36.7% in stuttering severity. Reduction in stuttering during reading was 48.9%. Participants who had not received prior PS treatment made greater gains following EMG intervention (67.1% vs. 30.1% reduction). Mean SPM in conversation at home 1 week pre-treatment and 1 day pre-treatment were 115 SPM and 102.5 SPM respectively. Mean SPM in conversation at home 1 week post treatment and 3 months post treatment were 113.5 SPM and 109.5 SPM respectively. Pooling pre-treatment and post-treatment measures, these data constitute an increase of 2.5% in SPM after the EMG treatment | |
| Block et al. 200537 Country: Australia Study design: before and after Data collection method: assessment measures/observation Aim: to evaluate a student-delivered intervention Detail of participants (number, any reported demographics): 80 adults who had completed the programme between 1998 and 2000. 68 males and 14 females, age range 16–70 years, mean age 28 years |
Block and Dacakis programme: a PS intervention. Programme is conducted in two stages. 12–15 participants, aged at least 16 years in each programme Number of hours: stage 1, participants attend the clinic for 9 hours each day for 5 days. Stage 2, weekly individual and group follow-up sessions conducted for 2 hours a week for 7 weeks. Total = approximately 60 hours Clients have unlimited access to a number of voluntary 7-hour ‘booster’ days, which occur at 6-monthly intervals Delivered by who? Student clinicians supervised by clinical educator Control: none Length of follow-up: immediate (after stage 1), 3 months (after stage 2), 6 months and 3.5 to 5 years Response and/or attrition rate: two were lost at follow-up. 50% of home data was not available at 3 months and 50% of clinic and home data not available at 12 months. 87% of data available at long-term follow-up. Return rate for speech naturalness questionnaire at 3- to 5-year follow-up was 44% |
Percentage of syllables that are stuttered Self-report inventory Attitude to Communication (S24) LCB scale Speech naturalness |
Stuttering was significantly lower immediately after treatment, both within and beyond the clinic, and also at 3 months post treatment. Follow-up stuttering in the clinic. During conversation stuttering was significantly higher within the clinic than beyond the clinic. Percentage of syllables that are stuttered data pre-treatment was 5.4% and immediately post treatment was 1.8%. The ES was large at 0.86. The mean 3.5- to 5-year follow-up stuttering rate was 1.6% of syllables that are stuttered. Speech naturalness mean pre-treatment 3.8 (SD 51.3, range 51.6–7.1). Mean immediately post treatment 4.5 (SD 51.3, range 51.9–8.7). Medium ES of 0.52 [sic]. Self-report inventory data single time point reported by comparison with another study. Self rating of how stuttering was before programme mean 6.5 (1 = no, 9 = extremely severe). Stuttering now 3.2 | Reports same study as Block et al. 2006,38 this one reports intervention detail in more depth and one additional measure |
| Block et al. 200638 Country: Australia Study design: before and after Data collection method: assessment measures/observed rating Aim: to investigate whether or not stuttering rate, attitude to communication and LOC are predictive of long-term outcomes Detail of participants (number, any reported demographics): 80 adults who had completed the programme between 1998 and 2000. 68 males and 14 females, age range 16–70 years, mean age 28 years |
Block and Dacakis programme: a PS intervention. Programme is conducted in two stages. 12–15 participants, aged at least 16 years in each programme To gather the follow-up data an investigator unexpectedly telephoned the participants and conducted a 10-minute conversation with them Number of hours: stage 1, participants attend the clinic for 9 hours each day for 5 days. Stage 2, weekly individual and group follow-up sessions conducted for 2 hours a week for 7 weeks. Total approximately 60 hours Clients have unlimited access to a number of voluntary 7-hour ‘booster’ days, which occur at 6-monthly intervals Delivered by who? Student clinicians under the supervision of clinical educators Control: none Length of follow-up: immediate, 3 months, 6 months and 3.5 to 5 years Response and/or attrition rate: two were lost at follow-up |
Percentage of syllables that are stuttered Attitude to Communication (S24) LCB scale Speech naturalness rating |
Pre-treatment mean percentage of syllables that are stuttered was 4.9% (SD 4.4%). Levels of stuttering reduced to a mean of 0.9% (SD 1.4%) of syllables that are stuttered immediately post treatment, and 1.5% (SD 2.2%) at 3-month follow-up. At 12 months the mean percentage of syllables that are stuttered was 2.6%, and at 3.5–5 years, during a surprise telephone call, the mean percentage of syllables that are stuttered was 1.6%. The pre-treatment rate of stuttering predicted immediate post-treatment rate. Regression modelling using two predictors (pre-intervention percentage of syllables that are stuttered and 3-month follow-up percentage of syllables that are stuttered) predicted 54% of the variance in 3.5- to 5-year data, with the latter predicting nearly 50% of the variance. The percentage of syllables that are stuttered at long-term follow-up was only predicted by immediate post-intervention percentage of syllables that are stuttered and 3-month follow-up percentage of syllables that are stuttered. Pre-treatment stuttering rate, attitude to communication, LOC, post-intervention speech naturalness and number of booster sessions attended were not predictors of long-term outcome. Authors highlight that 46% of variance at long-term follow-up remains unaccounted for | |
| Block et al. 199635 Country: Australia Study design: before and after Data collection method: reading, monologue, telephone, conversation tasks audiotaped. The masker was activated for half of the time that it was worn and switched off for the other half of the time Aim: to evaluate the Edinburgh masker Detail of participants (number, any reported demographics): 18 participants, four female and 14 male, aged 18–58 years. Fourteen had received previous treatment with a variety of therapies. 16 sound/syllable repetitions and two severe blocking |
Edinburgh Masker Number of hours: 200 minutes of operation Delivered by who? Device Control: none Length of follow-up: immediate Response and/or attrition rate: none |
Percentage of syllables that are stuttered Mean speech rate Speech naturalness rated by students |
More stuttering in non-masked condition (mean 5.1% of syllables that are stuttered across all conditions) than in masked condition (2.6%). Stuttering rate reduced by mean 50% in masking condition during conversation with familiar person. Increase in speaking rate when using masker for reading, but reduction in rate for all other conditions. Mean speaking rate across all condition during masking 184.4, non-masking 192.9. Listener judged masked speech to be less natural sounding | |
| Blomgren et al. 200539 Country: USA Study design: before and after Data collection method: recorded speech samples Aim: to evaluate an intensive stuttering programme Detail of participants (number, any reported demographics): 19 participants, 15 male and four female, mean age 26.3 years (range 16–52 years, SD 10.1 years) Seven of the participants had a prior history of fluency-shaping therapy, averaging 9.6 years prior to participation in the SSMP (range 1–22 years, SD 7.3 years) |
A 3-week intensive stuttering modification treatment programme (the SSMP). The programme consisted of three phases of treatment: (1) confrontation of stuttering, (2) modification of stuttering and (3) maintenance. Therapy was conducted within the Speech and Hearing Clinic at The University of Utah (Salt Lake City, UT, USA), and transfer practice took place in nearby public settings such as shopping malls Hours: the duration of each of the two SSMP offerings was 3.5 weeks. Group and individual therapy was offered for 3.5 hours (1 p.m. to 4:30 p.m.) during the weekdays. Clients were assigned numerous speaking tasks to complete during the mornings (usually in the form of conducting surveys). Group activities were also arranged on Saturdays Delivered by? Clinicians/students Control: none Length of follow-up: 6 months speaking samples were collected immediately pre and post treatment, and 6 months post treatment at the beginning of the 2-day refresher programme Response and/or attrition rate: none |
SSI PSI LCB scale Beck Depression Inventory MCAI-IV State–Trait Anxiety Inventory |
Statistically significant improvements were observed on 4 out of the total 14 measures immediately following treatment and on four measures at 6 months post treatment. Statistically significant improvements observed immediately post treatment included scores on the SSI and the Struggle, Avoidance, and Expectancy subscales of the PSI. Sustained statistically significant improvements at 6 months post treatment were observed only on client-reported perceptions of stuttering (the Avoidance and Expectancy subscales of the PSI; p < 0.001) and two specific affective functioning measures (the Psychic and Somatic Anxiety subscales of the MCAI-IV; p = 0.078 and p = 0.036, respectively) | Stuttering treatment efficacy measures should include client-reported treatment satisfaction data and self-measurement ratings, and data pertaining to the values and priorities of those within the stuttering population. The treatment programme was not described clearly (would not be easily replicable), the participants did not improve their speech fluency and the treatment time was extensive (estimated 6.5 hours per day × 6 days per week × 7 weeks plus a 2-day refresher of 12 hours = 284 hours × two clinicians per client = 568 hours of clinician time per client) See Blomgren et al.39 Response and discussion of terminology |
| Blood 199540 Country: USA Study design: before and after Data collection method: unclear Aim: to evaluate the efficacy of a behavioural–cognitive treatment program Detail of participants (number, any reported demographics): four participants, aged 20–25 years, all had received many years of prior therapy |
Behavioural–cognitive programme. First phase change in motor speech behaviour using the Computer Aided Fluency Establishment Trainer program. This targets diaphragmatic breathing, continuous airflow, pre-voice exhalation, easy onset, initial prolongation, continuous phonation, phrasing and monitored speech. Immediate feedback provided on computer screen. Second and third phases use POWER relapse management programme based on Bandura’s self-efficacy model working on feelings and attitudes Number of hours: 93–124 hours. Phase 1, 46–55 hours using computer program over maximum of 3 weeks, two or three times per week. Phases 2 and 3, 50-minute sessions three times per week for 6–8 months. Asked to maintain contact and return for assessment at 6 and 12 months Delivered by who? Not reported Control: none Length of follow-up: 6 and 12 months Response and/or attrition rate: none |
Percentage of syllables that are stuttered SPM SSI Personal Report of Communication Apprehension scale Assertiveness Scale Self-Efficacy Scale for Adult Stutterers S24 Scale |
At end of phase 1, all had reduced stuttering to criterion level of < 3% of syllables that are stuttered. Two increased percentage of syllables that are stuttered to > 3% during second and third phases but did not relapse to pre-treatment levels. Subject one 221% of syllables that are stuttered baseline to 3% at 6 and 12 month follow-up. Subject two 13% of syllables that are stuttered baseline to 3% at 6 and 12-month follow-up. Subject three 18% of syllables that are stuttered baseline to 1–2% at 6- and 12-month follow-up. Subject four 20% of syllables that are stuttered to 1–2% at 6- and 12-month follow-up. Feeling and thinking scales all showed positive changes that were maintained at 6 and 12 months. Individual scale scores reported for each individual participant only | |
| Boberg and Kully 199441 Country: USA Study design: before and after Data collection method: audio-recorded speech samples during telephone calls Aim: to evaluate the CSP Detail of participants (number, any reported demographics): 42 participants, two groups: adolescents and adults. Adults 14 males and three females, mean age 24.59 years, range 18–36 years. Adolescents 20 males and five females, mean age 14.28 years, range 11–17 years |
3-week intensive CSP. Behavioural strategies to teach prolongation, easy onset, soft contacts, appropriate phrasing, continuous airflow/blending. Gradual increase in syllable rate using techniques during establishment phase. Includes teaching of self-monitoring and transfer phase using speech outside clinic in situations of increasing difficulty. Includes identification of fears and reduction of avoidance, discussion with family/friends and social skills. Home maintenance programme for after the course. Self-help group, weekend and 5-day refresher clinics available Number of hours: 7 hours × 15 days. First 2 weeks residential final week choose residential or not Delivered by who? Clinician Control: none Length of follow-up: some had completed the intervention 24 months earlier some 12 months earlier. Response and/or attrition rate: seven not available at follow-up, data available for 42. Questionnaires available for 30 |
Percentage of syllables that are stuttered Speech Performance Questionnaire |
Pre- to immediate post-treatment mean percentage of syllables that are stuttered decreased from 19.59% to 1.29% for the adult group and 14.32% to 1.75% for the adolescent group. During the follow-up period, mean percentage of syllables that are stuttered for adults increased from 1.29% to 4.27% at 4 months and 6.03% at 12 months. For those seven who had received intervention 2 years before, mean percentage of syllables that are stuttered was 2.03% at 24 months. During the follow-up period, mean percentage of syllables that are stuttered for adolescent group was 1.75% at immediate post treatment to 3.65% at 4 months and 3.89% at 12 months. For the eight who had completed intervention 2 years earlier increase to 7.3% of syllables that are stuttered at 24 months. Individual variation in patterns, difficult to identify subcategories of individuals associated with different treatment outcomes. Immediate post treatment 93% indicated they were satisfied or very satisfied with their speech. At 12 out of 24 months, 80% described speech as fair or good and 80% poor or terrible. A total of 50% reported almost always able to speak normally without thinking about controlling their speech. A total of 40% reported they always or almost always felt like a normal speaker. A total of 77% reported skills learned in the clinic were effective most or all of the time. A total of 23% reported they no longer considered themselves to be stutterers | |
| Bonnelli et al. 200042 Country: Australia Study design: before and after Data collection method: tape recorded interactions Aim: to investigate any changes in parental or change language following the intervention Detail of participants (number, any reported demographics): nine participants, age range 34–60 months Taken part in the studies reported in Onslow et al. 199088 and 199429 |
LP Hours: not reported in this paper Delivered by: not reported in this paper Control: none Length of follow-up: immediate post intervention Response and/or attrition rate: none |
% syllables dysfluent Articulation rate Time between speaker turns Mean length utterance Development sentence score Number different words Requests for clarification Requests for information |
Data reported by individual participant only. All children showed a reduction in percentage of syllables that are dysfluent post intervention. No clear pattern in rate change for children with five showing reduction and four an increase. Seven mothers showed an increase in rate of articulation post intervention. No pattern of change in speaker’s turn time for children or mothers. No clear pattern for children or mothers in regard to MLU. No clear pattern for development sentence score, number of different words. No clear pattern for parental requests for clarification. Seven of the mothers showed reduction in requests for clarification. Children’s language within normal limits both before and after treatment | |
| Bray and James 200943 Country: UK Study design: two baseline measures before intervention. Third measure using device Data collection method: recording of telephone calls Aim: to evaluate the use of a telephone assistive device Detail of participants (number, any reported demographics): five participants, three males and two females, age range 40.6–70.5 years (mean 54.46 years, SD 11.57 years). All participants had previously had speech and language therapy at some time in their lives and one was receiving therapy at time of the study. One participant had some experience in using an AAF device |
VA609 Telephone Assistive Device, an AAF device (DAF) that is used with a regular landline telephone Participants asked to make three telephone calls prior to receiving device: (1) to someone who the participant felt comfortable speaking to, (2) to someone who was less comfortable to speak to and (3) a formal call, e.g. to request a brochure After receiving this recorded data, a request was made for three further recordings 1 month later. Following receipt of this second set of baseline recordings, the device was delivered and participant asked to use the device as much or as little as they wished and to record three further calls Number of hours: data not reported regarding how much participants used the device Delivered by who? Altered feedback device Control: none Length of follow-up: immediate Response and/or attrition rate: none |
Wright and Ayre Stuttering Self-Rating Profile Speaking Task Response Questionnaire Stuttering frequency Naturalness |
WASSP scores at the start of the study were: mean 97.4, SD 14.74, and at the end of the study these had dropped to: mean 80, SD 22.02. Changes in this general scale were minimal and variation in scores was considerable. Frequency of stuttering: group means and SDs – baseline 1, mean 8.62%, SD 3.73, and baseline 2, mean 8.28%, SD 3.74%. Using device during call led to reduction in the group mean to 4.82%, SD 2.54%. Individual reduction for four out of the five participants. No specific trend could be found before or after use of the Telephone Assistive Device in speech naturalness. Speaking Task Response Questionnaire: trend towards more positive ratings of self when using the Telephone Assistive Device. Change from 63.3%, SD 15.88%, to 82%, SD 9.96%. Descriptive statistics only. Large individual variation in usage of device hinted at in discussion. No data on usage reported so difficult to identify impact of device. Participants returned three recordings of their choice for analysis – bias in selection of these? | |
| Bray and Kehle 199844 Country: UK Study design: before and after Data collection method: videotaping of sessions plus observations around school Aim: to evaluate a self-modelling intervention Detail of participants (number, any reported demographics): four participants, three male and one female, aged 8, 9, 11 and 13 years Two learning disabilities, three moderate and one severe stutter |
Self-modelling: repeated viewing of oneself on edited videotape. Two 5-minute videos per participant of himself or herself exhibiting stutter-free speech Hours: seven, 15-minute, sessions over 6 weeks Delivered by: not reported, presumably the authors Control: none Length of follow-up: 4–8 weeks Response and/or attrition rate: none |
Speech rate Percentage of syllables that are stuttered Speech naturalness rating scale SSI Participant satisfaction scale |
Data reported by individual only. All participants reduced stuttering: subject one mean baseline 7.7% SS, follow-up mean 2.6% SS; subject two mean baseline 5.9% SS, follow-up mean 1.5% SS, subject three mean baseline, 9.1% SS follow-up mean 3.2% SS; subject four mean baseline 8.0% SS, follow-up mean 0.3% SS. SSI scores at baseline range from 5 to 7.5. At follow-up, scores on the Stuttering Severity Instrument ranged from 1 to 3.8. Gains ‘generalised to everyday situations’ (data not reported). Students satisfied with the intervention. Mean 4.8 on +5-point scale | |
| Carey et al. 201045 Country: Australia Study design: before and after Data collection method: speech sample analysis Aim: to investigate whether or not telehealth delivery of the Camperdown Program provides a non-inferior alternative to face-to-face treatment Detail of participants (number, any reported demographics): 40 participants. None had received speech restructuring treatment within the past 12 months |
Camperdown Program. This includes four components: (1) individual teaching sessions, (2) group practise day, (3) individual problem solving sessions and (4) maintenance. Participants in the telehealth arm received a slightly modified programme that was adapted for telehealth delivery; however, all of the concepts of the original programme were retained Hours contact: telehealth 221 minutes Delivered by: clinician/telehealth Control: the study had two intervention arms only and no control arm. 20 participants were in the telehealth arm and 20 in the face-to-face arm of the study Length of follow-up: 12 months post treatment Response and/or attrition rate: 3 out of the 40 randomised participants (7.5%) did not complete the trial |
Percentage of syllables that are stuttered Contact hours Speech naturalness Self-reported stuttering severity Treatment satisfaction |
There was no statistically or clinically significant difference in percentage of syllables that are stuttered between the two groups at 9 months post randomisation. ANCOVA adjusting for baseline percentage of syllables that are stuttered showed telehealth had 0.8% absolute lower percentage of syllables that are stuttered than face to face. (95% one-sided CI 0.7 higher percentage of syllables that are stuttered at most.) There were also no differences in percentage of syllables that are stuttered between groups immediately post treatment or at 6 months and 12 months post treatment (p = 0.9). In the second primary outcome measure, the telehealth group used statistically less contact time (221 minutes) on average than the face-to-face group (95% CI –387 to –56 minutes; p = 0.01). The key findings of the post-treatment questionnaire were (1) participants in both groups were equally likely to describe talking on the telephone as ‘extremely easy’ (p = 0.4), (2) learning the speech restructuring pattern was ‘extremely easy’ (p = 0.5), and (3) getting to know the speech pathologist was ‘easy’ (p = 0.2). The telehealth treatment was described significantly more frequently as ‘extremely convenient’ (p = 0.018) | |
| Cocomazzo et al. 201246 Country: Australia Study design: non-RCT Data collection method: unclear Aim: Phase I trial of the Camperdown Program Detail of participants (number, any reported demographics): 12 participants, 10 male and two female, aged 21–47 years (mean 29 years) |
Modified version of the Camperdown Program adapted for use in a student training clinic. The programme was modified in the following ways: (1) all treatment was provided by speech pathology students, under the supervision of clinical supervisors experienced in stuttering treatment; and (2) the programme was adapted to fit into a 20-hour clinic during a 10-week period, instead of time in treatment being performance contingent and, therefore, individualised to client need Hours contact: 10 weeks, total 20 hours Delivered by: student clinicians. Prior to commencement of treatment, student clinicians were familiarised with the programme and attended a 2-hour preparatory session with the clinical supervisors Control: not clear Length of follow-up: 12 months Response and/or attrition rate: none |
Percentage of syllables that are stuttered Speech naturalness |
Pooled percentage of syllables that are stuttered scores pre-treatment were 5.7, at immediate post treatment were 1.0 and at 12 months post treatment were 2.4. Mean percentage of syllables that are stuttered within-clinic pre-treatment was 5.9% (SD 7.8%), 0.8% (SD 0.7%) immediately post treatment and 2.6% (SD 3.1%) at 12 months post treatment. Mean percentage of syllables that are stuttered beyond clinic pre-treatment was 5.5% (SD 6.9%), 1.2% (SD 1.8%) immediately post treatment and 2.1% (SD 2.2%) at 12 months post treatment. The group speech naturalness scores post treatment did not increase to a clinically significant extent. The mean NAT score was 4.1 at pre-treatment and 4.5 immediately post treatment. This difference was not significant [t(9) = –0.897; p = 0.393] | |
| Craig et al. 199616 Country: Australia Study design: non-RCT Data collection method: speech samples in clinic at home and on the telephone, psychological measures Aim: to test the effectiveness of three interventions Detail of participants (number, any reported demographics): 97 participants, aged 9–14 years. Mean age 10.5–11.4 years across the groups, 75–88% male across the groups Two-thirds had received previous treatment in most cases consisting of response contingent stimulation or breathing and relaxation methods. None had received intervention in previous 3 months |
Compared three interventions EMG feedback which focused on speech muscle control through the use of computer feedback, intensive smooth speech which emphasised intensive treatment and rating sessions at gradually increasing speeds without intensive parental feedback, home-based smooth speech emphasised parental involvement and conducted in a home environment Number of hours: ISS – 5 hours practise, 1-week group intensive; HBSS – 1-week over 4 weeks, 6.5 hour sessions; EMG – 1 week, 6.5 hours per day Delivered by who? Clinicians Control: 20 children on waiting lists treatment delayed for 3 months Length of follow-up: immediate, 3 months, 1 year Response and/or attrition rate: none dropped out of the treatment. Three lost to follow-up at 3 months |
Percentage of syllables that are stuttered % improvement across time Speech naturalness State and trait anxiety inventory Speech rate |
No significant difference on stuttering scores between treatment groups across the three time points. Significant differences between control group and all treatment groups across all contexts (p < 0.001). Pre-treatment scores differed significantly from immediate post treatment (p < 0.001). Stuttering no better or worse depending on context measured (clinic or home). Speech rate significantly increased for all intervention groups (p < 0.001 conversation and telephone; p < 0.05 home). Intervention groups significantly increased speech rate compared with controls (p < 0.001). Decrease in percentage improvement across follow-up periods post treatment 90–95% of syllables that are stuttered, 75–80% 3-month follow-up, 65–75% 1-year follow-up. No improvement in stuttering for controls over this time period. ISS: 9 out of 10 children reduced stuttering to < 1% immediate post treatment, this reduced to 1 out of 10 at 1-year follow-up. EMG and HBSS: 6 out of 10 children reduced stuttering to < 1% immediate and 4 in 10 at 1-year follow-up. These two treatments superior at long-term follow-up if 2% threshold also applied. These two interventions therefore had less immediate effect but greater long-term effect than the intensive course. Those more severe at baseline higher risk of relapse, immediate post results not an indicator of long-term outcome, age and sex not predictors. Child and parent ratings of naturalness were lower than clinician ratings of naturalness (p < 0.01). Significant difference in naturalness baseline to 3 months for all interventions (p < 0.001). Significant difference baseline to 1-year follow-up in state and trait anxiety for all intervention groups compared with control (p < 0.05/p < 0.01) | Breathing techniques were observed directly in this study |
| Craig et al. 200247 Country: Australia Study design: before and after Data collection method: audio-taped speech sample in clinic, telephone, home Aim: to evaluate a relapse management programme for adolescents Detail of participants (number, any reported demographics): six adolescents who had taken part in an intervention at least 2 years earlier and had substantially increased their percentage of syllables that are stuttered following the intervention. Aged 11–17 years. 5–12.5% of syllables that are stuttered Two had received EMG intervention and four speech fluency shaping with 12-month maintenance sessions |
Group intervention including at least one parent consisting of combination of smooth speech, EMG feedback, self-management skills (importance of self-responsibility, self-evaluation, self-effort and motivation), cognitive techniques (self-talk, self-mastery enhancement/perceived control, methods of coping, resilience) and physical relaxation. Transfer activities such as games and shopping/telephone calls days 2 to 5, specific relapse management skills taught from day 2 encompassing self-control techniques and relaxation as well as CBT aimed at enhancing perceptions of control Number of hours: twice a week over 2 weeks, 9.30 a.m. to 4.00 p.m. with option of fifth day if inadequate transfer Delivered by who? Clinician initially, parents trained and assumed role of therapist Control: none Length of follow-up: 2 years following relapse programme Response and/or attrition rate: none |
Percentage of syllables that are stuttered Speech naturalness judged by an independent clinician Child/parent rating of naturalness State–Trait Anxiety Inventory for Children Communication Attitude Test-revised |
All participants had relapsed following their initial therapy 2–6 years earlier. Narrative describes two participants showing immediate improvement after the relapse programme but relapsed to > 5% of syllables that are stuttered at 2-year follow-up, two participants improved quickly and gains maintained (well below 5% of syllables that are stuttered) at 2 years, two participants improved more slowly and at 2 years remained ‘well below’ 5% of syllables that are stuttered. Speech naturalness increased for five participants and decreased for one participant. Anxiety scores were well below normal range for all participants. However, no trend for anxiety to be associated with relapse. The two participants who relapsed showed abnormally high Communication Attitude Test-revised scores at 2-year follow-up | |
| Cream et al. 200948 Country: Australia Study design: before and after Data collection method: conversation samples Aim: to investigate whether or not the use of VSM using restructured stutter-free speech reduces stuttering in adults who had learnt a speech restructuring technique and subsequently relapsed Detail of participants (number, any reported demographics): 12 participants, eight male and four female, aged 27–69 years (mean 50 years) All had previously had speech restructuring treatment for stuttering and relapsed |
Participants were video recorded for 1 hour within the clinic, practising their speech restructuring technique. The videos were then edited to remove all observable stuttering. Participants then viewed the resulting video of themselves using restructured stutter-free speech each day for 1 month and were instructed to speak as they did on the video Hours: 1 hour in clinic, 1 month home practise Delivered by? Clinician/self Length of follow-up: there were two assessments – (1) pre-intervention, several days to 2 weeks before the 1-hour videoed speaking session, and (2) post intervention, at the completion of the 4-week viewing period Response and/or attrition rate: 2 out of the 12 participants withdrew during the trial |
Percentage of syllables that are stuttered Self-reported severity ratings from nominated representative situations Speech naturalness. |
Very large ESs were found. The mean per cent syllables stuttered was 7.7 pre-intervention and 2.3 post intervention. For all but one participant there was a reduction in stuttering from pre-intervention to post intervention. These results were verified with self-report data. Speech naturalness was not compromised by the VSM procedure. For the 10 participants who remained in the study, mean stuttering frequency was 7.7% of syllables that are stuttered pre-intervention and 2.3% post intervention; a difference of 5.4% of syllables that are stuttered [95% CI 51.89% to 8.89% of syllables that are stuttered, t(9)53.49; p < 0.001]. For self-reported severity the group mean self-report was 5.2 pre-intervention and 3.5 post intervention; a difference of 1.7 [95% CI 2.13 to 2.13, t(9)510.15; p < 0.0001]. The mean naturalness score for the five raters for each sample was calculated. The grand mean was 3.8 for the pre-intervention speech samples and 3.9 for the post-intervention samples. This difference was not significant [t(9)50.86; p = 0.0.05]. Half the participants increased their NAT scores (speech was less natural) while half remained stable or decreased their NAT scores (speech was more natural) | |
| Cream et al. 201017 Country: Australia Study design: RCT Data collection method: conversational samples Aim: to evaluate the efficacy of VSM following speech restructuring treatment to improve the maintenance of treatment effects Detail of participants (number, any reported demographics): 89 adults, aged 12–74 years. Four times as many men as women. All had undertaken intensive speech restructuring treatment |
All participants received five consecutive days of intensive group speech restructuring treatment followed by a maintenance programme of seven weekly clinic visits These maintenance visits were individual and small group sessions. Three of the sites used the La Trobe Smooth Speech Program and three of the sites used a modified version of the Camperdown Program. Participants in the VSM intervention arm viewed stutter-free videos of themselves each day for 1 month Hours: 5 days followed by 7 visits Delivered by: clinician Control: two treatment arms – randomly assigned to either standard maintenance and standard maintenance plus VSM Length of follow-up: 6 months Response and/or attrition rate: five adults did not complete the study and their data were analysed with intention-to-treat procedures |
Percentage of syllables that are stuttered Self-rated anxiety Self-rated stuttering severity Avoidance Satisfaction with fluency Quality of life |
The addition of VSM did not improve speech outcomes, as measured by per cent syllables stuttered, at either 1 or 6 months post randomisation. At assessment 2, the percentage of syllables that are stuttered had decreased considerably for both groups. At assessment 3, the mean percentage of syllables that are stuttered was slightly higher for the VSM group; however, this difference was not statistically significant: 1.1% of syllables that are stuttered (95% CI –0.03% to 2.3% of syllables that are stuttered; p = 0.056). There was an apparent difference between groups for the primary outcome of percentage of syllables that are stuttered at assessment 4. However, when adjusted for percentage of syllables that are stuttered at assessments 1 and 2, this difference was not statistically significant (mean difference: 0.06 percentage of syllables that are stuttered with 95% CI –1.3% to 1.4% of syllables that are stuttered; p = 0.92). However, at the follow-up assessment, self-rating of worst stuttering severity by the VSM group was 10% better than that of the control group, and satisfaction with speech fluency was 20% better. Quality of life was also better for the VSM group, which was mildly to moderately impaired compared with moderate impairment in the control group | |
| De Veer et al. 200918 Country: the Netherlands Study design: RCT Data collection method: unclear Aim: to examine the psychological impact of the Mindfulness Program Detail of participants (number, any reported demographics): 37 participants, 29 male and eight female, mean age 36.57 (SD 12.97) years. All had undergone speech therapy, psychotherapy and a number of different stutter therapies |
Mindfulness-based Stress Reduction Program. A training course that has a focus on teaching its participants how to relax attentively. It aims to reduce stress, anxiety, trait anxiety, self-efficacy beliefs and develop coping responses and positive attitude towards speech situations. Included the following exercises: (1) a body scan, meant to get them to pay systematic attention to the whole body and simultaneously perceive sensations in various parts of the body, (2) yoga exercises involving stretching and striking poses to increase awareness of the muscular system and (3) sitting meditation, during which the participant’s attention is drawn to breathing, physical sensations, thoughts and emotions. After the first, third and fifth session, the participants were also given a compact disc with the body scan, yoga and sitting meditation exercises Hours: 8 weeks of 2.5-hour sessions. Participants expected to spend at least 45 minutes a day, six days a week doing one or more of the exercises Delivered by: first author who had attended a training programme for delivering the intervention Control: delayed intervention group Length of follow-up: 4 weeks Response and/or attrition rate: unclear |
Perceived Stress Scale Speech Situation Checklist PSI SESAS Condensed S Scale LCB scale |
Post intervention, there was a significant difference between intervention and control in measures of stress (F = 16.95; p < 0.001), anxiety about speech situations (F = 13.81; p < 0.01), self-efficacy trust (F = 10.66; p < 0.01), locus of control (F = 11.83; p < 0.01), coping (F = 5.05; p < 0.05) and attitude towards speech situations (F = 14.47; p < 0.01). No significant difference was found in self-efficacy fluency (F = 3.29; p = 0.08). ESs average for self-efficacy beliefs, coping and attitude towards speech situations (d = 0.55, 0.62 and 0.48, respectively). ESs large for stress, anxiety and locus of control. (d = 1.16, 1.07 and 0.76 respectively). At 4-week follow-up, no difference from immediate post intervention for anxiety (t = 1.65; p = 0.12; mean 1.99, SD 0.32 and mean 2.10, SD 0.51, respectively), self-efficacy trust (t = 0.18; p = 0.86; mean = 72.23, SD 11.75 and mean 72.43, SD 9.90, respectively), locus of control (t = 3.15; p = 0.76; mean = 75.00, SD 7.59 and mean = 75.38, SD 8.37, respectively) and attitude towards speech situations (t = 0.42; p = 0.68; mean 12.11, SD 4.67 and mean 11.95, SD 4.62, respectively). At 4-week follow-up, stress was significantly lower than immediate post intervention (t = –2.78; p < 0.05; mean 19.35, SD 3.74 and mean 17.82, SD 4.28, respectively), self-efficacy fluency was significantly higher than immediate post intervention (t = –2.40; p < 0.05; mean 63.80, SD 8.80 and mean 68.15, SD 10.82, respectively) and coping was significantly higher than immediate post test (t = –2.65; p < 0.05; mean 13.26, SD 3.57 and mean 14.58, SD 3.81, respectively). Some difference between response to intervention for both groups, with the delayed intervention group self-efficacy effect fading at second follow-up more than results obtained for the first group. No other difference in response of the two groups to the intervention | |
