
Notes
Article history
The research reported in this issue of the journal was funded by the HTA programme as project number 11/141/05. The contractual start date was in January 2013. The draft report began editorial review in January 2014 and was accepted for publication in April 2015. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HTA editors and publisher have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
Nefyn Williams, Rhiannon Tudor Edwards and Joanna Charles’s posts are part funded and Noel Craine is employed by Public Health Wales. Jane Noyes received grants from the National Institute for Health Research (NIHR) Health Technology Assessment programme during the conduct of the study and received other financial support for speaking at a Diabetes UK conference sponsored by Janssen-Cilag Ltd, AstraZeneca UK, Boehringer Ingelheim Ltd, Eli Lilly and Company, Merck Sharp & Dohme Corp., Novartis Pharmaceuticals UK Ltd and Roche who may produce and distribute contraceptives to the target population of this systematic review outside the submitted work. Jo Rycroft-Malone is a member of the NIHR Health Services and Delivery Research (HS&DR) Board (commissioned research) and, since completing this research, she has been appointed director of the NIHR HS&DR programme.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2016. This work was produced by Whitaker et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Introduction
Background
The World Health Organization reports that there are 16 million births annually to mothers aged 15–19 years. Complications from pregnancy and childbirth are a leading cause of death in this age group. Repeat pregnancy in adolescents is a significant public health concern across the world, since it frequently occurs in the context of economic constraints and poor maternal and child well-being. 1–3 Despite data from the UK that are consistent with a gradual decline in teenage conception rates, the UK continues to have one of the highest rates of teenage pregnancy in Western Europe. 4–6 Repeat pregnancies represent a considerable proportion of the overall rate of teenage pregnancy: one-fifth of births among girls under 18 years of age are estimated to result from repeat pregnancies7 and thus are a crucial focus for intervention. Around three-quarters of teenage pregnancies are unplanned with up to half resulting in abortion. 8 Within the UK, teenage pregnancy is strongly associated with social disadvantage. The social predictors of repeat adolescent pregnancy are varied and, previously, have been usefully grouped into predictors operating at individual, couple, family, community and social levels. 9 These predictors share much in common with those of first teenage pregnancies. ‘Unintended’ or ‘unplanned’ pregnancy have often been used as a proxy measure of poor sexual health. 10
Teenage pregnancies have a considerable impact on the individual well-being of teenage parents and their children. Inherent within the national strategy responses, and a range of other national policy documents addressing this issue, is the recognition that babies of teenage mothers have increased mortality in their first year and a significantly increased risk of living in poverty, poor achievement at school and being unemployed later in life,11 with substantial costs to society. Teenage pregnancies are a target for the England Teenage Pregnancy Strategy and their equivalents within the devolved governments of the UK. 8,12–14
Teenage pregnancy is associated with an almost threefold risk of preterm delivery and stillbirth. 1,15 Young mothers who have had repeat pregnancies are vulnerable to health risks associated with early childbearing,16,17 abortion outcomes and sexually transmitted infections, including human immunodeficiency virus (HIV) and acquired immunodeficiency syndrome (AIDS). 18 They also face a number of challenges, including interpersonal violence and abuse,19 inability to complete school and substance abuse. 17 This results in a significant socioeconomic cost to the adolescent, their families and societies at large. Societal costs result from the increased use of general and specialist health services for mother and child, programme implementation, educational and skills training for young mothers (and staff supporting them) to provide psychosocial and economic empowerment, welfare assistance for young mothers experiencing financial difficulties and lost tax revenues arising from reduced earnings. 20–24
Repeat pregnancy in adolescents is defined here as the incidence of two or more pregnancies before the age of 20 years. Defining ‘intended’ poses a challenge since this term is used inconsistently in the professional literature. For example, ‘intended’, ‘unintended’, ‘mistimed’, ‘wanted’, ‘unwanted’ and ‘planned’ are used interchangeably. A validated index has been developed to produce reliable estimates of intention in pregnancy, which also assesses if, or how, women’s accounts changed over time. 25 For this review, we have conceptualised unintendedness as a construct based on unwantedness and mistiming to mean any incidence of pregnancy when intention was not specifically stated. 26 We have included literature covering any repeat conception in young women that was not specifically planned. A woman’s perception of her pregnancy may change over time. The difference between an unintended conception and an unwanted child is not within the scope of this review. We have concentrated on interventions designed to reduce conceptions.
Description of the interventions
To address the short- and long-term consequences of unintended pregnancies for adolescents, their families and the society at large, various local and national public health programmes have been implemented for first-time pregnancies. It is not clear whether or not these interventions are effective at preventing repeat unintended pregnancies in teenagers. Such interventions may be population-based strategies or policies, or comprise simple interventions targeting specific groups, for example interventions may include contraception advice or provision, or complex interventions that include a combination of school- and community-based or targeted efforts. These interventions may, for example, be nurse-led interventions or occur in a group setting which includes peer support. The building blocks for these interventions could include, in differing combinations, elements of health education, skill building, contraception education and distribution, individual counselling, etc. Furthermore, they could be designed to increase adolescents’ knowledge and attitudes relating to the risk of unintended pregnancies and promote delaying the initiation of sexual intercourse and encourage the consistent use of birth control.
How the interventions might work
Interventions which have been shown to be effective at reducing first-time teenage pregnancies focused on sex education, skills training for jobs and personal development. 27–29 These complex interventions were intended to reduce teenage pregnancy by increasing self-confidence and work opportunities, combined with increasing access to contraception. With regard to repeat pregnancy, there is an additional concern for the well-being of a young mother’s other children. Therefore, complex interventions may aim to address parenting skills and a knowledge of child development, as well as meeting the goals and needs of the young mother.
Heller30 postulated that a multidimensional, theoretical model of adolescent pregnancy is conducive to the application of a preventative intervention research cycle to reduce the incidence of adolescent pregnancy. Other diverse theoretical models have been borrowed from different disciplines. Based on literature related to adolescent pregnancy, we have identified five candidate theories for consideration. These theories take differing, but not mutually exclusive, attitudes to the mechanisms and drivers at work: (1) social–cognitive–ecological theory; (2) developmental theories; (3) resilience theory; (4) recoil–rebound theory; and (5) resilience–recoil–rebound theory.
Social–cognitive–ecological theory
Social–cognitive–ecological theory31 addresses cultural norms, modelling and the concepts of self-efficacy and support. It is based on Bandura’s32 postulation that a person’s internalised standards for behaviour are developed from information conveyed by sources of social influence (parents, peers and characters portrayed in mass media) and their environment. For example, a young mother may desire a repeat pregnancy to seek a sense of fulfilment as a woman, to create a stable relationship with her partner or to improve connections within her family.
Developmental theories
Erikson33 posited that an adolescent has physical, cognitive, socioemotional and moral goals to accomplish during their transition to adulthood. Developmental theories described in repeat pregnancy literature address this transition. In addition, they address the management and perception of pregnancy by adolescents, and the relationship between risky sexual behaviour and pregnancy. These theories also examine the development of health promotion behaviours in families led by adolescent parents. 34
Resilience theory
The concept of resilience can be described as ‘the process of identifying or developing resources and strengths to flexibly manage stressors to gain a positive outcome, a sense of confidence or mastery, self-transcendence, and self-esteem’. 35 Adolescent resilience theory focuses particularly on the ‘assets and resources that enable some adolescents to overcome the negative effects of risk exposure’. 36
Recoil–rebound theory
The main focus of this theory is the parenting adolescent mother’s resilience, social influences, recoil (having a repeat adolescent pregnancy) and rebound (the use of contraception or abstinence to prevent a repeat adolescent pregnancy). 37
Resilience–recoil–rebound theory
This model, proposed by Porter and Holness,37,38 has four central concepts: the adolescent, pregnancy, recoil–rebound interactions and resilience. The external influences of family, peers, school, church and community, though incorporated, are not major concepts within this theory.
Why it is important to do this review
A Cochrane review27 on interventions for preventing unintended pregnancies among adolescents reported 41 randomised controlled trials (RCTs) and three mixed studies (individually and cluster randomised). The results showed that complex interventions, which were primarily a combination of educational and contraceptive interventions, lowered the rate of unintended pregnancy among adolescents.
The UK National Institute for Health Research (NIHR) Health Technology Assessment (HTA) characterised the necessity for this systematic review in its call for proposals as follows:
Numerous prevention strategies such as health education, skills-building and improving accessibility to contraceptives have been employed across the UK in an effort to prevent unintended teenage pregnancy.
Oringanje et al. (2009)27
The commissioners go on to characterise the question further: ‘. . . there is uncertainty regarding the effects of these interventions, and in many areas the problem persists despite co-ordinated efforts to halve the number of teenage pregnancies over recent years’. 27 They point out that ‘Some groups of adolescents are at risk of multiple unintended pregnancies and it is not known if specific interventions or approaches will help to reduce the risk of further pregnancies in girls who have already had one pregnancy’. 27
As well as considering the effectiveness of interventions, there are broader questions to answer such as values for money, acceptability of interventions and the facilitators of and barriers to uptake of intervention. In addition, consideration should be given to how specific interventions might work, under what circumstances and in which groups of teenagers.
Aims of the review: the hypotheses tested and the research questions
The overall aims of this review were to identify and evaluate the effectiveness of interventions for preventing repeat unintended pregnancies among adolescents, and to investigate the barriers to and facilitators of their implementation and uptake. Although these overall aims were broad, the focus was on the implementation of interventions.
The specific research objectives were to determine:
-
What factors characterise subgroups that are at greatest risk of repeat unintended pregnancies (i.e. what are the predictors of repeat unintended pregnancy)?
-
Which (elements of) interventions appear to be effective, how do they work, in what setting and for whom? (Conversely, why are they ineffective/why do they not work?)
-
What are the barriers to and facilitators of the acceptability, uptake and implementation of interventions?
-
What is the relative cost-effectiveness of interventions?
Overall plan of the research
To address the complexity of the topic, a four-phase approach to the review was adopted:
-
Phase 1 We identified and filtered the literature by first applying inclusion/exclusion criteria then making a basic quality appraisal and a mapping of the literature types.
-
Phase 2 We prioritised and selected records for in-depth review and data extraction.
-
Phase 3 We synthesised the evidence according to study type and by using design-appropriate tools.
-
Phase 4 Finally, we gathered service user and stakeholder feedback and conducted an overarching narrative synthesis.
The map of these phases, evidence streams and methods of syntheses is fully described and illustrated in Chapter 3.
Structure of this report
Following this introduction, Chapter 2 fully describes all aspects of the search strategies, the sifting of evidence, the assessment of quality and the integration of the stakeholder’s consultation exercises. The methods employed for synthesising the different evidence streams are then discussed and, finally, details of the realist synthesis are given; this realist synthesis adds an extra dimension to the review by attempting to enable learning about the key contexts and mechanisms in order to provide a conceptual framework for the development of future interventions to prevent repeat teenage pregnancy. As the realist element is relatively unusual, we have detailed the rationale, methodology and approach in some detail.
Chapter 3, the results section, is divided into the results of the extractions and mapping exercises, including the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) flow chart (see Figure 3), and the four basic review questions which address who is at risk, what is effective and cost-effective, and what are the barriers to and facilitators of implementation. We then report other outcomes of interest. The results we report here arise from both qualitative and qualitative evidence streams.
Chapter 4 brings a realist synthesis approach to bear on the evidence in order to draw out candidate theories of action of the interventions, and to identify barriers to and facilitators of intervention implementation.
In Chapter 5, the results reported in Chapter 4 are brought together in an overarching synthesis to enable the reader to see all the evidence summarised in matrix form.
In Chapter 6, the discussion and conclusions section, the findings are summarised. In addition, the review’s strengths and weaknesses are discussed, and the results are compared with existing literature before describing knowledge gaps, the implications for practice and policy, and identifying potential areas for future research.
Chapter 2 Methods
This chapter describes all aspects of the search strategies, the sifting of evidence, the assessment of quality and the integration of the stakeholder and service user consultation exercises. We then briefly discuss the methods employed for synthesising the different evidence streams. This is followed by an explanation of the realist synthesis, which adds an extra dimension to the review by attempting to enable learning about the key contexts and mechanisms in order to provide a conceptual framework for the development of future interventions to prevent repeat teenage pregnancy. As the realist element of this systematic review is relatively unusual, we have detailed the rationale, methodology and approach in some detail in this chapter.
Overall study design
Initial scoping searches informed a tailored, four-phase approach to the review (Figure 1). For the overall framework of the mixed-methods review, we drew on the structured, phased, Evidence for Policy and Practice Information and Co-ordinating Centre (EPPI-Centre) approach,39 and used their reviews of young people, pregnancy and social exclusion, and the barriers to and facilitators of children’s healthy eating as methodological exemplars. 40,41 After conducting extensive literature searches, screening the evidence against explicit inclusion and exclusion criteria and applying two initial screening criteria from our chosen quality appraisal tool, a mapping exercise was undertaken to organise and describe the evidence so as to give a clear picture of the body of research (phase 1). We presented the findings of our mapping exercise to our service provider consultation group; individual feedback regarding the focus of the in-depth review and possible gaps in the evidence were also presented.
FIGURE 1.
Overview of review methods.
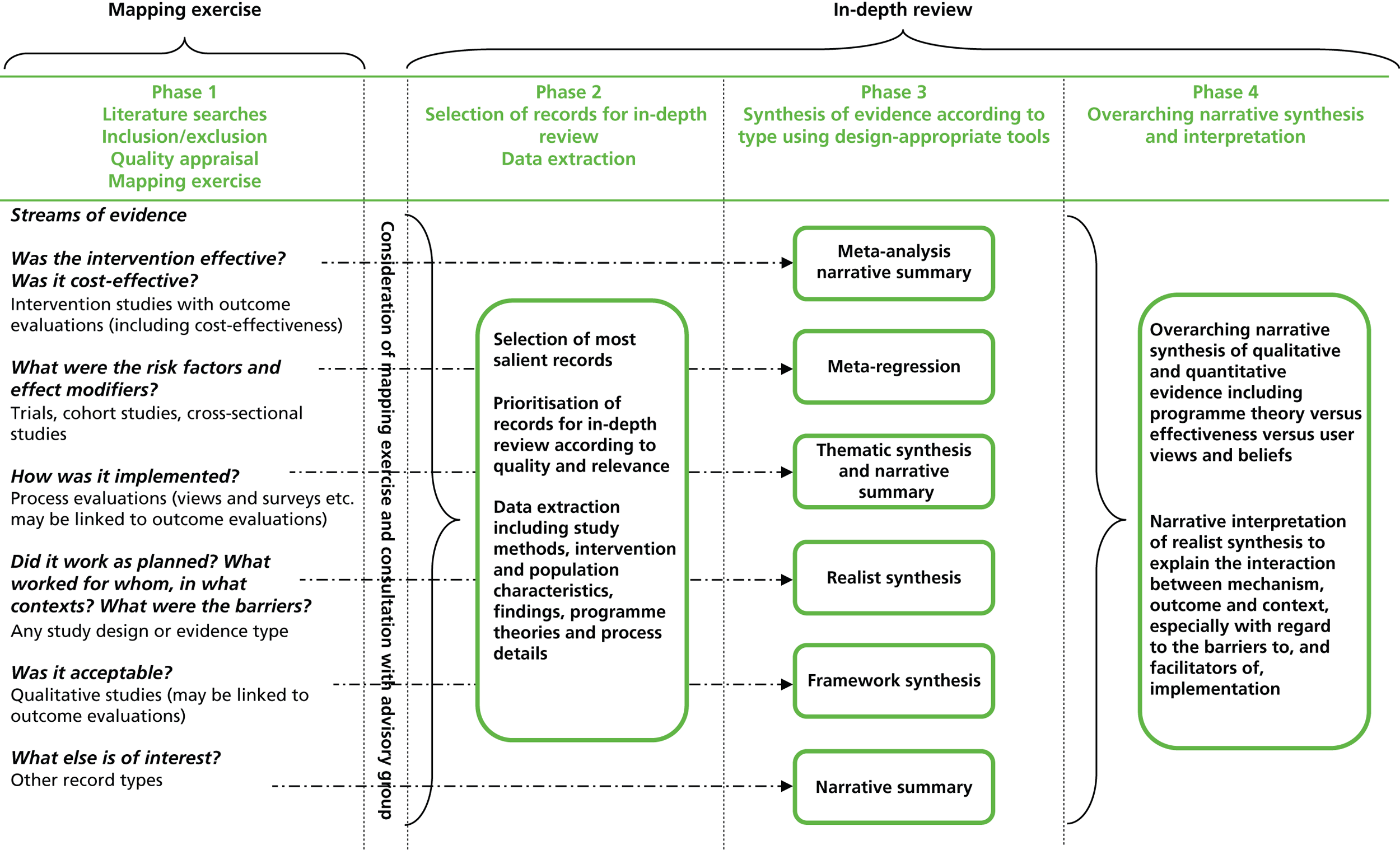
After the mapping exercise, we prioritised and selected records for in-depth review and data extraction (phase 2) before synthesising the evidence according to study type and by using design-specific methods which we describe in more detail later in this chapter. Members of the review team presented preliminary findings at a second meeting of the service provider consultation group and subsequently to a group of young women who had experience of teenage pregnancy and early parenthood at meetings facilitated by Flying Start staff members (phase 3). Finally, we conducted an overarching narrative synthesis and interpreted the results (phase 4).
Stakeholder engagement
Members of our team were involved in co-ordinating a project (the Empower to Choose project) targeting repeat teenage conceptions, which is part of the Welsh Government’s Sexual Health and Wellbeing Action Plan12 aimed at reducing the rate of unwanted teenage pregnancies. The project included the implementation of an intervention to (1) increase education and raise awareness of the benefits of long-acting reversible contraceptives (LARCs) in young women who present to services having conceived before their 18th birthday; and (2) provide a robust mechanism of referral to appropriate services for young women and capture patient-specific information that both supports individual patient care and allows audit of the number of looked-after children, the uptake of LARCs and pregnancy outcomes among this vulnerable group of young people. The work was guided by the Task and Finish Group, a group of practitioners, stakeholders, policy-makers and academics; Public Health Wales (PHW) co-ordinated this group and also facilitated the group engagement for this systematic review. The group also provided a route to engage with teenagers who had experienced pregnancy by utilising group members from two organisations that work with pregnant teenagers and young mothers: Barnardo’s Cymru (Cardiff, UK), which works with children, young people and families who are struggling to overcome the disadvantages caused by poverty, abuse and discrimination; and Flying Start (Swansea, UK), which is funded by the Welsh Government and brings together education, childcare, and health and social services to offer preventative interventions to improve outcomes for children. Both organisations work with pregnant teenagers and young mothers.
Literature searches
Databases searched
We conducted initial scoping searches to identify the volume and nature of the literature we were likely to encounter. Building on and revising those search strategies, we searched the major, relevant electronic databases (listed in Box 1) for published literature using strategies that combined thesaurus terms and keywords relating to pregnancy, termination of pregnancy (TOP) or parenthood with ‘adolescence’ and text word synonyms for ‘repeat’ or ‘subsequent’. These searches were conducted between May and July 2013 and updated in June 2014.
-
MEDLINE and MEDLINE In-Process & Other Non-Indexed Citations.
-
PsycINFO.
-
CINAHL (Cumulative Index to Nursing and Allied Health Literature).
-
NHS EED (NHS Economic Evaluation Database).
-
EMBASE (Excerpta Medica database).
-
BNI (British Nursing Index).
-
ERIC (Educational Resources Information Center).
-
SocAbs (Sociological Abstracts).
-
DARE (Database of Abstracts of Reviews of Effects).
-
CDSR (Cochrane Database of Systematic Reviews).
-
HTA Database.
-
SSCI (Social Sciences Citation Index).
-
ASSIA (Applied Social Sciences Index and Abstracts).
-
BiblioMap (the EPPI-Centre register of health promotion and public health research).
Design of search strategies
We used a search strategy developed and piloted in MEDLINE and subsequently modified for use in the other databases (full details of all the search strategies can be found in Appendix 1). Further modified versions of the same strategy were used to search the following databases for ‘grey’ literature: OpenGrey, Scopus, Scirus, Social Care Online, National Research Register, NIHR Clinical Research Network Portfolio and Index to THESES. To capture economic studies, we searched Research Papers in Economics (RePEc) and the American Economic Association’s electronic bibliography (EconLit). We applied an alternative search strategy specifically designed to capture the type of descriptive titles that are common in qualitative studies to the following selected databases: Sociological Abstracts (SocAbs), Applied Social Sciences Index and Abstracts (ASSIA), British Nursing Index (BNI) and the Social Science Citation Index (SSCI). This strategy combined additional synonyms for ‘pregnancy’, ‘adolescence’ and ‘repeat’ with a brief qualitative filter comprising three broad free-text terms, ‘qualitative’, ‘findings’ and ‘interview$’, that has been shown to be as effective as a more complex one. 42,43
A number of systematic reviews related to teenage pregnancy have been published in the last two decades. The earliest we found in our scoping search was dated 1997. 44 Therefore, after allowing for an additional conservative margin, we limited our searches to 1995 onwards. We intended to conduct a separate sensitive search excluding the terms for second or subsequent pregnancies but including a filter for systematic reviews as a means of capturing relevant data from earlier studies; however, our expert panel advised us that social norms and behaviours relating to teenage motherhood have changed dramatically and that they considered evidence related to contraception more than 10 years old to be of limited relevance. Therefore, we omitted this additional search.
Owing to the dearth of UK literature identified in the database searches, we developed an additional strategy to identify UK grey literature using the search engine Google (Google Inc., Mountain View, CA, USA). This strategy comprised 24 search terms that were variations on ‘repeat’ or ‘second’ and ‘teenage’, ‘teenager’, ‘teenagers’, etc. and ‘pregnancy’ or ‘pregnancies’, each prefaced by the term ‘site: UK’. This search was conducted in January 2014.
In July 2014, we conducted repeat searches by (1) rerunning or updating the searches from all the relevant databases; (2) citation tracking the RCTs and systematic reviews identified during the course of our literature searches using ‘forward chaining’ and ‘backward chaining’ techniques;45 and (3) using the Google Scholar alert function to indicate any new trials on repeat adolescent pregnancy.
The issues surrounding implementation of interventions are a primary focus of this systematic review; qualitative and process evaluation evidence associated with trials is highly relevant, particularly to better understand the facilitators of and barriers to implementation. 46 Therefore, a key feature of our search strategy was to identify ‘evidence clusters’, that is studies that investigated the implementation or acceptability of interventions related to key RCTs. 47 These studies have the potential to indicate the effectiveness of an intervention as well as its acceptability to users and barriers to its implementation and uptake. However, we were unable to capitalise on the full potential of the approach as we wished to explore UK-relevant implementation issues, and all but one of the trials we identified were conducted in the USA and the other was conducted in Australia.
Finally, also in July 2014, we compiled a list of journals that had published the RCTs and the qualitative studies included in our review and compared this list with the Master List of hand-searched journals and conference proceedings (journals/conference proceedings being hand-searched by Cochrane Entities);48 we hand-searched the online indexes of 17 English-language journals that did not appear in this Master List from January 2010 (see Appendix 1). Because of time constraints and practical difficulties we did not search the index of one foreign language journal.
References were managed using EndNote bibliographic reference management software (Thomson Reuters, CA, USA) and extracted data were organised in a database using Microsoft Access® (Microsoft Corporation, Redmond, WA, USA). Two reviewers independently screened titles and abstracts to identify potentially relevant documents, which were retrieved and assessed according to the inclusion criteria described below (see Study inclusion criteria). Disagreements were resolved by discussion or, when necessary, by a third reviewer.
Stakeholder engagement exercises
Mapping exercise
In November 2013, we facilitated a meeting with a group of stakeholders, including public health, primary care, sexual health, obstetrics and midwifery representatives, as well as the full review team. A report of the meeting, including a list of those who attended, can be found in Appendix 2. We presented initial results from our mapping exercise to describe the scope of the literature we had identified and we conducted a workshop with three discussion groups which focused on linking the different topics to the group members’ experiences. We asked the subgroups at the meeting a range of questions; these are listed below:
-
How relevant is evidence from different settings and particularly from non-UK studies to your context?
-
What components of complex interventions do you consider to be most important in relation to reducing repeat pregnancies?
-
How relevant are other outcomes (health-related, social, educational, maternal or child-related, etc.) to repeat pregnancies?
-
Are repeat teenage pregnancies truly unintended? (What are the differences between unintended, unplanned and unwanted pregnancies?)
-
In your experience, what are the differences between the motivating factors for repeat teenage pregnancies and first teenage pregnancies?
-
Which intervention components best address the factors that motivate young women to have (or not to avoid having) a repeat pregnancy?
-
What are the barriers to and facilitators for accessing interventions?
-
What is the best way of packaging and presenting an intervention to teenage mothers to ensure maximum uptake (such as pregnancy spacing, making healthy choices, using contraception effectively, planning your future or others)?
-
How is the success of a programme best measured in monetary terms?
The meeting was concluded with feedback from the groups and discussion.
Presentation of preliminary findings and feedback exercise
In June 2014, a second meeting was facilitated as part of the work of the Task and Finish Group which co-ordinates the PHW response to teenage conceptions. Members of this group included public health, primary care, sexual health, obstetrics and midwifery representatives, as well as members of the review team. A report of the meeting, including an attendee list and comments made by stakeholders, can be found in Appendix 3.
We presented an overview of the study and progress to date, together with Phase 3 results from the quantitative and qualitative syntheses of the study, as well as preliminary findings from our realist synthesis, and invited feedback from the delegates.
We then presented the delegates with the following questions and received comments:
-
What do these findings mean to you within your work context?
-
Who do you think should hear these findings?
-
How do you think these findings should be delivered to these audiences to maximise uptake?
-
Is there a policy message?
-
Do these findings make sense to you?
-
How similar are they to the interventions you are delivering locally?
The findings from these meetings contributed to the realist synthesis (see Chapter 4) and informed the overarching synthesis (see Chapter 5).
Service user engagement
Two members of our team presented the findings of the review to a group of 17 young mothers, ranging in age from 15 to 22 years in April 2014. Flying Start helped us to organise and facilitate this meeting. Based on the evidence generated during the review, we sought opinions on the following three areas: (1) contraception, (2) psychosocial programmes and (3) barriers to and facilitators of the uptake of interventions. The findings were presented to the group through a range of person-centred activities. For example, to present the findings regarding contraception we used pictures of each contraceptive method on a flipchart with space to record summary points and keywords. The views expressed and the discussion that was stimulated are summarised in Appendix 4 and were used to inform both the realist synthesis and the narrative synthesis of this report.
Study selection
Study inclusion criteria
We included published studies from any country. Our search strategy was designed to capture published studies of any type, including trials of interventions, effectiveness studies, interrupted time series studies, cost-effectiveness studies, process evaluations, surveys and qualitative studies of participants’ views and experiences of interventions. We also considered relevant grey literature of any type, such as unpublished reports, service evaluations and theses, but limited this to UK-based literature so as to be applicable to the NHS and UK public health bodies. We set the earliest date for published work as 1995 and excluded any studies that reported data collected prior to 1990. We described the inclusion criteria using the patient intervention comparison outcome (PICO) framework. 49
Population
The population of interest comprised young women, aged ≤ 19 years at the time of conception, who had had at least one unintended pregnancy, whether the outcome was termination, miscarriage or delivery. If study populations were mixed, we included studies if at least 75% of the reported populations were young mothers in our target age group. 27
Interventions or phenomena of interest
We included studies of any intervention designed to reduce or delay repeat pregnancies (also referred to as ‘birth-spacing’ or ‘pregnancy-spacing’) in these young women, delivered in any educational, health-care or community setting. Interventions could have single or multiple components, and could be delivered to individuals or communities. We included studies designed to identify risk factors or subgroups at increased risk of repeat unintended pregnancy, or qualitative studies describing the experience of repeat teenage pregnancy if there was no actual intervention.
We included studies that identified barriers to and facilitators of the implementation and uptake of interventions, and explored the views of intervention recipients, providers and health professionals, particularly when information on whether or not the intervention was implemented and worked in the way intended was available. We looked for studies that could help us to identify programme theories and logic, and we looked for, and developed, candidate theories to explain why some young women have more than one unplanned pregnancy, in order to explain the relative success or failure of particular interventions. 50
Comparators
The comparators were no intervention, standard practice or an alternative intervention. Qualitative studies and studies containing epidemiological data suitable for contribution to risk factor assessment without a comparator were also included.
Outcomes
For this review, we selected studies that met the inclusion criteria irrespective of the results found. We focused on studies that reported on any primary or secondary outcomes of interest.
Primary outcomes
-
Effectiveness of interventions (reducing unintended teenage pregnancy).
-
Acceptability of interventions (the proportion of participants that reported the intervention was acceptable or, in the absence of this, the proportion of participants who were willing to be recruited into the study).
-
Uptake of the interventions (the proportion of participants who were recruited and received the intervention compared with those recruited).
Secondary outcomes
-
Reported changes in knowledge and attitudes about the risk of unintended pregnancies.
-
Age at initiation of sexual intercourse.
-
Use of birth control methods.
-
Abortion.
-
Childbirth.
-
Morbidity related to pregnancy, abortion or childbirth.
-
Mortality related to pregnancy, abortion or childbirth.
-
Sexually transmitted infections (including HIV).
-
Risky behaviours.
-
Abuse.
-
Validated quality-of-life indices.
The other phenomena of interest for the qualitative synthesis and realist review were the views and experiences of young women, families and professionals, and the identification of barriers to and facilitators of interventions relating to (1) acceptability, (2) uptake and (3) feasibility of implementation.
Study exclusion criteria
We did not exclude quantitative studies found in non-English-language publications; we used English-language abstracts, if available, to help decide whether or not they met our inclusion criteria and an online language translation service, Google Translate, to aid data extraction. Abstracts in which results could not be confirmed in subsequent publications were excluded. We found that translation software was adequate for the quantitative data extraction of baseline variables and outcome data but we were not confident of its reliability for the quality appraisal of studies; therefore, we asked a Spanish-speaking team member to appraise the quality of the foreign-language studies (which were published in Spanish and Portuguese).
A priori we had decided to exclude non-English-language qualitative studies if we had no native speakers available because of the complex nature of the linguistic validation of translations on such nuanced work. We did not, however, encounter any such papers so there was no loss of data.
We limited our searches for unpublished material to the UK to enhance the direct applicability of the results to the NHS and UK public health bodies. This judgement was supported by advice from the advisory group obtained during the stakeholder engagement exercise. Once studies found in the grey literature had met a very basic quality standard (see Quality appraisal section) they were included in the in-depth review and we incorporated further judgements about study quality when interpreting the evidence.
Data extraction
We created a bespoke set of data extraction forms to collect data from each study on the following: study characteristics (design, sample type, sample size, etc.); a description of the intervention or risk factors; the contextual factors in the study setting; the outcomes, including the costs of implementing the intervention; and programme theories or mechanisms described by the authors in the rationale behind the intervention or postulated in the explanation of the results. For quantitative studies, data extraction of study characteristics was undertaken by one reviewer and checked by a second reviewer. The risk and outcome data were extracted independently by two reviewers and then compared; any disagreements were resolved by discussion and recourse to a third reviewer if necessary. Data extraction was performed on qualitative studies collaboratively by two reviewers.
Prioritising evidence for the in-depth review (further study inclusion criteria)
The review team, with advice from independent experts obtained during the stakeholder engagement exercises, prioritised the evidence for in-depth review. Beginning with evidence relating to primary outcomes and within each grouped set of data, we prioritised the best quality evidence of most relevance to address the research questions. In order to systematise this process we applied the completeness, accuracy, relevance and timeliness (CART) framework, whereby evidence is judged on the criteria of completeness, accuracy, relevance and timeliness. 51 We developed a protocol for applying CART criteria which can be found in Appendix 5. We screened all the studies using these criteria.
Study classification: Effective Practice and Organisation of Care classification
We classified all the quantitative papers using the flow chart shown in Appendix 6, in accordance with the Effective Practice and Organisation of Care (EPOC) Group’s non-randomised studies methods guidance on incorporating diverse types of evidence in a review (see Appendix 19). These guidelines classify the study designs to use for the evaluation of the effects of health-care interventions. If quantitative papers did not meet inclusion criteria for the quantitative effectiveness evaluation but did provide insights for either the qualitative or realist syntheses, they were transferred to that evidence stream for assessment. All studies that contained epidemiological data, no matter how they were classified according to EPOC criteria,52 were considered as part of the risk factor identification.
Quality appraisal
The protocol for part of this review is registered with Cochrane and we intend to be publish some of the findings as a Cochrane review. Therefore, RCTs and quasi-RCTs were assessed using Cochrane’s risk of bias tool. 53 We categorised and reported the overall risk of bias for each of the included trials as having:
-
a low risk of bias (plausible bias unlikely to seriously alter the results) if all criteria were met
-
an unclear risk of bias (plausible bias that gives rise to some doubt about the results) if one or more criteria were deemed unclear
-
a high risk of bias (plausible bias that seriously weakens confidence in the results) if one or more criteria were not met.
The Cochrane risk of bias tool was supplemented by the mixed-methods appraisal tool (MMAT)54 (see Appendix 7 for mixed studies reviews). This MMAT has the advantage of incorporating the appraisal of several different study designs (qualitative, RCT, non-RCT, observational and mixed methods) using a single tool with a coherent range of quality criteria. 55
We slightly amended the published version of the MMAT54 for the qualitative studies by adding an alternative response, ‘somewhat’, for items that were partially described if we considered that either a ‘yes’ or a ‘no’ response would be misleading. We used the MMAT assessment items relevant to the qualitative analysis as follows:
-
Are the sources of qualitative data (archives, documents, informants, observations) relevant to address the research question (objective)?
-
Is the process for analysing qualitative data relevant to address the research question (objective)?
-
Is appropriate consideration given to how findings relate to the context, for example the setting, in which the data were collected?
-
Is appropriate consideration given to how findings relate to researchers’ influence, for example through their interactions with participants?
Pilot studies suggested that the MMAT54 was an efficient and reliable tool. However, it does not cover economic evaluations; therefore, for such evaluations, we used the Drummond checklist, which is recommended for economic studies56 (see Appendix 8).
Certainty of evidence
We used the accepted Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach to assess the certainty of the findings of reviews on effectiveness. 46 This is an overall quality of evidence rating which is combined to categorise the quality of evidence across outcomes as:
-
high, meaning that further research is very unlikely to change confidence in the estimate of the effect
-
moderate, meaning that further research is likely to have an important impact on the estimate of the effect and may change the estimate
-
low, meaning that further research is very likely to have an important impact on the confidence in the estimate of the effect and is likely to change the estimate
-
very low, meaning that any estimate of the effect is very uncertain.
However, the GRADE approach is not suitable for appraising the certainty of qualitative evidence; therefore, for qualitative evidence, we used the recently developed CerQual (certainty of the qualitative evidence) method47 to assess our level of certainty in the findings of the qualitative synthesis. Using the CerQual approach, our assessment of certainty was based on two factors: the methodological limitations of the individual studies contributing to a review finding and the coherence of each finding. Firstly, we agreed on a set of 25 findings statements that covered the main key findings of interest from the thematic synthesis. For each finding statement, we made a note of the studies that made a contribution to that finding. We agreed on how many studies made a contribution and the relevance of their context, and attributed an overall rating to the specific finding (high, medium or low) with a statement to explain the rating. We then looked at the quality of the studies (as assessed by the MMAT)54 contributing to the specific finding and attributed an overall rating (high, medium or low). However, the MMAT assessments were so adversely affected by poor reporting of the study methods that we also considered the extent to which the findings of each study were supported by extracts from the original data (i.e. the ‘thickness’ and ‘richness’ of the supporting data). The final rating was a combination of the two (high, medium or low) and we recorded a brief explanation.
Using the MMAT54 and based on the richness and thickness of the data, we deemed the qualitative studies to be of moderate to high quality. All of the qualitative studies supported their findings by quoting extracts from the data and, in several cases, there was evidence of in-depth engagement with participants resulting in particularly rich data sets. We considered whether or not findings were seen in more than one study and in more than one country and, in view of the limited geographical spread of the evidence (seven studies from the USA, two from the UK and one from Australia), whether or not it seemed plausible that they would be transferable between these contexts and to other comparable settings. Overall, our confidence in the certainty of findings was high (for 18 findings) to moderate (for four findings), with only three findings achieving low certainty because they were found in only one study and either the data supporting the finding was relatively weak or the finding itself was equivocal. A table summarising the qualitative findings and indicating the level of certainty for each finding, and a brief explanation of the assessment, can be found in Appendix 17.
Whether or not evidence from studies was included in the realist synthesis conceptual framework was based on an assessment of its relevancy and rigour. 57 Pawson58 stated that ‘Judgements about rigour are made not on the basis of pre-formulated checklists, but in relation to the precise usage of each fragment of evidence within the review’. Hence, pieces of evidence from the included studies were used to help us make sense of the programme theories we were exploring.
Mapping the evidence
We undertook a mapping exercise in accordance with the EPPI-Centre method. 40 We categorised the studies according to the study design or type of record (intervention study, process evaluation, qualitative study, report, etc.), the country, the health, educational or community setting in which the study took place, the topic or focus of the study/report, the population focus of the study/report and the study design. From the grouping exercise, we developed a descriptive map of the literature and used it to identify gaps in the identified research. The map also provided a basis for refining the scope of the review by aiding the advisory group at a meeting held late in Phase 1 to identify areas for in-depth focus.
Analysis and synthesis
The data that we considered in this review are diverse, and the data analysis and synthesis were complex. The choice of synthesis method depended on the questions addressed and the type of data included. Figure 1 illustrates the method of synthesis proposed for each evidence type.
Descriptive study summaries
We present the full findings of the data extraction exercise for studies included in the meta-analysis of RCTs and in the qualitative synthesis in a table of study characteristics (see Appendix 18). These include the study details, the setting, the population, the quality appraisal and the methods. We present sociodemographic characteristics known to be important from an equity perspective. For this process, the PROGRESS (place, race, occupation, gender, religion, education, socioeconomic status and social status) framework was utilised. 59 For the studies that were included in the risk factor analysis, a brief summary table containing the study type and PROGRESS data is included (see Appendix 19).
Quantitative meta-analysis
Measures of intervention effect
We have presented quantitative continuous outcomes using the original scales that were reported in each individual study. When appropriate, if the studies used different scales, we standardised the scores by dividing the estimated mean difference by its standard deviation (SD). Dichotomous outcome data were fitted with a random effects model using the Mantel–Haenszel test and presented as risk ratios (RRs). All outcome data were reported as effect sizes with associated 95% confidence intervals (CIs).
Unit of assessment
In all studies, the unit of assessment was the individual.
Assessment of heterogeneity
We assessed both clinical and statistical heterogeneity. Clinical heterogeneity was assessed by examining the characteristics of the studies, the similarity between the types of participants and the interventions, while statistical heterogeneity was assessed using the I2-statistic. We have reported statistical heterogeneity as important if it is at least moderate to substantial (I2 > 30%) and we have not pooled data when statistical heterogeneity was severe (I2 > 90%); if statistical heterogeneity (I2 between 60% and 90%) could be explained by clinical reasoning and a coherent argument made for combining the studies, the data were entered into a meta-analysis. After exploring the heterogeneity, if a coherent scientific argument could not be found, the study causing the heterogeneity was excluded and the analysis was repeated as a sensitivity analysis. If the heterogeneity was not adequately explained, the data were not pooled in a meta-analysis. In this case, or when only single outcomes were reported, we presented study findings in tables (see Appendix 19) and explored the relationships within and between studies in a narrative summary. 60
Assessment of reporting biases
We performed an assessment of reporting bias if we found an adequate number of studies (at least 10) by observing funnel plot asymmetry. 61 Possible sources of asymmetry were explored with an additional sensitivity analysis and the studies at greatest risk of bias removed. The most likely unbiased intervention effects are summarised in the meta-analyses (see Appendix 11 for judgements of risks of bias).
Dealing with missing data
If data were missing or unclear, we contacted the investigators of the primary research (see Appendix 9). After such correspondence, if the degree of imbalance in dropout between the groups was small and could be argued to be completely missing at random, data would have been re-analysed in accordance with a treatment-by-allocation principle62 whenever possible. However, in no case could this assumption be made so we used the available case population for meta-analyses.
Subgroup analysis and heterogeneity
Subgroups included and highlighted within the primary research as important confounders were used to identify risk factors as well as explain heterogeneity. The following were considered important factors with regard to exploring differences in intervention effectiveness: the age of the young mother; the deprivation index of the area of residence; the length of follow-up; a history of substance misuse; and looked-after children (or care leavers). However, none of these factors was found to be informative so no subgroup analyses were performed.
Certainty of the findings
After the primary analysis, the quality of the overall evidence for each outcome was judged using the GRADE approach (Guyatt et al. ). 46 In this approach, evidence from each outcome is initially rated as high if from randomised trials but its quality may then be ‘down-graded’ depending on the following factors:
-
limitations in study design or execution (risk of bias)
-
inconsistency of results (based on between-study heterogeneity)
-
indirectness of evidence (i.e. how closely the outcome measures, interventions and participants match those of interest)
-
imprecision (based on the CIs around the effect size)
-
publication bias.
GRADE profiler software was used to grade the evidence and generate evidence profile tables, which include a summary of the findings, number of participants in each group, the quality of the evidence for each outcome and an estimate of the magnitude of the effect. An example of GRADE profiles is shown in Appendix 10.
Investigation of risk factors using metaregression
A key aim of the review was to search, identify and summarise the populations of young girls that are at greatest risk of repeat pregnancy (by, for example, considering income, social deprivation, ethnicity, degree of rurality, substance misuse, whether or not currently in care or care leavers, and those from vulnerable or at-risk communities). We expected that these factors would be considered and summarised as important confounding variables within RCTs, quasi-RCTs and cost–benefit analyses for studies investigating interventions to reduce repeat pregnancies. We also aimed to identify non-interventional studies that present epidemiological data (e.g. cohort studies, cross-sectional studies and policy documents) of effect modifiers associated with an increased risk of repeat pregnancy. We shortlisted possible risk factors from a review by Rigsby et al. 17 and added any risk factors which were supported by several studies. Data were extracted and summarised and, if possible (if 10 or more studies reported similar factors), presented in a metaregression summarising the standardised effectiveness by presenting the slope parameter, with the associated 95% CIs. Graphical representations of the metaregressions were plotted using the square root of the sample size for each of the studies.
Cost-effectiveness
We provide a narrative review of economic evaluations of interventions specifically designed to reduce the number of unintended repeat teenage conceptions. We planned to stratify any economic studies found by the public health lever mechanism used; examples of such mechanisms are government, statutory or legal mechanisms, public information mechanisms, school-based group or targeted interventions, and NHS- or charity-initiated mechanisms. We were particularly interested in the perspective of the analysis or the type of economic evaluation (e.g. cost analysis, cost–benefit analysis, cost-effectiveness analysis or cost–utility analysis). We documented the way in which these studies attempted to overcome the methodological challenges specifically associated with these types of complex, preventative, behavioural change based interventions. 63–66 We planned to conduct a meta-analysis of the economic evidence (if the data were sufficiently homogeneous to allow it).
Qualitative studies
For qualitative studies, we developed, a priori, a coding framework adapted from the Support Unit for Research Evidence (SURE) framework67 for identifying factors affecting the implementation of a policy option (see Appendix 12), which was successfully used in a qualitative systematic review of barriers and facilitators to the implementation of lay health worker programmes to improve child and maternal health. 47 Data were coded directly from the papers into the framework and thematic syntheses were conducted using a framework method developed by Ritchie and Spencer. 68
Surveys, process evaluations and other types of data
Data from surveys, process evaluations and other sources, such as reports, may be either semi-narrative or quantitative or both. Data were extracted to present evidence of acceptability and uptake of interventions, and were synthesised in a narrative summary and aggregated using thematic analysis. 69
Realist synthesis
We selected subsets of evidence and applied the principles of realist synthesis. 58,70,71 We identified explicit or implicit theories which postulate how an intervention has an underlying causal mechanism that works in a defined social context to result in a particular outcome. Such theories may also be used to explain the failure of an intervention. Additional theories were identified from the wider literature (e.g. policy documents), the advisory group members or personal contact with other experts in the field. Data synthesis involved individual reflection and team discussion in order to question the integrity of each theory, adjudicate between competing theories, consider the same theory in different settings and compare the particular theory with actual practice. 72 Coded data from the studies were then used to confirm, refute or refine the candidate theories. Thus, we attempted to explain which interventions work, for whom and under what circumstances.
Background
The study protocol73 outlines the plans to apply realist synthesis principles to the subsets of evidence that were included in the review, in order to provide an indication of the interventions’ causal mechanisms of action. Chapter 6 describes the findings, followed by implications for future intervention development and research.
Approach
A realist review adopts a theory-driven approach to evidence synthesis, which is underpinned by a realist philosophy of science and causality. 58,74 According to Pawson,58 any synthesis of evidence needs to investigate why and how interventions might work and in what contexts. The aim then is ‘to articulate underlying programme theories and then to interrogate the existing evidence to find out whether these theories are pertinent and productive.’58 In realism, theory is construed and framed in terms of a proposition about how and why interventions work (or not).
As this component was embedded in the broader evidence review and therefore not a full realist synthesis, we took the principles of realist synthesis and applied them in the interlinked stages described in the following sections.
Identifying the territory
During the full screening of the papers for inclusion in the full review, the realist synthesis team met to map the conceptual and theoretical territory of the literature being retrieved (see Appendix 13). This involved a high-level theming process managed through deliberative processes, which were informed by the original brief, review questions, emerging evidence and other policy documents. This process resulted in a list of questions of interest that covered a number of different domains. At the individual level, the overarching question was ‘What factors predict repeat unintended teenage pregnancy?’ For example, family support, community, having an older boyfriend, and drug and alcohol abuse were considered as potential predictors of teenage pregnancy. Other questions resulting from this process were:
-
What personal factors (e.g. age, level of education, ethnicity, family support or peer influence) influence successful contraceptive use?
-
How does lack of knowledge affect repeat unintended teenage pregnancy?
-
How does social connectedness affect repeat unintended teenage pregnancy?
-
How do social, community and environmental factors influence repeat unintended teenage pregnancy?
-
How does living in an area of socioeconomic deprivation affect repeat unintended teenage pregnancy?
-
How can empowerment and realistic goal-setting facilitate interventions to reduce unintended teenage pregnancy?
-
What affects a girl’s motivation to prevent a repeat unintended teenage pregnancy?
At an intervention level, the overarching question was ‘What factors facilitate intervention delivery?’ This question addressed, for example, which health professionals should deliver the intervention or the optimal time for delivering the intervention. Other questions included:
-
How do individual components of complex interventions impact on repeat unintended teenage pregnancy rates?
-
How do home visits as part of an intervention delay repeat unintended teenage pregnancy?
-
How can the delivery setting increase the success of an intervention?
-
When is the optimal time to deliver an intervention to reduce repeat unintended teenage pregnancy?
-
How can psychosocial models (e.g. Health Belief Model) be utilised in interventions to reduce repeat unintended teenage pregnancy?
-
What are the barriers to successful contraception use?
-
How does mentoring and counselling from another teenager or peer counsellor reduce repeat unintended teenage pregnancy?
-
How can tailoring be utilised in an intervention to reduce repeat unintended teenage pregnancy?
-
How does funding affect contraception use?
-
What factors influence attrition in interventions delivered to reduce repeat unintended teenage pregnancy?
-
Are multiple component interventions more effective than single component interventions at reducing repeat unintended teenage pregnancy?
-
Are group delivered interventions more effective than individually delivered interventions at reducing repeat unintended teenage pregnancy?
When considering the team delivering the intervention, the overarching question was ‘Who is the optimal practitioner to deliver an intervention to reduce repeat unintended teenage pregnancy?’ Other related questions are listed below:
-
What qualities does a practitioner need to have to deliver an intervention to reduce repeat unintended teenage pregnancy?
-
Are trained peer mentors more effective than older professional practitioners at delivering interventions to reduce unintended pregnancy?
Developing the conceptual platform for the review
Through further reading of the evidence that was emerging from the searching processes and a process of mapping, the realist review team constructed a series of conceptual maps that were linked to the questions outlined above. These maps represent the clustering of concepts, which, through further discussion and deliberation, were developed into four theory areas of interest for the realist review of evidence gathered. The theory elements identified are discussed in Chapter 3.
Stakeholder engagement
We had the opportunity to ‘test’ these theory areas with a group of stakeholders at the first stakeholder meeting (see Appendix 2). We gave the stakeholders an opportunity to add or amend the content of the theory areas through the use of an engaging process by which they could annotate the conceptual maps and provide a rationale for their suggestions. This resulted in some additions to the theory areas of connectedness and motivation.
Data extraction
The theory areas were made visible in the data extraction forms. We also developed a ‘crib sheet’ (see Appendix 13, Table 15) for the team to cross-reference as they were extracting data to act as an aide-memoire of the evidence they were searching for. The team met on a regular basis to discuss any further evidence they found in relation to the theory areas. As part of this process, the theory area ‘Targeting’ became ‘Tailoring’. ‘Setting/environment’ was spilt into evidence concerning the individual and evidence concerning the intervention. Two new areas were developed: ‘Other goals/aspirations’ and ‘Perceptions/ideas of parental responsibility’.
As extraction progressed, any new information found by the reviewers that did not fit into the theory headings was highlighted and given a new heading name, an explanation of what the theory area contained and keywords. As new theory areas emerged the ‘crib sheet’ was updated accordingly (see Appendix 13, Table 16).
Synthesis
Once the reviewers had completed their first and second extraction of assigned papers, they shared their summaries of the realist evidence. We used tables to state the author’s name, the verbatim extraction and the reviewer’s own commentary on the data. These commentaries were then pulled together into a single narrative for each theory area. We had an opportunity to present this emerging evidence at a further stakeholder group meeting (see Appendix 3). Summaries of the emerging evidence can be found in Appendix 13 (see Summary statements of emerging theory areas).
Summary of changes to protocol
We made the following minor changes to our protocol:
-
We added and developed the CART criteria to assess the completeness, accuracy, relevance and timeliness of studies to be included after the mapping exercise. This helped to focus our review aims.
-
We used only the Drummond checklist56 for economic studies, as the Phillips checklist75 was not needed.
-
We further refined the outcomes mentioned in the protocol to better reflect outcomes of our stakeholder consultations.
-
We used the SURE framework67 and realist synthesis instead of the Greenhalgh framework76 to map facilitators and barriers to intervention implementation, since we found it more appropriate for our review. Consequently, we made one minor addition to the methodological diagram.
-
We only formally translated RCTs and any study that we thought would make a significant contribution to the evidence, as Google Translate was sufficient for assessing the evidence and screening effectively.
-
We adopted EPOC criteria52 for defining quantitative evidence to ensure we included any studies yielding evidence of effect for inclusion in the sensitivity analysis, which was also an addition to the study protocol.
Chapter 3 Results
This section is divided into the results of the extractions and mapping exercises, including the PRISMA flow chart (see Figure 3), and the four basic review questions:
-
Who is at risk?
-
What is effective?
-
What is cost-effective?
-
What are the barriers to and facilitators of implementation?
We then report other outcomes of interest. The results we report here arise from both qualitative and qualitative evidence streams.
Search results
We identified 8668 study reports during the original search, and after deduplication and initial screening by title and abstract, 118 studies met our inclusion criteria for the mapping exercise. The vast majority of the studies in the mapping exercise (94 out of 118) were conducted in the USA, followed by eight in Brazil, seven in the UK, three in the Caribbean, two in Sweden, and one each in Mexico, South Africa, Taiwan and Australia. Fourteen of these studies were randomised trials, and the majority of studies were either set in health-care56 or community43 settings. The geographical diversity of these studies is illustrated in Figure 2, and study design and context are described in Table 1.
FIGURE 2.
Geographical spread of studies included in the mapping exercise.

| Characteristics | Number of studies (n = 118) |
|---|---|
| Study design | |
| RCTs | 14 |
| Cohort studies | 40 |
| Case–control studies | 16 |
| Quasi-experimental studies | 3 |
| Mixed-methods studies | 2 |
| Process evaluations | 15 |
| Qualitative/views studies | 11 |
| Other report types | 17 |
| Intervention context | |
| Community | 43 |
| Health | 52 |
| Education | 4 |
| Multiple settings | 8 |
| Not reported | 11 |
After the mapping exercise, 70 studies met the CART criteria51 and were included in the in-depth review. Full details of these studies can be found in Appendix 15. Updated database searches, citation searches and hand-searching identified a further 5243 studies or reports which, after screening, resulted in additional seven included studies. The 77 included studies were: 14 RCTs, 10 qualitative studies and 53 other quantitative studies. Publication dates ranged from 1995 to 2014 and the studies had predominantly been carried out in the USA.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram
The PRISMA diagram77 (Figure 3) describes the full flow of studies through the filtering process to our final 77, including seven studies that were added as a result of the updated literature searches. Excluded studies and reasons for exclusions can be found in Appendix 16.
FIGURE 3.
The PRISMA diagram illustrating the sifting of evidence from discovery to inclusion in the review.

