

Notes
Article history
The research reported in this issue of the journal was funded by the HTA programme as project number 14/26/08. The contractual start date was in September 2015. The draft report began editorial review in August 2017 and was accepted for publication in June 2019. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HTA editors and publisher have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
Rona Moss-Morris has published papers that met the criteria for inclusion in the review, and she was previously an advisor to the NHS Improving Access to Psychological Therapies programme. Peter White does consultancy work for a re-insurance company. He also is a member of the Independent Medical Experts Group, a non-departmental body, which advises the UK Ministry of Defence regarding the Armed Forces Compensation Fund. Peter White was also an unpaid chairperson of One Health between 2002 and 2010. One Health is a not-for-profit company that was set up to promote the British Psychological Society model within medicine. Andrew Booth is a member of the National Institute for Health Research (NIHR) Complex Reviews Advisory Board, the NIHR Health Services and Delivery Research Funding Board and the NIHR Systematic Review Advisory Group.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2020. This work was produced by Leaviss et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
2020 Queen’s Printer and Controller of HMSO
Chapter 1 Background
Definition of medically unexplained symptoms
The term ‘medically unexplained symptoms’ (MUS) is used to describe a wide range of persistent bodily complaints for which adequate examination does not reveal sufficient explanatory structural or other specified pathology (reproduced with permission from the Royal College of General Practitioners). 1 Henningsen et al. 2 describe three main types of MUS: pain in different locations, for example headache, back pain, non-cardiac chest pain; functional disturbance of organ systems; and complaints of fatigue or exhaustion. The term MUS may be applied to patients presenting with single symptoms, multiple symptoms or clusters of symptoms that are related to one another and are specific to a certain organ system or medical specialty; for example, chronic fatigue syndrome (CFS), irritable bowel syndrome (IBS) or fibromyalgia. CFS, IBS or fibromyalgia are often referred to as functional somatic syndromes (FSSs). 3 For patients reporting multiple symptoms, these may vary in range and type. MUS may also vary in terms of reported severity (i.e. number/duration of symptoms) and their effects on functional disability or quality of life.
The term MUS is controversial, and debate regarding its use is ongoing. To many patients with symptoms that are not readily explainable by disease, a diagnostic label is important, but the label ‘MUS’ can be regarded as offensive. 4 Creed et al. 5 suggest that the use of the term ‘MUS’ is a barrier to improved care and, presented a review of the challenges associated with terminology in this area. They suggested alternative terms, such as functional or persistent symptoms. ‘MUS’ is a portfolio term covering a wide range of presentations. The term ‘medically unexplained’ does not exclude physical pathology.
The debate surrounding an appropriate alternative to ‘MUS’ is ongoing and the current review does not seek to contribute to this, nor to address ‘causes’ of MUS.
Classification and diagnosis of medically unexplained symptoms
Diagnostic criteria for MUS are varied. Most of the FSSs are diagnosed according to published diagnostic criteria that include specified symptom criteria alongside the exclusion of medical and/or psychiatric conditions that may mimic similar symptoms [e.g. CFS may be diagnosed by the Fukuda Diagnostic Criteria,6 functional gastrointestinal disorders may be diagnosed by the Rome 111 Diagnostic Criteria,7 fibromyalgia may be diagnosed by the American College of Rheumatology (ACR) 2010 Diagnostic Criteria8]. Patients visiting their general practitioner (GP) frequently with unexplained symptoms are not necessarily offered a formal diagnosis. Where diagnosis of MUS is made, this may be either by use of a validated instrument, such as the Patient Health Questionnaire (PHQ) 15,9 Screening for Somatoform Symptoms (SOMS),10 the Brief Symptom Inventory (BSI),11 or by clinical judgement, usually by a GP. Hoedeman et al. 12 describe a continuum of severity for MUS, ranging from short term or incidental to persisting and recurrent. Fink et al. 13 argue that research into the FSSs and related disorders and their treatment is restricted by the lack of a valid and reliable diagnostic classification. There is overlap between the diagnostic categories of functional somatic disorders and, therefore, patients with similar symptoms and clinical presentations may receive different diagnostic labels. Fink et al. 13 have gone on to describe ‘bodily distress syndrome’ as an alternative to MUS.
The presence of MUS is also a key feature of a range of somatoform disorders. These include somatisation disorder, somatoform pain disorder, undifferentiated somatoform disorder and unspecified somatisation disorder. Diagnosis of any of the somatoform disorders is made by clinical structured interview, with patients meeting diagnostic criteria according to the Diagnostic and Statistical Manual of Mental Disorders (DSM)-IV,14 or V15 or the International Classification of Diseases (ICD)-916 or 10. 17 Although the DSM-IV specifically refers to symptoms being medically unexplained, the DSM-V classification no longer has a requirement that symptoms should lack an explanation. Somatic symptom disorder in the DSM-V is characterised by ‘the presence of one or more distressing and disabling somatic symptoms that disrupt daily functioning’. 18 Significant, moderate to severe somatic symptoms are required to be present, accompanied by excessive, illness-related thoughts, feelings or behaviours. Criticism of the DSM-V definition of somatic symptom disorder centres around the removal of the requirement for symptoms to be ‘unexplained’, and the focus on ‘excessive responses’. As the DSM-V classifies mental disorders, it is argued that this extended scope risks mislabelling many people with physical conditions, such as cancer, heart disease, IBS or fibromyalgia, as mentally ill. 19 Frances20 raises concerns that mislabelling a patient with somatic symptom disorder causes harms (e.g. missed diagnosis of underlying medical causes), subjecting patients to stigma, inappropriate drugs, psychotherapy and iatrogenic disease, and that it may also cause patients to be disadvantaged with regard to employment, education and health care. The 2016 Rome IV guidelines suggest removing the term ‘functional’ from gastrointestinal disorders such as IBS and replacing them with terminology relating to ‘brain–gut interaction’. 21,22 Smith and Dwamena23 propose a clinical spectrum of severity for MUS, from normal/mild, featuring few, minor transient symptoms and little accompanying depression/anxiety, to very severe, which includes the somatoform disorders. Other acknowledged somatoform disorders that have their own diagnostic criteria include bodily distress syndrome, bodily distress disorder and complex somatic symptom disorder.
The current review uses a broad definition of MUS, which encompasses all of the above definitions, so that the term MUS will be used to refer to any of the following definitions: (1) the occurrence of physical symptoms in the absence of clear physical pathology, (2) to FSSs, such as CFS, IBS or fibromyalgia, (3) the DSM-IV (and more recently V) somatoform disorders and (4) somatoform disorders that have their own diagnostic criteria (e.g. bodily distress syndrome). The rationale behind this broad definition is that there is clear overlap between these groups and as yet no consensus as to the validity of one syndrome (i.e. MUS) versus many (i.e. the various FSSs). Whether patients are diagnosed with MUS as opposed to a more specific diagnosis can be an artefact of clinician or researcher preference rather a defining feature of the included patients. 3,24 A final point about classification of MUS is that there is preliminary evidence that several single FSSs are in fact themselves composed of multiple different conditions, united only by common symptoms, which may complicate our understanding of whether or not interventions work for MUS.
Clinical guidelines for MUS (Joint Commissioning Panel for Mental Health 201725) encourage a philosophy of care where physical and mental health are integrated. A recognition that MUS are ‘mind–body problems’ is also encouraged. Some authors have suggested that the biopsychosocial model itself is responsible for dissatisfaction and harm in patients with CFS,26 arguing that its application is biased towards the psychological, framing patients as mentally ill. It is argued that this risks distraction from research into the biological aetiology of symptoms and syndromes, for example Ghoshal and Gwee,21 de Vega et al. 27 and Gur and Oktayoglu. 28 Imposing the biopsychosocial model on patients, it is argued, can lead to ‘disputes over diagnosis, rejection of psychiatric diagnosis, as well as doctors being dismissive, sceptical and lacking in knowledge about the condition’. 29 The alternative view is that the biopsychosocial model allows the inclusion and integration of biological, psychological and social factors in understanding and treatment particularly of chronic conditions. 30
Prevalence and costs of medically unexplained symptoms
A range of prevalence rates of MUS have been estimated. Edwards et al. 31 report worldwide prevalence rates of primary care patients presenting with MUS of 25–50%. In the UK, Taylor et al. 32 report a MUS prevalence rate of 18% of consecutive attenders to UK GP practices. It is estimated that this creates an annual cost to the UK NHS in excess of £3.1B. 33,34 Taking into account quality of life and sickness absence, wider costs to the economy were estimated at over £14B. 33 The inappropriate management of MUS may result in patients undergoing invasive and potentially harmful tests and treatments. Some patients with MUS have comorbid depression/anxiety. 35 Health-care utilisation varies between patients with MUS due to the wide variability in symptom experience. Collin et al. 36 used a case–control study of nearly 8000 matched pairs to show that GP consultation rates for patients with CFS were 50% higher in adult cases than in the controls 11–15 years before diagnosis, and 56% higher 6–10 years after diagnosis, with a peak difference of more than twofold higher in the year of diagnosis. Similarly, a study of health-care resource use for patients with fibromyalgia37 found that patients had considerably higher resource use at least 10 years prior to their diagnosis of fibromyalgia. At the time of diagnosis, patients recorded an average of 25 visits per year compared with 12 visits for the matched controls. For IBS, health-care visits are considerably lower, with one study estimating one extra visit to primary care per year compared with controls. 38
A systematic review of the course and prognosis of MUS and somatoform disorders39 suggested that the prognosis for patients with MUS is influenced by the severity of the condition at baseline and by the number of symptoms. Creed et al. 40 showed, in a large epidemiological study, that symptom count predicted later quality of life. It has been estimated that between 50% and 75% of patients with MUS will improve, whereas between 10% and 30% will see their condition deteriorate. 39
Interventions for medically unexplained symptoms
A wide range of interventions has been implemented in the treatment of MUS. Pharmacological interventions (e.g. antidepressants) are sometimes used. Reviews of pharmacological interventions have shown these to produce some improvement in responsive patients in terms of symptom severity and functioning,12,41,42 but significant heterogeneity of efficacy between different FSSs.
Psychological therapies
Several types of psychological therapies have been implicated. Cognitive–behavioural therapy (CBT) for treatment of MUS is based on the model of CBT proposed by Beck43 and is one of the most common interventions used for this group of patients. CBT for MUS focuses on the perpetuating cycle that maintains symptoms, distress and disability. This type of therapy targets the relationship between cognitive, behavioural and physiological responses that are proposed to maintain symptoms. 44 Reattribution for MUS, although no longer commonly delivered, was designed to be delivered by GPs and is based on providing a psychological explanation for somatised mental disorders. Patients are encouraged to reattribute their symptoms and relate them to psychosocial problems. The three stages of therapy are feeling understood, changing the agenda and making the link. 45 Behaviour therapy may be delivered to MUS patients. In these cases, therapy aims to modify behaviours such as increased vigilance in detecting physical symptoms, or reducing inappropriate coping behaviours such as reassurance-seeking or inactivity. 46 Relaxation therapies may be used as treatments for MUS – these include biofeedback,47,48 meditation-based stress reduction49 and qigong. 49 Third-wave CBTs include mindfulness and acceptance and commitment therapy (ACT), which focuses on psychological flexibility, self-regulation of attention and acceptance. 50 Other psychological therapies such psychodynamic therapy have also been adopted for the treatment of MUS. 51
Physical therapies
A further category of interventions for MUS are physical therapies. Such physical therapies include graded exercise therapy (GET), whereby exercise is started gradually and increased over time, and may incorporate the psychological component of graded exposure to exercise alongside a range of aerobic or non-aerobic exercise, such as walking, pool-based exercise or strength training. 52–56 More physiologically based physical activity interventions include aerobic exercises or non-aerobic exercise (e.g. yoga/qigong), which may also be offered to patients with MUS. 57–59 Our review distinguishes between graded and other physical activity interventions, with the former defined as exercise with a defined behavioural model and the latter defined as exercise with a physiological rationale. Physiotherapy-based exercise interventions were considered provided they included an element of active behavioural participation. Manual therapies were not considered for inclusion if they were predominantly passive.
Other therapies
Other therapies that have been adopted for the treatment of MUS include alternative therapies such as hypnotherapy60 or acupuncture. 61 These are usually passive therapies and were not included in the review.
Not all of these treatments are available on the NHS and, therefore, some patients with MUS may pay to access treatments that they perceive to improve their own symptoms, and where they feel they have more time to express their concerns without the pressure of a time-limited GP consultation.
Setting
Interventions for MUS may be delivered in primary care settings, or after referral to secondary care (e.g. to one or more specialists, such as general physicians, immunologists, neurologists, haematologists, or psychiatrists). 62 In primary care, GPs may deliver behavioural modification interventions to MUS patients as part of enhanced care (encompassing techniques including CBT, reattribution or reframing). Alternatively, patients with MUS may receive collaborative care, where for example a psychologist may deliver CBT within the primary care setting. Delivering interventions in a primary care setting may offer additional benefits, for example patients with MUS may refuse referral to services outside the primary care setting. 63
Evidence for the effectiveness of interventions for medically unexplained symptoms
To our knowledge, there are currently no published systematic reviews that specifically evaluate behavioural modification interventions for patients fulfilling the broad definition of MUS patients as outlined above, within a primary care setting. However, a number of reviews have been conducted for specific subgroups of interventions or patients. Reviews of evidence for the effectiveness of interventions for MUS in general are less common than reviews of individual FSS. Reviews of FSSs have shown that, in the case of CFS, CBT and GET can improve symptom severity and functioning following treatment and are acceptable to patients. 64–67 In the case of fibromyalgia, CBT has been shown to improve physical symptoms and functioning,68 as have exercise therapies69,70 and multicomponent therapy. 71 In the case of IBS, psychological therapies have been shown to reduce symptoms as effectively as pharmacological therapies,42 whereas Zijdenbos et al. 72 found psychological interventions to be slightly superior to usual care or waiting list controls. For other conditions, Aggarwal et al. 73 found only weak evidence of effectiveness of psychosocial interventions including CBT and biofeedback for patients with chronic orofacial pain. Champaneria et al. 74 found psychological interventions improved pain scores for patients with chronic pelvic pain compared with no psychological intervention. van Dessel et al. 75 conducted a review of all non-pharmacological interventions for somatoform disorders and MUS but identified only studies of psychological interventions. The authors found that compared with usual care, treatment resulted in less severe symptoms at the end of treatment. The evidence for CBT was similar to other psychotherapies.
Primary care reviews
The majority of studies included in these reviews were conducted within secondary care. Fewer reviews addressed the effects of interventions in a primary care setting. A review of psychological interventions for MUS76 found that short-term psychotherapy demonstrated small effects for the improvement of physical symptoms in patients with medically unexplained physical symptoms (MUPS), with type and mode of therapy and profession of the therapist moderating the results (e.g. inpatient therapy was more effective, as was therapy delivered by mental health professionals). However, GP-delivered interventions were found to be more effective at reducing health-care utilisation. Rosendal et al. 77 reviewed enhanced care delivered by generalists for patients with functional somatic symptoms and concluded that the current evidence does not answer the question of whether or not there is an effect for these types of interventions. Gerger et al. 78 reviewed psychological therapies for MUS and compared the effectiveness of such interventions when delivered by GPs versus psychologists. They found a small effect for psychological therapies at the end of treatment for physical symptoms, physical functioning and psychological functioning. This effect was moderated by the provider, with delivery by a psychologist found to be more effective, but only for physical symptoms. There was no robust evidence for any long-term effects. Metaregression also showed moderating effects for the number of sessions, with more sessions being more effective. There was no moderating effect of severity of symptoms, although exploratory analyses indicated that psychological intervention delivered by a GP was more effective for more patients with more severe symptoms. Garcia-Campayo et al. 79 reported that psychological interventions may be no less effective in primary care than when conducted in secondary care settings. Edwards et al. 31 provide a narrative review of the literature on the treatment of MUS in primary care, which outlines some of the issues related to the delivery of interventions in a primary care setting, for example the importance of the doctor–patient relationship, involving family members in interventions and the importance of cultural considerations. The authors concluded that no single approach would effectively treat all MUS patients in primary care, and that care must be taken to investigate which intervention is appropriate for individual patients. Our qualitative review and realist synthesis will add to these findings.
Definitions of behavioural modification interventions
As evidenced by the existing literature and described above, interventions for MUS are, in general, based around pharmacological, psychological or physical therapeutic models. Our review will focus specifically on interventions that aim to promote behavioural change. Although there are a number of theoretical models of behavioural change, attempting to assign interventions designed for patients with MUS to any of these theoretical frameworks presents difficulties. For example, for psychological therapies, there may be little behaviour modification theory or practice in ‘pure’ cognitive therapies but it has been shown empirically that in practice not many therapists will practice pure cognitive therapy – most will incorporate behavioural elements. 80 Similarly, for physical therapies, if an intervention is based around a model of physical fitness rather than behaviour re-engagement, then it could be argued that this no longer meets the criteria of a behavioural modification intervention. Many physical fitness methods involve predetermined goals based on a patient’s physiology, which are set by the physiologist or sport scientist and may not be considered as ‘therapy’, although they still constitute an intervention. We will therefore adopt a liberal definition of ‘behavioural modification interventions’ as ‘interventions aimed to achieve behavioural change’. Interventions will include ‘named’ behavioural interventions such as CBT, behavioural therapy and GET (GET incorporates principles of systematic desensitisation and behaviour modification with the aim of gradually increasing physical activity, see, for example, Bagnall et al. 62). However, we will also include any intervention that meets the criteria described above. Owing to wide variation in these interventions, we will categorise them by subtype rather than attempt to treat them as one homogeneous intervention type.
Modifying effects
Results of existing reviews suggest that the effectiveness of treatments for MUS may be modified by a number of factors and that treatment may depend on how MUS is defined. There is currently no consensus on whether or not to use a generic intervention protocol, where all patients with MUS receive the same treatment protocol regardless of key presenting symptoms and/or level of disability versus the use of a very specific protocol, developed for patients with a defined functional somatic or DSM syndrome. There is some suggestion from previous reviews that more specific protocols may have larger treatment effects but this has yet to be investigated systematically. 76
Furthermore, the type of control condition used in randomised controlled trials (RCTs) may influence an intervention’s effectiveness. Some studies have shown that patients with IBS respond well to placebo,72 whereas patients with CFS do not respond well. 81 This highlights the importance of recognising differences in the design and conduct of control conditions. Where the control condition is inactive (e.g. waiting list or treatment as usual), good effect sizes for the experimental intervention have been found, whereas trials with active control interventions have shown small effect sizes. 82 Our review will take account of these issues by extracting information from individual studies for a number of potential modifiers, including mode of delivery of the intervention, MUS population (e.g. diagnosed FSSs), multiple MUS, and chronic unexplained pain as described in Chapter 3, Description of the evidence. Potential modifying effects for intervention type will be explored by categorising by broad type of behavioural modification intervention (e.g. CBT, GET, behaviour therapy). Details of all types of controls will be synthesised for all included trials.
Acceptability of primary care interventions for medically unexplained symptoms
Several authors suggest that the relationship between service users and service providers is key to the success of primary care interventions. 83–85 Poor communication between the GP and the patient as well as lack of emotional and practical support are suggested as barriers to effective treatment of MUS. Creating a safe, therapeutic environment, and the importance of offering effective reassurance, are highlighted as important enabling factors for effective treatment of MUS. 84 Therefore, the current review aims to add greater depth to the clinical effectiveness data by retrieving qualitative data relating to potential barriers to and facilitators of effectiveness and conducting realist synthesis of these data. This is of particular importance as a good proportion of these patients hold strong views about the biological nature of their condition and view the suggestion of a more psychosocial approach to treatment as invalidating their symptoms. 86 Understanding ways in which to make behavioural approaches more acceptable may increase their uptake.
Chapter 2 Definition of the decision problem
Decision problem
The assessment addressed the question: what is the clinical effectiveness, cost-effectiveness and acceptability of behavioural modification interventions for MUS in primary care or community-based settings?
Intervention
Interventions that aimed to modify behaviour were sought. These included explicit behavioural interventions such as CBT, behaviour therapy and GET. Where the intervention was not explicitly named as a behavioural modification intervention (i.e. one of the above), a broad definition of behavioural change interventions was adopted. Interventions therefore included but were not exclusive to a range of psychotherapies, for example CBT, behavioural therapy, psychodynamic therapy, mindfulness and reattribution. Interventions also included other physical therapies, such as aerobic exercise and strengthening or stretching exercises. Interventions with multiple components were included where one of the components was considered a behavioural modification technique as defined by the above criteria. Individual and group interventions were noted as separate interventions; however, because of the limited number of studies per intervention type, both group and individual interventions of the same type were considered together for the purposes of the network meta-analyses, and sensitivity analyses conducted where possible. Interventions were also considered where primary care practitioners were trained to communicate a ‘behavioural’ message to patients during their consultations. In these cases, interventions required a stated explicit aim to train GPs to adopt a behavioural or biopsychosocial approach towards consultations with patients with MUS.
Population and relevant subgroups
Studies of populations meeting the criteria for MUS, MUPS, and somatoform disorders were included. Populations with defined FSSs were also included. Diagnostic/inclusion criteria used are discussed in more detail in Chapter 5, Scope the primary literature.
Relevant comparators
Any comparator was considered. Comparators are described in greater detail in Chapter 5, Scope the primary literature.
Overall aims and objectives of assessment
Research aim
This project evaluated the clinical effectiveness, cost-effectiveness and acceptability of behavioural modification interventions for MUS in primary care or community-based settings. The purpose of the project was to provide a comprehensive systematic review of both quantitative and qualitative studies, using rigorous methods for reviewing, evidence synthesis and cost-effectiveness modelling to evaluate the clinical effectiveness and cost-effectiveness of these interventions.
Research objectives
-
To determine the clinical effectiveness of behavioural modification interventions for MUS in primary care and community-based settings, by undertaking a full systematic review of quantitative literature.
-
To evaluate the barriers to and facilitators of effectiveness and acceptability of behavioural modification interventions for MUS from the perspective of both patients and service providers, by undertaking a realist synthesis following a systematic review of the available qualitative research literature.
-
To undertake a meta-analysis of the available evidence on clinical effectiveness, including a network meta-analysis (NMA) to allow simultaneous comparison of all identified intervention types where appropriate.
-
To identify and synthesise evidence on health economic outcomes such as health-care resource use (e.g. GP appointments), and health-related quality-of-life (HRQoL) data from the studies included in the clinical effectiveness review.
-
To provide new evidence on the cost-effectiveness of behavioural modification interventions for MUS conducted in a primary care or community setting, by conducting a systematic review of existing economic analyses and undertaking a de novo model-based evaluation where there is an absence of high-quality published analyses which are directly applicable to our research question.
-
To explain which circumstances influence the effects of behavioural interventions for MUS patients (via realist synthesis).
Patient and public involvement
Patients were involved throughout the review process. Two members of the public with a history of MUS contributed to the writing of the review protocol. They, along with a person with experience of fibromyalgia, went on to be active members of our Expert Advisory Group. The Expert Advisory Group was made up of subject experts, clinicians and our patient and public involvement (PPI) representatives (experts by experience). There were two whole-group meetings: the project team and one of the Expert Advisory Group, held at the School of Health and Related Research (ScHARR) but with an independent chairperson. These were at the beginning of the review to discuss plans and potential issues before the review got started, and at the end of the review to report the results of the review. Between these meetings, the Expert Advisory Group were e-mailed at key stages in the project to receive updates on progress and to be invited to contribute any feedback.
In addition to the two whole-group meetings, a meeting with JL, AS and MB was held in London solely for the PPI representatives. The purpose of this meeting was to allow a more informal discussion of the project, in particular the qualitative and quantitative reviews, with a focus on a patient point of view. The PPI representatives were also given a booklet containing plain English information on the systematic review process.
All of the PPI representatives made substantial and valuable contributions to the project. Providing a patient perspective at each stage of the review enabled the project team to gain a deeper understanding of the issues arising from the literature, and kept the importance of patient perceptions of their symptoms and health-care provision in focus.
One patient with MUS wrote:
Being involved with this review has opened up my understanding of how important it is when one has ‘unexplained symptoms’ to take part in one’s own recovery and health and how difficult it must be for doctors to have patients who look to them as saviours, not to be able to diagnose and then treat. I thoroughly enjoyed having an insight into both doctors’ and patients’ point of view into the frustrating world of MUS! It also gave me hope seeing the differing and varied interventions available. It was encouraging to see that nearly all symptoms under the various headings seemed to respond to CBT. It has been a great pleasure to be involved with this study and review. The team were brilliant in making a very complex subject accessible and interesting to a lay person.
The other patient with MUS wrote:
It has been a fascinating experience being a small part of a very carefully thought out and thorough review. Credit should go to the team that managed to filter through all of the studies and create a model that allowed for some conclusions to be made. While the review didn’t perhaps reach the clear conclusions it aimed for, there were a lot of interesting observations: From a patient-perspective, the fact that there were few significant effects for any GP intervention, i.e. reattribution, GP led CBT, or GP MUS management, is quite worrying. It is useful knowledge that multimodal and CBT interventions have an impact on the majority of MUS. These findings are something that should be embraced and addressed by the NHS (although it’s interesting to see that there is little evidence supporting the impact on long-term health). It seems that patient caution and stigma can still be attached to CBT and similar therapies so I would be interested to find how this problem could be tackled in the future. It’s also a pity that little could be found that would benefit patients with ‘somatisation and generic physical symptoms’. I’ve really enjoyed working on this project and would be happy to contribute to any further studies.
The person with experience of fibromyalgia wrote:
My experience of being part of the stakeholder group: It was an enormous piece of research that was undertaken and I observed that it was done with great care. I always felt that my opinions, written and oral, were taken seriously and followed-up. I am not sure how valuable my contributions were. I do know that I tried my best to look at all the information and paid attention to the details as much as I tried to look at the bigger picture. I do think that having patient representatives helps to keep the research grounded in the real world. I was astounded by some of the outcomes, as they seemed counter to generally held beliefs. This only shows how important it was to collate this evidence. I do hope that the report will help many people with pain and other unexplained symptoms to reach relief that they have not yet achieved.
Chapter 3 Assessment of clinical effectiveness
Methods for reviewing effectiveness
A systematic review of the literature and (network) meta-analysis (where appropriate) was undertaken to evaluate the clinical effectiveness of behavioural modification interventions for MUS, in a primary care or community setting. The review of the clinical evidence was undertaken in accordance with the general principles recommended in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.
Identification of studies
Searches were undertaken to identify relevant studies regarding clinical effectiveness, cost-effectiveness and acceptability (qualitative studies). The search strategies are reported separately for each below. Methods of searching for studies included in the realist synthesis are described in Chapter 7.
Screening and eligibility
A two-stage sifting process for inclusion of studies (title/abstract then full-paper sift) was undertaken. Titles and abstracts were scrutinised by one systematic reviewer (JL) according to the inclusion and exclusion criteria. There was no exclusion on the basis of quality. All studies identified for inclusion using the abstract alone, plus any study in which a decision on inclusion was not possible only from the abstract, were retrieved for more detailed appraisal. Agreement on inclusion at title/abstract sift was checked by a second systematic reviewer (CGC) for 20% of the total electronic search results. Further sifting processes were developed as it became apparent that there were many studies where inclusion/exclusion was unclear. A sifting meeting was held with all subject experts present to discuss general sifting issues and specific individual cases. A common issue was whether or not interventions met the primary care/community-based criteria. To address this issue, operational sifting criteria were developed in order to aid decision-making. Data were extracted regarding where diagnosis, recruitment and referral (to the study) took place and where the intervention took place, and outcomes were assessed. Inclusion was decided based on a combination of these factors and, where there was doubt, judgements were made via discussion among the review team. Inclusion of studies on setting was kept broad. Appendix 2, Table 40, shows the sifting criteria considered for setting for each included study. Another common issue was the nature of the symptoms meeting the ‘unexplained’ criteria. Studies were included if symptoms were explicitly described as ‘medically unexplained’, as were studies that explicitly stated that they included patients with ‘MUS’. Studies of populations with FSSs were included without a need for further reference to medical explanation. Inclusion issues became apparent in studies of patients with chronic pain but no description of whether or not the pain had a known organic cause. To address this issue, a sample of study authors of these papers were contacted to request further information about their populations. None of the studies of those who responded had lack of ‘medical explanation’ as a criterion for inclusion. Therefore, it would be impossible to determine whether the populations contained a mix of patients with chronic pain with known cause, for example arthritis, and patients with pain without known cause. Specifically, an explanation of the cause of pain was not deemed necessary in these studies, nor was it necessary for pain to be a target for the interventions. It was therefore decided to keep this inclusion criterion narrow, and to include only studies of patients with chronic pain that deliberately targeted pain of unknown or ‘unexplained’ origin.
Clinical effectiveness searches
A systematic search strategy was developed in consultation with the review team, to identify systematic reviews and RCTs relating to the defined population. The focus was on identifying studies in primary care or community-based settings; therefore, population terms were combined with terms to define the setting. A combination of free-text terms and thesaurus searching was used. Published methodological search filters to limit the study type (systematic review or RCT) were used where available. No other search limits were applied. Reference sections of included studies were scrutinised for additional potential studies to include, as were reference lists from relevant reviews.
Searches were conducted in the following sources:
-
MEDLINE via OvidSP (1946–20 November 2015)
-
MEDLINE In-Process & Other Non-Indexed Citations & Epub Ahead of Print & MEDLINE® without Revisions via OvidSP (2013–20 November 2015)
-
Cumulative Index to Nursing and Allied Health Literature (CINAHL) via EBSCOhost (1981–3 December 2015)
-
PsycINFO via OvidSP (1967–3 December 2015)
-
EMBASE via Ovid SP (1974–4 December 2015)
-
Cochrane Database of Systematic Reviews (CDSR) via the Cochrane Library (2005–4 December 2015)
-
Database of Abstracts of Reviews of Effects (DARE) via the Cochrane Library (1994–April 2015 – no longer updated, archive only searched 4 December 2015)
-
Cochrane Central Register of Controlled Trials (CENTRAL) via the Cochrane Library (1898–4 December 2015)
-
Health Technology Assessment (HTA) Database via the Cochrane Library (1989–4 December 2015)
-
Science Citation Index via Web of Science (1900–7 December 2015)
-
Social Sciences Citation Index via Web of Science (1956–7 December 2015).
Searches for systematic reviews and RCTs were conducted between 20 November and 7 December 2015. Detailed search strategies are provided in Appendix 1.
Qualitative searches
A systematic search strategy was developed in consultation with the review team to identify qualitative research relating to the defined population. The focus was on identifying studies in primary care or community-based settings; therefore, population terms were combined with terms to define the setting. A combination of free-text terms and thesaurus searching was used. Published methodological search filters to limit to study type (qualitative) were used where available. The qualitative research filter was combined with a geographic filter to identify UK studies only. No other search limits were applied.
Searches were conducted in the following sources:
-
MEDLINE via OvidSP (1946–4 July 2016)
-
MEDLINE In-Process & Other Non-Indexed Citations & Epub Ahead of Print & MEDLINE without Revisions via OvidSP (2013–4 July 2016)
-
EMBASE via Ovid SP (1974–4 July 2016)
-
CINAHL via EBSCOhost (1981–4 July 2016)
-
PsycINFO via OvidSP (1967–4 July 2016)
-
Science Citation Index via Web of Science (1900–4 July 2016)
-
Social Sciences Citation Index via Web of Science (1956–4 July 2016).
Searches for qualitative research were conducted on 4 July 2016. Detailed search strategies are provided in Appendix 1.
Economic searches
A systematic search strategy was developed in consultation with the review team to identify economic evaluations relating to the defined population. The focus was on identifying studies in primary care or community-based settings; therefore, population terms were combined with terms to define the setting. A combination of free-text terms and thesaurus searching was used. Published methodological search filters to limit to study type (economic evaluation) were used where available. No other search limits were applied.
Searches were conducted in the following sources:
-
MEDLINE via OvidSP (1946–15 August 2016)
-
MEDLINE In-Process & Other Non-Indexed Citations & Epub Ahead of Print & MEDLINE without Revisions via OvidSP (2013–15 August 2016)
-
EMBASE via Ovid SP (1974–25 August 2016)
-
CINAHL via EBSCOhost (1981–25 August 2016)
-
PsycINFO via OvidSP (1967–25 August 2016)
-
NHS Economic Evaluation Database (NHS EED) via the Cochrane Library (1968–April 2015 – no longer updated, archive only searched 25 August 2015)
-
Science Citation Index via Web of Science (1900–25 August 2015)
-
Social Sciences Citation Index via Web of Science (1956–25 August 2015).
Searches for economic evaluations were conducted between 15 and 25 August 2016. The search results were imported into EndNote [Clarivate Analytics (formerly Thomson Reuters), Philadelphia, PA, USA] and subsequently filtered to identify UK studies, using terms from line 29 of the EU economies search filter to search the EndNote library for potentially relevant references. Detailed search strategies are provided in Appendix 1.
Clinical effectiveness review
Details of the qualitative and cost-effectiveness review methods are detailed in Chapters 4–6.
Inclusion and exclusion criteria
Study design
Only RCTs were included as these represent the optimal study design for assessing intervention effectiveness. Scoping of the review indicated the availability of a substantial number of published RCTs. No minimum duration of follow-up was applied.
Intervention
A diverse range of interventions that met with our definition of behavioural interventions were identified. Interventions were subsequently ‘grouped’ by type. Definitions of intervention groups were created following review team discussions. These are presented in Table 1. Two reviewers initially grouped each included intervention into these groups. Where there were difficulties or disagreements, subject experts were consulted.
| Intervention group | Description |
|---|---|
| CBT – high intensity | CBT, delivered by a trained clinical specialist, ≥ 6 hours’ contact |
| CBT – low intensity | CBT, either delivered by a trained clinical specialist but < 6 hours’ contact time, or delivered by a non-specialist (may be > 6 contact hours) |
| Other psychotherapy | Any other psychotherapy (e.g. expressive, psychoanalytic) |
| Graded activity or exercise therapy | Exercise with a defined behavioural model |
| Strength, endurance, sport | Exercise with a physiological model (e.g. aerobic, strengthening) |
| Relaxation, stretching, social support/emotional support | Interventions designed to encourage relaxation or stress relief, general MUS-focused support, stretching |
| Guided self-help | Educational support, including information or self-management materials; visual presentations |
| Multimodal | An intervention that incorporates components from more than one category or was conceptualised as ‘multimodal’ by the study authors |
| GP interventions | |
| GP – reattribution | GP trained in reattribution according to Goldberg principles45 or modified reattribution |
| GP – CBT | GP trained in and delivered CBT |
| GP – other psychotherapy | GP trained in and delivered any other type of psychotherapy as described in general ‘other psychotherapy’ category |
| GP – MUS management | GP trained in the management of MUS. Must be focused on management using behavioural/biopsychosocial principles |
| GP – other | GP intervention consisting of multiple components, does not fit with any other category |
| Non-behavioural comparator interventions | |
| Medication | Any medication prescribed specifically as a comparator intervention (i.e. above patients’ usual regimen) |
| Usual care | Care as usual, also incorporates waiting list or treatment as usual |
| Usual care plus | Enhanced usual care or usual care with minor addition (e.g. a leaflet) |
Appendix 2, Table 28, describes the interventions at a study level, with a brief description, with their designated intervention groupings.
Population
Adults aged ≥ 18 years with MUS, MUPS or somatoform disorders were included. Diagnosis of MUS or MUPS could be either by validated instrument (e.g. PHQ-15, SOMS, BSI) or by clinician judgement. Diagnosis was not restricted by duration (except in the case of chronic pain the duration of which should be > 3 months) or severity (e.g. number of symptoms). Patients with single symptoms were included. Populations with FSSs were included (e.g. IBS, CFS, fibromyalgia). For somatoform disorders, diagnosis should have been made by formal clinical interview and should meet DSM-IV or DSM-V, or ICD-9 or ICD-10 criteria. Somatoform disorders included somatisation disorder, somatoform disorders, somatoform pain disorders, persistent physical symptoms, bodily distress syndrome, bodily distress disorder, FSS, medically unexplained syndrome.
Appendix 2, Tables 29–36, shows diagnostic/inclusion criteria used by condition for individual studies.
Comparator
Studies where ‘usual care’ was the comparator were included. Owing to variation in terminology, studies where the comparator is ‘treatment as usual’ or ‘waiting list’ ’were also included as usual care’. A ‘medication’ control group was included for studies where a comparator arm consisted of a specific medication regimen. Trials with a ‘placebo’ control (e.g. which control for time and attention) were also included. As a number of high-quality head-to-head trials of two or more experimental interventions were identified during scoping searches, head-to-head trials were also included where at least one intervention arm met the definitions outlined above.
Outcomes
Appendix 2, Table 37, presents information on primary and secondary outcomes measured in each study, with an indication of the scale used.
Primary outcomes
Patient level: improvement in symptoms, functioning and/or health-related quality of life (HRQoL). Measures of symptom improvement could be through assessment of severity or frequency and must have been assessed using a generic or symptom-specific validated instrument, for example EuroQol-5 Dimensions (EQ-5D)/Short Form questionnaire-36 items (SF-36) for HRQoL, symptom checklist for symptom severity and PHQ-15.
Health-care level: use of health-care resources (e.g. frequency of GP visits, diagnostic outpatient procedures, hospital admissions, emergency department attendances). Costs are reviewed in detail in the cost-effectiveness review Chapter 6.
Secondary outcomes
Emotional distress, including depression and anxiety as diagnosed by a validated instrument [e.g. Beck Depression Inventory (BDI) or Beck Anxiety Inventory (BAI)] or a composite measure, such as the mental health component from the SF-36; satisfaction with care; attrition (persistence and adherence).
Studies were diverse and, because of the differences in populations, types of symptoms measured were varied. Scales used to measure similar constructs (e.g. depression, quality of life) differed between studies. Appendix 2, Table 37, lists all the primary and secondary outcomes measured, with scales used, for all included studies. Outcome data for individual studies were extracted and commonalities were sought. Ten key outcomes were considered to have sufficiently similar data to be included in meta-analyses. These were individual physical symptoms: pain, fatigue and bowel symptoms; somatisation; composite measures of emotional distress; physical functioning; depression; anxiety; impact of symptoms on daily activities (including disability); and generic physical symptoms (e.g. severity of ‘main’ symptom, where no particular symptom is specified). In addition, data were extracted regarding satisfaction/adherence, adverse events and health-care utilisation. These outcomes were considered too heterogeneous to consider meta-analysis and are reported as a narrative synthesis only.
Outcome measurement time points
Studies measured outcomes at a range of time points. As well as variation in follow-up times (e.g. 3 months, 6 months, 1 year), there was variation in the definitions of these time points. As an example, Figure 1 shows three different ways of defining ‘6 months’ follow-up’.
FIGURE 1.
Variation in definitions of follow-up.
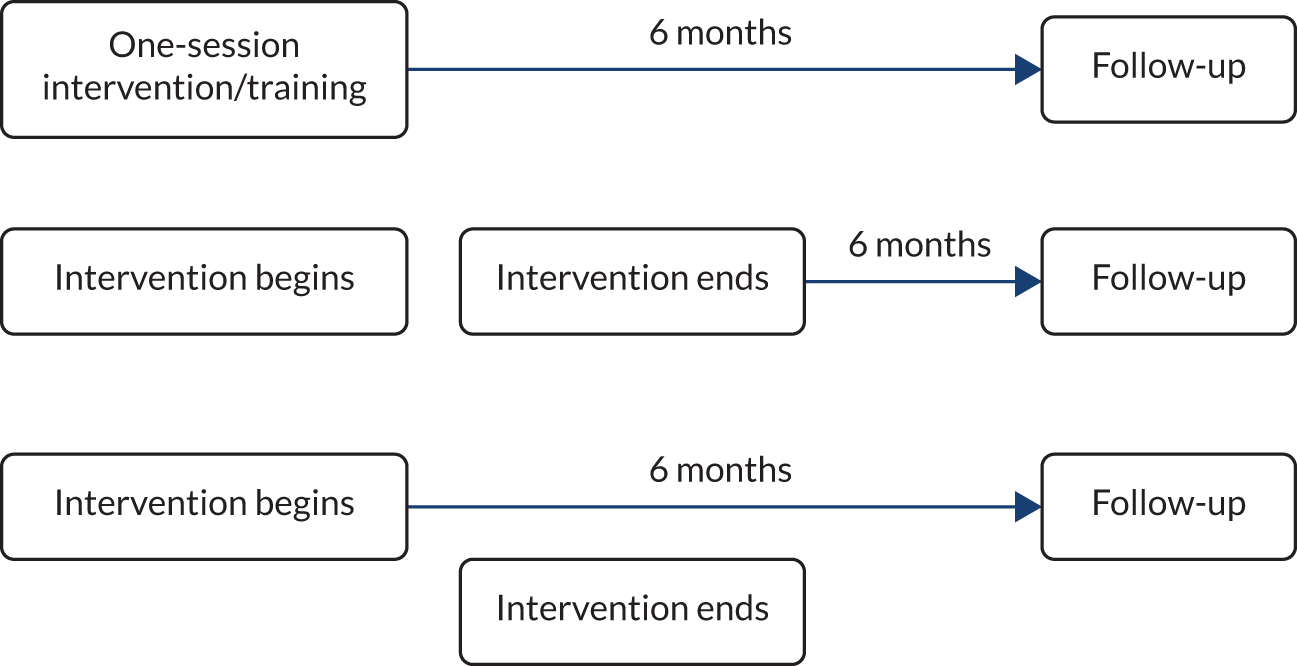
Although all of these variations may be described in individual studies as ‘6 months’ follow-up’, 6 months may refer to the time since one-off treatment, to the time since the end of treatment, to the time since the GP received training, or to the time since baseline (pre-treatment). As previous studies have shown that intervention effects can diminish once treatment has ended, time since end of treatment was considered important. Time points used in the meta-analyses were extracted as baseline, end of treatment (i.e. corresponding to duration of treatment), short-term follow-up (time since end of treatment < 6 months) or long-term follow-up (time since end of treatment ≥ 6 months). The longest follow-up time point within these categories was chosen where possible. Where studies did not explicitly report end-of-treatment time, this was calculated by subtracting duration from follow-up since baseline. Weeks were converted to months using a conversion of 1 week = 0.230137 months. Assessment time points as reported in individual studies are reported in the table of basic study design characteristics in Appendix 2, Table 42. Converted or calculated time points are reported for individual studies in Appendix 2, Table 39.
Settings
Studies in primary care or community-based settings were included. To be considered a primary care setting, interventions must have been conducted within a primary care or community-based setting, but they could have been delivered by any health-care discipline within that setting. Interventions could be face to face or delivered at a distance (e.g. via the internet or telephone), and may include computer-assisted interventions. However, to be considered primary care, a degree of involvement with primary health professionals (HPs) was necessary. Therefore studies of e-health, telephone interventions or self-help that were conducted by university research teams with no primary care practitioner involvement were excluded. For interventions delivered by a therapist (e.g. a psychologist or physiotherapist – not by the GP or primary care practice staff), these could have been delivered by the therapist while the patient was still regarded as a ‘primary care patient’, but not once the patient had been referred to secondary or tertiary care. Improving Access to Psychological Therapies (IAPT) interventions were included if delivered in a primary care or community-based setting.
Data extraction strategy
Data extraction was performed by one reviewer into a standardised data extraction form and independently checked for accuracy by a second. The extraction form was designed using the Template for Intervention Description and Replication (TIDieR) Checklist as a guide. Intervention information regarding setting, duration, provider (e.g. qualifications and training) and number of sessions, etc., was extracted. Basic demographic information for participants was also extracted. Discrepancies were resolved by discussion between the two reviewers and, if agreement could not be reached, then a third reviewer was consulted.
Critical appraisal strategy
The quality assessment of included RCTs was performed by one reviewer (JL) using Higgins’ risk-of-bias tool87 for RCTs, and 20% of completed checklists were independently checked for accuracy by a second reviewer (AS). Discrepancies were resolved by discussion between the two reviewers and, if agreement could not be reached, then a third reviewer was consulted.
Methods of data synthesis
Comparative effectiveness was evaluated using a NMA to allow a comprehensive synthesis of all evidence on all relevant interventions. NMA is an extension of pairwise meta-analysis and it can be used to combine direct and indirect evidence about treatment effects across studies to provide an internally consistent set of intervention effects while respecting the randomisation used in individual studies. 88 The NMAs were conducted using a Bayesian Markov chain Monte Carlo approach88 on the following outcomes: pain, fatigue, bowel symptoms, somatisation, generic physical symptoms, physical functioning, impact of illness on daily activities, anxiety, depression and emotional distress. This assumed a random-effects model to allow for heterogeneity in treatment effects across studies. Separate NMAs were performed for the three time points: immediately post treatment, short term (up to 6 months post treatment) and long term (> 6 months post treatment).
Definition of treatment effect (continuous outcome measures)
For each outcome of interest, the individual studies may have used one of several different (continuous) measurement scales (see Appendix 2, Table 38). To allow studies using different measurement scales to be included in a single NMA, standardised mean differences (SMDs) were computed for each study. The use of SMDs stems from the concept that the different reported measures are essentially quantifying the same effect and can be placed on a common scale by dividing the mean difference between the intervention and control arms in each study by the standard deviation (SD). Raw reported data, in the form of mean/median, SD/standard error (SE)/confidence interval (CI)/interquartile range (IQR), were used to calculate the SMD for each study using Hedges’ (corrected) g. 87 The SMD was computed based on absolute values at the end of follow-up rather than mean difference from baseline, as the within-study correlation would be needed for the latter and was not reported. All of the scales were transferred to be consistent across the scales used in the included studies so that a positive SMD indicates beneficial effect of a treatment in the intervention group when compared with the treatment in the control group.
Synthesis population
The synthesis population was defined following the inclusion criteria as all MUS. Condition groupings within MUS have been defined as chronic fatigue, chronic pain single site, chronic pain multiple sites, IBS or MUS/somatoform disorders. All condition groupings were synthesised in a single integrated analysis. Ideally, differential responses within each condition grouping would be explored through metaregression; however, the networks were too sparse to allow this.
Statistical model for the network meta-analysis
Let yik denote the observed SMD of arm k of trial i (i = 1 . . . ns, k = 1 . . . na), with variance Vik. We assume that the treatment effects are normally distributed such that:
The parameters of interest, θik, are modelled using the identity link function:
A random-effects model was assumed, so that the trial-specific treatment effects, δi,1k, are assumed to arise from a common population distribution with mean treatment effect relative to the reference treatment such that:
where dti1tik represents the mean effect of the treatment in arm k of study i (tik) compared with the treatment in arm 1 of study i (ti1) and τ2 represents the between-study variance in treatment effects (heterogeneity), which is assumed to be the same for all treatments.
Parameters were estimated in a Bayesian framework. Where there was sufficient sample data, conventional reference prior distributions were used:
-
between-study SD of treatment effects, τ ∼ U(0,1.1)
-
mean of treatment effects dti1tik∼N(0,1002).
In the case of there being relatively few studies, an informative prior distribution was assumed for the between-study SD. Rhodes et al. 89 proposed a t-distribution for log of the heterogeneity parameter for the SMD scale. The prior proposed by Rhodes et al. 89 still has probabilities of extremely high heterogeneity, which is implausible in the context that we are working on. For example, this prior represents the belief that the heterogeneity will be low, moderate, high or extremely high with probabilities of 22%, 41%, 16% or 20%, respectively. It has about 20% of the odds ratio in one study would be > 50 times greater than in another. Hence, the prior prosed by Ren et al. 90 is used, which is a truncated Turner et al. 91 prior [a log-normal (–2.56, 1.742)]. The truncation is based on the judgement that the odds ratio in one study would not be ≥ 50 times greater than in another. The resulting prior represents the belief that the heterogeneity will be low, moderate, high or extremely high with probabilities of 15%, 66%, 19% or 0%, respectively.
Inconsistency checking was performed by comparing the standard NMA consistency model with an inconsistency model. 92 In the inconsistency model, no consistency is assumed; that is, each of the pairwise comparisons represents an unrelated parameter to be estimated. The deviance information criteria (DIC) for both models are compared, as are the contributions to the deviance for both models, to determine if there is evidence to suggest inconsistency in the network.
All analyses were conducted in the freely available software packages WinBUGS93 (MRC Biostatistics Unit, Cambridge, UK) and R (The R Foundation for Statistical Computing, Vienna, Austria) using the R2Winbugs interface package. 94 Convergence to the target posterior distributions was assessed using the Gelman–Rubin statistic. 95 The chains converged within 18,000 iterations so a burn-in of 18,000 iterations was used. We retained a further 20,000 iterations of the Markov chain to estimate parameters using one chain. The absolute goodness of fit was checked by comparing the total residual deviance with the total number of data points included in an analysis.
Results are presented using the posterior median treatment effects, 95% credible intervals (CrIs) and 95% prediction interval (PrI). The 95% PrI indicates the extent of between-study heterogeneity by illustrating the range of SMDs that might be expected in a future study. The PrI is calculated based on the predictive distribution of the mean treatment effect. In a Bayesian Markov chain Monte Carlo setting, the predictive distribution is obtained by sampling from the distribution of effects N(d,τ2). Probabilities of treatment rankings were computed by counting the proportion of iterations of the Markov chain in which each intervention had each rank. Median treatment rankings and the probabilities of being the best treatment are presented.
Results
Quantity of research available
Characteristics of included studies
The searches identified 8925 citations for RCTs and 2929 citations for reviews. After deduplication, there were 5909 unique citations for RCTs and 2464 for reviews. For the RCTs, 281 full papers were retrieved as being potentially relevant. A total of 220 of these papers were excluded for at least one of the following reasons: pain was acute or subacute; symptoms did not meet the pre-defined review criteria for ‘unexplained’ as described above; pain was mixed explained/unexplained but populations could not be distinguished from one another in the results; setting was not primary care or insufficient primary care involvement; outcomes were not relevant; conference abstracts or dissertations; or not RCTs. Figure 2 shows the PRISMA flow chart. Studies excluded at full-paper stage are presented with reasons in Appendix 4.
FIGURE 2.
The PRISMA flow diagram.
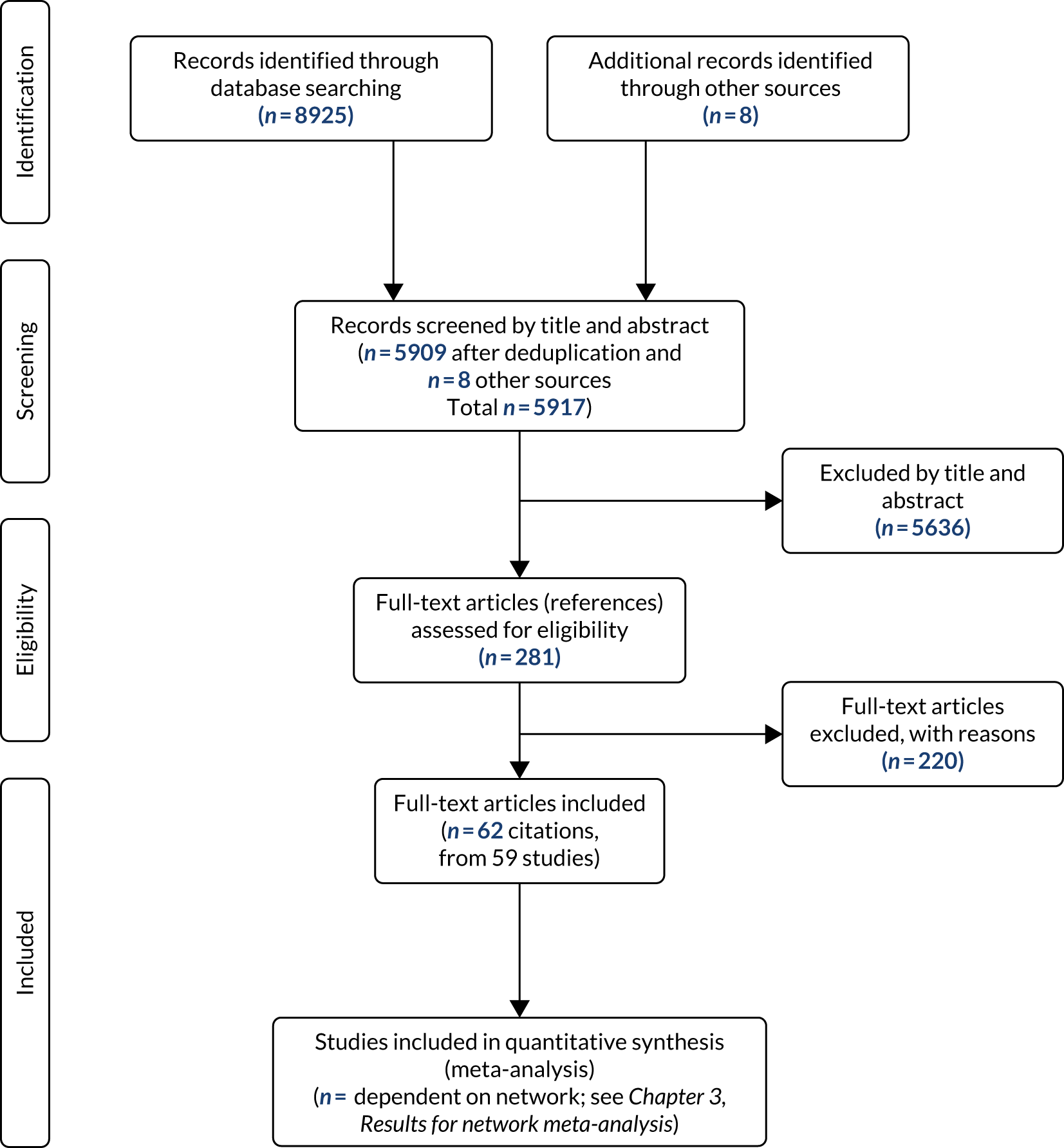
Sixty-two papers provided data from 59 trials. There were a total of 9077 participants across all trials that randomised numbers in each arm. The number of participants in a single trial ranged from 1096 to 524. 97 Owing to the nature of some of the interventions (i.e. where GPs received training to deliver treatment of MUS), some studies were cluster randomised, whereas the rest were randomised at patient level. Basic study characteristics are presented in Appendix 2, Table 42.
Description of the evidence
Study characteristics
Population
Appendix 2, Tables 29–36, shows the population inclusion criteria for individual studies by condition grouping. Condition groupings were MUS/somatoform disorder (including single MUS or mixed MUS), chronic fatigue (including but not exclusive to CFS), chronic pain (single site), chronic pain (multisite, including fibromyalgia) and IBS.
Of 59 studies that met the inclusion criteria, 29 studied either ‘MUS’ or ‘somatoform disorder’. Approximately half of these studies required participants to meet the diagnostic criteria for either somatoform disorder (DSM-III-R, DSM-IV, ICD-9, or ICD-10) or abridged somatisation disorder. 98 The remaining studies included populations of patients with ‘MUS’. Criteria for inclusion were varied, from number of unexplained symptoms within a set time (e.g. two or more within the past 6 months,99 lifetime history of 6–12 unexplained symptoms,100 five or more symptoms meeting the definition of unexplained during past 6 months101) to more general criteria (e.g. ‘multiple unexplained symptoms’,102 ‘symptoms rated by the GP as psychosomatic in origin’,103 ‘GP confirmed medically unexplained nature of symptoms’104 or ‘primary care providers had recognised that emotional status may have been related to their patient’s symptoms’105). The remaining studies set duration of unexplained symptoms as their inclusion criteria (e.g. duration of unexplained complaints of at least 12 months,106 no documented organic disease to explain symptoms of at least 6 months’ duration107 and ≥ 3 months’ physical symptoms not explained by physical pathology108).
One of the 59 studies109 had a population of mixed diagnoses that included any functional disorders, and one further study included participants with a single MUS: medically unexplained vaginal discharge. 110
Twelve of the 59 studies were of participants with chronic fatigue, and 7 of these 12 included populations meeting diagnostic criteria for CFS. Most of these used the US Centers for Disease Control and Prevention (CDC) criteria for CFS,6 but one study used the Oxford criteria. 111 Two of the 12 studies included participants who either met US CDC criteria for CFS or scored ≥ 4 on the Chalder Fatigue Scale. 112,113 The remaining three studies did not include participants with CFS, with two requiring a score of ≥ 4 on the Chalder Fatigue Scale,114,115 and one requiring a score of ≥ 35 on the fatigue subscale of the Dutch Checklist of Individual Strength. 116,117
Six of the 59 studies were of chronic pain at a single site on the body. Four of these were of back pain,118–121 one was of headache122 and one was of neck pain. 123 All required the duration of pain to be ≥ 3 months, apart from Loew et al. ,122 in which the requirement was for ≥ 12 months’ duration.
Seven of the 59 studies were of chronic pain at multiple sites of the body. Four of these studies were of participants with fibromyalgia, and these used the 1990 ACR diagnostic criteria as their inclusion criteria. 124 The remaining three studies were of chronic widespread pain125,126 or mixed chronic multisite pain, for example chronic generalised or regional pain where organic explanation had been ruled out. 127,128
The remaining three studies were of IBS. Inclusion criteria were that patients met the Rome I diagnostic criteria129 or Rome I and II diagnostic criteria. 130 The third IBS study required a diagnosis of functional gastrointestinal symptoms diagnosed as IBS, but participants did not necessarily have to meet Rome criteria. 131
Setting
Fifty-six of the included studies were defined as ‘primary care’, with the remaining three studies defined as ‘community based’. Appendix 2, Table 40, shows that there was considerable heterogeneity in the details of the setting of the studies. Studies varied in the primary care involvement, although all were designed for primary care patients rather than patients already in tertiary care or who self-referred to a university-based study without co-ordination with a primary care practitioner. Variation in setting detail included study designs where:
-
Patients were recruited and treated by their own GP at their own GP practice.
-
Patients were recruited by their GP, but treated by another health-care professional at their own GP practice.
-
Patients were recruited and assessed by their GP, but treated by another health-care professional at an outside facility; for example a gymnasium or park.
-
Patients were recruited and co-ordinated by their GP, but treatment was self-directed (e.g. home-based exercises).
-
Non-UK studies where the organisation of primary care may differ from the UK health-care system (e.g. ‘primary care physiotherapy clinic’). These clinics are described as working in close co-operation with ordinary primary health systems.
Studies where the intervention itself was not delivered within the primary care practice tended to be sport- or exercise-based interventions, or use of self-help materials. Community-based interventions were included only if the study was explicit in its description and aim of the intervention as being community based. Appendix 2, Table 40, shows setting details for individual studies.
Interventions
Intervention arms were coded into one of the 13 pre-defined intervention groupings. Appendix 2, Table 28, reports the detail of the intervention arms for each study, as described by the authors, and the intervention grouping that the arm has been coded into. Control arms that were active rather than passive were coded into one of the intervention groupings, therefore the numbers reported below for each intervention group add up to greater than the number of studies. Passive control arms were coded either as medication or as usual care/usual care plus. There were a total of 127 intervention arms. Of these, 80 were active intervention arms (or were categorised as such by the review team; for example, where an education booklet/presentation was called usual care by the authors, this was categorised as guided self-help and, therefore, an active intervention) and 47 were passive control arms. There was considerable heterogeneity both between and within groupings. Numbers for types of intervention groups are listed below. Appendix 2, Table 41, presents a summary of intervention groupings for each study arm.
Active intervention arms:
-
GP reattribution (including modified), n = 5
-
GP MUS management, n = 6
-
GP-CBT, n = 1
-
GP other psychotherapy, n = 1
-
GP other, n = 1
-
CBT high intensity, n = 8
-
CBT low intensity, n = 7
-
other psychotherapy, n = 11
-
graded activity (GA), n = 7
-
strength/endurance/sport (SES), n = 7
-
relaxation, stretching, social support, emotional support (RSSE), n = 8
-
guided self-help, n = 6
-
multimodal, n = 12.
Passive control arms:
-
medication, n = 3
-
usual care, n = 39
-
usual care plus, n = 5.
The most common active intervention was multimodal therapy. There was wide variation in the nature of the multimodal interventions, with various combinations of the individual interventions represented. These may be specifically defined in the paper as ‘multimodal’ (e.g. Smith et al. 107) or may consist of components from different groups (e.g. van der Roer et al. 120 sport/exercise + education + behavioural programme; McBeth et al. 125 CBT + sport/exercise). Not only did the RSSE group encompass a wide range of different types of intervention, but these types of intervention were also commonly used as active controls (or were classed as active controls by the review team), as were guided self-help interventions, which were often a self-management information/education booklet. There was an element of overlap between some of the guided self-help interventions and low-intensity CBT (CBTLI), with the latter providing more structure and support than the guided self-help interventions. Other psychotherapy was the next most common intervention, with high-intensity CBT (CBTHI) and CBTLI being the third and fourth most common. Graded activity and sport/exercise interventions were equally represented, with seven arms each. Some interventions were conducted in groups and some were conducted individually. Some were conducted face to face whereas others were conducted at a distance, either by telephone or by e-mail. Appendix 2, Table 41, presents these details by arm for each study.
For most interventions, treatment was directed at patients, in a set number of sessions, for a recommended duration. However, some interventions were directed primarily at the GP. GPs would receive training in methods of treating patients with MUS. This training aimed to enable the GP to communicate a behavioural/biopsychosocial approach to unexplained symptoms to their patients. In these cases, a set study period was usually specified, during which time the GP would conduct consultations with patients in their usual distribution of surgeries rather than at a set number of GP/patient sessions. This study period could last up to 2 years. 97
There was also heterogeneity within intervention groups. Appendix 2, Tables 43 and 44, presents details of planned duration of treatment sessions for each arm, and Table 44 presents details of planned duration of the treatment period. Greater detail by intervention arm for actual mean sessions/duration for each arm is reported in the cost analysis in Chapter 6. There was no typical treatment duration, either between or within intervention groups. Treatment sessions ranged from 1 × 10- to 15-minute session with a HP followed by self-management114 to 10 × 90-minute sessions of treatment plus booster sessions. 132 The shortest treatment periods were around 6–8 weeks (e.g. McCleod et al. ,105 LeFort128 – 6 weeks; Macedo et al. ,119 Moss-Morris et al. 130 – 8 weeks), with a mid-range of 12 weeks (e.g. Marques et al. 133 and Ridsdale et al. 112). Longer-term treatment periods ranged up to 1 year (e.g. Kocken et al. 103 and Smith et al. 107).
Differences in intervention provider and the contact time spent with patients are shown in Appendix 2, Table 45. Interventions were delivered by a range of health-care professionals (e.g. GPs, psychologists, practice nurses, physiotherapists, psychiatrists, psychiatric nurses and health educators). There was little consistency in contact time between provider and patient across the studies.
Most usual-care arms were not specific in their descriptions of care received – this probably varies between individual patients in response to their particular needs, but may consist of giving information leaflets/medication. Some controls defined as ‘usual care’ by the study authors were categorised into active intervention groups. For example, an active study intervention ‘self-help’ consisting of a self-management booklet and minimal contact with a HP114 is categorised as guided self-help. The same booklet is used as a part of a ‘usual-care’ control arm in another study115 but, for the purposes of the review, has been categorised as guided self-help.
Outcomes
All primary and secondary outcomes assessed in each study, together with the scales used for assessment, are reported in Appendix 2, Table 37. Owing to differences in populations, outcomes varied between studies. Key outcomes across studies were identified and are presented in Appendix 2, Table 38. Condition-specific symptoms were measured, for example bowel symptoms for IBS studies, fatigue for chronic fatigue studies, and pain for chronic pain studies. Some of these condition-specific symptoms were also recorded for studies of ‘MUS’ patients, most commonly for pain, but never for bowel symptoms. Pain was most frequently measured using a visual analogue scale (VAS) or numerical rating scale (NRS) in studies of chronic pain populations, whereas, for studies of MUS patients, the SF-36 bodily pain subscale was more frequently used. Fatigue was almost always assessed using the Chalder Fatigue Scale. Psychological symptoms, most commonly anxiety and depression, were measured across all condition groups. For depression, the Hospital Anxiety and Depression Scale – Depression (HADS-D), BDI, Hamilton Rating Scale for Depression (HAM-D) and Symptom Checklist-90 – Depression (SCL-90-D) were the most frequently used scales. For anxiety, the Hospital Anxiety and Depression Scale – Anxiety (HADS-A), Hamilton Anxiety Rating Scale (HAM-A) and Symptom Checklist-90 – Anxiety (SCL-90-A) were the most frequently used scales. Composite measures of emotional distress were also reported, most commonly using the SF-36 mental health subscale, but also HADS total scores, or the General Health Questionnaire (GHQ-30). For ‘MUS/somatoform’ studies, ‘somatisation’ was commonly measured to assess symptom load, using a number of scales but most commonly the SOMS or PHQ-15 or Brief Symptom Inventory (BSI). Severity of main symptoms or number of symptoms was also measured (generic physical symptoms) in a minority of studies, with severity VAS or number of symptoms used as methods of assessment. Physical function was measured in studies of all conditions, almost always using the Short Form questionnaire-12 items (SF-12) or SF-36 physical functioning subscale. Finally, illness impact on daily activities was measured across conditions, using disability scales such as the Roland–Morris Disability Questionnaire (RMDQ), the Neck Disability Index or Oswestry Disability Index (ODI), or, for fibromyalgia, the Fibromyalgia Impact Questionnaire (FIQ) total.
Quality of the evidence
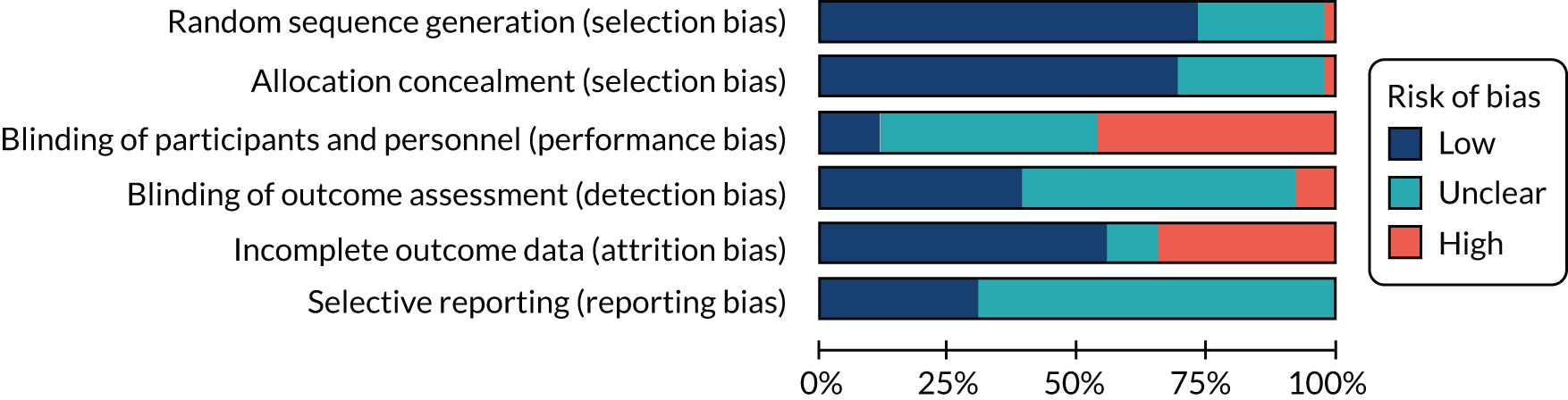
Individual risk-of-bias extractions and summary tables can be found in Appendix 3. The quality of individual studies ranged from low to high. Most commonly, studies were found to be at high risk of performance bias, with patients and intervention providers frequently not blinded because of the nature of the interventions and comparators. Over 25% of studies were at high risk of attrition bias, but over 50% of studies were found to be at low risk of attrition bias using the 20% cut-off point. 134 Reporting bias was assessed by reference to study protocols. Study protocols were sought using a number of methods and these are described, with success rates, in a separate paper. 135 Figure 3 shows the summary table for risk-of-bias assessments.
FIGURE 3.
Summary table of risk-of-bias assessments.
Study results
Raw data extracted from individual studies (means, SD/SE by outcome) can be found in Appendix 4. For the following reasons, studies do not contribute data to all outcomes in the NMA:
-
as is seen in Appendix 2, Table 38, key outcomes vary by study
-
as is seen in Appendix 2, Table 39, follow-up time points are not consistent between studies
-
studies could not be included in the NMA where both intervention arms were grouped into the same intervention category; for example, Aiarzeguena et al. 136 where both arms were grouped as GP reattribution (one arm being modified reattribution) or where both arms were GA (one arm being symptom contingent and one arm being time contingent)
-
data could not be included where no variance was given
-
data could not be included when only provided in graphical format
-
studies could not be included where no raw data were provided for non-significant outcomes.
For these reasons, results of the NMA should be interpreted with caution, and considered within the context of the narrative summaries of results from individual studies. Appendix 2, Tables 46–76, presents narrative summaries of results for key outcomes for individual studies.
Narrative overviews for key outcomes are presented below, complementing the summaries in Appendix 2, Tables 46–80. Studies varied in the manner in which they reported their results. Some presented information on significance of effects both within and between groups, whereas others reported only between-group differences. Some studies report significance controlling for baseline variables, or before and after controlling for multiple comparisons. Owing to these differences in reporting, it was considered inappropriate to present ‘counts’ or ‘percentages’ of significant effects for each outcome by time point. However, a summary of main effects by outcomes as reported in individual studies is presented in Appendix 2, Tables 46–80, along with key information regarding the patient population studied and the interventions being compared. Therefore, this indicates whether the trials had active or ‘do nothing’ (usual care/treatment as usual/waiting list) controls.
Physical symptoms
Pain
Twenty-three studies reported pain as an outcome. Thirteen of these were studies of the chronic pain population: six of single-site chronic pain118–123 and seven of chronic pain at multiple sites on the body. 125,127,128,137–140 The remaining 10 studies were in the MUS/somatoform disorder population (see Appendix 2, Table 46). 103,106,136,141–148 A number of intervention types were reported to show an improvement in pain intensity. These include CBTHI, SES, RSSE and multimodal (exercise + education). No other psychotherapy or any GP intervention showed a positive effect. There were no CBTLI studies. Narrative summaries for each individual study for pain results are presented in Appendix 2, Table 46.
Fatigue
Fourteen studies reported fatigue as an outcome. Most studies measured fatigue using the Chalder Fatigue Scale, although the Checklist of Individual Strength (CIS) fatigue severity subscale and the FIQ fatigue subscale were also used in a minority of studies. Twelve studies were undertaken in participants with chronic fatigue111–115,133,149–155 and two studies in a chronic multisite pain population. 125,139 Intervention types that were reported to show a positive improvement in fatigue included CBTLI, GA and RSSE. No GP interventions were found to be effective. There were no studies of CBTHI. Narrative summaries for each individual study for fatigue results are presented in Appendix 2, Table 47.
Bowel symptoms
Three studies reported bowel symptoms as an outcome and these were all in populations with IBS. Two studies used the IBS Symptom Severity Scale129,130 and one used the Clinical Global Impression Scale (CGIS) – Severity of Symptoms. 131 Two studies reported significant improvements in bowel symptoms after behavioural interventions. These were both CBTLI, with one also including medication, but CBT was reported to have a beneficial summary effect over medication alone, although the effect was lost by 12 months. The one study131 that found no significant effect for behavioural interventions compared an RSSE intervention with a multimodal intervention and a third arm of usual care. Narrative summaries for bowel symptoms results are presented in Appendix 2, Table 48.
Somatisation
Twenty-one studies reported somatisation as an outcome. Of these, 19 were of populations of patients in the MUS/somatoform disorder condition group,97,99,102,104–107,116,117,141–144,146–148,156–159 one study was of unexplained vaginal discharge110 and the remaining study was of patients with chronic fatigue. 133 Studies measured somatisation using the Symptom Checklist-90 – Somatisation (SCL-90-S), the BSI-somatic complaints, the PHQ-15 somatic complaints, the SOMS-7 and the Scale for Assessment of Somatic Symptoms (SASS)-somatisation. Intervention types that were reported to show positive improvement in somatic complaints after behavioural modification interventions included both CBTLI and CBTHI, other psychotherapy, multimodal therapy and GP reattribution, although this significant effect was lost after controlling for confounding factors. Narrative summaries for somatisation results are presented in Appendix 2, Table 49.
Generic physical symptoms
Five studies reported this outcome, which represents ‘symptom load’ or severity of unspecified symptoms where not measured by a validated scale (see ‘somatisation’ outcome for these). 96,104,109,156,160 This outcome includes measures such as ‘N unexplained symptoms’ or severity of ‘main’ symptom’ (where the symptom is not specified and not specific to a particular condition, e.g. IBS or fibromyalgia). All studies were of the MUS/somatoform disorder condition group. Intervention types that were reported to show positive improvement in symptom load included CBTLI, CBTHI and multimodal therapy.
Physical functioning and impact
Physical function
Thirty-two studies reported physical function as an outcome (see Table 38 for condition groups and scales used in individual studies). 97,100,106,107,111,114,118,119,125,127,128,131,133,136,139–153,155–158,161 Most of these studies used either the SF-12 or SF-36, either the physical functioning subscale or less commonly the physical component summary only. One study used the FIQ physical functioning subscale. Of the 32 studies, eight were in the chronic fatigue condition group, 16 were in the MUS/somatoform condition group, one was in the IBS group, and seven were in chronic pain populations (two single site and five multisite). A number of different intervention types showed significant positive improvement in physical function. These included RSSE, SES, CBTHI, GP reattribution and multimodal interventions. Narrative summaries for physical function results are presented in Appendix 2, Table 53.
Impact of illness on daily activities
Twenty-two studies reported measures of impact as an outcome (see Table 38 for conditions and scales used in individual studies). 103,112,113,115,118–121,123,127–130,137–141,146,154,159,160 These mostly used disability scales: the RMDQ, ODI, London Handicap Scale, NDI, or the SCL-90 – Global Wellness (SCL-90-G), the FIQ-total, or the Work and Social Adjustment Scale (WASA)162 impact subscale. Four studies were of populations in the chronic fatigue condition group, 11 in the chronic pain condition group (five single site and six multisite), two in IBS populations and five in the MUS/somatoform disorder condition group. A number of different intervention types showed significant improvements in ‘impact’ after behavioural interventions. These were both CBTLI and CBTHI, RSSE, SES and multimodal interventions.
Emotional distress
Anxiety
Thirty studies reported anxiety as an outcome. 102,104–108,110–113,115,127–130,133,137–139,141,142,144,145,148,149,151,154,156–159 A range of measures was used, most commonly the HADS-A and the HAM-A, but also the BAI, SCL-90-A, the BSI-anxiety and the FIQ anxiety subscale. Fifteen studies were in populations in the MUS/somatoform condition group, two were in populations of patients with IBS, eight studies were in populations in the chronic fatigue condition group, and four were in populations with chronic multisite pain. The remaining study was of unexplained vaginal discharge (see Table 38 for conditions and measures used for individual studies). A number of different intervention groups showed positive effects: CBTLI and CBTHI, RSSE, GP MUS management and GP reattribution, although the GP reattribution effect was lost when controlling for confounders. Narrative summaries for anxiety results are presented in Appendix 2, Table 51.
Depression
Depression, along with physical functioning, was the most commonly reported outcome, with 32 studies representing populations in four condition groups: seven for chronic fatigue, six for pain – multisite, one for IBS and 17 for the MUS/somatoform condition group, and one for unexplained vaginal discharge (see Table 38 for conditions and measures used for individual studies). 99,102,105–108,111–113,115,127–130,133,137–145,147,148,151,156–159 A range of measures were used, the most common being HADS-D, HAM-D and BDI, with other studies using CES-D, SCL-90-D and the PHQ-9. Studies reporting positive improvement in depression were found across a number of intervention types, including CBTHI, GA, SES and GP reattribution, although this effect was lost after controlling for confounders. Narrative summaries for depression are presented in Appendix 2, Table 52.
Emotional distress
Thirty studies reported composite measures of emotional distress. 97,100,103,106,107,114,116–119,125,128,129,131,133,136,140–148,150,153,155,157,158,160,161 All condition groups were represented, with five chronic pain studies (two single site, three multisite), four chronic fatigue studies, two IBS studies and 19 MUS/somatoform studies) (see Table 38 for conditions and measures used for individual studies). The majority of these studies used the SF-12 or SF-36 mental health subscale or mental component summary. HADS total, GHQ-30 psychological morbidity and sickness impact profile (SIP) psychological subscales were also used. Positive effects were found across a number of different intervention types: CBTLI and CBTHI, other psychotherapy, RSSE, GA, SES, GP reattribution and multimodal. Narrative summaries for emotional distress results are presented in Appendix 2, Table 50.
Satisfaction, acceptability and adherence
Satisfaction, acceptability and adherence were not measured or reported in a consistent way across studies and, therefore, no attempt was made to conduct a meta-analysis of the data. For GP interventions, ‘attendance’ (by patients to their treatment sessions) or by GPs (to their training) gave an indication of acceptability where no formal measure was taken. GPs were also asked for their confidence in dealing with patients with MUS, or their satisfaction with their training and its relevance to their practice. Patients were also asked about satisfaction with their care. For other interventions, satisfaction was rarely formally measured. Uptake, attendance and attrition data were presented for many studies, giving an indication of acceptability of the treatment offered. Appendix 2, Tables 54–62, presents a narrative synthesis of data relating to these outcomes for individual studies by intervention type. Narrative summaries of results for satisfaction, acceptability or adherence by intervention type are also presented in Appendix 2, Tables 54–62.
Health-care utilisation
The review of health economic literature in Chapter 6 presents data relating to costs associated with health-care utilisation. Owing to sparse reporting of health-care utilisation and heterogeneity of reported data, this is not included as an outcome in the NMA. Appendix 2, Tables 63–71, presents a narrative synthesis of data relating to this outcome, by intervention type. As most studies did not provide these data, only those that did are reported.
Adverse events
Very few studies reported adverse events in detail. It is unclear whether this is because of a lack of events or a lack of recording of events. Where data were reported, the most frequent adverse events were increase in pain with exercise interventions, increase in nausea and dry mouth for pharmaceutical interventions, and an increase in rumination for CBT in one study. One patient was found to have an incorrect diagnosis of CFS. Although other studies did report numbers of reported adverse events, the specific nature of these events was not reported. Appendix 2, Tables 72–76, presents a narrative summary of data relating to this outcome. As the majority of studies did not record/report adverse events, only those that did so are presented in the tables, by intervention type, where available.
Results for network meta-analysis
For all the results presented in this section, a positive SMD indicates a beneficial effect when compared with usual care. Cohen’s categories were used to describe the magnitude of the effect size, with SMD ≥ 0.2 to 0.5 being a small effect size, SMD ≥ 0.5 to 0.8 being a medium effect size, and SMD ≥ 0.8 being a large effect size. 163 SMD < 0.2 was labelled ‘not substantial’ effect size.
Physical symptom outcome measures immediately post treatment
Pain (post treatment)
Data were available from 10 studies presenting the pain score immediately post treatment. A NMA was used to compare the effects of usual care plus, medication, CBTHI, other psychotherapy, RSSE, guided self-help, SES and multimodal relative to usual care on pain score. Figure 4 presents the network of evidence.
FIGURE 4.
Pain score immediately post treatment: network of evidence. GSH, guided self-help; ME, medication; MM, multimodal; OP, other psychotherapy; UC, usual care; UC+, usual care plus.
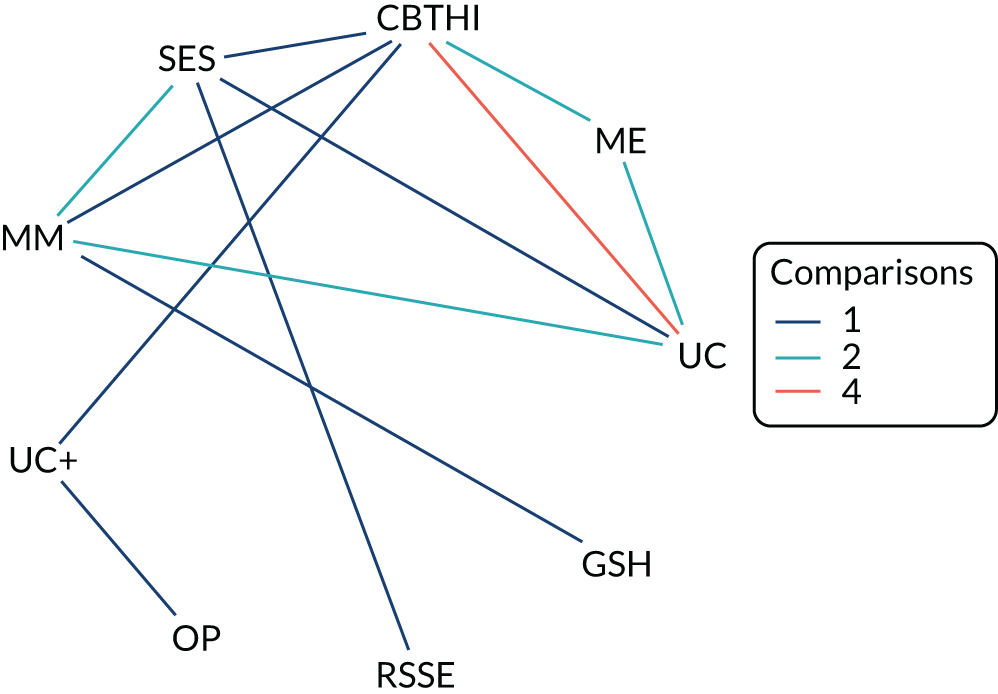
Figure 5 presents the SMD of each intervention relative to usual care, the median of treatment rankings and the probability of being the best treatment. For all interventions with the exception of guided self-help, the estimated SMD was greater than zero, suggesting a beneficial effect compared with usual care. However, only the effect of CBTHI (a medium effect size, SMD 0.54, with 95% CrI 0.28 to 0.84) and multimodal (a small effect size, SMD 0.52, with 95% CrI 0.19 to 0.89) were statistically significant at a conventional 5% level. CBTHI was also statistically significant compared with usual care, based on the 95% prediction intervals (which illustrate the range of SMDs that might be expected in a future study) (see Figure 5). The interventions with the highest probabilities of being the best were CBTHI and multimodal (probability 0.31 and 0.30, respectively). The between-study SD was estimated to be 0.19 (95% CrI 0.04 to 0.44), which implies moderate heterogeneity of intervention effects between studies.
FIGURE 5.
Pain score immediately post treatment: SMD for all interventions relative to usual care. a, Probability of being the best treatment. GSH, guided self-help; ME, medication; MM, multimodal; OP, other psychotherapy; UC, usual care; UC+, usual care plus.