| Druce and Debney et al. 199749 Country: Australia Study design: before and after Data collection method: videotaped speech sample Aim: to investigate the effects of an intensive, behaviourally oriented treatment programme for 6- to 8-year-old children who stutter Detail of participants (number, any reported demographics):15 participants, 13 male and two female. Age range 6 years 9 months to 8 years 1 month (mean age 7 years 4 months) |
The programme began with children identifying stutters in the speech pathologist’s speech and then in their own speech and a peer’s speech. Fluency acquisition phase followed when each child individually worked through a regimen of repeating single words, naming pictures and then producing monosyllabic words in response to a verbal cue followed by producing phrases of gradually increasing length, retelling a story first with pictures and then without the aid of a visual cue. Monologue tasks, asking and answering questions and conversational tasks. Reinforcement of the child’s success at each step was through a reinforcement system of stickers, games and social praise Hours: intensive week. Parents attended two 1-hour workshops during the programme in addition to a 45-minute session each day when they observed their child in an individual and group setting, and had an opportunity to discuss issues with the speech pathologist Delivered by: SLP Length of follow-up: 18 months Response and/or attrition rate: none |
Percentage of syllables that are stuttered Speech naturalness Subjective stuttering severity |
From pre-intervention, to after the intensive week, the mean percentage of syllables that are stuttered for the group decreased by 7.6% to 1.75% with a standard error of 0.54. This change in the percentage of syllables that are stuttered with treatment was statistically significant (95% CI –11.7% to –3.5% of syllables that are stuttered; p = 0.0015). Pre-intervention to immediate post-intervention speech rate increased by a mean of 20.5 SPM (from 92.3 to 112.8 SPM) (95% CI 13 to 28 SPM; p < 0.0001) | |
| Elliott et al. 199850 Country: US Study design: before and after (multiple baseline assessments) Data collection method: observed speech, assessment scales Aim: to evaluate the simplified regulated breathing method Detail of participants (number, any reported demographics): five participants, all male, aged 5–11 years. All referred by SLTs. Number of words stuttered ≥ 5% of the total words spoken, stuttering behaviours had occurred for at least 1 year. Two participants had been receiving therapy and had achieved lower stuttering rates but had relapsed to these rates since ending treatment. 1.5–8 years of stuttering, 1–6 years of previous treatment |
The simplified regulated breathing method. 1-hour session conducted individually in the home with parent present. Included awareness training, competing response (regulated breathing techniques) and social support procedures (praise/feedback). Delivered by clinical psychology students. Parents asked to carry out and record daily 10-minute practise sessions Number of hours: 1–5 half-hour booster sessions provided for three participants for 6–9 months post treatment. These participants had < 3% stuttered words at end of treatment period Delivered by: clinical psychology students Control: none Length of follow-up: 9 months was the longest Response and/or attrition rate: no attrition although reported one child poor co-operation during therapy and refused practise sessions |
% stuttered words Rate of speech SSI (physical concomitants and duration scales) Abbreviated acceptability rating profile Treatment credibility scale Social perception scale |
Four out of the five participants reduced their stuttering to below 3% of words (reading only, three only below 3% in conversation) after one session of intervention and this was maintained for up to 9 months with periodic booster sessions for three. The mean percentage of stuttered words during conversation was 8.58 at baseline, and post treatment had reduced to 3.43. The frequency of stuttered words during reading was 9.22 at baseline and post treatment had reduced to 2.86. During conversation, rate of speech increased from a baseline mean of 120.91 to a post-treatment mean of 136.36 words per minute across participants. SSI: during conversation, the baseline mean of 1.27 dropped to 0.79 following treatment. All subjects decreased the mean length of their blocks, with a mean rating of 2.29 during baseline to 1.17 during post treatment. All the parents found the treatment protocol to be credible and acceptable. The average rating of acceptability was 42.6 before treatment, and 42.5 following treatment implementation. The average rating of credibility was 38.9 before treatment and 43.6 following treatment implementation. Social perception ratings: the baseline mean of 19.11 (range 7.67–29.33) was lower than the post-treatment mean of 30.25 (range 26.17–32.33). Parents compliant with carrying out the practise sessions, one child non-compliant with the treatment and practise, parents discontinued practise | Booster sessions provided ‘as needed’ also seem to have been provided at different times for each participant according to a figure in Elliott et al.50 Descriptive statistics only. Two children had achieved low rates following previous therapy |
| Femrell et al. 201251 Country: Sweden Study design: before and after Data collection method: observed speech and questionnaire Aim: to report long-term follow-up data Detail of participants (number, any reported demographics): 10 participants, eight males and two females, aged from 2 years 9 months to 5 years, mean age 4.4 years. Had been stuttering for 9 months to 3 years and 3 months. Mean stuttering frequency of 10.1% syllables stuttered (range 0.8–33.9% of syllables that are stuttered) before treatment |
LP. Children referred to the clinic recruited consecutively. Number of hours: the median number of treatment visits at stage 1 was 32.5, the range was 9–46 visits (SD 14.9, mean 30.5). The median time spent at stage 1 was 55.5 weeks. Children placed in stage 2 when they achieved < 1% of syllables that are stuttered and the parents’ daily severity ratings 1 or 2, with at least four of these being 1, for about 3 weeks. Stage 2 included nine visits over a period of almost 2 years (2, 2, 4, 4, 8, 8, 16, 16, 24 weeks between clinic visits) Delivered by: treatment provided by the paper authors Control: none Length of follow-up: 2 years Response and/or attrition rate: two did not complete the programme as parents satisfied with progress made at 30- and 35-week stage |
Percentage of syllables that are stuttered Parent and teacher rating of child speech |
Significant [t(7) = 4.3; p < 0.01] decrease in mean percentage of syllables that are stuttered before and after treatment [7.6% (SD 4.9%) vs. 0.1% (SD 0.2%), respectively] with a large ES (d = 2.9) an average reduction of 97.8% after stage 2. Questionnaire data: significant difference (p < 0.01 or p < 0.05) parent and teacher rating stuttering rate, struggling with words, stuttering variation, parent worry about child stuttering. No significant difference rating of child bothered by speech, inhibited by stuttering, teacher worried about stuttering, child enjoys talking, child self-confidence. 62.5% of the parents reported treatment too time-consuming | |
| Foundas et al. 201352 Country: USA Study design: before and after Data collection method: observed speech Aim: to evaluate SpeechEasy in adults Detail of participants (number, any reported demographics): 24 males, aged 20–46 years, 14 who stuttered, 10 non-stutterers. Stutterers had conversational speech that contained three or more stutterings per 100 words and had stuttered continually to the present with the onset before 8 years of age |
SpeechEasy (Janus Development Group, Inc. Greenville, NC) is an electronic device designed to alleviate stuttering by manipulating auditory feedback via time delays and frequency shifts. Control condition: participant wore device but not switched on, two experimental condition device operating at manufacturers default setting with the DAF set at a 60-millisecond delay and the frequency shift function set at + 500 Hz, and device set to individual preference for comfort level Number of hours: not specified, one session Delivered by: electronic device, session overseen by paper authors Control: normal speakers Length of follow-up: none Response and/or attrition rate: N/A |
Stuttering rate | Among people who stutter, there was a significantly greater reduction in stuttering when wearing the SpeechEasy with custom settings than at baseline (mean –2.35, SE 0.54) compared with the non-altered feedback (control) condition (mean –1.72, SE 0.48; p = 0.014). Decreased stuttering was found for all device settings compared with baseline for people who stutter. The effect was most pronounced with the use of the self-prescribed (custom) setting. Despite this statistical effect, the mean reduction of 2.3 stuttering events per 100 syllables for the device custom setting reflected a relatively small change in actual frequency of stuttering. Stuttering was reduced the most during reading, followed by narrative and conversation. Those individuals with a more severe stuttering rate at baseline had a greater benefit from the use of the device than individuals with less severe stuttering | |
| Franken et al. 199253 Country: the Netherlands Study design: before and after Data collection method: recorded speech samples Aim: to examine the quality of post-treatment speech in stutters compared to non-stutterers Detail of participants (number, any reported demographics): 32 male stutterers, mean age 25.3 years, range 15–46 years. Severe stuttering, speech motoric component outweighed emotional components, 20 non-stutterers matched |
Dutch adaptation of Webster’s Precision Fluency Shaping Program. A systematic SMT programme that deals with the reconstruction of behaviour details involving respiration, voicing and articulation. Included overlearning, exaggeration, immediate informational feedback about response correctness, fading, parallel transfer, and client self-reliance and self-control. After fluency has been established in the clinic, it is generalised to the stutterer’s daily environment via ‘transfer-activities’ Number of hours: about 120 treatment hours followed by ‘elaborate home treatment programme’ Delivered by: clinician Control: non-stutterers Length of follow-up: 6 months Response and/or attrition rate: unclear |
Percentage of syllables that are stuttered Syllables per second 14 listener rating scales grouped into three dimensions: distorted speech, dynamics/prosody and voice |
Percentage of syllables that are stuttered pre-intervention 27.7%, post intervention 5.8%, follow-up 16.3%. Syllables per second pre-intervention 2.1, post intervention 2.1, follow-up 2.3. Post therapy, the stutterers’ scores on the Distorted Speech dimension are just about as low as those of the normal speakers owing to reduction in frequency of stuttered syllables. The judgments for the three conditions of the stutterers on nearly all rating scales show a V-shape, or inverted V-shape: a clear improvement or deterioration in the post-therapy condition, followed by a relapse or recovery in the follow-up therapy condition. Only two scales, unpleasant vs. pleasant and unnatural vs. natural, show a small but steady improvement going from pre-therapy to follow-up therapy. The speech of treated stutterers is different from the speech of non-stutterers; on the Dynamics/Prosody dimension the post-therapy stutterers did not move closer to the non-stutterers than the pre-therapy stutterers rating | |
| Franken et al. 200554 Country: the Netherlands Study design: before and after Data collection method: audio recording and questionnaires Aim: a pilot study to examine the feasibility of comparing the effectiveness of two programmes Detail of participants (number, any reported demographics): 23 participants, 17 males and six females, mean age 4 years 3 months, mean age at onset 2 years 9 months |
LP treatment or a DCM treatment. Recruited via SLTs Number of hours: LP – the mean number of treatment sessions was 11.5. Treatment lasted fewer than 12 weeks for 2 out of the 11 children. DCM – the mean number of treatment sessions was 11.0. Treatment lasted fewer than 12 weeks for 3 out of the 12 children Delivered by: therapist Control: two intervention arms only Length of follow-up: immediate Response and/or attrition rate: 30 randomised, four did not complete the intervention, further three did not collect all the required data |
Percentage of syllables that are stuttered Stuttering severity rating Bristol Stammering Questionnaire |
Stuttering frequency: for LP treatment, the means decreased from 7.2% (SD 2.0) to 3.7% (SD 2.1). For DCM treatment, the means decreased from 7.9% (SD 7.1) to 3.1% (SD 2.1). Stuttering severity: significant effect of time (pre to post treatment), F(1,21) = 15.18 (p < 0.01). No significant difference between interventions (p > 0.10). Parent ratings and therapist ratings: effects of time (pre- to post treatment) for the parent F(1,21) = 85.50 (p < 0.01), and for the therapist, F(1,21) = 73.73 (p < 0.01). No effects that involved the type of treatment (p > 0.10). Both treatments were found to be highly acceptable on all dimensions. No significant differences between the interventions in terms of acceptability | |
| Franklin et al. 200819 Country: Australia Study design: Quasi-RCT (randomised consecutively) Data collection method: tape-recorded speech Aim: to evaluate the effectiveness of time out response contingencies Detail of participants (number, any reported demographics): 60 adults, treatment participants averaging 32 years (range 16–61 years, SD 13 years and controls averaging 33 years range = 17–61 years, SD 12 years) Treatment participants averaged 26 months of previous treatment (range = 0–120 months, SD 28 months) and controls 36 months (range = 1–120 months, SD 35 months). All participants had received PS treatment, 14 treatment group and seven controls had received therapy in the last year |
Time-out individuals were instructed to cease talking whenever the red light was illuminated and to recommence conversation once it was switched off. The light remained on for 5 seconds and was contingent on each stuttering episode, as identified by the experimenter. During the time-out period, all social reinforcers in forms of eye contact, smiles, nods and conversation comments were ceased Number of hours 2 × 20-minute sessions of spontaneous speech Delivered by: first author Control: individuals had same 2 × 20-minute sessions with no response contingencies, encouraged to keep talking Length of follow-up: immediate retest Response and/or attrition rate: none |
Percentage of syllables that are stuttered Number of syllables stuttered and spoken fluently %WPWR |
Baseline percentage of syllables that are stuttered intervention group mean 5.8% (range 1.2–28.3%, SD 6.4%). Control group 4.9% (range 0.7–23.3%, SD 5%). Post-treatment percentage of syllables that are stuttered intervention group mean 3.9% (range 0.5–25.6%, SD 5.6%). Control group 6.4% (range 0.5–20.7%, SD 5.1%). Baseline SPM intervention group mean 211% (range 70–296%, SD 57%). Control group 236% (range 107–317%). Post-treatment intervention 234 SPM (range 77–300 SPM, SD 51 SPM), control 229 SPM (range 102–325 SPM, SD 54 SPM). Baseline %WPWR mean intervention 19.6 (range 0–66.7, SD 16). Control 32 (range 0–100, SD 29.5). Post-treatment intervention 30 (range 2.7–87.3, SD 22). Control 31.7 (range 2.5–100, SD 27.7). A between-groups analysis showed a significant difference between the two groups in percentage of syllables that are stuttered during the treatment condition, U = 85.5; p < 0.007, as well as a significant difference between the groups during post treatment, U = 234.5; p < 0.007. Time-out participants did not slow down their speech, but instead increased it. The increase in SPM relative to baseline was significant during both the treatment phase, F(1,58) = 4.09; p < 0.05, and post treatment, F(1,58) = 13.75; p < 0.05. Strong association between baseline stuttering severity and treatment outcomes, negative association between baseline speech rate and outcome, better responsiveness to this intervention moderately associated with higher amount of past therapy (but not a unique predictor) | |
| Gagnon and Ladouceur 199255 Country: Canada Study design: before and after Data collection method: speech sample, scaled measures Aim: to evaluate Modified Regulated Breathing Method intervention Detail of participants (number, any reported demographics): study 1 – four participants, male, aged 10–11 years, three moderate and one severe stutterer. Study 2 – four participants, male, aged 6–7 years, none received previous therapy, all classed as severe stutterers. Study 3 – three participants, male, aged 7–11 years, none previously received therapy, all had at least 5% of syllables that are stuttered (with a range of 14–35%), none received previous therapy |
Sessions consisted of awareness training, also Modified Regulated Breathing Method whereby children are instructed to stop speaking when a stutter occurs and to exhale and then inhale a deep breath. Built up from words to sentences and then conversation. Sessions also included EasySpeech – demonstration of tension/relaxation of facial muscles, and generalisation activities. Parents present for all sessions, received information and advice regarding attitudes and behaviours Study 3 also included group activities, 3-weekly booster sessions and parents taking part in sessions, moving to parents taking the entire session Number of hours: study 1, 2 × 1 hour per week, seven sessions needed to reach ‘clinically significant’ reduction of 3% in SS. From graph in Gagnon and Ladouceur,55 25 sessions delivered in total Study 2, 5–41 sessions needed to reach 3% reduction (mean 29 sessions) Delivered by who? Student therapist Control: none Length of follow-up: 1 and 6 months Response and/or attrition rate: none |
Percentage of syllables that are stuttered SPM Assessment of stutterer or not Ryan’s Stuttering Severity Scale |
Study 1. Clinically significant (–3% of syllables that are stuttered) improvement in all at 1- and 6-month follow-up. In addition, clinically significant (160 SPM) maintained at both follow-ups. R(n) significant reduction pre-immediate post p < 0.05. No data regarding significance reported for following time points. Judges did not identify as stutterers Study 2. R(n) significant reduction p < 0.05. Not reported at which time point. Below 3% of syllables that are stuttered maintained at first follow-up for three participants, the fourth participant had 3.5% of syllables that are stuttered. At second follow-up, two participants remained below 3% of syllables that are stuttered. SPM above 160 SPM for all participants at all follow-ups. Three classed as mild stutterers post intervention, one normal Study 3. Clinically significant reduction after 4 sessions for all participants, gains maintained at both follow-ups. No further statistical detail. SPM in normal range at end of treatment and follow-ups |
Limited statistical analysis |
| Gallop and Runyan 201256 Country: USA Study design: before and after Data collection method: telephone interview Aim: to examine the long-term effectiveness of SpeechEasy Detail of participants (number, any reported demographics): 11 participants, seven male and four female, aged 11–51 years (mean 28 years) |
SpeechEasy in-ear auditory feedback device the DAF was set at 150 millisecond delay and the FAF setting was + 500 Hz Number of hours: N/A Delivered by who? Device Control: none Length of follow-up: 13–59 months (mean 37 months) Response and/or attrition rate: data available for seven who were ongoing users of the device. Full data not available for one and three had ceased usage |
Stuttering frequency | All participants had exhibited reduction in stuttering frequency at the time of the fitting while wearing the device compared with when they were not wearing the device. Comparison of pre-fitting of device with current use or non use of the device showed a significant decrease in stuttering [F(1,6) = 17.44; p = 0.006]. Significant difference (t = 2.851; p = 0.017) for the group between baseline stuttering frequency prior to being fitted with the device and current stuttering frequency while not wearing the device. Nine maintained or had reduced stuttering level. Individual variation: two participants with the highest frequency of stuttering when fitted with the device showed the greatest improvement over time; the two with lesser dysfluency at fitting showed lesser change, and the remaining three who exhibited minimal dysfluency when first fitted with the device, exhibited an increase in dysfluency after having worn the device for almost 4 years or longer. For the eight participants who were still using the device, significant benefits were not found when wearing the device compared with not wearing the device (t = 1.949; p = 0.092). For six, the device had a positive impact, but for two it worsened the percentage of syllables that are stuttered. There was no significant difference (t = −0.074; p = 0.943) between stuttering frequency when first fitted with the device and current stuttering frequency with the device in place, indicating initial gains were maintained | |
| Hancock and Craig 199820 Country: Australia Study design: further associations analysis of RCT data Data collection method: examination of RCT data Aim: to examine predictors of intervention outcome Detail of participants (number, any reported demographics): 77 participants, 64 male and 13 female, aged 9–14 years (51 subjects were 9–11 years, 26 were 12–14 years) mean age 10.8 years. Two-thirds had received previous therapy |
See Craig et al.16 for details of interventions. Those who stuttered on at least 2% of their syllables were classified as having relapsed Number of hours: See Craig et al.16 Delivered by who? See Craig et al.16 for details of interventions. Control: See Craig et al.16 Length of follow-up: 1 year Response and/or attrition rate: N/A |
12 predictor variables including demographics, history of stutter, family history, previous therapy, anxiety Percentage of syllables that are stuttered SPM Anxiety |
Variables that significantly correlated with percentage of syllables that are stuttered at 1-year follow-up were pre-percentage of syllables that are stuttered (p = 0.01), age (p = 0.05) and years stuttered (p = 0.05). Those who had high pre-treatment percentage of syllables that are stuttered were aged 12–14 years and had been stuttering longer were likely to have higher 1-year post-treatment percentage of syllables that are stuttered scores. However, although age and years stuttered were moderately correlated to long-term percentage of syllables that are stuttered, they had little predictive value in the regression analysis. In regression analysis, only two of the independent variables contributed significantly to prediction of long-term percentage of syllables that are stuttered (at p < 0.01), including pre-percentage of syllables that are stuttered (sr2 = 0.144) and post-trait anxiety (sr2 = 0.08). Pre-treatment stuttering severity contribution to long-term outcome was 14.4%. The immediate post-trait anxiety measure contributed 8% to stuttering severity 1-year post treatment. The 13 variables explained 33% (21% adjusted) of the total variance in long-term percentage of syllables that are stuttered scores | |
| Hancock and Craig 200257 Country: Australia Study design: before and after Data collection method: assessment of talking in clinic, on telephone, in home environment. Method not described in this paper Aim: to examine the effectiveness of retreatment for adolescents who had previously received an intervention Detail of participants (number, any reported demographics): 12 participants, at least 2% of syllables that are stuttered. 11 males and one female, aged 11–17 years (mean 14 years). Had received EMG or smooth speech treatment as part of trial 2–6 years earlier. All had attended maintenance sessions post treatment for 12 months |
Group of up to four children and parents. Combined smooth speech and EMG intervention with CBT components such as relaxation, self-management and attitude or cognitive therapy. Main emphasis on the psychological-based techniques with use of speech diary. Transfer activities such as games and shopping/telephone calls. Groups for younger children more emphasis on games, older more group conversation Number of hours: twice a week over 2 weeks 9.30 p.m. to 4 p.m., optional fifth day if insufficient transfer of skills. Evening completion of self-rating scale Delivered by who? Experienced clinician Control: none Length of follow-up: immediate, 3 months, 12 months, 2 years following the second period of treatment Response and/or attrition rate: 22 (32%) of previous trial participants eligible, two unwilling to participate, six other commitments |
Child and parental and independent listener rating of speech naturalness on Likert scale Percentage of syllables that are stuttered SPM State–Trait Anxiety Inventory for Children Communication Attitude Test-Revised Perceptions of Control Scale |
Initial intervention outcomes: significant difference (p < 0.001) pre- to post initial intervention for percentage of syllables that are stuttered at immediate post intervention, 3 months post intervention, 12 months and 2 years post intervention. Significant difference for SPM (p < 0.001) also at all post initial intervention time points. Retreatment outcomes: four of group scored > 2% of syllables that are stuttered immediate post retreatment, five of group scored > 2% of syllables that are stuttered at 3 months, six of group scored > 2% of syllables that are stuttered at 12 months and three of group scored > 2% of syllables that are stuttered at 2 years. Significant difference pre- to post intervention for percentage of syllables that are stuttered (p < 0.001 or p < 01 across the different contexts). SPM only significant difference for at home measure (p < 001). Clinician rating of naturalness significantly increased (p < 0.01) pre- to post intervention. No significant difference for state/trait, communication attitude or perception of control scores over time. However, mean anxiety scores were within normal limits at baseline and maintained at follow-up. Immediate post retreatment, five participants were considered to have negative communication attitudes, six participants at 12 months and five participants at 2 years. Follow-up level of percentage of syllables that are stuttered at 12 months was no different for retreatment intervention than initial intervention. However, retreatment intervention resulted in significantly lower percentage of syllables that are stuttered at 2-year follow-up than initial intervention 2-year follow-up had. SPM scores also significantly better for retreatment at 2-year follow-up than initial treatment | |
| Hancock et al. 199821 Country: Australia Study design: follow-up of RCT Data collection method: speech samples, psychological measures Aim: to evaluate long-term outcomes of a RCT comparing three interventions Detail of participants (number, any reported demographics): 97 participants, 27 intensive smooth speech, 25 home-based smooth speech, 25 EMG treatment, 20 control. Seven had received additional treatment since the original RCT, but none in previous 3 months. Age at follow-up – range 11–18 years, mean 14.8 years. Mean time since assessment 4.2 years (median 4 years). Original inclusion criterion had been < 2% syllables stuttered |
Follow-up of Craig et al.16, that paper gives details. Intensive smooth speech, home-based smooth speech, EMG interventions Number of hours: see Craig et al.16 Delivered by who? see Craig et al.16 Control: no treatment for 3 months Length of follow-up: 2–6 years Response and/or attrition rate: 77 1-year follow-up, 62 of these (81%) assessed at 2- to 6-year follow-up |
Percentage of syllables that are stuttered SPM Speech naturalness Parent judgement State–Trait Anxiety Inventory for Children Communication Attitude Test-Revised |
At 12 months there had been no difference between effectiveness of the interventions, all had been more effective than control. At 4 to 6-year follow-up, there continued to be no significant difference between the interventions in terms of effectiveness. Speech rate for all intervention groups had increased from 1 year post treatment, no significant difference between any intervention and others. Long-term rates of improvement were similar to 1-year follow-up levels (75–79% long term vs. 70–74% 1 year). Relapse rates of around 30% similar at long-term follow-up to that reported at 1 year. At 2- to 6-year follow-up around half the children stuttered < 1% syllables, and 7 out of 10 children < 2% of syllables that are stuttered. Variability in parent report of whether or not child had relapsed, 71% reported speech varied at different times (was cyclical). Mean score of Communication Attitudes Test-Revised on long-term follow-up was 12.4 (SD 8.1), similar for all interventions. This is reported as slightly higher than non-stuttering children but lower than reported for stuttering children generally. Anxiety scores similar to 12-month follow-up, no significant difference between intervention types | |
| Harris et al. 200222 Country: Australia Study design: quasi-RCT (recruited consecutively) Data collection method: recorded speech Aim: to evaluate the LP compared with no intervention Detail of participants (number, any reported demographics): 23 children stuttering at a rate of ≥ 3.0% of syllables that are stuttered. 19 males and four females. Mean percentage of syllables that are stuttered was 8.5% (across both groups) at baseline. Mean time since onset 11 months |
LP Number of hours: 12 weeks of clinic visits Delivered by who? Not reported Control: 12-week wait for intervention Length of follow-up: immediate post intervention Response and/or attrition rate: 29 randomised |
Percentage of syllables that are stuttered | Intervention group mean percentage of syllables that are stuttered was 8.4% at baseline, mean percentage of syllables that are stuttered was 3.5% (SD 2.8%; range 0.6–9.2%) post intervention. Control group mean percentage of syllables that are stuttered was 8.4% at baseline, mean percentage of syllables that are stuttered was 5.8% (SD 3.6%; range 2.3–15.3%) post intervention. There was a significant decrease in stuttering from baseline to second measure for both intervention and no intervention groups. The treatment group improved significantly more than the control group (F = 5.02; p < 0.05). Therefore, the intervention group improved twice as much as controls. 9 out of the 10 intervention children reduced percentage of syllables that are stuttered between pre and post measures. 9 out of the 13 control children reduced percentage of syllables that are stuttered between pre- and post measures. The other participants increased scores in this time period | |
| Harrison et al. 200458 Country: Australia Study design: each group received period of intervention then period of no intervention. Before and after Data collection method: recorded speech Aim: to evaluate two components of the LP Detail of participants (number, any reported demographics): 38 pre-school children, stuttering rate > 2% of syllables that are stuttered, no previous treatment with Lidcombe, onset at least 6 months earlier. 27 males and 11 females, mean age at onset 33 months (range 12–44 months) |
Evaluates parental contingencies and parental severity rating Number of hours: weekly clinic visits for 4 weeks of treatment Delivered by who? Unclear Control: four groups – treatment with and without verbal contingencies and with and without parental severity rating Length of follow-up: immediate post treatment and 4-week follow-up Response and/or attrition rate: 46 were randomised |
Percentage of syllables that are stuttered | The two groups whose treatment included parental verbal contingencies either maintained the same level of reduced stuttering or decreased it further during the 4-week follow-up (mean 8.9 baseline, 4.9 immediate post and 4.1 at 4-week follow-up and second group mean 5.6, 3.6, 3.7). The two groups that did not receive parental verbal contingencies for stuttering increased percentage of syllables that are stuttered at the 4-week follow-up (mean 6.8%, 3.8% and 5.2% and 7.0%, 4.1%, 6.3%). This suggests parental contingencies may have more of an effect on outcome than the severity rating component. However, neither the difference between parental verbal contingencies and no parental verbal contingencies [F(1,34) = 0.85; p = 0.77], nor the difference between self-report and no self-report [F(1, 34) = 0.23; p = 0.63] were significant. The authors associate this with the study being under-powered | |
| Hasbrouck 199259 Country: USA Study design: before and after Data collection method: sample of spontaneous speech Aim: to evaluate an intensive programme Detail of participants (number, any reported demographics): 117 participants, 111 males and six females, aged 18–41 years (mean 25.7 years) |
Groups of 3–5, individual and group sessions. Programme included graded airflow procedure in 19 stages (learn to initiate utterance with airflow and maintain continuous flow). Participants required to reach criteria before moving forward in programme. Programme also included relaxation group sessions using tension/relaxation procedures. EMG biofeedback used during airflow procedure. Final stage a hierarchical desensitisation procedure (systematic desensitisation procedure) whereby each was discussed until the power of each to effect stuttering was perceived as being reduced Number of hours: 7 hours a day for first 2 days Delivered by who? Clinicians Control: none Length of follow-up: 3- to 36-month follow-up Response and/or attrition rate: 57 patients followed up, 25 at 6 months, 32 at 1 year, 10 at 18 months, five at 2 years, seven at 2.5 years and five at 3 years |
Mean number of stutterings Number of words Mean percentage stuttered words Mean number of WPM |
All reduced % stuttered words to below 1%. A total of 42 of the 57 followed up had maintained this level. Mean number of stuttering pre-intervention 123.77, post intervention 4.58, follow-up 30.14. Mean % stuttered words pre-intervention 5.43, post intervention 0.18, follow-up 2.11. Mean WPM pre-intervention 141.21 post intervention 143.86, follow-up 153.16. Further statistical analysis only compares those that regressed with those that maintained rather than pre-intervention and post intervention for all participants | |
| Hewat et al. 200623 Country: Australia Study design: non-RCT Data collection method: audio and video recording Aim: to evaluate the self-imposed time out intervention Detail of participants (number, any reported demographics): 30 participants, 22 males and eight females, 22 had received therapy but no previous therapy in preceding 12 months, age range 14–52 years (mean age 29.7 years) Mentions 23 controls but little information |
SITO has two stages: instatement and generalisation, and maintenance. Stage 1 individuals are taught the technique and clinician administers time out in situations from single word to conversation followed by assignments away from the clinic. Group day then self-rating phase and then participants use technique everyday and bring recordings to clinic sessions Stage 2 focuses on self-management, problem-solving and ongoing monitoring of fluency. Criteria for end of each stage specified Number of hours: stage 1 individual sessions plus an intensive 8-hour group day with up to six participants. Number of sessions not provided. Stage 2 six monthly visits Delivered by who? Clinician Control: 11 matched controls and 12 stutters at various stages of PS treatment. No further information about these participants Length of follow-up: 3 measures pre-treatment, one 1 week post intervention and one 6 months post intervention Response and/or attrition rate: 22 completed stage 1. Complete data across all time points for 18 |
Percentage of syllables that are stuttered SPM Speech naturalness Type of stuttering using Lidcombe Behavioural Data Language Self-report inventory developed for study |
For the participants who completed stage 1, the mean reduction in percentage of syllables that are stuttered scores from pre-treatment to post stage 1 was 53.6%. More than half (from source figure, total 13 out of 22) the participants reduced their stuttering frequency by > 50%. Numbers taken from figure – six participants 50–60%, three participants 60–70%, four participants 80–90% reduction. There was a wide range of responsiveness to the intervention, with some participants responding very well and others responding to a quite limited extent. Range taken from figure 0–90% reduction in percentage of syllables that are stuttered. The SITO participants were judged to sound more unnatural after treatment than the control subjects, but more natural than the subjects who were using prolonged speech. There was no change in the relative proportions of repeated movements, fixed postures or superfluous behaviours pre- to post intervention. Indication that participants whose stuttering was more severe tended to benefit more from SITO than those whose stuttering was less severe. 16 out of the 17 respondents answered ‘yes’ to the question, ‘Would you recommend SITO to other people who stutter?’; 14 out of the 17 respondents answered ‘yes’ to the question, ‘Is SITO difficult to do?’; and 12 out of the 17 respondents answered ‘sometimes’ to the question ‘Were you using SITO 6 months after Stage 1?’, with two answering ‘yes’ to this question and three answering ‘no’ | Two versions of the programme (one no group day), paper reports results for each similar so have been pooled. Limited analysis. Described as clinical trial but no real control group. Highlights already known that combining fluency training enhances effect of time out. In addition, lack of reporting of SPM means reduction in stuttering frequency may be result of slower rate. Furthermore, no data reported on whether or not participants did use time out. No claim for treatment being more effective when stuttering more severe due to Law of Initial Value Ratings of speech naturalness were influenced by the frequency and severity of stuttering moments. Therefore, it was not valid to measure speech naturalness only during fluent speech samples. Speech rate may be an unreliable measure for naturalistic samples. The optimal check for speech rate issues is speech naturalness and the purpose of this assessment requires examination of stutter-free speech only. The paper included % improvement only as a secondary outcome to show individual variation with % stuttered as primary. Treatment fidelity was included and was a criterion for progression |
