
Notes
Article history
The research reported in this issue of the journal was funded by the HTA programme as project number 14/72/01. The contractual start date was in June 2014. The draft report began editorial review in May 2015 and was accepted for publication in December 2015. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HTA editors and publisher have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
James Raftery is a member of the National Institute for Health Research (NIHR) Health Technology Assessment Editorial Board and the NIHR Journals Library Editorial Group. He was previously Director of the Wessex Institute and Head of the NIHR Evaluation, Trials and Studies Co-ordinating Centre (NETSCC). Amanda Blatch-Jones is a senior researcher at NETSCC.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2016. This work was produced by Raftery et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Introduction
Assessing the impact of health research has become a major concern, not least because of claims that the bulk of research currently undertaken is wasteful. 1 As publicly funded research is often organised in ‘programmes’, assessment of impact must consider a stream of projects, sometimes interlinked. The Health Technology Assessment (HTA) programme, as the name implies, is such a programme, funding mainly a mix of systematic reviews and randomised controlled trials (RCTs). In a previous review, Hanney et al. 2 assessed the impact of the first 10 years of the NHS HTA programme from its inception in 1993 to June 2003 and identified factors that helped make an impact, including, first, the fact that the topics tend to be relevant to the NHS and to have a policy customer and, second, the strengths of the scientific methods used coupled with strict peer review. 2,3 That assessment included a review of the literature published up to 2005 on the methods for assessing the impact from programmes of health research.
Evidence explaining why this research is needed now
Internationally, there has been a growing interest in assessing the impact of programmes of health research, and recent developments in the UK have created a new context for considering impact assessment. Besides the claim that much research is wasteful, other factors include pressure on higher education institutions to demonstrate accountability and value for money, the expansion in routine collection of research impact data and the large-scale assessment of research impact in higher education through case studies in the Research Excellence Framework (REF).
Aim
To review published research studies on tools and approaches to assessing the impact of programmes of health research and, specifically, to update the previous 2007 systematic review funded by the HTA programme. 2
Objective
Our objective was to build on the previous HTA review2 (published in 2007, covering the literature up to 2005) to:
-
identify the range of theoretical models and empirical approaches to measuring impact of health research programmes, and collate findings from studies assessing the impact of multiproject programmes
-
extend the review to examine (1) the conceptual and philosophical assumptions underpinning different models of impact and (2) emerging approaches that might be relevant to the HTA programme, such as studies focusing on monetised benefits and on the impact of new trials on systematic reviews
-
analyse different options for taking impact assessment forward in the National Institute for Health Research (NIHR)/HTA programme, including options for drawing on routinely collected data.
Structure of the report
Chapter 2 describes the methods used for the review, Chapter 3 reports the findings from the updated review, Chapter 4 presents a broader taxonomy of impact models, Chapter 5 provides the findings on the monetary value of the impact of health research, Chapter 6 reports on the impact of trials on systematic reviews, Chapter 7 summarises the impact of trials on discontinuing the use of technologies and Chapters 8 and 9 provide a discussion of the main findings, including options for NIHR/HTA to take research impact assessment forward and draw conclusions from the report, and discuss recommendations for future impact assessment.
Chapter 2 Methods
The work was organised into three streams: the first stream focused on updating and extending the previous 2007 review;2 the second stream involved an extension of the literature in relation to the conceptual and philosophical assumptions on different models of impact and their relevance to the HTA programme; and the third stream considered the different options for taking impact assessment forward in the NIHR/HTA programme.
This chapter provides an account of the methods common to these streams of work. Where there were differences because of the type of review conducted, further explanation is provided under the relevant work stream.
Review methods
Given the nature and scope of the reviews included, a range of methods were used to identify the relevant literature:
-
systematic searching of electronic databases
-
hand-searching of selected journals
-
citation tracking of relevant literature
-
literature known to the team (i.e. snowballing)
-
bibliographic searches of other reviews
-
bibliographic searches of references in identified relevant literature.
Search strategies
Although different search strategies were conducted for the different elements, details of the individual search strategies can be found below (see Appendix 1 for full listing of the search strategies used).
Update to the previous review methods
The previous assessment of the impact of the HTA programme2 was informed by a review of the literature on assessing the impact of health research. It found an initial list of approximately 200 papers, which was reduced to a final ‘body of evidence’ of 46 papers: five conceptual/methodology, 23 application and 18 combined conceptual and application (please refer to the original Hanney et al. 2 report for a full list of these references). (In that review, as in the current one, ‘paper’ refers generically to the full range of publications, including reports in the grey literature.) The discussion included an analysis of the strengths, and weaknesses, of the conceptual approaches. The Payback Framework, the most widely used approach, was considered the most appropriate framework to adopt when measuring the impact of the HTA programme, notwithstanding the limited progress made in various empirical studies in identifying the health and economic benefit categories from the framework.
The first question for the updated review was: ‘what conceptual or methodological approaches to assessing the impact of programmes of health research have been developed, and/or applied in empirical studies, since 2005?’. 2
The second question was: ‘what are the quantitative findings from studies (published since 2005) that assessed the impact from multiproject programmes (such as the HTA programme)?’.
Search strategy development
The information scientist (Alison Price) evaluated the search strategy run in the previous report. 2 We used the same search strategy, but checked to identify any new medical subject headings and other new indexing terms. We also reviewed Banzi’s search strategy,4 a modified version of our original strategy. The review by Banzi et al. 4 searched in only two bibliographic databases (MEDLINE and The Cochrane Library), whereas we searched a larger number (see Databases searched). By not including the EMBASE database, Banzi et al. 4 may have missed some relevant indexed journals. For example, the journal in which the Banzi review was published, Health Research Policy and Systems, was indexed in EMBASE and not in MEDLINE until later. We included EMBASE indexing terms, as applied to the Banzi et al. 4 paper, in our expanded EMBASE search strategy.
Any new and relevant indexing terms were evaluated and added to the revised search strategies. The search strategies used text words and indexing terms to capture the concept of the impact of health research programmes. The search results were filtered by study and publication types. The new terms increased the sensitivity of the search, while the filters improved the precision and study quality of the results.
Databases searched
The searches were run in August 2014 for the publication period from January 2005 to August 2014 in the following electronic databases: Ovid MEDLINE, MEDLINE In-Process & Other Non-Indexed Citations, EMBASE, Cumulative Index to Nursing and Allied Health Literature (CINAHL), The Cochrane Library, including the Cochrane Methodology Register, HTA Database, the NHS Economic Evaluation Database (NHS EED) and Health Management Information Consortium (HMIC), which includes grey literature such as unpublished papers and reports (see Appendix 1 for a full description of the search strategies).
Other sources to identify literature
A list of known studies, including those using a range of approaches in addition to the Payback Framework, was constructed by SH. This list was used to inform aspects of the database search and help identify which journals to hand-search. These journals were Health Research and Policy and Systems, Implementation Science, International Journal of Technology Assessment in Health Care and Research Evaluation.
A list of key publications was constructed and the references were searched for additional papers. The list consisted of major reviews published since 2005 (that were already known to the authors, and/or were identified in the search) and key empirical studies. 4–19
For studies reporting on the development and use of selected conceptual frameworks, we took the main publication from each as the source for citation tracking using Google Scholar (Google Inc., Mountain View, CA, USA). The list was supplemented by citation tracking of selected key publications, although we considered only post-2005 citations of any papers that were published before that date.
Inclusion/exclusion criteria
We included studies if they described:
-
conceptual or methodological approaches to evaluating the impact of programmes of health research
-
the empirical evaluation of the impact of a particular programme of health research.
Studies were excluded if they provided only speculation on the potential impact of proposed (future) research [including recent studies on the value of information (VOI)], discussed the impact of research solely in the context of wide and intangible benefits (such as for the good of society and for the overall benefit of the population), or only considered impact in terms of guidance implementation. These inclusion/exclusion criteria repeated those used for the original review that aimed to identify appropriate approaches for retrospective assessment of the impact from the first decade of the HTA programme. VOI studies were not seen as relevant for such a review. Similarly, our review focused on the impact of specific pieces and programmes of research; it was beyond the scope of this study to consider the impact of guidelines based on multiple studies from different programmes of research. Therefore, our focus was on the implementation of that specific research and not on the implementation of guidelines in general.
Our focus on programmes of research highlights the perspective of funders who are interested in identifying the impact of the body of work, at some level of aggregation. We also expanded the use of the term ‘programme’ to included empirical studies focusing on bodies of research conducted by research centres or groups, or a collection of studies around a common theme and conducted in a way that the researchers collectively might view as a programme.
In the 2007 report, we distinguished ‘first, studies that start with a body of research and examine its impact and, second, those that consider developments within the health sector, especially policy decisions, and analyse how far research, from whatever source, influenced those developments’. 2 The latter category of studies, which would have been large, was excluded to allow us to focus on studies that worked forwards to trace the impact from specific programmes of research. Since 2005, there have been further major reviews of studies of policy-making and how research evidence is used. 5,8,20,21 We examined these reviews to help identify studies to include. Again, we did not include studies that explored how research was utilised by policy-makers unless the focus was on the impact made by a specific body of research.
In relation to studies setting out options for research impact assessment, we generally included the study if it made some proposal based on the review or analysis, and if the proposed approach could, at least in theory, have a reasonable chance of being used to assess impact of health research programmes. 8 We also included reviews that usefully collated data on issues such as the methods and conceptual frameworks used in studies. 5
Steve Hanney and AY independently went through the papers and applied the criteria (set out above) to at least the abstract of each paper identified. The studies were classified using the same criteria as previously applied; ‘includes’, ‘possible includes’ and ‘interest papers’, with scope for iteration. Agreement on inclusion was resolved by discussion by SH and AY. Where agreement could not be made, the final decision was made through further discussion with JR and/or TG.
Data extraction
We constructed a data extraction sheet based on a simplified version of the one previously used. 2 It covered basic details such as author, title and date; type of study; conceptual framework and methods used in impact assessment; categories of impacts assessed and found; identification of whether or not the study attempted to assess the impact from each project in a multiproject programme; conflicts of interest declared; strengths and weaknesses; factors associated with impact; and other reviewer comments and quotes (see Appendix 2 for full details).
The data extraction sheet was applied to the papers by SH, TG, MG, JR and AY. Each member of the team considered the list of ‘includes’, avoiding papers on which he/she had been an author. As anticipated, some papers were removed following more detailed examination at the data extraction stage.
Extension of the literature methods
The second stream formed four parts:
-
exploring the conceptual and philosophical assumptions of models of impact
-
monetary value on the impact of health research
-
the impact of randomised trials on systematic reviews
-
the impact of randomised trials on stopping the use of particular technologies.
The methods for each part are discussed below.
Conceptual and philosophical assumptions of models of impact
This stream aimed not merely to update the previous review but to extend its scope. Although much has been published in the past 10 years on different models of impact, less attention has been paid to theorising these models and critically exploring their conceptual and philosophical assumptions. We sought to identify, and engage theoretically with, work from the social sciences that questioned the feasibility and value of measuring research impact at all.
For this extension, we captured key papers from the main search described above and added selected studies published before 2005 if they provided important relevant insights. A modified data extraction sheet was developed (see Appendix 2).
For the theoretical component, we grouped approaches primarily according to their underlying philosophical assumptions (distinguishing, for example, between ‘positivist’, ‘constructivist’, ‘realist’, and so on) and, within those headings, by their theoretical perspective. We compared the strengths and limitations of different philosophical and theoretical approaches using narrative synthesis.
This stream also sought to tease out any approaches from the sample of papers identified in the updated review that might be especially relevant to the HTA programme. We were already aware of some papers on monetisation of research impacts, quantifying the contribution of RCTs to secondary research and to discontinuation of ineffective technologies. These three topics were themes in our searches and analysis.
Monetary value on the impact of health research
We considered approaches to monetising the value of the health gain arising from medical research. We reviewed key recent developments in this field, in the context of prior knowledge of several recently published studies, including the Medical Research: What’s it Worth report,22 which was widely cited to support medical research funding in the Government’s 2010 Spending Review. 23 We also included work by members of the review team (SH and MG), and others, on the monetised benefits from cancer research, and studies from Australia. 24–26 These studies also provided the context for an analysis to examine a subset of research supported by HTA. 27 An additional, complementary, thorough search of the literature was performed using Buxton et al. 28 as a starting point.
The purpose of this additional search was to identify studies since 2004 that have used any methods to attempt to value (in monetary terms) the benefits (health and cost savings) of a body of health research (e.g. disease-specific level, programme level, country level) and link that with an investment in the body of research.
Economic returns from health research can be considered in two categories: (1) the population health gains from improvements in mortality and morbidity, which can be monetised using various approaches (cost savings or increases in cost of delivery of new technologies can be incorporated into this monetisation); and (2) the wider economic benefits that contribute to gross domestic product (GDP) growth through mechanisms such as innovation, new technologies and patents – ‘spill-over’ effects.
The focus was on identifying studies that have at least included a component concerned with the first category of returns. Although the main literature review was limited to programmes of health research, this extension included studies that considered other units of analysis, such as by disease.
Search strategy
A supplementary search to the main review was run in October 2014 to ensure that no relevant papers were omitted. Searches of the following databases were performed: Ovid MEDLINE, EMBASE, The Cochrane Library, NHS EED and the HMIC from January 2003 to October 2014 (see Appendix 1 for full details of the database searches).
Studies were included if they contained a component that quantified the returns from investment in medical research, by attaching a monetary value to hypothetical or realised health gains of conducted research. Studies that discussed or estimated the value of conducting future research to eliminate decision uncertainty (expected VOI) were excluded.
Impact of randomised trials on systematic reviews
The importance of summarising available evidence before conducting new trials and using new trials to update and correct systematic reviews has long been argued29 and was embraced by the HTA programme from its start. 30 Impact on policy, such as guidance from the National Institute for Health and Care Excellence (NICE), relies, where possible, on systematic reviews rather than on individual trials. Although some 70% of HTA-funded trials cite a preceding systematic review, little work has been done on the impact such trials have on updating and correcting systematic reviews. 31 This element of the review tried to identify examples of attempts to do this, and explore literature relating to how the contribution of a randomised trial to a subsequent systematic reviews might be established.
Search strategy
Alison Price conducted a supplementary search to the main review in October 2014. The search identified 54 articles (see Appendix 1 for search terms). Two were added based on the review of citations. In addition, the literature on VOI was reviewed, as variants of this rely heavily on systematic reviews.
The identified articles comprised those that were descriptive, those relating to the use of systematic reviews in designing future trials and relating to VOI (and its variants).
Impact of randomised trials on stopping the use of particular technologies
This considered the impact that single randomised trials might have in stopping the use of particular technologies. Examples of such trials funded by the HTA programme include trials of water softening for eczema,31 and larvae for wound healing. 32 Their negative findings were probably definitive, but conventional methods might not capture their full impact. We explored the relevant literature with a focus on trials that were ‘first in class’ or ‘biggest in class’.
Search strategy
Alison Price conducted two supplementary searches to the main literature review in March 2015 on the following databases: Ovid MEDLINE without Revisions from 1996 to March 2015, week 2; EMBASE from 1996 to 2015, week 10; and Ovid MEDLINE(R) In-Process & Other Non-Indexed Citations.
The first search (using Ovid MEDLINE) identified 52 articles (see Appendix 1 for full details of the database searches) and the second search (again using Ovid MEDLINE) identified 55 articles.
Data extraction
If there was more than one version of a report, only one version was included. For example, we included only one 2012 report from the Higher Education Funding Council for England (HEFCE) outlining plans for the assessment of the impact of research conducted in UK higher education through means of the REF. 33 Similarly, the same criteria applied to annual sets of publications of research impact from funders such as the Medical Research Council (MRC) and the Wellcome Trust.
Rather than having two lists of partially overlapping papers relating to Chapters 3 and 4, we merged the two emerging lists into one list of papers. Thus, the numbers in Chapter 3 represent the numbers for both the updated review plus key papers from those described in Chapter 4.
EndNote X7 (Thomson Reuters, CA, USA) reference management database was used to store the relevant papers obtained from the different sources used.
Chapter 3 Updated systematic review
The purpose of the current review was to update the previous review,2 including a summary of the range of approaches used in health research impact assessment, and to collate the quantitative findings from studies assessing the impact of multiproject programmes. First, we present a summary of the literature that is reported in the large number of studies. Second, we describe 20 conceptual frameworks, or approaches that are the most commonly used and/or have the most relevance for assessing the impact of programmes such as the HTA programme. Third, we briefly compare the 20 frameworks. Fourth, we discuss the methods used in the various studies, and describe a range of techniques that are evolving. Fifth, we collate the quantitative findings from studies assessing the impact of multiproject programmes, such as the HTA programme, and analyse the findings in light of the full body of evolving literature.
Review findings
The number of papers identified though each source is set in Table 1. A total of 513 records were identified, of which 161 were eligible; databases directly identified only 40 of these 161 (see Appendix 3, Table 14, for a brief summary of each of the 161 references) (Figure 1).
| Source used to identify the literature | Number of records identified |
|---|---|
| Database | 40 |
| Hand-search | 14 |
| Reference list | 41 |
| Citation track | 23 |
| Known to the team/snowballing | 43 |
| Total | 161 |
FIGURE 1.
Flow diagram of identified studies.

Summary of the literature identified
From the initial searching and application of the inclusion criteria, the number of publications identified this time was approximately three times the 46 included in the ‘body of evidence’ for the 2007 review. 2 Using wider criteria, we ended up with a list of 161.
We classified 51 as conceptual/methodological papers (including reviews), 54 as application papers and 56 as both conceptual and application papers (these are classified and reported in Appendix 3, Table 14, under column ‘Type’). The 51 conceptual and methodological papers not only reflect an increase in the discussion about appropriate frameworks to use but also reflect the wider criteria used in the extension to the update, including some pre-2005 publications. Thus, a simple comparison between the 51 conceptual papers in the update and the five in the previous review would not be appropriate.
The papers come predominantly from four English-speaking nations (Australia, Canada, the UK and the USA), with clusters from the Netherlands and Catalonia/Spain. We also identified an increasing number of health research impact assessment studies from individual low- and middle-income countries, as well as many covering more than one country, including European Union (EU) programmes and international development initiatives.
Some of the studies on this topic are published in the ‘grey literature’, which probably means they are even more likely to be published in local languages than they would be if they were in the peer-reviewed literature. This exacerbates the bias towards a selection of publications from English-speaking nations that arises from the inclusion of publications if they are available only in English.
Appendix 3 (see Table 14) lists the 161 included studies with a brief summary of each. We note basic data such as lead author, year, type of study (method, application, or both) and country. The last item has become more complicated with the increase in the range of studies conducted. We prioritised the location of the research in which impact was assessed rather than the location of the team conducting the impact assessment. Similarly, for reviews or other studies intended to inform the approach taken in a particular country, it is important to identify the location of the commissioner of the review, if different from the team conducting the study. We also recorded the programme/specialism of the research in which impact was assessed, and the conceptual frameworks and methods used to conduct the assessment. A further column covers the impacts examined and a brief account of the findings. The final column offers comments, and quotes, where appropriate, on the strengths and weaknesses of the impact assessment and factors associated with achieving impact.
We also identified a range of papers that were of some interest for the review, but the papers did not sufficiently meet the inclusion criteria (see Appendix 4 for further details of these papers).
The included studies demonstrate that the diversity and complexity of the field has intensified. It has long been recognised that research might be used in many ways, even in relation to just one impact category, such as informing policy-making. 34,35 Within any one impact assessment, there can be many different ways and circumstances in which research from a single programme might be used. Furthermore, as a detailed analysis of one of the case studies described in Wooding et al. 36 illustrated, even a single project or stream of research might make an impact in various different ways, some relying on interaction between the research team and potential users and some through other routes.
The diversity in the approaches is also linked to the different types of research (basic, clinical, health services research, etc.) and fields, the various modes of research funding (responsive, commissioned, core funding, research training), and the diverse purposes and audiences for impact assessments. These are considered at various points in this review.
The 51 conceptual/methodological papers in Table 14 (see Appendix 3) illustrate the diversity. Some of these 51 papers developed new conceptual frameworks and some reviewed empirical studies and used the review to propose new approaches. Others analysed existing frameworks trying to identify the most appropriate frameworks for particular purposes. RAND Europe conducted one of the major streams of such review work. These reviews include background material informing the framework for the Canadian Academy of Health Sciences (CAHS),37 an analysis commissioned by the HEFCE to inform the REF,38 and a review commissioned by the Association of American Medical Colleges. 9
Such reviews represent major advances in the analysis of methods and conceptual frameworks, and each compares a range of approaches. They often focus on a relatively small number of major approaches. Although Guthrie et al. 9 identified 21 frameworks, many are not health specific and they vary in how far the assessment of impact features in the broader research evaluation frameworks.
Our starting position was different, and aimed to complement this stream of review work. We collated and reviewed a much wider range of empirical studies, in addition to the methodological papers. We not only identified the impacts assessed, but also considered the findings from empirical studies, both to learn what they might tell us about approaches to assessing research impact in practice and also to provide a context for the assessment of the second decade of the HTA programme.
In selecting the conceptual frameworks and methods on which to focus, we thought it was important to reflect the diversity in the field as far as possible, but at the same time focus on analysis of approaches likely to be of greatest relevance for assessing the impact of programmes such as the HTA programme.
Conceptual frameworks developed and/or used
We identified a wider range of conceptual frameworks than in the previous review. How the 20 frameworks were used can be seen later (see Table 2). We have grouped the discussion of conceptual frameworks into three main sections. The data are presented in ways that allow analysis from several perspectives. First, we present a historical analysis that helps to identify which frameworks have developed from those included in the 2007 review. Second, we order the frameworks by the level of aggregation at which they can be applied. Having briefly introduced each of the frameworks we then present them in tabular form under headings, such as the methods used, impacts assessed, strengths and weaknesses. Finally, in our analysis comparing the frameworks we locate each one on a figure with two dimensions: categories of impacts assessed and focus/level of aggregation at which the framework has primarily been applied.
The three main groups of frameworks are:
-
Post-2005 application, and further development, of frameworks described in the 2007 review, and reported in the order first reported in 2007 (five frameworks).
-
Additional frameworks or approaches applied to assess the impact of programmes of health research, and mostly developed since 2005 (13 frameworks). (These are broadly ordered according to the focus of the assessment, starting with frameworks that are primarily used to assess the impact from the programmes of research of specific funders, then frameworks that are more relevant for the work of individual researchers and, finally, approaches for the work of centres or research groups.)
-
Recent generic approaches to research impact developed and applied in the UK at a high level of aggregation, namely regular monitoring of impacts [e.g. via researchfish® (researchfish Ltd, Cambridge, UK)] and the REF (two frameworks or approaches).
Post-2005 applications of frameworks described in the 2007 review
Five are listed as follows:
-
the Payback Framework39
-
monetary value approaches to estimating returns from research (i.e. return on investment, cost–benefit analysis, or estimated cost savings)
-
the approach of the Royal Netherlands Academy of Arts and Sciences (2002)40
-
a combination of the frameworks originally developed in the project funded by the UK’s Economic and Social Research Council (ESRC) on the non-academic impact of socioeconomic research41 and in the Netherlands in 199442 [this became the Social Impact Assessment Methods through the study of Productive Interactions (SIAMPI)]
-
detailed case studies and follow-up analysis, on HTA policy impacts and cost savings: Quebec Council of Health Care Technology assessments (CETS). 43,44
The Payback Framework
The Payback Framework consists of two main elements: a multidimensional categorisation of benefits and a model to organise the assessment of impacts. The five main payback categories reflect the range of benefits from health research, from knowledge production through to the wider social benefits of informing policy development, and improved health and economy. This categorisation, which has evolved, is shown in Box 1.
-
Journal articles, conference presentations, books, book chapters and research reports.
-
Better targeting of future research.
-
Development of research skills, personnel and overall research capacity.
-
A critical capacity to absorb and appropriately utilise existing research, including that from overseas.
-
Staff development and educational benefits.
-
Improved information bases for political and executive decisions.
-
Other political benefits from undertaking research.
-
Development of pharmaceutical products and therapeutic techniques.
-
Improved health.
-
Cost reduction in delivery of existing services.
-
Qualitative improvements in the process of delivery.
-
Improved equity in service delivery.
-
Wider economic benefits from commercial exploitation of innovations arising from R&D.
-
Economic benefits from a healthy workforce and reduction in working days lost.
Although a detailed account of the various impact categories is available elsewhere,2 key recent aspects of the framework’s evolution relate to headings number 2 and 5 in Box 1.
In the ‘Benefits to future research and research use’ category, the subcategory termed ‘A critical capacity to absorb and appropriately utilise existing research, including that from overseas’ had proven difficult to operationalise in applications of the Payback Framework. However, a more recent evidence synthesis46 incorporated this concept into a wider analysis of the benefits to the health-care performance that might arise when clinicians and organisations engage in research. Although the evidence base is disparate, a range of studies was identified that suggested when clinicians and health-care organisations engaged in research there was a likelihood of improved health-care performance. Identification of the mechanisms through which this occurs contributes to the understanding of how impacts might arise, and increases the validity of some of the findings from payback studies in which researchers claim that research is making an impact on clinical behaviour in their local health-care systems.
In the ‘Broader economic benefits’ category, recent developments emphasise approaches that monetise the health gains per se from research, rather than assessing the economic benefits from research in terms of valuing the gains from a healthy workforce. 26 Nason et al. 47 applied the Payback Framework in a way that highlighted the economic benefits category and identified various subcategories.
The payback model is intended to assist the assessment of impact and is not intended necessarily to be a model of how impact arises. It consists of seven stages and two interfaces between the research system and the wider environment, with feedback and also the level of permeability at the interfaces being key issues: developments do not necessarily flow smoothly, or even at all, from one stage to the next (Figure 2).
FIGURE 2.
The Payback Framework: model for organising the assessment of the outcomes of health research. Reproduced with permission. 48

As noted in the 2007 review,2 although the framework is presented as an ‘input–output model’, it ‘also captures many of the characteristics of earlier models of research utilisation’ such as those of Weiss34 and Kogan and Henkel. 49 The framework recognises that research might be utilised in various ways. It was devised to assess the impact of the Department of Health/NHS programme of research, a programme in which development was informed by Kogan and Henkel’s earlier analysis of the department’s research and development. 49 That analysis had promoted the idea that collaboration between potential users and researchers was important in encouraging the commissioning of research that was more likely to make an impact. Partly, the development of the Payback Framework was a joint enterprise between the Department of Health and the Health Economics Research Group. 50 The inclusion in the updated review of the findings from the application of the framework to the assessment of the first decade of the HTA programme illustrates the context within which the framework seems best suited.
The conceptual framework informs the methods used in an application; hence, documentary analysis, surveys and case study interview schedules are all structured according the framework, which is also used to organise the data analysis and present case studies in a consistent format. The various elements were devised both to reflect and capture the realities of the diverse ways in which impact arises, including as a product of interaction between researchers and potential users at agenda-setting and other stages. The emphasis on examining the state of the knowledge reservoir at the time of research commissioning enables some evidence to be gathered that might help explore issues of attribution, and possibly the counterfactual, because it forces consideration of whatever other work might have been going on in the relevant field.
One of the limitations of the Payback Framework, and various other frameworks, arises because of the focus on single projects as the unit of analysis, when it is often argued that many advances in health care should be attributed to a body of work. This ‘project fallacy’ is widely noted, including by many who apply the framework. In some studies applying the framework, for example to the research funded by Asthma UK,51 the problem was acknowledged in the way in which case studies that started with a focus on a single project were expanded to cover streams of work. Although some studies have been able to apply a version of the framework to demonstrate considerable impact from single studies,52 this has tended to be in particular types of research – in this case, intervention studies.
Some studies applied the framework in new ways, as noted in Table 14 (see Appendix 3). This might lead to welcome innovation, but also to applications that do not recognise the importance of features such as the interfaces between the research system and the wider environment and the desirability of capturing aspects such as the level of interaction prior to research commissioning.
Despite the challenges in application, 27 of our 110 empirical studies published since 20052,36,47,51–74 claim their framework is based either substantially or partly on the Payback Framework (Table 2).
| Framework/approach (in order presented in text of Chapter 3) | Empirical studies applying the framework or drawing on aspects of it |
|---|---|
| Payback Framework | Action Medical Research, 2009;54 Anderson, 2006;55 Aymerich et al., 2012;56 Bennett et al., 2013;57 Catalan Agency for Health Technology Assessment and Research, 2006;58 Bunn, 2010;59 Bunn and Kendall, 2011;60 Bunn et al., 2014;61 Cohen et al., 2015;52 Donovan et al., 2014;62 Engel-Cox et al., 2008;63 Expert Panel for Health Directorate of the European Commission’s Research Innovation Directorate General, 2013;53 Guinea et al., 2015;64 Hanney et al., 2007;2 Hanney et al., 2013;51 Kalucy et al., 2009;65 Kwan et al., 2007;66 Longmore, 2014;67 Nason et al., 2011;47 NHS SDO, 2006;68 Oortwijn, 2008;69 Reed et al., 2011;70 RSM McClure Watters et al., 2012;71 Schapper et al., 2012;72 Scott et al., 2011;73 The Madrillon Group, 2011;74 and Wooding et al., 201436 |
| Monetary value | Deloitte Access Economics, 2011;25 Guthrie et al., 2015;27 Johnston et al., 2006;75 MRC, 2013;76 Murphy, 2012;77 and Williams et al., 200878 |
| Royal Netherlands Academy of Arts and Sciences and others | Royal Netherlands Academy of Arts and Sciences 201079 |
| Social impact assessment model through the study of productive interactions | Meijer, 2012;80 and Spaapen et al., 201181 |
| Quebec Council of Health Care Technology’s assessments | Bodeau-Livinec et al., 2006;82 and Zechmeister and Schumacher, 201283 |
| CAHS | Adam et al., 2012;84 Aymerich et al., 2012;56 Cohen et al., 2015;52 Graham et al., 2012;85 Saskatchewan Health Research Foundation, 2013;86 and Solans-Domenèch et al., 201387 |
| Banzi’s research impact model | Laws et al., 2013;88 and Milat et al., 201389 |
| National Institute of Environmental Health Sciences’s logic model | Drew et al., 2013;90 Engel-Cox et al., 2008;63 Liebow et al. 2009;91 Orians et al. 200917 |
| Medical research logic model (Weiss) | Informed various approaches rather than being directly applied |
| National Institute for Occupational Health and Safety’s logic model | Williams et al., 200992 |
| The Wellcome Trust’s assessment framework | Wellcome Trust, 201493 |
| VINNOVA | Eriksen and Hervik, 200594 |
| Flows of knowledge, expertise and influence | Meagher et al., 200895 |
| Research impact framework | Bunn, 2010;59 Bunn and Kendall, 2011;60 Bunn et al., 2014;61 Caddell et al., 2010;96 Kuruvilla et al., 2007;97 Schapper et al., 2012;72 and Wilson et al., 201098 |
| Becker Medical Library model | Drew et al., 2013;90 and Sainty, 201399 |
| Societal quality score (Leiden University Medical Centre) | Meijer, 2012;80 and Mostert et al., 2010100 |
| Research performance evaluation framework | Schapper et al., 201272 |
| Realist evaluation | Evans et al., 2014;101 and Rycroft-Malone et al., 2013102 |
| Regular monitoring | Drew et al., 2013;90 MRC, 2013;103 MRC, 2013;76 and Wooding et al., 2009104 |
| REF (informed by Research Quality Framework) | Cohen et al., 2015;52 Group of Eight and Australian Technology Network of Universities, 2012;105 and the HEFCE, REF Main Panel A, 2015106 |
In addition, the Payback Framework also informed the development of several other frameworks, especially the framework from the CAHS. 7 Furthermore, the framework based on the review by Banzi et al. 4 built on both the Payback Framework and the CAHS’s Payback Framework. The Payback Framework also contributed to the development, by Engel-Cox et al. ,63 of the National Institute of Environmental Health Sciences (NIEHS) framework.
Monetary value approaches to estimating returns from research (i.e. return on investment, cost–benefit analysis or estimated cost savings)
These approaches differ in the scope of the impacts that are valued and the valuation method adopted. In particular, since 2007 further methods have been developed that apply a value to, or monetise, the health gain resulting from research. Much of this work assesses the impacts of national portfolios of research, and is thus at a higher level of aggregation than that of a programme of research. Most of the studies of this are, therefore, not included here in Chapter 3, but are described in Chapter 5, which looks specifically at such developments. Nevertheless, three studies25,27,75 from this stream do assess the value of a programme of work and so are included in the update. Of the three, Guthrie et al. 27 and Johnston et al. 75 are the clearest applications of this approach to specific research programmes.
Furthermore, many econometric approaches to assessing research impact do not relate to the impact of specific programmes of research. However, an increasing number of frameworks have been developed that propose ways of collecting data from specific projects or programmes that can be built up to provide a broader picture of economic impacts. For example, Muir et al. 107 developed an approach for measuring the economic benefits from programmes of public research in Australia. Other work includes the development of frameworks by the UK department responsible for science; the Department of Business, Innovation and Skills (BIS) and, earlier, the Department for Innovation, Universities and Science108 developed frameworks under which the department collects data on economic benefits from each research council’s programmes of research, including the MRC. 76 The impacts include patents, spin-offs, intellectual property income; and data collection overlaps with the approach of regular collection of data from the MRC described below (see Regular monitoring or data collection). 76
A further category in the BIS framework is data on the employment of research staff. The classification of such data as a category of impact is part of a wider trend, but is controversial. However, in political jurisdictions, such as Ireland47 or Northern Ireland,6 it might be appropriate to consider the increased employment that comes as a result of local expenditure of public funds leveraging additional research funds from other sources.
To varying degrees the assessment of economic impacts can form part of wider frameworks, including the Payback Framework, as in the two Irish examples above, and the VINNOVA approach described by Eriksen and Hervik94 (see VINNOVA).
The approach of the Royal Netherlands Academy of Arts and Sciences
The report from the Royal Netherlands Academy of Arts and Sciences79 updated the evaluation framework previously used by the academy to assess research, not just impact, at the level of research organisations and groups or programmes. The approach combines self-evaluation and external peer review, including a site visit every 6 years. The report listed a range of specific measures, indicators or more qualitative approaches that might be used in self-evaluation. They included the long-term focus on the societal relevance of research, defined as ‘how research affects specific stakeholders or specific procedures in society (for example, protocols, laws and regulations)’. 79 The report proceeds to give the website for the Evaluating Research in Context (ERiC) project, which is described in Spaapen et al. 109 as being driven partly by the need, and/or opportunity, to develop methods to assist faculty in conducting the self-evaluation required under the assessment system for academic research in the Netherlands.
A combination of the frameworks originally developed in 2000 in the project funded by the UK’s Economic and Social Research Council on the non-academic impact of socioeconomic research and in the Netherlands in 1994 (this became the Social Impact Assessment Methods through the study of Productive Interactions)
In 2000, a team led by Molas-Gallart,41 working on the project funded by the UK’s ESRC on the non-academic impact of socioeconomic research, developed an approach based on the interconnections of three major elements: the types of output expected from research; the channels through which their diffusion to non-academic actors occurs; and the forms of impact. Later the team combined forces with Spaapen, whose early work with Sylvain42 on the societal quality of research had long been influential in the Netherlands, and, collectively, they led the SIAMPI approach. 110 This overlaps also with the development of the SciQuest method by Spaapen et al. 109 that came from the ERiC project described in The approach of the Royal Netherlands Academy of Arts and Sciences.
Its authors described SciQuest as a ‘fourth-generation’ approach to impact assessment. The previous three generations were characterised, they suggested, by measurement (e.g. an unenhanced logic model), description (e.g. the narrative accompanying a logic model) and judgement (e.g. an assessment of whether the impact was socially useful or not). The authors suggested that fourth-generation impact assessment is fundamentally a social, political and value-oriented activity and involves reflexivity on the part of researchers to identify and evaluate their own research goals and key relationships.
SciQuest methodology requires a detailed assessment of the research programme in context and the development of bespoke metrics (both qualitative and quantitative) to assess its interactions, outputs and outcomes. These are then presented in a unique research embedment and performance profile, visualised in a radar chart.
In addition to these two papers,109,110 the study by Meijer80 was partly informed by SIAMPI (see Appendix 3).
Detailed case studies and follow-up analysis on Health Technology Assessment policy impacts and cost savings: Quebec Council of Health Care Technology assessments
In the 2007 review,2 we described a series of studies of the benefits from HTAs conducted by the CETS. 43,44 They conducted case studies based on documentary analysis and interviews, and developed a scoring system for an overall assessment of the impact on policy that went from 0 (no impact) to +++ (major impact). They also assessed the impact on costs. Bodeau-Livinec et al. 82 assessed the impact on policy of 13 HTAs conducted by the French Committee for the Assessment and Dissemination of Technological Innovations. Although they did not explicitly state that they were using a particular conceptual framework, their approach to scoring impact appears to follow the earlier studies of CETS in Quebec.
Zechmeister and Schumacher83 assessed the impact of all HTA reports produced in Austria at the Institute for Technology Assessment and Ludwig Boltzmann Institute for HTA aimed at use before reimbursement decisions were made or decisions for disinvestment. Again, they developed their own methods, but the impact of these HTA reports was analysed partly by descriptive quantitative analysis of administrative data informed by the Quebec studies. 43,44
Additional frameworks or approaches applied to assess the impact of programmes of health research and mostly developed since 2005
Many other conceptual frameworks have been developed to assess the impacts from programmes of health research, mostly since 2005. Some studies have combined several approaches. Below we list 13 frameworks that have also been applied at least once. Some frameworks combine elements of existing frameworks, an approach recommended by Hansen et al. 111 This means that in the list of studies that have applied different conceptual frameworks (see Table 2), there are some inevitable overlaps. Scope exists for different interpretations of exactly how far a specific study does draw on a certain framework. An important consideration in deciding how much detail to give on each framework has been its perceived relevance for a programme such as the HTA programme.
The 13 conceptual frameworks are presented as follows: first, frameworks applicable to programmes that have funded multiple projects; second, frameworks devised for application by individual researchers; third frameworks devised for application to groups of researchers or departments within an institution; and, finally, a generic evaluation approach that has been applied to assess the impact of a new type of funded programmes. Inevitably, it is not this clear-cut and there are some hybrids.
Canadian Academy of Health Sciences
The CAHS established an international panel of experts, chaired by Cyril Frank, to make recommendations on the best way to assess the impact of health research. Its report, Making an Impact: A Preferred Framework and Indicators to Measure Returns on Investment in Research,7 contained a main analysis, supported by a series of appendices by independent experts. The appendices discuss the most appropriate framework for different types of research and are analysed in Table 14 (see Appendix 3). 37,112–114
The CAHS framework was designed to track impacts from research through translation to end use. It also demonstrates how research influences feedback upstream and the potential effect on future research. It aims to capture specific impacts in multiple domains, at multiple levels and for a wide range of audiences. As noted in several of the appendices, it is based on the Buxton and Hanney Payback Framework (see Figure 2). 39 The framework tracks impacts under the following categories, which draw extensively on the Payback Framework: advancing knowledge; capacity building; informing decision-making; health impacts; broader economic; and social impacts. 7,115 The categories from the Payback Framework had already been adopted in Canada by the country’s main public funder of health research, the Canadian Institutes of Health Research, for use in assessing the payback from its research.
The main difference in the categorisation from that in the original Payback Framework is the substitution of ‘informing decision-making’ for ‘informing policy and product development’. The CAHS return on investment version,7 allows the categorisation to include decisions by both policy-makers and individual clinicians in the same category, whereas the Payback Framework distinguishes between policy changes and behavioural changes, and does not specifically include decisions by individual clinicians in the policy category. Therefore, the CAHS framework explicitly includes the collection of data about changes in clinical behaviour as a key impact category, but in studies applying the Payback Framework any assessments that can be made of behavioural changes by clinicians and/or the public in the adoption stage of the model help form the basis for an attempt to assess any health gain.
The CAHS’s logic model framework also builds on a Payback logic model, and combines the five impact categories into the model showing specific areas and target audiences where health research impacts can be found, including the health industry, other industries, government and public information groups. It also recognises that the impacts, such as improvements in health and well-being, can arise in many ways, including through health-care access, prevention, treatment and the determinants of health.
The Canadian Institutes of Health Research divided its research portfolio into four pillars. Pillars I–IV cover the following areas: biomedical; clinical; health services; and social, cultural, environmental and population health. The CAHS team conducted detailed work to identify the impact from the different outputs arising in each of these areas.
The team also developed a menu of 66 indicators that could be collected. It was intended for use across Canada, and has been adopted by the Canadian Institutes of Health Research and in some of the provinces, for example by Alberta Innovates: Health Solutions (AIHS), the main Albertan public funder of health research. AIHS also further developed the framework into a specific version for their organisation and explored how it would be implemented and developed. Implementation had to do with standardising indicators across programmes to track progress to impact. It was developed to improve the organisation’s ability to assess its contributions to health systems impacts, in addition to the contributions of its grantees. 85 The CAHS framework has also been applied in Catalonia by the Catalan Agency for Health Information and Quality. 84
Banzi’s research impact model
Banzi et al. ,4 in a review of the literature on research impact assessment, identified the Payback Framework as the most frequently used approach. They presented the CAHS’s payback approach in detail, including the five payback categories as listed above. Building on the CAHS report, Banzi et al. 4 set out a list of indicators for each domain of impact and a range of methods that could be used in impact assessment. The Banzi research impact model has been used as the organising framework for several detailed studies of programmes of research in Australia.
A number of the applications have suggested ways of trying to address some of the limitations noted in the earlier account of the Payback Framework. For example, the study by Laws et al. 88 applied the Banzi framework to assess the impact of a schools physical activity and nutrition survey in Australia. They found it difficult to attribute impacts to a single piece of research, particularly the longer-term impacts, and wondered whether or not the use of contribution mapping, as proposed by Kok and Schuit may provide an alternative way forward (see Chapter 4 for a description of Kok and Schuit116).
National Institute of Environmental Health Sciences’s logic model
The US NIEHS developed and applied a framework to assess the impact from the research and the researchers it funded. Engel-Cox et al. 63 developed the NIEHS logic framework and identified a range of outcomes by drawing on the Payback Framework and Bozeman’s public value mapping. 117 These outcomes included translation into policy, guidelines, improved allocation of resources, commercial development; new and improved products and processes; the incidence, magnitude and duration of social change; health and social welfare gain and national economic benefit from commercial exploration and a healthy workforce; and environmental quality and sustainability. They added metrics for logic model components. The logic model is complex; in addition to the standard logic model components of inputs, activities, outputs and outcomes (short term, intermediate, long term), there are also four pathways: NIEHS and other government pathways, grantee institutions, business and industry, and community. The model also included the knowledge reservoir and contextual factors (Figure 3).
FIGURE 3.
The NIEHS’s logic model. Reproduced with permission from Environmental Health Perspective. 63

The various pathways allow a broader perspective to be developed than that of individual projects, for example by the grantee institution pathway, and by focusing on streams of research from multiple funders. Challenges identified in the initial case studies included ‘the lack of direct attribution of NIEHS-supported work to many of the outcome measures’. 63 The NIEHS put considerable effort into developing, testing and using the framework. Orians et al. 17 used it as an organising framework for a web-based survey of 1151 asthma researchers who received funding from NIEHS or comparison federal agencies from 1975 to 2005. Although considerable data were gathered, the authors noted that ‘this method does not support attribution of these outcomes to specific research activities nor to specific funding sources’. 17
Furthermore, Liebow et al. 91 were funded to tailor the logic model of the NIEHS’s framework to inputs, outputs and outcomes of the NIEHS asthma portfolio. Data from existing National Institutes of Health databases were used and, in some cases, data matched with that from public data on, for example the US Food and Drug Administration website for the references in new drug applications, plus available bibliometric data and structured review of expert opinion stated in legislative hearings. Considerable progress was made that did not require any direct input form researchers. However, not all the pathways could be used and they found their aim to obtain readily accessible, consistently organised indicator data could not in general be realised.
A further attempt was made to gather data from databases. Drew et al. 90 developed a high-impacts tracking system: ‘an innovative, Web-based application intended to capture and track short-and long-term research outputs and impacts’. It was informed by the stream of work from NIEHS,17,63 but also by the Becker Library approach118 and by the development in the UK of researchfish. The high-impacts tracking system imports much data from existing National Institutes of Health databases of grant information, in addition to text of progress reports and notes of programme officers/managers.
This series of studies demonstrates both a substantial effort to develop an approach to assessing research impacts, and the difficulties encountered. The various attempts at application clearly suggest that the full logic model is difficult and too complex to apply as a whole. Although the stream of work has, nevertheless, had some influence on thinking beyond the NIEHS, apart from the in-house stream of work no further empirical studies were identified as claiming that their framework was based on the NIEHS’s logic model approach.
Medical research logic model (Weiss)
Anthony Weiss analysed ways of assessing health research impact, but, unlike many of the other approaches identified, his analysis was not undertaken in the context of aiming to develop an approach for any specific funding or any research-conducting organisation. He drew on the United Way model119 for measuring programme outcomes to develop a medical research logic model. As with standard logic models it moves from inputs, to activities, outputs, and outcomes: initial, intermediate, long term. He also discussed various approaches that could be used, for example surveys of practitioners to track awareness of research findings; changes in guidelines, and education and training; use of disability-adjusted life-years (DALYs) or quality-adjusted life-years (QALYs) to assess patient benefit. He also analysed a range of dimensions from the outputs, such as publications through to clinician awareness, guidelines, implementation and overall patient well-being. 120
Although this model was not developed for a specific organisation, it does overlap with the emphasis given to logic models in various frameworks and studies, including the W.K. Kellogg logic model. 121 Weiss’s account is included here because it has become quite high profile and is widely cited. It has informed a range of studies rather than being directly applied in empirical studies.
National Institute for Occupational Health and Safety’s logic model
Williams et al. ,92 from the RAND Corporation in the USA, with advice from colleagues in RAND Europe, developed a logic model to assess the impact from the research funded by the National Institute for Occupational Health and Safety (NIOSH). At one level the basic structure of the logic model was a standard approach, as described by Weiss120 and as in the logic model from W.K. Kellogg. 121 Its stages include inputs, activities, outputs, transfer, intermediate customs, intermediate outcomes, final customers, intermediate outcomes and end outcomes.
A novel feature of the NIOSH model was outcome worksheets based on the historical tracing approach,122 which reversed the order ‘articulated in the logic model and essentially places the burden on research programs to trace backward how specific outcomes were generated from research activities’. 92
Research programmes could apply these tools to develop an outcome narrative to demonstrate and communicate impact to the National Academies’ external expert review panels established to meet the requirements of the US Government’s Performance Assessment Rating Tool. Williams et al. 92The report stated that intermediate outcomes include adoption of new technologies; changes in workplace policies, practices, and procedures; changes in the physical environment and organisation of work; and changes in knowledge, attitudes and behaviour of the final customers (i.e. employees, employers). End outcomes include various items related specifically to occupational health, including reduced work-related hazardous exposures, and, in relation to morbidity and mortality, reductions in occupational injuries and in fatalities within a particular disease- or injury-specific area.
The outcome worksheet was primarily designed as a practical tool to help NIOSH researchers think through the causal linkages between specific outcomes and research activities, determine the data needed to provide evidence of impact, and provide an organisational structure for the evidence.
The combination of historical tracing with a logic model is interesting because previously historical tracing has been more associated with identifying the impact made by different types of research (i.e. basic vs. clinical), irrespective of how they were funded, rather than contributing to the analysis of the impact from specific programmes of research.
The Wellcome Trust’s assessment framework
The Wellcome Trust’s assessment framework has six outcome measures and 12 indicators of success. 93 A range of qualitative and quantitative measures are linked to the indicators and are collected annually. A wide range of internal and external sources is drawn on, including end-of-grant forms. The evaluation team leads the information gathering and production of the report with contributions from many staff from across the trust.
‘The Assessment Framework Report predominantly describes outputs and achievements associated with trust activities though, where appropriate, inputs are also included where considered a major Indicator of Progress.’93 To complement the more quantitative and metric-based information contained in volume 1 of the Assessment Framework Report, volume 2 contains a series of research profiles that describe the story of a particular outcome or impact associated with Wellcome Trust funding. The Wellcome Trust research profiles are agreed with the researchers involved and validated by senior trust staff.
Although there is no specific overall framework, it is a comprehensive approach. This is another example of a major funder including impact in the annual collection of data about the work funded. On the one hand, the importance of case studies is highlighted: ‘Case studies and stories have gained increasing currency as tools to support impact evaluation’,93 but, on the other hand, the report described an interest in also moving towards more regular data collection during the life of a project: ‘In future years, as the Trust further integrates its online grant progress reporting system throughout its funding activities . . . it will be easier to provide access to, and updates on grant-associated outputs throughout their lifecycle’. 93
VINNOVA
VINNOVA, the Swedish innovation agency, has been assessing the impact of its research funding for some time. The VINNOVA framework consists of two parts, an ongoing evaluation process and an impact analysis, as described in the review for CAHS by Brutscher et al. 37 The former defines the results and impact of a programme against which it can be evaluated. It allows the collection of data on various indicators. The impact analyses, the main element in the framework, are conducted to study the long-term impact of programmes or portfolios of research. There are various channels through which impacts arise, but each specific impact analysis can take a particular form.
In Table 14 (see Appendix 3) we describe one example: the analysis of the impacts of a long-standing programme of neck injuries research conducted at Chalmers University of Technology. 94 This considered the benefits to society through a cost–benefit analysis, the benefits to companies involved through an assessment of the profits expected in the future as a result of the research and the benefits to the research field through traditional academic approaches of considering the number and quality of articles and doctorates, and peer review of the quality of the institute. Eriksen and Hervik94
The aim has been, as far as possible to quantify the effects in financial terms, or in terms of other physically measurable effects, and to highlight the contribution made by the research from the point of view of the innovation system.
This approach is a hybrid in that it does relate to a stream of research funded by a specific funder, but it is at a single unit.
Flows of knowledge, expertise and influence
Meagher et al. 95 developed the ‘flows of knowledge, expertise and influence’ approach to assess the impact of ESRC-funded projects in the field of psychology research. As part of a major analysis of the ways in which research might make an impact, the authors pointed out that one limitation was that their study was on a collection of responsive-mode projects and while they did have a common funder (i.e. the ESRC), they had not been commissioned to be a ‘programme’. This again makes the example more of a hybrid, and the study is described in more detail in Chapter 4, but this is the only application of the approach that we identified in our search.
Research impact framework
The research impact framework (RIF) was developed at the London School of Hygiene and Tropical Medicine by Kuruvilla et al. ,123 who noted that researchers were increasingly required to describe the impact of their work, for example in grant proposals, project reports, press releases and research assessment exercises for which the researchers would be grouped into a department or unit within an organisation. They also thought that specialised impact assessment studies could be difficult to replicate and may require resources and skills not available to individual researchers. Researchers, they felt, were often hard-pressed to identify and describe research impacts, but ad hoc accounts do not facilitate comparison across time or projects.
A prototype of the framework was used to guide an analysis of the impact of selected research projects at the London School of Hygiene and Tropical Medicine. Additional areas of impact were identified in the process and researchers also provided feedback on which descriptive categories they thought were useful and valid vis-à-vis the nature and impact of their work.
The RIF has four main areas of impact: research-related, policy, service and societal. Within each of these areas, further descriptive categories were identified, as set out in Table 3. According to Kuruvilla et al. ,123 ‘Researchers, while initially sceptical, found that the RIF provided prompts and descriptive categories that helped them systematically identify a range of specific and verifiable impacts related to their work (compared to ad hoc approaches they had previously used).’123
| Research-related impacts | Policy impacts | Service impacts | Societal impacts |
|---|---|---|---|
| Type of problem/knowledge | Level of policy-making | Type of services: health/intersectoral | Knowledge, attitudes and behaviour |
| Research methods | Type of policy | Evidence-based practice | Health literacy |
| Publications and papers | Nature of policy impact | Quality of care | Health status |
| Products, patents and translatability potential | Policy networks | Information systems | Equity and human rights |
| Research networks | Political capital | Services management | Macroeconomic/related to the economy |
| Leadership and awards | Cost-containment and cost-effectiveness | Social capital and empowerment | |
| Research management | Culture and art | ||
| Communication | Sustainable development outcomes |
Although it is multidimensional in similar ways to the Payback Framework, the categories were broadened to cover health literacy, social capital and empowerment, and sustainable development.
Another major feature of the RIF is the intention that it could become a tool that researchers themselves could use to assess the impact of their research. This addresses one of the major concerns about other research impact assessment approaches. However, while the broader categorisation has been used, on its own or in combination, in an increasing number of studies124, we are not aware of any studies that have used it by adopting the self-assessment approach envisaged. Nevertheless, it could be useful to researchers having to prepare for exercises such as the REF in the UK.
The Becker Medical Library’s model/the translational research impact scale
Sarli et al. 118 developed a new approach called the Becker Medical Library model for assessment of research. Its starting point is the logic model of the W.K. Kellogg Foundation,121 ‘which emphasises inputs, activities, outputs, outcomes, and impact measures as a means of evaluating a programme’. 118
For each of a series of main headings, it lists the range of indicators and the evidence for each indicator. The main headings are research outputs knowledge transfer; clinical implementation; and community benefit. The main emphasis is on the indicators for which the data are to be collected, and referring to the website on which the indicators are made available the authors state: ‘Specific databases and resources for each indicator are identified and search tips are provided’. 118 The authors found during the pilot case study that some supporting documentation was not available. In such instances, the authors contacted the policy-makers or relevant others to retrieve the required information.
The Sarli et al. 118 article includes the case study in which the Becker team applied the model, but the Becker model is mainly seen as a tool for self-evaluation, with the suggestion that it ‘may provide a tool for research investigators not only for documenting and quantifying research impact, but also . . . noting potential areas of anticipated impact for funding agencies’. 118 It is generating some interest in the USA, including partially informing the Drew et al. 90 implementation of the NIEHS framework described above, and a UK application from Sainty. 99
More recently, Dembe et al. 124 proposed the translational research impact scale, which is informed not only by a logic model from the W.K. Kellogg Foundation and by the RIF,123 but also by the Becker Medical Library model. 118
The authors identified 79 possible indicators, used in 25 previous articles, and reduced them to 72 through consulting a panel of experts, but further work was being undertaken to develop the requisite measurement processes: ‘Our eventual goal is to develop an aggregate composite score for measuring impact attainment across sites’. 124 However, there is no indication provided about how a valid composite score could ever be devised. Although as far as we are aware an application of it has yet to be reported, from the perspective of our review it usefully illustrates how new models are being built on a combination of existing ones.
Societal quality score
Mostert et al. 100 developed the societal quality score using the theory of communication from Van Ark and Klasen. 125 Audiences are segmented into different target groups that need different approaches. Scientific quality depends on communication with the academic sector and societal quality depends on communication with groups in society; specifically, three groups: lay public, health-care professionals and private sector.
Three types of communication are identified: knowledge production, for example papers, briefings, radio/television services, products; knowledge exchange, for example running courses, giving lectures, participating in guideline development, responding to invitations to advise or give invited lectures (these can be divided into ‘sender to receiver’, ‘mutual exchange’ and ‘receiver to sender’); and knowledge use, for example citation of papers, purchase of products, and earning capacity (i.e. the ability of the research group to attract external funding). Four steps are then listed:
-
Step 1: count the relative occurrences of each indicator for each department.
-
Step 2: allocate weightings to each indicator (e.g. a television appearance is worth x, a paper is worth y).
-
Step 3: multiply 1 by 2 = ‘societal quality’ for each indicator.
-
Step 4: the average societal quality for each group is used to get the total societal quality score for each department.
It is a heavily quantitative approach and looks only at process, as the authors say that ultimate societal quality takes a long time to happen and is hard to attribute to a single research group. The approach does not appear to control for the size of the group but seems to be more applicable to research at an institution rather than project level.
Research performance evaluation framework
Schapper et al. 72 describe the research performance evaluation framework used at Murdoch Children’s Research Institute in Australia. It is ‘based on eight key research payback categories’ from the Payback Framework and also draws on the approach described in the RIF. 123
The centre has an annual evaluation overseen by the Performance Evaluation Committee, with a nominee from each of six themes and external member and chairperson. The evaluation ‘seeks to assess quantitatively the direct benefits from research, such as gains in knowledge, health sector benefits, and economic benefits’. 72 Data for the Research performance evaluation are gathered centrally by the research strategy office and verified by the relevant theme. The theme with highest score on a particular measure is awarded maximum points; others are ranked relative to this. Each theme nominates its best three research outcomes over 5 years, and is then interviewed by the research strategy team using detailed questionnaires to gain evidence and verify outcomes. Research outcomes are assessed using a questionnaire based on the RIF. There are three broad categories: knowledge creation; inputs to research; and commercial, clinical and health outcomes. The six major areas of outcomes are development of an intervention; development of new research methods or applications; communication to a broad audience; adoption into practice and development of guidelines and policy; translation into practice; and impact of translation and on health.
Realist evaluation
The final approach described in this subsection, realist evaluation, is a relatively new generic evaluation approach originally developed in the field of social policy. It has been applied to evaluating the impact of the NIHR-funded Collaborations for Leadership in Applied Health Research and Care (CLAHRCs). This evaluation by Rycroft-Malone et al. 102 is described in Chapter 4 [see Co-production models (e.g. multistakeholder research partnerships)]. Realist evaluation may be more widely applicable to other programmes in the NIHR. The realist evaluation approach was also used in the evaluation of public involvement in health research in England. 101
Generic approaches to research impact assessment developed and applied in the UK, and parallel developments in other countries
In this final section considering conceptual frameworks we focus on two generic approaches that have recently been introduced in the UK, namely researchfish and the REF, and in which the data collection from individual projects or research groups, respectively, is brought together at a high level of aggregation. Here we consider some of the accounts we gathered about them from reports and articles included in our review.
Regular monitoring or data collection
Research funders became increasingly interested in moving beyond one-off impact assessments of the type conducted through the Payback Framework and similar approaches. Of the various streams of work to develop such approaches one emerged from the application of the framework to assess the impact of the research funded by the Arthritis Research Campaign. 104 Developed in consultation with members of the research community, the RAND/Arthritis Research Campaign’s impact scoring system was loosely based on the questions asked on previous payback surveys, but evolved thereafter, simplifying the questions and increasing the number. According to Morgan Jones and Grant,126 this informed the development of researchfish.
Researchfish (formerly MRC’s e-Val) is the system used to collect information on the outputs, outcomes and impacts that have arisen from MRC-funded research. MRC’s e-Val was first launched in November 2009 and was used in three rounds of data collection. In 2011/12, the MRC worked with a group of approximately 10 other funders on a ‘federated’ version of e-Val that works across funders so that researchers can enter an output just once and then associate it with the relevant funder or funders.
Launched in 2012 as researchfish, by March 2014 there were more than 80 research organisations and funders using it, including more than 50 medical research charities and 10 universities. The fourth data-gathering period in 2012 – the first using researchfish – saw a 98% response rate.
The MRC plans to continue to co-ordinate use of researchfish closely with university support offices and/or research unit. It sees the data being used in a variety of ways, from funders returning it to universities so that they can be used for their REF submissions, to using data to inform funders’ strategic plans and as evidence for the Government’s spending reviews. 127
Researchfish is considered in the MRC’s report, Outputs, Outcomes and Impact of MRC Research. 103 Although it could have been included in the list above, it might be seen more appropriately as a tool. The researchfish web-based survey asks project principal investigators a series of questions under 11 major headings ranging from publications through to impact on the private sector.
These headings have some parallels with some of the models considered above, although no conceptual framework is made explicit. Given the nature of the requirements to complete the annual survey this approach results in a high level of compliance, at least in terms of principal investigator’s supplying some response.
A range of health research funders, including NIHR and the MRC, use researchfish. In addition to the description in MRC reports,103 the results are also included as some of the data required in the reporting for the BIS framework on economic impacts. 76
Research Excellence Framework impact assessment (Higher Education Funding Council for England) and the Research Quality Framework
The Research Quality Framework (RQF) was developed for the assessment of university research in Australia. 128 Owing mainly to a change of government, this framework was not actually used in Australia, but it affected developments for research impact assessment in the higher education sector in the UK. The Australian model proposed the use of narrative cases studies written by higher education institutes as the basis of expert peer review in national assessments of university research performance. 128 The key impacts to be assessed were wider economic, social, environmental and cultural benefits of research. The study by Kalucy et al. 65 piloted the expected introduction of the RQF and found the Payback Framework would be likely to be a suitable framework to use to gather the data to submit to the assessment.
In preparing for the REF in the UK, the HEFCE commissioned RAND Europe to review possible frameworks that might be adopted. 38 RAND Europe reviewed four methods for evaluating impact of university research against HEFCE criteria and recommended the adoption of a case study approach, drawing on the RQF from Australia. 128
In the 2014 REF,33 the HEFCE required universities to submit impact case studies in the form of a four-page description of a research project/programme and its ensuing impact, with references and corroborating sources. In relation to medicine and life sciences the report identified the kind of impacts that were sought:
. . . benefits to one or more areas of the economy, society, culture, public policy and services, health, production, environment, international development or quality of life, whether locally, regionally, nationally or internationally.