Fatigue (post treatment)
Data were available from nine studies presenting the fatigue score immediately post treatment. A NMA was used to compare the effects of GP-CBT, CBTLI, CBTHI, other psychotherapy, RSSE, guided self-help, GA, SES and multimodal relative to usual care on fatigue score. Figure 6 presents the network of evidence.
FIGURE 6.
Fatigue score immediately post treatment: network of evidence. GSH, guided self-help; ME, medication; MM, multimodal; OP, other psychotherapy; UC, usual care; UC+, usual care plus.
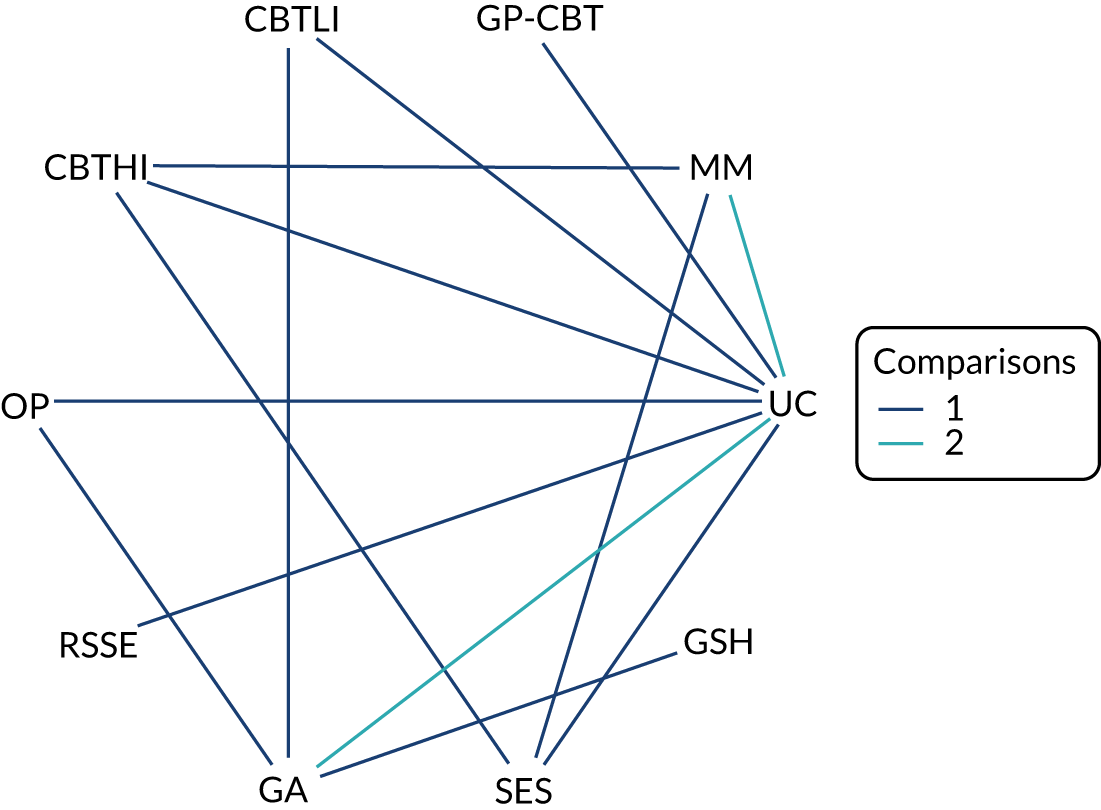
Figure 7 presents the SMD of each intervention relative to usual care, the median of treatment rankings and the probability of being the best treatment. For all interventions with the exception of guided self-help, the estimated SMD was greater than zero, suggesting a beneficial effect compared with usual care. However, only the effect of RSSE (a large effect size, SMD 0.87, with 95% CrI 0.20 to 1.55), CBTLI (a medium effect size, SMD 0.72, with 95% CrI 0.27 to 1.21), multimodal (a medium effect size, SMD 0.52, with 95% CrI 0.14 to 0.92) and GA (a medium effect size, SMD 0.51, with 95% CrI 0.14 to 0.93) were statistically significant at a conventional 5% level. Only the effects of RSSE and CBTLI were statistically significant compared with usual care based on the 95% prediction intervals (which illustrate the range of effect size that might be expected in a future study) (see Figure 7). The intervention with the highest probability of being the best was RSSE (probability 0.60). The between-study SD was estimated to be 0.18 (95% CrI 0.04 to 0.48), which implies moderate heterogeneity of intervention effects between studies.
FIGURE 7.
Fatigue score immediately post treatment: SMD for all interventions relative to usual care. a, Probability of being the best treatment. GSH, guided self-help; ME, medication; MM, multimodal; OP, other psychotherapy; UC, usual care; UC+, usual care plus.
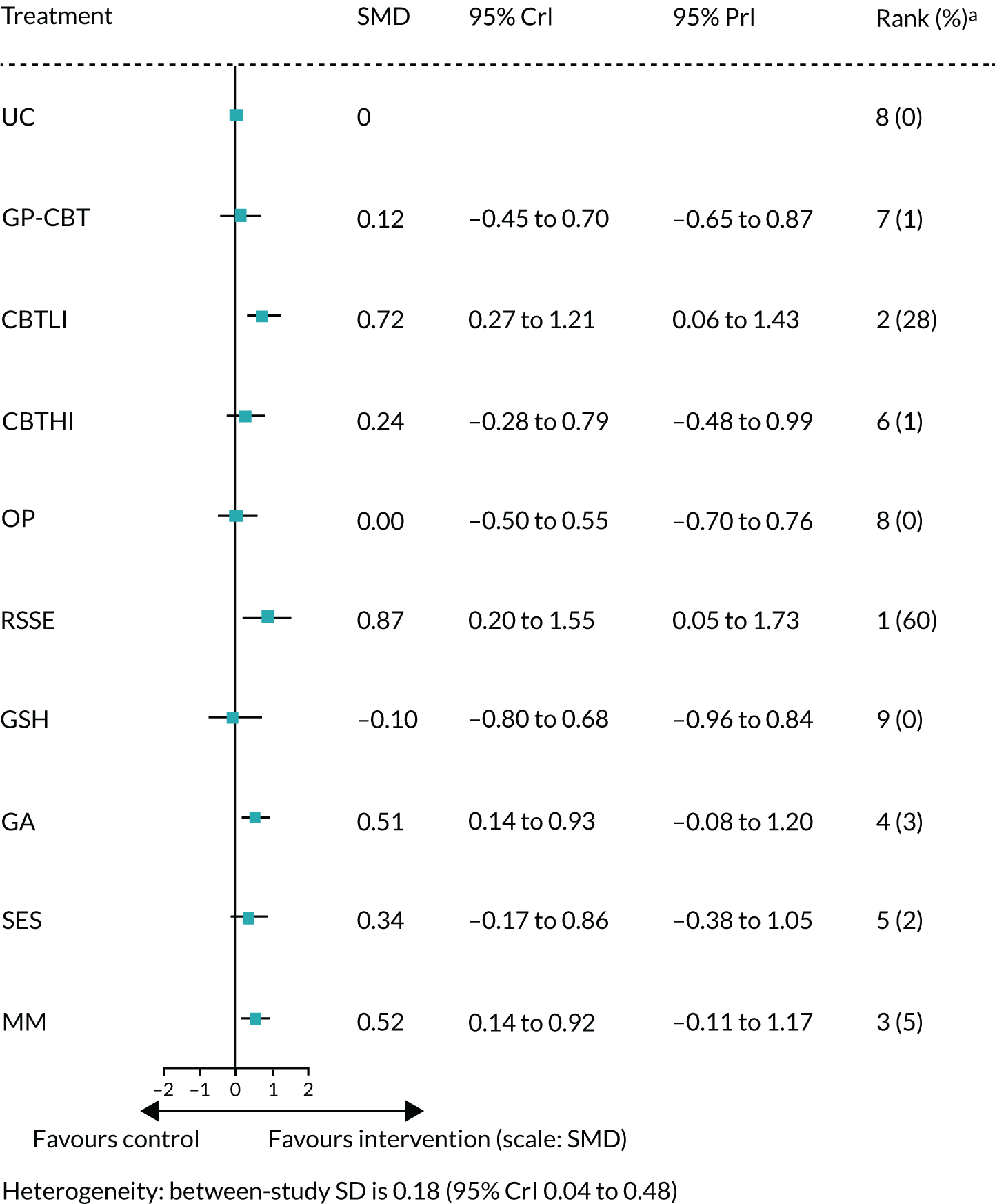
Bowel symptoms (post treatment)
Two studies (Kennedy et al. 129 compared multimodal with medication and Moss-Morris et al. 130 compared usual care vs. CBTLI) were available on the bowel symptoms outcome immediately post treatment. No NMA was performed because of the disconnect network. The estimated SMD of multimodal compared with medication was a small effect size, 0.45 (95% CI 0.13 to 0.77), from Kennedy et al. 129 The estimated SMD of CBTLI compared with usual care was a small effect size, 0.44 (95% CI –0.03 to 0.95), from Moss-Morris et al. 130
Somatisation (post treatment)
Data were available from 11 studies presenting the somatisation score immediately post treatment. A NMA was used to compare the effects of usual care plus, GP reattribution, CBTLI, CBTHI, other psychotherapy, RSSE and SES relative to usual care on somatisation score. Figure 8 presents the network of evidence.
FIGURE 8.
Somatisation score immediately post treatment: network of evidence. GPRE, general practitioner-delivered reattribution; GSH, guided self-help; OP, other psychotherapy; UC, usual care; UC+, usual care plus.
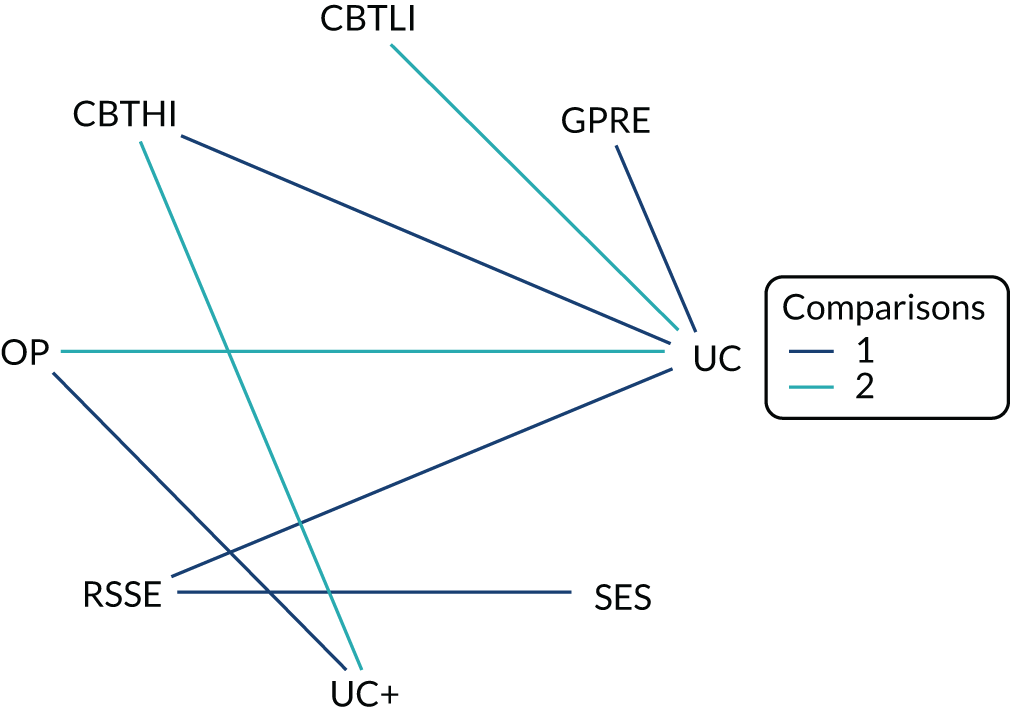
Figure 9 presents the SMD of each intervention relative to usual care, the median of treatment rankings and the probability of being the best treatment. For all interventions with the exception of usual care plus, the estimated SMD was greater than zero, suggesting a beneficial effect compared with usual care. However, none of the results was statistically significant at a conventional 5% level and the largest beneficial effect was associated with CBTHI with a small effect size (SMD 0.32, with 95% CrI –0.12 to 0.75). None of the results was statistically significant based on the prediction interval (PrI) (see Figure 9). The intervention with the highest probability of being the best was CBTHI (probability 0.39). The between-study SD was estimated to be 0.16 (95% CrI 0.03 to 0.43), which implies moderate heterogeneity of intervention effects between studies.
FIGURE 9.
Somatisation score immediately post treatment: SMD for all interventions relative to usual care. a, Probability of being the best treatment. GPRE, general practitioner-delivered reattribution; GSH, guided self-help; OP, other psychotherapy; UC, usual care; UC+, usual care plus.

Generic physical symptoms (post treatment)
Data were available from two studies presenting the generic physical symptoms score immediately post treatment. A NMA was used to compare the effects of other psychotherapy relative to usual care on generic physical symptoms score. Figure 10 presents the network of evidence.
FIGURE 10.
Generic physical symptoms score immediately post treatment: network of evidence. OP, other psychotherapy; UC, usual care.

Figure 11 presents the SMD of each intervention relative to usual care, the median of treatment rankings and the probability of being the best treatment. The estimated SMD of other psychotherapy was less effective than usual care (a small effect size, SMD –0.25, with 95% CrI –0.77 to 0.30). This effect was not statistically significant at a conventional 5% level, and it was also not statistically significant based on the PrI (see Figure 11). The intervention with the highest probability of being the best was usual care (probability 0.83). The between-study SD was estimated to be 0.13 (95% CrI 0.03 to 0.45), which implies moderate heterogeneity of intervention effects between studies.
FIGURE 11.
Generic physical symptoms score immediately post treatment: SMD for all interventions relative to usual care. a, Probability of being the best treatment. OP, other psychotherapy; UC, usual care.
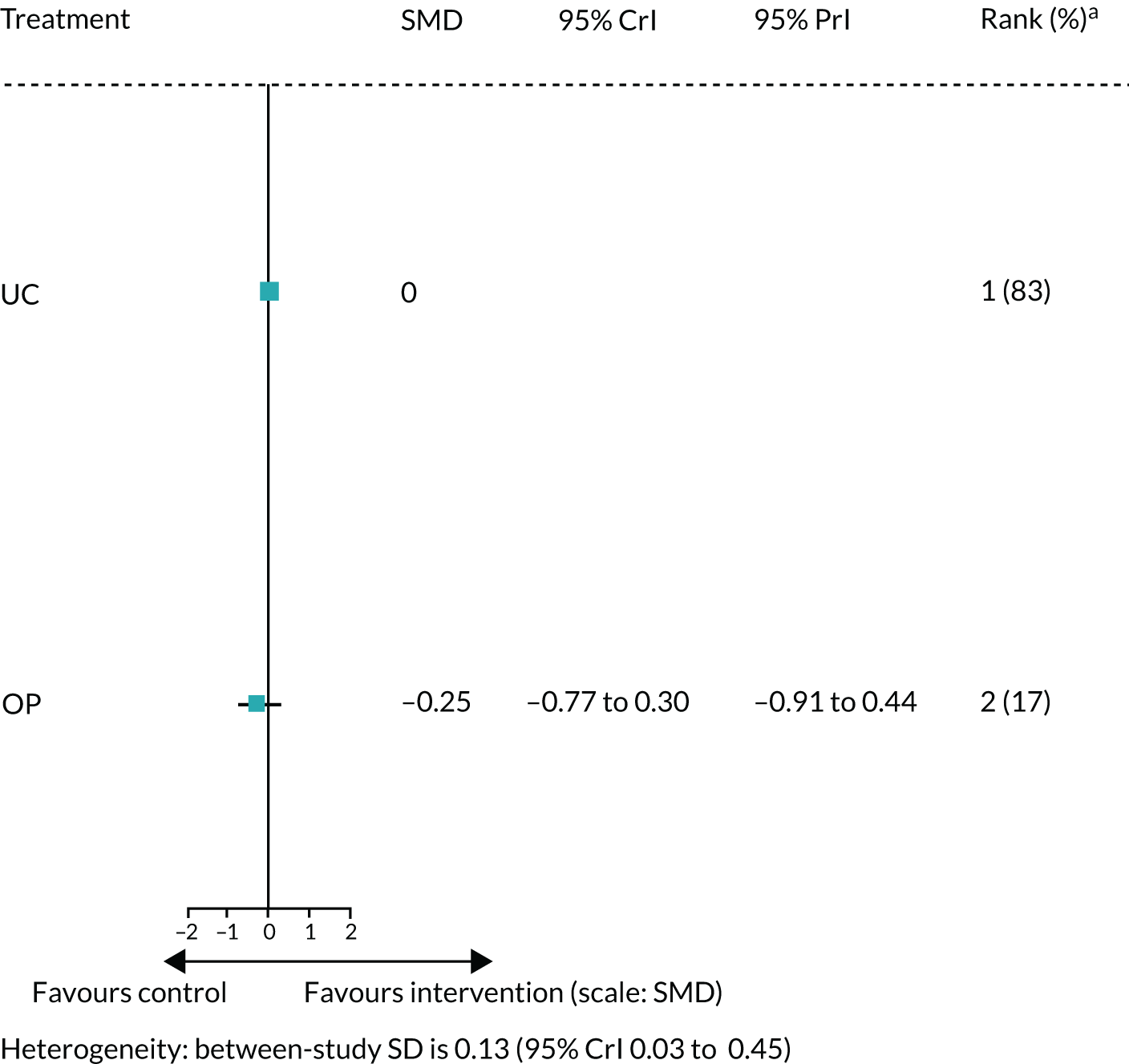
Physical functioning and impact outcome measures immediately post treatment
Physical functioning (post treatment)
Data were available from 14 studies presenting the physical functioning score immediately post treatment. A NMA was used to compare the effects of usual care plus, GP reattribution, GP-CBT, CBTLI, CBTHI, other psychotherapy, RSSE, guided self-help and GA, SES and multimodal relative to usual care on physical functioning score. Figure 12 presents the network of evidence.
FIGURE 12.
Physical functioning score immediately post treatment: network of evidence. GPRE, general practitioner-delivered reattribution; GSH, guided self-help; ME, medication; MM, multimodal; OP, other psychotherapy; UC, usual care; UC+, usual care plus.
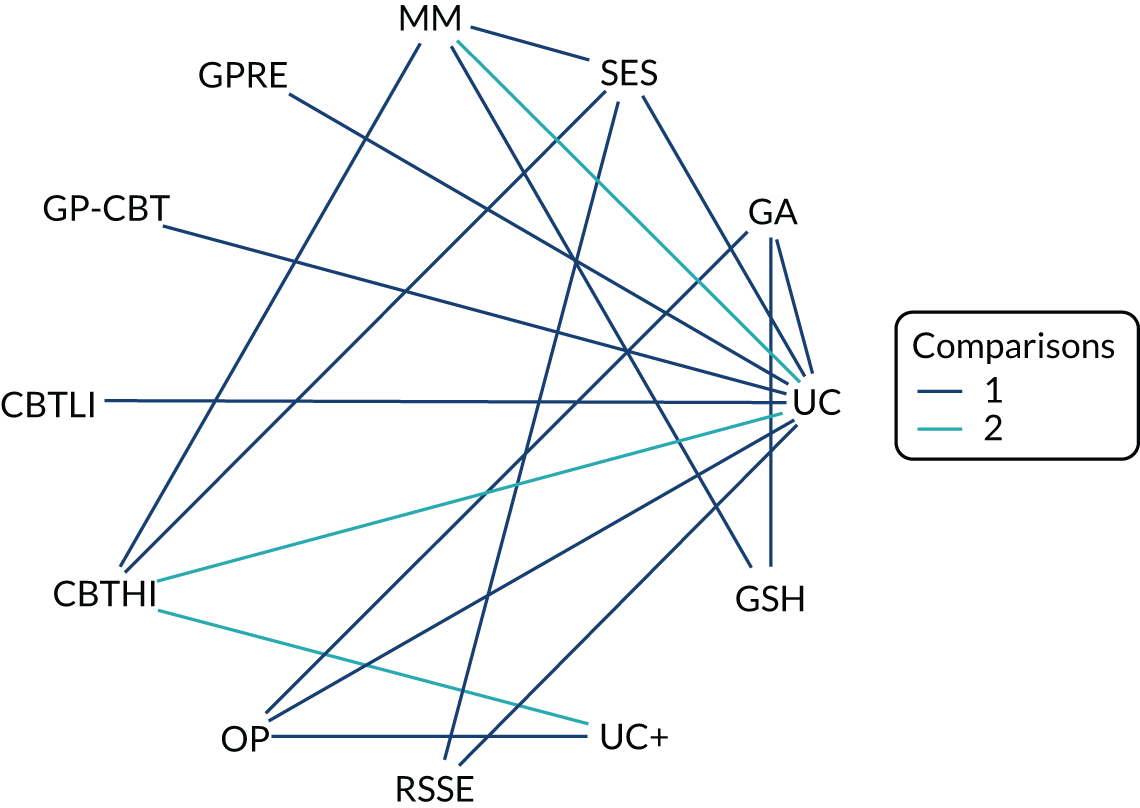
Figure 13 presents the SMD of each intervention relative to usual care, the median of treatment rankings and the probability of being the best treatment. For all interventions with the exception of usual care plus, GP-CBT, other psychotherapy and guided self-help, the estimated SMD was greater than zero, suggesting a beneficial effect compared with usual care. However, only the effect of multimodal (a small effect size, SMD 0.33, with 95% CrI 0.09 to 0.59) was statistically significant at a conventional 5% level, but none of the beneficial effects was statistically significant based on the PrI (see Figure 13). Guided self-help was significantly worse than usual care (a medium effect size, SMD –0.73, with 95% CrI –1.18 to –0.29), and this effect was also statistically significant on the PrI (see Figure 13). The intervention with the highest probability of being the best was multimodal (probability 0.35). The between-study SD was estimated to be 0.10 (95% CrI 0.03 to 0.29), which implies moderate heterogeneity of intervention effects between studies.
FIGURE 13.
Physical functioning score immediately post treatment: SMD for all interventions relative to usual care. a, Probability of being the best treatment. GPRE, general practitioner-delivered reattribution; GSH, guided self-help; ME, medication; MM, multimodal; OP, other psychotherapy; UC, usual care; UC+, usual care plus.
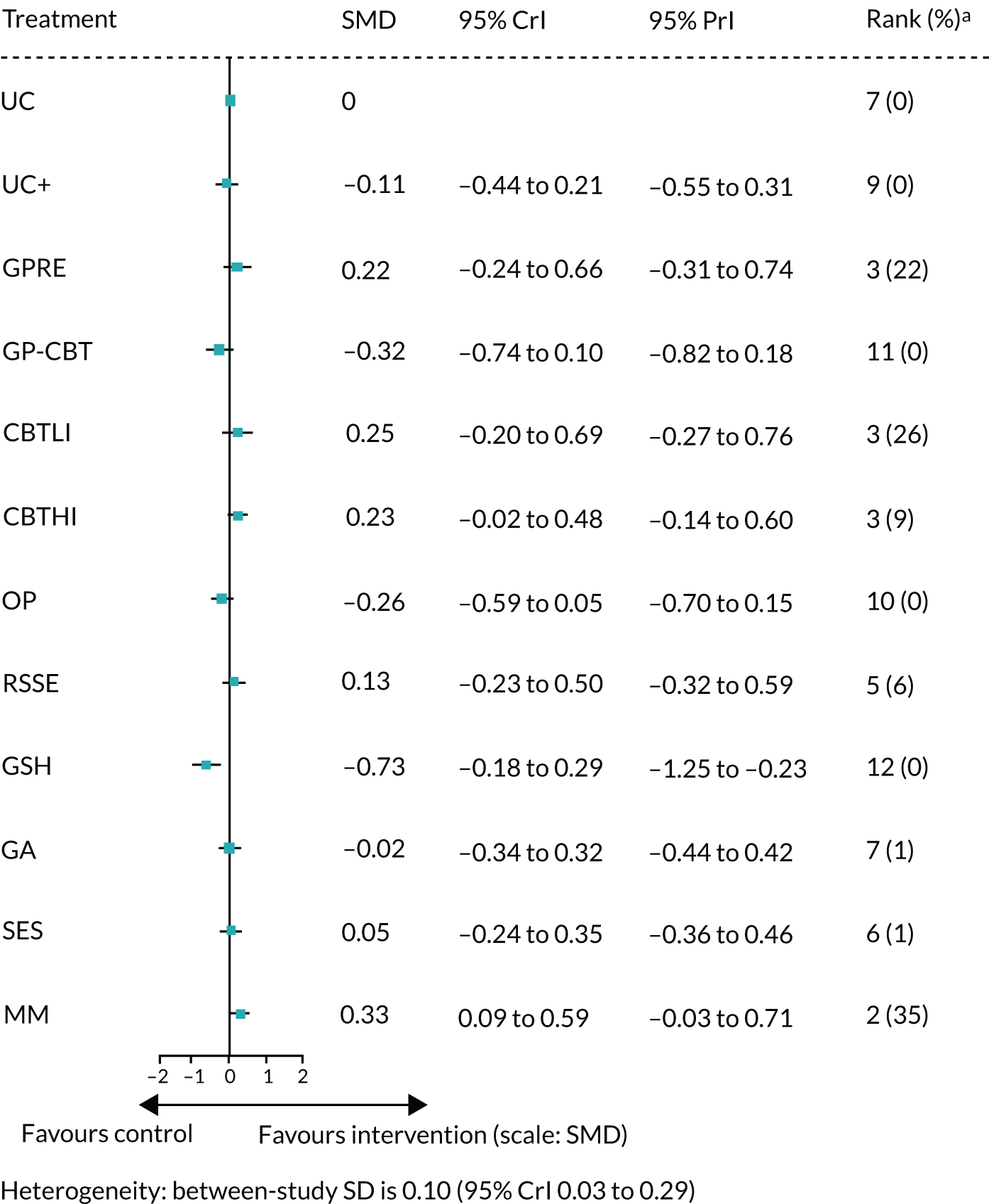
Impact of illness on daily activities (post treatment)
Data were available from nine studies presenting the impact score immediately post treatment. A NMA was used to compare the effects of medication, CBTLI, CBTHI, other psychotherapy, guided self-help, SES and multimodal relative to usual care on impact score. Figure 14 presents the network of evidence.
FIGURE 14.
Impact score immediately post treatment: network of evidence. GSH, guided self-help; ME, medication; MM, multimodal; OP, other psychotherapy; UC, usual care.

Figure 15 presents the SMD of each intervention relative to usual care, the median of treatment rankings and the probability of being the best treatment. For all interventions with the exception of guided self-help, SES and multimodal, the estimated SMD was greater than zero, suggesting a beneficial effect compared with usual care. However, only the effect of CBTHI (a large effect size, SMD 1.30, with 95% CrI 0.59 to 2.00) was statistically significant at a conventional 5% level, and it was also statistically significant based on the PrI (see Figure 15). The intervention with the highest probability of being the best was CBTHI (probability 0.72). The between-study SD was estimated to be 0.48 (95% CrI 0.31 to 0.55), which implies high heterogeneity of intervention effects between studies.
FIGURE 15.
Impact score immediately post treatment: SMD for all interventions relative to usual care. a, Probability of being the best treatment. GSH, guided self-help; ME, medication; MM, multimodal; OP, other psychotherapy.
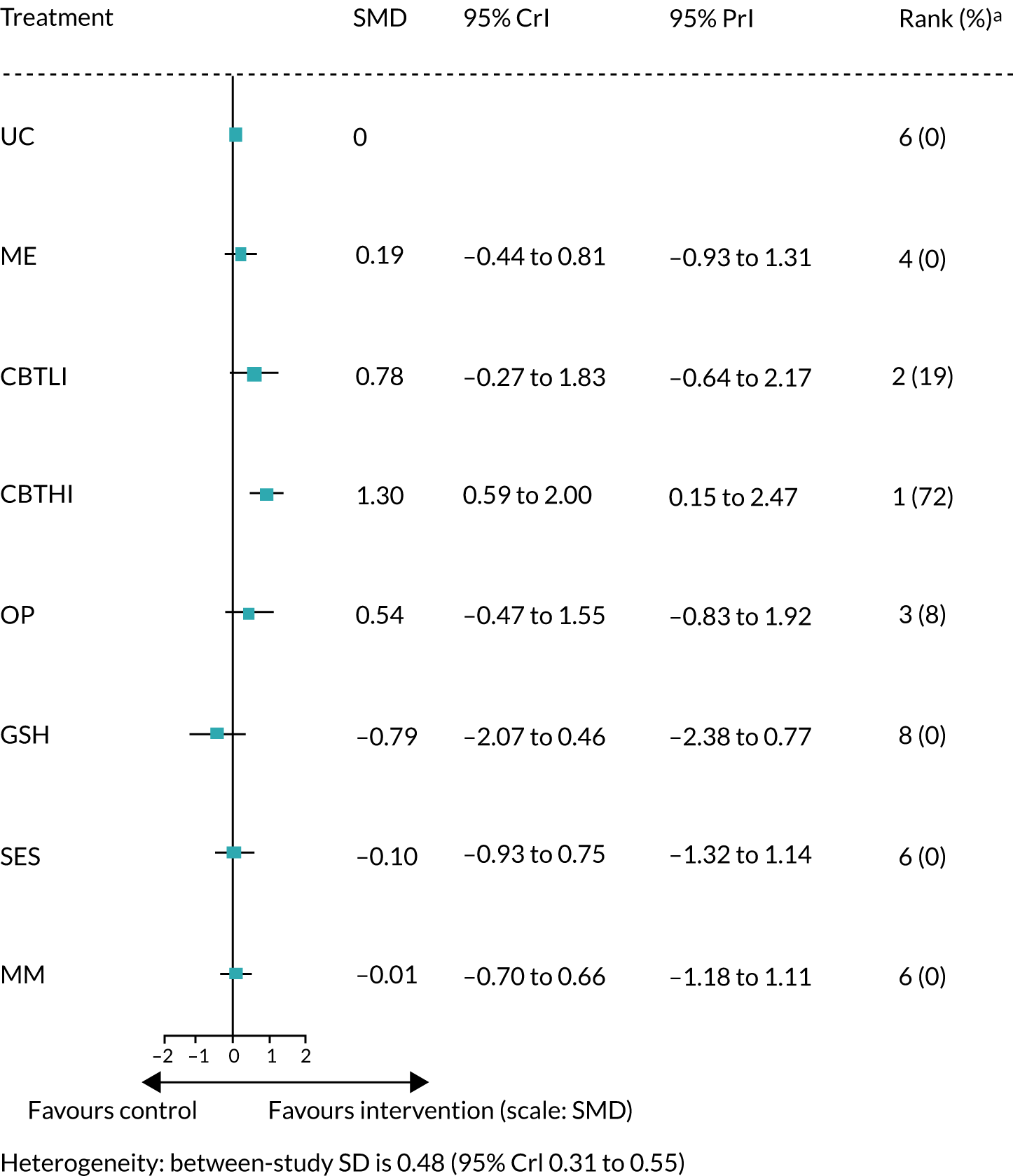
Emotional distress outcome measures immediately post treatment
Anxiety (post treatment)
Data were available from 14 studies presenting the anxiety score immediately post treatment. NMA was used to compare the effects of usual care plus, medication, GP reattribution, CBTLI, CBTHI, other psychotherapy, guided self-help, GA and multimodal relative to usual care on anxiety score. Figure 16 presents the network of evidence.
FIGURE 16.
Anxiety score immediately post treatment: network of evidence. GPRE, general practitioner-delivered reattribution; GSH, guided self-help; ME, medication; MM, multimodal; OP, other psychotherapy; UC, usual care; UC+, usual care plus.

Figure 17 presents the SMD of each intervention relative to usual care, the median of treatment rankings and the probability of being the best treatment. For all interventions with the exception of GP reattribution, guided self-help and GA, the estimated SMD was greater than zero, suggesting a beneficial effect compared with usual care. However, only the effect of CBTHI with a medium effect size (SMD 0.52, with 95% CrI 0.06 to 0.96) was statistically significant at a conventional 5% level, but this effect was not statistically significant based on the PrI (see Figure 17). The intervention with the highest probability of being the best was CBTHI (probability 0.48). The between-study SD was estimated to be 0.22 (95% CrI 0.05 to 0.45), which implies moderate heterogeneity of intervention effects between studies.
FIGURE 17.
Anxiety score immediately post treatment: SMD for all interventions relative to usual care. a, Probability of being the best treatment. GPRE, general practitioner-delivered reattribution; GSH, guided self-help; ME, medication; MM, multimodal; OP, other psychotherapy; UC, usual care; UC+, usual care plus.

Depression (post treatment)
Data were available from 13 studies presenting the depression score immediately post treatment. A NMA was used to compare the effects of usual care plus, medication, GP reattribution, CBTLI, CBTHI, other psychotherapy, GA and multimodal relative to usual care on depression score. Figure 18 presents the network of evidence.
FIGURE 18.
Depression score immediately post treatment: network of evidence. GPRE, general practitioner-delivered reattribution; GSH, guided self-help; ME, medication; MM, multimodal; OP, other psychotherapy; UC, usual care; UC+, usual care plus.
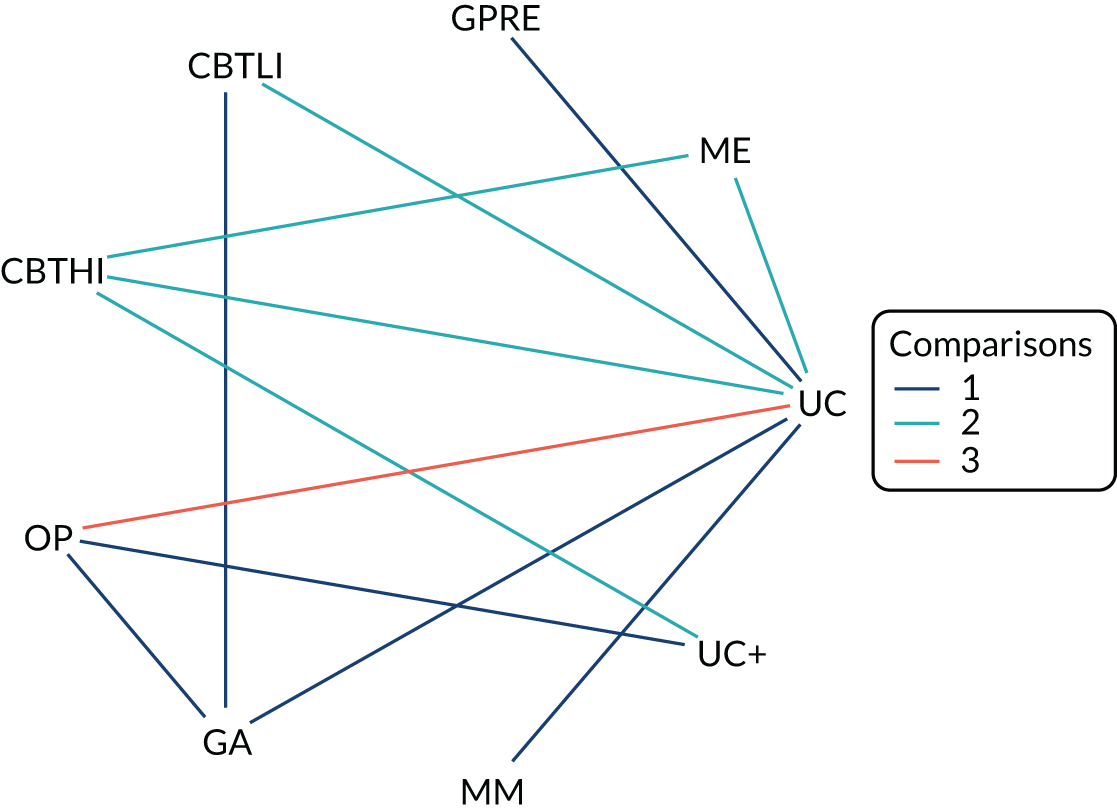
Figure 19 presents the SMD of each intervention relative to usual care, the median of treatment rankings and the probability of being the best treatment. For all interventions, the estimated SMD was greater than zero, suggesting a beneficial effect compared with usual care. However, only the effect of CBTHI, with a large effect size (SMD 0.80, with 95% CrI 0.26 to 1.38), was statistically significant at a conventional 5% level, but the result was not statistically significant based on the PrI (see Figure 19). The intervention with the highest probability of being the best was CBTHI (probability 0.66). The between-study SD was estimated to be 0.40 (95% CrI 0.24 to 0.54), which implies high heterogeneity of intervention effects between studies.
FIGURE 19.
Depression score immediately post treatment: SMD for all interventions relative to usual care. a, Probability of being the best treatment. GPRE, general practitioner-delivered reattribution; GSH, guided self-help; ME, medication; MM, multimodal; OP, other psychotherapy; UC, usual care; UC+, usual care plus.

Emotional distress (post treatment)
Data were available from 14 studies presenting the emotional distress score immediately post treatment. A NMA was used to compare the effects of usual care plus, medication, GP reattribution, GP-CBT, GP MUS management, CBTLI, CBTHI, other psychotherapy, RSSE, guided self-help, GA, SES and multimodal relative to usual care on emotional distress score. Figure 20 presents the network of evidence.
FIGURE 20.
Emotional distress score immediately post treatment: network of evidence. GPRE, general practitioner-delivered reattribution; GSH, guided self-help; ME, medication; MM, multimodal; OP, other psychotherapy; UC, usual care; UC+, usual care plus.
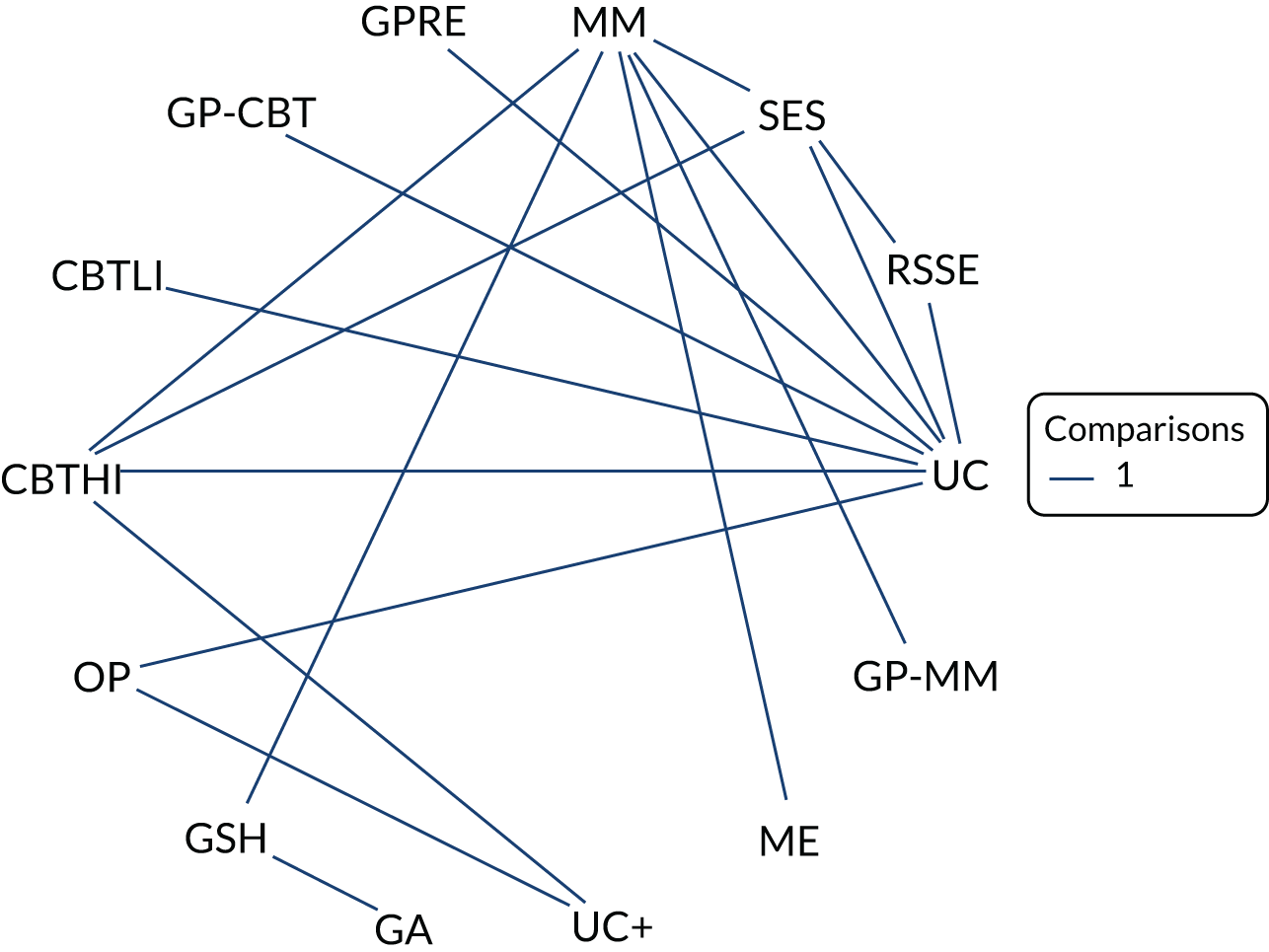
Figure 21 presents the SMD of each intervention relative to usual care, the median of treatment rankings and the probability of being the best treatment. For all interventions with the exception of GP reattribution, guided self-help and GA, the estimated SMD was greater than zero, suggesting a beneficial effect compared with usual care. However, only the effect of other psychotherapy (a medium effect size, SMD 0.58, with 95% CrI 0.05 to 1.13), RSSE (a medium effect size, SMD 0.66, with 95% CrI 0.18 to 1.28) and SES (a small effect size, SMD 0.49, with 95% CrI 0.03 to 1.01) were statistically significant at a conventional 5% level, but none of the effects was statistically significant based on the PrI (see Figure 21). Guided self-help was significantly worse than usual care (a large effect size, SMD –1.03, with 95% CrI –1.95 to –0.10), but the result was not statistically significant based on the PrI. The interventions with the highest probabilities of being the best were RSSE and CBTLI (probability 0.32 and 0.32, respectively), but the effect of CBTLI was inconclusive. The between-study SD was estimated to be 0.20 (95% CrI 0.04 to 0.49), which implies high heterogeneity of intervention effects between studies.
FIGURE 21.
Emotional distress score immediately post treatment: SMD for all interventions relative to usual care. a, Probability of being the best treatment. GPRE, general practitioner-delivered reattribution; GSH, guided self-help; ME, medication; MM, multimodal; OP, other psychotherapy; UC, usual care; UC+, usual care plus.

Physical symptom outcome measures at short term
Pain (short term)
Data were available from six studies presenting the pain score at short term. A NMA was used to compare the effects of medication, GP MUS management, CBTHI, guided self-help, SES and multimodal relative to usual care on pain score. Figure 22 presents the network of evidence.
FIGURE 22.
Pain score at short term: network of evidence. GSH, guided self-help; ME, medication; MM, multimodal; OP, other psychotherapy; UC, usual care; UC+, usual care plus.

Figure 23 presents the SMD of each intervention relative to usual care, the median of treatment rankings and the probability of being the best treatment. For all interventions with the exception of guided self-help, the estimated SMD was greater than zero, suggesting a beneficial effect compared with usual care. However, only the effect of CBTHI with a medium effect size (SMD 0.73, with 95% CrI 0.10 to 1.39) was statistically significant at a conventional 5% level, but this effect was not statistically significant based on the PrI (see Figure 23). The intervention with the highest probability of being the best was CBTHI (probability 0.41). The between-study SD was estimated to be 0.45 (95% CrI 0.27 to 0.55), which implies high heterogeneity of intervention effects between studies.
FIGURE 23.
Pain score at short term: SMD for all interventions relative to usual care. a, Probability of being the best treatment. GSH, guided self-help; ME, medication; MM, multimodal; UC, usual care.
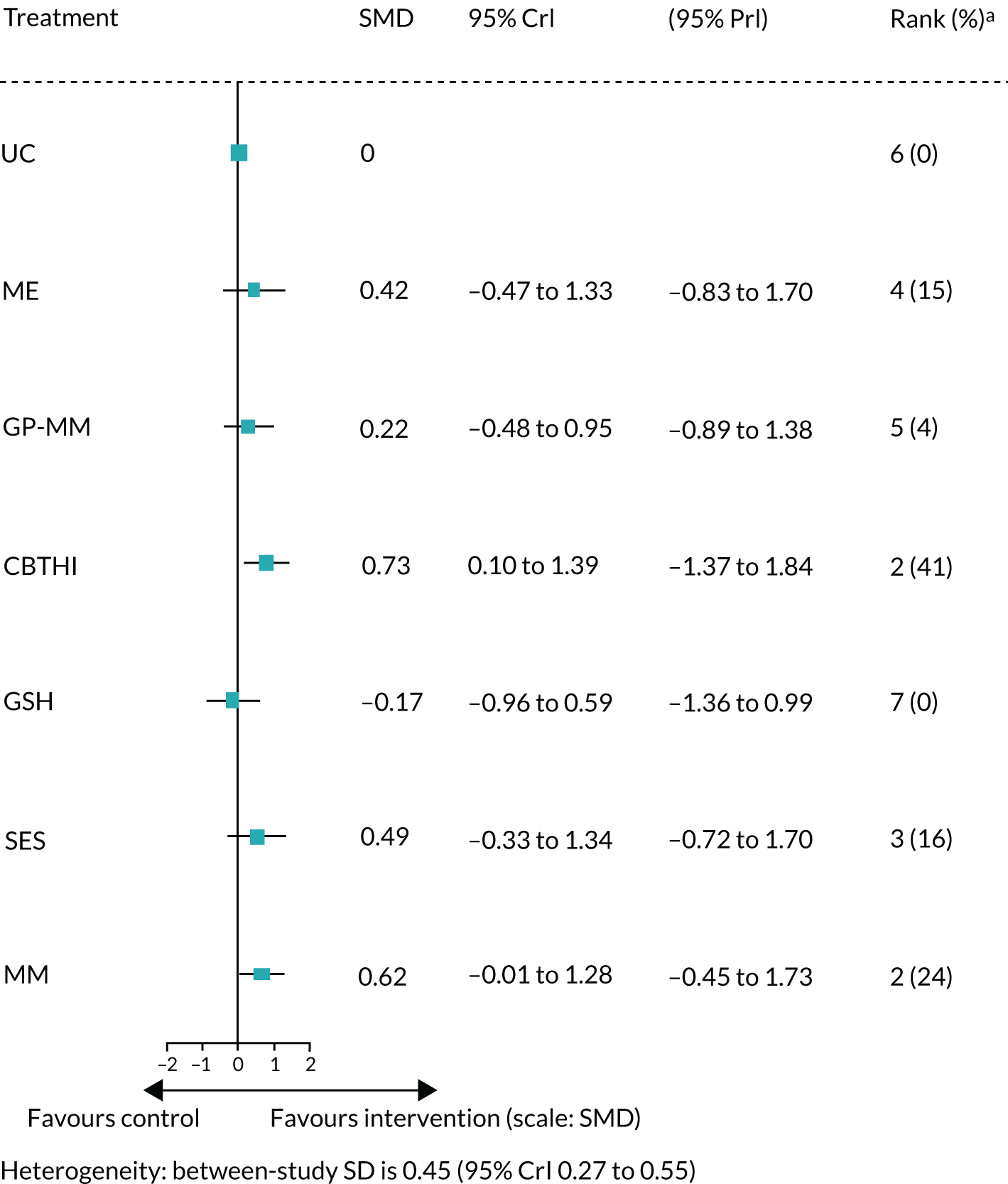
Fatigue (short term)
Data were available from seven studies presenting the fatigue score at short term. A NMA was used to compare the effects of usual care plus, CBTLI, CBTHI, other psychotherapy, RSSE, GA, SES and multimodal relative to usual care on fatigue score. Figure 24 presents the network of evidence.
FIGURE 24.
Fatigue score at short term: network of evidence. GSH, guided self-help; ME, medication; MM, multimodal; OP, other psychotherapy; UC, usual care; UC+, usual care plus.

Figure 25 presents the SMD of each intervention relative to usual care, the median of treatment rankings and the probability of being the best treatment. For all interventions, the estimated SMD was greater than zero, suggesting a beneficial effect compared with usual care. However, only the effect of CBTLI with a medium effect size (SMD 0.62 with 95% CrI 0.11 to 1.14) and RSSE with a medium effect size (SMD 0.51 with 95% CrI 0.06 to 1.00) were statistically significant at a conventional 5% level, but none of the results was statistically significant based on the PrI (see Figure 25). The interventions with the highest probability of being the best were CBTLI (probability 0.34). The between-study SD was estimated to be 0.18 (95% CrI 0.03 to 0.49), which implies moderate heterogeneity of intervention effects between studies.
FIGURE 25.
Fatigue score at short term: SMD for all interventions relative to usual care. a, Probability of being the best treatment. GSH, guided self-help; MM, multimodal; OP, other psychotherapy; UC, usual care.

Bowel symptoms (short term)
Two studies (Kennedy et al. 129 compared multimodal vs. medication and Moss-Morris et al. 130 compared usual care vs. CBTLI) were available on the bowel symptoms outcome immediately post treatment. No NMA was performed because of the disconnect network. The estimated SMD of multimodal compared with medication was a small effect size, 0.42 (95% CI 0.10 to 0.74), from Kennedy et al. 129 The estimated SMD of CBTLI compared with usual care was a medium effect size, 0.66 (95% CI 0.16 to 1.16), from Moss-Morris et al. 130
Somatisation (short term)
Data were available from six studies presenting the somatisation score at short term. A NMA was used to compare the effects of GP MUS management, GP reattribution and multimodal relative to usual care on somatisation score. Figure 26 presents the network of evidence.
FIGURE 26.
Somatisation score at short term: network of evidence. GPRE, general practitioner-delivered reattribution; MM, multimodal; UC, usual care.