Content or intervention type
Interventions were predominantly of two types: (1) those that focused solely on promoting the uptake, or facilitating the timely postpartum uptake, of contraception, usually long-acting reversible methods delivered by injection, implant or intra-uterine devices, or oral contraception; and (2) complex interventions comprising various combinations of health, social and educational elements, one of which was usually a contraception regimen. Complex interventions often had multiple objectives which included promoting parenting skills and infant health and nutrition, as well as preventing repeat pregnancy. Specific components that we identified included:
-
Fertility health-related components:
-
pregnancy testing and maternity counselling
-
primary and preventative health-care services (including prenatal and postnatal care)
-
counselling and referral for family planning services
-
-
Sexual health education and guidance:
-
referral for screening and treatment of sexually transmitted infections, including HIV/AIDS
-
educational services related to family life and problems associated with adolescent premarital sexual relations
-
-
Other maternal health components:
-
nutrition information and counselling
-
mental health services
-
-
Child health:
-
referral to appropriate paediatric care
-
-
Family support:
-
adoption counselling and referral services
-
addressing domestic violence and peer relationships
-
supportive counselling and social work services
-
-
General educational interventions:
-
Appropriate educational and vocational services including job skills training, tutoring and mentoring.
-
Overall summary of included studies and study quality
Studies used in the effectiveness evaluation
Using EPOC criteria,52 we identified 13 individual RCTs31,78–92 (one study reported in three papers82–84 and one in two papers85,86), one cluster RCT93 and two non-randomised trials94–96 (one of which was reported in two publications94,95) for potential inclusion in the meta-analysis. One of the ‘trials’78 was a meta-analysis of 12 smaller unpublished randomised and quasi-randomised trials and had an uncertain risk of bias; therefore, we did not include it in the primary analysis. As the non-randomised trials had a high risk of bias, we did not include them in the primary analysis either. 94–96 Therefore, we analysed 12 individually randomised trials31,79–81,85–92 in the principal analysis but have included the results obtained when the other four other studies were included as a sensitivity analysis. These studies were published between 1996 and 2012 (see Appendix 15).
Context/population
We used the PROGRESS framework to report on the sociodemographic characteristics. 59 All of the trials but one79 were based in the USA. The majority of the trials employed interventions for minority populations, for example African American, Hispanic and Latina American, and Pacific Islander populations. Three studies identified the socioeconomic status of the participants as ‘low’ or ‘poor’. 31,80,81
Interventions
The trials we included in the main analysis examined interventions that fell into two broad types: most were complex psychosocial programmes and one was a contraceptive programme. The psychosocial programmes offered an array of services, such as case management and referral; education about pregnancy, labour and delivery, contraception and infant health; child developmental training; contact facilitation with the health-care system; and individual counselling. These programmes were community based, or involved home visits or telephone counselling.
Studies used to identify risk factors
We used the criteria prescribed by EPOC52 to identify studies which reported on epidemiological risk factor data with a comparator. Thirty-four studies86,94,95,97–127 were used to identify risk factors in addition to the randomised trials discussed above. These 34 studies included 20 non-comparative studies,94,95,98–103,106,108,109,112–119,128 seven prospective cohort studies97,105,120–124 and eight retrospective cohort studies. 86,104,107,110,111,125–127
Qualitative studies
Ten studies published between 1998 and 2013 were included in the qualitative synthesis. 129–140 Two of the studies were reported in two papers, Clarke130,140 and Herrman. 132,133
Context/population
Participants in all 10 studies were pregnant or parenting teens. In one study, there was an additional group of teens who had had a recent abortion;137 in one study, parents or guardians of the teenage mothers were also recruited;129 and in two studies, key informants from health, community and educational organisations were included. 134,139 Seven studies were conducted in the USA,129,131–133,135,136,138,139 and the participants in five of these were predominantly of African-American and/or Hispanic ethnicity; in the remaining two US studies, the study participants were, in roughly equal proportions, white, African American or Asian/other. 131,139
Intervention/exposure
In one study, the participants were enrolled in a school-based intervention called the ‘Pregnancy free club’. In this intervention, public health nurses visited the school each day and delivered monthly pregnancy tests and surveys, health counselling and referral, and group health education classes. 136 In two studies, young mothers were participants in a mixed-methods observational study of African-American adolescent mothers’ contraceptive use and the risk of repeat pregnancy in the first postpartum year, known as the ‘Postpartum adolescent birth control study’. 135,138
Recruitment of participants
Participants in one study were recruited from a state supplemental nutritional programme for women, infants and children. 129 In another study, all participants were enrolled in high school and were receiving health care at an agency serving a low-income population and with specific expertise in caring for pregnant and parenting adolescents,131 and in two other studies participants were recruited from health, community, social service and educational agencies. 132,133,139 One study was carried out in Perth, Australia, where the participating teens were pregnant, parenting or had recently had an abortion. 137 One study focused on two study populations: (1) a group of teenage mothers of Caribbean ethnicity (from Barbados and Jamaica); and (2) a group of teenage mothers of various ethnicities (white, black, Asian and mixed race) in the UK. 130 For this latter study, we also included data relating to the London participants from the author’s doctoral thesis. 140 The final study was conducted in the UK and focused on abortion and repeat abortion. 134 A summary of the characteristics of included qualitative studies can be found in Appendix 18.
Quality appraisal of qualitative studies
We conducted quality appraisal using the appropriate questions for qualitative research in the MMAT. 54 We slightly amended the published version by adding an alternative response, ‘somewhat’, for items that were partially described, if we considered that either a ‘yes’ or a ‘no’ response would be misleading.
The MMAT54 assessment items relevant to qualitative studies are:
-
Item 1 Are the sources of qualitative data (archives, documents, informants, observations) relevant to addressing the research question (objective)?
-
Item 2 Is the process for analysing qualitative data relevant to addressing the research question (objective)?
-
Item 3 Is appropriate consideration given to how findings relate to the context, for example the setting in which the data were collected?
-
Item 4 Is appropriate consideration given to how findings relate to researchers’ influence through, for example, their interactions with participants?
In keeping with the MMAT authors’ suggestion that ‘an overall quality score may be not informative (in comparison to a descriptive summary using MMAT criteria)’,54 we have not calculated an overall score but make the following observations: only two studies score ‘yes’ for all four items (Bull and Hogue;129 Hoggart et al. 134); one scores ‘yes’ for three items (Hellerstedt and Story131); and there was only one ‘no’ response among all the studies (item 4 in Lewis et al. 135). These observations are summarised in Table 2. The predomination of ‘somewhat’ and ‘cannot tell’ responses largely reflect deficiencies in reporting.
| Author and year | Item 1 | Item 2 | Item 3 | Item 4 |
|---|---|---|---|---|
| Bull, 1998129 | Yes | Yes | Yes | Yes |
| Clarke, 2010130 | Yes | Cannot tell | Cannot tell | Cannot tell |
| Hellerstedt, 1998131 | Yes | Yes | Yes | Cannot tell |
| Herrman, 2006,132 2007133 | Somewhat | Somewhat | Cannot tell | Somewhat |
| Hoggart, 2010134 | Yes | Yes | Yes | Yes |
| Lewis, 2012135 | Yes | Yes | Somewhat | No |
| Schaffer, 2008136 | Somewhat | Somewhat | Cannot tell | Somewhat |
| Weston, 2012138 | Yes | Yes | Cannot tell | Cannot tell |
| Wilson, 2011139 | Yes | Cannot tell | Cannot tell | Cannot tell |
Economic findings
The search identified only one economic evaluation of an intervention for preventing repeat teenage pregnancy: a cost-effectiveness analysis of two home-based computer-aided motivational interviewing interventions were compared with usual care based on findings from a linked RCT. 82–84 Key et al. 141 also proposed cost-savings from a secondary teenage pregnancy prevention intervention that included school-based social work services co-ordinated with comprehensive health care for teenage mothers and their children.
Realist synthesis
The realist evidence stream utilised evidence from all the study types listed previously. Additional evidence was drawn from non-comparison studies which comprised the rest of the studies identified by the searches and included, but not utilised, to date. Policy documents from the UK were also used to explore elements of the theory areas under investigation, applying the criteria of relevance and rigor. Two policy documents (Teenage Pregnancy Strategy: Beyond 2010, Department of Health;8 Reducing Teenage Pregnancy, NHS Scotland142) provided useful further evidence for the theory areas, and were thus included in the evidence base for the realist chapter.
Identified quantitative studies that were not synthesised in any ‘pooled’ analysis
Twenty-one additional quantitative studies112–115,123–128,143–153 were identified as included studies, but were not synthesised in any ‘pooled’ analysis as they did not report on or contain data relevant to the outcomes under investigation.
Who is at greatest risk of repeat unintended pregnancies and why?
Quantitative data
Quantitative data related to potential risk factors for unintended repeat teenage conceptions were extracted from the 31 quantitative studies, as well as the RCTs, cohort studies and other, non-comparison longitudinal intervention studies if relevant and possible. The results of the metaregression showed inconsistent outcome reporting between studies that predominantly reported the repeat pregnancy proportion. Of all of the outcomes, only adequate data were provided to enable consideration of the factors that determine repeat pregnancy. Likewise, data were sparse for many other risk factors of interest and we were only able to evaluate the risks if at least 10 studies provided data. We extracted all the relevant risks, if data were available, if two or more papers included that risk factor. The risks we evaluated were the proportion of young people who:
-
had a minimum education
-
had been abused
-
smoked
-
lived with a partner (father of their children)
-
used LARCs
-
used oral contraception
-
used other forms of contraception.
We extracted data on other risk factors but had insufficient data to perform metaregression with any statistical integrity. All the studies and their study types included in this metaregression are listed in Appendix 14. The risk factors we extracted but had insufficient data to assess were:
-
teenage mothers’ age (mean and SD) at birth of first child
-
proportion of teenage mothers receiving support from friends and family
-
proportion of teenage mothers with reported depression or anxiety
-
proportion of teenage mothers misusing drugs or alcohol
-
proportion with partner reported as ‘older’ – (notionally a partner that is older by at least 3 years)
-
age (mean and SD) at first sexual intercourse in years
-
child mortality or loss related to previous pregnancy caused by miscarriage, stillbirth, abortion or child being taken into care
-
maternal morbidity related to pregnancy, abortion or childbirth (e.g. hypertension, haemorrhage, pulmonary embolism, pre-eclampsia or pelvic bone size)
-
proportion of teenage mothers reported to have had at least one sexually transmitted infection
-
proportion of teenage mothers whose first pregnancy was desired or intended
-
proportion of teenage mothers who failed to comply with a contraception regimen.
Despite the requirement for at least 10 studies to contain usable data for inclusion in the regressions, the 95% CIs around our estimates were very wide, indicating a low precision of the estimate. The results of these metaregressions cannot rule out that any of the experience factors may genuinely determine the risk of repeat pregnancy (Figures 4–10). However, from the data that we have found, there is little evidence to suggest that any of the seven risks we evaluated were helpful in determining the likelihood of repeat pregnancy.
FIGURE 4.
Prediction of repeat pregnancy (%) by continuation of education (%). The studies are plotted by the square root of their sample size. Slope parameter: –0.85, 95% CI –21.7 to 20.0; p-value = 0.93.
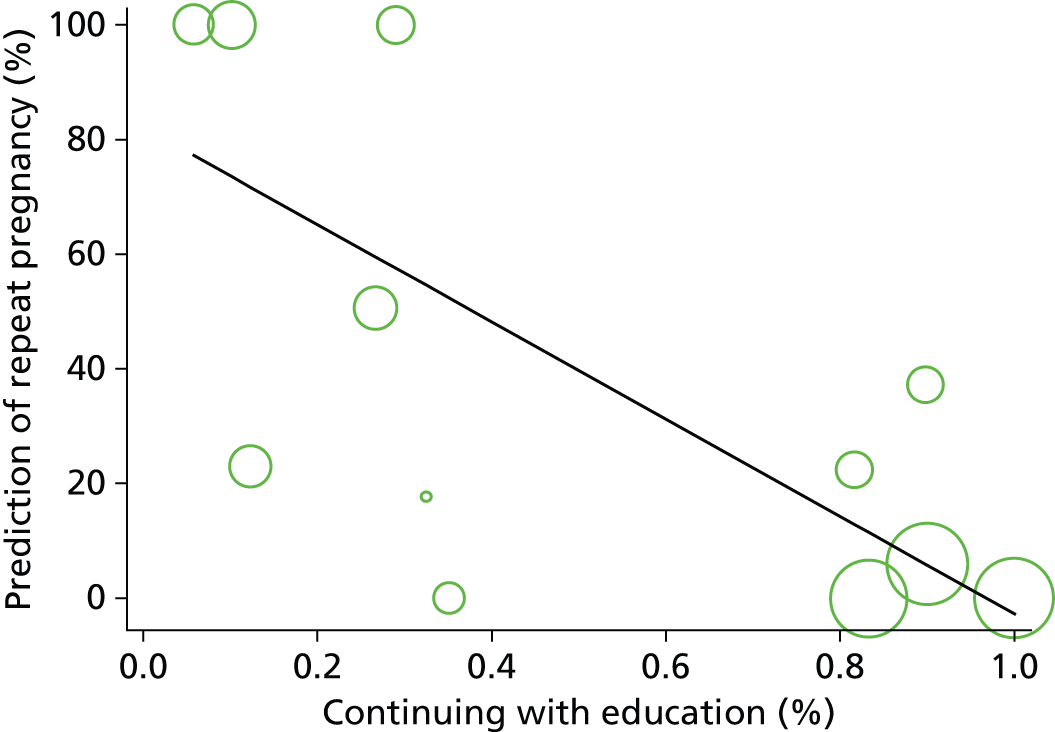
FIGURE 5.
Prediction of repeat pregnancy (%) by the level of abuse (%). The studies are plotted by the square root of their sample size. Slope parameter: –0.74, 95% CI –121.3 to 119.8; p-value = 0.99.
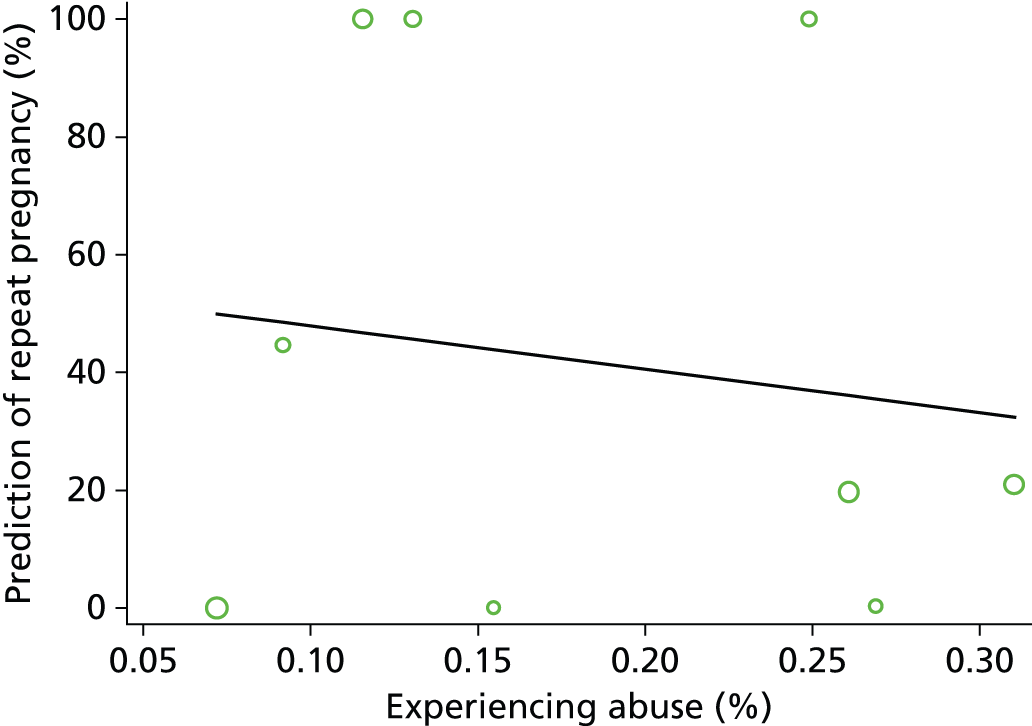
FIGURE 6.
Prediction of repeat pregnancy (%) by the level of smoking (%). The studies are plotted by the square root of their sample size. Slope parameter: 0.07, 95% CI –75.3 to 75.4; p-value = 1.00.
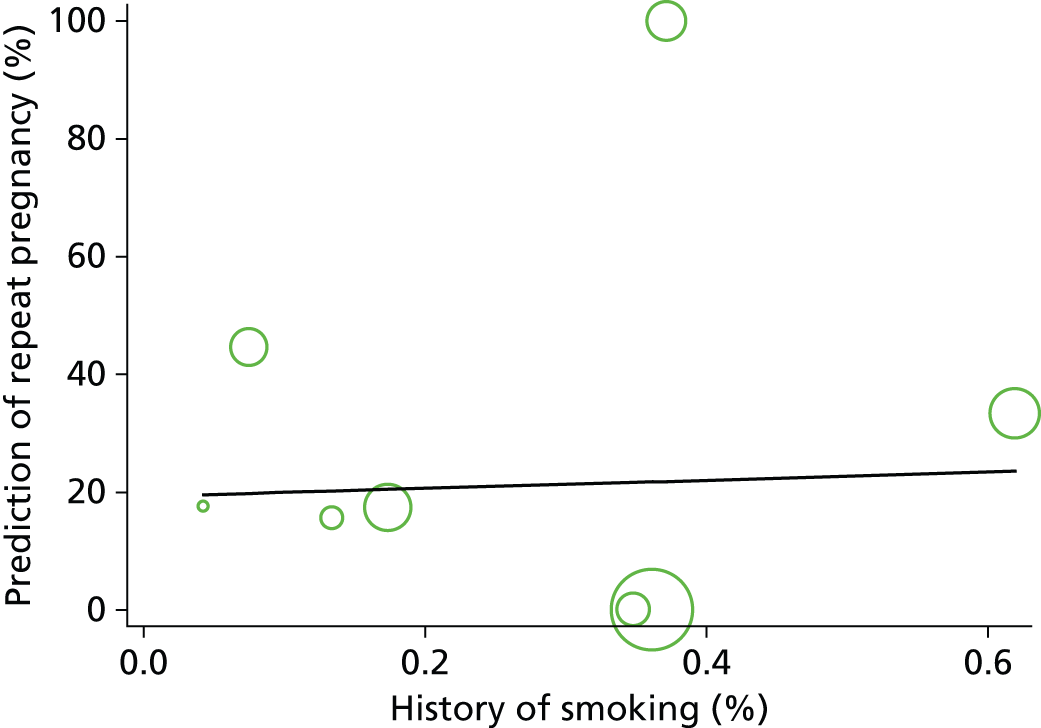
FIGURE 7.
Prediction of repeat pregnancy (%) by the proportion of young women that were living with their partner (%). The studies are plotted by the square root of their sample size. Slope parameter: 1.11, 95% CI –17.8 to 20.0; p-value = 0.90.
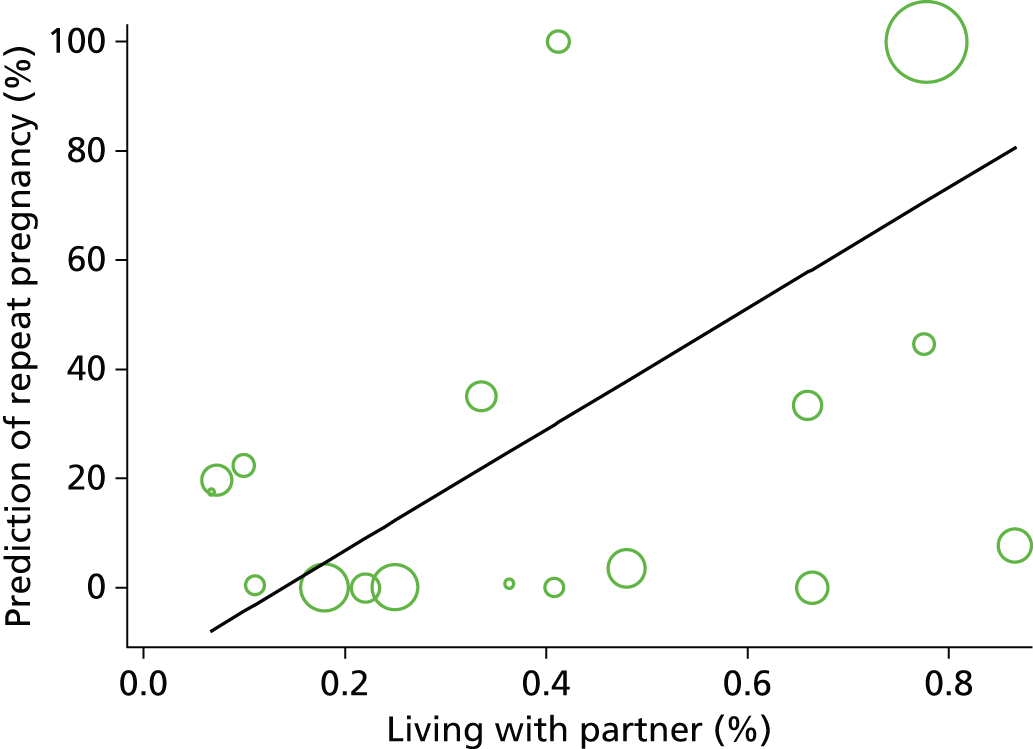
FIGURE 8.
Prediction of repeat pregnancy (%) by the proportion of young women and girls that were using long-acting reversible contraception (%). The studies are plotted by the square root of their sample size. Slope parameter: –0.74, 95% CI –27.0 to 25.3; p-value = 0.95.
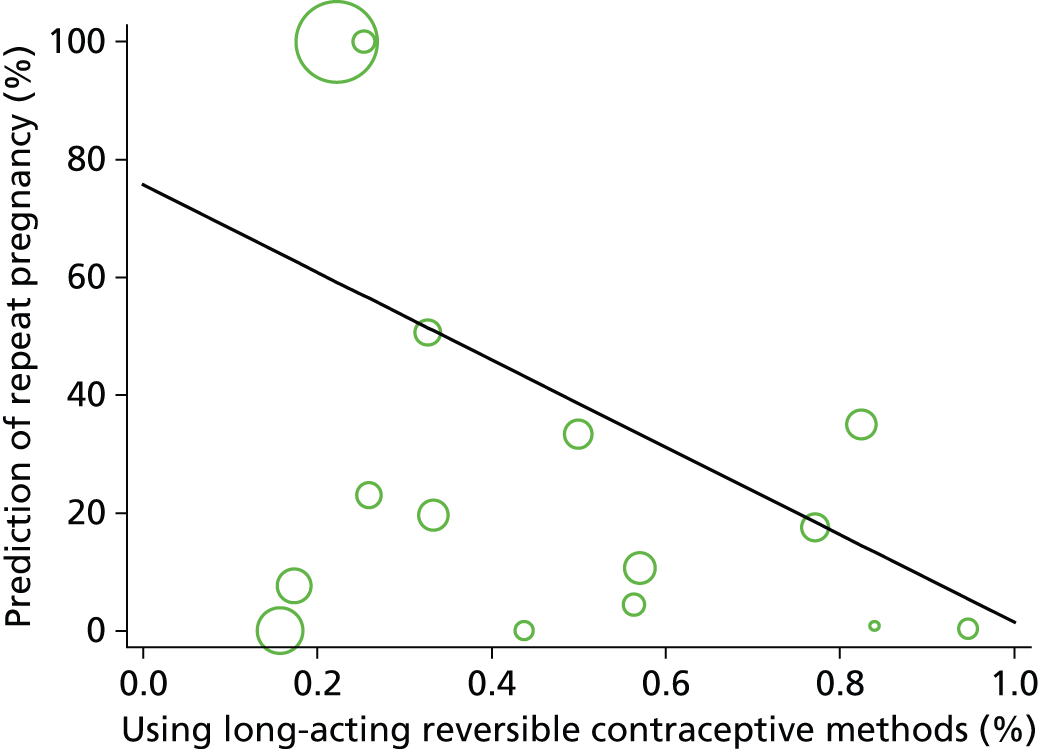
FIGURE 9.
Prediction of repeat pregnancy (%) by the proportion girls that were using oral contraception (%). The studies are plotted by the square root of their sample size. Slope parameter: 1.38, 95% CI –44.0 to 46.7; p-value = 0.94.