And:
. . . manifested in a wide variety of ways including . . . the many types of beneficiary (individuals, organisations, communities, regions and other entities).
p. 2633
The final report on the application of the REF to biomedical and health research from the REF 2014 Main Panel A, which had overseen the assessment of some 1600 case studies, concluded that the case study approach had been broadly successful. 106 The report noted, ‘International MPA [Main Panel A] members cautioned against attempts to “metricise” the evaluation of the many superb and well-told narrations describing the evolution of basic discovery to health, economic and societal impact’. 106 International members of the panel also produced a separate section for the report and described the REF as:
To our knowledge, the first systematic and extensive evaluation of research impact on a national level. We applaud this initiative by which impact, with its various elements, has received considerable emphasis.
p. 21106
The REF approach of assessing research impact through case studies prepared in institutions by groups of researchers, and assessed and graded by peer reviewers in accordance with the criteria of reach and significance, was adopted in Australia in a trial exercise by the Group of Eight and the Australian Technology Network of Universities. 105 Called Excellence in Innovation for Australia (EIA), this ‘replication’ of the REF approach was a small-scale trial, with 162 case studies, and was conducted much more rapidly, reporting in 2012. This study also reported that the case study methodology ‘to assess research impact is applicable as a way forward to a national assessment of impact’. 105
Comparing frameworks
The various analyses of research impact assessment frameworks conducted by RAND Europe involved making a series of detailed comparisons. 9,37,38 These included the scoring of 21 frameworks (e.g. SIAMPI, REF, CAHS/Payback) against 19 characteristics (e.g. formative, comprehensive, quantitative and transparency). 9
Over half of the 20 frameworks we described above were included in one or more of the three comparisons of frameworks noted here. Appendix 5 lists all the frameworks appearing at least once in the main analyses in these reviews, and identifies those we have included in our list of 20 frameworks, those for which we have included a later or alternative version, and those not included, with reasons, but some of these are described in Table 14 (see Appendix 3). The additional ones we have included that were not in the three reviews are generally more recent and have been applied specifically to assess the impact of programmes of health research.
In Table 4 we provide a brief analysis of the 20 frameworks described above. Much of the discussion of strengths and weaknesses focuses on specific aspects of particular frameworks, with more generic analysis in Chapter 4. The table of comparisons is intended to inform our assessment of options in Chapter 8.
| Framework/approach (in order presented in text of Chapter 3) | Methods of application typically used: can vary | Categories of impacts assessed | Types of programmes for which designed and applied | Key strengths | Main limitations | Potential applicability to NIHR programmes in future |
|---|---|---|---|---|---|---|
| Payback Framework | Case studies; interviews; surveys; documentary analysis; and bibliometrics | Multidimensional: knowledge production; future research and research use; informing policy and product development; health and health-care system; and broader economic benefits | Health services research; programmes of commissioned research, e.g. HTA; mixed portfolios of research covering many types and modes of funding | Applicable to a wide range of research; framework provides consistent structure for data collection, analysis and presentation especially through case studies; multidimensional categorisation of impacts included; focuses attention on context and interactions with potential users; and informed by collaborative approach | Resource intensive to apply, especially in the form of case studies; usual application is to projects, which intensifies attribution problems, despite focus on context and interactions in case studies; and often applied before a chance for most of any potential health and economic gains to have arisen | Wide range; and good for commissioned programmes, e.g. HTA; case studies usefully illustrate impact, but the surveys used previously become difficult because of researchfish |
| Monetary value | Desk analysis and case studies | Monetary value approaches: identifying or monetising the value of the health and/or GDP gains from research | Various approaches, often at high levels of aggregation; and one attempt to monetise health gain from the NIHR HTA programme | Findings of considerable interest to funders – in charity sector to show benefits to donors and in public sector to show government and public; and potentially comparable with returns on other public expenditure | Usually have to make many assumptions about attribution; resource intensive if attempt to monetise health gains; limited application at programme level; and controversy over some aspects of claimed impacts | The monetisation of health gains can only be applied to programmes where an assumption that health gains can be attributed |
| Royal Netherlands Academy of Arts and Sciences, and others | Self-evaluation and peer-review visits | Societal relevance: in relation to stakeholders or procedures ‘for example, protocols, laws, regulations’79 | Applied widely to institutions, research groups and programmes in the Netherlands | Evolved over many years and several rounds of application | In terms of application for assessing impacts, a comparatively small proportion of the approach relates to impact | Methods of application could possibly inform assessment of research centres |
| SIAMPI | Varies: audits of research groups (see Royal Netherlands Academy of Arts and Sciences above); stakeholder interviews; and bibliometrics | Productive interactions leading to societal quality. Social impact:the human well-being (‘quality of life’) and or the social relationships between people or organizationsSpaapen and van Drooge110 | Two health case studies during its development: an academic medical centre and an institute for health services research | Formative; flexible; innovative and intellectually engaging; sensitive to institutional goals; and avoids perverse incentives | Resource intensive; not comparable between institutions; and:challenging to implement, requires assessors to identify productive interactions, assumes interactions are a good indicator of impactGuthrie et al.9 | Possibly could inform approaches to evaluation of centres |
| CETS | Desk analysis to implement scoring; interviews; and case studies | Policy decisions (coverage of health technologies) and sometimes associated cost savings | HTA programmes with close links to user bodies | Used to quantify high levels of impact from several programmes | Highly specific use for measuring narrow range of impacts from some HTA programmes | Only relevant to programmes directly linked to decision-making bodies, possibly part of HTA |
| CAHS | Sets out the framework more than specific methods, but includes surveys and desk analysis | Multidimensional: advancing knowledge; capacity building; informing decision-making; health impacts; and broader health and social impacts | Been applied to a range of health research programmes, e.g. in Canada and Catalonia | Based on major analysis of options, including for different types of research, and wide stakeholder engagement and buy-in; very comprehensive; examines processes and outputs and impacts; concept of an indicator library | Resource intensive to establish mechanisms to gather data on the many indictors; and: complicated . . . [and] . . . requires participant expertise . . . definitional ambiguity between outputs and outcomesGuthrie et al.9 | Been designed for possible application to a wide range of health research programmes |
| Banzi’s research impact model | Range of methods: interviews, bibliometrics and documentary analysis | Multidimensional: advancing knowledge; capacity building; informing decision-making; health impacts; and, broader health and social impacts | Used to organise studies in Australia of a public health survey and a health promotion research grants scheme | Builds on existing frameworks (CAHS and Payback Framework), hence comprehensive list of impacts included; identifies list of indicators for each of the five Payback Framework categories; and helps organise in-depth studies of small schemes | Resource intensive to gather data on all the indicators identified; when applied at project-level it intensifies attribution problems; and application thus far has been to relatively small programmes | Possibly has potential for organising detailed impact assessments for small NIHR programmes |
| NIEHS’s logic model | Applied to NIEHS’s research in various studies: two desk analyses of databases; and one by survey | Multidimensional: including, policy; guidelines; products and processes; social change; health and social welfare gain; economic benefit; environmental quality; and sustainability | Applied to asthma portfolio of NIEHS and to careers of researchers who ever received NIEHS grants | Attempts to consider the various pathways through which impacts might arise and build the perspectives of a range of stakeholders into the logic model; and various applications attempted | Full logic model seems to have proven too complex to apply in its totality; and much of the focus has been on the total work of researchers who have ever received NIEHS’s funding, thus increasing attribution problems in relation to specific funders | Unlikely to be relevant as a full model, but some of the thinking could enrich other frameworks |
| Medical research logic model (Weiss) | Methods paper discusses options, for example surveys and desk analysis | Multidimensional: many discussed including publications; clinical awareness; guidelines; and patients’ well-being assessed by DALYs or QALYs | Informed several studies | Clearly sets out logic model for assessing range of dimensions; and seems simpler to implement than some others because it does not explicitly include the wider context of either the health/social/economic system or the wider knowledge reservoir | ‘Only covers medical research’ and not clear if it is appropriate for health research (CAHS,7 p. A-238); and it does not explicitly highlight the potentially problematic nature of the points where the researchers and the wider systems meet | Unlikely to be applied alone, but could help inform a range of studies |
| NIOSH’s logic model | Outcome worksheets to use in historical tracing back from impacts to research | Multidimensional: many including changes in workplace policies and practices; changes in knowledge and behaviour of employees/employers; and reductions in occupational injuries and fatalities | Applied to NIOSH research to develop outcome narratives for expert review panels | Combines a logic model that flows forwards from the research, with an historical tracing approach that works backwards from the impacts | Resource intensive; and not clear what happens when working backwards leads to research other than that funded by NIOSH | Unlikely to be used in this form, but historical tracing could possibly inform studies of NIHR’s impact on major health-care improvements |
| The Wellcome Trust’s assessment framework | Desk analysis by evaluation team to gather data from project reports, etc.; and case studies | Multidimensional: including knowledge/papers; products/devices; uptake into policy and practice; engagement; career development; and research environment | Used by the Wellcome Trust across its programmes | Wide-ranging main assessment of the trust’s research incorporates dimensions of impact; provides quantitative data and illuminated by case studies conducted by evaluation team, agreed by researchers and validated by senior trust staff | While being part of wide-ranging end-of-project assessment facilitates collection of impact data, it possibly means there is less focus on some aspects of impact; and it also limits time for impacts to have arisen | The careful production and use of case studies could inform the approach used in NIHR |
| VINNOVA | Impact analysis conducted in various ways in different assessments; includes economic analyses | Multidimensional: wide range but prime focus ‘to quantify the effects in financial terms, or other physically measurable effects’ and highlight contribution to innovation94 | Used by VINNOVA in a range of ways since 2003; applied to a range of innovation initiatives: we included example on neck injuries research | Flexible approach attempting to find best ways to assess long-term impacts of specific bodies of research; and a range of detailed economic approaches can be combined in each individual assessment | Many of the methods used are resource intensive; ‘there is a great deal of uncertainty in the calculations’;94 and difficult to identify ‘an approach’ that could be transferred | Is not a single approach that could easily be adopted in NIHR, but using a range of methods to assess the impact of specific bodies of research could provide lessons |
| Flows of knowledge, expertise and influence | Survey of PIs and others; focus groups; and semistructured interviews | Prime focus on flows of knowledge, expertise and influence on policy-making | Applied to the ESRC’s responsive mode projects in psychology | Comprehensive range of methods; approach informed by wide analysis; highlights the importance of conceptual (enlightenment-based, indirect) impacts; and identifies the limitations of a linear model | More resource intensive than some other approaches; and only one application identified and that was to responsive mode projects in one field, this reduced the scope for assessing interaction | The emphasis on conceptual impacts could have useful lessons |
| RIF | Originally through case studies by the RIF team who interviewed researchers; and intended for researcher use | Multidimensional: research-related impacts (papers, methods, products, etc.); policy (including policy networks and political capital, etc.); service impacts (evidence-based practice; quality of care, etc.); and societal impacts (health literacy, culture, sustainable development) | Originally applied to research conducted in one university department; and informed wider range of studies | Important additional impact categories beyond ones in the Payback Framework; devised as a do-it-yourself approach to meet the needs of researchers; adaptable and proved acceptable to researchers; and has been partially incorporated into various methodological analyses and empirical studies | Provides categories for capturing impacts, but the team’s own application study indicted some impacts not easily identifiable; others also ask how the will data be gathered on all the items;129 and our review did not identify examples of do-it-yourself application as intended | Designed for do-it-yourself by researchers, so application to programmes might be more limited, but impact categories could usefully enhance data gathering and inform questions asked |
| Becker Medical Library model | For self- evaluation by researchers: provides a list of indictors and databases, etc., that can be searched | Multidimensional – main headings: research outputs; knowledge transfer; clinical implementation; community benefits. Many indicators under each heading; and with 72 indicators in a spin-off framework | Developed as a tool for self-evaluation, but has informed sheets for ‘impact assessment’ sent to PIs in at least one UK organisation’s (small) research programme | Starting point was logic model that was used to generate/organise a list of indicators; comprehensive; and intended to assist researchers who are interested in conducting self-evaluation | Data for indicators are not always available; some categories are diverse and have an uncertain link with the framework; and difficult to establish ‘a clear pathway of diffusion of research output into knowledge transfer, clinical implementation, or community benefit outcomes’118 | Many survey items now covered by researchfish, but might have the potential to inform any bespoke survey planned by a NIHR programme |
| Societal quality score (Leiden University Medical Centre) | Surveys; benchmarking; and desk analysis | Prime focus on societal quality:depends on communication with groups in society – . . . lay public; healthcare professionals and private sectorMostert et al.100 | Application described is to research groups/departments in the one university medical centre (Leiden) | Based on considerable analysis of processes of communicating research; the focus on identifying who research is aimed at is:useful in trying to understand the processes around research translationCAHS et al.7 | Does not attempt to assess some categories of impacts such as health benefits; and heavily quantitative approach involves allocating weights to each indicator in a standardised way that might not reflect actual contribution | Focus is on comparing research groups rather than funded programmes; and might have some lessons on the importance of communications |
| Research performance evaluation framework | Desk analysis of each groups’ performance by central team using bibliometrics, documentary analysis; and then peer review | Multidimensional: eight categories drawn from Payback Framework, plus RIF:seeks to assess quantitatively the direct benefits from research, such as gains in knowledge, health sector benefits, and economic benefitsSchapper et al.72 | Designed by an Australian research institute for internal use to allocate funds: claim the evaluation is unique | Informed by existing approaches – Payback Framework and RIF; provides balanced analysis across range of impact categories; and:generally viewed positively by the researchers at the Institute . . . a powerful tool for evaluating the Institute’s progress towards achieving its strategic goalsSchapper et al.72 | Might appear rather formulaic; does not aim to provide assessment of all research from each group; can currently only be judged by the application in a single centre for which it was specifically designed; and potentially disruptive for centre cohesion | Designed to allocate funds between research groups in a centre, so potential application to NIHR programmes limited; and embeds impact assessment into centre management |
| Realist evaluation | Mixed-method case studies: interviews; ethnography; desk analysis; and participant observation | Not predefined; assumed to vary by study | One application to CLAHRCs | Identifies what works for whom in what circumstances; sensitive to the context within which research programme being implemented; and provides understanding about how impacts arise | Only one application to assess impact of a NIHR programme identified to date; resource intensive and can be expensive; and complex to undertake, i.e. requires detailed understanding of realist evaluation | Been applied to CLAHRCs; and might have potential for application in overall assessment of some programmes |
| Regular monitoring | Annual surveys to PIs during and after research funding | Multidimensional: publications; collaborations; further funding; career progression; engagement activities; influence on policy; research materials; IP; development of products or interventions; impacts on private sector; and, awards and recognition | Researchfish extensively used by NIHR, MRC and other health research funders | Reasonably comprehensive; high formal response rates; widely used, hence could facilitate comparability; and builds up fuller picture over succeeding years thus capturing some data a one-off bespoke survey might miss | Burden on researchers; danger of poorer response rate to key questions than can be obtained by bespoke surveys; and standardised questions to cover all research councils, etc. reduces specificity for aspects of health research | Researchfish extensively used by NIHR for its programmes |
| REF (informed by RQF) | Desk analysis to produce impact case studies based on research groups; and scored by peer review | Multidimensional: benefits to one or more areas of the economy, society, culture, public policy and services, health, production, environment, and international development or quality of life33 | Used to assess research groups in all UK higher education institutions; small replication study in Australia | ‘The narrative case study largely succeeded in capturing the complex links between research and impact’;106 the international members of the panel broadly endorsed the approach; and focused considerable policy-maker and international attention on the extensive impacts | Burden on institutions; not directly applicable to programmes of funded research, although case studies have been made searchable; selective inclusion of research; and many case studies in initial exercise did not provide (sufficient) quantification of the extent and reach of the impact | Potentially all NIHR programmes would be able to search the REF database of case studies with the aim of identifying the use of their research |
Figure 4 locates the various frameworks on two dimensions in an attempt to identify clusters of frameworks that might be attempting to do similar things. One dimension is the type of impact categories assessed. We have abstracted the key impact categories described in the frameworks: multidimensional (i.e. covers a range that can include health gains, economic impacts and policy impacts); economic impacts (value of improved health and GDP); policy impacts (including clinical policies); and communication/interactive processes. The other dimension is the level of aggregation at which the framework has primarily been applied and whether the focus is on programmes of work from funders or on the portfolio of work of individual researchers, groups of researchers or institutions. (We classed the REF as being in the producers of research category because the work assessed was funded by multiple organisations and conducted by institutions and their units, even though the assessment results will then be used to allocate the future funds from the specific funding organisation conducting the assessment, i.e. the HEFCE.) Where the focus is on programmes of funded research, the impact assessment is most likely to gather data from individual studies, but these are then pulled together and reported on at an aggregate programme level. Furthermore, there can be some data gathering about the whole programme.
FIGURE 4.
Twenty key frameworks: prime assessment focus/level and impact categories assessed.

Finally, in this section we draw attention to a very different approach: the balanced scorecard (BSC), which is analysed in the CAHS report. 7 Some studies describe health-care systems that include research as part of a BSC approach to assessing performance of their system,130,131 but it is argued that the approach is not a comprehensive impact assessment of research. 7 If, however, a BSC approach is used to assess health-care organisations, and includes research impact as one of the criteria, this could be a mechanism for encouraging health-care organisations to foster research activity in their facilities.
Methods used in empirical impact assessment studies
Our updated review identified several studies that undertook important analysis of the methods used in research impact evaluation. These include the UK Evaluation Forum,19 the CAHS report7 and the report from RAND for the Association of American Medical Colleges. 9 The last analysed 11 methods or tools used in a range of six major research evaluation frameworks; most relate to the collection of data and others to how data are presented. The authors provided a brief description of each with a suggestion of when and how it is used. The 11 methods/tools were set out in alphabetical order: bibliometrics, cases studies, data mining, data visualisation, document review, economic analysis, interviews, logic models, peer review, site visits and surveys. The review by Boaz et al. 5 of studies assessing the impact of research on policy-making identified 16 methods as having been used, with semistructured interviews, case study analysis and documentary analysis as the three most commonly adopted. Milat et al. 129 reported that typically mixed methods were used, which could include publications and citations analysis, interviews with principal investigators, peer assessment, case studies and documentary analysis.
Our review of 110 empirical studies also found that a wide range of methods were adopted, but in various combinations. Frequently used methods included desk analysis, surveys, interviews and case studies. The full range of methods used in the studies listed can be found in Table 14 (see Appendix 3), and below we note some interesting trends and show how our review provides further evidence on long-standing issues about the range of methods available for impact assessments. In relation to surveys, for example, there are concerns about the burden on researchers of completing them and on the accuracy of the data. The burden is widely viewed as having increased with the introduction of the above annual surveys, notwithstanding the attempts to reduce the burden by enabling the data entered to be attached to a range of grants. This increased burden might result in incomplete data in the response to specific questions within the overall survey, and might also have implications for the willingness of researchers to complete voluntary but bespoke surveys that specific funders might consider commissioning. The survey response rates in the included studies varied enormously. The compliance requirements in a survey such as researchfish result in very high formal response rate, but the rate has also been high in other surveys; for example, it was 87% in a study in Hong Kong. 66 The rate, however, was only 22% in a pilot study assessing the impact of the EU’s international development public health programme,27 but they did use a range of other methods as well.
In terms of the accuracy of the data from surveys of researchers, several studies report that, in general, the findings from users were similar to those from researchers, for example Guinea et al. 64 and Cohen et al. 52 When comparisons have been made between the responses to surveys, and the data gathered in subsequent case studies on the same project, researchers have been found not to routinely exaggerate. 2 Indeed, Gutman et al. 132 found that researchers interviewed claimed a higher level of impact on policy than was reported by researchers in a web survey, although the questions were slightly different. Meagher et al. 95 also reported that while, ‘case studies were crucial in illuminating the nature of policy and practice impacts . . . there were no evident contradictions between results obtained by different methods.’
Doubts have also been expressed as to how much researchers actually know about the impact their research might have made. One trend that might provide some reassurance about this is that some of the studies in Table 14 (see Appendix 3) report relatively small-scale research funding schemes in which much of the claimed impact arises from the adoption of the findings in the researcher’s own health-care unit, where researchers are well-placed to know the impact made. Some examples of this were reported by Caddell et al. 96
A balance must be found between coverage and resources. Several of the reported assessments relied on the programme office and/or impact evaluators gathering the data from databases, for example in the case of the evaluation of the impact from the EU’s public health programmes53 and in one of the NIEHS’s studies. 91 However, in both cases and others there were some doubts about whether or not sufficient data could be collected in this way, but one of the advantages was that it did not place the burden on researchers. Other attempts to increase practicality go in other directions. Individual researchers might be encouraged to construct accounts of the impact from their own work. In particular, Kuruvilla et al. 123 designed the RIF as a do-it-yourself approach, which prompts researchers to systematically think about the impact of their work using descriptive categories. The Becker Medical Library model was also primarily seen as a tool for self-evaluation. 118
Case studies tend to provide a wider and more rounded perspective on how the impact might have arisen and can address attribution. They tend to be resource intensive and usually conducted only selectively. One dilemma is case study selection, for which a purposive approach is often adopted. However, a stratified random selection has been used when applying the Payback Framework,2,36 and a recent study in Australia conducted case studies on all the projects in which the respondents had completed two surveys and an interview, thus avoiding any selection bias. 52 Case studies can, however, be conducted through self-assessment, perhaps based on desk analysis. They can then be evaluated by peers in an approach that seems to be becoming increasingly important and broadly successful. 33,105,106
There are also an increasing number of studies reporting attempts to score case studies. In addition to the examples of scoring of self-assessment described above, this also includes scoring case studies produced by impact assessors,36,52,89 or produced initially by central teams in the institution, including the cases produced for the research performance evaluation framework used at Murdoch Children’s Research Institute in Australia. 72
Whatever the method of data collection, attention has been given in several studies to expected benefits. We excluded studies that solely considered potential impact before research was commissioned, but some studies are considering aspects of ‘expected’ impacts in several ways. Some make a comparison between what was expected from a project and what had been achieved. Examples include studies from the EU studies,53,133 from Catalonia/Spain56,58 and from Australia. 70 Studies can also emphasise what impacts are expected from research that has already been completed, but which had not yet arisen at the time of the impact study: such questions are, for example, often a feature of surveys in studies applying the Payback Framework. This also includes the application of the framework to assess the impact of the funding provided for biomedical research by the annual TV3 Telethon in Catalonia. 58
Attempts are also being made to develop ways to consider the impact of programmes as a whole in addition to the impact that might come from the collation of data on individual projects. This overlaps with consideration of conceptual frameworks, where, for example, we discussed the role of realist evaluation in assessing one of the CLAHRCs,102 but it can also relate to the methods used in other studies. For example, in their assessment of the Austrian HTA programme, Schumacher and Zechmeister134 set out the methods they had used and the issues that could be addressed by each one, including attempts to identify the development of a HTA culture. Rispel and Doherty135 claimed that in their assessment of the impact of the Centre for Health Policy in South Africa, their own experiences gave them an ‘insider–outsider’ perspective, and that a rounded view of the Centre was provided by interviewing people with a predominantly ‘insider’ perspective, and others with an ‘outsider’ perspective.
Finally, in the 2007 report there was speculation regarding whether a conceptual framework was really needed or whether it might be possible just to apply some of the methods. It was claimed, however, that a conceptual framework could be most useful in informing the structure of a range of methods, such as documentary analysis, surveys and case study interviews. This was seen to be the case with the Payback Framework, and has remained so, as illustrated by the both the survey and the semistructured interview schedule included in the article describing the assessment of the impacts from Asthma UK funding. 51 This is also the case for newer frameworks such as the RIF.
Timing of assessments
Points about timing have sometimes been noted in the strengths and weaknesses column of Table 14 (see Appendix 3). As much of the impact from research is likely to arise some time after the completion of the research, any early one-off assessment is likely to capture less than regular monitoring that continues for some time after the completion of the project. Some impact assessments, for example Oortwijn,69 explicitly stated that they felt the early timing of the assessment had inhibited the level of impact that could have arisen and thus be recorded.
However, even this issue is not clear-cut and partly overlaps with the nature of the research approach. In the evaluation of the Africa Health Systems Initiative Support to African Research Partnerships, Hera136 reported that because the evaluation was before the end of the programme it was possible to observe the final workshop and present preliminary findings. It may have been too early for some of the expected impact to arise, but the interactive approach of the whole programme had led to some policy impact during project, and there were some advantages in analysing it while project meetings were still occurring. Nevertheless, the recent results from the UK’s REF clearly show that allowing up to 20 years for the impact to occur can contribute to assessments that show considerable impacts have been achieved by a range of research groups. 106
In the future, regular monitoring of research outcomes and continuous monitoring of uptake/coverage might provide ways of reducing at least some of the variations between studies in terms of the timing of assessments.
Summary findings from multiproject programmes
The findings from the analysis of multiproject programmes reported in the 2007 review provide a context for the current analysis. That review found that the six impact assessment studies that were focused on HTA programmes reported that the number of individual projects making an impact on policy ranged between 70% and 100%. The 10 impact assessment studies that were focused on ‘other health research programmes’, claimed that the number of individual projects making an impact on policy ranged between < 10% and 53%, and the number of projects making an impact on practice ranged between < 10% and 69%. These findings reflected the different roles of the two identified groups of programmes, but there was also considerable diversity within the nature of the programmes within each group.
The study of the impact of the first decade of the NHS HTA programme was reported as the main part of the 2007 report. However, the study was not included in the literature review chapter of that 2007 report because that review included studies published up to a cut-off point of mid-2005, and had been conducted in order to inform the assessment that was undertaken of the NHS HTA programme. Therefore, the findings below, from the survey of the lead researchers conducted as part of the assessment of the HTA programme, were not referred to in the review chapter. They show a similar pattern to that identified in the 2007 review, that is, an even higher level of impact being claimed for the Technology Assessment Reports (TARs) than for the other types of HTA-funded research, which, in the case of trials, are nearer to the research in the ‘other research programmes category’ than they are to appraisals that constitute the work of most HTA programmes (Table 5).
| Project type | Impact, n (%) | |||||
|---|---|---|---|---|---|---|
| Policy | Behaviour | |||||
| Already | Future | Combineda | Already | Future | Combineda | |
| Primary | 25 (66) | 27 (71) | 29 (76) | 17 (45) | 21 (55) | 23 (61) |
| Secondary | 27 (57) | 27 (57) | 36 (77) | 10 (21) | 22 (47) | 25 (53) |
| NICE TAR | 46 (96) | 29 (60) | 48 (100) | 29 (60) | 28 (58) | 37 (77) |
| Total | 97 (73) | 82 (62) | 113 (85) | 56 (42) | 70 (53) | 85 (64) |
In our current review a collation of the quantitative findings from studies assessing the impact from multiproject programmes (such as the HTA programme) and published since the previous review conducted in 2005 should provide a context for the results from the parallel study being conducted of the impact from the second decade of the HTA programme.
The diversity of circumstances makes it difficult to be certain about which studies to include, but we classified 26 studies as being empirical studies of the impact from multiproject programmes, and a further two studies of the impact from research training have been included because the impact assessment covered the wider impact made by the research conducted in each training award, as well as the impact on the trainees’ subsequent careers (see Table 6 for the included studies). Even for these 28 studies there is considerable diversity in a range of aspects, including:
-
types of research and modes of funding of the programmes of research assessment
-
timing of impact assessment (some while the programme was still continuing, some conducted years afterwards)
-
conceptual frameworks used for assessment (e.g. some ask about impact on policy, including guidelines, and separately ask about impact on practice; but others ask about a combined ‘decision-making’ and have that as an impact category)
-
methods used for collecting and presenting data in impact evaluations (e.g. some present percentage of projects claiming each type of impact and some present the total number of examples of each type of impact, making it impossible to tell how many projects are represented by the total number because some projects might have generated more than one example of a particular type of impact).
It is likely that there will be different levels of impact on policy achieved, for example by a programme of responsive mode basic research than by a programme of commissioned HTA research. However, studies assessing impact from research do not necessarily fall into such neat categories because different funders will have a different mix of research in their programmes and portfolios. Therefore, we have listed all 28 studies (Table 6), but do not include the figures for each study for the percentage of project principal investigators claiming to have made various impacts.
| Name and year | Location of original research conducted | Type of research/topic |
|---|---|---|
| Projects | ||
| Adam et al., 201284 | Catalonia | Clinical and health services |
| Aymerich et al., 201256 | Catalonia | Epidemiology and public health |
| Catalan Agency for HTA and Research, 200658 | Catalonia | Wide range |
| Bodeau-Livinec et al., 200682 | France | HTA |
| Brambila et al., 2007137 | Guatemala | Operational research in reproductive health |
| Caddell et al., 201096 | Canada | Women and children’s health |
| Cohen et al., 201552 | Australia | Intervention studies |
| Donovan et al., 201462 | Australia | Breast cancer research: wide range |
| Expert Panel, 201353 | EU | Public health |
| Gold et al., 2007138 | USA | Delivery systems: implementation |
| Gutman et al., 2009132 | USA | Active Living Research: transdisciplinary field |
| Hanney et al., 20072 | UK | HTA |
| Hanney et al., 201351 | UK | Asthma UK: wide-ranging portfolio |
| Hera, 2014136 | Africa | Research partnerships with users |
| Johnston et al., 200675 | USA | Stroke clinical trials |
| Kingwell et al., 2006139 | Australia | National Health and Medical Research Council: wide range (grants ending in 2003 and 1997) |
| Kwan et al., 200766 | Hong Kong | Health and Health Services Research Fund |
| Milat et al., 201389 | Australia | New South Wales Health Promotion Demonstration Research Grants Scheme |
| Oortwijn, 200869 | The Netherlands | Health Care Efficiency Research programme (HTA) |
| Poortvliet et al., 2010140 | Belgium | The Belgium Health Care Knowledge Centre, HTA, health services research and GCP |
| Reed et al., 201170 | Australia | Primary care research |
| RSM McClure Watters et al., 201271 | Northern Ireland | Northern Ireland Executive: Health and Social Care Research |
| Sainty, 201399 | UK | Occupational Therapy Research Foundation |
| The Madrillon Group, 201174 | USA | National Institutes of Health Mind Body Interactions and Health Programme |
| Wooding, 2009104 | UK | ARC: wide range |
| Zechmeister and Schumacher, 201283 | Austria | Institute for Technology Assessment and Ludwig Boltzmann Institute for HTA: HTA |
| Research training | ||
| Action Medical Research, 200954 | UK | Fellowships: wide range |
| Zachariah et al., 2014141 | International | Structured operational research and training initiative of World Health Organization/special programme for research and training in tropical diseases: adopted an existing training initiative |
All the data for the individual studies are available from Table 14 (see Appendix 3), but here in Table 7 we show the average figures for the 23 of the 26 multiproject programmes in which the data were presented in terms of the number, or percentage, of individual projects claiming to have made an impact in the categories being assessed. Presenting it in this way allows the overall picture from the quantitative analysis of multiproject programmes to be seen, but also allows a commentary to include some data from individual projects, while at the same time describing key features of a particular research programme, including sometimes the context in which it had been conducted. Table 7 presents the averages and the range on each of the following criteria: impact on policy; impact on practice; a combined category, for example policy and clinician impact, or impact on decision-making; and impact in terms of improved care/health gain/patient benefit.
| Type of impact | Studies number reporting on each impact category (n = 23) | Average achieving/claiming this impact in the studies reporting on it (%) | Range achieving/claiming this impact in the studies reporting on it (%) |
|---|---|---|---|
| Policy/organisation impact | 18 | 36 | 5–97 |
| Clinician change/informed practice | 10 | 31 | 10–43 |
| A combined category, e.g. policy and clinician impact, or impact on decision-making | 3 | 64 | 60–67 |
| Health gain/patient benefit/improved care | 8 | 28 | 6–49 |
These are considered in turn.
Policy impacts
As in the 2007 review, the HTA programmes analysed generally showed the highest percentage achieving or claiming an impact on policy, but various examples illustrate a range of issues. Although 97% of the assessments from the Austrian HTA programme were classified by Zechmeister and Schumacher83 as making some impact on coverage policies, other factors also played a role and in only 45% of reports ‘the recommendation and decision were totally consistent’. 83 There is some uncertainty about whether or not Bodeau-Livinec et al. 82 included all the studies available, but, assuming that they did, 10 out of 13 recommendations from the French HTA body explored ‘had an impact on the introduction of technology in health establishments’;82 in seven cases the impact was considerable and in three it was moderate.
In the case of the more mixed HTA programmes, we noted above the considerable impact made by the NHS HTA programme, but with the TARs having a higher figure than the primary studies. For the Belgium Health Care Knowledge Centre programme, Poortvliet et al. 140 reported that within the overall figure of 58% of project co-ordinators claiming the projects had made an impact, the figure for HTAs was higher than for the other two programmes. Finally, the Health Care Efficiency Research programme from the Netherlands was classified as a HTA programme, but included a large responsive mode element and most studies were prospective clinical trials. Furthermore, Oortwijn69 reported that the impact assessment was conducted soon after many of the projects had been completed. These various factors are likely to have contributed to the proportion claiming an impact on policy (in these cases mostly citation on a guideline) being lower than other HTA programmes at 29%.
In four non-HTA studies,66,70,74,136 more than one-third of the projects appeared to make an impact on policy, and generally interaction with potential users was highlighted as a factor in the impact being achieved. Of the principal investigators in four studies, ≤ 10% reported that their research had made an impact on policy, but three of these studies62,104,139 assessed the impact of wide-ranging research programmes that, in addition to clinical and other types of research, covered basic research from which policy impact would be much less likely to occur. However, some of these programmes also made an impact in areas not reported on the table. For example, Donovan et al. 62 reported that 11% of principal investigators from the research funded by the National Breast Cancer Foundation in Australia claimed to have made an impact on product development.
Informed practice
Of the 10 studies reporting on impact on clinical practice,2,53,62,66,69,84,96,99,139,140 the five highest were in a narrow band of 37–43% of the principal investigators claiming such impact. 2,66,84,96,99 The projects in these programmes generally incorporated factors associated with achieving impact, including being funded to meet the needs of the local health-care system and interaction with potential users. Two of the studies96,99 looked at small-scale funding initiatives, and found that the impact was often at the location where the research was conducted.
Combined category
The three studies89,137,138 in which the impact seemed best reported at a combined level covering policy and practice impact, all suggested considerable levels of impact from projects where partnerships with potential users were a key feature.
Health gain/patient benefit/improved care
Only eight studies went as far as attempting to assess impact in terms of health gain or improved care,51,53,66,70,71,74,75,96 and none of them reported a figure > 50%. Three studies66,74,96 were the only studies in which over one-third of principal investigators claimed an impact on health care, and, as noted, all three had features associated with impact being achieved. Also of note is Johnston et al. 75 because although only eight out of a programme of 28 RCTs (29%) were identified as having a measurable use, with six (21%) leading to a health gain, these health gains were monetised and provide a major example of valuing the benefits from a programme of health research. The study is fully reviewed and critiqued in Chapter 5.
Finally, both the studies assessing the impact of research training schemes54,141 indicate that between one-third and three-quarters of the former trainees claimed that a wider impact had arisen from the research conducted in each training award. Here, however, even more than with project funding, it can be difficult to discern the impact from the specific research conducted and that from subsequent research that built on it.
Analysis of the findings from multiproject programmes
The picture emerging from Tables 6 and 7, plus the equivalent one in the 2007 review, is that many multiproject programmes are being identified as resulting in a range of impacts, but levels are highly variable.
An analysis of the findings from quantitative studies contributes to the overall review in various ways.
-
It is recognised there are many limitations in reducing issues of influence on policy and the other areas to a tick-box survey, and recognition that case studies (externally conducted based on interviews and documentary review, or self-assessment through desk analysis, etc.) are likely to provide a richer and more nuanced analysis. However, we also noted above that a variety of studies that have used another method in addition to surveying researchers suggest that, on average, researchers do not seem to be making exaggerated claims in their survey responses. Therefore, surveys of researchers can play some role in research impact assessment, and do allow wider coverage than is usually possible through more resource-intensive methods such as case studies.
-
There is an undoubted desire from some to improve survey methods, for example by computer-assisted telephone interviews. Nevertheless, this portfolio of studies suggests impact assessment can be done to some degree across multiproject programmes.
-
The findings indicate that different types of research programmes are likely to lead to different levels and ranges of impact. With better understanding of the expectations of what might arise from different programmes, it might be possible to tailor impact assessments to focus on appropriate areas for the different types of research. Various studies of small-scale initiatives54,96,99 illustrate that there is now wide interest in assessing the impact of health research funding, but also illustrate that conducting research in a health-care setting can lead to impacts in that health-care setting.
-
Impact assessments are partly conducted to inform the approach to organising and managing research. Therefore, collating these studies can add weight to the comments made in individual studies. Quite frequent comments are made about impact being more likely when the research is focused on the needs of the health-care system and/or there is interaction or partnership with potential users. 2,66,84,89,132,136–138,141 The particular circumstances in which HTAs are conducted to meet very specific needs of organisations that are arranged to receive and use the findings as ‘receptor bodies’ are also associated with high levels of impact. 82,83,140 The qualitative study by Williams et al. ,78 which included observation of meetings, provides some verification of the finding in the assessment of the HTA programme that the TARs do inform decision-making. Looking specifically at the economic evaluations included in TARs they reported that, ‘economic analysis is highly integrated into the decision-making process of NICE’s technology appraisal programme’. 78
We looked for suitable comparators against which to consider these findings from assessments of multiproject programmes. Potentially this could have come from a large-scale regular assessment that could provide data about the proportion of projects claiming impacts in certain categories across a whole research system. However, this is not the way researchfish operates and we could find no other equivalent comparator.
Instead, the 2014 REF33 and the EIA105 offer illuminating comparators in that they show high levels of impact were achieved from the small percentage of the total research that was described in the case studies submitted by institutions for consideration through the REF and EIA. So, while the REF was based on the research conducted by groups of researchers, rather than, in most cases, being based on the work of a single funded programme, it is also of value as a comparator because of the amount of evidence gathered in support of the exercise. The findings from our collection of studies in some ways reflect aspects of the REF, for example in that the REF assumed only a minority of the research from groups over a 20-year period (in practice, 1993–2013) would be suitable for entry for using to demonstrate impact had been achieved. As described, some of the studies of the whole portfolios of research funders included in our review covered a wide range of projects, and usually, in such cases, the percentage of principal investigators reporting impacts on policy and practice was lower than in other studies. However, such studies often identified examples of research within the portfolio that had made major impacts, although these were best explored in depth through case studies. This reinforces the point that in most research programmes only a minority of research should be expected to make much impact, but the impact from that minority can sometimes be considerable.
Furthermore, the nature of some of the major impacts claimed in the impact assessments from around the globe are similar to those reported in REF cases, even if the impacts in the REF are generally the more substantial examples. For instance, the report on the impacts from the Main Panel A suggests that in the REF many cases reported citations in clinical guidelines as an impact, and this is frequently a focus of the impacts reported in the assessments of multiproject programmes.
Overall, therefore, the quantitative analysis of studies assessing multiproject programmes can contribute to understanding the role impact assessments might play, and the strengths and weaknesses of the methods available.
Discussion
The considerable growth of interest in assessing the impact from health research was captured in our review. We identified an increasing number and range of conceptual frameworks being developed and applied, and included 110 new empirical applications (see Appendix 3), in comparison with the 41 reported in the review published in 2007. 2 In particular, we described and compared 20 frameworks or approaches that had been applied since 2005, some of them having also been described in the previous review. Quite a few of the 20 frameworks, and others, built on earlier frameworks, and sometimes combine elements from several. This partly reflects the need to address the various challenges identified as facing attempts to assess the impact from research.
The Payback Framework39 remains the most widely used approach for evaluating the impact of funded research programmes. It has been widely applied, and sometimes adapted and refined, including in the CAHS framework115 and Banzi’s research impact model. 4 Other robust models that show promise in capturing the diverse forms of health and non-health impacts from research include the RIF123 and various approaches to considering the economic impacts of health research. A comparison of the 20 frameworks indicates that while most, if not all, could contribute something to the thinking about options for future assessment of impact by NIHR, some are more likely than others to be relevant for assessing the impact of the bulk of the portfolio.
There is considerable diversity in terms of the impacts measured in the studies examined. Some of them make no attempt to move beyond the assessment of impact on policy to consider whether or not there has been any health gain. Others that adopt a multidimensional categorisation often recognise the desirability of identifying health gains, but, in practice, lack the resources to make much progress in measuring the health gain even in those cases (usually a small minority) where some links can be established between the research being assessed and the eventual health gains. Finally, some studies, at least in a few of the case studies included in an overall assessment, do go on to attempt to assess the health gains that might be at least partially associated with particular research. The variations depend on combinations of (1) the type of research portfolio that is being assessed, for example if it is a commissioned programme; (2) the type of framework being used for the assessment; (3) the resources available; and (4) the actual outcomes from the particular examples of research assessed. The multidimensional categorisation of impacts, and the way it is applied in approaches such as the Payback Framework and CAHS framework, allows considerable flexibility. In each case study, for example, it might be appropriate to take the analysis as far along the categorisation as it is practical to go. So, for some it might be possible to show an impact on clinical policies, such as guidelines or screening policies, and then for a minority of those there might be opportunities to take the analysis further and explore whether or not there is evidence from databases of practice change, screening uptake rates, etc. that could feed into an estimate of possible health gain.
Although interviews, surveys, documentary analysis and cases studies remained the most frequently used methods to apply the models, the range of methods and ways in which they were combined also increased. The purpose behind a particular study often influenced the frameworks and methods adopted. We identified 28 studies that had reported the findings from an assessment of the impact from all the projects in multiproject programmes. We were able to compare the findings from 25 of these studies, and, as in the previous review, they varied markedly in the percentage of projects within each programme that seemed to make an impact on health policy and practice. Generally, the programmes with the highest levels of impact were HTA-type programmes in which the projects were primarily reviews or appraisals that fed directly into policy-making processes. Other programmes in which quite high proportions of projects were seen to be making some impact were ones in which there had been one or more of the following: thorough needs assessments conducted beforehand; frequent interactions with potential users; and the existence of ‘receptor’ bodies that would receive and potentially use the findings. A key conclusion from this is that impacts from such programmes were best assessed by frameworks devised to capture data about the context and interactions related to research programmes.
The consideration of the findings from studies and the role of the different possible frameworks and methods have to take account of the major recent developments in impact assessment described in the chapter, namely the introduction of regular monitoring of impact, for example through researchfish,76 and the major, and largely successful, REF exercise in the UK. 33 Both of these developments mean that any future additional assessment of impact by NIHR will take place in an environment in which there is already considerably more data available about impacts than was ever previously the case. Both developments also demonstrate that impact assessment can be conducted in ways that identify that a wide range of impacts come from health research and, therefore, provide a degree of endorsement of the previous smaller exercises. However, many challenges remain in assessing research impact and further consideration of the most appropriate approaches is highly desirable.
Chapter 4 Towards a broader taxonomy of impact models
This chapter attempts to make sense of the expanding array of impact models by offering a preliminary taxonomy based on two questions: (1) ‘who is the model for?’ and (2) ‘what are its underlying assumptions?’.
Different philosophical roots: five ‘ideal types’
Different approaches to measuring research impact also rest on different (usually implicit) assumptions about the nature of knowledge. To understand impact and measure it in a valid way, we need to clarify questions of ontology [what is (research) knowledge?], epistemology (how might we come to understand that knowledge), the purpose of scientific inquiry and the mechanism by which research is assumed to link to practice. The philosophical assumptions of different approaches to understanding scientific inquiry are summarised in Table 8.
| Philosophical assumptions | Positivist (unenhanced logic models) | Constructivist (interpretive and interactional models) | Realist (context–mechanism–outcome–impact models) | Critical (participatory models) | Performative (Co-production models) |
|---|---|---|---|---|---|
| Assumptions about what (research) knowledge is | Facts (especially, statements about the relationship between variables), independent of the researcher and (ideally) transferable to new contexts | Explanations and interpretations of a situation or phenomenon, taking account of historical, cultural and social context | Studies of how human actors process and interpret external social reality, producing statements about ‘what works for whom in what circumstances’ | Studies that reveal society’s inherent conflicts and injustices and give people the tools to challenge their own oppression | Knowledge is best thought of as something that is brought into being and enacted in practice by networks of people and technologies (‘actor–network theory’) |
| Assumed purpose of research | Predictive generalisations (‘laws’) | Meaning: perhaps in a single, unique case | Theoretical generalisation (what tends to work and why) | Learning, emancipation, challenge | To map the changing dynamics of actor–networks |
| Preferred research methods | Hypothesis testing; controlled experiments; modelling and measurement | Naturalistic inquiry (i.e. in real-world conditions) | Predominantly naturalistic, may combine qualitative and quantitative data | Participatory (action) research | Naturalistic, with a focus on change over time and network (in)stability |
| Assumed way to achieve quality in research | Hierarchy of preferred study designs; standardised instruments to help eliminate bias | Reflexive theorising; consideration of multiple interpretations; dialogue and debate | Abduction (asking what kind of reasoning by human actors could explain these findings in this context) | Measures to address power imbalances (ethos of democracy and inclusivity; conflict management) | Richness of description; plausible account of the network and how it changes over time |
| Assumed relationship between science and values | Science is inherently value-neutral (though research can be used for benign or malevolent motives) | Science can never be value-neutral; the researcher’s perspective must be made explicit and taken account of | Science may produce ‘facts’ but facts are interpreted and used by people who bring particular values and views | Science must be understood in terms of the historical conditions that gave rise to it and the interests it serves | Controversial. Arguably, actor–network theory is consistent with (but not centrally interested in) a value-laden view of science |
| Assumed mechanism through which impact is achieved | Direct (new knowledge will influence practice and policy if the principles and methods of implementation science are followed) | Mainly indirect (e.g. via interaction/enlightenment of policy-makers and influencing the ‘mindlines’ of clinicians) | Interaction between reasoning (of policy-makers, practitioners, change agents and others) and resources available for implementing research findings | Development of critical consciousness; strengthening of partnerships; research capacity building in community partner; lobbying; advocacy | Via ‘translations’ (stable changes in the actor–network), achieved by actors who mobilise other actors (human and non-human) into new configurations |
| Implications for the study of research impact | ‘Logic models’ will track how research findings (transferable facts about what works) are disseminated, taken up and used for societal benefit | Outcomes of social interventions are inherently unpredictable and hence impact studies should focus on ‘activities and interactions’ to build ongoing relationships with policy-makers | Impact studies should address variability in uptake and use of research outputs by exploring context–mechanism–outcome–impact configurations | Impact has a political dimension, as the purpose of (some) research is to challenge the status quo. Hence, some stakeholders stand to lose power; others stand to gain | For research to have impact, a realignment of actors (human and technological) is needed. Focus should be on the changing ‘actor scenario’ and how this becomes stabilised in the network |
Traditionally, HTA’s focus has been on experimental studies of drug treatments or surgical interventions from a positivist ‘hard science’ perspective. Mostly outwith HTA’s terms of reference, but within the wider scope of health services research [see, for example, the NIHR CLAHRC programme (www.clahrcprojects.co.uk/), the Wellcome Trust’s ‘Society and Ethics’ programme (https://wellcome.ac.uk/) or some elements of the European Commission’s Horizon 2020 programme (https://ec.europa.eu/programmes/horizon2020/)], are research designs such as collaborative codesign, policy analysis, health systems analysis and organisational case study that are built (variously) on constructivist, critical or performative assumptions (see Table 8). HTA has occasionally commissioned overviews of qualitative research from a constructivist perspective,142,143 systematic reviews with a realist component144 or a systematic review of action research that acknowledged (although it did not prescribe) a critical perspective. 145 However, even considering HTA’s main focus on clinical trials, few, if any, models of research impact assume a direct, linear and unproblematic link between a trial and its subsequent impact. Most begin with a basic logic model and enhance it with an interpretive account of the different relationships, interactions and contextual influences that affect the research–impact link.
In this chapter, we will outline some research approaches and models of research impact that draw on the wider range of philosophical assumptions set out in columns 3–6 in Table 8.
Different readers will have different views on the ‘correct’ or ‘preferred’ approach to research or the measurement of impact. However, it is important to note that these different philosophical positions tend to be linked to very different research topics and questions. Positivist assumptions tend to underpin quantitative and experimental studies (especially the question of if and for whom a particular intervention ‘works’, and what magnitude of benefit can be expected). In contrast, studies with a strong explanatory component (e.g. those that seek to build theory about a complex social intervention) may reject the positivist assumption that there is a transferable ‘effect size’ and focus instead on describing interactions and/or drawing out theoretical mechanisms of change. Studies that are driven by a passionate commitment to improve the lot of a marginalised or underserved group, such as refugees or the homeless, may find a critical perspective (and an action research study design) more appropriate and feasible than a randomised trial.
The literature on impact in health services research is increasingly philosophically diverse, attempting to combine the outputs of (positivist) evidence-based medicine (e.g. quantitative findings on the efficacy of tests and treatments) with a broader (constructivist, realist, performative), epistemology of research utilisation that incorporates various social science disciplines (notably, social psychology, organisational sociology, social policy, and science and technology studies). Some of these extended models sit more comfortably in a social policy paradigm than in implementation science. 146 In the following section (see ‘Logic models’ of research impact: strengths and limitations), we summarise these contrasting philosophical ideal types and suggest how the different models of research impact align with them, and the implications this has for assessing research impact in an increasingly diverse health research system.
Given that many of the models reviewed in this report draw on multiple philosophical assumptions, it is worth introducing a composite philosophical position (not shown in Table 8), which is pragmatism. Ontologically and epistemologically eclectic pragmatism proposes that when combining scientific and practical knowledge (e.g. when attempting to link a body of research with its application in the real world), the relevance of each competing position should be judged in terms of how well it addresses the problematic situation or issue at hand. 147
It should be noted that positivism is the only philosophical position that strongly supports a ‘model’ with ‘tools’ to apply it. Hence the perspectives in other philosophical schools might best be thought of as ‘approaches’ rather than as ‘models’.
‘Logic models’ of research impact: strengths and limitations
Most, although not all, approaches to assessing research impact in the health sciences include some kind of ‘logic model’ – defined as a depiction of the logical (implicitly, causal) relationships between the resources, activities, outputs and outcomes of a programme. However, few, if any, of these approaches assume that the link between research and impact is as linear and direct as the logic model implies. Different approaches enhance the logic model in different ways. In this section we summarise the approaches that include a logic model and review the strengths and limitations of the logic model.
Chapter 3 described a number of widely used approaches from the mainstream health services research (or ‘research on research’) literature, including the Payback Framework and its variants,39 the monetary value approach, the Quebec HTA approach,43,44 the CAHS approach,7 Banzi’s research impact model,4 the NIEHS logic model,63 the medical research logic model,120 the NIOSH logic model,92 the Wellcome Trust’s assessment framework,93 the VINNOVA framework,37 the RIF,123 the Becker Medical Library model,118 the research performance evaluation framework,72 the UK REF and the Australian RQF. 128 All these examples consist partly or wholly of a logic model (although Chapter 3 also includes some examples of constructivist, realist and performative approaches).
Similarly, all the models described in Chapter 5 on the monetary value are essentially logic models, whether ‘top down’ or ‘bottom up’, which link inputs (research funding) with the research process and then outputs and (monetised) impacts. Chapter 6 (the impact of RCTs via their role in systematic reviews and meta-analyses) and Chapter 7 (the impact of RCTs on stopping ineffective interventions) also relate exclusively to logic models.
The strengths of logic models are the way in which the links between inputs, processes, outputs and outcomes are carefully drawn out, and the fact that mediating and moderating variables can be added to the model to account for successes, failures and partial successes. A robust logic model, systematically applied, should produce valid and reliable statements about the relationship between these variables. However, in the real-world application of research evidence, it is widely recognised that not all research impact links can be predicted or reliably quantified. Part of the elegance of many frameworks that include a logic model is the sophistication of the caveats and nuances they accommodate to explain, for example how, why, by whom and influenced by what historical and contextual factors the impact unfolded as it did. In the Payback Framework, for example, the basic logic model is enhanced by a narrative account of factors and influences, including the context within which the research takes place and the interactions between potential users and the researchers. These are widely viewed as key features of the framework.
Although logic models are only ever an approximation of reality, they can be extremely helpful as conceptual tools. They generally cover a range of impacts considered important to stakeholders, and the various elements of the models provide a framework for organising data collection, analysis and data presentation consistently, taking account of inevitable variations between projects or programmes. A robust basic model, while being rigorously applied, can also be refined further in collaboration with the funders of particular studies and other stakeholders (e.g. patient organisations) to ensure that the assessment of impact focuses on the categories important to those stakeholders. Such models can often be applied flexibly in a way that is compatible with the values of the research funders and researchers, who are usually concerned to show that they are contributing to improved health care.
Even when they include such scope for flexibility and caveats, logic models may be criticised by social scientists who question their value for assessing research that is inherently non-linear (e.g. the evaluation of real-world social programmes that follow the non-linear dynamics of complex systems). We list below the alleged downsides of logic models as described by their critics. 5,6,14,95,115,116,148–151
-
Assumption of linear causality: to a greater or lesser extent (e.g. depending on the degree of ‘permeability’ acknowledged by their architects), logic models reflect a deterministic, research-into-practice mind set that is incapable of fully capturing the messiness and non-linearity of the relationship between research, practice and policy. The epistemological assumption behind unenhanced logic models is that with careful measurement and synthesis of input, process and context variables, it is possible to draw meaningful conclusions about the link between a research programme and subsequent impact, and predict comparable impact in the future. Critics say that this assumption is highly questionable in certain circumstances, notably when the context is complex and multiple input variables are rapidly changing.
-
Disciplinary bias: logic models are said to privilege ‘hard’ research, such as trials and epidemiological studies, over ‘soft’ research, such as qualitative or developmental studies, and to valorise easily monetised impacts such as licensing and start-up creation. Furthermore, the quest to measure the measurable in a rational, ‘objective’ way creates perverse incentives to overlook the unmeasurable elements in any research discipline.
-
Temporal bias: different kinds of research achieve impact over different time scales, and hence an overly rigid logic model will miss impacts at extremes of these scales. In general, the longer the time scale, the more diffuse the chain of causation. As Kok and Schuit stated: ‘pathways from research to ”impacts” are very diverse: sometimes short and traceable, but often long, through multiple reservoirs, and via utilization at untraceable times and places’. 116
-
Attribution: the extent to which an impact can be attributed to a particular research project is a matter of judgement. In reality, attribution is often an inexact science in which accuracy attenuates with each stage in the logic model.
-
Additionality: return on investment models are not designed to address whether or not the claimed impact would still have occurred had the research not been done. There is also the related question of opportunity costs – might the research budget have been spent differently, with greater benefit to the public good?
-
Excessive abstraction: according to critics, logic models are elegant and parsimonious in the abstract and convey the impression of rigour through ‘hard’ analytics, but (depending on how rigidly they are applied) they bear little relation to the messier real-world use of knowledge by human actors and how knowledge is interpreted, negotiated and valued by wider society.
-
Impracticality: application of logic models (which tend to be multimethod, multilevel and seek to build a rich picture of the numerous interacting influences on impact) is resource intensive, hence not a practical or affordable option in most situations. Reducing the rich, multimethod case study approach intended by the original authors to a crude inventory based on tick-box surveys and a handful of standardised interviews will not produce valid or reliable data.
-
Ethical issues: the impact of research may be significant and far-reaching but morally questionable (e.g. if it is achieved at the expense of environmental damage) or even harmful (e.g. if it distorts rather than informs decision-making). It has even been argued that the dominance of economic models of impact reflects a sinister development in which key moral questions about the public good (what kind of science is morally right) are downplayed in favour of instrumental practices aimed at a narrow range of utilitarian goals, especially innovation and economic growth.
The validity of all the above arguments will, of course, depend on context and specifics, but, as noted above, the crude and unenhanced logic model that depicts a naive and deterministic relationship between research and impact has long been rejected in favour of more pragmatic and flexible hybrids. As the range and diversity of research expands, the models reviewed in the next section should perhaps be viewed not as substitutes for (or competitors of) more widely used approaches based on logic models, but as complementary approaches that might prove fit for purpose in particular circumstances.
Alternatives to the logic model approach
Different models of research impact are more or less appropriate for different study designs and research themes – a finding that was evident in the previous HTA review. 2 Similarly, the CAHS panel commissioned separate analyses of how which approaches might work best for each of three of the four ‘pillars’ of research used to categorise health research in Canada: pillar II, clinical research;152 pillar III, health services research;113 and pillar IV, population and public health research. 114 (Pillar I, basic biomedical research, was excluded on the grounds that it ‘is the area where most has been said on understanding the impacts of health research’.)
Some Australian studies have also considered this issue. Cohen et al. 52 found that ‘single intervention research studies can and do have concrete and measurable post-research real-world impacts . . . on policy and practice’. 52 This recent study adds to the view that the degree of impact identified and reliably attributed (at least over relatively short time scales) might vary depending on the type or research, and context in which it is conducted and its findings presented. Kalucy et al. 65 used the Payback Framework to assess the impact of primary care research and reported that the ‘logic model’ of the framework worked better for a RCT than it did for an action research study.
Impact assessments are conducted for a variety of audiences (Table 9) and purposes [the ‘four As’ of advocacy (for research), accountability, analysis (of why and to what extent research is effective) and allocation]. 2,9
| Audience/stakeholder | Main concern |
|---|---|
| Research funder/donor | Was the money we invested in (donated to) research well spent? Were the benefits anticipated in the application actually realised? The audiences and purposes clearly overlap to a degree, but of course a major audience is likely to be the organisation funding the original research, who, according to our analysis, are the most likely to be funding the assessment. Research funders as an audience are likely to hope an assessment study would contribute to several purposes. Indeed, they might hope an assessment study would inform both analysis and allocation, but as shown above it is unlikely a single assessment approach would be best for both tasks |
| Patient/carer/research participant | Did the research address things of concern to people with the illness? Are we better off as a result of the research, and, if so, how? |
| Researcher | Who used the findings of my research and what benefit resulted? |
| Treasury/taxpayers | Is/was this programme of research a good use of public money? Were there cash-releasing or non-cash-releasing benefits elsewhere in the system? |
| Higher education institution | Was the research excellent (i.e. world-leading)? Did it lead to high-impact publications, reputational benefits, rise in university ranking, etc.? |
Guthrie et al. 9 examined six impact frameworks in detail and suggested that all six could be used if the purpose was advocacy or accountability. However, if the purpose were analysis, only three of the six frameworks would be fit and if the purpose were allocation, a different three would be fit. They applied the four As to inform a decision tree for developing a research evaluation framework.
Audiences and purposes clearly overlap to a degree. A major audience is likely to be the organisation funding the original research, who may also be funding the impact assessment. Research funders might hope a single impact assessment will inform both analysis and allocation, but may be unaware that different assessment tools are more or less suited to different purposes.
Bearing in mind the consistent evidence in favour of different models for different types of research, different audiences and different purposes, the next few sections address alternatives to the logic model for assessing research impact. Although many are only marginally relevant to the current remit of the HTA programme, they are nevertheless important components of a broader toolkit.
Constructivist models of impact (developed in social sciences)
As column 3 in Table 8 shows, constructivist (sometimes called interpretivist) research focuses on people’s interpretations of the world. This is important for the study of research impact because policy-makers, clinicians and patients interpret the world they inhabit – and they also interpret research evidence in ways that may not align with researchers’ perspectives.
This misalignment was systematically documented in a detailed ethnographic study undertaken in the 1970s,49 and more recently updated,153 of the interactions between national policy-makers and the university-based researchers from whom they commissioned research (the so-called ‘Rothschild experiment’ in the English Department of Health and Social Security). Kogan and Henkel’s49 landmark study demonstrated a number of key principles that are still relevant to the measurement of research impact today. First, science and government are from different cultural worlds; interaction between them is a ‘contact sport’, in which success depends on sustained linkage and exchange with ‘knowledge brokers’ playing a key role. 154
Second, despite the ubiquity of simple, linear models of research-into-policy, scientific research and the business of government is, in reality, highly complex. Simplistic models fail to capture their important nuances. In particular, science and government are interdependent and mutually shaping, hence even commissioned research does not follow a simple, customer–contractor logic.
Third, research priorities, even in applied fields, are rarely self-evident, partly because different stakeholders view the world differently and have competing vested interests.
Finally, the different perspectives within each ‘multimodal’ group of scientists and users can have major consequences; for example, if the chief scientist took a narrow, positivist and quantitative view of what science should look like, this would limit the scope for university researchers and research users to develop more emergent partnerships to address highly complex real-world problems.
In 1979, sociologist Carol Weiss34 challenged the prevailing assumption that research impact is direct and linear (and hence that it can be meaningfully summarised in logic models). Drawing on empirical studies in the social sciences, she argued that the assumed knowledge-driven mode of impact, along with problem-solving mode (research commissioned directly to solve particular policy problems – as in the Rothschild experiment) were rare, not least because the findings of social science research tend to illuminate the complexity and contingency of phenomena rather than providing simple and universal solutions to them.
