
Notes
Article history
The research reported in this issue of the journal was funded by the HTA programme as project number 10/80/01. The contractual start date was in February 2011. The draft report began editorial review in June 2014 and was accepted for publication in October 2015. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HTA editors and publisher have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
All review authors have applied for and received competitive research grants. Carl J Heneghan reports grants from the UK National Institute for Health Research (NIHR), the NIHR School of Primary Care, Wellcome Trust and the World Health Organization (WHO) during the conduct of the study, and has received expenses and payments for media work. In addition, he is an expert witness in an ongoing medical device legal case. He receives expenses for teaching evidence-based medicine and is paid for NHS general practitioner work in the out of hours service in Oxford. Tom Jefferson receives royalties from his books published by Blackwells and Il Pensiero Scientifico Editore, Rome. Tom Jefferson is occasionally interviewed by market research companies for anonymous interviews about Phase I or II pharmaceutical products. In 2011–13, Tom Jefferson acted as an expert witness in a labour case on influenza vaccines in health-care workers in Canada. In 1997–9, Tom Jefferson acted as a consultant for Roche, in 2001–2 for GlaxoSmithKline, and in 2003 for Sanofi-Synthelabo for pleconaril, which did not get approval from the US Food and Drug Administration (FDA). Tom Jefferson was a consultant for IMS Health in 2013, and in 2014 was retained as a scientific adviser to a legal team acting on the drug Tamiflu (oseltamivir, Roche). In 2014–15, Tom Jefferson was a member of two advisory boards for Boerhinger and is in receipt of a Cochrane Methods Innovations Fund grant to develop guidance on the use of regulatory data in Cochrane reviews. Tom Jefferson has a potential financial conflict of interest in the investigation of the drug oseltamivir. Tom Jefferson is acting as an expert witness in a medicolegal negligence case involving the drug oseltamivir (Roche). Peter Doshi received €1500 (£1241; US$2052) from the European Respiratory Society in support of his travel to the society’s September 2012 annual congress in Vienna, where he gave an invited talk on oseltamivir. Peter Doshi is an associate editor of the British Medical Journal (BMJ). Peter Doshi gratefully acknowledges the American Association of Colleges of Pharmacy for its funding support ($10,000) for a study to analyse written medical information regarding the possible harms of statins. Peter Doshi is also an unpaid member of the IMEDS steering committee at the Reagan–Udall Foundation for the FDA, which focuses on drug safety research. CDelM is the Co-ordinating Editor of the Acute Respiratory Infections Group of the Cochrane Collaboration. CDelM reports personal fees from Key Pharmaceuticals during the conduct of the study; grants from the National Health and Medical Research Council (Australia), grants from NIHR (UK), personal fees from Elsevier and BMJ Books, from conference organisers for International Viral Infections Conference, personal fees from GlaxoSmithKline Pharmaceuticals, personal fees from Key Pharmaceutical, outside the submitted work. Rokuro Hama provided scientific opinions and expert testimony on 11 adverse reaction cases related to oseltamivir for the applications by their families for adverse reaction relief by the Pharmaceuticals and Medical Devices Agency (PMDA) and in the lawsuits for revocation of the PMDA’s decision concerning with these reactions. Most of the cases were reported in the International Journal of Research Studies in Management (2008:20:5–36). Rokuro Hama was an expert witness in the lawsuit on the adverse reaction of (death from) gefitinib against AstraZeneca and Japanese Minister of Health Labour and Welfare, and provided scientific opinions and expert testimony. He argued that gefitinib’s fatal toxicity was known before approval in Japan, as shown in ‘Gefitinib story’ (http://npojip.org/english/The-gefitinib-story.pdf) and in other articles (http://npojip.org/). Plaintiffs finally lost the case on 12 April 2013 at the Supreme Court of Japan. Rokuro Hama has received royalties from a published book.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2016. This work was produced by Heneghan et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Introduction and rationale
Since the mid-2000s the use of neuraminidase inhibitors (NIs) has been endorsed and billions of pounds have been spent stockpiling the two anti-influenza drugs oseltamivir (Tamiflu®, Roche) and zanamivir [Relenza®, GlaxoSmithKline (GSK)] in preparation for an influenza pandemic. When the H1N1 pandemic emerged in 2009, the drugs were rolled out worldwide for the treatment and prevention of influenza and its complications. At that time, we were asked to conduct a systematic review for Cochrane to update evidence on their efficacy, during which it emerged that the validity of a key study underpinning the evidence on efficacy was unclear. After 3.5 years of making requests to the drug manufacturers, they provided us with full clinical study reports (CSRs).
Emergence of problems
The reasons for the stockpiling of oseltamivir and zanamivir are not well known, but the decision may be based on assumptions that the drugs would reduce hospital admissions and serious complications of influenza, such as pneumonia, by half and slow down the spread of the virus. 1–3 Some of these assumptions were supported by a peer-reviewed pooled analysis of 10 randomised trials of oseltamivir published in the Archives of Internal Medicine in 2003 by Kaiser et al. 4 This analysis seemed to be of high quality and formed a powerful scientific rationale for stockpiling,5 but during our review in 2009 it became apparent that the data underlying it were largely unpublished and inaccessible to independent scrutiny. Roche, the manufacturer of oseltamivir, funded the Kaiser review, employed some of its authors and had also sponsored the 10 trials. For 3.5 years Roche did not release the full CSRs despite a public pledge to do so made during the H1N1 ‘swine flu’ outbreak of 2009. 6,7
Research for our 2009 review also highlighted inconsistencies in decision-making. The US Food and Drug Administration (FDA), which had access to the full CSRs, concluded on the product label that ‘Tamiflu has not been shown to prevent such complications [serious bacterial infections]’. The European Medicines Agency (EMA), which had only partial reports, and another prominent US agency, the Centers for Disease Control and Prevention (CDC), came to the exact opposite conclusion – all apparently based on the same trials. 8
Owing to the risk of reporting bias as a result of the large amounts of unpublished data there are uncertainties about the stated benefits of oseltamivir and about the conclusions of previous Cochrane reviews of NIs in adults and children. 9,10 To address this, we worked for 4 years to obtain full CSRs of the oseltamivir trial programme. CSRs are considered to be the most exhaustive summaries of randomised controlled trials (RCTs) of drugs. They are usually composed of a main report of the trial (in introduction, methods, results and discussion style), with numerous appendices containing important supplementary data that are needed to understand and interpret the trial [e.g. protocol, protocol amendments, statistical analysis plan (SAP), blank case report forms (CRFs), certificates of analysis, randomisation list and informed consent forms]. 11 In the case of oseltamivir, CSRs were of a mean length of approximately 1300 pages (median around 900 pages). As a result of increasing availability, CSRs may in the future be incorporated into systematic reviews and other forms of evidence synthesis. 12,13
Rationale for this review
In the midst of the A/H1N1 influenza outbreak in June 2009, the Australian and UK governments commissioned an update of our long-standing Cochrane review on NIs for influenza in (otherwise) healthy adults (known as A047). At the time of publication of the 2009 update and its linked investigation by the British Medical Journal (BMJ), we underestimated the extent of the oseltamivir evidence development programme, expecting it to comprise around 36 trials, with only a proportion of these fitting our inclusion criteria. We were also unaware of the size and the level of detail that the CSRs contained.
Today, the obvious source of information on CSRs would be trial registries and company websites, but most trials of both NIs were carried out before inception or wide acceptance of centralised registries and company websites. In 2009–11, company websites did not, and still do not, have extensive lists of trials with downloadable CSRs. Many people had never heard of CSRs before media coverage of our work. We decided to construct our list by using multiple cross-referencing methods. We constructed a list beginning with clinical trials that were identified from previous review updates.
To ensure that the list did not include duplicate entries, we assigned to each trial a unique trial ID. ‘Author’ was insufficient to provide a unique trial ID, because different authors can be present across different versions of the same trial (i.e. the authors of CSRs can be different from publications arising from the same clinical trial).
Once we had as complete a list of trials as possible, we contacted manufacturers and sent them our draft list, asking them to check the accuracy and completeness of our list. Roche, GSK and BioCryst all did so, and informed us of additional trials.
We requested from Roche and GSK a series of regulatory documents under freedom of information (FOI) policies from both the FDA and the EMA. No substantial comments were made by Roche on the protocol of the Cochrane A159 review,14 which has been publicly available since December 2010.
Soon after the publication of the review, the BMJ agreed to publish our correspondence with Roche, GSK, EMA, CDC and World Health Organization (WHO), recording our attempts at retrieving the full reports without any conditions attached, and to understand the basis for promotion of the drugs (especially oseltamivir) by public health bodies. The correspondence (which is hundreds of pages long) formed the basis for what then became the BMJ Open Data Campaign and a stimulus for the later AllTrials campaign. Public exposure of this approach and considerable media coverage led to the unconditional release of 77 reports of oseltamivir of 82 studies sponsored by Roche and the equivalent of the 30 studies we had requested from GSK. For the full correspondence, see www.bmj.com/tamiflu and www.bmj.com/relenza. The reports (amounting to over 100,000 pages) are made available with this review for the first time at: https://datadryad.org/resource/doi:10.5061/dryad.77471/2, a positive step for open science. We have described the posting of these reports in a blog posting at: http://blog.datadryad.org/2014/04/17/tamiflu-data/, and a list of neuraminidase reviews, with peer review comments and responses relevant to review A159,14 is available at www.bmj.com/content/suppl/2014/04/09/bmj.g2545.DC1/jeft017746.ww8_default.pdf.
Before receiving the full reports, we resumed reviewing the remainder of the material that we had received in 2011. This mainly consisted of module 2s (Roche terminology for pre-study documents). Module 2s contained the information that was originally unavailable to us from Roche: study protocols with their amendments, randomisation lists, blank CRFs, certificates of analysis describing appearance and content of active and control capsules and, at times, SAPs. CRFs are containers for the rawest form of recorded data at the individual participant level.
While designing the tool to capture trial methods and assess bias, we also considered whether or not access to module 2 information (and later the full study reports) changed our perception of the trial and specifically our ‘risk-of-bias’ assessment. We found that access to what are supposed to be full study reports should provide clarity and remove the rationale for ‘unclear’ risk-of-bias judgements, and ideally remove the concept of risk leaving just ‘bias’, at least for certain study design elements, such as attrition bias. Either a design element introduces bias or it does not. In the case of the 15 full oseltamivir CSRs we reviewed when constructing our tool, only one report contained a protocol that predated the beginning of participant enrolment, only two reports had SAPs that clearly predated participants’ enrolment and three reports had clearly dated protocol amendments. No CSR reported a clear date of unblinding.
During the latter part of 2013, we received from the manufacturers tens of thousands of pages of full CSRs for both programmes combined.
These events form the basis for this review.
Aims and objectives
The main goals of the reviews included in this report were to:
-
describe the potential benefits and harms of NIs for influenza in all age groups by reviewing all CSRs of published and unpublished randomised, placebo-controlled trials and regulatory comments
-
determine the effect of oseltamivir on mortality in patients with 2009A/H1N1 influenza.
Research questions
The research questions addressed in this report are as follows:
-
What are the potential benefits and harms of NIs for the prevention and treatment of influenza in adults and children?
-
Does influenza virus-specific mechanism of action proposed by the producers fit the clinical evidence?
-
Does treatment with oseltamivir confer protection against mortality in patients with 2009A/H1N1 influenza?
Chapter 2 Neuraminidase inhibitors for preventing and treating influenza in adults and children
Abstract
Background
Neuraminidase inhibitors are stockpiled and recommended by public health agencies for treating and preventing seasonal and pandemic influenza. They are used clinically worldwide.
Objective
To describe the potential benefits and harms of NIs for influenza in all age groups by reviewing all CSRs of published and unpublished randomised, placebo-controlled trials and regulatory comments.
Search methods
We searched trial registries, electronic databases (to 22 July 2013) and regulatory archives, and corresponded with manufacturers to identify all trials. We also requested CSRs. We focused on the primary data sources of manufacturers but we checked that there were no published RCTs from non-manufacturer sources by running electronic searches in the following databases: the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, MEDLINE (via Ovid), EMBASE, EMBASE.com, PubMed (not MEDLINE), Database of Abstracts of Reviews of Effects (DARE), NHS Economic Evaluation Database (NHS EED) and Health Economic Evaluations Database (HEED).
Selection criteria
Randomised, placebo-controlled trials on adults and children with confirmed or suspected exposure to naturally occurring influenza.
Data collection and analysis
We extracted CSRs and assessed risk of bias using purpose-built instruments. We analysed the effects of zanamivir and oseltamivir on time to first alleviation of symptoms, influenza outcomes, complications, hospitalisations and adverse events in the intention-to-treat (ITT) population. All trials were sponsored by the manufacturers.
Main results
We obtained 107 CSRs from the EMA, GSK and Roche. We accessed comments by the FDA, EMA and Japanese regulator. We included 53 trials in stage 1 (a judgement of appropriate study design) and 46 in stage 2 (formal analysis), including 20 oseltamivir (9623 participants) and 26 zanamivir trials (14,628 participants). Inadequate reporting put most of the zanamivir studies and half of the oseltamivir studies at a high risk of selection bias. There were inadequate measures in place to protect 11 studies of oseltamivir from performance bias due to non-identical presentation of placebo. Attrition bias was high across the oseltamivir studies and there was also evidence of selective reporting for both the zanamivir and oseltamivir studies. The placebo interventions in both sets of trials may have contained active substances.
Time to first symptom alleviation
For the treatment of adults, oseltamivir reduced the time to first alleviation of symptoms by 16.8 hours [95% confidence interval (CI) 8.4 to 25.1 hours; p < 0.0001]. This represents a reduction in the time to first alleviation of symptoms from 7 to 6.3 days. There was no effect in asthmatic children, but in otherwise healthy children there was a reduction by a mean difference (MD) of 29 hours (95% CI 12 to 47 hours; p = 0.001). Zanamivir reduced the time to first alleviation of symptoms in adults by 0.60 days (95% CI 0.39 to 0.81 days; p < 0.00001), equating to a reduction in the mean duration of symptoms from 6.6 to 6.0 days. The effect in children was not significant. In subgroup analysis we found no evidence of a difference in treatment effect for zanamivir on time to first alleviation of symptoms in adults in the influenza-infected and non-influenza-infected subgroups (p = 0.53).
Hospitalisations
Treatment of adults with oseltamivir had no significant effect on hospitalisations [risk difference (RD) 0.15%, 95% CI –0.78% to 0.91%]. There was also no significant effect in children or in prophylaxis. Zanamivir hospitalisation data were unreported.
Serious influenza complications or those leading to study withdrawal
In adult treatment trials, oseltamivir did not significantly reduce those complications classified as serious or those that led to study withdrawal (RD 0.07%, 95% CI –0.78% to 0.44%), or in child treatment trials; neither did zanamivir in the treatment of adults or in prophylaxis. There were insufficient events to compare this outcome for oseltamivir in prophylaxis or zanamivir in the treatment of children.
Pneumonia
Oseltamivir significantly reduced self-reported, investigator-mediated, unverified pneumonia [RD 1.00%, 95% CI 0.22% to 1.49%, number needed to treat to benefit (NNTB) 100, 95% CI 67 to 451] in the treated population. The effect was not significant in the five trials that used a more detailed diagnostic form for pneumonia. There were no definitions of pneumonia (or other complications) in any trial. No oseltamivir treatment studies reported effects on radiologically confirmed pneumonia. There was no significant effect on unverified pneumonia in children. There was no significant effect of zanamivir on either self-reported or radiologically confirmed pneumonia. In prophylaxis, zanamivir significantly reduced the risk of self-reported, investigator-mediated, unverified pneumonia in adults (RD 0.32%, 95% CI 0.09% to 0.41%; NNTB 311, 95% CI 244 to 1086) but not oseltamivir.
Bronchitis, sinusitis and otitis media
Zanamivir significantly reduced the risk of bronchitis in adult treatment trials (RD 1.80%, 95% CI 0.65% to 2.80%; NNTB 56, 95% CI 36 to 155), but not oseltamivir. Neither NI significantly reduced the risk of otitis media and sinusitis in both adults and children.
Harms of treatment
Oseltamivir in the treatment of adults increased the risk of nausea [RD 3.66%, 95% CI 0.90% to 7.39%; number needed to treat to harm (NNTH) 28, 95% CI 14 to 112] and vomiting (RD 4.56%, 95% CI 2.39% to 7.58%; NNTH 22, 95% CI 14 to 42). The proportion of participants with fourfold increases in antibody titre was significantly lower in the treated group than in the control group (RR 0.92, 95% CI 0.86 to 0.97; I2 statistic = 0%) (5% absolute difference between arms). Oseltamivir significantly decreased the risk of diarrhoea (RD 2.33%, 95% CI 0.14% to 3.81%; NNTB 43, 95% CI 27 to 709) and cardiac events (RD 0.68%, 95% CI 0.04% to 1.0%; NNTB 148, 95% CI 101 to 2509) compared with placebo during the on-treatment period. There was a dose–response effect on psychiatric events in the two oseltamivir ‘pivotal’ treatment trials: WV15670 and WV15671, at 150 mg (standard dose) and 300 mg daily (high dose) (p = 0.038). In the treatment of children, oseltamivir induced vomiting (RD 5.34%, 95% CI 1.75% to 10.29%; NNTH 19, 95% CI 10 to 57). There was a significantly lower proportion of children on oseltamivir with a fourfold increase in antibodies (RR 0.90, 95% CI 0.80 to 1.00; I2 statistic = 0%).
Prophylaxis
In prophylaxis trials, oseltamivir and zanamivir reduced the risk of symptomatic influenza in individuals (oseltamivir RD 3.05%, 95% CI 1.83% to 3.88%; NNTB 33, 95% CI 26 to 55; zanamivir RD 1.98%, 95% CI 0.98% to 2.54%; NNTB 51, 95% CI 40 to 103) and in households (oseltamivir RD 13.6%, 95% CI 9.52% to 15.47%; NNTB 7, 95% CI 6 to 11; zanamivir RD 14.84%, 95% CI 12.18% to 16.55%; NNTB 7, 95% CI 7 to 9). There was no significant effect on asymptomatic influenza (oseltamivir, RR 1.14, 95% CI 0.39 to 3.33; zanamivir RR 0.97, 95% CI 0.76 to 1.24). Non-influenza, influenza-like illness (ILI) could not be assessed as a result of data not being fully reported. In oseltamivir prophylaxis studies, psychiatric adverse events were increased in the combined on- and off-treatment periods (RD 1.06%, 95% CI 0.07% to 2.76%; NNTH 94, 95% CI 36 to 1538) in the study treatment population. While on treatment, oseltamivir increased the risk of headaches (RD 3.15%, 95% CI 0.88% to 5.78%; NNTH 32, 95% CI 18 to 115), renal events (RD 0.67%, 95% CI –0.01% to 2.93%; NNTH 150, NNTH 35 to NNTB > 1000) and nausea (RD 4.15%, 95% CI 0.86% to 9.51%; NNTH 25, 95% CI 11 to 116).
Authors’ conclusions
Oseltamivir and zanamivir have small, non-specific effects on reducing the time to alleviation of influenza symptoms in adults, but not in asthmatic children. Using either drug as prophylaxis reduces the risk of developing symptomatic influenza. Treatment trials with oseltamivir or zanamivir do not settle the question of whether or not the complications of influenza (such as pneumonia) are reduced, because of a lack of diagnostic definitions. The use of oseltamivir increases the risk of adverse effects, such as nausea, vomiting, psychiatric effects and renal events in adults and vomiting in children. The lower bioavailability may explain the lower toxicity of zanamivir compared with oseltamivir. The balance between benefits and harms should be considered when making decisions about use of both NIs for either the prophylaxis or treatment of influenza. The influenza virus-specific mechanism of action proposed by the manufacturers does not match the observed clinical evidence.
Background
This review (known as A159) reports our work using unpublished CSRs (see Appendix 1, Glossary) and regulatory documents containing comments and reviews to evaluate the safety and efficacy of NIs. We have called the body of clinical studies and regulatory comments ‘regulatory information’. For the history and evolution of the review, see Appendix 1.
Description of the condition
Influenza is mostly a mild, self-limiting infection of the upper airways with local symptoms, including sniffles, nasal discharge, dry cough and sore throat, and systemic symptoms such as fever, headache, aches and pains, malaise and tiredness.
Occasionally, patients with influenza develop complications such as pneumonia, otitis media and dehydration or encephalopathy with or without liver failure, which may be due to the effects of the influenza virus itself or associated secondary bacterial infections and/or adverse effects of drugs such as antipyretics [including salicylates and other non-steroidal anti-inflammatory drugs (NSAIDs)]. 15
Influenza is not clinically distinguishable from ILI. 16 Epidemic influenza in humans is caused by influenza A and B viruses. Currently, influenza A/H1N1, influenza A/H3N2 and influenza B cause most influenza infections worldwide. 12
Description of the intervention
Neuraminidase inhibitors comprise inhaled zanamivir (Relenza®, GSK), oral oseltamivir (Tamiflu®, Gilead Sciences and F. Hoffman-La Roche), parenteral peramivir (Rapivab®, BioCryst Ltd), inhaled laninamivir (Inavir®, Daiichi Sankyo Co. Ltd)17 and others still under development. 18 The use of NIs has increased dramatically since the outbreak of A/H1N1 in April 2009, partly because of the rise in amantadine (Symmetrel®, Endo Pharmaceuticals Inc.)/rimantadine (Flumadine®, Forest Pharmaceuticals Inc.) resistance and, in the early stages of the outbreak, the lack of a vaccine, which meant that NIs became a widespread public health intervention. WHO had previously encouraged member states to stockpile and gain experience of using NIs. 19–21
How the intervention might work
Although NIs may reduce the ability of the virus to penetrate the mucus in the very early stage of infection,6,22–24 their main mechanism of action is thought to lie in their ability to inhibit influenza viruses from exiting host cells. 23,25 The manufacturers state that oseltamivir does not prevent infection or affect antibody production,26 but it reduces symptom duration probably by reducing viral load, spread and release of cytokines,8,27 diminishing the chance of complications and interrupting person–person viral spread. Oseltamivir phosphate (Tamiflu) is the prodrug of oseltamivir carboxylate, the effective form. Oseltamivir phosphate dissociates in the gastrointestinal tract to form oseltamivir, which is absorbed and metabolised into oseltamivir carboxylate by hepatic carboxylesterase. Oseltamivir may have a central depressant action15 and may also inhibit human sialidase,28 causing abnormal behaviour. Inhaled zanamivir reaches a far lower plasma concentration than its intravenous administration. 29
Any treatment that reduces the complications of influenza (e.g. pneumonia) and the excretion of the virus from infected people might be a useful public health measure to contain an epidemic by limiting the impact and spread of the virus. In addition to symptomatic treatment, prophylactic use for interrupting the spread of disease has informed pandemic planning over the past decade.
Why it is important to do this review
There are three major reasons for conducting this review, in addition to questions of efficacy associated with the clinical use of NIs for influenza:
-
Influenza antivirals are a commonly used and stockpiled drug against past and future pandemics on the basis of international and national recommendations. These recommendations are based on the claimed and assumed ability of the drug to reduce complications and transmission. 2,3 In theory, containing the spread of influenza allows time for an organised response with longer-term interventions (such as vaccines), which take time to produce. 3
-
The risk of reporting bias and publication bias leads to uncertainty about the effects of NIs and the results of previous Cochrane reviews of NIs in adults6,10,30,31 and children. 32
-
Oseltamivir is now on the list of WHO essential drugs. 33,34
Process
Review A159 is an amalgamation of two long-standing Cochrane reviews on the effects of NIs for influenza in healthy adults14 (also published in the BMJ31) and children,35 and it is based on the assessment of trials through their CSRs and other regulatory information; a decision we made after finding substantial reporting bias in the journal publications of the relevant trials.
For the full rationale for this process, see Appendix 1.
Examples of discrepancies and reporting bias
We identified that 60% (3145/5267) of patient data from randomised, placebo-controlled, Phase III treatment trials of oseltamivir have never been published. This includes M76001,36 the biggest treatment trial ever undertaken on oseltamivir (with just over 1400 people of all ages). Exclusion of unpublished data changed our previous findings regarding the ability of oseltamivir to reduce the complications of influenza. 8,31 In some cases, mistakes in the attribution of adverse events were discovered only through matching summary tables with individual participant listings. 37–39
A modified approach
We have modified the routine Cochrane processes to improve our previous methods, which we now consider to be inadequate. To resolve inconsistencies and under-reporting, we changed our approach by no longer including trial data as reported in papers published in biomedical journals. Instead, we treated CSRs as our basic unit of analysis. CSRs are often sent to national drug regulators, such as the FDA and the EMA (formerly the European Agency for the Evaluation of Medicinal Products), which require far more stringent standards for completeness and accuracy of reporting than biomedical journals. Journal articles can be regarded as a very succinct synthesis of a CSR. In addition to seeking CSRs, we decided to read and review regulatory documentation. The FDA in particular (and the EMA to a far lesser extent) makes many of its scientific reviews available on its website. Unlike Cochrane review authors, regulators can have access to the whole data set and their comments can provide useful insight, helping to achieve a better understanding of trial programmes.
Clinical study reports generally remain hidden from public view and are not readily available for wider scientific scrutiny, despite the wealth of information that they contain for those willing and able to spend the time reading them and despite calls to make all relevant trial data public,11,40 as well as the known problems with reporting biases. 41,42
Implications
This modified approach to a Cochrane review aims to provide patients, clinicians and policy-makers with the most transparent and independent information possible about NIs for influenza. In addition, it should contribute to improving a European regulatory and pharmacovigilance legal framework, which commentators consider weak. 40,43 We believe that as NIs have become public health drugs, recommended and stockpiled globally, independent scrutiny of all of the evidence relating to harms and effects on complications is necessary to provide patients, policy-makers and physicians with a complete and unbiased view of their risks and benefits.
Implication for A/H1N1 (2009) influenza
In response to our 2010 review,14,31 some have argued that its findings cannot be applied to the 2009 A/H1N1, suggesting that it is a new virus and that, we thus need new evidence. 44–48 Novel A/H1N1 is a new strain of a subtype that has been circulating since 1977, but it also resembles the A/H1N1 strain that has been circulating since before 195749 or before the 1918 pandemic. 50 Influenza subtype A/H1N1 was indeed circulating at the time when the clinical trials, included in our previous reviews, were recruiting. In addition, oseltamivir and zanamivir were approved by regulators worldwide for the treatment and prevention of influenza types A and B, not specific subtypes or strains of influenza A and B. The expectation of regulatory approval is thus that the effects of these drugs demonstrated in clinical trials will apply to future strains of influenza A and B. Use of these drugs during the pandemic was not off-label. It was approved use on the assumption that the clinical trial evidence underpinning regulatory approval applied to novel A/H1N1. We reviewed the clinical trial evidence with the expectation that our results, similar to regulators, will apply to all influenza viruses.
Wider implications
The modified approach in this Cochrane review developed from the realisation that prior methods used to review NIs were inadequate. There is little reason to think that the lessons learned are limited to these particular drugs. 40,42,51–53 On this basis, our independent scrutiny, using all possible trial information, may inform both the wider debate on the adequacy of existing regulatory frameworks in the adoption of new drugs and the question of whether or not other systematic reviews should move to this new, more rigorous, approach, which focuses on trial programmes rather than single trials54,55 (see Appendix 1, Glossary). Although there is substantial evidence for the effects of reporting bias in estimates of effectiveness, less is known of its impact on the evidence of harms. 56 We decided to quantify the additional resources required to follow our modified methodological approach to assess the feasibility of other systematic reviews proceeding in a similar fashion.
Objective
To describe the potential benefits and harms of NIs for influenza in all age groups by reviewing all CSRs of published and unpublished randomised, placebo-controlled trials and regulatory comments.
Methods
Criteria for considering studies for this review
Types of studies
We included evidence from RCTs testing the effects of NIs for prophylaxis, post-exposure prophylaxis (PEP) and treatment of influenza. Prophylaxis is the mode of use of NIs when there is expectation of possible near-future exposure to influenza.
Post-exposure prophylaxis is the use of NIs following probable exposure to influenza but before symptoms develop. Treatment is the use of NIs in persons showing probable signs of influenza.
Owing to discrepancies between published and unpublished reports of the same trials, we included only those trials for which we had unabridged CSRs (e.g. with consecutively numbered pages), even though they may be parts of CSRs (i.e. module 1 only) and information on reports of trials that were considered ‘pivotal’ (i.e. first- or second-line evidence to regulators in support of the registration application).
Types of participants
We included previously healthy people (children and adults). ‘Previously healthy’ includes people with chronic illness (such as asthma, diabetes, hypertension), but excludes people with illnesses with more significant effects on the immune system (such as malignancy or human immunodeficiency virus infection). We included only trials on people who were exposed to naturally occurring influenza with or without symptoms. We targeted the ITT and safety populations, as our prior review discovered compelling evidence that the intention-to-treat-influenza-infected (ITTI) subpopulation – the subpopulation deemed to be influenza-infected – was not balanced between treatment groups in the Roche oseltamivir trials. In addition, estimates from the ITT population will be more generalisable to clinical practice, where routine testing for influenza is not common in many countries (and even where it is used is of variable accuracy).
Types of interventions
Neuraminidase inhibitors administered by any route compared with placebo during the period in which medication was assumed and during the follow-up (on- and off-treatment) periods.
Types of outcome measures
Primary outcomes
-
Symptom relief.
-
Hospitalisation and complications.
-
Harms.
-
Influenza (symptomatic and asymptomatic, always with laboratory confirmation) and ILI.
-
Hospitalisation and complications.
-
Interruption of transmission (in its two components, reduction of viral spread from index cases and prevention of onset of influenza in contacts).
-
Harms.
Secondary outcomes
-
Symptom relapse after finishing treatment.
-
Drug resistance.
-
Viral excretion.
-
Mortality.
-
Drug resistance.
-
Viral excretion.
-
Mortality.
Although overall symptom reduction is well documented, our interest was particularly focused on complications and adverse events, as this is where evidence is currently scarce or inconclusive. 31,32 Our preliminary examination of some regulatory documents and some published versions of the studies had identified that some symptoms and sequelae of influenza (such as pneumonia) had been classified as either a ‘complication of influenza’ or as an ‘adverse event of the treatment’, or both. This is somewhat confusing and we intended to analyse ‘compliharms’ (see Appendix 1, Glossary) irrespective of the classification as a ‘complication of influenza’ or as an ‘adverse event of the treatment’ (see Appendix 2) in oseltamivir trials. Complications of particular interest included pneumonia, bronchitis, otitis media and sinusitis, as these were the secondary illnesses often collected in the Roche oseltamivir trials and we agreed that these events are clinically important. Initially, we constructed a table to illustrate the design methodology that was used for each complication by study (Table 1). The table included the following variables: definition of which events are termed complications; where complications are first defined in the CSR; diagnosis method; and availability of data. We then stratified our analysis by method of diagnosis with three possible criteria: (1) laboratory-confirmed diagnosis (e.g. based on radiologically or microbiologically confirmed evidence of infection); (2) clinical diagnosis without laboratory confirmation (diagnosed by a doctor after a clinical examination); and (3) other type of diagnosis, such as self-reported by patient. We conducted analysis of any complication (pneumonia, bronchitis, otitis media and sinusitis) that was classified as serious or led to study withdrawal.
| Study | Where in CRF (PDF p. #) | Data captured | Person reporting (participant/investigator) | Where reported | Specific field for recording confirmatory assessment (e.g. CXR) | Confirmation (including Px) |
|---|---|---|---|---|---|---|
| M7600136 | 1167 | Yes/no answer to question: ‘Is this event a secondary illness related to influenza?’ Secondary illness is defined: sinusitis, otitis, bronchitis, pneumonia plus other chest infections that are not diagnosed as bronchitis and/or pneumonia |
Investigator | In form for ‘Adverse events or intercurrent illness’ | No | Px |
| NV1687157 | 361, 389 | Form states: Have there been any changes in the patient’s health, including any new conditions or worsening of existing conditions since day 1 (please include secondary illnesses)? Yes/no: If ‘Yes’, please record the details on the ‘Adverse events or secondary illness’ form in the Additional Forms section of the CRF on p. 30.0. All serious adverse events must be reported within 1 working day of occurrence to Roche Page 30.0 of CRF (PDF p. 389) defines secondary illnesses as sinusitis, otitis media, bronchitis and pneumonia, and asks additional questions such as relationship to test drug and outcome, and leaves space for investigator’s comments on the adverse event |
Investigator | Secondary illness not listed as efficacy outcomes Recording of secondary illnesses was to occur in a form titled ‘Adverse event or secondary illness’ |
No | Px |
| WV156708 | 732, 754, 791, 832 | CRF (PDF p. 732) states: secondary illness reminder: has the patient reported any sinusitis, otitis, bronchitis, other chest infection or pneumonia since baseline? Yes [ ] Complete secondary illness page (not the adverse event page) No [ ] Secondary illness page CRF (PDF p. 754) requests information on date of onset, date resolved, whether or not treatment was given and, if so, what treatment or medical procedures, total daily dose, and start/end date of treatment or medical procedure In addition, participants could fill in information related to a secondary illness in their diary card in the free-text box called ‘Notes’, which prompts participants: ‘Please can you record below any extra information about your flu which may be of interest to us, (for example: did your flu symptoms re-occur, and if so when?), and have you taken any other treatments? If so please record the treatment name and the dates you took it.’ (PDF p. 791) |
Participant, mediated through investigator | For investigators, on ‘Secondary illness’ form For participants, on ‘Notes’ section of diary card |
No | |
| WV1567158 | 740, 889, 1018 | CRF (PDF p. 740) states: Secondary illness reminder: Has the patient reported any sinusitis, otitis, bronchitis, other chest infection or pneumonia since baseline? Yes [ ] Complete secondary illness page (not the adverse event page) No [ ] Secondary illness page CRF (PDF p. 889) requests information on date of onset, date resolved, whether or not treatment was given and, if so, what treatment or medical procedures, total daily dose and start/end date of treatment or medical procedure Secondary illnesses are listed as sinusitis, otitis, bronchitis, pneumonia and other chest infections that are not diagnosed as bronchitis and/or pneumonia In addition, participants could fill in information related to a secondary illness in their diary card in the free-text box called ‘Notes’, which prompts participants: ‘Please can you record below any extra information about your flu which may be of interest to us, (for example: did your flu symptoms re-occur, and if so when?), and have you taken any other treatments? If so please record the treatment name and the dates you took it.’ (PDF p. 1018) |
Participant, mediated through investigator | Mentioned in module 1 and RAP, as tertiary outcomes not mentioned in protocol | No | Px |
| WV15673/WV1569759 | From 483 | No mention of pneumonia, secondary illness, complications in the CRFs | Unclear | Secondary illnesses not listed in protocol as end points. They are listed as safety end points in the RAP, which states that ‘pre-defined’ secondary illnesses were ‘sinusitis, otitis, bronchitis, pneumonia, and other chest infections that are not diagnosed as bronchitis and/or pneumonia, plus recurrence of symptoms from the diary card once alleviation had occurred.’ (PDF p. 479) | ||
| WV1570760 | From 98 | Page 117: secondary illness reminder: Has the patient reported any sinusitis, otitis, bronchitis, other chest infection or pneumonia since baseline? Yes [ ] Complete secondary illness page (not the adverse event page) No [ ] Page 131: diagnostic procedures 1. Were there any diagnostic procedures or tests carried out since day 1 as a result of influenza or secondary illness that were not scheduled as part of protocol? Yes Type of diagnostic procedure or test: 1. Chest X-rays 2. ECG 3. Bacterial culture 4. Bronchoscopy 5. Pulmonary function test 6. Viral culture (other than influenza) 7. Blood tests (other than antibody sample) 8 Other specify No Secondary illness p. CRF (PDF p. 158) requests information on date of onset, date resolved, whether or not treatment was given and, if so, what treatment or medical procedures, total daily dose and start/end date of treatment or medical procedure |
Participant, mediated through investigator | Mentioned in RAP as tertiary end points, pp. 57–8 | Yes | Px |
| WV1570861 | From 460 | Secondary illness reminder, p. 474: Has the patient reported any new episodes of sinusitis, otitis, bronchitis, other chest infection or pneumonia since screening? Yes [ ] . . . Complete adverse event page No [ ] ‘Adverse events’ CRF collected data on date of onset, initial intensity, test drug adjustment, whether or not treatment was given (if so, what), most extreme intensity, relationship to test drug, outcome, whether or not it led to hospitalisation and a free-text line for recording ‘Comments on AE’ (e.g. PDF p. 479) |
Participant, mediated through investigator | Secondary illness not mentioned in protocol | No | Px |
| WV1573062 | From 340 | Secondary illness reminder: Has the patient reported any sinusitis, otitis, bronchitis, other chest infection or pneumonia since baseline? Yes [ ] . . . Complete secondary illness page (not the adverse event page) No [ ] The secondary illness page is descriptive of dates and Px |
Participant, mediated through investigator | Listed as tertiary end points in RAP, p. 297 | No | Px |
| WV1575863 | From 637 | Has the patient reported any new adverse events or symptoms (including intercurrent illnesses and secondary illnesses)? Yes [ ] record in the adverse events/intercurrent illness section of the case No [ ] report form Diagnostic confirmation of otitis media from p. 648 onwards |
Participant, mediated through investigator | Listed as secondary illnesses in core report modules 1 and 2, p. 36 | Yes | Px |
| WV15759/WV1587164 | From 665 | Has the subject reported any adverse events including secondary and intercurrent illnesses? | Participant, mediated through investigator | Secondary illnesses not mentioned in protocol, but secondary outcome in core report Note: worth looking at comparisons 1.49 to 1.51 in RM5. No effect but in bronchitis this study has a more conservative effect than NV16871, which has no definitions and no diagnostics |
Yes | Px |
| WV1579965 | From 642 | Secondary illness defined as in M76001.36 There is a generic physical examination form at p. 704, including ‘lungs’ normal/abnormal specify . . . . . At p. 709, has the patient reported any new AE, including intercurrent or secondary illnesses? Yes/no. If yes, record the adverse events/intercurrent illness section of the CRF (noted at p. 746 on the back of the CRF) with full history, physical examination and diagnostic work up questions for BRON ± PNUM ± LRTI ± SIN ± OM including questions about CXR, MRI, sputum, etc. |
Investigator | Proportion of contacts who are classified as having a secondary illness subsequent to a confirmed episode of influenza listed as tertiary end points | Yes | Px |
| WV15812/WV1587266 | From 285 | Has the patient reported any new adverse events or symptoms (including intercurrent illnesses and secondary illnesses)? Yes [ ] record in the adverse events/intercurrent illness section of the case No [ ] report form At pp. 450–74 is diagnosis of secondary illness page, which is very similar to the one at serial 10 Exhaustive list of diagnostic procedures |
Participant mediated through investigator | Listed as secondary tertiary in protocol at p. 252 | Yes | Px |
| WV15819/WV15978/WV1587667 | From 412 | Page 437 (adverse event reminder): Has the patient reported any new adverse events or symptoms (including intercurrent illnesses)? Yes [ ] record in the adverse events/intercurrent illness section of the case No [ ] report form In CRF p. 447 and p. 443, usual secondary illness reminder From p. 471, diagnosis of secondary illness. This is a one-page list of diagnostics similar to that at serial 10. The question is: ‘Were there any diagnostic procedures or tests carried out since day 1 as a result of influenza or secondary illness that were not scheduled as part of protocol?’ If yes, list per serial 10 From p. 486 is a list of diagnostic tests |
Participant, mediated through investigator | Secondary illness listed as secondary (required antibiotics) and tertiary outcomes in core report and as an addition in protocol amendment at p. 21 | Yes | Px |
| WV1582568 | From 389 | There is a usual note: please go to diagnosis of secondary illness at back of CRF, p. 487 Is this event a secondary illness related to influenza? Diagnosis of secondary illness From pp. 510–40 with exhaustive list of diagnostics as per serial 10 |
Participant, mediated through investigator | Secondary illness listed as secondary outcomes in protocol p. 346 Secondary illnesses recorded on ‘Adverse events’ CRF |
Yes | Px |
| WV1627769 | From 415 | Not found | Not found | Secondary illness not listed as efficacy outcomes |
In all cases of influenza complications reporting (pneumonia, bronchitis, sinusitis, otitis media) there is a variable degree of participant self-reporting, of investigator mediation (e.g. in writing down the details in the CRF) and lack of verification with investigations, such as culture or imaging. The ‘self-reported, investigator-mediated, unverified’ title is relevant to all complications but for brevity we use it as sparingly as possible.
For harms, we were limited by the frequency of occurrence of the adverse events collected in the trials. Consequently, we meta-analysed (1) all serious adverse events; (2) all adverse events leading to study withdrawal; (3) all withdrawals; (4) all adverse events within a CSR’s defined body system; and (5) a small group of common adverse events as defined in the FDA drug label for oseltamivir. There were too few events to meta-analyse: (1) deaths; (2) serious adverse events by body system; and (3) any events that had an overall incidence of < 0.5%. We did not meta-analyse outcomes with fewer than 10 events in total. We conducted analyses separately for on-treatment and off-treatment periods. However, in two cases for which (on-treatment) treatment effects were borderline statistically significant (prophylaxis with oseltamivir: renal body system on-treatment and psychiatric body system on-treatment), we conducted additional analysis combining on- and off-treatment periods to maximise statistical power. We conducted dose–response harms analysis for two treatment trials8,58 combined and one prophylaxis study,59 as these trials investigated the active agent at multiple doses. These studies8,58,59 included standard-dose and high-dose oseltamivir arms. For these analyses we used logistic regression, adjusting for study effects if appropriate (i.e. for the two treatment trials8,58) and testing for trend using a likelihood ratio test. We tested the hypothesis that increased dose of drug leads to increased incidence of adverse effects.
Search methods for identification of studies
To identify trials in the manufacturer-funded clinical trial programmes for NIs, as well as non-manufacturer-funded clinical trials of NIs, we used a variety of methods that were applied to a variety of sources from the literature, manufacturers and regulatory bodies. These methods, as well as our methodology for identifying and obtaining relevant CSRs, are detailed in Appendices 1, 4 and 5.
Electronic searches
We used electronic searches to identify trials that were not identified by the methods outlined in Appendix 1, particularly for non-manufacturer-funded clinical trials (see Appendix 3 for details). For the 2012 review, we updated our searches of the electronic databases of published studies that were previously carried out for the Cochrane reviews on NIs in children35 and healthy adults,14 and then updated the searches again on 22 July 2013.
Searching other resources
For the description of our searches for regulatory information (FDA, EMA, Roche, GSK, the Japanese Pharmaceuticals and Medical Devices Agency), see Appendix 4.
Data collection and analysis
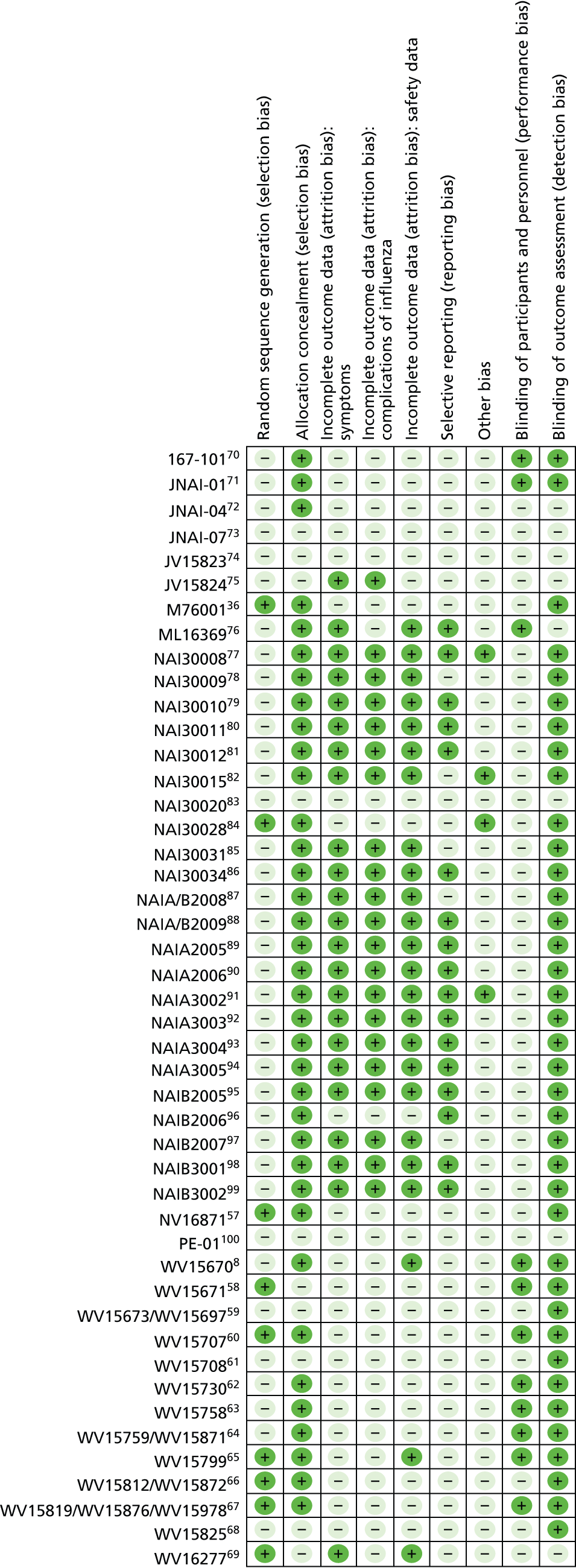
Collection and inventory of the evidence base was facilitated by the tools that were specifically developed for the review (see Appendix 5). The overall risk of bias is presented graphically in Figure 1 and summarised in Figure 2.
FIGURE 1.
Risk-of-bias graph: review of authors’ judgements about each risk-of-bias item, presented as percentages across all included studies. ‘Other bias’ includes potentially active placebos.
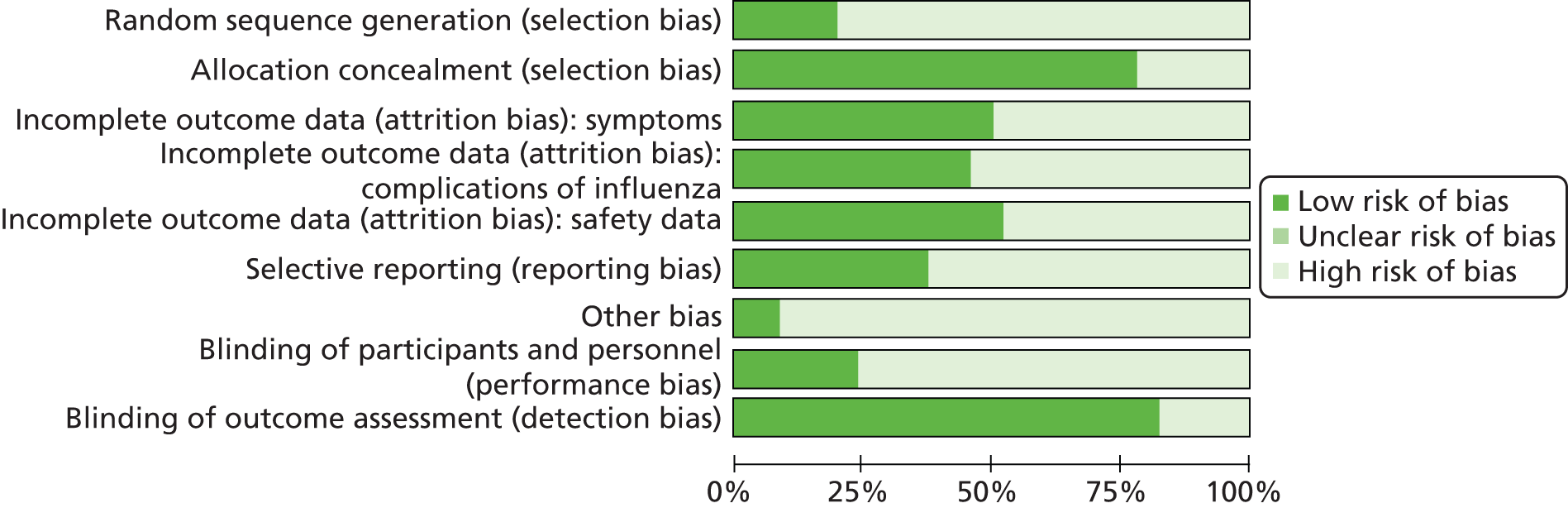
FIGURE 2.
Risk-of-bias summary: review of authors’ judgements about each risk-of-bias item for each included study. ‘Other bias’ includes potentially active placebos. +, low risk of bias; –, high risk of bias.
Selection of studies
For this 2013 review, two authors (PD and TJ) reapplied the inclusion criteria for the oseltamivir CSRs and resolved disagreements by discussion. Two review authors (ES and IO) applied the criteria for the zanamivir CSRs, whereas one review author (CH) arbitrated.
For the procedures followed in the 2012 review, see Appendix 7.
Data extraction and management
The sizeable quantity of available data led us to subdivide the extraction, appraisal and analysis of the data into a two-stage exercise. In stage 1 we assessed the reliability and completeness of the identified trial data. We decided to include in stage 2 of the review (full analysis following standard Cochrane methods) only data that satisfied the following three criteria:
-
Completeness CSRs/unpublished reports include both identifiable CONSORT (Consolidated Standards of Reporting Trials) statement-specified methods to enable replication of the study. Identifiable CONSORT statement-specified results (primary outcomes, tables, appendices) must be available.
-
Internal consistency All parts (e.g. denominators) of the same CSRs/unpublished report are broadly consistent.
-
External consistency Consistency of data as reported in regulatory documents, other versions of the same CSRs/unpublished reports and other references, to be established by cross-checking.
This was a different approach to that used in the previous version of the current review,9 as we had only incomplete information at that time and applied only the second and third criteria.
Stage 1
For details of the use of the CONSORT-based extraction template and the assessment for stage 1 inclusion in the A159 review,9 see Appendix 5. In this review, assessment for inclusion in stage 1 was part of the inclusion procedure.
Stage 2
In stage 2, one review author extracted data and a second review author checked it. We extracted data on to standard forms, checked and recorded it.
Use of regulatory information
We used regulatory information to assess the possible correlation between citation frequency of oseltamivir treatment trials in the FDA regulatory documents and trial size.
Post-protocol analyses
After publication of the A159 protocol in December 2010, but before validation of our CONSORT-based extractions in the spring of 2011, we decided to carry out analyses (which we called post-protocol analyses) to test five null hypotheses that we had formulated while reading, summarising and reconstructing the CSRs. The hypotheses originated from our observations of discrepancies and other unexpected observations in the CSRs’ data, and were informed by reading regulatory information. Appendix 8 reports the rationale, methods to formulate and test, and the results of the hypotheses.
The hypotheses reflect the uncertainty prevailing in the evidence base at a time when full CSRs were not available for all studies.
Assessment of risk of bias in included studies
Previous studies comparing regulatory with published or internal company sources of evidence have reported a variety of different biases that affect medical knowledge. 41,42,56,101 We will report in detail elsewhere our comments on using the Cochrane risk-of-bias tool102 to appraise CSRs and for trial programmes, and our efforts to construct an instrument for assessing risk of bias in complete CSRs. A full description of the methods used to quantify biases will be published in another paper.
Measures of treatment effect
To estimate treatment effects we first calculated the risk ratios (RRs) and used the average (mean) control event rate and the pooled RRs reported in the figures to calculate the RDs. For consistency, we adopted this method for both the ‘Summary of findings’ tables and for the RDs reported in the text. For the analysis we chose to report the RRs, as they are more consistent across the studies, and we have reported the heterogeneity for the pooled RR. We reinterpreted the results using the RD, as this result is applicable to clinical decision-making. We calculated MDs for time to first alleviation of symptoms. For time to first alleviation of symptoms we also estimated the treatment effect as the percentage reduction in the average time to first alleviation of symptoms in the placebo group. Most zanamivir CSRs stated treatment effects only in terms of medians in each treatment group, as well as p-values from a hypothesis test comparing the time-to-event distributions. These data are insufficient for conducting a meta-analysis. However, often sufficient time-to-event data were reported to allow us to estimate restricted means and standard deviations. Restricted means are based on the maximum time reported where alleviation occurred. There were some patients for whom alleviation was censored at the maximum follow-up time; therefore, restricted means are underestimates of the true means. However, the proportion of patients who were censored was generally low and similar in both treatment arms, hence this limitation is unlikely to have led to bias. The length of follow-up varied across trials and this has led to high variation in the estimated means and standard deviations across trials.
A post hoc analysis was undertaken after we discovered seven zanamivir trials that provided data on time to first alleviation of symptoms with and without relief medication. Each patient in the studies may or may not have taken relief medication [e.g. paracetamol (acetaminophen)] during the trial. Alleviation of symptoms may have occurred while the patient was taking relief medication and the ‘standard’ comparison was made using this scenario. However, an additional analysis used a stricter definition, for which alleviation of symptoms could be achieved only without the use of relief medication. For example, a patient may have achieved alleviation using relief medication after 5 days but took 7 days to achieve alleviation without the use of relief medication. The comparison we reported is for all patients for whom we used the stricter definition for the zanamivir group (alleviation without relief medication) and the less-strict definition for the placebo group (alleviation with relief medication).
We planned to use the tridimensional dose-relatedness, timing and patient susceptibility methodology to assess the likelihood of harms causality,103 but the quality of the data available did not allow for this.
Unit of analysis issues
Problems with unit of analysis are described in ‘Post-protocol hypotheses’ (see Appendix 8).
Dealing with missing data
We developed a comprehensive strategy for dealing with data that we know are missing at the trial level, that is, unpublished trials (see Search methods for identification of studies, above, and Appendices 1, 4 and 5) and unreliable published records, which are a very concentrated summary of CSRs. For example, in the oseltamivir trial programme, some trials’ CSRs (e.g. WP16263104) consist of 8545 pages. This has a 1000-fold greater length than its published version,105 which consists of seven pages. The purpose of this review is to provide as complete a picture as possible of trial programmes, without reliance on the published literature. Appendix 9 reports an example of the content of a typical Roche CSR.
Assessment of heterogeneity
We used tau-squared (inverse variance method) and the I2 statistic to estimate between-study variance as measures of the level of statistical heterogeneity, and the chi-squared test to test for heterogeneity.
Assessment of reporting biases
We carried out assessment of reporting biases (comparing CSR with the relevant publication) only in the first publication of A159. 106 For this version, as we had complete CSRs for the trial programmes of the two drugs, we expected to find all of the relevant information in these documents and adopted a binary assessment (high risk, low risk or unclear bias).
Data synthesis
We used the random-effects approach of DerSimonian and Laird107 based on MDs for analysis of time to first alleviation of symptoms. For all of the other outcomes we used the random-effects approach for binary data of DerSimonian and Laird107 where tau-squared was estimated using the inverse variance method.
Although overall symptom reduction is well documented, our interest was particularly focused on complications and adverse events, as this is where evidence is currently scarce or inconclusive. 31,32,35 Our preliminary examination of CSRs identified that some symptoms and sequelae of influenza (such as ‘pneumonia’) had been classified as either a ‘complication of influenza’ or as an ‘adverse event of the treatment’, or both. We called this somewhat confusing classification ‘compliharms’. We decided to deal with compliharms as follows. We identified complications of particular clinical interest as ‘pneumonia’, bronchitis, otitis media and sinusitis. We tabulated the type of data capture used for each complication (‘secondary illness’) by study, including the following variables: definition of what events are termed complications; which part of the CSR captured data on complications; who reported and captured the data; which diagnostic method was used; whether or not, and where, the diagnostic pathway was (usually a form); and whether or not prescriptions for treatment were captured. We then aimed to stratify our analysis by method of diagnosis with three possible criteria: (1) laboratory-confirmed diagnosis (e.g. based on radiologically or microbiologically confirmed evidence of infection); (2) clinical diagnosis without laboratory confirmation (diagnosed by a doctor/investigator after a clinical examination); and (3) other type of diagnosis, such as self-reported by patient. We also conducted analysis of any complication (such as ‘pneumonia’, bronchitis, otitis media and sinusitis) that was classified as serious or led to study withdrawal.
We tested the effects of oseltamivir in prophylaxis of influenza and ILI. However, the CSRs of prophylaxis trials do not define ILI but report eight different definitions for influenza with laboratory confirmation (see web extra influenza definitions, Appendix 11).
This is a complex and confusing set of definitions, in which, for example, the definition for upper respiratory tract infection with systemic disturbance is the same as one of the definitions for asymptomatic influenza. After discovering the absence of a definition for ILI, and the complex and confusing definitions for laboratory-confirmed influenza, we classified ILI as having two or more symptoms from the following: nasal congestion, headache, chills/sweats, sore throat, cough, fatigue, myalgia and fever. These were the symptoms reported in the efficacy listing of individual patients in module 3 of the prophylaxis trials CSRs.
In two oseltamivir treatment trials8,58 and one prophylaxis study59 there were three treatment arms comparing placebo, standard dose and high dose. For time to first alleviation of symptoms, we restricted comparison to placebo against standard dose (as this is how it was reported in the original report). However, for all other outcomes we combined the standard and high-dose treatment arms. There was little apparent difference in the incidence of outcomes between the standard- and high-dose arms, and combining the arms did not appear to cause heterogeneity. However, in two cases there was some evidence of a dose–response effect. These cases are described more fully below (see Results, Analysis of harms).
The majority of zanamivir trials compared placebo with inhaled zanamivir. However, some trials also included an intranasal zanamivir treatment arm and a combined arm of inhaled and intranasal treatment. The multiple zanamivir arms were generally combined for meta-analysis, as effects appeared similar and did not appear to cause heterogeneity.
Subgroup analysis and investigation of heterogeneity
We investigated the robustness of complications outcomes using subgroup analysis by method of diagnosis. We investigated high estimates of heterogeneity, where possible, using subgroup analysis. For example, we conducted a subgroup analysis of time to first alleviation of symptoms in studies of oseltamivir treatment in children by partitioning studies into those of otherwise healthy children and those of children with chronic illness (asthma). Based on a referee’s comment, we conducted a subgroup analysis on time to first alleviation of symptoms by infection status for zanamivir. We could not do a similar analysis for oseltamivir because we did not have data on the non-influenza-infected patients, and we could not correctly identify the patients with influenza infection as a result of the effect of oseltamivir on antibodies.
