
Notes
Article history
The research reported in this issue of the journal was funded by the HTA programme as project number 10/104/41. The contractual start date was in November 2012. The draft report began editorial review in November 2014 and was accepted for publication in July 2015. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HTA editors and publisher have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
Professor Glyn Lewis is a board member of the National Institute for Health Research (NIHR) Efficacy and Mechanism Evaluation programme. Dr Naomi Fineberg reports grants and non-financial support from NIHR during the conduct of the study; grants, personal fees, non-financial support and other from Lundbeck (Copenhagen, Denmark); grants and personal fees from GlaxoSmithKline (London, UK); non-financial support from Novartis (Basel, Switzerland); other from Transcept Pharmaceuticals (Boston, MA, USA); grants, personal fees, non-financial support and other from Servier (Suresnes, France); grants, non-financial support and other from Cephalon (Frazer, PA, USA); grants and personal fees from AstraZeneca (London, UK); personal fees and non-financial support from the European College of Neuropsychopharmacology (Utrecht, the Netherlands); grants from the Medical Research Council (London, UK); grants from the Wellcome Foundation (London, UK); personal fees, non-financial support and other from Jazz Pharmaceuticals (Dublin, Ireland); personal fees and non-financial support from Bristol-Myers Squibb (New York, NY, USA); non-financial support and other from the Royal College of Psychiatrists (London, UK); non-financial support from Janssen (Beerse, Belgium); non-financial support from International College of Obsessive Compulsive Spectrum Disorders; non-financial support and other from British Association for Psychopharmacology, non-financial support from the Journal of Behavioural Addiction; and non-financial support from World Health Organization (Geneva, Switzerland) outside the submitted work, and is medical lead to a NHS service that provides treatment for treatment-refractory obsessive–compulsive and related disorders, has been a Council member for the British Association for Psychopharmacology and sits on the Royal College of Psychiatrists Psychopharmacology Special Committee and the European College of Neuropsychopharmacology Education Committee and Research Network. Dr Deborah Caldwell reports grants from Medical Research Council Population Health Scientist fellowship (G0902118) during the conduct of the study.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2016. This work was produced by Skapinakis et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Background
Description of the health problem
Descriptions of obsessive–compulsive symptoms have been reported since the late medieval period, mainly in relation to religious or moral issues. 1 Several nineteenth- and early twentieth-century physicians showed great interest in these phenomena, including Carl Westphal in 1877 [who used the term ‘Zwangsvorstellung’ to describe obsessive–compulsive disorder (OCD)], Julius Donath in 1897 (who invented the term ‘anancasmus’ from the Greek word of the same root meaning ‘to compel’) and Pierre Janet in 1906 (who associated the symptom of obsessions with the ‘psychasthenic’ condition). 2 By 1906, the term ‘Obsessional Insanity’ had been included in the ‘Nomenclature of Diseases’ of the Royal College of Physicians in London, and Emil Kraepelin included in his textbooks the similar condition of ‘Zwangsneurose’. 2 It is interesting that all the main symptoms of the current description of OCD have been described very accurately in the past, including the egodystonic nature of obsessions, the presence of both obsessions and compulsions in the majority of patients, the preservation of insight (the ‘folie avec conscience’ – insanity with insight – of the French psychopathologists), the accompanying anxiety, the common comorbidity with depression, the chronic and fluctuating course, and the tendency of patients to hide their symptoms and not seek help from doctors.
Diagnostic criteria: disease classification
The first two versions of the Diagnostic and Statistical Manual of Mental Disorders (DSM) of the American Psychiatric Association were heavily influenced by the psychodynamic concepts of mental illness and defined obsessive and compulsive phenomena accordingly. In the first edition (DSM-I), the term ‘Obsessive Compulsive Reaction’ was used; the term ‘reaction’ referred to the way in which a person reacts to unconscious intrapsychic conflicts using defence mechanisms. 3 This was classified under the broader category of ‘Psychoneurotic Disorders’. In the second edition (DSM-II), the term ‘Obsessive Compulsive Neurosis’ was used. 4 Next editions of the manual abandoned the effort of classifying mental disorders in accordance with aetiology and adopted an atheoretical model based on descriptive phenomenology and empirical research. This was mainly done to increase the reliability of psychiatric diagnosis. The World Health Organization (WHO) followed along the same path and published clinical descriptions and specific diagnostic criteria for research. 5 From 1980 (DSM-III) to 2000, when the fourth edition of DSM was published (DSM-IV), there were few differences in the conceptualisation of OCD. 6 The disorder is classified under the broad category of ‘Anxiety Disorders’ and the two main characteristics are the presence of either obsessions or compulsions. Obsessions are defined as recurring and persistent thoughts, images or impulses that are intrusive and inappropriate and cause much distress and anxiety. Owing to their content, the patient tries to resist and control these thoughts or to suppress the resulting anxiety with compulsions. These are repetitive behaviours or mental acts that may aim to reduce the anxiety brought on by the obsession or that the person feels driven to perform in accordance with a rigid sequence or idiosyncratic rules. Quite often, these behaviours are not connected in a realistic way with what they aim to neutralise or prevent, or they are clearly excessive. In order for these symptoms to be considered clinically significant, they should have a considerable impact on the everyday functioning of the individual.
In the latest edition of the DSM (DSM-V),7 there have been some slight changes to the definition of the disorder, some of the most important of which are the following:
-
OCD has been separated from the broader category of ‘Anxiety Disorders’ and it is now described under the category of ‘Obsessive–Compulsive and Related Disorders’ which also includes body dysmorphic disorder, hoarding disorder, trichotillomania and excoriation disorder.
-
It is acknowledged that there is a spectrum of insight and that some patients may have absent insight or ‘delusional’ beliefs. Therefore, in DSM-V insight is coded as ‘good/fair’ (obsessions are recognised as excessive and abnormal ideas), ‘poor’ (obsessions take the form of overvalued ideas) or ‘absent’ (obsessions share some characteristics with delusions). An absent insight does not preclude the diagnosis of OCD. As Leckman et al. 8 point out, it is assumed that patients with currently absent insight have shown some insight in the past during the course of their disorder.
-
Hoarding disorder is now a separate disorder and not a subtype of OCD.
-
A form of OCD related to chronic tics is now included as a new subtype, as there is evidence that this subtype has a younger age at onset and different treatment response. 8
-
The definition of OCD according to the International Classification of Diseases, Tenth Edition (ICD-10), is very similar to that of the DSM, with slight and not essential differences. 8
-
The ICD-10 does not include separate definitions of obsessions and compulsions but the emphasis is placed on their shared characteristics.
-
The DSM implies that obsessions and compulsions have a functional relationship (in the sense that compulsions are behaviours that aim to reduce the distress caused by the obsessions), whereas the ICD does not suggest such a connection.
Form and content of obsessions and compulsions
Previous studies of the phenomenology of OCD have described both the form and the content of obsessions and compulsions. Khanna et al. 9 described the following forms for obsessions (in order of frequency): fears, thoughts, doubts, urges, convictions and images; and, for compulsion: repeating, rituals, checking and avoiding.
The thematic content of obsessions and compulsions has been described in detail by Rasmussen and Eisen10 and Foa et al. 11 Rasmussen and Eisen10 have used data from their large cohort of 560 OCD patients (diagnosed in accordance with DSM-III or DSM-III-R criteria), whereas Foa et al. 11 reported data from 425 patients with OCD (in accordance with DSM-IV criteria). Although there are some differences between these two studies, it is generally accepted that common themes of obsessions are (all figures from Foa et al. 11) worries about dirt/contamination (40%), aggressive obsessions (25%), content related to sexual or religious themes (12%), need for symmetry (10%), somatic/hypochondriac concerns (7%) and unacceptable urges (4%). In the Rasmussen and Eisen10 cohort, pathological doubt (regarding responsibility for a terrible event) was the second most common content, reported in 40% of patients (this theme is related to aggressive ideas or harm-related content in the Foa et al. 11 study). Regarding compulsions, common themes include checking (28%), cleaning/washing (27%), repeating/counting (13%), mental rituals (11%), ordering/symmetry compulsions (6%) and hoarding-related compulsions (4%).
Given that there may be a functional relationship between obsessions and compulsions, some studies have investigated the structure of symptoms using the statistical techniques of factor or cluster analysis. Recently, Bloch et al. 12 carried out a meta-analysis of all studies that used factor-analytic methods to investigate the symptom structure of the most commonly used symptom scale, the Yale–Brown Obsessive–Compulsive Scale (YBOCS) (n = 21 studies involving 5124 participants). They concluded that four distinct factors explained 79% of the variance in the total sample: (1) a symmetry factor, which included symmetry obsessions and ordering, repeating and counting compulsions; (2) a factor associated with ‘forbidden’ thoughts, which included aggressive, sexual and religious obsessions; (3) a cleaning factor, including dirt/contamination obsessions and cleaning compulsions; and (4) a hoarding factor. The results were quite similar in both the children and adolescents and adults subsamples.
Although most patients have a main/primary theme for their obsession or compulsion, it is not uncommon to report other themes of milder intensity or frequency. 9 Mataix-Cols et al. 13 investigated the longitudinal stability of symptoms in 117 adult patients and concluded that symptoms were quite stable at 2 years’ follow-up and that shifts between symptom dimensions were relatively rare.
Phenomenological differences between the two genders
The phenomenological differences between the two genders have been recently reviewed by de Mathis et al. 14 Men are younger at onset, and this is sometimes associated with the presence of chronic tics and a worse prognosis. Most phenomenological studies conclude that men are more likely to develop obsessions with a sexual/religious theme, whereas women more often develop dirt/contamination obsessions and cleaning compulsions. 15,16 Some studies also report that symmetry/ordering obsessions are more common in men,15,17 whereas in women the presence of obsessions (either fears or impulses) with an aggressive content may be more common. 15,18
Phenomenology in children and adolescents
Obsessive–compulsive disorder may start very early in childhood,19 and it is interesting to investigate differences in the presentation of symptoms between children and adults. Geller et al. 20 compared symptom dimensions in a sample of 101 patients aged < 18 years, including a subsample of children (n = 46) and a subsample of adolescents (n = 55), and compared this with a reference adult patient sample previously reported in Rasmussen and Eisen. 21 Regarding obsessions, they reported significant differences between both the children and adolescents samples and the adults sample as regards the presence of aggressive/catastrophic obsessions (less common in the adult sample) and sexual/religious obsessions (which were more common in the adolescent sample). In addition, they reported that confessing/asking compulsions were more common in children. Similar studies have also confirmed that contamination obsessions and washing/cleaning compulsions are very common in children and adolescents. 22,23
Measurement of disease severity
Several instruments have been developed to assess symptom severity in OCD. These include both clinician-administered interviews and self-report questionnaires (or parent report in the case of the paediatric population). Grabill et al. 24 included four clinician-administered instruments and 10 self-report questionnaires in their review of this issue.
Of the clinician-administered instruments, the YBOCS25 is the most widely used instrument to assess symptom severity and is considered the gold standard in OCD literature, especially to assess change in symptoms after treatment. 26 This is a semistructured clinician-administered instrument assessing the severity and frequency of obsessions and compulsions. It yields three scores, an obsessions severity score, a compulsions severity score and a total score (ranging from 0 to 40 for the total). Good psychometric properties have been reported for both clinical and non-clinical samples of patients. 24 A cut-off score of 16 is often used in clinical trials for patients to be eligible for inclusion in a study. This score distinguishes patients with moderate-to-severe symptoms from patients with mild or subclinical symptoms and has demonstrated good sensitivity. 26 Other versions of the YBOCS include a self-report version26 and a modified version (YBOCS-II)27 to take into account more recent research on the phenomenology of OCD. An adaptation of the same scale for children and adolescents has been also developed, the Children’s Yale–Brown Obsessive–Compulsive Scale (CYBOCS),28 which has been used extensively in paediatric OCD trials. Studies of the factor structure of the YBOCS have generally confirmed the existence of two factors (severity of obsessions and severity of compulsions), although a third factor of resistance has been replicated in some studies. 24,29
Aetiology
Obsessive–compulsive disorder is a complex neuropsychiatric disorder, and several genetic, biological and psychological factors may have an important role in the aetiology of the condition. Although aetiological research in the OCD field is very active, the clinical heterogeneity and complexity of the disorder have resulted in the limited translational capacity of basic research into clinical practice. 30
Genetic factors
Family studies among relatives of both adults and children and adolescents with OCD have consistently shown that OCD is familial and that the risk of OCD is higher in first-degree relatives of patients. For example, in the Pauls et al. study,31 the rate of OCD in relatives of patients was significantly higher than in controls (10.3% vs. 1.9%). Similar results were reported by Nestadt et al. 32 (11.7% vs. 2.7%). Studies in children have reported an even higher familial association, with odds ratios (ORs) ranging from 12 to 30. 33–35
Although family studies point to a possible genetic aetiology in OCD, twin studies are more suitable to distinguish between genetic and environmental factors. Adoption twin studies have not been conducted in the OCD field36 and, therefore, most twin studies have compared the concordance rates in monozygotic versus dizygotic twin pairs. van Grootheest et al. 36 reviewed these studies and a meta-analysis of all available twin studies has been published more recently. 37 The conclusion of these studies is that approximately 40% of the variance in OCD can be explained by additive genetic factors, whereas 50% of the variance can be explained by non-shared environmental factors. Surprisingly, shared environmental factors (e.g. parental style or practices) were not associated with phenotypic variance.
Genetic linkage studies and the two published genome-wide association studies have been recently reviewed by Pauls et al. 33 The genetic linkage studies have identified two genomic regions (on chromosomes 9 and 15) that may be associated with an increased risk of OCD. Given that OCD is most probably a multigenic disorder, genetic linkage studies have limited power to identify multiple genes with a small-to-moderate effect. Genome-wide association studies may be more suitable, but the results of two such studies are inconclusive. It has been suggested that larger samples may be needed for the results to reach genome-wide significance. 33
Taken together, findings from genetic research support the hypothesis that multiple genes, regulating parts of the serotonergic, dopaminergic and glutamatergic systems, may be related to an increased vulnerability to OCD, but non-shared environmental factors also play an important part in the development of the disorder.
Biological factors
There is a consensus, mainly due to functional imaging studies, that a dysregulation in the frontostriatal circuit is involved in the pathophysiology of OCD. 33 Studies have consistently shown an increased activation of the orbitofrontal and possibly the anterior cingulate cortex, and an hyperactivity of the head of the caudate nucleus. Increased activation of the caudate leads, through a positive feedback loop, to an increase in the excitatory glutamatergic output from the thalamus to the frontal cortex. 33 This results in exaggerated worries about danger, despite direct evidence from the senses that contradict this danger. 33,38 Recent experimental studies in animals using the technique of optogenetics have shown that repeated stimulation of the orbitofrontal cortex and the ventromedial striatum generates a progressive increase in compulsive behaviours in animals (e.g. increased grooming) that is reversed by the chronic, but not acute, administration of fluoxetine. 39
Psychological factors
The psychological model of OCD postulates that patients interpret their unwanted intrusive thoughts (obsessions) in a maladaptive way. Salkovskis40 suggested that faulty appraisals related to inflated responsibility are very important. Apart from inflated responsibility, other maladaptive appraisals include the overimportance of thoughts, the need to control those thoughts and the exaggerated estimate of the probability that an unwanted event will occur (thought–action fusion). 41 These appraisals lead to anxiety and the need to engage in neutralising behaviours (such as compulsions, avoidance and reassurance seeking) to prevent harm. Compulsions are positively reinforced because they reduce the anxiety caused by the faulty appraisals in the short term. However, in the long term they prevent habituation and fear extinction from happening and thereby help in the maintenance of obsessions. Therefore, compulsive behaviour is considered as a maladaptive response to obsessions. Based on these theories, both cognitive–behavioural therapy (CBT) and behavioural therapy (BT) [exposure and response prevention (ERP)] have been successfully used for the treatment of OCD.
Epidemiology
Prevalence in adults
The descriptive epidemiology of OCD has been recently reviewed by Fontenelle et al. 19 and Torres and Lima. 42 Before 1980, the prevailing view was that OCD is a relatively severe but rare psychiatric disorder. This view was mainly based on the frequently cited 1953 study by Rudin,43 which estimated a prevalence of 0.05% in the general population. 10 However, even in this early period, which preceded modern diagnostic criteria, some studies showed a different situation for OCD prevalence. Among them, the careful psychiatric epidemiological study by Brunetti,44 in the small community of Roussillon in south-east France, reported a higher prevalence of 1%, which is a figure very close to estimates in more recent studies. The view that OCD is a rare disease changed after the large American epidemiological study of the 1980s, the Epidemiologic Catchment Area (ECA) study. 45 This study used a fully structured diagnostic interview, designed to be used by lay interviewers, and included OCD in the assessment. The OCD data were analysed by Karno et al. 46 They reported a lifetime prevalence for OCD in adults of 2.5% and a 6-month prevalence of 1.5%, which was considerably higher than previous estimates. Prevalence of OCD was higher in women than in men (with a ratio of 1 : 4). The diagnostic interview schedule (DIS) that was used for the assessment has been criticised for its inability to assess reliably anxiety and phobic disorders. 47 Nelson and Rice48 in a subsequent study examined the stability of the OCD diagnosis in the ECA data set using longitudinal data from the second wave, 12 months after the baseline measurement. They found that 80% of the participants who met lifetime criteria for OCD at baseline did not meet the same criteria at the second assessment. A clinical revalidation of OCD diagnosis in a subset of the ECA study showed a prevalence of clinically validated OCD of 0.3%, which was considerably lower than the DIS assessment. 47 Similarly, in a German study,49 the lifetime prevalence in accordance with the DIS was 2%, whereas according to clinicians it was 1%. More recent epidemiological studies using the Composite International Diagnostic Interview have resulted in a much broader range of prevalence rates of OCD in adults, from 0.9% lifetime prevalence in the Netherlands50 to 3% 1-month prevalence in Canada. 51 In this Canadian study, a clinical revalidation of the data resulted in a lower prevalence of 0.6%, whereas another 0.6% of patients met criteria for ‘subclinical’ OCD. According to the authors,51 the differences between the results of the diagnostic interviews and clinicians’ diagnoses are attributable to the following factors: (1) common or everyday worries are sometimes confused with obsessions in diagnostic interviews; and (2) it is likely that epidemiological interviews may overestimate the intensity or frequency of obsessions or compulsions.
Apart from DIS and the Composite International Diagnostic Interview, other studies have used the revised Clinical Interview Schedule and the Mini International Neuropsychiatric Interview. In one study,52 the 1-month prevalence with the revised Clinical Interview Schedule was 1.1%. In Italy, Faravelli et al. 53 reported a lifetime prevalence of 2.4% using the Mini International Neuropsychiatric Interview. In Greece, Skapinakis et al. 54 reported a 1-month prevalence of 1.7% using the revised Clinical Interview Schedule.
There is great variability in the estimation of the prevalence of OCD in the general population and this is partly explained by the different samples and methodologies used. Taking into account the majority of the studies, a conservative estimate of the lifetime prevalence of OCD, using diagnostic interviews in the general population, is approximately 2%, and the 1- to 6-month prevalence is between 1% and 1.5%. These estimates would be reduced by approximately half if clinicians had been involved in the assessments.
Prevalence in children and adolescents
The prevalence of OCD in children and adolescents has been investigated in several studies either in the general population or in more selected samples (e.g. school-based surveys). Of the general population studies, three are particularly useful as a result of their large samples or their representativeness: (1) a British study55 in a nationally representative sample of 10,000 children aged 5–15 years, which reported a low prevalence of current OCD at 0.2%; (2) a US study56 in a sample of 4500 children aged 9, 11 and 13 years, which also reported a 3-month prevalence of 0.2%; and (3) a study from the Netherlands57 in a nationally representative sample of 2916 adolescents aged 13–18 years, which reported a 6-month prevalence of 1%. It is worth noting that in both the Dutch study57 and in another community study in the USA,58 the authors found that relying solely on parents’ reports of symptoms may underestimate the true burden of OCD symptoms. This is especially relevant for studies of children < 12 years old, in which it is less likely that children will be directly asked to report their symptoms.
Incidence
The incidence of OCD has been studied less than the prevalence. A review by Fontenelle et al. 19 reported four studies in adults with an annual incidence ranging from 0.05% to 0.7%. The two most prominent studies are (1) a longitudinal study undertaken in the USA using a subset of the original ECA study59 which specifically investigated the incidence of OCD; and (2) a longitudinal extension of the NEtherlands MEntal health Survey and Incidence Study (NEMESIS). 60 The former reported an incidence of 0.55 per 1000 person-years (approximately 0.05% per year), whereas the latter reported an incidence of 0.2% per year.
Regarding children and adolescent samples, a school-based study conducted in the USA among 488 adolescents aged 13–15 years61 reported an annual incidence of OCD of 0.7% [95% confidence interval (CI) 0.12% to 1.34%].
Prevalence differences between men and women
Most studies conducted in the general population have shown a higher prevalence in women than men, with the female-to-male ratio ranging between 1.2 and 3.8 in several studies. 42,62 In one British study,52 the ratio was 1.44. These findings show that the clinical observation that the number of women in clinical samples far outweighs the number of men is not the result of help-seeking bias.
Regarding children and adolescents, most studies in non-clinical samples seem to support a 1 : 1 ratio for prevalence in boys and girls,55,61,63 although there are some studies reporting a higher prevalence for boys. 64,65 In clinical samples, there is an excess of boys, possibly owing to younger age at onset and more severe symptomatology. 62,63
Socioeconomic status
Fontenelle and Hasler,62 in their review of the analytical epidemiology of OCD, mention several studies that have shown a positive association between a higher socioeconomic status or education and OCD. However, other studies did not confirm this, or found a negative association (e.g. the study by Torres et al. 52). It can be concluded from these studies that OCD, in contrast to other psychiatric disorders, displays no clear social gradient, although there is even a small possibility of a mild positive association. Regarding employment status, in most studies, individuals with OCD are more likely to be unemployed or economically inactive,46,52,62 although this possibly reflects the generally negative association of the common mental disorders with employment status and is not specific to OCD. A similar observation can be made for marital or family status: individuals with OCD are more likely to be unmarried or to live alone, as is common for all other mental disorders. 62
Comorbidity
Several studies with clinical samples have confirmed that OCD is often comorbid with other psychiatric disorders. 66–68 In most clinical studies, the most common comorbidity is mood disorders, a finding that is compatible with the view that patients with OCD will often seek help from a mental health specialist when they develop depression or some other psychiatric disorder. The reported prevalence of comorbid disorders differs from study to study depending on the methodology and the time frame used (e.g. 1 month, 1 year, lifetime). In a Dutch sample of 420 outpatients with OCD,67 24% had comorbid current depression/dysthymia and 13% had any anxiety disorder [most often social phobia (3.6%) and panic disorder (2.6%)]. These figures are much higher than the reported prevalence in the general population. One study reported that alcohol use disorders in patients with OCD were less common than in the general population. 67 Another study from the USA, which included 334 outpatients from the adult OCD clinic at the National Institute of Mental Health,66 assessed the lifetime prevalence of comorbid disorders. Approximately 66% of patients had experienced major depression at some time in their lives, whereas one in four had experienced social phobia, panic disorder or dysthymia. It is worth noting that in this cohort, lifetime alcohol dependence was high, at 25%. In women, the prevalence of eating disorders was increased (26% of the sample). Data from the Brown cohort68 showed that a minority of patients (< 10%) had not experienced any other disorder in their life. As reported elsewhere, depression was the most common comorbid condition (67% lifetime prevalence and 15% current episode). Other common diagnoses in this cohort were social phobia (28% lifetime, 19% current), panic disorder (18% lifetime, 7% current) and alcohol dependence (23% lifetime, 4.5% current). Eating disorders were also common in this cohort (10% lifetime prevalence for the entire sample).
Studies conducted in the general population have confirmed that these patterns of comorbidity are not the result of help-seeking bias. In the British Psychiatric Morbidity Survey,52 37% of participants with OCD also met criteria for current depression. In addition, comorbidity with anxiety disorders, such as panic disorder (22%) and social phobia (17%), and with alcohol dependence (33% in men, 11% in women) was particularly high. In the replication study of the National Comorbidity Survey in the USA,69 participants who met criteria for OCD had an increased lifetime prevalence for other mood and anxiety disorders (40% for depression, 44% for social phobia, 20% for panic disorder, 38% for alcohol dependence). These figures are very similar to those reported from the first large epidemiological survey of OCD in the US general population, the ECA study. 46
The association of OCD with bipolar disorder has attracted research interest over the past decade. Several studies have reported that OCD patients have a lifetime history of bipolar disorder, mainly type 2 bipolar disorder (bipolar II), with prevalence rates that are much higher than in the general population (up to 15% in some samples70). Conversely, an OCD history is often reported in patients with bipolar disorder (up to 35% in a German study71). In a recent review of this issue,72 it is pointed out that there are disagreements between studies regarding the extent of this comorbidity. For example, in a French study that included mainly type 1 bipolar disorder (bipolar I) patients,73 history of OCD was quite low (at 3%), in contrast to histories of panic disorder and phobic disorders, which were higher (16% and 11%, respectively).
The relationship between obsessive–compulsive symptoms and psychotic disorders in general, or schizophrenia in particular, has been noted since the early twentieth century,74,75 but only recently has this association been studied more systematically. 72 A recent meta-analysis of this topic identified 37 studies that aimed to estimate the prevalence of OCD in patients with schizophrenia and related disorders. 76 This analysis reported a mean OCD prevalence of 12.3% (95% CI 9.7% to 15.4%), which is much higher than that of the general population. Obsessive–compulsive symptoms were even more common. Eisen et al. ,77 in a study that used a very careful methodology, reported that the prevalence of OCD in 77 patients with psychotic disorders (schizophrenia, n = 52; schizoaffective disorder, n = 25) was 7.8% (6/77 patients). It is worth noting, however, that five of these six patients with OCD had schizoaffective disorder (5/25, 20%) and only one had schizophrenia (1/52 patients, 1.9%). Another interesting study from the Netherlands, among patients with first-episode psychosis or at ultra-high risk for developing psychosis,75 reported that the prevalence of OCD was 1.5%, whereas that of obsessive–compulsive symptoms not meeting full diagnostic criteria for OCD was 9.3%. The authors note that these figures are very similar to those reported from general population samples. The prevalence of both the disorder and the symptoms was lower in those patients who met criteria for schizophrenia rather than schizophreniform or schizoaffective disorders. No significant differences were found between the time of onset of obsessive–compulsive symptoms prior to or after the onset of the first episode of psychosis. OCD did not precede the onset of psychosis in patients with both disorders. These findings are compatible with the view that obsessive–compulsive symptoms may be either prodromal symptoms of first-episode psychosis or a secondary side effect of antipsychotic medications. 75 Studies that have investigated the presence of psychotic symptoms among patients with OCD are few. In the Brown cohort,78 6% of OCD patients had a comorbid psychotic disorder (4% schizophrenia; 2% delusional disorder). In NEMESIS,79 the presence of obsessive–compulsive symptoms at baseline predicted the onset of psychotic symptoms at follow-up and vice versa. From these studies, it is concluded that although there seems to be an association between symptoms of OCD and psychotic disorders, this association is bidirectional and complex.
Suicidality
In the past, OCD was considered a relatively rare condition,19 with a low risk for suicide, at least compared with other mental disorders. 80,81 More recent studies, however, have changed this view. In Brazil, a large clinical study of outpatients with OCD (n = 582) found that 11% of the sample had attempted suicide at least once in their lifetime. 81 Studies in unselected samples of the general population have confirmed these findings. In the UK, a history of suicide attempt was reported by 26% of the participants who met criteria for OCD, compared with 14.5% of those with other common mental disorders, a statistically significant difference. 52 These studies were cross-sectional and assessed suicidality retrospectively. There are few longitudinal studies that have reported suicidal behaviour. In a prospective clinical study in Spain,82 218 outpatients with OCD were followed up for a mean duration of 4 years. Two patients (0.9%) committed suicide and 11 (5%) attempted suicide. Risk factors for suicidal behaviour were the presence of symmetry/ordering obsessions and the initial severity of depressive symptoms. In NEMESIS,83 the cumulative incidence of suicide attempts in participants with OCD, after 3 years’ follow-up, was 0.4%, a very low figure compared with other common mental disorders and the lowest among the anxiety disorders. Incidence of suicidal behaviour was also low in a meta-analysis that used data from patients who had participated in randomised controlled trials (RCTs) submitted to the US Food and Drug Administration (FDA). 84 In that analysis, the annual incidence of suicide attempts in OCD patients was approximately 1.47% (1468/100,000 per year) and the suicide rate was 0.11% (105/100,000 per year). It is worth noting that these figures were comparable with the other anxiety disorders covered in this analysis and significantly lower compared with the figures for depression (2.9% and 0.8%, respectively) that have been reported in a separate paper with the same methodology. 85
In conclusion, the results of these studies show that suicide risk in OCD is higher than in the general population by a factor of 10 or more, but is comparable to risk in popuations with other anxiety disorders. It is lower than the risk associated with depression, but it should be pointed out that, because OCD is often comorbid with depression, the incidence in real clinical practice might be higher. In a secondary analysis of the NEMESIS sample, for example, the suicide risk (either attempt or ideation) was higher in participants who met criteria for both depression and anxiety disorders. 86
The study of suicidal behaviour in child/adolescent OCD samples is not so extensive. A recent study of 54 patients aged 7–17 years from a tertiary centre in the USA87 reported that 13% of the sample (n = 7) had clinically significant suicidal ideation during the past month. Significant associations were found with the presence of symmetry/ordering obsessions and obsessions of sexual or religious content, with increasing age and with the presence of depressive symptoms.
Natural history: prognosis
Historically, OCD was considered a disorder with a poor prognosis. This view was challenged by the seminal study of Pollitt. 88 Pollitt’s study used a very strict methodology in a period in which there was no specific form of treatment other than leucotomy (with uncertain effects). To avoid any possible treatment effects of this procedure, Pollitt presents his results on the course of OCD separately for patients with or without leucotomy. According to this study, the longitudinal course of the illness was good: complete remission was observed in 24% of the patients after a mean duration of follow-up of 3.4 years (range 0.5–15 years), whereas 36% had a mild illness (i.e. 60% of the patients had a benign course). A study conducted in Sweden by Skoog and Skoog89 included 144 patients with OCD who were examined by one of the authors between 1954 and 1956 by means of a semistructured clinical interview. The patients were re-examined by the same researcher after 40 years using the same methodology. Rates of complete remission (20%) were comparable to those in the Pollitt study,88 whereas 28% of patients had mild symptoms at follow-up. Therefore, in this study almost half of the patients had a good course.
With the advent of new and effective treatments in the 1980s [BT/CBT, clomipramine and selective serotonin reuptake inhibitors (SSRIs)], it is interesting to review longitudinal studies of the prognosis of OCD in patients who received such treatments. Two such studies have been published recently. Bloch et al. 90 investigated the longitudinal course of illness (10–20 years) in 83 patients with OCD who had participated in clinical trials in their centre (Yale). The authors reported that 20% of the sample experienced complete remission, whereas another 30% experienced partial remission. Almost half of the patients still had symptoms that would make them eligible for inclusion in a new clinical trial (a score on the YBOCS of ≥ 16). It is worth noting that 70% of these patients were receiving medication at follow-up and approximately half had received BT or CBT at some point in their lives (after the baseline assessment). Similar results were reported in the study of the Brown cohort that included 213 patients with OCD. 91 Complete remission at 5 years’ mean follow-up was observed in 17% of the sample, whereas partial remission was observed in 22% of patients. This study also assessed the rates of relapse after partial or complete remission, which were quite high (59%). In another study from Italy, which included 55 outpatients with OCD treated with SSRIs, the rates for complete and partial remission at 3 years’ follow-up were 22% and 34%, respectively. 92
The main conclusion that can be drawn from the above discussion is that remission rates in the modern era have not improved compared with those reported in earlier studies88,89 despite the wide availability of effective treatments. It is difficult, however, to interpret this finding, as changes in diagnostic preferences or criteria may have resulted in non-comparable groups of patients being selected for inclusion in these studies.
Regarding the factors that are associated with a poor prognosis, several studies report that an early onset, more severe initial symptoms, a longer duration of illness and comorbidity with depression are all associated with a poor prognosis. 89,92–95 In the Brown cohort,91 patients with primary hoarding obsessions/compulsions had a worse prognosis with very low remission rates, whereas patients with primary obsessions regarding an inflated sense of responsibility for harm had a better prognosis. In the Yale cohort,90 an initial good response to SSRIs was a good prognostic factor. In other studies, the presence of schizotypal92 or obsessive–compulsive personality disorder91 was associated with a poor prognosis.
The long-term prognosis of OCD in children and adolescents has been reviewed by Stewart et al. ,96 who included 16 studies from various settings. Stewart et al. 96 report a mean remission of 40% after a mean duration of 5.7 years’ follow-up. When including partial remission, this rate is increased to 59%. Focusing on the studies that have used non-clinical samples, the remission rate is even higher, at 74%. Some more recent studies from the USA97,98 and the UK99 have also been published. The results of more recent studies are similar to those seen in the Stewart et al. review,96 despite the use of selected samples from tertiary centres. In the Yale cohort,98 58% of the patients had complete remission after a mean follow-up duration of 9 years. In the Maudsley cohort,99 approximately 60% of the patients had at least a partial remission after 5 years’ mean follow-up. From these findings it can be concluded that remission rates in children and adolescents may be higher than those in adults. Regarding factors associated with a poor prognosis, the following have been reported: duration of illness,96,99 early onset96 and presence of hoarding obsessions/compulsions. 98 A better prognosis has been reported in patients with chronic tics98 and in patients who showed a good initial treatment response. 96
Impact on quality of life and functioning
As a chronic disorder, OCD can have a severe impact on everyday functioning and quality of life. Two systematic reviews have recently investigated the published literature on this issue. 100,101 Most studies have used clinical samples and compared several dimensions of quality of life in OCD and other psychiatric disorders, chronic physical disorders and the general population. Fewer studies have used non-selected samples in the community,101,102 but these have confirmed that OCD, even in individuals living in the community who have not made contact with services, can have a detrimental effect on quality of life compared with the healthy population. In a study in Asia, OCD was associated with a worse quality of life than in other common mental disorders. 103 Studies have reported that contact104 or relationships with family members103 may be more severely affected in patients with OCD than in patients with other mental disorders.
Most studies in clinical samples have compared quality of life in patients with OCD with that in patients with other mental disorders, chronic physical disorders or population norms. One of the most cited studies that compared the quality of life in patients with depression and anxiety disorders used data from patients who took part in several multicentre RCTs of sertraline. 105 According to this study, patients with OCD had a better overall quality of life compared with patients with depression and comparable to other anxiety disorders, with the exception of post-traumatic stress disorder. Olatunji et al. 106 carried out a meta-analysis of 33 studies that examined quality of life in patients with anxiety disorders. Six of these studies focused on OCD and their findings show that OCD is associated with a worse quality of life for patients than for the general population, but other anxiety disorders may have a more harmful effect (e.g. social phobia or post-traumatic stress disorder). In the clinical samples, the dimension of quality of life more severely affected in OCD is the one associated with social relationships. 101
Some studies have investigated quality of life as a long-term outcome in RCTs of psychopharmacological or psychosocial interventions. 100 These studies have concluded that changes in quality of life can be quite delayed and certainly are not expected in the short term. In the psychopharmacology trials, these changes may become evident after 1 year of continuous treatment. 107 It should be pointed out that because OCD is often comorbid with other disorders, in particular depression, this may lead to further worsening of quality of life and, generally, is an important factor in determining levels of functional impairment. 100
Studies conducted in child and adolescent samples are limited and assess functional impairment more often than quality of life. It should be noted that these are related but not identical concepts. 108 Two recent studies have investigated quality of life in children and adolescents with OCD. 108,109 Both confirmed the negative effect of the disorder on the quality of life of patients compared with healthy children. An important factor that predicted a worse quality of life was the presence of comorbid internalising or externalising disorders.
Current service provision
Treatment options
Primary care
General practitioners (GPs) encounter patients with a range of OCD severity; milder presentations are not uncommon, although the major influence on people with mental disorders seeking help from their doctor is severity. 110 Many patients who see their GP with OCD symptoms are also suffering from comorbid depression or anxiety. Data from the 2000 British National Psychiatric Morbidity Survey have shown that less than 15% of patients with non-comorbid OCD were receiving any treatment for emotional problems, compared with 56% of patients with comorbid OCD and depression or other anxiety disorders. 52
In recent years, it has been possible in the UK to refer patients with OCD to the Improving Access to Psychological Therapies service, and this has made both low-intensity and high-intensity CBT interventions more widely available. The National Institute for Health and Care Excellence (NICE) Clinical Guideline (CG) 31 states that low-intensity treatments, including ERP of up to 10 therapist hours per patient, are offered to those with milder degrees of functional impairment. This intervention includes brief self-help materials and may include group CBT. Those who do not respond to this or who find it difficult to engage are often treated with a SSRI. This also can have the benefit of treating coexisting symptoms of depression and anxiety. Although response may be seen fairly quickly for depressive symptoms, it is not uncommon for considerably longer response times to be seen for OCD symptoms, and SSRIs should be given at an adequate dose for at least 12 weeks and perhaps even longer before treatment can be said to be ineffective. 111 In more chronic and severe cases it may be necessary to go on to offer high-intensity individual CBT, including ERP, as well as a SSRI.
Secondary care
Those who do not experience a clinically significant improvement following these treatments are likely to be referred to secondary care for further assessment. Psychiatric services will often offer further CBT or BT and may switch medications from SSRIs to clomipramine. 112 If this is not successful, treatment with an antipsychotic in addition to the antidepressant may be considered. 111,113
Tertiary care for treatment-refractory patients
In order to be considered treatment refractory, patients are required to score very highly on symptoms scales such as the YBOCS (≥ 30/40) and to have received at least two courses of CBT from an accredited therapist as well as two courses of a SSRI (or one course of a SSRI and one of clomipramine) at maximally tolerated doses as well as one attempt at pharmacological augmentation. Many patients referred to specialised services (usually judged to be at level 5 of the NICE stepped care pathway and, therefore, not eligible for highly specialised services) give a history of not receiving adequate treatment locally, despite high levels of distress and disability. There would appear to be problems in finding suitably trained and experienced clinicians for patients with severe OCD nationwide. OCD is a severe, chronic mental disorder and patients in remission have a high chance of relapse even after specialist care (around 60% over 5 years91). Full relapse is associated with major loss in health-related quality of life. 114 Ongoing co-ordinated clinical care from local mental health services is required for long periods to reduce the risks of relapse or to ensure early intervention to prevent full relapse occurring. The need for long-term responsive care in local NHS community services for individuals with OCD needs to be better recognised.
Patients eligible for highly specialised services
In recognition of the high levels of distress and serious functional impairment associated with severe and enduring OCD (and body dysmorphic disorder), patients with severe illness who have not responded to substantial evidence-based treatment with medication or CBT (at level 6 of the NICE stepped care pathway) may be referred for treatment from the highly specialised Obsessive–Compulsive Disorder and Body Dysmorphic Disorder Service commissioned by NHS England (see www.england.nhs.uk/). The aim of the service is to improve the mental health state of both adolescents and adults suffering with the most profound OCD/body dysmorphic disorder, who have failed all previous evidence-based pharmacological and psychological treatments (including home-based treatments). The service provides treatment across the lifespan (children, adolescents and adults), including intensive clinic-based, home-based and inpatient CBT, as well as specialist pharmacotherapy at the following centres:
-
Hertfordshire Partnership NHS Foundation Trust, Queen Elizabeth II Hospital, Welwyn Garden City, UK (adults)
-
South London and Maudsley Hospital Anxiety Disorders Residential Unit; Centre for Anxiety Disorders and Trauma (adults); Child and Adolescent OCD Service, London, UK
-
South West London and St George’s NHS Trust, Springfield Hospital (adults), London, UK
-
The Priory Hospital Adolescent Inpatient Unit, London, UK.
A similar service is available in Scotland from the Advanced Interventions Service located at Ninewells Hospital, Dundee. This service additionally provides specialist neurosurgery for the most extreme cases of severe, refractory mental disorder including OCD (see www.advancedinterventions.org.uk/index.php/the-service).
Current guidelines
Table 1 presents the most recent published guidelines for the management of OCD. The most recent clinical practice guidelines for the pharmacological treatment of OCD have been published by the British Association for Psychopharmacology. 111 The Canadian Anxiety Disorders Association has also published guidelines for both pharmacological and psychological interventions for all anxiety disorders including a separate section for OCD. 115 The American Psychiatric Association had recently updated its previous detailed clinical practice guideline (see http://psychiatryonline.org). 116 The World Federation of Societies of Biological Psychiatry published its guidelines for all anxiety disorders, including OCD, in 2008. 117 In addition, NICE published a very comprehensive clinical practice guideline for OCD and body dysmorphic disorder in 2005 (NICE CG31). 118 NICE has recently placed the 2005 OCD guideline on a ‘static’ list of guidelines that will not be reviewed again within the next 5 years unless there is important new evidence of either efficacy or safety. NICE has also published a quick reference guide, which includes a detailed version of their stepped care model for treating OCD in all age groups (see www.nice.org.uk/nicemedia/live/10976/29945/29945.pdf).
| Authors, year, country | Organisation | Title | Citation |
|---|---|---|---|
| Baldwin et al. 2014, UK111 | British Association for Psychopharmacology | Evidence-based pharmacological treatment of anxiety disorders, post-traumatic stress disorder and obsessive–compulsive disorder: a revision of the 2005 guidelines from the British Association for Psychopharmacology | J Psychopharmacol 2014;28:403–39 |
| Katzman et al. 2014, Canada115 | Anxiety Disorders Association of Canada | Canadian clinical practice guidelines for the management of anxiety, posttraumatic stress and obsessive–compulsive disorders | BMC Psychiatry 2014;14(Suppl. 1):1 |
| Koran et al. 2007, USA116 | American Psychiatric Association | Practice guideline for the treatment of patients with obsessive–compulsive disorder | Am J Psychiatry 2007;164(Suppl. 7):5–53 (an updated supplement of this guideline up to March 2013 by the same authors is also available at: http://psychiatryonline.org/pb/assets/raw/sitewide/practice_guidelines/guidelines/ocd-watch.pdf) |
| Bandelow et al. 2008, worldwide117 | World Federation of Societies of Biological Psychiatry | World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for the pharmacological treatment of anxiety, obsessive–compulsive and post-traumatic stress disorders – first revision | World J Biol Psychiatry 2008;9:248–312 |
| NICE, 2005, UK118 | NICE/Royal College of Psychiatrists/British Psychological Society | Obsessive–Compulsive Disorder: Core Interventions in the Treatment of Obsessive–Compulsive Disorder and Body Dysmorphic Disorder CG31 | NICE. Obsessive–Compulsive Disorder: Core Interventions in the Treatment of Obsessive–compulsive Disorder and Body Dysmorphic Disorder CG31. London: NICE |
Description of technology under assessment
Medications
Pharmacotherapy with the tricyclic antidepressant clomipramine or a SSRI (paroxetine, fluvoxamine, fluoxetine, citalopram, escitalopram and sertraline) has shown efficacy in OCD. 119 Meta-analyses of seven RCTs of clomipramine120 and 17 randomised, double-blind placebo-controlled trials of various SSRIs121 have been performed. The trials were generally short term (i.e. of 4–12 weeks’ duration) and showed that all these compounds were superior to placebo. Patients were roughly twice as likely to respond to a SSRI as to placebo. Data on comparisons between different SSRIs and between SSRIs and clomipramine are limited but have shown no significant differences in efficacy. The SSRIs are recommended as the first-line pharmacological treatment for OCD, with clomipramine reserved for those who do not respond to or tolerate SSRIs, owing to the more favourable adverse event profile. 111,116,118 SSRIs tend to take longer to be effective (between 4 and 12 weeks) when used for OCD than when used for other disorders, such as depression and anxiety. A positive dose–response relationship has been observed with several SSRIs (paroxetine, fluoxetine and escitalopram), and higher doses of SSRI are often required. 116,118,119 Approximately 40–70% of patients respond to a SSRI, but the long-term improvement in total symptom severity is relatively low, averaging 20–40%,122,123 as is the remission rate, with full remission ranging from approximately 10%123 to 40%. 124 A long duration of untreated illness,94 coexisting tic116 and hoarding symptoms125 have all been associated with a poorer treatment response to clomipramine and the SSRIs.
The findings of acute treatment studies indicate that the proportion of responding patients increases steadily over time. Long-term (up to 12 months) double-blind RCTs demonstrate an advantage for continuing with medication in patients who have responded to acute treatment. 126,127 A randomised placebo-controlled trial with paroxetine as an active comparator found that a low dosage of escitalopram became efficacious only in the second half of a 24-week study. 124 Most (but not all) placebo-controlled relapse prevention studies in patients who have responded to previous acute treatment reveal a significant advantage for staying on active medication (escitalopram, fluoxetine at higher daily doses, paroxetine and sertraline), compared with switching to placebo, for up to 12 months,128 but the optimal duration of continuation treatment is uncertain. 129 For these reasons, it is recommended that clinicians continue drug treatment for at least 12 months in patients who have responded to treatment. 111 As approximately 50% of patients with OCD relapse if they discontinue medication after up to 1 year of successful treatment, it is advisable to counsel patients about the risk of relapse prior to drug discontinuation and, if relapse occurs, medication is usually reinstated and continued indefinitely. 130
Adverse events with medications
Selective serotonin reuptake inhibitors are generally safe and well tolerated, according to the placebo-referenced treatment trials that reported adverse event-related withdrawal rates of approximately 5–15%. As a group, however, SSRIs may cause unwanted nausea, insomnia, somnolence, dizziness and diarrhoea. Sexual side effects include reduced libido and delayed orgasm, and can affect up to 30% of individuals. 131 Fluoxetine has a long half-life and fewer discontinuation effects, which can be advantageous for patients who forget to take their tablets. It has also been extensively used in pregnancy and generally shown to be safe. 132 The recent demonstration of prolongation of the electrocardiogram QT-interval associated with higher dose levels of citalopram (and, to a lesser extent, escitalopram)133 argues for a degree of caution in using higher doses of these compounds in OCD, especially if individuals are taking other medications that increase the QT interval. However, a recent large study found no elevated risks of ventricular arrhythmia or all-cause, cardiac or non-cardiac mortality associated with citalopram doses exceeding 40 mg per day. 133
Clomipramine can also be associated with potentially dangerous side effects. Cardiotoxicity and cognitive impairment occur much more often with clomipramine than with SSRIs. In addition, there is an increased risk of convulsions in patients taking clomipramine (up to 2%). Overdose on clomipramine can prove fatal, and this needs to be borne in mind when prescribing for OCD, in view of the elevated suicide risk associated with the illness. Clomipramine is also associated with greater impairment of sexual performance (up to 80% of patients) compared with SSRIs, with weight gain and with troublesome anticholinergic effects. 134
Suicide in children with obsessive–compulsive disorder receiving selective serotonin reuptakes inhibitors
Meta-analyses examining the effects of SSRIs in children aged 6–18 years have been performed, following warnings from the US FDA that SSRIs in the young may increase the risk of suicidal thoughts and behaviours. A pooled analysis of childhood OCD studies comparing ‘numbers needed to treat’ with those ‘needed to harm’ revealed no suicidal actions and a positive risk ratio for the use of sertraline in children and adolescents with OCD. 135
In the recent study by Bridge et al. ,136 27 RCTs of SSRIs, of which six were in OCD, were identified. There were no completed suicides. The pooled absolute rates of either suicidal ideation or suicide attempt (treatment vs. placebo) in OCD (1% vs. 0.3%) compared favourably with the pooled absolute clinical response rates (treatment vs. placebo; 52% vs. 32%). The authors concluded that the benefits of SSRIs probably outweigh the risks in the OCD paediatric population, with the doctor–patient relationship playing an important part.
Psychotherapy
The general principles of the psychological model of OCD have been described (see Aetiology). Based on this model, a number of psychological treatments have been developed. A comprehensive historical review of these treatments is given by Abramowitz. 137 Two main treatments have been developed, a behaviourally oriented treatment (ERP) and a treatment based on the cognitive model of OCD. 40
Exposure and response prevention was first described in a clinical setting by Meyer,138 and the relative success of this method soon replaced other behaviourally oriented methods such as Wolpe’s systematic desensitisation. 137 According to Abramowitz,137 in ERP, first, the patient undergoes prolonged exposure to situations or stimuli that provoke obsessional fears and, second, the patient is advised to refrain from performing the compulsive behaviour (response prevention). Response prevention helps the patient learn that anxiety will eventually decrease on its own over time and also that obsessions are not really dangerous or do have catastrophic consequences. 137 The intensity of the treatment differs, but typical forms of therapy include at least 16 sessions over 8 weeks. Some of the sessions are supervised by the therapist and the patient also practises self-exposure between sessions. 137 Owing to the nature of the treatment, some patients may not tolerate the distress associated with the exposure or they may not be willing to refrain totally from the ritualistic behaviour. Despite the difficulties in applying this treatment, ERP has established its effectiveness both in research and practical settings. 118
The cognitive model of obsessions is primarily based on the work of Salkovskis,40 who suggested that, although disturbing, intrusive and unacceptable thoughts (normal obsessions) are experienced by all,139 patients with abnormal obsessions appraise the intrusions in a pathological way. Salkovskis suggested that such appraisals ‘appear to relate specifically to ideas of being responsible for damage or harm coming to oneself or to others’. 40 Compulsions are viewed as efforts by the individual to prevent any harmful consequences or to reduce the unwanted intrusions. Apart from Salkovskis’ ‘inflated responsibility’, other faulty appraisals of intrusions have been described by the Obsessive Compulsive Cognitions Working Group,140 such as the overimportance of thoughts, the excessive concern about the importance of controlling one’s thoughts, the overestimation of threat and the intolerance of uncertainty. Based on the cognitive model, cognitive therapy (CT) that does not require the use of ERP techniques has been developed, although behavioural experiments are used to help patients modify their views about the risks associated with obsessions. 137 CBT for OCD combines both ERP techniques and cognitive restructuring. 137 There is now evidence that both therapies are effective in the management of OCD and have comparable efficacy to ERP with a slightly improved tolerability. 118
Reasons for conducting this review
Two criteria have been taken into account in order to examine the need for a new review regarding the management of OCD:
-
the need to update previous systematic reviews and/or meta-analyses, especially if new trials have been conducted since the publication of previous reviews, which could potentially change current recommendations
-
the need to synthesise existing and updated evidence to answer the questions that matter most to clinicians and patients/carers using, if necessary, previously unavailable methodological techniques.
Although the number of new trials since previously published systematic reviews (e.g. NICE118) is relatively small, these were studies that reported direct comparisons between treatments that were not previously available. In addition, previous reviews have focused only on the available direct pairwise comparisons of active (either pharmacological or psychological) versus inactive interventions (drug placebo, waitlists, psychological placebo). Although these comparisons may be suitable for regulatory agencies or to establish efficacy, they may not be equally useful in directing real clinical practice or cost-effectiveness analyses. As a result, previous reviews could not rank the treatments depending on their efficacy or acceptability using all available evidence (both direct and indirect), and their results are inconclusive. Owing to these problems, it has been suggested that evidence for the superiority of a given treatment against another in OCD is absent and that clinicians’ or patients’ choices are based on preference, side-effect profile for drugs or comorbidity. The present review and economic evaluation aims to fill this gap in the knowledge, by applying appropriate statistical techniques of evidence synthesis that allow the ranking of treatments, taking into account both direct and indirect evidence, and will provide clinicians with a framework for decision-making for the optimum management of patients of all ages with OCD.
Chapter 2 Definition of the decision problem
This review addresses the research question: what is the clinical effectiveness, acceptability and cost-effectiveness of pharmacological and psychological (behavioural or cognitive–behavioural) interventions for the management of OCD?
Decision problem
Population
Children and adolescents, and adults with OCD.
Intervention and relevant comparators
Any antidepressant medication with some serotonergic properties used in the management of OCD (including amitriptyline, imipramine, clomipramine, all SSRIs, all serotonin–noradrenaline reuptake inhibitors, mirtazapine and hypericum), BT (therapy that includes some kind of exposure and/or response prevention), CT or CBT and any drug/psychotherapy combination of these interventions. Comparators included drug placebo, psychological placebo, waitlist and any other comparator from the list of interventions that would allow an indirect comparison with network meta-analysis (NMA).
Outcomes
The primary outcome for effectiveness was the reduction in symptoms of OCD as measured at the end of the study period by the YBOCS scale (or the CYBOCS). The secondary outcome was acceptability, as measured by the total number of dropouts in each intervention arm.
Subgroup analyses
Regarding the preplanned subgroup analyses, where sufficient data were available, metaregression/subgroup analyses were conducted to explore the impact of:
-
publication date
-
length of trial
-
inclusion of patients with comorbid depression
-
pharmaceutical sponsorship of drug trials.
Overall aims and assessment objectives
The main aim of this review was to determine the clinical effectiveness, acceptability and cost-effectiveness of pharmacological and psychological interventions for the treatment of OCD.
More specifically, the aims of this review were to:
-
undertake a systematic review of the clinical effectiveness and acceptability of pharmacological and psychological interventions (behavioural or cognitive–behavioural) for the treatment of OCD in children and adolescents, and in adults
-
use both direct and indirect evidence to simultaneously compare all multiple treatments (pharmacological and psychological) in a single analysis (multiple treatments meta-analysis) with the aim of ranking all treatments in terms of efficacy and acceptability
-
develop a probabilistic economic model of alternative treatments (pharmacological and psychological) for the management of OCD in order to evaluate the relative cost-effectiveness of these treatments.
Chapter 3 Systematic review methods: assessment of clinical effectiveness
Methods for reviewing clinical effectiveness
For this systematic review meta-analysis we followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) recommendations141 and the guidelines for conducting systematic reviews reported in the Cochrane Handbook. 142
The protocol is registered with PROSPERO database number CRD42012002441 and can be accessed at www.crd.york.ac.uk/PROSPERO/display_record.asp?ID = CRD42012002441.
Identification of trials: search strategy
Search dates
We carried out searches between 1 December 2012 and 31 May 2014. A detailed description of the specific search strategy used is given in Appendix 1.
Search strategy
Electronic databases
We searched the twin Cochrane Collaboration Depression, Anxiety and Neurosis (CCDAN) Controlled Trials Registers (CCDANCTR). The CCDAN maintain two clinical trials registers at its editorial base in Bristol, UK: a references register (CCDANCTR-References) and a studies-based register (CCDANCTR-Studies). The CCDANCTR-References Register contains more than 27,000 reports of trials in depression, anxiety disorders (including OCD) and other neurotic disorders. Approximately 65% of these references have been tagged to individual, coded trials. The coded trials are held in the CCDANCTR-Studies Register and records are linked between the two registers through the use of unique study identification (ID) tags. Coding of trials is based on the EU-Psi coding manual (see http://psitri.stakes.fi/). Reports of trials for inclusion in the Group’s registers are collated from routine (weekly), generic searches of MEDLINE, EMBASE and PsycINFO; quarterly searches of the Cochrane Central Register of Controlled Trials and review-specific searches of additional databases. Reports of trials are also sourced from international trials registers using WHO’s trials portal, the International Clinical Trials Registry Platform (see http://apps.who.int/trialsearch/), drug companies, the hand-searching of key journals, conference proceedings and other (non-Cochrane) systematic reviews and meta-analyses. Details of CCDAN’s generic search strategies can be found in the ‘Specialized Register’ section of the Cochrane Depression, Anxiety and Neurosis Group’s website.
The CCDANCTR-Studies Register was initially searched (September–December 2012) using the following index terms:
Condition = obsess* or compulsi*
AND
Intervention = (Citalopram or (Clomipramin* or Clorimipramin* or Chlomipramin* or Chlorimipramin*) or Escitalopram or Fluoxetine or Fluvoxamine or Paroxetine or Sertraline or Venlafaxine or Duloxetine or Mirtazapine or SSRI* or Serotonin or cognitive* or behavi* or exposure or “response prevention”).
The CCDANCTR-References Register was initially searched using a more sensitive set of free-text terms (to identify additional untagged/uncoded reports of trials):
((obsess* or compulsi* or OCD) AND (Citalopram or (Clomipramin* or Clorimipramin* or Chlomipramin* or Chlorimipramin*) or Escitalopram or Fluoxetine or Fluvoxamine or Paroxetine or Sertraline or Venlafaxine or Duloxetine or Mirtazapine or SSRI* or (Serotonin and (uptake or reuptake or re-uptake)) or SNRI* or CBT or cognitive* or behavioral or behavioural or exposure or ERP or “response prevention” or ((*therap* or train* or treatment*) and (behavi* or expos*)))).
As the number of studies retrieved in this initial search was not very large (643 studies), in order to increase the sensitivity of the search we decided to repeat the search using the condition only (obsess* or compulsi*) without any other terms.
Reference checking
The reference lists of all selected studies, as well as the references of previous systematic reviews, meta-analyses and evidence-based guidelines, were additionally inspected for potential studies or reports that had not been identified through our electronic search. We also searched papers that had cited previous meta-analyses or systematic reviews using Google Scholar (Google Inc., Mountain View, CA, USA) to identify potential new studies that had not been identified. No additional records were identified through this source.
Ongoing clinical trials
We also searched the controlled trials registers of the following organisations to identify ongoing studies that could potentially have published preliminary results or reports:
-
ClinicalTrials.gov
-
Controlled-Trials.com
-
WHO’s trials portal (International Clinical Trials Registry Platform).
We used the generic term (obsessive or compulsive) for these searches and we filtered the results by condition (OCD) and type of study (controlled intervention). We checked 145 records from https://clinicaltrials.gov, 19 from www.controlled-trials.com and 23 from WHO’s portal for ongoing clinical trials.
Abstract appraisal
All abstracts identified through the search process were transferred into a Microsoft Excel® 2013 (Microsoft Corporation, Redmond, WA, USA) spreadsheet and were independently screened for potential inclusion by two reviewers (PS and HB). In cases of uncertainty (or disagreement), the full text was obtained. Abstracts excluded at this stage were not relevant to the present study either because they were observational studies or the interventions were not covered by the report (e.g. if they had investigated lithium, electroconvulsive therapy or repetitive transcranial magnetic stimulation vs. placebo). The full texts of all controlled trials studies that included at least one intervention covered by the report were obtained even if it was clear from the abstract that this should be excluded (e.g. because the comparator intervention was not covered or the patient population was treatment refractory). These studies were excluded at the full-text stage. Similarly, we obtained the full text of studies with special populations of OCD (e.g. hoarding patients) even if these would be excluded at the full-text stage.
Study selection: inclusion and exclusion criteria
Studies were included (or excluded) in accordance with the following criteria:
-
Study design: RCT. Trials with a crossover design were not excluded and we tried to extract all available data up to the point of the crossover. Quasi-randomised trials (such as those allocating by using alternate days of week) were excluded. Owing to the aim of the review, we included trials irrespective of blinding (because otherwise a lot of psychotherapy trials might not be eligible for inclusion). Sensitivity analyses examined the possible effect of unblinded or single-blinded trials.
-
Patient population.
-
Age: all patients aged ≤ 74 years (if patients aged ≥ 75 years were included, mean age should be within the range).
-
Diagnosis: a primary diagnosis of OCD in accordance with standardised diagnostic criteria (ICD, DSM, Feighner or research diagnostic criteria). Studies that specifically focused on treatment-resistant OCD were excluded. Treatment resistance should have been defined within the study using specific criteria. Most often, studies will have used a first, uncontrolled, treatment phase, in which all patients received the same intervention and the non-responders (usually showing < 25% reduction in the YBOCS scale) were eligible for the second randomised phase. Studies that had included patients that could be considered refractory to treatment outside the context of the particular study (e.g. because they might have tried medications or other interventions in the past unsuccessfully) were not excluded. It is worth noting that most psychotherapy trials have included patients who were symptomatic despite being stable on medications before entering the study.
-
Comorbidities: these will be accepted if OCD was the primary disorder. However, studies that included patients with schizophrenia or bipolar disorder were excluded.
-
Diagnostic criteria: the authors should have used established diagnostic criteria to diagnose OCD (either ICD, or any version of DSM, or Research Diagnostic Criteria or Feigner criteria). The method of assessment of these criteria (either through typical clinical examination or use of more formal diagnostic interviews) was not a reason for exclusion.
-
-
Experimental intervention.
-
For pharmacological interventions: any antidepressant medication with some serotonergic properties (including: amitriptyline, imipramine, clomipramine, all SSRIs, all serotonin-noradrenaline reuptake inhibitors, mirtazapine). Studies that have used hypericum were included, whereas other non-standard approaches were excluded (e.g. studies that have used folic acid, herbal medicines other than hypericum, vitamins or omega-3 supplements). Studies that had used a mainly noradrenergic medication as the experimental intervention of interest [e.g. reboxetine (Edronax®, Pfizer) or nortriptyline] were excluded.
-
For psychological interventions: we included trials that have used as their main intervention (1) BT (therapy that included some kind of exposure and/or response prevention); (2) CBT; or (3) CT (therapy that included some kind of cognitive restructuring intervention). We excluded studies that used therapies based on psychodynamic principles (including interpersonal psychotherapy or other insight-oriented therapies exploring unconscious mental processes), Gestalt therapy, systemic therapy and family therapy. We also excluded studies that used behavioural-type therapies with no exposure component (e.g. behavioural activation, social skills training) and biofeedback as their experimental intervention.
-
-
Comparator intervention.
-
For pharmacological interventions: drug placebo or any other antidepressant with some serotonergic properties, or any other psychotherapy from those eligible (BT, CT, CBT), or other inactive type of therapy considered as ‘control’.
-
For psychological interventions: any type of psychological placebo (including attention placebo) or non-specific therapy (including supportive therapy), or waitlist/no treatment, or any other BT/CT/CBT type of therapy, or drug placebo, or any other antidepressant with some serotonergic properties.
-
-
Focus of analysis: Between-group comparison of treatments should be reported. Studies that report only additional secondary analyses (e.g. predictors of treatment outcome) were excluded. Studies that did not report continuous outcome were not included in the quantitative synthesis.
Study inclusion assessment
Inclusion/exclusion criteria were independently assessed by two reviewers (HB and PS) and validated by one reviewer (PS). The standardised data extraction form (see Data extraction) included a section on inclusion/exclusion criteria. This section was transferred to an Excel spreadsheet and we recorded all necessary information for the inclusion or exclusion of studies that had passed through abstract screening. For excluded studies, we noted the main reason for exclusion.
Data extraction
We used a standardised data extraction form to extract detailed information on included studies. This form also included a section on inclusion and exclusion criteria that was used for all studies that passed through the abstract screening. We originally developed this form in a Microsoft Word® 2013 (Microsoft Corporation, Redmond, WA, USA) document format, but to facilitate data extraction, we transferred the various sections of this form into several Excel spreadsheets. All information extracted was directly recorded onto these spreadsheets on a computer.
Initial data extraction was carried out independently by two reviewers (HB and PS). As the agreement between the reviewers was high, one reviewer independently extracted the remaining papers (HB) and a second reviewer (PS) validated the extraction. Potential discrepancies were discussed by the reviewers and, if necessary, by all other collaborators during the meetings.
Data extracted from papers included the following information:
-
inclusion and exclusion criteria (study design, experimental intervention, control intervention, age range, primary diagnosis, diagnostic criteria, focus of analysis)
-
details of participants (country, treatment setting, age, diagnostic classification, primary severity scale used, comorbidities)
-
details of experimental and control interventions
-
details of continuous outcome (primary scale used, end of treatment follow-up time)
-
risk-of-bias assessment
-
results [baseline, end of treatment continuous measures for YBOCS or other primary scale, change from baseline, mean difference (MD) between arms, completers analysis or use of methods for handling missing data such as last observation carried forward]
-
dropouts (total dropouts per arm).
Risk-of-bias assessment: quality assessment strategy
To assess the methodological quality of included trials we used the criteria for quality assessment recommended by the Cochrane Handbook for Systematic Reviews of Interventions. 142 Two reviewers independently assessed and a second reviewer validated these criteria, which mainly focus on descriptions of sequence generation, allocation concealment, blinding, completeness of outcome data and selective outcome reporting, and other potential sources of bias (such as attrition rates). Studies were given a quality rating of ‘low’, ‘unclear’ or ‘high’ risk of bias in accordance with these criteria. If there was disagreement on quality assessment, the final rating was made by consensus with the involvement (if necessary) of another member of the review group. Studies with a high risk of bias were included in the main analysis, but we also examined in a sensitivity analysis the effect of excluding them.
Methods of network meta-analysis
Primary outcome
Pairwise analysis and NMA were conducted for the primary outcomes of reduction in OCD symptoms (as measured by the YBOCS in adults or the CYBOCS in children and adolescents) and for acceptability (as measured by total number of dropouts per study). A NMA is the simultaneous comparison of multiple competing treatments in a single statistical model. 143,144 In exploiting both direct and indirect evidence, a NMA produces estimates of the relative effects of each treatment compared with all others in the network, even if treatments have not been directly compared. It is then possible to calculate the probability of a treatment being better, or worse, for a specific outcome.
Derivation of primary outcome and handling of missing data
For the primary outcome, data are continuous and were reported as either (1) mean scores at baseline and at follow-up for treatment and control groups; or (2) mean change from baseline scores in each group. If both formats were reported, we chose the mean change from baseline score as our preferred summary, which captures correlations in measures within individuals. 145 If mean change from baseline was not reported, we used mean score at follow-up for each group, as this gives an unbiased estimate of treatment effect if randomisation is adequate. 145 If data were missing on either the total number of patients randomised or mean YBOCS/CYBOCS scores, the study was excluded from the quantitative analysis. Where possible, missing standard deviations (SDs) were derived from reported statistics following guidance in the Cochrane Handbook for Systematic Reviews of Interventions. 142 If derivation of missing SDs was not possible, they were estimated based on a prediction from a hierarchical model for SDs in those studies that did report them. Here, we assumed that any missing SD is exchangeable (i.e. broadly similar) with the reported SDs. (Further detail and code is available in Appendix 8.) For the secondary outcome, data are dichotomous and were extracted on intention-to-treat principles. Any participant dropout that occurred after the point of randomisation was included in our analysis.
Assessment of transitivity
The assumption of transitivity is the crucial starting point for a NMA. 146 Transitivity suggests that intervention A is similar when it appears in A versus B and A versus C studies. 147 It can be examined by comparing the distribution of potential effect modifiers across the different comparisons148 because if there is an imbalance in the presence of effect modifiers across the A versus B and A versus C comparisons, the conclusions about B versus C may be in doubt.
Study-level characteristics that were considered potential effect modifiers were mean baseline symptom severity, gender, participant age, length of trial follow-up, proportion of participants with concurrent mental illness (depression) and year of trial publication. We examined the study characteristics tables (see Tables 10 and 11) and concluded that, with the exception of participant age, the assumption of transitivity was likely to hold across the trials and comparisons. We considered that the assumption may be breached on the basis of participant age, because it would appear that children and adolescents were more likely than adults to be randomised to a psychological therapy. Indeed, of pharmacological treatments, only sertraline and fluvoxamine are licensed for use in patients aged < 18 years in the UK, and NICE also mentions fluoxetine in cases with significant comorbid depression. 118 Therefore, we decided that, contrary to our protocol specification, we would analyse children and adolescents separately to adults.
Pairwise and network meta-analysis
Network diagrams were drawn using Stata version 13 (StataCorp LP, College Station, TX, USA) to ensure that treatments formed a connected network for both outcomes and populations considered. 149 Pharmacological placebo was considered as the reference treatment throughout all analyses.
All analyses were conducted in a Bayesian framework and were undertaken using OpenBUGS version 3.2.3 (members of OpenBUGS Project Management Group; see www.openbugs.net). Pairwise meta-analyses were conducted in a single model assuming independent treatment effects and a shared heterogeneity parameter. 150 We used the NMA programme code given by Dias et al. 145 and modified to incorporate an additional class hierarchy,151 such that interventions with a similar mechanism of action were grouped together in a class in which pooled effects might be assumed to be ‘similar’. This approach allows both the relative effectiveness of the individual treatments and that of the classes to be estimated. On the basis of the systematic review and clinical expertise, it was assumed that only the SSRIs citalopram, escitalopram, fluoxetine, fluvoxamine, paroxetine and sertraline could be considered a ‘class’ on this criterion. Psychological therapies were analysed as individual treatments. Non-specific psychological therapies (‘psychological placebo’) were distinguished from waitlist controls. In psychological therapies we did not distinguish between individual or group delivery format. In addition, we did not distinguish treatments based on drug dose or intensity of psychological treatment. (All OpenBUGS code is available in Appendix 8. )
Random-effects models were used, accounting for the correlation between trial-specific effects in multiarm studies. 145 Vague priors were used for all parameters, including the prior for within-class variability. Convergence was checked based on two chains using the Brooks–Gelman–Rubin diagnostic plots and visually using history plots available in OpenBUGS. In all cases, the first 50,000 iterations were discarded as ‘burn-ins’. Reported estimates are based in the subsequent 100,000 iterations. We report the relative effectiveness of each treatment versus every other treatment and also the probability that each treatment is the most effective on each outcome.
Model fit and assessment of statistical inconsistency
Heterogeneity was assessed by examining the posterior median of the between-studies heterogeneity parameter from the random-effects model. Goodness of fit was measured by the posterior mean of the residual deviance. In a well-fitting model, the residual deviance should be close to the number of data points. Model comparison was based on the deviance information criterion (DIC). 152 A difference of 3 or more points was considered meaningful. 145 A key assumption of NMA is that of consistency between the direct and indirect evidence. To assess inconsistency, we compared the fit of a model assuming consistency with that of a model assuming independent treatment effects. 153 In addition, we also compared the results of the pairwise meta-analysis with the NMA. As a further proxy measure, where the NMA effect estimate did not fall within the 95% credible intervals (CrIs) from the pairwise analysis, we defined these as inconsistent.
Sensitivity analysis and meta-regression
Sensitivity analyses were conducted, excluding studies at high risk of bias on the following domains as defined by the Cochrane Collaboration’s risk-of-bias assessment tool:142
-
allocation concealment
-
outcome assessor blinding
-
incomplete outcome data
-
studies with high levels of attrition (overall attrition > 25% or differential attrition > 15%).
Separate meta-regressions were also conducted assuming a common interaction term for the following study-level characteristics:
-
length of trial (including follow-up)
-
year of publication of trial
-
pharmaceutical sponsorship of drug trials.
Chapter 4 Results of the systematic review
Quantity of research available
Our initial search of CCDANCTR resulted in 1028 citations. An updated search in March 2014 yielded another 74 citations, bringing the total number of citations from this source to 1102. No additional trials that met the criteria of the review of having a projected end-of-study period before the end of the current project were identified from our search of the registers of ongoing clinical trials. After removing some duplicate entries, a total of 1083 abstracts were initially screened and 905 (84%) were excluded, as they were not relevant to the study aims.
A total of 178 full papers were retrieved as being potentially relevant to the study aims. Sixty-eight of these papers were excluded for one or more reasons (see Studies excluded).
Of the remaining 110 papers, 25 papers were assigned to the waiting status for one of the following reasons: (1) article written in Chinese (n = 17); (2) article written in Arabic (n = 1); (3) congress report with no further publication and no usable data reported (n = 2); (4) unable to locate articles in several languages (n = 1 in Japanese, n = 1 in Turkish and n = 1 in German); (5) inconsistent results reported in another publication (thesis) of the same data (n = 1, author has been contacted); and (6) unable to decide if paper reports duplicate data with previous publication (n = 1, authors have been contacted). A detailed list of the papers that have been assigned to the waiting status can be found in Appendix 3.
Eighty-five papers provided data for the analysis of at least one outcome. One paper154 reported the results of two clomipramine trials and, therefore, the included papers included data on 86 trials. Figure 1 presents the results of the search in the form of the PRISMA flow chart.
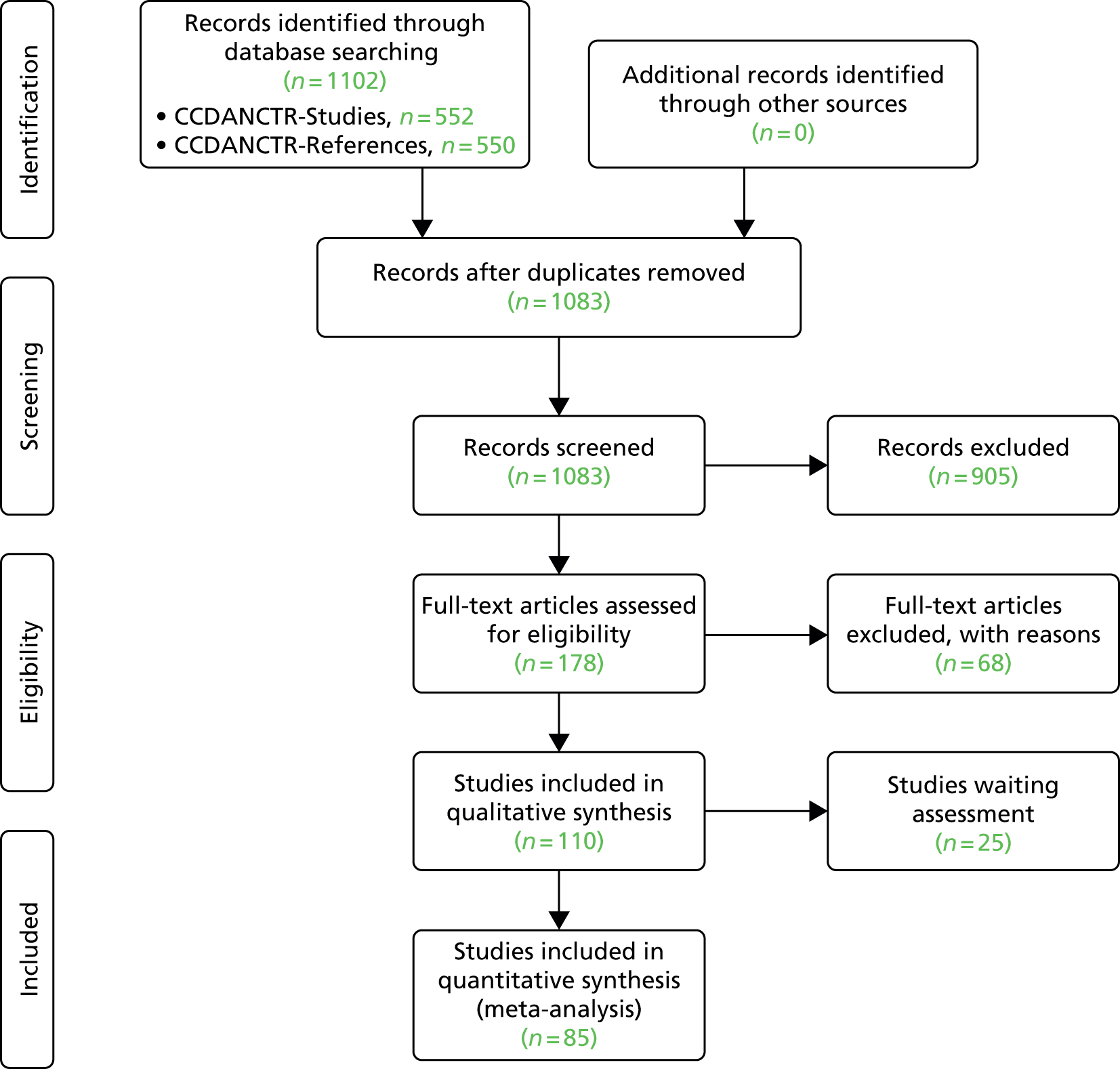
Studies excluded
Sixty-eight papers were excluded from the analysis. A detailed table of the excluded studies and the reasons for exclusion can be found in Appendix 2. Table 2 shows the main reasons for exclusion.
| Main reason for exclusion | Number of papers |
|---|---|
| Duplicate publication | 17 |
| Control intervention not covered | 11 |
| Non-randomised design | 10 |
| Data not usable | 9 |
| Preliminary congress abstract report | 8 |
| Aim of the study not relevant (secondary analyses, relapse prevention studies) | 5 |
| Diagnosis not focused on OCD | 4 |
| Treatment-refractory patient population | 2 |
| Main intervention not covered | 2 |
| Total | 68 |
General summary characteristics of the included studies
We included 86 unique studies reported in 85 publications. It can be seen from Table 3 that 64 studies (74%) were conducted in adult patients, whereas 22 studies (26%) were conducted in child and adolescent samples. The majority of the studies (84%) had only two arms. Approximately half of the studies were conducted after the 2000s and 14% were conducted before the 1990s.
| Characteristics of studies | n (%) |
|---|---|
| Total studies included | 86 (100) |
| Number of studies by age group | |
| Adults | 64 (74) |
| Children/adolescents | 22 (26) |
| Total number of arms | 194 |
| Adults | 148 (76) |
| Children/adolescents | 46 (24) |
| Number of studies by number of arms | |
| Two-arm studies: total | 72 (84 |
| Adults | 51 (80) |
| Children/adolescents | 21 (95) |
| Three-arm studies: total | 6 (7) |
| Adults | 6 (9) |
| Children/adolescents | 0 |
| Four-arm studies: total | 8 (9) |
| Adults | 7 (11) |
| Children/adolescents | 1 (5) |
| Total patients randomised | 8611 |
| Adults | 7306 (85) |
| Children/adolescents | 1305 (15) |
| Number of studies by date of publication | |
| 1980–90 | 12 (14) |
| 1991–2000 | 32 (37) |
| 2001–14 | 42 (49) |
In total, 8611 patients were randomised (7306 adults and 1305 children and adolescents) into 194 arms including 23 different interventions or combinations of interventions. Table 4 summarises data on the number of randomised patients in arms/studies.
| Type of study | Number of arms | Number of patients | Minimum | Maximum | Mean | SD |
|---|---|---|---|---|---|---|
| Per arm | 194 arms | 8611 | 5 | 241 | 44 | 40 |
| Per study/arm | ||||||
| Two-arm studies | 72 studies | 5745 | 10 | 325 | 80 | 72 |
| Three-arm studies | Six studies | 789 | 21 | 406 | 131 | 158 |
| Four-arm studies | Eight studies | 2077 | 29 | 466 | 260 | 155 |
Country of publication
Figure 2 presents summary data on the country of publication of included studies. The majority of the studies (52% in total; 48% in adults vs. 66% in children/adolescents) were conducted in North America (33 studies in the USA, eight in Canada and four in both for the total sample). Five studies (all in adults) were multinational, that is, defined as having recruited patients from three or more countries (one fluoxetine vs. placebo; one citalopram vs. placebo; one paroxetine vs. placebo and clomipramine; one escitalopram vs. placebo and paroxetine; and one fluvoxamine vs. clomipramine study). Countries with more than three studies were the Netherlands (five studies), and Australia, Brazil and UK (three studies each). A total of seven studies (six in adults and one in children/adolescents) were conducted in Asia (three in Japan, three in Iran and one in China). There were no studies from Africa.
FIGURE 2.
Country of publication [n (%) of included studies].
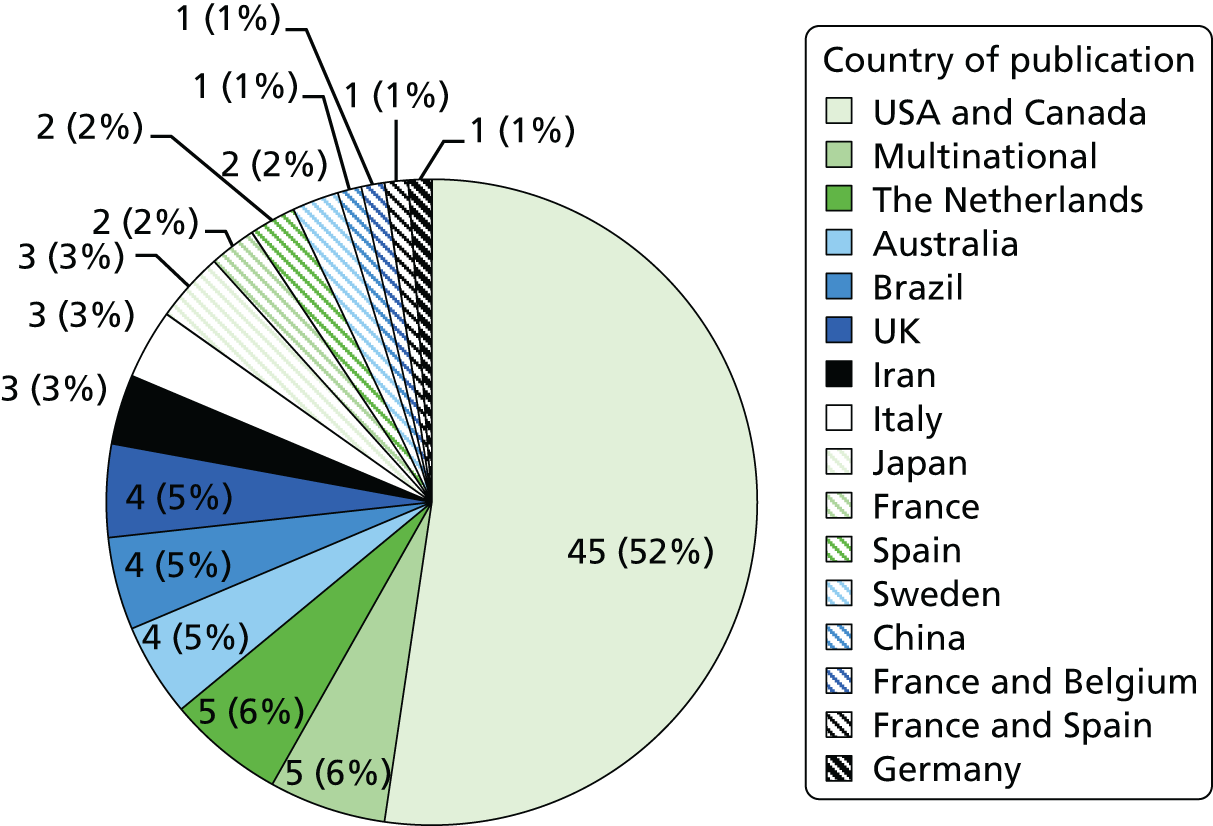
Types of interventions
Fifty-six of the included arms (29%) involved a supposedly inactive intervention, either drug placebo (18.5%) or psychological placebo (4.5%), or a waitlist control (6%). Table 5 shows the number of arms/number of patients per type of intervention in the total sample and Figure 3 presents a relevant bar diagram.
| Intervention | Number of arms | Number of patients | % of arms | % of patients | Mean per arm | Minimum | Maximum |
|---|---|---|---|---|---|---|---|
| Placebo | 36 | 2005 | 18.5 | 23.3 | 56 | 6 | 139 |
| Clomipramine | 21 | 1013 | 11 | 11.8 | 48 | 8 | 142 |
| CBT | 17 | 446 | 9 | 5.2 | 26 | 7 | 70 |
| Fluvoxamine | 17 | 641 | 9 | 7.5 | 38 | 5 | 127 |
| BT | 16 | 418 | 8 | 4.8 | 26 | 9 | 69 |
| Fluoxetine | 14 | 754 | 7 | 8.8 | 54 | 7 | 90 |
| Waitlist | 12 | 194 | 6 | 2.2 | 16 | 6 | 24 |
| Paroxetine | 11 | 1017 | 5.5 | 11.8 | 92 | 9 | 205 |
| Sertraline | 10 | 711 | 5 | 8.2 | 71 | 10 | 241 |
| CT | 9 | 252 | 5 | 2.9 | 28 | 10 | 49 |
| Psychological placebo | 8 | 251 | 4.5 | 2.9 | 31 | 9 | 75 |
| Citalopram | 5 | 325 | 2.5 | 3.8 | 65 | 11 | 102 |
| Other drug | 3 | 52 | 1.5 | 0.6 | 17 | 10 | 30 |
| Fluvoxamine and BT | 3 | 55 | 1.5 | 0.6 | 18 | 5 | 30 |
| Escitalopram | 2 | 232 | 1 | 2.7 | 116 | 116 | 116 |
| Sertraline and CBT | 2 | 42 | 1 | 0.5 | 21 | 14 | 28 |
| Venlafaxine | 2 | 101 | 1 | 1.2 | 50 | 26 | 75 |
| Clomipramine and BT | 1 | 33 | 0.5 | 0.4 | 33 | 33 | 33 |
| Fluvoxamine and CBT | 1 | 7 | 0.5 | 0.1 | 7 | 7 | 7 |
| Placebo + BT | 1 | 30 | 0.5 | 0.3 | 30 | 30 | 30 |
| Placebo + CBT | 1 | 16 | 0.5 | 0.2 | 16 | 16 | 16 |
| Serotonergic medication | 1 | 6 | 0.5 | 0.1 | 6 | 6 | 6 |
| Serotonergic medication + CBT | 1 | 10 | 0.5 | 0.1 | 10 | 10 | 10 |
FIGURE 3.
Number of arms per type of intervention: total sample. SRI, serotonin reuptake inhibitor.
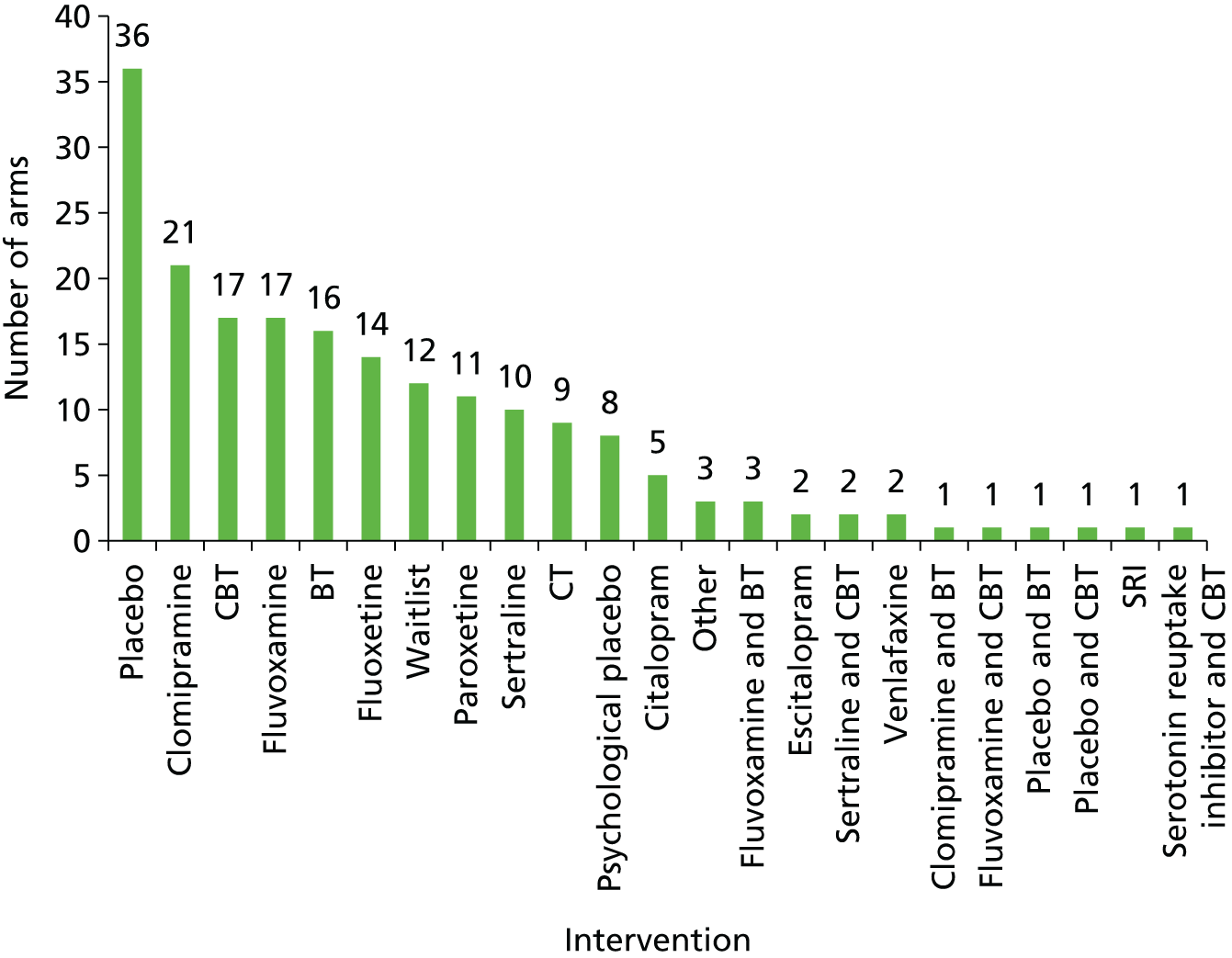
It can be seen that in adults (Table 6), the most used active intervention was clomipramine (12%), followed by fluvoxamine (10%). Paroxetine, however, had the second largest sample of randomised patients after clomipramine. Overall, 48% of the arms in the adult set involved an active drug intervention, 22% involved an active psychological intervention and 4% involved a combination treatment. In children and adolescents (Table 7), the most used active intervention was CBT (18% of the arms), followed by sertraline (11.5%, either alone or in combination with CBT) and fluoxetine (9% of the arms). Approximately 30% of the arms in children and adolescent samples included a medication, 25% of the arms included a psychological intervention and 7% included a combination of both types of treatments.
| Intervention | Number of arms | Number of patients | % of arms | % of patients | Mean per arm | Minimum | Maximum |
|---|---|---|---|---|---|---|---|
| Placebo | 26 | 1605 | 18 | 22.1 | 60 | 8 | 139 |
| Clomipramine | 17 | 955 | 12 | 13.2 | 53 | 8 | 142 |
| Fluvoxamine | 15 | 579 | 10 | 7.9 | 39 | 7 | 127 |
| BT | 14 | 395 | 9 | 5.4 | 28 | 9 | 69 |
| Fluoxetine | 10 | 640 | 6.7 | 8.6 | 64 | 23 | 90 |
| Paroxetine | 10 | 917 | 6.7 | 12.5 | 92 | 9 | 205 |
| CBT | 9 | 240 | 6 | 3.3 | 27 | 7 | 70 |
| CT | 9 | 252 | 6 | 3.4 | 28 | 10 | 49 |
| Sertraline | 7 | 571 | 4.7 | 7.8 | 82 | 10 | 241 |
| Waitlist | 7 | 111 | 4.7 | 1.5 | 16 | 6 | 24 |
| Psychological placebo | 6 | 209 | 4 | 2.8 | 35 | 9 | 75 |
| Citalopram | 4 | 311 | 2.8 | 4.2 | 78 | 11 | 102 |
| Other drug | 3 | 52 | 2 | 0.7 | 17 | 10 | 30 |
| Escitalopram | 2 | 232 | 1.3 | 3.2 | 116 | 116 | 116 |
| Fluvoxamine and BT | 2 | 50 | 1.3 | 0.7 | 25 | 20 | 30 |
| Venlafaxine | 2 | 101 | 1.3 | 1.4 | 50 | 26 | 75 |
| Clomipramine + BT | 1 | 33 | 0.7 | 0.5 | 33 | 33 | 33 |
| Fluvoxamine + CBT | 1 | 7 | 0.7 | 0.1 | 7 | 7 | 7 |
| Placebo + BT | 1 | 30 | 0.7 | 0.5 | 30 | 30 | 30 |
| Serotonergic medication | 1 | 6 | 0.7 | 0.1 | 6 | 6 | 6 |
| Serotonergic medication + CBT | 1 | 10 | 0.7 | 0.1 | 10 | 10 | 10 |
| Intervention | Number of arms | Number of patients | % of arms | % of patients | Mean per arm | Minimum | Maximum |
|---|---|---|---|---|---|---|---|
| Placebo | 10 | 400 | 20.4 | 30.3 | 43 | 6 | 107 |
| CBT | 8 | 206 | 18 | 16 | 26 | 11 | 49 |
| Waitlist | 5 | 83 | 11.3 | 6.4 | 17 | 10 | 24 |
| Fluoxetine | 4 | 114 | 9.1 | 8.9 | 28 | 7 | 71 |
| Clomipramine | 4 | 58 | 7 | 3.8 | 16 | 8 | 31 |
| Sertraline | 3 | 42 | 7 | 3.3 | 21 | 14 | 28 |
| BT | 2 | 23 | 4.5 | 1.8 | 11 | 10 | 13 |
| Fluvoxamine | 2 | 62 | 4.5 | 4.8 | 31 | 5 | 57 |
| Psychological placebo | 2 | 42 | 4.5 | 3.3 | 21 | 20 | 22 |
| Sertraline + CBT | 2 | 140 | 4.5 | 10.9 | 47 | 20 | 92 |
| Citalopram | 1 | 14 | 2.3 | 1.1 | 14 | 14 | 14 |
| Fluvoxamine + BT | 1 | 5 | 2.3 | 0.4 | 5 | 5 | 5 |
| Paroxetine | 1 | 100 | 2.3 | 7.8 | 100 | 100 | 100 |
| Placebo + CBT | 1 | 16 | 2.3 | 1.2 | 16 | 16 | 16 |
Specific characteristics of individual studies
Tables 8 and 9 present specific characteristics of individual studies for the adult (n = 64 studies) and child and adolescent (n = 22 studies) subsets of data, respectively. The following data are presented for each individual study: study ID (including year of publication), total sample size (original number of randomised patients), number of arms, type of included interventions (grouped into three categories: medication arms only, psychological therapy arms only and arms with a combination of treatment interventions), specific intervention used in each arm, duration of the trial in weeks (primary end point), mean age of the total sample of randomised patients, percentage of female patients, primary scale used for the assessment of obsessive–compulsive symptoms, percentage of patients with depression comorbidity (grouped into six categories: none, < 25%, 25–50%, > 50%, unspecified and unclear), sponsorship of the study from drug companies (grouped into three categories: yes, no and unclear. This is not applicable for studies with psychological arms only. It should be noted that specific details of the interventions (mean dose, range of dose, number of psychotherapeutic sessions and mean duration of each session) are given for all studies in Appendix 6.
For the adult subset, the median number of randomised patients per study was 66 (range 16–466); 60% of the studies included drug arms only and 12% included combined arms; median duration of follow-up per study was 12 weeks (range 3–24 weeks); median percentage of female patients per study was 52.5% (range 0–94%); 85% of the studies used the YBOCS as their primary symptom scale, 54% of the studies excluded patients with major depression, and 60% of the studies that used at least one drug or combined arm were sponsored by the pharmaceutical industry. Of the 12 psychotherapy studies that used an inactive control condition, seven (58%) used a waitlist control (five CBT trials, one BT and one CT trial).
| Study ID | n | Number of arms | Intervention type | Arm 1 | Arm 2 | Arm 3 | Arm 4 | Duration, weeks | Mean age, years | Female, % | Scale used | Comorbid depression | Sponsorship |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Albert et al., 2002155 | 73 | 2 | Drug | VEN | CLO | 12 | 29.65 | 47.9 | YBOCS | No | No | ||
| Ananth et al., 1981156 | 20 | 2 | Drug | CLO | AMI | 4 | 36.9 | 65 | Severity Questionnaire | Yes | Unclear | ||
| Anderson and Rees, 2007157 | 38 | 2 | Therapy | CBT | Waitlist | 10 | 33.18 | • | YBOCS | Yes | NA | ||
| Andersson et al., 2012158 | 101 | 2 | Therapy | CBT | PsychPLA | 10 | 34 | 66 | YBOCS | Yes | NA | ||
| Belloch et al., 2008159 | 33 | 2 | Therapy | BT | CT | 24 | 32 | • | YBOCS | Yes | NA | ||
| Belotto-Silva et al., 2012160 | 158 | 2 | Combination | FLX | CBT | 12 | 34.04 | 55 | YBOCS | Yes | No | ||
| Bergeron et al., 2002161 | 150 | 2 | Drug | FLX | SER | 24 | 36.53 | 54 | YBOCS | No | Yes | ||
| Bisserbe et al., 1997162 | 168 | 2 | Drug | SER | CLO | 16 | 39.77 | 63 | YBOCS | No | Yes | ||
| CCSG1, 1991154 | 239 | 2 | Drug | CLO | PLA | 10 | 35.4 | 61 | YBOCS | No | Yes | ||
| CCSG2, 1991154 | 281 | 2 | Drug | CLO | PLA | 10 | 35.6 | 51.5 | YBOCS | No | Yes | ||
| Chouinard et al., 1990163 | 87 | 2 | Drug | SER | PLA | 8 | 37.25 | 15 | YBOCS | No | Yes | ||
| Cordioli et al., 2003164 | 47 | 2 | Therapy | CBT | Waitlist | 12 | 36.5 | 51 | YBOCS | Yes | NA | ||
| Cottraux et al., 1993165 | 60 | 3 | Combination | FLV | BT | BT + FLV | 24 | • | 63 | OCD symptom scales | Yes | No | |
| Cottraux et al., 2001166 | 65 | 2 | Therapy | BT | CT | 16 | 35.78 | 74 | YBOCS | No | NA | ||
| Denys et al., 2003167 | 150 | 2 | Drug | PAR | VEN | 12 | 35 | 62 | YBOCS | No | Yes | ||
| Emmelkamp and Beens, 1991168 | 30 | 2 | Therapy | CT | BT | 4 | • | 76 | Maudsley OCI | Yes | NA | ||
| Emmelkamp et al., 1988169 | 20 | 2 | Therapy | CT | BT | 8 | 29.9 | • | Maudsley OCI | Yes | NA | ||
| Fals-Stewart et al., 1993170 | 66 | 2 | Therapy | BT | PsychPLA | 12 | 30.5 | 55 | YBOCS | No | NA | ||
| Foa et al., 2005171 | 149 | 4 | Combination | BT | CLO | BT + CLO | PLA | 12 | 34.8 | 48 | YBOCS | No | No |
| Freeman et al., 1994172 | 66 | 2 | Drug | FLV | CLO | 10 | 33.01 | 47 | YBOCS | No | Yes | ||
| Freeston et al., 1997173 | 29 | 2 | Therapy | CBT | Waitlist | 16 | 35.8 | 45 | YBOCS | Yes | NA | ||
| GlaxoSmithKline, 2005174 | 241 | 3 | Drug | PLA | PAR | CLO | 12 | 37.95 | 39 | YBOCS | No | Yes | |
| GlaxoSmithKline, 2005175 | 146 | 2 | Drug | PAR | CLO | 10 | 30.85 | 62 | YBOCS | No | Yes | ||
| Goodman et al., 1989176 | 46 | 2 | Drug | PLA | FLV | 6 | 37 | 55 | YBOCS | Yes | No | ||
| Goodman et al., 1996177 | 160 | 2 | Drug | PLA | FLV | 10 | 36.65 | 50 | YBOCS | No | Yes | ||
| Greist et al., 1995126 | 325 | 2 | Drug | SER | PLA | 12 | 38. 64 | 52 | YBOCS | No | Yes | ||
| Greist et al., 2002178 | 144 | 2 | Therapy | BT | PsychPLA | 10 | 39 | 42 | YBOCS | Yes | NA | ||
| Hohagen et al., 1998179 | 60 | 2 | Combination | BT + PLA | BT + FLV | 10 | 35.5 | 59 | YBOCS | Yes | No | ||
| Hollander et al., 2003180 | 253 | 2 | Drug | PLA | FLV | 12 | 37.4 | 64 | YBOCS | No | Yes | ||
| Hollander et al., 2003181 | 348 | 4 | Drug | PLA | PAR-20 | PAR-40 | PAR-60 | 12 | 41.36 | 26 | YBOCS | No | Yes |
| Jaurrieta et al., 2008182 | 38 | 2 | Therapy | CBT | Waitlist | 20 | 31.6 | 40.4 | YBOCS | Yes | NA | ||
| Jenike et al., 1990183 | 19 | 2 | Drug | SER | PLA | 10 | 39.7 | 21 | YBOCS | No | Yes | ||
| Jenike et al., 1990184 | 40 | 2 | Drug | PLA | FLV | 10 | 35.9 | 47 | YBOCS | No | Yes | ||
| Jenike et al., 1997185 | 44 | 2 | Drug | PLA | FLX | 10 | 34.86 | 48 | YBOCS | No | No | ||
| Jones and Menzies, 1998186 | 23 | 2 | Therapy | CT | Waitlist | 8 | 38.52 | 90 | Maudsley OCI | Unclear | NA | ||
| Kamijima et al., 2004187 | 191 | 2 | Drug | PLA | PAR | 12 | 37.8 | 62 | YBOCS | Yes | Unclear | ||
| Khodarahimi, 2009188 | 40 | 2 | Therapy | Waitlist | BT | 6 | 24.6 | 0 | YBOCS | No | NA | ||
| Kobak et al., 2005189 | 60 | 2 | Drug | PLA | Hypericum | 12 | 37.72 | • | YBOCS | No | No | ||
| Koran et al., 1996190 | 79 | 2 | Drug | FLV | CLO | 10 | • | 45 | YBOCS | No | Yes | ||
| Kronig et al., 1999191 | 167 | 2 | Drug | SER | PLA | 12 | 36.76 | 45 | YBOCS | No | Yes | ||
| Lindsay et al., 1997192 | 18 | 2 | Therapy | BT | PsychPLA | 3 | 32.8 | 66 | YBOCS | Yes | NA | ||
| López-Ibor et al., 1996193 | 55 | 2 | Drug | FLX | CLO | 8 | 34 | 62 | YBOCS | No | Yes | ||
| Mavissakalian et al., 1985194 | 16 | 2 | Drug | CLO | PLA | 12 | 35.9 | 56 | OCNS | Yes | Yes | ||
| McLean et al., 2001195 | 93 | 2 | Therapy | CT | BT | 12 | 35 | 48 | YBOCS | Yes | NA | ||
| Milanfranchi et al., 1997196 | 26 | 2 | Drug | CLO | FLV | 9 | 27.35 | 42 | YBOCS | No | Yes | ||
| Montgomery et al., 1993197 | 217 | 4 | Drug | PLA | FLX-20 | FLX-40 | FLX-60 | 8 | 37.16 | 47 | YBOCS | Yes | Yes |
| Montgomery et al., 2001198 | 401 | 4 | Drug | PLA | CIT-20 | CIT-40 | CIT-60 | 12 | 37.82 | 54 | YBOCS | Yes | Yes |
| Mundo et al., 1997199 | 30 | 3 | Drug | FLV | PAR | CIT | 10 | 30.78 | 30 | YBOCS | No | No | |
| Mundo et al., 2001200 | 227 | 2 | Drug | CLO | FLV | 10 | 35.2 | 45 | YBOCS | No | Yes | ||
| Nakajima et al., 1996201 | 94 | 2 | Drug | FLV | PLA | 8 | 34.38 | 46 | YBOCS | Unclear | Unclear | ||
| Nakatani et al., 2005202 | 31 | 3 | Combination | PsychPLA | FLV | BT | 12 | 33.66 | 68 | YBOCS | No | No | |
| O’Connor et al., 1999203 | 29 | 4 | Combination | SRI | Waitlist | CBT | CBT + SRI | 20 | 35.94 | 37 | YBOCS | Yes | No |
| O’Connor et al., 2006204 | 21 | 2 | Drug | PLA | FLV | 20 | 35.76 | 57 | YBOCS | No | No | ||
| Perse et al., 1987205 | 20 | 2 | Drug | PLA | FLV | 8 | • | • | Maudsley OCI | Yes | Yes | ||
| Shareh et al., 2010206 | 21 | 3 | Combination | FLV | CBT | FLV + CBT | 10 | 26.84 | 53 | YBOCS | No | No | |
| Sousa et al., 2006207 | 56 | 2 | Combination | SER | CBT | 12 | 38.5 | 77 | YBOCS | No | No | ||
| Stein et al., 2007124 | 466 | 4 | Drug | PLA | PAR | ESCIT-10 | ESCIT-20 | 12 | 37.75 | 57 | YBOCS | No | Yes |
| Thoren et al., 1980208 | 16 | 2 | Drug | CLO | PLA | 5 | 38.9 | 94 | OCD symptom scale | Yes | No | ||
| Tollefson et al., 1994127 | 355 | 4 | Drug | PLA | FLX-20 | FLX-40 | FLX-60 | 13 | 36.9 | 55.2 | YBOCS | Yes | Yes |
| Van Oppen et al., 1995209 | 71 | 2 | Therapy | CT | BT | 16 | 34.71 | 53 | YBOCS | Yes | NA | ||
| Volavka et al., 1985210 | 23 | 2 | Drug | CLO | IMI | 12 | 29.94 | 52 | SRONS | No | Yes | ||
| Whittal et al., 2005211 | 83 | 2 | Therapy | CT | BT | 12 | 34.89 | 62.5 | YBOCS | Yes | NA | ||
| Whittal et al., 2010212 | 73 | 2 | Therapy | CT | PsychPLA | 12 | 31.5 | 46.6 | YBOCS | Yes | NA | ||
| Zohar and Judge, 1996213 | 406 | 3 | Drug | PLA | PAR | CLO | 12 | 37.94 | 52 | YBOCS | No | Yes |
| Study ID | n | Number of arms | Arm 1 | Arm 2 | Arm 3 | Arm 4 | Duration, weeks | Mean age, years | Female, % | Scale used | Comorbid depression | Sponsorship |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Alaghband-Rad and Hakimshooshtary, 2009215 | 29 | 2 | FLX | CIT | 6 | • | 41 | CYBOCS | Unclear | Unclear | ||
| Asbahr et al., 2005216 | 40 | 2 | SER | CBT | 12 | 13.05 | 35 | CYBOCS | Yes | No | ||
| Barrett et al., 2004217 | 48 | 2 | CBT | Waitlist | 14 | 11.25 | 48 | CYBOCS | Yes | NA | ||
| Bolton and Perrin, 2008218 | 20 | 2 | BT | Waitlist | 7 | 13.2 | 30 | CYBOCS | Yes | NA | ||
| Bolton et al., 2011219 | 60 | 2 | CBT | Waitlist | 12 | 14.6 | 57 | CYBOCS | No | NA | ||
| de Haan et al., 1998220 | 23 | 2 | CLO | BT | 12 | 13.43 | 50 | CYBOCS | No | No | ||
| DeVeaugh-Geiss et al., 1992221 | 60 | 2 | CLO | PLA | 8 | 14.25 | 35 | CYBOCS | No | Yes | ||
| Flament et al., 1985222 | 19 | 2 | CLO | PLA | 5 | 14.5 | 26 | OCR scale | Yes | No | ||
| Freeman et al., 2008223 | 42 | 2 | CBT | PsychPLA | 14 | 7.11 | 57 | CYBOCS | Yes | NA | ||
| Geller et al., 2001224 | 103 | 2 | FLX | PLA | 13 | 11.4 | 52 | CYBOCS | Yes | Yes | ||
| GlaxoSmithKline, 2001225 | 207 | 2 | PAR | PLA | 10 | 11.3 | 42 | CYBOCS | Unclear | Yes | ||
| Liebowitz et al., 2002226 | 43 | 2 | FLX | PLA | 8 | 12.65 | 42 | CYBOCS | Yes | Yes | ||
| March et al., 1990227 | 16 | 2 | CLO | PLA | 10 | 15 | 31 | YBOCS | Yes | Yes | ||
| March et al., 1998228 | 187 | 2 | SER | PLA | 12 | 12.6 | • | CYBOCS | Yes | Yes | ||
| Neziroglu et al., 2000229 | 10 | 2 | FLV | FLV + BT | 43 | 14.5 | 40 | CYBOCS | Yes | Unclear | ||
| Piacentini et al., 2011230 | 71 | 2 | CBT | PsychPLA | 14 | 12.2 | 63.4 | CYBOCS | Yes | NA | ||
| Riddle et al., 1992231 | 13 | 2 | FLX | PLA | 8 | 12.7 | 61 | CYBOCS | Yes | No | ||
| Riddle et al., 2001232 | 120 | 2 | FLV | PLA | 10 | 13.03 | 47 | CYBOCS | No | Yes | ||
| Storch et al., 2011233 | 31 | 2 | CBT | Waitlist | 12 | 11.1 | 39 | CYBOCS | Yes | NA | ||
| Storch et al., 2013234 | 30 | 2 | SER + CBT | CBT + PLA | 18 | 12.13 | 40 | CYBOCS | Yes | No | ||
| Williams et al., 2010235 | 21 | 2 | CBT | Waitlist | 12 | 13.6 | 38 | CYBOCS | Yes | NA | ||
| The Pediatric OCD Treatment Study, 2004236 | 112 | 4 | SER | CBT | SER + CBT | PLA | 12 | 11.77 | 50 | CYBOCS | No | No |
For the children and adolescents subset, the median number of randomised patients per study was 42 (range 9–207); 43% of the studies included drug arms only and 24% included combined arms; median duration per study was 12 weeks (range 5–43 weeks); median percentage of female patients per study was 42% (range 30–63%); 95% of the studies used the CYBOCS as their primary symptom scale; 24% of the studies excluded patients with major depression; and 50% of the studies that used at least one drug or combined arm were sponsored by the pharmaceutical industry. Of the seven psychotherapy studies that used an inactive control condition, five (71%) used a waitlist control (four CBT trials and one BT trial).
Individual studies per included active intervention
For ease of reference, we also present separate tables with the included studies for each active intervention (Tables 10 and 11 for adults and children and adolescent subsets, respectively). We present the following information: study ID (including year of publication); total sample size (original number of randomised patients); specific intervention used in each arm; duration of the trial in weeks (primary end point); and primary scale used for the assessment of obsessive–compulsive symptoms. It should be noted that some studies appear more than once because they compared an active drug with another active drug.
| Study ID | n | Arm 1 | Arm 2 | Arm 3 | Arm 4 | Duration (weeks) | Scale used |
|---|---|---|---|---|---|---|---|
| Fluoxetine studies (n = 6) | |||||||
| Jenike et al., 1997185 | 44 | FLX | PLA | 10 | YBOCS | ||
| Montgomery et al., 1993197 | 217 | FLX-20 | FLX-40 | FLX-60 | PLA | 8 | YBOCS |
| Tollefson et al., 1994127 | 355 | FLX-20 | FLX-40 | FLX-60 | PLA | 13 | YBOCS |
| López-Ibor et al., 1996193 | 55 | FLX | CLO | 8 | YBOCS | ||
| Bergeron et al., 2002161 | 150 | FLX | SER | 24 | YBOCS | ||
| Belotto-Silva et al., 2012160 | 158 | FLX | CBT | 12 | YBOCS | ||
| Total | 979 | ||||||
| Fluvoxamine studies (n = 16) | |||||||
| Perse et al., 1987205 | 20 | FLV | PLA | 8 | Maudsley OCI | ||
| Goodman et al., 1989176 | 46 | FLV | PLA | 6 | YBOCS | ||
| Jenike et al., 1990184 | 40 | FLV | PLA | 10 | YBOCS | ||
| Goodman et al., 1996177 | 160 | FLV | PLA | 10 | YBOCS | ||
| Nakajima et al., 1996201 | 94 | FLV | PLA | 8 | YBOCS | ||
| Hollander et al., 2003181 | 253 | FLV | PLA | 12 | YBOCS | ||
| O’Connor et al., 2006204 | 21 | FLV | PLA | 20 | YBOCS | ||
| Freeman et al., 1994172 | 66 | FLV | CLO | 10 | YBOCS | ||
| Koran et al., 1996190 | 79 | FLV | CLO | 10 | YBOCS | ||
| Milanfranchi et al., 1997196 | 26 | FLV | CLO | 9 | YBOCS | ||
| Mundo et al., 2001200 | 227 | FLV | CLO | 10 | YBOCS | ||
| Mundo et al., 1997199 | 30 | FLV | PAR | CIT | 10 | YBOCS | |
| Nakatani et al., 2005202 | 31 | FLV | BT | PsychPLA | 12 | YBOCS | |
| Cottraux et al., 1993165 | 60 | FLV | FLV + BT | BT | 24 | OCD symptom scales | |
| Hohagen et al.,1998179 | 60 | FLV + BT | PLA + BT | 10 | YBOCS | ||
| Shareh et al., 2010206 | 21 | FLV | FLV + CBT | CBT | 10 | YBOCS | |
| Total | 1234 | ||||||
| Clomipramine studies (n = 17) | |||||||
| Thoren et al., 1980208 | 16 | CLO | PLA | 5 | OCD symptom scale | ||
| Mavissakalian et al., 1985194 | 16 | CLO | PLA | 12 | OCNS | ||
| CCSG1, 1991154 | 239 | CLO | PLA | 10 | YBOCS | ||
| CCSG2, 1991154 | 281 | CLO | PLA | 10 | YBOCS | ||
| Ananth et al., 1981156 | 20 | CLO | AMI | 4 | Severity questionnaire | ||
| Volavka et al., 1985210 | 23 | CLO | IMI | 12 | SRONS | ||
| Freeman et al., 1994172 | 66 | CLO | FLV | 10 | YBOCS | ||
| Koran et al., 1996190 | 79 | CLO | FLV | 10 | YBOCS | ||
| Milanfranchi et al., 1997196 | 26 | CLO | FLV | 9 | YBOCS | ||
| Mundo et al., 2001200 | 227 | CLO | FLV | 10 | YBOCS | ||
| López-Ibor et al., 1996193 | 55 | CLO | FLX | 8 | YBOCS | ||
| GlaxoSmithKline, 2005175 | 146 | CLO | PAR | 10 | YBOCS | ||
| GlaxoSmithKline, 2005174 | 241 | CLO | PAR | PLA | 12 | YBOCS | |
| Zohar and Judge, 1996213 | 406 | CLO | PAR | PLA | 12 | YBOCS | |
| Bisserbe et al., 1997162 | 168 | CLO | SER | 16 | YBOCS | ||
| Albert et al., 2002155 | 73 | CLO | VEN | 12 | YBOCS | ||
| Foa et al., 2005171 | 149 | CLO | CLO + BT | BT | PLA | 12 | YBOCS |
| Total | 2231 | ||||||
| Paroxetine studies (n = 8) | |||||||
| Hollander et al., 2003180 | 348 | PAR-20 | PAR-40 | PAR-60 | PLA | 12 | YBOCS |
| Kamijima et al., 2004187 | 191 | PAR | PLA | 12 | YBOCS | ||
| GlaxoSmithKline, 2005175 | 146 | PAR | CLO | 10 | YBOCS | ||
| GlaxoSmithKline, 2005174 | 241 | PAR | CLO | PLA | 12 | YBOCS | |
| Zohar and Judge, 1996213 | 406 | PAR | CLO | PLA | 12 | YBOCS | |
| Mundo et al., 1997199 | 30 | PAR | CIT | FLV | 10 | YBOCS | |
| Stein et al., 2007124 | 466 | PAR | ESCIT-10 | ESCIT-20 | PLA | 12 | YBOCS |
| Denys et al., 2003167 | 150 | PAR | VEN | 12 | YBOCS | ||
| Total | 1978 | ||||||
| Sertraline studies (n = 7) | |||||||
| Chouinard et al., 1990163 | 87 | SER | PLA | 8 | YBOCS | ||
| Jenike et al., 1990183 | 19 | SER | PLA | 10 | YBOCS | ||
| Greist et al., 1995126 | 325 | SER | PLA | 12 | YBOCS | ||
| Kronig et al., 1999191 | 167 | SER | PLA | 12 | YBOCS | ||
| Bisserbe et al., 1997162 | 168 | SER | CLO | 16 | YBOCS | ||
| Bergeron et al., 2002161 | 150 | SER | FLX | 24 | YBOCS | ||
| Sousa et al., 2006207 | 56 | SER | CBT | 12 | YBOCS | ||
| Total | 972 | ||||||
| Citalopram studies (n = 2) | |||||||
| Montgomery et al., 2001198 | 401 | CIT-20 | CIT-40 | CIT-60 | PLA | 12 | YBOCS |
| Mundo et al., 1997199 | 30 | CIT | FLV | PAR | 10 | YBOCS | |
| Total | 431 | ||||||
| Escitalopram studies (n = 1) | |||||||
| Stein et al., 2007124 | 466 | PLA | PAR | ESCIT-10 | ESCIT-20 | 12 | YBOCS |
| Other medications (n = 3) | |||||||
| Ananth et al., 1981156 | 20 | AMI | CLO | 4 | Severity questionnaire | ||
| Volavka et al., 1985210 | 23 | IMI | CLO | 12 | SRONS | ||
| Kobak et al., 2005189 | 60 | Hypericum | PLA | 12 | YBOCS | ||
| Total | 103 | ||||||
| Venlafaxine studies (n = 2) | |||||||
| Albert et al., 2002155 | 73 | VEN | CLO | 12 | YBOCS | ||
| Denys et al., 2003167 | 150 | VEN | PAR | 12 | YBOCS | ||
| Total | 223 | ||||||
| BT studies (n = 15) | |||||||
| Fals-Stewart et al., 1993170 | 66 | BT | PsychPLA | 12 | YBOCS | ||
| Lindsay et al., 1997192 | 18 | BT | PsychPLA | 3 | YBOCS | ||
| Greist et al., 2002178 | 144 | BT | PsychPLA | 10 | YBOCS | ||
| Khodarahimi, 2009188 | 40 | BT | Waitlist | 6 | YBOCS | ||
| Foa et al., 2005171 | 149 | BT | BT + CLO | CLO | PLA | 12 | YBOCS |
| Cottraux et al., 1993165 | 60 | BT | BT + FLV | FLV | 24 | OCD symptom scales | |
| Nakatani et al., 2005202 | 31 | BT | FLV | PsychPLA | 12 | YBOCS | |
| Hohagen et al., 1998179 | 60 | BT + FLV | BT + PLA | 10 | YBOCS | ||
| Emmelkamp and Beens, 1991168 | 30 | BT | CT | 4 | Maudsley OCI | ||
| Van Oppen et al., 1995209 | 71 | BT | CT | 16 | YBOCS | ||
| Emmelkamp et al., 1988169 | 20 | BT | CT | 8 | Maudsley OCI | ||
| Cottraux et al., 2001166 | 65 | BT | CT | 16 | YBOCS | ||
| McLean et al., 2001195 | 93 | BT | CT | 12 | YBOCS | ||
| Whittal et al., 2005211 | 83 | BT | CT | 12 | YBOCS | ||
| Belloch et al., 2008159 | 33 | BT | CT | 24 | YBOCS | ||
| Total | 963 | ||||||
| CBT studies (n = 9) | |||||||
| Andersson et al., 2012158 | 101 | CBT | PsychPLA | 10 | YBOCS | ||
| Freeston et al., 1997173 | 29 | CBT | Waitlist | 16 | YBOCS | ||
| Cordioli et al., 2003164 | 47 | CBT | Waitlist | 12 | YBOCS | ||
| Anderson and Rees, 2007157 | 38 | CBT | Waitlist | 10 | YBOCS | ||
| Jaurrieta et al., 2008182 | 38 | CBT | Waitlist | 20 | YBOCS | ||
| Belotto-Silva et al., 2012160 | 158 | CBT | FLX | 12 | YBOCS | ||
| Shareh et al., 2010206 | 21 | CBT | CBT + FLV | FLV | 10 | YBOCS | |
| Sousa et al., 2006207 | 56 | CBT | SER | 12 | YBOCS | ||
| O’Connor et al., 1999203 | 29 | CBT | CBT + SRI | SRI | Waitlist | 20 | YBOCS |
| Total | 517 | ||||||
| CT studies (n = 9) | |||||||
| Whittal et al., 2010212 | 73 | CT | PsychPLA | 12 | YBOCS | ||
| Jones and Menzies, 1998186 | 23 | CT | Waitlist | 8 | Maudsley OCI | ||
| Emmelkamp et al., 1988169 | 20 | CT | BT | 8 | Maudsley OCI | ||
| Emmelkamp and Beens, 1991168 | 30 | CT | BT | 4 | Maudsley OCI | ||
| Van Oppen et al., 1995209 | 71 | CT | BT | 16 | YBOCS | ||
| Cottraux et al., 2001166 | 65 | CT | BT | 16 | YBOCS | ||
| McLean et al., 2001195 | 93 | CT | BT | 12 | YBOCS | ||
| Whittal et al., 2005211 | 83 | CT | BT | 12 | YBOCS | ||
| Belloch et al., 2008159 | 33 | CT | BT | 24 | YBOCS | ||
| Total | 491 | ||||||
| Study ID | n | Arm 1 | Arm 2 | Arm 3 | Arm 4 | Duration (weeks) | Scale used |
|---|---|---|---|---|---|---|---|
| Fluoxetine studies (n = 4) | |||||||
| Riddle et al., 1992231 | 13 | FLX | PLA | 8 | CYBOCS | ||
| Geller et al., 2001224 | 103 | FLX | PLA | 13 | CYBOCS | ||
| Liebowitz et al., 2002226 | 43 | FLX | PLA | 8 | CYBOCS | ||
| Alaghband-Rad and Hakimshooshtary, 2009215 | 29 | FLX | CIT | 6 | CYBOCS | ||
| Total | 188 | ||||||
| Fluvoxamine studies (n = 2) | |||||||
| Riddle et al., 2001232 | 120 | FLV | PLA | 10 | CYBOCS | ||
| Neziroglu et al., 2000229 | 10 | FLV | FLV + BT | 43 | CYBOCS | ||
| Total | 130 | ||||||
| Clomipramine studies (n = 4) | |||||||
| Flament et al., 1985222 | 19 | CLO | PLA | 5 | OCR scale | ||
| March et al., 1990227 | 16 | CLO | PLA | 10 | YBOCS | ||
| DeVeaugh-Geiss et al., 1992221 | 60 | CLO | PLA | 8 | CYBOCS | ||
| de Haan et al., 1998220 | 23 | CLO | BT | 12 | CYBOCS | ||
| Total | 99 | ||||||
| Paroxetine studies (n = 1) | |||||||
| GlaxoSmithKline, 2001225 | 207 | PAR | PLA | 10 | CYBOCS | ||
| Sertraline studies (n = 4) | |||||||
| March et al., 1998228 | 187 | SER | PLA | 12 | CYBOCS | ||
| The Pediatric OCD Treatment Study, 2004236 | 112 | SER | SER + CBT | CBT | PLA | 12 | CYBOCS |
| Asbahr et al., 2005216 | 40 | SER | CBT | 12 | CYBOCS | ||
| Storch et al., 2013234 | 30 | SER + CBT | PLA + CBT | 18 | CYBOCS | ||
| Total | 369 | ||||||
| Citalopram studies (n = 1) | |||||||
| Alaghband-Rad and Hakimshooshtary, 2009215 | 29 | CIT | FLX | 6 | CYBOCS | ||
| BT studies (n = 3) | |||||||
| Bolton and Perrin, 2008218 | 20 | BT | Waitlist | 7 | CYBOCS | ||
| de Haan et al., 1998220 | 23 | BT | CLO | 12 | CYBOCS | ||
| Neziroglu et al., 2000229 | 10 | BT + FLV | FLV | 43 | CYBOCS | ||
| Total | 53 | ||||||
| CBT studies (n = 9) | |||||||
| Freeman et al., 2008223 | 42 | CBT | PsychPLA | 14 | CYBOCS | ||
| Piacentini et al., 2011230 | 71 | CBT | PsychPLA | 14 | CYBOCS | ||
| Barrett et al., 2004217 | 48 | CBT | Waitlist | 14 | CYBOCS | ||
| Williams et al., 2010235 | 21 | CBT | Waitlist | 12 | CYBOCS | ||
| Bolton et al., 2011219 | 60 | CBT | Waitlist | 12 | CYBOCS | ||
| Storch et al., 2011233 | 31 | CBT | Waitlist | 12 | CYBOCS | ||
| The Pediatric OCD Treatment Study, 2004236 | 112 | CBT | SER | 12 | CYBOCS | ||
| Asbahr et al., 2005216 | 40 | CBT | SER | 12 | CYBOCS | ||
| Storch et al., 2013234 | 30 | CBT + PLA | CBT + SER | 18 | CYBOCS | ||
| Total | 455 | ||||||
Quality of included trials (risk-of-bias assessment)
The methodological quality of included trials is summarised in Table 12 and Figure 4 for the adult subset and Table 13 and Figure 5 for the children and adolescents subset. We used the criteria for quality assessment recommended by the Cochrane Handbook for Systematic Reviews of Interventions. 142 We have included the following criteria: random sequence generation; allocation sequence concealment; blinding of participants; blinding of those delivering the intervention; blinding of the outcome assessor; completeness of outcome data; and selective outcome reporting and other potential sources of bias. Studies were given a quality rating of ‘low’, ‘unclear’ or ‘high’ risk of bias in accordance with these criteria. For the last criterion of ‘any other potential source of bias’, we categorised studies as high risk if the overall attrition rate was > 25% or if there was evidence of differential attrition between arms of > 15%. The tables present the summary results for each criterion, and a more detailed table in Appendix 7 includes a description of the reason behind the specific categorisation. Studies with a high risk of bias were included in the main analysis but we also examined, in a sensitivity analysis, the effect of excluding them.
FIGURE 4.
Methodological quality graph for the adult subset (n = 64): reviewers’ judgements about each criterion as percentages across all included studies.
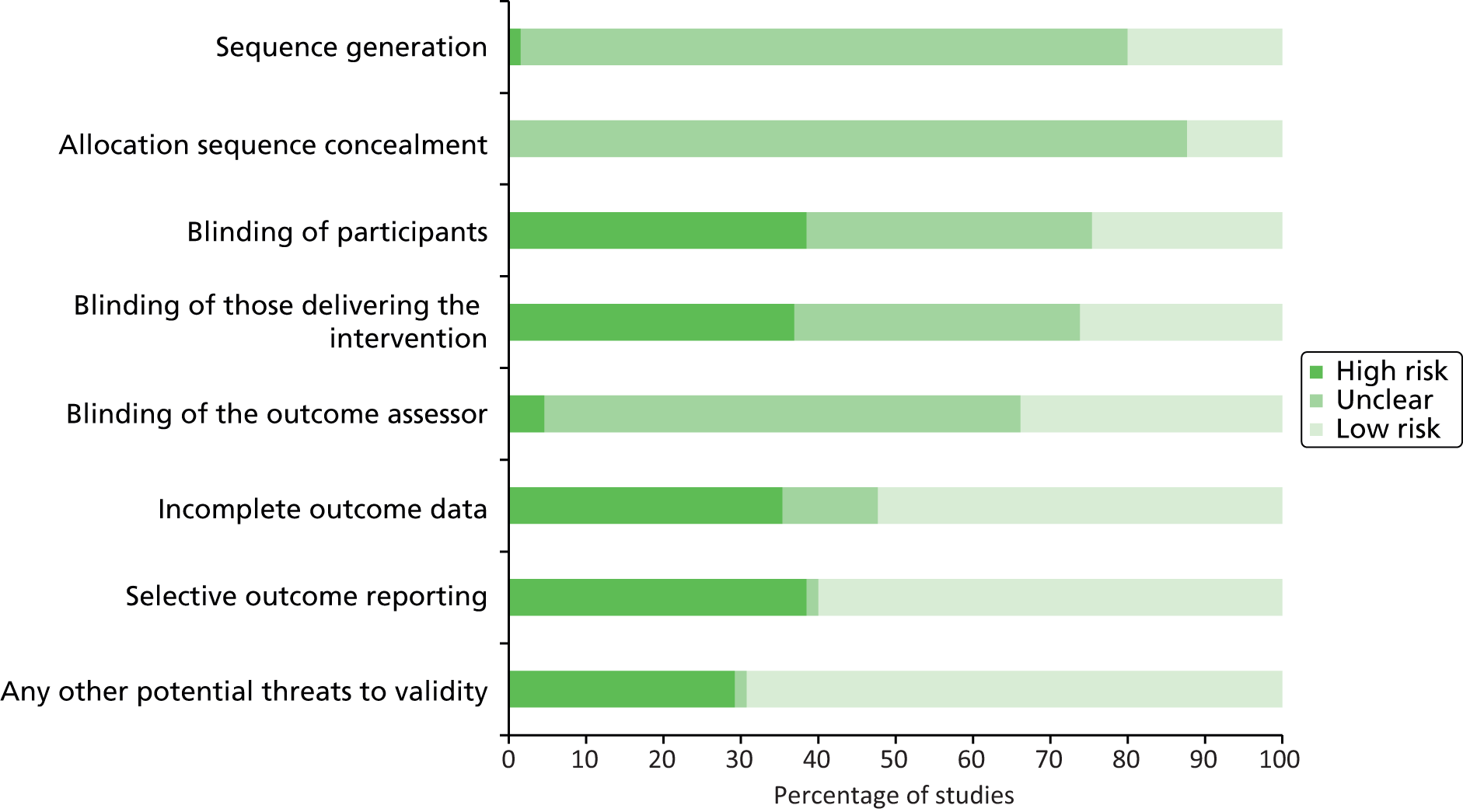
FIGURE 5.
Methodological quality graph for the children and adolescents subset (n = 22): reviewers’ judgements about each criterion as percentages across all included studies.