| Hudock and Kalinowski 201460 Country: USA Study design: before and after Data collection method: recordings of scripted telephone conversations Aim: to evaluate DAF and FAF combination interventions Detail of participants (number, any reported demographics): nine participants, eight males and one female, mean age 35.1 years, range 21–72 years. > 5% stuttering |
Two different combinations of DAF and FA: condition one – 50 millisecond delay and plus one half octave frequency; condition two – encompassed above condition together with 200 millisecond delay and minus one half octave. Speech collected via microphone and altered signal sent via digital signal processer to monaural receiver held to ear by participant Control: none Length of follow-up: immediate Response and/or attrition rate: none |
Total spoken and total stuttered syllables | Both conditions had significantly lower proportions of stuttered syllables than no altered feedback. No AF and condition one average 63% reduction p < 0.05. NAF and condition two p < 0.05 average 72% reduction. Second condition lower proportion of stuttered syllables than condition one | Scripted telephone conversation |
| Huinck et al. 200661 Country: the Netherlands Study design: before and after Data collection method: video and audio recording of speech during interview, self-report Aim: to identify the impact of stuttering intervention by individual subgroup Detail of participants (number, any reported demographics): 25 participants, 17 male and eight female. Mean age 29.6 years (range 17–53 years). Participants did not attend another treatment programme in at least year before onset of the study. 13 severe and 12 mild stutterers |
CSP integrates fluency enhancing techniques, tension and stuttering modification techniques, and cognitive–behavioural strategies to deal with the emotional and attitudinal aspects of stuttering. 73.3% of the therapy time was devoted primarily to skill-training exercises targeting speech motor control (e.g. prolongation or smooth blending); 26.7% was devoted primarily to the reduction of the negative emotions and cognitions associated with stuttering Number of hours: 3-week residential programme, two follow-up sessions Delivered by who? Author, clinicians, students, clinical co-ordinator at the centre Control: none Length of follow-up: immediate, 1 year and 2 year Response and/or attrition rate: none |
Nijmegen Speech Motor Test Naturalness judgements SSI PSI Inventory of Interpersonal Situations Percentage of syllables that are stuttered Distorted speech scale of the Speech Situation Checklist The emotional reaction scale of the Speech Situation Checklist Speech Satisfaction Rating Scale S24 Attitude Scale |
Significant overall main effect of therapy on all three measures of speech (percentage of syllables that are stuttered, Brutten distorted speech and dysdiadochokinesis). Percentage of syllables that are stuttered pre- to posttreatment mean difference 9.17% (SE 1.655%; p < 0.0001), pre-treatment to follow-up one 3.09% (SE 0.913%; p < 0.001) pre-treatment to follow-up two 3.79% (SE 0.866%; p < 0.0001). Although the mean scores of all speech measures showed a clear regression at both follow-ups, significant gains relative to pre-treatment levels were maintained. Significant effect of stuttering severity on the speech-related treatment results (F 9.17; p < 0.01). Severe stutterers at baseline gained more from the intervention but higher levels of regression at follow-up than the mild stutterers (p < 0.001). No significant difference between severe and mild stutterers in terms of severity of emotional and cognitive reactions | |
| Ingham et al. 201362 Country: USA Study design: before and after Data collection method: within and beyond clinic audio–visual recordings and a positron emission tomography scanning session Aim: to explore brain activity changes following intervention Detail of participants (number, any reported demographics): 30 participants (22 stutterers and eight controls), 17 males and five females, mean age 35.9 years, range 20–64 years. All had stuttered since childhood and had ‘chronic stuttering’ at least 3% of syllables that are stuttered. All had received a range of previous therapies, but none in the previous 3 years. Participants were part of a larger study |
Modifying Phonation Intervals and PS programmes Contained five phases: pre-treatment, establishment, transfer, maintenance and follow-up MPI: participants taught to reduce voicing. Participants required to meet performance criteria on speaking tasks with feedback via response-contingent auditory signals and counts in the boxes. If participants failed a task the program returned the participant to an earlier stage PS: participants taught to use PS at 40, 70, 100 and 130 SPM. They read aloud with an audio model followed by speaking tasks to gradually shape towards natural sounding speech. Same establishment phase as MPI but no feedback Both programs contained transfer phase with speaking tasks beyond the clinic Hours: varied across participants. Average 8 weeks pre-treatment, 8 weeks establishment, 27 weeks transfer and 64 weeks maintenance Delivered by who? Clinician Control: eight participants not stutterers. 12 stutterers received MPI and 10 PS program Length of follow-up: to completion of transfer phase average 33 weeks Response and/or attrition rate: one failed to complete establishment phase, 10 of the 22 failed to complete to transfer phase. Four in MPI program and five in PS program |
Percentage of syllables that are stuttered Stutter-free SPM Self rating on a naturalness scale Positron emission tomography scans |
This study considered only pre-treatment, establishment and transfer phases Data analysis compares the group who completed the intervention with those who did not and non-stutterers; therefore, aiming to consider a different question. However, from the tables for reading – pre-treatment mean percentage of syllables that are stuttered was 8.8% for those completed. At transfer phase those who completed 0.9 mean percentage of syllables that are stuttered. For monologue – pre-treatment mean 7.1% of syllables that are stuttered for those who completed. At transfer phase mean percentage of syllables that are stuttered was 1.0% for those completed. Reading – for those who completed baseline 186 stutter-free SPM and end transfer phase 225. Monologue – 175 pre-intervention and 199 post intervention. Naturalness baseline 4.8 and post 2.9 |
|
| Ingham et al. 200163 Country: USA Study design: before and after (multiple baseline measures) Data collection method: recording during speaking tasks Aim: to evaluate the MPI program Detail of participants (number, any reported demographics): five males |
Modifying Phonation Intervals a computer-based program that trains stutterers to reduce the frequency of short phonation intervals (maintain a continuous speech flow). Includes establishment, transfer and maintenance. The MPI includes software and an accelerometer and pre-amplifier that are worn on the throat. The system records speech and provides immediate auditory and visual feedback Number of hours: establishment phase daily or twice daily 2–3 hour sessions over 2–3 weeks. Transfer phase average 25 minutes per week over 8 weeks. 12–19 months required for maintenance phase Delivered by who? Clinician directs pre-treatment phase, treatment largely carried out by individual stutterer Control: none Length of follow-up: 1 year and 2 year Response and/or attrition rate: none |
Percentage of syllables that are stuttered Stutter-free SPM Speech naturalness Target range phonation interval frequency |
All participants achieved stutter-free speech and natural-sounding speech at the completion of maintenance | |
| Irani et al. 2012116 Country: USA Study design: mixed methods and also included in qualitative review Data collection method: interviews, clinical data (measures on assessments) Aim: to understand client perceptions of an intensive programme. Detail of participants (number, any reported demographics): seven participants, five males and two females, average age 27 years (range 22–39 years). All had attended the programme, three once or twice previously. Two had not received follow-up therapy. Four were students, one a residential specialist, one a teacher and one a SLP |
Phenomenological approach, retrospective clinical data and interviews Control: none Length of follow-up: participants had attended the programme in 2003–6 and 2008–9 Response and/or attrition rate: N/A Intervention: 9- or 15-day intensive therapy programme conducted during the summer. Utilises both fluency shaping and stuttering modification approaches in addition to CBT. Sessions last 5–7 hours each day with both group and individual sessions. Provided by graduate students, overseen by fluency specialist and clinicians on a 1 : 1patient-to-clinician ratio Four phases of therapy: awareness of stuttering behaviours, process of reducing stuttering behaviours, techniques to modify and improve fluency, and developing a personal maintenance programme. Follow-up therapy in form of weekend intensive workshops, regular therapy or telepractise |
Clinical data from case notes gathered retrospectively. Questionnaire assessing feeling and attitudes (LCB scale, Erickson S24, OASES). Speech samples – conversation, telephone call, reading analysed for % syllables stuttered, type of dysfluency, secondary behaviours, SSI. Current clinical data – LCB, S24, OASES, speech sample, attitudes questionnaire, SSI-3. Treatment outcomes measured via attitudes questionnaire and before/after speech sample. Views and perceptions | Clinical outcomes: SSI ES pre-intervention to post intervention 1.19 (Cohen’s d) (95% CI –0.01 to 2.24). Pre-intervention to time of interview 1.25 (95% CI 0.04 to 2.31). S24 ES pre-intervention to post intervention 1.79 (95% CI 0.46 to 2.89). The percentage of syllables that are stuttered pre-intervention to time of interview was 0.70% of syllables that are stuttered (95% CI –0.42% to 1.73% of syllables that are stuttered). LCB ES pre-intervention to post intervention 0.75 (95% CI –0.38 to 1.78). Pre-intervention to time of interview 0.07 (95% CI –0.99 to 1.11). Percentage of syllables that are stuttered pre-intervention to post intervention. Conversation: ES 1.12 (95% CI –0.07 to 2.17). Pre-intervention to time of interview 1.97 (95% CI 0.59 to 3.09). Reading pre-intervention to post intervention 0.59 (95% CI –0.52 to 1.62). Pre-intervention to time of interview 0.98 (95% CI –0.19 to 2.02). Telephone call pre-intervention to post intervention 0.72 (95% CI –0.40 to 1.75). Pre-intervention to time of interview 2.22 (95% CI 0.78 to 3.38). Descriptive attitude data indicates improvement on measures of attitude change pre- to post intervention | Unclear when the interviews were carried out. Follow-up interview up to 7 or 8 years for some, 2 or 3 years for others. 95% CI data across zero for many measures |
| Iverach et al. 200964 Country: Australia Study design: before and after Data collection method: questionnaires and speech sample Aim: to investigate whether or not the presence of mental health disorders contributes to poor long-term maintenance Detail of participants (number, any reported demographics): 64 participants, 51 males and 13 females, age range 18–73 years (mean 32.2, S.D. = 12). Pre-treatment stuttering severity range 0.3–27.6% of syllables that are stuttered (mean 8.3%, SD 6.5%). 78% (n = 50) had received previous treatment for stuttering |
Intervention consisted of PS and problem-solving to incorporate fluency in everyday life. Four sites used Camperdown Program others La Trobe Smooth Speech Program. Following the intervention half viewed a DVD of themselves using speech restructuring with no stuttering for 10 minutes twice daily for 6 months, whereas the other half did not Number of hours: 1-week intensive group speech restructuring programme followed by seven 2-hour weekly follow-up group sessions Delivered by who? At four of the sites, treatment was conducted by speech–language pathology students under supervision, while treatment at the other sites was conducted by experienced speech–language pathologists Control: none Length of follow-up: 6 months Response and/or attrition rate: none |
Computerised Version of the Composite International Diagnostic Interview The International Personality Disorder Examination Questionnaire Percentage of syllables that are stuttered Self-rated stuttering severity Self-reported avoidance of speaking situations |
There was no significant difference between groups with regard to the additional DVD element. 66% of participants were categorised as having a personality disorder. 30% were identified as having an anxiety disorder. 19% had a mood disorder. The presence of mental health disorders was not associated with higher or lower pre-treatment percentage of syllables that are stuttered. No single mental health disorder had an effect on short-term treatment outcome in terms of percentage of syllables that are stuttered. However, a test for trend suggested that an increase in the number of mental health disorders of any type was associated with poorer short-term treatment outcome for percentage of syllables that are stuttered, but this did not reach significance (p = 0.039). There was a significant association between having a mental health disorder of any type and poorer medium-term treatment outcome (p = 0.007). There was no significant association between having a personality, anxiety or mood disorder and medium-term treatment outcome in terms of self-rated stuttering severity Not possible to identify accurately from the data presented the overall effect of the intervention. Reported by disorder only. ESs (percentage of syllables that are stuttered) for these individuals with a disorder vs. individuals without a disorder ranged from –0.4 to 1.3 immediate post intervention and –1.1 to 2.2 at 6-month follow-up. Mean percentage of syllables that are stuttered for those without disorder approximately seven pre-treatment, 0.5 post intervention and one follow-up |
|
| Jones et al. 200065 Country: Australia Study design: before and after Data collection method: NR Aim: to examine potential predictors of stuttering intervention outcome Detail of participants (number, any reported demographics): 216 participants, 192 males and 58 females, mean age 46 months (SD 9.4 months) |
LP Control: none Length of follow-up: immediate Response and/or attrition rate: 250 out of 261 completed the programme |
Age Gender Period from onset to treatment Stuttering severity |
A median of 11 clinic visits was required to achieve zero or near zero stuttering. There was a significant relationship between stuttering severity (percentage of syllables that are stuttered at first treatment session) and time needed for treatment OR 4.1, 95% CI 2.1 to 7.8 (p < 0.001). There was no association with increasing age on increasing time to onset with longer treatment times | |
| Jones et al. 200524 Country: New Zealand Study design: RCT Data collection method: recorded speech samples Aim: to evaluate the efficacy of the LP in a controlled trial Detail of participants (number, any reported demographics): stuttering pre-school children aged 3–6 years and frequency of stuttering of at least 2% syllables stuttered. 43 males and 12 females. None had received treatment for stuttering during the previous 12 months. 54 randomised: 29 to the LP arm and 25 to the control arm |
LP Control: delayed intervention. Parents told they could receive treatment during the trial at other clinics providing it was not the LP while they were waiting Length of follow-up: 9 months Response and/or attrition rate: seven (13%); the participants withdrawing were on average 9 months older (p = 0.015) |
Frequency of stuttering was measured as the proportion of syllables stuttered, from audio-taped recordings of participants’ conversational speech outside the clinic | Analysis showed a highly significant difference (p = 0.003) at 9 months after randomisation. The mean proportion of syllables stuttered at nine months after randomisation was 1.5% (SD 1.4) for the treatment arm and 3.9% (SD 3.5) for the control arm, giving an ES of 2.3% of syllables stuttered (95% CI 0.8% to 3.9%; p = 0.003). This ES was more than double the minimum clinically worthwhile difference specified in the trial protocol. In an exploratory analysis of the proportion of children with less than 1.0% syllables stuttered at 9 months after randomisation. The proportion was higher in the Lidcombe arm than in the control arm when adjusted for the baseline severity score in a logistic regression model OR 0.13 (95% CI 0.03 to 0.63; p = 0.011) | Because of difficulty with recruitment it was decided to stop the trial before it had obtained the target 110 participants. Three participants allocated to the control arm received other treatment |
| Jones et al. 200825 Country: Australia/New Zealand/USA Study design: RCT (additional follow-up data) Data collection method: audio-recorded speech via telephone conversation and parental interview and questionnaires Aim: to follow-up the children in the Jones et al.24 trial to determine extended long-term outcomes of the programme Detail of participants (number, any reported demographics): 28 children, average age 9 years (range 7–12 years) Details given in Jones et al. 200524 not repeated in this paper |
LP. This paper linked to Jones et al. 200524 For the treatment group, the telephone interview involved questions relating to the children’s speech from the time they completed the LP until the time of the assessment, as well as how satisfied parents were with the LP and with the current speech of the children. Parents of the control children were asked about the treatment history since the children completed the trial Control: children not in the trial Length of follow-up: average 5 years since randomisation (up to 7 years) Response and/or attrition rate: 20 out of the 29 (69%) children in the treatment arm and eight of the 25 children in the control (no treatment) arm were able to be contacted |
Percentage of syllables that are stuttered Frequency of stuttering Parental report |
Of the children in the treatment group, one (5%) failed to complete treatment and 19 had completed treatment successfully and had zero or near-zero frequency of stuttering. Three of the children (16%) who had completed treatment successfully had relapsed after ≥ 2 years of speech that was below 1% syllables stuttered. Overall, there was a significant reduction in frequency of stuttering from randomisation to the time of extended follow-up for the 20 children (paired t-test: mean difference 55.5% of syllables that are stuttered; p = 0.0001). This represents an 80% reduction in stuttering frequency. Meaningful comparison with the control group was not possible because an insufficient number of control children were located and some of them received treatment after completing the trial. Results from the parent questionnaires indicated that eight (40%) children had stuttered at some time during the previous month and 12 (60%) children had not. 10 (50%) children had stuttered at some time since completing treatment and 10 (50%) children had not. Nineteen (95%) parents were satisfied or very satisfied with the LP and one (5%) parent was not satisfied. Seventeen (85%) parents were satisfied or very satisfied with their child’s speech and three (15%) parents were not satisfied | |
| Kaya and Alladin 201266 Country: Turkey Study design: before and after Data collection method: video recording of treatment sessions Aim: to evaluate a hypnosis intervention Detail of participants (number, any reported demographics): 59 participants, 28 had received therapy previously but with little benefit |
Purpose of hypnosis to alleviate anxiety, boost self-confidence and increase motivation for intervention. Consisted of hypnotic induction, relaxation, hypoamnesia, hyperamnesia, past and forward projections, hallucinations. While in deep hypnosis participants practised speaking fluently with positive reinforcement. This also included discussion of transferring fluency and confidence outside sessions. After each session participants practised abdominal weightlifting (with a dumbbell) to strengthen respiratory muscles and improve movement of the diaphragm Hours: eight sessions spread over 8 days each session 60–90 minutes. After each session abdominal weightlifting practised for 15–20 minutes in the clinic and 2 hours at home Delivered by: unclear, presumably a hypnotherapist Control: none Length of follow-up: followed up 1 year later by telephone call Response and/or attrition rate: none |
Occurrences of stuttering ranked on a scale of 1–10 by ‘experienced judges’ | At baseline stuttering severity ranked as 2.10 (SD 0.31) (30–46 occurrences), immediately following intervention stuttering rank 8.25 (SD 0.39) (5–8 occurrences). Mean difference –6.15 (SD 0.5); p < 0.000. 1-year follow-up ‘all improving well except 4 patients helped by family therapy’. These four reported that their stuttering had recurred after 2 months post intervention and attributed this to family-related stress particularly criticism from the family | |
| Kaya 201167 Country: Turkey Study design: before and after Data collection method: video recorded speech sample Aim: to investigate the combined effect of hypnosis and diaphragmatic exercises in the management of stuttering Detail of participants (number, any reported demographics): 93 participants, 79 males and 14 females, mean age 23 years (SD 7.95 years). 35% had received intervention previously, which they reported had achieved little or no benefit |
The purpose of the hypnotherapy component was to alleviate anxiety, boost self-confidence and increase motivation for abdominal weightlifting training. After each hypnotic session, the patient was instructed to practise abdominal weightlifting for two hours at home. The abdominal weightlifting exercises involved lifting a dumbbell (2.0–4.0 kg) with the abdomen for two hours in order to strength the respiratory muscles and the diaphragm. Hypnotic suggestions were utilised to increase motivation for the patient to practise abdominal weightlifting at home Hours: the hypnotherapy consists of eight sessions spread over 8 days and each session ranged from 60 to 90 minutes Delivered by: unclear, presumably the author Control: none Length of follow-up: immediate Response and/or attrition rate: none |
Occurrences of stuttering ranked on a scale of 1–10 by ‘experienced judges’ | At baseline stuttering rank judged as 3.06 (SD 1.33), after intervention 8.06 (SD 1.08). Mean difference –4.99 (SD 1.63). Pre and post measurements were found to be statistically significant (p < 0.000) | |
| Kingston et al. 200368 Country: UK Study design: before and after Data collection method: unclear Aim: to determine how long treatment is likely to take and whether or not treatment time can be predicted. This study, conducted independently in the UK, was designed to replicate an Australian study Detail of participants (number, any reported demographics): 78 participants, 46 males and 20 females, children who began treatment before 6 years of age: 66 completed stage 1. Mean age at first stage 1 clinic visit was 52 months (range 32–71 months) |
LP The data from both British and Australian cohorts were pooled in a meta-analysis Control: none Length of follow-up: unclear Response and/or attrition rate: 12 (15.3%) did not complete stage 1 |
Number of clinic visits required to complete stage 1 of the programme | Per cent syllables stuttered was a significant predictor of time to complete stage 1 (p = 0.029), with an OR of 3.8. There was a non-significant trend suggesting that onset-to-treatment interval is related to treatment time (p = 0.084), with an OR of 0.33. For the combined cohort (total), both percentage of syllables that are stuttered and onset-to-treatment interval are significant. There was a significant correlation between treatment time and both percentage of syllables that are stuttered at the first clinic visit (OR 3.5; p < 0.001) and onset-to-treatment interval (OR 0.52; p = 0.013) | |
| Koushik et al. 200969 Country: Canada Study design: before and after Data collection method: Lidcombe scale, audio-recorded speech sample, parent interview Aim: to evaluate the LP Detail of participants (number, any reported demographics): 11 participants, 9 males and 2 females, mean age 9 years (range 6–10 years). Pre-treatment percentage of syllables that are stuttered ranged from 2% to 27% |
LP: a behavioural treatment Involving verbal response contingent stimulation (acknowledgement, praise and request for self-evaluation) administered by parents Number of hours: weekly visits to clinic and parent home intervention. Median eight clinic visits (range 6–10) Delivered by who? Clinician and parents Control: none Length of follow-up: mean 70 weeks (range 9–187 weeks) Response and/or attrition rate: one child removed from analysis as required supplement to standard programme |
Percentage of syllables that are stuttered SPM Parent rating of severity |
Mean % syllables stuttered baseline 9.2 (SD 7.8) and 1.9 (SD 1.3, range 0.2–3.8%) at follow-up significant difference (p = 0.0002). No association between length of follow-up period and stuttering rate. Explained only 0.04% of the variance pre- to post intervention. Mean SPM baseline 145.8 (SD 22.7) and 179.3 (SD 20.5) follow-up. Significant difference pre- to post intervention (p = 0.0097). Parent data: 70% rated child’s stuttering as no or extremely mild stuttering post intervention. All parents reported enjoying taking part in the programme although 60% reported finding time to practise difficult | |
| Koushik et al. 2011121 Country: USA Study design: cross-sectional Data collection method: retrospective examination of case note data Aim: to examine predictors of length of treatment for the LP. Replicates Jones et al.65 USA study and combines data from an Australian and a UK study Detail of participants (number, any reported demographics): 134 participants, 105 males and 33 females, before one clinic (four children) excluded. All were children who attended one of four clinics 2002–9 and had achieved requirement for stage 2 of the programme. Percentage of syllables that are stuttered was < 1.0 within the clinic and severity rating scores for the previous week of 1 or 2. Mean age at first clinic visit 49.7 months (range 31–71 months) |
LP Number of hours: examines these data Delivered by who? Unclear Fifteen clinicians with varying levels of experience all received 2-day Lidcombe workshop Control: none Length of follow-up: immediate Response and/or attrition rate:165 cases examined 27 (13.5%) had not progressed to stage 2. Dropout for all but five due to families not attending sessions, five due to perception of slow progress |
Number of clinic visits Percentage of syllables that are stuttered |
Median number of clinic visits by which 50% of all children reached near zero stuttering were 11, 10, 14, and 23 visits for each clinic. Median across all was 12 visits. Mean across all clinics 14.1 (SD 7.5, range 4–44). Mean not including outlier 12.4 (SD 5.8, range 4–44). No evidence of an association between number of clinic sessions and age, sex or onset-to-treatment interval. Strong evidence that higher severity associated with more clinic visits (p = 0.004). Children with stuttering severity of 5% of syllables that are stuttered or more approximately a fourfold increased odds of requiring ≥ 12 visits. Some evidence that frequent clinic attendance associated with more clinic visits to stage 2 (p = 0.04). Children who attended more than every 11 days had more than twice the odds of requiring longer than 12 clinic sessions than children who attended the clinic infrequently. Association between frequency of attendance and number of clinic sessions was not significant (OR 0.47; p = 0.07). Association severity and number sessions (OR 0.37; p = 0.01). Meta-analysis of data from this study and two others (n = 444 cases) indicated no evidence of a correlation between age, sex, onset-to-treatment interval and treatment duration. Strong evidence of correlation between stuttering severity and treatment duration with increasing severity associated with increased number of clinic visits (p = 0.0001) | |
| Laiho and Klippi 200770 Country: Finland Study design: before and after Data collection method: videotaped speech sample, questionnaires Aim: to evaluate an intensive stuttering intervention Detail of participants (number, any reported demographics): 21 participants, 16 males and five females, aged 6 years 8 months to 14 years. Two groups those under 10 years (n = 8) and those over (n = 13). Four no previous therapy others 5–40 previous sessions. 29 parents |
Included practising oral motor abilities, examining the speech production system, and exploring the movements of tongue and lips and other articulators during speech. Included pantomime and pseudostuttering. Aimed also to deal with feelings and attitudes related to stuttering and to improve self-esteem and share information about stuttering. Parents worked in groups while children worked in speech groups Number of hours: under-10s course 14 days and over-10s 18 days 2.5–3 hours per day. In addition, parents practised therapy methods for 7.5 hours. Evening group social activities. Held in two parts beginning of summer holiday and end of summer holiday Delivered by who? Speech therapist and a psychologist Control: none Length of follow-up: 9 months. During follow-up period, six no other therapy, seven had 1–4 sessions, two had 12 sessions, four had 20–30 sessions and one had 45 sessions Response and/or attrition rate: none |
Percentage of syllables that are stuttered Characteristics of moments of stuttering Length of stuttering Escape behaviour Avoidance behaviour Above measures combined into stuttering severity classification % improvement |
Immediate post-intervention percentage of syllables that are stuttered had fallen in the case of 14 participants, no change four participants, three participants had a small rise. The mean baseline percentage of syllables that are stuttered as 4.4% and post 2.7%, (38.6% improvement). Statistically significant change (p = 0.01). Amount of avoidance reduced pre- to post 13.1% to 9.5% spoken syllables (p = 0.01). Proportion of repetitions reduced, prolongations and blocks rose slightly. Half had greater proportion of prolongations and repetitions at the end of the course than the beginning. Only avoidance statistically significant change in stuttering behaviour. Increased use of repair behaviours pre- to post intervention; p = 0.01. Four categorised as severe, 14 moderate, three mild pre-course, post intervention none were rated as severe, 14 moderate, three mild, one fluent. Twenty-two parents rated speech as more fluent. At 9-month follow-up, 24 parents rated speech as ‘more fluent’ but no reported changes were statistically significant at 9-month follow-up | |
| Langevin and Boberg 199371 Country: Canada Study design: before and after Data collection method: video- and audio-taped telephone speech samples Aim: to evaluate the CSP intervention Detail of participants (number, any reported demographics): 10 participants, eight males and two females, aged 16–38 years (mean 24.2 years) |
CSP Number of hours: 3-week intensive, 6.5 hours per day. Residential for 2 weeks, participants choose where to live for third. One refresher weekend included in the programme Delivered by who? Not reported Control: none Length of follow-up: 12–14 months Response and/or attrition rate: none Data reported on 10 of 21 who completed the intervention, others incomplete data |
Percentage of syllables that are stuttered SPM Revised Communication Attitude Inventory (S24) PSI SESAS Speech Performance Questionnaire |
Substantial decrease in percentage of syllables that are stuttered for all participants. Mean percentage of syllables that are stuttered during video recording reduced from 14.2 pre-treatment to 0.53 post treatment. Eight participants stuttered on < 1% of total syllables. The mean SPM increased from 126.5 pre-treatment to 140.7 post treatment. Small increase in mean percentage of syllables that are stuttered (2.4%) at follow-up telephone call compared with telephone call immediately after treatment (0.8%). Pre-treatment telephone call mean percentage of syllables that are stuttered was 15.3%. S24 scale scores revealed very negative attitudes (score of 19.6) before treatment. After treatment communication, attitudes were normal (score of 8.4) and remained so during follow-up (score of 12.4). PSI: before treatment high levels of struggle, expectancy and avoidance (56.3%). These levels decreased after therapy to 15.4% and showed only a small increase to 23.2% during the follow-up period. On the SESAS scale, pre-treatment scores showed a low confidence mean rating of 47%. This score almost doubled to 84.9% after therapy and then declined to 70.5 at follow-up. 80% were very or generally satisfied with their speech at the time of follow-up. 80% rated their current speech fluency as generally good | |
| Langevin and Boberg 199672 Country: Canada Study design: before and after Data collection method: videotaped conversation and reading, telephone speech sample Aim: to evaluate the outcomes of an intervention for clutter-stutterers Detail of participants (number, any reported demographics): four of a group of 39 who had taken part in an intervention, four males, aged 18–42 years |
CSP Number of hours: not reported in this paper Delivered by who? Not reported in this paper Control: none Length of follow-up: 1 year, but limited data Response and/or attrition rate: none |
Percentage of syllables that are stuttered SPM % improvement S24 PSI SESAS |
Pre-intervention percentage of syllables that are stuttered during conversation were 5.6%, 9.4%, 8.4% and 3.6%. Post-intervention percentage of syllables that are stuttered were 1.7%, 0.1%, 3.8% and 1.4%. Compared with stuttering participants, half the cluttering participants decreased more than stutterers and half less. The % improvement scores were lower for clutterers than stutterers. Non-speech data indicate that attitude and confidence scores improved for both groups, but the clutterer group improved less | Before immediate post-intervention data for all participants but long-term follow-up data only for one. Limited presentation of data |
| Langevin et al. 200673 Country: Canada and the Netherlands Study design: before and after Data collection method: video recorded in-clinic speech samples, telephone speech samples Aim: to compare treatment outcomes across cultures Detail of participants (number, any reported demographics): 25 participants in the Netherlands, 17 males and eight females, mean age 29.6 years (range 17–53 years). All 25 had received therapy previously, all but one > 5 years earlier. A total of 16 participants in Canada (follow-up data available for 14 participants), 13 males and three females, mean age 24.6 years (range 15–42 years), 15 reported previous therapy, all but one > 2 years earlier |
CSP. Combination of individual, small-group and large-group activities that targeted speech restructuring, stuttering management, self-management goals and attitudinal–emotional change. Three phases: acquisition of fluency and cognitive–behavioural skills (weeks 1 and 2); transfer (week 3); maintenance in months and years following the programme. Self-management integral to the programme. Dutch programme residential, Canadian students choose where to be housed on campus Number of hours: 3-week intensive group-therapy Clients received 90 hours of therapy (6 hours per day) Delivered by who? A clinical team that includes senior Institute for Stuttering Treatment and Research staff, student speech–language pathologists and practising speech–language pathologists who wish to obtain specialised experience. Clinician-to-client ratio varied over the course of the treatment day from 1 : 1 to 1 : 3 Control: none Length of follow-up: 2 years Response and/or attrition rate: 2 out of 18 Canadian cohort lost to immediate follow-up, two further to long term |
Percentage of syllables that are stuttered SPM Speech naturalness scale Maintenance of gains Revised Communication Attitude Inventory (S24) PSI SESAS Speech Performance Questionnaire |
Dutch group mean pre- to post-intervention percentage of syllables that are stuttered was 1.18% to 0.75% in-clinic measure. ES at 2 years 6.86. Beyond clinic telephone measure pre-intervention mean 12% of syllables that are stuttered (SD 10.73%), post intervention 3.24% of syllables that are stuttered (SD 5.25%), 2-year follow-up 7.04% of syllables that are stuttered (SD 8.99%). ES at 2 years. Canadian group beyond clinic telephone measure pre-intervention mean 11.99% of syllables that are stuttered (SD 5.72%), post intervention 0.91% of syllables that are stuttered (SD 0.83%), 2-year follow-up 4.38% of syllables that are stuttered (SD 7.31%). ES at 2 years was 7.62%. 17 (71%) of Dutch group classified as maintainers and 12 (86%) of Canadian group. The percentage of syllables that are stuttered d ESs were medium or typical (0.52) for the Dutch group, larger than typical (0.86) for the Canadian group, and typical to larger than typical (0.69) for the global treatment effect. Dutch group mean naturalness rating at 2-year follow-up 4.03 (SD 0.79; median 4.17; range 2.69–5.19). Canadian group mean naturalness rating at 2-year follow-up 2.85 (SD 0.73; median 2.86; range 1.70–3.77). These scores in range of that reported for non-stutterers. At 2 years post treatment, both groups were maintaining statistically significant reductions in stuttering frequency and improvements in attitudes, confidence and perceptions | |