FIGURE 10.
Prediction of repeat pregnancy (%) by the proportion of young women and girls that were using other contraception methods (%). The studies are plotted by the square root of their sample size. Slope parameter: 0.42, 95% CI –36.0 to 36.9; p-value = 0.98.
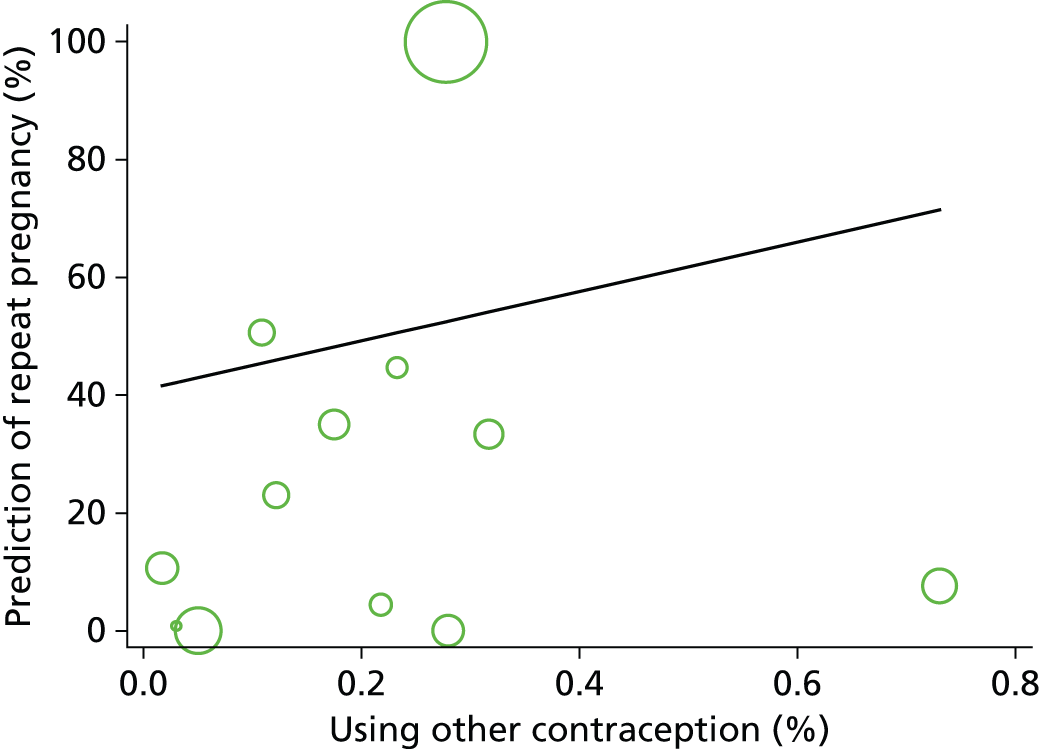
In Figures 4–10, we present the slope parameter of the linear regression; this indicates the increase (or decrease) in the percentage of young women and girls with repeat unintended pregnancy for each per cent increase in girls presenting a particular risk factor. A positive (or negative) value of the slope indicates an increase (or decrease) in the percentage of young women and girls with repeat unintended pregnancy. The slopes are presented as mean differences to highlight that we actually know very little about the actual percentage of increase (or decrease). That is why we also present the 95% CI, to highlight the level of uncertainty around the slope, and the p-value, to represent the statistical significance. A low p-value (p < 0.05) would indicate that a risk factor is likely to be a meaningful addition to our model because changes in the risk factor’s value are significantly related to changes in the repeat pregnancy rate.
Using Figure 4 as an example, the slope parameter of –0.85 can be interpreted to indicate that the percentage of teenagers with repeat unintended pregnancy reduces by 0.85% for every 1% increase in the proportion of young women and girls remaining in education. However, the 95% CI ranges from –21.7 (indicating a 21.7% decrease in pregnancy rate per 1% increase in the proportion in education) to +20.0 (indicating a 20% increase in the pregnancy rate per 1% increase in the proportion in education). These data result in a p-value of 0.93, which indicates that the mean decrease of 0.85% per 1% increase in those in education is meaningless. This interpretation also applies to Figures 5–10, taking into consideration the positive or negative values of the slope parameters accordingly.
As no quantitative evidence has emerged to help characterise the population at most risk of repeat unintended teenage conceptions, we turned to an examination of the in-depth qualitative studies which asked young women about their circumstances and motivations. Five of the 10 included qualitative studies shed light on the characteristics and life circumstances of young women, and some of the factors that help to explain why they had, or chose not to have, a repeat pregnancy. 85,129,130,134,136 Themes included contextual, motivational and emotional factors, and rationales for having a rapid repeat pregnancy.
Contextual factors: family, peer group and lifestyle
Many young mothers had unstable backgrounds, characterised by a lack of family support, insecure housing and chaotic lifestyles, and were lacking educational and vocational opportunities. Sex education and access to contraception alone could not effectively address the issue of unprotected sex in the context of these teenagers’ real lives, and they continued in their risky behaviours. 129 Although they understood the risks of unprotected sex, there was a complete lack of planning or consideration of the consequences; rather, teenage sex was a spontaneous activity132,133 and, in the context of some families and peer groups, teenage pregnancy was considered the norm. 129
You take chances, it’s just like gambling, if you keep doing it . . . I knew [about birth control]; I just wasn’t careful.
Teenage mother who received state food aid (USA)129
We’ve accepted [teen pregnancy and early childbearing]. Now it has become normal to become a parent while you’re a teenager, but I think it is time to take a role that this is not right.
Mother of teenage parent who received state food aid (USA)129
Motivational factors: goals and aspirations
A key feature of the lifestyles of young women whose environment offered little opportunity was a lack of goals and aspirations, and, in some cases, even a lack of expectation of any future achievement that could be planned for; they lived in the moment. However, some young mothers did have educational or career objectives, although there were significant barriers to achieving them. These barriers included the difficulty of combining the role of being a mother with that of being a student, particularly when children were ill, and having limited access to childcare. 129 Poorly paid work provided only a marginal improvement in income compared with state benefits for young mothers in the UK. This had to be weighed against the disadvantage of being out at work for several hours a day and thus being unable to spend much time with their children. 130 Nevertheless, those who had goals and aspirations were more likely not to have a rapid repeat pregnancy. 134 Some of the respondents recognised and reacted against the prevailing stereotypical views of teenage mothers (thoughtless, feckless, welfare-dependent, etc.) and were determined not to conform to that image. This was a powerful motivating factor behind their resolution to make a success of their lives, as was the desire to be a good role model and provide a better life for their children. 130,136
What am I supposed to do when my baby has a fever? I had already missed 2 days of school and the teacher told me that if I missed again I would get an F in history. Well, then he got sick, so I got an F.
Teenage mother who received state food aid (USA)129
So I did want to carry on not just to be like a stereotype you know, have kids young, sponging off the dole, sitting at home doing nothing. I wanted to show people that not all young people are just not worth it, they do want to help themselves.
Teenager of Caribbean ethnicity with two (or more) pregnancies (London)130
When I got pregnant, all my family was like you messed up – because I was the smartest one. And now I’m going to college . . . when I’m going to take a step I’m not only taking it for me. I’m taking that step for my daughter.
Teenage mother participating in a school-based intervention (USA)136
Emotional factors: replacing a loss; looking for love
In both studies from the UK,130,134 replacing a loss was a powerful theme. Young women whose first pregnancy had not reached term, as a result of miscarriage or abortion, or whose baby had been stillborn or taken into care, felt an overwhelming sense of loss and bereavement. This was particularly acute when the first baby had been wanted. 130,134 This was described as ‘unnoticed loss’ because the feelings of grief and loss were often not recognised by family, friends or service providers, and therefore these young women received no support or counselling. 130 Under these circumstances, young women intentionally became pregnant again in order to fill the emotional void. Some young women who had lacked emotional warmth in childhood tried to build themselves a family in order to achieve a sense of purpose and fulfilment in their lives, and to feel needed, loved and valued, which had not been provided by their own parents. 130
. . . I never got a chance with him for people to see how capable I was . . . I was just devastated carrying a baby for nine months and feeling it move, going through labour and everything and seeing him for the first time and him just going. It was horrible.
Teenager of Caribbean ethnicity with two (or more) pregnancies (London)130
I was just gonna go straight to the abortion place and my mother said no . . . my dad said . . . you not getting an abortion . . . if I get an abortion I have to leave . . . but in the back of my head . . . I didn’t want an abortion neither.
Teenage mother recruited from social service agency (USA)132
I didn’t go to school a lot because my mum was an alcoholic . . . so instead of me being her baby, she was my baby . . . I suppose I just fell pregnant because I didn’t have no one there with me. I thought I wanted someone to love and take care of.
Teenager of Caribbean ethnicity with two (or more) pregnancies (London)130
If young women’s own abortion decisions were supported, they were more likely to recover emotionally and move on with their lives. If, however, they were encouraged or coerced into having an abortion when they would have preferred to have the baby, they could be deeply distressed and were more likely to go on to have a repeat pregnancy. They would often conceal this pregnancy in order to avoid a second abortion and in order to replace their loss. 130 Furthermore, if young women had been persuaded against their wishes to have an abortion, the feelings of loss were compounded by feelings of guilt. 130,134 It appears that for young women who considered abortion, the choice was not an easy one to make and it was often made with little or no support from family, friends or service providers. If women’s choices were adequately supported, whatever their decision, those who chose to have an abortion would have a better chance of getting their lives back on track, returning to education and avoiding another pregnancy. UK service providers were very concerned about the emotional damage caused by persuading young women to have an abortion against their wishes and/or not providing the appropriate support and counselling before, at the time of, and after the abortion. 130,134 In the absence of adequate support, the emotional pain could sometimes only be alleviated by having another pregnancy and keeping the baby. 130
I felt really bad about what happened last time, when I found out that I was pregnant again I thought I am going to keep it a secret, because I knew that everyone was going to pressure me to have an abortion again, and I didn’t want to do it . . .
Teenager of Caribbean ethnicity with two (or more) pregnancies (London)130
Rationales for rapid repeat pregnancy: creating a family and reverse life-course rationalisation
For some young women, once they had embarked on becoming a mother, they felt it was appropriate to complete their family while still young and energetic, and before moving on with their lives. They felt an only child would be a lonely child and so wanted to provide him or her with siblings. 129 Some second babies were intentionally conceived in order to please a partner and, for some men, fatherhood was proof of their manhood and virility. Young women took this into account in their pregnancy decision-making, reasoning that pride in their achievement might encourage their partner’s commitment to the relationship. 85,129,130 Young women reasoned that they could go back to education and/or a career later on; it seemed to them a more sensible course of action than the traditional choice that other women made to focus on education and work objectives first and then have to interrupt their progress to start a family later, potentially just as their career was taking off. 85,129,130 According to this reverse life-course rationalisation, having one child as a teenager and then delaying completing a family until much later represented the worst of both worlds.
My baby needs a brother or sister – it is too sad to see him growing up without someone to play with.
Teenage mother who received state food aid (USA)129
Now that I’ve had one, I should just finish it, you know, before going back to school and dropping out all over again.
Teenage mother who received state food aid (USA)129
With my baby’s father he was happy when I got pregnant . . . He said it [having a baby] was the best present he could get from me.
Teenage mother who received state food aid (USA)129
I knew what I was doing, I thought he might stick with me if I had a baby so I didn’t want a baby, but I didn’t stop it neither . . . he has kids with other women, so I thought he could with me too . . . if it happened, it happened . . .’
Teenage mother recruited from social service agency (USA)132
Whether the explanation for repeat pregnancies was contextual, motivational, emotional or based on teenage mothers’ own rationale, as described in our findings, it is important to seek an understanding of the complex and diverse reasons that result in some teenage mothers being at a greater risk of repeat pregnancies than others, so that these reasons can be addressed through targeted interventions and the improved provision of services.
Assessment of the certainty of findings
We judged the qualitative studies to be of moderate to high quality; all supported their findings by quoting extracts from the data and in several cases there was evidence of in-depth engagement with participants resulting in particularly rich data sets. We considered whether or not findings were seen in more than one study and in more than one country and, in view of the limited geographical spread of the evidence (seven studies from the USA, two from the UK and one from Australia), whether or not it seemed plausible that they would be transferable between these contexts and to other comparable settings. Overall, our confidence in the certainty of findings was high (for 18 findings) to moderate (for four findings), with only three findings achieving low certainty because they were found in only one study and either the data supporting the finding was relatively thin or the finding itself was equivocal. A table summarising the qualitative findings and indicating the level of certainty for each finding, and a brief explanation of the assessment, can be found in Appendix 17.
Which interventions are effective and cost-effective and in what setting might they work?
Studies identified
We identified 14 RCTs that met our inclusion criteria31,78–93 and two studies that contained useful effectiveness evidence when EPOC criteria52 were applied. One of the randomised trials93 was a cluster randomised trial of poor quality and another was a large study that combined 12 smaller randomised and quasi-randomised studies on one multifactorial intervention into an RCT-style analysis. 78 Both of these studies were judged to have too large a risk of bias to include in the main analysis, but have been included in sensitivity analyses of outcomes as quasi-experimental studies.
Primary analysis
The trial we included in the main analysis examined interventions that fell into two broad types: most were multielement psychosocial programmes and one was a contraceptive programme. The psychosocial programmes offered an array of services, such as case management and referral; education about pregnancy, labour and delivery, contraception, and infant health; child developmental training; contact facilitation with the health-care system; and individual counselling. These programmes were community based, or involved home visits or telephone counselling: seven studies involved home visits,79–82,85,89,91 two studies were community based88,92 and one study used telephone counselling. 90 The contraceptive programme87 offered advanced provision of emergency contraception. The details of these programmes, their lengths and their findings are described in detail in Appendix 19.
The interventions based on home visits had counsellors,138 mentors,90 midwives,78 nurses79 or trained home visitors141 delivering the interventions to young mothers at their homes. These professionals and paraprofessionals could be state sponsored,78 recruited from the community141 or from the same ethnicity. 29,138
It was difficult to establish a definition of usual care or standard practice. Eleven31,80–82,85,87–92 of the 12 studies were from the USA (with the exception being an Australian study)79 where the provision of care for young mothers varies within and between each state. Usual care within each study is described in the study characteristics table.
Ten trials reported the effectiveness of interventions in terms of reducing repeat pregnancy and six trials reported on acceptability (see Appendix 19). The outcomes reported by these 12 studies are outlined in Table 3.
| Study | Outcome variable | |||||||
|---|---|---|---|---|---|---|---|---|
| A | B | C | D | E | F | G | H | |
| Psychosocial: home-based interventions | ||||||||
| Barnet et al., 200785 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Barnet et al., 200882 | ✓ | ✓ | ✓ | |||||
| Black et al., 200631 | ✓ | |||||||
| Cherniss and Herzog, 199680 | ✓ | ✓ | ||||||
| Havens et al., 199789 | ✓ | ✓ | ||||||
| Koniak-Griffin et al., 200381 | ✓ | ✓ | ||||||
| Quinlivan et al., 200379 | ✓ | |||||||
| Sims and Luster, 200291 | ✓ | |||||||
| Psychosocial: community-based interventions | ||||||||
| Ford et al., 200288 | ✓ | ✓ | ||||||
| Stevens-Simon et al., 199792 | ✓ | ✓ | ||||||
| Psychosocial: telephone-based interventions | ||||||||
| Katz et al., 201190 | ✓ | ✓ | ||||||
| Contraceptive programme | ||||||||
| Belzer et al., 200587 | ✓ | ✓ | ✓ | ✓ | ||||
Is there any evidence that supports effective interventions to reduce unintended repeat teenage pregnancies?
Nine of our included studies, involving 1126 young women, 628 of whom were receiving psychosocial interventions and 498 as control, reported the rate of unintended teenage pregnancy, as did the contraceptive intervention study (91 young women participated in this study, of whom 48 received the intervention). The data from psychosocial programmes were split into three subgroups dependent on the delivery of the intervention: home-based (597 participants), community-based (297 participants) and telephone-based (232 participants) interventions.
In none of the home visit studies did the proportion of young women and girls who experienced an unintended repeat teenage pregnancy differ between intervention and control arms. Figure 11 illustrates that, even when these results were pooled, no significant differences could be found between the psychosocial intervention arms and the control arms of the studies and that did not differ by mode of delivery.
FIGURE 11.
Forest plot of comparison: psychosocial intervention vs. usual experience following delivery. Outcome: the proportion of repeat pregnancies (i.e. the effectiveness of the intervention). M–H, Mantel–Haenszel.
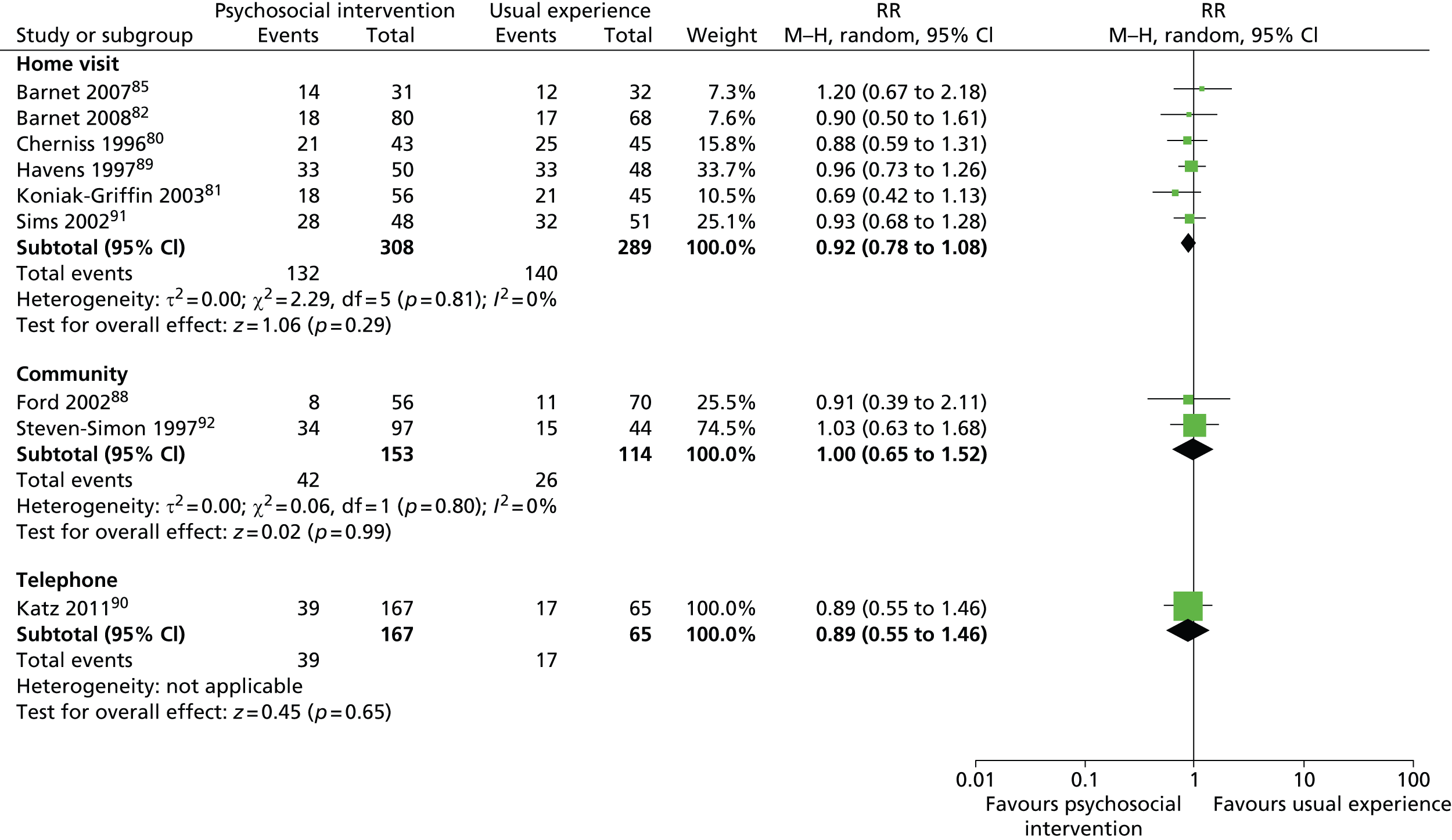
The contraception intervention study87 showed a reduction in the number of repeat pregnancies in the intervention group (10 of 48) compared with the control group (14 of 43), giving a RR of 0.69 (95% CI 0.34 to 1.14); however, this was not statistically significant.
Despite these negative findings, four studies31,81,82,85 went on to report the secondary outcome childbirth (75 events from 461 participants). The outcome ‘pregnancies’ covers all cases of known conception. These could have led to miscarriages, abortions, or still or live births. Three of the four studies reporting the outcome childbirth gave RRs of < 1; however, none was significant. Figure 12 illustrates these data.
FIGURE 12.
Forest plot of comparison: psychosocial intervention vs. usual experience following delivery, for the secondary outcome childbirth. M–H, Mantel–Haenszel.
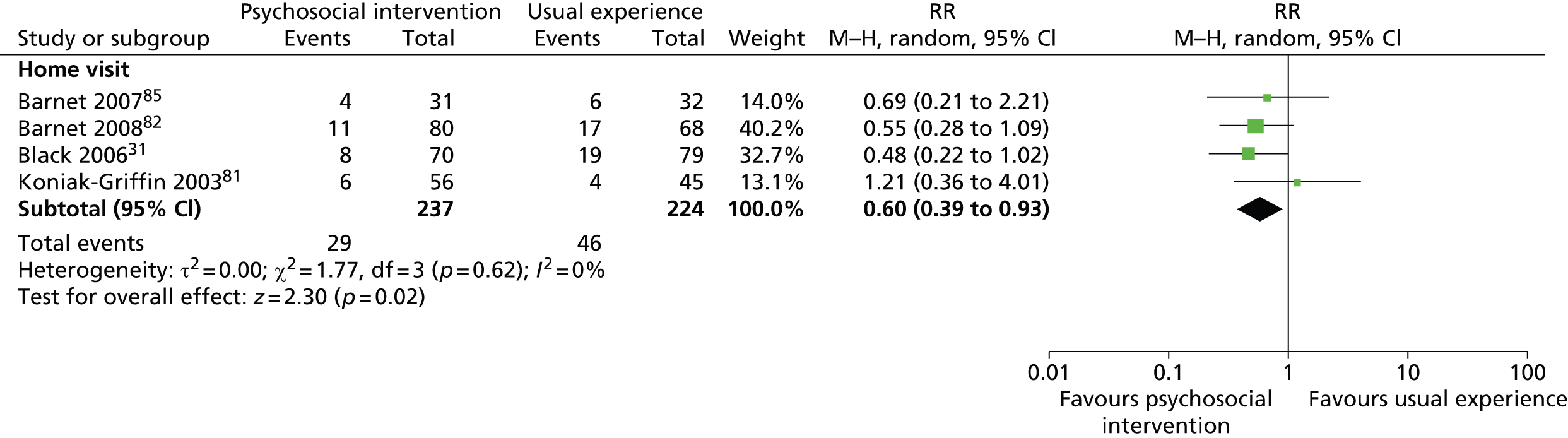
When these results were combined in our meta-analysis, we found a RR of 0.60 (95% CI 0.39 to 0.93) indicating a significant reduction of the number of births observed in the intervention arms of the studies.
Cost-effectiveness of a psychosocial intervention
Only one study investigated the cost-effectiveness of an intervention. 92 This study was a three-arm RCT investigating computer-assisted motivational interviewing (CAMI), with (CAMI+) or without a multipart home visit programme. In this study, the costs of both CAMI+ and any CAMI were evaluated and compared with the control arm.
The perspective of the analysis was not reported in the paper. Only direct intervention costs were included in the analysis, although intervention costs did include start up and implementation determined by programme personnel admin records adjusted to 2009 US dollars. Weighted mean costs were US$2064 per teenager for any CAMI (n = 167), US$2735 per teenager for CAMI+ (n = 80) and US$1449 per teenager for CAMI only (n = 87).
The costs associated with CAMI+ were higher than those for CAMI only because each CAMI+ interventionist carried a smaller caseload than CAMI-only interventionists (20 vs. 60 teenagers) to provide a greater frequency of the enhanced home-visiting components.
Incremental cost-effectiveness ratios (ICERs) were normalised to a sample of 100 teenagers for any CAMI versus usual care, CAMI+ versus usual care and CAMI only versus usual care. The cost per prevented repeated birth was calculated by dividing the cost of the intervention by the number of repeated births between the two groups (intervention and control groups). Unadjusted and adjusted ICERs were calculated. ICERs were adjusted for age, prior birth, continuous insurance, history of sexually transmitted infection and contraceptive-use intentions during pregnancy using logistic regression analyses. Table 4 shows the unadjusted and adjusted ICERs of cost per prevented repeated birth, as calculated by Barnet et al.,83 depending on the level of CAMI received.
| Intervention | Unadjusted ICERs | Adjusted ICERs with 95% CI | ||||
|---|---|---|---|---|---|---|
| Number of repeat births prevented | Estimated cost (US$) | Number of repeat births prevented | Estimated cost (US$) | Lower CI bound (US$) | Upper CI bound (US$) | |
| CAMI only | 8 | 18,672 | 10 | 15,078 | 11,546 | 21,092 |
| Any CAMI | 9 | 21,895 | 12 | 17,388 | 11,821 | 31,901 |
| CAMI+ | 11 | 24,313 | 14 | 19,247 | 15,085 | 26,072 |
Further ICERs were calculated based on a set of scenarios created for specific subpopulations of teenagers with respect to intervention group, age, insurance status and parity. The costs per prevented repeated birth were highest for the youngest teenage mothers in the CAMI+ group (12 years old) with continuous insurance (US$27,187) and lowest for the oldest teenage mothers in the CAMI-only (18 years old) group who were newly insured (US$6822).
This cost-effectiveness analysis was appraised using the Drummond checklist (see Appendix 8). 56 The analysis met certain checklist criteria. The analysis had a clearly defined question and the effectiveness of the intervention was assessed using a RCT. The costs and consequences were justified, credible and appropriate for the research question posed. ICERs were calculated for the two intervention arms and usual care. To test uncertainty further, analyses were conducted based on a set of scenarios created for specific subpopulations of teenagers with respect to intervention group, age, insurance status and parity. The authors considered issues of wider concern by comparing the large costs of unwanted teenage pregnancy on the state, with the costs of prevention, stating that the programme demonstrates good value for money in Maryland, USA. The authors also compared their results with other economic evaluations of teenage pregnancy prevention interventions, although the evidence base is constrained. However, the analysis failed to meet certain checklist criteria: no description of usual care was given; the perspective of the analysis was not stated; the authors considered the direct costs of the intervention, including start up and implementation, yet other costs, such as those to the individual and society, were not considered; no discount rate was reported, although the time horizon of the analysis exceeded 1 year; and the authors stated that the unadjusted and adjusted ICERs presented were normalised to a sample of 100, although no details of the methods and rationale for this normalisation were given. In their conclusion, the authors stated that the results have limited generalisability because of the setting, the population, the geographical area and the short follow-up period of 2 years.
Although the search identified only one economic evaluation, Key et al. 141 stated economic findings in their write-up of the effectiveness of a secondary teenage pregnancy prevention intervention that included school-based social work services co-ordinated with comprehensive health care for teenage mothers and their children. Key et al. 141 proposed that this secondary teenage pregnancy prevention intervention under investigation would result in societal cost savings to the state of approximately US$19,000 for each birth that was postponed until adulthood, which equated to cost savings of approximately US$60,000 for each year of intervention implementation.
Acceptability of interventions
The acceptability of interventions was not directly measured by any study; however, we inferred that if there were any differential dropout between the control and the intervention arms of a study, we might have a suitable proxy for acceptability. We observed that no study, except that of Ford et al. ,88 showed significant differences between arms, and, on combining that with the other trial reporting psychosocial interventions delivered in a community setting (Stevens-Simon et al. ),92 there were no overall significant differences between arms. Figure 13 illustrates these results in a forest plot.
FIGURE 13.
Forest plot of comparison: psychosocial intervention vs. usual experience following delivery. Outcome: the acceptability of the intervention. M–H, Mantel–Haenszel.
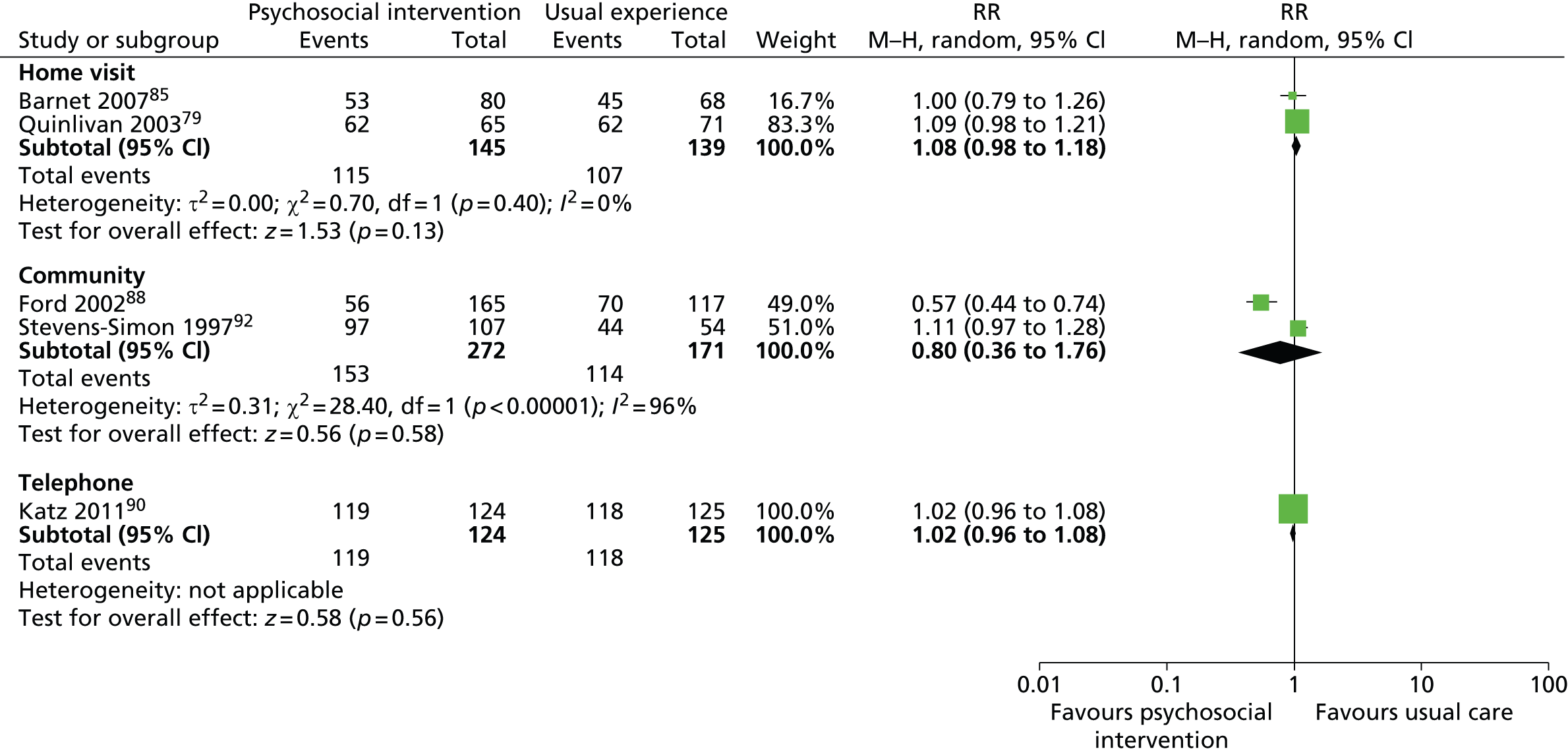
Contraception and unprotected sex
Two studies, one reporting a contraception intervention87 and one reporting a psychosocial intervention using trained home visitors,85 reported outcomes related to contraception use and unprotected sex. As these interventions were very different in nature, we did not combine the data in any way. Table 5 shows that the contraception intervention was unsuccessful in increasing either condom use or oral contraception, or in reducing unprotected sex. Although the results are non-significant, it should be noted that all three of these outcomes favour the control arm.
| Outcome measure | Number of events | RR | 95% CI | ||
|---|---|---|---|---|---|
| Intervention arm (n = 48) | Control arm (n = 43) | Random effects | Lower bound | Upper bound | |
| Number of repeat pregnancies | 10 | 13 | 0.69 | 0.34 | 1.14 |
| Condom use | 15 | 18 | 0.75 | 0.43 | 1.29 |
| Oral contraception | 5 | 8 | 0.56 | 0.56 | 1.58 |
| Unprotected sex | 28 | 22 | 1.14 | 0.78 | 1.66 |
In contrast to Belzer et al. ,87 Barnet et al. 85 did show some evidence of increased use of both condoms and oral contraception. While the use of condoms was not statistically greater in the intervention group, use of oral contraception was. Table 6 shows these results. The final comparison in this table is for ‘birth control’ and shows no difference between the study arms.
| Outcome measure | Number of events | RR | 95% CI | ||
|---|---|---|---|---|---|
| Intervention arm (n = 31) | Control arm (n = 32) | Random effects | Lower bound | Upper bound | |
| Condom use | 17 | 12 | 1.46 | 0.84 | 2.53 |
| Oral contraception | 22 | 14 | 1.62 | 1.03 | 2.55 |
| Birth control | 18 | 21 | 0.88 | 0.6 | 1.31 |
School dropout
As school dropout is considered to be related to first conceptions, several authors addressed this outcome in their intervention studies. Three studies reported the rates of either successful graduation or continuation in school, or actual dropout. 80,89,95 After re-scaling these variables to read in the same direction, we combined them in a meta-analysis. Barnet et al. 85 demonstrated a RR of 0.52 (95% CI 0.28 to 0.97) in favour of a psychosocial intervention implemented by home visitors to reduce school dropout. Neither of the other two studies replicate this finding; however, Havens et al. 89 did demonstrate marginally fewer dropouts in the intervention arm. When combined, these results demonstrate a RR of 0.74 (95% CI 0.51 to 1.07), which is marginally below the threshold for statistical significance. Figure 14 illustrates the full results of this analysis.
FIGURE 14.
Forest plot of comparison: psychosocial intervention vs. usual experience following delivery. Outcome: school dropout. M–H, Mantel–Haenszel.
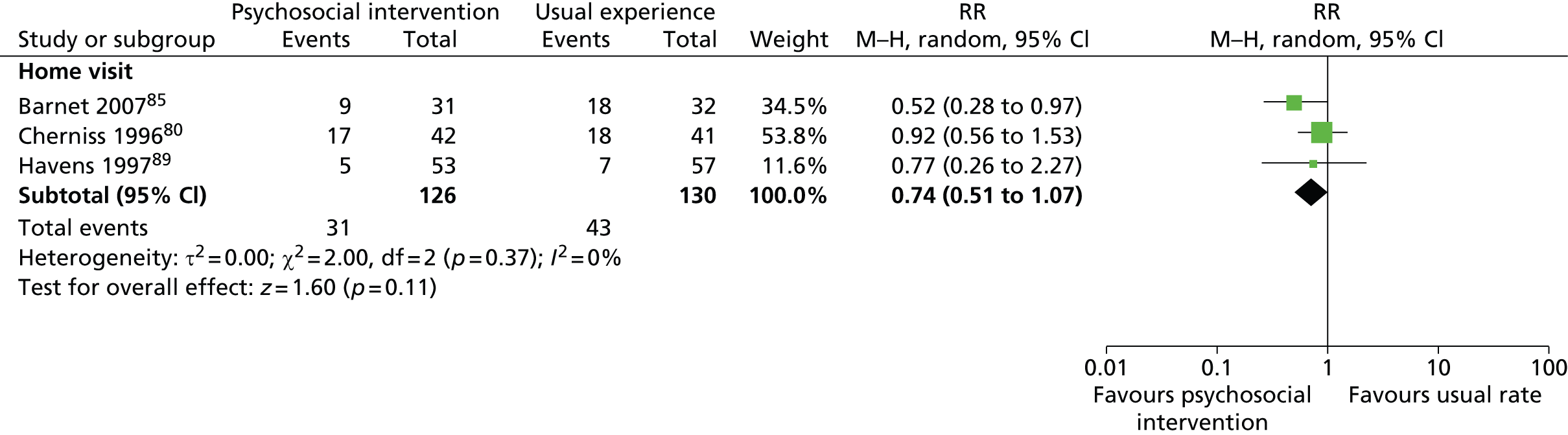
Overall completeness and applicability of the evidence
External validity
The limitations of this meta-analysis are the relatively small data sets available for the main outcomes of interest, and the likelihood of incomplete reporting of outcomes such as abortion and risky behaviour, which have the potential to affect the rates of unintended pregnancies reported. Furthermore, all of the trials were conducted in the USA (with the exception of the study by Quinlivan et al. ,79 which was carried out in Australia), which may limit the applicability of the results in the UK because of differences in the health systems. It also limits the applicability of these interventions in developing countries.
Another limitation is the small number of studies with a true control group, that is a group without any intervention designed to reduce the incidence of unintended repeat pregnancy or ‘usual care’.
Quality of the evidence
The studies had some overall strengths: most had sample sizes of more than 100 participants, most carried out 24-month follow-ups, most described data collection instruments, most used measures to ensure the validity of self-reported data, most controlled for baseline differences in statistical analyses, and most reported the causes and possible impacts of loss of follow-up.
The risk-of-bias table and figure (Table 7 and Figure 15) highlight that, for many of the studies, it was difficult to judge the methodological quality because of insufficient reporting of key methodological features.
| Study | Bias | ||||||
|---|---|---|---|---|---|---|---|
| A | B | C | D | E | F | G | |
| Koniak-Griffin et al., 200381 | + | ? | – | + | ? | ? | + |
| Barnet et al., 200785 | ? | – | – | + | + | + | ? |
| Quinlivan et al., 200379 | + | + | – | ? | ? | ? | ? |
| Belzer et al., 200587 | + | + | ? | ? | + | ? | – |
| Katz et al., 201190 | + | + | – | – | ? | ? | ? |
| Havens et al., 199789 | + | ? | – | ? | ? | ? | ? |
| Black et al., 200631 | – | – | – | + | + | ? | + |
| Cherniss and Herzog, 199680 | ? | ? | – | + | – | + | – |
| Sims and Luster, 200291 | ? | + | – | – | ? | ? | ? |
| Barnet et al., 200982 | + | ? | – | – | – | ? | ? |
| Ford et al., 200288 | ? | ? | – | – | ? | ? | – |
| Stevens-Simon et al., 199792 | – | – | – | – | ? | ? | ? |
FIGURE 15.
Risk-of-bias graph: review authors’ judgements about each risk of bias item presented as percentages across all included studies.
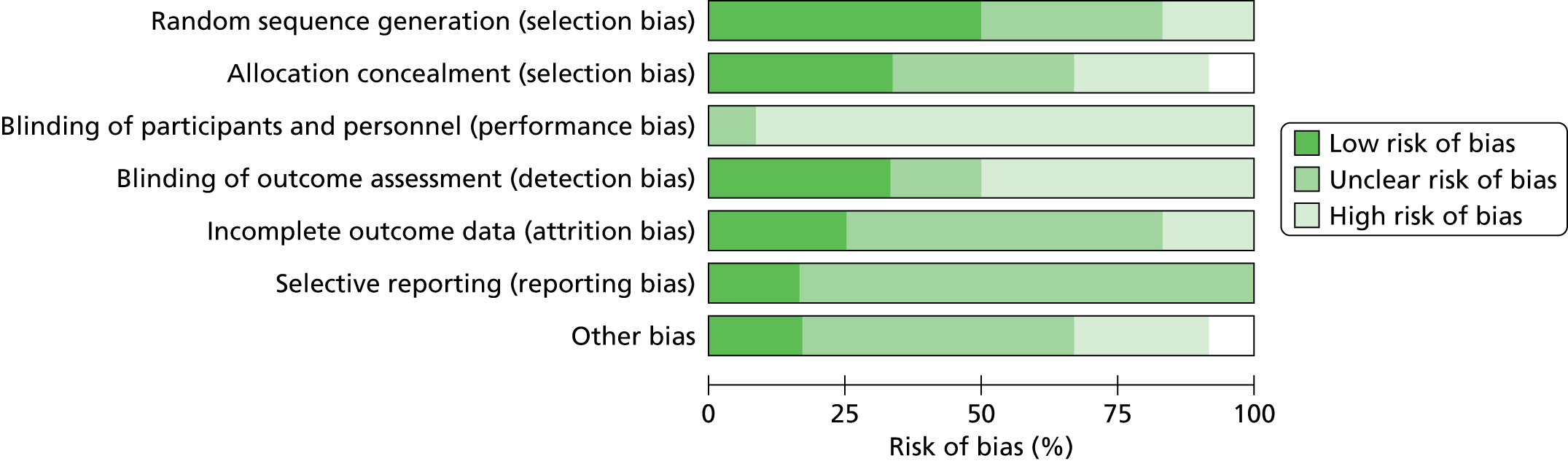
Four studies80,88,91,95 had insufficient information about the randomisation sequence to make a judgement and just said ‘participants were randomised’ or ‘randomly assigned’; one31 used a randomisation procedure stratified on maternal age and sex of the child; and Stevens-Simon et al. 92 assigned patients to the intervention group using a systematic, non-random approach. This study92 had a high risk of selection, detection and performance bias, and provided insufficient information for attrition and reporting concealed allocation, blinded outcome assessors or separated programme facilitators between the intervention and the control groups. Only one study79 reported adequate allocation concealment using sealed opaque envelopes.
Although these studies reported blinding of study participants and key personnel, it was not emphasised whether this blinding was broken or not. Pragmatic trials cannot use blinding because once randomised, it is impossible to blind the adolescent to her allocated group. Thus, the young woman and the personnel delivering the intervention cannot be blind to the intervention received. However, detection bias was circumvented by some studies that used research assistants to collect outcome data. 88,90,92
Limitations of outcome measures
From our three outcomes, effectiveness of intervention and acceptance of intervention were susceptible to self-report bias. There were some studies that validated the effectiveness of interventions indirectly, for example through hospital records. Self-reported behavioural outcomes unavoidably introduce self-report bias. Follow-up periods also ranged from 12 months to 24 months. There was an absence of a standardised set of outcome measures with explicit definitions; for example, while some studies used the term contraceptive, others differentiated it into condom use or hormone-based contraceptive pills.
Sensitivity analysis
We conducted sensitivity analyses of the primary outcomes (unintended repeat pregnancy and uptake of interventions) and secondary outcomes (birth control/contraception and school dropout), including quasi-experimental and observational study. Our EPOC screening identified four studies which contained comparative data that would inform an assessment of effect.
We identified three quasi-experimental studies (two randomised and one non-randomised): two reported the effectiveness and uptake of the interventions, and one reported on the acceptability of the intervention. We also identified one observational study with a population control which reported the effectiveness of the intervention, birth control/contraception and school dropout.
Effectiveness of the interventions
We added three studies78,93,135 to the 10 included in the primary analysis. 16,80–82,86,88–92 These three included 1484 teenagers (709 receiving psychosocial interventions and 715 receiving control) and reported the rate of unintended repeat pregnancy. All the reported studies reported a home visiting intervention.
By including these studies, and rerunning the meta-analysis, the results showed that the proportion of girls who experienced an unintended repeat teenage pregnancy in the home visit arms (288/1077) was lower than the proportion in the control group (297/1004); the associated RR was 0.88 (95% CI 0.78 to 1.00). By including these studies, there is an indication that psychosocial interventions delivered in the home setting are indeed effective. Sensitivity analyses forest plots are shown in Appendix 20.
When we added the one study of home-based psychosocial interventions reporting school dropout as an outcome,78 the meta-analysis changed a non-significant finding favouring the psychosocial intervention into a significant finding [65/635 (10%) dropping out from the intervention arm against 87 out of 659 (13%) from the control arm], with a RR of 0.76 (95% CI 0.6 to 0.96).
No other sensitivity analyses changed the significance of the outcome.
What are the barriers and facilitators to the uptake of interventions?
Qualitative findings
As there are no linked qualitative studies or process evaluations, we cannot say anything about implementation of included interventions in the review. One of the qualitative studies focused on a specific intervention (the school-based ‘pregnancy free club’),136 but it was not possible to assess the effect of this intervention as no quantitative evaluation has been published. All of the studies contributed data that helped to explain why young women failed to prevent second or subsequent pregnancies and, to some extent, what might have helped them to do so. Themes identified included barriers to understanding about both the nature of fertility and the properties and relative merits of different contraceptive methods; difficulties relating to access to and continuity of contraceptive care; and facilitators of contraceptive uptake, including choice, acceptability, support and encouragement.
Barriers to understanding: knowledge, information and misinformation
Some young women lacked even the most basic knowledge about contraceptive methods. In some cases, they found it difficult or embarrassing to talk to their mothers about sex and contraception even when the mothers were open and willing to discuss such matters;129,139 more open discussion between mothers and daughters sometimes became easier after the first pregnancy, in which case family could be a useful source of information and help. 139 In one US study, young mothers who were enrolled in a combined public health and educational intervention valued the daily presence of a nurse in school because she was considered a useful and easily accessible source of unbiased and authoritative knowledge and information. 136
After delivery, sex appeared to be a more open topic among some of the teenagers’ families . . . However, some parental communication about sex remained limited . . .
Wilson et al., 2011 (USA)139
I haven’t really talked to my mom [about contraceptives] . . . She just tells me to take care.
17-year-old Latina girl engaged in education/training (USA)139
Focus group participants appeared to be very comfortable talking [with nurses] about birth control methods and issues.
Schaffer et al., 2008 (USA)136
I think also birth control wise sometimes you have questions about – like am I bleeding too much, is this ok? . . . They help you find other resources.
Teenage mother participating in a school-based intervention (USA)136
There were some common misconceptions, particularly about fertility. Some young mothers thought it was not possible to get pregnant soon after a birth, miscarriage or abortion so, consequently, they did not perceive the need for contraception at that time. 130 One young woman, who had been using oral contraceptives when she got pregnant, supposed herself to be particularly fertile and, believing that no contraceptive method could provide adequate protection in her case, declined to use any; she believed that abstinence was the only solution, but was not successful in achieving it and so became pregnant again. 138 Others could not imagine that they would be interested in having sex so soon after the birth130,139 or overestimated the contraceptive effect of breastfeeding. 85 Misconceptions about the side effects of some types of contraception deterred young women from using them. Some of these were spread by rumour (‘the coil can rot your insides’, etc.), but some young women misinterpreted the product information on the packaging of contraceptives or the information given to them by health-care professionals, or focused on rare adverse effects, particularly infertility, and became quite fearful of contraceptive products. 130,131,138 Such misconceptions could lead them to use less reliable contraceptive methods, if any at all. One teenage mother said:
I mean, I’m gonna get pregnant if I have sex. That’s what I tell myself, so . . . I’m just gonna stop altogether. I have to. It’s gonna be hard, but, yeah. I got pregnant with my son on the pill . . .
Teenage mother who expressed an intention to obtain an intrauterine device (IUD) (USA)138
This particular teenager did go on to have another pregnancy. 138 Another teenage mother said:
I used the pill but I stopped, the injections make you bleed, the coil can rot you out and make you stink down below.
Teenager of Caribbean ethnicity with two (or more) pregnancies (London)130
This teenager ‘was so adamant about her views that no amount of attempt to convince her otherwise would have changed her mind’. 130
Additional concerns included having a foreign object inside of one’s body (‘something inside [me] that doesn’t belong for 5 years’) and the string check requirement (‘I don’t think I could do that. Like go up there, like every . . . [period].’).
Weston et al., 2012 (USA);138 study on teenage mothers who expressed an intention to obtain an intrauterine contraceptive device (IUCD)
The most common misconception about abortion was that, as a consequence, a woman would never be able to have a child. This misconception sometimes led directly to a rapid repeat pregnancy. Some young women believed it to be true and so saw no need for contraception. Others, because their anxiety about possible infertility was so acute, got pregnant in order to see whether or not they could, and to alleviate their distress. Information given by health professionals about the minor risks of infection leading to adverse effects on fertility after an abortion appeared to be overemphasised. This could have been with the intention of discouraging young women from putting themselves into the position of needing an(other) abortion, or, possibly, it was misinterpreted as a major threat. These fears were sometimes reinforced in schools where, in both sex and relationship education (SRE) and religious education, abortion was presented from a negative, moralistic stance. 130,134
After the second abortion my doctors told me that my chances of having kids would be slimmer . . . I was being a bit more careful thinking that I won’t get pregnant again, but at the same time sort of hoping that I would be, because then I would know that I could have children.
Teenager of Caribbean ethnicity with two (or more) pregnancies (London)130
. . . if doctors and nurses and other people spent less time telling women they were risking their fertility by having an abortion there would be less second abortions . . . I see people back pregnant just a few months after an abortion and they are really surprised.
Hoggart et al., 2010 (UK)134
One problem we do find, is that some of the girls have had some quite heavy handed sex education . . . they’ve obviously been exposed to something fairly dramatic in schools which has had quite an impact in terms of putting them off abortion.
Hoggart et al., 2010 (UK)134
Barriers to contraceptive uptake: access and continuity of care
For some young women, contraceptive counselling given during pregnancy, or immediately afterwards, together with prescription, facilitated timely uptake of effective contraception. These young women tended to have more frequent contact with the health-care system and received more information and counselling about contraceptive methods, particularly during pregnancy and shortly afterwards. They were often supplied with their method of choice at the hospital after delivery. 139 In contrast, other young women encountered significant barriers related to difficulties in accessing contraceptive care or the contraceptive method of choice, including missing appointments because of restrictive clinic hours, the requirement to obtain a referral letter, the requirement to be aged 18 years or over or have parental consent, health requirements [e.g. to remain sexually transmitted disease (STD) free for the preceding year], lack of provider training to supply the contraceptive device of choice (e.g. to fit an IUCD or hormonal implant) and lengthy gaps between requesting a device and having it fitted. 138,139 In the USA, lack of Medicaid cover was also a problem. 139 In the Australian study,137 however, it was stated that all the participants, whether they were pregnant, were parenting or had experienced a recent abortion, and whether the first pregnancy had been planned and wanted or unintended and unwanted, expressed firm intentions to be vigilant about their contraceptive use in the immediate future. Those who had had abortions experienced a heightened sense of pregnancy risk and consequently were keen to avoid repeating the experience; those who continued the pregnancy wanted to delay further childbearing.
They were just saying about the pill, the shot, like just different methods. And I just asked, ‘Could I get the pill?’ And they just prescribed me some pills.
Teenage mother engaged in education/training (USA)139
Barriers included limited clinic hours . . . ‘I missed my appointment . . . last month but I couldn’t do it ‘cause I couldn’t afford to miss any more days out of school.’
Weston et al., 2012 (USA);138 study on teenage mothers who expressed an intention to obtain an IUD
I’ve basically made the decision, like, for when the baby’s born, I’m getting straight back on the pill but I’m getting a different one and he’ll be wearing a condom as well ‘cause I’m not taking any more chances after this, I’ll be really cautious.
Smith et al., 2013 (Australia);131 study on pregnant, parenting and post-abortion teens
However, key informants in the UK were concerned about a lack of post-abortion follow-up care for teenagers that included establishing an effective contraceptive regime and addressing any social problems that had contributed to the girl getting pregnant. This could be associated with commissioning issues: primary care trusts varied regarding whether or not they commissioned contraceptive services at the time of abortion and whether or not this included LARCs. Continuity (including having referral, assessment, procedure and follow-up components all in place) was thought to be important so that intervention opportunities would not be missed. It was considered most important to use the referral consultation to begin supporting contraceptive choices after the abortion. Where continuous services were not available, young women could be left at risk of a repeat pregnancy. 134 According to Hoggart et al. (2010),134 one of their study participants, Yasmeen, ‘had plans for the future, and she wanted to ensure that she did not become pregnant again. She would have liked to have an injection at the clinic . . .’
They are sending you somewhere else, and I don’t even know where that is.
Teenager who had had an abortion (UK)134
Other findings of interest
Young women’s attitudes towards abortion
Among the qualitative studies, there were some additional data, largely from one UK study,134 relating to attitudes towards abortion. This did not strictly speaking address the issue of repeat pregnancy, rather it concerned first pregnancies, but nevertheless it is pertinent to our review questions. We have described how some young women were pressured into having an abortion and subsequently became pregnant again as a means of relieving their feelings of grief, loss and guilt. Conversely, if a young woman, finding herself unintentionally pregnant, decided that her best course of action was to have the pregnancy terminated, and if she was adequately supported in that decision, then she was not as likely to have a repeat pregnancy. However, if she felt unable to even consider the possibility of having an abortion, she would have the child and be at a greater risk of a second pregnancy. Abortion was often mentioned by study participants in negative, moralistic terms that did not allow them to consider it as a reasonable option. 129–133 They saw it as wrong or immoral,134 they ‘didn’t believe in abortion’,131 or the fathers of their children strongly opposed abortion. 129 Some young women reasoned that, because there are women who desperately wanted to have children and were unable to, it would not be right to have an abortion just because the timing of their pregnancy was inconvenient. Other young women thought that girls who were foolish enough to engage in risky sexual behaviour should take responsibility for the consequences. 134
. . . the same way murderers get sent to prison, people that abort their babies should get sent to prison as well because they’re murderers as well, simple as ABC.
Hoggart et al., 2010 (UK);134 study on teenagers who had had abortions, abortion providers and other stakeholders
I say quick enough to open your legs, take the consequences for it.
Hoggart et al., 2010 (UK);134 study on teenagers who had had abortions, abortion providers and other stakeholders
For some young women, the root of their negative opinions about abortion lay in deeply held religious or cultural beliefs. 130 However, many young women’s views seemed to have been influenced by the way abortion was presented in the context of SRE or, in some cases, framed as a moral issue in the context of religious education. 134 Some young women had been directed by their teacher to the internet to research abortion issues, where they had found a variety of information about what the abortion process entailed. They were equipped with neither the intellectual nor the emotional maturity necessary to evaluate this information, which included some horrific myths. 134
. . . there’s one where they put the hook in yeah, and they use the hook to shred the baby and it is nasty sometimes if they give birth to the child they cry they leave it to die.
Hoggart et al., 2010 (UK);134 study on teenagers who had had abortions, abortion providers and other stakeholders
Others, who might have been less put off by these negative views and beliefs, were deterred from considering abortion by a very poor level of knowledge about it, including the misconceptions that you had to pay for an abortion, that if you are under 16 your parents must be informed and that you need to be accompanied by someone over the age of 18 years134 (none of which are true in the UK). In contrast with these accounts, a group of 21 young Australian women who elected to terminate their pregnancies all indicated that their pregnancies were both unplanned and unwanted and therefore resolved to ‘escape’ pregnancy and motherhood. Most of them held little regret over this decision. 137
. . . if it’s gotta happen, it’s gotta happen. It’s best to get rid of it if you don’t really want it and you’re not ready for it . . . I was too young; I wasn’t ready for it so I am just grateful that it is there for me as an option.
Smith et al., 2013 (Australia);137 study on pregnant, parenting and post-abortion teens
The authors of this study137 did not offer any explanation for this pragmatic attitude (their focus was on pre- and postpregnancy birth control intentions), but it seemed to result in a less emotionally stressful experience for these young women. They did appear to have made their own decisions to terminate the pregnancy, but we do not know what support they received from either family or service providers. Nor do we know whether or not the Australian educational system or social attitudes are more supportive of abortion as a means of resolving an unplanned teenage pregnancy. Alternatively, it may be that young women who were coerced or unhappy with their abortion decisions did not consent to enter this study.
Chapter 4 Theory formation: why interventions might work and for whom (realist synthesis)
This chapter brings the principles of a realist synthesis to bear on the evidence, and draws out candidate theories of the action of interventions and identifies barriers to and facilitators of intervention implementation.
Findings
Each theory area was taken in turn and all the evidence relating to a particular programme theory was gathered. This facilitated a fuller understanding and refinement of the theory areas, for example ‘other goals and aspirations’ and ‘connectedness’, as the story from the theory area began to emerge and the researchers began to see common mechanisms and contexts. Further scrutiny and analysis of the emerging story across each theory area resulted in the emergence of a number of key mechanisms that seemed to be potentially important for increasing the likelihood of interventions working. We also identified a number of different contexts in which these mechanisms may (or may not) be triggered. From the evidence base that was reviewed, it was difficult to identify the contingencies between particular mechanisms and specific contexts, which resulted in actual outcomes. Below, we report on contexts (see Contexts) and mechanisms (see Attending to mechanisms), and outcomes related to these are integrated into the descriptions. These findings provide the conceptual platform on which we proposed interventions might be built to enhance their potential to be effective.
Contexts
We identified a number of different contexts that might help explain whether or not the mechanism(s) underpinning particular interventions may be ‘triggered’. Different types of contexts, uncovered in the evidence review, ranged from philosophical to physical and practical, through to emotional, including conceptualising the issue (who develops the intervention and their perspective on the issue of repeat pregnancy),133,142,154 home (evidence offered by stakeholders who attended the Shrewsbury Stakeholder mapping meeting), community,31 partner/relationship,97,155 family,98 ethnicity,99–101,156,157 previous pregnancies,102,130,139 preferences103,130 and the availability of different types of services. 104,131 These contexts, which are described in the following sections, may explain why some approaches might work (in certain circumstances), for whom and why, and also provide an indication of the factors that need to be taken into account when developing new interventions.
Conceptualising the issue
There was a polarisation in the evidence base with regards to the epistemology of interventions to prevent or delay subsequent teenage pregnancy. Authors of some of the quantitative evidence viewed teenage pregnancy from the perspective of irresponsible, problem behaviour, typically associated with alcohol use, socioeconomic deprivation and particular ethnic groups (in the USA) which are considered at high risk. 31,98–101,157 Conversely, writers of the qualitative reports viewed teenage pregnancy from the perspective of the adolescents themselves or health-care professionals who work closely with young mothers. From this perspective, sexual activity was often thought of as spontaneous, unplanned and sometimes involuntary. 85
Interventions developed from this issue, being based on the informed decision-making of young women who weigh up the consequences of pregnancy and motherhood, may be unrealistic. 85,154 Stakeholders agreed that for some adolescents there was no planning or consideration of consequences, and no planned behaviour: adolescents would prioritise carrying their mobile phone, but not contraception. Generally, it was felt that adolescents live for the moment and do not believe that they will get pregnant.
Evidence suggests that viewing repeat teenage pregnancy from a developmental approach, focusing on the individual’s level and abilities, cultural context, age-appropriate impulsive and rational decision-making styles, may be a better place to start with regard to conceptualising interventions. 85
The NHS Scotland strategy document Reducing Teenage Pregnancy142 states that promoting a culture of participation is one of many effective methods for reducing teenage pregnancy. In line with UNICEF’s UN Convention on the Rights of the Child,158 more successful interventions might be those that involve young people at a level that is both meaningful and appropriate. This culture of participation includes creating opportunities for young people’s individual experiences of education and services related to sex and relationships to be heard and influence their future direction. Opportunities to involve young people should be considered throughout the development and delivery of work, for example in scoping objectives, creating leaflets and marketing campaigns. 154,159 Framing the issue using adolescent views and opinions, rather than those of adults, and by focusing on their control and abilities to manage sexual relationships through engaging in discussion might provide conditions under which interventions will work because there is the opportunity for the young people to take responsibility for actions and choices.
Community
A community may value rapid repeat teenage pregnancies, believing motherhood to be a desirable and defining role for an adolescent. 31 Communities also play an important role in how pregnancies are perceived; stakeholders stated that in more deprived areas, pregnancy is viewed as normal and almost expected, while in less deprived, more privileged areas, teenage pregnancy is viewed as out of the ordinary and, in certain circumstances, shameful. The differing perceptions of teenage pregnancy could lead to differing ages of onset of sexual activity, differing use of contraception and different decisions regarding the outcome of pregnancy, such as termination, adoption or raising the child, depending on what the community regards as ‘normal’ or ‘acceptable’. 31 Aligned to the expectations of a person’s community, the teenager’s culture provides a context for sexual activity, use of contraception and terminations. This context might influence an adolescent’s decision-making and their opinions on the potential consequences of pregnancy, affecting their behaviour and, in some cases, limiting their options if they were to become pregnant unintentionally. 99–101,156,157
Communities can also hinder or facilitate intervention delivery. Stakeholders working closely with young mothers cited an example of an area in which there is little or no engagement in available services for young mothers. The area in question is one with a strong sense of community. Therefore, it might be more challenging to operationalise interventions in close, tight-knit communities in which service providers are viewed as ‘outsiders’; in such circumstances, attention should be paid to developing approaches and strategies from the ground up.
Family
The importance of understanding a teenager’s family context is also important. Stakeholders suggested that a difficult home life caused by, for example, disagreements with family members or a breakdown in family structure, as often experienced by looked-after children, can lead to the desire to create a family of one’s own, as a way of dealing with the feelings of family loss experienced by these adolescents. Herrman133 also suggested that pregnancy and the birth of a child may meet the needs of the adolescent, as they perceive this to enhance family closeness.
Teenage childbearing can also run in families, thereby influencing future generations. 98 If their own mothers had been teenage mums, teenage girls are more likely to experience teenage pregnancy, perhaps because childbearing is normalised from an early age and a large emphasis is placed on motherhood. If teenagers have helped to raise younger siblings, they may feel competent enough to raise children of their own, thus altering their perception and reducing the gravity of the consequences of becoming pregnant themselves. A mother attending a service user feedback group conducted by the study team stated that she was one of 10 children and had helped to raise her siblings from a very young age. When she had her first baby, she said it was no different: ‘I had basically been a mother since the age of 10 anyway.’
These findings point to the need to better understand the motivations of a teenager with regard to becoming pregnant, as these might be highly complex, and emotionally and socially embedded and therefore not necessarily visible to those providing services and support.
Peer influence
Peer influence can provide a context in which a teenager feels they do not fit if they are not sexually active or have not experienced a pregnancy. 97,129 Peer influence can be a significant driving force for sexual activity, as all teenagers want to fit in with their peer group.
Therefore, interventions that operate within the context of teenagers’ peer groups might have more impact than those that operate in isolation of this context.
Partner influence
The relationship between the young women and their partners also provides a further layer of context, particularly for the risk of rapid repeat teenage pregnancy. Stevens-Simon et al. 155 reported that the following partner variables were associated with repeat pregnancy: having an older boyfriend, having a new boyfriend since the conception of the first pregnancy and having a boyfriend who wanted a child. The main reason highlighted, as regards partner influence, in the evidence was the ability of the partner to influence child bearing intentions and contraception use. 97,99–101,155 Chapter 3 describes how partners and young women’s relationships with them influence contraception intentions and use, and views of pregnancy.
In summary:
-
Older partners may exert influence over an adolescent because of the adolescent’s limited experience and confidence; the adolescent trusts that their partner knows better than themselves.
-
Gender roles and cultural influences place women in passive roles, unable to state whether or not sex will occur and whether or not contraception will be used. 97,99–101
-
Those in long-term relationships with new partners since the birth of their first baby, may become pregnant again to give the partner a baby of their own as a way to repay them for helping to look after the older child, and to cement their relationship (stakeholders from the first meeting). Stakeholders also stated that young mothers want to give their new partner a baby and perceived this as a way of ‘keeping him’.
Female adolescents in relationships with older partners tend to be younger, less likely to use a condom at first intercourse, less likely to use condoms consistently and more likely to become pregnant than adolescents with partners of similar age . . .
Raneri and Wiemann (2007)97
Previous experiences
Relationships and a partner’s influence can have a powerful effect and, therefore, the effectiveness of interventions may be mediated by this context. This issue also highlights the need to pay attention to the context around the teenager when designing and delivering interventions.
Emotional context of previous experience
Pregnancies that resulted in miscarriage, stillbirth, adoption or a child being taken into care provide an emotional context for young women. Evidence suggests these circumstances can lead to feelings of loss, guilt and depression, and result in a subsequent pregnancy as the mother tries to replace what was lost. 102 This is conceptualised by Clarke130 as a ‘journey of search,’ in which meaning and fulfilment is brought to their lives after the loss of a previous child.
In cases of abortion, there were accompanying feelings of guilt . . . they spoke of the compelling need to fill the emotional void created by the loss by becoming pregnant again as quickly as possible they felt that the loss had a strong bearing on the second pregnancy. 130
. . . women whose first pregnancy ended in miscarriage were more likely to have a rapid repeat pregnancy. . . . history of miscarriage before the index pregnancy was associated with increased recidivism. . . . . Feelings of guilt or a desire to replace a lost pregnancy may be more important in these cases than in cases of pregnancy termination. 102
Those stakeholders attending our first engagement meeting whose first pregnancies had resulted in termination, stillbirth or the child being taken into care said that they wanted to replace the baby – and also to know that they could conceive again.
The evidence seems to suggest that when the choice was not the mother’s own, that is they were forced to terminate or coerced into terminating a pregnancy, or they had lost a baby through miscarriage or stillbirth, the likelihood of a repeat pregnancy is greater. 130 It would seem that, regardless of others wishes, if a mother wants to replace the loss, whether intentionally or unintentionally, the loss will be replaced. Therefore, the timing of interventions after such events would seem to be an important condition for outcomes. Counselling for mothers who have had a termination, a stillbirth or a child that has been taken into care has been proposed. Such counselling may help to counteract feelings of loss and/or help individuals to make appropriate and informed choices about how to respond to these feelings.
Summary
There are complex layers of context that have the potential to influence the motivations, intentions and behaviours of young women, with respect to sexual activity and pregnancy. These different contexts provide both an explanation and some signposting as regards what should be accounted for in the development and implementation of interventions so that they have the desired impact. Our analysis of the evidence leads us to suggest that ‘framing’ the issue from the perspective of the young person, which includes their active engagement in strategy development and implementation, may provide a more conducive context for an intervention to work. Furthermore, paying attention to the potential ways that communities, families, peers and partners can both be engaged in and influence intervention development and use could help situate the intervention in a context that is relevant to the individual. We also draw attention to the emotional aspects of the issues surrounding sexual activity, relationships and pregnancy (particularly in the context of previous losses), which may be more or less visible to those providing services, but which provide a powerful backdrop to the young person’s motivations, intentions and behaviours.
Attending to mechanisms
We purposively reviewed the evidence to see if we could uncover mechanisms that have been attended to in the design, implementation and evaluation of interventions for repeat teenage pregnancy. As has already been reported, the evidence base for this review was patchy. However, we have been able to both identify and hypothesise that there are four mechanisms that should be attended to if services want to engage participants in the issue of teenage pregnancy, and design and implement strategies and approaches that are more likely to have a desired impact. In the context of realism, it is the underlying mechanisms that give rise to an event or outcome. Pawson and Tilley160 use the analogy of a clock to illustrate the meaning of a mechanism – it is only by examining the inside of the clock that it would be possible to understand how it works, not by examining the clock face itself. Therefore, mechanisms may be more or less hidden from view.
Motivations
As described, different individuals will have different reasons for becoming pregnant; thus, attending to underlying motivations within the development of interventions would be a good starting point. These motivations are driven by community norms, social context, peer influence and past experiences, which all add to a complex mix. Working with these different motivations could lead to better engagment with the issue of sex and pregnancy, and enhance the potential of the young person responding to an intervention and making informed choices.
The motivation(s) to get pregnant – whether these are positive or negative – may be contingent on the issue of how young women plan for or view the future. Evidence suggests that some perceive a dichotomous choice between motherhood31,85,97,130 and other goals and aspirations. 31,91 In the absence of other goals and aspirations, some adolescents look to motherhood. Low educational attainment and disengagement with school may lead teenagers to believe that childbearing may provide them with an opportunity to experience success, gain autonomy and self-esteem that they cannot gain through academic and vocational routes. 31,91 Our stakeholders raised the concern that parenting skills and praise during pregnancy and the early years may be the only time that a teenage mother has felt as though she is good at something. Furthermore, in low-income communities, it has been observed that there may be ‘rewards’ (such as respect in the community) for bearing children, where the norms might not discourage having children at a young age. 85
Adolescents can also have low expectations of life. Our stakeholders suggested that teenagers may get pregnant as there are no jobs and no prospects. Girls sometimes ‘drift’ and are unsure of what to do when they find themselves pregnant, or they could be unaware that they are pregnant. In this context, they continue with pregnancy because they perceive that they have limited options.
There was also evidence to suggest that some adolescents perceive having children during their teenage years as a sensible and beneficial decision, which was coined by Clarke130 as a ‘reversed life course’. By having their children young, mothers have the rest of their lives to focus on a career; once their child is old enough to attend school full time, the majority of mothers who became pregnant as teenagers are still in their teenage years or early twenties. However, if they wait until they are in their mid to late thirties to begin a family, after they have established a career, it might be difficult or impossible to conceive. From this perspective, unintentional pregnancy is not viewed negatively, but as a positive decision to have children at a young age in order to provide more opportunities and choices in the future.
Therefore, interventions that focus on reducing repeat pregnancy should be considered within the broader context of the young person’s life, motivations, attainment and ambitions. It is important to note that the narratives of some may run counter to the policy discourse, in that pregnancy might have an ascribed positive meaning, which may also be contextually (within their community) accepted as the norm. Furthermore, interventions might usefully focus on alternative strategies (if appropriate) for achieving personal automony and acheivement other than pregnancy.
Taking control
Understanding and working with the different motivations that underpin decisions related to pregnancy could facilitate an adolescent’s ability to take (more) control. Designing and delivering interventions that provide opportunities for adolescents to take control of sexual encounters, contraception and decisions about pregnancy might empower them to make informed choices. This mechanism may, however, be mediated by culturally determined attitudes that have shaped adolescents’ identities and perceptions of sexual roles for males and females, which can also impact on their abilities to negotiate the use of contraception with partners. 97,99–101
Paying attention to self-esteem, self-efficacy (confidence in one’s ability to take action) and empowerment were all stated as ways that could increase the likelihood of an adolescent taking control. 31,81,85,105,129 Our stakeholders also highlighted the need for adolescents to increase their self-esteem, life skills and empowerment. They theorised that if adolescents feel that their options are limited and have low expectations of life, they may also believe that their choices do not impact on their life, leading to more impulsive decisions without thinking through the consequences; these views are also supported by research. 85,154 Policy documents from the UK8,142 also recognise the importance of raising self-esteem and empowerment as part of their strategies to reduce teenage pregnancy. Reducing Teenage Pregnancy (NHS Scotland, 2014)142 also highlights the roles that a wider context, such as the media, can have on influencing behaviour and promoting positive role models.
There are a range of theories that conceptualise the multiple levels of influence that an adolescent is under and that could help to build self-esteem, self-efficacy and empowerment. For example, Raneri and Wiemann97 used social–ecological theory as a basis to explain the influence of these multiple levels (e.g. individual, dyad, family, peer/community and social system) on behavioural outcomes. According to this theory, development and behaviour are influenced by a range of factors, from those that are closest to the individual, such as individual experiences and attitudes, to those that are part of the social environment, such as race, ethnicity and socioeconomic status. Based on this analysis, Raneri and Wiemann97 suggested that multifaceted interventions that target adolescent mothers and the communities in which they live, at delivery and during the early postpartum period, can help them to overcome outcomes such as repeat pregnancy. It was suggested that interventions might include policies, programmes and funding to intensify and lengthen services for young mothers and their children in the postpartum period, to strengthen connections with educational and occupational opportunities, to improve adolescents’ and their families’ understanding of the effects of partner selection and characteristics on their life course and to provide individual and partner health education or counselling on family planning and healthy relationships.
Mbambo et al. 106 drew on the Health Belief Model to provide a context for a teenage girl’s personal circumstances and stated their perceived susceptibility to getting pregnant again, the perceived severity of getting pregnant again, such as the likelihood of a breakdown in family relationships, and the perceived benefits of not getting pregnant again, such as the ability to complete school. In this study, 107 adolescent mothers, attending two clinics in Mkhondo, South Africa, were given a questionnaire that enquired about their biographic information and individual perceptions, and modifying factors and variables that could affect the likelihood of utilising contraceptives, such as age and educational attainment. The application of this theory resulted in the analysis described in the following sections, which may provide a useful heuristic guide to intervention development within specific contexts.
Individual perceptions
Lack of knowledge about contraceptives, as well as negative attitudes towards the use of contraceptives, might have influenced the participating adolescent mothers’ choice not to use contraceptives. Only 46% of the participants believed that contraceptives prevented pregnancies and as few as 13% believed that condoms prevented both pregnancies and STDs (including HIV). 106
Modifying factors
The adolescent mothers’ ages ranged from 14 to 19 years. Consequently, they required, but may have failed to receive, adequate health education about menstruation, sexual intercourse, pregnancy and contraception before they reached the age of 14. Although some participants knew that contraceptives prevent pregnancies, they did not use contraceptives effectively to prevent pregnancies. Another modifying factor could be that the majority (75%; n = 80) of the adolescent mothers received education about menstruation from their mothers. These adolescent participants’ mothers and other informants (clinic nurses, friends and educators) reportedly did not provide information about pregnancy and contraceptives, even if they informed the adolescents about menstruation and sexual intercourse. 106
Benefits
The major benefit of the use of contraceptives is that it grants a woman the ability to control her fertility and to bear children if and when she is ready to do so. Given that all the participants were adolescent mothers, none of them had used contraceptives effectively to delay their pregnancies until they had completed their studies. Although numerous factors can influence the decisions made by adolescents regarding whether or not to use contraceptives, they need knowledge about and access to contraceptives to be able to utilise them effectively. 106
Variables affecting the initiation of actions
Identified barriers which might have prevented the adolescent mothers from using contraceptives effectively to prevent unplanned pregnancies included contraceptives’ side effects, lack of knowledge about contraceptives and problems of accessing contraceptives if clinic hours coincided with school hours, as well as the misconception that contraceptives could only be obtained from clinics on one specific day. 106
Koniak-Griffin et al. 81 used a theory of social competence to further explore the effects of internal and external influences. The ‘Early Intervention Program’ was designed to help young mothers achieve programme objectives as a result of improved social competence. 81 Social competence was stated to have two facets: internal and external. A young mother’s internal competence (ability to handle her inner world) increased through training in self-management skills, including self-care, life planning and decision-making, handling emotions and coping with stress and depression. At the same time, they proposed that external competence (ability to interact effectively with partners, family, peers and social agencies) improved through training in communication and social skills. 81
A greater sense of control over self, choices and outcomes related to pregnancy may be achieved by working on and improving self-esteem, self-efficacy and empowerment. With regard to the mechanism underpinning taking control, there are two levels to consider: (1) the individual in relation to pregnancy and (2) how they are situated in their wider context. As outlined earlier, an adolescent faces many influences from multiple sources. Therefore, the pregnancy cannot be viewed in isolation; a more holistic approach is required, and, as such, any intervention needs to be situated within a broad context.
Situating the intervention
As previous sections and findings indicate, the issue of adolescent pregnancy involves family, societal, medical and educational components; therefore, interventions need to address the complex needs of the young women,107 that is not just the issue of early (repeat) pregnancy. Therefore, by paying attention to these wider issues, interventions would be situated within a wider context for the young person.
Failure to address the wider social and cultural influences on teenage pregnancy has contributed to the lack of progress made in reducing it in Scotland in the past . . . The most successful programmes therefore are multi-component and address a wide range of determinants of risk.
Reducing Teenage Pregnancy, NHS Scotland, 2014142
Evidence suggests that this could include medical and social service providers helping adolescents to think through the wider repercussions of childbearing: how their age, educational status (current level of schooling and qualifications), financial situation and relationship status may impact, not only on decisions affecting childbearing but also upon other areas of their life. 97 Interventions should take account of the individual’s internal/external social competence (their ability or inability to handle their inner and outer worlds),81 their community31 and their cultural99,100,156,157 and peer group norms. 97,129 Other relevant questions include those related to previous experiences of pregnancy, including how decisions were made about the outcomes (e.g. whether or not decisions were made for the pregnant adolescent), which might lead to beginning a ‘journey of search’. 130
These wider contextual issues have the potential to influence the outcome of an intervention, for example by making adolescents equate contraception use with obtaining the lifestyle they want. 161 However, they could also help to shape the intervention itself by situating it in the context of the young person, that is by providing elements which may be desired by the adolescents, such as skills development, and re-engagement with education or employment training. 99–101,108,129
The role of education in this group of individuals seems to be important; for example, Berenson and Wiemann108 reported that reliable contraception was observed to occur more frequently in adolescents who were doing well at school and who were enrolled in school within 6 months of delivery. Drayton et al. 99–101 also found that participation in their programme, the Women’s Centre of Jamaica Foundation Programme, exerted a protective effect against the occurrence of repeat pregnancy with key positive variables including the desire to continue education. This programme provides classroom instruction and support for adolescent mothers, aged 16 years and under, with the aim of returning them to the formal school system, and delaying the birth of a second child. The programme also provides skills training and job placement assistance to unmarried, unemployed mothers over the age of 18 years. Acceptance and use of a family planning method is a requirement for programme participation. The theory is that completing education is a motivator for not getting pregnant, and links to issues around achieving hope for the future.
The promotion of educational attainment needs to include practical considerations through, for example, a greater awareness of the challenges that young mothers face when trying to continue their education while parenting. 129 Difficulties include arranging childcare if they are the sole parent, inability to meet deadlines because of limited time to complete assignments, not being able to give tasks their undivided attention and issues of absences if their children are unwell.
Young mothers attending a service user feedback group stated that they wished to continue education, but the needs of their children would require a crèche, and for the intervention to be delivered at school. In the UK, this is currently not an option; however, evidence from the USA demonstrates positive results when interventions are delivered in schools. 97,107,109,162 This approach embeds the intervention in the mother’s lives, keeping the focus on education, but also allowing them to have contact with their children during the day. Providing childcare in a school as part of a wider intervention acknowledges the dual role of the adolescent mother; she is still an adolescent who needs to complete her education, but she is a mother who feels responsible for her child and needs to know that they are safe and well cared for while she is attending classes. 162
Situating the intervention in the broader context of the young person also means considering vulnerable and high-risk groups, such as victims of violence. Stakeholders attending a meeting in Shrewsbury stated that sexual exploitation can be a problem, particularly older men targeting vulnerable, looked-after children. They suggested that there should be appropriate sex education and services specifically for vulnerable children (e.g. looked-after children or victims of violence), because ‘basic’ services are not good enough in these cases. Because of an upheaval in family life and traumatic events in their past, such adolescents may drift and feel their options are limited. There is a risk that these young women will be exploited by men who promise them a stable, loving relationship, only to be manipulated as the relationship continues; with a lack of family, these adolescents could easily find themselves trapped in such relationships with no one to turn to. Policy documents have also highlighted the need to target vulnerable groups and undertake needs assessments in order to provide the support that these adolescents need. 8,142,163
The outcome of ‘situating the intervention’ within the broader context of the young person’s life and taking a wider view of pregnancy in adolescence may lead to a greater potential for ‘connectedness’ with the intervention,31,89,162,164–166 the issue108 and their own context90 and, therefore, the notion of ‘support’ may trigger their self-determination and active control. Feeling connected and supported can help an adolescent to feel that their life choices are being encouraged. 31,166 A supportive professional delivering the intervention, the group itself or family members can help to verbalise and confirm a mother’s skills,108 and help them to develop strategies and plans to change their attitudes and behaviour. 89 Feeling connected and supported as part of a group of mothers with whom they can relate to may inspire mothers to achieve and not feel limited because of their current situation. 166 Young mothers attending a service user feedback group also stated that being part of a group allowed them to hear others’ feelings and opinions, and let them know that they were ‘not alone’. Havens et al. 89 also found that the bond and the supportive relationship between a mentor and an adolescent could give pregnant teenagers the support that they needed to change attitudes and behaviours.
If an adolescent has limited support from family and friends, the connections made as part of an intervention could fill the gaps in their social networks, offering an avenue of support for adolescent mothers that they do not have in their day-to-day lives, which, without the intervention, would have remained unfulfilled. 162 Feelings of support and connectedness can increase self-esteem, self-competence and empowerment, which, as stated previously, can in turn lead to greater feelings of control over self, choices and outcomes. Being connected to the intervention, group or others can also have the added benefit of helping to keep mothers on track with the changes they propose to make. 166 Professionals delivering the intervention or group leaders are ideally placed to routinely check the adolescents’ progress.
Evidence from stakeholder meetings suggests that other opportunities and services (aside from specific interventions) from local government and authorities, such as additional visits from health-care professionals, access to nursery places and community playgroups, may enhance connection to the system, community and other young mothers. It allows young mothers to know that the system still cares, although there seems to be a need for a balance of providing support through different avenues, without the mothers relying on these services and having subsequent pregnancies in order to still qualify for them. Stakeholders attending a meeting in Shrewsbury gave stories of a service that provided young mothers with support through groups and crèche facilities until the child was 2 years old. Mothers enjoyed the service; they built friendships, gained support, felt as though they could share problems and issues, and gain advice in a nurturing environment. Once the child reached the cut-off age of 2 years, the mothers said that they felt lonely because they had become used to seeing their group leaders and the other mothers. In short, they felt abandoned and without support. Some mothers confessed later to having subsequent children in order to go back to the service, reconnect with their peers and regain the lost support.
Tailoring
Given the issues described above and the complexities inherent in tackling this issue, ‘tailoring’ interventions may provide a useful mechanism. This would require some individualised assessment of what is required (regarding the wider context of the person’s life and ambitions) and the availability of a suite of interventions, which would need some oversight and co-ordination. Key et al. 107 suggested that, given the many factors involved in multiple ways, a multifaceted approach should be employed. Traditional approaches for providing information will not necessarily result in contraceptive use or behaviour change. 167 If an adolescent is ambivalent or unmotivated, providing information on contraception and services is unlikely to motivate them; instead, they need to be engaged in the issue. 130 There may be many emotional and psychological barriers to contraceptive use; these barriers need to be explored when health-care professionals prescribe contraceptives. 130 Furthermore, a multidisciplinary and service approach is needed to meet the complex needs of adolescents. They need to understand how engaging in sexual activity could potentially affect them and their lives, whether or not they are already sexually active or planning on having sex for the first time. Their thoughts and feelings about sex, their choices of contraception and their level of maturity need to be considered.
There a number of ways that tailoring can operate. In the following sections (Contraception methods and preferences, Barriers and Facilitators), we outline tailoring in the context of contraception use, and in relation to minimising barriers and increasing facilitators in order to support engagement with the issue and with the intervention itself.
Contraception methods and preferences
Contraception advice and prescription is a specific example of the way in which tailoring, as a mechanism, might operate. Although there are a variety of contraceptive methods available, research104,131 and evidence from our two stakeholder group meetings and from young mothers at our service user feedback group agreed that LARCs, in the form of a contraceptive implant, IUDs or hormone injections, is better suited to adolescents, because they are likely to forget to take oral contraceptives daily. While health-care professionals have their own views on the best method for an adolescent to use, this may not be the right choice for the adolescent.
Health-care professionals need to be aware that they can greatly influence a young woman’s choices, sometimes by facilitating, but at other times by preventing, uptake. 138 Adolescents may switch methods or use a number of methods in conjunction; it is important to understand the types and combinations of contraceptives used by adolescents and tailor these accordingly. Therefore, interventions that consider adolescents’ contraceptive preferences may be more successful than interventions that focus on a purely medical model that provides information and then encourages hormone-based or long-acting reversible methods. 103
Knowledge and use of contraception may also vary among young women; therefore, it is important to assess knowledge and thoughts about sex, relationships and contraception on an individual basis. Policies in the UK encourage parents to engage in open discourse about sex and relationships with their children in order to increase knowledge and implementation of contraception so that adolescents practice safe sex. 8,142 There is also an argument that this individual-based approach should extend beyond the adolescent years, as young adulthood is considered a distinct developmental period with challenges, change and the exploration of life possibilities and decisions. 110
Previous experiences of pregnancy can also influence contraception preferences, with adolescents who have been pregnant before, regardless of the outcomes, being more likely to choose effective methods and be more motivated to use them consistently than never-pregnant adolescents. 111,168 The reality of motherhood may encourage an adolescent to better comply with contraceptives; however, rapid repeat pregnancy rates in adolescents are high. There is a need to understand what changes; it could be that, over time, as the adolescent becomes more settled in her mothering role she feels that she would be able to cope with another child, thus minimising the enormity of pregnancy and leading to a change in her contraception practices. As contraception is an individual choice, there is a need to understand the ‘longer journey’ of an adolescent.
As part of the service that medical professionals could provide, contraceptive counselling, as well as the actual contraceptives, tailored to encompass issues outside of the medical paradigm, including stress and depression, which have been shown to negatively affect contraception use. 85,169 This provides a more holistic approach, exploring the reasoning, motivation and context behind contraceptive use, especially as these could change over time. This would provide an opportunity to tailor prescriptions and support the adolescent’s decision-making, reducing the likelihood of discontinuing with methods, rather than seeking alternatives that may be better suited under the circumstances. Stakeholders attending a meeting in Cardiff stated that interventions need to be tailored to the individual according to their circumstances at the time; professionals need to find out what the adolescent really wants and understand what they are asking for. The stakeholders also stated that there is too much generalisation of the perceptions of what adolescents want, which may not be accurate, and that adolescents should be asked about their preferences directly.
Stakeholders and young mothers who participated in our consultation meetings suggested a number of barriers and facilitators that should be considered as part of intervention content and delivery.
Barriers
Young mothers often experience many barriers with regard to interventions, mainly associated with difficulties in arranging childcare or transport to intervention venues. Transport is particularly difficult if mothers are so young that they cannot legally drive, they have no family members or friends to rely on and the venue is not within walking distance; if young mothers are supported by the state, they receive only a small income, which often limits funds to the essentials, such as rent, bills, food and clothing, and therefore there is little or no money available for transport. In addition, there is the added difficulty of single-handedly getting children on and off a bus or having to arrange appointments at times in the day that allow them to take children to and from school.
Adolescents can sometimes experience delays and difficulties obtaining contraception, with multiple visits required before they are even given a prescription. Adolescents can lose patience and hope in services after two or three visits, and become so frustrated that they do not attend subsequent appointments and, therefore, remain unprotected against pregnancy.
There are additional barriers with regard to literacy difficulties. Our stakeholders suggested that many young mothers experience difficulties with reading and writing. The information leaflets on contraception that are issued by health-care professionals create a large barrier for adolescents with literacy difficulties, as they would not be able to understand and use the information, and the leaflet would most likely end up in the bin. Sex is often seen as a taboo subject; therefore, there is a lack of open discussion about sex and adolescents can sometimes feel embarrassed when trying to access contraception or emergency contraception. Young mothers attending a service user feedback meeting stated that they felt judged by ‘gatekeepers’, such as receptionists and other staff, when accessing services; being judged and stigmatised in this way stopped them from accessing services.
Facilitators
As a result of practical difficulties in travelling to venues, interventions that provide home visiting as part of the intervention delivery are championed, as they minimise such transport difficulties. 79,91,92,95 Home visiting interventions also reduce the need for mothers to have to organise leaving the house with their children at a certain time to attend an intervention session, which can be problematic. The issue of multiple visits to clinics in order to obtain contraception was also raised as an area that could be improved. Stakeholders suggested that more staff could be trained to administer a wider range of methods, including midwives to administer LARCs, such as the contraceptive implant, at home. This would minimise travel for mothers, as contraception could be administered as part of a routine appointment, thus integrating with mothers’ lives and schedules. As well as delivering interventions at home, young mothers attending a service user feedback group showed support for interventions delivered in school settings, which are currently more prevalent in the USA. The mothers felt that having the option of a school-based intervention that provided crèche facilities would allow them to stay in education more easily and would give them more options for the future. Some mothers discontinued education out of necessity rather than choice, either because there was no one to look after their child after the birth or because the school had no facilities to cater for pregnant adolescents or adolescent mothers and their children. However, as stated previously, the location of the service is only one component and the wider perspective of the mothers’ wants, needs, motivations and contexts should all be taken into consideration.
Open discussion of sex and relationships should be encouraged, and interventions should be delivered in multiple formats, using not only written information but also role play and discussion topics so that no mother is excluded because of literacy difficulties. These open discussions about sex, relationships and contraception should be conducted by professionals who are specially trained to work with adolescents, so that the adolescents can relate to them and they can tailor messages accordingly, improving understanding and delivering the intervention or service using the appropriate tone and level of information for the target population.
The use of incentives as part of services or interventions is also a form of facilitation. Many incentives are available, such as monetary incentives (e.g. the dollar-a-day programme,92 which gave American adolescents, under 18 years of age, US$1 for each day they were not pregnant), transport to and from the intervention location, and the availability of food, refreshments and crèche facilities. All of these incentives can increase engagement and improve attendance rates. Young mothers attending a service user feedback group stated that they found a crèche and free transport vital for attending services and interventions, as without these in place they would not be able to attend, even if they really wanted to. Their children’s care and safety was paramount, and they could not afford to pay for a taxi or bus. The majority of these mothers received state support and a round trip on public transport could cost as much as 10% of their income; therefore, it is not surprising that they would not pay for transport and other costs themselves.
Summary
Adolescents face pressure and influence from many sources: their families, peers, friends and partners all shape their views and experiences of sex, and the potential consequences of motherhood, some encouraging adolescent girls towards pregnancy and mothering, and others discouraging. Exposure to these influences helps to inform adolescent girls’ ‘contexts’ about sex and relationships, leading to their engagement with the issue of adolescent pregnancy. This context either motivates them to take control to consistently protect against pregnancy, or to take a more relaxed approach to these issues. Understanding how an adolescent views pregnancy (e.g. negatively or positively) can help policy-makers to tailor interventions to target key issues of importance for adolescents.
For example, using their preferred method of contraception may increase an adolescent’s compliance with contraception, and providing an individualised intervention that dispels myths and misconceptions previously adopted by the adolescent may lead to a better understanding of and engagement with the issue of pregnancy.
By attending to the issues that adolescents deem as key, policy-makers can enable adolescents to take or maintain control to protect against pregnancy. Empowering adolescents to steer their life course in their preferred direction is not easy and will require support, particularly in the absence of comprehensive sex education, the presence of difficult mother–daughter relationships or if alongside current parenting responsibilities. The evidence and contact with young mothers at a service user feedback group highlighted the importance of tailoring interventions within a broader context, with reference to the multiple roles that an adolescent mother has to play, including student, employee, friend and daughter.
Pregnancy in adolescence is a complex issue, with many factors to consider. Young women need to be engaged in the issue, they need to know that they are being listened to and that the choice to have safe sex is theirs, and thereby have some perception of control of their bodies, decisions and lives. The evidence base has highlighted that context, motivation, planning for the future, taking control, situating the intervention within a broad context, connectedness and tailoring provide a conceptual framework to help guide policy-makers and professionals towards the areas that need to be attended to in order to increase the likelihood that an intervention will be effective at preventing rapid repeat teenage pregnancy.
Chapter 5 Overarching synthesis
As none of the interventions reduced repeat teenage conceptions, in the overarching synthesis we juxtaposed mixed-method and consultation evidence with the programme theories and logic of included interventions to shed more light on why the interventions did not seem to work as intended. A programme theory is the theory of how an intervention is intended to work. 170 The programme logic comprises all the elements and components of an intervention, and how they fit together for the delivery of the intervention.
We found that the included interventions addressed some but not all of the issues in the lives of young women that may influence their behaviour. In addition, there were concerns about the ability of staff to deliver these interventions. The full details of these findings are given in Table 8.
| Intervention component | Programme theory/logic | Risk factors: metaregression | Teenage mothers’ experiences: qualitative evidence | Realist theory areaa/interpretation of the evidence base | Stakeholder feedback/indirect evidence | Service users’ feedback/indirect evidence |
|---|---|---|---|---|---|---|
| Randomised controlled trials | ||||||
CAMI82–84 |
MI emphasises personal goals and self-efficacy and addresses any discrepancies between them, thereby refocusing on goals that are incompatible with repeat pregnancy | Lack of goals/self-efficacy was not an identified risk factor | Young mothers with goals and aspirations were less likely to have a repeat pregnancy | Tailoring (1), connectedness (1) and perspective/context | Utilising MI techniques to make every contact with GP, midwife or health visitors count | Preference for home visits since it felt personal with more space to discuss things that could not be discussed in a group. Practical preparation time for child (dressed, fed, nappy changed, etc.) and self was short |
CAMI + monthly home visiting by paraprofessional82–84 |
Home visits by professionals lead to feelings of support and encouragement of life choices and the perception that others are encouraging life choices | Lack of life choices was not an identified risk factor | There was no evidence relating to home visits in any of the qualitative studies | Tailoring (1), connectedness (1) and perspective/context | Home visits are more likely to be useful than interventions that rely on young women travelling to a clinic | |
| Weekly home visiting by paraprofessional91 | Repeated home visits remove barriers to accessing services and are designed to address gaps in social support networks and sustain behaviour change by repeated contact to direct teenagers away from repeat pregnancy | Lack of access to services or social support were not identified as risk factors | There was no evidence relating to home visits by professional, para-professional or lay persons | Tailoring (2), connectedness (1) and perspective/context | ||
Trained volunteer mentors to give telephone support and social outings 12 hours per month89 |
Using the mentor as a role model, information/education resource and a source of social support for young mother and her family could reduce repeat pregnancy | Lack of social support was not an identified risk factor, but living with a partner was weakly associated with an increase in repeat pregnancy | There was no evidence relating to either trained mentors or role models; however, there was evidence that some young women perceived a negative stereotype of teenage motherhood, which they were determined not to conform to | Tailoring (1), connectedness (1) and perspective/context | No feedback | No feedback |
Small group educational intervention to promote antenatal care and well-baby care88 |
A peer support group prevents unplanned repeat pregnancies by addressing self-efficacy and improving self-concept among young mothers | Lack of peer support and self-efficacy were not identified as risk factors, but continued education was weakly associated with a reduction in repeat pregnancies | In some contexts, teenage pregnancy was perceived to be the norm | Connectedness (1, 3) and perspective/context | A ‘buddy’ system or peer support group could offer choices, empower young women and give them confidence, as well as create space for them to state what they want and need | The young mothers enjoyed taking part in a group as they can see everyone, hear everyone’s opinion and know that they are not alone |
Weekly supportive group meetings and monthly pregnancy test92 |
A peer support group helps build trusting relationships and prevents unplanned repeat pregnancies by addressing self-efficacy and improving self-concept among young mothers | Lack of peer support was not identified as a risk factor | There was no evidence relating to organised group support. Informal peer group influence tended to reinforce a view of teenage parenthood as the social norm | Connectedness (3) and perspective/context | ||
Monetary incentive, weekly supportive group meetings and monthly pregnancy test92 |
Monetary incentives seek to improve attendance for a peer support group that helps build trusting relationships and prevents unplanned repeat pregnancies by addressing self-efficacy and improving self-concept among young mothers | Finance was not an identified risk factor | There was no evidence regarding monetary incentives in this context | Tailoring (3), connectedness (1, 3) and perspective/context | No feedback | Transport to and from the location and the availability of food, refreshments and crèche facilities can all increase engagement and improve attendance rates |
Monetary incentive and monthly pregnancy test92 |
The monetary enticement designed to improve group attendance so in the absence of the group component the monetary incentive should have little effect on pregnancy avoidance | Finance was not an identified risk factor | Some young mothers in the UK complained of inadequate provision of childcare or financial support to allow them to continue their education or work. Time spent with their children was of higher value to them than the marginal difference in income between benefits and what they could earn from low-paid work | Tailoring (3) and perspective/context | No feedback | |
Forty-two telephone counselling sessions up to 18 months postpartum by Masters-level young women following a manual-based written curriculum90 |
Healthy communication skills and connectedness with community can influence repeat pregnancy by reducing negative behaviours through knowledge expansion and behaviour change | Lack of support and knowledge were not identified risk factors | There was no evidence relating to telephone counselling in any of the included qualitative studies. However, some young women lacked basic knowledge about fertility and contraception | Tailoring (1), connectedness (3) and perspective/context | No feedback | No feedback |
Trained professional home visitors who visited biweekly for first year and monthly for second year and delivered parenting skills, safe sex, pregnancy prevention and goal-setting support82,83 |
Home visiting aims to reduce rates of repeat pregnancy through education and support and may be suitable for adolescents who are hard to engage, at high risk and living under adverse conditions | Lack of pregnancy prevention skills was not an identified risk factor. However, evidence that LARC, oral or other types of contraceptive reduce repeat pregnancy was weak; education and support in the appropriate and consistent use of contraceptives could have been lacking | There was no evidence relating to professional home visiting in any of the included qualitative studies. However, some young women lacked basic knowledge about fertility and contraception | Connectedness (3) and perspective/context | Home visits are more likely to be useful than interventions that rely on young women travelling to a clinic | Preference for home visits since it felt personal with more space to discuss things that could not be discussed in group, and also helps to adjust to demands of motherhood. Practical preparation time for child (dressed, fed, nappy changed, etc.) and self was short |
Peer mentors (‘big sisters’) delivered 19-lesson home-based intervention with parenting skills, pregnancy prevention and condom provision31 |
The use of support and self-efficacy through peer mentors can influence repeat pregnancies by emphasising goal-setting and involving family members at home | Lack of self-efficacy and support were not identified risk factors | In the context of unstable backgrounds, chaotic lifestyles and lack of family support, sexual activity was spontaneous and without thought | Tailoring (1), connectedness (1, 3) and perspective/context | ||
Nurse midwives delivered six home visits for first 6 months postnatal; childcare, parenting skills and contraceptive advice79 |
Repeated home visits remove barriers to accessing services for improving care for young mothers and infants sustain behaviour change by repeated contact to direct young mothers away from repeat pregnancy | Evidence that contraceptive use reduced repeat pregnancies was weak; appropriate access, skills and knowledge to support consistent use of contraception could have been lacking | Inflexible appointment times and the inability of providers to promptly supply the contraceptive of choice led to gaps in postpartum contraceptive protection and when young women decided to change methods | Connectedness (1, 3), tailoring (2) and perspective/context | ||
Advance supply of emergency contraception87 |