| Study ID | Sequence generation | Allocation sequence concealment | Blinding of participants | Blinding of those delivering the intervention | Blinding of the outcome assessor | Incomplete outcome data | Selective outcome reporting | Any other potential threats to validity |
|---|---|---|---|---|---|---|---|---|
| Albert et al., 2002155 | Unclear | Unclear | High | High | Low | High | High | High |
| Ananth et al., 1981156 | Unclear | Unclear | Low | Low | Unclear | High | Low | Low |
| Anderson and Rees, 2007157 | Unclear | Unclear | High | High | Unclear | Low | High | Low |
| Andersson et al., 2012158 | Low | Unclear | High | High | Low | Low | Low | Low |
| Belloch et al., 2008159 | Unclear | Unclear | High | High | Low | High | Low | Low |
| Belotto-Silva et al., 2012160 | Low | Low | High | High | Low | Low | Low | Low |
| Bergeron et al., 2002161 | Unclear | Unclear | Unclear | Unclear | Unclear | Low | Low | High |
| Bisserbe et al., 1997162 | Unclear | Unclear | Unclear | Unclear | Unclear | Low | High | High |
| CCSG1, 1991154 | Unclear | Unclear | Low | Low | Unclear | Unclear | High | High |
| CCSG2, 1991154 | Unclear | Unclear | Low | Low | Unclear | Unclear | High | High |
| Chouinard et al., 1990163 | Unclear | Unclear | Unclear | Unclear | Unclear | Low | High | Low |
| Cordioli et al., 2003164 | Low | Low | High | High | Low | Low | Low | Low |
| Cottraux et al., 1993165 | Unclear | Unclear | Unclear | Unclear | Unclear | High | Low | High |
| Cottraux et al., 2001166 | Unclear | Unclear | High | High | Low | High | High | Low |
| Denys et al., 2003167 | Unclear | Unclear | Low | Low | Low | Low | Low | Low |
| Emmelkamp and Beens, 1991168 | Unclear | Unclear | High | High | Low | High | Low | High |
| Emmelkamp et al., 1988169 | Unclear | Unclear | High | High | Low | High | Low | Low |
| Fals-Stewart et al., 1993170 | Unclear | Unclear | High | High | Unclear | High | High | Low |
| Foa et al., 2005171 | Low | Unclear | Unclear | Low | Low | Low | Low | High |
| Freeman et al., 1994172 | Unclear | Unclear | Unclear | Unclear | Unclear | Low | High | High |
| Freeston et al., 1997173 | Unclear | Unclear | High | High | High | Low | Low | Low |
| GlaxoSmithKline, 2005174 | Unclear | Unclear | Unclear | Unclear | Unclear | Low | Low | High |
| GlaxoSmithKline, 2005175 | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | Low | High |
| Goodman et al., 1989176 | Unclear | Unclear | Low | Low | Low | Low | Low | High |
| Goodman et al., 1996177 | Unclear | Unclear | Unclear | Unclear | Unclear | Low | High | Low |
| Greist et al., 1995126 | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | Low | High |
| Greist et al., 2002178 | Unclear | Unclear | High | High | High | Low | Low | Low |
| Hohagen et al., 1998179 | Unclear | Unclear | Unclear | Unclear | Low | Unclear | Low | High |
| Hollander et al., 2003180 | Unclear | Unclear | Unclear | Unclear | Unclear | Low | High | Low |
| Hollander et al., 2003181 | Low | Low | Low | Low | Unclear | Low | High | Low |
| Jaurrieta et al., 2008182 | Low | Low | High | High | Unclear | Low | High | Low |
| Jenike et al., 1990183 | Unclear | Unclear | Low | Low | Unclear | Low | Low | Low |
| Jenike et al., 1990184 | Unclear | Unclear | Low | Low | Low | High | High | Low |
| Jenike et al., 1997185 | Unclear | Unclear | Unclear | Unclear | Unclear | Low | Low | Unclear |
| Jones and Menzies, 1998186 | Unclear | Unclear | High | High | High | Unclear | Low | Low |
| Kamijima et al., 2004187 | Unclear | Unclear | Unclear | Unclear | Unclear | Low | High | Low |
| Khodarahimi, 2009188 | Low | Unclear | High | High | Unclear | High | Low | Low |
| Kobak et al., 2005189 | Unclear | Unclear | Low | Low | Unclear | Low | Low | Low |
| Koran et al., 1996190 | Low | Unclear | Low | Low | Unclear | Low | Low | High |
| Kronig et al., 1999191 | Low | Unclear | Unclear | Unclear | Unclear | Low | High | High |
| Lindsay et al., 1997192 | Unclear | Unclear | High | High | Unclear | Unclear | Unclear | Low |
| López-Ibor et al., 1996193 | Unclear | Unclear | Unclear | Unclear | Unclear | Low | Low | Low |
| Mavissakalian et al., 1985194 | Unclear | Unclear | Unclear | Unclear | Unclear | High | High | Low |
| McLean et al., 2001195 | Low | Unclear | High | High | Unclear | High | Low | Low |
| Milanfranchi et al., 1997196 | Unclear | Unclear | Low | Low | Unclear | High | Low | Low |
| Montgomery et al., 1993197 | Unclear | Unclear | Unclear | Unclear | Unclear | Low | Low | Low |
| Montgomery et al., 2001198 | Unclear | Unclear | Unclear | Unclear | Unclear | Low | Low | Low |
| Mundo et al., 1997199 | Unclear | Unclear | High | High | Low | Low | Low | Low |
| Mundo et al., 2001200 | Unclear | Unclear | Unclear | Unclear | Unclear | Low | High | Low |
| Nakajima et al., 1996201 | Unclear | Unclear | Unclear | Unclear | Unclear | Low | Low | Low |
| Nakatani et al., 2005202 | Unclear | Low | High | Unclear | Low | High | Low | Low |
| O’Connor et al., 1999203 | High | Unclear | High | High | Low | High | High | Low |
| O’Connor et al., 2006204 | Unclear | Low | Low | Low | Low | High | Low | Low |
| Perse et al., 1987205 | Unclear | Unclear | Unclear | Unclear | Low | High | High | Low |
| Shareh et al., 2010206 | Unclear | Unclear | High | High | Unclear | High | Low | High |
| Sousa et al., 2006207 | Low | Unclear | High | High | Low | Low | High | Low |
| Stein et al., 2007124 | Low | Low | Low | Low | Low | Low | Low | Low |
| Thoren et al., 1980208 | Unclear | Unclear | Low | Low | Unclear | High | High | Low |
| Tollefson et al., 1994127 | Unclear | Unclear | Unclear | Unclear | Unclear | Low | High | High |
| Van Oppen et al., 1995209 | Unclear | Unclear | High | High | Unclear | High | High | Low |
| Volavka et al., 1985210 | Low | Low | Low | Low | Unclear | High | Low | Low |
| Whittal et al., 2005211 | Unclear | Unclear | High | High | Low | High | Low | Low |
| Whittal et al., 2010212 | Unclear | Unclear | High | High | Unclear | High | Low | Low |
| Zohar and Judge, 1996213 | Unclear | Unclear | Unclear | Unclear | Unclear | Low | Low | High |
| Study ID | Sequence generation | Allocation sequence concealment | Blinding of participants | Blinding of those delivering the intervention | Blinding of the outcome assessor | Incomplete outcome data | Selective outcome reporting | Any other potential threats to validity |
|---|---|---|---|---|---|---|---|---|
| Alaghband-Rad and Hakimshooshtary, 2009215 | Unclear | Unclear | Unclear | Unclear | Unclear | High | High | High |
| Asbahr et al., 2005216 | Unclear | Unclear | High | High | Low | Low | High | Low |
| Barrett et al., 2004217 | Low | Unclear | High | High | Unclear | Unclear | High | Low |
| Bolton and Perrin, 2008218 | Low | Low | High | High | High | Low | Low | Low |
| Bolton et al., 2011219 | Low | Low | High | High | Low | Low | Low | Low |
| de Haan et al., 1998220 | Unclear | Unclear | High | High | Unclear | Low | Low | Low |
| DeVeaugh-Geiss et al., 1992221 | Unclear | Unclear | Unclear | Unclear | Unclear | Low | High | Low |
| Flament et al., 1985222 | Unclear | Unclear | Low | Low | Low | Unclear | High | Low |
| Freeman et al., 2008223 | Unclear | Unclear | High | High | Low | Low | Low | High |
| Geller et al., 2001224 | Unclear | Unclear | Unclear | Unclear | Unclear | Low | Low | High |
| GlaxoSmithKline, 2001225 | Low | Unclear | Low | Low | Unclear | High | Low | High |
| Liebowitz et al., 2002226 | Unclear | Unclear | Unclear | Unclear | Low | Low | Low | Low |
| March et al., 1990227 | Unclear | Unclear | Low | Low | Unclear | Low | Low | Low |
| March et al., 1998228 | Low | Unclear | Low | Low | Unclear | Low | High | Low |
| Neziroglu et al., 2000229 | Unclear | Unclear | High | High | Unclear | Low | Low | Low |
| Piacentini et al., 2011230 | Unclear | Unclear | High | High | Low | Low | Low | Low |
| Riddle et al., 1992231 | Unclear | Low | Low | Low | Unclear | Low | Low | Low |
| Riddle et al., 2001232 | Unclear | Unclear | Low | Low | Low | Low | Low | High |
| Storch et al., 2011233 | Low | Unclear | High | High | Low | Low | Low | Low |
| Storch et al., 2013234 | Low | Unclear | Unclear | Unclear | Low | Low | Low | High |
| Williams et al., 2010235 | Low | Low | High | High | Low | Low | High | Low |
| The Pediatric OCD Treatment Study, 2004236 | Low | Low | Unclear | Unclear | Low | Low | Low | Low |
Figures 4 and 5 show that the majority of the studies in the adult subset have not described adequately the random sequence generation or the way in which they have concealed the allocation sequence. Similar findings are reported for the children and adolescents subset.
We have also extracted data on the type of analysis (whether or not the authors have performed an intention-to-treat analysis) and the method of handling missing data. Tables 14 and 15 present this information for adults and for children and adolescents, respectively. It can be seen that the majority (81%) of the children and adolescents studies have used intention-to-treat analysis, compared with 43% of the adult studies. The last observation carried forward was the most common method for imputing missing observations.
In the adult subset, 54% of the trials either did not report intention-to-treat results or did not describe the way in which missing data were handled. Tabulation per type of intervention showed that in studies with medication arms only, the percentage was 41% (16 out of 39), compared with 77% (14 out of 18) of trials with psychological interventions only and 62% (5/8) of trials with combined arms. The majority of the studies with medication arms only involved clomipramine (10/16 studies that did not report such data), whereas those studies of psychological interventions involved either CT or compared CT and BT (9/14 studies that did not report such data).
| Intention-to-treat analysis | Number of studies | % of studies |
|---|---|---|
| Yes | 28 | 44 |
| No | 26 | 41 |
| Unclear | 8 | 12 |
| Not applicable | 2 | 3 |
| Total | 64 | 100 |
| Imputation method | ||
| Last observation carried forward | 25 | 39 |
| Linear mixed-effects models | 1 | 2 |
| Unclear | 10 | 16 |
| No | 26 | 40 |
| Not applicable | 2 | 3 |
| Total | 64 | 100 |
| Intention-to-treat analysis | Number of studies | % of studies |
|---|---|---|
| Yes | 17 | 77 |
| No | 3 | 14 |
| Unclear | 2 | 9 |
| Total | 22 | 100 |
| Imputation method | ||
| Last observation carried forward | 14 | 65 |
| Mixed-effects models | 1 | 4 |
| Other | 1 | 4 |
| Unclear | 2 | 9 |
| No | 3 | 14 |
| Not applicable | 1 | 4 |
| Total | 22 | 100 |
Chapter 5 Network meta-analysis results (adults)
Clinical effectiveness: symptom reduction in the Yale–Brown Obsessive–Compulsive Scale
Description of the data set
Table 16 presents the raw data used for the YBOCS analysis in the adult subset of the data (a complete copy of the full data extraction is available in Appendix 4). Of the 64 studies eligible for inclusion in the NMA, 9 were excluded because they had not used the YBOCS scale. 156,165,168,169,186,194,205,208,210 This decision was made in light of the well-documented methodological and interpretational difficulties associated with the standardised MD. 142 The excluded studies are summarised here for completeness: these studies involved a total of 288 randomised patients (4% of the total randomised patients in the adult subset) and four clomipramine arms, three BT arms, three CT arms, two fluvoxamine arms, one amitriptyline arm, one imipramine arm and three placebo arms. One additional study was excluded because it was not part of the connected network. 179 Therefore, 54 studies were included in this analysis (see Table 16).
Table 17 presents summary data per type of intervention for the studies included in the NMA (number of arms and number of randomised patients per intervention).
| Study ID | t[i,1] | y[i,1] | n[i,1] | sd[i,1] | t[i,2] | y[i,2] | n[i,2] | sd[i,2] | t[i,3] | y[i,3] | n[i,3] | sd[i,3] | t[i,4] | y[i,4] | n[i,4] | sd[i,4] | Arms |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Albert et al., 2002155 | 8 | 18.36 | 25 | 7.11 | 9 | 17.3 | 40 | 6.15 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Anderson and Rees, 2007157 | 2 | 23.5 | 14 | 6.4 | 11 | 16.7 | 17 | 6.8 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Andersson et al., 2012158 | 11 | 12.94 | 49 | 6.26 | 17 | 18.88 | 51 | 4.18 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Belloch et al., 2008159 | 10 | 8.31 | 13 | 8.75 | 12 | 6.8 | 16 | 3.55 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Belotto-Silva et al., 2012160 | 3 | 20.29 | 88 | 8.05 | 11 | 19.97 | 70 | 8.48 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Bergeron et al., 2002161 | 3 | –9.7 | 72 | 7.7 | 6 | –9.6 | 76 | 7.9 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Bisserbe et al., 1997162 | 6 | –14.3 | 86 | NA | 9 | –11.71 | 81 | NA | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| CCSG1 1991154 | 1 | 25.11 | 108 | 6.34 | 9 | 16.23 | 102 | 7.37 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| CCSG2 1991154 | 1 | 25.59 | 119 | 5.78 | 9 | 14.7 | 120 | 7.45 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Chouinard et al., 1990163 | 1 | –1.48 | 44 | NA | 6 | –3.79 | 43 | NA | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Cordioli et al., 2003164 | 2 | 23.2 | 24 | 5.5 | 11 | 15.1 | 23 | 7.8 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Cottraux et al., 2001166 | 10 | –12.1 | 30 | 7.8 | 12 | –12.5 | 30 | 8.2 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Denys et al., 2003167 | 5 | –7.8 | 72 | 5.4 | 8 | –7.2 | 73 | 7.5 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Fals-Stewart et al., 1993170 | 10 | –8.1 | 31 | NA | 17 | –1.8 | 32 | NA | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Foa et al., 2005171 | 1 | 22.2 | 26 | 6.4 | 9 | 18.2 | 36 | 7.8 | 10 | 11 | 29 | 7.9 | 15 | 10.5 | 31 | 8.2 | 4 |
| Freeman et al., 1994172 | 4 | –8.6 | 28 | NA | 9 | –7.8 | 19 | NA | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Freeston et al., 1997173 | 2 | 22 | 14 | 6 | 11 | 12.2 | 15 | 9.6 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Goodman et al., 1989176 | 1 | 28 | 21 | 7 | 4 | 19.4 | 21 | 7 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Goodman et al., 1996177 | 1 | –1.71 | 78 | 4.88 | 4 | –3.95 | 78 | 6.28 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Greist et al., 1995126 | 1 | –3.41 | 84 | 6.19 | 6 | –5.57 | 240 | 6.19 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Greist et al., 2002178 | 10 | 17.6 | 55 | 6.2 | 17 | 24.1 | 66 | 6.7 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| GlaxoSmithKline, 2005174 | 1 | –4.61 | 75 | 7.53 | 5 | –5.61 | 79 | 7.47 | 9 | –7.73 | 78 | 7.42 | NA | NA | NA | NA | 3 |
| GlaxoSmithKline, 2005175 | 5 | –14.26 | 72 | 6.33 | 9 | –13.19 | 69 | 6.48 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Hollander et al., 2003180 | 1 | –5.6 | 120 | 7.67 | 4 | –8.5 | 117 | 7.57 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Hollander et al., 2003181 | 1 | –3.33 | 89 | NA | 5 | –4.14 | 88 | NA | 5 | –6.35 | 86 | NA | 5 | –7.34 | 85 | NA | 4 |
| Jaurrieta et al., 2008182 | 2 | 24.6 | 19 | 8.9 | 11 | 17.8 | 19 | 8.4 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Jenike et al., 1990183 | 1 | 22.3 | 9 | 7.8 | 6 | 20.6 | 10 | 9.2 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Jenike et al., 1990184 | 1 | 21.8 | 20 | 7.6 | 4 | 18.8 | 18 | 4 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Jenike et al., 1997185 | 1 | 18.7 | 18 | 6.1 | 3 | 16.2 | 19 | 6.3 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Kamijima et al., 2004187 | 1 | 20.3 | 94 | 7.38 | 5 | 15.8 | 94 | 8.09 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Khodarahimi, 2009188 | 2 | 36.45 | 20 | 2.24 | 10 | 5.58 | 20 | 2.39 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Kobak et al., 2005189 | 1 | 19.87 | 30 | 7.46 | 13 | 19.75 | 30 | 7.46 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Koran et al., 1996190 | 4 | 17.8 | 34 | 7.7 | 9 | 17 | 39 | 8.55 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Kronig et al., 1999191 | 1 | –4.14 | 79 | NA | 6 | –8.5 | 85 | NA | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Lindsay et al., 1997192 | 10 | 11 | 9 | 3.81 | 17 | 25.89 | 9 | 5.8 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| López-Ibor et al., 1996193 | 3 | –7.5 | 30 | 9.29 | 9 | –8.9 | 24 | 7.13 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| McLean et al., 2001195 | 12 | 16.1 | 31 | 6.7 | 10 | 13.2 | 32 | 7.2 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Milanfranchi et al., 1997196 | 4 | 18.4 | 13 | 9.2 | 9 | 16.5 | 12 | 11 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Montgomery et al., 1993197 | 1 | –3.7 | 56 | 5.98 | 3 | –5.13 | 52 | 6.41 | 3 | –4.76 | 52 | 6.89 | 3 | –6.07 | 54 | 6.92 | 4 |
| Montgomery et al., 2001198 | 1 | –5.6 | 101 | 6.9 | 7 | –8.4 | 102 | 7.3 | 7 | –8.9 | 98 | 7 | 7 | –10.4 | 100 | 6.9 | 4 |
| Mundo et al., 1997199 | 4 | 16.2 | 10 | 8.9 | 5 | 21.6 | 9 | 7.6 | 7 | 19.8 | 11 | 10.1 | NA | NA | NA | NA | 3 |
| Mundo et al., 2001200 | 4 | –12.2 | 115 | NA | 9 | –12 | 112 | NA | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Nakajima et al., 1996201 | 1 | –1.9 | 33 | 7.2 | 4 | –7.1 | 60 | 7.03 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Nakatani et al., 2005202 | 4 | 20.2 | 10 | 9.4 | 10 | 12.9 | 10 | 4.9 | 17 | 28.4 | 8 | 5.5 | NA | NA | NA | NA | 3 |
| O’Connor et al., 1999203 | 2 | 17.5 | 6 | 4 | 11 | 13.3 | 6 | 8.6 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| O’Connor et al., 2006204 | 1 | 25.4 | 10 | 3.5 | 4 | 24 | 11 | 4.7 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Shareh et al., 2010206 | 4 | 16.66 | 6 | 3.2 | 11 | 7 | 7 | 2.38 | 14 | 8.5 | 6 | 2.42 | NA | NA | NA | NA | 3 |
| Sousa et al., 2006207 | 6 | –7.36 | 25 | NA | 11 | –10.8 | 25 | NA | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Stein et al., 2007124 | 1 | –8.46 | 113 | 8.08 | 5 | –11.67 | 116 | 8.40 | 16 | –11.43 | 112 | 8.25 | 16 | –12.14 | 114 | 8.22 | 4 |
| Tollefson et al., 1994127 | 1 | –0.8 | 89 | 5.66 | 3 | –5.44 | 266 | 7.88 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Van Oppen et al., 1995209 | 10 | 17.9 | 29 | 9 | 12 | 13.4 | 28 | 9.4 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Whittal et al., 2005211 | 10 | 10.41 | 29 | 7.6 | 12 | 10.6 | 30 | 7.1 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Whittal et al., 2010212 | 12 | 6.43 | 37 | 4.77 | 17 | 9.1 | 30 | 6.48 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Zohar and Judge, 1996213 | 1 | –4.2 | 99 | 7.2 | 5 | –6.4 | 201 | 7.1 | 9 | –7 | 99 | 6.8 | NA | NA | NA | NA | 3 |
| Intervention | Number of arms | Number of patients |
|---|---|---|
| Placebo | 23 | 1515 |
| Waitlist | 6 | 97 |
| Fluoxetine | 8 | 633 |
| Fluvoxamine | 13 | 521 |
| Paroxetine | 10 | 902 |
| Sertraline | 7 | 565 |
| Citalopram | 4 | 311 |
| Venlafaxine | 2 | 98 |
| Clomipramine | 13 | 831 |
| BT | 11 | 287 |
| CBT | 9 | 231 |
| CT | 6 | 172 |
| Hypericum | 1 | 30 |
| CBT + fluvoxamine | 1 | 6 |
| BT + clomipramine | 1 | 31 |
| Escitalopram | 2 | 226 |
| Psychological placebo | 6 | 196 |
| Total | 123 | 6652 |
Network meta-analysis: results
Network geometry
Figure 6 shows the network geometry of the YBOCS outcome in the adult subset, and Table 18 presents summary data per type of intervention (number of patients randomised, total number of links with other treatments, number of unique treatments compared). Overall, of the 136 pairwise comparisons that can be made among the 17 treatment conditions, only 37 (27%) were studied directly by head-to-head comparison in 54 studies involving 6652 randomised patients. It should be noted, however, that 24 of these 37 direct comparisons are made in single trials. Each circle (node) represents an intervention and is proportional to the number of participants randomised to each treatment (i.e. the larger the node, the greater the number of participants randomised to each intervention). Placebo (n = 1515), paroxetine (n = 902), clomipramine (n = 831), fluoxetine (n = 633), sertraline (n = 565), fluvoxamine (n = 521), citalopram (n = 311), BT (n = 287), CBT (n = 231), escitalopram (n = 226), psychological placebo (n = 196), CT (n = 172), venlafaxine (n = 98) and waitlist (n = 97) had a sample approximately ≥ 100 (Table 18). Lines represent the available direct evidence and are proportional to the number of trials making a randomised comparison of each pair of treatments. Figure 6 includes 79 randomised pairwise comparisons and the most common comparisons are those between placebo versus paroxetine (n = 7), placebo versus fluvoxamine (n = 6), placebo versus fluoxetine, placebo versus clomipramine, CBT versus waitlist and BT versus psychological placebo (n = 5 each), placebo versus sertraline and fluvoxamine versus clomipramine (n = 4 each). Nodes with the most connections (links) in the network (see Table 24) are drug placebo (n = 35 links with 10 different interventions), clomipramine (n = 17 links with eight different interventions), fluvoxamine (n = 16 links with seven different interventions), paroxetine (n = 15 links with six different interventions), BT (n = 14 links with seven different interventions), CBT (n = 9 links with six different interventions), fluoxetine (n = 8 links with four different interventions), sertraline (n = 7 links with four different interventions), psychological placebo (n = 6 links with four different interventions), waitlist (n = 6 links with two different interventions), citalopram (n = 5 links with two different interventions) and CT (n = 5 links with two different interventions).
FIGURE 6.
Network diagram for YBOCS analysis representing individual treatments (adult subset). BTCLO, BT + clomipramine; CBTFLV, CBT + fluvoxamine; CIT, citalopram; CLO, clomipramine; ESCIT, escitalopram; FLV, fluvoxamine; FLX, fluoxetine; HYP, hypericum; PAR, paroxetine; PL, placebo; PSYPL, psychological placebo; SER, sertraline; VEN, venlafaxine; WL, waitlist. Reproduced from Skapinakis P, Caldwell DM, Hollingworth W, Bryden P, Fineberg N, Salkovskis P, et al. Pharmacological and psychotherapeutic interventions for management of obsessive-compulsive disorder in adults: a systematic review and network meta-analysis [published online ahead of print June 15 2016]. Lancet Psychiatry 2016. © Skapinakis et al. Open Access article distributed under the terms of CC BY. 214
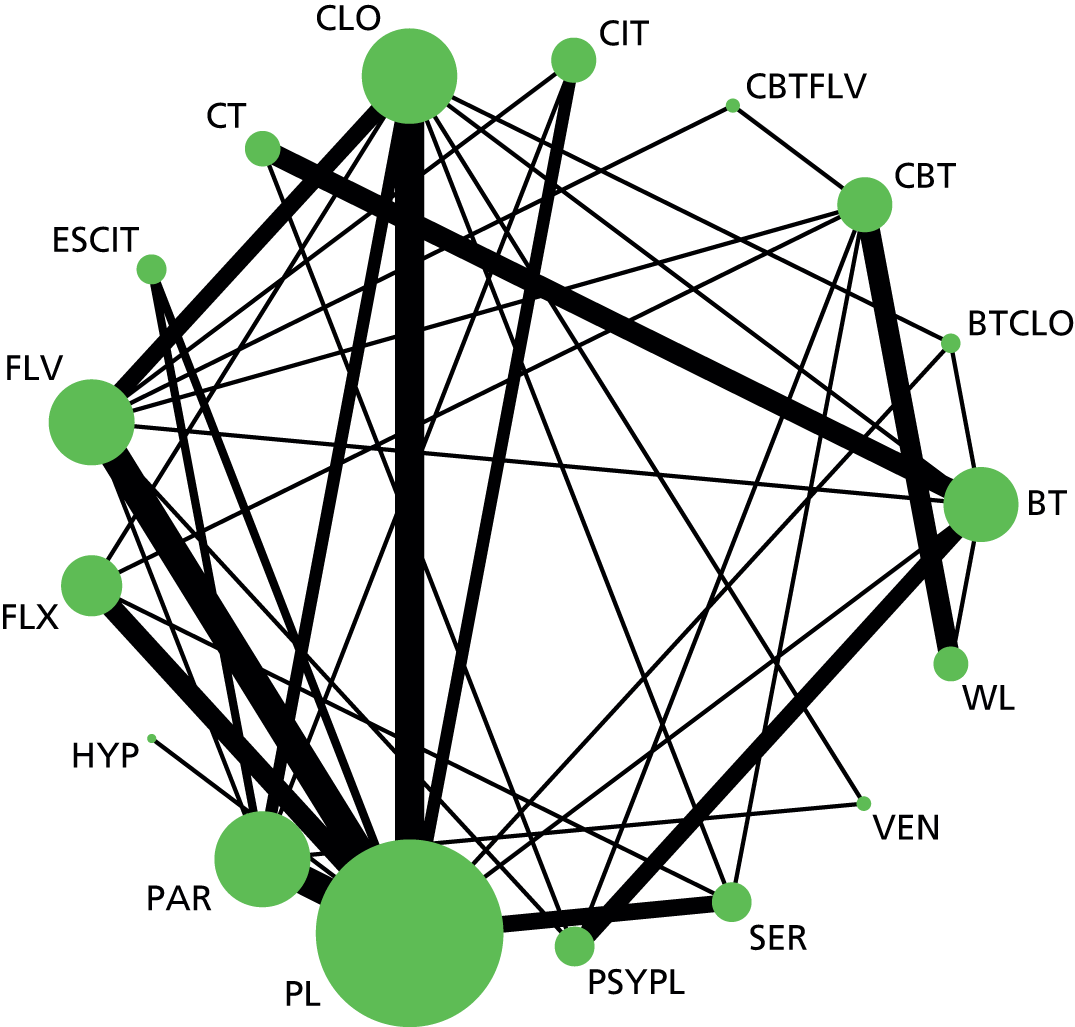
| Intervention | Number of patients randomised | Number of pairwise comparisons (links) | Number of unique treatment comparisons |
|---|---|---|---|
| Placebo | 1515 | 35 | 10 |
| Clomipramine | 831 | 17 | 8 |
| Fluvoxamine | 521 | 16 | 7 |
| Paroxetine | 902 | 15 | 6 |
| BT | 287 | 14 | 7 |
| CBT | 231 | 9 | 6 |
| Fluoxetine | 633 | 8 | 4 |
| Sertraline | 565 | 7 | 4 |
| Psychological placebo | 196 | 7 | 4 |
| Waitlist | 97 | 6 | 2 |
| Citalopram | 311 | 5 | 3 |
| CT | 172 | 5 | 2 |
| Escitalopram | 226 | 4 | 2 |
| Venlafaxine | 98 | 2 | 2 |
| CBT + fluvoxamine | 6 | 2 | 2 |
| BT + clomipramine | 31 | 2 | 3 |
| Hypericum | 30 | 1 | 1 |
Consistency of evidence
We examined model fit using the posterior mean of the residual deviance, the degree of between-study heterogeneity and the DIC. We compared a model assuming consistency of treatment effects with a model assuming independent treatment effects. Table 19 presents the results of this comparison for the adult population.
| Model | Number of data points | Residual deviance (posterior mean) | SD, posterior median (95% CrI) | DIC |
|---|---|---|---|---|
| Random-effects consistency | 107a | 104.6a | 3.10 (2.46 to 3.95) | 480.8 |
| Random-effects inconsistency | 107a | 105.8a | 1.75 (1.18 to 2.53) | 479.1 |
The posterior mean of the residual deviance was 104.6 in the NMA, assuming consistency, compared with 107 data points (equivalent to the number of trial arms/data observations), suggesting adequate model fit. The posterior mean residual deviance from the independent treatment-effects model was 105.8. In addition, figures for the DIC are similar in both models (differences of < 3 or 5 are not considered important145), suggesting that the model assuming consistency has a similar fit to the model assuming independent treatment effects. However, we note a considerable reduction in heterogeneity when we relax the consistency assumption – the upper bound of the 95% CrI for the posterior median SD for the independent effects model (upper credible limit 2.53) only just overlaps the lower bound of the 95% CrI for the consistency model (lower credible limit 2.46). We further explore this heterogeneity in subgroup and sensitivity analyses. As a further informal check, we note that the results of the NMA and the results of the pairwise comparisons (see Table 20) are in the same direction, with no evidence that the NMA effect estimate falls outside the 95% CrIs from the pairwise analysis. Overall, we conclude that there is no evidence for inconsistency in this network of trials, although heterogeneity may be moderate to high.
Data synthesis
The results of the NMA are presented in Table 20. We present the mean and 95% CrIs for the MD in YBOCS scores. We present both the direct, head-to-head and pairwise comparisons (as estimated from the independent effects model) and the results of the NMA (consistency model). All reported results for the NMA are at the class level, with the exception of the results for individual SSRIs, which are at the treatment level. Note that for treatments that did not form a class with multiple treatments (e.g. venlafaxine, clomipramine), the effect estimates from either the class or treatment level will be identical. For simplicity, we present only the MDs and 95% CrIs for all interventions compared with the reference intervention (drug placebo). A detailed table with all possible comparisons (both for the direct and NMA) is given in Appendix 8.
| Intervention | Posterior distribution of the treatment effect (mean YBOCS difference) | Posterior treatment rank, median (95% CrI) | |||
|---|---|---|---|---|---|
| Direct | NMA | ||||
| Mean | 95% CrI | Mean | 95% CrI | ||
| Placebo | 15 (14 to 16) | ||||
| Waitlist | NA | NA | 5.62 | 0.91 to 10.26 | 17 (16 to 17) |
| SSRIs (class effect) | –3.49 | –5.12 to –1.81 | |||
| Fluoxetine | –2.66 | –4.72 to –0.54 | –3.46 | –5.27 to –1.58 | 11 (6 to 14) |
| Fluvoxamine | –3.58 | –5.51 to –1.70 | –3.60 | –5.29 to –1.95 | 10 (6 to 14) |
| Paroxetine | –2.84 | –4.48 to –1.17 | –3.42 | –5.10 to –1.61 | 11 (6 to 14) |
| Sertraline | –2.85 | –5.18 to –0.50 | –3.50 | –5.30 to –1.63 | 10 (6 to 14) |
| Citalopram | –3.65 | –6.25 to –1.06 | –3.49 | –5.62 to –1.31 | 10 (5 to 14) |
| Escitalopram | –3.28 | –6.38 to –0.20 | –3.48 | –5.61 to –1.23 | 10 (5 to 14) |
| Venlafaxine | NA | NA | –3.22 | –8.26 to 1.88 | 12 (4 to 16) |
| Clomipramine | –6.28 | –8.15 to –4.34 | –4.72 | –6.85 to –2.60 | 7 (4 to 13) |
| BT | –11.76 | –16.87 to –6.62 | –14.48 | –18.61 to –10.23 | 1 (1 to 3) |
| CBT | NA | NA | –5.37 | –9.10 to –1.63 | 6 (4 to 14) |
| CT | NA | NA | –13.36 | –18.40 to –8.21 | 2 (1 to 4) |
| Hypericum | –0.08 | –5.30 to 5.11 | –0.15 | –7.46 to 7.12 | 15 (4 to 17) |
| CBT + fluvoxamine | NA | NA | –7.50 | –13.89 to –1.17 | 4 (2 to 14) |
| BT + clomipramine | –12.25 | –17.29 to –7.09 | –12.97 | –19.18 to –6.74 | 3 (1 to 4) |
| Psychological placebo | NA | NA | –4.15 | –8.65 to 0.49 | 8 (4 to 15) |
Waitlist was the only group that showed a statistically significant worse effect than drug placebo. All active interventions, apart from venlafaxine and hypericum, had a greater effect than drug placebo on OCD symptom reduction (as measured by the total YBOCS scores). Venlafaxine showed a similar non-significant trend, whereas the effect of hypericum was indistinguishable from that of placebo.
Regarding the pharmacological interventions, SSRIs as a class had greater effects than drug placebo (class effect MD –3.49, 95% CrI –5.12 to –1.81). Regarding the individual effects of SSRIs, they were very similar with small differences between them. However, this was not unexpected because the grouping of treatments into a ‘class’ will have the effect of drawing individual treatment effects towards the class mean. All remaining treatments were analysed as individual treatments (within the class-level model). The relative effect of clomipramine was also greater than drug placebo (MD –4.72, 95% CrI –6.85 to –2.60). There was a trend for clomipramine to have a greater effect than SSRIs, but the 95% CrI included the null value (MD –1.23, 95% CrI –3.41 to 0.94). Venlafaxine showed a trend for a greater effect than drug placebo, but the 95% CrI also included the null value (MD –3.21, 95% CrI –8.26 to 1.88). It should be noted, however, that this result is based on two trials without direct comparison to placebo and a total number of 98 randomised patients. Therefore, this result should be interpreted with caution.
Regarding psychological interventions, all active psychotherapies had greater effects than drug placebo, with BT and CT having the largest effects, with small differences between them (MD –1.12, 95% CrI –1.95 to 4.19). Regarding the comparison between psychological interventions and psychological placebo, both BT and CT had greater effects (MD –10.33, 95% CrI –13.38 to –7.29 and MD –9.21, 95% CrI –13.1 to –5.34, respectively) but the effect of CBT was not significantly different from psychological placebo (MD –1.22, 95% CrI –5.54 to 3.03). In addition, both BT and CT had greater effects than CBT (MD –9.11, 95% CrI –13.18 to –4.97 and MD –7.99, 95% CrI –12.97 to –3.01, respectively). It should be noted, however, that CBT has not been compared directly with any of the psychological interventions and CT has been compared directly with BT only.
Regarding the comparison between psychological and pharmacological interventions, both BT and CT had greater effects than SSRIs as a class (MD –10.99, 95% CrI –15.14 to –6.75 for the comparison between BT and SSRIs; class effect MD –9.87, 95% CrI –14.91 to –4.74 for the comparison between CT and SSRIs). The difference with CBT was smaller and the 95% CrI included the null value (MD –1.88, 95% CrI –5.52 to 1.76) for the comparison between CBT and SSRIs. It should be noted, however, that of the three types of psychotherapy, CBT has been directly compared with SSRIs more extensively, whereas for CT there is no such direct comparison.
Similar results were observed for the comparison between different types of psychotherapy and clomipramine (MD –9.76, 95% CrI –14.02 to –5.40 for the comparison between BT and clomipramine; MD –8.63, 95% CrI –13.79 to –3.38 for the comparison between CT and clomipramine; MD –0.65, 95% CrI –4.60 to 3.29 for the comparison between CBT and clomipramine).
Combinations of medications and psychotherapy show large effects compared with placebo, with small differences between the effects of psychotherapy as monotherapy. It should be noted, however, that these results are based on a very limited number of patients and/or comparisons, especially for the combination of CBT with fluvoxamine. We recommend extreme caution in the interpretation of these results.
Table 20 also presents the median posterior treatment ranks with 95% CrIs. BT and CT were the most highly ranked treatments, followed by combinations of drug and psychotherapy, CBT and clomipramine.
Sensitivity analyses: outcome 1 – YBOCS (adult subset)
Low overall attrition and no evidence of imbalanced attrition
For this analysis, we excluded 21 studies in the adult subset for which overall levels of attrition were > 25% or differential attrition was > 15%. The 33 studies included124,127,154,157–159,163,164,166,167,170,175,178,181–185,187,192,193,196,198–200,202,203,206,207,209,212 and the raw data used are presented in Appendix 9. Overall, 15 interventions (SSRIs were analysed individually and within a single class) were included and the total number of randomised patients was 3804 (57% of the patients originally used in our full analysis). MDs and 95% CrIs compared with placebo are presented in Table 21.
| Intervention | Posterior distribution of the treatment effect (mean YBOCS difference) | Posterior treatment rank, median (95% CrI) | |
|---|---|---|---|
| Mean | 95% CrI | ||
| Placebo | Reference | Reference | 15 (13 to 15) |
| Waitlist | –3.32 | –8.98 to 2.38 | 12 (5 to 15) |
| SSRIs (class effect) | –4.09 | –6.07 to –2.06 | |
| Fluoxetine | –4.10 | –6.31 to –1.84 | 10 (6 to 14) |
| Fluvoxamine | –4.26 | –6.64 to –2.00 | 9 (6 to 13) |
| Paroxetine | –4.10 | –6.03 to –2.09 | 10 (6 to 13) |
| Sertraline | –4.05 | –6.41 to –1.62 | 10 (6 to 14) |
| Citalopram | –4.01 | –6.25 to –1.63 | 10 (6 to 14) |
| Escitalopram | –4.03 | –6.30 to –1.61 | 10 (6 to 14) |
| Venlafaxine | –4.32 | –8.72 to 0.12 | 9 (3 to 14) |
| Clomipramine | –6.42 | –8.93 to –3.85 | 5 (3 to 10) |
| BT | –11.04 | –16.84 to –5.19 | 2 (1 to 5) |
| CBT | –10.13 | –14.52 to –5.69 | 3 (1 to 5) |
| CT | –10.63 | –17.08 to –4.16 | 2 (1 to 7) |
| CBT + fluvoxamine | –10.31 | –16.14 to –4.52 | 3 (1 to 7) |
| Psychological placebo | –2.85 | –8.33 to 2.77 | 13 (5 to 15) |
Compared with the results of the full data (see Table 20), there is a trend for a larger effect for SSRIs, clomipramine and CBT and a trend for a smaller effect for BT and CT. CBT (either as a monotherapy or in combination with fluvoxamine) has an effect that is very similar to the other psychological therapies. Clomipramine showed a non-statistically significant trend for superiority over SSRIs (MD –2.33, 95% CrI –4.94 to 0.29). All comparisons between clomipramine and psychological therapies had 95% CrIs that crossed zero (e.g. for the comparison between BT and clomipramine: MD –4.62, 95% CrI –4.63 to 1.46). However, the statistical power of these comparisons may be compromised as a result of the smaller number of studies/randomised patients included.
Low risk of bias in the domain: incomplete outcome assessment
Thirty-four studies from the adult subset were judged to be of ‘low risk’ in this domain (see Table 12) and were included in the analysis. The studies included and the raw data used are presented in Appendix 9. Overall, 15 interventions were included and the total number of randomised patients was 5074 (76% of the patients originally used in our full analysis). MDs and 95% CrIs relative to placebo are presented in Table 22.
| Intervention | Posterior distribution of the treatment effect (mean YBOCS difference) | Posterior treatment rank, median (95% CrI) | |
|---|---|---|---|
| Mean | 95% CrI | ||
| Placebo | Reference | Reference | 13 (12 to 15) |
| Waitlist | 2.06 | –1.51 to 5.61 | 15 (12 to 15) |
| SSRIs (class effect) | –3.32 | –4.25 to –2.46 | |
| Fluoxetine | –3.37 | –4.37 to –2.43 | 7 (4 to 11) |
| Fluvoxamine | –3.44 | –4.48 to –2.53 | 7 (4 to 11) |
| Paroxetine | –3.04 | –3.92 to –1.99 | 9 (5 to 12) |
| Sertraline | –3.49 | –4.66 to –2.50 | 6 (4 to 11) |
| Citalopram | –3.37 | –4.58 to –2.24 | 7 (4 to 11) |
| Escitalopram | –3.29 | –4.45 to –2.07 | 7 (4 to 11) |
| Venlafaxine | –2.46 | –5.49 to 0.57 | 11 (3 to 14) |
| Clomipramine | –3.16 | –4.39 to –1.95 | 9 (4 to 12) |
| BT | –8.70 | –11.78 to –5.75 | 2 (1 to 3) |
| CBT | –5.76 | –8.23 to –3.31 | 3 (2 to 7) |
| Hypericum | –0.10 | –4.34 to 4.11 | 13 (4 to 15) |
| BT + clomipramine | –10.67 | –14.42 to –6.90 | 1 (1 to 2) |
| Psychological placebo | –0.92 | –4.10 to 2.09 | 12 (4 to 14) |
Compared with the results of the full data (see Table 20), there is a trend for a smaller effect for clomipramine, which is similar to the effect of the SSRIs. However, the combination of clomipramine with BT is now the highest ranked treatment, although the CrIs for ranks suggest that it may have a similar effectiveness to BT as monotherapy. It should be noted that in this analysis all CT studies have been excluded (eight out of nine CT studies have been assessed as being at high risk of incomplete outcome assessment bias, mainly because they had performed a completers analysis).
Low risk of bias in the domain: blinding of the outcome assessor
Seventeen studies that had reported the YBOCS outcome from the adult subset were judged to be at ‘low risk’ in this domain and were included in the analysis. The studies included and the raw data used are presented in Appendix 9. Overall, 15 interventions were included and the total number of randomised patients was 1461 (22% of the patients originally used in our full analysis). MDs and 95% CrI compared with placebo are presented in Table 23.
Compared with the results of the full data (see Table 20), there are small differences and the power of this analysis, owing to the small number of included studies, is low.
| Intervention | Posterior distribution of the treatment effect (mean YBOCS difference) | Posterior treatment rank, median (95% CrI) | |
|---|---|---|---|
| Mean | 95% CrI | ||
| Placebo | Reference | Reference | 13 (11 to 15) |
| Waitlist | 3.23 | –2.16 to 8.44 | 15 (12 to 15) |
| SSRIs (class effect) | –3.30 | –5.59 to –0.65 | |
| Fluoxetine | –3.42 | –6.62 to 0.07 | 8 (4 to 12) |
| Fluvoxamine | –3.85 | –5.99 to –1.95 | 7 (4 to 11) |
| Paroxetine | –3.20 | –5.29 to –0.90 | 9 (5 to 12) |
| Sertraline | –2.71 | –5.65 to 2.03 | 10 (5 to 13) |
| Citalopram | –3.27 | –6.50 to 0.42 | 8 (4 to 13) |
| Escitalopram | –3.36 | –5.38 to –1.21 | 8 (4 to 12) |
| Venlafaxine | –2.73 | –5.97 to 0.47 | 10 (4 to 13) |
| Clomipramine | –4.05 | –7.30 to –0.73 | 6 (4 to 12) |
| BT | –11.79 | –15.17 to –8.28 | 2 (1 to 3) |
| CBT | –4.11 | –7.63 to –0.34 | 5 (4 to 12) |
| CT | –12.23 | –16.66 to –7.80 | 2 (1 to 3) |
| BT + clomipramine | –11.85 | –16.07 to –7.82 | 2 (1 to 3) |
| Psychological placebo | 2.33 | –1.49 to 6.36 | 14 (13 to 15) |
Acceptability (total dropouts)
Description of the data set
Table 24 presents the raw data used for the dropout analysis in the adult subset of the data. From the 64 studies eligible for inclusion in the NMA, 11 were excluded: eight studies either did not report dropout data or did not report dropout data separately for each arm;179,182,187,188,194,201,204,208 and three studies were excluded because there were no dropouts (zero dropouts) in all arms. 183,192,199 Therefore, 53 studies were included in this analysis. 124,126,127,154–178,180,181,184–186,189–191,193,195–198,200,202,203,205–207,209–213
Table 24 also presents raw dropout rates. It can be seen that the range of dropouts was 0–43%, with a median of 18%. Table 25 presents summary dropout rate per type of intervention (minimum, maximum and median of raw dropout rates).
| Study ID | t[i,1], % | r[i,1], % | n[i,1], % | dr[i,1], % | t[i,2], % | r[i,2], % | n[i,2], % | dr[i,2], % | t[i,3], % | r[i,3], % | n[i,3], % | dr[i,3], % | t[i,4], % | r[i,4], % | n[i,4], % | dr[i,4], % |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Albert et al., 2002155 | 8 | 1 | 26 | 4 | 9 | 7 | 47 | 15 | NA | NA | NA | NA | NA | NA | NA | NA |
| Ananth et al., 1981156 | 9 | 1 | 10 | 10 | 13 | 2 | 10 | 20 | NA | NA | NA | NA | NA | NA | NA | NA |
| Anderson and Rees, 2007157 | 2 | 3 | 17 | 18 | 11 | 4 | 21 | 19 | NA | NA | NA | NA | NA | NA | NA | NA |
| Andersson et al., 2012158 | 11 | 2 | 50 | 4 | 18 | 0 | 51 | 0 | NA | NA | NA | NA | NA | NA | NA | NA |
| Belloch et al., 2008159 | 10 | 2 | 15 | 13 | 12 | 2 | 18 | 11 | NA | NA | NA | NA | NA | NA | NA | NA |
| Belotto-Silva et al., 2012160 | 3 | 33 | 88 | 38 | 11 | 18 | 70 | 26 | NA | NA | NA | NA | NA | NA | NA | NA |
| Bergeron et al., 2002161 | 3 | 22 | 73 | 30 | 6 | 22 | 77 | 29 | NA | NA | NA | NA | NA | NA | NA | NA |
| Bisserbe et al., 1997162 | 6 | 23 | 86 | 27 | 9 | 35 | 82 | 43 | NA | NA | NA | NA | NA | NA | NA | NA |
| CCSG1, 1991154 | 1 | 13 | 121 | 11 | 9 | 17 | 118 | 14 | NA | NA | NA | NA | NA | NA | NA | NA |
| CCSG2, 1991154 | 1 | 12 | 139 | 9 | 9 | 14 | 142 | 10 | NA | NA | NA | NA | NA | NA | NA | NA |
| Chouinard et al., 1990163 | 1 | 4 | 44 | 9 | 6 | 6 | 43 | 14 | NA | NA | NA | NA | NA | NA | NA | NA |
| Cordioli et al., 2003164 | 2 | 1 | 24 | 4 | 11 | 1 | 23 | 4 | NA | NA | NA | NA | NA | NA | NA | NA |
| Cottraux et al., 1993165 | 4 | 7 | 20 | 35 | 10 | 5 | 20 | 25 | 14 | 4 | 20 | 20 | NA | NA | NA | NA |
| Cottraux et al., 2001166 | 10 | 3 | 33 | 9 | 12 | 2 | 32 | 6 | NA | NA | NA | NA | NA | NA | NA | NA |
| Denys et al., 2003167 | 5 | 9 | 75 | 12 | 8 | 4 | 75 | 5 | NA | NA | NA | NA | NA | NA | NA | NA |
| Emmelkamp and Beens, 1991168 | 10 | 4 | 15 | 27 | 12 | 5 | 15 | 33 | NA | NA | NA | NA | NA | NA | NA | NA |
| Emmelkamp et al., 1988169 | 10 | 1 | 10 | 10 | 12 | 1 | 10 | 10 | NA | NA | NA | NA | NA | NA | NA | NA |
| Fals-Stewart et al., 1993170 | 10 | 3 | 34 | 9 | 18 | 0 | 32 | 0 | NA | NA | NA | NA | NA | NA | NA | NA |
| Foa et al., 2005171 | 1 | 12 | 32 | 38 | 9 | 20 | 47 | 43 | 10 | 16 | 37 | 43 | 16 | 14 | 33 | 42 |
| Freeman et al., 1994172 | 4 | 6 | 34 | 18 | 9 | 13 | 32 | 41 | NA | NA | NA | NA | NA | NA | NA | NA |
| Freeston et al., 1997173 | 2 | 0 | 14 | 0 | 11 | 3 | 15 | 20 | NA | NA | NA | NA | NA | NA | NA | NA |
| GlaxoSmithKline, 2005174 | 1 | 20 | 77 | 26 | 5 | 28 | 82 | 34 | 9 | 28 | 82 | 34 | NA | NA | NA | NA |
| GlaxoSmithKline, 2005175 | 5 | 1 | 73 | 1 | 9 | 4 | 73 | 5 | NA | NA | NA | NA | NA | NA | NA | NA |
| Goodman et al., 1989176 | 1 | 6 | 23 | 26 | 4 | 2 | 23 | 9 | NA | NA | NA | NA | NA | NA | NA | NA |
| Goodman et al., 1996177 | 1 | 17 | 80 | 21 | 4 | 23 | 80 | 29 | NA | NA | NA | NA | NA | NA | NA | NA |
| Greist et al., 1995126 | 1 | 24 | 84 | 29 | 6 | 65 | 241 | 27 | NA | NA | NA | NA | NA | NA | NA | NA |
| Greist et al., 2002178 | 10 | 14 | 69 | 20 | 18 | 9 | 75 | 12 | NA | NA | NA | NA | NA | NA | NA | NA |
| Hollander et al., 2003180 | 1 | 31 | 126 | 25 | 4 | 43 | 127 | 34 | NA | NA | NA | NA | NA | NA | NA | NA |
| Hollander et al., 2003181 | 1 | 15 | 89 | 17 | 5 | 14 | 88 | 16 | 5 | 20 | 86 | 23 | 5 | 19 | 85 | 22 |
| Jenike et al., 1990184 | 1 | 0 | 20 | 0 | 4 | 2 | 20 | 10 | NA | NA | NA | NA | NA | NA | NA | NA |
| Jenike et al., 1997185 | 1 | 3 | 21 | 14 | 3 | 4 | 23 | 17 | NA | NA | NA | NA | NA | NA | NA | NA |
| Jones and Menzies, 1998186 | 2 | 1 | 11 | 9 | 12 | 1 | 12 | 8 | NA | NA | NA | NA | NA | NA | NA | NA |
| Kobak et al., 2005189 | 1 | 9 | 30 | 30 | 19 | 8 | 30 | 27 | NA | NA | NA | NA | NA | NA | NA | NA |
| Koran et al., 1996190 | 4 | 8 | 37 | 22 | 9 | 15 | 42 | 36 | NA | NA | NA | NA | NA | NA | NA | NA |
| Kronig et al., 1999191 | 1 | 25 | 81 | 31 | 6 | 25 | 86 | 29 | NA | NA | NA | NA | NA | NA | NA | NA |
| López-Ibor et al., 1996193 | 3 | 5 | 30 | 17 | 9 | 3 | 25 | 12 | NA | NA | NA | NA | NA | NA | NA | NA |
| McLean et al., 2001195 | 10 | 12 | 44 | 27 | 12 | 18 | 49 | 37 | NA | NA | NA | NA | NA | NA | NA | NA |
| Milanfranchi et al., 1997196 | 4 | 0 | 13 | 0 | 9 | 1 | 13 | 8 | NA | NA | NA | NA | NA | NA | NA | NA |
| Montgomery et al., 1993197 | 1 | 15 | 57 | 26 | 3 | 14 | 53 | 26 | 3 | 13 | 52 | 25 | 3 | 14 | 55 | 25 |
| Montgomery et al., 2001198 | 1 | 17 | 101 | 17 | 7 | 15 | 100 | 15 | 7 | 15 | 98 | 15 | 7 | 16 | 102 | 16 |
| Mundo et al., 2001200 | 4 | 19 | 115 | 17 | 9 | 26 | 112 | 23 | NA | NA | NA | NA | NA | NA | NA | NA |
| Nakatani et al., 2005202 | 4 | 1 | 11 | 9 | 10 | 1 | 11 | 9 | 18 | 1 | 9 | 11 | NA | NA | NA | NA |
| O’Connor et al., 1999203 | 2 | 0 | 6 | 0 | 11 | 1 | 7 | 14 | NA | NA | NA | NA | NA | NA | NA | NA |
| Perse et al., 1987205 | 1 | 2 | 10 | 20 | 4 | 2 | 10 | 20 | NA | NA | NA | NA | NA | NA | NA | NA |
| Shareh et al., 2010206 | 4 | 1 | 7 | 14 | 11 | 0 | 7 | 0 | 15 | 1 | 7 | 14 | NA | NA | NA | NA |
| Sousa et al., 2007208 | 6 | 3 | 28 | 11 | 11 | 3 | 28 | 11 | NA | NA | NA | NA | NA | NA | NA | NA |
| Stein et al., 2007124 | 1 | 16 | 115 | 14 | 5 | 29 | 119 | 24 | 17 | 24 | 116 | 21 | 17 | 21 | 116 | 18 |
| Tollefson et al., 1994127 | 1 | 13 | 89 | 15 | 3 | 12 | 87 | 14 | 3 | 22 | 89 | 25 | 3 | 22 | 90 | 24 |
| Van Oppen et al., 1995209 | 10 | 7 | 36 | 19 | 12 | 7 | 35 | 20 | NA | NA | NA | NA | NA | NA | NA | NA |
| Volavka et al., 1985210 | 9 | 3 | 11 | 27 | 20 | 4 | 12 | 33 | NA | NA | NA | NA | NA | NA | NA | NA |
| Whittal et al., 2005211 | 10 | 13 | 42 | 31 | 12 | 11 | 41 | 27 | NA | NA | NA | NA | NA | NA | NA | NA |
| Whittal et al., 2010212 | 12 | 3 | 40 | 8 | 18 | 3 | 33 | 9 | NA | NA | NA | NA | NA | NA | NA | NA |
| Zohar and Judge, 1996213 | 1 | 40 | 100 | 40 | 5 | 53 | 205 | 26 | 9 | 36 | 101 | 36 | NA | NA | NA | NA |
| Intervention | Dropout rates (%) | Number of arms | ||
|---|---|---|---|---|
| Minimum | Maximum | Median | ||
| Placebo | 0 | 40 | 21 | 20 |
| Waitlist | 0 | 18 | 4 | 5 |
| Fluoxetine | 14 | 38 | 25 | 10 |
| Fluvoxamine | 0 | 35 | 17 | 12 |
| Paroxetine | 1 | 34 | 23 | 8 |
| Sertraline | 11 | 29 | 27 | 6 |
| Citalopram | 15 | 16 | 15 | 3 |
| Venlafaxine | 4 | 5 | 4.5 | 2 |
| Clomipramine | 5 | 43 | 23 | 15 |
| BT | 9 | 43 | 20 | 12 |
| CBT | 0 | 26 | 12.5 | 8 |
| CT | 6 | 37 | 11 | 9 |
| Amitriptyline | 20 | 20 | NA | 1 |
| BT + fluvoxamine | 20 | 20 | NA | 1 |
| CBT + fluvoxamine | 14 | 14 | NA | 1 |
| BT + clomipramine | 42 | 42 | NA | 1 |
| Escitalopram | 18 | 21 | 19.5 | 2 |
| Psychological placebo | 0 | 12 | 9 | 5 |
| Hypericum | 27 | 27 | NA | 1 |
| Imipramine | 33 | 33 | NA | 1 |
Network meta-analysis: results
Network geometry
Figure 7 shows the network geometry for total dropouts in the adult subset. Overall, of the 190 comparisons that can be made among the 20 treatment conditions, only 38 (20%) were studied directly in 53 studies involving 6743 randomised patients. It should be noted, however, that 24 of the 38 direct comparisons are made in single trials. As before, circles (treatment nodes) represent the interventions used in the network and are proportional to the number of participants randomised to a treatment. Placebo (n = 1439), clomipramine (n = 937), paroxetine (n = 813), fluoxetine (n = 640), sertraline (n = 561), fluvoxamine (n = 497), BT (n = 366), citalopram (n = 300), escitalopram (n = 232), CBT (n = 221), psychological placebo (n = 200) and venlafaxine (n = 101) had a sample size of > 100. Lines (network edges) are proportional to the number of direct randomised comparisons. Figure 7 includes 79 randomised pairwise comparisons and the most common comparisons are those between placebo versus fluoxetine (n = 7) and BT versus CT (n = 7). Nodes with the most connections (links) in the network are drug placebo (n = 33 links), clomipramine (n = 19 links), BT (n = 16 links), fluvoxamine (n = 15 links), paroxetine (n = 11 links), fluoxetine (n = 10 links), CBT (n = 9 links) and CT (n = 9 links).
FIGURE 7.
Network diagram for dropouts representing individual treatments (adult subset). AMI, amitriptyline; BTCLO, BT + clomipramine; BTFLV, BT + fluvoxamine; CBTFLV, CBT + fluvoxamine; CIT, citalopram; CLO, clomipramine; ESCIT, escitalopram; FLV, fluvoxamine; FLX, fluoxetine; HYP, hypericum; IMI, imipramine; PAR, paroxetine; PL, placebo; PSYPL, psychological placebo; SER, sertraline; VEN, venlafaxine; WL, waitlist.
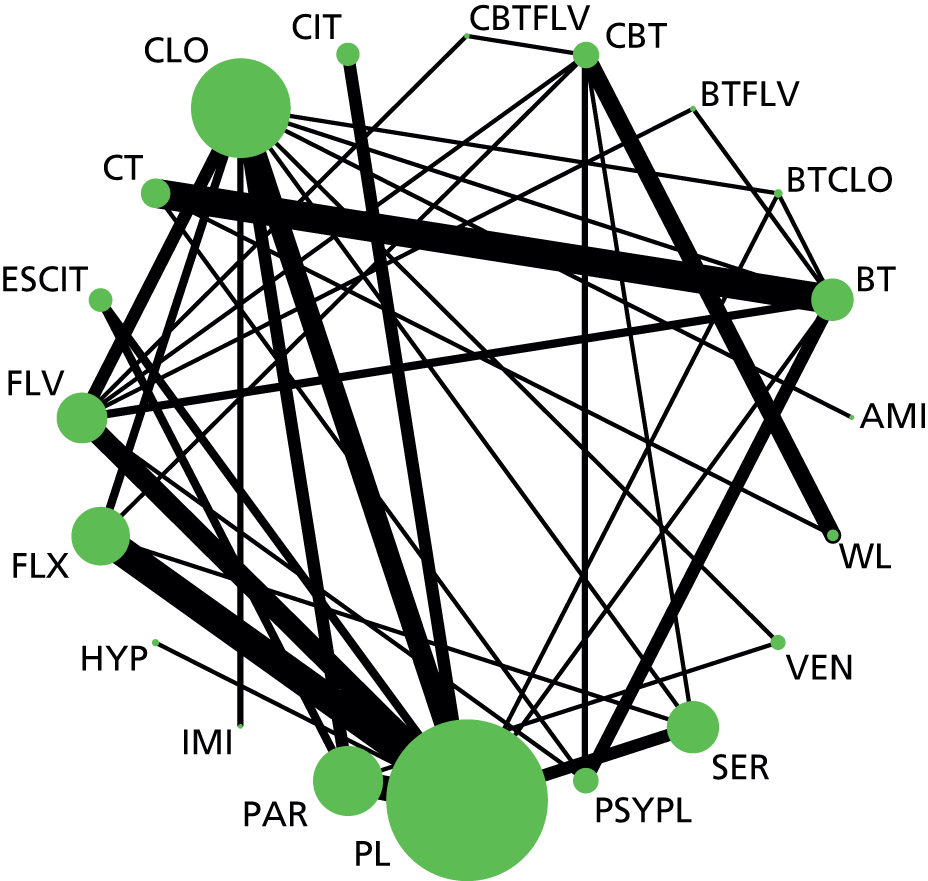
Consistency of evidence
We examined model fit using the posterior mean of the residual deviance, the degree of between-study heterogeneity and the DIC. We compared a model assuming consistency of treatment effects with a model assuming independent treatment effects. For the ‘consistency’ model all SSRIs were analysed as a class and individually. Table 26 presents the results of this comparison for the adult set.
| Model | Number of data points | Residual deviance, posterior mean | SD,a posterior median, (95% CrI) | DIC |
|---|---|---|---|---|
| Random-effects consistency | 123 | 118.2 | 0.13 (0.01 to 0.32) | 610.3 |
| Random-effects independent effect | 123 | 120.3 | 0.12 (0.01 to 0.32) | 626.0 |
The posterior mean of the residual deviance was 118.2 in model assuming consistency compared with the number of data points (n = 123), suggesting adequate model fit. The posterior mean residual deviance from the independent treatment-effects model was 120.3 In addition, the lower value of the DIC for the consistency model suggests that it is preferred over the independent effects model. In addition, the results of the NMA and the results of the pairwise comparisons (see Table 27) are in the same direction, with no evidence that the NMA effect estimate falls outside the 95% CrIs from the pairwise analysis. Overall, there is no evidence for inconsistency.
Data synthesis
The results of the NMA are presented in Table 27. We present posterior median ORs for dropouts relative to drug placebo (reference treatment). We present both the direct head-to-head comparisons from pairwise meta-analysis (from independent effects model) and the results of the NMA from the model assuming consistency. For simplicity, we present only the ORs compared with the drug placebo. A more detailed table with all possible comparisons (both for the direct and NMA) is given in Appendix 8.
| Intervention | Direct | NMA | Posterior treatment rank (median and 95% CrI) | ||
|---|---|---|---|---|---|
| Median OR | 95% CrI | Median OR | 95% CrI | ||
| Placebo | Reference | Reference | Reference | Reference | 9 (5 to 16) |
| Waitlist | NA | NA | 0.40 | 0.10 to 1.50 | 2 (1 to 17) |
| Psychological placebo | NA | NA | 0.52 | 0.19 to 1.45 | 4 (1 to 15) |
| SSRIs (class effect) | 1.08 | 0.85 to 1.36 | |||
| Fluoxetine | 1.25 | 0.79 to 2.03 | 1.12 | 0.88 to 1.54 | 13 (7 to 18) |
| Fluvoxamine | 1.38 | 0.88 to 2.18 | 1.09 | 0.85 to 1.41 | 12 (6 to 17) |
| Paroxetine | 1.08 | 0.78 to 1.52 | 1.09 | 0.86 to 1.38 | 12 (6 to 17) |
| Sertraline | 0.98 | 0.63 to 1.55 | 1.04 | 0.78 to 1.33 | 10 (5 to 16) |
| Citalopram | 0.90 | 0.49 to 1.75 | 1.06 | 0.74 to 1.41 | 11 (5 to 17) |
| Escitalopram | 1.09 | 0.64 to 1.97 | 1.08 | 0.80 to 1.46 | 12 (5 to 17) |
| Venlafaxine | NA | NA | 0.39 | 0.11 to 1.15 | 2 (1 to 13) |
| Clomipramine | 1.25 | 0.88 to 1.76 | 1.52 | 1.16 to 2.01 | 17 (13 to 19) |
| Amitriptyline | NA | NA | 4.51 | 0.30 to 138.6 | 19 (2 to 20) |
| Imipramine | NA | NA | 1.96 | 0.29 to 16.07 | 18 (2 to 20) |
| Hypericum | 0.83 | 0.25 to 2.80 | 0.85 | 0.25 to 2.73 | 7 (1 to 19) |
| BT | 1.27 | 0.52 to 3.08 | 1.04 | 0.52 to 2.08 | 10 (4 to 18) |
| CBT | NA | NA | 0.77 | 0.40 to 1.59 | 6 (2 to 17) |
| CT | NA | NA | 1.01 | 0.43 to 2.30 | 9 (3 to 19) |
| BT + fluvoxamine | NA | NA | 0.61 | 0.13 to 2.35 | 4 (1 to 19) |
| CBT + fluvoxamine | NA | NA | 2.13 | 0.04 to 74.15 | 18 (1 to 20) |
| BT + clomipramine | 1.23 | 0.48 to 3.05 | 1.27 | 0.53 to 2.93 | 15 (4 to 19) |
Clomipramine was the only intervention with a statistically significant higher likelihood of dropout than placebo, with an OR of 1.52 (95% CrI 1.16 to 2.01). Amitriptyline, imipramine and the combination of CBT with fluvoxamine had larger ORs than clomipramine, suggesting increased odds of dropout. However, these results are based on just one trial, the 95% CrIs are wide and include the null value of no difference. Therefore, these results should be interpreted with caution. SSRIs as a class were not more likely than placebo to lead to attrition. Differences with individual SSRIs were very small and insignificant. There was a non-significant trend for venlafaxine to be associated with a lower dropout rate than placebo but this was based on only two trials. All psychological therapies were not more likely than placebo to lead to dropout.
Table 27 also presents the posterior median treatment ranks with 95% CrIs. As before, it is the tricyclics, particularly clomipramine, that are ranked lowest (i.e. they are less tolerable). In general, all psychological therapies delivered as monotherapy are ranked more highly than pharmacological treatments. Combinations of psychological treatments with medication result in lower ranks than psychological monotherapy, but the evidence is based on single trials with small sample sizes. We again suggest caution in the interpretation of these findings.
Sensitivity analyses: outcome 2, dropouts – adult subset
Low overall attrition and no evidence of imbalanced attrition
For this analysis we included 40124,127,154,156–160,163,164,166,167,169–171,175,177,178,180,181,184–186,189,193,195–198,200,202,203,205–207,209–212 and excluded 13 studies. The studies included and the raw data used are presented in Appendix 9. Overall, 18 interventions were included and the total number of randomised patients was 4767 (70.7% of the patients originally used in our full analysis). MDs and 95% CrIs compared with placebo are presented in Table 28. It can be seen that compared with the full data set reported in Table 27, the results are essentially similar, with the tricyclic drugs, in particular clomipramine, being most poorly tolerated.
| Intervention | Posterior distribution of the treatment effect (mean YBOCS difference) | Posterior treatment rank, median (95% CrI) | |
|---|---|---|---|
| Median OR | 95% CrI | ||
| Placebo | Reference | Reference | 8 (4 to 12) |
| Waitlist | 0.36 | 0.09 to 1.43 | 3 (1 to 13) |
| SSRIs (class effect) | 1.28 | 0.94 to 1.73 | |
| Fluoxetine | 1.32 | 0.95 to 1.87 | 12 (7 to 17) |
| Fluvoxamine | 1.31 | 0.98 to 1.76 | 12 (7 to 16) |
| Paroxetine | 1.34 | 0.97 to 1.90 | 13 (7 to 17) |
| Sertraline | 1.28 | 0.80 to 1.97 | 12 (6 to 17) |
| Citalopram | 1.22 | 0.75 to 1.67 | 11 (5 to 16) |
| Escitalopram | 1.27 | 0.88 to 1.79 | 11 (6 to 16) |
| Venlafaxine | 0.52 | 0.10 to 1.84 | 5 (1 to 16) |
| Clomipramine | 1.58 | 1.04 to 2.59 | 15 (8 to 18) |
| BT | 0.44 | 0.05 to 2.77 | 4 (2 to 17) |
| CBT | 0.84 | 0.42 to 1.62 | 7 (3 to 15) |
| CT | 0.45 | 0.06 to 2.70 | 4 (1 to 16) |
| Amitriptyline | 3.94 | 0.23 to 162.7 | 17 (2 to 18) |
| CBT + fluvoxamine | 1.94 | 0.06 to 79.68 | 16 (1 to 18) |
| Psychological placebo | 0.24 | 0.02 to 1.46 | 2 (1 to 11) |
| Hypericum | 0.83 | 0.23 to 2.91 | 7 (1 to 17) |
| Imipramine | 2.05 | 0.27 to 15.90 | 16 (2 to 18) |
Low risk of bias in the domain: incomplete outcome assessment
For this analysis we included 29124,127,157,158,160–164,167,171–174,176–178,180,181,185,189–191,193,197,198,200,207,213 and excluded 24 studies. The studies included and the raw data used are presented in Appendix 9. Overall, 15 interventions were included and the total number of randomised patients was 4868 (72% of the patients originally used in our full analysis). MDs and 95% CrIs compared with placebo are presented in Table 29. It can be seen that compared with the full data set reported in Table 27, the results are essentially similar.
| Intervention | Posterior distribution of the treatment effect (mean YBOCS difference) | Posterior treatment rank, median (95% CrI) | |
|---|---|---|---|
| Median OR | 95% CrI | ||
| Placebo | Reference | Reference | 7 (3 to 12) |
| Waitlist | 0.39 | 0.08 to 1.81 | 2 (1 to 14) |
| SSRIs (class effect) | 1.10 | 0.84 to 1.43 | |
| Fluoxetine | 1.15 | 0.88 to 1.59 | 10 (5 to 14) |
| Fluvoxamine | 1.09 | 0.81 to 1.43 | 9 (4 to 13) |
| Paroxetine | 1.12 | 0.86 to 1.48 | 10 (5 to 14) |
| Sertraline | 1.07 | 0.76 to 1.42 | 8 (4 to 13) |
| Citalopram | 1.08 | 0.72 to 1.49 | 9 (3 to 14) |
| Escitalopram | 1.10 | 0.78 to 1.52 | 9 (4 to 14) |
| Venlafaxine | 0.44 | 0.10 to 1.61 | 2 (1 to 14) |
| Clomipramine | 1.55 | 1.10 to 2.17 | 14 (10 to 15) |
| BT | 1.23 | 0.50 to 2.91 | 12 (3 to 15) |
| CBT | 0.80 | 0.37 to 1.73 | 5 (2 to 14) |
| BT + clomipramine | 1.33 | 0.52 to 3.39 | 13 (3 to 15) |
| Psychological placebo | 0.51 | 0.14 to 1.82 | 3 (1 to 14) |
| Hypericum | 0.84 | 0.25 to 2.90 | 5 (1 to 15) |
Low risk of bias in the domain: blinding of the outcome assessor
For this analysis we included 18124,155,158–160,164,166–169,171,175,184,202,203,205,207,211 and excluded 35 studies. The studies included and the raw data used are presented in Appendix 9. Overall, 14 interventions were included and the total number of randomised patients was 1581 (23.5% of the patients originally used in our full analysis). MDs and 95% CrIs compared with placebo are presented in Table 30. The power of the analysis is compromised, but the results show the same trends with the full analysis.
| Intervention | Posterior distribution of the treatment effect (mean YBOCS difference) | Posterior treatment rank, median (95% CrI) | |
|---|---|---|---|
| Median OR | 95% CrI | ||
| Placebo | Reference | Reference | 6 (2 to 12) |
| Waitlist | 0.45 | 0.01 to 31.84 | 2 (1 to 14) |
| SSRIs (class effect) | 1.39 | 0.46 to 8.44 | |
| Fluoxetine | 1.60 | 0.45 to 47.92 | 11 (4 to 14) |
| Fluvoxamine | 1.11 | 0.36 to 2.71 | 7 (2 to 13) |
| Paroxetine | 1.55 | 0.67 to 3.74 | 10 (4 to 14) |
| Sertraline | 1.38 | 0.31 to 31.95 | 10 (2 to 14) |
| Escitalopram | 1.34 | 0.62 to 3.05 | 9 (3 to 14) |
| Venlafaxine | 0.48 | 0.10 to 1.79 | 3 (1 to 11) |
| Clomipramine | 1.36 | 0.46 to 4.24 | 9 (3 to 14) |
| BT | 1.23 | 0.39 to 3.83 | 8 (3 to 14) |
| CBT | 1.13 | 0.27 to 32.32 | 7 (2 to 14) |
| CT | 1.10 | 0.27 to 4.30 | 7 (2 to 14) |
| BT + clomipramine | 1.24 | 0.36 to 4.26 | 8 (2 to 14) |
| Psychological placebo | 0.31 | 0.01 to 4.51 | 2 (1 to 14) |
Rankograms (both outcomes)
Table 31 presents the probabilities that each treatment is among the best three or worst three for both outcomes (YBOCS/dropouts) – a dropout rate that is among the top three means better tolerability (i.e. fewer dropouts). In Appendix 8 we present complete data for all rank probabilities for both outcomes. Based on these data, we also present rankograms (plots of the probabilities for each treatment taking each possible rank) in Figure 8. These results show that there is a great deal of uncertainty surrounding the overall rankings of the active treatments used to treat OCD in adults. Although we observe that BT has a 50% probability of being the most effective treatment for reducing OCD symptoms, there is a 50% probability that it is not the best treatment, which represents a large degree of uncertainty.
| Outcomea | Treatment | Probability treatment being in: | |
|---|---|---|---|
| Top three | Bottom three | ||
| YBOCS | Placebo | 0.00 | 0.92 |
| Dropout | Placebo | 0.00 | 0.00 |
| YBOCS | Waitlist | 0.00 | 1.00 |
| Dropout | Waitlist | 0.66 | 0.02 |
| YBOCS | Fluoxetine | 0.00 | 0.02 |
| Dropout | Fluoxetine | 0.00 | 0.03 |
| YBOCS | Fluvoxamine | 0.00 | 0.01 |
| Dropout | Fluvoxamine | 0.00 | 0.01 |
| YBOCS | Paroxetine | 0.00 | 0.02 |
| Dropout | Paroxetine | 0.00 | 0.01 |
| YBOCS | Sertraline | 0.00 | 0.02 |
| Dropout | Sertraline | 0.00 | 0.00 |
| YBOCS | Citalopram | 0.00 | 0.02 |
| Dropout | Citalopram | 0.01 | 0.01 |
| YBOCS | Venlafaxine | 0.01 | 0.19 |
| Dropout | Venlafaxine | 0.69 | 0.00 |
| YBOCS | Clomipramine | 0.00 | 0.00 |
| Dropout | Clomipramine | 0.00 | 0.39 |
| YBOCS | BT | 1.00 | 0.00 |
| Dropout | BT | 0.01 | 0.06 |
| YBOCS | CBT | 0.00 | 0.01 |
| Dropout | CBT | 0.12 | 0.02 |
| YBOCS | CT | 0.95 | 0.00 |
| Dropout | CT | 0.03 | 0.08 |
| YBOCS | Hypericum | 0.00 | 0.66 |
| Dropout | Hypericum | 0.21 | 0.13 |
| YBOCS | CBT + fluvoxamine | 0.14 | 0.02 |
| Dropout | CBT + fluvoxamine | 0.20 | 0.56 |
| YBOCS | BT + clomipramine | 0.89 | 0.00 |
| Dropout | BT + clomipramine | 0.02 | 0.24 |
| YBOCS | Escitalopram | 0.00 | 0.02 |
| Dropout | Escitalopram | 0.01 | 0.02 |
| YBOCS | Psychological placebo | 0.00 | 0.09 |
| Dropout | Psychological placebo | 0.50 | 0.00 |
| Dropout | Amitriptyline | 0.06 | 0.76 |
| Dropout | BT + fluvoxamine | 0.41 | 0.06 |
| Dropout | Imipramine | 0.07 | 0.59 |
FIGURE 8.
Rankograms for adults: dropout (black lines); YBOCS (green lines). (a) placebo; (b) waitlist; (c) fluoxetine; (d) fluvoxamine; (e) paroxetine; (f) sertraline; (g) citalopram; (h) venlafaxine; (i) clomipramine; (j) BT; (k) CBT; (l) CT; (m) hypericum; (n) CBT + fluvoxamine; (o) BT + clomipramine; (p) escitalopram; (q) psychological placebo; (r) amitriptyline; (s) BT + fluvoxamine; and (t) imipramine. Reproduced from Skapinakis P, Caldwell DM, Hollingworth W, Bryden P, Fineberg N, Salkovskis P, et al. Pharmacological and psychotherapeutic interventions for management of obsessive-compulsive disorder in adults: a systematic review and network meta-analysis [published online ahead of print June 15 2016]. Lancet Psychiatry 2016. © Skapinakis et al. Open Access article distributed under the terms of CC BY. 214


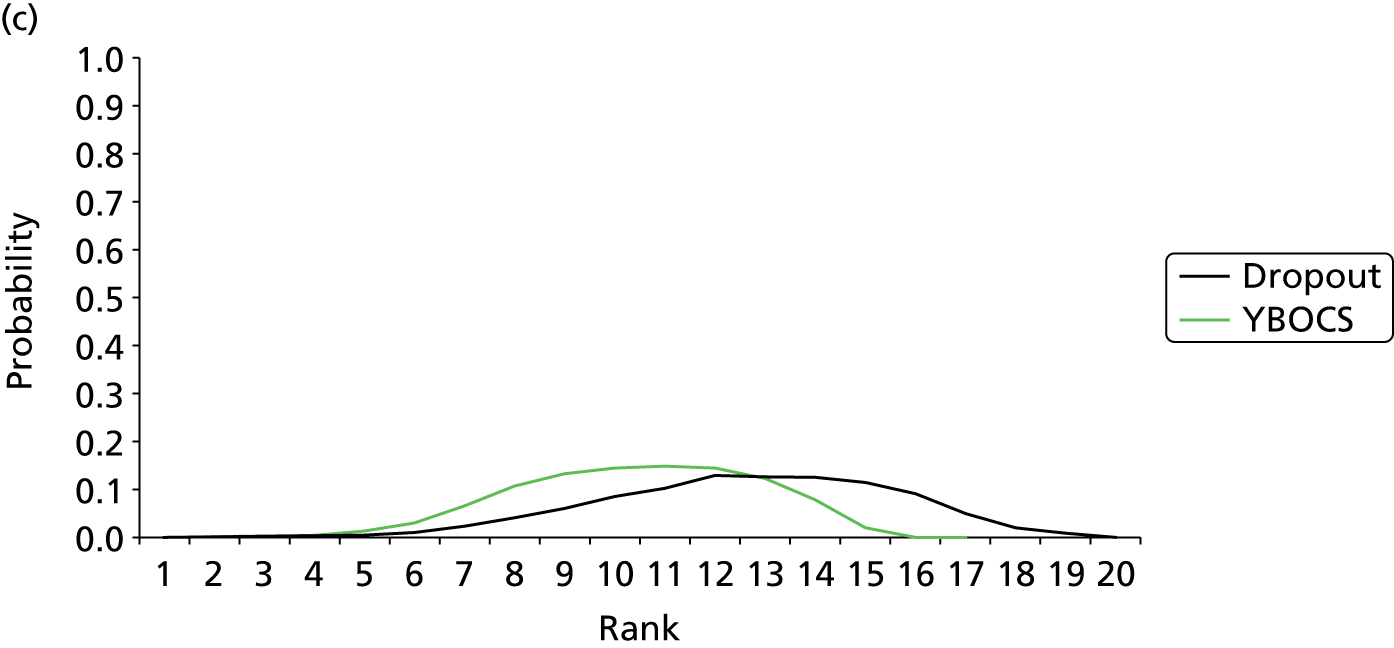



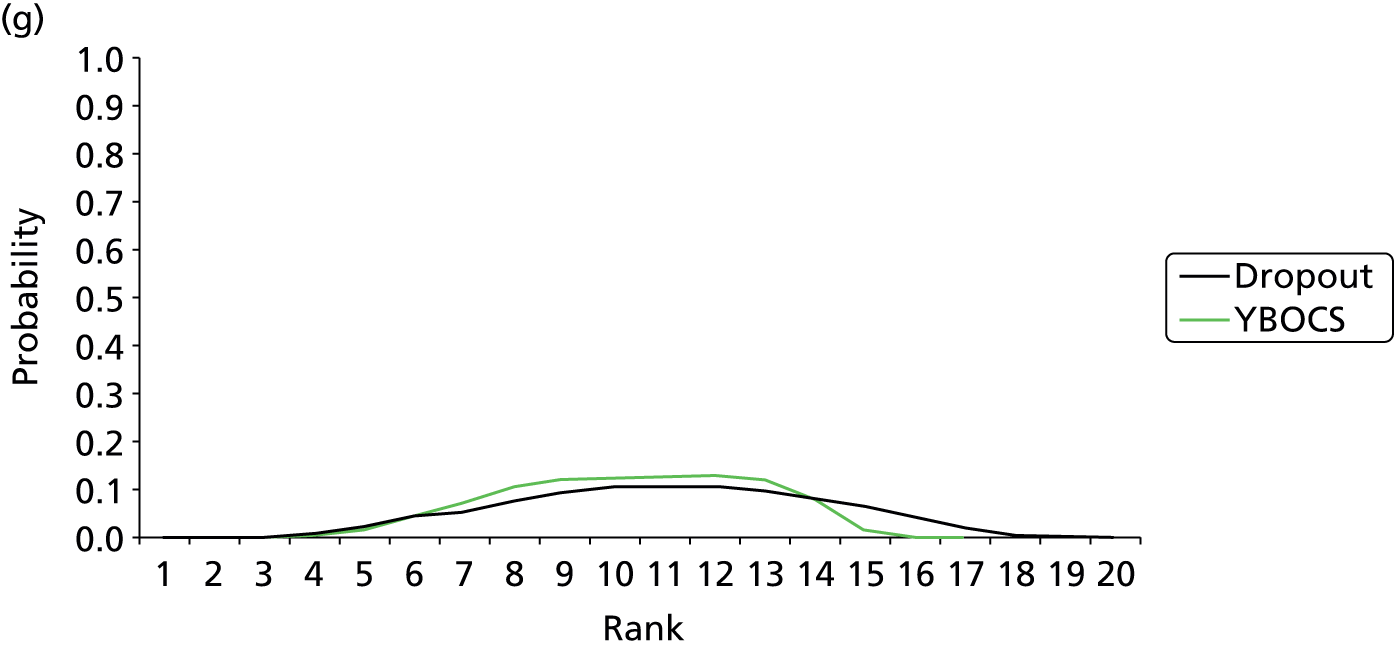



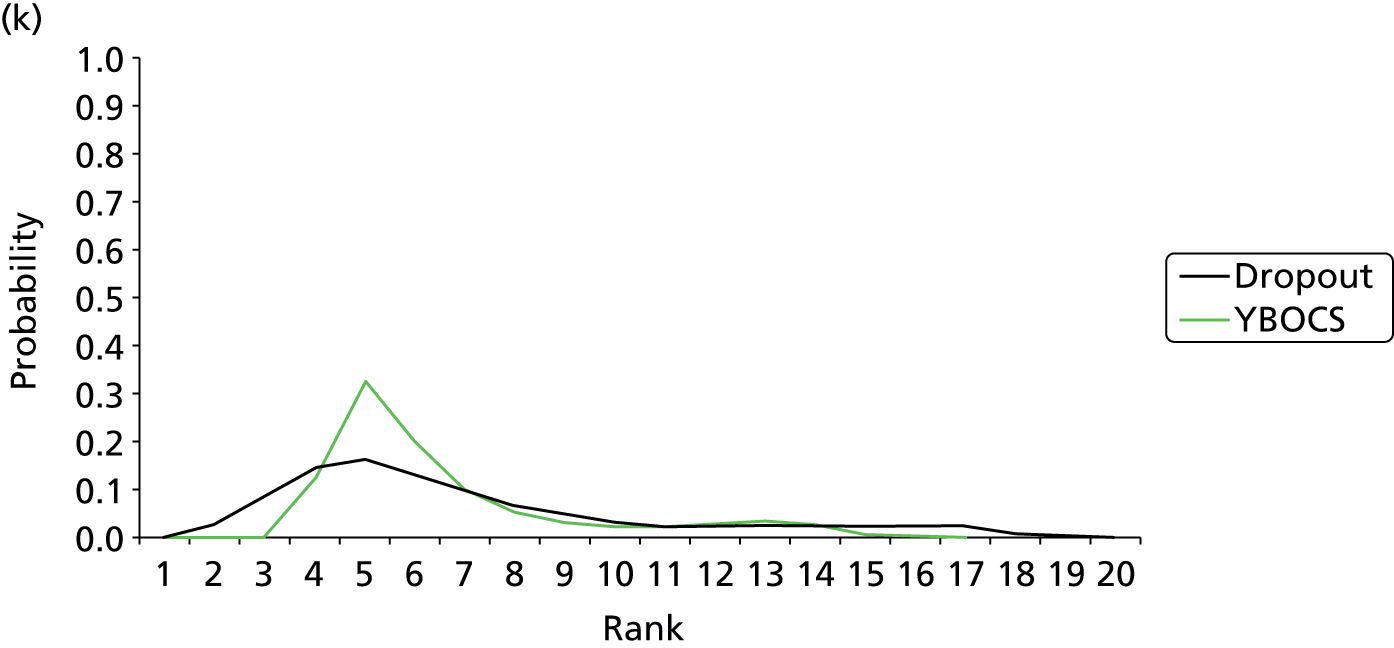
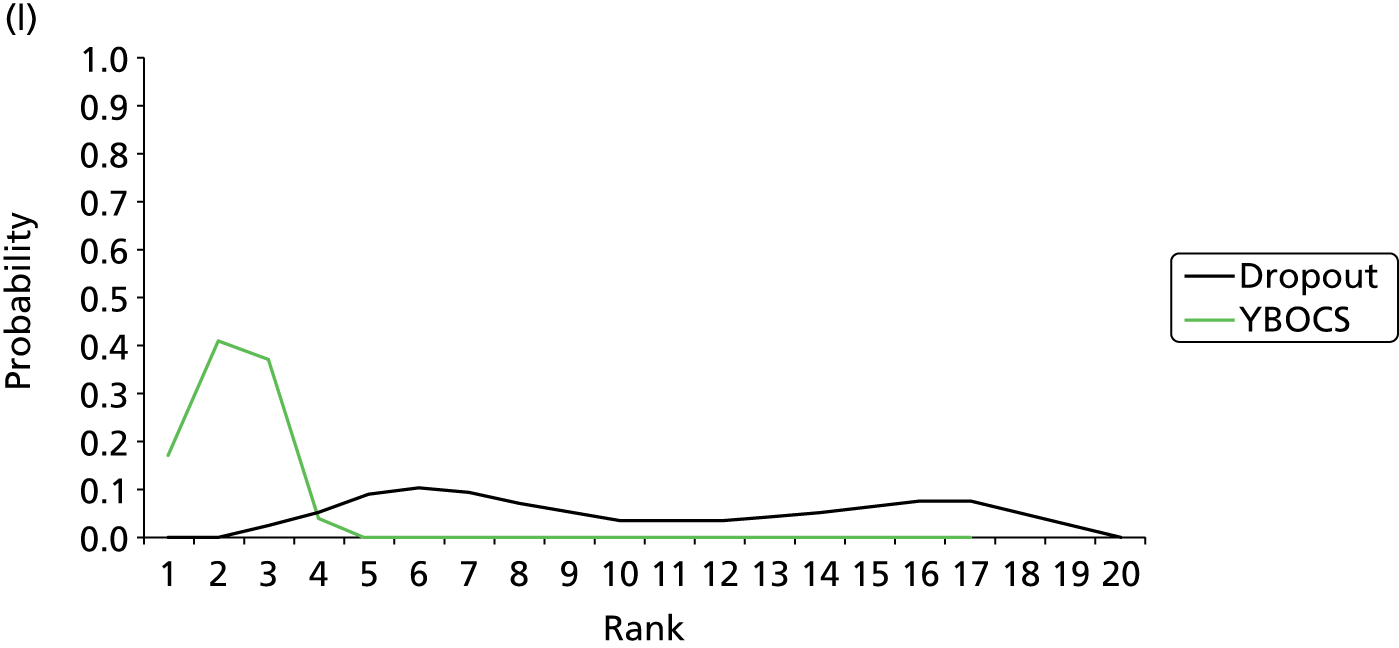
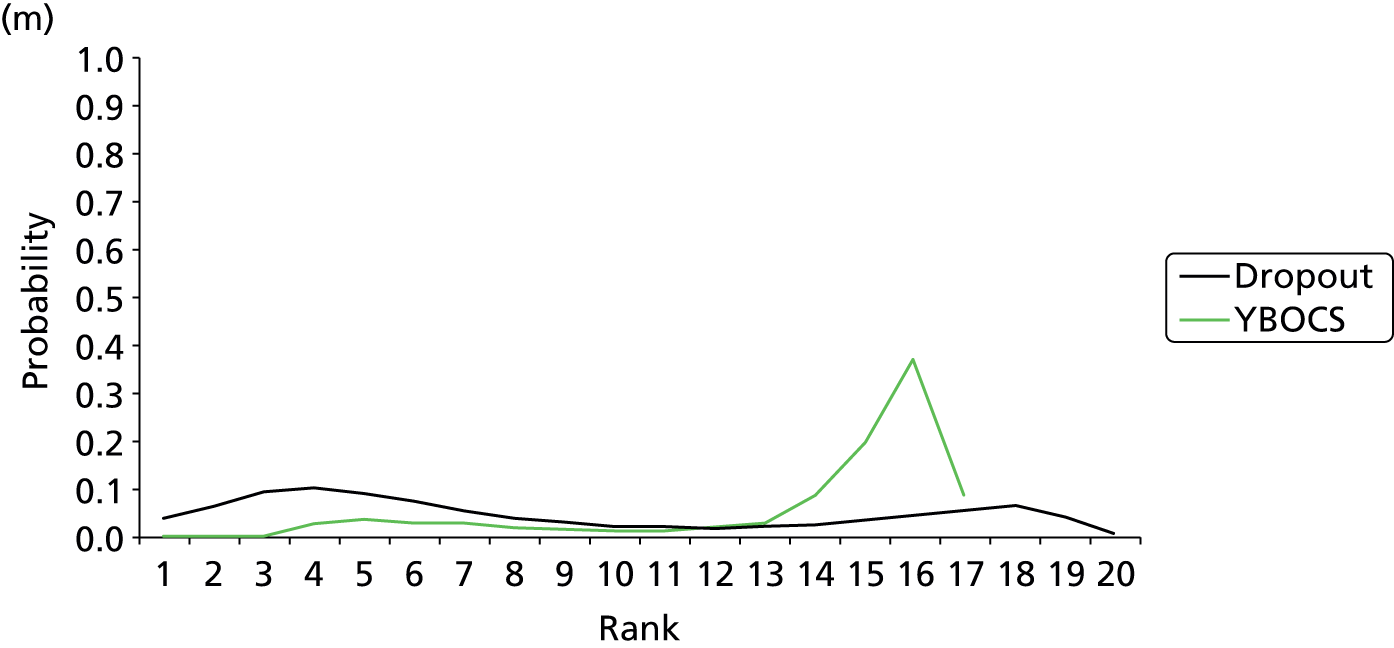

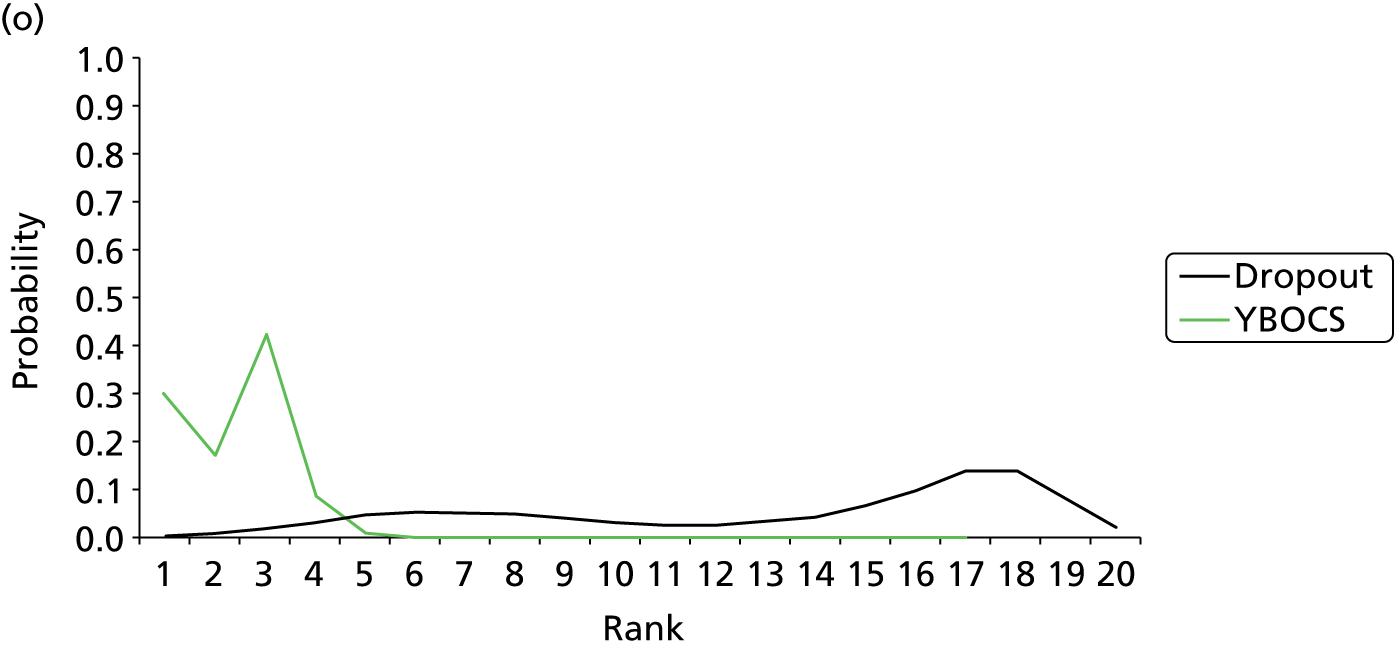
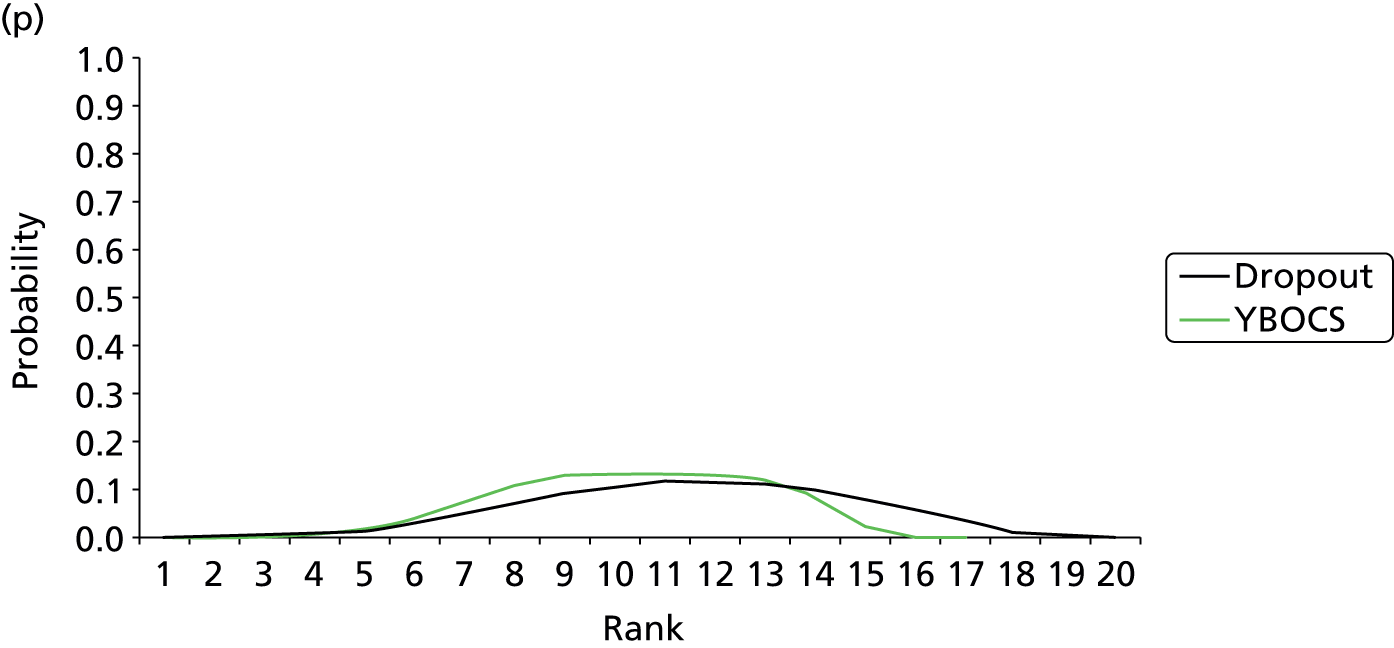

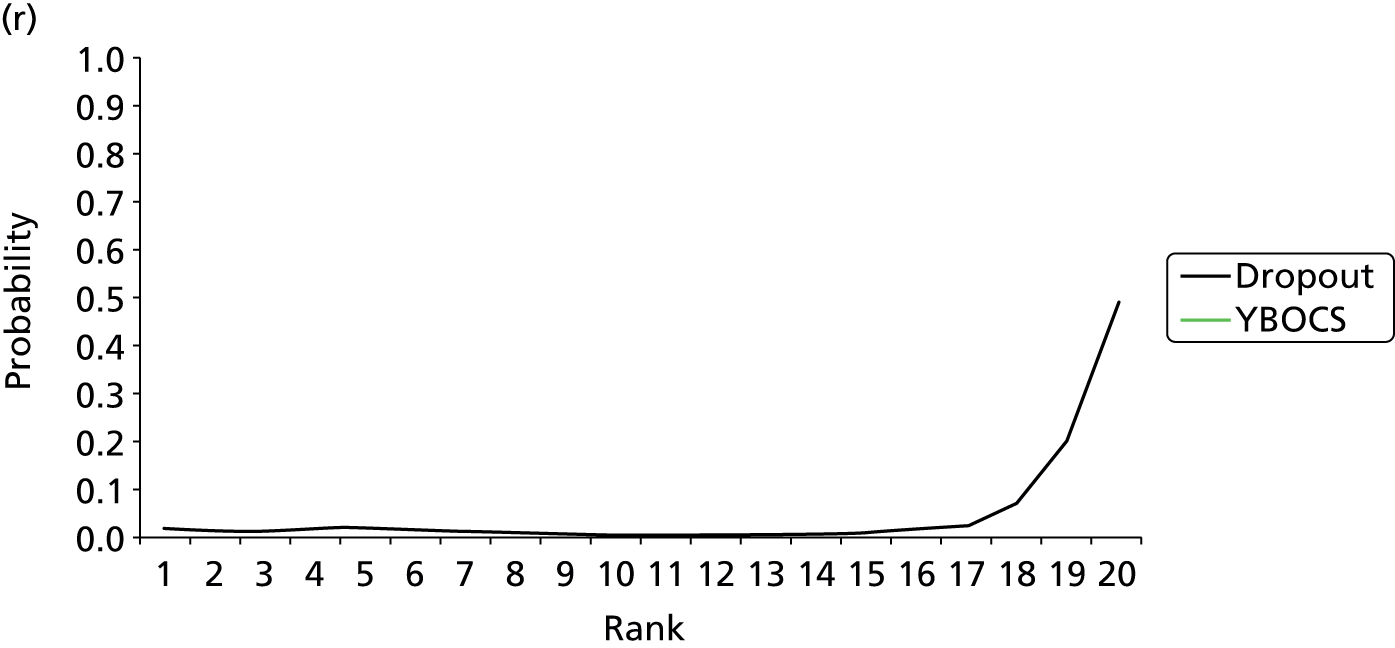
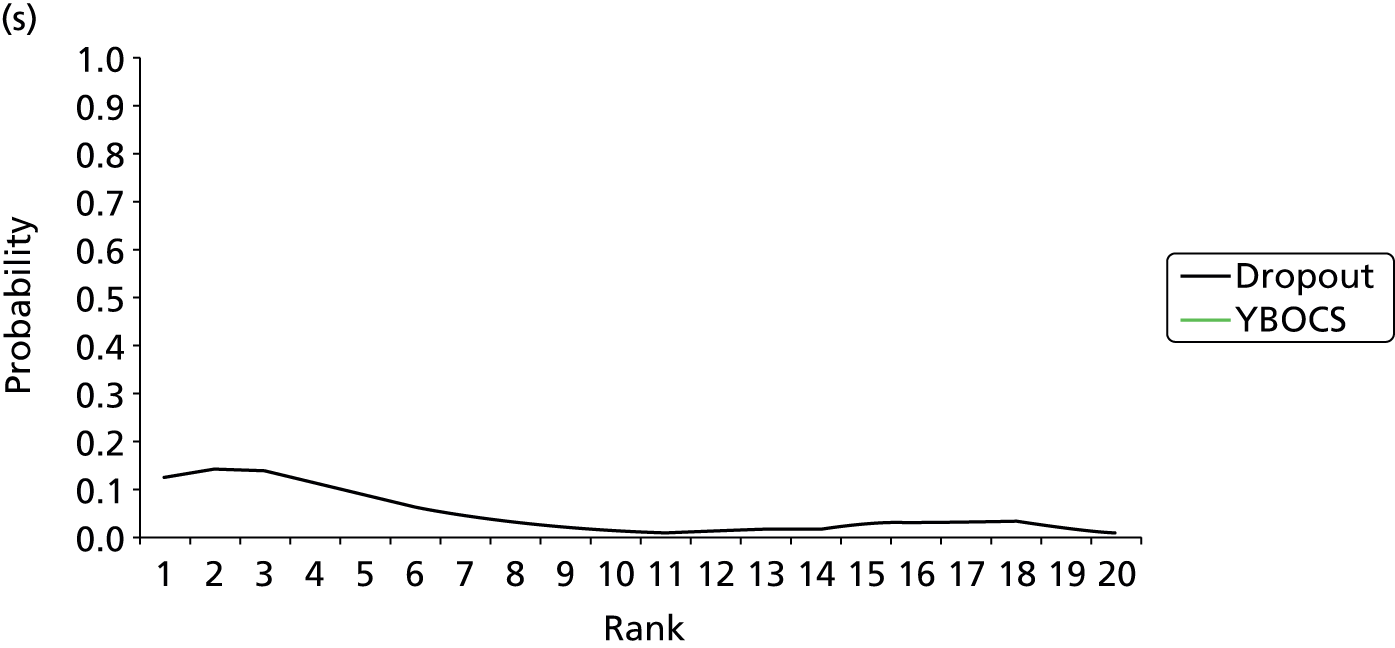

Meta-regression
Table 32 presents the study-level covariates that could potentially influence the treatment effect (effect modification). It can be seen that the meta-regressions do not suggest an effect of adjusting for each covariate and the 95% CrIs all cross the null value. In addition, model fit was not improved and heterogeneity was not reduced in the covariate models when compared with the main consistency model reported in Table 20.
| Included covariate | Coefficient (95% CrI) |
|---|---|
| Subset: adults (outcome: YBOCS) | |
| Publication date (continuous) | 0.14 (–0.11 to 0.39) |
| Trial length (continuous) | 0.31 (–0.26 to 0.86) |
| Comorbid depression (binary, 1 = yes) | –1.24 (–4.34 to 1.78) |
| Pharmaceutical industry sponsorship (binary, 1 = yes) | –0.40 (–4.33 to 3.41) |
| Subset: adult (outcome: dropouts) | |
| Publication date | 0.03 (–0.01 to 0.06) |
| Trial length | 0.05 (–0.07 to 0.18) |
| Comorbid depression (yes/no) | –0.13 (–0.68 to 0.36) |
| Pharmaceutical industry sponsorship (binary, 1 = yes) | 0.27 (–0.54 to 1.04) |
Chapter 6 Network meta-analysis results (children and adolescents)
Clinical effectiveness: symptom reduction (Children’s Yale–Brown Obsessive–Compulsive Scale)
Description of the data set
Table 33 presents the raw data used for the dropout analysis in the children and adolescents subset of the data (for a complete copy of the data extraction, see Appendix 5). Of the 22 studies eligible for inclusion in the NMA,215–236 four were excluded: Flament et al. did not use the CYBOCS scale; March et al. 228 contained a population of 10- to 18-year-olds and used the adult YBOCS rather than the CYBOCS to assess symptoms; Asbahr et al. 216 did not report the follow-up measures; Alaghband-Rad and Hakimshooshtary215 did not report the number at follow-up or any uncertainty around the CYBOCS; and GlaxoSmithKline225 did not report a follow-up CYBOCS or a change from baseline. The studies excluded from the analysis involved a total of 311 randomised patients, but 207 of whom were included in the GlaxoSmithKline225 paroxetine versus placebo study, whereas 104 patients were included in the remaining four studies. In total, 17 studies were included in the analysis. 217–221,223,224,228–236
| Study ID | t[,1] | y[,1] | n[,1] | sd[,1] | t[,2] | y[,2] | n[,2] | sd[,2] | t[,3] | y[,3] | n[,3] | sd[,3] | t[,4] | y[,4] | n[,4] | sd[,4] | Arms |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Barrett et al., 2004217 | 2 | 24.04 | 24 | 4.14 | 9 | 8.36 | 22 | 6.93 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Bolton and Perrin, 2008218 | 2 | 21.1 | 10 | 5.9 | 8 | 13.9 | 10 | 10.74 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Bolton et al., 2011219 | 2 | 23.3 | 24 | 8.3 | 9 | 9.5 | 36 | 8 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| de Haan et al., 1998220 | 7 | 17.6 | 10 | 11.8 | 8 | 9.1 | 12 | 9.1 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| DeVeaugh-Geiss et al., 1992221 | 1 | –2.4 | 29 | NA | 7 | –10 | 31 | NA | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Freeman et al., 2008223 | 3 | 17.1 | 20 | 7.57 | 9 | 14.45 | 22 | 8.16 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Geller et al., 2001224 | 1 | –5.2 | 32 | 7.4 | 4 | –9.5 | 71 | 9.2 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Liebowitz et al., 2002226 | 1 | 18.55 | 22 | 11.44 | 4 | 14.71 | 21 | 8.73 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| March et al., 1998228 | 1 | –3.4 | 95 | 7.99 | 6 | –6.8 | 92 | 8.34 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Neziroglu et al., 2000229 | 5 | 19.2 | 5 | 3.56 | 10 | 16.4 | 5 | 5.18 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Piacentini et al., 2011230 | 3 | 17.2 | 22 | 10.04 | 9 | 13.3 | 49 | 9.31 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Riddle et al., 1992231 | 1 | 14.8 | 6 | 7 | 4 | 13.6 | 7 | 5.7 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Riddle et al., 2001232 | 1 | 20.9 | 63 | 8.5 | 5 | 18.2 | 57 | 8.6 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Storch et al., 2011233 | 2 | 18.53 | 15 | 8.11 | 9 | 11.13 | 16 | 10.53 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Storch et al., 2013234 | 11 | 15.43 | 14 | 9.72 | 12 | 15.56 | 16 | 6.62 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| Williams et al., 2010235 | 2 | 19.6 | 10 | 6.42 | 9 | 12.09 | 11 | 7.46 | NA | NA | NA | NA | NA | NA | NA | NA | 2 |
| The Pediatric OCD Treatment Study, 2004236 | 1 | 21.5 | 28 | 5.4 | 6 | 16.5 | 28 | 9.1 | 9 | 14 | 28 | 9.5 | 11 | 11.2 | 28 | 8.6 | 4 |
Table 34 presents summary data per type of intervention for the studies included in the NMA (number of arms and number of randomised patients per intervention).
| Intervention | Number of arms | Number of patients |
|---|---|---|
| Placebo | 7 | 275 |
| Waitlist | 5 | 83 |
| Psychological placebo | 2 | 42 |
| Fluoxetine | 3 | 99 |
| Fluvoxamine | 2 | 62 |
| Sertraline | 2 | 120 |
| Clomipramine | 2 | 41 |
| BT | 2 | 22 |
| CBT | 7 | 184 |
| BT + fluvoxamine | 1 | 5 |
| CBT + sertraline | 2 | 42 |
| CBT + placebo | 1 | 16 |
| Total | 36 | 991 |
Network meta-analysis: results
Network geometry
Figure 9 shows the network geometry of the CYBOCS comparison in the children and adolescent subsets and Table 35 presents summary data per type of intervention (number of patients randomised, total number of links with other treatments, number of unique treatments compared). Overall, of the 66 pairwise comparisons that can be made among the 12 treatment conditions, only 15 (23%) were studied directly by head-to-head comparison in 17 studies involving 991 randomised patients. It should be noted, however, that 11 of these 15 direct comparisons were made in single trials. Figure 9 includes 22 randomised pairwise comparisons and the most common comparisons are those between CBT and waitlist (n = 4), fluoxetine and placebo (n = 3), sertraline and placebo (n = 2), and CBT and psychological placebo (n = 2). Placebo (n = 275), CBT (n = 184), sertraline (n = 120) and fluoxetine (n = 99) had a sample approximately ≥ 100 (Table 35). Nodes with the most connections (links) in the network (Table 35) are drug placebo (n = 9 links with six different interventions), CBT (n = 9 links with five different interventions), waitlist (n = 5 links with two different interventions), sertraline (n = 4 links with three different interventions), the combination of sertraline and CBT (n = 4 links with four different interventions) and fluoxetine (n = 3 links with placebo).
FIGURE 9.
Network diagram for CYBOCS analysis representing individual treatments (children and adolescents subset). Circles (nodes) represent the types of interventions compared in the network and they are proportional to the number of participants randomised to a treatment. Lines are proportional to the number of direct randomised comparisons. BTFLV, BT + fluvoxamine; CBTPL, CBT + placebo; CBTSER, CBT + sertraline; CLO, clomipramine; FLV, fluvoxamine; FLX, fluoxetine; PL, placebo; PSYPL, psychological placebo; SER, sertraline; WL, waitlist.
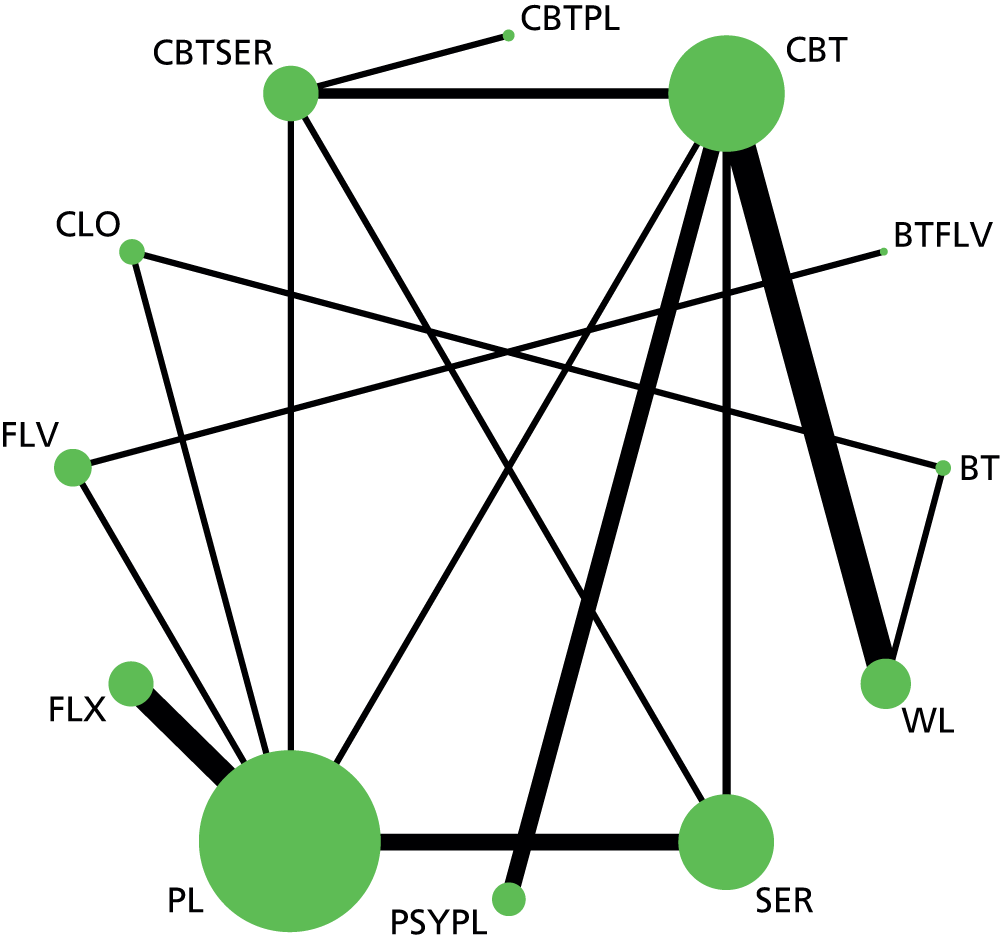
| Intervention | Number of patients randomised | Number of pairwise comparisons (links) | Number of unique treatment comparisons |
|---|---|---|---|
| Placebo | 275 | 9 | 6 |
| CBT | 184 | 9 | 5 |
| Sertraline | 120 | 4 | 3 |
| Fluoxetine | 99 | 3 | 1 |
| Waitlist | 83 | 5 | 2 |
| Fluvoxamine | 62 | 2 | 2 |
| Psychological placebo | 42 | 2 | 1 |
| CBT + sertraline | 42 | 4 | 4 |
| Clomipramine | 41 | 2 | 2 |
| BT | 22 | 2 | 2 |
| CBT + placebo | 16 | 1 | 1 |
| BT + fluvoxamine | 5 | 1 | 1 |
Consistency of evidence
We examined model fit using the posterior mean of the residual deviance, the degree of between-study heterogeneity and the DIC. We compared a model assuming consistency of treatment effects with a model assuming independent treatment effects. For the consistency model, all SSRIs were analysed as a class and individually. Table 36 presents the results of this comparison for the children and adolescents subset.
| Model | Number of data points | Residual deviance, posterior meana | SD,b posterior median (95% CrI) | DIC |
|---|---|---|---|---|
| Random-effects consistency | 34 | 35.04 | 1.88 (0.13 to 5.23) | 64.2 |
| Random-effects inconsistency | 34 | 34.27 | 1.81 (0.08 to 5.78) | 64.4 |
The posterior mean of the residual deviance was 35.04 compared with the number of data points (n = 34), suggesting adequate model fit. The posterior mean residual deviance was 34.27 in the independent effects model; however, heterogeneity was not reduced and may be considered low to moderate. In addition, the DIC suggests that we can select the model assuming consistency as our preferred choice. The results of the NMA and the results of the pairwise comparisons (see Table 37) are in the same direction, with no evidence that the NMA effect estimate falls outside the 95% CrIs from the pairwise analysis. Overall, we conclude that there is no evidence of inconsistency in this network of evidence.
Data synthesis
The results of the NMA are presented in Table 37. We present the mean and 95% CrIs for the MD in CYBOCS scores at the end of study between the treatments compared. We present both the direct, head-to-head and pairwise comparisons (from the model assuming independent effects) and the results of the NMA (consistency model). For simplicity, we present only the MD and 95% CrIs for all interventions compared with the reference intervention (drug placebo). A more detailed table with all possible comparisons (both for the direct analysis and NMA) is given in Appendix 8.
| Intervention | Direct | NMA | Posterior treatment rank, median (95% CrI) | ||
|---|---|---|---|---|---|
| Mean CYBOCS score | 95% CrI | Mean CYBOCS score | 95% CrI | ||
| Placebo | Reference | Reference | Reference | Reference | 11 (9 to 12) |
| Waitlist | NA | NA | 3.10 | –3.79 to 9.03 | 12 (8 to 12) |
| Psychological placebo | NA | NA | –5.37 | –12.9 to 2.01 | 6 (2 to 11) |
| SSRIs (class effect) | –3.57 | –8.57 to 1.51 | |||
| Fluoxetine | –3.52 | –7.59 to 0.81 | –3.58 | –7.01 to –0.08 | 8 (4 to 11) |
| Fluvoxamine | –2.69 | –8.73 to 3.35 | –3.27 | –7.39 to 1.13 | 9 (4 to 11) |
| Sertraline | –3.99 | –8.45 to 0.21 | –3.90 | –7.47 to –0.60 | 8 (4 to 10) |
| Clomipramine | –7.62 | –14.21 to –0.97 | –5.64 | –11.36 to 0.64 | 6 (2 to 11) |
| BT | NA | NA | –8.47 | –16.98 to –0.39 | 4 (1 to 10) |
| CBT | –7.30 | –13.95 to –0.88 | –8.66 | –14.38 to –3.14 | 3 (1 to 7) |
| BT + fluvoxamine | NA | NA | –6.12 | –14.49 to 2.45 | 6 (1 to 12) |
| CBT + sertraline | –10.12 | –16.58 to –3.84 | –10.30 | –16.16 to –4.58 | 2 (1 to 6) |
| CBT + placebo | NA | NA | –10.22 | –19.84 to –0.61 | 2 (1 to 10) |
Selective serotonin reuptake inhibitors as a class showed a trend for a greater effect than drug placebo, but the 95% CrIs included the null value. Individual SSRIs, however, reached marginal statistical significance, in particular sertraline (MD –3.90, 95% CrI –7.47 to –0.60). Although clomipramine showed a greater effect in the direct pairwise analysis (MD –7.62, 95% CrI –14.21 to –0.97), in the network analysis this effect was attenuated (MD –5.64, 95% CrI –11.36 to 0.64). It should be noted, however, that this result is based on two small studies with 41 patients randomised to clomipramine.
Behavioural therapy and CBT had greater effects than drug placebo (MD –8.47, 95% CrI –16.98 to –0.39 and MD –8.66, 95% CrI –14.38 to –3.14, respectively). Compared with psychological placebo, there was a trend for a greater effect, especially in CBT, but the 95% CrIs included the null value.
Compared with SSRIs as a class, both psychological therapies (BT and CBT) showed a trend for a greater effect, although the 95% CrIs included the null value (BT: MD –4.89, 95% CrI –14.6 to 4.28; CBT: MD –5.09, 95% CrI –12.33 to 1.86). Similar results were found for clomipramine.
The combination of sertraline with CBT was compared in four arms within two studies with a total number of 42 randomised patients. This was associated with the largest effect compared with drug placebo (MD –10.30, 95% CrI –16.16 to –4.58), but the same was observed for the combination of CBT with placebo (MD –10.22, 95% CrI –19.84 to –0.61). Compared with sertraline as monotherapy, the combination of sertraline and CBT had a greater effect (MD –6.40, 95% CrI –12.35 TO –0.40), but compared with CBT as monotherapy, the combination had similar effects (MD –1.64, 95% CrI –8.26 to 5.06). The combination of CBT with sertraline showed a trend for a greater effect than psychological placebo but the 95% CrI included the null value.
Table 37 also presents the posterior median treatment ranks with 95% CrIs. CBT as monotherapy or combined with sertraline or drug placebo were ranked as the highest performing treatments, followed by BT.
Sensitivity analyses: outcome 1, CYBOCS – subset (children and adolescents)
Low overall attrition and no evidence of imbalanced attrition
For this analysis, we excluded the five studies in the children and adolescents subset for which overall levels of attrition were > 25% or differential attrition was > 15%. The remaining 12 studies217,219–221,226–231,233,235,236 included and the raw data used are presented in Appendix 9. Overall, 11 interventions were included and the total number of randomised patients was 686 (69% of the patients originally used in our full analysis). MDs and 95% CrIs compared with placebo are presented in Table 38. The results are essentially similar to the original analysis with the full data reported in Table 37, but the power of the analysis is low owing to the small number of included studies.
| Intervention | Posterior distribution of the treatment effect (mean CYBOCS difference) | Posterior treatment rank, median (95% CrI) | |
|---|---|---|---|
| Mean | 95% CrI | ||
| Placebo | Reference | Reference | 9 (6 to 11) |
| Waitlist | 2.47 | –6.72 to 10.43 | 10 (6 to 11) |
| Psychological placebo | –4.88 | –16.98 to 6.95 | 6 (1 to 10) |
| SSRIs (class effect) | –3.65 | –12.37 to 5.01 | |
| Fluoxetine | –3.18 | –9.12 to 2.87 | 7 (3 to 10) |
| Fluvoxamine | –3.64 | –17.44 to 10.31 | 7 (1 to 11) |
| Sertraline | –4.10 | –9.47 to 1.10 | 6 (3 to 9) |
| Clomipramine | –5.28 | –12.97 to 3.28 | 5 (2 to 10) |
| BT | –8.75 | –19.24 to 1.43 | 3 (1 to 9) |
| CBT | –8.82 | –16.67 to –1.38 | 3 (1 to 7) |
| BT + fluvoxamine | Not estimable | ||
| CBT + sertraline | –10.37 | –18.48 to –2.396 | 2 (1 to 7) |
Low risk of bias in the domain: incomplete outcome assessment
For this analysis, we included 15218–221,223,224,226,228,230–236 and excluded two studies. The studies included and the raw data used are presented in Appendix 9. Overall, 12 interventions were included and the total number of randomised patients was 935 (94% of the patients originally used in our full analysis). MDs and 95% CrIs compared with placebo are presented in Table 39. It can be seen from the table that the results are essentially similar to the original analysis, with the full data reported in Table 37.
| Intervention | Posterior distribution of the treatment effect (mean CYBOCS difference) | Posterior treatment rank, median (95% CrI) | |
|---|---|---|---|
| Mean | 95% CrI | ||
| Placebo | Reference | Reference | 11 (9 to 12) |
| Waitlist | 1.36 | –5.01 to 7.12 | 11 (7 to 12) |
| Psychological placebo | –5.08 | –11.91 to 1.57 | 6 (3 to 11) |
| SSRIs (class effect) | –3.55 | –8.16 to 1.16 | |
| Fluoxetine | –3.59 | –6.53 to –0.56 | 8 (4 to 10) |
| Fluvoxamine | –3.21 | –6.80 to 0.57 | 8 (5 to 11) |
| Sertraline | –3.85 | –6.92 to –1.01 | 8 (4 to 10) |
| Clomipramine | –6.14 | –11.25 to –0.59 | 6 (2 to 10) |
| BT | –9.58 | –17.62 to –1.61 | 3 (1 to 9) |
| CBT | –8.36 | –13.52 to –3.48 | 4 (1 to 7) |
| BT + fluvoxamine | Not estimable | ||
| CBT + sertraline | –10.23 | –15.40 to –5.20 | 3 (1 to 6) |
| CBT + placebo | –10.06 | –18.84 to –1.32 | 3 (1 to 10) |
Low risk of bias in the domain: blinding of the outcome assessor
For this analysis, we included nine219,223,226–230,232–236 and excluded eight studies. The studies included and the raw data used are presented in Appendix 9. Overall, nine interventions were included and the total number of randomised patients was 530 (53% of the patients originally used in our full analysis). MDs and 95% CrIs compared with placebo are presented in Table 40. Owing to the small number of studies included, the power is compromised but the results show the same trends with the full analysis reported in Table 37.
| Intervention | Posterior distribution of the treatment effect (mean CYBOCS difference) | Posterior treatment rank, median (95% CrI) | |
|---|---|---|---|
| Mean | 95% CrI | ||
| Placebo | Reference | Reference | 8 (5 to 9) |
| Waitlist | 3.10 | –5.74 to 11.54 | 9 (5 to 9) |
| Psychological placebo | –3.94 | –13.04 to 5.26 | 5 (1 to 8) |
| SSRIs (class effect) | –3.79 | –10.55 to 2.97 | |
| Fluoxetine | –3.85 | –10.08 to 2.40 | 5 (2 to 8) |
| Fluvoxamine | –3.27 | –8.81 to 2.22 | 6 (2 to 8) |
| Sertraline | –4.27 | –9.96 to 1.42 | 5 (2 to 8) |
| CBT | –7.18 | –14.33 to 0.09 | 3 (1 to 6) |
| CBT + sertraline | –9.97 | –16.91 to –2.86 | 2 (1 to 5) |
| CBT + placebo | –9.76 | –20.78 to 1.46 | 2 (1 to 8) |
Acceptability (dropouts)
Description of the data set
Table 41 presents the raw data used for the dropout analysis in the children and adolescents subset of the data. Of the 22 studies eligible for inclusion in the NMA,215–236 four were excluded: three studies either did not report dropout data or did not report dropout data separately for each arm;215,217 and one study was excluded because there were no dropouts (zero dropouts) in all arms. 229 Therefore, 18 studies were included in this analysis. 216,218–221,223–228,230–236
Table 41 also presents raw dropout rates. It can be seen that the range of dropouts was 0–43%, with a median of 14%. Table 42 presents summary dropout rate per type of intervention (minimum, maximum and median of raw dropout rates).
| Study | t[,1] | r[,1] | n[,1] | dr[,]1, % | t[,2] | r[,2] | n[,2] | dr[,2], % | t[,3] | r[,3] | n[,3] | dr[,3], % | t[,4] | r[,4] | n[,4] | dr[,4], % |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Asbahr et al., 2005216 | 7 | 1 | 20 | 5 | 10 | 0 | 20 | 0 | NA | NA | NA | NA | NA | NA | NA | NA |
| Bolton and Perrin, 2008218 | 2 | 0 | 10 | 0 | 9 | 2 | 10 | 20 | NA | NA | NA | NA | NA | NA | NA | NA |
| Bolton et al., 2011219 | 2 | 3 | 24 | 13 | 10 | 2 | 36 | 6 | NA | NA | NA | NA | NA | NA | NA | NA |
| DeVeaugh-Geiss et al., 1992221 | 1 | 2 | 29 | 7 | 8 | 4 | 31 | 13 | NA | NA | NA | NA | NA | NA | NA | NA |
| Freeman et al., 2008223 | 3 | 5 | 20 | 25 | 10 | 6 | 22 | 27 | NA | NA | NA | NA | NA | NA | NA | NA |
| Geller et al., 2001224 | 1 | 12 | 32 | 38 | 4 | 22 | 71 | 31 | NA | NA | NA | NA | NA | NA | NA | NA |
| GlaxoSmithKline, 2001225 | 1 | 27 | 107 | 25 | 6 | 35 | 100 | 35 | NA | NA | NA | NA | NA | NA | NA | NA |
| de Haan et al., 1998220 | 8 | 0 | 10 | 0 | 9 | 1 | 13 | 8 | NA | NA | NA | NA | NA | NA | NA | NA |
| Liebowitz et al., 2002226 | 1 | 4 | 22 | 18 | 4 | 1 | 21 | 5 | NA | NA | NA | NA | NA | NA | NA | NA |
| March et al., 1990227 | 1 | 0 | 8 | 0 | 8 | 2 | 8 | 25 | NA | NA | NA | NA | NA | NA | NA | NA |
| March et al., 1998228 | 1 | 13 | 95 | 14 | 7 | 18 | 92 | 20 | NA | NA | NA | NA | NA | NA | NA | NA |
| Piacentini et al., 2011230 | 3 | 5 | 22 | 23 | 10 | 8 | 49 | 16 | NA | NA | NA | NA | NA | NA | NA | NA |
| Riddle et al., 1992231 | 1 | 1 | 6 | 17 | 4 | 1 | 7 | 14 | NA | NA | NA | NA | NA | NA | NA | NA |
| Riddle et al., 2001232 | 1 | 27 | 63 | 43 | 5 | 19 | 57 | 33 | NA | NA | NA | NA | NA | NA | NA | NA |
| Storch et al., 2011233 | 2 | 0 | 15 | 0 | 10 | 2 | 16 | 13 | NA | NA | NA | NA | NA | NA | NA | NA |
| Storch et al., 2013234 | 11 | 6 | 14 | 43 | 12 | 3 | 16 | 19 | NA | NA | NA | NA | NA | NA | NA | NA |
| Williams et al., 2010235 | 2 | 1 | 10 | 10 | 10 | 1 | 11 | 9 | NA | NA | NA | NA | NA | NA | NA | NA |
| The Pediatric OCD Treatment Study, 2004236 | 1 | 7 | 28 | 25 | 7 | 2 | 28 | 7 | 10 | 3 | 28 | 11 | 11 | 3 | 28 | 11 |
| Intervention | Dropout rates (%) | Number of arms | ||
|---|---|---|---|---|
| Minimum | Maximum | Median | ||
| Placebo | 0 | 43 | 18 | 9 |
| Waitlist | 0 | 12.5 | 5 | 4 |
| Psychological placebo | 23 | 25 | 24 | 2 |
| Fluoxetine | 5 | 31 | 14 | 3 |
| Fluvoxamine | 33 | 33 | NA | 1 |
| Paroxetine | 35 | 35 | NA | 1 |
| Sertraline | 5 | 20 | 7 | 3 |
| Clomipramine | 0 | 25 | 13 | 3 |
| BT | 8 | 20 | 14 | 2 |
| CBT | 0 | 27 | 11 | 7 |
| CBT + sertraline | 11 | 43 | 27 | 2 |
| CBT + placebo | 19 | 19 | NA | 1 |
Network meta-analysis: results
Network geometry
Figure 10 shows the network geometry for total dropouts in the children and adolescents subset. Overall, of the 66 comparisons that can be made among the 12 treatment conditions, only 15 (23%) were studied directly by head-to-head evidence in 18 studies involving 1199 randomised patients. It should be noted, however, that 9 of the 15 direct comparisons are associated with one study each. Placebo (n = 390), CBT (n = 182), sertraline (n = 140), paroxetine (n = 100) and fluoxetine (n = 99) are the treatments with the largest sample size. Figure 10 includes 23 randomised pairwise comparisons and the most common comparisons are those between placebo and fluoxetine (n = 3) and CBT and waitlist (n = 3). Nodes with the most connections (links) in the network are drug placebo (n = 11 links with seven different treatments), CBT (n = 9 links with four different treatments), sertraline (n = 5 links with three different treatments), combination of sertraline and CBT (n = 4 links with three different treatments) and waitlist (n = 4 links with two different treatments).
FIGURE 10.
Network diagram for dropouts representing individual treatments (children and adolescent subset). Circles represent the types of interventions used in the network and they are proportional to the number of participants randomised to a treatment. Lines (edges) are proportional to the number of direct randomised comparisons. CBTPL, CBT + placebo; CBTSER, CBT + sertraline; CLO, clomipramine; FLV, fluvoxamine; FLX, fluoxetine; PAR, paroxetine; PL, placebo; PSYPL, psychological placebo; SER, sertraline; WL, waitlist.

Consistency of evidence
We examined model fit using the posterior mean of the residual deviance, the degree of between-study heterogeneity and the DIC. We compared a model assuming consistency of treatment effects with a model assuming independent treatment effects. For the consistency model, all SSRIs were analysed as a class and individually. Table 43 presents the results of this comparison for the children and adolescents subset.
| Model | Number of data points | Residual deviance (posterior mean) | SD,a posterior median (95% CrI) | DIC |
|---|---|---|---|---|
| Random-effects consistency | 38 | 42.0 | 0.36 (0.02 to 1.19) | 169.3 |
| Random-effects independent effects | 38 | 41.4 | 0.58 (0.04 to 1.92) | 170.9 |
The posterior mean of the residual deviance was 42.0 in the NMA (the consistency model) compared with the number of data points (n = 38), suggesting adequate model fit. The posterior mean residual deviance was 41.4 in the independent effect model. The DIC does not differentiate between the two models. In addition, the results of the NMA and the results of the pairwise comparisons (Table 44) are in the same direction, with no evidence that the NMA effect estimate falls outside the 95% CrIs from the pairwise analysis. Overall, we conclude that there is no evidence of inconsistency.
Data synthesis
The results of the NMA are presented in Table 44. We present posterior median ORs for dropouts compared with drug placebo, which is the reference treatment. We present both pairwise comparisons (from the independent effects model) for the direct head-to-head comparisons and the results of the NMA. For simplicity, we present only the ORs compared with drug placebo. A more detailed table with all possible comparisons (both for the direct and NMA) is given in Appendix 8.
| Intervention | Direct | NMA | Posterior treatment rank, median (95% CrI) | ||
|---|---|---|---|---|---|
| Median OR | 95% CrI | Median OR | 95% CrI | ||
| Placebo | Reference | Reference | Reference | Reference | 8 (3 to 11) |
| Waitlist | NA | NA | 0.53 | 0.05 to 4.33 | 4 (1 to 11) |
| Psychological placebo | NA | NA | 0.58 | 0.07 to 4.44 | 5 (1 to 11) |
| SSRIs (class effect) | 0.87 | 0.23 to 3.00 | |||
| Fluoxetine | 0.56 | 0.09 to 2.57 | 0.74 | 0.25 to 1.68 | 6 (1 to 10) |
| Fluvoxamine | 0.66 | 0.06 to 6.95 | 0.79 | 0.24 to 2.07 | 6 (1 to 11) |
| Paroxetine | 1.59 | 0.16 to 16.65 | 1.12 | 0.37 to 3.42 | 9 (3 to 12) |
| Sertraline | 0.81 | 0.10 to 3.78 | 0.89 | 0.32 to 2.07 | 7 (2 to 11) |
| Clomipramine | 3.44 | 0.41 to 41.35 | 3.06 | 0.54 to 21.69 | 11 (4 to 12) |
| BT | NA | NA | 7.64 | 0.41 to 423.7 | 12 (4 to 12) |
| CBT | 0.44 | 0.02 to 5.08 | 0.49 | 0.09 to 2.41 | 4 (1 to 10) |
| Sertraline + CBT | 0.43 | 0.02 to 4.91 | 0.54 | 0.08 to 3.15 | 4 (1 to 11) |
| Placebo + CBT | NA | NA | 0.15 | 0.01 to 2.26 | 1 (1 to 10) |
There were no interventions with a statistically significant higher dropout than placebo. However, clomipramine and BT were associated with the largest median ORs. It should be noted, however, that the evidence for this comes from three220,221,227 and two studies,218,220 respectively, with small sample sizes (n = 49 for clomipramine and n = 23 for BT), and in the case of BT, there is no direct comparison with placebo. Paroxetine was the only SSRI with an OR greater than 1, but this was not statistically significant. SSRIs as a class were not more likely than placebo to lead to dropout.
Sensitivity analyses: outcome 2 – dropouts, children and adolescents subset
Low overall attrition and no evidence of imbalanced attrition
For this analysis, we included 13216,218–221,226–228,230,231,233,235,236 and excluded five studies. The studies included and the raw data used are presented in Appendix 9. Overall, nine interventions were included and the total number of randomised patients was 707 (59% of the patients originally used in our full analysis). MDs and 95% CrI compared with placebo are presented in Table 45. Compared with the full data set reported in Table 44, the results are essentially similar.
| Intervention | Median OR | 95% CrI | Posterior treatment rank, median (95% CrI) |
|---|---|---|---|
| Placebo | Reference | Reference | 6 (2 to 8) |
| Waitlist | 0.46 | 0.02 to 7.38 | 3 (1 to 8) |
| Psychological placebo | 0.68 | 0.02 to 23.59 | 4 (1 to 9) |
| SSRIs (class effect) | 0.58 | 0.0005 to 448.1 | |
| Fluoxetine | 0.41 | 0.03 to 3.62 | 3 (1 to 8) |
| Sertraline | 0.79 | 0.12 to 4.08 | 5 (1 to 8) |
| Clomipramine | 3.12 | 0.36 to 36.01 | 8 (2 to 9) |
| BT | 8.09 | 0.23 to 695.2 | 9 (3 to 9) |
| CBT | 0.47 | 0.04 to 4.39 | 3 (1 to 7) |
| CBT + sertraline | 0.54 | 0.03 to 7.33 | 4 (1 to 9) |
Low risk of bias in the domain: incomplete outcome assessment
For this analysis, we included 16216,218–221,223,224,226,228,230–236 and excluded two studies. The studies included and the raw data used are presented in Appendix 9. Overall, 11 interventions were included and the total number of randomised patients was 984 (82% of the patients originally used in our full analysis). MDs and 95% CrIs compared with placebo are presented in Table 46. Compared with the full data set, reported in Table 44, the results show the same trends.
| Intervention | Median | 95% CrI | Posterior treatment rank, median (95% CrI) |
|---|---|---|---|
| Placebo | Reference | Reference | 8 (4 to 11) |
| Waitlist | 0.48 | 0.04 to 4.17 | 4 (1 to 10) |
| Psychological placebo | 0.55 | 0.05 to 4.71 | 5 (1 to 10) |
| SSRIs (class effect) | 0.70 | 0.06 to 7.78 | |
| Fluoxetine | 0.64 | 0.19 to 1.70 | 5 (1 to 10) |
| Fluvoxamine | 0.69 | 0.18 to 2.31 | 6 (1 to 10) |
| Sertraline | 0.80 | 0.25 to 2.18 | 7 (2 to 10) |
| Clomipramine | 2.01 | 0.23 to 20.91 | 10 (2 to 11) |
| BT | 5.95 | 0.27 to 307.3 | 11 (3 to 11) |
| CBT | 0.48 | 0.07 to 2.39 | 4 (1 to 9) |
| CBT + sertraline | 0.52 | 0.06 to 3.50 | 5 (1 to 10) |
| CBT + placebo | 0.14 | 0.01 to 2.59 | 1 (1 to 10) |
Low risk of bias in the domain: blinding of the outcome assessor
For this analysis, we included 10216,219,223,226,230,232–236 and excluded eight studies. The studies included and the raw data used are presented in Appendix 9. Overall, nine interventions were included and the total number of randomised patients was 574 (48% of the patients originally used in our full analysis). MDs and 95% CrIs compared with placebo are presented in Table 47. Compared with the full data set reported in Table 44, the results show similar trends for the included interventions.
| Intervention | Median OR | 95% CrI | Posterior treatment rank, median (95% CrI) |
|---|---|---|---|
| Placebo | Reference | Reference | 8 (4 to 9) |
| Waitlist | 0.26 | 0.01 to 4.36 | 4 (1 to 9) |
| Psychological placebo | 0.32 | 0.01 to 5.32 | 5 (1 to 9) |
| SSRIs (class effect) | 0.38 | 0.01 to 15.56 | |
| Fluoxetine | 0.30 | 0.01 to 2.50 | 4 (1 to 9) |
| Fluvoxamine | 0.54 | 0.06 to 3.52 | 7 (2 to 9) |
| Sertraline | 0.33 | 0.03 to 2.43 | 5 (1 to 9) |
| CBT | 0.27 | 0.02 to 2.50 | 4 (1 to 8) |
| CBT + sertraline | 0.36 | 0.02 to 4.28 | 5 (2 to 9) |
| CBT + placebo | 0.10 | 0.01 to 4.01 | 1 (1 to 9) |
Rankograms (both outcomes)
Table 48 presents the probabilities that each treatment is among the best three or worst three for both outcomes (CYBOCS/dropouts: for dropouts, being in the top three means better tolerability, i.e. lower dropouts). In Appendix 8 we present complete data for all rank probabilities for both outcomes. Based on these data, we also present rankograms (plots of the probabilities for each treatment taking each possible rank) in Figure 11.
| Outcomea | Treatment | Probability of treatment being in the | |
|---|---|---|---|
| Top three | Bottom three | ||
| CYBOCS | Placebo | 0.00 | 0.95 |
| Dropout | Placebo | 0.03 | 0.18 |
| CYBOCS | Waitlist | 0.00 | 0.96 |
| Dropout | Waitlist | 0.42 | 0.14 |
| CYBOCS | Psychological placebo | 0.11 | 0.17 |
| Dropout | Psychological placebo | 0.36 | 0.15 |
| CYBOCS | Fluoxetine | 0.01 | 0.19 |
| Dropout | Fluoxetine | 0.21 | 0.06 |
| CYBOCS | Fluvoxamine | 0.01 | 0.26 |
| Dropout | Fluvoxamine | 0.17 | 0.09 |
| Dropout | Paroxetine | 0.05 | 0.35 |
| CYBOCS | Sertraline | 0.01 | 0.13 |
| Dropout | Sertraline | 0.07 | 0.12 |
| CYBOCS | Clomipramine | 0.14 | 0.11 |
| Dropout | Clomipramine | 0.02 | 0.84 |
| CYBOCS | BT | 0.48 | 0.05 |
| Dropout | BT | 0.02 | 0.89 |
| CYBOCS | CBT | 0.53 | 0.00 |
| Dropout | CBT | 0.43 | 0.03 |
| CYBOCS | CBT + sertraline | 0.78 | 0.00 |
| Dropout | CBT + sertraline | 0.40 | 0.11 |
| CYBOCS | CBT + placebo | 0.66 | 0.04 |
| Dropout | CBT + placebo | 0.82 | 0.04 |
| CYBOCS | BT + fluvoxamine | 0.27 | 0.14 |
FIGURE 11.
Rankograms for children and adolescents: dropout (black lines); CYBOCS (green lines). (a) Placebo; (b) waitlist; (c) psychological placebo; (d) fluoxetine; (e) fluvoxamine; (f) sertraline; (g) clomipramine; (h) BT; (i) CBT; (j) CBT + sertraline; (k) CBT + placebo; (l) BT + fluvoxamine; and (m) paroxetine.
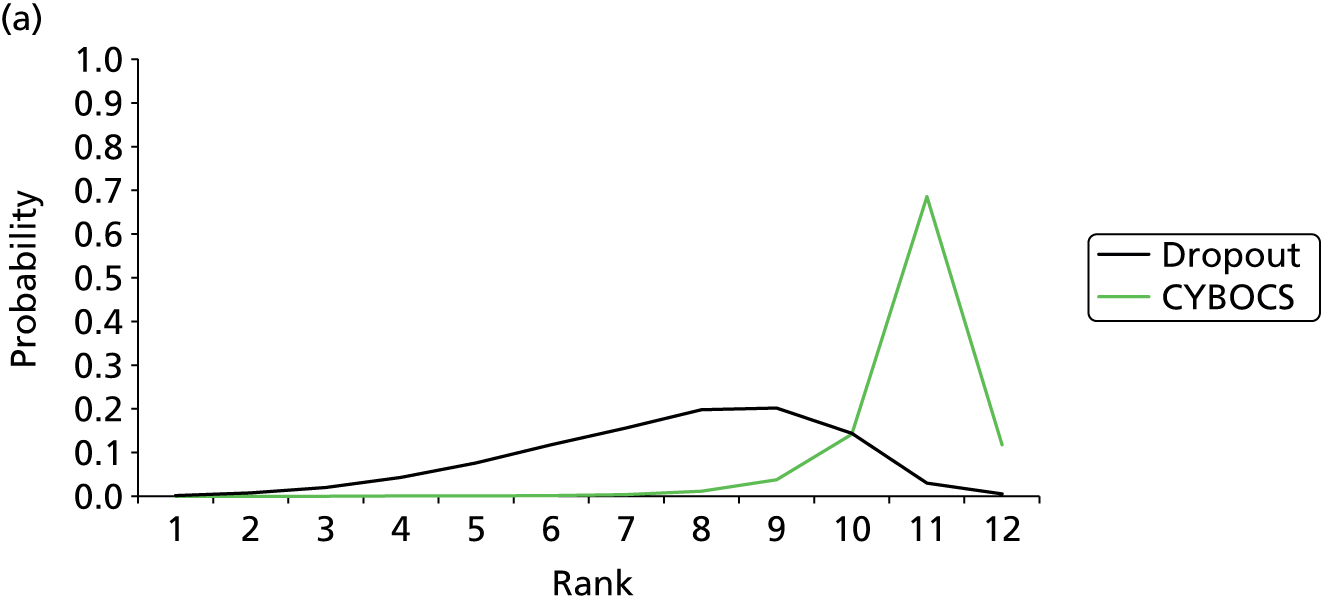




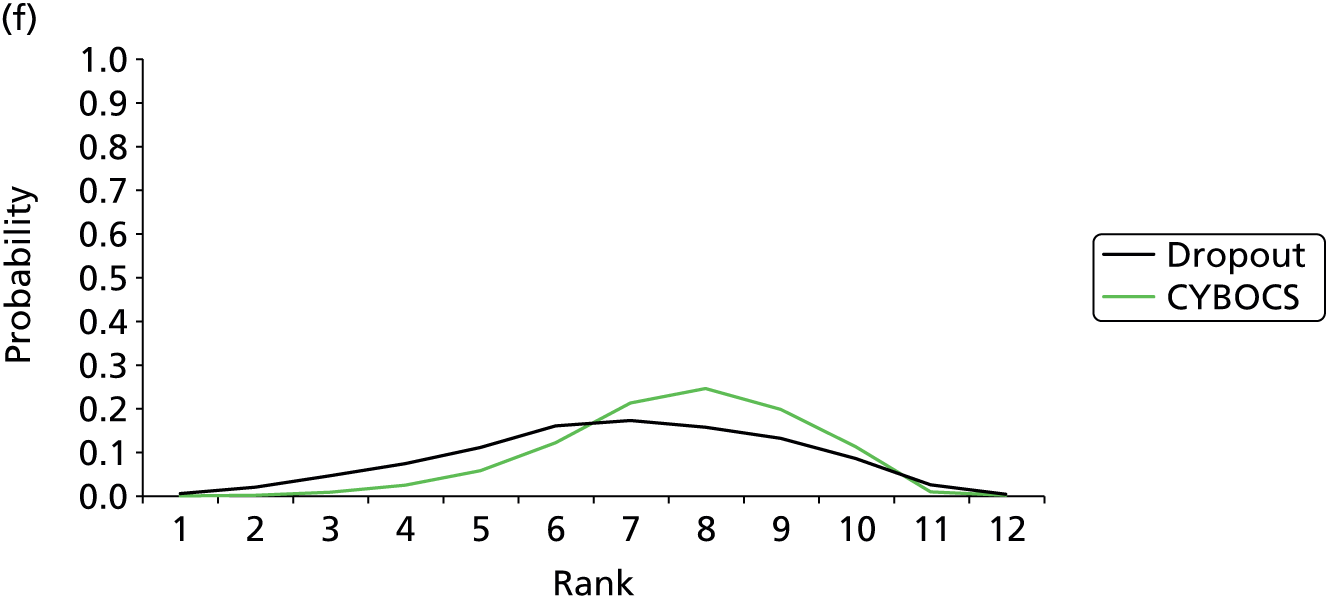

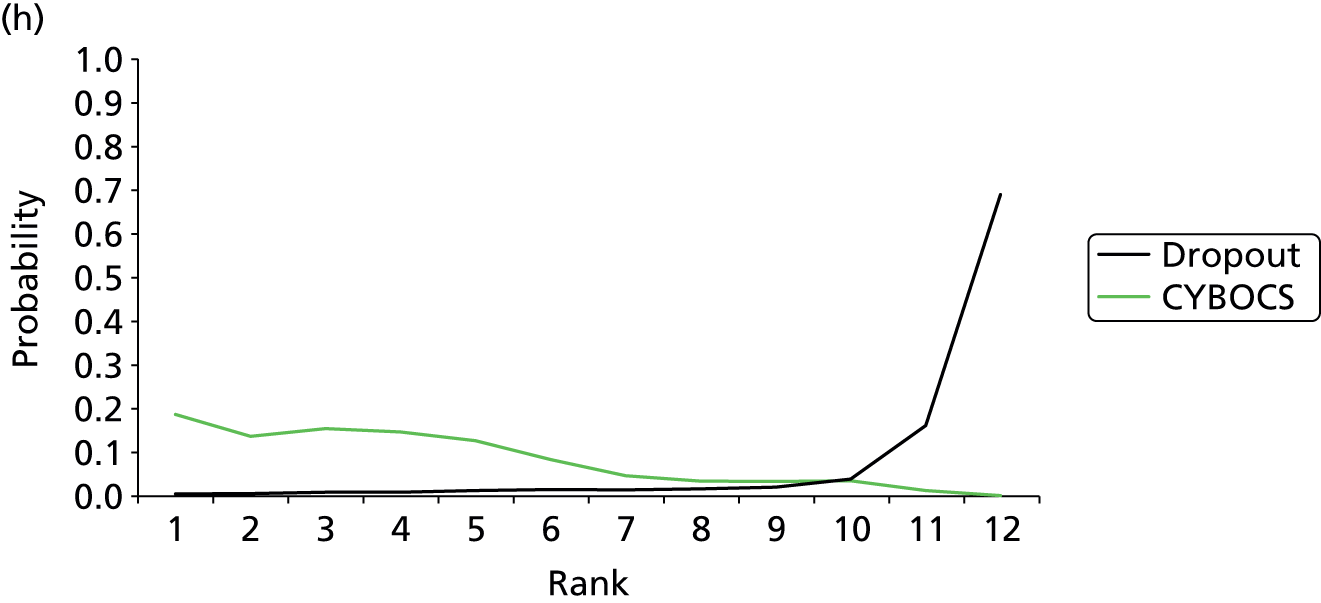


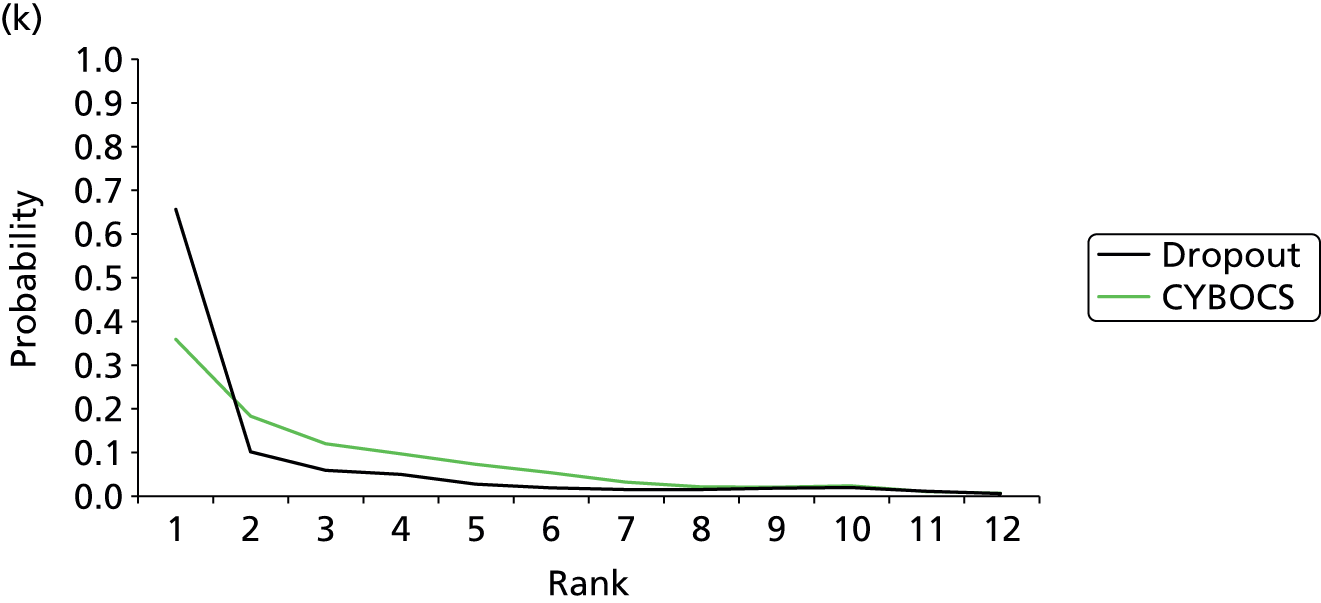


Meta-regression
We were not able to explore fully the impact of effect modifiers as we had originally planned, because in the children and adolescent networks, there were an insufficient number of studies (CYBOCS) and/or insufficient data (dropouts) for the analysis to be feasible. Therefore, these analyses were not undertaken.
Chapter 7 Assessment of cost-effectiveness
Background
The economic burden of obsessive–compulsive disorder
The total economic burden of OCD for the NHS and society in the UK is difficult to estimate and is not accurately known. 237 Work conducted in the USA during the 1990s suggests that the total costs of OCD equated to 5.7% of the estimated US$147.8B cost of all mental illness, and 18.0% of the costs of all anxiety disorders. 238 The direct costs to health services and patients of medical care represents only one aspect of the total burden. Indirect costs to patients and society as a result of lost productivity and wider impacts on informal care from friends and family members are also substantial. 239 Very few studies have estimated the per-patient health-care costs of OCD or the incremental costs compared with the general population or patients with other mental health problems. 240,241 The limited evidence available suggests that OCD has a similar health-care burden to depression, but with a relatively higher use of psychotropic medications. 240 The high cost of care for patients with OCD raises the possibility that therapies with a substantial and sustained effect on symptoms may reduce health-care costs in the long run.
Existing evidence on the cost-effectiveness of treatment for obsessive–compulsive disorder: primary studies
There are very few primary economic studies of interventions for patients with OCD, particularly economic evaluations conducted alongside RCTs likely to provide the most internally valid data. Tolin et al. 242 collected cost and outcome data alongside a trial comparing stepped with standard ERP therapy in 30 adults with moderate OCD symptoms (YBOCS score of ≥ 16) of at least 12 months’ duration. This study reported no statistically significant differences in efficacy between interventions, measured by mean improvement in YBOCS scores or response rates (defined as YBOCS score of ≤ 12) at 3 months’ follow-up. Total costs, including direct and indirect costs to patients, those who pay for health care (e.g. regional health-care authorities) and health-care providers (e.g. hospitals), were lower in the stepped care arm (US$2480 vs. US$4280; p < 0.05). An incremental cost-effectiveness ratio was not calculated and the small sample size limits interpretation. However, the authors conclude that their results suggest that stepped ERP care can significantly reduce treatment costs. McCrone et al. 243 report an economic evaluation of a three-arm RCT178 comparing computer-guided BT, clinician-guided BT and a relaxation control therapy in 218 adults with DSM-IV-defined OCD. In incremental analyses, the authors report that the cost per one point improvement in YBOCS score of computer-guided therapy (£64, 95% CI £36 to £249) and clinician-guided therapy (£90, 95% CI £61 to £167) was modest compared with relaxation control.
A Cochrane review of psychological treatments for OCD, noting the lack of evidence on efficiency, called for future trials to include an economic evaluation. 244 Such trials are under way, including the Obsessive Compulsive Treatment Efficacy Trial,245 which compares the cost-effectiveness of computerised CBT with guided self-help, and a Dutch trial comparing schema therapy versus clarification-oriented psychotherapy versus treatment as usual. 246 When published, these trials will improve the evidence base on cost-effective care for OCD. However, they will not answer many of the questions facing clinicians, policy-makers and health-care funders. A single trial cannot compare the large number of pharmacological and behavioural therapies available for OCD and typically will not have sufficient follow-up to determine whether or not initially expensive therapies are justified by better long-term outcomes. 247 A decision analysis based on a NMA of RCTs, estimating costs and outcomes beyond the end of trial follow-up is likely to provide the best evidence to inform this complex decision.
Existing evidence on the cost-effectiveness of treatment for obsessive–compulsive disorder: models
Previous work248 has developed decision-analytic models to evaluate the cost-effectiveness of therapy for patients with OCD underpinning the NICE appraisal of computerised CBT. These authors developed a decision tree comparing three interventions (computer-guided BT, clinician-led BT or relaxation) based predominantly on one RCT in 218 adults with DSM-IV-defined OCD. The decision model tracked compliance with BT, response among compliers and relapse among responders during 6-month cycles over an 18-month time horizon. The authors concluded that, subject to substantial uncertainties, therapist-led CBT is cost-effective compared with relaxation and that computerised CBT has the potential to be cost-effective, depending on the licence fees for health-care commissioners. 248 The authors acknowledged significant limitations in their model, particularly relating to the indirect method of estimating quality-of-life (utility) scores for calculating quality-adjusted life-years (QALYs) because data on this parameter are scarce.
In developing their clinical guidelines for the treatment of OCD, NICE118 also describe a crude model for comparing the cost-per-responder of usual care, SSRIs, CBT and combination therapy. Pooled effect sizes for each therapy were estimated based on separate pairwise meta-analyses. NICE concluded that CBT alone is dominated by SSRIs and combination therapy and, therefore, that CBT alone is unlikely to be cost-effective. However, this conclusion does not appear to be supported by the data (see table 3, p. 214118); furthermore, no probabilistic sensitivity analyses were conducted to estimate statistical uncertainty about this conclusion.
Our model addresses a broader question than the previous cost per QALY gained model248 by comparing behavioural and pharmacological interventions. We used a more comprehensive range of evidence, based on a NMA of RCTs, to inform model estimates of effect size and allowing a full probabilistic assessment of the relative cost-effectiveness of treatment strategies.
Cost-effectiveness model methods
Overview
The model evaluates the cost-effectiveness (cost per QALY gained) of pharmacotherapies, psychological interventions and combinations of both from a NHS perspective. In the final section of this chapter, we discuss the likely implications of a broader societal perspective. The primary model time horizon is 5 years. The interventions evaluated in trials are relatively inexpensive, meaning that therapies with a sustained effect on OCD symptoms would be expected to become cost-effective over a relatively short time horizon. Furthermore, as longitudinal cohort studies of patients with OCD over protracted periods of time are rare, any extrapolation of trial results over the lifetime of patients would be very speculative. Therefore, we elected to evaluate cost-effectiveness over a 5-year time horizon. The model uses probabilistic analysis to quantify the stochastic uncertainty around estimates of cost-effectiveness. The importance of parameter and structural uncertainty is also tested through sensitivity analyses.
Patient populations and interventions compared
The model evaluates the cost-effectiveness of interventions in two patient populations; children and adolescents, and adults. This reflects our NMA, which is also stratified by age. The weighted average age of patients recruited to adult trials is approximately 36 years, compared with 12 years in trials conducted in children or adolescents. The model structure is identical for the two populations; however, the parameter values vary to reflect differing treatment effects and long-term probabilities of response and relapse in these patient populations. All active interventions that were included in the NMA for both outcomes (dropout and YBOCS/CYBOCS scores) were compared in the cost-effectiveness model. We did not evaluate pharmacological and psychological placebos and the herbal remedy hypericum, as they are not directly relevant to NHS decision-makers. In total, there were 13 interventions compared in adult trials, including six SSRIs (see Table 20), and seven interventions evaluated in trials of children and adolescents, including three SSRIs (see Table 37). As the NMA revealed no clear difference within SSRIs in effect on symptoms or dropout rates, we elected to evaluate SSRIs at the class level in the cost-effectiveness analysis. Therefore, the cost-effectiveness of eight interventions in the adult model and five interventions in the child and adolescent model is compared. In sensitivity analyses, we reran the model restricting the evidence on treatment response and dropout rates to those RCTs considered to have (1) low attrition; (2) low risk of bias on ‘incomplete outcome assessment’; or (3) low risk of bias on ‘blinding of the outcome assessor’, to evaluate the potential impact of RCT bias on our findings and mirror the NMA. In the adult model, we also conducted a sensitivity analysis excluding RCTs that used a waitlist control group for psychological therapies. Blinding of participants is not possible in these trials and, therefore, they may be more prone to bias.
Model structure
The model comprises a decision tree covering the initial response to treatment at 12 weeks and a Markov model to simulate the course, costs and outcomes (utilities) of OCD from 12 weeks to 5 years. The initial 12-week period is chosen, as this represents the median follow-up period used in the trials summarised in our meta-analysis. The structure of the decision tree is the same for all interventions in both adult and child and adolescent models (Figure 12). Patients are assigned to treatment and will either continue to receive the prescribed course of treatment during the 12-week period or prematurely discontinue treatment (drop out). In our primary analysis, we assumed that if a patient drops out of treatment they get no benefit from treatment (‘no response’). Patients who continue treatment (comply) during the 12-week period are categorised in accordance with the degree to which their symptoms improve after treatment (‘full response’, ‘partial response’, ‘no response’). The appropriateness of the assumption that patients who drop out of treatment have no response depends on the statistical methods used in RCTs when analysing CYBOCS/YBOCS scores. It would be appropriate in trials reporting ‘per-protocol’ analyses, where mean CYBOCS/YBOCS scores exclude those who drop out. However, in trials reporting ‘intention-to-treat’ analyses where dropouts are already included in the CYBOCS/YBOCS effect estimate, it would effectively double-weight poorer outcomes in patients who drop out. It was often difficult to ascertain whether trials had conducted a pure ‘per-protocol’ analysis or a pure ‘intention-to-treat’ analysis. Therefore, in sensitivity analysis, we test this structural assumption.
After the initial 12 weeks, the course of patients’ OCD symptoms is tracked using a Markov model with four health states (Figure 13). The Markov model includes a ‘dead’ state; however, in a young cohort of patients with OCD over a 5-year time horizon this will be a very rare event. The remaining three health states are connected by bidirectional arrows, meaning that patients in the model can relapse to a more symptomatic state or achieve partial or full symptom response at any point during the 5 years. In order to estimate the pathway of a patient cohort through this Markov model, we need information on nine transition probabilities at each time point (cycle) of the model. The Markov model uses a 12-week (3-month) cycle length to track OCD symptom response at intervals from 12 weeks to 5 years.
FIGURE 12.
Decision tree structure over the first 12 weeks.