Figure 27 presents the SMD of each intervention relative to usual care, the median of treatment rankings and the probability of being the best treatment. Only the estimated SMD of multimodal was greater than zero, suggesting a beneficial effect compared with usual care. However, this is a not substantial effect size (SMD 0.18, with 95% CrI –0.28 to 0.61) and it was not statistically significant at a conventional 5% level. None of the results was statistically significant based on the PrI (see Figure 27). The intervention with the highest probability of being the best was multimodal (probability 0.74), but the result of treatment effect was inconclusive. The between-study SD was estimated to be 0.15 (95% CrI 0.03 to 0.42), which implies moderate heterogeneity of intervention effects between studies.
FIGURE 27.
Somatisation score at short term: SMD for all interventions relative to usual care. a, Probability of being the best treatment. GPRE, general practitioner-delivered reattribution; MM, multimodal; UC, usual care.
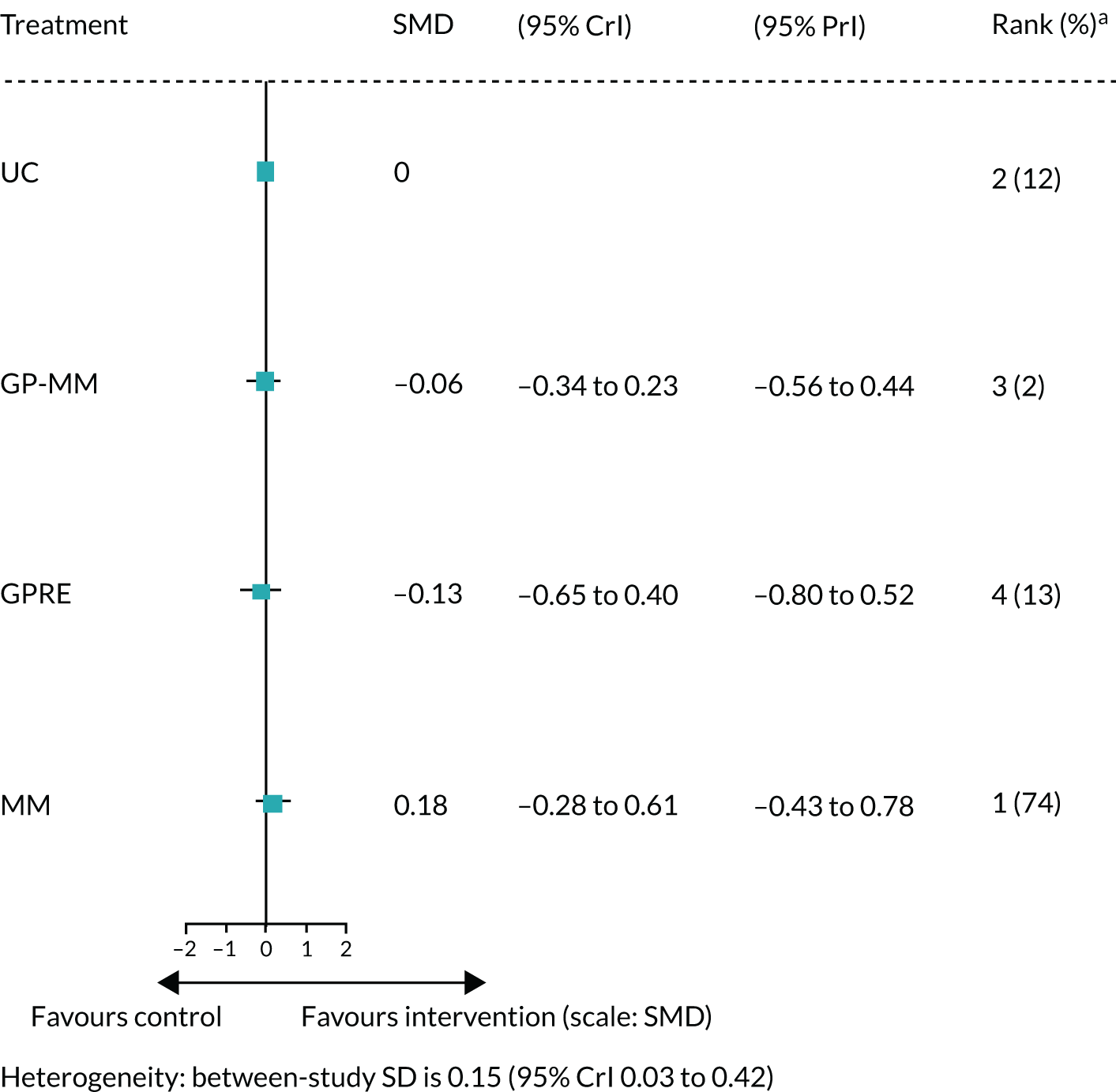
Generic physical symptoms (short term)
Only one study,160 which compared multimodal versus GP reattribution, was available on the generic physical symptoms at short term. No NMA was performed because of the disconnect network. The estimated SMD of multimodal compared with GP reattribution was a large effect size, 1.13 (95% CI 0.62 to 1.64), from van der Feltz-Cornelis et al. 160
Physical functioning and impact outcome measures at short term
Physical functioning (short term)
Data were available from 10 studies presenting the physical functioning score at short term. A NMA was used to compare the effects of GP reattribution, GP MUS management, CBTLI, CBTHI, RSSE, guided self-help, SES and multimodal relative to usual care on physical functioning score. Figure 28 presents the network of evidence.
FIGURE 28.
Physical functioning score at short term: network of evidence. GPRE, general practitioner-delivered reattribution; GSH, guided self-help; ME, medication; MM, multimodal; OP, other psychotherapy; UC, usual care.
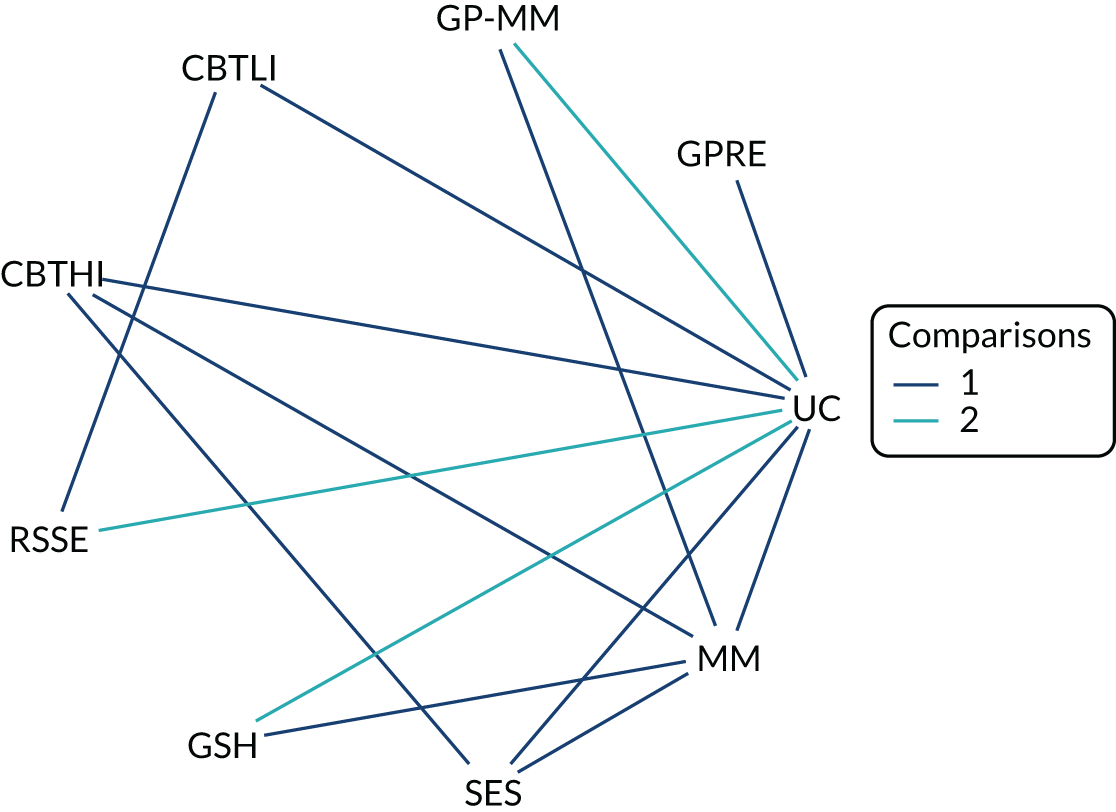
Figure 29 presents the SMD of each intervention relative to usual care, the median of treatment rankings and the probability of being the best treatment. For all interventions with the exception of GP reattribution, the estimated SMD was greater than zero, suggesting a beneficial effect compared with usual care. However, only the effect of multimodal, with a medium effect size (SMD 0.78, with 95% CrI 0.23 to 1.40), was statistically significant at a conventional 5% level, but none of the results was statistically significant based on the PrI (see Figure 29). The intervention with the highest probability of being the best was multimodal (probability 0.50). The between-study SD was estimated to be 0.40 (95% CrI 0.21 to 0.54), which implies high heterogeneity of intervention effects between studies.
FIGURE 29.
Physical functioning score at short term: SMD for all interventions relative to usual care. a, Probability of being the best treatment. GPRE, general practitioner-delivered reattribution; GSH, guided self-help; MM, multimodal; UC, usual care.
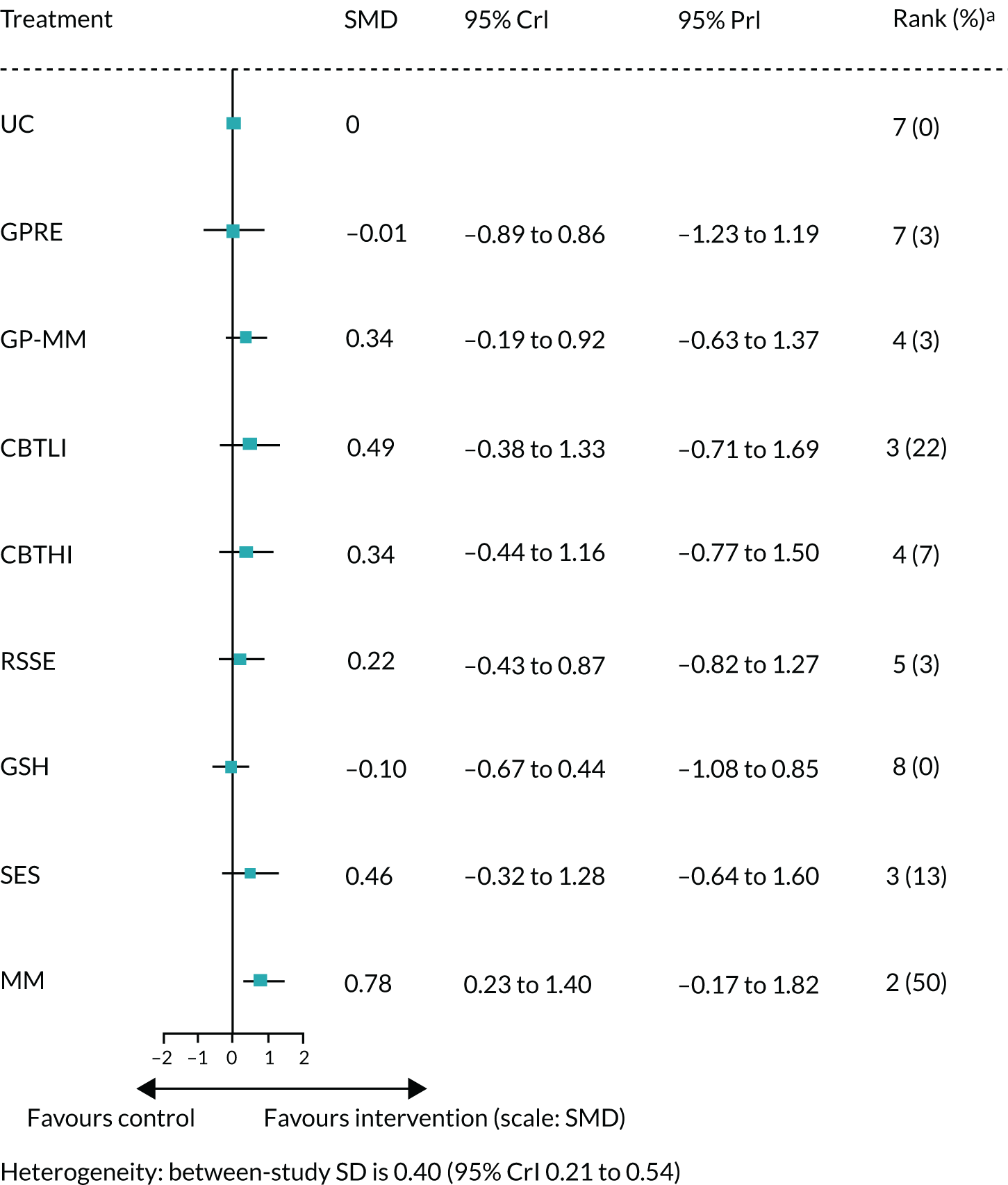
Impact (short term)
Data were available from seven studies presenting the impact score at short term. A NMA was used to compare the effects of medication, CBTLI, CBTHI, other psychotherapy, guided self-help, GA and multimodal relative to usual care on impact score. Figure 30 presents the network of evidence.
FIGURE 30.
Impact score at short term: network of evidence. GSH, guided self-help; ME, medication; MM, multimodal; OP, other psychotherapy.

Figure 31 presents the SMD of each intervention relative to usual care, the median of treatment rankings and the probability of being the best treatment. For all interventions, the estimated SMD was greater than zero, suggesting a beneficial effect compared with usual care. However, only the effect of CBTHI, with a large effect size (SMD 2.25, with 95% CrI 1.34 to 3.16), and the effect of medication with a medium effect size (SMD 0.79 with 95% CrI 0.02 to 1.56) were statistically significant at a conventional 5% level. The effect of CBTHI was also statistically significant based on the PrI (see Figure 31). The intervention with the highest probability of being the best was CBTHI (probability 0.98). The between-study SD was estimated to be 0.41 (95% CrI 0.20 to 0.54), which implies high heterogeneity of intervention effects between studies.
FIGURE 31.
Impact score at short term: SMD for all interventions relative to usual care. a, Probability of being the best treatment. GSH, guided self-help; ME, medication; MM, multimodal; OP, other psychotherapy; UC, usual care.

Emotional distress outcome measures at short term
Anxiety (short term)
Data were available from nine studies presenting the anxiety score at short term. A NMA was used to compare the effects of medication, GP reattribution, GP MUS management, CBTLI, CBTHI, other psychotherapy, RSSE, guided self-help and GA relative to usual care on anxiety score. Figure 32 presents the network of evidence.
FIGURE 32.
Anxiety score at short term: network of evidence. GPRE, general practitioner-delivered reattribution; GSH, guided self-help; ME, medication; MM, multimodal; OP, other psychotherapy; UC, usual care.

Figure 33 presents the SMD of each intervention relative to usual care, the median of treatment rankings and the probability of being the best treatment. For all interventions with the exception of GP reattribution, GP MUS management and RSSE, the estimated SMD was greater than zero, suggesting a beneficial effect compared with usual care. However, only the effect of CBTHI with a medium effect size (SMD 0.74 with 95% CrI 0.14 to 1.37) was statistically significant at a conventional 5% level, but this effect was not statistically significant based on the PrI (see Figure 33). The intervention with the highest probability of being the best was CBTHI (probability 0.59). The between-study SD was estimated to be 0.25 (95% CrI 0.06 to 0.51), which implies moderate heterogeneity of intervention effects between studies.
FIGURE 33.
Anxiety score at short term: SMD for all interventions relative to usual care. a, Probability of being the best treatment. GPRE, general practitioner-delivered reattribution; GSH, guided self-help; ME, medication; MM, multimodal; OP, other psychotherapy; UC, usual care.

Depression (short term)
Data were available from 12 studies presenting the depression score at short term. A NMA was used to compare the effects of medication, GP reattribution, GP MUS management, CBTLI, CBTHI, other psychotherapy, RSSE, guided self-help, GA and multimodal relative to usual care on depression score. Figure 34 presents the network of evidence.
FIGURE 34.
Depression score at short term: network of evidence. GPRE, general practitioner-delivered reattribution; GSH, guided self-help; ME, medication; MM, multimodal; OP, other psychotherapy; UC, usual care.

Figure 35 presents the SMD of each intervention relative to usual care, the median of treatment rankings and the probability of being the best treatment. For all interventions, with the exception of GP reattribution and GP MUS management, the estimated SMD was greater than zero, suggesting a beneficial effect compared with usual care. However, only the effect of CBTHI, with a large effect size (SMD 0.93, with 95% CrI 0.37 to 1.52), was statistically significant at a conventional 5% level, and this effect was also statistically significant based on the PrI (see Figure 35). The intervention with the highest probability of being the best was CBTHI (probability 0.64). The between-study SD was estimated to be 0.24 (95% CrI 0.07 to 0.49), which implies moderate heterogeneity of intervention effects between studies.
FIGURE 35.
Depression score at short term: SMD for all interventions relative to usual care. a, Probability of being the best treatment. GSH, guided self-help; ME, medication; MM, multimodal; OP, other psychotherapy; UC, usual care.
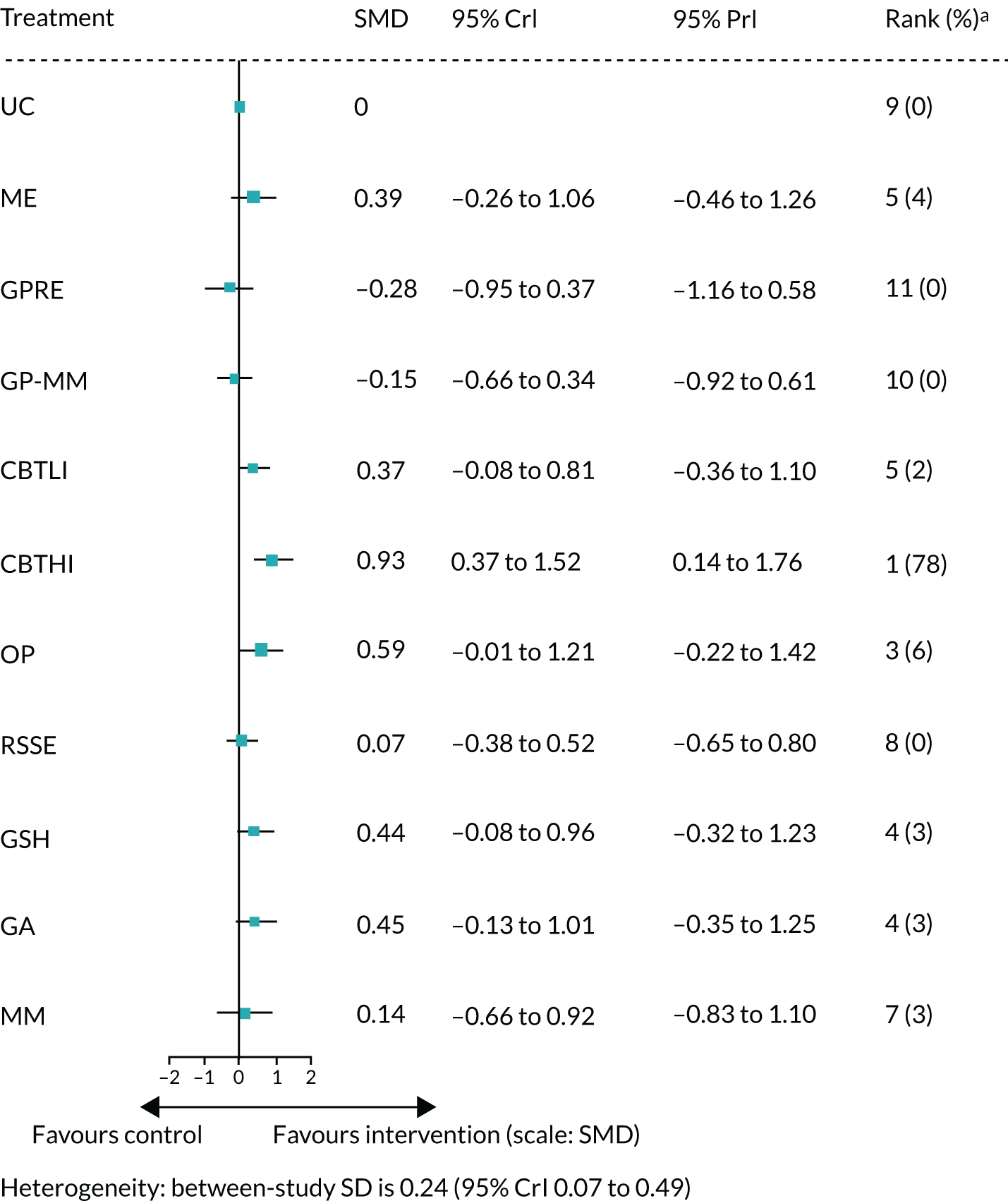
Emotional distress (short term)
Data were available from 12 studies presenting the emotional distress score at short term. A NMA was used to compare the effects of medication, GP reattribution, GP MUS management, CBTHI, RSSE, guided self-help, SES relative and multimodal relative to usual care on emotional distress score. Figure 36 presents the network of evidence.
FIGURE 36.
Emotional distress score at short term: network of evidence. GPRE, general practitioner-delivered reattribution; GSH, guided self-help; ME, medication; MM, multimodal; UC, usual care.
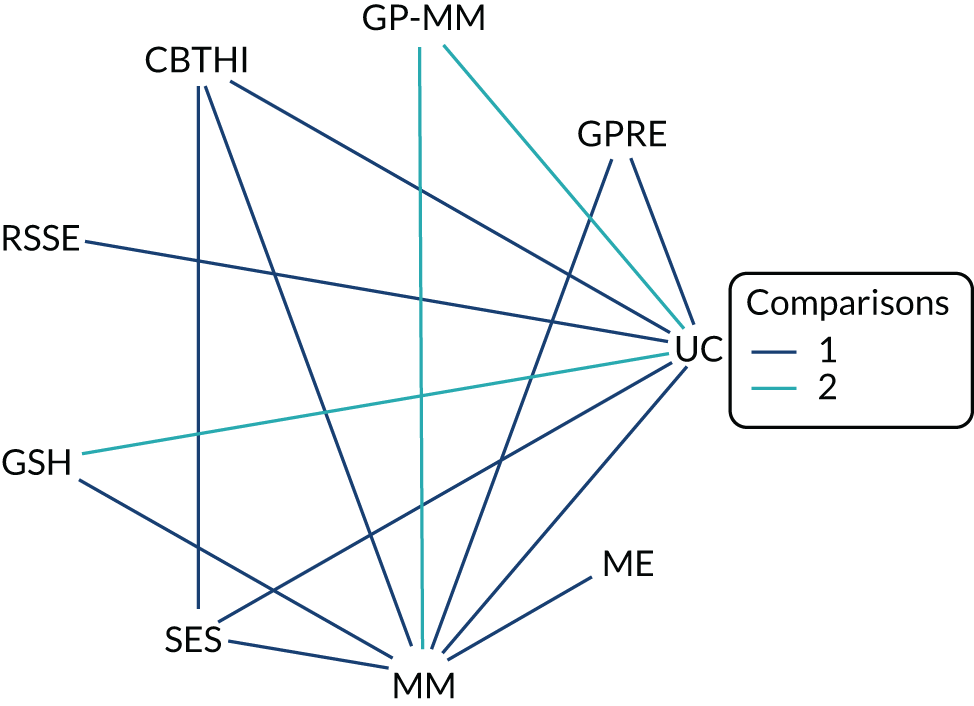
Figure 37 presents the SMD of each intervention relative to usual care, the median of treatment rankings and the probability of being the best treatment. For all interventions with the exception of GP reattribution, medication and GP MUS management, the estimated SMD was greater than zero, suggesting a beneficial effect compared with usual care. However, only the effect of RSSE (a large effect size, SMD 0.82, with 95% CrI 0.02, 1.65) and multimodal (a small effect size, SMD 0.43, with 95% CrI 0.04 to 0.91) were statistically significant at a conventional 5% level, but none of the results was statistically significant based on the PrI (see Figure 37). The intervention with the highest probability of being the best was RSSE (probability 0.68). The between-study SD was estimated to be 0.32 (95% CrI 0.11 to 0.52), which implies high heterogeneity of intervention effects between studies.
FIGURE 37.
Emotional distress score at short term: SMD for all interventions relative to usual care. a, Probability of being the best treatment. GPRE, general practitioner-delivered reattribution; GSH, guided self-help; ME, medication; MM, multimodal; OP, other psychotherapy; UC, usual care.

Physical symptom outcome measures at long term
Pain (long term)
Data were available from seven studies presenting the pain score at long term. A NMA was used to compare the effects of usual care plus, medication, GP MUS management, GP other, CBTHI, other psychotherapy, guided self-help and multimodal relative to usual care on pain score. Figure 38 presents the network of evidence.
FIGURE 38.
Pain score at long term: network of evidence. GP-O, GP – other; GSH, guided self-help; ME, medication; MM, multimodal; OP, other psychotherapy; UC, usual care; UC+, usual care plus.
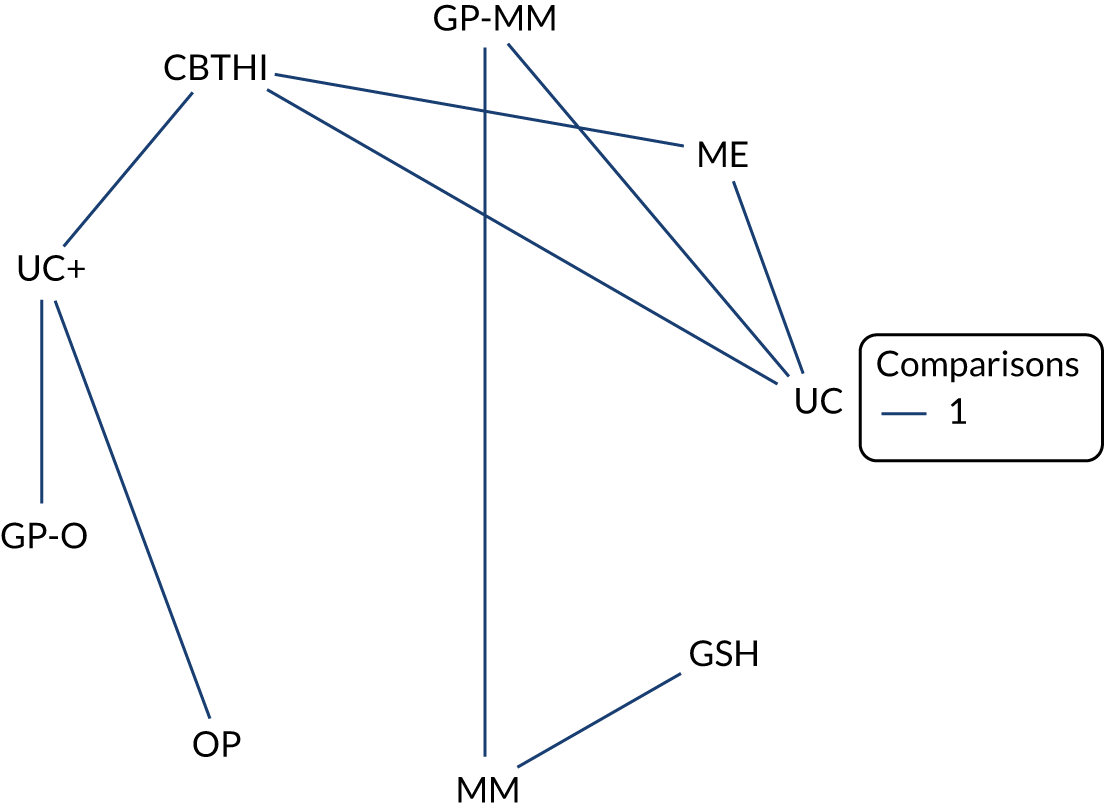
Figure 39 presents the SMD of each intervention relative to usual care, the median of treatment rankings and the probability of being the best treatment. For all interventions with the exception of guided self-help, GP MUS management, other psychotherapy, multimodal and usual care plus, the estimated SMD was greater than zero, suggesting a beneficial effect compared with usual care. The largest beneficial effects were associated with medication (a small effect size, SMD 0.41, with 95% CrI –0.16 to 0.98) and CBTHI (a small effect size, SMD 0.36, with 95% CrI –0.21 to 0.94). However, none of the beneficial effects was statistically significant at a conventional 5% level, and none of the beneficial effects was statistically significant based on the PrI (see Figure 39). Guided self-help was significantly worse than usual care (a large effect size, SMD –2.27, with 95% CrI –3.30 to –1.23). The intervention with the highest probabilities of being the best was medication and CBTHI (a probability of 0.49 and 0.28, respectively), but the results of treatment effects were inconclusive. The between-study SD was estimated to be 0.14 (95% CrI 0.03 to 0.48), which implies moderate heterogeneity of intervention effects between studies.
FIGURE 39.
Pain score at long term: SMD for all interventions relative to usual care. a, Probability of being the best treatment. GP-O, GP – other; GSH, guided self-help; ME, medication; MM, multimodal; OP, other psychotherapy; UC, usual care; UC+, usual care plus.
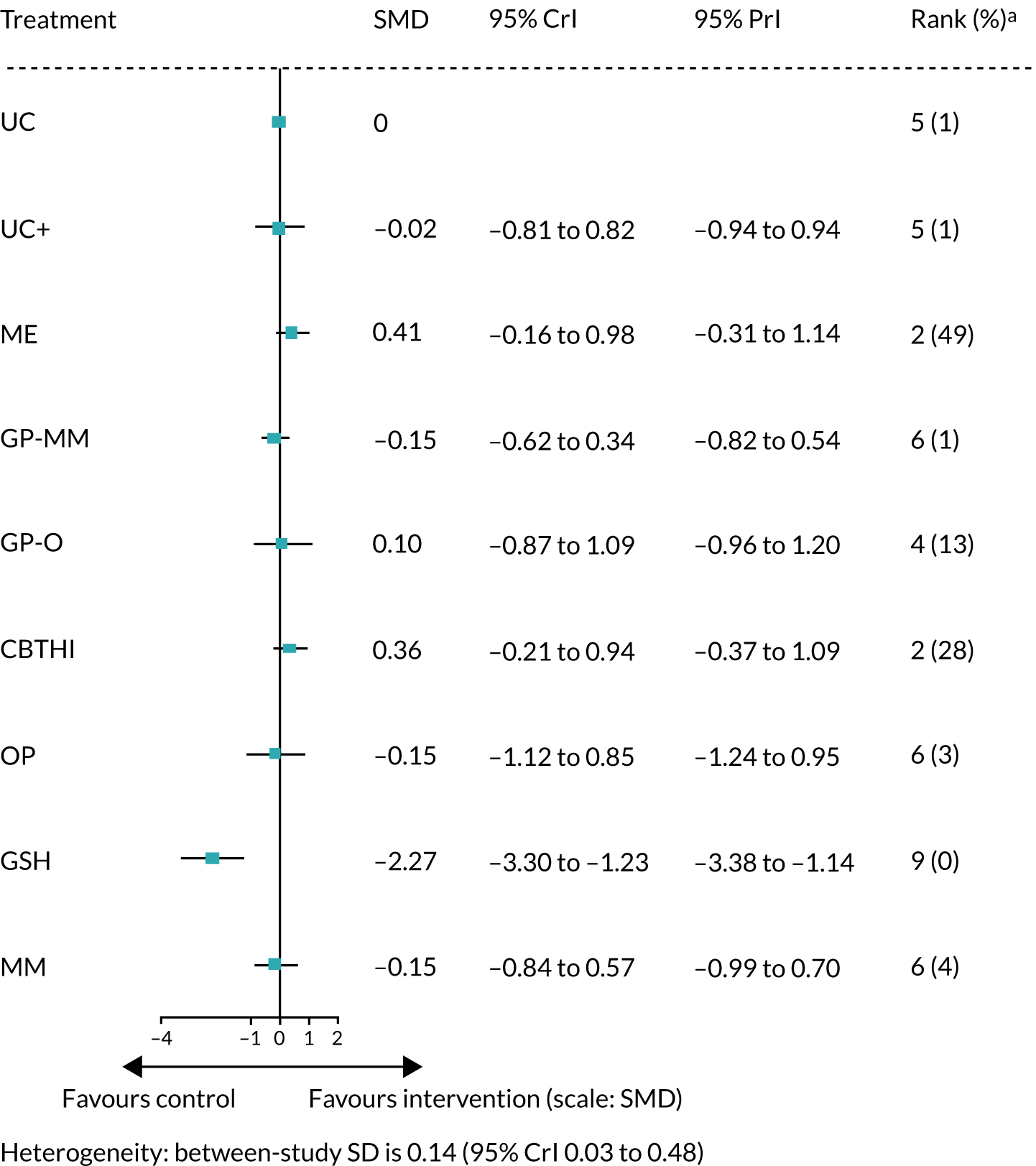
Fatigue (long term)
Data were available from five studies presenting the fatigue score at long term. A NMA was used to compare the effects of GP-CBT, CBTLI, CBTHI, other psychotherapy, RSSE, guided self-help, GA, SES and multimodal relative to usual care on fatigue score. Figure 40 presents the network of evidence.
FIGURE 40.
Fatigue score at long term: network of evidence. GSH, guided self-help; ME, medication; MM, multimodal; OP, other psychotherapy; UC, usual care.
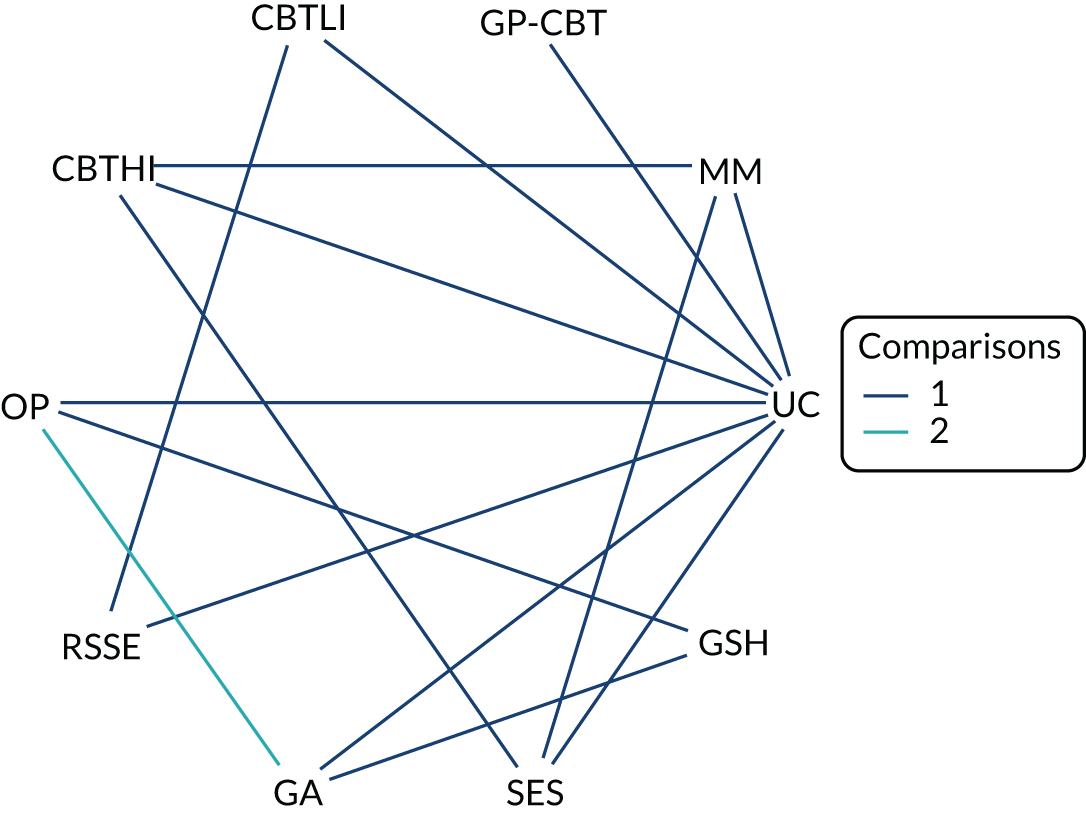
Figure 41 presents the SMD of each intervention relative to usual care, the median of treatment rankings and the probability of being the best treatment. For all interventions, with the exception of GP-CBT, the estimated SMD was greater than zero, suggesting a beneficial effect compared with usual care. However, only the effect of CBTLI, with a medium effect size (SMD 0.64, with 95% CrI 0.05 to 1.20), was statistically significant at a conventional 5% level, but none of the results was statistically significant based on the PrI (see Figure 41). The intervention with the highest probability of being the best was CBTLI (probability 0.73). The between-study SD was estimated to be 0.11 (95% CrI 0.03 to 0.42), which implies moderate heterogeneity of intervention effects between studies.
FIGURE 41.
Fatigue score at long term: SMD for all interventions relative to usual care. a, Probability of being the best treatment. GSH, guided self-help; ME, medication; MM, multimodal; OP, other psychotherapy; UC, usual care.

Bowel symptoms (long term)
Data were available from two studies presenting bowel symptoms at long term. A NMA was used to compare the effects of usual care plus, CBTLI and guided self-help relative to usual care on bowel symptoms. Figure 42 presents the network of evidence.
FIGURE 42.
Bowel symptoms at long term: network of evidence. GSH, guided self-help; UC, usual care.

Figure 43 presents the SMD of each intervention relative to usual care, the median of treatment rankings and the probability of being the best treatment. The estimated SMDs of both CBTLI and guided self-help were greater than zero, suggesting a beneficial effect compared with usual care. However, only the effect of CBTLI, with a large effect size (SMD 0.84, with 95% CrI 0.17 to 1.52), was statistically significant at a conventional 5% level, and also statistically significant based on the PrI (see Figure 43). The intervention with the highest probability of being the best was CBTLI (probability 0.95). The between-study SD was estimated to be 0.15 (95% CrI 0.03 to 0.49), which implies moderate heterogeneity of intervention effects between studies.
FIGURE 43.
Bowel symptoms at long term: SMD for all interventions relative to usual care. a, Probability of being the best treatment. GSH, guided self-help; UC, usual care.

Somatisation (long term)
Data were available from 11 studies presenting the somatisation score at long term. A NMA was used to compare the effects of usual care plus, GP MUS management, GP reattribution, GP other, CBTLI, CBTHI, other psychotherapy and multimodal relative to usual care on somatisation score. Figure 44 presents the network of evidence.
FIGURE 44.
Somatisation score at long term: network of evidence. GP-O, GP – other; GPRE, general practitioner-delivered reattribution; MM, multimodal; OP, other psychotherapy; UC, usual care; UC+, usual care plus.

Figure 45 presents the SMD of each intervention relative to usual care, the median of treatment rankings and the probability of being the best treatment. For all interventions with the exception of GP MUS management, GP reattribution, CBTLI and GP other, the estimated SMD was greater than zero, suggesting a beneficial effect compared with usual care. The largest beneficial effect was associated with CBTHI (a small effect size, SMD 0.47 with 95% CrI –0.30 to 1.29), but this effect was not statistically significant at a conventional 5% level, and it was also not statistically significant based on the PrI (see Figure 45). The intervention with the highest probability of being the best was CBTHI (probability 0.71), but the result of treatment effect was inconclusive. The between-study SD was estimated to be 0.11 (95% CrI 0.02 to 0.35), which implies moderate heterogeneity of intervention effects between studies.
FIGURE 45.
Somatisation score at long term: SMD for all interventions relative to usual care. a, Probability of being the best treatment. GP-O, GP – other; GPRE, general practitioner-delivered reattribution; GSH, guided self-help; MM, multimodal; OP, other psychotherapy; UC, usual care; UC+, usual care plus.

Generic physical symptoms (long term)
Only one study,104 which compared other psychotherapy and usual care, was available on the generic physical symptoms at short term. No NMA was performed because of the disconnect network. The estimated SMD of other psychotherapy compared with usual care was a small effect size, –0.30 (95% CI –0.76 to 0.16), from Kolk et al. 104
Physical functioning and impact outcome measures at long term
Physical functioning (long term)
Data were available from 13 studies presenting the physical functioning score at long term. A NMA was used to compare the effects of usual care plus, GP reattribution, GP MUS management, GP-CBT, CBTLI, CBTHI, other psychotherapy, RSSE, guided self-help, GA, SES and multimodal relative to usual care on physical functioning score. Figure 46 presents the network of evidence.
FIGURE 46.
Physical functioning score at long term: network of evidence. GPRE, general practitioner-delivered reattribution; GSH, guided self-help; MM, multimodal; OP, other psychotherapy; UC, usual care; UC+, usual care plus.
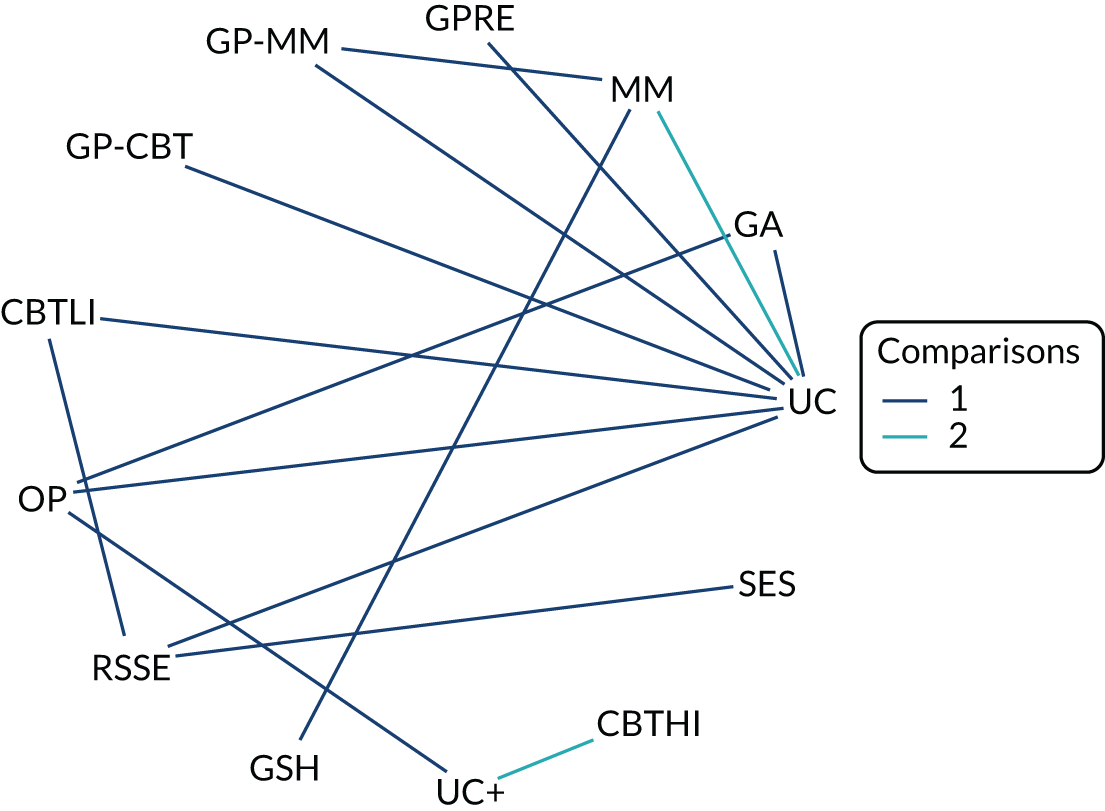
Figure 47 presents the SMD of each intervention relative to usual care, the median of treatment rankings and the probability of being the best treatment. For all interventions with the exception of GP-CBT, other psychotherapy and guided self-help, the estimated SMD was greater than zero, suggesting a beneficial effect compared with usual care. The largest beneficial effect was associated with CBTHI (a small effect size, SMD 0.47, with 95% CrI 0.19 to 1.44), but this effect was not statistically significant at a conventional 5% level, and none of the results was statistically significant based on the PrI (see Figure 47). Guided self-help was significantly worse than usual care (a large effect size, SMD –2.98, with 95% CrI –4.00 to –1.96), and the result was statistically significant based on the PrI. The intervention with the highest probability of being the best was CBTHI (probability 0.38). The between-study SD was estimated to be 0.21 (95% CrI 0.05 to 0.49), which implies moderate heterogeneity of intervention effects between studies.
FIGURE 47.
Physical functioning score at long term: SMD for all interventions relative to usual care. a, Probability of being the best treatment. GPRE, general practitioner-delivered reattribution; GSH, guided self-help; ME, medication; MM, multimodal; OP, other psychotherapy; UC, usual care; UC+, usual care plus.
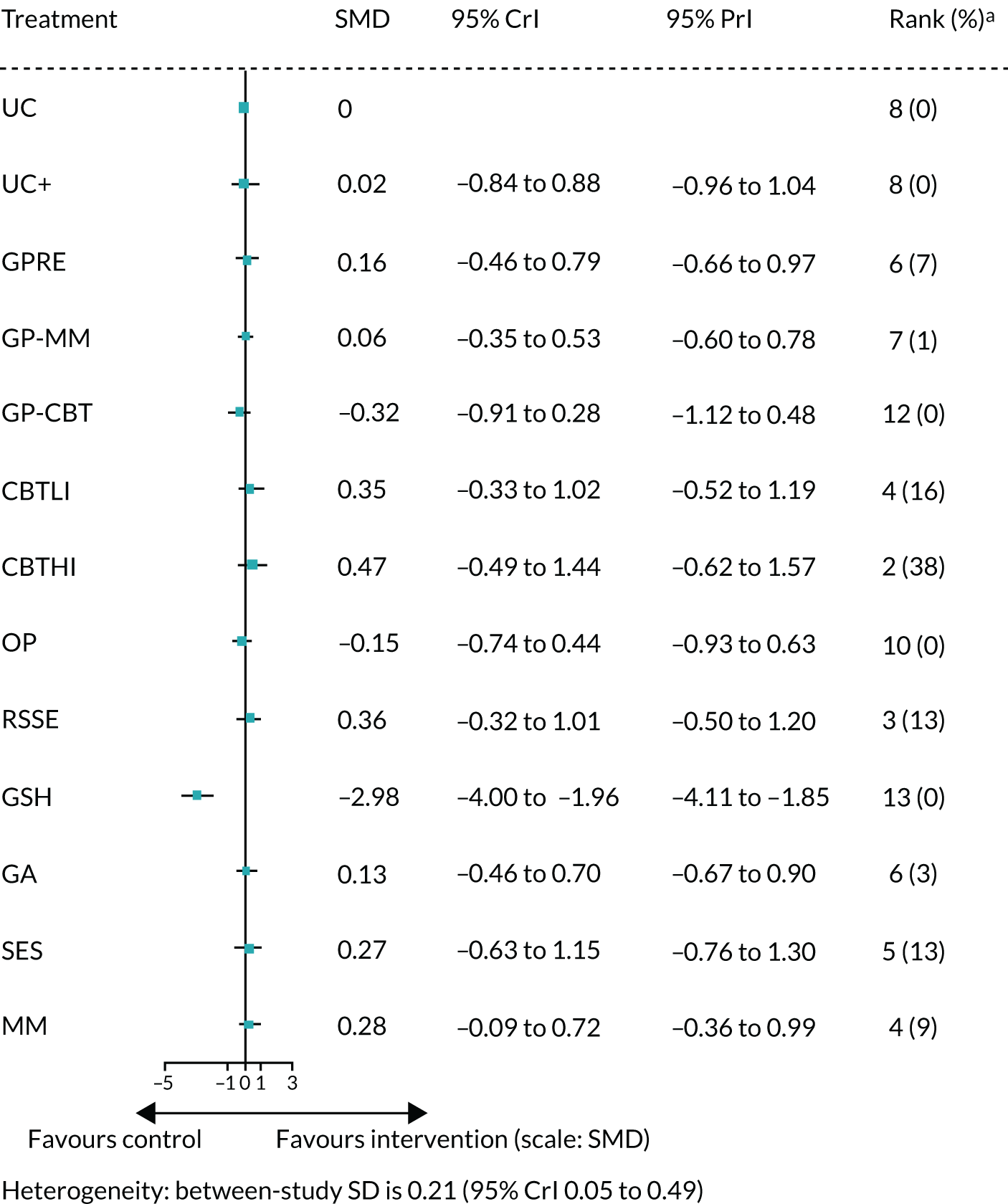
Impact (long term)
Data were available from four studies presenting the impact score at long term. A NMA was used to compare the effects of medication, CBTLI, CBTHI, guided self-help and multimodal relative to usual care on impact score. Figure 48 presents the network of evidence.
FIGURE 48.
Impact score at long term: network of evidence. GSH, guided self-help; ME, medication; MM, multimodal; UC, usual care.
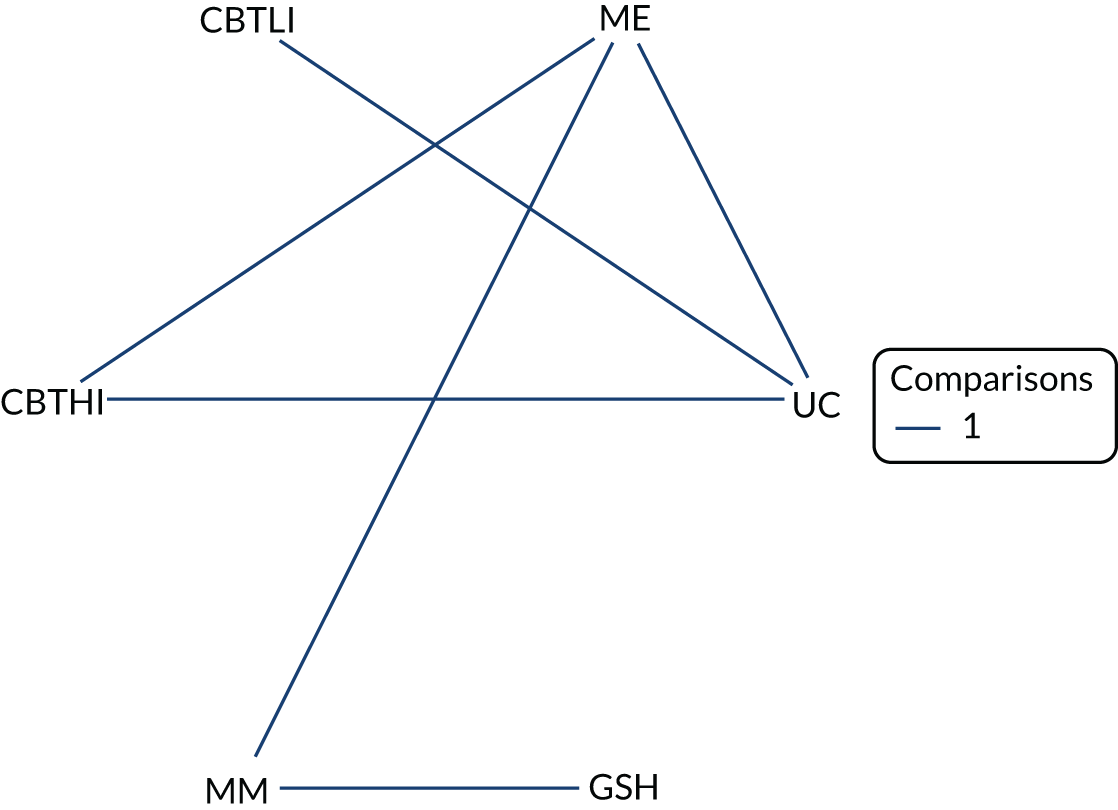
Figure 49 presents the SMD of each intervention relative to usual care, the median of treatment rankings and the probability of being the best treatment. For all interventions with the exception of guided self-help and multimodal, the estimated SMD was greater than zero, suggesting a beneficial effect compared with usual care. The largest beneficial effect was associated with CBTLI (a large effect size, SMD 0.89, with 95% CrI 0.22 to 1.55), and it was also statistically significant at a conventional 5% level. Guided self-help was significantly worse than usual care (and a large effect size, SMD –1.10, with 95% CrI –2.08 to –0.07 for guided self-help). However, this result was statistically significant based on the PrI (see Figure 49). The intervention with the highest probability of being the best was CBTLI (probability 0.92), but the result of treatment effect was inconclusive. The between-study SD was estimated to be 0.15 (95% CrI 0.03 to 0.48), which implies moderate heterogeneity of intervention effects between studies.
FIGURE 49.
Impact score at long term: SMD for all interventions relative to usual care. a, Probability of being the best treatment. GSH, guided self-help; ME, medication; MM, multimodal; UC, usual care.
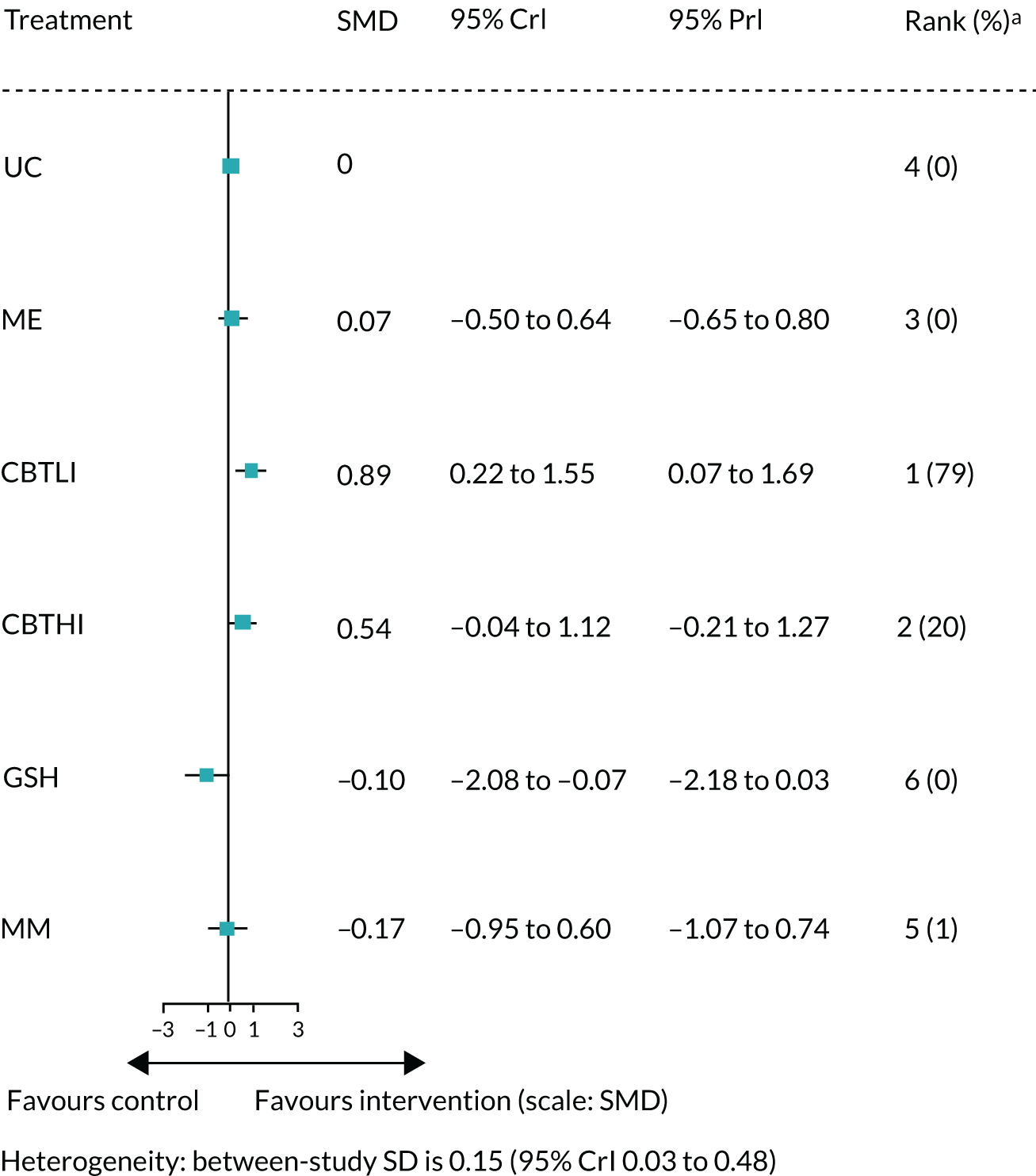
Emotional distress outcome measures at long term
Anxiety (long term)
Data were available from 11 studies presenting the anxiety score at long term. A NMA was used to compare the effects of usual care plus, medication, GP reattribution, GP MUS management, GP other, GP other psychotherapy, CBTLI, CBTHI, other psychotherapy, RSSE and GA relative to usual care on anxiety score. Figure 50 presents the network of evidence.
FIGURE 50.
Anxiety score at long term: network of evidence. GP-O, GP – other; GPRE, general practitioner-delivered reattribution; ME, medication; MM, multimodal; OP, other psychotherapy; UC, usual care; UC+, usual care plus.
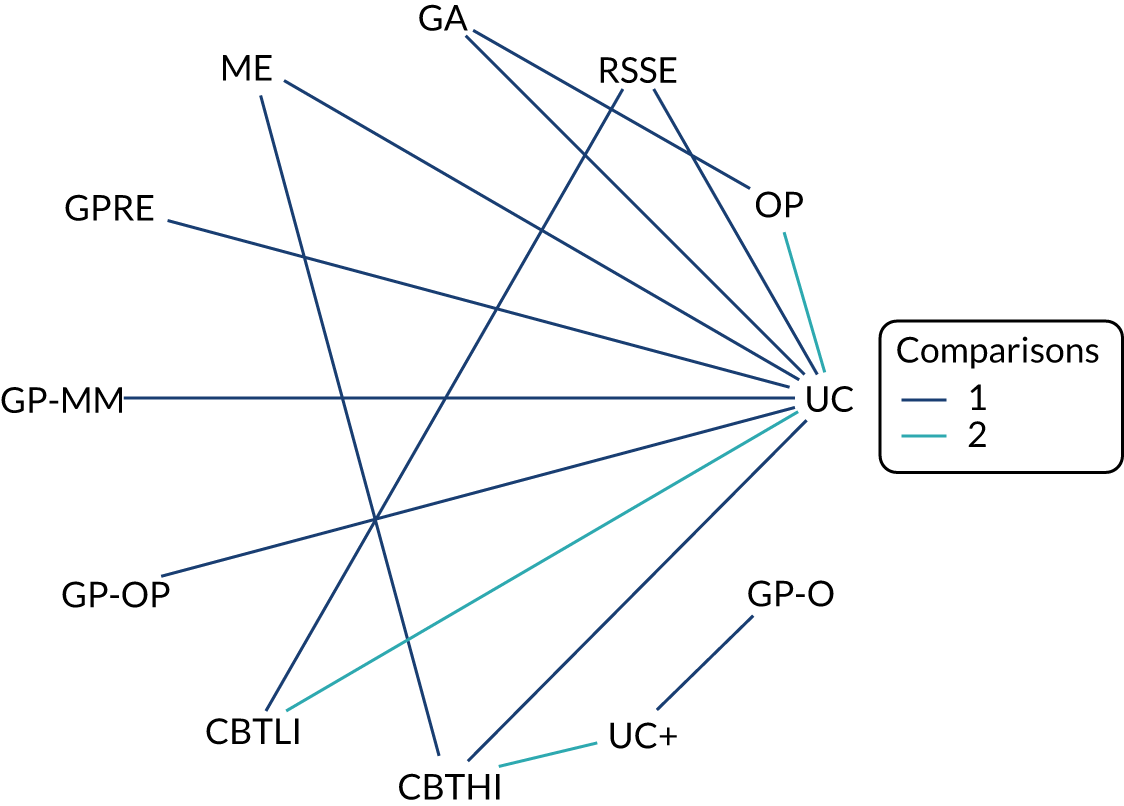
Figure 51 presents the SMD of each intervention relative to usual care, the median of treatment rankings and the probability of being the best treatment. For all interventions with the exception of medication, GP other psychotherapy and CBTHI, the estimated SMD was smaller than zero, suggesting a negative effect compared with usual care. None of the effects was statistically significant at a conventional 5% level and based on the PrI (see Figure 51). The largest beneficial effect was associated with GP other psychotherapy (a not substantial effect size, SMD 0.18, with 95% CrI –0.40 to 0.76). The intervention with the highest probability of being the best was GP other psychotherapy (probability 0.32). The between-study SD was estimated to be 0.19 (95% CrI 0.04 to 0.46), which implies moderate heterogeneity of intervention effects between studies.
FIGURE 51.
Anxiety score at long term: SMD for all interventions relative to usual care. a, Probability of being the best treatment. GP-O, GP – other; GPRE, general practitioner-delivered reattribution; ME, medication; MM, multimodal; OP, other psychotherapy; UC, usual care; UC+, usual care plus.

Depression (long term)
Data were available from 14 studies presenting the depression score at long term. A NMA was used to compare the effects of usual care plus, medication, GP reattribution, GP MUS management, GP other, GP other psychotherapy, CBTLI, CBTHI, other psychotherapy, RSSE, GA and multimodal relative to usual care on depression score. Figure 52 presents the network of evidence.
FIGURE 52.
Depression score at long term: network of evidence. GP-O, GP – other; GSH, guided self-help; ME, medication; MM, multimodal; OP, other psychotherapy; UC, usual care; UC+, usual care plus.
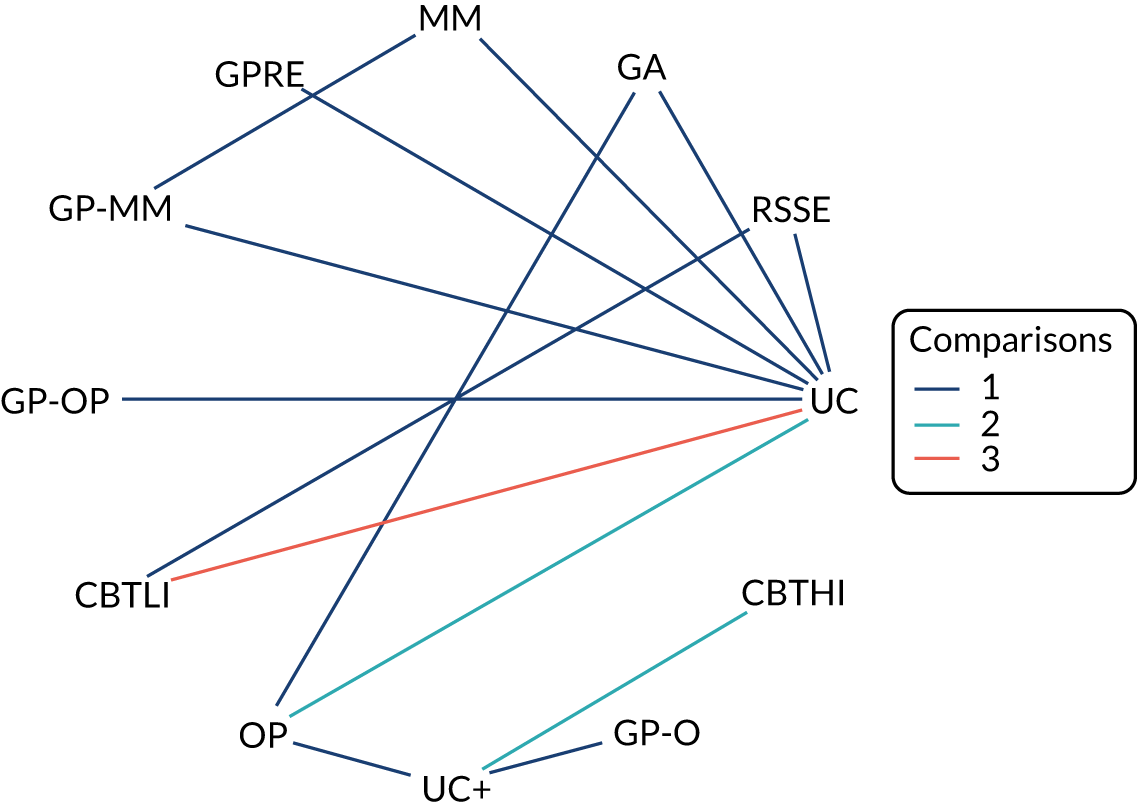
Figure 53 presents the SMD of each intervention relative to usual care, the median of treatment rankings and the probability of being the best treatment. For all interventions with the exception of usual care plus, GP reattribution, GP other, GP other psychotherapy, CBTLI, other psychotherapy, RSSE and GA, the estimated SMD was greater than zero, suggesting a beneficial effect compared with usual care. The largest beneficial effect was associated with multimodal (a small effect size, SMD 0.51, with 95% CrI –0.02 to 1.13), but this effect was not statistically significant at a conventional 5% level. None of the results was statistically significant based on the PrI (see Figure 53). The intervention with the highest probability of being the best was multimodal (probability 0.66). The between-study SD was estimated to be 0.20 (95% CrI 0.05 to 0.46), which implies moderate heterogeneity of intervention effects between studies.
FIGURE 53.
Depression score at long term: SMD for all interventions relative to usual care. a, Probability of being the best treatment. GP-O, GP – other; GPRE, general practitioner-delivered reattribution; MM, multimodal; OP, other psychotherapy; UC, usual care; UC+, usual care plus.

Emotional distress (long term)
Data were available from nine studies presenting the emotional distress score at long term. There were two separate networks for the emotional distress score at long term due to disconnect networks. A NMA was used to compare the effects of medication, GP reattribution, GP MUS management, GP-CBT, guided self-help and multimodal to usual care on emotional distress score. A separate NMA was used to compare the effect of CBTHI, other psychotherapy relative to usual case plus. Figure 54 presents the network of evidence.
FIGURE 54.
Emotional distress score at long term: network of evidence – (a) network 1; and (b) network 2. GPRE, general practitioner-delivered reattribution; GSH, guided self-help; ME, medication; MM, multimodal; OP, other psychotherapy; UC, usual care; UC+, usual care plus.
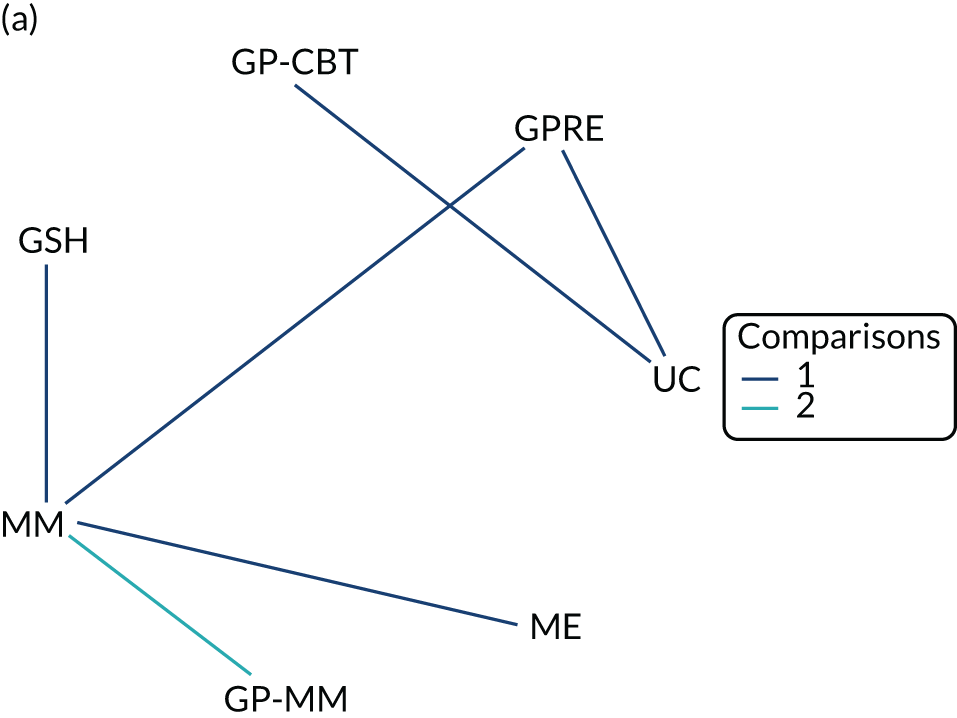
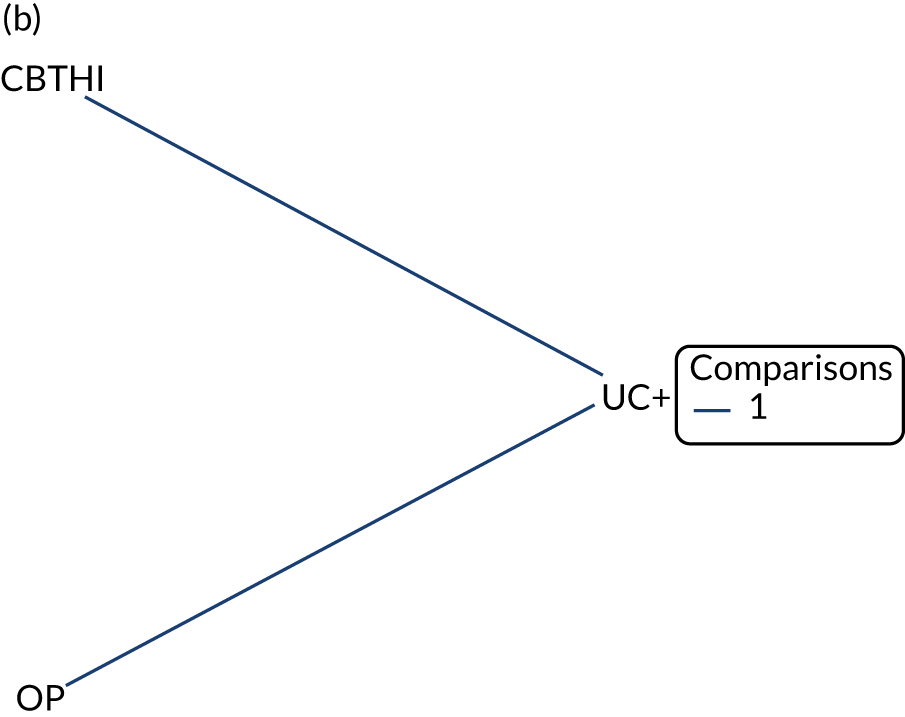
Figure 55 presents the SMD from network 1, the median of treatment rankings and the probability of being the best treatment. For all interventions with the exception of GP reattribution, guided self-help, the estimated SMD was greater than zero, suggesting a beneficial effect compared with usual care. However, none of the beneficial effects was statistically significant at a conventional 5% level and based on the PrIs. The largest beneficial effect was associated with multimodel (a small effect size, SMD 0.56, with 95% CrI –0.31 to 1.45). Guided self-help was significantly worse than usual care (a large effect size, SMD –1.44, with 95% CrI –2.60 to –0.30), and this effect was also statistically significant based on the PrI (see Figure 55). The intervention with the highest probability of being the best was multimodal (probability 0.73), but the result of treatment effect was inconclusive. The between-study SD was estimated to be 0.15 (95% CrI 0.03 to 0.47), which implies moderate heterogeneity of intervention effects between studies.
FIGURE 55.
Emotional distress score at long term: SMD for all interventions relative to usual care (network 1). a, Probability of being the best treatment. GPRE, general practitioner-delivered reattribution; GSH, guided self-help; ME, medication; MM, multimodal; UC, usual care.
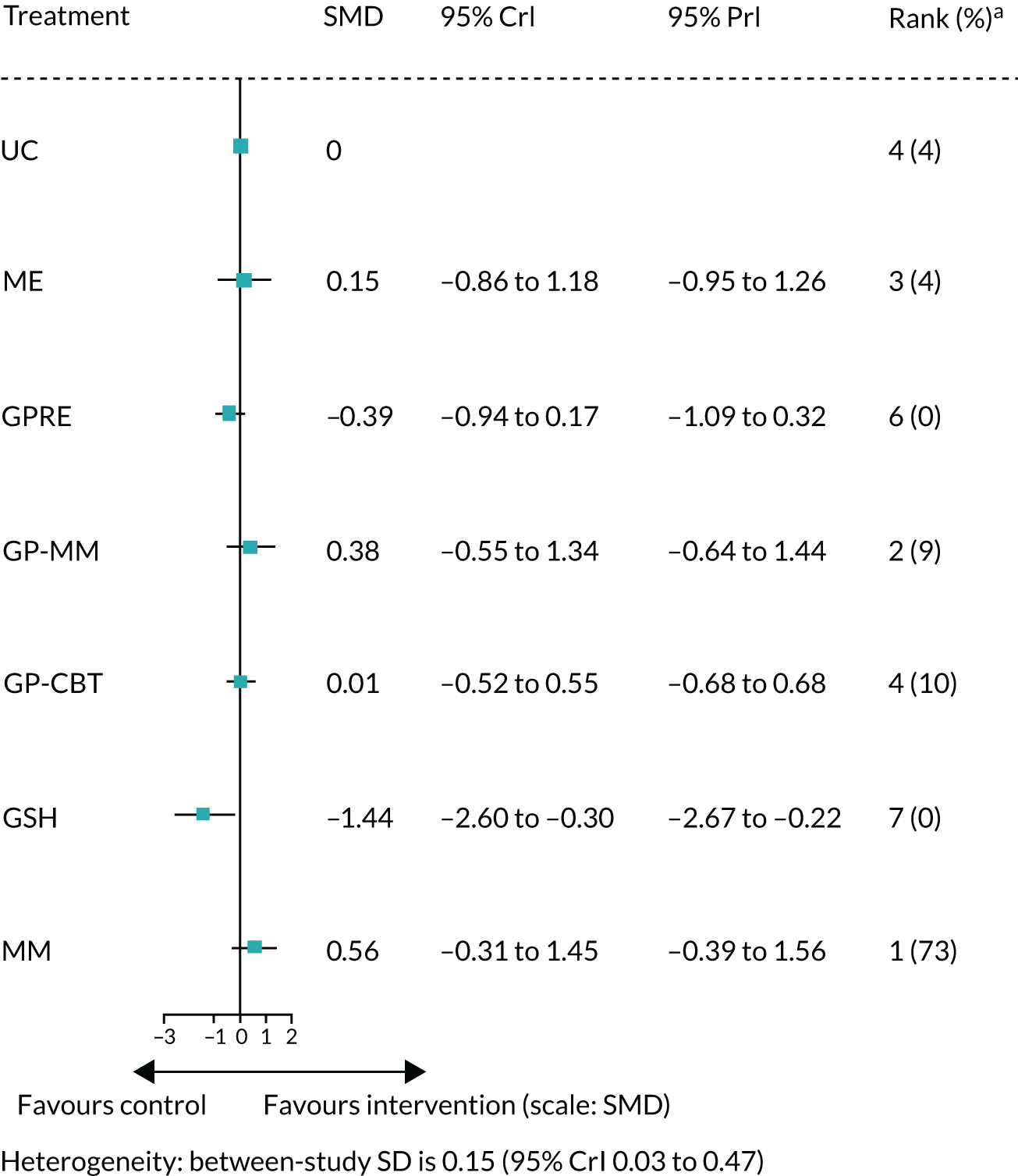
Figure 56 presents the SMD from network 2, the median of treatment rankings and the probability of being the best treatment. The estimated SMDs of CBTHI and other psychotherapy were both greater than zero, suggesting a beneficial effect compared with usual care. However, only the effect of CBTHI with a median effect size (SMD 0.61, with 95% CrI 0.05 to 1.18) was statistically significant at a conventional 5% level, but none of the results was statistically significant based on the PrI (see Figure 56). The intervention with the highest probability of being the best was CBTHI (probability 0.94). The between-study SD was estimated to be 0.19 (95% CrI 0.03 to 0.49), which implies moderate heterogeneity of intervention effects between studies.
FIGURE 56.
Emotional distress score at long term: SMD for all interventions relative to usual care plus (network 2). a, Probability of being the best treatment. OP, other psychotherapy; UC+, usual care plus.