In the trial programmes for both oseltamivir and zanamivir there was large variation in treatment effects for pneumonia across the populations studied (i.e. adults and children, as well as treatment and prophylaxis), hence we conducted a metaregression to investigate this heterogeneity. We included all of the studies that reported pneumonia (32 studies in total) and investigated the four binary factors: age group (adults vs. children), drug (oseltamivir vs. zanamivir): indication (treatment vs. prophylaxis) and method of diagnosis. For oseltamivir studies, the method of diagnosis was based on either data collected on non-specific adverse events or secondary/intercurrent illness forms, or data collected on specific ‘diagnosis of secondary illness’ forms that included objective criteria such as X-ray confirmation. For zanamivir, two trials included X-ray confirmation of pneumonia. We conducted the metaregression in Stata/SE, version 13 for Windows (StataCorp LP, College Station, TX, USA) using the metareg command. There were some studies where one treatment group had zero events, therefore we added 0.5 events to all treatment groups for all studies prior to analysis. The dependent variable in the regression was log-relative risk. A further post hoc analysis was undertaken after we discovered that seven trials provided data on time to first alleviation of symptoms with and without relief medication. Each patient in the studies may or may not have taken relief medication during the trial. Alleviation of symptoms may have occurred while the patient was taking relief medication, and the ‘standard’ comparison was made using this scenario. However, an additional analysis used a stricter definition, for which alleviation of symptoms could be achieved only without the use of relief medication. For example, a patient may have achieved alleviation using relief medication after 5 days but took 7 days to achieve alleviation without the use of relief medication. The comparison we reported is for all patients, for which we used the stricter definition for the zanamivir group (alleviation without relief medication) and the less strict definition for the placebo group (alleviation with relief medication).
Sensitivity analysis
Sensitivity analyses applicable to our post-protocol analyses have been covered above (see Methods). We used the fixed-effect method of Mantel and Haenszel as a sensitivity analysis to supplement our primary analyses using the random-effects method of DerSimonian and Laird. 107 Random-effects meta-analysis is known to be overly conservative with sparse data. Hence, we conducted sensitivity analysis using Peto’s method on two occasions for which we had sparse data and borderline statistically significant results (prophylaxis with oseltamivir: renal body system on-treatment and psychiatric body system on-treatment).
Results
Description of studies
We searched trial registries, electronic databases and regulatory archives, and corresponded with manufacturers to identify all trials and requested CSRs. Although this review focuses on the primary data sources of manufacturers, we checked that there were no published RCTs from non-manufacturer sources by running electronic searches in the following databases: CENTRAL 2013, Issue 6, limited to year published 2010–13 (20 search results); MEDLINE (January 2011 to July week 2, 2013) (56 search results) and MEDLINE (via Ovid) from 1 January 2011 to July week 2, 2013 (56 search results); EMBASE (January 2011 to July 2013) (90 search results) and EMBASE.com from 1 January 2011 to July 2013 (90 search results); and PubMed (not MEDLINE) with no date limit (21 records). We searched PubMed to identify publisher-submitted records that will never be indexed in MEDLINE and the most recently added records not yet indexed in MEDLINE. To identify reviews that may possibly have referenced further trials we searched DARE 2013, Issue 2 of 4 April (four search results); NHS EED, Issue 2 of 4 April 2013 (two search results); both resources parts of The Cochrane Library (accessed 22 July 2013); and HEED (searched 22 July 2013) (three search results).
Results of the search
Use of regulatory information
We were able to download 2673 pages from the FDA website. The table of contents (TOC) is provided in Tables 2–5. We used these pages to identify all of the trials that had been conducted within a drug’s trial programme. There was no correlation between citation frequency of oseltamivir treatment trials in the FDA regulatory documents and trial size. The biggest treatment trial36 is cited only four times in three documents, whereas other contemporary treatment trials are cited far more. 8,58,60,62,66 One trial,8 for example, is cited 46 times in the FDA documents. However, the combined enrolled denominator of the four treatment trials completed at the time8,58,60,62 was 1442, smaller than 1459. 36 This suggested that the FDA’s regulatory evaluation of Roche’s New Drug Application (NDA) was based predominantly on what Roche had presented to them as ‘pivotal’, or trials that best demonstrated the properties of oseltamivir, not the complete evidence base of all oseltamivir trials. One possible alternative explanation for this observation could have been the interval between trial completion, generation of the report and NDA submission. This explanation is supported by the relatively brief interval between completion of the M76001 trial36 (19 February 1999) and submission (on 30 April 1999) of NDA 021087 to the FDA. However, the core part of the submission (the clinical development programme) contains data from two (at the time of writing) ongoing trials. 66,67
| Mentioned study | File name | Pages on which study is mentioned (separated by commas) | Note |
|---|---|---|---|
| 113502 | |||
| 113625 | |||
| 113678 | |||
| 114045 | |||
| NAI108166 | |||
| 105934 | |||
| NAI106784 | |||
| 107485 | |||
| 108127 | |||
| 112311 | |||
| 112312 | |||
| 113268 | |||
| GCP/95/045 | |||
| NAI10901 | Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-admin2.pdf | 15.15 | |
| NAI10902 | |||
| NAI3000877 | Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-admin2.pdf | 15 | Seven documents with 14 instances |
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-admin3.pdf | 13 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview7.pdf | 19, 19, 20 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview8.pdf | 1, 1, 3, 4, 4 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview9.pdf | 7.7 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/21036ltr.pdf | 2 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/20000426_001/21–036-S001_RELENZA_MEDR.pdf | 33 | ||
| NAI3000978 | Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview8.pdf | 1.2 | Seven documents with 110 instances |
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/20000426_001/21–036-S001_RELENZA_ADMINCORRES_P1.pdf | 10, 10, 12, 13, 13, 14, 14, 17, 29, 42, 61, 62, 64, 64, 65, 65, 68 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/20000426_001/21–036-S001_RELENZA_ADMINCORRES_P2.pdf | 33, 34, 36, 43, 43, 43, 43, 52, 52, 52, 53, 53, 56, 57 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/20000426_001/21–036-S001_RELENZA_BIOPHARMR.pdf | 5, 5, 5, 6, 6, 8, 8 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/20000426_001/21–036-S001_RELENZA_MEDR.pdf | 3, 3, 3, 3, 3, 3, 3, 4, 4, 5, 8, 9, 9, 10, 10, 11, 11, 11, 14, 14, 15, 16, 17, 19, 19, 19, 20, 20, 22, 23, 23, 23, 24, 24, 24, 25, 25, 25, 25, 25, 25, 26, 26, 26, 27, 27, 28, 28, 28, 29, 29, 31, 31, 31, 31 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/20000426_001/21–036-S001_RELENZA_MICROBR.pdf | 3, 3, 4, 4, 4 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/20000426_001/21–036-S001_RELENZA_STATR.pdf | 2, 2, 2, 4, 7, 12, 18, 18, 18, 19 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/20000426_001/21–036-S001_RELENZA_ADMINCORRES_P1.pdf | 31.56 | One document with two instances | |
| NAI3001079 | Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview8.pdf | 1.2 | Six documents with 65 instances |
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/20000426_001/21–036-S001_RELENZA_ADMINCORRES_P1.pdf | 10, 12, 13, 14, 14, 15, 17, 62, 62, 62, 64 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/20000426_001/21–036-S001_RELENZA_ADMINCORRES_P2.pdf | 34, 34, 36, 43, 53 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/20000426_001/21–036-S001_RELENZA_BIOPHARMR.pdf | 5, 5, 6, 6 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/20000426_001/21–036-S001_RELENZA_MEDR.pdf | 3, 3, 3, 3, 3, 4, 5, 18, 19, 21, 21, 22, 23, 23, 23, 23, 24, 25, 25, 25, 26, 26, 26, 26, 27, 27, 27, 28, 28, 29, 29, 29, 30, 31, 31, 31, 32 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/20000426_001/21–036-S001_RELENZA_STATR.pdf | 2, 2, 13, 13, 13, 19 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/20000426_001/21–036-S001_RELENZA_BIOPHARMR.pdf | 6 | One document with one instance | |
| NAI3001281 | Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview7.pdf | 1 | One document with one instance |
| NAI3001582 | |||
| NAI3002083 | |||
| NAI3002884 | |||
| NAI3003486 | |||
| NAI40012 | |||
| NAIA1009 | Tamiflu and Relenza/Relenza/Relenza – NDA 021036/20000426_001/21–036-S001_RELENZA_ADMINCORRES_P1.pdf | 56 | Four documents with 17 instances |
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/20000426_001/21–036-S001_RELENZA_ADMINCORRES_P2.pdf | 1, 1, 1, 48, 49, 52 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/20000426_001/21–036-S001_RELENZA_BIOPHARMR.pdf | 5, 5, 6 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/20000426_001/21–036-S001_RELENZA_MEDR.pdf | 3, 3, 6, 7, 20, 31, 31 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview5.pdf | 18 | Five documents with five instances | |
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview6.pdf | 9 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/20000426_001/21–036-S001_RELENZA_ADMINCORRES_P2.pdf | 52 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/20000426_001/21–036-S001_RELENZA_BIOPHARMR.pdf | 11 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/20000426_001/21–036-S001_RELENZA_STATR.pdf | 2 | ||
| NAIA300291 | Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-admin1.pdf | 15 | Thirteen documents with 122 instances |
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-admin2.pdf | 6, 6, 7, 7, 14, 15, 22, 22, 23 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-admin3.pdf | 1, 4, 4, 12, 12, 12, 12, 17 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview1.pdf | 4, 14, 14, 14, 14, 14, 15, 15, 15, 15, 16 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview2.pdf | 1, 2, 3, 4, 4, 5, 6, 6, 6, 8, 8, 9, 9, 9, 12, 12, 15, 16, 16, 16, 17 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview3.pdf | 5, 5, 6, 6, 6, 7, 7, 7, 8, 8, 9, 9, 9, 10, 11, 12, 13, 13, 14, 15, 15, 17, 18, 18, 19, 20, 21 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview4.pdf | 1, 1, 1, 1, 2, 6 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview6.pdf | 4, 5, 10, 12 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview7.pdf | 1, 1, 2, 2, 2, 2, 3, 3, 4, 4, 5, 5, 7, 8, 10, 11, 12, 14, 16, 16, 16, 16, 16, 17 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview8.pdf | 2, 2, 6, 6, 8, 8, 9, 10 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview9.pdf | 10 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-stats.pdf | 7 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/20000426_001/21–036-S001_RELENZA_BIOPHARMR.pdf | 5 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview1.pdf | 15 | One document with one instance | |
| NAIA300392 | Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview7.pdf | 17, 17, 18 | Three documents with six instances |
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview8.pdf | 4.4 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview9.pdf | 22 | ||
| NAIA300493 | Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-admin3.pdf | 14 | Four documents with eight instances |
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview6.pdf | 7 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview7.pdf | 18, 18, 19 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview8.pdf | 4, 4, 4 | ||
| NAIA300594 | Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-admin3.pdf | 14 | Five documents with 12 instances |
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview1.pdf | 5 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview5.pdf | 12, 12, 12, 13, 14, 15, 15 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview7.pdf | 14.15 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/20000426_001/21–036-S001_RELENZA_ADMINCORRES_P2.pdf | 38 | ||
| NAIB1002 | |||
| NAIB300299 | Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-admin1.pdf | 15 | Fourteen documents with 99 instances |
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-admin2.pdf | 14, 15, 15, 15 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-admin3.pdf | 11.12 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview1.pdf | 4, 14, 14, 14, 14, 14, 14, 14, 14 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview2.pdf | 9, 9, 9, 9, 9, 9, 10, 11, 12, 12, 12, 12, 13, 13, 13, 14, 14, 14, 15, 15, 16, 16, 16, 17 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview3.pdf | 4, 5, 6, 6, 6, 7, 7, 7, 8, 8, 8, 9, 9, 11, 12, 12, 13, 13, 14, 15, 17, 18, 18, 19, 20, 21 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview4.pdf | 1, 1, 1, 1, 2 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview5.pdf | 4 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview6.pdf | 4, 5, 10, 12 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview7.pdf | 2, 3, 3, 7, 8, 10, 11, 14, 15, 16, 16, 16 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview8.pdf | 7, 8, 8, 8, 9, 9 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview9.pdf | 10.2 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-stats.pdf | 7 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/20000426_001/21–036-S001_RELENZA_BIOPHARMR.pdf | 5.5 | ||
| NAI3001180 | |||
| NAIB200797 | Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-admin1.pdf | 15 | Seven documents with 18 instances |
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-admin2.pdf | 15 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview1.pdf | 5 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview4.pdf | 14, 15, 15, 16, 16, 17, 17, 17, 18 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview6.pdf | 3 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview7.pdf | 8, 10, 10, 15 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview8.pdf | 2 | ||
| NAIA200690 | |||
| NAIB200696 | |||
| NAIB1007 | |||
| C94-009 | Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview5.pdf | 17 | One document with one instance |
| C94-085 | Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview5.pdf | 17 | Two documents with two instances |
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview9.pdf | 22 | ||
| NAIB1001 | Tamiflu and Relenza/Relenza/Relenza – NDA 021036/20000426_001/21–036-S001_RELENZA_BIOPHARMR.pdf | 17 | One document with one instance |
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/20000426_001/21–036-S001_RELENZA_BIOPHARMR.pdf | 6 | One document with one instance | |
| NAIA200589 | Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-admin1.pdf | 15 | Ten documents with 44 instances |
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-admin2.pdf | 7, 17, 10 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-admin3.pdf | 2.4 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview1.pdf | 4.5 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview4.pdf | 2, 2, 3, 3, 3, 3, 5, 6, 6, 6, 6, 8, 8, 8, 9, 11, 12, 12, 13, 14, 14, 14, 14, 14, 15, 18 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview5.pdf | 7.7 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview6.pdf | 3.4 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview7.pdf | 2, 5, 9, 15 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview8.pdf | 10 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-microbiology.pdf | 21 | ||
| NAIB200595 | Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-admin1.pdf | 15 | Nine documents with 43 instances |
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-admin2.pdf | 17, 20, 20, 22, 23 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview1.pdf | 5.5 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview4.pdf | 3, 3, 3, 7, 8, 8, 8, 9, 10, 11, 11, 11, 11, 11, 12, 12, 12, 13, 14, 14, 14, 14, 14, 14, 14, 15 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview5.pdf | 7.7 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview6.pdf | 3.4 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview7.pdf | 2, 9, 15 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview8.pdf | 2 | ||
| Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-microbiology.pdf | 21 | ||
| NAIA/B200878 | Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview6.pdf | 4 | One document with one instance |
| NAIA2010 | Tamiflu and Relenza/Relenza/Relenza – NDA 021036/19990726_000/021036-medreview5.pdf | 16 | One document with one instance |
| NAIA/B200988 | |||
| 167-02 | |||
| 167-03 | |||
| 167-05 | |||
| 167-04 | |||
| JNAI-03 | |||
| JNAI-02 | |||
| JNAI-0171 | |||
| JNAI-0773 | |||
| JNAI-0472 | |||
| PE-01100 | |||
| 167-10170 | |||
| 167T3-11 |
| Referenced study | File name | Pages on which study is mentioned (separated by commas) | Note |
|---|---|---|---|
| NP15717 | Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_bior.pdf | 46.46 | Six documents with 13 instances |
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_medr_P2.pdf | 14, 15, 15 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20040624_010/021087_S016_TAMIFLU CAPSULES – DRY POWDER_BIOPHARMR.pdf | 3 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_Admindocs_P2.pdf | 2 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_BioPharmr.pdf | 5, 8, 10, 13, 31 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20040624_010/021087_S016_TAMIFLU CAPSULES – DRY POWDER_BIOPHARMR.pdf | 3 | ||
| NP15718 | Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_bior.pdf | 17 | One document with one instance |
| NP15728 | Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_bior.pdf | 16.35 | Three documents with six instances |
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_medr_P1.pdf | 11 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_medr_P2.pdf | 45, 46, 47 | ||
| NP15757 | Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/20001117_002/21–087SE1–002_review.pdf | 92, 93, 104, 122, 126, 131, 144, 144, 145 | One document with nine instances |
| NP15826 | Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_medr_P2.pdf | 47 | Nine documents with 26 instances |
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/20040624_016/021087_S016_TAMIFLU CAPSULES – DRY POWDER_ADMINCORRES.pdf | 6 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20040624_010/021087_S016_TAMIFLU CAPSULES – DRY POWDER_BIOPHARMR.pdf | 3 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_Admindocs_P2.pdf | 2 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_BioPharmr.pdf | 4, 5, 5, 8, 8, 8, 10, 17, 29, 30, 30, 30, 30, 30, 31, 31 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_Medr.pdf | 9.1 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_Statr.pdf | 9.1 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/20040624_016/021087_S016_TAMIFLU CAPSULES – DRY POWDER_ADMINCORRES.pdf | 6 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20040624_010/021087_S016_TAMIFLU CAPSULES – DRY POWDER_BIOPHARMR.pdf | 3 | ||
| NP15827 | Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_medr_P1.pdf | 10.12 | Two documents with seven instances |
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_medr_P2.pdf | 16, 16, 17, 17, 17 | ||
| WP15525 | Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_bior.pdf | 21, 25, 26, 27, 27, 27, 27, 42, 42, 44 | Three document with 13 instances |
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_Admindocs_P2.pdf | 2.2 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_BioPharmr.pdf | 29 | ||
| WP15647 | Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_bior.pdf | 24, 27, 27 | Two documents with four instances |
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_medr_P2.pdf | 44 | ||
| WP15648 | Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_bior.pdf | 39 | Three documents with eight instances |
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_medr_P2.pdf | 44.44 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/20001117_002/21–087SE1–002_review.pdf | 94, 128, 153, 153, 154 | ||
| WP15676 | Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_bior.pdf | 28.33 | Three documents with four instances |
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_medr_P1.pdf | 11 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_medr_P2.pdf | 45 | ||
| WV156708 | Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_bior.pdf | 2, 44, 44 | Six documents with 45 instances |
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_medr_P1.pdf | 6, 19, 37, 38, 39, 39, 39, 39, 40, 41, 41, 42, 43, 44, 48, 48, 49, 49 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_medr_P2.pdf | 1, 25, 25, 35, 35, 39, 39, 47 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_Statr.pdf | 3, 3, 4, 4, 5, 5, 5, 8, 9, 10, 17, 17, 21, 22 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/20001117_002/21–087SE1–002_review.pdf | 189 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20040624_010/021087_S016_TAMIFLU CAPSULES – DRY POWDER_BIOPHARMR.pdf | 3 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20040624_010/021087_S016_TAMIFLU CAPSULES – DRY POWDER_BIOPHARMR.pdf | 3 | ||
| WV1567158 | Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_bior.pdf | 2, 44, 44 | Seven documents with 50 instances |
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_medr_P1.pdf | 6, 16, 19, 24, 24, 25, 25, 26, 27, 27, 28, 32, 34, 35, 36, 37, 38, 39, 39, 39, 40, 41, 46, 49, 49 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_medr_P2.pdf | 1, 25, 25, 35, 38, 47 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_Statr.pdf | 3, 4, 4, 5, 5, 5, 5, 9, 10, 10, 15, 17, 21 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/20001117_002/21–087SE1–002_review.pdf | 189 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20040624_010/021087_S016_TAMIFLU CAPSULES – DRY POWDER_BIOPHARMR.pdf | 3 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20040624_010/021087_S016_TAMIFLU CAPSULES – DRY POWDER_BIOPHARMR.pdf | 3 | ||
| WV1567359 | Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_medr_P1.pdf | 3 | Three documents with 50 instances |
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_medr_P2.pdf | 18, 18, 18, 20, 21, 21, 21, 22, 39 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/20001117_002/21–087SE1–002_review.pdf | 58, 59, 71, 71, 71, 71, 71, 72, 72, 73, 73, 76, 76, 76, 76, 76, 77, 77, 79, 82, 83, 83, 84, 122, 124, 125, 126, 128, 131, 131, 132, 133, 134, 134, 145, 145, 156, 169, 177, 189 | ||
| WV1569759 | Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_medr_P2.pdf | 39 | Two documents with 40 instances |
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/20001117_002/21–087SE1–002_review.pdf | 58, 59, 71, 71, 71, 71, 71, 72, 72, 73, 73, 76, 76, 76, 76, 76, 77, 77, 79, 82, 83, 83, 84, 122, 126, 128, 131, 131, 131, 132, 133, 134, 145, 145, 152, 153, 156, 162, 189 | ||
| WV1570861 | Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_medr_P1.pdf | 3 | Three documents with 39 instances |
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_medr_P2.pdf | 23, 35, 39, 41 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/20001117_002/21–087SE1–002_review.pdf | 71, 71, 71, 71, 71, 72, 72, 72, 72, 75, 75, 75, 75, 77, 77, 78, 79, 79, 82, 82, 122, 125, 125, 126, 131, 134, 134, 135, 135, 149, 151, 152, 152, 153 | ||
| WV15708D | Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_medr_P1.pdf | 3 | Two documents with three instances |
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_medr_P2.pdf | 23.35 | ||
| WV1573062 | Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_bior.pdf | 44.44 | Five documents with 15 instances |
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_medr_P1.pdf | 6, 9, 19, 49, 50, 50 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_medr_P2.pdf | 1, 1, 25, 25, 27 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/20001117_002/21–087SE1–002_review.pdf | 189 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20040624_010/021087_S016_TAMIFLU CAPSULES – DRY POWDER_BIOPHARMR.pdf | 3 | ||
| WV15731 | Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_Admindocs_P2.pdf | 17 | Four documents with nine instances |
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_Medr.pdf | 5, 30, 37 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_Microbr.pdf | 5.6 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_Statr.pdf | 5, 30, 37 | ||
| WV15758863 | Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_Admindocs_P1.pdf | 12, 19, 19, 36 | Nine documents with 92 instances |
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_Admindocs_P2.pdf | 2, 8, 17, 39, 39, 57, 57 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_BioPharmr.pdf | 3, 4, 5, 5, 5, 8, 10, 17, 27, 30 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_Corres.pdf | 6.9 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_Medr.pdf | 5, 5, 9, 9, 10, 11, 12, 12, 16, 18, 18, 18, 19, 19, 31, 31, 31, 33, 33, 35, 36, 37, 37, 37, 37, 37, 37, 37, 40, 43 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_Microbr.pdf | 2, 4, 5, 6 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_Statr.pdf | 5, 5, 9, 9, 10, 11, 12, 12, 16, 18, 18, 18, 19, 19, 31, 31, 31, 33, 33, 35, 36, 37, 37, 37, 37, 37, 37, 37, 40, 43 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/20040624_016/021087_S016_TAMIFLU CAPSULES – DRY POWDER_ADMINCORRES.pdf | 6, 6, 8 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20040624_010/021087_S016_TAMIFLU CAPSULES – DRY POWDER_BIOPHARMR.pdf | 2.3 | ||
| WV1575964 | Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_Admindocs_P1.pdf | 12.13 | Seven documents with 44 instances |
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_Admindocs_P2.pdf | 39 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_Medr.pdf | 5, 10, 30, 30, 30, 30, 31, 32, 32, 33, 34, 37, 37, 37, 40, 44 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_Microbr.pdf | 2, 4, 4, 5, 6 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_Statr.pdf | 5, 10, 30, 30, 30, 30, 31, 32, 32, 33, 34, 37, 37, 37, 40, 44 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/20040624_016/021087_S016_TAMIFLU CAPSULES – DRY POWDER_ADMINCORRES.pdf | 6, 6, 9 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20040624_010/021087_S016_TAMIFLU CAPSULES – DRY POWDER_BIOPHARMR.pdf | 2 | ||
| WV1579965 | Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/20001117_002/21–087SE1–002_review.pdf | 28, 28, 28, 28, 28, 29, 29, 30, 30, 30, 30, 30, 31, 31, 31, 31, 32, 32, 32, 32, 32, 33, 33, 34, 34, 35, 35, 35, 36, 37, 37, 37, 37, 37, 38, 38, 38, 39, 39, 40, 40, 40, 40, 40, 58, 60, 71, 71, 71, 71, 71, 72, 72, 73, 76, 76, 76, 77, 78, 79, 84, 85, 122, 125, 125, 126, 126, 128, 131, 140, 140, 140, 143, 147, 149, 156, 162, 169, 175, 187, 203, 208, 208 | Four documents with 89 instances |
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_Medr.pdf | 10.11 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_Statr.pdf | 10.11 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/20040624_016/021087_S016_TAMIFLU CAPSULES – DRY POWDER_ADMINCORRES.pdf | 6.7 | ||
| WV1581266 | Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_medr_P1.pdf | 3, 6, 10, 12 | Two documents with nine instances |
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_medr_P2.pdf | 6, 8, 10, 25, 35 | ||
| WV1581967 | Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_medr_P1.pdf | 6, 10, 12, 15 | Two documents with eight instances |
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/19991027_000/21087_Tamiflu_medr_P2.pdf | 2, 6, 6, 39 | ||
| WV1582568 | Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/20001117_002/21–087SE1–002_review.pdf | 41, 41, 41, 41, 42, 42, 42, 42, 42, 42, 43, 44, 58, 59, 71, 71, 71, 71, 71, 72, 72, 72, 72, 73, 73, 75, 75, 77, 77, 78, 79, 79, 79, 80, 80, 80, 81, 82, 85, 125, 125, 126, 126, 128, 131, 134, 134, 135, 135, 137, 137, 138, 145, 150, 151, 152, 152, 155, 156, 162, 169, 180, 204, 211 | One document with 64 instances |
| WV1587164 | Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_Admindocs_P1.pdf | 12.13 | Seven documents with 42 instances |
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_Admindocs_P2.pdf | 39 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_Medr.pdf | 5, 11, 30, 31, 31, 32, 32, 32, 33, 34, 37, 37, 37, 37, 37, 37, 40 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_Microbr.pdf | 2, 5, 6 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_Statr.pdf | 5, 11, 30, 31, 31, 32, 32, 32, 33, 34, 37, 37, 37, 37, 37, 37, 40 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021087/20040624_016/021087_S016_TAMIFLU CAPSULES – DRY POWDER_ADMINCORRES.pdf | 6 | ||
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20040624_010/021087_S016_TAMIFLU CAPSULES – DRY POWDER_BIOPHARMR.pdf | 2 | ||
| WV1587266 | Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_Medr.pdf | 11.33 | Two documents with four instances |
| Tamiflu and Relenza/Tamiflu/Tamiflu – NDA 021246/20001214_000/21–246_Tamiflu_Statr.pdf | 11.33 |
| Mentioned study | File name | Pages on which study is mentioned (separated by commas) | Note |
|---|---|---|---|
| NAI106784 | |||
| 107485 | |||
| 108127 | |||
| 112311 | |||
| 112312 | |||
| 113268 | |||
| GCP/95/045 | |||
| NAI10901 | |||
| NAI10902 | |||
| NAI30008 | Relenza treatment submission executive summary.pdf | 4 | Three documents with 10 instances |
| Relenza treatment submission full document.pdf | 5, 26, 26, 26, 146 | ||
| Relenza treatment submission main text.pdf | 5, 26, 26, 26 | ||
| NAI30009 | NAI30010 study report pdf\FINAL NAI30010 for sign-off.pdf | 102 | Seven documents with 461 instances |
| NAI30009 study report pdf\CSR30009.pdf | |||
| NAI30009 study report pdf\NAI 30009 HO final FSR.pdf | |||
| NAI30009 study report pdf\suptables.pdf | |||
| NAI30009 study report pdf\tables.pdf | |||
| Relenza treatment submission full document.pdf | 16, 16, 17, 18, 18, 18, 18, 19, 27, 30, 31 | ||
| Relenza treatment submission main text.pdf | 16, 16, 17, 18, 18, 18, 18, 19, 27, 30, 31, 76, 128, 130, 132, 134, 144 | ||
| NAI30010 | NAI30010 study report\Final NAI30010 for sign-off.pdf | Seven documents with 399 instances | |
| NAI30010 study report pdf\NAI30010 HO final FSR.pdf | |||
| NAI30010 study report pdf\suptables.pdf | |||
| NAI30010 study report pdf\tables.pdf | |||
| Relenza prophylaxis submission.pdf | 2, 5, 8, 11, 12, 19, 20, 21, 23, 24 | ||
| Relenza treatment submission full document.pdf | 16, 16, 17, 18, 18, 18, 27, 30, 31, 76, 135, 137, 139, 141, 143, 144 | ||
| Relenza treatment submission main text.pdf | 16, 16, 17, 18, 18, 18, 27, 30, 31 | ||
| NAI30012 | Relenza treatment submission executive summary.pdf | 4 | Three documents with eight instances |
| NAI30012 | Relenza treatment submission full document.pdf | 5, 26, 26, 146 | |
| NAI30012 | Relenza treatment submission main text.pdf | 5, 26, 26 | |
| NAI30015 | Relenza treatment submission full document.pdf | 146 | One document with one instance |
| NAI30020 | |||
| NAI30028 | |||
| NAI30031 | |||
| NAI30034 | |||
| NAI40012 | |||
| NAIA1009 | NAI30010 study report pdf\FINAL NAI30010 for sign-off.pdf | 101 | Two documents with three instances |
| NAI30009 study report pdf\CSR30009.pdf | 28.34 | ||
| NAIA300291 | NAI30010 study report pdf\FINAL NAI30010 for sign-off.pdf | 102 | Nine documents with 513 instances |
| NAI30009 study report pdf\CSR30009.pdf | 34.95 | ||
| NAI30009 study report pdf\NAI30009 HO final FSR.pdf | 22 | ||
| NAIA3002 study report pdf\NAIA3002 full study report.pdf | |||
| NAIA3002 study report pdf\NAIA3002 supporting tables 2.pdf | |||
| NAIA3005 study report pdf\A3005cr01.pdf | 25 | ||
| NAIB3002 study report pdf\NAIB3002 full study report.pdf | 28, 47, 49 | ||
| Relenza treatment submission full document.pdf | 16, 16, 17, 17, 18, 19, 27, 30, 31, 63, 63, 63, 76, 106, 106, 107, 107, 109, 109, 112, 112, 114, 114, 115, 115, 144 | ||
| Relenza treatment submission main text.pdf | 16, 16, 17, 17, 18, 19, 27, 30, 31 | ||
| NAIA3003 | Relenza prophylaxis submission.pdf | 10 | One document with one instance |
| NAIA3004 | Relenza prophylaxis submission.pdf | 10 | One document with one instance |
| NAIA3005 | NAI30010 study report pdf\FINAL NAI30010 for sign-off.pdf | 36, 94, 94, 94, 95, 96, 96, 101 | Five documents with 310 instances |
| NAI30010 study report pdf\NAI30010 HO FSR.pdf | 6.18 | ||
| NAIA3005 study report pdf\A3005cr01.pdf | |||
| NAIA3005 study report pdf\TABS.pdf | |||
| Relenza prophylaxis submission.pdf | 2, 5, 6, 12, 13, 13, 15, 15, 16, 16, 17, 17, 18, 18 | ||
| NAIB1002 | |||
| NAIB3001 | NAI30009 study report pdf\CSR30009.pdf | 34, 50, 95 | Eleven documents with 374 instances |
| NAI30009 study report pdf\NAI 30009 HO final FSR.pdf | 10.22 | ||
| NAI30010 study report pdf\FINAL NAI30010 for sign-off.pdf | 102 | ||
| NAI30010 study report pdf \NAI30010 HO FSR.pdf | 17.17 | ||
| NAIA3002 study report pdf\NAIA3002 full study report.pdf | 28 | ||
| NAIA3005 study report pdf\A3005cr01.pdf | 25 | ||
| NAIB3001 study report pdf\NAIB3001 full study report.pdf | |||
| NAIB3001 study report pdf\NAIB3001 supporting tables 1.pdf | |||
| NAIB3002 study report pdf\NAIB3002 full study report.pdf | 28 | ||
| Relenza treatment submission full document.pdf | 16, 16, 17, 18, 18, 18, 18, 27, 30, 31, 32, 63, 63, 63, 76, 99, 99, 101, 101, 103, 103, 105, 105, 144, 162 | ||
| Relenza treatment submission main text.pdf | 16, 16, 17, 18, 18, 18, 18, 27, 30, 31, 32 | ||
| NAIB3002 | NAI30009 study report pdf\CSR30009.pdf | 34.95 | Ten documents with 579 instances |
| NAI30009 study report pdf\NAI 30009 HO final FSR.pdf | 22 | ||
| NAI30010 study report pdf\FINAL NAI30010 for sign-off.pdf | 102 | ||
| NAIA3002 study report pdf\NAIA3002 full study report.pdf | 28, 48, 50 | ||
| NAIA3005 study report pdf\A3005cr01.pdf | 25 | ||
| NAIB3002 study report pdf\NAIB3002 full study report.pdf | |||
| NAIB3002 study report pdf\NAIB3002supporting tables 1.pdf | |||
| NAIB3002 study report pdf\NAIB3002supporting tables 2.pdf | |||
| Relenza treatment submission full document.pdf | 16, 16, 17, 17, 18, 19, 27, 30, 31, 63, 63, 63, 76, 117, 117, 117, 118, 118, 120, 120, 122, 122, 124, 124, 125, 125, 127, 127, 144 | ||
| Relenza treatment submission main text.pdf | 16, 16, 17, 17, 18, 19, 27, 30, 31 | ||
| NAI30011 | Relenza treatment submission full document.pdf | 146 | One document with one instance |
| NAIB2007 | NAI30009 study report pdf\CSR30009.pdf | 95 | 10 documents with 379 instances |
| NAI30009 study report pdf\NAI 30009 HO final FSR.pdf | 10 | ||
| NAIA3002 study report pdf\NAIA3002 full study report.pdf | 28, 28, 29 | ||
| NAIA3005 study report pdf\A3005cr01.pdf | 25 | ||
| NAIB2007 study report pdf\b2007cr.pdf | |||
| NAIB2007 study report pdf\TABLES.pdf | |||
| NAIB3001 study report pdf\NAIB3001 full study report.pdf | 25.26 | ||
| NAIB3002 study report pdf\NAIB3002 full study report.pdf | 28, 28, 29 | ||
| Relenza treatment submission full document.pdf | 16, 16, 17, 18, 18, 19, 27, 30, 31, 76, 91, 91, 92, 92, 94, 94, 96, 96, 98, 98, 144 | ||
| Relenza treatment submission main text.pdf | 16, 16, 17, 18, 18, 19, 27, 30, 31 | ||
| NAIA2006 | NAIA2005 study report pdf\a2005cr.pdf | 38, 73, 74 | Four documents with six instances |
| NAIA3002 study report pdf\NAIA3002 full study report.pdf | 28 | ||
| NAIA3005 study report pdf\A3005cr01.pdf | 25 | ||
| NAIB3002 study report pdf\NAIB3002 full study report.pdf | 28 | ||
| NAIB2006 | NAIA3002 study report pdf\NAIA3002 full study report.pdf | 28 | Three documents with three instances |
| NAIA3005 study report pdf\A3005cr01.pdf | 25 | ||
| NAIB3002 study report pdf\NAIB3002 full study report.pdf | 28 | ||
| NAIB1007 | |||
| C94-009 | |||
| C94-085 | |||
| NAIB1001 | |||
| NAIB_1001 | |||
| NAIA2005 | NAI30009 study report pdf\CSR30009.pdf | 95 | Twelve documents with 895 instances |
| NAIA2005 study report pdf\a2005cr.pdf | |||
| NAIA2005 study report pdf\APPS_ALL.pdf | |||
| NAIA2005 study report pdf\TBS_ALL.pdf | |||
| NAIA3002 study report pdf\NAIA3002 full study report.pdf | 28, 28, 48, 48 | ||
| NAIA3005 study report pdf\A3005cr01.pdf | 25 | ||
| NAIB2005 study report pdf\b2005cr.pdf | 7, 7, 22, 25, 26, 34, 34, 42, 71, 72, 72 | ||
| NAIB2007 study report pdf\b2007cr.pdf | 76 | ||
| NAIB3001 study report pdf\NAIB3001 full study report.pdf | 25 | ||
| NAIB3002 study report pdf\NAIB3002 full study report.pdf | 28, 28, 47, 47 | ||
| Relenza treatment submission full document.pdf | 16, 16, 16, 16, 17, 18, 27, 30, 76, 77, 77, 77, 79, 79, 79, 80, 80, 82, 82, 84, 84, 85, 144, 144 | ||
| Relenza treatment submission main text.pdf | 16, 16, 16, 16, 17, 18, 27, 30 | ||
| NAIB2005 | NAI30009 study report pdf\CSR30009.pdf | 95 | Twelve documents with 838 instances |
| NAIA2005 study report pdf\a2005cr.pdf | 7, 8, 8, 24, 24, 25, 43, 70, 74, 74 | ||
| NAIA3002 study report pdf\NAIA3002 full study report.pdf | 28, 28, 48, 48 | ||
| NAIA3005 study report pdf\A3005cr01.pdf | 25 | ||
| NAIB2005 study report pdf\APPSNEW.pdf | |||
| NAIB2005 study report pdf\b2005cr.pdf | |||
| NAIB2005 study report pdf\TBS_ALL.pdf | |||
| NAIB2007 study report pdf\b2007cr.pdf | 76 | ||
| NAIB3001 study report pdf\NAIB3001 full study report.pdf | 25 | ||
| NAIB3002 study report pdf\NAIB3002 full study report.pdf | 28, 28, 47, 47 | ||
| Relenza treatment submission full document.pdf | 16, 16, 16, 16, 17, 18, 27, 30, 76, 77, 79, 79, 85, 85, 85, 86, 86, 88, 88, 90, 90, 144, 144 | ||
| Relenza treatment submission main text.pdf | 16, 16, 16, 16, 17, 18, 27, 30 | ||
| NAIA/B2008 | NAI30009 study report pdf\CSR30009.pdf | 95 | Six documents with 16 instances |
| NAI30009 study report pdf\NAI 30009 HO final FSR.pdf | 10 | ||
| NAIA3002 study report pdf\NAIA3002 full study report.pdf | 28, 28, 29, 29 | ||
| NAIA3005 study report pdf\A3005cr01.pdf | 25 | ||
| NAIB3001 study report pdf\NAIB3001 full study report.pdf | 25, 26, 26, 26, 77 | ||
| NAIB3002 study report pdf\NAIB3002 full study report.pdf | 28, 28, 29, 29 | ||
| NAIA2010 | NAIA3005 study report pdf\A3005cr01.pdf | 25 | One document with one instance |
| NAIA/B200988 | NAIA3002 study report pdf\NAIA3002 full study report.pdf | 28 | Three documents with three instances |
| NAIA3005 study report pdf\A3005cr01.pdf | 25 | ||
| NAIB3002 study report pdf\NAIB3002 full study report.pdf | 28 | ||
| 167-02 | |||
| 167-03 | |||
| 167-05 | |||
| 167-04 | |||
| JNAI-03 | |||
| JNAI-02 | |||
| JNAI-01 | |||
| JNAI-07 | |||
| JNAI-04 | |||
| PE-01100 | |||
| 167-10170 | |||
| 167T3–11 |
| Referenced study | File name volumea | Pages where study is mentioned (separated by commas) | Note |
|---|---|---|---|
| GS97-802 | |||
| 133312 | |||
| GS-97-801 | |||
| JP15734 | |||
| JP15735 | |||
| JV1582374 | |||
| JV1582475 | |||
| JV16284 | |||
| M7600136 | 1 | 33, 36, 37, 37, 38, 38, 39, 67, 68, 94, 95, 224 | One document with 12 instances |
| M76006 | |||
| ML20910 | |||
| ML22789 | |||
| ML22879 | |||
| MV21118 | |||
| MV22841 | |||
| NCT00298233 | |||
| NCT00555893 | |||
| NCT00707941 | |||
| NCT00799760 | |||
| NCT00830323 | |||
| ML25018 | |||
| NCT00867139 | |||
| NCT00873886 | |||
| NCT01002729 | |||
| NP15717 | 6 | 32, 75, 76, 77 | Two documents with five instances |
| 8 | 68 | ||
| 6 | 73.98 | One document with two instances | |
| NP15718 | |||
| NP15728 | |||
| NP15757 | 8 | 68 | One document with one instance |
| NP15826 | 6 | 32, 75, 75, 75, 76, 76, 77, 78, 79, 80, 98 | One document with 11 instances |
| NP15827 | 8 | 68 | One document with one instance |
| NP22770 | |||
| NP25138 | |||
| NP25139 | |||
| NV16871 | |||
| NV20234 | |||
| NV20235 | |||
| NV20236 | |||
| NV20237 | |||
| NV22155 | |||
| NV25118 | |||
| NV25182 | |||
| PP16351 | |||
| WP15517 | 1 | 185.245 | One document with two instances |
| WP15525 | 1 | 185.245 | One document with two instances |
| WP15647 | |||
| WP15648 | |||
| WP15676 | |||
| WP15901 | |||
| WP22849 | |||
| WV144181 | |||
| WV156708 | 1 | 33, 36, 37, 37, 38, 38, 39, 47, 48, 48, 49, 49, 50, 53, 54, 54, 55, 163, 171, 188, 207, 209, 224, 245, 245, 252, 253, 253 | Seven documents with 1193 instances |
| 10 | 7, 36, 37, 37 | ||
| 2 | |||
| 3 | |||
| 4 | 90 | ||
| 6 | 35.98 | ||
| 8 | 65 | ||
| 2 | 20, 20, 20, 20, 20 | One document with five instances | |
| WV1567158 | 1 | 33, 36, 37, 37, 38, 38, 39, 47, 48, 49, 49, 50, 53, 54, 54, 55, 163, 171, 188, 207, 209, 224, 245, 245 | Seven documents with 1222 instances |
| 10 | 7, 36, 37, 37 | ||
| 2 | 82 | ||
| 4 | |||
| 5 | |||
| 6 | 35.98 | ||
| 8 | 66 | ||
| WV1567359 | 8 | 66 | One document with one instance |
| WV15673D | 8 | 66 | One document with one instance |
| WV1569759 | 8 | One document with one instance | |
| WV15697D | 8 | One document with one instance | |
| WV1570760 | 1 | 33, 36, 37, 37, 38, 67, 68, 224, 245, 245, 245, 246 | One document with 12 instances |
| WV1570861 | |||
| WV15708D | |||
| WV1573062 | 1 | 33, 36, 37, 37, 38, 38, 39, 47, 53, 54, 55, 186, 207, 224, 245, 245, 246 | Four documents with 22 instances |
| 10 | 7, 36, 37 | ||
| 2 | 82 | ||
| 4 | 90 | ||
| WV15731 | 6 | 98 | One document with one instance |
| WV1575863 | 1 | 36, 37, 82, 83, 84, 85, 86, 92, 94, 95, 97, 106, 224, 246 | Four documents with 424 instances |
| 6 | |||
| 7 | |||
| 8 | 68 | ||
| WV1575964 | 1 | 36, 37, 94, 95, 95, 109, 113, 114, 121, 122, 224, 246 | One document with 12 instances |
| WV1579965 | 1 | 137, 139, 139, 232, 233 | Three documents with 499 instances |
| 8 | |||
| 9 | |||
| WV1581266 | 1 | 36, 37, 37, 38, 38, 39, 67, 68, 68, 107, 107, 107, 108, 108, 121, 121, 122, 123, 224, 246 | Two documents with 197 instances |
| 10 | |||
| WV1581967 | 1 | 33, 36, 37, 37, 38, 58, 58, 59, 59, 60, 61, 62, 62, 65, 65, 67, 68, 224, 246 | Two documents with 173 instances |
| 10 | |||
| WV1582568 | 8 | 66, 66 | One document with two instances |
| WV1587164 | 1 | 109, 246 | One document with two instances |
| WV1587266 | 1 | 36, 37, 37, 38, 38, 39, 67, 68, 68, 107, 107, 108, 108, 121, 121, 122, 123, 224 | One document with 18 instances |
| WV1587667 | 1 | 246, 246 | One document with two instances |
| WV1597867 | 1 | 67, 70, 175, 246, 246 | One document with five instances |
| WV16193 | |||
| ML1636976 |
The basis of the selection of trials to regulators is therefore unclear but appears to be dictated by criteria other than availability and size. The importance of trials (to manufacturers and possibly to regulators) may not be based on the same criteria that systematic reviewers would use (i.e. the capability of the trial to answer questions).
Owing to the vast size of FDA documents, sometimes hundreds of pages long, it was difficult to determine important emerging themes solely by reading. To identify items of interest in the FDA comments we used word clouds. 108 Word clouds give greater prominence to words that appear more frequently in the source document. The resulting graphic representation showed words such as ‘diary’ and ‘baseline’ to be heavily mentioned in the relevant (abridged) text from the FDA’s Medical Officer Review. 109 Examining the ‘diary’ entry in more detail, we found the following FDA comment:
The majority of subjects participating in the treatment trials had only used the first diary card. The second diary card was issued in 15% to 20% of participants. In response to FDA’s request, the applicant provided a summary of diary card dispensing in the 8/6/99 submission. It became apparent that instructions on when to start a second diary card were not uniformly followed in three trials. 8,58,62 There were examples of patients who had alleviated symptoms yet also received a second diary card. Conversely, there were also examples of patients who did not alleviate all symptoms but did not receive a second diary card. Thus the second diary card was used inconsistently which is viewed as a flaw of these trials. The lack of consistency in collecting symptom information after alleviation precluded a complete documentation of symptom fluctuation. Also missing second diary cards in subjects who had not alleviated symptoms were responsible for the majority of censored data which may have potentially influenced the results of efficacy analysis. In order to address the impact of censoring, the applicant performed several sensitivity analyses, which will be summarized in the Integrated Summary of Efficacy.
This comment highlights problems with the follow-up procedure of treatments trials, which may have impaired the regulator’s ability to draw conclusions on the duration of effect of oseltamivir. It also provides a good example of how graphic methods can help to identify crucial comments in vast regulatory files.
Several other experiments with text from the same FDA document showed that the choice of text to be represented as a word cloud heavily influenced cloud construction, visibility of words and hence our ability to detect important comments. It is for this reason that we decided to adopt a mixed approach: mapping citations while reading FDA comments and integrating such comments in our appraisal of the evidence. Regulatory comments were all the more important because, at the time that we developed this method, we had few CSRs, and comments helped to identify the gaps in our knowledge of the trial programmes.
Once the TOC had been constructed, we postulated that, given the huge work involved in reviewing lots of regulatory files, our new instrument could also help us by indicating which parts were more important than others, thus focusing our efforts. We experimented with a variety of methods, which are reported above (see Data collection and analysis).
Clinical study reports
After prolonged correspondence and media pressure (see Appendix 1), we were able to access the trial programmes for both oseltamivir and zanamivir without clauses restricting their accessibility to third parties.
Electronic searches
Two review authors (CDM and MT) independently scanned the titles and abstracts of the electronic searches. Three identified studies110–112 were published versions of trials that were possibly unknown to us. We wrote to the first trial author to ask for CSRs, or equivalent, on 12 November 2013, and the author confirmed that the trials had not been completed.
Included studies
The absence of documentation of trial programmes for both drugs, listing all sponsored trials completed or under way, meant that we had to rely on a variety of sources for the reconstruction of the trial programmes and identification of relevant CSRs. This complexity is reflected in the flow chart presented in Figure 3, illustrating the study selection process for this review. The two main pathways were the spontaneous release of 77 full CSRs by Roche and the requests to regulatory authorities and GSK for all of the relevant reports.
FIGURE 3.
Flow diagram describing the number of studies identified, inclusion, exclusion and progression from identification to stage 1 to stage 2 of the review. PMDA, Japanese Pharmaceuticals and Medical Devices Agency.

We carried out the inclusion into stage 1 using the CSRs, titles, abstracts and any other relevant information. Through this process we identified 208 potentially relevant studies (139 oseltamivir trials, 61 zanamivir trials and eight peramivir trials). We excluded 123 studies (see Appendix 10, listed in the ‘characteristics of excluded studies’ table) as clearly ineligible. A further 19 studies are awaiting classification (Table 6). We requested 66 trials from study sponsors, the EMA and the FDA. From these different methods, the total number of trials available for assessment for inclusion in our review at stage 1 was 53.
| JPRN-JapicCTI-111647 | |
|---|---|
| Methods | A randomised, double-blind, placebo-controlled study to confirm the efficacy in the prevention of influenza virus infection (Phase 3 study) |
| Duration of the study | 1 October 2011 to 30 June 2012 |
| Sponsor | Daiichi Sankyo Co., Ltd |
| Participants | – |
| Interventions | Laninamivir, placebo |
| Outcomes | – |
| Notes | Awaiting assessment, as we do not yet have the clinical study reports for this study |
| ML20589 | |
| Methods | Economic and social benefits of treating and preventing influenza in aged care facilities |
| Sponsor | The University of Sydney, Australia anzctr.org.au number ACTRN12606000278538 |
| Participants | – |
| Interventions | Oseltamivir, three different regimens |
| Outcomes | – |
| Notes | Awaiting assessment, as we do not yet have the clinical study reports for this study |
| ML20910 | |
| Methods | A study of Tamiflu (oseltamivir) treatment in laboratory-confirmed influenza |
| Sponsor | Hoffmann-La Roche, NCT00436124 |
| Participants | – |
| Interventions | Oseltamivir |
| Outcomes | – |
| Notes | Awaiting assessment, as we do not yet have the clinical study reports for this study |
| ML21776 | |
| Methods | Study to evaluate nosocomial transmission of influenza |
| Sponsor | University Hospitals, Leicester |
| NCT00798421 | |
| Participants | – |
| Interventions | – |
| Outcomes | – |
| Notes | Awaiting assessment, as we do not yet have the clinical study reports for this study |
| MV21118 | |
| Methods | Early oseltamivir treatment of influenza in children aged 1–3 years |
| Sponsor | Hospital District of Southwestern Finland |
| NCT00593502 | |
| Participants | – |
| Interventions | Oseltamivir, placebo |
| Outcomes | – |
| Notes | Awaiting assessment, as we do not yet have the clinical study reports for this study |
| MV21737 | |
| Methods | Long-term influenza prophylaxis with inhaled zanamivir or oral oseltamivir |
| Sponsor | University of Oxford |
| NCT00980109 | |
| Participants | – |
| Interventions | Oseltamivir, zanamivir, placebo |
| Outcomes | – |
| Notes | Awaiting assessment as we do not yet have the clinical study reports for this study |
| MV21879 | |
| Methods | Oseltamivir randomised controlled efficacy trial |
| Sponsor | International Centre for Diarrhoeal Disease Research, Bangladesh |
| NCT00707941 | |
| Participants | – |
| Interventions | Oseltamivir, placebo |
| Outcomes | – |
| Notes | Awaiting assessment, as we do not yet have the clinical study reports for this study |
| MV22841 | |
| Methods | An observational clinical trial of influenza A/H1N1 2009 resistance under standard-duration oseltamivir treatment |
| Sponsor | Not known |
| Participants | – |
| Interventions | Oseltamivir |
| Outcomes | – |
| Notes | Awaiting assessment, as we do not yet have the clinical study reports for this study |
| MV22940 | |
| Methods | A randomised controlled trial on the effect of post-exposure oseltamivir prophylaxis on influenza transmission in nursing homes |
| Sponsor | National Institute for Public Health and the Environment (RIVM), The Netherlands |
| NCT01053377 | |
| Participants | – |
| Interventions | Oseltamivir, placebo |
| Outcomes | – |
| Notes | Awaiting assessment, as we do not yet have the clinical study reports for this study |
| NCT00419263 | |
| Methods | Evaluation of the efficacy and safety of peramivir in subjects with uncomplicated acute influenza |
| Sponsor | BioCryst Pharmaceuticals |
| Participants | – |
| Interventions | Peramivir |
| Outcomes | – |
| Notes | Awaiting assessment, as we do not yet have the clinical study reports for this study |
| NCT00453999 | |
| Methods | Evaluation of the efficacy and safety of peramivir in adults with acute serious or potentially life-threatening influenza |
| Sponsor | BioCryst Pharmaceuticals |
| Participants | – |
| Interventions | Peramivir |
| Outcomes | – |
| Notes | Awaiting assessment, as we do not yet have the clinical study reports for this study |
| NCT00486980 | |
| Methods | Intramuscular peramivir for the treatment of uncomplicated influenza |
| Sponsor | BioCryst Pharmaceuticals |
| Participants | – |
| Interventions | Peramivir |
| Outcomes | – |
| Notes | Awaiting assessment as we do not yet have the clinical study reports for this study |
| NCT00555893 | |
| Methods | Efficacy study of early versus late oseltamivir administration for treating and preventing influenza |
| Participants | – |
| Interventions | Oseltamivir, placebo |
| Outcomes | – |
| Notes | Awaiting assessment, as we do not yet have the clinical study reports for this study |
| NCT00610935 | |
| Methods | Intramuscular peramivir in subjects with uncomplicated acute influenza |
| Sponsor | Marshfield Clinic Research Foundation |
| Participants | – |
| Interventions | Peramivir, placebo |
| Outcomes | – |
| Notes | Awaiting assessment, as we do not yet have the clinical study reports for this study |
| NCT00705406 | |
| Methods | A Phase II, multicentre, randomised, placebo-controlled, study to evaluate the efficacy and safety of intramuscular peramivir 600 mg in subjects with uncomplicated acute influenza |
| Sponsor | BioCryst Pharmaceuticals |
| Participants | – |
| Interventions | Peramivir, placebo |
| Outcomes | – |
| Notes | Awaiting assessment, as we do not yet have the clinical study reports for this study |
| NCT00958776 | |
| Methods | A study to evaluate the efficacy and safety of IV peramivir in addition to standard of care compared to standard of care alone in adults and adolescents who are hospitalised due to influenza |
| Sponsor | BioCryst Pharmaceuticals |
| Participants | Peramivir |
| Interventions | – |
| Outcomes | – |
| Notes | Awaiting assessment, as we do not yet have the clinical study reports for this study |
| NCT00980109 | |
| Methods | Long-term influenza prophylaxis with inhaled zanamivir or oral oseltamivir |
| Sponsor | University of Oxford |
| Participants | – |
| Interventions | Oseltamivir, zanamivir, placebo |
| Outcomes | – |
| Notes | Awaiting assessment, as we do not yet have the clinical study reports for this study |
| NCT01032837 | |
| Methods | A study of Tamiflu (oseltamivir) for treatment of influenza with a focus on (H1N1) 2009 flu strain |
| Sponsor | Hoffmann-La Roche |
| Participants | – |
| Interventions | Oseltamivir, placebo |
| Outcomes | – |
| Notes | Awaiting assessment, as we do not yet have the clinical study reports for this study |
| NV20236 | |
| Methods | A study of Tamiflu (oseltamivir) for seasonal prophylaxis of influenza in children |
| Sponsor | Hoffmann-La Roche |
| NCT00412555 | |
| Participants | – |
| Interventions | Oseltamivir |
| Outcomes | – |
| Notes | Awaiting assessment, as we do not yet have the clinical study reports for this study |
Twenty-three studies of oseltamivir8,36,57–69,74–76 and 28 of zanamivir70–73,77–100 were included in stage 1. It was not uncommon for more than one trial to be reported in the same CSRs. This was either because of the amalgamation of two or more trials due to low influenza virus circulation and difficulties in recruitment (e.g. WV15812/WV1587266) or because the trials bore different ID numbers when, in reality, they followed the same protocol, albeit in two different hemispheres (e.g. WV15759/WV1587164).
We also identified six completed or ongoing studies of peramivir in dose–response or placebo-controlled studies. 113–118
The included trials were predominantly conducted in adults during influenza seasons in both hemispheres. A small number of studies were conducted in older people who were residing in care homes and in people with underlying respiratory diseases. All trials were sponsored by the manufacturers.
Oseltamivir
Of the 23 oseltamivir trials in stage 1, 15 were multicentre trials conducted in both the northern and southern hemispheres, whereas eight were carried out in only one country (USA, five; Japan, two; China, one). In total, 9623 participants were included (6574 in treatment trials and 3049 in prophylaxis trials). The age of the participants ranged from 1 to 82 years and the duration of follow-up varied from 6 to 42 days.
Two of the trials were conducted within nursing homes; 20 were within free-living populations; and one was performed in inpatient and outpatient departments. Three trials were conducted in children (two of the trials were among children with chronic asthma, n = 660; one trial was performed among otherwise healthy children, n = 669), whereas participants in 20 trials were adults. In some trials the eligible population included participants who were at increased risk of influenza complications, or with diagnoses of asthma or chronic obstructive pulmonary disease, but the majority included only otherwise healthy adults. In one trial,62 participants were stratified by smoking status, whereas those in another trial were stratified by the presence or absence of otitis media. 63
All trials compared orally administered oseltamivir (either as capsules or reconstituted powder) with placebo.
Of the 23 trials, we included 20 RCTs for the analysis examining the use of oseltamivir compared with placebo. Two RCTs were excluded from the meta-analysis because they were only synopsis reports74,75 and another because it was not a full CSR. 76
We finally included 20 oseltamivir trials into stage 2: 11 on treatment in adults,8,36,57,58,60–62,66,67,69,74–76,108–112 four in children57,63,64 and five on prophylaxis:51,61,65,68 two in adults,51 two in the elderly61,68 and one in households. 65 Of the 15 included treatment trials of oseltamivir, only three8,36,63 were successful in recruiting the a priori planned sample size.
Zanamivir
Of the 28 included zanamivir trials, 18 were multicentre trials that were conducted in both the northern and southern hemispheres and 10 were carried out in only one country (Japan, five; USA, three; Finland, one; Germany, one). In total 14,628 participants were included (7678 in treatment trials and 6950 in prophylaxis trials). Participants’ age ranged from 5 to 12 years to > 65 years, and duration of follow-up varied from 5 to 35 days.
Two of the trials were performed within nursing homes; several were within free-living populations; one was performed within a university student population. In some trials the eligible population included participants at increased risk of influenza complications, or with diagnoses of asthma or chronic obstructive pulmonary disease, but the majority included only adults who were otherwise healthy.