FIGURE 13.
Markov model structure for disease course from 12 weeks to 5 years.

Model parameters: dropouts and responses during the initial 12 weeks
The results of the NMA are used to estimate the probability that patients will drop out of treatment before 12 weeks. In the meta-analysis, the ORs for dropout, compared with drug placebo, were typically close to 1 and, with the exception of clomipramine in adults, had wide CrIs spanning unity (see Tables 27 and 44). The equivalent probability of dropout and associated CrIs for each intervention are provided in Table 49 (adults) and Table 50 (children/adolescents).
| Intervention | Source | Probability | 95% CrI | Probabilistic analysis |
|---|---|---|---|---|
| SSRIs | NMA | 0.21 | 0.15 to 0.28 | 5000 MCMC posterior distribution |
| Venlafaxine | NMA | 0.10 | 0.03 to 0.22 | 5000 MCMC posterior distribution |
| Clomipramine | NMA | 0.27 | 0.20 to 0.36 | 5000 MCMC posterior distribution |
| BT | NMA | 0.21 | 0.10 to 0.35 | 5000 MCMC posterior distribution |
| CBT | NMA | 0.17 | 0.08 to 0.29 | 5000 MCMC posterior distribution |
| CT | NMA | 0.21 | 0.09 to 0.37 | 5000 MCMC posterior distribution |
| Fluvoxamine + CBT | NMA | 0.41 | 0.01 to 0.96 | 5000 MCMC posterior distribution |
| Clomipramine + BT | NMA | 0.25 | 0.11 to 0.44 | 5000 MCMC posterior distribution |
| Intervention | Source | Probability | 95% CrI | Probabilistic analysis |
|---|---|---|---|---|
| SSRIs | NMA | 0.20 | 0.04 to 0.48 | 5000 MCMC posterior distribution |
| Clomipramine | NMA | 0.46 | 0.11 to 0.87 | 5000 MCMC posterior distribution |
| BT | NMA | 0.62 | 0.09 to 0.99 | 5000 MCMC posterior distribution |
| CBT | NMA | 0.14 | 0.02 to 0.42 | 5000 MCMC posterior distribution |
| CBT + sertraline | NMA | 0.16 | 0.02 to 0.49 | 5000 MCMC posterior distribution |
We also used the results of the NMA to estimate the initial probability of full, partial and no response to therapy. One challenge in using this modelling approach is that there is no consistent definition in the literature of how response should be measured or categorised. 249 Response may be defined based on the CYBOCS/YBOCS, using absolute (e.g. YBOCS score of ≤ 12) or relative (e.g. YBOCS score improves by ≥ 25 or 30% or 35% from baseline) thresholds,90,250,251 or using additional measures such as the Clinical Global Impressions252 scale assessment of overall illness improvement or psychiatric status ratings (PSRs). 91,97 Not all RCTs in the NMA reported response rates, and definitions of response varied among those that did. Therefore, it is not possible to directly estimate response rates from the meta-analysis. Instead, we indirectly estimate the initial response based on CYBOCS/YBOCS scores. In our primary analysis, we used a CYBOCS/YBOCS score threshold of < 16 to define full response and a CYBOCS/YBOCS score of ≥ 16 and < 20 to define partial response. The < 20 threshold corresponds to an approximately 25% improvement or 1 SD improvement upon the mean baseline YBOCS scores observed in trials. We tested a range of other values in sensitivity analysis.
We estimate a normal distribution for individual CYBOCS/YBOCS scores on placebo (reference). The mean of this distribution is estimated by fitting a standard normal random-effects meta-analysis model to all reference (placebo) arms of trials (included in the NMA) that recorded a mean score and standard error at follow-up. The mean score was estimated using a standard meta-analysis model in which each study provides an estimate of the mean with associated standard error. The SD of the distribution is estimated by fitting a normal random-effects distribution to the SDs at follow-up for all treatments that report this. Note that this assumes that the spread of CYBOCS/YBOCS scores does not depend on treatment. A prediction from these two random-effects distributions (i.e. predictive distribution for mean and SD response) is used to describe our uncertainty in the estimated normal distribution parameters. Relative treatment effects obtained from the NMA were added to the mean reference (placebo) CYBOCS/YBOCS scores, to obtain a predicted mean CYBOCS/YBOCS score for each intervention, and the SD in absolute scores is assumed to be equal for all interventions [and equal to that predicted for the reference (placebo)]. This gives us a prediction for the distribution of absolute CYBOCS/YBOCS scores across individuals for each intervention at follow-up. Assuming these scores follow a normal distribution, the proportion of patients achieving a CYBOCS/YBOCS score of < 16 (full response), between 16 and 20 (partial response), and > 20 (no response) were estimated using appropriate evaluations of the cumulative distribution function for the normal distribution. All of the above is computed at each iteration of a Bayesian Markov chain Monte Carlo simulation, so that we fully reflect uncertainty and correlations in our estimates of the proportions in each category for each intervention. The resulting probabilities for response at 12 weeks, stratified by intervention class and age, are provided in Tables 51 and 52.
| Intervention | Source | Probability of full response | 95% CrI | Probability of partial response | 95% CrI | Probabilistic analysis |
|---|---|---|---|---|---|---|
| SSRIs | NMA | 0.32 | 0.02 to 0.71 | 0.22 | 0.09 to 0.42 | 5000 MCMC posterior distribution |
| Venlafaxine | NMA | 0.32 | 0.01 to 0.78 | 0.20 | 0.05 to 0.40 | 5000 MCMC posterior distribution |
| Clomipramine | NMA | 0.39 | 0.04 to 0.79 | 0.22 | 0.10 to 0.43 | 5000 MCMC posterior distribution |
| BT | NMA | 0.84 | 0.50 to > 0.99 | 0.09 | < 0.01 to 0.23 | 5000 MCMC posterior distribution |
| CBT | NMA | 0.42 | 0.05 to 0.86 | 0.21 | 0.08 to 0.42 | 5000 MCMC posterior distribution |
| CT | NMA | 0.80 | 0.39 to > 0.99 | 0.11 | < 0.01 to 0.27 | 5000 MCMC posterior distribution |
| Fluvoxamine + CBT | NMA | 0.54 | 0.07 to 0.97 | 0.19 | 0.02 to 0.38 | 5000 MCMC posterior distribution |
| Clomipramine + BT | NMA | 0.78 | 0.33 to > 0.99 | 0.11 | < 0.01 to 0.29 | 5000 MCMC posterior distribution |
| Intervention | Source | Probability of full response | 95% CrI | Probability of partial response | 95% CrI | Probabilistic analysis |
|---|---|---|---|---|---|---|
| SSRIs | NMA | 0.53 | 0.05 to 0.97 | 0.16 | 0.02 to 0.31 | 5000 MCMC posterior distribution |
| Clomipramine | NMA | 0.62 | 0.08 to 0.99 | 0.14 | 0.01 to 0.29 | 5000 MCMC posterior distribution |
| BT | NMA | 0.71 | 0.13 to > 0.99 | 0.12 | < 0.01 to 0.26 | 5000 MCMC posterior distribution |
| CBT | NMA | 0.73 | 0.19 to > 0.99 | 0.11 | < 0.01 to 0.26 | 5000 MCMC posterior distribution |
| CBT + sertraline | NMA | 0.78 | 0.25 to > 0.99 | 0.10 | < 0.01 to 0.24 | 5000 MCMC posterior distribution |
Model parameters: initial pharmacological and psychological therapy costs
The mean daily dose of pharmacological interventions varied between and within trials (see Appendix 6). In order to estimate the initial costs of pharmacotherapy, we selected a daily dose close to the mean of the mean daily doses reported in RCTs, stratified by adults and children and adolescents populations (Table 53). This dose was rounded to the nearest multiple of a tablet/capsule size available. We also used data on mean daily dose reported in RCTs to define the plausible maximum and minimum daily dose, and tested the impact of these daily doses on incremental costs and cost-effectiveness in deterministic sensitivity analyses.
| Intervention | Mean dose across arms, daily (mg)a | Minimum dose during the study (mg) | Maximum dose during the study (mg) | Daily dose in model (mg) | 12-week cost in model (£) | Cost of pack (for dropouts) (£) |
|---|---|---|---|---|---|---|
| Adults | ||||||
| SSRIs | 31.43 | 9.25 | ||||
| Fluoxetine | 49.46 | 20 | 80 | 60 | 8.48 | 1.01 |
| Fluvoxamine | 252.32 | 50 | 300 | 250 | 117.81 | 33.66 |
| Paroxetine | 45.95 | 20 | 60 | 50 | 9.21 | 3.29 |
| Sertraline | 154.25 | 50 | 200 | 150 | 12.48 | 4.16 |
| Citalopram | 42.73 | 20 | 60 | 40 | 3.51 | 1.17 |
| Escitalopram | 15 | 10 | 20 | 15 | 71.10 | 23.70 |
| Venlafaxine | 282.5 | 225 | 350 | 300 | 14.46 | 2.41 |
| Clomipramine | 196.48 | 50 | 300 | 200 | 25.80 | 2.15 |
| Children/adolescents | ||||||
| SSRIs | 22.92 | 9.56 | ||||
| Fluoxetine | 32.35 | 20 | 80 | 40 | 5.66 | 1.01 |
| Fluvoxamine | 165 | 50 | 200 | 150 | 70.69 | 33.66 |
| Sertraline | 154.36 | 25 | 200 | 150 | 12.48 | 4.16 |
| Clomipramine | 190 | 75 | 200 | 200 | 25.80 | 2.15 |
The unit costs for pharmaceuticals were based on the British National Formulary estimates. 253 The cheapest combination of pack sizes was used to derive the cost of pharmacotherapy for 12 weeks (Table 54). The cost of the SSRI class was estimated by taking an average cost of the SSRIs used in the RCTs, weighted by the number of participants randomised to each SSRI. We assumed that patients who complied with therapy would incur pharmaceutical costs throughout the initial 12-week period. We assumed that patients who dropped out of pharmacotherapy incurred only the cost of one prescription (see Table 53).
| Intervention | Units I | Unit dose I (mg) | Cost I, £ | Units II | Unit dose II (mg) | Cost II (£) | Units III | Unit dose III (mg) | Cost III (£) |
|---|---|---|---|---|---|---|---|---|---|
| SSRIs | |||||||||
| Fluoxetine | 30 | 20 | 1.01 | 30 | 60 | 28.79 | |||
| Fluvoxamine | 60 | 50 | 16.83 | 30 | 100 | 16.83 | |||
| Paroxetine | 30 | 20 | 1.52 | 30 | 30 | 1.77 | |||
| Sertraline | 28 | 50 | 1.92 | 28 | 100 | 2.24 | |||
| Citalopram | 28 | 10 | 0.91 | 28 | 20 | 1.00 | 28 | 40 | 1.17 |
| Escitalopram | 28 | 5 | 8.97 | 28 | 10 | 14.73 | 28 | 20 | 25.20 |
| Venlafaxine | 56 | 37.5 | 2.15 | 56 | 75 | 2.41 | |||
| Clomipramine | 28 | 10 | 1.30 | 28 | 25 | 1.71 | 28 | 50 | 2.15 |
The number of psychological therapy sessions showed little consistency within or between BT, CT and CBT trials (see Appendix 6), ranging from a maximum of 40 to fewer than 10 sessions. Session duration, where reported, ranged from < 1 hour to 2.5 hours per session. We estimated typical therapist contact hours of psychological therapy, stratified by therapy type (BT, CT and CBT) and patient group (adults, children/adolescents) based on the mean number of contact hours estimated from trial reports (Table 55). We used the contact hours reported in RCTs to define the plausible maximum and minimum contact hours for use in sensitivity analyses. We used Personal Social Services Research Unit (PSSRU)254 unit costs to value initial psychological therapy. The estimated hourly face-to-face cost of conducting all types of psychological therapy (BT, CT and CBT) was assumed to be equal to the CBT hourly cost (£99; 2013 prices) estimated by the PSSRU. We assumed that patients who dropped out of psychological therapy did so after attending, on average, one-quarter of sessions, thereby incurring one-quarter of therapy costs. The cost of combinations of pharmacological and psychological therapies were estimated to be the sum of the components.
| Intervention | Mean hours across arms | Minimum hours | Maximum hours | Cost per therapy (£) | Cost for patients dropping out (£) |
|---|---|---|---|---|---|
| Adult | |||||
| BT | 17.17 | 10 | 46.5 | 1699.83 | 424.96 |
| CBT | 20.78 | 10 | 60 | 2057.22 | 514.31 |
| CT | 15.25 | 8 | 30 | 1509.75 | 377.44 |
| Children/adolescents | |||||
| BT | 22.5 | 15 | 30 | 2227.50 | 556.88 |
| CBT | 15 | 10 | 21 | 1485.00 | 371.25 |
Model parameters: mortality, symptoms, costs and utilities in the longer term
Mortality
Epidemiological evidence255 suggests that mortality rates are not higher in individuals with OCD; indeed, observed mortality rates may be lower than the expected rates. Therefore, we used the Office for National Statistics all-cause mortality life tables256 to estimate mortality, independent of OCD symptom severity. Mortality was estimated based on the mean age of patients recruited to the adult and child and adolescent RCTs, and mortality estimates were weighted to reflect their gender profile (see Appendix 10).
Symptoms
Most trials included in the NMA had relatively short periods of follow-up; there is little evidence from RCTs on how differences between interventions evident in the short term (e.g. 12 weeks) might be sustained in the longer term. 122 In our primary economic analysis, we assumed that, after the first 12-week period, the initial choice of therapy did not affect the probability of further remission or relapse. In other words, initial therapy affected the probability of being in each of the three health states in the Markov model (full, partial or no response) at 12 weeks, but did not affect transition probabilities thereafter. We tested other assumptions in sensitivity analyses.
In order to identify evidence on transition probabilities for OCD symptom severity, we conducted a rapid literature review. We used an adapted version of the Scottish Intercollegiate Guidelines Network MEDLINE filter for observational studies257 supplemented with text words for OCD and the YBOCS to identify studies reporting on the long-term course of OCD remission and relapse in adults and in children and adolescents (see Appendix 10). Of 561 articles initially identified, we selected 24 for full-text review, based on the title and abstract. On review of the full text, we selected two publications, Mancebo et al. 97 and Eisen et al. ,91 based on the Brown Longitudinal Obsessive–Compulsive Study (BLOCS) cohort study as containing the most relevant information on remission and relapse transition probabilities. The BLOCS recruited treatment-seeking subjects (325 adults and 70 children) with OCD from multiple psychiatric treatment settings in the USA (71% outpatient OCD clinic, 4% inpatient units, 25% community mental health centres). Subjects had annual assessments using a semistructured interview. Each assessment recorded a weekly PSR, which was used to define partial or full remission and any subsequent relapse. PSR is a rating of 6 points based on OCD symptom severity and functional impairment. A rating of 6 points indicates the most severe symptoms and impairment, and one indicates no OCD symptoms or impairment. BLOCS defined full remission as a PSR score of ≤ 2 (minimal or no symptoms and no impairment) for 8 consecutive weeks, partial remission as a score of 3 (symptoms present for less than 1 hour daily, but not impairing) for 8 consecutive weeks and relapse as a score of 4 or more for 4 consecutive weeks after achieving a full or partial response.
Eisen et al. 91 report the 5-year course of symptoms for 213 adults enrolled in the BLOCS who had at least 3 years of follow-up data. Over 5 years, 36 (16.9%) patients in the sample had full remission and a further 47 (22.1%) had partial remission. However, subsequent relapse was common in those who achieved partial remission (70%) or full remission (45%). Mancebo et al. 97 report the 3-year course of symptoms for 46 children and adolescents, aged 6–18 years, participating in the BLOCS who met the DSM-IV criteria for OCD at enrolment and completed at least 2 years of follow-up. Of these, 12 (27%) had achieved full remission by 3 years and a further 12 (27%) were in partial remission; five (21%) of these 24 individuals subsequently relapsed.
Data used to estimate ‘no response’ to ‘partial response’ and ‘no response’ to ‘full response’ time-varying transition probabilities in both adult and child and adolescent populations over the first 36 months post treatment were obtained from Mancebo et al. 97 From 36 to 60 months, in the absence of direct evidence from the BLOCS, the transition probabilities were assumed to remain constant (i.e. equal to the 31–36 month transition probabilities). Six-monthly probabilities were converted to 3-monthly probabilities to match the model cycle length.
A plot in Eisen et al. 91 displayed the probability of relapse after initial response, stratified by partial and full response, over 4 years in an adult population. Three-monthly transition probabilities were extracted from this plot using Digitizeit version 2.0 (Bormisoft, Braunschweig, Germany; www.digitizeit.de/) software that extracts numerical data from images. The 3-monthly transition probabilities between 48 and 60 months were assumed to remain constant (i.e. equal to the 46- to 48-month probabilities). In children and adolescents, Mancebo et al. 97 report that 5 of 24 subjects (21%) who had partial or full response subsequently relapsed over a study period of, on average, 88 weeks. However, this study did not provide further detail on relapse rates over time. Therefore, we assumed that the relapse probability was constant over the 5-year period and that the relative proportion of relapse from full or partial response was the same as that observed in the adult population.
These two articles provide evidence on the bidirectional time-varying transition probabilities between full response and no response (i.e. relapse) and between partial response and no response. However, they do not provide evidence on the transition probabilities between full and partial response. In our primary analysis, we arbitrarily assumed no transition between full and partial response, which is equivalent to assuming the proportion of patients moving from partial to full response is counterbalanced in each cycle by the proportion of patients moving from full to partial response. We tested other assumptions in sensitivity analyses. The time-varying transition probabilities for adults and children and adolescents are presented in Tables 56 and 57, respectively.
| Time period for Markov model (months) | Source | Rate | Aa | Ba | Probabilistic distribution |
|---|---|---|---|---|---|
| No response to partial or full response | |||||
| 0–6 | Mancebo et al., 201497 | 0.109 | 24 | 221 | Beta |
| 7–12 | Mancebo et al., 201497 | 0.091 | 18 | 197 | Beta |
| 13–18 | Mancebo et al., 201497 | 0.039 | 7 | 179 | Beta |
| 19–24 | Mancebo et al., 201497 | 0.070 | 12 | 172 | Beta |
| 25–30 | Mancebo et al., 201497 | 0.038 | 6 | 160 | Beta |
| 31–36 | Mancebo et al., 201497 | 0.052 | 8 | 154 | Beta |
| 37+b | Mancebo et al., 201497 | 0.052 | 8 | 154 | Beta |
| Proportion of responders who have full response | |||||
| 0–6 | Mancebo et al., 201497 | 0.208 | 5 | 24 | Beta |
| 7–12 | Mancebo et al., 201497 | 0.278 | 5 | 18 | Beta |
| 13–18 | Mancebo et al., 201497 | 0.571 | 4 | 7 | Beta |
| 19–24 | Mancebo et al., 201497 | 0.500 | 6 | 12 | Beta |
| 25–30 | Mancebo et al., 201497 | 0.667 | 4 | 6 | Beta |
| 31–36 | Mancebo et al., 201497 | 0.500 | 4 | 8 | Beta |
| 37+b | Mancebo et al., 201497 | 0.500 | 4 | 8 | Beta |
| Partial response to no response (relapse) | |||||
| 0–3 | Eisen et al., 201391 | 0.013 | 0.59 | 46.41 | Beta |
| 4–6 | Eisen et al., 201391 | 0.170 | 6.83 | 40.17 | Beta |
| 7–9 | Eisen et al., 201391 | 0.098 | 4.18 | 42.82 | Beta |
| 10–12 | Eisen et al., 201391 | 0.057 | 2.54 | 44.46 | Beta |
| 13–15 | Eisen et al., 201391 | 0.046 | 2.07 | 44.93 | Beta |
| 16–18 | Eisen et al., 201391 | 0.000 | 0.00 | 47.00 | Beta |
| 19–21 | Eisen et al., 201391 | 0.035 | 1.60 | 45.40 | Beta |
| 22–24 | Eisen et al., 201391 | 0.065 | 2.87 | 44.13 | Beta |
| 25–27 | Eisen et al., 201391 | 0.000 | 0.00 | 47.00 | Beta |
| 28–30 | Eisen et al., 201391 | 0.000 | 0.00 | 47.00 | Beta |
| 31–33 | Eisen et al., 201391 | 0.074 | 3.24 | 43.76 | Beta |
| 34–36 | Eisen et al., 201391 | 0.074 | 3.24 | 43.76 | Beta |
| 37–39 | Eisen et al., 201391 | 0.034 | 1.55 | 45.45 | Beta |
| 40–42 | Eisen et al., 201391 | 0.020 | 0.94 | 46.06 | Beta |
| 43–45 | Eisen et al., 201391 | 0.031 | 1.41 | 45.59 | Beta |
| 46–48 | Eisen et al., 201391 | 0.029 | 1.32 | 45.68 | Beta |
| 49+c | Eisen et al., 201391 | 0.029 | 1.32 | 45.68 | Beta |
| Full response to no response (relapse) | |||||
| 0–3 | Eisen et al., 201391 | 0.011 | 0.38 | 35.62 | Beta |
| 4–6 | Eisen et al., 201391 | 0.107 | 3.47 | 32.53 | Beta |
| 7–9 | Eisen et al., 201391 | 0.026 | 0.90 | 35.10 | Beta |
| 10–12 | Eisen et al., 201391 | 0.035 | 1.22 | 34.78 | Beta |
| 13–15 | Eisen et al., 201391 | 0.068 | 2.30 | 33.70 | Beta |
| 16–18 | Eisen et al., 201391 | 0.022 | 0.79 | 35.21 | Beta |
| 19–21 | Eisen et al., 201391 | 0.001 | 0.04 | 35.96 | Beta |
| 22–24 | Eisen et al., 201391 | 0.000 | 0.00 | 36.00 | Beta |
| 25–27 | Eisen et al., 201391 | 0.030 | 1.04 | 34.96 | Beta |
| 28–30 | Eisen et al., 201391 | 0.030 | 1.04 | 34.96 | Beta |
| 31–33 | Eisen et al., 201391 | 0.048 | 1.66 | 34.34 | Beta |
| 34–36 | Eisen et al., 201391 | 0.047 | 1.62 | 34.38 | Beta |
| 37–39 | Eisen et al., 201391 | 0.014 | 0.50 | 35.50 | Beta |
| 40–42 | Eisen et al., 201391 | 0.010 | 0.36 | 35.64 | Beta |
| 43–45 | Eisen et al., 201391 | 0.011 | 0.40 | 35.60 | Beta |
| 46–48 | Eisen et al., 201391 | 0.010 | 0.36 | 35.64 | Beta |
| 49+c | Eisen et al., 201391 | 0.010 | 0.36 | 35.64 | Beta |
| Time period for Markov model (months) | Source | Rate | Aa | Ba | Probabilistic distribution |
|---|---|---|---|---|---|
| No response to partial or full remission | |||||
| 0–6 | Mancebo et al., 201497 | 0.087 | 4 | 46 | Beta |
| 7–12 | Mancebo et al., 201497 | 0.143 | 6 | 42 | Beta |
| 13–18 | Mancebo et al., 201497 | 0.111 | 4 | 36 | Beta |
| 19–24 | Mancebo et al., 201497 | 0.156 | 5 | 32 | Beta |
| 25–30 | Mancebo et al., 201497 | 0.111 | 3 | 27 | Beta |
| 31–36 | Mancebo et al., 201497 | 0.083 | 2 | 24 | Beta |
| 37+b | Mancebo et al. 201497 | 0.091 | 2 | 22 | Beta |
| Proportion of responders who have full response | |||||
| 0–6 | Mancebo et al., 201497 | 0.500 | 2 | 4 | Beta |
| 7–12 | Mancebo et al., 201497 | 0.333 | 2 | 6 | Beta |
| 13–18 | Mancebo et al., 201497 | 0.500 | 2 | 4 | Beta |
| 19–24 | Mancebo et al., 201497 | 0.600 | 3 | 5 | Beta |
| 25–30 | Mancebo et al., 201497 | 0.667 | 2 | 3 | Beta |
| 31–36 | Mancebo et al., 201497 | 0.500 | 1 | 2 | Beta |
| 37+b | Mancebo et al., 201497 | 0.500 | 1 | 2 | Beta |
| Partial response to no response | |||||
| 88.2-week intervalc | Mancebo et al., 201497 and Eisen et al., 201391 | 0.333 | 3 | 9 | Beta |
| Full response to no response | |||||
| 88.2-week intervalc | Mancebo et al., 201497 and Eisen et al., 201391 | 0.200 | 2 | 10 | Beta |
Utilities
A rapid literature review was conducted to identify quality-of-life studies in OCD. The review identified 447 abstracts; after initial screening, 12 abstracts were selected for full-text review (see Appendix 10). Most studies did not use a generic preference-based outcome measure, such as the European Quality of Life-5 Dimensions (EQ-5D™) or Short Form questionnaire-6 Dimensions (SF-6D),258 both of which allow calculation of QALYs. Of those studies that did use these measures, several did not report results for the health states (full, partial, no response) that correspond to the Markov model. We did not find any studies reporting utility values in children and adolescents with OCD; therefore, we assume that the impact of OCD on health-related quality of life in adults is generalisable to children and adolescents and use one set of utility values for both age groups.
Hollander et al. 114 used data from two double-blind, placebo-controlled RCTs with similar eligibility criteria in adults with OCD. 124,128 Stein et al. 124 recruited 466 patients with a mean age of 23 years and a mean YBOCS score of 27, and Fineberg et al. 128 recruited 468 patients with a mean age of 23 years and a mean YBOCS score of 26.4. In this study, response was defined as a decrease in YBOCS score of ≥ 25% relative to baseline. In responders, relapse was defined as a subsequent increase in YBOCS score of 5 points or more, or an unsatisfactory treatment effect as judged by the investigators. Both studies collected Short Form questionnaire-36 Items data from which SF-6D utility scores were derived. The study estimates SF-6D utility values for adult patients at baseline (pre-randomisation) and for patients with response; no response; response and relapse; and response and no relapse at 16 weeks from the start of treatment. The definitions of response used by Hollander et al. 114 in measuring utility values do not correspond exactly with the definitions of response used by the BLOCS in defining symptom course. Therefore, we had to make assumptions about the most appropriate utility values to use in our Markov model. The utility values applied in our primary economic analysis are described in Table 58.
| Markov health state | Label used | Source | Mean utility value | SD | Probabilistic distribution |
|---|---|---|---|---|---|
| Pre-treatment | Baseline value | Hollander et al., 2010114 | 0.648 | 0.103 | 1 – gamma |
| Partial response | Response | Hollander et al., 2010114 | 0.725 | 0.108 | 1 – gamma |
| No response | No response | Hollander et al., 2010114 | 0.664 | 0.106 | 1 – gamma |
| Not used in Markov model | Relapse | Hollander et al., 2010114 | 0.684 | 0.116 | 1 – gamma |
| Full response | No relapse | Hollander et al., 2010114 | 0.776 | 0.113 | 1 – gamma |
Long-term costs of health care
Patients who fail to respond fully to initial therapy are likely to be prescribed a number of other pharmacological or psychological therapies with their attendant costs and benefits. Our cost-effectiveness model aims to predict the impact of initial therapy on longer-term costs and outcomes, but there is insufficient information to track all treatment switching or therapy combinations likely to occur in practice. We therefore assumed that the incremental differences in treatment cost after 12 weeks are driven solely by symptom severity. As previously discussed, the literature on the health-care costs of OCD is very sparse. The only study in the peer-reviewed literature that we are aware of which has estimated the per-patient costs of OCD used retrospective claims data from Medicaid enrolees in Florida. 248 Hankin et al. 240 used the ICD Ninth Edition diagnosis codes to identify 85 newly diagnosed patients with ‘pure OCD’ and 14,906 patients with newly diagnosed ‘pure depression’ in order to compare health-care costs over a 2-year period. The median 2-year cost of inpatient, outpatient and pharmacy health-care claims were similar in patients with OCD and depression (US$6588 for OCD vs. US$5347 for depression; Wilcoxon’s signed-rank p-value 0.27). However, the composition of costs differed; patients with OCD had higher use of psychotropic medications, whereas patients with depression had higher use of non-psychiatric outpatient care. The authors note that the long-term costs of OCD may be higher than those of depression because OCD is a chronic disorder requiring ongoing therapy, whereas depression is episodic in most cases. This study has limited value in informing our cost-effectiveness model, because it is based on findings from a selected subset of patients (i.e. eligible for Medicaid) in a US health-care setting in which unit costs are higher than in the NHS and the analysis does not stratify costs by symptom response to therapy.
In order to estimate a proxy NHS cost in our model for long-term OCD care, we assumed costs to be similar to patients treated for depression. In a study of 88,935 patients aged > 18 years, diagnosed with depression, Byford et al. 259 found that the mean 12-month NHS costs, including medications, primary care, psychological therapies and secondary care, were 33% lower among patients who achieved remission from depressive symptoms than in those who did not [£656 vs. £973 (2005/6 values) or £945 vs. £1402 at 2014 values; p < 0.001]. Therefore, we assumed that the annual NHS costs in patients with OCD who have no response to therapy were equivalent to patients with depression who do not achieve remission. Furthermore, in our primary analysis, we assumed that patients with OCD who have a full response to therapy will have 33% lower NHS costs, and we selected an arbitrary value (17% reduction) for patients with partial response to therapy. Owing to the weak and indirect evidence on costs, we tested these assumptions using a wide range of alternative values in our sensitivity analysis (Table 59).
| Health state | Source | Cost (£) | SE (£)a | Distribution |
|---|---|---|---|---|
| Full response | Byford et al., 2011259 | 236 | ||
| Partial response | Byford et al., 2011259 | 291 | ||
| No response | Byford et al., 2011259 | 351 | 88 | Log-normal |
| Dead | 0 |
Methods of analysis
The model was constructed in Microsoft Excel 2010. A half-cycle correction was applied to estimate costs and utilities for patients who move between health states during each cycle of the Markov model. Costs and utilities were discounted at 3.5%, in line with NICE guidelines. 260 Verification of the model’s internal validity was tested using extreme value analysis. The cost-effectiveness of each intervention is summarised using the net benefit statistic at thresholds of £20,000 and £30,000 (i.e. the amount the NHS is prepared to pay in order to produce a QALY). 260 Parametric uncertainty surrounding the point estimate is estimated using 95th-percentile intervals from a probabilistic analysis, generated using second-order Monte Carlo simulation taking 3000 random draws from parameter distributions. The probability that each intervention is the most cost-effective at a range of willingness-to-pay thresholds (£0–50,000 per QALY) is summarised using cost-effectiveness acceptability curves (CEACs). 261
Sensitivity analyses
We used a series of sensitivity analyses to evaluate the robustness of the cost-effectiveness results to several of the assumptions made within the model.
-
Risk of bias: we reran the model using the subset of studies that met the NMA criteria of low risk of bias in (1) overall attrition; (2) incomplete outcome assessment; or (3) blinding of outcome assessor to assess the potential impact of RCT bias on cost-effectiveness results. In the adult model, we also reran the model excluding RCTs that used a waitlist control for psychotherapy interventions.
-
Effectiveness in patients who drop out: we reran the model assuming that patients who dropped out of treatment had lower costs, but identical outcomes to those who completed treatment.
-
Definition of full response: we lowered the threshold for defining full response (≤ 12).
-
Cost of initial therapy: we used minimum and maximum dose and contact hours to assess the impact of initial therapy costs on cost-effectiveness estimates.
-
Sustained effect of initial therapy: we reduced the time horizon of the model to assess the impact on cost-effectiveness if treatment effects were sustained for fewer than 5 years.
-
Transition from full to partial response: we varied the net flow of patients from full to partial response in the Markov model to assess the impact on cost-effectiveness results.
-
Change cost of long-term care: we assessed the impact of assuming higher incremental long-term costs of care for patients with no response (compared with those with full and partial response).
-
SSRI costs: in both the adult and child and adolescent models we reran the model assuming that SSRI medication costs were equivalent to the cheapest SSRI, rather than the class average cost. Medication costs vary considerably among SSRIs and, therefore, if effectiveness is equivalent within the class, cheaper SSRIs will be more cost-effective.
-
Venlafaxine: in the adult model, we reran analyses excluding venlafaxine, which is not licensed for OCD despite being evaluated in a small number of RCTs for off-label use.
Cost-effectiveness results: adults
Primary cost-effectiveness analysis
The estimated NHS costs, QALYs and cost-effectiveness of each of the eight interventions in adults are reported in Table 60. Over a 5-year time period, the high upfront costs of psychological therapies are not completely offset by lower NHS costs in subsequent years. The three drug groups (SSRIs, clomipramine and venlafaxine) have the lowest NHS costs (range £5727–5788), strategies including CT and BT have higher costs (range £6590–6778), and strategies including CBT had the highest estimated costs (range £7206–7428). The difference in cost between CBT and the other two psychological therapies is partly attributable to the higher number of contact hours used in adult CBT trials (see Table 55) and partly attributable to the lower effect size of CBT estimated in the NMA (see Table 51).
| Intervention | Total costs (£) | Total QALYs | NMB (£20,000) (£) | Lower 95th percentile (£) | Upper 95th percentile (£) | NMB (£30,000) (£) |
|---|---|---|---|---|---|---|
| Fluvoxamine + CBT | 7206 | 3.219 | 57,174 | 53,043 | 61,108 | 89,364 |
| CBT | 7428 | 3.238 | 57,337 | 53,189 | 61,367 | 89,719 |
| SSRIs | 5788 | 3.208 | 58,373 | 54,498 | 62,047 | 90,453 |
| Clomipramine | 5751 | 3.215 | 58,549 | 54,768 | 62,061 | 90,699 |
| Venlafaxine | 5727 | 3.220 | 58,664 | 54,442 | 62,675 | 90,860 |
| Clomipramine + BT | 6778 | 3.299 | 59,208 | 55,120 | 62,692 | 92,201 |
| CT | 6590 | 3.313 | 59,668 | 55,571 | 63,112 | 92,797 |
| BT | 6715 | 3.320 | 59,695 | 55,718 | 63,168 | 92,899 |
Psychological therapies, particularly CT and BT, are estimated to result in the highest QALYs over the 5-year period. The absolute difference in QALYs is quite small [range from 3.208 (SSRIs) to 3.320 (BT)]. However, this range is approximately equivalent to an additional 365 days in ‘full response’ rather than ‘no response’ over the 5-year period. The net monetary benefit (NMB) (£20,000) column summarises cost-effectiveness if the NHS is willing to pay £20,000 for each QALY gained by patients, which is at the lower end of NICE’s stated threshold. Table 60 is ordered by this column, with interventions with the lowest estimated NMB (i.e. least cost-effective) at the top and interventions with the highest estimated NMB (i.e. most cost-effective) at the bottom. The interventions fall into three clusters based on NMB (£20,000). Strategies involving CT or BT are most cost-effective (NMB range £59,208–59,695). The additional upfront costs of the CT and BT strategies, compared with the pharmacological monotherapies are justified by better outcomes (QALYs). The pharmacological monotherapies have a similar range of cost-effectiveness [NMB range from £58,373 (SSRIs) to £58,664 (venlafaxine)]. Differences between the pharmacological monotherapies are driven by the slightly higher costs of SSRIs (see Table 53) and the low probability of dropout from venlafaxine estimated from two relatively small RCTs (see Table 49). The strategies including CBT have the poorest cost-effectiveness [NMB range from £57,174 (fluvoxamine + CBT) to £57,337 (CBT)]. The higher upfront costs of CBT, compared with pharmacotherapy, are not justified by the marginal improvement in symptom response (see Table 51). The 95th percentile intervals around the NMBs (£20,000) estimated by the probabilistic analysis overlap, indicate that there is no strong evidence that any single therapy is more cost-effective than the other therapies. The findings are not materially altered if the NHS is willing to pay more (NMB £30,000) for each QALY gained (Table 60).
The CEAC (Figure 14) depicts the probability that each intervention is the most cost-effective, on the vertical axis, as a function of increasing NHS willingness to pay for a QALY, on the horizontal axis. The CEAC demonstrates that at lower willingness-to-pay thresholds (i.e. < £10,000 per QALY), the cheaper pharmacotherapies (venlafaxine and clomipramine and, to a lesser extent, SSRIs) have higher probabilities of being most cost-effective. Once the willingness to pay exceeds NICE’s stated threshold (£20,000 per QALY), strategies involving CT and BT become the most likely to be cost-effective. The CEAC suggests that there is no clear ‘winner’ in terms of cost-effectiveness, with the difference in probability of being most cost-effective between the therapies ranked first and second rarely exceeding 0.1 across all willingness-to-pay values. Therapies including CBT had a very low probability of being most cost-effective across the range of willingness-to-pay values. These findings are supported by the cost-effectiveness acceptability frontier (Figure 15), which identifies, with a low degree of certainty, venlafaxine as the most cost-effective (optimal) therapy at low willingness-to-pay thresholds and BT as the optimal therapy at the thresholds (£20,000–30,000 per QALY) used by NICE.
FIGURE 14.
Cost-effectiveness acceptability curve: adults, primary analysis. CLO, clomipramine; FLV, fluvoxamine; VEN, venlafaxine.

FIGURE 15.
Cost-effectiveness acceptability frontier: adults, primary analysis. CLO, clomipramine; FLV, fluvoxamine; VEN, venlafaxine.

Sensitivity analyses
Full results of all sensitivity analyses are provided in Appendix 10. Here, we focus on the five sensitivity analyses that had most impact on the interpretation of the cost-effectiveness model.
The exclusion of evidence from RCTs that used waitlist controls decreased the probability that BT and CT strategies were most cost-effective at the thresholds (£20,000–30,000 per QALY) used by NICE (Figure 16). The difference in effectiveness between different types of psychological therapy was very small in this sensitivity analysis (Table 61). However, the higher estimated cost of CBT, owing to the higher number of contact hours used in adult CBT trials, meant that CBT strategies were less likely to be cost-effective. Clomipramine and BT had the highest probability of being cost-effective, although this did not exceed 0.4 (Figure 16).
FIGURE 16.
Cost-effectiveness acceptability curve: adults – excluding RCTs with waitlist controls. CLO, clomipramine; FLV, fluvoxamine; VEN, venlafaxine.
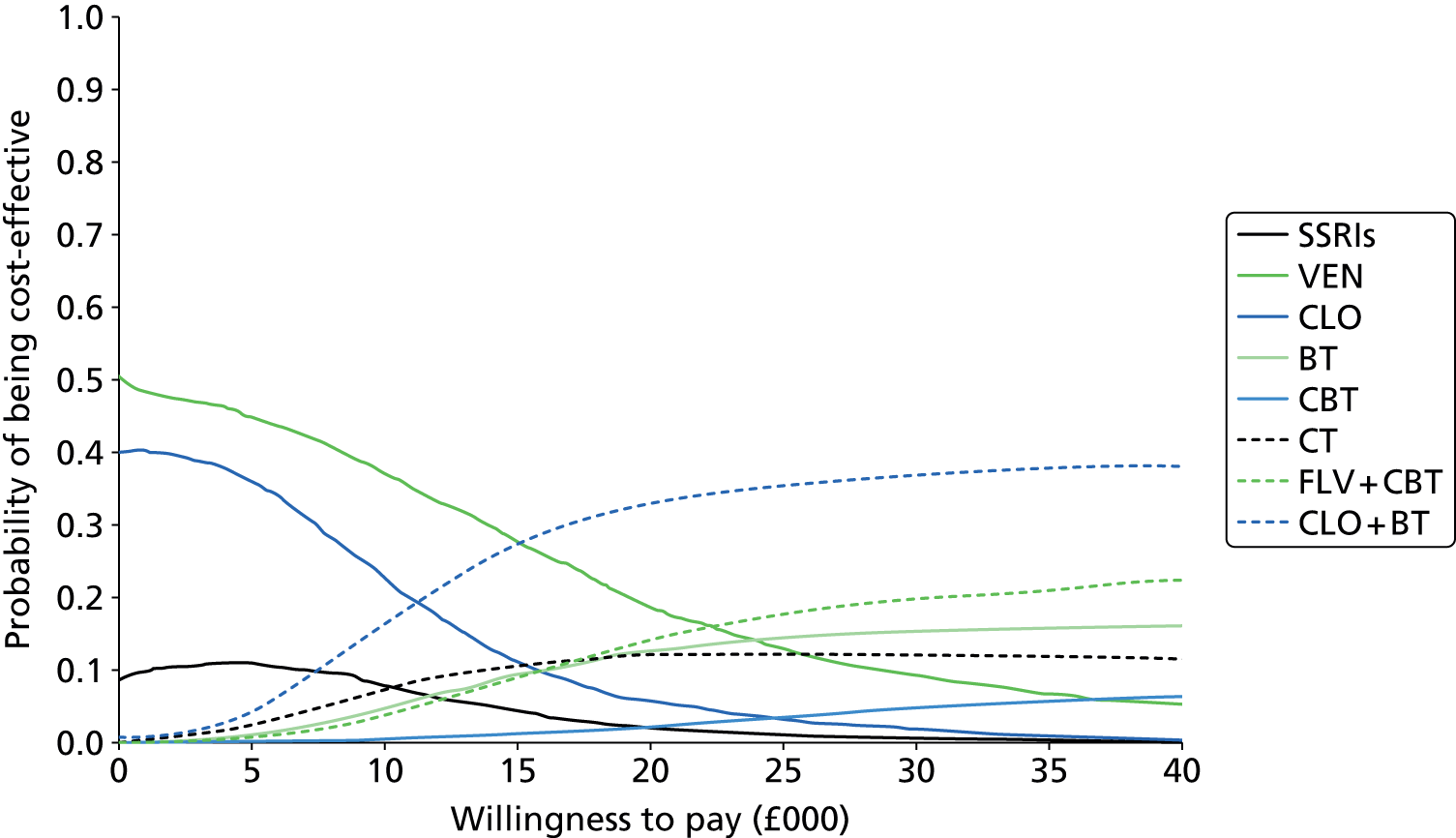
| Intervention | Total costs (£) | Total QALYs | NMB (£20,000) (£) | Lower 95th percentile (£) | Upper 95th percentile (£) | NMB (£30,000) (£) |
|---|---|---|---|---|---|---|
| CBT | 7385 | 3.256 | 57,743 | 53,805 | 61,290 | 90,307 |
| Fluvoxamine + CBT | 7438 | 3.266 | 57,883 | 53,879 | 61,846 | 90,543 |
| SSRIs | 5865 | 3.190 | 57,930 | 54,314 | 61,020 | 89,827 |
| Clomipramine | 5834 | 3.195 | 58,065 | 54,516 | 61,146 | 90,015 |
| Venlafaxine | 5822 | 3.197 | 58,115 | 54,344 | 61,527 | 90,084 |
| CT | 6818 | 3.256 | 58,296 | 54,354 | 61,773 | 90,853 |
| BT | 6920 | 3.265 | 58,380 | 54,612 | 61,851 | 91,030 |
| Clomipramine + BT | 6867 | 3.274 | 58,605 | 54,811 | 62,119 | 91,341 |
The most cost-effective pharmacotherapy was strongly dependent on assumptions about outcomes in patients who drop out. If we assume that the outcomes in patients who drop out are fully reflected in analyses of YBOCS scores in the meta-analysis (i.e. analyses were predominantly intention to treat), then clomipramine, rather than venlafaxine, is much more likely to be the most cost-effective pharmacotherapy at lower willingness-to-pay thresholds (Figure 17). The finding that strategies involving CT and BT become more cost-effective at higher willingness-to-pay thresholds is not affected by this assumption.
FIGURE 17.
Cost-effectiveness acceptability curve: adults – effectiveness in patients who drop out. CLO, clomipramine; FLV, fluvoxamine; VEN, venlafaxine.

The initial cost of therapy, particularly psychological therapies, was also influential. The number of contact hours of BT, CT and CBT differed greatly across RCTs (see Table 55). The impact of this on NHS costs of initial therapy was much greater than the range of daily doses used in pharmacotherapy trials. Therefore, if we assume that all psychological and pharmacological therapies have a cost at the upper end of the range evaluated in RCTs, pharmacotherapies become relatively cheaper and more cost-effective (Figure 18). Although psychological therapy (specifically CT) was still estimated to be cost-effective at higher willingness-to-pay thresholds, cheaper pharmacotherapies (e.g. venlafaxine and clomipramine) remain relatively cost-effective options at the £20,000-per-QALY threshold.
FIGURE 18.
Cost-effectiveness acceptability curve: adults – maximum cost of initial therapy. CLO, clomipramine; FLV, fluvoxamine; VEN, venlafaxine.

Assumptions about the sustainability of treatment effects observed in RCTs with short follow-up periods (e.g. 12 weeks) are influential on the cost-effectiveness results. Our primary analysis assumes that some of the benefits of more effective therapies (i.e. the psychological therapies, particularly CT and BT) are sustained beyond the end of the trial, although they gradually diminish as patients who had an initial response relapse. If we were to assume that all differences in intervention costs and benefits are limited to the within-trial period, then the initially cheaper pharmacotherapies (venlafaxine and clomipramine) are predominantly likely to be most cost-effective (Figure 19).
FIGURE 19.
Cost-effectiveness acceptability curve: adults – costs and benefits limited to the within-trial period. CLO, clomipramine; FLV, fluvoxamine; VEN, venlafaxine.

Excluding venlafaxine, which does not have a licensed indication in OCD, affected the choice of optimal intervention at lower willingness-to-pay thresholds (Figure 20). Under this scenario, clomipramine and, to a certain extent, SSRIs, become more likely to be cost-effective, but psychological therapies remain most likely to be cost-effective at the £20,000-per-QALY threshold.
FIGURE 20.
Cost-effectiveness acceptability curve: adults – excluding venlafaxine. CLO, clomipramine; FLV, fluvoxamine.
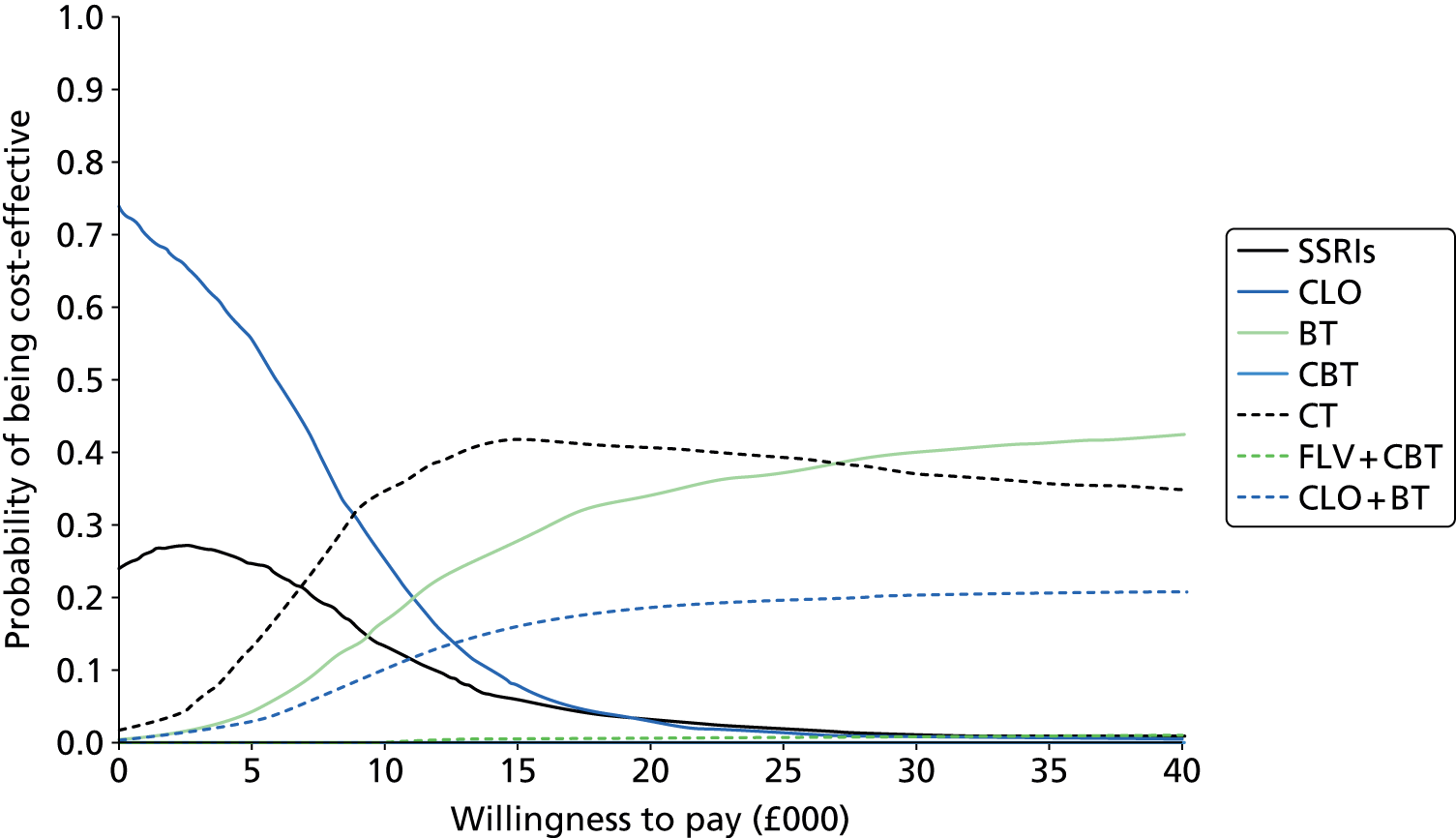
Cost-effectiveness results: children and adolescents
Primary cost-effectiveness analysis
The estimated NHS costs, QALYs and cost-effectiveness of each of the five interventions in children and adolescents are reported in Table 62. As with the adult population, over a 5-year time period, the high upfront costs of psychological therapies are not completely counterbalanced by lower NHS costs in subsequent years. The two pharmacotherapies (SSRIs and clomipramine) have the lowest NHS costs (range £5398–5515), and strategies including BT or CBT have higher costs (range £6418–6762). The cost of CBT was similar to BT, because RCTs in children and adolescents, unlike those in adults, used a similar number of contact hours to deliver CBT and BT (see Table 55).
In children and adolescents, strategies including CBT were estimated to result in the highest QALYs over the 5-year period. The absolute difference in QALYs is again relatively small [range from 3.254 (BT) to 3.376 (sertraline and CBT)]. However, this range is approximately equivalent to an additional 397 days in ‘full response’ rather than ‘no response’ over the 5-year period. The NMB (£20,000) column summarises cost-effectiveness if the NHS is willing to pay £20,000 for each QALY gained by patients, which is at the lower end of NICE’s stated threshold. Table 61 is ordered by this column, with interventions with the lowest estimated NMB (i.e. least cost-effective) at the top and interventions with the highest estimated NMB (i.e. most cost-effective) at the bottom. In contrast to findings in the adult population, BT was estimated to be least cost-effective (NMB £58,325). The additional upfront costs of BT, compared with the pharmacological monotherapies, were not justified by better outcomes (QALYs). In fact, the high dropout rate from BT among children and adolescents (see Table 50), albeit imprecisely estimated from two very small trials,218,220 led to BT being both more expensive and less effective than SSRIs and clomipramine. The pharmacological monotherapies have a similar range of cost-effectiveness [NMB range from £60,087 (clomipramine) to £60,828 (SSRIs)]. Differences between the pharmacological monotherapies are driven by higher dropout rates estimated for clomipramine than SSRIs (see Table 50). The cost-effectiveness of strategies including CBT was similar to pharmacotherapies [NMB range from £60,905 (CBT) to £61,107 (sertraline and CBT)]. The 95th percentile intervals around the NMBs (£20,000) estimated by the probabilistic analysis overlap, which indicates that there is no strong evidence that any single therapy is more cost-effective than any other therapy. Strategies including CBT became relatively more cost-effective if the NHS is willing to pay more (NMB £30,000) for each QALY gained (Table 62).
| Intervention | Total costs (£) | Total QALYs | NMB (£20,000) (£) | Lower 95th percentile (£) | Upper 95th percentile (£) | NMB (£30,000) (£) |
|---|---|---|---|---|---|---|
| BT | 6762 | 3.254 | 58,325 | 54,212 | 62,524 | 90,868 |
| Clomipramine | 5515 | 3.280 | 60,087 | 55,775 | 64,407 | 92,888 |
| SSRIs | 5394 | 3.311 | 60,828 | 56,298 | 65,162 | 93,934 |
| CBT | 6459 | 3.368 | 60,905 | 56,188 | 64,974 | 94,586 |
| Sertraline + CBT | 6418 | 3.376 | 61,107 | 56,510 | 65,215 | 94,869 |
The CEAC (Figure 21) depicts the probability that each intervention is the most cost-effective, on the vertical axis, as a function of increasing NHS willingness to pay for a QALY, on the horizontal axis. The CEAC demonstrates that at lower willingness-to-pay thresholds (i.e. < £15,000 per QALY), the pharmacotherapies (particularly SSRIs) are more likely to be most cost-effective. Once the willingness-to-pay threshold exceeds £20,000 per QALY, the combined strategy of CBT and sertraline becomes the most likely to be cost-effective, with a probability exceeding 0.5. BT had a very low probability of being most cost-effective across the range of willingness-to-pay values. These findings are supported by the cost-effectiveness acceptability frontier (Figure 22), which identifies SSRIs as probably the most cost-effective (optimal) therapy at low (< £15,000 per QALY) willingness-to-pay thresholds. At the thresholds (£20,000–30,000 per QALY) used by NICE, combined CBT and sertraline is the optimal therapy.
FIGURE 21.
Cost-effectiveness acceptability curve: children and adolescents – primary analysis. CLO, clomipramine; SER, sertraline.
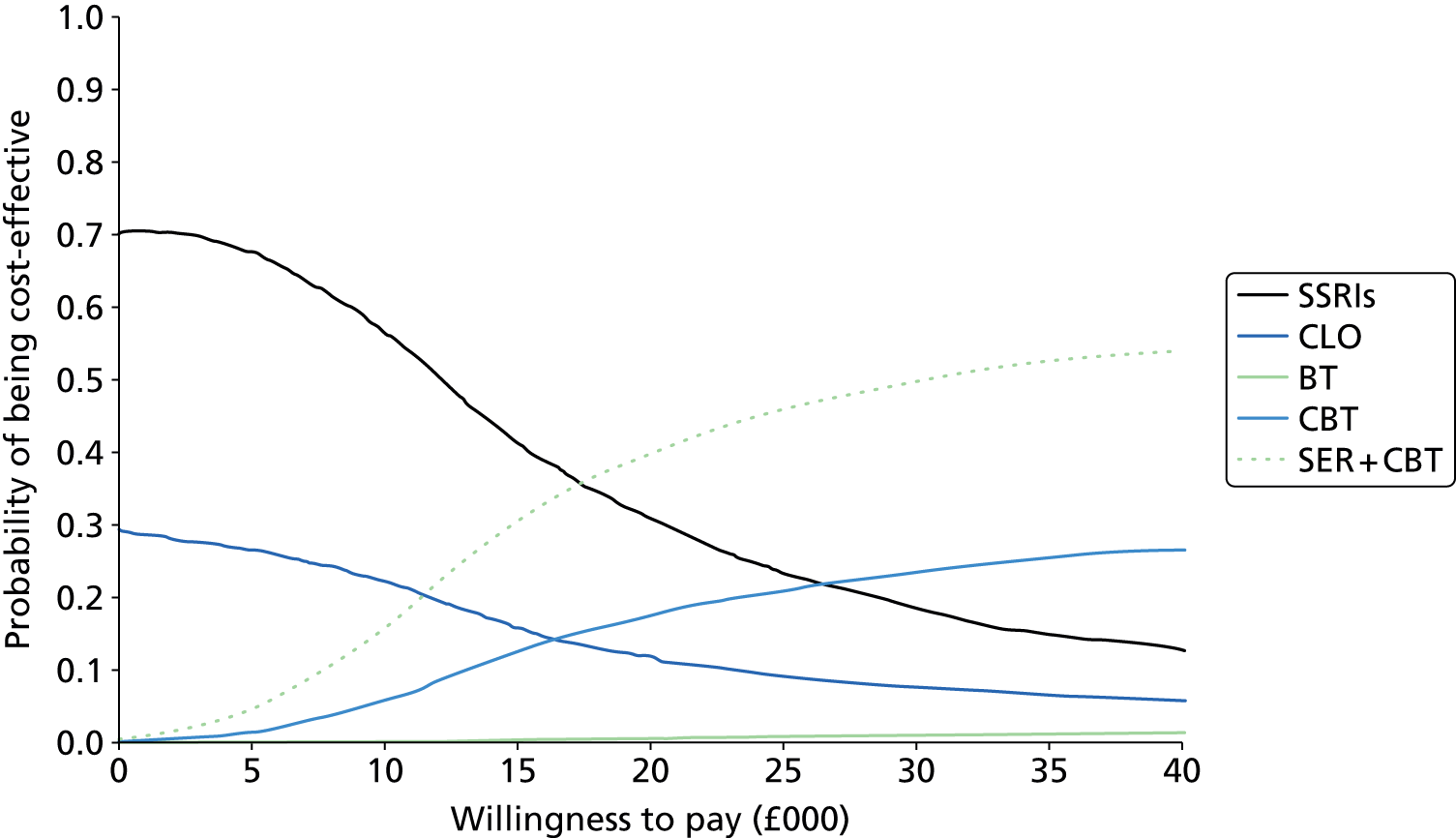
FIGURE 22.
Cost-effectiveness acceptability frontier: children and adolescents – primary analysis. CLO, clomipramine; SER, sertraline.

Sensitivity analyses
Full results of all sensitivity analyses are provided in Appendix 10. Here, we focus on the three sensitivity analyses that had most impact on the findings of the cost-effectiveness model.
The most cost-effective pharmacotherapy was again strongly dependent on assumptions about outcomes in patients who drop out. If we assume that the outcomes in patients who drop out are fully reflected in analyses of CYBOCS scores in the meta-analysis (i.e. analyses were predominantly intention to treat), then clomipramine, rather than SSRIs, is more likely to be the most cost-effective pharmacotherapy at lower willingness-to pay-thresholds (Figure 23) and continues to be more cost-effective than strategies including CBT even at higher willingness-to-pay thresholds.
FIGURE 23.
Cost-effectiveness acceptability curve: children and adolescents. Effectiveness in patients who drop out. CLO, clomipramine; SER, sertraline.

As with the adult RCTs, the initial cost of psychological therapies is difficult to estimate because the number of contact hours differed greatly across RCTs (see Table 55). The impact of this on NHS costs of initial therapy was much greater than the range of daily doses used in pharmacotherapy trials. Therefore, if we assume that all psychological and pharmacological therapies have a cost at the upper end of the range evaluated in RCTs, pharmacotherapies become relatively cheaper and more cost-effective (Figure 24). Although psychological therapy (specifically CBT and sertraline) was still estimated to be cost-effective at higher willingness-to-pay thresholds, SSRIs remain the most cost-effective option at the £20,000-per-QALY threshold.
FIGURE 24.
Cost-effectiveness acceptability curve: children and adolescents. Maximum cost of initial therapy. CLO, clomipramine; SER, sertraline.
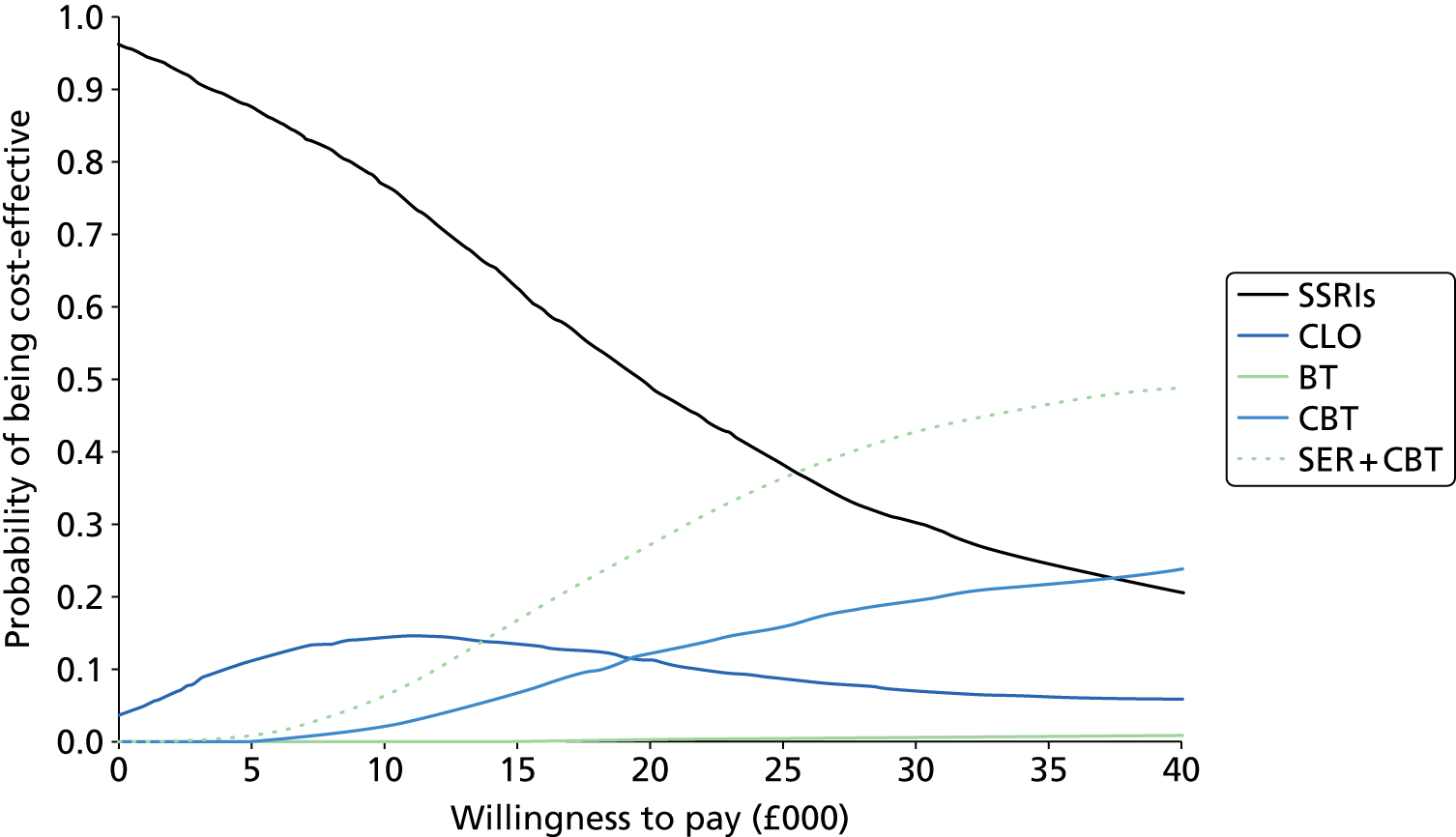
Assumptions about the sustainability of treatment effects observed in RCTs with short follow-up periods (e.g. 12 weeks) are influential on the cost-effectiveness results. Our primary analysis assumes that some of the benefits of more effective therapies (i.e. the psychological therapies, particularly CBT) are sustained beyond the end of the trial, although they gradually diminish as patients who had an initial response relapse. If we were to assume that all differences in intervention costs and benefits are limited to the within-trial period, then SSRIs are predominantly likely to be most cost-effective (Figure 25).
FIGURE 25.
Cost-effectiveness acceptability curve: children and adolescents. Costs and benefits limited to the within-trial period. CLO, clomipramine; SER, sertraline.