Model checking
The goodness of model fit is presented in Table 2. For all the analyses, the models fitted the data well, with the total residual deviance close to the total number of data points. Inconsistency checking was performed using the inconsistency model approach. 92 The DICs for both the consistency model and the inconsistency model are presented in Appendix 13, Figures 75–84. Plots of the posterior mean deviance of the individual data points in both the consistency model and the inconsistency model for each of the outcomes are presented in Appendix 11.
For all the outcomes, the consistency model provides a similar DIC as the inconsistency model, with the exception of physical functioning at post treatment and short term, and emotional distress at short term. The contributions to the deviance are very similar in the two models for all the outcomes, with the exception of pain short term (the comparison between guided self-help and multimodal, the comparison between usual care and medication, and the comparison between usual care and CBTHI), fatigue at short term (the comparison between usual care and RSSE), physical functioning at short term (the comparison between guided self-help and multimodal, and the comparison between usual care and GP MUS management), emotional distress at post treatment (the comparison between usual care and RSSE) and short term (the comparison between guided self-help and multimodal), and depression at short term (the comparison between usual care and medication, and the comparison between usual care and CBTHI). However, there are overlaps in the 95% CrIs for the estimates between the two models (see Appendix 11). Hence, overall there is no evidence to suggest inconsistency in the networks for all the outcomes.
| Outcome | Time point | Total number of data points | Total residual deviance | Inconsistency check | |
|---|---|---|---|---|---|
| Consistency model DIC | Inconsistency model DIC | ||||
| Pain | Post treatment | 14 | 16.21 | 4.27 | 6.19 |
| Short term | 9 | 10.38 | 0.96 | 1.25 | |
| Long term | 8 | 8.05 | 1.00 | 0.97 | |
| Fatigue | Post treatment | 12 | 13.38 | 2.95 | 3.79 |
| Short term | 11 | 13.54 | 3.96 | 4.60 | |
| Long term | 10 | 9.51 | –0.75 | 0.38 | |
| Bowel symptoms | Long term | 2 | 2.03 | 0.91 | 0.98 |
| Somatisation | Post treatment | 11 | 12.04 | 2.96 | 3.75 |
| Short term | 6 | 6.80 | –0.16 | –0.20 | |
| Long term | 11 | 10.99 | –0.90 | –0.74 | |
| Generic physical symptoms | Post treatment | 2 | 1.32 | 2.30 | 2.19 |
| Physical functioning | Post treatment | 17 | 16.32 | –1.44 | 2.74 |
| Short term | 13 | 15.16 | 4.57 | 1.39 | |
| Long term | 15 | 16.24 | 4.40 | 4.49 | |
| Impact | Post treatment | 11 | 11.51 | 9.34 | 10.15 |
| Short term | 9 | 10.43 | 9.34 | 10.15 | |
| Long term | 5 | 4.95 | 3.42 | 3.56 | |
| Emotional distress | Post treatment | 15 | 16.24 | 3.42 | 3.57 |
| Short term | 14 | 17.03 | 4.30 | 0.21 | |
| Long term for NMA1 | 7 | 7.23 | 3.21 | 3.15 | |
| Long term for NMA2 | 2 | 2.03 | 0.92 | No indirect evidence | |
| Anxiety | Post treatment | 17 | 19.05 | 7.78 | 8.70 |
| Short term | 12 | 13.35 | 6.95 | 5.45 | |
| Long term | 14 | 15.09 | 4.66 | 4.80 | |
| Depression | Post treatment | 16 | 17.39 | 6.20 | 7.33 |
| Short term | 15 | 16.11 | 5.69 | 2.04 | |
| Long term | 16 | 17.29 | 5.30 | 6.11 | |
All NMAs had moderate to high heterogeneity in treatment effects between studies. For most of the outcomes, there were only one or two studies to inform each of the pairwise comparisons/contrasts, with the exception for pain and anxiety both at post treatment, where one contrast was informed by four studies, somatisation at short term and depression at both post treatment and long term, where one contrast was informed by three studies. Hence, there were not enough data to update the prior for the heterogeneity parameter in most analyses. However, the use of plausible informative prior distribution for the heterogeneity ensures that the posterior distribution of the heterogeneity and treatment effects were in also in the plausible range.
It was not possible to perform a metaregression to explain the heterogeneity because there was insufficient replication of each treatment effect across studies. Hence, we compared the point estimate and CIs across condition groupings.
The outcome measures of pain, fatigue, physical functioning, anxiety, depression and emotional distress have been assessed in different condition groupings. For all of these outcomes, the point estimates of the pooled SMDs differed over condition groups, when they were estimated separately in each of these groups. The exceptions to this were for physical functioning score (guided self-help vs. usual care) at short term between the chronic fatigue group and the pain multiple sites group, and for depression score (CBTLI vs. usual care) at short term between the IBS group and the chronic fatigue group. In both of these cases, the SMDs for the individual condition groups were similar.
In all the cases, the CIs of the point estimates generally overlapped indicating that the difference in SMD between condition groups was not statistically significant. Overall, the evidence suggested that the relative treatment effects for the interventions listed in Table 3 were not significantly different across condition groupings.
| Time point | Outcome measure | Treatment (vs. usual care) | Condition grouping (first author and year of publication) | SMD (95% CI) | Comments |
|---|---|---|---|---|---|
| Immediately post treatment | Pain | CBTHI | MUS/somatoform (Zonneveld, 2012141) | 0.51 (0.20 to 0.82) | Different point estimates, but overlapping CIs |
| Pain multiple sites (Alda, 2011137) | 0.23 (–0.14 to 0.59) | ||||
| Pain multiple sites (Luciano, 2014138) | 1.20 (0.78 to 1.61) | ||||
| Pain multiple sites (McBeth, 2012125/Beasley 2015126) | 0.35 (0.08 to 0.61) | ||||
| Physical functioning | CBTHI | MUS/somatoform (Zonneveld, 2012141) | 0.39 (0.08 to 0.70) | Different point estimates, but overlapping CIs | |
| Pain multiple sites (McBeth, 2012125) | 0.15 (–0.11 to 0.41) | ||||
| Anxiety | CBTLI | Chronic fatigue (Tummers, 2012)149 | 0.14 (–0.21 to 0.50) | Different point estimates, but overlapping CIs | |
| IBS (Moss-Morris, 2010130) | –0.46 (–0.95 to 0.04) | ||||
| OP | MUS/somatoform (Kolk, 2004104) | –0.01 (–0.47 to 0.45) | Different point estimates, but overlapping CIs | ||
| MUS/somatoform (McLeod, 1997105) | 0.32 (–0.08 to 0.72) | ||||
| MUS/somatoform (Posse, 200496) | 0.46 (–0.67 to 1.59) | ||||
| Chronic fatigue (Wearden, 2010111) | –0.18 (–0.45 to 0.10) | ||||
| Depression | CBTLI | IBS (Moss-Morris, 2010130) | –0.03 (–0.51 to 0.45) | Different point estimates, but overlapping CIs | |
| MUS/somatoform (Martin, 200799) | –0.14 (–0.47 to 0.19) | ||||
| OP | MUS/somatoform (Kolk, 2004104) | –0.10 (–0.55 to 0.36) | Different point estimates, but overlapping CIs | ||
| MUS/somatoform (McLeod, 1997105) | 0.57 (0.16 to 0.97) | ||||
| Chronic fatigue (Wearden, 2010111) | –0.09 (–0.36 to 0.19) | ||||
| Short term | Physical functioning | GSH | Pain multiple sites (LeFort, 1998128) | 0.27 (–0.10 to 0.64) | Similar point estimates, and overlapping CIs |
| Chronic fatigue (Chalder, 1997114) | 0.26 (–0.06 to 0.58) | ||||
| Anxiety | CBTLI | IBS (Moss-Morris, 2010130) | –0.08 (–0.56 to 0.41) | Different point estimates, but overlapping CIs | |
| Chronic fatigue (Friedberg, 2013151) | 0.35 (–0.10 to 0.80) | ||||
| Depression | CBTLI | IBS (Moss-Morris, 2010130) | 0.29 (–0.20 to 0.78) | Similar point estimates, and overlapping CIs | |
| Chronic fatigue (Friedberg, 2013151) | 0.25 (–0.20 to 0.70) | ||||
| RSSE | MUVD (Kobeissi, 2012110) | 0.10 (–0.14 to 0.34) | Different point estimates, but overlapping CIs | ||
| Chronic fatigue (Friedberg, 2013151) | –0.02 (–0.48 to 0.42) | ||||
| Emotional distress | GSH | Pain multiple sites (LeFort, 1998128) | 0.38 (0 to 0.75) | Different point estimates, but overlapping CIs | |
| Chronic fatigue (Chalder, 1997114) | 0.28 (–0.37 to 0.60) | ||||
| Long term | Anxiety | OP | MUS/somatoform (Kolk, 2004104) | –0.34 (–0.80 to 0.13) | Different point estimates, but overlapping CIs |
| Chronic fatigue (Wearden, 2010111) | –0.15 (–0.42 to 0.13) | ||||
| CBTLI | IBS (Moss-Morris, 2010130) | –0.27 (–0.76 to 0.21) | Different point estimates, but overlapping CIs | ||
| Chronic fatigue (Friedberg, 2013151) | 0.18 (–0.26 to 0.63) | ||||
| Depression | OP | MUS/somatoform (Kolk, 2004104) | –0.31 (–0.77 to 0.15) | Different point estimates, but overlapping CIs | |
| Chronic fatigue (Wearden, 2010111) | –0.13 (–0.41 to 0.14) | ||||
| CBTLI | IBS (Moss-Morris, 2010130) | 0.35 (–0.14 to 0.83) | Different point estimates, but overlapping CIs | ||
| MUS/somatoform (Martin, 200799) | –0.26 (–0.60 to 0.06) | ||||
| Chronic fatigue (Friedberg, 2013151) | –0.07 (–0.52 to 0.37) |
Discussion of clinical effectiveness review
The review identified 59 studies that met the inclusion criteria. A broad approach to inclusion was taken, and this is reflected in the considerable heterogeneity found. Owing to the considerable differences in types of interventions, it was not appropriate to treat all interventions as one behavioural intervention group and, therefore, study arms were categorised into 13 types. Even within intervention types, there was variation in treatment duration and intensity, mode of delivery and intervention provider, and differences in the specifics of the primary care setting – from interventions delivered by the patient’s own GP within their own GP practice to those involving collaborative care with health-care professionals from outside the practice or primary care patients travelling to a gym or fitness facility. Studies included a range of populations, and this resulted in further heterogeneity, with, for example, several studies of CBTHI but these being in different populations. Ideally, these differences would have been explored through metaregression, but there was insufficient replication of each intervention type within the networks to allow this. These issues have resulted in limitations when drawing conclusions regarding clinical effectiveness. Further to this, studies did not measure the same outcomes at the same time points (i.e. end of treatment, short- and long-term follow-up) and, therefore, different studies inform the network at these different time points; these analyses are not repeated measures and do not account for correlations between time points.
The evaluation of clinical effectiveness necessitated making judgements regarding intervention groups, and inclusion judgements such as participants meeting ‘medically unexplained’ criteria (where populations did not meet the criteria for FSSs or other pre-defined diagnostic classifications) and primary care setting criteria. Although efforts were made to ensure that these judgements were made using objective criteria, and with consultation between project team members when borderline decisions were required, it is acknowledged that judgements could arguably have been made differently. A narrower scope may have reduced this possibility but using broad inclusion criteria has allowed a broader evaluation of the topic. With regard to setting, the review did not include studies of home-based or self-help behavioural interventions, such as e-health, where these had insufficient or no involvement of primary care practitioners (i.e. were conducted solely by university research teams). These interventions may well be feasible and effective in a primary care setting and when co-ordinated by primary care teams. However, as was evidenced by the wide variation in recruitment by GPs seen in the current review, it was considered inappropriate to include these interventions until they have been conducted in the ‘real world’ of primary care.
Appendix 12, Table 97, summarises the significant results identified in the NMAs, showing the SMDs for the significant intervention groups for each outcome and time point. Although the NMAs do not identify individual significant trials, SMDs for all individual trials are presented by outcomes in Appendix 12, Tables 98–107. For those intervention groups that were shown to have significant beneficial effects, a brief description of the key characteristics of the trials in those groups is presented below by outcome.
Pain
At the end of treatment, CBTHI and multimodal interventions were shown to be significantly more effective than usual care at reducing pain. CBTHI was the only intervention to be significantly more effective than usual care at short-term follow-up. No interventions were more effective than usual care at long-term follow-up.
High-intensity cognitive–behavioural therapy
There were four studies that informed the pain networks for CBTHI interventions. These were Zonneveld et al. ,141 Alda et al. ,137 Luciano et al. 138 and McBeth et al. 125 One of these studies141 was of a population of patients with unexplained physical symptoms, referred to the study by the GPs if their symptoms were considered to be unexplained by a physical condition. Patients were then included if they fulfilled the DSM-IV criteria for undifferentiated somatoform disorder or a chronic pain disorder. The CBT intervention was based on the consequences model, tailored for MUS in primary care, and delivered over 13 weeks by an outreaching mental health service. Patients in the control group were put on a waiting list. At the end of treatment, small to moderate SMDs were found in favour of the intervention for pain, physical functioning, emotional distress and somatisation.
The remaining three studies that informed this network were of populations of patients with chronic widespread pain. McBeth et al. 125 report results from the MUSICIAN trial [Managing Unexplained Symptoms (chronic widespread pain) In primary Care: Involving traditional and Accessible New approaches]. 125 Patients meeting the criteria were recruited from primary care practices in the UK and were allocated to one of four arms: (1) telephone CBT, consisting of seven weekly sessions of 45–60 minutes plus two further follow-up sessions. Patients were given a self-management CBT manual and offered some choice in the type of CBT they preferred, including behavioural activation, cognitive restructuring and lifestyle changes; (2) exercise, consisting of a leisure facility- and gym-based exercise programme, with recommended exercise duration of 20 to 60 minutes, at least twice per week; (3) combined, consisting of both the telephone CBT and exercise interventions; and (4) treatment as usual, consisting of usual care by their family physician. Small SMDs were found in favour of all three active intervention groups, with the SMDs for CBTHI and combined groups marginally larger.
Luciano et al. 138 studied a population of patients fulfilling the ACR 1990 criteria for fibromyalgia, recruited by GPs from primary health-care centres in Spain. The intervention arm received group ACT, adapted to fibromyalgia patients, consisting of sessions on mindfulness, cognitive defusion, committed action and observation of the self. Sessions were delivered by a therapist over eight 2.5-hour sessions, with daily homework exercises. A second intervention group received recommended pharmacological treatment, prescribed by the GP after a 2-hour training session. A third, control, group were put on a waiting list. At the end of treatment, large SMDs were found for patients in the CBTHI group, and moderate effects for those in the medication group, when compared with those on the waiting list.
Alda et al. 137 also included patients with fibromyalgia recruited by primary care doctors from primary health-care centres in Spain. The intervention arm received CBT based on Thorn’s model of pain catastrophising, adapted to people with fibromyalgia. The main components of the CBT were cognitive restructuring and coping. Ten 90-minute group CBT sessions were delivered over 10–12 weeks by trained therapists. A second intervention group received recommended pharmacological treatment, administered by a psychiatrist. A third, control, group received treatment as usual. At the end of treatment, SMDs showed no substantial effects on pain for CBT compared with usual care, although a small effect was found at long-term follow-up. There was a small effect for the medication group both at the end of treatment and in the long term.
Only the McBeth et al. 125 and Luciano et al. 138 studies informed the network for CBTHI at short-term follow-up, with the CBTHI group in Luciano et al. 138 continuing to show a large effect size, and McBeth et al. 125 showing a small effect size for CBTHI compared with usual care. By long-term follow-up, the NMA found no significant effects for CBTHI compared with usual care, with data from only one study remaining to inform the network (Alda et al. 137).
Multimodal interventions
Five studies informed the pain networks for multimodal (MM) interventions. These were Cuesta-Vargas et al. ,118 Schaefert et al. ,132 Walti et al. ,121 Luciano et al. 139 and McBeth et al. 125 McBeth et al. 125 had multiple arms and has been previously described under CBTHI. Cuesta-Vargas et al. 118 is described under guided self-help.
Schaefert et al. 132 reports results from the speciAL trial (specific collaborative group intervention for MUS patients in general practice). This was a cluster randomised trial including patients meeting the criteria of > 6 months’ bodily complaints without sufficient explanatory peripheral organ pathology, and with MUS as the main treatment issue. The multimodal group consisted of GP MUS management training, plus a syndrome-oriented psychosomatic group intervention for MUS patients conducted by GPs together with a psychosomatic specialist, in 10 weekly sessions of 90 minutes plus two booster sessions. The GP training consisted of a guideline-based curriculum in the diagnosis and management of patients with MUS. At follow-up, SMDs showed that there were no substantial differences between the two groups for pain scores.
Walti et al. 121 conducted a pilot RCT with a population of patients with non-specific lower back pain recruited and treated in a primary care physiotherapy centre in Switzerland. Patients had moderate to severe disability. The multimodal intervention group received patient education, sensory retraining and motor retraining. Sessions were delivered in 16 sessions over 8–12 weeks. The control group received usual physiotherapy care, which consisted primarily of active treatment, such as muscle-strengthening exercises and mobilisation or stretching exercises.
Luciano et al. 139 conducted a trial of 216 patients with fibromyalgia. The intervention was set in three general practices in Spain. GPs previously referred patients suspected of fibromyalgia for diagnosis at a rheumatology unit. A database of these patients is kept at the GP practice for monitoring. These patients were included in the trial, which was conducted by a multidisciplinary team within the three general practices. The multimodal intervention consisted of five 2-hour group sessions of education and four 2-hour sessions of autogenic training. The education element included information on symptoms, course of the condition, comorbidities and causes. The programme outlined the influence of psychosocial factors on pain, the benefits of exercise and behavioural change. The autogenic training focused on physical and mental relaxation, pain relief and stress reduction. The group sessions encouraged emotive exchange with other patients. The control group received usual care. The multimodal intervention group reported a greater reduction in pain than the control group. SMDs showed this to be a moderate effect.
Guided self-help
Guided self-help was shown to be less effective than usual care at long-term follow-up. Only one study of guided self-help informed the network. Cuesta-Vargas et al. 118 studied a population of 58 primary care patients with > 3 months of non-specific chronic lower back pain, who had been referred to the study by their GP. The intervention arm was deep-water running three times per week for 4 months plus an education intervention. This consisted of a 25-page educational booklet and verbal presentation on basic anatomy and physiology of the spine, principles of ergonomics for low back pain patients, and instructions for coping strategies. The booklet encouraged the patients to treat themselves instead of undergoing passive treatments. This was presented alongside usual care from their GP. Patients in the control arm received the education booklet and presentation alongside usual care from their GP. Both groups showed improvement over time, but the deep-water running/education group showed more improvement with large SMDs for pain, physical functioning, impact and emotional distress at all time points. The effect sizes for this study were particularly large, and inconsistency checking of the NMA showed that the direct evidence of this effect was not consistent with the indirect evidence.
Fatigue
At the end of treatment, RSSE, CBTLI, multimodal interventions and GA were shown to be significantly more effective than usual care at reducing fatigue. RSSE and CBTLI were significantly more effective than usual care at short-term follow-up. CBTLI was the only intervention more effective than usual care at long-term follow-up.
Relaxation/stretching/social support/emotional support interventions
Two RSSE interventions informed the fatigue network at the end of treatment. The first of these was Ho et al.,150 a Hong Kong study of people with CFS who were recruited from the community. Participants were recruited following screening via a web-based questionnaire and were required to meet the US CDC criteria for CFS; however, diagnosis was not confirmed by medical examination. The intervention group received 2-hour group qigong training for 5 weeks. The group sessions included basic theories of Chinese medicine and physiology of mind–body connections, mindful meditation for relaxation and gentle movement or body stretching in standing postures. A final session in qigong exercise training was delivered by a Daoist qigong master. Participants were also expected to continue to practise qigong exercise at home for the remaining 12 weeks of the study period. Participants in the control group received qigong training at the end of the study. SMDs showed a large beneficial effect on reduction in self-perceived fatigue at the end of the 5-week group training for the qigong group. At the 4-month follow-up, this beneficial effect remained, although it should be noted that it was expected that participants continued to practise qigong at home during this follow-up period.
A further RSSE intervention arm informed the network at short- and long-term follow-up (Friedberg et al. 151), which also included a CBTLI arm and is described below.
Low-intensity cognitive–behavioural therapy interventions
Two CBTLI interventions informed the fatigue network at the end of treatment,113,149 with a further study informing the network at short- and long-term follow-up. 151
Ridsdale et al. 113 studied a UK population of 123 patients presenting to their GPs with unexplained fatigue of > 3 months. The study compared two active interventions: CBT and graded exercise. Both treatments were delivered on the GP premises by CBT therapists and physiotherapists, in six 45-minute sessions over 12 weeks. The CBT treatment was manualised, based on a model of precipitating and perpetuating factors. It involved activity planning, establishing a sleep routine and other cognitive interventions, and addressed negative beliefs, self-expectations and self-esteem. The GA intervention (i.e. GET) was based on each individual patient’s physical capacity, and aimed to achieve a gradual but progressive increase in aerobic activity. A third, non-randomised cohort of patients received an educational booklet. Both groups saw a significant reduction in fatigue from baseline. SMDs showed a small beneficial effect for the CBT group compared with the GET group at the end of treatment, but showed no substantial difference between groups at follow-up. A total of 3% of patients in the CBT group showed an increase in fatigue after treatment, compared with 12% of patients in the GET group.
Tummers et al. 149 studied a population of 123 patients in Holland diagnosed with CFS (US CDC criteria) by either their GP or a consultant. The active intervention was a minimal intervention based on CBT, previously shown by the authors to be effective in a tertiary treatment setting. The intervention was applied in a community-based mental health centre, with no previous experience of treating patients with CFS. Psychiatric nurses were trained to deliver the intervention, which was based on a protocol for CBT for CFS, and was in the form of a guided self-instruction booklet delivered over 20 weeks. The programme focused on precipitating and perpetuating factors, challenging fatigue-related cognitions, reducing the focus of fatigue, establishing a sleep routine, assessing activity patterns and gradually increasing physical activity. The control group was put on a waiting list. A total of 12 out of the 123 randomised patients were found to have a misdiagnosis of CFS during the course of the trial but were not excluded from the analyses. Patients in the intervention group showed a significantly greater reduction in fatigue severity than those in the waiting list group at the end of treatment. SMDs showed this effect to be moderate.
Friedberg et al. 151 studied a population of 111 primary care patients with chronic fatigue, recruited from a family medicine/primary care practice in the USA. A total of 39% of the included sample met the US CDC criteria for CFS, and the remaining 61% did not meet the full criteria but had at least 6 months’ persistent fatigue not clearly attributable to identifiable medical conditions, with associated impairment in functioning. The study had three arms. The CBTLI intervention was ‘fatigue self-management’. This consisted of two nurse-led sessions based on a CBT treatment programme for CFS, with a self-help booklet for a period of home-based self-management. The nurse-led sessions covered diagnosis and possible causes, stress and sleep disturbance, balance between mental and physical exertion, unhelpful behaviours or illness beliefs, and development of more useful cognitive and behavioural strategies. The second arm was an attention control RSSE intervention. It included emotional support and self-monitoring of symptoms, affect and stress. The intervention also consisted of two sessions and a period of home-based activities. The third arm was usual medical care/no treatment. The results showed significantly greater reduction in fatigue in the CBTLI group than in both the RSSE attention control group and the usual-care group. SMDs showed moderate effects for the CBTLI group compared with usual care, and showed no substantial effects for the RSSE intervention compared with usual care.
Multimodal interventions
Two multimodal interventions informed the fatigue network, McBeth et al. 125 and Luciano et al. 139 For both of these studies, the populations were patients with chronic widespread pain/fibromyalgia. The studies are outlined above under Pain. For fatigue, SMDs showed a small effect for the intervention on reduction in fatigue at the end of treatment in Luciano et al. 139 compared with usual care, and a large effect at the end of treatment in McBeth et al. ,125 reducing to a small effect at long-term follow-up compared with usual care.
Graded activity
Four studies with GA arms informed the fatigue network: Ridsdale et al. 113 (described in Low-intensity cognitive–behavioural therapy interventions), Marques et al. ,133 Wearden et al. 111 and Ridsdale et al. 115
Marques et al. 133 included a study population of 99 patients meeting the CDC criteria for idiopathic chronic fatigue, recruited to the study by their medical doctor. The trial took place in four public primary care centres and one private practice, and in a patient association. The active intervention arm was the 4-STEPS programme, which was delivered by a health psychologist over a 12-week intervention period. The intervention was based on the use of self-regulation theory to promote physical activity. Features of the intervention were the use of motivational interviewing to increase motivation and confidence, and the formation of action plans with specific personal physical activity goals. The control condition (guided self-help) comprised an educational booklet containing information about the benefits of physical activity and physical activity guidelines for adults, and participants in this group were set a personal activity goal. At the end of the intervention, a significant beneficial effect for the GA intervention was found compared with the control of guided self-help. SMDs showed this to be a moderate effect.
Ridsdale et al. 115 included a study population of 222 primary care patients consulting with their GPs for fatigue of > 3 months’ duration as the main problem, but with no known physical condition that could explain the fatigue. The study had three arms. The graded exercise intervention was delivered by physiotherapists over eight 30-minute sessions at 2-weekly intervals in the patient’s own primary care practice. Patients were guided through supervised exercise (walking), tailored to their individual current physical capacity, and gradually building in intensity. A second arm was a psychotherapy intervention. This consisted of Rogerian client-centred non-directive counselling. The counselling was delivered by trained therapists in eight 50-minute sessions at 2-weekly intervals. The third arm was usual care with the addition of a booklet of self-help techniques based on CBT principles, and including information on the causes of fatigue (guided self-help). No significant differences in reduction in fatigue were found between the three intervention groups at either the 6- or the 12-month follow-up. SMDs showed no substantial effect for either guided self-help or GA when compared with other psychotherapy at either time point. The authors reported a high level of dissatisfaction with care, but less dissatisfaction in the GA group.
Wearden et al. 111 included a study population of 296 patients who met the Oxford criteria for CFS/myalgic encephalomyelitis, and who scored < 70% on the SF-36 physical functioning scale, and > 4 on the Chalder Fatigue Scale. Patients meeting these criteria were referred by their GP. The study had three intervention arms. The GA intervention (‘pragmatic rehabilitation’) consisted of a programme of graded return to activity, and a focus on regularising sleep patterns, addressing somatic symptoms of anxiety and addressing concentration and memory problems. The counselling intervention (‘other psychotherapy’) was a non-directive listening therapy, allowing the patient to discuss their concerns and problems. Both the GA and the counselling interventions were delivered over a 10-week period by general nurses with experience of working in primary care, but not of CFS/myalgic encephalomyelitis, in the patients’ own homes, with additional telephone sessions. Home visits were of 1 hour’s duration, and telephone sessions were of 30 minutes’ duration. The third arm was GP usual care. At the end of treatment, patients in the GA group had significantly reduced fatigue compared with patients in the usual-care group. This effect was no longer significant at long-term follow-up; however, at 70 weeks, GA was significantly better than usual care when the Chalder Scale was used with Likert scoring. There was no significant beneficial effect on fatigue of other psychotherapy compared with usual care at the end of treatment or follow-up. SMDs show small effects at the end of treatment and long-term follow-up for GA compared with usual care, but show no substantial effects for other psychotherapy compared with usual care at either time point.
Bowel symptoms
There were insufficient studies to form networks for bowel symptoms for end of treatment and short-term follow-up. Only two studies informed the network for long-term follow-up. Of these, only CBTLI was shown to have a significantly beneficial effect compared with usual care.
Low-intensity cognitive–behavioural therapy intervention
Moss-Morris et al. 130 reported results from a pilot study of a population of 64 patients meeting the Rome II criteria for IBS. Patients were recruited either from a database of known patients with IBS who had taken part in a previous primary care study or from patients presenting to the study GP with IBS symptoms. The study GP screened interested participants for eligibility. The intervention arm was a 7-week home-based manualised self-management programme. The programme included one 1-hour face-to-face session and two 1-hour telephone sessions with a health psychologist. The programme focused on assessment of symptoms and self-monitoring behaviours, behavioural management of symptoms and goal-setting, managing unhelpful thoughts, personal expectations and activity patterns, and relaxation and stress management. The control arm received treatment as usual, which included a sheet explaining that a range of tests had been conducted and had ruled out structural causes for their IBS. Results showed a significant reduction in bowel symptoms severity at the end of treatment and at long-term follow-up. SMDs showed this to be a moderate to large effect.
Somatisation
Data from 11 studies were available to inform the network for somatisation. Despite this, no interventions were found to have any significant beneficial effects on somatisation compared with usual care. Trials of a range of intervention types were identified. SMDs for individual trials show that, although a small number of trials found small beneficial effects at the end of treatment, these effects are mostly lost by long-term follow-up. One trial of CBTHI144,148 produced moderate beneficial effects both at end of treatment and at long-term follow-up. This was a study of patients meeting the criteria for Escobar’s Abridged Somatisation Disorder, recruited by GPs from 21 primary care centres in Spain. The CBT intervention was based on a protocol by Escobar et al. ,156 delivered over 10 weekly sessions. The programme included muscle relaxation, emotional mindfulness, cognitive restructuring and social skills.
Generic physical symptoms
Data from two studies were available to inform the network for generic physical symptoms at the end of treatment; however, no interventions showed significant beneficial effects. There were insufficient data to form networks for short- or long-term follow-ups.
Physical functioning
At the end of treatment and short-term follow-up, multimodal interventions were the only interventions that showed significant beneficial effects. No interventions showed significant beneficial effects at long-term follow-up. Studies that contributed data to the network for multimodal studies have been described previously. 107,118,125,132,139,142 SMDs for these studies showed that, in Cuesta Vargas et al.,118 large effects were found for multimodal compared with guided self-help at the end of both short- and long-term treatment; in Schaefert et al.,132 a small effect was found at short-term follow-up for multimodal compared with GP MUS management, but no substantial effect was found at long-term follow-up; in Luciano et al.,139 a small effect was found for multimodal compared with usual care at the end of treatment; and in McBeth et al.,125 a small effect was found in favour of multimodal compared with usual care at the end of treatment and at short-term follow-up.
Smith et al. 107 report results from a study of 206 high-utilising MUS patients recruited from a health maintenance organisation in the USA. MUS patients were identified through patient records, with eligibility assessed in patients who had more than eight visits per year. MUS was identified if symptoms of > 6 months’ duration were present that had no documented disease. Nurse practitioners with no prior experience in mental health received a 10-week training programme to deliver the intervention. The intervention consisted of patient-centred management to improve communication and establish positive patient–provider relationships, antidepressants, exercise, relaxation training, physical therapy and comorbid organic disease management. It was delivered in 12 20-minute visits with patients over a 1-year period. The control group received usual care. Patients in the intervention group were more likely to improve than those in the control group.
Smith et al. 142 report results from a pilot study of 30 high-utilising patients with MUS. Patients were identified from the Henry Ford Health System using ICD-9 codes to identify MUS. The intervention group received a multimodal intervention delivered by primary care physicians (PCPs) who had received training for the study. The intervention was similar to that of Smith et al.,107 with the exception that the prior study used nurse practitioners to deliver the intervention. It consisted of antidepressant medication (where PHQ-9 identified depression), structured CBT and patient-centred management aimed at maximising communication and the patient–provider relationship. The intervention was delivered over 1 year, with seven visits with the PCP, and three visits with a case manager. The intervention produced a significant beneficial effect on somatisation compared with the control group, which was usual care. SMDs show a moderate effect for the multimodal intervention compared with usual care at long-term follow-up.
Impact
At the end of treatment and at short-term follow-up, only the CBTHI interventions were shown to have a significant beneficial effect on impact of the illness on daily life. Two studies of CBTHI informed the network at the end of treatment. 137,138 Only data from Luciano et al. 138 informed the network at short-term follow-up. Both of these studies have been previously described.
Anxiety
At the end of treatment and at short-term follow-up, only the CBTHI interventions were shown to have a significant beneficial effect on anxiety compared with usual care. Four studies of CBTHI informed the network at the end of treatment. These were Escobar et al. ,156 Gili/Moreno,144,148 Alda et al. 137 and Luciano et al. 138 At short-term follow-up, only data from Luciano et al. 138 informed the network. Gili/Moreno,144,148 Alda et al. ,137 and Luciano et al. 138 have been previously described. No interventions showed significant beneficial effects on anxiety at long-term follow-up.
Escobar et al. 156 studied a population of patients meeting the criteria for Escobar’s abridged somatisation, recruited from primary care clinics in the USA. PCPs and nurses referred consecutive adult patients who had repeatedly sought care for MUS and for whom the symptoms were a source of distress. The intervention group received a CBT-type intervention delivered by therapists trained for the study. The intervention was delivered in 10 sessions of 45–60 minutes over 10–20 weeks. The control group received usual clinical care from their PCP, which included a consultation letter. SMDs showed a small beneficial effect on anxiety for the intervention group versus the control at the end of treatment. In Gili/Moreno,144,148 a moderate beneficial effect was found for the CBTHI group compared with usual care. For Alda et al.,137 no substantial effect was found compared with usual care. In Luciano et al.,138 a large beneficial effect was found for the CBTHI group compared with usual care.
Depression
At the end of treatment and at short-term follow-up, only the CBTHI interventions were shown to have significant beneficial effects. Four studies on CBTHI informed the network at the end of treatment. These were the same studies as for anxiety, and all have been described previously. 137,138,144,148,156 No interventions had significant beneficial effects at long-term follow-up. SMDs showed small beneficial effects in Escobar 2007156 and Gili/Moreno. 144,148 No substantial effects on depression were found in Alda et al.,137 but a large beneficial effect on depression was found in Luciano et al. 138 Only Luciano et al. 138 showed a beneficial effect at short-term follow-up.
Chapter 4 The acceptability of primary care or community-based behaviour modification interventions for medically unexplained symptoms: qualitative systematic review
This chapter aims to provide an overview of the evidence for patients’ and HPs’ perspectives on the acceptability, relative benefits and potential harms of primary care or community-based behaviour modification interventions for MUS.
Review methods
Screening and eligibility
A two-stage sifting process for inclusion of studies (title/abstract then full-paper sift) was undertaken. Titles and abstracts were scrutinised by one systematic reviewer (AS) according to the inclusion and exclusion criteria. There was no exclusion on the basis of quality. All studies identified for inclusion using the abstract, together with any in which a decision on inclusion was not possible from these brief details, was obtained for more detailed appraisal. Agreement on inclusion at title/abstract sift was checked by a second systematic reviewer (AB) for 20% of the total electronic search results; therefore, 345 records were sifted by both AS and AB. Agreement was calculated using the kappa statistic. Based on these data, the kappa statistic was 0.765. As the kappa statistic was above acceptable levels (i.e. 0.7), double-sifting was not deemed necessary. Where the reviewers disagreed on inclusion/exclusion at title/abstract sift, these records were retrieved to check at full text. In the event of disagreement regarding the inclusion of a study, the opinion of the MUS experts in the project team was sought.
The inclusion and exclusion criteria for the qualitative review are reported in Table 4. The inclusion and exclusion criteria for the project as a whole are presented in detail in Chapter 3. Any inclusion and exclusion criteria that are specific to the qualitative review are documented in more detail here.
| Inclusion criteria | Included | Excluded |
|---|---|---|
| P – population | Patients meeting the criteria for MUS, MUPS and somatoform disorders. Populations with FSSs were included (e.g. IBS, CFS, fibromyalgia). Health-care providers who had delivered behavioural modification interventions designed for these patients were also included | Subacute patients. Patients with intermittent pain (where current episode was < 3 months – or this information was not available from the paper/or they cannot be disentangled from the rest of the sample) |
| I – intervention | Behavioural modification interventions | Studies of management of MUS where evidence relating to a treatment of interest was not separately identifiable |
| C – comparator | N/A | N/A |
| O – outcomes | Qualitative data | N/A |
| S – study design | Qualitative research, mixed-methods research, qualitative data embedded in trial reports or process evaluations | Quantitative reports without qualitative evidence |
Evidence from health-care providers who delivered the behavioural interventions for included patients was sought, in addition to patients’ views. Studies were included only if they contained data related specifically to an intervention that met the review’s inclusion criteria, as the review was specifically aimed at evaluating perceptions of behavioural interventions delivered in a primary care setting. Studies containing qualitative data relating to general management of MUS and not to a specific included intervention were therefore excluded (e.g. Ax et al. ,164 Bayliss et al. ,165 Wallace et al. ,166 Deale and Wessely,167 Raine et al. 168).
Study types: (1) studies reporting qualitative research or qualitative data elicited via a survey or a mixed-methods study to include qualitative data on the perspectives and attitudes of patients who had received behaviour modification interventions in a primary care or community-based setting; (2) qualitative data, embedded in trial reports or in accompanying process evaluations, which can inform an understanding of how issues of acceptability are likely to affect the clinical effectiveness of eligible interventions; (3) qualitative data, either from separately conceived research or embedded within quantitative study reports, reporting the acceptability of interventions to health-care practitioners.
Quality assessment strategy
Assessment of confidence in the review findings:
The Confidence in the Evidence from Reviews of Qualitative (CERQual)169 research approach was used to summarise our confidence in the findings across the studies included in the review. CERQual is currently under development and draws on the principles used to develop the GRADE approach. An earlier version of this approach has been used in two Cochrane reviews169,170 and three non-Cochrane reviews. 171–173 CERQual assesses confidence in the evidence based on four key components:
-
The methodological limitations of included studies. Methodological quality of individual studies was appraised using an abbreviated version of the Critical Appraisal Skills Programme (CASP) quality assessment tool for qualitative studies. 174 Two reviewers (AS and AB) independently applied the set of quality criteria to each included study. In the event of a disagreement, a third reviewer (JL) was consulted. Studies were included in the review regardless of study quality.
-
The relevance of the included studies to the review question, which is the extent to which the review finding is applicable to the context (perspective or population, setting) specified in the review question.
-
The coherence of the review finding, which is the extent to which the pattern across the data that constitutes a review finding, is based on evidence that is consistent across multiple individual studies and/or incorporates convincing explanations for the patterns of evidence in the underlying studies, including explanations for variations across individual studies. The coherence of each review finding was assessed by looking at the extent to which a clear pattern across the data was identified and was contributed to by each individual study, and whether or not this was consistent across multiple contexts.
-
The adequacy of the data contributing to a review finding that refers to an overall determination of the degree of richness and quantity of data supporting a review finding.
Confidence in a finding will be weakened when:
-
the included studies have important methodological limitations
-
the contexts of the primary studies underlying a review finding are substantively different from the context of the review question (relevance)
-
variation is found across data from individual studies and there is no convincing explanation for this variation (coherence)
-
a review finding is supported by data from only one or few primary studies, settings or relevant groups, or the data supporting a finding are very thin (adequacy).
After assessing each of the four components, a judgement was made about the overall confidence in each review finding. Confidence was judged as high, moderate, low or very low. The starting point of ‘high confidence’ reflects a view that each review finding should be seen as a reasonable representation of the phenomenon of interest unless there are factors that would weaken this assumption.
Data extraction strategy
Data extraction from included qualitative studies was undertaken by one reviewer (AS) using a data extraction tool adapted and tailored for the purpose of this qualitative review. All data extractions were checked by a second reviewer (AB), with any discrepancies being discussed by both reviewers. Where data for included studies were missing, reviewers attempted to contact the authors at their last known e-mail addresses. For the purpose of data extraction, two principal approaches to decide what counts as qualitative evidence have been proposed. 175 In the first, only data from primary studies that are illustrated by a direct quotation from the respondent are extracted, whereas, in the second, all qualitative data identified in the primary studies and relevant to the review question are extracted. Given the anticipated paucity of relevant evidence (i.e. evidence relating specifically to behavioural modification interventions in primary care rather than perceptions and attitudes towards general management of MUS), the latter, more inclusive, approach to data type was adopted, together with a selective approach to extract data relevant to the specific research question. A framework for extraction was developed which focused specifically on data relating to the review question. This framework allowed the data to be extracted into broad themes relating to the research question, as illustrated in Table 5. Within these broad themes, more specific subthemes were then generated by coding the data. Although in a number of papers the authors had coded the data and had arranged it in themes, these themes were not always used in this review; in some cases, these themes were adapted and in other cases data were subsumed into other, different, themes.
| Source of data | Theme |
|---|---|
| Data from patients | Positive factors relating to behavioural modification interventions as reported by patients/what did you gain from being referred to a behavioural modification intervention? |
| Factors reported as important, wanted or expected in behavioural modification interventions | |
| What patients did not like about (being referred to) behavioural interventions | |
| Barriers – why patients did not want behavioural interventions/or could not engage with them | |
| Neutral effects (neither benefits or harms) | |
| Data from HPs | Positive factors relating to behavioural modification interventions as reported by HPs/what did you gain from being trained to deliver and/or delivering a behavioural modification intervention? |
| Factors reported as important, wanted or expected for training in and delivery of behavioural modification interventions | |
| What did not help or was detrimental to the patients or delivery of the intervention | |
| Barriers – from the perspective of HPs as to why patients did not want behavioural interventions/or could not engage with them, or barriers to delivery of the intervention | |
| Neutral effects (neither benefits or harms) |
Data synthesis strategy
Qualitative evidence synthesis was undertaken to provide added value to the quantitative analysis by indicating patient and service provider issues around the acceptability of interventions. Specifically, thematic synthesis was used to aggregate the findings. 176 The framework developed for data extraction was used to shape the synthesis of the findings. Themes were then developed within the framework elements.
Combining the quantitative and qualitative data
Methodological work to date has been unable to establish the superiority of conducting the qualitative and quantitative synthesis in parallel or of conducting quantitative followed by qualitative, qualitative followed by quantitative or some more iterative approach. Our choice of method of combining data was determined by the needs of this particular review, in which the quantitative data were the main focus and the qualitative data were used for their explanatory potential. We, therefore, employ methods similar to those described by Noyes et al. 177 to explore the effectiveness review in the light of supporting qualitative research data.
Results of the qualitative review
Included studies: qualitative review
From the 1735 citations identified from the initial searches, 42 remained after title and abstract sift and these citations were considered at full-paper sift for the qualitative review. Figure 57 shows the flow chart of studies included in the qualitative review. The sifting process resulted in the inclusion of 10 studies at full paper. These 10 papers reported evidence from eight studies. Two papers reported evidence from the same study but from some of the same participants; of these one reported evidence from both the patients and HPs178 and the other reported evidence only from patients. 179 A further two papers reported on the same study, with one paper reporting evidence from patients180 and the other reporting evidence from HPs. 181 Details of studies excluded at full-paper sift together with reasons are shown in Appendix 5. All included full papers were published between 2007 and 2016. A summary of the included studies and their sample and study characteristics can be found in Table 6.
FIGURE 57.
The PRISMA flow diagram for the MUS qualitative review.
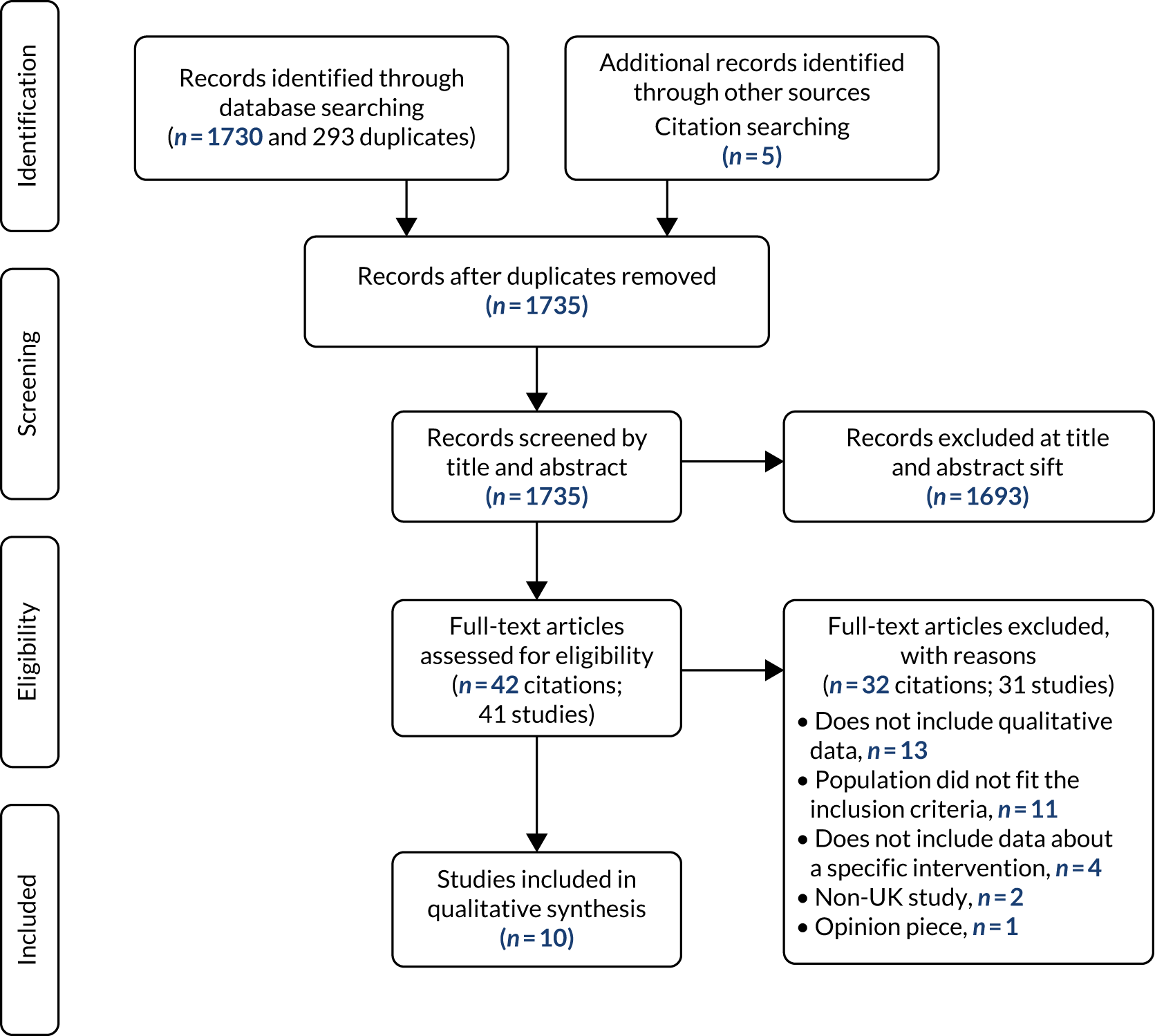
Study respondents
Eight studies assessed patients’ attitudes and three studies assessed HPs’ attitudes to the intervention (of these, two studies178,181 reported data from both patients and the HPs who had been involved in delivering the intervention). Altogether, the studies contained qualitative data from 130 patients and from 38 HPs. In terms of HPs, the data were specifically from 24 GPs, eight CBT therapists, three nurse therapists and three nurse therapist supervisors. A summary of HPs’ characteristics is shown in Table 7.
| First author and year of publication | Sample (contributing qualitative data) | Population being treated as described in the study | Data collection | Intervention |
|---|---|---|---|---|
| Burton, 2012157 | 11 patients | MUS | Interview | GP with special interest ‘symptoms’ clinic |
|
Chew-Graham, 2011179 Peters, 2011178 |
3 nurse therapists, 3 supervisors, 46 patients | CFS/myalgic encephalomyelitis | Semistructured interviews | Pragmatic rehabilitation and supportive listening |
|
Dowrick, 2008181 Peters, 2009180 (report different data from the study above) |
24 GPs 23 patients |
MUS | Semistructured interviews | Reattribution (by trained GPs) |
| Gerskowitch, 2015182 | 11 patients | MUPS | Semistructured interviews | CBT and mindfulness-based stress reduction |
| Graham, 2007183 | 6 patients | Somatisation | Self-reports – a series of open questions put to each patient in writing | Group counselling (humanistic) |
| Lewis, 2013184 | 8 CBT therapists | MUS | Semistructured interviews | Individual CBT |
| Morton, 2016185 | 17 patients | MUS | Semistructured interviews | GP with special interest ‘symptoms’ clinic |
| Payne, 2015186 | 16 patients | MUS | Case studies; qualitative data from a survey | The BodyMind Approach™ (Pathways2Wellbeing, University of Hertfordshire, Hatfield, UK) group intervention |
| First author and year of publication | Sample | Population being treated as described in the study | Sex | Age (years) |
|---|---|---|---|---|
| Peters, 2011178 | 3 nurse therapists, 3 supervisors | CFS/myalgic encephalomyelitis | Nurses = 3 women; NR for supervisors | NR for nurses and supervisors |
| Dowrick, 2008181 | 24 GPs | MUS | 16 female; 8 male | Three aged < 35; 14 between 35 and 50 and 7 > 50 |
| Lewis, 2013184 | 8 CBT therapists | MUS | Five female; three male | Mean 43.5 (SD = 9.04) (range 30–60) |
Respondent characteristics
Six studies focused on interventions for MUS/MUPS, one focused on interventions for CFS/myalgic encephalomyelitis and one focused on interventions for somatisation. The majority of patient participants met the criteria for MUS or MUPS (n = 78) as reported in the studies, with 46 patients diagnosed with CFS/myalgic encephalomyelitis and six who met the criteria for somatisation as reported in the studies. Reporting of patient characteristics was limited and incomplete in a number of studies. Details, where reported, are shown in Table 8. The general trend was that more women than men contributed data for the studies, and age varied widely, ranging from 19 to 84 years.
| First author and year of publication | Sample (contributing qualitative evidence) | Population being treated as described in the study | Sex | Age (years) |
|---|---|---|---|---|
| Burton, 2012157 | 11 patients | MUS | NR | NR |
|
Chew-Graham, 2011179 Peters, 2011178 |
46 patients | CFS/myalgic encephalomyelitis | 33 female; 13 male | Patients = mean 46.11 (range 20–73) |
| Gerskowitch, 2015182 | 11 patients | MUPS | 8 female; 3 male | Median age 50 (range 19–60) |
| Graham, 2007183 | 6 patients | Somatisation | NR | NR |
| Morton, 2016185 | 17 patients | MUS | NR | NR |
| Payne, 2015186 | 16 patients | MUS | 10 female; 6 male | Range 19–80 |
| Peters, 2009180 | 23 patients | MUS | 20 female; 3 male | Mean = 53 (range 32–84) |
For HP details, reporting of participant characteristics was also limited across the included primary studies. Again, more of the HPs who contributed data were women and the age of the participants ranged from 30 to 60 years, where reported.
Study setting
All interventions took place in primary care or in the community. One study reported on interventions that were delivered in patients’ homes,178,179 one in a primary care mental health trust,184 one in a primary care psychological therapies service,182 four in GP practices157,180,183,185,187 and one in a community setting. 186
Intervention description and facilitators
Three of the interventions described here were GP delivered; these included reattribution180,187 and special interest ‘symptoms’ clinic. 157,185 These interventions were delivered individually to patients and involved a series of structured consultations. Nurse-delivered interventions were reported in one study; these interventions were pragmatic rehabilitation, a therapist-facilitated self-management intervention178,179 and supportive listening,178 which were delivered individually to patients in their own home. Trained CBT therapists delivered one of the interventions investigated in two studies. 182,184 In one of these studies, the intervention that was delivered by a trained CBT therapist was described as high intensity182 and simply described as CBT in the other study. 184 A psychological well-being practitioner delivered a CBTLI intervention and a trained mindfulness-based stress reduction (MBSR) facilitator delivered a MBSR intervention in one of these studies. 182 All CBT interventions were delivered to patients individually, whereas the MBSR intervention was delivered in a group setting. The final two interventions included were also delivered in a group setting. 183,186 Group counselling (humanistic) was delivered by a facilitator described as a ‘group counsellor’ in one study,183 and the BodyMind Approach intervention was delivered by clinical psychologists together with facilitators who were psychotherapists or art therapists in the final study. 186
The reattribution intervention delivered by GPs180,187 was linked to the MUST trial,108 and the pragmatic rehabilitation and supportive listening interventions delivered by nurse therapists reported by Peters et al. 178 and Chew-Graham et al. 179 were linked to the Fatigue Intervention by Nurses Evaluation (FINE) trial. 111 Both of these trials are included in the quantitative review. A description of the interventions delivered in the included studies can be found in Table 9.
| First author and year of publication | Population being treated as described in the study | Intervention | Intervention provider | Intervention setting | Intervention duration | Individual or group |
|---|---|---|---|---|---|---|
| Burton, 2012157 | MUS | GP with special interest ‘symptoms’ clinic. The consultations were structured to first hear the patient’s experience of illness then to propose and negotiate constructive explanations of physical symptoms. These explanations were used as the basis for simple cognitive and behavioural actions to modify symptoms and their impact | GP | GP practice | Four appointments; the first was of 1-hour duration and the subsequent three lasted 20 minutes | Individual |
|
Chew-Graham, 2011179 Peters, 2011178 |
CFS/ME |
|
Primary care nurses trained to deliver the interventions | Patients’ homes | 90-minute session followed by 1-hour sessions on weeks 2, 4, 10 and 18. 30-minute telephone calls on weeks 3, 6, 8, 12 and 15 | Individual |
|
Dowrick, 2008181 Peters, 2009180 |
MUS | Reattribution – a structured intervention, designed to provide a simple explanation of the mechanism of a patient’s MUS, through negotiation and other features of patient-centred communication, and to be delivered during routine consultations | GP | GP practice | The time since the index consultation ranged from 8 to 55 weeks (mean 32 weeks) | Individual |
|
Gerskowitch, 2015182 Gerskowitch, 2015182 |
MUPS | CBT high intensity | HI-CBT therapist | Primary care psychological therapies service | Weekly 1-hour appointments. The median number of sessions attended was 17 (range 4–25) | Individual |
| CBT low intensity | Psychological well-being practitioner | Fortnightly with homework set between meetings | Individual | |||
| MBSR | Trained MBSR facilitator | An 8-week programme for 2 hours per week | Group | |||
| Graham, 2007183 | Somatisation | Group counselling (humanistic) | Group counsellor | GP practice | 1.5-hour weekly sessions for half a year | Group |
| Lewis, 2013184 | MUS | CBT | CBT therapists with a postgraduate diploma in CBT | Primary care mental health-care trust | Not specified | Individual |
| Morton, 2016185 | MUS | SCI – a structured series of consultations. The SCI comprises four key elements: recognition, explanation, action and learning | GP | GP practice | 3 or 4 consultations over a period of 6–8 weeks. The first lasts 50 minutes and subsequent consultations are shorter (15–20 minutes) | Individual |
| Payne, 2015186 | MUS | The BodyMind Approach, based on a biopsychosocial model derived from dance movement psychotherapy | Clinical psychologist/facilitators (psychotherapists or art therapists) | Community setting | 2 hours for 12 sessions over 8 weeks and other communication over a 12-month period. Total face-to-face contact is 27 hours | Group |
Quality of the included studies
The inclusion criteria for study design for the qualitative review were broad, in that any study presenting qualitative evidence was eligible. Therefore, it was evident at the outset that the majority of the included studies would not meet the quality criteria for qualitative research. Nevertheless, these data are important to assess the perceptions of patients and HPs who are receiving or delivering behavioural modification interventions for MUS. To this end, it is acknowledged that a number of the included studies did not have qualitative research aims as their primary aims. Furthermore, owing to journal word count limits, it may not have been possible to provide the level of detail relating to qualitative methods and analysis in the published papers that would be expected for qualitative research. Therefore, we have used an adaptation of the CASP assessment of study quality for qualitative studies to assess the included studies. This sought to provide some leeway in terms of reporting of the findings in order to account for studies with primary research designs that were not qualitative in nature. Studies were assessed in terms of the extent to which they met each of the seven CASP requirements. If the study met all seven requirements it was assessed as high quality, if it met six of the criteria it was assessed as moderate quality, and it was assessed as low quality if it met only five or fewer criteria. Results are presented in Table 10.
| Question | Yes/somewhat (N = 9 studies), % (n) | |
|---|---|---|
| 1 | Is the study qualitative research or does it provide qualitative data? | 100 (9) |
| 2 | Are the study context and aims clearly described? | 100 (9) |
| 3 | Is there evidence of research reflexivity? | 33 (3) |
| 4 | Are the sampling methods clearly described and appropriate for the research question? | 89 (8) |
| 5 | Are the methods of data collection clearly described and appropriate to the research question? | 89 (8) |
| 6 | Is the method of analysis clearly described and appropriate to the research question? | 67 (6) |
| 7 | Are the claims made supported by sufficient evidence (i.e. Did the data provide sufficient depth detail and richness)? | 56 (5) |
Certainty of the review findings: CERQual assessment
The CERQual assessment relied on the assessment of the methodological quality of each study contributing to the review finding, as assessed by CASP. The relevance of the individual studies contributing to the review finding was assessed by considering both the format of the intervention (whether it was individual or group based) and the facilitator who delivered the intervention (whether a GP, nurse therapist or psychological therapist). As the review inclusion criteria specified that the setting was primary care or community based, this criterion was not considered in the CERQual analysis of relevance. The coherence of each review finding was assessed by considering if all the data contributing to that finding supported the finding and whether or not there were any ambiguities or any plausible alternative explanations. Finally, the adequacy of the data was assessed by considering the richness and number of data supporting each review finding. The synthesis of evidence from patients yielded 22 findings overall. Only one finding was assessed as high confidence, six findings were assessed as moderate confidence, 13 were assessed as low confidence and two were assessed as very low confidence. The evidence from HPs yielded 16 findings overall. Four findings were assessed as high confidence, eight as moderate confidence and four as low confidence. The results of the CERQual assessment are set out alongside each review finding in Tables 11 and 12.
| Meta theme | Theme | Studies (first author) contributing to the finding | CERQual assessment of confidence in the evidence | Explanation CERQual assessment |
|---|---|---|---|---|
| Positive factors relating to behavioural modification interventions as reported by patients/what did you gain from being referred to a behavioural modification intervention. | ||||
| Support | Acceptance | Gerskowitch;182 Chew-Graham;179 Graham;183 Morton;185 Peters;180 Peters;178 Payne186 | High confidence | 6 studies, in general the studies were moderately well done. The finding was seen across most of the studies in the synthesis and across different intervention formats and facilitators. Included studies with thick data. Coherent data across the studies |
| Validation | ||||
| Empathy | ||||
| Being listened to | ||||
| Explanation leading to understanding | Accepting the treatment model | Gerskowitch;182 Chew-Graham179 | Moderate confidence | 2 studies, both of moderate quality, and including thick data. Evidence came from different intervention types, and different facilitators. Coherent data across the studies |
| Understanding the treatment model | Gerskowitch182 | |||
| Learning achieved/gains from the interventions | Self-management techniques | Gerskowitch;182 Graham;183 Morton;185 Payne186 | Moderate confidence | 4 studies of moderate to low quality. Evidence came from different settings. However, there were limited rich data. The data appeared to be coherent across the studies |
| Improved confidence | Graham;183 Payne186 | |||
| Improved communication with family and friends | Graham183 | |||
| Benefits from being part of a group (specific to group interventions) | Sharing experiences with other patients | Gerskowitch182 | Low confidence | 2 studies: one moderate quality with rich data and one low quality with thin data. Data were specific to group interventions. Coherent data across the studies |
| Learning from other patients | Gerskowitch;182 Graham183 | |||
| Factors reported as important, wanted or expected in behavioural modification interventions | ||||
| Balance between psychological and physical elements | Burton157 | Very low confidence | 1 one study of low quality with thin dataa | |
| Flexibility | Gerskowitch182 | Low confidence | 1 study of moderate quality with thick dataa | |
| Other factors such as diet/nutrition advice, the role of faith | Gerskowitch182 | Low confidence | 1 study of moderate quality with thick dataa | |
| Group-based treatment | Gerskowitch182 | Low confidence | 1 study of moderate quality with thick dataa | |
| More consultation time | Burton157 | Very low confidence | 1 one study of low quality with thin dataa | |
| More investigations | Peters180 | Low confidence | 1 study of moderate quality with thick dataa | |
| Explanation | Specialist knowledge of the symptoms | Gerskowitch;182 Peters180 | Moderate confidence | 2 studies, both of moderate quality with thick data. Data evident across different formats, and different facilitators. Coherent data across the studies |
| Explanation of the symptoms | ||||
| HPs’ understanding of the patient and symptoms | Reassurance | Peters180 | Low confidence | 1 study of moderate quality with thick dataa |
| Relationship with the GP | Peters180 | |||
| Learning skills to deal with the symptoms | Self-management techniques | Gerskowitch;182 Peters180 | Moderate confidence | 2 studies, both of moderate quality with thick data. Data evident across different formats, and different facilitators. Coherent data across the studies |
| Support for learning | ||||
| What patients did not like about (being referred to) behavioural interventions | ||||
| It made things worse/did not make any difference (adverse effects) | Frustration – things are not getting any better | Gerskowitch182 | Low confidence | 3 studies of moderate quality. Coherence is unclear as findings within the theme are diverse, thick data, consistent across different formats and facilitators |
| Negativity of the intervention | Gerskowitch182 | |||
| Made symptoms worse | Gerskowitch182 | |||
| Inflexibility of the model/not workable in everyday life | Chew-Graham;179 Peters180 | |||
| HPs’ lack of understanding | HP does not understand | Peters180 | Low confidence | 2 studies, both moderate quality, only one with thick data. Specific to, GP-delivered, individual interventions. Coherent data across the studies |
| Feeling of being blamed by the GP | Morton185 | |||
| It ended | A feeling of loss when the intervention ends/lost a friend | Peters;178 Chew-Graham179 | Low confidence |
1 study of moderate quality with thick dataa This finding was only seen in the one included study of patients with CFS and may only be specific to this group |
| Conflicts between HPs and patients | Intervention asserted as the only right answer | Chew-Graham179 | Low confidence |
1 study of moderate quality with thick dataa This finding was only seen in the one included study of patients with CFS and may only be specific to this group |
| Patients felt the intervention did not address their symptoms | Peters178 | |||
| A belief exercise is damaging despite HP advice | Chew-Graham179 | |||
| Barriers – why patients did not want behavioural interventions/or could not engage with them | ||||
| Lack of choice | Lack of information/choice given by referrers | Gerskowitch182 | Low confidence | 1 study of moderate quality with thick dataa |
| Sceptical of HPs | GPs aim is to assert problems are psychological | Burton157 | Moderate confidence | 4 studies, three of moderate quality, one low quality, three with thick data, across different intervention formats and facilitators. Coherent data across the studies |
| Mention of psychosocial problems diverts GPs attention from other problems (so should not mention them) | Peters180 | |||
| Simplistic explanations | Gerskowitch;182 Peters180 | |||
| Disagreements with HPs that illness is physical | Peters178 | |||
| Physical limitations | Cannot physically undertake the intervention | Gerskowitch182 | Low confidence | 1 study of moderate quality with thick dataa |
| HPs’ lack of knowledge/skill at treating the symptoms | GPs are unskilled | Peters180 | Moderate confidence | 2 studies, both moderate quality and with thick data, across different intervention formats and facilitators. Coherent data across the studies |
| Nurse therapists are novices | Peters178 | |||
| Patients beliefs that you should deal with it yourself | Patients should self-manage | Peters180 | Low confidence | 1 study of moderate quality with thick dataa Specific to a GP-delivered intervention |
| Inappropriate to discuss psychosocial problems (with GP) | Peters180 | |||
| Stigma related to psychosocial problems | Peters180 | |||
| Meta theme | Theme | Studies (first author) contributing to the finding | CERQual assessment of confidence in the evidence | Explanation CERQual assessment |
|---|---|---|---|---|
| Positive factors relating to behavioural modification interventions as reported by HPs/what did you gain from being trained to and/or delivering a behavioural modification intervention? | ||||
| Training and supervision was useful | Supervision in managing tensions | Peters178 | Moderate confidence | 2 studies, both of moderate quality, both including thick data. Evidence came from different intervention types with different facilitators. Coherent data across the studies |
| Therapist peer support | Peters178 | |||
| Increased GPs’ awareness and altered perceptions | Dowrick181 | |||
| Addressed professional and/or training needs | Dowrick181 | |||
| Extended knowledge and skill of the HP | Learning and applying boundaries of their role | Peters178 | High confidence | 3 studies: one high quality and two of moderate quality. All three including thick data. Evidence came from different intervention types with different facilitators. Coherent data across the studies |
| Flexibility of the therapist | Peters;178 Lewis184 | |||
| Increasing confidence in discussing MUS | Dowrick181 | |||
| Helped structure MUS consultations | Dowrick181 | |||
| The primary care/community setting was helpful | Secondary care may support a belief in a physical cause | Dowrick181 | Moderate confidence | 2 studies, both of moderate quality, both including thick data. Evidence came from different intervention types with different facilitators. Coherent data across the studies |
| Tool to protect patients (from secondary care) | Dowrick181 | |||
| Primary care allowed a more tailored approach | Peters178 | |||
| Being in patients’ homes was helpful in building a therapeutic relationship | Peters178 | |||
| Rewarding experience | Rewarding when patients engaged | Peters;178 Lewis184 | High confidence | 2 studies, one high quality, one of moderate quality, both including thick data. Evidence came from different intervention types with different facilitators. Coherent data across the studies |
| What did not help or were detrimental to the patients or delivery of the intervention? | ||||
| When HPs felt that they were a novice or did not have the required skill levels | Being a novice therapist/lack of experience | Peters;178 Lewis184 | High confidence | 2 studies, one high quality, one of moderate quality, both including thick data. Evidence came from different intervention types with different facilitators. Coherent data across the studies |
| Anxiety because of a lack of training/knowledge | Lewis184 | |||
| Unfamiliarity with MUS | Lewis184 | |||
| No specific MUS model to work with | Lewis184 | |||
| Not as comfortable with mental health aspects of the interventions (as physical health) | Peters178 | |||
| When HPs struggled to deal with their own or patient emotions | Not dealing well with failure | Peters178 | Moderate confidence | 2 studies, both of moderate quality, both including thick data. Evidence came from different intervention types with different facilitators. Coherent data across the studies |
| Pessimism (from HP) about dealing with MUS | Lewis184 | |||
| Angry patients | Peters178 | |||
| HPs’ anxieties that the intervention may have detrimental consequences for the patients | Nurse therapists worries about the interventions consequences | Peters178 | Moderate confidence | 2 studies, both of moderate quality, both including thick data. Evidence came from different intervention types with different facilitators. Coherent data across the studies |
| Could increase patient dependency | Dowrick181 | |||
| Too much complexity | Difficulty of applying when the patients have multiple symptoms/complaints | Dowrick181 | Low confidence | 1 study of moderate quality with thick dataa |
| The community setting was unhelpful | Difficulties of being in the patients’ home | Peters178 | Low confidence | 1 study of moderate quality with thick dataa |
| It’s nothing new (neutral effects) | Ride it out (when the intervention is not addressing needs and both parties know it) | Peters178 | Moderate confidence | 2 studies, both of moderate quality, both including thick data. Evidence came from different intervention types with different facilitators. Coherent data across the studies |
| Nothing new (HPs felt that they were already doing it) | Dowrick181 | |||
| Barriers – from the perspective of HPs why patients did not want behavioural interventions/or could not engage with them, or barriers to delivery of the intervention | ||||
| Resource constraints | Not enough time | Peters;178 Dowrick181 | Moderate confidence | 3 studies, all of moderate quality, both including thick data. Evidence came from different intervention types with different facilitators. Coherent data across the studies |
| Other time constraints/competing pressures | Dowrick181 | |||
| Other pressures go against applying reattribution (medicolegal) | Dowrick181 | |||
| Lack of clarity on service provision for MUS | Lewis184 | |||
| Patient beliefs | Patients’ belief in a physical cause | Dowrick181 | High confidence | 3 studies: one high quality and two of moderate quality. All three including thick data. Evidence came from different intervention types with different facilitators. Coherent data across the studies |
| Patients benefit from their symptoms (an agenda – secondary gain) | Dowrick181 | |||
| Patients have an agenda (e.g. target the locum)/patients’ pre-existing beliefs/an agenda | Dowrick;181 Lewis184 | |||
| Patients’ beliefs about not being able to do physical activity | Lewis184 | |||
| Patients’ resistance to intervention/patients did not want to engage with the model | Peters;178 Lewis184 | |||
| HP skill, beliefs and attitudes | Some GPs more skilled than others | Dowrick181 | Low confidence | 1 study of moderate quality with thick dataa |
| GPs’ prior expectations of patients | Dowrick181 | |||
| GPs’ mood | Dowrick181 | |||
| Personality clash (between HPs and patients) | Dowrick181 | |||
| Patient barriers | Patients not able/willing to share | Dowrick181 | Moderate confidence | 2 studies: one of high quality and one of moderate quality. Both including thick data. Evidence came from different intervention types with different facilitators. Coherent data across the studies |
| Patients’ physical difficulties were barriers to attendance and adherence | Lewis184 | |||
| Other factors | Not knowing if it is actually MUS | Dowrick181 | Low confidence | 1 study of moderate quality with thick dataa |
| Factors reported as important, wanted or expected for training in and delivery of behavioural modification interventions | ||||
| More training and supervision required | Supervision | Dowrick;181 Lewis184 | Moderate confidence | 2 studies: one of high quality and one of moderate quality. Both including thick data. Evidence came from different intervention types with different facilitators. Coherent data across the studies |
| More training | Lewis184 | |||
Synthesis of patient and health professional evidence
Findings were synthesised across all intervention types and organised in accordance with the questions outlined in the data extraction framework items as detailed in the methods section. The findings of the synthesis have been summarised and are presented in Figure 58 to demonstrate the expectations, perceived barriers and facilitators, and potential outcomes of the interventions. Thus, the figure represents the experience of having received the interventions rather than the anticipation of them. Within these, a number of important themes emerged. Each metatheme, together with subthemes where applicable, with examples and an estimate of the strength of the evidence, is presented in Tables 11 and 12. The themes are synthesised further within the following narrative synthesis. As illustrated in Table 11, the synthesis of evidence from patients yielded 22 findings overall. Only one finding, ‘support’, was assessed as high confidence and was derived from six studies, in which the quality was judged to be moderate, and the finding was seen across most of the studies in the synthesis and across different intervention formats and facilitators. Six findings were assessed as moderate confidence, with these each including evidence from more than one study, with some thick data. In addition, the overall quality was at least moderate, with coherence across different studies. Thirteen findings were assessed as low confidence and two as very low confidence, with evidence coming from only one study for each finding and, therefore, this paucity of evidence should be taken into account when interpreting the synthesis findings. The evidence from HPs yielded 16 findings overall. Four findings were assessed as high confidence, with evidence emerging from two or more studies, including some thick data. They were of moderate quality, and had coherence across studies. Eight were assessed as moderate confidence, with evidence coming from at least two studies (of moderate quality), including thick data and with coherence across studies. Finally, four studies were assessed as low confidence, with evidence only coming from one study for each finding and, again, the paucity of the evidence for these findings should be taken into account during interpretation.
FIGURE 58.
Patients’ and HPs’ perceptions of behavioural interventions for MUS in primary care settings. Model to show expectations, perceived barriers and facilitators, and potential outcomes, based on evidence from included studies.
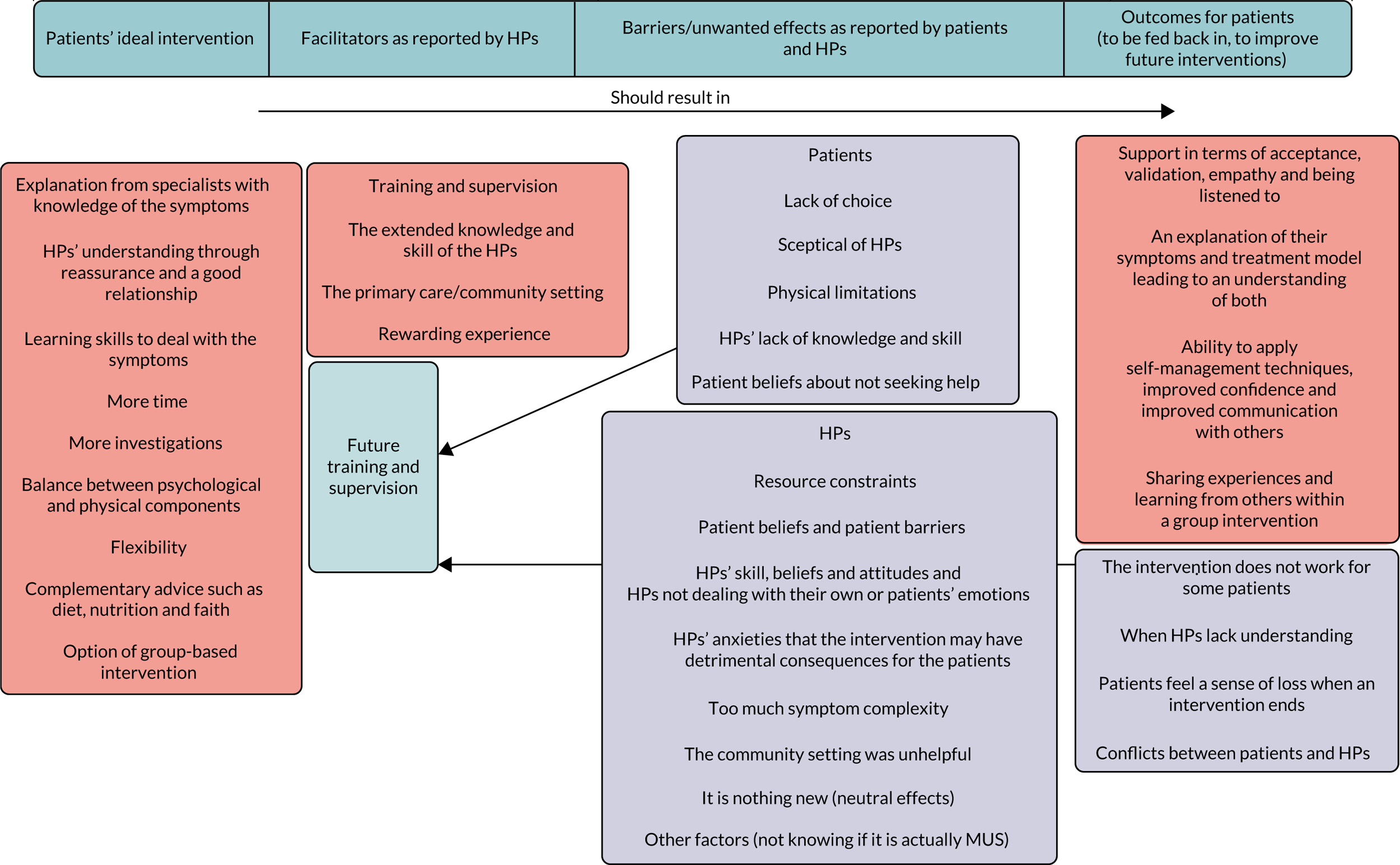
Factors identified as important in primary care-delivered behavioural modification interventions for medically unexplained symptoms from the perspective of patients who had received the interventions
Support
Support was defined by patients as being accepted and validated by HPs and fellow intervention participants, receiving empathy and being listened to. This was found across an array of intervention types and there was high confidence in this finding. 178,180,182,183,185,186 This type of support was described as the most positive part of the pragmatic rehabilitation intervention in one study, with ‘being believed and feeling understood by the therapist’ as a key part of the intervention. 179 Patients across various intervention types reported valuing a feeling of being understood and validated by the HP. 179,182 This was sometimes as a result of the knowledge that the HP had about the patient’s symptoms, which gave them a sense of having someone ‘on their side’. 180,182,185 In some instances, it appeared that no one else in their lives was able to provide such support, ‘It was just an understanding from her that I didn’t, haven’t had from anybody else’ (patient). 179 One patient reporting that the empathetic nature of the nurse delivering the supportive listening intervention was their most valued attribute. 178 This feeling of being understood also came from fellow participants with similar symptoms, as part of group interventions. 182,183,186 These factors were reported as key to patient engagement and contributed to whether or not the interventions were reported as acceptable to the participants. 179 Some participants thought that the ‘extra time’ afforded by the interventions allowed these aspects of support to be accessed. 185
Explanation
Patients also clearly valued explanations that they had been provided with as part of the interventions, and reported that this led to accepting and understanding the treatment model,179,182 with moderate confidence assessed in this finding. Patients felt that the pragmatic rehabilitation intervention helped them to come to terms with and accept a diagnosis (of CFS) and that having an explanation and understanding of their symptoms was key to this. ‘She explained all about CFS and the physiology of it really, which was the first time really that I understood why my energy was so low, so that made a lot of sense’ (patient). 179 Gaining new knowledge about their symptoms was reported to be reassuring to patients, enabling them to accept the idea that the pragmatic rehabilitation intervention might be appropriate for them and, therefore, facilitated the progress made with the intervention. 179 Similar factors were also identified in the data about what patients wanted from an intervention. Patients reported that they consulted their GP to seek an explanation for their symptoms180 and took part in interventions to see someone who had specialist knowledge and information about their symptoms. 182
Important intervention elements for the delivery and success of primary care-delivered behavioural modification interventions for MUS from the perspective of patients and health professionals
Intervention elements
An important feature of the evidence from patients was the reported benefit that they had gained from the behavioural self-management techniques that they had learned. This was evident across four of the studies that included the following interventions, with participants commenting on their improved confidence and improved communication with significant others: CBT, mindfulness, group counselling, GP interventions and the BodyMind Approach intervention. 182,183,185,186 This also emerged in the evidence around what was wanted or needed as part of any future intervention, with patients saying they needed to learn skills such as self-management techniques to deal with the symptoms and to have the support for learning such techniques. 180,182 Specific to group interventions, patients found sharing their experiences with other patients182 and learning skills from other patients182,183 valuable as part of the intervention.
A number of additional elements were suggested by patients in single studies as potentially important as part of any intervention for MUS. These elements included having a balance between the psychological and physical elements of an intervention in one GP-delivered intervention study,157 and incorporating other factors, such as diet and nutrition advice and the role of faith, in the management of symptoms in another study. 182 Patients also reported that flexibility in accessing the therapy was important to them in one study,182 as was the availability of group-based treatment. 182 Specific to a GP-delivered study, patients wanted more consultation time,157 which, in comparison with standard care, most of the behavioural interventions detailed here provided. Again specific to a GP-delivered intervention, some patients simply wanted to have further investigations. 180
Health professional training and supervision
From the point of view of the HPs, training and supervision in applying behaviour modification interventions was reported as helpful in two studies178,187 and was also recommended as useful for future training in two studies. 184,187 Supervision was reported as ‘fundamental’ and as key to resolving difficulties that might arise between the deliverer of the intervention and the patient receiving the intervention in a nurse therapist-delivered intervention. 178 Having the support of peers who were delivering the same intervention was also valued, ‘If we were having a really difficult time with a certain patient, then we would sort of pool ideas, and ask advice how they would cope with it, the other nurse therapists or what do they think is going on’ (nurse). 178 GPs delivering a reattribution intervention found the training useful in that it increased their awareness of MUS and suggested it ‘altered my perception a bit, it’s easy to get stale and view that group of patients as difficult or troublesome or irksome at times because we’re not always at our best every time (GP). 187 GPs also reported that it addressed their training needs and allowed them the opportunity it compare consultation skills with colleagues. 187
Primary care and community setting
The primary care or community setting was reported to be a helpful factor by the HPs in two studies. In one study, the reasons for this were that the primary care setting provided a tailored approach, and the setting (e.g. being in patients’ homes) was useful when trying to develop a therapeutic relationship. 178 In another case, this contrasted with the perceived failing of the secondary care setting. 187 ‘You see these people getting referred to the hospital with back pain and the next thing you know some bright spark is going to operate on them and you think ‘What!’ . . . Maybe we’re here in a way as a gateway to try and prevent harm as well as anything else’ (GP). 187 This appears to indicate that primary care practitioners see part of their role as protecting their patient from entering secondary care when they believe this is unnecessary. Although the evidence pointed towards favourable views regarding the primary care and community setting, it should be considered that the home setting could also be a source of difficulties (e.g. issues with privacy and interference from family members), but this finding was specific to the intervention for CFS/myalgic encephalomyelitis. 178
Important facilitating factors for intervention success by patients and health professionals
Good relationships
It was important that the HPs delivering an intervention had an understanding of the patients and their symptoms. Specifically, the patients in one study reported needing reassurance and a good relationship with the person delivering the intervention. 180 Patients liked the fact that they had a longstanding relationship with the HP. In a reattribution intervention, this gave them a feeling that they knew what type of treatment, if any, would be suitable for them: ‘He knows I like to keep myself to myself, knows I believe in self-help . . . knows I’m somebody that likes to work it out for myself’ (patient). 180 Others simply appreciated the understanding and reassurance they received from the HP and just wanted an opportunity to share their difficulties. 180
Health professional knowledge and skill
Health professionals across three different interventions reported that they found being involved in delivering behaviour modification interventions helped them to develop their knowledge and skills in the area of MUS. 178,184,187 This training helped them learn about the boundaries of their own role178 and to be flexible when delivering interventions. 178,184 GPs reported being able to structure consultations in an appropriate way for MUS and that the intervention, in this case reattribution, provided this structure and increased their confidence in discussing MUS with patients. 187 Although acknowledging that there can be difficulties in delivering MUS interventions, CBT therapists184 and nurse therapists178 both reported that it can be rewarding when it is evident that patients have gained benefit from the intervention.
Factors identified as barriers to intervention success by patients and health professionals
Difficult relationships
At the same time as good relationships facilitating intervention success, difficult relationships between patients and HPs appeared to undermine progress, and this was reported across five studies. Some patients, taking part in a reattribution intervention, felt that there was a lack of understanding on the part of the HP, with simplistic causes and resolutions to problems being proffered. 180 Sometimes, reported specifically in one GP-delivered intervention study, this extended to patients feeling that they were being blamed by the GP. 185 Specific to the intervention study for patients with CFS/myalgic encephalomyelitis, the relationship between HPs and patients also sometimes led to conflict, in some cases patients felt the HPs were asserting the intervention (in this case pragmatic rehabilitation) as the only right answer, and patients disagreed with this point of view, ‘I think my main reason is the fundamental theory behind it [the treatment model offered] just disregards it as illness’ (patient). 179 There was also a feeling from patients that some heath professionals were unskilled or lacked the knowledge to deal with their symptoms or provide appropriate intervention. 178,180
Patients in a GP-delivered intervention study also reported being sceptical of HPs, believing that the aim was to assert that their problems were psychological,157 and some patients reported having disagreements with their HP regarding the physical nature of their symptoms in an intervention for patients with CFS. 178 Patients were also sceptical that they would only be provided with simplistic explanations for their symptoms,182 and that if they were to mention any psychosocial problems this would divert the HP’s attention away from other problems associated with their symptoms. 180 Specific to a GP-delivered intervention, GPs reported that there might be a personality clash between them and their patients, meaning that insufficient rapport is built for reattribution to be successfully delivered. 187 Other factors reported by HPs included patients not being able or willing to communicate with their GP. 187
Attitudes and beliefs
In one study, some patients simply felt that the intervention did not address their symptoms and that they could not believe in the intervention,178 contrary to the HP view. It was also reported that several patients held a belief that an activity (as part of the pragmatic rehabilitation intervention) could be damaging to them, despite the fact that it was described in the intervention manual and recommended by the HP delivering the intervention. 179 Patients reported that the lack of information given to them by those who referred them meant that they did not know the remit of the intervention, and it was also reported that patients felt that the referring GP did not know what the intervention entailed. Patients were therefore surprised about the content of the intervention and found it difficult to see why they had been referred to a psychological therapy-based intervention when their problems were physical. 182 Furthermore, evidence suggested that some patients may hold the belief that they should deal with the symptoms themselves, and that they should self-manage without the input of HPs. 180 Patients had their own ideas around what they should be doing to self-manage: ‘I’ve started knitting – gets my mind occupied’ (patient). 180 Further barriers came from an opinion that it is inappropriate to discuss psychosocial problems (with the GP)180 and the idea of there being a stigma related to reporting psychosocial problems. 180 In addition to these beliefs, patients also reported physical limitations that represented barriers to physically undertaking the intervention. 182
Health professionals also reported that they felt patient beliefs could be significant barriers to engagement with behavioural modification interventions. 178,184,187 HPs described, and some appeared to expect, patients to have a belief in a physical cause. 187 HPs were reported in one reattribution study to suggest that this belief was a learned behaviour to deal with unhappiness. 187 HPs also reported in two studies that patients could be resistant to the intervention or the treatment model itself. 178,184 Furthermore, CBT therapists reported that patients sometimes held a belief that they were not able to take part in aspects of interventions that required physical activity, despite HPs’ reassurances otherwise. 184 Finally, it was suggested by HPs that patients might be benefiting materially from their MUS symptoms, in terms of family support and state benefits, which might have an impact on their willingness to engage with an intervention. 187
Health professionals’ lack of experience and skills
Nurse therapists and CBT therapists who had been trained to deliver MUS-specific interventions felt that they were novices and lacked the experience to deliver the interventions in two separate studies. 178,184 It was reported that they did not have a specific MUS model to work with, and they were unfamiliar with the symptoms. 184 Furthermore, they experienced anxiety because of this lack of training and experience in MUS184 and were not comfortable dealing with the mental health aspects as compared with the physical health aspects of the interventions they were delivering. 178 This also emerged as a barrier to service provision, with GPs acknowledging that the successful application of reattribution may be dependent on variations in the communication skills of the practitioner delivering the intervention. 187
Difficulty of dealing with emotions
Patient and HP emotions emerged as a source of difficulty in delivering MUS interventions in two studies. 178,184 Nurse therapists found at times that they did not deal well with failure, ‘One common theme I think with has come up is the difficult of accepting that you can’t get it right all the time’ (supervisor). 178 Sometimes patients became angry when an intervention could not address their needs, and this was also a source of difficulty for nurse therapists. 178 Conversely, some CBT therapists reported a level of pessimism when faced with patients with MUS. 184
Constraining factors
Health professionals reported that resource constraints, such as time constraints, and impositions about what data needed to be collected during a consultation presented barriers to delivering interventions in two studies. 178,187 The concerns regarding time constraints were associated with each consultation187 and also with the length of the course of therapy, with concerns expressed that too few sessions were available to deal with deep-seated issues. 178 Other constraining factors reported by HPs included physical difficulties preventing patients attending and adhering to interventions. 184
Problems of diagnosis
The GPs were also concerned about medicolegal issues in one study, such as overdiagnosing and overtreating patients. 187 It was also reported that a lack of information about service provision may have lowered the referral rate in another study. 184 Other constraining factors included situations in which HPs were unsure that the symptoms were actually medically unexplained,187 or in which there was too much symptom complexity. 187
Potential unwanted or adverse effects on patients as reported by patients and health professionals
The HPs in two studies reported that they had concerns that the intervention might be detrimental to patients. 184,187 These worries took the form in one case with a reattribution intervention that patients might form a dependent relationship with the GP and become reliant on them. 187 In another case, these worries took the form of the impact of the intervention (pragmatic rehabilitation and supportive listening) possibly being negatively felt in wider aspects of the patients’ lives. 184
Some patients considered that the psychological interventions made things worse, or were not making things any better in one study. 182 This manifested itself in the form of frustration in some cases,182 whereas, in others, patients found the intervention model negative in nature. 182 Some patients with CFS found the pragmatic rehabilitation intervention model inflexible and, therefore, were unable to make it work in everyday life. 179,180
Where good relationships were established between the two parties, as in a study of an intervention for CFS/myalgic encephalomyelitis, patients reported finding it difficult when the intervention came to an end, experiencing a feeling of loss when support was withdrawn. 178,179
In some cases, it was felt that the intervention was not suited to the patient and that both the HP delivering the intervention and the patient receiving the intervention had come to this realisation but both parties followed through with it despite this. 178 In another case, HPs felt that the intervention training on reattribution offered them nothing new and that they were already providing it in their consultations. 187
Table 13 shows a summary of the key findings.
| Patients | HPs | |
|---|---|---|
| Valuable results from intervention participation or training | Gaining support being validated | Developing knowledge and skills around MUS |
| Explanation | ||
| Support for self-management | Rewarding when patients engaged | |
| Facilitators | Good relationships between patients and HPs | Training and supervision |
| Primary care or community setting | ||
| Barriers | Patient attitudes and beliefs | Lack of confidence in their own skills and abilities to deal with MUS |
| Poor relationship with HPs | Patient attitudes and beliefs | |
| HP attitudes and beliefs | ||
| Resources constraints | ||
| Adverse effects | It ended | Detrimental intervention consequences for patients |
| Conflicts between HPs and patients, and HPs’ lack of understanding | Patient and HP emotions |
Discussion of the qualitative review
This review presents patients’ and HPs’ perspectives on the acceptability, relative benefits and potential harms of primary care or community-based behaviour modification interventions for MUS. The findings offer insight into what aspects of the interventions patients and HPs found helpful, what was unhelpful and what were the barriers to participation or intervention success, which could all contribute towards an understanding of what might make a more successful intervention.
Although the quality of the study reports included in the review was not universally high, studies were in general suitable for the purpose of the review. Although the quality of the studies would have been increased by limiting our review to studies that could be identified as qualitative research (i.e. using both accepted methods of qualitative data collection and data analysis), important data may have been missed had this criterion been applied.
The findings of the synthesis showed that, across all interventions, what patients thought was helpful was gaining support. Patients found being accepted and validated by the HP (and also other intervention participants, in the case of group interventions), together with receiving empathy and being listened to, helpful as part of an intervention. Patients also valued receiving an explanation for their symptoms and appeared to find interventions that offered this to be helpful. In terms of practical intervention elements, an important feature was the gains made from the self-management techniques they had learned, and patients reported that support for learning such techniques was important. The progress and perceived helpfulness of the intervention appeared to be facilitated by a good relationship between patients and the HPs delivering the intervention. In terms of findings relating exclusively to GP-delivered interventions, patients reported that helpful elements of an intervention included having a balance between psychological and physical elements,157 more consultation time157 and, in one study, further investigations. 180
Patients’ own attitudes and beliefs appeared to be potential barriers to their participation in the intervention and its success, with some patients reporting that they did not believe in the treatment model or found it unworkable, or had a belief in dealing with problems themselves. It also appeared that conflicts between HPs and patients could impede success. A small number of findings related exclusively to the intervention study for patients with CFS/ME. Patients reported finding it difficult when the intervention came to an end, experiencing a feeling of loss when support was withdrawn. 178,179 They also reported that the relationship between HPs and patients could sometimes lead to conflict – in some cases patients felt that the HPs were asserting the intervention (in this case pragmatic rehabilitation) as the only right answer and disregarded the patient’s point of view. 179 Specifically relating to GP-delivered interventions, patients reported that they felt that there was a lack of understanding from the GP,180 and they also reported a feeling of being blamed by the GP. 185 Again relating to GP-delivered interventions, the evidence suggested that some patients may hold a belief that you should deal with the symptoms yourself and that they should self-manage without the input of HPs. 180
Evidence from HPs described how they found being trained or delivering the interventions helped to develop their own knowledge and skills around MUS, and they reported that the experience was rewarding when patients engaged with them. They found important facilitators were training and supervision for the interventions and found primary care or the community an appropriate and helpful setting for the delivery of the intervention. Barriers to successful delivery of the intervention(s) were reported to include a lack of confidence in their own skills and abilities to deal with MUS, patient attitudes and beliefs that went against the intervention, their own attitudes and beliefs and resource constraints. HPs were also worried that the interventions might have inadvertent detrimental consequences for patients, and that they might be ill-equipped to deal with their own and the patient’s emotions. Although the evidence indicated favourable views regarding the primary care and community setting, it should be considered that the home setting could also be a source of difficulties (e.g. issues with privacy and interference from family members), but this finding was specific to the intervention for CFS/myalgic encephalomyelitis. 178
Barriers reported specifically from GP-delivered interventions included GPs feeling that there was too much condition complexity,187 GPs’ skills, beliefs and attitudes sometimes not helping,187 and GPs, on some occasions, not knowing if it was actually MUS did not help in the delivery of the intervention. 187
The implications of the findings suggest that, although a number of patients found the interventions helpful, with a number of key helpful factors that could inform the development of a future intervention, a minority did not find the intervention helpful or did not want to take part in the intervention at all. This links to one of the barriers to taking part in or engaging with interventions, which was reported as a lack of information and choice given by referrers. If patients do not have the information that they need to make an informed choice, it is less likely that the intervention will be suitable for them. Therefore, this requires consideration of the matching of intervention type to patients where possible. Other barriers that would need to be addressed in any future intervention include patients’ scepticism of HPs, with patients reporting disagreements with HPs regarding the nature of their symptoms, and an expectation that simplistic explanations will be provided. Patients also reported in some cases that they were not convinced that the HPs delivering the intervention had an appropriate level of knowledge and skill. Further barriers included physical limitations, problems of stigma around asking for help and a belief in dealing with problems oneself. A further consideration for all interventions, but specifically evidenced here from the patient evidence on the intervention for CFS/myalgic encephalomyelitis,178,179 is continuity of care from the same HP or team and that interventions should not end suddenly or without adequate follow-up.
Limitations
Limitations include the fact that some of the included studies were of moderate or low quality, as assessed using CASP,174 and that confidence in some of the findings was assessed as moderate or low using the CERQual assessment. 169 Word limits imposed by journals may have contributed to this. Such limitations may result in a lack of rich data consistently across all studies, limiting (to some degree) the interpretations that can be made, particularly for some of the minor themes identified. Although the metathemes identified were supported by a number of studies and were supported by the CERQual assessment, a number of other findings reported here did not offer the same strength of evidence. In addition, although the validity of these findings should not be understated, it may be the case that further research is required to ascertain their generalisability and importance in the development of future interventions. A further limitation concerns the inclusion criteria for the qualitative review. The scope of the qualitative review was to present evidence about the experience of the interventions rather than the anticipation of them; therefore, the data included were in the main from patients who had agreed to take part in an intervention. Evidence about the general management of MUS was not included in the qualitative review but these data did meet the inclusion criteria for the realist synthesis.
Summary of the findings of the qualitative review
-
Both patients and HPs reported positive gains from taking part or delivering interventions.
-
A number of reported barriers appeared to be underpinned by the relationship between the patients and HPs delivering the intervention, and by beliefs and attitudes held by both parties.
-
Both positive and negative experiences of the primary care setting were reported.
-
Detrimental effects of the intervention were associated with an abrupt end to the intervention and frustration attributable to symptoms not improving.
-
Some patients and HPs did not feel it could add anything for them.
Combining the quantitative and qualitative findings
The quantitative review did not consistently reveal one intervention as more successful than any other across the various outcomes, with the exception of GP-delivered interventions, which were rarely successful. Therefore, as suggested in the qualitative evidence, considered matching of intervention type to patients, taking into account patient preferences, should take place. Further to this, the qualitative evidence showed that patients’ own attitudes and beliefs may be barriers to intervention participation, with some patients reporting that they did not believe in the treatment model, found it unworkable or had a belief in dealing with problems themselves, again giving support for careful matching of intervention to patient. Although not frequently reported in the trials of clinical effectiveness, this theme was sometimes reflected in the numbers of eligible participants declining to take part, with reasons including beliefs that the interventions would not work, or would exacerbate symptoms.
Although the quantitative findings did not show that the GP-delivered interventions were generally effective, the qualitative review demonstrated that patients found that the GPs’ understanding of them and their symptoms and a good relationship with them was an important part of a successful intervention. However, the qualitative review also demonstrated that a key barrier for patients taking part in interventions, including those that were GP delivered, was a scepticism regarding the deliverer. Specifically, some patients reported disagreements with GPs regarding the physical or psychological nature of their symptoms and also that sometimes simplistic explanations were proffered by GPs.
Evidence outlined in the review of cost-effectiveness demonstrated a large variation in the number of patients recruited by GPs between studies. Evidence from the qualitative review showed that some HPs found delivering the interventions to be a rewarding experience, and it might therefore be assumed that such HPs would be more likely to recruit patients. Others had a contrasting view, that the training they were given for MUS interventions was nothing new, and some reported that they found it difficult to deal with failure and were ill-equipped to deal with angry patients. Some HPs worried that it could increase dependency and that it would be difficult to apply when symptoms were complex. Other factors that may prevent HPs from recruiting to interventions include resource constraints, medicolegal concerns and a lack of clarity around service provision. HPs were also concerned that it was not always clear that it was actually MUS that the patients had, and they wanted more training and supervision.
Findings from the cost-effectiveness review also demonstrated a large variation in the number of sessions the patients attended both within and between studies. Evidence from the qualitative review may provide explanations for this; for example, there were a number of things that patients felt that they did not like about the intervention or were barriers to them taking part or continuing with it. These factors included frustration that things were not getting any better after attending and finding the rationale of the intervention negative and that they could not work it into their everyday life. They also reported feeling that the HP did not understand, or that the HP was blaming them. There were also conflicts reported between HPs and patients, and a reported lack of understanding from the HP. This may include patients losing faith in the intervention when it was asserted as the only right answer to their problems and that their needs were not addressed.
Chapter 5 The contribution of contextual factors to the success or failure of behaviour modification interventions for medically unexplained symptoms: realist synthesis
This chapter aims to provide an overview and analysis of the evidence for the contribution of contextual factors associated with the ongoing primary care consultation and the patient’s interaction with primary care professionals to the success or failure of behaviour modification interventions (‘behavioural interventions’) for MUS. Given the complexity of the phenomenon and the interaction between HPs for a variety of purposes and at multiple levels, the review team has undertaken a review utilising realist principles. Realist reviews particularly offer a lens or strategy by which complex interventions can be examined and analysed.
This realist synthesis on behaviour modification interventions for MUS draws on three main sources:
-
study ‘clusters’ of primary studies, linking UK quantitative and qualitative reports, identified from the effectiveness review and from the qualitative synthesis, to all other published accounts that share a study context
-
the qualitative synthesis conducted for this HTA, which focused on UK intervention studies only
-
published narrative and systematic reviews, particularly qualitative evidence syntheses, covering the entire primary care pathway from making an appointment through to potential referral to secondary care.
In addition, further systematic reviews, qualitative research and conceptual papers were examined as referenced by any of the above, offering productive ‘forays’ into the relevant literature.
Evidence identification
Study ‘clusters’ of primary studies
When exploring complex interventions, a review team must seek to gain as full an understanding as possible of the essential characteristics of the context and the intervention. One possible way of acquiring such an understanding is by examining papers and additional studies that have been conducted alongside an effectiveness study, either as part of an integrated mixed-methods study or as a ‘sibling study’. Sibling studies may include qualitative research studies, economic evaluations or process evaluations associated with specific RCTs, whereas additional papers may offer commentaries on the programme theory or contextual issues. Sibling and associated studies are particularly valuable because they offer additional insights beyond the reporting limitations of the key index paper ‘in explaining contextual factors that influence implementation and/or outcomes’. 58 The systematic searches reported in Chapter 3 identified 59 RCTs, of which 15 were UK-based trials and 10 were UK-based qualitative intervention studies. From this initial yield of 24 citations, including one mixed-methods paper that featured in both sets, 19 ‘clusters’ were formed to reflect a proportion of overlap of three RCTs (five papers) with qualitative papers. Each of the 24 citations was searched using the ‘cited by’ facility on Google Scholar (Google Inc., Mountain View, CA, USA) via Publish or Perish software (Harzing.com, London, UK)188 to retrieve a total of 1182 citations. These were manually checked to identify associated study reports. Other methods of identification included author searching, checking of websites, and trial name and number searching. A total of 80 additional papers were identified to augment the original 24 papers, making a total of 104 papers spread across 19 different clusters (see Appendix 2, Table 69).
Qualitative synthesis
Findings from the qualitative synthesis conducted for this HTA (see Chapter 4), which focused on UK intervention studies only, were examined in addition to details of the interventions and contexts with additional data being extracted to templates for reporting interventions (see Appendix 6).
Review-level evidence
Qualitative syntheses on MUS and associated conditions were identified from the study register of the Cochrane Qualitative and Implementation Methods Group together with systematic reviews and narrative reviews (see Appendix 2, Table 68) identified from the PubMed Reviews subset.
Formulate review question
The realist review was framed within the overall study objectives for the HTA as a whole. However, within this broader aim it sought to address the following specific question:
To what extent do contextual factors associated with the ongoing primary care consultation between the PCP (GP) and the patient, or the patient’s interaction with other primary care professionals, collectively contribute to the success or failure of behavioural interventions for MUS?
Scope the primary literature
The team started by using a large number of narrative reviews and qualitative syntheses (see Appendix 2, Table 68) as key documents to be harvested as a source of potential programme theory. Once a generic pathway had been developed to map the patient’s journey, and challenging junctures throughout this process had been identified, the team moved on to interrogate ‘clusters’ of primary studies. According to previously published work, clusters represent multiple related outputs associated with a single project or, at the very least, with investigation within the same context. 58 These documents, labelled ‘sibling studies’, are considered particularly important because they remove variation in context among the set of studies while contributing collective detail and interpretation. By extension, a further group of related studies, identified as ‘kinship studies’, relate to the original cluster at a more conceptual level, not sharing the same context but sharing conceptual links. For example, kinship papers may share an underpinning theory of change or may seek to replicate, or indeed may have preceded the intervention or study design that are the focus of the index study.
Previous research, by ourselves and others, has found that these sets of cluster documents are often thickly populated; expenditure on a trial and the range of individual collaborators on a project act as catalysts for substantive collateral research activity. 135,189,190 Given the large number of trials identified, and anticipating multiple related reports per trial, the review team took a decision to focus on trials and/or qualitative intervention studies conducted in a UK context. To this extent our focus was more co-terminous with the qualitative synthesis for this project, rather than the review of effectiveness. Nevertheless, a major difference was that the realist synthesis extended its purview, not only by covering the entire primary care pathway, and not just the intervention itself, but by accessing non-intervention-based qualitative sibling studies and metasyntheses, narrative reviews and systematic reviews recording experiences from a diverse range of countries and settings.
The review team identified six UK-based potential clusters (Table 14). 157,182,184,185,191 However, ultimately only three of these represented viable clusters with at least one trial report and one qualitative study from within the same study context. The remaining interventions were centred on qualitative intervention studies already covered by the qualitative synthesis. Two independent studies examined the IAPT Long-Term Condition/MUPS intervention and were therefore linked to broaden their explanatory power. Similarly, studies by Burton et al. ,157 Morton et al. 185 and Morton et al. 191 related to the same intervention in the same context, but were not formally linked to the same project. For included studies, see Chapter 4.
| Cluster identifier | RCT | Other quantitative | Qualitative | Economic | Other evidence |
|---|---|---|---|---|---|
| The BodyMind Approach | Payne192,193 | Payne194–197 | Payne186 | Payne192,198 |
Lin202 Samaritter205 |
| FINE (2010) | Wearden111 | Wearden111,206–208 |
Chew-Graham179 [I]; Peters178 [I] Hannon214 Bayliss215 |
Bayliss165 (QES) |
|
| Humanistic group counselling for somatisation84 | Graham183 [I] | ||||
| IAPT long-term condition/MUPS85 |
Gerskowitch182 [I] Lewis184 [I] |
||||
| MUST reattribution training (2007) | Morriss63,108 |
Morriss223 |
Morriss220 [NI] Dowrick181 [I] Peters180 [I] Salmon226 [NI] |
Morriss221 |
Salmon222 Salmon226 [C] Gask85 [NR] |
| (Primary) SCI (2012/16) |
Burton157 [I] |
Decide on the scope of the review
In contrast to the qualitative systematic review, which focused on the direct treatment context (see Chapter 4), the realist review adopted a broad pathway-based perspective. Essentially this followed an input–processes–output logic, with input being the decision of the patient to present with symptoms to their GP, the processes covering all interactions with primary health-care services, including initial and repeat consultations and the treatment itself, and output occurring at the resolution of the initial situation through relief, recovery, resignation to the situation or referral (Table 15). McGowan et al. 227 describe a typical pathway in connection with chronic pelvic pain:
| Why will patients be more or less likely to present to their GP with MUS? | What will make the initial consultation more or less successful from the patient’s viewpoint? | What will make a patient more or less likely to benefit from being assigned the MUS label? | What will make a patient more or less likely to benefit from being assigned a diagnostic label? | How do patients/doctors benefit from more having a disease model? | What will make the initial consultation more or less successful from the GP’s viewpoint? | What will make the ongoing relationship between patient and GP/HP more or less successful? | What will make a patient likely to attend? | What will make a patient more or less likely to receive/accept behavioural treatment? | What will make a patient more or less likely to continue behavioural treatment? | What will make a patient more or less likely to respond to behavioural treatment? | What will make a patient more or less likely to be able to cope with unsuccessful behavioural treatment? | What will make a patient more or less likely to use/be referred to another service? | What will make the patient more or less likely to view the overall therapeutic process as successful? | What will make the GP more or less likely to view the overall therapeutic process as successful? |
The process of seeking medical advice followed a typical cycle of events: consultation with GP (initial investigations and treatment) – diagnosis – no resolution of symptoms – referral (further investigations and treatment) – diagnosis – back to the GP – diagnosis – (treatment and management). 227
Table 15 necessarily presents a simplified primary care pathway; the pathway to see a HP other than the GP for treatment involves various significant additional steps that have been omitted from the pathway as described.
Despite this broad perspective, which extends beyond that of the accompanying syntheses, this model might still be considered simplistic, in that therapeutic scenarios can include diagnosis and treatment in primary care, diagnosis in primary care and treatment within secondary or tertiary services, and referral to secondary care and subsequent treatment in primary care. The other observation to help unravel this complexity is that important issues such as trust and the continuity of the therapeutic relationship inform the context even prior to presentation to the GP (e.g. past experiences of the GP, practice or health services in general by either the patient or their friends and family). 103,104 Indeed, the decision as to whether or not to attend a GP appointment depends on the patient’s anticipation of the reception from the GP and practice to their particular presentation.
Mapping the programme theory/theories
Initially, seven programme theory statements were developed for testing from engagement with conceptual and qualitative literature. Such theory-driven evaluation aims to offer plausible explanations, not probabilistic statements:228
-
Belief (in the patient, doctor and symptoms) is key.
-
Focus on symptom management not labels.
-
A healthy professional–patient relationship is fundamental.
-
Congruity between disease models facilitates treatment.
-
Working together, professional and patient can exit the diagnostic cycle.
-
Psychosocial talk only to be cued by the patient.
-
Honesty helps more than certainty.
Following discussion within the team, and advice from a clinical expert, one of these statements was modified and another was added. The initial programme theory on ‘honesty’ was felt to imply some absolute value; in fact, what the patient responds to is a belief that the professional is offering an explanation for their symptoms that they (the professional) believe is congruent with the facts and uncertainties at that particular point in time, while acknowledging that this may change as new data or experience become available. This ‘explanation’ may include not being able to offer an explanation at all, and openly acknowledging this. The more relative statement ‘a useful explanation can be good enough’ was felt within the team to more accurately reflect the data in capturing the dynamic context within which the explanation is negotiated between GP and patient, therefore requiring that the prevalent explanation be more contingent, flexible and modifiable as new clinically relevant information or additional patient experience becomes apparent.
In addition, it was felt important to try to surface the specific impact of setting, given the exclusive focus of this project on primary care interventions. The team therefore explored the proposition that ‘a contextually sensitive therapeutic response (i.e. a setting within which a patient feels that their concerns are being addressed) facilitates resolution’. Three of the programme theory statements were prioritised for a fuller exploration [indicated below with a double asterisk (**)]. See the finalised list of exploratory programme statements in Box 1.
PT1: belief (in the patient, doctor and symptoms) is key.
PT2: focus on symptom management versus labels.
PT3: a healthy professional–patient relationship is fundamental.
PT4: a contextually sensitive therapeutic response facilitates resolution (**).
PT5: congruity between disease models facilitates treatment.
PT6: working together, professional and patient can exit the diagnostic cycle.
PT7: psychosocial talk only to be cued by the patient (**).
PT8: a useful explanation can be good enough (**).
Prioritised statements are indicated with a double asterisk (**). A fuller explanation of each programme statement follows below (see programme therories 1–8). PT, programme theory.
Finally, at a relatively late stage of the review, the wording of programme theory 2 was amended to read ‘focus on symptom management versus labels’. This was in direct response to the equivocation within the literature, and surfaced among stakeholders, regarding the utility of a label. In some contexts, a label was seen to offer validation to a patient or entry on a pathway, and there was some evidence of perceived differences in the value between two labels (e.g. CFS and myalgic encephalomyelitis). The revised wording offered a choice rather than a dogmatic course of action.
Propositional statements
A series of propositional statements were devised linking characteristics with key outcomes in the form of ‘if–then’ statements.
Programme theory 1: belief (in the patient, doctor and symptoms) is key
How might this work?
IF HPs show that they take the patient and their concerns seriously, THEN the patient will engage with treatment. 1
A consistent response from patients within qualitative studies, qualitative syntheses and the intervention clusters is that patients want their concerns to be taken seriously. Patients are more likely to feel that they are being taken seriously when the GP:
-
pays empathic attention to them as individuals, meaning that the GP knows their personal circumstances and has an open and empathic approach105–107
-
ensures a good conversation by treating the patient as an equal partner105,108
-
is attentive to their symptoms by exploring these symptoms in depth and by acting on them. 108,109
These findings cross-cut the foci of other programme theories, especially programme theory 2 (focus on symptom management vs. labels) and programme theory 3 (a healthy professional–patient relationship is fundamental). Furthermore, within a healthy climate for communication, there is increased likelihood that a further programme theory will be accessed [i.e. that doctor and patient will negotiate and reach a congruent understanding of the disease (programme theory 5)]. Locating or co-ordinating treatment within primary care is also described as being likely to activate a further programme theory, not as a location but in recognition of the GP role, namely that of better knowledge of personal circumstances, which is achieved through continuity of care.
Two further observations can be made. First, the trend away from the personal GP to more of a team-based approach, with the associated difficulties in making an appointment with the same GP, is likely to fragment this knowledge. Paradoxically, it may heighten the likelihood of meeting at least one GP with whom one has a rapport. Larger practices also extend the prospect of more flexible appointments and individual therapists. 110 Second, the need to be believed is often highlighted as key at the beginning of the consultation episode. However, patients also express a need for the GP to keep believing in them, even when negative test results or other modifiers challenge this therapeutic relationship. In group interventions, this feeling of being understood could alternatively derive from fellow participants with similar problems (see Chapter 465,84,85).
Conversely, not being believed may have a significant impact on individuals with myalgic encephalomyelitis/CFS. These patients have reported feelings of shame associated with invalidation of their symptoms,111 with patients sometimes attributing their feelings of shame to the attitudes encountered from medical professionals and others expressing the idea that they were made to feel that myalgic encephalomyelitis/CFS was ‘all in their heads’. 112
Contextually, there is reason to believe that the impact of non-belief by the HP may differ according to the amount of social support being received from friends and family by the individual. Kendrick229 cites the mechanism of the Stress Buffering Model in achieving an ameliorative role of social support so that any potentially shaming effects of illness invalidation are diminished. However, ‘illness invalidation’ must not only be considered in the context of the direct relationship between HP and patient; the GP is also a source of diagnosis that offers social identity, removing the patient from perceived isolation. 113 Such labels may be accessible for fibromyalgia or CFS, but are typically lacking for MUS/somatoform disorders, which are, in fact, characterised by an absence of diagnostic labels. In this context, ‘diagnosis’ lacks the precise use favoured by the biomedical model, instead referring to a number of unexplained symptoms making it challenging to pass these on to the patient. Recent commentators have remarked on the risk that the new somatic symptom disorder in DSM-5 may mislabel many people as mentally ill. 20 The absence of a label or diagnosis does not necessarily throw into question the GP’s belief in the validity of the patient’s symptoms. However, were this to translate into an expression of non-belief, verbal or non-verbal, by the HP this could indirectly undermine the patient’s credibility should the patient decide to disclose this non-belief to family members or significant others. 111
How the disease label is viewed within the medical profession and within society more generally is another source of potential variation. Doctors may be more likely to maintain their belief if they are able to map the patient’s symptoms to a disorder that they recognise or understand. Labels may also offer patients a communicative mechanism by which they can validate their experience with their family members, serving as a form of ‘shorthand’. The corollary is that where the label is perceived negatively, being associated with ‘skivers’73 or those who are ‘hysterical’,114,115 the label operates in a negative way, causing frustration, stigma and shame. Patients with unexplained neurological symptoms are reported to prefer the term ‘functional’ to MUS as it appears to offer a diagnostic category with which they can identify. 114 As Jutel230 observes, diagnosis, as a form of classification, valorises some points of view, and silences others.
How might this be explained?
Many studies confirm the need for a patient to feel heard, believed, accepted,118 and this aligns well with the Health Belief Model,119 which emphasises the importance of the patient feeling that the GP is gaining a true understanding of where they are coming from. According to the Health Belief Model, three factors explain whether or not a patient will decide to consult their GP:
-
the extent to which a person perceives a threat to his or her health
-
the degree to which a person believes that consultation with the GP will help to reduce that threat
-
‘cues to action’, prompting a person to consult the GP, either internal (symptoms) or external (e.g. mass media communications or interpersonal interactions). 231
When a patient feels that their GP understands them, this may pave the way for a healthy relationship between patient and professional that helps when subsequent challenges need to be ‘smoothed out’. As a corollary, the literature also reveals the unhelpfulness of the patient not being listened to and the psychological impact that this may have. 120 For example, Horton-Salway232 describes how a member of a myalgic encephalomyelitis support group attributed much of the associated depression with the challenge of trying to convince doctors that there is something wrong with them.
Therefore, a major role of the initial conversation may be in serving to validate the patient’s experience. 122,123 Numerous studies describe how this is critical to the receptivity and subsequent engagement of the patient within the treatment pathway. Hoedeman et al. 233 describe the contents of a ‘consultation letter’, which states that patients are best helped by having their symptoms taken seriously. Other content of this consultation letter implicitly confirms that the GP symbolises their belief by not telling the patient that their symptoms are ‘all in your head’; conducting a physical examination at each visit; and arranging to see the patient at regular intervals. However, this study does not address whether or not repeated examinations might have unintended consequences in contributing to patient concern that the doctor had previously missed significant physical pathology. Potentially, a pattern where further physical examination is directly triggered either by new symptoms or by exacerbation of existing symptoms may be more acceptable and more feasible within existing time and resource constraints.
What are the implications?
A key factor in whether or not a patient will engage with, and ultimately benefit from, a treatment is whether or not they believe that their concerns are being taken seriously and that their feelings are being respected. It is important that a GP works continuously on maintaining this belief beyond the initial consultation, making sure that any referrals and tests are justified123 and explained so that they are not misconstrued. However, the reality of demands of GP workload must understandably recognise instances where GP and patient negotiate an agreed explanation for and understanding of the patient’s symptoms (e.g. programme theory 8). Given the absence of a link between the patient’s symptoms and a serious pathology, both may agree that there is no need for ongoing review by the GP. In other more complex cases, regular review every few weeks by the same GP with whom the patient maintains a good relationship may be helpful in managing the patient’s concerns and may help to avoid superfluous investigations and referrals. 126 However, such complex cases probably constitute only a minority of patients presenting with MUS, and so such regular reviews need not place a substantial burden on already-pressed services. Some evidence suggests that preparing the patient for a negative or inconclusive outcome, in cases where the tests and investigations are predominantly for the purpose of ‘reassurance’, can be considered helpful. 127–129
Programme theory 2: focus on symptom management versus labels
How might this work?
IF HPs focus on the patient’s symptoms and how to manage them, THEN the patient feels that something is being done about their symptoms and that their symptoms are not being dismissed as all in the mind. 130
Several commentators have explored the importance of the label assigned to the patient’s symptoms. 113,114,125,131 Stone et al. 4 has reported on the potential of particular diagnostic labels to offend patients, particularly ‘when they imply a psychological rather than a physical explanation’. He observes that ‘Although “medically unexplained” is scientifically neutral, it had surprisingly negative connotations for patients’4 and proposes use of a preferred term ‘functional’. Jutel proposes reorientation from clinical diagnosis to clinical interpretation as a route to ‘reconcile medicine and the individual, the unexplained symptom and the patient distress’. 230 The objective becomes not accurate diagnosis but satisfactory interpretation (e.g. programme theory 8). More recently, Sharpe et al. 234 highlights the erosion of the uncertain boundaries between medically explained and MUS, with the latter having previously been seen as the traditional domain of the psychiatrist. 131 In doing so, he advocates a closer working relationship between psychiatrist and clinician consonant with the current professional movement towards a more integrated approach to physical and mental symptoms in primary care. 130
How might this be explained?
Medical diagnosis explains, legitimises and normalises. 113 The absence of diagnosis denies the patient an immediate explanatory framework, a treatment, access to the sick role and legitimisation of the complaint. 113 This factor surfaced during the project’s public involvement consultations (for details see Chapter 2, Patient and public involvement). Diagnosis of MUS is recognised as particularly challenging, with HPs demonstrating considerable uncertainty, particularly where symptoms are seen as particularly complex (see the qualitative review in Chapter 491). Jutel230 sees this as inevitable given that both practice and the literature have sought to reduce a diversity of symptoms into a single unitary term: ‘MUS’. In this context we can identify a demonstrable difference between IBS, fibromyalgia and CFS, where the clinician is able to pass on a definition in their transaction with the patient, and ‘MUS’, where a clinician seeks to explain that the patient has one or more symptoms for which the clinician does not have an explanation.
Jutel230 highlights circumstances where, when a patient presents with multiple unexplained causes, their doctor may translate these into ‘a unitary condition under an informal diagnostic category linked to psychiatric dysfunction’. Whether the new DSM-5 classification114 is practically useful or whether the label simply operates as a ‘secret’ label that facilitates coding of patients on administrative systems or for academic research purposes requires further exploration. However, this technical consideration should not be allowed to subvert recognition of overall resistance to the use of labels. Labels may be perceived as consigning patients to a metaphorical ‘scrapheap’132 and so it has been suggested that metaphors, models, informal terms or stories could productively be used as an alternative to labels. 132 Stone235 also describes how taking physical symptoms seriously helps to establish trust between the patient and the professional. 132 Some clinicians report not giving the patient a formal ‘label’, suggesting that there are circumstances when either patient or clinician, or even both, do not feel it productive to ‘trigger’ a label.
What are the implications?
Given that evidence on the value of either condition-specific labels or of the general MUS label is equivocal, GPs should seek to focus the consultation and subsequent treatment on symptoms. Use of labels is located firmly within a biomedical disease model which is not generally helpful within the context of MUS. If it becomes clear that the patient would value assignation of a label, then a GP can consider this possibility. In some cases, diagnostic labels will be required in order to access a particular treatment pathway.
Programme theory 3: a healthy professional–patient relationship is fundamental
How might this work?
IF HPs maintain a positive relationship with the patient, THEN professional and patient develop a shared understanding of the patient’s experience.
Many papers identify the importance of initiating and maintaining a healthy relationship between professional and patient as a key factor in successful resolution of MUS. Deale and Wessely29 confirmed this programme theory via a questionnaire survey of 68 patients with CFS. They found that dissatisfied patients were more likely to describe delay, dispute or confusion over diagnosis; to have received and rejected a psychiatric diagnosis; and to perceive doctors as dismissive, sceptical or lacking knowledge about CFS. Dissatisfied patients were also more likely to feel that the advice given was inadequate or conflicting. In contrast, satisfied patients were more likely to perceive doctors as caring, supportive and interested in their illness; to state that they did not expect their doctors to cure CFS; and to perceive their GP or hospital doctor as the source of greatest help during their illness. These findings support the view that medical care is evaluated less on the ability of doctors to treat CFS, and more on the interpersonal and informational skills of those delivering care. One apparent mechanism for improved satisfaction with care is ‘engagement’. 133 Such engagement uses a ‘five areas approach’ that ‘allows patient and therapist to develop a deeper understanding of the patient’s physical symptoms by integrating the full range of the patient’s experiences in areas of (1) situation, relationships, resources, and practical problems; (2) symptoms; (3) behaviour; (4) thinking; and (5) feeling’. 131 Extra time spent on such engagement is seen as critical. 86 However, this provides particular challenges within the pressured time and resource context of primary care.
How might this be explained?
Substantial numbers of studies have identified the importance of trust to the success of the primary care consultation. Although trust is key to most medical contexts, it becomes even more important within a context where epistemological incongruence and communication challenges are likely to occur. In this context, trust has both a supportive function and an enabling function, and it affects not only what is said but how it is said and interpreted.
Continuity of care is also related to the formation of trust. GPs feel that trust makes patients more likely to disclose problems and, in return, GPs feel more able to openly challenge patients. 160 In contrast, referral to other types of HP may subvert the trusting doctor–patient relationship; for example, referral to an orthopaedic surgeon for neck pain was seen to act contrary to a provisional psychosomatic cause. 141 Under other circumstances, however, referral to an orthopaedic surgeon offered reassurance and backup to the GP diagnosis. Collectively, this emphasises the importance of preparing the ground with clear communication of expectations of both GP and patient from the consultation.
Central to trust is empathy; this may be challenging if patients are felt to be ‘heartsink’132 or demanding of time and resources. 131 Wileman et al. 236 report how GPs, when interviewed, felt that showing an empathy with the patient, and taking an interest in them, enabled the patients to gain personal trust in the doctor.
Another sign of a healthy relationship is avoidance of destructive and unhealthy relationship behaviours. Commentators have highlighted the risk of what they have labelled the ‘duet of escalating antagonism’. 138 A similar challenge is posed by ‘looping effects’ (vicious cycles where the emotion of one person causes escalation within the relationship). 149
A contrary type of dysfunctional relationship is the ‘dependency relationship’. Salmon et al. 218 highlight the importance of ‘getting the balance right’ between meeting the patient’s support needs and encouraging dependency. It should also not be assumed that all patients experience an ongoing relationship with their GP72 or that they may not be simultaneously managed by multiple practitioners. 91,92
What are the implications?
The state of the professional–patient relationship is critical to the success of the primary care model, both in initiating a consultation and in maintaining engagement. Where a patient’s interaction persists beyond initial consultation and investigation, a GP must utilise communication behaviours that allow continual renegotiation of the patient’s understanding of their symptoms in the light of that patient’s ongoing experience and as new information becomes available. 98 A patient will be more likely to volunteer useful information within a climate of mutual trust. Increasingly, the general public appears to be becoming aware of the potentially debilitating effects of stress-related symptoms that do not have a clear organic basis. 237 At the same time, a GP must work hard to prevent the creation of a model of dependency.
Programme theory 4: a contextually sensitive therapeutic response facilitates resolution
How might this work?
IF diagnosis, management and treatment takes place within a primary care setting, THEN the patient experiences continuity of care that may lead to progress and resolution.
A key issue in assessing the value of primary care-based behavioural approaches relates to the perceived relative advantage of delivering treatment within a primary care setting. Within the literature the discourse revolves around two types of potential advantage, namely the operational and the conceptual. 139 It is noteworthy that many operational issues, relating to the logistics and practicality of a primary care setting, are stated explicitly, whereas perceived inherent advantages of the setting from a therapeutic perspective tend to be understated or even implicit.
Operational benefits of a primary care setting
Commentators express many potential benefits in favour of treating MUS in primary care. For example, Kroenke and Swindle238 suggest that primary care may be considered an appropriate care setting, highlighting how patients who do not wish to explore psychological attributions for their symptoms, and are therefore unwilling to accept psychological/psychiatric referral elsewhere, may find primary care more acceptable. 86 However, such a conclusion fails to acknowledge that a large proportion of MUS patients do not have underlying psychological causes or associations. 83 Foremost among identified benefits is the opportunity to understand the patient’s circumstances and context and to bring this understanding to bear when interpreting their symptoms. Personalised care is a fundamental value for general practice. Knowledge of the patient and his/her history and context is considered to facilitate recognition of MUS early in the consultation. 142,151,160 Other clues used by GPs to aid recognition of MUS in familiar patients include frequent and often prolonged consultations, with many frequent requests for referrals, and engendering subjective feelings such as irritability and frustration.
Huibers156 advances several reasons why GPs may be particularly suited to performing psychosocial interventions in primary care. First, GPs are able to exercise the ‘stepped-care’ principle so that all appropriate options are explored prior to referral to specialist care. Second, many GPs already provide general support to patients with stress, anxiety or depression. Offering GPs a behavioural toolkit to manage patients with MUS as well as those with more generalised complaints may simply be making better use of their time with a stronger likelihood of benefit or resolution. However, introducing additional demands on an already pressurised frontline service, with the associated demands on time, skills and motivation that such an approach might bring, may not be considered feasible. One alternative may lie with the availability of psychological practitioners based in primary care (e.g. through IAPT workers based in primary care), which is becoming an increasingly common model. These interventions offer an opportunity to build on an existing relationship of trust as an alternative to an unfamiliar provider in secondary care. Finally, provision in general practice could potentially disrupt the strongly entrenched split between psychological and physical forms of primary care.
Conceptual benefits of a primary care setting
Continuity of care is frequently cited as a benefit of locating treatments in a primary care setting239 and is particularly endorsed by the Royal Colleges (Psychiatrists, GPs and Physicians) which espouse the value of co-locating physical and mental health services. 240 It is frequently assumed in the literature that being seen repeatedly by the same professional is advantageous. Although this may be true from a service perspective (e.g. in perpetuating stable expectations and a consistent standard of care), there may also be negative consequences that become particularly important during the breakdown of the therapeutic relationship. Different personnel may be able to offer an alternative perspective, establish a different type of relationship or draw on a different set of intellectual and emotional ‘resources’ in seeking to address the symptoms. By way of a contrast, Peters et al. 180 report how patients may gravitate towards the doctor with whom they have had a longstanding relationship in the knowledge that they would ‘avoid challenging their current ways of managing their problem’. The long-term nature of the relationship, ‘time is on our side’, was seen as an opportunity to work together on resolving patient symptoms.
Although it is difficult to draw robust conclusions about continuity of care, given such variation within the professional–patient relationships, it is certainly worth recording that developments within UK general practice (e.g. larger practices, practice teamworking rather than personal GP provision, increasing front-line nurse roles, etc., to support improved access and out-of-hours coverage) may subvert this as a claimed advantage. 160
Contrary evidence
This realist review found some evidence that patients believed that primary care is an inappropriate setting for exploration of psychosocial issues. Murray et al. 241 offer multiple reasons why this might be the case, citing patient beliefs concerning the superiority of self-management of symptoms and assumptions that limited treatment options would be available. Past experiences of primary care may also be influential. 104 Patients may feel that their primary care provider does not have the ability to resolve such health problems. 92,137,228 Advocates of the BodyMind Approach, one suggested therapeutic intervention for disrupting the expression of MUS, attributed benefit from delivering the intervention in a setting that does not hold the negative connotations of health premises. 65
Murray et al. 241 further highlights other, practical, constraints that may negatively impact on diagnosis in primary care. Of particular resonance are the short consultation time available and a correspondingly heavy patient caseload. Patients may ‘second guess’ the receptivity of the primary care professional, based on prior familiarity with the practice context. Other considerations may relate to financial factors and a lack of local mental health resources.
How might this be explained?
Many factors used to endorse location of services in primary care are generic and seem determined by current models of service delivery, not by the specific requirements of these treatments. This ongoing discourse is currently taking place against a backdrop of service reconfiguration, new models of care and migration of services from secondary to primary care. A further argument relates to integration of physical and mental health services, for which MUS seems to have a particular case.
What are the implications?
A GP must seek to establish a role not as an expert on the patient’s symptoms, but as a co-ordinator and facilitator of the patient’s overall care, regardless of setting. Referral must not be used simply for respite, possibly signalling that the doctor has run out of ideas or patience. Conversely, demand for referral may be initiated by the patient, who requires some sort of ‘reassurance’ that nothing more sinister underlies their symptoms. Care therefore needs to be taken that referral is being initiated in response to need and that entry into the referral pathway will benefit the individual patient in the long run.
The main strength of a primary care setting appears to be the opportunity to offer continuity of care, contextualised within an understanding of a patient’s individual circumstances. However, recourse to external expertise or resources may help in exiting unproductive loops and in advancing the negotiation. Such a finding fits well with the collective body of effectiveness studies that cover a wide variety of primary care-based service models from those that deliver services on primary care premises through to those where the GP acts as initiator and co-ordinator of care but where the services are actually delivered by another professional.
Programme theory 5: congruity between disease models facilitates treatment
How might this work?
IF the disease model advanced by the HP matches, or is compatible with, that of the patient, THEN the patient will accept treatment. 20
Qualitative research has revealed that a dissonance frequently exists between the mental conception, or models, of disease held by the patient and those held by the GP. 242 In a qualitative study that accompanied a trial of training family practitioners in reattribution to manage patients with MUS (the MUST trial), Peters et al. 180 describe how patient explanatory models were ‘multifaceted, simultaneously incorporating disease and non-disease causes and the interaction between them’. This complexity was portrayed in fragmented and chaotic narratives ‘presenting multiple, seemingly unconnected and incoherent problems with no clear beginning or end’. In contrast, some patients viewed GPs as holding ‘more unidimensional, dualistic and hence simplistic models about cause and resolution of problems than their own’. 180
Other studies note how patients remark on the insufficiency of doctor’s illness models. 243 In their metasynthesis of 32 quantitative and qualitative studies of CFS/myalgic encephalomyelitis, Bayliss et al. 165 report that working within the biomedical model has led some GPs to be sceptical about the existence of CFS/myalgic encephalomyelitis. In contrast, GPs who provide a diagnosis were likely to hold a broader, multifactorial biopsychosocial model of CFS/myalgic encephalomyelitis and also to possess more positive attitudes to its symptoms.
Achieving greater congruity between disease models,244 reached through a process of negotiation as modelled by medical reattribution interventions, may thus contribute to improved communication and, potentially, to a healthier patient–professional relationship. 98 However, some evidence suggests that these improvements are not as far-reaching as intended, contributing only to improved patient satisfaction but not to more effective treatment.
van Ravenzwaaij et al. 245 identified nine different potential explanatory models for MUS. This examination concluded by identifying the superiority of a cognitive–behavioural metamodel, principally because it was the only model to include all four domains (i.e. somatic causes, perception, illness behaviour and predisposition) inhabited by the alternative models. 11 This metamodel proposes that the cause of MUS is a self-perpetuating multifactorial cycle, with interaction of different factors across the four domains. This model provides a framework to incorporate patients’ own personal perpetuating factors as well as predisposing and precipitating factors. These three categories offer a framework for understanding individual variation in MUS. Predisposing factors are individual characteristics that make people more vulnerable to distress, physiological arousal and bothersome physical symptoms. Precipitating factors are events or factors that initiate physically symptomatic episodes within vulnerable asymptomatic individuals or that increase disability or distress among those who are already symptomatic. Perpetuating factors maintain symptoms, distress and disability, and extend their period of duration. 246 Each factor can result in physical symptoms and/or distress. The doctor and patient collaborate to identify those elements of a patient’s personal circumstances that might contribute to the patient’s distress. The metamodel incorporates at least five different theories: sensitivity, sensitisation, somatosensory amplification, endocrine dysregulation and the illness behaviour model. The authors conclude that these explanatory models should be ‘integrated in the educational programs of all medical doctors in order to improve the quality of care for patients with persistent MUS’. 247
How might this be explained?
The conceptualisation of the ‘unexplained symptom’ has been seen ‘to shift responsibility for the inability to explain the symptom from the doctor to the patient’. Hadler248 describes a ‘contest of diagnosis’, with medicine ‘not [being] likely to accept blame for subjecting the patient to months of an exercise that turn[s] out to be flawed in design and iatrogenic in execution’. 248 Johansen and Risor242 identify what they term ‘epistemological incongruence’ between dominant disease models and the realities of encountering patients with persistent symptoms. When facing cognitive incongruence, GPs should strive to achieve relational or emotional congruence, through the establishment of good relations, alliances and partnerships with patients. 242 This is seen to contribute to positive experiences of mutual trust and validation.
Achieving congruity of models is also a key factor in treatment success. If a patient feels that a proposed treatment is compatible with their illness model and with their preferences/lifestyle (e.g. dance classes vs. exercise) then they are more likely to initiate the treatment and to persist with it. 249
What are the implications?
Successful resolution of, not necessarily recovery from, challenging MUS is largely dependent on a shared understanding of the problem. 250 There is clear evidence that the different mental models used by GPs and patients to understand the symptoms may contribute to communication difficulties. Ideally, professional and patient should arrive at a negotiated and necessarily contingent understanding; a biopsychosocial model, as proposed by Engel > 40 years ago,251 may offer a meeting point between initially conflicting or incompatible models.
Programme theory 6: working together, professional and patient can exit the diagnostic cycle99,102
How might this work?
IF patient and professional can avoid perpetuating extensive and unproductive diagnostic tests, THEN patient and professional achieve a sense of progress. 252
Patients appear to attach great importance to gaining a diagnosis, which was reported in one study of CFS patients as the single most helpful event. 253 However, the same study reveals this as another example of dissonance between patients and GPs, with GPs seeing a definitive diagnosis for CFS as disabling, potentially becoming a self-fulfilling prophecy. 253 Patients also find it frustrating if they have to wait for years before receiving a diagnosis. Diagnostic tests are viewed as a way of securing a diagnosis, but at the risk of increased frustration if a definitive diagnosis is not actually realised. Frustrations also accompany receiving the ‘wrong’ diagnosis, with some patients expressing a preference of myalgic encephalomyelitis over CFS. 253 Misdiagnosis also carries frustrations and risks. GPs therefore find themselves in a paradoxical situation where the ordering of diagnostic tests may be variously seen as a response to patient demand, a signal to the patient that they are unable to resolve the situation within their more immediate resources, an abdication of interest or commitment to the therapeutic relationship and a potential cause of additional frustration when faced with a subsequent negative result. Such frustration can be mediated if the GP or secondary care clinician has created clear expectations, with the patient being advised of the potential implications of a negative test. Avoidance of unnecessary tests carries further benefits for the patient and health-care system; it reduces costs, patient anxiety and the possibility of identifying ‘incidentalomas’, which then need further investigation but may not be of serious significance. 254,255
How might this be explained?
Several authors use the concept of the ‘diagnostic cycle’ in connection with MUS. Figure 59 shows a pictorial representation of diagnostic loops potentially leading to an unproductive diagnostic cycle. 257 This concept figures in the title of a study of chronic pelvic pain. 102 The authors describe the underpinning biomedical programme theory that diagnosis will, in turn, lead to a ‘suitable resolution of the problem’. However, the reality as revealed by the women’s narratives is that ‘many women do not complete this cycle, they become stuck at a certain point, or re-enter the cycle repeatedly. Women can only opt out of the cycle if the problem is resolved, or by choosing to disengage with medical care’. 227 Women enter the diagnostic cycle actively seeking an explanation for their pain and are consequently frustrated if this is not attained.
In a subsequent study, McGowan et al. 258 revisit this phenomenon, again in the context of chronic pelvic pain, describing how failure to receive a ‘medical explanation’ for their pain can lead women to enter ‘a cycle of re-investigation and re-referral’. Burton et al. 157 extend this concept to a wider group of symptoms to be addressed by a primary symptom clinic. The Symptom Clinic model ‘aims to negotiate a “medical” explanation for symptoms involving physiological processes’. 157 The Serene health organisation in Plymouth uses a diagram of the unproductive diagnostic cycle to illustrate the need to ensure that patients progress along the pathway and to not become becalmed within a cycle of successive tests and/or referrals. 257