| Langevin et al. 201074 Country: Canada Study design: before and after Data collection method: recorded telephone calls, postal questionnaires Aim: to explore long term impacts of an intervention Detail of participants (number, any reported demographics): long-term data from 17 participants (but this could be 16 according to source table) 18 pre- to post intervention, 14 males and four females, mean age 23.8 years (range 17–42 years). A total of 17 had received therapy previously up to 10 years earlier |
CSP. Integrates: prolongation and the use of other fluency enhancing techniques, stuttering management skills and cognitive–behavioural skills. Self-management strategies include goal setting, self-measurement, self-evaluation, self-monitoring and problem solving. Three phases: acquisition of fluency and cognitive–behavioural skills; transfer; maintenance. Includes refresher sessions, self-help groups Number of hours: 3-week intensive programme. No further details Delivered by who? Institute for Stuttering Treatment and Research, no further details Control: none Length of follow-up: up to 5 years Response and/or attrition rate: 21 potential participants, three lost to immediate follow-up (two not contactable, one multiple disorders). One further lost to 5-year follow-up? |
Percentage of syllables that are stuttered SPM Maintenance of treatment gains at 5-year follow-up Revised Communication Attitude Inventory (S24) PSI SESAS Speech Performance Questionnaire |
10 had not accessed any refresher sessions, those who had varied from one weekend to 2-week refresher courses. Statistically significant and clinically significant reductions in percentage of syllables that are stuttered and increases in SPM were achieved at immediate post treatment and were maintained over the 5-year follow-up period. Pre-intervention mean percentage of syllables that are stuttered was 15.86%, immediate post-intervention mean 0.9%, 5-year follow-up mean 4.98%. Pre- to post-intervention significant p < 0.001 (large ES –14.96), pre-intervention 5-year follow-up p = 0.002 (large ES –11.49). Pre-intervention mean SPM 117.81, immediate post-intervention mean 147.86. Pre- to post-intervention significant p = 0.005 (large ES 30.05), pre-intervention 5-year follow-up p = 0.004 [large ES 30.79, 15 out of the 18 (or 17/16)] participants classified as maintained speech gains at 5-year follow-up. There were no significant differences among the immediate post treatment and five follow-up measures, indicating that speech gains achieved by the end of the treatment programme were stable over the follow-up period. Low return rate for questionnaires (28%) for 5-year follow-up; therefore, longer-term data not reported. Statistically and clinically significant reductions in S24 and PSI scores and improvements in SESAS scores were achieved at immediate post-intervention measure and maintained at 1 year | |
| Lattermann et al. 200826 Country: Germany Study design: RCT Data collection method: recorded speech sample at home by parent and in clinic, parent rating scale Aim: to evaluate the LP in Germany Detail of participants (number, any reported demographics): 45 participants, 42 males and three females, aged 3 years to 5 years and 11 months. Mean age intervention group 53 months and in control 48 months. Nine had received previous therapy |
LP Number of hours: average 13 sessions attended once per week for 45-minute session. A 15-minute daily home practise Delivered by who? First author SLP and high level of training in programme, carried out by parent at home Control: waiting list. Assigned consecutively Length of follow-up: immediate post intervention Response and/or attrition rate: 58 recruited, 12 did not meet inclusion criteria, one further excluded as incomplete data |
Percentage of syllables that are stuttered at home and in clinic | Home measures. At baseline: mean percentage of syllables that are stuttered was 7.5% (SD 4.7%, range 1.8–20.2%) for the wait contrast group and 9.5% (SD 5.5%, range 2.8–26.6%) for the treatment group. Post-intervention mean percentage of syllables that are stuttered was 6.2% (SD 4.7%, range 0.7–17.4%) for the control group and 2.6% (SD 1.9%, range 0.0–7.3%) for the treatment group. Mean reduction in intervention group 6.9%, reduction in dysfluency rate of mean 70.3% from baseline. Control group mean reduction in percentage of syllables that are stuttered score of 3.6%, a reduction in dysfluency rate of mean 17.6% from baseline. ANCOVA: very significant effect for the interaction group by assessment occasion, F(1,41) = 10.300; p = 0.003, partial η2 = 0.201, the improvement in the treatment group was significantly more than in the control group. Clinic measures: mean reduction of 6.8% of syllables that are stuttered control group, a reduction in dysfluency rate of mean 70.6% from baseline. Control group mean reduction of 1.6% of syllables that are stuttered, a reduction in dysfluency rate of mean 25.4% from baseline. ANCOVA: the difference in improvement between the groups was significant – interaction group by assessment occasion, F(1,41) = 5.400; p = 0.025, partial η2 = 0.116. Both the treatment and control group increased their articulation rates from T1 to T2, treatment group mean of 3.49 at baseline to 3.58 syllables per second post intervention, the control group from 3.16 at baseline to 3.28 syllables | |
| Lawson et al. 199375 Country: UK Study design: before and after Data collection method: participant self-evaluation questionnaires, video recording for study two Aim: to evaluate attitudinal changes following an intensive course Detail of participants (number, any reported demographics): study 1 – 15 participants, 11 males and four females, mean age 16.8 years (SD 2.4 years, range 12–21 years). Four severe, six moderate, two mild, two very mild. Study 2 – 19 participants, 14 males and five females, mean age 16.5 years (SD 3.9 years, range 11–25 years). Three severe, seven moderate, four mild, five very mild |
Groups of similar age. Based on avoidance reduction and block modification. Some elements of PCP Number of hours: 5 days intensive further details not reported in this paper Delivered by who? Two therapists with students assisting Control: none Length of follow-up: 1 month Response and/or attrition rate: 22 recruited, incomplete follow-up data from four, three withdrew from course. 27 recruited for study 2, four did not attend, incomplete data for other four |
PSI Rate of speech Percentage of syllables that are stuttered |
Study 1: no significant change pre- to post intervention in struggle or expectancy scores. Avoidance scores before the course were significantly higher than post intervention [F(1,42) = 13.99; p < 0.001]. No significant change in scores immediate post intervention to 1-month follow-up Study 2: significant overall improvement on the PSI for all areas although avoidance greatest change. Struggle [F(3,122) = 3.03; p < 0.05), avoidance [F(3,122) = 14.02; p < 0.001], expectancy [F(3,122) = 4.80; p < 0.01]. No significant change in rate of speech or percentage of syllables that are stuttered (no further data reported) |
|
| Leahy and Collins 199176 Country: Ireland Study design: before and after Data collection method: speech samples using SSI. Completion of self-character sketch and repertory grid Aim: to evaluate a group intervention Detail of participants (number, any reported demographics): 5 participants, all male, aged 20–26 years |
Group therapy underpinned by Kelly’s personal construct theory. Exploration of theories and views, relationship between change in behaviour and in anticipation explored. Included conversation skills during role-play, experimenting with different fluency techniques, feedback on what most and least useful for individuals Hours: unclear Delivered by who? Student clinician supervised by authors Control: none Length of follow-up: 2 clients attended 5-month follow-up Response and/or attrition rate: none |
SSI Self-character sketch Situations grid |
Data reported for each client individually only. SSI at baseline 3, 24, 14, 10, 31. Post-intervention SSI 0, 10, 4, 0, 10. Character sketches received from three clients only and situation grids from three clients only. No major changes in these detectable. Informal feedback from clients: for two fluency no longer of concern (one fluency not changed but did not see it as much of a problem, other speech poorer but brushed it aside). Further participant reported speech really improved at work but other primary concerns (exams). One reported complete fluency and another reported feeling more optimistic about fluency control. Four reported technique work as important element, agreement regarding usefulness of focus on communication skills. At 5 months the two who attended had SSI of 4 (post intervention 4) and 8 (post intervention 10). Two did not attend but reported fluency going well, one emigrated | |
| Lewis et al. 200827 Country: Australia Study design: RCT Data collection method: audio-recorded speech sample by parents at home, parent questionnaire Aim: to evaluate telehealth delivery of the LP Detail of participants (number, any reported demographics): 18 participants, eight intervention, 10 controls, 14 males and eight females, aged 3–6 years, began intervention (four withdrew) |
LP. Regular telephone calls typically weekly, video demonstration, support via telephone/e-mail, feedback on audio recordings Number of hours: those who successfully completed stage 1 required mean 49 consultations over mean 62 weeks, of mean duration 33.1 minutes Delivered by who? First author, experienced with programme Control: waiting list for 9 months Length of follow-up: 9 months (and 12-month data for intervention group) Response and/or attrition rate: 37 recruited: seven recovered, five services locally, two parents withdrew. One child in intervention and three control lost owing to non-compliance |
Percentage of syllables that are stuttered A responder to treatment defined as a child who showed greater than an 80% reduction in percentage of syllables that are stuttered scores from time of randomisation to 9 months |
Baseline mean, pooled percentage of syllables that are stuttered scores 6.7 intervention group and 4.5 controls. Mean 9-month percentage of syllables that are stuttered scores 1.1 for the experimental and 1.9 for controls. ANCOVA: 69% decrease in frequency of stuttering intervention compared with controls (95% CI 13% to 89%; p = 0.04). Adjusted treatment effect (sex, age, family history, severity) estimated to be a 73% decrease in stuttering (95% CI 25% to 90%; p = 0.02). Six out of the eight experimental children responded, while only 2 of the 10 control children met the responder criterion through natural recovery (p = 0.054). 87% of parents reported telehealth process had been positive. At 6 months and 12 months 100% of parents rated themselves as very satisfied with their child’s speech | |
| Lincoln and Onslow 1997122 Country: Australia Study design: follow-up data only Data collection method: parent collected tape recording, request and details of how to collect sent annually Aim: to collect long-term follow-up data Detail of participants (number, any reported demographics): 43 participants, recruited from two treatment centres, mean age 6 years and 4 months, range 4 years and 9 months to 9 years and 8 months |
LP Number of hours: mean 10.5 clinic sessions Delivered by who? N/A Control: none Length of follow-up: 7-year data for two children, 4-year follow-up data for others Response and/or attrition rate: 59 out of 123 invited agreed to participate. 16 failed to supply recordings required and were removed from study |
Percentage of syllables that are stuttered Parent questionnaire |
Reported as two groups, one group who had taken part in previous research (n = 9) and second group who had received programme but not taken part in a research study. Group one reported by individual child range 0–1.4% of syllables that are stuttered, mean 0.3% of syllables that are stuttered. Group two mean 0.5% of syllables that are stuttered, range 0.3–0.5% of syllables that are stuttered. Parent report: no children had attended for treatment for stuttering in previous year, 44% reported carrying out techniques during previous year, 71% reported child had begun to stutter in previous year. 95% reported that someone had told them that their child may be stuttering in the previous year | |
| Lincoln et al. 199677 Country: Australia Study design: before and after Data collection method: tape-recorded speech sample during clinic visit, parent rating of severity, parent collected tape recording Aim: to evaluate an operant treatment for school-age children Detail of participants (number, any reported demographics): 11 participants, 10 male and one female, age range 6 years and 10 months to 12 years and 4 months, mean age 8 years and 3 months. Three severe, five moderate, three mild stutterers |
LP. Operant programme using parent-treated response contingent stimulation. Parents praised stutter free speech in a warm and enthusiastic manner. Stuttered speech corrected by requesting the child to repeat. Ratio of praise to correction individualised for each child. Following instatement phase child enrolled in maintenance programme when achieved 1% or 1.5% of syllables that are stuttered. If child failed to meet performance criteria causes discussed with parent and child and strategies implemented Number of hours: weekly 1-hour sessions during instatement programme. 3–4 week maintenance programme designed for each child, typically visit 2 × 2-weekly then 2 × 4-weekly, then 2 × 8-weekly, then 2 × 16-weekly, then 2 × 32-weekly. Median 12 sessions to reach maintenance (range 4–39) Delivered by who? Three clinicians. Both parents trained for three participants, mothers only for five and fathers only for three Control: none Length of follow-up: 2 years Response and/or attrition rate: 22 recruited, nine did not comply with data collection requirements, two did not comply with treatment programme requirements. Seven continued to participate in maintenance programme, four withdrew from study before completing maintenance owing to personal circumstances |
Percentage of syllables that are stuttered SPM Rating scale 1 = normal speech, 10 = extremely severe stuttering Parent survey |
Baseline mean 5% of syllables that are stuttered to 18.9% of syllables that are stuttered. One week to 12-month follow-up, mean 0% of syllables that are stuttered to 5.1% of syllables that are stuttered (data presented as figure only). Additional data for three children treatment most successful for and least successful. All children maintained decreased stuttering rates at 12-month follow-up. Reduction in percentage of syllables that are stuttered was not at the expense of SPM reduction | |
| Lutz 200978 Country: Germany Study design: before and after Data collection method: assessment through standardised questionnaires before and after the treatment, 3-month follow-up, also assessment of parents who were not involved in the workshop and speech and language therapists who were external therapists of the children from the parents who took part in the study Aim: to evaluate if the participation at a workshop for parents of children who stutter changes the thinking of parents positively, changes the support of parents in intervention positively, and has a positive effect on the stutter symptomatic of the child Detail of participants (number, any reported demographics): 11 parents of children who stutter |
Conversations between parents of children who stutter; lessons about the theory of stuttering; removal of taboos about stuttering; change of attitude towards stuttering; tricks and tips for parents – through tasks for self-awareness training, talks, reflections and group works Number of hours: one weekend workshop, duration 12 hours Delivered by who? Speech and language therapist specialised in stuttering Control: yes, parents of children who stutter who did not take part in the workshop Length of follow-up: 3 months Response and/or attrition rate: no dropouts |
Change of attitude towards stuttering Feedback about contents of the workshop Understanding of intervention programme Changes in symptomatic of stuttering of the child |
Change of attitude towards stuttering: 92% of the 11 participants confirmed that their attitude towards stuttering has changed immediately after the workshop and 3 month later. Feedback about contents of the workshop: 83% of the participants were happy about the contents of the workshops. In comparison with the control group a distinct difference is observable between the attitude of the parents from the control group and the parents who took part in the workshop: parents who took part in the workshop changed their attitude towards the phenomenon stuttering. External speech and language therapists were asked about the parents’ understanding of the intervention programme. Five out of six speech and language therapists confirmed a distinct improvement of parents’ understanding; four out of six described more interest of parents towards the therapy 5 out of 7 children observed a positive qualitative improvement of the stuttering symptomatic of their child |
|
| Mallard 199879 Country: USA Study design: before and after Data collection method: parent report Aim: to evaluate a family-orientated therapy programme Detail of participants (number, any reported demographics): 28 children, 21 males and seven females, age range 5–12 years. Furthermore, 34 parents |
South West Texas Program/Rustin Program. Emphasises social skills training and parental involvement. Parent groups and child groups. Fluency-shaping speech skills (such as adopting a slower rate of speech than normal, proper breathing, and starting the voice gently and stuttering modification procedures) and social skills in week one. Transfer, problem-solving and negotiation in week two. Each family developed a plan for managing stuttering upon their return home with tasks Number of hours: 2 weeks intensive Delivered by who? Therapist. Both parents and stuttering child had to attend and siblings also encouraged Control: none Length of follow-up: at least 1 year Response and/or attrition rate: none |
Percentage of children no longer needing formal therapy | 23 children (82%) did not require further therapy. Of the five enrolled in further therapy three received treatment for other speech and language problems. Most frequently mentioned topic identified by parents as most important for them in managing stuttering following therapy was letting child take responsibility (25 parents) followed by family discussion (13 parents), listening (12 parents) and desensitisation (11 parents) | |
| Menzies et al. 200828 Country: Australia Study design: RCT Data collection method: video recording and recorded telephone speech samples Aim: to study the effects of speech restructuring treatment on social anxiety, and study the effects on anxiety and stuttering of a cognitive–behaviour therapy package Detail of participants (number, any reported demographics): 30 participants, 25 males and five females, age range 18–66 years. Sixteen had never received treatment for their stuttering,14 had received some form of treatment for their stuttering but not in the previous 12 months. Complete follow-up data only for 14. At baseline mean stuttering severity 8.0% of syllables that are stuttered (SD 5.0%, range 0.9–27.6%) |
Intervention arm received speech restructuring and CBT. CBT focused on reducing speech-related anxiety. It incorporated cognitive restructuring, graded exposure and behavioural experiments. Speech restructuring: modified One-Day PS Instatement Program. Consisted of individual PS teaching sessions, a 7-hour group day in which participants instated stutter-free speech, and four further individual sessions in which participants practised their new speech pattern Number of hours: intervention arm – 10-week (15 hours) CBT followed by 14 sessions (14 hours) speech restructuring. Three months of maintenance sessions offered Delivered by who? CBT delivered by one of the authors a clinical psychologist, speech restructuring by SLP Control: speech restructuring only. Received no intervention for first 10 weeks then same speech restructuring sessions as intervention group Length of follow-up: 12 months Response and/or attrition rate: 32 recruited, two lost to follow-up. Five from control group withdrew from intervention. Data at 1-year follow-up available for 19 (speech) and 14 (psychological measures) |
Percentage of syllables that are stuttered Multiaxial psychiatric interview Diagnostic and Statistical Manual of Mental Disorders general assessment of functioning scale Clinical assessment of social anxiety Social Phobia Anxiety Inventory Fear of Negative Evaluation Scale Social Avoidance and Distress Scale Beck Anxiety Inventory Beck Depression Inventory-II Unhelpful Thoughts and Beliefs About Stuttering (UTBAS) measure |
Participants in the experimental group had superior, sustained and often continuously improving measures of psychological functioning in relation to the control group. Participants in the experimental group who had received the CBT package scored, on average, 21.3 points higher on the general assessment of functioning scale than those in the control group (95% CI 12.6 to 32.7 points; p < 0.005). The experimental group displayed significantly less avoidance at final follow-up than the control group (score: 95% CI 17 to 48). No participant in the experimental group retained a diagnosis of social phobia at follow-up, despite two-thirds being diagnosed with the condition at baseline. The control group intervention did little to eliminate the high rate of social phobia. No difference in percentage of syllables that are stuttered between the two groups at follow-up. The additional CBT treatment given to the experimental group had no further impact on the stuttering reduction resulting from their speech restructuring treatment. Post-treatment stuttering frequency (percentage of syllables that are stuttered) at follow-up was around half that at baseline. Group mean for intervention at recruitment 7% of syllables that are stuttered at follow-up 3–4% (taken from figure), for controls 8–9% baseline 3–4% follow-up | |
| Millard et al. 200880 Country: UK Study design: before and after Data collection method: video-recorded speech samples Aim: to evaluate parent–child interaction therapy Detail of participants (number, any reported demographics): six participants, four male and two female, aged 3 years and 3 months to 4 years and 10 months |
Parent–Child Interaction Therapy. Initial consultation followed by introduction of ‘Special Time’ during which parents practise interaction targets during play with the child. Programme includes parent management strategies based on behavioural methods together with parent-identified interaction targets. Home-based consolidation period following clinic sessions Number of hours: six sessions of clinic-based therapy and 6 weeks of home consolidation Delivered by who? Specialist SLTs Control: none Length of follow-up: 12 months Response and/or attrition rate: two completed follow-up to 7/8 months only |
Percentage of syllables that are stuttered Stuttering severity score (0–7) based on duration of three longest stutters, degree of tension and secondary behaviours |
Four out of the six children studied significantly reduced the frequency of their stuttering with both parents by the end of the therapy phase. Three children reduced stuttering severity level to zero (from 5, 3, 2) and were discharged. One reduced from 2 to 1 and was also discharged. Two children had severity scores of 2 at follow-up (reduced from 4 and 5) and required further intervention | Data reported by each individual child |
| Millard et al. 200981 Country: UK Study design: before and after Data collection method: video recording, parent questionnaire Aim: to evaluate Palin Parent–Child Interaction therapy Detail of participants (number, any reported demographics): 10 participants (six intervention and four control), nine male and one female, age range 3 years and 7 months to 4 years and 11 months |
Palin Parent–Child Interaction therapy. Initial assessment, followed by six sessions of clinic-based therapy (incorporating interaction strategies, family strategies and direct fluency strategies), 6 weeks of home-based therapy and regular review sessions for up to 1 year post therapy Number of hours: 6-week package of weekly 1-hour clinic sessions. Six weeks’ home practise. Progress reviewed at 3 weeks, 3 months, 6 months and 1 year Delivered by who? Specialist SLTs Control: no intervention, families completed video recordings Length of follow-up: 1 year Response and/or attrition rate: none |
% stuttered words Parent rating |
All six children who received therapy and one child in the no-treatment condition significantly reduced stuttering frequency over the period of the study. This was associated with therapy in four cases. Families who participated in therapy reported reduced impact and increased knowledge and confidence in managing stuttering at the end of the study | Data reported by each individual child |
| Miller and Guitar 200982 Country: USA Study design: before and after Data collection method: video recording in clinic and home Aim: to evaluate long-term outcomes of the LP Detail of participants (number, any reported demographics): 15 participants, 11 male and four female, mean age 3 years and 9 months (SD 8.1 months; range 2 years 5 months to 5 years 9 months) |
Standard Lidcombe treatment Number of hours: average number of clinic visits for the participants to reach the end of stage 1 (essentially stutter-free in all situations) was 19.8 (SD 10.7, range 6–44). The median number of sessions was 17 Delivered by who? SLPs who had not used the programme previously but received two days training, assisted by students Control: none Length of follow-up: 12 months Response and/or attrition rate: 17 had been recruited, one withdrew one lost to follow-up |
Percentage of syllables that are stuttered SSI |
Mean baseline percentage of syllables that are stuttered 12.6% (SD 7.38%, range 5.9–24%). Mean follow-up percentage of syllables that are stuttered 0.5% (SD 1.1%, range 0–3.7%). An average reduction in stuttering frequency of 96%. Significant pre- to post-intervention change; p < 0.001; ES 2.3. Baseline SSI-3 total overall score 24.9 (SD 5.7, range 18–37, moderate to very severe). Mean follow-up SSI-3 total overall score 3.5 (SD 5.8, range 0–16, normal fluency to mild). An 86% reduction in severity of stuttering. Eleven children evidenced no stuttering in the follow-up and 13 were considered to be completely fluent by their parents. The difference between the baseline and follow-up SSI scores was significant; p < 0.001; ES 3.7 | |
| Nilsen and Ramberg 199983 Country: Sweden Study design: before and after Data collection method: tape-recorded speech samples reading and retelling a story, visual analogue scales Aim: to evaluate an intensive programme for adolescents Detail of participants (number, any reported demographics): 13 participants, 11 males and two females, aged 13 years to 17 years and 9 months, mean age 15 years and 2 months. All referred to programme by SLTs all had received therapy or consultations previously. One mild, five moderate, seven severe stutterers |
Residential individual and group therapy encompassing dealing with stuttering, stuttering more fluently and development of social and communication skills. Individual therapy as well as group sessions. Each participant had own therapist. Individual sessions mostly focused on motor speech control, attitudes and emotional obstacles tailored for individual. Group sessions practised techniques, role play, group exercises Number of hours: 21 days divided into three sections over a 6-month period. Evening social activities, games and sports Delivered by who? Experienced therapists, a drama pedagogue and youth leaders (who stuttered and had experienced intervention) Control: none Length of follow-up: immediate post intervention Response and/or attrition rate: 15 had been recruited, one withdrew owing to personal problems, one withdrew owing to illness |
Rating of severity by independent listener (SLT) on 3-point criteria of mild, moderate or severe stuttering Rating of severity and communication problems by therapist on rating scale. Results measured by distance in millimetres on visual analogue scale. Social skills evaluated by youth leaders via rating scale LCB scale Questionnaire to participants |
Over all measures 12 had a change on at least one aspect measured. Independent rating: six participants positive change, seven did not change. Post-intervention rating two mild, nine moderate, two severe. Therapist rating five positive change, six no change, two negative change in stuttering severity. Social skills: nine positive change, one no change, three negative change. LCB: five positive change, one no change, seven negative change. No significant change for the group. Nine participants satisfied or very satisfied with the programme | |
| O’Brian et al. 200384 Country: Australia Study design: before and after Data collection method: video- and audio-recorded speech samples Aim: to evaluate the Camperdown Program Detail of participants (number, any reported demographics): 30 participants, 21 male and nine female, age range 17 to 58 years. 10 had received no previous treatment for stuttering. The other 20 had received some form of treatment 4–30 years previously. Average time since treatment was 12.8 years |
The Camperdown Program. Four stages: individual teaching sessions, a group practise day, individual problem-solving sessions and a performance-contingent maintenance stage. Participants learn PS and self-evaluation of stuttering severity. Progression through programme, dependent on achieving severity targets Number of hours: average 3.8 hours individual sessions during phase 1. Mean time required to reach the final phase was 20.1 hours (range 13–29 hours) Delivered by who? Clinician. At group practise day groups of three, with two clinicians for the first six cycles and with three clinicians for the remainder of the day Control: none for intervention, use of matched normal speakers for naturalness outcomes Length of follow-up: 12 months Response and/or attrition rate: 30 recruited, five lost during first phase, four withdrew after group practise day, five lost during final phase |
Percentage of syllables that are stuttered SPM Speech naturalness Self-report inventory |
Complete data for 16 to 1-year follow-up. By the end of the group practise day, all participants had achieved natural sounding speech that contained minimal stuttering (NAT rating 1–3, severity rating 1–2) while talking in a group situation in the clinic. Of those 25 participants, 21 subsequently generalised this result to situations beyond the clinic during the individual problem-solving sessions. Mean pre-treatment stuttering rate 7.9% of syllables that are stuttered (n = 21). At maintenance stage group mean decreased to 0.4% of syllables that are stuttered and remained stable at 0.5% of syllables that are stuttered at 6 months post-performance contingent maintenance stage (n = 18) and 0.4% of syllables that are stuttered at 12 months maintenance (n = 16). 10 participants (56%) achieved mean naturalness score either below or within one NAT scale value of matched control speakers. The mean naturalness rating was 4.5 (SD 1.9, range 1.3–7.3) and for matched control participants 3.6 (SD 2.1, range 2.0–4.7). The difference between the groups was significant (p = 0.025) but was less than one naturalness scale value. The reported group mean daily severity rating pre-treatment was 5.4 and post treatment 2.8. Majority of participants indicated that they had control over their stutter for ‘half’ or ‘more than half the time’. No participant reported control over stuttering all of the time. All but two participants scored the difficulty in learning PS on the midpoint of the scale or as easier than that. However, seven responded with the ‘difficult’ half of the scale when indicating how difficult it was to use PS outside the clinic and 10 reported the use of PS as moderately to very uncomfortable in settings beyond the clinic | |
| O’Brian et al. 200885 Country: Australia Study design: before and after Data collection method: telephone-recorded speech sample Aim: to evaluate telehealth delivery of an intervention Detail of participants (number, any reported demographics): 10 participants, eight male and two female, aged 22–48 years (mean 34 years). Six had attended speech restructuring treatment programmes as adults 5–25 years previously (mean 15 years previously), one had received a few sessions of speech restructuring treatment as an adult, two had received minimal treatment as children and one had never received treatment. Pre-treatment stuttering severity ranged from very mild (2.4% of syllables that are stuttered) to moderately severe (10.8% of syllables that are stuttered). Mean stuttering rate pre-treatment for the group was 6.9% of syllables that are stuttered |
Telehealth adaptation of the Camperdown Program. Phases of: teaching PS and self-evaluation scales; instatement of natural-sounding stutter-free speech; generalisation of stutter-free speech; maintenance of treatment gains via telephone contact Number of hours: ‘as little clinician contact as possible with telephone consultations if and when required’. Average 8 contact hours Delivered by who? Clinician Control: none Length of follow-up: 6 months Response and/or attrition rate: none |
Percentage of syllables that are stuttered SPM Self-reported stuttering severity Speech naturalness |
Mean 82% reduction in stuttering frequency from baseline to immediate follow-up and 74% reduction at 6 months. Significant individual variation in response. 7 out of the 10 participants achieved > 80% reduction in stuttering, but some individuals had a 33% reduction in stuttering. At 6-month follow-up only four retained > 80% reduction in percentage of syllables that are stuttered, three of these had previously completed an intensive PS programme, whereas the final one had received no prior treatment. All participants increased speech rate, group mean increased from 184 SPM to 228 SPM. It remained fairly stable at the 6-month post-treatment assessment occasion (224 SPM). Before commencing treatment, 9 out of the 10 participants reported situations in which their worst stuttering self-report was 7–9 on the 9-point scale (1 = no stuttering, 9 = extremely severe stuttering). However, immediately after treatment, four out of these nine reported a worst self-report of 4, four reported a worst self-report of 3 and one reported a worst self-report of 2. Those scores had reportedly decreased still further for eight out of the participants 6 months later | |
| O’Brian et al. 201386 Country: Australia Study design: before and after Data collection method: tape-recorded speech sample during clinic visit, parent rating of severity, parent collected tape recording Aim: to investigate efficacy of the programme in a community setting and factors associated with outcomes Detail of participants (number, any reported demographics): 57 children, 50 males and seven females, age range 2 years and 7 months to 6 years and 4 months (mean 4 years and 5 months) |
LP Number of hours: median number visits 11 over median 24 weeks Delivered by who? SLPs Control: none Length of follow-up: 9 months Response and/or attrition rate: 12 had withdrawn from treatment at 9 months (although supplied data) |
Percentage of syllables that are stuttered Parent-reported severity rating |
37 (64.9%) children had completed stage 1 of the programme by 9 months. For all 57 children at 9 months mean percentage of syllables that are stuttered was 1.7% (SD 2.1%; large range 0.1–13%), 47% had percentage of syllables that are stuttered of < 1%. Baseline mean 5.2 stuttering severity (scale 1–10). At 9 months mean 2.1. Issues with clinician adherence to recommended programme – 49% more likely to schedule 30-minute rather than 45- to 60-minute sessions and mean 15.4 days between visits rather than weekly. Pre-treatment stuttering severity associated with longer time to complete stage 1 (p < 0.001). SLPs who had received training in the programme associated with larger number of clinic visits (76% more) to complete stage 1 (p < 0.001). Training associated with 54% lower stuttering levels (p < 0.0003) than untrained clinicians | |
| O’Donnell et al. 200887 Country: Canada Study design: before and after Data collection method: telephone-recorded speech sample Aim: to evaluate SpeechEasy including consistency of effect Detail of participants (number, any reported demographics): seven, five males and two females, five had participated in a previous study on the efficacy of the device, aged 24–53 years (mean 36 years). Two participants were enrolled in therapy and another attended a self-help group for people who stutter for a portion of the study, all had received therapy in the past |
Participants were each fitted with a programmable SpeechEasy in-the-canal device Number of hours: participants varied with respect to average hours of daily use, ranging from 2 hours for participant 3 to 15 hours for participant 2. Participants 6 and 7 also reported large amounts of daily wearing time at 5.2 and 11.6 hours of use, respectively. The remaining participants did not record hours of use in their logbooks, although they verbally reported that they wore the device on a daily basis Delivered by who? Device Control: none Length of follow-up: 16 weeks Response and/or attrition rate: all but one participant experienced interruptions during the intervention, two terminated early |
PSI Self rated severity Erickson scale of communication attitudes Views of the device and frequency of use |
All participants exhibited less stuttering with the device than without at the beginning of the study, with a group mean reduction in stuttering of 87%. However, at the end of the study four experienced a reduction in stuttering when wearing the device, but three exhibited more stuttering with the device than without in the laboratory. In a home setting, five exhibited some instances of reduced stuttering when wearing the device and three of these exhibited relatively stable amounts of stuttering reduction during long-term use. Five participants reported a reduction in stuttering frequency while using SpeechEasy, found SpeechEasy easy to use and that it did not interfere with their ability to speak. Two participants reported that SpeechEasy was not beneficial. All but one participant reported that the physical sensation of wearing the device did not interfere with their ability to speak. The majority of participants in the current study indicated that using the device was easy and effortless. Five reported that they felt that the benefits of the device outweighed its costs and would be interested in acquiring a device of their own | Most data reported by individual participant, much of paper evaluates in-laboratory assessment |