Chapter 8 Discussion
Principal findings
In this NMA, we compared the effect of pharmacological and psychological interventions for the management of OCD in all age groups. As far as we know, this is the first time that all available interventions for OCD have been compared in a single analysis using mixed evidence (direct and indirect). Previous meta-analyses on this issue had examined only the direct evidence between different interventions and most are now outdated. 120,262–264 More recent meta-analyses comparing the full range of treatment options in depression and anxiety disorders did not focus specifically on OCD and also used the direct comparisons. 265,266 Overall, we included 86 studies reported in 85 papers (64 in adults and 22 in children and adolescents) involving 8611 randomised patients (7306 adults and 1305 children and adolescents). In the total sample, 23 different interventions were tested in 194 arms. Interventions with the most studies were, in adults, clomipramine (n = 17), fluvoxamine (n = 16) and BT (n = 15) and, in children and adolescents, CBT (n = 9), fluoxetine (n = 4); clomipramine (n = 4) and sertraline (n = 4).
Clinical effectiveness findings
Results in adults
In total, 54 studies were included in this analysis, involving 6652 randomised patients. All active interventions, apart from venlafaxine and hypericum, had a greater effect than drug placebo on OCD symptom reduction. It should be noted that venlafaxine has not been directly compared with placebo, and the result is based on indirect evidence only.
Regarding the pharmacological interventions, SSRIs as a class had greater effects than placebo (class effect MD –3.49, 95% CrI –5.12 to –1.81) with small differences between them confirming previous meta-analyses using pairwise comparisons only. 263 There was a trend for clomipramine to have a greater effect than SSRIs, but the 95% CrI included the null value. Previous meta-analyses have pointed to a possible superior effect of clomipramine over SSRIs. 120,263 Using the full data set we confirmed this trend, although this was not formally significant. Clomipramine studies, however, were more likely to report per-protocol and not intention-to-treat analyses (see Table 14). In our sensitivity analysis, including studies with low risk of bias in the domain ‘incomplete outcome assessment’, the effect of clomipramine was no longer different from those of other SSRIs (see Table 22). Therefore, our analysis cannot confirm the supposed superiority of clomipramine over other SSRIs.
Regarding the psychological interventions, all active psychotherapies had larger effects than drug placebo, with BT and CT having the largest effects, with small differences between them. However, CBT had a smaller effect than both BT and CT (MD –9.11, 95% CrI –13.18 to –4.97 and MD –7.99, 95% CrI –12.97 to –3.01, respectively). Regarding the comparison between psychological interventions and psychological placebo, both BT and CT had greater effects (MD –10.33, 95% CrI–13.38 to –7.29 and MD –9.21, 95% CrI –13.1 to –5.34, respectively) but the effect of CBT was not significantly different from psychological placebo (MD –1.22, 95% CrI –5.54 to 3.03).
It is difficult to explain why patients randomised to BT or CT fared better than those receiving CBT. It is worth noting that in the sensitivity analyses, excluding the studies with high overall attrition, all three psychotherapies had similar effects. In addition, CT has mainly been compared with BT, whereas CBT has been compared with other interventions in a more extensive network of trials. CBT has also been compared directly with several drugs in the same trial. Therefore, the differential effect found for CBT in the full data set should be interpreted with caution.
Regarding the comparison between psychological and pharmacological interventions, both BT and CT had larger effects than SSRIs and clomipramine. The difference in effect between drugs and CBT was smaller and the 95% CrI included the null value for both SSRIs and clomipramine. In a recent meta-analysis using direct data only, Cuijpers et al. 265 examined the differential effect of pharmacotherapy and psychotherapy in major depression, dysthymia, panic disorder, social anxiety disorder and OCD. A positive effect for psychotherapy over medications was reported for OCD only. The same finding was reported in a recent meta-analysis of head-to-head comparisons of behavioural psychotherapy versus medications. 267 Our NMA confirms this trend for BT and CT but not for CBT (which is a combination of the two therapies). However, there are two points that need to be taken into account. First, as mentioned, CT has been compared mainly with BT, and in the data used for the analysis, BT had very limited connections with drugs (one direct comparison with clomipramine and one with fluvoxamine). CBT, however, has several direct links with other drugs. Second, a major limitation of psychotherapy trials is that most patients in these trials were on a stable dose of a medication, usually a SSRI. Very few trials excluded patients on medications and these were mainly trials that compared psychological interventions with pharmacological interventions in the same trial (most often these were trials including CBT arms). Therefore, trials that have compared psychological interventions only (e.g. CT vs. BT) have essentially examined the effectiveness of these therapies in patients taking stable doses of antidepressant medications. Although patients were symptomatic and fulfilled the criteria for inclusion in the trials (for example a YBOCS score of ≥ 16), it is not known whether or not the concurrent use of medications could have influenced the results at the end of the study. There is some evidence that continuous use of medications beyond the 12 weeks of the short-term trials may reduce symptoms further. 268 It is also unknown whether or not the effect of a therapy would be different if patients were off medications, because such trials have not been performed. However, placebo-controlled studies that used antipsychotic augmentation of SSRIs in treatment-refractory patients have shown very small effects for ‘SSRIs + placebo’; this is against the hypothesis of a delayed effect of SSRIs in symptomatic patients in particular. In any case, the generalisability of these results in patients not taking a stable dose of medication should be made with caution.
Combinations of medications and psychotherapy showed greater effects than drug placebo. The combination of clomipramine with BT was also better than psychological placebo and clomipramine as monotherapy (although this evidence is based on a small number of patients). However, there was no evidence that the combinations were better than psychotherapy as monotherapy. In this respect, we did not confirm the results of a previous direct meta-analysis that the effects of psychotherapy and pharmacotherapy are largely independent and have additive effects. 266
One of the aims of the NMA is to rank the treatments relative to each other. We have produced ranking tables and rankograms. We would like to emphasise, however, that ranks are based on the calculated MDs and, in that sense, they are considered a supplementary analysis regarding treatment effectiveness. The rankograms in Figure 8 show the substantial uncertainty surrounding our estimates. In general, we did not achieve more than a 50% probability that any of the treatments were best (and this refers to BT). A more conservative interpretation is that there is a 50% probability that BT is the best treatment but this also means that there is a 50% probability that it is not. Detailed tables in Appendix 8 present all the rank probabilities.
Results in children
A total of 17 studies were included in the analysis, involving 991 randomised patients. CBT and BT had greater effects than drug placebo. Compared with psychological placebo, both psychotherapies, and in particular CBT, showed a trend for a greater effect, but the 95% CrIs included the null value. These results are in line with those reported in a recent direct meta-analysis for the effectiveness of CBT in paediatric OCD. 269
Selective serotonin reuptake inhibitors as a class showed a trend for a greater effect than drug placebo, but the 95% CrIs included the null value. Individual SSRIs (fluoxetine and sertraline, but in particular the latter), however, reached marginal statistical significance. Regarding clomipramine, taking into account both the direct and indirect evidence (i.e. the results of the NMA), the 95% CrIs included the null value. The results of the pairwise analysis were formally statistically significant, whereas the results of one of the sensitivity analyses (excluding studies with completers analyses) showed a greater effect than drug placebo. Taken together, these results confirm that there is a trend for clomipramine to have a greater effect than drug placebo. There is one previous meta-analysis of SSRIs and clomipramine conducted in 2003,264 but since then most recent trials have included psychological therapies, with the exception of one recent trial that compared CBT both alone and in combination with sertraline. 234 Considering all the evidence, both direct and indirect, our findings point to a possible advantage of some SSRIs and possibly clomipramine in children and adolescents compared with drug placebo, although we do not confirm any superiority for clomipramine as previously reported. 264
Compared with SSRIs as a class, both psychological therapies (BT and CBT) showed a trend for a greater effect, although the 95% CrIs included the null value. Similar results were found for clomipramine. The combination of sertraline with CBT was associated with the largest effect compared with drug placebo and showed marginal statistical significance compared with sertraline alone, but compared with CBT as monotherapy, the combination had similar effects.
Regarding ranking of treatments, taking into account the limitations mentioned in the discussion of the adult subset, CBT either as monotherapy or combined with sertraline were the best treatments, followed by BT. All sensitivity analyses gave results with similar trends.
Tolerability findings
There is less uncertainty regarding the results of tolerability in all age groups. In adults, clomipramine was clearly less well tolerated. All other drugs and therapies were not significantly different from placebo. There was no evidence that combination treatments fared worse than monotherapies, although the data are limited for these comparisons. In children and adolescents, clomipramine also showed a trend for worse tolerability. The same was observed for BT, although this result is based on a very limited number of patients and should be interpreted with caution. SSRIs in children and adolescents showed very good tolerability compared with placebo, and CBT had excellent acceptability either alone or in combination with sertraline.
Cost-effectiveness findings
Main findings
The selection of the most cost-effective therapy for adults or children and adolescents with OCD is not clear-cut. In both populations, the most effective therapies were also among the more expensive therapies; there is a trade-off between the higher upfront costs of psychological therapies and the potential for them to improve outcomes and reduce long-term costs of care.
In the primary economic evaluation in adults, psychological therapies, specifically CT and BT, had the highest probability of being most cost-effective at the conventional NICE thresholds (£20,000 to £30,000 per QALY) and above. Perhaps surprisingly, CBT had a low probability of being cost-effective in adults at all cost-effectiveness thresholds. This was predominantly a result of the substantially lower estimated effect size of CBT, compared with CT and BT, and the higher intensity and, therefore, higher cost of CBT evaluated in RCTs. However, the difference in estimated effectiveness between CBT and other psychotherapies was very sensitive to the inclusion of RCTs that used waitlist controls and in which, therefore, participants were unblinded. At lower willingness-to-pay thresholds (< £10,000 per QALY), pharmacotherapy, particularly clomipramine and venlafaxine, had a relatively high probability of being cost-effective. The cost-effectiveness of venlafaxine is particularly sensitive to the low dropout rate estimated from just two trials, which might be viewed as an anomaly. It should be noted that the dropout rate in these two trials (< 10%) is well below the average dropout rate of venlafaxine trials in depression or other anxiety disorders (usually > 20%). The finding that clomipramine is more likely to be more cost-effective than SSRIs should be considered in conjunction with the known toxicity and side-effect profile of clomipramine.
There is substantially less trial evidence in children and adolescents. Of the five interventions compared, SSRIs had the highest probability of being most cost-effective at lower willingness-to-pay thresholds (< £15,000 per QALY). At the conventional NICE thresholds (£20,000 to £30,000 per QALY) and above, CBT or CBT combined with a SSRI were more likely to be cost-effective.
The results of the economic evaluation reflect considerable uncertainty from many different sources. Although several thousand patients with OCD have participated in RCTs, the numbers randomised to each intervention varied considerably and were often small. The economic model is dependent on the validity of the NMA, which itself depends on the transitivity of interventions and methods between RCTs. Furthermore, we have demonstrated that cost-effectiveness results are sensitive to assumptions about the sustainability of treatment effects beyond the initial treatment period. Clinicians and policy-makers should bear this uncertainty in mind when developing treatment guidelines and prioritising future research.
Comparisons with previous studies
It is not possible to directly compare our results with those of the previous cost-effectiveness models. In developing NICE clinical guidelines for the treatment of OCD,118 researchers developed a crude model for comparing the cost-per-responder of SSRIs, CBT and combination therapy. They concluded that CBT alone is dominated by SSRIs and combination (CBT and SSRI) therapy and that combination therapy is likely to be a cost-effective option. Other work underpinning the NICE appraisal of computerised CBT compared three interventions (computer-guided BT, clinician-led BT or relaxation) and concluded that, subject to substantial uncertainties, therapist-led CBT is cost-effective compared with relaxation, and that computerised CBT has the potential to be cost-effective, depending on the licence fees for health-care commissioners. 248 Our work is different in that it draws on a network of evidence, stratifies analysis by adults and children and adolescents and provides a probabilistic analysis of treatment class options at various thresholds of willingness to pay for a QALY.
Main limitations
Main limitations: clinical effectiveness
-
In our NMA, we excluded studies that had not used the YBOCS to avoid using standardised MDs instead of the MDs. There were only a small number of older trials with small sample sizes that had not used the YBOCS. This decision was made in light of the well-documented methodological270 and interpretational difficulties142 associated with the standardised MD.
-
There were few studies (n = 5) that had used different fixed doses of the same drug in order to investigate the possibility of a dose–response association. Owing to the limited data in the NMA, we were unable to treat these dosing schemes as different nodes in the network and, therefore, we merged these treatment groups into one.
-
There is meta-epidemiological evidence that suggests that blinding is crucial to avoid bias for subjective and semi-objective outcome measures. 271 Blinding in psychotherapy trials is difficult owing to the nature of intervention, but in the case of waitlist controls, it is impossible. Therefore, trials that have used waitlist controls (e.g. most of the CBT trials in children and adolescent) are more prone to bias owing to a lack of blinding and this may have resulted in overestimation of the effect of psychotherapies. 272
-
We did not run additional tests, such as loop-specific examinations of inconsistency or a node-splitting approach, to examine inconsistency, as suggested by some authors. 149 However, given the good fit we have observed in all our analyses we think that this was not necessary.
-
Given that most trials were of a short-term duration rarely exceeding 12 weeks, generalisation of the results beyond this point should be made with caution.
Main limitations: cost-effectiveness
There has been very little research on the cost-effectiveness of therapy for OCD. Our work addresses a broader question than two previous cost-effectiveness models by estimating cost per QALY gained and by comparing behavioural therapies and pharmacotherapies. We use a more comprehensive range of evidence, based on a systematic review and a NMA of RCTs, to inform model estimates of effect size and allowing a full probabilistic assessment of the relative cost-effectiveness of treatment strategies. We also used rapid literature reviews to identify recent evidence on the life course of OCD symptoms91,97 and utility scores. 114
Any cost-effectiveness model is only as valid as the structural assumptions and evidence that underlie it. 273 We conducted the analysis from a NHS perspective, although it would be preferable to broaden it to also include Personal Social Services costs (the perspective recommended by NICE) and broader societal costs to patients, carers, employers and others. We could not identify any relevant data on the NHS costs of routine care of patients with OCD, and including costs to other sectors of society would have been even more speculative. However, it seems likely that if these costs had been available, the therapies that are initially expensive, but also effective (i.e. psychological therapies), would become more cost-effective, as reducing symptoms will reduce the impacts of OCD on wider society. Our model assesses the cost-effectiveness of initial therapy only in patients with moderate or severe OCD symptoms, whereas clinical guidelines need to consider appropriate treatment options for milder symptoms and where initial therapy has failed. Without individual patient data from RCTs, it is difficult to judge how the (cost-)effectiveness of therapy varies by initial symptom severity or to appropriately account for potential correlations between parameters, such as effectiveness and dropout rates, in probabilistic sensitivity analyses. Furthermore, RCTs often collect little detail on previous or concurrent treatment used by trial participants. Therefore, for example, an intervention described in a RCT as ‘CBT’ may in fact include patients who have failed or are still being prescribed various types of pharmacotherapies. In fact, our review showed that most of the patients who were included in RCTs of psychological interventions were also taking stable doses of medications.
We conducted our economic evaluation at the class level, combining different SSRIs and different intensities of psychological therapies. In part, this decision reflects the similarity of effect sizes within drug classes and also the scarcity of data for conducting sub-class analysis. However, there are important economic implications at the sub-class level. For example, although the average cost of SSRIs used in the model was higher than clomipramine, a number of SSRIs (e.g. fluoxetine, paroxetine, sertraline or citalopram) are cheaper and potentially more cost-effective. However, this was not confirmed from our sensitivity analysis, assuming that SSRI medication costs were equivalent to the cheapest SSRI rather than the class average cost. Likewise, psychological therapy might be delivered with different intensity (e.g. brief or stepped care) and in different formats (group/individual, face to face/telephone/computer) tailored to individual patients which may have important implications for cost-effectiveness.
Our model is based on relatively weak evidence on costs and outcomes in several areas, particularly for children and adolescents. The sustainability of treatment effects beyond the typical 12-week follow-up period observed in trials is particularly important. We relied on longitudinal data on response and relapse from cohort studies following relatively small numbers of patients over a 3- to 5-year period. 91,97 Long-term follow-up of trial participants, particularly those in trials comparing pharmacotherapy and psychological therapy, are essential to inform the cost-effectiveness of treatment options. We linked symptoms scores (YBOCS) to response rates (full, partial or none) in order to estimate utilities via a Markov model. This indirect approach would not have been necessary if utility scores, for instance the EQ-5D,274 were collected in RCTs or if robust mapping functions had been developed between the YBOCS and EQ-5D. 275 The estimation of patient outcomes was further complicated by the absence of information on utilities in children and adolescents and the widely differing definitions of full and partial response used in the OCD literature.
Our conclusions are sensitive to structural assumptions about patients who drop out of therapy. One example of this is the cost-effectiveness of venlafaxine at low willingness-to-pay thresholds in adults. The prominence of venlafaxine in our results is surprising, given the low effect size estimated in the NMA and the fact that venlafaxine is explicitly not recommended in NICE OCD clinical guidelines118 and is caused by the low apparent dropout rate for venlafaxine estimated in two trials. If the majority of RCTs report ‘intention to treat’ analyses where dropouts are already included in the CYBOCS/YBOCS effect size estimate, then our primary analysis effectively ‘double-weights’ poorer outcomes in patients who drop out, thereby unfairly favouring interventions such as venlafaxine with low dropout rates. This underlines the importance of considering the cost-effectiveness findings alongside other evidence on the toxicity and side effects of interventions.
Chapter 9 Conclusions
Conclusions: clinical effectiveness
The results of this review support a range of effective options, both pharmacological and psychological, for the management of OCD in all age groups. Regarding the relative effectiveness of treatments, our review highlighted the great uncertainty surrounding the published randomised evidence. Although specific psychological interventions were found to have greater effects than medications, there are important methodological limitations that need to be taken into account in future research before a final decision can be made.
Relevance of the findings to national guidelines: clinical effectiveness
The NICE guideline118 recommends a ‘stepped care’ approach towards managing OCD in both adults and young people. They recommend that those with mild symptoms should be offered low-intensity (< 10 sessions or group treatment) CBT including ERP. The evidence we found did not stratify the analyses in accordance with the severity of the illness so we could not justify this approach from the empirical data, although it might appear sensible from a clinical perspective.
For adults with moderate symptoms, the NICE guideline recommends either SSRIs or high-intensity CBT (including ERP). Our review finds evidence to support both these interventions. As discussed above, there was some indication that behavioural approaches were more effective than SSRIs but we cannot be certain of this conclusion. However, the combination of SSRIs and BT or CBT seemed an acceptable treatment, although we do not have sufficient evidence to suggest that the combination of medication and psychotherapy is better than psychotherapy alone. This is also relevant to the recommendation that for those with severe illness, the combination of SSRI and BT is used.
Our review supports the NICE decision to recommend SSRIs rather than clomipramine as the first-line antidepressant. Although clomipramine had a slightly larger effect size, we did not have any convincing statistical evidence to suggest that clomipramine is more effective. Given the increased tolerability of SSRIs, our review supports the recommendation that these should be used as a first-line treatment.
In conclusion, the evidence broadly supports the approach of the NICE guideline. At present, the trial evidence on effectiveness does not justify a stepped approach towards the recommendations, although, of course, other considerations would also have informed the NICE guideline group. The evidence suggested that behavioural interventions could be more effective than SSRI medication, but there is a great deal of uncertainty and we cannot confidently make that recommendation on the basis of the current evidence of clinical effectiveness.
Research implications: clinical effectiveness
-
More RCTs are needed comparing medications with psychotherapies in a single trial.
-
Issues of blinding in psychotherapy trials should be taken into account. The possibility of comparing combinations of mixed arms of the following types: ‘drug + psychological placebo’ and ‘drug placebo + psychotherapy’ should be better explored. In the reviewed literature, there was just one study that combined CBT with drug placebo. More studies of this design are needed.
-
The use of the waitlist as a control in psychotherapy trials should be re-examined and perhaps replaced with psychological placebo.
-
Psychotherapy trials should exclude patients taking concurrent medications during the period of the trial.
Conclusions: cost-effectiveness
Relevance of the findings to national guidelines: cost-effectiveness
In adults with OCD with moderate functional impairment, current NICE guidance recommends either a course of a SSRI or more intensive CBT (including ERP) with > 10 therapist hours per patient, noting that these treatments appear to be comparably efficacious. The findings of our cost-effectiveness model have important implications for guidance.
-
There is considerable uncertainty in the economic model; at current NICE thresholds (£20,000–30,000 per QALY), CrIs of all therapies overlap and, therefore, clinical guidance is necessarily a difficult judgement based on the balance of probabilities of costs, outcomes and risks of side effects and withdrawal.
-
The choice of the most cost-effective psychological therapy depends, to a large extent, on the subset of RCTs informing effect size estimates. If all RCTs are included, the considerably larger effect sizes of CT and BT (compared with CBT) make them most likely to be cost-effective options at current NICE thresholds. If trials with high risk of bias owing to ‘incomplete outcome assessment’ are excluded, no CT trials remain and the difference in effect size between BT and CBT is much smaller (see Appendix 10). Excluding trials that use waitlist controls also reduces the differences in effect size between these psychological therapies.
-
The choice of the most cost-effective pharmacological therapy also depends, to a large extent, on the subset of RCTs informing effect size estimates. In our primary analysis, clomipramine and venlafaxine are slightly more cost-effective than SSRIs because of somewhat greater effectiveness (clomipramine) or a lower dropout rate (venlafaxine). In sensitivity analyses, excluding trials with high risk of bias owing to ‘incomplete outcome assessment’ and assuming patients who drop out are incorporated in the intention-to-treat effect size estimates, SSRIs become relatively more cost-effective.
-
Therefore, current NICE recommendations [SSRI or intensive CBT (including ERP)] are not inconsistent with the evidence synthesised in this report, particularly if the focus is placed on trials with complete outcome assessment. Our analysis suggests that CBT might be slightly more efficacious that SSRIs but is initially more expensive. There is a fine balance between the relative costs and effects of SSRIs and CBT. Tailoring the format and intensity of CBT might make it more cost-effective.
-
If a SSRI is used, the choice of drug has important economic implications. Our analysis suggests that the within-class treatment effect is similar, but current prices vary substantially. NICE guidance does not currently distinguish between higher and lower cost SSRIs, but given that prescribing is recommended for extended periods (12 months and beyond), a focus on the cheaper SSRIs (e.g. fluoxetine, paroxetine, sertraline and citalopram) seems prudent.
In children and adolescents with OCD with moderate to severe functional impairment, NICE guidance recommends CBT (including ERP), involving family or carers and adapted to suit the developmental age of the child. Group or individual CBT should be offered based on patient and family preferences.
-
Based on the limited evidence available, our findings suggest that this is a reasonable initial treatment strategy. Again, there is considerable uncertainty in the economic model, which makes it impossible to definitively identify a single most cost-effective treatment strategy.
-
CBT is among the most effective treatment options, and the higher initial costs of CBT compared with SSRIs are counterbalanced by better outcomes and lower long-term costs of care at current NICE willingness-to-pay thresholds. Given the risk of withdrawal and side effects in this young population, a strategy of reserving SSRI and combined SSRI and CBT therapy to children and adolescents who have not responded to a full trial of CBT and who have had a multidisciplinary review seems appropriate.
-
As with adult patients, considering ways to tailor the format and intensity of CBT and, if SSRIs are used, selecting less expensive drugs licensed in children (e.g. sertraline) may improve the cost-effectiveness of care.
Research implications: cost-effectiveness
There are a number of areas of further research that would help policy-makers draw firmer conclusions about the most cost-effective interventions for OCD:
-
Observational research, most feasibly retrospective cohort studies based on routinely collected and electronically collated primary care records, could provide evidence, currently absent, on the costs of NHS care for patients with a diagnosis of OCD, stratified by symptom severity.
-
Cross-sectional surveys of patients with OCD and their families should be conducted to provide new information on the wider societal cost of OCD and might also be used to provide additional evidence on the quality-of-life (utility) impact of OCD. These studies are particularly needed in children and adolescents, where there is no strong evidence currently.
-
Existing RCT evidence could be further used in individual patient data meta-analyses to provide a fuller picture about any association between symptom severity and (cost) effectiveness of pharmacological and psychological therapies.
-
Long-term follow-up (i.e. at 12, 24 and 36 months) of published and ongoing high-quality RCTs, particularly those directly comparing psychological and pharmacological therapies, would be very valuable in establishing whether or not the initial high cost of psychological therapies is justified by sustained treatment effects.
-
New RCTs are needed to evaluate different formats and intensities of psychological therapies in direct comparison with pharmacotherapy and should include data on costs and quality of life (utilities) of patients over the course of the trial follow-up.
Acknowledgements
We would like to thank the following people for their assistance in the production of this report:
-
Petros Skapinakis would like to acknowledge his main affiliation with the Department of Psychiatry, University of Ioannina School of Medicine.
-
Lazaros Belbasis and Vanesa Bellou, School of Medicine, University of Ioannina, Ioannina, Greece, for their assistance in data extraction.
-
Sarah Dawson and the team at the CCDAN, University of Bristol, Bristol, UK, for their help in the search for files.
-
Joel Rose, OCD Action UK, for his comments on the final draft.
Contributions of authors
Petros Skapinakis led the review, was responsible for managing the project and drafted the report.
Deborah Caldwell provided statistical support, undertook the network meta-analyses with Peter Bryden and reviewed the final report.
William Hollingworth oversaw the economic modelling, drafted the economic synthesis and reviewed the final report.
Peter Bryden conducted the economic modelling, helped in the drafting of the economic synthesis, and undertook the NMA with Deborah Caldwell.
Naomi Fineberg provided expert clinical advice (psychopharmacology), made critical comments that helped in the interpretation of results, helped in writing sections of the report and reviewed the final report.
Paul Salkovskis provided expert clinical advice (psychotherapy) and reviewed the final report.
Nicky Welton provided statistical advice and helped with the statistical modelling.
Helen Baxter contributed to the data extraction and the systematic review.
David Kessler provided clinical advice, helped to write sections of the report and reviewed the final report.
Rachel Churchill provided advice for the systematic review and methodology, and reviewed the final report.
Glyn Lewis provided advice on the methodology and systematic review, made critical comments that helped in the interpretation of the results, helped in writing sections of the report and reviewed the final report.
All authors read and commented on draft versions of the report.
Publications
Skapinakis P, Caldwell DM, Hollingworth W, Bryden P, Fineberg N, Salkovskis P, et al. Pharmacological and psychotherapeutic interventions for management of obsessive-compulsive disorder in adults: a systematic review and network meta-analysis [published online ahead of print June 15 2016]. Lancet Psychiatry 2016. http://dx.doi.org/10.1016/S2215-0366(16)30069-4.
Data sharing statement
All data used for the analysis are included in tables in the main report (see Chapters 5 and 6) and detailed data extraction can be found in the Appendices.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HTA programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HTA programme or the Department of Health.
References
- Berrios GE. Our knowledge of anancasm (psychic compulsive states). Hist Psychiatry 2003;14:113-28. http://dx.doi.org/10.1177/0957154X03014001007.
- Berrios GE. The History of Mental Symptoms: Descriptive Psychopathology Since the Nineteenth Century. Cambridge: Cambridge University Press; 1995.
- Diagnostic and Statistical Manual of Mental Disorders. Washington, DC: American Psychiatric Association; 1952.
- Diagnostic and Statistical Manual of Mental Disorders. Washington, DC: American Psychiatric Association; 1968.
- The ICD-10 Classification of Mental and Behavioural Disorders: Diagnostic Criteria for Research. Geneva: World Health Organization; 1993.
- Diagnostic and Statistical Manual of Mental Disorders. Washington, DC: American Psychiatric Association; 2000.
- Diagnostic and Statistical Manual of Mental Disorders. Washington DC: American Psychiatric Association; 2013.
- Leckman JF, Denys D, Simpson HB, Mataix-Cols D, Hollander E, Saxena S, et al. Obsessive–compulsive disorder: a review of the diagnostic criteria and possible subtypes and dimensional specifiers for DSM-V. Depress Anxiety 2010;27:507-27. http://dx.doi.org/10.1002/da.20669.
- Khanna S, Kaliaperumal VG, Channabasavanna SM. Clusters of obsessive–compulsive phenomena in obsessive–compulsive disorder. Br J Psychiatry 1990;156:51-4. http://dx.doi.org/10.1192/bjp.156.1.51.
- Rasmussen SA, Eisen JL. Epidemiology of obsessive compulsive disorder. J Clin Psychiatry 1990;51:10-3.
- Foa EB, Kozak MJ, Goodman WK, Hollander E, Jenike MA, Rasmussen SA. DSM-IV field trial: obsessive–compulsive disorder. Am J Psychiatry 1995;152:90-6.
- Bloch MH, Landeros-Weisenberger A, Rosario MC, Pittenger C, Leckman JF. Meta-analysis of the symptom structure of obsessive–compulsive disorder. Am J Psychiatry 2008;165:1532-42. http://dx.doi.org/10.1176/appi.ajp.2008.08020320.
- Mataix-Cols D, Rauch SL, Baer L, Eisen JL, Shera DM, Goodman WK, et al. Symptom stability in adult obsessive–compulsive disorder: data from a naturalistic 2-year follow-up study. Am J Psychiatry 2002;159:263-8. http://dx.doi.org/10.1176/appi.ajp.159.2.263.
- de Mathis MA, Alvarenga PD, Funaro G, Torresan RC, Moraes I, Torres AR, et al. Gender differences in obsessive–compulsive disorder: a literature review. Rev Bras Psiquiatr 2011;33:390-9. http://dx.doi.org/10.1590/S1516-44462011000400014.
- Lensi P, Cassano GB, Correddu G, Ravagli S, Kunovac JL, Akiskal HS. Obsessive–compulsive disorder. Familial-developmental history, symptomatology, comorbidity and course with special reference to gender-related differences. Br J Psychiatry 1996;169:101-17. http://dx.doi.org/10.1192/bjp.169.1.101.
- Labad J, Menchon JM, Alonso P, Segalas C, Jimenez S, Jaurrieta N, et al. Gender differences in obsessive–compulsive symptom dimensions. Depress Anxiety 2008;25:832-8. http://dx.doi.org/10.1002/da.20332.
- Masi G, Millepiedi S, Perugi G, Pfanner C, Berloffa S, Pari C, et al. A naturalistic exploratory study of the impact of demographic, phenotypic and comorbid features in pediatric obsessive–compulsive disorder. Psychopathology 2010;43:69-78. http://dx.doi.org/10.1159/000274175.
- Torresan RC, Ramos-Cerqueira AT, Shavitt RG, do Rosário MC, de Mathis MA, Miguel EC, et al. Symptom dimensions, clinical course and comorbidity in men and women with obsessive–compulsive disorder. Psychiatry Res 2013;209:186-95. http://dx.doi.org/10.1016/j.psychres.2012.12.006.
- Fontenelle LF, Mendlowicz MV, Versiani M. The descriptive epidemiology of obsessive–compulsive disorder. Prog Neuropsychopharmacol Biol Psychiatry 2006;30:327-37. http://dx.doi.org/10.1016/j.pnpbp.2005.11.001.
- Geller DA, Biederman J, Faraone S, Agranat A, Cradock K, Hagermoser L, et al. Developmental aspects of obsessive compulsive disorder: findings in children, adolescents, and adults. J Nerv Ment Dis 2001;189:471-7. http://dx.doi.org/10.1097/00005053-200107000-00009.
- Rasmussen S, Eisen J, Jenike MA, Baer L, Minichiello WE. Obsessive–Compulsive Disorders: Practical Management. New York, NY: Mosby; 1998.
- Swedo SE, Rapoport JL, Leonard H, Lenane M, Cheslow D. Obsessive–compulsive disorder in children and adolescents. Clinical phenomenology of 70 consecutive cases. Arch Gen Psychiatry 1989;46:335-41. http://dx.doi.org/10.1001/archpsyc.1989.01810040041007.
- March JS, Leonard HL. Obsessive–compulsive disorder in children and adolescents: a review of the past 10 years. J Am Acad Child Adolesc Psychiatry 1996;35:1265-73. http://dx.doi.org/10.1097/00004583-199610000-00012.
- Grabill K, Merlo L, Duke D, Harford KL, Keeley ML, Geffken GR, et al. Assessment of obsessive–compulsive disorder: a review. J Anxiety Disord 2008;22:1-17. http://dx.doi.org/10.1016/j.janxdis.2007.01.012.
- Goodman WK, Price LH, Rasmussen SA, Mazure C, Fleischmann RL, Hill CL, et al. The Yale–Brown Obsessive Compulsive Scale. I. Development, use, and reliability. Arch Gen Psychiatry 1989;46:1006-11. http://dx.doi.org/10.1001/archpsyc.1989.01810110048007.
- Steketee G, Frost R, Bogart K. The Yale–Brown Obsessive–Compulsive Scale: interview versus self-report. Behav Res Ther 1996;34:675-84. http://dx.doi.org/10.1016/0005-7967(96)00036-8.
- Storch EA, Rasmussen SA, Price LH, Larson MJ, Murphy TK, Goodman WK. Development and psychometric evaluation of the Yale–Brown Obsessive–Compulsive Scale, 2nd edn. Psychol Assess 2010;22:223-32. http://dx.doi.org/10.1037/a0018492.
- Scahill L, Riddle MA, McSwiggin-Hardin M, Ort SI, King RA, Goodman WK, et al. Children’s Yale–Brown Obsessive–Compulsive Scale: reliability and validity. J Am Acad Child Adolesc Psychiatry 1997;36:844-52. http://dx.doi.org/10.1097/00004583-199706000-00023.
- Anholt GE, van Oppen P, Cath DC, Smit JH, den Boer JA, Verbraak MJ, et al. The Yale–Brown obsessive–compulsive scale: factor structure of a large sample. Front Psychiatry 2010;1. http://dx.doi.org/10.3389/fpsyt.2010.00018.
- Fineberg NA, Chamberlain SR, Hollander E, Boulougouris V, Robbins TW. Translational approaches to obsessive–compulsive disorder: from animal models to clinical treatment. Br J Pharmacol 2011;164:1044-61. http://dx.doi.org/10.1111/j.1476-5381.2011.01422.x.
- Pauls DL, Alsobrook JP, Goodman W, Rasmussen S, Leckman JF. A family study of obsessive–compulsive disorder. Am J Psychiatry 1995;152:76-84. http://dx.doi.org/10.1176/ajp.152.1.76.
- Nestadt G, Samuels J, Riddle M, Bienvenu OJ, Liang KY, LaBuda M, et al. A family study of obsessive–compulsive disorder. Arch Gen Psychiatry 2000;57:358-63. http://dx.doi.org/10.1001/archpsyc.57.4.358.
- Pauls DL, Abramovitch A, Rauch SL, Geller DA. Obsessive–compulsive disorder: an integrative genetic and neurobiological perspective. Nat Rev Neurosci 2014;15:410-24. http://dx.doi.org/10.1038/nrn3746.
- Hanna GL, Himle JA, Curtis GC, Gillespie BW. A family study of obsessive–compulsive disorder with pediatric probands. Am J Med Genet B Neuropsychiatr Genet 2005;134B:13-9. http://dx.doi.org/10.1002/ajmg.b.30138.
- do Rosario-Campos MC, Leckman JF, Curi M, Quatrano S, Katsovitch L, Miguel EC, et al. A family study of early-onset obsessive–compulsive disorder. Am J Med Genet B Neuropsychiatr Genet 2005;136B:92-7. http://dx.doi.org/10.1002/ajmg.b.30149.
- van Grootheest DS, Cath DC, Beekman AT, Boomsma DI. Twin studies on obsessive–compulsive disorder: a review. Twin Res Hum Genet 2005;8:450-8. http://dx.doi.org/10.1375/twin.8.5.450.
- Taylor S. Etiology of obsessions and compulsions: a meta-analysis and narrative review of twin studies. Clin Psychol Rev 2011;31:1361-72. http://dx.doi.org/10.1016/j.cpr.2011.09.008.
- Milad MR, Rauch SL. Obsessive–compulsive disorder: beyond segregated cortico-striatal pathways. Trends Cogn Sci 2012;16:43-51. http://dx.doi.org/10.1016/j.tics.2011.11.003.
- Ahmari SE, Spellman T, Douglass NL, Kheirbek MA, Simpson HB, Deisseroth K, et al. Repeated cortico-striatal stimulation generates persistent OCD-like behavior. Science 2013;340:1234-9. http://dx.doi.org/10.1126/science.1234733.
- Salkovskis PM. Obsessional-compulsive problems: a cognitive–behavoural analysis. Behav Res Ther 1985;23:571-83. http://dx.doi.org/10.1016/0005-7967(85)90105-6.
- Rachman S. A cognitive theory of obsessions. Behav Res Ther 1997;35:793-802. http://dx.doi.org/10.1016/S0005-7967(97)00040-5.
- Torres AR, Lima MCP. Epidemiology of obsessive–compulsive disorder: a review. Rev Bras Psiquiatr 2005;27:237-42. http://dx.doi.org/10.1590/S1516-44462005000300015.
- Rudin E. Beitrag zur frage der zwangskrankheit insbesondere ihrere editaren beziechungen. Arch Psychiatr Nervenkr 1953;191:14-5. http://dx.doi.org/10.1007/BF00345572.
- Brunetti PM. A prevalence survey of mental disorders in a rural commune in Vaucluse. Acta Psychiatr Scand 1964;40:323-58. http://dx.doi.org/10.1111/j.1600-0447.1964.tb05758.x.
- Robins LN, Helzer JE, Weissman MM, Orvaschel H, Gruenberg E, Burke JD, et al. Lifetime prevalence of specific psychiatric disorders in three sites. Arch Gen Psychiatry 1984;41:949-58. http://dx.doi.org/10.1001/archpsyc.1984.01790210031005.
- Karno M, Golding JM, Sorenson SB, Burnam MA. The epidemiology of obsessive–compulsive disorder in five US communities. Arch Gen Psychiatry 1988;45:1094-9. http://dx.doi.org/10.1001/archpsyc.1988.01800360042006.
- Anthony JC, Folstein M, Romanoski AJ, Von Korff MR, Nestadt GR, Chahal R, et al. Comparison of the lay Diagnostic Interview Schedule and a standardized psychiatric diagnosis. Experience in eastern Baltimore. Arch Gen Psychiatry 1985;42:667-75. http://dx.doi.org/10.1001/archpsyc.1985.01790300029004.
- Nelson E, Rice J. Stability of diagnosis of obsessive–compulsive disorder in the Epidemiologic Catchment Area study. Am J Psychiatry 1997;154:826-31. http://dx.doi.org/10.1176/ajp.154.6.826.
- Wittchen HU, Essau CA, von Zerssen D, Krieg JC, Zaudig M. Lifetime and 6-month prevalence of mental disorders in the Munich Follow-Up Study. Eur Arch Psychiatry Clin Neurosci 1992;241:247-58. http://dx.doi.org/10.1007/BF02190261.
- Bijl RV, Ravelli A, van Zessen G. Prevalence of psychiatric disorder in the general population: results of The Netherlands Mental Health Survey and Incidence Study (NEMESIS). Soc Psychiatry Psychiatr Epidemiol 1998;33:587-95. http://dx.doi.org/10.1007/s001270050098.
- Stein MB, Forde DR, Anderson G, Walker JR. Obsessive–compulsive disorder in the community: an epidemiologic survey with clinical reappraisal. Am J Psychiatry 1997;154:1120-6. http://dx.doi.org/10.1176/ajp.154.8.1120.
- Torres AR, Prince MJ, Bebbington PE, Bhugra D, Brugha TS, Farrell M, et al. Obsessive–compulsive disorder: prevalence, comorbidity, impact, and help-seeking in the British National Psychiatric Morbidity Survey of 2000. Am J Psychiatry 2006;163:1978-85. http://dx.doi.org/10.1176/ajp.2006.163.11.1978.
- Faravelli C, Abrardi L, Bartolozzi D, Cecchi C, Cosci F, D’Adamo D, et al. The Sesto Fiorentino study: background, methods and preliminary results. Lifetime prevalence of psychiatric disorders in an Italian community sample using clinical interviewers. Psychother Psychosom 2004;73:216-25. http://dx.doi.org/10.1159/000077740.
- Skapinakis P, Bellos S, Koupidis S, Grammatikopoulos I, Theodorakis PN, Mavreas V. Prevalence and sociodemographic associations of common mental disorders in a nationally representative sample of the general population of Greece. BMC Psychiatry 2013;13. http://dx.doi.org/10.1186/1471-244X-13-163.
- Heyman I, Fombonne E, Simmons H, Ford T, Meltzer H, Goodman R. Prevalence of obsessive–compulsive disorder in the British nationwide survey of child mental health. Br J Psychiatry 2001;179:324-9. http://dx.doi.org/10.1192/bjp.179.4.324.
- Costello EJ, Angold A, Burns BJ, Stangl DK, Tweed DL, Erkanli A, et al. The Great Smoky Mountains Study of Youth. Goals, design, methods, and the prevalence of DSM-III-R disorders. Arch Gen Psychiatry 1996;53:1129-36. http://dx.doi.org/10.1001/archpsyc.1996.01830120067012.
- Verhulst FC, van der Ende J, Ferdinand RF, Kasius MC. The prevalence of DSM-III-R diagnoses in a national sample of Dutch adolescents. Arch Gen Psychiatry 1997;54:329-36. http://dx.doi.org/10.1001/archpsyc.1997.01830160049008.
- Rapoport JL, Inoff-Germain G, Weissman MM, Greenwald S, Narrow WE, Jensen PS, et al. Childhood obsessive–compulsive disorder in the NIMH MECA study: parent versus child identification of cases. Methods for the Epidemiology of Child and Adolescent Mental Disorders. J Anxiety Disord 2000;14:535-48. http://dx.doi.org/10.1016/S0887-6185(00)00048-7.
- Nestadt G, Bienvenu OJ, Cai G, Samuels J, Eaton WW. A family study of obsessive–compulsive disorder. Arch Gen Psychiatry 2000;57:358-63. http://dx.doi.org/10.1001/archpsyc.57.4.358.
- De Graaf R, Bijl RV, Ravelli A, Smit F, Vollebergh WA. Predictors of first incidence of DSM-III-R psychiatric disorders in the general population: findings from the Netherlands Mental Health Survey and Incidence Study. Acta Psychiatr Scand 2002;106:303-13. http://dx.doi.org/10.1034/j.1600-0447.2002.01397.x.
- Valleni-Basile LA, Garrison CZ, Waller JL, Addy CL, McKeown RE, Jackson KL, et al. Incidence of obsessive–compulsive disorder in a community sample of young adolescents. J Am Acad Child Adolesc Psychiatry 1996;35:898-906. http://dx.doi.org/10.1097/00004583-199607000-00015.
- Fontenelle LF, Hasler G. The analytical epidemiology of obsessive–compulsive disorder: risk factors and correlates. Prog Neuropsychopharmacol Biol Psychiatry 2008;32:1-15. http://dx.doi.org/10.1016/j.pnpbp.2007.06.024.
- Flament MF, Whitaker A, Rapoport JL, Davies M, Berg CZ, Kalikow K, et al. Obsessive compulsive disorder in adolescence: an epidemiological study. J Am Acad Child Adolesc Psychiatry 1988;27:764-71. http://dx.doi.org/10.1097/00004583-198811000-00018.
- Canals J, Domenech E, Carbajo G, Blade J. Prevalence of DSM-III-R and ICD-10 psychiatric disorders in a Spanish population of 18-year-olds. Acta Psychiatr Scand 1997;96:287-94. http://dx.doi.org/10.1111/j.1600-0447.1997.tb10165.x.
- Zohar AH, Ratzoni G, Pauls DL, Apter A, Bleich A, Kron S, et al. An epidemiological study of obsessive–compulsive disorder and related disorders in Israeli adolescents. J Am Acad Child Adolesc Psychiatry 1992;31:1057-61. http://dx.doi.org/10.1097/00004583-199211000-00010.
- LaSalle VH, Cromer KR, Nelson KN, Kazuba D, Justement L, Murphy DL. Diagnostic interview assessed neuropsychiatric disorder comorbidity in 334 individuals with obsessive–compulsive disorder. Depress Anxiety 2004;19:163-73. http://dx.doi.org/10.1002/da.20009.
- Denys D, Tenney N, van Megen HJ, de Geus F, Westenberg HG. Axis I and II comorbidity in a large sample of patients with obsessive–compulsive disorder. J Affect Disord 2004;80:155-62. http://dx.doi.org/10.1016/S0165-0327(03)00056-9.
- Pinto A, Mancebo MC, Eisen JL, Pagano ME, Rasmussen SA. The Brown Longitudinal Obsessive Compulsive Study: clinical features and symptoms of the sample at intake. J Clin Psychiatry 2006;67:703-11. http://dx.doi.org/10.4088/JCP.v67n0503.
- Ruscio AM, Stein DJ, Chiu WT, Kessler RC. The epidemiology of obsessive–compulsive disorder in the National Comorbidity Survey Replication. Mol Psychiatry 2010;15:53-6. http://dx.doi.org/10.1038/mp.2008.94.
- Perugi G, Akiskal HS, Pfanner C, Presta S, Gemignani A, Milanfranchi A, et al. The clinical impact of bipolar and unipolar affective comorbidity on obsessive–compulsive disorder. J Affect Disord 1997;46:15-23. http://dx.doi.org/10.1016/S0165-0327(97)00075-X.
- Krüger S, Cooke RG, Hasey GM, Jorna T, Persad E. Comorbidity of obsessive compulsive disorder in bipolar disorder. J Affect Disord 1995;34:117-20. http://dx.doi.org/10.1016/0165-0327(95)00008-B.
- Pallanti S, Grassi G, Sarrecchia ED, Cantisani A, Pellegrini M. Obsessive–compulsive disorder comorbidity: clinical assessment and therapeutic implications. Front Psychiatry 2011;2. http://dx.doi.org/10.3389/fpsyt.2011.00070.
- Henry C, Van den Bulke D, Bellivier F, Etain B, Rouillon F, Leboyer M. Anxiety disorders in 318 bipolar patients: prevalence and impact on illness severity and response to mood stabilizer. J Clin Psychiatry 2003;64:331-5. http://dx.doi.org/10.4088/JCP.v64n0316.
- Achim AM, Maziade M, Raymond E, Olivier D, Mérette C, Roy MA. How prevalent are anxiety disorders in schizophrenia? A meta-analysis and critical review on a significant association. Schizophr Bull 2011;37:811-21. http://dx.doi.org/10.1093/schbul/sbp148.
- Sterk B, Lankreijer K, Linszen DH, de Haan L. Obsessive–compulsive symptoms in first episode psychosis and in subjects at ultra high risk for developing psychosis; onset and relationship to psychotic symptoms. Aust N Z J Psychiatry 2011;45:400-6. http://dx.doi.org/10.3109/00048674.2010.533363.
- Swets M, Dekker J, van Emmerik-van Oortmerssen K, Smid GE, Smit F, de Haan L, et al. The obsessive compulsive spectrum in schizophrenia, a meta-analysis and meta-regression exploring prevalence rates. Schizophr Res 2014;152:458-68. http://dx.doi.org/10.1016/j.schres.2013.10.033.
- Eisen JL, Beer DA, Pato MT, Venditto TA, Rasmussen SA. Obsessive–compulsive disorder in patients with schizophrenia or schizoaffective disorder. Am J Psychiatry 1997;154:271-3. http://dx.doi.org/10.1176/ajp.154.2.271.
- Eisen JL, Rasmussen SA. Obsessive compulsive disorder with psychotic features. J Clin Psychiatry 1993;54:373-9.
- Van Dael F, van Os J, de Graaf R, ten Have M, Krabbendam L, Myin-Germeys I. Can obsessions drive you mad? Longitudinal evidence that obsessive–compulsive symptoms worsen the outcome of early psychotic experiences. Acta Psychiatr Scand 2011;123. http://dx.doi.org/10.1111/j.1600-0447.2010.01609.x.
- Coryell W. Obsessive–compulsive disorder and primary unipolar depression. Comparisons of background, family history, course, and mortality. J Nerv Ment Dis 1981;169:220-4. http://dx.doi.org/10.1097/00005053-198104000-00003.
- Torres AR, Ramos-Cerqueira AT, Ferrão YA, Fontenelle LF, do Rosário MC, Miguel EC. Suicidality in obsessive–compulsive disorder: prevalence and relation to symptom dimensions and comorbid conditions. J Clin Psychiatry 2011;72:17-26. http://dx.doi.org/10.4088/JCP.09m05651blu.
- Alonso P, Segalàs C, Real E, Pertusa A, Labad J, Jiménez-Murcia S, et al. Suicide in patients treated for obsessive–compulsive disorder: a prospective follow-up study. J Affect Disord 2010;124:300-8. http://dx.doi.org/10.1016/j.jad.2009.12.001.
- ten Have M, de Graaf R, van Dorsselaer S, Verdurmen J, van’t Land H, Vollebergh W, et al. Incidence and course of suicidal ideation and suicide attempts in the general population. Can J Psychiatry 2009;54:824-33.
- Khan A, Leventhal RM, Khan S, Brown WA. Suicide risk in patients with anxiety disorders: a meta-analysis of the FDA database. J Affect Disord 2002;68:183-90. http://dx.doi.org/10.1016/S0165-0327(01)00354-8.
- Khan A, Warner HA, Brown WA. Symptom reduction and suicide risk in patients treated with placebo in antidepressant clinical trials: an analysis of the Food and Drug Administration database. Arch Gen Psychiatry 2000;57:311-17. http://dx.doi.org/10.1001/archpsyc.57.4.311.
- Sareen J, Cox BJ, Afifi TO, de Graaf R, Asmundson GJ, ten Have M, et al. Anxiety disorders and risk for suicidal ideation and suicide attempts: a population-based longitudinal study of adults. Arch Gen Psychiatry 2005;62:1249-57. http://dx.doi.org/10.1001/archpsyc.62.11.1249.
- Storch EA, Bussing R, Jacob ML, Nadeau JM, Crawford E, Mutch PJ, et al. Frequency and correlates of suicidal ideation in pediatric obsessive–compulsive disorder. Child Psychiatry Hum Dev 2015;46:75-83. http://dx.doi.org/10.1007/s10578-014-0453-7.
- Pollitt J. Natural history of obsessional states; a study of 150 cases. Br Med J 1957;1:194-8. http://dx.doi.org/10.1136/bmj.1.5012.194.
- Skoog G, Skoog I. A 40-year follow-up of patients with obsessive–compulsive disorder. Arch Gen Psychiatry 1999;56:121-7. http://dx.doi.org/10.1001/archpsyc.56.2.121.
- Bloch MH, Green C, Kichuk SA, Dombrowski PA, Wasylink S, Billingslea E, et al. Long-term outcome in adults with obsessive–compulsive disorder. Depress Anxiety 2013;30:716-22. http://dx.doi.org/10.1002/da.22103.
- Eisen JL, Sibrava NJ, Boisseau CL, Mancebo MC, Stout RL, Pinto A, et al. Five-year course of obsessive–compulsive disorder: predictors of remission and relapse. J Clin Psychiatry 2013;74:233-9. http://dx.doi.org/10.4088/JCP.12m07657.
- Catapano F, Perris F, Masella M, Rossano F, Cigliano M, Magliano L, et al. Obsessive compulsive disorder: a 3-year prospective follow-up study of patients treated with serotonin reuptake inhibitors OCD follow-up study. J Psychiatr Res 2006;40:502-10. http://dx.doi.org/10.1016/j.jpsychires.2005.04.010.
- Jakubovski E, Diniz JB, Valerio C, Fossaluza V, Belotto-Silva C, Gorenstein C, et al. Clinical predictors of long-term outcome in obsessive–compulsive disorder. Depress Anxiety 2013;30:763-72. http://dx.doi.org/10.1002/da.22013.
- Dell’Osso B, Benatti B, Buoli M, Altamura AC, Marazziti D, Hollander E, et al. The influence of age at onset and duration of illness on long-term outcome in patients with obsessive compulsive disorder: a report from the International College of Obsessive–compulsive Spectrum Disorders. Eur Neuropsychopharmacol 2013;23:865-71. http://dx.doi.org/10.1016/j.euroneuro.2013.05.004.
- Marcks BA, Weisberg RB, Dyck I, Keller MB. Longitudinal course of obsessive–compulsive disorder in patients with anxiety disorders: a 15-year prospective follow-up study. Compr Psychiatry 2011;52:670-7. http://dx.doi.org/10.1016/j.comppsych.2011.01.001.
- Stewart SE, Geller DA, Jenike M, Pauls D, Shaw D, Mullin B, et al. Long-term outcome of pediatric obsessive–compulsive disorder: a meta-analysis and qualitative review of the literature. Acta Psychiatr Scand 2004;110:4-13. http://dx.doi.org/10.1111/j.1600-0447.2004.00302.x.
- Mancebo MC, Boisseau CL, Garnaat SL, Eisen JL, Greenberg BD, Sibrava NJ, et al. Long-term course of pediatric obsessive–compulsive disorder: 3 years of prospective follow-up. Compr Psychiatry 2014;55:1498-504. http://dx.doi.org/10.1016/j.comppsych.2014.04.010.
- Bloch MH, Craiglow BG, Landeros-Weisenberger A, Dombrowski PA, Panza KE, Peterson BS, et al. Predictors of early adult outcomes in pediatric onset obsessive–compulsive disorder. Pediatrics 2009;124:1085-93. http://dx.doi.org/10.1542/peds.2009-0015.
- Micali N, Heyman I, Perez M, Hilton K, Nakatani E, Turner C, et al. Long-term outcomes of obsessive–compulsive disorder: follow-up of 142 children and adolescents. Br J Psychiatry 2010;197:128-34. http://dx.doi.org/10.1192/bjp.bp.109.075317.
- Macy AS, Theo JN, Kaufmann SC, Ghazzaoui RB, Pawlowski PA, Fakhry HI, et al. Quality of life in obsessive compulsive disorder. CNS Spectr 2013;18:21-33. http://dx.doi.org/10.1017/S1092852912000697.
- Subramaniam M, Soh P, Vaingankar JA, Picco L, Chong SA. Quality of life in obsessive–compulsive disorder: impact of the disorder and of treatment. CNS Drugs 2013;27:367-83. http://dx.doi.org/10.1007/s40263-013-0056-z.
- Roberts J, Lenton P, Keetharuth AD, Brazier J. Quality of life impact of mental health conditions in England: results from the adult psychiatric morbidity surveys. Health Qual Life Outcomes 2014;12. http://dx.doi.org/10.1186/1477-7525-12-6.
- Subramaniam M, Abdin E, Vaingankar JA, Chong SA. Obsessive–compulsive disorder: prevalence, correlates, help-seeking and quality of life in a multiracial Asian population. Soc Psychiatry Psychiatr Epidemiol 2012;47:2035-43. http://dx.doi.org/10.1007/s00127-012-0507-8.
- Cramer V, Torgersen S, Kringlen E. Quality of life and anxiety disorders: a population study. J Nerv Ment Dis 2005;193:196-202. http://dx.doi.org/10.1097/01.nmd.0000154836.22687.13.
- Rapaport MH, Clary C, Fayyad R, Endicott J. Quality-of-life impairment in depressive and anxiety disorders. Am J Psychiatry 2005;162:1171-8. http://dx.doi.org/10.1176/appi.ajp.162.6.1171.
- Olatunji BO, Cisler JM, Tolin DF. Quality of life in the anxiety disorders: a meta-analytic review. Clin Psychol Rev 2007;27:572-81. http://dx.doi.org/10.1016/j.cpr.2007.01.015.
- Koran LM, Bromberg D, Hornfeldt CS, Shepski JC, Wang S, Hollander E. Extended-release fluvoxamine and improvements in quality of life in patients with obsessive–compulsive disorder. Compr Psychiatry 2010;51:373-9. http://dx.doi.org/10.1016/j.comppsych.2009.10.001.
- Lack CW, Storch EA, Keeley ML, Geffken GR, Ricketts ED, Murphy TK, et al. Quality of life in children and adolescents with obsessive–compulsive disorder: base rates, parent-child agreement, and clinical correlates. Soc Psychiatry Psychiatr Epidemiol 2009;44:935-42. http://dx.doi.org/10.1007/s00127-009-0013-9.
- Vivan Ade S, Rodrigues L, Wendt G, Bicca MG, Cordioli AV. Quality of life in adolescents with obsessive–compulsive disorder. Rev Bras Psiquiatr 2013;35:369-74. http://dx.doi.org/10.1590/1516-4446-2013-1135.
- Bebbington PE, Brugha TS, Meltzer H, Jenkins R, Ceresa C, Farrell M, et al. Neurotic disorders and the receipt of psychiatric treatment. Psychol Med 2000;30:1369-76. http://dx.doi.org/10.1017/S0033291799002974.
- Baldwin DS, Anderson IM, Nutt DJ, Allgulander C, Bandelow B, den Boer JA, et al. Evidence-based pharmacological treatment of anxiety disorders, post-traumatic stress disorder and obsessive–compulsive disorder: a revision of the 2005 guidelines from the British Association for Psychopharmacology. J Psychopharmacol 2014;28:403-33. http://dx.doi.org/10.1177/0269881114525674.
- Stein DJ, Koen N, Fineberg N, Fontenelle LF, Matsunaga H, Osser D, et al. A 2012 evidence-based algorithm for the pharmacotherapy for obsessive–compulsive disorder. Curr Psychiatry Rep 2012;14:211-19. http://dx.doi.org/10.1007/s11920-012-0268-9.
- Skapinakis P, Papatheodorou T, Mavreas V. Antipsychotic augmentation of serotonergic antidepressants in treatment-resistant obsessive–compulsive disorder: a meta-analysis of the randomized controlled trials. Eur Neuropsychopharmacol 2007;17:79-93. http://dx.doi.org/10.1016/j.euroneuro.2006.07.002.
- Hollander E, Stein DJ, Fineberg NA, Marteau F, Legault M. Quality of life outcomes in patients with obsessive–compulsive disorder: relationship to treatment response and symptom relapse. J Clin Psychiatry 2010;71:784-92. http://dx.doi.org/10.4088/JCP.09m05911blu.
- Katzman MA, Bleau P, Blier P, Chokka P, Kjernisted K, Van Ameringen M. Canadian clinical practice guidelines for the management of anxiety, posttraumatic stress and obsessive–compulsive disorders. BMC Psychiatry 2014;14. http://dx.doi.org/10.1186/1471-244X-14-S1-S1.
- Koran LM, Hanna GL, Hollander E, Nestadt G, Simpson HB. Practice guideline for the treatment of patients with obsessive–compulsive disorder. Am J Psychiatry 2007;164:5-53.
- Bandelow B, Zohar J, Hollander E, Kasper S, Möller HJ. World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for the pharmacological treatment of anxiety, obsessive–compulsive and post-traumatic stress disorders – first revision. World J Biol Psychiatry 2008;9:248-312. http://dx.doi.org/10.1080/15622970802465807.
- Obsessive–Compulsive Disorder: Core Interventions in the Treatment of Obsessive–Compulsive Disorder and Body Dysmorphic Disorder CG31. London: NICE; 2005.
- Fineberg NA, Brown A, Reghunandanan S, Pampaloni I. Evidence-based pharmacotherapy of obsessive–compulsive disorder. Int J Neuropsychopharmacol 2012;15:1173-91. http://dx.doi.org/10.1017/S1461145711001829.
- Ackerman DL, Greenland S. Multivariate meta-analysis of controlled drug studies for obsessive–compulsive disorder. J Clin Psychopharmacol 2002;22:309-17. http://dx.doi.org/10.1097/00004714-200206000-00012.
- Soomro GM, Altman D, Rajagopal S, Oakley-Browne M. Selective serotonin re-uptake inhibitors (SSRIs) versus placebo for obsessive compulsive disorder (OCD). Cochrane Database Syst Rev 2008;1. http://dx.doi.org/10.1002/14651858.cd001765.pub3.
- Mancebo MC, Eisen JL, Pinto A, Greenberg BD, Dyck IR, Rasmussen SA. The Brown longitudinal obsessive compulsive study: treatments received and patient impressions of improvement. J Clin Psychiatry 2006;67:1713-20. http://dx.doi.org/10.4088/JCP.v67n1107.
- Reddy YC, Alur AM, Manjunath S, Kandavel T, Math SB. Long-term follow-up study of patients with serotonin reuptake inhibitor-nonresponsive obsessive–compulsive disorder. J Clin Psychopharmacol 2010;30:267-72. http://dx.doi.org/10.1097/JCP.0b013e3181dbfb53.
- Stein DJ, Andersen EW, Tonnoir B, Fineberg N. Escitalopram in obsessive–compulsive disorder: a randomized, placebo-controlled, paroxetine-referenced, fixed-dose, 24-week study. Curr Med Res Opin 2007;23:701-11. http://dx.doi.org/10.1185/030079907X178838.
- Stein DJ, Carey PD, Lochner C, Seedat S, Fineberg N, Andersen EW. Escitalopram in obsessive–compulsive disorder: response of symptom dimensions to pharmacotherapy. CNS Spectr 2008;13:492-8.
- Greist JH, Jefferson JW, Kobak KA, Chouinard G, DuBoff E, Halaris A, et al. A 1 year double-blind placebo-controlled fixed dose study of sertraline in the treatment of obsessive–compulsive disorder. Int Clin Psychopharmacol 1995;10:57-65. http://dx.doi.org/10.1097/00004850-199506000-00001.
- Tollefson GD, Birkett M, Koran L, Genduso L. Continuation treatment of OCD: double-blind and open-label experience with fluoxetine. J Clin Psychiatry 1994;55:69-76.
- Fineberg NA, Tonnoir B, Lemming O, Stein DJ. Escitalopram prevents relapse of obsessive–compulsive disorder. Eur Neuropsychopharmacol 2007;17:430-9. http://dx.doi.org/10.1016/j.euroneuro.2006.11.005.
- Donovan MR, Glue P, Kolluri S, Emir B. Comparative efficacy of antidepressants in preventing relapse in anxiety disorders – a meta-analysis. J Affect Disord 2010;123:9-16. http://dx.doi.org/10.1016/j.jad.2009.06.021.
- Grant JE. Clinical practice: obsessive–compulsive disorder. N Engl J Med 2014;371:646-53. http://dx.doi.org/10.1056/NEJMcp1402176.
- Monteiro WO, Noshirvani HF, Marks IM, Lelliott PT. Anorgasmia from clomipramine in obsessive–compulsive disorder. A controlled trial. Br J Psychiatry 1987;151:107-12. http://dx.doi.org/10.1192/bjp.151.1.107.
- Bairy KL, Madhyastha S, Ashok KP, Bairy I, Malini S. Developmental and behavioral consequences of prenatal fluoxetine. Pharmacology 2007;79:1-11. http://dx.doi.org/10.1159/000096645.
- Zivin K, Pfeiffer PN, Bohnert AS, Ganoczy D, Blow FC, Nallamothu BK, et al. Evaluation of the FDA warning against prescribing citalopram at doses exceeding 40 mg. Am J Psychiatry 2013;170:642-50. http://dx.doi.org/10.1176/appi.ajp.2013.12030408.
- Maina G, Albert U, Salvi V, Bogetto F. Weight gain during long-term treatment of obsessive–compulsive disorder: a prospective comparison between serotonin reuptake inhibitors. J Clin Psychiatry 2004;65:1365-71. http://dx.doi.org/10.4088/JCP.v65n1011.
- March JS, Klee BJ, Kremer CM. Treatment benefit and the risk of suicidality in multicenter, randomized, controlled trials of sertraline in children and adolescents. J Child Adolesc Psychopharmacol 2006;16:91-102. http://dx.doi.org/10.1089/cap.2006.16.91.
- Bridge JA, Iyengar S, Salary CB, Barbe RP, Birmaher B, Pincus HA, et al. Clinical response and risk for reported suicidal ideation and suicide attempts in pediatric antidepressant treatment: a meta-analysis of randomized controlled trials. JAMA 2007;297:1683-96. http://dx.doi.org/10.1001/jama.297.15.1683.
- Abramowitz JS. The psychological treatment of obsessive–compulsive disorder. Can J Psychiatry 2006;51:407-16.
- Meyer V. Modification of expectations in cases with obsessional rituals. Behav Res Ther 1966;4:273-80. http://dx.doi.org/10.1016/0005-7967(66)90023-4.
- Rachman S, de Silva P. Abnormal and normal obsessions. Behav Res Ther 1978;16:233-48. http://dx.doi.org/10.1016/0005-7967(78)90022-0.
- Obsessive Compulsive Cognitions Working Group . Cognitive assessment of obsessive–compulsive disorder. Obsessive Compulsive Cognitions Working Group. Behav Res Ther 1997;35:667-81. http://dx.doi.org/10.1016/S0005-7967(97)00017-X.
- Moher D, Liberati A, Tetzlaff J, Altman DG. PRISMA Group . Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLOS Med 2009;6. http://dx.doi.org/10.1371/journal.pmed.1000097.
- Higgins J, Green S. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.0.0. Chichester, UK: Cochrane Collaboration; 2008.
- Lu G, Ades AE. Combination of direct and indirect evidence in mixed treatment comparisons. Stat Med 2004;23:3105-24. http://dx.doi.org/10.1002/sim.1875.
- Caldwell DM, Ades AE, Higgins JPT. Simultaneous comparison of multiple treatments: combining direct and indirect evidence. BMJ 2005;331:897-900. http://dx.doi.org/10.1136/bmj.331.7521.897.
- Dias S, Sutton AJ, Ades AE, Welton NJ. Evidence synthesis for decision making 2: a generalized linear modeling framework for pairwise and network meta-analysis of randomized controlled trials. Med Decis Making 2013;33:607-17. http://dx.doi.org/10.1177/0272989X12458724.
- Caldwell DM. An overview of conducting systematic reviews with network meta-analysis. Syst Rev 2014;3. http://dx.doi.org/10.1186/2046-4053-3-109.
- Salanti G. Indirect and mixed-treatment comparison, network, or multiple-treatments meta-analysis: many names, many benefits, many concerns for the next generation evidence synthesis tool. Res Synth Method 2012;3:80-97. http://dx.doi.org/10.1002/jrsm.1037.
- Jansen J, Naci H. Is network meta-analysis as valid as standard pairwise meta-analysis? It all depends on the distribution of effect modifiers. BMC Med 2013;11. http://dx.doi.org/10.1186/1741-7015-11-159.
- Chaimani A, Higgins JPT, Mavridis D, Spyridonos P, Salanti G. Graphical tools for network meta-analysis in STATA. PLOS ONE 2013;8. http://dx.doi.org/10.1371/journal.pone.0076654.
- Dias S, Welton NJ, Sutton AJ, Ades AE. Evidence synthesis for decision making 1: introduction. Med Decis Making 2013;33:597-606. http://dx.doi.org/10.1177/0272989X13487604.
- Haas DM, Caldwell DM, Kirkpatrick P, McIntosh JJ, Welton NJ. Tocolytic therapy for preterm delivery: systematic review and network meta-analysis. BMJ 2012;345. http://dx.doi.org/10.1136/bmj.e6226.
- Spiegelhalter DJ, Best NG, Carlin BP, van der Linde A. Bayesian measures of model complexity and fit. J Roy Stat Soc B 2002;64:583-616. http://dx.doi.org/10.1111/1467-9868.00353.
- Dias S, Welton NJ, Sutton AJ, Caldwell DM, Lu G, Ades AE. Evidence synthesis for decision making 4: inconsistency in networks of evidence based on randomized controlled trials. Med Decis Making 2013;33:641-56. http://dx.doi.org/10.1177/0272989X12455847.
- Clomipramine Collaborative Study Group . Clomipramine in the treatment of patients with obsessive–compulsive disorder. Arch Gen Psychiatry 1991;48:730-8. http://dx.doi.org/10.1001/archpsyc.1991.01810320054008.
- Albert U, Aguglia E, Maina G, Bogetto F. Venlafaxine versus clomipramine in the treatment of obsessive–compulsive disorder: a preliminary single-blind, 12-week, controlled study. J Clin Psychiatry 2002;63:1004-9. http://dx.doi.org/10.4088/JCP.v63n1108.
- Ananth J, Pecknold JC, van den Steen N, Engelsmann F. Double-blind comparative study of clomipramine and amitriptyline in obsessive neurosis. Prog Neuropsychopharmacol 1981;5:257-62. http://dx.doi.org/10.1016/0364-7722(81)90077-1.
- Anderson RA, Rees CS. Group versus individual cognitive–behavoural treatment for obsessive–compulsive disorder: a controlled trial. Behav Res Ther 2007;45:123-37. http://dx.doi.org/10.1016/j.brat.2006.01.016.
- Andersson E, Enander J, Andrén P, Hedman E, Ljótsson B, Hursti T, et al. Internet-based cognitive behaviour therapy for obsessive–compulsive disorder: a randomized controlled trial. Psychol Med 2012;42. http://dx.doi.org/10.1017/S0033291712000244.
- Belloch A, Cabedo E, Carrio C. Cognitive versus behaviour therapy in the individual treatment of OCD: changes in cognitions and clinically significant outcomes at post-treatment and one-year follow-up. Behav Cogn Psychother 2008;36:521-40. http://dx.doi.org/10.1017/S1352465808004451.
- Belotto-Silva C, Diniz JB, Malavazzi DM, Valério C, Fossaluza V, Borcato S, et al. Group cognitive–behavioural therapy versus selective serotonin reuptake inhibitors for obsessive–compulsive disorder: a practical clinical trial. J Anxiety Disord 2012;26:25-31. http://dx.doi.org/10.1016/j.janxdis.2011.08.008.
- Bergeron R, Ravindran AV, Chaput Y, Goldner E, Swinson R, van Ameringen MA, et al. Sertraline and fluoxetine treatment of obsessive–compulsive disorder: results of a double-blind, 6-month treatment study. J Clin Psychopharmacol 2002;22:148-54. http://dx.doi.org/10.1097/00004714-200204000-00007.
- Bisserbe JC, Lane RM, Flament MF. A double-blind comparison of sertraline and clomipramine in outpatients with obsessive–compulsive disorder. Eur Psychiatry 1997;12:82-93. http://dx.doi.org/10.1016/S0924-9338(97)89646-0.
- Chouinard G, Goodman W, Greist J, Jenike M, Rasmussen S, White K, et al. Results of a double-blind placebo controlled trial of a new serotonin uptake inhibitor, sertraline, in the treatment of obsessive–compulsive disorder. Psychopharmacology Bull 1990;26:279-84.
- Cordioli AV, Heldt E, Braga Bochi D, Margis R, Basso de Sousa M, Fonseca Tonello J, et al. Cognitive–behavioural group therapy in obsessive–compulsive disorder: a randomized clinical trial. Psychother Psychosom 2003;72:211-16. http://dx.doi.org/10.1159/000070785.
- Cottraux J, Mollard E, Bouvard M, Marks I. Exposure therapy, fluvoxamine, or combination treatment in obsessive–compulsive disorder: 1-year follow up. Psychiatry Res 1993;49:63-75. http://dx.doi.org/10.1016/0165-1781(93)90030-K.
- Cottraux J, Note I, Yao SN, Lafont S, Note B, Mollard E, et al. A randomized controlled trial of cognitive therapy versus intensive behavior therapy in obsessive compulsive disorder. Psychother Psychosom 2001;70:288-97. http://dx.doi.org/10.1159/000056269.
- Denys D, van der Wee N, van Megen HJ, Westenberg HG. A double blind comparison of venlafaxine and paroxetine in obsessive–compulsive disorder. J Clin Psychopharmacol 2003;23:568-75. http://dx.doi.org/10.1097/01.jcp.0000095342.32154.54.
- Emmelkamp PM, Beens H. Cognitive therapy with obsessive–compulsive disorder: a comparative evaluation. Behav Res Ther 1991;29:293-300. http://dx.doi.org/10.1016/0005-7967(91)90120-R.
- Emmelkamp PM, Visser S, Hoekstra RJ. Cognitive therapy vs exposure in vivo in the treatment of obsessive–compulsives. Cognit Ther Res 1988;12:103-14. http://dx.doi.org/10.1007/BF01172784.
- Fals-Stewart W, Marks AP, Schafer J. A comparison of behavioral group therapy and individual behavior therapy in treating obsessive–compulsive disorder. J Nerv Ment Dis 1993;181:189-93. http://dx.doi.org/10.1097/00005053-199303000-00007.
- Foa EB, Liebowitz MR, Kozak MJ, Davies S, Campeas R, Franklin ME, et al. Randomized, placebo-controlled trial of exposure and ritual prevention, clomipramine, and their combination in the treatment of obsessive–compulsive disorder. Am J Psychiatry 2005;162:151-61. http://dx.doi.org/10.1176/appi.ajp.162.1.151.
- Freeman CP, Trimble MR, Deakin JF, Stokes TM, Ashford JJ. Fluvoxamine versus clomipramine in the treatment of obsessive compulsive disorder: a multicenter, randomized, double-blind, parallel group comparison. J Clin Psychiatry 1994;55:301-5.
- Freeston MH, Ladouceur R, Gagnon F, Thibodeau N, Rhéaume J, Letarte H, et al. Cognitive–behavioural treatment of obsessive thoughts: a controlled study. J Consult Clin Psychol 1997;65:405-13. http://dx.doi.org/10.1037/0022-006X.65.3.405.
- GlaxoSmithKline . Paroxetine Versus Clomipramine and Placebo in the Treatment of Obsessive–Compulsive Disorder n.d.
- GlaxoSmithKline . A Double Blind, Multicenter, Randomized, Drug-Controlled Study to Assess the Efficacy and Tolerance of Paroxetine Compared With Clomipramine in Treatment of Obsessive Compulsive Disorder n.d.
- Goodman WK, Price LH, Rasmussen SA, Delgado PL, Heninger GR, Charney DS. Efficacy of fluvoxamine in obsessive–compulsive disorder. A double-blind comparison with placebo. Arch Gen Psychiatry 1989;46:36-44. http://dx.doi.org/10.1001/archpsyc.1989.01810010038006.
- Goodman WK, Kozak MJ, Liebowitz M, White KL. Treatment of obsessive–compulsive disorder with fluvoxamine: a multicentre, double-blind, placebo-controlled trial. Int Clin Psychopharmacol 1996;11:21-9. http://dx.doi.org/10.1097/00004850-199603000-00003.
- Greist JH, Marks IM, Baer L, Kobak KA, Wenzel KW, Hirsch MJ, et al. Behavior therapy for obsessive–compulsive disorder guided by a computer or by a clinician compared with relaxation as a control. J Clin Psychiatry 2002;63:138-45. http://dx.doi.org/10.4088/JCP.v63n0209.
- Hohagen F, Winkelmann G, Rasche-Rüchle H, Hand I, König A, Münchau N, et al. Combination of behaviour therapy with fluvoxamine in comparison with behaviour therapy and placebo. Results of a multicentre study. Br J Psychiatry Suppl 1998;35:71-8.
- Hollander E, Allen A, Steiner M, Wheadon DE, Oakes R, Burnham DB, et al. Acute and long-term treatment and prevention of relapse of obsessive–compulsive disorder with paroxetine. J Clin Psychiatry 2003;64:1113-21. http://dx.doi.org/10.4088/JCP.v64n0919.
- Hollander E, Koran LM, Goodman WK, Greist JH, Ninan PT, Yang H, et al. A double-blind, placebo-controlled study of the efficacy and safety of controlled-release fluvoxamine in patients with obsessive–compulsive disorder. J Clin Psychiatry 2003;64:640-7. http://dx.doi.org/10.4088/JCP.v64n0604.
- Jaurrieta N, Jimenez-Murcia S, Menchón JM, Del Pino Alonso M, Segalas C, Alvarez-Moya EM, et al. Individual versus group cognitive–behavioural treatment for obsessive–compulsive disorder: a controlled pilot study. Psychother Res 2008;18:604-14. http://dx.doi.org/10.1080/10503300802192141.
- Jenike MA, Baer L, Summergrad P, Minichiello WE, Holland A, Seymour R. Sertraline in obsessive–compulsive disorder: a double-blind comparison with placebo. Am J Psychiatry 1990;147:923-8.
- Jenike MA, Hyman S, Baer L, Holland A, Minichiello WE, Buttolph L, et al. A controlled trial of fluvoxamine in obsessive–compulsive disorder: implications for a serotonergic theory. Am J Psychiatry 1990;147:1209-15. http://dx.doi.org/10.1176/ajp.147.9.1209.
- Jenike MA, Baer L, Minichiello WE, Rauch SL, Buttolph ML. Placebo-controlled trial of fluoxetine and phenelzine for obsessive–compulsive disorder. Am J Psychiatry 1997;154:1261-4. http://dx.doi.org/10.1176/ajp.154.9.1261.
- Jones MK, Menzies RG. Danger ideation reduction therapy (DIRT) for obsessive–compulsive washers. A controlled trial. Behav Res Ther 1998;36:959-70. http://dx.doi.org/10.1016/S0005-7967(98)00057-6.
- Kamijima K, Murasaki M, Asai M, Higuchi T, Nakajima T, Taga C, et al. Paroxetine in the treatment of obsessive–compulsive disorder: randomized, double-blind, placebo-controlled study in Japanese patients. Psychiatry Clin Neurosci 2004;58:427-33. http://dx.doi.org/10.1111/j.1440-1819.2004.01278.x.
- Khodarahimi S. Satiation therapy and exposure response prevention in the treatment of obsessive compulsive disorder. J Contemp Psychother 2009;39:203-7. http://dx.doi.org/10.1007/s10879-009-9110-z.
- Kobak KA, Taylor LV, Bystritsky A, Kohlenberg CJ, Greist JH, Tucker P, et al. St John’s wort versus placebo in obsessive–compulsive disorder: results from a double-blind study. Int Clin Psychopharmacol 2005;20:299-304. http://dx.doi.org/10.1097/00004850-200511000-00003.
- Koran LM, McElroy SL, Davidson JR, Rasmussen SA, Hollander E, Jenike MA. Fluvoxamine versus clomipramine for obsessive–compulsive disorder: a double-blind comparison. J Clin Psychopharmacol 1996;16:121-9. http://dx.doi.org/10.1097/00004714-199604000-00004.
- Kronig MH, Apter J, Asnis G, Bystritsky A, Curtis G, Ferguson J, et al. Placebo-controlled, multicenter study of sertraline treatment for obsessive–compulsive disorder. J Clin Psychopharmacol 1999;19:172-6. http://dx.doi.org/10.1097/00004714-199904000-00013.
- Lindsay M, Crino R, Andrews G. Controlled trial of exposure and response prevention in obsessive–compulsive disorder. Br J Psychiatry 1997;171:135-9. http://dx.doi.org/10.1192/bjp.171.2.135.
- López-Ibor JJ, Saiz J, Cottraux J, Note I, Viñas R, Bourgeois M, et al. Double-blind comparison of fluoxetine versus clomipramine in the treatment of obsessive compulsive disorder. Eur Neuropsychopharmacol 1996;6:111-18. http://dx.doi.org/10.1016/0924-977X(95)00071-V.
- Mavissakalian M, Turner SM, Michelson L, Jacob R. Tricyclic antidepressants in obsessive–compulsive disorder: antiobsessional or antidepressant agents? II. Am J Psychiatry 1985;142:572-6. http://dx.doi.org/10.1176/ajp.142.5.572.
- McLean PD, Whittal ML, Thordarson DS, Taylor S, Söchting I, Koch WJ, et al. Cognitive versus behavior therapy in the group treatment of obsessive–compulsive disorder. J Consult Clin Psychol 2001;69:205-14. http://dx.doi.org/10.1037/0022-006X.69.2.205.
- Milanfranchi A, Ravagli S, Lensi P, Marazziti D, Cassano GB. A double-blind study of fluvoxamine and clomipramine in the treatment of obsessive–compulsive disorder. Int Clin Psychopharmacol 1997;12:131-6. http://dx.doi.org/10.1097/00004850-199705000-00002.
- Montgomery SA, McIntyre A, Osterheider M, Sarteschi P, Zitterl W, Zohar J, et al. A double-blind, placebo-controlled study of fluoxetine in patients with DSM-III-R obsessive–compulsive disorder. Eur Neuropsychopharmacol 1993;3:143-52. http://dx.doi.org/10.1016/0924-977X(93)90266-O.
- Montgomery SA, Kasper S, Stein DJ, Bang Hedegaard K, Lemming OM. Citalopram 20 mg, 40 mg and 60 mg are all effective and well tolerated compared with placebo in obsessive–compulsive disorder. Int Clin Psychopharmacol 2001;16:75-86. http://dx.doi.org/10.1097/00004850-200103000-00002.
- Mundo E, Bianchi L, Bellodi L. Efficacy of fluvoxamine, paroxetine, and citalopram in the treatment of obsessive–compulsive disorder: a single-blind study. J Clin Psychopharmacol 1997;17:267-71. http://dx.doi.org/10.1097/00004714-199708000-00005.
- Mundo E, Rouillon F, Figuera ML, Stigler M. Fluvoxamine in obsessive–compulsive disorder: similar efficacy but superior tolerability in comparison with clomipramine. Hum Psychopharmacol 2001;16:461-8. http://dx.doi.org/10.1002/hup.317.
- Nakajima T, Kudo Y, Yamashita I. Clinical usefulness of fluvoxamine maleate (SME3110), a selective serotonin reuptake inhibitor, in the treatment of obsessive compulsive disorder: a double blind, placebo controlled study. J Clin Ther Med 1996;12:409-37.
- Nakatani E, Nakagawa A, Nakao T, Yoshizato C, Nabeyama M, Kudo A, et al. A randomized controlled trial of Japanese patients with obsessive–compulsive disorder – effectiveness of behavior therapy and fluvoxamine. Psychother Psychosom 2005;74:269-76. http://dx.doi.org/10.1159/000086317.
- O’Connor K, Todorov C, Robillard S, Borgeat F, Brault M. Cognitive–behavour therapy and medication in the treatment of obsessive–compulsive disorder: a controlled study. Can J Psychiatry 1999;44:64-71.
- O’Connor KP, Aardema F, Robillard S, Guay S, Pélissier MC, Todorov C, et al. Cognitive behaviour therapy and medication in the treatment of obsessive–compulsive disorder. Acta Psychiatr Scand 2006;113:408-19. http://dx.doi.org/10.1111/j.1600-0447.2006.00767.x.
- Perse TL, Greist JH, Jefferson JW, Rosenfeld R, Dar R. Fluvoxamine treatment of obsessive–compulsive disorder. Am J Psychiatry 1987;144:1543-8. http://dx.doi.org/10.1176/ajp.144.12.1543.
- Shareh H, Gharraee B, Atef-Vahid M, Eftekhar M. Metacognitive Therapy (MCT), fluvoxamine, and combined treatment in improving obsessive–compulsive, depressive and anxiety symptoms in patients with obsessive–compulsive disorder (OCD). IJPBS 2010;4:17-25.
- Sousa MB, Isolan LR, Oliveira RR, Manfro GG, Cordioli AV. A randomized clinical trial of cognitive–behavioural group therapy and sertraline in the treatment of obsessive–compulsive disorder. J Clin Psychiatry 2006;67:1133-9. http://dx.doi.org/10.4088/JCP.v67n0717.
- Thoren P, Asberg M, Cronholm B, Jornestedt L, Traskman L. Clomipramine treatment of obsessive–compulsive disorder. I. A controlled clinical trial. Arch Gen Psychiatry 1980;37:1281-5. http://dx.doi.org/10.1001/archpsyc.1980.01780240079009.
- Van Oppen P, de Haan E, van Balkom AJ, Spinhoven P, Hoogduin K, van Dyck R. Cognitive therapy and exposure in vivo in the treatment of obsessive compulsive disorder. Behav Res Ther 1995;33:379-90. http://dx.doi.org/10.1016/0005-7967(94)00052-L.
- Volavka J, Neziroglu F, Yaryura-Tobias JA. Clomipramine and imipramine in obsessive–compulsive disorder. Psychiatry Res 1985;14:85-93. http://dx.doi.org/10.1016/0165-1781(85)90092-7.
- Whittal ML, Thordarson DS, McLean PD. Treatment of obsessive–compulsive disorder: cognitive behavior therapy vs. exposure and response prevention. Behav Res Ther 2005;43:1559-76. http://dx.doi.org/10.1016/j.brat.2004.11.012.
- Whittal ML, Woody SR, McLean PD, Rachman SJ, Robichaud M. Treatment of obsessions: a randomized controlled trial. Behav Res Ther 2010;48:295-303. http://dx.doi.org/10.1016/j.brat.2009.11.010.
- Zohar J, Judge R. Paroxetine versus clomipramine in the treatment of obsessive–compulsive disorder. OCD Paroxetine Study Investigators. Br J Psychiatry 1996;169:468-74. http://dx.doi.org/10.1192/bjp.169.4.468.
- Skapinakis P, Caldwell DM, Hollingworth W, Bryden P, Fineberg N, Salkovskis P, et al. Pharmacological and psychotherapeutic interventions for management of obsessive-compulsive disorder in adults: a systematic review and network meta-analysis [published online ahead of print June 15 2016]. Lancet Psychiatry 2016. http://dx.doi.org/10.1016/S2215-0366(16)30069-4.
- Alaghband-Rad J, Hakimshooshtary M. A randomized controlled clinical trial of citalopram versus fluoxetine in children and adolescents with obsessive–compulsive disorder (OCD). Eur Child Adolesc Psychiatry 2009;18:131-5. http://dx.doi.org/10.1007/s00787-007-0634-z.
- Asbahr FR, Castillo AR, Ito LM, Latorre MR, Moreira MN, Lotufo-Neto F. Group cognitive–behavioural therapy versus sertraline for the treatment of children and adolescents with obsessive–compulsive disorder. J Am Acad Child Adolesc Psychiatry 2005;44:1128-36. http://dx.doi.org/10.1097/01.chi.0000177324.40005.6f.
- Barrett P, Healy-Farrell L, March JS. Cognitive–behavioural family treatment of childhood obsessive–compulsive disorder: a controlled trial. J Am Acad Child Adolesc Psychiatry 2004;43:46-62. http://dx.doi.org/10.1097/00004583-200401000-00014.
- Bolton D, Perrin S. Evaluation of exposure with response-prevention for obsessive compulsive disorder in childhood and adolescence. J Behav Ther Exp Psychiatry 2008;39:11-22. http://dx.doi.org/10.1016/j.jbtep.2006.11.002.
- Bolton D, Williams T, Perrin S, Atkinson L, Gallop C, Waite P, et al. Randomized controlled trial of full and brief cognitive–behaviour therapy and wait-list for paediatric obsessive–compulsive disorder. J Child Psychol Psychiatry 2011;52:1269-78. http://dx.doi.org/10.1111/j.1469-7610.2011.02419.x.
- de Haan E, Hoogduin KA, Buitelaar JK, Keijsers GP. Behavior therapy versus clomipramine for the treatment of obsessive–compulsive disorder in children and adolescents. J Am Acad Child Adolesc Psychiatry 1998;37:1022-9. http://dx.doi.org/10.1097/00004583-199810000-00011.
- DeVeaugh-Geiss J, Moroz G, Biederman J, Cantwell D, Fontaine R, Greist JH, et al. Clomipramine hydrochloride in childhood and adolescent obsessive–compulsive disorder: a multicenter trial. J Am Acad Child Adolesc Psychiatry 1992;31:45-9. http://dx.doi.org/10.1097/00004583-199201000-00008.
- Flament MF, Rapoport JL, Berg CJ, Sceery W, Kilts C, Mellström B, et al. Clomipramine treatment of childhood obsessive–compulsive disorder: a double-blind controlled study. Arch Gen Psychiatry 1985;42:977-83. http://dx.doi.org/10.1001/archpsyc.1985.01790330057007.
- Freeman JB, Garcia AM, Coyne L, Ale C, Przeworski A, Himle M, et al. Early childhood OCD: preliminary findings from a family-based cognitive–behavioural approach. J Am Acad Child Adolesc Psychiatry 2008;47:593-602. http://dx.doi.org/10.1097/CHI.0b013e31816765f9.
- Geller DA, Hoog SL, Heiligenstein JH, Ricardi RK, Tamura R, Kluszynski S, et al. Fluoxetine treatment for obsessive–compulsive disorder in children and adolescents: a placebo-controlled clinical trial. J Am Acad Child Adolesc Psychiatry 2001;40:773-9. http://dx.doi.org/10.1097/00004583-200107000-00011.
- GlaxoSmithKline . A Randomized, Multicenter, 10-Week, Double-Blind, Placebo-Controlled, Flexible-Dose Study to Evaluate the Efficacy and Safety of Paroxetine in Children and Adolescents With Obsessive–Compulsive Disorder (OCD) 2001.
- Liebowitz MR, Turner SM, Piacentini J, Beidel DC, Clarvit SR, Davies SO, et al. Fluoxetine in children and adolescents with OCD: a placebo-controlled trial. J Am Acad Child Adolesc Psychiatry 2002;41:1431-8. http://dx.doi.org/10.1097/00004583-200212000-00014.
- March JS, Johnston H, Jefferson JW, Kobak KA, Greist JH. Do subtle neurological impairments predict treatment resistance to clomipramine in children and adolescents with obsessive–compulsive disorder?. J Child Adolesc Psychopharmacol 1990;1:133-40. http://dx.doi.org/10.1089/cap.1990.1.133.
- March JS, Biederman J, Wolkow R, Safferman A, Mardekian J, Cook EH, et al. Sertraline in children and adolescents with obsessive–compulsive disorder: a multicenter randomized controlled trial. JAMA 1998;280:1752-6. http://dx.doi.org/10.1001/jama.280.20.1752.
- Neziroglu F, Yaryura-Tobias JA, Walz J, McKay D. The effect of fluvoxamine and behavior therapy on children and adolescents with obsessive–compulsive disorder. J Child Adolesc Psychopharmacol 2000;10:295-306. http://dx.doi.org/10.1089/cap.2000.10.295.
- Piacentini J, Bergman RL, Chang S, Langley A, Peris T, Wood JJ, et al. Controlled comparison of family cognitive behavioral therapy and psychoeducation/relaxation training for child obsessive–compulsive disorder. J Am Acad Child Adolesc Psychiatry 2011;50:1149-61. http://dx.doi.org/10.1016/j.jaac.2011.08.003.
- Riddle MA, Scahill L, King RA, Hardin MT, Anderson GM, Ort SI, et al. Double-blind, crossover trial of fluoxetine and placebo in children and adolescents with obsessive–compulsive disorder. J Am Acad Child Adolesc Psychiatry 1992;31:1062-9. http://dx.doi.org/10.1097/00004583-199211000-00011.
- Riddle MA, Reeve EA, Yaryura-Tobias JA, Yang HM, Claghorn JL, Gaffney G, et al. Fluvoxamine for children and adolescents with obsessive–compulsive disorder: a randomized, controlled, multicenter trial. J Am Acad Child Adolesc Psychiatry 2001;40:222-9. http://dx.doi.org/10.1097/00004583-200102000-00017.
- Storch EA, Caporino NE, Morgan JR, Lewin AB, Rojas A, Brauer L, et al. Preliminary investigation of web-camera delivered cognitive–behavioural therapy for youth with obsessive–compulsive disorder. Psychiatry Res 2011;189:407-12. http://dx.doi.org/10.1016/j.psychres.2011.05.047.
- Storch EA, Bussing R, Small BJ, Geffken GR, McNamara JP, Rahman O, et al. Randomized, placebo-controlled trial of cognitive–behavioural therapy alone or combined with sertraline in the treatment of pediatric obsessive–compulsive disorder. Behav Res Ther 2013;51:823-9. http://dx.doi.org/10.1016/j.brat.2013.09.007.
- Williams TI, Salkovskis PM, Forrester L, Turner S, White H, Allsopp MA. A randomised controlled trial of cognitive behavioural treatment for obsessive compulsive disorder in children and adolescents. Eur Child Adolesc Psychiatry 2010;19:449-56. http://dx.doi.org/10.1007/s00787-009-0077-9.
- The Pediatric OCD Treatment Study . Cognitive–behaviour therapy, sertraline, and their combination for children and adolescents with obsessive–compulsive disorder: the Pediatric OCD Treatment Study (POTS) randomized controlled trial. JAMA 2004;292:1969-76. http://dx.doi.org/10.1001/jama.292.16.1969.
- Knapp M, Henderson J, Patel A, Maj M, Sartorius N, Okasha A, et al. Obsessive–Compulsive Disorder. New York, NY: Wiley; 2002.
- DuPont RL, Rice DP, Shiraki S, Rowland CR. Economic costs of obsessive–compulsive disorder. Med Interface 1995;8:102-9.
- Greist JH, Bandelow B, Hollander E, Marazziti D, Montgomery SA, Nutt DJ, et al. WCA recommendations for the long-term treatment of obsessive–compulsive disorder in adults. CNS Spectr 2003;8:7-16.
- Hankin CS, Koran L, Sheehan DV, Hollander E, Culpepper L, Black DW, et al. Patients with obsessive–compulsive disorder vs depression have comparable health care costs: a retrospective claims analysis of Florida Medicaid enrollees. Ann Clin Psychiatry 2011;23:285-96.
- Koran LM, Leventhal J, Fireman B, Jacobsen A. Recognition and treatment of obsessive compulsive disorder in a pre-paid health plan: does adequate treatment reduce costs?. Eur Neuropsychopharmacol 1997;7. http://dx.doi.org/10.1016/S0924-977X(97)88803-7.
- Tolin DF, Diefenbach GJ, Gilliam CM. Stepped care versus standard cognitive–behavioural therapy for obsessive–compulsive disorder: a preliminary study of efficacy and costs. Depress Anxiety 2011;28:314-23. http://dx.doi.org/10.1002/da.20804.
- McCrone P, Marks IM, Greist JH, Baer L, Kobak KA, Wenzel KW, et al. Cost-effectiveness of computer-aided behaviour therapy for obsessive–compulsive disorder. Psychother Psychosom 2007;76:249-50.
- Gava I, Barbui C, Aguglia E, Carlino D, Churchill R, De Vanna M, et al. Psychological treatments versus treatment as usual for obsessive compulsive disorder (OCD). Cochrane Database of Syst Rev 2007;2. http://dx.doi.org/10.1002/14651858.cd005333.pub2.
- Gellatly J, Bower P, McMillan D, Roberts C, Byford S, Bee P, et al. Obsessive Compulsive Treatment Efficacy Trial (OCTET) comparing the clinical and cost effectiveness of self-managed therapies: study protocol for a randomised controlled trial. Trials 2014;15. http://dx.doi.org/10.1186/1745-6215-15-278.
- Bamelis LL, Evers SM, Arntz A. Design of a multicentered randomized controlled trial on the clinical and cost effectiveness of schema therapy for personality disorders. BMC Public Health 2012;12. http://dx.doi.org/10.1186/1471-2458-12-75.
- Petrou S, Gray A. Economic evaluation using decision analytical modelling: design, conduct, analysis, and reporting. BMJ 2011;342. http://dx.doi.org/10.1136/bmj.d1766.
- Kaltenthaler E, Brazier J, De Nigris E, Tumur I, Ferriter M, Beverley C, et al. Computerised cognitive behaviour therapy for depression and anxiety update: a systematic review and economic evaluation. Health Technol Assess 2006;10. http://dx.doi.org/10.3310/hta10330.
- Pallanti S, Hollander E, Bienstock C, Koran L, Leckman J, Marazziti D, et al. (International Treatment Refractory OCD Consortium). Treatment non-response in OCD: methodological issues and operational definitions. Int J Neuropsychopharmacol 2002;5:181-91. http://dx.doi.org/10.1017/s1461145702002900.
- Farris SG, McLean CP, Van Meter PE, Simpson HB, Foa EB. Treatment response, symptom remission, and wellness in obsessive–compulsive disorder. J Clin Psychiatry 2013;74:685-90. http://dx.doi.org/10.4088/JCP.12m07789.
- Storch EA, Lewin AB, De Nadai AS, Murphy TK. Defining treatment response and remission in obsessive–compulsive disorder: a signal detection analysis of the Children’s Yale–Brown Obsessive Compulsive Scale. J Am Acad Child Adolesc Psychiatry 2010;49:708-17. http://dx.doi.org/10.1016/j.jaac.2010.04.005.
- Guy W. ECDEU Assessment Manual for Psychopharmacology. Rockville, MD: National Institute for Mental Health; 1976.
- British National Formulary. London: BMJ Group and Pharmaceutical Press; n.d.
- Curtis L. Unit Costs of Health and Social Care. Canterbury: Personal Social Services Research Unit; 2013.
- Eaton WW, Roth KB, Bruce M, Cottler L, Wu L, Nestadt G, et al. The relationship of mental and behavioral disorders to all-cause mortality in a 27-year follow-up of 4 epidemiologic catchment area samples. Am J Epidemiology 2013;178:1366-77. http://dx.doi.org/10.1093/aje/kwt219.
- Office for National Statistics . National Life Tables 2010–12. Secondary National Life Tables, 2010–12 n.d. www.ons.gov.uk/ons/publications/re-reference-tables.html?edition=tcm%3A77-352834 (accessed 1 November 2014).
- Guidelines: Search Filters for Observational Studies. Edinburgh: Scottish Intercollegiate Network; n.d.
- Mulhern B, Mukuria C, Barkham M, Knapp M, Byford S, Soeteman D, et al. Using generic preference-based measures in mental health: psychometric validity of the EQ–5D and SF–6D. Br J Psychiatry 2014;205:236-43. http://dx.doi.org/10.1192/bjp.bp.112.122283.
- Byford S, Barrett B, Despiegel N, Wade A. Impact of treatment success on health service use and cost in depression: longitudinal database analysis. Pharmacoeconomics 2011;29:157-70. http://dx.doi.org/10.2165/11537360-000000000-00000.
- Guide to the Methods of Technology Appraisal 2013. London: National Institute for Health and Care Excellence; 2013.
- Barton GR, Briggs AH, Fenwick EA. Optimal cost-effectiveness decisions: the role of the cost-effectiveness acceptability curve (CEAC), the cost-effectiveness acceptability frontier (CEAF), and the expected value of perfection information (EVPI). Value Health 2008;11:886-97. http://dx.doi.org/10.1111/j.1524-4733.2008.00358.x.
- van Balkom Anton JLM, van Oppen P, Vermeulen Alexander WA, van Dyck R, Nauta Mary CE, Vorst Harne CM. A meta-analysis on the treatment of obsessive compulsive disorder: a comparison of antidepressants, behavior, and cognitive therapy. Clin Psychol Rev 1994;14:359-81. http://dx.doi.org/10.1016/0272-7358(94)90033-7.
- Piccinelli M, Pini S, Bellantuono C, Wilkinson G. Efficacy of drug treatment in obsessive–compulsive disorder. A meta-analytic review. Br J Psychiatry 1995;166:424-43. http://dx.doi.org/10.1192/bjp.166.4.424.
- Geller DA, Biederman J, Stewart SE, Mullin B, Martin A, Spencer T, et al. Which SSRI? A meta-analysis of pharmacotherapy trials in pediatric obsessive–compulsive disorder. Am J Psychiatry 2003;160:1919-28. http://dx.doi.org/10.1176/appi.ajp.160.11.1919.
- Cuijpers P, Sijbrandij M, Koole SL, Andersson G, Beekman AT, Reynolds CF. The efficacy of psychotherapy and pharmacotherapy in treating depressive and anxiety disorders: a meta-analysis of direct comparisons. World Psychiatry 2013;12:137-48. http://dx.doi.org/10.1002/wps.20038.
- Cuijpers P, Sijbrandij M, Koole SL, Andersson G, Beekman AT, Reynolds CF. Adding psychotherapy to antidepressant medication in depression and anxiety disorders: a meta-analysis. World Psychiatry 2014;13:56-67. http://dx.doi.org/10.1002/wps.20089.
- Romanelli RJ, Wu FM, Gamba R, Mojtabai R, Segal JB. Behavioral therapy and serotonin reuptake inhibitor pharmacotherapy in the treatment of obsessive–compulsive disorder: a systematic review and meta-analysis of head-to-head randomized controlled trials. Depress Anxiety 2014;31:641-52. http://dx.doi.org/10.1002/da.22232.
- Rasmussen S, Hackett E, DuBoff E, Greist J, Halaris A, Koran LM, et al. A 2-year study of sertraline in the treatment of obsessive–compulsive disorder. Int Clin Psychopharmacol 1997;12:309-16. http://dx.doi.org/10.1097/00004850-199711000-00003.
- Skarphedinsson G, Hanssen-Bauer K, Kornor H, Heiervang ER, Landro NI, Axelsdottir B, et al. Standard individual cognitive behaviour therapy for paediatric obsessive–compulsive disorder: a systematic review of effect estimates across comparisons. Nord J Psychiatry 2014;68:1-12. http://dx.doi.org/10.3109/08039488.2014.941395.
- Lu G, Kounali D, Ades AE. Simultaneous multioutcome synthesis and mapping of treatment effects to a common scale. Value Health 2014;17:280-7. http://dx.doi.org/10.1016/j.jval.2013.12.006.
- Wood L, Egger M, Gluud LL, Schulz KF, Jüni P, Altman DG, et al. Empirical evidence of bias in treatment effect estimates in controlled trials with different interventions and outcomes: meta-epidemiological study. BMJ 2008;336:601-15. http://dx.doi.org/10.1136/bmj.39465.451748.AD.
- Huhn M, Tardy M, Spineli LM, Kissling W, Förstl H, Pitschel-Walz G, et al. Efficacy of pharmacotherapy and psychotherapy for adult psychiatric disorders: a systematic overview of meta-analyses. JAMA Psychiatry 2014;71:706-15. http://dx.doi.org/10.1001/jamapsychiatry.2014.112.
- Weinstein MC, O’Brien B, Hornberger J, Jackson J, Johannesson M, McCabe C, et al. Principles of good practice for decision analytic modeling in health-care evaluation: report of the ISPOR task force on good research practices: modeling studies. Value Health 2003;6:9-17. http://dx.doi.org/10.1046/j.1524-4733.2003.00234.x.
- Oppe M, Devlin NJ, van Hout B, Krabbe PF, de Charro F. A program of methodological research to arrive at the new international EQ-5D-5L valuation protocol. Value Health 2014;17:445-53. http://dx.doi.org/10.1016/j.jval.2014.04.002.
- Longworth L, Yang Y, Young T, Mulhern B, Hernandez Alava M, Mukuria C, et al. Use of generic and condition-specific measures of health-related quality of life in NICE decision-making: a systematic review, statistical modelling and survey. Health Technol Assess 2014;18. http://dx.doi.org/10.3310/hta18090.
Appendix 1 Search strategy
The CCDANCTR-Studies Register was initially searched (September–December 2012) using the following index terms:
Condition = obsess* or compulsi*
AND
Intervention = (Citalopram or (Clomipramin* or Clorimipramin* or Chlomipramin* or Chlorimipramin*) or Escitalopram or Fluoxetine or Fluvoxamine or Paroxetine or Sertraline or Venlafaxine or Duloxetine or Mirtazapine or SSRI* or Serotonin or cognitive* or behavi* or exposure or “response prevention”)
The CCDANCTR-References Register was initially searched using a more sensitive set of free-text terms (to identify additional untagged/uncoded reports of trials):
((obsess* or compulsi* or OCD) AND (Citalopram or (Clomipramin* or Clorimipramin* or Chlomipramin* or Chlorimipramin*) or Escitalopram or Fluoxetine or Fluvoxamine or Paroxetine or Sertraline or Venlafaxine or Duloxetine or Mirtazapine or SSRI* or (Serotonin and (uptake or reuptake or re-uptake)) or SNRI* or CBT or cognitive* or behavioral or behavioural or exposure or ERP or “response prevention” or ((*therap* or train* or treatment*) and (behavi* or expos*))))
As the number of studies retrieved in this initial search was not very large (643 studies), in order to increase the sensitivity of the search we decided to repeat the search using the condition only, (obsess* or compulsi*), without any other terms.
Appendix 2 Table of excluded studies
| Number | Reference | Summary comment for exclusion |
|---|---|---|
| 1 | Aigner M, Demal U, Zitterl W, Bach M, Trappl E, Lenz G. Behavioural group therapy for obsessive–compulsive disorder. Verhaltenstherapie 2004;14:7–14 | Controlled but not randomised |
| 2 | Akouchekian S, Jamshidian Z, Maracy MR, Almasi A, Davarpanah Jazi AH. Religious cognitive behavioural therapy in religious oriented obsessive compulsive disorder. The 19th European Congress of Psychiatry, Vienna, Austria, 12–15 March 2011 | Duplicate: early congress abstract of the full paper |
| 3 | Akouchekian S, Jamshidian Z, Maracy MR, Almasi A, Davarpanah Jazi AH. Effectiveness of religious cognitive–behavioural therapy on religious oriented obsessive compulsive disorder and its co-morbidity. J Isfahan Med School 2011;28:1 | Special subgroup of OCD patients with religious-oriented symptoms (in Arabic) |
| 4 | Askin R, Turan M, Cilli AS, Kaya N. Clomipramine versus sertraline in the treatment of obsessive compulsive disorder. Bull Clin Psychopharmacol 1999;9:133–8 | Usable data only for dichotomous outcome. No variability measure for continuous outcome |
| 5 | van Balkom A, Haan ED, Oppen PV, Spinhoven P, Hoogduin L, Dyck RV. Cognitive–behavioural Therapy Versus the Combination with Fluvoxamine in the Treatment of OCD. 150th Annual Meeting of the American Psychiatric Association. San Diego, California, USA, 17–22 May 1997 | Duplicate reporting: early congress abstract of the van Balkom et al. 1998 paper |
| 6 | Belloch A, Cabedo E, Carrió C, Fernández-Alvarez H, García F, Larsson C. Group versus individual cognitive treatment for obsessive–compulsive disorder: changes in non-OCD symptoms and cognitions at post-treatment and 1-year follow-up. Psychiatry Res 2011;187:174–9 | Secondary analysis of Cabedo et al. 2010 paper, which has also been excluded |
| 7 | Black DW, Monahan P, Gable J, Blum N, Clancy G, Baker P. Hoarding and treatment response in 38 nondepressed subjects with obsessive–compulsive disorder. J Clin Psychiatry 1998;59:420–5 | Duplicate data, paroxetine vs. placebo already included in Hollander et al. 2003.180 CBT arm not randomised |
| 8 | Cabedo E, Belloch A, Carrio C, Larsson C, Fernández-Alvarez H, García F. Group versus individual cognitive treatment for obsessive–compulsive disorder: changes in severity at post-treatment and 1-year follow-up. Behav Cogn Psychother 2010;38:227–32 | Control intervention not covered (comparison between different forms of the same therapy) |
| 9 | Denys D, van Megen HJ, van der Wee N, Westenberg HG. A double-blind switch study of paroxetine and venlafaxine in obsessive–compulsive disorder. J Clin Psychiatry 2004;65:37–43 | Extension of the Denys et al. 2003167 study in non-responders (treatment refractory population) |
| 10 | Dougherty DD, Jameson M, Deckersbach T, et al. Open-label study of high (30 mg) and moderate (20 mg) dose escitalopram for the treatment of obsessive–compulsive disorder. Int Clin Psychopharmacol 2009;24:306–11 | Dose ranging study of the same drug: no comparator |
| 11 | Eli Lilly. Fluoxetine Treatment for Obsessive Compulsive Disorder in Children and Adolescents. Clinical Study Register. ID No. 3032. URL: www.lillytrials.com/results/prozac.pdf (accessed 5 February 2016) | Duplicate with Geller et al. 2001224 |
| 12 | Fineberg NA, Hughes A, Gale TM, Roberts A. Group cognitive behaviour therapy in obsessive–compulsive disorder (OCD): a controlled study. Int J Psychiatry Clin Pract 2005;9:257–63 | This paper used systematic and not random sampling |
| 13 | Franklin ME, Abramowitz JS, Bux DA Jr, Zoellner LA, Feeny NC. Cognitive–behavioural therapy with and without medication in the treatment of obsessive–compulsive disorder. Prof Psychol Res Pract 2002;33:162–8 | Observational study stratified by medication: not an experimental study |
| 14 | Giasuddini NA, Nahar JS, Morshed NM, Balhara YP, Sobhan MA. Efficacy of combination of fluoxetine and cognitive behavioural therapy and fluoxetine alone for the treatment of obsessive compulsive disorder. Pak J Pharm Sci 2013;26:95–8 | Uncertain if truly randomised (abstract does not mention randomised, baseline scores of the scale used almost marginally significantly different between the two groups with p = 0.07), unable to find if the symptom scale used (Dhaka University Obsessive–Compulsive Scale) has been validated or not – reference given unable to locate, this scale has not been used again in research |
| 15 | GlaxoSmithKline. Paroxetine versus Placebo in the Treatment of Obsessive–Compulsive Disorder. Clinical Study Register. 1993. URL: www.gsk-clinicalstudyregister.com/study/29060/116 (accessed 5 February 2016) | Early report of the Hollander et al. 2003180 data set |
| 16 | GlaxoSmithKline. A Double-Blind Study to Assess the Efficacy and Tolerance of a Flexible Dose of Paroxetine Compared with a Flexible Dose of Clomipramine and Placebo in the Treatment of Obsessive Compulsive Disorder. Clinical Study Register. Study No. MY-1037/BRL-029060/1/CPMS-136. 1993. URL: www.gsk-clinicalstudyregister.com/files2/2287.pdf (accessed 5 February 2016) | Duplicate of Zohar and Judge 1996213 |
| 17 | Goodman WK, Lydiard RB, Rubin A, Hackett E, Wolkow R, Londborg PD. Safety of sertraline in long-term OCD treatment: preliminary results of a multicenter study. 152nd Annual Meeting of the American Psychiatric Association, Washington, DC, 15–20 May 1999 | Relapse prevention study |
| 18 | Goodman WK, Price LH, Delgado PL, Palumbo J, Krystal JH, Nagy LM, et al. Specificity of serotonin reuptake inhibitors in the treatment of obsessive–compulsive disorder: comparison of fluvoxamine and desipramine. Arch Gen Psychiatry 1990;47:577–85 | See control intervention |
| 19 | Greist JH. Fluvoxamine in obsessive compulsive disorder: a multicenter parallel design double-blind placebo-controlled trial. Clin Neuropharm 1992;15(Suppl. 1):310B | Abstract report with no data given. This is one of the two pivotal studies of fluvoxamine from Solvay but only the second – Goodman et al. 1996177 – has been published. Greist et al. 1995126 in a meta-analysis has combined the two trials but no data can be used either |
| 20 | Greist JH, Jefferson JW, Kobak KA, Chouinard G, DuBoff E, Halaris A, et al. A 1 year double-blind placebo-controlled fixed dose study of sertraline in the treatment of obsessive–compulsive disorder. Int Clin Psychopharmacol 1995;10:57–65 | Duplicate of the CCSG 1991154 |
| 21 | Hewlett WA, Vinogradov S, Agras WS. Clomipramine, clonazepam, and clonidine treatment of obsessive–compulsive disorder. J Clin Psychopharmacol 1992;12:420–30 | Comparator not covered (clonazepam, clonidine) |
| 22 | Hoehn-Saric R, Ninan P, Black DW, Stahl S, Greist JH, Lydiard B, et al. Multicenter double-blind comparison of sertraline and desipramine for concurrent obsessive–compulsive and major depressive disorders. Arch Gen Psychiatry 2000;57:76–82 | See diagnosis and control not covered |
| 23 | Hohagen F, Konig A, Rasche-Rauchle H, Hand I, Rey E, Aldenhoff J, et al. Behaviour therapy and fluvoxamine versus behaviour therapy and placebo: results of a multicenter study. Sixth World Congress of Biological Psychiatry, Nice, France, 22–27 June 1997 | Duplicate: early congress abstract of the Hohagen et al. 1998179 paper |
| 24 | Holland R, Vardy A, Bolt G. A comparison of fluvoxamine (FL) and clomipramine (CLO) in the treatment of obsessive compulsive disorder (OCD). Clin Neuropharm 1992;15(Suppl. 1):311B | Abstract congress about tolerability including previously published data from Solvay |
| 25 | Insel TR, Murphy DL, Cohen RM, Alterman I, Kilts C, Linnoila M. Obsessive–compulsive disorder. A double-blind trial of clomipramine and clorgyline. Arch Gen Psychiatry 1983;40:605–12 | Control intervention not covered |
| 26 | Jakubovski E, Diniz JB, Valerio C, Fossaluza V, Belotto-Silva C, Gorenstein C, et al. Clinical predictors of long-term outcome in obsessive–compulsive disorder. Depress Anxiety 2013;30:763–72 | Duplicate of Belotto-Silva et al. 2012:160 secondary |
| 27 | Jenike MA, Baer L, Summergrad P, Weilburg JB, Holland A, Seymour R. Obsessive–compulsive disorder: a double-blind, placebo-controlled trial of clomipramine in 27 patients. Am J Psychiatry 1989;146:1328–30 | Duplicate of CCSG 1991154 |
| 28 | Jonsson H, Hougaard E, Bennedsen BE. Randomised comparative study of group versus individual cognitive behavioural therapy for obsessive compulsive disorder. Acta Psychiatr Scand 2011;123:387–97 | Control intervention not covered (comparison between different forms of the same therapy) |
| 29 | Karabanow O. Double-blind controlled study in phobias and obsessions. J Int Med Res 1977;5(Suppl. 5):42–8 | Not exclusively OCD (phobias): unstandardised diagnosis |
| 30 | Kearns C, Tone Y, Rush G, Lucey JV. Effectiveness of group-based cognitive–behavioural therapy in patients with obsessive–compulsive disorder. Psychiatrist 2010;34:6–9 | Uncontrolled case series (not randomised) |
| 31 | Khan MN, Hotiana UA, Ahmad S. Escitalopram in the treatment of obsessive–compulsive disorder: a double blind placebo control trial. J Ayub Med Coll Abbottabad 2007;19:58–63 | First phase of the study open label uncontrolled trial, second phase randomised responders only for relapse prevention |
| 32 | Koran LM, Cain JW, Dominguez RA, Rush AJ, Thiemann S. Are fluoxetine plasma levels related to outcome in obsessive–compulsive disorder? Am J Psychiatry 1996;153:1450–4 | Duplicate of Tollefson et al., 1994127 |
| 33 | Kudo Y. A placebo controlled double blind study in obsessive compulsive disorder with fluvoxamine. Eur Neuropsychopharmacol 1995;5:371–2 | Early congress report of the Nakajima et al. 1996201 paper |
| 34 | Leonard HL, Swedo SE, Rapoport JL, Koby EV, Lenane MC, Cheslow DL, et al. Treatment of obsessive–compulsive disorder with clomipramine and desipramine in children and adolescents. A double-blind crossover comparison. Arch Gen Psychiatry 1989;46:1088–92 | Comparator not covered |
| 35 | Ma JD, Wang CH, Li HF, Zhang XL, Zhang YL, Hou YH, et al. Cognitive-coping therapy for obsessive–compulsive disorder: a randomised controlled trial. J Psychiatr Res 2013;47:1785–90 | Non-extractable data for non-resistant patients: this study included patients who were treatment resistant within the study but no separate data are given for those who were non-resistant |
| 36 | Mallya GK, White K, Waternaux C, Quay S. Short and long term treatment of obsessive compulsive disorder with fluvoxamine. Ann Clin Psychiatry 1992;4:77–80 | Duplicate data also reported in Goodman et al. 1996177 |
| 37 | Marks IM, Lelliott P, Basoglu M, Noshirvani H, Monteiro W, Cohen D, et al. Clomipramine, self-exposure and therapist-aided exposure for obsessive–compulsive rituals. Br J Psychiatry 1988;152:522–34 | No extractable data for treatment comparisons |
| 38 | Marks IM, Stern RS, Mawson D, Cobb J, McDonald R. Clomipramine and exposure for obsessive–compulsive rituals. Br J Psychiatry 1980;136:1–25 | No extractable data for treatment comparisons: OCD diagnosis not standardised |
| 39 | Mavissakalian MR, Jones B, Olson S, Perel JM. Clomipramine in obsessive–compulsive disorder: clinical response and plasma levels. J Clin Psychopharmacol 1990;10:261–8 | Duplicate with CCSG 1991154 |
| 40 | Montgomery SA. Clomipramine in obsessional neurosis: a placebo-controlled trial. Pharmacol Med 1980;1:189–92 | Duplicate: crossover data at the point of cross-over, also reported later in Montgomery et al. 1990 |
| 41 | Mundo E, Bianchi L, Bellodi L. Efficacy of fluvoxamine, paroxetine, and citalopram in the treatment of obsessive–compulsive disorder: a single-blind study. J Clin Psychopharmacol 1997;17:267–71 | Dose-ranging study of the same drug: no comparator |
| 42 | Mundo E, Maina G, Uslenghi C. Multicentre, double-blind, comparison of fluvoxamine and clomipramine in the treatment of obsessive–compulsive disorder. Int Clin Psychopharmacol 2000;15:69–76 | Early report of a subset of the data that also reported in Mundo et al. 2001200 (14 out of the 40 centres) |
| 43 | Muroff J, Steketee G, Bratiotis C, Ross A. Group cognitive and behavioural therapy and bibliotherapy for hoarding: a pilot trial. Depress Anxiety 2012;29:597–604 | Hoarding disorder not OCD |
| 44 | Nazari H, Momeni N, Jariani M, Tarrahi MJ. Comparison of eye movement desensitization and reprocessing with citalopram in treatment of obsessive compulsive disorder. Int J Psychiatry Clin Pract 2011;15:270–4 | Main intervention not covered: eye movement desensitization and reprocessing |
| 45 | Olatunji BO, Rosenfield D, Tart CD, Cottraux J, Powers MB, Smits JA. Behavioural versus cognitive treatment of obsessive–compulsive disorder: an examination of outcome and mediators of change. J Consult Clin Psychol 2013;81:415–28 | Reports same data with Cottraux et al. 2001,166 but different method of analysis and treating missing data (multilevel instead of last observation carried forwards) |
| 46 | Omranifard V, Akuchakian S, Almasi A, Maraci MR. Effect of religious cognitive–behavour therapy on religious content obsessive compulsive disorder and marital satisfaction [conference abstract]. Eur Psychiatry 2011;26(Suppl. 1):1742 | Duplicate with the Akouchakian 2011 paper, which has been excluded |
| 47 | Pigott TA, L’Heureux F, Rubenstein CS, Bernstein SE, Hill JL, Murphy DL. A double-blind, placebo controlled study of trazodone in patients with obsessive–compulsive disorder. J Clin Psychopharmacol 1992;12:156–62 | Intervention not included (trazodone) |
| 48 | Pigott TA, Pato MT, Bernstein SE, Grover GN, Hill JL, Tolliver TJ, et al. Controlled comparisons of clomipramine and fluoxetine in the treatment of obsessive–compulsive disorder. Behavioural and biological results. Arch Gen Psychiatry 1990;47:926–32 | Data not extractable at the point of cross-over |
| 49 | Rapoport J, Elkins R, Mikkelsen E. Clinical controlled trial of chlorimipramine in adolescents with obsessive–compulsive disorder. Psychopharmacol Bull 1980;16:61–3 | Duplicate data - this is an early report of the Flament et al. 1985222 study (this is reported and cited in the later Flament study) |
| 50 | Richter P, Witheridge K, Daskalakis ZJ, Deluce J, Nebitt R, Rector N, et al. Investigation of predictors of drug response in obsessive compulsive disorder (OCD) [conference abstract]. Eur Neuropsychopharmacol 2010;20:529 | Congress abstract only: crossover of escitalopram versus clomipramine but no usable data given |
| 51 | Rouillon F. A double-blind comparison of fluvoxamine and clomipramine in OCD. 11th European College of Neuropyschopharmacology Congress. Paris, France, 31 October–4 November 1998 | Duplicate, early congress report of the Mundo et al. 2001200 study |
| 52 | Shareh H, Gharaie B, Vahid MKA. [Comparison between metacognitive therapy, fluvoxamine and combined therapy in the improvement of thought control strategies and stop signal criteria in obsessive compulsive disorder.] IJPCP 2011;17:199–207 | Duplicate publication of Shareh et al. 2010206 |
| 53 | Shareh H, Gharraee B, Vahid MKA. [Comparison of metacognitive therapy, fluvoxamine and combined treatment in improving metacognitive beliefs and subjective distress of patients with obsessive–compulsive disorder.] Adv Cog Sci 2011;12:45–59 | Secondary analysis of Sharreh et al. 2010206 |
| 54 | Shavitt R, Valerio C, Diniz JB, Fossaluza V, Belotto-Silva C, Jakubovski J, et al. Clinical predictors of treatment outcome in obsessive–compulsive disorder: a 2-year follow-up [conference abstract]. Eur Neuropsychopharmacol 2011;21(Suppl. 3):530 | Congress abstract: extension of the Belotto-Silva et al. 2012160 dataset |
| 55 | Sibon I, Leyton M, Gravel P, Sookman D, Pinard G, Diksic M, et al. CBT vs sertraline in OCD: effects on brain regional serotonin synthesis index. ACNP, Waikoloa, HI, 11–15 December 2005 | Congress abstract, data not given for analysis, unable to decide on inclusion criteria |
| 56 | Solyom L, Sookman D. A comparison of clomipramine hydrochloride (Anafranil) and behaviour therapy in the treatment of obsessive neurosis. J Int Med Res 1977;5(Suppl. 5):49–61 | Not randomised |
| 57 | Stein DJ, Hollander E, Mullen LS, DeCaria CM, Liebowitz MR. Comparison of clomipramine, alprazolam and placebo in the treatment of obsessive compulsive disorder. Hum Psychopharmacol 1992;7:389–95 | Continuous data not extractable for treatment comparisons |
| 58 | Stein DJ, Tonnior B, Andersen EW. Escitalopram in the treatment of OCD. Proceedings of the 159th Annual Meeting of the American Psychiatric Association, Toronto, ON, 20–25 May 2006 | Early congress abstract of the full Stein et al. 2007124 paper |
| 59 | Steketee G, Frost RO, Tolin DF, Rasmussen J, Brown TA. Waitlist-controlled trial of cognitive behaviour therapy for hoarding disorder. Depress Anxiety 2010;27:476–84 | Hoarding disorder not OCD |
| 60 | Tamimi Raed R, Mavissakalian Matig R, Jones B, Olson S. Clomipramine versus fluvoxamine in obsessive–compulsive disorder. Ann Clin Psychiatry 1991;3:275–9 | Unblinded (open-label) controlled trial |
| 61 | Turner SM, Jacob RG, Beidel DC, Himmelhoch J. Fluoxetine treatment of obsessive–compulsive disorder. J Clin Psychopharmacol 1985;5:207–12 | Uncontrolled study, only one fluoxetine arm |
| 62 | Vallejo J, Olivares J, Marcos T, Bulbena A, Menchón JM. Clomipramine versus phenelzine in obsessive–compulsive disorder. A controlled clinical trial. Br J Psychiatry 1992;161:665–70 | Comparator (phenelzine) not covered |
| 63 | van Balkom AJ, de Haan E, van Oppen P, Spinhoven P, Hoogduin KA, van Dyck R. Cognitive and behavioural therapies alone versus in combination with fluvoxamine in the treatment of obsessive compulsive disorder. J Nerv Ment Dis 1998;186:492–9 | The usable comparison (CBT vs. BT for 16 weeks) has been fully reported in Van Oppen et al. 1995209 study, therefore this reports is duplicate. Remaining arms cannot be used owing to the complexity of the design |
| 64 | Wheadon DE, Bushnell WD, Steiner MA. A fixed-dose comparison of 20, 40 or 60 mg paroxetine to placebo in the treatment of obsessive–compulsive disorder. The annual meeting of the American College of Neuropsychopharmacology, Honolulu, HI, 1993 | Early report of the Hollander et al. 2003180 data set |
| 65 | Wilhelm S, Steketee G, Fama JM, Buhlmann U, Teachman BA, Golan E. Modular cognitive therapy for obsessive–compulsive disorder: a wait-list controlled trial. J Cogn Psychother 2009;23:294–305 | Not random assignment (but ‘according to therapist availability’) |
| 66 | Williams TI, Salkovskis P, White H, Turner S, Forrester E, Allsopp M. Trialled cognitive behaviour therapy for children with OCD: a randomised controlled trial. 32nd Congress of the British Association for Behavioural and Cognitive Psychotherapies (jointly with the European Association of Behavioural and Cognitive Therapies), Manchester, 7–11 September 2004 | Duplicate: early congress abstract of the Williams et al. 2010236 full paper |
| 67 | Wootton BM, Dear BF, Johnston L, Terides MD, Titov N. Remote treatment of obsessive–compulsive disorder: a randomised controlled trial. J Obsess Compuls Relat Disord 2013;2:375–84 | Main aim of the paper to compare different form of same treatment |
| 68 | Yaryura-Tobias JA, Neziroglu FA. Venlafaxine in obsessive–compulsive disorder. Arch Gen Psychiatry 1996;53:653–4 | This is a letter from a small pilot study that, according to the authors, is double blind but the results have not been published. The authors report very general trends and the study is negative. It is not possible to extract any information |
Appendix 3 Publications in waiting status
| Study | Comment for waiting status |
|---|---|
| Bai X, Liu C, Li X. A comparative trial of paroxetine versus clomipramine in treatment of obsessive–compulsive neurosis. Pract Clin Med 2002;13:63–4 | In Chinese |
| Huang SN, Ji QM, Xie SP. A clinical comparative study of venlafaxine and paroxetine in the treatment of obsessive–compulsive disorder. Shandong Arch Psychiatry 2003;16:129–30 | In Chinese |
| Jianxun L, Hu X, Haiying D. Clinical controlled study of paroxetine and clomipramine in treatment of obsessive–compulsive disorder. Chin J Psychiatry 1998;31:215–17 | In Chinese |
| Jing Ping, ZA. Controlled study of clomipramine and amitriptyline for treating obsessive–compulsive disorder. Chin J Neurol Psychiatry 1990;23:68–70 | In Chinese |
| Lakatos A. Cognitive behaviour therapy of obsessive–compulsive neurosis. Praxis der Klinischen Verhaltensmedizin und Rehabilitation 1994;7:99–106 | Unable to locate (article in German): small study (n = 28) comparing BT with CBT – e-mailed author |
| Lei BS. A cross-over treatment of obsessive–compulsive neurosis with imipramine and chlorimipramine. Chin J Neurol Psychiatry 1986;19:275–8 | In Chinese |
| Li X, Li Z, Li Z, Huang K, Sun L. Comparative study of citalopram and clomipramine in treatment of obsessive–compulsive disorder. J Clin Psychological Med 2005;15:354–5 | In Chinese |
| Liu X, Liu J, Long J. Paroxetine combined with cognitive behaviour therapy in treatment of obsessive–compulsive disorder. Chin J Health Psychology 2005;13:86–7 | In Chinese |
| Liu Y, Yao C, Xu M. A comparative study of fluoxetine and sertraline in the treatment of obsessive–compulsive disorder. Shandong Arch Psychiatry 2004;17:204–6 | In Chinese |
| Marconi P, Pancheri P, Catapano F, Maj M. Fluvoxamine vs clomipramine in obsessive–compulsive disorder. 10th World Congress of Psychiatry, 23–28 August 1996, Madrid, Spain | Congress report, no further details, no usable data, no further publication |
| Montgomery SA, Montgomery DB, Fineberg N. Early response with clomipramine in obsessive compulsive disorder a placebo controlled study. Prog Neuro-Psychopharmacol Biol Psychiatry 1990;14:719–27 | Uncertain if duplicate data with the Montgomery SA. Clomipramine in obsessional neurosis: a placebo-controlled trial. Pharmacological Med 1980;1:189–92 study: e-mailed authors |
| Qing Y, Denghua T, Xiaoyang G. Comparative study of cognitive therapy on obsessional compulsive disorder. Chin Mental Health J 2004;18:421–2 | In Chinese |
| Rajagopalan R, Niveditha, Vijayakumar. A comparative study of efficacy and tolerability of fluvoxamine and sertraline in treatment of obsessive–compulsive disorder. Int J Pharm Pharm Sci 2013;5(Suppl. 2):629–32 | Another publication of the same study (the thesis of the first author) reports slightly different and inconsistent results, although it is the same study with the same patient population – e-mailed authors |
| Saboory S, Mehryar H, Ghareeb A. Comparing the effectiveness of cognitive–behavioural techniques, clomipramine and their combination in treatment of obsessive–compulsive disorder. Andeesheh Va Raftar 1998;4:25–34 | In Arabic |
| Shaomei L, Fenglia H. Combination of clomipramine with exposure therapy in treatment of obsessive–compulsive disorder. Chin Mental Health J 2001;15:239–40 | In Chinese |
| Song R, Zheng Z, Chen M. Contrast study of the effects of paroxetine and chlorimipramine on obsessive–compulsive disorder. J Linyi Med Coll 2005;27:327–8 | In Chinese |
| Todorov C, Brassard M, Fontaine R, Vezina M, Elie R. Fluoxetine vs clomipramine in obsessive–compulsive disorder. 10th World Congress of Psychiatry, 23–28 August 1996, Madrid, Spain | Congress: abstract – no further data |
| Ushijima S, Kamijima K, Asai M, Murasaki M, Nakajima T, Kudo Y, et al. Clinical evaluation of sertraline hydrochloride, a selective serotonin reuptake inhibitor in the treatment of obsessive–compulsive disorder. Jpn J Neuropsychopharmacol 1997;19:603–23 | In Japanese: unable to locate |
| Wang Y, Long J, Sun M. A comparative study of citalopram and clomipramine in the treatment of obsessive–compulsive disorder. J Clin Psychosomatic Dis 2005;11:17–18 | In Chinese |
| Wu H, Luo Y, Chen C. Control study of fluvoxamine and chlorimipramine in treatment of obsession. Nervous Dis Mental Health 2005;5:101–2 | In Chinese |
| Yargic LI, Enderer M, Imre H, Sen D, Yazici O. A randomised single blind comparison of clomipramine and fluvoxamine in OCD patients. Noropsikiyatri Arsivi 1995;32:70–5 | In Turkish: unable to locate |
| Yu L, Jin W. Clinical comparing study of sertraline and clomipramine in treatment of obsessive–compulsive disorder. Med J Chin People Health 2006;18:169–71 | In Chinese |
| Zhao JP. [A control study of clomipramine and amitriptyline for treating obsessive–compulsive disorder.] Chin J Neurol Psychiatry 1991;24:68–70 | In Chinese |
| Zhu J, Zhang F, Zhou D. A comparative study of mirtazapine and chlorimipramine in treatment of obsessive–compulsive disorder. Shandong Arch Psychiatry 2005;18:84–5 | In Chinese |
Appendix 4 Main data extraction: adult subset
| Study | Number of arms | Year | Intervention | Coding of intervention | Scale used | Original N randomised | BLn | BL_m | BL_sd | Dr_n | FU_n | FU_mean | FU_sd | CGEn | CGE_m | CGE_sd |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Albert et al., 2002155 | 2 | 2001 | VEN | 8 | YBOCS | 26 | 26 | 25 | 4.81 | 1 | 25 | 18.36 | 7.11 | |||
| Albert et al., 2002155 | 2 | 2001 | CLO | 9 | YBOCS | 47 | 47 | 25.7 | 5.07 | 7 | 40 | 17.3 | 6.15 | |||
| Ananth et al., 1981156 | 2 | 1981 | CLO | 9 | Severity Quest | 10 | 10 | 122 | NA | 1 | 9 | 43 | NA | |||
| Ananth et al., 1981156 | 2 | 1981 | AMI | 13 | Severity Quest | 10 | 10 | 113 | NA | 2 | 8 | 76 | NA | |||
| Anderson and Rees, 2007157 | 2 | 2007 | CBT | 11 | YBOCS | 21 | 17 | 24 | 6.2 | 4 | 17 | 16.7 | 6.8 | |||
| Anderson and Rees, 2007157 | 2 | 2007 | Waitlist | 2 | YBOCS | 17 | 14 | 24.1 | 5.1 | 3 | 14 | 23.5 | 6.4 | |||
| Andersson et al., 2012158 | 2 | 2012 | CBT | 11 | YBOCS | 50 | 50 | 21.42 | 4.59 | 2 | 49 | 12.94 | 6.26 | |||
| Andersson et al., 2012158 | 2 | 2012 | PsychPLA | 25 | YBOCS | 51 | 51 | 20.8 | 4.04 | 0 | 51 | 18.88 | 4.18 | |||
| Belloch et al., 2008159 | 2 | 2008 | BT | 10 | YBOCS | 15 | 13 | 24.69 | 5.72 | 2 | 13 | 8.31 | 8.75 | |||
| Belloch et al., 2008159 | 2 | 2008 | CT | 12 | YBOCS | 18 | 16 | 26.4 | 4.98 | 2 | 16 | 6.8 | 3.55 | |||
| Belotto-Silva et al., 2012160 | 2 | 2012 | FLX | 3 | YBOCS | 88 | 88 | 25.82 | 5.1 | 33 | 88 | 20.29 | 8.05 | |||
| Belotto-Silva et al., 2012160 | 2 | 2012 | CBT | 11 | YBOCS | 70 | 70 | 25.97 | 5.48 | 18 | 70 | 19.97 | 8.48 | |||
| Bergeron et al., 2002161 | 2 | 2002 | FLX | 3 | YBOCS | 73 | 72 | 26.1 | 5.1 | 22 | 72 | NA | NA | 72 | 9.7 | 7.7 |
| Bergeron et al., 2002161 | 2 | 2002 | SER | 6 | YBOCS | 77 | 76 | 25.3 | 5 | 22 | 76 | NA | NA | 76 | 9.6 | 7.9 |
| Bisserbe et al., 1997162 | 2 | 1997 | SER | 6 | YBOCS | 86 | 86 | 27.86 | NA | 23 | 86 | 13.56 | NA | |||
| Bisserbe et al., 1997162 | 2 | 1997 | CLO | 9 | YBOCS | 82 | 81 | 27.43 | NA | 35 | 81 | 15.72 | NA | |||
| CCSG1, 1991154 | 2 | 1991 | CLO | 9 | YBOCS | 118 | 118 | 26.3 | 5.5 | 17 | 102 | 16.23 | 0.73 | |||
| CCSG1, 1991154 | 2 | 1991 | PLA | 1 | YBOCS | 121 | 120 | 26 | 5.5 | 13 | 108 | 25.11 | 0.61 | |||
| CCSG1, 1991154 | 2 | 1991 | CLO | 9 | YBOCS | 142 | 134 | 26.2 | 4.9 | 14 | 120 | 14.7 | 0.68 | |||
| CCSG1, 1991154 | 2 | 1991 | PLA | 1 | YBOCS | 139 | 129 | 27.2 | 4.8 | 12 | 119 | 25.59 | 0.53 | |||
| Chouinard et al., 1990163 | 2 | 1990 | SER | 6 | YBOCS | 43 | 43 | 23.4 | 4.9 | 6 | 43 | 3.79 | 5.22 | |||
| Chouinard et al., 1990163 | 2 | 1990 | PLA | 1 | YBOCS | 44 | 44 | 22.6 | 6.1 | 4 | 44 | 1.48 | 5.22 | |||
| Cordioli et al., 2003164 | 2 | 2003 | CBT | 11 | YBOCS | 23 | 23 | 26.7 | 4.9 | 1 | 23 | 15.1 | 7.8 | |||
| Cordioli et al., 2003164 | 2 | 2003 | Waitlist | 2 | YBOCS | 24 | 24 | 24.7 | 5.2 | 1 | 24 | 23.2 | 5.5 | |||
| Cottraux et al., 1993165 | 3 | 1993 | FLV | 4 | NA | 20 | 13 | NA | 7 | 13 | NA | |||||
| Cottraux et al., 1993165 | 3 | 1993 | BT | 10 | NA | 20 | 15 | NA | 5 | 15 | NA | |||||
| Cottraux et al., 1993165 | 3 | 1993 | BT + FLV | 15 | NA | 20 | 16 | NA | 4 | 16 | NA | |||||
| Cottraux et al., 2001166 | 2 | 2001 | BT | 10 | YBOCS | 33 | 32 | 28.5 | 4.9 | 3 | 30 | 12.1 | 7.8 | |||
| Cottraux et al., 2001166 | 2 | 2001 | CT | 12 | YBOCS | 32 | 30 | 28.6 | 5.1 | 2 | 30 | 12.5 | 8.2 | |||
| Denys et al., 2003167 | 2 | 2003 | PAR | 5 | YBOCS | 75 | 72 | 25.3 | 5.6 | 9 | 72 | 17.5 | 8 | 72 | 7.8 | 5.4 |
| Denys et al., 2003167 | 2 | 2003 | VEN | 8 | YBOCS | 75 | 73 | 26.9 | 5 | 4 | 73 | 19.7 | 8.6 | 73 | 7.2 | 7.5 |
| Emmelkamp and Beens, 1991168 | 2 | 1991 | CT | 12 | Maudsley OCI | 15 | 10 | 17.2 | 6.2 | 5 | 10 | 12.3 | 7.3 | |||
| Emmelkamp and Beens, 1991168 | 2 | 1991 | BT | 10 | Maudsley OCI | 15 | 11 | 16.3 | 5.7 | 4 | 11 | 13.7 | 5.8 | |||
| Emmelkamp et al., 1988169 | 2 | 1988 | CT | 12 | Maudsley OCI | 10 | 9 | 15.6 | 2.9 | 1 | 9 | 11.3 | 1.7 | |||
| Emmelkamp et al., 1988169 | 2 | 1988 | BT | 10 | Maudsley OCI | 10 | 9 | 15.6 | 4 | 1 | 9 | 12.6 | 5.4 | |||
| Fals-Stewart et al., 1993170 | 2 | 1993 | BT | 10 | YBOCS | 34 | 31 | 20.2 | NA | 3 | 31 | 12.1 | NA | |||
| Fals-Stewart et al., 1993170 | 2 | 1993 | PsychPLA | 25 | YBOCS | 32 | 32 | 19.9 | NA | 0 | 32 | 18.1 | NA | |||
| Foa et al., 2005171 | 4 | 2005 | BT | 10 | YBOCS | 37 | 29 | 24.6 | 4.8 | 16 | 29 | 11 | 7.9 | |||
| Foa et al., 2005171 | 4 | 2005 | CLO | 9 | YBOCS | 47 | 36 | 26.3 | 4.4 | 20 | 36 | 18.2 | 7.8 | |||
| Foa et al., 2005171 | 4 | 2005 | BT + CLO | 18 | YBOCS | 33 | 31 | 25.4 | 4.6 | 14 | 31 | 10.5 | 8.2 | |||