Zanamivir was administered as an intranasal spray, an inhalation or a combination of both, and placebos were designed to match. Administration was by the participant in the majority of trials and by nursing staff in the trials within nursing homes. Twenty-two trials compared inhaled zanamivir with placebo and six trials compared inhaled zanamivir, or intranasal zanamivir, with placebo or usual care.
Of the 28 trials,70–73,77–100 we included 26 RCTs70–73,77–82,84–91,93–100 for the analysis, examining the use of zanamivir compared with placebo. Two trials83,92 were excluded from the meta-analysis because one was only a synopsis83 and one compared zanamivir to usual care and not placebo. 92
We finally included 26 zanamivir trials: 14 on treatment in adults,71–73,77,80–82,87,89,91,95,97–99 two in children78,84 and 10 trials in prophylaxis. 70,79,85,86,88,90,93,94,96,100
Our attempt at collecting sufficient information from regulatory files to reconstruct missing CSRs also failed because the information appeared to be insufficient for a reliable reconstruction.
Excluded studies
We excluded 123 studies from entering stage 1 for various reasons. Some were pharmacokinetic studies, had an active comparator, compared higher-dose schedules with lower-dose schedules or were ongoing trials. A further 19 trials are awaiting assessment (see Table 6).
Risk of bias in included studies
Study-level assessments are reported in the risk-of-bias tables (see Figure 2). To address the problem of reporting bias, we ignored published trial reports and directed our attention to CSRs and regulatory information. Our problems in reviewing the copious material at our disposal were how to identify and analyse important details in the midst of thousands of pages of information and how to construct a coherent appraisal of large and complex trial programmes.
In addition, as we gained unrestricted access to the full CSRs (apart from personal de-identifying redactions) we took the view that all information needed to judge risk of bias should be present. Therefore, when this information was not available, we judged the corresponding risk-of-bias element as at ‘high’ risk of bias. For example, when details of the random sequence generation are missing from journal publications of clinical trials, it is customary to record this as ‘unknown’ risk of bias. This judgement usually carries the assumption that the random sequence generation details are available in more detailed reports. But when these details were still missing, even in full CSRs, we chose to rate this risk-of-bias element at ‘high’ risk of bias.
In the following paragraphs we report some of the salient findings using the current Cochrane format but applying the logic of reviewing regulatory data.
Allocation (selection bias)
In 10 of the 20 oseltamivir studies included in stage 2, the description of random sequence generation is missing. All of the zanamivir trials but one84 had reporting bias due to the absence of description of random sequence generation.
Blinding (performance bias and detection bias)
The placebo and active drug capsule cap were not identical in 11 of the 20 trials of oseltamivir. This may have compromised blinding of participants. For all but one of the zanamivir trials we did not have the certificates of analysis to enable us to reconstruct the appearance, taste and texture of the two principles.
Incomplete outcome data (attrition bias)
In addition to the missing diary cards in three treatment trials (see Results of the search, above), we were unable to identify all of the data for all of the outcomes in all of the oseltamivir trials and in eight of the zanamivir trials. For example, hospitalisations were not reported in zanamivir trials and inconsistently reported in oseltamivir trials. The relevant data in this review come from a table of hospitalisations sent to us by Roche in late 2013. In addition, in some trials we were unable to track individual participants through tables, narratives and individual listings. The issue of compliharms impeded the ascertainment of harms in oseltamivir treatment trials (see Appendix 1). We had difficulty in following the logic of compliharms, even with access to full CSRs. The definition of adverse events in the RCTs of oseltamivir and zanamivir is different from the ordinary definition of the International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use E2D guideline, which is as follows: ‘An adverse event (AE) is any untoward medical occurrence in a patient administered a medicinal product and which does not necessarily have to have a causal relationship with this treatment. An adverse event can therefore be any unfavourable and unintended sign (e.g. an abnormal laboratory finding), symptom, or disease temporally associated with the use of a medicinal product, whether or not considered related to this medicinal product’ [www.ich.org/fileadmin/Public_Web_Site/ICH_Products/Guidelines/Efficacy/E2D/Ste p4/E2D_Guideline.pdf (accessed 27 December 2013)].
As an example, the definition of adverse events in one study58 is as follows: ‘following the alleviation of influenza-like symptoms, the recurrence of a single respiratory or constitutional symptom was recorded as an adverse event, however, the reappearance of more than one symptom was recorded as influenza-like syndrome (i.e. secondary illness) and therefore do not appear as adverse events’ (p. 35)58 and: ‘any adverse change from the subject’s baseline (pre-treatment) condition, which occurred during the course of the study after treatment had started, whether considered related to treatment or not’. Treatment included all investigational agents (including placebo and comparative agents) administered during the course of the study)’ (our emphasis). 8 As a consequence, adverse events that are similar to the symptoms of influenza (such as headache and mild gastrointestinal adverse events) tend to be excluded from the treatment trials.
We identified a report of a site inspection for one adult prophylaxis trial. 59 The FDA carried out the inspection in September 2000 at various trial sites in the USA, including the West Virginia site (which was responsible for enrolling many hundreds of participants). A FDA official letter reported several violations, including failure to report serious harms to the sponsor (Roche) as the protocol required and in addition stated: ‘. . . we view the statement in the payment section of the consent form used in the study that subjects . . . will receive $300.00 for participating in and completing the study. No payment will be made to you if you withdraw from the study for personal reasons . . . to be an improper procedure. When subjects are to be paid for participating in a study, the payment should be prorated for the subject’s actual participation in the study in order to avoid the possibility of coercion’ (p. 177). 119 However, the FDA allowed the data (which had been published 1 year earlier in a prime journal) to stand in support of Roche’s application for the prophylaxis indication. We do not know whether or not the participant contract was standard (i.e. whether or not the observation of possible improper procedures could be generalised to other sites and other trials) but the document cited by the FDA inspector is the subject of one of our (as yet unfulfilled) FOI requests. The possibility of financial pressure, if confirmed, could seriously confound dropout rates because of harms or any other causes in prophylaxis trials.
The significantly higher incidence of diarrhoea in placebo recipients of treatment trial WV1567158 was identified by the FDA reviewers who remarked ‘Diarrhea was reported more frequently among subjects receiving placebo than among subjects receiving Ro 64-0796 [oseltamivir]. Diarrhoea, although not specified as an inclusion criterion, has been documented to be a clinical manifestation of influenza infection. The reduction in the incidence of diarrhoea for the treatment groups compared with the placebo group could be considered as a possible treatment effect of Ro 64–0796’. 109 However, according to the Japanese Summary Basis for Approval of oseltamivir capsules for prophylaxis, diarrhoea was reported more frequently in the oseltamivir arm (49/986) than in the placebo group (38/973) in the summarised table of adverse events from three trials. 59,61,68 Our findings are inconsistent with the explanation by the FDA.
Selective reporting (reporting bias)
All of the oseltamivir trials and almost half of the zanamivir trials had selected reporting. The oseltamivir trials showed a consistent trend of missing original protocols (except for one trial36), changing outcome definitions while the trial was running, protocol amendments even after the trial had been completed, inconsistent approaches to outcome data collection, missing SAPs, missing date of unblinding and the use of self-reported outcomes such as pneumonia. 8,36,47,60,68,69 This represents 55% of pneumonia event data. As an example, in trial WV15670,8 secondary illnesses were patient reported. The body of the CSR states that complications requiring antibiotic treatment were specified a priori, but, even in the final version of the protocol, for which we have the full text, there is no predefined list of secondary illnesses (i.e. no mention of pneumonia, bronchitis, sinusitis or otitis in the protocol); complications did not have anything to do with antibiotic treatment according to the protocol; and the CRF did not mention specific secondary illnesses by name. Zanamivir trials reported outcomes that were not specified in the protocol provided.
We found evidence of possible selective reporting bias when we analysed the Japanese Summary Basis for Approval data on prophylaxis. The regulatory data report tables for individual trials, as well as 10 pages of summarised tables for three trials of prophylaxis. 59,61,70 Tables for individual trials include data for high-dose arms but report few psychiatric adverse events overall. However, the summarised tables list a variety of psychiatric adverse events, including psychotic and suicidal adverse events, but not adverse events from the high-dose group. As a preliminary exploratory analysis, we combined the following suspected serious adverse events collectively: hallucination and delusion, which are classified grade 3 (serious) by the National Cancer Institute-Common Toxicity Criteria Version 2.0 (NCI-CTC V2.0); psychosis (hallucination and delusion are the two major symptoms of this disease); suicidal attempt, which is classified grade 3 (serious) by the Common Terminology Criteria for Adverse Events Version 4.0 (CTCAE V4.0); and hostility, which includes aggression, hostility, violence and murder, commonly considered as serious events although not listed in the NCI-CTC V2.0 or CTCAE V4.0. Numbers of suspected serious psychotic/suicidal adverse events (including hallucination, psychosis, schizophrenia, paranoia, aggression/hostility and attempted suicide) were five in the oseltamivir group and zero in the placebo group during the on-treatment period; when the off-treatment period data are added, the total was eight compared with one. The prophylaxis programme is crucial in understanding the harms profile of the drug, as the potential for harms witnessed to be confounded by the apparently numerous symptoms and signs of influenza infection is far less, as many participants do not become infected with influenza. This makes a causality assessment more straightforward.
Other potential sources of bias
All but three of the oseltamivir treatment trials were under-recruited. Several of the zanamivir trials were also under-recruited. We noted the use of different relief medication across different centres within the same trial, and in one zanamivir trial,85 according to the protocol, participants receiving antibiotics for bacterial respiratory tract infection should have been excluded but in the trial this did not happen. In the zanamivir trial,86 the definition of ‘confirmed influenza’ was amended after protocol closure.
We also noted several other items that were not included in all full CSRs:
-
Study protocols dated prior to participant enrolment (missing for many oseltamivir trials).
-
Certificates of analysis for the intervention/placebo preparations.
-
Patient enrolment dates explicitly reported (only trial inception and cessation dates are given; in zanamivir trials these are partially redacted).
-
Explicitly reported date of trial unblinding. We frequently noted the statement ‘the database was authorised on xxxx’ to identify the unblinding date but an explicit date is important to report. In some cases, the date of unblinding was reported, but the actual date within the month was redacted. This practice also applied to zanamivir protocol amendments.
-
Authorship and accountability for the writing of the CSRs.
-
SAPs in some cases.
-
Patient consent forms (missing from most zanamivir trials).
-
Patient information form (missing from most zanamivir trials).
-
List of randomisation codes (variably included).
-
CRF templates in zanamivir trials do not allow for determining who completes the form (patient or clinician).
-
Core data sheet.
Other important documents that we did not have included:
-
study manual of procedures
-
minutes of safety data monitoring committee meetings.
The placebo interventions in both sets of trials may have contained active substances. The placebo for zanamivir trials contained lactose powder, which can potentially cause bronchospasm, whereas the placebo for oseltamivir trials contained dehydrocholic acid and dibasic calcium phosphate dehydrate, which can cause gastrointestinal symptoms.
Data on participants by influenza-infected status (in treatment trials) and for participants with ILI (in prophylaxis trials) were not reported in the oseltamivir CSRs.
Finally, data on the effects of rescue or relief medication (mainly paracetamol/acetaminophen) were incomplete in CSRs of oseltamivir trials and not reported separately in all of the zanamivir trials.
Effects of interventions
Analysis of time to first symptom alleviation
In adult treatment, oseltamivir reduced the time to first alleviation of symptoms by 16.8 hours (95% CI 8.4 to 25.1 hours; I2 statistic = 0%), representing a 10% reduction from 7 days to 6.3 days (Figure 4). There was no significant effect in asthmatic children: increased by 5.2 hours (95% CI 11.1 hours lower to 21.4 hours higher; I2 statistic = 0%). But there was an effect in otherwise healthy children, based on one trial (29 hours, 95% CI 12 to 47 hours; p = 0.001) (see Table 9). Zanamivir reduced time to first alleviation of symptoms in adults by 0.60 days (95% CI 0.39 to 0.81 days; I2 statistic = 9%), which equates to a 14.4-hour (10%) reduction in symptoms from 6.6 days to 6.0 days (Figure 5). There was no significant effect in children: time to first alleviation of symptoms was 1.08 days lower in the zanamivir group (95% CI 2.32 lower to 0.15 days higher; I2 statistic = 72%).
FIGURE 4.
Oseltamivir vs. placebo for treatment. Time (hours) to first alleviation of symptoms in adult treatment (ITT population). df, degrees of freedom; IV, inverse variance;SD, standard deviation.

FIGURE 5.
Zanamivir vs. placebo for treatment. Time (days) to first alleviation of symptoms in adult treatment. df, degrees of freedom; IV, inverse variance; SD, standard deviation.

In eight zanamivir trials that reported on use of relief medication, in all of the participants the median days to alleviation in both the placebo and the treatment arms was less than those who did not use relief medications (Table 7). In seven zanamivir trials, time to first alleviation of symptoms was also reported with and without rescue medication. Using these data we were able to compare zanamivir without rescue medication with placebo with rescue medication. Overall, there was a non-significant 0.41-day decrease (95% CI 0.47 days lower to 1.29 days higher; I2 statistic = 67%) in time to first alleviation of symptoms in the placebo with rescue medication group, suggesting that zanamivir itself is no better than rescue medication, and possibly even less effective, although the varying levels of use of rescue medication in the seven trials did give rise to large heterogeneity (Figure 6).
| Study | Sample size (n) | Median days to alleviation for all participants | Difference in days (p-value) | Median days to alleviation and no use of relief medication | Difference in days (p-value) | |||
|---|---|---|---|---|---|---|---|---|
| Zanamivir | Placebo | Zanamivir | Placebo | Zanamivir | Placebo | |||
| NAI3000877 | 262 | 263 | 6.0 | 7.0 | 1.0 (0.123) | 8.0 | 10.0 | 2.0 (0.037) |
| NAI3000978 | 224 | 247 | 4.5 | 5.0 | 0.5 (0.011) | 5.0 | 6.0 | 1.0 (0.002) |
| NAI3001079 | 76 | 81 | 4.5 | 5.5 | 1.0 (0.033) | 5.5 | 6.75 | 1.25 (0.150) |
| NAI3001180 | 237 | 229 | 4.50 | 5.00 | 0.50 (0.495) | 7.0 | 7.0 | 0.0 (0.623) |
| NAI3001281 | 191 | 167 | 6.5 | 7.5 | 1.0 (0.159) | 9.0 | 10.0 | 1.0 (0.131) |
| NAI3001582 | 293 | 295 | 2.17 | 2.67 | 0.5 (0.166) | 3.17 | 3.83 | 0.66 (0.058) |
| NAIA300291 | 412 | 365 | 5.5 | 6.0 | 0.5 (0.228) | 7.0 | 8.0 | 1.0 (0.054) |
| NAIB300299 | 174 | 182 | 5.0 | 7.5 | 2.5 (< 0.001) | 5.5 | 8.25 | 2.75 (< 0.001) |
FIGURE 6.
Zanamivir vs. placebo for treatment. Time (days) to first alleviation of symptoms in adults with/without relief medication. df, degrees of freedom; IV, inverse variance; SD, standard deviation.
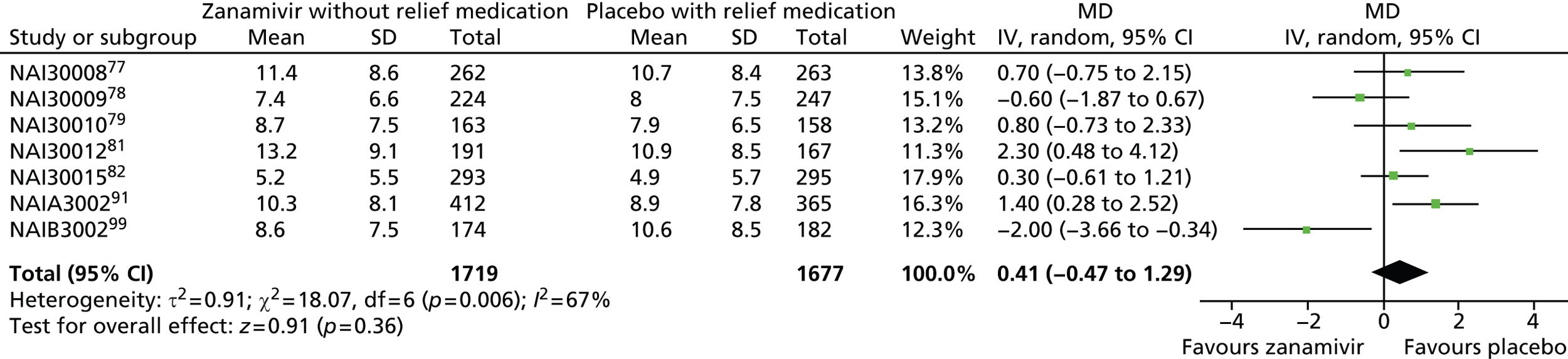
In a subgroup analysis of time to first alleviation of symptoms in adults by infection status, we found no evidence of a difference in treatment effect for zanamivir on the influenza-infected subgroup compared with the non-influenza-infected subgroup (p = 0.53). The treatment effect was 0.67 days (95% CI 0.35 to 0.99 days; I2 statistic = 17%) for influenza-infected patients and 0.52 days (95% CI 0.18 to 0.86 days; I2 statistic = 0%) for non-influenza-infected patients.
Analysis of hospitalisations
In oseltamivir treatment of adults, there was no significant difference in hospitalisation rate between treatment groups (RR 0.92, 95% CI 0.57 to 1.50; I2 statistic = 0%) or in treatment of children (RR 1.92, 95% CI 0.70 to 5.23; I2 statistic = 0%), with wide CIs; or in prophylaxis (RR 1.14, 95% CI 0.66 to 1.94; I2 statistic = 0%). Data on hospitalisations for the zanamivir studies were not reported.
Analysis of influenza complications
Pneumonia
In adult treatment trials, oseltamivir significantly reduced self-reported, investigator-mediated, unverified pneumonia (RR 0.55, 95% CI 0.33 to 0.90; I2 statistic = 0%; RD 1.00%, 95% CI 0.22% to 1.49%; NNTB 100, 95% CI 67 to 451) in the treated population. The effect was significant in the six trials that collected data on non-specific adverse events or secondary/intercurrent illness forms (RR 0.44, 95% CI 0.22 to 0.88; I2 statistic = 0%; RD 0.99%, 95% CI 0.21% to 1.38%; NNTB 101, 95% CI 73 to 470). However, it was not significant in the five trials (two CSRs) that used more detailed diagnostic data collection forms, and in no studies that reported on radiological confirmation of pneumonia (Figure 7). There was no significant effect on pneumonia in children (RR 1.06, 95% CI 0.62 to 1.83; I2 statistic = 0%). In two zanamivir adult trials,81,82 pneumonia reporting was based on a stricter definition of X-ray confirmation and there was also no significant treatment effect (RR 1.02, 95% CI 0.35 to 3.02; I2 statistic = 39%). In nine zanamivir trials,77,79,80,87,89,91,97–99 pneumonia was a self-reported, investigator-mediated, unverified outcome (see Figures 8 and 9). Overall, there was no significant effect of zanamivir on mixed verified and unverified pneumonia in adult treatment (RR 0.90, 95% CI 0.58 to 1.40; I2 statistic = 0%). In prophylaxis trials, zanamivir reduced the risk of self-reported, investigator-mediated, unverified pneumonia in adults (RR 0.30, 95% CI 0.11 to 0.80; I2 statistic = 0%; RD 0.32%, 95% CI 0.09% to 0.41%; NNTB 311, 95% CI 244 to 1086).
FIGURE 7.
Oseltamivir vs. placebo for treatment complications: pneumonia in adult treatment. df, degrees of freedom; IV, inverse variance.
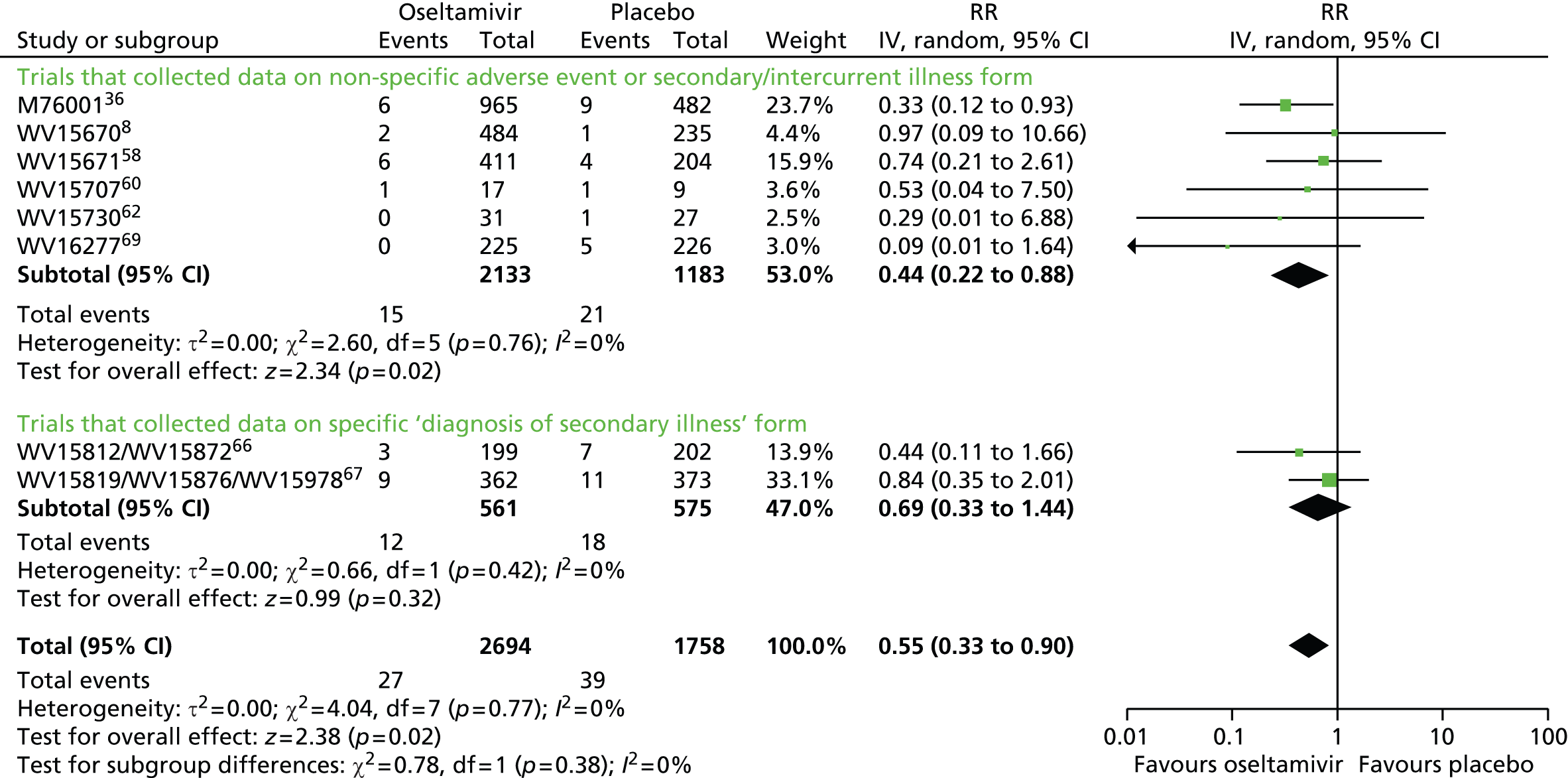
In a metaregression of ‘pneumonia’ based on 32 studies, treatment effects were not statistically different by age group (p = 0.22), drug (p = 0.89) or indication (p = 0.14). However, treatment effects were statistically different by method of diagnosis (p = 0.025). For unclear objective diagnosis of pneumonia, the treatment effect was RR 0.51 (95% CI 0.35 to 0.75; I2 statistic = 0%), whereas for objective diagnosis data collection of pneumonia, the treatment effect was 1.01 (95% CI 0.69 to 1.47; I2 statistic = 0%).
Serious complications and study withdrawals
In oseltamivir trials, treatment did not significantly affect complications classified as serious or those that led to withdrawal from the trial in adults (RR 0.91, 95% CI 0.40 to 2.06; I2 statistic = 0%) or in children (RR 1.98, 95% CI 0.58 to 6.72; I2 statistic = 0%). This outcome could not be assessed in oseltamivir prophylaxis because of an insufficient number of events. There was no significant effect of zanamivir, in adult treatment, in reducing the risk of any complication classified as serious or which led to study withdrawal (RR 1.10, 95% CI 0.46 to 2.63; I2 statistic = 0%) or in prophylaxis (RR 1.09, 95% CI 0.36 to 3.26; I2 statistic = 0%). This outcome could not be assessed in children because of an insufficient number of events.
Bronchitis, sinusitis and otitis media
Neither zanamivir nor oseltamivir significantly reduced the risk of bronchitis or sinusitis in prophylaxis trials. In adults, treatment with oseltamivir did not significantly reduce the risk of bronchitis (RR 0.75, 95% CI 0.56 to 1.01; I2 statistic = 36%), sinusitis (RR 1.03, 95% CI 0.76 to 1.40; I2 statistic = 0%) or otitis media (RR 1.11, 95% CI 0.57 to 2.15; I2 statistic = 0%). The result for bronchitis was sensitive to the methods used, as a fixed-effects analysis showed a significant effect (p = 0.02). Oseltamivir did not significantly affect complications in treatment of children, including otitis media (RR 0.80, 95% CI 0.62 to 1.02; I2 statistic = 0%).
Treatment with zanamivir significantly reduced the risk of bronchitis in adults (RR 0.75, 95% CI 0.61 to 0.91; I2 statistic = 0%; RD 1.80%, 95% CI 0.65% to 2.80%; NNTB 56, 95% CI 36 to 155), but did not reduce the risk of sinusitis or otitis media. In children, zanamivir treatment did not significantly reduce the risk of sinusitis (RR 0.87, 95% CI 0.12 to 6.45; I2 statistic = 40%) or otitis media (RR 1.00, 95% CI 0.59 to 1.72; I2 statistic = 0%).
See Table 1 for a summary of the methodology used for collecting and assessing complications in oseltamivir treatment trials. For the overall results for oseltamivir in adults see Table 8 and for children see Table 9. Table 10 shows the overall results for zanamivir in adults and Table 11 shows the results for children.
| Patient or population: healthy adults with influenza Settings: community, nursing homes Intervention: oseltamivir vs. placebo for treatment |
||||||
|---|---|---|---|---|---|---|
| Outcomes | Illustrative comparative risks,a study population (95% CI) | Relative effect (95% CI) | Number of participants (studies) | RD, % (95% CI) | NNTB or NNTH (95% CI) | |
| Assumed risk | Corresponding risk | |||||
| Placebo | Oseltamivir vs. placebo for treatment | |||||
| Time to first alleviation of symptoms in adult treatment (ITT population) (hours) | The mean time (hours) to first alleviation of symptoms adults in the intervention groups was 16.76 lower | 16.8 hours (8.4 to 25.1) | 3954 (8) | N/A | N/A | |
| Adverse events: nausea in adult treatment (on-treatment) | 64 per 1000 | 101 per 1000 (73 to 138) | RR 1.57 (1.14 to 2.15) | 4452 (8) | –3.66 (–7.39 to –0.9) | NNTH 28 (14 to 112) |
| Adverse events: vomiting in adult treatment (on-treatment) | 32 per 1000 | 77 per 1000 (56 to 108) | RR 2.43 (1.75 to 3.38) | 4452 (8) | –4.56 (–7.58 to –2.39) | NNTH 22 (14 to 42) |
| Adverse events: diarrhoea in adult treatment (on-treatment) | 71 per 1000 | 47 per 1000 (32 to 69) | RR 0.67 (0.46 to 0.98) | 4452 (8) | 2.33 (0.14 to 3.81) | NNTB 43 (27 to 709) |
| Complications: self reported, investigator-mediated, unverified pneumonia in adult treatment | 22 per 1000 | 12 per 1000 (7 to 20) | RR 0.55 (0.33 to 0.90) | 4452 (8) | 1.00 (0.22 to 1.49) | NNTB 100 (67 to 451) |
| Adverse events: cardiac body system in adult treatment (on-treatment) | 13 per 1000 | 7 per 1000 (3 to 13) | RR 0.49 (0.25 to 0.97) | 3943 (6) | 0.68 (0.04 to 1.00) | NNTB 148 (101 to 2509) |
| Adverse events: hospital admission in adult treatment | 18 per 1000 | 17 per 1000 (11 to 28) | RR 0.92 (0.57 to 1.50) | 4394 (7) | 0.15 (–0.78 to 0.91) | NNTB 687 (NNTB 110 to ∞ to NNTH 128) |
| Patient or population: healthy children with influenza Settings: community Intervention: oseltamivir vs. placebo for treatment |
||||||
|---|---|---|---|---|---|---|
| Outcomes | Illustrative comparative risks,a study population (95% CI) | Relative effect (95% CI) | Number of participants (studies) | RD, % (95% CI) | NNTB or NNTH (95% CI) | |
| Assumed risk | Corresponding risk | |||||
| Placebo | Oseltamivir vs. placebo for treatment | |||||
| Time to first alleviation of symptoms in child treatment (hours) | The mean time (hours) to first alleviation of symptoms in children in the intervention groups was 8.04 lower (33.34 lower to 17.26 higher) | 1329 (3) | Not significant | |||
| Hospital admission in child treatment (safety population) | 9 per 1000 | 17 per 1000 (6 to 46) | RR 1.92 (0.7 to 5.23) | 1359 (3) | –0.81 (–3.72 to 0.26) | NNTH 124 (NNTB 379 to ∞ to NNTH 27) |
| Complications: bronchitis in child treatment | 31 per 1000 | 20 per 1000 (8 to 48) | RR 0.65 (0.27 to 1.55) | 1359 (3) | 1.08 (–1.69 to 2.25) | NNTB 93 (NNTB 45 to ∞ to NNTH 59) |
| Complications: otitis media in child treatment | 163 per 1000 | 130 per 1000 (101 to 166) | RR 0.8 (0.62 to 1.02) | 1359 (3) | 3.26 (–0.33 to 6.18) | NNTB 31 (NNTB 17 to ∞ to NNTH 308) |
| Complications: pneumonia in child treatment | 37 per 1000 | 39 per 1000 (23 to 68) | RR 1.06 (0.62 to 1.83) | 1359 (3) | –0.22 (–3.07 to 1.41) | NNTH 450 (NNTB 71 to ∞ to NNTH 33) |
| Adverse events: diarrhoea in child treatment (on-treatment) | 72 per 1000 | 63 per 1000 (42 to 92) | RR 0.87 (0.58 to 1.28) | 1358 (3) | 0.93 (–2.01 to 3.02) | NNTB 108 (NNTB 34 to ∞ to NNTH 50) |
| Adverse events: vomiting in child treatment (on-treatment) | 76 per 1000 | 130 per 1000 (94 to 179) | RR 1.7 (1.23 to 2.35) | 1358 (3) | 5.34 (1.75 to 10.29) | NNTH 19 (10 to 57) |
| Patient or population: healthy adults with influenza Settings: community, nursing homes Intervention: zanamivir vs. placebo for treatment |
||||||
|---|---|---|---|---|---|---|
| Outcomes | Illustrative comparative risks,a study population (95% CI) | Relative effect (95% CI) | Number of participants (studies) | RD, % (95% CI) | NNTB or NNTH (95% CI) | |
| Assumed risk | Corresponding risk | |||||
| Placebo | Zanamivir vs. placebo for treatment | |||||
| Time to first alleviation of symptoms in adult treatment (days) | The mean time (days) to first alleviation of symptoms in adults in the intervention groups was 0.60 lower | 0.60 days (0.39 to 0.81) | 5411 (13) | N/A | N/A | |
| Complications: pneumonia confirmed with X-ray in adult treatment | 32 per 1000 | 33 per 1000 (11 to 98) | RR 1.02 (0.35 to 3.02) | 946 (2) | –0.06 (–6.56 to 2.11) | NNTH 1540 (NNTB 48 to ∞ to NNTH 16) |
| Adverse events: nausea/vomiting in adult treatment (on-treatment) | 41 per 1000 | 24 per 1000 (16 to 38) | RR 0.6 (0.39 to 0.94) | 6553 (15) | 1.63 (0.24 to 2.48) | NNTB 62 (41 to 411) |
| Adverse events: psychiatric body system in adult treatment (on-treatment) | 6 per 1000 | 6 per 1000 (3 to 13) | RR 1.16 (0.57 to 2.38) | 4732 (10) | –0.09 (–0.76 to 0.24) | NNTH 1132 (NNTB 421 to ∞ to NNTH 132) |
| Complications: bronchitis in adult treatment | 72 per 1000 | 54 per 1000 (44 to 65) | RR 0.75 (0.61 to 0.91) | 6072 (12) | 1.80 (0.65 to 2.80) | NNTB 56 (36 to 155) |
| Patient or population: healthy children with influenza Settings: community Intervention: zanamivir vs. placebo for treatment |
||||||
|---|---|---|---|---|---|---|
| Outcomes | Illustrative comparative risks,a study population (95% CI) | Relative effect (95% CI) | Number of participants (studies) | RD, % (95% CI) | NNTB or NNTH (95% CI) | |
| Assumed risk | Corresponding risk | |||||
| Placebo | Zanamivir vs. placebo for treatment | |||||
| Time to first alleviation of symptoms in children (days) | The mean time (days) to first alleviation of symptoms in children in the intervention groups was 1.08 lower (2.32 lower to 0.15 higher) | 723 (2) | N/A | N/A | ||
| Complications: sinusitis in child treatment | 15 per 1000 | 13 per 1000 (2 to 96) | RR 0.87 (0.12 to 6.45) | 737 (2) | 0.19 (–8.09 to 1.31) | NNTB 519 (NNTB 13 to ∞ to NNTH 77) |
| Complications: otitis media in child treatment | 71 per 1000 | 71 per 1000 (42 to 122) | RR 1.0 (0.59 to 1.72) | 737 (2) | 0.00 (–5.13 to 2.92) | NNTB ≥ 1000 (NNTB 35 to ∞ to NNTH 20) |
Analysis of influenza outcomes in prophylaxis studies
Symptomatic influenza was lower in the oseltamivir arms than the placebo arms in studies of prophylaxis (RR 0.45, 95% CI 0.30 to 0.67; I2 statistic = 0%; RD 3.05%, 95% CI 1.83% to 3.88%; NNTB 33,95% CI 26 to 55), but there were no differences for all other influenza outcomes, including overall ILI reported as an adverse event on-treatment. In household prophylaxis, one small study with missing outcome data and selective reporting, including 405 participants, showed a significant reduction of symptomatic influenza in the oseltamivir arm compared with placebo (RR 0.20, 95% CI 0.09 to 0.44; RD 13.6%, 95% CI 9.52% to 15.47%), but in the same study there was no significant reduction in asymptomatic influenza (RR 1.14, 95% CI 0.39 to 3.33). Asymptomatic influenza was not significantly reduced and there was no non-influenza ILI reported throughout the study period.
In prophylaxis trials we could not analyse effects on ILI because of a lack of definition in the CSRs. However, using our definition (see Methods), oseltamivir did not reduce ILI in participants (RR 0.95, 95% CI 0.86 to 1.06). See Appendix 11 for further analysis of symptomatic ILI.
The Roche trial programme assessing the effects of oseltamivir in PEP, submitted to the FDA on 22 May 2000, consisted of two trials. 65,120 We included only one trial65 because the other120 was not placebo controlled. WV1579965 was a double-blind, cluster-randomised trial in which contact clusters of index cases were randomised to oseltamivir 75 mg a day or placebo for 7 days. The manufacturer concluded that the trial proved that oseltamivir could prevent influenza in contacts by interrupting transmission from index cases. Interruption of transmission has two components: reduction of viral spread from index cases (measured by nasal shedding of influenza viruses) and prevention of onset of influenza in contacts measured with a mixture of symptoms and signs and ‘laboratory confirmation’ (i.e. viral culture from the upper airways and/or at least a fourfold rise in antibody titres measured between baseline and 2–3 weeks later). The design of the WV1579965 is weak. All index cases were left untreated except for a paracetamol rescue pack, making it impossible to assess the effect of oseltamivir on nasal voidance of index cases. Nasal viral voidance was measured only in symptomatic participants thereby missing out on potential asymptomatic infected people.
Zanamivir similarly significantly reduced the risk of symptomatic influenza for individuals (RR 0.39, 95% CI 0.22 to 0.70; I2 statistic = 45%; RD 1.98%, 95% CI 0.98% to 2.54%; NNTB 51, 95% CI 40 to 103), as well as households (RR 0.33, 95% CI 0.18 to 0.58; I2 statistic = 40%; RD 14.84%, 95% CI 12.18% to 16.55%; NNTB 7, 95% CI 6 to 9). However, it did not reduce the risk of asymptomatic influenza in the prophylaxis of individuals (RR 0.97, 0.76 to 1.24; I2 statistic = 0%) or asymptomatic individuals in PEP of households (RR 0.88, 95% CI 0.65 to 1.20; I2 statistic = 0%). See Table 10 for the overall results for zanamivir in adults and Table 11 for results in children. See Tables 12 and 13 for the overall results for zanamivir in adults.
| Patient or population: healthy adults without influenza Settings: community, nursing homes Intervention: zanamivir vs. placebo for prophylaxis |
||||||
|---|---|---|---|---|---|---|
| Outcomes | Illustrative comparative risks,a study population (95% CI) | Relative effect (95% CI) | Number of participants (studies) | RD, % (95% CI) | NNTB or NNTH (95% CI) | |
| Assumed risk | Corresponding risk | |||||
| Placebo | Zanamivir vs. placebo for prophylaxis | |||||
| Symptomatic influenza in prophylaxis of individuals | 33 per 1000 | 13 per 1000 (7 to 23) | RR 0.39 (0.22 to 0.70) | 5275 (4) | 1.98 (0.98 to 2.54) | NNTB 51 (40 to 103) |
| Asymptomatic influenza in prophylaxis of individuals | 50 per 1000 | 48 per 1000 (38 to 60) | RR 0.97 (0.76 to 1.24) | 5275 (4) | 0.14 (–1.1 to 1.1) | NNTB 729 (NNTB 91 to ∞ to NNTH 91) |
| Symptomatic influenza in household prophylaxis | 190 per 1000 | 42 per 1000 (25 to 68) | RR 0.22 (0.13 to 0.36) | 824 (2) | 14.84 (12.18 to 16.55) | NNTB 7 (6 to 9) |
| Asymptomatic influenza in household prophylaxis | 107 per 1000 | 97 per 1000 (64 to 145) | RR 0.90 (0.6 to 1.35) | 824 (2) | 1.32 (–2.2 to 3.84) | NNTB 76 (NNTB 26 to ∞ to NNTH 46) |
| Complications: pneumonia in adult prophylaxis | 5 per 1000 | 1.5 per 1000 (1 to 4) | RR 0.30 (0.11 to 0.8) | 7662 (6) | 0.32 (0.09 to 0.41) | NNTB 311 (244 to 1086) |
| Complications: bronchitis in adult prophylaxis | 15 per 1000 | 8 per 1000 (3 to 18) | RR 0.49 (0.02 to 1.19) | 7662 (6) | 0.79 (–0.29 to 1.24) | NNTB 127 (to NNTB 81 to ∞ to NNTH 341) |
| Patient or population: healthy adults without influenza Settings: community, nursing homes Intervention: oseltamivir vs .placebo for prophylaxis |
||||||
|---|---|---|---|---|---|---|
| Outcomes | Illustrative comparative risks,a study population (95% CI) | Relative effect (95% CI) | Number of participants (studies) | RD, % (95% CI) | NNTB or NNTH (95% CI) | |
| Assumed risk | Corresponding risk | |||||
| Placebo | Oseltamivir vs. placebo for prophylaxis | |||||
| Symptomatic influenza in adult prophylaxis of individuals | 55 per 1000 | 25 per 1000 (17 to 37) | RR 0.45 (0.30 to 0.67) | 2479 (3) | 3.05 (1.83 to 3.88) | NNTB 33 (26 to 55) |
| Symptomatic influenza in household prophylaxis | 170 per 1000 | 34 per 1000 (15 to 75) | RR 0.2 (0.09 to 0.44) | 405 (1) | 13.6 (9.52 to 15.47) | NNTB 7 (6 to 11) |
| Adverse events: psychiatric body systems in adult prophylaxis (all events on- and off-treatment) | 13 per 1000 | 23 per 1000 (14 to 40) | RR 1.80 (1.05 to 3.08) | 3434 (4) | –1.06 (–2.76 to –0.07) | NNTH 94 (36 to 1538) |
| Adverse events: headache in adult prophylaxis (on-treatment) | 175 per 1000 | 207 per 1000 (184 to 233) | RR 1.18 (1.05 to 1.33) | 3434 (4) | –3.15 (–5.78 to –0.88) | NNTH 32 (18 to 115) |
| Adverse events: nausea in adult prophylaxis (on-treatment) | 43 per 1000 | 85 per 1000 (52 to 138) | RR 1.96 (1.2 to 3.2) | 3434 (4) | –4.15 (–9.51 to –0.86) | NNTH 25 (11 to 116) |
| Adverse events: vomiting in adult prophylaxis (on-treatment) | 10 per 1000 | 20 per 1000 (7 to 55) | RR 1.91 (0.7 to 5.22) | 3434 (4) | –0.95 (–4.41 to 0.31) | NNTH 106 (NNTB 319 to ∞ to NNTH 23) |
| Adverse events: headache in adult prophylaxis (off-treatment) | 37 per 1000 | 33 per 1000 (23 to 46) | RR 0.88 (0.63 to 1.24) | 3434 (4) | 0.44 (–0.89 to 1.37) | NNTB 226 (NNTB 74 to ∞ to NNTH 113) |
Analysis of harms
Oseltamivir treatment
Oseltamivir in the treatment of adults is associated with increased risk of nausea (RR 1.57, 95% CI 1.14 to 2.15; I2 statistic = 43%; RD 3.66%, 95% CI 0.90% to 7.39%; NNTH 28, 95% CI 14 to 112) and vomiting (RR 2.43, 95% CI 1.75 to 3.38; I2 statistic = 12%; RD 4.56%, 95% CI 2.39% to 7.58%; NNTH 22, 95% CI 14 to 42). It is associated with a decreased risk of diarrhoea (RR 0.67, 95% CI 0.46 to 0.98; I2 statistic = 44%; RD 2.33%, 95% CI 0.14% to 3.81%; NNTB 43, 95% CI 27 to 709) compared with placebo during on-treatment periods. Both nausea and vomiting were associated with significant heterogeneity, when treatment effects appeared larger in otherwise healthy adults than in the elderly and the chronically ill. However, one trial of otherwise healthy adults69 also showed smaller effects. Vomiting was more common in those children on oseltamivir treatment than in those on placebo treatment (RR 1.70, 95% CI 1.23 to 2.35; I2 statistic = 0%; RD 5.34%, 95% CI 1.75% to 10.29%; NNTH 19, 95% CI 10 to 57).
The cardiac effects of oseltamivir are unclear. Exposure to oseltamivir may reduce cardiac general events compared with placebo (RR 0.49, 95% CI 0.25 to 0.97; I2 statistic = 0%; RD 0.68%, 95% CI 0.04% to 1.00%; NNTB 148, 95% CI 101 to 2509), excluding one trial70 in which electrocardiography was included in the safety parameters. However, exposure to oseltamivir may increase corrected QT interval prolongation (including borderline) as reported in trial WV1627770 (RD 4.0%, 95% CI 0.71% to 7.30%; NNTH 25, 95% CI 14 to 140) compared with placebo during on-treatment periods.
In treatment trials, there was no significant increase in risk between oseltamivir and on-treatment psychiatric adverse events overall (RR 0.93, 95% CI 0.43 to 2.03; I2 statistic = 0%). However, there was a dose–response effect in the two ‘pivotal’ treatment trials. 8,58 In the identically designed trials8,58 there were two active treatment groups: 150 mg (standard dose) and 300 mg (high dose) oseltamivir per day. In the dose–response analysis there was an increased risk of psychiatric body system adverse events over the entire follow-up period (p = 0.038, based on likelihood ratio test). In one trial,8 the event rates were 1 of 204, 1 of 206 and 4 of 205 in the placebo, 75-mg and 150-mg arms, respectively, whereas the second trial58 had rates of 2 of 235, 0 of 242 and 5 of 242, respectively.
The proportion of patients being diagnosed as influenza infected in oseltamivir treatment of adults was significantly lower in the treated group than in the control group (RR 0.95, 95% CI 0.91 to 0.99; I2 statistic = 0%). The proportion of patients with fourfold increases in antibody titre was significantly lower in the treated group than in the control group (RR 0.92, 95% CI 0.86 to 0.97; I2 statistic = 0%). This represents an absolute difference of 5% between treatment groups. There was a lower proportion of children on oseltamivir with a fourfold increase in antibodies (RR 0.90, 95% CI 0.80 to 1.00; I2 statistic = 0%).
Oseltamivir prophylaxis
In oseltamivir prophylaxis, there was an increased risk of headaches on-treatment (RR 1.18, 95% CI 1.05 to 1.33; I2 statistic = 0%; RD 3.15%, 95% CI 0.88% to 5.78%; NNTH 32, 95% CI 18 to 115) (Figure 8) and nausea on-treatment (RR 1.96, 95% CI 1.20 to 3.20; I2 statistic = 49%; RD 4.15%, 95% CI 0.86% to 9.51%; NNTH 25, 95% CI 11 to 116). There was also a dose–response effect for headaches in study52 (p = 0.013, based on likelihood ratio test), for which on-treatment rates were 202 of 519, 225 of 520 and 242 of 520 in the placebo, standard-dose and high-dose arms, respectively.
FIGURE 8.
Oseltamivir vs. placebo for prophylaxis, outcome: adverse events – headache in adult prophylaxis (on-treatment). df, degree of freedom; IV, inverse variance.
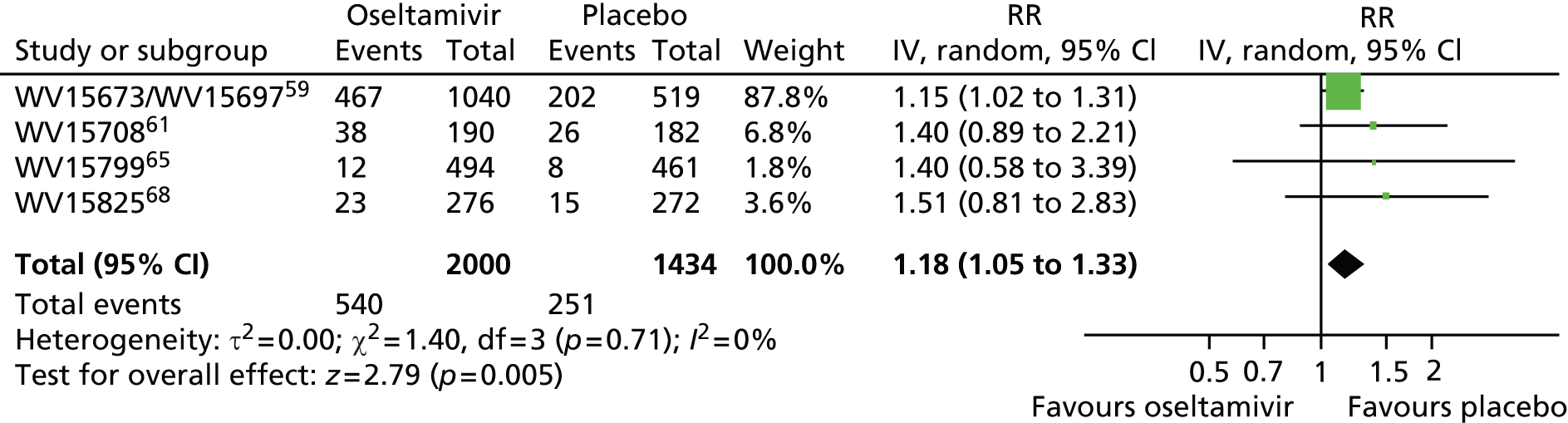
Figure 9 shows that in prophylaxis trials of oseltamivir there was a significant increase in patients with psychiatric adverse events over the on- and off-treatment periods (RR 1.80, 95% CI 1.05 to 3.08; I2 statistic = 0%; RD 1.06%, 95% CI 0.07% to 2.76%; NNTH 94, 95% CI 36 to 1538). Initial analysis of patients with psychiatric adverse events in the on-treatment period showed a borderline statistically significant result (p = 0.06), hence we conducted sensitivity analysis using Peto’s method (p = 0.05) as well as the analysis reported in Figure 9.
FIGURE 9.
Oseltamivir vs. placebo for prophylaxis: adverse events – psychiatric body system in adult prophylaxis (on- and off-treatment). df, degree of freedom; IV, inverse variance.

Table 14 shows a summary of all of the psychiatric adverse events in oseltamivir prophylaxis trials. Of particular note was an oseltamivir patient in one study68 who had severe confusion on day 27 and was hospitalised. On day 28 the patient was taken off medication and the event resolved. On day 29 the patient was discharged from hospital and subsequently resumed medication. However, confusion reappeared on day 32. The initial event was misclassified in the CSR as ‘mental impairment’ but has since been corrected in an erratum published in the same journal that published the original trial manuscript. 37,38
| Event type | Oseltamivir | Placebo | Total | |||
|---|---|---|---|---|---|---|
| Number of events | % | Number of events | % | Number of events | % | |
| Confusion | 5 | 0.25 | 1 | 0.07 | 6 | 0.17 |
| Depression | 14 | 0.7 | 6 | 0.42 | 20 | 0.58 |
| Hallucinations | 2 | 0.1 | 0 | 0.00 | 2 | 0.06 |
| Anxiety | 7 | 0.35 | 8 | 0.56 | 15 | 0.44 |
| Psychosis | 2 | 0.1 | 1 | 0.07 | 3 | 0.09 |
| Schizophrenia | 1 | 0.05 | 0 | 0.00 | 1 | 0.03 |
| Bipolar disorder | 0 | 0 | 1 | 0.07 | 1 | 0.03 |
| Sleeping disorder | 2 | 0.1 | 0 | 0.00 | 2 | 0.06 |
| Aggression | 1 | 0.05 | 0 | 0.00 | 1 | 0.03 |
| Stress symptoms | 3 | 0.15 | 0 | 0.00 | 3 | 0.09 |
| Restlessness | 1 | 0.05 | 0 | 0.00 | 1 | 0.03 |
| Nervousness | 1 | 0.05 | 0 | 0.00 | 1 | 0.03 |
| Suicide ideation | 1 | 0.05 | 0 | 0.00 | 1 | 0.03 |
| Paranoia | 1 | 0.05 | 0 | 0.00 | 1 | 0.03 |
| Alcohol related | 6 | 0.3 | 2 | 0.14 | 8 | 0.23 |
| Total | 47 | 2.35 | 19 | 1.32 | 66 | 1.92 |
There was a non-significant increase in renal events on-treatment (RR 3.17, 95% CI 0.96 to 10.49; I2 statistic = 0; RD 0.67%, 95% CI –0.01% to 2.93%; NNTH 150, 95% CI NNTH 35 to ∞ to NNTB > 1000). However, in sensitivity analysis using Peto’s method the result for renal events was statistically significant (p = 0.02).
Zanamivir
There was no significant effect on serious adverse events in adult treatment trials (RR 0.86, 95% CI 0.49 to 1.50; I2 statistic = 0%).
In treatment trials, there was no significant effect on diarrhoea in adults (RR 0.87, 95% CI 0.66 to 1.14; I2 statistic = 5%) or headache (RR 0.84, 95% CI 0.60 to 1.18; I2 statistic = 0). However, during the on-treatment phase, nausea and vomiting were significantly less frequent in the zanamivir arm (RR 0.60, 95% CI 0.39 to 0.94; I2 statistic = 0%; RD 1.63%, 95% CI 0.24% to 2.48%; NNTB 62, 95% CI 41 to 411).
There was no significant effect observed on the renal system (RR 0.84, 95% CI 0.41 to 1.72; I2 statistic = 0%) or the psychiatric system (RR 1.16, 95% CI 0.57 to 2.38; I2 statistic = 0%). In adult treatment trials of zanamivir, there was no significantly increased risk of any other reported adverse events, and there was no significant increase in adverse effects observed in prophylaxis trials, including psychiatric (RR 1.05, 95% CI 0.48 to 2.29; I2 statistic = 25%) and renal effects (RR 0.67, 95% CI 0.35 to 1.26; I2 statistic = 0%) on-treatment. There was no significant increase in harms associated with zanamivir treatment of children but data were sparse.
There was no significant effect of zanamivir treatment on influenza diagnosis (RR 1.02, 95% CI 0.98 to 1.06; I2 statistic = 0%) or probability of a fourfold increase in antibody titre (RR 1.06, 95% CI 0.96 to 1.06; I2 statistic = 0%).
Deaths
In oseltamivir treatment trials, there was one death overall. This event occurred as a result of acute respiratory syndrome in a placebo patient without influenza in study. 66 In prophylaxis trials, there were four deaths in total, all in elderly patients, with two in the placebo group and two in the oseltamivir group. Causes of death were reported as two cancers, one myocardial infarction and one intestinal perforation. However, for both deaths in the oseltamivir arms the participants experienced acute renal failure on-treatment prior to death.
There were eight deaths in total in the zanamivir trials. Six of the deaths were caused by neoplasias or cardiovascular events in elderly patients with multiple pathologies. However, two deaths were reported as being due to influenza A pneumonia. One participant was on inhaled rimantadine plus placebo and the other on zanamivir.
The results of post-protocol hypotheses are in Appendix 8.
Discussion
Oseltamivir and zanamivir have small, non-specific effects on reducing time to alleviation of ILI symptoms in adults but not in asthmatic children. Using either drug as prophylaxis reduces the risk of developing symptomatic influenza. Treatment trials with oseltamivir or zanamivir do not settle the question of whether or not complications of influenza, such as pneumonia, are reduced, because of a lack of diagnostic definitions. Use of oseltamivir increases the risk of adverse effects such as nausea, vomiting, psychiatric effects and renal events in adults, and the risk of vomiting in children. The lower bioavailability may explain the lower toxicity of zanamivir than that of oseltamivir. The influenza virus-specific mechanism of action proposed by the producers does not fit the clinical evidence, which shows no such effects.
Reconstructing trial lists and indexing regulatory comments
Calls for incorporating unpublished data to supplement published trial data in systematic reviews and meta-analyses highlight deficiencies in the current methods for obtaining the most complete understanding of a drug’s effects. 121 Our methodological approach entailed comprehensive searching of unpublished sources, with a particular emphasis on obtaining unpublished and internal reports from drug manufacturers, intended for regulatory submission, and comments from national regulatory bodies. Our decision not to use published evidence as a basis for trial appraisal and data extraction meant that we had to reconcile and synthesise information from multiple unpublished sources. We had to devise a new method of searching, indexing, retrieving and reviewing trial data, and to combine this understanding with regulatory comments to produce an informative review. The first step in this process entailed the need to develop our own reconstruction of the trial programme without initial help from outside sources. The reconstructed list of trials and then programmes took a whole-time equivalent researcher 20 days to compile. Owing to the complexity of the task, we suggest that, in the future, some of the essential phases, such as checking the trial identification number across multiple documents and databases, be conducted in pairs.
One of the comments received on our protocol suggested that discrepancies between published and unpublished versions of the same data set could be due to mistakes in the non-peer reviewed, unedited CSRs (which may be corrected by the time of publication). Our experience, especially with the non-reporting of serious adverse events, points to the opposite being the case. 122 Considering the fact that unintentional errors can occur, we believe that the response should not be a resort to published papers as ‘most accurate’ and best unit of analysis, but rather that CSRs – as by far the most comprehensive record of a trial – remain the key unit of analysis, with the expectation that they be amended and kept as accurate as possible over time, with complete documentation of reasons for any amendments. We believed that the results of our review would be undermined without accessing a more complete body of evidence that we knew to be outside the public domain.
In theory, trial registers would be expected to provide a comprehensive picture of a drug’s trial programme. However, registers were not our primary instruments to reconstruct zanamivir and oseltamivir trial programmes. Both drugs’ programmes were mainly run in the late 1990s, before trial registration became the norm. In addition, registers may suffer from some of the problems that we were trying to address. Bourgeois et al. 123 audited entries for 546 trials of five major classes of drugs on ClinicalTrials.gov, the biggest prospective register of clinical trials, and found evidence of risk of reporting bias and delay in reporting of results. Another review of 152 trials found that the description of 123 (or 81%) of the trials in the sample had been changed in at least one key element in the time between registration and publication. The most frequent changes regarded outcomes. 124 Despite the current limits of registers, both specifically to this review and in the way they are run and updated, we believe that registers are an obvious first choice to start reconstruction of trials programmes. Searching for unpublished material has not yet become standard practice in conducting Cochrane reviews,125 and is currently variably reported. 126
The indexing and review of regulatory files was also a very laborious task. It took a whole-time equivalent researcher 3 days to review the FDA regulator’s comments and gain a basic understanding of the content. Four additional days were needed to read and annotate the FDA zanamivir files and 28 days for reading and annotating the oseltamivir files and building the table of contents-evidence (see Appendix 11). The exercise had to be repeated several times to cross-check content and expand annotations. Construction of the TOC was laborious. A first attempt at electronic mapping the TOC content took 12 and 8 hours, respectively, for the FDA and National Institute for Health and Care Excellence (NICE) regulatory documents. This was carried out using the Adobe Acrobat (Adobe Systems; https://acrobat.adobe.com/us/en/acrobat/how-to/ocr-software-convert-pdf-to-text.htm) optical character recognition search facility, which enabled mapping of citation counts by document and by trial ID. Initially, we used the trial prefix followed by the serial number (‘WV15670’) as ID. This procedure, however, had one major drawback linked to the nature of regulatory documents. As regulatory documents consist of notes, correspondence and reviews, the same trial is cited in a non-standardised way. For example, trial WV156708 is cited as ‘WV15670’ 15 times, as ‘WV_15670’ 12 times and simply as ‘15670’ 19 times. Thorough searches must be conducted using all of the different terms. As this can be very time-consuming, we decided to compare an Acrobat search with a Boolean string strategy containing all of the possible citation formats (e.g. WV15758 OR WV 15758 OR Trial 15758 OR Trial15758 OR Trials 15758 OR Trials15758 OR 15758 OR study 15758 OR study15758) (this is logically equivalent to ‘WV 15758 OR WV 15758’) with a term-by-term search (i.e. separately searching for WV15758 and then for WV 15758 and so on). We reasoned that if the yield were comparable, the Boolean strategy would have been faster. The yield of citations of the two strategies was the same for six of seven ‘tracker’ studies, but use of a Boolean string was considerably faster (an average of 3 vs. 14 hours) than the term-by-term strategy. The NICE submission citations took 2 hours to list in a TOC using a Boolean strategy. We adopted the Boolean search strategy to construct our TOC. Ultimately, it is possible that a search with the trial numerals (‘15670’) may be sufficient to identify the vast majority of citations. To validate this method of searching further, our methods should be repeated on other sets of regulatory documents.