| Onslow et al. 199429 Country: Australia Study design: controlled before and after. Drawn from waiting list at two clinics, allocated to intervention or control arms at clinic level Data collection method: conversation during clinic visits, parental severity rating, tape-recorded speech sample Aim: to evaluate an intervention Detail of participants (number, any reported demographics): 11 controls, four male and seven female, mean age 3 years and 7 months. 12 intervention group, eight male and four female, mean age 3 years and 7 months |
The operant programme: parental verbal contingencies, positive input and prompting for target responses. In-clinic sessions and home practise. Maintenance programme over 92 weeks based on needing to continually meet speech performance targets Number of hours: median 10.5 1-hour clinic sessions, median 84.5 days from start of intervention to maintenance programme, 10- to 15-minute sessions at home carried out regularly Delivered by who? Clinician (first author) Control: children on a comparator clinic’s waiting list (majority withdrew and asked for treatment to begin) Length of follow-up: 12 months Response and/or attrition rate: 22 controls recruited, seven did not comply with assessment requirements, one relocated, three withdrew consent. 18 recruited intervention group, five treatment not completed |
Percentage of syllables that are stuttered SPM Parent views |
Parent survey returned by only five and sent to only three controls; therefore, data not extracted. Poor reliability for rating of SPM, data only for four reported and, therefore, not extracted. All children in intervention group showed decrease in percentage of syllables that are stuttered to ≤ 1% and an average severity rating of 2.0 and, therefore, progressed to the maintenance phase. Eight moved through this programme without any failures, two were lost to follow-up during maintenance, one failed to meet criteria at third assessment and one at fifth assessment. Data reported by individual as figures only | |
| Onslow et al. 199088 Country: Australia Study design: before and after Data collection method: audio recording in clinic and at home Aim: to evaluate the LP Detail of participants (number, any reported demographics): 4 participants, aged 3 years 2 months to 5 years 3 months |
Parent-administered verbal stimulation. Parent and child seated together and engaged in conversational speaking task, with stutter-free utterances rewarded with praise. Stuttered utterances noted by parents and request for repetition. During clinic sessions clinician trained parents in techniques. At conclusion of treatment placed on maintenance programme based on maintaining performance criteria Hours: sessions conducted at home regularly for 10-minute periods. Clinic sessions 5–7 ranging from 30 to 80 minutes Delivered by: clinician/parent Control: none Length of follow-up: up to 9 months Response and/or attrition rate: none |
Percentage of syllables that are stuttered SPM Stuttering per minute of speaking time Syllables spoken 10-point scale of severity 10 = most severe, 1 = least severe Speech naturalness |
Data reported for each participant individually and in graph form only. percentage of syllables that are stuttered in general data show reduced stuttering with improvement maintained over 9-month period. All showed an increase in syllable output during the post-treatment period. All parents reported no stuttering post treatment (although clinician ratings were of a small number of stutterings). Clinician ratings of naturalness varied however there was no increase in perceived unnaturalness | |
| Onslow et al. 199289 Country: Australia Study design: two studies before and after (controls not stutterers) Data collection method: recorded speech samples during conversation and monologue Aim: to compare speech naturalness of treated stutterers vs. non-stutterers Detail of participants (number, any reported demographics): study one – 14 participants, all male, Seven stutterers and seven who did not stutter, age range 13–36 years. Study two – 36 participants in same treatment programme, 33 males and three females, age range 9–50 years, mean age 21 years |
Clients in PS residential programme. Consisted of establishment phase shaping PS into normal sounding speech followed by self-evaluation one and transfer programme with second self-evaluation phase and finally maintenance Number of hours: 2 weeks residential phase, weekly visits transfer phase, 126-week maintenance programme Delivered by who? Clinician Control: seven non-stutterers matched for age Length of follow-up: 2 weeks after residential phase Response and/or attrition rate: none |
Speech naturalness scale Percentage of syllables that are stuttered SPM |
Mean naturalness score for treated stutterers was 5.49 (SD 1.01) and non-stutterers 3.25 (SD 0.77). The scores significantly differentiated the two groups (p < 0.001). Two weeks after residential naturalness scores were little changed. Pre-treatment percentage of syllables that are stuttered and SPM scores showed low but significant correlations with post-treatment naturalness scores (0.38% of syllables that are stuttered and –0.44 SPM). More severe stuttering pre-intervention = worse speech naturalness post intervention | |
| Onslow et al. 199690 Country: Australia Study design: before and after Data collection method: audio-taped speech sample, covert telephone sample (posing as hospital public relations staff) Aim: to evaluate a PS programme Detail of participants (number, any reported demographics): 18 participants, of these 12 completed the entire programme (3- to 7-year follow-up), 15 male and three female, mean age 21 years (SD 8.4 years, range 10.7–41.6 years). All had history of previous treatment with short-term partial benefit followed by complete relapse |
Residential and non-residential components. Residential phase client learns PS at increasing rates of SPM with criteria of speech naturalness required in order to progress to increased rate. Followed by transfer phase using techniques outside setting and self-evaluation phase 1. After approximately 2 weeks of residential second phase of self-evaluation with weekly clinic visits. Final maintenance phase 126 weeks of speaking tasks, recording and clinic visits. None attended a self-help group during study period. None attended booster or refresher courses during period of study Number of hours: during residential clients live in treatment setting 24 hours, 7 days a week, usually 2 weeks. Self-evaluation phase 2 usually weekly for 12 weeks. Maintenance 126 weeks Delivered by who? Clinicians Control: none Length of follow-up: up to 3 years Response and/or attrition rate: 32 recruited, six failed to learn the technique satisfactorily, eight declined to regularly attend and make recordings. 18 completed intensive phase. Data collected for 3 up to 7 years |
Percentage of syllables that are stuttered SPM Speech naturalness |
Those who withdrew after residential did not differ in terms of percentage of syllables that are stuttered 1 week post treatment from those who completed second self-evaluation phase. Percentage of syllables that are stuttered scores generally at or near zero for 9 out of the 12 clients, the other three scored > 1%. No reduction in SPM, indeed participants increased SPM during post-treatment phase. All achieved post-treatment naturalness scores in the range of 2–4 (non-stuttering speakers). The majority (eight) did not show a regression in percentage of syllables that are stuttered or naturalness during post-treatment period | |
| Onslow et al. 2002123 Country: Australia Study design: cross-sectional Data collection method: audio-recorded speech samples, conversation in clinic and at home Aim: to examine any acoustic changes associated with completing the programme Detail of participants (number, any reported demographics): eight males who completed the LP |
LP Number of hours: not reported in this paper Delivered by who? Not reported in this paper Control: none Length of follow-up: immediate Response and/or attrition rate: none |
Percentage of syllables that are stuttered Mean length of utterance Articulation rate Spectrogram acoustic analysis of speech timing measures (including inter-vocalic interval, vowel duration, voice onset time) |
No significant changes in any measures were detected after treatment. The reduction in stuttering achieved following the programme are not due to change in speech timing | |
| Pape-Neumann 200491 Country: Germany Study design: before and after Data collection method: questionnaires and speech samples directly before treatment, 4–6 weeks after end of treatment, 1 year and 2 years after treatment Aim: to evaluate stuttering intervention on a longitudinal basis Detail of participants (number, any reported demographics): 100 participants were first selected. No inclusion or exclusion criteria was chosen, just a stutter needed to be obvious (and participant in therapy with any speech and language therapist) |
No specific methods: different external speech and language therapist took part with their patients, the study focused on evaluation of any therapy approach (included were single, group and intensive intervention programmes) Number of hours: variable, depended on the therapy programme the individual speech and language therapist chose Delivered by who? Speech and language therapists Control: none Length of follow-up: 1 year and 2 years Response and/or attrition rate: from 100 participants results from 82 were analysed, as the other participants did not finish their intervention up to the second measurement point |
Avoidance of communication Attitude towards communication Self-judgement of stuttering in social situations Impact on all day life Speech samples for quantitative data about stutter symptomatic (including stutter frequency, naturalness of speech, speech rate) |
Children: ESs for speech samples for quantitative data about stutter symptomatic were calculated – stutter frequency = 0.63, naturalness of speech = 0.60, speech rate = 0.37. Additionally, ESs for avoidance of communication, attitude towards communication, self-judgement of stuttering in social situations and impact on all day life were 1.70 (one value for all ESs). Adolescents and adults: ESs for speech samples for quantitative data about stutter symptomatic were calculated – stutter frequency = 0.77, naturalness of speech = 0.44, speech rate = 0.35. Additionally, ESs for avoidance of communication (1.84), attitude towards communication (2.26), self-judgement of stuttering in social situations (2.15) and impact on all day (2.46). In general, improvement could be observed in all measured outcomes. A t-test result showed for every outcome a significant positive improvement from p < 0.1 or smaller | |
| Pollard et al. 200992 Country: USA Study design: before and after Data collection method: video- and audio-recorded speech samples, questionnaire, diary Aim: to evaluate SpeechEasy in a natural setting Detail of participants (number, any reported demographics): 12 participants, six males and six females, aged 18–62 years (mean 34.2 years). All had received treatment in the past and one attended a stuttering support group during the study period |
SpeechEasy in-the-canal units. Includes instructing the wearer to attend to the second speech signal and teaching several active techniques to alter one’s speech pattern, such as easy vocal onsets, prolongations, continuous phonation. DAF delay settings around 50–60 milliseconds were suggested but final settings were participant preference Number of hours: suggested 5 hours per day. Average wear time 5 hours. Range from none (one participant) to 10.4 hours per day. 9-week treatment phase with bi-weekly visits for recording speech Delivered by? Device Control: none Length of follow-up: 4 months Response and/or attrition rate: none |
SSI Percentage of syllables that are stuttered OASES PSI Logs of usage Participant views |
Data for nine included in analysis. A statistically significant effect of SpeechEasy immediately post fitting compared with baseline [PSI scores t(16) = 3.13; p = 0.014]. Effect not maintained at follow-up. No other pre- to post assessments reached significance (p > 0.05 for SSI and OASES). Large individual variation in response. Most commonly reported ‘likes’ were increased confidence in speaking (n = 6) and improvement in fluency (n = 6). Most commonly reported ‘dislikes’ of were irritating background noise (n = 8) and being unable to hear/understand one’s self and/or others (n = 5). Most common situations in which the device was reported to be helpful were using the telephone (n = 9) and speaking with strangers (n = 5). At end of study, four purchased the device, six reported they would use it if provided free of charge but would not purchase, and one could not be contacted for response | The study is criticised on the grounds that the study failed to maintain participant adherence to the treatment protocol of device usage; they utilised an inadequate question-asking task; and their conclusion of no significant treatment effect that is drawn from their inferential statistical analyses of group data only, and positive subjective findings |
| Ratynska et al. 2012124 Country: Poland Study design: cross-sectional Data collection method: assessment during reading and monologue/dialogue Aim: to evaluate the Digital Speech Aid Detail of participants (number, any reported demographics): 335 participants, 268 males and 67 females, aged 6–64 years, average age 17.9 years. All had received intervention but found them to be ineffective or insufficiently effective |
Digital Speech Aid incorporating DAF and FAF Number of hours: aid fitted by a clinician with trial at different settings over a 3-day period of hospitalisation Delivered by who? Device Control: none Length of follow-up: immediate Response and/or attrition rate: none |
Speech fluency with and without the aid Kurkowski Syllabic Test (number of dysfluent syllables in 100) |
Fluency in all speaking situations improved with the DSA (p < 0.005). The OR of dysfluency during reading without vs. with was 3.39. Immediate fluency in 82.1% of participants. In dialogue, the OR of dysfluency without vs. with was 3.19. Immediate fluency improvement in 84.5%. In monologue the OR of dysfluency without vs. with was 2.69. Immediate improvement in 81.2%. 17.9% of the group exhibited no change or deterioration in fluency during reading | |
| Reddy et al. 201093 Country: India Study design: before and after Data collection method: assessment scales Aim: to evaluate CBT intervention Detail of participants (number, any reported demographics): five participants, all male, aged 16–30 years |
Phase 1, eight sessions CBT training in relaxation techniques (mindfulness meditation, deep breathing) and speech techniques such as humming and prolongation. Phase 2 techniques including cognitive restructuring, problem solving and assertiveness. Sessions flexible according to client need Number of hours: 22/23 sessions over 4–6 weeks, 16–18 of these were intervention and the rest used for assessment. Each session 60 minutes Delivered by who? Not reported Control: none Length of follow-up: immediate post intervention only Response and/or attrition rate: none |
SSI PSI Becks Anxiety Inventory Dysfunctional Attitude Scale Fear of Negative Evaluation Assertiveness Scale Rosenberg’s Self-Esteem Scale WHO Quality of Life Scale |
Clinically significant change (50% and above). Improvement on SSI between pre and post assessment for three patients, no change at mid intervention point. Clinically significant reduction of struggle avoidance, expectancy in one case. Clinically significant reduction in anxiety seen in all cases. Self esteem two clients showed clinically significant improvement | Few data provided, general description of findings only |
| Riley and Ingham 200094 Country: USA Study design: before and after Data collection method: oral motor assessment scale recording of repeated syllable sets Aim: to examine speech motor changes following intervention Detail of participants (number, any reported demographics): 12 intervention + nine in reference group, 14 males and seven females, aged 3 years and 8 months to 8 years and 4 months (mean 6 years and 2 months in SMT group, 5 years and 9 months in ELU group) |
SMT and ELU treatment Number of hours: 24 sessions of SMT, 24 sessions of ELU Delivered by who? Clinician Control: two treatment arms, nine children with no stutter formed ‘reference group’ but baseline data only Length of follow-up: 8 weeks Response and/or attrition rate: none |
Measures of speech motor performance – vowel duration, stop gap duration, voice onset time, stop gap/vowel duration ratio, total token duration Percentage of syllables that are stuttered |
Following SMT increase in vowel duration (by 44 milliseconds) and some reduction in stop gap duration (but not significant). Significantly reduced vowel duration/stop gap ratios (by 50%). Median decrease in percentage of syllables that are stuttered following SMT intervention was 3.19 (a 36.5% reduction p < 0.05). One child increased. ELU treatment had no effect on acoustic measures pre- to post intervention. Median decrease in percentage of syllables that are stuttered following ELU intervention was 2.36 (a 63.5% reduction p < 0.04). Difference between SMT and ELU intervention significant (p = 0.04). At baseline children who stutter not different from normal matched controls on acoustic measures | |
| Rosenberger et al. 200795 Country: Germany Study design: before and after Data collection method: four assessment points – pre-treatment (T1); post treatment (T2); 2-month follow-up (T3); 9-month follow-up (T4) Aim: to analyse the clinical effectiveness of a intensive stuttering therapy programme for children and adolescents who stutter Detail of participants (number, any reported demographics): two groups – group A 19 participants (14 male, five female, mean age 14.5 years); group B 15 participants (10 male, five female, mean age 13 years) |
Stuttering modification therapy method amending awareness tasks in larger and smaller therapy groups; social interaction and activities Number of hours: 3 weeks intensive stutter therapy, one weekend of follow-up treatment after 2 months; one weekend of follow-up treatment after 9 months Delivered by who? Three experienced stuttering therapists, some internship candidates from speech and language therapy and to carer (for social activities) Control: none Length of follow-up: 2 months and 9 months Response and/or attrition rate: dropouts in group B – for T3 and T4 data from just 10 participants could be taken |
Suttering severity including stutter rate and stutter symptoms Assessment of child’s experience of stuttering |
Significantly reduced stutter rate and reduced anxiety of children when they stutter following intervention. Group A: 10 out of 19 participants showed distinct reduction of stuttering between T1 and T2 and 9 of 19 between T1 and T4. 18 out of 19 participants show reduced anxiety considering experience with stuttering. Group B: 8 out of 11 participants show a reduced stutter rate between T1 and T2, one participant showed reduced stutter rate between T1 and T3. Comparison for group A with group B: significant improvement of scores considering reduction of stutter rate (p < 0.001) for T1, T2 and T3. Additionally, significant reduction of anxiety measured via the child’s experience test (p < 0.001) for group A for T1, T2, T3, and T4 and (p < 0.025) for group B | |
| Rousseau et al. 200796 Country: Australia Study design: before and after Data collection method: language assessments, recorded speech samples Aim: to examine factors associated with response to treatment Detail of participants (number, any reported demographics): 29 participants completed programme, 21 male and eight female, three had received previous therapy |
LP Number of hours: once weekly session. Stage 1 completed in a median of 16 clinic visits (mean 18), and in a median of 27 weeks (mean 24). 90% completed stage 1 within 31 visits Delivered by who? SLP (first author) and parents Control: none Length of follow-up: 24 months Response and/or attrition rate: 34 enrolled |
Time taken to complete stage 1 of the programme. Clinical Evaluation of Language Fundamentals Peabody Picture Vocabulary Test Assessment of Phonological Processes MLU Percentage of syllables that are stuttered |
Phonological development does not predict treatment time. Stuttering severity, MLU and CELF receptive score predict 35–45% of the variance for time taken to complete stage 1 of the programme. For each 10-unit increase in CELF receptive score, the number of clinic visits to complete stage 1 is estimated to increase by 27% (95% CI 7% to 49%) and for each 1-unit increase in MLU, the number of clinic visits to complete stage 1 is estimated to decrease by 18% (95% CI 2% to 32%). Higher CELF receptive scores only a significant factor though when added to stuttering severity. Mean baseline 3.0% of syllables that are stuttered and mean immediate post intervention was, with few exceptions, < 1.0% of syllables that are stuttered. Difference between pre- and post-treatment percentage of syllables that are stuttered scores was significant (p < 0.0001). At 6 months, mean in three conditions (home, away from home, clinic) was 1.1, 1.0 and 0.8, respectively. At 12 months 1.0. 0.8 and 0.6, and at 24 months 0.3, 0.3 and 0.1, respectively. Mean number of syllables spoken 581 at baseline and 715 follow-up indicating that treatment outcome was not associated with reduced speech output | |
| Ryan and Van Kirk 199597 Country: USA Study design: before and after Data collection method: recorded speech samples in clinic, home and school Aim: to compare outcomes from DAF with GILCU establishment programs Detail of participants (number, any reported demographics): 24 participants, 20 male and four female, aged 7–17 years (mean 11.8 years) |
DAF with prolongation programme: taught slow PS aided by DAF equipment built up gradually in terms of reducing auditory feedback. No emphasis on increasing speaking rate. GILCU: gradual increase from one word utterances to 5 minutes of fluent speaking at normal rates. Participants received same transfer and maintenance program after this – increasing audience size, different settings. Maintenance consisted of 3 minutes each of reading, monologue and conversation fluently Number of hours: DAF – minimal time 110 minutes to complete programme; GILCU – minimal time 105 minutes. Transfer programme minimum 115 minutes. Maintenance minimal 36 minutes over 15-week period. Total 7.9 hours establishment and 10.4 hours transfer and maintenance. 11 out of the 20 who completed phase 1 successfully achieved it within 9 months Delivered by who? 12 clinicians in 4 sites supervised by authors Control: two intervention arms Length of follow-up: 7 months for 18, and 14 months for 11 Response and/or attrition rate: 20 completed the first phase and started transfer programme, 11 finished maintenance |
Stuttered words per minute Words spoken per minute These assessed during ‘Criterion test’ and Stuttering interview Views of parents, teachers and clinicians |
20 (11 DAF and 9 GILCU) achieved less than 0.5 stuttered words per minute at end of first intervention phase and stared transfer. Eleven out of 20 finished the transfer and maintenance programme. Both programmes reduced stuttering rate. DAF from 7.5 to 0.3 SWM to and GILCU 6.0 to 0.4 SWM. Significant effect pre- to post-intervention mean of both interventions SWM (6.6 vs. 3.1; p < 0.01). Difference (p < 0.01) between pre-means (7.0 and 6.4) and post-GILCU mean (1.5) indicating GILCU had better generalisation. Higher speaking rate for both groups pre- vs. post intervention. Significant difference in percentage of syllables that are stuttered pre- to post intervention (p < 0.01) for both interventions, with GILCU reducing percentage of syllables that are stuttered more than DAF (p < 0.05). At mean 7-month follow-up those who participated in the maintenance programme did better than those who did not (0.3 SWM vs. 2.8 SWM). No statistically significant difference between the intervention groups. At 14-month follow-up, 11 children who completed had reduced stuttering from 7.7 SWM to 0.8 SWM. Interview data found 7 out of 19 children who completed maintenance programme no longer viewed themselves as having a stutter and reduction in avoidance reported by children (from 74% to 47%) and by parents. All 12 clinicians reported that they planned to use the programmes again | |
| Sicotte et al. 200398 Country: Canada Study design: before and after Data collection method: recorded speech sample, questionnaires, interviews, observation Aim: to evaluate the use of a telemedicine-delivered intervention Detail of participants (number, any reported demographics): 6 participants, aged 4–19 years, at least 5% of syllables that are stuttered. No further details |
The type of therapy given ‘consisted of currently accepted and well used procedures documented by various authors’ Number of hours: 12 × 1-hour weekly sessions. Four received an additional eight sessions, to give a total of 20 hours of therapy. Maintenance phase = 5 × 1-hour sessions in weeks two, four and eight and then at the third and sixth month Delivered by who? SLP via videoconferencing Control: none Length of follow-up: 6 months Response and/or attrition rate: none |
Attendance Quality of session Patient/carer views Percentage of syllables that are stuttered |
Overall, the telemedicine unit was judged as adequate by the SLP to deliver a satisfactory intervention. Five patients/parents highly satisfied with therapeutic contact, none concerned about treatment at a distance. Stuttering ranged from 13% to 36% across participants before treatment and from 2% to 26% after treatment (mean 52% decrease in the frequency of stuttering). All participants maintained at least part of their improved fluency at the end of follow-up, when stuttering ranged from 4% to 32%. Data reported by individual only | |
| Smits-Bandstra and Yovetich 200399 Country: Canada Study design: before and after Data collection method: video speech sample retelling a story Aim: to evaluate an intervention Detail of participants (number, any reported demographics): three intervention (all male, aged 8/9 years, two severe and one mild stutter), and two control (both male, aged 11/12 years, severe and moderate stutter) |
CBT focused on the remediation of negative attitudes, thought processes and avoidance tendencies. Included cognitive techniques (employing self-monitoring, facilitating positive attitudes, desensitization) and behavioural stuttering therapeutic techniques (blending, easy onsets, cancellations, pull-outs and preparatory sets). All parents participated in a 3-hour group counselling session. Homework assignments were included in the programme (e.g. practising and delivering a speech) Number of hours: semi-intensive, 3 weeks Monday to Friday from 9.00 a.m. to 12.00 p.m. Delivered by who? Clinician Control: children of families willing to receive intervention but who had transport issues and unable to attend Length of follow-up: 2 months Response and/or attrition rate: one participant lost at 1-month follow-up |
% dysfluent speech time Dysfluent words per minute % words stuttered per minute Culture-Free Self-Esteem Inventory Communication Attitudes Test Revised Parent views |
The programme was partially effective in the alleviation of both behavioural and attitudinal stuttering symptoms. However, 90% of the participants went back into therapy after 2 months. The improvement in dysfluent time for participants was 79.4%, 59.6% and 67.5% for the intervention children, and 17.6% and 18% for control children. The percentage of words stuttered per minute comparing pre-intervention to 2 months post intervention was 22.8 to 23.5 for one child, 2.8 to 2.3 for another, and 9.5 to 7.4. The control child had increased from 30.5% to 35.8% of words stuttered. Experimental participants displayed improvement or normalised CAT-R scores after treatment. Control participants’ scores worsened or remained highly negative. Both experimental participants and control participants self-esteem scores fell well within the expected range for children of their age | |
| Stewart 1996100 Country: UK Study design: before and after Data collection method: recorded speech sample Aim: to explore factors underpinning the long-term maintenance of fluent speech Detail of participants (number, any reported demographics): 12 participants, 11 male and one female, aged 18–38 years, mean 26.1 years (SD 7.5 years). All but one had received previous intervention (six immediately prior), none had received group intervention |
Group intervention including phases of attitude change sessions that aimed to develop self-awareness, positive aspects of self, identification of aspects of fluency important for individuals, exploration of issues relating to generalisation and maintenance. In addition, technique sessions that taught prolongation, rate control, pausing, regular breathing, flow, light contacts and easy onset. Final phase of transfer and maintenance to establish techniques at acceptable speaking rate and in spontaneous utterances, transfer into non clinical situations and further examination of issues relating to relapse/non-use Hours: weekly sessions of 2 hours for 6 months then fortnightly for up to 12 months. After 12 months option of maintenance sessions (50% attended regularly) Delivered by who? Two therapists – one was the author, the second was a specialist SLT Control: none Length of follow-up: 2 years Response and/or attrition rate: 12 out of 15 approached recruited. Two lost to follow-up at 2-year reassessment |
Words spoken per minute % words stuttered Stuttered words per minute SSI S24 assessment of communication attitudes Attitude and intention assessment |
Assessed following attitude change sessions and again following the technique phase, third assessment 1 year post initial assessment and final assessment 2 years after initial assessment. At baseline for WSM the group mean was 83.6 (SD 69.09). After attitude change sessions WSM group mean 91.1 (SD 51.68). After 1 year WSM group mean 92.75 (SD 30.86). After 2 years group mean 103.5 (SD 33.67). Baseline SWM group mean 15.2 (SD 8.76). After attitude change sessions SWM group mean 12.8 (SD 6.18). After 1 year group mean 5.7 (SD 5.28). After 2 years group mean 3.7 (SD 3.86). Baseline % words stuttered 30.6 (SD 28.28). After attitude change sessions % words stuttered group mean 30.7 (SD 34.5). After 1 year group mean 12.6 (SD 25.78). After 2 years group mean 19.7 (SD 18.9). Conversation: baseline WSM mean 100.8 (SD 55.91). After attitude change sessions WSM group mean 91.3 (SD 46.38). After 1 year group mean 105.8 (SD 39.89). After 2 years group mean 107.2 (SD 40.2). Baseline SWM group mean 16.6 (SD 8.6). After attitude-change sessions SWM group mean 14.1 (SD 10.41). After 1 year group mean 7.0 (SD 6.85). After 2 years group mean 10.5 (SD 8.37). Baseline % words stuttered 23.4 (SD 16.78). After attitude change sessions % words stuttered group mean 25.6 (SD 27.02). After 1 year group mean 12.2 (SD 20.43). After 2 years group mean 19.7 (SD 18.9). SSI baseline range mild to very severe, after phase 1 range very mild to very severe, after technique phase all but three in very mild to mild/moderate, after 1 year all but three scored in very mild to mild-moderate, after 2 years severity ranged very mild to very severe six scored in very mild to mild range. S24 baseline mean 18.5 (SD 5.2), after phase 1 mean 17 (SD 4.6 non-significant difference baseline), after technique phase mean 16.8 (SD 5.9) significant change from baseline p < 0.02, after 1 year group mean 14.2 (SD 6.6 significant change from baseline; p < 0.05), after 2 years group mean 13.2 (SD 7.5 significant change from baseline; p < 0.05). Attitude to own speech baseline mean 1.67 (SD 0.85), after phase 1 mean 1.6 (SD 0.9), after technique phase mean 1.7 (SD 0.78 not significant), after 1 year mean 1.89 (SD 1.32 not significant), after 2 years mean 1.6 (SD 0.94 not significant). Attitude to technique speech baseline mean 1.98 (SD 0.91), mean 2.6 (SD 0.9), after phase 1 mean 1.7 (SD 0.9), after technique phase mean 3.4 (SD 1.51 significant change from baseline p < 0.02), at 1 year mean 3.7 (SD 1.32 significant change from baseline; p < 0.01), at 2 years mean 3.2 (SD 1.3 significant change from baseline; p < 0.05). Intention to use technique speech baseline mean 2.18 (1.12), after phase 1 mean 2.1 (SD 1.04), after technique phase mean 3.44 (SD 1.36 significant change from baseline; p < 0.05), at 1 year mean 3.48 (SD 0.9 significant change from baseline; p < 0.01), at 2 years mean 2.98 (SD 1.2 significant change from baseline; p < 0.05). Intention to use own speech baseline mean 2.83 (SD 1.09), after phase 1 mean 2.6 (SD 0.9), after technique phase mean 1.8 (SD 0.88 significant change from baseline; p < 0.05), after 1 year mean 1.95 (SD 1.04 significant difference from baseline; p < 0.05), after 2 years mean 2.16 (SD 1.3 not significant). Attitude change sessions did not seem to result in significant changes, the technique sessions in contrast resulted in significant changes. During transfer and maintenance group maintained speech gains however small number of participants had poor maintenance. Change apparent in most of the attitude measures following technique sessions | |
| Stidham et al. 2006101 Country: USA Study design: before and after Data collection method: recorded speech sample Aim: evaluate the effects of a prototype device using a modification of a currently used bone conduction hearing device with DAF on adult patients with significant stuttering problems Detail of participants (number, any reported demographics): 10 participants, eight male and two female, average age 38 years, range 18–58 years |
Bone conduction device on a headband with temporal feedback delayed according to patient preference between 5 and 130 milliseconds. Patients were allowed to choose their own DAF setting based on the naturalness of their speech and comfort at the initial fitting Hours: patients were asked to wear the device at least 4 hours per day for 4 weeks Delivered by? Device Control: none Length of follow-up: stuttering Severity Index-3 (SSI-3) tests were completed at pre-fit, immediate post fit, and at 2-week, 4-week, and 6-week intervals Response and/or attrition rate: nine patients completed the study |
SSI | A statistically significant decline in SSI-3 scores was documented from pre-fit compared with immediate post fit and 4-week follow-up (p < 0.001) using the Tukey test method. Before fitting, 78% (seven) of patients scored as very severe/severe and 22% (two) were moderate with 0% of patients scoring mild/very mild. At the immediate post-fitting scoring, 22% (two) were very severe/severe, 11% (one) was moderate and now 67% (six) scored as mild/very mild. Statistical significance was approached but not reached at 2 weeks. At 2 weeks, 33% (three) were very severe/severe, 44% (four) were moderate and 33% (three) were mild/very mild. At 4 weeks, 33% (three) scored very severe/severe, 11% (one) scored moderate and 56% (five) scored mild/very mild. There was no significant difference between pre-fit and the 6-week follow-up when patients had returned the device. At the 6-week scoring, 33% (three) of patients tested as very severe/severe, 56% (five) were moderate and 11% tested (one) mild/very mild. Patients subjectively noted improvement in their speech and confidence using the device | |
| Stuart et al. 2004102 Country: USA Study design: before and after Data collection method: video-recorded speech samples Aim: to examine the first therapeutic application of self-contained ear-level devices on the proportion of stuttered syllables and speech naturalness Detail of participants (number, any reported demographics): Experiment 1 – seven participants, six male and one female, five adults and two adolescents, mean age 21.9 years (SD 7.3 years). All presented with stuttering at ≥ 5% of syllables that are stuttered in either reading or monologue. All reported a history of therapy though none currently. Experiment 2 – eight participants, four adults (mean age 38.0 years, SD 15.9 years) and four youths (mean age 12.5 years, SD 2.6 years). None had been enrolled in experiment 1. Experiment 3 – 15 undergraduate students, four males and 11 females, mean age 23.1 years (SD 4.0 years) |
A self-contained in-the-ear AAF prosthetic fluency device was used. FAF was set up at 500 Hz and combined with a DAF setting of 60 milliseconds Experiment 1: each participant read different 300-syllable passages. Participants also produced 300 syllables of monologue speech. Both speech tasks were produced with and without a device. Reading and monologue conditions were counter balanced Experiment 2: apparatus were the same as that in experiment 1 with one exception – personal ear-level devices were constructed in either in the canal or completely in the canal custom-made shell designs Experiment 3: 12 speech samples were extracted from the video recordings of each participant in experiment 2. The listeners rated each track for naturalness in which ‘1’ was ‘highly natural’ and ‘9’ was ‘highly unnatural’. A 5-minute rest was provided at the end of 48 tracks Hours: every participant returned to the clinic, either once or twice for a follow-up session. These sessions typically lasted for approximately 30–45 minutes At 4 months post fitting (± 1 week), participants returned to the clinic for follow-up testing as before Control: none Length of follow-up: 4 months Response and/or attrition rate: none |
Number of stuttered syllables Rating of speech naturalness |
Experiment 1: a statistically significant main effect of device was found [F(1,6) ≈13.2, Huynh–Felt; p≈0.011, g2 ≈ 0.69]. The proportion of stuttered syllables was reduced by approximately 90% during reading and 67% during monologue Experiment 2: a significant main effect of device was found (p = 0.0028). All other main effects and interactions were not significant (p < 0.05). The proportion of stuttering events was significantly reduced with the device in place regardless of speech task or group and remained so after 4 months of time. Collapsed across speech task, time and group an approximately 81% reduction in the proportion of stuttered syllables occurred with the device in place compared with not in place. Although participants in experiments 1 and 2 displayed significant reductions in stuttering, not all individuals responded favourably or at all to AAF Experiment 3: mean naturalness ratings of speech samples generated with the device were judged to be more natural sounding than those without the device (p < 0.0001). There was no significant difference between the mean naturalness ratings of speech samples generated during the initial fitting with the device relative to that at 4 months with the device (p < 0.05) in all cases except with the youths while engaged in monologue. For that condition, raters judged the speech produced at the initial fitting as more natural Mean naturalness: comparison of device vs. no device p < 0.001 Initial visit with device vs. 4 months with device p = 0.012 Adult monologue Device vs. no device p < 0.0001 Initial visit with device vs. 4 months with device; p = 0.072 (not significant) |