Supplying emergency contraception is aimed at reducing repeat pregnancies by addressing frequent discontinuation or switching of contraceptive methods | Evidence that contraceptive use reduced repeat pregnancies was weak, but inconsistency of use was not investigated as a risk factor | Many young women experienced unwanted side effects of contraception unfortunately often associated with more reliable methods. Stopping one method before obtaining another was not uncommon and left them vulnerable to unwanted pregnancy in the period between | Tailoring (2) and perspective/context | Emergency contraception is not the answer for young women with chaotic lifestyles as there is a danger that they would not use it as intended but would rely on it as their sole method of contraception. Since LARCs are not easily accessible through GPs, or repeated appointments have to be made, it increases susceptibility to repeat pregnancy | The overlap of the 72 hour requirement of the emergency contraception with bank holidays or Christmas is a cause of concern. There was also hesitancy in asking for emergency contraception for fear of being judged. Preference for LARCs as well, since it takes care of things for a long time |
Intensive family-based therapy, home visits, developmental guidance and supportive counselling80 |
Repeated home visits by a profession involving other family members can improve engagement with dysfunctional families direct young mothers away from repeat pregnancy | Poor family relationships were not identified as a risk factor; history of abuse was not significantly associated with repeat pregnancy | In the context of unstable backgrounds, chaotic lifestyles and lack of family support, sexual activity was spontaneous and without thought | Tailoring (1, 2), connectedness (1, 2, 3) and perspective/context | Home visits are more likely to be useful than interventions that rely on young women travelling to a clinic | The decision to complete a family in the present than later could influence decision to forgo birth spacing. Partner abuse (some like to keep them pregnant) and sexual exploitation by older men targeting young looked-after women in the name of having a ‘family’ could form the basis for repeat pregnancies. Absence of life skills training makes young mothers more susceptible to repeat pregnancies. Preference for home-visits, etc. |
The individual treatment condition received home visits, developmental guidance, supportive counselling and help in acquiring other needed services80 |
Repeated home visits remove barriers to accessing services for improving care for young mothers and infants to sustain behaviour change by repeated contact to direct young mothers away from repeat pregnancy | Lack of support and access to services were not identified risk factors | There was no evidence relating to home visits in any of the included qualitative studies. But some young women complained of poor access and a lack of continuity in contraceptive care. Others were deficient in basic knowledge about fertility and contraception | Connectedness (3) and perspective/context | Home visits are more likely to be useful than interventions that rely on young women travelling to a clinic | Preference for home visits since it felt personal with more space to discuss things discussed in group, and also helps to adjust to demands of motherhood. Practical preparation time for child (dressed, fed, nappy changed, etc.) and self was short |
| Cluster randomised controlled trial | ||||||
Monthly individual contacts on campus and five yearly home visits plus case management with state-wide teaching component with additional curriculum details93 |
Repeated home and school visits remove barriers to accessing services and are designed to address gaps in social support networks and sustain behaviour change by repeated contact to direct teenagers away from repeat pregnancy | The evidence that remaining in education reduced repeat pregnancies was inconclusive | There was no evidence relating to home or school visits in any of the included qualitative studies. However, some young women lacked basic knowledge about fertility and contraception and had poor access to contraceptive care | Connectedness (1, 3), tailoring (1, 2) and perspective/context | Home visits are more likely to be useful than interventions that rely on young women travelling to a clinic | Preference for home visits since it felt personal with more space to discuss things that could not be discussed in group. Practical preparation time for child (dressed, fed, nappy changed, etc.) and self was short |
| Non-randomised trials | ||||||
Relationship-focused, intensive case management programme with bimonthly contacts for up to 3 years94,95 |
Repeated home visits by a mentor aimed at developing resilience could reduce repeat pregnancy by (1) developing personal goals and self-efficacy, and (2) using the mentor as a role model, information/education resource and a source of social support for the young mother | Lack of support was not an identified risk factor | There was no evidence relating to intensive case management in any of the included qualitative studies. There was a lack of continuity of care including contraceptive care and post-abortion care | Connectedness (1, 3), tailoring (1) and perspective/context | No feedback | No feedback |
Simple case management services |
Using the mentor as a role model, information/education resource and a source of social support for young mother could reduce repeat pregnancy | Lack of support was not an identified risk factor | There was no evidence relating to simple case management in any of the included qualitative studies | Connectedness (1, 3) and tailoring (1) | No feedback | No feedback |
Family planning methods by approaching beliefs about health (‘Health Belief Model’)96 |
Adherence to family planning methods may be influenced by addressing the personal beliefs or perceptions about health behaviours of young mothers | Health beliefs were not an identified risk factor | There was no evidence relating to family planning from a health belief perspective; failures in effective contraceptive use was attributed to lack of knowledge, understanding or access | Tailoring (1), perspective/context | The need to give each partner a child as a token of commitment | No feedback |
Family planning methods by approaching social contexts in which health/illness exists (PRECEDE)96 |
Adherence to family planning methods may be influenced by understanding the social context in which repeat pregnancy exists | Social contexts were not considered in terms of their relationship to contraceptive use | Repeat pregnancies were more likely to occur in the context of unstable backgrounds, lack of family support, insecure housing, and chaotic lifestyles lacking in educational or vocational opportunities, when there was no thought or planning; sexual activity was spontaneous and teenage pregnancy an accepted norm | Tailoring (1) | Contraception not portrayed in sex scenes in films. Social media encourages casual relationships. Partner abuse (some like to keep them pregnant) and sexual exploitation by older men targeting young looked-after girls in the name of having a ‘family’ could form the basis for repeat pregnancies. Absence of life skills training makes young mothers more susceptible to repeat pregnancies | No feedback |
For example, as shown in Table 8, repeated home visits, which constitute the main component of a psychosocial programme in seven of the interventions reported in the trials,31,79,80,85,86,91,93,171 were designed to remove barriers to accessing services, to address gaps in social support networks and to sustain behaviour change by repeated contact with teenagers, thereby directing them away from repeat pregnancy. Although these interventions did not reduce repeat teenage pregnancies (GRADE rating of moderate), three realist mechanisms were addressed by this type of intervention: (1) paying attention to adolescents’ life experiences as well as their developmental stage, cultural context, age-appropriate impulsive and rational decision-making styles and responses to stress (‘tailoring’); (2) considering that feeling supported and being connected to the professional may trigger feelings of self-determination and active control (‘connectedness’); and (3) exploring motivations (e.g. norms, peers and past experiences) that lead to better engagement with the issues of sex and pregnancy (‘perspective’/’context’). The qualitative evidence also offered insight into a risk factor that was addressed by the intervention programme theory, that is that young mothers with goals and aspirations are less likely to have a repeat pregnancy. Service users also stated a preference for home visits, since this approach allowed the expression of their individual needs. Nonetheless, to increase the likelihood of this intervention working, the staff conducting home visits should have specialist training. Two of the biggest concerns of the health-care professionals in our consultation group were (1) the inconsistent knowledge base of the health-care professionals who provide advice on contraception for young adolescents, and (2) the absence of life-skills training, making young mothers more susceptible to repeat pregnancies.
Another example is the use of peer support, a key component of the psychosocial programme used in two trials,88,92 to allow peers to build trusting relationships and prevent unplanned repeat pregnancies by addressing self-efficacy and improving self-concept among young mothers. Again, these interventions did not reduce repeat teenage conceptions (GRADE rating of moderate) and there were no qualitative studies to support their approach. From the realist synthesis, three mechanisms supported this programme theory: (1) offering incentives to increase engagement and attendance (‘tailoring’); (2) considering that feeling supported and being connected to the professional or group may trigger feelings of self-determination, active control and ‘being heard’ (‘connectedness’); and (3) exploring motivations (e.g. norms, peers and past experiences) that lead to better engagement with the issues of sex and pregnancy (‘perspective’/’context’). Health professionals stated that using a ‘buddy system’ or peer support group could offer choices that empower young women and give them confidence, as well as giving them the opportunity to state what they want and need. The adolescent mothers in the service user group appreciated being part of a peer group.
Importantly, Table 8 shows that issues such as the motivation for wanting a repeat pregnancy (CerQual: high); peer pressure and its influence on sexual behaviour (CerQual: high); questions of identity in adulthood with regard to, for example, masculinity and femininity; and not including young fathers as part of the focus of the programmes were not addressed by trial interventions and may help explain why no effect on the rate of repeat pregnancy was seen. For example, qualitative evidence shows that for some teenagers the second or subsequent pregnancy was planned or conceptualised to replace a previous pregnancy loss. This cognition and decision-making by teenagers was not mentioned in the reports of intervention outcomes, and may explain why psychosocial or contraceptive programmes did not appear to reduce repeat conceptions, as they were not specifically targeting the way in which teenagers rationalised their lives or the thinking that underpins their decision-making (CerQual: high).
We have summarised our findings in a matrix of outcomes (see Table 8). It should be noted that no qualitative evidence was found to support the programme theories developed in this synthesis. In Table 9, we have mapped the programme theories from evidence that was not directly linked to specific interventions evaluated by the trials.
| Qualitative findings | Stakeholder feedback |
|---|---|
| Planned pregnancies to please/keep a partner | The need to give each partner a child as a token of commitment |
| Pregnancies to replace a loss or fill an emotional void | Bereavement counselling is a necessary consideration for young mothers who have had abortions, miscarriages or a child taken into care |
| Pregnancies to provide a sibling or complete a family | No feedback |
| Misinformation/misconceptions about fertility | Notions of masculinity and womanhood attached to birth may influence repeat pregnancies in close relationships |
| Need for education about contraception and understanding fertility for both young people (especially within 2 weeks of birth or abortion) and health professionals | |
| Lack of literacy leading to difficulties in accessing ‘educational material’, such as contraception information given in leaflets | |
| Peer pressure and influence on sexual behaviour | Peer pressure against the use of LARC implants (often known as ‘slag tags’) |
| Absence of life skills training makes young mothers more susceptible to repeat pregnancies | |
| Lack of pre- and post-abortion counselling | Bereavement counselling is a necessary consideration for young mothers who have had abortions, miscarriages or a child taken into care |
| Good and neutral information about abortion in schools or, if this is not allowed, girls should be directed to reliable sources of information | |
| Realist theory area | Stakeholder and service user feedback |
| Taking control of sexual encounters and what happens in the future | No feedback |
| Perceptions of parental responsibility | Looking after a small baby is easy, so why not have another? |
| Young mothers felt judged as ‘bad mothers’ by professionals helping them, which was a common reason for non-engagement with services | |
| Contraception is not portrayed in sex scenes in films Social media encourages casual relationships |
|
| Girls feel special during pregnancy and enjoy the professional input, friendship group and status while it lasts |
Chapter 6 Discussion
Summary of the main findings
Despite extensive searches across different databases, the various streams of our review have yielded inconclusive and inconsistent answers to our research questions. We found no evidence from our metaregressions for an association of any of the following factors or variables with the risk of repeat unintended pregnancy, beyond their association with the risk of first adolescent pregnancy: age, education level, history of abuse, smoking, living with the father of the children or the use of oral contraception or LARCs. Qualitative evidence, however, suggests that risk factors for repeat unintended pregnancy included contextual factors, such as lack of family and peer support and a chaotic lifestyle; motivational factors, such as lack of personal goals and aspirations; emotional factors, related to, in particular, filling an emotional void after abortion or adoption; and also rational reasons for further pregnancy, such as the desire to complete one’s family while still young. With regard to interventions for reducing repeat unintended pregnancy, most RCTs were of psychosocial programmes conducted by home visits, community interventions or over the telephone. Meta-analyses found no convincing, statistically significant reduction in repeat pregnancy as a result of these programmes, although there was a reduction in live births. There was also a reduction in the number of young women dropping out of school as a result of these programmes, but, again, this was not statistically significant. Finally, qualitative studies found a number of themes explaining the barriers to the uptake of these services, namely poor knowledge, lack of information and misconceptions about contraceptive methods; poor access to services; and a lack of continuity of care.
Literature that we considered
We found comparatively little literature or other high-quality evidence that focused on whether or not intendedness of repeat teenage conceptions in the context of interventional studies. We found that, if the qualitative evidence discussed motivation, many conceptions were, to a limited extent, indeed intended by the young women. An accurate measurement of unintended pregnancy is essential to demographers seeking to understand fertility, to public health practitioners who aim to reduce the incidence of unwanted pregnancies among young mothers and to groups that promote women’s ability to determine whether or not and when to have children. This is demonstrated by the development of the Pregnancy Risk Assessment Monitoring System,172 a surveillance project of the Centers for Disease Control and Prevention and state health departments in the USA; in this regard, the definitions of ‘intendedness’ and ‘unwanted’ have undergone considerable changes. A validated index developed by Barnet82 offers a similar measure, but only a few studies we encountered used any tool to quantify or explore intention in a meaningful way.
In some cases, the authors of studies have used the words ‘pregnancy’ and ‘conception’ interchangeably. Most commonly, studies appear to use ‘conception’ to mean the fertilisation of the egg, ‘pregnancy’ to mean the time between conception and either abortion or birth, ‘birth’ to mean either live or stillbirth, and ‘abortion’ to mean the deliberate termination of a pregnancy. Our report reflects the terminology of the individual studies that we are reporting on.
From a pool of over 6000 articles, we filtered all out but 77 in a rigorous process of assessment for relevance and quality. Our time window, which included studies published from 1995 but contained no data obtained prior to 1990, was sufficiently wide to capture all studies not previously included in a systematic review of secondary pregnancy prevention programmes. 173 The standard for reporting RCTs has undergone a transformation over this time, with the introduction, and then subsequent revisions and extensions, of the CONSORT (Consolidated Standards of Reporting Trials) guidelines. 174 When we examined the randomised trials, we observed an increase in the quality of reporting over time. Studies reported after 2000 were generally more robustly designed to protect against bias, and the reporting of potential bias was more comprehensive.
Interventions and usual care
The majority of the interventions that have been evaluated were based on the concurrent application of preventative programme elements, such as home visiting, education, peer support, promoting contraception and skill building. These psychosocial programmes were delivered through a variety of media, such as computer- or telephone-based counselling, were home based or group based, and were driven by peers or professionals. There has been an underlying assumption that these elements, in some combination, should be effective. In many evaluations, it is not clear whether the intervention itself or the mode of delivery is being tested. Only one programme, the CAMI study, could be described as a dismantling study, examining different elements of a complex intervention. The study looked at the added value of a home visiting element of the programme compared with the standard intervention or care as usual. 92 Without exception, we found no effect of these interventions on our primary outcome measure of reducing repeat pregnancies. However, this finding does not imply that these programmes have no value. Our qualitative and realist streams of work have provided insights and points for consideration which reflect on why the interventions did not work as intended.
Context and population
Our initial mapping exercise revealed that the majority of the studies identified were generated in the USA, with only two other clusters, the UK and Brazil, being identified. All of the randomised trials, apart from one Australian study,79 were US studies. We did, however, identify three qualitative studies which included UK settings. This heavy focus on evidence derived from the USA caused some difficulties in interpreting comparisons made with usual care. The interventions in the USA vary between and within individual states, and often involved practices which are considered usual care in the UK. For example, experimenting with the provision of free birth control offers little insight into the effectiveness of this intervention in the UK, where free and easily accessible contraceptive provision is widely utilised. UK standard prenatal and postnatal care is more comprehensive than was previously available for Americans with low incomes, although President Obama’s health reforms are seeking to address this issue. 175 Americans with higher incomes and good medical insurance may be exposed to much greater levels of attention than their UK counterparts, but the studies we identified focused on ethnic minority populations from economically deprived areas, reflecting the readily available evidence worldwide which identifies social disadvantage as a primary risk factor for first adolescent conceptions. 176
Who is at greatest risk of repeat unintended pregnancies?
There is much evidence for a clear set of risk factors associated with first pregnancies in young women. Low socioeconomic status, being a care leaver, having low educational attainment and being the victim of abuse have all been identified as placing young women at increased risk of unintended first pregnancies. 31,87,92 We aimed to discover whether or not any risks could be identified for repeat conceptions, which would enable interventions to be targeted at subgroups and so maximise their effectiveness and cost-effectiveness. A large range of intervention studies that had various comparator groups, including cohort studies and trials, were analysed and the many risk factors reported were extracted. However, we found little consistency with regard to the factors that were considered important and many were inconsistently reported. In our metaregression analysis, we were only able to analyse seven potential risk factors, none of which was shown to be a predictor of repeated teenage conception. However, as all of these studies had comparator groups comprising women who had already had one teenage conception, they were, consequently, derived from populations that were at risk of first teenage conceptions. This could be interpreted to indicate that the outstanding risk of a second teenage conception is the occurrence of a first conception, and that, within a high-risk population, there are no particular additional features that will identify subgroups who are susceptible to further conceptions. One practice implication that may be drawn from this finding is that further targeting of interventions to particular groups of teenagers, within a high-risk population, who have had one conception will not be helpful, and that general interventions should be universally accessible to all young women who have already had one conception.
We carefully analysed qualitative evidence from young women which explored their perceptions of why they had repeated pregnancies. Whether the explanation for repeat pregnancies is contextual, motivational and emotional, or according to the teenage mothers’ own rationale (i.e. is an intended pregnancy or not) it is important to seek to understand the complex and diverse reasons that result in some teenage mothers having multiple pregnancies so that interventions can be developed to address individual issues through targeted, personalised interventions and improved provision of services.
Which interventions are effective and cost-effective, how do they work, in what setting and for whom?
We found no convincing evidence for the effectiveness of any intervention with regard to reducing the rate of pregnancies in young women who had already had a previous conception. The overarching synthesis of evidence showed that the programme theories of included interventions addressed some, but not all, of the important factors and issues that appear to lead to repeat teenage conception, which may explain why no evidence of effect was detected. The most promising of the interventions was examined in a study by Belzer et al. ;87 this study examined a contraceptive-based intervention, delivered by licenced health professionals, which enhanced the usual offering of 10–15 minutes of education about emergency contraception by actually providing advanced emergency contraception. 87 The study’s focus was to consider if supplying emergency contraception in advance would alter emergency contraception use, unprotected sex or condom use rather than to specifically enquire about the downstream effects on pregnancy rate. This study was not powered to show any effect on our primary outcome, but if it had been larger it may well have produced a significant effect.
Four studies31,81,82,85 of psychosocial interventions reported the outcome of childbirth and, while individually none of them showed a significant decrease in childbirth rates, when pooled, the outcome significantly favoured the intervention. Three of these studies81,82,85 also reported the outcome repeat pregnancies. None of the authors was specific about the reasons for the relative differences in conception and birth rate between the arms, and therefore we can only speculate that the interventions resulted in greater access to and information about abortion availability which, in turn, led to more pregnancies being terminated. It is possible, however, that this result could be entirely accounted for by the inclusion of a study by Black et al. ,31 which did not report the repeat pregnancy rate but only the birth rate.
One known risk factor for initial teenage conceptions, and one element often adversely affected by repeated conceptions, is educational status. Three studies52,85,89 reported the effects of their psychosocial interventions on the rate of high school completion, graduation or dropout. All three reported a slight reduction in dropout with their psychosocial interventions; however, only one reported statistically significant benefits. 95
There was almost a compete dearth of economic and cost evaluation in the included studies. Despite the Barnet study showing no significant effectiveness on teenage conception rates (but showing some tentative effect on school dropout) the study did provide data on costs. 83 Overall, the mean cost per adolescent was US$2064, with unadjusted and adjusted ICERs per prevented birth of US$21,895 and US$17,388, respectively. The authors concluded that the costs and cost-effectiveness ratios associated with CAMI compare favourably with other effective programmes aimed at pregnancy prevention, although the evidence base is limited.
As the search identified only one economic evaluation and the description of the cost–benefit analysis by Key et al. 141 was minimal, we cannot make any definitive conclusions about this particular evidence base; therefore, more research is needed in this regard. The unadjusted and adjusted ICERs presented by Barnet et al. 83 were normalised to a sample of 100; however, no detail is given of the methods or rationale for this normalisation in the paper. The ICERs assessed only the cost of the interventions compared with their prevention of subsequent births, and no wider perspectives of costs to society or other agencies, such as social care agencies, were considered in the analysis. A discount rate is also not reported, although the time horizon of the analysis exceeds 1 year. The further analysis conducted by Barnet et al. ,83 using a range of scenarios, does give us further insight into which subgroups may be considered in order to achieve the most cost-effective results when delivering CAMI-based interventions; however, there is limited generalisability of these findings because of the population and setting of the RCT, and the corresponding economic evaluation. The description of the cost–benefit analysis by Key et al. 141 was limited, as it formed part of a wider description of the effectiveness of the intervention under investigation; therefore, no definitive conclusions can be made about the economic evidence relating to interventions designed to prevent repeat teenage pregnancy.
The findings related to the effectiveness of interventions with regard to rates of contraceptive uptake, from both the psychosocial and the contraceptive-based intervention studies, were somewhat mixed. No effective interventions were revealed and there was a lack of clarity about overall contraception rates, with some papers reporting, for example, condom use or oral contraceptive use without providing information on the numbers of participants switching between different contraceptives or using more than one method. These data seem too unreliable to form any strong judgements regarding the overall effectiveness of psychosocial interventions on contraception.
After including further sources of effectiveness evidence in a sensitivity analysis, we found that psychosocial visits delivered in a home-based setting reached statistically significant effectiveness. This tentative quantitative finding was very much supported by the evidence and feedback from both stakeholders and service users who concluded that the home setting felt personal with more opportunity to discuss things that could not be discussed in a group setting. Home visits also impacted less on practical preparation time for the mothers with regard to organising themselves and their child or children to attend groups. Professionals suggested that home visits are more likely to be useful than interventions that rely on young women travelling to a clinic.
We postulate that there are several reasons why home visits are potentially effective beyond the obvious practical considerations of convenience and attendance. Repeated home visits by professionals:
-
foster feelings of support and encouragement of life choices, and the perception that others are encouraging life choices
-
reduce barriers to accessing services, thereby improving care for young mothers and infants
-
sustain behaviour change by repeated contact
-
encourage the involvement of other family members, which can improve engagement within dysfunctional families
-
foster the development of resilience, which could reduce repeat pregnancy by (1) promoting the development of personal goals and self-efficacy, and (2) encouraging the use, by the young mother, of the mentor as a role model, an information/education resource and a source of social support.
What are the barriers to and facilitators of the uptake of these interventions and their ultimate success in reducing repeat teenage conceptions?
Clearly, there is a lack of evidence, but no lack of theories and good intentions, with regard to the development of interventions that address the well-established problems of repeat teenage conceptions for the young mother, the child and wider society. Many of the interventions we examined seemed to be derived from concepts arising from the literature on risk factors for first teenage pregnancy. Our work on risk factors would suggest that this is a reasonable way to proceed, as we did not identify any factors beyond those accounted for by the risk of a first pregnancy in the quantitative work, although the qualitative evidence stream hypothesised several. There are several possible reasons for the fact that we found no successful interventions for repeat pregnancy. A lack of high-quality, well-powered research is a clear factor; however, it is possible that what causes well-principled interventions to fail are barriers to their successful implementation.
The pressures and influences facing young adults, from various sources, shape their views, experience and negotiation of relationships and motherhood. These factors either motivate them to take control and to consistently protect against pregnancy, or to take a more relaxed approach to these issues. The views from young mothers at a service user feedback group highlighted the importance of tailoring interventions within this broader context, with an appreciation of the multiple roles that an adolescent mother has to play, which include student, employee, friend and daughter. Young women need to be engaged in the issue, they need to know that they are being listened to and that the choice to have safe sex is theirs, and thereby have some perception of control of their bodies, decisions and lives. The evidence base has highlighted that context, motivation, planning for the future, taking control, situating the intervention within a broad context, connectedness and tailoring provide a conceptual framework to help guide future research.
Strengths and limitations of the review
The strengths of this review are that we undertook extensive literature searches of multiple sources using tailored search strategies for each. We did not exclude studies on the grounds of quality or language. Our inclusion criteria permitted published and unpublished quantitative and qualitative data. We used a mixed-method streamed approach to allow us to examine the research questions from different perspectives. We sought the perspectives of service providers and service users and integrated them with our findings from the literature. Finally, we conducted an overarching narrative synthesis allowing us to draw our findings together and present them as a rounded and coherent whole. A particular strength of our review is the support and input we received from our stakeholder group, with its wide variety of practitioners, policy-makers and public health professionals. The stakeholder group had a primarily Welsh focus, and the majority of our study team were based in Wales. However, there is unlikely to have been any bias related to this largely Celtic team, with regard to the review of the evidence, as most of the literature included was not based in the UK and both the stakeholders and the team of authors are widely experienced.
The limitations of the review are related to the literature available. The included studies rarely characterised conceptions and pregnancies in young women and girls as ‘unintended’ or as ‘planned’. The interventions were often in place to provide alternatives to second pregnancies through programmes of empowerment, education and social contact, but without regard to intention. As no interventions we found directly discriminated between those young people who ‘intended’ another conception and those who did not, we concluded that the word ‘unintended’ was not useful in the context of our review, although the qualitative evidence did point to reasons as to why young women planned or intended to have subsequent pregnancies. Furthermore, studies with complex interventions had multiple aims, often with regard to maternal and child health, and/or educational goals for the mother. Whether or not the provision of, or counselling about, contraceptives was included in these interventions is often unclear, and the mechanism by which the intervention was intended to achieve a reduction in repeat conceptions is usually not explicit. The realist element of our review shed some light on these questions, but it may be that the lack of clear effectiveness of these interventions (in terms of reducing repeat conceptions) was because their main focus was on other goals.
An important limitation of the review was the geographical spread of the literature, particularly the randomised trials, with the vast majority being conducted in the USA and, among those studies, the majority of populations being young African American or Latina women. This was mitigated to some extent by two good-quality UK qualitative studies, although both of these were based in London. However, there are some concerns about the transferability of the largely US-based findings to the UK NHS and other European health-care systems. The application of CerQual to qualitative findings reinforces the level of confidence in transferring findings across some cultural boundaries. Pragmatically, the UK and many other countries are now multicultural and contain significant transient migrant populations. Our search included much international evidence, and that increased the relevance and depth of the work’s cultural, multiethnic and religious perspectives.
Most of the RCTs we found had a low risk of bias because of the appropriate random sequence generation of allocations. However, as expected, the majority of the RCTs were found to have a high risk of bias because they were unable to adequately blind the teenage participants to their group allocations. The usefulness of the cohort studies that we found, in assessing the risk factors for second pregnancies, was limited. The data available were not of sufficient strength or depth to identify any specific risk factors beyond those which are associated with the risk of a first teenage pregnancy.
Our review demonstrates the lack of economic evidence for interventions designed to prevent repeat teenage pregnancies. There is scope to argue, given the implications on the state and publicly funded services of a pregnancy, for example, the costs to the NHS of health care during pregnancy, labour and the first few hours of a child’s life, that it is pertinent to create an evidence base with regard to multiple pregnancies, which would have greater cost implications than first pregnancies. By adopting a multiagency perspective in future economic analysis, the implications for social care could also be assessed. As noted in the qualitative literature, some young mothers experienced their child being taken into care and there are further considerations, such as state support, which can be an important source of income for young mothers who may still be attending school or be too young to legally work. 130,134 During these times of financial constraint for services, such as the NHS and social and community services, it is important that policy-makers are given evidence, not only for effectiveness, but also for cost-effectiveness so they can implement interventions that are considered the best use of their resources.
Gaps in the evidence
Clear definitions and explorations of the concept of ‘unintendedness’, especially in relation to repeat pregnancies were absent from the literature, but we included these in our report. There are some discussions, although limited, with regard to some young women’s poor understanding about being able to get pregnant straight away or while breastfeeding, and some thinking that having an abortion might make them infertile. Otherwise, although many pregnancies were unplanned, they do not appear be unintended, even if elements in society deem them to be unwise. Even if there were good interventions for unintended pregnancies (educational or contraceptive) these cannot be expected to address intended conceptions.
In the studies we included in our review, all the interventions targeted pregnant or parenting young women. We found no interventions directed towards young fathers, neither were male partners given a direct voice in any of the qualitative studies; their views about pregnancy (whether or not they desired either the first or any further pregnancies) and contraception were reported by the young women. There is anecdotal and some audit evidence to suggest that children who leave the care system are particularly vulnerable to multiple early conceptions; however, we found no studies which examined this group in detail so it was impossible for us to assess their excess risk. 177 There is very little evidence directly addressing repeat conceptions in young women who have substance abuse problems. Young women may feel pressured in two ways which influence their social and sexual behaviours: (1) within the family structure and (2) by peers. Within the family, some young women may feel pressured to provide a sibling or to complete a family with a partner. Young women who perceive that their peers are engaged in sexual practices are more likely to adopt these behaviours in order to be accepted. Addressing these components may empower young women to take control of sexual encounters, and what happens in the future. We suggest that interventions focused on empowering young women are key to influencing this mechanism.
We found no evidence from the studies that we identified to suggest that any consideration was given to the role of modern media, either as an influence on young women’s attitudes or as an intervention. In this age of apps and tweets, this avenue for potential interventions is ripe for investigation. A recent study178 (which did not meet our inclusion criteria) examined the influences of media on social outcomes and concluded that television programmes, such as the reality TV show ‘16 and Pregnant’,179 engaged at-risk adolescents and conveyed information that led to changes in their behaviour and prevented them from giving birth at such a young age. The authors of this study stated that there was a substantial change (a 5.7% reduction) in the rate of teenagers giving birth in the USA to babies that would have been conceived between June 2009, when the show began, and the end of 2010. This study highlights the fact that the mode of communication can be a powerful driver of social outcomes, as in this case when it led young women to search and tweet about birth control and abortion, indicating that it influenced them in a way that could potentially change their behaviour. For example, one tweet read:
. . . watching 16 and Pregnant is a great refresher on why NOT to get pregnant. Perfect birth control.
Kearney and Levine178
This study highlights that one gap in the current research agenda lies with the method of delivering information most effectively in order to influence young people’s attitudes in the context of a fast-moving, information-rich culture.
There were no RCTs of any interventions conducted in a UK setting at the time of our searches; however, we did identify a study that was currently under way in the UK, called the Building Blocks study, which targeted 1600 nulliparous pregnant women with the Family Nurse Partnership home visiting programme; one of the primary outcomes of this study was the number of second pregnancies within 2 years. 180 The study recruited 1645 participants, of which 426 of 643 in the intervention group went on to have a second pregnancy within 2 years and 427 of 646 in the control group went on to have a second pregnancy in this same period. The adjusted odds ratio for the intervention was 1.01 (95% CI 0.77 to 1.33). Therefore, although this intervention was previously deemed to be effective in the USA, it was not found to be effective in a UK setting.
We found no evidence from managers of interventional programmes or from policy-makers, except what appeared in policy documents, that provides a policy or service delivery perspective.
Comparison with previous literature
The evidence reported by previous systematic reviews on intervention programmes aimed at reducing repeat adolescent is inconsistent. Furey181 conducted a systematic review which sought to examine whether or not parenting programmes were of any value with regard to improving maternal or infant outcomes. This review cited two programmes79,81 that claimed to be successful in reducing the incidence of repeat pregnancy, however, our careful examination of the data in these studies did not find a statistically significant reduction in the incidence. Corcoran and Pillai173 performed a meta-analysis to investigate the effect of adolescent parent programmes on reducing repeat pregnancy; this showed a reduction in the incidence of repeat pregnancy at follow-up on average 19 months after the intervention. This meta-analysis showed the effects of the programmes that led to a reduction in the incidence of repeat pregnancy after the first follow-up, on average after 19 months of the intervention, and also showed a dissipating effect by second follow-up at 31 months. The difference between our findings and those of Corcoran and Pillai173 was that our review showed dissipation after 24 months. This disparity has arisen because we used slightly different inclusion criteria for our study, and employed more rigorous statistical methods for the analysis.
Although there are some published literature reviews on programmes trialled within the USA, there is a lack of systematic reviewing of the evidence that addresses programmes to reduce the incidence of repeat teenage pregnancy and the risk factors, and that scrutinises the reasons behind the success or failure of these programmes. 182–184 However, common themes that seem to be emerging from these literature reviews are that programmes would be more successful if they incorporated an increase in the choices available to young women, which would improve their social and economic circumstances, and a clear understanding of the motivation behind their pregnancy. The review of qualitative evidence supports these themes.
Our findings also echoed the recommendations contained within two major strategy documents currently being implemented in the UK. 8,163 They also highlight the absence of rigorous comparative studies that could strengthen the evidence base. A very interesting example of an underevaluated project is the Hackneys Assertive Outreach Nurse project,8 whose key methods of interaction are perseverance, being young-people friendly and having the flexibility to meet young people at times and locations that suit them. According to the report,8 between 2006 and 2007, the number of repeat abortions in girls under 18 years of age fell from 41 to 29. This finding was reflected in our results, which indicate that conception rates do decrease by half in the first year of an intervention, but the incidence rates do not differ after 24 months. This project, along with other ‘case studies’ section of the report,8 need careful evaluation in well-conducted trials so that they might yield valuable evidence regarding the effectiveness and cost-effectiveness of such interventions in the UK context.
Recent policy developments
The Department of Health’s Teenage Pregnancy Strategy: Beyond 20108 covers the same emerging theory areas in its guidance as we have identified from the literature, and contains an example of a repeat teenage pregnancy service with several features that appear to map onto evidence of what could potentially work.
Recent guidance185 from the National Institute for Health and Care Excellence (NICE) makes similar recommendations to our report, emphasising the need for services that are universal and inclusive. These guidelines also emphasise the need to offer additional tailored support to meet the particular needs and choices of those who are socially disadvantaged or who may find it difficult to use contraceptive services.
Reflections from primary care
In compiling this research, we were mindful to include reflections and perspectives from both stakeholders and users; however, one voice that had not been specifically heard was that of a general practitioner (GP). In order to rectify this omission, we specifically asked the GP (Dr Nefyn Williams) in our authorship team to reflect on his first-hand experiences in the context of the literature that we had found.
. . . and it seems to me that the components of a good intervention for young mothers and reducing unintended repeat pregnancies in young women are already in place. Namely: comprehensive primary care; free contraception; an extended primary healthcare team who are often co-located with primary care including midwives, health visitors, pharmacists providing emergency contraception; a range of community health services such as school nurses, contraception clinics and sexual health clinics; social work departments who are sometimes co-located with primary care or with other community services; third sector organisations such as Barnardo’s etc.
So why is there this problem? This is partly because there are access problems for teenagers as described in the user groups, provision of all contraceptive services particularly LARCs are patchy and inconsistent with only some GPs providing IUCDs and contraceptive implants and different mechanisms for accessing them, all of the different services in primary care, school, community clinics and social care have separate information systems that do not communicate well with each other.
There are good examples of good practice such as drop-in teenage clinics in primary care and with school nurses but these are not universal. Commissioners of services for teenagers need to pull these various components together to provide a coherent service with a single point of access. They particularly need to design easy access for hard to reach groups such as looked after children.
We also need to consider peer-led interventions and interventions that engage the youth involving social media, text messaging etc.
Finally, just after delivery or just after TOP are the times when behaviour change is most likely. The provision of LARCs immediately post-partum or immediately following TOP should be prioritised.
Future research and designing new interventions
The challenge for the research community is to take the tentative evidence and views of young people and design an intervention to address their motivations and beliefs, as well as their practical needs. This intervention should be designed with a sound theoretical basis and evaluated thoroughly by means of a high-quality, adequately powered randomised trial.
Studies that address how primary care in the UK, including care involving doctors, nurses, midwives and health visitors, might better support the young women most at risk of pregnancy, whether that be the first or subsequent conceptions, would be valuable.
There is a need for more research on hard-to-reach groups that may be particularly vulnerable to repeat teenage conceptions; we could not clearly identify such groups in this review because of the lack of evidence. These groups include looked-after children, problematic drug or alcohol users, sex workers, homeless young people, asylum seekers and those caught up in the justice system. It is likely that it will not be possible to conduct randomised trials in these subgroups because of the difficulties inherent in identifying, recruiting and retaining such young people in studies; therefore, high-quality qualitative research is recommended.
In designing interventions aimed at the service structure, we suggest that young mothers should be given the information they need to improve their attitude and self-efficacy towards contraception before and after they enter the postpartum period. Stakeholders highlighted that the timing of any educational messages relating to contraception or pregnancy in adolescents in schools should be considered, as well as the method of delivery.
Another important factor is the professional delivering these services. For more than 25 years, nurse-midwives have been shown to be particularly effective at engaging pregnant adolescents in maternal and child health activities. 186 Furthermore, the findings of a UK study indicate that general practices with more nurse time have lower teenage pregnancy rates than do those with little nursing input;187 however, whether or not they are important in reducing the incidence of repeat pregnancy has not been formally assessed. The importance of the quality and content of the services provided to the adolescent mother was highlighted by the stakeholders. It was considered important that professionals listen to adolescents and understand what they are asking for, as well as that emphasis be given to designing a way of eliciting the right information quickly through a few key questions. There was also thought to be a need for short educational courses to address the gap in knowledge and understanding about fertility among some health-care professionals.
The qualitative evidence had significant gaps, since there was no evidence from managers or policy-makers on repeat pregnancies.
Conclusions
We have found no conclusive evidence that any interventions to reduce repeat teenage pregnancy were effective. However, ‘the absence of evidence is not evidence of absence’. 188 We discovered very few well designed studies capable of providing good evidence of effect. There was some, weak quantitative evidence indicating that home delivered, multicomponent, complex psychosocial interventions may be effective in reducing teenage conceptions and subsequent births, and may help teenage mothers to remain in education. This evidence was strengthened and supported by the qualitative evidence and realist synthesis.
More rigorously conducted and better-reported studies are needed, and the other goals of adolescent parenting programmes, beyond simple reduction in the incidence of pregnancy, need to be subjected to rigorous quantitative scrutiny.
Acknowledgements
We thank the NIHR HTA panel for having faith that we were the right team to invest in, and to the staff at Southampton for being so open and approachable whenever we needed their assistance.
A review of this type cannot be completed without a great deal of help and assistance from a selection of people. The review team wish to gratefully acknowledge all their help and support: firstly, the young women of the service user group who so generously gave their time and opinions; secondly, all the participants of our stakeholder groups and the Empower to Choose group, co-ordinated by PHW, whose wise counsel was invaluable; and, thirdly, the voluntary organisations and their key personnel for facilitating our work. In particular, we would like to say a big ‘thank you’ to Sally Roberts of Flying Start and Rachel Lawton of Barnardo’s.
We are very grateful for the support received from Dr Marion Lyons of PHW and for including us in the Empower to Choose project, assisting us in the protocol development and permitting access to PHW’s information services.
Within Bangor University, we would like to thank Karen Hughes, Michelle Williams, Dr Huw Roberts, Roumen Kuncheva, Kirsty Pye, Annie Hendry and Nafees Din for administrative, managerial, IT and data extraction assistance – all very much appreciated. Thanks too to Dr Richa Sinha for her contribution to the development of the search strategies.
Contributions of authors
Rhiannon Whitaker (senior research fellow, clinical trials) initiated the study and led the study team, drafted and edited both the study protocol and the manuscript. She was a member of the PHW’s Empower to Choose project from which this project grew.
Maggie Hendry (research fellow and systematic reviewer) devised the overall study design and drafted the protocol. She designed and executed the searches, managed the project during the first year, contributed to the work of the realist team, and carried out the analysis and reporting of the qualitative data.
Dr Rabeea’h Aslam (senior research fellow and systematic reviewer) managed the project for the final 10 months, co-ordinated and contributed to the work of the quantitative, qualitative and realist teams, extracted and analysed data, and contributed text to all sections of the review.
Dr Andrew Booth (reader in evidence based information practice and director of information) designed the search strategies, advised the project team on all aspects of information retrieval, and was involved in developing the qualitative synthesis methodology and in the analysis and interpretation of the qualitative evidence synthesis.
Dr Ben Carter (lecturer in medical statistics) contributed to the protocol design and led the meta-analysis, metaregression and quantitative analysis.
Dr Joanna M Charles (research fellow in health economics) performed the economic analysis and contributed to the search strategies and realist synthesis.
Dr Noel Craine (research scientist) initiated the study and was closely involved in PHW’s Empower to Choose project from which this project grew. He contributed to the protocol development and advised on public health issues.
Professor Rhiannon Tudor Edwards (professor of health economics) contributed to the protocol development and led the economic analysis team.
Professor Jane Noyes (professor of health and social services research and child health) contributed to the original design and protocol development, supported the qualitative analysis and led the mixed-methods synthesis.
Dr Lupetu Ives Ntambwe (research fellow in statistics) supported the meta-analysis, metaregression and quantitative analysis.
Diana Pasterfield (research assistant and systematic reviewer) contributed to the protocol development and supported the data extraction, contributed to the work of the realist team, and synthesised and carried out the analysis and reporting of the qualitative data.
Professor Jo Rycroft-Malone (professor of implementation) contributed to the protocol development and led the realist synthesis.
Dr Nefyn Williams (senior clinical lecturer and practising GP) contributed to the protocol and provided the health-care perspective.
All authors contributed to the study design, revised the manuscript for important intellectual content, and read and approved the final manuscript.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HTA programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HTA programme or the Department of Health.
Publication
Craine N, Midgley C, Zou L, Evans H, Whitaker R, Lyons M. Elevated teenage conception risk amongst looked after children; a national audit. Public Health 2014;128:668–700.
Data sharing statement
This is a systematic review, therefore, there are no data to share. Further information can be obtained from the corresponding author.
References
- Nelson PB. Repeat pregnancy among adolescent mothers: a review of the literature. J Natl Black Nurses Assoc 1990;4:28-34.
- Fraser AM, Brockert JE, Ward RH. Association of young maternal age with adverse reproductive outcomes. N Engl J Med 1995;332:1113-17. http://dx.doi.org/10.1056/NEJM199504273321701.
- World Health Organization . Maternal, Newborn, Child and Adolescent Health. Adolescent Pregnancy 2015. www.who.int/maternal_child_adolescent/topics/maternal/adolescent_pregnancy/en/ (accessed 7 April 2015).
- Office for National Statistics . UK National Statistics Publication Hub: Conception and Fertility Rates 2011. www.statistics.gov.uk/hub/population/births-and-fertility/conception-and-fertility-rates/index.html (accessed 6 June 2013).
- Child Poverty and Perspective: An Overview of Child Well-being in Rich Countries. Florence: UNICEF Innocenti Research Centre; 2007.
- Child Well-being in Rich Countries: A Comparative Overview. Florence: UNICEF Innocenti Research Centre; 2013.
- The Teenage Pregnancy Independent Advisory Group (TPIAG) . Teenage Pregnancy: You Can Make a Real Difference to Teenage Pregnancy n.d. www.fpa.org.uk/media/uploads/professionals/talking-sense/teenage-pregnancy-briefing.pdf (accessed 6 June 2013).
- Department of Health . Teenage Pregnancy Strategy: Beyond 2010 2010. www.teachernet.gov.uk/publications (accessed 7 June 2013).
- Rowlands S. Social predictors of repeat adolescent pregnancy and focussed strategies. Best Pract Res Cl Ob 2010;24:605-16. http://dx.doi.org/10.1016/j.bpobgyn.2010.02.016.
- Trussell J, Wynn LL. Reducing unintended pregnancy in the United States. Contraception 2008;77:1-5. http://dx.doi.org/10.1016/j.contraception.2007.09.001.
- Wellings K, Wilkinson P, Grundy C, Kane R, Lachowycz, Jacklin P, et al. Teenage Pregnancy Strategy Evaluation: Final Report Synthesis 2005. http://webarchive.nationalarchives.gov.uk/20130401151715/http://www.education.gov.uk/publications/eOrderingDownload/RW38.pdf (accessed 28 June 2015).
- Welsh Assembly Government . Sexual Health and Wellbeing Action Plan for Wales 2010–2015 2010. www.shnwales.org.uk/Documents/485/Strategy%20(English).pdf (accessed 6 June 2013).
- Northern Ireland Department of Health, Social Services and Public Safety . Sexual Health Promotion: Strategy &Amp; Action Plan 2008–2013 2008. www.dhsspsni.gov.uk/dhssps_sexual_health_plan_front_cvr.pdf (accessed 6 June 2013).
- The Scottish Executive . Respect and Responsibility: Strategy and Action Plan for Improving Sexual Health 2005. www.scotland.gov.uk/Resource/Doc/35596/0012575.pdf (accessed 6 June 2013).
- Smith GC, Pell JP, Walsh D. Pregnancy complications and maternal risk of ischaemic heart disease: a retrospective cohort study of 129,290 births. Lancet 2001;357:2002-6. http://dx.doi.org/10.1016/S0140-6736(00)05112-6.
- Koniak-Griffin D, Turner-Pluta C. Health risks and psychosocial outcomes of early childbearing: a review of the literature. J Perinat Neonatal Nurs 2001;15:1-17. http://dx.doi.org/10.1097/00005237-200109000-00002.
- Rigsby DC, Macones GA, Driscoll DA. Risk factors for rapid repeat pregnancy among adolescent mothers: a review of the literature. J Pediatr Adolesc Gynecol 1998;11:115-26. http://dx.doi.org/10.1016/S1083-3188(98)70130-5.
- Meade CS, Ickovics JR. Systematic review of sexual risk among pregnant and mothering teens in the USA: pregnancy as an opportunity for integrated prevention of STD and repeat pregnancy. Soc Sci Med 2005;60:661-78. http://dx.doi.org/10.1016/j.socscimed.2004.06.015.
- Jacoby M, Gorenflo D, Wunderlich C, Eyler AE. Rapid repeat pregnancy and experiences of interpersonal violence among low-income adolescents. Am J Prev Med 1999;16:318-21. http://dx.doi.org/10.1016/S0749-3797(99)00029-X.
- Burt MR. Estimating the public cost of teenage childbearing. Fam Plann Perspect 1986;18:221-6. http://dx.doi.org/10.2307/2134980.
- Burt MR. Public cost and policy implications of teenage childbearing. Adv Adolesc Mental Health 1990;4:265-80.
- Hoffman SD, Foster ME, Furstenberg FF. Re-evaluating the costs of teenage childbearing. Demography 1993;30:1-13. http://dx.doi.org/10.2307/2061859.
- Hoffman SD, Maynard RA. Kids Having Kids: Economic Costs & Social Consequences of Teen Pregnancy. Washington, DC: The Urban Institute; 2008.
- Rich-Edwards J. Teen pregnancy is not a public health crisis in the United States: it is time we made it one. Int J Epidemiol 2002;31:555-6. http://dx.doi.org/10.1093/ije/31.3.555.
- Barrett G, Smith SC, Wellings K. Conceptualization, development, and evaluation of a measure of unplanned pregnancy. J Epidemiol Community Health 2004;58:426-33. http://dx.doi.org/10.1136/jech.2003.014787.
- Klerman LV. The intendedness of pregnancy: a concept in transition. Matern Child Health J 2000;4:163-9. http://dx.doi.org/10.1023/A:1009534612388.
- Oringanje C, Meremikwu MM, Eko H, Esu E, Meremikwu A, Ehiri JE. Interventions for preventing unintended pregnancies among adolescents. Cochrane Database Syst Rev 2009;4. http://dx.doi.org/10.1002/14651858.cd005215.pub2.
- Ramos C. Interventions for Preventing Unintended Pregnancies Among Adolescents. Geneva: the WHO Reproductive Health Library (RHL); 2011.
- DiCenso A, Guyatt G, Willan A, Griffith L. Interventions to reduce unintended pregnancies among adolescents: systematic review of randomised controlled trials. BMJ 2002;15. http://dx.doi.org/10.1136/bmj.324.7351.1426.
- Heller K. Coming of age of prevention science: comments on the 1994 National Institute of Mental Health Institute of Medicine prevention reports. Am Psychol 1996;51:1123-7. http://dx.doi.org/10.1037/0003-066X.51.11.1123.
- Black M, Bentley M, Papas M, Oberlander S, Teti L, McNary S, et al. Delaying second births among adolescent mothers: a randomized, controlled trial of a home-based mentoring program. Pediatrics 2006;118:e1087-99. http://dx.doi.org/10.1542/peds.2005-2318.
- Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev 1977;84:191-215. http://dx.doi.org/10.1037/0033-295X.84.2.191.
- Erikson EH. Childhood and Society. New York, NY: WW Norton & Company; 1993.
- Talashek ML, Alba ML, Patel A. Untangling the health disparities of teen pregnancy. J Spec Pediatr Nurs 2000;11:14-27. http://dx.doi.org/10.1111/j.1744-6155.2006.00040.x.
- Peterson SJ, Bredow TS. Middle Range Theories. Philadelphia, PA: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2009.
- Fergus S, Zimmerman MA. Adolescent resilience: a framework for understanding healthy development in the face of risk. Annu Rev Public Health 2005;26:399-41. http://dx.doi.org/10.1146/annurev.publhealth.26.021304.144357.
- Holness NA. The Effects of Resiliance and Social Influences on Preventing Repeat Adolescent Pregnancies in Parenting Adolescent Mothers. Florida, FL: Florida International University; 2014.
- Porter LS, Holness NA. Breaking the repeat teen pregnancy cycle. Nurs Womens Health 2011;15:368-81. http://dx.doi.org/10.1111/j.1751-486X.2011.01661.x.
- Gough D, Oliver S, Thomas J. Introduction to Systematic Reviews. London: Sage; 2012.
- Evidence for Policy and Practice Information and Co-ordinating Centre . EPPI-Centre Methods for Conducting Systematic Reviews 2007. http://eppi.ioe.ac.uk/cms/LinkClick.aspx?fileticket=hQBu8y4uVwI%3d&tabid=88&mid=6162 (accessed 7 June 2013).
- Thomas J, Sutcliffe K, Harden A, Oliver S, Rees R, Brunton G, et al. Children and Healthy Eating: A Systematic Review of Barriers and Facilitators. London: EPPI-Centre, Social Science Research Unit, Institute of Education, University of London; 2003.
- Flemming K, Briggs M. Electronic searching to locate qualitative research: evaluation of three strategies. J Adv Nurs 2006;57:95-100. http://dx.doi.org/10.1111/j.1365-2648.2006.04083.x.
- Shaw R, Booth A, Sutton A, Miller T, Smith J, Young B, et al. Finding qualitative research: an evaluation of search strategies. BMC Med Res Methodol 2004;4. http://dx.doi.org/10.1186/1471-2288-4-5.
- Preventing and Reducing the Adverse Effects of Unintended Teenage Pregnancies. York: Centre for Reviews and Dissemination; 1997.
- Booth A. Unpacking your literature search toolbox: on search styles and tactics. Health Info Libr J 2008;25:313-7. http://dx.doi.org/10.1111/j.1471-1842.2008.00825.x.
- Guyatt GH, Oxman AD, Schunemann HJ, Tugwell P, Knottnerus A. GRADE guidelines: a new series of articles in the Journal of Clinical Epidemiology. J Clin Epidemiol 2011;64:380-2. http://dx.doi.org/10.1016/j.jclinepi.2010.09.011.
- Glenton C, Colvin C, Carlsen B, Swartz A, Lewin S, Noyes J, et al. Barriers and facilitators to the implementation of lay health worker programmes to improve access to maternal and child heath: qualitative evidence synthesis (protocol). Cochrane Database Syst Rev 2013;10.
- Cochrane United States . Master List of Journals Being Searched n.d. http://us.cochrane.org/master-list (accessed 2 August 2014).
- Stone PW. Popping the (PICO) question in research and evidence-based practice. Appl Nurs Res 2002;15:197-8. http://dx.doi.org/10.1053/apnr.2002.34181.
- Rogers PJ. Using programme theory to evaluate complicated and complex aspects of interventions. Evaluation 2008;14:29-48. http://dx.doi.org/10.1177/1356389007084674.
- Tennison B, Pencheon D, Guest C, Melzer D, Muir Gray JA. Oxford Handbook of Public Health Practice. Oxford: Oxford University Press; 2006.
- Cochrane Effective Practice and Organisation of Care Group . EPOC Resources: Study Designs Accepted in EPOC Reviews 2013. http://epoc.cochrane.org/epoc-resources (accessed 9 September 2014).
- Higgins JPT, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011;343. http://dx.doi.org/10.1136/bmj.d5928.
- Pluye P, Robert E, Cargo M, Bartlett G, O’Cathain A, Griffiths F, et al. Proposal: A Mixed Methods Appraisal Tool for Systematic Mixed Studies Reviews 2011. http://mixedmethodsappraisaltoolpublic.pbworks.com (accessed 13 June 2013).
- Pace R, Pluye P, Bartlett G, Macaulay A, Salsberg J, Jagosh J, et al. Testing the reliability and efficiency of the pilot mixed methods appraisal tool (MMAT) for systematic mixed studies review. Int J Nurs Stud 2012;49:47-53. http://dx.doi.org/10.1016/j.ijnurstu.2011.07.002.
- Drummond MF, Sculpher MJ, Torrance GW, O’Brien BJ, Stoddart GL. Methods for the Economic Evaluation of Health Care Programmes. Oxford: Oxford University Press; 2005.
- Pawson R, Greenhalgh T, Harvey G, Walshe K. Realist review – a new method of systematic review designed for complex policy interventions. J Health Serv Res Policy 2005;10:21-34. http://dx.doi.org/10.1258/1355819054308530.
- Pawson R. Evidence-based Policy: A Realist Perspective. London: Sage; 2006.
- Ueffing E, Tugwell P, Welch V, Petticrew M, Kristjansson E. Campbell and Cochrane Equity Methods Group . Equity Checklist for Systematic Review Authors n.d. http://equity.cochrane.org/sites/equity.cochrane.org/files/uploads/EquityChecklist2012.pdf (accessed 7 June 2013).
- Deeks J, Higgins J, Altman D. Analysing Data and Undertaking Meta-Analyses 2011. www.cochrane-handbook.org (accessed 7 June 2013).
- Sterne J, Egger M, Moher D. Addressing Reporting Biases 2011. www.cochrane-handbook.org (accessed 12 June 2013).
- Higgins J, Deeks J, Altman D. Special Topics in Statistics 2011. www.cochrane-handbook.org (accessed 12 June 2013).
- Kelly M, McDaid D, Ludbrook A, Powell J. Economic Appraisal of Public Health Interventions. London: Health Development Agency; 2005.
- Medical Research Council . Guidance on the Development, Evaluation and Implementation of Complex Interventions to Improve Health 2008. www.mrc.ac.uk/Utilities/Documentrecord/index.htm?d=MRC004871 (accessed 7 June 2013).
- Vos T, Carter R, Barendregt J, Mihalopoulos C, Veerman L, Magnus A, et al. Assessing Cost-Effectiveness in Prevention ACE–Prevention n.d. www.sph.uq.edu.au/docs/BODCE/ACE-P/ACE-Prevention_final_report.pdf (accessed 7 June 2013).
- Payne K, McAllister M, Davies L. Valuing the economic benefits of complex interventions: when maximising health is not sufficient. Health Econ 2013;22:258-71. http://dx.doi.org/10.1002/hec.2795.
- The SURE (Supporting the Use of Research Evidence) Collaboration . SURE Guides for Preparing and Using Evidence-Based Policy Briefs: 5. Identifying and Addressing Barriers to Implementing the Policy Options 2011. http://global.evipnet.org/SURE-Guides/ (accessed 13 June 2013).
- Ritchie L, Spencer J, Bryman A, Burgess R. Analysing Qualitative Data. London: Routledge; 1994.
- Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol 2008;8. http://dx.doi.org/10.1186/1471-2288-8-45.
- Rycroft-Malone J, McCormack B, DeCorby K, Hutchinson A, Gerrish K, Lacey A. The Research Process in Nursing. Chichester: Wiley-Blackwell; 2010.
- Greenhalgh T, Kristjansson E, Robinson V. Realist review to understand the efficacy of school feeding programmes. BMJ 2007;335:858-61. http://dx.doi.org/10.1136/bmj.39359.525174.AD.
- Rycroft-Malone J, McCormack B, Hutchinson A, DeCorby K, Bucknall T, Kent B, et al. Realist synthesis: illustrating the method for implementation research. Implement Sci 2012;7. http://dx.doi.org/10.1186/1748-5908-7-33.
- Whitaker Rh, Hendry M, Booth A, Carter B, Charles J, Craine N, et al. Intervention Now To Eliminate Repeat Unintended Pregnancy in Teenagers (INTERUPT): a systematic review of intervention effectiveness and cost-effectiveness, qualitative and realist synthesis of implementation factors and user engagement. BMJ Open 2014;4.
- Wong G, Greenhalgh T, Westhorp G, Buckingham J, Pawson R. RAMESES publication standards: realist syntheses. BMC Med 2013;11. http://dx.doi.org/10.1186/1741-7015-11-21.
- Philips Z, Ginnelly L, Sculpher M, Claxton K, Golder S, Riemsma R, et al. Review of guidelines for good practice in decision-analytic modelling in health technology assessment. Health Technol Assess 2004;8. http://dx.doi.org/10.3310/hta8360.
- Greenhalgh T, Robert G, MacFarlane F, Bate P, Kyriakidou O. Diffusions of innovation in service organisations: systematic review and recommendations. Milbank Q 2004;82:581-629. http://dx.doi.org/10.1111/j.0887-378X.2004.00325.x.
- Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: the PRISMA statement. Ann Intern Med 2009;151:264-9. http://dx.doi.org/10.7326/0003-4819-151-4-200908180-00135.
- Kan ML, Silber Ashley O, LeTourneau KL, Williams JC, Jones SB, Hampton J, et al. The Adolescent Family Life Program: a multisite evaluation of federally funded projects serving pregnant and parenting adolescents. Am J Public Health 2012;102:1872-8. http://dx.doi.org/10.2105/AJPH.2012.300836.
- Quinlivan JA, Box H, Evans SF. Postnatal home visits in teenage mothers: a randomised controlled trial. Lancet 2003;361:893-900. http://dx.doi.org/10.1016/S0140-6736(03)12770-5.
- Cherniss C, Herzog E. Impact of home-based family therapy on maternal and child outcomes in disadvantaged adolescent mothers. Fam Relat 1996;45:72-9. http://dx.doi.org/10.2307/584772.
- Koniak-Griffin D, Verzemnieks IL, Anderson NLR, Brecht ML, Lesser J, Kim S, et al. Nurse visitation for adolescent mothers: two-year infant health and maternal outcomes. Nurs Res 2003;52:127-36. http://dx.doi.org/10.1097/00006199-200303000-00009.
- Barnet B, Liu J, DeVoe M, Duggan AK, Gold MA, Pecukonis E. Motivational intervention to reduce rapid subsequent births to adolescent mothers: a community-based randomized trial. Ann Fam Med 2009;7:436-45. http://dx.doi.org/10.1370/afm.1014.
- Barnet B, Rapp T, DeVoe M, Mullins CD. Cost-effectiveness of a motivational intervention to reduce rapid repeated childbearing in high-risk adolescent mothers a rebirth of economic and policy considerations. Arch Pediatr Adolesc Med 2010;164:370-6. http://dx.doi.org/10.1001/archpediatrics.2010.16.
- Johnston-Briggs BD, Liu J, Carter-Pokras O, Barnet B. Effect of partner relationship on motivation to use condoms among adolescent mothers. J Natl Med Assoc 2008;100:929-35.
- Barnet B, Liu J, DeVoe M, Alperovitz-Bichell K, Duggan AK. Home visiting for adolescent mothers: effects on parenting, maternal life course, and primary care linkage. Ann Fam Med 2007;5:224-32. http://dx.doi.org/10.1370/afm.629.
- Barnet B, Liu J, Devoe M. Double jeopardy – depressive symptoms and rapid subsequent pregnancy in adolescent mothers. Arch Pediatr Adolesc Med 2008;162:246-52. http://dx.doi.org/10.1001/archpediatrics.2007.60.
- Belzer M, Sanchez K, Olson J, Jacobs A, Tucker D. Advance supply of emergency contraception: a randomized trial in adolescent mothers. J Pediatr Adolesc Gynecol 2005;18:347-54. http://dx.doi.org/10.1016/j.jpag.2005.06.007.
- Ford K, Weglicki L, Kershaw T, Schram C, Hoyer PJ, Jacobson ML. Effects of a prenatal care intervention for adolescent mothers on birth weight, repeat pregnancy, and educational outcomes at one year postpartum. J Perinat Educ 2002;11:35-8. http://dx.doi.org/10.1624/105812402X88588.
- Havens KK, Wagstaff DA, Mercer PA, Longeway K, Gutman M. Lessons learned from a mentoring program for teenage mothers. Wisc Med J 1997;96:38-43.
- Katz KS, Rodan M, Milligan R, Tan S, Courtney L, Gantz M, et al. Efficacy of a randomized cell phone-based counseling intervention in postponing subsequent pregnancy among teen mothers. Matern Child Health J 2011;15:S42-S53. http://dx.doi.org/10.1007/s10995-011-0860-3.
- Sims K, Luster T. Factors related to early subsequent pregnancies and second births among adolescent mothers in a family support program. J Fam Issues 2002;23:1006-31. http://dx.doi.org/10.1177/019251302237301.
- Stevens-Simon C, Dolgen JI, Kelly L, Singer D. The effect of monetary incentives and peer support groups on repeat adolescent pregnancies. J Am Med Assoc 1997;277:977-82. http://dx.doi.org/10.1001/jama.1997.03540360045029.
- Scott AA, Amodeis N, Hoffman TJ. Preventing repeat pregnancies and other negative outcomes: among pregnant and parenting Hispanic adolescents. J Multicult Nurs Health 2004;10:32-8.
- Lewis LN, Doherty DA, Hickey M, Skinner SR. Predictors of sexual intercourse and rapid-repeat pregnancy among teenage mothers: an Australian prospective longitudinal study. Med J Aust 2010;193:338-42.
- Lewis LN, Doherty DA, Hickey M, Skinner SR. Implanon as a contraceptive choice for teenage mothers: a comparison of contraceptive choices, acceptability and repeat pregnancy. Contraception 2010;81:421-6. http://dx.doi.org/10.1016/j.contraception.2009.12.006.
- Nunez Rocha GM, Alanis Alanis MDJ, Alanis Salazar J, Salinas Martinez AM, Garza Elizondo ME, Villarreal Rios E. Differences in the use of family planning methods by adolescent females according to the education model utilized during pregnancy. Monterrey, Mexico. Rev Esp Salud Publica 2005;79:69-77. http://dx.doi.org/10.1590/S1135-57272005000100007.
- Raneri LG, Wiemann CM. Social ecological predictors of repeat adolescent pregnancy. Perspect Sex Reprod Health 2007;39:39-47. http://dx.doi.org/10.1363/3903907.
- Crittenden CP, Boris NW, Rice JC, Taylor CA, Olds DL. The role of mental health factors, behavioral factors, and past experiences in the prediction of rapid repeat pregnancy in adolescence. J Adolesc Health 2009;44:25-32. http://dx.doi.org/10.1016/j.jadohealth.2008.06.003.
- Drayton VLC, Montgomery SB, Modeste NN, Frye-Anderson BA, McNeil P. The impact of the Women’s Centre of Jamaica Foundation programme for adolescent mothers on repeat pregnancies. West Indian Med J 2000;49:316-26.
- Drayton VLC. Contraceptive use among Jamaican teenage mothers. Rev Panam Salud Publica 2002;11:150-7. http://dx.doi.org/10.1590/S1020-49892002000300003.
- Drayton VLC, Montgomery S, Modeste NN, Frye-Anderson BA. The Health Belief Model as a predictor of repeat pregnancies among Jamaican teenage mothers. Int Q Community Health Educ 2002;21:67-81.
- Stevens-Simon C, Kelly L, Singer D, Nelligan D. Reasons for first teen pregnancies predict the rate of subsequent teen conceptions. Pediatrics 1998;101. http://dx.doi.org/10.1542/peds.101.1.e8.
- Kershaw TS, Niccolai LM, Ickovics JR, Lewis JB, Meade CS, Ethier KA. Short and long-term impact of adolescent pregnancy on postpartum contraceptive use: implications for prevention of repeat pregnancy. J Adolesc Health 2003;33:359-68. http://dx.doi.org/10.1016/S1054-139X(03)00138-1.
- Paukku M, Quan J, Darney P, Raine T. Adolescents’ contraceptive use and pregnancy history: is there a pattern?. Obstet Gynecol 2003;101:534-8. http://dx.doi.org/10.1016/S0029-7844(02)02717-5.
- Sant’Anna MJC, Carvalho KAM, Melhado A, Coates V, Omar HA. Teenage pregnancy: impact of the integral attention given to the pregnant teenager and adolescent mother as a protective factor for repeat pregnancy. Scientific World J 2007;7:187-94. http://dx.doi.org/10.1100/tsw.2007.12.
- Mbambo DE, Ehlers VJ, Monareng LV. Factors influencing adolescent mothers’ non-utilisation of contraceptives in the Mkhondo area. Health SA Gesondheid 2006;11:22-31. http://dx.doi.org/10.4102/hsag.v11i4.227.
- Key JD, Barbosa GA, Owens VJ. The Second Chance Club: repeat adolescent pregnancy prevention with a school-based intervention. J Adolesc Health 2001;28:167-9. http://dx.doi.org/10.1016/S1054-139X(00)00186-5.
- Berenson A, Wiemann C. Contraceptive use among adolescent mothers at 6 months postpartum. Obstet Gynecol 1997;89:999-1005. http://dx.doi.org/10.1016/S0029-7844(97)00123-3.
- Williams EG, Sadler LS. Effects of an urban high school-based child care center on self-selected adolescent parents and their children. J Sch Health 2001;71:47-52. http://dx.doi.org/10.1111/j.1746-1561.2001.tb06489.x.
- Sangalang BB, Barth RP, Painter JS. First-birth outcomes and timing of second births: a statewide case management program for adolescent mothers. Health Soc Work 2006;31:54-63. http://dx.doi.org/10.1093/hsw/31.1.54.
- Falk G, Ostlund I, Magnuson A, Schollin J, Nilsson K. Teenage mothers – a high-risk group for new unintended pregnancies. Contraception 2006;74:471-5. http://dx.doi.org/10.1016/j.contraception.2006.07.014.
- Coard SI, Nitz K, Felice ME. Repeat pregnancy among urban adolescents: sociodemographic, family, and health factors. Adolescence 2000;35:193-200.
- Omar HA, Fowler A, McClanahan KK. Significant reduction of repeat teen pregnancy in a comprehensive young parent program. J Pediatr Adolesc Gynecol 2008;21:283-7. http://dx.doi.org/10.1016/j.jpag.2007.08.003.
- Persona L, Shimo AK, Tarallo MC. Profile of adolescents with repeated pregnancies attended at a prenatal clinic. Rev Lat-Am Enferm 2004;12:745-50. http://dx.doi.org/10.1590/S0104-11692004000500007.
- Salihu HM, August EM, Jeffers DF, Mbah AK, Alio AP, Berry E. Effectiveness of a federal healthy start program in reducing primary and repeat teen pregnancies: our experience over the decade. J Pediatr Adolesc Gynecol 2011;24:153-60. http://dx.doi.org/10.1016/j.jpag.2011.01.001.
- Stevens-Simon C, Wallis J, Allen-Davis J. Which teen mothers choose Norplant?. J Adolesc Health 1995;16:350-3. http://dx.doi.org/10.1016/S1054-139X(94)00048-J.
- Stevens-Simon C, Kelly L. Correlates and consequences of early removal of Levonorgestrel implants among teenaged mothers. Arch Pediatr Adolesc Med 1998;152:893-8. http://dx.doi.org/10.1001/archpedi.152.9.893.
- Stevens-Simon C, Kelly L, Singer D. Preventing repeat adolescent pregnancies with early adoption of the contraceptive implant. Fam Plann Perspect 1999;31:88-93. http://dx.doi.org/10.2307/2991646.
- Stevens-Simon C. The Second Chance Club. J Adolesc Health 2001;29. http://dx.doi.org/10.1016/S1054-139X(01)00299-3.
- Bruno Z, Feitosa F, Silveira K, de Morais I, Bezerra M. Subsequent pregnancy among adolescents. Rev Bras Ginecol Obstet 2009;31:480-4. http://dx.doi.org/10.1590/S0100-72032009001000002.
- Mears C, Hediger M, Martin S, Scholl T, Kramer J. Social factors prediciting postpartum choice of Norplant among African American and non-Hispanic white adolescents. J Adolesc Health 1997;21:167-71. http://dx.doi.org/10.1016/S1054-139X(97)00001-3.
- Mulsow MH, Murry VM. Parenting on edge: economically stressed, single, African American adolescent mothers. J Fam Issues 1996;17:704-21. http://dx.doi.org/10.1177/019251396017005007.
- Templeman CL, Cook V, Goldsmith LJ, Powell J, Hertweck SP. Postpartum contraceptive use among adolescent mothers. Obstet Gynecol 2000;95:770-6. http://dx.doi.org/10.1016/S0029-7844(00)00787-0.
- Thurman AR, Hammond N, Brown HE, Roddy ME. Preventing repeat teen pregnancy: postpartum depot medroxyprogesterone acetate, oral contraceptive pills, or the patch?. J Pediatr Adolesc Gynecol 2007;20:61-5. http://dx.doi.org/10.1016/j.jpag.2006.11.006.
- O’Dell CM, Forke CM, Polaneczky MM, Sondheimer SJ, Slap GB. Depot medroxyprogesterone acetate or oral contraception in postpartum adolescents. Obstet Gynecol 1998;91:609-14. http://dx.doi.org/10.1016/S0029-7844(97)00710-2.
- Patchen L, Caruso D, Lanzi RG. Poor maternal mental health and trauma as risk factors for a short interpregnancy interval among adolescent mothers. J Psychiatr Ment Health Nurs 2009;16:401-3. http://dx.doi.org/10.1111/j.1365-2850.2008.01353.x.
- Richio LJ, Phipps MG, Raker CA. Repeat teen birth: does delivery mode make a difference? American. J Obstet Gynecol 2010;203. http://dx.doi.org/10.1016/j.ajog.2010.06.027.
- Wang R, Wang H. Prebirth psychosocial factors as predictors of consistency in contraceptive use among Taiwanese adolescent mothers at 6 months postpartum. Public Health Nurs 2005;22:271-9. http://dx.doi.org/10.1111/j.0737-1209.2005.220402.x.
- Bull S, Hogue C. Exploratory analysis of factors associated with teens’ repeated childbearing. J Health Care Poor Underserved 1998;9:42-61. http://dx.doi.org/10.1353/hpu.2010.0511.
- Clarke J. Repeat teenage pregnancy in two cultures – the meanings ascribed by teenagers. Child Soc 2010;24:188-99.
- Hellerstedt WL, Story M. Adolescent satisfaction with postpartum contraception and body weight concerns. J Adolesc Health 1998;22:446-52. http://dx.doi.org/10.1016/S1054-139X(97)00258-9.
- Herrman JW. The voices of teen mothers: the experience of repeat pregnancy. Am J Mater Child Nurs 2006;31:243-9. http://dx.doi.org/10.1097/00005721-200607000-00009.
- Herrman JW. Repeat pregnancy in adolescence: intentions and decision making. Am J Mater Child Nurs 2007;32:89-94. http://dx.doi.org/10.1097/01.NMC.0000264288.49350.ed.
- Hoggart L, Phillips J, Birch A, Koffman O. Young People in London: Abortion and Repeat Abortion. London: Young London Matters Teenage Pregnancy Work Strand, Government Office for London; 2010.
- Lewis D, Martins SL, Gilliam M. Partner roles in contraceptive use: what do adolescent mothers say?. J Pediatr Adolesc Gynecol 2012;25:396-400. http://dx.doi.org/10.1016/j.jpag.2012.08.003.
- Schaffer MA, Jost R, Pederson BJ, Lair M. Pregnancy-free club: a strategy to prevent repeat adolescent pregnancy. Public Health Nurs 2008;25:304-11. http://dx.doi.org/10.1111/j.1525-1446.2008.00710.x.
- Smith JL, Skinner SR, Fenwick J. Preconception reflections, postconception intentions: the before and after of birth control in Australian adolescent females. Sex Health 2013;10:332-8. http://dx.doi.org/10.1071/SH13020.
- Weston MRS, Martins L, Neustadt AB, Gilliam ML. Factors influencing uptake of intrauterine devices among postpartum adolescents: a qualitative study. Am J Obstet Gynecol 2012;206:e1-7. http://dx.doi.org/10.1016/j.ajog.2011.06.094.
- Wilson EK, Samandari G, Koo HP, Tucker C. Adolescent mothers’ postpartum contraceptive use: a qualitative study. Perspect Sex Reprod Health 2011;43:230-7. http://dx.doi.org/10.1363/4323011.
- Clarke JE. Repeated Teenage Pregnancies – The Meanings Ascribed by Teenagers – A Comparison Between London and Two Caribbean Islands 2002.
- Key JD, Gebregziabher MG, Marsh LD, O’Rourke KM. Effectiveness of an intensive, school-based intervention for teen mothers. J Adolesc Health 2008;42:394-400. http://dx.doi.org/10.1016/j.jadohealth.2007.09.027.
- NHS Scotland . Reducing Teenage Pregnancy 2014. www.educationscotland.gov.uk/Images/teenage%20pregnancy%20web_tcm4–593480.pdf (accessed 13 June 2015).
- Rubin V, East P. Adolescents’ pregnancy intentions: relations to life situations and caretaking behaviors prenatally and 2 years postpartum. J Adolesc Health 1999;24:313-20. http://dx.doi.org/10.1016/S1054-139X(98)00082-2.
- Silva ADA, Coutinho IC, Katz L, Souza ASR. A case–control study of factors associated with repeat teen pregnancy based on a sample from a university maternity hospital. Cad Saude Publica 2013;29:496-50. http://dx.doi.org/10.1590/S0102-311X2013000300008.
- Teal SB, Sheeder J. IUD use in adolescent mothers: retention, failure and reasons for discontinuation. Contraception 2012;85:270-4. http://dx.doi.org/10.1016/j.contraception.2011.07.001.
- Key JD, O’Rourke K, Judy N, McKinnon SA. Efficacy of a secondary adolescent pregnancy prevention program: an ecological study before during and after implementation of the second chance club. Int Q Community Health Educ 2006;24:231-40. http://dx.doi.org/10.2190/1LC5-83MP-XT2W-PE40.
- Flynn L. The Adolescent Parenting Program: improving outcomes through mentorship. Public Health Nurs 1999;16:182-9. http://dx.doi.org/10.1046/j.1525-1446.1999.00182.x.
- Padin MDR, Silva RDE, Mitsuhiro SS, Chalem E, Barros MM, Guinsburg R, et al. Repeat pregnancies among adolescents in a tertiary hospital in Brazil. J Reprod Infant Psychol 2012;30:193-200. http://dx.doi.org/10.1080/02646838.2012.677139.
- Schaffer MA, Goodhue A, Stennes K, Lanigan C. Evaluation of a public health nurse visiting program for pregnant and parenting teens. Public Health Nurs 2012;29:218-31. http://dx.doi.org/10.1111/j.1525-1446.2011.01005.x.
- Stevens-Simon C, Kelly L, Kulick R. A village would be nice but. . .It takes a long-acting contraceptive to prevent repeat adolescent pregnancies. Am J Prev Med 2001;21:60-5. http://dx.doi.org/10.1016/S0749-3797(01)00316-6.
- Viellas EF, da Gama SG, Theme Filha MM, Leal Mdo C. Repeated pregnancy among adolescents and negative outcomes of the newborn: study in the city of Rio de Janeiro. Rev Bras Epidemiol 2012;15:443-54. http://dx.doi.org/10.1590/S1415-790X2012000300001.
- Wilson EK, Fowler CI, Koo HP. Postpartum contraceptive use among adolescent mothers in seven states. J Adolesc Health 2013;52:278-83. http://dx.doi.org/10.1016/j.jadohealth.2012.05.004.
- Patchen L, Letourneau K, Berggren E. Evaluation of an integrated services program to prevent subsequent pregnancy and birth among urban teen mothers. Soc Work Health Care 2013;52:642-55. http://dx.doi.org/10.1080/00981389.2013.797538.
- Haamid F, Wiemann C. You’re pregnant again?! Which adolescent mothers experience multiple repeat pregnancies?. J Adolesc Health 2010;46. http://dx.doi.org/10.1016/j.jadohealth.2009.11.076.
- Stevens-Simon C, Kelly L, Singer D. Absence of negative attitudes towards childbearing among pregnant teenagers. Arch Pediatr Adolesc Med 1996;150:1037-43. http://dx.doi.org/10.1001/archpedi.1996.02170350039006.
- Collins ME, Stevens JW, Lane TS. Teenage parents and welfare reform: findings from a survey of teenagers affected by living requirements. Soc Work 2000;45:327-38. http://dx.doi.org/10.1093/sw/45.4.327.
- Seamark C. Design or accident? The natural history of teenage pregnancy. J R Soc Med 2001;94:282-5.
- UNICEF . UN Convention on the Rights of the Child 1992. www.unicef.org.uk/UNICEFs-Work/UN-Convention/ (accessed 8 September 2014).
- Central Bedfordshire Health and Wellbeing Strategy 2012–2016. NHS Central Bedfordshire; 2012.
- Pawson R, Tilley N. Realistic Evaluation. London: Sage; 1997.
- Gray S, Sheeder J, O’Brien R, Stevens-Simon C. Having the best intentions is necessary but not sufficient: what would increase the efficacy of home visiting for preventing second teen pregnancies?. Prev Sci 2006;7:389-95. http://dx.doi.org/10.1007/s11121-006-0045-2.
- Sadler LS, Swartz MK, Ryan-Krause P, Seitz V, Meadows-Oliver M, Grey M, et al. Promising outcomes in teen mothers enrolled in a school-based parent support program and child care center. J Sch Health 2007;77:121-30. http://dx.doi.org/10.1111/j.1746-1561.2007.00181.x.
- Local Government Association . Tackling Teenage Pregnancy: Local Government’s New Public Health Role 2013. www.local.gov.uk/c/document_library/get_file?uuid=9f5ef790-eee2–422d-851c-6eb5c3562990&groupId=10180 (accessed 1 July 2014).
- Akers DD, Mince J, Card JJ, Benner T. Model Programs for Adolescent Sexual Health: Evidence-based HIV, STI And Pregnancy Prevention Interventions. New York, NY: Springer; 2008.
- Solomon R, Liefeld CP. Effectiveness of a family support centre approach to adolescent mothers: repeat pregnancy and school drop-out rates. Fam Relat 1998;47:139-44. http://dx.doi.org/10.2307/585617.
- Swedish KA, Rothenberg A, Fuchs K, Rosenberg G. Successful life navigation by former participants in a group for pregnant and parenting teens. Vulnerable Child Youth Stud 2010;5:310-21. http://dx.doi.org/10.1080/17450128.2010.507806.
- Mapanga KG, Andrews CM. The influence of family and friends’ basic conditioning factors and self-care agency on unmarried teenage primiparas’ enagagement in contraceptive practice. J Community Health Nurs 1995;12:89-100. http://dx.doi.org/10.1207/s15327655jchn1202_3.
- Truong HHM, Kellogg T, McFarland W, Kang MS, Darney P, Drey EA. Contraceptive intentions among adolescents after abortion. J Adolesc Health 2006;39:283-6. http://dx.doi.org/10.1016/j.jadohealth.2005.11.025.
- Carvajal D, Burrell L, Duggan A, Barnet B. Repeat pregnancy prevention self-efficacy in adolescents: associations with provider communication, provider type, and depression. South Med J 2012;105:591-7. http://dx.doi.org/10.1097/SMJ.0b013e31826ff173.
- Lewis SA, Noyes J. Effective process or dangerous precipice: qualitative comparative embedded case study with young people with epilepsy and their parents during transition from children’s to adult services. BMC Pediatr 2013;13. http://dx.doi.org/10.1186/1471-2431-13-169.
- Lewis CM, Faulkner M, Scarborough M, Berkeley B. Preventing subsequent births for low-income adolescent mothers: an exploratory investigation of mediating factors in intensive case management. Am J Public Health 2012;102:1862-5. http://dx.doi.org/10.2105/AJPH.2012.300914.
- Centers for Disease Control and Prevention (CDC) . PRAMS 2015. www.cdc.gov/prams/index.htm (accessed 2 October 2015).
- Corcoran J, Pillai VK. Effectiveness of secondary pregnancy prevention programs: a meta-analysis. Res Social Work Pract 2007;17:5-18. http://dx.doi.org/10.1177/1049731506291583.
- Schulz KF, Altman DG, Moher D. on behalf of the CONSORT Group . CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMC Med 2010;8. http://dx.doi.org/10.1186/1741-7015-8-18.
- Frey JJ. Is Obamacare working?. Br J Gen Pract 2014;64:360-1. http://dx.doi.org/10.3399/bjgp14X680653.
- Trivedi D, Bunn F, Graham M, Wentz R. Update on Review of Reviews on Teenage Pregnancy and Parenthood 2007. www.nice.org.uk/guidance/ph3/evidence/update-on-review-of-teenage-pregnancy-and-parenthood2 (accessed 28 September 2015).
- Craine N, Midgley C, Zou L, Evans H, Whitaker R, Lyons M. Elevated teenage conception risk amongst looked after children in Wales; a national audit. Public Health 2014;128:668-70. http://dx.doi.org/10.1016/j.puhe.2014.05.008.
- Kearney MS, Levine PB. Media Influences on Social Outcomes: the Impact of MTV’s 16 and pregnant on Teen Childbearing. Cambridge, MA: US National Bureau of Economic Research; 2014.
- MTV . 16 and Pregnant n.d. www.mtv.co.uk/16-and-pregnant (accessed 7 April 2015).
- Robling M, Bekkers M-J, Bell K, Butler CC, Cannings-John R, Channon S, et al. Effectiveness of a nurse-led intensive home-visitation programmes for first-time teenage mothers (Building Blocks): a pragmatic randomised controlled trial. Lancet 2015. http://dx.doi.org/10.1016/S0140-6736(15)00392-X.
- Furey A. Are support and parenting programmes of value for teenage parents? Who should provide them and what are the main goals?. Public Health 2004;118:262-7. http://dx.doi.org/10.1016/j.puhe.2003.09.005.
- Baldwin MK, Edelman AB. The effect of long-acting reversible contraception on rapid repeat pregnancy in adolescents: a review. J Adolesc Health 2012;52:S47-S53. http://dx.doi.org/10.1016/j.jadohealth.2012.10.278.
- Milne D, Glasier A. Preventing repeat pregnancy in adolescents. Curr Opin Obstet Gynecol 2008;20:442-6. http://dx.doi.org/10.1097/GCO.0b013e3283086708.
- Seitz V, Apfel NH. Effective interventions for adolescent mothers. Clin Psychol-Sci Pract 1999;6:50-66. http://dx.doi.org/10.1093/clipsy.6.1.50.
- Contraceptive Services with a Focus on Young People up to the Age of 25. NICE; 2014.
- Anon . 30,000 Florida rural poor receiving Ob Gyn care. Ob Gyn News 1973;8.
- Hippisley-Cox J, Allen J, Pringle M. Association between teenage pregnancy rates and the age and sex of general practitioners: cross sectional survey in Trent 1994–97. BMJ 2000;320:842-5. http://dx.doi.org/10.1136/bmj.320.7238.842.
- Alderson P. Absence of evidence is not evidence of absence. BMJ 2004;328. http://dx.doi.org/10.1136/bmj.328.7438.476.
- McNeill EH. Hope as a Strategy for Improving Student Achievement and Dissuading Repeat Pregnancy in Pregnant and Parenting Adolescents. Texas: A&M University; 2010.
Appendix 1 Search strategies
Electronic databases searched
MEDLINE and MEDLINE In-Process & Other Non-Indexed Citations.
PsycINFO.
Cumulative Index to Nursing and Allied Health Literature.
The Cochrane Library (Cochrane Database of Systematic Reviews, Database of Abstracts of Reviews of Effects, the HTA Database, NHS Economic Evaluation Database).
EMBASE (Excerpta Medica database).
BNI.
Educational Resources Information Center.
SocAbs.
ASSIA.
BiblioMap (the EPPI-Centre register of health promotion and public health research).
SSCI (supported by Web of Knowledge).
Additional databases used for grey literature
OpenGrey.
Scopus.
Scirus.
Social Care Online [via Science Citation Index Expanded website].
National Research Register.
NIHR Clinical Research Network Portfolio.
Index to THESES.
Google.
Databases searched for qualitative literature
ASSIA.
BNI.
SocAbs.
SSCI.
Search strategies
MEDLINE
-
exp pregnancy in adolescence/
-
Pregnancy, unplanned/
-
Pregnancy unwanted/
-
Abortion, induced/
-
Abortion, legal/
-
Or/2-5
-
Adolescent/
-
(Adolescen$ or teen$ or girl or girls or youth or youths or youthful or young or juvenile).ti,ab.
-
7 or 8
-
(Repeat or subsequent or second or secondary or further or additional).ti,ab.
-
1 and 10
-
6 and 9 and 10
-
11 or 12
-
Limit 13 to 1995 onwards and humans only
PsycINFO
S1 SU.EXACT(“Adolescent Pregnancy”)
S2 SU.EXACT(“Induced Abortion”)
S3 AB,TI(Adolescen* OR teen* OR girl or girls OR youth or youths or youthful OR young OR juvenile)
S4 AB,TI(Repeat OR subsequent OR second OR secondary OR further OR additional)
S5 S1 AND S4
S6 S2 AND S3 AND S4
S7 S5 OR S6
S8 Limit to 1995 to 2013
Cumulative Index to Nursing and Allied Health Literature
S1 (MM “Pregnancy in adolescence+”) OR (MM “Adolescent Mothers) OR (MM “Adolescent Parents+”)
S2 (MM “Pregnancy, unplanned”) OR (MM “Pregnancy unwanted”) OR (MM “Abortion, induced”)
S3 TI (Adolescen* or teen* or girl or girls or youth or youths or youthful or young or juvenile)
S4 AB (Adolescen* or teen* or girl or girls or youth or youths or youthful or young or juvenile)
S5 S3 OR S4
S6 TI (Repeat or subsequent or second or secondary or further or additional)
S7 AB (Repeat or subsequent or second or secondary or further or additional)
S8 S6 OR S7
S9 S1 AND S8
S10 S2 AND S5 AND S8
S11 >S9 OR S10
S12 Limit 11 to yr=”1995-current”
Cochrane Library
-
Pregnancy in adolescence/
-
Pregnancy, unplanned/
-
Pregnancy, unwanted/
-
Abortion, legal/
-
Abortion, induced/
-
OR/ 1-5
-
Adolescent/
-
(adolescen* or teen* or girls or girls or youth or youths or youthful or young or juvenile):ti,ab.
-
7 OR 8
-
(repeat or subsequent or second or secondary or further or additional):ti,ab.
-
1 AND 10
-
6 AND 9 AND 10
-
11 OR 12
-
Limit 13 to 1995 onwards
EMBASE
-
exp adolescent pregnancy/
-
unplanned pregnancy/ or unwanted pregnancy/
-
legal abortion/ or induced abortion/
-
2 or 3
-
adolescent/
-
(Adolescen$ or teen$ or girl or girls or youth or youths or youthful or young or juvenile).ti,ab.
-
5 or 6
-
(Repeat or subsequent or second or secondary or further or additional).ti,ab.
-
1 and 8
-
4 and 8 and 9
-
9 or 10
-
limit 12 to 1995 onwards and humans only
British Nursing Index (BNI)
S1 SU.EXACT(pregnancy : age factors)
S2 SU.EXACT(“Abortion”)
S3 SU.EXACT(“Adolescents”)
S4 AB,TI(Adolescen* OR teen* OR girl or girls OR youth or youths or youthful OR young OR juvenile)
S5 S3 OR S4
S6 AB,TI(Repeat OR subsequent OR second OR secondary OR further OR additional)
S7 S1 AND S6
S8 S2 AND S5 AND S6
S9 S7 OR S8
S10 Limit S9 to 1995-2013 and humans
Educational Resources Information Center
S1 SU.EXACT(“Early Parenthood”)
S2 AB,TI(Abortion)
S3 SU.EXACT(“Adolescents”)
S4 AB,TI(Adolescen* OR teen* OR girl or girls OR youth or youths or youthful OR young OR juvenile)
S5 S3 OR S4
S6 AB,TI(Repeat OR subsequent OR second OR secondary OR further OR additional)
S7 S1 AND S6
S8 S2 AND S5 AND S6
S9 S7 OR S8
S10 Limit S9 to 1995 onwards and humans
Sociological Abstracts
S1 SU.EXACT(“Adolescent Pregnancy”) OR SU.EXACT(“Adolescent Mothers”)
S2 SU.EXACT(“Abortion”)
S3 SU.EXACT(“Adolescents”)
S4 AB,TI(Adolescen* OR teen* OR girl or girls OR youth or youths or youthful OR young OR juvenile)
S5 S3 OR S4
S6 AB,TI(Repeat OR subsequent OR second OR secondary OR further OR additional)
S7 S1 AND S6
S8 S2 AND S5 AND S6
S9 S7 OR S8
S10 Limit S10 to 1995 onwards and humans
BiblioMap
-
Category: Focus of the report: pregnancy prevention
-
Freetext: pregnancy
-
Freetext: pregnancies
-
Freetext: pregnant
-
Freetext: conception
-
Freetext: conceptions
-
Freetext: abortion
-
Freetext: abortions
-
OR/1-8
-
Category: Characteristics of the study population: young people
-
Freetext: teen
-
Freetext: teens
-
Freetext: teenage
-
Freetext: teenagers
-
Freetext: adolescent
-
Freetext: adolescents
-
Freetext: adolescence
-
Freetext: youth
-
Freetext: young
-
Freetext: youthful
-
Freetext: juvenile
-
Freetext: girl
-
Freetext: girls
-
OR/10-23
-
Freetext: repeat
-
Freetext: subsequent
-
Freetext: second
-
Freetext: secondary
-
Freetext: further
-
Freetext: additional
-
OR/25-30
-
AND 24 AND 31
Applied Social Sciences Index and Abstracts
S1 SU.EXACT(“Pregnant adolescent girls”) OR SU.EXACT(“Adolescent mothers”)
S2 SU.EXACT(“Abortion”)
S3 SU.EXACT(“Adolescents”)
S4 AB,TI(Adolescen* OR teen* OR girl or girls OR youth or youths or youthful OR young OR juvenile)
S5 S3 OR S4
S6 AB,TI(Repeat OR subsequent OR second OR secondary OR further OR additional)
S7 S1 AND S6
S8 S2 AND S5 AND S6
S9 S7 OR S8
S10 Limit S10 to 1995 onwards and humans
Social Sciences Citation Index (Web of Science)
Free text search:
-
Pregnancy
-
Pregnancies
-
“conception*”
-
“abortion*”
-
OR 1-4
-
“teenage*”
-
“adolescent*”
-
6 or 7
-
Repeat
-
Subsequent
-
Secondary
-
OR 9-11
-
5 AND 8 AND 12
-
Limit to 1995 onwards
Additional databases for grey literature
OpenGrey
“teenage pregnancy” OR “teenage pregnancies” OR “teenage conception” OR ” “teenage conceptions"
Scopus
Teenge pregnancy AND repeat
Scirus
“repeat +pregnancy” AND (teenage* OR adolescen*)
Limit to 1995 onwards and excluding journal sources
Social Care Online (via Science Citation Index Expanded website)
Teenage pregnancy AND repeat
Limit to 1995 onwards
National Research Register archive
Keyword search: adolescence and pregnancy
National Institute for Health Research Clinical Research Network Portfolio
Reproductive health (all section screened)
Index to THESES
Title search: teenage pregnancy or teenage pregnancies or teenage abortions or teenage conceptions
Site:uk “repeat pregnancy” teenager
Site:uk “repeat pregnancy” teenagers
Site:uk “repeat pregnancies” teenagers
Site:uk “repeat pregnancies” teenager
Site:uk “repeat pregnancy” teenage
Site:uk “repeat pregnancies” teenage
Site:uk “repeat pregnancy” teen
Site:uk “repeat pregnancies” teen
Site:uk “repeat pregnancy” teens
Site:uk “repeat pregnancies” teens
Site:uk “repeat teen” pregnancy
Site:uk “repeat teen” pregnancies
Site:uk “repeat teenage” pregnancy
Site:uk “repeat teenage” pregnancies
Site:uk “second pregnancy” teen
Site:uk “second pregnancies” teen
Site:uk “second pregnancy” teens
Site:uk “second pregnancies” teens
Site:uk “second pregnancy” teenage
Site:uk “second pregnancies” teenage
Site:uk “second pregnancy” teenager
Site:uk “second pregnancies” teenager
Site:uk “second pregnancy” teenagers
Site:uk “second pregnancies” teenagers
Databases used for economics literature
Research Papers in Economics
Free text search:
(teen | adolescent | adolescence | girl | young | youth | juvenile) + (pregnancy | pregnancies | conception | abortion) + (repeat | subsequent | second | secondary | further | additional)
Limit to 1995 onwards
American Economic Association’s electronic bibliography (EconLit)
-
SU = pregnancy and teens or SU = adolescent mothers or SU = adolescent pregnancy
-
SU = pregnancy or SU = abortion or SU = conception
-
AB = (adolescen* or teen* or girl* or young or youth* or juvenile)
-
AB = (repeat or subsequent or second or secondary or further or additional)
-
1 and 4
-
2 and 3 and 4
-
5 or 6
-
Limit 7 to 1995 onwards
Additional searches for qualitative literature
-
ASSIA.
-
BNI.
-
SocAbs.
-
SCI.
The above databases were searched using alternative text terms for pregnancy, adolescence and repeat plus the short qualitative filter described in Shaw et al. ,43 as follows:
-
Conception or conceptions or pregnancy or pregnancies or abortion or abortions or birth or births or mother or mothers or motherhood or mum or mums or mom or moms or baby or babies
-
Adolescen* OR teen* OR girl or girls OR youth or youths or youthful OR young OR juvenile
-
Repeat or subsequent or second or secondary
-
(Pregnancy or birth) adj 2 spacing
-
1 and 2 and 3
-
2 and 4
-
5 or 6
-
Qualitative or findings or interview*
-
7 and 8
-
Limit 8 to 1995 onwards
Strategy for searching for evidence ‘clusters’ associated with randomised controlled trials
-
Check references in the trial paper.
-
Locate the trial in PubMed and use the “related articles” feature to find related studies and other studies by the same authors.
OR, if not found in PubMed, try the database where the study was found (some have a “related articles” feature but some do not).
-
Locate the RCT in the Science and Social Science Citation Index and check the list of studies citing the paper.
-
Search the study title or acronym in Google Scholar.
-
Contact the lead (or corresponding) author.
Contact with lead authors:
Request details of any associated reports (published or unpublished) that relate to the target trial. Principally, these may include process evaluations or qualitative research studies, although they could also include other useful data such as associated economic evaluations or cost details. Such requests should make it clear that it is the trial, not the lead author, that is the item of interest and that outputs associated with the trial are being sought regardless of whether the lead author has been attributed with authoring such ‘sibling’ studies. Indeed, such sibling studies may well be led by another research colleague, such as a qualitative researcher or a health economist.
| Database | Dates covered | Hits: 8–27 May 2013 | Updated hits: 10–19 June 2014 | Host |
|---|---|---|---|---|
| ASSIA | 1995–2013 | 187 | 3 | Child Support Agency |
| BiblioMap | 1995–2013 | 97 | 0 | EPPI-Centre |
| BNI | 1995–2013 | 83 | 13 | ProQuest |
| CINAHL | 1995–2013 | 479 | 8 | EBSCOhost |
| The Cochrane Library | 1995–2013 | 95 | 8 | Wiley |
| EMBASE | 1995–2013 | 977 | 105 | Elsevier |
| ERIC | 1995–2013 | 613 | 0 | ProQuest |
| MEDLINE/MEDLINE In-Process & Other Non-Indexed Citations | 1995–2013 | 1331 | 107 | Ovid |
| PsychINFO | 1995–2013 | 683 | 12 | ProQuest |
| SocAbs | 1995–2013 | 335 | 9 | ProQuest |
| SSCI | 1995–2013 | 583 | 6 | Web of Knowledge |
| Database | Dates covered | Hits: 7–21 May 2013 | Updated hits: 10–19 June 2014 | Host |
|---|---|---|---|---|
| OpenGrey | 1995–2013 | 56 | 0 | www.opengrey.eu |
| Scopus | 1995–2013 | 24 | 4 | Elsevier |
| Scirus | 1995–2013 | 1007 | Not available | www.scirus.com |
| Social Care Online | 1995–2013 | 4 | 1 | www.scie-socialcareonline.org.uk |
| NRR | 1995–2013 | 134 | 0 | www.nihr.ac.uk |
| NIHR Clinical Research Network Portfolio | 1995–2013 | 450 | 0 | www.crncc.nihr.ac.uk |
| Index to THESES | 1995–2013 | 27 | 0 | ProQuest |
| Database | Dates covered | Hits: 15–21 May 2013 | Updated hits: 17 June 2014 | Host |
|---|---|---|---|---|
| RePEc | 1995–2013 | 101 | 1 | http://repec.org/ |
| EconLit | 1995–2013 | 31 | 6 | EBSCOhost |
| Database | Dates covered | Hits: 18 July 2013 | Updated hits: 19–20 June 2014 | Host |
|---|---|---|---|---|
| ASSIA | 1995–2013 | 229 | 3 | Child Support Agency |
| BNI | 1995–2013 | 21 | 1 | ProQuest |
| SocAbs | 1995–2013 | 652 | 1 | ProQuest |
| SSCI | 1995–2013 | 1394 | 303 | Web of Knowledge |
| Search strategy | Number of results |
|---|---|
| Site:uk “repeat pregnancy” teenager | 117 |
| Site:uk “repeat pregnancy” teenagers | 109 |
| Site:uk “repeat pregnancies” teenagers | 151 |
| Site:uk “repeat pregnancies” teenager | 143 |
| Site:uk “repeat pregnancy” teenage | 205 |
| Site:uk “repeat pregnancies” teenage | 216 |
| Site:uk “repeat pregnancy” teen | 120 |
| Site:uk “repeat pregnancies” teen | 143 |
| Site:uk “repeat pregnancy” teens | 211 |
| Site:uk “repeat pregnancies” teens | 223 |
| Site:uk “repeat teen” pregnancy | 159 |
| Site:uk “repeat teen” pregnancies | 165 |
| Site:uk “repeat teenage” pregnancy | 95 |
| Site:uk “repeat teenage” pregnancies | 93 |
| Site:uk “second pregnancy” teen | 265 |
| Site:uk “second pregnancies” teen | 221 |
| Site:uk “second pregnancy” teens | 234 |
| Site:uk “second pregnancies” teens | 227 |
| Site:uk “second pregnancy” teenage | 215 |
| Site:uk “second pregnancies” teenage | 214 |
| Site:uk “second pregnancy” teenager | 225 |
| Site:uk “second pregnancies” teenager | 217 |
| Site:uk “second pregnancy” teenagers | 237 |
| Site:uk “second pregnancies” teenagers | 222 |
| Total | 4427 |
Summary of initial database search results: May–July 2013
Total number of hits: 8664.
Total after de-duplication: 5779.
Number rejected after screening titles and abstracts: 5551.
Number of relevant papers identified by screening titles and abstracts: 232.
Total number of included studies from database searches: 118 (127 articles).
Studies included in mapping exercise only: 48 (50 articles).
Studies carried forward to full review: 70 (78 articles).
Summary of grey literature (Google) search results: January 2014
Number of records identified by grey literature (Google) searches: 4427.
Number of full-text articles assessed after screening titles: 22.
Number included in the review: 1.
Summary of updated search results: June 2014
Total hits: 497.
Total after deduplication: 403.
Number rejected after screening titles and abstracts: 395.
Number of full records retrieved and assessed: 8.
Number included: 3.
Summary of citation search results: July 2014
Total hits: 1062.
Total after deduplication: 717.
Total published after 1995: 599.
Total new articles (not identified in previous database searches): 414.
Number rejected after screening titles and abstracts: 408.
Number of full records retrieved and assessed: 6.
Number included: 3.
Summary of hand searches: July 2014
The electronic indexes of 17 journals were searched by hand from January 2010.
Number of full records retrieved and assessed: 2.
Number included: 0.
Strategy for citation searches
We also conducted forwards and backwards citation searches based on the included RCTs and teenage pregnancy related systematic reviews we had identified during the course of our literature searches. We identified the relevant studies in Web of Science and used their electronic tools to find studies that had cited and been cited by them.
Hand searches
Journals were identified by comparing those that published RCTs and qualitative studies included in the review with a Cochrane register of journals and selecting those English-language journals not included in the register.
The electronic indexes of the journals listed below were screened for relevant article titles from January 2010 until June 2014.
-
Family Relations
-
Journal of Perinatal Education
-
Wisconsin Medical Journal
-
Annals Family Medicine
-
Maternal Child Health Journal
-
Journal of Family Issues
-
Health Care for Women International
-
Journal of Psychosocial Nursing
-
MIDIRIS Midwifery Digest
-
Community Practitioner
-
Journal of Adolescent Health
-
International Quarterly of Community Health Education
-
Nursing Connections
-
Journal of Health Care for the Poor and Underserved
-
Children & Society
-
Early Child Development and Care
-
Perspectives on Sexual and Reproductive Health.
Appendix 2 Report of the stakeholder mapping meeting (Prince Rupert Hotel, Shrewsbury)