| Foa et al., 2005171 | 4 | 2005 | PLA | 1 | YBOCS | 32 | 26 | 25 | 4 | 12 | 26 | 22.2 | 6.4 | |||
| Freeman et al., 1994172 | 2 | 1994 | FLV | 4 | YBOCS | 34 | 34 | 26.2 | NA | 6 | 8.6 | NA | ||||
| Freeman et al., 1994172 | 2 | 1994 | CLO | 9 | YBOCS | 32 | 30 | 25.5 | NA | 13 | 7.8 | NA | ||||
| Freeston et al., 1997173 | 2 | 1997 | CBT | 11 | YBOCS | 15 | 15 | 25.1 | 5 | 3 | 15 | 12.2 | 9.6 | |||
| Freeston et al., 1997173 | 2 | 1997 | Waitlist | 2 | YBOCS | 14 | 14 | 21.2 | 6 | 0 | 14 | 22 | 6 | |||
| GlaxoSmithKline, 2005174 | 3 | 1993 | PLA | 1 | YBOCS | 77 | 75 | 24.66 | NA | 20 | 75 | 4.61 | 0.87 | |||
| GlaxoSmithKline, 2005174 | 3 | 1993 | PAR | 5 | YBOCS | 82 | 79 | 23.28 | NA | 28 | 79 | 5.61 | 0.84 | |||
| GlaxoSmithKline, 2005174 | 3 | 1993 | CLO | 9 | YBOCS | 82 | 78 | 23.9 | NA | 28 | 78 | 7.73 | 0.84 | |||
| GlaxoSmithKline, 2005175 | 2 | 1999 | PAR | 5 | YBOCS | 73 | 72 | 25.11 | 6.07 | 1 | 72 | 10.85 | 6.85 | 72 | 14.26 | 6.33 |
| GlaxoSmithKline, 2005175 | 2 | 1999 | CLO | 9 | YBOCS | 73 | 69 | 24.07 | 5.74 | 4 | 69 | 10.88 | 6.86 | 69 | 13.19 | 6.48 |
| Goodman et al., 1989176 | 2 | 1989 | PLA | 1 | YBOCS | 23 | 21 | 25.6 | 6.6 | 6 | 21 | 28 | 7 | |||
| Goodman et al., 1989176 | 2 | 1989 | FLV | 4 | YBOCS | 23 | 21 | 25 | 6 | 2 | 21 | 19.4 | 7 | |||
| Goodman et al., 1996177 | 2 | 1996 | PLA | 1 | YBOCS | 80 | 78 | 24 | NA | 17 | 78 | 1.71 | 4.88 | |||
| Goodman et al., 1996177 | 2 | 1996 | FLV | 4 | YBOCS | 80 | 78 | 22.6 | NA | 23 | 78 | 3.95 | 6.28 | |||
| Greist et al., 1995126 | 2 | 1995 | SER | 6 | YBOCS | 241 | 240 | 23.8 | 5.3 | 65 | 240 | 5.57 | 6.19 | |||
| Greist et al., 1995126 | 2 | 1995 | PLA | 1 | YBOCS | 84 | 84 | 23.4 | 4.9 | 24 | 84 | 3.41 | 6.19 | |||
| Greist et al., 2002178 | 2 | 2002 | BT | 10 | YBOCS | 69 | 55 | 25.2 | 4.6 | 14 | 55 | 17.6 | 6.2 | |||
| Greist et al., 2002178 | 2 | 2002 | PsychPLA | 25 | YBOCS | 75 | 66 | 25.8 | 5.1 | 9 | 66 | 24.1 | 6.7 | |||
| Hohagen et al., 1998179 | 2 | 1998 | BT + PLA | 21 | YBOCS | 30 | 25 | 28.4 | 3.8 | NA | 25 | 15.9 | 7.9 | |||
| Hohagen et al., 1998179 | 2 | 1998 | BT + FLV | 15 | YBOCS | 30 | 24 | 27.9 | 2.9 | NA | 24 | 12.4 | 6.8 | |||
| Hollander et al., 2003181 | 2 | 2003 | PLA | 1 | YBOCS | 126 | 120 | 26.4 | 0.3 | 31 | 120 | 21 | 1 | 120 | 5.60 | 0.70 |
| Hollander et al., 2003181 | 2 | 2003 | FLV | 4 | YBOCS | 127 | 117 | 26.8 | 0.3 | 43 | 117 | 17.6 | 1.1 | 117 | 8.5 | 0.70 |
| Hollander et al., 2003181 | 4 | 2003 | PLA | 1 | YBOCS | 89 | 89 | 25.6 | NA | 15 | 89 | 3.33 | NA | |||
| Hollander et al., 2003180 | 4 | 2003 | PAR-20 | 5 | YBOCS | 88 | 88 | 25.9 | NA | 14 | 88 | 4.14 | NA | |||
| Hollander et al., 2003180 | 4 | 2003 | PAR-40 | 5 | YBOCS | 86 | 86 | 25.4 | NA | 20 | 86 | 6.35 | NA | |||
| Hollander et al., 2003180 | 4 | 2003 | PAR-60 | 5 | YBOCS | 85 | 85 | 25.3 | NA | 19 | 85 | 7.34 | NA | |||
| Jaurrieta et al., 2008182 | 2 | 2008 | CBT | 11 | YBOCS | 19 | 19 | 25.2 | 7.7 | NA | 19 | 17.8 | 8.4 | |||
| Jaurrieta et al., 2008182 | 2 | 2008 | Waitlist | 2 | YBOCS | 19 | 19 | 24.8 | 7.3 | NA | 19 | 24.6 | 8.9 | |||
| Jenike et al., 1990183 | 2 | 1990 | SER | 6 | YBOCS | 10 | 10 | 22.8 | 6 | 0 | 10 | 20.6 | 9.2 | |||
| Jenike et al., 1990183 | 2 | 1990 | PLA | 1 | YBOCS | 9 | 9 | 22.8 | 4.8 | 0 | 9 | 22.3 | 7.8 | |||
| Jenike et al., 1990184 | 2 | 1990 | PLA | 1 | YBOCS | 20 | 20 | 22.7 | 6.1 | 0 | 20 | 21.8 | 7.6 | |||
| Jenike et al., 1990184 | 2 | 1990 | FLV | 4 | YBOCS | 20 | 18 | 22.6 | 3.5 | 2 | 18 | 18.8 | 4 | |||
| Jenike et al., 1997185 | 2 | 1997 | PLA | 1 | YBOCS | 21 | 19 | 18.9 | 6.2 | 3 | 18 | 18.7 | 6.1 | |||
| Jenike et al., 1997185 | 2 | 1997 | FLX | 3 | YBOCS | 23 | 22 | 19 | 5.4 | 4 | 19 | 16.2 | 6.3 | |||
| Jones and Menzies, 1998186 | 2 | 1998 | CT | 12 | Maudsley OCI | 12 | 11 | 17.82 | NA | 1 | 11 | 14.27 | NA | |||
| Jones and Menzies, 1998186 | 2 | 1998 | Waitlist | 2 | Maudsley OCI | 11 | 10 | 17.6 | NA | 1 | 10 | 17.7 | NA | |||
| Kamijima et al., 2004187 | 2 | 2004 | PLA | 1 | YBOCS | 96 | 94 | 23.4 | 4.72 | NA | 94 | 20.3 | 7.38 | |||
| Kamijima et al., 2004187 | 2 | 2004 | PAR | 5 | YBOCS | 95 | 94 | 24.3 | 4.4 | NA | 94 | 15.8 | 8.09 | |||
| Khodarahimi, 2009188 | 2 | 2009 | Waitlist | 2 | YBOCS | 20 | 20 | 36.4 | 2.26 | 0 | 20 | 36.45 | 2.24 | |||
| Khodarahimi, 2009188 | 2 | 2009 | BT | 10 | YBOCS | 20 | 20 | 37.2 | 1.91 | 0 | 20 | 5.58 | 2.39 | |||
| Kobak et al., 2005189 | 2 | 2005 | PLA | 1 | YBOCS | 30 | 30 | 23.47 | 5.54 | 9 | 30 | 19.87 | 7.46 | |||
| Kobak et al., 2005189 | 2 | 2005 | HYP | 13 | YBOCS | 30 | 30 | 23.17 | 3.81 | 8 | 30 | 19.75 | 7.46 | |||
| Koran et al., 1996190 | 2 | 1996 | FLV | 4 | YBOCS | 37 | 34 | 25.5 | 5.97 | 8 | 34 | 17.8 | 7.7 | |||
| Koran et al., 1996190 | 2 | 1996 | CLO | 9 | YBOCS | 42 | 39 | 24.3 | 5.95 | 15 | 39 | 17 | 8.55 | |||
| Kronig et al., 1999191 | 2 | 1999 | SER | 6 | YBOCS | 86 | 86 | 25.21 | 3.79 | 25 | 85 | 8.5 | 10.50 | |||
| Kronig et al., 1999191 | 2 | 1999 | PLA | 1 | YBOCS | 81 | 81 | 25.05 | 4.09 | 25 | 79 | 4.14 | 10.50 | |||
| Lindsay et al., 1997192 | 2 | 1997 | BT | 10 | YBOCS | 9 | 9 | 28.7 | 4.56 | 0 | 9 | 11 | 3.81 | |||
| Lindsay et al., 1997192 | 2 | 1997 | PsychPLA | 25 | YBOCS | 9 | 9 | 24.44 | 6.98 | 0 | 9 | 25.89 | 5.8 | |||
| López-Ibor et al., 1996193 | 2 | 1996 | FLX | 3 | YBOCS | 30 | 30 | 27.6 | 5.2 | 5 | 30 | 30 | 7.5 | 9.29 | ||
| López-Ibor et al., 1996193 | 2 | 1996 | CLO | 9 | YBOCS | 25 | 24 | 25.6 | 6.09 | 3 | 24 | 24 | 8.9 | 7.13 | ||
| Mavissakalian et al., 1985194 | 2 | 1985 | CLO | 9 | OCNS | NA | 7 | 74.5 | 4.74 | NA | 7 | 48 | 6.94 | |||
| Mavissakalian et al., 1985194 | 2 | 1985 | PLA | 1 | OCNS | NA | 5 | 80 | 6.55 | NA | 5 | 69 | 8.51 | |||
| McLean et al., 2001195 | 2 | 2001 | CT | 12 | YBOCS | 49 | 33 | 21.9 | 5.8 | 18 | 31 | 16.1 | 6.7 | |||
| McLean et al., 2001195 | 2 | 2001 | BT | 10 | YBOCS | 44 | 40 | 21.8 | 4.6 | 12 | 32 | 13.2 | 7.2 | |||
| Milanfranchi et al., 1997196 | 2 | 1997 | CLO | 9 | YBOCS | 13 | 13 | 27.5 | 6.8 | 1 | 12 | 16.5 | 11 | |||
| Milanfranchi et al., 1997196 | 2 | 1997 | FLV | 4 | YBOCS | 13 | 13 | 29.7 | 5.5 | 0 | 13 | 18.4 | 9.2 | |||
| Montgomery et al., 1993197 | 4 | 1993 | PLA | 1 | YBOCS | 57 | 56 | 23.25 | 6.86 | 15 | 56 | 20.04 | NA | 56 | 3.7 | 5.98 |
| Montgomery et al., 1993197 | 4 | 1993 | FLX-20 | 3 | YBOCS | 53 | 52 | 23.79 | 4.91 | 14 | 53 | 18.66 | NA | 52 | 5.13 | 6.41 |
| Montgomery et al., 1993197 | 4 | 1993 | FLX-40 | 3 | YBOCS | 52 | 52 | 25.52 | 5.59 | 13 | 52 | 19.06 | NA | 52 | 4.76 | 6.89 |
| Montgomery et al., 1993197 | 4 | 1993 | FLX-60 | 3 | YBOCS | 55 | 54 | 22.98 | 7.18 | 14 | 54 | 17.71 | NA | 54 | 6.07 | 6.92 |
| Montgomery et al., 2001198 | 4 | 2001 | CIT-20 | 7 | YBOCS | 102 | 102 | 25.1 | 3.9 | 16 | 102 | 8.4 | 7.3 | |||
| Montgomery et al., 2001198 | 4 | 2001 | CIT-40 | 7 | YBOCS | 98 | 98 | 26 | 3.7 | 15 | 98 | 8.9 | 7.00 | |||
| Montgomery et al., 2001198 | 4 | 2001 | CIT-60 | 7 | YBOCS | 100 | 100 | 25.9 | 4.5 | 15 | 100 | 10.4 | 6.90 | |||
| Montgomery et al., 2001198 | 4 | 2001 | PLA | 1 | YBOCS | 101 | 101 | 25.4 | 3.9 | 17 | 101 | 5.6 | 6.90 | |||
| Mundo et al., 1997199 | 3 | 1997 | FLV | 4 | YBOCS | 10 | 10 | 25.4 | 6.5 | 0 | 10 | 16.2 | 8.9 | |||
| Mundo et al., 1997199 | 3 | 1997 | PAR | 5 | YBOCS | 9 | 9 | 30.5 | 3.9 | 0 | 9 | 21.6 | 7.6 | |||
| Mundo et al., 1997199 | 3 | 1997 | CIT | 7 | YBOCS | 11 | 11 | 29.3 | 3.9 | 0 | 11 | 19.8 | 10.1 | |||
| Mundo et al., 2001200 | 2 | 2001 | CLO | 9 | YBOCS | 112 | 112 | 25.4 | 6.1 | 26 | 112 | 13.4 | NA | |||
| Mundo et al., 2001200 | 2 | 2001 | FLV | 4 | YBOCS | 115 | 115 | 26.5 | 5.6 | 19 | 115 | 14.3 | NA | |||
| Nakajima et al., 1996201 | 2 | 1996 | FLV | 4 | YBOCS | 61 | 61 | 24.7 | 4.8 | NA | 61 | NA | NA | 61 | 7.1 | 7.03 |
| Nakajima et al., 1996201 | 2 | 1996 | PLA | 1 | YBOCS | 33 | 33 | 26.2 | 6.1 | NA | 33 | NA | NA | 33 | 1.9 | 7.20 |
| Nakatani et al., 2005202 | 3 | 2005 | PsychPLA | 25 | YBOCS | 9 | 8 | 30.5 | 3.7 | 1 | 8 | 28.4 | 5.5 | |||
| Nakatani et al., 2005202 | 3 | 2005 | FLV | 4 | YBOCS | 11 | 10 | 28.4 | 3.8 | 1 | 10 | 20.2 | 9.4 | |||
| Nakatani et al., 2005202 | 3 | 2005 | BT | 10 | YBOCS | 11 | 10 | 29.9 | 3.1 | 1 | 10 | 12.9 | 4.9 | |||
| O’Connor et al., 1999203 | 4 | 1999 | SRI | 14 | YBOCS | 6 | 5 | 21 | 2.9 | 1 | 5 | 12 | 4.5 | |||
| O’Connor et al., 1999203 | 4 | 1999 | Waitlist | 2 | YBOCS | 6 | 6 | 19.3 | 4.5 | 0 | 6 | 17.5 | 4 | |||
| O’Connor et al., 1999203 | 4 | 1999 | CBT | 11 | YBOCS | 7 | 6 | 23.5 | 4 | 1 | 6 | 13.3 | 8.6 | |||
| O’Connor et al., 1999203 | 4 | 1999 | CBT + SRI | 20 | YBOCS | 10 | 9 | 23.8 | 5.4 | 1 | 9 | 17.8 | 4.7 | |||
| O’Connor et al., 2006204 | 2 | 2006 | PLA | 1 | YBOCS | 10 | 10 | 27.3 | 4.3 | NA | 10 | 25.4 | 3.5 | |||
| O’Connor et al., 2006204 | 2 | 2006 | FLV | 4 | YBOCS | 11 | 11 | 28.3 | 3.9 | NA | 11 | 24 | 4.7 | |||
| Perse et al., 1987205 | 2 | 1987 | PLA | 1 | Maudsley OCI | 10 | 8 | NA | NA | 2 | NA | NA | ||||
| Perse et al., 1987205 | 2 | 1987 | FLV | 4 | Maudsley OCI | 10 | 8 | NA | NA | 2 | NA | NA | ||||
| Shareh et al., 2010206 | 3 | 2010 | FLV | 4 | YBOCS | 7 | 6 | 25.83 | 5.77 | 1 | 6 | 16.66 | 3.2 | |||
| Shareh et al., 2010206 | 3 | 2010 | CBT | 11 | YBOCS | 7 | 7 | 29 | 6.73 | 0 | 7 | 7 | 2.38 | |||
| Shareh et al., 2010206 | 3 | 2010 | FLV + CBT | 16 | YBOCS | 7 | 6 | 26.16 | 7.98 | 1 | 6 | 8.5 | 2.42 | |||
| Sousa et al., 2006207 | 2 | 2006 | SER | 6 | YBOCS | 28 | 25 | 26.12 | NA | 3 | 25 | 18.76 | NA | |||
| Sousa et al., 2006207 | 2 | 2006 | CBT | 11 | YBOCS | 28 | 25 | 25.08 | NA | 3 | 25 | 14.28 | NA | |||
| Stein et al., 2007124 | 4 | 2007 | PLA | 1 | YBOCS | 115 | 113 | 27.7 | 4.2 | 18 | 113 | 8.46 | 0.76 | |||
| Stein et al., 2007124 | 4 | 2007 | PAR | 5 | YBOCS | 119 | 116 | 27.3 | 4 | 29 | 116 | 11.67 | 0.78 | |||
| Stein et al., 2007124 | 4 | 2007 | ESCIT-10 | 19 | YBOCS | 116 | 112 | 26.6 | 3.7 | 24 | 112 | 11.43 | 0.78 | |||
| Stein et al., 2007124 | 4 | 2007 | ESCIT-20 | 19 | YBOCS | 116 | 114 | 26.6 | 3.9 | 21 | 114 | 12.14 | 0.77 | |||
| Thoren et al., 1980208 | 2 | 1980 | CLO | 9 | OCD symptom scale | NA | 8 | 4.38 | 1.22 | NA | 8 | 2.94 | 1.15 | |||
| Thoren et al., 1980208 | 2 | 1980 | PLA | 1 | OCD symptom scale | NA | 8 | 3.94 | 1.24 | NA | 8 | 3.69 | 1.46 | |||
| Tollefson et al., 1994127 | 4 | 1994 | PLA | 1 | YBOCS | 89 | 89 | 24.3 | 5.7 | 13 | 76 | 23.6 | 7.5 | 89 | 0.8 | 5.66 |
| Tollefson et al., 1994127 | 4 | 1994 | FLX-20 | 3 | YBOCS | 87 | 87 | 23.6 | 5.7 | 12 | 75 | 18.9 | 8.3 | |||
| Tollefson et al., 1994127 | 4 | 1994 | FLX-40 | 3 | YBOCS | 89 | 89 | 23.5 | 5.6 | 22 | 67 | 18.1 | 7.9 | |||
| Tollefson et al., 1994127 | 4 | 1994 | FLX-60 | 3 | YBOCS | 90 | 90 | 24.4 | 5.1 | 22 | 68 | 16.8 | 7.8 | |||
| Van Oppen et al., 1995209 | 2 | 1995 | CT | 12 | YBOCS | 35 | 28 | 28.7 | 5.3 | 7 | 28 | 13.4 | 9.4 | |||
| Van Oppen et al., 1995209 | 2 | 1995 | BT | 10 | YBOCS | 36 | 29 | 31.4 | 5 | 7 | 29 | 17.9 | 9 | |||
| Volavka et al., 1985210 | 2 | 1985 | CLO | 9 | SRONS | 11 | 8 | 61.5 | 13.6 | 3 | 8 | 41.9 | 13.9 | |||
| Volavka et al., 1985210 | 2 | 1985 | IMI | 13 | SRONS | 12 | 8 | 80.7 | 11.5 | 4 | 8 | 63.6 | 20.5 | |||
| Whittal et al., 2005211 | 2 | 2005 | CT | 12 | YBOCS | 41 | 34 | 23.5 | 4.3 | 11 | 30 | 10.6 | 7.1 | |||
| Whittal et al., 2005211 | 2 | 2005 | BT | 10 | YBOCS | 42 | 37 | 21.66 | 5.9 | 13 | 29 | 10.41 | 7.6 | |||
| Whittal et al., 2010212 | 2 | 2010 | CT | 12 | YBOCS | 40 | 40 | 18.03 | 6.29 | 3 | 37 | 6.43 | 4.77 | |||
| Whittal et al., 2010212 | 2 | 2010 | PsychPLA | 25 | YBOCS | 33 | 33 | 17.73 | 7.73 | 3 | 30 | 9.1 | 6.48 | |||
| Zohar and Judge, 1996213 | 3 | 1996 | PLA | 1 | YBOCS | 100 | 99 | NA | NA | 40 | 99 | 4.2 | 7.2 | |||
| Zohar and Judge, 1996213 | 3 | 1996 | PAR | 5 | YBOCS | 205 | 201 | NA | NA | 53 | 201 | 6.4 | 7.1 | |||
| Zohar and Judge, 1996213 | 3 | 1996 | CLO | 9 | YBOCS | 101 | 99 | NA | NA | 36 | 99 | 7 | 6.8 |
Appendix 5 Main data extraction: children and adolescents subset
| Study | Number of arms | Year | Intervention | Coding of intervention | Scale used | Original N randomised | BLn | BL_m | BL_sd | Dr_n | FU_n | FU_mean | FU_sd | CGEn | CGE_m | CGE_sd |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Alaghband-Rad and Hakimshooshtary, 2009215 | 2 | 2009 | FLX | 3 | CYBOCS | 15 | 15 | 26.66 | NA | NA | NA | 15 | NA | |||
| Alaghband-Rad and Hakimshooshtary, 2009215 | 2 | 2009 | CIT | 7 | CYBOCS | 14 | 14 | 28 | NA | NA | NA | 16.9 | NA | |||
| Asbahr et al., 2005216 | 2 | 2005 | SER | 6 | CYBOCS | 20 | 19 | 27 | 6.65 | 1 | 19 | NA | NA | |||
| Asbahr et al., 2005216 | 2 | 2005 | CBT | 11 | CYBOCS | 20 | 20 | 26.3 | 4.9 | 0 | 20 | NA | NA | |||
| Barrett et al., 2004217 | 2 | 2004 | CBT | 11 | CYBOCS | 24 | 22 | 23.64 | 4.3 | NA | 22 | 8.36 | 6.93 | |||
| Barrett et al., 2004217 | 2 | 2004 | Waitlist | 2 | CYBOCS | 24 | 24 | 22.95 | 5.49 | NA | 24 | 24.04 | 4.14 | |||
| Bolton and Perrin, 2008218 | 2 | 2008 | BT | 10 | CYBOCS | 10 | 10 | 24 | 4.78 | 2 | 10 | 13.9 | 10.74 | |||
| Bolton and Perrin, 2008218 | 2 | 2008 | Waitlist | 2 | CYBOCS | 10 | 10 | 22 | 8.25 | 0 | 10 | 21.1 | 5.9 | |||
| Bolton et al., 2011219 | 2 | 2011 | Waitlist | 2 | CYBOCS | 24 | 24 | 24,2 | 5 | 3 | 24 | 23.3 | 8.3 | |||
| Bolton et al., 2011219 | 2 | 2011 | CBT | 11 | CYBOCS | 36 | 36 | 22.3 | 5 | 2 | 36 | 9.5 | 8 | |||
| de Haan et al., 1998220 | 2 | 1998 | CLO | 9 | CYBOCS | 10 | 10 | 23.8 | 7.2 | 0 | 10 | 17.6 | 11.8 | |||
| de Haan et al., 1998220 | 2 | 1998 | BT | 10 | CYBOCS | 13 | 12 | 21.5 | 5.9 | 1 | 12 | 9.1 | 9.1 | |||
| DeVeaugh-Geiss et al., 1992221 | 2 | 1992 | CLO | 9 | CYBOCS | 31 | 31 | 27.1 | NA | 4 | 31 | 17.1 | NA | |||
| DeVeaugh-Geiss et al., 1992221 | 2 | 1992 | PLA | 1 | CYBOCS | 29 | 29 | 28.4 | NA | 2 | 29 | 26 | NA | |||
| Flament et al., 1985222 | 2 | 1985 | CLO | 9 | OCR scale | NA | NA | NA | NA | NA | NA | 9.1 | 3.6 | |||
| Flament et al., 1985222 | 2 | 1985 | PLA | 1 | OCR scale | NA | NA | NA | NA | NA | NA | 12.1 | 4 | |||
| Freeman et al., 2008223 | 2 | 2008 | CBT | 11 | CYBOCS | 22 | 22 | 22.95 | 3.84 | 6 | 22 | 14.45 | 8.16 | |||
| Freeman et al., 2008223 | 2 | 2008 | PsychPLA | 25 | CYBOCS | 20 | 20 | 21.7 | 4.52 | 5 | 20 | 17.1 | 7.57 | |||
| Geller et al., 2001224 | 2 | 2001 | PLA | 1 | CYBOCS | 32 | 32 | 26.3 | 4.6 | 12 | 32 | 5.2 | 7.4 | |||
| Geller et al., 2001224 | 2 | 2001 | FLX | 3 | CYBOCS | 71 | 71 | 24.5 | 5.1 | 22 | 71 | 9.5 | 9.2 | |||
| GlaxoSmithKline, 2001225 | 2 | 2001 | PAR | 5 | CYBOCS | 100 | 98 | 24.4 | 4.95 | 35 | 98 | |||||
| GlaxoSmithKline, 2001225 | 2 | 2001 | PLA | 1 | CYBOCS | 107 | 105 | 25.3 | 5.05 | 27 | 105 | |||||
| Liebowitz et al., 2002226 | 2 | 2002 | PLA | 1 | CYBOCS | 22 | 22 | 23.82 | 5.77 | 4 | 22 | 18.55 | 11.44 | |||
| Liebowitz et al., 2002226 | 2 | 2002 | FLX | 3 | CYBOCS | 21 | 21 | 22.5 | 4.16 | 1 | 21 | 14.71 | 8.73 | |||
| March et al., 1990227 | 2 | 1990 | CLO | 9 | YBOCS | 8 | 8 | 24.5 | 3.6 | 2 | 8 | 19.3 | 8.6 | |||
| March et al., 1990227 | 2 | 1990 | PLA | 1 | YBOCS | 8 | 8 | 27.4 | 3.4 | 0 | 8 | 25.6 | 2.4 | |||
| March et al., 1998228 | 2 | 1998 | SER | 6 | CYBOCS | 92 | 92 | 23.4 | NA | 18 | 92 | 6.8 | 0.87 | |||
| March et al., 1998228 | 2 | 1998 | PLA | 1 | CYBOCS | 95 | 95 | 22.2 | NA | 13 | 95 | 3.4 | 0.82 | |||
| Neziroglu et al., 2000229 | 2 | 2000 | FLV | 4 | CYBOCS | 5 | 5 | 22.8 | 4.21 | 0 | 5 | 19.2 | 3.56 | |||
| Neziroglu et al., 2000229 | 2 | 2000 | BT + FLV | 15 | CYBOCS | 5 | 5 | 28 | 6.2 | 0 | 5 | 16.4 | 5.18 | |||
| Piacentini et al., 2011230 | 2 | 2011 | CBT | 11 | CYBOCS | 49 | 49 | 24.7 | 0.71 | 8 | 49 | 13.3 | 1.33 | |||
| Piacentini et al., 2011230 | 2 | 2011 | PsychPLA | 25 | CYBOCS | 22 | 22 | 25.3 | 0.97 | 5 | 22 | 17.2 | 2.14 | |||
| Riddle et al., 1992231 | 2 | 1992 | PLA | 1 | CYBOCS | 6 | 6 | 20.2 | 7.7 | 1 | 6 | 14.8 | 7 | |||
| Riddle et al., 1992231 | 2 | 1992 | FLX | 3 | CYBOCS | 7 | 7 | 24.3 | 4.2 | 1 | 7 | 13.6 | 5.7 | |||
| Riddle et al., 2001232 | 2 | 2001 | PLA | 1 | CYBOCS | 63 | 63 | 24.2 | 4.8 | 27 | 63 | 20.9 | 8.5 | |||
| Riddle et al., 2001232 | 2 | 2001 | FLV | 4 | CYBOCS | 57 | 57 | 24.2 | 4.4 | 19 | 57 | 18.2 | 8.6 | |||
| Storch et al., 2011233 | 2 | 2011 | CBT | 11 | CYBOCS | 16 | 16 | 25.38 | 3.81 | 2 | 16 | 11.13 | 10.53 | |||
| Storch et al., 2011233 | 2 | 2011 | Waitlist | 2 | CYBOCS | 15 | 15 | 21.27 | 2.74 | 0 | 15 | 18.53 | 8.11 | |||
| Storch et al., 2013234 | 2 | 2013 | SER + CBT | 17 | CYBOCS | 14 | 14 | 23.64 | 4.48 | 6 | 14 | 15.43 | 9.72 | |||
| Storch et al., 2013234 | 2 | 2013 | CBT + PLA | 22 | CYBOCS | 16 | 16 | 25.06 | 4.01 | 3 | 16 | 15.56 | 6.62 | |||
| The Pediatric OCD Treatment Study, 2004236 | 4 | 2004 | SER | 6 | CYBOCS | 28 | 28 | 23.5 | 4.7 | 2 | 28 | 16.5 | 9.1 | |||
| The Pediatric OCD Treatment Study, 2004236 | 4 | 2004 | CBT | 11 | CYBOCS | 28 | 28 | 26 | 4.6 | 3 | 28 | 14 | 9.5 | |||
| The Pediatric OCD Treatment Study, 2004236 | 4 | 2004 | SER + CBT | 17 | CYBOCS | 28 | 28 | 23.8 | 3 | 3 | 28 | 11.2 | 8.6 | |||
| The Pediatric OCD Treatment Study, 2004236 | 4 | 2004 | PLA | 1 | CYBOCS | 28 | 28 | 25.2 | 3.3 | 7 | 28 | 21.5 | 5.4 | |||
| Williams et al., 2010235 | 2 | 2010 | CBT | 11 | CYBOCS | 11 | 11 | 23.09 | 1.22 | 1 | 11 | 12.09 | 2.25 | |||
| Williams et al., 2010235 | 2 | 2010 | Waitlist | 2 | CYBOCS | 10 | 10 | 21.05 | 1.84 | 1 | 10 | 19.6 | 2.03 |
Appendix 6 Additional extraction: intervention details
| Study | Settinga | Intervention | Average or mean dose at the end (mg) | SD of mean dose (mg) | Minimum dose during the study (mg) | Maximum dose during the study (mg) | Number of sessions | Duration of session (hours) |
|---|---|---|---|---|---|---|---|---|
| Albert et al., 2002155 | 1 | VEN | 265 | 52.5 | 225 | 350 | ||
| Albert et al., 2002155 | 1 | CLO | 168 | 28.9 | 150 | 225 | ||
| Ananth et al. 1981156 | 3 | CLO | 133.3 | NA | 75 | 300 | ||
| Ananth et al. 1981156 | 3 | AMI | 197.4 | NA | 75 | 300 | ||
| Anderson and Rees, 2007157 | 1 | CBT | 10 | 1 | ||||
| Anderson and Rees, 2007157 | 1 | Waitlist | Waitlist | Waitlist | ||||
| Anderson and Rees, 2007157 | 1 | CBT | 10 | NA | ||||
| Anderson and Rees, 2007157 | 1 | PsychPLA | PsychPLA | PsychPLA | ||||
| Belloch et al., 2008159 | 1 | BT | 20 | 1 | ||||
| Belloch et al., 2008159 | 1 | CT | 18 | 1 | ||||
| Belotto-Silva et al., 2012160 | 1 | FLX | 80 | Fixed | ||||
| Belotto-Silva et al., 2012160 | 1 | CBT | 12 | 2 | ||||
| Bergeron et al., 2002161 | 1 | FLX | 56.7 | 23 | 20 | 80 | ||
| Bergeron et al., 2002161 | 1 | SER | 139.5 | 58.5 | 50 | 200 | ||
| Bisserbe et al., 1997162 | 1 | SER | 136 | NA | 50 | 200 | ||
| Bisserbe et al., 1997162 | 1 | CLO | 110 | NA | 50 | 200 | ||
| CCSG1, 1991154 | 1 | CLO | 234.5 | NA | 100 | 300 | ||
| CCSG1, 1991154 | 1 | PLA | PLA | |||||
| CCSG2, 1991154 | 1 | CLO | 218.8 | NA | 100 | 300 | ||
| CCSG2, 1991154 | 1 | PLA | PLA | |||||
| Chouinard et al., 1990163 | 1 | SER | 185 | NA | 50 | 200 | ||
| Chouinard et al., 1990163 | 1 | PLA | PLA | PLA | PLA | PLA | ||
| Cordiolo et al., 2003164 | 1 | CBT | 12 | 2 | ||||
| Cordiolo et al., 2003164 | 1 | Waitlist | Waitlist | Waitlist | ||||
| Cottraux et al., 1993165 | 1 | FLV | 282 | NA | NA | 300 | ||
| Cottraux et al., 1993165 | 1 | BT | 25 | NA | ||||
| Cottraux et al., 1993165 | 1 | BT + FLV | 282 | NA | NA | 300 | 25 | NA |
| Cottraux et al., 2001166 | 1 | BT | 20 | 1 | ||||
| Cottraux et al., 2001166 | 1 | CT | 20 | 1 | ||||
| Denys et al., 2003167 | 1 | PAR | 60 | Fixed | 60 | |||
| Denys et al., 2003167 | 1 | VEN | 300 | Fixed | 300 | |||
| Emmelkamp and Beens, 1991168 | 1 | CT | 31 | NA | ||||
| Emmelkamp and Beens, 1991168 | 1 | BT | 31 | 1.5 | ||||
| Emmelkamp et al., 1988169 | 1 | CT | 10 | 1 | ||||
| Emmelkamp et al., 1988169 | 1 | BT | 10 | 1 | ||||
| Fals-Stewart et al., 1993170 | 1 | BT | 24 | 1 | ||||
| Fals-Stewart et al., 1993170 | 1 | PsychPLA | ||||||
| Foa et al., 2005171 | 1 | BT | 15 | 2 | ||||
| Foa et al., 2005171 | 1 | CLO | 235 | 34 | 250 | |||
| Foa et al., 2005171 | 1 | BT + CLO | 194 | 48 | 250 | 15 | 2 | |
| Foa et al., 2005171 | 1 | PLA | PLA | |||||
| Freeman et al., 1994172 | 1 | FLV | 200 | NA | 150 | 250 | ||
| Freeman et al., 1994172 | 1 | CLO | 200 | NA | 150 | 250 | ||
| Freeston et al., 1997173 | 1 | CBT | 40 | 1.5 | ||||
| Freeston et al., 1997173 | 1 | Waitlist | Waitlist | Waitlist | ||||
| GlaxoSmithKline, 2005174 | 1 | PLA | PLA | PLA | PLA | PLA | ||
| GlaxoSmithKline, 2005174 | 1 | PAR | NA | NA | 60 | |||
| GlaxoSmithKline, 2005174 | 1 | CLO | NA | NA | 250 | |||
| GlaxoSmithKline, 2005175 | 9 | PAR | NA | NA | 50 | |||
| GlaxoSmithKline, 2005175 | 9 | CLO | NA | NA | 275 | |||
| Goodman et al., 1989176 | 1 | PLA | PLA | |||||
| Goodman et al., 1989176 | 1 | FLV | 255 | 60 | 300 | |||
| Goodman et al., 1996177 | 1 | PLA | PLA | |||||
| Goodman et al., 1996177 | 1 | FLV | 245 | NA | 100 | 300 | ||
| Greist et al., 1995126 | 1 | SER | 50/100/200 | Fixed | ||||
| Greist et al., 1995126 | 1 | PLA | PLA | |||||
| Greist et al., 2002178 | 1 | BT | 11 | 1 | ||||
| Greist et al., 2002178 | 1 | PsychPLA | PsychPLA | PsychPLA | ||||
| Hohagen et al., 1998179 | 2 | BT + PLA | PLA | PLA | PLA | PLA | ||
| Hohagen et al., 1998179 | 2 | BT + FLV | 288.1 | NA | 300 | |||
| Hollander et al., 2003181 | 1 | PLA | PLA | |||||
| Hollander et al., 2003181 | 1 | FLV | 271 | NA | 100 | 300 | ||
| Hollander et al., 2003180 | 1 | PLA | PLA | PLA | PLA | PLA | ||
| Hollander et al., 2003180 | 1 | PAR-20 | 20 | Fixed | Fixed | Fixed | ||
| Hollander et al., 2003180 | 1 | PAR-40 | 40 | Fixed | Fixed | Fixed | ||
| Hollander et al., 2003180 | 1 | PAR-60 | 60 | Fixed | Fixed | Fixed | ||
| Jaurrieta et al., 2008182 | 1 | CBT | 20 | 0.75 hours (45 minutes) | ||||
| Jaurrieta et al., 2008182 | 1 | Waitlist | Waitlist | Waitlist | ||||
| Jenike et al., 1990183 | 9 | SER | 200 | Fixed | 200 | |||
| Jenike et al., 1990183 | 9 | PLA | PLA | PLA | ||||
| Jenike et al., 1990184 | 1 | PLA | PLA | |||||
| Jenike et al., 1990184 | 1 | FLV | 294 | 23.6 | 100 | 300 | ||
| Jenike et al., 1997185 | 1 | PLA | PLA | PLA | PLA | PLA | ||
| Jenike et al., 1997185 | 1 | FLX | 77.9 | 6.3 | 80 | |||
| Jones and Menzies, 1998186 | 1 | CT | 8 | 1 | ||||
| Jones and Menzies, 1998186 | 1 | Waitlist | ||||||
| Kamijima et al., 2004187 | 9 | PLA | PLA | PLA | PLA | PLA | ||
| Kamijima et al., 2004187 | 9 | PAR | 45 | 5 | 40 | 50 | ||
| Khodarahimi, 2009188 | 1 | Waitlist | Waitlist | Waitlist | ||||
| Khodarahimi, 2009188 | 1 | BT | 12 | 1.5 | ||||
| Kobak et al., 2005189 | 1 | PLA | PLA | |||||
| Kobak et al., 2005189 | 1 | HYP | 1663.64 | 303.22 | 600 | 1800 | ||
| Koran et al., 1996190 | 1 | FLV | 255 | NA | 100 | 300 | ||
| Koran et al., 1996190 | 1 | CLO | 201 | NA | 100 | 250 | ||
| Kronig et al., 1999191 | 1 | SER | 165 | 55 | 50 | 200 | ||
| Kronig et al., 1999191 | 1 | PLA | PLA | PLA | PLA | PLA | ||
| Lindsay et al., 1997192 | 1 | BT | 15 | 1 | ||||
| Lindsay et al., 1997192 | 1 | PsychPLA | PsychPLA | PsychPLA | ||||
| López-Ibor et al., 1996193 | 9 | FLX | 40 | Fixed | 40 | |||
| López-Ibor et al., 1996193 | 9 | CLO | 150 | Fixed | 150 | |||
| Mavissakalian et al., 1985194 | 1 | CLO | 228.5 | NA | 100 | 300 | ||
| Mavissakalian et al., 1985194 | 1 | PLA | PLA | |||||
| McLean et al., 2001195 | 1 | CT | 12 | 2.5 | ||||
| McLean et al., 2001195 | 1 | BT | 12 | 2.5 | ||||
| Milanfranchi et al., 1997196 | 1 | CLO | 300 | 0 | 300 | |||
| Milanfranchi et al., 1997196 | 1 | FLV | 300 | 0 | 300 | |||
| Montgomery et al., 1993197 | 9 | PLA | PLA | |||||
| Montgomery et al., 1993197 | 9 | FLX-20 | 20 | Fixed | ||||
| Montgomery et al., 1993197 | 9 | FLX-40 | 40 | Fixed | ||||
| Montgomery et al., 1993197 | 9 | FLX-60 | 60 | Fixed | ||||
| Montgomery et al., 2001198 | 9 | CIT-20 | 20 | Fixed | ||||
| Montgomery et al., 2001198 | 9 | CIT-40 | 40 | Fixed | ||||
| Montgomery et al., 2001198 | 9 | CIT-60 | 60 | Fixed | ||||
| Montgomery et al., 2001198 | 9 | PLA | PLA | |||||
| Mundo et al., 1997199 | 2 | FLV | 290 | 31 | 150 | 300 | ||
| Mundo et al., 1997199 | 2 | PAR | 53.3 | 10 | 20 | 60 | ||
| Mundo et al., 1997199 | 2 | CIT | 50.9 | 10.4 | 20 | 60 | ||
| Mundo et al., 2001200 | 9 | CLO | NA | NA | 150 | 300 | ||
| Mundo et al., 2001200 | 9 | FLV | NA | NA | 150 | 300 | ||
| Nakajima et al., 1996201 | 9 | FLV | 193.5 | 64 | NA | 150–300 | ||
| Nakajima et al., 1996201 | 9 | PLA | PLA | PLA | PLA | PLA | ||
| Nakatani et al., 2005202 | 1 | PsychPLA | ||||||
| Nakatani et al., 2005202 | 1 | FLV | 190 | 21 | 150 | 200 | ||
| Nakatani et al., 2005202 | 1 | BT | 12 | 0.75 hours (45 minutes) | ||||
| O’Connor et al., 1999203 | 1 | SRI | NA | NA | NA | NA | ||
| O’Connor et al., 1999203 | 1 | Waitlist | ||||||
| O’Connor et al., 1999203 | 1 | CBT | 20 | 1 | ||||
| O’Connor et al., 1999203 | 1 | CBT + SRI | NA | NA | NA | NA | 20 | 1 |
| O’Connor et al., 2006204 | 1 | PLA | PLA | |||||
| O’Connor et al., 2006204 | 1 | FLV | NA | NA | 100 | 300 | ||
| Perse et al., 1987205 | 1 | PLA | PLA | |||||
| Perse et al., 1987205 | 1 | FLV | Not reported | NA | 300 | |||
| Shareh et al., 2010206 | 1 | FLV | NA | NA | 50 | 300 | ||
| Shareh et al., 2010206 | 1 | CBT | 10 | 1 | ||||
| Shareh et al., 2010206 | 1 | FLV + CBT | NA | NA | 50 | 300 | 10 | 1 |
| Sousa et al., 2006207 | 1 | SER | 100 | Fixed | ||||
| Sousa et al., 2006207 | 1 | CBT | 12 | 2 | ||||
| Stein et al., 2007124 | 1 | PLA | PLA | PLA | PLA | PLA | ||
| Stein et al., 2007124 | 1 | PAR | 40 | Fixed | Fixed | Fixed | ||
| Stein et al., 2007124 | 1 | ESCIT-10 | 10 | Fixed | Fixed | Fixed | ||
| Stein et al., 2007124 | 1 | ESCIT-20 | 20 | Fixed | Fixed | Fixed | ||
| Thoren et al., 1980208 | 2 | CLO | 150 | Fixed | 150 | |||
| Thoren et al., 1980208 | 2 | PLA | PLA | |||||
| Tollefson et al., 1994127 | 1 | PLA | PLA | |||||
| Tollefson et al., 1994127 | 1 | FLX-20 | 20 | Fixed | ||||
| Tollefson et al., 1994127 | 1 | FLX-40 | 40 | Fixed | ||||
| Tollefson et al., 1994127 | 1 | FLX-60 | 60 | Fixed | ||||
| Van Oppen et al., 1995209 | 1 | CT | 16 | 0.75 hours (45 minutes) | ||||
| Van Oppen et al., 1995209 | 1 | BT | 16 | 0.75 hours (45 minutes) | ||||
| Volavka et al., 1985210 | 1 | CLO | 275 | 53.5 | 300 | |||
| Volavka et al., 1985210 | 1 | IMI | 262.5 | 74.4 | 300 | |||
| Whittal et al., 2005211 | 1 | CT | 12 | 1 | ||||
| Whittal et al., 2005211 | 1 | BT | 12 | 1 | ||||
| Whittal et al., 2010212 | 1 | CT | 12 | 1 | ||||
| Whittal et al., 2010212 | 1 | PsychPLA | PsychPLA | PsychPLA | ||||
| Zohar and Judge, 1996213 | 9 | PLA | PLA | |||||
| Zohar and Judge, 1996213 | 9 | PAR | 49.3 | 13.7 | 20 | 60 | ||
| Zohar and Judge, 1996213 | 9 | CLO | 204.5 | 65.1 | 50 | 250 |
| Study | Settinga | Intervention | Average or mean dose at the end (mg) | SD of mean dose (mg) | Minimum dose during the study (mg) | Maximum dose during the study (mg) | Number of sessions | Duration of session (hours) |
|---|---|---|---|---|---|---|---|---|
| Alaghband-Rad and Hakimshooshtary, 2009215 | 1 | FLX | 20 | Fixed | ||||
| Alaghband-Rad and Hakimshooshtary, 2009215 | 1 | CIT | 20 | Fixed | ||||
| Asbahr et al., 2005216 | 1 | SER | 137.5 | 57.1 | 25 | 200 | ||
| Asbahr et al., 2005216 | 1 | CBT | 12 | 1.5 | ||||
| Barrett et al., 2004217 | 1 | CBT | 14 | 1.5 | ||||
| Barrett et al., 2004217 | 1 | PsychPLA | Waitlist | Waitlist | ||||
| Bolton and Perrin, 2008218 | 1 | BT | 10 | 1 to 1.5 | ||||
| Bolton and Perrin, 2008218 | 1 | PsychPLA | Waitlist | Waitlist | ||||
| Bolton et al., 2011219 | 1 | PsychPLA | Waitlist | Waitlist | ||||
| Bolton et al., 2011219 | 1 | CBT | 12 | 1 | ||||
| de Haan et al., 1998220 | 1 | CLO | 2.5 mg/kg | 0.63 | NA | 3 mg/kg | ||
| de Haan et al., 1998220 | 1 | BT | ||||||
| DeVeaugh-Geiss et al., 1992221 | 1 | CLO | NA | NA | 75 | 200 | ||
| DeVeaugh-Geiss et al., 1992221 | 1 | PLA | PLA | |||||
| Flament et al., 1985222 | 1 | CLO | 141 | 30 | 100 | 200 | ||
| Flament et al., 1985222 | 1 | PLA | PLA | |||||
| Freeman et al., 2008223 | 1 | CBT | 12 | 1 | ||||
| Freeman et al., 2008223 | 1 | PsychPLA | 12 | 1 | ||||
| Geller et al., 2001224 | 1 | PLA | PLA | |||||
| Geller et al., 2001224 | 1 | FLX | 24.6 | NA | 20 | 60 | ||
| GlaxoSmithKline, 2001225 | 1 | PAR | NA | NA | 20 | 50 | ||
| GlaxoSmithKline, 2001225 | 1 | PLA | PLA | PLA | PLA | PLA | ||
| Liebowitz et al., 2002226 | 9 | PLA | PLA | |||||
| Liebowitz et al., 2002226 | 9 | FLX | 64.8 | 18.9 | 20 | 80 | ||
| March et al., 1990227 | 1 | CLO | 190 | NA | 200 | |||
| March et al., 1990227 | 1 | PLA | PLA | |||||
| March et al., 1998228 | 1 | SER | 167 | NA | 200 | |||
| March et al., 1998228 | 1 | PLA | 180 | |||||
| Neziroglu et al., 2000229 | 9 | FLV | 200 | Fixed | 200 | |||
| Neziroglu et al., 2000229 | 9 | BT + FLV | 200 | Fixed | 200 | 20 | 1.5 | |
| Piacentini et al., 2011230 | 1 | CBT | 12 | 1.5 | ||||
| Piacentini et al., 2011230 | 1 | PsychPLA | 12 | 1.5 | ||||
| Riddle et al., 1992231 | 1 | PLA | PLA | |||||
| Riddle et al., 1992231 | 1 | FLX | 20 | Fixed | ||||
| Riddle et al., 2001232 | 9 | PLA | PLA | |||||
| Riddle et al., 2001232 | 9 | FLV | 165 | 50 | 50 | 200 | ||
| Storch et al., 2011233 | 1 | CBT | 12 | 1–1.5 hours | ||||
| Storch et al., 2011233 | 1 | PsychPLA | Waitlist | Waitlist | ||||
| Storch et al., 2013234 | 1 | SER + CBT | 164.3 | NA | 200 | 14 | 1 | |
| Storch et al., 2013234 | 1 | CBT + PLA | 14 | 1 | ||||
| The Pediatric OCD Treatment Study, 2004236 | 1 | SER | 170 | 33 | 200 | |||
| The Pediatric OCD Treatment Study, 2004236 | 1 | CBT | 12 | 1 | ||||
| The Pediatric OCD Treatment Study, 2004236 | 1 | SER + CBT | 133 | 64 | 200 | 14 | 1 | |
| The Pediatric OCD Treatment Study, 2004236 | 1 | PLA | PLA | PLA | PLA | PLA | ||
| Williams et al., 2010235 | 1 | CBT | 10 | 1 | ||||
| Williams et al., 2010235 | 1 | PsychPLA | PsychPLA | PsychPLA |
Appendix 7 Quality assessment of trials
| Study | Sequence generation | Sequence generation comment | Allocation concealment | Allocation concealment comment |
|---|---|---|---|---|
| Alaghband-Rad and Hakimshooshtary, 2009215 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’, etc. (‘consenting subjects were randomly assigned to start with either’) | Unclear | No description |
| Albert et al., 2002155 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Ananth et al. 1981156 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Anderson and Rees 2007157 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Andersson et al., 2012158 | Low risk | Computer-based randomisation | Unclear | No description |
| Asbahr et al., 2005216 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Barrett et al., 2004217 | Low risk | Block randomisation | Unclear | No description |
| Belloch et al., 2008159 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Belotto-Silva et al., 2012160 | Low risk | Minimisation using computer program | Low risk | Allocation for each group was determined without the knowledge of the professionals responsible for screening and recruitment of patients |
| Bergeron et al., 2002161 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’, etc. (‘patients were randomised to 24 weeks of double-blind treatment with flexible doses of . . .’) | Unclear | No description |
| Bisserbe et al., 1997162 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Bolton and Perrin, 2008218 | Low risk | Participants were randomly assigned to ERP or a waitlist control condition by use of random number tables. A colleague independent of the trial selected a random sequence of 20 numbers including 10 even and 10 odd numbers, and then made each kind represent 1 of the 2 conditions on a database containing 20 separate pages, the assignment sequence being unknown to the trial team. Assignment of the nth case was made after informed consent to participate in the trial by accessing the relevant separate page of the assignment database | Low risk | Participants were randomly assigned to ERP or a waitlist control condition by use of random number tables. A colleague independent of the trial selected a random sequence of 20 numbers including 10 even and 10 odd, and then made each kind represent one of the two conditions on a database containing 20 separate pages, the assignment sequence being unknown to the trial team. Assignment of the nth case was made after informed consent to participate in the trial by accessing the relevant separate page of the assignment database |
| Bolton et al., 2011219 | Low risk | Randomisation was carried out independently of the study team using sampling without replacement in blocks of six. The randomisation was stratified depending on whether or not the participant was receiving current stable medication for OCD | Low risk | Assignment of the next recruited participant was placed in a sealed envelope and held by an independent administrator, and this information was provided to the research assessor in written form or by telephone following consent to enter the trial |
| CCSG1, 1991154 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| CCSG2, 1991154 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Chouinard et al., 1990163 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Cordioli et al., 2003164 | Low risk | Computer-based randomisation | Low risk | The random allocation was done by a researcher not involved in the clinical trial |
| Cottraux et al., 1993165 | Unclear | Description only includes ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Cottraux et al., 2001166 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| de Haan et al., 1998220 | Unclear | Description only includes ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Denys et al., 2003167 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| DeVeaugh-Geiss et al., 1992221 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Emmelkamp and Beens 1991168 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Emmelkamp et al., 1988169 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Fals-Stewart et al., 1993170 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Flament et al., 1985222 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Foa et al., 2005171 | Low risk | Block randomisation | Unclear | No description |
| Freeman et al., 1994172 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Freeman et al., 2008223 | Unclear | Description only includes ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Freeston et al., 1997173 | Unclear | The authors describe the process but they do not present how they got the random numbers. Therefore unclear | Unclear | No description |
| Geller et al., 2001224 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’, etc. | Unclear | No description |
| GlaxoSmithKline, 2005174 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| GlaxoSmithKline, 2005175 | Unclear | Description only includes ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| GlaxoSmithKline, 2001225 | Low risk | Stratified by age randomisation | Unclear | No description |
| Goodman et al., 1989176 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Goodman et al., 1996177 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Greist et al., 1995126 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Greist et al., 2002178 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Hohagen et al., 1998179 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’, etc. | Unclear | No description |
| Hollander et al., 2003181 | Unclear | Description only includes ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Hollander et al., 2003180 | Low risk | A computer-based randomisation | Low risk | Central randomisation by SmithKline Beecham plc |
| Jaurrieta et al., 2008182 | Low risk | Tables of random numbers | Low risk | The random allocation was performed by a researcher not involved in the clinical trial |
| Jenike et al., 1990183 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Jenike et al., 1990184 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Jenike et al., 1997185 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’, etc. | Unclear | No description |
| Jones and Menzies, 1998186 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Kamijima et al., 2004187 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Khodarahimi, 2009188 | Low risk | Description includes block randomisation in groups of three | Unclear | No description |
| Kobak et al., 2005189 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Koran et al., 1996190 | Low risk | Patients were randomly assigned to double-blind treatment with fluvoxamine or clomipramine in approximately equal numbers in accordance with a randomisation schedule | Unclear | No description |
| Kronig et al., 1999191 | Low risk | Randomly assigned via computer-generated codes | Unclear | No description |
| Liebowitz 2002226 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’, etc. | Unclear | No description |
| Lindsay et al., 1997192 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| López-Ibor et al., 1996193 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| March 1990227 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| March 1998228 | Low risk | Computer-generated randomisation algorithm | Unclear | No description |
| Mavissakalian et al., 1985194 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| McLean et al., 2001195 | Low risk | Block randomisation | Unclear | No description |
| Milanfranchi et al., 1997196 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’, etc. | Unclear | No description |
| Montgomery et al., 1993197 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’, etc. | Unclear | No description |
| Montgomery et al., 2001198 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Mundo et al., 1997199 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Mundo et al., 2001200 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’, etc. | Unclear | No description |
| Nakajima et al., 1996201 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’, etc. | Unclear | No description |
| Nakatani et al., 2005202 | Unclear | Description only includes ‘random’, ‘randomly generated’, ‘randomised’ | Low risk | Central randomisation:A study coordinator who did not know any further information of the subjects randomly assigned them to one of three treatment conditions |
| Neziroglu et al., 2000229 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| O’Connor et al., 1999203 | High risk | Three clients had definite preferences (at least initially) regarding whether they preferred medication or non-medication. This choice was respected, so allocation to groups was not entirely random | Unclear | No description |
| O’Connor et al., 2006204 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Low risk | Pharmacy-controlled randomisation:The code was controlled through random allocation by the hospital pharmacy who revealed the code only at the end of follow-up |
| Perse et al., 1987205 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Piacentini et al., 2011230 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Riddle et al., 1992231 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’, etc. | Low risk | Pharmacy-controlled randomisation |
| Riddle et al., 2001232 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Shareh et al., 2010206 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’, etc. (‘21 patients who met all the conditions to participate in the study were randomly assigned to one of the three’) | Unclear | No description |
| Sousa et al., 2006207 | Low risk | Computer-generated random numbers | Unclear | No description |
| Stein et al., 2007124 | Low risk | A computer-generated randomisation list | Low risk | Sealed opaque envelopes |
| Storch et al., 2011233 | Low risk | Computer-based randomisation | Unclear | No description |
| Storch et al., 2013234 | Low risk | A computer-based randomisation | Unclear | No description |
| The Pediatric OCD Treatment Study, 2004236 | Low risk | Patients were randomly assigned (within site) to treatment using a computer-generated randomised permuted blocking procedure using a block size of four | Low risk | Concealment methods followed standard recommendations |
| Thoren et al., 1980208 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Tollefson et al., 1994127 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’, etc. | Unclear | No description |
| Van Oppen et al., 1995209 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Volavka et al., 1985210 | Low risk | Computer-generated random numbers were used in blocks | Low risk | Central randomisation by the manufacturer of the drug |
| Whittal et al., 2005211 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Whittal et al., 2010212 | Unclear | Description includes only ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Williams et al., 2010235 | Low risk | Tables of random numbers | Low risk | Only the trial administrator was aware which participants were in which group |
| Zohar and Judge 1996213 | Unclear | Description only includes ‘random’, ‘randomly generated’, ‘randomised’ | Unclear | No description |
| Study | Blinding of participants | Blinding of participants comment | Blinding of those delivering the intervention | Blinding of those delivering comment | Blinding of the outcome assessor | Blinding of outcome assessors comment |
|---|---|---|---|---|---|---|
| Alaghband-Rad and Hakimshooshtary, 2009215 | Unclear | Description includes only ‘double blind’ | Unclear | Description includes only ‘double blind’ | Unclear | The CYBOCS was administrated by an experienced clinician (MS) |
| Albert et al., 2002155 | High risk | Open-label treatment, as in the outcome assessment the authors report that the patients were instructed not to reveal their current treatment to evaluators | High risk | Open label treatment for clinicians; the term single blind was used to refer to independent evaluators | Low risk | Independent evaluators and patients were also instructed not to reveal their current treatment |
| Ananth et al. 1981156 | Low risk | Identical pills and description includes ‘double blind’ | Low risk | Identical pills and description includes ‘double blind’ | Unclear | No description |
| Anderson and Rees 2007157 | High risk | Psychological interventions not possible to blind | High risk | Psychological interventions not possible to blind | Unclear | No description |
| Andersson et al., 2012158 | High risk | Psychological interventions not possible to blind | High risk | Psychological interventions not possible to blind | Low risk | The assessors were blinded to treatment allocation at the post-treatment interview and were instructed to guess to which treatment condition the participant had been randomised in order to control for blinding integrity |
| Asbahr et al., 2005216 | High risk | No description of blindness regarding the drug and not possible to blind the psychological intervention | High risk | No description of blindness regarding the drug and not possible to blind the psychological intervention | Low risk | Two independent evaluators who were blinded to treatment assignment, performed all clinician-rated instruments. Subjects were not assessed by their own therapist and were asked not to reveal any information about their treatment to the independent evaluators |
| Barrett et al., 2004217 | High risk | Psychological interventions not possible to blind | High risk | Psychological interventions not possible to blind | Unclear | No description |
| Belloch et al., 2008159 | High risk | Psychological interventions not possible to blind | High risk | Psychological interventions not possible to blind | Low risk | The evaluator was blind to the treatment received by patients |
| Belotto-Silva et al., 2012160 | High risk | Psychological intervention in group format compared with drug | High risk | The principal CBT therapist was the main author of the manuscript | Low risk | Follow-up assessments administered by a rater who was blind to the patient treatment condition |
| Bergeron et al., 2002161 | Unclear | Description includes only ‘double blind’ | Unclear | Description only includes ‘double blind’ | Unclear | Efficacy assessments were conducted exclusively by psychiatrists with expertise in treatment research. Rater training on the primary outcome measures was conducted at an investigator meeting. As often as possible the same rater completed all of the ratings of a given patient |
| Bisserbe et al., 1997162 | Unclear | Description includes only ‘double blind’ | Unclear | Description includes only ‘double blind’ | Unclear | No description |
| Bolton and Perrin, 2008218 | High risk | Psychological interventions not possible to blind | High risk | Psychological interventions not possible to blind | High risk | The rater undertaking the CYBOCS assessment was not involved in the treatment of the case, but no attempt was made to achieve blindness of rater to condition because of the great difficulty associated with preserving it in this intensive treatment condition, especially in children |
| Bolton et al., 2011219 | High risk | Psychological interventions not possible to blind | High risk | Psychological interventions not possible to blind | Low risk | CYBOCS and ADIS–C/P assessments were made by trained independent evaluators in the research team, masters’ or doctoral-level psychologists, kept blinded to the randomisation status |
| CCSG1, 1991154 | Low risk | Identical capsules | Low risk | Identical capsules and states double blind | Unclear | No description |
| CCSG2, 1991154 | Low risk | Identical capsules | Low risk | Identical capsules and states double blind | Unclear | No description |
| Chouinard et al., 1990163 | Unclear | Description includes only ‘double blind’ | Unclear | Description includes only ‘double blind’ | Unclear | No description |
| Cordioli et al., 2003164 | High risk | Psychological interventions not possible to blind | High risk | Psychological interventions not possible to blind | Low risk | Patients of both groups were rated by three independent raters, blinded for patient group allocation |
| Cottraux et al., 1993165 | Unclear | Stated as double blind (expect FLV + BT group which is single blind) | Unclear | Stated as double blind (expect FLV + BT group which is single blind) | Unclear | No description |
| Cottraux et al., 2001166 | High risk | Psychological interventions not possible to blind | High risk | Psychological interventions not possible to blind | Low risk | The evaluator was independent and did not take part in the treatment. He or she had no information about the treatment under way |
| de Haan et al., 1998220 | High risk | Abstract says that open clomipramine was used and BT not possible to blind | High risk | Abstract says that open clomipramine was used and BT not possible to blind | Unclear | No description |
| Denys et al., 2003167 | Low risk | The study drugs were packaged so that the units were identical, and each subject received the appropriate dosage | Low risk | The study drugs were packaged so that the units were identical, and each subject received the appropriate dosage | Low risk | Two trained investigators, blind to the patient’s assigned condition, completed the scales at baseline and on each visit |
| DeVeaugh-Geiss et al., 1992221 | Unclear | Description includes only ‘double blind’ | Unclear | Description includes only ‘double blind’ | Unclear | No description |
| Emmelkamp and Beens 1991168 | High risk | Psychological interventions not possible to blind | High risk | Psychological interventions not possible to blind | Low risk | In addition, an independent assessor, a clinical psychologist who was blind with respect to the treatment condition rated the patients at assessment II (pretest) and after the first (assessment III) and second (assessment V) treatment block |
| Emmelkamp et al., 1988169 | High risk | Psychological interventions not possible to blind | High risk | Psychological interventions not possible to blind | Low risk | In addition, an independent assessor, a clinical psychologist who was blind with respect to the treatment condition, rated the patients at pre- and post-test |
| Fals-Stewart et al., 1993170 | High risk | Psychological interventions not possible to blind | High risk | Psychological interventions not possible to blind | Unclear | No description |
| Flament et al., 1985222 | Low risk | Identical pills and description includes ‘double blind’ | Low risk | Identical pills and description includes ‘double blind’ | Low risk | Two independent psychiatrists blinded to the patients’ treatment |
| Foa et al., 2005171 | Unclear | Description includes only double blind for medication and placebo. Blinding not possible for psychological intervention | Low risk | Independent evaluators, who remained blind to treatment assignment, conducted the assessments. Psychiatrists were blind to patients’ medication assignment and therapy status. The therapists who provided exposure and ritual prevention were blind to patients’ medication status. Patients were reminded not to discuss their treatment in order to maintain the blinding | Low risk | Independent evaluators, who remained blind to treatment assignment, conducted the assessments. Psychiatrists were blind to patients’ medication assignment and therapy status. The therapists who provided exposure and ritual prevention were blind to patients’ medication status. Patients were reminded not to discuss their treatment in order to maintain the blinding |
| Freeman et al., 1994172 | Unclear | Description includes only ‘double blind’ | Unclear | Description includes only ‘double blind’ | Unclear | No description |
| Freeman et al., 2008223 | High risk | Psychological interventions not possible to blind | High risk | Psychological interventions not possible to blind | Low risk | Trained independent evaluators (i.e. child clinical psychologists and child psychiatrists) who were blind |
| Freeston et al., 1997173 | High risk | Psychological interventions not possible to blind | High risk | Psychological interventions not possible to blind | High risk | The rater was aware of treatment status |
| Geller et al., 2001224 | Unclear | Description includes only ‘double blind’ | Unclear | Description includes only ‘double blind’ | Unclear | No description |
| GlaxoSmithKline, 2005174 | Unclear | Description only includes ‘double blind’ | Unclear | Description only includes ‘double blind’ | Unclear | Description includes only ‘double blind’ |
| GlaxoSmithKline, 2005175 | Unclear | Description only includes ‘double blind’ | Unclear | Description only includes ‘double blind’ | Unclear | Description includes only ‘double blind’ |
| GlaxoSmithKline, 2001225 | Low risk | Both double-blind medications (i.e. paroxetine and placebo) were in the form of white, oval, film-coated tablets for oral administration once daily. They were identical in size, shape and colour | Low risk | Both double-blind medications (i.e. paroxetine and placebo) were in the form of white, oval, film-coated tablets for oral administration once daily. They were identical in size, shape and colour | Unclear | No description |
| Goodman et al., 1989176 | Low risk | ‘Identical appearing tablets’ and double blind | Low risk | ‘Identical appearing tablets’ and double blind | Low risk | Experienced raters blind to drug assignment assessed symptoms of OCD |
| Goodman et al., 1996177 | Unclear | Description only includes ‘double blind’ | Unclear | Description only includes ‘double blind’ | Unclear | No description |
| Greist et al., 1995126 | Unclear | Description only includes ‘double blind’ | Unclear | Description only includes ‘double blind’ | Unclear | No description |
| Greist et al., 2002178 | High risk | Psychological interventions not possible to blind | High risk | Psychological interventions not possible to blind | High risk | Self-rated YBOCS by patients |
| Hohagen et al., 1998179 | Unclear | Description includes only ‘double blind’ | Unclear | Description includes only ‘double blind’ | Low risk | The YBOCS was used weekly by an independent rater to rate patients’ symptoms |
| Hollander et al., 2003181 | Unclear | Description includes only ‘double blind’ | Unclear | Description includes only ‘double blind’ | Unclear | No description |
| Hollander et al., 2003180 | Low risk | Description includes ‘double blind’ and ‘identical tablets and identical coded bottles’ | Low risk | Description includes ‘double blind’ and ‘identical tablets and identical coded bottles’ | Unclear | No description |
| Jaurrieta et al., 2008182 | High risk | Psychological interventions not possible to blind | High risk | Psychological interventions not possible to blind | Unclear | Vague description unable to decide if high risk or not; therefore, unclear |
| Jenike et al., 1990183 | Low risk | Identically appearing placebo capsules | Low risk | Identically appearing placebo capsules | Unclear | No description |
| Jenike et al., 1990184 | Low risk | Identical appearing placebo capsules | Low risk | Identical appearing placebo capsules | Low risk | The authors give details on the rigorous procedure they followed about measuring YBOCS (giving intraclass correlation coefficients) and they state that:the raters were provided with standardized instructions and the same rater assessed each individual patient throughout the course of the study |
| Jenike et al., 1997185 | Unclear | No description | Unclear | No description | Unclear | No description |
| Jones and Menzies, 1998186 | High risk | Psychological interventions not possible to blind | High risk | Psychological interventions not possible to blind | High risk | Self-rated instruments |
| Kamijima et al., 2004187 | Unclear | Description includes only ‘double blind’ | Unclear | Description only includes ‘double blind’ | Unclear | No description |
| Khodarahimi, 2009188 | High risk | Psychological interventions not possible to blind | High risk | Psychological interventions not possible to blind | Unclear | No description |
| Kobak et al., 2005189 | Low risk | The authors describe ‘matched’ placebo | Low risk | The authors describe ‘matched’ placebo | Unclear | No description |
| Kobak et al., 2005189 | Low risk | Blinding was accomplished by having all study patients take the same number of capsules daily and medications supplied in identical capsules for oral administration | Low risk | Blinding was accomplished by having all study patients take the same number of capsules daily and medications supplied in identical capsules for oral administration | Unclear | No description |
| Kronig et al., 1999191 | Unclear | Description includes only ‘double blind’ | Unclear | Description includes only ‘double blind’ | Unclear | No description |
| Liebowitz et al., 2002226 | Unclear | Study is only described as ‘placebo-controlled’ | Unclear | Study is only described as ‘placebo-controlled’ | Low risk | Independent evaluators assessing symptoms were blind to treatment assignment |
| Lindsay et al., 1997192 | High risk | Psychological interventions not possible to blind | High risk | Psychological interventions not possible to blind | Unclear | No description |
| López-Ibor et al., 1996193 | Unclear | Description includes only ‘double blind’ | Unclear | Description includes only ‘double blind’ | Unclear | No description |
| March et al., 1990227 | Low risk | Identical pills and description includes ‘double blind’ | Low risk | Identical pills and description includes ‘double blind’ | Unclear | No description |
| March et al., 1998228 | Low risk | Identical blisters | Low risk | Identical blisters | Unclear | No description |
| Mavissakalian et al., 1985194 | Unclear | Description only includes ‘double blind’ | Unclear | Description only includes ‘double blind’ | Unclear | No description |
| McLean et al., 2001195 | High risk | Psychological interventions not possible to blind | High risk | Psychological interventions not possible to blind | Unclear | No description |
| Milanfranchi et al., 1997196 | Low risk | Description includes ‘double blind’ and also the authors note how the two drugs were similar (‘the drugs were administered in capsules containing either 50 mg of FLV or 50 mg of CLO; the clomipramine dose was distributed in two comfits of 25 mg in the same capsule’) | Low risk | Description includes ‘double blind’ and also the authors note how the two drugs were similar (‘the drugs were administered in capsules containing either 50 mg of FLV or 50 mg of CLO; the clomipramine dose was distributed in two comfits of 25 mg in the same capsule’) | Unclear | No description |
| Montgomery et al., 1993197 | Unclear | Description includes only ‘double blind’ | Unclear | Description includes only ‘double blind’ | Unclear | No description |
| Montgomery et al., 2001198 | Unclear | Description includes only ‘double blind’ | Unclear | Description includes only ‘double blind’ | Unclear | No description |
| Mundo et al., 1997199 | High risk | Mentioned that patients were not blinded for medication | High risk | The authors report that this is a single blind study, with the blinding referring to independent raters, therefore we can assume that the health-care providers were not blinded | Low risk | The ratings were all made under blind conditions |
| Mundo et al., 2001200 | Unclear | Description includes only ‘double blind’ | Unclear | Description includes only ‘double blind’ | Unclear | No description |
| Nakajima et al., 1996201 | Unclear | Description includes only ‘double blind’ | Unclear | Description includes only ‘double blind’ | Unclear | No description |
| Nakatani et al., 2005202 | High risk | No description but due to the nature of intervention this is high risk | Unclear | No description | Low risk | Clinical ratings were undertaken blindly at baseline, week 4, 8 and 12 by 4 clinically experienced psychiatrists |
| Neziroglu et al., 2000229 | High risk | Psychological intervention was added to one of the groups and, therefore, blinding was not possible | High risk | Psychological intervention was added to one of the groups and, therefore, blinding was not possible | Unclear | No description |
| O’Connor et al., 1999203 | High risk | Psychological interventions not possible to blind | High risk | Psychological interventions not possible to blind | Low risk | The same clinician carried out all ratings post treatment and was blind to treatment-group membership |
| O’Connor et al., 2006204 | Low risk | Paper discusses how placebos were similar (‘The active and inactive medication was given in identical tablet form of 50 mg units and were identical in appearance’) | Low risk | Paper discusses how placebos were similar (‘The active and inactive medication was given in identical tablet form of 50 mg units and were identical in appearance’) | Low risk | An independent assessor administered the YBOCS at pre-, mid- and post-treatment and follow-ups |
| Perse et al., 1987205 | Unclear | Description includes only ‘double blind’ | Unclear | Description includes only ‘double blind’ | Low risk | Each of the three physician investigators made independent blind clinical ratings |
| Piacentini et al., 2011230 | High risk | Psychological interventions not possible to blind | High risk | Psychological interventions not possible to blind | Low risk | Trained evaluators blinded to treatment condition conducted assessments with families |
| Riddle et al., 1992231 | Low risk | Paper discusses how placebos were similar (‘placebo capsules were prepared by filling identical opaque jackets with lactose powder’) | Low risk | Paper discusses how placebos were similar (‘placebo capsules were prepared by filling identical opaque jackets with lactose powder’) | Unclear | No description |
| Riddle et al., 2001232 | Low risk | Description includes ‘double blind’ and ‘identical placebo capsule’ | Low risk | Description includes ‘double blind’ and ‘identical placebo capsule’ | Low risk | The authors give details on the rigorous procedure they followed about measuring CYBOCS |
| Shareh et al., 2010206 | High risk | No description but owing to the nature of intervention this is high risk | High risk | No description of blindness in the paper, therefore high risk | Unclear | No description |
| Sousa et al., 2006207 | High risk | Psychological intervention was added to one of the groups and, therefore, blinding was not possible | High risk | Psychological intervention was added to one of the groups and, therefore, blinding was not possible | Low risk | Two psychiatrists blind to the type of treatment were used as independent evaluators |
| Stein et al., 2007124 | Low risk | Double blind and identical appearance of study medications | Low risk | Double blind and identical appearance of study medications | Low risk | The authors give details on the rigorous procedure they followed about measuring YBOCS (‘Only those investigators who had actively participated in rater training sessions prior to inclusion of patients into the study were allowed to rate patients. Rater training was undertaken to increase inter-rater reliability, and was chaired by an experienced psychiatrist’). Patient ratings were assessed by the same investigator at each visit, whenever possible |
| Storch et al., 2011233 | High risk | Psychological interventions not possible to blind | High risk | Psychological interventions not possible to blind | Low risk | Independent evaluators blinded to treatment |
| Storch et al., 2013234 | Unclear | Description includes only ‘double blind’ | Unclear | Description includes only ‘double blind’ | Low risk | Independent evaluators trained by the authors in the administration of scales |
| Thoren et al., 1980208 | Low risk | Identical pills and description includes ‘double blind’ | Low risk | Identical pills and description includes ‘double blind’ | Unclear | No description |
| Tollefson et al., 1994127 | Unclear | No description | Unclear | ‘Patients were examined by the treating clinicians who were blinded to the study medication’ but no further information | Unclear | No description |
| Van Oppen et al., 1995209 | High risk | Psychological interventions not possible to blind | High risk | Psychological interventions not possible to blind | Unclear | No description |
| Volavka et al., 1985210 | Low risk | Identical capsules | Low risk | Identical capsules and double blind | Unclear | No description |
| The Pediatric OCD Treatment Study, 2004236 | Unclear | Except in emergencies, participants and clinicians remained masked in the pills-only conditions. However, it is not possible to blind the psychological intervention | Unclear | Except in emergencies, participants and clinicians remained masked in the pills-only conditions. However, it is not possible to blind the psychological intervention | Low risk | Independent evaluators |
| Whittal et al., 2005211 | High risk | Psychological interventions not possible to blind | High risk | Psychological interventions not possible to blind | Low risk | The assessors were blind to treatment type. With few exceptions, the same assessor was used at pre- and post-treatment, and follow-up |
| Whittal et al., 2010212 | High risk | Psychological interventions not possible to blind | High risk | Psychological interventions not possible to blind | Unclear | No description |
| Williams et al., 2010235 | High risk | Psychological interventions not possible to blind | High risk | Psychological interventions not possible to blind | Low risk | Assessors were blind to the allocation of the participants, and the participants were instructed not to reveal whether or not they had received treatment |
| Zohar and Judge 1996213 | Unclear | Description includes only ‘double blind’ | Unclear | Description includes only ‘double blind’ | Unclear | Description includes only ‘double blind’ |
| Study ID (author and year) | Incomplete outcome data | Incomplete outcome comment | Selective outcome reporting | Selective outcome comment | Any other potential threats to validity | Any other comment |
|---|---|---|---|---|---|---|
| Alaghband-Rad and Hakimshooshtary, 2009215 | High risk | No description of how the handled missing data, no ITT analysis. Overall attrition 17%; no further details | High risk | SDs not given for CYBOCS | High risk | No data for number of children screened initially, excluded because not eligible. Standard of reporting not high despite this being a relatively recent trial |
| Albert et al., 2002155 | High risk | Missing data not imputed, completers analysis. Differential attrition almost reached 15% | High risk | Data for completers only, even though they reported that they have also carried out LOCF as well, they only present the results for the visitwise analysis | High risk | Differential attrition ≈15% |
| Ananth et al. 1981156 | High risk | Completers analysis | Low risk | Low risk | Not any other | |
| Anderson and Rees, 2007157 | Low risk | Completers analysis reported in detail although the authors have also used ITT but only giving F-statistics and p-values | High risk | The results of the ITT analysis are not given in full; therefore, only the completers analysis can be included | Low risk | Not any other |
| Andersson et al., 2012158 | Low risk | One dropout only and therefore they performed completers analysis. Unlikely that this may have influenced their results, and also they examined blinding integrity. Therefore, could be low risk | Low risk | Low risk | Not any other | |
| Asbahr et al., 2005216 | Low risk | The authors reported that they did not use ITT because only one patient dropped out. Could be low risk for this reason | High risk | No detailed measures for CYBOCS for follow-up measurements, only F-tests and figures | Low risk | Not any other |
| Barrett et al., 2004217 | Unclear | It is not clear from the description whether this is a completers or ITT analysis | High risk | Dropouts not per arm | Low risk | Not any other |
| Belloch et al., 2008159 | High risk | Completers analysis | Low risk | Low risk | Not any other | |
| Belotto-Silva et al., 2012160 | Low risk | Missing data have been imputed using appropriate methods (‘Intention-to-treat and last-observation-carried-forward analyses were conducted in order to make conservative estimates of symptom severity for individuals whose outcome measures were missing’). Dropout rates were 25.7% in the CBT (n = 18) and 37.5% in the SSRI group (n = 33). Overall attrition > 20% and some evidence of differential attrition but reasons for dropouts given and judgement is that there is no serious risk for differential bias. Overall, low risk | Low risk | Low risk | Not any other serious risk (see comment for differential attrition in column 3 – Incomplete outcome comment – of this table) | |
| Bergeron et al., 2002161 | Low risk | Missing data have been imputed using appropriate methods (ITT and LOCF). However, overall attrition rate high (> 30%) without differential attrition | Low risk | High risk | Overall attrition high (> 30%) | |
| Bisserbe et al., 1997162 | Low risk | The authors report that they used ITT and ‘last efficacy assessment’ for those who dropped out | High risk | SDs not given | High risk | High attrition 35% and evidence of differential attrition > 15% (27% vs. 43%) |
| Bolton and Perrin, 2008218 | Low risk | ITT analysis and LOCF as stated in the methods section | Low risk | Low risk | Not any other | |
| Bolton et al., 2011219 | Low risk | ITT analysis and LOCF as stated in the methods section | Low risk | Low risk | Not any other | |
| CCSG1, 1991154 | Unclear | In the methods section they do not mention how they handled missing data. In the results, although they mention that in the efficacy analysis that all patients and not just the completers have been used, it is not clear from figures and tables that this is the case | High risk | In the results, although they mention that in the efficacy analysis all patients and not just the completers have been used, it is not clear from figures and tables that this is the case. Therefore, evidence for selective reporting | High risk | They report deviations from the protocol:Because the physicians’ and patients’ global ratings did not satisfy the statistical assumptions for logistic regression, i.e., the analysis that had been intended, these scores were analysed by the Wilcoxon rank-sum test |
| CCSG2, 1991154 | Unclear | In the methods section they do not mention how they handled missing data. In the results, although they mention that in the efficacy analysis all patients and not just the completers have been used it is not clear from figures and tables that this is the case | High risk | In the results, although they mention that in the efficacy analysis all patients and not just the completers have been used it is not clear from figures and tables that this is the case. Therefore, evidence for selective reporting | High risk | They report deviations from the protocol:Because the physicians’ and patients’ global ratings did not satisfy the statistical assumptions for logistic regression, i.e., the analysis that had been intended, these scores were analysed by the Wilcoxon rank-sum test |
| Chouinard et al., 1990163 | Low risk | The authors report that ‘no patients were excluded from analysis’ and LOCF was used to handle missing data – low attrition | High risk | SDs not given | Low risk | Not any other |
| Cordioli et al., 2003164 | Low risk | ITT analysis and LOCF as stated in the methods section. Overall attrition low | Low risk | Low risk | Not any other | |
| Cottraux et al., 1993165 | High risk | No description of how the handled missing data, completers and no ITT analysis. High attrition rate: 45% | Low risk | High risk | Very high attrition (45%). Not standardised scale of overall OCD symptoms | |
| Cottraux et al., 2001166 | High risk | Completers analysis reported although the authors point out that they have also used ITT with LOCF | High risk | Completers analysis only reported. Regarding the results of the ITT, there were no differences | Low risk | Not any other |
| de Haan et al., 1998220 | Low risk | Although this is completers analysis, just one dropout so possibly no effect | Low risk | Low risk | Not any other | |
| Denys et al., 2003167 | Low risk | ITT analysis and LOCF as stated in the methods section | Low risk | Low risk | Not any other | |
| DeVeaugh-Geiss et al., 1992221 | Low risk | Missing data have been imputed using appropriate methods (ITT and LOCF). Low attrition and no evidence of differential attrition | High risk | SDs not given | Low risk | Not any other |
| Emmelkamp and Beens 1991168 | High risk | There were dropouts but the authors focused only on the completers analysis | Low risk | High risk | Dropout rate 8/31 = 26% | |
| Emmelkamp et al., 1988169 | High risk | Two dropped out but the authors conducted completers analysis | Low risk | Low risk | Not any other | |
| Fals-Stewart et al., 1993170 | High risk | Completers analysis | High risk | SDs not reported | Low risk | Not any other |
| Flament et al., 1985222 | Unclear | Crossover trial | High risk | Not sufficient data for baseline and first crossover | Low risk | Not any other |
| Foa et al., 2005171 | Low risk | Linear mixed-effects model to account for missing data | Low risk | High risk | Overall attrition high (29%) and evidence of > 15% differential attrition between placebo and BT + CLO groups | |
| Freeman et al., 1994172 | Low risk | Missing data have been imputed using appropriate methods (ITT and LOCF). Overall attrition high (26%) and some evidence for differential attrition (17% vs. 34%) | High risk | SDs not given | High risk | Overall attrition high (26%) and evidence for differential attrition > 15% (17% FLV vs. 34% CLO) |
| Freeman et al., 2008223 | Low risk | ITT analysis and LOCF as stated in the methods section. Overall attrition moderate 26% but no evidence of differential attrition | Low risk | High risk | Overall attrition > 25% ( = 26%); no differential attrition however | |
| Freeston et al., 1997173 | Low risk | ITT analysis although not exactly sure which method they have used for missing data, possibly LOCF though | Low risk | Low risk | Not any other | |
| Geller et al., 2001224 | Low risk | Missing data have been imputed using appropriate methods (ITT and LOCF). Overall attrition high (33%); no evidence of differential attrition | Low risk | High risk | Overall attrition high (> 33%) | |
| GlaxoSmithKline, 2005174 | Low risk | Missing data have been imputed using appropriate methods (ITT and LOCF). Overall high attrition (32%), but no evidence of differential attrition > 15% | Low risk | High risk | No publication: high attrition of 32% | |
| GlaxoSmithKline, 2005175 | Unclear | Report describes ITT as the method of the analysis but from the table it is not clear | Low risk | High risk | No publication: company report | |
| GlaxoSmithKline, 2001225 | High risk | Missing data have been imputed using appropriate methods (ITT and LOCF). Overall high attrition (31%) but no evidence of differential attrition > 15% | Low risk | High risk | No publication: high attrition of 31% | |
| Goodman et al., 1989176 | Low risk | ‘Dropouts were subjected to endpoint analysis’ | Low risk | High risk | Differential attrition (8% vs. 26%) but in favour of active treatment rather than placebo | |
| Goodman et al., 1996177 | Low risk | Missing data have been imputed using appropriate methods (ITT and LOCF). Overall attrition moderate (23%), but no evidence for differential attrition | High risk | Absolute values for YBOCS at follow-up not given for the ITT population, only figures and change values | Low risk | Not any other |
| Greist et al., 1995126 | Unclear | Tables for end-point analysis report N for all patients randomised, but there is no discussion of how the missing data were handled or if they used ITT, although it seems that this is ITT analysis | Low risk | High risk | High attrition of 27% overall with no evidence of differential attrition | |
| Greist et al., 2002178 | Low risk | LOCF and ITT | Low risk | Low risk | Not any other | |
| Hohagen et al., 1998179 | Unclear | No discussion of dropouts | Low risk | High risk | The authors state that owing to significant imbalance in the two groups at baseline, they dropped the outliers in both therefore reducing the sample for analysis to 25 and 24, respectively | |
| Hollander et al., 2003181 | Low risk | Missing data have been imputed using appropriate methods (LOCF, ITT). Overall attrition 31%, but no evidence of differential attrition (> 15% between treatments) | High risk | SEs given instead of SDs, high attrition | Low risk | Not any other |
| Hollander et al., 2003180 | Low risk | ITT analysis and LOCF as stated in the methods section | High risk | SDs not given | Low risk | Not any other |
| Jaurrieta et al., 2008182 | Low risk | ITT analysis and LOCF as stated in the methods section. Overall attrition < 25% ( = 21%) | High risk | Dropouts not per arm | Low risk | Not any other |
| Jenike et al., 1990183 | Low risk | No dropouts | Low risk | Low risk | Not any other | |
| Jenike et al., 1990184 | High risk | No description of how the handled missing data, completers and no ITT analysis. Low attrition rate (45%) | High risk | Baseline data only for completers | Low risk | Not any other |
| Jenike et al., 1997185 | Low risk | No methods for imputing but the authors note that ‘All analyses were conducted for both patients who completed the study and all patients in intent-to-treat analyses. In all cases, the pattern of results was identical across both analyses’. Therefore, one can assume low risk | Low risk | Unclear | ITT analysis not reported but they mention that results were similar with completers | |
| Jones and Menzies, 1998186 | Unclear | No discussion of dropouts, possibly no dropouts | Low risk | Low risk | Not any other | |
| Kamijima et al., 2004187 | Low risk | Missing data have been imputed using appropriate methods (ITT and LOCF) | High risk | No description of dropouts per arm reported | Low risk | Not any other |
| Khodarahimi, 2009188 | High risk | No discussion of dropouts | Low risk | Low risk | Not any other | |
| Kobak et al., 2005189 | Low risk | ITT and LOCF | Low risk | Low risk | Not any other | |
| Kobak et al., 2005189 | Low risk | Missing data have been imputed using appropriate methods (ITT and LOCF). Overall attrition however high (29%) and some evidence for differential attrition | Low risk | High risk | Differential attrition despite missing data handling (21% FLV vs. 36% CLO) | |
| Kronig et al., 1999191 | Low risk | The authors report LOCF | High risk | No detailed follow-up data, figures only and F-tests and p-values | High risk | High attrition (30%) but no evidence of differential attrition |
| Liebowitz et al., 2002226 | Low risk | Missing data have been imputed using appropriate methods. Low overall attrition (12%) and low differential attrition | Low risk | Low risk | Not any other serious risk | |
| Lindsay et al., 1997192 | Unclear | The authors do not discuss any dropouts but it is unclear if this was a completers analysis or there were no dropouts | Unclear | No discussion of dropouts, therefore unable to decide if completers or not | Low risk | Not any other |
| López-Ibor et al., 1996193 | Low risk | ITT and LOCF | Low risk | Low risk | Not any other | |
| March et al., 1990227 | Low risk | There were two dropouts and the authors say that they did an ITT analysis by using the mean treatment score of the treatment group | Low risk | Low risk | Not any other | |
| March et al., 1998228 | Low risk | Missing data have been imputed using appropriate methods (ITT and LOCF). Low attrition of 16% and no evidence of differential attrition | High risk | SDs not given | Low risk | Not any other |
| Mavissakalian et al., 1985194 | High risk | Completers analysis | High risk | Original number randomised not reported | Low risk | Not any other |
| McLean et al., 2001195 | High risk | Completers analysis | Low risk | Low risk | Not any other | |
| Milanfranchi et al., 1997196 | High risk | One dropout only but no LOCF | Low risk | Low risk | Not any other | |
| Montgomery et al., 1993197 | Low risk | Missing data have been imputed using appropriate methods (ITT and LOCF). Overall attrition high (25%), no evidence of differential attrition | Low risk | Low risk | Not any other | |
| Montgomery et al., 2001198 | Low risk | Missing data have been imputed using appropriate methods (ITT and LOCF). Low attrition and no evidence of differential attrition | Low risk | Low risk | Not any other | |
| Mundo et al., 1997199 | Low risk | No dropouts, therefore no need to handle missing data | Low risk | Low risk | Not any other | |
| Mundo et al., 2001200 | Low risk | Missing data have been imputed using appropriate methods (ITT and LOCF). Attrition 20% | High risk | SDs not given for follow-up | Low risk | Not any other |
| Nakajima et al., 1996201 | Low risk | Missing data have been imputed using appropriate methods (ITT and LOCF) | Low risk | Low risk | Not any other | |
| Nakatani et al., 2005202 | High risk | No description of how missing data were handled, completers and no ITT analysis | Low risk | Low risk | Not any other | |
| Neziroglu et al., 2000229 | Low risk | No dropouts according to the authors | Low risk | Low risk | Not any other | |
| O’Connor et al., 1999203 | High risk | Completers analysis | High risk | No baseline data for dropouts, only for completers | Low risk | Not any other |
| O’Connor et al., 2006204 | High risk | No description of how the handled missing data, completers and no ITT analysis | Low risk | Low risk | Not any other | |
| Perse et al., 1987205 | High risk | Missing data not imputed, completers analysis | High risk | Not full reporting of means and SDs | Low risk | Not any other |
| Piacentini et al., 2011230 | Low risk | ITT analysis and LOCF as stated in the methods section. Moderate attrition and no evidence of differential attrition | Low risk | Low risk | Not any other | |
| Riddle et al., 1992231 | Low risk | Missing data have been imputed using appropriate methods (‘Intention-to-treat’ and ‘the 4-week data for those two subjects were carried over to week 8’) | Low risk | Low risk | Very small sample size, initial protocol for crossover not feasible in the end, but no evidence for risk for the first 8 weeks of analysis included in this meta-analysis | |
| Riddle et al., 2001232 | Low risk | Missing data have been imputed using appropriate methods (ITT and LOCF). Overall attrition high (38%) but no evidence for differential attrition | Low risk | High risk | Very high attrition (38%) | |
| Shareh et al., 2010206 | High risk | No description of how the handled missing data, completers and no ITT analysis | Low risk | High risk | No standard reporting despite this being a recent trial, no flow chart, potentially high risk | |
| Sousa et al., 2006207 | Low risk | No dropouts with at least one baseline evaluation, therefore it can be considered that there are no missing data | High risk | SDs not given | Low risk | Not any other |
| Stein et al., 2007124 | Low risk | Missing data have been imputed using appropriate methods (ITT and LOCF) | Low risk | Low risk | Not any other | |
| Storch et al., 2011233 | Low risk | ITT analysis and LOCF as stated in the methods section | Low risk | Low risk | Not any other | |
| Storch et al., 2013234 | Low risk | Missing data have been imputed using appropriate methods [random-effects models in SAS (SAS Institute Inc., Cary, NC, USA) with MLE instead of LOCF, which is more conservative]. Overall high attrition (30%) and evidence of differential attrition (> 15%) | Low risk | High risk | High attrition (30%) and evidence of differential attrition (> 15%) between some of the arms | |
| The Pediatric OCD Treatment Study, 2004236 | Low risk | Missing data have been imputed using appropriate methods (ITT and LOCF) | Low risk | Low risk | Not any other | |
| Thoren et al., 1980208 | High risk | Completers analysis | High risk | No details for dropouts | Low risk | Not any other |
| Tollefson et al., 1994127 | Low risk | They have used appropriate methods (LOCF and ITT) but see reporting issues | High risk | SDs not given for ITT analysis, therefore only completers analysis can be used | High risk | Reporting should be better, reliance on secondary outcomes |
| Van Oppen et al., 1995209 | High risk | Completers analysis | High risk | Baseline data only for completers | Low risk | Not any other |
| Volavka et al., 1985210 | High risk | Completers analysis | Low risk | Low risk | Not any other | |
| Whittal et al., 2005211 | High risk | Completers analysis | Low risk | Low risk | Not any other | |
| Whittal et al., 2010212 | High risk | Completers analysis | Low risk | Low risk | Not any other | |
| Williams et al., 2010235 | Low risk | ITT analysis and LOCF as stated in the methods section. Moderate attrition and no evidence of differential attrition | High risk | SEs given instead of SDs | Low risk | Not any other |
| Zohar and Judge, 1996213 | Low risk | Missing data have been imputed using appropriate methods (ITT and LOCF). Overall high attrition (30%), but no evidence of differential attrition > 15% | Low risk | High risk | High attrition (30%) |
| Study | Imputation for missing data | Imputation method | ITT analysis |
|---|---|---|---|
| Alaghband-Rad and Hakimshooshtary, 2009215 | No | No | |
| Albert et al., 2002155 | No | No | |
| Ananth et al. 1981156 | No | No | |
| Anderson and Rees, 2007157 | Unclear | No description given | Unclear |
| Andersson et al., 2012158 | No | No | |
| Asbahr et al., 2005216 | No | No | |
| Barrett et al., 2004217 | Unclear | Unclear | Unclear |
| Belloch et al., 2008159 | No | No | |
| Belotto-Silva et al., 2012160 | Yes | LOCF | Yes |
| Bergeron et al., 2002161 | Yes | LOCF | Yes |
| Bisserbe et al., 1997162 | Yes | LOCF | Yes |
| Bolton and Perrin, 2008218 | Yes | LOCF | Yes |
| Bolton et al., 2011219 | Yes | LOCF | Yes |
| CCSG1, 1991154 | Unclear | Unclear | Unclear |
| CCSG2, 1991154 | Unclear | Unclear | Unclear |
| Chouinard et al., 1990163 | Yes | LOCF | Yes |
| Cordioli et al., 2003164 | Yes | LOCF | Yes |
| Cottraux et al., 1993165 | No | No | |
| Cottraux et al., 2001166 | No | No | |
| de Haan et al., 1998220 | No | No | |
| Denys et al., 2003167 | Yes | LOCF | Yes |
| DeVeaugh-Geiss et al., 1992221 | Yes | LOCF | Yes |
| Emmelkamp and Beens 1991168 | No | No | |
| Emmelkamp et al., 1988169 | No | No | |
| Fals-Stewart et al., 1993170 | No | No | |
| Flament et al., 1985222 | Unclear | Unclear | Unclear |
| Foa et al., 2005171 | Yes | Linear mixed-effects models | Yes |
| Freeman et al., 1994172 | Yes | LOCF | Yes |
| Freeman et al., 2008223 | Yes | LOCF | Yes |
| Freeston et al., 1997173 | Yes | Unclear | Yes |
| Geller et al., 2001224 | Yes | LOCF | Yes |
| GlaxoSmithKline, 2005174 | Yes | LOCF | Yes |
| GlaxoSmithKline, 2005175 | Unclear | Unclear | Unclear |
| GlaxoSmithKline, 2001225 | Yes | LOCF | Yes |
| Goodman et al., 1989176 | Yes | LOCF | Yes |
| Goodman et al., 1996177 | Yes | LOCF | Yes |
| Greist et al., 1995126 | Unclear | Unclear | Unclear |
| Greist et al., 2002178 | Yes | LOCF | Yes |
| Hohagen et al., 1998179 | Unclear | Unclear | No |
| Hollander et al., 2003180 | Yes | LOCF | Yes |
| Hollander et al., 2003181 | Yes | LOCF | Yes |
| Jaurrieta et al., 2008182 | Yes | LOCF | Yes |
| Jenike et al., 1990183 | NA | NA | NA |
| Jenike et al., 1990184 | No | No | |
| Jenike et al., 1997185 | No | No | |
| Jones and Menzies, 1998186 | Unclear | Unclear | Unclear |
| Kamijima et al., 2004187 | Yes | LOCF | Yes |
| Khodarahimi, 2009188 | No | Unclear | Unclear |
| Kobak et al., 2005189 | Yes | LOCF | Yes |
| Koran et al., 1996190 | Yes | LOCF | Yes |
| Kronig et al., 1999191 | Yes | LOCF | Yes |
| Liebowitz et al., 2002226 | Yes | LOCF | Yes |
| Lindsay et al., 1997192 | Unclear | Unclear | Unclear |
| López-Ibor et al., 1996193 | Yes | LOCF | Yes |
| March et al., 1990227 | Yes | Other | Yes |
| March et al., 1998228 | Yes | LOCF | Yes |
| Mavissakalian et al., 1985194 | No | No | |
| McLean et al., 2001195 | No | No | |
| Milanfranchi et al., 1997196 | No | No | |
| Montgomery et al., 1993197 | Yes | LOCF | Yes |
| Montgomery et al., 2001198 | Yes | LOCF | Yes |
| Mundo et al., 1997199 | No | Yes | |
| Mundo et al., 2001200 | Yes | LOCF | Yes |
| Nakajima et al., 1996201 | Yes | LOCF | Yes |
| Nakatani et al., 2005202 | No | No | |
| Neziroglu et al., 2000229 | NA | NA | Yes |
| O’Connor et al., 1999203 | No | No | |
| O’Connor et al., 2006204 | No | No | |
| Perse et al., 1987205 | No | No | |
| Piacentini et al., 2011230 | Yes | LOCF | Yes |
| Riddle et al., 1992231 | Yes | LOCF | Yes |
| Riddle et al., 2001232 | Yes | LOCF | Yes |
| Shareh et al., 2010206 | No | No | |
| Sousa et al., 2006207 | NA | NA | NA |
| Stein et al., 2007124 | Yes | LOCF | Yes |
| Storch et al., 2011233 | Yes | LOCF | Yes |
| Storch et al., 2013234 | Yes | MLE | Yes |
| The Pediatric OCD Treatment Study, 2004236 | Yes | LOCF | Yes |
| Thoren et al., 1980208 | No | No | |
| Tollefson et al., 1994127 | No | No | |
| Van Oppen et al., 1995209 | No | No | |
| Volavka et al., 1985210 | No | No | |
| Whittal et al., 2005211 | No | No | |
| Whittal et al., 2010212 | No | No | |
| Williams et al., 2010235 | Yes | LOCF | Yes |
| Zohar and Judge, 1996213 | Yes | LOCF | Yes |
Appendix 8 Detailed results of network meta-analysis
Adult subset: clinical effectiveness (Yale–Brown Obsessive–Compulsive Scale)
Network geometry
FIGURE 26.
Network plot for class effects (the plot for individual effects is included in the main report). BTCLO, BT + clomipramine; CBTFLV, CBT + fluvoxamine; CLO, clomipramine; HYP, hypericum; PL, placebo; PSYPL, psychological placebo; VEN, venlafaxine; WL, waitlist.
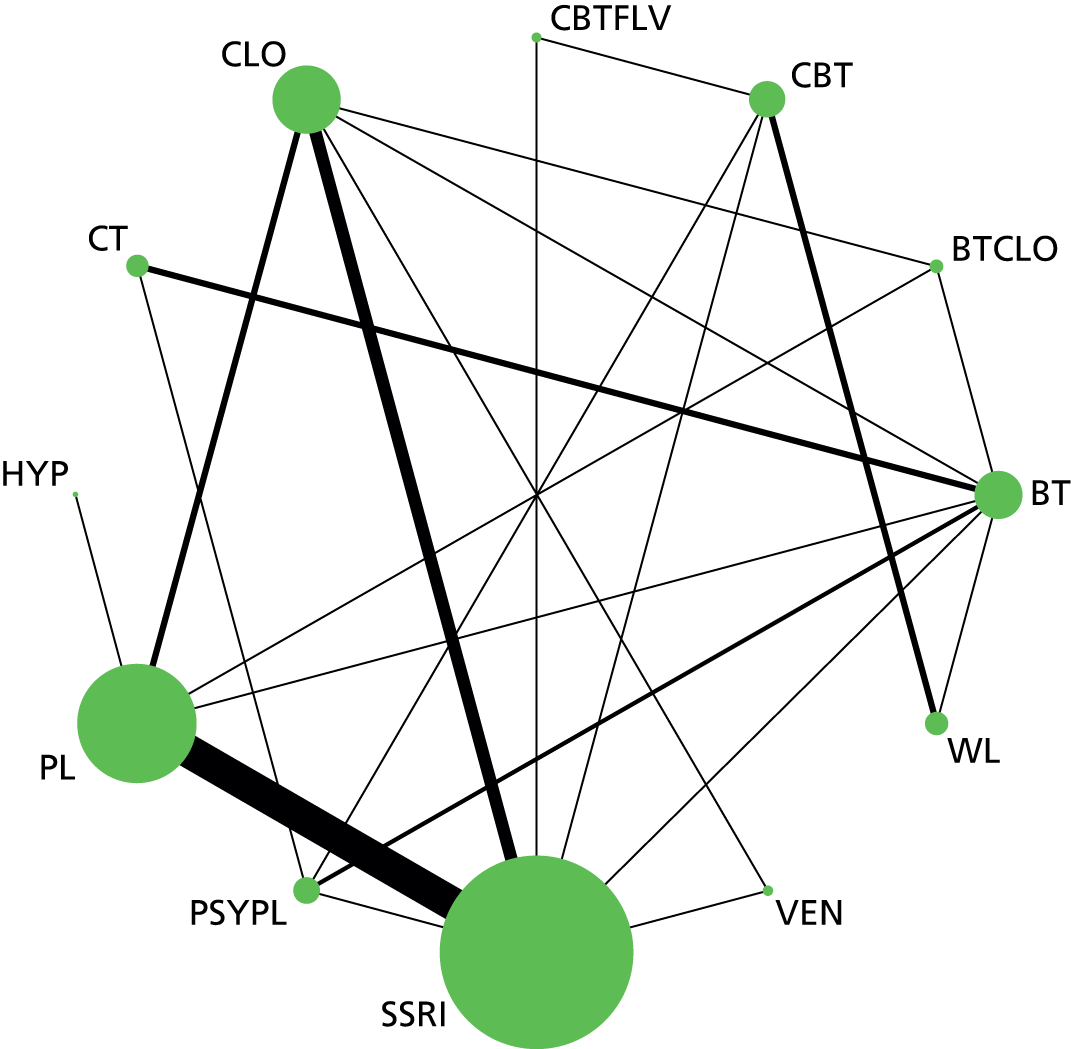
| Model fit | ||||||||
|---|---|---|---|---|---|---|---|---|
| Dbar | Dhat | DIC | pD | |||||
| mu.sd | 2.773 | 2.773 | 2.773 | 4.24 × 10–12 | ||||
| sd1 | 386.1 | 382.1 | 390.2 | 4.046 | ||||
| y | 370.1 | 259.4 | 480.8 | 110.7 | ||||
| total | 759 | 644.2 | 873.7 | 114.7 | ||||
| Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample | |
| sdev | 3.128 | 0.3794 | 0.002615 | 2.462 | 3.102 | 3.95 | 50,001 | 100,000 |
| totresdev | 104.6 | 14.35 | 0.06465 | 78.34 | 103.9 | 134.6 | 50,001 | 100,000 |
| Model fit | ||||||||
|---|---|---|---|---|---|---|---|---|
| Dbar | Dhat | DIC | pD | |||||
| mu.sd | 2.773 | 2.773 | 2.773 | 5.16 × 10–12 | ||||
| sd1 | 386.1 | 382.1 | 390.2 | 4.054 | ||||
| y | 370.8 | 262.6 | 479.1 | 108.3 | ||||
| total | 759.8 | 647.4 | 872.1 | 112.3 | ||||
| Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample | |
| sdev | 1.78 | 0.3462 | 0.003119 | 1.18 | 1.755 | 2.534 | 60,001 | 120,000 |
| totresdev | 105.8 | 14.46 | 0.06664 | 79.48 | 105.2 | 135.8 | 60,001 | 120,000 |
Data synthesis: consistency model (network meta-analysis)
Key: intervention (class)
-
Placebo (1).
-
Waitlist (2).
-
Fluoxetine (3).
-
Fluvoxamine (3).
-
Paroxetine (3).
-
Sertraline (3).
-
Citalopram (3).
-
Venlafaxine (4).
-
Clomipramine (5).
-
BT (6).
-
CBT (7).
-
CT (8).
-
Hypericum (9).
-
Fluvoxamine + CBT (10).
-
BT+ clomipramine (11).
-
Escitalopram (3).
-
Psychological placebo (12).
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| class.mean.diff[1,2] | 5.62 | 2.378 | 0.02451 | 0.9106 | 5.635 | 10.26 | 50,001 | 100,000 |
| class.mean.diff[1,3] | –3.493 | 0.8465 | 0.0126 | –5.116 | –3.503 | –1.814 | 50,001 | 100,000 |
| class.mean.diff[1,4] | –3.217 | 2.577 | 0.01525 | –8.262 | –3.225 | 1.885 | 50,001 | 100,000 |
| class.mean.diff[1,5] | –4.724 | 1.078 | 0.009793 | –6.851 | –4.728 | –2.601 | 50,001 | 100,000 |
| class.mean.diff[1,6] | –14.48 | 2.131 | 0.02531 | –18.61 | –14.51 | –10.23 | 50,001 | 100,000 |
| class.mean.diff[1,7] | –5.374 | 1.898 | 0.02087 | –9.098 | –5.377 | –1.632 | 50,001 | 100,000 |
| class.mean.diff[1,8] | –13.36 | 2.59 | 0.02797 | –18.4 | –13.39 | –8.21 | 50,001 | 100,000 |
| class.mean.diff[1,9] | –0.1555 | 3.716 | 0.01768 | –7.456 | –0.1629 | 7.124 | 50,001 | 100,000 |
| class.mean.diff[1,10] | –7.521 | 3.222 | 0.02186 | –13.89 | –7.517 | –1.173 | 50,001 | 100,000 |
| class.mean.diff[1,11] | –12.97 | 3.165 | 0.01717 | –19.18 | –12.97 | –6.738 | 50,001 | 100,000 |
| class.mean.diff[1,12] | –4.147 | 2.324 | 0.02623 | –8.649 | –4.171 | 0.4895 | 50,001 | 100,000 |
| class.mean.diff[2,3] | –9.114 | 2.349 | 0.02079 | –13.67 | –9.133 | –4.459 | 50,001 | 100,000 |
| class.mean.diff[2,4] | –8.838 | 3.395 | 0.02372 | –15.47 | –8.856 | –2.141 | 50,001 | 100,000 |
| class.mean.diff[2,5] | –10.34 | 2.462 | 0.02028 | –15.14 | –10.36 | –5.475 | 50,001 | 100,000 |
| class.mean.diff[2,6] | –20.1 | 2.272 | 0.01427 | –24.52 | –20.13 | –15.55 | 50,001 | 100,000 |
| class.mean.diff[2,7] | –10.99 | 1.715 | 0.008719 | –14.31 | –11.01 | –7.601 | 50,001 | 100,000 |
| class.mean.diff[2,8] | –18.98 | 2.694 | 0.01744 | –24.21 | –19 | –13.62 | 50,001 | 100,000 |
| class.mean.diff[2,9] | –5.776 | 4.413 | 0.0298 | –14.44 | –5.784 | 2.911 | 50,001 | 100,000 |
| class.mean.diff[2,10] | –13.14 | 3.501 | 0.01671 | –19.98 | –13.15 | –6.262 | 50,001 | 100,000 |
| class.mean.diff[2,11] | –18.59 | 3.719 | 0.02054 | –25.88 | –18.6 | –11.23 | 50,001 | 100,000 |
| class.mean.diff[2,12] | –9.768 | 2.455 | 0.01473 | –14.51 | –9.796 | –4.857 | 50,001 | 100,000 |
| class.mean.diff[3,4] | 0.2759 | 2.553 | 0.01126 | –4.731 | 0.2721 | 5.325 | 50,001 | 100,000 |
| class.mean.diff[3,5] | –1.231 | 1.109 | 0.00638 | –3.408 | –1.231 | 0.9418 | 50,001 | 100,000 |
| class.mean.diff[3,6] | –10.99 | 2.129 | 0.02277 | –15.14 | –11.01 | –6.752 | 50,001 | 100,000 |
| class.mean.diff[3,7] | –1.88 | 1.85 | 0.01643 | –5.517 | –1.878 | 1.763 | 50,001 | 100,000 |
| class.mean.diff[3,8] | –9.866 | 2.587 | 0.02559 | –14.91 | –9.878 | –4.739 | 50,001 | 100,000 |
| class.mean.diff[3,9] | 3.338 | 3.815 | 0.02117 | –4.134 | 3.339 | 10.82 | 50,001 | 100,000 |
| class.mean.diff[3,10] | –4.028 | 3.19 | 0.01734 | –10.36 | –4.016 | 2.212 | 50,001 | 100,000 |
| class.mean.diff[3,11] | –9.476 | 3.211 | 0.01784 | –15.78 | –9.473 | –3.137 | 50,001 | 100,000 |
| class.mean.diff[3,12] | –0.6541 | 2.312 | 0.02379 | –5.139 | –0.6794 | 3.949 | 50,001 | 100,000 |
| class.mean.diff[4,5] | –1.507 | 2.519 | 0.01091 | –6.501 | –1.502 | 3.436 | 50,001 | 100,000 |
| class.mean.diff[4,6] | –11.26 | 3.229 | 0.02526 | –17.57 | –11.29 | –4.862 | 50,001 | 100,000 |
| class.mean.diff[4,7] | –2.156 | 3.074 | 0.0198 | –8.191 | –2.164 | 3.879 | 50,001 | 100,000 |
| class.mean.diff[4,8] | –10.14 | 3.547 | 0.02778 | –17.08 | –10.16 | –3.114 | 50,001 | 100,000 |
| class.mean.diff[4,9] | 3.062 | 4.517 | 0.02292 | –5.836 | 3.084 | 11.9 | 50,001 | 100,000 |
| class.mean.diff[4,10] | –4.304 | 4.033 | 0.02118 | –12.26 | –4.292 | 3.584 | 50,001 | 100,000 |
| class.mean.diff[4,11] | –9.752 | 3.988 | 0.01997 | –17.62 | –9.746 | –1.905 | 50,001 | 100,000 |
| class.mean.diff[4,12] | –0.93 | 3.354 | 0.02612 | –7.449 | –0.9471 | 5.711 | 50,001 | 100,000 |
| class.mean.diff[5,6] | –9.756 | 2.191 | 0.02149 | –14.02 | –9.771 | –5.404 | 50,001 | 100,000 |
| class.mean.diff[5,7] | –0.6494 | 2.008 | 0.016 | –4.604 | –0.642 | 3.293 | 50,001 | 100,000 |
| class.mean.diff[5,8] | –8.635 | 2.638 | 0.02443 | –13.79 | –8.651 | –3.385 | 50,001 | 100,000 |
| class.mean.diff[5,9] | 4.569 | 3.876 | 0.02024 | –3.072 | 4.582 | 12.15 | 50,001 | 100,000 |
| class.mean.diff[5,10] | –2.797 | 3.291 | 0.01753 | –9.323 | –2.794 | 3.677 | 50,001 | 100,000 |
| class.mean.diff[5,11] | –8.245 | 3.177 | 0.01566 | –14.48 | –8.238 | –1.984 | 50,001 | 100,000 |
| class.mean.diff[5,12] | 0.577 | 2.384 | 0.02248 | –4.048 | 0.559 | 5.333 | 50,001 | 100,000 |
| class.mean.diff[6,7] | 9.106 | 2.089 | 0.01435 | 4.97 | 9.109 | 13.18 | 50,001 | 100,000 |
| class.mean.diff[6,8] | 1.12 | 1.561 | 0.008178 | –1.955 | 1.122 | 4.192 | 50,001 | 100,000 |
| class.mean.diff[6,9] | 14.32 | 4.282 | 0.03056 | 5.879 | 14.34 | 22.7 | 50,001 | 100,000 |
| class.mean.diff[6,10] | 6.959 | 3.54 | 0.0212 | –0.04063 | 6.976 | 13.87 | 50,001 | 100,000 |
| class.mean.diff[6,11] | 1.511 | 3.379 | 0.01985 | –5.158 | 1.517 | 8.135 | 50,001 | 100,000 |
| class.mean.diff[6,12] | 10.33 | 1.547 | 0.006452 | 7.289 | 10.33 | 13.38 | 50,001 | 100,000 |
| class.mean.diff[7,8] | –7.986 | 2.532 | 0.01758 | –12.97 | –7.981 | –3.008 | 50,001 | 100,000 |
| class.mean.diff[7,9] | 5.218 | 4.167 | 0.02699 | –2.976 | 5.23 | 13.37 | 50,001 | 100,000 |
| class.mean.diff[7,10] | –2.147 | 3.121 | 0.01332 | –8.307 | –2.136 | 3.987 | 50,001 | 100,000 |
| class.mean.diff[7,11] | –7.596 | 3.495 | 0.01823 | –14.46 | –7.606 | –0.7485 | 50,001 | 100,000 |
| class.mean.diff[7,12] | 1.226 | 2.173 | 0.01469 | –3.029 | 1.22 | 5.541 | 50,001 | 100,000 |
| class.mean.diff[8,9] | 13.2 | 4.535 | 0.03276 | 4.261 | 13.19 | 22.11 | 50,001 | 100,000 |
| class.mean.diff[8,10] | 5.838 | 3.814 | 0.02375 | –1.666 | 5.839 | 13.33 | 50,001 | 100,000 |
| class.mean.diff[8,11] | 0.3902 | 3.698 | 0.02294 | –6.854 | 0.3933 | 7.678 | 50,001 | 100,000 |
| class.mean.diff[8,12] | 9.212 | 1.973 | 0.009613 | 5.341 | 9.213 | 13.1 | 50,001 | 100,000 |
| class.mean.diff[9,10] | –7.366 | 4.933 | 0.02833 | –17.08 | –7.357 | 2.351 | 50,001 | 100,000 |
| class.mean.diff[9,11] | –12.81 | 4.871 | 0.02431 | –22.35 | –12.81 | –3.281 | 50,001 | 100,000 |
| class.mean.diff[9,12] | –3.992 | 4.379 | 0.03134 | –12.55 | –3.996 | 4.653 | 50,001 | 100,000 |
| class.mean.diff[10,11] | –5.448 | 4.415 | 0.02175 | –14.08 | –5.445 | 3.286 | 50,001 | 100,000 |
| class.mean.diff[10,12] | 3.374 | 3.619 | 0.02194 | –3.661 | 3.354 | 10.53 | 50,001 | 100,000 |
| class.mean.diff[11,12] | 8.822 | 3.563 | 0.02118 | 1.849 | 8.797 | 15.84 | 50,001 | 100,000 |
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| treat.mean.diff[1,2] | 5.62 | 2.378 | 0.02451 | 0.9106 | 5.635 | 10.26 | 50,001 | 100,000 |
| treat.mean.diff[1,3] | –3.463 | 0.9264 | 0.01216 | –5.268 | –3.478 | –1.584 | 50,001 | 100,000 |
| treat.mean.diff[1,4] | –3.604 | 0.8429 | 0.01194 | –5.292 | –3.594 | –1.947 | 50,001 | 100,000 |
| treat.mean.diff[1,5] | –3.416 | 0.878 | 0.01195 | –5.105 | –3.431 | –1.611 | 50,001 | 100,000 |
| treat.mean.diff[1,6] | –3.498 | 0.9257 | 0.0124 | –5.304 | –3.506 | –1.628 | 50,001 | 100,000 |
| treat.mean.diff[1,7] | –3.488 | 1.065 | 0.01272 | –5.622 | –3.498 | –1.309 | 50,001 | 100,000 |
| treat.mean.diff[1,8] | –3.217 | 2.577 | 0.01525 | –8.262 | –3.225 | 1.885 | 50,001 | 100,000 |
| treat.mean.diff[1,9] | –4.724 | 1.078 | 0.009793 | –6.851 | –4.728 | –2.601 | 50,001 | 100,000 |
| treat.mean.diff[1,10] | –14.48 | 2.131 | 0.02531 | –18.61 | –14.51 | –10.23 | 50,001 | 100,000 |
| treat.mean.diff[1,11] | –5.374 | 1.898 | 0.02087 | –9.098 | –5.377 | –1.632 | 50,001 | 100,000 |
| treat.mean.diff[1,12] | –13.36 | 2.59 | 0.02797 | –18.4 | –13.39 | –8.21 | 50,001 | 100,000 |
| treat.mean.diff[1,13] | –0.1555 | 3.716 | 0.01768 | –7.456 | –0.1629 | 7.124 | 50,001 | 100,000 |
| treat.mean.diff[1,14] | –7.521 | 3.222 | 0.02186 | –13.89 | –7.517 | –1.173 | 50,001 | 100,000 |
| treat.mean.diff[1,15] | –12.97 | 3.165 | 0.01717 | –19.18 | –12.97 | –6.738 | 50,001 | 100,000 |
| treat.mean.diff[1,16] | –3.483 | 1.088 | 0.01272 | –5.611 | –3.498 | –1.234 | 50,001 | 100,000 |
| treat.mean.diff[1,17] | –4.147 | 2.324 | 0.02623 | –8.649 | –4.171 | 0.4895 | 50,001 | 100,000 |
| treat.mean.diff[2,3] | –9.083 | 2.36 | 0.02061 | –13.68 | –9.102 | –4.405 | 50,001 | 100,000 |
| treat.mean.diff[2,4] | –9.225 | 2.329 | 0.02016 | –13.77 | –9.237 | –4.628 | 50,001 | 100,000 |
| treat.mean.diff[2,5] | –9.036 | 2.384 | 0.02101 | –13.68 | –9.06 | –4.306 | 50,001 | 100,000 |
| treat.mean.diff[2,6] | –9.118 | 2.358 | 0.02042 | –13.73 | –9.134 | –4.45 | 50,001 | 100,000 |
| treat.mean.diff[2,7] | –9.108 | 2.451 | 0.0212 | –13.89 | –9.127 | –4.253 | 50,001 | 100,000 |
| treat.mean.diff[2,8] | –8.838 | 3.395 | 0.02372 | –15.47 | –8.856 | –2.141 | 50,001 | 100,000 |
| treat.mean.diff[2,9] | –10.34 | 2.462 | 0.02028 | –15.14 | –10.36 | –5.475 | 50,001 | 100,000 |
| treat.mean.diff[2,10] | –20.1 | 2.272 | 0.01427 | –24.52 | –20.13 | –15.55 | 50,001 | 100,000 |
| treat.mean.diff[2,11] | –10.99 | 1.715 | 0.008719 | –14.31 | –11.01 | –7.601 | 50,001 | 100,000 |
| treat.mean.diff[2,12] | –18.98 | 2.694 | 0.01744 | –24.21 | –19 | –13.62 | 50,001 | 100,000 |
| treat.mean.diff[2,13] | –5.776 | 4.413 | 0.0298 | –14.44 | –5.784 | 2.911 | 50,001 | 100,000 |
| treat.mean.diff[2,14] | –13.14 | 3.501 | 0.01671 | –19.98 | –13.15 | –6.262 | 50,001 | 100,000 |
| treat.mean.diff[2,15] | –18.59 | 3.719 | 0.02054 | –25.88 | –18.6 | –11.23 | 50,001 | 100,000 |
| treat.mean.diff[2,16] | –9.103 | 2.457 | 0.02115 | –13.9 | –9.118 | –4.223 | 50,001 | 100,000 |
| treat.mean.diff[2,17] | –9.768 | 2.455 | 0.01473 | –14.51 | –9.796 | –4.857 | 50,001 | 100,000 |
| treat.mean.diff[3,4] | –0.1412 | 0.8752 | 0.004168 | –2.196 | –0.04312 | 1.62 | 50,001 | 100,000 |
| treat.mean.diff[3,5] | 0.04729 | 0.8874 | 0.003442 | –1.843 | 0.009691 | 2.033 | 50,001 | 100,000 |
| treat.mean.diff[3,6] | –0.03457 | 0.8854 | 0.00315 | –2.019 | –0.00726 | 1.857 | 50,001 | 100,000 |
| treat.mean.diff[3,7] | –0.02461 | 1.042 | 0.004036 | –2.315 | –0.00442 | 2.256 | 50,001 | 100,000 |
| treat.mean.diff[3,8] | 0.2457 | 2.602 | 0.01119 | –4.871 | 0.2425 | 5.377 | 50,001 | 100,000 |
| treat.mean.diff[3,9] | –1.261 | 1.182 | 0.006338 | –3.63 | –1.254 | 1.055 | 50,001 | 100,000 |
| treat.mean.diff[3,10] | –11.02 | 2.155 | 0.0226 | –15.23 | –11.04 | –6.742 | 50,001 | 100,000 |
| treat.mean.diff[3,11] | –1.911 | 1.853 | 0.01622 | –5.549 | –1.902 | 1.728 | 50,001 | 100,000 |
| treat.mean.diff[3,12] | –9.896 | 2.606 | 0.02546 | –14.98 | –9.912 | –4.757 | 50,001 | 100,000 |
| treat.mean.diff[3,13] | 3.308 | 3.832 | 0.02092 | –4.217 | 3.312 | 10.81 | 50,001 | 100,000 |
| treat.mean.diff[3,14] | –4.058 | 3.21 | 0.01732 | –10.43 | –4.039 | 2.225 | 50,001 | 100,000 |
| treat.mean.diff[3,15] | –9.506 | 3.231 | 0.01754 | –15.86 | –9.5 | –3.137 | 50,001 | 100,000 |
| treat.mean.diff[3,16] | –0.01967 | 1.048 | 0.003805 | –2.314 | –0.0041 | 2.276 | 50,001 | 100,000 |
| treat.mean.diff[3,17] | –0.6843 | 2.33 | 0.02355 | –5.218 | –0.7018 | 3.94 | 50,001 | 100,000 |
| treat.mean.diff[4,5] | 0.1885 | 0.8269 | 0.004488 | –1.409 | 0.06661 | 2.146 | 50,001 | 100,000 |
| treat.mean.diff[4,6] | 0.1066 | 0.8689 | 0.003919 | –1.676 | 0.02994 | 2.116 | 50,001 | 100,000 |
| treat.mean.diff[4,7] | 0.1166 | 0.9929 | 0.004682 | –1.94 | 0.03256 | 2.417 | 50,001 | 100,000 |
| treat.mean.diff[4,8] | 0.3869 | 2.571 | 0.0118 | –4.653 | 0.377 | 5.462 | 50,001 | 100,000 |
| treat.mean.diff[4,9] | –1.12 | 1.083 | 0.005907 | –3.24 | –1.131 | 1.036 | 50,001 | 100,000 |
| treat.mean.diff[4,10] | –10.88 | 2.099 | 0.02222 | –14.96 | –10.91 | –6.69 | 50,001 | 100,000 |
| treat.mean.diff[4,11] | –1.769 | 1.831 | 0.01591 | –5.365 | –1.776 | 1.866 | 50,001 | 100,000 |
| treat.mean.diff[4,12] | –9.755 | 2.557 | 0.0251 | –14.73 | –9.778 | –4.697 | 50,001 | 100,000 |
| treat.mean.diff[4,13] | 3.449 | 3.816 | 0.02111 | –4.032 | 3.454 | 10.95 | 50,001 | 100,000 |
| treat.mean.diff[4,14] | –3.917 | 3.147 | 0.01687 | –10.14 | –3.912 | 2.281 | 50,001 | 100,000 |
| treat.mean.diff[4,15] | –9.365 | 3.198 | 0.01756 | –15.62 | –9.371 | –3.02 | 50,001 | 100,000 |
| treat.mean.diff[4,16] | 0.1215 | 1.012 | 0.004475 | –1.937 | 0.02962 | 2.493 | 50,001 | 100,000 |
| treat.mean.diff[4,17] | –0.5431 | 2.283 | 0.02332 | –4.964 | –0.566 | 4.005 | 50,001 | 100,000 |
| treat.mean.diff[5,6] | –0.08186 | 0.8859 | 0.003587 | –2.096 | –0.0227 | 1.769 | 50,001 | 100,000 |
| treat.mean.diff[5,7] | –0.0719 | 0.9897 | 0.004086 | –2.309 | –0.01626 | 2.029 | 50,001 | 100,000 |
| treat.mean.diff[5,8] | 0.1984 | 2.501 | 0.01046 | –4.704 | 0.1935 | 5.125 | 50,001 | 100,000 |
| treat.mean.diff[5,9] | –1.309 | 1.101 | 0.005826 | –3.508 | –1.304 | 0.848 | 50,001 | 100,000 |
| treat.mean.diff[5,10] | –11.06 | 2.156 | 0.023 | –15.27 | –11.08 | –6.784 | 50,001 | 100,000 |
| treat.mean.diff[5,11] | –1.958 | 1.898 | 0.0166 | –5.704 | –1.955 | 1.762 | 50,001 | 100,000 |
| treat.mean.diff[5,12] | –9.944 | 2.61 | 0.02578 | –15.06 | –9.961 | –4.784 | 50,001 | 100,000 |
| treat.mean.diff[5,13] | 3.26 | 3.821 | 0.02081 | –4.243 | 3.263 | 10.76 | 50,001 | 100,000 |
| treat.mean.diff[5,14] | –4.105 | 3.218 | 0.0176 | –10.49 | –4.092 | 2.212 | 50,001 | 100,000 |
| treat.mean.diff[5,15] | –9.554 | 3.214 | 0.01765 | –15.88 | –9.547 | –3.232 | 50,001 | 100,000 |
| treat.mean.diff[5,16] | –0.06696 | 0.9761 | 0.003684 | –2.261 | –0.01811 | 2.024 | 50,001 | 100,000 |
| treat.mean.diff[5,17] | –0.7316 | 2.342 | 0.02399 | –5.301 | –0.7494 | 3.927 | 50,001 | 100,000 |
| treat.mean.diff[6,7] | 0.009959 | 1.039 | 0.003995 | –2.271 | 0.001729 | 2.285 | 50,001 | 100,000 |
| treat.mean.diff[6,8] | 0.2803 | 2.596 | 0.01146 | –4.789 | 0.2729 | 5.417 | 50,001 | 100,000 |
| treat.mean.diff[6,9] | –1.227 | 1.173 | 0.006392 | –3.552 | –1.224 | 1.095 | 50,001 | 100,000 |
| treat.mean.diff[6,10] | –10.98 | 2.153 | 0.02246 | –15.16 | –11.01 | –6.708 | 50,001 | 100,000 |
| treat.mean.diff[6,11] | –1.876 | 1.859 | 0.01605 | –5.532 | –1.881 | 1.798 | 50,001 | 100,000 |
| treat.mean.diff[6,12] | –9.862 | 2.604 | 0.0253 | –14.93 | –9.871 | –4.706 | 50,001 | 100,000 |
| treat.mean.diff[6,13] | 3.342 | 3.835 | 0.02118 | –4.181 | 3.344 | 10.86 | 50,001 | 100,000 |
| treat.mean.diff[6,14] | –4.023 | 3.209 | 0.01722 | –10.39 | –4.009 | 2.274 | 50,001 | 100,000 |
| treat.mean.diff[6,15] | –9.472 | 3.23 | 0.01747 | –15.82 | –9.468 | –3.113 | 50,001 | 100,000 |
| treat.mean.diff[6,16] | 0.0149 | 1.044 | 0.003616 | –2.26 | 0.001961 | 2.338 | 50,001 | 100,000 |
| treat.mean.diff[6,17] | –0.6497 | 2.333 | 0.02343 | –5.19 | –0.6678 | 3.987 | 50,001 | 100,000 |
| treat.mean.diff[7,8] | 0.2703 | 2.644 | 0.01148 | –4.932 | 0.262 | 5.48 | 50,001 | 100,000 |
| treat.mean.diff[7,9] | –1.237 | 1.304 | 0.007012 | –3.847 | –1.229 | 1.338 | 50,001 | 100,000 |
| treat.mean.diff[7,10] | –10.99 | 2.24 | 0.0231 | –15.36 | –11.01 | –6.56 | 50,001 | 100,000 |
| treat.mean.diff[7,11] | –1.886 | 1.982 | 0.01693 | –5.806 | –1.884 | 2.029 | 50,001 | 100,000 |
| treat.mean.diff[7,12] | –9.872 | 2.677 | 0.02598 | –15.12 | –9.893 | –4.573 | 50,001 | 100,000 |
| treat.mean.diff[7,13] | 3.332 | 3.87 | 0.02124 | –4.254 | 3.332 | 10.93 | 50,001 | 100,000 |
| treat.mean.diff[7,14] | –4.033 | 3.265 | 0.01785 | –10.52 | –4.013 | 2.361 | 50,001 | 100,000 |
| treat.mean.diff[7,15] | –9.482 | 3.281 | 0.01792 | –15.91 | –9.484 | –3.001 | 50,001 | 100,000 |
| treat.mean.diff[7,16] | 0.004941 | 1.13 | 0.003898 | –2.469 | –3.77 × 10–4 | 2.509 | 50,001 | 100,000 |
| treat.mean.diff[7,17] | –0.6597 | 2.418 | 0.02409 | –5.361 | –0.6761 | 4.163 | 50,001 | 100,000 |
| treat.mean.diff[8,9] | –1.507 | 2.519 | 0.01091 | –6.501 | –1.502 | 3.436 | 50,001 | 100,000 |
| treat.mean.diff[8,10] | –11.26 | 3.229 | 0.02526 | –17.57 | –11.29 | –4.862 | 50,001 | 100,000 |
| treat.mean.diff[8,11] | –2.156 | 3.074 | 0.0198 | –8.191 | –2.164 | 3.879 | 50,001 | 100,000 |
| treat.mean.diff[8,12] | –10.14 | 3.547 | 0.02778 | –17.08 | –10.16 | –3.114 | 50,001 | 100,000 |
| treat.mean.diff[8,13] | 3.062 | 4.517 | 0.02292 | –5.836 | 3.084 | 11.9 | 50,001 | 100,000 |
| treat.mean.diff[8,14] | –4.304 | 4.033 | 0.02118 | –12.26 | –4.292 | 3.584 | 50,001 | 100,000 |
| treat.mean.diff[8,15] | –9.752 | 3.988 | 0.01997 | –17.62 | –9.746 | –1.905 | 50,001 | 100,000 |
| treat.mean.diff[8,16] | –0.2654 | 2.646 | 0.0116 | –5.501 | –0.2571 | 4.944 | 50,001 | 100,000 |
| treat.mean.diff[8,17] | –0.93 | 3.354 | 0.02612 | –7.449 | –0.9471 | 5.711 | 50,001 | 100,000 |
| treat.mean.diff[9,10] | –9.756 | 2.191 | 0.02149 | –14.02 | –9.771 | –5.404 | 50,001 | 100,000 |
| treat.mean.diff[9,11] | –0.6494 | 2.008 | 0.016 | –4.604 | –0.642 | 3.293 | 50,001 | 100,000 |
| treat.mean.diff[9,12] | –8.635 | 2.638 | 0.02443 | –13.79 | –8.651 | –3.385 | 50,001 | 100,000 |
| treat.mean.diff[9,13] | 4.569 | 3.876 | 0.02024 | –3.072 | 4.582 | 12.15 | 50,001 | 100,000 |
| treat.mean.diff[9,14] | –2.797 | 3.291 | 0.01753 | –9.323 | –2.794 | 3.677 | 50,001 | 100,000 |
| treat.mean.diff[9,15] | –8.245 | 3.177 | 0.01566 | –14.48 | –8.238 | –1.984 | 50,001 | 100,000 |
| treat.mean.diff[9,16] | 1.242 | 1.316 | 0.006932 | –1.352 | 1.236 | 3.89 | 50,001 | 100,000 |
| treat.mean.diff[9,17] | 0.577 | 2.384 | 0.02248 | –4.048 | 0.559 | 5.333 | 50,001 | 100,000 |
| treat.mean.diff[10,11] | 9.106 | 2.089 | 0.01435 | 4.97 | 9.109 | 13.18 | 50,001 | 100,000 |
| treat.mean.diff[10,12] | 1.12 | 1.561 | 0.008178 | –1.955 | 1.122 | 4.192 | 50,001 | 100,000 |
| treat.mean.diff[10,13] | 14.32 | 4.282 | 0.03056 | 5.879 | 14.34 | 22.7 | 50,001 | 100,000 |
| treat.mean.diff[10,14] | 6.959 | 3.54 | 0.0212 | –0.04063 | 6.976 | 13.87 | 50,001 | 100,000 |
| treat.mean.diff[10,15] | 1.511 | 3.379 | 0.01985 | –5.158 | 1.517 | 8.135 | 50,001 | 100,000 |
| treat.mean.diff[10,16] | 11 | 2.241 | 0.02308 | 6.548 | 11.01 | 15.4 | 50,001 | 100,000 |
| treat.mean.diff[10,17] | 10.33 | 1.547 | 0.006452 | 7.289 | 10.33 | 13.38 | 50,001 | 100,000 |
| treat.mean.diff[11,12] | –7.986 | 2.532 | 0.01758 | –12.97 | –7.981 | –3.008 | 50,001 | 100,000 |
| treat.mean.diff[11,13] | 5.218 | 4.167 | 0.02699 | –2.976 | 5.23 | 13.37 | 50,001 | 100,000 |
| treat.mean.diff[11,14] | –2.147 | 3.121 | 0.01332 | –8.307 | –2.136 | 3.987 | 50,001 | 100,000 |
| treat.mean.diff[11,15] | –7.596 | 3.495 | 0.01823 | –14.46 | –7.606 | –0.7485 | 50,001 | 100,000 |
| treat.mean.diff[11,16] | 1.891 | 1.985 | 0.0168 | –2.03 | 1.891 | 5.813 | 50,001 | 100,000 |
| treat.mean.diff[11,17] | 1.226 | 2.173 | 0.01469 | –3.029 | 1.22 | 5.541 | 50,001 | 100,000 |
| treat.mean.diff[12,13] | 13.2 | 4.535 | 0.03276 | 4.261 | 13.19 | 22.11 | 50,001 | 100,000 |
| treat.mean.diff[12,14] | 5.838 | 3.814 | 0.02375 | –1.666 | 5.839 | 13.33 | 50,001 | 100,000 |
| treat.mean.diff[12,15] | 0.3902 | 3.698 | 0.02294 | –6.854 | 0.3933 | 7.678 | 50,001 | 100,000 |
| treat.mean.diff[12,16] | 9.877 | 2.678 | 0.02587 | 4.591 | 9.889 | 15.14 | 50,001 | 100,000 |
| treat.mean.diff[12,17] | 9.212 | 1.973 | 0.009613 | 5.341 | 9.213 | 13.1 | 50,001 | 100,000 |
| treat.mean.diff[13,14] | –7.366 | 4.933 | 0.02833 | –17.08 | –7.357 | 2.351 | 50,001 | 100,000 |
| treat.mean.diff[13,15] | –12.81 | 4.871 | 0.02431 | –22.35 | –12.81 | –3.281 | 50,001 | 100,000 |
| treat.mean.diff[13,16] | –3.327 | 3.874 | 0.02134 | –10.94 | –3.331 | 4.227 | 50,001 | 100,000 |
| treat.mean.diff[13,17] | –3.992 | 4.379 | 0.03134 | –12.55 | –3.996 | 4.653 | 50,001 | 100,000 |
| treat.mean.diff[14,15] | –5.448 | 4.415 | 0.02175 | –14.08 | –5.445 | 3.286 | 50,001 | 100,000 |
| treat.mean.diff[14,16] | 4.038 | 3.274 | 0.01775 | –2.386 | 4.023 | 10.51 | 50,001 | 100,000 |
| treat.mean.diff[14,17] | 3.374 | 3.619 | 0.02194 | –3.661 | 3.354 | 10.53 | 50,001 | 100,000 |
| treat.mean.diff[15,16] | 9.487 | 3.285 | 0.01803 | 3.003 | 9.481 | 15.93 | 50,001 | 100,000 |
| treat.mean.diff[15,17] | 8.822 | 3.563 | 0.02118 | 1.849 | 8.797 | 15.84 | 50,001 | 100,000 |
| treat.mean.diff[16,17] | –0.6646 | 2.418 | 0.0241 | –5.384 | –0.6767 | 4.141 | 50,001 | 100,000 |
| d | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| d[1,3] | –2.656 | 1.064 | 0.006615 | –4.722 | –2.666 | –0.5367 | 60,001 | 120,000 |
| d[1,4] | –3.577 | 0.9644 | 0.005258 | –5.513 | –3.566 | –1.704 | 60,001 | 120,000 |
| d[1,5] | –2.839 | 0.8353 | 0.004452 | –4.48 | –2.844 | –1.174 | 60,001 | 120,000 |
| d[1,6] | –2.85 | 1.188 | 0.006132 | –5.182 | –2.854 | –0.503 | 60,001 | 120,000 |
| d[1,7] | –3.653 | 1.32 | 0.008286 | –6.255 | –3.651 | –1.056 | 60,001 | 120,000 |
| d[1,9] | –6.278 | 0.9656 | 0.004634 | –8.154 | –6.291 | –4.34 | 60,001 | 120,000 |
| d[1,10] | –11.76 | 2.598 | 0.0167 | –16.87 | –11.77 | –6.617 | 60,001 | 120,000 |
| d[1,13] | –0.0795 | 2.658 | 0.01658 | –5.297 | –0.08029 | 5.112 | 60,001 | 120,000 |
| d[1,15] | –12.25 | 2.599 | 0.01664 | –17.29 | –12.26 | –7.094 | 60,001 | 120,000 |
| d[1,16] | –3.281 | 1.563 | 0.008429 | –6.38 | –3.275 | –0.1997 | 60,001 | 120,000 |
| d[2,10] | –30.86 | 1.945 | 0.00709 | –34.72 | –30.86 | –27 | 60,001 | 120,000 |
| d[2,11] | –7.392 | 1.452 | 0.0107 | –10.25 | –7.395 | –4.542 | 60,001 | 120,000 |
| d[3,6] | 0.1054 | 2.22 | 0.009702 | –4.27 | 0.106 | 4.466 | 60,001 | 120,000 |
| d[3,9] | –1.422 | 2.862 | 0.0203 | –7.063 | –1.414 | 4.208 | 60,001 | 120,000 |
| d[3,11] | –0.3179 | 2.244 | 0.01055 | –4.766 | –0.3078 | 4.083 | 60,001 | 120,000 |
| d[4,5] | 5.399 | 4.21 | 0.0448 | –2.866 | 5.41 | 13.59 | 60,001 | 120,000 |
| d[4,7] | 3.603 | 4.507 | 0.05032 | –5.237 | 3.594 | 12.44 | 60,001 | 120,000 |
| d[4,9] | –0.1027 | 1.331 | 0.007964 | –2.735 | –0.1039 | 2.515 | 60,001 | 120,000 |
| d[4,10] | –7.277 | 3.785 | 0.05031 | –14.74 | –7.247 | 0.05766 | 60,001 | 120,000 |
| d[4,11] | –9.656 | 2.408 | 0.01619 | –14.4 | –9.656 | –4.914 | 60,001 | 120,000 |
| d[4,14] | –8.149 | 2.426 | 0.0168 | –12.92 | –8.147 | –3.367 | 60,001 | 120,000 |
| d[4,17] | 8.227 | 3.961 | 0.05129 | 0.4291 | 8.253 | 15.93 | 60,001 | 120,000 |
| d[5,7] | Not estimable | |||||||
| d[5,8] | 0.6068 | 2.106 | 0.008706 | –3.561 | 0.6089 | 4.744 | 60,001 | 120,000 |
| d[5,9] | 1.06 | 2.109 | 0.009106 | –3.096 | 1.06 | 5.213 | 60,001 | 120,000 |
| d[5,16] | Not estimable | |||||||
| d[6,9] | 2.581 | 2.123 | 0.009151 | –1.611 | 2.584 | 6.762 | 60,001 | 120,000 |
| d[6,11] | –3.44 | 2.711 | 0.01678 | –8.768 | –3.438 | 1.924 | 60,001 | 120,000 |
| d[8,9] | –1.071 | 2.502 | 0.0164 | –5.988 | –1.08 | 3.865 | 60,001 | 120,000 |
| d[9,10] | Not estimable | |||||||
| d[9,15] | Not estimable | |||||||
| d[10,12] | –0.3039 | 1.246 | 0.008738 | –2.747 | –0.3015 | 2.147 | 60,001 | 120,000 |
| d[10,15] | Not estimable | |||||||
| d[10,17] | 8.424 | 1.437 | 0.008111 | 5.641 | 8.405 | 11.31 | 60,001 | 120,000 |
| d[11,14] | Not estimable | |||||||
| d[11,17] | 5.937 | 2.105 | 0.01018 | 1.741 | 5.942 | 10.06 | 60,001 | 120,000 |
| d[12,17] | 2.673 | 2.301 | 0.01049 | –1.86 | 2.686 | 7.185 | 60,001 | 120,000 |
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk.class[1] | 10.37 | 0.6439 | 0.003308 | 9 | 10 | 11 | 50,001 | 100,000 |
| rk.class[2] | 11.89 | 0.3477 | 0.001867 | 11 | 12 | 12 | 50,001 | 100,000 |
| rk.class[3] | 7.882 | 1.128 | 0.007899 | 5 | 8 | 10 | 50,001 | 100,000 |
| rk.class[4] | 7.852 | 2 | 0.009506 | 4 | 8 | 11 | 50,001 | 100,000 |
| rk.class[5] | 6.353 | 1.27 | 0.007864 | 4 | 6 | 9 | 50,001 | 100,000 |
| rk.class[6] | 1.585 | 0.6645 | 0.002948 | 1 | 1 | 3 | 50,001 | 100,000 |
| rk.class[7] | 5.892 | 1.42 | 0.008825 | 4 | 6 | 9 | 50,001 | 100,000 |
| rk.class[8] | 2.294 | 0.8118 | 0.004527 | 1 | 2 | 4 | 50,001 | 100,000 |
| rk.class[9] | 9.666 | 2.042 | 0.01036 | 4 | 10 | 12 | 50,001 | 100,000 |
| rk.class[10] | 4.733 | 1.776 | 0.007904 | 2 | 4 | 9 | 50,001 | 100,000 |
| rk.class[11] | 2.369 | 1.104 | 0.00559 | 1 | 3 | 4 | 50,001 | 100,000 |
| rk.class[12] | 7.116 | 1.826 | 0.01607 | 4 | 7 | 10 | 50,001 | 100,000 |
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk[1] | 15.36 | 0.6554 | 0.00344 | 14 | 15 | 16 | 50,001 | 100,000 |
| rk[2] | 16.89 | 0.3588 | 0.00192 | 16 | 17 | 17 | 50,001 | 100,000 |
| rk[3] | 10.46 | 2.306 | 0.01013 | 6 | 11 | 14 | 50,001 | 100,000 |
| rk[4] | 10.03 | 2.199 | 0.01102 | 6 | 10 | 14 | 50,001 | 100,000 |
| rk[5] | 10.61 | 2.204 | 0.01088 | 6 | 11 | 14 | 50,001 | 100,000 |
| rk[6] | 10.35 | 2.314 | 0.009603 | 6 | 10 | 14 | 50,001 | 100,000 |
| rk[7] | 10.35 | 2.498 | 0.01192 | 5 | 10 | 14 | 50,001 | 100,000 |
| rk[8] | 10.56 | 4.078 | 0.01757 | 4 | 12 | 16 | 50,001 | 100,000 |
| rk[9] | 7.078 | 2.24 | 0.01174 | 4 | 7 | 13 | 50,001 | 100,000 |
| rk[10] | 1.585 | 0.6645 | 0.002947 | 1 | 1 | 3 | 50,001 | 100,000 |
| rk[11] | 6.683 | 2.744 | 0.01967 | 4 | 6 | 14 | 50,001 | 100,000 |
| rk[12] | 2.295 | 0.8165 | 0.004561 | 1 | 2 | 4 | 50,001 | 100,000 |
| rk[13] | 13.71 | 3.736 | 0.01859 | 4 | 15 | 17 | 50,001 | 100,000 |
| rk[14] | 5.252 | 2.984 | 0.01282 | 2 | 4 | 14 | 50,001 | 100,000 |
| rk[15] | 2.38 | 1.168 | 0.005787 | 1 | 3 | 4 | 50,001 | 100,000 |
| rk[16] | 10.35 | 2.504 | 0.01141 | 5 | 10 | 14 | 50,001 | 100,000 |
| rk[17] | 9.053 | 3.823 | 0.03553 | 4 | 8 | 15 | 50,001 | 100,000 |
Children and adolescent/clinical effectiveness (CYBOCS)
Network geometry
FIGURE 27.
Network plot for class effects (the plot for individual effects is included in the main report). BTFLV, BT + fluvoxamine; CBTPL, CBT + placebo; CBTSER, CBT + sertraline; CLO, clomipramine; PL, placebo; PSYPL, psychological placebo; WL, waitlist.
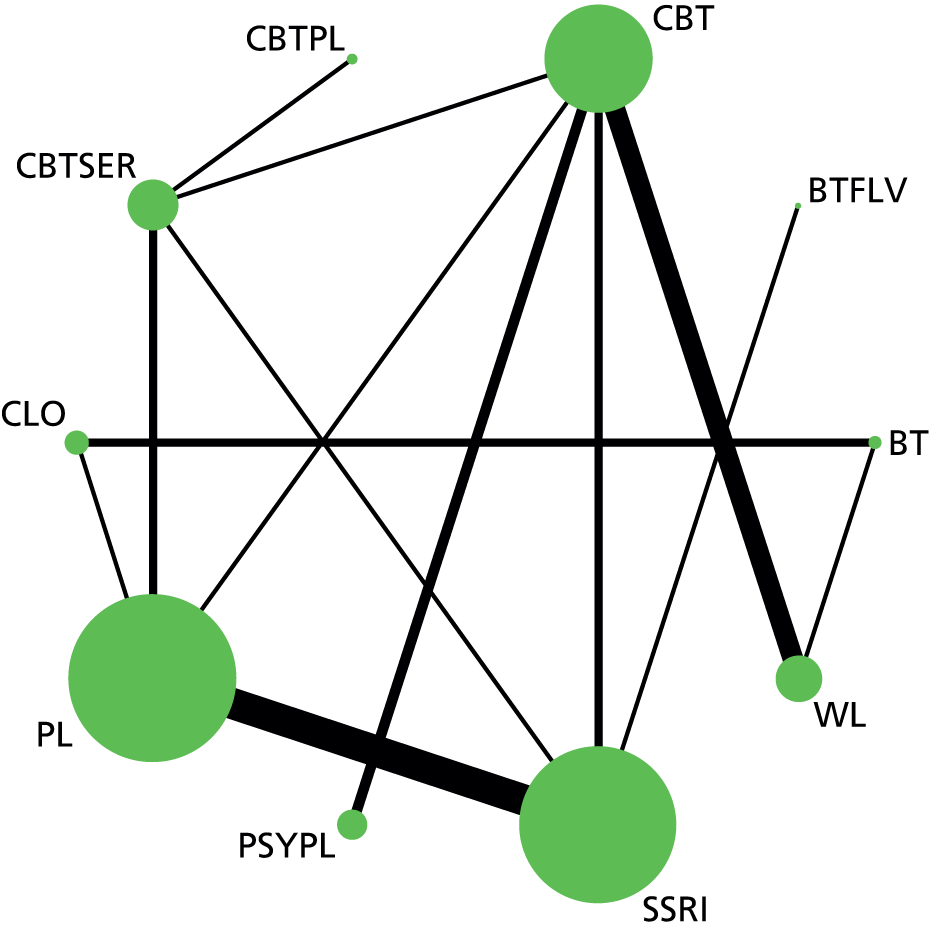
| Model fit | ||||||||
|---|---|---|---|---|---|---|---|---|
| Dbar | Dhat | DIC | pD | |||||
| mu.sd | 2.773 | 2.773 | 2.773 | 4.24 × 10–12 | ||||
| sd1 | 139.7 | 135.2 | 144.2 | 4.505 | ||||
| y | 156.2 | 110.9 | 201.6 | 45.36 | ||||
| total | 298.7 | 248.8 | 348.5 | 49.87 | ||||
| Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample | |
| sdev | 2.083 | 1.352 | 0.0313 | 0.1306 | 1.888 | 5.233 | 50,001 | 100,000 |
| totresdev | 35.04 | 7.992 | 0.07331 | 20.81 | 34.58 | 52.19 | 50,001 | 100,000 |
| Model fit | ||||||||
|---|---|---|---|---|---|---|---|---|
| Dbar | Dhat | DIC | pD | |||||
| mu.sd | 2.773 | 2.773 | 2.773 | 6.30 × 10–12 | ||||
| sd1 | 139.7 | 135.2 | 144.2 | 4.504 | ||||
| y | 558.8 | 108.9 | 1009 | 449.9 | ||||
| total | 701.2 | 246.8 | 1156 | 454.4 | ||||
| Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample | |
| sdev | 2.062 | 1.506 | 0.02984 | 0.07666 | 1.809 | 5.782 | 70,000 | 140,001 |
| totresdev | 34.27 | 7.881 | 0.0579 | 20.53 | 33.71 | 51.36 | 70,000 | 140,001 |
Data synthesis: consistency model (network meta-analysis)
Key
| Treatment | Treatment ID | Class ID |
|---|---|---|
| Placebo | 1 | 1 |
| Waitlist | 2 | 2 |
| Psychological placebo | 3 | 3 |
| Fluoxetine | 4 | 4 |
| Fluvoxamine | 5 | 4 |
| Sertraline | 6 | 4 |
| Clomipramine | 7 | 5 |
| BT | 8 | 6 |
| CBT | 9 | 7 |
| BT + fluvoxamine | 10 | 8 |
| CBT + sertraline | 11 | 9 |
| CBT + placebo | 12 | 10 |
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| class.mean.diff[1,2] | 3.10E + 00 | 3.212 | 0.05846 | –3.792 | 3.275 | 9.03 | 50,001 | 100,000 |
| class.mean.diff[1,3] | –5.374 | 3.736 | 0.05499 | –12.9 | –5.318 | 2.011 | 50,001 | 100,000 |
| class.mean.diff[1,4] | –3.577 | 2.379 | 0.01829 | –8.57 | –3.586 | 1.515 | 50,001 | 100,000 |
| class.mean.diff[1,5] | –5.645 | 3.004 | 0.03301 | –11.36 | –5.736 | 0.6411 | 50,001 | 100,000 |
| class.mean.diff[1,6] | –8.467 | 4.206 | 0.06413 | –16.98 | –8.355 | –0.3873 | 50,001 | 100,000 |
| class.mean.diff[1,7] | –8.664 | 2.798 | 0.04855 | –14.38 | –8.643 | –3.139 | 50,001 | 100,000 |
| class.mean.diff[1,8] | –6.123 | 4.247 | 0.04411 | –14.49 | –6.139 | 2.453 | 50,001 | 100,000 |
| class.mean.diff[1,9] | –10.3 | 2.899 | 0.03269 | –16.16 | –10.27 | –4.582 | 50,001 | 100,000 |
| class.mean.diff[1,10] | –10.22 | 4.864 | 0.0634 | –19.84 | –10.19 | –0.6097 | 50,001 | 100,000 |
| class.mean.diff[2,3] | –8.474 | 3.04 | 0.03171 | –14.15 | –8.61 | –2.028 | 50,001 | 100,000 |
| class.mean.diff[2,4] | –6.678 | 3.848 | 0.05634 | –13.96 | –6.843 | 1.556 | 50,001 | 100,000 |
| class.mean.diff[2,5] | –8.745 | 4.027 | 0.06251 | –16.1 | –9.018 | –0.08619 | 50,001 | 100,000 |
| class.mean.diff[2,6] | –11.57 | 3.843 | 0.04655 | –19.04 | –11.63 | –3.788 | 50,001 | 100,000 |
| class.mean.diff[2,7] | –11.77 | 1.782 | 0.02223 | –14.91 | –11.91 | –7.83 | 50,001 | 100,000 |
| class.mean.diff[2,8] | –9.223 | 5.273 | 0.07134 | –19.09 | –9.409 | 1.857 | 50,001 | 100,000 |
| class.mean.diff[2,9] | –13.41 | 3.719 | 0.05122 | –20.39 | –13.52 | –5.562 | 50,001 | 100,000 |
| class.mean.diff[2,10] | –13.32 | 5.388 | 0.07379 | –23.62 | –13.42 | –2.244 | 50,001 | 100,000 |
| class.mean.diff[3,4] | 1.796 | 4.285 | 0.05382 | –6.692 | 1.727 | 10.48 | 50,001 | 100,000 |
| class.mean.diff[3,5] | –0.2708 | 4.495 | 0.05865 | –8.874 | –0.3962 | 9.083 | 50,001 | 100,000 |
| class.mean.diff[3,6] | –3.093 | 4.648 | 0.05348 | –12.43 | –3.028 | 6.046 | 50,001 | 100,000 |
| class.mean.diff[3,7] | –3.291 | 2.472 | 0.02408 | –8.218 | –3.284 | 1.637 | 50,001 | 100,000 |
| class.mean.diff[3,8] | –0.7488 | 5.572 | 0.06654 | –11.55 | –0.7911 | 10.54 | 50,001 | 100,000 |
| class.mean.diff[3,9] | –4.931 | 4.171 | 0.05001 | –13.15 | –4.954 | 3.422 | 50,001 | 100,000 |
| class.mean.diff[3,10] | –4.842 | 5.686 | 0.07099 | –16.03 | –4.884 | 6.517 | 50,001 | 100,000 |
| class.mean.diff[4,5] | –2.067 | 3.803 | 0.03652 | –9.524 | –2.189 | 5.901 | 50,001 | 100,000 |
| class.mean.diff[4,6] | –4.889 | 4.752 | 0.06341 | –14.6 | –4.8 | 4.28 | 50,001 | 100,000 |
| class.mean.diff[4,7] | –5.087 | 3.497 | 0.04683 | –12.33 | –5.027 | 1.864 | 50,001 | 100,000 |
| class.mean.diff[4,8] | –2.545 | 4.413 | 0.04026 | –11.24 | –2.6 | 6.461 | 50,001 | 100,000 |
| class.mean.diff[4,9] | –6.727 | 3.563 | 0.03146 | –14.02 | –6.7 | 0.4664 | 50,001 | 100,000 |
| class.mean.diff[4,10] | –6.638 | 5.296 | 0.06311 | –17.16 | –6.637 | 3.873 | 50,001 | 100,000 |
| class.mean.diff[5,6] | –2.822 | 4.143 | 0.0641 | –11.37 | –2.708 | 4.944 | 50,001 | 100,000 |
| class.mean.diff[5,7] | –3.02 | 3.772 | 0.05265 | –10.9 | –2.876 | 4.19 | 50,001 | 100,000 |
| class.mean.diff[5,8] | –0.478 | 5.187 | 0.05526 | –11.06 | –0.4075 | 9.66 | 50,001 | 100,000 |
| class.mean.diff[5,9] | –4.66 | 4.054 | 0.04384 | –13.04 | –4.557 | 3.127 | 50,001 | 100,000 |
| class.mean.diff[5,10] | –4.571 | 5.637 | 0.07232 | –15.96 | –4.49 | 6.375 | 50,001 | 100,000 |
| class.mean.diff[6,7] | –0.1977 | 3.979 | 0.04858 | –7.957 | –0.2628 | 7.793 | 50,001 | 100,000 |
| class.mean.diff[6,8] | 2.344 | 5.954 | 0.07583 | –9.139 | 2.32 | 14.35 | 50,001 | 100,000 |
| class.mean.diff[6,9] | –1.838 | 4.766 | 0.06176 | –11.08 | –1.904 | 7.805 | 50,001 | 100,000 |
| class.mean.diff[6,10] | –1.749 | 6.167 | 0.08015 | –13.74 | –1.834 | 10.65 | 50,001 | 100,000 |
| class.mean.diff[7,8] | 2.542 | 5.002 | 0.06231 | –7.198 | 2.474 | 12.75 | 50,001 | 100,000 |
| class.mean.diff[7,9] | –1.64 | 3.354 | 0.04181 | –8.257 | –1.633 | 5.06 | 50,001 | 100,000 |
| class.mean.diff[7,10] | –1.551 | 5.131 | 0.06601 | –11.68 | –1.547 | 8.672 | 50,001 | 100,000 |
| class.mean.diff[8,9] | –4.182 | 5.044 | 0.05016 | –14.35 | –4.165 | 5.715 | 50,001 | 100,000 |
| class.mean.diff[8,10] | –4.093 | 6.354 | 0.06923 | –16.77 | –4.056 | 8.517 | 50,001 | 100,000 |
| class.mean.diff[9,10] | 0.08868 | 3.909 | 0.04742 | –7.601 | 0.1137 | 7.812 | 50,001 | 100,000 |
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| treat.mean.diff[1,2] | 3.101 | 3.212 | 0.05846 | –3.792 | 3.275 | 9.03 | 50,001 | 100,000 |
| treat.mean.diff[1,3] | –5.374 | 3.736 | 0.05499 | –12.9 | –5.318 | 2.011 | 50,001 | 100,000 |
| treat.mean.diff[1,4] | –3.58 | 1.693 | 0.01926 | –7.014 | –3.588 | –0.08378 | 50,001 | 100,000 |
| treat.mean.diff[1,5] | –3.273 | 2.073 | 0.02171 | –7.39 | –3.334 | 1.127 | 50,001 | 100,000 |
| treat.mean.diff[1,6] | –3.903 | 1.69 | 0.01729 | –7.466 | –3.845 | –0.5958 | 50,001 | 100,000 |
| treat.mean.diff[1,7] | –5.645 | 3.004 | 0.03301 | –11.36 | –5.736 | 0.6411 | 50,001 | 100,000 |
| treat.mean.diff[1,8] | –8.467 | 4.206 | 0.06413 | –16.98 | –8.355 | –0.3873 | 50,001 | 100,000 |
| treat.mean.diff[1,9] | –8.664 | 2.798 | 0.04855 | –14.38 | –8.643 | –3.139 | 50,001 | 100,000 |
| treat.mean.diff[1,10] | –6.123 | 4.247 | 0.04411 | –14.49 | –6.139 | 2.453 | 50,001 | 100,000 |
| treat.mean.diff[1,11] | –10.3 | 2.899 | 0.03269 | –16.16 | –10.27 | –4.582 | 50,001 | 100,000 |
| treat.mean.diff[1,12] | –10.22 | 4.864 | 0.0634 | –19.84 | –10.19 | –0.6097 | 50,001 | 100,000 |
| treat.mean.diff[2,3] | –8.474 | 3.04 | 0.03171 | –14.15 | –8.61 | –2.028 | 50,001 | 100,000 |
| treat.mean.diff[2,4] | –6.68 | 3.558 | 0.06036 | –13.32 | –6.846 | 0.9085 | 50,001 | 100,000 |
| treat.mean.diff[2,5] | –6.373 | 3.71 | 0.05793 | –13.18 | –6.567 | 1.58 | 50,001 | 100,000 |
| treat.mean.diff[2,6] | –7.004 | 3.324 | 0.05219 | –13.24 | –7.145 | 0.04082 | 50,001 | 100,000 |
| treat.mean.diff[2,7] | –8.745 | 4.027 | 0.06251 | –16.1 | –9.018 | –0.08619 | 50,001 | 100,000 |
| treat.mean.diff[2,8] | –11.57 | 3.843 | 0.04655 | –19.04 | –11.63 | –3.788 | 50,001 | 100,000 |
| treat.mean.diff[2,9] | –11.77 | 1.782 | 0.02223 | –14.91 | –11.91 | –7.83 | 50,001 | 100,000 |
| treat.mean.diff[2,10] | –9.223 | 5.273 | 0.07134 | –19.09 | –9.409 | 1.857 | 50,001 | 100,000 |
| treat.mean.diff[2,11] | –13.41 | 3.719 | 0.05122 | –20.39 | –13.52 | –5.562 | 50,001 | 100,000 |
| treat.mean.diff[2,12] | –13.32 | 5.388 | 0.07379 | –23.62 | –13.42 | –2.244 | 50,001 | 100,000 |
| treat.mean.diff[3,4] | 1.794 | 4.023 | 0.05669 | –5.995 | 1.719 | 10.03 | 50,001 | 100,000 |
| treat.mean.diff[3,5] | 2.101 | 4.162 | 0.05531 | –6.055 | 2.018 | 10.64 | 50,001 | 100,000 |
| treat.mean.diff[3,6] | 1.47 | 3.83 | 0.05047 | –6.121 | 1.457 | 9.187 | 50,001 | 100,000 |
| treat.mean.diff[3,7] | –0.2708 | 4.495 | 0.05865 | –8.874 | –0.3962 | 9.083 | 50,001 | 100,000 |
| treat.mean.diff[3,8] | –3.093 | 4.648 | 0.05348 | –12.43 | –3.028 | 6.046 | 50,001 | 100,000 |
| treat.mean.diff[3,9] | –3.291 | 2.472 | 0.02408 | –8.218 | –3.284 | 1.637 | 50,001 | 100,000 |
| treat.mean.diff[3,10] | –0.7488 | 5.572 | 0.06654 | –11.55 | –0.7911 | 10.54 | 50,001 | 100,000 |
| treat.mean.diff[3,11] | –4.931 | 4.171 | 0.05001 | –13.15 | –4.954 | 3.422 | 50,001 | 100,000 |
| treat.mean.diff[3,12] | –4.842 | 5.686 | 0.07099 | –16.03 | –4.884 | 6.517 | 50,001 | 100,000 |
| treat.mean.diff[4,5] | 0.307 | 2.246 | 0.01943 | –4.344 | 0.1259 | 5.191 | 50,001 | 100,000 |
| treat.mean.diff[4,6] | –0.3238 | 1.993 | 0.01728 | –4.802 | –0.129 | 3.582 | 50,001 | 100,000 |
| treat.mean.diff[4,7] | –2.065 | 3.406 | 0.03578 | –8.647 | –2.177 | 5.01 | 50,001 | 100,000 |
| treat.mean.diff[4,8] | –4.887 | 4.487 | 0.06599 | –14.04 | –4.789 | 3.696 | 50,001 | 100,000 |
| treat.mean.diff[4,9] | –5.085 | 3.17 | 0.05022 | –11.62 | –5.016 | 1.052 | 50,001 | 100,000 |
| treat.mean.diff[4,10] | –2.543 | 4.315 | 0.04213 | –11.05 | –2.564 | 6.081 | 50,001 | 100,000 |
| treat.mean.diff[4,11] | –6.725 | 3.245 | 0.03557 | –13.33 | –6.666 | –0.326 | 50,001 | 100,000 |
| treat.mean.diff[4,12] | –6.636 | 5.077 | 0.06581 | –16.73 | –6.632 | 3.319 | 50,001 | 100,000 |
| treat.mean.diff[5,6] | –0.6308 | 2.251 | 0.01714 | –5.809 | –0.3063 | 3.693 | 50,001 | 100,000 |
| treat.mean.diff[5,7] | –2.372 | 3.627 | 0.03927 | –9.412 | –2.481 | 5.184 | 50,001 | 100,000 |
| treat.mean.diff[5,8] | –5.194 | 4.632 | 0.06495 | –14.65 | –5.112 | 3.752 | 50,001 | 100,000 |
| treat.mean.diff[5,9] | –5.392 | 3.358 | 0.04913 | –12.33 | –5.295 | 1.14 | 50,001 | 100,000 |
| treat.mean.diff[5,10] | –2.85 | 3.731 | 0.03711 | –10.18 | –2.877 | 4.587 | 50,001 | 100,000 |
| treat.mean.diff[5,11] | –7.032 | 3.437 | 0.03377 | –14.08 | –6.998 | –0.2872 | 50,001 | 100,000 |
| treat.mean.diff[5,12] | –6.943 | 5.199 | 0.06297 | –17.36 | –6.922 | 3.356 | 50,001 | 100,000 |
| treat.mean.diff[6,7] | –1.741 | 3.389 | 0.03599 | –8.13 | –1.877 | 5.471 | 50,001 | 100,000 |
| treat.mean.diff[6,8] | –4.563 | 4.383 | 0.06104 | –13.39 | –4.497 | 3.961 | 50,001 | 100,000 |
| treat.mean.diff[6,9] | –4.761 | 2.92 | 0.043 | –10.69 | –4.737 | 1.034 | 50,001 | 100,000 |
| treat.mean.diff[6,10] | –2.22E+ 00 | 4.337 | 0.04293 | –10.64 | –2.267 | 6.639 | 50,001 | 100,000 |
| treat.mean.diff[6,11] | –6.401 | 2.992 | 0.02854 | –12.35 | –6.394 | –0.4037 | 50,001 | 100,000 |
| treat.mean.diff[6,12] | –6.312 | 4.927 | 0.06145 | –16.05 | –6.315 | 3.455 | 50,001 | 100,000 |
| treat.mean.diff[7,8] | –2.822 | 4.143 | 0.0641 | –11.37 | –2.708 | 4.944 | 50,001 | 100,000 |
| treat.mean.diff[7,9] | –3.02 | 3.772 | 0.05265 | –10.9 | –2.876 | 4.19 | 50,001 | 100,000 |
| treat.mean.diff[7,10] | –0.478 | 5.187 | 0.05526 | –11.06 | –0.4075 | 9.66 | 50,001 | 100,000 |
| treat.mean.diff[7,11] | –4.66 | 4.054 | 0.04384 | –13.04 | –4.557 | 3.127 | 50,001 | 100,000 |
| treat.mean.diff[7,12] | –4.571 | 5.637 | 0.07232 | –15.96 | –4.49 | 6.375 | 50,001 | 100,000 |
| treat.mean.diff[8,9] | –0.1977 | 3.979 | 0.04858 | –7.957 | –0.2628 | 7.793 | 50,001 | 100,000 |
| treat.mean.diff[8,10] | 2.344 | 5.954 | 0.07583 | –9.139 | 2.32 | 14.35 | 50,001 | 100,000 |
| treat.mean.diff[8,11] | –1.838 | 4.766 | 0.06176 | –11.08 | –1.904 | 7.805 | 50,001 | 100,000 |
| treat.mean.diff[8,12] | –1.749 | 6.167 | 0.08015 | –13.74 | –1.834 | 10.65 | 50,001 | 100,000 |
| treat.mean.diff[9,10] | 2.542 | 5.002 | 0.06231 | –7.198 | 2.474 | 12.75 | 50,001 | 100,000 |
| treat.mean.diff[9,11] | –1.64 | 3.354 | 0.04181 | –8.257 | –1.633 | 5.06 | 50,001 | 100,000 |
| treat.mean.diff[9,12] | –1.551 | 5.131 | 0.06601 | –11.68 | –1.547 | 8.672 | 50,001 | 100,000 |
| treat.mean.diff[10,11] | –4.182 | 5.044 | 0.05016 | –14.35 | –4.165 | 5.715 | 50,001 | 100,000 |
| treat.mean.diff[10,12] | –4.093 | 6.354 | 0.06923 | –16.77 | –4.056 | 8.517 | 50,001 | 100,000 |
| treat.mean.diff[11,12] | 0.08868 | 3.909 | 0.04742 | –7.601 | 0.1137 | 7.812 | 50,001 | 100,000 |
| d | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| d[1,4] | –3.525 | 2.099 | 0.0166 | –7.589 | –3.553 | 0.8077 | 70,000 | 140,001 |
| d[1,5] | –2.687 | 2.984 | 0.01831 | –8.731 | –2.705 | 3.354 | 70,000 | 140,001 |
| d[1,6] | –3.989 | 2.122 | 0.01392 | –8.452 | –3.963 | 0.2112 | 70,000 | 140,001 |
| d[1,7] | –7.623 | 3.303 | 0.02624 | –14.21 | –7.667 | –0.9719 | 70,000 | 140,001 |
| d[1,9] | –7.299 | 3.282 | 0.02647 | –13.95 | –7.278 | –0.8807 | 70,000 | 140,001 |
| d[1,11] | –10.12 | 3.166 | 0.02212 | –16.58 | –10.09 | –3.844 | 70,000 | 140,001 |
| d[2,8] | –7.051 | 4.672 | 0.05982 | –16.17 | –7.073 | 2.047 | 70,000 | 140,001 |
| d[2,9] | –12.34 | 1.828 | 0.01991 | –15.6 | –12.47 | –8.35 | 70,000 | 140,001 |
| d[3,9] | –3.206 | 2.514 | 0.02367 | –8.194 | –3.214 | 1.915 | 70,000 | 140,001 |
| d[5,10] | –2.811 | 3.829 | 0.04023 | –10.26 | –2.79 | 4.759 | 70,000 | 140,001 |
| d[6,9] | Not estimable | |||||||
| d[6,11] | Not estimable | |||||||
| d[7,8] | –8.57 | 5.227 | 0.07107 | –18.81 | –8.609 | 1.701 | 70,000 | 140,001 |
| d[9,11] | Not estimable | |||||||
| d[11,12] | 0.1554 | 3.988 | 0.04839 | –7.703 | 0.1543 | 7.952 | 70,000 | 140,001 |
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk.class[1] | 8.879 | 0.7007 | 0.007675 | 7 | 9 | 10 | 50,001 | 100,000 |
| rk.class[2] | 9.707 | 0.7274 | 0.009997 | 7 | 10 | 10 | 50,001 | 100,000 |
| rk.class[3] | 5.887 | 1.851 | 0.02335 | 2 | 6 | 9 | 50,001 | 100,000 |
| rk.class[4] | 6.933 | 1.447 | 0.0142 | 3 | 7 | 9 | 50,001 | 100,000 |
| rk.class[5] | 5.574 | 1.831 | 0.02318 | 2 | 6 | 9 | 50,001 | 100,000 |
| rk.class[6] | 3.808 | 2.143 | 0.03 | 1 | 4 | 8 | 50,001 | 100,000 |
| rk.class[7] | 3.44 | 1.435 | 0.01966 | 1 | 3 | 6 | 50,001 | 100,000 |
| rk.class[8] | 5.212 | 2.385 | 0.02745 | 1 | 5 | 10 | 50,001 | 100,000 |
| rk.class[9] | 2.555 | 1.41 | 0.01666 | 1 | 2 | 6 | 50,001 | 100,000 |
| rk.class[10] | 3.005 | 2.204 | 0.0301 | 1 | 2 | 8 | 50,001 | 100,000 |
| Mean | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk[1] | 10.84 | 0.7791 | 0.008764 | 9 | 11 | 12 | 50,001 | 100,000 |
| rk[2] | 11.64 | 0.9671 | 0.01322 | 8 | 12 | 12 | 50,001 | 100,000 |
| rk[3] | 6.508 | 2.503 | 0.03344 | 2 | 6 | 11 | 50,001 | 100,000 |
| rk[4] | 7.963 | 1.701 | 0.02002 | 4 | 8 | 11 | 50,001 | 100,000 |
| rk[5] | 8.28 | 1.734 | 0.01771 | 4 | 9 | 11 | 50,001 | 100,000 |
| rk[6] | 7.667 | 1.621 | 0.01517 | 4 | 8 | 10 | 50,001 | 100,000 |
| rk[7] | 6.065 | 2.39 | 0.02953 | 2 | 6 | 11 | 50,001 | 100,000 |
| rk[8] | 4.057 | 2.571 | 0.03552 | 1 | 4 | 10 | 50,001 | 100,000 |
| rk[9] | 3.519 | 1.598 | 0.02183 | 1 | 3 | 7 | 50,001 | 100,000 |
| rk[10] | 5.701 | 2.976 | 0.03297 | 1 | 6 | 12 | 50,001 | 100,000 |
| rk[11] | 2.587 | 1.512 | 0.01737 | 1 | 2 | 6 | 50,001 | 100,000 |
| rk[12] | 3.171 | 2.57 | 0.03467 | 1 | 2 | 10 | 50,001 | 100,000 |
Adults/acceptability (total dropouts)
Network geometry
FIGURE 28.
Network plot for class effects (the plot for individual effects is included in the main report). AMI, amitriptyline; BTCLO, BT + clomipramine; BTFLV, BT + fluvoxamine; CBTFLV, CBT + fluvoxamine; CLO, clomipramine; HYP, hypericum; IMI, imipramine; PL, placebo; PSYPL, psychological placebo; VEN, venlafaxine; WL, waitlist.