Stone235 extends this analogy, using the words of a GP informant, to that of a spiral or cascade effect, where ‘someone sees a specialist, and because the thing is not within the specialty for which they are trained [they] don’t feel able to exclude organic pathology, and will therefore either make a referral or intimate that a referral would be required . . .’.
The consultation letter intervention described by Hoedeman et al. 259 specifically seeks to avoid unproductive tests, with the psychiatrist providing detailed recommendations to the GP concerning management, that is, to avoid unnecessary diagnostic procedures and hospitalisation.
Embarking on such a diagnostic cascade, where the clinician feels out of control of the decision-making process, has previously been identified as a source of particular stress and anxiety, both for the GP and for those experiencing the symptoms. 260 This further explains why non-resolution of MUS can be perceived as threatening to the professional–patient relationship. However, a counterargument relates to the persistent ‘niggling biomedical doubt’ that may be held by a GP, or a prevalent fear of litigation, requiring them to rule out symptoms related to such conditions as cancer, thus precipitating further tests or referral. 132
The literature reflects an ambiguous attitude towards referral to a specialist and/or for further tests. Use of referral appears to differ according to whether the GP seeks resolution, reassurance or respite. In the first context, the GP may genuinely feel, operating within a culture of ‘medical certainty’, that the patient simply needs a label to attach to their symptoms and then this will serve as a passport to their legitimate entry into a treatment pathway. If they communicate this prospect to the patient, then the result of a negative test can prove frustrating to patient and professional alike. On the other hand, it may be valuable to forewarn, and thereby prepare, the patient when a negative result from investigations may be expected. 261 In the second context, the GP is seeking a second opinion, either to confirm or to disconfirm a putative diagnosis or to offer an additional ‘resource’ that they would otherwise not be able to access. Confirmation or negation of a GP’s diagnosis may reassure the GP that they are not missing or overlooking something, but may not necessarily advance the patient’s agenda. 129 In the final context, the GP feels unable to sustain their interaction with the patient in a healthy manner and so looks for respite during which they are able to reorganise their resources and plan a future strategy. Shattock et al. 262 describes circumstances under which frustration and hopelessness may precipitate referral.
The verdict resulting from the external referral either to a specialist or for diagnostic tests may or may not provide useful additional information, but in a way that is only a secondary objective. Being referred to a specialist or for further diagnostic tests holds considerable potential for frustration – from a negative test result, from a narrowing down of possibilities or from being assigned a label that is either unhelpful or unwelcome.
If the patient seeks a referral, in the quest to receive a clear and ambiguous diagnosis, they may find any persistent medical uncertainty unfulfilling and unrewarding. 263 From the patient’s perspective, there are potential unintended consequences. Referral from the GP to an external source may undermine the GP’s credibility, creating the impression that the GP is unable to address the patient’s symptoms within their own expertise or resources. Alternatively, the patient may perceive that the GP is trying to obviate responsibility, whether or not this is actually the case, or is beginning to find the professional–patient relationship too demanding and thus requires respite.
What are the implications?
Being tied into the diagnostic cycle can prove frustrating for GP and patient alike and can result in unwarranted utilisation of referral and/or tests. Ongoing referral from an inconclusive consultation with a first specialist to subsequent additional specialists may perpetuate and exacerbate this problem. When tests or referral are being ordered, GP and patient should share an understanding of how they will potentially advance the patient’s circumstances. 123 Tests should not be used in a symbolic way, nor as a manifestation of GP, or even patient, power.
Programme theory 7: psychosocial talk only to be cued by the patient
How might this work?
IF HPs introduce psychosocial explanations, THEN the patient feels that they are being problematised.
If GPs conduct a physical examination for any new symptoms at each consultation, this may signal to the patient that the GP is resisting a tendency for early closure by offering an expeditious psychosocial explanation. 264 Some GP trainees describe how they try to initiate discussion as early as possible about underlying psychological factors. 265 This opens the way for future consultations to be able to legitimately return to these possibilities without appearing a course of last recourse. This illustrates an important contextual determinant in how programme theory 7 is seen to operate. 141
Doctors have also described how CFS/myalgic encephalomyelitis patients resisted any attempt to attribute their disorder to psychological factors. Patients may feel that a physical explanation for a symptom does not imply that the doctor is attributing personal responsibility for its onset. Conversely, patients may feel that, when a doctor provides a psychological explanation, they are implying that the patient might be able to control, or even reverse, the physical symptoms. 113 Given that the patient has sought help for their distress in the first place, such an interpretation may seem impossible to the sufferer, and several commentators85,158 observe that this may precipitate stigma and shame. Recent literature on the causes of CFS reveals a vigorous and ongoing debate about the extent to which the condition may be explained by physiological findings. The extent to which physiological explanations might offer a challenge to the stigma associated with specific labels is not yet clear and may, in fact, vary across the conditions associated with MUS.
In particular, patients may show themselves as reluctant to engage with follow-up that attributes a psychological explanation to their symptoms. 266 Lewis184 describes how patients were less likely to engage with CBT if they had strong ideas about what was causing their symptoms, perceiving that their problem was purely a physical one. The literature contrasts this response to that for other applications of CBT where patients accept that there is a psychological element to their symptoms. 184
Murray et al. 241 describe how some GPs are reluctant to suggest a significant influence of psychosocial factors fearing that this will have adverse consequences. For example, patients may feel that a psychosocial-oriented discussion will deflect attention away from some serious underlying pathology. 180 Indeed, some patients may avoid discussing psychosocial factors for this reason.
Evidence suggests that patients often actively resist reattribution. 267 Even when they experience anxiety and depression, patients with MUS may see these as associated with, rather than causal to, their physical symptoms. 268 Patients’ reasons for not wanting to share psychosocial information may be sensitive to context; for example, some patients may want to protect their GP from burden. 92 However, such caveats do not, in themselves, represent sufficient reason for not asking the patients about possible anxiety or depression symptoms when taking a medical history.
The GPs may be reluctant to hand the onus of initiating discussion of psychosocial cues to patients, feeling that the patient is unlikely to volunteer such information within the time-limited constraints of a brief consultation. 269 However, qualitative analysis of audiotaped consultations between patients and GPs revealed that in > 95% of the consultations with patients with MUS, patients presented signals or cues of one or more psychosocial problems. 270 Many patients with MUS presented psychosocial cues that their GPs tended to ignore until they encountered a physical symptom that offered a rationale for exploring or investigating. Salmon et al. 271 found that patients with MUS appeared to be seeking emotional reassurance more than patients with clear organic problems.
Thus, GPs have cause to reflect on their own communication skills with such patients. 272
How might this be explained?
Traditionally, GPs have sought to rule out an organic illness before exploring a possible psychological origin. This focus on organic illness has been suggested as a potential reason for low detection rates for mental health problems in primary care generally. 273 It has also been suggested that this approach can reinforce the patient’s view that the cause is physical, which could exacerbate the symptoms – especially if the doctor and patient have not previously discussed the possibility of something other than an organic cause. 274,275 By contrast, current GP training places emphasis on taking a proper biopsychosocial history, acknowledging that even when a patient appears to have a physical problem this may be associated with accompanying psychological symptoms or exacerbating social difficulties. 130 This approach is further underpinned by the philosophy of ‘parity of esteem’ between physical and mental health problems currently endorsed by the same Royal Colleges. 276
Promising initial results in reattribution training from poorly designed studies have probably been unduly influential in supporting the hypothesis that patients will achieve better outcomes if the GP and patient are able to establish a clear link between psychological distress and physical symptoms. 277 This remains an area where the literature and the theoretical base underpinning particular interventions demonstrate largely unresolved dissonance. Rosendal77 highlights potential explanations for these conflicting results, citing the heterogeneity of both patients and their disorders and the differential effects that psychosocial interpretations and interventions may have in the short term. 278
What are the implications?
Most patients presenting to HPs with MUS believe that they have a physical health problem, rather than a mental health problem. They therefore feel more able to trust a physician to respond appropriately to their ‘physical’ health problems. 279 In a sizeable proportion of cases, patients with MUS may in fact have an underlying psychological cause for their physical symptoms. What is less clear is the extent to which psychological problems are the consequences of a patient having unexplained physical symptoms. In the light of this, doctors may choose to respond to patient cues of emotional distress rather than directly asking patients about their feelings, unless doing so in the context of understanding how their symptoms have affected their mood. The increased risk of suicide reported among patients with MUS suggests that elucidation of mood and associated risks, by one means or another, is important in any assessment of such patients. However, GPs need to ensure that the approaches that they typically use in consultation and diagnosis do not in themselves generate or maintain MUS. 132,280
Programme theory 8: a useful explanation can be good enough
How might this work?
IF HPs offer an explanation that they believe is congruent with current facts and uncertainties AND this explanation makes sense to, and is accepted by, the patient, THEN the patient believes that it is possible to maintain the therapeutic relationship. 274
Patients frequently express dissatisfaction with explanations that are provided for their symptoms. 20,129 However, where explanations are effective and empowering, making sense to both patient and clinician, patients feel a corresponding sense of satisfaction. 20 Salmon et al. 281 describe how empowering explanations are tangible, exculpating and involving. 20 Conversely, primary care providers sometimes feel unable to explain symptoms. 272,282 Numerous reasons are advanced to seek to explain this inability. 139 These include feeling unsure or inadequate. Doctors frequently resort to the use of multiple tests in the pursuit of certainty or may refer to a specialist to compensate for their own perceived uncertainties or inadequacies in relation to this complex range of symptoms and explanations. Kirmayer et al. 283 observe that lack of explanation reflects ‘the limits of medical knowledge, available technology and the epistemological difficulties of assigning a clear cause to subjective complaints like pain and fatigue, which may have no objectively measurable correlates and may change rapidly over time in quality and intensity’. Additionally, clinicians, including GPs, are unlikely to have received any training in providing effective explanations for MUS. 159,265
This uncertainty is seen to persist to subsequent stages of the pathway, namely to access to treatment or referral. 139 In the intervention studies, patients clearly valued explanations that helped them to come to terms with and accept a diagnosis (see Chapter 4). Where this explanation is not forthcoming within a primary care setting, patients valued being able to access specialist knowledge and information on their symptoms and what they might mean. 85
The converse is that if the GP and patient feel able to accommodate uncertain or ‘good enough’ explanation at the stage of diagnosis, they may jointly feel able to carry this forward, given their ongoing relationship, to the subsequent stage of action, making that equally contingent and pragmatic. 20 For example, Lewis184 describes how therapists were prepared for ‘having a go’ rather than feeling sure about their approach, acknowledging, however, that working in such an ad hoc way can feel uncomfortable. Under such contingency, patients may modify their expectations and may seek to self-manage their symptoms rather than necessarily resolve them. In a trial of self-management for chronic fatigue in primary care, Friedberg et al. 151 contrast the theory of illness with a more common physical deconditioning and avoidance model, particularly emphasising that their model makes no assumptions about recovery or cure.
How might this be explained?
Although GPs may feel a compulsion to seek a definitive diagnosis and thus achieve ‘closure’ of the consultation, several commentators describe the unhelpfulness of this ‘myth of certainty’. 284,285 Howman286 characterises the prevailing need for GP trainees to want to ‘fix things’ as evidenced in contemporary medical training. Where distrust is initially present, either of doctors or of HPs more generally, providing a frank and bounded explanation, even if acknowledged as contingent or incomplete, may be seen as a form of propitiation.
Some commentators have located that doctors, including GPs, experience difficulty with admitting uncertainty within a prevalent discourse of power. 236 Medical training and the role of the GP assert the importance of the GP appearing competent and knowledgeable168,287 as a way of ensuring their medical authority. 241 Jutel230 highlights that, specifically, diagnosis is the foundation of that social authority. MUS, and their associated uncertainty, can pose a direct challenge to this authority. 181,288
Furthermore, some commentators describe how truthfulness about the limitations of medical options can enable patients to discard the likelihood of medical resolution of their symptoms. This can serve to reduce their dependence on their GP and encourage self-reliance. 288 In this way, patients are facilitated in building up their resilience, adaptability and defiance. 187 However, it may also have the unintended consequence of steering the patient to seek resolution from complementary therapies, often at great personal expense and with limited evidence of effectiveness. 289
The value of a contingent ‘good enough’ explanation, rather than a more definite conclusive verdict, is that it keeps open the possibility of medical options. Clinicians may be concerned about the possibility of missing a serious diagnosis, and this risk-averse culture may influence their test-ordering behaviour. Lines of communication between GP and patient remain open without offering a solid prospect of immediate resolution by medical means.
Caution must be expressed, however, against the presumption that it is simply the apparent agreement of doctor and patient with a ‘shared’ explanation that underpins satisfactory resolution. In a qualitative analysis, Stanley et al. 290 demonstrated that agreement between patients and their doctors in assigning symptoms to broadly defined ‘syndromes’ appears to reflect collaboration that is largely expedient, implying that something more pervasive than superficial compromise is required.
What are the implications?
While the evidence relating to the value of the GP’s explanation for the patient’s symptoms is broad and diverse, it offers a strong theme relating to providing a contingent and sincere explanation. This explanation needs to be seen, by both GP and patient, to be compatible with available facts and experiences but to remain flexible to future adaptation and modification as further information and experience becomes available. Above all, the explanation must keep open possible physical explanations as a potentially viable line of inquiry. The explanation should be jointly owned and the product of ongoing negotiation between GP and patient. 98
Specific evidence exists for the value of specific management techniques in improving clinician communication skills for patients with MUS with the aim of reducing investigations and health-care costs. 152 For example, in a multicentre RCT, Weiland et al. 291 describe how medical specialists received a 14-hour training programme based around experiential learning and feedback. Using techniques from CBT, those in the intervention group were stimulated to ‘seek interrelating factors (symptoms, cognitions, emotions, behaviour, and social environment) that reinforced a patient’s symptoms’. 291 The specialists were taught to explain MUPS understandably, reassure patients effectively and avoid unnecessary diagnostic testing.
Rief et al. 102 describe a training package entitled ‘How to Manage Patients With Unexplained Physical Symptoms’, which utilises guidelines that embody much of the programme theory elicited by this realist review (Table 16 maps programme theory components to the guidelines). This 1-day workshop included how to communicate with MUPS patients, when to start and stop medical examinations, and treatment options. GPs valued this workshop as highly relevant to their daily practice. Patients in the study reported a small reduction in general psychopathology between the index visit and the 6-month follow-up. Data suggesting better outcomes for the patients of trained GPs were inconclusive, given that the attribution of this improvement to the GP training is less clear and could potentially be confounded by time effects as GPs become more experienced or attuned to patients with unexplained physical symptoms. 29
| Stage | Approach |
|---|---|
| General aspects |
Show empathy and understanding for the complaints and frustrating experiences the patient has had so far (PT1) Develop a good patient–physician relationship (PT3) |
| Diagnosis |
Explore not only history of complaints and former treatments, but impairment, (health) anxiety, psychosocial issues Use symptom diaries to assess course and influencing factors on symptoms (PT7) When patient presents with a new symptom, examine the relevant organ system (PT2) Show results of investigations to explain absence of pathology and to give clear reassurance that there is no serious physical disease (PT8) Avoid unnecessary diagnostic tests or surgical procedures (PT6) |
| Treatment |
Provide regularly scheduled visits (e.g. every 4–6 weeks), especially in cases of very frequent health-care utilisation (PT1) Explain that treatment is coping, not curing (when pathology cannot be found or does not explain degree of complaints) (PT8) Suggest coping strategies (e.g. regular physical activity, relaxation, distraction) |
| Referral | If referral is necessary to start psychotherapy or psychopharmacotherapy, prepare the patient for the treatment. Reassure him/her that you will continue to be his/her ‘doctor’ (PT3) |
Programme components
Generically speaking, behavioural intervention programmes follow a similar process:
-
sensitisation of the HP to the patient’s symptoms and circumstances
-
selection of resources or strategies
-
initiation of the treatment
-
review and evaluation of the treatment
-
continuation or discontinuation of the treatment.
A previous meta-analysis found that psychological interventions can be effective for patients with MUS, but the effects were modest and of probable short duration. 78 Analysis demonstrated that psychotherapists achieved larger effects on unexplained physical symptoms than GPs. However, it was unclear whether or not this advantage is attributable to a larger number of psychotherapist-led sessions. Evidence for the effectiveness of teaching GPs skills in brief CBT for depression suggests that CBT training has little effect on GPs’ knowledge and attitudes or on overall treatment outcomes at 6 months. 292 This may equally be the case for MUS. The authors conclude that GPs may require more training and support than a basic educational package on brief CBT to acquire requisite skills. 292 Current training does not equip junior doctors with the necessary knowledge and skills to effectively and confidently manage patients with MUS. 293
Providing patients with a convincing explanation for their symptoms (programme theory 8) is seen as a key component of the FINE Supportive Listening Intervention. 206 This initial session also involves indicating how symptoms may be targeted for treatment (programme theory 2).
Interventions may differ in the extent to which stages 1 and 2 of the behavioural components listed occur within or outside a typical primary care consultation. Furthermore, where treatment is being delivered by a HP other than the patient’s GP, it seems inevitable that there will be some overlap or repetition of these two stages across both HPs. In other cases, the gatekeeper role of the GP is simply to channel the patient towards a particular pathway and then the selection of resources is fundamental to the actual treatment. This personalised tailoring of resources could contribute to a feeling of individualised care and of being taken seriously. This element of personalisation is commonly believed to be more likely to be achieved if the HP is able to gain an understanding of the patient’s individualised personal circumstances.
What is absent from this generic five-stage model for behavioural intervention programmes is a formal stage of ‘labelling’ to achieve matching of strategy to label in stage 2. As itemised above, Burton et al. 157 point out the shared limitation of approaches that ‘concentrate on making the link between physical symptoms and underlying psychological cause’ (cp. Hubley et al. 277). Instead, professionals are encouraged to base the selection of resources and strategies on the patient’s symptoms (see Programme theory 2). Burton suggests that there is value in initially providing conventional biomedical (i.e. contingent ‘good enough’) explanations for MUS (see Programme theory 8). 157 However, it remains unclear if such a biomedical model offers advantages over a biopsychosocial model as endorsed by other commentators. Similarly, the suggestion to embark on psychosocial talk only when cued by the patient (see Programme theory 7)157 receives an equivocal response from the literature and from practitioners. For example, initiating psychosocial talk only when cued by the patient contrasts with reattribution approaches that specifically aim to ‘encourage people to reattribute their MUS to physiological or psychosocial causes rather than to somatic causes’. 294
Another CBT-based approach to MUS is problem-solving treatment. The aim is to reduce complaints associated with unresolved problems in daily life by enhancing a person’s problem-solving capacities in a step-by-step manner. This approach is not explicitly addressed by any of our focal programme theories. Nevertheless, it is firmly grounded implicitly in several of these programme theory assumptions. For example, maintenance of a healthy professional–patient relationship (programme theory 3) is essential in creating a climate in which the patient is prepared to share their problems. Similarly, being provided with a ‘good enough’ explanation may allow a patient to metaphorically draw a line under a potentially futile quest for a definitive explanation and to move on to adopt self-management and problem-solving strategies.
Neither does this staged approach acknowledge a recursive and unproductive loop, with the patient requiring legitimation of their symptoms through a definitive result from a diagnostic test in order to be admitted to the treatment pathway (see programme theory 6, below). Where the diagnosis cycle is repeated, particularly with non-productive results, then not only does the patient feel frustrated, but concerns about the professional–patient relationship (programme theory 3) may be exacerbated. The patient may start to question the skills, abilities and resources possessed by their GP or may feel that they are becoming a ‘guinea pig’295 for diagnostic testing or that they are being ‘fobbed off’. 296 The ‘consultation letter’ intervention259 includes three specific provisions that can be seen as tackling some of these concerns. Unnecessary tests are to be avoided (programme theory 6), the patient is to be monitored regularly and a physical examination is to be conducted at each consultation. This last provision may help to confirm that the professional is still taking physical symptoms seriously (programme theory 1). 297 However, it is recognised that regular physical examination, outside the specific context of new symptoms, may be prohibitive in terms of time and may add little additional useful information. Collectively, avoidance of unnecessary tests and physical examination for new symptoms may serve to maintain a healthy relationship between GP and patient (programme theory 3) although, in this particular study, intervention by an external specialist (i.e. a psychiatrist) precipitated this series of measures. Focusing entry into the treatment pathway on symptoms, not on labels or test results, appears to be key to making progress.
The consultation letter approach259 includes three components that may contribute to the effect of the intervention and that could explain how the intervention might work:
-
confirmation of the persistent diagnosis MUPS
-
management rules for communication
-
management rules for case management.
It should be emphasised that it is the mechanisms that underpin this intervention that may be generalisable to primary care and not the exact intervention that was targeted at secondary care and delivered by psychiatrists. Hoedeman et al. 259 conclude that it is not known which of these components is effective or whether a synergistic effect exists.
Burton et al. 157 claim several advantages for components of his symptom clinic approach. Unlike the consultation letter approach, the symptom clinic model aims to negotiate a ‘medical’ explanation for symptoms involving physiological processes (programme theory 8), thus reducing uncertainty and permitting an exit from the diagnostic cycle (programme theory 6). They describe how this explanation is followed up over a series of shorter consultations, offering the prospect of the professional demonstrating belief in the patient (programme theory 1), of maintaining a healthy professional–patient relationship (programme theory 3) and, above all, of negotiating a shared mental model (programme theory 5). However, as demonstrated throughout this chapter, avoidance of psychosocial cues unless initiated by the patient is more equivocal and does not receive substantive support from within the literature as a whole.
In addition, Burton et al. ’s157 underlying epidemiological approach, identifying patients from a combination of their symptoms and health-care resource use, may be felt to negate recognition of the individualised experience of MUS. Individual symptoms may be common but may present in an almost infinite variety of combinations. Patients may therefore resist any attempt to pigeonhole their experience through strictly epidemiological means.
Another group of therapies offered to people with MUS, and examined in a Cochrane review,77 relates to ‘enhanced care’. Usual care, typically delivered by GPs, is enhanced by the addition of ‘participant education, structured counselling moments, a psychiatric interview, or a reattribution training of the doctor’. 77 These therapies offer no specific treatment agenda or structure. Instead, they aim to offer the person tools to assist them in the recovery process, stimulating self-management (programme theory 8).
Although validation of patient symptoms is primarily invoked within the context of the patient–professional consultation,298 other types of treatment offer alternative forms of validation. 179,182 Group-based sessions can lead to the discovery of a shared experience thereby legitimating patients’ symptoms. Such findings have been reported for fibromyalgia,299 low back pain,300 CFS,301 pelvic pain227 and MUS. 302 However, group sessions do not privilege a particular worldview and, therefore, dissonant explanations and disease models across a group of patients may prove threatening or divisive. As with other treatments, the patient often requires some form of ‘label’ to access a pathway leading to group treatment, again emphasising the potential value of employing a symptom-based approach (programme theory 2) rather than assigning patients by label or test result. Notably, the BodyMind Approach focuses only on symptoms and does not utilise labels. 186 In doing so it acknowledges the personalised and individualised nature of the patient experience, harnessing an almost exclusively somatic frame of reference when offering potential physical explanations (negating programme theory 7). Searches of the literature identified no RCTs of this intervention.
Summary statements
Programme theory 1: take concerns seriously
There is consistent evidence across multiple studies and intervention packages that it is necessary for the GP to take patients’ concerns seriously both at the time of initial consultation and at subsequent visits.
Programme theory 2: focus on symptom management
Many interventions focus on symptoms rather than labels. Evidence for the effect of patients being given a label in general, or a specific diagnostic label, is equivocal and dependent on the needs of the patient, public perceptions of particular labels and the link with subsequent action/inaction.
Programme theory 3: maintain positive relationship
Irrespective of outcome, a GP must seek to maintain a positive relationship characterised by the presence of empathy, trust and good communication.
Programme theory 4: provide a context-sensitive response
Claimed benefits for treating MUS in a primary care setting include enhanced knowledge of the patient and their particular circumstances. However, evidence for these advantages of the primary care setting is equivocal, with some patients feeling that a GP does not have the skills, expertise or resources to manage their symptoms. In turn, doctors may feel that the practical constraints of the consultation, against a backdrop of moves to extended opening and a consequent reduction in access to a personal GP, may run counter to such a direction of travel. Access to psychological practitioners in primary care, as under the IAPT programme, may help to ameliorate such concerns.
Programme theory 5: share congruent disease models
The literature is consistent in highlighting the shortcomings of the biomedical model for MUS. A cognitive–behavioural metamodel136 offers an alternative way of explaining what is happening that may be useful in bridging the incompatibility of professional and patient models.
Programme theory 6: avoid futile diagnostic cycle
There is widespread agreement in the literature, and incorporated within the components of particular interventions, that the HP should seek to avoid perpetuating an unhelpful cycle of tests. However, professional and patient attitudes towards tests or referral are complex and may be construed positively or negatively. In some cases, a diagnostic label can function as a pass key to a particular treatment pathway.
Programme theory 7: consider the appropriateness of initiating psychosocial cues
We were unable to identify definitive evidence in support of this initial programme theory. The literature is equivocal regarding the value of the GP making a connection between the physical symptoms and psychosocial factors. Some treatments are predicated on this connection whereas others purposefully circumvent it. It is likely that this factor is very dependent on the context in which these cues operate. It can be helpful not to exclude this possibility too prematurely. Patient-initiated psychosocial cues have been shown to be more prevalent than doctors think. Further research is required to explore those contexts in which initiation of psychosocial cues by the GP is helpful and those where it might be more appropriate to have such issues raised by the patient. At present, recommendations for each approach in the literature appear determined by the prevailing philosophy of the intervention and not by more salient contextual characteristics of the doctor–patient consultation and ongoing interaction.
Programme theory 8: offer useful explanations
A GP must seek a balance between their expected role of medical authority and the considerable uncertainty that accompanies MUS. Plausible and believable explanations, constructed through negotiation between GP and patient, can offer a contingent way forward, particularly in encouraging an expectation of coping rather than curing.
Discussion of the realist review
The therapeutic relationship is key to a satisfactory interaction between patient and HP and to successful engagement with the treatment. Establishing trust, believing and valuing the patient and developing an empathetic style of communication may all contribute to a positive experience, irrespective of treatment outcome.
Patient and professionals must feel that they are not entering into a destructive diagnostic cycle that may lead to unnecessary or uninformative tests or to referral to secondary care. Such a cycle may lead to excess health-care costs, unnecessary anxiety and frustration and, ultimately, may threaten the therapeutic relationship.
It is challenging to try to extricate the differential effects of a productive consultation, interaction according to behavioural principles and a manualised approach to behavioural modification. Attention must be directed to all three if one is to optimise clinician–patient interaction.
A CBT metamodel136 may offer a useful frame for analysis of an individual presentation and a tool for communication and a constructive dialogue. This may challenge existing mental models, relieve epistemological incongruence and acknowledge individual differences in MUPS.
Limitations
The realist review served a subsidiary, explanatory function for the overall intervention-focused HTA. It focused on a UK context and accessed large bodies of qualitative data through existing rich metasyntheses (Table 17), including the tailored qualitative systematic review reported in Chapter 4. It was not possible to engage with all available primary qualitative studies (Table 18) and the focus was necessarily limited to interventions trialled within a UK setting. Descriptions of interventions were variable, making it challenging to identify intervention components and putative mechanisms of effect. Lewis184 describes how many published RCTs give only brief descriptions of the techniques used, with treatment manuals being rarely published.
| Study (first author and year of publication) | Patient group | Number of included studies/references | Principal themes |
|---|---|---|---|
| Anderson, 2012303 | Myalgic encephalomyelitis/CFS | 34 qualitative studies | Three substantive thematic areas:
|
| Bayliss, 2014165 | CFS/myalgic encephalomyelitis | 21 studies | HPs report a limited understanding of CFS/myalgic encephalomyelitis. Working within the biomedical model has led some GPs to be sceptical about the existence of CFS/myalgic encephalomyelitis. GPs who provide a diagnosis tend to have a broader, multifactorial, model of CFS/myalgic encephalomyelitis and more positive attitudes towards CFS/myalgic encephalomyelitis. GPs collaborate with patients to reach agreement on symptom management, and use their therapeutic skills to promote self-care |
| Burton, 2003304 | MUPS | 77 references | Neither somatised mental distress nor somatisation disorders, based on symptom counts, account for most MUPS patients. With substantial overlap between symptoms/syndromes, suggesting much commonality, patients with MUPS may best be viewed as having complex adaptive systems in which cognitive and physiological processes interact with each other and with their environment. CBT and antidepressant drugs can be effective. Their effects may be greatest when the patient feels empowered by their doctor to tackle their problem |
| Drachler, 2009305 | CFS/myalgic encephalomyelitis | 32 quantitative and qualitative studies | Identified support needs:
|
| Edwards, 201031 | MUS | 109 references | No single approach will be effective in all patients. Chronic, high-utilising patients with MUS need care that is patient centred and attentive to their biopsychosocial needs. Requires careful assessment of the following: psychological concerns, family and cultural issues, a history of a dysfunctional childhood and symptoms of depression, anxiety and post-traumatic stress disorder. To be followed with confirmation that symptoms are real even when linked to psychosocial stress. GPs should clarify appropriate options for individual patients [e.g. reattribution, progressive muscle relaxation/related techniques, CBT (group/individual, by GP/mental health clinician) or medication]. Clinicians require patience and empathic communication. Multiple methods available but territory is unfamiliar/uncharted. Time taken to develop one’s clinical approach can contribute to welfare of patients and their family and to GPs’ personal and professional growth |
| Gask, 201185 | MUS | 25 publications from 13 studies | The reattribution model is too simplistic in its current form to address the needs of many people presenting with MUS in primary care. Reattribution of physical symptoms to psychological causes is often unnecessary. Further research is required into the effectiveness of stepped and collaborative care models that include the education of primary care practitioners. The consultation process is best seen as a conversation and ongoing negotiation between doctor and patient in which there are no certainties about the presence/absence of organic pathology |
| Hubley, 2016277 | MUS | 62 references | Challenges include complex symptom presentations, strained patient–physician relationships and treatment-resistant symptoms that challenge clinician competency. Emphasises importance of co-creating plausible explanations for MUS, understanding the pitfalls of consultations involving MUS and developing multimodal treatment plans |
| Johansen, 2017242 | MUS | 13 studies | Epistemological incongruence between dominant disease models and reality of meeting patients suffering from persistent illness. GPs have used flexible approaches to manage the situation, yet patients and doctors have parallel negative experiences of being stuck, untrustworthy and helpless. When facing cognitive incongruence, GPs strive to achieve relational congruence with patients. This has led to parallel positive experiences of mutual trust and validation. With more experience, some GPs overcome incongruences; later studies point towards reframing of problem |
| Larun, 2007301 | CFS | 20 studies | Symptom experiences and responses from significant others could jeopardise the patient’s sense of identity; feeling severely ill, yet blamed and dismissed. Patients’ beliefs and causal attributions oppose the doctor’s understanding of CFS. For the patient, getting a diagnosis and knowing more was necessary for recovery. Doctors were reluctant towards the diagnosis, and struggle to maintain professional authority. For patients, experience of discreditation could lead to withdrawal and behavioural disengagement |
| MacNeela, 2013187 | Chronic low back pain | 38 studies | Proposes four themes:
|
| Murray, 2016241 | Somatoform disorders | 42 studies | Identified 379 barriers within 77 barrier-level codes, 16 thematic categories and five overarching themes (i.e. patient-related, primary care practitioner-related, doctor–patient interactional, situational, and conceptual and operational barriers |
| Pinxsterhuis, 2015306 | CFS | 15 studies | Coping strategies, including activity management and the use of cognitive and emotional strategies, and psychological processes, such as acceptance and the rebuilding of identities and lives, may promote coping with CFS. Use of adequate coping strategies facilitated by progress in these psychological processes. Coping facilitated mainly by self-management, occasionally complemented by treatments and social support |
| Toye, 2013307–309 | Chronic non-malignant musculoskeletal pain; fibromyalgia | 77 studies of musculoskeletal pain including 28 on fibromyalgia | Concept of adversarial struggle (includes struggle to affirm self and construct self over time; find an explanation for pain; negotiate the health-care system while feeling compelled to stay in it; be valued and believed; and find the right balance between sick/well and hiding/showing pain). Some people move forward by listening to their body rather than fighting it, letting go of old self and finding a new self, becoming part of a community and not feeling like the only one, telling others about pain and redefining relationships, realising that pain is here to stay rather than focusing on diagnosis and cure, and becoming the expert and making choices |
| van Ravenzwaaij, 2011247 | MUS | 24 papers | Identified nine specific explanatory models of MUS: somatosensory amplification, sensitisation, sensitivity, immune system sensitisation, endocrine dysregulation, signal filter model, illness behaviour model, autonomous nervous system dysfunction and abnormal proprioception. Explanatory models focus on four domains: somatic causes, perception, illness behaviour and predisposition. One metamodel, incorporates all four domains: the CBT model. May help GPs in providing explanations to patients |
| Study (first author and year of publication) | Publication type | Contribution |
|---|---|---|
| Aiarzaguena, 2007136 | RCT | Primary care-based intervention |
| Aiarzaguena, 2009310 | RCT | Primary care-based intervention |
| Arnold, 2009311 | Controlled trial | Primary care-based intervention |
| Blane, 2014312 | ||
| Chew-Graham, 2017313 | Editorial | |
| Corbett, 2007300 | ||
| Deary, 200744 | Conceptual model | |
| den Boeft, 2017314 | Doctor–patient communication | |
| den Boeft, 2016315 | ||
| den Boeft, 2017316 | ||
| Dimsdale, 201319 | Diagnostic background | |
| Finset, 2009317 | Doctor–patient communication | |
| Gerger, 201578 | Meta-analysis | |
| Graugaard, 2003318 | Doctor–patient communication | |
| Hoedeman, 2010259 | Systematic review | Cochrane review |
| Howman, 2016286 | GP trainee perspectives | |
| Huibers, 2007319 | Systematic review | Cochrane review |
| Jutel, 2010230 | Literature review | Effects of ‘labelling’ |
| Kromme, 2016320 | Doctor perspective | |
| Layard, 2006321 | Editorial | Trends in psychological treatment centres |
| Malins, 2016322 | ||
| McDermott, 2011323 | Qualitative research | Patient perspective |
| Picariello, 2017324 | Qualitative research | Patient perspective |
| Rask, 2014325 | Mixed methods | GP perspective |
| Reid, 2001261 | ||
| Rosendal, 201377 | Systematic review | Cochrane review |
| Schweickhardt, 2005326 | ||
| Shattock, 2013262 | Qualitative research | Trainee perspective |
| Sirri, 2017327 | Qualitative research | Doctor perspective |
| Stone, 2014235 | Qualitative research | Trainers’ and trainees’ perspective |
| van Dessel, 2014294 | Systematic review | Cochrane review |
| Weiland, 2015291 | RCT | Doctor training programme |
| Ziadni, 2018328 | RCT |
Nevertheless, the realist review has expanded the analytical lens beyond the UK intervention studies included in the qualitative systematic review and extends beyond delivery of the intervention to include the entire pathway from initiation of the consultation through to resolution or referral. In particular, the realist review has engaged at a higher level of theorising with a view to helping to highlight promising candidate interventions or components. A valuable contribution of the realist review is the completion of the TIDieR templates for each of the focal interventions150 (see Appendix 6). The TIDieR checklist and guide was developed to improve the completeness of reporting, and ultimately the replicability, of interventions and can be used by reviewers to assess completeness of intervention descriptions and by readers who want to access more detailed information on the focal interventions.
Conclusions
This realist review was able to identify eight key programme theories (Table 19) that underpin the likely success of current UK-based interventions as explored in clinical trials (see Table 70). Confirmatory evidence was found for the majority of these programme theories, primarily in qualitative research and expert commentary. Few of these component theories have been explored empirically and, indeed, many of them would challenge current trial design. The two remaining programme theories, regarding the role of labels (programme theory 2) and avoidance of psychosocial cues unless initiated by the patient (programme theory 7), present more equivocal evidence – with the literature and our clinical experts equally being split on both the theoretical underpinnings and the practical usefulness of such theories. Although it seems that the value of such strategies would ultimately be determined by the characteristics of the patient, the nature of their symptoms and the context of the clinician–patient interaction, it remains unclear how these strategies might be differentially selected according to patient need. Reasons for this include the fact that these strategies are inextricably tied up with particular types of intervention (e.g. reattribution or the primary care symptom clinic) and not to some underlying theory-informed differentiation. Nevertheless, this chapter has been able to identify where and to what extent current intervention components seem to engage with our prioritised programme theories (Table 20). In doing this, we extend the usefulness of the realist review beyond existing UK trials to include all interventions covered by the effectiveness review and inform possible future intervention design.
| Cluster identifier | PT1 | PT2 | PT3 | PT4 | PT5 | PT6 | PT7 | PT8 |
|---|---|---|---|---|---|---|---|---|
| IF HPs show that they take the patient and their concerns seriously, THEN the patient will engage with treatment | IF HPs focus on patient’s symptoms and how to manage them, THEN patient feels something is being done about their symptoms and that their symptoms are not being dismissed as all in the mind | IF HPs maintain a positive relationship with the patient, THEN professional and patient develop a shared understanding of the patient’s experience | IF diagnosis, management and treatment takes place within a primary care setting, THEN the patient experiences continuity of care that may lead to progress and resolution | IF the disease model advanced by the HP matches, or is compatible with, that of the patient, THEN the patient will accept treatment | IF patient and professional can avoid perpetuating extensive and unproductive diagnostic tests, THEN patient and professional achieve a sense of progress | IF HPs introduce psychosocial explanations, THEN the patient feels that they are being problematised | IF HPs offer an explanation that they believe is congruent with current facts and uncertainties THEN the patient, believes that it is possible to maintain the therapeutic relationship | |
| The BodyMind Approach | By validating the symptom helps patients to feel believed. Utilises patient’s strengths and resources rather than focusing on remediation and deficits (cp. other mental health approaches) | Validates the symptom [cp. other approaches that invalidate and/or negate symptoms (e.g. terms such as psychological therapies/psychosomatic conditions that result in patients not feeling believed)]. By starting where patient is, sensory, physical, bodily symptom is acknowledged and worked with as an ally, promoting positive reassociation with the body, which is often viewed as the ‘enemy’ | Alternative: relationship with other members of the group is important in combating isolation | Group sessions conducted in a non-stigmatising, non-medical venue in the community, designed to be more anonymous than GP setting or a room within psychological services setting | Frames sessions as social rather than medical model, promoting inclusion | Case study states that frequent referrals for tests and scans increase patient’s belief that there would be a physical, medical explanation | Negating: biopsychosocial model is fundamental. Relies on somatic awareness, a normal part of consciousness, to resolve body–mind dualism inherent in conventional multidisciplinary approaches | Works on principle of recovery, giving hope to people to live well with their symptom rather than promising a cure or having to learn to live with it. Empowers patient to self-manage their symptoms |
| FINE (2010) (pragmatic rehabilitation) | No details | Nurses give patients detailed physiological explanation of symptom patterns, followed by treatment programme focusing on graded exercise, sleep and relaxation | No details | No details | No details | No details | Patients keep a diary of their progress on the exercise programme, together with a note of their daily activities, rest and sleep, and any problems encountered and how they were dealt with. Diaries are reviewed at each contact with the nurse | Initial session, which provides patients with convincing explanations for their symptoms and also indicates how they can be targeted in treatment, is crucial to the success of the intervention |
| FINE (2010) (supportive listening) | Patients may improve if they feel that the therapist empathises with them and takes their concerns seriously. Aims to provide emotional support and validation for the patient | No details | Aims to develop a collaborative relationship in which the patient is held in unconditional positive regard, and encouraged to talk about his or her experience of CFS/myalgic encephalomyelitis and problems which he or she has in dealing with it | No details | No details | No details | No details | Patients encouraged to find their own approach to addressing their symptoms |
| IAPT long-term condition/MUPS85 | No details | Seeks to elicit patient beliefs and concerns about symptoms, provide positive diagnosis if possible, biopsychosocial explanation of symptoms | No details | Describes importance of centring on setting and integration with existing services. Physical and mental health-care provision should be co-located to address:
|
No details | Proposes that MUPS are caused by a self-perpetuating multifactorial cycle, based on interaction of different factors in several domains, including somatic (physical) aspects, cognitions (thoughts), behaviour, emotions and environment. Important not to continue to look for possible disease once rigorous diagnostic workup has been completed. Ongoing referral and testing increases patient anxiety and can be iatrogenic preventing patients from moving forward into appropriate treatment | GPs have an important role in ensuring people experiencing FSS engage with IAPT services. GPs are usually first point of contact for people with FSS. They may need to prepare patients who present with FSS for psychological therapies by explaining the biopsychosocial model of FSS | No details |
| MUST reattribution training (2007) | No details | No details | No details | No details | Aims to generate information to provide a simple three-stage psychological explanation (symptom, psychosocial problem, physiological or temporal mechanism linking symptom to psychosocial problem) for the patient’s MUS through negotiation between the GP and patient | No details | Explores social and family factors. explores possibility that physical symptoms might be linked to psychosocial factors. Links physical symptom to an underlying psychosocial or lifestyle issue using normalising physiological, temporal or social link | Three elements to explanation: the symptom (e.g. backache), the psychosocial issue (e.g. stress at home) and mechanism (e.g. muscles held tight by stress for long time start to ache) |
| (Primary) symptoms clinic intervention (2012/16) | No details | No specific attempt is made to screen for common mental disorders; however, patients are encouraged to describe their emotional responses to symptoms and other events, and diagnostic labels such as depression were discussed collaboratively with the patient rather than imposed by the doctor | No details | No details | Consultations are structured to first hear the patient’s experience of illness then to propose and negotiate constructive explanations of physical symptoms. Aims to negotiate a ‘medical’ explanation for symptoms involving physiological processes | Aims to reduce uncertainty and thereby permit an exit from the diagnostic cycle | Focuses on biological (including neurological and cognitive) mechanisms rather than psychological cause | GP explores acceptable explanations for symptoms in terms of biological (including neurological and cognitive) mechanisms rather than psychological cause |
| Intervention | PT1 | PT2 | PT3 | PT4 | PT5 | PT6 | PT7 | PT8 |
|---|---|---|---|---|---|---|---|---|
| The BodyMind Approach | ✓✓ | ✓✓ | ✓ | ✓✓ | ✓ | ✓ | ✗✗ | ✗ |
| FINE (pragmatic rehabilitation) | ? | ✓ | ? | ? | ✓ | ? | ✓ | ✓✓ |
| FINE (supportive listening) | ✓✓ | ? | ✓✓ | ? | ? | ? | ? | ✓ |
| IAPT | ✓✓ | ✓✓ | ✓ | ✓ | ? | ✓✓ | ✗✗ | ✓ |
| MUST | ✓✓ | ✓✓ | ✓ | ✓ | ✓ | ? | ✗✗ | ✓ |
| Symptom clinic intervention | ✓✓ | ✓✓ | ✓✓ | ? | ✓✓ | ✓✓ | ✓✓ | ✓✓ |
Chapter 6 Assessment of cost-effectiveness
Systematic review of existing cost-effectiveness evidence
Objective
A systematic review was conducted to identify published economic evaluations examining the cost-effectiveness of behavioural modification interventions in patients with MUS.
Inclusion/exclusion criteria
Populations, interventions and comparators were defined as per the clinical effectiveness review (see Chapter 3) with the additional requirement that the study population was restricted to patients treated in the UK NHS as estimates of resource use, and costs may not be transferable between different health-care settings. In terms of study design, we restricted the review to cost-effectiveness studies. In terms of outcomes, we restricted the review to studies that measured benefits using quality-adjusted life-years (QALYs), as the QALY has been defined by the National Institute for Health and Care Excellence (NICE) as the reference case measure for benefit for UK cost-effectiveness studies and the NICE methods guide provides guidance on the range of cost per QALY values that can be considered to represent good value for money within the UK NHS. 244 Cost–consequences studies that reported incremental costs but did not report benefits as QALYs were excluded from the cost-effectiveness review, but are narratively summarised in Narrative summary of cost-consequences studies as these studies provide evidence on whether behavioural modification interventions have a negative or positive impact on net health-care costs.
Search strategy
A systematic search strategy was developed in consultation with the review team, to identify economic evaluations relating to the defined population. The focus was on identifying studies in primary care or community-based settings; therefore, population terms were combined with terms to define the setting. A combination of free-text terms and thesaurus searching was used. Published methodological search filters329 to limit to study type (economic evaluation) were used where available. No other search limits were applied.
Searches were conducted in the following sources:
-
MEDLINE via OvidSP (1946–15 August 2016)
-
MEDLINE In-Process & Other Non-Indexed Citations and Epub Ahead of Print & MEDLINE® without Revisions via OvidSP (2013–15 August 2016)
-
EMBASE via Ovid SP (1974–25 August 2016)
-
CINAHL via EBSCOhost (1981–25 August 2016)
-
PsycINFO via OvidSP (1967–25 August 2016)
-
NHS EED via the Cochrane Library (1968–April 2015 – no longer updated, archive only searched 25 August 2015)
-
Science Citation Index via Web of Science (1900–25 August 2015)
-
Social Sciences Citation Index via Web of Science (1956–25 August 2015).
Searches for economic evaluations were conducted between 15 and 25 August 2016. The search results were imported into EndNote [Clarivate Analytics (formerly Thomson Reuters), Philadelphia, PA, USA] and subsequently filtered to identify UK studies, using terms from line 29 of the EU economies search filter,249 to search the EndNote library for potentially relevant references. Detailed search strategies are provided in Appendix 1.
Methods
The citations were sifted by a single reviewer. Full-text articles were examined for those studies that could not be excluded based on the title or the abstract and the reason for exclusion was recorded for all articles for which the full text was examined. Those studies that were also identified in the search for relevant RCTs were cross-checked to ensure that the population, intervention and comparator inclusion criteria were being consistently applied across the clinical effectiveness and cost-effectiveness reviews. The applicability of the studies to the NICE reference case and their methodological quality was addressed using the checklist provided in the NICE guidelines manual. 250
Results
The search identified 1606 unique citations, of which 1541 were excluded at either the title or the abstract searching stage. The exclusion of papers at each stage is summarised in Figure 60. One paper reported clinical outcomes for a study that reported the economic analysis in a separate paper. 112 Three papers were excluded because they reported a population not recruited from primary care. 252,330 Six papers were excluded because they reported a population that did not meet the requirements to be classified as MUS253–256,331,332 and 14 papers were excluded because they reported non-UK populations. 109,138,260,263,265–270,272,273,333,334 One study was excluded because it was not considered to be a behavioural modification intervention. 274 Six papers were classified as cost–consequence studies131,275,276,278–280 and 30 papers were classified as providing only costing or resource use data. Reasons for exclusion for each paper examined at full text are provided in Appendix 7.
FIGURE 60.
The PRISMA flow diagram for identification of cost-effectiveness studies.