Once we had reconstructed the trial programmes, we submitted the results to GSK and Roche for their input. We received detailed feedback from both but, into 2011, Roche’s list of trials was still incomplete. Despite the laboriousness of the methods, we believe that we ended up with a far more comprehensive and less biased set of evidence than that available through the current system of journal-based publications. This shift in our data synthesis paradigm was made necessary by the numerous and documented discrepancies between regulatory and published evidence and by the sizeable risk of publication bias of the oseltamivir trial programme. The importance of reconstructing the trial programme by first generating a complete trial list was further reinforced upon discovering bias and oversights in regulators’ handling of the trial programme. Regulators focus on a few mutually agreed ‘pivotal’ trials, the data analyses of which are replicated by the FDA but not by the EMA. Both largely ignored trial M76001,36 the largest oseltamivir treatment trial that was conducted prior to initial registration of the drug (and still unpublished). Although the manufacturer may not have offered it as a ‘pivotal’ trial, far smaller and even ongoing studies were included in the evidence base to support Roche’s year 1999 NDA number 021087 (treatment of uncomplicated acute illness due to influenza infections in adults who have been symptomatic for no more than 2 days). The history of the EMA scrutiny is harder to assess as we could find no reports of trial site visits or of data analysis replication, but we identified a pooled analysis of treatment trials, very similar to the Kaiser 2003 analysis,4 which formed the basis for the EMA conclusion that oseltamivir affected complications reported, for example on EMA’s 4 October 2012 Summary of Product Characteristics (www.bmj.com/tamiflu/ema). We requested modules 3–5 (individual listings, demographic data and the statistical analysis report) from the EMA. However, for most oseltamivir trials, the EMA does not have the relevant documents and neither apparently does the National Competent Authorities (e-mail from the EMA, 24 May 2011; e-mail from Dutch regulator Medicines Evaluation Board, 20 July 2011). This means that the modules do not appear to have been either submitted to or requested by regulators, raising questions as to the extent of scrutiny of the clinical trials during the regulatory review of oseltamivir in Europe.
Our new method
Reviewing large quantities of complicated data and linked comments is a very difficult and delicate process. The main problem is not so much the appraisal following standard rules and possible synthesis of data (as when we review published information), but the reconstructions and logical threading of a trial programme generating huge amounts of data needing appraisal. Also the manufacturer’s full regulatory submission, which may have even more information than a full CSR, remains confidential. Most of the essential data required are available in CSRs, together with masses of less important data, but, as we have explained, even in this case there may be important omissions, such as mislaid diary cards (Figures 10 and 11) for follow-up. Manufacturers are under obligation to provide regulators with all of the data requested to enable them to reach a decision: in doing so they produce vast submissions. None of the authors (all experienced systematic reviewers) had any experience of reviewing regulatory information, but we could not find any workable shortcuts. We believe that providing a critical overview of a trial programme rather than minute dissection of each trial is necessary. This can be done by identifying the important topics in the trial programme (such as the effects of the drug on symptoms, infection, complications, transmission and well-being) and following them throughout the programme, putting the evidence together coherently. This includes carrying out a high-level overview of the mode of action of the drug in different populations for different indications. Understanding a drug’s mode of action underpins correct reporting of its strengths and limitations. In addition, a large part of the regulatory submission is made up of chemistry, microbiological, animal model pharmacodynamic and pharmacokinetic studies, which are important for shedding light on the trial programme but which seldom feature in systematic reviews. We are unsure whether or not this information could be considered as core information, but an exhaustive review of a trial programme should include reviews dedicated to such topics.
FIGURE 10.
Example diary card from CRF for zanamivir trial (1).

FIGURE 11.
Example diary card from CRF for zanamivir trial (2).
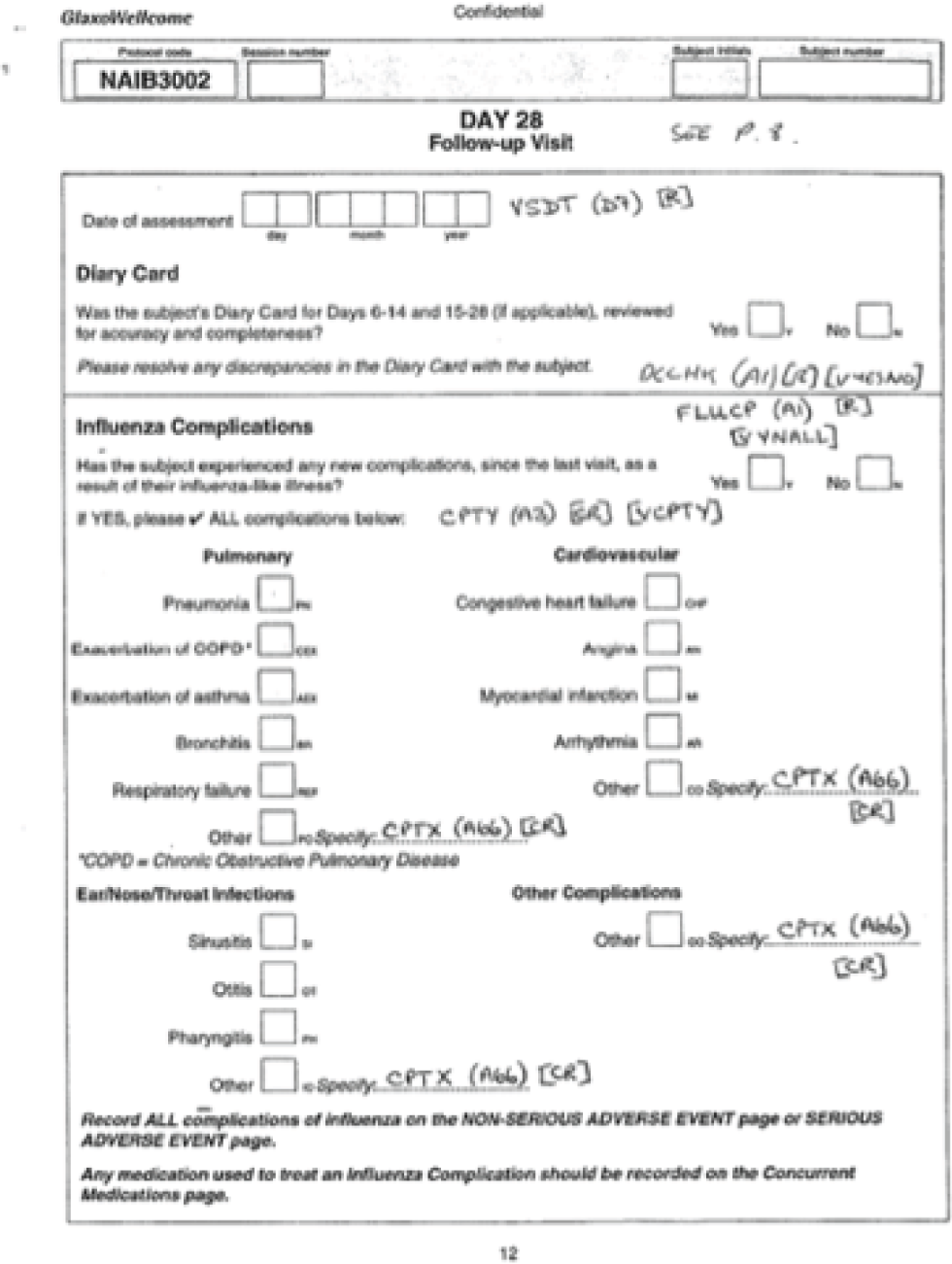
These methods revealed possible problems in trial conduct and validity, including the lack of comparability between arms induced by subset analysis and by the randomisation analysis fork, high positivity rate of influenza, high gastrointestinal events in the placebo arms, possibly active placebo content and possible procedural breaches in several trials. The ideal option is to carry out analyses on the basis of the ITT population, in which units of randomisation and analysis are the same and many of the potential problems listed are either not present or minimised. We are continuing to develop further methods for using such data.
Regulatory comments
Reviewing regulatory comments was essential to expand our understanding of the trial programme. We expected that detailed reading of regulatory material would allow us to understand discrepancies between US and European regulators’ conclusions regarding the effects of oseltamivir, particularly (but not limited to) their putative effect on complications. 8 We were interested in what led the FDA to have far more cautious and conservative statements – as witnessed in the Tamiflu product label and FDA letters – in comparison with European regulators. Our access to huge amounts of FDA regulatory data allowed for many insights but gave us little visibility of manufacturers’ responses.
Some of the statements (such as NIs reduce bacterial complications) made by the manufacturer in the CSRs, and, subsequently, in contemporaneous publications and advertisements, appeared unsupported by the evidence provided at the time. The FDA drug regulatory reviewers’ comments, although laborious to summarise and contextualise (because of the non-availability of the whole pharmaceutical submission), were confirmed by our reading of the CSRs. However, we were unable to find a statement explaining how the FDA reviewed each NDA. FDA reviewing methods appeared to be a mixture of spot checks, re-run of statistical analyses and on-site inspections. A FDA methods volume or standard operational procedure may be among the documents not available from the web but accessible through a FOI request. Neither the FDA nor the EMA have inventories of held documents, making it very difficult to know what to ask for under FOI rules. We concentrated on downloading or asking for specific CSRs and related documents or reviewers’ comments on a particular NDA. The quantity of information held by regulators is likely to be large. For example, NDA 21–246, regarding the use of Tamiflu in the treatment of influenza in children, submitted to the FDA on 15 June 2000, consisted of 137 volumes of study documents and possibly several electronic files. Although we do not know exactly how long a volume was, we have seen references to up to hundreds of pages in each volume.
Requesting specific documents and packages of information is especially important to allow a more efficient and timely reviewing process when confronted with a large volume of evidence, most of which could be of peripheral value. A request for a specific document is likely to be dealt with far more efficiently than a generic request for ‘all documentation relating to oseltamivir’. This is one of the reasons why developing a TOC for any drug or family of drugs (no matter how time-consuming) is an absolute prerequisite for any serious attempt at reviewing regulatory evidence. This introduces another very difficult problem: how to handle huge quantities of structured information and the ethics of drawing conclusions from what is still a fragmentary (albeit sizeable) evidence base.
Overall, the FDA assessment of the performance of oseltamivir was ‘modest’. This adjective appears six times in a 50-page review document. 109 For example, in the Division Director Memorandum dated 25 October 1999, under the heading ‘Public health role of antiviral treatment’ the FDA109 states: ‘The clinical relevance of the modest treatment benefit is a highly subjective question’ (p. 3). The FDA refused to accept claims of oseltamivir’s effects on influenza complications as ‘false or misleading’ statements in promotional materials. 122 A FDA warning letter seems to imply, for example, that oseltamivir’s mode of action is ‘proposed’ or ‘possibly’ (that proposed by the manufacturers) (i.e. not certain). 127 However, FDA reviewers appear to have missed important problems in Roche’s clinical trials (such as the imbalance in the numbers of individuals classified as influenza infected in oseltamivir treatment trials). Importantly, there appears to have been no investigation into the coherence of the evidence with the proposed mode of action of the drug.
Summary of main results
For the first time, a Cochrane review is based on all relevant full CSRs of a class of drugs integrated by regulatory comments. Also for the first time, all CSRs of trials in a manufacturer’s programme (regardless of their relevance to the review) are available to readers without any restriction (apart from minimal redactions to protect anonymity further). The role of Roche and GSK in making this possible should be recognised, as well as that of the BMJ, which kept the issue in the public eye until it was resolved.
The evidence we have presented and synthesised shows that both of the NIs in this review have symptom-relieving effects, especially for self-reported outcomes. They appear to have symptom-relieving properties that make people with ILI and self-reported, investigator-mediated, unverified pneumonia feel better by shortening symptom duration and reducing the frequency of symptoms, such as cough. For oseltamivir, this effect perhaps extends to cardiac symptoms, despite the short duration of treatment (5 days). We are unsure what to make of this finding but we think it deserves further investigation.
The issue which triggered our change of evidence-seeking methods is partly resolved: no definitions of secondary illnesses were given anywhere in the CSRs [e.g. ‘pneumonia’ was defined as ‘pneumonia’ in the CRFs (see Table 1) and diagnostic criteria were not given]; clinical diagnosis in the absence of criteria and without X-ray has only a moderate chance of being correct.
We could not decide the level of diagnostic ascertainment of diagnosis of pneumonia and other complications, as it is unclear from the CSRs. Definitions of pneumonia were not given and the algorithm for classification of an event as pneumonia was not supplied. In oseltamivir trials, the CRF trigger for recording of adverse events and secondary illness was a question to the participant posed by the investigator. A typical phrasing is as follows: ‘Secondary illness reminder: Has the patient reported any sinusitis, otitis, bronchitis, other chest infection or pneumonia since baseline?’ This was followed by a yes/no box to be ticked and an additional form was to be filled out by the investigator for collecting details on the secondary illness. A record of medications outside trial allocation was elicited in addition to the participant’s diary card. The original and Medical Dictionary for Regulatory Activities terms suggest diagnoses for all secondary illnesses and adverse events but there is no indication as to how the original and preferred terms were assigned. We therefore considered these outcomes to be ‘self-reported, investigator-mediated, unverified’ outcomes. For a subset of trials, secondary/intercurrent illness and adverse event data were collected on a single, one-page form. In our meta-analyses, we called this subanalysis ‘Trials which collected data on non-specific adverse events or secondary/intercurrent illness form’. For a different subset of trials, CRFs contained space to record diagnostic tests, such as chest X-rays, tympanometry and sinus X-rays for all secondary illness but there was no reporting of such variables in the CSRs (Figures 12–15). In our meta-analyses, we called this subanalysis ‘Trials which collected data on specific “Diagnosis of Secondary Illness” form’. None of the complications was defined as primary outcomes in any trial, which may explain the poverty of data definition.

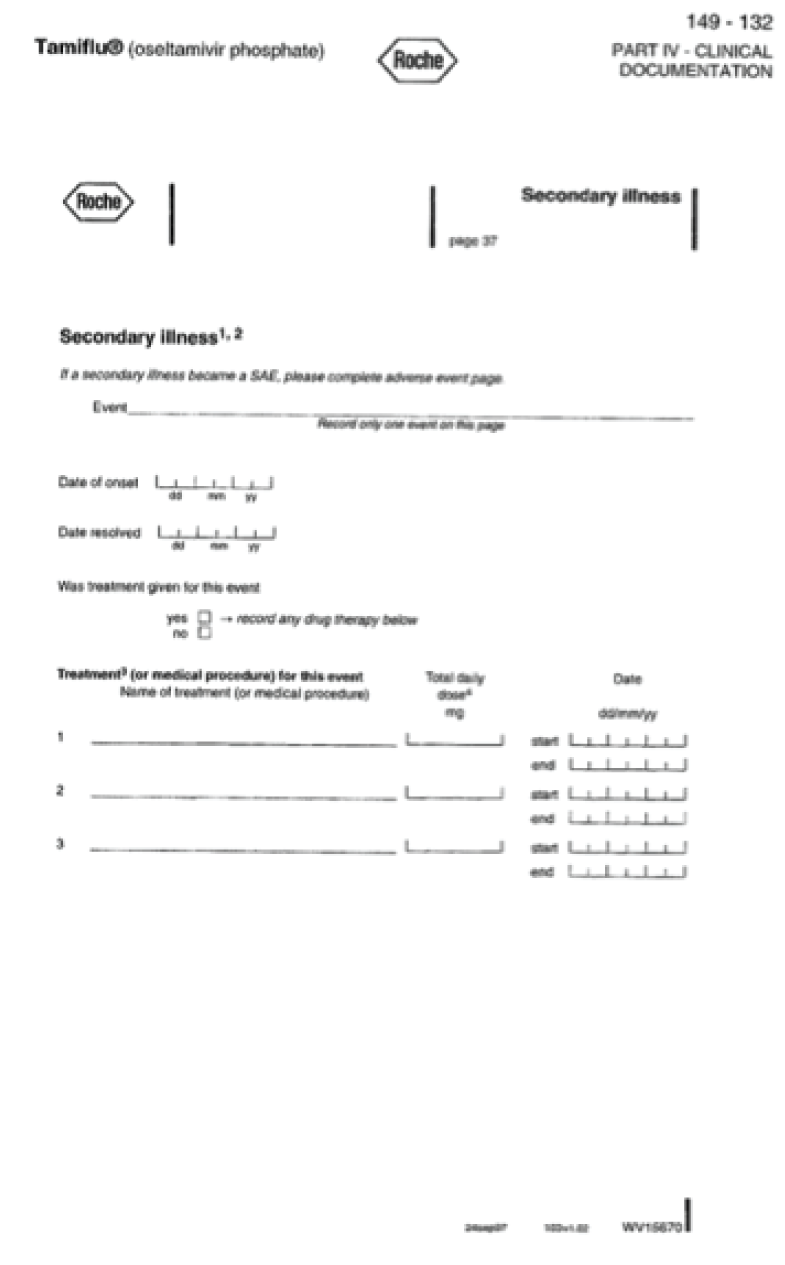

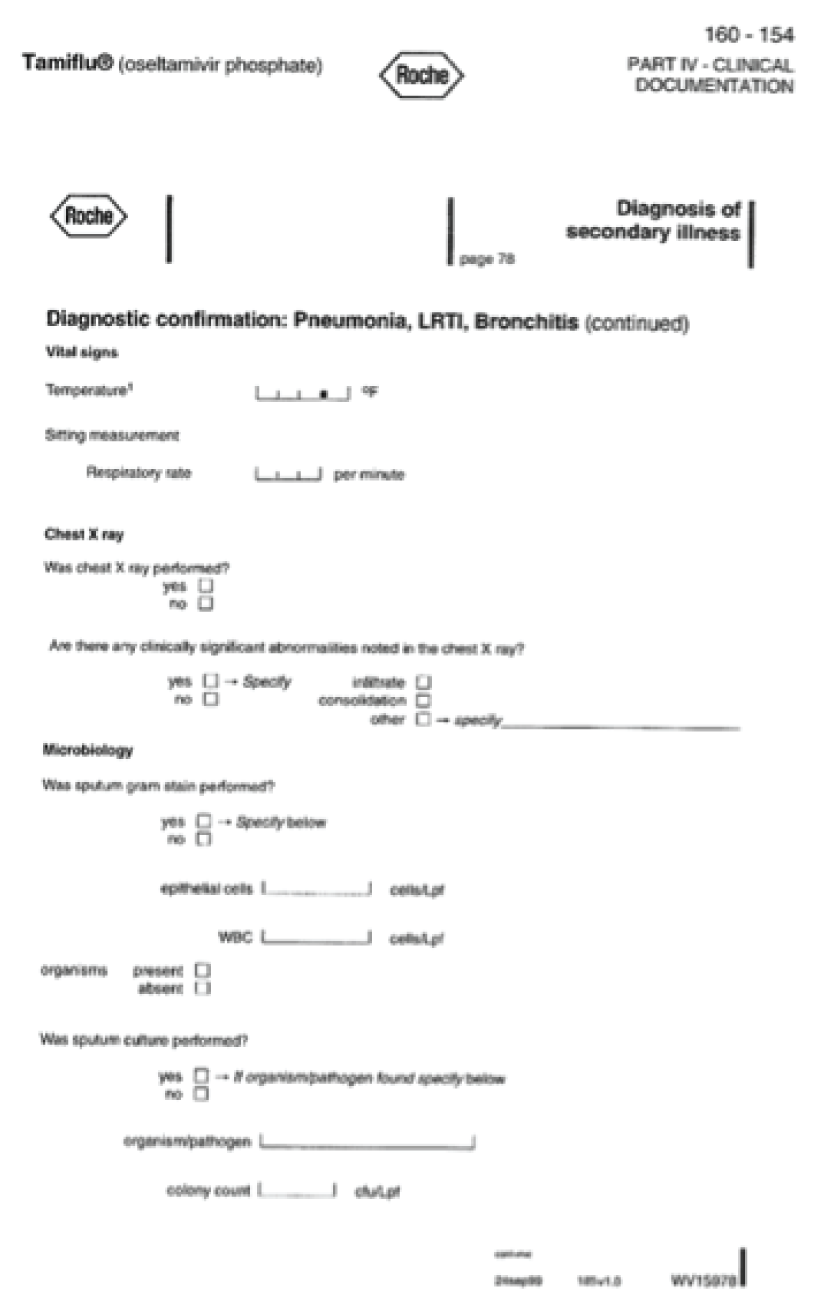
In a metaregression of all of the 32 included studies that reported on ‘pneumonia’, we found evidence that treatment effects for pneumonia are statistically different depending on the method of diagnosis. Unclear objective diagnosis was associated with an apparent 46% reduction in pneumonia as a result of treatment with NIs, whereas the use of objective criteria in the data collection showed no evidence of effect, with a RR of 1.0. Age group (adults vs. children), drug (oseltamivir vs. zanamivir) and indication (treatment vs. prophylaxis) showed no evidence of association with treatment effect.
Meaningful conclusions on the effect of either NI on complications of influenza are difficult to draw based on the trial evidence. In part, this was due to the lack of standardised definitions. In addition, meta-analyses of these outcomes that lacked definitions were based on few events and therefore not robust. Caution is therefore urged in interpreting the meta-analysis result, which suggests that 100 patients (95% CI 67 to 451 patients) need to be treated with oseltamivir for one less self-reported, investigator-mediated, unverified pneumonia. The same applies to the zanamivir treatment result, which suggests a reduced risk of self-reported, investigator-mediated, unverified bronchitis in adults (NNTB 56, 95% CI 36 to 155). The evidence suggested that oseltamivir had a similar effect, although the result was non-significant.
As stated above, there is no evidence that definitions of complications in paediatric, elderly or adult trials were ever prepared and incorporated in the trials’ design. Therefore, the reporting of cases of ‘otitis media’, ‘pneumonia’, ‘sinusitis’ or ‘bronchitis’ are of unclear significance and importance, making it impossible to attribute a cause and draw conclusions. 128 This is probably why the FDA-approved oseltamivir package insert, since 17 November 2000, has consistently stated: ‘serious bacterial infections may begin with influenza-like symptoms or may coexist with or occur as complications during the course of influenza. TAMIFLU has not been shown to prevent such complications’. The original product label did not contain such a statement but, on 14 April 2000, after oseltamivir was approved for sale in the USA, the FDA sent Roche an untitled letter about ‘Misleading Efficacy Claims’, which the FDA had noted in Roche’s promotional materials (p. 3129). One of the statements that Roche made was: ‘Tamiflu reduces incidence of secondary complications (i.e. bacterial infections) by 45%’. The FDA commented: ‘Further, you have claimed reductions in severity and incidence of secondary infections with Tamiflu that are misleading because they are not supported by substantial evidence’ (p. 3129). We do not know how Roche responded to the FDA but in subsequently available Roche promotional material information, Roche’s statements were consistent with the FDA’s demands. 8
There is uncertainty in the ‘complications’ and ‘secondary illnesses’ outcome definition, therefore we carried out an analysis on the data from adult treatment trials on those complications classified as serious or those which led to study withdrawal. For oseltamivir, there was no evidence that treatment affected such complications (RD 0.07%, 95% CI –0.78% to 0.44%). This outcome could not be assessed in oseltamivir prophylaxis due to an insufficient number of events. For zanamivir, there was no significant evidence of a treatment effect on such complications (RD –0.04%, 95% CI –0.64% to 0.24%). This outcome could not be assessed in children because of an insufficient number of events.
Contrary to the FDA, the EMA’s oseltamivir Summary of Product Characteristics states that oseltamivir significantly reduces the incidence of ‘specified lower respiratory tract complications (mainly bronchitis) treated with antibiotics’ in individuals aged ≥ 13 years. This claim is based on ‘a pooled analysis of all influenza-positive adults and adolescents (N = 2413) enrolled into treatment studies’, of which 1063 were in the placebo group and 1350 were in the oseltamivir-treated population. 130 This statement appears in the EMA files as early as 2001. 131 These exact denominators appear in the Kaiser et al. 4 2003 meta-analysis.
The design of the trials – as defined in the protocol with amendments, SAP and CRFs – does not allow any further inferences. The effect on outcomes that were originally considered of secondary or tertiary importance (such as bronchitis and pneumonia) would have been clarified with better clinical definitions and investigations, as were some of the serious adverse events. These benefited from a paragraph-length narrative, which reported most of the salient features of the event.
Our previous decision to analyse the effects of oseltamivir and zanamivir on the ITT population has been confirmed for oseltamivir, with the demonstration of the effect on antibody responses in participants in treatment trials, although no such effect is discernible for zanamivir. This effect leads to the introduction of selection bias, with a significantly reduced probability of being diagnosed with influenza and an imbalance in the two arms if the ITTI population is analysed. The effect of oseltamivir on antibodies appears to be carried over to children with ILI. Its finding contradicts statements made by the manufacturer.
The apparent incomparability between arms of the influenza-infected subpopulations in the oseltamivir trials raises the question of how an appropriate analysis should be conducted. If influenza-infected groups are comparable (as appears to be the case in zanamivir treatment trials) then an appropriate analysis strategy (based on Senn132) would be to first determine the effect of treatment in the ITT population. If there is evidence of a treatment effect then treatment by infected status interaction could be tested. If there was evidence of an interaction then estimates of treatment effect could be derived separately for the influenza-infected and non-influenza-infected subpopulations. However, this analysis should be conducted on the ITT population using a single appropriate statistical model, obviating the need to conduct separate analysis on the influenza-infected subpopulation. Roche used geometric mean titres indicating antibody responses in the ITTI population to support their statement that oseltamivir does not affect antibody responses (e.g. in Table 15 and linked text of module 1 of trial WV1579965). However, the use of such measures can be misleading. What are required for such an analysis are data on how many ITT population participants responded by arm, at what level of antibody response and how many were tested. Such data could not be identified with certainty. A further effect of choosing a subpopulation analysis (ITTI in treatment trials and ITTIINAB (ITT influenza-infected index cases who had negative virology at baseline) in prophylaxis trials) as the primary analysis is the restriction of the generalisability of results. This is especially so in the case of design flaws (e.g. in the case of the PEP trial WV15799,65 in which all index cases were not treated and around 55% of participants were dropped from the ITTIINAB analysis). In this cluster trial design, households should be included as random effects in the analysis to take account of within-household correlations.
| Positive serology | Group | Total | |
|---|---|---|---|
| Placebo, n (%) | Tamiflu, n (%) | ||
| No | 166 (83.0) | 192 (93.7) | 358 |
| Yes | 34 (17.0) | 13 (6.3) | 47 |
| Total | 200 | 205 | 405 |
A significant but slight reduction of the proportion with serum antibody (mostly haemagglutination inhibition antibody) titre rise by fourfold or more among those who were tested was shown in this review. This was consistent with the evidence from animal tests using a subclinical dose of oseltamivir in influenza A/H1N1-infected mice. 133 Takahashi et al. 133 reported a non-significant slight reduction of haemagglutinin-specific secretory immunoglobulin G antibody in the serum and spleen, whereas they reported about an 80% significant reduction of haemagglutinin-specific secretory immunoglobulin A antibody in the nasal wash and bronchoalveolar fluids on day 12. From this evidence, they warned that the risk of reinfection may increase in patients showing a low mucosal immunoglobulin A antibody response following oseltamivir administration. These experiments were done because they had the unexpected finding that patients with paediatric influenza who were treated orally with oseltamivir for 5 days had significantly low levels (about 60% reduction on day five) of anti-influenza secretory-immunoglobulin A nasopharyngeal fluids compared with levels in patients who were not treated with oseltamivir. 134 Their findings are consistent with our findings that serum haemagglutinin inhibition antibody response was decreased by oseltamivir administration, although secretory immunoglobulin G antibody could not be analysed in our study because the data were not reported in the CSRs. 133,134 These findings are also consistent with the evidence on the mode of action of oseltamivir from animal models8,58,135 and from viral challenge, randomised, placebo-controlled studies in humans. 27
Pro-inflammatory cytokines, including interleukin 6, tumour necrosis factor alpha and interferon gamma, were completely suppressed by oseltamivir administered 28 hours after the experimental inoculation of influenza virus, whereas the reduction of viral titre in nasal lavages was partial. 27
There is decisive evidence that administration of oseltamivir in animals challenged by respiratory syncytial virus, which lacks a neuraminidase gene, showed a symptom-relieving effect (decreased weight loss) and inhibition of viral clearance. 136 These effects were accompanied by a decreased cluster of differentiation +8 T-cell surface sialoglycosphingolipid GM1 level, which is regulated by the endogenous sialidase/neuraminidase in response to viral challenge along with suppression of cytokine expression. 136 They are consistent with those findings from the pharmaceutical company and their investigators. The findings of the study by Moore et al. 136 suggest a risk of infection and exacerbation of infection by pathogens other than influenza virus despite the apparent reduction of symptoms from infection.
Sufficient plasma concentration of oseltamivir carboxylate from orally administered oseltamivir phosphate may act directly on the host endogenous neuraminidase to reduce (or suppress) the immune response even at the dose of 20 mg twice a day for 5 days. However, the bioavailability of inhaled zanamivir seems to be very broad: about 10–70%, as estimated by the area-under-the-curve data from the inhalation and intravenous study from the Japanese Summary Basis for Approval. The difference in peak concentration (Cmax) was much larger (sixfold to 37-fold). This means that inhaled zanamivir could reach a high enough concentration to reduce the immune response, if it is administered at a high dose or for a long period, or if the patient is very susceptible. In fact, a double-blind, placebo-controlled trial137 using healthy volunteers to investigate the effect of zanamivir treatment (20 mg/day for 14 days) on the humoral immune response to influenza vaccine showed that the zanamivir group responded with significantly lower antibody titres to the H1N1. Pro-inflammatory cytokines, including interleukin 6, tumour necrosis factor alpha, interferon gamma and other chemokines, were almost completely suppressed in the viral challenge RCT using a very high dose (600 mg) of intravenous zanamivir before inoculation of the influenza virus in human adults. 138
These findings all suggest that the low immune response, with a low level of pro-inflammatory cytokines, induced by the action of oseltamivir carboxylate, may reduce the symptoms of influenza irrespective of an inhibition of influenza virus replication, which is widely believed to be the main mode of action of NIs.
In addition, the potential hypothermic or antipyretic effect of oseltamivir (but not zanamivir) as a central nervous system depressant may also contribute to the apparent reduction of host symptoms. 139,140
Zanamivir had no effect on pneumonia symptoms in treatment trials, even when the diagnosis was supported by a chest radiograph, nor did it affect antibody responses, but it did affect bronchitis. We think that this shows a symptom-relieving effect of both drugs, which also applies to more severe, if undefined, syndromes. Both drugs relieve ILI symptoms by around 0.6–0.7% day’s reduction although this is first relief and not necessarily complete relief. In the case of oseltamivir, the mix-up with the follow-up cards does not allow us to draw any conclusions on a possible length of the duration of symptom relief. Also of note is the fact that this important information came to light from the FDA reports and not from the CSRs of the relevant trials. 8,58 This points to the incomplete nature of reporting in the CSRs and the important role of Summary Basis of Approval (SBA) regulatory information.
In a subgroup analysis we found no evidence of a difference in treatment effect for zanamivir on time to first alleviation of symptoms in adults in the influenza- and non-influenza-infected subgroups. Both subgroups showed strong evidence of treatment effect of 0.5–0.7% day’s reduction in time to first alleviation of symptoms. This strongly supports our hypothesis that these drugs do not have an influenza-specific effect.
Oseltamivir relieves symptoms in otherwise healthy children, but no effect was noted with zanamivir, which may be because of the limited power of the two eligible trials, with just over 700 children in total. However, oseltamivir does not have any effect on asthmatic children with ILI, a population that should benefit most from its use. One explanation for this finding is in the nature of the young asthmatic population, which is well cared for and used to regular powerful medications and close follow-up. The incremental benefit of oseltamivir is thus likely to be undetectable in such a population. An alternative explanation could be the higher susceptibility of the immune system to suppression by oseltamivir carboxylate in asthmatic children compared with those in the placebo group. The finding that oseltamivir administered to asthmatic children reduces symptoms faster than in placebo recipients at the beginning of the study, but during the off-treatment period more recovered later than those administered placebo, gives some support to this explanation.
There is no evidence of an effect of oseltamivir on hospitalisations. Hospitalisations are an important but poorly defined outcome in the oseltamivir protocols, inconsistently reported in the CSRs and overlooked in the zanamivir protocols and reports.
The oseltamivir trials did not detect any influenza-related deaths, reflecting the relatively benign nature of influenza in the study populations. The zanamivir trials detected eight deaths, of which only two were likely to be caused by influenza and both occurred in the intervention arms. All of the trials were likely to be underpowered to detect differential effects on mortality, but the absence of deaths in placebo recipients again underlines the benign nature of influenza. In fact, mortality in Japan during the 2009A/H1N1 influenza outbreak was 198 among about 20 million patients with influenza (1 in 100,000 infected). Early deterioration leading to death was observed more frequently in oseltamivir recipients than in zanamivir recipients or no antiviral recipients. 141
Overall, the two drugs have similar benefits but markedly different toxicity profiles. On average, for every 28 (95% CI 14 to 112) adults treated with oseltamivir there will be one more report of nausea and for every 22 (95% CI 14 to 42) adults and 19 (95% CI 10 to 57) children there will be one more report of vomiting. Oseltamivir seems to have an apparent protective effect on diarrhoea, contrary to the other evidence of gastrointestinal disturbance. This finding might be as an effect of a placebo containing dehydrocholic acid or it might be one of the results of the ILI symptom-relieving effects (similar to relief of tachycardia and palpitation). The other apparent gastrointestinal events, such as nausea and vomiting, may be the result of central nervous disorders indicated by ‘only day 1 increase of vomiting’ in treatment trials in children.
For every 62 (95% CI 41 to 411) adults exposed to zanamivir there will be one fewer case of nausea and vomiting, but no such effect was visible in children, probably because of a lack of power. Zanamivir does not appear to affect the frequency of bowel movements.
In the prophylaxis data set, ‘influenza without laboratory confirmation’ (i.e. ILI) was only partially reported in the oseltamivir CSRs and not reported in the zanamivir CSRs, except for one report,86 in which no significant reduction was observed (zanamivir 9% vs. placebo 10%). As a consequence we are unable to report on that outcome. The size of the reduction in influenza symptoms in oseltamivir prophylactic trials is inferior in magnitude to that seen in hand washing to prevent severe acute respiratory syndrome, based on seven case–control studies [odds ratio (OR) 0.77, 95% CI 0.70 to 0.84; I2 statistic = 68%; RD –0.12, –0.16 to 0.08; I2 statistic = 26%], the NNTB being approximately ‘50’ for prophylaxis with oseltamivir and ‘8’ with handwashing. 142
There is a significant reduction in the proportion of patients with symptomatic influenza with both NIs. However, these findings do not reflect the true efficacy for prevention of influenza because they conceal the positivity of laboratory testing (measured through tests of viral shedding and fourfold antibody titre rise).
We found an apparent prophylactic effect of zanamivir on pneumonia (which was not defined in CRFs) when it was used for 14–28 days. However, we found no evidence of significant effects on other complications and no evidence of an effect of oseltamivir on complications or hospitalisations.
Oseltamivir induced nausea in people who were undergoing prophylaxis but there was insufficient evidence to show an association with vomiting.
On-treatment renal adverse events were three times more common in the oseltamivir arms than in the placebo arms, with 150 treated patients leading to one additional event. The two participants who died in the oseltamivir arms both experienced acute renal failure while on-treatment, although only one of those events was listed as an adverse event. The unlisted event was in a 91-year-old female who was ‘withdrawn from the study on Study Day 15 because her estimated creatinine clearance was less than 30 ml/minute (WV15708, p. 44). 61 The screening laboratory examinations, that were carried out 10 days before the start of study treatment, were normal’. Hyperglycaemic adverse events (aggravated diabetes mellitus or hyperglycaemia) were also more common in the oseltamivir arms, with eight events in total (one in WV15673/WV15697,59 two in WV1570861 and five in WV1582568) compared with none in the corresponding placebo arms. These data are only presented descriptively, as they are too few (< 10) to meta-analyse formally, as prespecified in our analysis plan.
Finally, oseltamivir caused headaches and psychiatric harms in adult prophylaxis trials. Headaches are one of the most prominent harms of oseltamivir. There is evidence of a dose–response effect in prophylaxis trials (p = 0.013),59 in which headaches were observed in 202 of 519, 225 of 520 and 242 of 520 participants in the placebo, oseltamivir 75 mg once daily and twice daily arms, respectively.
In the psychiatric category, several rare and severe single events (nervousness, aggression, hallucinations, psychosis, suicide ideation and paranoia) were reported significantly more frequently in the intervention arm. Added to other more frequently reported but not significantly different events (such as depression and confusion), this gave a large effect and a relatively small NNTH of 94 (95% CI 36 to 1538). The importance of such a finding lies in the distribution of oseltamivir to large numbers of asymptomatic individuals following pandemic plans. There were no prophylaxis trials in children that met our inclusion criteria, therefore we cannot report on prophylaxis harms in this important population.
The question of why oseltamivir treatment trials failed to identify a clear association between oseltamivir and psychiatric harms, although a weak dose-dependent association was observed, is a moot point. It is possible that ILI and influenza symptoms masked the harms in those who were already symptomatic and therefore recruited in the treatment trials (and influenza-type symptoms were excluded as adverse events to be reported). The reporting issue of compliharms may have helped to mask such events. Alternatively, it could be that these events are rare in the populations studied and that there was insufficient power to detect an association. The CI was wide (0.43 to 2.03) and does not rule out a doubling in risk as a result of treatment, as was found in the prophylaxis trials. It is also possible that the risk of psychiatric harm increases with increasing dose (as the data from two trials8,58 suggest) and increasing duration of treatment (as the prophylaxis trials suggest).
Toovey et al. 143 assessed the issue and failed to find an association between neurological and psychiatric adverse events and oseltamivir exposure. The outcomes studied were not based on the a priori definition of psychiatric adverse events as defined in the CSRs. The definition was constructed post hoc, based on a selected group of adverse events taken from the psychiatric, neurological and injury body systems in the reports. The issues are described fully in another report144 and Toovey’s response. 145 Toovey et al. 143 reviewed only retrospective observational studies and did not review three prospective cohort studies conducted in Japan.
A meta-analysis of three prospective cohort studies of neuropsychiatric adverse events (NPAEs) in Japanese children show a pooled OR for abnormal behaviours due to oseltamivir exposure of 1.55 (95% CI 1.21 to 1.98; p = 0.0005) without significant heterogeneity. 146 In one prospective study147 of several thousand children with influenza, carried out to test the hypothesis of a causal relation between oseltamivir and neuropsychiatric events, abnormal behaviour was observed more frequently in oseltamivir recipient children than in control subjects (RR 1.57, 95% CI 1.34 to 1.83). Abnormal behaviour was observed in 3.4 per 100 person-days (or 13.8%) in the oseltamivir group compared with 2.2 per 100 person-days (or 8.8%) in the control group. Reanalysis of this study population, focusing on delirium and unconsciousness, also showed a significant association between oseltamivir and neuropsychiatric events, especially in the very early phase of the illness within a day of commencement of fever. 148 These indicate that prospective and intentional collection with this scale of participants may be necessary in treatment RCTs.
Animal toxicity study results firmly support the effect of oseltamivir on the central nervous system. One of these is the hypothermic effect of oseltamivir (but not zanamivir) administered orally, intraperitoneally139,140 and intracerebroventricularly. 140 The other is that intraduodenal or intravenous administration of oseltamivir to mature rats induced respiratory arrest shortly followed by cardiac arrest. These studies clearly show central depressant effects of oseltamivir. 149 Moreover, in the post-marketing toxicology phase studies by Roche, many symptoms that the manufacturer considered ‘item-related’ were observed: alterations in respiration including decreased respiratory rate/gasping and altered mucous membrane/skin colour (pale) prior to death. Although the manufacturer denied the causality,150 symptoms at 2 hours after administration that showed dose-related increase were lack of olfactory orientation, lack of cliff aversion and low/very low arousal. Twenty-four of 52 pups that did not exhibit cliff aversion were later found dead. Fourteen of 17 animals with low or very low arousal died thereafter. These findings are consistent with the clinically observed psychiatric symptoms in the RCTs and post-marketing spontaneous reports.
Zanamivir was well tolerated. However, a potentially active placebo may have masked the occurrence of bronchospasm in zanamivir trials.
Treatment trials were mostly under-recruited and often their results pooled post hoc in two, or even three, trials, and yet they showed very high influenza positivity rates. One possible explanation for this lies in the intensive surveillance carried out in the predefined trial centre areas and the restricted time span of recruitment during high likelihood of positivity periods. This may be why many centres with low levels of recruitment are listed in the CSRs; this limits the generalisability of the results to everyday life.
In a primary or secondary prophylaxis indication the postulated central effect of oseltamivir is confined to suppressing symptoms, as infection was not prevented even when oseltamivir was administered prior to the inoculation of influenza virus both in animals135 and in humans,27 and the prophylaxis trials. However, the central problem remains the incompatibility of the two contrasting claims of its activity against antibody production. If, as reported in many documents, oseltamivir does not interfere with antibody production (e.g. see FDA151 and Roche Investigators’ Guide152), how is it possible that oseltamivir prevents cases of influenza when part of the definition of prevented cases in oseltamivir trials was based on the absence of antibody response?
The apparent ability of oseltamivir to interfere with antibody response calls into question the mode of action of the drug and puts in doubt the proposed effects of oseltamivir. One possibility in treatment trials is that oseltamivir administration, by interfering with antibody production, has the effect of selecting the strongest antibody responders in the ITTI subpopulation. These individuals are classified as influenza cases and are included in the oseltamivir arm of the ITTI population. This selected subpopulation probably represents the healthiest or those least likely to experience complications. An alternative consequence could be that interference with antibody production in the oseltamivir arm led to active arm participants being more likely to develop complications as a result of impaired immune function.
Evidence from prophylaxis and secondary prophylaxis trials suggests that in addition to the apparent similar mode of action as in the treatment studies, suppression of viral shedding in nasal swabs may be of importance. In the former, participants who become positive (i.e. who are subsequently classified as cases of influenza) in the oseltamivir arms are the few who mount a strong response despite oseltamivir interference. The remainder (who are significantly more than in the placebo arm) are classified as prevented or avoided cases. However, as prophylaxis CSRs do not report antibody responses and viral isolate results for the ITT populations either, it is impossible to tell whether or not this proposed mode of action fits all of the evidence. The effect of oseltamivir on nasal shedding is consistent with the proposed mode of action of NIs in preventing the virus from leaving the host respiratory epithelial cells, which are covered by a mucous layer. Compared with the rather small reduction of symptoms of ILI and reduction in antibody rise (up to 10%) by both oseltamivir and zanamivir, the extent of the reduction of symptomatic influenza is almost half. This may be as a result of reduction of influenza viruses in the nasal swab sample.
In prophylaxis there is no evidence that oseltamivir reduces symptomatic ILI. Oseltamivir reduces the number of prophylaxis participants testing positive (based on antibody rise and/or culture test). However, this finding is weakened by oseltamivir’s interference with the viral replication on the swab and effect on antibody production. In addition oseltamivir does not affect asymptomatic influenza and there is no evidence that it interferes with person-to-person spread.
Similar to the FDA,109,153 because of the problems with the design of study WV1579965 we could not draw any conclusions on the ability of oseltamivir to interrupt viral transmission.
This is important as the results of the trial65 formed part of the WHO3 rationale for use of the drug to interrupt transmission from person to person, and allow time before the arrival of vaccines in the event of a pandemic furnishing a seemingly powerful rationale for stockpiling oseltamivir.
This shows the importance of availability of full CSRs, something the WHO did not have.
Antibody suppression seems stronger for oseltamivir than zanamivir, probably because of the difference in bioavailability. It may be that evidence of other effects, such as hyperglycaemia and renal impairment (though significance was marginal) in the prophylaxis trials may be due to inhibition of the host’s endogenous neuraminidase, which impairs the cell function of various organs. 15 Overall, the significance of oseltamivir for nasal shedding is unclear but problems with sampling and culture undermine any claims as to its secondary prophylactic properties, as the FDA made clear in its response. 109
The dose–response increase in psychiatric events in the ‘pivotal’ oseltamivir treatment trials and the increase in vomiting only on day 1 in treatment trials in children may be caused by the sudden onset of the central action of unchanged oseltamivir. 15 Brain concentration of unchanged oseltamivir increases during the early phase of influenza in juvenile animals150 as a result of a reduced or low function of p-glycoprotein, a major transporter of oseltamivir at the blood–brain barrier. 15,149 The likely centrally mediated mode of action of oseltamivir is supported by the finding of adverse events in healthy people in prophylaxis trials. However, these effects may also be derived from a delayed action that is associated with host endogenous neuraminidase inhibition by oseltamivir,15 because this appeared after more than 1 week’s exposure to the drug and lasted for > 2 weeks. Other effects, such as pain in the limbs, hyperglycaemia or diabetic events, reduction of antibody rise and reduction of cytokine induction, may also result from the suppression of the host’s endogenous neuraminidase by oseltamivir. 136 Pain in the limbs and metabolic control events (mainly hyperglycaemia) were in excess in the oseltamivir arms, but we did not carry out a formal meta-analysis, as they were not prespecified in our analysis plan and the number of events was < 10 for metabolic events.
Statements made about the capacity of oseltamivir to interrupt viral transmission and reduce complications are not supported by any data that we have been able to access.
We have not reviewed other NIs, such as laninamivir and peramivir, or other antivirals, such as the adamantanes (amantadine and rimantadine) or antipyretic/anti-inflammatory agents. Laninamivir and peramivir may be more potent as NIs because their bioavailability is far higher than zanamivir and may affect the host’s endogenous neuraminidase. Adamantanes are well known centrally active agents and may be more harmful than oseltamivir and zanamivir. Anti-inflammatory antipyretics (except paracetamol) may be more toxic than NIs. 15 Hence, the other NIs, adamantanes and anti-inflammatory antipyretics may not be alternatives to oseltamivir and zanamivir.
Overall completeness and applicability of evidence
We used the Cochrane seven-domain risk-of-bias instrument to assess bias. The availability of partial or complete CSRs decreased the uncertainty and allowed definitive judgements to be made. Previous unclear risk of bias became certainty of bias or certainty of absence of bias. Certainty or low levels of uncertainty are due to our expectations regarding the complete CSRs. We were expecting to have all relevant and consistent information available for our reviews, but, when it was not, our judgements changed because we found gaps in the availability of information and inconsistent information. We are still uncertain as to whether or not the complete study reports represent an exhaustive and coherent source of trial narrative and data.
In the case of treatment trials, conclusions and generalisations are drawn from a subpopulation in which the two arms do not appear comparable as a result of the apparent ability of oseltamivir to interfere with influenza antibody production. The effect of oseltamivir on the gastrointestinal tract appears to be notable, although a definitive statement will be possible only once the mode of action and dosage of dibasic calcium phosphate dihydrate and dehydrocholic acid have been clarified. The high percentage of influenza infections appears to be in contrast with the need to pool or delay several trials and the small recruitment size of others because of a lack of influenza circulation. In the case of PEP trials, the selection of the infected population has the effect of excluding from the analysis large percentages (in some cases > 50%) of participants. This brings the generalisability of the results of these trials into question.
Much has been made in the trial programmes of viral nasal voidance as a marker of effect. However, its measurement was unreliable in treatment trials, as this verbatim quote from the FDA review shows:FDA, p.14109
Duration of viral shedding was measured from treatment initiation to the time of the first negative virus culture with no subsequent positive cultures. Upon reviewing a list of viral shedding patterns provided by the applicant on 8/16/99, two problems emerged: (1) the pattern of virus shedding was fluctuating in at least 33 subjects (i.e. pos-neg-pos-neg, with or without a subsequent negative result). (2) In at least 100 subjects, the last virus shedding sample was the first negative sample in sequence, meaning there was not a subsequent negative confirmation. Given the fluctuating pattern of virus shedding, to estimate the duration of viral shedding based on the occurrence of a single first negative data poses a high level of uncertainty.
In all of the programmes, the effect on complications was based on unclear and potentially unreliable definitions, often at the discretion of local clinicians, and confirmation (e.g. radiological confirmation of pneumonia) was not consistently reported when it did occur. In the ITT population, the correct population for analysis, there is no credible effect of oseltamivir against pneumonia as the significance of the term ‘pneumonia’ is not clarified.
In the case of PEP trial,65 nasal voidance was measured only in symptomatic subjects, as an adjunct to the protocol version. However, this does not prevent the manufacturers from making claims of effect for all of these outcomes.
Other general requirements, such as presentation within 36–48 hours, raise questions about the generalisability of the research evidence. However, underlying all our doubts is the conflicting evidence on the mode of action of the drug.
Most of the trials were substantially under-recruited and so had insufficient power individually to answer the research question.
Quality of the evidence
We assessed all full CSRs of relevant trials. An example of the kind of detail available in complete CSRs and the importance of the trial timeline in assessing the presence of bias is the observation that of the CSRs for the included trials, only one contained a protocol that predated the beginning of participant enrolment, only two had SAPs that clearly predated participant enrolment and three had clearly dated protocol amendments. No oseltamivir CSR included a clear date of unblinding.
All reports in our review were sponsored by the manufacturers. It is known that published studies sponsored by the pharmaceutical industry are more likely to have outcomes favouring the sponsor than studies that have other sponsors. 154,155 As the evidence relates to published studies, we do not know whether or not the findings are applicable to CSRs.
Potential biases in the review process
The main limitation of our study is our relative inexperience in dealing with large quantities of information and our lack of familiarity with certain trial documents, such as randomisation lists. Randomisation lists appeared to be of two types. The first was a pre-randomisation list of random codes with which participants’ IDs cannot be matched with the participant IDs used within other sections of the CSR. The second was a post hoc randomisation list to which individual participants can be matched but the original generated codes are not shown. In both cases the truly random generation of the sequence could not be properly assessed because either the original codes are not provided or the original codes cannot be matched to patients.
We have created methods and procedures to address the risk of reporting bias that we identified in published trials, but remain uncertain about the success of these new methods.
Agreements and disagreements with other studies or reviews
Several reviews of NIs are now available,156–160 including several separate versions of our previous reviews. 30–32,35 All are mainly based on published information and reach similar conclusions to our 2006 review, which sparked the reader’s comment and subsequent investigation and change of methods.
Following publication of our review update in December 2009, Roche asked the Harvard-based academics Hernan and Lipsitch161 to repeat the Kaiser analysis4 to confirm or reject Kaiser’s conclusions. They were not provided with any funding to carry out this analysis and Roche ultimately provided them with patient-level data sets and module 1 for the 10 Kaiser trials and one more treatment trial. 69 An important methodological difference between Hernan and Lipsitch’s analysis161 and that of Kaiser4 was Hernan and Lipsitch’s decision to privilege a true ITT analysis over the subpopulation analysis featured in the Kaiser analysis. Our Cochrane review also analyses the ITT population.
The Kaiser analysis4 concluded that oseltamivir provided two statistically significant reductions: in lower respiratory tract complications and in hospitalisations.
Hernan and Lipsitch161 evaluated lower respiratory tract complications and found a statistically significant, but smaller, reduction in the risk of these complications.
Hernan and Lipsitch161 omitted evaluating the Kaiser paper’s conclusion that oseltamivir reduced the risk of hospitalisation. They wrote, ‘it was not possible to assess the potential benefit for high-risk participants who are hospitalised, because the sample size of most studies was too small to consider hospitalisation as an outcome’.
Hernan and Lipsitch161 do not elaborate on or highlight their apparent methodological disagreement with the Kaiser 2003 analysis4 and it is not reflected in the news article published on the Harvard website entitled ‘Oseltamivir effect on complications confirmed by reanalysis’ (http://ccdd.hsph.harvard.edu/NewsEvents/Oseltamivir-reanalysis). In fact, Hernan and Lipsitch161 did not confirm one of the key conclusions of the Kaiser paper. 4
Unfortunately, the Hernan–Lipsitch analysis161 has been cited by influential bodies, such as the European Centre for Disease Prevention and Control, as ‘confirmation of the original Kaiser meta-analysis’ (http://ecdc.europa.eu/en/activities/sciadvice/_layouts/forms/Review_DispForm.aspx?ID=561&List=a3216f4c%2Df040%2D4f51%2D9f77%2Da96046dbfd72) despite the fact that Hernan and Lipsitch161 did not confirm one of the key conclusions of the Kaiser paper. 4
For complications, although Hernan and Lipsitch161 clearly produced similar results to Kaiser,4 we do not think that this means that the result is more credible. In view of our findings, we suggest that these results should be interpreted with caution. We have published our preliminary comments. 162 The approach Hernan and Lipsitch161 took in analysing data was insufficient to provide a credible, independent check on validity, and reinforces the importance of detailed, critical assessment of entire trial programmes, with access to full-length study reports. Our analysis questions the coherence between the evidence and the proposed mode of action of oseltamivir.
The Ebell et al. 163 review concluded that there was ‘no evidence that oseltamivir reduces the likelihood of hospitalisation, pneumonia or the combined outcome of pneumonia, otitis media and sinusitis in the ITT population’. This conclusion was based on module 1 of the 10 Kaiser trials plus WV16277. 69 These are the same 11 trials included by Hernan and Lipsitch. 161
Conclusions
Main conclusions
These data show that oseltamivir and zanamivir cause small reductions in the time to alleviation of influenza symptoms in adults, but not in asthmatic children. The use of oseltamivir increases the risk of nausea, vomiting and psychiatric events in adults and vomiting in children and may reduce risk of diarrhoea and cardiac events in adults. Observational studies fail to show that oseltamivir has a protective effect on mortality among patients with 2009A/H1N1 influenza. Prophylaxis with either oseltamivir or zanamivir may reduce symptomatic influenza in individuals and in households but there was no reduction in all other influenza outcomes, including overall ILI reported as an adverse event on-treatment. In previous Cochrane reviews it is likely that evidence from published data was insufficient to fully assess risk of bias within the trials. Our results do not discount a potential benefit of using zanamivir and oseltamivir in individuals under particular situations, for example in immunocompromised or in compassionate cases, for which few other therapeutic options may exist. However, NIs themselves may be immunosuppressants.
The balance between benefits and harms should be considered when making decisions about use of NIs for either prophylaxis or treatment of influenza.
Implications for practice
These results show that both oseltamivir and zanamivir reduce the time to symptomatic improvement in adults (but not asthmatic children) with ILI. The size of this effect is small – approximately half a day. We have no data comparing oseltamivir or zanamivir with paracetamol and other antipyretics. We did not find convincing evidence that either oseltamivir or zanamivir reduces the risk of complications of influenza, particularly pneumonia, or reduce risk of hospitalisation or death. Even in individuals at higher risk of complications, such as children with asthma or the elderly, there was no evidence of a beneficial effect for reducing risks of complications.
The findings demonstrate a minimal effect on prevention of influenza by oseltamivir or zanamivir among individuals or families. This suggests little support for their use as prophylactic agents, for example during influenza epidemics. 164
Implications for research
The considerable body of evidence from RCTs included in this review indicates either no effect or a relatively small absolute effect size against the complications of influenza. Such an effect, even if statistically significant, would be too small to warrant treatment with NIs in a primary care setting, especially as effective diagnosis and treatments for rare complications (such as pneumonia) are available. Lack of evidence of an effect on hospitalisations probably indicates lack of severity in the first place. Assuming an influenza incidence rate of 2% (similar to that in the control arms of oseltamivir treatment trials) to detect a 25% clinically significant reduction in pneumonia, 21,500 participants would have to be enrolled in a clinical trial.
Our findings have implications for research on the mechanism of action of NIs, with special regard to any direct central action of oseltamivir and the inhibitory effect of the host endogenous neuraminidase of various organs and systems. We could not reach a consensus on whether or not further trials are warranted and whether or not current trials should be discontinued.
Published trials are unlikely to provide the level of detail to allow the results of a drug trial to be properly evaluated and risk presenting a partial and potentially biased report of trial conduct and findings. This has implications not only for the reporting of trials but also the weight that can be applied to published studies alone.
Our calculation is likely to underestimate population size, as the 2% incidence rate was derived from trials that used enhanced ad hoc surveillance systems. Any trial design would have to ensure that the presence of complications is ascertained using objective diagnostic criteria (e.g. with confirmation using imaging or laboratory testing for pneumonia). Such trials would also have to consider the ethical implications of conducting studies for which the estimate of benefit (based on 11 RCTs) in otherwise healthy people is likely to be small, and would have to be balanced against the apparent risks of adverse effects from NIs. We think research should be aimed at more effective preventative measures and early identification of complications.
The methods used to conduct our evidence synthesis need to be repeated across further interventions and by other researchers, and may need to be refined further. Given the considerable resources involved in using these methods, a system is needed to prioritise reviews of important drugs so that such methods are reserved for drugs that meet certain conditions. Priority could perhaps be given to first drugs of a new family, drugs considered to be innovative or those that are likely to have a big market impact. Such reviews should be publicly funded and be independent of both regulators and manufacturers. Researchers who conduct these ‘high-scrutiny’ reviews need to be free of recent ties to either government or the pharmaceutical industry. Systematic review groups such as The Cochrane Collaboration should consider adopting these methods for other drugs and whether, perhaps, to scrutinise the published reviews of prioritised drugs.