Model fit
| Model fit | ||||||||
|---|---|---|---|---|---|---|---|---|
| Dbar | Dhat | DIC | pD | |||||
| r | 537.2 | 464.1 | 610.3 | 73.1 | ||||
| total | 537.2 | 464.1 | 610.3 | 73.1 | ||||
| Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample | |
| sd | 0.1379 | 0.08448 | 0.002286 | 0.008152 | 0.1295 | 0.3204 | 100,001 | 200,000 |
| totresdev | 118.2 | 12.81 | 0.1327 | 94.43 | 117.7 | 144.7 | 100,001 | 200,000 |
| Model fit | ||||||||
|---|---|---|---|---|---|---|---|---|
| Dbar | Dhat | DIC | pD | |||||
| r | 539.3 | 452.5 | 626 | 86.73 | ||||
| total | 539.3 | 452.5 | 626 | 86.73 | ||||
| Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample | |
| SD | 0.1304 | 0.08595 | 0.001213 | 0.007238 | 0.1197 | 0.3231 | 100,001 | 200,000 |
| totresdev | 120.3 | 13.96 | 0.1046 | 94.57 | 119.7 | 149.3 | 100,001 | 200,000 |
Data synthesis: consistency model (network meta-analysis)
Key: intervention (class)
-
Placebo (1).
-
Waitlist (11).
-
Fluoxetine (3).
-
Fluvoxamine (3).
-
Paroxetine (3).
-
Sertraline (3).
-
Citalopram (3).
-
Venlafaxine (2).
-
Clomipramine (4).
-
BT (5).
-
CBT (6).
-
CT (7).
-
Amitriptyline (10).
-
BT + fluvoxamine (13).
-
CBT + fluvoxamine (9).
-
BT + clomipramine (8).
-
Escitalopram (3).
-
Psychological placebo (12).
-
Hypericum (14).
-
Imipramine (15).
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| OR.D[1,2] | 0.4546 | 0.2824 | 0.006189 | 0.1095 | 0.3921 | 1.148 | 100,001 | 200,000 |
| OR.D[1,3] | 1.087 | 0.1338 | 0.002307 | 0.8511 | 1.081 | 1.363 | 100,001 | 200,000 |
| OR.D[1,4] | 1.539 | 0.2175 | 0.004003 | 1.163 | 1.521 | 2.015 | 100,001 | 200,000 |
| OR.D[1,5] | 1.105 | 0.411 | 0.01157 | 0.5177 | 1.041 | 2.085 | 100,001 | 200,000 |
| OR.D[1,6] | 0.8339 | 0.3076 | 0.007419 | 0.4018 | 0.7748 | 1.595 | 100,001 | 200,000 |
| OR.D[1,7] | 1.103 | 0.4937 | 0.01353 | 0.4341 | 1.009 | 2.301 | 100,001 | 200,000 |
| OR.D[1,8] | 1.383 | 0.6327 | 0.01068 | 0.5262 | 1.267 | 2.931 | 100,001 | 200,000 |
| OR.D[1,9] | 11.39 | 59.29 | 1.302 | 0.04345 | 2.128 | 74.15 | 100,001 | 200,000 |
| OR.D[1,10] | 31.64 | 294 | 8.646 | 0.2991 | 4.513 | 138.6 | 100,001 | 200,000 |
| OR.D[1,11] | 0.5054 | 0.3846 | 0.01051 | 0.09958 | 0.402 | 1.502 | 100,001 | 200,000 |
| OR.D[1,12] | 0.5986 | 0.3323 | 0.008996 | 0.1878 | 0.5216 | 1.451 | 100,001 | 200,000 |
| OR.D[1,13] | 0.7691 | 0.6121 | 0.01333 | 0.1304 | 0.6073 | 2.353 | 100,001 | 200,000 |
| OR.D[1,14] | 1.018 | 0.6868 | 0.01217 | 0.2476 | 0.8517 | 2.729 | 100,001 | 200,000 |
| OR.D[1,15] | 3.486 | 4.934 | 0.1183 | 0.2908 | 1.965 | 16.07 | 100,001 | 200,000 |
| OR.D[2,3] | 3.437 | 2.555 | 0.0562 | 0.9351 | 2.754 | 9.894 | 100,001 | 200,000 |
| OR.D[2,4] | 4.848 | 3.603 | 0.0798 | 1.342 | 3.893 | 14.07 | 100,001 | 200,000 |
| OR.D[2,5] | 3.479 | 2.973 | 0.06704 | 0.7327 | 2.697 | 10.99 | 100,001 | 200,000 |
| OR.D[2,6] | 2.647 | 2.323 | 0.05077 | 0.5758 | 1.969 | 8.62 | 100,001 | 200,000 |
| OR.D[2,7] | 3.461 | 3.038 | 0.0705 | 0.655 | 2.641 | 11.18 | 100,001 | 200,000 |
| OR.D[2,8] | 4.347 | 3.974 | 0.07893 | 0.82 | 3.254 | 14.34 | 100,001 | 200,000 |
| OR.D[2,9] | 35.55 | 169.6 | 4.153 | 0.09668 | 5.559 | 245.3 | 100,001 | 200,000 |
| OR.D[2,10] | 88.25 | 763.8 | 19.5 | 0.6283 | 11.4 | 457.7 | 100,001 | 200,000 |
| OR.D[2,11] | 1.642 | 2.047 | 0.05398 | 0.1755 | 1.02 | 6.745 | 100,001 | 200,000 |
| OR.D[2,12] | 1.875 | 1.793 | 0.04252 | 0.3112 | 1.352 | 6.566 | 100,001 | 200,000 |
| OR.D[2,13] | 2.416 | 2.889 | 0.05796 | 0.2337 | 1.567 | 9.449 | 100,001 | 200,000 |
| OR.D[2,14] | 3.21 | 4.582 | 0.06746 | 0.4138 | 2.186 | 11.82 | 100,001 | 200,000 |
| OR.D[2,15] | 10.94 | 21.64 | 0.5357 | 0.6329 | 5.165 | 55.38 | 100,001 | 200,000 |
| OR.D[3,4] | 1.429 | 0.2256 | 0.003166 | 1.049 | 1.409 | 1.92 | 100,001 | 200,000 |
| OR.D[3,5] | 1.025 | 0.3859 | 0.0103 | 0.4757 | 0.9626 | 1.96 | 100,001 | 200,000 |
| OR.D[3,6] | 0.7713 | 0.2807 | 0.006354 | 0.3736 | 0.7205 | 1.458 | 100,001 | 200,000 |
| OR.D[3,7] | 1.022 | 0.4608 | 0.01212 | 0.398 | 0.9287 | 2.164 | 100,001 | 200,000 |
| OR.D[3,8] | 1.285 | 0.5984 | 0.009415 | 0.482 | 1.171 | 2.763 | 100,001 | 200,000 |
| OR.D[3,9] | 10.52 | 57.29 | 1.231 | 0.04033 | 1.96 | 68.64 | 100,001 | 200,000 |
| OR.D[3,10] | 28.96 | 266.4 | 7.609 | 0.281 | 4.165 | 130.1 | 100,001 | 200,000 |
| OR.D[3,11] | 0.4677 | 0.3561 | 0.009647 | 0.09169 | 0.3746 | 1.387 | 100,001 | 200,000 |
| OR.D[3,12] | 0.5544 | 0.3075 | 0.008097 | 0.1734 | 0.4835 | 1.343 | 100,001 | 200,000 |
| OR.D[3,13] | 0.7128 | 0.5665 | 0.01217 | 0.1194 | 0.5624 | 2.177 | 100,001 | 200,000 |
| OR.D[3,14] | 0.9489 | 0.6533 | 0.01133 | 0.2263 | 0.7891 | 2.598 | 100,001 | 200,000 |
| OR.D[3,15] | 3.239 | 4.603 | 0.1088 | 0.2702 | 1.82 | 15.01 | 100,001 | 200,000 |
| OR.D[4,5] | 0.725 | 0.2687 | 0.007152 | 0.3367 | 0.6836 | 1.365 | 100,001 | 200,000 |
| OR.D[4,6] | 0.5495 | 0.2096 | 0.00475 | 0.2521 | 0.5112 | 1.066 | 100,001 | 200,000 |
| OR.D[4,7] | 0.7238 | 0.3236 | 0.008512 | 0.279 | 0.6648 | 1.517 | 100,001 | 200,000 |
| OR.D[4,8] | 0.9061 | 0.4111 | 0.006424 | 0.3459 | 0.8282 | 1.912 | 100,001 | 200,000 |
| OR.D[4,9] | 7.599 | 40.91 | 0.893 | 0.02825 | 1.385 | 49.55 | 100,001 | 200,000 |
| OR.D[4,10] | 21.27 | 209 | 6.016 | 0.2031 | 2.94 | 90.76 | 100,001 | 200,000 |
| OR.D[4,11] | 0.3326 | 0.2554 | 0.006912 | 0.06458 | 0.2654 | 1.007 | 100,001 | 200,000 |
| OR.D[4,12] | 0.3925 | 0.2165 | 0.005704 | 0.1237 | 0.3411 | 0.9491 | 100,001 | 200,000 |
| OR.D[4,13] | 0.5061 | 0.4044 | 0.008782 | 0.08497 | 0.3978 | 1.579 | 100,001 | 200,000 |
| OR.D[4,14] | 0.6731 | 0.4673 | 0.008039 | 0.1572 | 0.5572 | 1.846 | 100,001 | 200,000 |
| OR.D[4,15] | 2.256 | 3.113 | 0.07227 | 0.1957 | 1.294 | 10.07 | 100,001 | 200,000 |
| OR.D[5,6] | 0.8443 | 0.4219 | 0.01039 | 0.3086 | 0.7506 | 1.904 | 100,001 | 200,000 |
| OR.D[5,7] | 1.002 | 0.2496 | 0.00467 | 0.598 | 0.9733 | 1.573 | 100,001 | 200,000 |
| OR.D[5,8] | 1.362 | 0.693 | 0.01231 | 0.4607 | 1.223 | 3.091 | 100,001 | 200,000 |
| OR.D[5,9] | 11.3 | 70.18 | 1.397 | 0.04308 | 2.05 | 77.11 | 100,001 | 200,000 |
| OR.D[5,10] | 31.6 | 283.5 | 8.307 | 0.2778 | 4.329 | 133.7 | 100,001 | 200,000 |
| OR.D[5,11] | 0.5049 | 0.4307 | 0.01168 | 0.0914 | 0.3873 | 1.65 | 100,001 | 200,000 |
| OR.D[5,12] | 0.5443 | 0.2164 | 0.004716 | 0.2302 | 0.506 | 1.06 | 100,001 | 200,000 |
| OR.D[5,13] | 0.7347 | 0.5717 | 0.01167 | 0.1261 | 0.5881 | 2.234 | 100,001 | 200,000 |
| OR.D[5,14] | 1.048 | 0.8506 | 0.01773 | 0.1978 | 0.8174 | 3.252 | 100,001 | 200,000 |
| OR.D[5,15] | 3.483 | 5.141 | 0.1092 | 0.2599 | 1.923 | 16.52 | 100,001 | 200,000 |
| OR.D[6,7] | 1.467 | 0.8041 | 0.01971 | 0.4573 | 1.292 | 3.472 | 100,001 | 200,000 |
| OR.D[6,8] | 1.862 | 1.1 | 0.0206 | 0.5442 | 1.614 | 4.707 | 100,001 | 200,000 |
| OR.D[6,9] | 14.49 | 73.24 | 1.588 | 0.05081 | 2.72 | 96.33 | 100,001 | 200,000 |
| OR.D[6,10] | 40.64 | 335.9 | 10.24 | 0.3673 | 5.493 | 195.3 | 100,001 | 200,000 |
| OR.D[6,11] | 0.614 | 0.4048 | 0.01061 | 0.1467 | 0.526 | 1.641 | 100,001 | 200,000 |
| OR.D[6,12] | 0.7916 | 0.4931 | 0.01244 | 0.2065 | 0.6677 | 2.035 | 100,001 | 200,000 |
| OR.D[6,13] | 1.037 | 0.94 | 0.02044 | 0.1448 | 0.7629 | 3.418 | 100,001 | 200,000 |
| OR.D[6,14] | 1.372 | 1.075 | 0.01909 | 0.2664 | 1.09 | 4.156 | 100,001 | 200,000 |
| OR.D[6,15] | 4.731 | 7.86 | 0.2071 | 0.3283 | 2.57 | 21.78 | 100,001 | 200,000 |
| OR.D[7,8] | 1.442 | 0.8391 | 0.01591 | 0.4264 | 1.251 | 3.555 | 100,001 | 200,000 |
| OR.D[7,9] | 11.77 | 72.72 | 1.422 | 0.04379 | 2.1 | 80.25 | 100,001 | 200,000 |
| OR.D[7,10] | 32.96 | 305.2 | 8.652 | 0.2665 | 4.467 | 145.6 | 100,001 | 200,000 |
| OR.D[7,11] | 0.527 | 0.4687 | 0.0128 | 0.09104 | 0.3952 | 1.767 | 100,001 | 200,000 |
| OR.D[7,12] | 0.5707 | 0.2543 | 0.005342 | 0.2155 | 0.525 | 1.178 | 100,001 | 200,000 |
| OR.D[7,13] | 0.7775 | 0.6611 | 0.01371 | 0.1214 | 0.601 | 2.464 | 100,001 | 200,000 |
| OR.D[7,14] | 1.107 | 0.9609 | 0.02076 | 0.1875 | 0.847 | 3.562 | 100,001 | 200,000 |
| OR.D[7,15] | 3.674 | 5.679 | 0.1201 | 0.2566 | 1.99 | 17.86 | 100,001 | 200,000 |
| OR.D[8,9] | 9.921 | 60.43 | 1.178 | 0.03375 | 1.735 | 65.2 | 100,001 | 200,000 |
| OR.D[8,10] | 28.5 | 317.4 | 7.988 | 0.2241 | 3.573 | 120 | 100,001 | 200,000 |
| OR.D[8,11] | 0.4387 | 0.4185 | 0.009987 | 0.06539 | 0.3156 | 1.566 | 100,001 | 200,000 |
| OR.D[8,12] | 0.5026 | 0.3446 | 0.006854 | 0.1265 | 0.4141 | 1.405 | 100,001 | 200,000 |
| OR.D[8,13] | 0.6512 | 0.6021 | 0.01046 | 0.09153 | 0.4819 | 2.245 | 100,001 | 200,000 |
| OR.D[8,14] | 0.894 | 0.7887 | 0.01299 | 0.1541 | 0.671 | 2.934 | 100,001 | 200,000 |
| OR.D[8,15] | 2.957 | 4.606 | 0.08921 | 0.1993 | 1.574 | 14.18 | 100,001 | 200,000 |
| OR.D[9,10] | 59.82 | 684.1 | 14.32 | 0.02385 | 2.139 | 291.7 | 100,001 | 200,000 |
| OR.D[9,11] | 2.12 | 27.16 | 0.6386 | 0.004269 | 0.1896 | 11.94 | 100,001 | 200,000 |
| OR.D[9,12] | 2.971 | 52.54 | 1.085 | 0.006906 | 0.2424 | 12.3 | 100,001 | 200,000 |
| OR.D[9,13] | 3.417 | 53.45 | 1.251 | 0.005859 | 0.2718 | 16.1 | 100,001 | 200,000 |
| OR.D[9,14] | 4.489 | 62.3 | 1.452 | 0.009721 | 0.3928 | 23.35 | 100,001 | 200,000 |
| OR.D[9,15] | 10.21 | 84.75 | 1.67 | 0.01887 | 1.002 | 74.09 | 100,001 | 200,000 |
| OR.D[10,11] | 0.3217 | 1.189 | 0.02484 | 0.002413 | 0.08551 | 1.913 | 100,001 | 200,000 |
| OR.D[10,12] | 0.3608 | 1.521 | 0.02863 | 0.003334 | 0.117 | 2.003 | 100,001 | 200,000 |
| OR.D[10,13] | 0.4583 | 2.107 | 0.03533 | 0.003304 | 0.1371 | 2.633 | 100,001 | 200,000 |
| OR.D[10,14] | 0.6583 | 3.664 | 0.05761 | 0.005043 | 0.1925 | 3.699 | 100,001 | 200,000 |
| OR.D[10,15] | 1.952 | 8.639 | 0.1464 | 0.009582 | 0.4587 | 12.83 | 100,001 | 200,000 |
| OR.D[11,12] | 1.834 | 1.712 | 0.04359 | 0.254 | 1.325 | 6.453 | 100,001 | 200,000 |
| OR.D[11,13] | 2.458 | 3.08 | 0.07976 | 0.2077 | 1.47 | 10.96 | 100,001 | 200,000 |
| OR.D[11,14] | 3.319 | 4.124 | 0.09609 | 0.354 | 2.132 | 13.53 | 100,001 | 200,000 |
| OR.D[11,15] | 11.59 | 22.71 | 0.5601 | 0.4562 | 4.985 | 64.95 | 100,001 | 200,000 |
| OR.D[12,13] | 1.557 | 1.423 | 0.02744 | 0.2142 | 1.16 | 5.396 | 100,001 | 200,000 |
| OR.D[12,14] | 2.248 | 2.206 | 0.0467 | 0.3217 | 1.628 | 7.927 | 100,001 | 200,000 |
| OR.D[12,15] | 7.492 | 12.33 | 0.255 | 0.4661 | 3.715 | 38.18 | 100,001 | 200,000 |
| OR.D[13,14] | 2.288 | 3.079 | 0.05419 | 0.2268 | 1.417 | 9.682 | 100,001 | 200,000 |
| OR.D[13,15] | 7.571 | 17.92 | 0.3625 | 0.3497 | 3.417 | 38.12 | 100,001 | 200,000 |
| OR.D[14,15] | 5.008 | 9.252 | 0.2034 | 0.2605 | 2.337 | 26.58 | 100,001 | 200,000 |
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| OR[1,2] | 0.5054 | 0.3846 | 0.01051 | 0.09958 | 0.402 | 1.502 | 100,001 | 200,000 |
| OR[1,3] | 1.146 | 0.1657 | 0.00323 | 0.8801 | 1.125 | 1.539 | 100,001 | 200,000 |
| OR[1,4] | 1.101 | 0.1416 | 0.00298 | 0.852 | 1.092 | 1.409 | 100,001 | 200,000 |
| OR[1,5] | 1.099 | 0.1324 | 0.002389 | 0.8648 | 1.09 | 1.385 | 100,001 | 200,000 |
| OR[1,6] | 1.042 | 0.1368 | 0.002443 | 0.785 | 1.039 | 1.326 | 100,001 | 200,000 |
| OR[1,7] | 1.063 | 0.1678 | 0.002733 | 0.7366 | 1.059 | 1.413 | 100,001 | 200,000 |
| OR[1,8] | 0.4546 | 0.2824 | 0.006189 | 0.1095 | 0.3921 | 1.148 | 100,001 | 200,000 |
| OR[1,9] | 1.539 | 0.2175 | 0.004003 | 1.163 | 1.521 | 2.015 | 100,001 | 200,000 |
| OR[1,10] | 1.105 | 0.411 | 0.01157 | 0.5177 | 1.041 | 2.085 | 100,001 | 200,000 |
| OR[1,11] | 0.8339 | 0.3076 | 0.007419 | 0.4018 | 0.7748 | 1.595 | 100,001 | 200,000 |
| OR[1,12] | 1.103 | 0.4937 | 0.01353 | 0.4341 | 1.009 | 2.301 | 100,001 | 200,000 |
| OR[1,13] | 31.64 | 294 | 8.646 | 0.2991 | 4.513 | 138.6 | 100,001 | 200,000 |
| OR[1,14] | 0.7691 | 0.6121 | 0.01333 | 0.1304 | 0.6073 | 2.353 | 100,001 | 200,000 |
| OR[1,15] | 11.39 | 59.29 | 1.302 | 0.04345 | 2.128 | 74.15 | 100,001 | 200,000 |
| OR[1,16] | 1.383 | 0.6327 | 0.01068 | 0.5262 | 1.267 | 2.931 | 100,001 | 200,000 |
| OR[1,17] | 1.091 | 0.1666 | 0.002681 | 0.7961 | 1.081 | 1.461 | 100,001 | 200,000 |
| OR[1,18] | 0.5986 | 0.3323 | 0.008996 | 0.1878 | 0.5216 | 1.451 | 100,001 | 200,000 |
| OR[1,19] | 1.018 | 0.6868 | 0.01217 | 0.2476 | 0.8517 | 2.729 | 100,001 | 200,000 |
| OR[1,20] | 3.486 | 4.934 | 0.1183 | 0.2908 | 1.965 | 16.07 | 100,001 | 200,000 |
| OR[2,3] | 3.64 | 2.864 | 0.07925 | 0.7702 | 2.818 | 11.32 | 100,001 | 200,000 |
| OR[2,4] | 3.521 | 2.808 | 0.07836 | 0.7258 | 2.7 | 10.95 | 100,001 | 200,000 |
| OR[2,5] | 3.52 | 2.818 | 0.07883 | 0.7285 | 2.702 | 11.11 | 100,001 | 200,000 |
| OR[2,6] | 3.337 | 2.688 | 0.07447 | 0.6859 | 2.541 | 10.6 | 100,001 | 200,000 |
| OR[2,7] | 3.41 | 2.764 | 0.07634 | 0.6762 | 2.605 | 10.82 | 100,001 | 200,000 |
| OR[2,8] | 1.476 | 1.646 | 0.03985 | 0.1483 | 0.9807 | 5.698 | 100,001 | 200,000 |
| OR[2,9] | 4.933 | 3.982 | 0.1111 | 0.9928 | 3.768 | 15.49 | 100,001 | 200,000 |
| OR[2,10] | 3.423 | 2.827 | 0.07772 | 0.6061 | 2.582 | 10.94 | 100,001 | 200,000 |
| OR[2,11] | 2.409 | 1.719 | 0.04724 | 0.6094 | 1.901 | 6.815 | 100,001 | 200,000 |
| OR[2,12] | 3.364 | 2.856 | 0.07542 | 0.566 | 2.531 | 10.98 | 100,001 | 200,000 |
| OR[2,13] | 85.96 | 665.7 | 19.86 | 0.5226 | 11.69 | 414.6 | 100,001 | 200,000 |
| OR[2,14] | 2.458 | 3.08 | 0.07976 | 0.2077 | 1.47 | 10.96 | 100,001 | 200,000 |
| OR[2,15] | 32.47 | 174.6 | 3.61 | 0.08373 | 5.275 | 234.4 | 100,001 | 200,000 |
| OR[2,16] | 4.379 | 4.156 | 0.09986 | 0.6387 | 3.168 | 15.29 | 100,001 | 200,000 |
| OR[2,17] | 3.487 | 2.807 | 0.07781 | 0.7085 | 2.674 | 11.01 | 100,001 | 200,000 |
| OR[2,18] | 1.834 | 1.712 | 0.04359 | 0.254 | 1.325 | 6.453 | 100,001 | 200,000 |
| OR[2,19] | 3.319 | 4.124 | 0.09609 | 0.354 | 2.132 | 13.53 | 100,001 | 200,000 |
| OR[2,20] | 11.59 | 22.71 | 0.5601 | 0.4562 | 4.985 | 64.95 | 100,001 | 200,000 |
| OR[3,4] | 0.9715 | 0.1316 | 0.002139 | 0.6796 | 0.9855 | 1.246 | 100,001 | 200,000 |
| OR[3,5] | 0.9703 | 0.1269 | 0.00171 | 0.6966 | 0.9837 | 1.235 | 100,001 | 200,000 |
| OR[3,6] | 0.9206 | 0.1304 | 0.002143 | 0.6268 | 0.9486 | 1.143 | 100,001 | 200,000 |
| OR[3,7] | 0.9392 | 0.1547 | 0.002319 | 0.5827 | 0.9685 | 1.229 | 100,001 | 200,000 |
| OR[3,8] | 0.4023 | 0.2532 | 0.00544 | 0.09534 | 0.3422 | 1.015 | 100,001 | 200,000 |
| OR[3,9] | 1.362 | 0.2279 | 0.00366 | 0.9379 | 1.35 | 1.853 | 100,001 | 200,000 |
| OR[3,10] | 0.9754 | 0.3665 | 0.009627 | 0.4438 | 0.9183 | 1.871 | 100,001 | 200,000 |
| OR[3,11] | 0.7303 | 0.2527 | 0.005679 | 0.36 | 0.6864 | 1.332 | 100,001 | 200,000 |
| OR[3,12] | 0.973 | 0.4383 | 0.01139 | 0.3734 | 0.8857 | 2.06 | 100,001 | 200,000 |
| OR[3,13] | 27.29 | 237.7 | 7.204 | 0.2683 | 3.99 | 123.8 | 100,001 | 200,000 |
| OR[3,14] | 0.6805 | 0.5435 | 0.01177 | 0.111 | 0.5364 | 2.114 | 100,001 | 200,000 |
| OR[3,15] | 10.01 | 53.13 | 1.166 | 0.03831 | 1.855 | 65.45 | 100,001 | 200,000 |
| OR[3,16] | 1.224 | 0.5745 | 0.00902 | 0.4514 | 1.117 | 2.648 | 100,001 | 200,000 |
| OR[3,17] | 0.962 | 0.1468 | 0.001912 | 0.6432 | 0.9805 | 1.264 | 100,001 | 200,000 |
| OR[3,18] | 0.5276 | 0.2913 | 0.007611 | 0.1619 | 0.4604 | 1.291 | 100,001 | 200,000 |
| OR[3,19] | 0.9042 | 0.6268 | 0.01106 | 0.2144 | 0.7482 | 2.495 | 100,001 | 200,000 |
| OR[3,20] | 3.092 | 4.437 | 0.1049 | 0.2544 | 1.739 | 14.15 | 100,001 | 200,000 |
| OR[4,5] | 1.008 | 0.1307 | 0.001907 | 0.7557 | 1 | 1.317 | 100,001 | 200,000 |
| OR[4,6] | 0.9556 | 0.1308 | 0.002129 | 0.6772 | 0.9749 | 1.219 | 100,001 | 200,000 |
| OR[4,7] | 0.9742 | 0.1561 | 0.002078 | 0.6388 | 0.9871 | 1.315 | 100,001 | 200,000 |
| OR[4,8] | 0.4177 | 0.2622 | 0.005638 | 0.09918 | 0.3575 | 1.062 | 100,001 | 200,000 |
| OR[4,9] | 1.412 | 0.2153 | 0.00355 | 1.037 | 1.393 | 1.884 | 100,001 | 200,000 |
| OR[4,10] | 1.01 | 0.3718 | 0.009983 | 0.4754 | 0.9506 | 1.922 | 100,001 | 200,000 |
| OR[4,11] | 0.7633 | 0.2812 | 0.006348 | 0.3663 | 0.7095 | 1.458 | 100,001 | 200,000 |
| OR[4,12] | 1.008 | 0.4471 | 0.0118 | 0.3998 | 0.9185 | 2.137 | 100,001 | 200,000 |
| OR[4,13] | 28.57 | 260.8 | 7.54 | 0.2757 | 4.066 | 128.8 | 100,001 | 200,000 |
| OR[4,14] | 0.7001 | 0.5479 | 0.01173 | 0.1206 | 0.555 | 2.117 | 100,001 | 200,000 |
| OR[4,15] | 10.38 | 55.63 | 1.208 | 0.03995 | 1.935 | 66.97 | 100,001 | 200,000 |
| OR[4,16] | 1.268 | 0.5865 | 0.009184 | 0.4781 | 1.158 | 2.714 | 100,001 | 200,000 |
| OR[4,17] | 0.999 | 0.1534 | 0.001928 | 0.6945 | 0.9973 | 1.354 | 100,001 | 200,000 |
| OR[4,18] | 0.5467 | 0.3009 | 0.007949 | 0.1747 | 0.4782 | 1.328 | 100,001 | 200,000 |
| OR[4,19] | 0.9389 | 0.6505 | 0.01133 | 0.2231 | 0.7757 | 2.577 | 100,001 | 200,000 |
| OR[4,20] | 3.182 | 4.486 | 0.1031 | 0.2699 | 1.79 | 14.34 | 100,001 | 200,000 |
| OR[5,6] | 0.9554 | 0.1262 | 0.001717 | 0.6835 | 0.9739 | 1.212 | 100,001 | 200,000 |
| OR[5,7] | 0.974 | 0.1515 | 0.001814 | 0.6456 | 0.987 | 1.296 | 100,001 | 200,000 |
| OR[5,8] | 0.4147 | 0.2534 | 0.005529 | 0.1012 | 0.3593 | 1.029 | 100,001 | 200,000 |
| OR[5,9] | 1.412 | 0.2086 | 0.003072 | 1.046 | 1.397 | 1.868 | 100,001 | 200,000 |
| OR[5,10] | 1.013 | 0.3773 | 0.01014 | 0.4664 | 0.9546 | 1.92 | 100,001 | 200,000 |
| OR[5,11] | 0.7637 | 0.2809 | 0.006426 | 0.3654 | 0.7111 | 1.456 | 100,001 | 200,000 |
| OR[5,12] | 1.011 | 0.4524 | 0.01199 | 0.3923 | 0.9218 | 2.121 | 100,001 | 200,000 |
| OR[5,13] | 28.58 | 259.1 | 7.517 | 0.2763 | 4.13 | 128.4 | 100,001 | 200,000 |
| OR[5,14] | 0.704 | 0.5564 | 0.01195 | 0.1189 | 0.5555 | 2.131 | 100,001 | 200,000 |
| OR[5,15] | 10.44 | 56.56 | 1.22 | 0.03955 | 1.935 | 68.25 | 100,001 | 200,000 |
| OR[5,16] | 1.269 | 0.5876 | 0.009358 | 0.4772 | 1.162 | 2.725 | 100,001 | 200,000 |
| OR[5,17] | 0.9973 | 0.1375 | 0.001376 | 0.7274 | 0.9967 | 1.314 | 100,001 | 200,000 |
| OR[5,18] | 0.548 | 0.3014 | 0.007975 | 0.1702 | 0.4789 | 1.329 | 100,001 | 200,000 |
| OR[5,19] | 0.9384 | 0.6472 | 0.01124 | 0.2231 | 0.7797 | 2.568 | 100,001 | 200,000 |
| OR[5,20] | 3.203 | 4.561 | 0.109 | 0.2661 | 1.807 | 15.02 | 100,001 | 200,000 |
| OR[6,7] | 1.029 | 0.1702 | 0.002173 | 0.7202 | 1.007 | 1.453 | 100,001 | 200,000 |
| OR[6,8] | 0.4412 | 0.276 | 0.005935 | 0.104 | 0.3794 | 1.118 | 100,001 | 200,000 |
| OR[6,9] | 1.495 | 0.2482 | 0.003963 | 1.081 | 1.469 | 2.061 | 100,001 | 200,000 |
| OR[6,10] | 1.073 | 0.4116 | 0.01112 | 0.4918 | 1.001 | 2.077 | 100,001 | 200,000 |
| OR[6,11] | 0.8072 | 0.2982 | 0.006886 | 0.386 | 0.7514 | 1.533 | 100,001 | 200,000 |
| OR[6,12] | 1.071 | 0.4889 | 0.01292 | 0.412 | 0.9697 | 2.306 | 100,001 | 200,000 |
| OR[6,13] | 30.42 | 280.2 | 8.141 | 0.2922 | 4.339 | 135.4 | 100,001 | 200,000 |
| OR[6,14] | 0.7473 | 0.5986 | 0.01322 | 0.1243 | 0.5863 | 2.329 | 100,001 | 200,000 |
| OR[6,15] | 10.95 | 59.74 | 1.273 | 0.04193 | 2.042 | 72.71 | 100,001 | 200,000 |
| OR[6,16] | 1.344 | 0.6319 | 0.01025 | 0.4972 | 1.223 | 2.886 | 100,001 | 200,000 |
| OR[6,17] | 1.057 | 0.179 | 0.002455 | 0.7688 | 1.017 | 1.504 | 100,001 | 200,000 |
| OR[6,18] | 0.5804 | 0.3238 | 0.008627 | 0.1792 | 0.5024 | 1.394 | 100,001 | 200,000 |
| OR[6,19] | 0.9924 | 0.6832 | 0.01197 | 0.2337 | 0.8286 | 2.725 | 100,001 | 200,000 |
| OR[6,20] | 3.385 | 4.835 | 0.1141 | 0.2827 | 1.911 | 15.34 | 100,001 | 200,000 |
| OR[7,8] | 0.4375 | 0.2814 | 0.006025 | 0.1004 | 0.3746 | 1.148 | 100,001 | 200,000 |
| OR[7,9] | 1.48 | 0.3017 | 0.004631 | 1.012 | 1.439 | 2.205 | 100,001 | 200,000 |
| OR[7,10] | 1.062 | 0.4309 | 0.01126 | 0.4743 | 0.9828 | 2.105 | 100,001 | 200,000 |
| OR[7,11] | 0.7997 | 0.3172 | 0.007052 | 0.3729 | 0.7357 | 1.593 | 100,001 | 200,000 |
| OR[7,12] | 1.059 | 0.5044 | 0.01298 | 0.3995 | 0.9528 | 2.318 | 100,001 | 200,000 |
| OR[7,13] | 29.9 | 277.2 | 7.74 | 0.287 | 4.276 | 134.2 | 100,001 | 200,000 |
| OR[7,14] | 0.7391 | 0.6056 | 0.01274 | 0.1215 | 0.5756 | 2.286 | 100,001 | 200,000 |
| OR[7,15] | 10.8 | 56.9 | 1.236 | 0.04037 | 2.015 | 71.57 | 100,001 | 200,000 |
| OR[7,16] | 1.329 | 0.6467 | 0.0102 | 0.4849 | 1.199 | 2.929 | 100,001 | 200,000 |
| OR[7,17] | 1.044 | 0.2045 | 0.002524 | 0.7223 | 1.007 | 1.576 | 100,001 | 200,000 |
| OR[7,18] | 0.5749 | 0.3338 | 0.008727 | 0.1733 | 0.4948 | 1.418 | 100,001 | 200,000 |
| OR[7,19] | 0.9805 | 0.688 | 0.01158 | 0.229 | 0.8131 | 2.729 | 100,001 | 200,000 |
| OR[7,20] | 3.351 | 4.772 | 0.1112 | 0.2727 | 1.868 | 15.43 | 100,001 | 200,000 |
| OR[8,9] | 4.848 | 3.603 | 0.0798 | 1.342 | 3.893 | 14.07 | 100,001 | 200,000 |
| OR[8,10] | 3.479 | 2.973 | 0.06704 | 0.7327 | 2.697 | 10.99 | 100,001 | 200,000 |
| OR[8,11] | 2.647 | 2.323 | 0.05077 | 0.5758 | 1.969 | 8.62 | 100,001 | 200,000 |
| OR[8,12] | 3.461 | 3.038 | 0.0705 | 0.655 | 2.641 | 11.18 | 100,001 | 200,000 |
| OR[8,13] | 88.25 | 763.8 | 19.5 | 0.6283 | 11.4 | 457.7 | 100,001 | 200,000 |
| OR[8,14] | 2.416 | 2.889 | 0.05796 | 0.2337 | 1.567 | 9.449 | 100,001 | 200,000 |
| OR[8,15] | 35.55 | 169.6 | 4.153 | 0.09668 | 5.559 | 245.3 | 100,001 | 200,000 |
| OR[8,16] | 4.347 | 3.974 | 0.07893 | 0.82 | 3.254 | 14.34 | 100,001 | 200,000 |
| OR[8,17] | 3.446 | 2.587 | 0.05629 | 0.9096 | 2.768 | 9.988 | 100,001 | 200,000 |
| OR[8,18] | 1.875 | 1.793 | 0.04252 | 0.3112 | 1.352 | 6.566 | 100,001 | 200,000 |
| OR[8,19] | 3.21 | 4.582 | 0.06746 | 0.4138 | 2.186 | 11.82 | 100,001 | 200,000 |
| OR[8,20] | 10.94 | 21.64 | 0.5357 | 0.6329 | 5.165 | 55.38 | 100,001 | 200,000 |
| OR[9,10] | 0.725 | 0.2687 | 0.007152 | 0.3367 | 0.6836 | 1.365 | 100,001 | 200,000 |
| OR[9,11] | 0.5495 | 0.2096 | 0.00475 | 0.2521 | 0.5112 | 1.066 | 100,001 | 200,000 |
| OR[9,12] | 0.7238 | 0.3236 | 0.008512 | 0.279 | 0.6648 | 1.517 | 100,001 | 200,000 |
| OR[9,13] | 21.27 | 209 | 6.016 | 0.2031 | 2.94 | 90.76 | 100,001 | 200,000 |
| OR[9,14] | 0.5061 | 0.4044 | 0.008782 | 0.08497 | 0.3978 | 1.579 | 100,001 | 200,000 |
| OR[9,15] | 7.599 | 40.91 | 0.893 | 0.02825 | 1.385 | 49.55 | 100,001 | 200,000 |
| OR[9,16] | 0.9061 | 0.4111 | 0.006424 | 0.3459 | 0.8282 | 1.912 | 100,001 | 200,000 |
| OR[9,17] | 0.719 | 0.1298 | 0.001756 | 0.4905 | 0.7096 | 1.006 | 100,001 | 200,000 |
| OR[9,18] | 0.3925 | 0.2165 | 0.005704 | 0.1237 | 0.3411 | 0.9491 | 100,001 | 200,000 |
| OR[9,19] | 0.6731 | 0.4673 | 0.008039 | 0.1572 | 0.5572 | 1.846 | 100,001 | 200,000 |
| OR[9,20] | 2.256 | 3.113 | 0.07227 | 0.1957 | 1.294 | 10.07 | 100,001 | 200,000 |
| OR[10,11] | 0.8443 | 0.4219 | 0.01039 | 0.3086 | 0.7506 | 1.904 | 100,001 | 200,000 |
| OR[10,12] | 1.002 | 0.2496 | 0.00467 | 0.598 | 0.9733 | 1.573 | 100,001 | 200,000 |
| OR[10,13] | 31.6 | 283.5 | 8.307 | 0.2778 | 4.329 | 133.7 | 100,001 | 200,000 |
| OR[10,14] | 0.7347 | 0.5717 | 0.01167 | 0.1261 | 0.5881 | 2.234 | 100,001 | 200,000 |
| OR[10,15] | 11.3 | 70.18 | 1.397 | 0.04308 | 2.05 | 77.11 | 100,001 | 200,000 |
| OR[10,16] | 1.362 | 0.693 | 0.01231 | 0.4607 | 1.223 | 3.091 | 100,001 | 200,000 |
| OR[10,17] | 1.115 | 0.4284 | 0.01116 | 0.4918 | 1.038 | 2.147 | 100,001 | 200,000 |
| OR[10,18] | 0.5443 | 0.2164 | 0.004716 | 0.2302 | 0.506 | 1.06 | 100,001 | 200,000 |
| OR[10,19] | 1.048 | 0.8506 | 0.01773 | 0.1978 | 0.8174 | 3.252 | 100,001 | 200,000 |
| OR[10,20] | 3.483 | 5.141 | 0.1092 | 0.2599 | 1.923 | 16.52 | 100,001 | 200,000 |
| OR[11,12] | 1.467 | 0.8041 | 0.01971 | 0.4573 | 1.292 | 3.472 | 100,001 | 200,000 |
| OR[11,13] | 40.64 | 335.9 | 10.24 | 0.3673 | 5.493 | 195.3 | 100,001 | 200,000 |
| OR[11,14] | 1.037 | 0.94 | 0.02044 | 0.1448 | 0.7629 | 3.418 | 100,001 | 200,000 |
| OR[11,15] | 14.49 | 73.24 | 1.588 | 0.05081 | 2.72 | 96.33 | 100,001 | 200,000 |
| OR[11,16] | 1.862 | 1.1 | 0.0206 | 0.5442 | 1.614 | 4.707 | 100,001 | 200,000 |
| OR[11,17] | 1.468 | 0.5409 | 0.01177 | 0.6645 | 1.389 | 2.759 | 100,001 | 200,000 |
| OR[11,18] | 0.7916 | 0.4931 | 0.01244 | 0.2065 | 0.6677 | 2.035 | 100,001 | 200,000 |
| OR[11,19] | 1.372 | 1.075 | 0.01909 | 0.2664 | 1.09 | 4.156 | 100,001 | 200,000 |
| OR[11,20] | 4.731 | 7.86 | 0.2071 | 0.3283 | 2.57 | 21.78 | 100,001 | 200,000 |
| OR[12,13] | 32.96 | 305.2 | 8.652 | 0.2665 | 4.467 | 145.6 | 100,001 | 200,000 |
| OR[12,14] | 0.7775 | 0.6611 | 0.01371 | 0.1214 | 0.601 | 2.464 | 100,001 | 200,000 |
| OR[12,15] | 11.77 | 72.72 | 1.422 | 0.04379 | 2.1 | 80.25 | 100,001 | 200,000 |
| OR[12,16] | 1.442 | 0.8391 | 0.01591 | 0.4264 | 1.251 | 3.555 | 100,001 | 200,000 |
| OR[12,17] | 1.178 | 0.5401 | 0.01398 | 0.4475 | 1.076 | 2.559 | 100,001 | 200,000 |
| OR[12,18] | 0.5707 | 0.2543 | 0.005342 | 0.2155 | 0.525 | 1.178 | 100,001 | 200,000 |
| OR[12,19] | 1.107 | 0.9609 | 0.02076 | 0.1875 | 0.847 | 3.562 | 100,001 | 200,000 |
| OR[12,20] | 3.674 | 5.679 | 0.1201 | 0.2566 | 1.99 | 17.86 | 100,001 | 200,000 |
| OR[13,14] | 0.4583 | 2.107 | 0.03533 | 0.003304 | 0.1371 | 2.633 | 100,001 | 200,000 |
| OR[13,15] | 5.556 | 28.5 | 0.6176 | 0.003429 | 0.4675 | 41.93 | 100,001 | 200,000 |
| OR[13,16] | 0.8363 | 3.329 | 0.06118 | 0.008335 | 0.2799 | 4.463 | 100,001 | 200,000 |
| OR[13,17] | 0.676 | 2.681 | 0.05176 | 0.007658 | 0.2391 | 3.617 | 100,001 | 200,000 |
| OR[13,18] | 0.3608 | 1.521 | 0.02863 | 0.003334 | 0.117 | 2.003 | 100,001 | 200,000 |
| OR[13,19] | 0.6583 | 3.664 | 0.05761 | 0.005043 | 0.1925 | 3.699 | 100,001 | 200,000 |
| OR[13,20] | 1.952 | 8.639 | 0.1464 | 0.009582 | 0.4587 | 12.83 | 100,001 | 200,000 |
| OR[14,15] | 23.43 | 123.1 | 2.653 | 0.06213 | 3.679 | 170.7 | 100,001 | 200,000 |
| OR[14,16] | 3.005 | 3.138 | 0.05922 | 0.4455 | 2.075 | 10.93 | 100,001 | 200,000 |
| OR[14,17] | 2.437 | 2.294 | 0.04934 | 0.4563 | 1.778 | 8.501 | 100,001 | 200,000 |
| OR[14,18] | 1.247 | 1.316 | 0.02774 | 0.1854 | 0.8621 | 4.669 | 100,001 | 200,000 |
| OR[14,19] | 2.288 | 3.079 | 0.05419 | 0.2268 | 1.417 | 9.682 | 100,001 | 200,000 |
| OR[14,20] | 7.571 | 17.92 | 0.3625 | 0.3497 | 3.417 | 38.12 | 100,001 | 200,000 |
| OR[15,16] | 7.697 | 133.4 | 3.041 | 0.01534 | 0.5764 | 29.64 | 100,001 | 200,000 |
| OR[15,17] | 4.798 | 59.05 | 1.332 | 0.01439 | 0.509 | 25.01 | 100,001 | 200,000 |
| OR[15,18] | 2.971 | 52.54 | 1.085 | 0.006906 | 0.2424 | 12.3 | 100,001 | 200,000 |
| OR[15,19] | 4.489 | 62.3 | 1.452 | 0.009721 | 0.3928 | 23.35 | 100,001 | 200,000 |
| OR[15,20] | 10.21 | 84.75 | 1.67 | 0.01887 | 1.002 | 74.09 | 100,001 | 200,000 |
| OR[16,17] | 0.9526 | 0.4623 | 0.007213 | 0.3544 | 0.8549 | 2.11 | 100,001 | 200,000 |
| OR[16,18] | 0.5026 | 0.3446 | 0.006854 | 0.1265 | 0.4141 | 1.405 | 100,001 | 200,000 |
| OR[16,19] | 0.894 | 0.7887 | 0.01299 | 0.1541 | 0.671 | 2.934 | 100,001 | 200,000 |
| OR[16,20] | 2.957 | 4.606 | 0.08921 | 0.1993 | 1.574 | 14.18 | 100,001 | 200,000 |
| OR[17,18] | 0.557 | 0.3131 | 0.008084 | 0.1705 | 0.4845 | 1.358 | 100,001 | 200,000 |
| OR[17,19] | 0.9535 | 0.6646 | 0.01152 | 0.2234 | 0.7871 | 2.615 | 100,001 | 200,000 |
| OR[17,20] | 3.27 | 4.723 | 0.1144 | 0.267 | 1.825 | 15.75 | 100,001 | 200,000 |
| OR[18,19] | 2.248 | 2.206 | 0.0467 | 0.3217 | 1.628 | 7.927 | 100,001 | 200,000 |
| OR[18,20] | 7.492 | 12.33 | 0.255 | 0.4661 | 3.715 | 38.18 | 100,001 | 200,000 |
| OR[19,20] | 5.008 | 9.252 | 0.2034 | 0.2605 | 2.337 | 26.58 | 100,001 | 200,000 |
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| or[1,3] | 1.293 | 0.3195 | 0.003551 | 0.7902 | 1.251 | 2.035 | 100,001 | 200,000 |
| or[1,4] | 1.422 | 0.3342 | 0.00321 | 0.8762 | 1.385 | 2.177 | 100,001 | 200,000 |
| or[1,5] | 1.097 | 0.1883 | 0.001546 | 0.7836 | 1.078 | 1.521 | 100,001 | 200,000 |
| or[1,6] | 1.009 | 0.2379 | 0.001747 | 0.6274 | 0.9797 | 1.549 | 100,001 | 200,000 |
| or[1,7] | 0.9585 | 0.3273 | 0.003297 | 0.4869 | 0.9016 | 1.751 | 100,001 | 200,000 |
| or[1,9] | 1.267 | 0.2235 | 0.001783 | 0.8794 | 1.25 | 1.756 | 100,001 | 200,000 |
| or[1,10] | 1.406 | 0.6698 | 0.005369 | 0.5194 | 1.274 | 3.08 | 100,001 | 200,000 |
| or[1,16] | 1.371 | 0.683 | 0.006053 | 0.4762 | 1.23 | 3.049 | 100,001 | 200,000 |
| or[1,17] | 1.147 | 0.3434 | 0.002527 | 0.6416 | 1.092 | 1.971 | 100,001 | 200,000 |
| or[1,19] | 1.009 | 0.6816 | 0.007816 | 0.2523 | 0.8358 | 2.8 | 100,001 | 200,000 |
| or[2,11] | 3.016 | 2.536 | 0.04166 | 0.6695 | 2.329 | 9.441 | 100,001 | 200,000 |
| or[2,12] | 7.359 | 77.39 | 1.501 | 0.0235 | 0.9059 | 37.32 | 100,001 | 200,000 |
| or[3,6] | 0.9992 | 0.4135 | 0.003322 | 0.4231 | 0.9231 | 1.998 | 100,001 | 200,000 |
| or[3,9] | 0.9222 | 0.9469 | 0.01388 | 0.1094 | 0.6574 | 3.308 | 100,001 | 200,000 |
| or[3,11] | 0.6126 | 0.2452 | 0.001872 | 0.2643 | 0.5702 | 1.209 | 100,001 | 200,000 |
| or[4,9] | 2.063 | 0.5714 | 0.005245 | 1.177 | 1.986 | 3.404 | 100,001 | 200,000 |
| or[4,10] | 0.8249 | 0.602 | 0.007823 | 0.1737 | 0.6654 | 2.401 | 100,001 | 200,000 |
| or[4,11] | 0.1916 | 2.693 | 0.0376 | 3.22 × 10–29 | 3.71 × 10–08 | 0.9807 | 100,001 | 200,000 |
| or[4,14] | 0.6066 | 0.5124 | 0.005516 | 0.093 | 0.4648 | 1.954 | 100,001 | 200,000 |
| or[4,15] | 9.598 | 112.2 | 1.093 | 0.0197 | 1.011 | 55.18 | 100,001 | 200,000 |
| or[4,18] | 2.525 | 7.221 | 0.08789 | 0.02603 | 0.9102 | 14.75 | 100,001 | 200,000 |
| or[5,8] | 0.4725 | 0.3376 | 0.003374 | 0.09511 | 0.3896 | 1.333 | 100,001 | 200,000 |
| or[5,9] | 24.61 | 164.5 | 2.297 | 0.6354 | 5.26 | 137.3 | 100,001 | 200,000 |
| or[5,17] | Not estimable | |||||||
| or[6,9] | 2.218 | 0.8519 | 0.00654 | 1.009 | 2.069 | 4.304 | 100,001 | 200,000 |
| or[6,11] | 1.593 | 2.08 | 0.02623 | 0.1562 | 1.01 | 6.675 | 100,001 | 200,000 |
| or[8,9] | 34.05 | 274.8 | 3.707 | 0.8065 | 6.109 | 186.5 | 100,001 | 200,000 |
| or[9,10] | Not estimable | |||||||
| or[9,13] | 37.43 | 957.5 | 15.96 | 0.1695 | 2.827 | 106.7 | 100,001 | 200,000 |
| or[9,16] | Not estimable | |||||||
| or[9,20] | 2.254 | 3.057 | 0.0391 | 0.1999 | 1.345 | 9.741 | 100,001 | 200,000 |
| or[10,12] | 1.115 | 0.296 | 0.003279 | 0.6476 | 1.079 | 1.802 | 100,001 | 200,000 |
| or[10,14] | Not estimable | |||||||
| or[10,16] | Not estimable | |||||||
| or[10,18] | 0.4653 | 0.2291 | 0.002258 | 0.1581 | 0.4214 | 1.031 | 100,001 | 200,000 |
| or[11,15] | Not estimable | |||||||
| or[11,18] | 0.02907 | 0.4428 | 0.00551 | 5.48 × 10–34 | 1.47 × 10–10 | 0.2107 | 100,001 | 200,000 |
| or[12,18] | 1.886 | 2.371 | 0.02685 | 0.2005 | 1.216 | 7.628 | 100,001 | 200,000 |
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk.class[1] | 8.085 | 1.946 | 0.05168 | 4 | 8 | 12 | 100,001 | 200,000 |
| rk.class[2] | 3.071 | 2.329 | 0.0511 | 1 | 2 | 10 | 100,001 | 200,000 |
| rk.class[3] | 9.087 | 1.926 | 0.0441 | 5 | 9 | 12 | 100,001 | 200,000 |
| rk.class[4] | 12.04 | 1.439 | 0.03463 | 9 | 12 | 14 | 100,001 | 200,000 |
| rk.class[5] | 8.67 | 2.485 | 0.0615 | 4 | 9 | 13 | 100,001 | 200,000 |
| rk.class[6] | 6.351 | 2.659 | 0.0627 | 2 | 6 | 12 | 100,001 | 200,000 |
| rk.class[7] | 8.397 | 2.913 | 0.07246 | 3 | 8 | 14 | 100,001 | 200,000 |
| rk.class[8] | 10.04 | 3.093 | 0.0506 | 3 | 11 | 14 | 100,001 | 200,000 |
| rk.class[9] | 10.27 | 5.291 | 0.1756 | 1 | 13 | 15 | 100,001 | 200,000 |
| rk.class[10] | 12.73 | 3.762 | 0.09555 | 2 | 14 | 15 | 100,001 | 200,000 |
| rk.class[11] | 3.386 | 2.829 | 0.07809 | 1 | 2 | 12 | 100,001 | 200,000 |
| rk.class[12] | 4.019 | 2.365 | 0.05665 | 1 | 4 | 10 | 100,001 | 200,000 |
| rk.class[13] | 5.306 | 3.719 | 0.08131 | 1 | 4 | 14 | 100,001 | 200,000 |
| rk.class[14] | 7.223 | 3.919 | 0.07868 | 1 | 7 | 14 | 100,001 | 200,000 |
| rk.class[15] | 11.32 | 3.987 | 0.08988 | 2 | 13 | 15 | 100,001 | 200,000 |
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk[1] | 9.484 | 2.829 | 0.06994 | 5 | 9 | 16 | 100,001 | 200,000 |
| rk[2] | 3.757 | 3.831 | 0.1029 | 1 | 2 | 17 | 100,001 | 200,000 |
| rk[3] | 12.69 | 2.82 | 0.04927 | 7 | 13 | 18 | 100,001 | 200,000 |
| rk[4] | 11.83 | 2.771 | 0.04972 | 6 | 12 | 17 | 100,001 | 200,000 |
| rk[5] | 11.82 | 2.792 | 0.05045 | 6 | 12 | 17 | 100,001 | 200,000 |
| rk[6] | 10.51 | 2.987 | 0.05807 | 5 | 10 | 16 | 100,001 | 200,000 |
| rk[7] | 10.99 | 3.276 | 0.05719 | 5 | 11 | 17 | 100,001 | 200,000 |
| rk[8] | 3.245 | 2.897 | 0.05979 | 1 | 2 | 13 | 100,001 | 200,000 |
| rk[9] | 16.92 | 1.568 | 0.03531 | 13 | 17 | 19 | 100,001 | 200,000 |
| rk[10] | 10.95 | 4.431 | 0.1165 | 4 | 10 | 18 | 100,001 | 200,000 |
| rk[11] | 7.263 | 4.037 | 0.09317 | 2 | 6 | 17 | 100,001 | 200,000 |
| rk[12] | 10.55 | 4.908 | 0.1263 | 3 | 9 | 19 | 100,001 | 200,000 |
| rk[13] | 16.92 | 5.446 | 0.1358 | 2 | 19 | 20 | 100,001 | 200,000 |
| rk[14] | 6.362 | 5.435 | 0.1197 | 1 | 4 | 19 | 100,001 | 200,000 |
| rk[15] | 13.53 | 7.524 | 0.2471 | 1 | 18 | 20 | 100,001 | 200,000 |
| rk[16] | 13.23 | 5.061 | 0.08111 | 4 | 15 | 19 | 100,001 | 200,000 |
| rk[17] | 11.53 | 3.142 | 0.05114 | 5 | 12 | 17 | 100,001 | 200,000 |
| rk[18] | 4.438 | 3.362 | 0.08106 | 1 | 4 | 15 | 100,001 | 200,000 |
| rk[19] | 8.965 | 5.926 | 0.1137 | 1 | 7 | 19 | 100,001 | 200,000 |
| rk[20] | 15.02 | 5.952 | 0.1315 | 2 | 18 | 20 | 100,001 | 200,000 |
Children and adolescents/acceptability (total dropouts)
Network geometry
FIGURE 29.
Network plot for class effects (the plot for individual effects is included in the main report). CBTPL, CBT + placebo; CBTSER, CBT + sertraline; CLO, clomipramine; PL, placebo; PSYPL, psychological placebo; WL, waitlist.