Four papers met the criteria for inclusion in the review. 125,126,282,335 Two papers125,126 described results from the MUSICIAN trial at different periods of follow-up, and one paper335 was a conference abstract for the FINE study that was reported in full in another included paper. 282 Clinical outcomes for the FINE study were reported by Wearden et al. 111 and clinical outcomes for the MUSICIAN trial were reported in the same two papers that reported the economic evaluation. Therefore, our review identified two unique cost-effectiveness studies (referred to in this review as Beasley et al. 126 and Richardson et al. 282). The characteristics of the two included studies are summarised in Table 21.
| First author and year of publication | Population | Interventions and comparators | Study design | Incremental costs (£) (mean, 95% CI) | Incremental QALYs (mean, 95% CI) | Cost-effectiveness | Uncertainty | Applicability and limitationsa |
|---|---|---|---|---|---|---|---|---|
| Richardson, 2013282 | CFS/ME |
|
Within-trial analysis |
1 vs. 3 = 218 (–474 to 911) 2 vs. 3 = 460 (–250 to 1169) |
1 vs. 3 = –0.012 (–0.09 to 0.07) 2 vs. 3 = –0.042 (–0.12 to 0.04) |
1 and 2 were dominated by 3 |
Probability that 3 was cost-effective was 0.645 at £20,000 per QALY and 0.626 at £30,000 per QALY 1 not dominated by 3 for sensitivity analysis using complete cases (ICER for 1 vs. 3 = £39,583), but 2 remained dominated |
Directly applicable. Minor limitations |
| Beasley, 2015126 (short-term outcomes in McBeth, 2012125) | Chronic pain |
|
Within-trial analysisb |
1 vs. 4 = 574 (–441 to 1554) 2 vs. 4 = 1924 (782 to 3295) 3 vs. 4 = 1778 (690 to 3009) |
1 vs. 4 = 0.097 (–0.05 to 0.24) 2 vs. 4 = 0.025 (–0.10 to 0.15) 3 vs. 4 = 0.047 (–0.09 to 0.18) |
1 vs. 4 = £5917 2 dominated by 1 3 dominated by 1 |
1 had approximately a 75% chance of being optimal at £20,000 per QALY Sensitivity analysis using multiple imputation to handle missing data gave similar results with 1 vs. 4 having an ICER of £3957 and 2 and 3 remaining dominated by 1 |
Directly applicable. Minor limitations |
Each of the included analyses examined a different population, with Richardson et al. 282 examining patients with chronic fatigue and Beasley et al. 126 examining patients with chronic pain. Both of the studies included treatment as usual as a comparator and both evaluated more than one behavioural modification intervention. In terms of the interventions examined, there were some common elements, with both studies including a psychological intervention and both including an intervention that involved some form of activity or exercise. However, the interventions examined by Richardson et al. 282 have been categorised in the clinical review as GA and other psychotherapy, whereas the interventions examined by Beasley et al. 126 have been categorised as CBTHI and SES. In addition, Beasley et al. 126 examined a multimodal intervention combining both CBTHI and exercise, whereas Richardson et al. 282 did not examine any multimodal interventions. The two studies were not judged to be sufficiently similar in their population, interventions and comparators to allow a direct comparison of outcomes but similar issues were identified when assessing the applicability and quality of the studies. Therefore, a narrative summary of methodological quality across both studies is provided followed by a summary of results from each individual study.
There were significant similarities in the studies in terms of the methods employed. Both were within-trial economic analyses. The duration of the analysis period was 70 weeks for Richardson et al. 282 and 2 years for Beasley et al. ,126 which are both relatively short time horizons for a population with chronic symptoms. Both studies applied the discount rate recommended in the NICE methods guide (3.5% per annum). 244 Owing to the inclusion criteria of the review, both were conducted in the UK and valued outcomes using QALYs. Both measured HRQoL using the EQ-5D and restricted benefits to those accrued by patients. Both studies used patient self-report to assess resource use, which may be subject to recall bias.
Richardson et al. 282 stated that they took an NHS and PSS perspective. The approach taken by Beasley et al. 126 is consistent with an NHS perspective. In terms of the assessment of broader costs falling outside the stated perspective, Richardson et al. 282 examined the costs to patients and families, including lost working days, but excluded these from the cost-effectiveness analysis. Both studies evaluated the uncertainty surrounding the cost-effectiveness estimates by using bootstrapping to generate a cost-effectiveness acceptability curve (CEAC), which shows the probability that the intervention is cost-effective for various willingness-to-pay thresholds. Both studies used multiple imputation to handle missing data either in their base-case analysis or in a sensitivity analysis, but no other sensitivity analyses were reported. Overall, both of the studies were assessed to be directly applicable and to have minor limitations.
The MUSICIAN trial compared CBTHI alone, SES alone and CBTHI combined with SES against treatment as usual in patients with chronic widespread pain. This study was originally reported by McBeth et al. 125 using data from a 9-month follow-up, but here we focus on the results at 24 months post intervention, which were reported by Beasley et al. 126 When using the complete-case analysis, all three active strategies (i.e. CBTHI alone, SES alone and CBTHI with SES) provided more benefits than usual care but at an additional cost. However, SES alone and CBTHI with SES were both dominated by CBTHI alone, which had an incremental cost-effectiveness ratio (ICER) of £5917 compared with treatment as usual and approximately a 75% chance of being optimal at £20,000 per QALY. Sensitivity analysis using multiple imputations to handle missing data resulted in qualitatively similar results but with an ICER of £3957 for CBTHI compared with treatment as usual. These results were more favourable than the short-term results reported by McBeth et al. ,125 suggesting that the cost-effectiveness is improved by considering a longer time frame.
The FINE study282 compared pragmatic rehabilitation (GA), supportive listening (other psychotherapy) and treatment as usual in patients with CFS or myalgic encephalomyelitis/encephalitis. Richardson et al. 282 reported that both pragmatic rehabilitation (GA) and supportive listening (other psychotherapy) provided less benefit than treatment as usual but at an additional cost and, therefore, both strategies were dominated by treatment as usual, which had a 65.5% probability of being cost-effective at £20,000 per QALY. In the complete-case analysis, pragmatic rehabilitation (GA) was no longer dominated by treatment as usual but the ICER versus treatment as usual was £39,583. Supportive listening (other psychotherapy) remained dominated in the complete-case analysis.
Conclusions
The review found relatively few UK-based cost-effectiveness analyses in comparison with the number of RCTs included in the clinical effectiveness review. The studies that were identified both used a within-trial analysis to examine the short-term cost-effectiveness of behavioural modification interventions. Although both studies assessed the cost-effectiveness of behavioural modification interventions in patients with MUS, the two studies examined different behavioural modification interventions in different populations. Richardson et al. 282 found that neither GA nor other psychotherapy provided more benefit than usual care in patients with CFS/myalgic encephalomyelitis. Beasley et al. 126 found that CBTHI was cost-effective compared with usual care when valuing a QALY at £20,000 in patients with chronic pain. In addition Beasley et al. 126 found that CBTHI provided more benefit than both SES and a multimodal intervention combining both CBTHI and SES. The studies were all generally applicable to the stated aims of this review and were mostly of reasonable quality, although their short-term nature is a potential limitation.
Narrative summary of cost–consequences studies
Six of the papers131,275,276,278–280 excluded from the review of cost-effectiveness were classified as cost–consequence studies, as they reported the impact of behavioural modification interventions on both costs and benefits but did not measure benefits using QALYs and, therefore, did not meet the inclusion criteria for the review of cost-effectiveness studies. However, these studies do provide evidence regarding whether behavioural modification interventions result in an overall reduction or increase in health-care costs. Two of these papers276,278 reported results from the same study. This resulted in a total of five unique cost–consequence studies being included.
We applied relevant aspects of the applicability and quality criteria used in the cost-effectiveness review250 to the cost element of these studies. The findings for each study are provided in Appendix 8 and are narratively summarised below. The incremental costs reported by each study are summarised in Table 22 and discussed in turn for each study.
| First author and year of publication | Population | Interventions and comparators | Study design | Incremental costs (£) (mean, 95% CI) | Applicability and limitationsa |
|---|---|---|---|---|---|
| Chisholm, 2001275 | Chronic fatigue |
|
Within-trial analysis | 1 vs. 2 = –63 (–258 to 42) (health care only) | Directly applicable for health service cost outcomes. Minor limitations |
| Kennedy, 2005129 | IBS (not responded to drug therapy) |
|
Within-trial analysis | 1 vs. 2 = –64b (–201 to 83) at 12 months [does not include intervention costs, which were 308 (SD 202)] | Directly applicable for health service cost outcomes. Minor limitations |
| McCrone, 2004279 (clinical paper is Ridsdale, 2004113) | Chronic fatigue |
|
Within-trial analysis |
1 vs. 2 = 193 (–946 to 458), 0.589 probability of 2 being cost-saving vs. 1 Therapy (1 or 2) vs. 3 = 149 (–708 to 1001)c |
Partly applicable. Potentially serious limitations for the comparison against 3. Minor limitations for 1 vs. 2 |
| Robinson, 2006131 | IBS |
|
Within-trial analysis |
Effect of guidebook = –72.74 (–102.63 to –42.84); p = 0.000d Effect of self-help group (over and above effect of guidebook) = 7.53 (–20.41 to 35.48); p = 0.591 |
Directly applicable for health service cost outcomes. Potentially serious limitations |
| Sabes-Figuera, 2012280 (clinical paper is Ridsdale, 2012115) | Chronic fatigue |
|
Within-trial analysis |
1 vs. 3 = 261 (141 to 382) 2 vs. 3 = 423 (288 to 559) 1 vs. 2 = –202 (–362 to –43) |
Directly applicable for health service cost outcomes. Minor limitations |
All of the studies had a UK setting as this was one of the inclusion criteria. All five were economic evaluations conducted alongside a RCT, although one paper279 reported a non-randomised comparison against usual care in addition to the randomised comparison of two behavioural modification interventions. All five studies had a time horizon of ≤ 1 year and, therefore, costs were not discounted. The perspectives were often not reported explicitly. Robinson et al. 131 included only NHS costs, but the remaining four studies275,276,279,280 included costs for alternative/complementary therapies within health service costs. Three papers reported the broader costs falling on patients or their carers including lost employment275,276 or informal care-giving275,279 and one paper275 did not report health service costs separately from these societal costs. Four papers relied on patient self-report for resource using some form of the Client Service Receipt Inventory275,276,279,280 Robinson et al. 131 used GP records for primary care resource use but relied on patient self-report for secondary care consultations. Kennedy et al. 129 reported the intervention costs separately from the costs for other resource use. All five used bootstrapping to estimate the uncertainty around the difference in costs between trial arms. Four papers131,276,279,280 used regression analysis to estimate differences in costs and three papers131,279,280 adjusted for baseline costs or resource use in their regression analysis. All five studies reported using standard sources for unit costs, such as NHS Reference Costs336 or Personal Social Services Research Unit (PSSRU)337 costs, but two papers279,280 reporting using a nominal cost for the self-help booklet provided alongside usual care.
One study279 was considered to be partly applicable because, although it did report informal care separately for each treatment arm, it did not report incremental costs falling on the health service separately from total incremental costs, which included costs of informal care. This study was also considered to have potentially serious limitations, but only for the comparison against usual care with self-help booklet as this comparison was non-randomised. However, the randomised comparison of two behavioural modification interventions was considered to have only minor limitations. The other four studies131,275,276,280 were considered to be directly applicable because they reported health service costs separately from broader societal costs. Three of these four papers were considered to have minor limitations. 275,276,280 The remaining paper, by Robinsons et al. ,131 was found to have potentially serious limitations because it did not appear to include the costs of the intervention in the analysis.
Chisholm et al. 275 report results from a RCT that compared CBTHI with counselling (classified as other psychotherapy) for patients with chronic fatigue. The clinical results are reported by Ridsdale et al. 112 and have been included in the clinical effectiveness review. Costs at baseline are compared with costs at 6 months to estimate the change in costs for each therapy and the difference between arms is calculated for change from baseline. CBTHI resulted in a statistically significant increase in health-care costs from baseline (mean change in cost from baseline £129, 95% CI £23 to £242). Other psychotherapy (counselling) resulted in a non-significant increase from baseline (mean change in cost from baseline £65, 95% CI –£6 to £146). The difference in change from baseline for health-care costs was not statistically significantly different between the two active interventions (mean change in cost from baseline –£63, 95% CI –£258 to £42).
Kennedy et al. 129 reported the results of a RCT that compared CBTLI with mebeverine to mebeverine alone in patients who continue to report moderate to severe IBS symptoms after 4 weeks of drug therapy with mebeverine. Mean costs for resource use (other than that associated with CBT) were lower in the CBTLI with mebeverine arm at 12 months than in the mebeverine-alone arm, but the difference was not statistically significant. The cost of CBT was reported to be £308 (SD £202), but these costs do not appear to have been combined with the costs of other resource use to estimate the overall incremental cost for CBT with mebeverine versus mebeverine alone.
McCrone et al. 279 report results from a RCT that compared GA with CBTLI. A non-randomised comparison against usual care plus (self-help booklet) is also reported but was considered to have potentially serious limitations. The clinical results are reported by Ridsdale et al. 113 and the results from the randomised comparison have been included in the clinical effectiveness review. GA was found to have a lower mean cost than CBTLI but the difference was not statistically significant. Behavioural modification interventions (CBTLI or GA) were found to have higher costs than usual care plus (self-help booklet) when results from the two therapies were combined but the comparison against usual care plus was non-randomised.
Robinson et al. 131 reported a comparison of a self-help guidebook (guided self-help) and a self-help group in addition to a guidebook (multimodal combining guided self-help and RSSE) with usual care in patients with IBS. In addition to reporting the mean costs across each of the arms, regression was also used to estimate the individual impact on costs of the guidebook and the self-help group. The guidebook was found to have statistically significantly lower costs by £72.74 (a 40% reduction) but the addition of the self-help group was found not to have a statistically significant impact on costs. The results were not sensitive to whether or not the patients met the Rome criteria for IBS.
Sabes-Figuera et al. 280 report results from a RCT that compared two behavioural modification interventions [i.e. GA and counselling (classified as other psychotherapy)] against usual care plus self-help booklet (classified as guided self-help) for patients with chronic fatigue. The clinical results are reported by Ridsdale et al. 115 and have been included in the clinical effectiveness review. Both GA and other psychotherapy (counselling) resulted in additional costs relative to guided self-help. GA resulted in significantly lower costs than other psychotherapy (counselling). The authors conclude that GA dominates (has lower cost and better outcomes) other psychotherapy (counselling), but this conclusion is made on the basis of a single clinical effectiveness outcome measure and, therefore, should be interpreted with caution.
Overall, the impact of behavioural modification interventions on net health-care costs was found to vary between studies. Only two studies131,280 reported a statistically significant difference in health-care costs between trial arms. From the study by Robinson et al. ,131 we can conclude that the self-help guidebook used in this study is likely to be cost-saving for patients with IBS provided that it has a low cost per patient (i.e. < £72). From the study by Sabes-Figuera et al. ,280 we can conclude that the choice of behavioural modification intervention is important as some interventions may achieve similar effectiveness results while having a lower impact on overall costs than other interventions. However, two other studies275,279 were unable to show a statistically significant difference in overall health-care costs when comparing one behavioural modification against another. From the study by Kennedy et al. ,129 we can conclude that CBT does not lead to a statistically significant increase in health service costs over and above those associated with the intervention.
Independent economic assessment
The general approach taken in our independent economic assessment was to generate a within-study estimate of cost-effectiveness for individual trials included in the clinical effectiveness review. The four main steps required were to:
-
estimate the incremental costs relative to usual care of delivering the behavioural modification interventions (and any active comparator interventions) reported in the individual studies
-
estimate health-utility outcomes from the clinical outcomes reported in the individual studies
-
estimate the difference in benefits between trial arms in terms of the incremental QALYs gained
-
combine these to estimate the cost-effectiveness.
The methods for each of these steps are described in Inclusion/exclusion criteria to Methods, respectively, and the results are described in sections Results: intervention and comparator costs to Results: cost-effectiveness analysis. Information on the impact of interventions on other NHS resource use (i.e. resource not directly related to the delivery of the intervention) has also been incorporated in the estimates of cost-effectiveness described in Results: cost-effectiveness analysis, where this was identified within the economic studies described in Systematic review of existing cost-effectiveness evidence.
Our decision to focus on within-trial estimates of cost-effectiveness rather than using the outcomes of the NMA to conduct a single incremental analysis covering all of the different categories of behavioural modification interventions is discussed further in Chapter 7, Cost-effectiveness.
Methods used to estimate intervention costs
Each of the included studies was examined to determine the resources required to deliver the intervention and any active comparators (i.e. comparators that were not usual care/treatment as usual or waiting list control). We have assumed that usual care (or treatment as usual/waiting list control) has zero cost so that any intervention or active comparator is costed relative to usual care. Six studies100,113,118,151,159,160 had comparator arms that were categorised as ‘usual care plus’, and these have been costed where possible. Information was extracted on the number of sessions, duration of sessions and the health-care professionals involved in delivering or facilitating the intervention. For interventions delivered to groups, information was also extracted on the number of individuals who started the intervention and either the group size or the number of groups to allow an estimation of the average cost per patient. Unit costs were taken from the most recent edition of the PSSRU Unit Costs of Health and Social Care 2016338 with three exceptions: the unit costs for clinical psychologists, counsellors and mindfulness trainers were reported in the 2014 edition of PSSRU unit costs (Unit Costs of Health and Social Care 2014339) but not in the 2016 edition, so the costs from the 2014 edition have been uplifted to 2016 prices using the Hospital and Community Health Service Pay and Prices index. 338 We have used unit costs including qualification costs where these are reported. The ratio of direct to indirect time is the ratio of time spent in direct contact with patients relative to time spent on other activities. As the resource use in our studies is based on face-to-face time with patients, we have used the cost per minute of face-to-face time where this has been reported. Where this has not been reported we have used the ratio of direct to indirect time to estimate the cost per minute of face-to-face time. For example, the ratio of direct to indirect time for a nurse in general practice is 1 : 0.20, so for each hour spent in contact with a patient an additional 12 minutes is spent on other activities. Therefore, if the cost per working hour is £43 then the cost per minute of face-to-face time is £0.86 (= 1.2 × £43/60). An exception was made for the time that GPs spent training in the GP interventions, which included a training element. For these interventions, the training time was based on the cost per minute across all GP activity, but the time spent with patients was still based on the cost per minute of face-to-face time with patients. Unit costs are summarised in Table 23.
| Health-care staff | Unit cost | Ratio of direct to indirect time | Cost per minute (£)a | Source |
|---|---|---|---|---|
| CBT | £97 per 55 minutes of contact time | NAb | 1.76 | Unit Costs of Health and Social Care 2016 338 |
| Clinical psychologist | £138 per hour of client contact | NAb | 2.35c | Unit Costs of Health and Social Care 2014 339 |
| Counsellor | £50 per hour | Not reported | 0.85c | Unit Costs of Health and Social Care 2014 339 |
| Consultant, medicine | £135 per working hour | 1 : 0.61d | 3.62 | Unit Costs of Health and Social Care 2016 338 |
| Consultant, psychiatry | £138 per working hour | 1 : 0.61d | 3.70 | Unit Costs of Health and Social Care 2016 338 |
| GP (training) | £147 per hour of GMS activity | NA | 2.45 | Unit Costs of Health and Social Care 2016 338 |
| GP (treating) | £3.90 per minute of patient contact time | 1 : 0.61 | 3.90 | Unit Costs of Health and Social Care 2016 338 |
| Mindfulness-based cognitive therapy | £172 per 2-hour session | NAb | 1.47c | Unit Costs of Health and Social Care 2014 339 |
| Nurse practitioners | £61 per hour | 1 : 0.33 | 1.35 | Unit Costs of Health and Social Care 2016 338 |
| Physiotherapist | £45 per hour | 1 : 0.37 | 1.03 | Unit Costs of Health and Social Care 2016 338 |
| Primary care nurse | £43 per hour | 1 : 0.20 | 0.86 | Unit Costs of Health and Social Care 2016 338 |
| Social worker adult services | £98 per hour of client-related work | NAb | 1.63 | Unit Costs of Health and Social Care 2016 338 |
Interventions delivered to groups and interventions delivered to individuals have been split into separate categories as interventions delivered to groups are usually cheaper on a cost per patient basis. A list of the detailed assumptions used in the costing analysis is provided in Appendix 9.
Methods used to estimate utility values from study outcomes
The method for estimating treatment benefit recommended by NICE is to estimate the difference in QALYs between groups receiving different interventions. 244 Health utility is a measure of HRQoL on a scale of zero to one; one represents full health and zero represents a state equivalent to death. When calculating QALYs, the patient’s estimated survival is adjusted to reflect their health utility during that period of survival. Therefore, an estimate of health utility is needed to estimate treatment benefit using QALYs. Some generic measures of HRQoL, such as the EQ-5D, come with a tariff that allows utility to be estimated from an individual’s response to the EQ-5D using preferences obtained from a UK general population sample. The EQ-5D is NICE’s preferred measure of health utility for estimating QALYs. 244 When health-utility values based on the EQ-5D are not available, NICE recommends that these are estimated by using mapping functions that estimate EQ-5D utility values from the other HRQoL measure or health-related benefits observed in the trials. 244
It was our aim to measure health benefits using QALYs based on EQ-5D outcomes valued with UK preferences whenever this was feasible from the data collected, as this is consistent both with the NICE methods guide and with the data reported in those studies included in our systematic review of published cost-effectiveness studies. We examined the generic preference and non-preference-based measures of HRQoL reported in the included studies. For studies that did not report EQ-5D directly, we looked to identify mapping algorithms that would allow us to estimate EQ-5D utility values from the other measures of HRQoL reported. Studies that reported EQ-5D utility values obtained with a non-UK preference set were considered acceptable where it was not possible to obtain EQ-5D values obtained using the UK preference set. Estimates obtained from alternative generic quality-of-life instruments were also considered acceptable if they met NICE’s requirement that health-utility values should be based on a valuation of public preferences from a representative sample of the UK population using a choice-based method.
Summary of generic preference and non-preference-based measures reported
Both of the published cost-effectiveness analyses identified in our systematic review126,282 measured QALYs using the EQ-5D with UK preferences. A further six studies108,115,137,138,143,340 reported EQ-5D outcomes in their clinical or economic papers but did not meet the inclusion criteria for our systematic review of published cost-effectiveness analyses. Morriss et al. 108 reported both the EQ-5D utility index and resource use but did not conduct a full economic evaluation. Furthermore, the scale on which the EQ-5D score is reported does not appear to be the standard zero to one scale and, therefore, it is unclear if the value reported is based on the UK tariff or some other method for scoring the EQ-5D. Luciano et al. 138 (the economic paper for Alda et al. )137 present a full economic evaluation, but the setting was the USA rather than the UK. In addition, Luciano et al. 138 used a Spanish tariff rather than the UK tariff to calculate utility values from the EQ-5D. van Ravesteijn et al. 143 reported only the VAS part of the EQ-5D, which is not a preference-based measure of health utility and, therefore, cannot be used to calculate QALYs. The related economic paper341 reported QALY gains, but these were obtained using a different measure of health utility rather than the EQ-5D. A second study by Luciano et al. 138 also reported only the VAS part of the EQ-5D. van der Roer et al. 340 reported QALY gains calculated using the EQ-5D in their within-trial economic evaluation,340 but the utility values were estimated using the Dutch rather than the UK tariff. Ridsdale et al. 115 reported EQ-5D values at baseline only within the related economic paper,280 stating that there was an ‘unexpected unavailability of EQ-5D questionnaire data for the six-month follow-up’. Therefore, although eight studies reported some aspect of the EQ-5D, only the two studies included in the systematic review of cost-effectiveness analyses126,282 reported EQ-5D values that can be used to calculate QALYs based on UK preferences, although a further two studies reported EQ-5D utility values based on non-UK preferences. 137,340
Twenty-five of the studies included in the systematic review of clinical effectiveness reported some aspect of the Medical Outcomes Survey (MOS) Short Form questionnaire-36 items (SF-36). 97,103,106,107,111,112,114,119,125,131,136,140,141,143–147,149,151–153,156,342,343 This is a generic measure of HRQoL that is usually reported as either eight domain scores (i.e. physical functioning, role physical, role emotional, vitality, mental health, social functioning, bodily pain and general health) or a pair of higher-level summary scores described as the mental component summary (MCS) score and the physical component summary (PCS) score. An additional five studies reported outcomes from the MOS SF-12. 118,133,150,157,158 This is a shortened version of the SF-36 that is able to produce MCS and PCS scores similar to those reported by the SF-36 with less respondent burden. 344 The Short Form questionnaire-6 Dimensions (SF-6D) is a shortened version of the SF-36 that contains only six items. 345 A preference-based measure of utility exists for the SF-6D, which was derived using preferences expressed by a sample representative of the UK general population. Although this is not NICE’s preferred method for estimating utility, it has similarities with the EQ-5D in that it provides a measure of HRQoL that is based on public preferences from a representative sample of the UK population using a choice-based method. The study by van Ravesteijn et al. 143 used the SF-6D to estimate QALYs for the within-trial economic analysis, and one further study by Aiarzaguena et al. 136 reported outcomes using the SF-6D (although the utility values appear to have been reported on a 0 to 100 scale rather than a 0 to 1 scale).
Identification and selection of mapping algorithms
‘Mapping’ or ‘cross-walking’ algorithms exist that allow the expected outcomes from the EQ-5D instrument to be calculated from other generic or disease-specific HRQoL instruments. These have been systematically reviewed by Dakin et al. 346,347 and a database of instruments that map to the EQ-5D is provided on the website of the Health Economic Research Centre (HERC) at the University of Oxford (version 5.0, last updated 16 May 2016). We examined this database to identify algorithms that would allow us to map trial outcomes measured using the SF-36 to utility values measured using the EQ-5D with the UK tariff. We also examined the list of titles identified during a systematic review of mapping studies that was ongoing at ScHARR at the time to find any studies not picked up in the HERC database.
Six studies that mapped from the SF-36 to the EQ-5D were identified from the HERC database and no additional studies were identified from the list of titles taken from the ongoing ScHARR systematic review. One of these studies was discounted because it used preferences from a Korean population rather than a UK population. 348 Three others were discounted because they used a data set for a specific condition, which may limit the generalisability of the results to patients with a more diverse range of health conditions. 349–351 Of the two remaining papers, the paper by Ara and Brazier352 was selected in preference to the paper by Rowen et al. 353 because it specifically validated the algorithm for use in predicting mean EQ-5D scores from mean SF-36 domain scores in situations where the patient-level data are not available. It was also noted that the data sets used by Ara and Brazier352 covered a range of conditions, including some conditions, such as IBS, which would be managed in primary care, whereas the data set used by Rowen et al. 353 was limited to secondary care inpatients and outpatients and, therefore, it might be less generalisable to our target primary care population. Ara and Brazier352 examined seven different ordinary least squares (OLS) models and concluded the simplest model (referred to as eq1) was the preferred model for estimating group EQ-5D scores from group domain scores, whereas the model referred to as eq4, which contained second-order terms, was preferred for estimating between-group differences and changes over time. However, after discussion with the corresponding author, we decided that as there was little difference between the performances of these two models, it was best to use the simplest model, which contained only linear functions of the domain scores, as this allowed us to calculate changes from baseline and differences between groups where the absolute scores were not reported.
Eight studies that mapped from SF-12 to EQ-5D were identified from the HERC database and two additional studies were identified from the list of titles taken from the ongoing ScHARR systematic review. Of these 10 studies, five354–358 used US preferences for the EQ-5D and three359–361 mapped to the actual EQ-5D responses rather than to the preference-based EQ-5D index. The remaining three papers362–364 used US samples to derive the mapping algorithm, but they used UK preferences for the EQ-5D index as they were developed before the US preference set was published. All three studies used a similar methodology of OLS regression to map from the MCS and PCS scores of the SF-12 to the UK preference-based index for EQ-5D. One study used a sample (n = 240) from a single health centre to examine the validity of the EQ-5D in a low-income minority population. 364 The other two papers362,363 used larger general population samples and these were considered more generalisable to our target population. The algorithm reported by Lawrence and Fleishman362 was selected in preference to the one reported by Franks et al. 363 because Lawrence and Fleishman362 explicitly validated whether or not the algorithm could predict the mean EQ-5D score across a group from the mean PCS and MCS score for that group. This was carried out for groups of patients stratified by age and for groups stratified according to the presence of six different conditions. 362 Although the algorithm developed by Franks et al. 363 was validated using an external data set, the validation did not explicitly examine whether or not the algorithm could predict group mean EQ-5D scores for different groups of patients. 363 Lawrence and Fleishman362 examined two-, three- and six-variable algorithms but found that two- and three-variable models performed better than the six-variable model and there was not much difference in performance between the two- and three-variable models. 362 We therefore decided to use the two-variable model, which predicted the EQ-5D score as a linear function of MCS and PCS. This had the added advantage that differences in EQ-5D scores (over time or between groups) could be calculated from the differences in MCS and PCS when the absolute scores are not reported.
Twelve of the included studies reported outcomes on only one or two domains of the SF-36. 97,103,107,111,112,114,149,151–153,156,343 We considered whether or not it was feasible to use these outcomes to estimate changes in EQ-5D based on changes in a single SF-36 domain by using the linear algorithm presented by Ara and Brazier352 and assuming no changes on any other domains. The study by Wearden et al. 111 provided an opportunity to validate if this approach provided reasonable estimates as it reported only a single domain of the SF-36 in the clinical paper, but also reported EQ-5D scores in the accompanying economic analysis by Richardson et al. 282 We found that the changes in utility from baseline based on changes in the single domain of SF-36 (physical functioning in this case) were a factor of 10 smaller than the changes in utility measured on the EQ-5D. This discrepancy may be due to the intervention having an effect on multiple aspects of HRQoL and these effects not being constrained to the single domain reported, as changes in other domains may influence the overall EQ-5D score. For these reasons, the approach of mapping EQ-5D changes from changes in a single domain of the SF-36 was not considered to be valid and we did not explore applying this mapping approach any further.
Three studies reported SF-36 MCS and PCS scores but did not report the scores for all eight domains. A study by Maund et al. 351 used OLS regression to estimate a mapping algorithm for SF-36 MCS and PCS to EQ-5D in a population with shoulder pain. The median duration of shoulder pain in the population used to derive the algorithm was < 12 weeks, with population being acute pain and, therefore, this population would not have been categorised as having chronic pain according to the definition used in our clinical effectiveness review. Although other studies were chosen in preference to the study by Maund et al. 351 for mapping between eight domains of SF-36 to EQ-5D, no alternatives were found in the HERC database that mapped SF-36 MCS and PCS to EQ-5D. We used the data from McBeth et al. 125 to validate whether or not using the algorithm presented by Maund et al. 351 generated QALY gains similar to those estimated directly using the EQ-5D in the McBeth et al. 125 study. We found that the utility values estimated indirectly from the SF-36 MCS and PCS scores varied from those estimated directly by up to 20% with lower absolute utility values predicted. The QALY gains between active intervention and the treatment-as-usual arm were up to 70% smaller than those estimated directly and the ordering of interventions in terms of the QALY gain was not consistent, with combined CBTHI and GA having the largest QALY gain when measuring utility indirectly from SF-36 MCS and PCS scores and CBTHI alone having the largest QALY gain based on direct EQ-5D scores. For these reasons, we did not explore applying this mapping approach any further.
The paper by Franks et al. 363 suggested that algorithms that map MCS and PCS scores from the SF-12 to the EQ-5D may be suitable for use with summary scores from the SF-36, but Franks et al. 363 recommended that this approach be validated further. Given that the algorithm by Lawrence and Fleishman362 for mapping between SF-12 MCS and PCS scores and EQ-5D has been developed and validated in a data set covering a more diverse population than the algorithm reported by Maund et al. ,351 we decided to explore the validity of using the SF-36 MCS and PCS scores in the algorithm intended for SF-12 MCS and PCS scores developed by Lawrence and Fleishman. 362 Again, we validated this approach using the data from McBeth et al. ,125 which reported both EQ-5D and SF-36 MCS and PCS scores. We found that the utility values calculated from the SF-36 MCS and PCS scores using the algorithm published by Lawrence and Fleishman362 were not similar to those measured directly using the EQ-5D with differences of 34% to 38% in the absolute utility values predicted. Furthermore, the incremental QALY gains differed by up to 80%, and again the ordering of interventions in terms of the greatest QALY gain versus treatment as usual was not consistent with the directly measured EQ-5D values. Therefore, this mapping approach was not considered to be valid and was not explored further.
Overall, there were 19 studies that reported either EQ-5D (four studies reported utility using UK or non-UK preferences),111,125,137,340 the SF-6D (two studies),136,143 all eight domains of the SF-36 (eight studies)106,131,141,144–147,342 or both the MCS and PCS of the SF-12 (five studies). 118,133,150,157,158 There were 41 studies remaining either that did not report any generic measures of HRQoL or for which we were unable to estimate preference-based utilities from the generic measures of HRQoL reported using a mapping algorithm. We considered if it was feasible to estimate QALY gains for these remaining studies by mapping from a single key symptom measure, such as fatigue, pain or disability. However, this was considered to potentially have limitations similar to mapping from a single domain of the SF-36; an improvement in one symptom may underestimate the overall benefit if other symptoms improve but the opposite could be true if an intervention improved one symptom but caused others to worsen. We therefore decided that this was not a valid approach as it could provide misleading results.
In summary, utility values over time have been extracted for those studies reporting utility values directly from the EQ-5D (using either UK preferences or non-UK preferences and the SF-6D (using UK preferences). For those studies reporting all eight domains of the SF-36 or the MCS and PCS of the SF-12, utility values have been estimated using algorithms provided by Ara and Brazier352 and Lawrence and Fleishman,362 respectively.
For studies that reported both SF-6D outcomes and all eight domains of the SF-36, we have conducted a sensitivity analysis to determine whether or not the estimates of utilities differed substantially when using utility values based on mapping to the EQ-5D from the SF-36 rather than those obtained directly from the SF-6D.
Methods used to estimate quality-adjusted life-years from utility values
The QALY gains have been estimated by assuming a linear change in utility values between each reported value and using an area under the curve approach to estimate QALYs for each arm. Where the absolute utility values were not reported, we have used data on the change in utility values from baseline or data on the difference in utilities between arms to estimate the QALY gains relative to usual care (or the lowest cost comparator arm if no usual-care arm was included).
We calculated the QALY gains using both the raw utility values and the utility values adjusted for baseline differences. We adjusted for utility differences at baseline using one of the following methods. Where the difference between arms has been reported after adjustment for differences in baseline characteristics, these have been used in preference to the raw values. Where these data are not available, the baseline value in all arms has been set to that observed in the comparator arm and then values thereafter have been determined using the difference from baseline for each study arm.
The time frame for estimating QALYs has been restricted to the last time point with comparative utility data for each study. Given the differences in populations and interventions across the studies being considered, it did not seem reasonable to use data from studies with a longer follow-up period to make predictions about the long-term persistence of treatment effects beyond the study period for studies with shorter follow-up times. Only two studies reported utility values beyond 12 months. Both of these were within-trial economic evaluations that reported QALY gains after discounting at 3.5% per annum. 111,125,126,282 Therefore, no further adjustments for discounting were required.
A full probabilistic assessment of the uncertainty around the estimates of QALY gains has not been conducted. This is because to do so for those studies where utility values have been estimated by applying a mapping algorithm to the mean SF-36 or SF-12 scores would have required the covariance matrix for the regression coefficients, which we did not have. Instead, we have used the estimates of variance for the SF-36 and SF-12 scores to derive the IQR for each score used in the mapping algorithm. We have then estimated the output of the mapping algorithm when all of the SF-36 (or both SF-12) scores are at their lower IQR and the output when they are all at their upper IQR. These utility values have been used as the upper and lower IQR for the utility values. The utility values in the comparator arm were kept fixed at their mean values and the lower and upper IQR for the QALY gain versus the comparator were calculated by setting the utility values in the intervention arm to their upper and lower IQR. (Note: if the lower IQR for both intervention and comparator are compared then the incremental QALY gains remain broadly similar as both the intervention and the comparator move a similar amount in a similar direction.) The IQR was used instead of the 95% CI because our method assumes that all eight domains of the SF-36 (or both summary component scores of the SF-12) are perfectly correlated (i.e. change in the same direction all of the time), which is unlikely to be true. So while the variability in the QALY gains is presented as an IQR, it is possible that the variance for the QALY gains is overestimated. Using the broader 95% CI as inputs to the mapping algorithm would have further exacerbated this potential overestimation of variance. Where studies have reported the 95% CI for QALYs directly, these have been used in preference to our IQR estimate.
Methods used to estimate cost-effectiveness
We sought to obtain a within-trial estimate of cost-effectiveness for each of those studies for which we were able to obtain an estimate of incremental QALYs, either from utilities/QALYs reported directly in the study or from mapping from SF-36/SF-12 outcomes to utility values (described previously in this chapter). The estimates of incremental QALYs described in Results: estimates of quality-adjusted life-year gains have been combined with the estimates of intervention costs described in Results: comparator costs. Where there were data from the published cost-effectiveness studies and cost–consequence studies, described in Systematic review of existing cost-effectiveness evidence, to indicate that an intervention increased or decreased other NHS resource use (e.g. GP consultations, hospital visits, etc. not related directly to delivery of the intervention), these have also been incorporated in the incremental cost used to calculate the ICER. However, the estimates of intervention costs from earlier in this chapter have been used, rather than any estimates of intervention costs reported in the studies themselves, for two reasons: first, it allowed a consistent costing methodology to be employed across all studies and, second, it allowed us to apply up-to-date unit costs. A fully probabilistic assessment of uncertainty was not feasible as the QALY estimates were based on a mapping algorithm and no information was available on the correlation between different quality-of-life domains used as inputs to the mapping algorithm (see Results: estimates of health utility). Instead, the lower and upper IQR range for the incremental QALYs, estimated as described in Results: estimates of quality-adjusted life-year gains, were used to calculate an IQR for the ICERs. For studies involving more than two treatment options, the IQR for the ICER was calculated only versus the lowest cost treatment option (usual care or lowest cost active comparator if no usual-care arm).
Results: intervention and comparator costs
Tables of costs estimated for each behavioural modification intervention (or active comparator, e.g. medication) by intervention types are provided in Tables 77–96 of Appendix 11. Costs could not be estimated for three studies105,146,149 because no information was provided in the publications on the duration of sessions with health-care providers. In addition, costs for the training element of two GP interventions101,159,365 could not be estimated because of a lack of information on the nature of the training, so costs for these interventions exclude training costs and total costs are therefore underestimated. For three studies that were classified as guided self-help,115,131,133 one of the study arms consisted of providing materials to patients without any sessions with health-care providers. One of these studies reported a nominal cost for a CBT booklet of £5 in its economic analysis. 115 No costs were reported for the materials provided in the other two studies. 131,133 In the study by Smith et al. ,100 GPs were provided with a consultation letter that gave advice on how to manage patients with somatisation disorder, but no cost was provided for this consultation letter. Consultation letters were also provided to GPs as part of ‘usual care plus’ in four other studies but the associated costs were not provided and could not be estimated from the papers. 143,144,156,161 Two studies137,138 had active comparator arms that consisted of recommended pharmacological management, which was costed as £217.60 and £214.03 respectively for the 6-month trial period (see Appendix 11, Table 96, for details). In Kennedy et al. ,129 both the intervention and the comparator arms received medication, but this was not costed as the medication was considered to form part of usual care. Overall, a cost was estimated for at least one arm of 55 studies that included a total of 77 intervention or active comparator arms. The median costs according to intervention type are summarised in Table 24. For GP interventions, the costs are summarised both by the type of intervention (e.g. CBT, reattribution) and by the mode of delivery (e.g. whether or not there was GP training and whether the intervention involved any interventions delivered to individual patients or groups of patients). We have summarised the other interventions according to whether they are delivered to a group of patients or to individuals.
| Intervention type | Group or individual intervention for patients | Number of study armsb | Median cost (£) |
|---|---|---|---|
| CBT low intensity | Group | 1 | 123 |
| Individual | 5 | 317 | |
| CBT high intensity | Group | 4 | 216 |
| Individual | 4 | 794 | |
| Other psychotherapy | Group | 2 | 228 |
| Individual | 8 | 462 | |
| GA | Individual | 7 | 564 |
| SES | Group | 1 | 128 |
| Individual | 6 | 740 | |
| RSSE | Group | 7 | 62 |
| Individual | 1 | 212 | |
| Guided self-help | Group | 1 | 143 |
| Individual | 2 | 240 | |
| Multimodal | Group | 3 | 193 |
| Individual | 5 | 892 | |
| Pharmacological | Individual | 2 | 216 |
| GP interventions summarised by delivery mode | |||
| GP training | NA | 7 | 337 |
| GP training with group intervention for patients | Group | 1 | 1299 |
| GP interventions for individuals | Individual | 2 | 505 |
| GP training with individual GP intervention | Individual | 8 | 871 |
| GP interventions summarised by intervention type | |||
| CBT | One individual | 1 | 939 |
| Reattribution (including modified) | Individual | 5 | 793 |
| Multimodal | Three individual and one group | 4 | 1288 |
| MUS management | Individual | 7 | 337 |
| Other psychotherapy | Individual | 1 | 802 |
| All GP interventions | NA | 18 | 546 |
The costs for interventions are summarised in Figures 61–64 as box-and-whisker plots. The green box for each intervention type shows the IQR, with the line dividing it indicating the median value. The upper and lower whiskers show the maximum and minimum values for interventions of that type. Means are shown on the plot as individual points sitting on the line between the maximum and minimum values.
FIGURE 61.
Distribution of costs for interventions delivered to individuals.
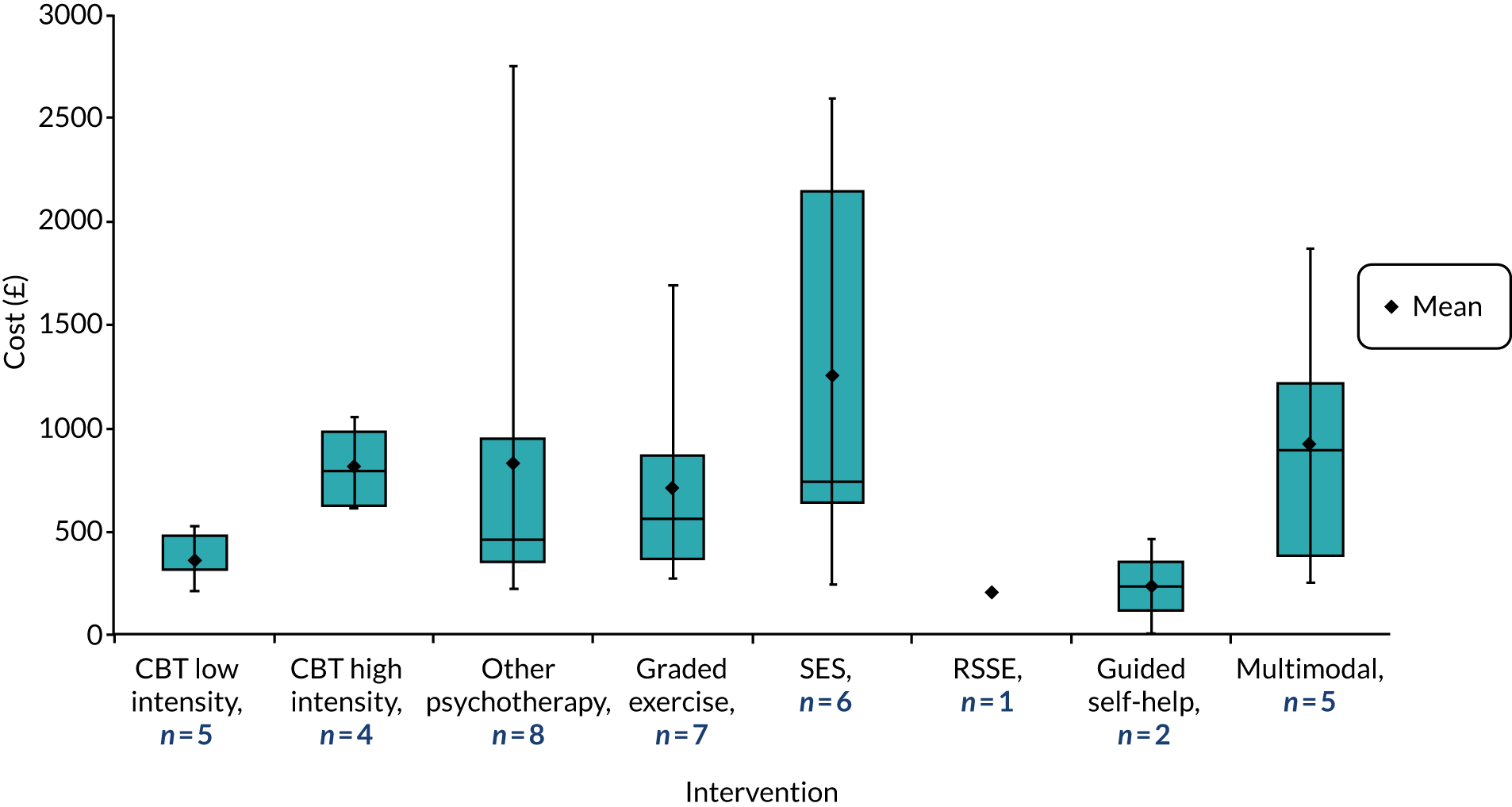
FIGURE 62.
Distribution of costs for interventions delivered to groups.