Implications for policy
These findings suggest that the current recommendations for oseltamivir as an essential medicine for the treatment of seriously ill patients or those in higher-risk groups with influenza 2009A/H1N1 need revision. 33,34 The small benefits in symptomatic improvement and the lack of evidence for an effect on serious complications need to be balanced with the adverse effects found with these drugs in meta-analyses, especially diabetic/hyperglycaemic, renal and neuropsychiatric effects in all of those people for whom the WHO recommends its use.
Policy-makers should be cautious in interpreting and using the findings of systematic reviews including only published studies, particularly those that comprise only a portion of an entire drug trial programme or which contain only a portion of the results of trials. The current findings suggest that numerous national and international bodies may have been based on inadequate or poor-quality information. 165 This could be obviated by ensuring that documentary evidence relating to a trial on humans (including CSRs, regulatory documents, evidence syntheses) should be archived electronically with no statute of limitations.
Several steps are required to provide patients, clinicians and policy-makers with the most transparent assessment of the relative benefits and risks of new drugs.
Based on the length of time it has taken to provide a definitive answer on the efficacy of the NIs, the challenges in obtaining the full information and the methods that we needed to develop to conduct the evidence synthesis, we believe the main implication of our review is the need for reform of multiple components of the research and development, regulatory and assessment pathway of new drugs.
Pharmaceutical sponsors of drug trials should follow a data access and sharing procedure which is similar to that of the EMA, and sponsors should make all full CSRs available to be downloaded from their websites and shared freely once a regulatory decision has been made. Redactions should be kept to the minimum. Part of this process needs to include a full list of the entire drug development programme to avoid assessment of an incomplete set of trials. Researchers and industry employees who are listed in trial documents should be considered to have legal responsibility for the conduct and reporting of a trial.
Regulators should post an inventory of their documentary holdings on their websites with a brief description of the main content and size of each file. They should make all information available shortly after making a registration decision on a drug and within a reasonable time period. The information should be in electronic format and anonymised (i.e. participants’ details should be removed to prevent each person being identified but no further).
Trial registries have improved the reporting of new trials. However, on their own they will not be adequate to resolve the problems we encountered. The completeness of trial registries needs to be tested with a random sampling procedure. Clear instructions for the reporting and updating of their content should be promulgated and penalties imposed on breaches of these procedures. Trial registration should include the original and final versions of a trial protocol, with a full declaration of dated amendments. Procedures for trial unblinding and dates of unblinding should be routinely reported. Registration should be made compulsory for all studies in which human beings are randomly assigned to experimental arms. Ethical and consent procedures for all trials should include obligations of the trial sponsor to ensure that results are made public. Failure to report the existence of a trial on humans and to make results available should be considered as an ethical breach of conduct and be subject to appropriate penalties.
Authors’ note: In reviewing over 2 GB of data there is the possibility of mistakes. The authors would be grateful if readers could identify these. We promise that, if we concur, the record will be amended accordingly.
Chapter 3 Effect of oseltamivir on mortality in patients with 2009A/H1N1 influenza: a systematic review and individual patient data meta-analysis of observational studies
Abstract
Objectives
To determine the effect of oseltamivir on mortality in 2009A/H1N1 influenza patients.
Design
Systematic review of observational studies.
Data sources
Summary and individual patient data (IPD) from published observational studies.
Eligibility criteria for selecting studies
Any study of 2009A/H1N1 influenza patients reporting mortality outcomes and exposure to oseltamivir with at least 5% of patients untreated with influenza antivirals and five or more deaths overall.
Main outcome measures
Mortality.
Results
A total of 1117 studies were identified and screened, with 154 full-text articles assessed for eligibility. Of these, 30 observational studies of hospitalised patients were eligible and a total of 11,013 patients were available for qualitative synthesis. Overall there were 1301 deaths (12%) with the percentage of deaths receiving oseltamivir similar to that of survivors (83% vs. 82%). We found evidence of time-dependent bias in the summary data and the IPD. The IPD came from four studies including 3071 patients and 242 (8%) deaths. After taking account of time-dependent bias, potential confounding variables, and the competing risk of hospital discharge, analysis of the IPD showed insufficient evidence that oseltamivir reduced the risk of mortality [hazard ratio (HR) 1.03, 95% CI 0.64 to 1.65].
Conclusions
We found insufficient evidence from 30 observational studies to support oseltamivir having a protective effect on 2009A/H1N1 influenza patients for mortality. However, the included studies were observational and IPD analysis was based on only four studies without adjustment for baseline severity of illness or other drug use hence the findings should be interpreted with caution. Observational studies with time-dependent treatment exposure appear to be at a high risk of time-dependent bias unless an appropriate analysis is conducted.
Introduction
Influenza is a seasonal, mostly mild and self-limiting infection of the upper airways. Occasionally, patients with influenza develop complications, including pneumonia, encephalopathy and multiorgan failure, often requiring hospitalisation and, in a small number of cases, patients die. Influenza is mainly caused by influenza A and B viruses and the predominant subtype of viruses changes from season to season. A novel strain of influenza 2009A/H1N1 was the predominant cause of influenza infections worldwide resulting in the WHO declaring a pandemic in April 2009.
Oral oseltamivir is an antiviral and a NI. It has been used primarily in Japan and the USA prior to 2009. However, its use increased dramatically in the A/H1N1 pandemic when oseltamivir became a widespread public health intervention. 166
Mortality is a generally rare, but important, outcome of influenza and RCTs have not been powered to address this outcome. To our knowledge, there have been five deaths in comparative Phase II/III RCTs of oseltamivir;167,168 however, none of the deaths was in a patient with confirmed influenza. Reviews of observational studies of influenza 2009A/H1N1 have shown protective effects of NIs on mortality169–173 and oseltamivir is now listed as an essential medicine,174 although there is insufficient evidence based on randomised studies to show that oseltamivir reduces complications of influenza106 and case series have suggested increased mortality. 15,141
The objective of this systematic review was to determine the effect of oseltamivir treatment on mortality in patients with 2009A/H1N1 influenza. We focused on 2009A/H1N1 influenza specifically because WHO and others have suggested that studies of antivirals for seasonal influenza may not be relevant to the current novel form of circulating influenza,46,47 and current antiviral treatment policies have been largely influenced by the results of observational studies of 2009A/H1N1 influenza.
Methods
Ethics approval was not required for this research because it is a systematic review of published studies. Any study comparing oseltamivir with no treatment in patients with confirmed 2009A/H1N1 influenza and reporting mortality outcomes was eligible for inclusion. The definitions for mortality and treatment exposure were as used in the individual studies. We did not include studies where < 5% of patients or < 10 patients were untreated and studies in which fewer than five patients in total died. If there were multiple publications of the same or overlapping cohorts of patients we included the largest cohort in our review. Studies reported in languages other than English were potentially eligible for inclusion but only if data were clearly reported by mortality and treatment status. Studies that were reported in abstracts but not published in full were not eligible for inclusion. We searched MEDLINE, EMBASE, Cumulative Index to Nursing and Allied Health Literature, Web of Science and Latin American and Caribbean Health Sciences Literature databases (see Appendix 12 for details of our search strategy). We also hand-searched bibliographies from two relevant documents published by WHO169,175 and two previous reviews. 171,172
Three reviewers separately assessed the studies identified during the search and applied inclusion criteria. Any disagreements were resolved by discussion. Data from included studies were extracted and checked by a second reviewer. Variables included in the extraction were citation; study design; study setting (country, city, institution); study population (sex, age groups, types of patients, severity of disease); time period of study; how and if influenza was confirmed; number of patients (by survival status and antiviral treatment received); and timing of hospital admission and treatment from onset of symptoms.
To address the limitations of using summary information from observational studies for meta-analysis, we requested IPD from the corresponding authors of all of the included studies and kept a record of all of the correspondence that ensued (see Appendix 13 for a template of the letters that we sent to the corresponding authors).
Our primary analysis was to compare use or non-use of oseltamivir as a binary exposure between patients with fatal and non-fatal outcome. We planned to use Cochran’s Q chi-squared statistic to test for statistical heterogeneity and the I2 statistic to estimate heterogeneity and perform a random-effects meta-analysis of the primary outcome using the method of DerSimonian and Laird. 107 For studies with no events in one of the treatment groups we added a continuity correction of one event to all four cells of the study to enable estimation of ORs. Small study effects were intended to be formally assessed using the method of Harbord et al. 176 and investigated using a funnel plot. In fact we used the method of Rucker et al. 177 to test for small studies effect as a result of their method of moments test being the only one we could find that is appropriate when heterogeneity is substantial (τ2 > 0.1]. The Meta-analysis of Observational Studies in Epidemiology guidelines were followed in the reporting of this systematic review. 178 A protocol outlining our proposed study is available from: www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42012002245.
In the subgroup of studies for which we obtained IPD we planned to investigate the time-dependent effect of oseltamivir on mortality (by fitting treatment as a time-dependent exposure in a Cox regression model), adjust for potential confounding variables and identify predictors of treatment using logistic regression. A detailed example of the methodology we used for fitting a time-dependent variable in SAS version 9.4 (SAS Institute Inc., Cary, NC, USA) is provided in the following web link: http://support.sas.com/documentation/cdl/en/statug/63347/HTML/default/viewer.htm#statug_phreg_sect049.htm. Analysis 1 is appropriate for our study because we had one time-dependent exposure variable and a number of baseline covariates. Potential confounding variables that were investigated included patient comorbidities (respiratory, cancer, obesity, heart disease, infection, immunosuppression, diabetes, neurological), age and time from onset of symptoms to hospital presentation. After taking account of time-dependent bias (using proper hazard-based analyses for which oseltamivir is included as a time-dependent exposure) and missing data (using multiple imputation and adjusting for potential confounding variables), we planned to report the overall estimate of treatment effect of oseltamivir on mortality, as well as the treatment effect by the timing of treatment categorised into early (≤ 2 days from onset of symptoms) or late (> 2 days from onset of symptoms). Survival analyses were stratified by study, and logistic models were adjusted for study. Multivariable analysis was conducted when all potential confounders were included in the models. Multiple imputation was implemented in a sensitivity analysis to assess the potential influence of missing data using proc mi and proc mianalyze commands in SAS. We specified multivariate imputation by a fully conditional specification method using regression models that we developed for predicting the missing data and created 20 imputed data sets. Covariates included in the regression models were mortality status, age, study, treatment group, time from onset to presentation and comorbidities (as detailed above).
On the basis of a recommendation by Wolkewitz and Schumacher,179 we conducted competing risks survival analysis on the IPD, for which the competing risks were death and hospital discharge. Wolkewitz and Schumacher179 suggest that a fundamental assumption in survival analysis is that the death hazard remains the same after censoring. This may be violated because discharged patients are usually in a better health condition than patients who remain in hospital. Hence, discharge from hospital should be directly modelled and treated as a competing event for dying in hospital. We performed competing risks analysis using the method of Fine and Gray180 on the three cohorts that provided data on hospital discharge, with adjustment for all potential confounders but no imputation for missing data. Oseltamivir treatment was fitted as a time-dependent exposure because time-dependent bias may also occur for hospital discharge because, for example, patients who recover quickly may not get the opportunity for antiviral treatment.
Results
On the basis of searches conducted on 15–18 February 2013, we identified 1107 potential studies for inclusion. We identified a further 10 studies through hand-searching. After assessing the abstracts of these studies, we agreed that 154 full manuscripts were required for further assessment. Of these 154 full manuscripts, 124 were excluded for the reasons given in Figure 16 and references are provided in Appendix 14. We initially excluded 18 studies because they did not present a breakdown of numbers of patients dying as a result of oseltamivir exposure. We wrote to the corresponding authors of these studies requesting this additional summary data and received replies from 12, of which six provided data that we were able to use. In total, 30 studies181–210 are included in the qualitative synthesis (Table 16 and see Figure 16).
FIGURE 16.
Flow diagram showing process for inclusion and analysis of observational studies examining the effect of oseltamivir on mortality in patients with 2009A/H1N1 influenza.
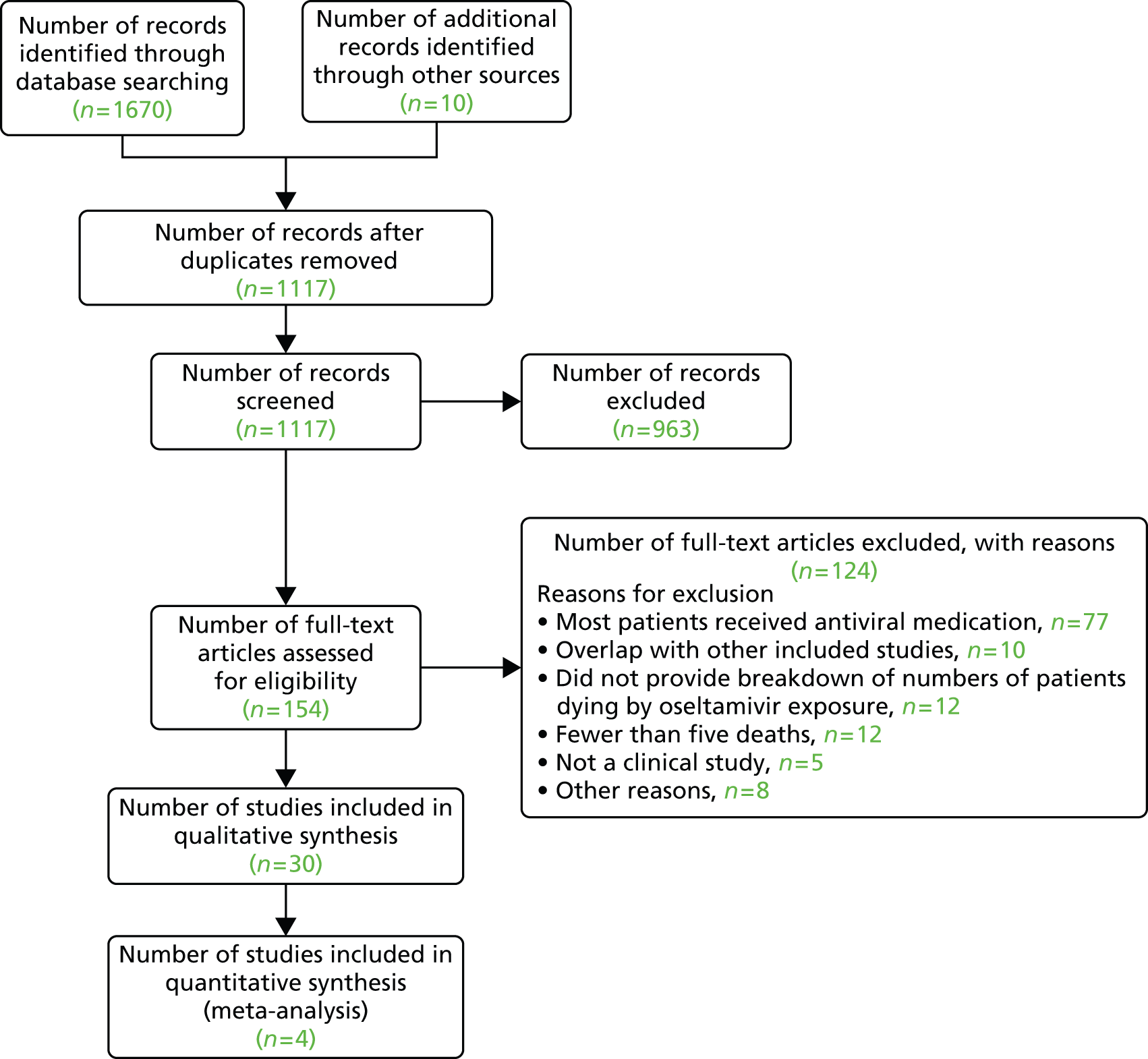
| Study | Setting and population | Time period | Definition for death | Description of treatment exposure | Drug use before admission |
|---|---|---|---|---|---|
| Siston et al.183 | USA, pregnant women | April to December 2009 | Maternal influenza deaths | Antiviral (492/496 received oseltamivir) | Not reported |
| Louie et al.181 | California, all ages, critically ill | 3 April 2009 to 10 August 2010 | Died from pandemic H1N1 infection | One dose of antiviral (1671/1675 received oseltamivir)a | Not reported |
| Jain et al.189 | USA, all ages, hospitalised | April to June 2009 | Not reported | Antiviral (188/200 received oseltamivir) | Antiviral, antibiotic |
| Farias et al.190 | Argentina, children, critical | 15 June to 31 July 2009 | Mortality at 28 days | Oseltamivir | Not reported |
| Yang et al.191 | Beijing, all ages, hospitalised | Up to 31 December 2009 | Cause of death 2009 H1N1 influenza | NI | Not reported |
| Altmann et al.185 | Germany, children, critically ill | August 2009 to 30 April 2010 | Not reported | Oseltamivir | Not reported |
| Enstone et al.192 | UK, all ages, hospitalised | 11 May 2009 to 31 January 2010 | Deaths attributed to pandemic (H1N1) 2009 | Received antiviral as inpatients | Patients infected in hospital |
| Dominguez-Cherit et al.184 | Mexico, all ages, critically ill | 24 March to 1 June 2009 | ICU and hospital mortality at 14, 28, 60 days | NI (44/45 received oseltamivir) | Not reported |
| Kumar et al.187 | Canada, adults, critically ill | 16 April to 12 August 2009 | 28- and 90-day mortality | Oseltamivir | Not reported |
| Nguyen-Van-Tam et al.186 | UK, all ages, hospitalised | 27 April to 30 September 2009b | In-hospital death | Oseltamivir | Antiviral |
| Chitnis et al.193 | Wisconsin, USA, all ages, hospitalised | 23 April 23 to 15 August 2009 | Not reported | Antiviral (99% got oseltamivir) | Not reported |
| ANZIC194 | Australasia, pregnant women, intensive care | 1 June to 31 August 2009 | Maternal death | Oseltamivir | Not reported |
| Yung et al.195 | Australasia | From 1 June to 31 August 2009 | In-hospital death | Oseltamivir | Not reported |
| Javadi et al.196 | Iran, all ages, hospitalised | September 2009 to February 2010 | Not reported | Oseltamivir | Not reported |
| Miranda-Choque et al.197 | Peru, children, hospitalised | June to September 2009 | Death related to pandemic influenza | Oseltamivir | Antibiotics |
| Poeppl et al.198 | Austria, all ages, hospitalised | 20 September 2009 to 2 February 2010 | In-hospital death | Oseltamivir | Not reported |
| Riquelme et al.199 | International, all ages, hospitalised | April to October 2009 | In-hospital all-cause mortality | Oseltamivir | Not reported |
| Yokota et al.200 | Brazil, all ages, hospitalised | July 2009 | Death caused by pandemic (H1N1) 2009 | Oseltamivir | Oseltamivir |
| Thompson et al.188 | USA, all ages, hospitalised | 14 September 2009 to 13 January 2010 | Influenza-related in-hospital death | Neuraminidase antiviral | Not reported |
| Bagdure et al.201 | Colorado, USA, children, hospitalised | 1 May to 30 November 2009 | Death in hospital or emergency room | Oseltamivir | Not reported |
| Blumental et al.202 | Belgium, children > 2 years, hospitalisedc | 1 July 2009 to 31 January 2010 | Not reported but all were due to influenza | Oseltamivir | Not reported |
| Chemaly et al.203 | International, hospitalised cancer patients | During the 2009–10 H1N1 pandemic | Death within 60 days of onset of symptoms | Oseltamivir | Not reported |
| Çiftçi et al.204 | Turkey, children, hospitalised | 17 July 2009 to 10 February 2010 | Not reported but causes described | Oseltamivir | Not reported |
| del Rosal et al.205 | Spain, children, hospitalised | 1 May to 30 November 2009 | Not reported but causes described | Oseltamivir | Not reported |
| Kusznierz et al.206 | Argentina, all ages, hospitalised | May to December 2009 | Not reported | Oseltamivir | Not reported |
| Mickienė et al.207 | Lithuania, adults, hospitalised | 1 November 2009 to 15 March 2010 | Not reported | Antiviral (all received oseltamivir) | Not reported |
| Moretti et al.208 | Brazil, all ages, hospitalised | 28 April to 31 December 2009 | Not reported | Oseltamivir | Not reported |
| Brink et al.209 | Sweden, all ages, critically ill | August 2009 to February 2010 | Mortality at 28 and 90 days after admission | Oseltamivir | Oseltamivir, antibiotics |
| Rahamat-Langendoen et al.210 | Netherlands, all ages, hospitalised | June 2009 to July 2010 | Not reported | Oseltamivir | Not reported |
| Yang et al.182 | China, children, hospitalised with pneumoniad | 1 September to 31 December 2009 | In-hospital and 60-day mortality | 1-day oseltamivira | Not reported |
Quality of the included studies
We included observational studies that reported on series of cases with laboratory-confirmed 2009A/H1N1 influenza. There were no randomised or prospective cohort studies or case–control studies comparing death or severe cases with matched uncomplicated patients despite the call for this type of study. 211,212 Table 16 shows information on the design characteristics of the included studies and Table 17 provides details on outcomes and analysis methods used. The proportion of patients treated in the studies ranged from 35% to 94%, with a median of 82%.
| Study | Time from symptom onset to admissiona | Time from symptom onset to treatmenta | Time from admission to treatmenta | Oseltamivir exposure for deaths, n/N (%) | Oseltamivir exposure for survivors, n/N (%) | Not included because of missing data | Statistical analysis method used |
|---|---|---|---|---|---|---|---|
| Siston et al.183 | Not reported | 2 (–2 to 21)b | Not reported | 25/30 (83) | 471/545 (86) | 200 patients | Mantel–Haenszel test, Fisher’s exact test |
| Louie et al.181 | 3 (0–42) | 4 (0–52) | Not reported | 416/492 (85) | 1260/1367 (92) | 91 patients | Chi-squared test, Fisher’s exact test, Cochran–Armitage test |
| Jain et al.189 | 3 (0–18) | 3 (0–29) | 46% after admission | 17/19 (89) | 183/249 (73) | 4 patients | Multivariate logistic regression |
| Farias et al.190 | Not reported | Not reported | 86% within 24 hours | 52/57(91) | 83/90 (92) | 0 patients | Multivariate logistic regression |
| Yang et al.191 | 30% after 48 hours | 71% not within 48 hours | Not reported | 54/69 (78) | 355/436 (81) | 112 patients | Multivariate logistic regression |
| Altmann et al.185 | 2 (IQR 1–5) | 4 (IQR 1–7) | Not reported | 7/10 (70) | 44/74 (59) | 9 patients | Logistic regression |
| Enstone et al.192 | Not applicable | Range 0–8 | Not applicable | 5/6 (83) | 15/20 (75) | 4 patients | No statistical analysis performed |
| Dominguez-Cherit et al.184 | 6 (IQR 4–8) | Not reported | Not reported | 14/18 (78) | 31/34 (91) | 6 patients | Multiple logistic regression, Kaplan–Meier |
| Kumar et al.187 | 4 (IQR 2–7) | Not reported | Not reported | 105/117 (90) | 435/461 (94) | 23 patients | No analysis by treatment performed |
| Nguyen-Van-Tam et al.186 | 2 (0–33) | Not reported | Not reported | 60/80 (75) | 1023/1440 (71) | 0 patients | Multivariable logistic regression |
| Chitnis et al.193 | 50% < 48 hours | 38% within 48 hours | 77% within 24 hours | 9/11 (82) | 206/239 (86) | 2 patients | Chi-squared test, Fisher’s exact test, Mantel–Haenszel test |
| ANZIC194 | 6 (0–35) | 6 (0–37) | Not reported | 7/7 (100) | 45/57 (79) | 0 patients | Descriptive analysis |
| Yung et al.195 | 5 (IQR 2–8) | Not reported | Not reported | 5/6 (83) | 58/72 (81) | 5 patients | Multivariable logistic regression |
| Javadi et al.196 | Mean (range) 5 (1–15) | Not reported | Not reported | 34/36 (94) | 166/180 (92) | 0 patients | Multivariable logistic regression |
| Miranda-Choque et al.197 | 5 (1–10) | Time of treatment unknown | Time of treatment unknown | 11/12 (92) | 50/62 (81) | 0 patients | Multivariable logistic regression |
| Poeppl et al.198 | Not reported | Not available | Not reported | 9/14 (64) | 232/327 (71) | 2 patients | Multivariable logistic regression |
| Riquelme et al.199 | Not reported | Not reported | Not reported | 40/41 (98) | 193/206 (93) | 0 patients | Chi-squared test, Fisher’s exact test, bivariate analysis |
| Yokota et al.200 | 5 (0–15) | Deaths 6 (1–16); survivors 5 (0–19) | Not reported | 25/52 (48) | 64/105 (61) | 0 patients | Multivariate unconditional logistic regression |
| Thompson et al.188 | Mean 2.1 days (95% CI 2.0 to 2.3 days) | Mean 3.2 days (95% CI 3.0 to 3.5 days) | Mean 1.3 days (95% CI 1.2 to 1.5 days) | 23/32 (72) | 646/869 (74) | 25 patients | Multivariable Poisson regression |
| Bagdure et al.201 | 3 (IQR 1–5) | 2 (IQR 1–4) | 0 (IQR 0–1) | 7/8 (88) | 262/299 (88) | 0 patients | Multiple logistic regression |
| Blumental et al.202 | 2 (IQR 1–4) | Not reported | 79% started on admission | 4/5 (80) | 36/110 (33) | 0 patients | Chi-squared test, Fisher’s exact test |
| Chemaly et al.203 | 2 (0–21) | 2 (0–24) | Not reported | 11/11 (100) | 89/104 (86) | 0 patients | Survival analysis |
| Çiftçi et al.204 | Not reported | Median 24 hours (range 3–240 hours) | Not reported | 33/35 (91) | 718/786 (91) | 0 patients | Chi-squared test, Fisher’s exact test |
| del Rosal et al.205 | 3 (IQR 1–5) | Not reported | Not reported | 4/5 (80) | 385/512 (75) | 0 patients | Multiple logistic regression |
| Kusznierz et al.206 | Not reported | Mean (range) 3 (0–30) | Not reported | 70/81 (86) | 157/161 (97) | 0 patients | Mantel–Haenszel test, chi-squared test, bivariate analysis |
| Mickienė et al.207 | 2 (0–7) | 3 (0–10) | Not reported | 6/6 (100) | 63/115 (55) | 4 patients | Multivariate logistic regression |
| Moretti et al.208 | Mean 2.3 days | Mean 4 days | Not reported | 7/10 (70) | 59/129 (46) | 0 patients | Chi-squared test, Fisher’s exact test |
| Brink et al.209 | 6 (IQR 3–7) | Not reported | Not reported | 11/14 (79) | 100/108 (93) | 14 patients | Relative risk for death, Kaplan–Meier curves |
| Rahamat-Langendoen et al.210 | 2 (IQR 1–4) | Not reported | Not reported | 7/7 (100) | 58/78 (74) | 0 patients | Multinomial logistic regression |
| Yang et al.182 | Not reported | 13% within 48 hours, 39% within 5 days | Not reported | 7/10 (70) | 485/531 (91) | 0 patients | Survival analysis |
Although all 30 studies classified patients by treatment exposure, only two defined it: one as ‘at least one dose of oseltamivir’181 and the other as ‘at least one day of treatment’182 [although it was unclear how they classified patients who received one dose only; there were 26 such patients excluded from the study [Iratxe Puebla, PLOS ONE journal editor, 7 August 2012, personal e-mail communication)]. It is unknown how many other studies failed to report excluded patients but we note that a number of studies had missing information on mortality status and/or treatment status (for 200 patients in one study,183 for which missing data were more common in patients with less-severe disease), whereas other studies reported complete information. None of the included studies reported over-the-counter medication use prior to hospital presentation. This may be important as, for example, NSAIDs have been shown to increase mortality in influenza-infected animals. 213
Although a number of the included studies conducted analyses adjusting for potential confounding variables, such as patient comorbidities, they used logistic regression or standard survival analysis, which may not be appropriate for observational studies in which treatment exposure is time dependent. This type of analysis misallocates the time from initiation of the study (e.g. hospital admission) to start of antiviral treatment and leads to time-dependent bias. Beyersmann et al. 214 provide mathematical proof that analyses which ignore the time-dependent nature of an exposure variable lead to biased estimates of treatment effect in favour of treatment. Time-dependent bias is also referred to as immortal time bias,215 survivor treatment selection bias216 and survival bias. 217 It causes selection bias because patients who die early do not get an opportunity to receive treatment. In addition, patients who are extremely sick may not be given the opportunity to receive treatment because other more critical procedures take priority. Only two of the included studies182,184 attempted to take account of time-dependent bias but they appeared to have used flawed approaches. One study excluded all deaths within 3 days of onset of symptoms and the other obtained results that appear incorrect because their analysis – taking into account time-dependent bias – increased the treatment effect in favour of oseltamivir. Only six studies reported data on time from hospital admission to treatment initiation (see Table 17). Beyersmann et al. 214 suggest that time-dependent bias can be avoided by proper hazard-based analyses. See Appendix 15 for a detailed description and example of time-dependent bias.
Analysis of summary data from included studies
Table 17 shows a summary of the numbers and percentages of patients with oseltamivir exposure by survival status for each of the 30 included studies. In total there are 11,013 patients included and 1301 deaths (12%). Overall, the percentage receiving oseltamivir among deceased patients (1085/1301 = 83%) was similar to the percentage receiving oseltamivir among survivors (7918/9712 = 82%). Meta-analysis of the included studies showed moderate heterogeneity [I2 = 44%, χ2 = 51.93, degrees of freedom (df) = 29, p = 0.006, τ2 = 0.217] and no evidence of small study effects (p = 0.25). Figure 17 shows a funnel plot of the 30 included studies.
FIGURE 17.
Funnel plot of the 30 included studies. Please note that the pseudo 95% confidence limits are shown by the dotted lines. The funnel shape, bounded by the confidence limits, represents the expected distribution of studies where, assuming no heterogeneity, 95% of the treatment effect estimates should lie.
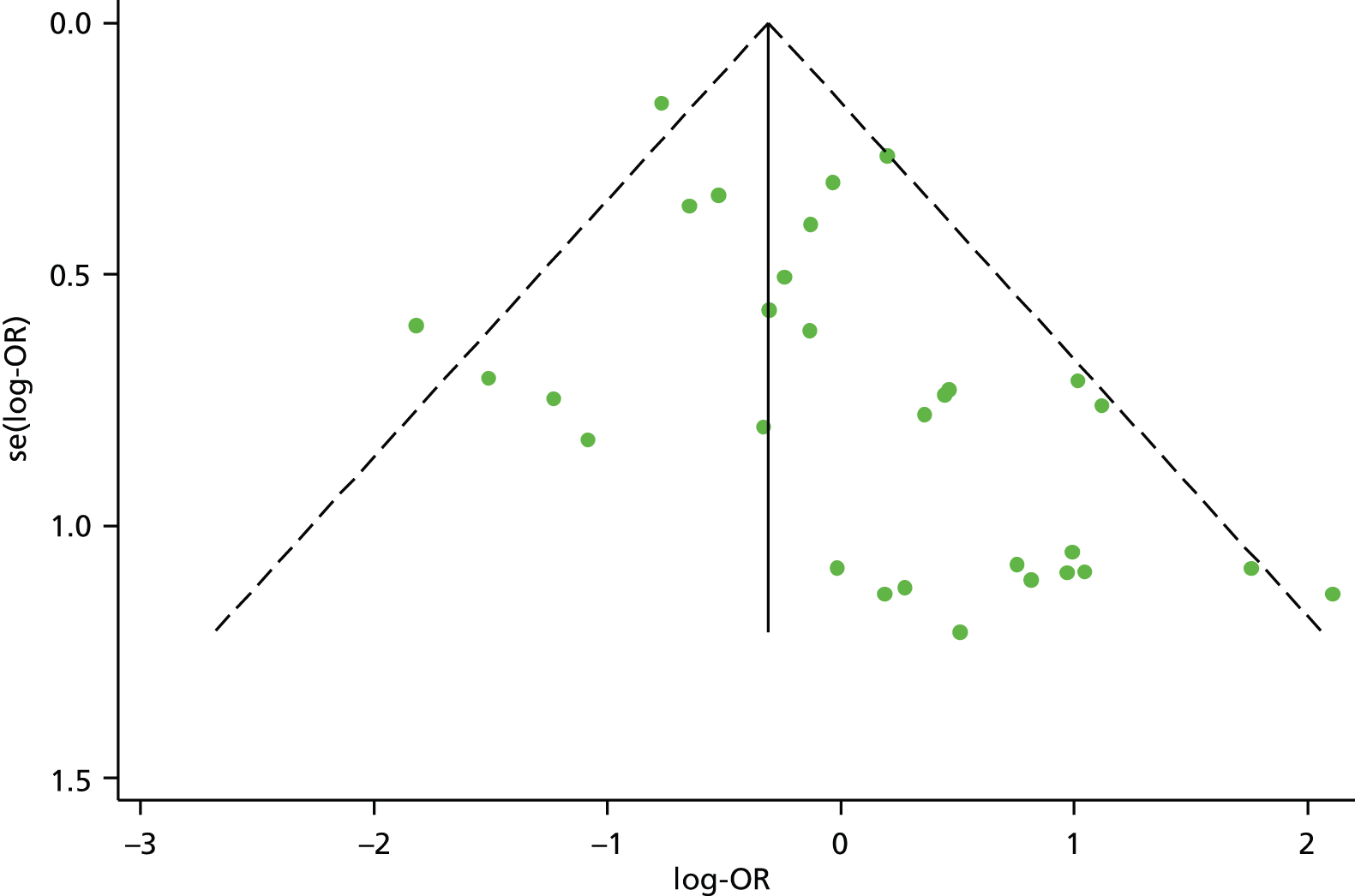
To investigate heterogeneity we conducted a random-effects metaregression using the metareg command in Stata/IC. Factors investigated included age group (adults vs. children), severity of illness (critically ill vs. hospitalised), log-odds of death (another measure of severity of illness) and log-odds of treatment. This last factor was included to investigate the potential effect of time-dependent bias on treatment effects. If time-dependent bias is apparent then we would expect it to have a greater influence in cohorts that had higher odds of treatment. This is because if few patients were untreated then patients dying before initiation of treatment would tend to have a large influence on the odds of patients dying in the untreated group. Results showed no effect of age group (p = 0.40) or severity of illness (p = 0.38), but evidence of an effect of log-odds of death (p = 0.024) when, as odds of death increases, the treatment effect in favour of oseltamivir increases, and log-odds of treatment (p = 0.003), when, as odds of treatment increases, the treatment effect in favour of oseltamivir increases. These effects appear to be independent as p-values in multivariable analysis are 0.031 and 0.006, respectively.
To illustrate these effects we conducted subgroup analysis by odds of treatment: ‘< 5’ compared with ‘≥ 5’ and percentage of death: ‘< 10%’ compared with ‘≥ 10%’. An odds of treatment of ‘≥ 5’ equates to a percentage of ≥ 83.3%. Results show treatment effect is in favour of oseltamivir and more heterogeneous in cohorts when odds of treatment were ‘≥ 5’. Conversely, in cohorts for which odds were ‘< 5’, heterogeneity is smaller and overall effect is in favour of no treatment (Figure 18). Similarly, treatment effect is in favour of oseltamivir and more heterogeneous in cohorts in which percentage of death was ≥ 10%; conversely, in cohorts in which the percentage is < 10%, heterogeneity is smaller and overall effect is in favour of no treatment (Figure 19).
FIGURE 18.
Meta-analysis of included studies by odds of treatment with oseltamivir.
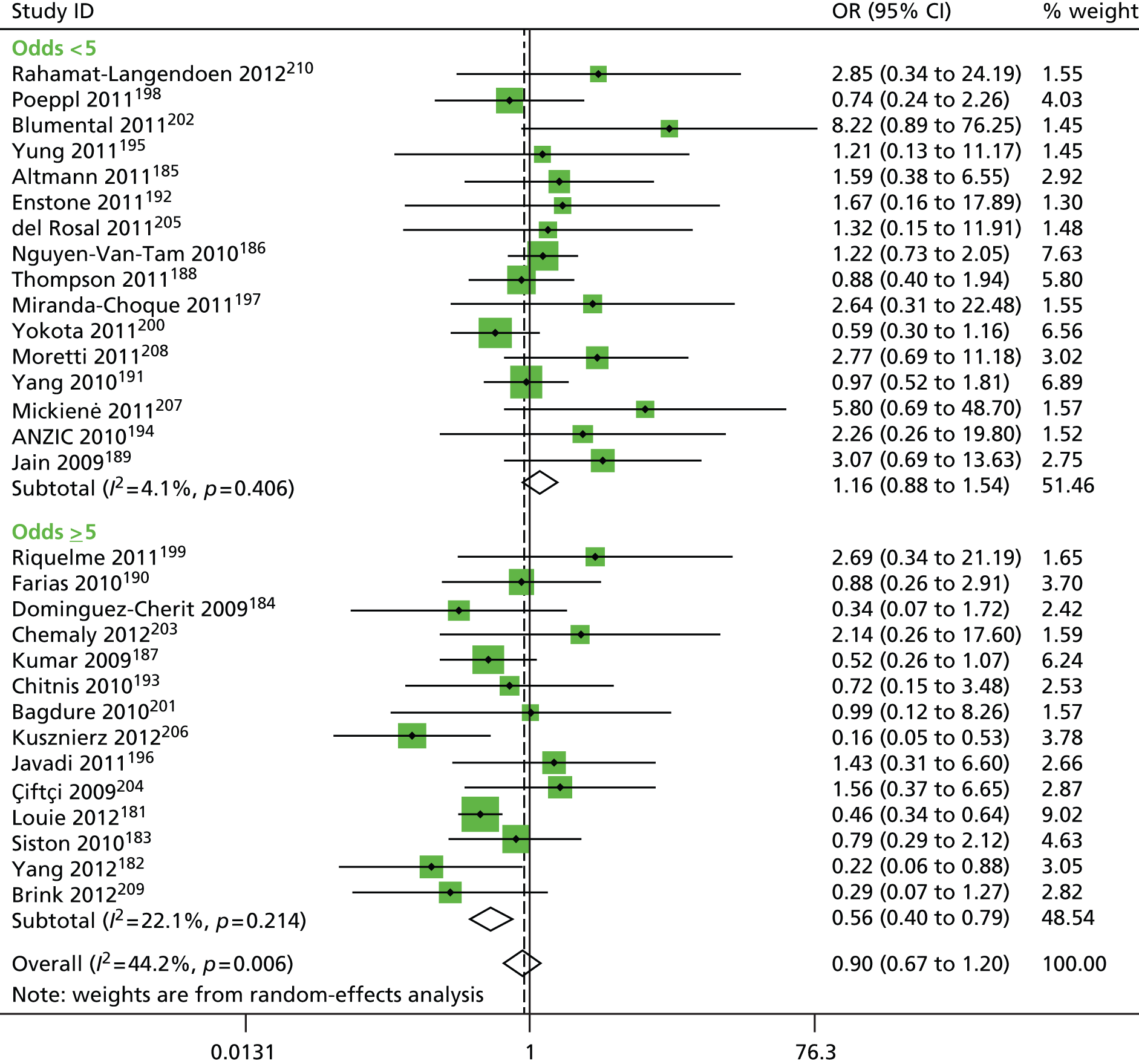
FIGURE 19.
Meta-analysis of included studies by proportion of death.
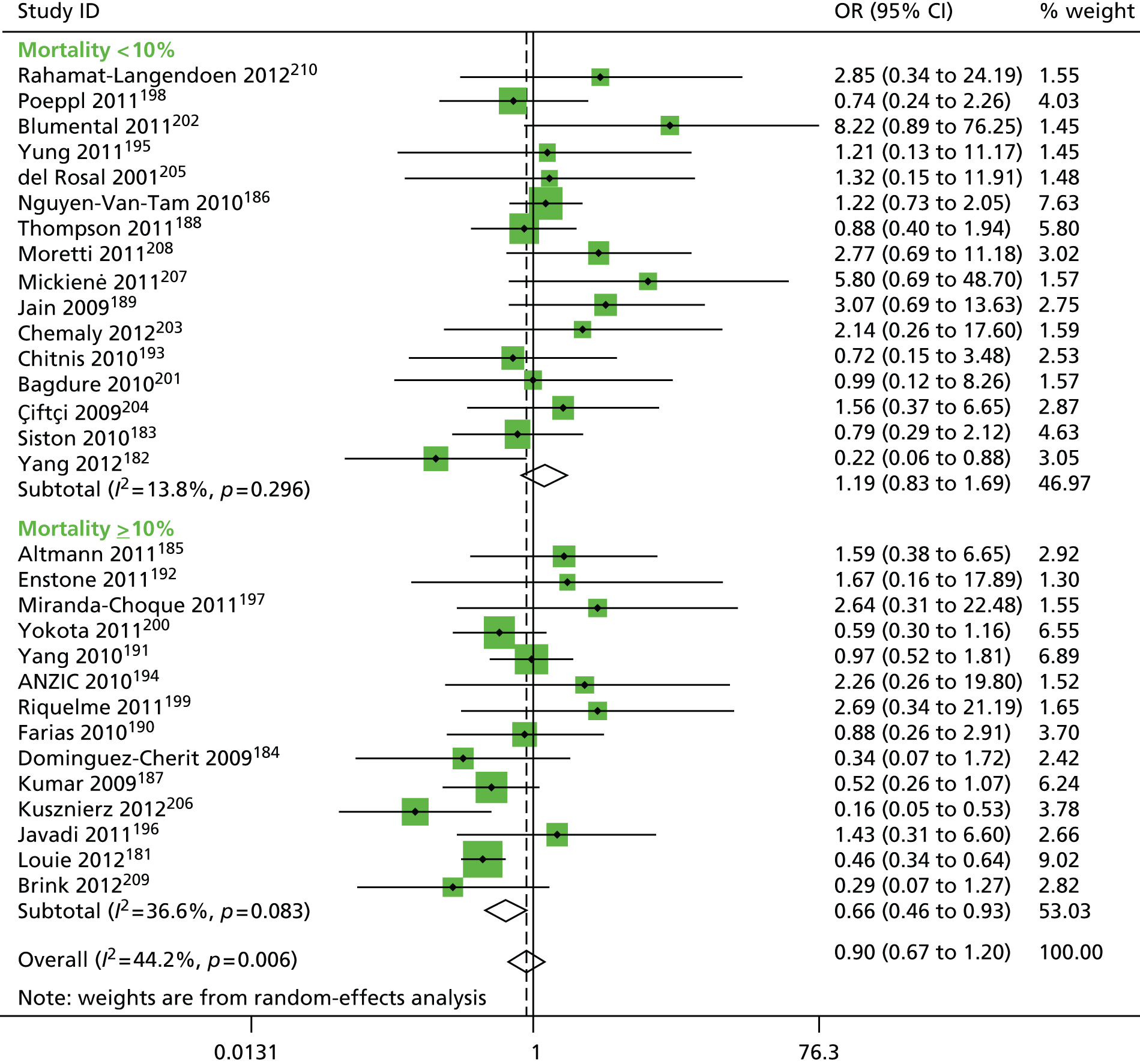
Meta-analysis of individual patient data
We were able to obtain IPD from four included studies. 185–188 One was a German study of 93 critically ill children;185 another was a UK study of 1520 hospitalised patients of all ages;186 another was a Canadian study187 of 605 critically ill adults; and the last study188 was a US study of 926 hospitalised patients of all ages. After removing data from patients who received zanamivir and patients with missing death status (n = 73, 2%), we had data for 3071 patients, of whom 242 (8%) died, 1803 (59%) were discharged, 140 (4%) remained in hospital and 886 (29%) had missing date of discharge. Details of responses and non-responses from corresponding authors of included studies to our request for IPD are shown in Table 18.
In Table 19 we present results of analysis of our primary outcome using five different methods. The first is logistic regression; the second is standard Cox regression; the third is Cox regression including treatment as a time-dependent exposure (td-Cox); the fourth is td-Cox with inclusion of potential confounders as covariates; and the fifth is td-Cox with inclusion of covariates as well as imputing missing time from hospital admission to death/discharge (for which 33% of values are missing, mainly due to the US study not providing date of discharge for survivors), time from hospital admission to oseltamivir exposure (for which 10% of values of the patients treated with oseltamivir are missing) and time from onset of symptoms to hospital admission (16% missing). The percentages of missing data were smaller for the deaths than the survivors (0.4% vs. 36% for time to death/discharge for example), suggesting that data collection was more thorough for patients who died.
| Outcome from our request | Number of studies |
|---|---|
| Obtained IPD | 4 |
| No response to request | 20 |
| Response to our request but did not provide IPDa | 6 |
| Method | Estimatea | 95% CI | p-value | |
|---|---|---|---|---|
| 1. | Logistic regression | 0.93 | 0.65 to 1.33 | 0.71 |
| 2. | Standard Cox regressionb | 0.75 | 0.51 to 1.10 | 0.14 |
| 3. | Cox regression with time-dependent treatment exposure (td-Cox)b | 1.11 | 0.75 to 1.65 | 0.59 |
| 4. | td-Cox adjusting for covariatesb | 1.10 | 0.74 to 1.63 | 0.64 |
| 5. | td-Cox with imputation and adjusting for covariates | 1.11 | 0.77 to 1.62 | 0.57 |
Results show that when the time-dependent nature of treatment is taken into account appropriately the treatment effects change direction, although none of the results is statistically significant. Adjusting for potential confounders and imputing missing data made little difference to the results. Table 20 shows results of the first three analysis methods by study, and a detailed analysis of the Canadian study,187 shown in Appendix 15, further illustrates why the time-dependent nature of treatment needs to be taken account of appropriately. This study was used for illustration because it had the most deaths and 93% of patients were treated, hence we would expect time-dependent bias to be large. However, bias is also apparent in the other studies if treatment is incorrectly assumed to be time independent (see Table 20). Table 21 shows distributions of potential confounding variables by treatment received stratified by study with p-values based on the chi-squared test. Detailed examination suggests a possible explanation for the reason oseltamivir is associated with greater risk of mortality in the Altmann et al. 185 and Nguyen-Van-Tam et al. 186 studies. In these two studies,185,186 comorbidities are generally more prevalent in the group that received treatment.
In Table 22 we show the variables that were associated with oseltamivir treatment. Respiratory and neurological comorbidities, as well as cancer, were all associated with increased odds of treatment, whereas the ages of < 20 years and > 64 years, as well as missing time from symptom onset to hospital presentation, were associated with lower odds of treatment. Early presentation was not associated with increased odds of treatment. In multivariable competing risks analysis, respiratory comorbidity was protective for mortality irrespective of exposure to treatment (HR 0.60, 95% CI 0.43 to 0.84) and each 10 years increase in age was associated with increased risk of death by 22% (95% CI 10% to 35%). Respiratory comorbidity was also associated with 15% (95% CI 3% to 28%) increased likelihood of discharge suggesting despite the comorbidity these patients had a good prognosis. Furthermore, a two-sample t-test showed respiratory comorbidity was associated with slightly lower Acute Physiology and Chronic Health Evaluation (APACHE) II scores in the Kumar et al. 187 study [mean (SD) 20 (10)10 vs. 22 (10)10; p = 0.014].
The results of mortality analyses by timing of treatment (Table 23) further illustrate the importance of appropriate analysis of a time-dependent treatment exposure. Logistic regression shows a statistically significant reduced odds of death associated with early treatment compared with no treatment, and estimates from standard Cox regression suggest treatment reduces risk of death compared with no treatment, although the result is not statistically significant. However, when time-dependent exposure to treatment is included appropriately in the Cox model, the results show no evidence treatment is beneficial. There is a suggestion that patients receiving late treatment do worse than those who received early treatment; however, this can be at least partially explained by the patients receiving late treatment having worse prognosis due to being older and having increased likelihood of a number of comorbidities, including infection, cardiovascular, diabetes and obesity (Table 24).
Competing risks survival analysis on the three cohorts that provided date of hospital discharge showed insufficient evidence that oseltamivir is associated with mortality (HR 1.03, 95% CI 0.64 to 1.65) but the results showed an association with increased likelihood of hospital discharge for survivors (HR 1.44, 95% CI 1.26 to 1.64).
| Study | Number of patients | Age in yearsa | Days admission to treatmenta | Percentage treated | Percentage died | OR from logistic regression | HRb from Cox regression | HRc from td-Cox regression |
|---|---|---|---|---|---|---|---|---|
| Altmann et al.185 | 88 | 5 (0–14) | 0.85 (0–6) | 60 | 16 | 1.23 | 1.36 | 1.67 |
| Nguyen-Van-Tam et al.186 | 1480 | 29 (0–95) | 1.7 (0–79) | 73 | 5 | 1.13 | 0.84 | 1.22 |
| Kumar et al.187 | 583 | 47 (19–92) | 0.62 (0–45) | 93 | 20 | 0.54 | 0.52 | 0.87 |
| dThompson et al.188 | 936 | 30 (0–02) | 1 (0–34) | 74 | 4 | 0.99 | d | d |
| Variable | No-treatment group, n (%) | Oseltamivir group, n (%) | p-value |
|---|---|---|---|
| Altmann et al.185 | |||
| Age group (years) | |||
| < 20 | 35 (100) | 53 (100) | – |
| 20–64 | 0 (0) | 0 (0) | |
| 65+ | 0 (0) | 0 (0) | |
| Presentation timing | |||
| < 2 days | 17 (48) | 21 (40) | 0.65 |
| > 2 days | 15 (43) | 28 (53) | |
| Missing | 3 (9) | 4 (7) | |
| Infection | 25 (71) | 49 (92) | 0.019 |
| Cardiovascular | 5 (14) | 6 (11) | 0.93 |
| Neurological | 17 (49) | 37 (70) | 0.075 |
| Cancer | 1 (3) | 4 (8) | 0.65 |
| Immunosuppression | 3 (9) | 8 (15) | 0.56 |
| Respiratory | 13 (37) | 32 (60) | 0.055 |
| Obesity | 0 (0) | 0 (0) | – |
| Diabetes | 0 (0) | 0 (0) | – |
| Nguyen-Van-Tam et al.186 | |||
| Age group (years) | |||
| < 20 | 216 (54) | 355 (33) | < 0.0001 |
| 20–64 | 163 (41) | 656 (61) | |
| 65+ | 18 (5) | 72 (7) | |
| Presentation timing | |||
| < 2 days | 140 (35) | 467 (43) | < 0.0001 |
| > 2 days | 97 (25) | 346 (32) | |
| Missing | 160 (40) | 270 (25) | |
| Infection | – | – | – |
| Cardiovascular | 31 (8) | 159 (15) | 0.0006 |
| Neurological | 39 (10) | 170 (16) | 0.005 |
| Cancer | 8 (2) | 43 (4) | 0.096 |
| Immunosuppression | 10 (3) | 34 (3) | 0.65 |
| Respiratory | 115 (29) | 496 (46) | < 0.0001 |
| Obesity | 9 (2) | 40 (4) | 0.23 |
| Diabetes | 24 (6) | 77 (7) | 0.55 |
| Kumar et al.187 | |||
| Age group (years) | |||
| < 20 | 0 (0) | 8 (2) | 0.23 |
| 20–64 | 32 (82) | 480 (88) | |
| 65+ | 7 (18) | 56 (10) | |
| Presentation timing | |||
| < 2 days | 11 (28) | 135 (25) | 0.26 |
| > 2 days | 26 (67) | 402 (74) | |
| Missing | 2 (5) | 7 (1) | |
| Infection | 22 (56) | 332 (61) | 0.69 |
| Cardiovascular | 16 (41) | 215 (40) | 0.99 |
| Neurological | 1 (3) | 30 (6) | 0.67 |
| Cancer | 0 (0) | 36 (7) | 0.19 |
| Immunosuppression | 2 (5) | 33 (6) | 1.0 |
| Respiratory | 18 (46) | 298 (55) | 0.38 |
| Obesity | 8 (21) | 135 (25) | 0.68 |
| Diabetes | 9 (23) | 138 (25) | 0.90 |
| Thompson et al.188 | |||
| Age group (years) | |||
| < 20 | 96 (40) | 292 (43) | 0.001 |
| 20–64 | 104 (43) | 327 (48) | |
| 65+ | 42 (17) | 59 (9) | |
| Presentation timing | |||
| < 2 days | 137 (57) | 362 (53) | 0.048 |
| > 2 days | 90 (37) | 295 (44) | |
| Missing | 15 (6) | 21 (3) | |
| Infection | – | – | – |
| Cardiovascular | 46 (19) | 94 (14) | 0.071 |
| Neurological | 23 (10) | 79 (12) | 0.43 |
| Cancer | 3 (1) | 22 (3) | 0.16 |
| Immunosuppression | 10 (4) | 73 (11) | 0.003 |
| Respiratory | 89 (37) | 275 (41) | 0.34 |
| Obesity | 42 (17) | 149 (22) | 0.15 |
| Diabetes | 50 (21) | 101 (15) | 0.048 |
| Variable | OR for treatment | 95% CI | p-value |
|---|---|---|---|
| Age (years) | |||
| < 20a | 0.61 | 0.50 to 0.74 0.38 to 0.72 |
< 0.0001 |
| > 64 | 0.52 | ||
| Time from onset of symptoms to hospital presentationb | 0.89 (early vs. late) | 0.72 to 1.09 0.34 to 0.57 |
< 0.0001 |
| 0.44 (missing vs. late) | |||
| Neurological comorbidity | 1.57 | 1.18 to 2.09 | 0.002 |
| Cancer | 2.93 | 1.55 to 5.54 | 0.001 |
| Respiratory comorbidity | 1.56 | 1.30 to 1.88 | < 0.0001 |
| Method | Estimatea,b | 95% CI | p-value |
|---|---|---|---|
| 1. Logistic regression | 0.54 (early vs. none) | 0.33 to 0.89 | 0.008 |
| 1.12 (late vs. none) | 0.76 to 1.66 | ||
| 1.11 (missing vs. none) | 0.73 to 1.71 | ||
| 2. Standard Cox regressionc | 0.68 (early vs. none) | 0.40 to 1.16 | 0.12 |
| 0.85 (late vs. none) | 0.56 to 1.29 | ||
| 0.69 (missing vs. none) | 0.44 to 1.06 | ||
| 3. Cox regression with time-dependent treatment exposure (td-Cox)c | 0.89 (early vs. none) | 0.52 to 1.52 | 0.69 |
| 1.15 (late vs. none) | 0.74 to 1.77 | ||
| 1.25 (missing vs. none) | 0.72 to 2.16 | ||
| 4. td-Cox adjusting for covariatesc | 0.92 (early vs. none) | 0.54 to 1.57 | 0.76 |
| 1.16 (late vs. none) | 0.75 to 1.79 | ||
| 1.14 (missing vs. none) | 0.65 to 1.99 | ||
| 5. td-Cox with imputation and adjusting for covariates | 1.10 (early vs. none) | 0.60 to 1.47 | 0.64 |
| 1.28 (late vs. none) | 0.86 to 1.90 |
| Variable | Early treatment group, n (%) | Late treatment group, n (%) | p-value |
|---|---|---|---|
| Age group (years) | |||
| < 20 | 313 (42) | 237 (23) | < 0.0001 |
| 20–64 | 375 (51) | 686 (68) | |
| 65+ | 55 (7) | 90 (9) | |
| Infectiona | 80 (19) | 201 (30) | 0.0001 |
| Cardiovascular | 106 (14) | 235 (23) | < 0.0001 |
| Neurological | 101 (14) | 133 (13) | 0.83 |
| Cancer | 24 (3) | 42 (4) | 0.38 |
| Immunosuppression | 51 (7) | 63 (6) | 0.66 |
| Respiratory | 344 (46) | 486 (48) | 0.52 |
| Obesity | 87 (12) | 179 (18) | 0.0007 |
| Diabetes | 78 (11) | 159 (16) | 0.002 |
Discussion
We have systematically reviewed the literature on the relationship between mortality from influenza 2009A/H1N1 and oseltamivir exposure. We included 30 studies in our review and obtained IPD for four of those studies. Analysis of both the summary data of the 30 studies, as well as the IPD, showed evidence of time-dependent bias, with bias increasing with increasing odds of treatment. Analysis of the IPD using Cox regression, with treatment exposure included as a time-dependent variable, adjusting for covariates and imputing missing data, has shown insufficient evidence that oseltamivir is associated with a reduction in mortality. Furthermore, early treatment with oseltamivir did not appear to have a beneficial effect on survival compared with no treatment. Competing risks survival analysis also showed insufficient evidence of association of treatment with mortality but the results showed an association with increased likelihood of hospital discharge for survivors.
Analysis of the IPD using logistic regression included 3071 patients and showed an OR of 0.93, whereas standard Cox regression on the 2056 patients with survival times gave a HR of 0.75, reflecting that untreated subjects who died did so earlier than those treated. When the time-dependent nature of oseltamivir exposure was incorporated into the Cox model, results showed a HR of 1.11, a marked difference from 0.75, illustrating the large time-dependent bias associated with standard Cox regression. After adjusting for covariates, the HR was virtually unchanged (1.10) and multiple imputation of the missing data had a negligible effect (HR 1.11). A competing risks survival analysis showed a consistent result, with a HR of 1.03 for mortality. We suggest that the competing risks analysis result may be the most appropriate because it takes into account the competing risk of discharge for treated patients, although a limitation is that it is based on only three studies because the fourth (US) study did not have data available for date of discharge.
The metaregression result that showed increasing mortality rate is associated with an increasingly favourable outcome for treatment is difficult to interpret because of the presence of time-dependent bias that cannot be quantified with access to only summary data. The metaregression result suggests that increasingly severe patients may lead to a better efficacy/toxicity trade-off of treatment. However, without the IPD it is unknown where, if anywhere, oseltamivir becomes a beneficial treatment. An alternative explanation is that cohorts with higher mortality rates were associated with greater time-dependent bias, as a greater proportion of patients died before they had the opportunity to receive antiviral treatment.