Intervention Now to Eliminate Repeat Unintended Pregnancy in Teenagers (INTERUPT) Mapping Day – 21 November 2013
Agenda
Morning session: presentations by the review team to the stakeholders
Introduction and background to the study
Rhiannon Whitaker (chief investigator) welcomed delegates, introduced the investigators and the review team and gave an overview of the objectives of the day. She also presented the background to the study and its conception and its aims.
Overview of study methods
Maggie Hendry (lead reviewer) explained the research brief and outlined the mixed-methods approach to the study. For this review, 118 studies have been included and key for this meeting is to discover the relevance to stakeholders of the evidence we have and to identify relevant UK evidence that is missing.
Professor Jane Noyes presented examples of one quantitative and one qualitative study and explained the typical limitations of these types of studies.
Outline of the mapping exercise and overview of the literature
Rabeea’h Aslam (systematic reviewer) described the 118 studies in terms of:
-
geography
-
94 studies from USA
-
seven studies from the UK
-
the rest from around the world
-
-
study design
-
14 RCTs
-
40 cohort studies
-
16 case control studies
-
quasi-experimental studies
-
two mixed-methods studies
-
15 process evaluations
-
11 qualitative/views studies of girls and health professionals
-
-
context/setting
-
43 community
-
52 health
-
education
-
eight multiple
-
-
content/intervention type
-
contraceptive advice or education
-
LARCs or oral contraception
-
54 complex interventions, with examples of the different types given
-
-
outcomes measured
-
primary outcomes, namely identification of at risk group; identification of barriers and facilitators of interventions relating to acceptability, uptake and feasibility of implementation; and views and experiences of young women, families and professionals
-
other outcomes, namely identification of, access to and uptake of reproductive services and social care; feasibility of widespread adoption of interventions in health and social care; cost of interventions; effectiveness of interventions – (1) change in validated quality of life indices and (2) change in the rate of abortion – and cost-effectiveness of interventions.
-
Realist synthesis
Joanna Charles (health economist) gave an outline of the realist element of the review and examples of the mid-range theories developed. She explained that the realist research question is often summarised as ‘What works for whom, under what circumstances, how and why?’. The mind map of the evidence was presented, and a poster of this displayed with participants invited to use sticky notes to add any elements they saw, during meal breaks.
Example of service to teen mums
Sally Roberts (specialist midwife for pregnant teenagers Abertawe Bro Morgannwg University Health Board) presented details about ‘Teenstart’, which is a bespoke project that provides additional antenatal and postnatal support to pregnant teenagers and teenage parents aged 18 years and under at the time for booking for maternity care and then up to the age of 20 years or the child’s second birthday. She also presented data from the annual report from the programme.
Summary of review methods
Phase 1
-
Literature searches, inclusion/exclusion, quality appraisal and mapping exercise.
-
Consideration of mapping exercise and consultation with advisory group and stakeholders.
Phase 2
-
Selection of records for in-depth review and data extraction.
Phase 3
-
Synthesis of evidence according to type using design appropriate tools.
Phase 4
-
Overarching narrative synthesis and interpretation.
Questions following team presentations: summary of comments and questions
Maggie Hendry
‘Are there any issues comparing studies from the 1980s with recently published material say from 2007?’
Jane Noyes responded, saying that:
there is an issue within this field of a lack of longitudinal follow-up to long-term interventions/strategies/programmes, which could provide insight to changes in health behaviour over time and longer term outcomes. The team could use methods such as targeted sub-group and sensitivity analyses to look at differences between the studies over time.
Context: comparing the USA and UK may not be that different after all, the USA has great difficulty with contraception availability. We assume that the UK has good availability, but this is not always the case. How do we get this information? It is not usually reported in papers.
Maggie Hendry responded:
the aim of this day is to gain this information from the stakeholders we have present today as the evidence only tells us so much.
Generalisability: are the pressures and experiences of the population under study the same now as they were in the 1980s/1990s? There could be a difference in teenage morals/values, use of technology (mobiles, internet), availability of contraception and cost of contraception.
The team responded that the evidence does not report these issues and that the majority of the time, we have to infer and make assumptions about these factors. The team are aware that the life of a teenager was different in 1980 than now. We will be discussing specific questions later and the stakeholders’ experience and opinions would be extremely valuable for discussions such as these.
A question was raised regarding the limited economic evidence and whether or not any NICE guidance exists.
Sara Thomas said that NICE guidance on teenage pregnancy exists, but there is a limited amount of information contained about repeat pregnancies. Sara worked on a large review with Rhiannon Tudor Edwards and Joanna Charles for PHW and offered to share information from that review with the team.
The team said that they would look at this guidance.
Rabeea’h Aslam
‘Are terminations included in our study? There is a lack of data in general about this.’
Maggie Hendry responded:
we used a search strategy and definition based on teen conceptions and included the terms termination in our review. However, the evidence in relation terminations is low
There was a generally positive response relating to the Hope project,189 with people asking Rabeea’h Aslam to further emphasise the details of this study.
Joanna Charles
It was requested that the following points be added to the mind map for inclusion in the realist review:
-
abuse
-
exploitation
-
housing (including homelessness)
-
substance misuse
-
looked-after children
-
known to family services
-
financial issues (joblessness, frequent use of food banks)
-
no use of contraception
-
access to contraception (issues of multiple appointments to get contraception).
Joanna Charles stated that she would add these to the mind map for inclusion in the realist review and asked that if anyone had any further points, to please add them to the mind map poster.
Has the published evidence looked at social service involvement? Figures show that 60% of families who have teenage pregnancies and repeat teenage pregnancies are known to social services and have had involvement from social services at some point in their lives. Also, a trend for ‘family files’ continued social service records spanning generations of families.
The team responded that the evidence has not shown papers with social service involvement; however, some research uses targeted samples from areas of high socioeconomic deprivation.
Lunch and networking
Afternoon session
Participants were divided into three groups for discussion and feedback of three each of the key questions, listed below.
Key questions for stakeholders
-
How relevant is evidence from different settings and particularly from non-UK studies?
-
What components of complex interventions are most important in relation to reducing repeat pregnancies?
-
How relevant are other outcomes (health, social, educational, maternal or child-related) to repeat pregnancies?
-
Are repeat teenage pregnancies truly unintended? (What is the difference between unintended, unplanned and unwanted?)
-
What are the differences in motivating factors between first and repeat teenage pregnancies?
-
Which intervention components best address the factors that motivate young women to have (or not to avoid having) a repeat pregnancy?
-
What are the barriers to and facilitators of accessing interventions?
-
What is the best way of packaging and presenting the intervention to teenagers to ensure maximum take-up? (such as pregnancy spacing, making healthy choices, using contraception effectively, planning your future, others)
-
How is the success of a programme best measured in monetary terms?
Group 1 feedback
How relevant is evidence from different settings and particularly from non-UK studies?
-
Different settings can be useful, providing readers are informed of the differences.
-
Research found has focused on samples that are from areas of high socioeconomic deprivation and low educational attainment, which could provide continuity with the areas with the highest rates of conceptions in the UK.
-
There were some success stories in Wales that could be used as case studies of good practice. For example, Blaenau Gwent, South Wales, has seen a significant reduction in teenage conception rates since Louise Taylor (a midwife specialising in teenage pregnancies) was appointed. There were no other changes in the area other than this new post.
What components of complex interventions are most important in relation to reducing repeat pregnancies?
-
Self-esteem and goal-setting
-
One participant mentioned a project called the Genesis project that provided child care so teenage mothers could go to school or enrol in a training course; unfortunately, the funding for this project has been pulled.
-
-
Assured education.
-
Life skills.
-
Teenagers may be getting pregnant as there are no jobs or prospects. Young women and girls sometimes ‘drift’ and are unsure of what to do when they find themselves pregnant or they could be unaware they are pregnant. Thus, they just continue the pregnancies because they do not know there are other options. Sometimes this ‘drifting’ may result in reduced options as the teenager is unable to have a termination.
How relevant are other outcomes (health, social, educational, maternal or child-related) to repeat pregnancies?
-
Absenteeism Repeat pregnancies reduce the chances of the teenager attending school regularly.
-
Location of services Reducing barriers to access and multiple appointments before receiving contraception. Midwives ask the mothers soon after birth about their future plans and contraception needs and wants, but they cannot administer some forms of contraception resulting in a lapse of time between intention and action. Unless the mothers are seen on the maternity or gynaecology ward in which case contraception can be given the same day (Ward 18 in Singleton Hospital, Swansea, can often see the mother on the same day if she has attended a morning appointment). One participant reiterated this point ‘it’s key to bring the teenager to the service in order to receive the requested contraception’.
-
Families and family situation Some families are in social service records for 20–30 years, the subsequent generations seem to just be getting added to larger and larger files.
-
Social services and court outcomes There are cases in which teenage mothers request contraception such as having a coil fitted in order to gain favour with a court or social services to increase their likelihood of having their child who was taken into care returned, rather than being motivated to reduce the chance of repeat pregnancies.
-
Outcomes for the child Our group discussed two outcomes
-
Using outcomes for the child can be a motivating factor, for example ‘doing the best for my baby’ may motivate the mother to use contraception; also motivations using the child (e.g. providing a better life for the child) seem to be more effective than the teenagers own personal motivations (e.g. I want to return to school to see my friends). One or two children may allow a mother to go back to school or further training but three or four children reduces a mother’s prospects.
-
Low birthweight. Some mothers see low birthweight as a positive thing, meaning a less difficult birth; however, low-birthweight babies cost the health system significantly and it is a priority of PHW to reduce the number of these births.
-
-
Class differences These could be linked with a locus of control, educational attainment, family norms and vulnerability. It is typically teenagers from more impoverished backgrounds that have higher rates of teenage pregnancy. There may be stigma in these areas of terminating pregnancies, as the ‘norm’ is to carry to term, most young mothers have multiple children. Girls who terminate pregnancies may be perceived as ‘stuck up’.
Group 2 feedback
Are repeat pregnancies truly intended (what is the difference between unintended, unplanned and unwanted)?
This was not easy to tease this out as comments from participants were more general:
-
Unplanned
-
Accessing contraceptive services is difficult. In cases of repeat pregnancies, they do not take up opportunities to access contraceptive services.
-
-
Similar to first time around
-
Contraception is not a priority. They just do not think it’s going to happen to them/as a result of opportunistic sex with no thought of consequences.
-
They do not come from regular families and there is a lot of ignorance.
-
Access to contraception through GPs is a problem; the process is difficult because they have to make an appointment to ask for contraception. This can be off putting as they have to discuss this with a doctor (possibly male). Also then sometimes given a leaflet and told to make another appointment, by which time it may be too late.
-
-
There is a literacy problem. They are given a leaflet and lots cannot read.
-
Health workers try to help as much as they can with information on contraceptive methods (what is a coil, how to use a condom, etc.).
-
Important to break down barriers; this should not be a taboo subject and therefore embarrassing.
-
Partner abuse; some partners like to keep the girls pregnant.
-
They live for the moment and do not believe they will get pregnant.
-
Social factors
-
in deprived areas they felt it was expected of them
-
in privileged areas it brings shame
-
ignorance (do not want contraception as do not have partners).
-
-
Empowerment/education
-
these girls do not have any life skills
-
no planned behaviour (e.g. prioritise phone but not contraception)
-
they have low expectations.
-
-
It is a circle
-
to break out of the cycle, need to start at school, including biology.
-
-
Education programmes in schools have now had funding reduced.
-
In social media, contraception is not visible
-
In films, etc., no contraception in sex scenes
-
Message should be aimed at younger ones, but watershed prevents.
-
-
That services are not integrated was perceived as a major problem.
What are the differences in motivating factors between repeat teenage pregnancies and first pregnancies?
-
Partner (first baby) often goes off, but they meet another partner and they want to give this partner a baby.
-
The effect and influence of social media was discussed [Facebook (www.facebook.com), etc.] on ways of meeting new people and the casualness of relationships.
-
Girls generally have low expectations of life.
-
They want to give new partner a baby and perceive this as a way of keeping him.
-
The midwives and health workers did not agree that there is a financial motivation to having another pregnancy as they do not get enough to make this a factor.
-
If their first pregnancy resulted in termination, stillbirth or the child was taken into care, they want to replace a baby and also to know they can conceive again. These young women do not receive any bereavement counselling.
-
The girls enjoy having more professional input/attention (although some do not like the ‘interference’)
-
However, the rapport with services (during first pregnancy and immediately after birth) then ends.
-
They feel special during the pregnancy and they get attention, which they enjoy.
-
It can bring a friendship group (with others in the same situation).
-
It gives them a sort of status.
-
Therefore, they want another pregnancy.
-
-
They think it’s easy having a baby (this is when the child is very young and sleeps a lot, etc.) so why not have another?
-
Some also see the sense in completing their family now rather than later.
-
For many of these girls, it is the ‘norm’; their mothers had lots of children, so that’s normal.
Which intervention components best address factors that motivate young women to have (or not to avoid having) a repeat pregnancy?
The group gave suggestions of elements that might help:
-
Sexual health education, of teachers too. The participants felt it is very important to break down barriers and make sex and contraception an open subject/normal/accessible. This should start with young children.
-
We should pay attention to literacy and realise that many of these girls cannot necessarily read a leaflet.
-
We should use social media/Facebook, etc. to engage in promoting contraception.
-
There are condom schemes but it is very difficult to get boys to go in. Usually mothers or girlfriends go with.
-
There are dads groups but the young men usually come with girlfriend.
-
When asked ‘what makes you a man?’ They reply: ‘having a baby, especially a girl’.
-
Girls expected to solve the problem.
-
We need to empower girls; give them confidence and buddy/peer support.
-
Sexual exploitation can be a problem: older men targeting vulnerable, looked-after children.
-
The girls are not worried about STDs; pregnancy is more of a worry.
-
Problems
-
parents not educated, and do not know/care what kids are doing.
-
Group 3 feedback
What are the barriers and facilitators to accessing interventions?
-
Considering emphasis on access to interventions.
-
Schemes that involve home visits are likely to be more successful than involving people getting to clinics and using public transport.
-
Knowledge of services helps, but internet medium may not be the best way of advertising this.
-
Comment from Nefyn Williams:
As part of QOF all women and girls who receive contraception care should receive advice about LARCs. Some but by no means all GPs are able to provide this in terms of contraceptive implants and IUCDs. When these are provided in primary care, this avoids delay in referral and waiting for secondary care provision. They are also provided in a more familiar community setting.
-
Are we looking at barriers for different risk groups, or are we looking at barriers that effect all children?
-
Who drives the social norms? Peers, community, parents? Wider? It’s the community because it relates to educational attainment, it lends to aspiration, and the whole package that goes together, as well as lifestyle issues.
-
Social norms were discussed in two ways. The first related to considering pregnancy as a possible positive choice. The second related to social norms and acceptability to different methods of contraception. There was a mention of some resistance to using LARC implants because peers, friends, etc., call them ‘SlagTags’.
-
Different issues in terms of a first pregnancy as compared with a second pregnancy relate to pressures of caring for the little ones, and life being more chaotic generally so problems to make time to go and make the appointment for contraception.
-
Age differences of mothers; 13 year old would make different choices from a 19 year old.
-
Loss of pregnancy and having another pregnancy to fill that loss and having the support available for that loss and the decision she makes.
-
Long-term consequences are not a powerful motivator.
What is the best ways of packaging and presenting interventions to teenage mothers to ensure maximum take-up? (such as pregnancy spacing, making health choices using contraception effectively, planning your future and others)
-
Talking about it, more in school, early age, talking about relationships.
-
Personal social education.
-
Teachers, experts into schools, young mums to young mums. In-school education more relevant in first pregnancy.
-
Childcare to support young mothers going back into education should be more supported and facilitated.
-
Drama, role playing but not preaching to them.
-
Making all contacts count using motivational interviewing techniques; a repeated message, by different services, GP, midwife, health visitors, childcare.
-
Access to information, support and contraception.
-
Consider that the more support the young mothers have, the more they do not have to deal with the consequences of their decisions. If they have a good support network, the pressure of having a baby is reduced.
How is the success of a programme best measured in monetary terms?
-
Participants found this a difficult question because cost of service and cost benefits need to be measured against the costs of bringing a child into the world; it’s a moral question.
-
LARCs have significant costs, but if you consider the long-term costs, they are cheap.
-
A child from these adolescent mothers may be involved in a deprivation cycle, so may be a victim of child abuse or have more disabilities, etc., but we have to take care as that may be a form of eugenics at play, for example preventing pregnancies where the child may have a disability. Is it right to prevent a birth if we think they will not be in a good socioeconomic status?
-
We ought to record delaying as an outcome measure.
-
How is the success of a programme measured? Delaying? In terms of costing? Does this mean that a mother has re-entered society and joined the work force?
-
Or would we define success as contribution to society, uptake of LARCs or achievements like exam results or training programmes. Those stats, as well pregnancy ones, need to go side by side.
Our final questions to the stakeholders
What is important, what should we know, key issues, things to consider and comments
-
Proper sex education and services, there should be services specific for the vulnerable (looked-after children, substance misuse, victims of violence). Basic services are not good enough.
-
Outreach, that is bringing the intervention to a person’s home. Midwives are trained to deliver the contraceptive injection but not to fit the implant or coils. This is something that could have a great impact if midwives were trained and able to provide all methods of contraception at a home visit.
-
To have implant or coils, girls have to be referred to GP and fall through the net.
-
Outreach was the icing on the cake. First there is a need for a flood of LARCs in the population for those who have fewer barriers to accessing services. For those who find accessing services difficult, then there is a need for outreach.
-
These would be great but sexual health is viewed as a ‘Cinderella service’, with a lack of funding in general.
-
There is a serious lack of education in schools. Vulnerable students often have high levels of absenteeism or if they are in attendance but are disruptive then they are often removed when guest speakers come in to give sex education classes.
-
There is often an issue of literacy when providing sexual health information, leaflets are often not good enough.
-
Key Stage 4 should be the key stage to target these sexual health messages. Unfortunately, a lot of kids are disruptive and removed from sexual health lessons.
-
Teenage girls are vulnerable.
-
There is a lack of services and service availability (services thin and patchy).
-
The importance of financial concerns, particularly assessing services. Anecdotal evidence from Swansea was presented explaining that women from Swansea were expected to travel to Bridgend for emergency contraception.
-
The problem of no money or capacity to put intentions into action. Women were expected to pay £4.10 for a bus ticket to travel to clinics for appointments to discuss and receive contraception. For some of these women who receive only Income Support, this equates to 10% of their income.
-
Early involvement with social services is important.
-
The girls are mostly looked-after children, young and homeless.
-
Wales is considered a poor country compared with other UK countries, and has the highest looked-after children rate, low education attainment rates and many deprived areas.
-
Increased self-esteem, life skills and empowerment of girls is important.
-
Girls live a chaotic lifestyle and do not have the capacity to be organised.
-
Termination rates are not counted but they might give an indication of the number of repeat pregnancies that are not wanted.
-
Interventions are driven by the desire to get the number of low-birthweight babies down.
-
We should look at NICE guidelines.
-
Sex under 16 years old not perceived as a problem; it is illegal. Occasionally, a girl will make a complaint.
-
This is about delaying a second pregnancy – not preventing it; maybe to motivate – what is best for my baby is delaying second pregnancy.
-
Need to empower the girls to make choices – message to be given by all services consistently.
-
Messages to be given as early as possible (before birth of first child).
-
Higher rate of lower birth rate in second pregnancies and more stillbirths and defects which relates directly to cost of services.
-
What are the motivations for services to put money/time into these services?
-
Young people have different perception of risk.
-
In terms of research, very young girls would not have been interviewed (evidence gap).
-
Educate about relationships (not just sex)
-
The Netherlands has early personal and social education with open cultural discussions which normalises relationship discussions.
-
Outcome should be: future, timely, intended appropriate pregnancy.
-
Promising interventions might be:
-
young mothers coming into schools to talk
-
bereavement counselling for mothers who have terminations, abortions, stillbirths or child taken into care
-
selling it to young mothers: ‘doing the best for your baby’; for example, getting more education will help give your child a better life.
-
-
The review focuses so much on girls, where are the interventions for boys? The point is just not stable relationships, since the responsibility just falls on the teenage mother, but should also lie on the male and consider the legality of the sexual behaviour.
-
Sometimes the aim of an intervention can be contradictory. Parenting skills and praise during pregnancy and early years may be the only time where a teenage mother has felt as though she is good at something, this could have a knock-on effect that the girl feels that the only she is good at is being mother which could lead to repeat pregnancies – the exact thing the intervention is trying to prevent.
List of attendees
| Name | Organisation | |
|---|---|---|
| Sarah Andrews | PHW | Sarah.Andrews2@wales.nhs.uk |
| Rabeea’h Aslam | NWORTH, BU | r.w.aslam@bangor.ac.uk |
| Andrew Booth | Sheffield University | A.Booth@sheffield.ac.uk |
| Ben Carter | Cardiff University | carterbr@cardiff.ac.uk |
| Joanna Charles | CHEME, BU | j.charles@bangor.ac.uk |
| Helen Davies | Barnardo’s | helen.davies@barnardos.org.uk |
| Yvonne Harding | BCUHB | YVONNE.HARDING@wales.nhs.uk |
| Maggie Hendry | NWCPCR, BU | m.hendry@bangor.ac.uk |
| Ceri Jones | Action for Children | Ceri.Jones@actionforchildren.org.uk |
| Louise Massey | BCUHB | Louise.Massey@wales.nhs.uk |
| Christine Mcknight | Aneurin Bevan Health Board | Christine.Mcknight@wales.nhs.uk |
| Julie Morgan | Midwife | Julie.morgan13@wales.nhs.uk |
| Jane Noyes | Health Care Sciences, BU | Jane.noyes@bangor.ac.uk |
| Diana Pasterfield | NWCPCR, BU | d.pasterfield@bangor.ac.uk |
| Sally Roberts | ABM ULHB/Midwife | Sally.Roberts3@wales.nhs.uk |
| Jane Shakespeare | BCUHB | Jane.Shakespeare@wales.nhs.uk |
| Jacqui Slee | Health visitor | Jacqui.slee@wales.nhs.uk |
| Sara Thomas | PHW | Sara.Thomas4@wales.nhs.uk |
| Hayley Todd | Health visitor | Hayley.todd@wales.nhs.uk |
| Rhiannon Tudor-Edwards | CHEME, BU | r.t.edwards@bangor.ac.uk |
| Rhiannon Whitaker | NWORTH, BU | r.whitaker@bangor.ac.uk |
| Nefyn Williams | NWCPCR/NWORTH, BU | Nefyn.williams@bangor.ac.uk |
| Bridget Osborne | GP | brosborne@doctors.org.uk |
| Rhian Rouse | Barnardo’s | Rhian.rouse@barnardos.org.uk |
Appendix 3 Report of the stakeholder meeting (Hayden Ellis Building, Cardiff)
INTERUPT Stakeholder Consultation Meeting (as part of Task and Finish Group Meeting, PHW) – 3 June 2014
Agenda
Introduction, background and study update
Rhiannon Whittaker (chief investigator) thanked the Task and Finish Group for facilitating this meeting with stakeholders and thanked everyone for attending. She gave an overview of the objectives of the session and added that comments and questions would be requested at each stage of the meeting. These would be noted and circulated to all later with the report of the meeting and with a request for comments on accuracy or omissions. Following the presentations, the team had some questions to pose to stakeholders.
Overview of study methods
Maggie Hendry (lead reviewer) explained the research brief and outlined the mixed-methods approach to the study with a brief outline of systematic review methodology. Summary of review methods:
-
Phase 1
-
literature searches, inclusion/exclusion, quality appraisal and mapping exercise
-
consideration of mapping exercise and consultation with advisory group and stakeholders.
-
-
Phase 2
-
selection of records for in-depth review and data extraction.
-
-
Phase 3
-
synthesis of evidence according to type using design appropriate tools.
-
-
Phase 4
-
overarching narrative synthesis and interpretation.
-
The results presented at this meeting are the Phase 3 results.
Overview of mapping exercise and final numbers of included studies
Rabeea’h Aslam (INTERUPT project manager and systematic reviewer) gave an overview of the mapping exercise and explained how papers were sifted using CART criteria to achieve the final number of included studies. Details of intervention types identified and outcomes measured were given.
A total of 118 studies were identified for the mapping exercise. Through the process of discussion and development of the CART criteria, the team culled the final number of papers to 12 RCTs, 10 qualitative studies and 49 non-randomised observational studies.
Components for complex interventions:
-
pregnancy testing and maternity counselling
-
adoption counselling and referral services
-
primary and preventative health-care services (including prenatal and postnatal care)
-
nutrition information and counselling
-
referral for screening and treatment of sexually transmitted infections, including HIV/AIDS
-
referral to appropriate paediatric care
-
educational services related to family life and problems associated with adolescent premarital sexual relations
-
appropriate educational and vocational services
-
mental health services
-
counselling and referral for family planning services
-
job skills training
-
tutoring
-
mentoring
-
addressing domestic violence and peer-relationships
-
supportive counselling and social work services.
Outcomes measured
Primary outcomes:
-
identification of at-risk group
-
identification of barriers to and facilitators of interventions relating to acceptability, uptake and feasibility of implementation
-
views and experiences of young women, families and professionals.
Other outcomes:
-
identification of, access to and uptake of reproductive services and social care
-
feasibility of widespread adoption of interventions in health and social care
-
cost of interventions
-
effectiveness of interventions
-
change in validated quality of life indices
-
change in rate of abortion
-
-
cost-effectiveness of interventions.
There was discussion about the appropriateness of the use of the word ‘unintended’ in this review. It was agreed that a large part of repeat pregnancies were not unintended and that it is difficult to establish a definition of ‘intent’.
Overview of quantitative data synthesis
Ben Carter (statistician) gave an overview.
The interventions considered were:
-
control group (usual care or usual experience)
-
counselling (home visit, community, telephone or in person)
-
contraception.
The primary outcomes considered were:
-
acceptability of interventions
-
proportion of participants who reported that the intervention was acceptable or, in the absence of this, the proportion of participants who were willing to be recruited into the study.
-
-
effectiveness of interventions
-
proportion of unintended repeat teenage pregnancies.
-
-
uptake of the interventions
-
proportion of participants who were recruited and allocated to the intervention, compared with those recruited.
-
Summary of findings
It was noted that the evidence showed some effectiveness of interventions vs. usual care. Stakeholders were keen to have more information about the context and details of interventions.
Stakeholders debated the use of the word ‘counselling’ as an overarching term. For this group, it meant educational interventions. They wanted to know if there could be a different division of studies since that would have policy and funding implications.
Stakeholders wondered about teenage mums’ motivation to receive or not receive the additional element (counselling or whatever).
Stakeholders wondered how participants were recruited into the studies.
Stakeholders wondered how we tease out ‘unintended’ in quantitative studies.
Phase 3: qualitative results
Maggie Hendry (lead reviewer) presented the qualitative results from the study.
We included nine studies, published between 1998 and 2012, seven of which were conducted in the USA, one in the UK and one in the UK and the Caribbean. Participants in the US studies were predominantly African American or Hispanic, UK participants were of mixed ethnicity, but all were in London. Only one study addressed an intervention (the Pregnancy Free Club). 136
Three main themes were identified:
-
‘Attitudes towards repeat pregnancy’, which included lifestyle and aspirations, no planning or consideration of consequences, teenage pregnancy being the norm for some, whereas some had education or career aspirations, but had problems achieving them. Others did not want to conform to stereotypes and wanted to do the best for themselves and their children. It also included rationales for repeat pregnancy which included reverse life-course rationalisation (completing their family before moving on), partners’ desire to have a baby and that it might make them stay with them, or replacing a loss (after stillbirth, abortion or a child being taken into care).
-
‘Barriers and facilitators to effective postpartum contraceptive use’ relating to knowledge, information and misinformation (lack of knowledge about contraception and understanding of fertility, misconceptions about side effects of contraceptives, experience of side effects prompting method change or discontinuation with potential for gaps in protection, partners’ influence – positive and negative), access and continuity of care (timely contraceptive counselling together with supply of the preferred method was ideal; there were perceived barriers, such as restrictive clinic hours and requirement for a referral letter).
-
‘Abortion and repeat abortion’ which included negative attitudes towards abortion (viewed from a moral stance and negative attitudes reinforced in school), influences on the abortion choice (partners, parents, peers community and lack of knowledge and misinformation and horror stories and fears for future fertility) and the need for pre- and post-abortion support and that services were patchy.
Summary of qualitative results
There is a need for:
-
more information and less misinformation
-
better sex and relationships education in schools
-
education about abortion not framed as a moral issue
-
more timely and more joined up services
-
better provision of emergency contraception.
However, the qualitative results also suggest that:
-
repeat pregnancies are mainly intended or semi-intended
-
there is no distinction between subgroups
-
there is little or no overlap with other issues, such as those associated with care leavers, victims of abuse, alcohol or substance abuse, gang culture, etc.
The team welcomed questions and comments from delegates to help the team present the review to enhance its usefulness to stakeholders.
Stakeholders agreed with the findings that there was no planning or consideration of consequences and that for some teenage pregnancy was the norm.
They agreed that some had educational or career aspirations, but that most of the girls they dealt with had already disengaged with school and that there were problems to stay in school.
Stakeholders did not comment on findings concerning partner influence, reverse life-course rationalisation or replacing a loss as a rationale for repeat pregnancy.
Stakeholders very much agreed with and stressed the importance of the findings about lack of knowledge about contraception and understanding of fertility; this was also poor among health-care professionals! It is important to understand ovulatory cycles.
Stakeholders endorsed the findings regarding the fear of side effects and said that girls did not compare the risks of contraception (possible side effects) with the risks of pregnancy (i.e. health risks).
A lot depends on how information is delivered.
Stakeholders thought timely contraceptive counselling (critical 2 weeks after birth or abortion) were very important and at the core of what needs to be done.
There was discussion relating to the finding reported that one girl was pleased to have asked for the pill and been given it straight away. It was felt that it was necessary to have discussion and health checks before prescribing it, while recognising that any delay (i.e. requesting the girl to come to second or third appointment) can result in the girl not returning and remaining unprotected.
Not all GPs are able to do implants and there is considerable time pressure on GPs. It was suggested that perhaps practice nurses could be trained to do this.
Assessing the needs and targeting education and training of health-care professionals was considered a priority (and generally those who interface with the teenagers).
Generally the findings about concerns about accessibility of services for girls were considered relevant.
Stakeholders agreed it is important to give good (neutral) information about abortion. Where schools do not allow information about abortion to be given, stakeholders direct girls to reliable sources of information.
Post-abortion counselling is variable in quality and amount given. This needs to be addressed.
Emergency contraception was discussed. It is available at pharmacies, clinics, etc. Although it is legal (according to a doctor present) to prescribe emergency contraception for people to have at home, concern was expressed that girls would use this as an alternative to regular contraception.
Misinformation and misunderstandings and fears about future fertility post abortion was considered highly relevant to repeat pregnancies.
It was agreed that services can be patchy and that this needs to be addressed.
Stakeholders agreed with the summary of qualitative findings with the exception of the needs for ‘better sex and relationships education in schools’. They did not feel that the evidence reflected this.
As stated earlier, girls have often disengaged with schools. One stakeholder mentioned a European paper regarding the delivery of this information in the home, working with the parents.
Some stakeholders reported that they had tried to form parent groups at schools, but the parents simply did not turn up.
Teenage pregnancy correlates with education (rather than sex education).
Service user feedback and overview of realist synthesis methods and preliminary findings
Rabeea’h Aslam presented details of our service user feedback session.
A meeting was facilitated by Flying Start, Barnardo’s and Swansea Young Families with a group of 17 young mothers aged 15–22 years. We sought their opinions on the following issues.
Contraception
The young mothers find LARCs useful because they have trouble remembering to take the pill, they thought sterilisation should be available as an option and they liked to have the availability of emergency contraception.
Complex interventions
The young mothers agreed that in group interventions they would not feel alone, but one-to-one would be more personal and they would be able to say things they cannot in a group. They would rather speak to their Teen Start case worker, as they found health-care professionals judgemental. The young mothers favoured the idea of home visits. For those seeking to continue education, postnatal and prenatal care needs to include crèche facilities and interventions need to occur at school.
Barriers to and facilitators of uptake of interventions
Barriers included difficulty in accessing services, absence of open sexual discourse, absence of supportive relationships and societal and familial pressures.
Facilitators included care providers addressing multiple needs of young mothers, positive perceptions of different contraceptives, and services and incentives
Findings reported from service user feedback resonated with the stakeholders.
It was commented that, regarding sterilisation, it may be offered to someone over 30 years old with two or more children, but there are no legal limitations and the cut-off point of six children was an example of misinformation.
Emergency contraception has already been discussed above.
The girls’ perception of ‘being judged’ was discussed. Stakeholders felt that the fact that girls were in fact also ‘judging themselves’ should be taken into account.
Stakeholders also commented that remarks such as the midwife had called a girl ‘a bad mother’ may be misreported and a reflection of a perceived criticism.
Stakeholders agreed with the summary of barriers and facilitators.
There was a discussion about SRE. Stakeholders seemed to agree that conversations about sex needed to occur much sooner, since young mothers tend to drop out of school before these classes, or pastoral care, are offered.
Overview of realist theory areas
Rabeea’h Aslam also presented an overview of realist synthesis methods and some preliminary findings. Realist review has developed from the philosophical traditions of critical realism, which question and address the perceived or assumed interrelationship between science, knowledge and reality. The realist research question is often summarised as ‘What works for whom, under what circumstances, how and why?’. The evidence mind map was presented. Preliminary middle-range theories are:
-
motivation (reasons for getting pregnant)
-
the government’s view of teenage pregnancy
-
economic factors
-
family situation
-
question of unintended, unplanned, unwanted versus ambivalence.
-
-
connectedness
-
to peer group
-
to family
-
to school
-
to the intervention itself
-
to the person delivering the intervention
-
mentorship
-
personal care.
-
-
targeting
-
tailoring (including who delivers the intervention)
-
timing of the intervention
-
nature of the intervention
-
person focused rather than programme focused
-
collaborative decision-making.
-
-
setting/environment
-
stigma
-
‘norms’ (societal and family)
-
partner influence
-
education setting
-
intervention setting.
-
Regarding tailoring, stakeholders felt that interventions need to be tailored to the individual according to circumstances at the time – girls complain that they are not listened to by professionals.
We really need to find out what they really need and want and understand what they are asking for – there is too much generalisation, and perceptions of what girls want are not accurate.
INTERUPT team questions to stakeholders
What do these findings mean to you within your work context?
Responsible professionals should be more responsive and reactive (particularly with reference to primary care).
Lack of information and incidence of misinformation is a big problem which needs urgently addressing.
Who do you think should hear these findings?
Policy-makers in the Assembly:
-
Comments were made that people at the delivery end are aware of the problems but no-one takes ownership of sexual health and that unless something lands on the Chief Executive’s desk from on high, then nothing gets done.
Commissioners.
Royal College of General Practitioners.
Professional educationalists (those who plan at Key Stage 2).
Should form part of the National Health Delivery Plan.
Anna Soubry, MP, who has a special interest in underage pregnancy.
Faculty of family planning and reproductive health.
Royal College of Obstetricians and Gynaecologists.
How do you think these findings should be delivered to these audiences to maximise uptake?
Target (relevant) government minister and/or department.
Participants mentioned talking to Welsh Assembly Government, different divisions.
Is there a policy message?
Underage pregnancy is still a huge problem which feeds into societal deprivation at every level.
It is extremely important that there is well-funded and organised research into that will work rather than spending money on initiatives with no idea of whether or not they might work: there is no evidence for interventions being implemented.
Evaluation of projects is essential, and this is not happening in spite of funding offers to do so. Which outcomes are valuable needs to be more carefully examined.
Sustaining short-term projects is unethical as money is given to one project, and then not to another.
We are letting young people down by allowing them to be ill-informed. This is the responsibility of the services. (This especially related to the fact the young people are ignorant about fertility.)
The timing of any educational messages in schools should be considered (while the girls still ‘trust’ their teachers).
Various ways of information provision should be researched. There is a lack of evidence of how it should/could be provided.
As mentioned above, stakeholders would emphasise that professionals need to listen to girls and understand what they are asking for. There is a need to design a way of eliciting the right information quickly through a few key questions.
Do these findings make sense to you?
The evidence presented regarding lack of information and misinformation was very relevant to stakeholders’ experiences. Lack of knowledge and understanding about fertility was very familiar to stakeholders’ experiences. The importance of educating health-care professionals is vital so they pass on good and comprehensible information.
Stakeholders agreed that the word ‘unintended’ is poorly defined.
Problems with access and continuity of care also resonated with stakeholders’ experiences.
Caution was advocated that findings should be totally evidence based and not interpretations.
How similar are they to the interventions you are delivering locally?
Lots of projects do not survive the short-term funding.
Stakeholders said they knew certain interventions work, but then they end up being offered to one teenager and not another, which raises ethical issues.
List of attendees
| Name | Organisation | Role | |
|---|---|---|---|
| Sarah Andrews | PHW | Sarah.Andrews2@wales.nhs.uk | Principal in public health |
| Jean Beard | ABM ULHB | Jean.Beard@wales.nhs.uk | Lead nurse manager |
| Zoe Couzens | PHW | Zoe.couzens@wales.nhs.uk | Health protection specialist |
| Angela Jones | Cwm Taf Public Health Team | Angela.jones26@wales.nhs.uk | Consultant in public health |
| Rebecca Lewis | Cardiff and Vale Public Health Team | Rebecca.lewis2@wales.nhs.uk | Senior health promotion specialist |
| Louise Massey | BCUHB | Louise.Massey@wales.nhs.uk | |
| Christine McNight | ABUHB | Christine.mcnight@wales.nhs.uk | Sexual health outreach worker |
| Bridget Osborne | RCGP Wales | brosborne@doctors.org.uk | GP |
| Sally Roberts | ABM ULHB | Sally.Roberts3@wales.nhs.uk | Flying Start/Teen Start midwife |
| Annette Schaudraff | Cardiff and Vale Public Health Team | Annette.schlaudraff@wales.nhs.uk | Consultant in sexual and reproductive health |
| Jane Shakespeare | BCUHB | Jane.Shakespeare@wales.nhs.uk | Specialist nurse, children and young people |
| Claire Thompson | ABM Public Health Team | Claire.thompson@wales.nhs.uk | Health promotion specialist |
| Hayley Todd | Communities First | Hayley.todd@wales.nhs.uk | Teen Start, nursery nurse |
| INTERUPT TEAM | |||
| Noel Craine | PHW | noel.craine@wales.nhs.uk | |
| Rhiannon Whitaker | NWORTH, BU | r.whitaker@bangor.ac.uk | |
| Ben Carter | Cardiff University | carterbr@cardiff.ac.uk | |
| Maggie Hendry | NWCPCR, BU | m.hendry@bangor.ac.uk | |
| Rabeea’h Aslam | NWORTH, BU | r.w.aslam@bangor.ac.uk | |
| Diana Pasterfield | NWCPCR, BU | d.pasterfield@bangor.ac.uk | |
Appendix 4 INTERUPT service user meeting (Swansea)
Meeting time: 1 hour 30 min; 12:15–14:30
Introduction to the project (5 minutes)
Ask permission for recording
Aim
Hello everyone, I hope you’re comfortable. Are from Bangor University.
We are working on a research project with Bangor University. Our research looks into different things that can assist young mothers make their own choices relating to themselves, their children and their lives. This research which will help inform services for young mothers. This where you as our expert consultants come in. We want to know what you think of our findings. Because at the end of the day, the services are and should be about you. We are very grateful that you have agreed to take time out and come meet with us. We will give you a certificate in the end for participation. This certificate will be useful when applying for different jobs, or courses. We also bought Tesco vouchers as a thank you as well. There are also some chocolates in the middle of the table.
Exercise
Quick exercise with flipchart, so we can establish ground rules like respect, not talking over one another, etc., be respectful to any other persons point of view give them the opportunity to finish. If they don’t like something, they’re allowed to say it. Cell phones silent. Allowed to pass.
Icebreaker (10 minutes)
Outline of conversation and exercise
Go around the room and ask everyone to introduce themselves, and then either of the below: tell us their favourite TV show or ‘something (interesting?) about yourself’.
Views on contraception
Outline of conversation
According to our review findings, if they use contraception consistently, it reduces multiple pregnancies.
-
Authors suggest wide usage of LARCs such as injection or implants in young mums. The reason they give is say that the possibility of forgetting to take the pill is increased in this age group (13–19 years). What do you think of this finding?
-
Researchers argue that pills are not a good method because it requires daily compliance and young mums fear weight gain and other side effects. What do you think of this finding?
-
Advanced supply of emergency contraception emergency contraception should be provided with primary contraception. Y/N
-
Let’s we think about the argument that increasing access to emergency contraception means that young mums use emergency contraception as a primary contraceptive method.
Exercise
Picture of each contraceptive methods on a flipchart, with space to jot down summary points keywords, etc. We will lead them through the above statements, and work accordingly.
Views on complex intervention (20 minutes)
Contraception isn’t magic; there are other factors to supports decision-making in young mothers.
Main interventions (for research group, not young mothers) (2 minutes).
-
Mentorship by an older role model. What do you think of this finding?
-
Our review suggests that, peer support group with a central role model works best.
-
The reason people fear peer-support is that it can reinstates the same thought process. The positive of peer-support is that they have group to relate to who have has similar experiences, and are the same age. Role models in a peer group situation can provide guidance.
-
School. If they are looking to continue education, then postnatal and prenatal care needs to include crèche facilities and intervention needs occur at school.
-
Motivational interviewing with curriculum guided the young mum providing case management help with housing, day care, school, and health-care issues, and sought to help teenagers to learn skills to negotiate daily challenges from adverse personal circumstances (e.g. abusive relationships and drug trafficking within home).
-
Motivational interviewing guides teenagers
-
Time for interventions (how long?)
Exercise with young mums
Using the above seven points as guidance, we will use like and dislike votes (flash cards which have the Facebook sign of like and dislike) and then speak to them in easy language about those main interventions from our study.
Break (20 minutes)
Views on barriers and facilitators and risk factors (20–30 minutes)
Outline of conversation
We’ve talked about complex intervention, now what we want to know, what things support young mothers’ decisions or choices?
Exercise
Mid, Family, Services, Opportunities (thought boxes on flipcharts, and comments below) Access to services means, when do they access, do they have access, do they know about the services? What stops from accessing?
Sum up, opportunity for questions, comments, anonymous comments in the box/Twitter feed (10 minutes)
Close with certificates and gift vouchers of £10 for a well-known retail company (Tesco PLC, Cheshunt, UK)
Background
A group of 17 very interesting young mothers, aged from 15 to 22 years, attended the service user feedback group. This was the first of the two meetings planned.
The following groups helped us to organise and facilitate the meetings. (We are thankful for their patience with us.)
-
Flying Start
-
Barnardo’s
-
Swansea Young Families.
Based on the evidence generated, we sought their opinions on the following three areas:
-
views on contraception
-
views on complex intervention
-
views on barriers to and facilitators of the uptake of interventions.
Views on contraception
-
The use of LARCs, such as injections or implants, was particularly useful in young mums since the possibility of forgetting to take the pill was increased in the age group of 13–19 years. Most of the young mums agreed with this finding, saying that it was one appointment, and it was already taken care of for 3 years. Some cited fear of needles saying that they would ‘rather give birth again than have a needle’. The issue of weight gain and side effects, such as mood swings, depression and emotional instability, was also highlighted in a discussion of oral contraceptives such as the pill.
-
Although not reflected in the research, sterilisation was brought up as a viable intervention. The young mothers felt that it should be available as an option for young mothers, and the ‘cut-off’ point after six children should not be a strict requirement. This was a much debated topic. For example, one mother said ‘I’m 23 and I have six children, I know I do not want any more children’.
-
The availability of emergency contraception at the sexual health clinic, from doctors, over the counter or given to them at their next appointment with a health professional seemed to have firm support. The prime concern had been an overlap of the 72-hour requirement for emergency contraception with bank holidays or Christmas. They also stated hesitancy in asking for or acquiring the emergency contraception for fear of being judged.
Views on complex interventions
There are other factors which support decision-making in young mothers. This is where complex interventions come in, for which there is some conflicting evidence.
Our findings showed that mentorship in a group setting, rather than a one-on-one setting could be more effective. The young mothers agreed that in a group they can see everyone, they can hear everyone’s opinion, and said if ‘I feel something, I’m not alone’.
However, one-on-one interaction would be more personal, and they would be able to say things that they could not say in a group. If they had goals, aspirations or wanted advice, there were some things they thought they could not speak to a health visitor about. They would rather speak to their Teen Start case worker, instead of their midwives or health visitor. This was because they found both of these professionals to be very judgemental.
The young mothers favoured the idea of home visitation. This is because they needed assistance adjusting and negotiating with the various realities of motherhood. They did not realise the difficulties with their children, their sleeping patterns, etc. One young mother said that she expected that ‘. . . all I would have to do is change them in the morning, and change them in the evening, and they’ll sleep all night . . .’
The use of role models was also highlighted as a positive, whether they be from outside their group or peers who attended these groups previously.
Views on complex interventions continued
The young mothers also said that they had trouble dealing with tantrums and screaming. They agreed that someone coming to their house once or twice a month would be very helpful.
Who do you speak to when you’re going out of your mind?
She called me a bad mother because she was constipated when she went from breast feeding to normal milk.
They found there was a difference between the health visitor and a Teen Start visitor, and would prefer a person who was specialised in working with young mothers.
They also said many were seeking to continue education, then postnatal and prenatal care needs to include crèche facilities and intervention needs to occur at school. They would have liked support after a second child was born because it is hard each time.
Barriers and facilitators
The young mothers attending the group cited a number of factors that stop them accessing contraception or services, which were supported by the evidence base. Reasons given by the mothers included:
-
Some forms of contraception are available in only hospitals or clinics which they have difficulty accessing because of the distance of these venues and transport issues.
-
They felt stigma and judgement from ‘gate keepers’, such as receptionists, when trying to access services; common forms of judgement were looks, barbed comments and condescending tones of voice.
-
Appointments also needed to be arranged to fit in with mothers’ other commitments, such as dropping off and collecting their children from school.
FIGURE 16.
Barriers to effective and consistent contraceptive use.