|
| Stuart et al. 2006103 Country: USA Study design: before and after Data collection method: recorded speech samples Aim: to measure the effect of a self-contained ear-level device delivering AAF at 12-month follow-up Detail of participants (number, any reported demographics): nine individuals with developmental stuttering participated. Five participants were adults (mean age 41.4 years, SD 14.7 years) and four were youths (mean age 13.5 years, SD 2.6 years) |
In experiment 1, the proportion of stuttering was examined during reading and monologue. A self-report inventory inquiring about behaviour related to struggle, avoidance and expectancy associated with stuttering was examined in experiment 2. In experiment 3, native listeners rated the speech naturalness of speech produced by the participants during reading and monologue Control: none Length of follow-up: 12 months Response and/or attrition rate: none |
Proportion of stuttering events Self-reported perceptions of stutter Speech naturalness |
The proportions of stuttering events were significantly (p < 0.05) reduced at initial fitting and remained so 12 months post follow-up. After using the device for 12 months, self-reported perception of struggle, avoidance and expectancy were significantly (p < 0.05) reduced relative to pre-fitting. Native listeners rated the speech samples produced by those who stutter while wearing the device significantly more natural sounding than those produced without the device for both reading and monologue (p < 0.0001) | |
| Trajkovski et al. 2011104 Country: Australia Study design: Phase II clinical trial Data collection method: audio-taped speech samples Aim: to extend evidence on treatment using STS. To determine the percentage of children who would achieve clinically significant reductions of stuttering by using non-programmed STS Detail of participants (number, any reported demographics): 17 participants, 11 male and six female, age range 3 years to 5 years 9 months (mean 3 years 9 months) No previous stuttering treatment |
Westmead programme. STS involves speaking with minimal differentiation of stress between syllables. Each syllable is spoken in time with a rhythmic beat. During STS practice sessions, parents are instructed to occasionally praise the child for using STS. Initially, STS is taught with imitation and closed picture description tasks. Once the child can maintain the STS pattern, open and natural conversation using STS occurs in and around the home. Progression to stage 1b occurs once the parents and child are implementing the STS practice correctly and consistently each day. The aim of stage 2 is to maintain low levels of stuttering while the child and parent attend the clinic less frequently for 1 year. During stage 2, parents are instructed to gradually withdraw the STS practice sessions, over a period of months. Each day the parent assigns a self-report score for average stuttering severity for that day Hours: during stage 1a, the child and parent attend the clinic once a week for between 30–60 minutes to master the STS technique and to establish a treatment routine Parent and child are instructed to practise STS four to six times per day for 5- to 10-minute intervals in everyday situations. Stage 1b frequency of clinic visits decreases to fortnightly and last 30–45 minutes Control: none Length of follow-up: 12 months Response and/or attrition rate: nine children (52.9%) withdrew before completing stage 1. Author’s impression is that families tended to withdraw from treatment at the point when low-level stuttering severity had been attained but not stabilised |
Percentage of syllables that are stuttered Treatment time Speech quality Parent severity ratings |
For the eight children who progressed to stage 2, the mean pre-treatment percentage of syllables that are stuttered was 6.0% and the mean at stage 2 entry was 1.3%, resulting in a 78.3% reduction in stuttering. At 12-month follow-up, the mean had further reduced to 0.2%, which represented a mean stuttering reduction of 96% in beyond-clinic conversations. The ES was large, at 1.8 for log-transformed data. For the nine children who did not progress to stage 2, the mean pre-treatment percentage of syllables that are stuttered was 6.7% and the mean within-clinic at the last clinic session was 2.6%. As a group, for these children stuttering had reduced by a mean of 58.7% at the time of withdrawal. This ES was large at 0.9 for log-transformed data. The eight children who completed the treatment did so with a mean of 12.4 (range 4–17) clinic visits to complete stage 1, over a mean period of 27 weeks (range 6–40). The mean number of clinical hours taken to complete stage 1 was 8.0 (range 2.6–12.8). For the nine children who did not complete the treatment, the mean number of hours in treatment before withdrawal was 8.6 (range 4.0–16.1) over a mean period of 18.7 weeks (range 6–36) and 11.3 clinic visits (range 4–20). Of the 17 participants recruited, 47% achieved and maintained a mean stuttering reduction of 96% for up to 12 months post entry to stage 2, with a decrease of stuttering to 0.2% of syllables that are stuttered | |
| Unger et al. 2012125 Country: Germany Study design: cross-sectional Data collection method: recorded speech samples Aim: to examine the immediate effect of DAF and FAF on people who stutter Detail of participants (number, any reported demographics): 30 adults (≥ 18 years), 23 male and seven female, age range 18–68 years (mean 36.5 years, SD 15.2 years). All diagnosed with stuttering. All had therapy in the past but not AAF |
Four experimental conditions: (1) no device (no AAF), (2) inactive [DAF/FAF was set to 0 (the participants were under the impression that the setting was active], (3) device A (active settings) DAF 50-millisecond delay; FAF upwards shift of 250 MHz, and (4) device B (active settings) DAF 50-millisecond delay; downwards shift 0.4 octaves Control: no device Length of follow-up: immediate Response and/or attrition rate: none |
Percentage of syllables that are stuttered SPM Frequency of repetitions, prolongations, blocks SSI |
Results show a statistically significant main effect in the occurrence of stuttered syllables between the control (no device) and active DAF/FAF conditions F(1.76, 51.08) = 4.89; p = 0.014, η2p = 0.145. Pairwise comparisons between the control and the two with-device conditions show that stuttering was reduced significantly while using both Device A (p = 0.000) and Device B (p = 0.000) Duration: there was no significant difference in the average length of moments of stuttering F(2, 58) = 0.27; p = 0.762, η2p = 0.009 when speaking while using a device. These results suggest that even though moments of stuttering appeared less often during the with-device conditions, the average lengths of the still-occurring dysfluencies remained essentially unaltered Speech rate: results revealed that there was no significant effect in speech rate F(2.08, 60.18) = 1.18; p = 0.323, η2p = 0.038. This result indicates that the evaluated participant group did not experience a notably slower speech rate while exposed to AAF. This conclusion is strengthened when considering the descriptive statistics, which prove that there was minimal variability in speech rate figures between the control (mean 174.61, SD 51.93) and with-device conditions (device A: mean 177.28, SD 45.03; device B: mean 176.77, SD 43.45). Articulatory rate: results revealed that there was no significant effect in articulatory rate F(2.09, 60.54) = 1.98; p = 0.145, η2p = 0.064. There were no statistically significant changes in articulatory rate when comparing the control (mean 197.99, SD 52.13) to the with-device (device A: mean 191.41, SD 51.63; device B: mean 192.88, SD 47.50) experimental conditions. This indicates that while using an AAF device set to display minimally invasive alterations, fluent speech output is produced at an unaltered speed Total repetitions: there was no significant effect in the frequency of total repetitions among the two with-device conditions F(1.52, 44.11) = 0.861; p = 0.402, η2p = 0.029, indicating that the use of a device does not impact the occurrence of repetitions Prolongations: there was also no significant effect in the occurrence of prolongations throughout the no-device, Device A and device B conditions F(1.75, 50.62) = 0.645; p = 0.508, η2p = 0.022 Total blocks: there was a significant effect in the occurrence of total blocks among the two with-device conditions F(1.73, 50.06) = 9.35; p = 0.001, η2p = 0.244. Results show that blocks were reduced significantly during both with-device conditions (Device A: p = 0.017; Device B: p = 0.049). Based on these results, the AAF devices appeared to decrease the occurrence of blocks during the administered speech samples. However, the frequency of the core behaviours prolongations and repetitions were not affected significantly by the use of a device Reading: findings suggest that there was a significant effect in the frequency of stuttering during the reading task F(1.86,54.17) = 7.29; p = 0.002, η2p = 0.201. The participant group experienced a significant reduction in stuttering while using both devices during the scripted speech task (Device A: p = 0.002; Device B: p = 0.007) Monologue: there was also a significant decrease in dysfluencies during the monologue F(2, 58) = 9.64; p = 0.000, η2p = 0.249. A decline in stuttering was evident during both device conditions (device A: p = 0.009; device B: p = 0.001) Dialogue: the evaluated participant group further appeared to benefit from the device use during the conversational speech task F(2,58) = 7.63; p = 0.001, η2p = 0.208. Stuttering was reduced significantly when using both devices (device A: p = 0.048; device B: p = 0.005). The use of a device significantly lowered dysfluencies during all administered speech samples. However, reductions in percentage of syllables that are stuttered varied between speech tasks; reading: mean 2.33, SD 3.75; monologue: mean 2.26, SD 3.32; dialogue: mean 1.49, SD 2.71. Although participants appeared to benefit from the use of a device during scripted and spontaneous speech, the mean reduction in dysfluencies did not result in stutter-free speech within any sample. Descriptive statistics show that stuttering remained most evident during the spontaneous speech tasks (monologue: mean 3.97, SD 4.10; dialogue: mean 4.32, SD 4.25), indicating that an AAF device had a dominant impact on stuttering during scripted speech tasks (reading: mean 2.99, SD 4.82) SSI: results revealed a significant group effect in the SSI severity ratings when comparing the no device to the Device A rating z-value = 3.75; p = 0.000, r = −0.48 and the no device to Device B severity rating z-value = 3.63; p = 0.000, r = −0.47. More specifically, for Device A 17 participants showed a decline in their stuttering severity rating while the use of this device did not result in a lowered SSI score for 13 participants. Throughout the Device B experimental condition, the SSI-4 rating decreased for 16 participants, remained unaltered for 14. Results showed that the mild severity group experienced statistically significant reductions in stuttering exclusively during the spontaneous speech tasks. Those clients within the moderate–severe category presented with significant decreases in stuttering during all recorded speech samples |
|
| Van Borsel et al. 2003105 Country: Belgium Study design: before and after Data collection method: videotaped speech samples Aim: to investigate the effects of DAF outside a clinical environment Detail of participants (number, any reported demographics): nine participants, four male and five female, age range 18–45 years (mean 26.5 years). Recruited from a self-help group. All had a history of therapy but with no durable results. Stuttering severity: very severe = seven, severe = one, mild = one |
Repeated exposure to DAF consisted of daily and weekly speech tasks. An examiner called participants randomly four times a month to ask about compliance. Delay times range = 13 to 187 minutes. Delay time used most frequently = 93, then 120, then 133 then 147 minutes Hours: each day participants used DAF during a 5-minute monologue, a 15 minute conversation and during 5 minutes reading aloud. Once a week they made a telephone call using DAF. Participants spent an average of 260 minutes per week using DAF. (mean individual duration 131 to 408 minutes; overall range 30–480 minutes) Delivered by who? DAF device, minimal instruction and clinical guidance in a non-clinical environment Control: none Length of follow-up: 3 months Response and/or attrition rate: none |
% stuttered words Diaries were kept of compliance and time spent carrying out tasks A summary evaluation sheet was completed at the end of each week |
Speaking during DAF resulted in a reduction of the number of dysfluencies in people who stutter. The percentage of stuttered words during no auditory feedback was significantly lower than before repeated exposure to DAF in all speech tasks. Pairwise comparisons (Wilcoxon rank-sum test) to test before and after effects: automatic speech: z-value = –2.371; p = 0.018; reading aloud: z-value = –2.666; p = 0.008; repeating words and sentences: z-value = –2.521; p = 0.012; picture description: z-value = –2.521; p = 0.012; conversation with an examiner: z-value = –2.310; p = 0.021 After 3 months before and after dropped to non-significant apart from reading aloud: automatic speech: z-value = –1.473; p = 0.141; reading aloud: z-value = –2.552; p = 0.011; repeating words and sentences: z-value = –0.676; p = 0.499; picture description: z-value = –1.859; p = 0.063; conversation with an examiner: z-value = –1.363; p = 0.173 Comparison (Wilcoxon test) of stuttered words before (NAF) and after DAF: automatic speech: z-value = –2.117; p = 0.034; reading aloud: z-value = –2.668; p = 0.008; repeating words and sentences: z-value = –2.313; p = 0.021; picture description: z-value = –1.960; p = 0.050; conversation with an examiner: z-value = –1.836; p = 0.066 After 3 months, comparison (Wilcoxon test) of stuttered words before (NAF) and after DAF: automatic speech: z-value = –0365; p = 0.715; reading aloud: z-value = –0.178; p = 0.859; repeating words and sentences: z-value = –0.843; p = 0.399; picture description: z-value = –0.560; p = 0.575; conversation with an examiner: z-value = –1.051; p = 0.293 A Spearman rank-order correlation showed a modest correlation (rho = 0.667; p = 0.05) between the amount of reduction and the time spent practising participant’s perceptions; almost all participants experienced fluency under DAF as better than speech fluency before the experiment. However, at least some participants at some point during the experiment found that their fluency or emotional state was worse (score 2) than before. Participants were generally positive about the device. In addition, some reported a positive effect when speaking without DAF. S2, for instance, wrote that already after 3 weeks her speech was remarkably better ‘even without the apparatus’. However, variation in perceptions. S8 wrote ‘Personally I experienced little improvement’ and ‘I certainly did not start speaking more fluently’. Some participants (S2, S7, S8, S9) also mentioned that at some point they faced a decline of the speech fluency they had initially experienced and several participants pointed out the importance of regular practise to obtain a good result. Some participants commented on the positive influence on their affective or cognitive status. For several participants, using the apparatus had reduced their fear to speak on the telephone, leading to its more-frequent use. Some of the comments were less positive. Although S7 mentioned that the apparatus gave her the feeling of being helped, she also added that this feeling was ‘not so familiar’ and that the small stutters now sounded in her ears as big stutters. S8 commented that the apparatus did not give him the feeling that his stuttering had now completely disappeared. A longer exposure to DAF does not reduce stuttering frequency further during DAF. It is possible that there is a limit after which longer exposure to DAF does not further reduce stuttering frequency during NAF |
|
| von Gudenberg 2006106 Country: Germany Study design: before and after Data collection method: measurement before therapy, after therapy, after 3 years and after 5 years Aim: to evaluate the therapy approach of Kassel (fluency shaping) and show long-term effectiveness Detail of participants (number, any reported demographics): unclear |
Fluency shaping therapy with focus on how to speak fluently and awareness tasks Number of hours: 3 weeks intensive programme with 1 year aftercare therapy Delivered by who? Speech and language therapists Control: none Length of follow-up: unclear (at least 1 year) Response and/or attrition rate: unclear, no defined participant group. Collected data over several years was compared for different outcomes |
Dysfluency in speech Self-judgement of treatment Natural speech Speech rate |
Dysfluency in speech: over a time period of 3 years a reduction of dysfluent speech was observable in 50 participants. Self-judgement of treatment: 46 out of 77 participants reported that they spoke horribly before they started the treatment; after 2 years only 6 out of 62 participants spoke about their own speech like this. Natural speech: directly after therapy the naturalness of the speech did not change, but after 1 year the speech becomes more natural (measured in 29 participants) Speech rate: all clients of the programme showed either the same speech rate after the treatment as before or even improved speech rate |
|
| von Gudenberg et al. 2006107 Country: Germany Study design: before and after Data collection method: before treatment, after treatment and for some after 1 year Aim: to evaluate if the computer-based intensive therapy approach is effective for children between the ages of 9 and 13 years Detail of participants (number, any reported demographics): 32 children between 9 and 13 years Additionally, longitudinal comparisons between this group and older groups (14–18 years and > 18 years) |
Fluency-shaping techniques, including computer-based training and awareness training Number of hours: 2-week intensive therapy programme (100 hours), one aftercare weekend after 1 month, and two refreshment weekends after 5 and 10 months Delivered by who? Speech and language therapists Control: none Length of follow-up: unclear up to 1 year Response and/or attrition rate: unclear |
Interview about therapy Reading Speaking on the telephone Interview of random people on the street Objective and subjective data about stuttering |
In general, an improvement can be observed in all described measured outcomes. 4 out of 23 participants suffer from a backslide into severe stuttering after 1 year; on the other hand, 5 out of these 23 children did not show any stuttering after 1 year. Speaking on the telephone improved distinctly. Comparing data from 9- to 13-year-olds and 14- to 19-year-olds shows that 9- to 13-year-old children stutter more after the therapy programme than 14- to 19-year-old participants, ESs were calculated between stutter rate before the treatment and after 1 year: 9- to 13-year-olds show an effect of d = 0.96, and 14- to 19-year-olds of d = 0.88. All ESs show a large effect | |
| Wagaman et al. 1993108 Country: USA Study design: before and after Data collection method: audio-taped speech samples Aim: to investigate the effectiveness of a treatment programme based on awareness training, response training and social support Detail of participants (number, any reported demographics): eight participants, six male and two female, aged 6–10 years Mean duration of stuttering = 3.9 years (range 1–7 years, mean 2.2 years) |
Three elements: awareness training, response training, social support. Awareness training: participant and parent identify stuttering events from audio-recorded speech samples by verbal response or hand raising. Response training: discussion and modelling of diaphragmatic breathing. Social support: at least one parent attended sessions and learned the techniques being taught. They were advised to practise at home with the participants and remind them to use techniques when stuttering was heard. Praise was used for good progress and daily records were kept Hours: initial training session 2 hours. Following sessions 45–60 minutes. Three treatment sessions per week until < 3% of syllables that are stuttered had been achieved Delivered by? Speech pathologist Control: N/A Length of follow-up: 10–13 months Response and/or attrition rate: none |
Percentage of syllables that are stuttered Rate of speech Treatment Evaluation Inventory Short Form |
Criterion of < 3% was used as a measure of treatment success. Baseline: all participants showed varied but relatively stable levels of stuttering. Post treatment, all participants achieved < 3% of syllables that are stuttered which were maintained for 10–13 months. The results show 89% reduction in stuttering across the sample. Speech rates were mainly equivalent from baseline to post treatment, showing that the success was not associated with changed rates. The intervention was acceptable to parents, particularly post treatment and speech pathologists assessed that speech was improved post treatment. Parents found the treatment acceptable: score 27 on description of the study, rising to 33.9 (range 32–37) before treatment and 39.5 (range 36–45) post treatment. t(7) = 4.11; p < 0.01. Parents and speech pathologists rated the children high on the five social validity questions post treatment, suggesting that their speech was unimpaired and natural, their dysfluencies were not noticeable and that they were not in need of further intervention for stuttering. For speech pathologists, the post-treatment mean score of 34 (range 32–35) was almost perfect and was significantly higher than the pre-treatment mean score of 16.3 (range 10.3–22.6), t(7) = 11.07; p < 0.001. For parents, the post-treatment mean of 25.7 (range 15.5–33) was lower than for the speech pathologists, but was significantly higher than the pre-treatment mean of 14.2 (range 7.3–25), t(7) = 3.90; p < 0.01 | |
| Wagaman et al. 1995109 Country: USA Study design: before and after Data collection method: audio-taped speech samples Aim: 3- to 5-year follow-up of investigation into the effectiveness of a treatment programme based on awareness training, response training and social support Detail of participants (number, any reported demographics): seven participants, aged 9–14 years All had participated in a previous research study. Two participants had received < 6 months of speech therapy since the original follow-up |
Three core elements of the programme. First, awareness training: participant and parent identify stuttering events from audio-recorded speech samples by verbal response or hand raising. Second, response training: discussion and modelling of diaphragmatic breathing. Third, social support: at least one parent attended sessions and learned the techniques being taught. They were advised to practise at home with the participants and remind them to use techniques when stuttering was heard. Praise was used for good progress and daily records were kept Hours of intervention: each participant received an average of 10 treatment sessions Delivered by: unclear Control: N/A Length of follow-up: 3–5 years Response and/or attrition rate: 1/8 from original study |
Percentage of syllables that are stuttered Speech rate |
All participants had increased their rate of speech since 1 year post treatment. For five out of seven participants the follow-up mean percentage of syllables that are stuttered was lower than at 1 year. For one participant, the follow-up increased score was well below their original baseline score. For the other participant the increased score was still close to 3%. The percentage of syllables that are stuttered results from baseline to follow-up (speech rate in brackets) for individual participants Nicky, % SS (speech rate)
|
|
| Ward 1992110 Country: UK Study design: before and after Data collection method: audio- and videotaped speech samples Aim: preliminary evaluation of SIFT intervention Detail of participants (number, any reported demographics): four participants, no other information reported |
SIFT has three phases: identification, prolongation, transfer. The purpose of the identification phase is to more fully acquaint participants with an understanding of normal phonatory processes to help stutterers become more aware of what is happening in motor speech and perceptual terms when dysfluencies occur. Prolongation phase: participants produce carefully monitored timed blocks of slowed speech while maintaining the required fluency skills. Transfer: client and clinician decide together on the appropriate rate ranges to be finally adopted for each individual. There is a group discussion on day 12 about clients’ perceptions and fears about transferring the new speech style to the ‘real’ world. Hours of intervention: participants attend clinic for two hours each day (4.30 p.m. to 6.30 p.m.), Monday to Friday for 3 weeks Delivered by who? Unclear Clinician control: none Length of follow-up: 3 months Assessment at 2 weeks, 4 weeks and 2 months post clinic then at 2 months, then monthly for first year Response and/or attrition rate: none |
SPM Percentage of syllables that are stuttered S24 |
Oral reading baseline to post intervention SH: SPM 170; percentage of syllables that are stuttered 8.2%, post SPM 187; percentage of syllables that are stuttered 2.0% WN: SPM 175; percentage of syllables that are stuttered 10.8%, post SPM 183; percentage of syllables that are stuttered 3.8% BW: SPM 216; percentage of syllables that are stuttered 7.2%, post SPM 182; percentage of syllables that are stuttered 0.8% BR: SPM 191; percentage of syllables that are stuttered 11.6%, post SPM 225; percentage of syllables that are stuttered 1.1% Group pre-oral reading: SPM 188; percentage of syllables that are stuttered 9.4% Post-intervention oral reading group: SPM 194; percentage of syllables that are stuttered 1.9% Monologue SH: SPM 222; percentage of syllables that are stuttered 9.0%, post SPM 223; percentage of syllables that are stuttered 4.7% WN: SPM 166; percentage of syllables that are stuttered 13.8%, post SPM 184; percentage of syllables that are stuttered 4.4% BW: SPM 210; percentage of syllables that are stuttered 9.7%, post SPM 221; percentage of syllables that are stuttered 1.6% BR: SPM 146; percentage of syllables that are stuttered 23.3%, post SPM 196; percentage of syllables that are stuttered 1.3% Group pre-monologue: SPM 186; percentage of syllables that are stuttered 13.9% Post-intervention monologue: group – SPM 206; percentage of syllables that are stuttered 3.0% Conversation SH: SPM 210; percentage of syllables that are stuttered 6.4%, post SPM 222; percentage of syllables that are stuttered 5.8% WN: SPM 191; percentage of syllables that are stuttered 10.5%, post SPM 183;% percentage of syllables that are stuttered 4.1% BW: SPM 200; percentage of syllables that are stuttered 5.7%, post SPM 207; percentage of syllables that are stuttered 1.9% BR: SPM 157 percentage of syllables that are stuttered 18.3%, post SPM 183; percentage of syllables that are stuttered 1.6% Group pre-intervention conversation: SPM 189; percentage of syllables that are stuttered 10.2% Post intervention conversation: group – SPM 196; percentage of syllables that are stuttered 3.3% Telephone conversation SH: SPM 166; percentage of syllables that are stuttered 10.8%, post SPM 228; percentage of syllables that are stuttered 3.7% WN: SPM 104; percentage of syllables that are stuttered 16.5%, post SPM 220; percentage of syllables that are stuttered 3.9% BW: SPM 198; percentage of syllables that are stuttered 12.4%, post SPM 229; percentage of syllables that are stuttered 2.8% BR: SPM 92; percentage of syllables that are stuttered 29.1%, post SPM 238; percentage of syllables that are stuttered 7.4% Group baseline telephone conversation: SPM 140; percentage of syllables that are stuttered 17.2% Post-intervention telephone conversation: group – SPM 228; percentage of syllables that are stuttered 4.4% S24 Score baseline SH, 7; WN, 17; BW, 23; BR, 23 Group mean: 17.5 S24 Score follow-up: SH, 7; WN, 9; BW, 11; BR, 8; group mean: 8.7 All clients achieved normal speaking rates though not consistently for all participants |
|
| Wille 1999111 Country: Germany Study design: before and after Data collection method: videotaped sample of spontaneous speech, reading and interviews with parents of participants Aim: to evaluate whether or not bioresonance therapy is more successful than standard therapy care Detail of participants (number, any reported demographics): 14 participants, aged 9–18 years |
The 14 participants were randomly allocated into two groups. One group first had bioresonance therapy, whereas the other group had standard speech therapy intervention. After a phase of 4 months the groups switched intervention types for another 4 months. Evaluation of stuttering severity was assessed before the first intervention, between the interventions and after the second intervention by interviewing parents, teachers and speech therapists Number of hours: 10 hours bioresonance therapy and 4 months of speech therapy (hours unclear) Delivered by who? By speech and language therapists using bioresonance therapy instrument Control: none Length of follow-up: no follow-up Response and/or attrition rate: unclear |
Spontaneous speech Reading Controlled speech |
Parental report suggested improvements in the behaviour of young children regarding social contacts. Improvement of fluency during the first 4 months of therapy, but no further improvement in the second therapy phase where intervention programmes changed. Considerable variation in individual response to the intervention. Not possible to conclude whether or not bioresonance therapy was more effective | |
| Wilson 2004112 Country: Australia Study design: before and after Data collection method: speech samples. Use of audio recorders or video recorders (depending on equipment available at home) to assess speech. 10-minute recordings Aim: to evaluate a telehealth version of the LP Detail of participants (number, any reported demographics): five participants, aged 3–7 years |
LP replacement of clinic visits with telehealth consultations. Videos provided for use by parents Number of hours: number of weeks from beginning to end of stage 1, range 11–30 Number of consultations required to reach stage 2: range 3–26 Duration of consultations (minutes): range 22.3–40.5 Total clinician time for each consultation (minutes): range 32.6–67.9 Frequency of consultations (days): range 9.1–38 Delivered by who? Clinician/parent Control: none Length of follow-up: 12 months Measured at: 2 months, 1 month, 1 week pre-treatment; 1 week, 1 month, 2 months, 4 months, 6 months, 8 months and 12 months post treatment Response and/or attrition rate: 18 families originally; attrition of 13 families Reasons: child stuttering reduced pre-treatment to non-significant levels (n = 2), serious illness or death in the family (n = 4), objection to protocol of no treatment during pre-treatment phase (n = 1), relocation (n = 1), unwilling to comply with beyond-clinic recording (n = 4), child not motivated (n = 1) |
Percentage of syllables that are stuttered SPM Parent questionnaires |
Mean 12–13 months post treatment were below or slightly above the LP criterion of 1.0%. Data reported by individual participant. Pre-treatment SPM and post-treatment SPM means: J.L. = 144, 191 A.C. = 101, 185 T.L. = 150, 175 G.H. = 186, 194 J.W. = 136, 167 Pre-treatment percentage of syllables that are stuttered: J.L. = 3.2 – 15.1 A.C. = 12.1 – 23.3 T.L. = 3.0 – 12.5 G.H. = 0.7 – 3.0 J.W. = 2.0 – 9.7 Range of percentage of syllables that are stuttered over 12 month follow-up: J.L. = 0.0 – 0.9 A.C. = 0.2 – 3.8 T.L. = Not reported G.H. = 0.0 – 0.6 J.W. = 1-week data only, near zero J.L. experienced slight increase in stuttering at 3 months post treatment. This was associated with stress at school. However, near zero rate was then achieved and maintained A.C. experienced some short-lived increases in stuttering at 1 week, 1 month, 8 months and 12 months post treatment T.L. experienced increases in stuttering at 1 week, 2 months and 8 months post treatment. This was associated with her mother’s lack of compliance, ceasing Lidcombe procedures once stage 2 was reached. Advice was not taken on board J.W. may have recovered naturally, as near zero stuttering was obtained at 1 week. The remaining data is unavailable owing to lack of attendance and compliance Parental questionnaires: three out of five questionnaires were returned at the end of stage 1, four out of five were returned in month 6, and five out of six were returned in month 12. Positive responses to satisfaction overall. Most parents were still praising stutter-free speech at 6- and 12-month follow-up. Satisfaction with child’s speech showed mainly satisfaction at 6 and 12 months, with one dissatisfied at 12 months |
|
| Woods et al. 2002113 Country: Australia Study design: before and after Data collection method: scores on questionnaire assessment tools Aim: to identify psychological effects of participating in the LP Detail of participants (number, any reported demographics): eight participants (child and parent), seven male and one female, age range 35–63 months (mean 54.4 months) Middle socioeconomic status area |
Evaluation of the LP. Assessment at 1 week pre-treatment, during treatment and 1 month post treatment Number of hours: all children had received the LP for a mean 12.3 months from stuttering onset to starting the programme Delivered by who? Clinician/parent Control: N/A Length of follow-up: 1 month Response and/or attrition rate: none |
Attachment Q-Set Screening tools completed by parents |
Total problems score
|
May have been some contamination in completing the checklist from parental positive attitude to decreased stuttering; however, the Attachment Q-Set scores are not consistent with bias |
| Yairi and Ambrose 1992114 Country: USA Study design: before and after Data collection method: recorded speech sample taken at clinic visits Aim: to provide long-term data on children who stutter Detail of participants (number, any reported demographics): 27 participants, 19 male and eight female, age range 23–52 months (mean 36.96 months, SD 6.73 months). Number of stuttering-like dysfluencies per 100 syllables: 3.64–32.32. Three mild, three mild/moderate, 11 moderate and nine severe. No more than 1 year post onset |
Treatment offered to all, 18 received a short programme of 5–12 sessions within first 4 months. Consisted of modelling slowed speech Number of hours: not specified Delivered by who? Not specified Control: untreated – not interested, preferred waiting, lived distant Length of follow-up: 2 years for all, up to 12 years Response and/or attrition rate: none |
Stuttering-like dysfluency Other dysfluency Total dysfluency |
No significant difference between groups over time, both had downwards trend in stuttering-like dysfluency (p = 0.4). Considerable variation between individuals but all followed the overall pattern. Much of the reduction took place near end of first year post onset with group differences suggested by 20 months post onset | |
| Yaruss et al. 2006115 Country: USA Study design: before and after Data collection method: speech sample, parent questionnaire Aim: to evaluate the Camperdown Program Detail of participants (number, any reported demographics): 17 participants, 12 male and five female, age range 31–62 months (mean 40.8 months SD 9.1 months). Three mild, one mild/moderate, six moderate, six moderate/severe and one severe stuttering |
Camperdown: a family-focused treatment approach consisting of parent–child training programme and child-focused treatment. Sessions once per week or twice weekly. Consists of education and counselling, communication modification training (parents learn to implement strategies to facilitate child fluent speech including easy talking, reduced time pressure, reduced demands, providing positive communication model), review and reassessment (parents evaluate strategies) Number of hours: nine children received 6–8 sessions of 45 minutes parent sessions, two received parent sessions and treatment for other communication problems, six received parent programme and child programme and, of these, one received five sessions, two received four and three received ‘considerably more’ or 6 months’ intervention Delivered by who? Speech and language pathologist (second author) Control: none Length of follow-up: 1–3 years (mean 2.3 years, SD 0.8 years) Response and/or attrition rate: 11 completed questionnaires, before-and-after data available for 16 children |
% stuttered words Parent views of programme Parent rating of fluency |
Baseline mean stuttering frequency 16.4% (SD 6.6%), after treatment 3.2% (SD 2.0%). Significant reduction (z-value = 3.517; p < 0.001). Parent questionnaire: most parents (91%) were very satisfied with the programme, parent education about stuttering was judged to be the most helpful component (10 rated as helpful to a high degree). Videotaping of sessions rated as least helpful. Children judged by parents to speak significantly more fluently at home following treatment (z-value = 2.64; p = 0.008) and more fluently in new speaking situations (z-value = 2.64; p = 0.008). Speaking more fluently at school was not significant. For 11 children (64.7%), the parent training sessions were sufficient for them to achieve child fluency within normal limits. These children continued to exhibit normal fluency at follow-ups. For the six who also received the child programme by follow-up, all but one had been discharged from formal treatment (one received occasional refresher sessions) | |