Confounding by indication is a possibility in observational studies and it is possible that sicker patients were more likely to get treatment. We were not able to adjust for severity of illness at baseline, as this information was not generally available for the included studies. However, APACHE II score was available for Kumar et al. 187 and comparison of treated with untreated patients showed no evidence of a difference in severity of illness (see Appendix 15). Prevalence of some comorbidities appeared higher for treated patients than untreated patients for two of the studies for which we had IPD, and this is reflected in the higher odds of mortality for treated patients in those studies. We adjusted for variables associated with treatment in the IPD analysis and this made little difference to the results. In addition, the competing risks survival analysis showed that treated patients who survived were discharged sooner than untreated patients. It is plausible that late treatment could indicate a sicker patient, as normally it takes time for patients to become severely ill. Patients who were treated late were older, and had greater prevalence of some comorbidities than patients who were treated early. This could at least partially explain why these patients had an increased risk of mortality.
Our results are different from those of three other recent reviews. Hsu et al. 172 included studies of seasonal influenza and 2009A/H1N1 influenza and based their primary analysis of mortality on three small studies of 681 patients, none of whom had 2009A/H1N1. They did not consider the time-dependent nature of treatment exposure and reported an OR of 0.23 (95% CI 0.13 to 0.43) based on summary data only. Muthuri et al. 171 focused on 2009A/H1N1 influenza, included 20 studies, did not consider time-dependent treatment exposure and reported an OR of 0.72 (95% CI 0.51 to 1.01) based on summary data only. Muthuri et al. 170 conducted an analysis of almost 30,000 patients from 78 studies using IPD; of the 78 studies included, only 22 would have been eligible for our study. For example, all included patients in 27 studies received NIs and 16 studies had no mortality. It is unclear how these studies were included in a mortality comparison between NIs and no treatment because, in meta-analyses, studies with no events and studies without a control group are dropped from the analysis. Muthuri et al. ’s crude analysis results170 are consistent with ours but the results from their analysis taking into account the time-dependent treatment exposure are different and appear to be incorrect, as they result in an increased protective effect of treatment. As Beyersmann et al. 214 show, mathematically time-dependent bias is always in the same direction (i.e. in the direction of showing a larger protective effect of treatment than is actually the case). Furthermore, the authors’ reply to criticisms of their analysis218 shows a crude HR of 0.36 (95% CI 0.32 to 0.41) for antiviral use modelled as a time-constant exposure without taking into account clustering or immortal time bias. However, this result is logically inconsistent with the descriptive data, which show that crude mortality in the antiviral group is larger than that of the no-treatment group (9.7% vs. 9.2%).
The results of this systematic review of observational studies are consistent with a recent Cochrane review9 of NIs for influenza based on a full set of manufacturer compiled CSRs of RCTs and regulatory information. The Cochrane review9 showed no evidence that NIs reduce the risk of hospitalisation or risk of complications classified as serious or leading to study withdrawal, a result consistent with oseltamivir not having a protective effect on mortality. The likelihood of treated survivors being discharged earlier is inconsistent with these findings, but is consistent with symptomatic relief that is not specific to influenza infection. The reasons for this inconsistency is unclear.
The problem of time-dependent bias is not confined to survival outcomes. For example, Beyersmann et al. 214 show time-dependent bias for the effect of hospital-acquired pneumonia on hospital length of stay. Yorifuji et al. 147 show the importance of taking account of time-dependent exposure of oseltamivir appropriately in a prospective observational study of Japanese children for which the outcomes related to abnormal behaviours. In the case of observational studies of 2009A/H1N1 influenza, outcomes by oseltamivir exposure – including pneumonia, hospitalisation and intensive care unit admission – have been compared and reported171,172 without regard to the time-dependent nature of treatment exposure. Beyersmann et al. 214 state that ‘because time-dependent bias inevitably leads to erroneous findings, it is a major concern that it is common in the clinical literature’. Van Walraven et al. 219 surveyed the medical literature and found that ‘in medical journals, time-dependent bias is concerningly common and frequently affects key factors and the study’s conclusion’. It is critical that analyses of all outcomes reported from observational studies with time-dependent exposures take account of time-dependent bias appropriately.
Strengths
We systematically searched five widely used databases over a 4-year period, as well as hand-searched relevant WHO documents and previous reviews. There were no restrictions on the type of research articles or studies considered for inclusion in the review. Studies from the Americas, UK and Europe, Australasia, Asia and the Middle East were included. We were able to obtain IPD for four studies that included > 3000 patients and more than 240 deaths. Using the IPD we were able to take account of the time-dependent nature of treatment exposure appropriately, impute missing time to event data and adjust for important covariates in the analysis. We were also able to take account of the competing risk of hospital discharge in estimating the effect of oseltamivir on mortality.
Limitations
Limitations of this review include the observational nature and quality of the included studies. All included studies were of hospitalised patients, and severity of illness of patients at baseline was not always reported. Limited information was provided on drug use prior to admission and no study reported NSAID use. Only two studies reported a definition for treatment and the comparison groups were assumed to be the subsets of patients who were not exposed to antivirals. The percentage of unexposed patients was often small (median 18%). Reasons for non-treatment with antivirals were not provided and none of the studies described a policy or criteria used for selecting patients for treatment. Our IPD analysis showed that patients with certain comorbidities were more likely to be treated, whereas children, the elderly and patients with unknown duration of symptoms were less likely to be treated.
We were able to obtain IPD for only four of the included studies, thus limiting the amount of statistical power that we had for our IPD analysis and potentially resulting in a biased subset of the 30 included studies. However, some of the responses to our request for IPD suggest critical data to assess the impact of oseltamivir on mortality were not collected. Furthermore, the IPD we obtained appears to be a representative sample of the 30 included studies as the ORs for mortality were similar for the IPD (0.93 – see Table 19) and the summary data (0.90 – see Figure 19). These estimates are also consistent with the crude OR of 0.92 reported by Muthuri et al. 170 Furthermore, the studies were from four different countries with varying mortality rates (4–20%), varying odds of treatment (60–93%) and included patients with ages from 0 to 102 years.
There were missing data for time to death/discharge and time to treatment (33% and 10% missing, respectively) in the four studies for which we had IPD. The majority of missing data for time to death/discharge was due to one study that did not report date of discharge for survivors. Analysis excluding this study showed similar results to those based on all four studies, hence we do not believe the missing time to discharge data has introduced a significant bias.
Conclusion
Our systematic review has found insufficient evidence that oseltamivir is associated with a reduced risk of mortality. However, this result is based primarily on an IPD analysis of just 4 of 30 eligible observational studies without adjustment for baseline severity of illness or other drug use. Analysis of all 30 included observational studies using summary data showed evidence of time-dependent bias that had an increasing effect with increasing odds of treatment. Observational studies with time-dependent treatment exposure are at high risk of time-dependent bias unless an appropriate analysis is conducted.
Acknowledgements
Thanks to Jon Deeks, Timothy Aoki, Carlo Di Pietrantonj, Vittorio Demicheli, Janet Wale, John Bartlett, Sree Nair, Tom Fahey, Matthew Shun-Shin, Anthony Harnden, Nigel Matheson, M Symmonds-Abrahams and Aziz Sheikh for input and advice on earlier versions of related reviews.
Thanks to Ruth Foxlee, Alex Rivetti and Nia Roberts for helping out with the searches.
Peter Collignon and Marcus Muellner helped us with aspects of the review.
Thanks to Nicola Ring and Ruth Jepson for advice on the inclusion of qualitative data.
We thank Toby Lasserson for providing advice and an independent check of our risk-of-bias judgements.
The EMA (formerly EMEA) provided all CSRs and reviewers’ comments in their archive.
Hoffman-La Roche SA and GSK provided us with full CSRs and answered our queries.
Thanks also to the Australian National Health and Medical Research Council and the UK NHS Research and Development fund for grants to enable the 2009 healthy adults review update.
Philip Carter and Deborah Cohen shared some of their FOI material.
Eliana Ferroni helped develop and cross-check the TOC.
We are very grateful to Sarah Thorning (clinical librarian) for running the literature searches; Anand Kumar and Rob Fowler for providing the Canadian IPD; Jonathan Van Tam and Puja Myles for providing the UK IPD; Mathias Altmann for providing the German IPD; and Deborah Thompson for providing the US IPD.
Finally, we wish to thank the following people for commenting on the draft protocol: Maryann Napoli, Janet Wale, Paul Glasziou, David Boltz, Elaine Beller, Anca Zalmanovici Trestioreanu and Marcus Muellner.
We also thank the following people for commenting on:
-
the draft 2012 review – Chris Cates, Janet Wale, Paul Glasziou, David Boltz and Robert Ware
-
the draft 2014 review – Chris Cates, Elizabeth Dooley, Janet Wale, David Boltz and Robert Ware.
Contributions of authors
Carl J Heneghan (Professor, Evidence-Based Medicine) amended the review protocol, applied the inclusion criteria to the zanamivir CSRs and contributed to the draft.
Igho Onakpoya (Research Fellow, Evidence-Based Practice and Pharmacovigilance) applied the inclusion criteria to the zanamivir CSRs, extracted data from the CSRs and contributed to the draft.
Mark A Jones (Senior Research Fellow, Biostatistics) amended the review protocol, arbitrated the process for inclusion of studies where necessary, performed statistical analyses and contributed to the draft.
Peter Doshi (Assistant Professor, Pharmaceutical Health Services Research) amended the review protocol, applied the inclusion criteria to the oseltamivir CSRs and contributed to the draft.
Chris B Del Mar (Professor, Public Health) amended the review protocol, screened the electronic search updates and contributed to the draft.
Rokuro Hama (Chairperson, Japan Institute of Pharmacovigilance) amended the review protocol and contributed to the draft.
Matthew J Thompson (Helen D Cohen Endowed Professorship in Family Medicine) amended the review protocol, screened the electronic search updates and contributed to the draft.
Elizabeth A Spencer (Epidemiologist) extracted data from the CSRs and contributed to the draft.
Kamal R Mahtani (National Institute for Health Research Academic Lecturer in General Practice) extracted data from the CSRs and contributed to the draft.
David Nunan (Research Fellow, Evidence-Based Practice and Physical Activity) extracted data from the CSRs and contributed to the draft.
Jeremy Howick (Research Fellow, Centre for Evidence-Based Medicine) extracted data from the CSRs and contributed to the draft.
Tom Jefferson (Reviewer, Cochrane) amended the review protocol, applied the inclusion criteria to the oseltamivir CSRs and prepared the final text.
Publications
Doshi P, Jefferson T, Del Mar C. The imperative to share clinical study reports: recommendations from the Tamiflu experience. PLOS Med 2012;9:e1001201.
Heneghan CJ, Onakpoya I, Thompson M, Spencer EA, Jones M, Jefferson T. Zanamivir for influenza in adults and children: systematic review of clinical study reports and summary of regulatory comments. BMJ 2014;348:g2547.
Jefferson T, Jones M, Doshi P, Spencer EA, Onakpoya I, Heneghan CJ. Oseltamivir for influenza in adults and children: systematic review of clinical study reports and summary of regulatory comments. BMJ 2014;348:g2545.
Jefferson T, Jones MA, Doshi P, Del Mar CB, Hama R, Thompson MJ, et al. Neuraminidase inhibitors for preventing and treating influenza in healthy adults and children. Cochrane Database Syst Rev 2014;4:CD008965.
Jefferson T, Jones MA, Doshi P, Del Mar CB, Hama R, Thompson MJ, et al. Risk of bias in industry-funded oseltamivir trials: comparison of core reports versus full clinical study reports. BMJ Open 2014;4:e005253.
Jones M, Jefferson T, Doshi P, Del Mar C, Heneghan C, Onakpoya I. Commentary on Cochrane review of neuraminidase inhibitors for preventing and treating influenza in healthy adults and children. Clin Microbiol Infect 2015;21:217–21.
Data sharing statement
The full set of CSRs for the NI Tamiflu (Oseltamivir) and Reenza (Zanamivir) produced by Roche were made available to the Cochrane collaboration for the production of their meta-analysis of neuraminidase inhibitors for preventing and treating influenza in adults and children are available at http://datadryad.org/resource/doi:10.5061/dryad.77471. (Jefferson T, Jones MA, Doshi P, Del Mar CB, Hama R, Thompson MJ, et al. Data from: Neuraminidase inhibitors for preventing and treating influenza in healthy adults and children. Dryad Digital Repository, 2014. http://dx.doi.org/10.5061/dryad.77471).
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HTA programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HTA programme or the Department of Health.
References
- UK Department of Health . UK Influenza Pandemic Contingency Plan 2005. www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_4121744.Pdf (accessed 27 June 2013).
- US Department of Health and Human Services . HHS Pandemic Influenza Plan 2005. www.pandemicflu.gov/planning-preparedness/federal/hhspandemicinfluenzaplan.pdf (accessed 27 June 2013).
- World Health Organization . WHO Interim Protocol: Rapid Operations to Contain the Initial Emergence of Pandemic Influenza n.d. www.who.int/entity/csr/disease/avian_influenza/guidelines/RapidContProtOct15.pdf (accessed 27 June 2013).
- Kaiser L, Wat C, Mills T, Mahoney P, Ward P, Hayden F. Impact of oseltamivir treatment on influenza-related lower respiratory tract complications and hospitalizations. Arch Intern Med 2003;63:1667-72. http://dx.doi.org/10.1001/archinte.163.14.1667.
- Jefferson T, Demicheli V, Rivetti D, Jones M, Di Pietrantonj C, Rivetti A. Antivirals for influenza in healthy adults: systematic review. Lancet 2006;367:303-13. http://dx.doi.org/10.1016/S0140-6736(06)67970-1.
- Doshi P, Jefferson T, Del Mar C. The imperative to share clinical study reports: recommendations from the Tamiflu experience. PLOS Med 2012;9. http://dx.doi.org/10.1371/journal.pmed.1001201.
- Thomas K. Breaking the Seal on Drug Research. New York Times 2013. www.nytimes.com/2013/06/30/business/breaking-the-seal-on-drug-research.html (accessed 20 October 2013).
- Doshi P. Neuraminidase inhibitors: the story behind the Cochrane review. BMJ 2009;339. http://dx.doi.org/10.1136/bmj.b5164.
- Jefferson T, Jones MA, Doshi P, Del Mar CB, Heneghan CJ, Hama R, et al. Neuraminidase inhibitors for preventing and treating influenza in healthy adults and children. Cochrane Database Syst Rev 2014;4. http://dx.doi.org/10.1590/1516-3180.20141324t2.
- Doshi P, Jones MA, Jefferson T. Rethinking credible evidence synthesis. BMJ 2012;344. http://dx.doi.org/10.1136/bmj.d7898.
- Doshi P, Jefferson T. Clinical study reports of randomised controlled trials: an exploratory review of previously confidential industry reports. BMJ Open 2013;3. http://dx.doi.org/10.1136/bmjopen-2012-002496.
- European Medicines Agency . European Medicines Agency Policy on Access to Documents (Related to Medicinal Products for Human and Veterinary Use) POLICY 0043 2010. www.ema.europa.eu/docs/en_GB/document_library/Other/2010/11/WC500099473.pdf (accessed 20 October 2013).
- Godlee F. Clinical trial data for all drugs in current use. BMJ 2012;345. http://dx.doi.org/10.1136/bmj.e7304.
- Jefferson T, Jones M, Doshi P, Del Mar C, Dooley L, Foxlee R. Neuraminidase inhibitors for preventing and treating influenza in healthy adults. Cochrane Database Syst Rev 2010;2. http://dx.doi.org/10.1002/14651858.cd001265.pub3.
- Hama R. Fatal neuropsychiatric adverse reactions to oseltamivir: case series and overview of causal relationships. Int J Risk Saf Med 2008;20:5-36.
- Call SA, Vollenweider MA, Hornung CA, Simel DL, McKinney WP. Does this patient have influenza?. JAMA 2005;8:987-97. http://dx.doi.org/10.1001/jama.293.8.987.
- Sugaya N, Ohashi Y. Long-acting neuraminidase inhibitor laninamivir octanoate (CS-8958) versus oseltamivir as treatment for children with influenza virus infection. Antimicrob Agents Chemother 2010;54:2575-82. http://dx.doi.org/10.1128/AAC.01755-09.
- Hayden F. Developing new antiviral agents for influenza treatment: what does the future hold?. Clin Infect Dis 2009;48:3-13. http://dx.doi.org/10.1086/591851.
- World Health Organization . Global Agenda on Influenza: Adopted Version. Part I. Weekly Epidemiological Record Health Section of the Secretariat of the League of Nations 2002;77:179-82.
- World Health Organization . Adoption of Global Agenda on Influenza. Part II. Weekly Epidemiological Record Health Section of the Secretariat of the League of Nations 2002;77:191-5.
- World Health Organization . WHO Guidelines on the Use of Vaccines and Antivirals During Influenza Pandemics 2009. www.who.int/csr/resources/publications/influenza/11_29_01_A.pdf (accessed 30 November 2009).
- Matrosovich MN, Matrosovich TY, Gray T, Roberts NA, Klenk H. Neuraminidase is important for the initiation of influenza virus infection in human airway epithelium. J Virol 2004;78:12665-7. http://dx.doi.org/10.1128/JVI.78.22.12665-12667.2004.
- Moscona A. Neuraminidase inhibitors for influenza. N Engl J Med 2005;353:1363-73. http://dx.doi.org/10.1056/NEJMra050740.
- Ohuchi M, Asaoka N, Sakai T, Ohuchi R. Roles of neuraminidase in the initial stage of influenza virus infection. Microbes Infect 2006;8:1287-93. http://dx.doi.org/10.1016/j.micinf.2005.12.008.
- Liu C, Eichelberger MC, Compans RW, Air GM. Influenza type A virus neuraminidase does not play a role in viral entry, replication, assembly, or budding. J Virol 1995;69:1099-106.
- Smith J, Dutkowski R, Ward P. Antivirals for influenza in healthy adults. Lancet 2006;367. http://dx.doi.org/10.1016/S0140-6736(06)68683-2.
- Hayden FG, Treanor JJ, Fritz RS, Lobo M, Betts RF, Miller M, et al. Use of the oral neuraminidase inhibitor oseltamivir in experimental human influenza: randomized controlled trials for prevention and treatment. JAMA 1999;282:1240-6. http://dx.doi.org/10.1001/jama.282.13.1240.
- Li C, Yu Q, Ye Z, Sun Y, He Q, Li X, et al. A nonsynonymous SNP in human cytosolic sialidase in a small Asian population results in reduced enzyme activity: potential link with severe adverse reactions to oseltamivir. Cell Res 2007;17:357-62. http://dx.doi.org/10.1038/cr.2007.27.
- Cass LM, Efthymiopoulos C, Bye A. Pharmacokinetics of zanamivir after intravenous, oral, inhaled or intranasal administration to healthy volunteers. Clin Pharmacokinet 1999;36:1-11. http://dx.doi.org/10.2165/00003088-199936001-00001.
- Jefferson TO, Demicheli V, Di Pietrantonj C, Jones M, Rivetti D. Neuraminidase inhibitors for preventing and treating influenza in healthy adults. Cochrane Database Syst Rev 2006;3. http://dx.doi.org/10.1002/14651858.cd001265.pub2.
- Jefferson T, Jones M, Doshi P, Del Mar C. Neuraminidase inhibitors for preventing and treating influenza in healthy adults: systematic review and meta-analysis. BMJ 2009;339. http://dx.doi.org/10.1136/bmj.b5106.
- Shun-Shin M, Thompson M, Heneghan C, Perera R, Harnden A, Mant D. Neuraminidase inhibitors for treatment and prophylaxis of influenza in children: systematic review and meta-analysis of randomised controlled trials. BMJ 2009;339. http://dx.doi.org/10.1136/bmj.b3172.
- World Health Organization . WHO Model List of Essential Medicines. ADULTS, 18th Edition (April 2013) 2013. www.who.int/medicines/publications/essentialmedicines/18th_EML_Final_web_8Ju_l13.pdf (accessed 25 November 2013).
- World Health Organization . WHO Model List of Essential Medicines for Children. 4th List (April 2013) 2013. http://apps.who.int/iris/bitstream/10665/93143/1/EMLc_4_eng.pdf (accessed 25 November 2013).
- Matheson NJ, Harnden AR, Perera R, Sheikh A, Symmonds-Abrahams M. Neuraminidase inhibitors for preventing and treating influenza in children. Cochrane Database Syst Rev n.d.;1.
- McGarty T. A Randomized, Double-Blind, Placebo-Controlled, Multicenter Study of Efficacy Based on the Time to Treatment of Influenza Infection With the Neuraminidase Inhibitor Ro 64–0796 (also Known As GS 4104) n.d.
- Gravenstein S, Peters P. Long-term use of oseltamivir for the prophylaxis of influenza in a vaccinated frail older population. J Am Geriatr Soc 2001;49:1025-31. http://dx.doi.org/10.1111/jgs.12250.
- Peters PH, Gravenstein S, Norwood P, De Bock V, Van Couter A, Gibbens M, et al. Long-term use of oseltamivir for the prophylaxis of influenza in a vaccinated frail older population. J Am Geriatr Soc 2001;49:1025-31. http://dx.doi.org/10.1046/j.1532-5415.2001.49204.x.
- A Double-Blind, Randomised, Placebo-Controlled Study of Ro 64–0796 (also Known As GS4104) Used in Elderly Subjects for the Prevention of Clinical Influenza During the Influenza Season n.d.
- Godlee F, Clarke M. Why don’t we have all the evidence on oseltamivir?. BMJ 2009;339. http://dx.doi.org/10.1136/bmj.b5351.
- McGauran N, Wieseler B, Kreis J, Schuler Y, Kolsch H, Kaiser T. Reporting bias in medical research: a narrative review. Trials 2010;11. http://dx.doi.org/10.1186/1745-6215-11-37.
- Wieseler B, Wolfram N, McGauran N, Kerekes MF, Vervölgyi V, Kohlepp P, et al. Completeness of reporting of patient-relevant clinical trial outcomes: comparison of unpublished clinical study reports with publicly available data. PLOS Med 2013;10.
- Cohen D. Complications: tracking down the data on oseltamivir. BMJ 2009;339. http://dx.doi.org/10.1136/bmj.b5387.
- Japanese Association for Infectious Diseases . Question and Answers on the Japanese Association for Infectious Diseases Urgent Recommendation ‘Handling Pandemic Influenza in Routine Care Institutions’ 2010. www.kansensho.or.jp/topics/090525influenza_qanda.html (accessed 9 May 2010).
- Maugh TH. British Medical Journal Questions Efficacy of Tamiflu for Swine Flu – Or Any Flu 2009. http://latimesblogs.latimes.com/booster_shots/2009/12/british-medical-journal-questions-efficacy-of-tamiflu-for-swine-flu-or-any-flu.html (accessed 8 December 2009).
- Nebehay S. WHO Backs Findings on Tamiflu for Seasonal Flu 2009. www.reuters.com/article/idUSGEE5BA0UY20091211?type=marketsNews (accessed 11 December 2009).
- NHS Choices . Antivirals and Swine Flu 2009. www.nhs.uk/news/2009/12December/Pages/Antivirals-and-swine-flu.aspx (accessed 17 May 2010).
- NHS Choices . Swine Flu – Questions and Answers 2010. www.nhs.uk/Conditions/Pandemic-flu/Pages/QA.aspx (accessed 17 May 2010).
- US Centers for Disease Control and Prevention . Serum cross-reactive antibody response to a novel influenza A (H1N1) virus after vaccination with seasonal influenza vaccine. MMWR Morb Mortal Wkly Rep 2009;58:521-4.
- Itoh Y, Shinya K, Kiso M, Watanabe T, Sakoda Y, Hatta M, et al. In vitro and in vivo characterization of new swine-origin H1N1 influenza viruses. Nature 2009;460:1021-5. http://dx.doi.org/10.1038/nature08260.
- Rodgers MA, Brown JVE, Heirs MK, Higgins JPT, Mannion RJ, Simmonds MC, et al. Reporting of industry funded study outcome data: comparison of confidential and published data on the safety and effectiveness of rhBMP-2 for spinal fusion. BMJ 2013;346. http://dx.doi.org/10.1136/bmj.f3981.
- Vedula SS, Bero L, Scherer RW, Dickersin K. Outcome reporting in industry-sponsored trials of gabapentin for off-label use. N Engl J Med 2009;361:1963-71. http://dx.doi.org/10.1056/NEJMsa0906126.
- Vedula SS, Li T, Dickersin K. Differences in reporting of analyses in internal company documents versus published trial reports: comparisons in industry-sponsored trials in off-label uses of gabapentin. PLOS Med 2013;10. http://dx.doi.org/10.1371/journal.pmed.1001378.
- Eyding D, Lelgemann M, Grouven U, Harter M, Kromp M, Kaiser T, et al. Reboxetine for acute treatment of major depression: systematic review and meta-analysis of published and unpublished placebo and selective serotonin reuptake inhibitor controlled trials. BMJ 2010;341. http://dx.doi.org/10.1136/bmj.c4737.
- Ioannidis JPA, Karassa FB. The need to consider the wider agenda in systematic reviews and meta-analyses: breadth, timing, and depth of the evidence. BMJ 2010;341. http://dx.doi.org/10.1136/bmj.c4875.
- Chou R, Helfand M. Challenges in systematic reviews that assess treatment harms. Ann Intern Med 2005;142:1090-9. http://dx.doi.org/10.7326/0003-4819-142-12_Part_2-200506211-00009.
- A Double-Blind, Randomized, Stratified, Placebo-Controlled Study of Oseltamivir in the Treatment of Influenza in Children With Asthma n.d.
- Dorkings J. Efficacy and Safety of the Oral Neuraminidase Inhibitor Oseltamivir in Treating Acute Influenza: A Randomized Controlled Trial n.d.
- Efficacy of RO 64–0796 When Used As Chemoprophylaxis Against Natural Influenza Infection n.d.
- Grosse M. A Multi-Center, Randomized, Double-Blind, Placebo-Controlled, Parallel Group Study of Oseltamivir Treatment in Elderly Patients With Influenza n.d.
- A Double-Blind Randomised Placebo Controlled Study of RO 64–0796 (also Known As GS4104) Used in Elderly Subjects for the Prevention of Clinical Influenza During Influenza Season n.d.
- Dorkings J. A Double-Blind, Stratified, Randomized, Placebo Controlled Study of Ro 64–0796 (GS4104) in the Treatment of Influenza Infection in Adults n.d.
- A Double-Blind, Randomized, Stratified, Placebo-Controlled Study of Ro 64–0796 (also Known As GS 4104) in the Treatment of Children With Influenza n.d.
- Gerster T. A Double-Blind, Randomized, Stratified, Placebo-Controlled Study of Oseltamivir Phosphate (Ro 64–0796, Also Known As GS 4104) in the Treatment of Influenza in Children With Chronic Asthma n.d.
- A Double-Blind Randomised Placebo Controlled Study of Ro 64–0796 (also Known As GS4104) for the Prevention of Clinical Influenza Post Exposure in Families n.d.
- McCarvil M. A Double-Blind, Stratified, Randomised, Placebo Controlled Study of Ro 64–0796 (also Known As GS4104) in the Treatment of Influenza in Chronically Ill Adults n.d.
- A Double-Blind, Randomized, Stratified, Placebo-Controlled Study of Ro 64–0796 (also Known As GS4104) in the Treatment of Influenza Infection in Elderly Patients n.d.
- A Double-Blind, Randomised, Placebo-Controlled Study of Ro 64–0796 (also Known As GS4104) Used in Elderly Subjects for the Prevention of Clinical Influenza During the Influenza Season n.d.
- A Double-Blind, Randomised, Stratified, Placebo-Controlled Study of Oseltamivir in the Treatment of Influenza Infection in Patients n.d.
- GSK . Investigation of the Efficacy of GG167 (Zanamivir) in the Treatment of Influenza Viral Infections (Late Phase II Study: Dose Comparison Study) n.d.
- GSK . Investigation of the Efficacy of CG167 in the Treatment of Influenza Viral Infections (Phase II Study) (Protocol NoJNAI-01). Double Blind, Double Dummy, Randomized, Placebo Controlled, Parallel Group, Multicenter Study to Investigate Safety and Route of Administration of CG167 When Inhaled, CG167 10 mg, or the Combination of Inhaled CG167 10 mg Plus Intranasal CG167 6.4 mg, Administered Twice Daily for 5 Days in the Treatment of Influenza A and B Viral Infections n.d.
- GSK . A Multicenter Two Way Layout Randomized Placebo-Controlled Double-Blind Trial Parallel Group Comparative Trial on the Efficacy and Safety of GG167 (zanamivir) 10 mg Twice a Day and 20 mg Twice a Day in the Treatment of Influenza Type A and Type B Infections (Late Phase II Study: Dose Comparison Study) (Protocol No. JNAI-04) n.d.
- GSK . A Multicenter Two Way Layout Randomized Placebo-Controlled Double-Blind Trial Parallel Group Comparative Trial on the Efficacy and Safety of GG167 (zanamivir) 10 mg Twice a Day and 20 mg Twice a Day in the Treatment of Influenza Type A and Type B Infections (Late Phase II Study: Dose Comparison Study) (Protocol No. JNAI-07) n.d.
- A Randomized, Placebo-Controlled, Multicenter Study of Oseltamivir (Ro 64–0796) in the Treatment of Influenza in Japanese Subjects (Translation of Summary Japanese Report – of 29 Pages) n.d.
- Phase 3 Study for Prophylaxis of Influenza With Ro64–0796 (15 Page Summary From Japanese) n.d.
- A Double-Blind, Randomized, Placebo-Controlled Multicenter Study of Oseltamivir Phosphate in the Treatment of Influenza Infection in China n.d.
- A Double-Blind, Randomized, Placebo-Controlled, Parallel Group, Multi-Center Study to Investigate the Efficacy and Safety of Inhaled Zanamivir 10 mg Administered Twice Daily for Five Days in the Treatment of Influenza in Patients 12 Years or over Diagnosed With Asthma or Chronic Obstructive Pulmonary Disease n.d.
- Alfors S, Keene O, Grice R, Hammond J, Hendricks V, Martin N, et al. A Double-Blind, Randomized, Placebo-Controlled, Parallel-Group, Multicenter Study to Investigate the Efficacy and Safety of Zanamivir (GG167) 10 mg Administered by Inhalation Twice Daily for Five Days in the Treatment of Symptomatic Influenza A and B Viral Infections in Children Ages 5–12 n.d.
- Hunter S, Reilly L, Sharp S, West M, Alfors S, Hammond J, et al. A Double-Blind, Randomized, Placebo-Controlled, Parallel-Group, Multicenter Study to Investigate the Efficacy and Safety of Inhaled Zanamivir (GG167) 10 mg Administered Once a Day for 10 Days in the Prevention of Transmission of Symptomatic Influenza A and B Viral Infections Within Families n.d.
- A Randomised, Double-Blind, Placebo-Controlled Study to Evaluate the Impact of Inhaled Zanamivir Treatment on Workplace Attendance Due to Influenza A and B Infections n.d.
- A Double-Blind, Randomised, Placebo-Controlled, Parallel-Group, Multicentre Study to Investigate the Efficacy and Safety of Inhaled Zanamivir 10 mg Administered Twice Daily for Five Days in the Treatment of Symptomatic Influenza A and B Viral Infections in Subjects Aged over 65 Years n.d.
- A Double-Blind, Randomised, Placebo-Controlled, Parallel-Group, Multicentre Study to Investigate the Efficacy and Safety of Inhaled Zanamivir 10 mg Administered Twice Daily for Five Days in the Treatment of Symptomatic Influenza A and B Viral Infections in Armed Services Personnel n.d.
- A Double-Blind, Randomised, Placebo-Controlled, Multicenter Study in 2 Parallel Groups, to Investigate the Efficacy and Safety of Inhaled Zanamivir (10 mg Bd. via Diskhaler), for 5 Days, in High Risk Patients With Symptomatic Influenza A and Or B Infection n.d.
- A Double-Blind, Randomised, Placebo-Controlled, Multicenter Study in 2 Parallel Groups, to Investigate the Efficacy and Safety of Inhaled Zanamivir (10 mg Bd via Diskhaler), for 5 Days, in Children Aged 5 to 12 Years With Symptomatic Influenza A and Or B Infection n.d.
- A Double-Blind, Randomised, Placebo-Controlled, Parallel-Group, Multicentre Study to Investigate the Efficacy and Safety of Inhaled Zanamivir 10 mg Administered Once a Day for 10 Days in the Prevention of Transmission of Symptomatic Influenza A and B Viral Infections Within Households n.d.
- A Double-Blind, Randomized, Placebo-Controlled, Parallel-Group, Multicentre Study to Investigate the Efficacy and Safety of Inhaled Zanamivir 10 mg Administered Once a Day for 28 Days in the Prevention of Symptomatic Influenza A and B Viral Infections in Community-Dwelling High-Risk Populations n.d.
- A Double-Blind, Randomized, Placebo-Controlled, Multicenter, Parallel-Group Study to Investigate the Efficacy and Safety of Zanamivir Administered Twice or Four Times a Day for the Treatment of Influenza A and B Viral Infections n.d.
- A Double-Blind, Randomised, Placebo-Controlled, Multicentre, Parallel-Group Study to Demonstrate the Efficacy and Safety of Zanamivir in the Prevention and Or Progression of Influenza A and B Viral Infections n.d.
- MacLeod A, Gummer M, Raniga K, Hirst H, Keene O, Ossi M, et al. A Double-Blind, Randomised, Placebo-Controlled Multi-Centre Study to Investigate the Efficacy and Safety of Inhaled and Intranasal Zanamivir in the Treatment of Influenza A and B Viral Infections n.d.
- A Double-Blind, Randomised, Placebo-Controlled Multicentre Study to Investigate the Efficacy and Safety of Zanamivir Therapy in the Prevention of Progression of Influenza A and B Viral Infections n.d.
- Elliott M, Flack N, Keene O, Szymborski P, Vega R. (PharmaResearch, Inc.) . A Double-Blind, Randomized, Placebo-Controlled, Parallel-Group, Multicenter Study to Investigate the Efficacy and Safety of Inhaled Zanamivir (GG167) 10 mg Administered Twice a Day for Five Days in the Treatment of Symptomatic Influenza A and B Viral Infections in Adolescents and Adults n.d.
- A Double-Blind, Randomized, Parallel-Group, Multi-Center Study to Investigate the Efficacy and Safety of Inhaled Zanamivir 10 mg Administered Once a Day Compared to the Standard of Care in Controlling Nursing Home Influenza Outbreaks n.d.
- A Double-Blind, Randomized, Placebo-Controlled, Parallel-Group, Multi-Center Study to Investigate the Efficacy and Safety of Inhaled Zanamivir 10 mg Once a Day in Controlling Nursing Home Influenza Outbreaks n.d.
- Elliott M, Hunter S, Flack N, Crisp A, Szymborski P, Vega R. A Double-Blind, Randomized, Placebo-Controlled, Parallel-Group, Multicenter Study to Investigate the Efficacy and Safety of Zanamivir (GG167) 10 mg Administered Once a Day for 28 Days in the Prevention of Symptomatic Influenza A and B Viral Infections in Community Dwelling Adults n.d.
- Leong J, Brennan J, Gummer M, Keene O, Wightman K. A Double-Blind, Randomised, Placebo-Controlled, Parallel-Group, Multi-Centre Study to Investigate the Efficacy and Safety of Inhaled Plus Intranasal Zanamivir in the Treatment of Influenza A and B Viral Infections n.d.
- A Double-Blind, Randomised, Placebo-Controlled, Parallel-Group, Multicentre Study to Investigate the Efficacy and Safety of Inhaled Zanamivir in Preventing Progression of Influenza A and B Viral Infections n.d.
- Perich R, Solterbeck A, Keene O, Leong J, Raniga K, MacLeod A. A Double-Blind, Randomised, Placebo-Controlled, Parallel-Group, Multi-Centre Study to Investigate the Efficacy and Safety of Inhaled and Inhaled Plus Intranasal Zanamivir in the Treatment of Influenza A and B Viral Infections n.d.
- Campion K, Gummer M, Keene O. A Double-Blind, Randomized, Placebo-Controlled, Parallel-Group, Multicenter Study to Investigate the Efficacy and Safety of Zanamivir Administered Twice Daily in the Treatment of Influenza A and B Viral Infections in Adults n.d.
- Man CY, Keene ON, Challoner T. Challoner Associates . A Double-Blind, Randomised, Placebo-Controlled, Parallel-Group, Multicentre Study to Investigate the Efficacy and Safety of Inhaled Zanamivir (GG167) 10 mg Administered Twice a Day for Five Days in the Treatment of Symptomatic Influenza A and B Viral Infections in Adolescents and Adults n.d.
- A Trial to Investigate Efficacy to Reduce Development of Influenza Symptoms in Influenza Infected Patients Treated With GG167 (protocol Number PE-01 Phase II Clinical Trial). A Double-Blind Double-Dummy, Randomized, Placebo-Controlled, Parallel Group, Multicenter Study to Investigate the Efficacy Reducing Development of Influenza Symptoms And, Safety and Route of Administration of GG 157 When Orally Inhaled GG 167 10 mg, 6.4 mg Nebulized Intranasally or the Combination of Inhaled GG167 10 mg Plus Intranasal GG167 6.4 mg Was Administered Twice Day for 5 Days in the Treatment of Influenza A and B Viral Infections n.d.
- MacLean CH, Morton SC, Ofman JJ, Roth EA, Shekelle PG. How useful are unpublished data from the Food and Drug Administration in meta-analysis?. J Clin Epidemiol 2003;56:44-51.
- Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions 2011. www.cochrane-handbook.org.
- Aronson JK, Ferner RE. Joining the DoTS: new approach to classifying adverse drug reactions. BMJ 2003;327:1222-5. http://dx.doi.org/10.1136/bmj.327.7425.1222.
- A Randomized, Double Blind, Parallel Group, Placebo Controlled Study of the Effect of Oseltamivir on ECG Intervals in Healthy Subjects n.d.
- Dutkowski R, Smith JR, Davies BE. Safety and pharmacokinetics of oseltamivir at standard and high dosages. Int J Antimicrob Agents 2010;35:461-7. http://dx.doi.org/10.1016/j.ijantimicag.2009.12.023.
- Jefferson T, Jones, M, Doshi, P, Del Mar CB, Heneghan CJ, Hama R, et al. Neuraminidase inhibitors for preventing and treating influenza in healthy adults and children. Cochrane Database Syst Rev 2012;1. http://dx.doi.org/10.1002/14651858.cd008965.pub3.
- DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials 1986;7:177-88. http://dx.doi.org/10.1016/0197-2456(86)90046-2.
- Feinberg J. Wordle n.d. www.wordle.net/2009 (accessed 15 September 2010).
- Food and Drug Administration . Tamiflu (Oseltamivir Phosphate) Capsule 1999. www.accessdata.fda.gov/drugsatfda_docs/nda/99/21087_Tamiflu_medr_P1.pdf (accessed 26 August 2009).
- Anekthananon T, Pukritayakamee S, Ratanasuwan W, Jittamala P, Werarak P, Charunwatthana P, et al. Oseltamivir and inhaled zanamivir as influenza prophylaxis in Thai health workers: A randomized, double-blind, placebo-controlled safety trial over 16 weeks. J Antimicrob Chemother 2013;68:697-70. http://dx.doi.org/10.1093/jac/dks418.
- Dharan NJ, Fry AM, Kieke BA, Coleman L, Meece J, Vandermause M, et al. Clinical and virologic outcomes in patients with oseltamivir-resistant seasonal influenza A (H1N1) infections: results from a clinical trial. Influenza Other Respir Viruses 2012;6:153-8. http://dx.doi.org/10.1111/j.1750-2659.2011.00312.x.
- Kashiwagi S, Watanabe A, Ikematsu H, Awamura S, Okamoto T, Uemori M, et al. Laninamivir octanoate for post-exposure prophylaxis of influenza in household contacts: A randomized double blind placebo controlled trial. J Infect Chemother 2013;19:740-9. http://dx.doi.org/10.1007/s10156-013-0622-9.
- A Phase II, Multicenter, Randomized, Double-Mask, Placebo-Controlled Study to Evaluate the Efficacy and Safety of Intramuscular Peramivir in Subjects With Uncomplicated Acute Influenza n.d.
- A Phase II, Multicenter, Randomized, Double-Mask, Double-Dummy Study Comparing the Efficacy and Safety of Peramivir Administered Intravenously Once Daily Versus Oseltamivir Administered Orally Twice Daily in Adults With Acute Serious or Potentially Life-Threatening Influenza n.d.
- A Phase 3 Multicenter, Randomized, Double Blind, Placebo-Controlled Study to Evaluate the Efficacy and Safety of Intramuscular Peramivir in Subjects With Uncomplicated Acute Influenza n.d.
- A Phase 3 Multicenter, Randomized, Double-Blind, Placebo-Controlled Study to Evaluate the Efficacy and Safety of Intramuscular Peramivir in Subjects With Uncomplicated Acute Influenza n.d.
- A Phase II, Multicenter, Randomized, Placebo-Controlled, Study to Evaluate the Efficacy and Safety of Intramuscular Peramivir 600 mg in Subjects With Uncomplicated Acute Influenza n.d.
- A Phase 3, Multicenter, Randomized, Double-Blind, Controlled Study to Evaluate the Efficacy and Safety of Peramivir Administered Intravenously in Addition to Standard of Care Compared to Standard of Care Alone in Adults and Adolescents Who Are Hospitalized Due to Serious Influenza n.d.
- Food and Drug Administration . Site Inspection Report in Review. Tamiflu (oseltamivir) 2000. www.accessdata.fda.gov/drugsatfda_docs/nda/2000/21–087SE1–002_review.pdf (accessed 26 August 2009).
- (Oseltamivir Trial. Title Unknown) n.d.
- Godlee F, Loder E. Missing clinical trial data: setting the record straight. BMJ 2010;341. http://dx.doi.org/10.1136/bmj.c5641.
- Jefferson T, Doshi P, Thompson M, Heneghan C. Ensuring safe and effective drugs: who can do what it takes?. BMJ 2011;342. http://dx.doi.org/10.1136/bmj.c7258.
- Bourgeois FT, Murthy S, Mandl KD. Outcome reporting among drug trials registered in ClinicalTrials.gov. Ann Intern Med 2010;153:158-66. http://dx.doi.org/10.7326/0003-4819-153-3-201008030-00006.
- Huic M, Marusic M, Marusic A. Completeness and changes in registered data and reporting bias of randomized controlled trials in ICMJE journals after trial registration policy. PLOS ONE 2011;6. http://dx.doi.org/10.1371/journal.pone.0025258.
- Van Driel ML, De Sutter A, De Maeseneer J, Christiaens T. Searching for unpublished trials in Cochrane reviews may not be worth the effort. J Clin Epidemiol 2009;62:838-44. http://dx.doi.org/10.1016/j.jclinepi.2008.09.010.
- Ghersi D, Clarke MJ, Reveiz L. Do Cochrane Reviews Search Databases of Ongoing Trials, and How Well Do They Report These Searches? Oral Presentation at the Joint Cochrane and Campbell Collaboration 2010:45-6. www.cochrane.org/sites/default/files/uploads/abstract_book_keystone_2010.pdf (accessed 1 August 2015).
- Food and Drug Administration . Faxed Letter to Roche (file UCM166329) [NDA 21–087TAMIFLU (oseltamivir Phosphate) MACMIS ID#8675] 2000. www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/EnforcementActivitiesbyFDA/WarningLettersandNoticeofViolationLetterstoPharmaceuticalCompanies/UCM166329.pdf (accessed 19 October 2010).
- Food and Drug Administration . Review. Tamiflu (Oseltamivir). NDA 021087 Supplement 002 2000. www.accessdata.fda.gov/drugsatfda_docs/nda/2000/21–087SE1–002_review.pdf (accessed 26 August 2009).
- Food and Drug Administration . Letter from FDA to Hoffman-La Roche Inc. Re ‘NDA 21–087 TAMIFLU (Oseltamivir Phosphate) MACMIS ID#8675 2000. www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Enfo rcementActivitiesbyFDA/WarningLettersandNoticeofViolationLetterstoPharmaceuticalCompanies/UCM166329.pdf (accessed 14 April 2000).
- European Medicines Agency . Annex I. Summary of Product Characteristics (Tamiflu 30 mg Hard Capsule) n.d. www.ema.europa.eu/ema/pages/includes/document/open_document.jsp?webContentId=WC500033106 (accessed 21 January 2010).
- European Agency for the Evaluation of Medicinal Products . Tamiflu. Oseltamivir Phosphate. (EMEA H C 402) CPMP Recommendation &Amp; Scientific Discussion Consolidated List of Questions (28 June 2001) n.d. www.ema.europa.eu/.
- Senn SJ. Added values: controversies concerning randomization and additivity in clinical trials. Stat Med 2004;23:3729-53. http://dx.doi.org/10.1002/sim.2074.
- Takahashi E, Kataoka K, Fujii K, Chida J, Mizuno D, Fukui M, et al. Attenuation of inducible respiratory immune responses by oseltamivir treatment in mice infected with influenza A virus. Microbes 2010;12:778-83. http://dx.doi.org/10.1016/j.micinf.2010.04.013.
- Sawabuchi T, Suzuki S, Iwase K, Ito C, Mizuno D, Togari H, et al. Boost of mucosal secretory immunoglobulin A response by clarithromycin in paediatric influenza. Respirology 2009;14:1173-9. http://dx.doi.org/10.1111/j.1440-1843.2009.01639.x.
- Mendel DB, Tai CY, Escarpe PA, Li W, Sidwell RW, Huffman JH, et al. Oral administration of a prodrug of the influenza virus neuraminidase inhibitor GS 4071 protects mice and ferrets against influenza infection. Antimicrob Agents Chemother 1998;42:640-6.
- Moore ML, Chi MH, Zhou W, Goleniewska K, O’Neal JF, Higginbotham JN, et al. Cutting edge: oseltamivir decreases T cell GM1 expression and inhibits clearance of respiratory syncytial virus: potential role of endogenous sialidase in antiviral immunity. J Immunol 2007;178:2651-4. http://dx.doi.org/10.4049/jimmunol.178.5.2651.
- Cox RJ, Mykkeltvedt E, Sjursen H, Haaheim LR. The effect of zanamivir treatment on the early immune response to influenza vaccination. Vaccine 2001;19:4743-9. http://dx.doi.org/10.1016/S0264-410X(01)00219-5.
- Fritz RS, Hayden FG, Calfee DP, Cass LM, Peng AW, Alvord WG, et al. Nasal cytokine and chemokine responses in experimental influenza A virus infection: results of a placebo-controlled trial of intravenous zanamivir treatment. J Infect Dis 1999;180:586-93. http://dx.doi.org/10.1086/314938.
- Ono H, Nagano Y, Matsunami N, Sugiyama S, Yamamoto S, Tanabe M. Oseltamivir, an anti-influenza virus drug, produces hypothermia in mice. Biol Pharm Bull 2008;31:638-42. http://dx.doi.org/10.1248/bpb.31.638.
- Ono H, Iwajima Y, Nagano Y, Chazono K, Maeda Y, Ohsawa M, et al. Reduction in sympathetic nerve activity as a possible mechanism for the hypothermic effect of oseltamivir, an anti-influenza virus drug, in normal mice. Basic Clin Pharmacol Toxicol 2013;113:25-30. http://dx.doi.org/10.1111/bcpt.12058.
- Hama R, Jones M, Hayashi K, Sakaguchi K. Oseltamivir and early deterioration leading to death. Int J Risk Saf Med 2011;23:201-15. http://dx.doi.org/10.3233/JRS-2011-0545.
- Jefferson T, Del Mar CB, Dooley L, Ferroni E, Al-Ansary LA, Bawazeer GA, et al. Physical interventions to interrupt or reduce the spread of respiratory viruses. Cochrane Database Syst Rev 2011;7.
- Toovey S, Rayner C, Prinssen E. Assessment of neuropsychiatric adverse events in influenza patients treated with oseltamivir. A comprehensive review. Drug Saf 2008;31:1097-114. http://dx.doi.org/10.2165/0002018-200831120-00006.
- Jones M, Hama R, Jefferson T, Doshi P. Neuropsychiatric adverse events and oseltamivir for prophylaxis. Drug Saf 2012;35:1187-8. http://dx.doi.org/10.1007/BF03262007.
- Toovey S. The author’s reply. Drug Saf 2012;35:1188-90. http://dx.doi.org/10.1007/BF03262008.
- Hama R, Jones M, Hayashi K, Yanagi K, Sakaguchi K. Oseltamivir: A Systematic Review and Meta-Analysis of Adverse Effects in Prospective Cohort Studies n.d.
- Yorifuji T, Suzuki E, Tsuda T. Oseltamivir and abnormal behaviors: true or not?. Epidemiology 2009;20:619-21. http://dx.doi.org/10.1097/EDE.0b013e3181a3d3f6.
- Fujita T, Fujii Y, Watanabe Y, Mori M, Yokota S. A pharmacoepidemiological study on the relationship between neuropsychiatric symptoms and therapeutic drugs after influenza infection. Jpn J Pharmacoepidemiol 2010;15:73-92. http://dx.doi.org/10.3820/jjpe.15.73.
- Kimura S, Niwa Y, Iwajima Y, Nagano Y, Yamamoto S, Ohi Y, et al. High doses of oseltamivir phosphate induce acute respiratory arrest in anaesthetized rats. Basic Clin Pharmacol Toxicol 2012;111:232-9. http://dx.doi.org/10.1111/j.1742-7843.2012.00889.x.
- Freichel C, Prinssen E, Hoffmann G, Gand L, Beck M, Weiser T, et al. Oseltamivir is devoid of specific behavioral and other central nervous system effects in juvenile rats at supratherapeutic oral doses. Int J Virol 2009;5:119-30. http://dx.doi.org/10.3923/ijv.2009.119.130.
- F. Hoffman-La Roche . Tamiflu Label (for FDA NDA No. 021087 2011. www.accessdata.fda.gov/drugsatfda_docs/label/2011/021087s057lbl.pdf (accessed 7 February 2011).
- Roche . Investigators Guide 2014. www.roche.be/fmfiles/re7189007/CU056/10_Investigators_brochure.pdf.
- Food and Drug Administration . Drug Approval Package. Tamiflu (Oseltamivir). Application No.: 021087-SE1–002 2000. www.accessdata.fda.gov/drugsatfda_docs/nda/2000/21–087SE1–002_review.pdf (accessed 27 August 2009).
- Lexchin J, Bero LA, Djulbegovic B, Clark O. Pharmaceutical industry sponsorship and research outcome and quality: systematic review. BMJ 2003;326:1167-70. http://dx.doi.org/10.1136/bmj.326.7400.1167.
- Lundh A, Sismondo S, Lexchin J, Busuioc OA, Bero L. Industry sponsorship and research outcome. Cochrane Database Syst Rev 2012;12. http://dx.doi.org/10.1002/14651858.mr000033.pub2.
- Burch J, Corbett M, Stock C, Nicholson K, Elliot AJ, Duffy S, et al. Prescription of anti-influenza drugs for healthy adults: a systematic review and meta-analysis. Lancet 2009;9:537-45. http://dx.doi.org/10.1016/S1473-3099(09)70199-9.
- Cooper NJ, Sutton AJ, Abrams KR, Wailoo A, Turner D, Nicholson KG. Effectiveness of neuraminidase inhibitors in treatment and prevention of influenza A and B: systematic review and meta-analyses of randomised controlled trials. BMJ 2003;326. http://dx.doi.org/10.1136/bmj.326.7401.1235.
- Falagas ME, Koletsi PK, Vouloumanou EK, Rafailidis PI, Kapaskelis AM, Rello J. Effectiveness and safety of neuraminidase inhibitors in reducing influenza complications: a meta-analysis of randomized controlled trials. J Antimicrob Chemother 2010;65:1330-46. http://dx.doi.org/10.1093/jac/dkq158.
- Tappenden P, Jackson R, Cooper K, Rees A, Simpson E, Read R, et al. Amantadine, oseltamivir and zanamivir for the prophylaxis of influenza (including a review of existing guidance no. 67): a systematic review and economic evaluation. Health Technol Assess 2009;13. http://dx.doi.org/10.3310/hta13110.
- Turner D, Wailoo A, Nicholson K, Cooper N, Sutton A, Abrams K. Systematic review and economic decision modelling for the prevention and treatment of influenza A and B. Health Technol Assess 2003;7. http://dx.doi.org/10.3310/hta7350.
- Hernan MA, Lipsitch M. Oseltamivir and risk of lower respiratory tract complications in patients with flu symptoms: a meta-analysis of eleven randomized clinical trials. Clin Infect Dis 2011;53:277-9. http://dx.doi.org/10.1093/cid/cir400.
- Cochrane Neuraminidase Inhibitors Review Team . Does oseltamivir really reduce complications of influenza?. Clin Infect Dis 2011;53:1302-3. http://dx.doi.org/10.1093/cid/cir706.
- Ebell MH, Call M, Shinholser J. Effectiveness of oseltamivir in adults: a meta-analysis of published and unpublished clinical trials. Fam Pract 2012;30:125-33. http://dx.doi.org/10.1093/fampra/cms059.
- Longini IM, Halloran ME, Nizam A, Yang Y. Containing pandemic influenza with antiviral agents. Am J Epidemiol 2004;159:623-33. http://dx.doi.org/10.1093/aje/kwh092.
- International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use . Structure and Content of Clinical Study Reports: E3 [Internet] 1995. www.ich.org/fileadmin/Public_Web_Site/ICH_Products/Guidelines/Efficacy/E3/E3_Guideline.pdf (accessed 12 July 2012).
- Jack A. Roche steps up production of Tamiflu after virus scare. Financial Times 2009.
- Chugai Pharmaceutical Company . Summary Basis of Approval; Tamiflu Capsule for Treatment 2001 n.d. http://211.132.8.246/shinyaku/g0012/07/53039900_21200AMY00238.html (accessed 12 July 2012).
- Chugai Pharmaceutical Company . Summary Basis of Approval; Oseltamivir Capsule for Prevention (2004) 2004. www.info.pmda.go.jp/shinyaku/P200400015/index.html (accessed 20 April 2009).
- World Health Organization . 18th Expert Committee on the Selection and Use of Essential Medicines: Section 6.4.3: Other Antivirals. November 2010 Update 2010. www.who.int/selection_medicines/committees/expert/18/en/index.html (accessed 16 November 2013).
- Muthuri S, Venkatesan S, Myles P, Leonardi-Bee J, Al Khuwaitir TS, Al Mamum A, et al. Effectiveness of neuraminidase inhibitors in reducing mortality in patients admitted to hospital with influenza A H1N1pdm09 virus infection: a meta-analysis of individual participant data. Lancet Respir Med 2014;2:395-404. http://dx.doi.org/10.1016/S2213-2600(14)70041-4.
- Muthuri S, Myles P, Venkatesan S, Leonardi-Bee J, Nguyen-Van-Tam J. Impact of neuraminidase inhibitor treatment on outcomes of public health importance during the 2009–10 influenza A(H1N1) pandemic: a systematic review and metaanalysis in hospitalized patients. J Infect Dis 2013;207:553-63. http://dx.doi.org/10.1093/infdis/jis726.
- Hsu J, Santesso N, Mustafa R, Brozek J, Chen YL, Hopkins JP, et al. Antivirals for treatment of influenza: a systematic review and meta-analysis of observational studies. Ann Intern Med 2012;156:512-24. http://dx.doi.org/10.7326/0003-4819-156-7-201204030-00411.
- Fiore A, Fry A, Shay D, Gubareva L, Bresee J, Uyeki T. Antiviral agents for the treatment and chemoprophylaxis of influenza: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep 2011;60:1-24.
- World Health Organization . Unedited Report of the 18th Expert Committee on the Selection and Use of Essential Medicines 2011. www.who.int/medicines/publications/unedited_trs/en/index.html (accessed 13 November 2013).
- World Health Organization . WHO Guidelines for Pharmacological Management of Pandemic Influenza A(H1N1) 2009 and Other Influenza Viruses n.d. www.who.int/csr/resources/publications/swineflu/h1n1_use_antivirals_20090820/en/index.html (accessed 20 November 2013).
- Harbord R, Egger M, Sterne J. A modified test for small-study effects in meta-analyses of controlled trials with binary endpoints. Stat Med 2006;25:3443-57. http://dx.doi.org/10.1002/sim.2380.
- Rucker G, Schwarzer G, Carpenter J. Arcsine test for publication bias in meta-analyses with binary outcomes. Stat Med 2008;27:746-63. http://dx.doi.org/10.1002/sim.2971.
- Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson D, . Meta-analysis of observational studies in epidemiology: a proposal for reporting. JAMA 2000;283:2008-12. http://dx.doi.org/10.1001/jama.283.15.2008.
- Wolkewitz W, Schumacher M. Statistical and methodological concerns about the beneficial effect of neuraminidase inhibitors on mortality. Lancet Respir Med 2014;2. http://dx.doi.org/10.1016/S2213-2600(14)70115-8.
- Fine J, Gray R. A proportional hazards model for the subdistribution of a competing risk. J Am Stat Assoc 1999;94:496-509. http://dx.doi.org/10.1080/01621459.1999.10474144.
- Louie J, Yang S, Acosta M, Yen C, Samuel M, Schechter R, et al. Treatment with neuraminidase inhibitors for critically ill patients with influenza A (H1N1) pdm09. Clin Infect Dis 2012;55:1198-204. http://dx.doi.org/10.1093/cid/cis636.
- Yang SG, Cao B, Liang LR, Li XL, Xiao YH, Cao ZX, et al. Antiviral therapy and outcomes of patients with pneumonia caused by influenza A pandemic (H1N1) virus. PLOS ONE 2012;7. http://dx.doi.org/10.1371/journal.pone.0029652.
- Siston A, Rasmussen S, Honein M, Fry AM, Seib K, Callaghan WM, et al. Pandemic 2009 influenza A (H1N1) virus illness among pregnant women in the United States. JAMA 2010;303:1517-25. http://dx.doi.org/10.1001/jama.2010.479.