Model fit
| Model fit | ||||||||
|---|---|---|---|---|---|---|---|---|
| Dbar | Dhat | DIC | pD | |||||
| r | 147.2 | 116.9 | 177.5 | 30.29 | ||||
| total | 147.2 | 116.9 | 177.5 | 30.29 | ||||
| Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample | |
| sd | 0.5147 | 0.3715 | 0.006303 | 0.02217 | 0.4515 | 1.403 | 100,001 | 200,000 |
| totresdev | 37.05 | 8.216 | 0.06423 | 22.75 | 36.44 | 54.83 | 100,001 | 200,000 |
| Model fit | ||||||||
|---|---|---|---|---|---|---|---|---|
| Dbar | Dhat | DIC | pD | |||||
| r | 149.1 | 115.7 | 182.6 | 33.43 | ||||
| total | 149.1 | 115.7 | 182.6 | 33.43 | ||||
| Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample | |
| sd | 0.8612 | 0.6323 | 0.01195 | 0.04502 | 0.7421 | 2.443 | 70,001 | 140,000 |
| totresdev | 38.99 | 8.76 | 0.07706 | 23.62 | 38.36 | 57.84 | 70,001 | 140,000 |
Data synthesis: consistency model (network meta-analysis)
Key: intervention (class)
-
Placebo (1).
-
Waitlist (2).
-
Psychological placebo (3).
-
Fluoxetine (4).
-
Fluvoxamine (4).
-
Paroxetine (4).
-
Sertraline (4).
-
Clomipramine (5).
-
BT (6).
-
CBT (7).
-
Sertraline + CBT (8).
-
CBT + placebo (9).
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| OR.D[1,2] | 0.9559 | 1.936 | 0.01895 | 0.05486 | 0.5295 | 4.328 | 100,001 | 200,000 |
| OR.D[1,3] | 1.033 | 2.564 | 0.01631 | 0.0683 | 0.5781 | 4.439 | 100,001 | 200,000 |
| OR.D[1,4] | 6.742 | 851.4 | 1.95 | 0.227 | 0.872 | 2.997 | 100,001 | 200,000 |
| OR.D[1,5] | 5.094 | 8.9 | 0.08637 | 0.5404 | 3.061 | 21.69 | 100,001 | 200,000 |
| OR.D[1,6] | 107.2 | 1453 | 24.67 | 0.4076 | 7.645 | 423.7 | 100,001 | 200,000 |
| OR.D[1,7] | 0.6919 | 0.8371 | 0.008558 | 0.09176 | 0.4952 | 2.415 | 100,001 | 200,000 |
| OR.D[1,8] | 0.8625 | 9.133 | 0.02526 | 0.07651 | 0.5374 | 3.148 | 100,001 | 200,000 |
| OR.D[1,9] | 0.5534 | 13.27 | 0.03814 | 0.008114 | 0.1486 | 2.26 | 100,001 | 200,000 |
| OR.D[2,3] | 2.018 | 8.554 | 0.03339 | 0.1509 | 1.081 | 8.872 | 100,001 | 200,000 |
| OR.D[2,4] | 17.42 | 2021 | 4.562 | 0.1446 | 1.628 | 20.15 | 100,001 | 200,000 |
| OR.D[2,5] | 18.19 | 156.2 | 0.6924 | 0.4662 | 5.804 | 95.46 | 100,001 | 200,000 |
| OR.D[2,6] | 280.2 | 4183 | 76.79 | 0.8716 | 14.28 | 785.2 | 100,001 | 200,000 |
| OR.D[2,7] | 1.323 | 1.526 | 0.0146 | 0.2087 | 0.9368 | 4.786 | 100,001 | 200,000 |
| OR.D[2,8] | 3.04 | 106.5 | 0.2573 | 0.08032 | 0.9982 | 13.51 | 100,001 | 200,000 |
| OR.D[2,9] | 2.462 | 174.6 | 0.4081 | 0.01024 | 0.2817 | 7.587 | 100,001 | 200,000 |
| OR.D[3,4] | 11.87 | 1088 | 2.437 | 0.1354 | 1.491 | 16.49 | 100,001 | 200,000 |
| OR.D[3,5] | 17.02 | 193.3 | 0.6174 | 0.4127 | 5.315 | 85.68 | 100,001 | 200,000 |
| OR.D[3,6] | 258.7 | 3404 | 54.9 | 0.5696 | 13.49 | 922 | 100,001 | 200,000 |
| OR.D[3,7] | 1.087 | 1.212 | 0.006656 | 0.2347 | 0.8582 | 3.236 | 100,001 | 200,000 |
| OR.D[3,8] | 2.277 | 15.15 | 0.05515 | 0.07783 | 0.9071 | 11.15 | 100,001 | 200,000 |
| OR.D[3,9] | 1.817 | 122.3 | 0.2775 | 0.009615 | 0.257 | 6.481 | 100,001 | 200,000 |
| OR.D[4,5] | 76.63 | 12,040 | 26.87 | 0.4338 | 3.553 | 38.72 | 100,001 | 200,000 |
| OR.D[4,6] | 554.3 | 89,330 | 205.4 | 0.374 | 8.929 | 635.8 | 100,001 | 200,000 |
| OR.D[4,7] | 10.86 | 2349 | 5.272 | 0.07641 | 0.5772 | 4.21 | 100,001 | 200,000 |
| OR.D[4,8] | 15.5 | 3969 | 8.915 | 0.06728 | 0.6203 | 5.557 | 100,001 | 200,000 |
| OR.D[4,9] | 9.836 | 2643 | 5.916 | 0.007736 | 0.1714 | 3.576 | 100,001 | 200,000 |
| OR.D[5,6] | 31.56 | 471.1 | 7.974 | 0.1311 | 2.483 | 114.1 | 100,001 | 200,000 |
| OR.D[5,7] | 0.315 | 0.9211 | 0.006088 | 0.01411 | 0.163 | 1.498 | 100,001 | 200,000 |
| OR.D[5,8] | 0.5014 | 23.49 | 0.0536 | 0.01133 | 0.172 | 2.019 | 100,001 | 200,000 |
| OR.D[5,9] | 0.3448 | 22.67 | 0.06146 | 0.001491 | 0.04777 | 1.189 | 100,001 | 200,000 |
| OR.D[6,7] | 0.2088 | 3.232 | 0.009925 | 0.001165 | 0.06527 | 1.222 | 100,001 | 200,000 |
| OR.D[6,8] | 0.543 | 86.68 | 0.195 | 9.79 × 10–04 | 0.06738 | 1.925 | 100,001 | 200,000 |
| OR.D[6,9] | 0.6371 | 137.2 | 0.42 | 1.67 × 10–04 | 0.01871 | 1.026 | 100,001 | 200,000 |
| OR.D[7,8] | 2.104 | 52.45 | 0.124 | 0.1312 | 1.076 | 8.83 | 100,001 | 200,000 |
| OR.D[7,9] | 1.357 | 36.53 | 0.1004 | 0.01429 | 0.3014 | 5.617 | 100,001 | 200,000 |
| OR.D[8,9] | 0.5331 | 6.051 | 0.01487 | 0.0303 | 0.284 | 2.25 | 100,001 | 200,000 |
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| OR[1,2] | 0.9559 | 1.936 | 0.01895 | 0.05486 | 0.5295 | 4.328 | 100,001 | 200,000 |
| OR[1,3] | 1.033 | 2.564 | 0.01631 | 0.0683 | 0.5781 | 4.439 | 100,001 | 200,000 |
| OR[1,4] | 0.794 | 0.4219 | 0.0038 | 0.2479 | 0.7371 | 1.685 | 100,001 | 200,000 |
| OR[1,5] | 0.8868 | 1.63 | 0.005053 | 0.2456 | 0.7863 | 2.068 | 100,001 | 200,000 |
| OR[1,6] | 1.33 | 1.974 | 0.006881 | 0.3738 | 1.118 | 3.416 | 100,001 | 200,000 |
| OR[1,7] | 0.9712 | 0.6798 | 0.004586 | 0.3211 | 0.8925 | 2.069 | 100,001 | 200,000 |
| OR[1,8] | 5.094 | 8.9 | 0.08637 | 0.5404 | 3.061 | 21.69 | 100,001 | 200,000 |
| OR[1,9] | 107.2 | 1453 | 24.67 | 0.4076 | 7.645 | 423.7 | 100,001 | 200,000 |
| OR[1,10] | 0.6919 | 0.8371 | 0.008558 | 0.09176 | 0.4952 | 2.415 | 100,001 | 200,000 |
| OR[1,11] | 0.8625 | 9.133 | 0.02526 | 0.07651 | 0.5374 | 3.148 | 100,001 | 200,000 |
| OR[1,12] | 0.5534 | 13.27 | 0.03814 | 0.008114 | 0.1486 | 2.26 | 100,001 | 200,000 |
| OR[2,3] | 2.018 | 8.554 | 0.03339 | 0.1509 | 1.081 | 8.872 | 100,001 | 200,000 |
| OR[2,4] | 3.042 | 18.91 | 0.1008 | 0.1342 | 1.361 | 14.35 | 100,001 | 200,000 |
| OR[2,5] | 3.507 | 39.05 | 0.1307 | 0.1436 | 1.457 | 16.19 | 100,001 | 200,000 |
| OR[2,6] | 5.1 | 30.22 | 0.1806 | 0.2113 | 2.137 | 24.52 | 100,001 | 200,000 |
| OR[2,7] | 3.307 | 10.22 | 0.07605 | 0.1953 | 1.669 | 15.4 | 100,001 | 200,000 |
| OR[2,8] | 18.19 | 156.2 | 0.6924 | 0.4662 | 5.804 | 95.46 | 100,001 | 200,000 |
| OR[2,9] | 280.2 | 4183 | 76.79 | 0.8716 | 14.28 | 785.2 | 100,001 | 200,000 |
| OR[2,10] | 1.323 | 1.526 | 0.0146 | 0.2087 | 0.9368 | 4.786 | 100,001 | 200,000 |
| OR[2,11] | 3.04 | 106.5 | 0.2573 | 0.08032 | 0.9982 | 13.51 | 100,001 | 200,000 |
| OR[2,12] | 2.462 | 174.6 | 0.4081 | 0.01024 | 0.2817 | 7.587 | 100,001 | 200,000 |
| OR[3,4] | 2.608 | 11.99 | 0.06187 | 0.1282 | 1.249 | 11.67 | 100,001 | 200,000 |
| OR[3,5] | 3.004 | 34.47 | 0.1066 | 0.1356 | 1.335 | 13.25 | 100,001 | 200,000 |
| OR[3,6] | 4.512 | 42.92 | 0.1743 | 0.1992 | 1.953 | 20.02 | 100,001 | 200,000 |
| OR[3,7] | 2.829 | 9.741 | 0.05322 | 0.1882 | 1.533 | 12.37 | 100,001 | 200,000 |
| OR[3,8] | 17.02 | 193.3 | 0.6174 | 0.4127 | 5.315 | 85.68 | 100,001 | 200,000 |
| OR[3,9] | 258.7 | 3404 | 54.9 | 0.5696 | 13.49 | 922 | 100,001 | 200,000 |
| OR[3,10] | 1.087 | 1.212 | 0.006656 | 0.2347 | 0.8582 | 3.236 | 100,001 | 200,000 |
| OR[3,11] | 2.277 | 15.15 | 0.05515 | 0.07783 | 0.9071 | 11.15 | 100,001 | 200,000 |
| OR[3,12] | 1.817 | 122.3 | 0.2775 | 0.009615 | 0.257 | 6.481 | 100,001 | 200,000 |
| OR[4,5] | 1.35 | 3.422 | 0.01122 | 0.3257 | 1.03 | 3.962 | 100,001 | 200,000 |
| OR[4,6] | 2.156 | 10.46 | 0.03006 | 0.5414 | 1.398 | 7.302 | 100,001 | 200,000 |
| OR[4,7] | 1.495 | 2.231 | 0.01093 | 0.4176 | 1.127 | 4.38 | 100,001 | 200,000 |
| OR[4,8] | 8.423 | 26.44 | 0.1767 | 0.6242 | 4.257 | 39.7 | 100,001 | 200,000 |
| OR[4,9] | 181.7 | 3674 | 42.78 | 0.5159 | 10.75 | 682.9 | 100,001 | 200,000 |
| OR[4,10] | 1.104 | 2.866 | 0.01676 | 0.1108 | 0.6883 | 4.419 | 100,001 | 200,000 |
| OR[4,11] | 1.452 | 21.8 | 0.05584 | 0.09549 | 0.7402 | 5.771 | 100,001 | 200,000 |
| OR[4,12] | 1.014 | 51.89 | 0.1321 | 0.01033 | 0.2054 | 3.781 | 100,001 | 200,000 |
| OR[5,6] | 2.072 | 13.12 | 0.03253 | 0.4542 | 1.306 | 6.815 | 100,001 | 200,000 |
| OR[5,7] | 1.471 | 19.68 | 0.04918 | 0.3417 | 1.074 | 4.143 | 100,001 | 200,000 |
| OR[5,8] | 8.204 | 37.83 | 0.179 | 0.5597 | 3.976 | 37.72 | 100,001 | 200,000 |
| OR[5,9] | 1076 | 402,800 | 920.1 | 0.4583 | 10.06 | 630.1 | 100,001 | 200,000 |
| OR[5,10] | 1.17 | 37.78 | 0.09073 | 0.09699 | 0.6418 | 4.208 | 100,001 | 200,000 |
| OR[5,11] | 1.425 | 23.22 | 0.0606 | 0.08489 | 0.6927 | 5.429 | 100,001 | 200,000 |
| OR[5,12] | 3.115 | 968.3 | 2.163 | 0.009302 | 0.1932 | 3.573 | 100,001 | 200,000 |
| OR[6,7] | 0.9465 | 3.136 | 0.008293 | 0.1962 | 0.8573 | 2.296 | 100,001 | 200,000 |
| OR[6,8] | 6.161 | 239.5 | 0.5562 | 0.3643 | 2.717 | 26.15 | 100,001 | 200,000 |
| OR[6,9] | 142.6 | 12,870 | 38.12 | 0.3133 | 6.805 | 423.3 | 100,001 | 200,000 |
| OR[6,10] | 0.7211 | 2.777 | 0.01193 | 0.06349 | 0.4408 | 2.793 | 100,001 | 200,000 |
| OR[6,11] | 0.9726 | 17.57 | 0.05602 | 0.05624 | 0.4719 | 3.725 | 100,001 | 200,000 |
| OR[6,12] | 0.8511 | 65.25 | 0.1538 | 0.006448 | 0.1303 | 2.479 | 100,001 | 200,000 |
| OR[7,8] | 6.738 | 28.23 | 0.1415 | 0.5278 | 3.444 | 31.11 | 100,001 | 200,000 |
| OR[7,9] | 136.3 | 3712 | 24.62 | 0.4528 | 8.661 | 528.2 | 100,001 | 200,000 |
| OR[7,10] | 0.7998 | 1.026 | 0.008957 | 0.1085 | 0.5644 | 2.844 | 100,001 | 200,000 |
| OR[7,11] | 1.013 | 8.437 | 0.0233 | 0.09035 | 0.6052 | 3.916 | 100,001 | 200,000 |
| OR[7,12] | 0.769 | 46.44 | 0.1119 | 0.00959 | 0.1673 | 2.794 | 100,001 | 200,000 |
| OR[8,9] | 31.56 | 471.1 | 7.974 | 0.1311 | 2.483 | 114.1 | 100,001 | 200,000 |
| OR[8,10] | 0.315 | 0.9211 | 0.006088 | 0.01411 | 0.163 | 1.498 | 100,001 | 200,000 |
| OR[8,11] | 0.5014 | 23.49 | 0.0536 | 0.01133 | 0.172 | 2.019 | 100,001 | 200,000 |
| OR[8,12] | 0.3448 | 22.67 | 0.06146 | 0.001491 | 0.04777 | 1.189 | 100,001 | 200,000 |
| OR[9,10] | 0.2088 | 3.232 | 0.009925 | 0.001165 | 0.06527 | 1.222 | 100,001 | 200,000 |
| OR[9,11] | 0.543 | 86.68 | 0.195 | 9.79 × 10–4 | 0.06738 | 1.925 | 100,001 | 200,000 |
| OR[9,12] | 0.6371 | 137.2 | 0.42 | 1.67 × 10–4 | 0.01871 | 1.026 | 100,001 | 200,000 |
| OR[10,11] | 2.104 | 52.45 | 0.124 | 0.1312 | 1.076 | 8.83 | 100,001 | 200,000 |
| OR[10,12] | 1.357 | 36.53 | 0.1004 | 0.01429 | 0.3014 | 5.617 | 100,001 | 200,000 |
| OR[11,12] | 0.5331 | 6.051 | 0.01487 | 0.0303 | 0.284 | 2.25 | 100,001 | 200,000 |
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| or[1,4] | 0.8024 | 4.62 | 0.01388 | 0.0948 | 0.5591 | 2.567 | 70,001 | 140,000 |
| or[1,5] | 4.409 | 395.2 | 1.456 | 0.06265 | 0.6615 | 6.949 | 70,001 | 140,000 |
| or[1,6] | 17.57 | 1645 | 4.528 | 0.1618 | 1.59 | 16.65 | 70,001 | 140,000 |
| or[1,7] | 1.265 | 19.6 | 0.06121 | 0.1058 | 0.807 | 3.784 | 70,001 | 140,000 |
| or[1,8] | 10.7 | 484.8 | 1.345 | 0.415 | 3.437 | 41.35 | 70,001 | 140,000 |
| or[1,10] | 4.49 | 505.5 | 1.392 | 0.02441 | 0.441 | 5.079 | 70,001 | 140,000 |
| or[1,11] | 2.774 | 246.6 | 0.6614 | 0.02385 | 0.4328 | 4.915 | 70,001 | 140,000 |
| or[2,9] | 78,230 | 1.39E+ 07 | 60,100 | 0.2729 | 12.92 | 9205 | 70,001 | 140,000 |
| or[2,10] | 1.948 | 9.336 | 0.03735 | 0.1654 | 1.04 | 7.907 | 70,001 | 140,000 |
| or[3,10] | 1.549 | 12.69 | 0.04082 | 0.1434 | 0.8612 | 5.475 | 70,001 | 140,000 |
| or[7,10] | 4.438 | 634.4 | 1.722 | 2.25 × 10–4 | 0.1758 | 10.21 | 70,001 | 140,000 |
| or[7,11] | Not estimable | |||||||
| or[8,9] | 6840 | 643,600 | 2588 | 0.06813 | 4.448 | 2504 | 70,001 | 140,000 |
| or[10,11] | Not estimable | |||||||
| or[11,12] | 16.02 | 3927 | 10.53 | 0.01717 | 0.2818 | 4.169 | 70,001 | 140,000 |
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk.class[1] | 5.769 | 1.498 | 0.0213 | 2 | 6 | 8 | 100,001 | 200,000 |
| rk.class[2] | 4.003 | 2.107 | 0.02918 | 1 | 4 | 8 | 100,001 | 200,000 |
| rk.class[3] | 4.27 | 2.069 | 0.02356 | 1 | 4 | 8 | 100,001 | 200,000 |
| rk.class[4] | 5.184 | 1.858 | 0.01989 | 1 | 5 | 8 | 100,001 | 200,000 |
| rk.class[5] | 7.725 | 1.361 | 0.01701 | 3 | 8 | 9 | 100,001 | 200,000 |
| rk.class[6] | 8.35 | 1.377 | 0.0248 | 4 | 9 | 9 | 100,001 | 200,000 |
| rk.class[7] | 3.678 | 1.502 | 0.01782 | 1 | 4 | 7 | 100,001 | 200,000 |
| rk.class[8] | 4.059 | 1.958 | 0.02073 | 1 | 4 | 8 | 100,001 | 200,000 |
| rk.class[9] | 1.961 | 1.752 | 0.01679 | 1 | 1 | 7 | 100,001 | 200,000 |
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk[1] | 7.652 | 1.96 | 0.02736 | 3 | 8 | 11 | 100,001 | 200,000 |
| rk[2] | 4.993 | 3.158 | 0.04543 | 1 | 4 | 11 | 100,001 | 200,000 |
| rk[3] | 5.321 | 3.121 | 0.0377 | 1 | 5 | 11 | 100,001 | 200,000 |
| rk[4] | 5.741 | 2.404 | 0.02741 | 1 | 6 | 10 | 100,001 | 200,000 |
| rk[5] | 6.099 | 2.48 | 0.02415 | 1 | 6 | 11 | 100,001 | 200,000 |
| rk[6] | 8.067 | 2.388 | 0.02601 | 3 | 9 | 12 | 100,001 | 200,000 |
| rk[7] | 6.873 | 2.174 | 0.02246 | 2 | 7 | 11 | 100,001 | 200,000 |
| rk[8] | 10.43 | 1.945 | 0.02452 | 4 | 11 | 12 | 100,001 | 200,000 |
| rk[9] | 11.11 | 2.012 | 0.03567 | 4 | 12 | 12 | 100,001 | 200,000 |
| rk[10] | 4.467 | 2.351 | 0.0305 | 1 | 4 | 10 | 100,001 | 200,000 |
| rk[11] | 4.97 | 2.906 | 0.02952 | 1 | 4 | 11 | 100,001 | 200,000 |
| rk[12] | 2.283 | 2.458 | 0.02273 | 1 | 1 | 10 | 100,001 | 200,000 |
Complete data for rank probabilities by type of intervention
| Adults | Rank (YBOCS: 17 treatments; dropouts: 20 treatments) | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | Sum | ||
| YBOCS | Placebo | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1.00 × 10–5 | 5.00 × 10–5 | 5.50 × 10–4 | 0.00586 | 0.07351 | 0.4772 | 0.4383 | 0.00453 | 1 | |||
| Dropout | Placebo | 0.00 | 0.00 | 0.00 | 0.02 | 0.04 | 0.08 | 0.12 | 0.14 | 0.14 | 0.13 | 0.10 | 0.08 | 0.06 | 0.04 | 0.03 | 0.02 | 0.01 | 0.00 | 0.00 | 0.00 | 1 |
| YBOCS | Waitlist | 0 | 0 | 0 | 0 | 0 | 1.00 × 10–5 | 3.00 × 10–5 | 1.00 × 10–5 | 2.00 × 10–5 | 0 | 1.00 × 10–5 | 4.00 × 10–5 | 1.30 × 10–4 | 0.00135 | 0.0063 | 0.09427 | 0.8978 | 1 | |||
| Dropout | Waitlist | 0.29 | 0.21 | 0.15 | 0.10 | 0.06 | 0.04 | 0.03 | 0.02 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.00 | 1 |
| YBOCS | Fluoxetine | 0 | 0 | 8.00 × 10–5 | 0.00223 | 0.01146 | 0.03125 | 0.06575 | 0.1076 | 0.1323 | 0.1413 | 0.146 | 0.1426 | 0.1258 | 0.07633 | 0.01688 | 3.30 × 10–4 | 0 | 1 | |||
| Dropout | Fluoxetine | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.01 | 0.02 | 0.04 | 0.06 | 0.08 | 0.10 | 0.13 | 0.13 | 0.13 | 0.12 | 0.09 | 0.05 | 0.02 | 0.01 | 0.00 | 1 |
| YBOCS | Fluvoxamine | 0 | 0 | 0 | 0.00166 | 0.01125 | 0.0377 | 0.08082 | 0.1311 | 0.1591 | 0.1571 | 0.1451 | 0.1246 | 0.09534 | 0.04741 | 0.00875 | 2.00 × 10–5 | 0 | 1 | |||
| Dropout | Fluvoxamine | 0.00 | 0.00 | 0.00 | 0.00 | 0.01 | 0.02 | 0.04 | 0.06 | 0.08 | 0.11 | 0.13 | 0.13 | 0.13 | 0.11 | 0.09 | 0.06 | 0.03 | 0.01 | 0.00 | 0.00 | 1 |
| YBOCS | Paroxetine | 0 | 0 | 1.00 × 10–5 | 0.00139 | 0.00764 | 0.02466 | 0.05581 | 0.09689 | 0.1297 | 0.1461 | 0.1559 | 0.1563 | 0.1355 | 0.07485 | 0.01502 | 1.20 × 10–4 | 0 | 1 | |||
| Dropout | Paroxetine | 0.00 | 0.00 | 0.00 | 0.00 | 0.01 | 0.02 | 0.04 | 0.06 | 0.09 | 0.11 | 0.12 | 0.13 | 0.13 | 0.11 | 0.09 | 0.06 | 0.03 | 0.01 | 0.00 | 0.00 | 1 |
| YBOCS | Sertraline | 0 | 0 | 6.00 × 10–5 | 0.00275 | 0.01315 | 0.03431 | 0.06953 | 0.1118 | 0.137 | 0.1448 | 0.1448 | 0.1386 | 0.116 | 0.07135 | 0.01556 | 2.60 × 10–4 | 0 | 1 | |||
| Dropout | Sertraline | 0.00 | 0.00 | 0.00 | 0.01 | 0.03 | 0.05 | 0.07 | 0.10 | 0.11 | 0.12 | 0.12 | 0.11 | 0.09 | 0.07 | 0.05 | 0.03 | 0.01 | 0.00 | 0.00 | 0.00 | 1 |
| YBOCS | Citalopram | 0 | 1.00 × 10–5 | 2.10 × 10–4 | 0.00634 | 0.02091 | 0.04177 | 0.07302 | 0.1076 | 0.125 | 0.129 | 0.132 | 0.133 | 0.1248 | 0.08273 | 0.02196 | 0.00169 | 7.00 × 10–5 | 1 | |||
| Dropout | Citalopram | 0.00 | 0.00 | 0.01 | 0.01 | 0.03 | 0.05 | 0.06 | 0.08 | 0.10 | 0.11 | 0.11 | 0.11 | 0.10 | 0.09 | 0.07 | 0.05 | 0.03 | 0.01 | 0.00 | 0.00 | 1 |
| YBOCS | Venlafaxine | 2.00 × 10–4 | 5.90 × 10–4 | 0.00452 | 0.05998 | 0.09522 | 0.08724 | 0.08047 | 0.06269 | 0.03474 | 0.03017 | 0.03238 | 0.0416 | 0.07623 | 0.199 | 0.1285 | 0.06263 | 0.00382 | 1 | |||
| Dropout | Venlafaxine | 0.28 | 0.25 | 0.16 | 0.11 | 0.07 | 0.04 | 0.03 | 0.02 | 0.01 | 0.01 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.01 | 0.00 | 0.00 | 0.00 | 0.00 | 1 |
| YBOCS | Clomipramine | 0 | 0 | 8.60 × 10–4 | 0.06048 | 0.1751 | 0.2376 | 0.2215 | 0.1153 | 0.05586 | 0.03749 | 0.02873 | 0.02559 | 0.02463 | 0.01445 | 0.00242 | 1.00 × 10–5 | 0 | 1 | |||
| Dropout | Clomipramine | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.01 | 0.02 | 0.04 | 0.08 | 0.17 | 0.28 | 0.26 | 0.11 | 0.02 | 1 |
| YBOCS | BT | 5.11 × 10–1 | 0.3972 | 0.08817 | 0.00367 | 3.00 × 10–5 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | |||
| Dropout | BT | 0.00 | 0.00 | 0.01 | 0.03 | 0.06 | 0.10 | 0.11 | 0.09 | 0.06 | 0.04 | 0.04 | 0.04 | 0.05 | 0.08 | 0.09 | 0.08 | 0.07 | 0.04 | 0.02 | 0.00 | 1 |
| YBOCS | CBT | 0 | 6.00 × 10–5 | 0.00445 | 0.1258 | 0.33 | 0.1982 | 0.1035 | 0.05264 | 0.03062 | 0.02482 | 0.02428 | 0.03059 | 0.03744 | 0.02797 | 0.00867 | 9.80 × 10–4 | 0 | 1 | |||
| Dropout | CBT | 0.00 | 0.03 | 0.09 | 0.15 | 0.16 | 0.14 | 0.10 | 0.07 | 0.05 | 0.03 | 0.03 | 0.02 | 0.02 | 0.02 | 0.03 | 0.03 | 0.02 | 0.01 | 0.00 | 0.00 | 1 |
| YBOCS | CT | 0.1726 | 0.4096 | 0.3718 | 0.04326 | 0.0021 | 3.70 × 10–4 | 1.00 × 10–4 | 7.00 × 10–5 | 2.00 × 10–5 | 2.00 × 10–5 | 1.00 × 10–5 | 1.00 × 10–5 | 2.00 × 10–5 | 0 | 0 | 0 | 0 | 1 | |||
| Dropout | CT | 0.00 | 0.01 | 0.02 | 0.06 | 0.09 | 0.11 | 0.10 | 0.07 | 0.05 | 0.04 | 0.03 | 0.03 | 0.04 | 0.05 | 0.07 | 0.08 | 0.08 | 0.05 | 0.03 | 0.00 | 1 |
| YBOCS | Hypericum | 3.10 × 10–4 | 7.10 × 10–4 | 0.00299 | 0.02795 | 0.03718 | 0.03148 | 0.02984 | 0.02298 | 0.0172 | 0.01398 | 0.01413 | 0.01878 | 0.03187 | 0.08821 | 0.196 | 0.3728 | 0.09357 | 1 | |||
| Dropout | Hypericum | 0.04 | 0.07 | 0.10 | 0.10 | 0.09 | 0.08 | 0.06 | 0.04 | 0.03 | 0.02 | 0.02 | 0.02 | 0.02 | 0.03 | 0.04 | 0.05 | 0.06 | 0.07 | 0.05 | 0.01 | 1 |
| YBOCS | CBT + fluvoxamine | 0.0151 | 0.02434 | 0.09851 | 0.5006 | 0.1236 | 0.06653 | 0.03564 | 0.01945 | 0.01279 | 0.01009 | 0.0107 | 0.01376 | 0.02199 | 0.02712 | 0.01438 | 0.00538 | 1.10 × 10–4 | 1 | |||
| Dropout | CBT + fluvoxamine | 0.12 | 0.05 | 0.04 | 0.03 | 0.03 | 0.02 | 0.02 | 0.02 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.02 | 0.03 | 0.09 | 0.20 | 0.27 | 1 |
| YBOCS | BT + clomipramine | 0.3009 | 0.1674 | 0.4262 | 0.08548 | 0.01209 | 0.00361 | 0.00154 | 6.30 × 10–4 | 3.60 × 10–4 | 3.40 × 10–4 | 3.00 × 10–4 | 4.20 × 10–4 | 3.40 × 10–4 | 3.10 × 10–4 | 1.10 × 10–4 | 1.00 × 10–5 | 0 | 1 | |||
| Dropout | BT + clomipramine | 0.00 | 0.01 | 0.02 | 0.03 | 0.05 | 0.05 | 0.05 | 0.05 | 0.04 | 0.03 | 0.03 | 0.03 | 0.03 | 0.04 | 0.07 | 0.10 | 0.14 | 0.14 | 0.08 | 0.02 | 1 |
| YBOCS | Escitalopram | 0 | 2.00 × 10–5 | 2.40 × 10–4 | 0.00669 | 0.02092 | 0.04178 | 0.07282 | 0.1064 | 0.1263 | 0.1309 | 0.1329 | 0.1308 | 0.1215 | 0.08387 | 0.02289 | 0.00203 | 2.00 × 10–5 | 1 | |||
| Dropout | Escitalopram | 0.00 | 0.00 | 0.00 | 0.01 | 0.02 | 0.03 | 0.05 | 0.07 | 0.09 | 0.10 | 0.12 | 0.11 | 0.11 | 0.10 | 0.08 | 0.06 | 0.03 | 0.01 | 0.00 | 0.00 | 1 |
| YBOCS | Psychological placebo | 0 | 0 | 0.00195 | 0.07178 | 0.1394 | 0.1635 | 0.1096 | 0.06475 | 0.03905 | 0.03389 | 0.03261 | 0.04278 | 0.08253 | 0.1316 | 0.06533 | 0.02116 | 5.00 × 10–5 | 1 | |||
| Dropout | Psychological placebo | 0.09 | 0.19 | 0.21 | 0.17 | 0.12 | 0.06 | 0.04 | 0.03 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.00 | 0.00 | 0.00 | 1 |
| Dropout | Amitriptyline | 0.02 | 0.02 | 0.02 | 0.02 | 0.02 | 0.02 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.02 | 0.03 | 0.07 | 0.20 | 0.49 | 1 |
| Dropout | BT + fluvoxamine | 0.13 | 0.14 | 0.14 | 0.12 | 0.09 | 0.06 | 0.04 | 0.03 | 0.02 | 0.01 | 0.01 | 0.01 | 0.02 | 0.02 | 0.03 | 0.03 | 0.03 | 0.04 | 0.02 | 0.01 | 1 |
| Dropout | Imipramine | 0.02 | 0.02 | 0.03 | 0.03 | 0.03 | 0.03 | 0.03 | 0.02 | 0.02 | 0.01 | 0.01 | 0.01 | 0.01 | 0.02 | 0.02 | 0.04 | 0.06 | 0.15 | 0.27 | 0.17 | 1 |
| Children and adolescents | Rank (CYBOCS: 12 treatments; dropouts: 12 treatments) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | Sum | ||
| CYBOCS | Placebo | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.01 | 0.04 | 0.14 | 0.69 | 0.12 | 1.00 |
| Dropout | Placebo | 0.00 | 0.01 | 0.02 | 0.04 | 0.08 | 0.12 | 0.16 | 0.20 | 0.20 | 0.14 | 0.03 | 0.00 | 1.00 |
| CYBOCS | Waitlist | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.01 | 0.01 | 0.02 | 0.04 | 0.10 | 0.82 | 1.00 |
| Dropout | Waitlist | 0.12 | 0.16 | 0.14 | 0.11 | 0.10 | 0.06 | 0.05 | 0.05 | 0.06 | 0.10 | 0.04 | 0.00 | 1.00 |
| CYBOCS | Psychological placebo | 0.02 | 0.03 | 0.06 | 0.11 | 0.17 | 0.16 | 0.12 | 0.08 | 0.08 | 0.11 | 0.05 | 0.00 | 1.00 |
| Dropout | Psychological placebo | 0.08 | 0.14 | 0.14 | 0.13 | 0.10 | 0.06 | 0.05 | 0.06 | 0.07 | 0.09 | 0.05 | 0.02 | 1.00 |
| CYBOCS | Fluoxetine | 0.00 | 0.00 | 0.01 | 0.02 | 0.05 | 0.10 | 0.17 | 0.23 | 0.22 | 0.17 | 0.02 | 0.00 | 1.00 |
| Dropout | Fluoxetine | 0.03 | 0.07 | 0.10 | 0.11 | 0.13 | 0.16 | 0.14 | 0.10 | 0.08 | 0.05 | 0.01 | 0.00 | 1.00 |
| CYBOCS | Fluvoxamine | 0.00 | 0.00 | 0.01 | 0.02 | 0.04 | 0.08 | 0.14 | 0.21 | 0.24 | 0.21 | 0.04 | 0.01 | 1.00 |
| Dropout | Fluvoxamine | 0.03 | 0.06 | 0.09 | 0.10 | 0.12 | 0.15 | 0.14 | 0.12 | 0.09 | 0.06 | 0.02 | 0.01 | 1.00 |
| Dropout | Paroxetine | 0.01 | 0.02 | 0.03 | 0.04 | 0.06 | 0.09 | 0.11 | 0.13 | 0.16 | 0.22 | 0.10 | 0.03 | 1.00 |
| CYBOCS | Sertraline | 0.00 | 0.00 | 0.01 | 0.02 | 0.06 | 0.12 | 0.21 | 0.25 | 0.20 | 0.11 | 0.01 | 0.00 | 1.00 |
| Dropout | Sertraline | 0.01 | 0.02 | 0.05 | 0.07 | 0.11 | 0.16 | 0.17 | 0.16 | 0.13 | 0.09 | 0.03 | 0.00 | 1.00 |
| CYBOCS | Clomipramine | 0.02 | 0.04 | 0.08 | 0.12 | 0.17 | 0.18 | 0.13 | 0.08 | 0.07 | 0.08 | 0.02 | 0.01 | 1.00 |
| Dropout | Clomipramine | 0.00 | 0.01 | 0.01 | 0.01 | 0.01 | 0.02 | 0.02 | 0.03 | 0.05 | 0.10 | 0.51 | 0.23 | 1.00 |
| CYBOCS | BT | 0.19 | 0.14 | 0.15 | 0.15 | 0.13 | 0.08 | 0.05 | 0.03 | 0.03 | 0.03 | 0.01 | 0.00 | 1.00 |
| Dropout | BT | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.02 | 0.01 | 0.02 | 0.02 | 0.04 | 0.16 | 0.69 | 1.00 |
| CYBOCS | CBT | 0.09 | 0.17 | 0.26 | 0.24 | 0.13 | 0.06 | 0.02 | 0.01 | 0.01 | 0.00 | 0.00 | 0.00 | 1.00 |
| Dropout | CBT | 0.04 | 0.15 | 0.23 | 0.19 | 0.11 | 0.07 | 0.06 | 0.06 | 0.05 | 0.03 | 0.01 | 0.00 | 1.00 |
| CYBOCS | CBT + sertraline | 0.24 | 0.35 | 0.19 | 0.11 | 0.06 | 0.03 | 0.01 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 1.00 |
| Dropout | CBT + sertraline | 0.03 | 0.25 | 0.12 | 0.12 | 0.12 | 0.07 | 0.06 | 0.05 | 0.06 | 0.07 | 0.03 | 0.01 | 1.00 |
| CYBOCS | CBT + placebo | 0.36 | 0.18 | 0.12 | 0.10 | 0.07 | 0.05 | 0.03 | 0.02 | 0.02 | 0.02 | 0.01 | 0.01 | 1.00 |
| Dropout | CBT + placebo | 0.66 | 0.10 | 0.06 | 0.05 | 0.03 | 0.02 | 0.02 | 0.02 | 0.02 | 0.02 | 0.01 | 0.01 | 1.00 |
| CYBOCS | BT + fluvoxamine | 0.08 | 0.08 | 0.11 | 0.11 | 0.12 | 0.13 | 0.10 | 0.06 | 0.07 | 0.08 | 0.04 | 0.03 | 1.00 |
WinBUGs code
Appendix 9 Detailed results of the sensitivity analyses
Adults
Adults: clinical effectiveness (YBOCS) – sensitivity analysis 1 (low overall attrition)
See Table 21 for a summary.
| Study | y[,1] | n[,1] | sd[,1] | y[,2] | n[,2] | sd[,2] | y[,3] | n[,3] | sd[,3] | y[,4] | n[,4] | sd[,4] | na[] | out[] | t[,1] | t[,2] | t[,3] | t[,4] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Albert et al., 2002155 | 18.36 | 25 | 7.11 | 17.3 | 40 | 6.15 | NA | NA | NA | NA | NA | NA | 2 | 2 | 8 | 9 | NA | NA |
| Anderson and Rees, 2007157 | 23.5 | 14 | 6.4 | 16.7 | 17 | 6.8 | NA | NA | NA | NA | NA | NA | 2 | 2 | 2 | 11 | NA | NA |
| Andersson et al., 2012158 | 12.94 | 49 | 6.26 | 18.88 | 51 | 4.18 | NA | NA | NA | NA | NA | NA | 2 | 2 | 11 | 17 | NA | NA |
| Belloch et al., 2008159 | 8.31 | 13 | 8.75 | 6.8 | 16 | 3.55 | NA | NA | NA | NA | NA | NA | 2 | 2 | 10 | 12 | NA | NA |
| CCSG1, 1991154 | 25.11 | 108 | 6.34 | 16.23 | 102 | 7.37 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 9 | NA | NA |
| CCSG2, 1991154 | 25.59 | 119 | 5.78 | 14.7 | 120 | 7.45 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 9 | NA | NA |
| Chouinard et al., 1990163 | –1.48 | 44 | NA | –3.79 | 43 | NA | NA | NA | NA | NA | NA | NA | 2 | 1 | 1 | 6 | NA | NA |
| Cordioli et al., 2003164 | 23.2 | 24 | 5.5 | 15.1 | 23 | 7.8 | NA | NA | NA | NA | NA | NA | 2 | 2 | 2 | 11 | NA | NA |
| Cottraux et al., 2001166 | –12.1 | 30 | 7.8 | –12.5 | 30 | 8.2 | NA | NA | NA | NA | NA | NA | 2 | 1 | 10 | 12 | NA | NA |
| Denys et al., 2003167 | –7.8 | 72 | 5.4 | –7.2 | 73 | 7.5 | NA | NA | NA | NA | NA | NA | 2 | 1 | 5 | 8 | NA | NA |
| Fals-Stewart et al., 1993170 | –8.1 | 31 | NA | –1.8 | 32 | NA | NA | NA | NA | NA | NA | NA | 2 | 1 | 10 | 17 | NA | NA |
| GlaxoSmithKline, 2005175 | –14.26 | 72 | 6.33 | –13.19 | 69 | 6.48 | NA | NA | NA | NA | NA | NA | 2 | 1 | 5 | 9 | NA | NA |
| Greist et al., 2002178 | 17.6 | 55 | 6.2 | 24.1 | 66 | 6.7 | NA | NA | NA | NA | NA | NA | 2 | 2 | 10 | 17 | NA | NA |
| Hollander et al., 2003181 | –3.33 | 89 | NA | –4.14 | 88 | NA | –6.35 | 86 | NA | –7.34 | 85 | NA | 4 | 1 | 1 | 5 | 5 | 5 |
| Jaurrieta et al., 2008182 | 24.6 | 19 | 8.9 | 17.8 | 19 | 8.4 | NA | NA | NA | NA | NA | NA | 2 | 2 | 2 | 11 | NA | NA |
| Jenike et al., 1990183 | 22.3 | 9 | 7.8 | 20.6 | 10 | 9.2 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 6 | NA | NA |
| Jenike et al., 1990184 | 21.8 | 20 | 7.6 | 18.8 | 18 | 4 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 4 | NA | NA |
| Jenike et al., 1997185 | 18.7 | 18 | 6.1 | 16.2 | 19 | 6.3 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 3 | NA | NA |
| Kamijima et al., 2004187 | 20.3 | 94 | 7.38 | 15.8 | 94 | 8.09 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 5 | NA | NA |
| Lindsay et al., 1997192 | 11 | 9 | 3.81 | 25.89 | 9 | 5.8 | NA | NA | NA | NA | NA | NA | 2 | 2 | 10 | 17 | NA | NA |
| López-Ibor et al., 1996193 | –7.5 | 30 | 9.29 | –8.9 | 24 | 7.13 | NA | NA | NA | NA | NA | NA | 2 | 1 | 3 | 9 | NA | NA |
| Milanfranchi et al., 1997196 | 18.4 | 13 | 9.2 | 16.5 | 12 | 11 | NA | NA | NA | NA | NA | NA | 2 | 2 | 4 | 9 | NA | NA |
| Montgomery et al., 2001198 | –5.6 | 101 | 6.9 | –8.4 | 102 | 7.3 | –8.9 | 98 | 7 | –10.4 | 100 | 6.9 | 4 | 1 | 1 | 7 | 7 | 7 |
| Mundo et al., 1997199 | 16.2 | 10 | 8.9 | 21.6 | 9 | 7.6 | 19.8 | 11 | 10.1 | NA | NA | NA | 3 | 2 | 4 | 5 | 7 | NA |
| Mundo et al., 2001200 | –12.2 | 115 | NA | –12 | 112 | NA | NA | NA | NA | NA | NA | NA | 2 | 1 | 4 | 9 | NA | NA |
| Nakatani et al., 2005202 | 20.2 | 10 | 9.4 | 12.9 | 10 | 4.9 | 28.4 | 8 | 5.5 | NA | NA | NA | 3 | 2 | 4 | 10 | 17 | NA |
| O’Connor et al., 1999203 | 17.5 | 6 | 4 | 13.3 | 6 | 8.6 | NA | NA | NA | NA | NA | NA | 2 | 2 | 2 | 11 | NA | NA |
| Shareh et al., 2010206 | 16.66 | 6 | 3.2 | 7 | 7 | 2.38 | 8.5 | 6 | 2.42 | NA | NA | NA | 3 | 2 | 4 | 11 | 14 | NA |
| Sousa et al., 2006207 | –7.36 | 25 | NA | –10.8 | 25 | NA | NA | NA | NA | NA | NA | NA | 2 | 1 | 6 | 11 | NA | NA |
| Stein et al., 2007124 | –8.46 | 113 | 8.08 | –11.67 | 116 | 8.40 | –11.43 | 112 | 8.25 | –12.14 | 114 | 8.22 | 4 | 1 | 1 | 5 | 16 | 16 |
| Tollefson et al., 1994127 | –0.8 | 89 | 5.66 | –5.44 | 266 | 7.88 | NA | NA | NA | NA | NA | NA | 2 | 1 | 1 | 3 | NA | NA |
| Van Oppen et al., 1995209 | 17.9 | 29 | 9 | 13.4 | 28 | 9.4 | NA | NA | NA | NA | NA | NA | 2 | 2 | 10 | 12 | NA | NA |
| Whittal et al., 2010212 | 6.43 | 37 | 4.77 | 9.1 | 30 | 6.48 | NA | NA | NA | NA | NA | NA | 2 | 2 | 12 | 17 | NA | NA |
Key: intervention (class)
-
Placebo (1).
-
Waitlist (2).
-
Fluoxetine(3).
-
Fluvoxamine(3).
-
Paroxetine (3).
-
Sertraline (3).
-
Citalopram (3).
-
Venlafaxine (4).
-
Clomipramine(5).
-
BT (6).
-
CBT (7).
-
CT (8).
-
CBT + fluvoxamine (9).
-
Escitalopram (3).
-
Psychological placebo (10).
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| class.mean.diff[1,2] | –3.317 | 2.875 | 0.03854 | –8.983 | –3.324 | 2.38 | 50,001 | 100,000 |
| class.mean.diff[1,3] | –4.091 | 1.005 | 0.0165 | –6.066 | –4.092 | –2.061 | 50,001 | 100,000 |
| class.mean.diff[1,4] | –4.319 | 2.234 | 0.01698 | –8.719 | –4.321 | 0.1204 | 50,001 | 100,000 |
| class.mean.diff[1,5] | –6.419 | 1.284 | 0.01173 | –8.932 | –6.435 | –3.852 | 50,001 | 100,000 |
| class.mean.diff[1,6] | –11.04 | 2.971 | 0.0506 | –16.84 | –11.04 | –5.186 | 50,001 | 100,000 |
| class.mean.diff[1,7] | –10.13 | 2.241 | 0.03435 | –14.52 | –10.15 | –5.687 | 50,001 | 100,000 |
| class.mean.diff[1,8] | –10.63 | 3.282 | 0.05325 | –17.08 | –10.62 | –4.16 | 50,001 | 100,000 |
| class.mean.diff[1,9] | –10.31 | 2.939 | 0.0301 | –16.14 | –10.31 | –4.521 | 50,001 | 100,000 |
| class.mean.diff[1,10] | –2.851 | 2.811 | 0.04821 | –8.334 | –2.868 | 2.771 | 50,001 | 100,000 |
| class.mean.diff[2,3] | –0.7743 | 2.771 | 0.03045 | –6.23 | –0.776 | 4.688 | 50,001 | 100,000 |
| class.mean.diff[2,4] | –1.002 | 3.487 | 0.03399 | –7.916 | –0.9951 | 5.826 | 50,001 | 100,000 |
| class.mean.diff[2,5] | –3.102 | 2.984 | 0.03305 | –9.001 | –3.116 | 2.781 | 50,001 | 100,000 |
| class.mean.diff[2,6] | –7.725 | 3.195 | 0.0332 | –13.98 | –7.734 | –1.385 | 50,001 | 100,000 |
| class.mean.diff[2,7] | –6.816 | 1.816 | 0.01158 | –10.38 | –6.819 | –3.22 | 50,001 | 100,000 |
| class.mean.diff[2,8] | –7.31 | 3.461 | 0.03576 | –14.15 | –7.299 | –0.5329 | 50,001 | 100,000 |
| class.mean.diff[2,9] | –6.996 | 3.24 | 0.01976 | –13.41 | –6.997 | –0.6501 | 50,001 | 100,000 |
| class.mean.diff[2,10] | 0.466 | 2.969 | 0.03005 | –5.327 | 0.4427 | 6.392 | 50,001 | 100,000 |
| class.mean.diff[3,4] | –0.2282 | 2.198 | 0.011 | –4.59 | –0.2308 | 4.143 | 50,001 | 100,000 |
| class.mean.diff[3,5] | –2.328 | 1.324 | 0.009057 | –4.944 | –2.333 | 0.2878 | 50,001 | 100,000 |
| class.mean.diff[3,6] | –6.951 | 2.883 | 0.04368 | –12.63 | –6.943 | –1.295 | 50,001 | 100,000 |
| class.mean.diff[3,7] | –6.042 | 2.109 | 0.02551 | –10.19 | –6.048 | –1.89 | 50,001 | 100,000 |
| class.mean.diff[3,8] | –6.535 | 3.202 | 0.04661 | –12.84 | –6.513 | –0.2369 | 50,001 | 100,000 |
| class.mean.diff[3,9] | –6.222 | 2.844 | 0.02163 | –11.91 | –6.212 | –0.651 | 50,001 | 100,000 |
| class.mean.diff[3,10] | 1.24 | 2.713 | 0.04085 | –4.066 | 1.227 | 6.595 | 50,001 | 100,000 |
| class.mean.diff[4,5] | –2.1 | 2.15 | 0.01099 | –6.334 | –2.103 | 2.167 | 50,001 | 100,000 |
| class.mean.diff[4,6] | –6.723 | 3.562 | 0.04667 | –13.7 | –6.73 | 0.3361 | 50,001 | 100,000 |
| class.mean.diff[4,7] | –5.814 | 2.977 | 0.02942 | –11.63 | –5.837 | 0.1271 | 50,001 | 100,000 |
| class.mean.diff[4,8] | –6.307 | 3.83 | 0.04946 | –13.81 | –6.314 | 1.295 | 50,001 | 100,000 |
| class.mean.diff[4,9] | –5.994 | 3.524 | 0.02539 | –12.98 | –5.999 | 0.9386 | 50,001 | 100,000 |
| class.mean.diff[4,10] | 1.468 | 3.43 | 0.04404 | –5.222 | 1.436 | 8.318 | 50,001 | 100,000 |
| class.mean.diff[5,6] | –4.623 | 3.072 | 0.04576 | –10.65 | –4.629 | 1.457 | 50,001 | 100,000 |
| class.mean.diff[5,7] | –3.714 | 2.374 | 0.02835 | –8.372 | –3.718 | 0.9799 | 50,001 | 100,000 |
| class.mean.diff[5,8] | –4.207 | 3.377 | 0.04856 | –10.86 | –4.196 | 2.451 | 50,001 | 100,000 |
| class.mean.diff[5,9] | –3.894 | 3.039 | 0.02453 | –9.925 | –3.889 | 2.079 | 50,001 | 100,000 |
| class.mean.diff[5,10] | 3.568 | 2.914 | 0.04304 | –2.132 | 3.547 | 9.364 | 50,001 | 100,000 |
| class.mean.diff[6,7] | 0.909 | 2.631 | 0.02946 | –4.294 | 0.9241 | 6.055 | 50,001 | 100,000 |
| class.mean.diff[6,8] | 0.4155 | 1.699 | 0.01145 | –2.946 | 0.4231 | 3.735 | 50,001 | 100,000 |
| class.mean.diff[6,9] | 0.7288 | 3.549 | 0.03566 | –6.29 | 0.7441 | 7.672 | 50,001 | 100,000 |
| class.mean.diff[6,10] | 8.191 | 1.441 | 0.007783 | 5.408 | 8.173 | 11.1 | 50,001 | 100,000 |
| class.mean.diff[7,8] | –0.4935 | 2.951 | 0.0326 | –6.361 | –0.4901 | 5.267 | 50,001 | 100,000 |
| class.mean.diff[7,9] | –0.1802 | 2.679 | 0.01381 | –5.513 | –0.1689 | 5.036 | 50,001 | 100,000 |
| class.mean.diff[7,10] | 7.282 | 2.346 | 0.02592 | 2.708 | 7.252 | 12 | 50,001 | 100,000 |
| class.mean.diff[8,9] | 0.3133 | 3.799 | 0.03858 | –7.207 | 0.3088 | 7.792 | 50,001 | 100,000 |
| class.mean.diff[8,10] | 7.776 | 1.919 | 0.0128 | 4.082 | 7.744 | 11.64 | 50,001 | 100,000 |
| class.mean.diff[9,10] | 7.462 | 3.377 | 0.03274 | 0.9321 | 7.425 | 14.23 | 50,001 | 100,000 |
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| treat.mean.diff[1,2] | –3.317 | 2.875 | 0.03854 | –8.983 | –3.324 | 2.38 | 50,001 | 100,000 |
| treat.mean.diff[1,3] | –4.103 | 1.11 | 0.01554 | –6.307 | –4.106 | –1.837 | 50,001 | 100,000 |
| treat.mean.diff[1,4] | –4.259 | 1.141 | 0.0184 | –6.642 | –4.224 | –1.997 | 50,001 | 100,000 |
| treat.mean.diff[1,5] | –4.096 | 0.9845 | 0.01555 | –6.032 | –4.098 | –2.095 | 50,001 | 100,000 |
| treat.mean.diff[1,6] | –4.048 | 1.193 | 0.01704 | –6.413 | –4.065 | –1.62 | 50,001 | 100,000 |
| treat.mean.diff[1,7] | –4.009 | 1.149 | 0.01604 | –6.247 | –4.031 | –1.633 | 50,001 | 100,000 |
| treat.mean.diff[1,8] | –4.319 | 2.234 | 0.01698 | –8.719 | –4.321 | 0.1204 | 50,001 | 100,000 |
| treat.mean.diff[1,9] | –6.419 | 1.284 | 0.01173 | –8.932 | –6.435 | –3.852 | 50,001 | 100,000 |
| treat.mean.diff[1,10] | –11.04 | 2.971 | 0.0506 | –16.84 | –11.04 | –5.186 | 50,001 | 100,000 |
| treat.mean.diff[1,11] | –10.13 | 2.241 | 0.03435 | –14.52 | –10.15 | –5.687 | 50,001 | 100,000 |
| treat.mean.diff[1,12] | –10.63 | 3.282 | 0.05325 | –17.08 | –10.62 | –4.16 | 50,001 | 100,000 |
| treat.mean.diff[1,13] | –10.31 | 2.939 | 0.0301 | –16.14 | –10.31 | –4.521 | 50,001 | 100,000 |
| treat.mean.diff[1,14] | –4.031 | 1.169 | 0.01598 | –6.304 | –4.05 | –1.609 | 50,001 | 100,000 |
| treat.mean.diff[1,15] | –2.851 | 2.811 | 0.04821 | –8.334 | –2.868 | 2.771 | 50,001 | 100,000 |
| treat.mean.diff[2,3] | –0.7862 | 2.858 | 0.0316 | –6.418 | –0.7947 | 4.886 | 50,001 | 100,000 |
| treat.mean.diff[2,4] | –0.9422 | 2.714 | 0.02867 | –6.295 | –0.9318 | 4.388 | 50,001 | 100,000 |
| treat.mean.diff[2,5] | –0.7796 | 2.819 | 0.03121 | –6.333 | –0.7792 | 4.795 | 50,001 | 100,000 |
| treat.mean.diff[2,6] | –0.7312 | 2.776 | 0.02917 | –6.191 | –0.7352 | 4.749 | 50,001 | 100,000 |
| treat.mean.diff[2,7] | –0.6924 | 2.87 | 0.03127 | –6.315 | –0.6962 | 4.98 | 50,001 | 100,000 |
| treat.mean.diff[2,8] | –1.002 | 3.487 | 0.03399 | –7.916 | –0.9951 | 5.826 | 50,001 | 100,000 |
| treat.mean.diff[2,9] | –3.102 | 2.984 | 0.03305 | –9.001 | –3.116 | 2.781 | 50,001 | 100,000 |
| treat.mean.diff[2,10] | –7.725 | 3.195 | 0.0332 | –13.98 | –7.734 | –1.385 | 50,001 | 100,000 |
| treat.mean.diff[2,11] | –6.816 | 1.816 | 0.01158 | –10.38 | –6.819 | –3.22 | 50,001 | 100,000 |
| treat.mean.diff[2,12] | –7.31 | 3.461 | 0.03576 | –14.15 | –7.299 | –0.5329 | 50,001 | 100,000 |
| treat.mean.diff[2,13] | –6.996 | 3.24 | 0.01976 | –13.41 | –6.997 | –0.6501 | 50,001 | 100,000 |
| treat.mean.diff[2,14] | –0.7137 | 2.869 | 0.03115 | –6.355 | –0.721 | 4.963 | 50,001 | 100,000 |
| treat.mean.diff[2,15] | 0.466 | 2.969 | 0.03005 | –5.327 | 0.4427 | 6.392 | 50,001 | 100,000 |
| treat.mean.diff[3,4] | –0.156 | 1.103 | 0.007438 | –2.735 | –0.04447 | 2.038 | 50,001 | 100,000 |
| treat.mean.diff[3,5] | 0.006609 | 1.008 | 0.004452 | –2.178 | 0.001402 | 2.213 | 50,001 | 100,000 |
| treat.mean.diff[3,6] | 0.05504 | 1.172 | 0.005662 | –2.451 | 0.01024 | 2.699 | 50,001 | 100,000 |
| treat.mean.diff[3,7] | 0.09385 | 1.146 | 0.005167 | –2.324 | 0.02365 | 2.704 | 50,001 | 100,000 |
| treat.mean.diff[3,8] | –0.2163 | 2.266 | 0.01135 | –4.703 | –0.2168 | 4.258 | 50,001 | 100,000 |
| treat.mean.diff[3,9] | –2.316 | 1.4 | 0.008942 | –5.099 | –2.322 | 0.4748 | 50,001 | 100,000 |
| treat.mean.diff[3,10] | –6.939 | 2.965 | 0.04455 | –12.8 | –6.929 | –1.119 | 50,001 | 100,000 |
| treat.mean.diff[3,11] | –6.03 | 2.224 | 0.02668 | –10.45 | –6.035 | –1.652 | 50,001 | 100,000 |
| treat.mean.diff[3,12] | –6.524 | 3.276 | 0.04749 | –13 | –6.5 | –0.07921 | 50,001 | 100,000 |
| treat.mean.diff[3,13] | –6.21 | 2.931 | 0.02268 | –12.05 | –6.2 | –0.4791 | 50,001 | 100,000 |
| treat.mean.diff[3,14] | 0.0725 | 1.149 | 0.004902 | –2.351 | 0.01609 | 2.679 | 50,001 | 100,000 |
| treat.mean.diff[3,15] | 1.252 | 2.802 | 0.04176 | –4.238 | 1.242 | 6.796 | 50,001 | 100,000 |
| treat.mean.diff[4,5] | 0.1626 | 0.9883 | 0.007063 | –1.784 | 0.05258 | 2.498 | 50,001 | 100,000 |
| treat.mean.diff[4,6] | 0.211 | 1.126 | 0.006667 | –1.972 | 0.06478 | 2.911 | 50,001 | 100,000 |
| treat.mean.diff[4,7] | 0.2498 | 1.135 | 0.00808 | –1.907 | 0.082 | 2.999 | 50,001 | 100,000 |
| treat.mean.diff[4,8] | –0.06028 | 2.248 | 0.01251 | –4.467 | –0.07289 | 4.436 | 50,001 | 100,000 |
| treat.mean.diff[4,9] | –2.16 | 1.354 | 0.01034 | –4.79 | –2.18 | 0.5713 | 50,001 | 100,000 |
| treat.mean.diff[4,10] | –6.783 | 2.794 | 0.04167 | –12.26 | –6.785 | –1.267 | 50,001 | 100,000 |
| treat.mean.diff[4,11] | –5.874 | 2.03 | 0.02349 | –9.855 | –5.887 | –1.842 | 50,001 | 100,000 |
| treat.mean.diff[4,12] | –6.368 | 3.122 | 0.04471 | –12.5 | –6.361 | –0.2322 | 50,001 | 100,000 |
| treat.mean.diff[4,13] | –6.054 | 2.75 | 0.01995 | –11.5 | –6.054 | –0.6226 | 50,001 | 100,000 |
| treat.mean.diff[4,14] | 0.2285 | 1.147 | 0.007522 | –1.963 | 0.06855 | 3.003 | 50,001 | 100,000 |
| treat.mean.diff[4,15] | 1.408 | 2.624 | 0.0388 | –3.693 | 1.395 | 6.616 | 50,001 | 100,000 |
| treat.mean.diff[5,6] | 0.04843 | 1.075 | 0.005323 | –2.252 | 0.01349 | 2.452 | 50,001 | 100,000 |
| treat.mean.diff[5,7] | 0.08724 | 1.032 | 0.004494 | –2.071 | 0.02513 | 2.433 | 50,001 | 100,000 |
| treat.mean.diff[5,8] | –0.2229 | 2.108 | 0.009994 | –4.415 | –0.2219 | 3.938 | 50,001 | 100,000 |
| treat.mean.diff[5,9] | –2.323 | 1.29 | 0.008259 | –4.891 | –2.327 | 0.2327 | 50,001 | 100,000 |
| treat.mean.diff[5,10] | –6.946 | 2.924 | 0.04461 | –12.71 | –6.928 | –1.22 | 50,001 | 100,000 |
| treat.mean.diff[5,11] | –6.037 | 2.17 | 0.02639 | –10.31 | –6.04 | –1.745 | 50,001 | 100,000 |
| treat.mean.diff[5,12] | –6.53 | 3.238 | 0.04748 | –12.91 | –6.51 | –0.1723 | 50,001 | 100,000 |
| treat.mean.diff[5,13] | –6.217 | 2.888 | 0.02244 | –11.99 | –6.207 | –0.5708 | 50,001 | 100,000 |
| treat.mean.diff[5,14] | 0.06589 | 0.9877 | 0.003986 | –1.993 | 0.01554 | 2.29 | 50,001 | 100,000 |
| treat.mean.diff[5,15] | 1.246 | 2.755 | 0.04179 | –4.146 | 1.231 | 6.695 | 50,001 | 100,000 |
| treat.mean.diff[6,7] | 0.03881 | 1.182 | 0.005654 | –2.523 | 0.008911 | 2.675 | 50,001 | 100,000 |
| treat.mean.diff[6,8] | –0.2713 | 2.316 | 0.01176 | –4.882 | –0.2655 | 4.303 | 50,001 | 100,000 |
| treat.mean.diff[6,9] | –2.371 | 1.494 | 0.009976 | –5.379 | –2.368 | 0.5962 | 50,001 | 100,000 |
| treat.mean.diff[6,10] | –6.994 | 2.914 | 0.0427 | –12.72 | –6.991 | –1.266 | 50,001 | 100,000 |
| treat.mean.diff[6,11] | –6.085 | 2.115 | 0.02415 | –10.27 | –6.088 | –1.935 | 50,001 | 100,000 |
| treat.mean.diff[6,12] | –6.579 | 3.23 | 0.04573 | –12.97 | –6.57 | –0.2254 | 50,001 | 100,000 |
| treat.mean.diff[6,13] | –6.265 | 2.887 | 0.02079 | –12.02 | –6.243 | –0.6345 | 50,001 | 100,000 |
| treat.mean.diff[6,14] | 0.01746 | 1.187 | 0.005286 | –2.536 | 0.001934 | 2.635 | 50,001 | 100,000 |
| treat.mean.diff[6,15] | 1.197 | 2.741 | 0.03985 | –4.157 | 1.18 | 6.626 | 50,001 | 100,000 |
| treat.mean.diff[7,8] | –0.3101 | 2.3 | 0.01147 | –4.911 | –0.3019 | 4.232 | 50,001 | 100,000 |
| treat.mean.diff[7,9] | –2.41 | 1.48 | 0.009452 | –5.408 | –2.4 | 0.4917 | 50,001 | 100,000 |
| treat.mean.diff[7,10] | –7.033 | 2.977 | 0.04466 | –12.92 | –7.021 | –1.186 | 50,001 | 100,000 |
| treat.mean.diff[7,11] | –6.124 | 2.235 | 0.02647 | –10.56 | –6.122 | –1.743 | 50,001 | 100,000 |
| treat.mean.diff[7,12] | –6.617 | 3.285 | 0.04754 | –13.1 | –6.593 | –0.1509 | 50,001 | 100,000 |
| treat.mean.diff[7,13] | –6.304 | 2.939 | 0.02248 | –12.17 | –6.28 | –0.5407 | 50,001 | 100,000 |
| treat.mean.diff[7,14] | –0.02135 | 1.154 | 0.004668 | –2.562 | –0.00565 | 2.516 | 50,001 | 100,000 |
| treat.mean.diff[7,15] | 1.158 | 2.811 | 0.04188 | –4.36 | 1.148 | 6.676 | 50,001 | 100,000 |
| treat.mean.diff[8,9] | –2.1 | 2.15 | 0.01099 | –6.334 | –2.103 | 2.167 | 50,001 | 100,000 |
| treat.mean.diff[8,10] | –6.723 | 3.562 | 0.04667 | –13.7 | –6.73 | 0.3361 | 50,001 | 100,000 |
| treat.mean.diff[8,11] | –5.814 | 2.977 | 0.02942 | –11.63 | –5.837 | 0.1271 | 50,001 | 100,000 |
| treat.mean.diff[8,12] | –6.307 | 3.83 | 0.04946 | –13.81 | –6.314 | 1.295 | 50,001 | 100,000 |
| treat.mean.diff[8,13] | –5.994 | 3.524 | 0.02539 | –12.98 | –5.999 | 0.9386 | 50,001 | 100,000 |
| treat.mean.diff[8,14] | 0.2888 | 2.288 | 0.01111 | –4.217 | 0.2814 | 4.854 | 50,001 | 100,000 |
| treat.mean.diff[8,15] | 1.468 | 3.43 | 0.04404 | –5.222 | 1.436 | 8.318 | 50,001 | 100,000 |
| treat.mean.diff[9,10] | –4.623 | 3.072 | 0.04576 | –10.65 | –4.629 | 1.457 | 50,001 | 100,000 |
| treat.mean.diff[9,11] | –3.714 | 2.374 | 0.02835 | –8.372 | –3.718 | 0.9799 | 50,001 | 100,000 |
| treat.mean.diff[9,12] | –4.207 | 3.377 | 0.04856 | –10.86 | –4.196 | 2.451 | 50,001 | 100,000 |
| treat.mean.diff[9,13] | –3.894 | 3.039 | 0.02453 | –9.925 | –3.889 | 2.079 | 50,001 | 100,000 |
| treat.mean.diff[9,14] | 2.389 | 1.476 | 0.009127 | –0.5044 | 2.379 | 5.359 | 50,001 | 100,000 |
| treat.mean.diff[9,15] | 3.568 | 2.914 | 0.04304 | –2.132 | 3.547 | 9.364 | 50,001 | 100,000 |
| treat.mean.diff[10,11] | 0.909 | 2.631 | 0.02946 | –4.294 | 0.9241 | 6.055 | 50,001 | 100,000 |
| treat.mean.diff[10,12] | 0.4155 | 1.699 | 0.01145 | –2.946 | 0.4231 | 3.735 | 50,001 | 100,000 |
| treat.mean.diff[10,13] | 0.7288 | 3.549 | 0.03566 | –6.29 | 0.7441 | 7.672 | 50,001 | 100,000 |
| treat.mean.diff[10,14] | 7.012 | 2.978 | 0.04446 | 1.171 | 6.995 | 12.9 | 50,001 | 100,000 |
| treat.mean.diff[10,15] | 8.191 | 1.441 | 0.007783 | 5.408 | 8.173 | 11.1 | 50,001 | 100,000 |
| treat.mean.diff[11,12] | –0.4935 | 2.951 | 0.0326 | –6.361 | –0.4901 | 5.267 | 50,001 | 100,000 |
| treat.mean.diff[11,13] | –0.1802 | 2.679 | 0.01381 | –5.513 | –0.1689 | 5.036 | 50,001 | 100,000 |
| treat.mean.diff[11,14] | 6.103 | 2.241 | 0.02636 | 1.693 | 6.095 | 10.55 | 50,001 | 100,000 |
| treat.mean.diff[11,15] | 7.282 | 2.346 | 0.02592 | 2.708 | 7.252 | 12 | 50,001 | 100,000 |
| treat.mean.diff[12,13] | 0.3133 | 3.799 | 0.03858 | –7.207 | 0.3088 | 7.792 | 50,001 | 100,000 |
| treat.mean.diff[12,14] | 6.596 | 3.285 | 0.04743 | 0.1353 | 6.576 | 13.06 | 50,001 | 100,000 |
| treat.mean.diff[12,15] | 7.776 | 1.919 | 0.0128 | 4.082 | 7.744 | 11.64 | 50,001 | 100,000 |
| treat.mean.diff[13,14] | 6.283 | 2.939 | 0.02256 | 0.5358 | 6.257 | 12.18 | 50,001 | 100,000 |
| treat.mean.diff[13,15] | 7.462 | 3.377 | 0.03274 | 0.9321 | 7.425 | 14.23 | 50,001 | 100,000 |
| treat.mean.diff[14,15] | 1.18 | 2.812 | 0.04166 | –4.332 | 1.171 | 6.716 | 50,001 | 100,000 |
Median ranks
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk.class[2] | 7.601 | 1.575 | 0.01425 | 5 | 8 | 10 | 50,001 | 100,000 |
| rk.class[3] | 7.167 | 1.017 | 0.01022 | 5 | 7 | 9 | 50,001 | 100,000 |
| rk.class[4] | 6.893 | 1.61 | 0.01281 | 3 | 7 | 9 | 50,001 | 100,000 |
| rk.class[5] | 5.127 | 1.116 | 0.01217 | 2 | 5 | 7 | 50,001 | 100,000 |
| rk.class[6] | 2.287 | 1.195 | 0.0116 | 1 | 2 | 5 | 50,001 | 100,000 |
| rk.class[7] | 2.823 | 1.135 | 0.008796 | 1 | 3 | 5 | 50,001 | 100,000 |
| rk.class[8] | 2.695 | 1.437 | 0.0147 | 1 | 2 | 6 | 50,001 | 100,000 |
| rk.class[9] | 2.778 | 1.518 | 0.009753 | 1 | 3 | 6 | 50,001 | 100,000 |
| rk.class[10] | 7.933 | 1.469 | 0.02014 | 5 | 8 | 10 | 50,001 | 100,000 |
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk[1] | 14.69 | 0.6014 | 0.007856 | 13 | 15 | 15 | 50,001 | 100,000 |
| rk[2] | 10.65 | 3.606 | 0.03481 | 5 | 12 | 15 | 50,001 | 100,000 |
| rk[3] | 9.634 | 2.297 | 0.01488 | 6 | 10 | 14 | 50,001 | 100,000 |
| rk[4] | 9.255 | 2.115 | 0.01239 | 6 | 9 | 13 | 50,001 | 100,000 |
| rk[5] | 9.658 | 2.098 | 0.0142 | 6 | 10 | 13 | 50,001 | 100,000 |
| rk[6] | 9.753 | 2.28 | 0.01095 | 6 | 10 | 14 | 50,001 | 100,000 |
| rk[7] | 9.853 | 2.321 | 0.01454 | 6 | 10 | 14 | 50,001 | 100,000 |
| rk[8] | 9.188 | 3.559 | 0.02113 | 3 | 9 | 14 | 50,001 | 100,000 |
| rk[9] | 5.38 | 1.585 | 0.01406 | 3 | 5 | 10 | 50,001 | 100,000 |
| rk[10] | 2.335 | 1.398 | 0.01375 | 1 | 2 | 5 | 50,001 | 100,000 |
| rk[11] | 2.844 | 1.207 | 0.009126 | 1 | 3 | 5 | 50,001 | 100,000 |
| rk[12] | 2.807 | 1.829 | 0.0191 | 1 | 2 | 7 | 50,001 | 100,000 |
| rk[13] | 2.86 | 1.799 | 0.0103 | 1 | 3 | 7 | 50,001 | 100,000 |
| rk[14] | 9.787 | 2.316 | 0.01366 | 6 | 10 | 14 | 50,001 | 100,000 |
| rk[15] | 11.31 | 3.409 | 0.04808 | 5 | 13 | 15 | 50,001 | 100,000 |
Adults: clinical effectiveness (Yale–Brown Obsessive–Compulsive Scale) – sensitivity analysis 2 (incomplete outcome data)
See Table 22 for a summary.
| Study | y[,1] | n[,1] | sd[,1] | y[,2] | n[,2] | sd[,2] | y[,3] | n[,3] | sd[,3] | y[,4] | n[,4] | sd[,4] | na[] | out[] | t[,1] | t[,2] | t[,3] | t[,4] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Anderson and Rees, 2007157 | 23.5 | 14 | 6.4 | 16.7 | 17 | 6.8 | NA | NA | NA | NA | NA | NA | 2 | 2 | 2 | 11 | NA | NA |
| Andersson et al., 2012158 | 12.94 | 49 | 6.26 | 18.88 | 51 | 4.18 | NA | NA | NA | NA | NA | NA | 2 | 2 | 11 | 15 | NA | NA |
| Belotto-Silva et al., 2012160 | 20.29 | 88 | 8.05 | 19.97 | 70 | 8.48 | NA | NA | NA | NA | NA | NA | 2 | 2 | 3 | 11 | NA | NA |
| Bergeron et al., 2002161 | –9.7 | 72 | 7.7 | –9.6 | 76 | 7.9 | NA | NA | NA | NA | NA | NA | 2 | 1 | 3 | 6 | NA | NA |
| Bisserbe et al., 1997162 | –14.3 | 86 | NA | –11.71 | 81 | NA | NA | NA | NA | NA | NA | NA | 2 | 1 | 6 | 9 | NA | NA |
| Chouinard et al., 1990163 | –1.48 | 44 | NA | –3.79 | 43 | NA | NA | NA | NA | NA | NA | NA | 2 | 1 | 1 | 6 | NA | NA |
| Cordioli et al., 2003164 | 23.2 | 24 | 5.5 | 15.1 | 23 | 7.8 | NA | NA | NA | NA | NA | NA | 2 | 2 | 2 | 11 | NA | NA |
| Denys et al., 2003167 | –7.8 | 72 | 5.4 | –7.2 | 73 | 7.5 | NA | NA | NA | NA | NA | NA | 2 | 1 | 5 | 8 | NA | NA |
| Foa et al., 2005171 | 22.2 | 26 | 6.4 | 18.2 | 36 | 7.8 | 11 | 29 | 7.9 | 10.5 | 31 | 8.2 | 4 | 2 | 1 | 9 | 10 | 13 |
| Freeman et al., 1994172 | –8.6 | 28 | NA | –7.8 | 19 | NA | NA | NA | NA | NA | NA | NA | 2 | 1 | 4 | 9 | NA | NA |
| Freeston et al., 1997173 | 22 | 14 | 6 | 12.2 | 15 | 9.6 | NA | NA | NA | NA | NA | NA | 2 | 2 | 2 | 11 | NA | NA |
| GlaxoSmithKline, 2005174 | –4.61 | 75 | 7.53 | –5.61 | 79 | 7.47 | –7.73 | 78 | 7.42 | NA | NA | NA | 3 | 1 | 1 | 5 | 9 | NA |
| Goodman et al., 1989176 | 28 | 21 | 7 | 19.4 | 21 | 7 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 4 | NA | NA |
| Goodman et al., 1996177 | –1.71 | 78 | 4.88 | –3.95 | 78 | 6.28 | NA | NA | NA | NA | NA | NA | 2 | 1 | 1 | 4 | NA | NA |
| Greist et al., 2002178 | 17.6 | 55 | 6.2 | 24.1 | 66 | 6.7 | NA | NA | NA | NA | NA | NA | 2 | 2 | 10 | 15 | NA | NA |
| Hollander et al., 2003180 | –5.6 | 120 | 7.67 | –8.5 | 117 | 7.57 | NA | NA | NA | NA | NA | NA | 2 | 1 | 1 | 4 | NA | NA |
| Hollander et al., 2003181 | –3.33 | 89 | NA | –4.14 | 88 | NA | –6.35 | 86 | NA | –7.34 | 85 | NA | 4 | 1 | 1 | 5 | 5 | 5 |
| Jaurrieta et al., 2008182 | 24.6 | 19 | 8.9 | 17.8 | 19 | 8.4 | NA | NA | NA | NA | NA | NA | 2 | 2 | 2 | 11 | NA | NA |
| Jenike et al., 1990183 | 22.3 | 9 | 7.8 | 20.6 | 10 | 9.2 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 6 | NA | NA |
| Jenike et al., 1997185 | 18.7 | 18 | 6.1 | 16.2 | 19 | 6.3 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 3 | NA | NA |
| Kamijima et al., 2004187 | 20.3 | 94 | 7.38 | 15.8 | 94 | 8.09 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 5 | NA | NA |
| Kobak et al.,189 | 19.87 | 30 | 7.46 | 19.75 | 30 | 7.46 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 12 | NA | NA |
| Koran et al., 1996190 | 17.8 | 34 | 7.7 | 17 | 39 | 8.55 | NA | NA | NA | NA | NA | NA | 2 | 2 | 4 | 9 | NA | NA |
| Kronig et al., 1999191 | –4.14 | 79 | NA | –8.5 | 85 | NA | NA | NA | NA | NA | NA | NA | 2 | 1 | 1 | 6 | NA | NA |
| López-Ibor et al., 1996193 | –7.5 | 30 | 9.29 | –8.9 | 24 | 7.13 | NA | NA | NA | NA | NA | NA | 2 | 1 | 3 | 9 | NA | NA |
| Montgomery et al., 1993197 | –3.7 | 56 | 5.98 | –5.13 | 52 | 6.41 | –4.76 | 52 | 6.89 | –6.07 | 54 | 6.92 | 4 | 1 | 1 | 3 | 3 | 3 |
| Montgomery et al., 2001198 | –5.6 | 101 | 6.9 | –8.4 | 102 | 7.3 | –8.9 | 98 | 7 | –10.4 | 100 | 6.9 | 4 | 1 | 1 | 7 | 7 | 7 |
| Mundo et al., 1997199 | 16.2 | 10 | 8.9 | 21.6 | 9 | 7.6 | 19.8 | 11 | 10.1 | NA | NA | NA | 3 | 2 | 4 | 5 | 7 | NA |
| Mundo et al., 2001200 | –12.2 | 115 | NA | –12 | 112 | NA | NA | NA | NA | NA | NA | NA | 2 | 1 | 4 | 9 | NA | NA |
| Nakajima et al., 1996201 | –1.9 | 33 | 7.2 | –7.1 | 60 | 7.03 | NA | NA | NA | NA | NA | NA | 2 | 1 | 1 | 4 | NA | NA |
| Sousa et al., 2006207 | –7.36 | 25 | NA | –10.8 | 25 | NA | NA | NA | NA | NA | NA | NA | 2 | 1 | 6 | 11 | NA | NA |
| Stein et al., 2007124 | –8.46 | 113 | 8.08 | –11.67 | 116 | 8.40 | –11.43 | 112 | 8.25 | –12.14 | 114 | 8.22 | 4 | 1 | 1 | 5 | 14 | 14 |
| Tollefson et al., 1994127 | –0.8 | 89 | 5.66 | –5.44 | 266 | 7.88 | NA | NA | NA | NA | NA | NA | 2 | 1 | 1 | 3 | NA | NA |
| Zohar and Judge, 1996213 | –4.2 | 99 | 7.2 | –6.4 | 201 | 7.1 | –7 | 99 | 6.8 | NA | NA | NA | 3 | 1 | 1 | 5 | 9 | NA |
Key: intervention (class)
-
Placebo (1).
-
Waitlist (2).
-
Fluoxetine (3).
-
Fluvoxamine (3).
-
Paroxetine (3).
-
Sertraline (3).
-
Citalopram (3).
-
Venlafaxine (4).
-
Clomipramine (5).
-
BT (6).
-
CBT (7).
-
Hypericum (8).
-
BT + clomipramine (9).
-
Escitalopram (3).
-
Psychological placebo (10).
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| class.mean.diff[1,2] | 2.063 | 1.806 | 0.03318 | –1.509 | 2.067 | 5.611 | 50,001 | 100,000 |
| class.mean.diff[1,3] | –3.332 | 0.4591 | 0.006652 | –4.25 | –3.329 | –2.456 | 50,001 | 100,000 |
| class.mean.diff[1,4] | –2.458 | 1.533 | 0.01317 | –5.492 | –2.461 | 0.5665 | 50,001 | 100,000 |
| class.mean.diff[1,5] | –3.156 | 0.6228 | 0.008235 | –4.392 | –3.151 | –1.95 | 50,001 | 100,000 |
| class.mean.diff[1,6] | –8.7 | 1.541 | 0.02275 | –11.78 | –8.686 | –5.747 | 50,001 | 100,000 |
| class.mean.diff[1,7] | –5.758 | 1.254 | 0.02213 | –8.232 | –5.744 | –3.314 | 50,001 | 100,000 |
| class.mean.diff[1,8] | –0.103 | 2.164 | 0.02634 | –4.344 | –0.1013 | 4.112 | 50,001 | 100,000 |
| class.mean.diff[1,9] | –10.67 | 1.916 | 0.02438 | –14.42 | –10.68 | –6.9 | 50,001 | 100,000 |
| class.mean.diff[1,10] | –0.9254 | 1.563 | 0.02449 | –4.097 | –0.8947 | 2.087 | 50,001 | 100,000 |
| class.mean.diff[2,3] | –5.395 | 1.808 | 0.03138 | –8.945 | –5.391 | –1.829 | 50,001 | 100,000 |
| class.mean.diff[2,4] | –4.52 | 2.351 | 0.03469 | –9.157 | –4.511 | 0.08525 | 50,001 | 100,000 |
| class.mean.diff[2,5] | –5.219 | 1.856 | 0.0317 | –8.904 | –5.21 | –1.566 | 50,001 | 100,000 |
| class.mean.diff[2,6] | –10.76 | 2.04 | 0.0285 | –14.87 | –10.74 | –6.858 | 50,001 | 100,000 |
| class.mean.diff[2,7] | –7.821 | 1.32 | 0.01947 | –10.41 | –7.816 | –5.23 | 50,001 | 100,000 |
| class.mean.diff[2,8] | –2.166 | 2.825 | 0.04148 | –7.694 | –2.138 | 3.396 | 50,001 | 100,000 |
| class.mean.diff[2,9] | –12.73 | 2.55 | 0.03768 | –17.77 | –12.72 | –7.707 | 50,001 | 100,000 |
| class.mean.diff[2,10] | –2.988 | 1.838 | 0.02496 | –6.636 | –2.964 | 0.5565 | 50,001 | 100,000 |
| class.mean.diff[3,4] | 0.8747 | 1.533 | 0.0124 | –2.121 | 0.8695 | 3.917 | 50,001 | 100,000 |
| class.mean.diff[3,5] | 0.1763 | 0.6482 | 0.005658 | –1.104 | 0.1775 | 1.444 | 50,001 | 100,000 |
| class.mean.diff[3,6] | –5.368 | 1.564 | 0.02109 | –8.483 | –5.36 | –2.357 | 50,001 | 100,000 |
| class.mean.diff[3,7] | –2.425 | 1.253 | 0.02014 | –4.891 | –2.417 | 0.03083 | 50,001 | 100,000 |
| class.mean.diff[3,8] | 3.229 | 2.214 | 0.02709 | –1.126 | 3.233 | 7.557 | 50,001 | 100,000 |
| class.mean.diff[3,9] | –7.339 | 1.948 | 0.02407 | –11.16 | –7.34 | –3.519 | 50,001 | 100,000 |
| class.mean.diff[3,10] | 2.407 | 1.569 | 0.02221 | –0.7641 | 2.435 | 5.452 | 50,001 | 100,000 |
| class.mean.diff[4,5] | –0.6984 | 1.605 | 0.01404 | –3.883 | –0.6939 | 2.453 | 50,001 | 100,000 |
| class.mean.diff[4,6] | –6.242 | 2.159 | 0.02455 | –10.57 | –6.21 | –2.064 | 50,001 | 100,000 |
| class.mean.diff[4,7] | –3.3 | 1.947 | 0.0237 | –7.165 | –3.296 | 0.5222 | 50,001 | 100,000 |
| class.mean.diff[4,8] | 2.354 | 2.654 | 0.03049 | –2.853 | 2.366 | 7.492 | 50,001 | 100,000 |
| class.mean.diff[4,9] | –8.214 | 2.448 | 0.02614 | –13.03 | –8.188 | –3.395 | 50,001 | 100,000 |
| class.mean.diff[4,10] | 1.532 | 2.161 | 0.02547 | –2.839 | 1.562 | 5.704 | 50,001 | 100,000 |
| class.mean.diff[5,6] | –5.544 | 1.569 | 0.02063 | –8.669 | –5.542 | –2.494 | 50,001 | 100,000 |
| class.mean.diff[5,7] | –2.602 | 1.326 | 0.02093 | –5.179 | –2.603 | 0.01789 | 50,001 | 100,000 |
| class.mean.diff[5,8] | 3.053 | 2.244 | 0.0267 | –1.368 | 3.063 | 7.418 | 50,001 | 100,000 |
| class.mean.diff[5,9] | –7.516 | 1.923 | 0.02344 | –11.28 | –7.513 | –3.713 | 50,001 | 100,000 |
| class.mean.diff[5,10] | 2.231 | 1.604 | 0.02237 | –0.9882 | 2.245 | 5.346 | 50,001 | 100,000 |
| class.mean.diff[6,7] | 2.942 | 1.563 | 0.01848 | –0.05385 | 2.929 | 6.044 | 50,001 | 100,000 |
| class.mean.diff[6,8] | 8.597 | 2.65 | 0.03238 | 3.396 | 8.619 | 13.8 | 50,001 | 100,000 |
| class.mean.diff[6,9] | –1.971 | 2.152 | 0.02598 | –6.188 | –1.968 | 2.292 | 50,001 | 100,000 |
| class.mean.diff[6,10] | 7.775 | 1.342 | 0.01406 | 5.142 | 7.772 | 10.43 | 50,001 | 100,000 |
| class.mean.diff[7,8] | 5.655 | 2.499 | 0.03332 | 0.7631 | 5.664 | 10.58 | 50,001 | 100,000 |
| class.mean.diff[7,9] | –4.914 | 2.18 | 0.02919 | –9.214 | –4.906 | –0.6075 | 50,001 | 100,000 |
| class.mean.diff[7,10] | 4.832 | 1.278 | 0.01355 | 2.256 | 4.847 | 7.284 | 50,001 | 100,000 |
| class.mean.diff[8,9] | –10.57 | 2.89 | 0.03667 | –16.23 | –10.58 | –4.859 | 50,001 | 100,000 |
| class.mean.diff[8,10] | –0.8223 | 2.675 | 0.0347 | –6.086 | –0.8262 | 4.44 | 50,001 | 100,000 |
| class.mean.diff[9,10] | 9.746 | 2.279 | 0.02926 | 5.261 | 9.76 | 14.22 | 50,001 | 100,000 |
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| treat.mean.diff[1,2] | 2.063 | 1.806 | 0.03318 | –1.509 | 2.067 | 5.611 | 50,001 | 100,000 |
| treat.mean.diff[1,3] | –3.374 | 0.4854 | 0.007081 | –4.367 | –3.369 | –2.426 | 50,001 | 100,000 |
| treat.mean.diff[1,4] | –3.44 | 0.4873 | 0.007192 | –4.479 | –3.422 | –2.535 | 50,001 | 100,000 |
| treat.mean.diff[1,5] | –3.038 | 0.4909 | 0.007551 | –3.924 | –3.067 | –1.993 | 50,001 | 100,000 |
| treat.mean.diff[1,6] | –3.486 | 0.5394 | 0.007976 | –4.662 | –3.455 | –2.499 | 50,001 | 100,000 |
| treat.mean.diff[1,7] | –3.366 | 0.5748 | 0.006907 | –4.579 | –3.357 | –2.24 | 50,001 | 100,000 |
| treat.mean.diff[1,8] | –2.458 | 1.533 | 0.01317 | –5.492 | –2.461 | 0.5665 | 50,001 | 100,000 |
| treat.mean.diff[1,9] | –3.156 | 0.6228 | 0.008235 | –4.392 | –3.151 | –1.95 | 50,001 | 100,000 |
| treat.mean.diff[1,10] | –8.7 | 1.541 | 0.02275 | –11.78 | –8.686 | –5.747 | 50,001 | 100,000 |
| treat.mean.diff[1,11] | –5.758 | 1.254 | 0.02213 | –8.232 | –5.744 | –3.314 | 50,001 | 100,000 |
| treat.mean.diff[1,12] | –0.103 | 2.164 | 0.02634 | –4.344 | –0.1013 | 4.112 | 50,001 | 100,000 |
| treat.mean.diff[1,13] | –10.67 | 1.916 | 0.02438 | –14.42 | –10.68 | –6.9 | 50,001 | 100,000 |
| treat.mean.diff[1,14] | –3.289 | 0.583 | 0.007209 | –4.447 | –3.3 | –2.07 | 50,001 | 100,000 |
| treat.mean.diff[1,15] | –0.9254 | 1.563 | 0.02449 | –4.097 | –0.8947 | 2.087 | 50,001 | 100,000 |
| treat.mean.diff[2,3] | –5.437 | 1.783 | 0.03076 | –8.956 | –5.432 | –1.929 | 50,001 | 100,000 |
| treat.mean.diff[2,4] | –5.503 | 1.822 | 0.03167 | –9.106 | –5.493 | –1.918 | 50,001 | 100,000 |
| treat.mean.diff[2,5] | –5.101 | 1.841 | 0.03199 | –8.726 | –5.093 | –1.483 | 50,001 | 100,000 |
| treat.mean.diff[2,6] | –5.549 | 1.804 | 0.03141 | –9.099 | –5.545 | –2 | 50,001 | 100,000 |
| treat.mean.diff[2,7] | –5.429 | 1.854 | 0.03184 | –9.071 | –5.426 | –1.759 | 50,001 | 100,000 |
| treat.mean.diff[2,8] | –4.52 | 2.351 | 0.03469 | –9.157 | –4.511 | 0.08525 | 50,001 | 100,000 |
| treat.mean.diff[2,9] | –5.219 | 1.856 | 0.0317 | –8.904 | –5.21 | –1.566 | 50,001 | 100,000 |
| treat.mean.diff[2,10] | –10.76 | 2.04 | 0.0285 | –14.87 | –10.74 | –6.858 | 50,001 | 100,000 |
| treat.mean.diff[2,11] | –7.821 | 1.32 | 0.01947 | –10.41 | –7.816 | –5.23 | 50,001 | 100,000 |
| treat.mean.diff[2,12] | –2.166 | 2.825 | 0.04148 | –7.694 | –2.138 | 3.396 | 50,001 | 100,000 |
| treat.mean.diff[2,13] | –12.73 | 2.55 | 0.03768 | –17.77 | –12.72 | –7.707 | 50,001 | 100,000 |
| treat.mean.diff[2,14] | –5.352 | 1.854 | 0.0316 | –8.987 | –5.35 | –1.699 | 50,001 | 100,000 |
| treat.mean.diff[2,15] | –2.988 | 1.838 | 0.02496 | –6.636 | –2.964 | 0.5565 | 50,001 | 100,000 |
| treat.mean.diff[3,4] | –0.06626 | 0.535 | 0.004969 | –1.276 | –0.02218 | 1.039 | 50,001 | 100,000 |
| treat.mean.diff[3,5] | 0.3363 | 0.5731 | 0.006438 | –0.5877 | 0.1992 | 1.711 | 50,001 | 100,000 |
| treat.mean.diff[3,6] | –0.1113 | 0.5238 | 0.004289 | –1.318 | –0.04389 | 0.9157 | 50,001 | 100,000 |
| treat.mean.diff[3,7] | 0.007895 | 0.6048 | 0.004594 | –1.315 | 0.001216 | 1.316 | 50,001 | 100,000 |
| treat.mean.diff[3,8] | 0.9167 | 1.561 | 0.01295 | –2.149 | 0.9082 | 3.996 | 50,001 | 100,000 |
| treat.mean.diff[3,9] | 0.2183 | 0.682 | 0.006852 | –1.122 | 0.2135 | 1.565 | 50,001 | 100,000 |
| treat.mean.diff[3,10] | –5.326 | 1.561 | 0.02122 | –8.441 | –5.316 | –2.31 | 50,001 | 100,000 |
| treat.mean.diff[3,11] | –2.383 | 1.218 | 0.01932 | –4.777 | –2.374 | 0.0129 | 50,001 | 100,000 |
| treat.mean.diff[3,12] | 3.271 | 2.216 | 0.02696 | –1.086 | 3.276 | 7.605 | 50,001 | 100,000 |
| treat.mean.diff[3,13] | –7.297 | 1.954 | 0.02443 | –11.13 | –7.303 | –3.467 | 50,001 | 100,000 |
| treat.mean.diff[3,14] | 0.08549 | 0.6104 | 0.004855 | –1.127 | 0.02296 | 1.507 | 50,001 | 100,000 |
| treat.mean.diff[3,15] | 2.449 | 1.553 | 0.02204 | –0.6869 | 2.479 | 5.475 | 50,001 | 100,000 |
| treat.mean.diff[4,5] | 0.4026 | 0.5837 | 0.006677 | –0.4634 | 0.2551 | 1.823 | 50,001 | 100,000 |
| treat.mean.diff[4,6] | –0.04508 | 0.5522 | 0.004903 | –1.264 | –0.01395 | 1.109 | 50,001 | 100,000 |
| treat.mean.diff[4,7] | 0.07415 | 0.6022 | 0.004913 | –1.168 | 0.02271 | 1.449 | 50,001 | 100,000 |
| treat.mean.diff[4,8] | 0.9829 | 1.567 | 0.01313 | –2.052 | 0.9648 | 4.119 | 50,001 | 100,000 |
| treat.mean.diff[4,9] | 0.2846 | 0.632 | 0.006125 | –0.9381 | 0.274 | 1.548 | 50,001 | 100,000 |
| treat.mean.diff[4,10] | –5.26 | 1.56 | 0.02093 | –8.352 | –5.257 | –2.247 | 50,001 | 100,000 |
| treat.mean.diff[4,11] | –2.317 | 1.273 | 0.02044 | –4.816 | –2.322 | 0.2033 | 50,001 | 100,000 |
| treat.mean.diff[4,12] | 3.337 | 2.225 | 0.02755 | –1.029 | 3.333 | 7.673 | 50,001 | 100,000 |
| treat.mean.diff[4,13] | –7.231 | 1.944 | 0.02369 | –11.05 | –7.235 | –3.392 | 50,001 | 100,000 |
| treat.mean.diff[4,14] | 0.1518 | 0.6232 | 0.005332 | –1.029 | 0.05458 | 1.642 | 50,001 | 100,000 |
| treat.mean.diff[4,15] | 2.515 | 1.571 | 0.02206 | –0.6391 | 2.533 | 5.588 | 50,001 | 100,000 |
| treat.mean.diff[5,6] | –0.4477 | 0.638 | 0.007698 | –2.005 | –0.2799 | 0.4829 | 50,001 | 100,000 |
| treat.mean.diff[5,7] | –0.3284 | 0.632 | 0.006024 | –1.869 | –0.1792 | 0.7137 | 50,001 | 100,000 |
| treat.mean.diff[5,8] | 0.5804 | 1.459 | 0.0117 | –2.292 | 0.5793 | 3.454 | 50,001 | 100,000 |
| treat.mean.diff[5,9] | –0.118 | 0.67 | 0.006758 | –1.489 | –0.101 | 1.153 | 50,001 | 100,000 |
| treat.mean.diff[5,10] | –5.662 | 1.586 | 0.02154 | –8.832 | –5.647 | –2.628 | 50,001 | 100,000 |
| treat.mean.diff[5,11] | –2.72 | 1.301 | 0.02126 | –5.327 | –2.709 | –0.195 | 50,001 | 100,000 |
| treat.mean.diff[5,12] | 2.935 | 2.222 | 0.02774 | –1.443 | 2.948 | 7.263 | 50,001 | 100,000 |
| treat.mean.diff[5,13] | –7.634 | 1.961 | 0.02443 | –11.48 | –7.632 | –3.774 | 50,001 | 100,000 |
| treat.mean.diff[5,14] | –0.2508 | 0.5732 | 0.004741 | –1.606 | –0.1365 | 0.7843 | 50,001 | 100,000 |
| treat.mean.diff[5,15] | 2.113 | 1.601 | 0.02298 | –1.129 | 2.149 | 5.188 | 50,001 | 100,000 |
| treat.mean.diff[6,7] | 0.1192 | 0.6287 | 0.005016 | –1.128 | 0.04269 | 1.588 | 50,001 | 100,000 |
| treat.mean.diff[6,8] | 1.028 | 1.588 | 0.01362 | –2.061 | 1.012 | 4.194 | 50,001 | 100,000 |
| treat.mean.diff[6,9] | 0.3296 | 0.6914 | 0.006814 | –1.012 | 0.3196 | 1.732 | 50,001 | 100,000 |
| treat.mean.diff[6,10] | –5.214 | 1.573 | 0.02119 | –8.353 | –5.202 | –2.172 | 50,001 | 100,000 |
| treat.mean.diff[6,11] | –2.272 | 1.245 | 0.01989 | –4.715 | –2.262 | 0.1749 | 50,001 | 100,000 |
| treat.mean.diff[6,12] | 3.383 | 2.232 | 0.02709 | –0.9925 | 3.391 | 7.727 | 50,001 | 100,000 |
| treat.mean.diff[6,13] | –7.186 | 1.961 | 0.02443 | –11.03 | –7.189 | –3.335 | 50,001 | 100,000 |
| treat.mean.diff[6,14] | 0.1968 | 0.6542 | 0.005736 | –0.9927 | 0.07337 | 1.795 | 50,001 | 100,000 |
| treat.mean.diff[6,15] | 2.56 | 1.568 | 0.02219 | –0.6208 | 2.576 | 5.595 | 50,001 | 100,000 |
| treat.mean.diff[7,8] | 0.9088 | 1.587 | 0.01318 | –2.186 | 0.898 | 4.079 | 50,001 | 100,000 |
| treat.mean.diff[7,9] | 0.2104 | 0.7561 | 0.006955 | –1.273 | 0.2016 | 1.732 | 50,001 | 100,000 |
| treat.mean.diff[7,10] | –5.334 | 1.615 | 0.02169 | –8.531 | –5.319 | –2.209 | 50,001 | 100,000 |
| treat.mean.diff[7,11] | –2.391 | 1.321 | 0.02061 | –4.996 | –2.384 | 0.1972 | 50,001 | 100,000 |
| treat.mean.diff[7,12] | 3.263 | 2.24 | 0.02707 | –1.131 | 3.268 | 7.622 | 50,001 | 100,000 |
| treat.mean.diff[7,13] | –7.305 | 1.986 | 0.02454 | –11.2 | –7.309 | –3.41 | 50,001 | 100,000 |
| treat.mean.diff[7,14] | 0.0776 | 0.6677 | 0.004748 | –1.278 | 0.01998 | 1.616 | 50,001 | 100,000 |
| treat.mean.diff[7,15] | 2.441 | 1.624 | 0.02278 | –0.8331 | 2.466 | 5.593 | 50,001 | 100,000 |
| treat.mean.diff[8,9] | –0.6984 | 1.605 | 0.01404 | –3.883 | –0.6939 | 2.453 | 50,001 | 100,000 |
| treat.mean.diff[8,10] | –6.242 | 2.159 | 0.02455 | –10.57 | –6.21 | –2.064 | 50,001 | 100,000 |
| treat.mean.diff[8,11] | –3.3 | 1.947 | 0.0237 | –7.165 | –3.296 | 0.5222 | 50,001 | 100,000 |
| treat.mean.diff[8,12] | 2.354 | 2.654 | 0.03049 | –2.853 | 2.366 | 7.492 | 50,001 | 100,000 |
| treat.mean.diff[8,13] | –8.214 | 2.448 | 0.02614 | –13.03 | –8.188 | –3.395 | 50,001 | 100,000 |
| treat.mean.diff[8,14] | –0.8312 | 1.566 | 0.01265 | –3.945 | –0.8274 | 2.228 | 50,001 | 100,000 |
| treat.mean.diff[8,15] | 1.532 | 2.161 | 0.02547 | –2.839 | 1.562 | 5.704 | 50,001 | 100,000 |
| treat.mean.diff[9,10] | –5.544 | 1.569 | 0.02063 | –8.669 | –5.542 | –2.494 | 50,001 | 100,000 |
| treat.mean.diff[9,11] | –2.602 | 1.326 | 0.02093 | –5.179 | –2.603 | 0.01789 | 50,001 | 100,000 |
| treat.mean.diff[9,12] | 3.053 | 2.244 | 0.0267 | –1.368 | 3.063 | 7.418 | 50,001 | 100,000 |
| treat.mean.diff[9,13] | –7.516 | 1.923 | 0.02344 | –11.28 | –7.513 | –3.713 | 50,001 | 100,000 |
| treat.mean.diff[9,14] | –0.1328 | 0.7567 | 0.006481 | –1.614 | –0.1446 | 1.413 | 50,001 | 100,000 |
| treat.mean.diff[9,15] | 2.231 | 1.604 | 0.02237 | –0.9882 | 2.245 | 5.346 | 50,001 | 100,000 |
| treat.mean.diff[10,11] | 2.942 | 1.563 | 0.01848 | –0.05385 | 2.929 | 6.044 | 50,001 | 100,000 |
| treat.mean.diff[10,12] | 8.597 | 2.65 | 0.03238 | 3.396 | 8.619 | 13.8 | 50,001 | 100,000 |
| treat.mean.diff[10,13] | –1.971 | 2.152 | 0.02598 | –6.188 | –1.968 | 2.292 | 50,001 | 100,000 |
| treat.mean.diff[10,14] | 5.411 | 1.614 | 0.02145 | 2.293 | 5.403 | 8.617 | 50,001 | 100,000 |
| treat.mean.diff[10,15] | 7.775 | 1.342 | 0.01406 | 5.142 | 7.772 | 10.43 | 50,001 | 100,000 |
| treat.mean.diff[11,12] | 5.655 | 2.499 | 0.03332 | 0.7631 | 5.664 | 10.58 | 50,001 | 100,000 |
| treat.mean.diff[11,13] | –4.914 | 2.18 | 0.02919 | –9.214 | –4.906 | –0.6075 | 50,001 | 100,000 |
| treat.mean.diff[11,14] | 2.469 | 1.322 | 0.02055 | –0.08331 | 2.457 | 5.096 | 50,001 | 100,000 |
| treat.mean.diff[11,15] | 4.832 | 1.278 | 0.01355 | 2.256 | 4.847 | 7.284 | 50,001 | 100,000 |
| treat.mean.diff[12,13] | –10.57 | 2.89 | 0.03667 | –16.23 | –10.58 | –4.859 | 50,001 | 100,000 |
| treat.mean.diff[12,14] | –3.186 | 2.244 | 0.02729 | –7.572 | –3.188 | 1.22 | 50,001 | 100,000 |
| treat.mean.diff[12,15] | –0.8223 | 2.675 | 0.0347 | –6.086 | –0.8262 | 4.44 | 50,001 | 100,000 |
| treat.mean.diff[13,14] | 7.383 | 1.987 | 0.02431 | 3.48 | 7.389 | 11.3 | 50,001 | 100,000 |
| treat.mean.diff[13,15] | 9.746 | 2.279 | 0.02926 | 5.261 | 9.76 | 14.22 | 50,001 | 100,000 |
| treat.mean.diff[14,15] | 2.363 | 1.623 | 0.02262 | –0.9254 | 2.397 | 5.517 | 50,001 | 100,000 |
Median ranks
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk.class[1] | 8.313 | 0.814 | 0.01061 | 7 | 8 | 10 | 50,001 | 100,000 |
| rk.class[2] | 9.576 | 0.7913 | 0.01062 | 7 | 10 | 10 | 50,001 | 100,000 |
| rk.class[3] | 4.78 | 0.8116 | 0.006447 | 4 | 5 | 6 | 50,001 | 100,000 |
| rk.class[4] | 5.846 | 1.456 | 0.01269 | 3 | 6 | 9 | 50,001 | 100,000 |
| rk.class[5] | 5.085 | 0.9136 | 0.007409 | 4 | 5 | 7 | 50,001 | 100,000 |
| rk.class[6] | 1.853 | 0.4327 | 0.003828 | 1 | 2 | 3 | 50,001 | 100,000 |
| rk.class[7] | 3.069 | 0.4784 | 0.004582 | 2 | 3 | 4 | 50,001 | 100,000 |
| rk.class[8] | 7.963 | 1.677 | 0.01967 | 4 | 8 | 10 | 50,001 | 100,000 |
| rk.class[9] | 1.191 | 0.4275 | 0.004097 | 1 | 1 | 2 | 50,001 | 100,000 |
| rk.class[10] | 7.323 | 1.297 | 0.01672 | 4 | 7 | 9 | 50,001 | 100,000 |
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk[1] | 13.31 | 0.814 | 0.0106 | 12 | 13 | 15 | 50,001 | 100,000 |
| rk[2] | 14.57 | 0.8591 | 0.01129 | 12 | 15 | 15 | 50,001 | 100,000 |
| rk[3] | 7.109 | 2.014 | 0.01435 | 4 | 7 | 11 | 50,001 | 100,000 |
| rk[4] | 6.782 | 1.983 | 0.01532 | 4 | 7 | 11 | 50,001 | 100,000 |
| rk[5] | 8.675 | 1.881 | 0.01767 | 5 | 9 | 12 | 50,001 | 100,000 |
| rk[6] | 6.617 | 2.041 | 0.01592 | 4 | 6 | 11 | 50,001 | 100,000 |
| rk[7] | 7.154 | 2.19 | 0.01599 | 4 | 7 | 11 | 50,001 | 100,000 |
| rk[8] | 9.42 | 3.3 | 0.02823 | 3 | 11 | 14 | 50,001 | 100,000 |
| rk[9] | 8.087 | 2.534 | 0.0223 | 4 | 9 | 12 | 50,001 | 100,000 |
| rk[10] | 1.856 | 0.4524 | 0.003938 | 1 | 2 | 3 | 50,001 | 100,000 |
| rk[11] | 3.219 | 1.074 | 0.01102 | 2 | 3 | 7 | 50,001 | 100,000 |
| rk[12] | 12.59 | 2.633 | 0.02894 | 4 | 13 | 15 | 50,001 | 100,000 |
| rk[13] | 1.192 | 0.4339 | 0.00412 | 1 | 1 | 2 | 50,001 | 100,000 |
| rk[14] | 7.441 | 2.19 | 0.01384 | 4 | 7 | 11 | 50,001 | 100,000 |
| rk[15] | 11.98 | 2.151 | 0.02675 | 4 | 12 | 14 | 50,001 | 100,000 |
Adults: clinical effectiveness (Yale–Brown Obsessive–Compulsive Scale) – sensitivity analysis 3 (blinding)
See Table 23 for a summary.
| Study | y[,1] | n[,1] | sd[,1] | y[,2] | n[,2] | sd[,2] | y[,3] | n[,3] | sd[,3] | y[,4] | n[,4] | sd[,4] | na[] | out[] | t[,1] | t[,2] | t[,3] | t[,4] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Albert et al., 2002155 | 18.36 | 25 | 7.11 | 17.3 | 40 | 6.15 | NA | NA | NA | NA | NA | NA | 2 | 2 | 8 | 9 | NA | NA |
| Andersson et al., 2012158 | 12.94 | 49 | 6.26 | 18.88 | 51 | 4.18 | NA | NA | NA | NA | NA | NA | 2 | 2 | 11 | 15 | NA | NA |
| Belloch et al., 2008159 | 8.31 | 13 | 8.75 | 6.8 | 16 | 3.55 | NA | NA | NA | NA | NA | NA | 2 | 2 | 10 | 12 | NA | NA |
| Belotto-Silva et al., 2012160 | 20.29 | 88 | 8.05 | 19.97 | 70 | 8.48 | NA | NA | NA | NA | NA | NA | 2 | 2 | 3 | 11 | NA | NA |
| Cordioli et al., 2003164 | 23.2 | 24 | 5.5 | 15.1 | 23 | 7.8 | NA | NA | NA | NA | NA | NA | 2 | 2 | 2 | 11 | NA | NA |
| Cottraux et al., 2001166 | –12.1 | 30 | 7.8 | –12.5 | 30 | 8.2 | NA | NA | NA | NA | NA | NA | 2 | 1 | 10 | 12 | NA | NA |
| Denys et al., 2003167 | –7.8 | 72 | 5.4 | –7.2 | 73 | 7.5 | NA | NA | NA | NA | NA | NA | 2 | 1 | 5 | 8 | NA | NA |
| Foa et al., 2005171 | 22.2 | 26 | 6.4 | 18.2 | 36 | 7.8 | 11 | 29 | 7.9 | 10.5 | 31 | 8.2 | 4 | 2 | 1 | 9 | 10 | 13 |
| Goodman et al., 1989176 | 28 | 21 | 7 | 19.4 | 21 | 7 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 4 | NA | NA |
| Jenike et al., 1990184 | 21.8 | 20 | 7.6 | 18.8 | 18 | 4 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 4 | NA | NA |
| Mundo et al., 1997199 | 16.2 | 10 | 8.9 | 21.6 | 9 | 7.6 | 19.8 | 11 | 10.1 | NA | NA | NA | 3 | 2 | 4 | 5 | 7 | NA |
| Nakatani et al., 2005202 | 20.2 | 10 | 9.4 | 12.9 | 10 | 4.9 | 28.4 | 8 | 5.5 | NA | NA | NA | 3 | 2 | 4 | 10 | 15 | NA |
| O’Connor et al., 1999203 | 17.5 | 6 | 4 | 13.3 | 6 | 8.6 | NA | NA | NA | NA | NA | NA | 2 | 2 | 2 | 11 | NA | NA |
| O’Connor et al., 2006204 | 25.4 | 10 | 3.5 | 24 | 11 | 4.7 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 4 | NA | NA |
| Sousa et al., 2006207 | –7.36 | 25 | NA | –10.8 | 25 | NA | NA | NA | NA | NA | NA | NA | 2 | 1 | 6 | 11 | NA | NA |
| Stein et al., 2007124 | –8.46 | 113 | 8.08 | –11.67 | 116 | 8.40 | –11.43 | 112 | 8.25 | –12.14 | 114 | 8.22 | 4 | 1 | 1 | 5 | 14 | 14 |
| Whittal et al., 2005211 | 10.41 | 29 | 7.6 | 10.6 | 30 | 7.1 | NA | NA | NA | NA | NA | NA | 2 | 2 | 10 | 12 | NA | NA |
Key
-
Placebo (1).
-
Waitlist (2).
-
Fluoxetine (3).
-
Fluvoxamine (3).
-
Paroxetine (3).
-
Sertraline (3).
-
Citalopram (3).
-
Venlafaxine (4).
-
Clomipramine (5).
-
BT (6).
-
CBT (7).
-
CT (8).
-
BT + clomipramine (9).
-
Escitalopram (3).
-
Psychological placebo (10).
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| class.mean.diff[1,2] | 3.235 | 2.714 | 0.06924 | –2.16 | 3.238 | 8.44 | 50,001 | 100,000 |
| class.mean.diff[1,3] | –3.305 | 1.234 | 0.02794 | –5.59 | –3.349 | –0.6521 | 50,001 | 100,000 |
| class.mean.diff[1,4] | –2.728 | 1.632 | 0.0314 | –5.968 | –2.7 | 0.4702 | 50,001 | 100,000 |
| class.mean.diff[1,5] | –4.046 | 1.674 | 0.03403 | –7.303 | –4.023 | –0.73 | 50,001 | 100,000 |
| class.mean.diff[1,6] | –11.79 | 1.762 | 0.04753 | –15.17 | –11.81 | –8.279 | 50,001 | 100,000 |
| class.mean.diff[1,7] | –4.112 | 1.842 | 0.04886 | –7.631 | –4.125 | –0.3389 | 50,001 | 100,000 |
| class.mean.diff[1,8] | –12.23 | 2.231 | 0.05662 | –16.66 | –12.24 | –7.796 | 50,001 | 100,000 |
| class.mean.diff[1,9] | –11.85 | 2.064 | 0.03817 | –16.07 | –11.85 | –7.821 | 50,001 | 100,000 |
| class.mean.diff[1,10] | 2.328 | 1.991 | 0.0483 | –1.486 | 2.28 | 6.364 | 50,001 | 100,000 |
| class.mean.diff[2,3] | –6.539 | 2.542 | 0.05609 | –11.41 | –6.547 | –1.448 | 50,001 | 100,000 |
| class.mean.diff[2,4] | –5.963 | 2.911 | 0.06212 | –11.5 | –5.948 | –0.1066 | 50,001 | 100,000 |
| class.mean.diff[2,5] | –7.28 | 2.983 | 0.06417 | –12.95 | –7.338 | –1.344 | 50,001 | 100,000 |
| class.mean.diff[2,6] | –15.02 | 2.918 | 0.06588 | –20.59 | –15.07 | –9.151 | 50,001 | 100,000 |
| class.mean.diff[2,7] | –7.347 | 1.969 | 0.04063 | –11.07 | –7.404 | –3.352 | 50,001 | 100,000 |
| class.mean.diff[2,8] | –15.47 | 3.237 | 0.07454 | –21.74 | –15.48 | –9.029 | 50,001 | 100,000 |
| class.mean.diff[2,9] | –15.09 | 3.247 | 0.06687 | –21.38 | –15.13 | –8.626 | 50,001 | 100,000 |
| class.mean.diff[2,10] | –0.9071 | 2.429 | 0.04743 | –5.577 | –0.9553 | 4.094 | 50,001 | 100,000 |
| class.mean.diff[3,4] | 0.5765 | 1.669 | 0.02399 | –2.802 | 0.5924 | 3.827 | 50,001 | 100,000 |
| class.mean.diff[3,5] | –0.7409 | 1.845 | 0.03034 | –4.413 | –0.7264 | 2.846 | 50,001 | 100,000 |
| class.mean.diff[3,6] | –8.486 | 1.902 | 0.04269 | –12.2 | –8.487 | –4.694 | 50,001 | 100,000 |
| class.mean.diff[3,7] | –0.8074 | 1.611 | 0.03221 | –3.942 | –0.8267 | 2.399 | 50,001 | 100,000 |
| class.mean.diff[3,8] | –8.929 | 2.349 | 0.05339 | –13.58 | –8.912 | –4.286 | 50,001 | 100,000 |
| class.mean.diff[3,9] | –8.55 | 2.272 | 0.03812 | –13.14 | –8.521 | –4.061 | 50,001 | 100,000 |
| class.mean.diff[3,10] | 5.632 | 1.883 | 0.03501 | 1.957 | 5.593 | 9.45 | 50,001 | 100,000 |
| class.mean.diff[4,5] | –1.317 | 1.645 | 0.02532 | –4.541 | –1.319 | 1.944 | 50,001 | 100,000 |
| class.mean.diff[4,6] | –9.062 | 2.129 | 0.04457 | –13.15 | –9.064 | –4.827 | 50,001 | 100,000 |
| class.mean.diff[4,7] | –1.384 | 2.151 | 0.03957 | –5.588 | –1.387 | 2.924 | 50,001 | 100,000 |
| class.mean.diff[4,8] | –9.506 | 2.52 | 0.0536 | –14.52 | –9.486 | –4.519 | 50,001 | 100,000 |
| class.mean.diff[4,9] | –9.126 | 2.363 | 0.03643 | –13.85 | –9.098 | –4.476 | 50,001 | 100,000 |
| class.mean.diff[4,10] | 5.056 | 2.304 | 0.0404 | 0.6046 | 5.021 | 9.779 | 50,001 | 100,000 |
| class.mean.diff[5,6] | –7.745 | 1.937 | 0.03849 | –11.47 | –7.768 | –3.863 | 50,001 | 100,000 |
| class.mean.diff[5,7] | –0.06652 | 2.247 | 0.04401 | –4.412 | –0.07668 | 4.391 | 50,001 | 100,000 |
| class.mean.diff[5,8] | –8.188 | 2.369 | 0.04925 | –12.86 | –8.214 | –3.489 | 50,001 | 100,000 |
| class.mean.diff[5,9] | –7.809 | 2.119 | 0.03235 | –12.02 | –7.798 | –3.656 | 50,001 | 100,000 |
| class.mean.diff[5,10] | 6.373 | 2.334 | 0.04407 | 1.879 | 6.35 | 11.12 | 50,001 | 100,000 |
| class.mean.diff[6,7] | 7.678 | 2.142 | 0.04823 | 3.483 | 7.676 | 11.91 | 50,001 | 100,000 |
| class.mean.diff[6,8] | –0.4437 | 1.39 | 0.02557 | –3.137 | –0.472 | 2.314 | 50,001 | 100,000 |
| class.mean.diff[6,9] | –0.0644 | 2.231 | 0.04198 | –4.457 | –0.09329 | 4.256 | 50,001 | 100,000 |
| class.mean.diff[6,10] | 14.12 | 2.108 | 0.04427 | 10.07 | 14.1 | 18.22 | 50,001 | 100,000 |
| class.mean.diff[7,8] | –8.122 | 2.542 | 0.05765 | –13.14 | –8.119 | –3.13 | 50,001 | 100,000 |
| class.mean.diff[7,9] | –7.743 | 2.583 | 0.04772 | –12.93 | –7.699 | –2.677 | 50,001 | 100,000 |
| class.mean.diff[7,10] | 6.44 | 1.4 | 0.01987 | 3.792 | 6.404 | 9.349 | 50,001 | 100,000 |
| class.mean.diff[8,9] | 0.3793 | 2.612 | 0.05047 | –4.818 | 0.3555 | 5.518 | 50,001 | 100,000 |
| class.mean.diff[8,10] | 14.56 | 2.518 | 0.05403 | 9.674 | 14.52 | 19.51 | 50,001 | 100,000 |
| class.mean.diff[9,10] | 14.18 | 2.643 | 0.04615 | 9.044 | 14.14 | 19.53 | 50,001 | 100,000 |
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| treat.mean.diff[1,2] | 3.235 | 2.714 | 0.06924 | –2.16 | 3.238 | 8.44 | 50,001 | 100,000 |
| treat.mean.diff[1,3] | –3.416 | 1.611 | 0.03769 | –6.618 | –3.456 | 0.06601 | 50,001 | 100,000 |
| treat.mean.diff[1,4] | –3.849 | 1.018 | 0.02311 | –5.988 | –3.813 | –1.948 | 50,001 | 100,000 |
| treat.mean.diff[1,5] | –3.203 | 1.103 | 0.02543 | –5.291 | –3.238 | –0.8988 | 50,001 | 100,000 |
| treat.mean.diff[1,6] | –2.713 | 1.897 | 0.04831 | –5.647 | –3.041 | 2.035 | 50,001 | 100,000 |
| treat.mean.diff[1,7] | –3.272 | 1.64 | 0.03575 | –6.501 | –3.333 | 0.4173 | 50,001 | 100,000 |
| treat.mean.diff[1,8] | –2.728 | 1.632 | 0.0314 | –5.968 | –2.7 | 0.4702 | 50,001 | 100,000 |
| treat.mean.diff[1,9] | –4.046 | 1.674 | 0.03403 | –7.303 | –4.023 | –0.73 | 50,001 | 100,000 |
| treat.mean.diff[1,10] | –11.79 | 1.762 | 0.04753 | –15.17 | –11.81 | –8.279 | 50,001 | 100,000 |
| treat.mean.diff[1,11] | –4.112 | 1.842 | 0.04886 | –7.631 | –4.125 | –0.3389 | 50,001 | 100,000 |
| treat.mean.diff[1,12] | –12.23 | 2.231 | 0.05662 | –16.66 | –12.24 | –7.796 | 50,001 | 100,000 |
| treat.mean.diff[1,13] | –11.85 | 2.064 | 0.03817 | –16.07 | –11.85 | –7.821 | 50,001 | 100,000 |
| treat.mean.diff[1,14] | –3.356 | 1.058 | 0.02341 | –5.376 | –3.374 | –1.212 | 50,001 | 100,000 |
| treat.mean.diff[1,15] | 2.328 | 1.991 | 0.0483 | –1.486 | 2.28 | 6.364 | 50,001 | 100,000 |
| treat.mean.diff[2,3] | –6.65 | 2.408 | 0.05065 | –11.19 | –6.696 | –1.818 | 50,001 | 100,000 |
| treat.mean.diff[2,4] | –7.084 | 2.684 | 0.06565 | –12.27 | –7.059 | –1.813 | 50,001 | 100,000 |
| treat.mean.diff[2,5] | –6.437 | 2.643 | 0.06003 | –11.49 | –6.466 | –1.121 | 50,001 | 100,000 |
| treat.mean.diff[2,6] | –5.948 | 2.585 | 0.05411 | –10.79 | –5.974 | –0.701 | 50,001 | 100,000 |
| treat.mean.diff[2,7] | –6.507 | 2.826 | 0.06123 | –11.91 | –6.538 | –0.7908 | 50,001 | 100,000 |
| treat.mean.diff[2,8] | –5.963 | 2.911 | 0.06212 | –11.5 | –5.948 | –0.1066 | 50,001 | 100,000 |
| treat.mean.diff[2,9] | –7.28 | 2.983 | 0.06417 | –12.95 | –7.338 | –1.344 | 50,001 | 100,000 |
| treat.mean.diff[2,10] | –15.02 | 2.918 | 0.06588 | –20.59 | –15.07 | –9.151 | 50,001 | 100,000 |
| treat.mean.diff[2,11] | –7.347 | 1.969 | 0.04063 | –11.07 | –7.404 | –3.352 | 50,001 | 100,000 |
| treat.mean.diff[2,12] | –15.47 | 3.237 | 0.07454 | –21.74 | –15.48 | –9.029 | 50,001 | 100,000 |
| treat.mean.diff[2,13] | –15.09 | 3.247 | 0.06687 | –21.38 | –15.13 | –8.626 | 50,001 | 100,000 |
| treat.mean.diff[2,14] | –6.591 | 2.672 | 0.0623 | –11.7 | –6.581 | –1.299 | 50,001 | 100,000 |
| treat.mean.diff[2,15] | –0.9071 | 2.429 | 0.04743 | –5.577 | –0.9553 | 4.094 | 50,001 | 100,000 |
| treat.mean.diff[3,4] | –0.4335 | 1.539 | 0.03259 | –4.176 | –0.1464 | 2.393 | 50,001 | 100,000 |
| treat.mean.diff[3,5] | 0.213 | 1.507 | 0.02551 | –2.921 | 0.07384 | 3.508 | 50,001 | 100,000 |
| treat.mean.diff[3,6] | 0.7025 | 1.613 | 0.02607 | –1.828 | 0.274 | 4.886 | 50,001 | 100,000 |
| treat.mean.diff[3,7] | 0.1434 | 1.802 | 0.02922 | –3.65 | 0.03283 | 4.281 | 50,001 | 100,000 |
| treat.mean.diff[3,8] | 0.6875 | 1.981 | 0.032 | –3.29 | 0.6776 | 4.713 | 50,001 | 100,000 |
| treat.mean.diff[3,9] | –0.6299 | 2.107 | 0.03662 | –4.804 | –0.6254 | 3.512 | 50,001 | 100,000 |
| treat.mean.diff[3,10] | –8.375 | 2.085 | 0.04425 | –12.47 | –8.381 | –4.207 | 50,001 | 100,000 |
| treat.mean.diff[3,11] | –0.6964 | 1.413 | 0.025 | –3.48 | –0.6962 | 2.101 | 50,001 | 100,000 |
| treat.mean.diff[3,12] | –8.818 | 2.498 | 0.05483 | –13.73 | –8.806 | –3.848 | 50,001 | 100,000 |
| treat.mean.diff[3,13] | –8.439 | 2.477 | 0.04285 | –13.47 | –8.4 | –3.502 | 50,001 | 100,000 |
| treat.mean.diff[3,14] | 0.05968 | 1.528 | 0.0269 | –3.238 | 0.01872 | 3.303 | 50,001 | 100,000 |
| treat.mean.diff[3,15] | 5.743 | 1.812 | 0.02962 | 2.273 | 5.698 | 9.405 | 50,001 | 100,000 |
| treat.mean.diff[4,5] | 0.6465 | 1.14 | 0.02204 | –1.226 | 0.3928 | 3.394 | 50,001 | 100,000 |
| treat.mean.diff[4,6] | 1.136 | 1.944 | 0.04714 | –1.374 | 0.5156 | 6.365 | 50,001 | 100,000 |
| treat.mean.diff[4,7] | 0.5769 | 1.558 | 0.03087 | –2.189 | 0.24 | 4.473 | 50,001 | 100,000 |
| treat.mean.diff[4,8] | 1.121 | 1.692 | 0.02782 | –2.14 | 1.081 | 4.632 | 50,001 | 100,000 |
| treat.mean.diff[4,9] | –0.1964 | 1.813 | 0.03407 | –3.689 | –0.2383 | 3.494 | 50,001 | 100,000 |
| treat.mean.diff[4,10] | –7.941 | 1.858 | 0.04794 | –11.5 | –7.995 | –4.206 | 50,001 | 100,000 |
| treat.mean.diff[4,11] | –0.2629 | 1.804 | 0.04362 | –3.538 | –0.3853 | 3.639 | 50,001 | 100,000 |
| treat.mean.diff[4,12] | –8.385 | 2.298 | 0.05613 | –12.94 | –8.403 | –3.759 | 50,001 | 100,000 |
| treat.mean.diff[4,13] | –8.005 | 2.195 | 0.0387 | –12.36 | –7.983 | –3.628 | 50,001 | 100,000 |
| treat.mean.diff[4,14] | 0.4932 | 1.107 | 0.02017 | –1.358 | 0.2504 | 3.153 | 50,001 | 100,000 |
| treat.mean.diff[4,15] | 6.177 | 1.97 | 0.04435 | 2.515 | 6.081 | 10.36 | 50,001 | 100,000 |
| treat.mean.diff[5,6] | 0.4895 | 1.708 | 0.03427 | –2.301 | 0.1156 | 5.021 | 50,001 | 100,000 |
| treat.mean.diff[5,7] | –0.06957 | 1.463 | 0.02327 | –3.284 | –0.02529 | 3.131 | 50,001 | 100,000 |
| treat.mean.diff[5,8] | 0.4744 | 1.39 | 0.01956 | –2.333 | 0.4868 | 3.177 | 50,001 | 100,000 |
| treat.mean.diff[5,9] | –0.8429 | 1.7 | 0.02827 | –4.188 | –0.834 | 2.518 | 50,001 | 100,000 |
| treat.mean.diff[5,10] | –8.588 | 1.872 | 0.04338 | –12.34 | –8.598 | –4.862 | 50,001 | 100,000 |
| treat.mean.diff[5,11] | –0.9094 | 1.761 | 0.0377 | –4.336 | –0.9386 | 2.646 | 50,001 | 100,000 |
| treat.mean.diff[5,12] | –9.031 | 2.325 | 0.05383 | –13.77 | –9.029 | –4.414 | 50,001 | 100,000 |
| treat.mean.diff[5,13] | –8.652 | 2.21 | 0.03778 | –13.1 | –8.625 | –4.289 | 50,001 | 100,000 |
| treat.mean.diff[5,14] | –0.1533 | 0.8776 | 0.01126 | –2.036 | –0.06866 | 1.617 | 50,001 | 100,000 |
| treat.mean.diff[5,15] | 5.53 | 1.963 | 0.03868 | 1.663 | 5.47 | 9.495 | 50,001 | 100,000 |
| treat.mean.diff[6,7] | –0.559 | 1.947 | 0.03412 | –5.537 | –0.1474 | 2.741 | 50,001 | 100,000 |
| treat.mean.diff[6,8] | –0.01503 | 2.163 | 0.04166 | –4.997 | 0.178 | 3.768 | 50,001 | 100,000 |
| treat.mean.diff[6,9] | –1.332 | 2.291 | 0.04468 | –6.485 | –1.177 | 2.757 | 50,001 | 100,000 |
| treat.mean.diff[6,10] | –9.077 | 2.281 | 0.05002 | –13.99 | –8.955 | –4.8 | 50,001 | 100,000 |
| treat.mean.diff[6,11] | –1.399 | 1.721 | 0.03463 | –5.105 | –1.283 | 1.726 | 50,001 | 100,000 |
| treat.mean.diff[6,12] | –9.521 | 2.677 | 0.0606 | –15.06 | –9.402 | –4.468 | 50,001 | 100,000 |
| treat.mean.diff[6,13] | –9.141 | 2.662 | 0.05178 | –14.85 | –9.002 | –4.184 | 50,001 | 100,000 |
| treat.mean.diff[6,14] | –0.6428 | 1.768 | 0.03724 | –5.344 | –0.2007 | 2.104 | 50,001 | 100,000 |
| treat.mean.diff[6,15] | 5.041 | 2.089 | 0.03947 | 0.7185 | 5.109 | 8.958 | 50,001 | 100,000 |
| treat.mean.diff[7,8] | 0.544 | 1.983 | 0.03284 | –3.508 | 0.5492 | 4.486 | 50,001 | 100,000 |
| treat.mean.diff[7,9] | –0.7733 | 2.131 | 0.03768 | –5.113 | –0.7453 | 3.389 | 50,001 | 100,000 |
| treat.mean.diff[7,10] | –8.518 | 2.207 | 0.05009 | –12.94 | –8.523 | –4.154 | 50,001 | 100,000 |
| treat.mean.diff[7,11] | –0.8399 | 2.024 | 0.0397 | –4.941 | –0.8563 | 3.252 | 50,001 | 100,000 |
| treat.mean.diff[7,12] | –8.962 | 2.606 | 0.05965 | –14.2 | –8.937 | –3.861 | 50,001 | 100,000 |
| treat.mean.diff[7,13] | –8.582 | 2.506 | 0.04391 | –13.64 | –8.573 | –3.58 | 50,001 | 100,000 |
| treat.mean.diff[7,14] | –0.08376 | 1.496 | 0.02316 | –3.474 | –0.01512 | 3.063 | 50,001 | 100,000 |
| treat.mean.diff[7,15] | 5.6 | 2.232 | 0.04279 | 1.03 | 5.56 | 10.09 | 50,001 | 100,000 |
| treat.mean.diff[8,9] | –1.317 | 1.645 | 0.02532 | –4.541 | –1.319 | 1.944 | 50,001 | 100,000 |
| treat.mean.diff[8,10] | –9.062 | 2.129 | 0.04457 | –13.15 | –9.064 | –4.827 | 50,001 | 100,000 |
| treat.mean.diff[8,11] | –1.384 | 2.151 | 0.03957 | –5.588 | –1.387 | 2.924 | 50,001 | 100,000 |
| treat.mean.diff[8,12] | –9.506 | 2.52 | 0.0536 | –14.52 | –9.486 | –4.519 | 50,001 | 100,000 |
| treat.mean.diff[8,13] | –9.126 | 2.363 | 0.03643 | –13.85 | –9.098 | –4.476 | 50,001 | 100,000 |
| treat.mean.diff[8,14] | –0.6278 | 1.588 | 0.0237 | –3.819 | –0.6289 | 2.551 | 50,001 | 100,000 |
| treat.mean.diff[8,15] | 5.056 | 2.304 | 0.0404 | 0.6046 | 5.021 | 9.779 | 50,001 | 100,000 |
| treat.mean.diff[9,10] | –7.745 | 1.937 | 0.03849 | –11.47 | –7.768 | –3.863 | 50,001 | 100,000 |
| treat.mean.diff[9,11] | –0.06652 | 2.247 | 0.04401 | –4.412 | –0.07668 | 4.391 | 50,001 | 100,000 |
| treat.mean.diff[9,12] | –8.188 | 2.369 | 0.04925 | –12.86 | –8.214 | –3.489 | 50,001 | 100,000 |
| treat.mean.diff[9,13] | –7.809 | 2.119 | 0.03235 | –12.02 | –7.798 | –3.656 | 50,001 | 100,000 |
| treat.mean.diff[9,14] | 0.6896 | 1.772 | 0.02976 | –2.805 | 0.6723 | 4.18 | 50,001 | 100,000 |
| treat.mean.diff[9,15] | 6.373 | 2.334 | 0.04407 | 1.879 | 6.35 | 11.12 | 50,001 | 100,000 |
| treat.mean.diff[10,11] | 7.678 | 2.142 | 0.04823 | 3.483 | 7.676 | 11.91 | 50,001 | 100,000 |
| treat.mean.diff[10,12] | –0.4437 | 1.39 | 0.02557 | –3.137 | –0.472 | 2.314 | 50,001 | 100,000 |
| treat.mean.diff[10,13] | –0.0644 | 2.231 | 0.04198 | –4.457 | –0.09329 | 4.256 | 50,001 | 100,000 |
| treat.mean.diff[10,14] | 8.434 | 1.879 | 0.04381 | 4.725 | 8.445 | 12.12 | 50,001 | 100,000 |
| treat.mean.diff[10,15] | 14.12 | 2.108 | 0.04427 | 10.07 | 14.1 | 18.22 | 50,001 | 100,000 |
| treat.mean.diff[11,12] | –8.122 | 2.542 | 0.05765 | –13.14 | –8.119 | –3.13 | 50,001 | 100,000 |
| treat.mean.diff[11,13] | –7.743 | 2.583 | 0.04772 | –12.93 | –7.699 | –2.677 | 50,001 | 100,000 |
| treat.mean.diff[11,14] | 0.7561 | 1.794 | 0.04019 | –2.931 | 0.7941 | 4.193 | 50,001 | 100,000 |
| treat.mean.diff[11,15] | 6.44 | 1.4 | 0.01987 | 3.792 | 6.404 | 9.349 | 50,001 | 100,000 |
| treat.mean.diff[12,13] | 0.3793 | 2.612 | 0.05047 | –4.818 | 0.3555 | 5.518 | 50,001 | 100,000 |
| treat.mean.diff[12,14] | 8.878 | 2.324 | 0.05373 | 4.27 | 8.853 | 13.55 | 50,001 | 100,000 |
| treat.mean.diff[12,15] | 14.56 | 2.518 | 0.05403 | 9.674 | 14.52 | 19.51 | 50,001 | 100,000 |
| treat.mean.diff[13,14] | 8.499 | 2.213 | 0.03778 | 4.126 | 8.485 | 12.94 | 50,001 | 100,000 |
| treat.mean.diff[13,15] | 14.18 | 2.643 | 0.04615 | 9.044 | 14.14 | 19.53 | 50,001 | 100,000 |
| treat.mean.diff[14,15] | 5.684 | 1.997 | 0.04124 | 1.801 | 5.616 | 9.757 | 50,001 | 100,000 |
Median ranks
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk.class[1] | 8.137 | 0.6112 | 0.01187 | 7 | 8 | 10 | 50,001 | 100,000 |
| rk.class[2] | 9.508 | 0.7976 | 0.01363 | 8 | 10 | 10 | 50,001 | 100,000 |
| rk.class[3] | 5.739 | 0.9598 | 0.01586 | 4 | 6 | 7 | 50,001 | 100,000 |
| rk.class[4] | 6.292 | 1.061 | 0.01519 | 4 | 7 | 8 | 50,001 | 100,000 |
| rk.class[5] | 5.078 | 1.096 | 0.01975 | 4 | 5 | 7 | 50,001 | 100,000 |
| rk.class[6] | 2.151 | 0.6964 | 0.01172 | 1 | 2 | 3 | 50,001 | 100,000 |
| rk.class[7] | 5.029 | 1.128 | 0.02361 | 4 | 5 | 7 | 50,001 | 100,000 |
| rk.class[8] | 1.817 | 0.8127 | 0.01454 | 1 | 2 | 3 | 50,001 | 100,000 |
| rk.class[9] | 2.042 | 0.9115 | 0.01683 | 1 | 2 | 3 | 50,001 | 100,000 |
| rk.class[10] | 9.207 | 0.6445 | 0.009085 | 8 | 9 | 10 | 50,001 | 100,000 |
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk[1] | 13 | 0.8523 | 0.01843 | 11 | 13 | 15 | 50,001 | 100,000 |
| rk[2] | 14.45 | 1.038 | 0.01616 | 12 | 15 | 15 | 50,001 | 100,000 |
| rk[3] | 8.025 | 2.379 | 0.03519 | 4 | 8 | 12 | 50,001 | 100,000 |
| rk[4] | 7.033 | 2.123 | 0.042 | 4 | 7 | 11 | 50,001 | 100,000 |
| rk[5] | 8.577 | 1.988 | 0.02899 | 5 | 9 | 12 | 50,001 | 100,000 |
| rk[6] | 9.308 | 2.443 | 0.04107 | 5 | 10 | 13 | 50,001 | 100,000 |
| rk[7] | 8.341 | 2.554 | 0.04085 | 4 | 8 | 13 | 50,001 | 100,000 |
| rk[8] | 9.542 | 2.724 | 0.04309 | 4 | 10 | 13 | 50,001 | 100,000 |
| rk[9] | 6.822 | 2.859 | 0.05316 | 4 | 6 | 12 | 50,001 | 100,000 |
| rk[10] | 2.153 | 0.7003 | 0.01172 | 1 | 2 | 3 | 50,001 | 100,000 |
| rk[11] | 6.548 | 2.704 | 0.06183 | 4 | 5 | 12 | 50,001 | 100,000 |
| rk[12] | 1.82 | 0.8264 | 0.01462 | 1 | 2 | 3 | 50,001 | 100,000 |
| rk[13] | 2.047 | 0.9274 | 0.01687 | 1 | 2 | 3 | 50,001 | 100,000 |
| rk[14] | 8.16 | 2.132 | 0.03462 | 4 | 8 | 12 | 50,001 | 100,000 |
| rk[15] | 14.17 | 0.7426 | 0.01001 | 13 | 14 | 15 | 50,001 | 100,000 |
Adults: clinical effectiveness (Yale–Brown Obsessive–Compulsive Scale) – sensitivity analysis 4 (post hoc), excluding studies that have used a waitlist as control
This is a post-hoc analysis.
| Study | y[,1] | n[,1] | sd[,1] | y[,2] | n[,2] | sd[,2] | y[,3] | n[,3] | sd[,3] | y[,4] | n[,4] | sd[,4] | na[] | out[] | t[,1] | t[,2] | t[,3] | t[,4] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Albert et al., 2002155 | 18.36 | 25 | 7.11 | 17.3 | 40 | 6.15 | NA | NA | NA | NA | NA | NA | 2 | 2 | 7 | 8 | NA | NA |
| Andersson et al., 2012158 | 12.94 | 49 | 6.26 | 18.88 | 51 | 4.18 | NA | NA | NA | NA | NA | NA | 2 | 2 | 10 | 16 | NA | NA |
| Bisserbe et al., 1997162 | –14.3 | 86 | NA | –11.71 | 81 | NA | NA | NA | NA | NA | NA | NA | 2 | 1 | 5 | 8 | NA | NA |
| Belloch et al., 2008159 | 8.31 | 13 | 8.75 | 6.8 | 16 | 3.55 | NA | NA | NA | NA | NA | NA | 2 | 2 | 9 | 11 | NA | NA |
| Belotto-Silva et al., 2012160 | 20.29 | 88 | 8.05 | 19.97 | 70 | 8.48 | NA | NA | NA | NA | NA | NA | 2 | 2 | 2 | 10 | NA | NA |
| Bergeron et al., 2002161 | –9.7 | 72 | 7.7 | –9.6 | 76 | 7.9 | NA | NA | NA | NA | NA | NA | 2 | 1 | 2 | 5 | NA | NA |
| CCSG1, 1991154 | 25.11 | 108 | 6.34 | 16.23 | 102 | 7.37 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 8 | NA | NA |
| CCSG2, 1991154 | 25.59 | 119 | 5.78 | 14.7 | 120 | 7.45 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 8 | NA | NA |
| Chouinard et al., 1990163 | –1.48 | 44 | NA | –3.79 | 43 | NA | NA | NA | NA | NA | NA | NA | 2 | 1 | 1 | 5 | NA | NA |
| Cottraux et al., 2001166 | –12.1 | 30 | 7.8 | –12.5 | 30 | 8.2 | NA | NA | NA | NA | NA | NA | 2 | 1 | 9 | 11 | NA | NA |
| Denys et al., 2003167 | –7.8 | 72 | 5.4 | –7.2 | 73 | 7.5 | NA | NA | NA | NA | NA | NA | 2 | 1 | 4 | 7 | NA | NA |
| Fals-Stewart et al., 1993170 | –8.1 | 31 | NA | –1.8 | 32 | NA | NA | NA | NA | NA | NA | NA | 2 | 1 | 9 | 16 | NA | NA |
| Foa et al., 2005171 | 22.2 | 26 | 6.4 | 18.2 | 36 | 7.8 | 11 | 29 | 7.9 | 10.5 | 31 | 8.2 | 4 | 2 | 1 | 8 | 9 | 14 |
| Freeman et al., 1994172 | –8.6 | 28 | NA | –7.8 | 19 | NA | NA | NA | NA | NA | NA | NA | 2 | 1 | 3 | 8 | NA | NA |
| GlaxoSmithKline, 2005174 | –4.61 | 75 | 7.53 | –5.61 | 79 | 7.47 | –7.73 | 78 | 7.42 | NA | NA | NA | 3 | 1 | 1 | 4 | 8 | NA |
| GlaxoSmithKline, 2005175 | –14.26 | 72 | 6.33 | –13.19 | 69 | 6.48 | NA | NA | NA | NA | NA | NA | 2 | 1 | 4 | 8 | NA | NA |
| Goodman et al., 1989176 | 28 | 21 | 7 | 19.4 | 21 | 7 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 3 | NA | NA |
| Goodman et al., 1996177 | –1.71 | 78 | 4.88 | –3.95 | 78 | 6.28 | NA | NA | NA | NA | NA | NA | 2 | 1 | 1 | 3 | NA | NA |
| Greist et al., 1995126 | –3.41 | 84 | 6.19 | –5.57 | 240 | 6.19 | NA | NA | NA | NA | NA | NA | 2 | 1 | 1 | 5 | NA | NA |
| Greist et al., 2002178 | 17.6 | 55 | 6.2 | 24.1 | 66 | 6.7 | NA | NA | NA | NA | NA | NA | 2 | 2 | 9 | 16 | NA | NA |
| Hollander et al., 2003180 | –5.6 | 120 | 7.67 | –8.5 | 117 | 7.57 | NA | NA | NA | NA | NA | NA | 2 | 1 | 1 | 3 | NA | NA |
| Hollander et al., 2003181 | –3.33 | 89 | NA | –4.14 | 88 | NA | –6.35 | 86 | NA | –7.34 | 85 | NA | 4 | 1 | 1 | 4 | 4 | 4 |
| Jenike et al., 1990183 | 22.3 | 9 | 7.8 | 20.6 | 10 | 9.2 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 5 | NA | NA |
| Jenike et al., 1990184 | 21.8 | 20 | 7.6 | 18.8 | 18 | 4 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 3 | NA | NA |
| Jenike et al., 1997185 | 18.7 | 18 | 6.1 | 16.2 | 19 | 6.3 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 2 | NA | NA |
| Kamijima et al., 2004187 | 20.3 | 94 | 7.38 | 15.8 | 94 | 8.09 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 4 | NA | NA |
| Kobak et al., 2005189 | 19.87 | 30 | 7.46 | 19.75 | 30 | 7.46 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 12 | NA | NA |
| Koran et al., 1996190 | 17.8 | 34 | 7.7 | 17 | 39 | 8.55 | NA | NA | NA | NA | NA | NA | 2 | 2 | 3 | 8 | NA | NA |
| Kronig et al., 1999191 | –4.14 | 79 | NA | –8.5 | 85 | NA | NA | NA | NA | NA | NA | NA | 2 | 1 | 1 | 5 | NA | NA |
| Lindsay et al., 1997192 | 11 | 9 | 3.81 | 25.89 | 9 | 5.8 | NA | NA | NA | NA | NA | NA | 2 | 2 | 9 | 16 | NA | NA |
| López-Ibor et al., 1996193 | –7.5 | 30 | 9.29 | –8.9 | 24 | 7.13 | NA | NA | NA | NA | NA | NA | 2 | 1 | 2 | 8 | NA | NA |
| McLean et al., 2001195 | 16.1 | 31 | 6.7 | 13.2 | 32 | 7.2 | NA | NA | NA | NA | NA | NA | 2 | 2 | 11 | 9 | NA | NA |
| Milanfranchi et al., 1997196 | 18.4 | 13 | 9.2 | 16.5 | 12 | 11 | NA | NA | NA | NA | NA | NA | 2 | 2 | 3 | 8 | NA | NA |
| Montgomery et al., 1993197 | –3.7 | 56 | 5.98 | –5.13 | 52 | 6.41 | –4.76 | 52 | 6.89 | –6.07 | 54 | 6.92 | 4 | 1 | 1 | 2 | 2 | 2 |
| Montgomery et al., 2001198 | –5.6 | 101 | 6.9 | –8.4 | 102 | 7.3 | –8.9 | 98 | 7 | –10.4 | 100 | 6.9 | 4 | 1 | 1 | 6 | 6 | 6 |
| Mundo et al., 1997199 | 16.2 | 10 | 8.9 | 21.6 | 9 | 7.6 | 19.8 | 11 | 10.1 | NA | NA | NA | 3 | 2 | 3 | 4 | 6 | NA |
| Mundo et al., 2001200 | –12.2 | 115 | NA | –12 | 112 | NA | NA | NA | NA | NA | NA | NA | 2 | 1 | 3 | 8 | NA | NA |
| Nakajima et al., 1996201 | –1.9 | 33 | 7.2 | –7.1 | 60 | 7.03 | NA | NA | NA | NA | NA | NA | 2 | 1 | 1 | 3 | NA | NA |
| Nakatani et al., 2005202 | 20.2 | 10 | 9.4 | 12.9 | 10 | 4.9 | 28.4 | 8 | 5.5 | NA | NA | NA | 3 | 2 | 3 | 9 | 16 | NA |
| O’Connor et al., 2006203 | 25.4 | 10 | 3.5 | 24 | 11 | 4.7 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 3 | NA | NA |
| Shareh et al., 2010206 | 16.66 | 6 | 3.2 | 7 | 7 | 2.38 | 8.5 | 6 | 2.42 | NA | NA | NA | 3 | 2 | 3 | 10 | 13 | NA |
| Sousa et al., 2006207 | –7.36 | 25 | NA | –10.8 | 25 | NA | NA | NA | NA | NA | NA | NA | 2 | 1 | 5 | 10 | NA | NA |
| Stein et al., 2007124 | –8.46 | 113 | 8.08 | –11.67 | 116 | 8.40 | –11.43 | 112 | 8.25 | –12.14 | 114 | 8.22 | 4 | 1 | 1 | 4 | 15 | 15 |
| Tollefson et al., 1994127 | –0.8 | 89 | 5.66 | –5.44 | 266 | 7.88 | NA | NA | NA | NA | NA | NA | 2 | 1 | 1 | 2 | NA | NA |
| Van Oppen et al., 1995209 | 17.9 | 29 | 9 | 13.4 | 28 | 9.4 | NA | NA | NA | NA | NA | NA | 2 | 2 | 9 | 11 | NA | NA |
| Whittal et al., 2005211 | 10.41 | 29 | 7.6 | 10.6 | 30 | 7.1 | NA | NA | NA | NA | NA | NA | 2 | 2 | 9 | 11 | NA | NA |
| Whittal et al., 2010212 | 6.43 | 37 | 4.77 | 9.1 | 30 | 6.48 | NA | NA | NA | NA | NA | NA | 2 | 2 | 11 | 16 | NA | NA |
| Zohar and Judge, 1996213 | –4.2 | 99 | 7.2 | –6.4 | 201 | 7.1 | –7 | 99 | 6.8 | NA | NA | NA | 3 | 1 | 1 | 4 | 8 | NA |
Key
-
Placebo (1).
-
Fluoxetine (2).
-
Fluvoxamine (2).
-
Paroxetine (2).
-
Sertraline (2).
-
Citalopram (2).
-
Venlafaxine (3).
-
Clomipramine (4).
-
BT (5).
-
CBT (6).
-
CT (7).
-
Hypericum (8).
-
Fluvoxamine + CBT (9).
-
BT + clomipramine (10).
-
Escitalopram (2).
-
Psychological placebo (11).
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| D[2] | –3.619 | 0.6562 | 0.008122 | –4.889 | –3.616 | –2.341 | 72,201 | 140,000 |
| D[3] | –3.211 | 1.965 | 0.01096 | –7.068 | –3.222 | 0.6873 | 72,201 | 140,000 |
| D[4] | –4.665 | 0.8162 | 0.00625 | –6.264 | –4.668 | –3.046 | 72,201 | 140,000 |
| D[5] | –10.41 | 1.854 | 0.02225 | –14.04 | –10.41 | –6.774 | 72,201 | 140,000 |
| D[6] | –7.981 | 1.544 | 0.01264 | –11.02 | –7.982 | –4.93 | 72,201 | 140,000 |
| D[7] | –9.452 | 2.179 | 0.02475 | –13.76 | –9.447 | –5.195 | 72,201 | 140,000 |
| D[8] | –0.1281 | 2.957 | 0.01417 | –5.932 | –0.125 | 5.678 | 72,201 | 140,000 |
| D[9] | –8.808 | 2.5 | 0.01532 | –13.75 | –8.8 | –3.879 | 72,201 | 140,000 |
| D[10] | –11.68 | 2.565 | 0.01434 | –16.73 | –11.68 | –6.655 | 72,201 | 140,000 |
| D[11] | –1.896 | 1.923 | 0.02168 | –5.621 | –1.901 | 1.908 | 72,201 | 140,000 |
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| d[2] | –3.668 | 0.7231 | 0.008129 | –5.126 | –3.655 | –2.26 | 72,201 | 140,000 |
| d[3] | –3.658 | 0.6577 | 0.007807 | –4.964 | –3.648 | –2.375 | 72,201 | 140,000 |
| d[4] | –3.513 | 0.6774 | 0.007931 | –4.809 | –3.528 | –2.137 | 72,201 | 140,000 |
| d[5] | –3.684 | 0.717 | 0.007973 | –5.141 | –3.67 | –2.296 | 72,201 | 140,000 |
| d[6] | –3.602 | 0.83 | 0.008281 | –5.251 | –3.606 | –1.906 | 72,201 | 140,000 |
| d[7] | –3.211 | 1.965 | 0.01096 | –7.068 | –3.222 | 0.6873 | 72,201 | 140,000 |
| d[8] | –4.665 | 0.8162 | 0.00625 | –6.264 | –4.668 | –3.046 | 72,201 | 140,000 |
| d[9] | –10.41 | 1.854 | 0.02225 | –14.04 | –10.41 | –6.774 | 72,201 | 140,000 |
| d[10] | –7.981 | 1.544 | 0.01264 | –11.02 | –7.982 | –4.93 | 72,201 | 140,000 |
| d[11] | –9.452 | 2.179 | 0.02475 | –13.76 | –9.447 | –5.195 | 72,201 | 140,000 |
| d[12] | –0.1281 | 2.957 | 0.01417 | –5.932 | –0.125 | 5.678 | 72,201 | 140,000 |
| d[13] | –8.808 | 2.5 | 0.01532 | –13.75 | –8.8 | –3.879 | 72,201 | 140,000 |
| d[14] | –11.68 | 2.565 | 0.01434 | –16.73 | –11.68 | –6.655 | 72,201 | 140,000 |
| d[15] | –3.593 | 0.8384 | 0.008388 | –5.247 | –3.598 | –1.861 | 72,201 | 140,000 |
| d[16] | –1.896 | 1.923 | 0.02168 | –5.621 | –1.901 | 1.908 | 72,201 | 140,000 |
Median ranks
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk.class[1] | 10.31 | 0.661 | 0.003972 | 9 | 10 | 11 | 72,201 | 140,000 |
| rk.class[2] | 7.593 | 0.8419 | 0.004448 | 6 | 8 | 9 | 72,201 | 140,000 |
| rk.class[3] | 7.828 | 1.488 | 0.007127 | 5 | 8 | 11 | 72,201 | 140,000 |
| rk.class[4] | 6.379 | 0.7793 | 0.003608 | 5 | 6 | 8 | 72,201 | 140,000 |
| rk.class[5] | 2.299 | 0.959 | 0.00593 | 1 | 2 | 4 | 72,201 | 140,000 |
| rk.class[6] | 4.237 | 1.006 | 0.004598 | 2 | 4 | 6 | 72,201 | 140,000 |
| rk.class[7] | 3.263 | 1.244 | 0.008831 | 1 | 3 | 5 | 72,201 | 140,000 |
| rk.class[8] | 9.763 | 1.565 | 0.007451 | 6 | 10 | 11 | 72,201 | 140,000 |
| rk.class[9] | 3.587 | 1.605 | 0.007865 | 1 | 4 | 7 | 72,201 | 140,000 |
| rk.class[10] | 1.861 | 1.25 | 0.005406 | 1 | 1 | 5 | 72,201 | 140,000 |
| rk.class[11] | 8.882 | 1.297 | 0.01203 | 6 | 9 | 11 | 72,201 | 140,000 |
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk[1] | 15.31 | 0.6624 | 0.003989 | 14 | 15 | 16 | 72,201 | 140,000 |
| rk[2] | 9.917 | 2.111 | 0.007922 | 6 | 10 | 14 | 72,201 | 140,000 |
| rk[3] | 9.955 | 2.012 | 0.007881 | 6 | 10 | 14 | 72,201 | 140,000 |
| rk[4] | 10.49 | 1.975 | 0.007702 | 7 | 11 | 14 | 72,201 | 140,000 |
| rk[5] | 9.856 | 2.095 | 0.007831 | 6 | 10 | 14 | 72,201 | 140,000 |
| rk[6] | 10.12 | 2.242 | 0.008465 | 6 | 10 | 14 | 72,201 | 140,000 |
| rk[7] | 10.74 | 3.543 | 0.01511 | 5 | 12 | 16 | 72,201 | 140,000 |
| rk[8] | 6.998 | 1.73 | 0.007727 | 5 | 6 | 12 | 72,201 | 140,000 |
| rk[9] | 2.301 | 0.9668 | 0.006013 | 1 | 2 | 4 | 72,201 | 140,000 |
| rk[10] | 4.254 | 1.063 | 0.004597 | 2 | 4 | 6 | 72,201 | 140,000 |
| rk[11] | 3.288 | 1.35 | 0.00982 | 1 | 3 | 6 | 72,201 | 140,000 |
| rk[12] | 14.14 | 2.944 | 0.01332 | 6 | 15 | 16 | 72,201 | 140,000 |
| rk[13] | 3.684 | 1.935 | 0.008808 | 1 | 4 | 8 | 72,201 | 140,000 |
| rk[14] | 1.868 | 1.287 | 0.00547 | 1 | 1 | 5 | 72,201 | 140,000 |
| rk[15] | 10.14 | 2.236 | 0.008085 | 6 | 10 | 14 | 72,201 | 140,000 |
| rk[16] | 12.94 | 2.84 | 0.02645 | 6 | 14 | 16 | 72,201 | 140,000 |
Adults: acceptability (dropouts) – sensitivity analysis 1 (low overall attrition)
See Table 28 for a summary.
| Study | r[,1] | n[,1] | r[,2] | n[,2] | r[,3] | n[,3] | r[,4] | n[,4] | na[] | t[,1] | t[,2] | t[,3] | t[,4] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ananth et al. 1981156 | 1 | 10 | 2 | 10 | NA | NA | NA | NA | 2 | 9 | 13 | NA | NA |
| Anderson and Rees, 2007157 | 3 | 17 | 4 | 21 | NA | NA | NA | NA | 2 | 2 | 11 | NA | NA |
| Andersson et al., 2012158 | 2 | 50 | 0 | 51 | NA | NA | NA | NA | 2 | 11 | 16 | NA | NA |
| Belloch et al., 2008159 | 2 | 15 | 2 | 18 | NA | NA | NA | NA | 2 | 10 | 12 | NA | NA |
| Belotto-Silva et al., 2012160 | 33 | 88 | 18 | 70 | NA | NA | NA | NA | 2 | 3 | 11 | NA | NA |
| CCSG1, 1991154 | 13 | 121 | 17 | 118 | NA | NA | NA | NA | 2 | 1 | 9 | NA | NA |
| CCSG2, 1991154 | 12 | 139 | 14 | 142 | NA | NA | NA | NA | 2 | 1 | 9 | NA | NA |
| Chouinard et al., 1990163 | 4 | 44 | 6 | 43 | NA | NA | NA | NA | 2 | 1 | 6 | NA | NA |
| Cordioli et al., 2003164 | 1 | 24 | 1 | 23 | NA | NA | NA | NA | 2 | 2 | 11 | NA | NA |
| Cottraux et al., 2001166 | 3 | 33 | 2 | 32 | NA | NA | NA | NA | 2 | 10 | 12 | NA | NA |
| Denys et al., 2003167 | 9 | 75 | 4 | 75 | NA | NA | NA | NA | 2 | 5 | 8 | NA | NA |
| Emmelkamp et al., 1988169 | 1 | 10 | 1 | 10 | NA | NA | NA | NA | 2 | 10 | 12 | NA | NA |
| Fals-Stewart et al., 1993170 | 3 | 34 | 0 | 32 | NA | NA | NA | NA | 2 | 10 | 16 | NA | NA |
| Freeston et al., 1997173 | 0 | 14 | 3 | 15 | NA | NA | NA | NA | 2 | 2 | 11 | NA | NA |
| GlaxoSmithKline, 2005175 | 1 | 73 | 4 | 73 | NA | NA | NA | NA | 2 | 5 | 9 | NA | NA |
| Goodman et al., 1996177 | 17 | 80 | 23 | 80 | NA | NA | NA | NA | 2 | 1 | 4 | NA | NA |
| Greist et al., 2002178 | 14 | 69 | 9 | 75 | NA | NA | NA | NA | 2 | 10 | 16 | NA | NA |
| Hollander et al., 2003180 | 31 | 126 | 43 | 127 | NA | NA | NA | NA | 2 | 1 | 4 | NA | NA |
| Hollander et al., 2003181 | 15 | 89 | 14 | 88 | 20 | 86 | 19 | 85 | 4 | 1 | 5 | 5 | 5 |
| Jenike et al., 1990184 | 0 | 20 | 2 | 20 | NA | NA | NA | NA | 2 | 1 | 4 | NA | NA |
| Jenike et al., 1997185 | 3 | 21 | 4 | 23 | NA | NA | NA | NA | 2 | 1 | 3 | NA | NA |
| Jones and Menzies, 1998186 | 1 | 11 | 1 | 12 | NA | NA | NA | NA | 2 | 2 | 12 | NA | NA |
| Kobak et al., 2005189 | 9 | 30 | 8 | 30 | NA | NA | NA | NA | 2 | 1 | 17 | NA | NA |
| López-Ibor et al., 1996193 | 5 | 30 | 3 | 25 | NA | NA | NA | NA | 2 | 3 | 9 | NA | NA |
| McLean et al., 2001195 | 12 | 44 | 18 | 49 | NA | NA | NA | NA | 2 | 10 | 12 | NA | NA |
| Milanfranchi et al., 1997196 | 0 | 13 | 1 | 13 | NA | NA | NA | NA | 2 | 4 | 9 | NA | NA |
| Montgomery et al., 1993197 | 15 | 57 | 14 | 53 | 13 | 52 | 14 | 55 | 4 | 1 | 3 | 3 | 3 |
| Montgomery et al., 2001198 | 17 | 101 | 15 | 100 | 15 | 98 | 16 | 102 | 4 | 1 | 7 | 7 | 7 |
| Mundo et al., 2001200 | 19 | 115 | 26 | 112 | NA | NA | NA | NA | 2 | 4 | 9 | NA | NA |
| Nakatani et al., 2005202 | 1 | 11 | 1 | 11 | 1 | 9 | NA | NA | 3 | 4 | 10 | 16 | NA |
| O’Connor et al., 1999203 | 0 | 6 | 1 | 7 | NA | NA | NA | NA | 2 | 2 | 11 | NA | NA |
| Perse et al., 1987205 | 2 | 10 | 2 | 10 | NA | NA | NA | NA | 2 | 1 | 4 | NA | NA |
| Shareh et al., 2010206 | 1 | 7 | 0 | 7 | 1 | 7 | NA | NA | 3 | 4 | 11 | 14 | NA |
| Sousa et al., 2006207 | 3 | 28 | 3 | 28 | NA | NA | NA | NA | 2 | 6 | 11 | NA | NA |
| Stein et al., 2007124 | 16 | 115 | 29 | 119 | 24 | 116 | 21 | 116 | 4 | 1 | 5 | 15 | 15 |
| Tollefson et al., 1994127 | 13 | 89 | 12 | 87 | 22 | 89 | 22 | 90 | 4 | 1 | 3 | 3 | 3 |
| Van Oppen et al., 1995209 | 7 | 36 | 7 | 35 | NA | NA | NA | NA | 2 | 10 | 12 | NA | NA |
| Volavka et al., 1985210 | 3 | 11 | 4 | 12 | NA | NA | NA | NA | 2 | 9 | 18 | NA | NA |
| Whittal et al., 2005211 | 13 | 42 | 11 | 41 | NA | NA | NA | NA | 2 | 10 | 12 | NA | NA |
| Whittal et al., 2010212 | 3 | 40 | 3 | 33 | NA | NA | NA | NA | 2 | 12 | 16 | NA | NA |
Key: intervention
-
Placebo (1).
-
Waitlist (2).
-
Fluoxetine (3).
-
Fluvoxamine (3).
-
Paroxetine (3).
-
Sertraline (3).
-
Citalopram (3).
-
Venlafaxine (4).
-
Clomipramine (5).
-
BT (6).
-
CBT (7).
-
CT (8).
-
Amitriptyline (9).
-
CBT + fluvoxamine (10).
-
Escitalopram (3).
-
Psychological placebo (11).
-
Hypericum (12).
-
Imipramine (13).
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| OR.D[1,2] | 0.4606 | 0.3501 | 0.01443 | 0.08904 | 0.3605 | 1.427 | 60,001 | 120,000 |
| OR.D[1,3] | 1.302 | 0.5778 | 0.005701 | 0.9421 | 1.284 | 1.726 | 60,001 | 120,000 |
| OR.D[1,4] | 0.6364 | 0.4778 | 0.01466 | 0.1053 | 0.5162 | 1.844 | 60,001 | 120,000 |
| OR.D[1,5] | 1.639 | 0.389 | 0.0117 | 1.039 | 1.584 | 2.588 | 60,001 | 120,000 |
| OR.D[1,6] | 0.6941 | 0.7862 | 0.03535 | 0.04697 | 0.441 | 2.772 | 60,001 | 120,000 |
| OR.D[1,7] | 0.8902 | 0.3111 | 0.0109 | 0.4249 | 0.8389 | 1.623 | 60,001 | 120,000 |
| OR.D[1,8] | 0.6763 | 0.773 | 0.03433 | 0.05704 | 0.4481 | 2.699 | 60,001 | 120,000 |
| OR.D[1,9] | 21.37 | 93.67 | 2.768 | 0.2314 | 3.94 | 162.7 | 60,001 | 120,000 |
| OR.D[1,10] | 13.73 | 153.6 | 3.737 | 0.06158 | 1.936 | 79.68 | 60,001 | 120,000 |
| OR.D[1,11] | 0.371 | 0.4034 | 0.01803 | 0.02338 | 0.244 | 1.463 | 60,001 | 120,000 |
| OR.D[1,12] | 1.001 | 0.6832 | 0.01939 | 0.2341 | 0.825 | 2.914 | 60,001 | 120,000 |
| OR.D[1,13] | 3.569 | 4.944 | 0.1543 | 0.2675 | 2.05 | 15.9 | 60,001 | 120,000 |
| OR.D[2,3] | 4.455 | 4.03 | 0.1474 | 0.9014 | 3.545 | 14.27 | 60,001 | 120,000 |
| OR.D[2,4] | 2.197 | 2.781 | 0.08812 | 0.1703 | 1.383 | 9.484 | 60,001 | 120,000 |
| OR.D[2,5] | 5.704 | 5.164 | 0.2038 | 1.073 | 4.326 | 18.4 | 60,001 | 120,000 |
| OR.D[2,6] | 2.033 | 2.669 | 0.1063 | 0.1405 | 1.197 | 8.662 | 60,001 | 120,000 |
| OR.D[2,7] | 2.756 | 1.927 | 0.07397 | 0.7092 | 2.258 | 8.006 | 60,001 | 120,000 |
| OR.D[2,8] | 1.982 | 2.625 | 0.1042 | 0.1675 | 1.155 | 8.94 | 60,001 | 120,000 |
| OR.D[2,9] | 63.9 | 294.6 | 7.505 | 0.4477 | 11.69 | 446.1 | 60,001 | 120,000 |
| OR.D[2,10] | 57.78 | 656.4 | 18.21 | 0.1507 | 5.399 | 223.4 | 60,001 | 120,000 |
| OR.D[2,11] | 1.086 | 1.332 | 0.05339 | 0.07371 | 0.6644 | 4.877 | 60,001 | 120,000 |
| OR.D[2,12] | 3.482 | 4.569 | 0.1517 | 0.4019 | 2.181 | 14.26 | 60,001 | 120,000 |
| OR.D[2,13] | 12.08 | 19.77 | 0.6272 | 0.5223 | 5.667 | 66.09 | 60,001 | 120,000 |
| OR.D[3,4] | 0.4951 | 0.3906 | 0.0112 | 0.08368 | 0.4031 | 1.472 | 60,001 | 120,000 |
| OR.D[3,5] | 1.287 | 0.4541 | 0.01003 | 0.7809 | 1.23 | 2.132 | 60,001 | 120,000 |
| OR.D[3,6] | 0.5391 | 0.6117 | 0.02709 | 0.0379 | 0.3446 | 2.155 | 60,001 | 120,000 |
| OR.D[3,7] | 0.6934 | 0.2743 | 0.007734 | 0.3377 | 0.6553 | 1.251 | 60,001 | 120,000 |
| OR.D[3,8] | 0.5248 | 0.6027 | 0.02624 | 0.04514 | 0.3496 | 2.17 | 60,001 | 120,000 |
| OR.D[3,9] | 16.58 | 71.88 | 2.044 | 0.1758 | 3.1 | 132.5 | 60,001 | 120,000 |
| OR.D[3,10] | 10.97 | 124.1 | 3.095 | 0.04991 | 1.508 | 62.93 | 60,001 | 120,000 |
| OR.D[3,11] | 0.2879 | 0.3122 | 0.01373 | 0.01926 | 0.1913 | 1.117 | 60,001 | 120,000 |
| OR.D[3,12] | 0.7896 | 0.567 | 0.01591 | 0.1776 | 0.6382 | 2.362 | 60,001 | 120,000 |
| OR.D[3,13] | 2.803 | 4.134 | 0.1232 | 0.2114 | 1.603 | 12.64 | 60,001 | 120,000 |
| OR.D[4,5] | 4.285 | 4.116 | 0.13 | 0.8094 | 3.101 | 15.29 | 60,001 | 120,000 |
| OR.D[4,6] | 1.825 | 2.953 | 0.1114 | 0.06651 | 0.8913 | 9.311 | 60,001 | 120,000 |
| OR.D[4,7] | 2.344 | 2.488 | 0.07862 | 0.3828 | 1.623 | 8.663 | 60,001 | 120,000 |
| OR.D[4,8] | 1.778 | 2.949 | 0.1098 | 0.06723 | 0.8737 | 9.341 | 60,001 | 120,000 |
| OR.D[4,9] | 54.1 | 250 | 7.15 | 0.3928 | 7.709 | 437.8 | 60,001 | 120,000 |
| OR.D[4,10] | 38.58 | 467.8 | 10.23 | 0.1029 | 3.557 | 226.3 | 60,001 | 120,000 |
| OR.D[4,11] | 0.9715 | 1.567 | 0.05868 | 0.03401 | 0.4878 | 4.693 | 60,001 | 120,000 |
| OR.D[4,12] | 2.707 | 3.643 | 0.1184 | 0.2615 | 1.635 | 12.61 | 60,001 | 120,000 |
| OR.D[4,13] | 9.49 | 19.25 | 0.6017 | 0.3936 | 4.032 | 53.97 | 60,001 | 120,000 |
| OR.D[5,6] | 0.4444 | 0.5035 | 0.02233 | 0.02804 | 0.2835 | 1.882 | 60,001 | 120,000 |
| OR.D[5,7] | 0.5686 | 0.2302 | 0.007678 | 0.239 | 0.5306 | 1.114 | 60,001 | 120,000 |
| OR.D[5,8] | 0.4333 | 0.5018 | 0.02191 | 0.03094 | 0.2805 | 1.759 | 60,001 | 120,000 |
| OR.D[5,9] | 13.6 | 61.38 | 1.756 | 0.1445 | 2.417 | 105.6 | 60,001 | 120,000 |
| OR.D[5,10] | 8.955 | 98.02 | 2.421 | 0.03736 | 1.17 | 54.48 | 60,001 | 120,000 |
| OR.D[5,11] | 0.2376 | 0.2609 | 0.01146 | 0.01275 | 0.1516 | 0.9647 | 60,001 | 120,000 |
| OR.D[5,12] | 0.6426 | 0.4697 | 0.01298 | 0.1333 | 0.5216 | 1.873 | 60,001 | 120,000 |
| OR.D[5,13] | 2.139 | 2.853 | 0.08707 | 0.1799 | 1.305 | 9.181 | 60,001 | 120,000 |
| OR.D[6,7] | 3.074 | 4.322 | 0.2128 | 0.3113 | 1.847 | 14.04 | 60,001 | 120,000 |
| OR.D[6,8] | 1.008 | 0.276 | 0.008877 | 0.5775 | 0.9644 | 1.685 | 60,001 | 120,000 |
| OR.D[6,9] | 55.97 | 262 | 7.207 | 0.3638 | 8.582 | 383.7 | 60,001 | 120,000 |
| OR.D[6,10] | 37.52 | 470.2 | 11.27 | 0.09105 | 4.489 | 194 | 60,001 | 120,000 |
| OR.D[6,11] | 0.5831 | 0.2309 | 0.007426 | 0.2459 | 0.5486 | 1.149 | 60,001 | 120,000 |
| OR.D[6,12] | 3.557 | 6.237 | 0.2474 | 0.1934 | 1.878 | 17.05 | 60,001 | 120,000 |
| OR.D[6,13] | 16.09 | 45.9 | 2.105 | 0.3054 | 4.402 | 121.9 | 60,001 | 120,000 |
| OR.D[7,8] | 0.7888 | 0.9077 | 0.03755 | 0.0783 | 0.5294 | 2.995 | 60,001 | 120,000 |
| OR.D[7,9] | 26.38 | 112.3 | 3.388 | 0.2515 | 4.747 | 189.2 | 60,001 | 120,000 |
| OR.D[7,10] | 17.54 | 206.1 | 4.953 | 0.07379 | 2.26 | 92.65 | 60,001 | 120,000 |
| OR.D[7,11] | 0.4352 | 0.478 | 0.02037 | 0.03298 | 0.2954 | 1.739 | 60,001 | 120,000 |
| OR.D[7,12] | 1.259 | 1.006 | 0.02827 | 0.2463 | 0.969 | 3.995 | 60,001 | 120,000 |
| OR.D[7,13] | 4.393 | 6.19 | 0.1776 | 0.2817 | 2.437 | 20.19 | 60,001 | 120,000 |
| OR.D[8,9] | 58.61 | 362.6 | 8.542 | 0.3793 | 9.009 | 409.6 | 60,001 | 120,000 |
| OR.D[8,10] | 40.73 | 655.4 | 14.48 | 0.09474 | 4.631 | 193 | 60,001 | 120,000 |
| OR.D[8,11] | 0.6139 | 0.2895 | 0.009711 | 0.235 | 0.5527 | 1.364 | 60,001 | 120,000 |
| OR.D[8,12] | 3.634 | 6.27 | 0.2406 | 0.2045 | 1.937 | 16.93 | 60,001 | 120,000 |
| OR.D[8,13] | 15.06 | 36.71 | 1.509 | 0.3086 | 4.474 | 119.3 | 60,001 | 120,000 |
| OR.D[9,10] | 5.53 | 39.52 | 0.9571 | 0.003667 | 0.4567 | 44.15 | 60,001 | 120,000 |
| OR.D[9,11] | 0.2245 | 0.5699 | 0.02051 | 0.001242 | 0.06062 | 1.593 | 60,001 | 120,000 |
| OR.D[9,12] | 0.7359 | 2.279 | 0.08093 | 0.005101 | 0.1999 | 4.611 | 60,001 | 120,000 |
| OR.D[9,13] | 2.564 | 9.984 | 0.3729 | 0.01042 | 0.4719 | 17.31 | 60,001 | 120,000 |
| OR.D[10,11] | 0.8251 | 3.825 | 0.1046 | 0.00282 | 0.1198 | 5.837 | 60,001 | 120,000 |
| OR.D[10,12] | 3.228 | 37.11 | 0.9332 | 0.01088 | 0.4266 | 14.55 | 60,001 | 120,000 |
| OR.D[10,13] | 11.66 | 192.3 | 3.894 | 0.01944 | 1.045 | 59.85 | 60,001 | 120,000 |
| OR.D[11,12] | 6.769 | 12 | 0.4891 | 0.3975 | 3.357 | 35.34 | 60,001 | 120,000 |
| OR.D[11,13] | 29.51 | 82.34 | 3.567 | 0.5747 | 7.942 | 243.2 | 60,001 | 120,000 |
| OR.D[12,13] | 5.49 | 10.53 | 0.3723 | 0.2458 | 2.469 | 32.39 | 60,001 | 120,000 |
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| OR[1,2] | 0.4606 | 0.3501 | 0.01443 | 0.08904 | 0.3605 | 1.427 | 60,001 | 120,000 |
| OR[1,3] | 1.338 | 0.23 | 0.007745 | 0.9537 | 1.316 | 1.874 | 60,001 | 120,000 |
| OR[1,4] | 1.325 | 0.2049 | 0.006246 | 0.9793 | 1.309 | 1.76 | 60,001 | 120,000 |
| OR[1,5] | 1.361 | 0.2378 | 0.006944 | 0.9756 | 1.336 | 1.901 | 60,001 | 120,000 |
| OR[1,6] | 1.31 | 0.2954 | 0.007809 | 0.8018 | 1.279 | 1.972 | 60,001 | 120,000 |
| OR[1,7] | 1.222 | 0.2357 | 0.006839 | 0.7468 | 1.224 | 1.672 | 60,001 | 120,000 |
| OR[1,8] | 0.6364 | 0.4778 | 0.01466 | 0.1053 | 0.5162 | 1.844 | 60,001 | 120,000 |
| OR[1,9] | 1.639 | 0.389 | 0.0117 | 1.039 | 1.584 | 2.588 | 60,001 | 120,000 |
| OR[1,10] | 0.6941 | 0.7862 | 0.03535 | 0.04697 | 0.441 | 2.772 | 60,001 | 120,000 |
| OR[1,11] | 0.8902 | 0.3111 | 0.0109 | 0.4249 | 0.8389 | 1.623 | 60,001 | 120,000 |
| OR[1,12] | 0.6763 | 0.773 | 0.03433 | 0.05704 | 0.4481 | 2.699 | 60,001 | 120,000 |
| OR[1,13] | 21.37 | 93.67 | 2.768 | 0.2314 | 3.94 | 162.7 | 60,001 | 120,000 |
| OR[1,14] | 13.73 | 153.6 | 3.737 | 0.06158 | 1.936 | 79.68 | 60,001 | 120,000 |
| OR[1,15] | 1.281 | 0.2332 | 0.006379 | 0.878 | 1.265 | 1.795 | 60,001 | 120,000 |
| OR[1,16] | 0.371 | 0.4034 | 0.01803 | 0.02338 | 0.244 | 1.463 | 60,001 | 120,000 |
| OR[1,17] | 1.001 | 0.6832 | 0.01939 | 0.2341 | 0.825 | 2.914 | 60,001 | 120,000 |
| OR[1,18] | 3.569 | 4.944 | 0.1543 | 0.2675 | 2.05 | 15.9 | 60,001 | 120,000 |
| OR[2,3] | 4.535 | 3.746 | 0.1472 | 0.9427 | 3.642 | 14.33 | 60,001 | 120,000 |
| OR[2,4] | 4.557 | 3.911 | 0.1555 | 0.9225 | 3.604 | 14.98 | 60,001 | 120,000 |
| OR[2,5] | 4.672 | 4.012 | 0.157 | 0.9489 | 3.659 | 15.04 | 60,001 | 120,000 |
| OR[2,6] | 4.503 | 4.001 | 0.1537 | 0.8925 | 3.537 | 15.34 | 60,001 | 120,000 |
| OR[2,7] | 4.175 | 3.561 | 0.1368 | 0.8044 | 3.323 | 13.4 | 60,001 | 120,000 |
| OR[2,8] | 2.197 | 2.781 | 0.08812 | 0.1703 | 1.383 | 9.484 | 60,001 | 120,000 |
| OR[2,9] | 5.704 | 5.164 | 0.2038 | 1.073 | 4.326 | 18.4 | 60,001 | 120,000 |
| OR[2,10] | 2.033 | 2.669 | 0.1063 | 0.1405 | 1.197 | 8.662 | 60,001 | 120,000 |
| OR[2,11] | 2.756 | 1.927 | 0.07397 | 0.7092 | 2.258 | 8.006 | 60,001 | 120,000 |
| OR[2,12] | 1.982 | 2.625 | 0.1042 | 0.1675 | 1.155 | 8.94 | 60,001 | 120,000 |
| OR[2,13] | 63.9 | 294.6 | 7.505 | 0.4477 | 11.69 | 446.1 | 60,001 | 120,000 |
| OR[2,14] | 57.78 | 656.4 | 18.21 | 0.1507 | 5.399 | 223.4 | 60,001 | 120,000 |
| OR[2,15] | 4.389 | 3.735 | 0.1444 | 0.8639 | 3.497 | 14.32 | 60,001 | 120,000 |
| OR[2,16] | 1.086 | 1.332 | 0.05339 | 0.07371 | 0.6644 | 4.877 | 60,001 | 120,000 |
| OR[2,17] | 3.482 | 4.569 | 0.1517 | 0.4019 | 2.181 | 14.26 | 60,001 | 120,000 |
| OR[2,18] | 12.08 | 19.77 | 0.6272 | 0.5223 | 5.667 | 66.09 | 60,001 | 120,000 |
| OR[3,4] | 1.007 | 0.1715 | 0.004519 | 0.6857 | 0.9984 | 1.409 | 60,001 | 120,000 |
| OR[3,5] | 1.034 | 0.195 | 0.005247 | 0.6817 | 1.006 | 1.522 | 60,001 | 120,000 |
| OR[3,6] | 0.9938 | 0.2267 | 0.005706 | 0.5629 | 0.993 | 1.539 | 60,001 | 120,000 |
| OR[3,7] | 0.9296 | 0.191 | 0.005216 | 0.4989 | 0.9628 | 1.292 | 60,001 | 120,000 |
| OR[3,8] | 0.481 | 0.3614 | 0.01066 | 0.08211 | 0.3942 | 1.418 | 60,001 | 120,000 |
| OR[3,9] | 1.253 | 0.3481 | 0.01095 | 0.7396 | 1.207 | 2.032 | 60,001 | 120,000 |
| OR[3,10] | 0.5243 | 0.5968 | 0.02639 | 0.03664 | 0.3399 | 2.07 | 60,001 | 120,000 |
| OR[3,11] | 0.6685 | 0.2146 | 0.006749 | 0.3502 | 0.6374 | 1.17 | 60,001 | 120,000 |
| OR[3,12] | 0.5101 | 0.5863 | 0.02546 | 0.04024 | 0.343 | 2.073 | 60,001 | 120,000 |
| OR[3,13] | 16.42 | 72.74 | 2.059 | 0.1734 | 2.999 | 133.2 | 60,001 | 120,000 |
| OR[3,14] | 10.93 | 124.9 | 3.106 | 0.04764 | 1.444 | 64.07 | 60,001 | 120,000 |
| OR[3,15] | 0.9728 | 0.1811 | 0.004307 | 0.6006 | 0.9846 | 1.378 | 60,001 | 120,000 |
| OR[3,16] | 0.2794 | 0.3017 | 0.01329 | 0.01756 | 0.1876 | 1.066 | 60,001 | 120,000 |
| OR[3,17] | 0.7725 | 0.5588 | 0.01624 | 0.1732 | 0.6238 | 2.326 | 60,001 | 120,000 |
| OR[3,18] | 2.725 | 3.754 | 0.119 | 0.2046 | 1.568 | 12.24 | 60,001 | 120,000 |
| OR[4,5] | 1.04 | 0.1851 | 0.004175 | 0.7257 | 1.008 | 1.519 | 60,001 | 120,000 |
| OR[4,6] | 0.9987 | 0.2174 | 0.004848 | 0.5927 | 0.9933 | 1.526 | 60,001 | 120,000 |
| OR[4,7] | 0.9345 | 0.1836 | 0.004833 | 0.5292 | 0.964 | 1.312 | 60,001 | 120,000 |
| OR[4,8] | 0.4881 | 0.3765 | 0.01151 | 0.08158 | 0.3935 | 1.493 | 60,001 | 120,000 |
| OR[4,9] | 1.254 | 0.309 | 0.008943 | 0.7896 | 1.209 | 1.985 | 60,001 | 120,000 |
| OR[4,10] | 0.5274 | 0.5936 | 0.02646 | 0.03597 | 0.3396 | 2.098 | 60,001 | 120,000 |
| OR[4,11] | 0.6807 | 0.2425 | 0.008035 | 0.3265 | 0.6393 | 1.234 | 60,001 | 120,000 |
| OR[4,12] | 0.5136 | 0.582 | 0.02564 | 0.04066 | 0.3445 | 2.115 | 60,001 | 120,000 |
| OR[4,13] | 16.35 | 69.19 | 2.013 | 0.1728 | 3.009 | 132.8 | 60,001 | 120,000 |
| OR[4,14] | 10.72 | 118.9 | 2.998 | 0.04838 | 1.447 | 61.97 | 60,001 | 120,000 |
| OR[4,15] | 0.9791 | 0.1807 | 0.004128 | 0.637 | 0.9842 | 1.408 | 60,001 | 120,000 |
| OR[4,16] | 0.2818 | 0.3034 | 0.01341 | 0.01743 | 0.1898 | 1.093 | 60,001 | 120,000 |
| OR[4,17] | 0.7761 | 0.5589 | 0.0163 | 0.1644 | 0.6268 | 2.395 | 60,001 | 120,000 |
| OR[4,18] | 2.719 | 3.716 | 0.1167 | 0.2096 | 1.582 | 11.92 | 60,001 | 120,000 |
| OR[5,6] | 0.9767 | 0.2187 | 0.004774 | 0.5448 | 0.9825 | 1.484 | 60,001 | 120,000 |
| OR[5,7] | 0.9141 | 0.1865 | 0.004695 | 0.4873 | 0.9492 | 1.26 | 60,001 | 120,000 |
| OR[5,8] | 0.4677 | 0.3404 | 0.01036 | 0.0822 | 0.3879 | 1.358 | 60,001 | 120,000 |
| OR[5,9] | 1.231 | 0.3318 | 0.009517 | 0.7223 | 1.177 | 2.023 | 60,001 | 120,000 |
| OR[5,10] | 0.5186 | 0.5976 | 0.02638 | 0.03615 | 0.3292 | 2.094 | 60,001 | 120,000 |
| OR[5,11] | 0.6658 | 0.2411 | 0.007683 | 0.3142 | 0.6253 | 1.23 | 60,001 | 120,000 |
| OR[5,12] | 0.5051 | 0.5922 | 0.02574 | 0.04422 | 0.3302 | 2.083 | 60,001 | 120,000 |
| OR[5,13] | 16.03 | 71.8 | 1.987 | 0.1715 | 2.959 | 130.4 | 60,001 | 120,000 |
| OR[5,14] | 10.56 | 117.2 | 2.956 | 0.04809 | 1.426 | 61.86 | 60,001 | 120,000 |
| OR[5,15] | 0.953 | 0.1584 | 0.003553 | 0.6321 | 0.9693 | 1.296 | 60,001 | 120,000 |
| OR[5,16] | 0.2773 | 0.3066 | 0.01344 | 0.01786 | 0.1819 | 1.115 | 60,001 | 120,000 |
| OR[5,17] | 0.7562 | 0.5426 | 0.01551 | 0.1654 | 0.6113 | 2.296 | 60,001 | 120,000 |
| OR[5,18] | 2.693 | 3.755 | 0.1195 | 0.1985 | 1.542 | 12.09 | 60,001 | 120,000 |
| OR[6,7] | 0.9652 | 0.2306 | 0.005611 | 0.4897 | 0.9798 | 1.465 | 60,001 | 120,000 |
| OR[6,8] | 0.5048 | 0.3955 | 0.01208 | 0.08244 | 0.4028 | 1.552 | 60,001 | 120,000 |
| OR[6,9] | 1.308 | 0.4288 | 0.01178 | 0.7103 | 1.236 | 2.365 | 60,001 | 120,000 |
| OR[6,10] | 0.5458 | 0.6266 | 0.02732 | 0.03707 | 0.3446 | 2.157 | 60,001 | 120,000 |
| OR[6,11] | 0.7041 | 0.2758 | 0.008852 | 0.3121 | 0.6567 | 1.343 | 60,001 | 120,000 |
| OR[6,12] | 0.5317 | 0.6163 | 0.02655 | 0.04695 | 0.3458 | 2.212 | 60,001 | 120,000 |
| OR[6,13] | 16.76 | 73.57 | 2.06 | 0.1745 | 3.127 | 128.8 | 60,001 | 120,000 |
| OR[6,14] | 10.93 | 122.7 | 3.062 | 0.05071 | 1.504 | 62.55 | 60,001 | 120,000 |
| OR[6,15] | 1.014 | 0.2603 | 0.005967 | 0.586 | 0.9945 | 1.63 | 60,001 | 120,000 |
| OR[6,16] | 0.2918 | 0.3188 | 0.01384 | 0.01922 | 0.1913 | 1.155 | 60,001 | 120,000 |
| OR[6,17] | 0.8007 | 0.5925 | 0.01636 | 0.1752 | 0.6381 | 2.444 | 60,001 | 120,000 |
| OR[6,18] | 2.841 | 3.933 | 0.1263 | 0.2084 | 1.595 | 12.91 | 60,001 | 120,000 |
| OR[7,8] | 0.5383 | 0.4246 | 0.01233 | 0.0867 | 0.4241 | 1.649 | 60,001 | 120,000 |
| OR[7,9] | 1.395 | 0.4565 | 0.0139 | 0.8077 | 1.295 | 2.6 | 60,001 | 120,000 |
| OR[7,10] | 0.5839 | 0.67 | 0.02938 | 0.0424 | 0.3661 | 2.397 | 60,001 | 120,000 |
| OR[7,11] | 0.7506 | 0.2931 | 0.009336 | 0.3527 | 0.6948 | 1.449 | 60,001 | 120,000 |
| OR[7,12] | 0.5688 | 0.6636 | 0.02858 | 0.0535 | 0.3705 | 2.348 | 60,001 | 120,000 |
| OR[7,13] | 17.57 | 76.02 | 2.141 | 0.1826 | 3.355 | 132.3 | 60,001 | 120,000 |
| OR[7,14] | 11.64 | 134.1 | 3.27 | 0.05443 | 1.656 | 65.3 | 60,001 | 120,000 |
| OR[7,15] | 1.079 | 0.2661 | 0.00615 | 0.7005 | 1.016 | 1.797 | 60,001 | 120,000 |
| OR[7,16] | 0.3115 | 0.3437 | 0.01492 | 0.02298 | 0.2047 | 1.219 | 60,001 | 120,000 |
| OR[7,17] | 0.8511 | 0.6209 | 0.01708 | 0.1888 | 0.6856 | 2.547 | 60,001 | 120,000 |
| OR[7,18] | 3.05 | 4.215 | 0.1368 | 0.2239 | 1.714 | 14.33 | 60,001 | 120,000 |
| OR[8,9] | 4.285 | 4.116 | 0.13 | 0.8094 | 3.101 | 15.29 | 60,001 | 120,000 |
| OR[8,10] | 1.825 | 2.953 | 0.1114 | 0.06651 | 0.8913 | 9.311 | 60,001 | 120,000 |
| OR[8,11] | 2.344 | 2.488 | 0.07862 | 0.3828 | 1.623 | 8.663 | 60,001 | 120,000 |
| OR[8,12] | 1.778 | 2.949 | 0.1098 | 0.06723 | 0.8737 | 9.341 | 60,001 | 120,000 |
| OR[8,13] | 54.1 | 250 | 7.15 | 0.3928 | 7.709 | 437.8 | 60,001 | 120,000 |
| OR[8,14] | 38.58 | 467.8 | 10.23 | 0.1029 | 3.557 | 226.3 | 60,001 | 120,000 |
| OR[8,15] | 3.366 | 3.382 | 0.1159 | 0.6569 | 2.438 | 11.92 | 60,001 | 120,000 |
| OR[8,16] | 0.9715 | 1.567 | 0.05868 | 0.03401 | 0.4878 | 4.693 | 60,001 | 120,000 |
| OR[8,17] | 2.707 | 3.643 | 0.1184 | 0.2615 | 1.635 | 12.61 | 60,001 | 120,000 |
| OR[8,18] | 9.49 | 19.25 | 0.6017 | 0.3936 | 4.032 | 53.97 | 60,001 | 120,000 |
| OR[9,10] | 0.4444 | 0.5035 | 0.02233 | 0.02804 | 0.2835 | 1.882 | 60,001 | 120,000 |
| OR[9,11] | 0.5686 | 0.2302 | 0.007678 | 0.239 | 0.5306 | 1.114 | 60,001 | 120,000 |
| OR[9,12] | 0.4333 | 0.5018 | 0.02191 | 0.03094 | 0.2805 | 1.759 | 60,001 | 120,000 |
| OR[9,13] | 13.6 | 61.38 | 1.756 | 0.1445 | 2.417 | 105.6 | 60,001 | 120,000 |
| OR[9,14] | 8.955 | 98.02 | 2.421 | 0.03736 | 1.17 | 54.48 | 60,001 | 120,000 |
| OR[9,15] | 0.8194 | 0.2235 | 0.006122 | 0.4373 | 0.795 | 1.327 | 60,001 | 120,000 |
| OR[9,16] | 0.2376 | 0.2609 | 0.01146 | 0.01275 | 0.1516 | 0.9647 | 60,001 | 120,000 |
| OR[9,17] | 0.6426 | 0.4697 | 0.01298 | 0.1333 | 0.5216 | 1.873 | 60,001 | 120,000 |
| OR[9,18] | 2.139 | 2.853 | 0.08707 | 0.1799 | 1.305 | 9.181 | 60,001 | 120,000 |
| OR[10,11] | 3.074 | 4.322 | 0.2128 | 0.3113 | 1.847 | 14.04 | 60,001 | 120,000 |
| OR[10,12] | 1.008 | 0.276 | 0.008877 | 0.5775 | 0.9644 | 1.685 | 60,001 | 120,000 |
| OR[10,13] | 55.97 | 262 | 7.207 | 0.3638 | 8.582 | 383.7 | 60,001 | 120,000 |
| OR[10,14] | 37.52 | 470.2 | 11.27 | 0.09105 | 4.489 | 194 | 60,001 | 120,000 |
| OR[10,15] | 4.669 | 6.306 | 0.3041 | 0.4554 | 2.871 | 26.53 | 60,001 | 120,000 |
| OR[10,16] | 0.5831 | 0.2309 | 0.007426 | 0.2459 | 0.5486 | 1.149 | 60,001 | 120,000 |
| OR[10,17] | 3.557 | 6.237 | 0.2474 | 0.1934 | 1.878 | 17.05 | 60,001 | 120,000 |
| OR[10,18] | 16.09 | 45.9 | 2.105 | 0.3054 | 4.402 | 121.9 | 60,001 | 120,000 |
| OR[11,12] | 0.7888 | 0.9077 | 0.03755 | 0.0783 | 0.5294 | 2.995 | 60,001 | 120,000 |
| OR[11,13] | 26.38 | 112.3 | 3.388 | 0.2515 | 4.747 | 189.2 | 60,001 | 120,000 |
| OR[11,14] | 17.54 | 206.1 | 4.953 | 0.07379 | 2.26 | 92.65 | 60,001 | 120,000 |
| OR[11,15] | 1.599 | 0.5897 | 0.01878 | 0.7501 | 1.502 | 3.001 | 60,001 | 120,000 |
| OR[11,16] | 0.4352 | 0.478 | 0.02037 | 0.03298 | 0.2954 | 1.739 | 60,001 | 120,000 |
| OR[11,17] | 1.259 | 1.006 | 0.02827 | 0.2463 | 0.969 | 3.995 | 60,001 | 120,000 |
| OR[11,18] | 4.393 | 6.19 | 0.1776 | 0.2817 | 2.437 | 20.19 | 60,001 | 120,000 |
| OR[12,13] | 58.61 | 362.6 | 8.542 | 0.3793 | 9.009 | 409.6 | 60,001 | 120,000 |