| Zimmerman et al. 1997126 Country: USA Study design: cross-sectional Data collection method: video recordings of telephone conversations under three conditions Aim: to investigate the effects of two types of AAF on stuttering during scripted telephone interactions Detail of participants (number, any reported demographics): nine participants, six male and three female, mean age 35 years (SD 9.2 years) |
AAF delivered by a digital signal processor. Binaural headset used with boom microphone so that participants could hear binaural sidetone amplification. Two intervention arms: DAF (50-millisecond delay) and FAF (frequency shift half octave down) Number of hours: not clear Delivered by who? AAF device Control: no auditory feedback Length of follow-up: immediate Response and/or attrition rate: none |
Stuttering episodes (divided by total number of syllables) | Mean proportion of stuttering events across nine participants:
|
Appendix 6 Extraction tables qualitative studies
| Study details | Method | Outcome measures | Main results | Limitations/comments |
|---|---|---|---|---|
| Anderson and Felsenfeld 2003128 Country: USA Study design: qualitative Data collection method: audio-recorded interviews Aim: to gain a better understanding of individuals who reported recovering from stuttering after the age of 10 years Detail of participants (number, any reported demographics): six participants (formerly n = 7), adults (18–55 years), mean age 21 years; range 17–30 years Recovered from stuttering and not participating in treatment. Mean % of dysfluent behaviours ranged from 0.6 to 2.0, overall mean 1.4 |
Recruitment: letters sent to participants of a stuttering intervention at a clinic. Flyers distributed at a local meeting of the National Stuttering Association as well as in several public areas. 60- to 90-minute interviews Analysis: interviews transcribed verbatim Familiarisation with the data and quotations that were salient to the research question identified. Thematically related material sorted together into categories. Modification of preliminary categories. Inter-rater reliability determined by second researcher categorising 20% of quotes Control: N/A Length of follow-up: N/A Response and/or attrition rate: one participant excluded following interview owing to not fitting inclusion criteria |
Recollections of past stuttering Representations of recovery Perceptions of the recovery process Perceptions of current speaking performance |
Relating to the review question: five participants had received some form of treatment for stuttering at some point in their lives. Perceptions of the treatment (which varied in type and duration) varied across the group Description of treatment: ‘Reading a lot of words’ KL ‘Saying words and making telephone calls’ AG ‘Reading, making telephone calls and pretending to stutter’ KP Of the five reporting formal treatment in the past, three attributed recovery to the treatment process. ME reported that being involved in a fluency shaping programme gave him the tools to become more fluent: ‘when I got through the programme – that’s when I knew that I had the mechanics’ KP attributed being in speech treatment as directly responsible for increasing her fluency: ‘I think there were people that helped me all of those years’ PC described how speech treatment as a child and public speaking courses in graduate school had assisted his recovery. At the age of 30 years, ME started a treatment programme at the suggestion of his girlfriend at the time. This was his first encounter with formal speech treatment and he reported feeling almost immediate positive changes in his speech as a result: ‘I began to see benefits of learning how to . . . not to force out sounds’ The treatment became ‘a power within not to stutter’ that allowed him to recognise that he ‘wasn’t helpless’. ME reported that he practised the techniques regularly at home for about a year after treatment ended using a voice monitor to signal the occurrence and smooth voice onsets and to monitor speaking rate. He reports that although now fluent most of the time, he still practises occasionally to keep his speech ‘on track’ |
Perceptions of the recovery process may or may not reflect the factors that were in reality responsible for their improvement. The study therefore identifies factors that participants believed were important in their recovery. Difficult to establish whether the participants were truly ‘recovered’ or whether they had learned to manage their condition effectively. There was an inability to fully verify past and present speaking behaviour as past speech was described through self-report |
| Beilby et al. 2013129 Country: Australia Study design: mixed methods, interviews, OASES and SF-36 Data collection method: audio recordings of interviews Aim: to investigate what personal experiences and themes exist for both members of a couple dyad when one member of the couple stutters. To examine whether or not the partners have different experiences with respect to the impact of stuttering on their lives Detail of participants (number, any reported demographics): 10 couple dyads (n = 20) in a > 1 year relationship. Adults ≥ 21 years. Relationship duration range 2–42 years. Participants who stuttered:
|
Interviews carried out with both partners present (at the choice of the people who stutter) Duration: 1–2 hours Analysis: open, axial and selective coding to develop a set of themes. Interview transcripts were read and segmented into sections of text containing one main meaning. Each of the meaning units was then assigned a theme that identified discrete ideas and phenomena. After initial themes were stipulated, a subset of text was selected for analysis of inter-rater reliability. The three researchers agreed on the coding of themes and subthemes in 94% of the passages. Reiterative comparison within and across groups were made. Emergent themes and subthemes were examined and agreed upon by all three authors Control: N/A Length of follow-up: N/A Response and/or attrition rate: not reported |
Questions relating to this review Fluent partner: what have you done to help your partner with their speech? What role did you play in them obtaining any help for their speech? How did/does the therapy affect your relationship? What advice would you offer to someone contemplating marrying a person who stutters? People who stutter: what have you done to work on improving your speech? Have you received therapy since beginning this relationship? How did/does the therapy affect your relationship? What advice would you offer to someone who stuttered if they were contemplating (a) beginning a relationship, (b) wanting to get married? |
Themes relating to this review question A number of participants indicated their preference for treatment including what they perceived was important in the therapeutic process: ‘We’re both involved. The individual who stutters and their partner, or whoever’s supporting them, should be involved in some pre-treatment workshops and discussions. And the discussions should be completely honest. Honest in that the therapy is not going to cure you. There is no cure. You’re starting on a journey that’s going to be life-long’. People who stutter were asked to describe previous and relevant intervention programmes that had been undertaken and there was a wide range of treatments and strategies that were detailed. ‘We had all those old wives tales, peas under the tongue . . .’ ‘I went to speech therapy, came out, thought I was cured. But then I crashed, it was so much harder . . . I was still hiding my stutter behind my newfound fluency’ One adult who stuttered flew to America to participate in an intensive, residential workshop. Financial and emotional consequences were outlined in his attempts to find a ‘cure’ for his stutter. ‘I went to the states and had therapy there. I did an intensive course for 14 days straight because I really wanted to improve my speech. That was big bucks as well. I heard about it from the internet. I saw their website and they claimed to have pretty good results from their clients. It worked for me for only a short time’ Discussion The fluent partners reflected on the perceived impact of the stutter upon communication with their spouse and explained the support that they felt they provided on a regular basis. This type of support varied from explicit provision of a target word, to broader concepts of patience in allowing the people who stutter to express themselves without pressure. They encouraged their spouse to seek therapy and described the support they provided regarding the range of decisions their partner made in the pursuit of fluency. The fluent partners described a strong and unfailing acceptance of their spouse and their stutter. Throughout the interviews there evolved a profile of individually tailored and personal approaches to successfully building a secure and supportive partnership |
This study attempted to obtain a randomly selected, representative sample of participants, but the recruited sample reflected only 10 couple dyads. A larger cohort may provide different insights regarding diverse life experiences, though analyses revealed that saturation of themes was reached with these 10 dyads. The treatment histories of the adults who stuttered in the study were not explored. Such background information about the types of treatments attempted, and details regarding the amount of time, money and resources expended in the past may have provided additional contexts for the responses and reactions described. It is possible that the results were biased by the fact that all dyads of participants and their partners opted to conduct their interviews together, rather than separately. This could be addressed through the use of independent interviews for speakers and their partners |
| Boberg and Boberg 1990130 Country: USA Study design: qualitative interviews Data collection method: audio-recorded interviews face to face (n = 12) and telephone (n = 3) Aim: to determine how wives of people who stutter were affected by their spouses’ stuttering, how they coped, and what advice they could offer to clinicians and wives of other stutterers Detail of participants (number, any reported demographics): 15 participants. Wives of people who stutter. Age range mid 20s to early 60s. Married for 6 months to 5 years. Educational status varied from diploma to PhD. Seven of the husbands who stuttered had completed a 3-week intensive CSP. Three had completed an intensive 3.5-week modified Precision Fluency Shaping Program. Three had participated in various types of avoidance-reduction programmes. Two had never received therapy |
Method: semi-structured interviews approximately 40 minutes in duration, face to face or by telephone Control: N/A Length of follow-up: N/A Response and/or attrition rate: not reported |
Outcome measures: questions related to how the couple met, did he stutter at the time, what was the wife’s first impression, how speech affected various stages of the relationship, whether or not there are children and if so how have they reacted to their father’s stuttering Relevant to the review: what role did you play in his obtaining therapy? How did the therapy affect your relationship? |
Eight wives said that at their first meeting with their future spouses, they noticed no stuttering. In some cases this was because the couple was alone: only in the presence of a third person would stuttering occur. In other cases, it was because the stutterer generally succeeded in hiding his problem from his future wife, and in one case the stutterer had been successful in therapy and was fluent, only to break down some months later in a devastating relapse. One very severe stutterer, unable to utter a word to anyone except his fiancée, went to a psychiatrist to be hypnotized for his wedding day. The psychiatrist did not believe hypnosis would help and prescribed instead a series of sedative pills, one to be taken each day leading up to the wedding and an extra powerful super pill for the day itself. The minister was also consulted and assured the stutterer that he would speak the vows in chorus with him. As a result, the bridegroom’s vows were the first fluent words his bride’s parents heard him speak. One wife described how a friend who was a speech pathologist had drilled her husband for several hours before the ceremony, going over and over the words he would have to say and ‘brainwashing’ him into believing he could be fluent. The most surprising discovery from the interviews was that many of the couples did not discuss stuttering until the husband announced his decision to take an intensive therapy course or, in two cases, until he became active in a self-help group for stutterers. In some cases, it was the prospect of having children that drove the stutterers to therapy. They did not want to be unable to read a bedtime story or communicate freely with their children, nor did they want to be a stuttering role model. Two spouses reported that they had delayed having children until the husband gained control over his speech. Once their father had been through effective therapy, some children took part in the maintenance programme by reminding him to use his fluency skills. Keeping track of speech rate or stutters, and even in a couple of cases fining him 2% for every uncorrected dysfluency. An endearing 3 year old, in her eagerness to help him speak, would hold her stepfather’s face when he struggled with a block. Such unaffected concern led to active participation in the post-therapy maintenance stage by both her and her siblings, which was reported to be very helpful to the stutterer. Only one wife reported obtaining professional advice to help relieve the impact of stuttering on her relationship. Before her marriage, she had sought out a speech pathologist in the school where she taught. From her she had learned helpful techniques for responding to her husband’s blocks and struggle behaviour. She also benefited for many years from confiding in a close friend who was a speech pathologist. Two wives said that they were amazed when their spouses expressed interest in attending a 3-week intensive clinic for stutterers because they had never realised that the slight dysfluency they saw was a matter of any concern to their husbands. They said their husbands seemed so outgoing and competent that they could not understand how they would benefit from therapy. The pre-treatment videotapes showing their husbands stuttering in a stressful situation were a revelation to them, as were the discussions they had with their husbands as a result of therapy. The striking fact running through all the interviews is that the wives took the lead from the husbands: ‘He didn’t seem embarrassed so I wasn’t’, ‘He didn’t seem to want to talk about it’, ‘I was afraid it might upset him if I mentioned it’. With one exception, only if the husband introduced the topic was it discussed. Another wife, unusually perceptive, tried to encourage her husband to tell people when he met them that he was a stutterer and might have difficulty speaking, instead of exerting great effort to hide the fact. She felt that it would be less embarrassing for the listeners if they were prepared for possible dysfluencies in advance, and her husband would be under less stress if he had nothing to hide. Unwittingly she had hit on one of the key points in many therapy programmes, but it was not until her husband had experienced therapy and received the same advice from a clinician that he was able to heed it. Several said they had believed there was nothing that could be done to help a stutterer until they read newspaper articles about the success of intensive therapy programmes. The spouses’ comments demonstrated the difficulty of obtaining accurate and up-to-date information about the problem and the availability of therapy. In addition to advising therapy, three wives advised that the wife become involved in the therapy procedures so that she can actively help her husband by slowing her speech to match his and reinforcing his appropriate use of fluency skills | |
| Bricker-Katz et al. 2010152 Country: Australia Study design: qualitative Data collection method: focus groups (n = 2) Aim: to investigate perceptions of limitations to activity and participation in a group of older people who stuttered into adulthood Detail of participants (number, any reported demographics): 11 participants, eight male and three female, all > 55 years of age, mean age = 70.7 (± 9.13) years. Six were retired, two semi-retired and three employed. Five had no past therapy, two had speech pathology only, and three and speech pathology, psychotherapy, hypnotherapy and medication Marital status
|
Recruited from general population via press releases to local and community newspapers and seniors’ newspapers inviting to contact researcher by telephone Control: N/A Length of follow-up: N/A Response and/or attrition rate: 16 suitable participants; 11 available for the focus groups |
Perspectives of older people who stutter about their experience of stuttering as an older person, how stuttering impacts on their communication, what barriers they foresee as they grow older with a stutter and what, if any, their treatment needs are | Participants spoke of impact of stuttering in the past as well as currently. Some felt that their experiences had improved since retiring because they did not have to talk to strangers and felt less self-conscious and fearful. Acceptance was linked with stuttering having less impact for them than in the past. They were less judgemental of themselves and more patient than in the past even when stuttering. Resignation to the fact that a solution in old age is less probable. Participants described spending time thinking about their speech; they are never sure when it will occur or how severe it will be. Therefore, they need to be constantly vigilant and this has not changed. Coping was described in two ways; coping with speech and coping with feelings. Fear can become a habit; some described facing that fear so that fear itself does not cause more dysfluency. Coping included strategies to manage speech and feelings. Some were taught on programmes, but increased age meant that a repertoire had been built up. There were several techniques for speech management reported such as slow or smooth speech; consideration about how to maintain this is needed in old age. Fear of speaking continued, particularly on the telephone, with other communication methods such as e-mail being used more There was also fear that others perceived them as mentally ill or intellectually disabled, though this was less prominent in those who had accepted themselves or were resigned to their stutter. Fear has consequences for social interaction following retirement when new relationships are likely to be made. Suggestions for improving their situation included ‘removing fear’ – through medication or reducing anxiety. Building confidence was linked to this. Self-disclosure as a strategy was valued as people who stutter felt more at ease. Support from others was helpful, particularly where the condition was understood. Growing older, others may attribute the speech problem to old age or a stroke. There is constant concern about what others are thinking, though with older age there may be less reactivity to problems. There was regret that opportunities to improve speech were missed when they were children. This was compared with more proactive treatment that can be accessed currently for children. Treatment needs and preferences were individual, with an experienced and knowledgeable clinician. Working in a group could be considered later in the treatment. Feeling understood was an important aspect of the therapeutic relationship. Motivation was linked to the perception that treatment would be effective. There was an expressed desire for a solution that is not complicated or time-consuming. Feelings of being misunderstood by speech pathologists led to disappointment with the treatment. Lack of understanding had also been experienced from teachers, relatives and work colleagues. Some felt let down by therapy, perhaps because of the need for ongoing work. Support at the emotional level was also cited as a need from therapy if maintenance was to succeed. This supports findings from studies with younger people who stutter | None reported |
| Butler 2013131 Country: UK Study design: qualitative Data collection method: focus groups and interviews Aim: to explore how individuals who experience speech dysfluency manage personal discrediting in their identity work in the intermittent emergence of a stigmatised characteristic (stuttering) Detail of participants (number, any reported demographics): 38 participants, 82% male, age range 19–90 years |
Recruitment was through ‘open microphone’ sessions at stuttering awareness events and by contacting members of stuttering self-help groups. Data were collected during stuttering self-help groups (led as focus groups) lasting average of 75 minutes and through 17 interviews, either face to face or via telephone. Interview duration was 30–75 minutes (mean 60 minutes). For interviews, questions were provided in advance for two participants so that they could prepare. Analysis was through a grounded approach that included familiarisation, coding to construct abstract categories. Broader themes were identified in the final stage Control: N/A Length of follow-up: N/A Response and/or attrition rate: not reported |
Ways in which people who stutter manage identity work given that stuttering can be stigmatised yet it is intermittent | Identity cloaking A randomised identity conflict was identified based on the evaluation of those who stutter of societal and personal forces as well as consideration of locus of control. Identity work is negotiated via a range of approaches the author describes as ‘identity cloaking’, taken from participant data. The cloak represents a veil which occupies the space between society and self or within the self. Each form of cloaking enables the use of space in a different way depending on use of personal and social space Hiding space: forestallers Theme of exclusion through being controlled by others and through self-exclusion from social situations. Felt stigma was reported as being experienced more often by those around the people who stutter than the people who stutter themselves. Avoidance by others could be due to fear of ‘courtesy stigma’ or stigma by association and controls the ability of those who stutter to be social. People who stutter are aware that in their deviant role in interactions, they disrupt the dual responsibility and take the blame for this, accepting the subsequent social exclusion. Yet people who stutter desire to be seen as an individual. Distinctiveness was afforded though was suboptimal ‘you just stand out like a sore thumb . . . what I want most is an invisibility cloak like Harry Potter’ Mental space to exchange words: converters Theme of concealing dysfluency by converting or avoiding words. Concealment can result in near fluency, presenting as ‘normal’ to observers. A range of methods were described to achieve this such as paving the way with easy sounds or words or switching words around. These people who stutter did not want to discuss these behaviours, seeing them as covert or ‘underhand’. They described the behaviour as reciprocal form of social-personal-social control and represented it as a struggle between their self-identity as a person who stutter and a perceived need to conceal to display an acceptable identity Social space as a prop cupboard: heeders One-fifth of people who stutter identified themselves as a ‘person who sometimes stammers’, reporting being ready to call upon approaches in social situations, but sometimes not needing them. They accepted this identity and were proud of their ability to heed and react to societal cues (‘special powers’). More than half talked of having advanced in other ways (‘I’m a far nicer person . . .’) They saw themselves as increasingly responsive to the personal and social contexts, as part of a wider group that have to face challenges Bodily space: exercisers Range of experiences includes shame, embarrassment and guilt, with strong reference to the views of others. Stuttering afforded low status in personal and working lives, with the reputational self being impacted by the stutter. Some demonstrated anger towards the self and hatred towards the stutter. Rather than conceal, they would try ‘anything that was out there’ which typically involved bodily techniques. This group represent in-group identity created by agreeing what the in-group is or is not (e.g. not identifying with concealment). They were controlled by or controlled the personal space rather than the social (as in concealers) Space for it: segregators Separation between self (and social stigmatised identity) and stutter through identity work. The onset was described as the arrival of ‘it’ (‘when it came back I was about twelve . . .’) disidentification (e.g. ‘them’ and ‘us’) is evidenced in a focus on being embodied in an external entity. References to being ‘odd’ or a ‘freak’ suggested a detrimental influence on identity work from social stigmatisation Space as a place to perform: narrators Behaviour is impacted by context and also the perception of role in that context. Leading roles in sport or as expert, for example, impacted positively on fluency and vice versa. However, with family and friends there were divided reports as being more relaxed could impact either positively or negatively on fluency. In role-playing, social identity was different from self-identity yet integrated (‘it’s just another me’) |
None reported |
| Crichton-Smith 2002136 Country: UK Study design: qualitative Data collection method: interviews Aim: to explore the experiences of adults who stutter Detail of participants (number, any reported demographics): 14 participants, 11 male and three female, age range 26–86 years, mean age 56 years. Thirteen had developmental stutter, one acquired, two had received no intervention and the remainder had received a wide variety of interventions |
Eleven recruited via newspaper advert and three via local self-help group. Semi-structured interview, framework analysis Control: N/A Length of follow-up: N/A Response and/or attrition rate: N/A |
Views and perceptions | Data reported as two groups, those received therapy during adulthood and those not. Perceptions of stutter limiting academic potential, working lives and exclusion from available activities. Respondents anticipated speech breakdown in social communicative situations and majority would avoid such situations if possible. References to low self-esteem commonplace, most perceived stuttering as an adult in social situations as unacceptable even though few described overtly negative reactions. All referred to episodes during childhood of negative reactions. Adults use a variety of speech management strategies, these strategies used equally by those who had received therapy as an adult and those who had not. Strategies: no change (no prior planning), intuitive change (not taught), taught change (use of therapy technique) and highlighting (commenting on their stutter). Heavy reliance on intuitive strategies such as word and situation avoidance; however, participants indicated that this avoidance not desirable therefore a mismatch between what they believed and what they practised. Belief that avoidance not desirable seemed to be what they had been told by SLT. Those who felt had experienced successful SLT cited more examples of adopting intuitive changes than taught changes. Many commented on useful strategies learnt in therapy yet did not cite them as current functional management strategies. Techniques gave sense of control, providing an opportunity to talk about stuttering. All those who had received therapy felt overloaded by either effort to think and control speech at same time or the responsibility of transferring fluency in to their daily routine, cited lack of dedication to practise or preference for habitual way of talking. Few dissatisfied with therapy. Need to discuss coping strategies as a therapeutic tool | |
| Corcoran and Stewart 1995132 Country: Canada Study design: qualitative Data collection method: interview Aim: to investigate adult stutterers’ perceptions of beneficial or adverse experiences Detail of participants (number, any reported demographics): five male and two female stutterers, age range 25–50 years. Three high school graduates, one at university, one had a degree. Range of occupations from farmer to engineer. All had been or were currently receiving stuttering therapy (four fluency shaping, two stuttering modification, one both). Two severe, two moderate, three mild stutterers. Level of stuttering not related to type of therapy received. None had received therapy as children |
Two interviews with each person conducted 1 month apart (one person had three). Purposive sampling of participants Control: N/A Length of follow-up: N/A Response and/or attrition rate: N/A |
Views and perceptions | Importance of understanding and establishing a relationship in therapy. One participant described a therapist using ‘tricks’ rather than having an understanding of stuttering. Another described failure of a therapist to establish a relationship with them – described as not wanting to get involved. Beneficial relationships were characterised by a therapist or fellow stutterer sharing their knowledge of stuttering. This led to feelings of hope, a sense of being supported and an awareness of not being alone. Interaction with fellow stutterers broke down the feeling of isolation. Those who had overcome stuttering gave beacons of hope. Support and understanding of another stuttering person added feeling of being truly understood. Positive aspects of therapy: having experience of stuttering understood by others, new understanding of the dynamics of their stuttering and ways to modify. Importance of clients understanding the rationale underpinning techniques. Other important aspect: a decrease in fears. Progress in therapy could change participant’s view of themselves which could lead to changed relationship with others, or highlight the need for psychological therapy | |
| Corcoran et al. 1998133 Country: Canada Study design: qualitative Data collection method: interview Aim: to investigate the experiences of adults who stutter Detail of participants (number, any reported demographics): same seven participants as in Corcoran 1995 study132 plus one additional person who was not receiving therapy. Five male and three female stutterers, age range 25–50 years. Three high school graduates, one at university, two had a degree. Range of occupations from farmer to engineer. All but one were currently receiving stuttering therapy (four fluency shaping, two stuttering modification, one both). Two severe, two moderate, three mild stutterers. Level of stuttering not related to type of therapy received. None had received therapy as children |
Two interviews with each person conducted 1 month apart (one person had three). Purposive sampling of participants Control: N/A Length of follow-up: N/A Response and/or attrition rate: N/A |
Views and perceptions | Ongoing experience of stuttering had resulted in a profound sense of helplessness. Effects of stuttering were so powerful they no longer felt in control of the direction of their lives. Powerful emotional components resulting from feelings of uncertainty and helplessness. Deep sense of shame reported. Positive aspects of themselves obscured or discounted as presence of stuttering became the primary focus. Insensitivity of listeners led to pain resulting from shame. Having a lack of explanation for stuttering led to guilt and self-blame for their stuttering. Participants spoke of fear and tension physically upsetting them | |
| Cream et al. 2003134 Country: Australia Study design: qualitative Data collection method: interviews Aim: to investigate the experiences of adults who received therapy for PS Detail of participants (number, any reported demographics): 10 people who had received treatment with PS therapy as an adult and who had experienced zero stuttering at the end of treatment. Nine male and one female, aged 24–54 years Nine had intensive PS treatment and four had treatment programmes on more than one occasion. Time since treatment 4–20 years. Six had accessed support groups/networks since treatment |
Phenomenology, open-ended conversational interview approach, purposive sample. Data collected over 2-year period. Two people had only one interview (one moved away, contact lost with other). In total 34 interviews carried out Control: N/A Length of follow-up: N/A Response and/or attrition rate: N/A |
Views and perceptions | All participants continued to stutter at times after intervention even those highly proficient in using the technique. Behavioural control provided by PS has to be balanced against sounding unnatural and different. Key importance of adults who stutter needing to protect themselves from the harmful consequences associated with stuttering which does not diminish following therapy with PS. Control of the speech motor system became a means of protecting themselves from harm while taking part in speaking situations. Participants continued to experience feelings of being different from people who do not stutter. Use of PS could exacerbate the feeling of being different. Participants could control stuttering by using an exaggerated version of PS but this was not considered acceptable to speaker or listener. Participants were prepared to use the technique in situations where the desire to not stutter over-rides the consequence of sounding unnatural and different. In other situations sounding unnatural in order to avoid stuttering was not considered personally or socially acceptable. Use of the technique could be reserved for high-risk situations rather than consistent use. Participants sought to control situations/environments, which were high risk. Perception of using PS as not sounding themselves. Fear of being discredited or caught out. Controlling stuttering using PS boosted self-confidence and self esteem however stutterers still felt different from non-stutterers. PS rewarded speakers with control over stuttering but also distinguished them from people who do not stutter. The effort required to maintain proficiency with PS could not be maintained constantly or in the long term | |
| Cream et al. 2004135 Country: Australia Study design: qualitative Data collection method: 34 interviews. Two focus groups Aim: 10 adults who stutter were interviewed to investigate their experience of treatment Detail of participants (number, any reported demographics): 10 people who had received treatment with PS therapy as an adult and who had experienced zero stuttering at the end of treatment. Nine male and one female, aged 24–54 years Nine had intensive PS treatment and four had treatment programmes on more than one occasion. Time since treatment 4–20 years. Six had accessed support groups/networks since treatment |
Phenomenology, open-ended conversational interview approach, purposive sample Data collected over 2-year period. Two people had only one interview (one moved away, contact lost with other). In total 34 interviews carried out Control: N/A Length of follow-up: N/A Response and/or attrition rate: NR |
Views and perceptions | People who stutter focus on doing what they can to protect themselves from the harmful consequences of stuttering. PS is only one of a variety of skills and strategies that they use in order to protect themselves. The essence of experiences after treatment was an active process of seeking balance between being different and being in control. The control people achieve with PS is subject to fluctuation because of the range and extent of demands in communication at the same time. Metaphor of a four-way rocker used to describe differing demands on communication in different speaking situations and need for PS to be one of a number of tools. May choose to use PS and not stutter or to participate naturally in a conversation and stutter | Same participants as 2003 study,134 findings also overlap with this study |
| Daniels et al. 2012138 Country: USA Study design: qualitative Data collection method: interviews and focus groups Aim: to explore the school experiences of adults who stutter Detail of participants (number, any reported demographics): 21 participants, 11 interviewed, eight male and three female, aged 29–69 years, mean 47 years. Eight mild, two moderate and one severe stutterer. One was receiving therapy currently and eight had received prior therapy, two had never had therapy. 10 participants in the focus group: one group of six participants – two male and six female, aged 30–58 mean 37 years, five mild and one moderate stutterer, five received prior therapy, one never had therapy. The second group had four participants: three male and one female, age range 21–34 years, mean 27 years, three moderate and one mild severity, all had received therapy in the past |
Participants purposively selected for diversity by advertising via stuttering association and personal contact Control: N/A Length of follow-up: N/A Response and/or attrition rate: N/A |
Views and perceptions | Physical (behaviours such as tapping and speech modification techniques), linguistic (word avoidance or substitution) and social-interactional (saying I do not know, developing signals to teacher, writing, talking in character) coping strategies reported | |
| Daniels et al. 2006137 Country: USA Study design: qualitative interviews Data collection method: videotapes of interviews Aim: to explore how African–American men who stutter view communication, identity and life choices Detail of participants (number, any reported demographics): six participants, age range 24–58 years, adult African–American males who stutter. Living in Texas, USA. Varied educational status from ‘some college’ to graduate degree (Masters). Recruitment through verbal announcements and flyers in universities, colleges and community buildings (libraries, churches, bookshops, barber shops etc.) |
Semi-structured interviews approximately 1 hour each Analysis: transcription of videotapes. Reading and coding each line. Abstraction of major and minor themes from codes. Credibility through two researchers carrying out review of transcripts Control: N/A Length of follow-up: N/A Response and/or attrition rate: not reported |
Questions: How has stuttering affected the way you live your life? How has stuttering affected the important relationships in your life? Prompts: Did you ever have speech therapy? How did that impact on your life at the time? |