The mothers cited the following facilitators as factors that would encourage them to access services:
-
Childcare and food being provided as part of the service, as this would be beneficial both for the mothers and the children.
-
Options of having interventions in schools or colleges so that mothers could continue education as this was important to some of them, but they had experienced limited choices in the past with colleges not allowing mothers to attend a course or offering only certain courses to mothers. An example was given from the group of a mother’s own experience:
-
I wanted to study fashion and textiles and I was told when she applied and enrolled at college that this would be possible; however, on her first day I was told that I couldn’t do textiles and fashion and could only enrol on a dance course . . . I had to be lifted as part of routines while I was 6 months pregnant, it was crazy and quite scary.
-
-
Flexibility of venues and times so the intervention fits in with a mother’s life and responsibilities, especially when they do not have childcare during group time.
The young mothers stated that they wanted positive discussions about contraception choices, with teen-centred groups who they could relate to and specially trained counsellors who had experience of working with teenagers, so they felt they were understood by the group leader.
FIGURE 17.
Facilitators and effective contraceptive use.
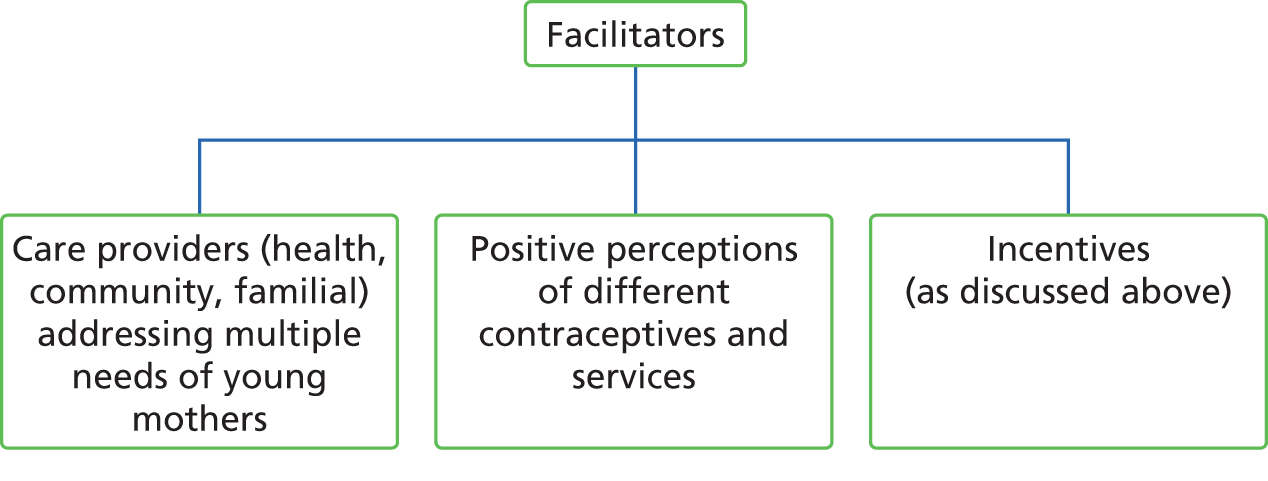
Appendix 5 Protocol for applying completeness, accuracy, relevance and timeliness criteria
INTERUPT
Phase 1 of the study was broad and inclusive; the aim was to identify, map and describe the full range of literature relating to repeat unintended teenage pregnancy. In Phase 2, we narrowed the review with the aim of focusing in depth on the data that best addresses the research questions to concentrate the available time and resources on the most relevant and fruitful areas. In order to achieve this narrowing, we were guided by our advisory group of experts, and adapted the CART criteria51 as a method for systematising the selection of studies for in-depth review. To be included, studies must meet all four criteria outlined in the following sections.
C: completeness
We will not include any reports in the in-depth review that are incomplete, that is:
-
those that, after exhaustive searches, only a partial record, such as an abstract or short report, can be obtained for
-
a report of an intervention where the components of the intervention are not fully described
-
a report of an evaluation that does not fully describe the methods used
-
a report that does not contain data that address the review question.
A: accuracy
Accuracy is generally assessed using quality appraisal criteria. Studies will not be excluded from in-depth review on the grounds of poor quality as long as they pass the screening questions of the MMAT,54 since further appraisal may be not feasible or appropriate when the answer is ‘no’ or ‘can’t tell’ to one or both of the following screening questions:
-
Are there clear qualitative and/or quantitative research questions (or objectives), or a clear mixed-methods question (or objective)?
-
Do the collected data allow the research question (or objective) to be addressed? For example, consider whether or not the follow-up period is long enough for the outcome to occur (for longitudinal studies or study components).
Studies that pass the screening questions and meet the criteria for completeness, relevance and timeliness will be included for in-depth review and undergo full quality appraisal, and the quality of studies will be addressed in the discussion.
R: relevance
Stakeholders agreed that, while there were some commonalities between study populations in different countries, contextual variations placed limitations on the applicability of their findings to UK settings. Therefore, we will limit the inclusion of non-UK studies in the in-depth review to those published in peer-reviewed journals. However, since published literature from the UK in this field is scarce, we will conduct additional targeted searches to identify grey literature, which we will include in the in-depth review if it meets the criteria for completeness, accuracy and timeliness.
T: timeliness
Stakeholders commented that, because of changes in social norms, behaviours, etc., studies should be reasonably up to date. Our cut-off date for literature searches was 1995; we will not include studies where data were collected before 1990.
Appendix 6 Effective Practice and Organisation of Care study design
Cochrane Effective Practice and Organisation of Care Group http://epoc.cochrane.org/
FIGURE 18.
Study designs for evaluating the effects of health-care interventions. (Shaded boxes are study designs that should be considered for inclusion in EPOC reviews).