- Dominguez-Cherit G, Lapinsky SE, Macias AE, Pinto R, Espinosa-Perez L, de la Torre A, et al. Critically Ill patients with 2009 influenza A(H1N1) in Mexico. JAMA 2009;302:1880-7. http://dx.doi.org/10.1001/jama.2009.1536.
- Altmann M, Fiebig L, Soyka J, von Kries R, Dehnert M, Haas W. Severe cases of pandemic (H1N1) 2009 in children, Germany. Emerg Infect Dis 2011;17:186-92. http://dx.doi.org/10.3201/eid1702.101090.
- Nguyen-Van-Tam J, Openshaw P, Hashim A, Gadd EM, Lim WS, Semple MG, et al. Risk factors for hospitalisation and poor outcome with pandemic A/H1N1 influenza: United Kingdom first wave. Thorax 2010;65:645-51. http://dx.doi.org/10.1136/thx.2010.135210.
- Kumar A, Zarychanski R, Pinto R, Cook DJ, Marshall J, Lacroix J, et al. Critically ill patients with 2009 influenza A(H1N1) infection in Canada. JAMA 2009;302:1872-9. http://dx.doi.org/10.1001/jama.2009.1496.
- Thompson DL, Jungk J, Hancock E, Smelser C, Landen M, Nichols M, et al. Risk factors for 2009 pandemic influenza A (H1N1)-related hospitalization and death among racial/ethnic groups in New Mexico. Am J Public Health 2011;101:1776-84. http://dx.doi.org/10.2105/AJPH.2011.300223.
- Jain S, Kamimoto L, Bramley A, Schmitz AM, Benoit SR, Louie J, et al. Hospitalised patients with 2009 H1N1 influenza in the United States, April–June 2009. N Engl J Med 2009;361:1935-44. http://dx.doi.org/10.1056/NEJMoa0906695.
- Farias J, Fernandez A, Monteverde E, Vidal N, Arias P, Montes MJ, et al. Critically ill infants and children with influenza A (H1N1) in pediatric intensive care units in Argentina. ICM 2010;36:1015-22. http://dx.doi.org/10.1007/s00134-010-1853-1.
- Yang P, Deng Y, Pang X, Shi W, Li X, Tian L, et al. Severe, critical and fatal cases of 2009 H1N1 influenza in China. J Infect 2010;61:277-83. http://dx.doi.org/10.1016/j.jinf.2010.07.010.
- Enstone J, Myles P, Openshaw P, Gadd E, Lim, W, Semple M, et al. Nosocomial pandemic (H1N1) 2009, United Kingdom, 2009–2010. Emerg Infect Dis 2011;17:592-8. http://dx.doi.org/10.3201/eid1704.101679.
- Chitnis A, Truelove S, Druckenmiller J, Heffernan R, Davis J. Epidemiologic and clinical features among patients hospitalized in Wisconsin with 2009 H1N1 influenza A virus infections, April to August 2009. WMJ 2010;109:201-8.
- ANZIC . Critical illness due to 2009 A/H1N1 influenza in pregnant and postpartum women: population based cohort study. BMJ 2010;340. http://dx.doi.org/10.1136/bmj.c1279.
- Yung M, Slater A, Festa M, Williams G, Erickson S, Pettila V, et al. Pandemic H1N1 in children requiring intensive care in Australia and New Zealand during winter 2009. Pediatrics 2011;127:e156-63. http://dx.doi.org/10.1542/peds.2010-0801.
- Javadi AA, Ataei B, Khorvash F, Babak A, Rostami M, Mostafavizadeh K, et al. Clinical features of novel 2009 influenza a (H1N1) infection in Isfahan, Iran. J Res Med Sci 2011;16:1550-4.
- Miranda-Choque E, Ramírez C, Candela-Herrera J, Díaz J, Fernández A, Kolevic L, et al. Niños hospitalizados con neumonía por influenza AH1N11/2009 pandémico en un hospital de referencia de Perú Children hospitalized with influenza pneumonia AH1N1/2009 pandemic in the INSN. Rev Peru Med Exp Salud Publica 2011;28:610-16.
- Poeppl W, Hell M, Herkner H, Stoiser B, Fritsche G, Schurz-Bamieh N, et al. Clinical aspects of 2009 pandemic influenza A (H1N1) virus infection in Austria. Infection 2011;39:341-52. http://dx.doi.org/10.1007/s15010-011-0121-9.
- Riquelme R, Jimenez P, Videla AJ, Lopez H, Chalmers J, Singanayagam A, et al. Predicting mortality in hospitalized patients with 2009 H1N1 influenza pneumonia. Int J Tuberc Lung Dis 2011;15:542-6. http://dx.doi.org/10.5588/ijtld.10.0539.
- Yokota R, Skalinski L, Igansi C, de Souza LR, Iser BP, Reis PO, et al. Risk factors for death from pandemic (H1N1) 2009, Southern Brazil. Emerg Infect Dis 2011;17:1467-71. http://dx.doi.org/10.3201/eid1708.101233.
- Bagdure D, Curtis DJ, Dobyns E, Glode MP, Dominguez SR. Hospitalized children with 2009 pandemic influenza A (H1N1): comparison to seasonal influenza and risk factors for admission to the ICU. PLOS ONE 2010;5. http://dx.doi.org/10.1371/journal.pone.0015173.
- Blumental S, Huisman E, Cornet MC, Ferreiro C, De Schutter I, Reynders M, et al. Pandemic A/H1N1v influenza 2009 in hospitalized children: a multicenter Belgian survey. BMC Infect Dis 2011;11. http://dx.doi.org/10.1186/1471-2334-11-313.
- Chemaly RF, Vigil KJ, Saad M, Vilar-Compte D, Cornejo-Juarez P, Perez-Jimenez C, et al. A multicenter study of pandemic influenza A (H1N1) infection in patients with solid tumors in 3 countries: early therapy improves outcomes. Cancer 2012;118:4627-33. http://dx.doi.org/10.1002/cncr.27447.
- Çiftçi E, Tuygun N, Ozdemir H, Tezer H, Sensoy G, Devrim I, et al. Clinical and epidemiological features of Turkish children with 2009 pandemic influenza A (H1N1) infection: experience from multiple tertiary paediatric centres in Turkey. Scand J Infect Dis 2011;43:923-9. http://dx.doi.org/10.3109/00365548.2011.598872.
- del Rosal T, Baquero-Artigao F, Calvo C, Mellado MJ, Molina JC, Santos MDM, et al. Pandemic H1N1 influenza-associated hospitalizations in children in Madrid, Spain. Influenza Other Respir Viruses 2011;5:e544-51. http://dx.doi.org/10.1111/j.1750-2659.2011.00272.x.
- Kusznierz G, Uboldi A, Sosa G, Torales S, Colombo J, Moyano C, et al. Clinical features of the hospitalized patients with 2009 pandemic influenza A (H1N1) in Santa Fe, Argentina. Influenza Other Respir Viruses 2012;7:410-17. http://dx.doi.org/10.1111/j.1750-2659.2012.00405.x.
- Mickienė A, Daniuseviciute L, Vanagaite N, Velyvyte D, Blauzdziuniene O, Nadisauskiene R, et al. Hospitalized adult patients with 2009 pandemic influenza A (H1N1) in Kaunas, Lithuania. Medicina (Kaunas) 2011;47:11-8.
- Moretti ML, Sinkoc V, Cardoso LG, Camargo GJ, Bachur LF, Hofling CC, et al. Lessons from the epidemiological surveillance program, during the influenza A (H1N1) virus epidemic, in a reference university hospital of Southeastern Brazil. Rev Soc Bras Med Trop 2011;44:405-11. http://dx.doi.org/10.1590/S0037-86822011005000048.
- Brink M, Hagberg L, Larsson A, Gedeborg R. Respiratory support during the influenza A (H1N1) pandemic flu in Sweden. Acta Anaesthesiol Scand 2012;56:976-86. http://dx.doi.org/10.1111/j.1399-6576.2012.02727.x.
- Rahamat-Langendoen JC, Tutuhatunewa ED, Scholvinck EH, Hak E, Koopmans M, Niesters HG, et al. Influenza in the immediate post-pandemic era: a comparison with seasonal and pandemic influenza in hospitalized patients. J Clin Virol 2012;54:135-40. http://dx.doi.org/10.1016/j.jcv.2012.02.010.
- Herxheimer A, Clarke M, Edwards R, Jefferson T, Loke Y. A/H1N1 flu: time for case–control studies of NSAIDs and oseltamivir. BMJ 2009;339. http://dx.doi.org/10.1136/bmj.b3048.
- Hama R. Potential Harm of Oseltamivir and NSAIDs Should Be Discussed, Before the Threat of a 2009A H1N1 Influenza-Caused Pandemic Is Feared. (Rapid Response) 2009. www.bmj.com/cgi/eletters/338/may12_3/b1962#214206 (accessed 9 April 2014).
- Eyers S, Weatherall M, Shirtcliffe P, Perrin K, Beasley R. The effect on mortality of antipyretics in the treatment of influenza infection: systematic review and meta-analysis. J R Soc Med 2010;103:403-11. http://dx.doi.org/10.1258/jrsm.2010.090441.
- Beyersmann J, Gastmeier P, Wolkewitz M, Schumacher M. An easy mathematical proof showed that time-dependent bias inevitably leads to biased effect estimation. J Clin Epidemiol 2008;61:1216-21. http://dx.doi.org/10.1016/j.jclinepi.2008.02.008.
- Suissa S. Immortal time bias in pharmacoepidemiology. Am J Epidemiol 2007;167:492-9. http://dx.doi.org/10.1093/aje/kwm324.
- Laupacis A. Observational studies of treatment effectiveness: some cautions. Ann Intern Med 2004;140:923-4. http://dx.doi.org/10.7326/0003-4819-140-11-200406010-00014.
- Zhou Z, Rahme E, Abrahamowicz M, Pilote L. Survival bias associated with time-to-treatment initiation in drug effectiveness evaluation: a comparison of methods. Am J Epidemiol 2005;162:1016-23. http://dx.doi.org/10.1093/aje/kwi307.
- Leonardi-Bee J, Venkatesan S, Muthuri S, Nguyen-Van Tam J, Myles P. Statistical and methodological concerns about the beneficial effect of neuraminidase inhibitors on mortality. Lancet Respir Med 2014;2:e10-12. http://dx.doi.org/10.1016/S2213-2600(14)70137-7.
- Van Walraven C, Davis D, Forster A, Wells G. Time-dependent bias was common in survival analyses published in leading clinical journals. J Clin Epidemiol 2004;57:672-82. http://dx.doi.org/10.1016/j.jclinepi.2003.12.008.
- Nicholson KG, Aoki FY, Osterhaus AD, Trottier S, Carewicz O, Mercier CH, et al. Efficacy and safety of oseltamivir in treatment of acute influenza: a randomised controlled trial. Neuraminidase Inhibitor Flu Treatment Investigator Group. Lancet 2000;355:1845-50. http://dx.doi.org/10.1016/S0140-6736(00)02288-1.
- Treanor JJ, Hayden FG, Vrooman PS, Barbarash R, Bettis R, Riff D, et al. Efficacy and safety of the oral neuraminidase inhibitor oseltamivir in treating acute influenza: a randomized controlled trial. US Oral Neuraminidase Study Group. JAMA 2000;283:1016-24. http://dx.doi.org/10.1001/jama.283.8.1016.
- Gøtzsche PC, Jørgensen AW. Opening up data at the European Medicines Agency. BMJ 2011;342. http://dx.doi.org/10.1136/bmj.d2686.
- Lefebvre C, Manheimer E, Glanville J, Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions. The Cochrane Collaboration; 2011.
- Food and Drug Administration . Drugs@FDA n.d. www.accessdata.fda.gov/scripts/cder/drugsatfda/2011 (accessed 17 May 2016).
- Food and Drug Administration . Warning Letters n.d. www.fda.gov/ICECI/EnforcementActions/WarningLetters/default.htm 2011 (accessed 17 May 2016).
- Brown JKM. Experimental Design Generator and Randomiser n.d. www.edgarweb.org.uk/2011 (accessed 24 August 2011).
- Simon R, Makuch RW. Non-parametric graphical representation of the relationship between survival and the occurrence of an event: application to responder versus non-responder bias. Stat Med 1984;3:35-44. http://dx.doi.org/10.1002/sim.4780030106.
Appendix 1 The story of A159
The 2009 review: from A047 to A159
In the midst of the A/H1N1 influenza outbreak in June 2009, the Australian and UK governments commissioned an update of our long-standing Cochrane review on NIs for influenza in (otherwise) healthy adults (known as A047). Prior to the emergence of influenza A/H1N1 in 2009, governments worldwide stockpiled nearly CHF (Swiss francs) 7.6B worth of oseltamivir. 166 The WHO considered antivirals for influenza important (WHO has recently added oseltamivir to the list of essential medicines169,174,175). Oseltamivir and zanamivir have been prescribed for the treatment of influenza worldwide since the outbreak of 2009 A/H1N1 influenza. The review (on healthy adults) had first been published in 1999 (as A047) and was updated in 2006 and 2008. At the same time a similar review on children32 (or A046) had also been published.
As the review had been updated the previous year, we initially anticipated that the commissioned 2009 update would not require substantial effort and would probably reflect only updated pharmacovigilance data and not the incorporation of new trial evidence. 6
In the end, the 2009 update was inconclusive regarding whether or not oseltamivir reduced the risk of complications of influenza,14 as we were unable to verify the data underlying manufacturer and government claims to this effect. The claims were based on clinical trial evidence included in a published pooled analysis of 10 manufacturer-funded clinical trials of oseltamivir for the treatment of influenza in people aged ≥ 13 years. 4 Eight of the 10 trials in the Kaiser et al. 4 pooled analysis have never been published,31 and their complete data sets were not available from either the authors or the manufacturers. Some of the published trials had been ghost written. 43 The largest of the 10 Kaiser trials (M7600136), involving over 1400 people, had been briefly reported in conference abstract format but the person whose name appeared on the abstract could not recall ever presenting its results or being involved with the study. 43 Our early requests for data from the 10 Kaiser studies were met with an offer from Roche to sign a confidentiality agreement with an embedded secrecy clause preventing us from mentioning the existence of the agreement. The unsigned agreement can be seen at www.bmj.com/highwire/filestream/440792/field_highwire_adjunct_files/0.
At the time of publication of the 2009 update and its linked investigation by the BMJ, we were unaware of the size and depth of the oseltamivir evidence development programme. We thought it comprised around 36 trials and we expected that only a proportion of these would fit our inclusion criteria. We also did not realise the size and the level of detail that the CSRs contained.
On 31 December 2009, Roche released the core reports (or module 1s) of the 10 Kaiser trials with no legal agreement signed (only a web-based agreement that we would not share the documents with other commercial companies). After requesting Roche to provide us with the full study reports, Roche said that the module 1s were all that were needed for us to complete our job. 6 The missing modules (or parts), numbered 3–4 according to the trial in question, contained protocols, amendments, individual listings and demographic information. It seemed to us that these documents would have contained some important additional material for understanding the trials, their design and interpretation but we were not sure.
In 2010 we started exploring the relationship between the available module 1s for the only two Kaiser trials that had been published (Doshi8 or Nicholson et al. ,220 and WV1567158 or Treanor et al. 221).
At about this time we started getting concerned that the oseltamivir trial programme was considerably larger than we first thought. Our interest was awakened by the casual discovery of a confidential 2009 Roche Tamiflu Investigator’s Brochure, which was freely accessible on the web. This reported a clinical trial programme of over 60 studies. Searching for an unpublished and hitherto unseen data set requires constructing a reasonably accurate list of all studies of the drug in question. The Roche Investigator’s Brochure did not mention some studies that we were aware of and reinforced an idea that we had become clear was essential: the need to develop our own list of trials, because a single, authoritative, up-to-date and complete list of all clinical trials conducted on humans using both drugs did not seem to exist.
When thinking about our next update we decided not to use publications because the majority of treatment trial evidence for Tamiflu remained unpublished; we had found some discrepancies between CSRs and published equivalents; and, mostly, CSRs were so much more detailed and comprehensive than short journal articles, enabling a more thorough critical analysis of the trials. We also decided to expand the scope of A047 by including evidence relating to people of all ages except for immune-suppressed individuals. This, de facto, amounted to the creation of one new review (A159) with a new protocol subsuming A047 and A046. The protocol for A159 was publicly posted in December 2010.
A new source of evidence for A159
Today, the obvious source of information on CSRs would be trial registries and company websites, but most trials of both NIs were carried out before inception or wide acceptance of centralised registries and company websites. In 2009–11, company websites did not, and still do not, have extensive lists of trials with downloadable CSRs. Most people had never heard of CSRs before media coverage of our efforts.
We decided to construct our list by using multiple cross-referencing methods. We constructed a list beginning with clinical trials identified from previous review updates. To this end, we added additional trials in humans from multiple sources, including manufacturer submissions to regulators, drug product information sheets, previous published reviews, Health Technology Assessment (HTA) documents and public and manufacturers’ registers,5,156,157,159,160 such as www.ClinicalTrials.gov and www.roche-trials.com. Regulatory documents also aided the identification of unknown trials. Finally, we also conducted traditional database and grey literature searches (see Appendix 3) to identify previously unknown trials.
One of the first things we learned was that to ensure that the list did not include duplicate entries, we had to assign to each trial a unique trial ID. ‘Author’ is not a good choice of unique trial ID, as different authors can be present across different versions of the same trial (i.e. the authors of CSRs can be different from publications arising from the same clinical trial). Nor are any other details connected to publications a good option for unique trial ID because not all studies are published. Some trials will have company-specific codes and some will have public clinical trial registry numbers, or both, or neither. To simplify recognition and terminology we used the manufacturer protocol ID as our unique trial ID.
Our list was going to be useful only if it had sufficient details to enable us to decide whether or not it met our inclusion criteria. For each unique trial ID, we gathered the following details:
-
unique trial ID
-
other IDs
-
phase of study
-
sponsor
-
short description
-
official trial title
-
first authors (name and e-mail)
-
type of trial
-
comparator
-
outcomes assessed
-
date of trial
-
study period (days)
-
population
-
number of participants planned
-
number of participants enrolled
-
number of participants completing
-
trial status (e.g. completed, ongoing or early termination)
-
publication status (a citation or understanding of why it was not published)
-
how identified (to record how the trial was discovered)
-
notes.
Once we had as complete a list of trials as possible, we contacted manufacturers and sent them our draft list, asking them to check the accuracy and completeness of our list. Roche, GSK and BioCryst all did so and, in doing so, we learned of hitherto unknown trials.
Occasionally, the existence of further unknown trials was detected weeks and months after we thought we had a ‘complete’ list. This may be inevitable, given that trial identification often takes place in unpredictable ways, for example while reading through detailed regulatory reports.
We engaged in prolonged correspondence with Roche and GSK, and requested a series of regulatory documents under freedom of information policies from both the FDA and EMA. No substantial comments were made by Roche on the protocol of 159, which has been publicly available in one form or another since December 2010.
Specifically, we applied to EMA under their new release policy for 26 CSRs in their holdings relating to oseltamivir and GSK’s zanamivir. The result was the delivery (starting in late March 2011) of 16 CSRs, all containing modules 1 and 2 plus one complete report for oseltamivir (trial WP16263104). (See table 1 in Doshi et al. 6) None was available for zanamivir, as the EMA had not played a part in its market authorisation. These formed the basis for the 2012 version of A159.
At the date of completion of data searches for A159 (12 April 2011), Roche had provided us with only partial CSRs despite five requests for full CSRs. The material obtained from Roche included the first section (or so-called ‘module 1′ or ‘core report’) of a full CSR, each of which contain four to five modules (see Appendix 9) for the 10 oseltamivir treatment trials included in the Kaiser et al. 4 meta-analysis. Not contained in the provided module 1s are trial protocols with the list of amendments and original reporting analysis plans (RAPs). These module 1s comprise 3195 pages. Roche had not made available any further material and indicated that it did not intend to answer our requests for clarification on aspects of trials and for availability of the missing parts of complete CSRs. In addition we had a 53-page report in English of the treatment trial ML16369,76 sponsored by Shanghai Roche Pharmaceutical Ltd. Regardless of success with our requests to obtain full CSRs, we decided to update our review with available material and subsequently update it as and when additional data became available.
Our searches of publication databases did not add any significant information.
Following a change of policy at the EMA, prompted by similar efforts of the Nordic Cochrane Centre,222 we received an additional eight CSRs (10,737 pages) in response to a FOI request. An additional 14,700 pages of further CSRs and 33 pages of regulators’ comments arrived after our search deadline. All of the materials received from the EMA are related to oseltamivir. The EMA has no access to information for zanamivir, as it is a nationally authorised product in Europe (correspondence with Xavier Luria, 23 March 2011, and David Mackay, 20 July 2011). At present, we hold all of the module 1s and module 2s of oseltamivir trials we have requested. From GSK we have received the promise of IPD. Many of the CSRs used in this review were obtained via FOI requests.
We still await a FDA decision regarding similar requests sent to FDA in January 2011.
We were able to download 2673 pages of SBA documents from the FDA website, 31 from EMA and 508 pages of Japanese SBA. We indexed the content and then constructed an extended table of contents, giving a summary of each file, thereby facilitating navigation of these complex documents. Once the table of contents had been constructed, we postulated that, given the huge work involved in reviewing lots of regulatory files, including CSRs, we needed new instruments to indicate which parts were more important than others, thus focusing our efforts. We experimented with a variety of methods reported in the earlier version of the review. We have now devised and used what, for us, is a satisfactory instrument for critically assessing CSRs in their entirety. We intend to publish this separately.
The EMA releases, coupled with documents from the FDA SBA for both drugs, formed the basis for the version of A159 that we eventually published in January 2012. The review reported our efforts to get to the bottom of the issue of the effects of NIs by appraising evidence from unpublished CSRs (see Appendix 1) and regulatory documents containing comments and reviews. We called the body of clinical studies and regulatory comments ‘regulatory information’, as all of these documents are either created for, or by, regulators. To our knowledge, this was the first Cochrane review ever conducted on the basis of regulatory documents only.
Owing to funding timelines and the sizeable amount of regulatory information already available to us, we decided to review material available as at 12 April 2011. This meant reviewing FDA SBA material and core reports (module 1s) in our possession from EMA data releases received by this time.
Study selection and extraction in 2011
In 2011 our methods were a mixture of established and novel, reflecting the size of the task, our lack of experience in dealing with large amounts of very detailed regulatory information and the lack of a complete set of CSRs. For example, scanning of titles and abstracts was doubled, but selection of studies for inclusion from the list constructed during our search was quadrupled, with disagreements resolved by discussion.
For many studies we had only titles and, in some cases, a very brief description of content, thus we assigned three categories to our trials:
-
definitely included
-
definitely excluded
-
trials for which we needed further information.
We excluded studies that were definitely not meeting the inclusion criteria on the basis of the available information (e.g. the title described the trial as a pharmacokinetic study). Where appropriate we requested further information from the trials’ sponsor: usually copies of the CSRs (minus participant identification) for each trial that was definitely included or for which we needed further information. We did not contact first/corresponding authors of published versions of the trials on the basis of our experience with the 2009 review.
Data extraction and management reflected the lack of established methods for reviewing regulatory material. We subdivided the extraction, appraisal and analysis of the data into a two-stage exercise, including studies in the analysis phase only if we judged their reports to be reliable and complete. To help structure the information we used CONSORT statement-based extraction forms aimed at assembling a concise version of the CSRs, which included all of the important methods, as well as defined and extracted all relevant outcomes. We colour-coded the original text to flag up uncertainty or lack of clarity or need for more information from other (then inaccessible) parts of the CSR.
During this process we excluded all six peramivir trials, as we were informed by the manufacturers that no CSRs would be available. The 2012 A159 review was based on 15 oseltamivir clinical study core reports and 10 very brief zanamivir study reports. The former came from EMA, whereas the latter had been part of a GSK submission to UK NICE, which the BMJ had passed on to us together with the SBA material. Our 2010 protocol for A159 was not very detailed on how we would handle this mass of information for the simple reason that no one had ever done it before. We quite literally were learning as we were going along, and our understanding of the structure and content of CSRs evolved. We created and tested five post-protocol hypotheses (see Appendix 8), which had originated from the findings in the reports. The best example was our finding of an unnaturally high (up to 80%) influenza positivity rate in treatment trials, which, in some cases, had been pooled because of lack of viral circulation. We hypothesised that screening for influenza positivity had been carried out prior to enrolment of people with ILI. This was not borne out by the evidence available to us. We know now that a far simpler explanation is more likely: careful selection of the time period for trial participant enrolment, based on when surveillance data suggested that high influenza activity led to the recruitment of small numbers of participants from each of many centres with a high likelihood of influenza positivity, but at the time we had limited information available.
The 2012 A159 review analyses were based on the ITT population, which we had found to be the only reliable analysis unit, as oseltamivir appeared to have an effect on antibody production in people with influenza, leading to an imbalance in numbers of subjects in the influenza-infected (so-called ITTI) subpopulation. This, in effect, introduced confounding in what otherwise should have been well-designed double-blind trials. The only effect that was clearly identifiable was a modest shortening of ILI symptoms by less than a day. This led us to believe that oseltamivir had an aspecific powerful effect on symptoms, not mediated by any action on influenza viruses but possibly via an anti-inflammatory mechanism. Clearly, the trials had been designed with a commercial focus in mind and some of the claims made by the manufacturer (especially on the effect on interruption of transmission and on pneumonia) were not supported by the evidence in our possession.
2012 to the present day
Soon after the publication of the review, the BMJ agreed to publish our correspondence with Roche, GSK, the EMA, the CDC and WHO, recording our attempts at retrieving the full reports without any conditions attached and to understand the basis for promotion of the drugs (especially oseltamivir) by public health bodies. The correspondence (which is hundreds of pages long) formed the basis for what then became the BMJ Open Data Campaign and a stimulus for the later AllTrials campaign. Public exposure of our efforts and copious media coverage had the direct effect of ensuring the unconditional release of 77 reports of oseltamivir of 82 studies sponsored by Roche, and the equivalent of the 30 studies we had requested from GSK. For the full correspondence, see www.bmj.com/tamiflu and www.bmj.com/relenza. The reports (amounting to over 140,000 pages) are made available with this review for the first time (at https://datadryad.org/resource/doi:10.5061/dryad.77471/2, p. 3), marking a small but significant victory for open science.
Before receiving the full reports, we resumed reviewing the remainder of the material that we had received in 2011. This mainly consisted of module 2s (Roche terminology for pre-study documents). Module 2s contained the information originally denied to us by Roche: study protocols with their amendments, randomisation lists, blank CRFs, certificates of analysis describing appearance and content of active and control capsules and, at times, SAPs. CRFs are containers for the rawest form of recorded data at the individual participant level.
We had no tools for reviewing and synthesising this information so, again, we had to create our own. The instrument is made up of three parts each with a separate function. In the first part there is a template for a brief summary description of the trial. The format fits into the RevMan (RevMan 5.3; The Cochrane Collaboration, The Nordic Cochrane Centre, Copenhagen, Denmark) Characteristics of Included Studies Table (CIST) and is mainly descriptive. The second part is the appraisal of the trial following the Cochrane risk-of-bias format. The third part reconstructs the trial timeline and provides a checklist and position in the document of the various elements, such as protocol, protocol amendments and study period with dates. The last part aims to check the internal consistency and coherence of each element (such as numbers screened, numbers randomised, interventions, comparators) across all the different documents, starting from the earliest available version of the protocol. The form also contains suggestions on where to look for the information. This is based on our experience gained in this review and in a descriptive review11 of 78 CSRs of 14 different drugs and biologicals.
While designing the tool, we also asked ourselves whether or not access to module 2 information (and later the full study reports) changed our perception of the trial and specifically our risk-of-bias assessment. We found that access to what are supposed to be full study reports should provide clarity and remove the rationale for ‘unclear’ risk-of-bias judgements, and, ideally, remove the concept of risk leaving just ‘bias’, at least for certain study design elements, such as attrition bias. Either a design element introduces bias or it does not. In the case of the 15 full oseltamivir CSRs we reviewed when constructing our tool, only one contained a protocol that predated the beginning of participant enrolment, only two had SAPs that clearly predated participants’ enrolment and three had clearly dated protocol amendments. No CSR reported a clear date of unblinding.
During the latter part of 2013, we received from the manufacturers tens of thousands of pages of full CSRs for both programmes combined.
The history and conclusions form the backdrop to this version of A159.
Oseltamivir studies received from Hoffman La Roche SA in CSR format:
-
WV1627769
-
WV15819/WV15876/WV1597867
-
WV1570760
-
WV15812/WV1587266
-
WV1573062
-
M7600136
-
WV156708
-
WV1567158
-
NV1687157
-
WV15759/WV1587164
-
WV16193
-
WV1582568
-
WV1570861
-
WV1579965
-
WV15673/WV1569759
-
WV1575863
-
NV20235
-
M76006
-
NV20236
-
NP15717
-
PV15616 (= GS-97-801)
-
PV15615 (= GS-97-802)
-
JV16284
-
WV15731
-
NV22155
-
NP15719
-
WP16254
-
WP16094
-
WP18308
-
WP16225
-
WP16134
-
PP15974
-
NP16472
-
NP15718
-
WP16226
-
NP25139
-
NP25138
-
NP15901
-
WP15525
-
NP25140
-
NP15728
-
NP15810
-
NP15826
-
PP16351
-
WP22849
-
NP22770
-
WP20727
-
PP16361
-
WP15517
-
NP15729
-
BP21288
-
WP21272
-
JP15735
-
WP15647
-
WP15648
-
WP15676
-
WP16263
-
NP15757
-
NV25118
-
NP15743
-
NP15881
-
NP15912
-
WP15979
-
WP16137
-
WP16295
-
NP15827
-
NV25655
-
JV21490
-
JP15734
-
NV22158
-
ML17713
-
ML22789
-
NV25182
-
ML17279 – publication only
-
ML19340 – publication only
-
JV1582374 – English translation of Gaiyo summary
-
JV1582475 – English translation of Gaiyo summary
-
ML17279 (= WV17052)
-
ML19340 (= COSMOS Study).
Zanamivir studies received from GSK in CSR format:
-
167-10170
-
JNAI-0171
-
JNAI-0472
-
JNAI-0773
-
NAI3000877
-
NAI3000978
-
NAI3001079
-
NAI3001180
-
NAI3001281
-
NAI3001582
-
NAI3002083
-
NAI3002884
-
NAI3003185
-
NAI3003486
-
NAIA/B200887
-
NAIA/B200988
-
NAIA200589
-
NAIA200690
-
NAIA300291
-
NAIA300392
-
NAIA300493
-
NAIA300594
-
NAIB200595
-
NAIB200696
-
NAIB200797
-
NAIB300198
-
NAIB300299
-
PE-01100
-
167T3–11
-
NAIA2010.
Appendix 2 Compliharms: events alternatively recorded as complications or harms
Roche clinical study report of oseltamivir treatment trial
The following symptoms, signs and common sequelae associated with influenza were excluded from specific adverse event reporting if they occurred during the period of drug treatment provided their appearance was in conjunction with one or more other influenza-related symptoms. The recrudescence of single discrete signs/symptoms associated with influenza syndrome were recorded as adverse events. 61
[Event by body system]
Respiratory cough, pneumonia, bronchitis/tracheitis, sinusitis, dyspnoea/difficulty breathing
Cardiovascular tachycardia
Eyes, ears, nose and throat sore throat, nasal obstruction, earache, otitis, coryza, conjunctivitis
Central nervous system headache, fatigue
Musculoskeletal myalgia
Other fever, rigor, malaise/asthenia, chills
Source: ‘Appendix 1. Events Associated with Influenza Syndrome’. Roche Clinical Study Report No. W-144117, Protocol WV15707, module I-43.
A 1999 Food and Drug Administration medical review of oseltamivir
As symptoms and common sequelae of influenza were collected as end point data, these symptoms, signs and common complications were specifically excluded from reporting as adverse events. The following table [above] lists events associated with influenza syndrome which were excluded from adverse event reporting. . .In addition, following the alleviation of influenza-like symptoms, the recurrence of a single respiratory or constitutional symptom was recorded as an adverse event; however, the reappearance of more than one symptom was recorded as influenza-like syndrome (i.e. secondary illness). Comment: As the applicant [Hoffman-La Roche] stated in a written response dated 6/11/99, some sites incorrectly reported symptoms occurring prior to the cessation of the primary illness as secondary illness. 109
Emphasis in the original. Oseltamivir Medical Review. US FDA Center for Drug Evaluation and Research, Application No. 021087, 25 October 1999, p. 15. www.accessdata.fda.gov/drugsatfda_docs/nda/99/21087_Tamiflu_medr_P1.pdf.
Appendix 3 Searches of the electronic databases
Although this review focuses on the primary data sources of manufacturers, we ran electronic searches in the following databases to check that there were no published RCTs from non-manufacturer sources:
-
CENTRAL (2013, issue 6) limited to year published 2010–13 (20 search results).
-
MEDLINE (January 2011 to July week 2, 2013) (56 search results) and MEDLINE (via Ovid) from 1 January 2011 to July week 2, 2013 (56 search results).
-
EMBASE (January 2011 to July 2013) (90 search results) and EMBASE.com from 1 January 2011 to July 2013 (90 search results).
-
PubMed (not MEDLINE) no date limit (21 records). We searched PubMed to identify publisher submitted records that will never be indexed in MEDLINE and the most recently added records not yet indexed in MEDLINE.
To identify reviews that may possibly have referenced further trials we searched:
-
DARE (2013 issue 2 of 4 April; four search results)
-
NHS EED (issue 2 of 4 April 2013; two search results) – both resources are part of The Cochrane Library, www.thecochranelibrary.com (accessed 22 July 2013).
-
HEED (searched 22 July 2013; three search results).
Previously, we had searched CENTRAL (eight search results); MEDLINE (via Ovid) from 1 May 2009 to 12 April 2011 (31 search results); EMBASE from 1 January 2010 to 12 April 2011 (54 search results); DARE (five search results) and NHS EED (five search results). CENTRAL, DARE and NHS EED are part of The Cochrane Library, www.thecochranelibrary.com (issue 2, 2011, accessed 1 June 2011). All search results were loaded to an electronic library (EndNote X4; Thomson Reuters, CA, USA).
We used the following search strategy to search MEDLINE and CENTRAL. We combined the MEDLINE search with the Cochrane Highly Sensitive Search Strategy for identifying randomised trials in MEDLINE: sensitivity- and precision-maximising version (2008 revision); Ovid format. 223 We adapted the search strategy for EMBASE. We imposed no publication or language restrictions.
MEDLINE (via Ovid)
-
Influenza, Human/
-
exp Influenzavirus A/
-
exp Influenzavirus B/
-
(influenza* or flu).tw.
-
or/1-4
-
Oseltamivir/
-
Zanamivir/
-
neuraminidase inhibitor*.tw.
-
(oseltamivir or zanamivir or tamiflu or relenza or peramivir or gs4071).tw,nm.
-
or/6-9
-
5 and 10
EMBASE.com
17 #13 AND #16
16 #14 OR #15 833616
15 random*:ab,ti OR placebo*:ab,ti OR factorial*:ab,ti OR crossover*:ab,ti OR ‘cross over’:ab,ti OR ‘cross-over’:ab,ti OR volunteer*:ab,ti OR assign*:ab,ti OR allocat*:ab,ti OR ((singl* OR doubl*) NEAR/1 blind*):ab,ti
14 ‘randomised controlled trial’/exp OR ‘single blind procedure’/exp OR ‘double blind procedure’/exp OR ‘crossover procedure’/exp
13 #4 AND #12
12 #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11
11 oseltamivir:ab,ti OR zanamivir:ab,ti OR tamiflu:ab,ti OR relenza:ab,ti OR peramivir:ab,ti OR laninamivir:ab,ti OR gs4071:ab,ti
10 ‘sialidase inhibitor’:ab,ti OR ‘sialidase inhibitors’:ab,ti
9 ‘neuraminidase inhibitor’:ab,ti OR ‘neuraminidase inhibitors’:ab,ti
8 ‘sialidase inhibitor’/exp
7 ‘peramivir’/de
6 ‘zanamivir’/de
5 ‘oseltamivir’/de
4 #1 OR #2 OR #3
3 influenza*:ab,ti OR flu:ab,ti
2 ‘influenza virus a’/exp OR ‘influenza virus b’/de
1 ‘influenza’/exp
Appendix 4 Searches for regulatory information
We searched the following sources:
-
the FDA
-
the EMA
-
Roche
-
the Japanese regulator [Pharmaceuticals and Medical Devices Agency (PMDA)] SBA.
We conducted a search of the FDA regulatory documentation of the NDAs and supplementary NDAs (sNDAs) of both drugs. 224 The FDA NDA documentation includes medical, statistical, microbiological and other reviews, product labels, reports of site inspections, meetings with manufacturers and records of the decision-making leading to registration and post-marketing requirements. We also searched ‘Warning Letters’ dispatched by the FDA. 225
To organise receipt of FDA materials, we created a TOC listing all of the regulatory and pharmaceuticals documents that were accessible to us. The TOC’s function was that of an index, searchable quick reference guide and research tool to enable us to carry out quantitative (e.g. citation density analysis) and qualitative analyses (e.g. theme summaries) of the content. We also needed a rapid aide-memoire with brief summaries of the evidence contained in each regulatory document listed in the TOC. We called this aide-memoire the table of contents evidence (TOCE). As the TOCE contains copious working personal notes aiming to assist the understanding of the regulatory narrative, we have not reproduced it here but its content is woven into the narrative of this review.
Owing to the length and format of regulatory documents, we realised in building the TOC that there was a need to formalise the search and identification methods of trials referenced in the FDA documentation. We concentrated on where each trial is mentioned in the documentation by its pharmaceutical code. So, for example, if trial WV156708 is mentioned 60 times by that code in a particular file then the TOC will report the page numbers in which it is cited, which could be any number up to 60. The unit of search was the file, as a FDA PDF file can contain many different types of documents scanned into the same file. TOC and TOCE are among the tools we specifically constructed for the review (see Appendix 1).
We wanted to validate our new methods, therefore we compared the yield of OCR searching and hand-searching of the PDF files of the FDA regulatory material using the same trial ID as a working example.
We also searched the material sent to us by Roche for our 2009 update.
We searched the website of the Japanese PMDA (www.info.pmda.go.jp/shinyaku/shinyaku_previous_index.html) for data relating to NIs approved in 1999 and 2000 and www.info.pmda.go.jp/approvalSrch/PharmacySrchInit for NIs approved since 2001. We identified 1575 pages of documents relating to the regulatory review by the PMDA and the Japanese Ministry of Health, Labour and Welfare (JMHLW) and the Japanese SBA of oseltamivir capsules for treatment (2000), prophylaxis of oseltamivir dry syrup for children (2002) and oseltamivir capsules for prophylaxis of influenza (2004), and their re-examination results. The Japanese regulatory body introduced a system to disclose their examination results and SBA in 1999 instead of the prior system, ‘full disclosure requirement system’, which had been introduced in 1967. Although these documents included preclinical, methodological, clinical (pharmacological, toxicity and pharmacokinetics with metabolism) data and clinical (Phase I–III) studies and contain more precise data than the published papers, no complete CSRs were publicly available. Therefore, one review author (RH) asked the JMHLW on 29 July 2010 to disclose all of the documents reporting the evidence base for the approval of oseltamivir for these indications. The JMHLW sent RH a letter of refusal dated 2 September 2010, with the explanation ‘because the disclosure of such documents might hurt the right, position or other fair benefit in the competition of the corporation concerned’. We waited for 6 months to take further action hoping that the required CSRs would be forthcoming from the manufacturers. When this did not happen, RH filed a suit to overturn the JMHLW decision with the Osaka (Japan) District Court on 28 February 2011. The District Court petition was rejected on 19 April 2013 and the Osaka High Court rejected it on 29 November 2013. No appeal to the Supreme Court was made because substantial CSRs had already disclosed from various sources.
Appendix 5 Modified Consolidated Standards of Reporting Trials statement-based extraction template for clinical study reports
| Title and drug name Include source documents used: |
||
|---|---|---|
| Modified CONSORT extraction template www.consort-statement.org/ | ||
| Introduction CONSORT number | ||
| Background and objectives | 2a | Scientific background and explanation of rationale |
| 2b | Specific objectives or hypotheses | |
| Insert text: | ||
| Methods | ||
| Trial design | 3a | Description of trial design (such as parallel, factorial) including allocation ratio |
| 3b | Important changes to methods after trial commencement (such as eligibility criteria), with reasons | |
| Insert text: | ||
| Participants | 4a | Eligibility criteria for participants |
| 4b | Settings and locations where the data were collected | |
| Insert text: | ||
| Interventions | 5 | The interventions for each group with sufficient details to allow replication, including how and when they were actually administered |
| Insert text: | ||
| Outcomes | 6a | Completely defined prespecified primary and secondary outcome measures, including how and when they were assessed |
| 6b | Any changes to trial outcomes after the trial commenced, with reasons | |
| Insert text: | ||
| Sample size | 7a | How sample size was determined |
| 7b | When applicable, explanation of any interim analyses and stopping guidelines | |
| Randomisation: | ||
| Sequence generation | 8a | Method used to generate the random allocation sequence |
| 8b | Type of randomisation; details of any restriction (such as blocking and block size) | |
| Allocation concealment mechanism | 9 | Mechanism used to implement the random allocation sequence (such as sequentially numbered containers), describing any steps taken to conceal the sequence until interventions were assigned |
| Implementation | 10 | Who generated the random allocation sequence, who enrolled participants and who assigned participants to interventions |
| Insert text: | ||
| Blinding | 11a | If done, who was blinded after assignment to interventions (e.g. participants, care providers, those assessing outcomes) and how |
| 11b | If relevant, description of the similarity of interventions | |
| Statistical methods | 12a | Statistical methods used to compare groups for primary and secondary outcomes |
| 12b | Methods for additional analyses, such as subgroup analyses and adjusted analyses | |
| Insert text: | ||
| Results | ||
| Participant flow (a diagram is strongly recommended) | 13a | For each group, the numbers of participants who were randomly assigned, received intended treatment and were analysed for the primary outcome |
| 13b | For each group, losses and exclusions after randomisation, together with reasons | |
| Recruitment | 14a | Dates defining the periods of recruitment and follow-up |
| 14b | Why the trial ended or was stopped | |
| Insert text: | ||
| Baseline data | 15 | A table showing baseline demographic and clinical characteristics for each group |
| Numbers analysed | 16 | For each group, number of participants (denominator) included in each analysis and whether the analysis was by original assigned groups |
| Insert text: | ||
| Outcomes and estimation | 17a | For each primary and secondary outcome, results for each group and the estimated effect size and its precision (such as 95% CI) |
| 17b | For binary outcomes, presentation of both absolute and relative effect sizes is recommended | |
| Insert text: | ||
| Ancillary analyses | 18 | Results of any other analyses performed, including subgroup analyses and adjusted analyses, distinguishing prespecified from exploratory |
| Insert text: | ||
| Harms | 19 | All important harms or unintended effects in each group (for specific guidance see CONSORT for harms) |
| Insert text: | ||
| Other information | ||
| Registration | 23 | Registration number and name of trial registry |
| Protocol | 24 | Where the full trial protocol can be accessed, if available |
| Funding | 25 | Sources of funding and other support (such as supply of drugs), role of funders |
| Insert text: | ||
| First author Date of completion Conflicts of interest Second author check Date of check Conflicts of interest |
||
Appendix 6 Stage 1 of the 2012 A159 review
Two review authors assessed each study (with studies allocated randomly to three pairs of review authors). The lists of included studies (33 for oseltamivir, 30 for zanamivir, six for peramivir) were randomly created by the program Edgar II (www.edgarweb.org.uk/2011). 226 Every study was openly allocated to each group according to its number.
We initially included six peramivir trials in the randomisation/allocation sequence but subsequently decided not to proceed further, as we were informed by the manufacturers that no CSRs would be available until after registration with the FDA (Bill Sheridan, BioCryst Pharmaceuticals Inc., 20 August 2010, personal communication). One review author (TJ) was assigned to the attempted reconstruction of CSRs from the FDA documents.
Two weeks before ‘time lock’ (see Appendix 1) we received the first batch of CSRs from the EMA (formerly EMEA), containing an additional four CSRs (including one complete four-module CSR) of studies we wanted to include. This time, random allocation was achieved by writing trial IDs on one set of tickets and asking an external researcher to allocate them to groups, the names of which had been written on another set of tickets.
Authors in pairs separately extracted data from the same CSRs of studies included in stage 1 of the review. When we had more than one copy of the same CSRs from different sources (e.g. CSRs submitted to a regulatory body and CSRs from a pharmaceutical company), we independently extracted data from each of the copies and then compared the results. We aimed to record and tabulate disagreements between data extracted from the same source and between different sources. We extracted data using a modified CONSORT statement-based extraction template (see Appendix 5).
The modified CONSORT-based extraction template aimed to assemble a concise version of the CSRs, which would include all important methods as well as define and extract all relevant outcomes. The CONSORT-based extraction template includes the features that would be expected to be found in a published trial report but in far greater detail. Our reconstructions do not include introduction or discussion sections. We extracted the following for each trial:
-
Background and objectives.
-
Methods: including trial design, important changes to methods after trial commencement (such as eligibility criteria), with reasons.
-
Participants: including eligibility criteria for participants and settings and locations where the data were collected.
-
Interventions: the interventions for each group with sufficient details to allow replication, including how and when they were actually administered.
-
Outcomes: prespecified primary and secondary outcome measures, including how and when they were assessed and changes to trial outcomes after the trial commenced, with reasons.
-
Sample size: how it was determined and explanation of any interim analyses and stopping guidelines.
-
Randomisation: including sequence generation and method used to generate the random allocation sequence.
-
Blinding: who was blinded after assignment to treatment groups.
-
Statistical methods: methods used to compare groups for primary and secondary outcomes and methods for additional analyses, such as subgroup analyses and adjusted analyses.
-
Results: participant flow, numbers of participants randomly assigned, losses and exclusions after randomisation, together with reasons. Baseline demographic and clinical characteristics for each group.
-
Outcomes: primary and secondary outcome results for each group.
-
Ancillary analyses: results of any other analyses performed, including subgroup analyses and adjusted analyses, distinguishing prespecified from exploratory.
-
Harms: all important harms or unintended effects in each group.
One review author completed the CONSORT-based extraction on the template in full (see Appendix 5), with the name and date of completion and a statement of conflict of interests. A second review author checked the extraction. We extracted data, text, tables and figures directly from the relevant sections of the CSRs into the appropriate section of the template. We did not change the text in any way apart from clarifying abbreviations or spellings, but we highlighted some text. We used three types of text highlighting in the document.
-
Yellow Where text, figures or tables need to be checked with further information (e.g. if an adverse event is referred to in appendices or a further CSRs module).
-
Red Where text or comments were inserted by one or both review authors but required an additional opinion because of concerns that there is the potential for discrepancies in the CSRs.
-
Green Any text or tables added by us to the template (e.g. a reconstructed table of adverse events).
Two review authors (CH and MT) independently piloted the reconstruction method on oseltamivir trial WV1567158 with data from module 1 of the CSR from Roche and data submitted to UK NICE. We discussed the pilot reconstruction among the whole review team for clarification. At a face-to-face meeting we discussed the reliability and completeness of each reconstructed trial in the light of comments and other information from regulatory sources with a view to inclusion of the trial in stage 2. We resolved all of the differences in opinion by consensus. We reached decisions on whether or not a trial moved to stage 2 by consensus. We planned to record dissent when consensus was not possible.
Appendix 7 Applying inclusion criteria for the A159 2012 review
For the 2012 A159 review, two review authors (CDM and MT) independently scanned the titles and abstracts identified from the searches of the published literature. None of the identified items was a published version of a trial unknown to us. Four review authors (TJ, CH, MJ and RH) independently read all of the data relating to the studies on the list constructed during our search and selected studies that seemingly fulfilled our inclusion criteria. One review author (PD) compiled the assessments into a single sheet for another review author (CDM). One review author (CDM) resolved disagreements by discussion.
We assigned three categories to identified trials from our complete list:
-
definitely included
-
definitely excluded
-
trials for which we needed further information.
We excluded studies definitely not meeting inclusion criteria on the basis of available information (e.g. the title described the trial as a pharmacokinetic study). Where appropriate, we requested further information from the trial’s sponsor, usually copies of the CSRs (minus participant identification) for each trial that was definitely included or for which we needed further information. We did not contact first/corresponding authors of published versions of the trials on the basis of our experience with the 2009 A047 review.
Appendix 8 Post-protocol hypotheses: methods and results
Appendix 9 Example of contents of a Clinical Study Report (from p. 1 of WV15670 report)
Final study report modules
This report consists of five modules. Those not supplied in this submission were obtainable from the sponsor on request.
Module 1: core report and study publications
Introduction.
Rationale.
Objectives.
Methodology.
Efficacy results.
Safety results.
Discussion/conclusions.
Appendices.
Module 2: prestudy documents and study methodology
Protocol and amendment history.
Blank CRF.
Subject information sheet.
Glossary of original and preferred terms.
Randomisation list RAP.
Certificates of analysis.
List of investigators.
List of responsible ethics committees.
Module 3: individual subject listings of demographic and efficacy data
Demographic data listings.
Previous and concomitant diseases.
Previous and concomitant medications.
Efficacy listings.
Module 4: individual subject listings of safety data
Laboratory parameters.
Vital signs data.
Module 5: statistical report
Appendix 10 List of excluded studies and reasons for exclusion
| Study | Reason for exclusion |
|---|---|
| 105934 | Post-marketing study |
| 107485 | Dose-ranging study |
| 108127 | Non-randomised study |
| 112311 | Pharmaco-availability study |
| 112312 | Pharmaco-availability study |
| 113268 | Pharmaco-availability study |
| 113502 | Non-comparative study |
| 113625 | Pharmacokinetics study |
| 113678 | Non-comparative study |
| 114045 | Survey |
| 114373 | Not placebo/do nothing controlled |
| 167-02 | Dose-ranging Phase I in volunteers, no influenza exposure |
| 167-03 | Dose-ranging Phase I in volunteers, no influenza exposure |
| 167-04 | Dose-ranging Phase I in volunteers, no influenza exposure |
| 167-05 | Dose-ranging Phase I in volunteers, no influenza exposure |
| 167T3-11 | An open-label trial of 20 mg CG167 (zanamivir) in the treatment of influenza viral infection in children aged ≤ 5 and < 15 years old (open-label study). Non-randomised; the intervention group was compared with a survey group; 18-page summary available with no title |
| ADS-TCAD-PO206 | Not placebo/do nothing controlled |
| BP21288 | Pharmacokinetics study |
| C94–009 | Pharmacokinetics study |
| C94–085 | Pharmacokinetics study |
| GCP/95/045 | Pharmacokinetics study |
| JNAI-02 | Unknown study. Only ID traced |
| JNAI-03 | Unknown study. Only ID traced |
| JP15734 | Pharmacokinetics non-comparative study |
| JP15735 | Does not test treatment, prophylaxis or PEP and there was no exposure to influenza |
| JV16284 | Open-label, no control |
| JV21490 | No influenza circulation, Phase IV study with unusual oseltamivir dosages |
| M76006 | Not placebo/do nothing controlled |
| ML17279 | CSR bears no title. Study of community pharmacist availability |
| ML17713 | Non-comparative study |
| ML19340 | Text in French. Community pharmacist availability study |
| ML20542 | Not placebo/do nothing controlled |
| ML21954 | Not placebo/do nothing controlled |
| ML22789 | Not placebo/do nothing controlled |
| ML22872 | Not placebo/do nothing controlled |
| ML22879 | Not placebo/do nothing controlled |
| ML25018 | Bioavailability study |
| ML25087 | Not placebo/do nothing controlled |
| ML25094 | Non-comparative study |
| ML25157 | Pharmacokinetics study |
| ML25176 | Pharmacokinetics study |
| ML25179 | Not placebo/do nothing controlled |
| ML25265 | Non-comparative observational study |
| ML25266 | Pharmacokinetics study |
| MP20691 | Pharmacokinetics study |
| MV20043 | Transmission study |
| MV20050 | Dose-ranging study |
| MV22926 | Non-comparative study |
| MV22949 | Pharmacokinetics study |
| MV22951 | Pharmacokinetics study |
| MV22963 | Pharmacokinetics study |
| MV22970 | Pharmacokinetics study |
| NAI106784 | Pharmacokinetics study |
| NAI108166 | Pharmacokinetics study |
| NAI10901 | Comparator is vaccine |
| NAI10902 | Pharmacokinetics study |
| NAI40012 | Instructional leaflet study |
| NAIA1009 | Pharmacokinetics study |
| NAIA2010 | Open-label, rimantadine-controlled, cluster randomised trial |
| NAIB1001 | Pharmacokinetics study |
| NAIB1002 | Pharmacokinetics study |
| NAIB1007 | Pharmacokinetics study |
| NCT00297050 | Dose-ranging study |
| NCT00416962 | Not placebo/do nothing controlled |
| NCT00867139 | Not placebo/do nothing controlled in immunocompromised people |
| NCT00957996 | Peramivir study – does not have placebo/do nothing comparator |
| NCT01063933 | Pharmacokinetics study |
| Not applicable (registry) | Unknown study. Only ID traced. Identified from Reddy D. J Antimicrob Chemother 2010;65(Suppl. 2):ii35–40 (doi: http://dx.doi.org/10.1093/jac/dkq014) table 2. http://jac.oxfordjournals.org/cgi/content/full/65/suppl_2/ii35/DKQ014TB2) |
| NP15525 | Pharmacokinetics study |
| NP15717 | Pharmacokinetics study |
| NP15718 | Pharmacokinetics study |
| NP15719 | Pharmacokinetics study |
| NP15728 | Pharmacokinetics study |
| NP15729 | Pharmacokinetics study |
| NP15743 | Palatability study, open-label |
| NP15757 | Pharmacokinetics study |
| NP15810 | Pharmacokinetics study |
| NP15826 | Pharmacokinetics study |
| NP15827 | Pharmacodynamics study |
| NP15881 | Palatability study in children |
| NP15901 | Pharmacokinetics study |
| NP15912 | Palatability study in children |
| NP16472 | Not placebo/do nothing controlled |
| NP22770 | Pharmacokinetics study |
| NP25138 | Not placebo/do nothing controlled |
| NP25139 | Not placebo/do nothing controlled |
| NP25140 | Pharmacokinetics study |
| NV20234 | Immunocompromised participants |
| NV20235 | Immunocompromised participants |
| NV20237 | Resistance study |
| NV22155 | Not placebo/do nothing controlled |
| NV22158 | Registry study |
| NV25118 | Pharmacokinetics study |
| NV25182 | Not placebo/do nothing controlled |
| NV25655 | Open-label pharmacokinetics study |
| PP15974 | Pharmacokinetics study |
| PP16351 | Pharmacokinetics study |
| PP16361 | Pharmacokinetics study |
| PV15615 | Viral challenge study |
| PV15616 | Viral challenge study |
| WP15517 | Pharmacokinetics study |
| WP15525 | Pharmacokinetics study |
| WP15647 | Pharmacokinetics study |
| WP15648 | Pharmacokinetics study |
| WP15676 | Pharmacokinetics study |
| WP15979 | Bioavailability study |
| WP16094 | Pharmacokinetics study |
| WP16134 | Bioequivalence study |
| WP16137 | Bioequivalence study |
| WP16225 | Bioequivalence study |
| WP16226 | Pharmacokinetics study |
| WP16254 | Pharmacokinetics study |
| WP16263 | No influenza circulation, Phase IV study |
| WP16295 | Open-label absorption study |
| WP17721 | Pharmacokinetics study |
| WP18308 | Pharmacokinetics study |
| WP20727 | Pharmacokinetics study |
| WP20749 | Not placebo/do nothing controlled |
| WP21272 | Pharmacokinetics study |
| WP22849 | Pharmacokinetics study |
| WV15731 | No placebo arm |
| WV16139 | Unknown study. Only ID traced. ID could be a typo |
| WV16193 | Not placebo/do nothing controlled |
Appendix 11 Symptomatic influenza-like illness in prophylaxis trials
Introduction
Among the CSRs of prophylaxis studies that we included, no oseltamivir study and only one study of zanamivir (NAI 3003486) reported the relevant primary outcome ‘symptomatic ILI irrespective of positivity of laboratory testing’. In the zanamivir CSR (NAI 30034) no significant reduction was observed (9% vs. 10%). Furthermore, no definition was provided for ILI in the oseltamivir CSRs; however, individual patient data on symptoms of influenza were provided in module 3.
Methods
Examples of the definitions of categories for lab-confirmed influenza used in the oseltamivir trials (p. 33, CSR for WV15673–697;59 p. 31, CSR for WV1582568) are given below:
| Category | Oral temperature | Constitutional symptoms | Respiratory symptoms |
|---|---|---|---|
| Clinical influenza | ≥ 99 °F | One or more | One or more |
| Non-clinical influenza | |||
| Non-clinical URTI | |||
| Febrile URTI | ≥ 99 °F | None | One or more |
| URTI without systematic disturbance | < 99 °F | None | One or more |
| URTI with systematic disturbance | < 99 °F | One or more | None |
| Febrile constitutional | ≥ 99 °F | One or more | None |
| Asymptomatic influenza | < 99 °F | None | None |
| ≥ 99 °F | None | None | |
| < 99 °F | One or more | None | |
| Category | Oral temperature | Constitutional symptoms | Respiratory symptoms |
|---|---|---|---|
| Clinical influenza | ≥ 99 °F | One or more | One or more |
| Non-clinical influenza | |||
| Non-clinical URTI | |||
| Febrile URTI | ≥ 99 °F | None | One or more |
| URTI without systematic disturbance | < 99 °F | None | One or more |
| URTI with systematic disturbance | < 99 °F | One or more | One or more |
| Febrile constitutional | ≥ 99 °F | One or more | None |
| Asymptomatic influenza | < 99 °F | None | None |
| ≥ 99 °F | None | None | |
| < 99 °F | One or more | None | |
These are complex and confusing definitions, in which, for example, the definition for ‘URTI with systemic disturbance’ is the same as one of the definitions for asymptomatic influenza in WV15673–697. 59 Furthermore, the definition for ‘URTI with systemic disturbance’ in WV1582568 and WV15673/WV1569759 is different. No definition is provided for ILI without confirmation of influenza. Asymptomatic influenza includes those with some symptoms.