Effects of race and communication on identity Effects of race and communication on life choices Communicative coping strategies of African–American men who stutter Identity construction: major and minor themes of African–American men who stutter
|
Not reported |
| Goodhue et al. 2010139 Country: New Zealand Study design: qualitative Data collection method: interviews Aim: to explore the experiences of mothers during the LP Detail of participants (number, any reported demographics): 16 mothers, children between 3 and 6 years, stuttering severity more than 2% at assessment, no previous stuttering treatment, mother and child proficient in English, no intellectual impairment of other SLT disorder |
Interviews pre-treatment and then at regular intervals during the programme. Each interviewed nine times. Work based on phenomenology. Interviews face to face and via telephone. Treatment provided by two SLTs independent of the interviewer. Thematic analysis process. Control: N/A Length of follow-up: N/A Response and/or attrition rate: N/A |
Views and perceptions | Five obstacles to impede participants’ ability to implement the programme: finding time to fit in therapy, forgetting to implement, presence of siblings. Other two obstacles not identified in the paper. Regular clinic sessions and/or telephone calls helped as reminders to do the treatment, using a previously established routine such a story time to carry it out was reported as helpful, another family member taking sibling in to another room or including them or carrying session out when sibling asleep reported as potentially helpful. Beneficial outcomes reported following programme: increase in quality time, increase in knowledge and management of stuttering, improved parenting skills. Report of increased child confidence. Adverse outcomes: several children did not like hearing feedback on their speech, did not like the word ‘smooth’, two children reportedly felt they had done something wrong by stuttering. Although many reported being empowered, some parents troubled by the responsibility leading to anxiety/pressure and guilt over not doing the therapy. Distress reported by eight mothers linked to severity of stutter and seeing child struggle, some distressed by relapse or process of conducting programme. Confidence improved if child’s speech improved however deteriorated if speech got worse. Parental expectations for all but one were that improvements would be quicker than they experienced, also surprise at their role in delivering the therapy. Perception that the programme was effective by all but one mother. Programme described as requiring commitment, dedication and consistent focus. Programme not difficult to carry out but implementation was a struggle. Perception that parent needed knowledge regarding the next steps in the programme, some wanted more written material, a few suggested a support group. Report of children enjoying the intervention, often reminded parent to carry out the sessions or give praise/reward for smooth speech | |
| Hayhow 2009140 Country: UK Study design: qualitative Data collection method: interviews Aim: to explore parental experiences of the LP Detail of participants (number, any reported demographics): parents of 14 children receiving the programme. Participant numbers not clear, included mothers, two fathers, one nanny, one partner |
21 interviews carried out, six participants interviewed twice Control: N/A Length of follow-up: N/A Response and/or attrition rate: N/A |
Views and perceptions | Some surprised by parental role in therapy. Most felt a sense of responsibility which, for some, was a positive feeling. Treatment times referred to by many as special times. However, some children tired of talk times after a while so they did not always retain this special quality. Positive aspects: stuttering reduced quite quickly and consistently, parents found own ways of implementing procedures into everyday lives, parents and children overall enjoyed the treatment, in some cases gradual shift from parent taking responsibility to child taking more responsibility, problems that arose were resolved by consultation with SLT or by experimentation. Issues identified: difficult to keep momentum of treatment going, setbacks, feelings of guilt, support needed in implementing treatment at home, weekly visits to clinic became a burden over a longer timescale, as children older school began to have an impact, children became less responsive over time and could become irritated by requests for self-correction. Those children who were less responsive to correction appeared to retain a greater vulnerability to persistent stuttering. Description of guilt/concern for parent when child progress halts. When progress not straightforward parents faced with long-term implications of stuttering and need help in adapting treatment. Two parents ambivalent about the programme and experienced difficulty in implementing procedures. These experienced difficulty in taking a firm lead, doubted their ability to help their child, had a more problem-orientated orientation, talked more about anxiety/guilt and had beliefs about stuttering at odds with the programme | Limited data presented, findings reported as lists of points with small number of quotes to illustrate |
| Hearne et al. 2008141 Country: Australia Study design: qualitative Data collection method: focus group and interviews Aim: to examine the impact of stuttering during adolescence Detail of participants (number, any reported demographics): 13 young adults/adolescents, 12 male and one female, aged 13–26 years. All stuttered during adolescence. Varying experiences of therapy, seven in maintenance having completed 1-week intensive Smooth Speech treatment, two in treatment (PS), one in maintenance PS, one completed Camperdown, two completed 1-day PS |
Purposive sampling across Australia. Two focus groups and seven interviews completed Control: N/A Length of follow-up: N/A Response and/or attrition rate: N/A |
Views and perceptions | Lack of awareness and knowledge regarding stuttering among significant others. Lack of own awareness of what stuttering is, who else stutters. Therapy had increased knowledge, variety of misconceptions and not sure whether or not what they did was stuttering. Many reported never having met anyone else that stuttered and thought they were the only person. Parental/teacher lack of knowledge, not talked about in the home, never spoke to friends about it. View that it should be spoken about, teachers should have more knowledge. Participants began attending therapy at a variety of ages however it was a decision that they made on their own. The participants all reached a point where they decided they needed to do something about it. Some had reached this point sooner than others. For some career aspirations spurred them to seek therapy. Participants reported that they preferred group therapy – an advantage to be with others of same age and interests and more representative of the real world. Felt they could learn from each other and know they were not the only one with this kind of problem. Participants found intensive therapy positive, emphasised easy-to-forget techniques. Struggle to keep skills once regular visits finished, leaving supportive environment, blamed lack of practise owing to forgetting, being busy or self-conscious. Not using when comfortable talking to friends/family, could not be bothered, getting lazy. Their busy lives meant speech practise slipped down their list of priorities, felt self-conscious using techniques. Family significant in helping them practise, others, however, viewed it as being up to them. Most useful part of therapy viewed as transfer tasks, need to experience talking to different people, therapy needs to focus on how going to use speech when leave, more follow-up days perceived as useful | |
| Hughes et al. 2011142 Country: Canada Study design: qualitative Data collection method: interviews Aim: to examine family experiences of adults who stutter Detail of participants (number, any reported demographics): seven adults who stutter who had received treatment at some point in their lives, five male and two female, aged 22–53 years. Range of therapies moderate or severe stutter |
Recruited via support groups and speech therapy clinics Control: none Length of follow-up: N/A Response and/or attrition rate: N/A |
Views and perceptions | Participants described a wish for support concerning the emotional aspects of stuttering ‘deep support’. Wanted to be able to discuss their feelings associated with stuttering. Voiced a desire for a role model, to know an older child or adult who had overcome their stuttering or someone more knowledgeable regarding stuttering who would help them cope more effectively. Felt a need to identify with others who stutter or individuals who stutter in order to obtain support not provided by their families. Participants reported a generally supportive home environment, e.g. assistance locating speech therapists, transportation and financial assistance. However, stuttering seldom discussed with family. Barriers to receiving help: pressure to be fluent around families, lack of communication regarding therapy and family overemphasising techniques taught in speech therapy. Assistance provided by family and SLT well-meaning but unhelpful. Four felt the treatments had not been beneficial to long-term recovery. Majority had received misguided assistance from family regarding their stuttering | |
| Irani et al. 2012116 Country: USA Study design: mixed methods Data collection method: interviews, clinical data (measures on assessments) Aim: to understand client perceptions of an intensive programme Detail of participants (number, any reported demographics): seven participants, five male and two female, average age 27 years (range 22–39 years). All had attended the programme, three once or twice previously. Two had not received follow-up therapy. Four were students, one a residential specialist, one a teacher and one a SLP |
Phenomenological approach, retrospective clinical data and interviews Control: none Length of follow-up: participants had attended the programme in 2003–6, 2008 and 2009 Response and/or attrition rate: N/A Intervention: 9- or 15-day intensive therapy programme conducted during the summer. Utilises both fluency-shaping and stuttering modification approaches in addition to CBT. Sessions last 5–7 hours each day with both group and individual sessions. Provided by graduate students, overseen by fluency specialist and clinicians on a 1 : 1 patient-to-clinician ratio. Four phases of therapy: awareness of stuttering behaviours, process of reducing stuttering behaviours, techniques to modify and improve fluency, and developing a personal maintenance programme. Follow-up therapy in form of weekend intensive workshops, regular therapy or telepractise |
Clinical data from case notes gathered retrospectively: questionnaire assessing feeling and attitudes (LCB scale, Erickson S24, OASES). Speech samples: conversation, telephone call, reading analysed for % syllables stuttered, type of dysfluency, secondary behaviours, SSI. Current clinical data: LCB, S24, OASES, speech sample, attitudes questionnaire, SSI-3. Treatment outcomes measured via attitudes questionnaire and before/after speech sample. Views and perceptions | Participant’s positive regarding benefit of an intensive clinic, found residential nature of course helpful. Speech techniques learned helpful, all reported benefit from learning a variety of techniques. Preference for slow PS. Participants reported difficult to use techniques in all speaking situations but important to know how to use them and practise in a variety of settings. Reported benefits of strategies such as CBT and motivational quotes. Benefited from exploring their own attitudes towards communication and stuttering. In many ways a foundation for the techniques. Perceived benefits of completing activities that pushed participants outside comfort zone and addressed transfer of techniques to typically feared speaking situations. Follow-up perceived as beneficial. Importance of personal motivation to attend the therapy impacting on perceived benefits. Importance of good clinician–client relationship with clinician responses and demeanour having a positive or negative impact. Clinical outcomes: SSI ES pre- to post intervention 1.19 (Cohen’s d), 95% CI –0.01 to 2.24. Pre-intervention to time of interview 1.25 (95% CI 0.04 to 2.31). S24 ES pre- to post intervention 1.79 (95% CI 0.46 to 2.89). Pre-intervention to time of interview 0.70 (95% CI –0.42 to 1.73). LCB ES pre- to post intervention 0.75 (95% CI –0.38 to 1.78). Pre-intervention to time of interview 0.07 (95% CI –0.99 to 1.11). Percentage of syllables that are stuttered pre- to post intervention: conversation – ES of 1.12 (95% CI –0.07 to 2.17). Pre-intervention to time of interview 1.97 (95% CI 0.59 to 3.09). Reading pre- to post intervention 0.59 (95% CI –0.52 to 1.62). Pre-intervention to time of interview 0.98 (95% CI –0.19 to 2.02). Telephone call pre- to post intervention 0.72 (95% CI –0.40 to 1.75). Pre-intervention to time of interview 2.22 (95% CI 0.78 to 3.38). Descriptive attitude data indicates improvement on measures of attitude change pre- to post intervention | Follow-up interview up to 7 or 8 years for some, 2 or 3 years for others. CI data across zero for many measures |
| Kathard et al. 2004143 Country: South Africa Study design: qualitative Data collection method: repeated interviews Aim: to explore processes shaping self-identity formation as dis-other and the actions of participants who stutter Detail of participants (number, any reported demographics): seven participants, five male and two female, age range 19–65 years, ethnicity: three black, two Indian and two white |
Participation invited via local hospitals, private practices, the university and a local self-help group. Semi-structured, open-ended life history interviews lasting on average 2 hours. Each participant was interviewed on average three times (total 6–10 hours per participant). Interviews were audio taped and recordings transcribed verbatim. Analysis was at two levels: (1) representational narrative analysis, where raw data are configured by means of a plot, into a story to explain a particular end, (2) grounding the analysis within the individual case; constant comparison across cases Control: N/A Length of follow-up: N/A Response and/or attrition rate: none reported |
Biographical stories and the representation of self-identity | All participants began to stutter in the pre-school years. The contexts for discovering difference were homes and school. Parents, teachers and peers drew attention to stuttering as being different from normal and as a disorder by reacting in a negative way. Though experiences at home and at school could differ, by adolescence the participants gained an understanding of themselves as different.
|
|
| Klompas and Ross 2004144 Country: South Africa Study design: qualitative Data collection method: interviews Aim: to investigate the life experiences of adults who stutter Detail of participants (number, any reported demographics): 16 adults, nine male and seven female, mean age 29 years (20–59 years). Four attending speech therapy at time of study. Fifteen had previously received therapy for periods ranging two sessions to 10 years, one not received any therapy; 13 single, 10 employed, mix of stuttering severity from one recovered to three varied mild to severe |
Recruited via stuttering association, university clinic and personal contacts Control: N/A Length of follow-up: N/A Response and/or attrition rate: N/A |
Views and perceptions | Data relating to perceived effects on education, social life, employment, family and married life. Only one participant viewed speech therapy as being helpful in terms of enhancing fluency; 14 perceived speech therapy as non-helpful. Frustration, anger, lack of carry-over to real-life situations, lack of belief trust between therapist and client, boredom and hatred towards therapy described. One person reported she went to speech therapy out of curiosity, four attended other forms of treatment such as speech and drama, which was described as a confidence booster. While holding negative opinions of therapy helped them become more fluent, eight viewed speech therapy as exerting a positive effect on their quality of life and three perceiving positive and negative effects. Three reported no effect on quality of life. Therapy described as boosting confidence, self-esteem, having techniques to fall back on, viewing and understanding stuttering, and identification with others. Thirteen reported using techniques or strategies to help them cope with their stuttering. Two of these did not use them all the time but it depended who the listener was. Varying the speech rate most common strategy used followed by changing words or phrases, advertising stuttering, taking a deep breath, word avoidance, avoiding eye contact and avoiding situations. Body language was also used as a strategy. Strategies perceived as helpful by nine participants were Easy Relaxed Approach and Easy Relaxed Approach Smooth Movement, shortening sentences, changing words/phrases, using airflow, interjections/filler sounds, light contacts, advertising and deep breathing. Techniques described as difficult and non-helpful by three people were airflow, rehearsing and deep breathing. Half reported that they had tried to find a cure for their stuttering, the other half described there being no cure/learning to live with it/accepted fact they stuttered. They gave their reasons for not trying to find a cure as making use of medication, a lack of facilities and had given up hope finding a cure. Three participants had not come to terms with their stuttering, others had to a greater or lesser extent | |
| Plexico et al. 2009146 Country: USA Study design: qualitative Data collection method: semi-structured interviews Aim: to develop a model of coping and a better understanding of the complexities within the coping responses of people who stutter Detail of participants (number, any reported demographics): nine adults, seven male and two female, age range 19–63 years. All reported to be coping with stuttering. Six Caucasian, two African American, one Indian; four educated to degree level, five some college education. Diverse occupations. Recruited through university clinical facilities |
Open-ended questions that were designed to elicit the participants’ personal experiences about coping with stuttering. Interviews were audio recorded and transcribed. Grounded theory analysis Control: N/A Length of follow-up: N/A Response and/or attrition rate: 13 originally contacted to participate. One did not turn up for initial interview, two could not be scheduled and one was excluded post interview owing to professional involvement with fluency disorders |
Interview transcripts were broken down into 1008 meaning units. However, because a meaning unit could be placed into more than one subcategory, there were a total of 1206 meaning units in the final hierarchy. The ‘core category’, the highest layer, subsumed four ‘clusters’ that constituted the second layer. The four clusters were developed from layer three that contained a total of 15 categories. Finally, the categories were derived from the fourth level that consisted of 39 ‘subcategories’ | This article describes the two clusters that address methods of escape as a coping response, and focuses on the categories and subcategories therein. Cluster 1: in an attempt to assuage the listener and protect myself, I devote a large amount of time and effort strategizing ways to prevent aversive communicative experiences Feelings of threat and anxiety result from a fear of being penalised by my listeners, and these feelings create inconsistency in my ability to manage stuttering and a desire to escape To protect myself from hurt and the listener from a stressful interaction, I try to take the perspective of the listener and assume responsibility for putting him/her at ease To protect myself from hurt and feeling a loss of control, I put a lot of effort into thinking about different ways to manage stuttering and speaking situations I cope with the urgency and fear associated with the need to respond to listeners in a timely manner by resisting the urge to speak immediately Cluster 2: using methods of escape provides relief and control but hazards the risk of isolation, frustration and emotional suffering I often withdraw from communicative situations because stuttering is inefficient and out of my control, and withdrawal results in a diminished quality of life Methods of escape provide momentary relief and distance from stuttering, but result in frustration from miscommunication and a narrowing of options Core category: coping with stuttering is a struggle to replace concerns to assuage listeners with a sense of self-acceptance that can lead to approach-oriented behaviours Conclusions: aside from one participant who professed that stuttering was ‘not a big deal’, the participants currently felt negatively towards stuttering or described how they had reacted negatively towards stuttering in the past. They stressed how they found stuttering to be extremely inefficient when attempting to communicate and how they experienced a variety of negative emotions including fear, frustration, shame, embarrassment, helplessness and anger |
Although the sample of participants is broad and diverse in terms of demographics, education, age, sex and therapy experience, the inclusion of participants who had never thought about seeking services would make the findings of this study more diverse. Second, the results of this study are based on the participants’ beliefs about their experience in coping with stuttering, not on formal observations of how the participants cope with stuttering. It is possible that the participants’ beliefs about how they cope with stuttering do not entirely match how they actually cope with the experience of stuttering |
| Plexico et al. 2009147 Country: USA Study design: qualitative (grounded theory) Data collection method: semi-structured interviews Aim: to identify patterns of coping responses by adults responding to the stress resulting from the threat of stuttering Detail of participants (number, any reported demographics): as Plexico et al.146 |
As Plexico et al. 2009146 Control: N/A Length of follow-up: N/A Response and/or attrition rate: as Plexico 2009147 |
As Plexico et al. 2009146 | Cluster 1: to improve my self-concept Cluster 2: when I focus on my own needs and experience of stuttering versus the listener’s needs, I have more agency and self-confidence, which in turn improves my fluency and self-concept Core category: coping with stuttering is a struggle to replace concerns to assuage listeners with a sense of self-acceptance that can lead to approach-oriented behaviours |
As Plexico et al. 2009146 |
| Plexico and Burrus 2012149 Country: USA Study design: qualitative. Phenomenological approach Data collection method: semi-structured interviews Aim: to describe in detail the underlying factors that may be relevant to being a parent of a child who stutters Detail of participants (number, any reported demographics): 12 participants, all with a child who stutters (aged 5–14 years), two male and 10 female, age range 25–49 years (mean 36.58 years ± 7.77 years). Six Caucasian and six African American |
Participants were recruited through either personal contact of the researcher, through word of mouth, or through personal contact of regional clinics and fluency programmes. The interviews did not have a pre-established time frame and took as long as it was necessary for the interviewer to feel that she had adequately captured the phenomenon of interest. The interviewer used a series of open-ended questions and unplanned prompts to elicit the participants’ personal experiences with the process of coping with having a child who stutters. Interviews were audio recorded and transcribed. Phenomenological analysis Control: N/A Length of follow-up: N/A Response and/or attrition rate: N/A |
What is the essential structure of coping with being the parent of a child who stutters? | Uncertainty about nature and cause of stuttering Coping strategies used to manage stuttering Parents cope with fear that their child will have negative experiences or live a restrictive lifestyle |
The participant pool cannot be viewed as a representation of all parents of all children who stutter. In addition, the results of this study are based on the participants’ descriptions about their experience in coping with a child who stutters, not upon formal observation. It is possible that the participants’ descriptions about how they cope with having a child who stutters do not entirely match how they actually cope with the experience. The results of the study were not enhanced by participant feedback. Questionnaires were sent to each of the participants, but none were returned. The poor response rate was a result of the intensive and time-consuming analysis and the time it took to later contact the participants |
| Plexico et al. 2005145 Country: USA Study design: qualitative Data collection method: interviews Aim: to understand how adults manage their stuttering Detail of participants (number, any reported demographics): seven participants, six male and one female, all history of stuttering well in to adulthood. Wide range of treatments experienced, age 38–59 years. All participants rated themselves as experiencing little or no handicap from the stuttering. On SSI-3 all were in the ‘very mild’ range. All were professionals and had at least one degree. Five of them were speech pathologists actively involved in providing services to stutterers, the other two participants were actively involved in self-help organisations |
Phenomenology approach. Interviews and assessment of stuttering using the Stuttering Severity Instrument (SSI-3) Control: N/A Length of follow-up: N/A Response and/or attrition rate: N/A |
Views and perceptions | Analysed data according to temporal stages – past if describing events from past when stuttering was essentially unsuccessfully managed, current if describing current situation when stuttering was successfully managed – transition describing transition from unsuccessful management to successful management of stuttering. Six consistent themes associated with transition – support from others, successful therapy, self-therapy and behavioural change, cognitive change, utilisation of personal experience, high levels of motivation/determination. Support systems provided a chance to connect with others who stuttered, disclose their stuttering and exchange information. Counselling support helped participants revise negative attitudes, feelings and thoughts related to stuttering. Some had mentors who respected them, were knowledgeable about stuttering, encouraging, supportive and understanding. Participants described helpful therapy during the transition process – provided behavioural tools and cognitive and affective elements needed to change fluency and how they felt about themselves as speakers. Self-therapy an instrumental part of transition. Described how had to take it upon themselves to work on their speech. Self-therapy could involve risk taking and self-disclosure. Importance of self-disclosure (letting participants know often by voluntary stuttering) provided a sense of freedom, diminished fear of discovery and reduced amount of avoidance behaviours. Cognitive change part of transition process – more willing to take risks, take responsibility, learn more about themselves as a speaker, adopt a positive attitude. Importance of recognising positive attributes in themselves to help compensate for negative impact stuttering having on their lives. Participants sought help for themselves and had an overwhelming desire to succeed with high levels of motivation and determination. Past experiences dominated by struggle and suffering, anxiety and negative emotions. Outcomes: current experience themes were optimistic and positive interpretation of life with stuttering no longer a major theme; a sense of freedom to act and speak on ones behalf | |
| Plexico et al. 2010148 Country: USA Study design: qualitative Data collection method: written responses to four questions Aim: to describe factors that contribute to successful or unsuccessful therapeutic interactions Detail of participants (number, any reported demographics): 28 participants, 19 males and nine females, age range 21–77 years, mean 39 years. Had received from 6 months to 12 years of therapy for stuttering; 21 had a degree |
Phenomenology. Recruitment via National Stuttering Association conference and support groups, personal contacts. Questions asked were: describe characteristics of effective SLP, describe how you felt in that interaction, describe an interaction with a SLP you felt not effective, describe how you felt in that interaction Control: N/A Length of follow-up: N/A Response and/or attrition rate: N/A |
View and perceptions | Characteristics distinguishing effective from ineffective clinicians were: communicate a passion for helping and genuine understanding, be client focused and pay attention to client goals and capabilities, foster a strong therapeutic alliance based on acceptance understanding and trust. Characteristics of effective clinicians: passionate, committed, have belief in the therapeutic process, have belief in the client’s ability to accomplish change. Effective clinicians are perceived as flexible and client centred in their approach to treatment. Customise treatment to meet needs of client and work closely to determine goals, needs and readiness for change. Need to provide the client with knowledge about the treatment process and are sensitive to what client needs at a particular moment in timer rather than having a pre-determined agenda for each session. Need to have a confident professional manner and possess a thorough and comprehensive understanding of stuttering and its treatment, including understanding physical and emotional aspects. Importance of establishing a therapeutic alliance with clients through being supportive and building a trusting relationship. Seeing client as a whole person and empathetic, honest and supportive. Actively listen to clients with a patient and caring demeanour. Need to encourage participation and urge action via encouragement and exhortation. Expectations should be communicated firmly and be realistic, that clients must practise and take responsibility for their own progress. Clients should be challenged beyond their comfort zone, to feel empowered to take risks and take charge of their communication abilities. Effective clinicians managed more than the speech dysfluency and emphasised effective communication rather than ideal fluency. Clients of effective therapists were more motivated and desired to attend therapy and achieve gains. Effective clinicians perceived as leading to increase in self-understanding and confidence resulting in stuttering being less dominant, increased fluency and reduced pressure to maintain complete fluency. Not effective – judgemental, lacking interest, knowledge or understanding, failed to show patience or to actively listen or focus on client’s goals and needs. Seen as dogmatic in their approach to therapy and likely to focus on techniques. This could lead to clients feeling misunderstood and a decreased interest in attending therapy; also created feelings of shame, inadequacy, hopelessness, frustration, anger, guilt, embarrassment and discouragement | |
| Stewart and Richardson 2004150 Country: UK Study design: qualitative Data collection method: interviews Aim: to investigate the experiences of adults who had completed therapy Detail of participants (number, any reported demographics): eight participants, seven male and one female, age range 23–59 years, mean 41 years, range of occupations, all had received the same programme of therapy individually and group with the same two specialist clinicians. Therapy received was combination of speak more fluently and stutter more fluently approaches grounded in client centred and PCP therapies. None of the participants were still receiving therapy, one had been discharged in 1996 and the rest in either 1998 or 1999 |
Selected from 77 clients receiving group therapy and who had been discharged from therapy between 1995 and 1999, also local self-help group. Thirteen volunteered, three did not attend the interview, two not met criteria Control: N/A Length of follow-up: N/A Response and/or attrition rate: N/A |
Views and perceptions | Effect of therapy: reduced isolation, a chance to meet like-minded people in group therapy and share experiences was greatly valued. In addition, the support received from others who stuttered. Support and empathetic understanding considered essential, feeling of being at ease. Seven out of the eight described significant changes experienced while attending the group sessions, group therapy more effective than individual. Seven perceived their fluency had increased but there was a lack of agreement on which techniques were helpful. Relaxation, rate control, desensitisation and focusing on content of utterance described as helpful. Two felt block modification and voluntary stuttering unhelpful. Some group experiences did not transfer to situations outside the group. Group considered ‘artificial’. Not a sense that skills were built on and situations became easier with time, application to everyday situations difficult. Half discussed usefulness of establishing a ‘toolbox’ of strategies, one could not remember having established these, another was not convinced therapy gave him the ability to continue to control his speech. Variability in speech control among participants; however, for many, outcome was attitudinal – fluency less of an issue of concern. Changes apparent in what clients felt able to do, feeling less fearful and stuttering less impact on being able to see themselves in positive light. Some discussed significant changes in training/employment opportunities and social activities as a result of having greater confidence. Content of therapy: suggestion that all possible interventions available should be outlined. Difference of opinion regarding balance of counselling and skills-based work during sessions. Three suggested generalisation/transfer work on interview, telephone and giving presentations needed. Need for support after sessions ended emphasised – booster sessions or weekends, periodic follow-up appointments, advanced group sessions or day courses | |
| Trichon and Tetnowski 2011151 Country: USA Study design: qualitative Data collection method: interviews Aim: to understand the experiences of individuals who attended a self-help conference Detail of participants (number, any reported demographics): 12 participants, seven male and five female, aged early 20s to mid-50s. Had taken part in self-help conferences for between 1 and 8 years |
Phenomenology, participants recruited from self-help conference and the self-help community. Interviews conducted 4–18 months after individual’s last conference Control: N/A Length of follow-up: N/A Response and/or attrition rate: N/A |
Views and perceptions | Socialising with others: self-help conferences a forum for conversing and building friendships with other people who stutter. Description of belonging, being in a place where not shunned or alone. Sense of becoming part of a community of people who stutter. Being there was an opportunity to redefine oneself, to accept themselves as a stutterer to be themselves. Participants described disclosure of their stutter as being a new experience or became easier after attending a conference, which could lead to being easier to talk with others after the conference about the participant’s stuttering |
Glossary
- Articulation
- The mechanism for producing speech sounds.
- Cluttering
- A fluency disorder characterised by a rapid and/or irregular speaking rate, excessive dysfluencies, disordered stress and pausing during speaking. It may co-exist with language or phonological errors and attention deficits. Cluttering is a different fluency disorder from stuttering, but it might occur alongside stuttering.
- Developmental stuttering
- Dysfluency of speech which has been present since childhood, this is distinguished from acquired stuttering which appears later in life.
- Effect size
- A way of measuring the size of the difference between two groups. An effect size of 0 indicates that two groups are the same. The convention for rating effect sizes is: a ‘small’ effect size is 20, a ‘medium’ effect size is 50 and a ‘large’ effect size is 80.
- Erickson S24 Scale
- This is an attitudinal scale for adults.
- p-value
- Probability value: the strength of evidence supporting that assumption that any difference found between groups is not the result of chance. A smaller p-value provides stronger evidence that the difference is not due to chance. The convention is to use levels of significance of p < 0.05 and p < 0.01.
- Speech and language pathologist
- A clinician who has completed an accredited training programme and specialises in treating people with communication difficulties.
- Speech and language therapist
- The term for a speech and language pathologist in the UK.
- Stutter
- Dysfluency of speech that may be characterised by repetition of the initial sound of words, repetition of whole words, ‘getting stuck’ and being unable to say a word, or avoiding certain words or situations because of a fear of stuttering.
List of abbreviations
- AAF
- altered auditory feedback
- ACT
- Acceptance and Commitment Therapy
- ANOVA
- analysis of variance
- CBT
- cognitive–behavioural therapy
- CSP
- Comprehensive Stuttering Program
- DAF
- delayed auditory feedback
- DCM
- Demands and Capacities Model
- ELU
- extended length of utterance
- EMG
- electromyography
- ES
- effect size
- FAF
- frequency altered feedback
- GILCU
- Gradual Increase in Length and Complexity of an Utterance
- LCB
- locus of control of behaviour
- LP
- Lidcombe Program
- MCAI-IV
- Multicomponent Anxiety Inventory IV
- OASES
- Overall Assessment of the Speaker’s Experience of Stuttering Questionnaire
- OECD
- Organisation for Economic Co-operation and Development
- OR
- odds ratio
- PCP
- personal construct psychology
- PS
- prolonged speech
- PSI
- Perceptions of Stuttering Inventory
- RCT
- randomised controlled trial
- SD
- standard deviation
- SESAS
- Self-Efficacy Scaling by Adult Stutterers
- SIFT
- semi-intensive fluency therapy
- SMT
- speech motor training
- SPM
- syllables per minute
- SSI
- Stuttering Severity Index
- STS
- syllable timed speech
- VSM
- video self-modelling