Weiss and others have shown that research in the social sciences (which includes much applied health research) is generally characterised by an interactional mode of impact in which researchers and policy-makers, through repeated interaction over time, come to understand each other’s worlds and develop shared goals and approaches. 34 Impact may also occur by other non-linear mechanisms including enlightenment – as Hanney et al. 35 stated, drawing on the work of Thomas,155 ‘the gradual “sedimentation” of insight, theories, concepts and perspectives’, as a result of continuing exposure to research insights and ideas. Finally, research findings may be used by policy-makers symbolically (either politically to support a particular course of action or tactically to delay a decision, perhaps commissioning new research in order to buy political breathing space). 34,35,156
Knowledge in the social sciences has complex properties. It is fluid, context dependent, embodied by individuals and embedded in organisational routines and norms. Hence social scientists are uncomfortable with models of impact that rest heavily on the ‘transfer’ or ‘implementation’ of an assumed fixed body of knowledge. Conversely, they are often keen to explore the processes by which knowledge, which is assumed to take multiple forms, is interpreted, negotiated, transformed and applied in practice, and how context may profoundly affect these processes. 149
Meagher et al. ,95 for example, applied a model with some parallels to the Payback Framework, but resting on interpretivist assumptions and placing more emphasis on processes and activities, to study the impacts of ESRC-funded research in a number of detailed case studies. They found that conceptual (e.g. indirect, enlightenment based) impacts were more common than instrumental (e.g. direct, knowledge driven) ones. They also found that most principal investigators had a naive and linear view of the research–impact link (e.g. few knew about interactive or enlightenment mechanisms or the need for ongoing linkage and exchange with policy-makers). They questioned the value of tracking impacts in the absence of specific activities aimed at facilitating uptake. Indeed, they felt it might be inappropriate to try to measure something that one has not expressly tried to bring about. They commented:
It was extremely difficult to attribute with certainty a particular impact to a particular project’s research findings. It was often more feasible to attach an impact to a particular researcher’s full body of research [. . .] Changes in practice or policy often appear to stem from a general ‘awareness-raising’ or conceptual shift.
p. 17095
The ‘full body of research’ referred to in the above quote has been described by RAND as a ‘research cloud’ and explored using electronic bibliometrics. 157
Brambila et al. 137 used a rare longitudinal case study methodology to demonstrate Weiss’s ‘incremental’ mechanism of impact in a sample of 44 community-based health care projects in Guatemala between 1988 and 2001. Like Meagher et al. ,95 they found few linear impacts directly attributable to single projects. Rather, policy change occurred through ‘a gradual process of information sharing, where researchers influence decision-makers through a continual stream of information rather than a single set of findings’. 137
de Goede et al. 158 developed a three-phase framework for capturing the complexity of research utilisation: (1) describe the research network and the policy network; (2) describe the types of research utilisation (classified as instrumental, conceptual and symbolic); and (3) describe the (reciprocal) interactions between researchers and policy-makers. Barriers to the effective uptake of research may occur at the level of expectation (are policy-makers ‘ready’ for these findings?), transfer (how effectively and appropriately are findings communicated?), acceptance (are findings seen as credible and true?) and interpretation (what value do policy-makers place on them?). Using three detailed case studies, these authors showed, like Meagher et al. ,95 and Kogan and Henkel earlier,49 that most research utilisation was conceptual and that non-uptake could often be explained by a mismatch of world view and problem definition between researchers and policy-makers.
de Jong et al. 159 developed a model for incorporating context into impact assessment (Figure 5), as different fields of inquiry provide very different contexts for research and impact. (This finding resonates with Nicolini et al. 160 on the different nature of knowing in different clinical specialties.)
FIGURE 5.
de Jong et al. ’s framework for assessing impact in context. Reproduced from de Jong SP, van Arensbergen P, Daemen F, van der Meulen B, van den Besselaar P. Evaluation of research in context: an approach and two cases. Res Eval 2011;20:61–72, by permission of Oxford University Press. 159
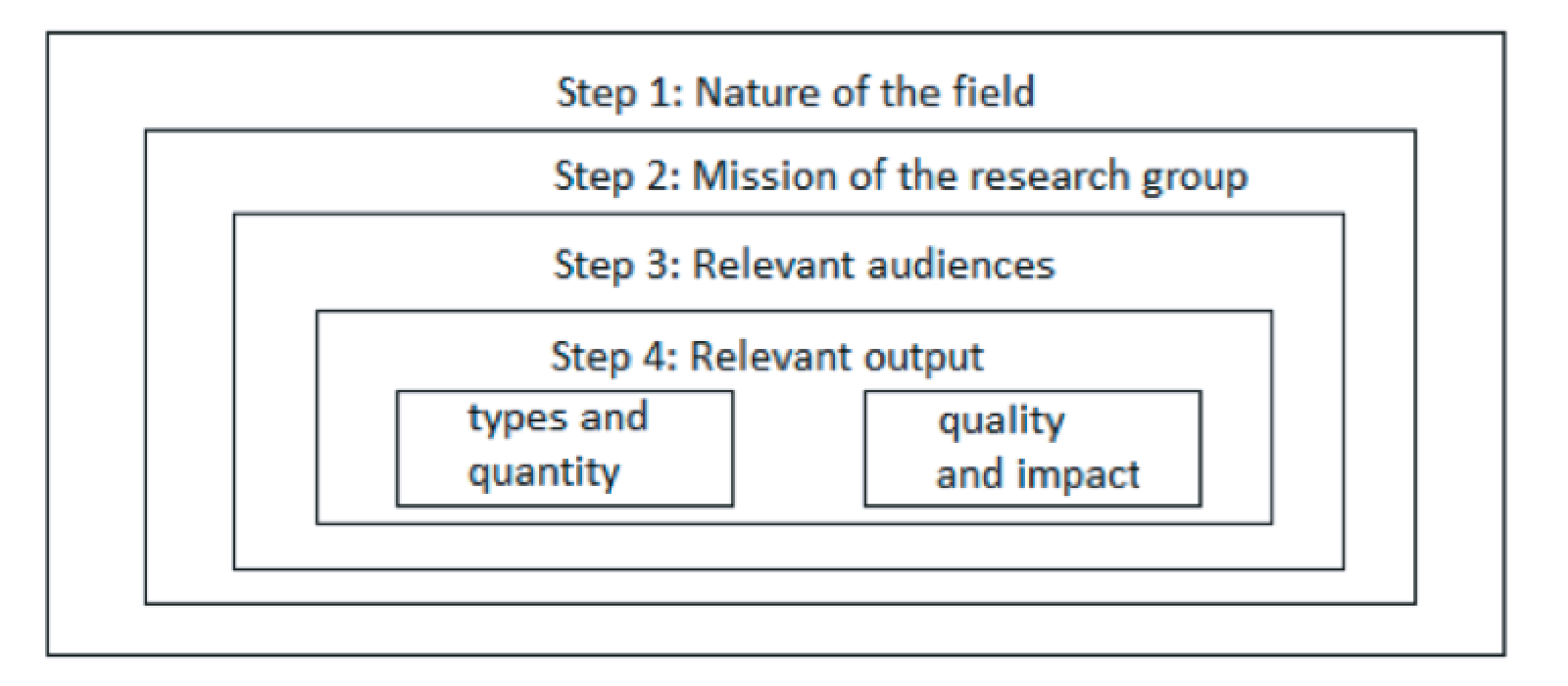
Step 1 considers ‘research field context’: nature and range of research, how quality is defined, and implications for agenda-setting, collaboration, knowledge dissemination and impact. Steps 2–4 consider missions of the research group, audiences and outputs within this wider context. Contrasting examples of architecture and law illustrate that attempts to assess research impact make little sense without preliminary contextualisation of the field.
A study from Australia based on five case studies in contrasting disciplines found similarly that ‘disciplinary and methodological context matters when it comes to understanding the translation, dissemination, and utilization of academic social research.’161
More recently, Lemay and Sá162 depict research utilisation as having the non-linear dynamics of a complex adaptive system, composed of multiple interacting entities, coevolving, locally adaptive, self-organising, path-dependent and sensitive to initial conditions. They view research users as active problem-solvers and generators of knowledge, not passive receptacles. They propose that impact may (theoretically at least) be modelled using computational techniques such as agent-based modelling, data mining or socionics. Such approaches would require a shift in the policy mind set.
Normative policy development and implementation are about directing, controlling and minimising uncertainty about outcomes. Taking into account the contingent, emergent and unpredictable nature of research use would imply acknowledging and accommodating unpredictable outcomes that might emerge over time.
p. 480162
In a widely cited systematic review of knowledge utilisation, Contandriopoulos et al. 163 depicted knowledge in two essential forms: individual, that is, held in people’s heads and translated (or not) into action by human will and agency (a conception of knowledge that rests largely on positivist assumptions); and collective, that is, socially shared and organisationally embedded (a conception that rests on more constructivist assumptions). They reviewed the mechanisms by which knowledge may become collectivised, including efforts to make it relevant, legitimate and accessible and to take account of the values and priorities of a particular audience. If there is broad agreement on what the problem is and what a solution would look like, arguments can proceed through logic models along the lines of conventional scientific inquiry (e.g. strength of research evidence). If not, the research impact challenge must take account of people’s interpretations, and hence enters the more fluid and subjective realm of political science in which research use is, in Weiss’s taxonomy, instrumental and/or tactical rather than knowledge driven. 34
In summary, whereas the natural sciences can be thought of as trading in more or less universal truths, knowledge in the social sciences (including the study of how individuals interact and how organisations and communities operate) is more fluid, dynamic and value-laden. The uptake and use of knowledge depend heavily on context; impacts may be diffuse, subtle, diverse and unpredictable; and causality tends to be explanatory rather than probabilistic.
Realist models: impact as ‘theory of change’
The studies described in the previous sections applied an interpretivist lens to explore the research–impact link in (mostly) single case studies without making predictions about other cases. A different approach, realist evaluation, uses case study methodology but through abductive theorising about context–mechanism–outcome configurations, seeks to make generalisable statements about what tends to work for whom in what circumstances. A preliminary paper purporting to apply realist methods to the study of impact has been published, although this monograph would more accurately be described as an introduction to realist methodology in general. 164 The principles of the realist approach are summarised below.
Realist evaluation was developed by Pawson and Tilley in the 1990s for the evaluation of ‘what works for whom in what circumstances and how?’165 This early work made the following points.
-
Complex interventions (what Pawson and Tilley call ‘social programmes’, e.g. an intervention to encourage people to consult their general practitioner rather than attend the emergency department) are an attempt to create some level of social change.
-
These interventions ‘work’ by enabling participants to make different choices.
-
Making and sustaining different choices requires a change in a participant’s reasoning (e.g. in their values, beliefs and attitudes or the logic they apply to a particular situation) and/or the resources (e.g. information, skills, material resources, support) they have available to them. This combination of ‘reasoning and resources’ is what enables the intervention to ‘work’ and is known as a ‘mechanism’.
-
Complex interventions ‘work’ in different ways for different people because contexts (social, economic, organisational, interpersonal) have different influence on different people, triggering different mechanisms: context + mechanism = outcome.
-
As complex interventions work differently in different contexts and through different change mechanisms, programmes cannot simply be replicated from one context to another and automatically achieve the same outcomes (i.e. impacts). Theory-based understandings about ‘what works for whom, in what contexts, and how’ are, however, transferable.
-
Therefore, one of the tasks of evaluation is to learn more about ‘what works for whom’, ‘in which contexts particular programmes do and don’t work’, and ‘what mechanisms are triggered by what programmes in what contexts’.
In summary, a realist approach to research impact is centrally concerned with looking at how different research programmes may have different impacts in different settings. Empirical studies applying realist methodology to the evaluation of research impact are currently sparse,166 but the approach is rapidly growing in popularity in the health-care field, and hence we flag it here as a potential (if largely untested) option.
Participatory and critical emancipatory models of impact
One of the most striking developments in UK health services research since the publication of the 2007 HTA report has been the increased emphasis on patient and public involvement as a contributory factor in research impact. 167 User involvement on grant applications and study steering groups is widely promoted and an important criterion against which studies are evaluated. However, this involvement is sometimes under-theorised, depicted as instrumental (aimed at increasing recruitment to clinical trials) and couched in strongly positivistic terminology, with an emphasis on standardisation and formal measurement of variables. One study, for example, was entitled Involving Service Users in Trials: Developing a Standardised Operating Procedure. 168 Another offered a 31-point checklist to ensure uniformity in this aspect of research. 169
An alternative approach to public involvement in research has been presented in the critical social science literature. 170 From this perspective, research impact is centrally concerned with achieving social justice and improving the lives of disadvantaged groups. Action research, sometimes known as community-based participatory research (CBPR), seeks to redress the adverse influence of social determinants of health (e.g. poverty, sex, ethnicity, education/literacy, citizenship status and access to services) through collaborative, multistakeholder activity. 171
A key challenge of CBPR is ensuring that the research process should remain democratic despite imbalances of resources and power, so some tools have been designed to measure the extent of power sharing. White,172 for example, writing in the CBPR literature, distinguishes nominal involvement of the lay public (undertaken to confer legitimacy on a project), instrumental involvement (to improve its delivery and/or efficiency), representative involvement (to avoid creating dependency) and transformative involvement (to enable people to influence their own destiny).
Additional dimensions of the CBPR process may also be assessed to estimate the level of democratic decision-making, such as the extent to which research designs are culturally and logistically appropriate; the extent of measures to develop capacity and capability in stakeholder groups; how, and to what extent, conflicts are managed; and the extent to which mutual trust builds over time. 173
Martin174 classifies involvement of practitioners (e.g. clinicians) in collaborative research on a five-point scale: informant (‘type 1 co-production’ – supplying data for a mode 1 research study but no other involvement); receiver (‘type 2 co-production’ – involved at the end of a mode 1 study to receive the findings, usually on terms set by the researchers); endorser (‘type 3 co-production’ – involved from an early stage to endorse, but not influence, priority setting and research programmes); commissioner (‘type 4 co-production’ – involved from the outset to conceive and initiate studies that are taken forward by researchers); or co-researcher (‘type 5 co-production’ – working democratically alongside researchers at every stage in the research).
Macaulay et al. 171 applied CBPR to health care. They proposed some indicators of whether or not a community–campus partnership was truly democratic, including (1) ‘Were the research goals, objectives and methods negotiated among all partners?’; (2) ‘Were the terms of the community–researcher partnership made explicit and agreed?’; (3) ‘Who evaluated the project and how?’; (4) ‘Where were the data filed and who had control over their subsequent analysis and publication?’; (5) ‘What were the arrangements for resolving disagreements?’; and (6)’ How and to whom were the findings disseminated?’.
In CBPR, partnerships succeed largely through partnership synergy – defined as combining people’s perspectives, resources and skills to ‘create something new and valuable together – a whole that is greater than the sum of its individual parts’. 175 Partnerships are often characterised, at least initially, by conflict, but synergy may increase as cogoverning partners work together, leading to convergence of perspectives by progressive alignment of purpose, values and goals and growth of mutual understanding and respect. 173
Cacari-Stone et al. 176 linked the CBPR approach to policy-making by linking CBPR contexts (political–societal and specific collaborative histories) and partnership processes (e.g. equitable decision-making or leadership) to intermediate research and system or capacity outcomes, and more distally to health outcomes (Figure 6). 176 They depict the policy process as iterative, non-linear and characterised by windows of opportunity. CBPR may influence this both instrumentally (by generating evidence) and interactively (through civic engagement).
FIGURE 6.
Conceptual model for illustrating the link between CBPR and policy-making. Cacari-Stone L, Wallerstein N, Garcia AP, Minkler M. The Promise of Community-Based Participatory Research for Health Equity: A Conceptual Model for Bridging Evidence With Policy. Am J Public Health 2014;104:1615–23, with permission from The Sheridan Press (on behalf of The American Public Health Association). 176
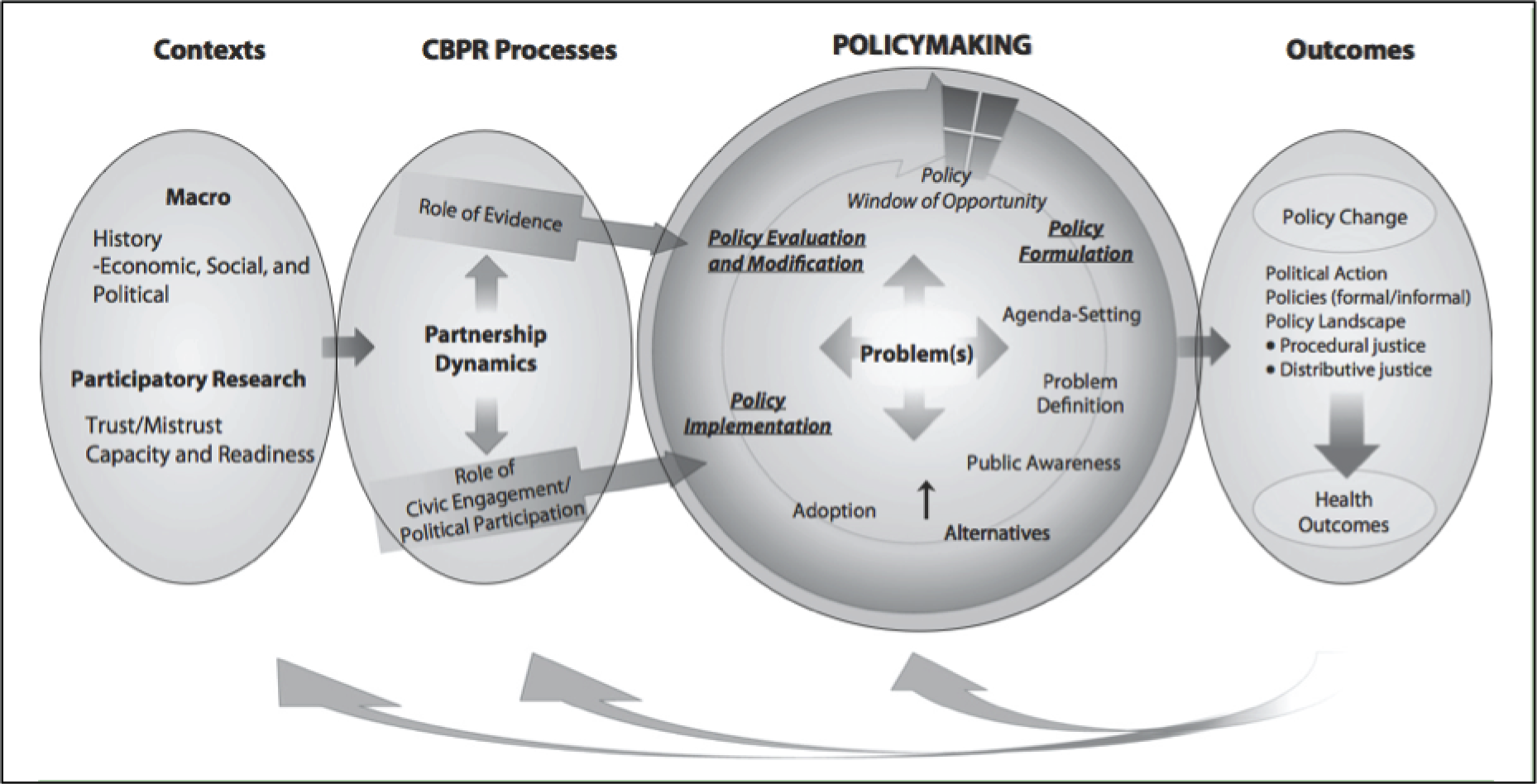
Community-based participatory research depicts sustainability of research impact in synergistic terms as progressive strengthening of the community–campus partnership for further collaborative knowledge production (hence the feedback arrows from the outcomes of one project to the context for the next project in Figure 6).
The literature on CBPR, and on ‘socially engaged’ research more generally, uses the language of critical sociology and critical public health. It is a world away from most clinical research, which remains dominated by the language and logic of epidemiology and RCTs. However, while the RCT is predicated on the positivist assumption that knowledge is fixed and stable and political issues lie beyond the analytic frame (see Table 8), the use of evidence from RCTs requires attention to the policy process and hence to interpretation (see the ‘constructivist’ column in Table 8) and the balance of power (see the ‘critical’ column in Table 8).
In 2011, Kessler and Glasgow177 famously called for a 10-year moratorium on RCTs to allow the health services research community to learn and apply the concepts of a more applied and socially engaged approach. They subsequently drew the disparate paradigms of RCTs and CBPR together in an evidence integration triangle designed to ‘[marry] rigorous design focused on internal validity and theory-driven hypotheses with an increased focus on external validity, contextual considerations, and stakeholder relevance’. 178
Glasgow et al. ’s ‘evidence implementation triangle’ (Figure 7)178 is an example of how the research tradition of knowledge translation has sought to embrace a wider range of paradigms. The triangle comprises an evidence-based intervention or policy (perhaps tested in a RCT), a participatory implementation process (perhaps using CBPR or some other developmental approach), and practical (i.e. feasible, affordable, actionable and sensitive to change) progress measures, all studied with attention to context. Although this is a worthy attempt to link the different cultural worlds of clinical trials and real-world implementation, the depiction of CBPR as an ‘implementation process’ for the findings of mode 1 research spectacularly misses the central emancipatory principle of this approach.
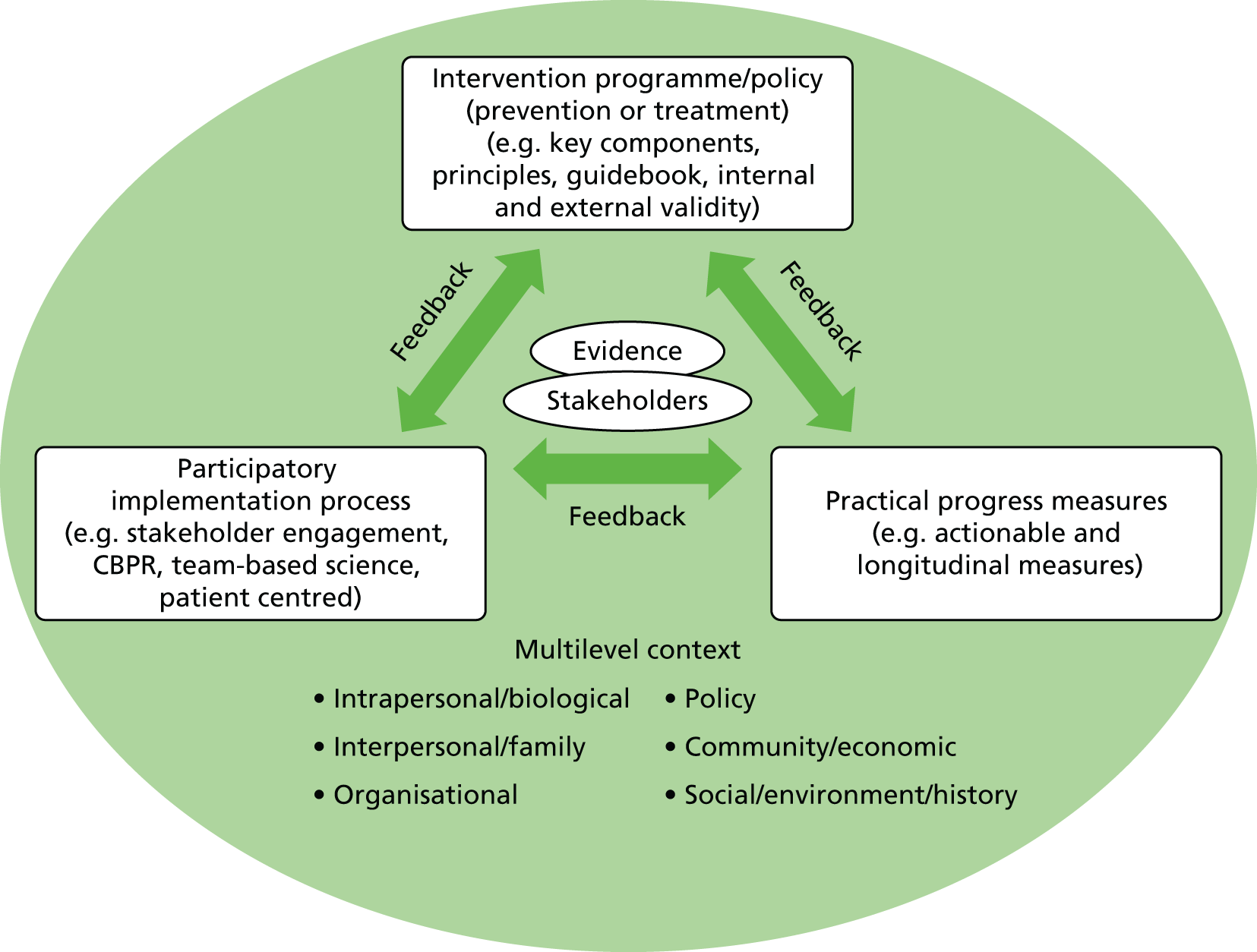
Many writers in social science traditions consider that a focus on ‘translation’ or ‘dissemination’ of pre-existing research knowledge offers only limited purchase on the phenomenon of impact. In this section, we review approaches that focus instead on knowledge production.
Co-production models (e.g. multistakeholder research partnerships)
In 1994, a book entitled The New Production of Knowledge: The Dynamics of Science and Research in Contemporary Societies introduced a new taxonomy: ‘mode 1 scientific discovery’ and ‘mode 2 knowledge production’. 179 This centred on the practices through which knowledge is produced rather than the mechanisms by which it was subsequently disseminated. The book had much influence in the social sciences, but less so in health-care fields. However, with the emergence of complex organisational forms (such as Academic Health Sciences Networks,180 funded by the NHS, and CLAHRC, funded jointly by the NHS and NIHR181–186) oriented towards the collaborative production of research knowledge between universities, the NHS and other partners, the literature on mode 2 research is increasingly relevant for the UK research community – though perhaps less so for the HTA programme in which the commissioning model remains largely mode 1.
Mode 1 research equates to traditional academic science, led by university researchers and then disseminated to stakeholders beyond higher education. In contrast, mode 2 knowledge is generated within its context of application – what Gibbons et al. 179 refer to as a ‘multi-stakeholder transaction space’ – embracing state, economy, culture and the wider public sphere, as well as academic institutions (of which Academic Health Service Networks and CLAHRCs are good examples). In this ‘transaction space’ (the formal board meetings of AHSNs and CLAHRCs, as well as the informal interactions that go on behind the scenes to keep these shows on the road), problems are identified, questions debated, methodologies developed and outcomes disseminated. There are many players, many experts (of different kinds) and an evolving collective view (though rarely a consensus) on what the questions and challenges are.
Gibbons et al. 179 emphasise that in mode 2 research, a range of theoretical perspectives and practical approaches – including, but not limited to, specialist scientific techniques – is mobilised and managed, often for only a limited period, to address a particular set of problems. The planning, execution, dissemination and implementation of research are not separate and linear phases but interwoven, and the relationship between scientists and research users (industry, policy-makers, citizens, patients) is one of Co-production rather than ‘producer’ and ‘consumer’ or ‘commissioner’ and ‘contractor’. The authors of the mode 2 hypotheses depicted the process as highly reflexive.
The research process can no longer be characterised as an ‘objective’ investigation of the natural (or social) world, or as a cool and reductionist interrogation of arbitrarily defined ‘others’. Instead it has become a dialogic process, an intense (and perhaps endless) ‘conversation’ between research actors and research subjects.
p. 4187
The emergence of complex forms for mode 2 research in health care in the UK is mirrored in other countries, for example the Canadian Community–University Research Alliances,188 the Dutch Academic Collaborative Centres for Public Health189 and the Australian Accreditation Collaborative for the Conduct of Research, Evaluation and Designated Investigations through Teamwork. 190 One recent publication coined the term ‘multi-stakeholder health services research collaborations’ to describe the increasingly complex, intersectoral and networked structure of contemporary medical and health services research. 190 These complex forms should be seen as part of the wider emergence of ‘health research systems’ – organised networks of researchers, knowledge intermediaries, policy-makers and others who provide a context for health sciences research and its uptake and application. 35,191 We include brief mention of them here, as even though the HTA programme is not directly linked to such forms, it must take account of their indirect influence on the UK research landscape.
While logic models tend to centre on demonstrating more or less causal connections in the temporal sequence of inputs (research funding), processes (execution of discrete projects or programmes of research, usually following a predefined protocol), outputs (e.g. publications and presentations) and outcomes (impacts on end-users of research), the study of knowledge production has emphasised the non-linearity, messiness and unpredictability of the collaborative knowledge production process. It has also surfaced the importance of power relations and governance for the success of such partnerships, as each partner brings different expectations and goals and the generation of robust and useful research will inevitably depend on managing these conflicts. Evaluations of multistakeholder research collaborations have consistently found that ‘colliding institutional logics’,192 ‘ambiguous loyalties . . . different interests . . . competing goals’193 and ‘multiple accountabilities’. 189 Hinchcliff et al. 190 distinguish between the sanitised written accounts of multistakeholder interactions (‘draped in the formal collaborative language and procedures prescribed by funding agency protocols’) and the reality in which ‘participants . . . view each other pragmatically as consultants, clients or even competitors, rather than partners’. 190
The analysis of developments such as CLAHRCs has (rightly) drawn on a range of different perspectives, approaches and models. Although they are empirically diverse and philosophically heterogeneous, they have in common recognition that the logic model approach is inadequate to capture the multiple (and bidirectional) interactions occurring within the system. These include:
-
approaches based on an in-depth case study that emphasised the formative role of real-time evaluation findings in shaping the emergence of CLAHRC activities185
-
approaches based on a complex adaptive systems perspective, including that proposed by the World Health Organization Alliance for Health Policy and Systems Research194 and Shepherd’s model of the evidence ecosystem in health and social care195
-
adaptation of complex systems theory that focus specifically on conflict, including Bennet et al. ’s196 metaphor of collaborative entanglement (depicting the conflict-ridden, messy, unpredictable and evolving interactions among stakeholders in contemporary mode 2 activity), explored further by Phipps et al. 197,198
-
Kislov et al. ’s199 theorisation of CLAHRCs as communities of practice
-
Caldwell and Mays’ application of sociological ‘frame analysis’ (Goffman200) to analyse a CLAHRC from macro (policy context), meso (organisational activities and interactions) and micro (individual behaviour) perspectives182
-
Currie et al. ’s201 application of neo-institutional theory to explore the interplay between knowledge brokering and professional power dynamics in CLAHRCs (‘Professional hierarchy means that some change agents or knowledge brokers are accorded greater legitimacy than others’) and question the level of policy commitment to the CLAHRC model
-
Rycroft-Malone et al. ’s102,166 adaptation of realist evaluation to look at context–mechanism–outcome configurations in a CLAHRC.
Critics have questioned if, and to what extent, mode 2 knowledge production (in which multiple stakeholders negotiate a research agenda that may not meet scientists’ standards of rigour) counts as science at all. 202 These reservations might be partially assuaged by Van de Ven and Johnson’s paper on engaged scholarship,203 in which they apply the concept of mode 2 to organisational academics working alongside managers. Using the philosophical lens of pragmatism, they argue that mode 2 is essentially a dialectical process of bringing competing perspectives (academic and practical) to bear on a problem – a task they term arbitrage and others have called ‘bricolage’. 204 They explain:
By exploiting multiple perspectives, the robust features of reality become salient and can be distinguished from those features that are merely a function of one particular view or model.
p. 810203
Such an approach is invariably conflict ridden; the key to its success is encouraging task-oriented conflict (which is creative and productive) while managing the potentially destructive influence of interpersonal conflict.
Discussion
In summary, the landscape of applied health research in the UK is changing. A great deal of research remains unambiguously university led, university based and funded (in either ‘responsive’ or ‘commissioned’ mode) from research councils, NIHR and the Department of Health (e.g. via the HTA programme). However, such mode 1 research (in which impact can often be effectively evaluated through logic models) increasingly coexists with mode 2 programmes of activity that are jointly led and governed by multiple (university and non-university) stakeholders, organised in a more neutral transaction space and characterised by organic, non-linear dynamics and focus on the ‘production’ rather than ‘translation’ of knowledge.
These findings are discussed further in Chapter 8.
Chapter 5 Estimating the monetary value of the impact of health research
Introduction
The economic impacts from medical research form a subset of many of the logic models presented in Chapter 3. A section of the literature has addressed the specific issues relating to undertaking exercises to determine economic impacts or the returns on investment from medical research and development spending. Previous reviews of the literature, which form a starting point for this review, have highlighted work that has been done to advance the field. 2,205 The methods used to assess these impacts or returns on investment are born from the economic evaluation literature, and the difference in approaches lies largely in the scope of the cost and benefits assessed, and the valuation methods for seemingly non-monetary components of the impact. As stated in Chapter 2, the purpose of this review was, using Buxton et al. 28 as a starting point, to identify studies since 2004 that have used any methods to attempt to value (in monetary terms) the benefits (health and cost savings) of a body of health research and link that with an investment in the body of research. Articles were included only if they contained a component that attempted to value the impact of research and development investment on population health.
The article in the Bulletin of the World Health Organization by Buxton et al. 28 attempted to learn from previous studies that had estimated ‘monetary values for the societal benefits obtained from health research, especially those studies that have attempted to link (and value) benefits to a specific society from a specified (and costed) body of research’.
The authors characterised the identified methods into four categories:
-
valuing direct cost savings to the health-care system
-
valuing benefits to the economy from a healthy workforce
-
valuing benefits to the economy from commercial development
-
measuring the intrinsic value to society from health gain.
Studies were identified that had considered the benefit of medical research and development as direct cost savings to the health-care system, brought about by a reduced number of people requiring treatment or reductions in per patient treatment costs. This approach had been predominant in estimating the benefits of vaccination research, which had the potential to eradicate subsequent disease and associated treatment costs. 205–208 Cost savings could be included as part of cost–benefit analysis, but these studies did not always link this to an investment period or country-specific research.
One of the earliest studies to attempt to calculate a rate of return from medical research was conducted by Mushkin and Landefeld. 209 A human capital approach (equating the value of life to market values, i.e. wages) was used to value gains from US biomedical research, characterised by a healthier workforce. The limitations of such an approach were acknowledged by the authors and others28,209,210 and tend to overstate benefits when lost labour can be replaced, while understating benefits for those sections of the population not of working age.
Buxton et al. 28 drew largely on a review conducted by Salter and Martin,211 which explored the commercial economic benefits from basic research. Salter and Martin noted progress made by Mansfield212,213 that estimated a worldwide social rate of return (benefits accrued to the whole of society, as opposed to one firm or funders of one project) of 28% for research undertaken 1975–78. Studies have also demonstrated the economic benefits of medical research through industrial applications to other industries. 214
An emerging field highlighted by a number of studies in the Buxton et al. 28 review had measured the intrinsic value of health gains brought about by research and development. A US initiative of the Mary Woodard Lasker Charitable Trust, Funding First,215 produced a series of papers that formed a subsequent book. 216 An informal approach used willingness-to-pay methods to value the increased longevity of life experienced by the US population, attributing a fraction of these gains to medical research. The results suggested ‘exceptional returns’ of nearly 20 times the investment in US medical research. This type of analysis was performed in a more systematic fashion in an Australian study, taking a similar ‘top-down’ approach to valuing health gains, to produce an estimate of the annual rate of return to investment in research and development. 217 They estimated a favourable benefit-to-cost ratio of 2.40 (i.e. AUS$1 invested creates an additional AUS$1.40 benefit); however, this work has been subsequently criticised because the time for investment in medical research to produce health gains was not considered. 218
Buxton et al. 28 noted that there is significant scope for these methods to be extended and refined to allow more robust estimation of the economic benefits from medical research. In particular, a widely acknowledged central challenge that must be addressed in this kind of analysis relates to the attribution problem; the relationship between investment in research and health outcomes. 15,22,28,115 This manifests itself as several related issues regarding the contribution of health research in improving health outcomes and what would have happened without research, that is the unobservable counterfactual. Assumptions must be made regarding the share of health gains attributable to health research, and given there is an international pool of health research, the contribution of any particular country to particular health gains. Finally, assumptions must be made regarding the temporal relationship between a period of investment and a period of health gains. Different approaches face somewhat different problems in dealing with attribution, but methods have continued to be developed to address these issues.
Review findings
The search of databases produced 413 articles, which were initially screened by a reviewer by title (Figure 8). After initial screening and deduplication, 102 articles were screened by abstract. Seventeen articles were reviewed in full, with five included. 22,26,75,218,219 Two of these articles were included in the main literature review. 26,75 One additional report that was not picked up by the supplementary search was included from the main literature review. 25 One additional article and one report known to the authors was also added. 24,220 One in-press article that the authors kindly gave us access to was also included. 27 In total, the review produced nine articles/reports. The studies and methods of assessing return on investment, that included a component that attached a monetary value to health gains, are summarised in Table 16 (see Appendix 6).
FIGURE 8.
Flow diagram of included studies.

The nine studies identified in the review can be split into two categories in terms of how health gains are measured: those taking a top-down approach and those taking a bottom-up approach. There are several other important issues that must be addressed in quantifying the returns; this simple taxonomy allows us to explore the different methodologies. Figure 9 depicts the basic methodologies.
FIGURE 9.
Approaches to identifying health gains from research. R&D, research and development.

Studies have been compared on a number of key facets of the analysis and assumptions that have to be made regarding measuring and valuing net health gains and how to attribute a proportion of health gains to a body of research as follows: How were health gains measured? How were health gains valued? Were health gains ex post or ex ante? Were the costs of delivery accounted for? Was the lag between investment and health gain considered? How was the attribution problem addressed?
Top down
A stream of work undertaken by Access Economics (now Deloitte Access Economics) assessed the benefits of medical research in terms of the intrinsic value of the health gains to society. Two studies were conducted to estimate the returns on investment from Australian research and development. 24,25 Access Economics considered all Australian health research and development spending both public and private between 1992 and 2005. 24 Building on their approach in an earlier report,217 they used projections from the Australian Institute of Health and Welfare to estimate DALYs averted in the period 2033–45 relative to 1993 levels and calculate a return on investment of 117%. 24 The authors assume that the lag between investment and realisation of health gains is 40 years, although the rationale for this figure is unclear.
To calculate the return on investment the authors considered the proportion of DALYs averted attributable to research and development, as opposed to other factors claimed not to be a result of research and development. The authors state that other factors include ‘public health awareness and preventive programs such as ‘Slip Slop Slap’ or ‘Quit’, screening and early intervention initiatives, the public subsidy of drugs and interventions through the Pharmaceutical Benefits Scheme and the Medicare Benefits Schedule, and so on’. 24 The extent to which these examples are not research and development-based interventions could be heavily debated, especially screening programmes; however, the premise that external factors other than research and development are responsible for health gain has been widely acknowledged. 221 They attributed 50% of health gains to research, as they had in their previous study, but have acknowledged that this was not robust. 217 The return was highly sensitive to the value of this parameter. The authors take account of research and development conducted in others countries and its contribution to Australian health gains by using bibliometric techniques to estimate a proxy, based on Australia’s share of publications in the clinical sciences. They estimated that 3% of health gains could be attributed to Australian research and development. The DALYs averted were monetised using a willingness-to-pay methodology, attaching the value of a statistical life-year [AUS$266,843 – £124,300 (converted at 2015 purchasing power parity exchange rate)]. 222
A further study estimated the returns from National Health and Medical Research Council (NHMRC) funding in five disease areas (cardiovascular disease, cancer, sudden infant death syndrome, asthma and muscular dystrophy) using the same methodology. 25 They estimated that the return on investment ranged from 509% in cardiovascular research to –30% for muscular dystrophy. These returns also included the value of avoiding direct health system expenditure, the value of avoiding indirect costs (through productivity losses), the value of direct commercial gains from the NHMRC-funded research and development, and benefits of NHMRC-supported commercialisation. Neither of the Deloitte Access Economics studies considered potential increased costs borne by the health-care system from expensive new technologies. 24,25
Health gains were measured using DALYs averted in 2040–50 relative to 2000 levels. 25 The time between investment (2000–10) and health gains (2040–50) was again assumed to be 40 years. It was assumed that the proportion of gains as a result of research and development was 50%, and 3.14% of these gains were assumed to be attributable to Australian research and development (re-estimated using bibliometric techniques). However, the authors were presented with an additional necessary estimation; the proportion of health gains that were a result of this programme of NHMRC research, rather than the whole body of Australian health research and development. Using bibliometric techniques they found that 25.04% of Australian research publications were funded through the NHMRC and used this as a proxy. The DALYs averted were monetised using a willingness-to-pay methodology (based on individual’s valuation of avoiding mortality/morbidity) attaching a value of a statistical life-year [AUS$168,166 – £78,300 (converted at 2015 purchasing power parity exchange rate)]. 222
Roback et al. 218 used a broadly similar approach to value Swedish gains from all public and private research and development spending on clinical and health research in the year 2005. In this tentative modelling exercise, average annual increases in life expectancy (population utility adjusted) were used to estimate QALY gains in 2015. This implies a lag of 10 years, but the authors did not explicitly discuss this. QALY gains were valued using the value of a statistical life-year [SEK500,000 – £37,900 (converted at 2015 purchasing power parity exchange rate)]. 222 The returns were estimated at a socioeconomic level, including a whole range of non-health benefits where they could be quantified, resulting in a return on investment of 1.08 (8%). In making this estimate, the authors did account for ‘more expensive healthcare due to new methods’. They assumed that 50% of health gains were attributable to research and development, referencing estimates made by various authors that suggest the range may be between 25% and 67%. 216,223–225 The proportion of health gains attributable to Swedish research and development was assumed to be 3% based loosely on an estimate of Sweden’s share of global expenditure and global medical publications.
A significant drawback of Roback et al. 218 and the Access Economics24,25,217 work is the ex ante nature of health gains: the reliance on predictions based on previous trends in population health improvement. This assumes the impact of as of yet unobserved future usage of interventions and hence improvements in health. Ex post studies use retrospective data, either by directly observing population health gains or by compiling data on observed uptake and modelled per patient incremental net health benefits. Although many of these studies require pragmatism in assumption making, the reliance on unknown unknowns requires a leap of faith. 24,25,217,218
Lakdawalla et al. 220 assessed the social surplus arising from the ‘war on cancer’ in the USA from all public cancer research and development spending between 1971 and 2000. An upper bound of this investment was estimated to be US$300B, based on National Cancer Institute spending (which was assumed to make up approximately one-quarter of cancer research and development spending). Ex post life-year gains in survival between 1988 and 2000 were identified and valued at individual willingness-to-pay [US$30,737 – £21,300 (converted at 2015 purchasing power parity exchange rate)]. 222 This produced an estimate of the net gains at US$1.6T. Lakdawalla et al acknowledge the likely lag between investment and health gain and suggest that they may have overestimated the size of investment and hence conservatively estimate social surplus, but did not explicitly investigate the lag. The survival gains were estimated based on cancer-specific improvements in detection and treatment, although the potential for non-research and development contributions to these improvements was not considered.
Bottom up
Informed by methodological frameworks, such as the Payback Framework, studies have used a different approach to build the benefits up from individual interventions to estimate the sum of the health gains, rather than starting from an estimate of overall health gains. 39 It, in part, theoretically deals with the attribution problem presented when trying to estimate the contributions of research and development and non-research and development factors in producing health gains, although it produces a different challenge in identifying only those interventions that are known to have been research driven.
Johnston et al. 75 applied such an approach to the US National Institute of Neurological Disorders and Stroke’s funding of 28 Phase III RCTs prior to 2000. They estimated a return on investment of 46% per year based on 10-year estimates of post-funding QALYs. Available cost–utility analyses were used to estimate the per-patient QALY gains for eight interventions, and data on use were gathered to estimate population gains. Implicitly, it was assumed that all changes in use post trial were a result of that clinical research. Although the examination of the use of the eight interventions suggests some lag, with use fairly stable for at least 2 years after the completion of funding, it might be considered shorter than other estimates. 226 Data presented by the authors suggest that use is not zero during the period when funding ends, which might be indicative that other research not funded by the National Institute of Neurological Disorders and Stroke could have played a role in health gains. By using cost per QALY utility data, the authors were able to present monetised health gains [valued at GDP per head of US$40,310 – £27,900 (converted at 2015 purchasing power parity exchange rate)]222 net of costs of delivery (net monetary benefits) for each intervention. The study was able to find adequate data for only 8 of the 28 Phase III trials, which highlights the data-heavy nature of this exercise and the reliance on published literature. In some instances, a paucity of data may limit the ability for such a study to be undertaken or at least limit the generalisability of findings.
Two studies published by authors of the Payback Framework have adopted an approach that is similar with respect to the identification of health gains to the work of Johnston et al. ,75 but have focused on quantifying the returns in different disease areas. 22,26
Buxton et al. 22 estimated the return on investment [presented as an internal rate of return (IRR) that considers the flow of cost and benefits] from publicly and charitably funded cardiovascular research in the UK to be 9% per year (£1 investment yields health gains equivalent to £1.09). They estimated the health gains between 1986 and 2005 and linked this with a period of investment between 1975 and 1988, based on a lag of 17 years. The lag was estimated based on citation analysis of UK guidelines, using mean time between citation and guideline publication (‘knowledge cycle time’) as a proxy for the time between investment and health gain. Research-led interventions in the cardiovascular field were identified and a timeline of usage assembled. For each of the interventions, per-patient QALY gains and net costs (increases from delivery and potential savings from reduced sequelae) were identified through published cost–utility analyses. QALY gains were valued at the health-care service opportunity cost based on implied cost-effectiveness thresholds of NICE (£25,000) and presented net of costs, to produce an estimate of the net monetary benefits produced per year. The NICE threshold value was chosen to reflect the competing nature of funding of health research over provision of existing technologies. It was assumed that 17% of the health gain was attributable to UK research, based on bibliometric analysis of cardiovascular guidelines that identified the proportion of cited work that contained a UK corresponding author. Buxton et al. 22 combined this IRR with the wider GDP spill over effects of research and development, estimated to be 30%, to give an overall IRR of 39%.
Glover et al. 26 applied the same methodology to publicly and charitably funded cancer research in the UK, re-estimating the lag between investment and health gain and the proportion of health gains attributable to UK research based on cancer guidelines. An IRR of 10% was estimated, based on the monetised net health gains for 1991–2010 for research-driven interventions, linked to cancer funding between 1976 and 1995 (15-year lag). This work highlighted the difficulty in identifying all of the important research-driven interventions. An additional publication227 used accompanying case studies to highlight the complex and heterogeneous relationship between research and health gains. There is a need in a field such as cancer to narrow the scope to complete such a resource-intensive exercise, where there have been widespread improvements in detection and treatment brought about by research, and where the benefits are realised across a heterogeneous patient population (for instance there are over 200 types of cancer). Although developing a method that used changes in incidence and survival gains as a predictor of which cancer types were likely to have contributed largely to overall gains, the authors assumed that interventions not represented in the analysis produced zero net benefit.
A study by de Oliveira et al. 219 largely replicated the methods presented in Buxton et al. 22 to assess the return from Canadian publicly and charitably funded cardiovascular research, which they estimated to be 21% per year based on QALY gains in 1994–2005. Using similar bibliometric techniques, a time lag of 13 years was estimated and 6% of overall health gains were attributed to Canadian research and development. They also argued that an additional component should be considered as part of the attribution problem, assuming that 70% of the health gains were attributable to medical research. However, if the identified interventions were research led and studies used to estimate per patient health gains produced incremental differences brought about by the specific intervention, it is not clear why non-research and development factors ought to be considered in this context.
Guthrie et al. 27 estimated the benefits of the NIHR HTA programme funding from 1993 to 2013. They selected 10 key HTA studies, which were largely made up of randomised trials but also systematic reviews. They identified the per-patient QALY gains associated with the interventions. QALY gains were monetised at the health-care opportunity cost (£20,000 and £30,000) net of health service costs, but total actualised gains were not estimated. Instead, a net monetary benefit associated with a hypothetical 1 year of full implementation for the patient population of the interventions was calculated; therefore, the lag between investment and gains was not considered. The HTA studies were considered to be responsible for all post-HTA research implementation, as they were seen to constitute ‘definitive’ evidence. The authors suggest that only 12% of potential net benefit would cover the £367M invested by the NIHR HTA programme. Although indicative of potential gains, this analysis does not adequately address the attribution problem and makes no consideration of when benefits accrue. It also raises the interesting problems posed when the research takes the form of systematic reviews and the role of such a study in changing clinical practice and hence leading to health gain.
Discussion
There have been contributions to the literature that estimate the impacts of health research using methods to attach a monetary value to health gains. Approaches have attempted to estimate the resultant health gains from investment in bodies of research, and, in doing so, must deal with several problems relating to attributing health gains to particular investments. Techniques that attempt to deal with the problems of attribution have been established. However, authors have acknowledged a simplification of the relationship that is required and the reliance on a logic model view of research impacts. Some of these contributions also consider non-health sector benefits falling on the wider economy, although the scope of the benefits considered often differs, as does the valuation.
Only a few studies specifically considered programmes of health research. 25,27,75 Guthrie et al. 27 estimated the gains of the NIHR HTA programme, but made cautious conclusions on the returns based on hypothetical uptake of a subset of HTA-funded research. 27 Clearly there is scope for these types of methods to be applied to estimate returns from programmes such as NIHR HTA, but several additional considerations need to be taken into account. Conversely, there are advantages to having a well-defined unit of analysis.
It would appear that assessing monetised impact at a programme level is conducive to the bottom-up approach, when the set of interventions is well defined and the task of identifying those that are ‘important’ could be avoided. To an extent, data feasibility issues that limit the bottom-up approach should be mitigated by programmes such as NIHR HTA in that most of its research includes cost–utility estimates. However, issues of scale are present if the number of studies undertaken by a programme is large, such as in the NIHR HTA programme. This might be mitigated to an extent by the need to consider only those trials that showed a significant effect, but this makes a bold assumption about the nature of evidence being used in clinical practice.
When attempting to measure health gains from a programme of research, the attribution problem manifests itself as an added layer of uncertainty regarding the proportion of total health gains that should be attributed to the specific programme. Using a top-down approach, Deloitte Access Economics25 dealt with this by using the percentage of total citations in clinical sciences that were studies funded by the programme as a proxy. This additional attribution problem is not circumvented by the bottom-up approach and a consideration must be still be made. The view taken in Johnston et al. 75 and Guthrie et al. ,27 that National Institute of Neurological Disorders and Stroke’s trials and HTA studies are definitive in terms of changes in uptake, is insufficient, especially in developed countries with multiple funding streams and complex and evolved research ecosystems. The use of the weights attached to particular RCTs in meta-analyses could provide a more systematic way of considering the relative impact of different clinical research supported by multiple funders. Regarding the proportion of health gains that should be attributed to world research and development, this could be used as an intervention-specific replacement for guideline analysis or used as an adjunct. Although time lags must be included, it is not clear how best to estimate these.
An additional problem for programmes that fund only clinical research is dealing with the role of basic research in health gains. This is unclear and constitutes a major potential limitation in these methods. No study looking at a programme has yet encompassed these kinds of considerations into the approach dealing with attribution of health gains to a programme, using either top-down or bottom-up methods.
Although it would clearly be possible to estimate the returns on investment from the NIHR HTA programme, significant challenges remain.
Chapter 6 Assessing the impact of trials on systematic reviews
Introduction
This chapter considers how the impact of a randomised trial might be measured in terms of its contribution to a subsequent systematic review. After an introduction, the results of the literature search are presented. The results of a search of The Cochrane Library for systematic reviews that include randomised trials funded by the HTA programme are then presented and the implications of these findings are discussed.
The HTA programme aims to fund research on technologies that matter to the NHS. In doing so, it funds mainly systematic reviews and randomised trials. Given the widely used hierarchy of evidence, which privileges randomised trials, most systematic reviews are composed of only randomised trials. Meta-analysis provides a synthesised estimate of the effectiveness of the technology. Results from systematic reviews are seen as more robust than those from particular trials and are the preferred basis of decisions by NICE and similar bodies. The two relate in that new trials are rarely funded without a prior systematic review about what current evidence exists. Many of these identify weaknesses in the body of research and recommend new research, usually randomised trials.
Systematic reviews can also provide a way of retrospectively assessing the impact that such trials made to the evidence on the clinical effectiveness and cost-effectiveness of the technology involved. Systematic reviews and their linked meta-analyses provide quantitative measures of the quality and impact of individual trials. Trials are assessed for quality to be included. The included trials indicate not only how many have reported but also the contribution (weight) of each. The resulting synthesised effect size may be statistically significant even though none of the contributing trials was, or, despite some trials showing statistically significant differences, the synthesised effect may not be statistically significant.
Although the HTA programme uses systematic reviews to identify topics for randomised trials, it does not review the impact that those trials have on any subsequent systematic reviews. To some extent it relies on this happening automatically, as the programme partly funds the Cochrane Collaboration, which has pioneered impartial, thorough systematic reviews that are in the public domain. However, the HTA programme keeps no record on the extent to which relevant systematic reviews include trials it has funded (whether new or updates). Updating systematic reviews varies widely, reflecting developments in science. Some HTA journal reports include updated systematic reviews by the triallists and others take a long time to be updated. Some updates adopt slightly different, narrower foci. No guarantee exists that a trial funded by the programme in response to an earlier systematic review will be included in that review’s update, if and when it is updated.
The HTA programme’s early adoption of the process whereby systematic reviews preceded new trials implied a cycle in which new RCTs would contribute to the updated meta-analysis so that uncertainty was reduced if not eliminated. Although methods of measuring such progress were not available when the programme started, this chapter explores if that has remained the case.
Many of the early projects commissioned by HTA were systematic reviews, all recommending further research (usually RCTs), some of which the programme went on to commission and fund. Of 109 projects that included a randomised trial to March 2011, 62 (57%) were recorded as quoting a prior systematic review in its monograph report. 228 Most [109/125 (87%)] of the RCTs funded by the HTA programme were superiority, not equivalence (non-inferiority), trials. Superiority trials also made up the bulk of systematic reviews.
Owing to the time lag between identification of topic and publication in HTA Journal, almost all trials published to 2011 had been commissioned pre-2006 when researcher-initiated bids began to be funded. Therefore, almost all were on topics identified and prioritised by the programme. For RCTs that are ‘commissioned’ (i.e. defined) by HTA, the research question, the existing evidence and the need for a trial are specified.
To explore the scope for measuring the impact of randomised trials through their contribution to systematic reviews, one needs to know what the literature offers in terms of methods and the extent to which systematic reviews that include trials funded by the HTA programme exist.
Literature searches
The methods used in the literature search were, as outlined in Chapter 2, supplemented by the team’s knowledge. The search of The Cochrane Library of Systematic Reviews was based on the relevant technology and disease. Reviews that included both the technology and disease were searched to locate randomised trials funded by the HTA programme, using the lead author as the link. For each review including a trial funded by the programme, the following items were extracted: technologies compared, whether or not the difference was statistically significant and the weight attached to the trial.
Results
The results of the literature search were divided into descriptive studies, those that explored the use of systematic reviews in designing trials, those regarding VOI [and its York/Patient-Centered Outcomes Research Institute (PCORI) variant] and those assessing systematic reviews in relation to their use in clinical guidelines.
Descriptive studies
Gouldie et al. 229 showed that a minority of trials published in leading journals cited previous RCTs (6/27) or systematic reviews (10/27) in determining their target sample size.
Jones et al. ,230 in a review of randomised trials funded by the HTA programme between 2006 and 2008, found that 77% (37/48) cited a previous systematic review. A follow-on of this study231 found that almost all of those that lacked a prior systematic review did so for good reasons. Some were new topics (first in class), in which case a formal systematic review might not be necessary. In other instances, the previous trials were judged to be of low quality.
Use of systematic reviews in designing new trials: literature
Sutton et al. 232 employed simulation methods to estimate the trial sample size linked to probability of conclusive result in meta-analyses. Their results favoured several small RCTs, rather than a single large conclusive trial.
Roloff et al. 233 used a random-effect meta-analysis to estimate conditional power, which is needed to detect a specified mean effect size for a given meta-analytic result. This work showed that, in the presence of heterogeneity, no trial could be large enough to be conclusive. Instead, several separate trials would be needed.
Heterogeneity was defined as relating to genuine differences underlying the results of RCTs (heterogeneity) as opposed to variation as a result entirely of chance (homogeneity). The degree of heterogeneity has become widely used in Cochrane reviews.
Value of information literature
Value of information, a concept from decision analysis, relates to the extent of uncertainty and the types of information that would reduce that uncertainty relative to perfect information. Wikipedia provides an entertaining definition: ‘Value of Information is sometimes distinguished into value of perfect information, also called value of clairvoyance, and value of imperfect information. They are closely related to the widely known expected value of perfect information and expected value of sample information’. More formal accounts of VOI have recently been puplished. 234–236
Cost-effectiveness acceptability curves, an element of the VOI approach, have been used in almost all the economic analyses in HTA-funded trials. They have also been adopted by NICE in its technology appraisal programme.
The HTA programme has made use of the VOI approach. It decided not to fund a trial based on a form of VOI from the preliminary assessment of technology for health services model. 237 It funded a review of the ‘role of modelling in planning trials’,238 which favoured VOI. It also reported the results of a pilot study of the use of VOI by the programme. 239 This was successful according to the authors, a University of York team that carried out the relevant analyses. A more recent review240 found that 25 of approximately 500 studies (≈5%) published by the programme had used VOI method(s).
Overall, VOI appears more useful in assessing the gaps in research than in assessing the impact of RCTs. Projects that are developed on the basis of VOI should produce less uncertain estimates of the cost-effectiveness of particular technologies. The extent to which this results in greater impact, however measured, is unknown. Research on this forms one of PCORI recommendations below.
Patient-Centered Outcomes Research Institute
The PCORI was authorised by the US Patient Protection and Affordable Care Act of 2010241 to conduct research to provide the best available evidence to help patients and those who care for them to make better-informed health-care decisions.
The PCORI was explicitly prohibited from using QALYs and cost-effectiveness in determining research priorities. 242 Instead of using VOI, which implies use of cost per QALY, it developed (along with Claxton et al. 234 from the University of York) an amended version that relies on cumulative meta-analysis and minimum clinical difference. This, combined with incidence/prevalence, can be used to assess the worth of funding new research. It involves asking if the expected net health benefits of additional evidence are sufficient to regard a particular research proposal as worth prioritising.
The scale of uncertainty is assessed from systematic reviews and meta-analysis, combined with baseline risk and incidence. These are used to express the expected consequences of uncertainty in terms of health outcomes. The approach also assumes degree of implementation.
The York/PCORI package was offered as a software package to the HTA programme in 2013, which has been exploring its use. No formal evaluation appears to be taking place.
This approach shares the VOI emphasis on prospectively prioritising elements of research. Whether or not reduced uncertainty leads to greater impact remains unknown.
Literature on systematic reviews and clinical guidelines
A different approach for valuing trials considers the scope for basing clinical guidelines on systematic reviews. The Grading of Recommendations Assessment, Development and Evaluation (GRADE) group provides tools to assess the quality of information in relation to its use in guidelines. GRADE ‘is a well-developed formal process to rate the quality of scientific evidence in systematic reviews and to develop recommendations in guidelines that are as evidence-based as possible’. 243
The GRADE tool is used by NICE along with many similar organisations elsewhere. Given the aim of the HTA programme in relation to meeting the needs of the NHS with high-quality evidence, GRADE provides a tool for assessing the extent the usefulness of that evidence for clinical guidelines.
The GRADE tool recommends that:
-
The strength of recommendations should be expressed using two categories (weak/conditional and strong) for or against a management option and the definitions for each category should be consistent with those used by the GRADE Working Group.
-
Decisions about the strength of the recommendations should be transparently reported.
However, an evaluation of GRADE suggests that it has had little impact on which systematic reviews are included in clinical guidelines. 244
Results of search of The Cochrane Library for systematic reviews that included trials funded by the Health Technology Assessment programme
The Cochrane Library was searched to explore the extent to which systematic reviews that included randomised trials funded by the HTA programme existed. This section provides preliminary results. As shown in Table 10, 28 (around one-quarter) out of the 121 eligible trials (excluding four feasibility or pilot trials) published up to 2011 featured in a subsequent Cochrane systematic review. This indicates that subsequent systematic reviews cannot be assumed.
| First author (volume:issue) | Subsequent Cochrane review | Comparison | Disease | Superior | Weight (%) |
|---|---|---|---|---|---|
| Simpson et al.238 (4:36) | Bower et al.245 | Counselling | Depression | No | 32 |
| Suri et al.246 (6:34) | Wark and McDonald247 | Daily rhDNase vs. alternate-day rhDNase vs. hypertonic saline | Cystic fibrosis | Yes | 64 |
| Garry et al.248 (8:26) | Nieboer et al.249 | Laparoscopic vs. abdominal hysterectomy | Menorrhagia | Yes | 36 |
| No | 40 | ||||
| Vickers et al.250 (8:48) | Linde et al.251 | Acupuncture vs. treatment as usual | Migraine | Yes (short and long term) | |
| Ozolins et al.252 (9:1) | Garner et al.253 | Antimicrobials | Acne | Yes (short and long term) | 100 |
| Cochrane et al.254 (9:31) | Bartels et al.255 | Hydrotherapy short term | Osteoarthritis | Yes (short and long term) | 100 |
| Thomas et al.256 (9:32) | Furlan et al.257 | Acupuncture/control | Lower back pain | Yes (short and long term) | 40 |
| Hobbs et al.258 (9:40) | Moran et al.259 | Atrial fibrillation detection | Atrial fibrillation | Yes | 100 |
| Dennis et al.260 (10:2) | Gomes et al.261 | Percutaneous endoscopic gastrostomy vs. nasogastric feeding | Post stroke | No | |
| Kennedy et al.262 (10:19) | Zijdenbos et al.263 | Cognitive–behavioural therapy + treatment as usual, short term | Irritable bowel syndrome | Yes (short and long term) | 52 |
| Nixon et al.264 (10:22) | McInnes et al.265 | Pressure mattress vs. underlay | Pressure ulcers | No | 100 |
| O’Dowd et al.266 (10:37) | Price et al.267 | Cognitive–behavioural therapy vs. treatment as usual | Chronic fatigue syndrome | No | 24 |
| Hewison et al.268 (10:50) | Mujezinovic et al.269 | Communication strategies | Amniocentesis | Yes | 100 |
| Jolly et al.270 (11:35) | Taylor et al.271 | Home vs. hospital | Cardiac rehabilitation | No | 9 |
| Fader et al.272 (12:29) | Fader et al.273 | Absorbent pads comparison 1 | Incontinence | Yes | 100 |
| Absorbent pads comparison 2 | No | 100 | |||
| Grant et al.274 (12:31) | Wileman et al.275 | Medical vs. surgical management | Gastro-oesophageal reflux disease | Yes | 96 |
| Potter et al.276 (13:9) | Bath and Krishnan277 | Hypertension control vs. treatment as usual | Post stroke | No | |
| Morrell et al.278 (13:30) | Dennis and Dowswell279 | Psychological intervention vs. treatment as usual | Postpartum depression | Yes | 39 |
| Grey et al.280 (13:33) | Vital et al.281 | Non-invasive ventilation methods (continuous positive airway pressure vs. non-invasive positive-pressure ventilation) | Cardiogenic pulmonary oedema | Yes | 31 |
| Williamson et al.282 (13:37) | Simpson et al.283 | Steroids: intranasal | Otitis media | No | 100 |
| Sullivan et al.284 (13:47) | Salinas et al.285 | Corticosteroids/control | Bell’s palsy | Yes | 18 |
| Jeffcoate et al.286 (13.54) | Dumville et al.287 | Dressings | Diabetes foot ulcer | Yes | 46 |
| Michaels et al.288 (13.56) | O’Meara et al.289 | Antimicrobial silver dressings vs. non-adherent control dressings | Venous leg ulcers | Yes (short and long term) | 77 |
| Lock et al.290 (14.13) | Burton et al.291 | Tonsillectomy | Tonsillectomy | Yes | 25 |
| Peek et al.292 (14.35) | Tramm et al.293 | No meta-analyses possible | N/A | ||
| Lamb et al.294 | Williams et al.295 | Not included as insufficient psychotheraptic content | Chronic pain | ||
| Sharp et al.296 (14.43) | Molyneaux et al.297 | Antidepressant drug therapy vs. psychosocial intervention | Postnatal depression | No | 100 |
| Antidepressant drug therapy vs. treatment as usual | Yes | 100 | |||
| Cockayne et al.298 (15.32) | Kwok et al.299 | Cryotherapy vs. salicylic acid | Verruca warts | No | 16 |
Caveats relate to the limited nature of the search and its restriction of the search to The Cochrane Library. Although a more thorough search might reveal a few more instances, we are confident the results presented here indicate the limited extent to which trials funded by the HTA programme feature in systematic reviews.