In the absence of a definition provided in the CSRs for ILI and the complex and confusing definitions of categories for lab-confirmed influenza, we classified ILI as two or more symptoms out of nasal congestion, headache, chills/sweats, sore throat, cough, fatigue, myalgia and fever. Fever was defined as reported in the original protocols for each trial. We counted the number of patients with ILI during the trial follow-up for each prophylaxis study of oseltamivir in adults.
Results
Oseltamivir did not reduce ILI (RR 0.95, 95% CI 0.86 to 1.06) (Figure 20). In additional analysis we found that fever is reduced (RR 0.62, 95% CI 0.42 to 0.93) (Figure 21), proportion with laboratory confirmation is reduced (RR 0.59, 95% CI 0.41 to 0.85) (Figure 22) but symptoms other than fever are not reduced (RR 0.96, 95% CI 0.86 to 1.07) (Figure 23).
FIGURE 20.
All symptomatic ILI in adult prophylaxis. ILI is classified as two or more symptoms out of: nasal congestion, headache, chills/sweats, sore throat, cough, fatigue, myalgia and fever (with or without lab confirmation). IV, inverse variance.

FIGURE 21.
Fever in adult prophylaxis. Temperature ≥ 100 °F (WV15673/69759) or ≥ 37.5 °C (WV15825/15708) as originally defined in the trial protocols. IV, inverse variance.
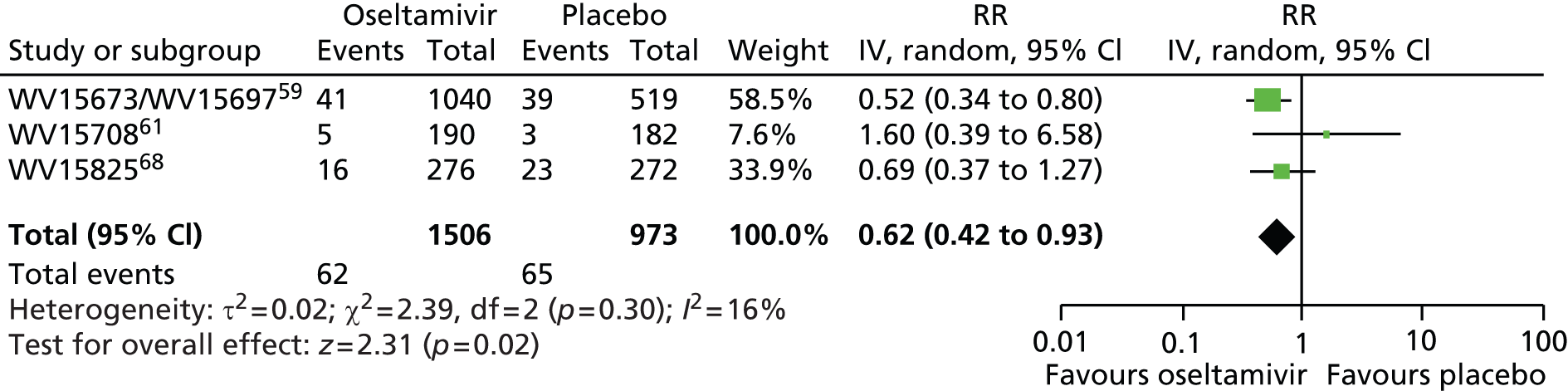
FIGURE 22.
Lab confirmation of influenza (symptomatic and asymptomatic). IV, inverse variance.

FIGURE 23.
Two or more symptoms (other than fever) of ILI in adult prophylaxis. Other than fever defined as nasal congestion, headache, chills/sweats, sore throat, cough, fatigue and myalgia. IV, inverse variance.

Interpretation
These results suggest oseltamivir suppresses fever, reduces antibody response and viral shedding but does not reduce the risk of symptomatic illness.
Appendix 12 Oseltamivir observational studies review search strategies
Database: Ovid MEDLINE (1946 to February Week 1 2013)
Search strategy
-
Influenza, Human/
-
influenzavirus a/ or influenza a virus/ or influenza a virus, h1n1 subtype/
-
(influenza* or flu or h1n1).tw.
-
or/1-3
-
Oseltamivir/
-
(oseltamivir or tamiflu or neuraminidase inhibitor*).tw,nm.
-
Antiviral Agents/
-
antiviral*.tw.
-
or/5-8
-
4 and 9
-
Hospitalization/
-
hospitali*.tw.
-
exp Mortality/
-
mortality.tw.
-
Death/
-
fatal outcome/
-
(death* or died or fatal*).tw.
-
Critical Illness/
-
(critical* adj2 ill*).tw.
-
or/11-19
-
10 and 20
-
epidemiologic studies/
-
epidemiology.fs.
-
epidemiol*.tw.
-
exp case-control studies/
-
exp Cohort Studies/
-
cohort*.tw.
-
((“follow up” or “follow-up”) adj2 (study or studies)).tw.
-
observational*.tw.
-
longitudinal*.tw.
-
retrospectiv*.tw.
-
prospectiv*.tw.
-
Cross-Sectional Studies/
-
(cross-section* or cross section*).tw.
-
(control* adj2 (group* or study or studies or patient* or case*)).tw.
-
or/22-35
-
21 and 36
EMBASE (Elsevier)
| #15 834 | ||
| #15.34 #15.19 AND #15.33 | #15.33 #15.20 OR #15.21 OR #15.22 OR #15.23 OR #15.24 OR #15.25 OR #15.26 OR #15.27 OR #15.28 OR #15.29 OR #15.30 OR #15.31 OR #15.32 | |
| #15.32 ‘control group’:ab,ti | ||
| #15.31 ‘cross-sectional’:ab,ti OR ‘cross sectional’:ab,ti | ||
| #15.30 ‘cross-sectional study’/de | ||
| #15.29 prospectiv*:ab,ti | ||
| #15.28 retrospectiv*:ab,ti | ||
| #15.27 longitudinal:ab,ti | ||
| #15.26 observational*:ab,ti | ||
| #15.25 ((‘follow up’ OR ‘follow-up’) NEAR/2 (study OR studies)):ab,ti | ||
| #15.24 cohort*:ab,ti | ||
| #15.23 ‘cohort analysis’/de | ||
| #15.22 ‘case control study’/exp | ||
| #15.21 epidemiol*:ab,ti | ||
| #15.20 ‘epidemiology’/de | ||
| #15.19 #15.9 AND #15.18 | ||
| #15.18 #15.10 OR #15.11 OR #15.12 OR #15.13 OR #15.14 OR #15.15 OR #15.16 OR #15.17 | ||
| #15.17 (critical* NEAR/2 ill*):ab,ti | ||
| #15.16 ‘critical illness’/de | ||
| #15.15 death*:ab,ti OR died:ab,ti OR fatal*:ab,ti | ||
| #15.14 ‘death’/de OR ‘fatality’/de | ||
| #15.13 mortality:ab,ti | ||
| #15.12 ‘mortality’/exp | ||
| #15.11 hospitali*:ab,ti | ||
| #15.10 ‘hospitalization’/de | ||
| #15.9 #15.3 AND #15.8 | ||
| #15.8 #15.4 OR #15.5 OR #15.6 OR #15.7 | ||
| #15.7 antiviral*:ab,ti | ||
| #15.6 ‘antivirus agent’/de AND [embase]/lim | ||
| #15.5 oseltamivir:ab,ti OR tamiflu:ab,ti OR ‘neuraminidase inhibitor’:ab,ti OR ‘neuraminidase inhibitors’:ab,ti | ||
| #15.4 ‘oseltamivir’/de | ||
| #15.3 #15.1 OR #15.2 | ||
| #15.2 influenza*:ab,ti OR flu:ab,ti OR h1n1:ab,ti | ||
| #15.1 ‘influenza’/de OR ‘influenza a’/de OR ‘2009 h1n1 influenza’/de OR ‘influenza a (h1n1)’/de OR ‘pandemic influenza’/de OR ‘swine influenza’/de |
Cumulative Index to Nursing and Allied Health Literature (EBSCOhost)
| Friday, February 15, 2013 2:30:38 AM | |
|---|---|
| # Query Limiters/Expanders Last Run Via Results Action | |
| S35 | S21 AND S34 |
| S34 | S22 OR S23 OR S24 OR S25 OR S26 OR S27 OR S28 OR S29 OR S30 OR S31 OR S32 OR S33 |
| S33 | TI ((control* N2 (group* or study or studies or patient* or case*))) OR AB ((control* N2 (group* or study or studies or patient* or case*))) |
| S32 | TI (cross section* or cross-section*) OR AB (cross section* or cross-section*) |
| S31 | TI prospectiv* OR AB prospectiv* |
| S30 | TI retrospectiv* OR AB retrospectiv* |
| S29 | TI longitudinal* OR AB longitudinal* |
| S28 | TI observational* OR AB observational* |
| S27 | TI (((“follow up” or “follow-up”) N2 (study or studies))) OR AB (((“follow up” or “follow-up”) N2 (study or studies))) |
| S26 | TI cohort* OR AB cohort* |
| S25 | (MH “Prospective Studies+”) |
| S24 | (MH “Case Control Studies+”) |
| S23 | TI epidemiol* OR AB epidemiol* |
| S22 | (MH “Epidemiological Research”) |
| S21 | S10 AND S20 |
| S20 | S11 OR S12 OR S13 OR S14 OR S15 OR S16 OR S17 OR S18 OR S19 |
| S19 | TI critical* N2 ill* OR AB critical* N2 ill* |
| S18 | (MH “Critical Illness”) |
| S17 | TI (death* or died or fatal*) OR AB (death* or died or fatal*) |
| S16 | (MH “Fatal Outcome”) |
| S15 | (MH “Death”) |
| S14 | TI mortality OR AB mortality |
| S13 | (MH “Mortality+”) |
| S12 | TI hospitali* OR AB hospitali* |
| S11 | (MH “Hospitalization”) |
| S10 | S4 AND S9 |
| S9 | S5 OR S6 OR S7 OR S8 |
| S8 | TI antiviral* OR AB antiviral* |
| S7 | (MH “Antiviral Agents”) |
| S6 | TI ( oseltamivir or tamiflu or neuraminidase inhibitor* ) OR AB ( oseltamivir or tamiflu or neuraminidase inhibitor* ) |
| S5 | (MH “Oseltamivir”) |
| S4 | S1 OR S2 OR S3 |
| S3 | TI (influenza* or flu or h1n1) OR AB (influenza* or flu or h1n1) |
| S2 | (MH “Influenzavirus A”) OR (MH “Influenza A Virus”) OR (MH “Influenza A Virus, H1N1 Subtype”) |
| S1 | (MH “Influenza”) OR (MH “Influenza, Human”) OR (MH “Influenza, Pandemic (H1N1) 2009”) |
Latin American and Caribbean Health Sciences Literature (BIREME)
(mh:“Influenza, Human” OR grippe OR “influenza humana” OR “gripe humana” OR influenza* OR flu OR h1n1 OR mh:“Influenzavirus A” OR mh:“Influenza A virus” OR mh:“Influenza A Virus, H1N1 Subtype”) AND (mh:oseltamivir OR oseltamivir OR tamiflu OR “neuraminidase inhibitor” OR “neuraminidase inhibitors” OR “inhibe la neuraminidasa” OR “inibe a neuraminidase” OR mh:“Antiviral Agents” OR antivirales OR antivirais OR antiviral*) AND (mh:“Epidemiologic Studies” OR “Estudios Epidemiológicos” OR epidemiol* OR mh:“Case-Control Studies” OR “Estudios de Casos y Controles” OR “Estudos de Casos e Controles” OR “Case-Base Studies” OR “Case-Comparison Studies” OR “Case-Referent Studies” OR “Matched Case-Control Studies” OR “Nested Case-Control Studies” OR “Combined Case-Control Studies” OR “Grupos de Estudio” OR “Estudios de Comparación de Casos” OR “Estudios de Referencia de Casos” OR “Estudios de Casos y Controles por Apareamiento” OR “Estudios de Casos y Controles Anidados” OR “Estudios de Casos y Controles Combinados” OR “Grupos de Estudo” OR “Estudos de Comparação de Casos” OR “Estudos de Referência de Casos” OR “Estudos de Caso-Controle com Emparelhamento” OR “Estudos de Caso-Controle Aninhados” OR “Estudos de Caso-Controle Combinados” OR mh:“Cohort Studies” OR “Estudios de Cohortes” OR “Estudos de Coortes” OR “Cohort Analysis” OR “Closed Cohort Studies” OR “Concurrent Studies” OR “Historical Cohort Studies” OR “Incidence Studies” OR “Análisis de Cohortes” OR “Estudios Cerrados de Cohortes” OR “Estudios de Concurrencia” OR “Estudios Históricos de Cohortes” OR “Estudios de Incidencia” OR “Análise de Coortes” OR “Estudos Fechados de Coortes” OR “Estudos Históricos de Coortes” OR “Estudos de Incidência” OR cohort* OR longitudinal OR retrospectiv* OR prospectiv* OR “follow up” OR “follow-up” OR “control group” OR mh:“Cross-Sectional Studies” OR “Estudios Transversales” OR “Estudos Transversais” OR “cross sectional” OR “cross- sectional”) AND db:(“LILACS”)
Web of Science (Thomson Reuters)
| #7 | 452 | #6 AND #5 Databases=SCI-EXPANDED, CPCI-S Timespan=All Years |
| #6 | 1,897,044 | Topic=(epidemiol* or cohort* or ((“follow up” or “follow-up”) NEAR/2 (study or studies)) or observational* or longitudinal or retrospectiv* or prospectiv* or “cross section*” or “cross-section*” or (control* NEAR/2 (group* or study or studies or patient* or case*))) Databases=SCI-EXPANDED, CPCI-S Timespan=All Years |
| #5 | 1527 | #4 AND #3 Databases=SCI-EXPANDED, CPCI-S Timespan=All Years |
| #4 | 1,158,683 | Topic=(hospitali* or mortality or death* or fatal* or died or (critical* NEAR/2 ill*)) Databases=SCI-EXPANDED, CPCI-S Timespan=All Years |
| #3 | 6592 | #2 AND #1 Databases=SCI-EXPANDED, CPCI-S Timespan=All Years |
| #2 | 56,113 | Topic=(oseltamivir or tamiflu or “neuraminidase inhibitor” or “neuraminidase inhibitors” or antiviral*) Databases=SCI-EXPANDED, CPCI-S Timespan=All Years |
| #1 | 86,524 | Topic=(influenza* or flu or h1n1) Databases=SCI-EXPANDED, CPCI-S Timespan=All Years |
Appendix 13 Template of letter sent to corresponding authors of included studies
Appendix 14 Reasons for exclusion of studies based on full manuscripts
| Reason for exclusion | Number of studies | Citationsa |
|---|---|---|
| Most (or all) patients received antiviral medication | 77 | 1–57, 59–61, 63, 67, 68, 71–73, 102–111 |
| Overlap with other included studies | 10 | 58, 62, 64–66, 69, 70, 74–76 |
| Did not provide a breakdown of numbers of patients dying by oseltamivir exposure | 12 | 77–88 |
| Fewer than five deaths | 12 | 89–100 |
| Not a clinical study | 5 | 101, 112–115 |
| Other reasons | 8 | 116–123 |
References
1. Metan G, Bozkurt I, Agkus C, Coskun R, Alp E, Sungur M, et al. Hospitalised pandemic influenza A (H1N1) patients in a university hospital. Cent Eur J Med 2010;6:83–8.
2. Chien Y, Su C, Tsai H, Huang AS, Lien CE, Hung MN, et al. Predictors and outcomes of respiratory failure among hospitalised pneumonia patients with 2009 H1N1 influenza in Taiwan. J Infect 2010;60:168–74.
3. Paredes G, Cevallos C. Acute respiratory distress syndrome during the 2009 H1N1 influenza A pandemic in Ecuador. Med Intensiva 2010;34:310–17.
4. Choi W, Kim WY, Kim S, Oh BJ, Kim W, Lim KS, et al. Clinical characteristics of pneumonia in hospitalised patients with novel influenza A (H1N1) in Korea. Scand J Infect Dis 2010;42:311–14.
5. Rello J, Rodriguez A, Ibanez P, Socias L, Cebrian J, Marques A, et al. Intensive care adult patients with severe respiratory failure caused by Influenza A (H1N1)v in Spain. Crit Care 2009;13:R148.
6. Kumar S, Havens P, Chusid M, Willoughby RE Jr, Simpson P, Henrickson KJ, et al. Clinical and epidemiologic characteristics of children hospitalised with 2009 pandemic H1N1 influenza A infection. Pediatr Infect Dis J 2010;29:591–4.
7. Creanga A, Johnson T, Graitcer S, Hartman LK, Al-Samarrai T, Schwarz AG, et al. Severity of 2009 pandemic influenza a (H1N1) virus infection in pregnant women. Obstet Gynecol 2010;115:717–26.
8. Dubar G, Azria E, Tesniere A, Dupont H, Le Ray C, Baugnon T, et al. French experience of 2009 A/H1N1v influenza in pregnant women. PLOS ONE 2010;5:e13112.
9. Cui W, Zhao H, Lu X, Wen Y, Zhou Y, Deng B, et al. Factors associated with death in hospitalized pneumonia patients with 2009 H1N1 influenza in Shenyang, China. BMC Infect Dis 2010;10:145.
10. Estenssoro E, Rios FG, Apezteguia C, Reina N, Neira J, Cerasso D, et al. Pandemic 2009 influenza A(H1N1) in Argentina: a study of 337 patients on mechanical ventilation. Am J Respir Crit Care Med 2010;182:41–8.
11. Wei J, Chen F, Jin J, Mai WY, Qian WB, Meng HT, et al. Novel influenza A (H1N1) in patients with hematologic disease. Leuk Lymphoma 2010;51:2079–83.
12. Lee E, Wu C, Lee E, Mai WY, Qian WB, Meng HT, et al. Fatalities associated with the 2009 H1N1 influenza a virus in New York City. Clin Infect Dis 2010;50:1498–504.
13. Kute V, Godara S, Goplani K, Gumber M, Shah P, Vanikar A, et al. High mortality in critically ill patients infected with 2009 pandemic influenza A (H1N1) with pneumonia and acute kidney injury. Saudi J Kidney Dis Transpl 2011;22:83–9.
14. Paganini H, Parra A, Ruvinsky S, Viale D, Baumeister E, Bologna R, et al. Clinical features and outcome of 2009 influenza A (H1N1) virus infections in children with malignant diseases: a case–control study. J Pediatr Hematol Oncol 2011;33:e5–8.
15. Smud A, Nagel C, Madsen E, Rial Mdel C, Barcan LA, Gomez AA, et al. Pandemic influenza A/H1N1 virus infection in solid organ transplant recipients: a multicenter study. Transplantation 2010;90:1458–62.
16. Abdulkader R, Ho Y, De Sousa Santos S, Caires R, Arantes M, Andrade L. Characteristics of acute kidney injury in patients infected with the 2009 influenza A (H1N1) virus. Clin J Am Soc Nephrol 2010;5:1916–21.
17. Louriz M, Mahraoui C, Azzouzi A, El Fassy Fihri MT, Zeggwagh AA, Abidi K, et al. Clinical features of the initial cases of 2009 pandemic influenza A (H1N1) virus infection in an university hospital of Morocco. Int Arch Med 2010;3:26.
18. Tutuncu E, Ozturk B, Gurbuz Y, Haykir A, Sencan I, Kuscu F, et al. Clinical characteristics of 74 pandemic H1N1 influenza patients from Turkey: risk factors for fatality. Saudi Med J 2010;31:993–8.
19. Satterwhite L, Mehta A, Martin G. Novel findings from the second wave of adult pH1N1 in the United States. Crit Care Med 2010;38:2059–61.
20. Venkata C, Sampathkumar P, Afessa B. Hospitalized patients with 2009 H1N1 influenza infection: The Mayo Clinic experience. Mayo Clin Proc 2010;85:798–805.
21. Siau C, Law J, Tee A, Poulose V, Raghuram J. Severe refractory hypoxaemia in H1N1 (2009) intensive care patients: initial experience in an Asian regional hospital. Singapore Med J 2010;51:490–5.
22. Abouchacra S, Chaaban A, Gebran N, Hassan M, Paul A, Eid H, et al. Acute kidney injury in patients with H1N1 admitted to ICU: incidence, patient and renal outcomes. A multi-center perspective. Anaesth Pain Intensive Care 2010;14:13–16.
23. Miller R, Markewitz B, Rolfs R, Brown SM, Dascomb KK, Grissom CK, et al. Clinical findings and demographic factors associated with ICU admission in Utah due to novel 2009 influenza a(H1N1) infection. Chest 2010;137:752–8.
24. Koegelenberg C, Irusen E, Cooper R, Diacon A, Taljaard J, Mowlana A, et al. High mortality from respiratory failure secondary to swine-origin influenza A (H1N1) in South Africa. QJM 2010;103:319–25.
25. Mu Y, Zhang Z, Chen X, Xi X, Lu Y, Tang Y, et al. Clinical features, treatments and prognosis of the initial cases of pandemic influenza H1N1 2009 virus infection in Shanghai China. QJM 2010;103:311–17.
26. Al-Khuwaitir TS, Al-Abdulkarim AS, Abba AA, Yousef AM, El-Din MA, Rahman KT, et al. H1N1 influenza A: preliminary evaluation in hospitalized patients in a secondary care facility in Saudi Arabia. Saudi Med J 2010;30:1532–6.
27. Naseem A, Satti S, Khan M, Saeed W. A clinical account of hospitalized 2009 pandemic influenza a (H1N1) cases. J Coll Physicians Surg Pak 2011;21:97–102.
28. Binsaeed A. Characteristics of pandemic influenza A (H1N1) infection in patients presenting to a university hospital in Riyadh, Saudi Arabia. Ann Saudi Med 2010;30:59–62.
29. Anand R, Gupta A, Gupta A, Wadhawan S, Bhadoria P, et al. Management of swine-flu patients in the intensive care unit: our experience. J Anaesthesiol Clin Pharmacol 2012;28:51–5.
30. Bhatt KN, Jethw SC, Bhadiyadar D, Patel D, Joshi K, et al. Study of clinical profile in patients with H1N1 influenza in Surat district, June 2009-March 2010. J Assoc Physicians India 2012;60:15–19.
31. Camargo LFA, de Sandes-Freitas TV, Silva CD, Bittante CD, Ono G, Corrêa L, et al. Morbimortality of pandemic influenza a H1N1 infection in kidney transplant recipients requiring hospitalization: a comparative analysis with nonimmunocompromised patients. Transplantation 2012;93:69–72.
32. Carrillo-Esper R, Sosa-Garcia JO, Arch-Tirado E. [Experience in the management of the severe form of human influenza A H1N1 pneumonia in an intensive care unit.] Cirugia y Cirujanos 2011;79:409–16.
33. Choi WI, Yim JJ, Park J, Kim SC, Na MJ, Lee WY, et al. Clinical characteristics and outcomes of H1N1-associated pneumonia among adults in South Korea. Int J Tuberc Lung Dis 2011;15:270–5.
34. Cordero E, Aydillo T, Farinas MC, Panio-Pardo JR, Pachon J, Viasus D, et al. Immunosuppressed patients with pandemic influenza A 2009 (H1N1) virus infection. Eur J Clin Microbiol Infect Dis 2012;31:547–56.
35. Damak H, Chtara K, Bahloul M, Kallel H, Chaari A, Ksibi H, et al. Clinical features, complications and mortality in critically ill patients with 2009 influenza A(H1N1) in Sfax, Tunisia. Influenza Other Respir Viruses 2011;5:230–40.
36. Dashti-Khavidaki S, Khalili H, Gholamalipour F, Soudbakhsh A, Talazaz AH, Hajabdolbaghi M, et al. Approach to pandemic 2009 influenza: first report from a main referral hospital for Pandemic H1N1 influenza care in Iran. J Infec Dev Ctries 2010;4:629–35.
37. Ellington SR, Hartman LK, Acosta M, Martinez-Romo M, Rubinson L, Jamieson DJ, et al. Pandemic 2009 influenza A (H1N1) in 71 critically ill pregnant women in California. Am J Obstetr Gynecol 2011;204(6 Suppl. 1):21–30.
38. Farooq O, Faden HS, Cohen ME, Ramanathan M, Barrett H, Farkas MK, et al. Neurologic complications of 2009 influenza: A H1N1 infection in children. J Child Neurol 2012;27:431–8.
39. Han K, Ma H, An X, Su Y, Chen J, Lian Z, et al. Early use of glucocorticoids was a risk factor for critical disease and death from pH1N1 infection. Clin Infect Dis 2011;53:326–33.
40. Hung IFN, To KK, Lee CK, Lee KL, Chan K, Yan WW, et al. Convalescent plasma treatment reduced mortality in patients with severe pandemic influenza A (H1N1) 2009 virus infection. Clin Infect Dis 2011;52:447–56.
41. Jung JY, Park BH, Hong SB, Koh Y, Su GY, Jeon K, et al. Acute kidney injury in critically ill patients with pandemic influenza A pneumonia 2009 in Korea: a multicenter study. J Crit Care 2011;26:577–85.
42. Kaya S, Yilmaz G, Arslan M, Oztuna F, Ozlu T, Koksal I, et al. Predictive factors for fatality in pandemic influenza A (H1N1) virus infected patients. Saudi Med J 2012;33:146–51.
43. Kim SH, Hong SB, Yun SC, Choi WI, Ahn JJ, Lee YJ, et al. Corticosteroid treatment in critically ill patients with pandemic influenza A/H1N1 2009 infection: analytic strategy using propensity scores. Am J Resp Crit Care Med 2011;183:1207–14.
44. Kirakli C, Tatar D, Cimen P, Edipoglu O, Coskun M, Celikten E, et al. Survival from severe pandemic H1N1 in urban and rural Turkey: a case series. Resp Care 2011;56:790–5.
45. Kumar D, Michaels MG, Morris MI, Green M, Avery RK, Liu C, et al. Outcomes from pandemic influenza A H1N1 infection in recipients of solid-organ transplants: a multicentre cohort study. Lancet Infect Dis 2010;10:521–6.
46. Kumar TCN, Shivakumar NS, Deepak TS, Krishnappa R, Goutam NS, et al. H1N1-infected patients in ICU and their clinical outcome. N Am J Med Sci 2012;4:394–8.
47. Lee N, Chan PK, Lui JC, Wong BC, Sin WW, Choi KW, et al. Complications and outcomes of pandemic 2009 influenza A (H1N1) virus infection in hospitalized adults: how do they differ from those in seasonal influenza? J Infect Dis 2011;203:1739–47.
48. Lenzi L, Wiens A, Pontarolo R. Clinical manifestations, outcomes and prognostic factors of the 2009 pandemic influenza A (H1N1) in children. Rev Paulista Pediatr 2012;30:346–52.
49. Li F, Chen G, Wang J, Liu H, Wu J. A case–control study on risk factors associated with death in pregnant women with severe pandemic H1N1 infection. BMJ Open 2012;2:e000827.
50. Linko R, Wiens A, Pontarolo R. Corticosteroid therapy in intensive care unit patients with PCR-confirmed influenza A(H1N1) infection in Finland. Acta Anaesthesiol Scand 2011;55:971–9.
51. Maravi-Poma E, Martin-Loeches I, Regidor E, Laplaza C, Cambra K, Aldunate S, et al. Severe 2009 A/H1N1v influenza in pregnant women in Spain. Crit Care Med 2011;39:945–51.
52. Minnema BJ, Patel M, Rotstein C, Mazzulli T, Hota S, Cole EH, et al. Comparison of hospitalized solid organ transplant recipients and nonimmunocompromised patients with pandemic H1N1 infection: a retrospective cohort study. Transplantation 2011;92:230–4.
53. Morales-Garcia G, Falfán-Valencia R, Garcia-Ramirez RA, Camarena Á, Ramirez-Venegas A, Castillejos-López M, et al. Pandemic influenza A/H1N1 virus infection and TNF, LTA, IL1B, IL6, IL8, and CCL polymorphisms in Mexican population: a case–control study. BMC Infect Dis 2012;12:299.
54. Nelliyanil M, Basha R, Sharada MP. Profile of novel flu patients admitted in two government hospitals in Bangalore. Aus Med J 2010;3:340–3.
55. Ormsby CE, de la Rosa-Zamboni D, Vasquez-Perez J, Ablanedo-Terrazas Y, Vega-Barrientos R, et al. Severe 2009 pandemic influenza A (H1N1) infection and increased mortality in patients with late and advanced HIV disease. AIDS 2011;25:435–9.
56. Paño-Pardo JR, Rodriguez-Baño A, Martinez-Sánchez N, Viasus D, Fariñas MC, Leyes M, et al. Prognosis of 2009 A(H1N1) influenza in hospitalized pregnant women in a context of early diagnosis and antiviral therapy. Antiviral Ther 2012;17:719–28.
57. Protheroe RE, Kirkland KE, Pearce RM, Kaminaris K, Bloor A, Potter MN, et al. The clinical features and outcome of 2009 H1N1 influenza infection in allo-SCT patients: a British Society of Blood and Marrow Transplantation study. Bone Marrow Transplant 2012;47:88–94.
58. Raboni SM, Stella V, Cruz CR, França JB, Moreira S, Gonçalves L, et al. Laboratory diagnosis, epidemiology, and clinical outcomes of pandemic influenza A and community respiratory viral infections in Southern Brazil. J Clin Microbiol 2011;49:1287–93.
59. Ramakrishna K, Sampath S, Chacko J, Chacko B, Narahari DL, Veerendra HH, et al. Clinical profile and predictors of mortality of severe pandemic (H1N1) 2009 virus infection needing intensive care: a multi-centre prospective study from South India. J Glob Infect Dis 2012;4:145–52.
60. Randolph AG, Vaughn F, Sullivan R, Rubinson L, Thompson BT, Yoon G, et al. Critically ill children during the 2009–2010 influenza pandemic in the United States. Pediatrics 2011;128:e1450–8.
61. Reyes S, Montull B, Martínez R, Córdoba J, Molina JM, Martí V, et al. Risk factors of A/H1N1 etiology in pneumonia and its impact on mortality. Resp Med 2011;105:1404–11.
62. Rhim JW, Go EJ, Lee KY, Youn YS, Kim MS, Park SH, et al. Pandemic 2009 H1N1 virus infection in children and adults: a cohort study at a single hospital throughout the epidemic. Int Arch Med 2012;5:13.
63. Rhim JW, Lee KY, Youn YS, Kang JH, Kim JC. Epidemiological and clinical characteristics of childhood pandemic 2009 H1N1 virus infection: an observational cohort study. BMC Infect Dis 2011;11:225.
64. Rice TW, Rubinson L, Uyeki TM, Vaughn FL, John BB, Miller RR III, et al. Critical illness from 2009 pandemic influenza A virus and bacterial coinfection in the United States. Crit Care Med 2012;40:1487–98.
65. Samra T, Pawar M, Yadav A. Comparative evaluation of acute respiratory distress syndrome in patients with and without H1N1 infection at a tertiary care referral center. Indian J Anaesth 2011;55:47–51.
66. Sertogullarindan B, Ozbay B, Gunini H, Sunnetcioglu A, Arisoy A, Bilgin HM, et al. Clinical and prognostic features of patients with pandemic 2009 influenza A (H1N1) virus in the intensive care unit. Afr Health Sci 2011;11:163–70.
67. Shah DP, El Taoum KK, Shah JN, Vigil KJ, Adachi JA, Granwehr BP, et al. Characteristics and outcomes of pandemic 2009/H1N1 versus seasonal influenza in children with cancer. Pediatr Infect Dis J 2012;31:373–8.
68. Souza TM, Salluh JIF, Bozza FA, Mesquita M, Soares M, Motta FC, et al. H1N1pdm influenza infection in hospitalized cancer patients: clinical evolution and viral analysis. PLOS ONE 2010;5:e14158.
69. Tabarsi P, Moradi A, Marjani M, Baghaei P, Hashemian SM, Nadji SA, et al. Factors associated with death or intensive care unit admission due to pandemic 2009 influenza A (H1N1) infection. Ann Thorac Med 2011;6:91–5.
70. Teke T, Coskun R, Sungur M, Guven M, Bekci T, Maden E, et al. 2009 H1N1 influenza and experience in three critical care units. Int J Med Sci 2011;8:270–7.
71. To KK, Wong SS, Li IW, Hung IF, Tse F, Woo PC, et al. Concurrent comparison of epidemiology, clinical presentation and outcome between adult patients suffering from the pandemic influenza A (H1N1) 2009 virus and the seasonal influenza A virus infection. Postgrad Med J 2010;86:515–21.
72. Torres SF, Iolster T, Schnitzler EJ, Farias J, Bordogna AC, Rufach D, et al. High mortality in patients with influenza A pH1N1 2009 admitted to a pediatric intensive care unit: a predictive model of mortality. Pediatr Crit Car Med 2012;13:e78–83.
73. Viasus D, Cordero W, Rodriguez-Bano, J, Oteo JA, Fernandez-Navarro A, Ortega L, et al. Changes in epidemiology, clinical features and severity of influenza A (H1N1) 2009 pneumonia in the first post-pandemic influenza season. Clin Microbiol Infect 2012;18:E55–62.
74. Vidovic J, Kovacevic P, Stanetic M, Rajkovaca Z, Zlojutro B. Treatment of critically ill patients with influenza a H1N1 in university hospital Banja Luka. Acta Med Saliniana 2011;40(Suppl. 1):49–51.
75. Zhang PJ, Li XL, Cao B, Yang SG, Liang AR, Gu L, et al. Clinical features and risk factors for severe and critical pregnant women with 2009 pandemic H1N1 influenza infection in China. BMC Infect Dis 2012;12:29.
76. Perez-Padilla R, De La Rosa-Zamboni D, Ponce De Leon S, Hernandez M, Quiniones-Falconi F, Bautista E, et al. Pneumonia and respiratory failure from swine-origin influenza A (H1N1) in Mexico. N Engl J Med 2009;361:680–9.
77. Schellongowski P, Ullrich R, Hieber C, Hetz H, Losert H, Hermann M, et al. A surge of flu-associated adult respiratory distress syndrome in an Austrian tertiary care hospital during the 2009/2010 influenza A H1N1v pandemic. Wien Klin Wochenschr 2011;123:209–14.
78. Louie J, Acosta M, Jamieson D, Honein M. Severe 2009 H1N1 influenza in pregnant and postpartum women in California. N Engl J Med 2010;362:27–35.
79. Xi X, Xu Y, Jiang L, Li A, Duan J, Du B. Hospitalized adult patients with 2009 influenza A(H1N1) in Beijing, China: risk factors for hospital mortality. BMC Infect Dis 2010;10:256.
80. Louie J, Gavali S, Acosta M, Samuel M, Winter K, Jean C, et al. Children hospitalized with 2009 novel influenza A(H1N1) in California. Arch Pediatr Adolesc Med 2010;164:1023–31.
81. Libster R, Bugna J, Coviello S, Hijano D, Dunaiewsky M, Reynoso N, et al. Pediatric hospitalizations associated with 2009 pandemic influenza A (H1N1) in Argentina. N Engl J Med 2010;362:45–55.
82. Altmann M, Fiebig L, Buda S, von Kries R, Dehnert M, Haas W. Unchanged severity of influenza A(H1N1)pdm09 infection in children during first postpandemic season. Emerg Infect Dis 2012;18:1755–62.
83. Bramley AM, Dasgupta S, Skarbinski J, Kamimoto L, Fry AM, Finelli L, et al. Intensive care unit patients with 2009 pandemic influenza A (H1N1pdm09) virus infection: United States, 2009. Influenza Other Respir Viruses 2012;6:e134–42.
84. Jain S, Benoit R, Skarbinski J, Bramley AM, Finelli L, 2009 Pandemic Influenza A(H1N1) Virus Hospitalizations Investigation Team. Influenza-associated pneumonia among hospitalized patients with 2009 pandemic influenza A (H1N1) virus: United States, 2009. Clin Infect Dis 2012;54:1221–9.
85. Peters PJ, Skarbinski J, Louie JK, Jain S, New York Department of Health Swine Flu Investigation Team, Roland M, et al. HIV-infected hospitalized patients with 2009 pandemic influenza A (pH1N1): United States, spring and summer 2009. Clin Infect Dis 2011;52(Suppl. 1):183–8.
86. Yen CJ, Louie JK, Schechter R. Infants hospitalized in intensive care units with 2009 H1N1 influenza infection, California, 2009–2010. Pediatr Infect Dis J 2012;31:e52–5.
87. Louie JK, Acosta M, Winter K, Jean C, Gavali S, Schechter R, et al. Factors associated with death or hospitalization due to pandemic 2009 influenza A(H1N1) infection in California. JAMA 2009;302:1896–902.
88. Subramony H, Lai F, Ang L, Cutter J, Lim P, James L. An epidemiological study of 1348 cases of pandemic H1N1 influenza admitted to Singapore hospitals from July to September 2009. Ann Acad Med Singapore 2010;39:283–8.
89. Yates L, Pierce M, Stephens S, Mill AC, Spark P, Kurinczuk JJ, et al. Influenza A/H1N1v in pregnancy: an investigation of the characteristics and management of affected women and the relationship to pregnancy outcomes for mother and infant. Health Technol Assess 2010;14(34).
90. Donaldson L, Rutter P, Ellis B, Greaves FE, Mytton OT, Pebody RG, et al. Mortality from pandemic A/H1N1 2009 influenza in England: Public health surveillance study. BMJ 2010;339:b5213.
91. Sachedina N, Donaldson L. Paediatric mortality related to pandemic influenza A H1N1 infection in England: an observational population-based study. Lancet 2010;376:1846–52.
92. Santa-Olalla Peralta P, Cortes-Garcia M, Vicente-Herrero M, Castillo-Villamandos C, Arias-Bohigas P, Pachon-Del Amo I, et al. Risk factors for disease severity among hospitalised patients with 2009 pandemic influenza A (H1N1) in Spain, April-December 2009. Euro Surveill 2010;15:19667.
93. Moghadami M, Kazeroni P, Honarvar B, Ebrahimi M, Bakhtiari H, Akbarpour MA, et al. Influenza A (H1N1) virus pandemic in Fars province: a report from Southern Iran, July–December 2009. Iran Red Crescent Med J 2010;12:231–8.
94. Morgan O, Bramley A, Fowlkes A, Freedman DS, Taylor TH, Gargiullo P, et al. Morbid obesity as a risk factor for hospitalization and death due to 2009 pandemic influenza A(H1N1) disease. PLOS ONE 2010;5:e9694.
95. Cortes Garcia M, Sierra Moros MJ, Santa-Olalla Peralta P, Hernandez-Baverra V, Jiminez-Garcia R, Pachon I, et al. Clinical characteristics and outcomes of diabetic patients who were hospitalised with 2009 pandemic influenza A H1N1 infection. J Infect 2012;64:218–24.
96. Gauzere BA, Bussienne F, Buchet B, Jabot J, Roussiaux J, Drouet D, et al. [Severe cases of A(H1N1)v2009 infection in Reunion Island in 2009 and 2010.] Bull Soc Pathol Exot 2011;104:97–104.
97. Hsann YM, Thang SP, Abdul Salam ZH, Yang Y, Su-Leong Lim V, Yang KS. Clinical characteristics and outcomes of hospitalized patients with 2009 H1N1 influenza in a large acute care tertiary hospital, Singapore. Am J Infect Cont 2011;39:e49–51.
98. Oersted I, Molvadgaard M, Linde Nielsen H, Nielsen H. The first, second and third wave of pandemic influenza A (H1N1) in North Denmark region, 2009–2011: a population-based study of hospitalisations. Clin Microbiol Infect 2012;18:217.
99. Pano-Pardo JR, Viasus D, Pachon J, Campins A, Lopez-Medrano F, Villoslada A, et al. Pandemic 2009 A(H1N1) infection requiring hospitalization of elderly Spanish adults. J Am Geriatr Soc 2012;60:740–4.
100. Aguirre E, Papenburg J, Ouakki M, Fontela PS, Guimont C, De Serres G, et al. Comparison of pandemic and seasonal influenza in the pediatric emergency department. Pediatr Infect Dis J 2011;30:633–9.
101. Cho JH, Kim CD, Kim MS, Kang ES, Kim YH, Kim JI, et al. The impact of A(H1N1)pdm09 infection on renal transplant recipients: a multicenter cohort study. J Infect 2012;65:88–90.
102. Choi SM, Boudreault AA, Xie H, Englund JA, Corey L, Boeckh M. Differences in clinical outcomes after 2009 influenza A/H1N1 and seasonal influenza among hematopoietic cell transplant recipients. Blood 2011;117:5050–6.
103. Fabbiani M, Sali M, De Cristo V, Pignataro G, Prete V, Farina S, et al. Prospective evaluation of epidemiological, clinical, and microbiological features of pandemic influenza A (H1N1) virus infection in Italy. J Med Virol 2011;83:2057–65.
104. Lee IK, Liu JW, Wang L, Yang KD, Li CC, Eng HL. 2009 pandemic influenza A (H1N1): clinical and laboratory characteristics in pediatric and adult patients and in patients with pulmonary involvement. Influenza Other Respir Viruses 2012;6:e152–61.
105. Morgan CI, Hobson MJ, Seger B, Rice MA, Staat MA, Wheeler DS. 2009 pandemic influenza A (H1N1) in critically ill children in Cincinnati, Ohio. Pediatr Crit Care Med 2012;13:e140–4.
106. Osoro EM, Munyua P, Muthoka P, Gikundi S, Njenga MK, Lifumo S, et al. Hospitalized patients with pandemic (H1N1) 2009, Kenya. Emerg Infect Dis 2011;17:1744–6.
107. Shlomai A, Nutman A, Kotlovsky T, Schechner V, Carmeli Y, Guzner-Gur H. Predictors of pandemic (H1N1) 2009 virus positivity and adverse outcomes among hospitalized patients with a compatible syndrome. Isr Med Assoc J 2010;12:622–7.
108. Bettinger J, Sauve L, Scheifele D, Moore D, Vaudry W, Tran D, et al. Pandemic influenza in Canadian children: a summary of hospitalised pediatric cases. Vaccine 2010;28:3180–4.
109. Hewagama S, Walker S, Stuart R, Gordon C, Johnson PD, Friedman ND, et al. 2009 H1N1 influenza A and pregnancy outcomes in Victoria, Australia. Clin Infect Dis 2010;50:686–90.
110. Stein M, Tasher D, Glikman D, Shachor-Meyouhas Y, Barkal G, Yochal AB, et al. Hospitalization of children with influenza A(H1N1) virus in Israel during the 2009 outbreak in Israel: a multicenter survey. Arch Pediatr Adolesc Med 2010;164:1015–22.
111. Bassetti M, Parisini A, Calzi A, Pallavicini F, Cassola G, Artioli S, et al. Risk factors for severe complications of the novel influenza A (H1N1): analysis of patients hospitalized in Italy. Clin Microbiol Infect 2011;17:247–50.
112. Chowell G, Viboud C, Simonsen L, Miller Ma, Echevarria-Zuno S, Gonzalez-Leon M, et al. Impact of antiviral treatment and hospital admission delay on risk of death associated with 2009 A/H1N1 pandemic influenza in Mexico. BMC Infect Dis 2012;12:97.
113. Gilca R, De Serres G, Boulianne N, Ouhoummane N, Papenburg J, Douville-Fradet M, et al. Risk factors for hospitalization and severe outcomes of 2009 pandemic H1N1 influenza in Quebec, Canada. Influenza Other Respir Viruses 2011;5:247–55.
114. Gouya MM, Nabavi M, Soroush M, Haghdoust AA, Ghalehee S, Hemmati P, et al. Mortality from pandemic influenza A (H1N1) in Iran. Iran Red Crescent Med J 2011;13:698–701.
115. Rana H, Parikh P, Shah AN, Ghandi S. Epidemiology and clinical outcome of H1N1 in Gujarat from July 2009 to March 2010. J Assoc Physicians India 2012;60:95–7.
116. Schout D, Hajjar LA, Galas FR, Uip DE, Levin AS, Caiaffa Filho HH, et al. Epidemiology of human infection with the novel virus influenza A (H1N1) in the Hospital das Clinicas, Sao Paulo, Brazil: June-September 2009. Clinics (Sao Paulo, Brazil) 2009;64:1025–30.
117. Wilking H, Buda S, von der Lippe E, Altmann D, Krause G, Eckmanns T, et al. Mortality of 2009 pandemic influenza A(H1N1) in Germany. Eur Surveill 2010;15:19741.
118. Rodriguez A, Socias L, Guerrero J, Figueira JC, Gonzalez N, Maravi-Poma E, et al. Pandemic influenza A in the ICU: experience in Spain and Latin America. Med Intensiva 2010;34:87–94.
119. Adisasmito W, Chan P, Lee N, Oner AF, Gasimov V, Aghayev F, et al. Effectiveness of antiviral treatment in human influenza A(H5N1) infections: analysis of a global patient registry. J Infect Dis 2010;202:1154–60.
120. Marcelli D, Marelli C, Richards N. Influenza A(H1N1)v pandemic in the dialysis population: first wave results from an international survey. Nephrol Dial Transplant 2010;24:3566–72.
121. Nukiwa N, Kamigaki T, Oshitani H. Fatal cases of pandemic (H1N1) 2009 influenza despite their early antiviral treatment in Japan. Clin Infect Dis 2010;51:993–4.
122. Fuhrman C, Bonmarin I, Bitar D, Cardoso T, Duport N, Herida M, et al. Adult intensive-care patients with 2009 pandemic influenza A(H1N1) infection. Epidemiol Infect 2011;139:1202–9.
123. Echevarria-Zuno S, Mejia-Arangure J, Mar-Obeso A, Grajales-Muniz C, Robles-Perez E, Gonzalez-Leon M, et al. Infection and death from influenza A H1N1 virus in Mexico: a retrospective analysis. Lancet 2009;374:2072–9.
124. Martin-Loeches I, Rodriguez A, Bonastra J, Zaragoza R, Sierra R, Marques A, et al. Severe pandemic (H1N1)v influenza A infection: report on the first deaths in Spain. Respirology 2011;16:78–85.
Appendix 15 Illustration of time-dependent bias using individual patient data from the Canadian study
We illustrate the effect of time-dependent bias using the data from one of the included studies. Of 578 patients with a survival time, 540 received oseltamivir [of which 105 (19%) died] compared with 38 who did not receive an antiviral [of which 12 (32%) died]. A simple chi-squared test gives weak evidence of a difference in survival (p = 0.072) and Cox regression, assuming that treatment exposure uniformly occurs at hospital admission provides evidence of reduced risk of death for patients receiving oseltamivir (HR 0.52, 95% CI 0.29 to 0.95; p = 0.033). See Table 27 for a life table and Figure 24 for a Kaplan–Meier plot of the data assuming treatment exposure occurred at hospital admission.
An alternative analysis that takes into account the fact that treatment with oseltamivir does not occur at hospital admission but rather occurred at a mean of 0.62 days (range 0–45 days) after hospital admission shows a markedly different result. Cox regression assuming time-dependent treatment exposure gives no evidence of reduced risk of death for patients receiving oseltamivir (HR 0.87, 95% CI 0.48 to 1.61; p = 0.66). See Table 28 for a life table and Figure 25 for a survival plot of the data using the method of Simon and Makuch. 227
The life tables and survival plots are shown for the first 11 days, as this is where most of the mortality occurred. When standard survival analysis is used there is an implicit assumption that treatment exposure begins at baseline, which, in this case, is hospital admission. Therefore, at baseline there were 540 patients at risk in the oseltamivir group and 38 patients at risk in the no-treatment group (see Table 27 and see Figure 24). This incorrect assumption is what leads to time-dependent bias.
In the alternative analysis the timing of exposure to treatment is taken account of correctly by considering how many patients were exposed or unexposed to treatment on a daily basis. If the data were available the computation could be done more accurately, for example on an hourly basis. Table 28 shows that in fact there were only 423 patients exposed to oseltamivir in the first 24 hours of hospital stay. By simple subtraction we also know that 155 patients had no exposure to oseltamivir during the first 24 hours of hospitalisation. This more accurate data then leads to more accurate estimates of the cumulative mortality. If we were to use hourly data then we would obtain more accurate estimates and reduce time-dependent bias further.
Severity of illness and competing risks analysis
Of 578 patients, 517 had an APACHE II score recorded, with the proportion missing being greater for the untreated patients than the treated patients (37% vs. 9%; p < 0.0001). Mortality was not significantly higher in the patients with missing APACHE II score (25% vs. 20%; p = 0.35). In those with an APACHE II score recorded there was no evidence of a difference between treated and untreated patients [untreated mean (SD) 19 (10)12 vs. treated mean (SD) 21 (10);10 p = 0.39]. Owing to the large difference in proportion missing between untreated and treated patients combined with similar observed scores in the two groups, unadjusted competing risks analysis was conducted using the method of Fine and Gray. 180 Results show insufficient evidence of a difference in mortality (HR 0.84, 95% CI 0.41 to 1.73; p = 0.64) or discharge (HR 1.41, 95% CI 0.73 to 2.74; p = 0.31).
| Days since admission | Number at risk (AV) | Number dead (AV) | Cumulative mortality (%) (AV) | Number at risk (no AV) | Number dead (no AV) | Cumulative mortality (%) (no AV) |
|---|---|---|---|---|---|---|
| 1 | 540 | 4 | 0.7 | 38 | 3 | 7.9 |
| 2 | 536 | 14 | 3.3 | 35 | 3 | 15.8 |
| 3 | 519 | 4 | 4.1 | 32 | 0 | 15.8 |
| 4 | 507 | 2 | 4.5 | 31 | 0 | 15.8 |
| 5 | 498 | 3 | 5.0 | 29 | 0 | 15.8 |
| 6 | 485 | 4 | 5.8 | 27 | 1 | 18.9 |
| 7 | 467 | 6 | 7.0 | 26 | 1 | 22.0 |
| 8 | 449 | 4 | 7.9 | 25 | 0 | 22.0 |
| 9 | 441 | 4 | 8.7 | 23 | 1 | 25.4 |
| 10 | 422 | 8 | 10.4 | 22 | 0 | 25.4 |
| 11 | 394 | 7 | 12.0 | 22 | 1 | 28.8 |
| 12 | 375 | 6 | 13.4 | 20 | 0 | 28.8 |
FIGURE 24.
Kaplan–Meier plot of time to death. AV, antiviral; TF, Tamiflu (oseltamivir).

| Days since admission | Number at risk (AV) | Number dead (AV) | Cumulative mortality (%) (AV) | Number at risk (no AV) | Number dead (no AV) | Cumulative mortality (%) (no AV) |
|---|---|---|---|---|---|---|
| 1 | 423 | 4 | 1.0 | 155 | 3 | 2.0 |
| 2 | 484 | 14 | 3.9 | 87 | 3 | 5.5 |
| 3 | 487 | 4 | 4.7 | 64 | 0 | 5.5 |
| 4 | 485 | 2 | 5.1 | 53 | 0 | 5.5 |
| 5 | 481 | 3 | 5.7 | 46 | 0 | 5.5 |
| 6 | 472 | 4 | 6.6 | 40 | 1 | 8.0 |
| 7 | 459 | 6 | 7.9 | 34 | 1 | 11.0 |
| 8 | 442 | 4 | 8.8 | 32 | 0 | 11.0 |
| 9 | 434 | 4 | 9.7 | 30 | 1 | 14.4 |
| 10 | 415 | 8 | 11.7 | 28 | 0 | 14.4 |
| 11 | 388 | 7 | 13.5 | 28 | 1 | 18.0 |
| 12 | 370 | 6 | 14.8 | 25 | 0 | 18.0 |
FIGURE 25.
Survival plot for time-dependent treatment exposure. AV, antiviral; TF, Tamiflu (oseltamivir).

Appendix 16 Feedback
Glossary
- Clinical study reports
- Detailed reports of a clinical trial, usually submitted to regulators, following a prescribed International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use format. Roche’s reports follow a modular structure (see Appendix 9). Reports can be several hundred pages long and contain details of the planned design, conduct (protocol), analysis (reporting analysis plan) and results of the trial.
- Compliharm
- Term describing events defined as either complications or harms according to ambiguous criteria that appeared to include time of analysis (with times either unspecified or inconsistent among trials) and whether or not participants were infected (by influenza). In oseltamivir treatment trials some potential harms or complications could be caused by both medication or influenza infection (e.g. vomiting), hence our classification as a compliharm.
- Consolidated Standards of Reporting Trials-based extraction
- Extraction, synthesis and appraisal method used in this review for data from clinical study reports. Reconstructions were done by pairs of review authors and assessed in the authors’ plenary session to decide whether or not included trials could proceed to stage 2 of the analysis. The structure of the reconstruction follows that of the Consolidated Standards of Reporting Trials statement.
- Freedom of information
- Enshrined by law in the US and European Medicines Agency policy in Europe. Freedom-of-information requests in this review have been a means of access to clinical study reports and regulatory comments (regulatory information).
- Individual patient data
- Anonymised individual data listings of characteristics and results, which form the basis for the synthetic analyses in clinical study reports.
- Japanese Summary Basis for Approval (of a drug)
- Summary of the application dossiers included as one of the documents that is prepared and attached by the sponsoring pharmaceutical company. These are submitted to the regulatory body for approval of a new drug.
- Modules
- Basic structure of Roche’s trial reports. Today, the term ‘Modules’ refers to the components of a regulatory submission, as set by the International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use (2011). Clinical study reports are just one ‘module’ of a regulatory submission.
- Protocol
- Document reporting the trial’s planned design and conduct, with amendments (when relevant). Confusingly, also used in submissions and regulatory documents as synonymous with study.
- Public health drugs
- Drugs in which a considerable quantity of public money has been invested and/or are on the World Health Organization essential drugs list.
- Regulatory information
- Term comprising clinical study reports (data) and regulatory comments and reviews.
- Reporting Analysis Plan
- Plan of analysis that is usually linked to the trial protocol, explaining what and how the authors intend to analyse.
- Table of content of regulatory reviews and comments on industry submissions
- Our table of content indicates which trial is cited, in which document, on which page and how many times.
- Table of contents-evidence
- Annotated version of the table of contents. Comments and annotation are preliminary and form the basis for the weaving of the important aspects into the review narrative.
- Time lock
- Date (12 April 2011) after which no documentation would be reviewed in the January 2012 version of the review. A cut-off was made necessary by the sheer scale of our data holdings. We were initially funded to review the full clinical study reports of the 10 treatment trials included in the Kaiser et al. paper (Kaiser L, Wat C, Mills T, Mahoney P, Ward P, Hayden F. Impact of oseltamivir treatment on influenza-related lower respiratory tract complications and hospitalizations. Arch Intern Med 2003;63:1667–72). We were able to access the 10 module 1s and regulatory comments (approximately 6000 pages in total). As the funder-stipulated deadline to producing our review progressively shortened, and our understanding of the issues evolved, we received notification that although the balance of the 10 study reports was unlikely to be accessible by our deadline, we would receive substantial quantities of regulatory documents from the European Medicines Agency in four tranches. When we held our second face-to-face meeting in April 2011 we had just received our first tranche of clinical study reports, consisting of just over 10,000 pages, bringing our total holdings to 16,000 pages. We decided that we did not have the resources to review any further documentation within our current funding and imposed a data time lock. Any documentation received after this date would be reviewed if and when we had more resources. The balance of documents (a further 14,000 pages) are included in this review.
- Trial ID
- Means of identifying a trial. Usually made up of letters and numbers (WV15799). At times the ID bears a letter suffix indicating the last version of the protocol followed in the trial (e.g. WV15799H, i.e. trial carried out following amendment H).
- Trial programme
- Series of trials designed and carried out to achieve registration or to answer specific questions. Usually, programmes of the same drug or intervention focus on the same indication or the same study population.
List of abbreviations
- APACHE
- Acute Physiology and Chronic Health Evaluation
- BMJ
- British Medical Journal
- CDC
- US Centers for Disease Control and Prevention
- CENTRAL
- Cochrane Central Register of Controlled Trials
- CI
- confidence interval
- CONSORT
- Consolidated Standards of Reporting Trials
- CRF
- case report form
- CSR
- clinical study report
- CTCAE V4.0
- Common Terminology Criteria for Adverse Events Version 4.0
- DARE
- Database of Abstracts of Reviews of Effects
- df
- degrees of freedom
- EMA
- European Medicines Agency
- FDA
- US Food and Drug Administration
- FOI
- freedom of information
- GSK
- GlaxoSmithKline
- HEED
- Health Economic Evaluations Database
- HR
- hazard ratio
- ILI
- influenza-like illness
- IPD
- individual patient data
- ITT
- intention to treat
- ITTI
- intention-to-treat-influenza-infected
- ITTIINAB
- intention-to-treat influenza-infected index cases who had negative virology at baseline
- MD
- mean difference
- NCI-CTC V2.0
- National Cancer Institute-Common Toxicity Criteria Version 2.0
- NDA
- New Drug Application
- NHS EED
- National Health Service Economic Evaluation Database
- NI
- neuraminidase inhibitor
- NICE
- National Institute for Health and Care Excellence
- NNTB
- number needed to treat to benefit
- NNTH
- number needed to treat to harm
- NSAID
- non-steroidal anti-inflammatory drug
- OR
- odds ratio
- PEP
- post-exposure prophylaxis
- RCT
- randomised controlled trial
- RD
- risk difference
- RR
- risk ratio
- SAP
- statistical analysis plan
- SBA
- Summary Basis of Approval
- td-Cox
- Cox regression including treatment as a time-dependent exposure
- TOC
- table of contents
- WHO
- World Health Organization