Appendix 7 Mixed-methods appraisal tool
Appendix 8 Economic evaluation appraisal tool responses (Drummond et al., 2005)56
| Checklist question | Response |
|---|---|
| Was a well-defined question posed in an answerable form? | Yes, the analysis assessed the costs and effects of two interventions with usual care |
| Was a comprehensive description of the competing alternatives given? | The two interventions are well explained; however, no information given for usual care |
| Was the effectiveness of the programmes or services established? | Yes, this was established from a RCT (Barnet et al., 2009).82 However the quality of the RCT was queried using the MMAT |
| Were all the important and relevant costs and consequences for each alternative identified? | The cost per prevented birth was identified for each alternative in line with the research question, but no other costs were considered, such as patient, social and third party costs and consequences |
| Were costs and consequences measured accurately in appropriate physical units? | The costs and consequences were justified and appropriate for the research question and sourced from an associated RCT |
| Were costs and consequences valued credibly? | Costs and consequences were clearly identified, and appropriate for the research question |
| Were costs and consequences adjusted for differential timing? | Although repeat birth was defined as a subsequent birth within 24 months, no discount rate was reported in the paper |
| Was an incremental analysis of costs and consequences of alternatives performed? | ICERs were calculated by dividing the cost of the intervention by the number of repeated births between the two groups (I and C) |
| Was allowance made for uncertainty in the establishments of costs and consequences? | Further analyses were conducted based on a set of scenarios created for specific subpopulations of teenagers with respect to intervention group, age, insurance status and parity |
| Did the presentation and discussion of study results include all issues of concern to users? | Conclusions were based on the cost-effectiveness ratios calculated. The authors compared the results with other economic evaluations of teenage pregnancy prevention interventions, although the evidence base is constrained. The authors note the limited generalisability of their conclusion because of setting, population, geographical area and short follow-up period of 2 years. The authors compare the large costs of unwanted teenage pregnancy on the state, with the costs of prevention, stating the programme demonstrates good value for money in Maryland, USA |
Appendix 9 Correspondence with authors of primary research
E-mail from Dr Ben Carter to Dr Beth Barnet
From: Ben Carter [mailto:]
Sent: Monday, January 13, 2014 12:34 PM
To: Barnet, Beth
Subject: Motivational Intervention to reduce rapid subsequent births
Dear Dr Barnet
I am a statistician trying to carry out a systematic review of the effectiveness of interventions for reducing repeat teenage pregnancies. We have found your paper from our searches, but we have many outcomes, that I believe that your raw data could help us with. Is there any way that you could answer the following or send me the raw data so that I can address these outcomes.
I have attached our data extraction sheet so you can see what we are looking for. Many thanks for all your help.
Bw
Ben
E-mail from Dr Beth Barnet to Dr Ben Carter
Ben,
I am attaching some tables that may meet your needs (or maybe not). I don’t have the information that you are requesting readily available. We did this project a number of years ago and my statistician no longer works here.
Hopefully this is helpful to you.
Regards,
Beth
Beth Barnet, M.D.
Professor of Family and Community Medicine
University of Maryland School of Medicine
Dr Ben Carter
Lecturer in Medical Statistics
Institute of Primary Care & Public Health
Cardiff University School of Medicine
Neuadd Meirionnydd, Heath Park
Cardiff, CF14 4YS
E-mail from Kirstie Pye to Dr Cox
From: Kirstie Pye
Sent: 29 July 2014 15:50
To: xxx@childrens.harvard.edu
Subject: Article query – Evaluation of Raising Adolescent Families Together Program: A Medical Home for Adolescent Mothers and Their Children
Dear Dr Cox,
We are conducting a systematic review to find and evaluate interventions designed to reduce repeat unintended teen pregnancies. Your article ‘Evaluation of Raising Adolescent Families Together Program: A Medical Home for Adolescent Mothers and Their Children’ has come up in our search and I have a question concerning your study sample. Please could you clarify whether 181 or 183 mothers were enrolled in the program, as the results section states 181 were enrolled, yet table 1 refers to a sample size of 183. If 183 is the total sample size, please could you tell me the reason for the dropout of 2 participants?
Many thanks in advance,
Kirstie Pye
(No response received)
Appendix 10 GRADE profiles
Appendix 11 Judgement for risks of bias
Barnet et al., 200785
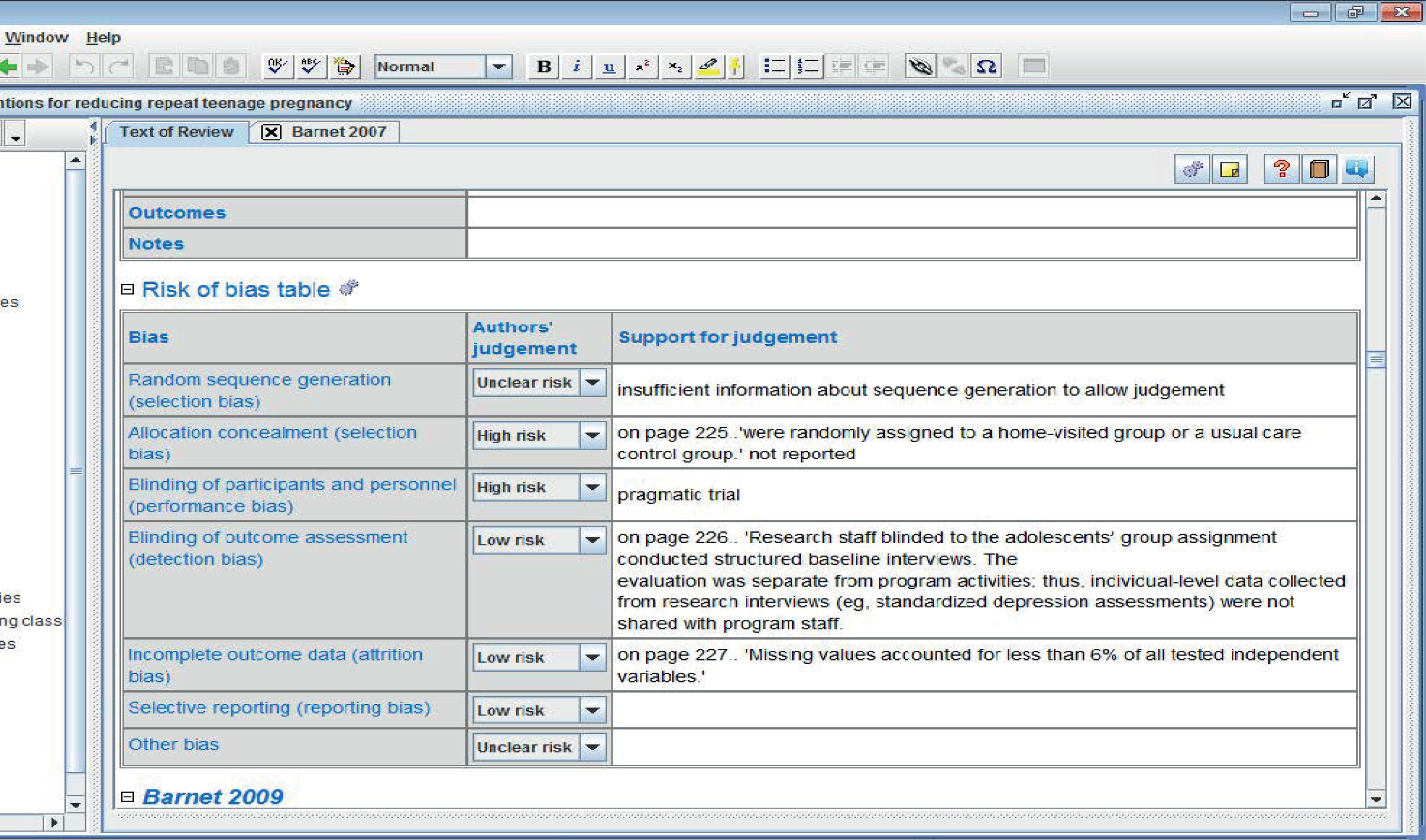
Barnet et al., 200992
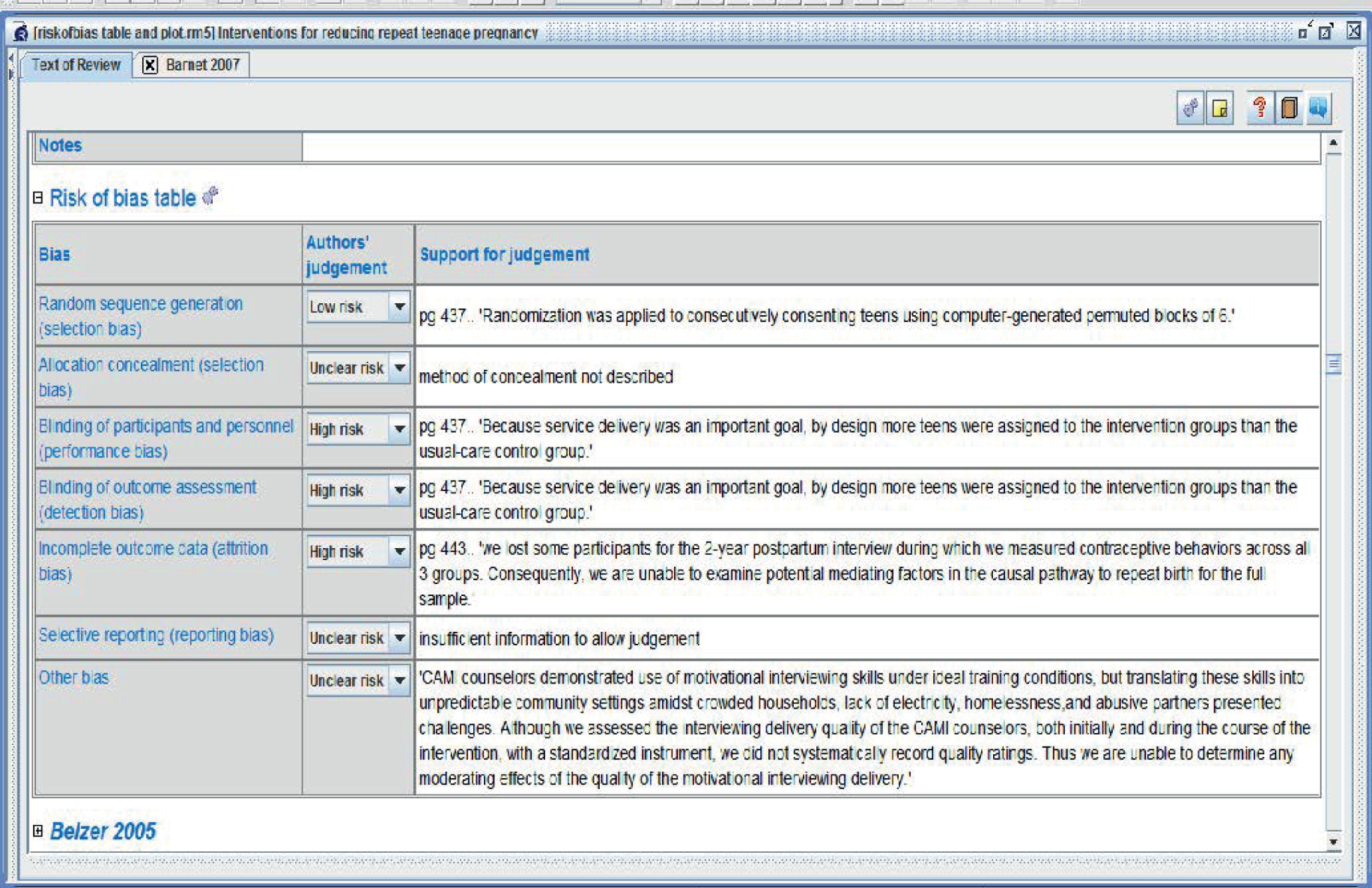
Belzer et al., 200587
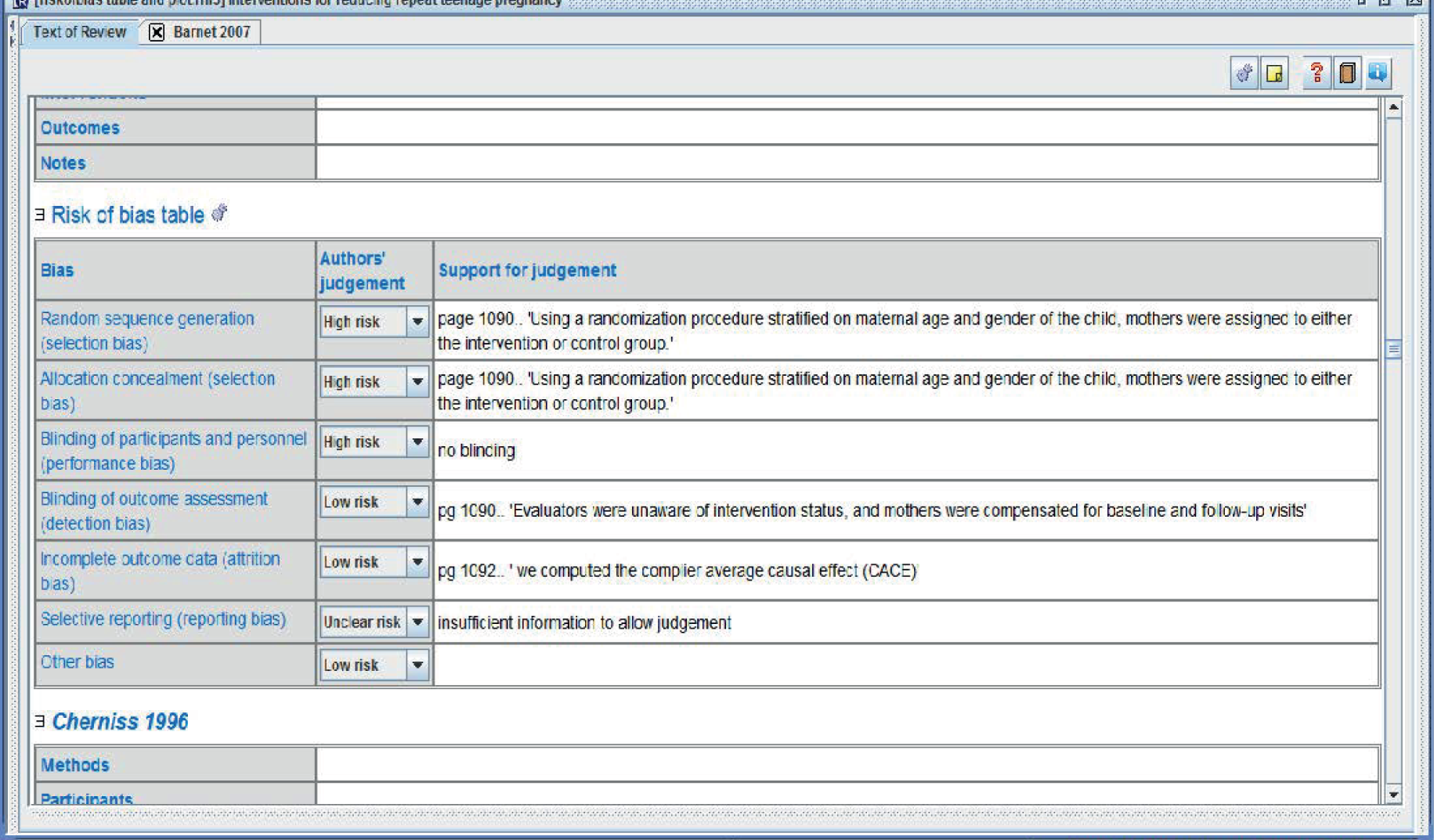
Cherniss and Herzog, 199680

Ford et al., 200288

Havens et al., 199789

Katz et al., 201190
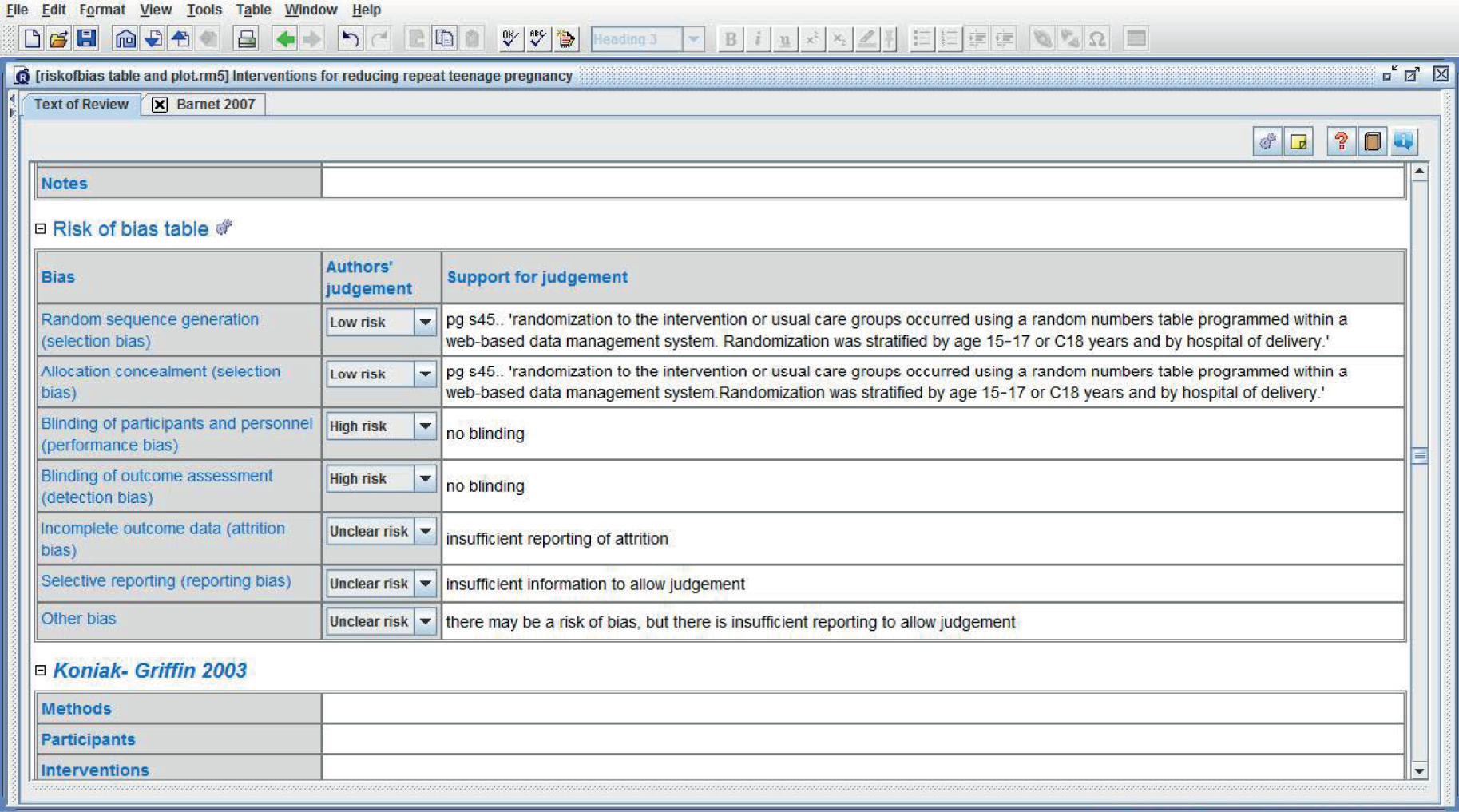
Koniak-Griffin et al., 200381

Quinlivan et al., 200379

Sims and Luster, 200291
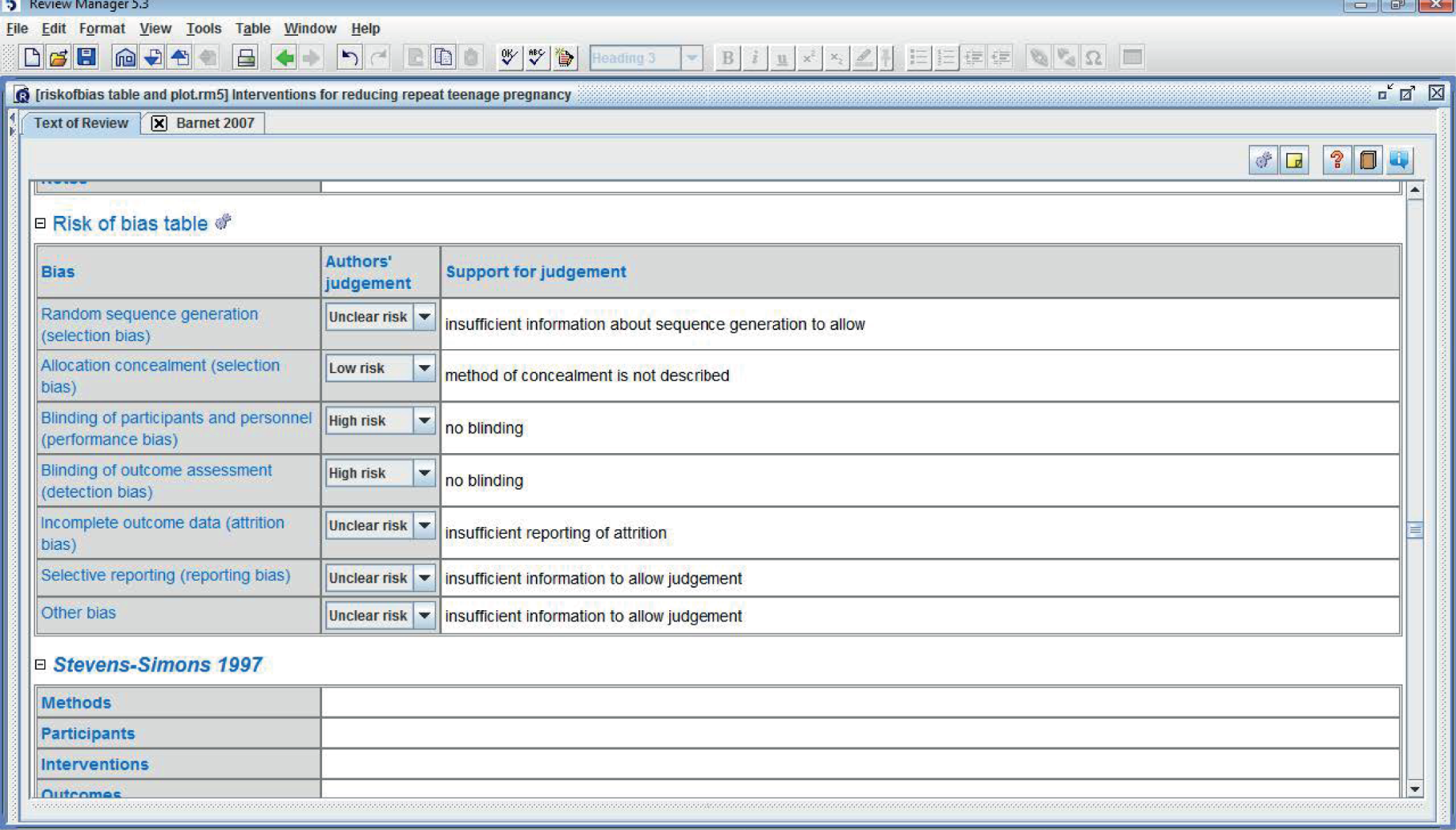
Stevens-Simons et al., 199792
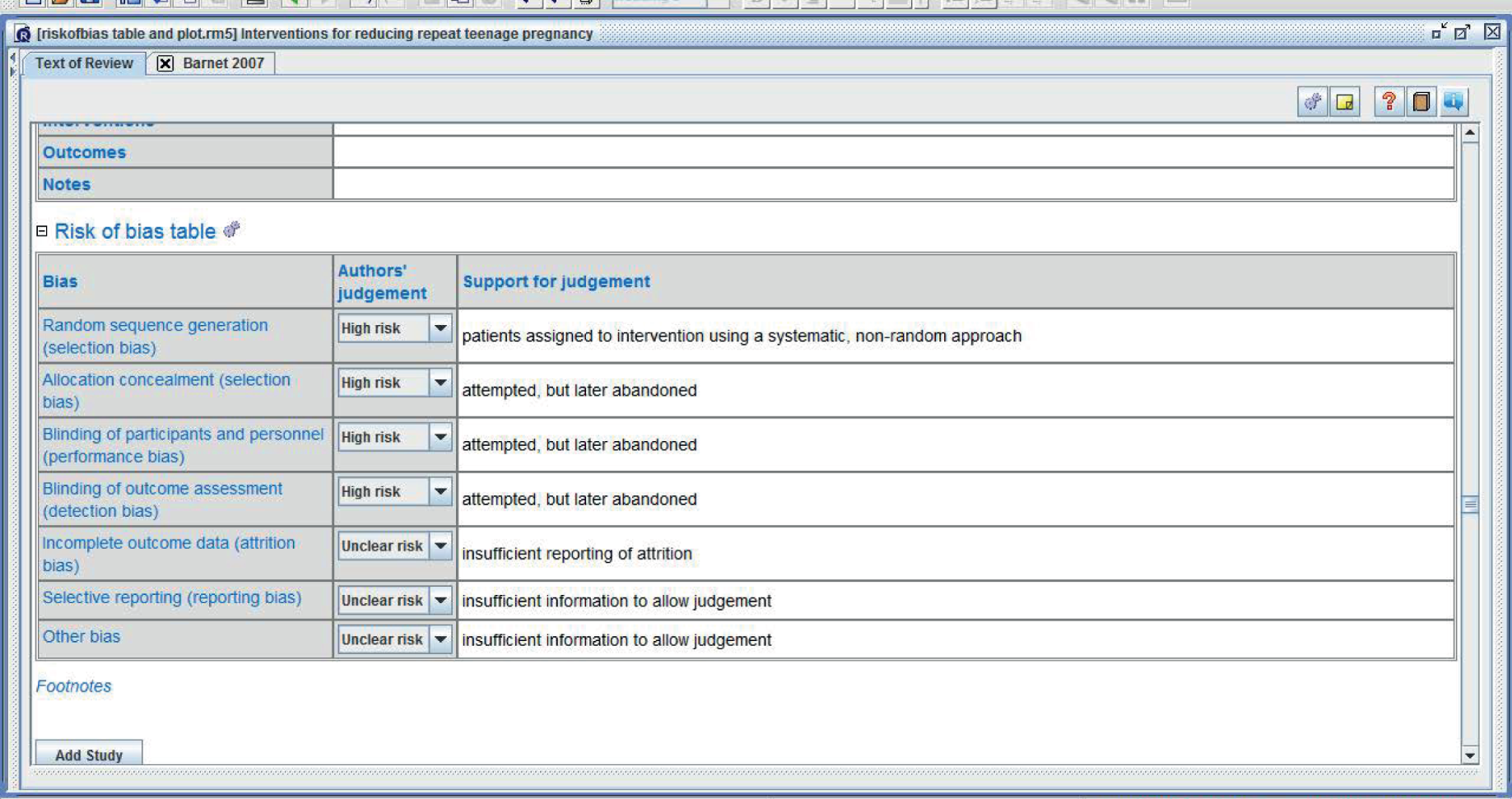
Appendix 12 Modified SURE framework67 for qualitative data extraction
Study name, year and ID number:______________________ Reviewers 1:________________________ Reviewer 2:_______________________
Part A Guidance
| Level | Barriers and enablers | Examples |
|---|---|---|
| Recipients of care | Knowledge and skills | Teenage mothers may have varying degrees of knowledge about sex, contraception, family planning services or support services or may not have the skills to know how to access services or use a contraceptive device correctly |
| Attitudes regarding intervention acceptability, appropriateness and credibility | Teenage mothers may have opinions about the intervention, including views about the acceptability and appropriateness of the intervention and the credibility of the provider | |
| Motivation to change or adopt new behaviour | Teenage mothers may have varying degrees of motivation to change behaviour or adopt new behaviours (i.e. to avoid a subsequent pregnancy). They may be ambivalent or they may actively want to get pregnant again | |
| Providers of care | Knowledge and skills | Providers of care may not understand or appreciate teenage mothers’ points of view or may not have the personal skills to approach them appropriately or with sensitivity, or the ability to judge the right time to initiate an intervention |
| Attitudes regarding programme acceptability, appropriateness and credibility | Providers may have opinions regarding the intervention, including views about its acceptability and appropriateness, and about the credibility of the provider and the health-care system. For example, health workers may not agree with the choice of intervention or may not trust the reasons behind it | |
| Motivation to change or adopt new behaviour | Providers may have varying degrees of motivation to change behaviour or adopt new behaviours. For example, they may be more or less motivated to take on new tasks | |
| System constraints | Accessibility of care | The accessibility of intervention facilities may affect implementation of the option, for instance because of financial (user fees), geographic (distance to services) or social (access for certain ethnic or low-income groups) factors |
| Financial resources | Additional financial resources may be needed to implement the option | |
| Human resources | An increased supply or distribution of health or social workers may be needed to implement the option | |
| Educational system | Aspects of the educational system may need to be modified to accommodate teenage mothers | |
| Professional supervision, support structures and guidelines | Health, social or education workers may require more supervision than is currently provided to implement the option; structural support or guidelines may be needed | |
| Incentives | Reimbursement systems for patients, health workers or others may need to be structured to facilitate rather than hinder implementation of the option | |
| Bureaucracy | Paperwork and procedures may need to be structured to facilitate rather than hinder implementation of the option | |
| Relationship with norms and standards | Current norms and standards of practice need to be in line with the relevant option |
Part B Data extraction table
| Level | Barriers and enablers | Extracts from papers (specify which type of respondent the data comes from) | Possible solutions (specify who made suggestions) |
|---|---|---|---|
| Recipients of care | Knowledge and skills | ||
| Attitudes regarding intervention acceptability, appropriateness and credibility | |||
| Motivation to change or adopt new behaviour | |||
| Providers of care | Knowledge and skills | ||
| Attitudes regarding programme acceptability, appropriateness and credibility | |||
| Motivation to change or adopt new behaviour | |||
| System constraints | Accessibility of care | ||
| Financial resources | |||
| Human resources | |||
| Educational system | |||
| Professional supervision, support structures and guidelines | |||
| Incentives | |||
| Bureaucracy | |||
| Relationship with norms and standards |
Appendix 13 Realist work
FIGURE 19.
The first iteration of the mind map of theory areas.