Only around half of the meta-analyses in these systematic reviews indicated that the intervention was superior, in that the 95% confidence interval for the primary outcome excluded no difference. 300 For the rest of the comparisons, the difference was not statistically significant. Non-superiority cannot be interpreted statistically as proof of no difference (whether non-inferiority or equivalence). However, although some authors claimed non-inferiority, this was not strictly justified. The policy implications resulting from systematic reviews that do not demonstrate superiority deserve separate attention, if only because such results are so common.
Several other points are worth noting from Table 10. First, the weight of the HTA trials in the meta-analysis varied widely. For some comparisons in eight reviews,252,254,258,264,269,273,283,297 the trial funded by the HTA programme had a weight of 100%, indicating that it provided the only evidence for that particular comparison. For the others in Table 10,252,254,258,264,268,272,282,296 the weight was much lower, indicating a lower contribution of that trial to the synthesised result. This is partly because of other trials reporting after the HTA trial was funded.
Second, the HTA-funded trials tended to have higher weights for comparisons relating to patient-related outcomes and/or longer time frames. This indicates that the contribution of a trial to a systematic review can take many forms, some of which may be more relevant to those commissioning health services than others.
Given that only around one-quarter of HTA-funded trials are included in a subsequent systematic review, more work is required on their contribution to knowledge.
Discussion
The chapter has shown that the HTA programme contributes only one side of the loop linking systematic reviews and trials. Although it usually carries out a systematic review before funding a trial, it does not follow up with any analysis of the contribution that trial makes to any subsequent systematic review.
The York/PCORI approach used in 2015 by the HTA programme for deciding when to fund trials is important and deserves to be evaluated. However, without subsequent analysis of the trials funded, this will not help with assessing the contribution any trial funded makes to the body of evidence.
The GRADE tool offers a way to assess how complete the evidence in systematic reviews is for the purpose of drawing up clinical guidelines. This may offer a way for the HTA programme to assess the extent to which a particular trial has contributed and if another is required.
The finding that only around one-quarter of HTA-funded trials are included in a subsequent systematic review shows that a contribution by a trial to systematic reviews cannot be assumed. Furthermore, the fact that around half of the Cochrane systematic reviews to which a trial contributes do not demonstrate superiority prompts questions as to how to assess the value of these.
Research recommendations
There is merit in using existing systematic reviews to assess the impact of trials funded by the programme. When systematic reviews of important topics are lacking, the programme should consider funding them.
When the topic of a trial may become part of a clinical guideline, GRADE should be employed to assess the completeness of the evidence. The exploration by the HTA programme of the PCORI/York approach of assessing the need for a trial in relation to existing systematic reviews should be evaluated.
Research on the extent to which projects and programmes that employ either VOI or the PCORI approach achieve greater impact would be valuable. As the HTA programme has made some use of both VOI and PCORI, the relevant projects might be considered for case studies as well as for bibliometric analysis.
Work is also required on the policy implications of non-superiority results in systematic reviews of superiority trials.
Chapter 7 The impact of randomised trials on stopping the use of particular health technologies
Introduction
This chapter was prompted by the suggestion that the impact of some RCTs funded by the HTA programme were mainly concerned with stopping new technologies. 30 The two cases cited were water softeners for eczema and larvae for wound healing. 31,32 Both were novel technologies, funded by the HTA programme. Both were negative in the sense that neither demonstrated that the technology added value to current treatments. Subsequently, neither technology appears to have been used much by the NHS, although no formal evaluation has been carried out.
To discredit or stop the diffusion of a technology, a randomised trial must be definitive; being one of the first and biggest in the field can do this. The water softener trial was both the first and biggest, whereas the larvae healing trial was the biggest but not the first.
This chapter explores the related literature and briefly reviews the HTA portfolio of randomised trials in terms of how many were ‘first in class’. In brief, it finds little of relevance in the literature on trials stopping technologies. It found that, of the 121 eligible trials published up to 2011, 30 could be considered first in class. A further 10 projects had three or fewer prior randomised trials (see Table 10 for these references). 228
Literature searches
Two searches were carried out, the terms of which are provided in Chapter 2. The first focused on terms such as ‘randomised controlled trials’ and ‘disinvestment/rationing’ and the second widened the terms to include The Lancet article,30 which included the water softening and larvae cases. Between them they identified 78 articles, of which 38 were deemed relevant. Of these:
-
six were on programme budgeting and marginal analysis316–321
-
one analysed a RCT in terms of discontinuation of a particular drug. 332
Four systematic reviews were identified, three of which were concerned with disinvestment. Leggatt et al. 333 found that eight countries had some evidence of such work but no clear findings. Polisena et al. ’s334 review of case studies of disinvestment found 14 cases, with programme budgeting marginal analysis used in six. Neilsen et al. 335 reviewed HTA in European countries, indicating the priority many attached to disinvestment. The final systematic review, by Watt et al. ,336 reviewed the use of safety and effectiveness in a single service, assisted reproduction.
Points arising from the descriptive papers included: the asymmetry between existing and new services in terms of assessment and scope for disinvestment,318 and the importance of safety concerns in decisions to stop use of particular technologies. 336 Stepped-wedge trials were advocated as a means of evaluating new technologies before/during implementation. 304
Overall, with the exception of the advocacy of the stepped-wedge design, the literature review offered little on the scope for using trials to prevent the diffusion of new technologies. The literature was focused on disinvestment and was concerned mainly with the removal of older, less effective technologies.
First in class
A term usually referring to the first pharmaceutical in a class to be authorised for marketing, the term acquires a gradation of meanings applied to HTA programme trials. The interventions are often complex packages, parts of which differ from trial to trial. Furthermore, such interventions can often be provided in different settings (hospital or community) or by different people (doctor or nurse). All those randomised trials with a reasonable claim to be first in their class, based on the background provided in each HTA journal, were included.
Forty-four out of a total of 121 trials involving a RCT that did not have a preceding systematic review were identified from the metadata database228 and examined in terms of preceding evidence. Twenty-two could be considered ‘first in class’. Systematic reviews that had a weight of 100% were added to these. As discussed in Chapter 6, eight fell into this category. Therefore, 30 out of 121 (around one-quarter) eligible trials could be considered first in class.
Few of these were novel technologies such as water softeners or larvae. The nearest to a new technology was a befriending service for people with dementia. 337 Many interventions were new only in the sense of being the variants of existing procedures. In surgery, these included different methods for performing tonsillectomy290 and for reconstructive surgery for limb ischaemia. 338 Some were the first in a particular setting, mainly in general practice, while others were new diagnostic tests,339 referrals for pain and for lumbar spine radiography,340,341 and screening for atrial fibrillation. 258
A further 10 had three or fewer preceding randomised trials. These were usually small trials, most of which were deemed of poor quality.
Discussion
The role of randomised trials in stopping the diffusion of particular technologies has received almost no attention in the literature. To have scope to prevent diffusion, any such trial needs to be definitive: this implies being either the first or the largest trial. Given the paucity of literature, a preliminary search was carried out to establish how many HTA trials could be considered first in class. This search showed that around 30 trials funded by the HTA programme could be titled ‘first in class’. However, many of these involved small variations on existing treatments. Very few were studies of completely new types of technology. The programme may wish to consider identifying trials that might be considered first in class and on the extent to which they can be considered definitive.
Chapter 8 Discussion
This chapter discusses the findings of each element of the work reported above, exploring their implications for the HTA programme. Recommendations are made for research priorities.
Updated systematic review
This updated systematic review identified and described 161 publications on research impact (see Appendix 3, Table 14). Most of these were published since the previous original review that included studies published up to 2005. 2 The earlier review2 described 46 publications from the period from 1990 to 2005 and hence the number of studies has grown, as has the range of approaches used (please refer to the original Hanney et al. 2 report for a full list of these references).
Continuities exist between this and the previous review. 2 Some older frameworks continued to be used, but with variations, particularly the Payback Framework and the monetary valuation of benefits. Additional frameworks have been developed and applied, often drawing on and combining earlier approaches. Major work building on previous frameworks was conducted by the CAHS,7 summarised in Frank and Nason. 115 This was further developed and built into the performance measurement system by the Alberta health research system. 85
The scale of application varied enormously, with some frameworks using small-scale approaches designed for use by individual researchers, such as the RIF developed by Kuruvilla et al. 97 At the other end of the spectrum national schemes continue in the Netherlands,79 and have developed with the UK’s REF. 106 This reflects the growing interest by research funders from national governments through to small funding organisations. For example, the Addenbrooke’s Charitable Trust commissioned a study to assess the impact of its fellowship scheme, which invested less than £1M. 67
Much of the literature comes from the English-speaking nations of Australia, Canada, the UK and the USA, perhaps partly reflecting the search restriction to English on pragmatic grounds. However, we also include ongoing work conducted in many other countries, including the Netherlands and Austria, and published in English. We also identified assessments of the impact of health research in international development programmes, including programmes of research training.
Some core methods continue to be widely used: interviews, surveys, documentary analysis and case studies. Case studies are of interest for several reasons. They have confirmed responses to surveys suggesting that researchers do not generally exaggerate the impact they report in surveys. 2,51,52,62,95 Case studies have enabled the capture of the wider impacts from research training programmes, such as that funded by the National Institutes of Health Fogarty International Centre. 57 Case studies have also incorporated qualitative findings in mixed-method approaches such as that adopted by the Wellcome Trust. 93 Finally, although the 2014 REF and the EIA exercises were based on the outputs of groups of researchers rather than funded programmes, they too demonstrated the advantages of using case studies. Those conducting the REF warned of the danger of excluding case studies in favour of metrics in future such exercises. 33
We also noted attempts to develop the methods used, owing, in part, to the recognition of limitations with the existing methods. One limitation frequently noted is that most of the studies have been funded by the same organisations that funded the original research. Potential for conflicts of interest can also arise owing to the involvement in impact assessments of members of the research organisation whose research is being assessed.
The impact assessment studies reported in our review (see Table 14, Appendix 3) generally start with specific pieces of research and work forwards to identify impacts. Many of them suggest that research has made a larger impact on policy than is often reported in reviews of studies that start with policy-making and work backwards to consider how far research might have impacted on those policies. 13 This might reinforce the suggestion that the best way to identify research impacts is to start from a body of research and work forwards to trace any impact that it might have had. 2 Tracing forwards provides a different focus from studies that start from impacts, such as on policy, and work backwards. For example, a researcher interested in their research being used might have better recall about how, and to whom, the findings were disseminated than a busy policy-maker would have of which research influenced him or her. The growing portfolio of case studies supports the claims that a range of impacts can be identified as coming from research. Sensitivity analyses have generally indicated the robustness of these estimates. On balance, differences in method rather than conflicts of interest seem to account for the high impact reported in some studies included in our review.
Not all types of programmes have the same potential for delivering impact. There is considerable evidence that programmes based on a prior assessment of needs by funders, or which have been commissioned by an authoritative ‘receptor body’, are likely to have more impact than programmes driven by researchers’ interests. This was, of course, the rationale for establishing the HTA programme in which the commissioning of research was linked to the needs of the NHS. 2,49 It is also seen internationally. This suggests that the frameworks to assess the impacts from these programmes should take account of the context within which the research occurs.
Many studies indicate that the impacts of research are often slow and incremental, and that many factors impinge on potential users. 137 Some highlight the importance of personal interactions between actors to achieve impact. We have shown that the programmes with the strongest interactions are among those reporting highest levels of impact. Does this suggest that a greater emphasis on interactions might be having some successes? Some of the studies described might indicate this is the case. 66,89,132,136–138,141 More detailed assessments might play a useful role in understanding the processes involved. However, initiatives informed by concepts such as linkage and exchange342,343 do not necessarily make an impact if, for example, there is a high turnover among the government officials. 344 Iteration at an organisational level may be required for interactions to be successful. Impact assessment requires attention to scale and context. The validity and reliability of different data sources also needs to be assured.
Taxonomy of approaches
The extended review of the social sciences literature revealed a wide variety of approaches which reflected a range of philosophical positions: positivist (e.g. the unenhanced logic model), constructionist (interpretative and interactionist), realist (context–mechanism–outcome–impact models), critical (participatory models) and performative (or Co-production models). However, these ‘ideal type’ positions are often used eclectically in combination. For example, the Payback approach is a hybrid, including a central logic model but enhanced by a focus on case study methods, reflecting the importance of an interpretative narrative and paying attention to context.
Approaches that emphasise ‘co-production’ of research findings are becoming more popular, particularly in Europe. These approaches may be less appropriate for the HTA programme than for some types of NIHR programmes such as CLAHRCs and Academic Health Science Networks.
Monetary value on the impact of health research
The literature on the economic returns from medical research has also expanded since 2005. Health gains have been monetised by putting a value on each QALY gained, net of the cost of delivery to produce estimates of net monetary benefit and linked to specific investments in research. Some of these analyses have also considered wider non-health benefits from research investments. These analyses have been performed at various levels from programmes to specific diseases. All these analyses required major assumptions relating to attribution, first of the contribution of research to health over specified time periods and then attribution by country. Each analysis has provided its own challenges in finding estimates to meet these assumptions.
A new method for identifying health gains has used a ‘bottom-up’ as opposed to a ‘top-down’ approach, building the totality of health gain based on individual research-led interventions. 22,26,27,75,219 Most of these assessed health gains ex post. The ‘top-down’ approach that formed much of the earlier work in the field has also continued to develop. 24,25,218,220
The bottom-up approach has produced more conservative returns and helps deal with some of the research/health attribution problems specific to the top-down approach, in that only research-driven interventions need be included in the analysis. In the latter, it is clear that estimates rely heavily on the fraction of health gains that are attributed to research and development, for which robust estimates do not exist. Although the bottom-up approach may be better able to address this attribution problem, it struggles with the issue of scale. This has often narrowed its scope because of the richness and level of data required.
Most of the identified studies acknowledge the time lag between the investment and health gains but based on different assumptions. The most robust estimates have been informed by guideline analysis,22,26,219 but even these share uncertainties about time lags and implementation.
Assessing the impact of trials on systematic reviews
The HTA programme contributes one side of the loop, from a systematic review to the need for new trials but not vice versa. The impact of a new trial on the subsequent systematic review is not routinely examined. Only by completing this side of the loop can it be established if further research is required. Clinical guidelines are the main ‘customer’ for systematic reviews. Both the York/PCORI (which is being used by the programme) and the GRADE toolkit consider systematic reviews and guidelines to assess if further research is required.
However, it remains the case that many trials funded by the HTA programme do not show statistically significant differences in their primary outcomes. When included in systematic reviews, these often also fail to show superiority of the intervention in question. Non-superiority, however, cannot be interpreted statistically as non-inferiority. A preliminary search showed that around only one-quarter of trials funded by the HTA programme were included in subsequent systematic reviewed by Cochrane; of these reviews, around half showed superiority. For the rest, the 95% confidence interval included a measure of no difference.
Although each trial has value in contributing to a meta-analysis, the policy implications are unclear when the meta-analysis fails to indicate superiority of any compared intervention. Work is required to assess what further research might indicate if non-superiority can reasonably be taken as indicating non-inferiority. The implications can be considerable. For instance, if two interventions had no difference in efficacy, a choice might be offered if the cost was similar. If the costs are materially different, the less costly might be preferred. More generally, funding trials and systematic reviews on the basis of hypothesised differences but being unwilling (or unable) to draw conclusions when such differences are not proven amounts to waste.
Cost-effectiveness modelling, such as that funded by the HTA programme, to support NICE’s technology appraisal programme, goes beyond systematic reviews to synthesise data on costs and effectiveness often projected to cover patients’ lifetimes. Such models can have a major impact on decisions made by NICE. Although we have not considered these models, we believe that assessment of their impact should be included in future.
Impact of randomised trials on stopping the use of particular health technologies
Although disinvestment has attracted considerable interest in the literature, it has been largely concerned with existing rather than new technologies. The literature provides no instances of a randomised trial playing a major role in stopping the diffusion of a new technology. A few trials funded by the HTA programme related to water softeners and larval healing may have played such a role. 31,32 One was first in class and both were the biggest trials of each topic. Around one-quarter of trials funded by the HTA programme can be considered first in class, but many of these were concerned with small changes in existing treatments. The term ‘first in class’ is usually used in discussing pharmaceuticals where ‘class’ may be defined more rigorously than for other interventions.
Limitations of the Health Technology Assessment review
In conducting this review we faced various challenges, and, although we attempted to address them, some limitations remain. The precise inclusion/exclusion criteria were difficult to define and apply, especially around issues such as what is meant by a ‘programme’ of research. For many programmes from specific funders they were, of course, clear-cut. However, the boundaries were less clear in relation to the collective work supported by multiple funders and conducted by a group of individual researchers at one end of the spectrum, and a large part of the research system at the other.
The nature of the review was also complex because we wished to not only update the earlier 2007 review,2 but also extend the focus of the review to include a wider range of analysis and address issues of particular (policy) relevance to the HTA programme. Therefore, inevitably, there were some issues in which the boundaries became fuzzy. At the same time, we wanted to maintain a degree of coherence by presenting just one main list of included studies before delving into the more specialist areas covered by Chapters 5–7. In addition, to ensure as wide a range of papers as possible was included in the main list, we drew on the knowledge of the team and snowballing to a considerable extent. These methods provided over one-quarter of the papers (43/161 included studies), a higher proportion than for many reviews. Although this might create some difficulties for any replication of the review, and the diversity of papers did present challenges for the analysis, the importance of these limitations was reduced because there was no possibility that a meta-analysis could have been meaningfully conducted in a field such as this. Nevertheless, the scope of the review remained challenging, especially in view of the resource constraints within which we operated.
Finally, as discussed below (see Options for the National Institute for Health Research/Health Technology Assessment to take research impact assessment forward), we were aware that the whole field has become increasingly controversial in recent years. Furthermore, there have been major developments at the system-wide level that, while they have not been fully evaluated, are having an increasing impact on what assessment might be undertaken at the level of specific funded programmes.
Options for the National Institute for Health Research/Health Technology Assessment to take research impact assessment forward
What do the findings of our review tell us about approaches to assessing the impact of multiproject programmes such as the Health Technology Assessment programme?
Our findings strongly support the recommendation that the HTA programme should continue to assess the impact of its research. The findings of this review support the use of the Payback Framework. The fact that the programme’s funding, like the rest of NIHR, comes from the funds allocated to the Department of Health, means that a major part of the impact must concerned with meeting the needs of the NHS. The HTA programme has succeeded in meeting the research needs of some key NHS bodies, such as the National Screening Committee and NICE. Changes in the structure of the NHS, the development of NHS England and changes in NICE’s remit pose new challenges relating to identifying and meeting current and future research needs.
In recent years, the NIHR has supplemented its focus on trials by embracing an explicitly interdisciplinary and mixed-method approach to the study of health policy and health services delivery (drawing on the assumptions and methods of the social sciences). The literature highlights the importance of building and maintaining relationships between different stakeholders in the research process (including, sponsors, researchers, the public and policy-makers) in order to build a shared understanding of research priorities and create interest and engagement in a programme of work (hence, improve dissemination and impact after it is complete). Sponsors of complex programmes of research with a strong social science element and/or those that emphasise collaborative Co-production of research may find this wider literature helpful.
However, enhanced logic models that assume a broadly direct and linear link between a programme of work and its impact, but which include scope for interpretive case study to explain unique and/or non-linear influences, may be appropriate for the bulk of HTA-funded research, especially systematic reviews and trials. These models may be less applicable to the study of organisational change or collaborative research such as CLAHRCs. Although many promising alternative models now exist in the social science literature, further work is needed to determine the most appropriate models and tools to use for different research programmes and study designs.
What might be the consequences of the introduction of the Research Excellence Framework, and what might it contribute to impact assessments for National Institute for Health Research programmes?
Future assessments of the impact of the HTA programme will have to take account of wider changes in research policy, notably the REF. The REF has become more important as a major and regular quality assurance mechanism. Its extension in 2014 to include impact appears to have been a success and hence likely to continue, possibly using a similar case study approach to that employed in 2014. 106,345 Besides learning from the REF case studies, the HTA programme should consider how these should be structured in the future. The selection of topics for case studies is often ad hoc, different methods are used and data are often either unavailable or retrospective. The selection of case studies, such as in the REF but also more generally, tends to be biased towards ‘good news’ stories. Other fields indicate that much can be learnt from failures. Appendix 7 gives brief details of some early research studies on impact case studies from the 2014 REF, which were published after the cut-off date for our census.
What might be the consequences of the introduction of researchfish, and what might it contribute to impact assessments for National Institute for Health Research programmes?
This review did not identify any independent evaluations of the use of researchfish in impact assessment. The adoption of researchfish by all major UK research funders also has implications for future assessments of impact. While the routine capture of indexed research publications has merit, the degree to which researchfish will succeed in collecting other, non-indexed outputs and activities remains to be established. Further, the focus on individual projects means the more macro aspect of the impact of research projects may receive less attention. These higher levels include the overall impact of the HTA programme on both the NHS and on the universities. The evolution of NIHR to be the main funder of most late-stage health research has plausibly changed how it is perceived by universities, not least in relation to REF. How this might affect how the NHS sees the programme remains to be established.
Options for the National Institute for Health Research/Health Technology Assessment for health research impact and research recommendations
One option for the HTA programme is to plan how best to meet the data requirements of future impact assessments, both by the programme but also in external assessments such as any future REF exercises. The data on the management of the HTA programme, held by NIHR Evaluation, Trials and Studies Coordinating Centre, focus on administration and management of the programme. Development of its electronic management information system has been slow and uneven. The programme has invested in projects that quality assures the data, and enables comparisons and trends to be analysed,228 but these have applied only to the randomised trials. The likely data requirements of future assessments of impact and of the REF need to be planned for and included either in management information systems or in special projects.
Research recommendations
We recommend research prioritised as ordered below.
-
Given the importance of case studies and the criticisms that can be levelled against them (selection and methods bias), research on the extent to which case studies in general and the REF impact case studies in particular provide sufficiently rich, complete, accurate, honest stories of the impact of a team’s research is required. We recommend a review of case studies and their application to health research, including the 2014 REF, combined with independent selection and preparation of case studies of HTA projects.
This should include both successful and unsuccessful projects. It should also include cases focusing on the monetisation of impact and on linking trials to systematic reviews and guidelines. Particular case studies might contrast the tracing forward/backward methods of linking particular research projects to policy changes. The aim should be the development of evidence-based case studies, as well as appropriate frameworks and examples of good practice. As case studies have importance in other NIHR research programmes, the remit of the proposed research should include the relevant NIHR research programmes.
-
Research is required on the role of ongoing electronic data collection of the sort involved with researchfish. This should assess the strengths and weaknesses of this approach, the extent of bias, such as towards indexed publications, and the extent of researchers’ compliance and support. A careful assessment of the completeness, accuracy, technical properties, usability and user experiences of researchfish is needed. Researchers’ responses on researchfish might be compared with previous studies (typically based on semistructured interviews) of principal investigators to ascertain their views on the impact of their research.
-
Research is also required on optimal methods for assessing the impact of randomised trials on systematic reviews and guidelines. The York/PCORI methods currently being piloted by the HTA programme should be evaluated along with the scope for use of GRADE. This research should also address ways of assessing the value of randomised trials and meta-analyses that indicate the non-superiority of particular interventions.
-
Research would be valuable on the extent to which projects and programmes that employ either VOI or the PCORI approach achieve greater impact, as discussed in Chapter 6. As the HTA programme has made use of both VOI and PCORI, the relevant projects might be considered for case studies as well as for bibliometric analysis.
-
Research might also usefully explore the impact of cost-effectiveness models, such as those used by NICE’s technology appraisal programme.
-
With regard to NIHR, research is required on the appropriate measures of impact for research programmes other than the HTA programme.
Chapter 9 Conclusions
We concluded that the HTA programme should continue to monitor and evaluate the impacts of the studies it funds. Such analyses should be informed by considering, in parallel, the assessment of the impact of the first decade of the HTA programme by Hanney et al. 2 and the findings from the RAND review of the second decade. 27 It should consider the scope for building on the analysis in the RAND Europe report of the wider, overall impact of the HTA programme as a long-standing programme. It should also consider the findings of this current review of methods and frameworks for assessing research programmes, including the analysis that the HTA programme contains several key features that increase the likelihood of impact arising.
Although it is important to consider the impact of a programme by gathering opinions from stakeholders about its overall impact, it is also desirable to collate data from a range of individual studies funded by the programme. For this, we recommend a review of case study methods and their application to health research, including the 2014 REF, combined with independent preparation of case studies of new HTA projects. They should include both successful and unsuccessful projects. They should include cases focusing on the monetisation of impact and on linking trials to systematic reviews and guidelines. Particular case studies might contrast the tracing forward/backward methods of linking particular research projects to policy changes. The aim should be to develop better, deeper case studies as well as appropriate frameworks and examples of good practice. As case studies have importance in other NIHR research programmes, the remit of the proposed research should include these.
The HTA programme should continue to expand its work on linking trials to meta-analyses and to guidelines. The York/PCORI methods currently being piloted by the HTA programme should be evaluated along with the scope for use of GRADE. This research should also address ways of assessing the value of randomised trials and meta-analyses that indicate the non-superiority of particular interventions.
The range of NIHR research programmes should consider the relevance of the broader literature, which suggests a range of approaches are appropriate in different circumstances. The menu of approaches should be taken into account in assessing the impact of NIHR research programmes and projects, particularly those that can be seen as involving ‘co-production’ of research.
The HTA programme should continue to support routine collection of data from researchers, such as researchfish, on aspects of impact but should be cautious of its effects. It should research researchers’ perceptions of this tool including what they include and exclude. Periodic case studies that provide a more detailed analysis of the impacts achieved and a greater understanding of the factors that contribute to achieving impact should support the routine collection of data by researchfish.
Financial constraints on health services mean that health research must demonstrate societal impact and value for money. Methods for doing so have developed significantly in the last few years. While not without caveats, these methods should be applied routinely to help safeguard the effectiveness and cost-effectiveness of research programmes.
Acknowledgements
We would like to thank Alison Price from the University of Southampton for developing all of the systematic literature searches, providing EndNote and data extraction support, and contributing to early drafts of the report. We are grateful to the HTA editor and referees for their valuable comments during the editorial stage of the report. The research team also acknowledge the funding supplied by the HTA programme.
Contributions of authors
James Raftery (Professor of HTA) was the chief investigator, originated the proposal, was project lead on Chapters 6 and 7, assisted with data extraction for Chapter 3 and prepared the report for publication.
Steve Hanney (Professorial Research Fellow) was a member of the research team, contributed to the development of the proposal, was project lead on Chapter 3, including literature searching, data extraction and write-up, and contributed and reviewed drafts of the report.
Trish Greenhalgh (Professor of Primary Care Health Sciences) was a member of the research team, contributed to the development of the proposal, was project lead on Chapter 4, including literature searching and write-up, assisted with data extraction for Chapter 3 and contributed and reviewed drafts of the report.
Matthew Glover (Research Fellow) was a member of the research team, was project lead on Chapter 5, assisted with data extraction for Chapter 3 and contributed and reviewed drafts of the report.
Amanda Blatch-Jones (Senior Research Fellow) was a member of the research team, contributed to the development of the proposal, collaborated on Chapter 3 with Steve Hanney including literature searching and data extraction, contributed and reviewed drafts of the report, worked closely with James Raftery to keep the project running and prepared the report for publication.
Data sharing statement
All available data, in addition to what is provided in the appendices, can be obtained from the corresponding author.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HTA programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HTA programme or the Department of Health.
References
- Chalmers I, Glasziou P. Avoidable waste in the production and reporting of research evidence. Lancet 2009;374:86-9. http://dx.doi.org/10.1016/S0140-6736(09)60329-9.
- Hanney S, Buxton M, Green C, Coulson D, Raftery J. An assessment of the impact of the NHS Health Technology Assessment Programme. Health Technol Assess 2007;11. http://dx.doi.org/10.3310/hta11530.
- Raftery J, Hanney S, Green C, Buxton M. Assessing the impact of England’s National Health Service R&D Health Technology Assessment program using the ‘payback’ approach. Int J Technol Assess Health Care 2009;25:1-5. http://dx.doi.org/10.1017/S0266462309090011.
- Banzi R, Moja L, Pistotti V, Facchini A, Liberati A. Conceptual frameworks and empirical approaches used to assess the impact of health research: an overview of reviews. Health Res Policy Syst 2011;9. http://dx.doi.org/10.1186/1478-4505-9-26.
- Boaz A, Fitzpatrick S, Shaw B. Assessing the impact of research on policy: a literature review. Sci Public Policy 2009;36:255-70. http://dx.doi.org/10.3152/030234209X436545.
- Bornmann L. What is societal impact of research and how can it be assessed? A literature survey. J Am Soc Inf Sci Technol 2013;64:217-33. http://dx.doi.org/10.1002/asi.22803.
- Making an Impact, A Preferred Framework and Indicators to Measure Returns on Investment in Health Research. Ottawa, ON: CAHS; 2009.
- What is the Evidence on the Impact of Research on International Development?. London: DFID; 2014.
- Guthrie S, Wamae W, Diepeveeen S, Wooding S, Grant J. Measuring Research: A Guide to Research Evaluation Frameworks and Tools. Santa Monica, CA: RAND Corporation; 2013.
- Harris R. Impact of Research on Development Policy and Practice: An Annotated Bibliography 2013. www.rogharris.org/uploads/5/0/5/4/5054025/impact_of_research_on_development_policy_and_practice_annotated_bibliography.pdf (accessed 16 July 2016).
- Moore G, Redman S, Haines M, Todd A. What works to increase the use of research in population health policy and programmes: a review. Evid Policy 2011;7:277-305. http://dx.doi.org/10.1332/174426411X579199.
- Neufeld V, Cole DC, Boyd A, Njelesani D, Bates I, Hanney SR. Perspectives on Evaluating Global Health Research for Development: A Background Paper. Ottawa, ON: Canadian Coalition for Global Health Research; 2014.
- Oliver K, Innvar S, Lorenc T, Woodman J, Thomas J. A systematic review of barriers to and facilitators of the use of evidence by policymakers. BMC Health Serv Res 2014;14. http://dx.doi.org/10.1186/1472-6963-14-2.
- Penfield T, Baker MJ, Scoble R, Wykes MC. Assessment, evaluations, and definitions of research impact: a review. Res Eval 2014;23:21-32. http://dx.doi.org/10.1093/reseval/rvt021.
- Yazdizadeh B, Majdzadeh R, Salmasian H. Systematic review of methods for evaluating healthcare research economic impact. Health Res Policy Syst 2010;8. http://dx.doi.org/10.1186/1478-4505-8-6.
- Measuring the Impacts of Federal Investments in Research. A Workshop Summary. Washington, DC: The National Academies; 2011.
- Orians CE, Abed J, Drew CH, Rose SW, Cohen JH, Phelps J. Scientific and public health impacts of the NIEHS Extramural Asthma Research Program: insights from primary data. Res Eval 2009;18:375-85. http://dx.doi.org/10.3152/095820209X480698.
- Thornton I, Shaw A. Evaluating the Impact of Research Programmes. London: UK Collaboration on Development Sciences; 2013.
- Medical Research: Assessing the Benefits to Society. London: UK Evaluation Forum; 2006.
- Oliver K, Innvar S, Lorenc T, Woodman J, Thomas J. Barriers and facilitators of the use of evidence by policy makers: an updated systematic review. BMC Health Serv Res 2014;14.
- Innvær S, Vist G, Trommald M, Oxman A. Health policy-makers’ perceptions of their use of evidence: a systematic review. J Health Serv Res Policy 2002;7:239-44. http://dx.doi.org/10.1258/135581902320432778.
- Buxton M, Hanney S, Morris S, Sundmacher L, Mestre-Ferrandiz J, Garau M, et al. Medical Research: What’s it Worth?: Estimating the Economic Benefits from Medical Research in the UK. London: UK Evaluation Forum; 2008.
- Spending Review 2010. Norwich: The Stationery Office; 2010.
- Exceptional Returns: The Value of Investing in Health Research in Australia 11. Canberra, ACT: ASMR; 2008.
- Deloitte Access Economics . Returns on NHMRC Funded Research and Development 2011. www.asmr.org.au/NHMRCReturns.pdf (accessed 14 October 2014).
- Glover M, Buxton M, Guthrie S, Hanney S, Pollitt A, Grant J. Estimating the returns to UK publicly funded cancer-related research in terms of the net value of improved health outcomes. BMC Med 2014;12. http://dx.doi.org/10.1186/1741-7015-12-99.
- Guthrie S, Hafner M, Bienkowska-Gibbs T, Wooding S. Returns on research funded under the NIHR Health Technology Assessment (HTA) Programme. Health Technol Assess 2015;19.
- Buxton M, Hanney S, Jones T. Estimating the economic value to societies of the impact of health research: a critical review. Bull World Health Organ 2004;82:733-9.
- Chalmers I, Haynes B. Systematic reviews: reporting, updating, and correcting systematic reviews of the effects of health care. BMJ 1994;309:862-5. http://dx.doi.org/10.1136/bmj.309.6958.862.
- Raftery J, Powell J. Health Technology Assessment in the UK. Lancet 2013;382:1278-85. http://dx.doi.org/10.1016/S0140-6736(13)61724-9.
- Thomas KS, Koller K, Dean T, O’Leary CJ, Sach TH, Frost A, et al. A multicentre randomised controlled trial and economic evaluation of ion-exchange water softeners for the treatment of eczema in children: the Softened Water Eczema Trial (SWET). Health Technol Assess 2011;15. http://dx.doi.org/10.3310/hta15080.
- Dumville JC, Worthy G, Soares M, Bland J, Cullum N, Dowson C, et al. VenUS II: a randomised controlled trial of larval therapy in the management of leg ulcers. Health Technol Assess 2009;13. http://dx.doi.org/10.3310/hta13550.
- 2014 REF: Assessment Framework and Guidance on Submissions. Panel A Criteria. London: HEFCE; 2012.
- Weiss C. The many meanings of research utilization. Public Admin Rev 1979;39:426-31.
- Hanney SR, Gonzalez-Block MA, Buxton MJ, Kogan M. The utilisation of health research in policy-making: concepts, examples and methods of assessment. Health Res Policy Syst 2003;1. http://dx.doi.org/10.1186/1478-4505-1-2.
- Wooding S, Hanney SR, Pollitt A, Grant J, Buxton MJ. Understanding factors associated with the translation of cardiovascular research: a multinational case study approach. Implement Sci 2014;9. http://dx.doi.org/10.1186/1748-5908-9-47.
- Brutscher PB, Wooding S, Grant J. Health Research Evaluation Frameworks; An International Comparison Making an Impact: A Preferred Framework and Indicators to Measure Returns in Investment in Health Research. Appendix A. Ottawa, ON: CAHS; 2009.
- Grant J, Brutscher BP, Kirk SE, Butler L, Wooding S. Capturing Research Impacts: A Review of International Practice. Santa Monica, CA: RAND Europe; 2009.
- Buxton M, Hanney S. How can payback from health services research be assessed?. J Health Serv Res 1996;1:35-43.
- The Societal Impact of Applied Research Towards a Quality Assessment System. Amsterdam: Royal Netherlands Academy of Arts and Sciences; 2002.
- Molas-Gallart J, Tang P, Morrow S. Assessing the non-academic impact of grant-funded socio-economic research: results from a pilot study. Res Eval 2000;9:171-82. http://dx.doi.org/10.3152/147154400781777269.
- Spaapen J, Sylvain C. Societal Quality of Research: Toward a Method for the Assessment of the Potential Value of Research for Society. London: Science Policy Support Group; 1994.
- Jacob R, Battista RN. Assessing technology assessment: early results of the Quebec experience. Int J Technol Assess Health Care 1993;9:564-72. http://dx.doi.org/10.1017/S0266462300005481.
- Jacob R, McGregor M. Assessing the impact of health technology assessment. Int J Technol Assess Health Care 1997;13:68-80. http://dx.doi.org/10.1017/S0266462300010242.
- Donovan C, Hanney S. The ‘Payback Framework’ explained. Res Eval 2011;20:181-3. http://dx.doi.org/10.3152/095820211X13118583635756.
- Hanney S, Boaz A, Jones T, Soper B. Engagement in research: an innovative three stage review of the benefits for health-care performance. Health Serv Deliv Res 2013;1.
- Nason E, Curran B, Hanney S, Janta B, Hastings G, O’Driscoll M, et al. Evaluating health research funding in Ireland: assessing the impacts of the Health Research Board of Ireland’s funding activities. Res Eval 2011;20:193-200. http://dx.doi.org/10.3152/095820211X12941371876823.
- Hanney SR, Grant J, Wooding S, Buxton MJ. Proposed methods for reviewing the outcomes of health research: the impact of funding by the UK’s ’Arthritis Research Campaign’. Health Res Policy Syst 2004;2. http://dx.doi.org/10.1186/1478-4505-2-4.
- Kogan M, Henkel M. Government and Research: The Rothschild Experiment in a Government Department. London: Heinemann Educational Books; 1983.
- Henshall C. The impact of Payback research: developing and using evidence in policy. Res Eval 2011;20:257-8. http://dx.doi.org/10.3152/095820211X13118583635873.
- Hanney SR, Watt A, Jones TH, Metcalf L. Conducting retrospective impact analysis to inform a medical research charity’s funding strategies: the case of Asthma UK. Allergy Asthma Clin Immunol 2013;9. http://dx.doi.org/10.1186/1710-1492-9-17.
- Cohen G, Schroeder J, Newson R, King L, Rychetnik L, Milat AJ, et al. Does health intervention research have real world policy and practice impacts: testing a new impact assessment tool. Health Res Policy Syst 2015;13. http://dx.doi.org/10.1186/1478-4505-13-3.
- Review of Public Health Research Projects Financed under the Commission’s Framework Programmes for Health Research. Brussels: European Commission; 2013.
- Investing in Our Future: Following Up the Impact of Research Training Fellowship Awards from Action Medical Research. Horsham: Action Medical Research; 2009.
- Anderson R. The policy impact of population health surveys: an illustration of the measurement challenges using the NSW Health Survey. Evid Policy 2006;2:167-83. http://dx.doi.org/10.1332/174426406777068975.
- Aymerich M, Carrion C, Gallo P, Garcia M, Lopez-Bermejo A, Quesada M, et al. Measuring the payback of research activities: a feasible ex-post evaluation methodology in epidemiology and public health. Soc Sci Med 2012;75:505-10. http://dx.doi.org/10.1016/j.socscimed.2012.03.044.
- Bennett S, Paina L, Ssengooba F, Waswa D, M’Imunya JM. The impact of Fogarty International Center research training programs on public health policy and program development in Kenya and Uganda. BMC Public Health 2013;13:1-11. http://dx.doi.org/10.1186/1471-2458-13-770.
- Berra S, Pons JMV. Impact Assessment of the TV3 Telethon on Biomedical Research in Catalonia. Barcelona: Fundació La Marató de TV3, Agència d’Avaluació de Tecnologia i Recerca Mèdiques (AATRM); 2006.
- Bunn F. The Impact of Systematic Reviews on Health Care Policy In England 2010.
- Bunn F, Kendall E. Does nursing research impact on policy? A case study of health visiting research and UK health policy. J Res Nurs 2011;16:169-91. http://dx.doi.org/10.1177/1744987110392627.
- Bunn F, Trivedi D, Alderson P, Hamilton L, Martin A, Iliffe S. The impact of cochrane systematic reviews: a mixed method evaluation of outputs from Cochrane Review Groups supported by the UK National Institute for Health Research. Syst Rev 2014;3. http://dx.doi.org/10.1186/2046-4053-3-125.
- Donovan C, Butler L, Butt AJ, Jones TH, Hanney SR. Evaluation of the impact of National Breast Cancer Foundation-funded research. Med J Aust 2014;200:214-18. http://dx.doi.org/10.5694/mja13.10798.
- Engel-Cox JA, Van Houten B, Phelps J, Rose SW. Conceptual model of comprehensive research metrics for improved human health and environment. Environ Health Perspect 2008;116:583-92. http://dx.doi.org/10.1289/ehp.10925.
- Guinea J, Sela E, Gómez-Núñez A, Mangwende T, Ambali A, Ngum N, et al. Impact oriented monitoring: a new methodology for monitoring and evaluation of international public health research projects. Res Eval 2015;24:131-45. http://dx.doi.org/10.1093/reseval/rvu034.
- Kalucy EC, Jackson-Bowers E, McIntyre E, Reed R. The feasibility of determining the impact of primary health care research projects using the Payback Framework. Health Res Policy Syst 2009;7. http://dx.doi.org/10.1186/1478-4505-7-11.
- Kwan P, Johnston J, Fung AY, Chong DS, Collins RA, Lo SV. A systematic evaluation of payback of publicly funded health and health services research in Hong Kong. BMC Health Serv Res 2007;7. http://dx.doi.org/10.1186/1472-6963-7-121.
- Longmore J. Evaluation Of The Fellowship Scheme 2007–2012 2014.
- The Impact of the NHS Service Delivery and Organisation Research and Development Programme 2001–2006. London: National Coordinating Centre for Service and Delivery Organisation; 2006.
- Oortwijn J. Assessing the impact of health technology assessment in the Netherlands. Int J Technol Assess Health Care 2008;24:259-69. http://dx.doi.org/10.1017/S0266462308080355.
- Reed RL, Kalucy EC, Jackson-Bowers E, McIntyre E. What research impacts do Australian primary health care researchers expect and achieve?. Health Res Policy Syst 2011;9. http://dx.doi.org/10.1186/1478-4505-9-40.
- Hanney S, Nason E. Evaluation of the impact of HSC R&D Funding in Northern Ireland, Including Benchmarking with other Countries. Belfast: RSM McClure Watters; 2012.
- Schapper CC, Dwyer T, Tregear GW, Aitken M, Clay MA. Research performance evaluation: the experience of an independent medical research institute. Aust Health Rev 2012;36:218-23. http://dx.doi.org/10.1071/AH11057.
- Scott JE, Blasinsky M, Dufour M, Mandal RJ, Philogene GS. An evaluation of the Mind Body Interactions and Health Program: assessing the impact of an NIH program using the Payback Framework. Res Eval 2011;20:185-92. http://dx.doi.org/10.3152/095820211X12941371876661.
- The Mind–Body Interactions and Health Program Outcome Evaluation. Final Report. Office of Behavioral and Social Sciences Research, National Institutes of Health: Bethesda, MD; 2011.
- Johnston SC, Rootenberg JD, Katrak S, Smith WS, Elkins JS. Effect of a US National Institutes of Health programme of clinical trials on public health and costs. Lancet 2006;367:1319-27. http://dx.doi.org/10.1016/S0140-6736(06)68578-4.
- Economic Impact Report 2012/13. Swindon: MRC; 2013.
- Murphy L. The Value of Clinical Trials: A New Zealand Case Study 2012.
- Williams I, McIver S, Moore D, Bryan S. The use of economic evaluations in NHS decision-making: a review and empirical investigation. Health Technol Assess 2008;12. http://dx.doi.org/10.3310/hta12070.
- Standard Evaluation Protocol 2009–2015. Protocol for Research Assessment in the Netherlands. Amsterdam: Association of Universities in the Netherlands; 2010.
- Meijer I. Societal Returns of Scientific Research. How Can we Measure it?. Leiden: Centre for Science and Technology Studies, Leiden University; 2012.
- Spaapen J, van Drooge L, Propp T, van der Meulen B, Shinn T, Marcovich A, et al. Social Impact Assessment Methods for Research and Funding Instruments Through the Study of Productive Interactions (SIAMPI): Final Report on Social Impacts of Research. Amsterdam: Royal Netherlands Academy of Arts and Sciences; 2011.
- Bodeau-Livinec F, Simon E, Montagnier-Petrissans C, Joël M-E, Féry-Lemonnier E. Impact of CEDIT recommendations: an example of health technology assessment in a hospital network. Int J Technol Assess Health Care 2006;22:161-8. http://dx.doi.org/10.1017/S0266462306050975.
- Zechmeister I, Schumacher I. The impact of health technology assessment reports on decision making in Austria. Int J Technol Assess Health Care 2012;28:77-84. http://dx.doi.org/10.1017/S0266462311000729.
- Adam P, Solans-Domènech M, Pons JMV, Aymerich M, Berra S, Guillamon I, et al. Assessment of the impact of a clinical and health services research call in Catalonia. Res Eval 2012;21:319-28. http://dx.doi.org/10.1093/reseval/rvs024.
- Graham KER, Chorzempa HL, Valentine PA, Magnan J. Evaluating health research impact: development and implementation of the Alberta Innovates – Health Solutions impact framework. Res Eval 2012;21:354-67. http://dx.doi.org/10.1093/reseval/rvs027.
- Measuring the Value of Saskatchewan’s Health Research. Saskatoon, SK: SHRF; 2013.
- Solans-Domènech M, Adam P, Guillamon I, Permanyer-Miralda G, Pons JMV, Escarrabill J. Impact of clinical and health services research projects on decision-making: a qualitative study. Health Res Policy Syst 2013;11. http://dx.doi.org/10.1186/1478-4505-11-15.
- Laws R, King L, Hardy LL, Milat A, Rissel C, Newson R, et al. Utilization of a population health survey in policy and practice: a case study. Health Res Policy Syst 2013;11. http://dx.doi.org/10.1186/1478-4505-11-4.
- Milat AJ, Laws R, King L, Newson R, Rychetnik L, Rissel C, et al. Policy and practice impacts of applied research: a case study analysis of the New South Wales Health Promotion Demonstration Research Grants Scheme 2000–2006. Health Res Policy Syst 2013;11. http://dx.doi.org/10.1186/1478-4505-11-5.
- Drew CH, Pettibone KG, Ruben E. Greatest ‘HITS’: A new tool for tracking impacts at the National Institute of Environmental Health Sciences. Res Eval 2013;22:307-15. http://dx.doi.org/10.1093/reseval/rvt022.
- Liebow E, Phelps J, Van Houten B, Rose S, Orians C, Cohen J, et al. Toward the assessment of scientific and public health impacts of the National Institute of Environmental Health Sciences Extramural Asthma Research Program using available data. Environ Health Perspect 2009;117:1147-54. http://dx.doi.org/10.1289/ehp.0800476.
- Williams V, Eiseman E, Landree E, Adamson D. Demonstrating and Communicating Research Impact. Preparing NIOSH Programs for External Review. Ann Arbor, MI: University of Michigan, RAND; 2009.
- Assessment Framework Report 2012/13. London: Wellcome Trust; 2014.
- Eriksen KS, Hervik A. Impacts of Neck Injuries Research at Chalmers University of Technology. Summary. Stockholm: VINNOVA – Swedish Agency for Innovation Systems; 2005.
- Meagher L, Lyall C, Nutley S. Flows of knowledge, expertise and influence: a method for assessing policy and practice impacts from social science research. Res Eval 2008;17:163-73. http://dx.doi.org/10.3152/095820208X331720.
- Caddell AJ, Hatchette JE, McGrath PJ. Examining the impact of health research facilitated by small peer-reviewed research operating grants in a women’s and children’s health centre. BMC Res Notes 2010;3. http://dx.doi.org/10.1186/1756-0500-3-107.
- Kuruvilla S, Mays N, Walt G. Describing the impact of health services and policy research. J Health Serv Res Policy 2007;12:23-31. http://dx.doi.org/10.1258/135581907780318374.
- Wilson P, Petticrew M, Calnan M, Nazareth I. Disseminating research findings: what should researchers do? A systematic scoping review of conceptual frameworks. Implement Sci 2010;5. http://dx.doi.org/10.1186/1748-5908-5-91.
- Sainty M. Research impact: a United Kingdom Occupational Therapy Research Foundation perspective. Br J Occup Ther 2013;76:528-37. http://dx.doi.org/10.4276/030802213X13861576675204.
- Mostert SP, Ellenbroek S, Meijer I, van Ark G, Klasen EC. Societal output and use of research performed by health research groups. Health Res Policy Syst 2010;8. http://dx.doi.org/10.1186/1478-4505-8-30.
- Evans D, Coad J, Cottrell K, Dalrymple J, Davies R, Donald C, et al. Public involvement in research: assessing impact through a realist evaluation. Health Serv Delivery Res 2014;2.
- Rycroft-Malone J, Wilkinson J, Burton CR, Harvey G, McCormack B, Graham I, et al. Collaborative action around implementation in Collaborations for Leadership in Applied Health Research and Care: towards a programme theory. J Health Servs Res Policy 2013;18:13-26. http://dx.doi.org/10.1177/1355819613498859.
- Outputs, Outcomes and Impact of MRC Research: 2012 Report. Swindon: MRC; 2013.
- Wooding S, Nason E, Starkey T, Hanney S, Grant J. Mapping the Impact: Exploring the Payback of Arthritis Research. Santa Monica, CA: RAND Corporation; 2009.
- Excellence in Innovation: Research Impacting our Nation’s Future: Assessing the Benefits. Adelaide, SA: Australian Technology Network of Universities; 2012.
- Research Excellence Framework 2014: Overview Report by Main Panel A and Sub-panels 1 to 6. London: HEFCE; 2015.
- Muir R, Arthur E, Berman T, Sedgley S, Herlick Z, Fullgrabe H. Metrics for Research Commercialisation: A Report to the Coordination Committee on Science and Technology. Canberra, ACT: Coordination Committee on Science and Technology; 2005.
- Economic Impacts of Investment in Research & Innovation. London: DIUS; 2007.
- Spaapen J, Dijstelbloem H, Wamelink F. Evaluating Research in Context. A Method for Comprehensive Assessment. The Hague: Consultative Committee of Sector Councils for Research and Development; 2007.
- Spaapen J, van Drooge L. Introducing ‘productive interactions’ in social impact assessment. Res Eval 2011;20:211-18. http://dx.doi.org/10.3152/095820211X12941371876742.
- Hansen J, Muscat N, Keskimaki L. Measuring and improving the societal impact of health care research. Eurohealth 2013;19:32-5.
- Hage J. Making an Impact: A Preferred Framework and Indicators to Measure Returns in Investment in Health Research. Appendix A (Commissioned Papers). Ottawa, ON: CAHS; 2009.
- Lewis S MP, Barre L. Pillar III. Estimating the Return on Investment for Health Services Research: A Theoretical and Empirical Analysis. Appendix A (Commissioned Papers). Ottawa, ON: CAHS; 2009.
- Shiel A, Di Ruggiero E. Pillar IV: Population and Public Health Research – ’Assessing the Return on Canada’s Public Investment in Population and Public Health Research: Methods and Metrics’. Ottawa, ON: CAHS; 2009.
- Frank C, Nason E. Health research: measuring the social, health and economic benefits. CMAJ 2009;180:528-34. http://dx.doi.org/10.1503/cmaj.090016.
- Kok MO, Schuit AJ. Contribution mapping: a method for mapping the contribution of research to enhance its impact. Health Res Policy Syst 2012;10. http://dx.doi.org/10.1186/1478-4505-10-21.
- Bozeman B, Bozeman B, Sarewitz D, Feinson S, Foladori G, Gaughan M, et al. Knowledge Flows and Knowledge Collectives: Understanding the Role of Science and Technology Policies in Development. Washington, DC: Center for Science Policy and Outcomes; 2003.
- Sarli CC, Dubinsky EK, Holmes KL. Beyond citation analysis: a model for assessment of research impact. J Med Lib Assoc 2010;98:17-23. http://dx.doi.org/10.3163/1536-5050.98.1.008.
- Measuring Program Outcomes: A Practical Approach. Alexandria, VA: United Way of America; 1996.
- Weiss AP. Measuring the impact of medical research: moving from outputs to outcomes. Am J Psychiatry 2007;164:206-14. http://dx.doi.org/10.1176/ajp.2007.164.2.206.
- W.K. Kellogg Foundation . Using Logic Models to Being Together Planning, Evaluation and Action: Logic Model Development Guide 2004. www.smartgivers.org/uploads/logicmodelguidepdf.pdf (accessed 10 June 2016).
- David PA, Mowery D, Steinmueller WE. Analysing the economic payoffs from basic research. Econ Innov New Technol 1992;2:73-90. http://dx.doi.org/10.1080/10438599200000006.
- Kuruvilla S, Mays N, Pleasant A, Walt G. Describing the impact of health research: a research impact framework. BMC Health Serv Res 2006;6. http://dx.doi.org/10.1186/1472-6963-6-134.
- Dembe AE, Lynch MS, Gugiu PC, Jackson RD. The translational research impact scale: development, construct validity, and reliability testing. Eval Health Prof 2014;37:50-7. http://dx.doi.org/10.1177/0163278713506112.
- Van Ark G, Klasen E. Societal impact of health research. J Health Sci 2007;85:259-61.
- Morgan Jones M, Grant J, Dean A, Wykes M, Stevens H. 7 Essays on Impact. DESCRIBE Project Report for Jisc. Exeter: University of Exeter; 2013.
- Medical Research Council . About Researchfish n.d. www.mrc.ac.uk/funding/guidance-for-mrc-award-holders/researchfish/about-researchfish/ (accessed 6 May 2015).
- Donovan C. The Australian Research Quality Framework: a live experiment in capturing the social, economic, environmental, and cultural returns of publicly funded research. New Directions Eval 2008:47-60.
- Milat AJ, Bauman AE, Redman S. A narrative review of research impact assessment models and methods. Health Res Policy Syst 2015;13. http://dx.doi.org/10.1186/s12961-015-0003-1.
- Chang W-C, Tung Y-C, Huang C-H, Yang M-C. Performance improvement after implementing the balanced scorecard: a large hospital’s experience in Taiwan. Total Qual Manag Bus Excellence 2008;19:1143-54. http://dx.doi.org/10.1080/14783360802323560.
- University Health Network . Achieving Our Vision: Balanced Scorecard n.d. www.uhn.ca/corporate/AboutUHN/AchievingOurVision/Pages/balanced_scorecard.aspx (accessed 7 October 2014).
- Gutman MA, Barker DC, Samples-Smart F, Morley C. Evaluation of active living research: progress and lessons in building a new field. Am J Prev Med 2009;36:22-33. http://dx.doi.org/10.1016/j.amepre.2008.10.009.
- Arnold E. Understanding long-term impacts of R&D funding: the EU Framework Programme. Res Eval 2012;21:332-43. http://dx.doi.org/10.1093/reseval/rvs025.
- Schumacher I, Zechmeister I. Assessing the impact of health technology assessment on the Austrian healthcare system. Int J Technol Assess Health Care 2013;29:84-91. http://dx.doi.org/10.1017/S0266462312000748.
- Rispel LC, Doherty J. Research in support of health systems transformation in South Africa: The experience of the Centre for Health Policy. J Public Health Policy 2011;32:10-29. http://dx.doi.org/10.1057/jphp.2011.33.
- End of Programme Summative Evaluation of the Africa Health Systems Initiative Support to African Research Partnerships. Reet: Hera; 2014.
- Brambila C, Ottolenghi E, Marin C, Bertrand JT. Getting results used: evidence from reproductive health programmatic research in Guatemala. Health Policy Plan 2007;22:234-45. http://dx.doi.org/10.1093/heapol/czm013.
- Gold M, Taylor EF. Moving research into practice: lessons from the US Agency for Healthcare Research and Quality’s IDSRN program. Implement Sci 2007;2. http://dx.doi.org/10.1186/1748-5908-2-9.
- Kingwell BA, Anderson GP, Duckett SJ, Hoole EA, Jackson-Pulver LR, Khachigian LM, et al. Evaluation of NHMRC funded research completed in 1992, 1997 and 2003: gains in knowledge, health and wealth. Med J Aust 2006;184:282-6.
- Poortvliet EP, Vijfvinkel D, Vennekens A, van Hoesel P, Daue F. Study into the Impact of the Belgian Health Care Knowledge Centre. Brussels: Belgian Health Care Knowledge Centre; 2010.
- Zachariah R, Guillerm N, Berger S, Kumar AMV, Satyanarayana S, Bissell K, et al. Research to policy and practice change: is capacity building in operational research delivering the goods?. Trop Med Int Health 2014;19:1068-75. http://dx.doi.org/10.1111/tmi.12343.
- Murphy E, Dingwall R, Greatbatch D, Parker S, Watson P. Qualitative research methods in health technology assessment: a review of the literature. Health Technol Assess 1998;2.
- Britten N, Campbell R, Pound P, Morgan M, Daker-White G, Pill R, et al. Evaluating meta ethnography: systematic analysis and synthesis of qualitative research. Health Technol Assess 2011;15.
- Nyssen OP, Taylor SJC, Wong G, Higgins A, Steed EM, Bourke L, et al. Does therapeutic writing help people with long-term conditions? Systematic review, realist synthesis and economic considerations. Health Technol Assess 2016;20. http://dx.doi.org/10.3310/hta20270.
- Waterman H, Tillen D, Dickson R, De Koning K. Action research: a systematic review and guidance for assessment. Health Technol Assess 2000;5.
- Nilsen P, Stahl C, Roback K, Cairney P. Never the twain shall meet? – a comparison of implementation science and policy implementation research. Implement Sci 2013;8. http://dx.doi.org/10.1186/1748-5908-8-63.
- Dewey J. The Theory Of Inquiry. New York, NY: Holt, Rinehart & Wiston; 1938.
- Martin BR. The Research Excellence Framework and the ‘impact agenda’: are we creating a Frankenstein monster?. Res Eval 2011;20:247-54. http://dx.doi.org/10.3152/095820211X13118583635693.
- Upton S, Vallance P, Goddard J. From outcomes to process: evidence for a new approach to research impact assessment. Res Eval 2014;23:352-65. http://dx.doi.org/10.1093/reseval/rvu021.
- Bozeman B, Rogers JD. A churn model of scientific knowledge value: internet researchers as a knowledge value collective. Res Policy 2002;31:769-94. http://dx.doi.org/10.1016/S0048-7333(01)00146-9.
- Briggle AR. Opening the black box: the social outcomes of scientific research. Social Epistemol 2014;28:153-66. http://dx.doi.org/10.1080/02691728.2013.782584.
- Meyer RM. Pillar II: Clinical Research. How to Optimally Measure the Impact of Health Research Funding in Clinical Research. Ottawa, ON: CAHS; 2009.
- Kogan M, Henkel M, Hanney S. Government and Research: 30 Years of Evolution. Dordrecht: Springer; 2006.
- Lomas J. The in-between world of knowledge brokering. BMJ 2007;334:129-32. http://dx.doi.org/10.1136/bmj.39038.593380.AE.
- Thomas P. The Aims and Outcomes of Social Policy Research. London: Croom Helm; 1985.
- Amara N, Ouimet M, Landry R. New evidence on instrumental, conceptual, and symbolic utilization of university research in government agencies. Sci Commun 2004;26:75-106. http://dx.doi.org/10.1177/1075547004267491.
- Wooding S, Pollitt A, Diepeveen S, Guthrie S, Jones MM, Chonaill SN, et al. Mental Health Retrosight 2013. http://lbr.rand.org/content/dam/rand/pubs/research_reports/RR400/RR452/RAND_RR452.pdf (accessed 2 December 2014).
- de Goede J, Putters K, van Oers H. Utilization of epidemiological research for the development of local public health policy in the Netherlands: a case study approach. Soc Sci Med 2012;74:707-14. http://dx.doi.org/10.1016/j.socscimed.2011.11.014.
- de Jong SP, van Arensbergen P, Daemen F, van der Meulen B, van den Besselaar P. Evaluation of research in context: an approach and two cases. Res Eval 2011;20:61-72. http://dx.doi.org/10.3152/095820211X12941371876346.
- Nicolini D, Powell J, Conville P, Martinez-Solano L. Managing knowledge in the healthcare sector. A review. Int J Manag Rev 2008;10:245-63. http://dx.doi.org/10.1111/j.1468-2370.2007.00219.x.
- Cherney A, Head B, Boreham P, Povey J, Ferguson M. Research utilization in the social sciences a comparison of five academic disciplines in Australia. Sci Commun 2013;35:780-809. http://dx.doi.org/10.1177/1075547013491398.
- Lemay MA, Sá C. Complexity sciences: towards an alternative approach to understanding the use of academic research. Evid Policy 2012;8:473-94. http://dx.doi.org/10.1332/174426412X660133.