FIGURE 63.
Distribution of costs for GP interventions by delivery model.

FIGURE 64.
Distribution of costs for GP interventions by type of intervention.
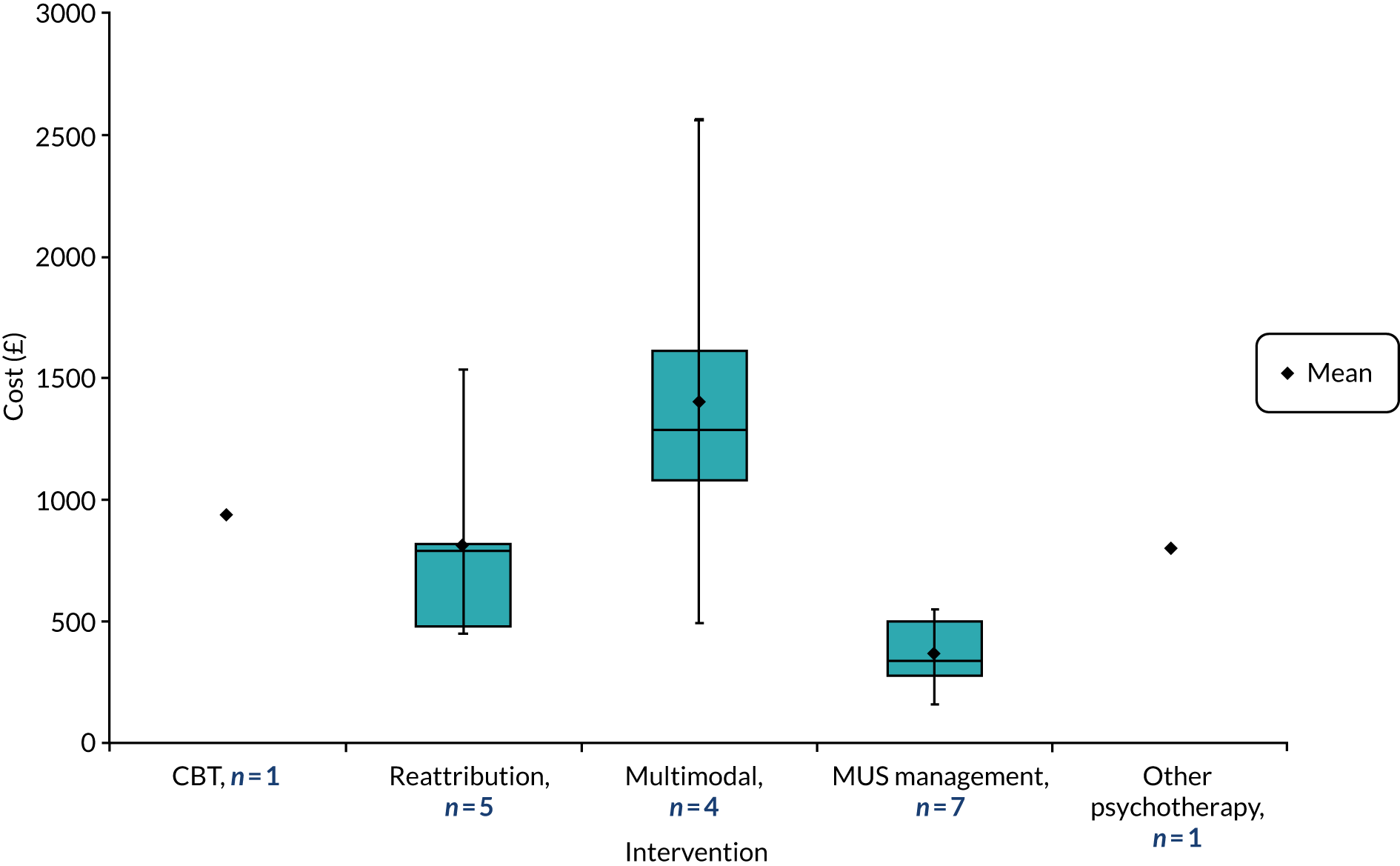
The costs for interventions delivered to individuals are summarised in Figure 61. It can be seen that within each intervention type there is typically a broad range of costs, with the greatest range being for other psychotherapy because of one very high-cost outlier. 96 There was also a wide IQR for the SES intervention type because of the results from two of the six interventions, which came from the same study,140 having a very high cost. However, the median values were less variable and ranged from £212 for RSSE to £892 for multimodal interventions.
A similar picture is seen for interventions delivered to groups in Figure 62. The median costs for group interventions range from £62 for RSSE to £227 for other (i.e. not CBT) psychotherapy interventions. The multimodal group intervention had a broad range of costs because of the results from one study, which had a very high cost (£2088), possibly because it combined both group and individual sessions. In general, the mean and median costs per patient for each intervention type are lower for interventions delivered to groups than for interventions delivered to individuals.
The costs for GP interventions by delivery mode are presented in Figure 63. The most common mode of delivery was one that involved training for GPs followed by a specific intervention for individual patients (eight study arms),101,136,153,154,159,160,311,343 which had a median cost £871 but a wide range of costs (£500–2561). It should be noted that training costs were not estimable for two of the studies included so the costs of this delivery model may have been underestimated. The next most common delivery mode was GP training with no specific intervention for patients (seven study arms),97,102,108,146,147,158,160 which had a median cost of £337 (range £160–821). The highest median cost was for GP training followed by a group intervention for patients, but the estimate was based on a single study. 147,365
When summarising the GP interventions according to the type of intervention (see Figure 64) rather than the mode of delivery, the most common intervention type was MUS management with a median cost of £337 and a range of £160–550. The other intervention types generally had higher costs and a greater spread of cost estimates, ranging from approximately £450 to £2500.
When considering all GP interventions (18 study arms), the median cost was £546 and the range was £160–2561. Part of the reason for the large variation in cost per patient is due to significant variation in the number of patients treated by each GP who was trained. In the studies that included a training element, the cost per patient is based on the number of patients treated by the GP within the study. However, this may overestimate the long-term cost per patient if GPs continue to use the training to improve their management of additional patients who were not recruited to the trial. Variation in the number of patients treated per GP trained is an important factor driving variation in the cost per patient. For example, van der Feltz-Cornelis et al. 160 included 18 GPs in the arm that received GP training but only 23 patients were enrolled in this arm. This was partly explained by a fall-off in recruitment once GPs discovered that they had been allocated to the control arm. For this reason, we used the number recruited in the intervention arm (n = 58) to estimate the cost per patient. However, even when using this latter figure, the cost per patient was very high in the control arm (i.e. £821). Conversely, Rosendal et al. 146 had a slightly higher duration of training but 506 patients were treated by 22 GPs, resulting in a much lower cost per patient (i.e. £160).
Results: estimates of health utility
Figures 65–72 show the profile of utility values over time for the 14 studies for which we were able to estimate absolute utility values either directly from the studies or via mapping from the SF-36 or the SF-12 outcomes reported. It can be seen from these figures that the utility at baseline is not always equal between arms taken from the same study, with clear baseline differences in 8 out of the 14 studies. 111,118,125,133,144,147,157,158
FIGURE 65.
Utility values for studies comparing CBTHI with usual care.
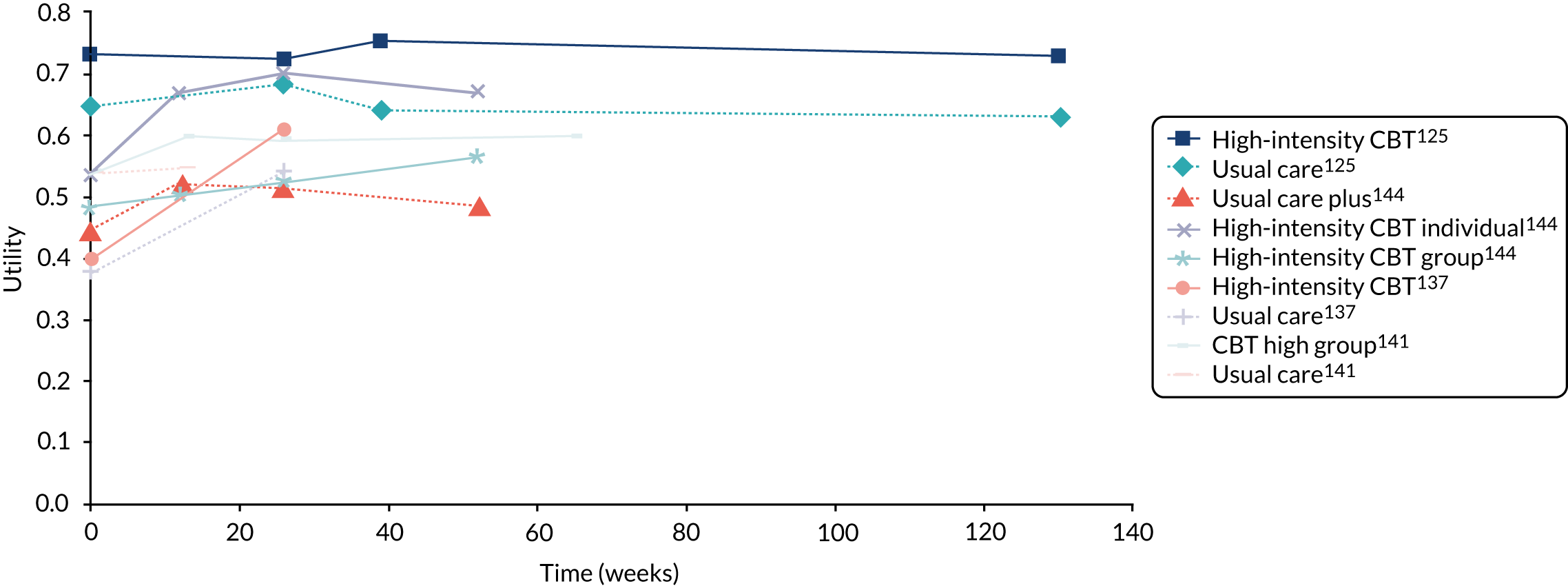
FIGURE 66.
Utility values for studies comparing GA with usual care or guided self-help.
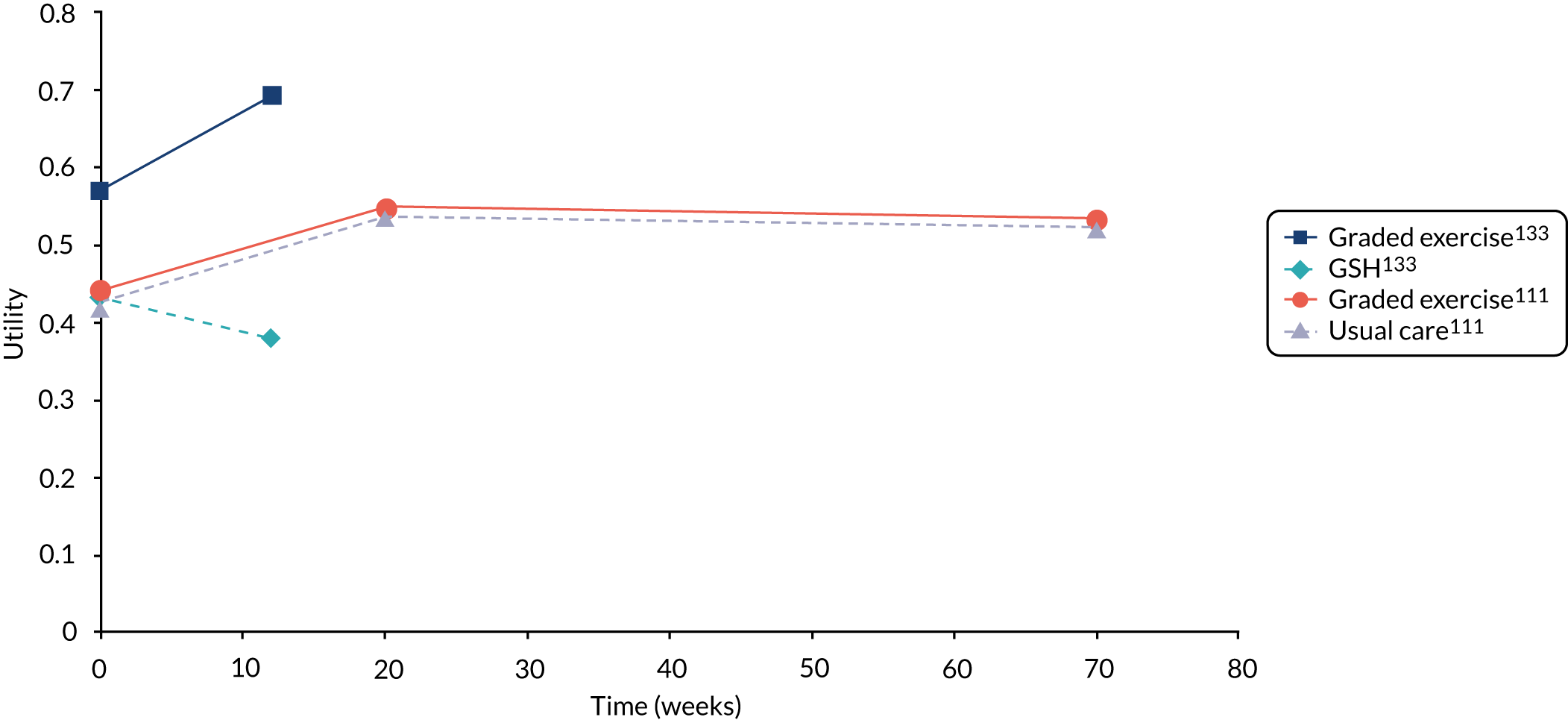
FIGURE 67.
Utility values for studies comparing other psychotherapy with usual care.

FIGURE 68.
Utility values for studies comparing RSSE with usual care.

FIGURE 69.
Utility values for studies comparing guided self-help with usual care.
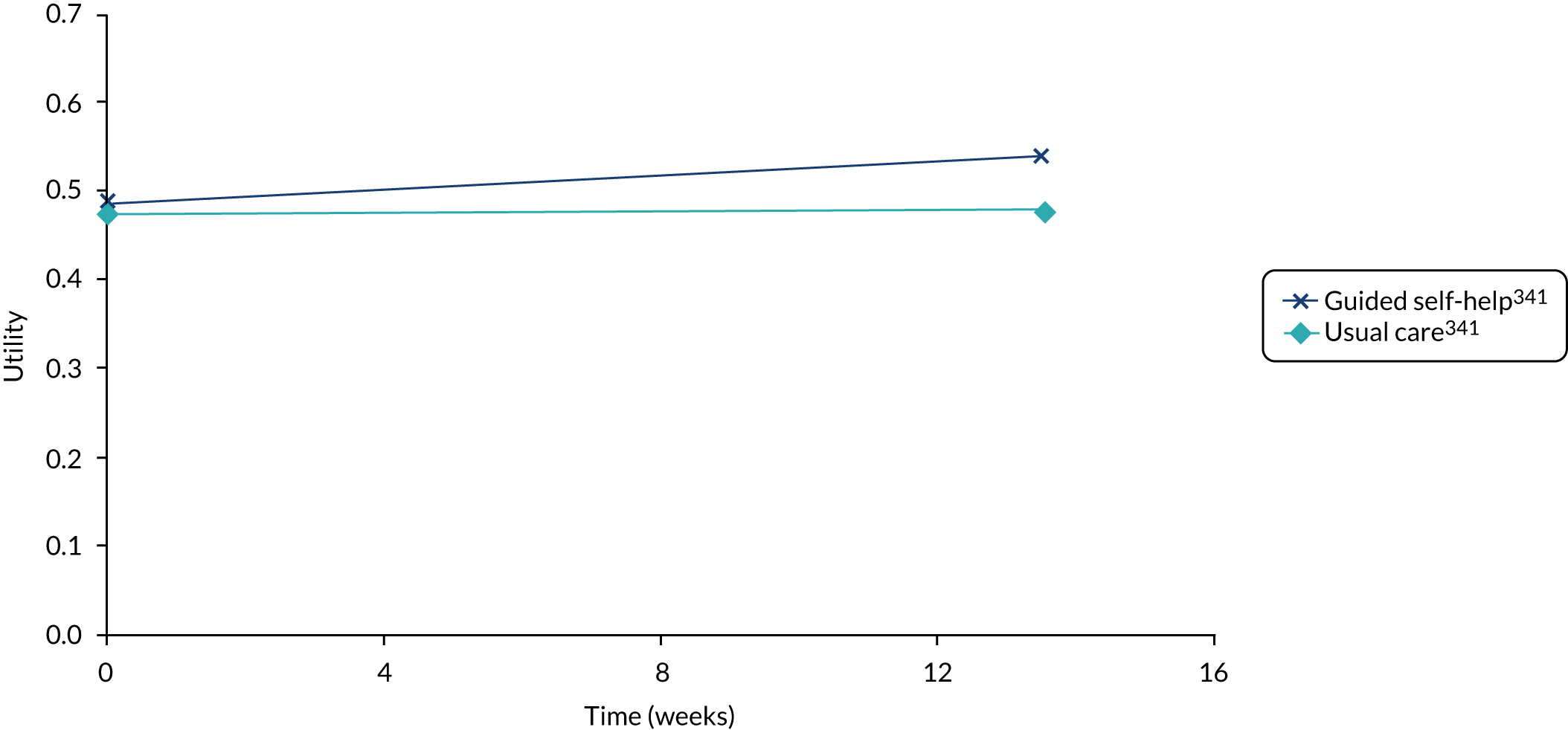
FIGURE 70.
Utility values for studies comparing SES with usual care.
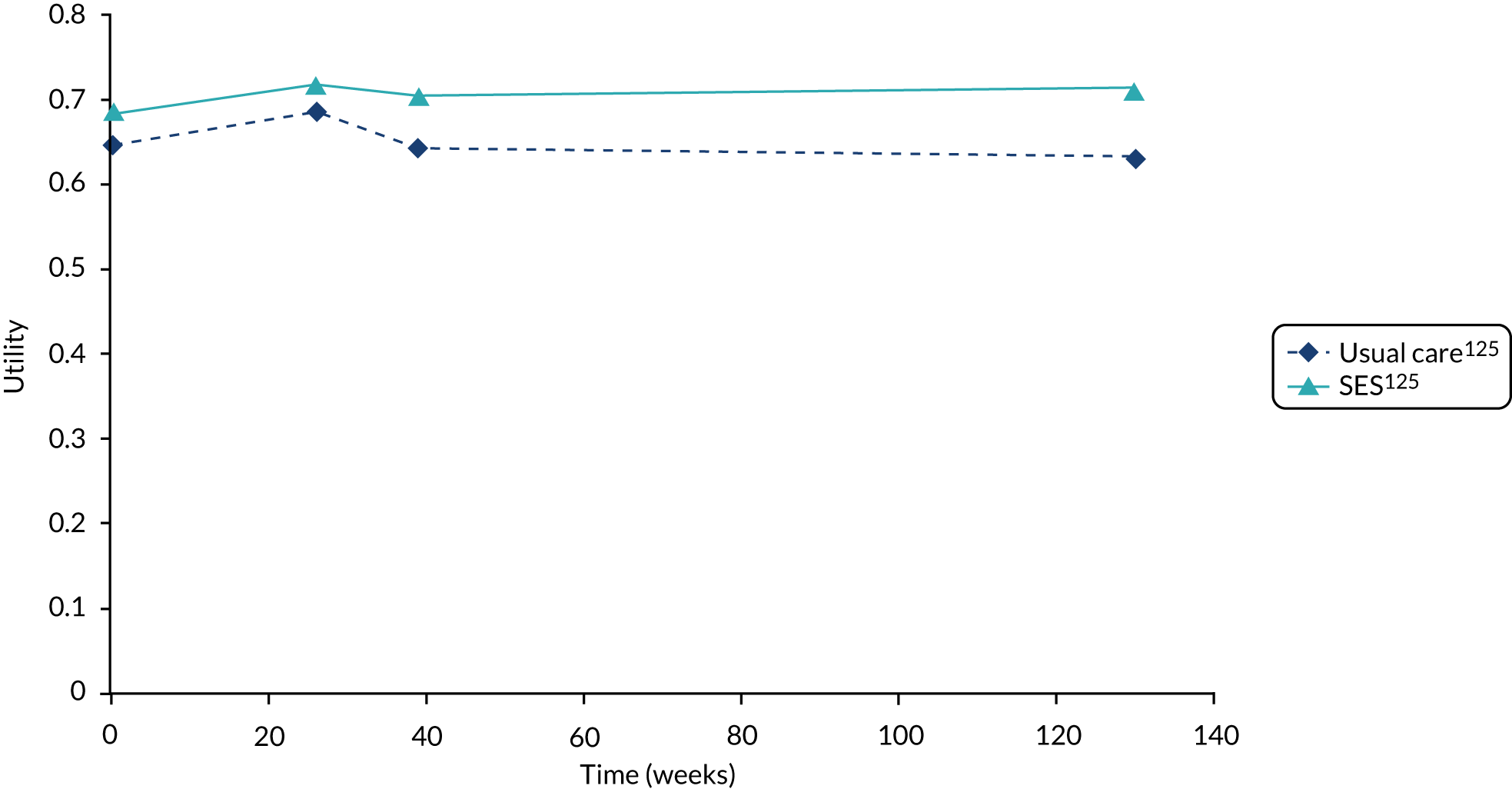
FIGURE 71.
Utility values for studies comparing multimodal treatments with single modality treatments.