FIGURE 20.
The second iteration of the mind map of theory areas.

FIGURE 21.
The third iteration of the mind map of theory areas with suggestions of other areas from the stakeholder meeting.
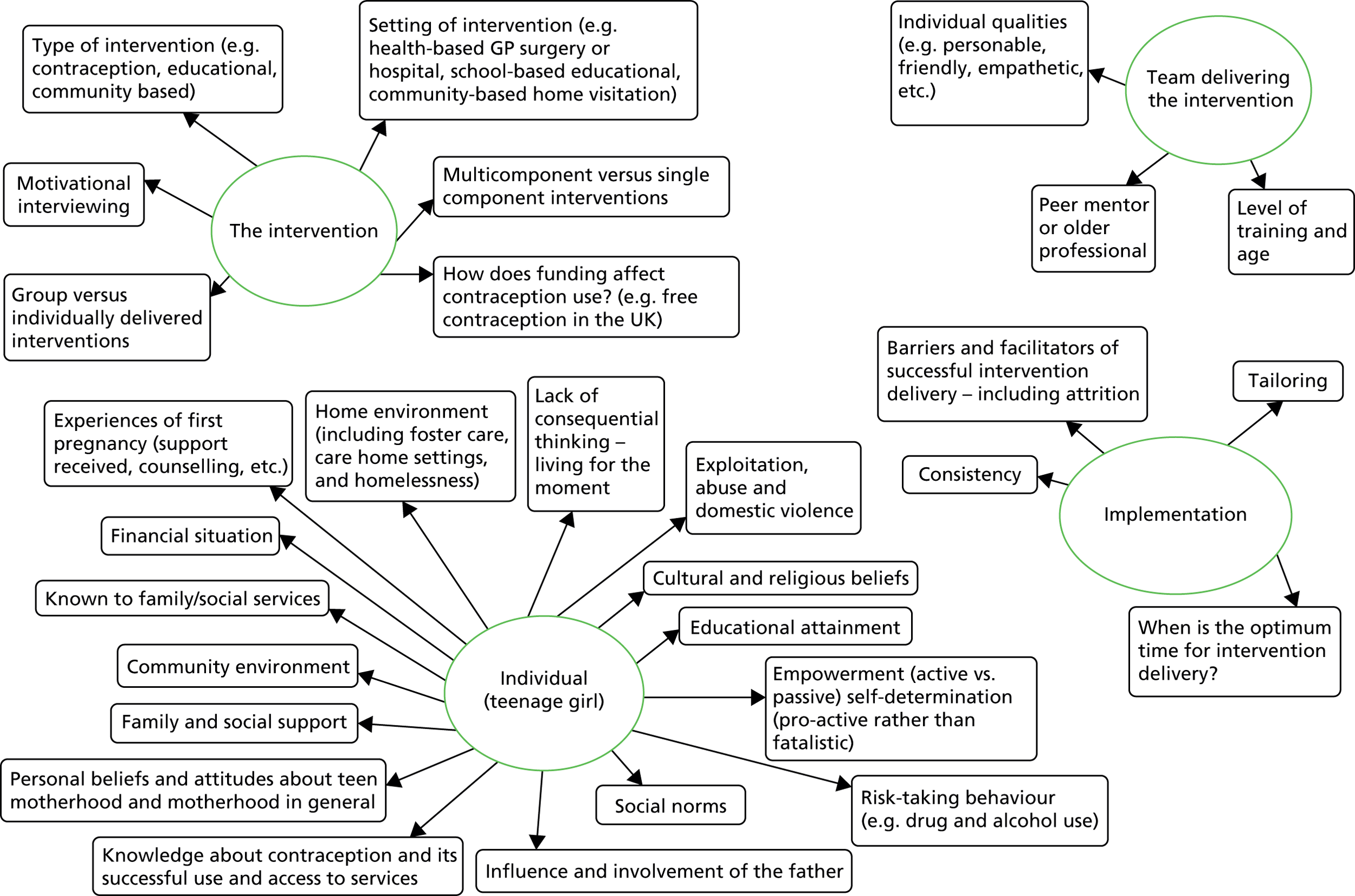
| Theory heading | Explanation, meaning and keywords to assist data extraction |
|---|---|
| Connectedness | Feeling connected as part of a family group or peer group may provide feelings of belonging and attachment which could lead to feelings of empowerment |
| Keywords: positive strong relationships, belonging, attachment and empowerment | |
| Structure | Consistent intervention delivery, format or personnel provides a structure and routine that could lead to feelings of security and support providing the teenager with a safe platform/space where she can discuss issues and take control of her life |
| Keywords: consistency, structure, support, fidelity and security | |
| Tailoring | Allowing for certain aspects of the intervention to be adapted and tailored e.g., timing, location of the intervention can minimise barriers to attendance and increase engagement and intervention adherence |
| Keywords, tailoring, targeting, personalisation/personalised intervention, adaptations, modifications, minimising barriers, increasing facilitators, engagement, timing, location and adherence | |
| Setting/environment: individual | The individual may be raised in a setting where the family and peer group norm is one that states multiple teenage pregnancies is common, normal and acceptable without any stigma The individual may be influenced by their partner with regards to family size or the likelihood of subsequent pregnancy may be increased by the desire to build a new family with their current partner if they have children from previous relationships |
| Keywords: social norms, family norms, peer group norms, partner influence, social class, living in an area of low socioeconomic status and living in an area of low educational attainment | |
| Motivation: reasons for getting pregnant | Is the pregnancy unplanned, unwanted or was the teenager ambivalent to motherhood and/or contraception use? |
| What are the state/economic views of teenage pregnancy (negative because of financial dependence on the state) versus individual views of teenage pregnancy (independence, positive experience that did not result in reliance on the state)? | |
| How do first pregnancy experiences, for example access to services, support received, issues of vulnerability (homelessness, exploitation, domestic/partner abuse), empowerment versus lack of control or consequential thinking, increase the likelihood of repeat teenage pregnancy? | |
| Keywords: unplanned, unwanted, ambivalence, drifting, lack of consequential thinking, lack of control/exploitation, vulnerability (homelessness, exploitation, domestic/partner abuse and violence), access to services during first pregnancy, support received during first pregnancy, influence and involvement of the father, self-determination, control, independence and social norms | |
| Other goals/aspirations | Having a more attractive alternative than teenage parenting (e.g. education or career goal) |
| Keywords: goal-setting, education, career, empowerment, control, achievement and attainment | |
| Being a good mother | Wanting to do the best for the child(ren) you already have setting limits on family size at the point when they think it would be detrimental to have another one (though this is probably more likely to be after 2 or 3 when the family can be considered complete) |
| Keywords: caring, maternal, family orientated, mothering, child-orientated goals, putting the children first and providing a good life for the family |
| Theory heading | Explanation, meaning and key words to assist data extraction | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Connectedness | Feeling connected as part of a family group or peer group may provide feelings of belonging and attachment which could lead to feelings of empowerment | ||||||||||||||||||||
| Keywords: positive strong relationships, belonging, attachment and empowerment | |||||||||||||||||||||
| Structure | Consistent intervention delivery, format or personnel provides a structure and routine that could lead to feelings of security and support providing the teenager with a safe platform/space where she can discuss issues and take control of her life | ||||||||||||||||||||
| Keywords: consistency, structure, support, fidelity and security | |||||||||||||||||||||
| Tailoring | Allowing for certain aspects of the intervention to be adapted and tailored e.g., timing, location of the intervention can minimise barriers to attendance and increase engagement and intervention adherence | ||||||||||||||||||||
| Keywords: tailoring, targeting, personalisation/personalised intervention (including addressing of fears and side effects of contraception), adaptations, modifications, minimising barriers (including addressing of fears and side effects of contraception), increasing facilitators, engagement, timing, location and adherence | |||||||||||||||||||||
| Setting/environment: individual | The individual may be raised in a setting where the family and peer group norm is one that states multiple teenage pregnancies is common, normal and acceptable without any stigma | ||||||||||||||||||||
| The individual may be influenced by their partner with regards to family size or the likelihood of subsequent pregnancy may be increased by the desire to build a new family with their current partner if they have children from previous relationships | |||||||||||||||||||||
| Keywords: social norms, family norms, peer group norms, partner influence, social class, living in an area of low socioeconomic status and living in an area of low educational attainment | |||||||||||||||||||||
| Setting/environment: intervention | Intervention Setting may influence the likelihood of repeat teenage pregnancy providing the intervention in settings such as the home, community or in school may minimise barriers to participation and attendance, increasing the likelihood of overall intervention engagement and continued attendance | ||||||||||||||||||||
| Keywords: minimising barriers, maximising facilitators, ease of access, reduced travel and additional services (e.g. on-site childcare facilities) | |||||||||||||||||||||
| Motivation: reasons for getting pregnant | Is the pregnancy unplanned, unwanted or was the teenager ambivalent to motherhood and/or contraception use? | ||||||||||||||||||||
| What are the state/economic views of teenage pregnancy (negative because of financial dependence on the state) versus individual views of teenage pregnancy (independence, positive experience that did not result in reliance upon the state)? | |||||||||||||||||||||
| How do first pregnancy experiences, for example access to services, support received, issues of vulnerability (homelessness, exploitation, domestic/partner abuse), empowerment, versus lack of control or consequential thinking increase the likelihood of repeat teenage pregnancy? | |||||||||||||||||||||
| Keywords: unplanned, unwanted, ambivalence, drifting, lack of consequential thinking, lack of control/exploitation, vulnerability (homelessness, exploitation, domestic/partner abuse and violence), access to services during first pregnancy, support received during first pregnancy, influence and involvement of the father, self-determination, control, independence and social norms | |||||||||||||||||||||
| Other goals/aspirations | Having a more attractive alternative than teenage parenting (e.g. education or career goal) | ||||||||||||||||||||
| Keywords: goal-setting, education, career, empowerment, control, achievement and attainment | |||||||||||||||||||||
| Perceptions/ideas of parental responsibility | Wanting to do the best for the child(ren) you already have, setting limits on family size at the point when they think it would be detrimental to have another one (although this is probably more likely to be after two or three when the family can be considered complete) | ||||||||||||||||||||
| Keywords: caring, maternal, family orientated, mothering, child-orientated goals, putting the children first and providing a good life for the family | |||||||||||||||||||||
| Health Belief Model | The Health Belief Model is a psychological model that attempts to explain and predict health behaviours, can be used to reduce the likelihood of repeat pregnancy | ||||||||||||||||||||
| The model has six components representing the perceived threat and net benefits: perceived susceptibility, perceived severity, perceived benefits and perceived barriers. These concepts were proposed as accounting for people’s ‘readiness to act.’ An added concept, ‘cues to action’, would activate that readiness and stimulate overt behaviour. A recent addition to the Health Belief Model is the concept of ‘self-efficacy’, or one’s confidence in the ability to successfully perform an action | |||||||||||||||||||||
| The model is summarised below: ConceptDefinitionApplicationPerceived susceptibilityOne’s opinion of chances of getting a conditionDefine population(s) at risk, risk levels; personalise risk based on a person’s features or behaviour; heighten perceived susceptibility if too lowPerceived severityOne’s opinion of how serious a condition and its consequences areSpecify consequences of the risk and the conditionPerceived benefitsOne’s belief in the efficacy of the advised action to reduce risk or seriousness of impactDefine action to take; how, where, when; clarify the positive effects to be expectedPerceived barriersOne’s opinion of the tangible and psychological costs of the advised actionIdentify and reduce barriers through reassurance, incentives and assistanceCues to actionStrategies to activate ‘readiness’Provide how-to information, promote awareness and remindersSelf-efficacyConfidence in one’s ability to take actionProvide training and guidance in performing action |
Concept | Definition | Application | Perceived susceptibility | One’s opinion of chances of getting a condition | Define population(s) at risk, risk levels; personalise risk based on a person’s features or behaviour; heighten perceived susceptibility if too low | Perceived severity | One’s opinion of how serious a condition and its consequences are | Specify consequences of the risk and the condition | Perceived benefits | One’s belief in the efficacy of the advised action to reduce risk or seriousness of impact | Define action to take; how, where, when; clarify the positive effects to be expected | Perceived barriers | One’s opinion of the tangible and psychological costs of the advised action | Identify and reduce barriers through reassurance, incentives and assistance | Cues to action | Strategies to activate ‘readiness’ | Provide how-to information, promote awareness and reminders | Self-efficacy | Confidence in one’s ability to take action | Provide training and guidance in performing action |
| Concept | Definition | Application | |||||||||||||||||||
| Perceived susceptibility | One’s opinion of chances of getting a condition | Define population(s) at risk, risk levels; personalise risk based on a person’s features or behaviour; heighten perceived susceptibility if too low | |||||||||||||||||||
| Perceived severity | One’s opinion of how serious a condition and its consequences are | Specify consequences of the risk and the condition | |||||||||||||||||||
| Perceived benefits | One’s belief in the efficacy of the advised action to reduce risk or seriousness of impact | Define action to take; how, where, when; clarify the positive effects to be expected | |||||||||||||||||||
| Perceived barriers | One’s opinion of the tangible and psychological costs of the advised action | Identify and reduce barriers through reassurance, incentives and assistance | |||||||||||||||||||
| Cues to action | Strategies to activate ‘readiness’ | Provide how-to information, promote awareness and reminders | |||||||||||||||||||
| Self-efficacy | Confidence in one’s ability to take action | Provide training and guidance in performing action |
Summary statements of emerging theory areas
Motivation: reasons for getting pregnant
-
Political view (i.e. the state’s view of teenage pregnancy).
-
Economic.
-
Family situation.
-
Question of unintended, unplanned or unwanted pregnancy, or ambivalence.
The likelihood of teenage pregnancy might be affected by paying attention to ‘motivation’; in particular, the reasons why a girl is pregnant, asking whether the pregnancy was unplanned, unintended or unwanted, or whether or not the girl in question was ambivalent to motherhood and/or contraception use. Interventions that pay attention to these factors may be more effective.
The likelihood of teenage pregnancy might be affected by paying attention to ‘state and economic views of teenage pregnancy.’ The Government and the media tend to view teenage pregnancy as a negative phenomenon, as teenage motherhood increases the likelihood of financial dependence on the state, thus perpetuating the negative view; however, in certain cases, teenage pregnancy can be a positive experience that does not result in financial dependence on the state.
Connectedness
-
To peer group.
-
To family.
-
To school.
-
To the intervention itself.
-
To the person delivering the intervention.
-
Mentorship.
-
Personal care.
-
Collaborative decision-making.
The likelihood of teenage pregnancy might be affected by paying attention to ‘connectedness’: positive/good relationships with family members, peers, their school and, in certain cases, the person delivering an intervention can provide a teenage girl with a sense of belonging and attachment to a group (which could in turn lead to feelings of empowerment). Therefore, interventions that pay attention to these factors may be more effective.
Targeting
-
Tailoring (including who delivers the intervention).
-
Timing of the intervention.
-
Nature of the intervention (e.g. single component vs. multicomponent).
-
Person focused rather than programme focused.
-
Collaborative decision-making.
The likelihood of teenage pregnancy might be affected by paying attention to ‘tailoring’: allowing for certain aspects of the intervention to be tailored (e.g. timing, location and intervention focus) can provide a personalised intervention that reduces barriers to attendance, increasing the likelihood of engagement and adherence to an intervention.
Setting/environment
-
Stigma.
-
‘Norms’ (i.e. society norm, family norm, etc.).
-
Partner influence.
-
Family setting.
-
Education setting.
-
Intervention setting.
The likelihood of teenage pregnancy might be affected by paying attention to ‘setting/environment’: family and education settings may create a social norm in which teenage pregnancy is deemed an acceptable and a common occurrence without stigma, leading to the ‘normalisation’ of teenage pregnancy.
The likelihood of teenage pregnancy might be affected by paying attention to ‘partner influence’: a partner may have their own ideals on family size or, in cases where the teenage girl in question has given birth to a previous partner’s child, the current partner may have his own desires to build a family with the girl. Both of these scenarios could influence the teenage girl.
The likelihood of teenage pregnancy might be affected by paying attention to ‘intervention setting’: providing the intervention in settings such as the home, community or school could minimise barriers to participation and attendance, increasing the likelihood of overall intervention engagement and continued attendance.
As part of the Cardiff Task and Finish Group meeting, summary statements were prepared and presented for each theory area to explain the emerging themes of evidence to the attendees. These summary statements are shown below.
Connectedness
The likelihood of teenage pregnancy might be affected by paying attention to ‘connectedness’. Adolescents need social support from parents, partners, friends and peers to develop their self-esteem, in order to increase their self-efficacy and to reinforce their choices regarding the delay or avoidance of repeat pregnancy with regard to, for example, accessing and consistent use of contraception. Adolescents without at least two people in their lives to verbalise their importance as a person or confirm their parenting skills were less likely to use birth control consistently. Interventions that provide social support through relatable sources to the mother, such as peers, mentors or role models, can assist with filling the gap in social support. Social support that builds trusting relationships can provide an adolescent mother with assistance, guidance, and confirmation of her self-worth. Interventions that use peers, mentors and role models may be more successful if they adopt a supportive ‘big sister’ role, rather than an authoritarian ‘mother’ or ‘teacher’ role, as many adolescents have fractured relationships with their own mother or conflicts with authority (e.g. teachers or law enforcement).
Intervention content
The likelihood of teenage pregnancy might be affected by paying attention to ‘intervention content’. Because of multiple levels of influence upon adolescents, from families, peers and the community, knowledge and information of contraception is, alone, not enough and often does not lead to implementation. Some have argued for the use of social ecological theory to examine individual, dyad, family, peer/community and social system factors in order to develop intervention frameworks. The issue of adolescent pregnancy involves family, societal, medical and educational components. Therefore, interventions should be multifaceted providing a range of support and services that address the complex needs of young mums. Common components that have been consistently found in effective programmes include peer counselling, case management, school completion and career strategies, and contraceptive availability.
Intervention delivery
The likelihood of teenage pregnancy might be affected by paying attention to ‘intervention delivery’. Interventions delivered in schools encourage a strong focus on remaining in education, as the adolescent mother usually needs to be enrolled in school to access these services and interventions. Engagement in school-based activities has been found to be a protective factor against pregnancy in adolescence. This could see a shift in resources in schools from downstream, reactive interventions to more upstream, proactive interventions that aim to prevent an initial pregnancy in adolescence rather than repeat pregnancies in adolescence. The dichotomy between the access and availability of services for urban versus rural adolescents was also evident, demonstrating a need for better access in rural areas.
Perspective/context
The likelihood of teenage pregnancy might be affected by paying attention to ‘perspective/context’. Family dynamics, past experiences and expectations of gender roles can influence an adolescent girl’s perceptions of motherhood. Interventions should be sensitive to these personal experiences when developing and delivering interventions; for example, an adolescent who has experienced multiple miscarriages may experience feelings of guilt, loss and depression leading to thoughts of repeat pregnancy to replace the baby or babies that she has lost. If an intervention pays attention to this history and its potential effect on decision-making, the appropriate counselling may be delivered as a part of the intervention allowing the adolescent to deal with these feelings of loss without resulting in a repeat pregnancy.
Other goals and aspirations
The likelihood of teenage pregnancy might be affected by paying attention to ‘other goals and aspirations’. Other goals and aspirations, outside of motherhood, may help teenagers to equate consistent contraception use with obtaining the lifestyle they want. Without other alternatives, motherhood may become the only option to provide girls with an opportunity for success and autonomy. However, if the adolescent is already a mother there is a need for flexibility and additional support to help these girls achieve their goals through intervention tailoring and structure, and providing, for example, extended deadlines for school or college course work or graduation requirements. Interventions that provide a range of services, such as birth control, social support, service co-ordination, health education, life skills and employment training, may equip adolescents with the skills they need to seek out alternative life choices.
Perceptions of parental responsibility
The likelihood of teenage pregnancy might be affected by paying attention to ‘perceptions of parental responsibility’. Adolescent mothers report their desire to provide a better upbringing for their own child than they experienced themselves; they see an opportunity to rectify the mistakes made in their own childhood. There is also a difficulty for adolescent mothers in developing autonomy and self-sufficiency in parenting, as maternal grandmothers often undermine the adolescent’s self-sufficiency by taking over the parenting role. This clash for parental responsibility can lead the adolescent to a repeat pregnancy in order to gain autonomy and the sole parenting role of a child, as the grandparent is now needed to parent the older sibling(s). Interventions should aim to support self-sufficiency by equipping parents with the skills they need to be the capable, competent parents they wish to be.
Setting/environment individual
The likelihood of teenage pregnancy might be affected by paying attention to ‘setting/environment individual’. Personal characteristics and circumstances influence an adolescent girl’s ideas about the likelihood, implications and potential benefits of becoming a mother during adolescence. The personality of an adolescent is important. There are sexually active adolescents who do not become pregnant. It has been suggested that exploring the characteristics and personalities of never-pregnant, sexually active adolescents to uncover exactly why they do not get pregnant, despite sexual activity, could provide insights into effective interventions. For example, do these never-pregnant sexually active adolescents feel they can speak openly about sex with mothers, friends and partners? Do they feel the personal cost of stigma when accessing emergency contraception is less than the personal cost of a pregnancy during adolescence?
Tailoring
The likelihood of teenage pregnancy might be affected by paying attention to ‘tailoring’. There are multiple levels of influence upon an adolescent and thus interventions should be geared towards an adolescent’s readiness to change, rather than standardised messages and advice. Interventions that pay attention to adolescents’ life experiences, as well as their developmental stage, cultural context, age-appropriate impulsive and rational decision-making styles and responses to stress, may be more successful than interventions based upon a medical model. Medical models of interventions are defined as interventions that focus mainly on information and access to contraception only. An example of this type of model is the suggestion that the most effective way to help adolescent mothers might be to encourage them to use long-acting injectable or implant contraceptive methods. Interventions should also be sensitive to barriers, including practical, emotional and psychological barriers, and should overcome these barriers; for example, interventions should address practical issues of access by providing interventions at home or by providing transport if the intervention is to be delivered in another setting, such as a community centre. Interventions also need to understand adolescent sexual behaviour from the point of view of the adolescents themselves. Many interventions are designed based upon adult beliefs of adolescent sexual activity and the consequences of adolescent pregnancy, which may lack relevance to the adolescent population that the intervention aims to serve. Interventions should be modelled using adolescent principles and perceptions of sex and relationships, and the potential consequences of pregnancy during adolescence.
These findings resonated with attendees at the stakeholder group, the stakeholders only wished to add, with regards to tailoring, that they felt interventions needed to be tailored to the individual according to their circumstances at the time. They said ‘girls complain that they are not listened to by professionals’. They also stated ‘we really need to find out what they really need and want, and understand what they are asking for – there is too much generalisation, and perceptions of what girls want are not accurate’.
Appendix 14 Studies in metaregression according to Effective Practice and Organisation of Care criteria52
| Author, Year | EPOC |
|---|---|
| Berenson and Wiemann, 1997108 | Non-comparative study |
| Coard et al., 2000112 | Non-comparative study |
| Crittenden et al., 200998 | Non-comparative study |
| Drayton et al., 2000;99 Drayton, 2002;100 Drayton et al., 2002101 | Non-comparative study |
| Kershaw et al., 2003103 | Non-comparative study |
| Lewis et al., 2010;94 Lewis et al., 201095 | Non-comparative study |
| Mbambo et al., 2006106 | Non-comparative study |
| Omar et al., 2008113 | Non-comparative study |
| Persona et al., 2004114 | Non-comparative study |
| Salihu et al., 2011115 | Non-comparative study |
| Stevens-Simon et al., 1995116 | Non-comparative study |
| Stevens-Simon et al., 1998117 | Non-comparative study |
| Stevens-Simon et al., 1999118 | Non-comparative study |
| Stevens-Simon, 2001119 | Non-comparative study |
| Wang and Wang, 2005128 | Non-comparative study |
| Williams et al., 2001109 | Non-comparative study |
| Mulsow and Murry, 1996122 | Prospective cohort study |
| Ranieri and Wiemann, 200797 | Prospective cohort study |
| Sant’Anna et al., 2007105 | Prospective cohort study |
| Templeman et al., 2000123 | Prospective cohort study |
| Thurman et al., 2007124 | Prospective cohort study |
| Mears et al., 1997121 | Prospective cohort study |
| Bruno et al., 2009120 | Prospective cohort study |
| Falk et al., 2006111 | Retrospective cohort study |
| Key et al., 2001107 | Retrospective cohort study |
| O’Dell et al., 1998125 | Retrospective cohort study |
| Patchen et al., 2009126 | Retrospective cohort study |
| Paukku et al., 2003104 | Retrospective cohort study |
| Richio et al., 2010127 | Retrospective cohort study |
| Sangalang et al., 2006110 | Retrospective cohort study |
| Barnet et al., 200886 | Retrospective cohort study |
Appendix 15 Details of included studies
Randomised controlled trials
Barnet B, Liu J, DeVoe M, Alperovitz-Bichell K, Duggan AK. Home visiting for adolescent mothers: effects on parenting, maternal life course and primary care linkage. Ann Fam Med 2007;5:224–32.
Barnet B, Liu J, Devoe M. Double jeopardy – depressive symptoms and rapid subsequent pregnancy in adolescent mothers. Arch Pediatr Adolesc Med 2008;162:246–52.
Belzer M, Sanchez K, Olson J, Jacobs A, Tucker D. Advance supply of emergency contraception: a randomized trial in adolescent mothers. J Pediatr Adolesc Gynecol 2005;18:347–54.
Black M, Bentley M, Papas M, Oberlander S, Teti L, McNary S, et al. Delaying second births among adolescent mothers: a randomized controlled trial of a home-based mentoring program. Pediatrics 2006;118:e1087–99.
Cherniss C, Herzog E. Impact of home-based family therapy on maternal and child outcomes in disadvantaged adolescent mothers. Fam Relat 1996;45:72–9.
Ford K, Weglicki L, Kershaw T, Schram C, Hoyer PJ, Jacobson ML. Effects of a prenatal care intervention for adolescent mothers on birth weight, repeat pregnancy and educational outcomes at one year postpartum. J Perinat Educ 2002;11:35–8.
Havens KK, Wagstaff DA, Mercer PA, Longeway K, Gutman M. Lessons learned from a mentoring program for teenage mothers. Wisc Med J 1997;96:38–43.
Katz KS, Rodan M, Milligan R, Tan S, Courtney L, Gantz M, et al. Efficacy of a randomized cell phone-based counseling intervention in postponing subsequent pregnancy among teen mothers. Matern Child Health J 2011;15:S42–S53.
Koniak-Griffin D, Verzemnieks IL, Anderson NLR, Brecht ML, Lesser J, Kim S, et al. Nurse visitation for adolescent mothers: two-year infant health and maternal outcomes. Nurs Res 2003;52:127–36.
Quinlivan JA, Box H, Evans SF. Postnatal home visits in teenage mothers: a randomised controlled trial. Lancet 2003;361:893–900.
Sims K, Luster T. Factors related to early subsequent pregnancies and second births among adolescent mothers in a family support program. J Fam Issues 2002;23:1006–31.
Stevens-Simon C, Dolgen JI, Kelly L, Singer D. The effect of monetary incentives and peer support groups on repeat adolescent pregnancies. J Am Med Assoc 1997;277:977–82.
Randomised controlled trials with multiple studies
Kan ML, Silber Ashley O, LeTourneau KL, Williams JC, Jones SB, Hampton J, et al. The adolescent family life program: a multisite evaluation of federally funded projects serving pregnant and parenting adolescents. Am J Public Health 2012;102:1872–8.
Randomised controlled trials and cost-effectiveness study
Barnet B, Liu J, DeVoe M, Duggan AK, Gold MA, Pecukonis E. Motivational intervention to reduce rapid subsequent births to adolescent mothers: a community-based randomized trial. Ann Fam Med 2009;7:436–45.
Barnet B, Rapp T, DeVoe M, Mullins CD. Cost-effectiveness of a motivational intervention to reduce rapid repeated childbearing in high-risk adolescent mothers a rebirth of economic and policy considerations. Arch Pediatr Adolesc Med 2010;164:370–6.
Johnston-Briggs BD, Liu J, Carter-Pokras O, Barnet B. Effect of partner relationship on motivation to use condoms among adolescent mothers. J Natl Med Assoc 2008;100:929–35.
Cluster randomised controlled trials
Scott AA, Amodeis N, Hoffman TJ. Preventing repeat pregnancies and other negative outcomes: among pregnant and parenting Hispanic adolescents. J Multicult Nurs Health 2004;10:32–8.
Non-randomised trials
Lewis LN, Doherty DA, Hickey M, Skinner SR. Predictors of sexual intercourse and rapid-repeat pregnancy among teenage mothers: An Australian prospective longitudinal study. Med J Aust 2010;193:338–42.
Lewis LN, Doherty DA, Hickey M, Skinner SR. Implanon as a contraceptive choice for teenage mothers: a comparison of contraceptive choices, acceptability and repeat pregnancy. Contraception 2010;81:421–26.
Nunez Rocha GM, Alanis Alanis MdJ, Alanis Salazar J, Salinas Martinez AM, Garza Elizondo ME, Villarreal Rios E. [Differences in the use of family planning methods by adolescent females according to the education model utilized during pregnancy. Monterrey, Mexico]. Rev Esp Salud Publica 2005;79:69–77.
Prospective cohort studies
Bruno Z, Feitosa F, Silveira K, de Morais I, Bezerra M. Subsequent pregnancy among adolescents. [Reincidencia de gravidez em adolescentes]. Rev Bras Ginecol Obstet 2009;31:480–4.
Cavazos-Rehg PA, Krauss MJ, Spitznagel EL, Schootman M, Cottler LB, Bierut LJ. Associations Between Multiple Pregnancies and Health Risk Behaviors Among U.S. Adolescents. J Adolesc Health 2010;47:600–3.
Key JD, Gebregziabher MG, Marsh LD, O’Rourke KM. Effectiveness of an intensive, school-based intervention for teen mothers. J Adolesc Health 2008;42:394–400.
Lewis CM, Faulkner M, Scarborough M, Berkeley B. Preventing subsequent births for low-income adolescent mothers: an exploratory investigation of mediating factors in intensive case management. Am J Public Health 2012;102:1862–5.
Mears C, Hediger M, Martin S, Scholl T, Kramer J. Social factors predicting postpartum choice of Norplant among African American and non-Hispanic white adolescents. J Adolesc Health 1997;21:167–71.
Mulsow MH, Murry VM. Parenting on edge: economically stressed single, African American adolescent mothers. J Fam Issues 1996;17:704–21.
Raneri LG, Wiemann CM. Social ecological predictors of repeat adolescent pregnancy. Perspect Sex Reprod Health 2007;39:39–47.
Rubin V, East P. Adolescents’ pregnancy intentions: relations to life situations and caretaking behaviors prenatally and 2 years postpartum. J Adolesc Health 1999;24:313–20.
Sant’Anna MJC, Carvalho KAM, Melhado A, Coates V, Omar HA. Teenage pregnancy: impact of the integral attention given to the pregnant teenager and adolescent mother as a protective factor for repeat pregnancy. Scientific World J 2007;7:187–94.
Silva ADA, Coutinho IC, Katz L, Souza ASR. A case–control study of factors associated with repeat teen pregnancy based on a sample from a university maternity hospital. Cad Saude Publica 2013;29:496–506.
Stevens-Simon C, Wallis J, Allen-Davis J. Which teen mothers choose Norplant? J Adolesc Health 1995;16:350–35
Stevens-Simon C and Kelly L, Correlates and consequences of early removal of Levonorgestrel implants among teenaged mothers. Arch Pediatr Adolesc Med 1998a;152:893–8.
Stevens-Simon C, Kelly L, Singer D. Preventing repeat adolescent pregnancies with early adoption of the contraceptive implant. Fam Plann Perspect 1999;31:88–93.
Teal SB, Sheeder J. IUD use in adolescent mothers: retention, failure and reasons for discontinuation. Contraception 2012;85:270–4.
Templeman CL, Cook V, Goldsmith LJ, Powell J, Hertweck SP. Postpartum contraceptive use among adolescent mothers. Obstet Gynecol 2000;95:770–6.
Thurman AR, Hammond N, Brown HE, Roddy ME. Preventing repeat teen pregnancy: postpartum depot medroxyprogesterone acetate, oral contraceptive pills, or the patch? J Pediatr Adolesc Gynecol 2007;20:61–5.
Retrospective cohort studies
Falk G, Ostlund I, Magnuson A, Schollin J, Nilsson K. Teenage mothers – a high-risk group for new unintended pregnancies. Contraception 2006;74:471–5.
Key JD, Barbosa GA, Owens VJ. The Second Chance Club: repeat adolescent pregnancy prevention with a school-based intervention. J Adolesc Health 2001;28:167–69.
Key JD, O’Rourke K, Judy N, A MS. Efficacy of a secondary adolescent pregnancy prevention program: an ecological study before during and after implementation of the second chance club. Int Q Community Health Educ 2006;24:231–40.
O’Dell CM, Forke CM, Polaneczky MM, Sondheimer SJ, Slap GB. Depot medroxyprogesterone acetate or oral contraception in postpartum adolescents. Obstet Gynecol 1998;91:609–14.
Patchen L, Caruso D, Lanzi RG. Poor maternal mental health and trauma as risk factors for a short interpregnancy interval among adolescent mothers. J Psychiatr Ment Health Nurs 2009;16:401–03.
Paukku M, Quan J, Darney P, Raine T. Adolescents’ contraceptive use and pregnancy history: is there a pattern? Obstet Gynecol 2003;101:534–8.
Richio LJ, Phipps MG, Raker CA. Repeat teen birth: does delivery mode make a difference? Am J Obstet Gynecol 2010;203:453.e1–e5.
Sangalang BB, Barth RP, Painter JS. First-birth outcomes and timing of second births: a statewide case management program for adolescent mothers. Health Soc Work 2006;31:54–63.
Non-comparison studies
Berenson A, Wiemann C. Contraceptive use among adolescent mothers at 6 months postpartum. Obstet Gynecol 1997;89:999–1005.
Carvajal D, Burrell L, Duggan A, Barnet B. Repeat pregnancy prevention self-efficacy in adolescents: associations with provider communication, provider type and depression. South Med J 2012;105:591–7.
Coard SI, Nitz K, Felice ME. Repeat pregnancy among urban adolescents: sociodemographic, family and health factors. Adolescence 2000;35:193–200.
Collins ME, Stevens JW, Lane TS. Teenage parents and welfare reform: findings from a survey of teenagers affected by living requirements. Soc Work 2000;45:327–38.
Crittenden CP, Boris NW, Rice JC, Taylor CA, Olds DL. The role of mental health factors, behavioral factors and past experiences in the prediction of rapid repeat pregnancy in adolescence. J Adolesc Health 2009;44:25–32.
da Silva KS, Rozenberg R, Bonan C, Chuva VCC da Costa SF, Gomes M. Repeated pregnancy among adolescents and social vulnerability in Rio de Janeiro (RJ, Brazil): data analysis of information system on live births. Cienc Saude Coletiva 2011;16:2485–93.
Drayton VLC, Montgomery SB, Modeste NN, Frye-Anderson BA, McNeil P. The impact of the Women’s Centre of Jamaica Foundation programme for adolescent mothers on repeat pregnancies. West Indian Med J 2000;49:316–26.
Drayton VLC. Contraceptive use among Jamaican teenage mothers. Pan Am J Public Health 2002a;11:150–7.
Drayton VLC, Montgomery SB, Modeste NN, Frye-Anderson BA. The Health Belief Model as a predictor of repeat pregnancies among Jamaican teenage mothers. Int Q Community Health Educ 2002b;21:67–81. 2000.
Flynn L. The Adolescent Parenting Program: improving outcomes through mentorship. Public Health Nurs 1999;16:182–9.
Gray S, Sheeder J, O’Brien R, Stevens-Simon C. Having the best intentions is necessary but not sufficient: what would increase the efficacy of home visiting for preventing second teen pregnancies? Prev Sci 2006;7:389–95.
Kershaw TS, Niccolai LM, Ickovics JR, Lewis JB, Meade CS, Ethier KA. Short and long-term impact of adolescent pregnancy on postpartum contraceptive use: implications for prevention of repeat pregnancy. J Adolesc Health 2003;33:359–68.
Lewis LN, Doherty DA, Nickey M, Skinner SR. Predictors of sexual intercourse and rapid-repeat pregnancy among teenage mothers: an Australian prospective longitudinal study. Med J Aust 2010;193:338–42.
Lewis LN, Doherty DA, Nickey M, Skinner SR. Implanon as a contraceptive choice for teenage mothers: a comparison of contraceptive choices acceptability and repeat pregnancy. Contraception 2010;81:421–6.
Mapanga KG, Andrews CM. The influence of family and friends’ basic conditioning factors and self-care agency on unmarried teenage primiparas’ enagagement in contraceptive practice. J Community Health Nurs 1995;12:89–100.
Mbambo DE, Ehlers VJ, Monareng LV. Factors influencing adolescent mothers’ non-utilisation of contraceptives in the Mkhondo area. Health SA Gesondheid 2006;11:22–31.
Omar HA, Fowler A, McClanahan KK. Significant reduction of repeat teen pregnancy in a comprehensive young parent program. J Pediatr Adolesc Gynecol 2008;21:283–7.
Padin MDR, Silva RDE, Mitsuhiro SS, Chalem E, Barros MM, Guinsburg R, et al. Repeat pregnancies among adolescents in a tertiary hospital in Brazil. J Reprod Infant Psychol 2012;30:193–200.
Persona L, Shimo AK, Tarallo MC. [Profile of adolescents with repeated pregnancies attended at a prenatal clinic]. Rev Lat-Am Enferm 2004;12:745–50.
Sadler LS, Swartz MK, Ryan-Krause P, Seitz V, Meadows-Oliver M, Grey M, et al. Promising outcomes in teen mothers enrolled in a school-based parent support program and child care center. J Sch Health 2007;77:121–30.
Salihu HM, August EM, Jeffers DF, Mbah AK, Alio AP, Berry E. Effectiveness of a federal healthy start program in reducing primary and repeat teen pregnancies: our experience over the decade. J Pediatr Adolesc Gynecol 2011;24:153–60.
Schaffer MA, Goodhue A, Stennes K, Lanigan C. Evaluation of a public health nurse visiting program for pregnant and parenting teens. Public Health Nurs 2012;29:218–31.
Stevens-Simon C, Kelly L, Singer D. Absence of negative attitudes towards childbearing among pregnant teenagers. Arch Pediatr Adolesc Med 1996;150:1037–43.
Stevens-Simon C, Kelly L, Kulick R. A village would be nice but . . . It takes a long-acting contraceptive to prevent repeat adolescent pregnancies. Am J Prev Med 2001;21:60–5.
Stevens-Simon C, Kelly L, Singer D, Nalligan D. Reasons for first teen pregnancies predict the rate of subsequent teen conceptions. Pediatrics 1998;101:e8.
Swedish KA, Rothenberg A, Fuchs K, Rosenberg G. Successful life navigation by former participants in a group for pregnant and parenting teens. Vulnerable Children Youth Stud 2010;5:310–21.
Truong HHM, Kellogg T, McFarland W, Kang MS, Darney P, Drey EA. Contraceptive intentions among adolescents after abortion. J Adolesc Health 2006;39:283–6.
Viellas EF, da Gama SG, Theme Filha MM, Leal Mdo C. Repeated pregnancy among adolescents and negative outcomes of the newborn: study in the city of Rio de Janeiro. Rev Bras Epidemiol 2012;15:443–54.
Wang R, Wang H. Prebirth psychosocial factors as predictors of consistency in contraceptive use among Taiwanese adolescent mothers at 6 months postpartum. Public Health Nurs 2005;22:271–9.
Williams EG, Sadler LS. Effects of an urban high school-based child care center on self-selected adolescent parents and their children. J Sch Health 2001;71:47–52.
Wilson EK, Fowler CI, Koo HP. Postpartum contraceptive use among adolescent mothers in seven states. J Adolesc Health 2013;52:278–83.
Patchen L, Letourneau K, Berggren E. Evaluation of an integrated services program to prevent subsequent pregnancy and birth among urban teen mothers. Soc Work Health Care 2013;52:642–55.
Qualitative studies
Bull S, Hogue C. Exploratory analysis of factors associated with teens’ repeated childbearing. J Health Care Poor Underserved 1998;9:42–61.
Clarke J. Repeat teenage pregnancy in two cultures – the meanings ascribed by teenagers. Child Soc 2010;24:188–99.
Clarke JE. Repeated Teenage Pregnancies – The Meanings Ascribed by Teenagers – A Comparison Between London and Two Caribbean Islands. PhD thesis. London: Brunel University; 2002.
Hellerstedt WL, Story M. Adolescent satisfaction with postpartum contraception and body weight concerns. J Adolesc Health 1998;22:446–52.
Herrman JW. The voices of teen mothers: the experience of repeat pregnancy. Am J Matern Child Nurs 2006;31:243–9.
Herrman JW. Repeat pregnancy in adolescence: intentions and decision making. Am J Matern Child Nurs 2007;32:89–94.
Hoggart L, Phillips J, Birch A, Koffman O. Young People in London: Abortion and Repeat Abortion. London: Young London Matters Teenage Pregnancy Work Strand, Government Office for London; 2010.
Lewis D, Martins SL, Gilliam M. Partner roles in contraceptive use: what do adolescent mothers say? J Pediatr Adolesc Gynecol 2012;25:396–400.
Schaffer MA, Jost R, Pederson BJ, Lair M. Pregnancy-free club: a strategy to prevent repeat adolescent pregnancy. Public Health Nurs 2008;25:304–11.
Smith JL, Skinner SR, Fenwick J. Preconception reflections, postconception intentions: the before and after of birth control in Australian adolescent females. Sex Health 2013;10:332–8.
Weston MRS, Martins L, Neustadt AB, ML G. Factors influencing uptake of intrauterine devices among postpartum adolescents: a qualitative study. Am J Obstet Gynecol 2012;206:e1–7.
Wilson EK, Samandari G, Koo HP, Tucker C. Adolescent mothers’ postpartum contraceptive use: a qualitative study. Perspect Sex Reprod Health 2011;43:230–7.
Appendix 16 Excluded studies with reasons
Full-text articles retrieved from database searches assessed and excluded (n = 105)
Excluded because of study type (usually the article did not report research with useable data) (n = 44)
Akinbami LJ, Cheng TL, Kornfeld D. A review of teen–tot programs: comprehensive clinical care for young parents and their children. Adolescence 2001;36:381–93.
Alford S, Rutledge A, Huberman B. Science and Success: Programs that Work to Prevent Subsequent Pregnancy Among Adolescent Mothers. Washington, DC: Advocates for Youth; 2009.
Bailey PE, Bruno ZV, Bezerra MF, Queiroz I, Oliveira CM, Chen-Mok M. Adolescent pregnancy 1 year later: the effect of abortion vs. motherhood in Northeast Brazil. J Adolesc Health 2001;29:223–32.
Baldwin MK, Edelman AB. The effect of long-acting reversible contraception on rapid repeat pregnancy in adolescents: a review. J Adolesc Health 2012;52:S47–53.
Barlow J. Young mothers: contraception choices and other concerns. Practice Nurse 2005;29:24.
Baytop CM. Evaluating the effectiveness of programs to improve educational attainment of unwed African American teen mothers: a meta analysis. J Negro Educ 2006;75:458–77.
Bouris A, Guilamo-Ramos V, Cherry K, Dittus P, Michael S, Gloppen K. Preventing rapid repeat births among Latina adolescents: the role of parents. Am J Public Health 2012;102:1842–7.
Childree J. Abstract and Critique for Repeat Pregnancies Among Adolescent Mothers. Abstract and research proposal for a thesis. West Florida: University of West Florida; 2007.
Collier J, Blake H. Sexual and reproductive health in pregnant teenagers presenting for antenatal care or for termination. Curr Paediatr 2006;16:211–15.
Corcoran J, Pillai VK. Effectiveness of secondary pregnancy prevention programs: a meta-analysis. Res Soc Work Pract 2007;17:5–18.
Coren C. Some teenage mothers place high priority on avoiding repeat pregnancy in their early postpartum months. Perspect Sex Reprod Health 2004;36:34–5.
Dailard C. Reviving interest in policies and programs to help teens prevent repeat births. Guttmacher Rep Public Policy 2000;3:1–11.
Edwards S. Incentives draw teenage mothers to support groups, but participation does not prevent repeat pregnancy. Fam Plann Perspect 1997;29:191–2.
Núñez-Urquiza RM, Hernández-Prado B, García-Barrios C, González D, Walker D. Embarazo no deseado en adolescentes, y utilizacion de metodos anticonceptivos posparto. Salud Publica Mexico 2003;45:S92–S102.
Florida State University Center for Prevention and Early Intervention Policy. Subsequent Pregnancies and Births Among Adolescent Mothers FACT SHEET. 2005. URL: www.cpeip.fsu.edu/resourceFiles/resourceFile_76.pdf (accessed 20 June 2014).
Furey A. Are support and parenting programmes of value for teenage parents? Who should provide them and what are the main goals? Public Health 2004;118:262–7.
Greer F, Levin-Epstein J. One Out of Every Five: Teen Mothers and Subsequent Childbearing. Washington, DC: Center for Law and Social Policy; 1998.
Klerman LV, Baker BA, Howard G. Second births among teenage mothers: program results and statistical methods. J Adolesc Health 2003;32:452–5.
Knafl K. Effectiveness of a family support center approach to adolescent mothers: repeat pregnancy and school drop-out rates. J Child Fam Nurs 1998;1:88–90.
Lopez LM, Hiller JE, Grimes DA, Chen M. Education for contraceptive use by women after childbirth. Cochrane Database Syst Rev 2012;8:CD001863.
Madden T. Long-acting removable contraceptives prevent teen pregnancy. J Adolesc Health 2013;52:255–6.
Meade CS, Ickovics JR. Systematic review of sexual risk among pregnant and mothering teens in the USA: pregnancy as an opportunity for integrated prevention of STD and repeat pregnancy. Soc Sci Med 2005;60:661–78.
Milne D, Glasier A. Preventing repeat pregnancy in adolescents. Curr Opin Obstet Gynecol 2008;20:442–6.
Mims BL. Afrocentric perspective of adolescent pregnancy in African American families: a literature review. ABNF J 1998;9:80–8.
Nunez-Urquiza RM, Hernandez-Prado B, Garcia-Barrios C, Gonzalez D, Walker D. Unwanted adolescent pregnancy and post-partum utilization of contraceptive methods. Salud Publica Mexico 2003;45:S92–S102.
Omar HA, Fowler A, McClanahan KK. Significant reduction of repeat teen pregnancy in a comprehensive young parent program. J Pediatr Adolesc Gynecol 2008;21:283–7.
Oxtoby K. The Moat House Centre for Teenage Mums in Stockport. Community Care; 2008. URL www.communitycare.co.uk/2008/06/24/the-moat-house-centre-for-teenage-mums-in-stockport/ (accessed 13 October 2015).
Perrow F. Teenagers and double buggies: preventing a second pregnancy. RCM Midwives J 2004;7:508–9.
PhysOrg.com. Repeat Pregnancies Among UK Teenagers on the Increase. University of Nottingham; 2010. URL: http://phys.org/news152204668.html (accessed 20 June 2014).
Plastino KA. Commentary on repeat pregnancy prevention self-efficacy in adolescents: associations with provider communication, provider type and depression. South Med J 2012;105:598–9.
Porter LS, Holness NA. Breaking the repeat teen pregnancy cycle. Nurs Womens Health 2011;15:368–81.
Riera KC. Living Arrangements and the Outcomes of a Teen or Young Adult Birth. PhD thesis. College Park, MD: Department of Family Science, University of Maryland; 2011.
Rigsby DC, Macones GA, Driscoll DA. Risk factors for rapid repeat pregnancy among adolescent mothers: a review of the literature. J Pediatr Adolesc Gynecol 1998;11:115–26.
Rosengard C. Confronting the intendedness of adolescent rapid repeat pregnancy. J Adolesc Health 2009;44:5–6.
Rowlands S. Social predictors of repeat adolescent pregnancy and focussed strategies. Best Pract Res Clin Obstet Gynaecol 2010;24:605–16.
Ruedinger E, Cox JE. Adolescent childbearing: consequences and interventions. Curr Opin Pediatr 2012;24:446–52.
Seitz V, Apfel NH. Effective interventions for adolescent mothers. Clin Psychol-Sci Pract 1999;6:50–66.
Smith P, Buzi R. Workforce development as a promising approach to pregnancy prevention. J Adolesc Health 2013;1:S108.
Snow T. Pregnant pause for teenage mums. Nurs Stand 2006;20:14–15.
Nursing Standard Clinical Digest. Aggression is a predictor of rapid repeat teen pregnancy: pubertal onset age and conflict management key considerations in prevention strategies. Nurs Stand 2009;23:16.
Nursing Standard Clinical Digest. Two-times teen mothers face high risks for second baby. Nurs Stand 2008;22:16.
Stevens-Simon C. A cautionary note: letter to the editor. J Adolesc Health 2003;33:322–3.
Stevens-Simon C. The Second Chance Club. J Adolesc Health 2001;29:80.
Women’s Centre of Jamaica Foundation. Programme for Adolescent Mothers. Advocates for Youth; 2012. URL: www.aed.org/en/RH/Pubs/wsp/caseStudies/JamaicaCS.htm (accessed 30 May 2013).
Excluded because of study focus (usually the focus was on primary teenage pregnancy, not repeat) (n = 33)
Alcindo José R. Novamente grávida: adolescentes com maternidades sucessivas em Rondonópolis. [MT Pregnancy Again: Consecutive Motherhood in Rondonópolis]. PhD thesis. São Paulo: Faculdade de Saúde Pública; 2007. URL: www.teses.usp.br/teses/disponiveis/6/6136/tde-11022008–222655/pt-br.php (accessed 2 June 2013).
Aracena M, Krause M, Perez C, Mendez MJ, Salvatierra L, Soto M, et al. A cost-effectiveness evaluation of a home visit program for adolescent mothers. J Health Psychol 2009;14:878–87.
Balcazar H, Peterson G, Cobas JA. Acculturation and health-related risk behaviors among Mexican American pregnant youth. Am J Health Behav 1996;20:425–33.
Beenhakker B, Becker S, Hires S, Molano Di Targiana N, Blumenthal P, Huggins G. Are partners available for post-abortion contraceptive counseling? A pilot study in a Baltimore city clinic. Contraception 2004;69:419–23.
Birch DML. The adolescent parent: a fifteen year longitudinal study of school-age mothers and their children. Int J Adolesc Med Health 1998;10:141–53.
Blank L, Baxter SK, Payne N, Guillaume LR, Pilgrim H. Systematic review and narrative synthesis of the effectiveness of contraceptive service interventions for young people, delivered in educational settings. J Pediatr Adolesc Gynecol 2010;23:341–51.
Blank L, Baxter SK, Payne N, Guillaume LR, Squires H. Systematic review and narrative synthesis of the effectiveness of contraceptive service interventions for young people, delivered in health care settings. Health Educ Res 2012;27:1102–19.
Bond L, Lavelle K, Lauby J. A comparison of the risk characteristics of ever-pregnant and never-pregnant sexually active adolescents. J HIV AIDS Prev Educ Adolesc Child 2002;5:123–37.
Bowman KG, Ruchala PL. A comparison of the postpartum learning needs of adolescent mothers and their mothers. J Obstet Gynecol Neonatal Nurs 2006;35:250–6.
Breheny M, Stephens C. Barriers to effective contraception and strategies for overcoming them among adolescent mothers. Public Health Nurs 2004;21:220–7.
Collins ME, Lemon C, Street E. A consumer view of teen living programs: teen parents’ satisfaction with program components and services. Fam Soc 2000;81:284–93.
Dallas CM. Rapid repeat pregnancy among unmarried, African American adolescent parent couples. West J Nurs Res 2013;35:177–92.
de Sousa MCR, Gomes KRO. Objective and perceived knowledge of oral contraceptive methods among adolescent mothers. Cad Saúde Pública 2009;25:645–54.
Degazon-Johnson R. A New Door Opened: a Tracer Study of the Teenage Mothers Project, Jamaica. Early Childhood Development: Practice and Reflections 13. Following Footsteps. The Hague: Bernard van Leer Foundation; 2001.
Felton GM, Parsons MA, Hassell JS. Health behavior and related factors in adolescents with a history of abortion and never-pregnant adolescents. Health Care Women Int 1998;19:37–47.
Kaufman CE, de Wet T, Stadler J. Adolescent pregnancy and parenthood in South Africa. Stud Fam Plann 2001;32:147–60.
Lee MC, Lee SH, Chou MC. Association of risk-taking behaviors with adolescent childbearing. J Formos Med Assoc 2001;100:533–8.
McGaha-Garnett V. Needs assessment for adolescent mothers: building resiliency and student success towards high school completion. In Walz GR, Bleuer J, Yep R, editors. Compelling Counseling Interventions: Celebrating VISTAS’ Fifth Anniversary. Ann Arbour, MI: Counseling Outfitters; 2008. pp. 11–20.
Meyrick J. Repeat use of contraceptive crisis services among adolescent women. J Fam Plann Reprod Health Care 2001;27:33–6.
Mims BL. Communication Patterns in African-American Families with Repeat Adolescent Pregnancy. PhD thesis. Ann Arbour, MI: University of Michigan; 1996. URL: http://0-search.ebscohost.com.unicat.bangor.ac.uk/login.aspx?direct=true&db=c8h&AN=1999063948&site=ehost-live (accessed 16 July 2013).
Molina RC, Roca CG, Zamorano JS, Araya EG. Family planning and adolescent pregnancy. Best Pract Res Clin Obstet Gynaecol 2010;24:209–22.
Moriarty Daley A, Sadler LS, Dawn Reynolds H. Tailoring clinical services to address the unique needs of adolescents from the pregnancy test to parenthood. Curr Probl Pediatr Adolesc Health Care 2013;43:71–95.
Obare F, van der Kwaak A, Birungi H. Factors associated with unintended pregnancy, poor birth outcomes and post-partum contraceptive use among HIV-positive female adolescents in Kenya. BMC Womens Health 2012;12:34.
Phipps MG, Rosengard C, Weitzen S, Meers A, Billinkoff Z. Age group differences among pregnant adolescents: sexual behavior, health habits and contraceptive use. J Pediatr Adolesc Gynecol 2008;21:9–15.
Rome ES, Rybicki LA, Durant RH. Pregnancy and other risk behaviors among adolescent girls in Ohio. J Adolesc Health 1998;22:50–5.
Ross M. Health and Social Services Provision to Pregnant and Parenting Adolescents in Southern New Brunswick. MA thesis. Fredericton, New Brunswick: University of New Brunswick; 2009.
Rotermann M. Second or subsequent births to teenagers. Health Rep Stat Canada 2007;18:39–42.
Sadler LS, Chen JY, Daley AM, Leventhal JM, Reynolds H. Reproductive care and rates of pregnancy in teenagers with negative pregnancy test results. J Adolesc Health 2006;38:222–9.
Taffa N, Omollo D, Matthews Z. Teenage pregnancy experiences in rural Kenya. Int J Adolesc Med Health 2003;15:331–40.
Tomlinson K. Repeat Pregnancy in Teenage Mothers. PhD thesis. Hull: University of Hull; 2008. URL: https://hydra.hull.ac.uk/assets/hull:1597a/content (accessed 20 June 2014).
Trivedi D, Brooks F, Graham M, Bunn F, Wentz R. Teenage Pregnancy and Parenthood: A Descriptive Mapping of Research Studies Exploring the Role of General Practitioners, Nurses, Health Visitors or Midwives; Young Fathers/Young Men; and Peers. 2012. URL: www.herts.ac.uk/fms/documents/research/health-and-human-science-research-institutes/nice_review.pdf (accessed 30 May 2013).
Ventura W, Ventura-Laveriano J, Nazario-Redondo C. Perinatal outcomes associated with subsequent pregnancy among adolescent mothers in Peru. Int J Gynecol Obstet 2012;117:56–60.
Vishneski S. Content validation of an instrument used to measure contraceptive knowledge, attitudes and usage in adolescents with a rapid repeat pregnancy. J Womens Health 2010;19:637.
Excluded because of study population (usually the study population was not clearly defined according to our criteria for ‘teenage’) (n = 22)
Akinbami LJ, Schoendorf KC, Kiely JL. Risk of preterm birth in multiparous teenagers. Arch Pediatr Adolesc Med 2000;154:1101–7.
Boardman L, Allsworth J, Phipps M, Lapane K. Risk factors for unintended versus intended rapid repeat pregnancies among adolescents. J Adolesc Health 2006;39:e1–8.
Gilliam M, Knight S, McCarthy M. Success with oral contraceptives: a pilot study. Contraception 2004;69:413–18.
Gilliam ML, Warden MM, Tapia B. Young Latinas recall contraceptive use before and after pregnancy: a focus group study. J Pediatr Adolesc Gynecol 2004;17:279–87.
Jacoby M, Gorenflo D, Wunderlich C, Eyler AE. Rapid repeat pregnancy and experiences of interpersonal violence among low-income adolescents. Am J Prev Med 1999;16:318–21.
Kanku T. Attitudes, perceptions and understanding amongst teenagers regarding teenage pregnancy sexuality and contraception in Taung. S Afr Fam Pract 2010;52:563–72.
Kelly LS, Sheeder J. Why lightning strikes twice: postpartum resumption of sexual activity during adolescence. J Pediatr Adolesc Gynecol 2005;18:327–35.
Kuroki LM, Allsworth JE, Redding CA, Blume JD, Peipert JF. Is a previous unplanned pregnancy a risk factor for a subsequent unplanned pregnancy? Am J Obstet Gynecol 2008;199:517.e1–7.
Lemay CA, Cashman SB, Elfenbein DS, Felice M. Adolescent mothers’ attitudes towards contraceptive use before and after pregnancy. J Paediatr Adolesc Gynecol 2007;20:233–40.
Matsuda Y, Masho S, McGrath JM. The relationship between repeated unintended pregnancies and current contraceptive use: National Survey of Family Growth (NSFG) 2006–2008 data. J Community Health Nurs 2012;29:163–72.
Mentula MJ, Niinimäki M, Suhonen S, Hemminki E, Gissler M, Heikinheimo O. Young age and termination of pregnancy during the second trimester are risk factors for repeat second-trimester abortion. Am J Obstet Gynecol 2010;203:107.e1–7.
Mims B, Biordi DL. Communication patterns in African-American families with adolescent mothers of single or repeat pregnancies. J Natl Black Nurses Assoc 2001;12:34–41.
Omar H, Fowler A, D’Angelo S. Improved continuation rate of depot-medroxyprogesterone acetate in adolescent mothers. Int J Adolesc Med Health 2002;14:149–52.
Peipert JF, Madden T, Allsworth JE, Secura GM. Preventing unintended pregnancies by providing no-cost contraception. Obstet Gynecol 2012;120:1291–7.
Qin J-P, Chen S, Di N, Yang Y-P, Zhou L, Zhang D-k. Evaluation of the effect of post-abortion counseling and education among unmarried abortion adolescents. Chung Hua Fu Chan Ko Tsa Chih 2010;45:201–4.
Rose SB, Cooper AJ, Baker NK, Lawton B. Attitudes toward long-acting reversible contraception among young women seeking abortion. J Womens Health 2011;20:1729–35.
Sundby J, Svanemyr J, Maehre T. Avoiding unwanted pregnancy-the role of communication, information and knowledge in the use of contraception among young Norwegian women. Patient Educ Couns 1999;38:11–19.
Tocce KM, Sheeder JL, Teal SB. Rapid repeat pregnancy in adolescence: do immediate postpartum contraceptive implants make a difference? Am J Obstet Gynecol 2012;206:e1–7.
Tocce K, Sheeder J, Python J, Teal SB. Long-acting reversible contraception in postpartum adolescents: early initiation of etonogestrel implant is superior to IUDs in the outpatient setting. J Pediatr Adolsc Gynecol 2012;25:59–63.
Torjesen I. Jinny had a real desire to make a difference. Nurs Times 2008;104:24–5.
Waggoner MR, Lanzi RG, Klerman LV. Pregnancy intentions, long-acting contraceptive use and rapid subsequent pregnancies among adolescent and adult first-time mothers. J Child Adolesc Psychiatr Nurs 2012;25:96–104.
Whitaker AK, Dude AM, Neustadt A, Gilliam ML. Correlates of use of long-acting reversible methods of contraception among adolescent and young adult women. Contraception 2010;81:299–303.
Unobtainable report (usually because a web page was no longer available) or full citation details missing (n = 6)
Baltimore Region Community Programs, Government and Community Affairs. College Park, MD: University of Maryland; 2012.
Community-based computer-assisted motivational intervention reduces repeat births to adolescents. J Natl Med Assoc 2010;102:154.
King-Marshall E. Achievement Motivation Association with Teen Birth and Repeat Birth: A Qualitative Study. Gainesville, FL: University of Florida; 2012.
Nottingham University Hospitals NHS Trust. Reducing Repeat Pregnancies: A Randomised Control Trial Of A Targeted Family Planning Intervention For Teenage Mothers & For Teenagers Who Have A Termination Of Pregnancy.
Barrett, The Honors College. Student Spotlight on Kaydi Flowers. 2012.
VioPro Database Record #3616. The Mission of Abuelas y Jovenes is to Mobilize Older Women as Abuelas to Visit Young Pregnant and Parenting Latina Women. 2010.
Studies included in the mapping exercise that did not meet the CART criteria and were excluded from the in-depth review (n = 48)
Completeness (n = 6)
Coard S, Nitz K, Parks P, Felice M. Predictors of repeat pregnancy in urban adolescent mothers. J Adolesc Health 1998;22:173.
Damle LF, McEvoy AK, Gohari A, Desale SY, Patchen L, Gomez-Lobo V. Early contraception initiation in first time adolescent mothers: does it decrease rapid repeat pregnancy? J Pediatr Adolesc Gynecol 2012;25:e52.
de Carvalho GM, Merighi MAB, de Jesus MCP. Repeated adolescent parenthood from the perspective of the subjects involved. Texto Contexto Enferm 2009;18:17–24.
Haamid F, Wiemann C. You’re pregnant again?! Which adolescent mothers experience multiple repeat pregnancies? J Adolesc Health 2010;46:S32.
Hayter M. Preventing unplanned repeat pregnancy in teenage mothers: a qualitative study of patients’ and professionals’ experiences of nurse led home based sexual health care. UKCRN portfolio database Record ID 14336, 2013. URL: www.nihr.ac.uk/funding/fundingdetails.htm?postid=1626 (accessed 13 October 2015).
Sakharkar VP, Frankson MA. Impact of the ‘providing access to continued education’ programme on repeat teenage pregnancy in The Bahamas. West Indian Med J 2012;61:33.
Accuracy (n = 15)
Blackman T, Wistow J, Byrne D. Towards a new understanding of how local action can effectively address health inequalities; Report for National Institute for Health Research Service Delivery and Organisation programme. Wolfson Research Institute, Durham University; 2011. NIHR Portfolio record. URL: www.nets.nihr.ac.uk/projects/hsdr/081716203 (accessed 20 June 2014).
Britner P, Reppucci N. Prevention of child maltreatment: evaluation of a parent education program for teen mothers. J Child Fam Stud 1997;6:165–75.
Brown H, Saunders R, Dick J. Preventing secondary pregnancy in adolescents: a model program. Health Care Women Int 1999;20:5–15.
Daly JZ, Ziegler R, Goldstein DJ. Adolescent postabortion groups: risk reduction in a school-based health clinic. J Psychosoc Nurs Ment Health Serv 2004;42:48–54.
Doherty E, Smith A. Postnatal contraception planning for young women. MIDIRS Midwifery Digest 2006;16:237–9.
Falk G, Brynhildsen J, Ivarsson AB. Contraceptive counselling to teenagers at abortion visits – a qualitative content analysis. Eur J Contracept Reprod Health Care 2009;14:357–64.
Fernandez M, Ruch-Ross HS. Ecological analysis of program impact: a site analysis of programs for pregnant and parenting adolescents in Illinois. J Appl Sociol 1998;15:104–33.
Fischer RL. Evaluating the delivery of a teen pregnancy and parenting program across two settings. Res Social Work Pract 1997;7:350–69.
Fuscaldo D, Kaye JW, Philliber S. Evaluation of a program for parenting. Fam Soc 1998;79:53–61.
Harris S, Koukos C. Sure Start: delivering a needs-led service in Swansea introduction the focus on play and stimulation helps. Community Pract 2007;80:24–7.
Hewell SW, Andrews JL. Contraceptive use among female adolescents. Clin Nurs Res 1996;5:356–63.
Kafka Brigade UK and Ireland. Swansea Young Parents: A look at Service Delivery; Phase 1 Action Plan 2012, Young Mothers’ Stories and Emerging Service Delivery Issues. Sponsor: Swansea Young Parents Strategy Group; 2012.
O’Rourke KM, Key JD. Process evaluation of a repeat pregnancy prevention program for African-American adolescent mothers. Int Q Community Health Educ 2004;23:253–62.
Philliber S, Brooks L, Lehrer L, Oakley M, Waggoner S. Outcomes of teen parenting programs in New Mexico. Adolescence 2003;38:536–53.
Saunders RB, Brown HN. Innovative collaboration to prevent repeated adolescent pregnancies. Nurs Connect 1997;10:5–11.
Relevance (n = 15)
Cavalier Y. Factors Associated with Repeat Teen Pregnancy Prevention Among Teen Mothers During 1996 and 2002 Using Longitudinal Survey of Adolescent Health Data. PhD thesis. Baltimore, MD: Morgan State University; 2009. URL: http://search.proquest.com/docview/622193489?accountid=14874 (accessed 28 May 2013).
Collier County Health Department. Teen Choices Program Details. 2003. URL: www.naccho.org/topics/modelpractices/database/practice.cfm?practiceID=48 (accessed 20 June 2014).
Conroy K, Engelhart T, Martins Y, To W, Snyder A, Coletti K, et al. The repeat pregnancy enigma: a qualitative study: exploring teen mothers’ motivation and planning for a second pregnancy. The Society for Adolescent Health and Medicine, 2012 Annual Meeting, New Orleans, LA, 14–17 March 2012.
Edwards CA. Predictors of Repeat Adolescent Motherhood: The Role of Beliefs Attitudes Subjective Norm, Perceived Control and Intention. PhD thesis. Lorna Linda, CA: Loma Linda University; 1996. URL: http://0-web.a.ebscohost.com.unicat.bangor.ac.uk/ehost/detail?sid=fbd12552–5402–4fea-a4ba-851a9b6f2b1f%40sessionmgr4002&vid=1&hid=4206&bdata=JnNpdGU9ZWhvc3QtbGl2ZQ%3d%3d#db=c8h&AN=2004076859 (accessed 30 May 2013).
Fenyk JM. An Evaluation of a School-based Program for Pregnant and Parenting Adolescents. PhD thesis. Minneapolis, MN: University of Minnesota; 2007. URL: http://search.proquest.com/docview/622020488?accountid=14874 (accessed 30 May 2013).
Kelsey MC. The Role of Home Visitation in Improving Outcomes for Teenage Mothers and their Children: Evidence from the Teenage Parent Home Visitor Services Demonstration. PhD thesis. Philadelphia, PA: University of Pennsylvania; 2000. URL: http://repository.upenn.edu/dissertations/AAI9965502/ (accessed 2 August 2013).
Kelsey M, Johnson A, Maynard R. The Potential of Home Visitor Services to Strengthen Welfare-to-Work Programs for Teenage Parents on Cash Assistance. University of Pennsylvania, Mathematica Policy Research, Inc., and the Health Federation, Philadelphia; 2001. URL: http://mathematica-mpr.com/publications/pdfs/potential.pdf (accessed 20 June 2014).
McNeill EH. Hope as a Strategy for Improving Student Achievement And Dissuading Repeat Pregnancy in Pregnant and Parenting Adolescents. PhD thesis. College Station, TX: Texas A&M University; 2010. URL: http://repository.tamu.edu/bitstream/handle/1969.1/ETD-TAMU-2010–05–7832/MCNEILL-DISSERTATION.pdf?sequence=3 (accessed 4 August 2013).
Montgomery AE. The Distinction Between First and Higher-Order Pregnancies Among Low-Income Adolescents. PhD thesis. Tuscaloosa, AL: University of Alabama; 2009. URL: http://gradworks.umi.com/33/66/3366905.html (accessed 2 August 2013).
Moses A. Teenage Pregnancy Prevention in California. 1995 Policy Roundtable Series Report. Sacramento, CA: California State Library Foundation; 1995. URL: www.library.ca.gov/crb/cafis/reports/95-01/95-01.pdf (accessed 14 October 2015).
O’Connell J. Expectant and Parenting Students. Cal-SAFE Report to the Legislature. California Department of Education; 2005. URL: www.cde.ca.gov/re/pr/calsafe.asp (accessed 14 October 2015).
O’Connell J. Cal-SAFE Reference Handbook – Child Development. Reference Handbook. California Department of Education; 2005. URL: http://4teenparents.com/School%20and%20You%20Rights%20PDF/Cal-SAFE%20reference%20handbook.pdf (accessed 14 October 2015).
Quint J, Bos J, Polit D. New Chance: Final Report on a Comprehensive Program for Young Mothers in Poverty and their Children. 1997. URL: www.mdrc.org/publication/new-chance (accessed 20 June 2014).
Shearer DL. Cognitive Ability and its Association with Early Childbearing and Second Teen Births. PhD thesis preview. Birmingham, AL: University of Alabama at Birmingham, 1999. URL: http://search.proquest.com/docview/619555688?accountid=14874 (accessed 13 October 2013).
Steinberg JK. Pregnant and Parenting Adolescents: Predictors of Success or Failure in a Community-Based Treatment Program. PhD thesis. New Brunswick, NJ: Rutgers State of New Jersey University; 1996. URL: http://search.proquest.com/docview/618996561?accountid=14874 (accessed 13 October 2013).
Therrien KJ. Repeat Pregnancies During Adolescence Factors that Influence Teens’ Decisions to Have More than One Child. Master’s thesis. Northampton, MA: Smith College School for Social Work; 2009. URL: https://dspace.smith.edu/handle/11020/10146 (accessed 4 November 2013).
United States General Accounting Office. Teen Pregnancy: State and Federal Efforts to Implement Prevention Programs and Measure their Effectiveness. Report to the Chairman, Committee on Labor and Human Resources, US Senate. US Washington, DC: US General Accounting Office; 1998.
Timeliness (n = 12)
Davis TM. An examination of repeat pregnancies using problem behavior theory: is it really problematic? J Youth Stud 2002;5:337–51.
East PL, Felice ME. Adolescent Pregnancy and Parenting: Findings from a Racially Diverse Sample (Research Monographs in Adolescence Series). Mahwah, NJ: Lawrence Erlbaum Associates Publishers; 1996.
Erickson PI. Latina Adolescent Childbearing in East Los Angeles. 1998. URL: http://search.proquest.com/docview/618996561?accountid=14874 (accessed 10 October 2013).
Finkel ML, Thompson S. Focus on teenage motherhood: an innovative response to a growing problem. Early Child Dev Care 1997;129:105–13.
Gillmore MR, Lewis SM, Lohr MJ, Spencer MS, White RD. Repeat pregnancies among adolescent mothers. J Marriage Fam 1997;59:536–50.
Gurdin JB, Mallari A, Park MJ, Mince J. Queens Hospital Center’s Teenage Program: a second pregnancy prevention program for young men and women. In Card JJ, Benner T, editors. Model Programs for Adolescent Sexual Health: Evidence-Based HIV, STI and Pregnancy Prevention Interventions. New York, NY: Springer; 2008. pp. 131–42.
Gurdin JB, Niego S, Mince J. A health care program for first-time adolescent mothers and their infants: a second pregnancy prevention program for teen mothers. In Card JJ, Benner T, editors. Model Programs for Adolescent Sexual Health: Evidence-Based HIV, STI and Pregnancy Prevention Interventions. New York, NY: Springer; 2008. pp. 121–9.
Manlove J. Subsequent fertility among teen mothers: longitudinal analyses of recent national data. J Marriage Fam 2000;62:430–48.
Pfitzner MA, Hoff C, McElligott K. Predictors of repeat pregnancy in a program for pregnant teens. J Pediatr Adolesc Gynecol 2003;16:77–81.
Seamark C. Design or accident? The natural history of teenage pregnancy. J R Soc Med 2001;94:282–5.
Seitz V, Apfel NH. Creating effective school-based interventions for pregnant teenagers. In Peters R deV, Leadbeater B, McMahon RJ, editors. Resilience in Children, Families and Communities: Linking Context to Practice and Policy. New York, NY: Kluwer Academic/Plenum Publishers; 2005. pp. 65–82.
Thompson PJ, Powell MJ, Patterson RJ, Ellerbee SM. Adolescent parenting: outcomes and maternal perceptions. J Obstet Gynecol Neonatal Nurs 1995;24:713–18.
Grey literature identified in Google search that did not meet the CART criteria (n = 21)
Completeness (n = 20)
Barlow J, McMillan AS, Kirkpatrick S, Ghate D, Smith M, Barnes J. Health-led Parenting Interventions in Pregnancy and Early Years. Research report DCSF-RW070. Warwick: Department for Children, Schools and Families, University of Warwick; 2008.
Bedfordshire Clinical Commissioning Group. Central Bedfordshire Health & Wellbeing Strategy 2012–2016. Bedfordshire Clinical Commissioning Group; 2012. URL: www.centralbedfordshire.gov.uk/Images/110213CBCHWBStrategyFinal_tcm6–40628.pdf (accessed 17 February 2014).
Bristol Public Health with the Bristol Partnership, NHS Bristol, Bristol City Council Bristol Public Health and Wellbeing Factsheet, January 2010. URL: www.bristol.gov.uk/sites/default/files/documents/health_and_adult_care/health_and_medical_advice/Bristol%20public%20health%20factsheet%20-%20teenage%20pregnancy.pdf (accessed 14 October 2015).
Gloucestershire Children’s Partnership. Gloucestershire Teenage Pregnancy Partnership Business Plan 2011/14. URL: www.gloucestershire.gov.uk/extra/CHttpHandler.ashx?id = 38556&p (accessed 16 February 2014).
Hallgarten L, Misaljevich N. Education for Choice, Reducing Repeat Teenage Conceptions: A Review of Practice. Education for Choice; 2007. URL: www.efc.org.uk/PDFs/reducing-repeat-teenage-conceptions-review-of-practice.pdf (accessed 17 February 2014).
Hertfordshire Children’s Trust Partnership. Hertfordshire Teenage Pregnancy Strategy Action Plan 2009 – 2010. URL: www.hertsdirect.org/teenpregnancy (accessed 16 February 2014).
Lewisham Strategic Partnership. Lewisham’s Children and Young People’s Plan 2009–12: Review at April 2011. URL: www.lewishamstrategicpartnership.org.uk/docs/LewishamsChildrenAndYoungPeoplesPlan20092012ReviewApril2011.pdf (accessed 17 February 2014).
Medway Council. Making Life Better: Children’s Services in Medway APA Self-Assessment. Medway Council; 2008. URL: http://medway.gov.uk/pdf/och20090921r-8.pdf (accessed 14 October 2015).
Mollidor CM. ‘I Deserve Respect Because I’m a Good Mum.’ Social Representations of Teenage Motherhood and the Potential for Social Change. PhD thesis. London: London School of Economics; 2013. URL: http://etheses.lse.ac.uk/621/ (accessed 16 February 2014).
NHS Islington. Islington JSNA 2010/11: Teenage Pregnancy. URL: www.islingtonccg.nhs.uk/JSNA2011/06._Teenage_pregnancy_long_version.pdf (accessed 17 February 2014).
NHS Wales. Teenage Conception Intervention and Audit:Empower to Choose. URL: www.wales.nhs.uk/sitesplus/documents/888/Empower%20to%20Choose%20Technical%20Book%20%283%29.pdf (accessed 16 February 2014).
Ormston R, McConville S. Evaluation of the Family Nurse Partnership Programme in NHS Lothian, Scotland: 3rd Report – Infancy. Scottish Government Social Research; 2012. URL: www.scotland.gov.uk/Publications/2012/12/4237 (accessed 16 February 2014).
Peterborough City Council. Scrutiny Review of Teenage Pregnancy. Peterborough City Council, Health Overview and Scrutiny Committee; 2007. URL: www.peterborough.gov.uk/pdf/cou-dem-teenagepregnancy-review-finalrpt.pdf (accessed 17 February 2014).
Report to The Chair and Members of the Health Scrutiny Committee, Redcar & Cleveland Borough Council, January 2013. Report unavailable.
Robinson J. Medway Teenage Pregnancy Annual Report 2009/2010. Medway Teenage Pregnancy Partnership; 2010. URL: www.medwaycan.co.uk/documents/medway-teenage-pregnancy-annual-report-20092010–1271852034.pdf (accessed 17 February 2014).
Southampton City Primary Care Trust. Health in Southampton 2006: Report of the Public Health Director. Southampton City Primary Care Trust; 2006. URL: www.publichealth.southampton.gov.uk/Images/Southampton%20PHAR%202006.pdf (accessed 16 February 2014).
Children and Young People’s Services. St Helens Teenage Pregnancy Strategy 2009–11. 2009. URL: http://moderngov.sthelens.gov.uk/%28S%28sayuwtrq5j4tsh45xi54xr55%29%29/mgConvert2PDF.aspx?ID=2053 (accessed 16 February 2014).
Teenage Pregnancy Strategy Partnership Board Workgroup. Children and Young People’s Strategic Partnership for Plymouth. 2006. URL: www.plymouth.gov.uk/teen_preg_agenda_setting_and_planning_report_march_06.pdf (accessed 16 February 2014).
Robinson D. The Annual Report of the Director of Public Health for Newcastle 2008–2009. URL: www.ntw.nhs.uk/fileUploads/1432652213NTW%20AD-PH%20Annual%20Report%202008-9.pdf (accessed 14 October 2015).
Torbay Council. Reducing Teenage Conceptions in Torbay: Annual Report April 2011–March 2012. URL: www.torbay.gov.uk/tp-annualreport0910.pdf (accessed 17 February 2014).
Relevance (n = 1)
Marie Stopes United Kingdom. Abortion, Contraceptive Uptake and Use Among Young Women: Findings From a Quantitative Surveyin Collaboration with the University of Greenwich. 2014. URL: http://mariestopes.org/sites/default/files/MSUK%20Contraception%20Uptake%20research.pdf (accessed 15 March 2014).
Studies identified in update searches and excluded (n = 5)
Excluded because of study type (n = 2)
Aventin A, Lohan M. ‘You’re wha . . .?!’. Pract Midwife 2013;16:21–3.
Centers for Disease Control and Prevention. Vital signs: repeat births among teens – United States, 2007–2010. Morb Mortal Wkly Rep 2013;62:249–55.
Excluded because of study focus (n = 2)
Barr AB, Simons RL, Simons LG, Gibbons FX, Gerrard M. Teen motherhood and pregnancy prototypes: the role of social context in changing young African American mothers’ risk images and contraceptive expectations. J Youth Adolesc 2013;42:1884–97.
DeSocio JE, Holland ML, Kitzman HJ, Cole RE. The influence of social-developmental context and nurse visitation intervention on self-agency change in unmarried adolescent mothers. Res Nurs Health 2013;36:158–70.
Excluded because of study population (n = 1)
Bajos N, Prioux F, Moreau C. Increase of repeat abortion in France: from contraceptive issues to postponement of childbearing age. Rev Epidemiol Sante Publique 2013;61:291–8.
Studies identified in citation searches and excluded (n = 3)
Excluded because of study type (n = 2)
Belzer M, Yoshida E, Teijirian T, Tucker D, Chung K, Sanchez K. Advanced supply of emergency contraception for adolescent mothers increased utilization without reducing condom or primary contraception use. J Adolesc Health 2003;32:122–3.
Cox JE, Buman MP, Woods ER, Famakinwa O, Harris SK. Evaluation of raising adolescent families together program: a medical home for adolescent mothers and their children. Am J Public Health 2012;102:1879–85.
Excluded because of study focus (n = 1)
SmithBattle L, Lorenz R, Leander S. Listening with care: using narrative methods to cultivate nurses’ responsive relationships in a home visiting intervention with teen mothers. Nurs Inq 2013;20:188–98.
Appendix 17 Certainty of the qualitative evidence (CerQual)
Method
Using the CerQual approach, our assessment of certainty is based on two factors: the methodological limitations of the individual studies contributing to a review finding and the coherence of each finding. Firstly, we agreed on a set of finding statements that covered the main key findings of interest from the thematic synthesis. For each finding statement, we made a note of the studies that made a contribution to that finding. We agreed on how many studies made a contribution and the relevance of their context, and attributed an overall rating to the specific finding (high, medium or low) with a statement to explain the rating. We then looked at the quality of studies (as assessed by the MMAT)54 contributing to the specific finding and attributed an overall rating (high, medium or low). However, the MMAT assessments were so adversely affected by poor reporting of the study methods that we also considered the extent to which the findings of each study were supported by extracts from the original data (i.e. the ‘thickness’ and ‘richness’ of the supporting data). The final rating was a combination of the two (high, medium or low) and we recorded a brief explanation.
| Summary statement | Certainty of the evidence | Explanation of the certainty in the evidence assessment |
|---|---|---|
| In the context of unstable backgrounds, lack of family support, insecure housing and chaotic lifestyles lacking in educational or vocational opportunities, there was no thought or planning; sexual activity was spontaneous and teenage pregnancy an accepted norm | High certainty | The finding was from two moderate- and high-quality US studies; however, the finding is plausible and likely to be transferable to UK settings |
| Some repeat pregnancies did not result from chaotic lifestyles but were conceived to provide a sibling for the first-born or to complete childbearing before going back to education or training or employment | High certainty | The finding was seen across two moderate- and high-quality US studies and one high-quality UK study |
| Some repeat pregnancies were conceived with the father in mind, either because he wanted a baby or because the mother felt it would help to consolidate the relationship | High certainty | The finding was from three studies of moderate- and high-quality; two were from the US and one from the UK |
| Some young mothers were determined not to get pregnant again and to manage their own sexual behaviour and contraception | High certainty | The finding was from four studies of moderate- to high-quality. All four were conducted in the USA but the finding is plausible and likely transferable to UK settings |
| Young mothers with goals and aspirations were less likely to have a repeat pregnancy; being a role model for their child was a motivating factor | High certainty | The finding was from three studies of moderate- and high-quality; two were from the USA and one from the UK |
| Attempts to achieve educational or employment goals were frustrated by lack of childcare, inflexible school authorities and limited earning capacity in comparison with benefits | High certainty | The finding was from one US and one UK study, both of high quality |
| Lack of love, or the loss of a baby through miscarriage, abortion, stillbirth or being taken into care was a powerful motivator not to avoid a subsequent pregnancy | High certainty | The finding was from two high-quality UK studies and one moderate-quality US study |
| Being persuaded to have an abortion against a young woman’s wishes was traumatic and very likely to result in a rapid repeat pregnancy being kept secret to avoid repeating the experience | High certainty | The finding was from two high-quality UK studies |
| Young women who made their own abortion decision and were supported were less likely to be traumatised or to regret their actions and more likely to take effective measures to avoid another pregnancy | High certainty | The finding was seen in only one high-quality UK study and one moderate-quality Australian study, but is plausible and likely to be transferable to other settings |
| Young women lacked basic understanding about fertility and knowledge about contraceptive methods | High certainty | The finding was seen across six moderate- to high-quality US studies and one high-quality study from the UK |
| Young women enrolled in a school-based intervention had daily access to a public health nurse who provided information and with whom they felt comfortable in discussing contraception | Low certainty | The finding was from one moderate-quality US study and the supporting data for this finding were relatively thin |
| A prevalent myth that deterred some young women from having an abortion, and led others to neglect to use contraception after having an abortion, was that following an abortion a woman would never be able to conceive again. This misunderstanding largely derived from sex and relationship education in schools and from abortion clinic staff | High certainty | The finding was from two high-quality UK studies |
| Timely contraceptive counselling and the provision to young mothers of the contraceptive method of their choice helped them to prevent a rapid repeat pregnancy | High certainty | The finding was seen in only one moderate- quality US study, but nevertheless seems extremely plausible |
| Inflexible appointment times and the inability of providers to counsel, prescribe and supply the method of choice in a single appointment were barriers to the timely uptake of effective contraception | High certainty | The finding was from two high- and moderate-quality US studies and one high-quality UK study |
| Young women frequently changed contraceptive methods and this, along with the difficulty in accessing contraceptive services described above, led to gaps in protection | High certainty | The finding was from two US studies of moderate and high quality, but seems plausible and likely to be transferable to other settings |
| Some young women were deterred from using or discontinued using some types of contraception because of side effects, particularly weight gain or disruption of the menstrual cycle | High certainty | The finding was seen in four US studies of moderate and highquality and seems likely to be transferable to other settings |
| Young women’s partners influenced their contraceptive choices and could support them (e.g. remind them to take the pill or persuade them to use LARCs). However, some wanted another baby and others objected to specific contraceptive methods (e.g. IUD) | High certainty | The finding was seen across five moderate- and high-quality studies. All were in the US but the finding seems likely to be transferable to other settings |
| Doctors or family members could also be supportive of contraceptive uptake and continued use | Moderate certainty | The finding was from only one high-quality US study but is likely to be transferable to other settings |
| Consistent use of oral contraceptives was a particular problem for young women with sometimes chaotic lifestyles and therefore many of them preferred LARCs | High certainty | The finding was seen in one high-quality UK study, two moderate- and high-quality US studies, and one Australian study of moderate-quality |
| Some young women who had previously failed to use oral contraception consistently enough to prevent pregnancy still chose it after their baby was born. Some (but not all) found better ways of remembering to take it, e.g. a reminder alarm on their mobile phone | Moderate certainty | The finding was from only one Australian study of moderate quality, but appears plausible |
| For some young women, even medroxyprogesterone acetate (Depo-Provera®, Pfizer) injections were unreliable because they entailed making and keeping regular doctor’s appointments; they preferred IUDs, which required minimum follow-up care | Moderate certainty | The finding was from one high-quality US study |
| Young women enrolled in a school-based intervention had monthly pregnancy tests and a monthly questionnaire about their sexual activity and contraceptive use. They found this useful but complained of its intrusiveness | Low certainty | This equivocal finding was from one moderate- quality US study |
| The idea of peer mentors had a mixed response. Some thought that, having had similar experiences, they might be more effective than older, more authoritative figures; others saw them as negative role models who had no right to preach | Low certainty | This equivocal finding was from one high-quality UK study |
| The provision of abortion services was patchy and access for vulnerable groups, including teenagers, was particularly difficult | Moderate certainty | The study was from two high-quality UK studies but both were set in London and might not be representative of services UK wide |
| Among the young women interviewed in these studies, there was a prevalence of negative, moralistic attitudes towards abortion that, in some cases, were related to religious or cultural beliefs, but often appeared to have been influenced by the presentation of abortion in the context of sex and relationship education or religious education in schools | High certainty | The study was from two high-quality UK studies and one high-quality US study |
Appendix 18 Summary of qualitative studies
| Study and location | Data collection method and date | Participant details | Setting (including intervention if any) | Analysis method | Study focus/research question |
|---|---|---|---|---|---|
| Bull and Hogue, 1998;129 USA (three urban and two rural counties in Georgia) | Focus groups; recorded and transcribed verbatim; date not reported | 40 teen mothers, aged 16–19 years; 29 African American, 9 white and 2 Hispanic; 24 mothers/guardians (1 male); 18 African American, 6 white | A state supplemental nutritional programme for women, infants and children that served > 70% of teen mothers in Georgia | Content analysis using grounded theory and Text Tally (version 1, Harmony Hollow Software) for thematic coding | Factors associated with repeat pregnancy including pregnancy plans, contraceptive use, education, aspirations, relationships between teen mothers and their parents and the fathers of their children. Influence of the nutrition programme and other social service agencies |
| Clarke, 2010,130 and Clarke, 200239 (thesis); UK and the Caribbean (London, Barbados and Jamaica) | Interviews; recorded and transcribed verbatim; date not reported | 52 teens who had had two or more pregnancies | Antenatal clinics, statutory and voluntary social service agencies in 14 London boroughs; social work department of major hospital in Barbados; antenatal clinics of two public hospitals and two polyclinics in Kingston, Jamaica | Framework analysis | To explore the psychosocial, emotional and economic factors which lead to repeat pregnancies |
| London: 26 teens (11 white, 10 black, 3 Asian and 3 mixed race)a aged 16–20 years; 9 with no formal exam passes, 19 in receipt of benefits and 11 living with a partner | |||||
| Barbados and Jamaica: 26 ethnic Caribbean teens aged 15–19 years; 22 with no formal exam passes, 21 with financial reliance on family and putative fathers and 4 living with a partner | |||||
| Hellerstedt and Story, 1998;131 USA (Minnesota) | Focus groups; recorded and transcribed verbatim; date not reported | 22 teen mothers (7 African American, 6 Asian, 7 white and 2 other) aged 13–19 years; 6 living with a partner, 6 had been pregnant more than once, all were enrolled in secondary school and 19 received medroxyprogesterone acetate post delivery | All participants received health care at an agency serving a low income population, and with specific expertise in pregnant and parenting adolescents | Thematic analysis | Decision-making about contraceptive use and factors that would influence contraceptive discontinuation, particularly side effects of medroxyprogesterone acetate |
| Herrman, 2006,132 and Herrman, 2007;133 USA (urban location, city not named) | Interviews; recorded and transcribed verbatim; date not reported | 16 teen mothers (15 African American, 1 Hispanic) aged 16–19 years; 2 were pregnant for the first time and 14 had been pregnant more than once | Recruited from social service agencies | Coding of data using Ethnograph (version 5.0) software (Qualis Research Associates, Colorado Springs) and thematic analysis | Intentions and decision-making associated with repeat pregnancy |
| Hoggart et al., 2010;134 UK (London) | Interviews, focus groups and discussion groups; method of recording the data not reported; date not reported | 23 teenage pregnancy strategy co-ordinators; 14 providers of abortion referrals; 8 abortion providers; 16 school-based focus groups of 8–10 female participants aged 14–16 years; 10 women aged 16–19 who had terminated pregnancies | 10 local health authorities in London and schools in the study area; seven of the young women who had had abortions were recruited from the British Pregnancy Advisory Service | Coding of data using NVivo software (QSR International, Warrington, UK) and thematic analysis | Teenage sexual behaviour and becoming pregnant, abortion decision-making and repeat abortion |
| Lewis et al., 2012;135 USA (Chicago) | Interviews and follow-up surveys at 6 and 12 months; recorded and transcribed; October 2006–August 2008 | 40 teen mothers aged 15–18 years; all African American; all primiparous and ≤ 13 weeks postpartum; 24 in relationships | The Postpartum Adolescent Birth Control Study. A longitudinal mixed-methods study of African American adolescent mothers’ contraceptive use and risk of repeat pregnancy in the postpartum year | Coding of data using ATLAS.ti (version 5.0) software (Scientific Software Development GmbH, Berlin) and thematic analysis | Partners’ roles in the use of non-coital dependent contraceptive methods (oral contraceptives, IUDs and medroxyprogesterone acetate) |
| Schaffer et al., 2008;136 USA (Minnesota urban location, city not named) | Focus groups; recorded and transcribed | 9 teen mothers (5 African American, 2 Latina and 2 Caucasian), age not reported | The Pregnancy Free Club. Delivered by Public Health Nurses and teachers in school, including monthly pregnancy tests, counselling, mentoring, contraception | Thematic analysis | Satisfaction with the experience of the Pregnancy Free Club |
| Smith et al., 2013;137 Australia (Perth) | Interviews; recorded and transcribed verbatim; May 2007–January 2009 | 56 teens aged 14–19 years; 16 were pregnant, 19 had a baby, 21 had had recent terminations, 8 were Aboriginal, 40 had dropped out of school; 18 were living with partner | Recruited from clinical and community-based antenatal and postnatal services | Additional thematic analyses were applied to a subset of data from a larger study which did not set out to explore pregnancy intentions but this theme inherently emerged in discussions | The relationship between pregnancy intentions and contraceptive behaviour |
| Weston et al., 2012;138 USA (Chicago) | Interviews at baseline, 3, 6, 9 and 12 months postpartum; recorded and transcribed verbatim | 20 teen mothers (all African American), aged 15–18 years, who expressed an intention to obtain an IUD in at least one interview | The Postpartum Adolescent Birth Control Study. A longitudinal mixed-methods study of African American adolescent mothers’ contraceptive use and risk of repeat pregnancy in the postpartum year | Coding of data using ATLAS.ti 5.0 software and thematic analysis using a grounded theory approach | Barriers and facilitators to uptake of IUDs |
Appendix 19 Study characteristics of included quantitative studies
| Study and location | Sample size and PROGRESS data | Type of programme and length of intervention | Programme description | Usual care | Main narrative findings |
|---|---|---|---|---|---|
| Belzer et al., 2005;87 USA | N = 160 (69 lost to follow-up; 91 analysed); intervention group, n = 43; control group, n = 48. Hispanic, n = 131; non- Hispanic (African American, Caucasian, Asian Pacific Islander), n = 29 | Contraceptive; 10–15 minutes of education about emergency contraception plus unspecified amount of family planning services | Provision of emergency contraception was provided by a licensed health professional | Education about emergency contraception for 10–15 minutes | The advance provision of emergency contraception in young mothers increases the likelihood of its use, and does not affect the use of other contraceptive methods, like condoms or hormonal methods, of birth control |
| Barnet et al., 2009;82 USA | N = 235 (predominantly African American); CAMI+, n = 80; CAMI only, n = 87; control, n = 68 | Psychological, home visit: CAMI sessions were initiated by 6 weeks postpartum and continued quarterly through 24 months postpartum | Delivered by African American counsellors. (1) CAMI+: home visiting with CAMI; training through a 16-module curriculum specifically for urban African-American adolescent mothers which addressed age- and developmentally appropriate feeding, growth, play and discipline; three modules focused on safer sex, negotiation and goal-setting. (2) CAMI only: single component intervention motivational interviewing | Usual care | Receipt of two or more CAMI sessions, either alone or within a multicomponent home-based intervention, reduced the risk of rapid subsequent birth to adolescent mothers (not statistically significant) |
| Black et al., 2006;31 USA | Initially recruited to intervention, n = 87; control, n = 94. African American with low-income SES | Psychosocial, home visit: received home visits every other week until the infant’s first birthday, for a maximum of 19 visits | Intervention delivered by college-educated, black single mothers who served as mentors (‘big sisters’). Curriculum focused on interpersonal negotiation skills, adolescent development and parenting. Condoms were provided at every contact | Initial information on services for young mothers and children | A home-based intervention founded on a mentorship model and targeted towards adolescent development, including negotiation skills, was effective in preventing rapid repeat. At the 2-year evaluation, there were no other differences in pregnancy rates between intervention- and control-group mothers |
| Barnet et al., 2007;85 USA | Home-visited group, n = 44; control group, n = 40 | Psychosocial, home visit: started in the third trimester and then biweekly for the first year of the child’s life and then monthly until the child’s second birthday | Trained home visitors, recruited from local communities, delivered a parenting curriculum, an adolescent curriculum, encouraged contraceptive use, connected the teen with primary care and promoted school continuation. Training was also geared towards improving communication and negotiation with partners. Visitors taught to identify depression and partner violence | Usual care | This community-based home-visiting programme improved adolescent mothers’ parenting attitudes and school continuation, but it did not reduce their odds of repeat pregnancy or depression, or achieve co-ordination with primary care. Co-ordinated care may require explicit mechanisms to promote communication between the community programme and primary care |
| Stevens-Simon et al., 1997;92 USA | N = 286; place: USA. 44% white, 25% black, 29% Hispanic and 2% other races | Psychosocial, community | Four interventions: (1) monetary incentive and peer-support; (2) peer-support; (3) monetary incentive; and (4) no intervention. Peer-based incentive programme ‘Dollar-a-Day’: meet weekly, mentor-led peer group environment; guest speakers, free contraceptive services and supplies and information about jobs and job-shadowing experiences are available on-site | The control group received three different versions of the intervention: (1) peer-support; (2) monetary incentive; and (3) usual care | Adolescent mothers participating in a weekly peer support group meeting during which they learn about the advantages of delaying further childbearing and the costs of repeat pregnancy have fewer second pregnancies during the 2 years following birth. However, this was not statistically significant |
| Ford et al., 2002;88 USA | N = 282 (93.1% African American); experimental, n = 165 (95.7% African American); control, n = 117 (89.4% African American). Years of schooling (range): 8–14 | Psychosocial, community: scheduled clinic time | Peer-centred prenatal care programme for adolescent mothers | Usual care and a box of educational materials that included written information on the three trimesters of pregnancy | Adolescents in the experimental group had fewer infants with low birthweight and were more likely to continue their education than those in the control group. However, this was not statistically significant |
| Havens et al., 1997;89 USA | N = 110; experimental, n = 53 (3 white, 47 black, 2 Hispanic, 1 native American); control, n = 57 (3 white, 53 black, 0 Hispanic, 1 native American). Occupation: students | Psychosocial, home visit: minimum of 12 hours each month with teens over the 2-year period of the project | Focus on telephone conversations and social outings. Mentors were expected to develop relationships with their teens that fostered trust and friendship then focus on goal-setting: contraception, continuing in school, day-care, parenting and budgeting and to deal with young mothers problems | Assistance from the community agency and social support from family and friends | The mentoring programme did not significantly impact repeat pregnancy rates |
| Koniak-Griffin et al., 2003;81 USA | Experimental group, n = 56; control group, n = 45. Latina, n = 63; African American, n = 13; non-Hispanic white, n = 18; other, n = 4. SES: ‘poor’ | Psychosocial, home visit: gestation age of 28 weeks or more from pregnancy to 1 year postpartum. The ‘Early Intervention Program’ was designed to include a maximum of 17 home visits: 2 prenatal and 15 postpartum (1.5 to 2 hours each); however, the number of visits varied among families depending on the mother’s availability | Comprehensive interventions were provided by public health nurses in five major areas: health, sexuality and family planning, maternal role, life skills, and social support. Prenatal visits focused on health care during pregnancy and preparation for childbirth, and maternal roles and mental health issues. Postpartum visits focused on family planning, infant care, and well-baby health care, demonstration of the Neonatal Behaviour Assessment Scale, educational and vocational goals, and video instruction for promoting appropriate maternal behaviours | The TPHNC mothers received services available in county health departments. One prenatal visit was made shortly after the participant’s entry into the study and a second during the third trimester. Visits focused on (1) assessment and counselling related to prenatal health care, (2) self-care, (3) preparation for childbirth, (4) education planning, and (5) well-baby care, including immunizations | The lower repeat pregnancy rate in adolescent mothers who received home visitation, although not statistically significant, is clinically important because of the negative impact short-interval births may have on the life course of these mothers and their children |
| Quinlivan et al., 2003;79 Australia | Experimental, n = 65 (21 indigenous Australians); control group, n = 71 (12 indigenous Australians) | Psychosocial, home visit: 6 months postpartum visits were undertaken at 1 week, 2 weeks, 1 month, 2 months, 4 months and 6 months after birth. Each visit lasted 1–4 hours | Postnatal home visits by midwives, routine postnatal support, counselling and information services provided by the hospital, including access to routine hospital support services: teach breastfeeding and maternal infant bonding skills; provide advice and information on contraception and on vaccination of infant; discuss postnatal mood disorders and mother’s feelings; follow up abnormalities detected in the antenatal period, such as pap smear problems, infectious diseases, substance misuse or family violence issues; ensure appointments are made for vaccination of infant; provide training in parenting skills, covering issues that will emerge with the increasing mobility of the child, and talk about child safety in the home | All participants were provided with routine postnatal support, counselling and information services provided by the hospital, including access to routine hospital support services | Postnatal home-visiting services by nurse midwives reduce adverse neonatal events and improve contraception outcomes, but do not affect breastfeeding or infant vaccination knowledge or compliance |
| Katz et al., 2011;90 USA | N = 249 (221 African American, 28 Latina); intervention group, n = 124; usual care, n = 125. Place: USA. SES: 166 on Medicaid 48 undertaking non-school-based job-training and 126 held back in school | All of the family advocates were female and African American. Biweekly phone sessions were scheduled during the subsequent 12 months with a maximum projected number of 42 phone counselling sessions over an 18-month postpartum interval | Counsellors were Masters-level young women of similar ethnic backgrounds as the teens. Curriculum content focused on building knowledge of health risks and developing positive teen attitudes and skills for future orientation and self-regulation. Other issues addressed included improving communication and negotiation skills with sexual partner, resisting peer pressures for risk behaviours, and increasing connectedness with family, health provider, school and work settings. Minimal content addressed parenting or child development. A workbook with visual support materials for the topics slated for discussion. Two-hour dinner group sessions at one of the centrally located hospitals serving pregnant and parenting teens | Participants randomised to usual care received the health and education services generally provided through their schools or health-care facilities | GirlTalk intervention did not reduce the time before a subsequent pregnancy for the 15–19-year-old sample as a whole. Among adolescent mothers aged 15–17 years, the rate of subsequent pregnancy was 26% in the intervention group and 39% in the usual care group. Subsequent analysis suggested that increased participation in the GirlTalk counselling programme was associated with postponing a second pregnancy among teen mothers aged 15–17 years, but not those ≥ 18 years |
| Sims and Luster, 2002;91 USA | Experimental group, n = 48; standard programme, n = 51. 64% of the teens who participated in the 24-month assessment were African American, 29% were European American, 3% were Hispanic and 4% indicated that they were of mixed race | Psychosocial, home: designed for home visitation 6 months postpartum | The family support programme involved weekly home visits from a paraprofessional family advocate. The family advocate attempted to establish a trusting relationship with the teens and their families, provided information about services available in the community (e.g. family planning) and the care of children, provided emotional and instrumental support (e.g. transportation), and encouraged young mothers to pursue the goals of the programme (e.g. high school completion and limiting further childbearing), which included helping the young mothers to return to school and addressing the psychological well-being of the adolescents. needed in the community, provided emotional and instrumental support, and encouraged the teens to complete school | In the standard programme, an advocate was housed at the health centre and worked with the teens almost exclusively via the phone and mail. Contact was less intensive and focused on crisis management, thus the rates of subsequent pregnancies and births were expected to be higher in the standard programme group. All the family advocates were female, African American, had at least a high school education when the programme began, and were from the community where the intervention took place | The two treatment groups did not differ in their rates of second pregnancies and second births. The repeat pregnancy rate was 58% for the home-visited group and 63% for the standard programme group. The rates of second births were 31% and 35%, respectively |
| Cherniss and Herzog, 1996;80 USA | N = 116 (50% African Americans; 27% Latina; 17% white/non-Latina). Place: USA; SES: low | Psychosocial – home-based family therapy. No set time limit for treatment | Intensive family-based therapy home visits, developmental guidance, supportive counselling, and help in acquiring other needed services. The family therapy clients received these services, the home-based family therapy intervention | Individual treatment group received home visits, developmental guidance, supportive counselling and help in acquiring other needed services | The intervention with the family improved the caring environment for the infant during the first 12 months of treatment |
Appendix 20 Sensitivity analysis forest plots
Sensitivity analysis
We conducted sensitivity analysis of the primary outcomes (unintended repeat pregnancy and uptake of interventions) and secondary outcomes (birth control/contraception and school dropout), including quasi-experimental and observational study.
We identified three quasi-experimental studies:78,93,135 two reported the effectiveness and uptake of the interventions, and one reported on the acceptability of the intervention. We also identified one observational study which reported the effectiveness of the intervention, birth control/contraception and school out drop.
Effectiveness of the interventions
We added three studies78,93,135 in addition to the nine included in the primary analysis. Three of the four included studies, concerning 1484 teenagers, 709 receiving psychosocial interventions and 715 receiving control, reported the rate of unintended repeat pregnancy. All the reported participants were in the home visit subgroup.
By including additional studies, the results of the sensitivity analysis in Figure 22 show that, in the home visit subgroup, the proportion of girls who experienced an unintended repeat teenage pregnancy was further lower than the primary analysis [288/1077 for the home visit intervention vs. 297/1004 for the control group, with a RR of 0.88 (95% CI 0.78 to 1)].
FIGURE 22.
Psychosocial vs. usual care for the proportion of participants experiencing a repeat pregnancy (i.e. the effectiveness of the intervention), including RCTs and quasi-experimental studies (sensitivity analysis of Figure 11). M–H, Mantel–Haenszel.

Uptake of the interventions
We added two studies in addition to the two studies included in the primary analysis. Two of the four included studies, concerning 446 teenagers, 260 receiving psychosocial interventions and 186 receiving control, reported the rate of uptake of the intervention. All the reported participants were in the home visit subgroup.
The results of the sensitivity analysis in Figure 23 show that, in the home visit subgroup, the proportion of girls who were recruited and received the intervention increased compared with the primary analysis [280/405 for the home visit intervention vs. 218/325 in the control group, with a RR of 1.07 (95% CI 0.99 to 1.16)].
FIGURE 23.
Psychosocial vs. usual care for the acceptability of the intervention including RCTs, quasi-experimental studies and observational studies (sensitivity analysis of Figure 13). M–H, Mantel–Haenszel.

Secondary outcomes
Birth control
One study has been added, in addition to the one study included in the primary analysis. The study, concerning 1038 teenagers, 509 receiving psychosocial interventions and 529 controls, reported the rate of birth control. All the reported participants were in the home visit subgroup.
The results of the sensitivity analysis in Figure 24 show that, in the home visit subgroup, the proportion of girls who were using birth control shows a lower uptake rate in the control group than the primary analysis [218/540 for the home visit intervention vs. 194/561 in the control group, with a RR of 1.09 (95% CI 0.82 to 1.44)].
FIGURE 24.
Psychosocial vs. usual care for the usage of birth control including RCTs, quasi-experimental studies and observational studies. M–H, Mantel–Haenszel.

School dropout
One study has been added in addition to the three studies included in the primary analysis. The study, concerning 1038 teenagers, 509 receiving psychosocial interventions and 529 controls, reported the rate of school dropout. All the reported participants were in the home visit subgroup.
The results of the sensitivity analysis in Figure 25 show that, in the home visit subgroup, the proportion of girls who dropped out of school is still in favour of psychosocial care, compared with the primary analysis [96/635 for the home visit intervention vs. 130/659 for the control group, with a RR of 0.76 (95% CI 0.60 to 0.96)].
FIGURE 25.
Psychosocial vs. usual care for the proportion who have dropped out of school including data from RCTs, quasi-experimental studies and observational studies (sensitivity analysis of Figure 14). M–H, Mantel–Haenszel.
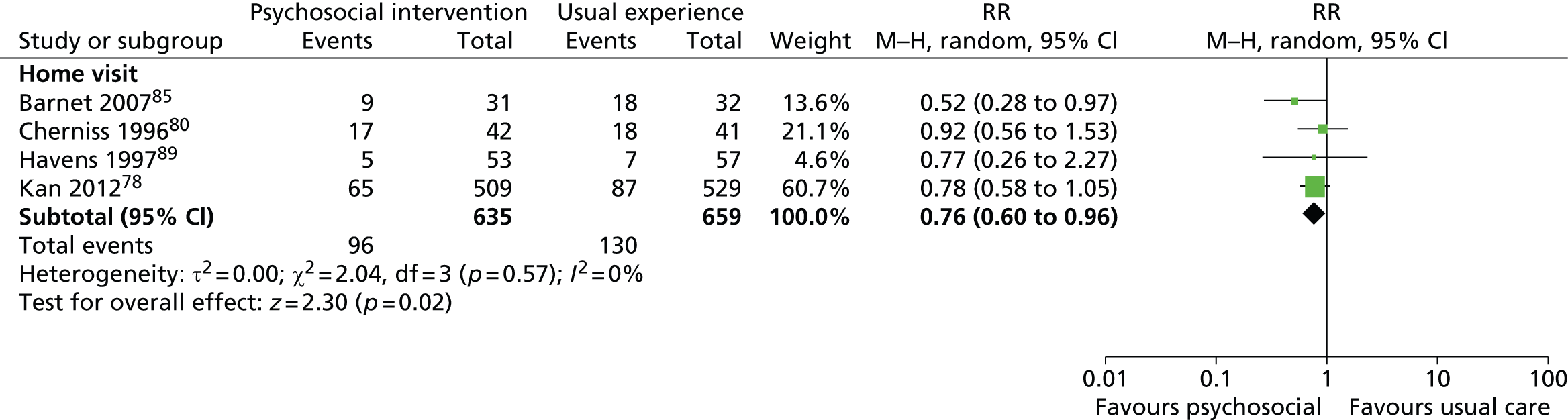
List of abbreviations
- AIDS
- acquired immunodeficiency syndrome
- ASSIA
- Applied Social Sciences Index and Abstracts
- BiblioMap
- the EPPI-Centre register of health promotion and public health research
- BNI
- British Nursing Index
- CAMI
- computer-assisted motivational interviewing
- CAMI+
- computer-assisted motivational interviewing with a multipart home visit programme
- CART
- completeness, accuracy, relevance and timeliness
- CerQual
- certainty of the qualitative evidence
- CI
- confidence interval
- EconLit
- American Economic Association’s electronic bibliography
- EPOC
- Effective Practice and Organisation of Care
- EPPI-Centre
- Evidence for Policy and Practice Information and Co-ordinating Centre
- GP
- general practitioner
- GRADE
- Grading of Recommendations Assessment, Development and Evaluation
- HIV
- human immunodeficiency virus
- HTA
- Health Technology Assessment
- ICER
- incremental cost-effectiveness ratio
- INTERUPT
- Intervention Now to Eliminate Repeat Unintended Pregnancy in Teenagers
- IUCD
- intrauterine contraceptive device
- IUD
- intrauterine device
- LARC
- long-acting reversible contraceptive
- MMAT
- mixed methods appraisal tool
- NICE
- National Institute for Health and Care Excellence
- NIHR
- National Institute for Health Research
- PHW
- Public Health Wales
- PRISMA
- Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- PROGRESS
- place, race, occupation, gender, religion, education, socioeconomic status and social status
- RCT
- randomised controlled trial
- RePEc
- Research Papers in Economics
- RR
- risk ratio
- SD
- standard deviation
- SocAbs
- Sociological Abstracts
- SRE
- sex and relationship education
- SSCI
- Social Sciences Citation Index
- STD
- sexually transmitted disease
- SURE
- Support Unit for Research Evidence
- TOP
- termination of pregnancy