- Contandriopoulos D, Lemire M, Denis JL, Tremblay E. Knowledge exchange processes in organizations and policy arenas: a narrative systematic review of the literature. Milbank Q 2010;88:444-83. http://dx.doi.org/10.1111/j.1468-0009.2010.00608.x.
- Realist Impact Evaluation – An Introduction. London: Overseas Development Institute; 2014.
- Pawson R, Tilley N. Realistic Evaluation. New York, NY: Sage; 1997.
- Rycroft-Malone J, Wilkinson JE, Burton CR, Andrews G, Ariss S, Baker R, et al. Implementing health research through academic and clinical partnerships: a realistic evaluation of the Collaborations for Leadership in Applied Health Research and Care (CLAHRC). Implement Sci 2011;6. http://dx.doi.org/10.1186/1748-5908-6-74.
- Brett J, Staniszewska S, Mockford C, Herron-Marx S, Hughes J, Tysall C, et al. A systematic review of the impact of patient and public involvement on service users, researchers and communities. Patient 2014;7:387-95. http://dx.doi.org/10.1007/s40271-014-0065-0.
- Evans BA, Bedson E, Bell P, Hutchings H, Lowes L, Rea D, et al. Involving service users in trials: developing a standard operating procedure. Trials 2013;14. http://dx.doi.org/10.1186/1745-6215-14-219.
- Staniszewska S, Brett J, Mockford C, Barber R. The GRIPP checklist: strengthening the quality of patient and public involvement reporting in research. Int J Technol Assess Health Care 2011;27:391-99. http://dx.doi.org/10.1017/S0266462311000481.
- Ward PR, Thompson J, Barber R, Armitage CJ, Boote JD, Cooper CL, et al. Critical perspectives on ‘consumer involvement’ in health research Epistemological dissonance and the know-do gap. J Sociol 2010;46:63-82. http://dx.doi.org/10.1177/1440783309351771.
- Macaulay AC, Commanda LE, Freeman WL, Gibson N, McCabe ML, Robbins CM, et al. Participatory research maximises community and lay involvement. BMJ 1999;319. http://dx.doi.org/10.1136/bmj.319.7212.774.
- White SC. Depoliticising development: the uses and abuses of participation. Dev Pract 1996;6:6-15. http://dx.doi.org/10.1080/0961452961000157564.
- Jagosh J, Macaulay AC, Pluye P, Salsberg J, Bush PL, Henderson J, et al. Uncovering the benefits of participatory research: implications of a realist review for health research and practice. Milbank Q 2012;90:311-46. http://dx.doi.org/10.1111/j.1468-0009.2012.00665.x.
- Martin S. Co-production of social research: strategies for engaged scholarship. Public Money Manag 2010;30:211-18. http://dx.doi.org/10.1080/09540962.2010.492180.
- Lasker RD, Weiss ES, Miller R. Partnership synergy: a practical framework for studying and strengthening the collaborative advantage. Milbank Q 2001;79:179-205. http://dx.doi.org/10.1111/1468-0009.00203.
- Cacari-Stone L, Wallerstein N, Garcia AP, Minkler M. The promise of community-based participatory research for health equity: a conceptual model for bridging evidence with policy. Am J Public Health 2014;104:1615-23. http://dx.doi.org/10.2105/AJPH.2014.301961.
- Kessler R, Glasgow RE. A proposal to speed translation of healthcare research into practice: dramatic change is needed. Am J Prev Med 2011;40:637-44. http://dx.doi.org/10.1016/j.amepre.2011.02.023.
- Glasgow RE, Green LW, Taylor MV, Stange KC. An evidence integration triangle for aligning science with policy and practice. Am J Prev Med 2012;42:646-54. http://dx.doi.org/10.1016/j.amepre.2012.02.016.
- Gibbons M, Limoges C, Nowotny H, Schwartzman S, Scott P, Trow M. The New Production of Knowledge: The Dynamics of Science and Research in Contemporary Societies. London: Sage; 1994.
- McGough R, Rubenstein S. Academia. Shaping the new science networks. Health Serv J 2013;123:32-3.
- Currie G, Lockett A, El Enany N. From what we know to what we do: lessons learned from the translational CLAHRC initiative in England. J Health Serv Res Policy 2013;18:27-39. http://dx.doi.org/10.1177/1355819613500484.
- Caldwell SE, Mays N. Studying policy implementation using a macro, meso and micro frame analysis: the case of the Collaboration for Leadership in Applied Health Research & Care (CLAHRC) programme nationally and in North West London. Health Res Policy Syst 2012;10. http://dx.doi.org/10.1186/1478-4505-10-32.
- Evans S, Scarbrough H. Supporting knowledge translation through collaborative translational research initiatives: ‘Bridging’ versus ‘blurring’ boundary-spanning approaches in the UK CLAHRC initiative. Soc Sci Med 2014;106:119-27. http://dx.doi.org/10.1016/j.socscimed.2014.01.025.
- Kislov R, Waterman H, Harvey G, Boaden R. Rethinking capacity building for knowledge mobilisation: developing multilevel capabilities in healthcare organisations. Implement Sci 2014;9. http://dx.doi.org/10.1186/s13012-014-0166-0.
- Soper B, Yaqub O, Hinrichs S, Marjanovich S, Drabble S, Hanney S, et al. CLAHRCs in practice: combined knowledge transfer and exchange strategies, cultural change, and experimentation. J Health Serv Res Policy 2013;18:53-64. http://dx.doi.org/10.1177/1355819613499903.
- Ling T, Soper B, Marjanovic S, Celia C, Yaqub O, Reding A, et al. Delivering the Aims of the CLAHRCs: Evaluating CLAHRCs’ Strategies and Contributions. Santa Monica, CA: RAND Corporation; 2011.
- Nowotny H, Scott P, Gibbons M. Mode 2 revisited: the new production of knowledge. Minerva 2003;41:179-94. http://dx.doi.org/10.1023/A:1025505528250.
- King G, Servais M, Forchuk C, Chalmers H, Currie M, Law M, et al. Features and impacts of five multidisciplinary community-university research partnerships. Health Soc Care Community 2010;18:59-6.
- Wehrens R, Bekker M, Bal R. Hybrid management configurations in joint research. Sci Technol Human Values 2014;39:6-41. http://dx.doi.org/10.1177/0162243913497807.
- Hinchcliff R, Greenfield D, Braithwaite J. Is it worth engaging in multi-stakeholder health services research collaborations? Reflections on key benefits, challenges and enabling mechanisms. Int J Qual Health Care 2014;26:124-8. http://dx.doi.org/10.1093/intqhc/mzu009.
- Hanney S, Kuruvilla S, Soper B, Mays N. Who needs what from a national health research system: lessons from reforms to the English Department of Health’s R&D system. Health Res Policy Syst 2010;8. http://dx.doi.org/10.1186/1478-4505-8-11.
- Swan J, Bresnen M, Robertson M, Newell S, Dopson S. When policy meets practice: colliding logics and the challenges of ‘mode 2’ initiatives in the translation of academic knowledge. Organ Stud 2010;31:1311-40. http://dx.doi.org/10.1177/0170840610374402.
- Orr K, Bennett M. Public Administration scholarship and the politics of coproducing academic–practitioner research. Public Adm Rev 2012;72:487-95. http://dx.doi.org/10.1111/j.1540-6210.2011.02522.x.
- De Savigny D, Adam T. Systems Thinking For Health Systems Strengthening. Geneva: Alliance for Health Policy and Systems Research, World Health Organization; 2009.
- Shepherd J. How to Achieve More Effective Services: The Evidence Scosystem. Cardiff: What Works Network/Cardiff University; 2014.
- Bennet A, Bennet D, Fafard K, Fonda M, Lomond T, Messier L, et al. Knowledge Mobilization in the Social Sciences and Humanities. Frost, WV: MQI Press; 2007.
- Phipps D. A report detailing the development of a university-based knowledge mobilization unit that enhances research outreach and engagement. Scholar Res Commun 2012;2.
- Phipps D, Jensen K, Myers JG, Lopez-Varela A. Theoretical and Methodological Approaches to Social Sciences and Knowledge Management. New York, NY: InTech; 2012.
- Kislov R, Harvey G, Walshe K. Collaborations for Leadership in Applied Health Research and Care: lessons from the theory of communities of practice. Implement Sci 2011;6. http://dx.doi.org/10.1186/1748-5908-6-64.
- Goffman E. Frame Analysis: An Essay on the Organization of Experience. Cambridge, MA: Harvard University Press Frame analysis; 1974.
- Currie G, Fitzgerald L, Keen J, McBride A, Martin G, Rowley E, et al. An Organizational Behaviour Perspective Upon CLAHRCs (Collaboratives for Leadership in Health Research and Care): Mediating Institutional Callenges through Change Agency 2010. www.download.bham.ac.uk/hsmc/graeme-currie.pdf (accessed 25 March 2015).
- Ziman J. Is science losing its objectivity?. Nature 1996;382:751-4. http://dx.doi.org/10.1038/382751a0.
- Van de Ven AH, Johnson PE. Knowledge for theory and practice. Acad Manage Rev 2006;31:802-21. http://dx.doi.org/10.5465/AMR.2006.22527385.
- Kincheloe JL. Describing the bricolage: conceptualizing a new rigor in qualitative research. Qual Inquiry 2001;7:679-92. http://dx.doi.org/10.1177/107780040100700601.
- Fudenberg HH. Biomedical Institutions, Biomedical Funding, And Public Policy. New York, NY: Plenum Press; 1983.
- Afseth J. On the value of research in health care. Eur J Oral Sci 1997;105:454-6. http://dx.doi.org/10.1111/j.1600-0722.1997.tb00229.x.
- Weisbrod BA. Costs and benefits of medical research: a case study of poliomyelitis. J Polit Econ 1971:527-44. http://dx.doi.org/10.1086/259766.
- Second Report in Science Policy. London: HSMO; 1967.
- Mushkin SJ, Landefeld JS. Biomedical Research: Costs and Benefits. Pensacola, FL: Ballinger Publishing; 1979.
- Drummond MF, Davies LM, Ferris FL. Assessing the costs and benefits of medical research: the diabetic retinopathy study. Soc Sci Med 1992;34:973-81. http://dx.doi.org/10.1016/0277-9536(92)90128-D.
- Salter AJ, Martin BR. The economic benefits of publicly funded basic research: a critical review. Res Policy 2001;30:509-32. http://dx.doi.org/10.1016/S0048-7333(00)00091-3.
- Mansfield E. Academic research and industrial innovation. Res Policy 1991;20:1-12. http://dx.doi.org/10.1016/0048-7333(91)90080-A.
- Mansfield E. Academic research and industrial innovation: an update of empirical findings. Res Policy 1998;26:773-6. http://dx.doi.org/10.1016/S0048-7333(97)00043-7.
- Silverstein SC, Garrison HH, Heinig SJ. A few basic economic facts about research in the medical and related life sciences. FASEB J 1995;9:833-40.
- Exceptional Returns: The Economic Value of America’s Investment in Medical Research. New York, NY: Lasker Foundation; 2000.
- Murphy KM, Topel RH. Measuring The Gains From Medical Research: An Economic Approach. Chicago, IL: University of Chicago Press; 2003.
- Exceptional Returns: The Value of Investing in Health R&D in Australia. Sydney, NSW: Australian Society for Medical Research; 2003.
- Roback K, Dalal K, Carlsson P. Evaluation of health research: measuring costs and socioeconomic effects. Int J Prev Med 2011;2:203-15.
- de Oliveira C, Nguyen HV, Wijeysundera HC, Wong WW, Woo G, Grootendorst P, et al. Estimating the payoffs from cardiovascular disease research in Canada: an economic analysis. Can Med Assoc Open Access J 2013;1:E83-90. http://dx.doi.org/10.9778/cmajo.20130003.
- Lakdawalla DN, Sun EC, Jena AB, Reyes CM, Goldman DP, Philipson TJ. An economic evaluation of the war on cancer. J Health Econ 2010;29:333-46. http://dx.doi.org/10.1016/j.jhealeco.2010.02.006.
- McKeown T. The Role Of Medicine. Oxford: Blackwell; 1979.
- OECD.Stat . PPPs and Exchange Rates n.d. https://stats.oecd.org/Index.aspx?DataSetCode=SNA_TABLE4 (accessed 11 July 2016).
- Cutler DM, McClellan M. Is technological change in medicine worth it?. Health Aff (Millwood) 2001;20:11-29. http://dx.doi.org/10.1377/hlthaff.20.5.11.
- Lichtenberg FR. The impact of new drug launches on longevity: evidence from longitudinal, disease-level data from 52 countries, 1982–2001. Int J Health Care Finance Econ 2005;5:47-73. http://dx.doi.org/10.1007/s10754-005-6601-7.
- Luce BR, Mauskopf J, Sloan FA, Ostermann J, Paramore LC. The return on investment in health care: from 1980 to 2000. Value Health 2006;9:146-56. http://dx.doi.org/10.1111/j.1524-4733.2006.00095.x.
- Hanney SR, Castle-Clarke S, Grant J, Guthrie S, Henshall C, Mestre-Ferrandiz J, et al. How long does biomedical research take? Studying the time taken between biomedical and health research and its translation into products, policy, and practice. Health Res Policy Syst 2015;13. http://dx.doi.org/10.1186/1478-4505-13-1.
- Guthrie S, Pollitt A, Hanney S, Grant J. Investigating Time Lags and Attribution in the Translation of Cancer Research: A Case Study Approach. Santa Monica, CA: RAND Corporation; 2014.
- Raftery J, Young A, Stanton L, Milne R, Cook A, Turner D, et al. Clinical trial metadata: defining and extracting metadata on the design, conduct, results and costs of 125 randomised clinical trials funded by the National Institute for Health Research Health Technology Assessment programme. Health Technol Assess 2015;19. http://dx.doi.org/10.3310/hta19110.
- Goudie AC, Sutton AJ, Jones DR, Donald A. Empirical assessment suggests that existing evidence could be used more fully in designing randomized controlled trials. J Clin Epidemiol 2010;63:983-91. http://dx.doi.org/10.1016/j.jclinepi.2010.01.022.
- Jones AP, Conroy E, Williamson PR, Clarke M, Gamble C. The use of systematic reviews in the planning, design and conduct of randomised trials: a retrospective cohort of NIHR HTA funded trials. BMC Med Res Methodol 2013;13. http://dx.doi.org/10.1186/1471-2288-13-50.
- Bhurke S, Cook A, Tallant A, Young A, Williams E, Raftery J. Are Systematic Reviews used in the Planning and Design of NIHR HTA Trials? A Retrospective Cohort. Oxford: Evidence Live Oxford; 2015.
- Sutton AJ, Cooper NJ, Jones DR, Lambert PC, Thompson JR, Abrams KR. Evidence-based sample size calculations based upon updated meta-analysis. Stat Med 2007;26:2479-500. http://dx.doi.org/10.1002/sim.2704.
- Roloff V, Higgins J, Sutton AJ. Planning future studies based on the conditional power of a meta-analysis. Stat Med 2013;32:11-24. http://dx.doi.org/10.1002/sim.5524.
- Claxton K, Griffin S, Koffijberg H, McKenna C. Expected Health Benefits of Additional Evidence Principles, Methods and Applications. York: University of York, Centre for Health Economics; 2013.
- Griffin S, Welton NJ, Claxton K. Exploring the research decision space: the expected value of information for sequential research designs. Med Decis Making 2010;30:155-62. http://dx.doi.org/10.1177/0272989X09344746.
- Claxton K, Eggington S, Ginnelly L, Griffin S, McCabe C, Philips Z, et al. A Pilot Study of Value of Information Analysis to Support Research Recommendations for NICE. York: Centre for Health Economics, University of York; 2005.
- Chilcott J, Brennan A, Booth A, Karnon J, Tappenden P. The role of modelling in prioritising and planning clinical trials. Health Technol Assess 2003;7. http://dx.doi.org/10.3310/hta7230.
- Simpson S, Corney R, Fitzgerald P, Beecham J. A randomised controlled trial to evaluate the effectiveness and cost-effectiveness of counselling patients with chronic depression. Health Technol Assess 2000;4.
- Claxton K, Ginnelly L, Sculpher M, Philips Z, Palmer S. A pilot study on the use of decision theory and value of information analysis as part of the NHS Health Technology Assessment programme. Health Technol Assess 2004;8. http://dx.doi.org/10.3310/hta8310.
- Mohiuddin S, Fenwick E, Payne K. Use of value of information in UK Health Technology Assessments. Int J Technol Assess Health Care 2014;30:553-70. http://dx.doi.org/10.1017/S0266462314000701.
- United States Senate . The Patient Protection and Affordable Care Act Detailed Summary n.d. www.dpc.senate.gov/healthreformbill/healthbill04.pdf (accessed 15 June 2016).
- Neumann PJ, Weinstein MC. Legislating against use of cost-effectiveness information. N Engl J Med 2010;363:1495-97. http://dx.doi.org/10.1056/NEJMp1007168.
- Dijkers M. Introducing GRADE: a systematic approach to rating evidence in systematic reviews and to guideline development. KT Update 2013;1.
- Gartlehner G, Swinson Evans T, Dobrescu A, Sommer I, Thaler K, Lohr K. The Predictive Validity of GRADE. Oxford: Evidence Live Oxford; 2015.
- Bower P, Knowles S, Coventry PA, Rowland N. Counselling for mental health and psychosocial problems in primary care. Cochrane Database Syst Rev 2011;9. http://dx.doi.org/10.1002/14651858.cd001025.pub3.
- Suri R, Wallis C, Bush A, Thompson S, Normand C. A comparative study of hypertonic saline, daily and alternate-day rhDNase in children with cystic fibrosis. Health Technol Assess 2003;6.
- Wark P, McDonald VM. Nebulised hypertonic saline for cystic fibrosis. Cochrane Database Syst Rev 2009;2. http://dx.doi.org/10.1002/14651858.cd001506.pub3.
- Garry R, Fountain J, Brown J, Manca A, Mason S. EVALUATE hysterectomy trial: a multicentre randomised trial comparing abdominal, vaginal and laparoscopic methods of hysterectomy. Health Technol Assess 2004;8. http://dx.doi.org/10.3310/hta8260.
- Nieboer TE, Johnson N, Lethaby A, Tavender E, Curr E, Garry R, et al. Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst Rev 2009;3. http://dx.doi.org/10.1002/14651858.cd003677.pub4.
- Vickers A, Rees R, Zollman C, McCarney R, Smith C. Acupuncture of chronic headache disorders in primary care: randomised controlled trial and economic analysis. Health Technol Assess 2004;8. http://dx.doi.org/10.3310/hta8480.
- Linde K, Allais G, Brinkhaus B, Manheimer E, Vickers A, White AR. Acupuncture for migraine prophylaxis. Cochrane Database Syst Rev 2009;1. http://dx.doi.org/10.1002/14651858.cd001218.pub2.
- Ozolins M, Eady E, Avery A, Cunliffe W, O’Neill C. Randomised controlled multiple treatment comparison to provide a cost-effectiveness rationale for the selection of antimicrobial therapy in acne. Health Technol Assess 2005;9. http://dx.doi.org/10.3310/hta9010.
- Garner SE, Eady A, Bennett C, Newton JN, Thomas K, Popescu CM. Minocycline for acne vulgaris: efficacy and safety. Cochrane Database Syst Rev 2012;8. http://dx.doi.org/10.1002/14651858.cd002086.pub2.
- Cochrane T, Davey R, Matthes Edwards S. Randomised controlled trial of the cost-effectiveness of water-based therapy for lower limb osteoarthritis. Health Technol Assess 2005;9. http://dx.doi.org/10.3310/hta9310.
- Bartels EM, Lund H, Hagen KB, Dagfinrud H, Christensen R, Danneskiold-Samsøe B. Aquatic exercise for the treatment of knee and hip osteoarthritis. Cochrane Database Syst Rev 2007;4. http://dx.doi.org/10.1002/14651858.cd005523.pub2.
- Thomas K, MacPherson H, Ratcliffe J, Thorpe L, Brazier J. Longer term clinical and economic benefits of offering acupuncture care to patients with chronic low back pain. Health Technol Assess 2005;9. http://dx.doi.org/10.3310/hta9320.
- Furlan AD, van Tulder MW, Cherkin D, Tsukayama H, Lao L, Koes BW, et al. Acupuncture and dry-needling for low back pain. Cochrane Database Syst Rev 2005;1. http://dx.doi.org/10.1002/14651858.cd001351.pub2.
- Hobbs FDR, Fitzmaurice DA, Mant J, Murray E, Jowett S, Bryan S, et al. A randomised controlled trial and cost-effectiveness study of systematic screening (targeted and total population screening) versus routine practice for the detection of atrial fibrillation in people aged 65 and over. The SAFE study. Health Technol Assess 2005;9. http://dx.doi.org/10.3310/hta9400.
- Moran PS, Flattery MJ, Teljeur C, Ryan M, Smith SM. Effectiveness of systematic screening for the detection of atrial fibrillation. Cochrane Database Syst Rev 2013;4. http://dx.doi.org/10.1002/14651858.cd009586.pub2.
- Dennis M, Lewis S, Cranswick G, Forbes J. FOOD: a multicentre randomised trial evaluating feeding policies in patients admitted to hospital with a recent stroke. Health Technol Assess 2006;10. http://dx.doi.org/10.3310/hta10020.
- Gomes CAR, Lustosa SAS, Matos D, Andriolo RB, Waisberg DR, Waisberg JW. Percutaneous endoscopic gastrostomy versus nasogastric tube feeding for adults with swallowing disturbances. Cochrane Database Syst Rev 2012;3. http://dx.doi.org/10.1002/14651858.cd008096.pub3.
- Kennedy T, Chalder T, McCrone P, Darnley S, Knapp M. Cognitive behavioural therapy in addition to antispasmodic therapy for irritable bowel syndrome in primary care: a randomised controlled trial. Health Technol Assess 2006;10. http://dx.doi.org/10.3310/hta10190.
- Zijdenbos IL, de Wit NJ, van der Heijden GJ, Rubin G, Quartero AO. Psychological treatments for the management of irritable bowel syndrome. Cochrane Database Syst Rev n.d.;1. http://dx.doi.org/10.1002/14651858.cd006442.pub2.
- Nixon J, Nelson A, Cranny G, Iglesias Urrutia C, Hawkins K. Pressure relieving support surfaces: a randomised evaluation. Health Technol Assess 2006;10. http://dx.doi.org/10.3310/hta10220.
- McInnes E, Dumville JC, Jammali-Blasi A, Bell-Syer SEM. Support surfaces for treating pressure ulcers. Cochrane Database Syst Rev 2011;12. http://dx.doi.org/10.1002/14651858.cd009490.
- O’Dowd H, Gladwell P, Rogers C, Hollinghurst S, Gregory A. Cognitive behavioural therapy in chronic fatigue syndrome: a randomised controlled trial of an outpatient group programme. Health Technol Assess 2006;10. http://dx.doi.org/10.3310/hta10370.
- Price JR, Mitchell E, Tidy E, Hunot V. Cognitive behaviour therapy for chronic fatigue syndrome in adults. Cochrane Database Syst Rev 2008;3. http://dx.doi.org/10.1002/14651858.cd001027.pub2.
- Hewison J, Nixon J, Fountain J, Cocks K, Jones C. Amniocentesis results: investigation of anxiety. The ARIA trial. Health Technol Assess 2006;10. http://dx.doi.org/10.3310/hta10500.
- Mujezinovic F, Prosnik A, Alfirevic Z. Different communication strategies for disclosing results of diagnostic prenatal testing. Cochrane Database Syst Rev 2010;11. http://dx.doi.org/10.1002/14651858.cd007750.pub2.
- Jolly K, Taylor R, Lip G, Greenfield S, Raftery J. The Birmingham Rehabilitation Uptake Maximisation Study (BRUM). Home-based compared with hospital-based cardiac rehabilitation in a multi-ethnic population: cost-effectiveness and patient adherence. Health Technol Assess 2007;11. http://dx.doi.org/10.3310/hta11350.
- Taylor RS, Dalal H, Jolly K, Moxham T, Zawada A. Home-based versus centre-based cardiac rehabilitation. Cochrane Database Syst Rev 2010;1. http://dx.doi.org/10.1002/14651858.cd007130.pub2.
- Fader M, Cottenden A, Getliffe K, Gage H, Clarke-O’Neill S. Absorbent products for urinary/faecal incontinence: a comparative evaluation of key product designs. Health Technol Assess 2008;12.
- Fader M, Cottenden AM, Getliffe K. Absorbent products for moderate-heavy urinary and/or faecal incontinence in women and men. Cochrane Database Syst Rev 2008;4. http://dx.doi.org/10.1002/14651858.cd007408.
- Grant A, Wileman S, Ramsay C, Bojke L, Epstein D. The effectiveness and cost-effectiveness of minimal access surgery amongst people with gastro-oesophageal reflux disease – a UK collaborative study. The REFLUX Trial. Health Technol Assess 2008;12. http://dx.doi.org/10.3310/hta12310.
- Wileman SM, McCann S, Grant AM, Krukowski ZH, Bruce J. Medical versus surgical management for gastro-oesophageal reflux disease (GORD) in adults. Cochrane Database Syst Rev 2010;3. http://dx.doi.org/10.1002/14651858.cd003243.pub2.
- Potter J, Mistri A, Brodie F, Chernova J, Wilson E. Controlling Hypertension and Hypotension Immediately Post-Stroke (CHHIPS) – a randomised controlled trial. Health Technol Assess 2009;13. http://dx.doi.org/10.3310/hta13090.
- Bath PMW, Krishnan K. Interventions for deliberately altering blood pressure in acute stroke. Cochrane Database Syst Rev 2014;10. http://dx.doi.org/10.1002/14651858.cd000039.pub3.
- Morrell CJ, Warner R, Slade P, Dixon S, Walters S. Psychological interventions for postnatal depression: cluster randomised trial and economic evaluation. The PONDER trial. Health Technol Assess 2009;13. http://dx.doi.org/10.3310/hta13300.
- Dennis CL, Dowswell T. Psychosocial and psychological interventions for preventing postpartum depression. Cochrane Database Syst Rev 2013;2. http://dx.doi.org/10.1002/14651858.cd001134.pub3.
- Gray AJ, Goodacre S, Newby DE, Masson MA, Sampson F. A multicentre randomised controlled trial of the use of continuous positive airway pressure and non-invasive positive pressure ventilation in the early treatment of patients presenting to the emergency department with severe acute cardiogenic pulmonary oedema: the 3CPO Trial. Health Technol Assess 2009;13. http://dx.doi.org/10.3310/hta13330.
- Vital FMR, Ladeira MT, Atallah ÁN. Non-invasive positive pressure ventilation (CPAP or bilevel NPPV) for cardiogenic pulmonary oedema. Cochrane Database Syst Rev 2013;5. http://dx.doi.org/10.1002/14651858.cd005351.pub3.
- Williamson I, Benge S, Barton S, Petrou S, Letley L. A double-blind randomised placebo controlled trial of topical intranasal corticosteroids in 4- to11-year-old children with persistent bilateral otitis media with effusion in primary care. Health Technol Assess 2009;13. http://dx.doi.org/10.3310/hta13370.
- Simpson SA, Lewis R, van der Voort J, Butler CC. Oral or topical nasal steroids for hearing loss associated with otitis media with effusion in children. Cochrane Database Syst Rev 2011;5. http://dx.doi.org/10.1002/14651858.cd001935.pub3.
- Sullivan FM, Swan IR, Donnan PT, Morrison JM, Smith BH, McKinstry B, et al. A randomised controlled trial of the use of aciclovir and/or prednisolone for the early treatment of Bell’s palsy: the BELLS study. Health Technol Assess 2009;13. http://dx.doi.org/10.3310/hta13470.
- Salinas RA, Alvarez G, Daly F, Ferreira J. Corticosteroids for Bell’s palsy (idiopathic facial paralysis). Cochrane Database Syst Rev 2010;3. http://dx.doi.org/10.1002/14651858.cd001942.pub4.
- Jeffcoate WJ, Price PE, Phillips CJ, Game FL, Mudge E. Randomised controlled trial of the use of three dressing preparations in the management of chronic ulceration of the foot in diabetes. Health Technol Assess 2009;13. http://dx.doi.org/10.3310/hta13540.
- Dumville JC, O’Meara S, Deshpande S, Speak K. Hydrogel dressings for healing diabetic foot ulcers. Cochrane Database Syst Rev 2013;7. http://dx.doi.org/10.1002/14651858.cd009101.pub3.
- Michaels JA, Campbell WB, King BM, MacIntyre J, Palfreyman SJ. A prospective randomised controlled trial and economic modelling of antimicrobial silver dressings versus non-adherent control dressings for venous leg ulcers: the VULCAN trial. Health Technol Assess 2009;13. http://dx.doi.org/10.3310/hta13560.
- O’Meara S, Al-Kurdi D, Ologun Y, Ovington LG, Martyn-St James M, Richardson R. Antibiotics and antiseptics for venous leg ulcers. Cochrane Database Syst Rev 2014;1. http://dx.doi.org/10.1002/14651858.cd003557.pub5.
- Lock C, Wilson J, Steen N, Eccles M, Mason H. North of England and Scotland Study of Tonsillectomy and Adeno-tonsillectomy in Children (NESSTAC): a pragmatic randomised controlled trial with a parallel non-randomised preference study. Health Technol Assess 2010;14.
- Burton MJ, Glasziou PP, Chong LY, Venekamp RP. Tonsillectomy or adenotonsillectomy versus non-surgical treatment for chronic/recurrent acute tonsillitis. Cochrane Database Syst Rev 2014;11. http://dx.doi.org/10.1002/14651858.cd001802.pub3.
- Peek G, Elbourne D, Mugford M, Tiruvoipati R, Wilson A. Randomised controlled trial and parallel economic evaluation of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR). Health Technol Assess 2010;14. http://dx.doi.org/10.3310/hta14350.
- Tramm R, Ilic D, Davies AR, Pellegrino VA, Romero L, Hodgson C. Extracorporeal membrane oxygenation for critically ill adults. Cochrane Database Syst Rev 2015;1. http://dx.doi.org/10.1002/14651858.cd010381.pub2.
- Lamb S, Lall R, Hansen Z, Castelnuovo E, Withers E. A multicentred randomised controlled trial of a primary-care based cognitive behavioural programme for low back pain. The Back Skills Training (BeST) trial. Health Technol Assess 2010;14. http://dx.doi.org/10.3310/hta14410.
- Williams AC, Eccleston C, Morley S. Psychological therapies for the management of chronic pain (excluding headache) in adults. Cochrane Database Syst Rev 2012;11. http://dx.doi.org/10.1002/14651858.cd007407.pub3.
- Sharp D, Chew-Graham C, Tylee A, Lewis G, Howard L. A pragmatic randomised controlled trial to compare antidepressants with a community-based psychosocial intervention for the treatment of women with postnatal depression: the RESPOND trial. Health Technol Assess 2010;14. http://dx.doi.org/10.3310/hta14430.
- Molyneaux E, Howard LM, McGeown HR, Karia AM, Trevillion K. Antidepressant treatment for postnatal depression. Cochrane Database Syst Rev 2014;9. http://dx.doi.org/10.1002/14651858.cd002018.pub2.
- Cockayne E, Curran M, Denby G, Hashmi F, Hewitt C. EVerT: cryotherapy versus salicylic acid for the treatment of verrucae – a randomised controlled trial. Health Technol Assess 2011;15. http://dx.doi.org/10.3310/hta15320.
- Kwok CS, Gibbs S, Bennett C, Holland R, Abbott R. Topical treatments for cutaneous warts. Cochrane Database Syst Rev 2012;9. http://dx.doi.org/10.1002/14651858.cd001781.pub3.
- Schumi J, Wittes JT. Through the looking glass: understanding non-inferiority. Trials 2011;12. http://dx.doi.org/10.1186/1745-6215-12-106.
- Aberegg SK, Arkes H, Terry PB. Failure to adopt beneficial therapies caused by bias in medical evidence evaluation. Med Decis Making 2006;26:575-82. http://dx.doi.org/10.1177/0272989X06295362.
- Elshaug AG, Hiller JE, Moss JR. Exploring policy-makers’ perspectives on disinvestment from ineffective healthcare practices. Int J Technol Assess Health Care 2008;24:1-9. http://dx.doi.org/10.1017/S0266462307080014.
- García-Armesto S, Campillo-Artero C, Bernal-Delgado E. Disinvestment in the age of cost-cutting sound and fury. Tools for the Spanish National Health System. Health Policy 2013;110:180-85. http://dx.doi.org/10.1016/j.healthpol.2013.01.007.
- Haines T, O’Brien L, McDermott F, Markham D, Mitchell D, Watterson D, et al. A novel research design can aid disinvestment from existing health technologies with uncertain effectiveness, cost-effectiveness, and/or safety. J Clin Epidemiol 2014;67:144-51. http://dx.doi.org/10.1016/j.jclinepi.2013.08.014.
- Henshall C, Schuller T, Mardhani-Bayne L. Using health technology assessment to support optimal use of technologies in current practice: The challenge of ‘disinvestment’. Int J Technol Assess Health Care 2012;28:203-10. http://dx.doi.org/10.1017/S0266462312000372.
- Hodgetts K, Elshaug AG, Hiller JE. What counts and how to count it: physicians’ constructions of evidence in a disinvestment context. Soc Sci Med 2012;75:2191-9. http://dx.doi.org/10.1016/j.socscimed.2012.08.016.
- Hodgetts K, Hiller JE, Street JM, Carter D, Braunack-Mayer AJ, Watt AM, et al. Disinvestment policy and the public funding of assisted reproductive technologies: outcomes of deliberative engagements with three key stakeholder groups. BMC Health Serv Res 2014;14. http://dx.doi.org/10.1186/1472-6963-14-204.
- Ibargoyen-Roteta N, Gutiérrez-Ibarluzea I, Asua J. Guiding the process of health technology disinvestment. Health Policy 2010;98:218-26. http://dx.doi.org/10.1016/j.healthpol.2010.06.018.
- Karnon J, Carlton J, Czoski-Murray C, Smith K. Informing disinvestment through cost-effectiveness modelling: is lack of data a surmountable barrier?. Appl Health Econ Health Policy 2009;7:1-9. http://dx.doi.org/10.1007/BF03256137.
- Nuti S, Vainieri M, Bonini A. Disinvestment for re-allocation: a process to identify priorities in healthcare. Health Policy 2010;95:137-43. http://dx.doi.org/10.1016/j.healthpol.2009.11.011.
- Rooshenas L, Owen-Smith A, Hollingworth W, Badrinath P, Beynon C, Donovan JL. ‘I won’t call it rationing. . .’: an ethnographic study of healthcare disinvestment in theory and practice. Soc Sci Med 2015;128:273-81. http://dx.doi.org/10.1016/j.socscimed.2015.01.020.
- Watt AM, Hiller JE, Braunack-Mayer AJ, Moss JR, Buchan H, Wale J, et al. The ASTUTE health study protocol: Deliberative stakeholder engagements to inform implementation approaches to healthcare disinvestment. Implement Sci 2012;7. http://dx.doi.org/10.1186/1748-5908-7-101.
- Watt AM, Willis CD, Hodgetts K, Elshaug AG, Hiller JE. Engaging clinicians in evidence-based disinvestment: role and perceptions of evidence. Int J Technol Assess Health Care 2012;28:211-19. http://dx.doi.org/10.1017/S0266462312000402.
- Wilson MG, Ellen ME, Lavis JN, Grimshaw JM, Moat KA, Shemer J, et al. Processes, contexts, and rationale for disinvestment: a protocol for a critical interpretive synthesis. Syst Rev 2014;3. http://dx.doi.org/10.1186/2046-4053-3-143.
- de Souza ALC, de Assis Acurcio F, Júnior AAG, do Nascimento RCRM, Godman B, Diniz LM. Insulin glargine in a Brazilian state: should the government disinvest? An assessment based on a systematic review. Appl Health Econ Health Policy 2014;12:19-32. http://dx.doi.org/10.1007/s40258-013-0073-6.
- Cornelissen E, Mitton C, Davidson A, Reid C, Hole R, Visockas A-M, et al. Determining and broadening the definition of impact from implementing a rational priority setting approach in a healthcare organization. Soc Sci Med 2014;114:1-9. http://dx.doi.org/10.1016/j.socscimed.2014.05.027.
- Edwards RT, Charles JM, Thomas S, Bishop J, Cohen D, Groves S, et al. A national Programme Budgeting and Marginal Analysis (PBMA) of health improvement spending across Wales: disinvestment and reinvestment across the life course. BMC Public Health 2014;14. http://dx.doi.org/10.1186/1471-2458-14-837.
- Haas M, Hall J, Viney R, Gallego G. Breaking up is hard to do: why disinvestment in medical technology is harder than investment. Aust Health Rev 2012;36:148-52. http://dx.doi.org/10.1071/AH11032.
- Mitton C, Dionne F, Damji R, Campbell D, Bryan S. Difficult decisions in times of constraint: criteria based resource allocation in the Vancouver Coastal Health Authority. BMC Health Serv Res 2011;11. http://dx.doi.org/10.1186/1472-6963-11-169.
- Mortimer D. Reorienting programme budgeting and marginal analysis (PBMA) towards disinvestment. BMC Health Serv Res 2010;10. http://dx.doi.org/10.1186/1472-6963-10-288.
- Bohmer P, Pain C, Watt A, Abernethy P, Sceats J. Maximising health gain within available resources in the New Zealand public health system. Health Policy 2001;55:37-50. http://dx.doi.org/10.1016/S0168-8510(00)00107-X.
- Daniels T, Williams I, Robinson S, Spence K. Tackling disinvestment in health care services: the views of resource allocators in the English NHS. J Health Organ Manag 2013;27:762-80. http://dx.doi.org/10.1108/JHOM-11-2012-0225.
- Robinson S, Glasby J, Allen K. ‘It ain’t what you do it’s the way that you do it’: lessons for health care from decommissioning of older people’s services. Health Soc Care Community 2013;21:614-22. http://dx.doi.org/10.1111/hsc.12046.
- Robinson S, Williams I, Dickinson H, Freeman T, Rumbold B. Priority-setting and rationing in healthcare: evidence from the English experience. Soc Sci Med 2012;75:2386-93. http://dx.doi.org/10.1016/j.socscimed.2012.09.014.
- Williams IP, Bryan S. Cost-effectiveness analysis and formulary decision making in England: findings from research. Soc Sci Med 2007;65:2116-29. http://dx.doi.org/10.1016/j.socscimed.2007.06.009.
- Eddama O, Coast J. Use of economic evaluation in local health care decision-making in England: a qualitative investigation. Health Policy 2009;89:261-70. http://dx.doi.org/10.1016/j.healthpol.2008.06.004.
- Chamberlain CA, Martin RM, Busby J, Gilbert R, Cahill DJ, Hollingworth W. Trends in procedures for infertility and caesarean sections: was NICE disinvestment guidance implemented? NICE recommendation reminders. BMC Public Health 2013;13. http://dx.doi.org/10.1186/1471-2458-13-112.
- Garner S, Docherty M, Somner J, Sharma T, Choudhury M, Clarke M, et al. Reducing ineffective practice: challenges in identifying low-value health care using Cochrane systematic reviews. J Health Serv Res Policy 2013;18:6-12. http://dx.doi.org/10.1258/jhsrp.2012.012044.
- Garner S, Littlejohns P. Disinvestment from low value clinical interventions: NICEly done?. BMJ 2011;343. http://dx.doi.org/10.1136/bmj.d4519.
- Pearson S, Littlejohns P. Reallocating resources: how should the National Institute for Health and Clinical Excellence guide disinvestment efforts in the National Health Service?. J Health Serv Res Policy 2007;12:160-5. http://dx.doi.org/10.1258/135581907781542987.
- Walker S, Palmer S, Sculpher M. The role of NICE technology appraisal in NHS rationing. Br Med Bull 2007;81:51-64. http://dx.doi.org/10.1093/bmb/ldm007.
- Hopper I, Samuel R, Hayward C, Tonkin A, Krum H. Can Medications be Safely Withdrawn in Patients With Stable Chronic Heart Failure? Systematic Review and Meta-analysis. J Card Fail 2014;20:522-32. http://dx.doi.org/10.1016/j.cardfail.2014.04.013.
- Leggett L, Noseworthy TW, Zarrabi M, Lorenzetti D, Sutherland LR, Clement FM. Health technology reassessment of non-drug technologies: current practices. Int J Technol Assess Health Care 2012;28:220-7. http://dx.doi.org/10.1017/S0266462312000438.
- Polisena J, Clifford T, Elshaug AG, Mitton C, Russell E, Skidmore B. Case studies that illustrate disinvestment and resource allocation decision-making processes in health care: a systematic review. Int J Technol Assess Health Care 2013;29:174-84. http://dx.doi.org/10.1017/S0266462313000068.
- Nielsen CP, Funch TM, Kristensen FB. Health technology assessment: research trends and future priorities in Europe. J Health Serv Res Policy 2011;16:6-15. http://dx.doi.org/10.1258/jhsrp.2011.011050.
- Watt AM, Elshaug AG, Willis CD, Hiller JE. ASTUTE Health study group . Assisted reproductive technologies: a systematic review of safety and effectiveness to inform disinvestment policy. Health Policy 2011;102:200-13. http://dx.doi.org/10.1016/j.healthpol.2011.07.007.
- Charlesworth G, Shepstone L, Wilson E, Thalanany M, Mugford M, Poland F. Does befriending by trained lay workers improve psychological well-being and quality of life for carers of people with dementia, and at what cost? A randomised controlled trial. Health Technology Assessment 2008. http://dx.doi.org/10.3310/hta12040.
- Bradbury AW, Adam DJ, Bell J, Forbes JF, Fowkes FGR. Multicentre randomised controlled trial of the clinical and cost-effectiveness of a bypass-surgery-first versus a balloon-angioplasty-first revascularisation strategy for severe limb ischaemia due to infrainguinal disease. The Bypass versus Angioplasty in Severe Ischaemia of the Leg (BASIL) trial. Health Technol Assess 2010;14. http://dx.doi.org/10.3310/hta14140.
- Little P, Turner S, Rumsby K, Warner G, Moore M. Dipsticks and diagnostic algorithms in urinary tract infection: development and validation, randomised trial, economic analysis, observational cohort, and qualitative study. Health Technol Assess 2009;13. http://dx.doi.org/10.3310/hta13190.
- Kerry S, Dundas D, Hilton S, Rink E, Patel S. Routine referral for radiography of patients presenting with low back pain: is patients’ outcome influenced by GPs’ referral for plain radiography?. Health Technol Assess 2000;4.
- Kendrick D, Fielding K, Bentley E, Miller P, Kerslake R. The role of radiography in primary care patients with low back pain of at least 6 weeks’ duration: a randomised (unblinded) controlled trial. Health Technol Assess 2001;5. http://dx.doi.org/10.3310/hta5300.
- Lomas J. Improving Research Dissemination and Uptake in the Health Sector: Beyond the Sound of One Hand Clapping. Ottawa, ON: Canadian Health Services Research Foundation; 1997.
- Weiss CH. Have we learned anything new about the use of evaluation?. Am J Eval 1998;19:21-33. http://dx.doi.org/10.1016/S1098-2140(99)80178-7.
- Pittman P, Almeida C. Cross-sector learning among researchers and policy-makers: the search for new strategies to enable use of research results. Cadernos Saude Publica 2006;22:97-108. http://dx.doi.org/10.1590/S0102-311X2006001300019.
- Hinrichs S, Grant J. A new resource for identifying and assessing the impacts of research. BMC Med 2015;13. http://dx.doi.org/10.1186/s12916-015-0364-x.
- Barnhoorn F, McCarthy M, Deville W, Alexanderson K, Voss M, Conceicao C. PHIRE (Public Health Innovation and Research in Europe): methods, structures and evaluation. Eu J Public Health 2013;23:6-11. http://dx.doi.org/10.1093/eurpub/ckt148.
- Battles JB, Farr SL, Weinberg DA. From research to nationwide implementation: the impact of AHRQ’s HAI prevention program. Med Care 2014;52:91-6. http://dx.doi.org/10.1097/MLR.0000000000000037.
- Bernstein A, Hicks V, Borbey P, Campbell T. A Framework to Measure the Impact of Investments in Health Research n.d.
- Bumgarner R, Hattaway D, Lamb G, McGann J, Wise H. Center for Global Development: Evaluation of Impact. Washington, DC: Arabella Philanthropic Investment Advisors; 2006.
- Glennerster R, Kremer M, Williams H. Creating markets for vaccines. Innovations 2006;67. http://dx.doi.org/10.1162/itgg.2006.1.1.67.
- Bunn F. The Cochrane Injuries Group celebrates the publication of its 100th review: time to reflect on impact. Inj Prev 2010;16:208-9. http://dx.doi.org/10.1136/ip.2010.027136.
- Buykx P, Humphreys J, Wakerman J, Perkins D, Lyle D, McGrail M, et al. Making evidence count: a framework to monitor the impact of health services research. Aust J Rural Health 2012;20:51-8. http://dx.doi.org/10.1111/j.1440-1584.2012.01256.x.
- Lavis JN, Robertson D, Woodside JM, McLeod CB, Abelson J. How can research organizations more effectively transfer research knowledge to decision makers?. Milbank Q 2003;81:221-48. http://dx.doi.org/10.1111/1468-0009.t01-1-00052.
- Lavis J, Ross S, McLeod C, Gildiner A. Measuring the impact of health research. J Health Serv Res 2003;8:165-70. http://dx.doi.org/10.1258/135581903322029520.
- Developing a CIHR Framework to Measure The Impact of Health Research. Ottawa, ON: CIHR; 2005.
- Carden F. Knowledge to Policy: Making the Most of Development Research. Ottawa, ON: International Centre for Development Research; 2009.
- Currie M, King G, Rosenbaum P, Law M, Kertoy M, Specht J. A model of impacts of research partnerships in health and social services. Eval Program Plann 2005;28:400-12. http://dx.doi.org/10.1016/j.evalprogplan.2005.07.004.
- de Goede J, van Bon-Martens MJ, Putters K, van Oers HA. Looking for interaction: quantitative measurement of research utilization by Dutch local health officials. Health Res Policy Syst 2012;10. http://dx.doi.org/10.1186/1478-4505-10-9.
- Druce N, Gopalan A, Moree M, Nathanson N, Plotkin S, Skolnik R. Evaluation of the International AIDS Vaccine 2003–2007. New York, NY: IAVI; 2009.
- Bozeman B. Public Value Mapping of Science Outcomes: Theory and Method n.d. http://cspo.org/legacy/library/110215F3AQ_lib_BozemanPVMKnowle.pdf (accessed 14 July 2016).
- Ensor T, Clapham S, Prasai DP. What drives health policy formulation: insights from the Nepal maternity incentive scheme?. Health Policy 2009;90:247-53. http://dx.doi.org/10.1016/j.healthpol.2008.06.009.
- Garfinkel MS, Sarewitz D, Porter AL. A societal outcomes map for health research and policy. Am J Public Health 2006;96:441-6. http://dx.doi.org/10.2105/AJPH.2005.063495.
- Gibson B, Ehrlich D, Graff J, Dubois R, Farr M, Chernew M, et al. Real-world impact of comparative effectiveness research findings on clinical practice. Am J Manag Care 2014;20:e208-20.
- Godin B, Doré C. Measuring the Impacts of Science; Beyond the Economic Dimension. Helsinki: Helsinki Institute for Science and Technology Studies; 2005.
- Grazier KL, Trochim WM, Dilts DM, Kirk R. Estimating return on investment in translational research: methods and protocols. Eval Health Prof 2013;36:478-91. http://dx.doi.org/10.1177/0163278713499587.
- Morgan Jones M, Castle-Clarke S, Manville C, Gunashekar S, Grant J. Assessing Research Impact. An International Review of the Excellence in Innovation for Australia Trial. Santa Monica, CA: RAND Corporation; 2013.
- Largent MA, Lane JI. STAR METRICS and the science of science policy. Rev Policy Res 2012;29:431-8. http://dx.doi.org/10.1111/j.1541-1338.2012.00567.x.
- El Turabi A, Hallsworth M, Ling T, Grant J. A novel performance monitoring framework for health research systems: experiences of the National Institute for Health Research in England. Health Res Policy Syst 2011;9. http://dx.doi.org/10.1186/1478-4505-9-13.
- Ottoson JM, Green LW, Beery WL, Senter SK, Cahill CL, Pearson DC, et al. Policy-contribution assessment and field-building analysis of the Robert Wood Johnson Foundation’s active living research program. Am J Prev Med 2009;36:34-43. http://dx.doi.org/10.1016/j.amepre.2008.10.010.
- Hanney SR, Home PD, Frame I, Grant J, Green P, Buxton MJ. Identifying the impact of diabetes research. Diabet Med 2006;23:176-84. http://dx.doi.org/10.1111/j.1464-5491.2005.01753.x.
- Home PD. Impact of the UKPDS – an overview. Diabet Med 2008;25:2-8. http://dx.doi.org/10.1111/j.1464-5491.2008.02501.x.
- Embedding Impact Analysis in Research. Bristol: National Coordinating Centre for Public Engagement, University of Bristol, University of the West of England; 2013.
- Morton S. Exploring and Assessing Research Impact 2012.
- Kagan JM, Kane M, Quinlan KM, Rosas S, Trochim WM. Developing a conceptual framework for an evaluation system for the NIAID HIV/AIDS clinical trials networks. Health Res Policy Syst 2009;7. http://dx.doi.org/10.1186/1478-4505-7-12.
- King G, Servais M, Kertoy M, Specht J, Currie M, Rosenbaum P, et al. A measure of community members’ perceptions of the impacts of research partnerships in health and social services. Eval Program Plann 2009;32:289-99. http://dx.doi.org/10.1016/j.evalprogplan.2009.02.002.
- Caplan N, Morrison A, Stamburgh RJ. The Use of Social Science Knowledge in Policy Decisions at the National Level: A Report to Respondents. Ann Arbor, MI: Center for Research on Utilization of Scientific Knowledge, University of Michigan; 1975.
- Kryl D, Allen L, Dolby K, Sherbon B, Viney I. Tracking the impact of research on policy and practice: investigating the feasibility of using citations in clinical guidelines for research evaluation. BMJ Open 2012;2. http://dx.doi.org/10.1136/bmjopen-2012-000897.
- Latour B. Reassembling the Social – An Introduction to Actor-Network-Theory. Oxford: Oxford University Press; 2005.
- Martin B, Tang P. The Benefits from Publicly Funded Research. Brighton: SPRU, University of Sussex; 2007.
- McCarthy M. Public health research support through the European structural funds in central and eastern Europe and the Mediterranean. Health Res Policy Syst 2012;10. http://dx.doi.org/10.1186/1478-4505-10-12.
- McLean RK, Graham I, Bosompra K, Choudhry Y, Coen S, MacLeod M, et al. Understanding the performance and impact of public knowledge translation funding interventions: protocol for an evaluation of Canadian Institutes of Health Research knowledge translation funding programs. Implement Sci 2012;7. http://dx.doi.org/10.1186/1748-5908-7-57.
- Moreira T. The Transformation of Contemporary Health Care: The Market, the Laboratory, and the Forum. London: Routledge; 2013.
- Morlacchi P, Nelson RR. How medical practice evolves: learning to treat failing hearts with an implantable device. Res Policy 2011;40:511-25. http://dx.doi.org/10.1016/j.respol.2011.01.001.
- Niederkrotenthaler T, Dorner T, Maier M. Development of a practical tool to measure the impact of publications on the society based on focus group discussions with scientists. BMC Public Health 2011;11. http://dx.doi.org/10.1186/1471-2458-11-588.
- Oliver TR, Singer RF. Health services research as a source of legislative analysis and input: the role of the California health benefits review program. Health Serv Res 2006;41:1124-58. http://dx.doi.org/10.1111/j.1475-6773.2006.00523.x.
- Wilson JQ. Political Organizations. New York, NY: Basic Books; 1973.
- Wilson JQ, Wilson JQ. The Politics of Regulation. New York, NY: Basic Books; 1990.
- Arnold RD. The Logic of Congressional Action. New Haven, CT: Yale University Press; 1990.
- Ovseiko PV, Oancea A, Buchan AM. Assessing research impact in academic clinical medicine: a study using Research Excellence Framework pilot impact indicators. BMC Health Serv Res 2012;12. http://dx.doi.org/10.1186/1472-6963-12-478.
- Percy-Smith J, Speller V, Nutley S. Evidence Informed Policy and Practice: A Review of Approaches used in Health Improvement in Scotland. Edinburgh: NHS Health Scotland; 2006.
- Walter I, Nutley S, Percy-Smith J, McNeish D, Frost S. Improving the Use of Research in Social Care Practice. London: Social Care Institute for Excellence; 2004.
- Ritter A, Lancaster K. Measuring research influence on drug policy: a case example of two epidemiological monitoring systems. Int J Drug Policy 2013;24:30-7. http://dx.doi.org/10.1016/j.drugpo.2012.02.005.
- Hass PM. Introduction: epistemic communities and international policy coordination. International Organization 1992;46:1-35. http://dx.doi.org/10.1017/S0020818300001442.
- Lomas J. Using ‘linkage and exchange’ to move research into policy at a Canadian foundation. Health Aff 2000;19:236-40. http://dx.doi.org/10.1377/hlthaff.19.3.236.
- Rosas SR, Schouten JT, Cope MT, Kagan JM. Modeling the dissemination and uptake of clinical trials results. Res Eval 2013;22:179-86. http://dx.doi.org/10.1093/reseval/rvt005.
- Runyan C, Garrettson M, Yee SL. Development of a set of indicators to evaluate injury control research centers. Eval Rev 2014;38:133-59. http://dx.doi.org/10.1177/0193841X14529287.
- Logic Model Development Guide. Battle Creek, MI: The Foundation; 2004.
- Sarli CC, Holmes KL. Update to ‘Beyond citation analysis: a model for assessment of research impact’. J Med Libr Assoc 2012;100. http://dx.doi.org/10.3163/1536-5050.100.2.002.
- Report on Approaches to Assess the Value of Biomedical Research Supported by the NIH. Bethesda, MD: National Institutes of Health; 2014.
- Spoth RL, Schainker LM, Hiller-Sturmhöefel S. Translating family-focused prevention science into public health impact: illustrations from partnership-based research. Alcohol Res Health 2011;34.
- Sridharan S, Maplazi J, Vijendran M, Richardson E, Nichols J, Parekh H. Final Report: Evaluation of Teasdale-Corti Initiative. Toronto, ON: The Evaluation Centre for Complex Health Interventions (TECCHI); 2013.
- Sullivan R, Lewison G, Purushotham AD. An analysis of research activity in major UK cancer centres. Eur J Cancer 2011;47:536-44. http://dx.doi.org/10.1016/j.ejca.2010.10.015.
- Sutherland WJ, Goulson D, Potts SG, Dicks LV. Quantifying the impact and relevance of scientific research. PLOS ONE 2011;6. http://dx.doi.org/10.1371/journal.pone.0027537.
- Theobald S, Taegtmeyer M, Squire SB, Crichton J, Simwaka BN, Thomson R, et al. Towards building equitable health systems in sub-Saharan Africa: lessons from case studies on operational research. Health Res Policy Syst 2009;7. http://dx.doi.org/10.1186/1478-4505-7-26.
- Tremblay G, Zohar S, Bravo J, Potsepp P, Barker M. The Canada Foundation for Innovation’s outcome measurement study: a pioneering approach to research evaluation. Res Eval 2010;19:333-45. http://dx.doi.org/10.3152/095820210X12809191250960.
- Trochim WM, Marcus SE, Masse LC, Moser RP, Weld PC. The evaluation of large research initiatives – a participatory integrative mixed-methods approach. Am J Eval 2008;29:8-28. http://dx.doi.org/10.1177/1098214007309280.
- Sherwin CW, Isenson RS. Project Hindsight: a Defense Department study of the utility of research. Science 1967;156:1571-7. http://dx.doi.org/10.1126/science.156.3782.1571.
- Technology in Retrospect and Critical Events in Science. Chicago, IL: IIT Research Institute; 1968.
- Wilson PM, Petticrew M, Calnan MW, Nazareth I. Does dissemination extend beyond publication: a survey of a cross section of public funded research in the UK. Implement Sci 2010;5. http://dx.doi.org/10.1186/1748-5908-5-61.
- Xia AD. Comparative effectiveness reviews and their potential impact on formulary access in the United States. Value Health 2011;14. http://dx.doi.org/10.1016/j.jval.2011.02.172.
- ERA 2012 Submission Guidelines, Excellence in Research for Australia. Canberra, ACT: Australian Research Council; 2011.
- Morgan B. Research impact: income for outcome. Nature 2014;511:S72-75.
- Manville C, Guthrie S, Henham M-L, Garrod B, Sousa S, Kirtley A, et al. Assessing Impact Submissions for REF 2014: An Evaluation. Cambridge: RAND Europe; 2015.
- Greenhalgh T, Fahy N. Research impact in the community based health sciences: an analysis of 162 case studies from the 2014 UK Research Excellence Framework. BMC Med 2015;13. http://dx.doi.org/10.1186/s12916-015-0467-4.
Appendix 1 Literature search strategies
Search strategy for the update to the 2007 systematic review (impact of Health Technology Assessment research)
Search date: August 2014.
| Database | Search strategy | Download file |
|---|---|---|
| Ovid MEDLINE(R) without Revisions Search range: 1996 to August, week 2 2014 Saved as med-impact-final-strategy |
|
494 |
| Ovid MEDLINE(R) In-Process & Other Non-Indexed Citations Search date: 13 August 2014 |
|
17 |
| EMBASE Search range: 1996 to 2014 week 33 |
|
120 |
| Cochrane Methodology Register, issue 3 of 4, July 2012 | Impact AND research | 61 |
| HMIC Search range: 1979 to present Records from The King’s Fund and Department of Health (August 2014) |
(impact AND “health research”).ti,ab Limited from 2005 to date |
67 |
| CINAHL | (impact AND “health research”).ti,ab [Limit to: Publication Year 2005-2014] | 188 |
| Total records downloaded | 947 | |
| Total records after duplicates removed and initial screening | 297 | |
Search strategy for monetary value on the impact of research
Search date: October 2014.
| Database | Search strategy | Download file |
|---|---|---|
| Ovid MEDLINE(R) without Revisions Search range: 1996 to September, week 4 2014 |
|
178 |
| EMBASE Search range: 1996 to 2014 week 40 |
|
76 |
| Ovid MEDLINE(R) In-Process & Other Non-Indexed Citations Search date: 7 October 2014 |
|
47 |
| The Cochrane Library including NHS EED and Methodology | Monetisation or “value of research” or payback or payoff | No additional records identified |
| HMIC | Monetisation or “value of research” or payback or payoff | 112 |
| Total records identified | 413 | |
| Total records downloaded after initial screening and duplicates removed | 102 | |
Search strategy for randomised trials impact on systematic reviews
Search date: October 2014.
| Database | Search strategy | Download file |
|---|---|---|
| Ovid MEDLINE(R) without Revisions Search range: 1996 to October, week 1 2014 |
|
40 |
| EMBASE Serach range: 1996 to 2014 week 41 |
|
8 |
| Cochrane methodology | cumulative meta-analysis | 6 |
| Total records identified after initial screening and duplicates removed | 54 | |
Search strategy for impact of randomised trials on stopping health technologies
Database: Ovid MEDLINE(R) without Revisions
Search date: March 2015.
Search range: 1996 to week 2 March 2015.
Search strategy
-
disinvestment.mp. (86)
-
discontinue.mp. (3569)
-
(disinvest and technology).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] (1)
-
(discontinu* and technolog*).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] (522)
-
1 or 3 or 4 (608)
-
*“Efficiency, Organizational”/ (6431)
-
“Biomedical Technology”/ (3230)
-
6 and 7 (15)
-
from 8 keep 5,11 (2)
-
from 1 keep 1-2,7-8,11,16-18,20,22,27-29,33-34,40,43,45,50,52,56-57,61,64,68 (25)
-
optimization.mp. (50,487)
-
7 and 11 (10)
-
from 12 keep 1-3 (3)
-
Technology Assessment, Biomedical/ec, og [Economics, Organization & Administration] (1048)
-
7 or 14 (4203)
-
1 and 15 (17)
-
from 16 keep 1-8,12-16 (13)
-
impact.mp. (422,537)
-
5 and 18 (45)
-
10 or 15 (38)
-
19 or 20 (52)
Database: Ovid MEDLINE(R) without Revisions
Search date: March 2015.
Search range: 1996 to week 2 March 2015.