| OR[12,14] | 40.73 | 655.4 | 14.48 | 0.09474 | 4.631 | 193 | 60,001 | 120,000 |
| OR[12,15] | 4.685 | 5.933 | 0.2691 | 0.4509 | 2.817 | 20.32 | 60,001 | 120,000 |
| OR[12,16] | 0.6139 | 0.2895 | 0.009711 | 0.235 | 0.5527 | 1.364 | 60,001 | 120,000 |
| OR[12,17] | 3.634 | 6.27 | 0.2406 | 0.2045 | 1.937 | 16.93 | 60,001 | 120,000 |
| OR[12,18] | 15.06 | 36.71 | 1.509 | 0.3086 | 4.474 | 119.3 | 60,001 | 120,000 |
| OR[13,14] | 5.53 | 39.52 | 0.9571 | 0.003667 | 0.4567 | 44.15 | 60,001 | 120,000 |
| OR[13,15] | 0.9641 | 2.463 | 0.1004 | 0.007295 | 0.3162 | 5.661 | 60,001 | 120,000 |
| OR[13,16] | 0.2245 | 0.5699 | 0.02051 | 0.001242 | 0.06062 | 1.593 | 60,001 | 120,000 |
| OR[13,17] | 0.7359 | 2.279 | 0.08093 | 0.005101 | 0.1999 | 4.611 | 60,001 | 120,000 |
| OR[13,18] | 2.564 | 9.984 | 0.3729 | 0.01042 | 0.4719 | 17.31 | 60,001 | 120,000 |
| OR[14,15] | 4.573 | 61.1 | 1.488 | 0.01533 | 0.6399 | 20.1 | 60,001 | 120,000 |
| OR[14,16] | 0.8251 | 3.825 | 0.1046 | 0.00282 | 0.1198 | 5.837 | 60,001 | 120,000 |
| OR[14,17] | 3.228 | 37.11 | 0.9332 | 0.01088 | 0.4266 | 14.55 | 60,001 | 120,000 |
| OR[14,18] | 11.66 | 192.3 | 3.894 | 0.01944 | 1.045 | 59.85 | 60,001 | 120,000 |
| OR[15,16] | 0.2941 | 0.3242 | 0.01412 | 0.02061 | 0.194 | 1.15 | 60,001 | 120,000 |
| OR[15,17] | 0.8049 | 0.5781 | 0.01617 | 0.1844 | 0.6472 | 2.337 | 60,001 | 120,000 |
| OR[15,18] | 2.859 | 3.935 | 0.1259 | 0.2136 | 1.645 | 13.11 | 60,001 | 120,000 |
| OR[16,17] | 6.769 | 12 | 0.4891 | 0.3975 | 3.357 | 35.34 | 60,001 | 120,000 |
| OR[16,18] | 29.51 | 82.34 | 3.567 | 0.5747 | 7.942 | 243.2 | 60,001 | 120,000 |
| OR[17,18] | 5.49 | 10.53 | 0.3723 | 0.2458 | 2.469 | 32.39 | 60,001 | 120,000 |
Median ranks
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk.class[1] | 7.457 | 1.605 | 0.06546 | 4 | 8 | 10 | 60,001 | 120,000 |
| rk.class[2] | 3.591 | 2.242 | 0.08864 | 1 | 3 | 9 | 60,001 | 120,000 |
| rk.class[3] | 9.338 | 1.524 | 0.05377 | 6 | 9 | 12 | 60,001 | 120,000 |
| rk.class[4] | 4.774 | 2.818 | 0.09714 | 1 | 5 | 11 | 60,001 | 120,000 |
| rk.class[5] | 10.43 | 1.414 | 0.05074 | 7 | 11 | 13 | 60,001 | 120,000 |
| rk.class[6] | 4.989 | 2.772 | 0.1259 | 2 | 4 | 12 | 60,001 | 120,000 |
| rk.class[7] | 6.753 | 1.942 | 0.06629 | 3 | 7 | 11 | 60,001 | 120,000 |
| rk.class[8] | 4.741 | 2.78 | 0.1243 | 1 | 4 | 12 | 60,001 | 120,000 |
| rk.class[9] | 10.93 | 3.089 | 0.1193 | 2 | 12 | 13 | 60,001 | 120,000 |
| rk.class[10] | 8.913 | 4.313 | 0.1881 | 1 | 11 | 13 | 60,001 | 120,000 |
| rk.class[11] | 2.372 | 1.863 | 0.07739 | 1 | 2 | 8 | 60,001 | 120,000 |
| rk.class[12] | 6.763 | 2.945 | 0.09328 | 1 | 7 | 12 | 60,001 | 120,000 |
| rk.class[13] | 9.952 | 3.188 | 0.1145 | 2 | 11 | 13 | 60,001 | 120,000 |
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk[1] | 7.887 | 1.915 | 0.07426 | 4 | 8 | 12 | 60,001 | 120,000 |
| rk[2] | 3.761 | 2.776 | 0.1071 | 1 | 3 | 13 | 60,001 | 120,000 |
| rk[3] | 12.22 | 2.477 | 0.06913 | 7 | 12 | 17 | 60,001 | 120,000 |
| rk[4] | 12.11 | 2.432 | 0.06942 | 7 | 12 | 16 | 60,001 | 120,000 |
| rk[5] | 12.52 | 2.476 | 0.06783 | 7 | 13 | 17 | 60,001 | 120,000 |
| rk[6] | 11.73 | 2.851 | 0.07212 | 6 | 12 | 17 | 60,001 | 120,000 |
| rk[7] | 10.79 | 2.817 | 0.07826 | 5 | 11 | 16 | 60,001 | 120,000 |
| rk[8] | 5.227 | 3.785 | 0.1255 | 1 | 5 | 16 | 60,001 | 120,000 |
| rk[9] | 14.39 | 2.566 | 0.07931 | 8 | 15 | 18 | 60,001 | 120,000 |
| rk[10] | 5.667 | 4.145 | 0.1894 | 2 | 4 | 17 | 60,001 | 120,000 |
| rk[11] | 7.337 | 2.8 | 0.08787 | 3 | 7 | 15 | 60,001 | 120,000 |
| rk[12] | 5.38 | 4.108 | 0.1849 | 1 | 4 | 16 | 60,001 | 120,000 |
| rk[13] | 14.78 | 4.979 | 0.1917 | 2 | 17 | 18 | 60,001 | 120,000 |
| rk[14] | 11.89 | 6.55 | 0.2844 | 1 | 16 | 18 | 60,001 | 120,000 |
| rk[15] | 11.47 | 2.615 | 0.06606 | 6 | 11 | 16 | 60,001 | 120,000 |
| rk[16] | 2.55 | 2.49 | 0.1019 | 1 | 2 | 11 | 60,001 | 120,000 |
| rk[17] | 7.968 | 4.593 | 0.1354 | 1 | 7 | 17 | 60,001 | 120,000 |
| rk[18] | 13.32 | 5.238 | 0.1872 | 2 | 16 | 18 | 60,001 | 120,000 |
Adults: acceptability (dropouts) – sensitivity analysis 2 (incomplete outcome data)
See Table 29 for a summary.
| Study | r[,1] | n[,1] | r[,2] | n[,2] | r[,3] | n[,3] | r[,4] | n[,4] | na[] | t[,1] | t[,2] | t[,3] | t[,4] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Anderson and Rees, 2007157 | 3 | 17 | 4 | 21 | NA | NA | NA | NA | 2 | 2 | 11 | NA | NA |
| Andersson et al., 2012158 | 2 | 50 | 0 | 51 | NA | NA | NA | NA | 2 | 11 | 14 | NA | NA |
| Belotto-Silva et al., 2012160 | 33 | 88 | 18 | 70 | NA | NA | NA | NA | 2 | 3 | 11 | NA | NA |
| Bergeron et al., 2002161 | 22 | 73 | 22 | 77 | NA | NA | NA | NA | 2 | 3 | 6 | NA | NA |
| Bisserbe et al., 1997162 | 23 | 86 | 35 | 82 | NA | NA | NA | NA | 2 | 6 | 9 | NA | NA |
| Chouinard et al., 1990163 | 4 | 44 | 6 | 43 | NA | NA | NA | NA | 2 | 1 | 6 | NA | NA |
| Cordioli et al., 2003164 | 1 | 24 | 1 | 23 | NA | NA | NA | NA | 2 | 2 | 11 | NA | NA |
| Denys et al., 2003167 | 9 | 75 | 4 | 75 | NA | NA | NA | NA | 2 | 5 | 8 | NA | NA |
| Foa et al., 2005171 | 12 | 32 | 20 | 47 | 16 | 37 | 14 | 33 | 4 | 1 | 9 | 10 | 12 |
| Freeman et al., 1994172 | 6 | 34 | 13 | 32 | NA | NA | NA | NA | 2 | 4 | 9 | NA | NA |
| Freeston et al., 1997173 | 0 | 14 | 3 | 15 | NA | NA | NA | NA | 2 | 2 | 11 | NA | NA |
| GlaxoSmithKline, 2005174 | 20 | 77 | 28 | 82 | 28 | 82 | NA | NA | 3 | 1 | 5 | 9 | NA |
| Goodman et al., 1989176 | 6 | 23 | 2 | 23 | NA | NA | NA | NA | 2 | 1 | 4 | NA | NA |
| Goodman et al., 1996177 | 17 | 80 | 23 | 80 | NA | NA | NA | NA | 2 | 1 | 4 | NA | NA |
| Greist et al., 2002178 | 14 | 69 | 9 | 75 | NA | NA | NA | NA | 2 | 10 | 14 | NA | NA |
| Hollander et al., 2003180 | 31 | 126 | 43 | 127 | NA | NA | NA | NA | 2 | 1 | 4 | NA | NA |
| Hollander et al., 2003181 | 15 | 89 | 14 | 88 | 20 | 86 | 19 | 85 | 4 | 1 | 5 | 5 | 5 |
| Jenike et al., 1997185 | 3 | 21 | 4 | 23 | NA | NA | NA | NA | 2 | 1 | 3 | NA | NA |
| Kobak et al., 2005189 | 9 | 30 | 8 | 30 | NA | NA | NA | NA | 2 | 1 | 15 | NA | NA |
| Koran et al., 1996190 | 8 | 37 | 15 | 42 | NA | NA | NA | NA | 2 | 4 | 9 | NA | NA |
| Kronig et al., 1999191 | 25 | 81 | 25 | 86 | NA | NA | NA | NA | 2 | 1 | 6 | NA | NA |
| López-Ibor et al., 1996193 | 5 | 30 | 3 | 25 | NA | NA | NA | NA | 2 | 3 | 9 | NA | NA |
| Montgomery et al., 1993197 | 15 | 57 | 14 | 53 | 13 | 52 | 14 | 55 | 4 | 1 | 3 | 3 | 3 |
| Montgomery et al., 2001198 | 17 | 101 | 15 | 100 | 15 | 98 | 16 | 102 | 4 | 1 | 7 | 7 | 7 |
| Mundo et al., 2001200 | 19 | 115 | 26 | 112 | NA | NA | NA | NA | 2 | 4 | 9 | NA | NA |
| Sousa et al., 2006207 | 3 | 28 | 3 | 28 | NA | NA | NA | NA | 2 | 6 | 11 | NA | NA |
| Stein et al., 2007124 | 16 | 115 | 29 | 119 | 24 | 116 | 21 | 116 | 4 | 1 | 5 | 13 | 13 |
| Tollefson et al., 1994127 | 13 | 89 | 12 | 87 | 22 | 89 | 22 | 90 | 4 | 1 | 3 | 3 | 3 |
| Zohar and Judge, 1996213 | 40 | 100 | 53 | 205 | 36 | 101 | NA | NA | 3 | 1 | 5 | 9 | NA |
Key: intervention
-
Placebo (1).
-
Waitlist (2).
-
Fluoxetine (3).
-
Fluvoxamine (3).
-
Paroxetine (3).
-
Sertraline (3).
-
Citalopram (3).
-
Venlafaxine (4).
-
Clomipramine (5).
-
BT (6).
-
CBT (7).
-
BT + clomipramine (8).
-
Escitalopram (3).
-
Psychological placebo (9).
-
Hypericum (10).
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| OR.D[1,2] | 0.5368 | 0.4823 | 0.01184 | 0.08188 | 0.3911 | 1.806 | 60,001 | 120,000 |
| OR.D[1,3] | 1.107 | 0.1536 | 0.002988 | 0.8368 | 1.098 | 1.435 | 60,001 | 120,000 |
| OR.D[1,4] | 0.5482 | 0.4165 | 0.007525 | 0.1029 | 0.4439 | 1.609 | 60,001 | 120,000 |
| OR.D[1,5] | 1.578 | 0.2737 | 0.004665 | 1.105 | 1.554 | 2.175 | 60,001 | 120,000 |
| OR.D[1,6] | 1.349 | 0.6253 | 0.01276 | 0.5019 | 1.227 | 2.91 | 60,001 | 120,000 |
| OR.D[1,7] | 0.8623 | 0.3524 | 0.0076 | 0.3689 | 0.8054 | 1.729 | 60,001 | 120,000 |
| OR.D[1,8] | 1.499 | 0.7573 | 0.01471 | 0.5177 | 1.335 | 3.386 | 60,001 | 120,000 |
| OR.D[1,9] | 0.6353 | 0.4454 | 0.009881 | 0.1439 | 0.5159 | 1.824 | 60,001 | 120,000 |
| OR.D[1,10] | 1.033 | 0.7204 | 0.01341 | 0.2466 | 0.8391 | 2.896 | 60,001 | 120,000 |
| OR.D[2,3] | 3.815 | 3.673 | 0.09655 | 0.6073 | 2.788 | 13.19 | 60,001 | 120,000 |
| OR.D[2,4] | 1.869 | 2.563 | 0.0522 | 0.1416 | 1.115 | 8.087 | 60,001 | 120,000 |
| OR.D[2,5] | 5.456 | 5.307 | 0.1369 | 0.8413 | 3.947 | 19.32 | 60,001 | 120,000 |
| OR.D[2,6] | 4.58 | 5.203 | 0.123 | 0.5442 | 3.133 | 17.44 | 60,001 | 120,000 |
| OR.D[2,7] | 2.586 | 2.153 | 0.05721 | 0.5407 | 2.029 | 8.078 | 60,001 | 120,000 |
| OR.D[2,8] | 5.132 | 5.82 | 0.1341 | 0.5515 | 3.441 | 20.35 | 60,001 | 120,000 |
| OR.D[2,9] | 2.14 | 2.932 | 0.07268 | 0.1828 | 1.331 | 8.937 | 60,001 | 120,000 |
| OR.D[2,10] | 3.588 | 4.987 | 0.1072 | 0.3084 | 2.14 | 15.8 | 60,001 | 120,000 |
| OR.D[3,4] | 0.4992 | 0.377 | 0.006642 | 0.09421 | 0.4054 | 1.454 | 60,001 | 120,000 |
| OR.D[3,5] | 1.439 | 0.2575 | 0.003114 | 1.001 | 1.419 | 2.002 | 60,001 | 120,000 |
| OR.D[3,6] | 1.234 | 0.5833 | 0.01131 | 0.4517 | 1.122 | 2.671 | 60,001 | 120,000 |
| OR.D[3,7] | 0.7845 | 0.3168 | 0.006195 | 0.3418 | 0.7308 | 1.563 | 60,001 | 120,000 |
| OR.D[3,8] | 1.373 | 0.711 | 0.01355 | 0.4659 | 1.219 | 3.129 | 60,001 | 120,000 |
| OR.D[3,9] | 0.582 | 0.4177 | 0.009214 | 0.1306 | 0.4704 | 1.69 | 60,001 | 120,000 |
| OR.D[3,10] | 0.9491 | 0.6783 | 0.01254 | 0.2175 | 0.7669 | 2.715 | 60,001 | 120,000 |
| OR.D[4,5] | 4.676 | 4.245 | 0.07812 | 0.9583 | 3.507 | 15.3 | 60,001 | 120,000 |
| OR.D[4,6] | 4.001 | 4.251 | 0.07371 | 0.5536 | 2.785 | 14.51 | 60,001 | 120,000 |
| OR.D[4,7] | 2.559 | 2.626 | 0.04798 | 0.4166 | 1.785 | 9.203 | 60,001 | 120,000 |
| OR.D[4,8] | 4.444 | 4.824 | 0.08092 | 0.6143 | 3.099 | 16.47 | 60,001 | 120,000 |
| OR.D[4,9] | 1.876 | 2.358 | 0.04325 | 0.1961 | 1.195 | 7.612 | 60,001 | 120,000 |
| OR.D[4,10] | 3.051 | 4.041 | 0.06462 | 0.3062 | 1.987 | 12.39 | 60,001 | 120,000 |
| OR.D[5,6] | 0.8661 | 0.3962 | 0.00754 | 0.3192 | 0.7938 | 1.839 | 60,001 | 120,000 |
| OR.D[5,7] | 0.559 | 0.2404 | 0.004717 | 0.2273 | 0.5175 | 1.143 | 60,001 | 120,000 |
| OR.D[5,8] | 0.9636 | 0.4861 | 0.009502 | 0.3366 | 0.8614 | 2.165 | 60,001 | 120,000 |
| OR.D[5,9] | 0.4083 | 0.2862 | 0.006212 | 0.09316 | 0.3321 | 1.166 | 60,001 | 120,000 |
| OR.D[5,10] | 0.673 | 0.4854 | 0.008825 | 0.1504 | 0.5407 | 1.922 | 60,001 | 120,000 |
| OR.D[6,7] | 0.7694 | 0.4893 | 0.009361 | 0.2154 | 0.6592 | 2.02 | 60,001 | 120,000 |
| OR.D[6,8] | 1.262 | 0.7268 | 0.01311 | 0.3817 | 1.095 | 3.066 | 60,001 | 120,000 |
| OR.D[6,9] | 0.4793 | 0.2494 | 0.004438 | 0.1582 | 0.425 | 1.107 | 60,001 | 120,000 |
| OR.D[6,10] | 0.9297 | 0.8433 | 0.01443 | 0.1532 | 0.6931 | 3.107 | 60,001 | 120,000 |
| OR.D[7,8] | 2.018 | 1.363 | 0.02948 | 0.5075 | 1.673 | 5.575 | 60,001 | 120,000 |
| OR.D[7,9] | 0.8405 | 0.7029 | 0.01594 | 0.1544 | 0.6413 | 2.658 | 60,001 | 120,000 |
| OR.D[7,10] | 1.391 | 1.216 | 0.02328 | 0.2467 | 1.06 | 4.459 | 60,001 | 120,000 |
| OR.D[8,9] | 0.505 | 0.4269 | 0.009518 | 0.09524 | 0.3845 | 1.649 | 60,001 | 120,000 |
| OR.D[8,10] | 0.8652 | 0.8256 | 0.01346 | 0.1305 | 0.6307 | 2.967 | 60,001 | 120,000 |
| OR.D[9,10] | 2.438 | 2.821 | 0.04791 | 0.2808 | 1.604 | 9.457 | 60,001 | 120,000 |
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| OR[1,2] | 0.5368 | 0.4823 | 0.01184 | 0.08188 | 0.3911 | 1.806 | 60,001 | 120,000 |
| OR[1,3] | 1.169 | 0.1838 | 0.003938 | 0.8761 | 1.146 | 1.592 | 60,001 | 120,000 |
| OR[1,4] | 1.097 | 0.1559 | 0.002968 | 0.808 | 1.092 | 1.434 | 60,001 | 120,000 |
| OR[1,5] | 1.132 | 0.1558 | 0.003222 | 0.8646 | 1.121 | 1.48 | 60,001 | 120,000 |
| OR[1,6] | 1.071 | 0.1659 | 0.003257 | 0.7602 | 1.067 | 1.423 | 60,001 | 120,000 |
| OR[1,7] | 1.082 | 0.19 | 0.003507 | 0.7187 | 1.077 | 1.49 | 60,001 | 120,000 |
| OR[1,8] | 0.5482 | 0.4165 | 0.007525 | 0.1029 | 0.4439 | 1.609 | 60,001 | 120,000 |
| OR[1,9] | 1.578 | 0.2737 | 0.004665 | 1.105 | 1.554 | 2.175 | 60,001 | 120,000 |
| OR[1,10] | 1.349 | 0.6253 | 0.01276 | 0.5019 | 1.227 | 2.91 | 60,001 | 120,000 |
| OR[1,11] | 0.8623 | 0.3524 | 0.0076 | 0.3689 | 0.8054 | 1.729 | 60,001 | 120,000 |
| OR[1,12] | 1.499 | 0.7573 | 0.01471 | 0.5177 | 1.335 | 3.386 | 60,001 | 120,000 |
| OR[1,13] | 1.11 | 0.1839 | 0.003213 | 0.7808 | 1.099 | 1.517 | 60,001 | 120,000 |
| OR[1,14] | 0.6353 | 0.4454 | 0.009881 | 0.1439 | 0.5159 | 1.824 | 60,001 | 120,000 |
| OR[1,15] | 1.033 | 0.7204 | 0.01341 | 0.2466 | 0.8391 | 2.896 | 60,001 | 120,000 |
| OR[2,3] | 3.991 | 3.791 | 0.09895 | 0.6527 | 2.937 | 13.81 | 60,001 | 120,000 |
| OR[2,4] | 3.794 | 3.701 | 0.097 | 0.5932 | 2.773 | 13.15 | 60,001 | 120,000 |
| OR[2,5] | 3.905 | 3.762 | 0.09781 | 0.6172 | 2.862 | 13.56 | 60,001 | 120,000 |
| OR[2,6] | 3.692 | 3.59 | 0.09489 | 0.5807 | 2.662 | 12.9 | 60,001 | 120,000 |
| OR[2,7] | 3.739 | 3.647 | 0.09542 | 0.5739 | 2.678 | 13.1 | 60,001 | 120,000 |
| OR[2,8] | 1.869 | 2.563 | 0.0522 | 0.1416 | 1.115 | 8.087 | 60,001 | 120,000 |
| OR[2,9] | 5.456 | 5.307 | 0.1369 | 0.8413 | 3.947 | 19.32 | 60,001 | 120,000 |
| OR[2,10] | 4.58 | 5.203 | 0.123 | 0.5442 | 3.133 | 17.44 | 60,001 | 120,000 |
| OR[2,11] | 2.586 | 2.153 | 0.05721 | 0.5407 | 2.029 | 8.078 | 60,001 | 120,000 |
| OR[2,12] | 5.132 | 5.82 | 0.1341 | 0.5515 | 3.441 | 20.35 | 60,001 | 120,000 |
| OR[2,13] | 3.832 | 3.737 | 0.09732 | 0.5977 | 2.802 | 13.37 | 60,001 | 120,000 |
| OR[2,14] | 2.14 | 2.932 | 0.07268 | 0.1828 | 1.331 | 8.937 | 60,001 | 120,000 |
| OR[2,15] | 3.588 | 4.987 | 0.1072 | 0.3084 | 2.14 | 15.8 | 60,001 | 120,000 |
| OR[3,4] | 0.9513 | 0.1428 | 0.001887 | 0.6309 | 0.9736 | 1.231 | 60,001 | 120,000 |
| OR[3,5] | 0.9816 | 0.1408 | 0.001805 | 0.6889 | 0.9904 | 1.287 | 60,001 | 120,000 |
| OR[3,6] | 0.9279 | 0.1403 | 0.002183 | 0.6145 | 0.9568 | 1.183 | 60,001 | 120,000 |
| OR[3,7] | 0.9381 | 0.166 | 0.002505 | 0.5664 | 0.969 | 1.254 | 60,001 | 120,000 |
| OR[3,8] | 0.475 | 0.3604 | 0.006235 | 0.08722 | 0.3866 | 1.368 | 60,001 | 120,000 |
| OR[3,9] | 1.371 | 0.2641 | 0.004059 | 0.8972 | 1.355 | 1.933 | 60,001 | 120,000 |
| OR[3,10] | 1.175 | 0.5591 | 0.01119 | 0.4245 | 1.065 | 2.573 | 60,001 | 120,000 |
| OR[3,11] | 0.7401 | 0.2838 | 0.005498 | 0.3331 | 0.6928 | 1.429 | 60,001 | 120,000 |
| OR[3,12] | 1.308 | 0.6796 | 0.01321 | 0.4356 | 1.159 | 2.983 | 60,001 | 120,000 |
| OR[3,13] | 0.9621 | 0.1596 | 0.002065 | 0.6226 | 0.9799 | 1.296 | 60,001 | 120,000 |
| OR[3,14] | 0.5536 | 0.3971 | 0.008822 | 0.1239 | 0.4479 | 1.616 | 60,001 | 120,000 |
| OR[3,15] | 0.9016 | 0.6488 | 0.01197 | 0.2064 | 0.7282 | 2.592 | 60,001 | 120,000 |
| OR[4,5] | 1.045 | 0.1606 | 0.001942 | 0.7871 | 1.012 | 1.458 | 60,001 | 120,000 |
| OR[4,6] | 0.9862 | 0.1509 | 0.001856 | 0.6917 | 0.9905 | 1.331 | 60,001 | 120,000 |
| OR[4,7] | 0.9956 | 0.1725 | 0.0022 | 0.6618 | 0.9961 | 1.396 | 60,001 | 120,000 |
| OR[4,8] | 0.5063 | 0.3878 | 0.006808 | 0.09506 | 0.4095 | 1.498 | 60,001 | 120,000 |
| OR[4,9] | 1.454 | 0.2553 | 0.003461 | 1.022 | 1.431 | 2.02 | 60,001 | 120,000 |
| OR[4,10] | 1.247 | 0.5898 | 0.01119 | 0.4577 | 1.13 | 2.704 | 60,001 | 120,000 |
| OR[4,11] | 0.7959 | 0.3325 | 0.006539 | 0.337 | 0.7346 | 1.629 | 60,001 | 120,000 |
| OR[4,12] | 1.387 | 0.7133 | 0.01317 | 0.4674 | 1.234 | 3.15 | 60,001 | 120,000 |
| OR[4,13] | 1.023 | 0.1789 | 0.00188 | 0.7168 | 1.002 | 1.463 | 60,001 | 120,000 |
| OR[4,14] | 0.5875 | 0.4199 | 0.008943 | 0.1324 | 0.4735 | 1.7 | 60,001 | 120,000 |
| OR[4,15] | 0.9589 | 0.687 | 0.01226 | 0.2199 | 0.7747 | 2.737 | 60,001 | 120,000 |
| OR[5,6] | 0.9545 | 0.143 | 0.002086 | 0.6513 | 0.9749 | 1.247 | 60,001 | 120,000 |
| OR[5,7] | 0.9639 | 0.1642 | 0.002669 | 0.5953 | 0.9834 | 1.306 | 60,001 | 120,000 |
| OR[5,8] | 0.4835 | 0.3548 | 0.006231 | 0.09376 | 0.3971 | 1.384 | 60,001 | 120,000 |
| OR[5,9] | 1.406 | 0.2432 | 0.00348 | 0.9812 | 1.391 | 1.931 | 60,001 | 120,000 |
| OR[5,10] | 1.206 | 0.5681 | 0.01112 | 0.4422 | 1.094 | 2.618 | 60,001 | 120,000 |
| OR[5,11] | 0.7681 | 0.3133 | 0.006304 | 0.3297 | 0.7112 | 1.549 | 60,001 | 120,000 |
| OR[5,12] | 1.34 | 0.6853 | 0.01281 | 0.456 | 1.194 | 3.065 | 60,001 | 120,000 |
| OR[5,13] | 0.9871 | 0.1463 | 0.00173 | 0.6905 | 0.9916 | 1.323 | 60,001 | 120,000 |
| OR[5,14] | 0.5689 | 0.4066 | 0.008892 | 0.1267 | 0.4592 | 1.653 | 60,001 | 120,000 |
| OR[5,15] | 0.9261 | 0.6579 | 0.01213 | 0.2148 | 0.7519 | 2.654 | 60,001 | 120,000 |
| OR[6,7] | 1.022 | 0.1854 | 0.00209 | 0.6825 | 1.003 | 1.475 | 60,001 | 120,000 |
| OR[6,8] | 0.5196 | 0.398 | 0.006908 | 0.09647 | 0.4196 | 1.524 | 60,001 | 120,000 |
| OR[6,9] | 1.494 | 0.2823 | 0.003616 | 1.026 | 1.468 | 2.14 | 60,001 | 120,000 |
| OR[6,10] | 1.281 | 0.6112 | 0.01176 | 0.4633 | 1.166 | 2.792 | 60,001 | 120,000 |
| OR[6,11] | 0.8147 | 0.3334 | 0.006708 | 0.3517 | 0.756 | 1.641 | 60,001 | 120,000 |
| OR[6,12] | 1.428 | 0.7528 | 0.0149 | 0.4745 | 1.261 | 3.296 | 60,001 | 120,000 |
| OR[6,13] | 1.051 | 0.1945 | 0.002293 | 0.7376 | 1.012 | 1.553 | 60,001 | 120,000 |
| OR[6,14] | 0.6038 | 0.4332 | 0.009467 | 0.1343 | 0.4885 | 1.768 | 60,001 | 120,000 |
| OR[6,15] | 0.9866 | 0.7084 | 0.01321 | 0.2251 | 0.7914 | 2.783 | 60,001 | 120,000 |
| OR[7,8] | 0.5197 | 0.4061 | 0.007301 | 0.09568 | 0.4155 | 1.563 | 60,001 | 120,000 |
| OR[7,9] | 1.493 | 0.3328 | 0.004181 | 0.968 | 1.455 | 2.273 | 60,001 | 120,000 |
| OR[7,10] | 1.28 | 0.6299 | 0.01196 | 0.4493 | 1.159 | 2.853 | 60,001 | 120,000 |
| OR[7,11] | 0.8157 | 0.356 | 0.006692 | 0.3403 | 0.7491 | 1.697 | 60,001 | 120,000 |
| OR[7,12] | 1.426 | 0.7698 | 0.01575 | 0.4687 | 1.25 | 3.443 | 60,001 | 120,000 |
| OR[7,13] | 1.048 | 0.22 | 0.002709 | 0.7105 | 1.007 | 1.594 | 60,001 | 120,000 |
| OR[7,14] | 0.6042 | 0.4461 | 0.009913 | 0.1318 | 0.4899 | 1.769 | 60,001 | 120,000 |
| OR[7,15] | 0.9865 | 0.7245 | 0.01403 | 0.22 | 0.7862 | 2.868 | 60,001 | 120,000 |
| OR[8,9] | 4.676 | 4.245 | 0.07812 | 0.9583 | 3.507 | 15.3 | 60,001 | 120,000 |
| OR[8,10] | 4.001 | 4.251 | 0.07371 | 0.5536 | 2.785 | 14.51 | 60,001 | 120,000 |
| OR[8,11] | 2.559 | 2.626 | 0.04798 | 0.4166 | 1.785 | 9.203 | 60,001 | 120,000 |
| OR[8,12] | 4.444 | 4.824 | 0.08092 | 0.6143 | 3.099 | 16.47 | 60,001 | 120,000 |
| OR[8,13] | 3.291 | 2.989 | 0.05449 | 0.665 | 2.462 | 10.7 | 60,001 | 120,000 |
| OR[8,14] | 1.876 | 2.358 | 0.04325 | 0.1961 | 1.195 | 7.612 | 60,001 | 120,000 |
| OR[8,15] | 3.051 | 4.041 | 0.06462 | 0.3062 | 1.987 | 12.39 | 60,001 | 120,000 |
| OR[9,10] | 0.8661 | 0.3962 | 0.00754 | 0.3192 | 0.7938 | 1.839 | 60,001 | 120,000 |
| OR[9,11] | 0.559 | 0.2404 | 0.004717 | 0.2273 | 0.5175 | 1.143 | 60,001 | 120,000 |
| OR[9,12] | 0.9636 | 0.4861 | 0.009502 | 0.3366 | 0.8614 | 2.165 | 60,001 | 120,000 |
| OR[9,13] | 0.7191 | 0.1477 | 0.001776 | 0.4735 | 0.703 | 1.057 | 60,001 | 120,000 |
| OR[9,14] | 0.4083 | 0.2862 | 0.006212 | 0.09316 | 0.3321 | 1.166 | 60,001 | 120,000 |
| OR[9,15] | 0.673 | 0.4854 | 0.008825 | 0.1504 | 0.5407 | 1.922 | 60,001 | 120,000 |
| OR[10,11] | 0.7694 | 0.4893 | 0.009361 | 0.2154 | 0.6592 | 2.02 | 60,001 | 120,000 |
| OR[10,12] | 1.262 | 0.7268 | 0.01311 | 0.3817 | 1.095 | 3.066 | 60,001 | 120,000 |
| OR[10,13] | 0.9975 | 0.4961 | 0.009793 | 0.3615 | 0.8927 | 2.249 | 60,001 | 120,000 |
| OR[10,14] | 0.4793 | 0.2494 | 0.004438 | 0.1582 | 0.425 | 1.107 | 60,001 | 120,000 |
| OR[10,15] | 0.9297 | 0.8433 | 0.01443 | 0.1532 | 0.6931 | 3.107 | 60,001 | 120,000 |
| OR[11,12] | 2.018 | 1.363 | 0.02948 | 0.5075 | 1.673 | 5.575 | 60,001 | 120,000 |
| OR[11,13] | 1.483 | 0.6185 | 0.01323 | 0.6176 | 1.365 | 3.009 | 60,001 | 120,000 |
| OR[11,14] | 0.8405 | 0.7029 | 0.01594 | 0.1544 | 0.6413 | 2.658 | 60,001 | 120,000 |
| OR[11,15] | 1.391 | 1.216 | 0.02328 | 0.2467 | 1.06 | 4.459 | 60,001 | 120,000 |
| OR[12,13] | 0.9261 | 0.4948 | 0.00824 | 0.3177 | 0.8191 | 2.185 | 60,001 | 120,000 |
| OR[12,14] | 0.505 | 0.4269 | 0.009518 | 0.09524 | 0.3845 | 1.649 | 60,001 | 120,000 |
| OR[12,15] | 0.8652 | 0.8256 | 0.01346 | 0.1305 | 0.6307 | 2.967 | 60,001 | 120,000 |
| OR[13,14] | 0.586 | 0.4309 | 0.009998 | 0.1292 | 0.4709 | 1.713 | 60,001 | 120,000 |
| OR[13,15] | 0.9556 | 0.6968 | 0.0132 | 0.2162 | 0.7649 | 2.795 | 60,001 | 120,000 |
| OR[14,15] | 2.438 | 2.821 | 0.04791 | 0.2808 | 1.604 | 9.457 | 60,001 | 120,000 |
Median ranks
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk.class[1] | 5.78 | 1.344 | 0.02774 | 3 | 6 | 8 | 60,001 | 120,000 |
| rk.class[2] | 2.664 | 2.226 | 0.05422 | 1 | 2 | 9 | 60,001 | 120,000 |
| rk.class[3] | 6.692 | 1.38 | 0.02303 | 4 | 7 | 9 | 60,001 | 120,000 |
| rk.class[4] | 2.837 | 2.135 | 0.0419 | 1 | 2 | 9 | 60,001 | 120,000 |
| rk.class[5] | 8.961 | 1.021 | 0.01685 | 7 | 9 | 10 | 60,001 | 120,000 |
| rk.class[6] | 7.226 | 2.173 | 0.04225 | 3 | 8 | 10 | 60,001 | 120,000 |
| rk.class[7] | 4.771 | 1.969 | 0.04022 | 2 | 4 | 9 | 60,001 | 120,000 |
| rk.class[8] | 7.578 | 2.311 | 0.04114 | 3 | 8 | 10 | 60,001 | 120,000 |
| rk.class[9] | 3.207 | 2.094 | 0.0453 | 1 | 3 | 9 | 60,001 | 120,000 |
| rk.class[10] | 5.285 | 2.857 | 0.05624 | 1 | 5 | 10 | 60,001 | 120,000 |
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk[1] | 7.092 | 2.338 | 0.05465 | 3 | 7 | 12 | 60,001 | 120,000 |
| rk[2] | 3.149 | 3.453 | 0.08171 | 1 | 2 | 14 | 60,001 | 120,000 |
| rk[3] | 10.17 | 2.411 | 0.03526 | 5 | 10 | 14 | 60,001 | 120,000 |
| rk[4] | 8.965 | 2.477 | 0.02875 | 4 | 9 | 13 | 60,001 | 120,000 |
| rk[5] | 9.624 | 2.378 | 0.03381 | 5 | 10 | 14 | 60,001 | 120,000 |
| rk[6] | 8.449 | 2.552 | 0.03386 | 4 | 8 | 13 | 60,001 | 120,000 |
| rk[7] | 8.675 | 2.786 | 0.03903 | 3 | 9 | 14 | 60,001 | 120,000 |
| rk[8] | 3.268 | 3.238 | 0.0601 | 1 | 2 | 14 | 60,001 | 120,000 |
| rk[9] | 13.78 | 1.326 | 0.01856 | 10 | 14 | 15 | 60,001 | 120,000 |
| rk[10] | 10.24 | 4.218 | 0.08325 | 3 | 12 | 15 | 60,001 | 120,000 |
| rk[11] | 5.78 | 3.485 | 0.06809 | 2 | 5 | 14 | 60,001 | 120,000 |
| rk[12] | 10.86 | 4.307 | 0.07552 | 3 | 13 | 15 | 60,001 | 120,000 |
| rk[13] | 9.121 | 2.662 | 0.03399 | 4 | 9 | 14 | 60,001 | 120,000 |
| rk[14] | 3.817 | 3.428 | 0.07177 | 1 | 3 | 14 | 60,001 | 120,000 |
| rk[15] | 7.009 | 4.923 | 0.09658 | 1 | 5 | 15 | 60,001 | 120,000 |
Adults/acceptability (dropouts): sensitivity analysis 3 (blinding)
See Table 30 of the main report for a summary.
| Study | r[,1] | n[,1] | r[,2] | n[,2] | r[,3] | n[,3] | r[,4] | n[,4] | na[] | t[,1] | t[,2] | t[,3] | t[,4] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Albert et al., 2002155 | 1 | 26 | 7 | 47 | NA | NA | NA | NA | 2 | 7 | 8 | NA | NA |
| Andersson et al., 2012158 | 2 | 50 | 0 | 51 | NA | NA | NA | NA | 2 | 10 | 14 | NA | NA |
| Belloch et al., 2008159 | 2 | 15 | 2 | 18 | NA | NA | NA | NA | 2 | 9 | 11 | NA | NA |
| Belotto-Silva et al., 2012160 | 33 | 88 | 18 | 70 | NA | NA | NA | NA | 2 | 3 | 10 | NA | NA |
| Cordioli et al., 2003164 | 1 | 24 | 1 | 23 | NA | NA | NA | NA | 2 | 2 | 10 | NA | NA |
| Cottraux et al., 2001166 | 3 | 33 | 2 | 32 | NA | NA | NA | NA | 2 | 9 | 11 | NA | NA |
| Denys et al., 2003167 | 9 | 75 | 4 | 75 | NA | NA | NA | NA | 2 | 5 | 7 | NA | NA |
| Emmelkamp and Beens, 1991168 | 4 | 15 | 5 | 15 | NA | NA | NA | NA | 2 | 9 | 11 | NA | NA |
| Emmelkamp et al., 1988169 | 1 | 10 | 1 | 10 | NA | NA | NA | NA | 2 | 9 | 11 | NA | NA |
| Foa et al., 2005171 | 12 | 32 | 20 | 47 | 16 | 37 | 14 | 33 | 4 | 1 | 8 | 9 | 12 |
| Goodman et al., 1989176 | 6 | 23 | 2 | 23 | NA | NA | NA | NA | 2 | 1 | 4 | NA | NA |
| Jenike et al., 1990184 | 0 | 20 | 2 | 20 | NA | NA | NA | NA | 2 | 1 | 4 | NA | NA |
| Nakatani et al., 2005202 | 1 | 11 | 1 | 11 | 1 | 9 | NA | NA | 3 | 4 | 9 | 14 | NA |
| O’Connor et al., 1999203 | 0 | 6 | 1 | 7 | NA | NA | NA | NA | 2 | 2 | 10 | NA | NA |
| Perse et al., 1987205 | 2 | 10 | 2 | 10 | NA | NA | NA | NA | 2 | 1 | 4 | NA | NA |
| Sousa et al., 2006207 | 3 | 28 | 3 | 28 | NA | NA | NA | NA | 2 | 6 | 10 | NA | NA |
| Stein et al., 2007124 | 16 | 115 | 29 | 119 | 24 | 116 | 21 | 116 | 4 | 1 | 5 | 13 | 13 |
| Whittal et al., 2005211 | 13 | 42 | 11 | 41 | NA | NA | NA | NA | 2 | 9 | 11 | NA | NA |
Key: intervention
-
Placebo (1).
-
Waitlist (2).
-
Fluoxetine (3).
-
Fluvoxamine (3).
-
Paroxetine (3).
-
Sertraline (3).
-
Venlafaxine (4).
-
Clomipramine (5).
-
BT (6).
-
CBT (7).
-
CT (8).
-
BT + clomipramine (9).
-
Escitalopram (3).
-
Psychological placebo (10).
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| OR.D[1,2] | 152 | 4922 | 87.87 | 0.008968 | 0.4497 | 31.84 | 51,001 | 100,000 |
| OR.D[1,3] | 3979 | 1.23E+ 06 | 3875 | 0.4603 | 1.393 | 8.446 | 51,001 | 100,000 |
| OR.D[1,4] | 0.6071 | 0.6553 | 0.009367 | 0.1033 | 0.4765 | 1.792 | 51,001 | 100,000 |
| OR.D[1,5] | 1.613 | 1.243 | 0.02013 | 0.4567 | 1.365 | 4.242 | 51,001 | 100,000 |
| OR.D[1,6] | 1.454 | 0.9819 | 0.02283 | 0.389 | 1.23 | 3.832 | 51,001 | 100,000 |
| OR.D[1,7] | 73.75 | 1239 | 32.56 | 0.2699 | 1.13 | 32.32 | 51,001 | 100,000 |
| OR.D[1,8] | 1.401 | 1.288 | 0.02571 | 0.2702 | 1.102 | 4.305 | 51,001 | 100,000 |
| OR.D[1,9] | 1.534 | 1.585 | 0.01918 | 0.3576 | 1.245 | 4.265 | 51,001 | 100,000 |
| OR.D[1,10] | 0.7989 | 2.118 | 0.04562 | 0.01122 | 0.3155 | 4.512 | 51,001 | 100,000 |
| OR.D[2,3] | 32.22 | 1103 | 10.24 | 0.08203 | 3.185 | 147.4 | 51,001 | 100,000 |
| OR.D[2,4] | 11.11 | 83.76 | 2.895 | 0.01178 | 1.078 | 63.15 | 51,001 | 100,000 |
| OR.D[2,5] | 28.7 | 224 | 4.765 | 0.04023 | 3.027 | 173.3 | 51,001 | 100,000 |
| OR.D[2,6] | 23.47 | 169 | 3.246 | 0.0359 | 2.674 | 154.7 | 51,001 | 100,000 |
| OR.D[2,7] | 17.79 | 105.6 | 3.952 | 0.1951 | 2.643 | 96.55 | 51,001 | 100,000 |
| OR.D[2,8] | 22.5 | 164.5 | 2.995 | 0.02847 | 2.397 | 154.9 | 51,001 | 100,000 |
| OR.D[2,9] | 27.55 | 231.1 | 4.559 | 0.03399 | 2.699 | 168.1 | 51,001 | 100,000 |
| OR.D[2,10] | 10 | 88.01 | 1.697 | 0.006203 | 0.6522 | 58.37 | 51,001 | 100,000 |
| OR.D[3,4] | 0.5516 | 6.26 | 0.02648 | 0.03969 | 0.3283 | 1.64 | 51,001 | 100,000 |
| OR.D[3,5] | 1.548 | 21.95 | 0.08582 | 0.1324 | 0.9603 | 4.349 | 51,001 | 100,000 |
| OR.D[3,6] | 1.394 | 18.9 | 0.084 | 0.1135 | 0.8725 | 3.93 | 51,001 | 100,000 |
| OR.D[3,7] | 165.2 | 17080 | 104 | 0.2389 | 0.8059 | 10.16 | 51,001 | 100,000 |
| OR.D[3,8] | 1.339 | 17.54 | 0.08425 | 0.08769 | 0.7797 | 4.174 | 51,001 | 100,000 |
| OR.D[3,9] | 1.51 | 20.48 | 0.08574 | 0.1038 | 0.879 | 4.469 | 51,001 | 100,000 |
| OR.D[3,10] | 0.7554 | 19.39 | 0.1018 | 0.005801 | 0.2135 | 3.12 | 51,001 | 100,000 |
| OR.D[4,5] | 4.067 | 5.741 | 0.07591 | 0.6797 | 2.888 | 14.33 | 51,001 | 100,000 |
| OR.D[4,6] | 3.969 | 7.597 | 0.09576 | 0.5143 | 2.581 | 15.37 | 51,001 | 100,000 |
| OR.D[4,7] | 162.5 | 5480 | 72.81 | 0.3688 | 2.529 | 77.18 | 51,001 | 100,000 |
| OR.D[4,8] | 3.851 | 10.3 | 0.1033 | 0.3951 | 2.334 | 15.66 | 51,001 | 100,000 |
| OR.D[4,9] | 4.291 | 28.47 | 0.1184 | 0.4971 | 2.638 | 16.23 | 51,001 | 100,000 |
| OR.D[4,10] | 2.209 | 11.24 | 0.1245 | 0.01927 | 0.6745 | 12.7 | 51,001 | 100,000 |
| OR.D[5,6] | 1.063 | 0.8671 | 0.01063 | 0.2796 | 0.9051 | 2.705 | 51,001 | 100,000 |
| OR.D[5,7] | 53.63 | 1217 | 23.62 | 0.1463 | 0.8476 | 25.91 | 51,001 | 100,000 |
| OR.D[5,8] | 1.027 | 1.064 | 0.01292 | 0.1933 | 0.825 | 3.082 | 51,001 | 100,000 |
| OR.D[5,9] | 1.174 | 21.38 | 0.06714 | 0.2696 | 0.9156 | 3.015 | 51,001 | 100,000 |
| OR.D[5,10] | 0.6488 | 2.325 | 0.03773 | 0.007115 | 0.2285 | 3.77 | 51,001 | 100,000 |
| OR.D[6,7] | 51.09 | 980.7 | 21.95 | 0.1649 | 0.9436 | 28.15 | 51,001 | 100,000 |
| OR.D[6,8] | 0.9692 | 0.419 | 0.006677 | 0.399 | 0.8962 | 1.974 | 51,001 | 100,000 |
| OR.D[6,9] | 1.261 | 1.79 | 0.01434 | 0.2964 | 1.01 | 3.552 | 51,001 | 100,000 |
| OR.D[6,10] | 0.6732 | 1.755 | 0.03503 | 0.008585 | 0.2545 | 3.894 | 51,001 | 100,000 |
| OR.D[7,8] | 1.511 | 2.605 | 0.04271 | 0.0287 | 0.9467 | 6.442 | 51,001 | 100,000 |
| OR.D[7,9] | 1.693 | 2.819 | 0.04429 | 0.03419 | 1.07 | 7.002 | 51,001 | 100,000 |
| OR.D[7,10] | 0.5852 | 1.228 | 0.02428 | 0.004288 | 0.2484 | 3.305 | 51,001 | 100,000 |
| OR.D[8,9] | 1.557 | 3.091 | 0.02495 | 0.2675 | 1.11 | 5.031 | 51,001 | 100,000 |
| OR.D[8,10] | 0.8188 | 2.603 | 0.04028 | 0.009494 | 0.2793 | 4.781 | 51,001 | 100,000 |
| OR.D[9,10] | 0.7617 | 3.158 | 0.04598 | 0.007292 | 0.2495 | 4.548 | 51,001 | 100,000 |
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| OR[1,2] | 152 | 4922 | 87.87 | 0.008968 | 0.4497 | 31.84 | 51,001 | 100,000 |
| OR[1,3] | 150.8 | 3586 | 68.23 | 0.4545 | 1.596 | 47.92 | 51,001 | 100,000 |
| OR[1,4] | 1.217 | 0.6273 | 0.01446 | 0.3597 | 1.111 | 2.71 | 51,001 | 100,000 |
| OR[1,5] | 1.72 | 0.8848 | 0.01686 | 0.6758 | 1.553 | 3.743 | 51,001 | 100,000 |
| OR[1,6] | 73.78 | 1696 | 31.3 | 0.3077 | 1.379 | 31.95 | 51,001 | 100,000 |
| OR[1,7] | 0.6071 | 0.6553 | 0.009367 | 0.1033 | 0.4765 | 1.792 | 51,001 | 100,000 |
| OR[1,8] | 1.613 | 1.243 | 0.02013 | 0.4567 | 1.365 | 4.242 | 51,001 | 100,000 |
| OR[1,9] | 1.454 | 0.9819 | 0.02283 | 0.389 | 1.23 | 3.832 | 51,001 | 100,000 |
| OR[1,10] | 73.75 | 1239 | 32.56 | 0.2699 | 1.13 | 32.32 | 51,001 | 100,000 |
| OR[1,11] | 1.401 | 1.288 | 0.02571 | 0.2702 | 1.102 | 4.305 | 51,001 | 100,000 |
| OR[1,12] | 1.534 | 1.585 | 0.01918 | 0.3576 | 1.245 | 4.265 | 51,001 | 100,000 |
| OR[1,13] | 1.471 | 0.689 | 0.01231 | 0.6171 | 1.345 | 3.052 | 51,001 | 100,000 |
| OR[1,14] | 0.7989 | 2.118 | 0.04562 | 0.01122 | 0.3155 | 4.512 | 51,001 | 100,000 |
| OR[2,3] | 34.22 | 264 | 10.73 | 0.2374 | 3.935 | 156.5 | 51,001 | 100,000 |
| OR[2,4] | 18.5 | 134.4 | 2.619 | 0.02751 | 2.502 | 122.5 | 51,001 | 100,000 |
| OR[2,5] | 32.51 | 244.1 | 9.505 | 0.05415 | 3.514 | 165.2 | 51,001 | 100,000 |
| OR[2,6] | 23.97 | 159.1 | 4.641 | 0.1471 | 3.286 | 138.2 | 51,001 | 100,000 |
| OR[2,7] | 11.11 | 83.76 | 2.895 | 0.01178 | 1.078 | 63.15 | 51,001 | 100,000 |
| OR[2,8] | 28.7 | 224 | 4.765 | 0.04023 | 3.027 | 173.3 | 51,001 | 100,000 |
| OR[2,9] | 23.47 | 169 | 3.246 | 0.0359 | 2.674 | 154.7 | 51,001 | 100,000 |
| OR[2,10] | 17.79 | 105.6 | 3.952 | 0.1951 | 2.643 | 96.55 | 51,001 | 100,000 |
| OR[2,11] | 22.5 | 164.5 | 2.995 | 0.02847 | 2.397 | 154.9 | 51,001 | 100,000 |
| OR[2,12] | 27.55 | 231.1 | 4.559 | 0.03399 | 2.699 | 168.1 | 51,001 | 100,000 |
| OR[2,13] | 27.22 | 192.5 | 7.15 | 0.04512 | 3.027 | 143.9 | 51,001 | 100,000 |
| OR[2,14] | 10 | 88.01 | 1.697 | 0.006203 | 0.6522 | 58.37 | 51,001 | 100,000 |
| OR[3,4] | 0.7975 | 0.8508 | 0.01561 | 0.01678 | 0.7818 | 2.066 | 51,001 | 100,000 |
| OR[3,5] | 1.117 | 1.496 | 0.02527 | 0.03745 | 0.9739 | 3.523 | 51,001 | 100,000 |
| OR[3,6] | 0.998 | 1.358 | 0.01299 | 0.1535 | 0.905 | 2.805 | 51,001 | 100,000 |
| OR[3,7] | 0.4126 | 0.6574 | 0.01098 | 0.008698 | 0.2753 | 1.595 | 51,001 | 100,000 |
| OR[3,8] | 1.143 | 1.597 | 0.02741 | 0.02543 | 0.8109 | 4.296 | 51,001 | 100,000 |
| OR[3,9] | 1.027 | 1.388 | 0.02688 | 0.02361 | 0.7378 | 3.823 | 51,001 | 100,000 |
| OR[3,10] | 0.7776 | 0.6861 | 0.007148 | 0.2685 | 0.6659 | 1.917 | 51,001 | 100,000 |
| OR[3,11] | 0.9895 | 1.62 | 0.02709 | 0.01931 | 0.6511 | 4.049 | 51,001 | 100,000 |
| OR[3,12] | 1.104 | 2.034 | 0.02713 | 0.02211 | 0.7441 | 4.324 | 51,001 | 100,000 |
| OR[3,13] | 0.9643 | 1.043 | 0.02005 | 0.03015 | 0.8941 | 2.856 | 51,001 | 100,000 |
| OR[3,14] | 0.4151 | 0.9116 | 0.01623 | 0.002788 | 0.17 | 2.337 | 51,001 | 100,000 |
| OR[4,5] | 1.757 | 1.566 | 0.03598 | 0.5864 | 1.268 | 5.632 | 51,001 | 100,000 |
| OR[4,6] | 100.8 | 3975 | 44.84 | 0.3373 | 1.112 | 39.76 | 51,001 | 100,000 |
| OR[4,7] | 0.6237 | 0.8566 | 0.01435 | 0.08239 | 0.4301 | 2.36 | 51,001 | 100,000 |
| OR[4,8] | 1.643 | 1.742 | 0.02581 | 0.324 | 1.26 | 5.148 | 51,001 | 100,000 |
| OR[4,9] | 1.459 | 1.268 | 0.02568 | 0.2825 | 1.133 | 4.615 | 51,001 | 100,000 |
| OR[4,10] | 101.5 | 2850 | 47.36 | 0.2779 | 0.9784 | 38.56 | 51,001 | 100,000 |
| OR[4,11] | 1.41 | 1.592 | 0.02855 | 0.202 | 1.021 | 4.845 | 51,001 | 100,000 |
| OR[4,12] | 1.57 | 2.265 | 0.02606 | 0.2494 | 1.15 | 5.256 | 51,001 | 100,000 |
| OR[4,13] | 1.478 | 1.2 | 0.02542 | 0.5054 | 1.121 | 4.393 | 51,001 | 100,000 |
| OR[4,14] | 0.785 | 2.859 | 0.05705 | 0.01034 | 0.2822 | 4.699 | 51,001 | 100,000 |
| OR[5,6] | 45.35 | 1173 | 19.2 | 0.1867 | 0.9605 | 18.74 | 51,001 | 100,000 |
| OR[5,7] | 0.3742 | 0.3079 | 0.004739 | 0.07501 | 0.3054 | 1.066 | 51,001 | 100,000 |
| OR[5,8] | 1.102 | 1.129 | 0.01452 | 0.2359 | 0.8748 | 3.306 | 51,001 | 100,000 |
| OR[5,9] | 1.003 | 1.032 | 0.01642 | 0.1985 | 0.7967 | 3.013 | 51,001 | 100,000 |
| OR[5,10] | 44.66 | 887.9 | 19.56 | 0.1731 | 0.7456 | 17.27 | 51,001 | 100,000 |
| OR[5,11] | 0.9724 | 1.31 | 0.01864 | 0.1458 | 0.7106 | 3.291 | 51,001 | 100,000 |
| OR[5,12] | 1.07 | 1.631 | 0.01582 | 0.1884 | 0.7991 | 3.444 | 51,001 | 100,000 |
| OR[5,13] | 0.9188 | 0.4319 | 0.003572 | 0.4308 | 0.8998 | 1.647 | 51,001 | 100,000 |
| OR[5,14] | 0.5317 | 1.788 | 0.02894 | 0.0069 | 0.2026 | 2.868 | 51,001 | 100,000 |
| OR[6,7] | 0.5237 | 1.113 | 0.01673 | 0.01317 | 0.3253 | 2.155 | 51,001 | 100,000 |
| OR[6,8] | 1.436 | 2.266 | 0.03625 | 0.04136 | 0.9614 | 5.728 | 51,001 | 100,000 |
| OR[6,9] | 1.29 | 1.995 | 0.03352 | 0.03558 | 0.8692 | 5.076 | 51,001 | 100,000 |
| OR[6,10] | 1.13 | 1.371 | 0.02336 | 0.2315 | 0.8161 | 3.98 | 51,001 | 100,000 |
| OR[6,11] | 1.241 | 2.215 | 0.0338 | 0.03067 | 0.7737 | 5.315 | 51,001 | 100,000 |
| OR[6,12] | 1.398 | 2.809 | 0.03729 | 0.03484 | 0.8787 | 5.802 | 51,001 | 100,000 |
| OR[6,13] | 1.247 | 1.877 | 0.03297 | 0.04378 | 0.9897 | 4.4 | 51,001 | 100,000 |
| OR[6,14] | 0.5442 | 1.333 | 0.02444 | 0.003587 | 0.2063 | 3.131 | 51,001 | 100,000 |
| OR[7,8] | 4.067 | 5.741 | 0.07591 | 0.6797 | 2.888 | 14.33 | 51,001 | 100,000 |
| OR[7,9] | 3.969 | 7.597 | 0.09576 | 0.5143 | 2.581 | 15.37 | 51,001 | 100,000 |
| OR[7,10] | 162.5 | 5480 | 72.81 | 0.3688 | 2.529 | 77.18 | 51,001 | 100,000 |
| OR[7,11] | 3.851 | 10.3 | 0.1033 | 0.3951 | 2.334 | 15.66 | 51,001 | 100,000 |
| OR[7,12] | 4.291 | 28.47 | 0.1184 | 0.4971 | 2.638 | 16.23 | 51,001 | 100,000 |
| OR[7,13] | 3.887 | 5.254 | 0.058 | 0.7515 | 2.852 | 12.69 | 51,001 | 100,000 |
| OR[7,14] | 2.209 | 11.24 | 0.1245 | 0.01927 | 0.6745 | 12.7 | 51,001 | 100,000 |
| OR[8,9] | 1.063 | 0.8671 | 0.01063 | 0.2796 | 0.9051 | 2.705 | 51,001 | 100,000 |
| OR[8,10] | 53.63 | 1217 | 23.62 | 0.1463 | 0.8476 | 25.91 | 51,001 | 100,000 |
| OR[8,11] | 1.027 | 1.064 | 0.01292 | 0.1933 | 0.825 | 3.082 | 51,001 | 100,000 |
| OR[8,12] | 1.174 | 21.38 | 0.06714 | 0.2696 | 0.9156 | 3.015 | 51,001 | 100,000 |
| OR[8,13] | 1.235 | 1.519 | 0.01609 | 0.2701 | 0.9917 | 3.478 | 51,001 | 100,000 |
| OR[8,14] | 0.6488 | 2.325 | 0.03773 | 0.007115 | 0.2285 | 3.77 | 51,001 | 100,000 |
| OR[9,10] | 51.09 | 980.7 | 21.95 | 0.1649 | 0.9436 | 28.15 | 51,001 | 100,000 |
| OR[9,11] | 0.9692 | 0.419 | 0.006677 | 0.399 | 0.8962 | 1.974 | 51,001 | 100,000 |
| OR[9,12] | 1.261 | 1.79 | 0.01434 | 0.2964 | 1.01 | 3.552 | 51,001 | 100,000 |
| OR[9,13] | 1.413 | 1.623 | 0.024 | 0.2926 | 1.088 | 4.286 | 51,001 | 100,000 |
| OR[9,14] | 0.6732 | 1.755 | 0.03503 | 0.008585 | 0.2545 | 3.894 | 51,001 | 100,000 |
| OR[10,11] | 1.511 | 2.605 | 0.04271 | 0.0287 | 0.9467 | 6.442 | 51,001 | 100,000 |
| OR[10,12] | 1.693 | 2.819 | 0.04429 | 0.03419 | 1.07 | 7.002 | 51,001 | 100,000 |
| OR[10,13] | 1.496 | 1.557 | 0.0339 | 0.04613 | 1.2 | 4.728 | 51,001 | 100,000 |
| OR[10,14] | 0.5852 | 1.228 | 0.02428 | 0.004288 | 0.2484 | 3.305 | 51,001 | 100,000 |
| OR[11,12] | 1.557 | 3.091 | 0.02495 | 0.2675 | 1.11 | 5.031 | 51,001 | 100,000 |
| OR[11,13] | 1.732 | 3.124 | 0.03549 | 0.2743 | 1.219 | 5.876 | 51,001 | 100,000 |
| OR[11,14] | 0.8188 | 2.603 | 0.04028 | 0.009494 | 0.2793 | 4.781 | 51,001 | 100,000 |
| OR[12,13] | 1.45 | 2.263 | 0.02083 | 0.26 | 1.089 | 4.543 | 51,001 | 100,000 |
| OR[12,14] | 0.7617 | 3.158 | 0.04598 | 0.007292 | 0.2495 | 4.548 | 51,001 | 100,000 |
| OR[13,14] | 0.6143 | 2.41 | 0.03865 | 0.007926 | 0.2316 | 3.491 | 51,001 | 100,000 |
Median ranks
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk.class[1] | 5.418 | 1.917 | 0.05405 | 2 | 5 | 9 | 51,001 | 100,000 |
| rk.class[2] | 3.984 | 3.344 | 0.1012 | 1 | 2 | 10 | 51,001 | 100,000 |
| rk.class[3] | 7.261 | 2.131 | 0.04101 | 3 | 8 | 10 | 51,001 | 100,000 |
| rk.class[4] | 2.994 | 1.916 | 0.04307 | 1 | 2 | 8 | 51,001 | 100,000 |
| rk.class[5] | 7.046 | 2.182 | 0.04165 | 3 | 7 | 10 | 51,001 | 100,000 |
| rk.class[6] | 6.563 | 2.13 | 0.05017 | 2 | 7 | 10 | 51,001 | 100,000 |
| rk.class[7] | 6.274 | 2.66 | 0.07429 | 2 | 6 | 10 | 51,001 | 100,000 |
| rk.class[8] | 5.941 | 2.536 | 0.06181 | 2 | 6 | 10 | 51,001 | 100,000 |
| rk.class[9] | 6.526 | 2.477 | 0.04874 | 2 | 7 | 10 | 51,001 | 100,000 |
| rk.class[10] | 2.993 | 2.676 | 0.07246 | 1 | 2 | 10 | 51,001 | 100,000 |
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk[1] | 6.415 | 2.601 | 0.07389 | 2 | 6 | 12 | 51,001 | 100,000 |
| rk[2] | 4.926 | 4.714 | 0.1413 | 1 | 2 | 14 | 51,001 | 100,000 |
| rk[3] | 10.39 | 3.102 | 0.07114 | 4 | 11 | 14 | 51,001 | 100,000 |
| rk[4] | 7.418 | 3.237 | 0.07896 | 2 | 7 | 13 | 51,001 | 100,000 |
| rk[5] | 10.12 | 2.676 | 0.05522 | 4 | 10 | 14 | 51,001 | 100,000 |
| rk[6] | 9.112 | 3.418 | 0.07303 | 2 | 10 | 14 | 51,001 | 100,000 |
| rk[7] | 3.345 | 2.514 | 0.0553 | 1 | 3 | 11 | 51,001 | 100,000 |
| rk[8] | 8.995 | 3.442 | 0.06933 | 3 | 9 | 14 | 51,001 | 100,000 |
| rk[9] | 8.296 | 3.405 | 0.08337 | 3 | 8 | 14 | 51,001 | 100,000 |
| rk[10] | 7.695 | 3.817 | 0.1051 | 2 | 7 | 14 | 51,001 | 100,000 |
| rk[11] | 7.492 | 3.872 | 0.09628 | 2 | 7 | 14 | 51,001 | 100,000 |
| rk[12] | 8.291 | 3.806 | 0.07692 | 2 | 8 | 14 | 51,001 | 100,000 |
| rk[13] | 8.951 | 2.766 | 0.05694 | 3 | 9 | 14 | 51,001 | 100,000 |
| rk[14] | 3.546 | 3.729 | 0.09996 | 1 | 2 | 14 | 51,001 | 100,000 |
Children and adolescents: clinical effectiveness (Children’s Yale–Brown Obsessive–Compulsive Scale) – sensitivity analysis 1 (low overall attrition)
See Table 38 for a summary.
| Study | y[,1] | n[,1] | sd[,1] | y[,2] | n[,2] | sd[,2] | y[,3] | n[,3] | sd[,3] | y[,4] | n[,4] | sd[,4] | na[] | out[] | t[,1] | t[,2] | t[,3] | t[,4] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Barrett et al., 2004217 | 24.04 | 24 | 4.14 | 8.36 | 22 | 6.93 | NA | NA | NA | NA | NA | NA | 2 | 2 | 2 | 9 | NA | NA |
| Bolton et al., 2011219 | 23.3 | 24 | 8.3 | 9.5 | 36 | 8 | NA | NA | NA | NA | NA | NA | 2 | 2 | 2 | 9 | NA | NA |
| de Haan et al., 1998220 | 17.6 | 10 | 11.8 | 9.1 | 12 | 9.1 | NA | NA | NA | NA | NA | NA | 2 | 2 | 7 | 8 | NA | NA |
| DeVeaugh-Geiss et al., 1992221 | –2.4 | 29 | NA | –10 | 31 | NA | NA | NA | NA | NA | NA | NA | 2 | 1 | 1 | 7 | NA | NA |
| Liebowitz et al., 2002226 | 18.55 | 22 | 11.44 | 14.71 | 21 | 8.73 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 4 | NA | NA |
| March et al., 1998228 | –3.4 | 95 | 7.99 | –6.8 | 92 | 8.34 | NA | NA | NA | NA | NA | NA | 2 | 1 | 1 | 6 | NA | NA |
| Neziroglu et al., 2000229 | 19.2 | 5 | 3.56 | 16.4 | 5 | 5.18 | NA | NA | NA | NA | NA | NA | 2 | 2 | 5 | 10 | NA | NA |
| Piacentini et al., 2011230 | 17.2 | 22 | 10.04 | 13.3 | 49 | 9.31 | NA | NA | NA | NA | NA | NA | 2 | 2 | 3 | 9 | NA | NA |
| Riddle et al., 1992231 | 14.8 | 6 | 7 | 13.6 | 7 | 5.7 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 4 | NA | NA |
| Storch et al., 2011233 | 18.53 | 15 | 8.11 | 11.13 | 16 | 10.53 | NA | NA | NA | NA | NA | NA | 2 | 2 | 2 | 9 | NA | NA |
| The Pediatric OCD Treatment Study, 2004236 | 21.5 | 28 | 5.4 | 16.5 | 28 | 9.1 | 14 | 28 | 9.5 | 11.2 | 28 | 8.6 | 4 | 2 | 1 | 6 | 9 | 11 |
| Williams et al., 2010235 | 19.6 | 10 | 6.42 | 12.09 | 11 | 7.46 | NA | NA | NA | NA | NA | NA | 2 | 2 | 2 | 9 | NA | NA |
Key
-
Placebo (1).
-
Waitlist (2).
-
Psychological placebo (3).
-
Fluoxetine (4).
-
Fluvoxamine (4).
-
Sertraline (4).
-
Clomipramine (5).
-
BT (6).
-
CBT (7).
-
BT + fluvoxamine (8).
-
CBT + sertraline (9).
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| class.mean.diff[1,2] | 2.471 | 4.254 | 0.04991 | –6.717 | 2.678 | 10.43 | 60,001 | 120,000 |
| class.mean.diff[1,3] | –4.879 | 5.939 | 0.05252 | –16.98 | –4.833 | 6.948 | 60,001 | 120,000 |
| class.mean.diff[1,4] | –3.651 | 4.109 | 0.02343 | –12.37 | –3.65 | 5.012 | 60,001 | 120,000 |
| class.mean.diff[1,5] | –5.281 | 4.024 | 0.02711 | –12.97 | –5.438 | 3.279 | 60,001 | 120,000 |
| class.mean.diff[1,6] | –8.746 | 5.186 | 0.05006 | –19.24 | –8.693 | 1.434 | 60,001 | 120,000 |
| class.mean.diff[1,7] | –8.815 | 3.767 | 0.04254 | –16.67 | –8.731 | –1.379 | 60,001 | 120,000 |
| class.mean.diff[1,8] | 0.2639 | 99.73 | 0.2666 | –195.2 | 0.2606 | 196.1 | 60,001 | 120,000 |
| class.mean.diff[1,9] | –10.37 | 3.942 | 0.0225 | –18.48 | –10.34 | –2.396 | 60,001 | 120,000 |
| class.mean.diff[2,3] | –7.35 | 5.144 | 0.0299 | –17.29 | –7.525 | 3.555 | 60,001 | 120,000 |
| class.mean.diff[2,4] | –6.122 | 5.605 | 0.04701 | –17.24 | –6.272 | 5.586 | 60,001 | 120,000 |
| class.mean.diff[2,5] | –7.752 | 5.155 | 0.04911 | –17.15 | –8.051 | 3.338 | 60,001 | 120,000 |
| class.mean.diff[2,6] | –11.22 | 4.622 | 0.03467 | –20.2 | –11.3 | –1.699 | 60,001 | 120,000 |
| class.mean.diff[2,7] | –11.29 | 2.292 | 0.01522 | –15.49 | –11.43 | –6.302 | 60,001 | 120,000 |
| class.mean.diff[2,8] | –2.207 | 99.82 | 0.2719 | –197.7 | –2.057 | 193.8 | 60,001 | 120,000 |
| class.mean.diff[2,9] | –12.84 | 4.905 | 0.03839 | –22.23 | –13.05 | –2.42 | 60,001 | 120,000 |
| class.mean.diff[3,4] | 1.229 | 6.964 | 0.05114 | –12.77 | 1.218 | 15.34 | 60,001 | 120,000 |
| class.mean.diff[3,5] | –0.4019 | 6.707 | 0.05144 | –13.43 | –0.5988 | 13.56 | 60,001 | 120,000 |
| class.mean.diff[3,6] | –3.867 | 6.664 | 0.04516 | –17.32 | –3.806 | 9.334 | 60,001 | 120,000 |
| class.mean.diff[3,7] | –3.936 | 4.597 | 0.02564 | –13.3 | –3.925 | 5.317 | 60,001 | 120,000 |
| class.mean.diff[3,8] | 5.143 | 99.92 | 0.2723 | –190.4 | 5.036 | 201.1 | 60,001 | 120,000 |
| class.mean.diff[3,9] | –5.492 | 6.376 | 0.04277 | –18.37 | –5.508 | 7.428 | 60,001 | 120,000 |
| class.mean.diff[4,5] | –1.63 | 5.688 | 0.03357 | –12.95 | –1.782 | 10.29 | 60,001 | 120,000 |
| class.mean.diff[4,6] | –5.095 | 6.439 | 0.04859 | –18.23 | –5.069 | 7.824 | 60,001 | 120,000 |
| class.mean.diff[4,7] | –5.165 | 5.235 | 0.04034 | –15.99 | –5.112 | 5.531 | 60,001 | 120,000 |
| class.mean.diff[4,8] | 3.915 | 99.81 | 0.2666 | –191.6 | 3.966 | 199.8 | 60,001 | 120,000 |
| class.mean.diff[4,9] | –6.72 | 5.336 | 0.02461 | –17.73 | –6.691 | 4.15 | 60,001 | 120,000 |
| class.mean.diff[5,6] | –3.465 | 4.932 | 0.04626 | –13.73 | –3.342 | 5.82 | 60,001 | 120,000 |
| class.mean.diff[5,7] | –3.534 | 4.916 | 0.04128 | –13.94 | –3.353 | 5.827 | 60,001 | 120,000 |
| class.mean.diff[5,8] | 5.545 | 99.8 | 0.2687 | –190.2 | 5.557 | 201.4 | 60,001 | 120,000 |
| class.mean.diff[5,9] | –5.09 | 5.429 | 0.03003 | –16.57 | –4.93 | 5.561 | 60,001 | 120,000 |
| class.mean.diff[6,7] | –0.06935 | 4.832 | 0.03434 | –9.674 | –0.08316 | 9.604 | 60,001 | 120,000 |
| class.mean.diff[6,8] | 9.01 | 99.88 | 0.2713 | –186.5 | 9.135 | 205.2 | 60,001 | 120,000 |
| class.mean.diff[6,9] | –1.625 | 6.011 | 0.04339 | –13.52 | –1.671 | 10.61 | 60,001 | 120,000 |
| class.mean.diff[7,8] | 9.079 | 99.81 | 0.2712 | –186.3 | 9.163 | 204.8 | 60,001 | 120,000 |
| class.mean.diff[7,9] | –1.556 | 4.423 | 0.03107 | –10.42 | –1.609 | 7.512 | 60,001 | 120,000 |
| class.mean.diff[8,9] | –10.64 | 99.8 | 0.2678 | –206.6 | –10.73 | 185 | 60,001 | 120,000 |
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| treat.mean.diff[1,2] | 2.471 | 4.254 | 0.04991 | –6.717 | 2.678 | 10.43 | 60,001 | 120,000 |
| treat.mean.diff[1,3] | –4.879 | 5.939 | 0.05252 | –16.98 | –4.833 | 6.948 | 60,001 | 120,000 |
| treat.mean.diff[1,4] | –3.182 | 2.968 | 0.02477 | –9.123 | –3.215 | 2.866 | 60,001 | 120,000 |
| treat.mean.diff[1,5] | –3.642 | 6.385 | 0.02701 | –17.44 | –3.651 | 10.31 | 60,001 | 120,000 |
| treat.mean.diff[1,6] | –4.095 | 2.574 | 0.01928 | –9.473 | –4.04 | 1.102 | 60,001 | 120,000 |
| treat.mean.diff[1,7] | –5.281 | 4.024 | 0.02711 | –12.97 | –5.438 | 3.279 | 60,001 | 120,000 |
| treat.mean.diff[1,8] | –8.746 | 5.186 | 0.05006 | –19.24 | –8.693 | 1.434 | 60,001 | 120,000 |
| treat.mean.diff[1,9] | –8.815 | 3.767 | 0.04254 | –16.67 | –8.731 | –1.379 | 60,001 | 120,000 |
| treat.mean.diff[1,10] | 0.2639 | 99.73 | 0.2666 | –195.2 | 0.2606 | 196.1 | 60,001 | 120,000 |
| treat.mean.diff[1,11] | –10.37 | 3.942 | 0.0225 | –18.48 | –10.34 | –2.396 | 60,001 | 120,000 |
| treat.mean.diff[2,3] | –7.35 | 5.144 | 0.0299 | –17.29 | –7.525 | 3.555 | 60,001 | 120,000 |
| treat.mean.diff[2,4] | –5.653 | 5.001 | 0.05007 | –15.18 | –5.845 | 4.865 | 60,001 | 120,000 |
| treat.mean.diff[2,5] | –6.113 | 7.448 | 0.04875 | –21.47 | –6.269 | 9.754 | 60,001 | 120,000 |
| treat.mean.diff[2,6] | –6.566 | 4.444 | 0.04359 | –14.99 | –6.748 | 2.867 | 60,001 | 120,000 |
| treat.mean.diff[2,7] | –7.752 | 5.155 | 0.04911 | –17.15 | –8.051 | 3.338 | 60,001 | 120,000 |
| treat.mean.diff[2,8] | –11.22 | 4.622 | 0.03467 | –20.2 | –11.3 | –1.699 | 60,001 | 120,000 |
| treat.mean.diff[2,9] | –11.29 | 2.292 | 0.01522 | –15.49 | –11.43 | –6.302 | 60,001 | 120,000 |
| treat.mean.diff[2,10] | –2.207 | 99.82 | 0.2719 | –197.7 | –2.057 | 193.8 | 60,001 | 120,000 |
| treat.mean.diff[2,11] | –12.84 | 4.905 | 0.03839 | –22.23 | –13.05 | –2.42 | 60,001 | 120,000 |
| treat.mean.diff[3,4] | 1.697 | 6.507 | 0.05416 | –11.24 | 1.662 | 14.9 | 60,001 | 120,000 |
| treat.mean.diff[3,5] | 1.237 | 8.525 | 0.05203 | –16.21 | 1.204 | 18.89 | 60,001 | 120,000 |
| treat.mean.diff[3,6] | 0.784 | 6.073 | 0.04761 | –11.36 | 0.7809 | 13.12 | 60,001 | 120,000 |
| treat.mean.diff[3,7] | –0.4019 | 6.707 | 0.05144 | –13.43 | –0.5988 | 13.56 | 60,001 | 120,000 |
| treat.mean.diff[3,8] | –3.867 | 6.664 | 0.04516 | –17.32 | –3.806 | 9.334 | 60,001 | 120,000 |
| treat.mean.diff[3,9] | –3.936 | 4.597 | 0.02564 | –13.3 | –3.925 | 5.317 | 60,001 | 120,000 |
| treat.mean.diff[3,10] | 5.143 | 99.92 | 0.2723 | –190.4 | 5.036 | 201.1 | 60,001 | 120,000 |
| treat.mean.diff[3,11] | –5.492 | 6.376 | 0.04277 | –18.37 | –5.508 | 7.428 | 60,001 | 120,000 |
| treat.mean.diff[4,5] | –0.4598 | 6.181 | 0.01977 | –14.4 | –0.1438 | 13.03 | 60,001 | 120,000 |
| treat.mean.diff[4,6] | –0.913 | 3.208 | 0.02058 | –7.98 | –0.5303 | 5.333 | 60,001 | 120,000 |
| treat.mean.diff[4,7] | –2.099 | 4.957 | 0.03573 | –11.63 | –2.261 | 8.27 | 60,001 | 120,000 |
| treat.mean.diff[4,8] | –5.564 | 5.862 | 0.05201 | –17.46 | –5.511 | 5.995 | 60,001 | 120,000 |
| treat.mean.diff[4,9] | –5.633 | 4.583 | 0.0439 | –15.09 | –5.557 | 3.418 | 60,001 | 120,000 |
| treat.mean.diff[4,10] | 3.446 | 99.76 | 0.2674 | –192.1 | 3.492 | 199 | 60,001 | 120,000 |
| treat.mean.diff[4,11] | –7.189 | 4.714 | 0.02868 | –16.81 | –7.143 | 2.24 | 60,001 | 120,000 |
| treat.mean.diff[5,6] | –0.4533 | 6.174 | 0.01938 | –14.45 | –0.1494 | 13.01 | 60,001 | 120,000 |
| treat.mean.diff[5,7] | –1.639 | 7.493 | 0.03619 | –17.22 | –1.765 | 14.15 | 60,001 | 120,000 |
| treat.mean.diff[5,8] | –5.104 | 8.093 | 0.05014 | –21.92 | –5.037 | 11.51 | 60,001 | 120,000 |
| treat.mean.diff[5,9] | –5.173 | 7.174 | 0.04209 | –20.44 | –5.091 | 9.874 | 60,001 | 120,000 |
| treat.mean.diff[5,10] | 3.906 | 99.94 | 0.2665 | –191.8 | 3.929 | 199.6 | 60,001 | 120,000 |
| treat.mean.diff[5,11] | –6.729 | 7.247 | 0.02775 | –22.07 | –6.672 | 8.425 | 60,001 | 120,000 |
| treat.mean.diff[6,7] | –1.186 | 4.666 | 0.0301 | –10.21 | –1.375 | 8.722 | 60,001 | 120,000 |
| treat.mean.diff[6,8] | –4.651 | 5.503 | 0.04559 | –15.79 | –4.608 | 6.166 | 60,001 | 120,000 |
| treat.mean.diff[6,9] | –4.72 | 3.962 | 0.03644 | –12.9 | –4.687 | 3.202 | 60,001 | 120,000 |
| treat.mean.diff[6,10] | 4.359 | 99.76 | 0.266 | –191 | 4.419 | 200.1 | 60,001 | 120,000 |
| treat.mean.diff[6,11] | –6.276 | 4.071 | 0.01856 | –14.61 | –6.278 | 2.007 | 60,001 | 120,000 |
| treat.mean.diff[7,8] | –3.465 | 4.932 | 0.04626 | –13.73 | –3.342 | 5.82 | 60,001 | 120,000 |
| treat.mean.diff[7,9] | –3.534 | 4.916 | 0.04128 | –13.94 | –3.353 | 5.827 | 60,001 | 120,000 |
| treat.mean.diff[7,10] | 5.545 | 99.8 | 0.2687 | –190.2 | 5.557 | 201.4 | 60,001 | 120,000 |
| treat.mean.diff[7,11] | –5.09 | 5.429 | 0.03003 | –16.57 | –4.93 | 5.561 | 60,001 | 120,000 |
| treat.mean.diff[8,9] | –0.06935 | 4.832 | 0.03434 | –9.674 | –0.08316 | 9.604 | 60,001 | 120,000 |
| treat.mean.diff[8,10] | 9.01 | 99.88 | 0.2713 | –186.5 | 9.135 | 205.2 | 60,001 | 120,000 |
| treat.mean.diff[8,11] | –1.625 | 6.011 | 0.04339 | –13.52 | –1.671 | 10.61 | 60,001 | 120,000 |
| treat.mean.diff[9,10] | 9.079 | 99.81 | 0.2712 | –186.3 | 9.163 | 204.8 | 60,001 | 120,000 |
| treat.mean.diff[9,11] | –1.556 | 4.423 | 0.03107 | –10.42 | –1.609 | 7.512 | 60,001 | 120,000 |
| treat.mean.diff[10,11] | –10.64 | 99.8 | 0.2678 | –206.6 | –10.73 | 185 | 60,001 | 120,000 |
Median ranks
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk.class[1] | 7.268 | 1.042 | 0.00809 | 5 | 7 | 9 | 60,001 | 120,000 |
| rk.class[2] | 7.974 | 1.049 | 0.008874 | 5 | 8 | 9 | 60,001 | 120,000 |
| rk.class[3] | 5.095 | 1.939 | 0.01367 | 1 | 5 | 9 | 60,001 | 120,000 |
| rk.class[4] | 5.551 | 1.746 | 0.01018 | 2 | 6 | 9 | 60,001 | 120,000 |
| rk.class[5] | 4.854 | 1.675 | 0.01267 | 2 | 5 | 8 | 60,001 | 120,000 |
| rk.class[6] | 3.335 | 1.728 | 0.01424 | 1 | 3 | 7 | 60,001 | 120,000 |
| rk.class[7] | 3.156 | 1.264 | 0.009132 | 1 | 3 | 6 | 60,001 | 120,000 |
| rk.class[8] | 5.168 | 3.9 | 0.01086 | 1 | 7 | 9 | 60,001 | 120,000 |
| rk.class[9] | 2.598 | 1.455 | 0.009453 | 1 | 2 | 6 | 60,001 | 120,000 |
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk[1] | 9.028 | 1.221 | 0.00986 | 6 | 9 | 11 | 60,001 | 120,000 |
| rk[2] | 9.741 | 1.4 | 0.01252 | 6 | 10 | 11 | 60,001 | 120,000 |
| rk[3] | 5.932 | 2.619 | 0.02003 | 1 | 6 | 10 | 60,001 | 120,000 |
| rk[4] | 6.881 | 1.901 | 0.01429 | 3 | 7 | 10 | 60,001 | 120,000 |
| rk[5] | 6.491 | 2.716 | 0.01087 | 1 | 7 | 11 | 60,001 | 120,000 |
| rk[6] | 6.311 | 1.659 | 0.009755 | 3 | 6 | 9 | 60,001 | 120,000 |
| rk[7] | 5.552 | 2.245 | 0.01702 | 2 | 5 | 10 | 60,001 | 120,000 |
| rk[8] | 3.706 | 2.199 | 0.0186 | 1 | 3 | 9 | 60,001 | 120,000 |
| rk[9] | 3.397 | 1.542 | 0.01208 | 1 | 3 | 7 | 60,001 | 120,000 |
| rk[10] | 6.2 | 4.881 | 0.01359 | 1 | 9 | 11 | 60,001 | 120,000 |
| rk[11] | 2.76 | 1.678 | 0.01035 | 1 | 2 | 7 | 60,001 | 120,000 |
Children and adolescents: clinical effectiveness (Children’s Yale–Brown Obsessive–Compulsive Scale) – sensitivity analysis 2 (incomplete outcome data)
See Table 39 for a summary.
| Study | y[,1] | n[,1] | sd[,1] | y[,2] | n[,2] | sd[,2] | y[,3] | n[,3] | sd[,3] | y[,4] | n[,4] | sd[,4] | na[] | out[] | t[,1] | t[,2] | t[,3] | t[,4] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Bolton and Perrin, 2008218 | 21.1 | 10 | 5.9 | 13.9 | 10 | 10.74 | NA | NA | NA | NA | NA | NA | 2 | 2 | 2 | 8 | NA | NA |
| Bolton et al., 2011219 | 23.3 | 24 | 8.3 | 9.5 | 36 | 8 | NA | NA | NA | NA | NA | NA | 2 | 2 | 2 | 9 | NA | NA |
| de Haan et al., 1998220 | 17.6 | 10 | 11.8 | 9.1 | 12 | 9.1 | NA | NA | NA | NA | NA | NA | 2 | 2 | 7 | 8 | NA | NA |
| DeVeaugh-Geiss et al., 1992221 | –2.4 | 29 | NA | –10 | 31 | NA | NA | NA | NA | NA | NA | NA | 2 | 1 | 1 | 7 | NA | NA |
| Freeman et al., 2008223 | 17.1 | 20 | 7.57 | 14.45 | 22 | 8.16 | NA | NA | NA | NA | NA | NA | 2 | 2 | 3 | 9 | NA | NA |
| Geller et al., 2001224 | –5.2 | 32 | 7.4 | –9.5 | 71 | 9.2 | NA | NA | NA | NA | NA | NA | 2 | 1 | 1 | 4 | NA | NA |
| Liebowitz et al., 2002226 | 18.55 | 22 | 11.44 | 14.71 | 21 | 8.73 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 4 | NA | NA |
| March et al., 1998228 | –3.4 | 95 | 7.99 | –6.8 | 92 | 8.34 | NA | NA | NA | NA | NA | NA | 2 | 1 | 1 | 6 | NA | NA |
| Piacentini et al., 2011230 | 17.2 | 22 | 10.04 | 13.3 | 49 | 9.31 | NA | NA | NA | NA | NA | NA | 2 | 2 | 3 | 9 | NA | NA |
| Riddle et al., 1992231 | 14.8 | 6 | 7 | 13.6 | 7 | 5.7 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 4 | NA | NA |
| Riddle et al., 2001232 | 20.9 | 63 | 8.5 | 18.2 | 57 | 8.6 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 5 | NA | NA |
| Storch et al., 2011233 | 18.53 | 15 | 8.11 | 11.13 | 16 | 10.53 | NA | NA | NA | NA | NA | NA | 2 | 2 | 2 | 9 | NA | NA |
| Storch et al., 2013234 | 15.43 | 14 | 9.72 | 15.56 | 16 | 6.62 | NA | NA | NA | NA | NA | NA | 2 | 2 | 11 | 12 | NA | NA |
| The Pediatric OCD Treatment Study, 2004236 | 21.5 | 28 | 5.4 | 16.5 | 28 | 9.1 | 14 | 28 | 9.5 | 11.2 | 28 | 8.6 | 4 | 2 | 1 | 6 | 9 | 11 |
| Williams et al., 2010235 | 19.6 | 10 | 6.42 | 12.09 | 11 | 7.46 | NA | NA | NA | NA | NA | NA | 2 | 2 | 2 | 9 | NA | NA |
Key: intervention (class)
-
Placebo (1).
-
Waitlist (2).
-
Psychological placebo (3).
-
Fluoxetine (4).
-
Fluvoxamine (4).
-
Sertraline (4).
-
Clomipramine (5).
-
BT (6).
-
CBT (7).
-
BT + fluvoxamine (8).
-
CBT + sertraline (9).
-
CBT + placebo (10).
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| class.mean.diff[1,2] | 1.363 | 3.049 | 0.05907 | –5.013 | 1.444 | 7.121 | 60,001 | 120,000 |
| class.mean.diff[1,3] | –5.085 | 3.408 | 0.06288 | –11.91 | –5.098 | 1.569 | 60,001 | 120,000 |
| class.mean.diff[1,4] | –3.548 | 2.208 | 0.01677 | –8.156 | –3.565 | 1.161 | 60,001 | 120,000 |
| class.mean.diff[1,5] | –6.145 | 2.705 | 0.03675 | –11.25 | –6.214 | –0.5892 | 60,001 | 120,000 |
| class.mean.diff[1,6] | –9.581 | 4.048 | 0.07981 | –17.62 | –9.588 | –1.608 | 60,001 | 120,000 |
| class.mean.diff[1,7] | –8.365 | 2.526 | 0.0484 | –13.52 | –8.269 | –3.482 | 60,001 | 120,000 |
| class.mean.diff[1,8] | 0.4373 | 100.3 | 0.2885 | –195.9 | 0.2245 | 197.4 | 60,001 | 120,000 |
| class.mean.diff[1,9] | –10.23 | 2.556 | 0.03305 | –15.4 | –10.18 | –5.203 | 60,001 | 120,000 |
| class.mean.diff[1,10] | –10.06 | 4.455 | 0.06724 | –18.84 | –10.04 | –1.324 | 60,001 | 120,000 |
| class.mean.diff[2,3] | –6.448 | 2.971 | 0.04237 | –12.22 | –6.502 | –0.4866 | 60,001 | 120,000 |
| class.mean.diff[2,4] | –4.911 | 3.642 | 0.05624 | –11.91 | –5.009 | 2.769 | 60,001 | 120,000 |
| class.mean.diff[2,5] | –7.508 | 3.7 | 0.06175 | –14.38 | –7.615 | 0.277 | 60,001 | 120,000 |
| class.mean.diff[2,6] | –10.94 | 3.667 | 0.06444 | –18.06 | –10.93 | –3.692 | 60,001 | 120,000 |
| class.mean.diff[2,7] | –9.727 | 1.92 | 0.02752 | –13.36 | –9.745 | –5.811 | 60,001 | 120,000 |
| class.mean.diff[2,8] | –0.9256 | 100.3 | 0.294 | –197.3 | –1.027 | 195.9 | 60,001 | 120,000 |
| class.mean.diff[2,9] | –11.59 | 3.526 | 0.05615 | –18.31 | –11.63 | –4.384 | 60,001 | 120,000 |
| class.mean.diff[2,10] | –11.42 | 5.085 | 0.07934 | –21.21 | –11.46 | –1.213 | 60,001 | 120,000 |
| class.mean.diff[3,4] | 1.537 | 3.955 | 0.062 | –6.206 | 1.52 | 9.541 | 60,001 | 120,000 |
| class.mean.diff[3,5] | –1.06 | 4.09 | 0.06442 | –8.793 | –1.139 | 7.256 | 60,001 | 120,000 |
| class.mean.diff[3,6] | –4.496 | 4.464 | 0.07391 | –13.16 | –4.444 | 4.25 | 60,001 | 120,000 |
| class.mean.diff[3,7] | –3.279 | 2.249 | 0.03004 | –7.671 | –3.273 | 1.118 | 60,001 | 120,000 |
| class.mean.diff[3,8] | 5.523 | 100.3 | 0.2939 | –190.7 | 5.457 | 202.6 | 60,001 | 120,000 |
| class.mean.diff[3,9] | –5.142 | 3.815 | 0.05885 | –12.49 | –5.151 | 2.435 | 60,001 | 120,000 |
| class.mean.diff[3,10] | –4.97 | 5.277 | 0.07936 | –15.19 | –4.989 | 5.491 | 60,001 | 120,000 |
| class.mean.diff[4,5] | –2.597 | 3.469 | 0.0402 | –9.328 | –2.655 | 4.54 | 60,001 | 120,000 |
| class.mean.diff[4,6] | –6.033 | 4.535 | 0.07846 | –15.04 | –6.033 | 2.981 | 60,001 | 120,000 |
| class.mean.diff[4,7] | –4.816 | 3.221 | 0.04684 | –11.51 | –4.736 | 1.559 | 60,001 | 120,000 |
| class.mean.diff[4,8] | 3.986 | 100.3 | 0.2891 | –192.4 | 3.761 | 201.1 | 60,001 | 120,000 |
| class.mean.diff[4,9] | –6.68 | 3.239 | 0.03296 | –13.41 | –6.659 | –0.1466 | 60,001 | 120,000 |
| class.mean.diff[4,10] | –6.507 | 4.878 | 0.06746 | –16.16 | –6.535 | 3.121 | 60,001 | 120,000 |
| class.mean.diff[5,6] | –3.436 | 3.95 | 0.07453 | –11.41 | –3.362 | 4.149 | 60,001 | 120,000 |
| class.mean.diff[5,7] | –2.219 | 3.42 | 0.05284 | –9.22 | –2.15 | 4.204 | 60,001 | 120,000 |
| class.mean.diff[5,8] | 6.583 | 100.3 | 0.2923 | –189.9 | 6.298 | 203.6 | 60,001 | 120,000 |
| class.mean.diff[5,9] | –4.083 | 3.628 | 0.0451 | –11.48 | –4.054 | 2.863 | 60,001 | 120,000 |
| class.mean.diff[5,10] | –3.91 | 5.151 | 0.07278 | –14.44 | –3.836 | 5.87 | 60,001 | 120,000 |
| class.mean.diff[6,7] | 1.216 | 3.842 | 0.06653 | –6.371 | 1.209 | 8.742 | 60,001 | 120,000 |
| class.mean.diff[6,8] | 10.02 | 100.4 | 0.2999 | –186.6 | 9.879 | 207 | 60,001 | 120,000 |
| class.mean.diff[6,9] | –0.6469 | 4.525 | 0.07643 | –9.481 | –0.5944 | 8.237 | 60,001 | 120,000 |
| class.mean.diff[6,10] | –0.474 | 5.83 | 0.09455 | –11.89 | –0.4557 | 11.04 | 60,001 | 120,000 |
| class.mean.diff[7,8] | 8.802 | 100.3 | 0.2931 | –187.7 | 8.671 | 205.9 | 60,001 | 120,000 |
| class.mean.diff[7,9] | –1.863 | 3.047 | 0.04461 | –7.749 | –1.912 | 4.25 | 60,001 | 120,000 |
| class.mean.diff[7,10] | –1.691 | 4.754 | 0.07025 | –11.01 | –1.702 | 7.813 | 60,001 | 120,000 |
| class.mean.diff[8,9] | –10.67 | 100.3 | 0.2919 | –207.5 | –10.56 | 185.8 | 60,001 | 120,000 |
| class.mean.diff[8,10] | –10.49 | 100.4 | 0.2988 | –207.9 | –10.35 | 185.9 | 60,001 | 120,000 |
| class.mean.diff[9,10] | 0.1729 | 3.673 | 0.05314 | –7.111 | 0.1936 | 7.347 | 60,001 | 120,000 |
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| treat.mean.diff[1,2] | 1.363 | 3.049 | 0.05907 | –5.013 | 1.444 | 7.121 | 60,001 | 120,000 |
| treat.mean.diff[1,3] | –5.085 | 3.408 | 0.06288 | –11.91 | –5.098 | 1.569 | 60,001 | 120,000 |
| treat.mean.diff[1,4] | –3.59 | 1.493 | 0.02012 | –6.527 | –3.608 | –0.5575 | 60,001 | 120,000 |
| treat.mean.diff[1,5] | –3.21 | 1.824 | 0.01881 | –6.796 | –3.282 | 0.5665 | 60,001 | 120,000 |
| treat.mean.diff[1,6] | –3.849 | 1.457 | 0.01748 | –6.925 | –3.797 | –1.009 | 60,001 | 120,000 |
| treat.mean.diff[1,7] | –6.145 | 2.705 | 0.03675 | –11.25 | –6.214 | –0.5892 | 60,001 | 120,000 |
| treat.mean.diff[1,8] | –9.581 | 4.048 | 0.07981 | –17.62 | –9.588 | –1.608 | 60,001 | 120,000 |
| treat.mean.diff[1,9] | –8.365 | 2.526 | 0.0484 | –13.52 | –8.269 | –3.482 | 60,001 | 120,000 |
| treat.mean.diff[1,10] | 0.4373 | 100.3 | 0.2885 | –195.9 | 0.2245 | 197.4 | 60,001 | 120,000 |
| treat.mean.diff[1,11] | –10.23 | 2.556 | 0.03305 | –15.4 | –10.18 | –5.203 | 60,001 | 120,000 |
| treat.mean.diff[1,12] | –10.06 | 4.455 | 0.06724 | –18.84 | –10.04 | –1.324 | 60,001 | 120,000 |
| treat.mean.diff[2,3] | –6.448 | 2.971 | 0.04237 | –12.22 | –6.502 | –0.4866 | 60,001 | 120,000 |
| treat.mean.diff[2,4] | –4.952 | 3.313 | 0.0598 | –11.14 | –5.064 | 1.913 | 60,001 | 120,000 |
| treat.mean.diff[2,5] | –4.573 | 3.463 | 0.05694 | –11.05 | –4.669 | 2.673 | 60,001 | 120,000 |
| treat.mean.diff[2,6] | –5.212 | 3.132 | 0.05392 | –11.14 | –5.286 | 1.235 | 60,001 | 120,000 |
| treat.mean.diff[2,7] | –7.508 | 3.7 | 0.06175 | –14.38 | –7.615 | 0.277 | 60,001 | 120,000 |
| treat.mean.diff[2,8] | –10.94 | 3.667 | 0.06444 | –18.06 | –10.93 | –3.692 | 60,001 | 120,000 |
| treat.mean.diff[2,9] | –9.727 | 1.92 | 0.02752 | –13.36 | –9.745 | –5.811 | 60,001 | 120,000 |
| treat.mean.diff[2,10] | –0.9256 | 100.3 | 0.294 | –197.3 | –1.027 | 195.9 | 60,001 | 120,000 |
| treat.mean.diff[2,11] | –11.59 | 3.526 | 0.05615 | –18.31 | –11.63 | –4.384 | 60,001 | 120,000 |
| treat.mean.diff[2,12] | –11.42 | 5.085 | 0.07934 | –21.21 | –11.46 | –1.213 | 60,001 | 120,000 |
| treat.mean.diff[3,4] | 1.496 | 3.655 | 0.06534 | –5.54 | 1.487 | 8.809 | 60,001 | 120,000 |
| treat.mean.diff[3,5] | 1.875 | 3.798 | 0.0631 | –5.363 | 1.842 | 9.512 | 60,001 | 120,000 |
| treat.mean.diff[3,6] | 1.236 | 3.49 | 0.05974 | –5.649 | 1.255 | 8.097 | 60,001 | 120,000 |
| treat.mean.diff[3,7] | –1.06 | 4.09 | 0.06442 | –8.793 | –1.139 | 7.256 | 60,001 | 120,000 |
| treat.mean.diff[3,8] | –4.496 | 4.464 | 0.07391 | –13.16 | –4.444 | 4.25 | 60,001 | 120,000 |
| treat.mean.diff[3,9] | –3.279 | 2.249 | 0.03004 | –7.671 | –3.273 | 1.118 | 60,001 | 120,000 |
| treat.mean.diff[3,10] | 5.523 | 100.3 | 0.2939 | –190.7 | 5.457 | 202.6 | 60,001 | 120,000 |
| treat.mean.diff[3,11] | –5.142 | 3.815 | 0.05885 | –12.49 | –5.151 | 2.435 | 60,001 | 120,000 |
| treat.mean.diff[3,12] | –4.97 | 5.277 | 0.07936 | –15.19 | –4.989 | 5.491 | 60,001 | 120,000 |
| treat.mean.diff[4,5] | 0.3796 | 2.009 | 0.02054 | –3.652 | 0.1615 | 4.763 | 60,001 | 120,000 |
| treat.mean.diff[4,6] | –0.2596 | 1.749 | 0.01835 | –4.184 | –0.093 | 3.129 | 60,001 | 120,000 |
| treat.mean.diff[4,7] | –2.556 | 3.06 | 0.04071 | –8.389 | –2.637 | 3.633 | 60,001 | 120,000 |
| treat.mean.diff[4,8] | –5.991 | 4.271 | 0.0814 | –14.44 | –5.982 | 2.48 | 60,001 | 120,000 |
| treat.mean.diff[4,9] | –4.775 | 2.846 | 0.05069 | –10.58 | –4.674 | 0.6795 | 60,001 | 120,000 |
| treat.mean.diff[4,10] | 4.027 | 100.3 | 0.2895 | –192.2 | 3.917 | 200.9 | 60,001 | 120,000 |
| treat.mean.diff[4,11] | –6.638 | 2.862 | 0.03593 | –12.41 | –6.611 | –1.025 | 60,001 | 120,000 |
| treat.mean.diff[4,12] | –6.465 | 4.648 | 0.07035 | –15.64 | –6.48 | 2.628 | 60,001 | 120,000 |
| treat.mean.diff[5,6] | –0.6391 | 1.982 | 0.01744 | –5.16 | –0.3132 | 3.009 | 60,001 | 120,000 |
| treat.mean.diff[5,7] | –2.935 | 3.26 | 0.04117 | –9.154 | –2.966 | 3.687 | 60,001 | 120,000 |
| treat.mean.diff[5,8] | –6.371 | 4.394 | 0.07759 | –15.11 | –6.364 | 2.291 | 60,001 | 120,000 |
| treat.mean.diff[5,9] | –5.154 | 3.018 | 0.04755 | –11.34 | –5.07 | 0.6257 | 60,001 | 120,000 |
| treat.mean.diff[5,10] | 3.647 | 100.3 | 0.2892 | –192.8 | 3.437 | 200.6 | 60,001 | 120,000 |
| treat.mean.diff[5,11] | –7.018 | 3.045 | 0.03503 | –13.23 | –6.992 | –1.057 | 60,001 | 120,000 |
| treat.mean.diff[5,12] | –6.845 | 4.756 | 0.06888 | –16.18 | –6.841 | 2.535 | 60,001 | 120,000 |
| treat.mean.diff[6,7] | –2.296 | 3.041 | 0.04011 | –7.992 | –2.375 | 4.008 | 60,001 | 120,000 |
| treat.mean.diff[6,8] | –5.732 | 4.171 | 0.07775 | –13.95 | –5.759 | 2.71 | 60,001 | 120,000 |
| treat.mean.diff[6,9] | –4.515 | 2.629 | 0.04471 | –9.766 | –4.472 | 0.6213 | 60,001 | 120,000 |
| treat.mean.diff[6,10] | 4.286 | 100.3 | 0.2887 | –192 | 4.05 | 201.2 | 60,001 | 120,000 |
| treat.mean.diff[6,11] | –6.379 | 2.655 | 0.0324 | –11.66 | –6.391 | –1.043 | 60,001 | 120,000 |
| treat.mean.diff[6,12] | –6.206 | 4.519 | 0.0671 | –15.09 | –6.259 | 2.72 | 60,001 | 120,000 |
| treat.mean.diff[7,8] | –3.436 | 3.95 | 0.07453 | –11.41 | –3.362 | 4.149 | 60,001 | 120,000 |
| treat.mean.diff[7,9] | –2.219 | 3.42 | 0.05284 | –9.22 | –2.15 | 4.204 | 60,001 | 120,000 |
| treat.mean.diff[7,10] | 6.583 | 100.3 | 0.2923 | –189.9 | 6.298 | 203.6 | 60,001 | 120,000 |
| treat.mean.diff[7,11] | –4.083 | 3.628 | 0.0451 | –11.48 | –4.054 | 2.863 | 60,001 | 120,000 |
| treat.mean.diff[7,12] | –3.91 | 5.151 | 0.07278 | –14.44 | –3.836 | 5.87 | 60,001 | 120,000 |
| treat.mean.diff[8,9] | 1.216 | 3.842 | 0.06653 | –6.371 | 1.209 | 8.742 | 60,001 | 120,000 |
| treat.mean.diff[8,10] | 10.02 | 100.4 | 0.2999 | –186.6 | 9.879 | 207 | 60,001 | 120,000 |
| treat.mean.diff[8,11] | –0.6469 | 4.525 | 0.07643 | –9.481 | –0.5944 | 8.237 | 60,001 | 120,000 |
| treat.mean.diff[8,12] | –0.474 | 5.83 | 0.09455 | –11.89 | –0.4557 | 11.04 | 60,001 | 120,000 |
| treat.mean.diff[9,10] | 8.802 | 100.3 | 0.2931 | –187.7 | 8.671 | 205.9 | 60,001 | 120,000 |
| treat.mean.diff[9,11] | –1.863 | 3.047 | 0.04461 | –7.749 | –1.912 | 4.25 | 60,001 | 120,000 |
| treat.mean.diff[9,12] | –1.691 | 4.754 | 0.07025 | –11.01 | –1.702 | 7.813 | 60,001 | 120,000 |
| treat.mean.diff[10,11] | –10.67 | 100.3 | 0.2919 | –207.5 | –10.56 | 185.8 | 60,001 | 120,000 |
| treat.mean.diff[10,12] | –10.49 | 100.4 | 0.2988 | –207.9 | –10.35 | 185.9 | 60,001 | 120,000 |
| treat.mean.diff[11,12] | 0.1729 | 3.673 | 0.05314 | –7.111 | 0.1936 | 7.347 | 60,001 | 120,000 |
Median ranks
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk.class[1] | 8.648 | 0.8166 | 0.01045 | 7 | 9 | 10 | 60,001 | 120,000 |
| rk.class[2] | 9.054 | 0.9307 | 0.01243 | 7 | 9 | 10 | 60,001 | 120,000 |
| rk.class[3] | 6.049 | 1.573 | 0.02325 | 3 | 6 | 9 | 60,001 | 120,000 |
| rk.class[4] | 6.821 | 1.339 | 0.01517 | 4 | 7 | 9 | 60,001 | 120,000 |
| rk.class[5] | 5.334 | 1.626 | 0.02244 | 2 | 5 | 8 | 60,001 | 120,000 |
| rk.class[6] | 3.359 | 1.859 | 0.03424 | 1 | 3 | 7 | 60,001 | 120,000 |
| rk.class[7] | 3.873 | 1.331 | 0.01948 | 1 | 4 | 6 | 60,001 | 120,000 |
| rk.class[8] | 5.719 | 4.398 | 0.01267 | 1 | 9 | 10 | 60,001 | 120,000 |
| rk.class[9] | 2.856 | 1.325 | 0.01815 | 1 | 3 | 6 | 60,001 | 120,000 |
| rk.class[10] | 3.287 | 1.987 | 0.02956 | 1 | 3 | 8 | 60,001 | 120,000 |
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk[1] | 10.63 | 0.8384 | 0.01047 | 9 | 11 | 12 | 60,001 | 120,000 |
| rk[2] | 10.93 | 1.222 | 0.01717 | 7 | 11 | 12 | 60,001 | 120,000 |
| rk[3] | 6.699 | 2.218 | 0.0375 | 3 | 6 | 11 | 60,001 | 120,000 |
| rk[4] | 7.809 | 1.556 | 0.02128 | 4 | 8 | 10 | 60,001 | 120,000 |
| rk[5] | 8.164 | 1.645 | 0.01718 | 5 | 8 | 11 | 60,001 | 120,000 |
| rk[6] | 7.589 | 1.473 | 0.01721 | 4 | 8 | 10 | 60,001 | 120,000 |
| rk[7] | 5.689 | 2.069 | 0.02781 | 2 | 6 | 10 | 60,001 | 120,000 |
| rk[8] | 3.501 | 2.162 | 0.04068 | 1 | 3 | 9 | 60,001 | 120,000 |
| rk[9] | 3.935 | 1.45 | 0.02115 | 1 | 4 | 7 | 60,001 | 120,000 |
| rk[10] | 6.75 | 5.384 | 0.01547 | 1 | 11 | 12 | 60,001 | 120,000 |
| rk[11] | 2.872 | 1.381 | 0.0184 | 1 | 3 | 6 | 60,001 | 120,000 |
| rk[12] | 3.426 | 2.298 | 0.03362 | 1 | 3 | 10 | 60,001 | 120,000 |
Children and adolescents: clinical effectiveness (Children’s Yale–Brown Obsessive–Compulsive Scale) – sensitivity analysis 3 (blinding)
See Table 40 for a summary.
| Study | y[,1] | n[,1] | sd[,1] | y[,2] | n[,2] | sd[,2] | y[,3] | n[,3] | sd[,3] | y[,4] | n[,4] | sd[,4] | na[] | out[] | t[,1] | t[,2] | t[,3] | t[,4] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Bolton et al., 2011219 | 23.3 | 24 | 8.3 | 9.5 | 36 | 8 | NA | NA | NA | NA | NA | NA | 2 | 2 | 2 | 7 | NA | NA |
| Freeman et al., 2008223 | 17.1 | 20 | 7.57 | 14.45 | 22 | 8.16 | NA | NA | NA | NA | NA | NA | 2 | 2 | 3 | 7 | NA | NA |
| Liebowitz et al., 2002226 | 18.55 | 22 | 11.44 | 14.71 | 21 | 8.73 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 4 | NA | NA |
| Piacentini et al., 2011230 | 17.2 | 22 | 10.04 | 13.3 | 49 | 9.31 | NA | NA | NA | NA | NA | NA | 2 | 2 | 3 | 7 | NA | NA |
| Riddle et al., 2001232 | 20.9 | 63 | 8.5 | 18.2 | 57 | 8.6 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 5 | NA | NA |
| Storch et al., 2011233 | 18.53 | 15 | 8.11 | 11.13 | 16 | 10.53 | NA | NA | NA | NA | NA | NA | 2 | 2 | 2 | 7 | NA | NA |
| Storch et al., 2013234 | 15.43 | 14 | 9.72 | 15.56 | 16 | 6.62 | NA | NA | NA | NA | NA | NA | 2 | 2 | 8 | 9 | NA | NA |
| The Pediatric OCD Treatment Study, 2004236 | 21.5 | 28 | 5.4 | 16.5 | 28 | 9.1 | 14 | 28 | 9.5 | 11.2 | 28 | 8.6 | 4 | 2 | 1 | 6 | 7 | 8 |
| Williams et al., 2010235 | 19.6 | 10 | 6.42 | 12.09 | 11 | 7.46 | NA | NA | NA | NA | NA | NA | 2 | 2 | 2 | 7 | NA | NA |
Key: intervention (class)
-
Placebo (1).
-
Waitlist (2).
-
Psychological placebo (3).
-
Fluoxetine (4).
-
Fluvoxamine (4).
-
Sertraline (4).
-
CBT (5).
-
CBT + sertraline (6).
-
CBT + placebo (7).
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| class.mean.diff[1,2] | 3.103 | 4.279 | 0.05724 | –5.736 | 3.191 | 11.54 | 61,001 | 129,600 |
| class.mean.diff[1,3] | –3.943 | 4.497 | 0.05359 | –13.04 | –3.963 | 5.258 | 61,001 | 129,600 |
| class.mean.diff[1,4] | –3.795 | 3.219 | 0.02787 | –10.55 | –3.782 | 2.974 | 61,001 | 129,600 |
| class.mean.diff[1,5] | –7.18 | 3.555 | 0.04741 | –14.33 | –7.206 | 0.08779 | 61,001 | 129,600 |
| class.mean.diff[1,6] | –9.972 | 3.442 | 0.03088 | –16.91 | –10 | –2.862 | 61,001 | 129,600 |
| class.mean.diff[1,7] | –9.758 | 5.575 | 0.05763 | –20.78 | –9.741 | 1.458 | 61,001 | 129,600 |
| class.mean.diff[2,3] | –7.046 | 3.673 | 0.02754 | –14.15 | –7.139 | 0.6016 | 61,001 | 129,600 |
| class.mean.diff[2,4] | –6.898 | 4.989 | 0.05415 | –16.72 | –6.996 | 3.421 | 61,001 | 129,600 |
| class.mean.diff[2,5] | –10.28 | 2.417 | 0.02076 | –14.83 | –10.37 | –5.221 | 61,001 | 129,600 |
| class.mean.diff[2,6] | –13.07 | 4.567 | 0.04721 | –21.98 | –13.16 | –3.638 | 61,001 | 129,600 |
| class.mean.diff[2,7] | –12.86 | 6.334 | 0.06788 | –25.26 | –12.89 | 0.008206 | 61,001 | 129,600 |
| class.mean.diff[3,4] | 0.1485 | 5.165 | 0.05022 | –10.34 | 0.1485 | 10.63 | 61,001 | 129,600 |
| class.mean.diff[3,5] | –3.237 | 2.788 | 0.02048 | –8.806 | –3.246 | 2.374 | 61,001 | 129,600 |
| class.mean.diff[3,6] | –6.029 | 4.778 | 0.04467 | –15.67 | –6.047 | 3.646 | 61,001 | 129,600 |
| class.mean.diff[3,7] | –5.815 | 6.489 | 0.0665 | –18.68 | –5.803 | 7.188 | 61,001 | 129,600 |
| class.mean.diff[4,5] | –3.385 | 4.379 | 0.04524 | –12.36 | –3.378 | 5.519 | 61,001 | 129,600 |
| class.mean.diff[4,6] | –6.177 | 4.328 | 0.03163 | –15.06 | –6.185 | 2.796 | 61,001 | 129,600 |
| class.mean.diff[4,7] | –5.964 | 6.165 | 0.0578 | –18.28 | –5.939 | 6.432 | 61,001 | 129,600 |
| class.mean.diff[5,6] | –2.792 | 3.9 | 0.03758 | –10.6 | –2.81 | 5.091 | 61,001 | 129,600 |
| class.mean.diff[5,7] | –2.578 | 5.867 | 0.0621 | –14.14 | –2.525 | 9.12 | 61,001 | 129,600 |
| class.mean.diff[6,7] | 0.2136 | 4.395 | 0.04491 | –8.512 | 0.2153 | 8.938 | 61,001 | 129,600 |
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| treat.mean.diff[1,2] | 3.103 | 4.279 | 0.05724 | –5.736 | 3.191 | 11.54 | 61,001 | 129,600 |
| treat.mean.diff[1,3] | –3.943 | 4.497 | 0.05359 | –13.04 | –3.963 | 5.258 | 61,001 | 129,600 |
| treat.mean.diff[1,4] | –3.846 | 3.071 | 0.0307 | –10.08 | –3.821 | 2.399 | 61,001 | 129,600 |
| treat.mean.diff[1,5] | –3.268 | 2.696 | 0.02486 | –8.812 | –3.27 | 2.223 | 61,001 | 129,600 |
| treat.mean.diff[1,6] | –4.268 | 2.802 | 0.03029 | –9.965 | –4.217 | 1.422 | 61,001 | 129,600 |
| treat.mean.diff[1,7] | –7.18 | 3.555 | 0.04741 | –14.33 | –7.206 | 0.08779 | 61,001 | 129,600 |
| treat.mean.diff[1,8] | –9.972 | 3.442 | 0.03088 | –16.91 | –10 | –2.862 | 61,001 | 129,600 |
| treat.mean.diff[1,9] | –9.758 | 5.575 | 0.05763 | –20.78 | –9.741 | 1.458 | 61,001 | 129,600 |
| treat.mean.diff[2,3] | –7.046 | 3.673 | 0.02754 | –14.15 | –7.139 | 0.6016 | 61,001 | 129,600 |
| treat.mean.diff[2,4] | –6.948 | 5.017 | 0.05902 | –16.83 | –7.039 | 3.328 | 61,001 | 129,600 |
| treat.mean.diff[2,5] | –6.371 | 4.811 | 0.05586 | –15.88 | –6.456 | 3.49 | 61,001 | 129,600 |
| treat.mean.diff[2,6] | –7.371 | 4.452 | 0.05062 | –15.96 | –7.468 | 1.824 | 61,001 | 129,600 |
| treat.mean.diff[2,7] | –10.28 | 2.417 | 0.02076 | –14.83 | –10.37 | –5.221 | 61,001 | 129,600 |
| treat.mean.diff[2,8] | –13.07 | 4.567 | 0.04721 | –21.98 | –13.16 | –3.638 | 61,001 | 129,600 |
| treat.mean.diff[2,9] | –12.86 | 6.334 | 0.06788 | –25.26 | –12.89 | 0.008206 | 61,001 | 129,600 |
| treat.mean.diff[3,4] | 0.09769 | 5.192 | 0.05513 | –10.48 | 0.09801 | 10.5 | 61,001 | 129,600 |
| treat.mean.diff[3,5] | 0.6747 | 5.009 | 0.05222 | –9.585 | 0.6688 | 10.71 | 61,001 | 129,600 |
| treat.mean.diff[3,6] | –0.3247 | 4.648 | 0.0465 | –9.636 | –0.3322 | 9.015 | 61,001 | 129,600 |
| treat.mean.diff[3,7] | –3.237 | 2.788 | 0.02048 | –8.806 | –3.246 | 2.374 | 61,001 | 129,600 |
| treat.mean.diff[3,8] | –6.029 | 4.778 | 0.04467 | –15.67 | –6.047 | 3.646 | 61,001 | 129,600 |
| treat.mean.diff[3,9] | –5.815 | 6.489 | 0.0665 | –18.68 | –5.803 | 7.188 | 61,001 | 129,600 |
| treat.mean.diff[4,5] | 0.5771 | 3.215 | 0.02133 | –5.973 | 0.279 | 7.537 | 61,001 | 129,600 |
| treat.mean.diff[4,6] | –0.4224 | 3.286 | 0.02684 | –7.602 | –0.1731 | 6.282 | 61,001 | 129,600 |
| treat.mean.diff[4,7] | –3.335 | 4.417 | 0.05087 | –12.21 | –3.336 | 5.573 | 61,001 | 129,600 |
| treat.mean.diff[4,8] | –6.126 | 4.357 | 0.03743 | –15 | –6.131 | 2.769 | 61,001 | 129,600 |
| treat.mean.diff[4,9] | –5.913 | 6.179 | 0.06194 | –18.22 | –5.884 | 6.419 | 61,001 | 129,600 |
| treat.mean.diff[5,6] | –0.9994 | 3.068 | 0.02282 | –7.796 | –0.5784 | 4.947 | 61,001 | 129,600 |
| treat.mean.diff[5,7] | –3.912 | 4.194 | 0.04733 | –12.31 | –3.896 | 4.609 | 61,001 | 129,600 |
| treat.mean.diff[5,8] | –6.704 | 4.128 | 0.033 | –14.98 | –6.721 | 1.816 | 61,001 | 129,600 |
| treat.mean.diff[5,9] | –6.49 | 6.022 | 0.05815 | –18.43 | –6.527 | 5.726 | 61,001 | 129,600 |
| treat.mean.diff[6,7] | –2.912 | 3.743 | 0.04114 | –10.37 | –2.903 | 4.544 | 61,001 | 129,600 |
| treat.mean.diff[6,8] | –5.704 | 3.671 | 0.02713 | –13.02 | –5.727 | 1.755 | 61,001 | 129,600 |
| treat.mean.diff[6,9] | –5.49 | 5.729 | 0.05522 | –16.8 | –5.502 | 6.003 | 61,001 | 129,600 |
| treat.mean.diff[7,8] | –2.792 | 3.9 | 0.03758 | –10.6 | –2.81 | 5.091 | 61,001 | 129,600 |
| treat.mean.diff[7,9] | –2.578 | 5.867 | 0.0621 | –14.14 | –2.525 | 9.12 | 61,001 | 129,600 |
| treat.mean.diff[8,9] | 0.2136 | 4.395 | 0.04491 | –8.512 | 0.2153 | 8.938 | 61,001 | 129,600 |
Median ranks
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk.class[1] | 5.879 | 0.8012 | 0.008782 | 4 | 6 | 7 | 61,001 | 129,600 |
| rk.class[2] | 6.662 | 0.714 | 0.007736 | 5 | 7 | 7 | 61,001 | 129,600 |
| rk.class[3] | 4.332 | 1.189 | 0.01151 | 1 | 4 | 6 | 61,001 | 129,600 |
| rk.class[4] | 4.285 | 1.223 | 0.01049 | 1 | 4 | 7 | 61,001 | 129,600 |
| rk.class[5] | 2.799 | 0.9752 | 0.009909 | 1 | 3 | 5 | 61,001 | 129,600 |
| rk.class[6] | 1.85 | 0.905 | 0.008695 | 1 | 2 | 4 | 61,001 | 129,600 |
| rk.class[7] | 2.193 | 1.424 | 0.01474 | 1 | 2 | 6 | 61,001 | 129,600 |
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk[1] | 7.744 | 0.9853 | 0.01082 | 5 | 8 | 9 | 61,001 | 129,600 |
| rk[2] | 8.541 | 1.04 | 0.01128 | 5 | 9 | 9 | 61,001 | 129,600 |
| rk[3] | 5.303 | 1.899 | 0.02138 | 1 | 5 | 8 | 61,001 | 129,600 |
| rk[4] | 5.239 | 1.737 | 0.01652 | 2 | 5 | 8 | 61,001 | 129,600 |
| rk[5] | 5.641 | 1.567 | 0.01309 | 2 | 6 | 8 | 61,001 | 129,600 |
| rk[6] | 4.989 | 1.469 | 0.01242 | 2 | 5 | 8 | 61,001 | 129,600 |
| rk[7] | 3.137 | 1.399 | 0.01545 | 1 | 3 | 6 | 61,001 | 129,600 |
| rk[8] | 1.951 | 1.119 | 0.01031 | 1 | 2 | 5 | 61,001 | 129,600 |
| rk[9] | 2.456 | 1.907 | 0.01931 | 1 | 2 | 8 | 61,001 | 129,600 |
Children and adolescents: clinical effectiveness (Children’s Yale–Brown Obsessive–Compulsive Scale) – sensitivity analysis 4 (post hoc), excluding studies that have used a waitlist as control
This is a post hoc analysis.
| Study | y[,1] | n[,1] | sd[,1] | y[,2] | n[,2] | sd[,2] | y[,3] | n[,3] | sd[,3] | y[,4] | n[,4] | sd[,4] | na[] | out[] | t[,1] | t[,2] | t[,3] | t[,4] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| de Haan et al., 1998220 | 17.6 | 10 | 11.8 | 9.1 | 12 | 9.1 | NA | NA | NA | NA | NA | NA | 2 | 2 | 6 | 7 | NA | NA |
| DeVeaugh-Geiss et al., 1992221 | –2.4 | 29 | NA | –10 | 31 | NA | NA | NA | NA | NA | NA | NA | 2 | 1 | 1 | 6 | NA | NA |
| Freeman et al., 2008223 | 17.1 | 20 | 7.57 | 14.45 | 22 | 8.16 | NA | NA | NA | NA | NA | NA | 2 | 2 | 2 | 8 | NA | NA |
| Geller et al., 2001224 | –5.2 | 32 | 7.4 | –9.5 | 71 | 9.2 | NA | NA | NA | NA | NA | NA | 2 | 1 | 1 | 3 | NA | NA |
| Liebowitz et al., 2002226 | 18.55 | 22 | 11.44 | 14.71 | 21 | 8.73 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 3 | NA | NA |
| March et al., 1998228 | –3.4 | 95 | 7.99 | –6.8 | 92 | 8.34 | NA | NA | NA | NA | NA | NA | 2 | 1 | 1 | 5 | NA | NA |
| Neziroglu et al., 2000229 | 19.2 | 5 | 3.56 | 16.4 | 5 | 5.18 | NA | NA | NA | NA | NA | NA | 2 | 2 | 4 | 9 | NA | NA |
| Piacentini et al., 2011230 | 17.2 | 22 | 10.04 | 13.3 | 49 | 9.31 | NA | NA | NA | NA | NA | NA | 2 | 2 | 2 | 8 | NA | NA |
| Riddle et al., 1992231 | 14.8 | 6 | 7 | 13.6 | 7 | 5.7 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 3 | NA | NA |
| Riddle et al., 2001232 | 20.9 | 63 | 8.5 | 18.2 | 57 | 8.6 | NA | NA | NA | NA | NA | NA | 2 | 2 | 1 | 4 | NA | NA |
| Storch et al., 2013234 | 15.43 | 14 | 9.72 | 15.56 | 16 | 6.62 | NA | NA | NA | NA | NA | NA | 2 | 2 | 10 | 11 | NA | NA |
| The Pediatric OCD Treatment Study, 2004236 | 21.5 | 28 | 5.4 | 16.5 | 28 | 9.1 | 14 | 28 | 9.5 | 11.2 | 28 | 8.6 | 4 | 2 | 1 | 5 | 8 | 10 |
Key
-
Placebo (1).
-
Psychological placebo (2).
-
Fluoxetine (3).
-
Fluvoxamine (3).
-
Sertraline (3).
-
Clomipramine (4).
-
BT (5).
-
CBT (6).
-
BT + fluvoxamine (7).
-
Sertraline + CBT (8).
-
Placebo + CBT (9).
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| D[2] | –3.815 | 3.248 | 0.04646 | –10.08 | –3.845 | 2.654 | 101,001 | 186,000 |
| D[3] | –3.475 | 2.094 | 0.01409 | –7.803 | –3.513 | 1.013 | 101,001 | 186,000 |
| D[4] | –7.621 | 2.641 | 0.03338 | –12.82 | –7.61 | –2.436 | 101,001 | 186,000 |
| D[5] | –16.08 | 5.547 | 0.1055 | –26.99 | –16.05 | –5.252 | 101,001 | 186,000 |
| D[6] | –7.066 | 2.5 | 0.03558 | –11.88 | –7.105 | –2.151 | 101,001 | 186,000 |
| D[7] | –5.892 | 3.626 | 0.0444 | –13.01 | –5.914 | 1.201 | 101,001 | 186,000 |
| D[8] | –9.898 | 2.383 | 0.02919 | –14.5 | –9.936 | –5.157 | 101,001 | 186,000 |
| D[9] | –9.725 | 4.246 | 0.0648 | –17.96 | –9.716 | –1.401 | 101,001 | 186,000 |
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| d[2] | –3.815 | 3.248 | 0.04646 | –10.08 | –3.845 | 2.654 | 101,001 | 186,000 |
| d[3] | –3.561 | 1.385 | 0.01635 | –6.31 | –3.564 | –0.7715 | 101,001 | 186,000 |
| d[4] | –3.17 | 1.635 | 0.0186 | –6.288 | –3.24 | 0.2024 | 101,001 | 186,000 |
| d[5] | –3.725 | 1.299 | 0.01303 | –6.36 | –3.714 | –1.192 | 101,001 | 186,000 |
| d[6] | –7.621 | 2.641 | 0.03338 | –12.82 | –7.61 | –2.436 | 101,001 | 186,000 |
| d[7] | –16.08 | 5.547 | 0.1055 | –26.99 | –16.05 | –5.252 | 101,001 | 186,000 |
| d[8] | –7.066 | 2.5 | 0.03558 | –11.88 | –7.105 | –2.151 | 101,001 | 186,000 |
| d[9] | –5.892 | 3.626 | 0.0444 | –13.01 | –5.914 | 1.201 | 101,001 | 186,000 |
| d[10] | –9.898 | 2.383 | 0.02919 | –14.5 | –9.936 | –5.157 | 101,001 | 186,000 |
| d[11] | –9.725 | 4.246 | 0.0648 | –17.96 | –9.716 | –1.401 | 101,001 | 186,000 |
Median ranks
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk.class[1] | 8.771 | 0.5095 | 0.004998 | 7 | 9 | 9 | 101,001 | 186,000 |
| rk.class[2] | 6.852 | 1.472 | 0.01982 | 3 | 7 | 9 | 101,001 | 186,000 |
| rk.class[3] | 7.017 | 1.181 | 0.01059 | 4 | 7 | 9 | 101,001 | 186,000 |
| rk.class[4] | 4.436 | 1.615 | 0.0214 | 2 | 4 | 8 | 101,001 | 186,000 |
| rk.class[5] | 1.524 | 1.233 | 0.01822 | 1 | 1 | 5 | 101,001 | 186,000 |
| rk.class[6] | 4.633 | 1.35 | 0.01805 | 2 | 5 | 7 | 101,001 | 186,000 |
| rk.class[7] | 5.448 | 1.985 | 0.02561 | 2 | 6 | 9 | 101,001 | 186,000 |
| rk.class[8] | 2.945 | 1.156 | 0.01379 | 1 | 3 | 6 | 101,001 | 186,000 |
| rk.class[9] | 3.375 | 1.905 | 0.02738 | 1 | 3 | 8 | 101,001 | 186,000 |
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk[1] | 10.77 | 0.5484 | 0.005578 | 9 | 11 | 11 | 101,001 | 186,000 |
| rk[2] | 7.767 | 2.226 | 0.03217 | 3 | 8 | 11 | 101,001 | 186,000 |
| rk[3] | 7.969 | 1.473 | 0.0173 | 5 | 8 | 10 | 101,001 | 186,000 |
| rk[4] | 8.389 | 1.435 | 0.01459 | 5 | 9 | 10 | 101,001 | 186,000 |
| rk[5] | 7.819 | 1.391 | 0.01456 | 5 | 8 | 10 | 101,001 | 186,000 |
| rk[6] | 4.564 | 1.873 | 0.02389 | 2 | 4 | 9 | 101,001 | 186,000 |
| rk[7] | 1.55 | 1.372 | 0.01955 | 1 | 1 | 6 | 101,001 | 186,000 |
| rk[8] | 4.79 | 1.629 | 0.02138 | 2 | 5 | 9 | 101,001 | 186,000 |
| rk[9] | 5.913 | 2.565 | 0.03303 | 2 | 6 | 11 | 101,001 | 186,000 |
| rk[10] | 2.959 | 1.215 | 0.01403 | 1 | 3 | 6 | 101,001 | 186,000 |
| rk[11] | 3.512 | 2.227 | 0.0313 | 1 | 3 | 10 | 101,001 | 186,000 |
Children and adolescents: acceptability (dropouts) – sensitivity analysis 1 (low overall attrition)
See Table 45 for a summary.
| Study | r[,1] | n[,1] | r[,2] | n[,2] | r[,3] | n[,3] | r[,4] | n[,4] | na[] | t[,1] | t[,2] | t[,3] | t[,4] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Asbahr et al., 2005216 | 1.5 | 21 | 0.5 | 21 | NA | NA | NA | NA | 2 | 5 | 8 | NA | NA |
| Bolton and Perrin, 2008218 | 0.5 | 11 | 2.5 | 11 | NA | NA | NA | NA | 2 | 2 | 7 | NA | NA |
| Bolton et al., 2011219 | 3 | 24 | 2 | 36 | NA | NA | NA | NA | 2 | 2 | 8 | NA | NA |
| de Haan et al., 1998220 | 0.5 | 11 | 1.5 | 14 | NA | NA | NA | NA | 2 | 6 | 7 | NA | NA |
| DeVeaugh-Geiss et al., 1992221 | 2 | 29 | 4 | 31 | NA | NA | NA | NA | 2 | 1 | 6 | NA | NA |
| Liebowitz et al., 2002226 | 4 | 22 | 1 | 21 | NA | NA | NA | NA | 2 | 1 | 4 | NA | NA |
| March et al., 1990227 | 0.5 | 9 | 2.5 | 9 | NA | NA | NA | NA | 2 | 1 | 6 | NA | NA |
| March et al., 1998228 | 13 | 95 | 18 | 92 | NA | NA | NA | NA | 2 | 1 | 5 | NA | NA |
| Piacentini et al., 2011230 | 5 | 22 | 8 | 49 | NA | NA | NA | NA | 2 | 3 | 8 | NA | NA |
| Riddle et al., 1992231 | 1 | 6 | 1 | 7 | NA | NA | NA | NA | 2 | 1 | 4 | NA | NA |
| Storch et al., 2011233 | 0.5 | 16 | 2.5 | 17 | NA | NA | NA | NA | 2 | 2 | 8 | NA | NA |
| The Pediatric OCD Treatment Study, 2004236 | 7 | 28 | 2 | 28 | 3 | 28 | 3 | 28 | 4 | 1 | 5 | 8 | 9 |
| Williams et al., 2010235 | 1 | 10 | 1 | 11 | NA | NA | NA | NA | 2 | 2 | 8 | NA | NA |
Key: intervention (class)
-
Placebo (1).
-
Waitlist (2).
-
Psychological placebo (3).
-
Fluoxetine (4).
-
Sertraline (4).
-
Clomipramine (5).
-
BT (6).
-
CBT (7).
-
CBT + sertraline (8).
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| OR.D[1,2] | 2.004 | 47.63 | 0.1619 | 0.0234 | 0.4655 | 7.378 | 100,001 | 200,000 |
| OR.D[1,3] | 88.6 | 16,920 | 37.98 | 0.01715 | 0.6795 | 23.59 | 100,001 | 200,000 |
| OR.D[1,4] | 684,500 | 2.78 × 108 | 620,500 | 5.23 × 10– 4 | 0.5795 | 448.1 | 100,001 | 200,000 |
| OR.D[1,5] | 8.66 | 154.5 | 0.4221 | 0.3588 | 3.12 | 36.01 | 100,001 | 200,000 |
| OR.D[1,6] | 549.4 | 82,090 | 215.8 | 0.2338 | 8.088 | 695.2 | 100,001 | 200,000 |
| OR.D[1,7] | 1.066 | 8.235 | 0.03168 | 0.04269 | 0.4677 | 4.388 | 100,001 | 200,000 |
| OR.D[1,8] | 3.44 | 437.9 | 0.9819 | 0.03391 | 0.5395 | 7.327 | 100,001 | 200,000 |
| OR.D[2,3] | 51,760 | 2.31 × 107 | 51,600 | 0.05413 | 1.464 | 46.74 | 100,001 | 200,000 |
| OR.D[2,4] | 4.72E+ 06 | 1.89 × 109 | 4.23 × 106 | 8.12 × 10– 4 | 1.253 | 1366 | 100,001 | 200,000 |
| OR.D[2,5] | 144.4 | 12,320 | 31.54 | 0.2732 | 6.881 | 254.4 | 100,001 | 200,000 |
| OR.D[2,6] | 3556 | 442,300 | 2258 | 0.6616 | 17.25 | 1572 | 100,001 | 200,000 |
| OR.D[2,7] | 2.059 | 65.74 | 0.1484 | 0.1543 | 1 | 7.432 | 100,001 | 200,000 |
| OR.D[2,8] | 112.1 | 25,660 | 58.84 | 0.04329 | 1.134 | 36.74 | 100,001 | 200,000 |
| OR.D[3,4] | 3.44 × 106 | 1.21 × 109 | 2.70 × 106 | 4.15 × 10– 4 | 0.8422 | 1197 | 100,001 | 200,000 |
| OR.D[3,5] | 10,220 | 3.81 × 106 | 8978 | 0.08597 | 4.645 | 328.6 | 100,001 | 200,000 |
| OR.D[3,6] | 19,690 | 3.17 × 106 | 7701 | 0.1442 | 12.25 | 2389 | 100,001 | 200,000 |
| OR.D[3,7] | 10.39 | 1595 | 3.596 | 0.04189 | 0.6821 | 10.91 | 100,001 | 200,000 |
| OR.D[3,8] | 903.2 | 224100 | 500.6 | 0.01527 | 0.7741 | 43.04 | 100,001 | 200,000 |
| OR.D[4,5] | 3.91 × 106 | 8.33 × 108 | 1.85 × 106 | 0.005661 | 5.669 | 8118 | 100,001 | 200,000 |
| OR.D[4,6] | 3.32 × 107 | 6.47 × 109 | 1.52 × 107 | 0.01022 | 15.05 | 43550 | 100,001 | 200,000 |
| OR.D[4,7] | 2.91 × 106 | 1.12 × 109 | 2.50 × 106 | 8.74 × 10– 4 | 0.8002 | 1087 | 100,001 | 200,000 |
| OR.D[4,8] | 999,300 | 2.49 × 108 | 555,300 | 9.15 × 10– 4 | 0.923 | 1347 | 100,001 | 200,000 |
| OR.D[5,6] | 83.25 | 4380 | 29.29 | 0.0845 | 2.501 | 180.1 | 100,001 | 200,000 |
| OR.D[5,7] | 0.8665 | 32.12 | 0.07764 | 0.005902 | 0.1475 | 2.731 | 100,001 | 200,000 |
| OR.D[5,8] | 26.11 | 10530 | 23.55 | 0.004559 | 0.1674 | 4.631 | 100,001 | 200,000 |
| OR.D[6,7] | 1.037 | 169.8 | 0.3847 | 6.35 × 10– 4 | 0.05713 | 1.861 | 100,001 | 200,000 |
| OR.D[6,8] | 20.67 | 5441 | 12.17 | 4.50 × 10– 4 | 0.0643 | 4.102 | 100,001 | 200,000 |
| OR.D[7,8] | 7.098 | 382.1 | 0.8866 | 0.06605 | 1.146 | 20.08 | 100,001 | 200,000 |
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| OR[1,2] | 2.004 | 47.63 | 0.1619 | 0.0234 | 0.4655 | 7.378 | 100,001 | 200,000 |
| OR[1,3] | 88.6 | 16,920 | 37.98 | 0.01715 | 0.6795 | 23.59 | 100,001 | 200,000 |
| OR[1,4] | 0.8653 | 5.695 | 0.01689 | 0.02994 | 0.4078 | 3.622 | 100,001 | 200,000 |
| OR[1,5] | 1.241 | 15.18 | 0.03805 | 0.1239 | 0.7938 | 4.08 | 100,001 | 200,000 |
| OR[1,6] | 8.66 | 154.5 | 0.4221 | 0.3588 | 3.12 | 36.01 | 100,001 | 200,000 |
| OR[1,7] | 549.4 | 82,090 | 215.8 | 0.2338 | 8.088 | 695.2 | 100,001 | 200,000 |
| OR[1,8] | 1.066 | 8.235 | 0.03168 | 0.04269 | 0.4677 | 4.388 | 100,001 | 200,000 |
| OR[1,9] | 3.44 | 437.9 | 0.9819 | 0.03391 | 0.5395 | 7.327 | 100,001 | 200,000 |
| OR[2,3] | 51,760 | 2.31 × 107 | 51,600 | 0.05413 | 1.464 | 46.74 | 100,001 | 200,000 |
| OR[2,4] | 35.04 | 5064 | 11.88 | 0.02154 | 0.851 | 32.7 | 100,001 | 200,000 |
| OR[2,5] | 9.823 | 567.3 | 1.408 | 0.1006 | 1.676 | 30.07 | 100,001 | 200,000 |
| OR[2,6] | 144.4 | 12,320 | 31.54 | 0.2732 | 6.881 | 254.4 | 100,001 | 200,000 |
| OR[2,7] | 3556 | 442,300 | 2258 | 0.6616 | 17.25 | 1572 | 100,001 | 200,000 |
| OR[2,8] | 2.059 | 65.74 | 0.1484 | 0.1543 | 1 | 7.432 | 100,001 | 200,000 |
| OR[2,9] | 112.1 | 25,660 | 58.84 | 0.04329 | 1.134 | 36.74 | 100,001 | 200,000 |
| OR[3,4] | 1408 | 510,700 | 1142 | 0.008377 | 0.5765 | 38.53 | 100,001 | 200,000 |
| OR[3,5] | 1087 | 261,300 | 582.5 | 0.03144 | 1.155 | 38.62 | 100,001 | 200,000 |
| OR[3,6] | 10,220 | 3.81 × 106 | 8978 | 0.08597 | 4.645 | 328.6 | 100,001 | 200,000 |
| OR[3,7] | 19,690 | 3.17 × 106 | 7701 | 0.1442 | 12.25 | 2389 | 100,001 | 200,000 |
| OR[3,8] | 10.39 | 1595 | 3.596 | 0.04189 | 0.6821 | 10.91 | 100,001 | 200,000 |
| OR[3,9] | 903.2 | 224,100 | 500.6 | 0.01527 | 0.7741 | 43.04 | 100,001 | 200,000 |
| OR[4,5] | 10.07 | 389.9 | 0.9028 | 0.1496 | 1.74 | 36.51 | 100,001 | 200,000 |
| OR[4,6] | 257 | 44,410 | 101.2 | 0.364 | 8.065 | 255 | 100,001 | 200,000 |
| OR[4,7] | 6226 | 402,100 | 3626 | 0.3259 | 21.21 | 3037 | 100,001 | 200,000 |
| OR[4,8] | 12.04 | 957.4 | 2.632 | 0.05211 | 1.163 | 32.01 | 100,001 | 200,000 |
| OR[4,9] | 36.51 | 5828 | 13.04 | 0.04467 | 1.339 | 48.11 | 100,001 | 200,000 |
| OR[5,6] | 31.28 | 1904 | 4.73 | 0.2996 | 4.02 | 82.71 | 100,001 | 200,000 |
| OR[5,7] | 1133 | 117,700 | 330.8 | 0.2693 | 10.45 | 1099 | 100,001 | 200,000 |
| OR[5,8] | 1.351 | 13 | 0.04127 | 0.06476 | 0.601 | 5.613 | 100,001 | 200,000 |
| OR[5,9] | 5.107 | 431.8 | 0.964 | 0.04742 | 0.6859 | 10.67 | 100,001 | 200,000 |
| OR[6,7] | 83.25 | 4380 | 29.29 | 0.0845 | 2.501 | 180.1 | 100,001 | 200,000 |
| OR[6,8] | 0.8665 | 32.12 | 0.07764 | 0.005902 | 0.1475 | 2.731 | 100,001 | 200,000 |
| OR[6,9] | 26.11 | 10,530 | 23.55 | 0.004559 | 0.1674 | 4.631 | 100,001 | 200,000 |
| OR[7,8] | 1.037 | 169.8 | 0.3847 | 6.35 × 10–4 | 0.05713 | 1.861 | 100,001 | 200,000 |
| OR[7,9] | 20.67 | 5441 | 12.17 | 4.50 × 10–4 | 0.0643 | 4.102 | 100,001 | 200,000 |
| OR[8,9] | 7.098 | 382.1 | 0.8866 | 0.06605 | 1.146 | 20.08 | 100,001 | 200,000 |
Median ranks
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk.class[1] | 4.718 | 1.504 | 0.01493 | 2 | 5 | 7 | 100,001 | 200,000 |
| rk.class[2] | 3.238 | 1.793 | 0.0165 | 1 | 3 | 7 | 100,001 | 200,000 |
| rk.class[3] | 4.044 | 2.134 | 0.01497 | 1 | 4 | 8 | 100,001 | 200,000 |
| rk.class[4] | 3.814 | 2.477 | 0.01057 | 1 | 4 | 8 | 100,001 | 200,000 |
| rk.class[5] | 6.438 | 1.479 | 0.01284 | 2 | 7 | 8 | 100,001 | 200,000 |
| rk.class[6] | 7.125 | 1.44 | 0.01217 | 3 | 8 | 8 | 100,001 | 200,000 |
| rk.class[7] | 3.128 | 1.385 | 0.009781 | 1 | 3 | 6 | 100,001 | 200,000 |
| rk.class[8] | 3.495 | 1.948 | 0.01222 | 1 | 3 | 7 | 100,001 | 200,000 |
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk[1] | 5.523 | 1.667 | 0.01742 | 2 | 6 | 8 | 100,001 | 200,000 |
| rk[2] | 3.66 | 2.179 | 0.02084 | 1 | 3 | 8 | 100,001 | 200,000 |
| rk[3] | 4.599 | 2.555 | 0.01836 | 1 | 4 | 9 | 100,001 | 200,000 |
| rk[4] | 3.355 | 2.229 | 0.01983 | 1 | 3 | 8 | 100,001 | 200,000 |
| rk[5] | 4.82 | 1.842 | 0.01277 | 1 | 5 | 8 | 100,001 | 200,000 |
| rk[6] | 7.444 | 1.66 | 0.01503 | 2 | 8 | 9 | 100,001 | 200,000 |
| rk[7] | 8.128 | 1.631 | 0.01371 | 3 | 9 | 9 | 100,001 | 200,000 |
| rk[8] | 3.518 | 1.677 | 0.01318 | 1 | 3 | 7 | 100,001 | 200,000 |
| rk[9] | 3.953 | 2.31 | 0.01463 | 1 | 4 | 9 | 100,001 | 200,000 |
Children and adolescents: acceptability (dropouts) – sensitivity analysis 2 (incomplete outcome data)
See Table 46 for a summary.
| Study | r[,1] | n[,1] | r[,2] | n[,2] | r[,3] | n[,3] | r[,4] | n[,4] | na[] | t[,1] | t[,2] | t[,3] | t[,4] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Asbahr et al., 2005216 | 1.5 | 21 | 0.5 | 21 | NA | NA | NA | NA | 2 | 6 | 9 | NA | NA |
| Bolton and Perrin, 2008218 | 0.5 | 11 | 2.5 | 11 | NA | NA | NA | NA | 2 | 2 | 8 | NA | NA |
| Bolton et al., 2011219 | 3 | 24 | 2 | 36 | NA | NA | NA | NA | 2 | 2 | 9 | NA | NA |
| de Haan et al., 1998220 | 0.5 | 11 | 1.5 | 14 | NA | NA | NA | NA | 2 | 7 | 8 | NA | NA |
| DeVeaugh-Geiss et al., 1992221 | 2 | 29 | 4 | 31 | NA | NA | NA | NA | 2 | 1 | 7 | NA | NA |
| Freeman et al., 2008223 | 5 | 20 | 6 | 22 | NA | NA | NA | NA | 2 | 3 | 9 | NA | NA |
| Geller et al., 2001224 | 12 | 32 | 22 | 71 | NA | NA | NA | NA | 2 | 1 | 4 | NA | NA |
| Liebowitz et al., 2002226 | 4 | 22 | 1 | 21 | NA | NA | NA | NA | 2 | 1 | 4 | NA | NA |
| March et al., 1998228 | 13 | 95 | 18 | 92 | NA | NA | NA | NA | 2 | 1 | 6 | NA | NA |
| Piacentini et al., 2011230 | 5 | 22 | 8 | 49 | NA | NA | NA | NA | 2 | 3 | 9 | NA | NA |
| Riddle et al., 1992231 | 1 | 6 | 1 | 7 | NA | NA | NA | NA | 2 | 1 | 4 | NA | NA |
| Riddle et al., 2001232 | 27 | 63 | 19 | 57 | NA | NA | NA | NA | 2 | 1 | 5 | NA | NA |
| Storch et al., 2011233 | 0.5 | 16 | 2.5 | 17 | NA | NA | NA | NA | 2 | 2 | 9 | NA | NA |
| Storch et al., 2013234 | 6 | 14 | 3 | 16 | NA | NA | NA | NA | 2 | 10 | 11 | NA | NA |
| The Pediatric OCD Treatment Study, 2004236 | 7 | 28 | 2 | 28 | 3 | 28 | 3 | 28 | 4 | 1 | 6 | 9 | 10 |
| Williams et al., 2010235 | 1 | 10 | 1 | 11 | NA | NA | NA | NA | 2 | 2 | 9 | NA | NA |
Key: intervention (class)
-
Placebo (1).
-
Waitlist (2).
-
Psychological placebo (3).
-
Fluoxetine (4).
-
Fluvoxamine (4).
-
Sertraline (4).
-
Clomipramine (5).
-
BT (6).
-
CBT (7).
-
CBT + sertraline (8).
-
CBT + placebo (9).
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| OR.D[1,2] | 0.9409 | 8.238 | 0.0271 | 0.04177 | 0.4769 | 4.166 | 100,001 | 200,000 |
| OR.D[1,3] | 1.162 | 20.74 | 0.05403 | 0.05146 | 0.5519 | 4.709 | 100,001 | 200,000 |
| OR.D[1,4] | 323.1 | 74,690 | 167.2 | 0.05674 | 0.7056 | 7.78 | 100,001 | 200,000 |
| OR.D[1,5] | 4.559 | 31.82 | 0.1309 | 0.2264 | 2.013 | 20.91 | 100,001 | 200,000 |
| OR.D[1,6] | 130.6 | 11,210 | 55.65 | 0.2705 | 5.953 | 307.3 | 100,001 | 200,000 |
| OR.D[1,7] | 0.6984 | 2.111 | 0.01182 | 0.07205 | 0.4809 | 2.387 | 100,001 | 200,000 |
| OR.D[1,8] | 0.8992 | 4.497 | 0.01937 | 0.06399 | 0.519 | 3.502 | 100,001 | 200,000 |
| OR.D[1,9] | 0.9197 | 47.47 | 0.1255 | 0.006346 | 0.1373 | 2.595 | 100,001 | 200,000 |
| OR.D[2,3] | 2.362 | 16.71 | 0.04775 | 0.1402 | 1.159 | 10.14 | 100,001 | 200,000 |
| OR.D[2,4] | 693.5 | 140,500 | 313.1 | 0.06187 | 1.48 | 38.89 | 100,001 | 200,000 |
| OR.D[2,5] | 19.6 | 260.4 | 0.9916 | 0.258 | 4.276 | 99 | 100,001 | 200,000 |
| OR.D[2,6] | 546.2 | 100,600 | 378.3 | 0.7216 | 12.23 | 775.6 | 100,001 | 200,000 |
| OR.D[2,7] | 1.451 | 3.293 | 0.01678 | 0.2085 | 0.9965 | 5.226 | 100,001 | 200,000 |
| OR.D[2,8] | 4.23 | 172.5 | 0.4978 | 0.07702 | 1.073 | 17.45 | 100,001 | 200,000 |
| OR.D[2,9] | 7.159 | 916 | 2.08 | 0.008978 | 0.2873 | 10.88 | 100,001 | 200,000 |
| OR.D[3,4] | 1253 | 324,800 | 724.4 | 0.05251 | 1.285 | 32.02 | 100,001 | 200,000 |
| OR.D[3,5] | 44.45 | 6459 | 14.47 | 0.2018 | 3.748 | 92.32 | 100,001 | 200,000 |
| OR.D[3,6] | 525 | 70,130 | 275.8 | 0.3997 | 10.81 | 842 | 100,001 | 200,000 |
| OR.D[3,7] | 1.161 | 2.123 | 0.008579 | 0.208 | 0.8647 | 3.616 | 100,001 | 200,000 |
| OR.D[3,8] | 4.912 | 612.9 | 1.385 | 0.06947 | 0.9334 | 13.59 | 100,001 | 200,000 |
| OR.D[3,9] | 9.693 | 1846 | 4.138 | 0.008141 | 0.2491 | 8.657 | 100,001 | 200,000 |
| OR.D[4,5] | 2292 | 4.33 × 105 | 965.6 | 0.1206 | 2.9 | 83.47 | 100,001 | 200,000 |
| OR.D[4,6] | 1.10 × 104 | 1.64 × 106 | 3716 | 0.1866 | 8.626 | 893.3 | 100,001 | 200,000 |
| OR.D[4,7] | 891.5 | 222,800 | 501.7 | 0.03788 | 0.6786 | 11.68 | 100,001 | 200,000 |
| OR.D[4,8] | 1501 | 500,300 | 1136 | 0.03585 | 0.7311 | 15.94 | 100,001 | 200,000 |
| OR.D[4,9] | 512.7 | 151,200 | 340.3 | 0.004535 | 0.1964 | 9.29 | 100,001 | 200,000 |
| OR.D[5,6] | 30.75 | 618.7 | 5.422 | 0.1535 | 2.88 | 138.2 | 100,001 | 200,000 |
| OR.D[5,7] | 1.345 | 281.2 | 0.6446 | 0.01375 | 0.2306 | 3.039 | 100,001 | 200,000 |
| OR.D[5,8] | 1.186 | 57.18 | 0.1337 | 0.01204 | 0.2456 | 4.467 | 100,001 | 200,000 |
| OR.D[5,9] | 2.598 | 552.8 | 1.244 | 0.001577 | 0.06598 | 2.639 | 100,001 | 200,000 |
| OR.D[6,7] | 0.344 | 17.33 | 0.04053 | 0.001409 | 0.08033 | 1.582 | 100,001 | 200,000 |
| OR.D[6,8] | 0.5686 | 11.68 | 0.03208 | 0.001141 | 0.08434 | 2.951 | 100,001 | 200,000 |
| OR.D[6,9] | 1.336 | 220.7 | 0.5204 | 1.77 × 10–4 | 0.02216 | 1.646 | 100,001 | 200,000 |
| OR.D[7,8] | 2.403 | 28.68 | 0.08785 | 0.1208 | 1.076 | 10.36 | 100,001 | 200,000 |
| OR.D[7,9] | 3.044 | 271.4 | 0.6238 | 0.01256 | 0.2917 | 7.321 | 100,001 | 200,000 |
| OR.D[8,9] | 0.6063 | 7.055 | 0.01773 | 0.0269 | 0.2772 | 2.556 | 100,001 | 200,000 |
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| OR[1,2] | 0.9409 | 8.238 | 0.0271 | 0.04177 | 0.4769 | 4.166 | 100,001 | 200,000 |
| OR[1,3] | 1.162 | 20.74 | 0.05403 | 0.05146 | 0.5519 | 4.709 | 100,001 | 200,000 |
| OR[1,4] | 0.7185 | 0.5733 | 0.003248 | 0.1921 | 0.6427 | 1.702 | 100,001 | 200,000 |
| OR[1,5] | 0.8515 | 2.364 | 0.00837 | 0.18 | 0.6874 | 2.306 | 100,001 | 200,000 |
| OR[1,6] | 0.9138 | 0.9901 | 0.005231 | 0.2467 | 0.7994 | 2.183 | 100,001 | 200,000 |
| OR[1,7] | 4.559 | 31.82 | 0.1309 | 0.2264 | 2.013 | 20.91 | 100,001 | 200,000 |
| OR[1,8] | 130.6 | 11,210 | 55.65 | 0.2705 | 5.953 | 307.3 | 100,001 | 200,000 |
| OR[1,9] | 0.6984 | 2.111 | 0.01182 | 0.07205 | 0.4809 | 2.387 | 100,001 | 200,000 |
| OR[1,10] | 0.8992 | 4.497 | 0.01937 | 0.06399 | 0.519 | 3.502 | 100,001 | 200,000 |
| OR[1,11] | 0.9197 | 47.47 | 0.1255 | 0.006346 | 0.1373 | 2.595 | 100,001 | 200,000 |
| OR[2,3] | 2.362 | 16.71 | 0.04775 | 0.1402 | 1.159 | 10.14 | 100,001 | 200,000 |
| OR[2,4] | 4.048 | 85 | 0.293 | 0.1189 | 1.332 | 16.43 | 100,001 | 200,000 |
| OR[2,5] | 5.451 | 303.6 | 0.7032 | 0.1237 | 1.429 | 19.91 | 100,001 | 200,000 |
| OR[2,6] | 3.901 | 29.03 | 0.135 | 0.1811 | 1.673 | 18.02 | 100,001 | 200,000 |
| OR[2,7] | 19.6 | 260.4 | 0.9916 | 0.258 | 4.276 | 99 | 100,001 | 200,000 |
| OR[2,8] | 546.2 | 100,600 | 378.3 | 0.7216 | 12.23 | 775.6 | 100,001 | 200,000 |
| OR[2,9] | 1.451 | 3.293 | 0.01678 | 0.2085 | 0.9965 | 5.226 | 100,001 | 200,000 |
| OR[2,10] | 4.23 | 172.5 | 0.4978 | 0.07702 | 1.073 | 17.45 | 100,001 | 200,000 |
| OR[2,11] | 7.159 | 916 | 2.08 | 0.008978 | 0.2873 | 10.88 | 100,001 | 200,000 |
| OR[3,4] | 3.342 | 67.2 | 0.1859 | 0.1036 | 1.16 | 13.52 | 100,001 | 200,000 |
| OR[3,5] | 4.468 | 155.6 | 0.4065 | 0.1076 | 1.245 | 16.12 | 100,001 | 200,000 |
| OR[3,6] | 3.579 | 146 | 0.3305 | 0.161 | 1.453 | 14.04 | 100,001 | 200,000 |
| OR[3,7] | 44.45 | 6459 | 14.47 | 0.2018 | 3.748 | 92.32 | 100,001 | 200,000 |
| OR[3,8] | 525 | 70,130 | 275.8 | 0.3997 | 10.81 | 842 | 100,001 | 200,000 |
| OR[3,9] | 1.161 | 2.123 | 0.008579 | 0.208 | 0.8647 | 3.616 | 100,001 | 200,000 |
| OR[3,10] | 4.912 | 612.9 | 1.385 | 0.06947 | 0.9334 | 13.59 | 100,001 | 200,000 |
| OR[3,11] | 9.693 | 1846 | 4.138 | 0.008141 | 0.2491 | 8.657 | 100,001 | 200,000 |
| OR[4,5] | 1.589 | 7.636 | 0.02302 | 0.2631 | 1.031 | 5.289 | 100,001 | 200,000 |
| OR[4,6] | 1.713 | 8.746 | 0.02764 | 0.351 | 1.155 | 5.412 | 100,001 | 200,000 |
| OR[4,7] | 10.99 | 613.5 | 1.773 | 0.3015 | 3.197 | 44.76 | 100,001 | 200,000 |
| OR[4,8] | 281.9 | 29,060 | 112 | 0.3747 | 9.569 | 575 | 100,001 | 200,000 |
| OR[4,9] | 1.335 | 7.801 | 0.03151 | 0.1006 | 0.7536 | 5.269 | 100,001 | 200,000 |
| OR[4,10] | 1.919 | 35.42 | 0.09533 | 0.08909 | 0.8093 | 7.612 | 100,001 | 200,000 |
| OR[4,11] | 3.761 | 465.6 | 1.106 | 0.009238 | 0.2194 | 5.183 | 100,001 | 200,000 |
| OR[5,6] | 1.689 | 10.48 | 0.02893 | 0.2646 | 1.09 | 5.342 | 100,001 | 200,000 |
| OR[5,7] | 10.61 | 303.4 | 0.7695 | 0.2478 | 2.978 | 43.33 | 100,001 | 200,000 |
| OR[5,8] | 232 | 14,570 | 74.32 | 0.3297 | 8.827 | 556.1 | 100,001 | 200,000 |
| OR[5,9] | 1.332 | 9.608 | 0.03469 | 0.08188 | 0.7004 | 5.164 | 100,001 | 200,000 |
| OR[5,10] | 2.526 | 133.9 | 0.32 | 0.07279 | 0.7585 | 7.397 | 100,001 | 200,000 |
| OR[5,11] | 5.982 | 1149 | 2.583 | 0.008041 | 0.2022 | 4.912 | 100,001 | 200,000 |
| OR[6,7] | 7.599 | 152.4 | 0.4333 | 0.249 | 2.535 | 33.89 | 100,001 | 200,000 |
| OR[6,8] | 188.7 | 13,640 | 73.49 | 0.3203 | 7.444 | 430.4 | 100,001 | 200,000 |
| OR[6,9] | 0.8856 | 1.744 | 0.01158 | 0.1004 | 0.6035 | 3.192 | 100,001 | 200,000 |
| OR[6,10] | 1.227 | 16.02 | 0.04059 | 0.08275 | 0.6481 | 4.863 | 100,001 | 200,000 |
| OR[6,11] | 1.85 | 310.7 | 0.7309 | 0.008378 | 0.1736 | 3.568 | 100,001 | 200,000 |
| OR[7,8] | 30.75 | 618.7 | 5.422 | 0.1535 | 2.88 | 138.2 | 100,001 | 200,000 |
| OR[7,9] | 1.345 | 281.2 | 0.6446 | 0.01375 | 0.2306 | 3.039 | 100,001 | 200,000 |
| OR[7,10] | 1.186 | 57.18 | 0.1337 | 0.01204 | 0.2456 | 4.467 | 100,001 | 200,000 |
| OR[7,11] | 2.598 | 552.8 | 1.244 | 0.001577 | 0.06598 | 2.639 | 100,001 | 200,000 |
| OR[8,9] | 0.344 | 17.33 | 0.04053 | 0.001409 | 0.08033 | 1.582 | 100,001 | 200,000 |
| OR[8,10] | 0.5686 | 11.68 | 0.03208 | 0.001141 | 0.08434 | 2.951 | 100,001 | 200,000 |
| OR[8,11] | 1.336 | 220.7 | 0.5204 | 1.77 × 10–4 | 0.02216 | 1.646 | 100,001 | 200,000 |
| OR[9,10] | 2.403 | 28.68 | 0.08785 | 0.1208 | 1.076 | 10.36 | 100,001 | 200,000 |
| OR[9,11] | 3.044 | 271.4 | 0.6238 | 0.01256 | 0.2917 | 7.321 | 100,001 | 200,000 |
| OR[10,11] | 0.6063 | 7.055 | 0.01773 | 0.0269 | 0.2772 | 2.556 | 100,001 | 200,000 |
Median ranks
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk.class[1] | 6.095 | 1.553 | 0.02176 | 3 | 6 | 9 | 100,001 | 200,000 |
| rk.class[2] | 4.004 | 2.131 | 0.02932 | 1 | 4 | 8 | 100,001 | 200,000 |
| rk.class[3] | 4.418 | 2.155 | 0.02419 | 1 | 4 | 9 | 100,001 | 200,000 |
| rk.class[4] | 4.886 | 2.138 | 0.01902 | 1 | 5 | 9 | 100,001 | 200,000 |
| rk.class[5] | 7.119 | 1.902 | 0.02102 | 2 | 8 | 9 | 100,001 | 200,000 |
| rk.class[6] | 8.213 | 1.55 | 0.02074 | 3 | 9 | 9 | 100,001 | 200,000 |
| rk.class[7] | 3.877 | 1.582 | 0.01946 | 1 | 4 | 7 | 100,001 | 200,000 |
| rk.class[8] | 4.272 | 2.058 | 0.02425 | 1 | 4 | 8 | 100,001 | 200,000 |
| rk.class[9] | 2.117 | 1.903 | 0.01846 | 1 | 1 | 8 | 100,001 | 200,000 |
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk[1] | 7.678 | 1.802 | 0.02494 | 4 | 8 | 11 | 100,001 | 200,000 |
| rk[2] | 4.73 | 2.867 | 0.04154 | 1 | 4 | 10 | 100,001 | 200,000 |
| rk[3] | 5.226 | 2.898 | 0.03468 | 1 | 5 | 10 | 100,001 | 200,000 |
| rk[4] | 5.403 | 2.308 | 0.02558 | 1 | 5 | 10 | 100,001 | 200,000 |
| rk[5] | 5.733 | 2.417 | 0.02381 | 1 | 6 | 10 | 100,001 | 200,000 |
| rk[6] | 6.491 | 2.104 | 0.02158 | 2 | 7 | 10 | 100,001 | 200,000 |
| rk[7] | 8.794 | 2.463 | 0.02683 | 2 | 10 | 11 | 100,001 | 200,000 |
| rk[8] | 10.04 | 2.015 | 0.02746 | 3 | 11 | 11 | 100,001 | 200,000 |
| rk[9] | 4.523 | 2.189 | 0.02989 | 1 | 4 | 9 | 100,001 | 200,000 |
| rk[10] | 5.013 | 2.748 | 0.03233 | 1 | 5 | 10 | 100,001 | 200,000 |
| rk[11] | 2.369 | 2.431 | 0.02302 | 1 | 1 | 10 | 100,001 | 200,000 |
Children and adolescents: acceptability (dropouts) – sensitivity analysis 3 (blinding)
See Table 47 for a summary.
| Study | r[,1] | n[,1] | r[,2] | n[,2] | r[,3] | n[,3] | r[,4] | n[,4] | na[] | t[,1] | t[,2] | t[,3] | t[,4] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Asbahr et al., 2005216 | 1.5 | 21 | 0.5 | 21 | NA | NA | NA | NA | 2 | 6 | 7 | NA | NA |
| Bolton et al., 2011219 | 3 | 24 | 2 | 36 | NA | NA | NA | NA | 2 | 2 | 7 | NA | NA |
| Freeman et al., 2008223 | 5 | 20 | 6 | 22 | NA | NA | NA | NA | 2 | 3 | 7 | NA | NA |
| Liebowitz et al., 2002226 | 4 | 22 | 1 | 21 | NA | NA | NA | NA | 2 | 1 | 4 | NA | NA |
| Piacentini et al., 2011230 | 5 | 22 | 8 | 49 | NA | NA | NA | NA | 2 | 3 | 7 | NA | NA |
| Riddle et al., 2001232 | 27 | 63 | 19 | 57 | NA | NA | NA | NA | 2 | 1 | 5 | NA | NA |
| Storch et al., 2011233 | 0.5 | 16 | 2.5 | 17 | NA | NA | NA | NA | 2 | 2 | 7 | NA | NA |
| Storch et al., 2013234 | 6 | 14 | 3 | 16 | NA | NA | NA | NA | 2 | 8 | 9 | NA | NA |
| The Pediatric OCD Treatment Study, 2004236 | 7 | 28 | 2 | 28 | 3 | 28 | 3 | 28 | 4 | 1 | 6 | 7 | 8 |
| Williams et al., 2010235 | 1 | 10 | 1 | 11 | NA | NA | NA | NA | 2 | 2 | 7 | NA | NA |
Key: intervention (class)
-
Placebo (1).
-
Waitlist (2).
-
Psychological placebo (3).
-
Fluoxetine (4).
-
Fluvoxamine (4).
-
Sertraline (4).
-
CBT (5).
-
CBT + sertraline (6).
-
CBT + placebo (7).
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| OR.D[1,2] | 3.763 | 305.6 | 0.9887 | 0.008369 | 0.2633 | 4.365 | 91,001 | 200,000 |
| OR.D[1,3] | 82.62 | 19,310 | 44.19 | 0.01173 | 0.3215 | 5.323 | 91,001 | 200,000 |
| OR.D[1,4] | 372.9 | 54,740 | 121.5 | 0.006197 | 0.3773 | 15.56 | 91,001 | 200,000 |
| OR.D[1,5] | 1.043 | 40.1 | 0.1593 | 0.01888 | 0.2756 | 2.5 | 91,001 | 200,000 |
| OR.D[1,6] | 4.388 | 634.1 | 2.031 | 0.02267 | 0.3584 | 4.282 | 91,001 | 200,000 |
| OR.D[1,7] | 2549 | 906,900 | 2023 | 0.001884 | 0.09901 | 4.014 | 91,001 | 200,000 |
| OR.D[2,3] | 37.09 | 4857 | 10.85 | 0.09322 | 1.202 | 20.43 | 91,001 | 200,000 |
| OR.D[2,4] | 7017 | 1.49E+ 06 | 3328 | 0.01486 | 1.384 | 168.8 | 91,001 | 200,000 |
| OR.D[2,5] | 2.246 | 36.64 | 0.08773 | 0.1656 | 1.041 | 8.465 | 91,001 | 200,000 |
| OR.D[2,6] | 350.7 | 56,730 | 127.7 | 0.05515 | 1.332 | 47.05 | 91,001 | 200,000 |
| OR.D[2,7] | 40,130 | 1.12E+ 07 | 25,170 | 0.005716 | 0.3793 | 35.75 | 91,001 | 200,000 |
| OR.D[3,4] | 6359 | 1.40E+ 06 | 3131 | 0.01157 | 1.136 | 130.7 | 91,001 | 200,000 |
| OR.D[3,5] | 2.005 | 53.18 | 0.125 | 0.1408 | 0.8544 | 5.568 | 91,001 | 200,000 |
| OR.D[3,6] | 773.2 | 221,200 | 495.5 | 0.04658 | 1.104 | 32.98 | 91,001 | 200,000 |
| OR.D[3,7] | 49,850 | 2.04E+ 07 | 45,660 | 0.004622 | 0.3091 | 24.7 | 91,001 | 200,000 |
| OR.D[4,5] | 1407 | 168,400 | 372.8 | 0.01008 | 0.7556 | 50.93 | 91,001 | 200,000 |
| OR.D[4,6] | 1829 | 232,900 | 522.6 | 0.01211 | 0.974 | 87.08 | 91,001 | 200,000 |
| OR.D[4,7] | 5410 | 1.32E+ 06 | 2957 | 0.001433 | 0.2713 | 56.51 | 91,001 | 200,000 |
| OR.D[5,6] | 30.1 | 4063 | 9.31 | 0.08929 | 1.287 | 21.18 | 91,001 | 200,000 |
| OR.D[5,7] | 1781 | 433,200 | 979.3 | 0.007595 | 0.3615 | 18.66 | 91,001 | 200,000 |
| OR.D[6,7] | 449.2 | 191,700 | 427.9 | 0.01618 | 0.285 | 4.439 | 91,001 | 200,000 |
| Interventions compared | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| OR[1,2] | 3.763 | 305.6 | 0.9887 | 0.008369 | 0.2633 | 4.365 | 91,001 | 200,000 |
| OR[1,3] | 82.62 | 19,310 | 44.19 | 0.01173 | 0.3215 | 5.323 | 91,001 | 200,000 |
| OR[1,4] | 0.7078 | 9.981 | 0.02973 | 0.01278 | 0.2972 | 2.497 | 91,001 | 200,000 |
| OR[1,5] | 1.361 | 39.79 | 0.09724 | 0.0647 | 0.542 | 3.524 | 91,001 | 200,000 |
| OR[1,6] | 2.148 | 550.9 | 1.256 | 0.03273 | 0.3309 | 2.428 | 91,001 | 200,000 |
| OR[1,7] | 1.043 | 40.1 | 0.1593 | 0.01888 | 0.2756 | 2.5 | 91,001 | 200,000 |
| OR[1,8] | 4.388 | 634.1 | 2.031 | 0.02267 | 0.3584 | 4.282 | 91,001 | 200,000 |
| OR[1,9] | 2549 | 906,900 | 2023 | 0.001884 | 0.09901 | 4.014 | 91,001 | 200,000 |
| OR[2,3] | 37.09 | 4857 | 10.85 | 0.09322 | 1.202 | 20.43 | 91,001 | 200,000 |
| OR[2,4] | 909.1 | 322,300 | 726.3 | 0.0211 | 1.063 | 49.41 | 91,001 | 200,000 |
| OR[2,5] | 759.3 | 114,200 | 268.3 | 0.07927 | 2.04 | 83.19 | 91,001 | 200,000 |
| OR[2,6] | 56.27 | 9489 | 22.25 | 0.07649 | 1.23 | 31.66 | 91,001 | 200,000 |
| OR[2,7] | 2.246 | 36.64 | 0.08773 | 0.1656 | 1.041 | 8.465 | 91,001 | 200,000 |
| OR[2,8] | 350.7 | 56,730 | 127.7 | 0.05515 | 1.332 | 47.05 | 91,001 | 200,000 |
| OR[2,9] | 40,130 | 1.12E+ 07 | 25170 | 0.005716 | 0.3793 | 35.75 | 91,001 | 200,000 |
| OR[3,4] | 326.9 | 50,620 | 116.6 | 0.01739 | 0.8772 | 36.11 | 91,001 | 200,000 |
| OR[3,5] | 472.8 | 64,440 | 151.3 | 0.0607 | 1.665 | 61.34 | 91,001 | 200,000 |
| OR[3,6] | 75.49 | 11,180 | 25.07 | 0.06565 | 1.011 | 21.89 | 91,001 | 200,000 |
| OR[3,7] | 2.005 | 53.18 | 0.125 | 0.1408 | 0.8544 | 5.568 | 91,001 | 200,000 |
| OR[3,8] | 773.2 | 221,200 | 495.5 | 0.04658 | 1.104 | 32.98 | 91,001 | 200,000 |
| OR[3,9] | 49,850 | 2.04E+ 07 | 45,660 | 0.004622 | 0.3091 | 24.7 | 91,001 | 200,000 |
| OR[4,5] | 94.89 | 12,400 | 29.51 | 0.1718 | 1.59 | 59.8 | 91,001 | 200,000 |
| OR[4,6] | 135.6 | 24,550 | 54.73 | 0.07889 | 1.074 | 32.55 | 91,001 | 200,000 |
| OR[4,7] | 55.09 | 9875 | 22.29 | 0.04075 | 0.9672 | 34.13 | 91,001 | 200,000 |
| OR[4,8] | 164.9 | 25,630 | 57.6 | 0.04778 | 1.253 | 54.58 | 91,001 | 200,000 |
| OR[4,9] | 2876 | 4.79E+ 05 | 1121 | 0.004735 | 0.3589 | 37.53 | 91,001 | 200,000 |
| OR[5,6] | 10.24 | 1850 | 4.172 | 0.04129 | 0.6941 | 6.434 | 91,001 | 200,000 |
| OR[5,7] | 20.95 | 5141 | 11.65 | 0.02488 | 0.5203 | 8.125 | 91,001 | 200,000 |
| OR[5,8] | 96.62 | 19,130 | 46.34 | 0.029 | 0.6658 | 14.55 | 91,001 | 200,000 |
| OR[5,9] | 1.35E+ 06 | 6.03E+ 08 | 1.35E+ 06 | 0.002772 | 0.1847 | 12.21 | 91,001 | 200,000 |
| OR[6,7] | 1.954 | 31.68 | 0.1074 | 0.07761 | 0.8458 | 7.118 | 91,001 | 200,000 |
| OR[6,8] | 7.992 | 449.5 | 1.027 | 0.07516 | 1.106 | 14.78 | 91,001 | 200,000 |
| OR[6,9] | 893.2 | 206,200 | 460.9 | 0.006087 | 0.3081 | 13.37 | 91,001 | 200,000 |
| OR[7,8] | 30.1 | 4063 | 9.31 | 0.08929 | 1.287 | 21.18 | 91,001 | 200,000 |
| OR[7,9] | 1781 | 433,200 | 979.3 | 0.007595 | 0.3615 | 18.66 | 91,001 | 200,000 |
| OR[8,9] | 449.2 | 191,700 | 427.9 | 0.01618 | 0.285 | 4.439 | 91,001 | 200,000 |
Median ranks
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk.class[1] | 6.162 | 1.207 | 0.01402 | 3 | 7 | 7 | 91,001 | 200,000 |
| rk.class[2] | 3.612 | 1.885 | 0.02214 | 1 | 3 | 7 | 91,001 | 200,000 |
| rk.class[3] | 4.006 | 1.792 | 0.01616 | 1 | 4 | 7 | 91,001 | 200,000 |
| rk.class[4] | 4.123 | 1.991 | 0.01434 | 1 | 4 | 7 | 91,001 | 200,000 |
| rk.class[5] | 3.587 | 1.341 | 0.01295 | 1 | 4 | 6 | 91,001 | 200,000 |
| rk.class[6] | 4.209 | 1.688 | 0.01611 | 1 | 4 | 7 | 91,001 | 200,000 |
| rk.class[7] | 2.3 | 1.794 | 0.01636 | 1 | 1 | 7 | 91,001 | 200,000 |
| Intervention code | Mean | SD | MC_error | val2.5pc | Median | val97.5pc | Start | Sample |
|---|---|---|---|---|---|---|---|---|
| rk[1] | 7.961 | 1.434 | 0.01674 | 4 | 8 | 9 | 91,001 | 200,000 |
| rk[2] | 4.425 | 2.559 | 0.03144 | 1 | 4 | 9 | 91,001 | 200,000 |
| rk[3] | 4.918 | 2.445 | 0.02401 | 1 | 5 | 9 | 91,001 | 200,000 |
| rk[4] | 4.472 | 2.465 | 0.02435 | 1 | 4 | 9 | 91,001 | 200,000 |
| rk[5] | 6.116 | 2.142 | 0.01966 | 2 | 7 | 9 | 91,001 | 200,000 |
| rk[6] | 4.821 | 2.033 | 0.01934 | 1 | 5 | 9 | 91,001 | 200,000 |
| rk[7] | 4.374 | 1.862 | 0.02014 | 1 | 4 | 8 | 91,001 | 200,000 |
| rk[8] | 5.18 | 2.29 | 0.02194 | 2 | 5 | 9 | 91,001 | 200,000 |
| rk[9] | 2.733 | 2.384 | 0.02166 | 1 | 1 | 9 | 91,001 | 200,000 |
Appendix 10 Economic evaluation
Office for National Statistics life tables stratified by age and gender
| Age (years) | Males | Females |
|---|---|---|
| 12 (mean age of children and adolescents) | 0.0001 | 0.0001 |
| 13 | 0.0001 | 0.0001 |
| 14 | 0.0001 | 0.0001 |
| 15 | 0.0002 | 0.0001 |
| 16 | 0.0002 | 0.0001 |
| 17 | 0.0004 | 0.0002 |
| 18 | 0.0005 | 0.0002 |
| 36 (mean age of adults) | 0.0011 | 0.0006 |
| 37 | 0.0012 | 0.0007 |
| 38 | 0.0013 | 0.0008 |
| 39 | 0.0014 | 0.0008 |
| 40 | 0.0016 | 0.0009 |
| 41 | 0.0016 | 0.0010 |
| 42 | 0.0018 | 0.0011 |
PubMed search strategy for longitudinal studies of the course of obsessive–compulsive disorder symptom severity conducted October 2014
| Search | Search term | Hits |
|---|---|---|
| #1 | Case control studies [MeSH Terms] | 667,981 |
| #2 | Cohort studies [MeSH Terms] | 1,355,328 |
| #3 | Case control [Text Word] | 210,456 |
| #4 | Cohort analy*[Text Word] | 4462 |
| #5 | Longitudinal [Text Word] | 186,703 |
| #6 | #1 Or #2 Or #3 Or #4 Or #5 | 1,605,453 |
| #7 | #6 AND (obsessive*AND compulsi*) | 1995 |
| #8 | #7 AND (yale Or brown or scale) | 561 |
Search strategy for studies of utility scores in patients with obsessive–compulsive disorder conducted August 2014
| Date | Database | Number of hits | Total hits this database | Total hits overall |
|---|---|---|---|---|
| 5 August 2013 | MEDLINE 1950 to present on Ovid | 403 | 403 | |
| 6 August 2013 | MEDLINE In-Process & Other Non-Indexed Citations – current week | 44 | 44 | 447 |
Database: MEDLINE 1950 to present
Date of search: 5 August 2014.
Search strategy
-
exp quality of life/ (119,318)
-
quality of life.tw. (137,047)
-
life quality.tw. (3389)
-
hql.tw. (81)
-
(sf 36 or sf36 or sf thirtysix or sf thirty six or short form 36 or short form thirty six or short form thirty-six or short form 36).tw. (15,158)
-
qol.tw. (17,845)
-
(euroqol or eq5d or eq 5d).tw. (3723)
-
qaly$.tw. (4832)
-
quality adjusted life year$.tw. (5700)
-
hye$.tw. (630)
-
health$ year$ equivalent$.tw. (38)
-
health utilit$.tw. (1062)
-
hui.tw. (643)
-
quality of wellbeing$.tw. (6)
-
quality of well being.tw. (323)
-
qwb.tw. (166)
-
(qald$ or qale$ or qtime$).tw. (110)
-
standard gamble$.tw. (650)
-
time trade off.tw. (728)
-
time tradeoff.tw. (199)
-
tto.tw. (576)
-
visual analog$ scale$.tw. (26,566)
-
discrete choice experiment$.tw. (414)
-
(sf6 or sf 6 or short form 6 or shortform 6 or sf six or sfsix or short form six or short form six).tw. (984)
-
health state$ utilit$.tw. (281)
-
health state$ value$.tw. (128)
-
health state$ preference$.tw. (83)
-
or/1-27 (213341)
-
obsessive compulsive disorder/ (11,322)
-
(obsess$ and (personalit$ or compuls$)).tw. (11,266)
-
or/29-30 (15,018)
-
28 and 31 (403)
Database: MEDLINE In-Process & Other Non-Indexed Citations – current week
Date of search: 6 August 2014.
Search strategy
-
exp quality of life/ (0)
-
quality of life.tw. (15,810)
-
life quality.tw. (385)
-
hql.tw. (5)
-
(sf 36 or sf36 or sf thirtysix or sf thirty six or short form 36 or short form thirty six or short form thirty-six or short form 36).tw. (1455)
-
qol.tw. (2086)
-
(euroqol or eq5d or eq 5d).tw. (601)
-
qaly$.tw. (563)
-
quality adjusted life year$.tw. (649)
-
hye$.tw. (69)
-
health$ year$ equivalent$.tw. (1)
-
health utilit$.tw. (113)
-
hui.tw. (81)
-
quality of wellbeing$.tw. (2)
-
quality of well being.tw. (11)
-
qwb.tw. (6)
-
(qald$ or qale$ or qtime$).tw. (16)
-
standard gamble$.tw. (39)
-
time trade off.tw. (56)
-
time tradeoff.tw. (7)
-
tto.tw. (62)
-
visual analog$ scale$.tw. (3247)
-
discrete choice experiment$.tw. (80)
-
(sf6 or sf 6 or short form 6 or shortform 6 or sf six or sfsix or short form six or short form six).tw. (398)
-
health state$ utilit$.tw. (35)
-
health state$ value$.tw. (11)
-
health state$ preference$.tw. (10)
-
or/1-27 (20097)
-
obsessive compulsive disorder/ (0)
-
(obsess$ and (personalit$ or compuls$)).tw. (1072)
-
or/29-30 (1072)
-
28 and 31 (44)
Results of other sensitivity analyses: adults
| Intervention | Total costs, £ | Total QALYs | NMB (£20,000), £ | NMB (£30,000), £ |
|---|---|---|---|---|
| FLV + CBT | 7273 | 3.221 | 57,144 | 89,352 |
| CBT | 7477 | 3.234 | 57,212 | 89,557 |
| SSRIs | 5845 | 3.195 | 58,045 | 89,990 |
| VEN | 5801 | 3.202 | 58,229 | 90,244 |
| CLO | 5719 | 3.223 | 58,744 | 90,975 |
| CT | 6579 | 3.335 | 60,131 | 93,486 |
| BT | 6713 | 3.343 | 60,139 | 93,566 |
| CLO + BT |
| Intervention | Total costs, £ | Total QALYs | NMB (£20,000), £ | NMB (£30,000), £ |
|---|---|---|---|---|
| CBT | 7451 | 3.221 | 56,972 | 89,183 |
| CLO | 5894 | 3.180 | 57,711 | 89,514 |
| SSRIs | 5866 | 3.189 | 57,909 | 89,796 |
| BT | 6963 | 3.244 | 57,909 | 90,345 |
| VEN | 5846 | 3.191 | 57,965 | 89,870 |
| CLO + BT | 6892 | 3.260 | 58,318 | 90,923 |
| CT | ||||
| FLV + CBT |
| Intervention | Total costs, £ | Total QALYs | NMB (£20,000), £ | NMB (£30,000), £ |
|---|---|---|---|---|
| CBT | 7533 | 3.180 | 56,063 | 87,861 |
| SSRIs | 5937 | 3.172 | 57,495 | 89,210 |
| VEN | 5902 | 3.177 | 57,639 | 89,409 |
| CLO | 5894 | 3.181 | 57,721 | 89,528 |
| BT | 6915 | 3.271 | 58,514 | 91,228 |
| CLO + BT | 6929 | 3.272 | 58,516 | 91,238 |
| CT | 6744 | 3.277 | 58,803 | 91,576 |
| FLV + CBT |
| Intervention | Total costs, £ | Total QALYs | NMB (£20,000), £ | NMB (£30,000), £ |
|---|---|---|---|---|
| CBT | 7567 | 3.207 | 56,565 | 88,631 |
| FLV + CBT | 7306 | 3.196 | 56,619 | 88,582 |
| SSRIs | 5901 | 3.182 | 57,745 | 89,568 |
| CLO | 5869 | 3.188 | 57,897 | 89,779 |
| VEN | 5852 | 3.191 | 57,970 | 89,881 |
| CLO + BT | 6891 | 3.274 | 58,579 | 91,314 |
| CT | 6707 | 3.286 | 59,021 | 91,885 |
| BT | 6820 | 3.297 | 59,111 | 92,076 |
| Intervention | Total costs, £ | Total QALYs | NMB (£20,000), £ | NMB (£30,000), £ |
|---|---|---|---|---|
| FLV + CBT | 6412 | 3.219 | 57,968 | 90,158 |
| CBT | 6498 | 3.238 | 58,267 | 90,649 |
| SSRIs | 5770 | 3.208 | 58,390 | 90,471 |
| CLO | 5737 | 3.215 | 58,563 | 90,713 |
| VEN | 5724 | 3.220 | 58,668 | 90,863 |
| CLO + BT | 6186 | 3.299 | 59,799 | 92,792 |
| CT | 5986 | 3.313 | 60,272 | 93,401 |
| BT | 6119 | 3.320 | 60,291 | 93,495 |
| Intervention | Total costs, £ | Total QALYs | NMB (£20,000), £ | NMB (£30,000), £ |
|---|---|---|---|---|
| FLV + CBT | 7047 | 3.255 | 58,051 | 90,601 |
| CBT | 7233 | 3.283 | 58,418 | 91,243 |
| SSRIs | 5585 | 3.254 | 59,494 | 92,033 |
| CLO | 5558 | 3.259 | 59,614 | 92,200 |
| VEN | 5521 | 3.266 | 59,801 | 92,462 |
| CLO + BT | 6665 | 3.325 | 59,830 | 93,078 |
| BT | 6620 | 3.342 | 60,218 | 93,637 |
| CT | 6483 | 3.337 | 60,259 | 93,629 |
| Intervention | Total costs, £ | Total QALYs | NMB (£20,000), £ | NMB (£30,000), £ |
|---|---|---|---|---|
| FLV + CBT | 6615 | 3.219 | 57,765 | 89,955 |
| CBT | 6774 | 3.238 | 57,991 | 90,373 |
| SSRIs | 5237 | 3.208 | 58,924 | 91,004 |
| CLO | 5176 | 3.215 | 59,124 | 91,274 |
| VEN | 5137 | 3.220 | 59,254 | 91,450 |
| CLO + BT | 5912 | 3.299 | 60,074 | 93,067 |
| CT | 5678 | 3.313 | 60,580 | 93,709 |
| BT | 5777 | 3.320 | 60,633 | 93,838 |
| Intervention | Total costs, £ | Total QALYs | NMB (£20,000), £ | NMB (£30,000), £ |
|---|---|---|---|---|
| FLV + CBT | 7206 | 3.219 | 57,174 | 89,364 |
| CBT | 7428 | 3.238 | 57,337 | 89,719 |
| SSRIs | 5764 | 3.208 | 58,396 | 90,477 |
| CLO | 5751 | 3.215 | 58,549 | 90,699 |
| VEN | 5727 | 3.220 | 58,664 | 90,860 |
| CLO + BT | 6778 | 3.299 | 59,208 | 92,201 |
| CT | 6590 | 3.313 | 59,668 | 92,797 |
| BT | 6715 | 3.320 | 59,695 | 92,899 |
Results of other sensitivity analyses: children and adolescents
| Intervention | Total costs, £ | Total QALYs | NMB (£20,000), £ | NMB (£30,000), £ |
|---|---|---|---|---|
| BT | 6905 | 3.257 | 58,242 | 90,816 |
| CLO | 5578 | 3.266 | 59,735 | 92,392 |
| SSRIs | 5538 | 3.277 | 59,993 | 92,758 |
| CBT | 6615 | 3.339 | 60,166 | 93,556 |
| SER + CBT | 6562 | 3.350 | 60,437 | 93,936 |
| Intervention | Total costs, £ | Total QALYs | NMB (£20,000), £ | NMB (£30,000), £ |
|---|---|---|---|---|
| BT | 6780 | 3.268 | 58,580 | 91,259 |
| CLO | 5457 | 3.294 | 60,431 | 93,375 |
| CBT | 6469 | 3.365 | 60,829 | 94,478 |
| SSRIs | 5390 | 3.312 | 60,848 | 93,967 |
| SER + CBT | 6422 | 3.374 | 61,052 | 94,789 |
| Intervention | Total costs, £ | Total QALYs | NMB (£20,000), £ | NMB (£30,000), £ |
|---|---|---|---|---|
| CBT | 6732 | 3.298 | £59,223 | £92,201 |
| SSRIs | 5610 | 3.259 | £59,574 | £92,166 |
| SER + CBT | 6618 | 3.319 | £59,754 | £92,940 |
| Intervention | Total costs, £ | Total QALYs | NMB (£20,000), £ | NMB (£30,000), £ |
|---|---|---|---|---|
| BT | 6807 | 3.244 | 58,080 | 90,523 |
| CLO | 5590 | 3.263 | 59,677 | 92,311 |
| SSRIs | 5506 | 3.286 | 60,216 | 93,077 |
| CBT | 6572 | 3.343 | 60,289 | 93,719 |
| SER + CBT | 6518 | 3.354 | 60,561 | 94,101 |
| Intervention | Total costs, £ | Total QALYs | NMB (£20,000), £ | NMB (£30,000), £ |
|---|---|---|---|---|
| BT | 6376 | 3.254 | 58,710 | 91,254 |
| CLO | 5508 | 3.280 | 60,094 | 92,895 |
| SSRIs | 5381 | 3.311 | 60,840 | 93,951 |
| CBT | 6017 | 3.368 | 61,347 | 95,028 |
| SER + CBT | 5976 | 3.376 | 61,549 | 95,311 |
| Intervention | Total costs, £ | Total QALYs | NMB (£20,000), £ | NMB (£30,000), £ |
|---|---|---|---|---|
| BT | 6619 | 3.286 | 59,102 | 91,963 |
| CLO | 5360 | 3.315 | 60,931 | 94,077 |
| CBT | 6328 | 3.397 | 61,616 | 95,588 |
| SER + CBT | 6302 | 3.402 | 61,739 | 95,760 |
| SSRIs | 5220 | 3.350 | 61,776 | 95,274 |
| Intervention | Total costs, £ | Total QALYs | NMB (£20,000), £ | NMB (£30,000), £ |
|---|---|---|---|---|
| BT | 6073 | 3.254 | 59,014 | 91,557 |
| CLO | 4740 | 3.280 | 60,862 | 93,663 |
| SSRIs | 4515 | 3.311 | 61,707 | 94,818 |
| CBT | 5383 | 3.368 | 61,980 | 95,662 |
| SER + CBT | 5314 | 3.376 | 62,210 | 95,972 |
| Intervention | Total costs, £ | Total QALYs | NMB (£20,000), £ | NMB (£30,000), £ |
|---|---|---|---|---|
| BT | 6762 | 3.254 | 58,325 | 90,868 |
| CLO | 5515 | 3.280 | 60,087 | 92,888 |
| SSRIs | 5378 | 3.311 | 60,844 | 93,954 |
| CBT | 6459 | 3.368 | 60,905 | 94,586 |
| SER + CBT | 6418 | 3.376 | 61,107 | 94,869 |
List of abbreviations
- BLOCS
- Brown Longitudinal Obsessive–Compulsive Study
- BT
- behavioural therapy
- CBT
- cognitive–behavioural therapy
- CCDAN
- Cochrane Collaboration Depression, Anxiety and Neurosis
- CCDANCTR
- Cochrane Collaboration Depression, Anxiety and Neurosis Controlled Trials Registers
- CEAC
- cost-effectiveness acceptability curve
- CG
- clinical guideline
- CI
- confidence interval
- CrI
- credible interval
- CT
- cognitive therapy
- CYBOCS
- Children’s Yale–Brown Obsessive–Compulsive Scale
- DIC
- deviance information criterion
- DIS
- diagnostic interview schedule
- DSM
- Diagnostic and Statistical Manual of Mental Disorders
- ECA
- Epidemiologic Catchment Area
- EQ-5D
- European Quality of Life-5 Dimensions
- ERP
- exposure and response prevention
- FDA
- Food and Drug Administration
- GP
- general practitioner
- ICD-10
- International Classification of Diseases, Tenth Edition
- MD
- mean difference
- NEMESIS
- NEtherlands MEntal health Survey and Incidence Study
- NICE
- National Institute for Health and Care Excellence
- NMA
- network meta-analysis
- NMB
- net monetary benefit
- OCD
- obsessive–compulsive disorder
- OR
- odds ratio
- PRISMA
- Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- PSR
- psychiatric status rating
- PSSRU
- Personal Social Services Research Unit
- QALY
- quality-adjusted life-year
- RCT
- randomised controlled trial
- SD
- standard deviation
- SF-6D
- Short Form questionnaire-6 Dimensions
- SSRI
- selective serotonin reuptake inhibitor
- WHO
- World Health Organization
- YBOCS
- Yale–Brown Obsessive–Compulsive Scale