Search strategy
-
larval therapy in the management of leg ulcers.m_titl. (1)
-
“Treatment Outcome”/ (626,908)
-
water softening for eczema.m_titl. (0)
-
(water softening and eczema).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] (6)
-
((impact adj5 RCTs) or trial*) and (stop* adj5 technolog*)).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] (3)
-
(impact adj5 (RCTs or trial*)).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] (2608)
-
(impact adj2 (RCTs or trial*)).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] (396)
-
(impact adj2 (RCTs or trial*)).ti. (131)
-
Decision Making, Organizational/ (7820)
-
exp Resource Allocation/og, td [Organization & Administration, Trends] (1228)
-
9 or 10 (8959)
-
6 and 11 (0)
-
evidence.mp. (814,371)
-
11 and 13 (889)
-
from 4 keep 3-4 (2)
-
from 8 keep 10-11,30,32 (4)
-
from 14 keep 1,11,16 (3)
-
(evidence and disinvestment).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] (34)
-
from 18 keep 1-2,5,8,11-15,18-19,21,27-28,30 (15)
-
“Disinvestment”.kw. (2)
-
9 or 10 (8959)
-
2 and 21 (67)
-
*“Diffusion of Innovation”/ (6307)
-
9 or 10 or 23 (15,112)
-
(trial* and disinvest*).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] (4)
-
from 22 keep 30 (1)
-
from 25 keep 1-4 (4)
-
(trial* and (technolog* adj4 discontinu*)).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] (0)
-
(trial* and (technolog* adj4 stop*)).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] (3)
-
(against technolog* and trial*).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] (0)
-
(technolog* and (against or stop* or reject*)).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] (11,240)
-
(RCT* or trial).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] (620,530)
-
31 and 32 (566)
-
24 and 33 (4)
-
from 34 keep 3 (1)
-
26 or 27 or 35 (6)
-
2 and 24 (139)
-
from 37 keep 2,15,17-18,22,36,48,71,75 (9)
-
*“Technology Assessment, Biomedical”/ (2925)
-
*“Decision Support Techniques”/ (6218)
-
“Randomized Controlled Trials as Topic”/ (86,973)
-
40 and 41 (163)
-
from 42 keep 2 (1)
-
11 and 41 (29)
-
from 44 keep 1,8,13,16 (4)
-
discontinu*.mp. (54,765)
-
41 and 46 (1359)
-
39 and 47 (0)
-
39 and 41 (117)
-
from 49 keep 1-2,15,20-22,25,49 (8)
-
2 and 41 (20,759)
-
39 and 51 (18)
-
from 52 keep 5 (1)
-
31 and 39 and 41 (7)
-
from 54 keep 7 (1)
-
from 22 keep 30 (1)
-
32 and 39 and 41 (43)
-
from 57 keep 6-9 (4)
-
15 or 16 or 17 or 19 or 27 or 35 or 38 or 43 or 45 or 50 or 53 or 55 or 56 or 58 (53)
-
(disuse adj3 technolog*).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] (1)
-
(disuse or cancel*).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] (13,164)
-
2 and 61 (1199)
-
39 and 62 (0)
-
41 and 62 (13)
-
“raftery$”.fc_auts. and “lancet$”.fc_jour. (7)
-
“Program Evaluation”/ (40,717)
-
39 and 66 (72)
-
from 59 keep 1-53 (53)
-
from 67 keep 5-6 (2)
-
59 or 69 (55)
Appendix 2 Data extraction sheet
| Number | |
|---|---|
| Authors | |
| Title of paper | |
| Journal (journal, year, volume, etc.) | |
| Source summary | |
| Type of study or description of method/application/both | |
| Country | |
| Programme/specialty | |
| Conceptual framework used in impact assessment | |
| Methods used in impact assessment | |
| Brief description of aspects/dimensions of impacts assessed and found | |
| Attempts to assess the impact from each of the projects in a multiproject programme | |
| Conflicts of interest | |
| Meeting inclusion criteria | |
| Strengths and weaknesses | |
| Factors associated with impact | |
| Other comments (reviewer) and quotes |
Appendix 3 The included studies in the updated review
| Number | Authors | Year | Type | Location of research assessed (or to be assessed) | Programme/specialty | Concepts and techniques/methods for assessing health research impact | Impact: examined and found | Comments: strengths/weaknesses; factors associated with impact |
|---|---|---|---|---|---|---|---|---|
| 1 | Action Medical Research54 | 2009 | Application | UK | Action Medical Research: training fellowships | Payback Framework. Survey to past fellows (130: 72% completed) | Furthering medical science and developing research capacity; knowledge production; patient and health-care sector benefits; economic benefits; and benefits to the charity | There was a good response rate; however, it relied solely on self-reported data. Example of assessing capacity building/training award that moves beyond the capacity building – also consider impact of the research conducted, but as here, such studies sometimes take a career perspective, making comparisons with projects more difficult |
| Found: impact on career development – 78% had some research involvement; 30% had an impact on clinical guidelines; 42% on clinical practice or service improvements; and 46% patient benefit, much from follow-on research | ||||||||
| 2 | Adam et al.84 | 2012 | Application | Catalonia | Catalan Agency for Health Information, Assessment and Quality: clinical and HSR | ROI payback model from CAHS. Bibliometric analysis; surveys to researchers [99 (71%) response]; interviews – researchers (n = 15), decision-makers (n = 8); in-depth case study of translation pathways. Include the ROI focus on assessment in relation to targets the programme intended to reach | The article focused on two of the impact categories: advancing knowledge and impact on informed decision-making by policy-makers, managers, health-care professionals, patients, etc. | Achieved aim of filling a gap in the knowledge needs; study informed funding agency’s subsequent actions, but both internal and external validity ‘have room for improvement’. Noted limitations of attribution, time lags, counterfactual Factors: the studies ‘provide reasons to advocate for oriented research to fill specific knowledge gaps’. Interactions and participation of health-care and policy decision-makers in the projects was crucial |
| Found: 40 out of 70 said decision-making changes been induced by research results: 29 of those said research had changed clinical practice, a maximum of 16 said that there had been organisational/management/policy changes | ||||||||
| 3 | Anderson55 | 2006 | Application | Australia | NSW health survey | Payback Framework adapted. Subanalysis of a survey of users of the health survey; follow-up telephone survey of selected respondents; case studies using supplementary data sources | Categories adapted from Payback Framework. Emphasis on policy impacts | Useful analysis of assessment problems because diverse potential users of population surveys. Low response rate and difficult to go beyond policy impact:Simpler surveys of whether and how data are used by policy makers may be the only realistic option |
| Found: some examples of uses to inform policy. Most of the information could not have come from other sources | ||||||||
| 4 | Arnold133 | 2012 | Both | EU | EU FPs: including brain research | Developed a list of expected impacts from FP in terms of outputs, outcomes, mid-term impacts and long-term impacts. Attempted a more systematic approach to the role of funding in the social shaping of the research and innovation system. Limited account of methods in this paper that draws on a range of reports | Expected impacts – particular emphasis on knowledge and commercialisation | Fuller account given in a report |
| Found: ‘impact mechanisms’ in the brain research FP case study area included: knowledge, agenda-setting, promoting self-organisation of stakeholder communities; co-ordinating or influencing policy; leveraging funding for R&D; mobility and development of human capital; behavioural additionality – learning a ‘new’ innovation model | ||||||||
| 5 | Aymerich et al.56 | 2012 | Both | Catalonia | Network centre for research in epidemiology and public health | Adaption of Payback Framework, informed by CAHS and Berra et al.58 Survey of PIs of 217 small-scale projects (173 responded: 80%) ‘on the outcomes and potential impact of each project’; and a survey of external reviewers, with the aim of assessing the performance of each project in terms of how far the objectives were met | Survey to PIs covered three main categories of social impact, each with various dimensions, e.g. knowledge translation (including ‘To carry out clinical trials’ ‘To the development of synthesis reports of scientific evidence, clinical practice or public health guidelines, or similar products’ | Good response rate; opinions of external reviewers and researchers. Claim to report:a tool for ex-post evaluation with good discriminating ability that makes it possible to measure the extent to which a project’s objectives have been met . . . and the extent to which the project contributed benefits in terms of impact on the group’s scientific performance and social paybackHowever, considered potential not actual health-care benefits. Mixing of data for impact on synthesis reports in the same category as guidelines makes comparisons with other studies difficult |
| Found: PIs reported on ‘knowledge translation’. From the 173 projects, 59 examples contributing to synthesis reports or guidelines, many projects thought to have potential health-care benefits | ||||||||
| 6 | Banzi et al.4 | 2011 | Methodological | N/A | All health research | Cochrane review of approaches: highlighted five categories of impact from the CAHS/Payback Framework approach | Highlighted the payback categories: knowledge; capacity building; informing policies and product development; health and health sector; economic and social | Independent review confirmed findings from HTA review2 that the Payback Framework is the most frequently used approach. Limitations in previous studies: often based on information from researchers or funders; attribution; counterfactual and rarely a control situation; choosing appropriate timeA shared and comprehensive conceptual framework does not seem to be available yet and its single components (epidemiological, economic, and social) are often valued differently in different models |
| 7 | Barnhoorn et al.346 | 2013 | Methodological | EU | EU: public health innovation projects | Described the development and operation of a web survey of country informants | General focus on uptake of the innovations but no details given of the specific impacts. No details supplied about results | Illustrates increased interest in assessing impact; encouraged more thinking on the issue |
| 8 | Battles et al.347 | 2014 | Application | USA | AHRQ: Healthcare-Associated Infections Prevention Programme | No conceptual framework stated and no methods explicitly described as the account appears in a section of the journal headed: Agency Perspective. Presumably an ‘insider account’ | Examined: explored the knowledge produced, potential and actual impacts in terms of improved health care | Being conducted from within the agency provided an understanding of how the programme developed. However, it is not a formal or independent study of impact. As an agency covering both health-care research and quality, AHRQ seemed to be well placed to be involved in implementing/rolling out findings of a successful project |
| Found: a range of projects with notable findings and others that were promising. Some considerable impact:CUSP for CLABSI [central line-associated bloodstream infections] achieved a successful national roll-out and significant results, reducing CLABSI rates by 40% from baseline | ||||||||
| 9 | Bennett et al.57 | 2013 | Both | Kenya and Uganda | FIC: research training programmes | Informed by the Payback Framework and contribution mapping, and by approaches to assessing research capacity building. Case studies based on semistructured interviews (53 trainees and others), focus groups (26 participants), structured surveys, document review, e.g. reviewing policy documents for citations to trainees’ publications | Contribution to policy and programme developmentThere were numerous examples of work conducted by former FIC trainees that influenced national and global policiesImpact not solely as a result of FIC training grants, but that support often critical. Various barriers to policy impacts | Multimethod approach. An important example is that it shows considerable impacts from development training grants. However, some of the lines of attribution are particularly difficult to establish for training grantsFacilitators for this influence included . . . professional networks spanning research and policy communities |
| 10 | Bernstein et al.348 | 2006 | Methodological | Canada | CIHR | Payback Framework: describes how CIHR adapted the multidimensional categorisation of benefits from the Payback Framework. Describes the sources of information that might be used for each category | Five main categories of Payback Framework with some adaptions in the details: knowledge production; research targeting and capacity building; informing policy; health and health sector benefits; economic benefits | Could be seen as an important step between the Payback Framework and its adoption/adaptation in the ROI report by the CAHS |
| 11 | Catalan Agency for Health Technology Assessment and Research58 | 2006 | Application | Catalonia | TV3 telethon for biomedical research in Catalonia (different specialty each year) | Payback Framework: adapted and applied somewhat differently from how the original categorisation and model were brought together. Review of documents related to all projects (320) funded from 1993 to 2002. Survey of researchers for all completed projects (164 PIs = 72%). Bibliometric analysis. Desk analysis for comparisons with other programmes | Examined: patents, publications, research training and targeting of future research, application of the results in health care and health gain | Multimethods approach provides an assessment of how the programme contributed significantly to the Catalan health research system. However, difficulties were encountered with collecting the diverse data and most of the data on impacts on health care seemed to be potential impacts. Findings were presented in a way that makes it difficult to compare with some other quantitative assessments of multiproject programmes, but built on in a series of later studies |
| Found: considerable impact in terms of primary results (publications), secondary results (PhDs, targeting further research), and potentially on health care | ||||||||
| 12 | Boaz et al.5 | 2009 | Methodological | N/A | Review covering policy-making in any field but particular focus on strategic levels and on waste, environment and pollution policy | A total of 14 frameworks revealed: many little used; the lower in the list, the more it is used (as at 2007):
|
Very few frameworks are actually being used In the international development literature, studies traditionally favour ‘qualitative, participatory evaluations with a focus on learning and service improvement’. Methods such as ethnographic site visits and storytelling are used to capture multiple voices in what are usually presented as ‘positive utilisation narratives’. However, government donors, in particular, increasingly question the veracity of such narratives and favour external evaluations that use quantitative methods and predefined performance indicators EU research programmes – usually assessed by panel reviews |
Extensive systematic search of multiple databases to identify primary papers. Good review of difficulties assigning attributionThe approach selected to evaluate the impact of research programmes on policy also needs to be sensitive to the context in which the evaluation will be undertakenPanel reviews attract criticism for their reliance on experts, but they do have the advantage of building ownership through the participation of individuals from diverse EU countries. This is particularly important in a European context and underlines the importance of selecting methods that are fit for purpose and appropriate to the needs of key stakeholders |
| 13 | Bodeau-Livinec et al.82 | 2006 | Application | France | French Committee for the Assessment and Dissemination of Technological Innovations: HTA | None stated, but approach to scoring impact appears to follow the earlier studies of the HTA Council (CETS) in Quebec reported in the 2007 review: Jacob.43,44 Semidirective interviews with stakeholders affected by the recommendations (n = 14); and case studies that used surveys in hospitals to examine the impact of the recommendations (n = 13) | Examined: the impact in terms of interest in the recommendations and how they are used in decision-making, etc. | Using two mutually supportive approaches to data collection increases credibility. However, small numbers were interviewed and there was difficulty in establishing attribution. Main factor fostering compliance with recommendations ‘appears to be the existence of a system of regulation’. Reviewed other studies:All these experiences together with our own work suggest that the impact of HTA on practices and introduction of new technologies is higher the more circumscribed is the target of the recommendation |
| Found: widespread interest, ‘used as decision-making tools by administrative staff and as a negotiating instrument by doctors in their dealings with management . . . ten of thirteen recommendations had an impact on the introduction of technology in health establishments’: seven considerable and three moderate | ||||||||
| 14 | Brambila et al.137 | 2007 | Both | Guatemala | Population council: programme of operation research projects in reproductive health in Guatemala | Developed an approach that considered process, impact and contextual factors. Drew on literature such as Weiss.34 Key informant interviews; document review; and site visits to health centres and NGOs implementing or testing one or more operations research interventions. Based on the information collected the evaluation team scored 22 projects (out of 44 conducted between 1988–2001). Used a 3-point scale to score each project on 14 process indicators, 11 impact indicators and six context indicators | Aim:to evaluate ‘impact’ (the extent to which change occurred)Indicators included: was the intervention effective in improving service delivery; did the organisation act on the results after the operations research study; if effective, was it scaled up; was it replicated in another country; did the donor, or other donors, fund new activities based on the results | Used the impact literature to inform detailed analysis of a programme. However, no indication given on how the 22 projects were selected for scoring. The several 5-year cycles of funding:allowed for the accumulation of evidence in addition to the development of collaborative ties between researchers and practitioners, which ultimately resulted in changes to the service delivery environmentIn highlighting how impact can arise from a long-term approach it refers to the even longer-term projects such as Matlab in Bangladesh, which has hada profound impact on national health policy, donor priorities and public health action |
| Found: out of the 22, 13 projects found that the intervention was effective in improving results, three found interventions were not effective; in 14 studies, implementing agency acted on the results; nine interventions scaled up in the same organisation; five were adopted by another organisation in Guatemala; some studies led to policy changes, mainly at the programme level | ||||||||
| 15 | Brutscher et al.37 | 2009 | Methodological | Canada (review conducted from UK for CAHS report) | Conducted for health research by reviewing approaches in all fields | Reviews eight frameworks for evaluating research. (For a full analysis of how we drew on these see Appendix 5). Four are health specific: Leiden University Medical Centre (in our review see Mostert et al.100); measure of research impact and achievement – Australia, but ex ante; Payback Framework; and congressionally directed medical research programmes. Three are for research in general: VINNOVA (Swedish government agency for innovation – see Eriksen and Hervik94); UK Department for Innovation, Universities and Skills (economic impacts – see Department for Innovation, Universities and Skills106); and EU FP. One is used widely for USA government programmes: programme assessment rating tool (see Williams et al.92) | Analysed: five key elements in the frameworks: evaluation objectives; outcome measures; levels of aggregation; timing and evaluation methods | Identified there were likely to be trade-offs in the choice of key elements of evaluation frameworksIn particular, the choice of an evaluation objective, we find, is immensely important. It, directly or indirectly, influences the appropriateness of all other key elements |
| Found: significant differences between the evaluation frameworks. Only four frameworks go as far as assessing actual impacts | ||||||||
| 16 | Bumgarner et al.349 | 2006 | Application | International research (USA research organisation and review conducted by team from USA) | Center for Global Development: international development | No framework stated. In-depth interviews (more than 150); worldwide audience survey (more than 1200 respondents); documentary analysis and mapping; and case studies | Does research agenda meet the needs of its policy-making targets? Is the research high quality? Does it influence other researchers? Is the communications strategy achieving its desired impact? Is it building appropriate partnerships? | Comprehensive evaluation of impact of the programme of work of the Centre, independently conducted, and commissioned by a consortium of organisations that fund the centre. Having a large number of interviews addressed the challenge of showing impact on policy. In addition, evidence was cross-checked with publication dates and the perceived relevance of the research was important. However, the wide range of activities and the large potential audience were challenging to address. Much of this international research was not in health. Center for Global Development’s research and advocacy work for policy influence widely seen as ‘timely, empirically or analytically based, and highly effective among its audience’ |
| Found: many policy-makers in the audience survey discuss or use Center for Global Development’s policy research and analysis, which is generally well respected (though some complaints). Some limitations on the extent of outreach. Some work had a major impact on policy, including on the Making Markets for Vaccines Initiative350 where its work turned an existing idea into a concrete policy proposal | ||||||||
| 17 | Bunn59 | 2010 | Both | UK | Various health topics covered by systematic reviews | Payback Framework and RIF (Kuruvilla et al.123). Bibliometrics and documentary review | Knowledge production, research targeting, informing policy development, impact on practice | Limitations discussed; many factors associated with impact identified. PhD study examining impact of authors’ own systematic reviews and links to the author’s wider attempt to highlight the impact of Cochrane reviews351 |
| Found:The reviews had influenced the development of national and international policy, although much of the impact was at a ‘micro’ level in the form of practice guidelines | ||||||||
| 18 | Bunn and Kendall60 | 2011 | Both | UK | Health visiting | Informed by aspects of Payback Framework and RIF. Mixture of working forwards and backwards. Documentary and literature review (starting with 30 published policy documents and checking for impact from research), citation tracking (Web of Science, Scopus, and Google Scholar) and interviews with researchers (n = 7) about the impact of their own research | Impact on policy | Range of methods. Drew on analysis in Hanney et al.2 to combine mostly working backwards from policy documents in the specific field, but also forwards from individual researchers. However, not focused on a specific programme of research |
| Found:Although there were examples of policy documents being informed by health visiting research it was not always clear what role research had played in the development of recommendationsResearchers gave examples of impact on local, national and international policy impact, though often from bodies of research | ||||||||
| 19 | Bunn et al.61 | 2014 | Application | UK | NIHR: Cochrane systematic reviews from the supported CRGs | Applied same framework as developed in Bunn59 that was informed by aspects of Payback Framework and RIF. Questionnaires to review groups (20; 87% responded); documentary review; data verification and analysis; semistructured telephone interviews with users (i.e. eight guideline developers); detailed study of 60 reviews: questionnaire to review lead authors (60; 48% responded) and bibliometric analysis | As above on Bunn et al.:59 knowledge production, research targeting, informing policy development, impact on practice | Strength that overall considerable data collection using a range of methods, with interviews providing explanations for figures showing the impact being made on policies:Results from the semi-structured interviews suggest that searching for relevant Cochrane reviews is part of the guideline development processAlso limitations on use of reviews, e.g. out of date or not fit for the guideline scope. Possible weakness: only able to conduct detailed analysis on 60 of the 1502 reviews. Identified limited evidence on impact on practice:more work is needed to develop suitable methods for evaluating the impact of systematic reviews |
| Found: 1502 reviews between 2007–11. Of the 60 reviews, 27 had been cited > 100 times. Identified 40 examples where reviews informed further primary research. Thirteen (22%) of the surveys from authors said had influenced primary studies. Overall, there were 722 citations in 248 guidelines or evidence reviews behind them. A total of 481 reviews were in at least one guideline. Eight CRGs and 12 authors gave examples of impact on practice or services, but most did not know | ||||||||
| 20 | Buykx et al.352 | 2012 | Methodological | Australia | HSR | Developed the health services RIF, synthesising RIF (Kuruvilla et al.123), Lavis et al.,353,354 and the Payback Framework – the version developed by Kalucy et al.65 | Identified main areas of impact to assess: research related, policy, service and societal. Also planned to consider whether the impact originated with the researcher (i.e. producer push) or the end-user (i.e. user pull) | Planned to use to evaluate own research |
| 21 | Cacari-Stone et al.176 | 2014 | Both | USA | Public (ethnic) research | CBPR policy-making framework. Consists of four linked circles: context (which sets the stage for) the CBPR process (which feeds into) the policy-making process (which influences) outcomes Six case studies (using multiple methods – individual in-person interviews, focus groups, policy-maker telephone interviews, archival media and document review, and participant observation) |
Outcomes include political action, policies (formal/informal), changed policy landscape (e.g. improved distributive justice) and hence health outcomes | Strong, trusting pre-existing community–campus relationships. Tension for change (e.g. widespread local awareness of injustice). Dedicated funding for the CBPR activity. Wide range of research methods used to collect multiple data sources (‘street science’ and academic research) to produce robust and credible account of local inequalities. Effective use of these data in civic engagement activities including media campaign and broad-based public awareness with different sectors of the community Diverse and effective networking with intersectoral partners including advocacy organisations |
| 22 | Caddell et al.96 | 2010 | Application | Canada | IWK Health Centre, Halifax, NS, Canada. Research operating grants (small grants): women and children’s health | RIF: adapted. Online questionnaire to 64 principal investigators and co-principal investigators (39 completed surveys: 61%) | Five subsections: impact on research; policy; practice; society; personal: self or career development | Pioneering study of small grants. However, relatively low response rate and sample size, and reliant on a single data collection method – self report from researchers. An association between presenting at conferences and practice impacts. Authors stress the link between research and excellence in health care:It is essential that academic health centres engage actively in ensuring that a culture of research inquiry is maintained and that support is available to those researchers that may ultimately contribute to the excellence in health care |
| Found: 16% policy impact: 8% in health centre; 8% beyond; 32% said resulted in a change in clinical practice; 55% informed clinical practice by providing broader clinical understanding and increased awareness; 46% improved quality of care; 87% improved research skills | ||||||||
| 23 | CAHS7 | 2009 | Methodological | Canada | All health research | Appendix C reviewed a range of frameworks starting with Payback Framework on which the framework in the main report built. Other frameworks reviewed: Walt and Gilson’s analytical model, RIF, research utilisation ladder, Lavis’s decision-making model, the AP Weiss logic model approach, HTA organisation assessment framework, societal impact framework, and the BSC | Appendix E identifies indicators of impact organised according to the five categories of impact from the Payback Framework | The full report is probably the most systematic and important analysis of research impact assessment in the review period. An account of the report’s key recommendations is contained in our comments below on the article by Frank and Nason.115 Appendix D analyses a series of key issues facing research evaluation including: attribution (and the role of logic models and case studies in addressing this); the counterfactual (‘Having a framework that can understand the different external contextual factors that may have been involved in impacts makes understanding the counterfactual easier’; internal and external threats to evaluation validity; time lags to impact |
| 24 | CIHR355 | 2005 | Methodological | Canada | All CIHR health research | All three approaches to measuring research impact reviewed were found to have intellectual agreement on key issues, although the ways of conceptualising returns differed. It was decided to adapt the five-dimensional categorisation in the Buxton and Hanney’s payback model39 for CIHR’s framework. Recommended methods include a variety of approaches should be used as appropriate for subject area and stakeholder concerns. Include case studies or narratives and indicators of achievement in specific areas defined by the five impact categories | Adapted the five-dimensional categorisation in the Buxton and Haney’s payback model39 | Following an expert meeting, a draft framework was developed. It was reconciled with CIHR’s Common Performance Measurement and Evaluation Framework to ensure consistency with existing evaluation activities and to build on initiatives under way within the 13 institutes of CIHR |
| 25 | Carden356 | 2009 | Application | International studies (Canadian report) | International development: wide range (one case study health) | Case studies (n = 23): interviews and documentary analysis | Policy | Full report from International Development Research Centre allows detailed analysis of strengths and weaknesses of case study approach. Seems to be separate from funder(s) of projects |
| 26 | Cohen et al.52 | 2015 | Both | Australia | NHMRC: intervention studies in various programmes | Adapted categories from the Payback Framework and the CAHS framework, and aspects of case study scoring from UK’s REF. Mixed-method sequential methodology. Chief investigators of 70 eligible intervention studies who completed two surveys and an interview were included in the final sample (n = 50; 71%), on which post-research impact assessments were conducted. Data from the surveys and interviews triangulated with additional documentary analysis to develop comprehensive case studies. Case studies that indicated policy and practice impacts were summarised and the reported impacts were scored by an expert panel using criteria for four impact dimensions: corroboration, attribution, reach and importance. The scoring system separately considered reach and importance/significance ‘so as not to downplay the potential impact of smaller studies, or studies with small target groups’ | Developed a categorisation of impacts and mapped it onto the Payback categories. There were four main categories: scholarly outputs, translational outputs, policy and practice impacts, and long-term outcomes. Each has subcategories, five of which relevant to this study: within the translational outputs subcategory ‘intervention packaged for implementation’, and within policy and practice:changes to practice, changes to services, policy change, commercialisation | Case studies on all of the projects that met the inclusion criteria rather than applying any selection criteria. Multiple methods combined to form an innovative approach that included attempting independent verification of claimed impacts and advances in the approach to scoring impact case studies. Addressed issues such as attribution and corroboration by the data collection methods used and the scoring system. However, overall, there were issues with the scoring; the whole process was resource intensive. Had sufficient time been allowed for the impacts to occur? Authors note that:We found that single intervention research studies can and do have concrete and measurable post-research real-world impacts . . . on policy and practiceThis study adds to the view that the degree of impact identified (at least over relatively short time scales) might vary depending on the type or research, and context in which it is conducted and the findings presented |
| Found: 19 (38%) of studies had at least one impact in the categories listed. There were a total of 21 translational impacts and 21 policy and practice impacts. Examples given of each. Scoring resulted in projects being classified into high, medium and low impact score groups. Case studies provided illustrations of high impact | ||||||||
| 27 | Contandriopoulos et al.163 | 2010 | Methodological | N/A | HSR | Review of knowledge exchange; evidence into policy | How research knowledge is taken up and used in health-care organisations and policy settings – and why this process often fails | Knowledge may be individual or collective. Collective knowledge exchange differs when there is disagreement on values and priorities. If this is the case, scientific criteria, such as ‘strength of evidence’, may be overshadowed by political ones |
| 28 | Currie et al.357 | 2005 | Both | Canada | Health promotion and community development | Impact model for community–campus partnerships. Methods not clearly stated. Implicitly, the model is used to guide the development of bespoke metrics and indicators that can be used to track the project. A brief example sketched of the work of the Research Alliance for Children with Special Needs. See King et al.188 for a later application | Three domains of impact in community campus partnerships:
|
Strength: ‘systems’ model that recognises multidirectional influence, direct and indirect. Impact at multiple levels (individual, organisational, system) Limitation (to some extent acknowledged by researchers): model is outcome focused and does not address ‘structural elements of partnerships and audiences, nor processes that could be utilized to enhance research impacts’. (Hence does not look at partnership dynamics, absorptive capacity, social capital, or engage with literature on CBPR or with the political/emancipatory nature of much CBPR) |
| 29 | de Goede et al.158 | 2012 | Both | The Netherlands | Epidemiology and public health | Adaptation of Weiss’s model of research utilisation (meaning most policy impact is indirect and non-linear, achieved via interaction and enlightenment). Three case studies: interviews, ethnography and document analysis, with special focus on analysing the interactions in deliberative meetings among policy-makers | Model is more focused on processes than end-impacts: assumption that much of the impact is indirect and diffuse, hence it is the interactions and influences that matter. Structured framework for capturing the complexity of research utilisation, consisting of three phases:
|
Explore barriers to effective uptake of research: expectation (are policy-makers ‘ready’ for these findings?), transfer (how effectively and appropriately are findings communicated?), acceptance (are findings seen as credible and true?) and interpretation (what value do policy-makers place on them?). A significant barrier to uptake was different framings of problems (epidemiologists focused on ‘healthy behaviours’ whereas policy-makers took a more social framing and considered things like school drop-outs or domestic violence). Some policy-makers found the local health messages so irrelevant to their view of the problem that they did not use them at all. Early involvement of policy-makers in the process of producing local health messages appeared to make it more likely that they would be used |
| Found: most impacts were conceptual. Case studies considered the fate of ‘local health messages’ produced by researchers but intended for local policy influence. Policy-makers rarely took a local health message and immediately implemented it in ways that resonated with researchers’ model of the problem | ||||||||
| 30 | de Goede et al.358 | 2012 | Both | The Netherlands | Epidemiology and public health | Extension of de Goede158 described above. Again adaptation of Weiss’s model of research utilisation. Extended above study by including a quantitative scale for measuring kinds of utilisation. Case studies. This paper reports development and use of a questionnaire to 155 local policy-makers. Sets of questions linked to each of the three ways evidence used (see the next column) | Use of epidemiological evidence instrumentally (in specific and direct ways to solve a particular problem), conceptually (in a more general way to improve understanding of problems) or symbolically | More about how research is used than the impact of a programme of research. The various ways that the research was used were treated as dependent variables, with various independent variables tested for correlation (e.g. whether the policy-maker had previous experience of research or was involved in the research process) |
| 31 | Deloitte Access Economics25 | 2011 | Both | Australia | NHMRC: subset – cardiovascular disease, cancer, sudden infant death syndrome, asthma and muscular dystrophy | ROI analysis (cost–benefit analysis). Outcomes measured as: net benefit and benefit-to-cost ratio. Collation of funding data and estimation of projected benefits | Gains in well-being measured as reductions in DALYs gains in averted costs incorporated as well as productivity and indirect gains. Benefit-to-cost ratio: cardiovascular disease, 6.1; cancer, 2.7; sudden infant death syndrome, 1.2; and muscular dystrophy, 0.7 | Valid attempt to value monetised health benefits and equate with a lagged investment period, also accounting to some extent for problems of attribution. However, weaknesses include the use of projected health gains – ‘unknown unknowns’ and a weak basis for time lag between R&D and health gains. Does not seem to account for delivery costs of new interventions. Some disagreement about robustness of DALYs |
| 32 | Dembe et al.124 | 2014 | Methodological | USA | All health | The translational research impact scale: informed by a logic model from W.K. Kellogg Foundation, by the RIF (Kuruvilla et al.123) and the Becker Library (Sarli et al.118). Identified 79 possible indicators used in 25 previous articles and reduced them to 72 through consulting a panel of experts, but further work was being undertaken to develop the requisite measurement processesOur eventual goal is to develop an aggregate composite score for measuring impact attainment across sites | Three main domains: research-related impacts; translational impacts (that include ‘improvements result in better quality of care’); societal impacts | Would be comprehensive; however, feasibility yet to be reported on and number of subdomains and indicators in each domain varies considerably |
| 33 | Department for International Development8 | 2014 | Methodological | International studies (review conducted in UK) | Review of studies assessing impact of international development research, including health | Devised own theory of change that combines four major pathways by which research has been hypothesised to contribute to development. There are four pathways going from the supply of research and from the demand for research outputs towards poverty reduction and improved quality of life: economic growth, human capital, products and technologies, and evidence-informed policy/practice | Broadly structured review around the pathways developed: economic growth, human capital, pro-poor products and technologies, evidence-informed policy/practice, quantifying economic impact | Reviewed and organised a large number of papers and usefully challenges some assumptions about the benefits from research, but did not include some important papers from the health sector, e.g. Brambila et al.,137 showing how long-term programmes of health research can make an impact |
| 34 | Donovan128 | 2008 | Methodological | Australia | All research fields | RQF recommended the impact of Australian higher education could be assessed by research groups producing:A statement of claims against impact criteria, up to four case studies illustrating examples of impact, and details of end users who can verify the impact claimsAssessment panels would review the evidence portfolios and:apply their collective expert judgement to determine the validity of the claims made against the impact criteria. Impact ratings will be assigned . . . The Working Group recommended the Payback consensus scoring approach as particularly suited for this purpose | Wider economic, social, environmental and cultural benefits of research | Describes the RQF that became a key element in the development of methods to assess the impact of research in a national scheme across the entire system of higher education. Although it was not eventually introduced in Australia, it was drawn on in recommendations that the REF adopt impact case studies |
| 35 | Donovan et al.62 | 2014 | Application | Australia (assessment by UK team) | National Breast Cancer Foundation: key programmes | Payback Framework. Documentary analysis, bibliometrics, survey (242 sent – 63% response rate), 16 case studies and cross-case analysis. Applied to a range of funding schemes used by the charity | The five payback categories: knowledge, research, policy and product development, health and economy | Thorough study funded by the charity that announced the findings would be used to inform their research strategy; however, many projects had only recently been completed |
| Found: citation rate between 2006 and 10 was double the world benchmark; 185 higher degrees (121 PhDs); 46% career progression; 66% generated tools for future research use; leveraged additional AUS$1.4 for each dollar spent; 10% impact on policy – 29% expected to do so; 11% contributed to product development; 14% impact on practice/behaviour, 39% expected. Brief accounts of case studies included some important examples of impacts achieved | ||||||||
| 36 | Drew et al.90 | 2013 | Both | USA | NIEHS: all programmes of environmental health sciences research | High-impacts tracking system. A framework informed by stream of work from NIEHS (Engel-Cox et al.,63 Orians et al.17), also the Becker Library approach (Sarli et al.118) ‘closely aligned with the categories we used in our logic models, and also informed our ontology’. Also informed by the development in the UK of researchfish. High-impacts tracking system:an innovative, Web-based application intended to capture and track short- and long-term research outputs and impactsImports much of the data from existing NIH databases of grant information, also text of progress reports and notes of programme officers/manager | Outputs: scientific findings, publications, patents, collaborations, animal models, biomarkers, curricula and guidelines, databases and software, measurement instruments and sensors | This is one part of ambitious plans being developed by NIEHS for use by them. However, they are still evolving and recognise the need to develop ways to capture long-term impacts and ‘expert opinion and review of specific program areas’. A growing interest in UK developments in impact assessment illustrated by fact that informed by the researchfish approach |
| Impacts: improved health/disease reduction, exposure reduction, policies and regulations, community benefit, economic benefit | ||||||||
| 37 | Druce et al.359 | 2009 | Application | International | IAVI | None stated beyond assessing the extent to which IAVI met its strategic objectives over period 2003–7. Qualitative and quantitative: documentary review; interviews (100+); and field visits | Assessed initiative’s accomplishments in the following: R&D; clinical trials; advocacy and communications; policy | Comprehensive evaluation independently commissioned and conducted, using a range of methods. Denied access to individual partnership agreements for reasons of confidentiality. Not specifically an assessment of impacts, but the IAVI objectives included items such as policy. However, IAVI produces policy analysis more than producing research used in policy |
| Found: added scientific knowledge; built capacity; been a leader in advocacy for HIV vaccines; ‘important value-adding contributions to policy issues’ | ||||||||
| 38 | Engel-Cox et al.63 | 2008 | Both | USA | NIEHS: intended for all programmes of environmental health sciences research | NIEHS logic framework developed and identified a range of outcomes informed by the Payback Framework and Bozeman’s public value mapping;360 then added a list of metrics for logic model components. The logic model is complex, as in addition to inputs, activities, outputs, and outcomes (short term, intermediate and long term), there are also four pathways: NIEHS and other government pathways; grantee institutions; business and ‘industry; and community. Each pathway illustrates the research process that would be carried out most directly by a given institutional partner that is being evaluated.’ The model also included the knowledge reservoir, and contextual factors. No explicit description of methods used to conduct the illustrative case studies, but implied documentary review and ‘expert elicitation’ | From payback and value mapping: translation into policy, guidelines, improved allocation of resources, commercial development; new and improved products and processes; the incidence, magnitude, and duration of social change; HSC welfare gain and national economic benefit from commercial exploration and a healthy workforce; environmental quality and sustainability. Range of impacts identified in cases studies | Important methodological development, illustrated in two case studies rather than a full application. Builds comprehensively on earlier work. Having the various pathways allows a broader perspective to be developed (e.g. by the grantee institution pathway) than that of individual projects. However, challenges include:the lack of direct attribution of NIEHS-supported work to many of the outcome measures and the lack of robust electronic databases that can be easily searched to help establish these linkagesThe logic model is complex and:Distinctions drawn between the institutional pathways are artificial to some degree, and there is considerable cross-over between sub-models |
| 39 | Ensor et al.361 | 2009 | Application | Nepal | Maternity: skilled attendance | None stated. Key informant interviews to identify the role of specific research in a key policy | Policy: specific area of financing of skilled attendance at birth | Factors for rapid utilisation: the research processes helped ensure wide communication of the findings; political expediency meant that there was a key political champion advocating a strong policy response |
| 40 | Eriksen and Hervik94 | 2005 | Application | Sweden | VINNOVA: neck injuries research | VINNOVA approach. Mixed approach: economic analysis of benefits for Swedes, the industry and the world compared with the costs. Classic R&D assessment of contribution to the research field: publications, research training, quality of the research, development of networks, etc.: desk analysis followed by review by a panel. Best estimates also made of value of future research | Benefits to society, the companies involved and the research field | Wide-ranging approach including important long-term impacts from long-term funding of a centre. Admitted ‘there is a great deal of uncertainty in these calculations’. Perhaps it is even more challenging than is acknowledged in the report |
| Found:The main impression, therefore, is that the systems for protection against injury described above provide major economic benefits | ||||||||
| 41 | Evans et al.101 | 2014 | Application | UK | Public involvement in health research | Realist evaluation. Mixed-method case study | Factors and interactions that influence successful involvement of patients and the public in research | Strength – clear and rigorous application of realist method supplemented with other perspectives where appropriate. Various mechanisms – collaborative action, relationship building, engagement, motivation, knowledge exchange and learning – which interact with context to produce different outcomes in different parts of the programme |
| 42 | Expert Panel for Health Directorate of the European Commission’s Research Innovation Directorate General53 | 2013 | Application | EU | EU FPs 5, 6 and 7: public health projects | Payback Framework. Documentary review: all 70 completed projects; 120 ongoing; key informant interviews with particularly successful and underperforming projects (n = 16). A data extraction form was constructed based on the categories from the Payback Framework, with each of the main categories broken down into a series of specific questions. Distinction made between expected and achieved | Dimensions adapted from Payback Framework: knowledge production; research capacity building; informing health policy (and practice added after pilot); health and health sector benefits; economic and social impact; dissemination | Used documentary review, therefore, for completed projects had data about whole set. However,Extensive follow-up of the post-project impact of completed projects was not possible . . . we were unable to determine whether project deliverables were accessed and used by the relevant end-users, nor could we examine possible effects on population healthThe study did not include the health equity aspect included in the Payback Framework, or some aspects that could help analysis of the level of attribution. Illustrates a way of conducting impact assessment broadly (apart from the selected interviews) using a framework to interrogate documents and thus have comprehensive coverage of a programme without requiring additional data from the researchers. Also shows the limitations of such an approach |
| Found: only six out of the 70 completed projects did not achieve the primary intended output; 56 peer-reviewed publication; 42% took actions to engage or inform policy-makers; four projects change of policy (22% expected to do so); six impact on health service delivery; seven impact on health practitioners; six impact on health; one beneficial impact on small and medium enterprise | ||||||||
| 43 | Frank and Nason115 | 2009 | Methodological | Canada | All health | Adapted the Payback Framework to develop the CAHS framework. No application but identified 66 validated indicators. Framework based on a report overseen by an expert international panel and supported by a series of commissioned appendices. The panel recognised that ‘The 66 validated indictors currently listed do not cover the full spectrum of possibilities’ and identified a series of implementation challenges | Adapted the five categories in the dimensional categorisation of the Buxton and Hanney’s payback model:advancing knowledge, capacity building, informing decision-making [changed from the original informing policy and product development]; health benefits; and broad economic and social benefits [changed from broader economic benefits]’The authors report the CAHS panel:recommend a method that builds on the advantages of the ‘payback model’ but adapts it to target-specific impacts in multiple domains at multiple levels | Based on the work of an international panel of experts informed by a major review and analysis of many aspects of impact assessment. Highlighted a series of challenges facing any assessment of research impacts, including: attribution, the counter-factual and time lags. The CAHS framework has informed a series of studies. Attempting to develop an inclusive set of indicators has generated additional challenges, whereas the Payback Framework put more emphasis on addressing issues such as attribution through use of case studies |
| 44 | Garfinkel et al.362 | 2006 | Methodological | USA | Perinatal health | Societal outcomes map. ‘Technology road mapping’ can be described as ‘graphical overviews of potential solutions over time to specific concerns’, aimed at clarifying what inputs are needed to produce desired outcomes | Start by cataloguing desired outcomes, then specify inputs, identify potential research and policy paths, and mine the academic literature quantitatively to profile a research domain | Essentially an ‘engineering’ theory. Speculative and deterministic, seems to be a formalised brainstorming process that generates complicated (but not complex) boxes-and-arrows diagrams. Marginal for our review and does not link to assessment of specific programmes of research |
| 45 | Gibbons et al.179 | 1994 | Methodological | N/A | University–society relationships | Co-production. ‘Mode 2’ knowledge is:
|
Reframing of impact in terms of the increasingly complex and diverse infrastructures and relationships that support knowledge production rather than as dissemination, implementation or translation of research ‘findings’ | Pre-dates the current review period, but important for the philosophical taxonomy. Strength: novel and important reconceptualisation. Weakness: few detailed empirical examples hence (when initially published) largely speculative |
| 46 | Gibson et al.363 | 2014 | Application | USA | Comparative effectiveness research: four technologies | Before/after. Time trend. Each of the Comparative Effectiveness Trials identified a clinical practice guideline citing it and included the publication date of each in the analysis | Practice change | ‘This study demonstrates that evaluating the impact on clinical practice, based on results of published CER trials and CPGs, is complex’ |
| Found: no clear pattern of utilisation in the first four quarters after publication. (While this study was not measuring impact by inclusion on a guideline, all four were rapidly cited on one and would have been counted as making an impact in other studies) | ||||||||
| 47 | Glasgow et al.178 | 2012 | Methodological | N/A | Health research | Implementation science. New model proposed | Alignment of mode 1, research-based evidence, with mode 2, socially engaged implementation process | Strength: attempt to integrate mode 1 and mode 2. Weakness: may have inadvertently compromised core assumptions and principles of some models in producing the hybrid. Speculates that by aligning the ‘internal validity’ of RCTs with the ‘external validity’ of social engagement, will have greater impact |
| 48 | Godin and Doré364 | 2005 | Methodological | N/A | Science in general, including health | Developed an approach based on a range of dimensions of society, beyond the economic one, on which science has an impact. Challenges identified (see columns 8 and 9) might help inform methods for impact assessment | Identified a very preliminary list of 72 impacts and indicators within 11 dimensions on which impact could be assessed: science, technology, economy, culture, society, policy, organisation, health, environment, symbolic and training | Suggests three challenges must be met before one conducts any measurement of these types of impact:One is to distinguish conceptually between output and impact (or outcome). The second is to identify specifically the transfer mechanisms by which science translates into impact. The last is to develop appropriate and reliable instruments and indicators |
| 49 | Gold and Taylor138 | 2007 | Application | USA | AHRQ: Integrated Delivery Systems Research Network | Documentary review; descriptive interviews (85); four case studies. Mixed | Changes in operations. ‘Of the 50 completed projects studied, 30 had an operational effect or use’ | Partnerships. Success factors: responsiveness of project work to delivery system needs, ongoing funding, development of tools that helped users see their operational relevance |
| 50 | Graham et al.85 | 2012 | Both | Canada | AlHS: tested on several programmes, e.g. independent investigators to programme (all fields) | Developed and tested an AIHS version of the CAHS framework. Archival review of applications, progress reports, etc. For example, from 215 grantees on independent investigators programme whose awards ended 2004–8 | Started with the five CAHS categories (knowledge, capacity, decision-making, health, social and economic). Added additional one on organisational performance and additional indicators on items such as innovation | Mainly methodological describing how developed AIHS version of CAHS framework, with a particular focus on developing data capture approaches for the many indicators identified. The products and tools generated by AIHS through the framework’s implementation included:(1) a performance measurement system that tracks progress to impact; (2) aggregated and pooled reporting capabilities through the standardization of indicators and metrics across programsThe third point highlights the organisational focus:adoption of additional impact categories, indicators, and measures which improved the organization’s ability to assess and demonstrate its contributions to health system impacts in addition to the contribution of its grantees |
| Found (for independent investigators programme): advancing knowledge, e.g. 3901 publications; building capacity, e.g. CAD$217M leveraged in additional funding; informing decision-making, e.g. guidelines were developed in collaborations with health authorities, industry, government, and non-profit organisations; health care, e.g. 42 improvements to health care were identified through improvements to 30 therapeutics and 12 diagnosis/prognosis techniques; economic and social, e.g. 10 products in development, 5 spin-offs | ||||||||
| 51 | Grant et al.38 | 2009 | Methodological | UK | Review for HEFCE: all university research | Four methods for evaluating impact of university research. Reviewed against HEFCE criteria. Recommended adoption of case study approach as set out in the RQF from Australia (see Donovan128) | Wide range of impacts | Methodological review funded by HEFCE to inform its plans for assessing university research impact. Recommendation informed the development of the REF – see HEFCE33 |
| 52 | Grazier et al.365 | 2013 | Methodological | USA | NIH CTSA: clinical research units programme | ROI analysis (cost–benefit analysis) Essentially adopts a traditional cost–benefit approach. Paper details development of a ROI protocol to enable project-based evaluations of CTSA programme awards. Model development as an iterative process involving stakeholders to identify important components – beginning simple and may be limited by difficulties in identifying, measuring and monetising benefits/costs, hence qualitative data can support quantitative | ROI – timing and magnitude of expected gains/timing and magnitude of expected costs. Proposes methods (e.g. survey, scoping, interviews) for identify availability, accessibility and quality of data and suggests supplementing with qualitative data | Acknowledges that although not all benefits can be quantitatively measured, it is important for wider understanding of impact. Does it add much in comparison to other, more formal/considered approaches? Conjecture: value of return will be a function of a number of characteristics. These include awards through the CTSA and other sources; the institutions at the time of the award, before it and after; the investigator; number of collaborations in the award; length and extent of ‘exposure’ to the clinical research unit of research programmes; all dependant on the scope and boundary discussions with stakeholders and on the synthesised model constructed. Note difficulties in attribution if there are multiple sources of funding, and time lag between investment and health gain |
| 53 | Group of Eight and Australian Technology Network of Universities105 | 2012 | Both | Australia | All research fields | EIA based on the REF. Case studies (n = 162) developed by researchers in institutions to describe the impact achieved from 2007 to mid-2012 by their research conducted from 1992. Case studies then assessed and scored by expert panels containing many people from outside higher education. Panels rated the impacts according to their reach and significance | Explicitly adopted the definition of impact set out in the UK’s 2014 REF assessment exercise. (The EIA trial was designed after the criteria for the REF had been set out, but was conducted before the REF). Focus on measuring the innovation dividend in areas of: defence, economic development, society (including health) and environment | Had the strength of building on the 2014 REF. Reported that the case study methodology ‘to assess research impact is applicable as a way forward to a national assessment of impact’. Weaknesses or problems related to the time taken to put together the case studies, especially if the exercise was scaled up to a national impact assessment exercise, and given the time involved in assessing the case studies ‘more extensive Panel briefings would be essential should this assessment method be adopted at national level’ |
| Found: 87% of cases rated as being in the top three categories out of five (plus a not classified category)High quality research carried out in Australian universities has had enormous benefits for the health, security, prosperity, cultural and environmental wellbeing of Australia, the region and the world | ||||||||
| 54 | Guinea et al.64 | 2015 | Both | International | Seventh EU FP: international development public health research project | Impact-oriented monitoring informed by Payback Framework. Tested and propose elements: (1) project results framework (to be developed by each project co-ordinator during grant negotiation process to help link objectives with activities, results, impacts, and can be updated throughout life of the project); and (2) co-ordinators survey (web based and linked to five payback categories plus dissemination; completed at end of project and after 3 years, and in middle of projects of ≥ 4 years); end-user survey (web based, to people identified by project co-ordinator at end of project); assessment tool (online/web to assess individual projects at end of project and 3 years after on the basis of data gathered as above). In developing tool also conducted nine case studies | Based on five dimensions of Payback multidimensional categorisation, but with the additional category being ‘Pathway to impact’: advancing knowledge; capacity building and research targeting; informing decision-making, practice and policy; population health and health sector benefits; broad economic and social benefits; dissemination and knowledge transfer | Developed own comprehensive methodology informed by existing frameworks and tested a range of methods, but had a low response rate: 28 out of 116 projects. Large-scale EU project funded in the light of EU Court of Auditors criticism of lack of evaluation of EU FP4, FP5 and part of FP6. Aim:Structured information is intended to facilitate and underpin the decision-making of EC officers in charge of project management, and support them in the design of future research topics and programmesSome interesting methodological observations:results from case studies revealed a high concordance with the coordinators’ survey on several facets, for instance, in . . . providing evidence of project performance, and revealing some types of impacts |
| Found: generally findings mentioned only in relation to commenting on methodology | ||||||||
| 55 | Guthrie et al.9 | 2013 | Methodological | USA (review conducted in UK) | All fields | A total of 14 frameworks, six reviewed in detail (REF,33 Excellence in Research for Australia,366 STAR METRICS®,367 CAHS,7 NIHR Dashboard,368 Productive Interactions81). Criteria analysed included purpose: analysis, accountability, advocacy, allocation | The research evaluation frameworks and tools examined covered evaluation in general, not just impacts. Found considerable variety in role and potential of the different frameworks. Suggested CAHS payback could have advantages | Full report analysing many aspects of research evaluation systems. Conducted for Association of American Medical Colleges. In various places our review draws on aspects of this analysis |
| 56 | Guthrie et al.27 | 2015 | Both | UK | HTA programme | ROI. Selected 10 key HTA studies, mostly RCTs but a few systematic reviews, and applied desk analysis | Key impact: per patient QALY gains associated with the intervention monetised at a health-care opportunity cost of between £20,000–30,000 net of health-care costs. Net benefit calculated as a hypothetical full year implementation | Has the strength compared with most other ROI studies of having a clear picture of the cost of the research inputs and detailed case study analysis. Weaknesses: small sample size (10/743); does not adequately address attribution problems but assumes HTA studies were responsible for all post-HTA research implementation as they were considered to be ‘definitive’ evidence |
| Found: only 12% of potential net-benefit would cover the £367M invested in HTA programme | ||||||||
| 57 | Gutman et al.132 | 2009 | Both | USA | RWJF: ALR programme (see also Ottoson et al.369 on the same programme) | The conceptual model used in the ALR programme ‘was used to guide the evaluation’ but aspects needed refinement to give more emphasis to context, attracting additional research funding, and translating research into policy change. Aspects of Weiss’s model used for analysing policy contributions. A retrospective, in-depth, descriptive study utilising multiple methods, both qualitative and quantitative. Qualitative data derived mainly from 88 interviews with key informants: a random sample of grantees; other funding organisations; policy and advocacy organisations; programme leadership and RWJF staff. Quantitative data derived primarily from a web-based survey of grantee investigators (sent to PIs, chief investigators and applicants); of the 74 projects, 68 responses analysed. Analysed the early examples of policy impacts by using Weiss’s framework and found examples of instrumental, political and conceptual use | Building knowledge base, including creation of a new field; building human resources; growing financial resources; contribution to policy debate and change | Comprehensive data collection from diverse sources attempted to assess the impact of the research programme as part of a wider intervention; however, only 16% of competitively awarded grants had been completed prior to the year of the evaluation. The author commended on the limitations:the study design is descriptive rather than quasi-experimental, and therefore does not include a comparison group composed of other RWJF national programsThe author also commented:some approaches utilised by the program worked well, including developing a multifaceted, ongoing, interactive relationship with advocacy and policy-maker organisationsGrantees who completed both interviews and surveys generally gave similar responses, but researchers included in the random sample of interviewees gave a higher percentage of policy impact than researchers surveyed; questions bit different |
| Found:ALR was the catalyst to build a new field of transdisciplinary research focused on policy and environmental factors conducive to physical activityALR investigators leveraged more than two-thirds of the ALR investment; dissemination included synthesis and translation activities by the programme office, 55% of PIs produced policy-related products, effective two-way liaison with some organisations brokered by the ALR programme, interviewees from various organisations reported relationship with the ALR programme beneficial including bolstered the case for action, provided materials, etc. Generally thought to be too early for much policy impact, but 25% of survey, 43% of interviewees reported a policy impact | ||||||||
| 58 | Hage112 | 2009 | Methodological | Canada (part of appendix A of the CAHS report) | Treatment sector of the Canadian health care system | Informed development of CAHS framework | Identifies a series of meso-level metrics of impact that identify, for example, the detailed aspects of impacts on health care that might arise from different phases of research and shows how these might help an impact assessment | Referred to in the main CAHS report which states:This aligns with the paper by Hage (appendix A, p. A79), which argues that meso-level factors—those at the health category level—are vital in understanding the impacts and pathways to impacts of health researchCAHS7Although only a few aspects of the proposals seem to have been taken up in the final main CAHS report, it did inform the thinking |
| 59 | Hanney et al.2 | 2007 | Both | UK | NHS: HTA programme | Payback Framework. Multiple methods approach, literature review, funder documents, survey, case studies, interviews (n = 16) (between 1993 and 2003) | The review found that the Payback Framework is the most widely used approach/model. Impact on knowledge generation can be quantified more than that on policy, behaviour or health gain. A higher level of impact on policy than is often assumed. Primary study: used categories from Payback Framework. The HTA programme had considerable impact in terms of publications, dissemination, policy and behaviour. Different parts of the programme had different impacts, as expected: NICE TARs had 96% impact on past policy compared to 60% for primary and secondary HTA research. The mean number of publications per project is 2.93. Case studies showed large diversity in levels and forms of impacts and the way in which they arise. NICE TARs demonstrate the importance of having a customer (receptor) body for having impact on policy | The survey showed that the data on payback can be collected but more than one-third of the projects did not respond. The review conducted as part of the study identified the Payback Framework as the most appropriate approach to use to assess the impact of the HTA programme. It facilitated capture of key factors in achieving high levels of impact, i.e. the agenda setting to meet the needs of the health-care system, the generally high scientific quality of the research; and the existence of a range of ‘receptor bodies’ to receive and use the findings |
| 60 | Hanney et al.370 | 2006 | Application | UK | One diabetes researcher’s body of research over a certain period | Bibliometrics, surveys to key authors, semistructured interviews with the researcher and experts/users. The bibliometric analysis traced citations through first-, second- and third- generation papers with qualitative analysis of the importance of the work in citing papers | Partly informed by informed by the categories from the Payback Framework, with the articles describing the knowledge produced being particularly important | Qualitative approaches important alongside the bibliometric analysis |
| Found: various examples of impact, and not all papers thought to have make an impact were highly cited | ||||||||
| 61 | Hanney et al.51 | 2013 | Both | UK | Asthma UK: all programmes of asthma research | Payback. Survey, documents, case studies, some expanding the approach | Five categories from the Payback Framework: publications, including follow on; targeting further research and capacity building; policy influence and product development; health and health sector benefits; broader economic benefits | Extended Payback Framework to assess impact from long-term professorial chair funding and cofunding with MRC of a research centre. Also, as intended, informed strategy of the medical research charity |
| Found: various categories of social impact arose from only a minority of projects (13% on policy, 17% on product development, 6% on health gain) but some important influence on guidelines, potentially major breakthroughs in several asthma therapies, establishment of pioneering collaborative research centre | ||||||||
| 62 | Hanney et al.46 | 2013 | Methodological | N/A | Involvement in research in any health field/impact on health-care performance | The review identified papers assessing how far there were improvements in health-care performance associated with engagement in research. Hourglass review – focused and wide review. Built a matrix using an iterative approach:our initial planning and mapping exercise explored several major theoretical approaches that could, potentially, contribute to informing the conduct of the review and to building a framework within which to analyse the mechanisms through which engagement in research can improve performance | To map and explore plausible mechanisms through which research engagement might improve health services performance at clinician, team, service or organisational levels. (Improve understanding of the impact of engagement in health research.) Identified two main dimensions to categorise studies that assessed whether research engagement led to improved performance or not:We have called these two dimensions the degree of intentionality and the scope of the impactOf the 33 studies, 28 studies were positive in showing impacts: 13 described broader impact and 15 described specific impact | The focused review collated more evidence than previously thought, and although it was generally positive it was difficult to interpret One difficulty of applying the matrix arose because some of the papers in our focused review have features that fitted into more than one category on a certain dimension. Nevertheless, it was:important to attempt to make such categorisations because of the potentially very different mechanisms that may be at work in these different circumstances on the two dimensions |
| 63 | Hansen et al.111 | 2013 | Methodological | The European Observatory on Health Systems and Policies | Public health | Summarises four conceptual frameworks: Payback; RIF; European Commission seventh Framework (see next column); and research utilisation ladder. All essentially variants of case study | European Commission FP7: Description of main dissemination activities and exploitation of results; synergies with science education (involving students or creating science material); engagement with civil society and policy-makers (e.g. NGOs, government, patient groups) and production of outputs which could be used by policy-makers; use of dissemination mechanisms to reach the general public in appropriate languages; use and dissemination (peer-reviewed journal articles, patent applications, intellectual property rights, spin-offs); and the employment consequences of the project | Non-systematic review that usefully summarises some approaches but omits others. Importantly suggests:it may not be necessary to develop another version, but rather find clever ways to combine elements from different frameworks to best fit the particularities of a certain research topic |
| 64 | Hera136 | 2014 | Application | Africa | AHSI-RES | Key element of the design: adoption of an interactive model of knowledge translation. A theory-driven approach was used by constructing post hoc results frameworks for 6 of the 10 research projects according to a generic theory of change model for the programme. Then participatory workshops were held with the research teams to test the frameworks against the reality of implementation. Data gathered by a range of methods including documentary review; interviews at programme level; project-level information – for six projects workshops (see next column), and for the remaining four a total of 12 interviews with 16 members of research teams; participant observation of end-of-programme workshop, at which the team also presented some preliminary findings | Relevance; research capacity building; policy impact; social and gender equity; sustainability | There was a range of methods and it did assess using the logic model of the programme; however, it was completed just before the end of the programme, therefore, only identifying early impact. Abstract:Research teams who started the policy dialogue early and maintained it throughout the study, and teams that engaged with decision-makers at local level, district and national levels simultaneously were more successful in translating research results into policy actionTiming of evaluation raises interesting questions. Positive – were able to observe the final programme workshop and present preliminary findings. Negative – too early for some of the impact, but interactive approach of whole programme led to some policy impact during project |
| Found: a highly relevant structure that responded to the needs for research capacity building (but mainly only in institutions with little background in the field) and knowledge translation. Policy impact was created during the research process: 7/10 projects reported policy impact already. More progress in focusing research on pro-poor issues than on gender. . . the uptake of generated evidence in national health policy or international policy guidelines. Because of the interactive nature of AHSI-RES significant results have already been achieved, but the policy dialogue is not yet complete and further uptake can be anticipated | ||||||||
| 65 | HEFCE33 | 2012 | Methodological | UK | REF: Medicine and Life Sciences | REF Impact Assessment. Impact template is a description of the environment and activities in a higher education institution oriented to maximising impact Impact case study is a four-page description of a research project/programme and ensuing impact, with references and corroborating sources |
. . . benefits to one or more areas of the economy, society, culture, public policy and services, health, production, environment, international development or quality of life, whether locally, regionally, nationally or internationally. . . manifested in a wide variety of ways including, but not limited to: the many types of beneficiary (individuals, organisations, communities, regions and other entities); impacts on products, processes, behaviours, policies, practices; and avoidance of harm or the waste of resources | At the time that this guidance was published, the approach was largely untested, though there had been a ‘dry run’. The development of the approach can be traced through from the RQF in Australia (Donovan128), through the HEFCE commissioned review (Grant et al.38) to these plans |
| 66 | Home371 | 2008 | Application | UK | UK prospective diabetes study: type 2 diabetes mellitus | Drew on application of aspects of the Payback Framework Home had coauthored in Hanney et al.370 Narrative review by expert diabetes ‘insider’ | Publications, guidelines, education material, changes in monitoring, treatment and health outcomes | The UK Prospective Diabetes Study resembled a programme in that it consisted of a group of clinical trials, epidemiological analyses and health modelling studies. Not a formal impact assessment but more of an insider’s review drawing on author’s experience as a leading diabetes medical academic, and his involvement in a previous research impact assessment in the field |
| Found: 85 full papers, 78% in leading journals; cited in many guidelines, and not just in those relating to diabetes, but traces a complex picture of how citations of papers can get overtaken by citation of reviews that cite the papers: ‘considerable impact on available educational material’. Influenced monitoring and treatment:By inference it must be responsible for a significant part of the improvement in health outcomes in people with Type 2 diabetes over the last decade | ||||||||
| 67 | Jagosh et al.173 | 2012 | Both | N/A | CBPR | CBPR. Systematic review using realist principles | If delivered effectively, CBPR can:
|
Strength: rigorous application of realist methodology. Weakness: findings pertain only to CBPR; relatively small sample of high-quality studies. Factors: extent to which research designs are culturally and logistically appropriate; extent of measures to develop capacity and capability in stakeholder groups; how and to what extent conflicts are managed; and extent to which mutual trust builds over time |
| 68 | JISC372 | 2013 | Both | UK | Jisc Business and Community Engagement programme: partnership projects in a range of fields including health | The central team provided projects with an evaluation framework designed to help projects ‘to target and identify the emerging impact of their project’. Various projects drew on existing frameworks and tools including the Research Contribution Framework,373 stakeholder analysis. This report is based on detailing the learning from nine tripartite partnership projects set up to develop capacity in universities to embed impact analysis in research using the expertise of business and community engagement practitioners and information management specialists. Projects were ‘experiential and action learning approaches’ | Progress in the individual projects including: drawing on existing knowledge and frameworks about impact; developing and testing a model; delivering a system that is theoretically robust, practical to use and meets needs of stakeholders | Not health specific but some projects related to health, e.g. the Emphasising Research Impacts project at Newcastle University faculty of Medical Sciences. Of marginal relevance because not a standard research impact assessment because the programme consisted of projects developing the capacity to enhance and assess impact. However, this is another dimension of the increasing emphasis on impact assessment |
| Found: the overall accounts report challenges, but, ‘in spite of these challenges, the projects reported many positive outcomes’ – improved understanding of impact, improved evaluation strategies embedded within research groups, greater awareness of training needs, ‘improved focus on who to engage to maximise the potential of the impact of the research’ | ||||||||
| 69 | Johnston et al.75 | 2006 | Both | USA | National Institute of Neurological Disorders and Stroke: programme of clinical trials – all pre 2000 Phase III RCTs | ROI analysis. Health economic modelling used to estimate ROI from 28 RCTs | NIH funding of Phase III trials equated with quasi-societal returns (aggregate treatment costs/savings and health gains measured in QALYs, valued based on USA GDP per capita) based on projected usage. Eight RCTs had adequate data to estimate usage/cost/effects. Twenty-eight trials with a total cost of US$335M were included. Six trials (21%) led to improvements in health. Four (14%) resulted in cost savings. There were 470,000 QALY in 10 years since funding of trials at cost of US$3.6B. The projected net benefit was US$15.2B. Yearly ROI 46% | Innovative quantitative attempt to value benefits of a specific programme of research, net the costs of delivery of new interventions. Incorporate standard health economic information. However, limited by incomplete data and reliance on published work for model inputs. Inherent problems with cost–utility analyses and imprecise estimates. Unclear about the quality of data on usage, in particular. Another example of economic value assessment showing large gains, and an important development in the field because of its application to the programme level |
| 70 | Kagan et al.374 | 2009 | Methodological | Global research (analysis conducted in USA) | NIH: global HIV clinical trials research programme | Construct a new conceptual framework through a participatory process for an evaluation system for the National Institute of Allergy and Infectious Diseases HIV/AIDS clinical trials programme | Developed a concept map of success factors. The evaluation framework depicts a broad range of factors that affect the success of the clinical research networks. There is an average importance rating for each of the ideas (on a 1–5 scale) and average importance rating of the statements within each cluster, biomedical objectives (highest average rating score: 4.11), scientific agenda setting (4.06), collaboration communication and harmonisation (3.81), operations and management (3.80), Division of AIDS policies and procedures (3.96), resource utilisation (4.00), community involvement (4.05) and relevance to participants | Strengths: careful analysis of a pioneering and participatory process to develop a new conceptual framework mapping success factors Limitations: the results of the development of the conceptual framework are context specific. The ideas generated, organised and prioritised by the stakeholders were specific to the Division of AIDS clinical networks, thus limiting the generalisability of the results |
| 71 | Kalucy et al.65 | 2009 | Application | Australia | Primary health care | Payback. Telephone interviews (n = 13) plus bibliometric analysis of publications and analysis of range of project documents | Payback categories | Pioneering application of the Payback Framework – tested in the context of plans for the introduction of RQF in Australia (see Donovan128). Some limitations:
|
| Found: in testing the approach the Payback Framework was found to be robust and applicable. Advantage over bibliometric analysis – picked up many more publications especially in applied research where most outputs were not indexed on Web of Science. Four case studies consisted of one RCT, one action research study and two case note audits. The ‘logic model’ of the Payback Framework worked better for the RCT than for the action research study where there was input from ‘users’ at every stage in the research | ||||||||
| 72 | King et al.375 | 2009 | Methodological | Canada | HSC, community–campus partnerships | CIROP questionnaires. (See King et al.84 for application as part of wider study) | Four domains, psychometrically independent: personal knowledge development; personal research skill development; organisational/group access to and use of information; community and organisational development (for research), i.e.:
|
Seems psychometrically ‘internally valid’ (76% of variance was accounted for by the principal component analysis) but seems to measure a very small range of possible impacts, and only measures people’s perceptions of these. The aim was ‘to develop a generic survey measure of the influence of research partnerships on skills, decisions, and community capacity, in the eyes of target audience members’, i.e. it was intended to measure research-oriented outputs, not service-oriented ones. Hence very researcher-focused |
| 73 | King et al.188 | 2010 | Application | Canada | Community development for HSC | Impact model for community–campus partnerships: see Currie et al.357 The impact model specifies:
|
The study analysed community partnerships’ structure, process and outcomes. Structure measured by number and types of partner, local/national orientation, ratio of university: community staff and grant income. Process measured by indicators of research utilisation. Outcome measured using CIROP scale (see King et al.375). CIROP items used as dependent variables in a regression analysis. Main findings: mean impact scores indicate that research partnerships have small to moderate impacts on community and organisational development, and personal research skill development, but moderate to fairly great levels of impact on personal knowledge development | Innovative because it applies an ambitious impact model (Currie et al.357) and outcome measure scale (King et al.375), but convenience sample. Could be questions about how far the instruments have captured the key dimensions of the partnerships – very quantitative and tick-list focused. The finding that ‘personal knowledge development’ increased more than other dependent variables may be an artefact of the study design (asking personal recall of what happened) |
| 74 | Kingwell et al.139 | 2006 | Application | Australia | NHMRC: projects completed in 1992, 1997 and 2003 | No framework explicitly described, but used the new end-of-grant form developed by the NHMRC to capture impacts. Expert panel review of end-of-grant reports from researchers completing in 2003: 139 reports out of 454 expected (29%); retrospective surveys of investigators of earlier projects using a simplified version of new end-of grant report as the survey instrument: 1997 – 131/259 in contactable sample (51%); 1992 – response too low to use for full analysis but examples of impact identified. Separately computer-assisted telephone interview survey of recipients of people awards: 596 of 1897 (31%) completed survey | Knowledge gain; health gain: any research with a self-reported effect on clinical practice or other health service delivery practice or outcomes, changes in public health practice, or changes in health policy. Wealth gain: any research with self-reported commercial activity, including commercial potential and patents. People award recipients: career prospects | Helped identify ways to take impact assessment forward, e.g. on issues of timing, but generally quite low response rates. Also highlighted some projects with clinically relevant outcomes for showcasing to the community |
| Findings: papers per grant for 1997 ranged from basic research (7.0) to health services (3.0). For 2003, basic (7.5) and health services (4.3). For 1997, 24% of grants were deemed to have affected clinical practice, 14% public health practice and 9% health policy. Commercial potential: 41% of grants were deemed to have such potential. Patents arose from 20%. 89% of people award recipients thought career prospects improved (but there are barriers) | ||||||||
| 75 | Kogan and Henkel49 | 1983 | Both | UK | Department of Health and Social Security- funded programmes: wide range | Developed a collaborative approach informed by Weiss’s taxonomy of research utilisation, Caplan et al.376 etc. Case study of the new ‘Rothschild’ approach to organising and funding of Department of Health and Social Security research: including ethnography, participant observation, document analysis | Evaluation of the model introduced by Rothschild in which government departments had a chief scientific officer charged with commissioning research from scientists. Assessment of how far the department could successfully commission research to meet the needs of policy-makers | Rigorous and extensive ethnography of the process of government commissioning of research/policy-making, more so than on impacts of specific programmes. Now somewhat dated, but likely that key principles are still transferable. Science and government are very different cultural ‘worlds’, but also mutually shaping and interdependent. The key to success is sustained interaction over time. Linear models fail to do justice to the sheer complexity of both research and government. The policy timescale fits poorly to the research cycle |
| 76 | Kok and Schuit116 | 2012 | Methodological | N/A | Health research | Contribution Mapping. A three-phase process map that includes actors, activities and alignment efforts during research formulation (vision, aims, set-up), research production and ‘knowledge extension’ (dissemination and utilisation by both linked and unlinked actors). The contribution map is produced in a four-stage process beginning with an in-depth interview with the lead researcher, covering the three phases above and showing the contribution of the research to the realignment of actors and activities | ‘Impact’ is conceptualised as a new alignment of people, ideas, theories and artefacts. Knowledge may be formalised in journal articles but may also be captured more diffusely as ‘the knowledge available to a group of people’ or inscribed in technologies, e.g. magnetic resonance imaging | Elegant and richly theorised framework based on actor–network theory; however, no empirical application described in this paper (but contributed to thinking in Bennett et al.57). It challenges the view that impact can be attributed to a single research project:Research does not work like a cannon shooting knowledge into the world of action, where the targeting and force of the knowledge determines its ‘impact’.Instead, the productivity of research for health ultimately lies with the users who have to pick up and combine knowledges (in the plural), using them for their own purposes . . .The consequence is that achieved changes cannot realistically be attributed to a single research project as ‘source’ |
| 77 | Kryl et al.377 | 2012 | Both | UK | NICE guidelines: dementia, chronic obstructive pulmonary disease | Analysis of the papers cited on guidelines to check for the origin/funder of the research | Identified if papers had an author from UK institution. Checked funder acknowledgement and categorised by type/organisation | It argues that it is possible to track the source of funding, but improved accessibility of data and reporting of funding neededWe found that there is great potential for national and international guidelines to be used as sources of information to help further our understanding on the impact of research on practice: the challenge is to be able to harness that information in an efficient way |
| Found: over one-third of papers have at least one UK-based author. In over 40% of cited papers, no funding acknowledgement was found. The MRC, Department of Health/NHS and the Wellcome Trust ‘were overtly linked to only a small proportion of papers cited in the guidelines’ | ||||||||
| 78 | Kuruvilla et al.123 | 2006 | Methodological | UK | Health research | RIF. Policy impact assessment element was informed by Weiss’s taxonomy. Semistructured interview and document analysis leading to one-page ‘researcher narrative’, which was sent to the researcher for validation | Four broad areas of impact:
|
Pragmatic, carefully tested and richly informed by an extensive literature review. Designed to help researchers develop their narratives of impact. Inclusive and imaginative, and has strong face validity. The way RIF intended to be used as follows:designed as a ‘DIY’ approach with descriptive categories that prompt researchers to systematically think through and describe the impact of their work.While initially sceptical, LSHTM researchers found [it] prompted them to identify a wide range of impacts related to their work in a relatively systematic manner (compared to the ad hoc approaches they had previously used) |
| 79 | Kuruvilla et al.97 | 2007 | Application | UK | Health research | RIF. (See Kuruvilla et al.123) Case studies: 11 projects in total, selected for maximum variety. Semistructured interview and document analysis leading to one-page ‘researcher narrative’ which was sent to the researcher for validation | See companion paper above123 Prior relationships with policy-makers, reputation in field meaning invitation to bid for funding. Research networks, collaborations were key in helping communication Communication with other academics was straightforward but communication with policy-makers was challenging. Media and funders’ websites/reports were important channels. Policy impact occurred through different mechanisms, theorised using Weiss’s 1998 taxonomy.343 Instrumental use (research findings drive policy-making); mobilisation of support (research provides support for policy proposals); conceptual use; redefining/wider influence. The structured impact narratives facilitated analysis across projects |
Describes the successful application of above framework. The framework helped develop researcher impact narratives which were mostly found to be objectively verifiable ‘and facilitated comparisons across projects, highlighting issues for research management and assessment,’ but some ‘putative impacts were not as easily verifiable within the scope of this study, for example social capital or economic impact’. It was useful to help researchers ‘think through and describe the impact of their work across a range of instances when they are asked to account for these: in writing grant proposals, in research assessment exercises and in contributing to complex research, policy and service interventions aimed at improving health and promoting societal development’. Despite many strengths, not specifically designed for application to assess impact of programmes of funded research |
| 80 | Kwan et al.66 | 2007 | Application | Hong Kong | Health and HSR fund | Payback Framework. Adapted Payback survey sent to 205 PIs of completed projects: 178 (87%) responded. Statistical analysis including multivariate analysis | Knowledge production; research targeting and capacity building; informing policy- and decision-making; application of the findings through changed behaviour; health and health services benefit | Rigorous adaptation and application of existing framework plus detailed statistical analysis. High response rate and some real examples very briefly described, however it relied solely on self-reports by PIs. Multivariate analysis found investigators’ participation in policy committees as a result of the research and liaison with potential users before and during research were significantly associated with health service benefit, policy and decision-making, and change in behaviour |
Found: 5.4 publications per project
|
||||||||
| 81 | Latour378 | 2005 | Methodological | N/A | Critical social science | Actor–network theory. Case study | An actor–network consists of both people and technologies (or artefacts); they are inherently unstable. ‘Impact’ is conceptualised as achieving a new alignment of the actor-network through a process called ‘translation’ | Strength: novel, imaginative and potentially useful framework for considering multistakeholder research networks. Weakness: the claim that ‘objects have agency’ is widely contested; exclusive focus on ‘network effects’ mean that human agency is undertheorised |
| 82 | Laws et al.88 | 2013 | Application | Australia | Schools Physical Activity and Nutrition Survey | Banzi’s research impact model. Used the framework proposed by Banzi et al.,4 which has a range of potential areas of impact ‘which largely reflect the range of other commonly used models, for example, the payback framework’. Semistructured interviews with PIs (n = 3) and users (n = 9) of Schools Physical Activity and Nutrition Survey data; bibliometric analysis; verification using documentary evidence. Triangulation of data to produce case studies | Five categories: advancing knowledge; capacity building; policy impacts; practice impacts; broader impacts | Combined several methods and triangulated data to produce detailed analysis including illustrative quotes, but noted may have been some social desirability response bias. Discusses difficulty of attributing impacts to a single piece of research, particularly the longer-term societal, health and economic impacts. ‘The use of “contribution mapping” as proposed by Kok and colleagues may provide an alternative way forward.’ Factors: perceived credibility of survey findings; active dissemination; contextual factors, including continuity and partnerships between researchers and end-users, mechanisms and structures in place to implement recommendations; good fit with organisational culture |
| Found: each of the three surveys reported in multiple peer-review articles (32 in total); two PhDs and two post-doc positions; broad agenda-setting for policy and some examples of underpinning new policies; informed programme planning; more difficult to identify broader health, economic or societal impacts | ||||||||
| 83 | Lewis et al.113 | 2009 | Both | Canada | Manitoba Centre for Health Policy | ROI analysis. Stakeholder interviews; bibliometrics/altmetrics; cost analysis | Policy and culture of decision-making; financial; health status; public confidence; capacity building. The impact of Manitoba Centre for Health Policy demonstrated in ‘numerous ways, including reputation, research revenues and productivity, varying influence on policy and system management, and a major cultural and intellectual influence on the Manitoba environment’. Quantifiable ROI was 200% | Relatively explicit set of criteria/framework from which to evaluate. Problems of attribution. Described as ROI, akin to Payback Framework in many respects |
| 84 | Liebow et al.91 | 2009 | Application | USA | NIEHS: Extramural Asthma Research Programme | NIEHS logic model (see Engel-Cox et al.63). The logic model tailored to inputs, outputs and outcomes of the NIEHS asthma portfolio. Data from existing NIH databases were used and in some cases data matched with that from public data on, for example, the US Food and Drug Administration website for the references in new drug applications, plus available bibliometric data and structured review of expert opinion stated in legislative hearings | Publications, clinical policy and application of findings, community interventions, environmental policy and practice, health outcomes, and technology developments | Based on key aspects of the framework specifically developed previously for the research funder. Aim to obtain readily accessible, consistently organised indicator data could not in general be realised:Beyond publications, indicators of other activities, outputs, and outcomes are not as well supportedDid not use all the pathways set out in the original Engel-Cox framework. Highlights that other activities beyond current databases would be needed to gather the data |
| Found: PI publications from 0 to > 100; 2057 publications attributable to 30 years’ funding; PI membership of various advisory panels, etc.; four patents; matching of databases identified NIEHS-funded trials cited in new drug applications, but not able to link trends in environmental impacts or health and social impacts to specific research activity | ||||||||
| 85 | Lomas154 | 2007 | Methodological | N/A | HSR | Knowledge brokering; linkage and exchange | How the link between researchers and policy-makers works – and why it so often fails to work | Strength: clear and authoritative summary of a component of the literature. Weakness: ‘non-systematic’ review, hence omits other perspectivesResearchers and policy-makers come from different worlds and do not understand each other. There is much evidence that effective knowledge exchange occurs through sustained linkage and dialogue |
| 86 | Longmore67 | 2014 | Application | UK | Addenbrooke’s Charitable Trust: fellowship scheme | Payback Framework informed the study. Developed a fellowship review form based on items such as researchfish and the Payback Framework. Used the form to gather data from fellows through face-to-face interviews or via e-mails (14/18 fellows participated) | Career development; publications and dissemination; leveraged funding; capacity building; patient or health-care benefits; intellectual property/research tools/spinouts | The fellowship scheme was a small-scale (support for 1 year or less) attempt to nurture future clinical academics. Total value of 18 awards < £1M. The way the evaluation of such a small-scale scheme conducted reflects growing interest in impact assessment |
| Found: most secured external fellowships leading to PhDs; research projects have ‘potential to inform future research that may ultimately deliver benefits for patients’. Some fellows reported the research improved aspects of how they approached patients | ||||||||
| 87 | Martin and Tang379 | 2007 | Both | UK | Range of UK publicly funded research, e.g. the social benefit of preventative dental care | Updates the earlier Science Policy Research Unit framework for assessing the channels that might lead to economic and social benefits from public funding of basic research. Channels are: useful knowledge; skilled graduates and researchers; new instruments and methodologies; enhanced problem-solving capacity; new firms; provision of social knowledge. Desk analysis. Examined a series of case studies to identify the elements of the framework that might apply in each one | Key focus is on the channels, but some channels are items sometimes included in lists of impacts | Important analysis, informed by a review of case studies, of the exploitation channels to consider when assessing the benefits from publicly funded research. Shows the linear model has shortcomings, and highlights how some impacts will take a long time to move through the various channels and that incorrect science policy options might be adopted unless the long-term impacts are taken into account |
| Found: the social benefit of preventative dental care would be improved oral health care and avoidance of fillings – identified two exploitation channels for this research: spin-off; scientific instrumentation. Despite problems facing research impact assessment:a growing body of empirical work demonstrates that those benefits are substantial | ||||||||
| 88 | Martin174 | 2010 | Methodological | UK | Social research | Co-production (focus on practitioners) | Practitioner involvement in research. Involvement may be nominal (to confer legitimacy on a project), instrumental (to improve delivery), representative (to avoid creating dependency) or transformative (to enable people to influence their own destiny). The greater the involvement, the greater the potential impact in HSR | An elegant and simple tool for assessing (semiquantitatively) the level of lay involvement in a study. Weakness: not tested |
| 89 | McCarthy380 | 2012 | Application | EU | EU: Public Health Innovation and Research in Europe | None stated. Through the European Public Health Association, experts assessed the uptake of the eight public health collaborative projects (within areas of health promotion, health threats and health services), for 30 European countries. National public health associations reviewed the reports. Methods varied between countries. Following stakeholder workshops, or internal and external consultations, 11 national reports discussed impacts of the public health innovations | Focus on uptake of the innovations: impact on policy and practice | Quite wide-ranging input into the study: in total, 111 stakeholders were involved in workshops. Reports only produced for 11 countries. Methods varied: in Ireland, one person provided information. Strategies noted most often to spread the results were: reports; websites and national conferences; and seminars and lectures. Background: European Court of Auditors critical of the first EU Public Health Programme – project co-ordinators could not demonstrate ‘take up’ by target groups |
| Found: in 11 countries, there were reports on the eight innovations for 45 (51%) of the possible public health markets. The innovations contributed positively to policy, practice and research, across different levels and in different ways, in 35 (39%) markets, while competing innovation activities were recorded in 10 (11%) markets | ||||||||
| 90 | McLean et al.381 | 2012 | Methodological | Canada | CIHR: knowledge translation funding programmes | A framework inspired by the principles of integrated knowledge translation. Develops a logic model for evaluating the knowledge translation funding programme. The paper is a protocol but sets out planned methods:study will employ a novel method of participatory, utilisation-focused evaluationMixed methods using quantitative and qualitative data with participation from researchers, knowledge users, knowledge translation experts, other health research funding organisations. Environment scan, documentary review, interviews, targeted surveys, case studies and an expert review panel | Immediate outcomes:(knowledge user and researcher partnerships established; knowledge generated; relevant research results are disseminated and/or applied by partners and knowledge users; advancement of knowledge translation science)Intermediate outcomes (knowledge users and researchers learn from each other; knowledge users are informed by relevant research; generalisable knowledge is created and disseminated)Long-term outcomes (improved health, more effective health services and products and a strengthened health-care system) | The logic model used includes a focus on the processes as intermediate outcomes |
| 91 | Meagher et al.95 | 2008 | Both | UK | ESRC: all responsive mode funded projects in psychology | Flows of knowledge, expertise and influenceSurvey of chief investigators, survey of heads of department, two focus groups, 20 semistructured interviews, media-related searches, case studies. The team reported:no evident contradictions between results obtained by different methods. However, the level of detail provided did vary; unsurprisingly, some methods, such as the survey, enabled us to achieve greater breadth of data while others, such as the case study interviews, enabled us to probe issues in more depth | Collected data on six domains:
|
Thorough methods, but noted as a limitation, that the exclusive focus on responsive mode projects:meant there was no special research orientation towards users or ‘relevant themes’Authors question the value of tracking impacts in the absence of specific activities aimed at facilitating uptakeChanges in practice or policy often appear to stem from a general ‘awareness-raising’ or conceptual shift. Precise measurement of the impact of research upon a particular change in practice is likely to be unattainable |
| Found: conceptual (indirect, enlightenment-based) impacts were more common than instrumental (direct, knowledge-driven) ones | ||||||||
| 92 | MRC76 | 2013 | Both | UK | MRC: all programmes | The MRC economic impact report ‘is part of the research council’s performance management framework implemented by the Department for Business, Innovation and Skills (BIS)’. Combination of information from the MRC’s own databases and data gathered from PIs through researchfish | The BIS metrics framework 2011/12 includes range of items: budget allocation and funding leveraged from other sources; expenditure on different types of research; number of researchers funded in various categories; publications; research training; knowledge exchange activities; commercialisation: patents, spin-off, IP income; policy influence | Broad picture of activity and some key impacts by drawing on extensive data gathering through researchfish, etc. Questions about some of the data categories, e.g. classifying systematic reviews as a policy document, and questions of definition of economic impact. The MRC Economic Impact Report has been published each year since 2005. It illustrates several themes:
|
| Found: data collected for all items, including:2,879 reports of policy influences between 2006 and 2012 . . . in 1,083 awardsA total of 2267 were influences on policy setting processes, e.g. participation in an advisory committee; ‘610 reports of value/policy changes induced through citation in key policy documents between 2006 and 2012’, including clinical guidelines, systematic reviews. Some examples described | ||||||||
| 93 | MRC103 | 2013 | Application | UK | MRC: all programmes | Researchfish |
|
Can be implemented regularly and collects data from a wide range of researchers but possibly neglects some areas of impact. Also questions about how far it is fully completed |
| 94 | Meijer80 | 2012 | Methodological | The Netherlands | Dutch research but EU perspective: all fields | Scientific and societal quality of research. Combines three approaches:
|
Creating societal relevance is a four-step process:
|
Methodologically innovative but not published in peer-reviewed journal and speculative. Seems tied in with a wider Dutch-led effort to measure effect of research funding in context of competitiveness of EU countries. See also Mostert et al.100 |
| 95 | Meyer152 | 2009 | Methodological | Canada: (part of appendix A of CAHS report) | Clinical research | Starting point is the Payback Framework, as amended in CIHR versions | Provides details about health and economic gains being the most important of Payback Framework categories, and can be important for assessing the impact of clinical research to work towards showing them but that is more difficult | Part of the evidence base that encouraged the CAHS panel to adopt an adapted version of Payback Framework. It contributes to the discussion about assessing negative impacts |
| 96 | Milat et al.89 | 2013 | Application | Australia | New South Wales Health Promotion Demonstration Research Grants Scheme | Banzi’s research impact model. This draws on the range of five potential areas of impact set out in the Payback Framework (see also Laws et al.88 above for a parallel study). Semistructured interviews with CIs (n = 17) and end-users (n = 29) of the 15 projects. Thematic coding of interview data and triangulation with other data sources to produce case studies for each project. Case studies individually assessed against four impact criteria and discussed to reach group assessment consensus at a verification panel meeting where key influences of research impact also identified | Advancing knowledge and better targeting of future research; capacity building; informing policies and product development; health, societal and economic impacts | Detailed multimethod case study analysis of all (n = 15) projects in the programme, including a range of elements in the various payback categories. An independent panel conducted scoring. Illustrative quotes were supplied. Some potential for social response bias as some end-users may have been inclined to over-inflate positive impacts. The team identified a range of factors linked to high-impact projects. These included:the nature and quality of the intervention itself . . . high quality research, champions who advocated for adoption, and active dissemination strategies. Our findings also highlight the need for strong partnerships between researchers and policy makers/practitioners to increase ownership over the findings and commitment to action |
| Found: both CIs and end-users indicated capacity building occurred through staff development, partnership building and follow-on research funding; 13/15 projects scored above the minimum for impact on policy and practice combined, and 10/15 were in the moderate or high categories; no project independently assesses as high impact in health, societal and economic impacts category, but 13/15 were above the minimum | ||||||||
| 97 | Milat et al.129 | 2015 | Methodological | N/A | All health, but started with focus on public health and health promotion | Review:A total of 16 different impact assessment models were identified, with the ‘payback model’ being the most frequently used conceptual frameworkThe most frequently applied methods: publications and citations analysis, interviews with PIs, peer assessment, case studies and documentary analysis. Only four of the included studies interviewed non-academic end-users of research | The review notes the growth of hybrids of previous conceptual frameworks that categorise impacts and benefits in many dimensions and try to integrate them. Of the main frameworks analysed, ‘all attempted to quantify a mix of more proximal research and policy and practice impacts, as well as more distal societal and economic benefits of research’ | While the review identified just 31 primary studies and one systematic review that met their review criteria, ‘88% of studies that met the review criteria were published since 2006’ The attempts to broaden evaluation of research ‘raise an important question of how to construct an impact assessment process that can assess multidimensional impacts while being feasible to implement on a system level’. The potential for bias because of the involvement of PIs in impact assessments means end-users should routinely be interviewed in impact assessments and claims should be verified by documentary evidence |
| 98 | Moreira382 | 2013 | Application | N/A | Health care | Co-production. Case study with extensive ethnography of health service researchers and systematic reviewers | Intersectoral interaction between university, society and market | Strength: rigorous application of the ‘mode 1 vs. mode 2’ taxonomy to a detailed case study. ‘Impact’ occurs through the coevolution of three activities: market-driven reforms oriented to efficiency (‘market’), epidemiologically driven research oriented to clinical effectiveness (‘laboratory’) and patient and public involvement (‘forum’). This process is messy, organic, largely unpredictable and contested |
| 99 | Morlacchi and Nelson383 | 2011 | Both | USA-focused international study | National Heart Lung and Blood Institute stream of research on the LVAD | Propose medical practice evolves as a result of progress along three pathways: ‘improvements in the ability to develop effective medical technologies, learning in medical practice, and advances in biomedical scientific understanding of disease’. Longitudinal and contextual case study of the development of the LVAD using interviews with key actors, direct observation and documentary analysis to produce an historical analysis | Study analyses sources of advances in medical practice, and challenges the idea that scientific understanding of disease is the single source | Study has a different focus than most others: it attempts to show the impact on advances in medical practice made by three pathways, of which scientific understanding is only one |
| Found: case study of the emergence of the LVAD therapy showed the importance of progress along all three pathways, though an essential aspect was the collective and cumulative learning that requires experience that can only be gained through the use of the LVAD | ||||||||
| 100 | Mostert et al.100 | 2010 | Both | The Netherlands | Leiden University Medical Centre: various departments/groups including public health | Societal quality score. Van Ark and Klasen’s125 theory of communication in which audiences are segmented into different target groups needing different approaches. Scientific quality depends on communication with the academic sector; societal quality depends on communication with groups in society – specifically, three groups: lay public, health-care professionals and private sector
|
Three types of communication: knowledge production, e.g. papers, briefings, radio/television, services, products; knowledge exchange, e.g. running courses, giving lectures, participating in guideline development, responding to invitations to advise or give invited lectures (these can be divided into ‘sender to receiver’, ‘mutual exchange’ and ‘receiver to sender’); and knowledge use, e.g. citation of papers, purchase of products; earning capacity, i.e. the ability of the research group to attract external funding | Careful development of a new approach to assessing research impact appropriate for the specific circumstances of the medical faculties being integrated with their academic hospitals. Heavily quantitative – basically a counting exercise ‘how many of x have you done?’ Only looks at process as they say ultimate societal quality takes a long time to happen and is hard to attribute to a single research group. Did not control for the size of the group. Only a weak correlation was found between social and scientific quality |
| 101 | Muir et al.107 | 2005 | Methodological | Australia | All public research | None explicitly stated: focus on ‘measurements/indictors to monitor economic benefit flowing from commercialisation of research funded by the public sector’ | Metrics for commercialisation of public research need to be broadened to match understanding that commercialisation contributes ‘to Australia’s economic, social and environmental well-being. This is achieved through developing intellectual property, ideas, know-how and research-based skills resulting in new and improved products, services and business processes transferable to the private sector.’ Fourteen metrics covering: IP, consultancies and contracts, skills development and transfer. They form the basis of future data collection | Commissioned by the Australian government to inform policy on impact assessment in an area that has been important in Australia |
| 102 | Murphy77 | 2012 | Both | New Zealand | New Zealand publicly sponsored clinical trials | Multistrand mixed methods. Survey; cost–benefit analysis | Health outcomes; stakeholder perceptions (perceived value); economic outcomes (CBA) with QALYs as measurement of health benefit. QALYs valued using societal valuation of statistical life and health-care system opportunity cost (based on average Pharmaceutical Management Agency positive recommendation). Suggestion that benefit outweighs costs for all stakeholders | Triangulation methods. Use of well-validated QALYs in economic modelling. But only applied to two trials as a PhD study, and limited to assessing the benefits that accrued for patients in the trial |
| 103 | Nason et al.47 | 2011 | Application | Ireland | Health Research Board: all health fields | Payback Framework
|
|
Several of the case studies were expanded to consider whole streams of research to more comprehensively identify wider benefits. However, difficult to compare across case studies, because of the limited number owing to the resource-intensive nature of exercise. Article expands concept of economic impact to consider: major growth in funding and focus on ‘knowledge economy’ strategy, enabling international sources of funding to be attracted |
| Found: a range of impacts in all categories including: world-class articles; new clinical assays; improved recovery time; development of new drug company | ||||||||
| 104 | NHS SDO68 | 2006 | Application | UK | NIHR: SDO programme | Informed by the Payback Framework. Purposive selection of 23 projects to reflect the range of SDO research and where some evidence of impact was known to be available. Data collected in two stages, starting with primary outputs (publications); snowballing to capture data on secondary outputs (policy and practice impact). Internal sources used first: annual reports, projects database, programme managers and leads. External databases checked and all non-case study PIs e-mailed to provide data. Secondary outputs (policy documents, etc.) identified using web searches and sent to PI for verification. Eleven of the 23 projects purposively selected as case studies, including semistructured interviews with researchers and users | Two main categories taken from the Payback Framework: primary outputs (publications: SDO reports, academic papers, policy); and secondary outputs (citing in policy documents, practice guidance, newsletters, website and the media). In the 11 case studies, the impact and utilisation of the research is presented in five domains: services, policy, practice, research and capacity building | The range of methods used did identify a range of impacts, and the accounts of the case studies provide good examples. However, 2006 was quite early to conduct an impact assessment of first 5 years of programme from 2001 to 2006 |
| Found: publications – all had at least one published by SDO and average of 1.7 articles; policy and practice guidelines: 12 projects cited in total of 24 documents, e.g. five citations in NICE guidance | ||||||||
| 105 | Niederkrotenthaler et al.384 | 2011 | Methodological | Austria | All fields | Societal impact factor tool developed to consider the effect of a publication on a wide set of non-scientific areas, and also the motivation behind the publication, and efforts by the authors to translate their findings. Self-evaluation of papers by authors: in three main categories they score their paper, and provide textual justification/evidence for the score (see dimensions assessed). The self-evaluation sheet would then be sent to a reviewer for independent checking. Authors would be invited to submit their publications for reassessment if any developments | It was intended that the tool would be refined, but the version tested had three main elements: the aim of the publication (1 point if aim was gain of knowledge, application of knowledge or increase in awareness); the authors efforts to translate their research into social action (1 point); size of translation (geographical area: 1, 2 or 3 points; status: 1 or 2 points; target group: 1 point for individuals, 2 points for subgroups or 3 points for whole population) | Niederkrotenthaler et al.384 claim an advantage of their tool over that developed, for example by Sarli et al.,118 is that the tool does not specify the precise nature of any kind of translation (e.g. devices, guidelines) but leaves that to the author applying for a score to describe. But, as they admit, the tool ‘cannot be considered ready for routine implementation’. Because it aims to develop the equivalent to the scientific impact factor, the focus is at the publication level, which might seem even more limiting than a focus on projects |
| 106 | Oliver and Singer385 | 2006 | Application | USA | CHBRP: HSR | Informed by framework for analysis of policy design and political feasibility based on the typologies of Wilson386,387 and Arnold.388 Sixteen interviews with 20 key informants and documentary analysis | Impact of HSR on legislative debates and decisions | Theoretically informed analysis of the role of research identified various examples of use in Californian health policy-making; however, few details were given on the precise methods used. It uses a range of models from political science to help analyse the theoretical and actual role for a university-based body specifically designed to feed research and analysis into the legislative process around health insurance mandates |
| Found:participants inside and outside of state government have used the [CHBRP] . . . reports as both guidance in policy design and as political ammunition . . . Almost every respondent noted that CHBRP reports, however authoritative, served as ‘political ammunition’ in the manner described by Weiss (1989) | ||||||||
| 107 | Oortwijn69 | 2008 | Application | The Netherlands | ZonMw Health Care Efficiency Research programme: HTA | Payback Framework. Logic model; survey data collected from PIs of 43 studies conducted using health-care efficiency research funds (response rate 79%); case study analysis (including 14 interviews) of five HTA projects. Developed and applied a two-round scoring system | Knowledge production Research benefits Informing policy Changing health practice Broader impact on health There was a total of 101 papers, 25 PhD theses, citation in guidelines in six projects, implementation of new treatment strategies in 11 projects |
Use of triangulation methods and presentation of scores that account for wider range of impacts. Potentially not long enough to witness benefits for many of projects. The programme was mainly conducted in academic hospitals, with a large responsive mode element and most studies were prospective clinical trials |
| 108 | Orians et al.17 | 2009 | Application | USA | NIEHS: Extramural Asthma Research Programme | NIEHS logic model (see Engel-Cox et al.63). Web-based survey of 1151 asthma researchers who received funding from the NIEHS or comparison federal agencies from 1975–2005. A total of 725 responded (63%). While the researchers all received federal funds, most of the questions covered respondents’ body of research. Key informant interviews with end-users (n = 16). Analysis of the NIEHS model in the light of the findings. Companion article to Liebow et al.91 that described the attempt to apply the NIEHS framework using databases | Wide range of impacts considered as set out in Engel-Cox et al.63 Examples set out below from survey findings of asthma researchers | Large numbers surveyed and the focus on their role as researchers rather than on specific projects allowed nuanced assessment of dissemination and product development. However, the contribution to understanding outcomes is more limited:this method does not support attribution of these outcomes to specific research activities nor to specific funding sources. Nor did we gain many insights from the survey into the pathways by which research is translated and used to affect these outcomesAsking about research from any funder reduces the relevance for assessing the impact of specific programmes of research, but study concluded:the model guiding this assessment, with its “pathways”, is a reasonable representation of how research may result in such impacts, at least as they pertain to asthma research |
| Found: include: papers – 96%; research tool and methods – 29%; improved environmental measurement techniques – 20%; spin-off companies – 4%; licensing a patent – 38% of patent holder; changes in guidelines – 19%; changes in environmental standards/regulations indoor air – 8%; changes in business practices regarding air – 8%; changes in public knowledge – 33%; changes in clinical practice – 27%. End-users saw research use being in various categories: professional development; intervention/regulation, e.g. reducing environmental tobacco smoke and exposures to lead, etc.; new drug development and regulation; clinical practice | ||||||||
| 109 | Ottoson et al.369 | 2009 | Application | USA | RWJF: ALR programme | Utilisation-focused evaluation. Telephone interviews with 136 key informants (first-line consumers and implementers, policy-shapers) representative of four out of five levels in logic model (professional community, policy, scientific community, funders); bibliometric analysis | Is a field emerging? (If so, what is its name?) Is there an awareness of ALR within the field? Has ALR contributed to policy discussions? | Neat logic model. Limitations of snowball sampling in being representative of opinions. It makes five recommendations, which imply association with impact/greater utilisation, e.g. bridging research and policy (‘substantial and coordinated investment’); boosting visibility and relevance of policy (engage end-users and intermediaries early in research process); emphasising collaboration and co-ordination. Pair of evaluations of the same initiative – Gutman et al.132 |
| Found: it had contributed to development of transdisciplinary field; ‘ALR’s contributions to policy discussions were found across a spectrum of policy-development phases’ | ||||||||
| 110 | Ovseiko et al.389 | 2012 | Both | UK | Oxford University Clinical Medicine | REF pilot impact indicators. Describes survey (48% response) and other approaches used for data collection for this piloting of the REF | Delivering highly skilled people; creating new businesses, improving the performance of existing businesses, or commercialising new products or processes; attracting R&D investment from global business; better-informed public policy-making or improved public services; improved patient care or health outcomes; cultural enrichment, including improved public engagement with science and research; improved social welfare, social cohesion or national security | Important contribution to the analysis of the development of the REF. Problems with retrospective collection of data. Existence of self-selection bias? All known REF gaming issues. It concluded that:Assessing impact is feasible |
| Found:While the majority of the proposed indicators have some validity, there are significant challenges in refining the current indicators and methodologies in a number of ways | ||||||||
| 111 | Penfield et al.14 | 2014 | Methodological | UK in particular | All fields | Frameworks examined: Payback; SIAMPI; Australian RQF; RAND report that led to REF impact case study approach (Grant et al.38). Plus overview of specific indicators. Metrics, e.g. social ROI; narrative (case study) surveys and testimonies; citations outside academia/documentation. Also describes history of the impact component of the REF | Cites the REF definition of impact:an effect on, change or benefit to the economy, society, culture, public policy or services, health, the environment or quality of life, beyond academia | Rounded analysis led to the conclusion:While aspects of impact can be adequately interpreted using metrics, narratives, and other evidence, the mixed-method case study approach is an excellent means of pulling all available information, data, and evidence together, allowing a comprehensive summary of the impact within context |
| 112 | Percy-Smith et al.390 | 2006 | Application | Scotland | Health Scotland: five evidence informed policy and practice initiatives | Not restricted to a single framework but drew heavily on Social Care Institute for Excellence taxonomy (see Walter et al.391). Also drew on and amended Health Development Agency framework in the light of findings to produce a new, more complex model (see next column). ‘Mixed method’: literature review plus document analysis plus stakeholder seminar (n = 1) plus stakeholder interviews (n = 22) plus survey of participants in learning networks (631 completed forms received). Evaluated at three levels: the programme as a whole, the five separate initiatives and the individual practitioners | Impact was assessed in terms of:
|
Successful programmes were characterised by a high degree of opportunism (i.e. use policy windows). Extensive ‘reach’ into professional and other stakeholder groups. Clarity and accessibility of presentation of key messages
Some case studies produced to showcase good practice may have been questionable in some aspects of quality: hence, there is a quality control issue in relation to ‘practice based evidence’ |
| 113 | Pittman and Almeida344 | 2006 | Both | International | International Development Research Centre and Pan American Health Organization: programme on social protection in health in Latin America and the Caribbean | Research programme informed by concept of linkage between researchers and users (Lomas342) and therefore was structured with the intention of achieving impact. Not described in detail but appears to be mostly an insider account while the initiative was still under way and drawing also on early papers and discussions with researchers | The linkage model aims to ensure opportunities for users to be involved throughout a project, and that as a consequence impacts will arise | The detailed knowledge of the programme enabled an informed analysis; however, there were timing problems. The programme itself ran into difficulties of providing incentives for decision-makers:to remain active in the project, when their timelines tend to be more short-termAlso authors recognised it was too early for a final assessment of whether or not the type of research design will have an impact on innovation in social protection in health. The linkages between researchers and users seen as very important to achieving the impacts that had already arisen. Interesting contribution to debates about whether or not scientific quality and impacts are associated:all but one team felt the scientific rigor of the projects had improved as a result of the extended planning and interaction with decision-makers as well |
| Found: a negotiated research question that influenced ‘not only the project design, but the decision-makers’ ways of thinking about the problem as well’. In four out of the five cases, turnover among government officials impaired the process, but in the fifth team:the interaction has led to use of data in decision-making, as well as a clear recognition by both parties that different kinds of evidence were at play | ||||||||
| 114 | Poortvliet et al.140 | 2010 | Both | Belgium | KCE: HTA, HSR and good clinical practice | Developed own framework. Documentary review; two group discussions, with 11 KCE experts, with two KCE mangers; interviews with stakeholders (n = 20); web-based survey to project managers: 66 external (28% responded) and 101 KCE (72% responded) – a total of 88 managers reported on 126 projects; nine detailed case studies selected by stratified random approach; and international comparisons with three agencies using documentary/literature review and interviews (n = 3) | Dissemination (outputs, dissemination activities, stakeholders addressed, engagement of stakeholders in outputs, actual take-up of outputs); contribution to the decision-making process (familiarity with research projects, research utilisation, relevance of projects for policy-making/practice, reactions on finished projects from stakeholders); external image of KCE | Comprehensive range of methods and analysis that focused on the processes as well as impacts. However, in addition to some conflicts of interest, the data collection phases were simultaneous, thus reducing scope for triangulation through a sequence of data collection activities. While some important conditions for achieving impact were not realised, the report concludes that KCE had established some:Research questions come from primary stakeholders. There is involvement from these stakeholders in agenda and priority setting. The quality of KCE research itself is high and in general beyond discussion. The relevance of KCE research findings is generally judged as highSome similarities with other/earlier findings about the HTA impact: of the three fields included, more HTA project co-ordinators thought research made a policy impact than in GCP or HSR |
| Found: 16 stakeholders said findings influenced decision-making, four said not in their organisation; 58% of project co-ordinators thought projects contributed to policy development: more for HTA than Good Clinical Practice or HSR | ||||||||
| 115 | Reed et al.70 | 2011 | Application | Australia | Primary care research | Payback Framework. Online survey to 41 contactable CIs (out of 59 projects). Asked impacts expected, how many achieved. Some projects excluded as still under way, others refused. Out of 23 completed, 17 were relevant | Five domains: research transfer (including knowledge production); research targeting, capacity building and absorption; informing policy and product development; health and health sector benefits; and broader economic benefits | Inclusion of questions about what expectations CIs had had about impact: allowed interesting comparison with what achieved. However, quite a large number of CIs could not be located, or refused to participate. For those who did, there may have been ‘risks of a bias towards positive benefits’ and relied solely on survey. Interesting, comparison with Kalucy et al.65 from the same team:In an earlier study we collected qualitative data through interviews with CIs and gathered copious information that provided more context to better understand the results |
| Found: 13 CIs (76%) considered achieved at least half impacts expected; 11 PhDs came from 10 projects; further research, 65% achieved; 13 projects (76%) expected to influence national/state policy-making, four (24%) did so, but eight (47%) influenced decision-making at organisational, local or regional level [combined nine separate projects (53%) had policy/decision impact]; 10 (59%) expected to lead to improved health outcomes, five (29%) did so. Few broader economic impacts achieved. Three of the examples of impact overall were unexpected | ||||||||
| 116 | Higher Education Funding Council106 | 2015 | Both | UK | All medical, health, biological, agricultural, veterinary and food sciences | REF 2014. Panel reflections on the methods and results of the REF 2014 exercise. However, did not have access to the findings of the analysis funded by HEFCE of the impact case studies that was still on-going at the time of publication of the report | All aspects of impacts assessed in the REF | Given the scale and apparent success of the REF, the comments supporting the case study approach are highly important. The main panel recognised the difficulties in demonstrating the link between research and impact which may be non-linear, but thought that the narrative case study largely succeeded in capturing the complex links between research and impact Submissions could be strengthened in futureif HEIs were proactive in collecting more qualitative and quantitative data evidencing the reach and significance of the impact. International MPA members cautioned against attempts to ‘metricise’ the evaluation of the many superb and well-told narrations describing the evolution of basic discovery to health, economic and societal impactp. 11While cautioning against attempts to metricise the evaluation, MPA said in future exercises should attempt to provide more accurate quantification of the extent and reach of the impact, and also about the proportionality of an individual contribution to ‘impact’ |
| Found: MPAbelieves that the collection of impact case studies provide a unique and powerful illustration of the outstanding contribution that research in the fields covered by this panel is making to health, wellbeing, wealth creation and society within and beyond the UKInternational members described it as:the boldest, largest and most comprehensive exercise of its kind of any country’s assessment of its science . . . to our knowledge, [it is] the first systematic and extensive evaluation of research impact on a national level. We applaud this initiative by which impact, with its various elements, has received considerable emphasisMPA said best case studies had a:clear and compelling narrative linking the research programme to the claimed impact; verifiable evidence (qualitative or quantitative) to support the claimed impact provided within the text . . . and (where appropriate) spread of the impact beyond the immediate beneficiaries to a much broader and possibly global audience | ||||||||
| 117 | Rispel and Doherty135 | 2011 | Application | South Africa | CHP | None explicitly stated. Interviews with 25 purposively selected key informants (12 CHP alumni, seven current members of staff, six external stakeholders); documentary review; aspects of ‘insider account’ as both researchers had spent some time at CHP – but also time working elsewhere | Contribution to health policy development and implementation. Found: CHP ‘has contributed directly to health policy development and implementation while also changing the way government understood or approached policy issues’. ‘All key informants acknowledged that CHP had a significant impact on national health policy at one point or another’ | Authors claim that:there is great value in comparing and contrasting our own ‘insider-outsider’ perspectives with those of pure “insiders and outsiders” as this has helped to clarify the reasons behind differences of opinionA range of methods:triangulating information from the interviews, earlier evaluations, and external review reportsOnly able to interview a few government officials with no prior link to CHP. Factors: research quality and trustworthiness; strategic alliances and networking; capacity building – training future policy leadersAt CHP, discussing research ideas and the possible implementation of research findings with policy makers at the start-up of projects, and then presenting findings face-to-face, became a powerful mode of influencing policyReported examples of instrumental and conceptual impact on policy |
| 118 | Ritter and Lancaster392 | 2013 | Both | Australia | National Drug and Alcohol Research Centre: illicit drug epidemiological monitoring systems | Informed by previous frameworks, developed a three-component approach to assessing research influence:examination of the use of research in policy documents (which speaks to research utilisation theory); use of research in policy processes (which speaks to interactive engagement theories) and dissemination of research in the public sphere via the mediaRetrospective systematic review of data sourced from the public domain (using the names of the centre’s two monitoring systems as search terms): policy documents; policy processes; media mentions. The review considers the number of mentions and ‘type of mention’: ways in which the research being used (e.g. conceptually), purpose for which referenced (e.g. informing priority areas), value placed on the research (e.g. providing important knowledge in decision-making process) | Use of research in policy documents, policy processes and media | Developed an original framework and successfully used it to structure and implement their study. Then also analysed the findings in relation to a series a key theoretical perspectives on the link between policy and research, e.g. epistemic communities393 and linkage and exchange.394 Had the strength of being entirely independent of the researchers for data collection. However, it recognised that the approach did not extend to considering how far the research findings have changed drug policies in AustraliaThe approach is less complicated than others that have been suggested (Donovan and Hanney;45 Hanney et al., 2003;35 Lavis et al., 2003354) but goes beyond a simple checklist approach (Smith, 2001), whilst also being grounded in policy theory |
| Found: the majority of major drug strategy documents do not reference research, but the monitoring systems referenced in more detailed policy documents. In terms of policy processes, it found that 18 parliamentary committees and inquiries contained a total of 87 mentions of one of the monitoring systems, and often these were in submissions from other bodies. Sixty-eight mentions in the media: 0.2 of total drug mentions, but only 7.4% of drug-related media stories refer to any research | ||||||||
| 119 | Rosas et al.395 | 2013 | Both | USA | NIH: HIV/AIDS Clinical Trials Network | Process marker approach. Out of 419 publications in 2006–8, selected 22 from the network’s flagship studies in terms of scientific priority as primary interventional clinical trials. Obtained data about protocol dates from the network database. Identified publication date and citations on Web of Science. Used PubMed database to identify which citations were meta-analyses, reviews, and guidelines. Operationalises ‘date markers’ in citation data to track dissemination progress by selecting key end points | Citation of research in reviews, meta-analyses and guidelines | Does not need any direct input from the researchers of the projects assessed. However, used a very small sample and the simple citation metrics used have limitations. The time from study approval to citation in guidelines is shorter than identified in some other papers, but the HIV/AIDS field ‘is quite specialized’ |
| Found: 11 of the 22 publications were cited in guidelines within 2 years of publication, mean time from study approval to first guideline citation: 74.1 months | ||||||||
| 120 | Royal Netherlands Academy of Arts and Sciences79 | 2010 | Application | The Netherlands | All fields | Update of evaluation framework previously used by the organisations to assess research, not only its impact, at the level of research organisations and groups or programmes. Self-evaluation and external review, including site visit every 6 years | List a range of specific measures, indicators or more qualitative, that might be used in the self-evaluation. Also for assessment of societal relevance: ‘Several methods have been developed for specific areas (the payback methods for health research, for example) and new methods are being developed’ and here gives a link to the website for the ERiC project – see Spaapen et al.109 Uses the concept of societal quality to refer to productive interactions (as with some other Dutch studies) | As the major approach to assessing publicly funded research in the Netherlands has the strength of ‘a broad scope’ including a focus on the societal relevance of research. However, while the range of options of methods to show societal relevance provides flexibility, there might be uncertainties for institutions and programmes in deciding the best approach for a formal assessment |
| 121 | RSM McClure Watters et al.71 | 2012 | Application | UK | Northern Ireland Executive: HSC research | Payback Framework. Desk analysis of documents and literature, consultations with stakeholders, survey informed by Payback Framework, three case studies, benchmarking. Surveys to all 169 PIs for projects funded between 1998 and 2011 who could be contacted. There was a response rate of 84 (50%) | Used five Payback categories: knowledge/dissemination; benefits to future research (career development, qualifications, extended category to include jobs supported by the research funding); informing policy; health and health sector benefits (health gain, improved service delivery, cost reductions, increased equity); economic benefits (note: main factor considered here was additional funding brought in to support the HSC-funded projects, and leveraging for further funds) | Wide range of methods used to provide comprehensive picture of the context and impact of HSC research funding. There were both strengths and weaknesses in the focus on the economic impact. Given the clear geographic focus of the HSC R&D funding, it was valid to demonstrate the role of the funding from the Northern Ireland Executive in leveraging funding from outside Northern Ireland to support health research in Northern Ireland, but, ‘Much more detailed analysis would be necessary to demonstrate what proportion of this follow-on money was fully leveraged by the original HSC funding’. The case studies ‘provide good examples of the incremental nature of the impacts associated with research within the Health and Social Care field’ |
| Found: 66 PhDs/master’s/MDs supported; considerable career progression; over 100 posts supported; 19% impact on policy development; 20% health gain; 13% cost reductions; 17% increased equity; additional funding covered as much as HSC-funding on projects, substantial leveraged funds for follow-on projects came from outside Northern Ireland | ||||||||
| 122 | Runyan et al.396 | 2014 | Both | USA | Injury Control Research Centers | Not explicitly stated beyond noting that further refinement and identification of systems to support their use:should consider carefully the correspondence of the indicators with the agency’s implementation logic modelArticle mainly describes the methods used to develop the set of 58 indicators (27 priority, 31 supplemental) | The background refers to ‘impacts of academic research centres’: they have a teaching role as well as research role; therefore, indicators are comprehensive. Proposed indicators include: scholarly products; funding (including leveraged funds); policy-related work in relation to government and/or organisational policies (including both consultations and actual impact on policies); technical assistance (including consultation requests, e.g. participation on planning committees for community initiatives); improving community capacity (e.g. collaborations with community members involving collecting or evaluating data); interventions developed | Despite detailed work to develop the list of indicators, the process still needed further refinement and piloting. While the authors reflect the view that the richness of centres’ contributions exceeds the sum of the individual components, it is not clear how far the list of indicators reflect previous theoretical discussions about how this perspective can inform research impact assessments. A growing number of studies assess the impact of long-term funding for research centres, and might take a broader perspective than that applied to specific programmes of research. This feeds into discussion about the role of impact assessment within wider assessment of research:centers will be more receptive to the evaluation process if it is clear how the data are being used and if the information is considered in the context of how centers are designed and operate |
| 123 | Rycroft-Malone et al.102 | 2013 | Application | UK | NIHR: CLAHRCs – HSR | Realist evaluation. Mixed-method case study including interviews, ethnography, document analysis and participant observation | What works for whom in what circumstances in multistakeholder research collaborations, using a CLAHRC as a worked example | Strength: clear and rigorous application of realist method supplemented with other perspectives where appropriate. Weakness: not yet replicated in other CLAHRCs or similar models. Various mechanisms – collaborative action, relationship-building, engagement, motivation, knowledge exchange and learning – which interact with context to produce different outcomes in different parts of the programme |
| 124 | Sainty99 | 2013 | Application | UK | Occupational Therapy Research Foundation | Becker Medical Library model. All 11 grantees who had completed a UK Occupational Therapy Research Foundation-funded project were invited to complete a ‘personalised impact assessment form’ (equivalent to a survey). Eight responded (73%). Two researchers were invited to provide an independent review of the collated findings | Based on the Becker Model, four main categories: research output/advancement of knowledge (e.g. publications, PhD completion, career progression, follow-on funding); clinical implementation (e.g. assessment tools/outcome measures generated, guidelines, loan of final report from library, training materials, clinicians report change in practice); community or public benefits (e.g. service users engagement activities in project, presentations to public); economic benefits | Study informed by a literature review and based on a model. Possibility of recall and selection bias in responses from researchers – the only data source. In relation to the clinically related activities of three projects:Important to note, was the extent to which respondents highlighted this as being in the context of the participating services or host organisationsThis links with a growing number of examples where it is the local application that is recorded which important. It has credibility in that claiming impact in relation to local area know best and fits with the claims that engaging in research is likely to improve health care |
| Found: one PhD, one MPhil, six career progression, four further grants; and three projects – local clinical application | ||||||||
| 125 | Sarli et al.118 | 2010 | Methodological (plus case study) | USA | All health | Developed a new approach called The Becker Medical Library model for Assessment of Research. Started from the logic model of W.K. Kellogg Foundation397 ‘which emphasises inputs, activities, outputs, outcomes, and impact measures as a means of evaluating a program’. Methods proposed in the new model: main emphasis is on the indicators for which the data are to be collected (see column Impact: examined and found), but referring to the website on which indicators made available authors state:Specific databases and resources for each indicator are identified and search tips are provided’. However, in relation to their pilot case study state; ‘For some indicators, supporting documentation was not publicly available. In these instances, contact with policy makers or other officials was required | For each of a series of main headings lists the range of indicators, and the evidence for each indicator. Main headings: research outputs; knowledge transfer; clinical implementation; and community benefit | A comprehensive list, but could be questions about the diversity of items included in some of the categories, and how far they have been fully linked with the organising framework. It was also challenging to establish a clear pathway of diffusion of research output into knowledge transfer, clinical implementation or community benefit outcomes as a result of a research study. This was, in part, due to ‘the difficulty of establishing a direct correlation from a research finding to a specific indicator’. The Becker Model is mainly seen as a tool for self-evaluation:may provide a tool for research investigators not only for documenting and quantifying research impact, but also . . . noting potential areas of anticipated impacts for funding agencies |
| 126 | Sarli and Holmes398 | 2012 | Methodological | USA | All health | The Becker Medical Library model for Assessment of Research – update | Same basic method as in original model, but updated ‘to include additional indicators of research impact based on review of other research projects’ | Claimed that the changes also ‘reflect the authors’ intention to make the model more user friendly’. It has similarities with researchfish. After this, the web version updated on regular basis: https://becker.wustl.edu/impact-assessment (accessed 19 July 2016) |
| 127 | SHRF86 | 2013 | Application | Canada | SHRF | CAHS. Review by external consultant: 22 interviews, including with five researchers whose SHRF-funded work formed the basis of case studies | Five categories from CAHS’s framework: research capacity (e.g. personnel, additional research activity funding, infrastructure); advancing knowledge; informing decision-makers; health impacts; broad economic and social impacts (e.g. research activity) | Applies a framework SHRF had helped develop, but framework applied to just five case studies. Among the claimed facilitators of impact are SHRF’s ‘group-building grants, creation of research groups and networks’. The emphasis on the economic benefits in terms of research jobs attracted is linked to research infrastructure |
| Found: examples of capacity building and researcher retention: three out of five research groups reported limited impact on clinical and policy decision-makers, but one case study describes how a clinic launched as a demonstration project has now been used as the model by others; some guidelines been developed; ‘for every dollar awarded the researcher attains four dollars from external sources of funding . . . suggested that with the presence of special research infrastructure . . . comes higher paying jobs, resulting in a higher tax base and a highly sought knowledge economy’ | ||||||||
| 128 | Schapper et al.72 | 2012 | Both | Australia | Murdoch Children’s Research Institute | Institute’s own research performance evaluation framework ‘based on eight key research payback categories’ from the Payback Framework and draw on the RIF (Kuruvilla et al.123). A committee oversees the annual evaluation with a nominee from each of six themes and external member and chairperson. Evaluation ‘seeks to assess quantitatively the direct benefits from research’. Data are gathered centrally and verified by the relevant theme. Theme with highest score on a particular measure are awarded maximum points, others are ranked relative to this. Each theme nominates the best three research outcomes over 5 years, then interviewed by research strategy team using detailed questionnaire to gain evidence and verify outcomes. Research outcomes assessed using a questionnaire based on the RIF | Three broad categories: knowledge creation; inputs to research; and commercial, clinical and health outcomes. The six major areas of outcomes: development of an intervention; development of new research methods or applications; communication to a broad audience; adoption into practice and development of guidelines and policy; translation into practice – implementation of guidelines and policy; and impact of translation and on health | Framework developed for use in the institute to provide a balanced assessment across the wide range of modes of research conducted in the institute. Despite issues of the weighting to give various factors, and the relative scoring of data the evaluation ‘is generally viewed positively by researchers at the Institute’. However, it might appear rather formulaic. Impact embedded into the performance evaluation and strategic management of a research institute; ‘provides a fair and transparent means of disbursing internal funding. It is also a powerful tool for evaluating the Institute’s progress towards achieving its strategic goals, and is therefore a key driver for research excellence.’ It claims that the evaluation ‘is unique’ |
| 129 | Schumacher and Zechmeister134 | 2013 | Both | Austria | Institute for Technology Assessment and Ludwig Boltzmann Institute for HTA: HTA | An account that goes with the Zechmeister and Schumacher83 study in developing a framework informed by various strands of previous work including Weiss’s enlightenment concept and a ‘multidimensional concept of impact’. Combination of interviews (same 15 as Zechmeister and Schumacher83), download analysis, retrospective routine data analysis and media analysis | Whether or not the HTA research programmes ‘have had an impact on the Austrian healthcare system’. Considered seven impact categories: awareness, acceptance, process, decision, practice, final outcomes (i.e. economic impact), and enlightenment | Comprehensive methods. They developed a matrix to show the methods used, the impact categories to which they relate and the indicators addressed by each method. ‘The strength of our approach is that it takes into account that HTA research may affect all system levels, in a multi-dimensional manner rather than a linear one.’ However, there were only 15 interviews so they were not able to cover all target groups and ‘selection bias may have occurred . . . Further limitations are a lack of benchmarks.’ The study seems to underplay extent to which earlier studies used a combination of methods |
| Found: rising downloads, some reports high media interest; increasingly used for investment decisions and negotiation; ‘Economic impact was indicated by reduced expenditures due to HTA recommendation . . . in places, an “HTA culture” can be recognized’ | ||||||||
| 130 | Scientific Management Review Board399 | 2014 | Methodological | USA | NIH | Describes early stages in developing an approach. Assessments should:examine connections between the generation and communication of basic and clinical knowledge and the impact of this knowledge along different translational pathways | Assessments should attribute outcomes to all contributors, allow sufficient time to have elapsed and ‘begin with identifying the purpose of the study and its audiences’ | Identified issues but progress limited. Relevance for our current review is that it highlights the view from the world’s largest health research funder that considerable further work is required to develop an approach to assess the value of biomedical research supported by the NIH. Referring to data systems such as STAR METRICS says:NIH’s data infrastructure was built primarily to manage grants and contracts during their life cycle, not to track outcomes |
| 131 | Scott et al.73 | 2011 | Both | USA | NIH: Mind–Body Interactions and Health programme | Payback Framework incorporated into the design as a conceptual framework and adapted with greater focus on how the agenda for the programme was shaped and the extent of community outreach and engagement. Centres: documentary review, database analysis, interviews (centre PIs), bibliometric data, construction of narrative templates for centres based on the combined data. Similar approach for projects | Main payback categories as related to the stages of the payback model: primary outputs (knowledge production; research targeting and capacity building – including an emphasis on the effect on the host institution); secondary outputs; final outcomes (improvements in health, well-being and quality of life, changes to health-care service delivery, and broader social and economic impacts) | Adaption of conceptual framework to meet needs of specific evaluation, and use of wide range of complementary methods, but no findings presented in this paper. They considered the range of issues facing impact assessment: timing of evaluation with many outcomes not likely to be evident at the time evaluations usually requested – used term latency to describe that situation; attribution |
| 132 | Shiel and Di Ruggiero114 | 2009 | Methodological | Canada (part of appendix A of CAHS report) | Population and public health research | Recommends that the CAHS should adopt the Payback Framework, as amended by CIHR. Identifies sources for data for the various payback categories: bibliometrics; case studies; evaluation studies of clinical guidelines; database analysis; special studies of specific items | Shows how framework could be introduced to cover population and public health research. Covers the main payback categories: knowledge production; research targeting and capacity; informing policy; health and health sector benefits; and economic impacts | Analyses and contrasts payback studies and ROI studies (and by ROI mean the economic valuation studies, and not the broader use of the term by the CAHS who put the term ROI in the title of their report that recommended a variation of Payback). Also briefly highlights receptor capacity benefits from conducting research (e.g. p. 53) |
| 133 | Solans-Domènech et al.87 | 2013 | Application | Catalonia | Agency for Health Quality and Assessment of Catalonia: respiratory disease | ROI model from CAHS: this paper describes a study within the overall study described in Adam et al.84 Interviews with 23 key informants: researchers and decision-makers. Differences between achieved and expected impact described: expected defined as what hoped to achieve at start | Five main categories from CAHS: advancing knowledge; capacity building; informed decision-making; health and social; and broad economic | The detailed case studies allowed a thorough analysis of expected and achieved impacts, but there were only six cases:teams that include decision-makers or users of health of health information were more effective in achieving outcomes in health policy or practice from the research findings |
| Found: 3/6 projects achieved all expected impacts; there were some unexpected impacts, and some expected impacts not achieved in final outcomes and adoption phase | ||||||||
| 134 | Soper et al.185 | 2013 | Both | UK | NIHR: CLAHRCs – HSR | Did not start with a specific theoretical perspective in the evaluation – adopted a formative and emergent approach, but it informed by various studies: Quebec Social Research Council, Quality Enhancement Research Initiative, Need to Know project. Stakeholder survey of CLAHRCs, in-depth case studies of two CLAHRCs, validation interviews with nine CLAHRCs | From the two CLAHRC case studies they looked at 1. Establishing the CLAHRC, 2. Working as a CLAHRC, and 3. Emerging impacts and legacies. Stated that ‘both CLAHRCs had some comparatively rapid success in making an impact on health care provided locally and more widely across the NHS’. A common feature was use of range of knowledge transfer and exchange strategies. Authors used Mannion et al.’s framework to assess CLAHRCs efforts to encourage cultural change and explain variable success with different groups. Four types of culture: clan, hierarchical, developmental and rational | Did not specify which theories they would test, they considered how best to relate their data to existing theories. Instead they used a formative and emergent approach to analyse whether CLAHRCs met their remit or not. Limited to two case studies of CLAHRCs and people closely associated with them |
| 135 | Spaapen et al.109 | 2007 | Both | The Netherlands | Mostly describes methodological development, illustrated by earlier case studies, including one on the pharmaceutical science programme at Groningen University | SciQuest approach of the ERiC initiative. Mixed-method case studies using qualitative methods, a quantitative instrument called contextual response analysis and quantitative assessment of financial interactions (grants, spin-outs, etc.). SciQuest methodology is deliberately non-prescriptive and context-sensitive. There are four key stages:
|
Productive interactions (direct, indirect and financial) must happen for impact to occur. There are three social domains: science and certified knowledge; industry and market; and policy and societal. For the REPP in the pharmaceutical sciences example they set 15 benchmarks – five for each domain. For each benchmark there were five levels. The faculty had the highest benchmark in: relative citation impact; representation in editorial boards, involvement in industry/market; and additional grants societal/policy | It focuses the assessment on the context and is designed to overcome what were seen as the linear and deterministic assumptions of logic models. The primary goal of the study of the pharmaceutical sciences faculty was to support the faculty in conducting the self-evaluation required under the assessment system for academic research in the Netherlands. SciQuest is described as a ‘fourth generation’ evaluation approach. It draws on the work of Gibbons et al.179 on ‘Mode 2 knowledge production’. SciQuest is theoretically elegant but there are concerns about its feasibility for regular use:The REPP profiles represent the various existing constellations of interactions between a program and its environment. Because of the large quantity of indicators, it is not always easy to transform them interpretatively in the profile to construct such a constellationHowever, as noted, a link to this 2007 report was included in the new evaluation guidelines drawn up by Royal Netherlands Academy of Arts and Sciences79 |
| 136 | Spaapen et al.81 | 2011 | Both | EU – led from the Netherlands | Four case studies: health, ICT, nanotech, social/human sciences | Productive interactions. Based on SIAMPI collaboration. SIAMPI ‘involves two central tasks: to enlighten the mechanisms by which social impact occurs and to develop methods to assess social impact. SIAMPI . . . developed an analytical framework for the study of productive interactions and social impact’. Productive interactions, based on three categories of interaction:
|
The focus of the study was mainly on assessing the interactions. They found:
|
Definition:Social impact of scientific research refers to measurable effects of the work of a research group or program or a research funding instrument in a relevant social domain. The effect regards the human well-being (‘quality of life’) and or the social relations between people or organisationsThe SIAMPI/ERiC stream is widely seen as a major, innovative contribution to the field and is sensitive to institutional goals, however, it is resource intensive, challenging to implement and ‘assumes interactions are good indicators of impact’ (Guthrie et al.9) |
| 137 | Spoth et al.400 | 2011 | Methodological | USA | Family-focused prevention science | Primarily a review. Brief account of the PROSPER model ‘for the delivery of evidence-based intervention’, but also involves evaluation of interventions that are community–university partnerships. Collection of outcome data | Includes analysis of long-term effects. Explores four translational impact factors: effectiveness of interventions; extensiveness of their population coverage; efficiency of interventions; and engagement of populations | Not a traditional model for assessing research impact, but the review covers a range of issues |
| 138 | Sridharan et al.401 | 2013 | Both | International | Teasdale-Corti Global Health Research Partnership Programme | The evaluation was informed by a theory-driven approach (from Pawson et al. 2004) that emphasised iterative learning and assessing performance in light of anticipated timelines of impact. Interviews with planners of the programme. Analysis of the 8/14 final reports then available, and their proposals. Surveys: 1–87 grant recipients attending an initiative symposium; second to four different groups: co-PIs from Canada, co-PIs from southern countries, users, leadership award recipients; each group receiving a different version. Filmed interviews with some grantees. Bibliometric analysis. Brief case studies of three grantees including skype™ (Microsoft Corporation, Redmond, WA, USA) interviews. Documentary analysis and iterative development of the theory of change | Wide range of impacts identified in the proposals and linked to the activities that supported the theory of change. Included knowledge production, capacity building to conduct and use research, enhanced recognition of the role for research in policy and practice and alignment with local needs, strengthened health systems and enhanced health equity, improved health | Very wide-ranging and aimed to conduct a theory-driven evaluation, but limitations in how far they were able to implement a theory-driven approach and the timing limited what impacts could be identified, including from those projects that had not finished at the time of the evaluation. Again, increasing desire to include impacts in programme evaluation, but the timing of such evaluations is too soon for many of the impacts to have arisen. Also the findings mainly presented in terms of the different methods of data collection, which add clarity in terms of the report on each method, but reduces the overall description of how far the various impacts achieved |
| Found:wide range of research [publication], capacity building and knowledge translation outputsCase studies show examples of impact on policies and practice. The proposal analysis identified various discussions about addressing health inequalities, the evaluation found little seemed to have been done on this | ||||||||
| 139 | Sullivan et al.402 | 2011 | Both | UK | UK cancer centres (part of international programme of accreditation – but not a specific stream of funding) | Scientometric/bibliometric analysis, including guidelines. Broad bibliometric analysis but key issue:introduces two new indicators of a centre’s impact, namely the percentages of their papers that are cited on a set of 43 UK cancer clinical guidelines and in stories appearing on the BBC website | Found:We have found substantial variation in the propensity of papers originating from UK cancer centres to be cited on guidelines and in the media. There does not appear to be a correlation with the conventional citation impact of the papers, nor indeed with the size of the centre | Method not applied to funded programmes in this study but might have potential for such application |
| 140 | Sutherland et al.403 | 2011 | Both | UK | Any field: but example on research into means of conserving wild bee populations in UK | Propose ‘a quantitative approach in which impact scores for individual research publications are derived according to their contribution to answering questions of relevance to research end users’. Tested the proposed approach by evaluating the impact of the bee research. Identified key interventions (n = 54), searched for publications (n = 159) that test the interventions. Forty-four stakeholders allocated 1000 points between the different interventions according to how they should be prioritised. Three experts assessed the evidence for each intervention and contribution and relevance of each publication. Finally an impact score was calculated for each paper using an equation that incorporated the various elements (priority score, certainty of knowledge, contribution of knowledge, relevance and number of interventions for which the paper provides evidence) | How far the knowledge would be relevant, etc. for important policies and practice | Developed a new approach having discussed the problems with either assessing impact through stages to direct benefits to society or by counting the amount of communication. The approach could possibly be adapted for application to a programme of research It does not face the problems identified with attempts to track the actual impact from research, but the method is time-consuming. The authors report ‘A potential bias is introduced by the practitioners’ prior knowledge’, but the attempt to identify ways to reduce this suggest that the approach is attempting to identify a way of scoring impact that is insulated from the very context within which knowledge has in reality to exist if it is to make a real-world impact |
| 141 | The Madrillon Group74 | 2011 | Application | USA | NIH: Mind–Body Interactions and Health Programme | Payback Framework incorporated into the design as a conceptual framework (called the Research Payback Framework) and adapted with greater focus on how the agenda for the programme was shaped and the extent of community outreach and engagement (see Scott et al.73). Mixed-methods cross-sectional evaluation design. Used qualitative and quantitative data to build three snapshots of the programme as a whole, the research centres and the research projects. The request for semistructured interviews received 100% response rate from PIs of all 15 centres and all 44 investigator-initiated projects. Impacts of centres scored by adapting the scales used previous in payback studies and presenting the scores as radar graphs | Main payback categories: knowledge production; research targeting and capacity building; influence on policy; influence on health outcomes and health-care delivery; and broader economic and social impacts) | Thorough multimethod study applying and adapting conceptual framework. Conducted innovative analysis through examining three overlapping levels (programme, centre and projects), but while interviews were used rather than a survey, most of the data on wider benefits came from researchers and ‘[d]etermining whether a research project could be credited with an effect within a given benefit category still involved a degree of subjectivity’. The NIH feasibility study had led to a call stating that the Payback Framework should be used for this assessment:As a conceptual framework, the Payback Framework drew attention to a range of outcomes less often considered in other NIH program evaluations and ordered these in a logical manner |
| Found: achieved the programmatic goals and objectives of facilitating interdisciplinary collaboration in research ideas and building research capacity for mind–body research through the development of research personnel and funding of research core services. The centres and projects ‘produced clear and positive effects across all five of the Payback Framework research benefits categories’. Projects: 34% influenced policies; 48% led to improved health outcomes | ||||||||
| 142 | Theobald et al.404 | 2009 | Application | Kenya/Malawi/Nigeria | Liverpool School of Tropical Medicine’s Global Health Development Group: three operational research projects | Case studies organised using RAPID framework from Overseas Development Institute. They selected three cases using pre-defined criteria, including that it was known they had demonstrated an impact on health policy and practice. Analysed the research impact process using RAPID framework for research-policy links, which focuses on: the political context; links between policy-makers and other stakeholders; and the evidence. External influences examined as the wider context. Desk analysis with inputs from the PIs and the Global Health Development Working Group | Impact on health system strengthening and promotion of equity in health service provision | Using a common framework for the analysis of three case studies allowed the analysis to go further than had been reported in individual accounts of the projects, but there were only three case studies and were from one research group rather than a single funder’s programme – paper is at margins of meeting inclusion criteria Key factor:working in partnership with all relevant stakeholders to refine and develop research agendas and undertake research builds an appreciation of research that intensifies the effectiveness of the research to policy and practice interface |
| Found: in all cases, new knowledge and approaches were needed to fulfil policy requirements; they all involved partnerships between researchers and users; the links with policy-makers were not only at policy agenda setting but developing partnerships at multiple levels and with multiple players was key in all cases; the use of equity considerations was central in each case. Also capacity building was important | ||||||||
| 143 | Tremblay et al.405 | 2010 | Both | Canada | CFI: research infrastructure in a range of fields | Developed their own method: the Outcome Measurement Study Unit of analysis is multidisciplinary research themes at individual institutions. A theme includes CFI expenditures in a range of research infrastructure, laboratories, etc., data and computing platforms. Methods combine: research institution completes an in-depth questionnaire covering a series of indicators – the 50 plus questions cover quantitative and qualitative data; expert panel review of the survey data plus other documents followed by a visit to the institution | Evaluates contributions of CFI expenditure to improving outcomes in five categories: strategic research planning; research capacity (physical and human); training of highly qualified personnel; research productivity; and innovation and extrinsic benefits. The indicators listed for each include for the final category: leverage of CFI expenditures; type and amount of knowledge and technology exchange; key innovations – economic, social and organisational, evolving industrial clusters. Panel report for each outcome measurement study | Thorough analysis of approaches to impact assessment led to an approach that combines a range of methods and multiple outcome categories and ‘provides for a richness of analysis’. However, it is quite resource intensive for those being assessed and the assessors; some of the categories of outcomes, and indicators, relate to items such as recruitment of researchers that in other approaches would probably be viewed as inputs because they are directly paid for by the research funding. Perhaps different factors come into play because this is infrastructure funding, which might therefore facilitate the recruitment of researchers |
| Found: examples of social and economic benefits include:Improvements in health care (e.g. improved surgical treatment of brain tumours through pre-op MRI and intra-op ultrasound) | ||||||||
| 144 | Trochim et al.406 | 2008 | Both | USA | Pilot application to National Cancer Institute’s TTURC | Evaluation of large initiatives – a logic model. Concept mapping, logic modelling, a detailed researcher survey, content analysis and systematic peer-evaluation of progress reports, bibliometric analysis and peer evaluation of publications and citations, and financial expenditures analysis | Concept mapping produced domains of collaboration, scientific integration, professional validation, communication and health impacts. Some of these were mainly short-term and process oriented; others were medium or longer term, and outcome oriented This paper mostly about the short-term processes and interactions (details of managing the research programme and, especially, how to measure transdisciplinary collaboration). Brief on long-term markers:TTURC researchers report considerable impact on policies at the state and local levels and on practice with respect to tobacco control |
Describes just a single worked example. Authors also noted that the researchers surveyed expressed:optimism that their research will help lead to significant positive health outcomes, especially for consumption and prevalence [however] they reflect researcher attitudes but do not constitute evidence of long-term impact |
| 145 | UK Evaluation Forum19 | 2006 | Methodological | UK | All health fields | Discusses a range of approaches to assessing impact of medical research, but uses the categorisation of economic impacts from Buxton et al.28 as an organising framework for key sections | Reviewed a range of dimensions of impact but argued the socioeconomic benefits were an area where there was particular need for further studies | An important step in developing health research impact assessment as a field of study, in particular assessment of economic impacts. Key recommendations included:Research funders should identify and fund further research into evaluation methods with a rigour and quality equivalent to other research fields . . . UK research funders should support research to assess the economic impact of UK medical research, which should include critiques of existing economic approachesSubsequently a consortium of funders was formed under the umbrella of the UK Evaluation Forum to advance such studies |
| 146 | Upton et al.149 | 2014 | Methodological | UK | All fields: especially in relation to knowledge exchange | Propose an approach that would shift the focus from the outcomes of knowledge exchange to the process of engagement between academics and external audiences. They claim:by rewarding the process of knowledge exchange, rather than specific impacts, this approach would incentivize participation by a broader range of academics | Focused on analysing roles for assessing outcomes or processes | Recommendations for assessing impact, in particular, related to the higher education innovation funding, knowledge exchange funding It was based on responses from many academics, but the situation might have changed as a result of the REF. Addresses key issue of assessment of processes or outcomes |
| Found:evidence on the varied types of knowledge exchange activity undertaken by academics in different disciplines and institutional types calls into question the likely effectiveness of knowledge exchange drivers based on outcomes | ||||||||
| 147 | Van de Ven and Johnson203 | 2006 | Methodological | N/A | General: could be applied to HSR | Co-production. Interdisciplinarity and productive intersectoral conflict enable the salient features of reality to surface in the Co-production process through ‘arbitrage’ (see Chapter 4) | Intersectoral conflict, especially the ‘two cultures’ of academia and policy-making | Strength: introduces and justifies the pragmatic approach to exploring and achieving impact. Weakness: no well worked-up examples |
| 148 | Walter et al.391 | 2004 | Methodological | Scotland | Social care | Social Care Institute for Excellence | Three models of research utilisation:
|
Pre-dates our review period, but thought important to include because applied in Percy-Smith et al.390 |
| 149 | Weiss120 | 2007 | Methodological | USA | All health | Draws on the United Way model for measuring programme outcomes to develop a medical research logic model. Moves from inputs to activities, outputs and outcomes: initial, intermediate and long term. Discusses various approaches that could be used, e.g. surveys of practitioners to track awareness of research findings; changes in guidelines and education and training; use of DALYs or QALYs to assess patient benefit | Range of dimensions from the outputs such as publications, to clinician awareness, to guidelines, etc., to implementation and patient well-being | While it draws on much existing literature, it is seen as important article in moves towards increased interest in assessment of research impact, especially through the use of logic models |
| 150 | Weiss34 | 1979 | Methodological | N/A | Social science | Weiss’s taxonomy of research utilisation. Impact is rarely direct (either knowledge-driven or problem-solving). It is usually indirect, through sustained interaction between policy-makers and scientists, and occurs through conceptual changes (e.g. ‘enlightenment’). Research findings may be used instrumentally, and also symbolically to support a political decision, or a study may be commissioned tactically to delay a decision | Utilisation of research findings in policy-making | Plausible explanatory model for successes and failures of efforts to get social science research to influence policy. May be less relevant for other types of research/impact |
| 151 | Wellcome Trust93 | 2014 | Both | UK | Wellcome Trust: all funding, some health programmes highlighted | Framework has six outcome measures and 12 indicators of success. Range of qualitative and quantitative measures linked to the indicators and collected annually. Wide range of internal and external sources, including end of grant forms. The information gathering and report production led by the evaluation team though it is reliant on many sources Complementing the quantitative and metric-based information contained in volume 1 of the report, volume 2 contains a series of research profiles that describe the story (to date) of a particular outcome or impact. The Wellcome Trust research profiles – taking the form of highlights and histories – are agreed with the researchers involved and validated by senior trust staff |
The Assessment Framework Report predominantly describes outputs and achievements associated with Trust activities though, where appropriate, inputs are also included where considered a major Indicator of Progress | Another example of a major funder including impact in annual collection of data about the work fundedCase studies and stories have gained increasing currency as tools to support impact evaluation, and are a core component of institution submissions within the UK Research Excellence FrameworkIn future years, as the Trust further integrates its online grant progress reporting system throughout its funding activities (through Wellcome Trust e-Val and MInet) it will be easier to provide access to, and updates on grant-associated outputs throughout their lifecycle |
| Discoveries: applications of research – contributions to the development of enabling technologies, products and devices, uptake of research into policy and practice; engagement; research leaders; research environment; influence | ||||||||
| Found: 6% of grants ending 2012/13 reported filing a patent; 17% engaged with commercial collaborators during their research; £218M in venture capital; 40 inventions during 2012/13. A total of 28% of grants that ended in 2012/13 reported engagement with policy-makers and health-care professionals; 14% reported production of software and/or databases | ||||||||
| 152 | Westhorp164 | 2014 | Methodological | N/A | Evaluation and programme planning | Realist evaluation. This approach involves mixed-method case studies aimed at developing and testing programme theories about what works for whom in what circumstances | No empirical examples given. It does not specifically refer to research impact, but impact in general. Reading across to research, the assumption is that different research findings will have different impacts in different contexts because the context–mechanism–outcome link will be different | Strength: clear and authoritative summary of the realist approach and how it might be applied in impact assessment. Weakness: no examples given, and is for programme evaluation in general |
| 153 | White172 | 1996 | Methodological | N/A | CBPR | CBPR | Lay involvement in research. Involvement may be nominal (to confer legitimacy on a project), instrumental (to improve delivery), representative (to avoid creating dependency) or transformative (to enable people to influence their own destiny) | Elegant and simple tool for assessing (semiquantitatively) the level of lay involvement in a study. Weakness: not tested in HSR. The greater the involvement, the greater the potential impact |
| 154 | Williams et al.78 | 2008 | Application | UK | NHS HTA TARs: economic evaluations | The whole study focused on the use of economic evaluations in NHS decision-making. The part that is relevant for this review is the specific case study on the use of economic evaluations by NICE technology appraisal committees because they explicitly drew on one programme of research, i.e. the HTA TARs. In that case study, the economic evaluations were specifically commissioned to be used in the committee’s decision-making. Data collection informed by grounded theory. Documentary review for the seven identified appraisal topics included; 30 semistructured interviews with members of the NICE appraisal committee; group discussion with NICE technical support team; observation of meetings related to the selected topics. Triangulation of data | Use of economic evaluations in decision-making by NICE about whether or not to recommend specific interventions were made available for patients treated by the NHS | Provides an interesting contrast with many other studies in which the evidence is not produced so directly to be used by formal decision-making structures operating as a ‘receptor body’. However, the economic evaluation was just one part of the evidence from the TAR |
| Found:economic analysis is highly integrated into the decision-making process of NICE’s technology appraisal programme | ||||||||
| 155 | Williams et al.92 | 2009 | Both | USA | NIOSH | Developed the NIOSH logic model: inputs, activities, outputs, transfer, intermediate customs, intermediate outcomes, final customers, intermediate outcomes and end outcomes. Also developed outcome worksheets based on the historical tracing approach (see Project Hindsight407 and TRACES408), which reverse the order:This reversal of order moves beyond the program theory articulated in the logic model and essentially places the burden on research programs to trace backward how specific outcomes were generated from research activitiesThe report describes the development of tools that research programmes could apply to develop an outcome narrative to demonstrate and communicate impact to the National Academies’ external expert review panels established to meet the requirements of the Government’s Performance Assessment Rating Tool The expert panels receiving the documents would score the impact on a 5–0 scale, and separately score relevance of the research, i.e. did the programme appropriately set priorities among research needs and how engaged is the programme in transfer activities? |
Intermediate outcomes include: adoption of new technologies; changes in workplace policies, practices and procedures; changes in the physical environment and organisation of work; and changes in knowledge, attitudes, and behaviour of the final customers (i.e. employees, employers). End outcomes include:reduced work-related hazardous exposures or reductions in occupational injuries, illnesses, and fatalities within a particular disease- or injury-specific area | Thorough account of the development and implementation of tools to prepare data for an outcome narrative for expert panel assessment that has the strength of involving analysis that moves both forwards from the research and backwards from the outcomes. However, inevitably, this account provides only a partial picture and does not provide a complete example of what was prepared for the panel by any programme, or how the panel scored it. Also, while working backwards was seen as a strength in that it focused attention on a collective body of research rather than individual projects, it is not entirely clear what happens to the data identified when working backwards that comes from research programmes other than the one for which the narrative is being prepared. This places the report in the context of increased interest in the USA in evaluating/accounting for the outcomes from publicly funded programmes: Government Performance and Results Act and the Performance Assessment Rating Tool. Quotes from Government document on the Programme Assessment Rating Tool:The most significant aspect of program effectiveness is impact- the outcome of the program, which otherwise would not have occurred without the program intervention |
| Found: the report provides a few examples of impacts found by some NIOSH programmes, but they are illustrations and not full presentation of findings, e.g. the Hearing Loss Prevention programme initially identified 44 outcomes across 10 major research areas | ||||||||
| 156 | Wilson et al.409 | 2010 | Application | UK | Applied and public health research but from a range of UK programmes | As part of a wider survey the questions related to impact informed by questions from RIF. Survey to 485 PIs (232 completed) mainly focusing on dissemination of their research in general, but asked PIs to select one example of a project they had disseminated and answer more questions including some on research impact. It compared the responses to the various questions to analyse dissemination factors associated with the reporting of research impact | Impact on policy, health services and citation in clinical guidelines | Comparison of data from separate questions on (a) aspects of dissemination and (b) impacts claimed provides interesting findings, but only partially relevant for impact from programmes because the focus was on PIs from a range of programmes and they could chose examples of research on which to concentrate, etc. Those ‘receiving dissemination advice and support, and/or who believe that researchers need to do more than publish academic journal articles were more likely to report policy impacts . . . having access to dissemination support . . . appears to increase the chance that research findings are misreported’. ‘Although only a minority indicated that they routinely recorded formal or informal feedback about the impact of their research, when asked about impact in relation to specific research they had recently completed most respondents were able to provide examples’ |
| Found: 70% provided some details on impact on health policy and practice; 51% research led to discussions or interactions with policy-makers or cited in policy documents; 28% cited in clinical guidelines; 49% research had, or likely to have, influence on the acceptability or availability of a health intervention or on the organisation of health service: evidence claimed for this included citation in guidelines, or named specific interventions where acceleration anticipated. A total of 29 respondents felt their findings had been misrepresented or used in ways they felt inappropriate; 15 of which referred to the media | ||||||||
| 157 | Wooding et al.36 | 2014 | Both | Australia/Canada/UK | Leading medical research funders: cardiovascular and stroke | The study, called Project Retrosight, built on Payback Framework – developed new methods to expand analysis. Web-based survey, interviews, bibliometric analysis A total of 29 case studies (12 Canadian, nine UK and eight Australian). Scoring of case studies by experts and research team. Analysis of factors associated with impact by comparing the scores with features of the research processes recorded in the case studies |
Assessed factors associated with impact in two groupings of the five payback categories – academic impact and wider impact. The 29 case studies revealed a number of findings: diverse range of impacts, variations between the impacts of basic biomedical and clinical research, no correlation between knowledge production and wider impacts, engagement with practitioners and patients is associated with high academic impact and high wider impacts, etc. Biomedical research = more academic impact, clinical research = more wider impacts (on health policies and health gain). Collaboration = wider impact | Using case studies enabled Project Retrosight to identify paybacks which otherwise would not have been detected. A complex set of steps, methods and innovation were required to understand success and translation. These methods allowed a large and robust data set which, when applied, developed new approaches to understand factors associated with high and low payback. However, there were only 29 case studies, so there could have been inconsistencies between projects and countries. Health research funder wishing to achieve wider impacts should not use academic impacts as a proxy. Pathways to impact = funders should consider ways to assist researchers to maximise potential for research to be translated |
| 158 | Wooding et al.104 | 2009 | Both | UK | ARC: wide range | The framework developed and applied in this study subsequently was named the RAND/ARC Impact Scoring System – see Grant et al.,38 although that name not used in this report. It was developed from the Payback Framework and linked to research pathways developed to show the roles of different types of research within an overall portfolio. A web-based tick-list survey completed by PIs. It was piloted in 2007 on 136 grants ending in 2002 and 2006 (118 replies: 87% response rate). All data from each grant presented on one sheet called an ‘impact array’ in which each row of blocks shows all the answers from one grant, and each column represents all the answers to a single question. Each coloured block shows a positive response to the question. The research pathway and impact array data were then combined to explore which types of research gave rise to particular types of impact | Included: future research (e.g. further funding/new collaborations, contribution to careers, new tools); dissemination; health policy (citations on guidelines, contribution to guideline committees and discussion of health policy); training (undergraduates and health professionals); interventions/products (new treatments, public health advice, etc.) | The author’s claim:Overall the indications are that the instrument is an effective and low burden way of collecting an overview of the impacts arising from a portfolio of research . . . [But] depends on the researchers’ knowledge and honesty, and simplifies quantification of impacts and their attributionWhile the presentation of the data in an impact array clearly shows the overall picture in which some types of impact are much more common than others, it provides a rather complex picture. Quantification was recognised as an issue because while adopting a ticklist approach provided simplicity, it limited the information obtained, e.g. could not record if more than one example of an impact from the same grant. Development work on the Research Impact Questionnaire fed in further developments of surveys for routine assessment such as e-Val |
| Found: > 80% of grants generated new research tools, 50% of which were shared; 2.5% of research led ‘to diagnostics, therapeutics or public health advice that is in or nearing use, and 7.6% has generated intellectual property that has been protected or is in the process of being so’ and six projects (5%) to policy impact | ||||||||
| 159 | Xia410 | 2011 | Application | USA | AHRQ: The Effective Health Care Programme | None stated. Database analysis: they examined the AHRQ online database and compiled a list of conclusions from completed comparative effectiveness reviews in various therapy areas. Then they compared these conclusions to the current access of these therapies in a selection of the largest US plans by lines covered using their online formulary databases | Impact of AHRQ findings on formulary decisions of health-care organisations | Very little detail available from abstract and findings not strong, but potentially relevant for analysis of NIHR HTA programme |
| Found:It appears that these comparative effectiveness reviews by the AHRQ have some indirect impact on formulary access in the US. However, price and contracting, in addition to efficacy and safety are among the key determinants for plans | ||||||||
| 160 | Zachariah et al.141 | 2014 | Application | International | World Health Organization/ Special Programme for Research and Training in Tropical Diseases Structured Operational Research and Training Initiative: adopted an existing training initiative | None stated. Retrospective cohort study, by survey, of attendees of eight operational research capacity building courses: 93 enrolled, 83 completed. A total of 89 published papers and 88 replied about policy and practice. For each reported impact claimed from a published paper, a description of the attributed effect was requested. Categorisation was done by two independent researchers | Course completion (i.e. capacity building); attendees published papers assessed for impact on policy and practice | High response rate to survey; rare example of assessing wider impacts from capacity building course and range of example briefly described. However, the effects were self-reported and may have been responder bias. Possible factors for rapid translation include:participant selection that favours programme staff, studies being focused on healthcare delivery; research questions being of direct programme relevance; early engagement and buy-in of programme managers and/or policy makers; and inclusion of stakeholders as co-authors on publications |
| Found: 65 (74%) stated impact on policy and practice, including: 11 influenced national strategic policy and/or national guidelines; 12 national data monitoring was adapted; 13 change in routine implementation of a national programme; 14 change in routine implementation of a local programme | ||||||||
| 161 | Zechmeister and Schumacher83 | 2012 | Both | Austria | Institute for Technology Assessment and Ludwig Boltzmann Institute for HTA: HTA | Developed own methods but were partly informed by the work in Quebec described in our 2007 review,2 i.e. Jacob.43,44 Identified all HTA reports aimed at use before re-imbursement decisions made (category 1) or for disinvestment of oversupplied technologies (category 2). There were 11 full HTA reports, 58 rapid assessments. Descriptive quantitative analysis of administrative data informed by studies such as Jacob (1993, 1997) and 15 interviews with administrators and payers | Impact on ‘reimbursements/investment and disinvestment decisions that may have consequences for volume supplied, expenditure/or resource distribution . . . an impact in terms of rationalisation (reducing oversupply) or re-distribution of resources into evidence-based technologies, and we attempt to calculate this in monetary dimensions’ | It uses two main methods and ‘were able to present a rich picture of different perspectives’. The report provides a brief narrative of a range of examples and the calculations of the cost savings. However, while they were able to claim the majority of reports ‘have been used in decision processes’ the wording about the level of impact is much less clear:they had at least a selective effect on volumes supplied, expenditure and/or resource distributionIt raises a series of important questions about the nature of informing decisions: 67 of the 69 reports ‘were used for’ decisions and other factors also played a role in most cases. It look at both investment and disinvestment decisions |
| Found: five full HTA reports and 56 rapid assessments ‘were used for reimbursement decisions’. Four full HTAs and two rapid assessments ‘used for disinvestment decisions and resulted in reduced volumes and expenditure’. Two full HTAs had no impact. Other factors also played a role, but in only 45% of reports ‘the recommendation and decision were totally consistent’ and 53% partially consistent |
Appendix 4 List of interesting studies
The papers listed below are ones that were identified but either did not meet inclusion criteria for the updated review or they were reports or other publications covering the same material as publications that were included either in the current review or in our review conducted in 2005 and published in 2007. 2 Some papers on monetised health gains were excluded from the update, as they did not assess the value of the health gain from specific programmes of research. However, these were included in Chapter 5 on the monetary value of health research because that provided a broader analysis. The list below is only a selection of the potentially relevant papers that we reviewed but were not included in the final 161 included studies.
Access Economics. Exceptional Returns: The Value of Investing in Health Research in Australia. Prepared for the Australian Society for Medical Research. Canberra, ACT: ASMR; 2008.
Al-Kwifi, Osama S. Improving the accuracy of measuring the impact of health research: a global perspective. J Global Bus Adv 2012;5:271–84.
Australian Research Council. ERA 2012 Submission Guidelines, Excellence in Research for Australia. Canberra, ACT: Australian Research Council; 2011. 411
Basu A, Jena A. The impact of comparative effectiveness research on health and health care spending. J Health Econ 2011;30:695–706.
Boaz A. Systematic Reviews as a Source of Evidence for Policy: An In-depth Exploration of a Review on Mentoring. PhD thesis. London: University of London; 2006.
Boaz A, Fitzpatrick S, Shaw B. Assessing the Impact of Research on Policy: A Review of the Literature for a Project on Bridging Research and Policy through Outcome Evaluation. London: Policy Studies Institute; 2008.
Bornmann L. What is societal impact of research and how can it be assessed? A literature survey. J Am Soc Inf Sci Technol 2013;64:217–33.
Bornmann L, Marx W. How should the societal impact of research be generated and measured? A proposal for a simple and practicable approach to allow interdisciplinary comparisons. Scientometrics 2014;98:211–19.
Brazil K. From theory to practice: improving the impact of health services research. BMC Health Serv Res 2005;5:1.
Health Economics Research Group, Office of Health Economics, RAND Europe. Medical Research: What’s it Worth? Estimating the Economic Benefits from Medical Research in the UK. London: UK Evaluation Forum; 2008.
Canadian Health Services Research Foundation. Measuring the Impact of Research: What Do We Know? Part 1. Ottawa, ON: Canadian Health Services Research Foundation; 2008.
Chalkidou K, Tunis S, Lopert R, Rochaix L, Sawicki PT, Nasser M, et al. Comparative effectiveness research and evidence-based health policy: experience from four countries. Milbank Q 2009;87:339–67.
Chaney EF, Rubenstein LV, Liu CF, Yano EM, Bolkan C, Lee M, et al. Implementing collaborative care for depression treatment in primary care: a cluster randomized evaluation of a quality improvement practice redesign. Implement Sci 2011;6:15.
Chang W-C, Tung Y-C, Huang C-H, Yang M-C. Performance improvement after implementing the balanced scorecard: a large hospital’s experience in Taiwan. Total Qual Manag Bus Excellence 2008;19:1143–54.
Clarke A, Royle P. Feeling the impact. Eur J Public Health 2012;22:614–15.
Committee on Measuring Economic Investments Other Returns on Federal Research. Measuring the Impacts of Federal Investments in Research. A Workshop Summary. Washington, DC: The National Academies; 2011.
Corbacho B, Pinto-Prades JL. Health economic decision-making: a comparison between UK and Spain. Br Med Bull 2012;103:5–20.
Council for the Humanities, Arts and Social Sciences. Measures of Quality and Impact of Publicly Funded Research in the Humanities, Arts and Social Sciences. Canberra, ACT: CHASS, Department of Education, Science and Training; 2005.
de Campos A. A study on methodologies for research impact assessment: responses of the UK Research Councils to the Warry Report. Ind Higher Educ 2010;24:393–7.
de Oliveira C, Nguyen HV, Wijeysundera HC, Wong WW, Woo G, Grootendorst P, et al. Estimating the payoffs from cardiovascular disease research in Canada: an economic analysis. Can Med Assoc Open Access J 2013;1:E83–90.
Dean A, Wykes M, Stevens H. 7 Essays on Impact. DESCRIBE Project Report for Jisc. Exeter: University of Exeter; 2013.
Department for Innovation, Universities and Science. Economic Impacts of Investment in Research & Innovation. London: DIUS; 2007.
Donovan C, Hanney S. The ‘Payback Framework’ explained. Res Eval 2011;20:181–3.
Dorendorf E, Gerhardus A. A systematic review of the impact of HTA reports [abstract]. IV Annual Meeting of Health Technology Assessment International 2007:233. URL: www.htai.org/meetings/annual-meetings/past-annual-meetings/htai-2007-barcelona/barcelona-spain.html (accessed 15 July 2016).
van Drooge L, van den Besselaar P, Elsen GMF, de Haas M, van den Heuvel JJ, Maassen van den Brink H, et al. Evaluating the Societal Relevance of Academic Research: A Guide. Den Haag: Evaluating Research in Context, Rathenau Instituut; 2010.
European Science Foundation. Evaluation in National Research Funding Agencies: Approaches, Experiences and Case Studies. Strasbourg: European Science Foundation; 2009.
European Science Foundation. The Challenges of Impact Assessment. A report by the ESF MO Forum on Evaluation of Publicly funded Research – Working Group 2: Impact Assessment. Strasbourg: European Science Foundation, 2012.
Fournier MF. Knowledge mobilization in the context of health technology assessment: an exploratory case study. Health Res Policy Syst 2012;10:10.
Fronsdal KB, Facey K, Klemp M, Norderhaug IN, Morland B, Rottingen JA. Health technology assessment to optimize health technology utilization: using implementation initiatives and monitoring processes. Int J Technol Assess Health Care 2010;26:309–16.
Frontier Economics. Rates of Return to Investment in Science and Innovation. A report prepared for the Department for Business, Innovation and Skills (BIS). London: Frontier Economics Ltd; 2014. URL: www.gov.uk/government/uploads/system/uploads/attachment_data/file/333006/bis-14-990-rates-of-return-to-investment-in-science-and-innovation-revised-final-report.pdf (accessed 15 July 2016).
Glover M, Buxton M, Guthrie S, Hanney S, Pollitt A, Grant J. Estimating the returns to UK publicly funded cancer-related research in terms of the net value of improved health outcomes. BMC Med 2014;12:99.
Graham I, Tetroe J. Learning from the U.S. Department of Veterans Affairs Quality Enhancement Research Initiative: QUERI Series. Implement Sci 2009;4:13.
Hanney SR, González-Block MA. Four centuries on from Bacon: progress in building health research systems to improve health systems? Health Res Policy Syst 2014;12:56.
Harris R. Impact of Research on Development Policy and Practice: An Annotated Bibliography. 2013. URL: www.rogharris.org/uploads/5/0/5/4/5054025/impact_of_research_on_development_policy_and_practice_annotated_bibliography.pdf (accessed 15 July 2016).
Hegger I, Janssen SW, Keijsers JF, Schuit AJ, van Oers HA. Analyzing the contributions of a government-commissioned research project: a case study. Health Res Policy Syst 2014;12:8.
Hovland I. Making a Difference: M&E of Policy Research. Overseas Development Institute Working Paper 281. London: ODI; 2007.
Hughes A, Martin B. Enhancing Impact. Council for Industry and Higher Education and UK Innovation Research Centre, University of Cambridge; 2012. URL: www.cbr.cam.ac.uk/fileadmin/user_upload/centre-for-business-research/downloads/special-reports/specialreport-enhancingimpact.pdf (accessed 15 July 2016).
Jansen MW, Ruwaard D. Making an impact instead of ‘publish or perish’. Eur J Public Health 2012;22:613–14.
Jones T, Donovan C, Hanney S. Tracing the wider impacts of biomedical research: a literature search to develop a novel citation categorisation technique. Scientometrics 2012;93:125–34.
Kalucy L, Jackson-Bowers E, McIntyre E, Hordacre A, Reed R. Exploring the impact of primary health care research. Final Report Stage 2 Primary Health Care Research Impact Project. Primary Health Care Research and Information Practice; 2009. URL: www.nodo50.org/fadsp/archivos/ImpactoINvestigacionAP.pdf (accessed 15 July 2016).
Lafortune L, Farand L, Mondou I, Sicotte C, Battista R. Assessing the performance of health technology assessment organizations: a framework. Int J Technol Assess Health Care 2008;24:76–86.
Lane J, Bertuzzi S. Measuring the results of science investments. Science 2011;331:678–80.
Research Australia. The Economic Value of Australia’s Investment in Health and Medical Research: Reinforcing the Evidence for Exceptional Returns. Melbourne, VIC: Lateral Economics; 2010.
Leclerc A, Chastang J-F, Kaniewski N, Cyr D, Ozguler A, Descatha A. The bibliographic impact of epidemiological studies: what can be learnt from citations? J Occup Environ Med 2010;67:213–16.
Lewison G, Sullivan R. The impact of cancer research: how publications influence UK cancer clinical guidelines. Br J Cancer 2008;98:1944–50.
Liverani M, Hawkins B, Parkhurst JO. Political and institutional influences on the use of evidence in public health policy. A systematic review. PLOS ONE 2013;8:e77404.
Miller FA, Mentzakis E, Axler R, Lehoux P, French M, Tarride JE, et al. Do Canadian researchers and the lay public prioritize biomedical research outcomes equally? A Choice Experiment. Acad Med 2013;88:519–26.
Mohammadi E, Thelwall M. Assessing non-standard article impact using F1000 labels. Scientometrics 2013;97:383–95.
Moore G, Redman S, Haines M, Todd A. What works to increase the use of research in population health policy and programmes: a review. Evid Policy 2011;7:277–305.
Moses H 3rd, Dorsey ER, Matheson DH, Thier SO. Financial anatomy of biomedical research. JAMA 2005;294:1333–42.
Nason E, Janta B, Hastings G, Hanney S, O’Driscoll M, Wooding S. Health Research – Making an Impact: The Economic and Social Benefits of HRB Funded Research. Dublin: RAND Europe; 2008.
Neufeld V, Cole D, Boyd A, Njelesani D, Bates I, Hanney SR. Perspectives on Evaluating Global Health Research for Development: A Background Paper. Ottawa, ON: Canadian Coalition for Global Health Research; 2014.
Oliver K, Innvaer S, Lorenc T, Woodman J, Thomas J. A systematic review of barriers to and facilitators of the use of evidence by policymakers. BMC Health Serv Res 2014;14.
Peach I, Marshall J. The Economic Benefits of Health Research in Saskatchewan. Regina, SK: Saskatchewan Health Research Foundation; 2008. URL: http://shrf.ca/common/pdf/Benefits_of_Health_Research.pdf (accessed 15 July 2016).
Peckham S, Willmott M, Allen P, Anderson S, Goodwin N. Assessing the impact of the NHS Service Delivery and Organisation Research and Development Programme. Evid Policy 2008;4:313–30.
Raftery J, Hanney S, Green C, Buxton M. Assessing the impact of England’s National Health Service R&D Health Technology Assessment program using the ‘payback’ approach. Int J Technol Assess Health Care 2009;25:1–5.
Roback K, Dalal K, Carlsson P. Evaluation of health research: measuring costs and socioeconomic effects. Int J Prev Med 2011;2:203–15.
Torrens A, Thompson A. The social impact of research conducted in Russell Group universities. Russell Group Papers 2012:3.
Mateu PF, Hobson KA, Coryn S, Schröter DC. Key Issues and Trends in Evaluating Research Excellence in Applied Development Contexts: A Review and Synthesis of the Serial and Grey Literature. Kalamazoo, MI: Western Michigan University; 2012.
Scoble R, Dickson K, Fisher J, Hanney SR. Research Impact Evaluation, a Wider Context: Findings from a Research Impact Pilot. Uxbridge: Brunel University; 2010.
Scoble R, Dickson K, Hanney S, Rodgers GJ. Institutional strategies for capturing socio-economic impact of academic research. J Higher Education Policy Manag 2010;32:499–510.
Spaapen J, van Drooge L. Introducing ‘productive interactions’ in social impact assessment. Res Eval 2011;20:211–18.
Stevens H, Dean A, Wykes M. DESCRIBE Project: Final Project Report. Exeter: University of Exeter; 2013.
Stone V, Lane J. Modeling technology innovation: how science, engineering, and industry methods can combine to generate beneficial socioeconomic impacts. Implement Sci 2012;7:44.
Sweet S, Ginis KA, Estabrooks P, Latimer-Cheung A. Operationalizing the RE-AIM framework to evaluate the impact of multi–sector partnerships. Implement Sci 2014;9:74.
Thorton I, Shaw A. Evaluating the Impact of Research Programmes. London: UK Collaboration on Development Sciences; 2013.
Tran NI, Hyder AA, Kulanthayan S, Singh S, Umar RSR. Engaging policy makers in road safety research in Malaysia: a theoretical and contextual analysis. Health Policy 2009;90:58–65.
UK Collaboration on Development Sciences (UKCDS). Evaluating the Impact of Research Programmes – Approaches and Methods. Report of an international Workshop. London: UKCDS; 2013.
University Health Network. Achieving Our Vision: Balanced Scorecard. URL: www.uhn.ca/corporate/AboutUHN/AchievingOurVision/Pages/balanced_scorecard.aspx (accessed 7 October 2014).
Wells R, Whitworth J. Assessing outcomes of health and medical research: do we measure what counts or count what we can measure? Aust New Zealand Health Policy 2007;4:1.
Wooding S, Hanney S, Buxton M, Grant J. Payback arising from research funding: evaluation of the Arthritis Research Campaign. Rheumatology 2005;44:1145–56.
Wooding S, Pollitt A, Diepeveen S, Guthrie S, Jones MM, Chonaill SN, et al. Mental Health Retrosight. RAND for the Alliance of Mental Health Research Funders; 2013. URL: http://lbr.rand.org/content/dam/rand/pubs/research_reports/RR400/RR452/RAND_RR452.pdf (accessed 2 December 2014).
Yazdizadeh B, Majdzadeh R, Salmasian H. Systematic review of methods for evaluating healthcare research economic impact. Health Res Policy Syst 2010;8:6.
Appendix 5 Frameworks included in previous analyses by RAND Europe
Below we set out a range of conceptual frameworks or approaches that were included in the main comparative analysis described in at least one of the three studies from RAND Europe: Brutscher et al. ,37 Grant et al. 38 and Guthrie et al. 9 In each case we note if the framework was included in the list of frameworks in Chapter 3, and if it was not we briefly describe the reason(s).
| Framework for assessing impact from health research (country) | Description of whether or not it was included in account of frameworks in Chapter 3, or the reason for not including framework in list of those described in detail and compared in Chapter 3 |
|---|---|
| CAHS (Canada) | Included in the list of frameworks in Chapter 3 |
| Congressionally directed medical research programme (USA) | Designed to track the annual progress of projects conducted for the US Army Medical Research and Material Command. Perhaps it was too specific for wider application. The ‘research product’ is a central element:One rationale is that the pressure on the CDMRP (as a military command) is even higher to develop productsBrutscher et al. 2009, p. 6237 |
| Department for Innovation, Universities and Skills (UK) | Included in the list of frameworks in Chapter 3 as part of the background to the current approaches to monetary value approaches; specifically the previous version of the data collection undertaken by the MRC (2013) |
| EU FPs | Several studies included in Table 14 describe approaches previously used to assess EU FPs (e.g. Arnold et al.;133 Hansen et al.111) but the Court of Auditors criticised the lack of information on impacts from FPs’ health research and several studies in Table 14 describe work to develop new approaches (Expert Panel;53 Guinea et al.64). Hence, the position seems uncertain, and we have not included this |
| ERiC (the Netherlands) | While this was not directly included in the list of 20 frameworks in Chapter 3, some of the team conducting this Dutch study also led a parallel EU FR7 project that produced the Productive Interactions (SIAMPI) framework that is included in Chapter 3 (see also an account of ERiC in Spaapen et al.140 in Table 14) |
| ERA (Australia) | The criteria for the ERA framework are described in a report by the Australian Research Council,411 but ERA is not comprehensive in terms of impacts, and has an academic focus (Guthrie et al.9), which is why the EIA was developed to complement it (Group of Eight and Australian Technology Network of Universities105) |
| Leiden University Medical Centre (the Netherlands) | Included in the list of frameworks in Chapter 3 as the Societal Quality Score |
| MOIRA and NHMRC (Australia) | MOIRA was reported in Brutscher et al.37 2009 as an approach developed at the Australian NHMRC as a possible way of introducing impact into ex ante assessment of proposals. Of potentially more relevance to our review, it was thought it might inform the development of a new NHMRC end of grant form. While a new form was developed, and applied 6 months after project competition, as described in one of our included studies, i.e. Kingwell et al.,139 it was not included in the recent review from Australia by Milat et al.129 |
| NIHR Dashboard (UK) | Although developed for use by NIHR and has comprehensive coverage of financial data and internal and external processes, it is not designed to capture data for impact assessments (see Guthrie et al.)9 |
| PART (USA) | Partially included in the list of frameworks in Chapter 3, in that the NIOSH logic model described by Williams et al.92 was developed in order to gather data for an assessment under PART. However, PART is used widely to assess publicly funded programmes in general, and covers many issues such as programme design, so it takes a somewhat different form in relation to research than to most other areas |
| Payback Framework (UK) | Included in the list of frameworks in Chapter 3 |
| Productive Interactions (the Netherlands) | Included in the list of frameworks in Chapter 3 as SIAMPI |
| RAND/Arthritis Research Campaign Impact Scoring System (UK) | Included in the list of frameworks in Chapter 3, but as part of the background to regular monitoring |
| REF (UK) | Included in the list of frameworks in Chapter 3 |
| RQF (Australia) | Included in the list of frameworks in Chapter 3 but as part of the background to the REF |
| STAR METRICS (USA) | Developed for regular monitoring of US publicly funded research but not fully developed. The Scientific Management Review Board of the NIH said in relation to STAR METRICS and other developments:NIH’s data infrastructure was built primarily to manage grants and contracts during their life cycle, not to track outcomesScientific Management Review Board, NIH, p. 19399 |
| VINNOVA (Sweden) | Included in the list of frameworks in Chapter 3 |
Appendix 6 Summary of methods for estimating the monetary value of the impact of health research
| Authors | Publication year | Country | Unit of analysis | Investment | How were health gains measured? | How were health gains valued? | Were health gains ex post or ex ante? | Were the costs of delivery accounted for? | Was the lag between investment and health gains considered? | How was the attribution problem addressed? | Results |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Johnston et al.75 | 2006 | USA | Programme (NIH) | 28 Phase III RCTs funded by National Institute of Neurological Disorders and Stroke prior to 2000 | 10 year and 30 year post funding QALYS (identified through cost–utility analyses) | QALYs valued at GDP per head (US$40,310) | Ex post | Yes; societal costs | Yes; implicitly as usage post trial | Assumed that all changes in usage are prompted by Phase III RCTs | ROI of 46% per year (US$335M investment; 470,000 QALYS net US$3.3B treatment costs) |
| Buxton et al.22 | 2008 | UK | Disease (cardiovascular R&D) | Publicly and charitably funded cardiovascular research (1975–88 in base case) | QALY gains 1986–2005 (identified through cost–utility analyses) | QALYs valued at health-care opportunity cost (£25,000) | Ex post | Yes; health service costs | Yes; 17-year lag between investment and health gain (investment 1975–88, heath gains 1992–2005) | Assumed that 17% of health gain attributable to UK cardiovascular disease R&D | IRR of 9% per year (£2B investment 1975–1992; 2.76M QALYS, net £781 treatment costs per year 1986–2005) |
| Access Economics24 | 2008 | Australia | Country (Australian R&D) | All R&D spending public and private between 1992/3 and 2004/5 | DALYs averted relative to 1993 levels | DALYs valued at willingness-to-pay for statistical life-year (AU$266,843) | Ex ante | No | Yes; 40-year lag between investment and health gain (investment 1993–2005, health gains 2033–45) | Assumed that 50% of health gains are attributable R&D, of which 3.04% is Australian R&D | ROI: 117% per dollar invested |
| Lakdawalla et al.220 | 2010 | USA | Disease (‘The war on cancer’) | All cancer R&D funding 1971–2000 | Life-year gains in cancer survival 1988 to 2000 | Inframarginal changes in survival valued at willingness to pay (US$30,737) | Ex post | Yes; lifetime cancer spending | No; not explicitly, but acknowledged | Implicitly assumed that all gains were result of US R&D | Social surplus US$1.6–US$1.9T (US$2.3T health gains, US$30B investment) |
| Robacket al.218 | 2011 | Sweden | Country (Swedish R&D) | All R&D spending public and private on clinical and health research in 2005 | QALY gains – based on average annual increase in life expectancy, utility (0.75) adjusted and multiplied by 2015 population | QALYs valued at value of statistical life (assumed to be SEK500,000) | Ex ante | Yes; estimation of effect of more expensive methods of treatment | Unclear; implicitly assumed 10-year lag? | Assumed that 50% of health gains are attributable R&D, of which 3% is Swedish R&D | ROI of 1.08 (SEK21B investment in 2005, SEK14B QALYs but also including other socioeconomic returns) |
| Deloitte Access Economics25 | 2011 | Australia | Programme (NHMRC) | NHMRC funding 2000–2010 (cardiovascular disease, cancer, sudden infant death syndrome, asthma and muscular dystrophy R&D) | DALYs averted relative to 2000 levels | DALYs valued at willingness to pay for statistical life-year (AU$168,166) | Ex ante | No | Yes; 40-year lag between investment and health gain (investment between 2000–2010, health gains between 2040–50) | Assumed that 50% of health gains are attributable R&D, of which 3.14% is Australian R&D and 25% of which is NHMRC | ROI of 509% in cardiovascular disease, 170% in cancer, 12% in sudden infant death syndrome, 23% in asthma and –30% for muscular dystrophy, but also included indirect benefits |
| de Oliveira et al.219 | 2013 | Canada | Disease (cardiovascular R&D) | Publicly and charitably funded cardiovascular research 1981–92 | QALY gains 1994–2005 (identified through cost–utility analyses) | QALYs valued at CA$50,000 | Ex post | Yes; health service costs | Yes; 13-year lag between investment and health gain (investment 1981–92, health gains 1994–2005) | Assumed that 70% of health gains are attributable to R&D, of which 6% is attributable to Canadian R&D | ROI: IRR 21% per year (CA$392M investment 1981–1992; 2.21M QALYS net CA$20M treatment costs 1994–2005) |
| Glover et al.26 | 2014 | UK | Disease (cancer R&D) | Publicly and charitably funded cardiovascular research (1976–95 in base case) | QALY gains 1991–2010 (identified through cost–utility analyses) | QALYs valued at health-care opportunity cost (£25,000) | Ex post | Yes; health service costs | Yes; 15-year lag between investment and health gain (investment 1976–95, health gains 1991–2010) | Assumed that 17% of health gain attributable to UK cancer R&D | IRR of 10% per year (£15B investment 1970–2009, 5.9M QALYs net £24B treatment costs) |
| Guthrie et al.27 | 2015 | UK | Programme (HTA) | NIHR HTA funding (1993–2013) | QALY gains from ten ‘key’ studies (through cost–utility analyses) | QALYs valued at health-care opportunity cost (£20,000) | Ex ante | Yes; health service costs | No; hypothetical gains based on 1 year’s full implementation | Assumed that HTA trials were definitive (i.e. 100% attribution) | Net benefit £3B (£367M investment 1993–2013) |
Appendix 7 Studies of impact assessment in the 2014 Research Excellence Framework
The census date for this systematic review (2005–15) meant that our search just captured the reports from the HEFCE on the 2014 REF, but not evaluations published soon afterwards that assessed the success of that exercise. As the approach to impact assessment in the 2014 REF is widely viewed as an important innovation (e.g. other countries are looking to emulate the REF model for impact assessment105,412), we include an account of the REF and brief description of the published evaluations here.
The 2014 REF was an extensive exercise to assess UK universities’ research performance with a view to informing the allocation of a central budget (‘quality in research’ funding). It built on similar exercises held in 2008, 2001 and earlier years. Unlike previous exercises, in which scores had been allocated on the basis of publications, infrastructure and ‘prestige’, the 2014 REF introduced an additional category: 20% of the total score (and hence funding) was awarded for research impact. 106
Accordingly, as part of its REF submission, each higher education institution submitted an ‘impact template’ describing its strategy and infrastructure for achieving research impact, along with a sample (between 2 and 49, depending on the size of the submission) of impact case studies. Each case study was four pages long and described a programme of research along with the claimed impacts from that programme and supporting evidence. Impact case studies were required to follow a sequential and time-bound structure (describe research undertaken between 1993 and 2013 and then describe impact occurring between 2008 and 2013). In the REF, impact templates and case studies were peer reviewed by an intersectoral assessment panel representing academia and research users (industry and policy-makers). 106
The final report from the Medicine Panel in the 2014 REF106 concluded that the impact assessment component had been very successful – in that it had been possible to undertake a systematic evaluation of research impact using a structured case study format (although it also expressed the panel’s reservations about the usefulness and discriminatory ability of the impact template). 106 One important reason why the approach worked appears to have been the strong financial and reputational incentive to higher education institutions to engage with the REF, including putting significant effort into writing the case studies and linking them to externally verifiable evidence of impact. Whether or not such an exercise would work equally well if the financial component of that incentive were not present (e.g. in countries where the ranking would be purely reputational) is questionable.
The cost to HEFCE of the REF was high in absolute terms (£55M), though relatively modest as a proportion of quality in research funding (1.3%); however, these figures may not fully take account of the full costs to institutions of preparing their submissions.
An independent evaluation of the REF impact assessment process by RAND Europe (based on focus groups, interviews, survey and documentary analysis) concluded that panel members perceived it as fair and robust and valued the intersectoral discussions, though many felt the somewhat crude scoring system (in which 84% of case studies in medicine were awarded 3, 3.5 or 4) lacked granularity. 413
The 6679 non-redacted impact case studies submitted to the REF (1594 in Main Panel A, which covered medically related fields) have been placed in the public domain (see http://results.ref.ac.uk) and provide a unique data set for further analysis (around 4% of case studies, deemed commercial-in-confidence or otherwise sensitive, remain unpublished). The final report from Main Panel A commended the richness of the impact case study narratives and noted that ‘International Main Panel A members cautioned against attempts to “metricise” the evaluation of the many superb and well-told narrations describing the evolution of basic discovery to health, economic and societal impact’. 106
A preliminary analysis of all 6679 REF impact case studies, based mainly, but not exclusively, on automated text mining, identified 60 different kinds of impact and 3709 ‘pathways to impact’ through which these had been achieved; every country in the world was mentioned in the data set at least once, suggesting wide geographical spread of at least some UK research. 345 The authors of that analysis felt that attempts in the case studies to monetise health gains (using QALYs, for example) and other impacts from research were, by and large, crude and speculative, though in some cases the evaluation team were able (with additional efforts) to produce monetised estimates of return on investment. They commented that ‘the information presented in the [REF impact] case studies was neither consistent nor standardised’, and that there is probably considerable potential to improve the data collection and reporting process for future exercises.
A reviewer of this report, who is leading the ongoing analysis of impact case studies from 2014 REF, commented that, in his view, one of the most significant emerging findings was the difference between the great diversity of impacts and mechanisms for achieving it described in the REF impact case studies and the much more limited range and mechanisms of impact implicit in the frameworks covered in this report. He commented:
I wonder if we have over simplified our understanding of impact through the use of these frameworks and that as we apply more sophisticated empirically driven text mining methods (which I stress are not without limitations) we will radically rethink the way we need to conceptualise impact.
Professor Jonathan Grant, Director of the Policy Institute at King’s College London, personal communication, 2015
While text mining holds considerable promise for generating ‘big data’ on this important data set, there is likely to be a trade-off between breadth and depth, as automated analysis of several thousand documents would be unable to explore the detail of impact narratives or the complex and sometimes non-linear mechanisms through which impact may be achieved. A complementary approach, involving manual content and interpretive analysis of a smaller sample of REF impact case studies, has recently been published. 414
In summary, the impact case study as used in the 2014 REF, peer reviewed by mixed panels that included both academics and research end-users, is widely considered to have effectively captured the impacts of research at UK higher education institutions. The main limitation may have been lack of granularity in the scoring system used. As this exercise generated a large data set that has been placed in the public domain, it is also now methodologically innovative approaches to analysis, including (but not limited to) automated text mining. The future for research impact assessment is to include developments in this subfield.
List of abbreviations
- AIHS
- Alberta Innovates: Health Solutions
- BIS
- Business, Innovation and Skills
- BSC
- balanced scorecard
- CAHS
- Canadian Academy of Health Sciences
- CBPR
- community-based participatory research
- CETS
- Quebec Council of Health Care Technology assessments
- CINAHL
- Cumulative Index to Nursing and Allied Health Literature
- CLAHRC
- Collaborations for Leadership in Applied Health Research and Care
- DALY
- disability-adjusted life-year
- EIA
- Excellence in Innovation for Australia
- ERiC
- Evaluating Research in Context
- ESRC
- Economic and Social Research Council
- EU
- European Union
- GDP
- gross domestic product
- GRADE
- Grading of Recommendations Assessment, Development and Evaluation
- HEFCE
- Higher Education Funding Council for England
- HMIC
- Health Management Information Consortium
- HTA
- Health Technology Assessment
- IRR
- internal rate of return
- MRC
- Medical Research Council
- NHMRC
- National Health and Medical Research Council
- NHS EED
- NHS Economic Evaluation Database
- NICE
- National Institute for Health and Care Excellence
- NIEHS
- National Institute of Environmental Health Sciences
- NIHR
- National Institute for Health Research
- NIOSH
- National Institute for Occupational Health and Safety
- PCORI
- Patient-Centered Outcomes Research Institute
- QALY
- quality-adjusted life-year
- RCT
- randomised controlled trial
- REF
- Research Excellence Framework
- RIF
- research impact framework
- RQF
- Research Quality Framework
- SIAMPI
- Social Impact Assessment Methods through the study of Productive Interactions
- TAR
- Technology Assessment Report
- VOI
- value of information