FIGURE 72.
Utility values for studies comparing GP interventions with usual care or other GP interventions.
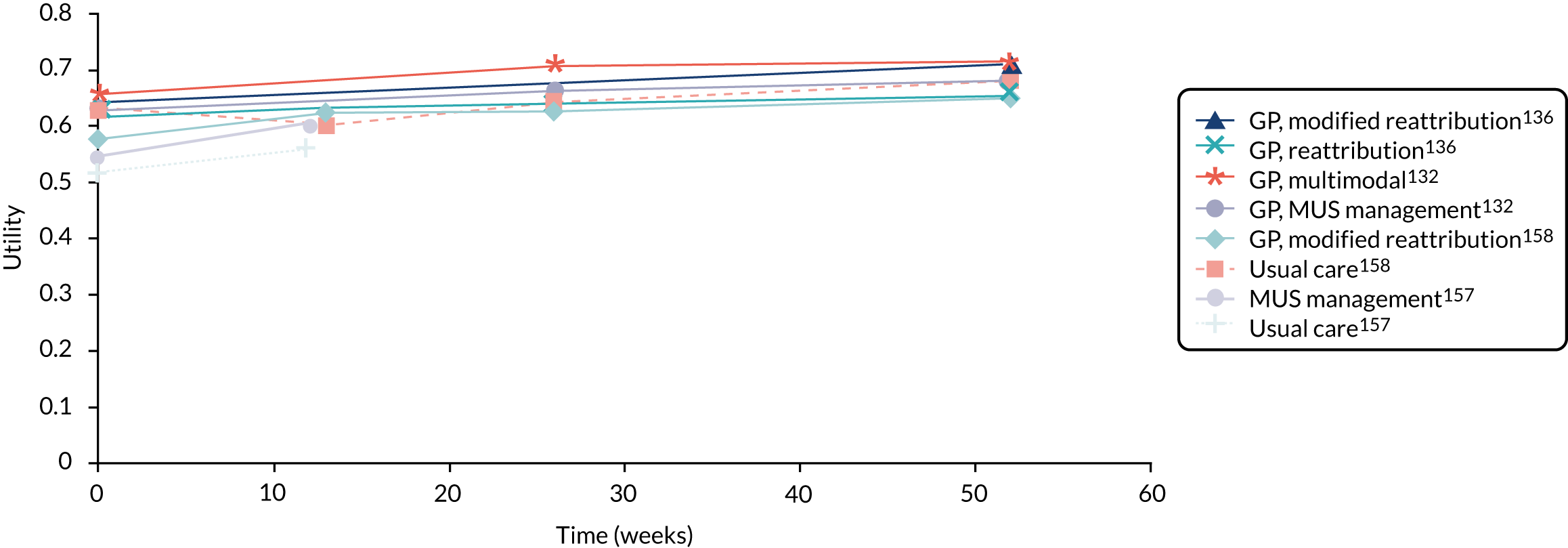
In general, those interventions that achieved a difference in utility at short-term follow-up were able to maintain that utility gain in the long term. 118,125,147,150 However, given that the populations and interventions varied considerably across the studies, it was not considered reasonable to assume that a similar maintenance of treatment effects would be seen across other behavioural modification interventions where long-term data were lacking.
We were unable to estimate absolute utility values for 5 of the 19 studies identified as including EQ-5D, SF-6D, SF-12 or SF-36 data, so these studies are not included in Figures 65–72. 106,131,145,146,340 Three of these studies131,145,146 provided data that allowed us to estimate the utility difference between trial arms, by assuming a common utility at baseline. Pols and Battersby145 reported the difference from baseline for each study arm. Robinson et al. 131 reported the difference between trial arms at 12 months, and Rosendal et al. 146 reported the difference from baseline for each arm and the adjusted difference between trial arms, with the adjusted difference between trial arms being used in the analysis. For one study,106 which reported SF-36 outcomes, we were unable to apply the utility mapping algorithm from SF-36 to EQ-5D as a mixture of mean and median SF-36 domain scores. Therefore, no utility values or QALYs could be estimated for this one study. The remaining study reported incremental QALYs directly, in the accompanying economic paper,340 so it was not necessary to calculate absolute or incremental utility values.
A sensitivity analysis was conducted to explore whether or not the utility values differed substantially when using EQ-5D-based utility values obtained via mapping from the SF-36 compared with using utility values based directly on the SF-6D. The results for the studies by Aiarzaguena et al. 136 and van Ravesteijn et al. 143 are shown in Figures 73 and 74, respectively.
FIGURE 73.
Sensitivity analysis comparing utility values mapped from SF-36 to EQ-5D with those obtained directly from SF-6D for Aiarzaguena et al. 136
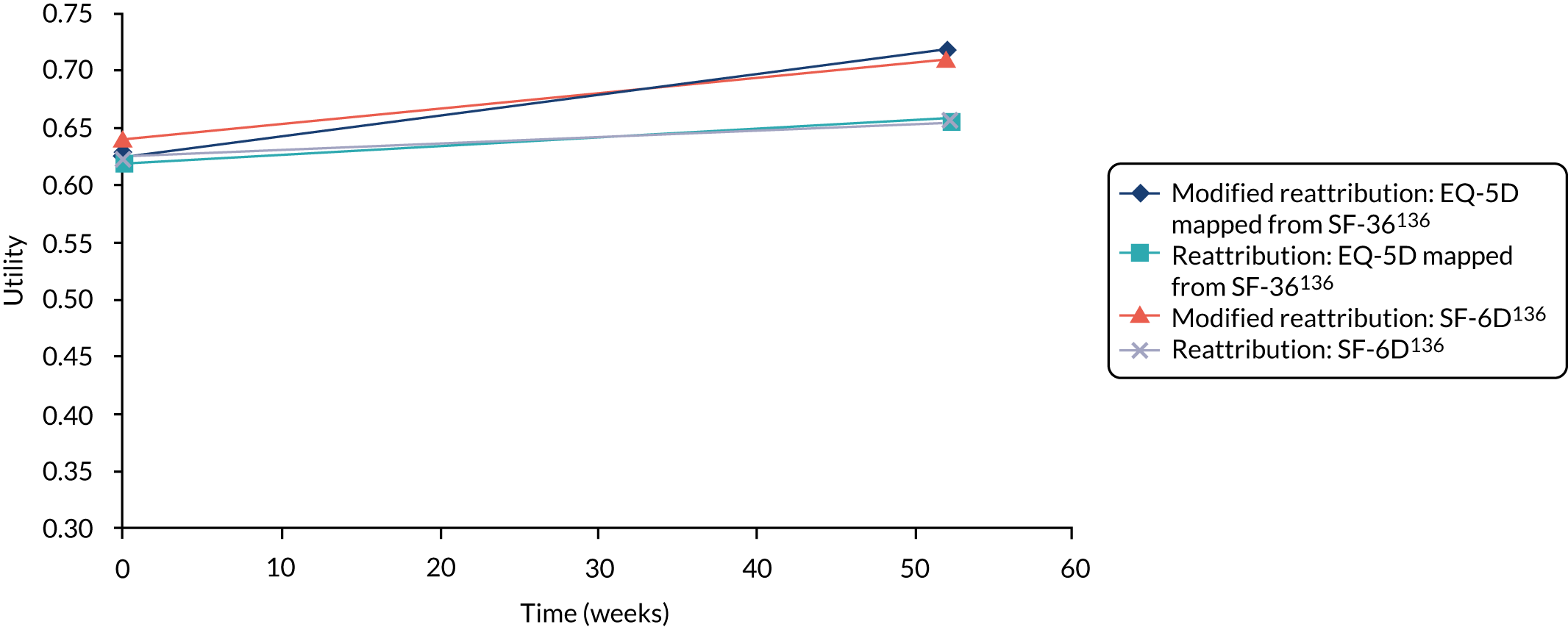
FIGURE 74.
Sensitivity analysis comparing utility values mapped from SF-36 to EQ-5D with those obtained directly from SF-6D for van Ravesteijn et al. 143
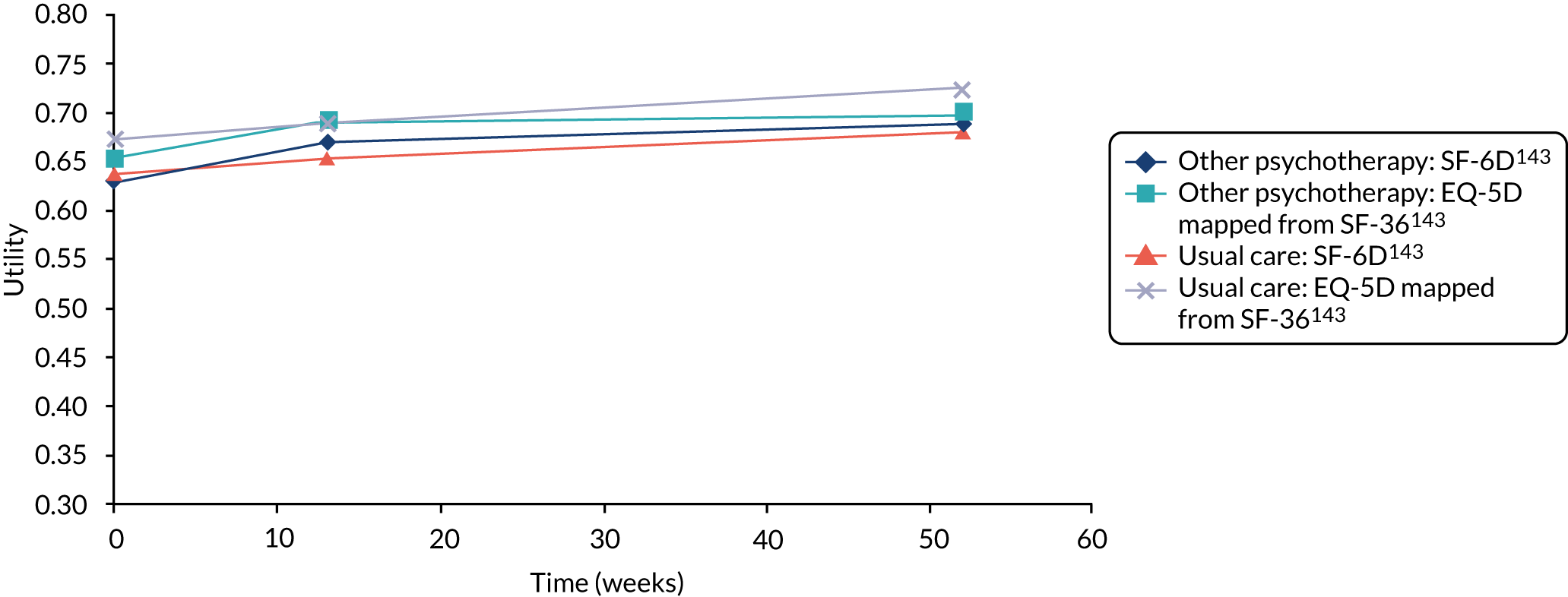
In the study by Aiarzaguena et al. ,136 the utility values obtained by mapping from the SF-36 to the EQ-5D and those obtained directly from the SF-6D are similar in the reattribution arm. In the modified reattribution arm, the values at baseline are lower when obtained by mapping from the SF-36 and the gain in utility values is slightly larger.
In the study by van Ravesteijn et al. ,143 the absolute utility values are higher in both arms when using the values obtained by mapping from the SF-36 to the EQ-5D. The ordering of the intervention and comparator arms in terms of absolute utility is different at final follow-up between the two methods for estimating health utility, with other psychotherapy having greater utility at final follow-up when using the values obtained directly from the SF-6D and usual care having greater utility at final follow-up when using the values mapped from SF-36 to EQ-5D. However, in both cases the differences between trial arms are small and the utility profiles cross during the duration of the study.
Results: estimates of quality-adjusted life-year gains
The QALY gains estimated for each study are provided in Table 25. It can be seen that the mean estimates of QALY gains are generally small and are consistently under 0.1 QALYs. In the five studies that directly reported the QALY gains and their 95% CI,111,125,126,137,143,282,340 it was found that there was no statistically significant difference in QALYs between trial arms. In the studies where the IQRs for the QALY gains were estimated from the IQRs for the SF-36/SF-12 outcomes, we found that the lower IQR was above zero for all but three comparisons. 144,146,147
| First author and year of publication | Treatment strategies | Utility measurement method | Baseline utility | Utility at last follow-up | ΔQALYs using unadjusted data | ΔQALYs using adjustment for baseline differences |
|---|---|---|---|---|---|---|
| Aiarzaguena, 2007136 |
|
SF-6D at baseline and 1 year |
|
|
1 vs. 2: 0.036 |
1 vs. 2: 0.019a (95% CI 0.002 to 0.036)a (mid-point of 0.028 when using EQ-5D mapped from SF-36) |
| Alda, 2011137 |
|
EQ-5D with Spanish tariff at baseline and 6 months and QALYs reported directly |
|
|
1 vs. 3: 0.02 2 vs. 3: 0.00 |
1 vs. 3: 0.02 (95% CI –0.00 to 0.03)b 2 vs. 3: 0.00 (95% CI –0.01 to 0.02)b |
| Burton, 2012157 |
|
EQ-5D mapped from SF-12 using Lawrence and Fleishman’s362 algorithm |
|
|
1 vs. 2: 0.008 | 1 vs. 2: 0.004 (IQR –0.015 to 0.023) |
| Cuesta-Vargas, 2012118 |
|
EQ-5D mapped from SF-12 using Lawrence and Fleishman’s362 algorithm |
|
|
NR | 1 vs. 2: 0.074c (IQR 0.049 to 0.100)d |
| Gili, 2014144 |
|
EQ-5D mapped from SF-36 using Ara and Brazier352 |
|
|
1 vs. 3: 0.164 2 vs. 3: 0.025 |
|
| Ho, 2012150 |
|
EQ-5D mapped from SF-12 using Lawrence and Fleishman’s362 algorithm |
|
|
1 vs. 2: 0.029 | 1 vs. 3: 0.027e (IQR 0.020 to 0.033)d |
| Larisch, 2004158 |
|
EQ-5D mapped from SF-12 using Lawrence and Fleishman’s362 algorithm |
|
|
1 vs. 2: –0.015 | 1 vs. 2: 0.041f (IQR 0.01 to 0.068)d |
| LeFort, 1998342 |
|
EQ-5D mapped from SF-36 using Ara and Brazier352 |
|
|
1 vs. 2: 0.009 | 1 vs. 2: 0.007e (IQR 0.005 to 0.009)d |
| Marques, 2015133 |
|
EQ-5D mapped from SF-12 using Lawrence and Fleishman’s362 algorithm |
|
|
1 vs. 2: 0.052 | 1 vs. 2: 0.020e (IQR 0.010 to 0.031)d |
| McBeth, 2012125 |
|
EQ-5D measured in study |
|
|
1 vs. 4: 0.1272 vs. 4: 0.2293 vs. 4: 0.151 |
1 vs. 4: 0.047 (95% CI –0.086 to 0.182)b 2 vs. 4: 0.097 (95% CI –0.048 to 0.240)b 3 vs. 4: 0.025 (95% CI –0.099 to 0.154)b (Discounted) |
| Peters, 2002106 |
|
EQ-5D mapped from SF-36 using Ara and Brazier352 | NEg | NEg | NEg | NEg |
| Pols, 2008145 |
|
EQ-5D mapped from SF-36 using Ara and Brazier352 | NEh | NEh | NEh | 1 vs. 2: –0.003i (IQR NE as no measure of variance presented) |
| Robinson, 2006131 |
|
EQ-5D mapped from SF-36 using Ara and Brazier352 | NEj | NEj | NEj | 2 vs. 3: 0.013i (IQR 0.006 to 0.020)d |
| Rosendal, 2007146 |
|
EQ-5D mapped from SF-36 using Ara and Brazier352 | NEj | NEj | NEj | 1 vs. 2: –0.018i (IQR –0.023 to –0.003)d |
| Schaefert, 2013147 |
|
EQ-5D mapped from SF-36 using Ara and Brazier352 |
|
|
1 vs. 2: 0.039 | 1 vs. 2: 0.008d (IQR –0.004 to 0.020)d |
| van der Roer, 2008340 |
|
QALY gains estimated from EQ-5D with Dutch tariff reported but not utility values | NE | NE | NE | 1 vs. 2: 0.03 (95% CI –0.06 to 0.12)b |
| van Ravesteijn, 2013143 |
|
SF-6D utility values reported in study |
|
|
1 vs. 2: 0.010k |
1 vs. 2: 0.012 (95% CI −0.019 to 0.041)b (mid-point of 0.015 when using EQ-5D mapped from SF-36) |
| Wearden, 2010111 |
|
EQ-5D reported in study |
|
|
1 vs. 3: 0.016 2 vs. 3: –0.019 |
1 vs. 3 = –0.012 (95% CI –0.088 to 0.065)b 2 vs. 3 = –0.042 (95% CI –0.122 to 0.038)b (Discounted) |
| Zonneveld, 2012141 |
|
EQ-5D mapped from SF-36 using Ara and Brazier352 |
|
2 vs. 1: 0.006l | 2 vs. 1: 0.007l (IQR 0.005 to 0.008)d |
A sensitivity analyses was conducted in which the utility values obtained by mapping from the SF-36 to the EQ-5D were used to calculate QALY gains for the two studies that reported SF-6D utility values. 136,143 For Aiarzaguena et al. 136 the QALY using the utility value obtained by mapping from SF-36 to EQ-5D was 0.028, after adjusting for baseline differences, whereas the equivalent estimate when using the SF-6D utility values reported directly in the paper was 0.019. For the study by van Ravesteijn et al. ,143 the QALY gain was calculated to be 0.015, after adjusting for baseline differences, whereas the equivalent figure when using the SF-6D was reported to be 0.012 in the paper. Therefore, the choice of method to obtain utility estimates does appear to be important and the mid-point ICERs for these two studies may be overestimated in the base-case analysis because of the use of utility values measured using the SF-6D rather than the EQ-5D.
Results: cost-effectiveness analysis
A summary of the cost-effectiveness evidence is provided in Table 26, with the detailed results for each study reported in Table 27. In the summary table, for each comparison we have recorded whether the mid-point ICER is under or over £30,000 per QALY (denoted by ‘< £30K’ or ‘> £30K’, respectively). This cut-off point has been chosen as it is the upper limit of the range considered to be cost-effective by NICE (£20,000 to £30,000 per QALY)244 so interventions with a mid-point ICER above this range are unlikely to be considered cost-effective when applying the NICE threshold. Where the mid-point ICER is under £30,000 but the upper range of the ICER is above £30,000, then the intervention may not be considered cost-effective because of the degree of uncertainty in the ICER. For this reason, where the IQR crosses £30,000, we have added ‘W’ to indicate that there is a wide IQR and there may be uncertainty regarding the cost-effectiveness. Comparisons where one intervention was dominated are also indicated (denoted by ‘Dom’); an intervention is dominated by another if it has higher costs but lower QALY gains.
| Intervention | UC | UC+ | CBTHI | GSH | SES | Graded activity | GP reattribution | GP MUS management |
|---|---|---|---|---|---|---|---|---|
| CBTHI |
< £30KW137 < £30KW125 > £30K141 |
< £30K144 Dom144 |
< £30K144a | |||||
| Other psychotherapy | Dom111 | < £30KW143 | Dom111 | |||||
| GA | Dom111 | < £30KW133 | ||||||
| SES | > £30K125 | Dom125 | ||||||
| GSH |
< £30KW131 < £30KW342 |
|||||||
| RSSE | < £30KW150 | |||||||
| GP modified reattribution | < £30KW158 | > £30KW136 | ||||||
| Pharmaceutical | Dom137 | |||||||
| Multimodal |
> £30K125 Dom145 |
Dom125 | < £30K118 |
< £30KW125 > £30KW340 |
||||
| GP MUS |
Dom146 > £30KW157 |
|||||||
| GP multimodal | > £30K147 |
| First author and year of publication | Treatment strategies | ΔQALYs using adjustment for baseline differences | Intervention costsa | Other costs | ICER | IQR for ICER |
|---|---|---|---|---|---|---|
| Aiarzaguena, 2007136 |
|
1 vs. 2: 0.019b (95% CI 0.002 to 0.036)b |
|
NR | 1 vs. 2: £39,142 (£26, 638 when using EQ-5D mapped from SF-36 instead of SF-6D) | 1 vs. 2: £20,719 to £353,214 |
| Alda, 2011137 |
|
1 vs. 3: 0.02 (95% CI 0.00 to 0.03)c 2 vs. 3: 0.00 (95% CI –0.01 to 0.02)c |
|
Non-UK resource use |
1 vs. 3: £10,025 2 vs. 1: 2 is dominated by 1 |
1 vs. 3: £6683 to > £40,000 |
| Burton, 2012157 |
|
1 vs. 2: 0.004 (IQR –0.103 to 0.018) |
|
NR | 1 vs. 2: £129,267 | 1 vs. 2: £20,658 to dominated |
| Cuesta-Vargas, 2012118 |
|
1 vs. 2: 0.074d (IQR 0.049 to 0.100)e |
|
NR | 2 vs. 1: £18,641 | 2 vs. 1: £13,883 to £28,261 |
| Gili, 2014144 |
|
|
NR |
1 vs. 3: £14,146 2 is dominated by 3 1 vs. 2: £9502 |
1 vs. 3: £10,928 to £20,049 2 vs. 3: £23,199 to dominated |
|
| Ho, 2012150 |
|
1 vs. 2: 0.027f (IQR 0.020 to 0.033)e |
|
NR | 1 vs. 2: £1397 (£23,048 if sessions are one to one) | 1 vs. 2: £1124 to £1843 (£18,558 to £30,406 if group sessions are two to one) |
| Larisch, 2004158 |
|
1 vs. 2: 0.041g (IQR 0.01 to 0.068)e |
|
Non-UK resource use | 1 vs. 2: £11,863 | 1 vs. 2: £7,115 to £47,022 |
| LeFort, 1998342 |
|
1 vs. 2: 0.007f (IQR 0.005 to 0.009)e |
|
NR | 1 vs. 2: £21,755 | 1 vs. 2: £16,632 to £31,437 |
| Marques, 2015133 |
|
1 vs. 2: 0.020f (IQR 0.010 to 0.031)e |
|
NR | 1 vs. 2: £27,894 | 1 vs. 2: £18.358 to £58,052 |
| McBeth, 2012125,126 |
|
1 vs. 4: 0.047 (95% CI –0.086 to 0.182)c 2 vs. 4: 0.097 (95% CI –0.048 to 0.240)c 3 vs. 4: 0.025 (95% CI –0.099 to 0.154)c (Discounted) |
Estimated from resource use:
|
2 vs. 4: £9797 3 and 1 are dominated by 2 3 vs. 4: £56,064 1 vs. 4: £39,387 1 vs. 3: £20,436 |
2 vs. 4: £3,959 to dominated | |
| Peters, 2002106 |
|
NEg |
|
No significant difference in resource use between arms (costs not reported) | NE | NE |
| Pols, 2008145 |
|
1 vs. 2: –0.003i (IQR NE as no measure of variance presented) |
|
Some resource use reported but non-UK | 1 dominated by 2 | NE |
| Robinson, 2006131 |
|
2 vs. 3: 0.013i (IQR 0.006 to 0.020)e 1 vs. 2: NE |
|
2 vs. 3: –£72.741 vs. 2: £7.53 |
2 vs. 3: NE (Guidebook would dominate UC if it cost under £72.74) 1 vs. 2: NE |
NE |
| Rosendal, 2007146 |
|
1 vs. 2: –0.018i (IQR –0.023 to –0.003)e |
|
NR | 1 is dominated by 2 | 1 vs. 2: dominated to dominated |
| Schaefert, 2013147 |
|
1 vs. 2: 0.008f (IQR –0.004 to 0.020)e |
|
Some resource use reported but non-UK | 1 vs. 2: £124,535 | 1 vs. 2: £51,184 to dominated |
| van der Roer, 2008340 |
|
1 vs. 2: 0.03 (95% CI –0.06 to 0.12)c |
|
Some resource use reported but non-UK | 1 vs. 2: £42,887 | 1 vs. 2: £10,722 to dominated |
| van Ravesteijn, 2013143 |
|
1 vs. 2: 0.012 (95% CI −0.019 to 0.041)c |
|
Some resource use reported but non-UK | 1 vs. 2: £13,825 (£11,171 when using EQ-5D mapped from SF-36 instead of SF-6D) | £4046 to dominated |
| Wearden, 2010111 |
|
1 vs. 3 = –0.012 (95% CI –0.088 to 0.065)c 2 vs. 3 = –0.042 (95% CI –0.122 to 0.038)c (Discounted) |
Estimated from resource use
|
1 vs. 3: dominated 2 vs. 3: dominated |
1 vs. 3: £2182 to dominated 2 vs. 3: £8653 to dominated |
|
| Zonneveld, 2012141 |
|
2 vs. 1: 0.007j (IQR 0.005 to 0.008)e |
|
NR | 1 vs. 2: £56,792 | 2 vs. 1: £45,400 to £76,816 |
There is a large degree of heterogeneity in the estimates of cost-effectiveness for individual studies, with some interventions having mid-point ICERs in the range that would normally be considered cost-effective by NICE (i.e. below £20,000 to £30,000 per QALY) and others having ICERs well above this range. Some interventions were also found to be dominated by usual care or dominated by other behavioural modification interventions.
Where there was more than one study providing an estimate of cost-effectiveness for a particular comparison, the evidence was often inconsistent. For example, the ICERs for two studies125,137 that compared CBTHI with usual care were below £20,000 with an upper IQR above £30,000, suggesting that CBTHI is potentially cost-effective. However, a third study141 had an ICER of £56,792 (IQR £45,400–£76,816). This was despite the Zonneveld et al. 141 study having a higher intervention cost than one of the other two studies, indicating a higher intensity of CBT. These inconsistencies may be driven by differences in the response of different study populations to CBT or differences in the delivery of the CBT that are not reflected in the cost estimates. In this case, the two studies with favourable mid-point ICERs125,137 were both studies in patients with chronic pain (fibromyalgia in both cases), whereas the study141 with the higher ICER had a broader population that included both patients with chronic pain and those with somatoform disorder.
High-intensity CBT was also found to have inconsistent cost-effectiveness compared with usual care plus, although it should be noted that this was based on a single study144 that found that individual CBTHI had an ICER < £30,000 compared with usual care plus, whereas group CBTHI was dominated by usual care plus. 144 This suggests that, although these interventions have been grouped together under the heading of CBTHI, the particular mode of delivery (i.e. group vs. individual) is capable of producing important differences in the estimates of benefits and the estimates of cost-effectiveness. Therefore, caution should be exercised when comparing interventions that have been grouped together but that may differ significantly.
The two studies that provide ICERs for guided self-help versus usual care suggest that this intervention has the potential to be cost-effective but there remains some uncertainty regarding its cost-effectiveness as the CIs crossed £30,000 per QALY. The study by Robinson et al. 131 found that guided self-help, delivered as a guidebook, was cost-saving and produced a QALY gain and, therefore, guided self-help would dominate usual care provided the guidebook cost less than the cost-saving (£72.74). It seems likely, therefore, that this intervention would be cost-effective but this cannot be confirmed without an estimate of the cost of the guidebook (the ICER has been summarised in Table 26 as ‘< £30KW’). The other study comparing guided self-help with usual care, by LeFort et al. ,342 gave a mid-point ICER of £21,775 with an IQR of £16,632–£31,437. These two studies also had different populations (i.e. IBS and chronic pain), suggesting that guided self-help has the potential to be cost-effective across a number of different subsets of the MUS population, but the cost-effectiveness remains uncertain.
The ICER for RSSE versus usual care based on the study by Ho et al. 150 was £1397 with a narrow IQR (£1124–£1843), but there was additional uncertainty related to this study because the intervention was described as being a group intervention but the group size was not indicated. The mid-point estimate was calculated assuming that the intervention was delivered to all patients at the same time in a single group but a sensitivity analysis exploring the impact of lower group sizes (two patients per group) gave a mid-point ICER of £23,048 (IQR £18,558–£30,406). For this reason, this study has been denoted as having wide uncertainty in Table 26.
Two studies provided estimates of the cost-effectiveness of GA in patients with chronic fatigue, but the comparator arms differed. The analysis based on Wearden et al. 111 found that GA was dominated by usual care. Conversely, the analysis based on Marques et al. 133 found a positive QALY gain but an ICER at the upper limit of the NICE cost-effectiveness range (£27,894) for GA compared with guided self-help, which in this study consisted of usual care plus the provision of information about physical activity. These two studies therefore appear to give inconsistent results. However, it should be noted that, in the study by Wearden et al. ,111 the QALY gains were estimated from directly measured EQ-5D utility values, whereas, in the study by Marques et al. ,133 the QALY gains were estimated via mapping from SF-36 MCS and PCS scores to EQ-5D utilities, which is associated with additional uncertainty.
The analysis based on the study by Wearden et al. 111 also found that GA dominated other psychotherapy, but other psychotherapy itself was also dominated by usual care. The only other study to examine other psychotherapy, by van Ravesteijn et al. ,143 had usual care plus as the comparator, and for this study we estimated a low mid-point ICER but a broad IQR, with other psychotherapy being dominated at the upper limit. The study by van Ravesteijn et al. 143 also had a broader MUS population than the study by Wearden et al,111 which was restricted to patients with chronic fatigue.
The evidence of cost-effectiveness for SES versus usual care was limited to a single study by McBeth et al. ,125 from which we estimated a high ICER versus usual care in patients with chronic pain. The same study also found that SES was dominated by CBTHI.
Pharmaceutical therapy was only included in one study, by Alda et al. ,137 and was found to be dominated by CBTHI in patients with chronic pain.
In general, the GP interventions were not particularly cost-effective. Modified reattribution had a high ICER versus reattribution in patients with MUS based on the study by Aiarzaguena et al. ,136 although the mid-point ICER was reduced to < £30,000 when EQ-5D utility values obtained by mapping from the SF-36 to the EQ-5D were used instead of using SF-6D utility values. GP MUS management was dominated by usual care in patients with somatoform disorder based on the study by Rosendal et al. ,146 and GP MUS management had a higher ICER (£129,000) with a wide IQR based on the pilot study by Burton et al. ,157 also in patients with MUS. GP multimodal intervention had a high ICER (£124,000) versus GP MUS management in patients with MUS, based on the study by Schaefert et al. 147 However, there was an exception for GP-modified reattribution compared with usual care that was found to have an ICER of £11,863 (IQR £7115–47,022) in patients with somatoform disorder based on the paper by Larisch et al. 158
Only one study118 compared a multimodal intervention combining guided self-help and SES with guided self-help alone in patients with back pain. The mid-point ICER was < £20,000 per QALY and the upper limit of the IQR for the ICER was < £30,000 per QALY, suggesting reasonable confidence in the cost-effectiveness of the multimodal intervention.
Two studies compared a multimodal intervention with SES in patients with chronic pain. van der Roer et al. 340 compared a multimodal intervention combining sport, education and a behavioural programme to SES in patients with back pain, but the ICER estimated for this comparison was above the range usually considered cost-effective. McBeth et al. 125 compared a combination of CBTHI with SES against SES alone in patients with chronic widespread pain. Multimodal intervention versus SES alone had an ICER in the range usually considered cost-effectiveness by NICE. However, the same study also included a CBTHI arm and multimodal therapy was dominated by CBTHI alone. Therefore, CBTHI would be the optimal intervention based on this study in preference to SES.
Conclusions and discussion
The behavioural modification interventions for patients with MUS identified in our review were found to have a very broad range of interventions costs. Interventions delivered to groups were generally found to have a cost per patient that is lower than the cost per patient for interventions of the same type delivered to individuals. For interventions delivered to groups, the cost per patient is dependent on the group size. In studies where the group size or number of groups was not reported, we have assumed that all patients received the intervention as part of a single group that may have underestimated the cost per patient if smaller groups were in fact used. The cost per patient for interventions that involve training GPs to manage MUS in a particular way is very dependent on the number of patients treated by each GP who is trained. The broad range of intervention costs is indicative of the high degree of heterogeneity in the behavioural modification interventions included in our review. In future research, it would be helpful to investigate whether or not more intensive interventions with higher costs generate greater QALY gains.
Utility estimates were often not equal at baseline, making adjustment for baseline differences necessary. Where outcomes adjusted for baseline differences were not reported in the study paper, adjustment for baseline differences was achieved by setting the starting utility of the intervention arm equal to that of the control arm and using either the difference from baseline or the difference between arms to estimate utility thereafter. This is a fairly crude method for adjusting for baseline differences and may have introduced bias, particularly if the utility changes that can be achieved in an individual are not independent of their baseline utility.
In general, those interventions that achieved a difference in utility at short-term follow-up were able to maintain that utility gain in the long term. However, as different interventions may have different capacities to achieve treatment effects that persist, we decided not to extrapolate the maintenance of treatment effects from those studies with long-term data to other studies with only short-term data. For this reason, our analysis of QALYs gained was limited to the last study time point reporting a randomised comparison of outcomes for each individual study.
Using a different time frame for each study was considered appropriate when the focus was on the within-trial estimates of cost-effectiveness for each study. However, the use of differing time frames for each study makes the estimates of QALY gains not comparable across studies. It would therefore not have been appropriate to have used these estimates of QALY gain to conduct an incremental analysis that compared interventions across multiple studies.
In general, the QALY gains estimated for behavioural modification interventions from individual studies were small, but our analysis may have underestimated the true long-term QALY gains if the differences between trial arms observed during the trial period persist in the long term beyond the trial follow-up.
The uncertainty in the QALY estimates has been captured in a fairly crude manner by using the upper and lower IQR for the HRQoL scores going into the utility mapping algorithm to explore the uncertainty in the incremental QALYs gained. The IQR values presented for the QALY gains are intended to give only an indication of the potential variation in the QALY gain that arises from uncertainty in the SF-36/SF-12 scores used within the mapping algorithm to calculate utilities. A more complex approach would have been necessary to allow a full probabilistic assessment of the uncertainty in the QALY gains but we felt that this may not provide a more unbiased estimate because of a lack of information on the correlation between changes in the various domain scores used in the mapping algorithm. Although our method assumes that changes in these domains are perfectly correlated and may therefore overestimate the variance, the use of the IQR rather than the full distribution for each input to the algorithm should mitigate any overestimation of the uncertainty. However, the true uncertainty around the QALY gains may be greater as our approach does not quantify uncertainty around the mapping algorithm itself.
This set of within-trial estimates of cost-effectiveness has several important limitations. The estimates of QALYs are based on the data and time points reported for each individual study rather than the outputs of the NMA. We have therefore not been able to benefit from pooling clinical efficacy data across studies, but this was considered to be a fairly minor limitation given that, in general, there were only one or two studies for each comparison in the NMA. The conclusions that can be drawn are also limited to the direct comparisons presented in the individual studies whereas the NMA allows indirect comparisons to be made regarding the clinical effectiveness of interventions not compared directly in a single study.
The included studies cover many different populations classified as having MUS including those with chronic pain, chronic fatigue, IBS and somatoform disorders. It is not clear from the evidence that we have identified if interventions that are cost-effective in one population would be similarly cost-effective in another population with MUS. Many of the interventions that have received the same intervention classification differ considerably in terms of their intensity or in terms of their content, owing to the broad intervention groupings. Although differences in intensity are easier to identify, as these usually translate into differences in cost, it may be harder to identify where differences in the content are responsible for inconsistencies in the cost-effectiveness evidence.
Very few of the studies reported UK estimates of resource use so the cost-effectiveness of the interventions may be overestimated or underestimated depending on whether the interventions reduced or increased health service resource use not directly related to the delivery of the intervention. Although several studies reported non-UK resource use or costs, we did not convert these to UK NHS costs as we were concerned that changes in the number of health-care contacts in one health-care system may not translate into an equivalent change in a different health-care system.
Finally, the estimates of uncertainty around the ICER should be considered to be providing only an indication of the potential uncertainty around the ICERs in a manner similar to a univariate sensitivity analysis because of the limitations in method used to estimate the uncertainty in the QALY gains, as described above.
We had originally planned to use the outcomes of the NMA to conduct an incremental cost-effectiveness analysis for each of the intervention categories included in the NMA. However, there were several issues with this approach. First, the individual interventions grouped within the same categories for the purposes of the NMA were often very different in terms of the resources that would be required to deliver them, as demonstrated in the costing analysis. Therefore, an individual estimate of cost-effectiveness would be required even if we assumed a consistent treatment effect across each category; an assumption that may not itself be justified given that we were not able to explore whether or not differences in the interventions or the population led to differences in effectiveness within the NMA because of the sparsity of the data informing the networks. Second, it was unclear how to generate a single estimate of health utility from the diverse range of outcomes analysed, particularly given that all of the outcomes have the potential to influence quality of life and their influence may not be independent of each other. This complication was avoided in the within-study estimates of cost-effectiveness by limiting the analysis to those studies that provided either a direct estimate of health utility (or incremental QALYs) or a generic measure of HRQoL that could be mapped to provide an estimate of health utility. The main disadvantage of the approach that we have used is that we have not been able to provide estimates of cost-effectiveness for all of the comparisons represented within the full set of clinical trials, as not all of the studies reported a generic measure of HRQoL.
Chapter 7 Discussion
Statement of principal findings
A total of 59 studies were identified that met the inclusion criteria for the clinical effectiveness review. These studies covered a broad and diverse range of populations, interventions and outcomes. A series of network meta-analyses of clinical effectiveness compared intervention types with usual care. There was moderate to high heterogeneity of intervention effects between studies. Networks were sparse and the results of the meta-analysis must therefore be evaluated with caution. In terms of symptom severity outcomes, results indicated some beneficial effects for behavioural interventions targeting specific physical symptoms (e.g. pain, fatigue, bowel symptoms), but not somatisation or generic physical symptom measures. Results also indicated beneficial effects of some behavioural interventions on physical functioning, impact of symptoms on daily activities and psychological symptoms (depression, anxiety and emotional distress). Across outcomes, significant beneficial effects were most frequently seen for CBTHI and multimodal therapy interventions. There were no significant effects for any of the GP interventions (e.g. reattribution or GP MUS management).
Pain
At the end of treatment, only CBTHI and multimodal interventions were statistically more beneficial than usual care, with medium effect sizes. At short-term follow-up, only CBTHI was statistically more beneficial than usual care, with large effect size. By long-term follow-up, no interventions were statistically more beneficial than usual care. The number of studies included at the end of treatment was 10, and by long-term follow-up this had reduced to seven.
Fatigue
At the end of treatment, CBTLI (large effect size), multimodal interventions (large effect size), GA (medium effect size) and RSSE interventions (medium effect size) were statistically more beneficial than usual care. At short-term follow-up, only CBTLI (medium effect size) and RSSE (small effect size) were statistically more beneficial than usual care. By long-term follow-up, only CBTLI was statistically more beneficial than usual care. The number of studies included at the end of treatment was nine and by long-term follow-up this had reduced to five.
Bowel symptoms
There were insufficient data to conduct meta-analyses for end-of-treatment or short-term follow-up. At long-term follow-up, only CBTLI had a statistically significant beneficial effect compared with usual care.
Somatisation and generic physical symptoms
There were no significant beneficial effects for any intervention types for somatisation at end-of-treatment, short-term or long-term follow-up. There were no significant beneficial effects found for generic physical symptoms at any time point.
Physical functioning
At the end of treatment, only the multimodal therapy intervention type was statistically more beneficial than usual care, with a small effect size. This effect was also found at short-term follow-up, with medium effect size, but no intervention types were statistically more beneficial than usual care at long-term follow-up. This outcome was well represented, with 13 out of 14 studies remaining in the network at long-term follow-up.
Impact of symptoms on daily activities
At the end of treatment, only CBTHI was statistically more beneficial than usual care (large effect size). This effect was also found at short-term follow-up (large effect size), but by long-term follow-up there were no statistically significant results. The number of studies informing the network reduced from nine at the end of treatment to four at long-term follow-up.
Anxiety
At the end of treatment, only CBTHI was statistically more beneficial than usual care (medium effect size). This was repeated at both short- and long-term follow-up (large effect, 14 studies informed the network at the end of treatment, reducing to 11 by long-term follow-up).
Depression
At the end of treatment, only CBTHI was statistically more beneficial than usual care (large effect size). At short-term follow-up, only CBTHI (large effect size) was statistically more beneficial than usual care. At long-term follow-up, only the multimodal intervention type was statistically significant (small effect size). Depression was well represented in the network, with 13 studies at the end of treatment and 14 studies by long-term follow-up.
Emotional distress
At the end of treatment, CBTHI, other psychotherapy, RSSE and SES intervention types were statistically more beneficial than usual care (small to medium effect sizes). Only RSSE and multimodal interventions were statistically more beneficial at short-term follow-up (large and small effect sizes, respectively). By long-term follow-up, no intervention was statistically more beneficial than usual care. The number of studies in the network reduced from 15 at the end of treatment to only nine at long-term follow-up.
Results were not consistent across intervention type and outcome. Across outcomes, significant beneficial effects were most frequently seen for CBTHI and multimodal interventions. The outcome on which positive benefits were demonstrated across behavioural interventions was emotional distress, where four different intervention types were seen to have significant beneficial effects at the end of treatment. The outcome that appeared least affected by the interventions was somatisation, with no statistically significant treatment effects, despite there being 13 studies that measured this outcome at the end of treatment. No effects were found for generic physical symptoms, although this outcome was poorly represented in the network (three studies). It was not possible to explore the observed moderate to high heterogeneity seen across all outcomes with metaregression because of insufficient replication of each treatment effect across studies. There were no significant effects for any of the GP interventions (i.e. reattribution) or GP MUS management.
Although there was variation in the study population, these were all patients with chronic conditions. The nature of these conditions has implications for the interpretation of results. Long-term follow-up time periods were generally no longer than 1 year, which is relatively short within the context of a chronic condition. Symptoms may wax and wane over time. A number of individual studies reported significant improvements for both the intervention and the control groups, and this was seen in studies with active control arms as well as studies with passive control arms (i.e. usual care and waiting list control). Improvement in passive control groups over time may indicate natural remission of symptoms. Many of the observed effects seen at the end of treatment and at short-term follow-up were no longer apparent at long-term follow-up. This may in part be influenced by a lack of long-term follow-up data for studies for which the final follow-up was < 6 months after the end of intervention. However, it may also indicate a decline in the beneficial effects of behavioural interventions once treatment has ceased. A review of CBT for CFS366 found a slight trend to suggest that effect size increased with longer follow-up. This could be explained by the possibility that patients in waiting list control groups were able to access the trial interventions once the study period was completed; however, this was not tested in the current review. The NMA allowed active control arms to be categorised into intervention types, where appropriate, and evaluated alongside all other interventions. These active controls were often classified into the RSSE intervention type or guided self-help, and the RSSE category of interventions was found to have a small effect size for fatigue, which suggests that, when interventions are compared against active controls with a RSSE component, this may influence the relative effect size measured.
Behavioural interventions appeared to be more beneficial for specific physical symptoms compared with outcomes where multiple symptoms were measured (i.e. somatisation and generic physical symptoms). This finding is consistent with other meta-analyses that evaluated the effectiveness of psychotherapies for specific physical symptoms. Kleinstäuber et al. 76 highlight that meta-analyses evaluating specific physical symptoms (e.g. Kisely et al. 367 for non-cardiac chest pain) report larger effect sizes than those that evaluate psychotherapies for multiple MUS. They suggest that psychotherapies for somatoform disorders are more likely to focus on coping strategies rather than on curing specific symptoms. These results may be an artefact of either classification of condition or type of protocol. In terms of condition, measures of somatisation were more frequently used in populations classified as having ‘MUS/somatoform disorder’ rather than IBS, chronic pain or chronic fatigue. Studies of ‘MUS/somatoform disorder’ populations may have also measured individual symptoms, but it is not clear which symptoms were dominant at that time. Studies were also statistically powered based on their primary outcome, which was often the predominant symptom in the target population (e.g. fatigue in chronic fatigue populations); therefore, it is possible that they were insufficiently powered to detect differences in secondary outcomes. Alternatively, it may be that treatment protocols that focus on a specific diagnosis of a functional condition or specific symptom group are more effective than interventions that are designed to focus more broadly on the concept of somatisation or MUS. There is a substantive literature showing that the term MUS is offensive to many patients so these interventions may also seem less acceptable. 4,368 The observed statistical lack of effectiveness of GP interventions may in part be due to these interventions mainly targeting MUS/somatoform patients, with somatisation perhaps more complex and appearing to be more difficult to treat.
Although the current review is, to our knowledge, the first to look at a broad range of behavioural interventions for diverse populations of patients meeting our broad inclusion criteria for ‘MUS’, specifically within a primary care setting, results are consistent with other reviews in this area. The current review found no significant beneficial effects for GP-delivered interventions included in the meta-analysis. Although there were some significant effects for GP interventions in individual studies, this is consistent with the review by Rosendal et al. ,77 who found no conclusive evidence to show any beneficial effects for enhanced generalist care, and Gerger et al. ,78 who found psychological therapy to be effective only when delivered by psychologists rather than GPs. Price et al. 66 found significant effects for CBT for CFS at the end of treatment, not only when compared with usual care, but also when compared with other psychological therapies (which included relaxation, counselling, educational support – which would be defined as RSSE/guided self-help in the current review). However, by follow-up, effects were heterogeneous and inconsistent. For IBS, Pajak et al. 369 found minimal contact CBT to show promise in symptom management. The results of the current review are not consistent with van Dessel et al. ,75 who reported less severe somatic symptoms for all psychotherapies (with no superiority of CBT over other psychotherapies) at the end of treatment. However, their review was not restricted to primary care and it may be that differences in setting (i.e. inclusion of tertiary care) contribute to different treatment effects. A review of GA and graded exposure for non-specific low back pain370 found GA to be slightly more effective than minimal intervention, but the effect was no greater than other types of exercise for pain. The most populated networks were for psychological symptoms (i.e. depression, anxiety and emotional distress). Examination of baseline scores showed some variation in anxiety and depression, with, for example, HADS-A baseline scores ranging from 6 to 12 (normal to moderate), whereas HADS-D scores generally fell within the range from 5 to 9 (normal to mild), although Escobar et al. 156 reported severe baseline depression. When baseline psychological symptoms are low, one would not generally expect to find large effect sizes.
Although the behavioural interventions reviewed in the current review showed some effectiveness for improvement of specific physical symptoms compared with usual care, there was less success at improvement in subjective ratings of physical functioning. Furthermore, few studies reported objective measures of functioning, such as return to work. The variability in range and severity of symptoms means that, although some patients with MUS may be able to work, others may not. The Action for M.E. survey371 found that only 10% of respondents were in full-time work, education or training, and a further 14% were in part-time work, education or training. Rask et al. 372 found both patients with MUS of recent onset and those with persistent somatoform disorders to be at increased risk of sick leave and work disability over a 10-year period. It was not possible to explore severity of symptoms as a moderator of treatment effects because of the sparsity of the networks; however, it is unlikely that the interventions explored in this study were trialled on patients at the more severe end of the spectrum, who would be more likely to be treated in tertiary care. It is unlikely that patients in the studies reviewed here would, for example, be non-ambulatory and, therefore, the results should not be generalised to these patients. Furthermore, few of the included studies framed their effectiveness in terms of ‘cure’ or ‘recovery’ and, therefore, the findings should not be interpreted as such.
The qualitative review focused on the perceptions of patients who had received a specific behavioural intervention for MUS. It did not include the perspectives of patients about their general care, or of those patients who had not received such an intervention.
Prior perceptions of behavioural interventions are important as they may influence patient acceptance/uptake. The current review summarised information on acceptance/uptake from the included trials. There was wide variability in the number of patients declining to take part in the studies, and in the number of participants dropping out of the studies. Where reasons were given, these often included lack of time, a lack of faith in therapy,113,133,143,149 or an exacerbation in symptoms. 121 In the study by Robinson et al. ,131 most participants did not attend the group meeting, some of whom stated that they were unwilling to discuss bowel symptoms with strangers. Some participants dropped out because they felt that the intervention was not helping120 or that their symptoms had reduced. 109 Some of these themes were reflected in the qualitative review, with patients reporting that they did not believe that behavioural interventions would address their symptoms178 or that they felt that the intervention would do harm or make things worse. 179,182 The issue of acceptability of behavioural interventions is further highlighted by a recent feasibility study of an early intervention for patients with a history of fatigue lasting 1 to 4 months. 373,374 The intervention consisted of an information booklet and support from a fatigue specialist. The study was able to recruit fewer than half of the participants it aimed to and the authors therefore concluded that this type of study was not feasible and that the type of intervention was not acceptable to many of the participants.
Few of the studies in the clinical effectiveness review reported adverse events, and it is not clear if this is a result of there being no adverse events or if adverse events were not reported. A concern identified in the realist synthesis was that of potential misdiagnosis. Few of the trials included in the clinical effectiveness review reported on whether participants were misdiagnosed with MUS or one of the functional somatic disorders. Tummers et al. 149 reported that 12 participants had received an incorrect diagnosis of CFS, with four having an identified somatic explanation for their fatigue and eight found to have a psychiatric disorder. The potential for a wrong diagnosis is a concern for both GPs and for patients. In general, adverse events have not been reported systematically in psychological therapy trials and deterioration rates are rarely reported. 375,376 This should be addressed in future trials.
A pragmatic approach to the treatment of MUS has been suggested that takes account of patient preferences. Studies included in the current review offered behavioural interventions to primary care patients; however, there was a large range of variability in the nature of the primary care settings. At one end of the spectrum, GP practices were randomised and participating GPs were trained to manage patients with MUS within the course of their everyday practice. Other GP-delivered interventions were more structured, with GPs delivering a specific intervention to patients over a prescribed number of sessions. At the opposite end of the spectrum, participants were recruited in primary care but received an intervention from a specialist HP, sometimes on the GPs’ premises, but alternatively the intervention may have been delivered elsewhere – in community health centres, or gymnasiums or swimming pools. These differences are one of many sources of heterogeneity within the review, and they offer an opportunity to explore issues around pragmatism in clinical trials. There has been increasing interest in how well the results of clinical trials can be applied to everyday clinical practice. Explanatory trials test the efficacy of interventions under conditions strictly controlled for errors and biases. At the opposite end of the continuum, pragmatic trials are designed to test the effectiveness of an intervention when applied to real-world conditions. 377 Although the GP interventions were not shown to be effective compared with usual care in this review, it is possible that these trials represent the most pragmatic end of the continuum. In particular, this review may represent those trials that involved the cluster randomisation of GP practices and where the GPs used MUS training in their everyday practice, rather than with specific patients considered to need to be treated in a prescribed way at a prescribed time. In this review, trials of interventions delivered to primary care patients by other professionals showed more of a trend towards reducing physical symptoms. It is possible that these trials were, in fact, less pragmatic and, therefore, may be less likely to be effective when delivered in a less controlled manner. That having been said, we have no definitive evidence for or against this view. Thorpe et al. 378 developed the PRagmatic Explanatory Continuum Indicator Summary (PRECIS) tool to evaluate trials according to relevant domains, including flexibility in the experimental and comparator interventions, practitioner expertise, the intensity of follow-up, clinical meaningfulness of outcomes, flexibility in practitioner adherence to the protocol, and strictness of eligibility criteria. For example, many of the trials included in this review required the application of diagnostic criteria to their patients to screen for eligibility. In practice, general practice ‘Read’ codes for MUS may not always be applied. A future review could apply the PRECIS criteria to included trials to assess to what extent they are pragmatic and more likely to be effective when applied to real-world clinical practice.
Cost-effectiveness
A range of methods were utilised to evaluate the cost-effectiveness of behavioural modification interventions for MUS, including a systematic literature review of cost-effectiveness studies using QALYs as the measure of benefit, an evaluation of cost–consequence studies and an independent economic assessment. With only two relevant studies,131,284 findings from UK studies of cost-effectiveness were heterogeneous, although differences in the findings may be explained by differences in the populations and interventions studied. For cost–consequence studies, the net impact on health-care costs varied between studies, with some but not all the interventions being found to have a favourable impact on either overall costs or costs unrelated to delivery of the intervention. From this we can conclude that future studies should measure the impact of behavioural modification interventions on health-care costs. Although exploring possible approaches for estimating QALY gains from study outcomes, we found that estimating QALY differences based on mapping from changes on a single domain of the SF-36 to changes on the EQ-5D was unlikely to provide a robust estimate of QALY differences. This may be because the interventions may affect more than one domain of quality of life (e.g. vitality and physical functioning) such that using a single domain would overestimate or underestimate the QALY gain depending on the correlation between changes in different domains. We therefore conclude that future studies should include either a direct measure of utility such as the EQ-5D or a generic measure of HRQoL that covers all relevant domains and that allows utility values to be estimated via mapping, such as the SF-36. Cost analysis of all studies included in the clinical effectiveness review revealed a broad range of costs per patient within each intervention type. Although the ranges for each type of intervention were wide, the median values across different types of interventions were less variable, with median costs of intervention influenced by group versus individual mode of delivery. The median costs ranged from £62 for seven studies106,110,122,123,150,161 that examined RSSE delivered to groups (see Table 87), to £892 for five studies107,118,121,125,145 of multimodal interventions delivered to individuals. GP interventions had a wide range of costs, from £160 to £2560 (median £546) (see Table 91). Variation in costs was influenced by significant variation in the number of patients treated for each GP trained.
In general, the QALY gains estimated for behavioural modification interventions from individual studies were small, with mid-point estimates consistently < 0.1. None of the studies that reported 95% CIs for QALY gains measured directly in the study found a statistically significant difference between trial arms. The method used to estimate the uncertainty around the QALY gains for studies where utility values were mapped from the SF-36 or SF-12 was crude, so although some studies had a positive lower IQR for the QALY gain, this does not allow us to conclude that a statistically significant difference in QALYs was observed.
The independent economic assessment found a large degree of heterogeneity in estimates of cost-effectiveness. Some studies had mid-point ICERs in the range that NICE considers cost-effective, whereas others had ICERs that were above the NICE threshold. Two studies of CBTHI suggest that this intervention is cost-effective, although a third study had an ICER above the NICE threshold. The cost-effective ICERs were for populations with chronic pain, whereas the intervention with the higher ICER had a population that included both patients with chronic pain and those with somatoform disorders. Two studies suggested that guided self-help has the potential to be cost-effective, but one of these studies131 was associated with some uncertainty as there was no estimate of the cost of the self-help guidebook. One study suggested that RSSE has the potential to be cost-effective; however, additional uncertainty arose from the fact that the intervention was delivered to groups, but there was no indication of group size, which is an important determinant of cost per person. Evidence for GA interventions was inconsistent, with one study showing a positive QALY gain compared with guided self-help, albeit with an ICER at the upper limit of the NICE threshold, and the other finding that GA was dominated by usual care. CBTHI dominated medication in one study of a population with chronic pain. CBTHI was also shown to dominate SES in one study. GP interventions were generally not found to be cost-effective, with the exception of modified reattribution compared with usual care in patients with somatoform disorder, where the mid-point ICER was < £30,000 per QALY but was associated with significant uncertainty. Multimodal interventions were inconsistent in patients with chronic pain, with one study showing an estimated ICER above the NICE limit and another within the range considered cost-effective when compared with SES. However, the same study found that the multimodal intervention was dominated by CBTHI, which was estimated to be the optimal intervention based on that study, as seen in Table 27.
Discussion of qualitative findings
In identifying qualitative intervention studies conducted in a UK setting, we were able to explore the perspectives of patients and health-care providers of interventions delivered within a UK setting. However, we acknowledge that this perspective is necessarily limited by including only intervention-based studies and by operating within a tight geographical definition. The value of qualitative studies examining the experience of a condition and of studies from a broader range of geographical contexts and settings could prove valuable. Generally, the qualitative evidence base has identified features considered important by those receiving interventions. However, our ability to identify the most useful, acceptable or efficacious components of intervention packages was constrained by the limited detail of reporting of each intervention. Nevertheless, we believe that the qualitative synthesis, informed and enhanced by the wider scope of the realist synthesis that extends beyond intervention-based studies, offers a potentially useful contribution to the design of future primary care-based interventions.
Implications for individual interventions
Several hypothesised features for successful inclusion in a primary care-based intervention for MUS are presented within the realist synthesis. Many of these features receive clear support, with the exception of the value of ‘labelling’ and the ongoing controversy regarding initiation of psychosocial cues. At a minimum, an intervention should allow patient and care provider to maintain a relationship in which the patient feels supported and believed. Avoidance of an unproductive diagnostic cycle and a seemingly endless pattern of referral are key. The important role of non-intervention-specific factors has been recognised in a variety of contexts for treatment of chronic disease more generally in primary care, and this has been confirmed in this review. Above all, patients should be encouraged to pursue opportunities for self-management while drawing on the resources and skills available via the primary care provider.
Strengths and limitations of the assessment
We undertook a rigorous systematic review following accepted standards for the conduct and reporting of an effects review and using comprehensive search strategies to identify relevant trials evaluating the clinical effectiveness of interventions to treat MUS in primary care. Although we appraised and summarised a relatively large number of trials, much of the evidence was inconclusive because of heterogeneity within interventions and across groups of interventions. Pragmatically, we have employed an approach that differs from that typically used in Cochrane reviews and other reviews by not distinguishing between interventions within trials in terms of the control or comparator interventions. A further strength was the use of multiple review strategies to address diverse questions relating to the overall review aim. Hence, the qualitative data were able to explore the acceptability of interventions to patients, and the economic evaluation studies were able to explore cost implications while the realist synthesis examined features of the patient–clinician consultation in primary care.
Inclusion criteria were kept broad for many elements of the review. This was because of variation in the use of labels for MUS; inconsistencies in diagnostic criteria; a range of interventions meeting our a priori definition of ‘behavioural modification’; a range of ways of incorporating the primary care setting into the intervention; and multiple and diverse outcomes measures employed in the studies. The use of broad criteria has allowed a comprehensive presentation of the potential sources of heterogeneity both within and between studies and these are apparent from the narrative synthesis. The NMA also identified moderate to high heterogeneity of intervention effects between studies. Insufficient replication of treatment effects across studies made it impossible to perform a metaregression to statistically explain the heterogeneity of effects, and this represents a key limitation of the analysis of clinical effectiveness. Differences in point estimates for treatments (vs. usual care), however, indicate that the effectiveness of the interventions may differ by condition grouping, although overlapping CIs demonstrate uncertainty around this finding.
Despite the large number of studies, the network was sparse because of the considerable heterogeneity between interventions and the resulting large number of intervention types. Individual studies also varied in follow-up time periods and this meant that data from many studies were not available for all three time points. Additional reasons why it was not possible to include data from some of the included studies included both arms being categorised into the same intervention type, incomplete reporting of data for non-significant outcomes, only graphical data presented, or no reported variance. Sparsity of the networks meant that the observed effects were often informed by only one study in each intervention type for each outcome at each time point. Results from the network meta-analyses can therefore only give an indication of effects and should be considered within the context of the narrative summaries of individual studies, with consideration to the considerable heterogeneity identified. Evidence from both the network meta-analyses and the narrative summaries of all individual studies suggests the presence of differences in effects between intervention types. However, scrutiny of the individual studies shows variability in their design and conduct, to such an extent that interpretation of the results is not straightforward and, therefore, firm conclusions cannot be drawn. Although combining all intervention types into one ‘behavioural modification’ intervention type would have potentially allowed a metaregression to identify moderators of effects, it was considered that this would be inappropriate because of these differences.
The diversity in the interventions meant that to synthesise the data, individual interventions needed to be categorised into broader intervention groups. This process necessitated subjective judgements. Although every effort was made to reach decisions on intervention groupings by expert consensus, the prevalence of borderline cases resulted in the inclusion within one category of interventions that could have arguably met the criteria of a different category. With a sparse network, it is possible that such borderline cases could influence the results of the meta-analysis. However, while this is to our knowledge the first review to address this specific research question, the results are generally consistent with existing reviews that have addressed similar questions. We were unable to investigate publication bias via funnel plots owing to there being < 10 trials per comparison (of the same interventions) (Cochrane handbook)87 for all outcomes, and we are therefore unable to address the possibility of small study effects.
Owing to the diversity of interventions and sparsity of the network, we were unable to address the question as to which components of effective interventions were most influential. Results from the NMA suggest that multimodal therapy interventions have beneficial effects across outcomes and time points, but there was considerable diversity in the individual components across multimodal interventions and it has not been possible to identify if specific components were driving the effectiveness or if the effects were due to the combination of components or increased intensity of the treatment.
There was limited information available from published cost-effectiveness analyses that reported outcomes using QALYs. The main strength of our approach to the independent economic assessment is that we have been able to provide an indication of within-study cost-effectiveness for a large number of studies covering a diverse range of interventions and populations. The main disadvantages of the approach that we have used is that we have not been able to provide estimates of cost-effectiveness for all of the comparisons represented within the full set of clinical trials, as not all of the studies reported a generic measure of HRQoL and we have been unable to conduct a full incremental analysis to identify the optimal behavioural modification intervention using evidence from multiple studies.
The review is further limited by the dates of the searches, which were conducted between November 2015 and August 2016. Studies published since this time may therefore offer more evidence to inform the research questions addressed in this review.
Conclusions
Evidence from the current review offers some support for the value of behavioural interventions in primary care for improvement in specific symptoms (pain, fatigue and bowel symptoms), with both CBTLI and CBTHI showing some beneficial effects in different conditions, and multimodal therapy supported across a number of outcomes. No one intervention was found to be effective across all MUS, suggesting that there is no generic treatment that can be applied across all MUS. Only CBTHI had support over usual care for anxiety, but a range of therapies showed effects in emotional distress including other psychotherapies. The beneficial effects shown for chronic pain were short term. There was no clear evidence for these interventions in somatisation disorders and multiple symptoms. GP-led interventions, such as reattribution, were not supported by the evidence. Further interrogation of the results may indicate whether or not this is because of a lack of effectiveness of the more pragmatic trials. Developing a clear referral pathway in primary care to therapist-supported CBT or multimodal therapy for specific symptoms or FSSs may be most indicated at this point. The synthesis of qualitative evidence on process suggests that the quality of relationship between the service user and their GP is vital, and this ‘therapeutic alliance’ is the determining factor for how successfully these interventions can be implemented. These conclusions must be read with caution because of the large degree of heterogeneity of studies. There was also a low level of replication of intervention types within the networks, which coupled with the observed between-study heterogeneity of effects means that conclusions on specific therapies could be altered by addition or exclusion of one study. These findings were mirrored in the economic analysis, which found that where there was more than one study providing an estimate of cost-effectiveness for a particular comparison, the evidence was often inconsistent.
Suggested research priorities
The following research priorities are suggested, based on the findings of the review:
-
Explanation of observed between-study differences in effects within the same intervention type. This may be addressed by –
-
More detailed reporting of information regarding the defined mechanisms of the behavioural interventions under study, and how these map onto a theoretical and empirical understanding of the conditions.
-
More research on potentially influencing factors such as effective dosage and therapist competency within the more promising behavioural interventions.
-
Within-trial comparisons of interventions targeting specific syndromes with those targeting general somatic symptoms.
-
-
Testing the therapeutic effect of the GP–patient relationship. This may be addressed by –
-
Increased awareness of likely GP effects by researchers conducting trials of behavioural interventions for MUS, with planned assessment of these as potential confounders.
-
More research aimed at better understanding the therapeutic elements behind a successful therapeutic GP–patient alliance, which are key to a successful outcome, and how these elements can be formalised as GP (and health-care practitioner) skills.
-
Development of standardised measures of adverse effects in trials of behavioural interventions for MUS.
-
Acknowledgements
The authors would like to thank the advisors who have contributed to the project Expert Advisory Group:
-
Professor Else Guthrie, Professor of Psychological Medicine, University of Leeds
-
Professor Chris Dowrick, Professor of Primary Medical Care, University of Liverpool
-
Dr Nick Read, Psychoanalytical Psychotherapist. Previously, Professor of Gastrointestinal Physiology, Human Nutrition and Integrated Medicine, University of Sheffield.
Three experts by experience also contributed to all stages of the project and were members of the Expert Advisory Group, and Professor Chris Burton, ScHARR, University of Sheffield, for his comments on the realist review.
The authors would also like to thank Matt Stevenson, Professor of Health Technology Assessment, ScHARR, for providing advice on the cost-effectiveness modelling; Andrea Shippam, Programme Manager, ScHARR, for her help in formatting the report; and Carmen Galvan de la Cruz for her help with data extraction and protocol searching.
Contributions of authors
Joanna Leaviss (https://orcid.org/0000-0002-5632-6021) (Research Fellow in Evidence Synthesis) was the principal investigator and undertook the quantitative review.
Sarah Davis (https://orcid.org/0000-0002-6609-4287) (Senior Lecturer in Health Economics) conducted the cost-effectiveness modelling.
Shijie Ren (https://orcid.org/0000-0003-3568-7124) (Research Fellow in Bayesian Statistics, NMA and Survival Analysis) and Jean Hamilton (https://orcid.org/0000-0003-3326-9842) (Research Associate in Statistics) conducted the network meta-analyses.
Alison Scope (Research Fellow in Evidence Synthesis) undertook the qualitative review.
Andrew Booth (https://orcid.org/0000-0003-4808-3880) (Reader in Evidence-based Information Practice and Director of Information) conducted the realist synthesis.
Anthea Sutton (https://orcid.org/0000-0003-2449-2516) (Information Resources Group Manager) designed and conducted the literature searches.
Glenys Parry (https://orcid.org/0000-0002-4339-0577) (Professor of Applied Psychological Therapies), Marta Buszewicz (https://orcid.org/0000-0003-4016-5857) (Reader in Primary Care), Rona Moss-Morris (https://orcid.org/0000-0002-2927-3446) (Professor of Health Psychology) and Peter White (https://orcid.org/0000-0002-8193-5355) (Emeritus Professor of Psychological Medicine) provided subject expertise and were involved in writing the final report.
Data-sharing statement
Data are archived at ScHARR. All data requests should be submitted to the corresponding author for consideration. Access to anonymised data may be granted following review.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HTA programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HTA programme or the Department of Health and Social Care.
References
- Chitnis A, Dowrick C, Byng R, Turner P, Shiers D. Guidance for Health Professionals on Medically Unexplained Symptoms – 2011. London: Royal College of General Practitioners and Royal College of Psychiatrists; 2014.
- Henningsen P, Jakobsen T, Schiltenwolf M, Weiss MG. Somatization revisited: diagnosis and perceived causes of common mental disorders. J Nerv Ment Dis 2005;193:85-92. https://doi.org/10.1097/01.nmd.0000152796.07788.b6.
- Wessely S, Nimnuan C, Sharpe M. Functional somatic syndromes: one or many?. Lancet 1999;354:936-9. https://doi.org/10.1016/S0140-6736(98)08320-2.
- Stone J, Wojcik W, Durrance D, Carson A, Lewis S, MacKenzie L, et al. What should we say to patients with symptoms unexplained by disease? The ‘number needed to offend’. BMJ 2002;325:1449-50. https://doi.org/10.1136/bmj.325.7378.1449.
- Creed F, Guthrie E, Fink P, Henningsen P, Rief W, Sharpe P, et al. Is there a better term than ‘medically unexplained symptoms’?. J Psychosom Res 2010;68:5-8. https://doi.org/10.1016/j.jpsychores.2009.09.004.
- Fukuda K, Straus SE, Hickie I, Sharpe MC, Dobbins JG, Komaroff A. The chronic fatigue syndrome: a comprehensive approach to its definition and study. Ann Int Med 1994;121:953-9. https://doi.org/10.7326/0003-4819-121-12-199412150-00009.
- Drossman DA, Dumitrascu DL. Rome III: new standard for functional gastrointestinal disorders. J Gastrointestinal Liver Dis 2006;15.
- Wolfe F, Clauw DJ, Fitzcharles MA, Goldenberg DL, Katz RS, Mease P, et al. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res 2010;62:600-10. https://doi.org/10.1002/acr.20140.
- Kroenke K, Spitzer RL, Williams JB. The PHQ-15: validity of a new measure for evaluating the severity of somatic symptoms. Psychosom Med 2002;64:258-66. https://doi.org/10.1097/00006842-200203000-00008.
- Rief W, Heuser J, Hiller W. SOMS: das Screening für Somatoforme Störungen. Manual zum Fragebogen; mit zusätzlichen Informationen zur Hypochondrie-Messung und zum Einsatz von Tagesprotokollen. Bern: Verlag Hans Huber; 1997.
- Mumford DB, Bavington JT, Bhatnagar KS, Hussain Y, Mirza S, Naraghi MM. The Bradford Somatic Inventory. A multi-ethnic inventory of somatic symptoms reported by anxious and depressed patients in Britain and the Indo-Pakistan subcontinent. Br J Psychiatry 1991;158:379-86. https://doi.org/10.1192/bjp.158.3.379.
- Hoedeman R, Blankenstein AH, Krol B, Koopmans PC, Groothoff JW. The contribution of high levels of somatic symptom severity to sickness absence duration, disability and discharge. J Occup Rehabil 2010;20:264-73. https://doi.org/10.1007/s10926-010-9239-3.
- Fink P, Rosendal M, Olesen F. Classification of somatization and functional somatic symptoms in primary care. Aust N Z J Psychiatry 2005;39:772-81. https://doi.org/10.1080/j.1440-1614.2005.01682.x.
- American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders 2000.
- American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders 2013. https://doi.org/10.1176/appi.books.9780890425596.
- World Health Organization . International Classification of Diseases 1978.
- World Health Organization . International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10) 1992.
- Newby JM, Hobbs MJ, Mahoney AEJ, Wong SK, Andrews G. DSM-5 illness anxiety disorder and somatic symptom disorder: Comorbidity, correlates, and overlap with DSM-IV hypochondriasis. J Psychosom Res 2017;101:31-7. https://doi.org/10.1016/j.jpsychores.2017.07.010.
- Dimsdale JE, Creed F, Escobar J, Sharpe M, Wulsin L, Barsky A, et al. Somatic symptom disorder: an important change in DSM. J Psychosom Res 2013;75:223-8. https://doi.org/10.1016/j.jpsychores.2013.06.033.
- Frances A. The new somatic symptom disorder in DSM-5 risks mislabeling many people as mentally ill. BMJ 2013;346. https://doi.org/10.1136/bmj.f1580.
- Ghoshal UC, Gwee KA. Post-infectious IBS, tropical sprue and small intestinal bacterial overgrowth: the missing link. Nat Rev Gastroenterol Hepatol 2017;14:435-41. https://doi.org/10.1038/nrgastro.2017.37.
- Drossman DA, Hasler WL. Rome IV-Functional GI disorders: disorders of gut–brain interaction. Gastroenterology 2016;150:1257-61. https://doi.org/10.1053/j.gastro.2016.03.035.
- Smith RC, Dwamena FC. Classification and diagnosis of patients with medically unexplained symptoms. J Gen Intern Med 2007;22:685-91. https://doi.org/10.1007/s11606-006-0067-2.
- Fink P, Schröder A. One single diagnosis, bodily distress syndrome, succeeded to capture 10 diagnostic categories of functional somatic syndromes and somatoform disorders. J Psychosom Res 2010;68:415-26. https://doi.org/10.1016/j.jpsychores.2010.02.004.
- Joint Commissioning Panel for Mental Health . Guidance for Commissioners of Services for People With Medically Unexplained Symptoms 2017. www.jcpmh.info/wp-content/uploads/jcpmh-mus-guide.pdf (accessed 5 November 2019).
- Geraghty KJ, Esmail A. Chronic fatigue syndrome: is the biopsychosocial model responsible for patient dissatisfaction and harm?. Br J Gen Pract 2016;66:437-8. https://doi.org/10.3399/bjgp16X686473.
- de Vega WC, Herrera S, Vernon SD, McGowan PO. Epigenetic modifications and glucocorticoid sensitivity in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). BMC Med Genomics 2017;10. https://doi.org/10.1186/s12920-017-0248-3.
- Gur A, Oktayoglu P. Status of immune mediators in fibromyalgia. Curr Pain Headache Rep 2008;12:175-81. https://doi.org/10.1007/s11916-008-0031-4.
- Deale A, Wessely S. Patients’ perceptions of medical care in chronic fatigue syndrome. Soc Sci Med 2001;52:1859-64. https://doi.org/10.1016/S0277-9536(00)00302-6.
- White P. Biopsychosocial Medicine: An Integrated Approach to Understanding Illness. Oxford: Oxford Uniersity Press; 2005.
- Edwards TM, Stern A, Clarke DD, Ivbijaro G, Kasney LM. The treatment of patients with medically unexplained symptoms in primary care: a review of the literature. Ment Health Fam Med 2010;7:209-21.
- Taylor RE, Marshall T, Mann A, Goldberg DP. Insecure attachment and frequent attendance in primary care: a longitudinal cohort study of medically unexplained symptom presentations in ten UK general practices. Psychol Med 2012;42:855-64. https://doi.org/10.1017/S0033291711001589.
- Bermingham SL, Cohen A, Hague J, Parsonage M. The cost of somatisation among the working-age population in England for the year 2008–2009. Ment Health Fam Med 2010;7:71-84.
- Barsky AJ, Orav EJ, Bates DW. Somatization increases medical utilization and costs independent of psychiatric and medical comorbidity. Arch Gen Psychiatry 2005;62:903-10. https://doi.org/10.1001/archpsyc.62.8.903.
- Li CT, Chou YH, Yang KC, Yang CH, Lee YC, Su TP. Medically unexplained symptoms and somatoform disorders: diagnostic challenges to psychiatrists. J Chin Med Assoc 2009;72:251-6. https://doi.org/10.1016/S1726-4901(09)70065-6.
- Collin SM, Sterne JA, Hollingworth W, May MT, Crawley E. Equity of access to specialist chronic fatigue syndrome (CFS/ME) services in England (2008–2010): a national survey and cross-sectional study. BMJ Open 2012;2. https://doi.org/10.1136/bmjopen-2012-001417.
- Hughes G, Martinez C, Myon E, Taïeb C, Wessely S. The impact of a diagnosis of fibromyalgia on health care resource use by primary care patients in the UK: an observational study based on clinical practice. Arthritis Rheum 2006;54:177-83. https://doi.org/10.1002/art.21545.
- Akehurst RL, Brazier JE, Mathers N, O’Keefe C, Kaltenthaler E, Morgan A, et al. Health-related quality of life and cost impact of irritable bowel syndrome in a UK primary care setting. PharmacoEconomics 2002;20:455-62. https://doi.org/10.2165/00019053-200220070-00003.
- olde Hartman TC, Borghuis MS, Lucassen PL, van de Laar FA, Speckens AE, van Weel C. Medically unexplained symptoms, somatisation disorder and hypochondriasis: course and prognosis. A systematic review. J Psychosom Res 2009;66:363-77. https://doi.org/10.1016/j.jpsychores.2008.09.018.
- Creed FH, Davies I, Jackson J, Littlewood A, Chew-Graham C, Tomenson B, et al. The epidemiology of multiple somatic symptoms. J Psychosom Res 2012;72:311-17. https://doi.org/10.1016/j.jpsychores.2012.01.009.
- Kroenke K. Efficacy of treatment for somatoform disorders: a review of randomized controlled trials. Psychosom Med 2007;69:881-8. https://doi.org/10.1097/PSY.0b013e31815b00c4.
- Ford AC, Talley NJ, Schoenfeld PS, Quigley EM, Moayyedi P. Efficacy of antidepressants and psychological therapies in irritable bowel syndrome: systematic review and meta-analysis. Gut 2009;58:367-78. https://doi.org/10.1136/gut.2008.163162.
- Beck AT, Therapy C. The Emotional Disorders. New York, NY: International University Press; 1976.
- Deary V, Chalder T, Sharpe M. The cognitive behavioural model of medically unexplained symptoms: a theoretical and empirical review. Clin Psychol Rev 2007;27:781-97. https://doi.org/10.1016/j.cpr.2007.07.002.
- Goldberg D, Gask L, O’Dowd T. The treatment of somatization: teaching techniques of reattribution. J Psychosom Res 1989;33:689-95. https://doi.org/10.1016/0022-3999(89)90084-6.
- Nezu AM, Nezu CM, Lombardo ER. Cognitive-behavior therapy for medically unexplained symptoms: a critical review of the treatment literature. Behavior Therapy 2001;32:537-83. https://doi.org/10.1016/S0005-7894(01)80035-6.
- Buckelew SP, Conway R, Parker J, Deuser WE, Read J, Witty TE, et al. Biofeedback/relaxation training and exercise interventions for fibromyalgia: a prospective trial. Arthritis Care Res 1998;11:196-209. https://doi.org/10.1002/art.1790110307.
- Keefer L, Blanchard EB. The effects of relaxation response meditation on the symptoms of irritable bowel syndrome: results of a controlled treatment study. Behav Res Ther 2001;39:801-11. https://doi.org/10.1016/S0005-7967(00)00078-4.
- Creamer P, Singh BB, Hochberg MC, Berman BM. Sustained improvement produced by nonpharmacologic intervention in fibromyalgia: results of a pilot study. Arthritis Care Res 2000;13:198-204. https://doi.org/10.1002/1529-0131(200008)13:4<198::AID-ANR4>3.0.CO;2-P.
- van Ravesteijn HJ, Suijkerbuijk YB, Langbroek JA, Muskens E, Lucassen PL, van Weel C, et al. Mindfulness-based cognitive therapy (MBCT) for patients with medically unexplained symptoms: process of change. J Psychosom Res 2014;77:27-33. https://doi.org/10.1016/j.jpsychores.2014.04.010.
- Abbass A, Kisely S, Kroenke K. Short-term psychodynamic psychotherapy for somatic disorders. Systematic review and meta-analysis of clinical trials. Psychother Psychosom 2009;78:265-74. https://doi.org/10.1159/000228247.
- de Jong JR, Vlaeyen JW, Onghena P, Cuypers C, den Hollander M, Ruijgrok J. Reduction of pain-related fear in complex regional pain syndrome type I: the application of graded exposure in vivo. Pain 2005;116:264-75. https://doi.org/10.1016/j.pain.2005.04.019.
- Heymans MW, de Vet HC, Bongers PM, Knol DL, Koes BW, van Mechelen W. The effectiveness of high-intensity versus low-intensity back schools in an occupational setting: a pragmatic randomized controlled trial. Spine 2006;31:1075-82. https://doi.org/10.1097/01.brs.0000216443.46783.4d.
- Smeets RJ, Vlaeyen JW, Hidding A, Kester AD, van der Heijden GJ, van Geel AC, et al. Active rehabilitation for chronic low back pain: cognitive-behavioral, physical, or both? First direct post-treatment results from a randomized controlled trial. BMC Musculoskelet Disord 2006;7. https://doi.org/10.1186/1471-2474-7-5.
- White P, Chalder T, Sharpe M. The PACE trial: results of a large trial of nonpharmacological treatments. J Psychosom Res 2011;70.
- Jason LA, Torres-Harding S, Friedberg F, Corradi K, Njoku MG, Donalek J, et al. Non-pharmacologic interventions for CFS: a randomized trial. J Clin Psychol Med Settings 2007;14:275-96. https://doi.org/10.1007/s10880-007-9090-7.
- Gowans SE, deHueck A, Voss S, Silaj A, Abbey SE, Reynolds WJ. Effect of a randomized, controlled trial of exercise on mood and physical function in individuals with fibromyalgia. Arthritis Rheum 2001;45:519-29. https://doi.org/10.1002/1529-0131(200112)45:6<519::AID-ART377>3.0.CO;2-3.
- Jentoft ES, Kvalvik AG, Mengshoel AM. Effects of pool-based and land-based aerobic exercise on women with fibromyalgia/chronic widespread muscle pain. Arthritis Rheum 2001;45:42-7. https://doi.org/10.1002/1529-0131(200102)45:1<42::AID-ANR82>3.0.CO;2-A.
- Jones AC, Coulson L, Muir K, Tolley K, Lophatananon A, Everitt L, et al. A nurse-delivered advice intervention can reduce chronic non-steroidal anti-inflammatory drug use in general practice: a randomized controlled trial. Rheumatology 2002;41:14-21. https://doi.org/10.1093/rheumatology/41.1.14.
- Witthöft M, Hiller W. Psychological approaches to origins and treatments of somatoform disorders. Annu Rev Clin Psychol 2010;6:257-83. https://doi.org/10.1146/annurev.clinpsy.121208.131505.
- Paterson C, Taylor RS, Griffiths P, Britten N, Rugg S, Bridges J, et al. Acupuncture for ‘frequent attenders’ with medically unexplained symptoms: a randomised controlled trial (CACTUS study). Br J Gen Pract 2011;61:e295-305. https://doi.org/10.3399/bjgp11X572689.
- Bagnall AM, Whiting P, Richardson R, Sowden AJ. Interventions for the treatment and management of chronic fatigue syndrome/myalgic encephalomyelitis. Qual Saf Health Care 2002;11:284-8. https://doi.org/10.1136/qhc.11.3.284.
- Morriss R, Gask L, Dowrick C, Dunn G, Peters S, Ring A, et al. Randomized trial of reattribution on psychosocial talk between doctors and patients with medically unexplained symptoms. Psychol Med 2010;40:325-33. https://doi.org/10.1017/S0033291709990353.
- Bagnall A-M, Hempel S, Chambers D, Forbes C. The Treatment and Management of Chronic Fatigue Syndrome (CFS) Myalgic Encephalomyelitis (ME) in Adults and Children. CRD Report 35 2007.
- Clark MR, McCarberg BH, Mease PJ. Fibromyalgia in primary care: what you need to know now! Practical applications for patient care. Johns Hopkins Adv Stud Med 2011;11:4-22.
- Price JR, Mitchell E, Tidy E, Hunot V. Cognitive behaviour therapy for chronic fatigue syndrome in adults. Cochrane Database Syst Rev 2008;3. https://doi.org/10.1002/14651858.CD001027.pub2.
- Chambers D, Bagnall AM, Hempel S, Forbes C. Interventions for the treatment, management and rehabilitation of patients with chronic fatigue syndrome/myalgic encephalomyelitis: an updated systematic review. J R Soc Med 2006;99:506-20. https://doi.org/10.1177/014107680609901012.
- Arnold B, Häuser W, Arnold M, Bernateck M, Bernardy K, Brückle W, et al. Multicomponent therapy of fibromyalgia syndrome. Systematic review, meta-analysis and guideline. Schmerz 2012;26:287-90. https://doi.org/10.1007/s00482-012-1173-1.
- Marcus DA. Fibromyalgia: diagnosis and treatment options. Gend Med 2009;6:139-51. https://doi.org/10.1016/j.genm.2009.01.004.
- Busch AJ, Barber KA, Overend TJ, Peloso PM, Schachter CL. Exercise for treating fibromyalgia syndrome. Cochrane Database Syst Rev 2007;4. https://doi.org/10.1002/14651858.CD003786.pub2.
- Häuser W, Bernardy K, Arnold B, Offenbächer M, Schiltenwolf M. Efficacy of multicomponent treatment in fibromyalgia syndrome: a meta-analysis of randomized controlled clinical trials. Arthritis Rheum 2009;61:216-24. https://doi.org/10.1002/art.24276.
- Zijdenbos IL, de Wit NJ, van der Heijden GJ, Rubin G, Quartero AO. Psychological treatments for the management of irritable bowel syndrome. Cochrane Database Syst Rev 2009;1. https://doi.org/10.1002/14651858.CD006442.pub2.
- Aggarwal VR, Lovell K, Peters S, Javidi H, Joughin A, Goldthorpe J. Psychosocial interventions for the management of chronic orofacial pain. Cochrane Database Syst Rev 2011;11. https://doi.org/10.1002/14651858.CD008456.pub2.
- Champaneria R, Daniels JP, Raza A, Pattison HM, Khan KS. Psychological therapies for chronic pelvic pain: systematic review of randomized controlled trials. Acta Obstet Gynecol Scand 2012;91:281-6. https://doi.org/10.1111/j.1600-0412.2011.01314.x.
- van Dessel N, den Boeft M, van der Wouden JC, Kleinstäuber M, Leone SS, Terluin B, et al. Non-pharmacological interventions for somatoform disorders and medically unexplained physical symptoms (MUPS) in adults. Cochrane Database Syst Rev 2014;11. https://doi.org/10.1002/14651858.CD011142.pub2.
- Kleinstäuber M, Witthöft M, Hiller W. Efficacy of short-term psychotherapy for multiple medically unexplained physical symptoms: a meta-analysis. Clin Psychol Rev 2011;31:146-60. https://doi.org/10.1016/j.cpr.2010.09.001.
- Rosendal M, Blankenstein AH, Morriss R, Fink P, Sharpe M, Burton C. Enhanced care by generalists for functional somatic symptoms and disorders in primary care. Cochrane Database Syst Rev 2013;10. https://doi.org/10.1002/14651858.CD008142.pub2.
- Gerger H, Hlavica M, Gaab J, Munder T, Barth J. Does it matter who provides psychological interventions for medically unexplained symptoms? A meta-analysis. Psychother Psychosom 2015;84:217-26. https://doi.org/10.1159/000380914.
- Garcia-Campayo J, Magdalena J, Magallón R, Fernández-García E, Salas M, Andrés E. A meta-analysis of the efficacy of fibromyalgia treatment according to level of care. Arthritis Res Ther 2008;10. https://doi.org/10.1186/ar2455.
- Castonguay LG, Hayes AM, Goldfried MR, DeRubeis RJ. The focus of therapist interventions in cognitive therapy for depression. Cog Ther Res 1995;19:485-503. https://doi.org/10.1007/BF02230510.
- Cho HJ, Hotopf M, Wessely S. The placebo response in the treatment of chronic fatigue syndrome: a systematic review and meta-analysis. Psychosom Med 2005;67:301-13. https://doi.org/10.1097/01.psy.0000156969.76986.e0.
- Williams AC, Eccleston C, Morley S. Psychological therapies for the management of chronic pain (excluding headache) in adults. Cochrane Database Syst Rev 2012;11. https://doi.org/10.1002/14651858.CD007407.pub3.
- Smith RC, Lein C, Collins C, Lyles JS, Given B, Dwamena FC, et al. Treating patients with medically unexplained symptoms in primary care. J Gen Intern Med 2003;18:478-89. https://doi.org/10.1046/j.1525-1497.2003.20815.x.
- Heijmans M, Olde Hartman TC, van Weel-Baumgarten E, Dowrick C, Lucassen PL, van Weel C. Experts’ opinions on the management of medically unexplained symptoms in primary care. A qualitative analysis of narrative reviews and scientific editorials. Fam Pract 2011;28:444-55. https://doi.org/10.1093/fampra/cmr004.
- Gask L, Dowrick C, Salmon P, Peters S, Morriss R. Reattribution reconsidered: narrative review and reflections on an educational intervention for medically unexplained symptoms in primary care settings. J Psychosom Res 2011;71:325-34. https://doi.org/10.1016/j.jpsychores.2011.05.008.
- Broom DH, Woodward RV. Medicalisation reconsidered: toward a collaborative approach to care. Sociol Health Illness 1996;18:357-78. https://doi.org/10.1111/1467-9566.ep10934730.
- Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions 2011. http://handbook-5-1.cochrane.org (accessed 27 March 2020).
- Dias S, Sutton AJ, Ades AE, Welton NJ. Evidence synthesis for decision making 2: a generalized linear modeling framework for pairwise and network meta-analysis of randomized controlled trials. Med Decis Making 2013;33:607-17. https://doi.org/10.1177/0272989X12458724.
- Rhodes KM, Turner RM, Higgins JP. Predictive distributions were developed for the extent of heterogeneity in meta-analyses of continuous outcome data. J Clin Epidemiol 2015;68:52-60. https://doi.org/10.1016/j.jclinepi.2014.08.012.
- Ren S, Oakley JE, Stevens JW. Incorporating genuine prior information about between-study heterogeneity in random effects pairwise and network meta-analyses. Med Decis Making 2018;38:531-42. https://doi.org/10.1177/0272989X18759488.
- Turner RM, Davey J, Clarke MJ, Thompson SG, Higgins JP. Predicting the extent of heterogeneity in meta-analysis, using empirical data from the Cochrane Database of Systematic Reviews. Int J Epidemiol 2012;41:818-27. https://doi.org/10.1093/ije/dys041.
- Dias S, Welton NJ, Sutton AJ, Caldwell DM, Lu G, Ades AE. NICE DSU Technical Support Document 4: Inconsistency in Networks of Evidence Based on Randomised Controlled Trials. Bristol: Decision Support Unit, University of Bristol and University of Sheffield; 2011.
- Lunn DJ, Thomas A, Best N, Spiegelhalter D. WinBUGS – a Bayesian modelling framework: concepts, structure, and extensibility. Stat Comput 2000;10:325-37. https://doi.org/10.1023/A:1008929526011.
- Stutrtz S, Ligges U, Gelman A. R2WinBUGS: a package for running WinBUGS from R. J Stat Software 2005;12:1-16. https://doi.org/10.18637/jss.v012.i03.
- Brooks S, Gelman A. Alternative methods for monitoring convergence of iterative simulations. J Comput Graph Stat 1998;7:434-55. https://doi.org/10.1080/10618600.1998.10474787.
- Posse M. Jungian psychotherapy for somatization. Eur J Psychiatr 2004;18:23-9.
- Toft T, Rosendal M, Ørnbøl E, Olesen F, Frostholm L, Fink P. Training general practitioners in the treatment of functional somatic symptoms: effects on patient health in a cluster-randomised controlled trial (the Functional Illness in Primary Care study). Psychother Psychosom 2010;79:227-37. https://doi.org/10.1159/000313691.
- Escobar JI, Gara M, Waitzkin H, Silver RC, Holman A, Compton W. DSM-IV hypochondriasis in primary care. Gen Hosp Psychiatry 1998;20:155-9. https://doi.org/10.1016/S0163-8343(98)00018-8.
- Martin A, Rauh E, Fichter M, Rief W. A one-session treatment for patients suffering from medically unexplained symptoms in primary care: a randomized clinical trial. Psychosomatics 2007;48:294-303. https://doi.org/10.1176/appi.psy.48.4.294.
- Smith GR, Rost K, Kashner TM. A trial of the effect of a standardized psychiatric consultation on health outcomes and costs in somatizing patients. Arch Gen Psychiatry 1995;52:238-43. https://doi.org/10.1001/archpsyc.1995.03950150070012.
- Sumathipala A, Siribaddana S, Hewege S, Sumathipala K, Prince M, Mann A. Understanding the explanatory model of the patient on their medically unexplained symptoms and its implication on treatment development research: a Sri Lanka Study. BMC Psychiatry 2008;8. https://doi.org/10.1186/1471-244X-8-54.
- Rief W, Martin A, Rauh E, Zech T, Bender A. Evaluation of general practitioners’ training: how to manage patients with unexplained physical symptoms. Psychosomatics 2006;47:304-11. https://doi.org/10.1176/appi.psy.47.4.304.
- Kocken PL, Zwanenburg EJ, de Hoop T. Effects of health education for migrant females with psychosomatic complaints treated by general practitioners. A randomised controlled evaluation study. Patient Educ Couns 2008;70:25-30. https://doi.org/10.1016/j.pec.2007.09.016.
- Kolk AM, Schagen S, Hanewald GJ. Multiple medically unexplained physical symptoms and health care utilization: outcome of psychological intervention and patient-related predictors of change. J Psychosom Res 2004;57:379-89. https://doi.org/10.1016/S0022-3999(04)00036-4.
- McLeod CC, Budd MA, McClelland DC. Treatment of somatization in primary care. Gen Hosp Psychiatry 1997;19:251-8. https://doi.org/10.1016/S0163-8343(97)00047-9.
- Peters S, Stanley I, Rose M, Kaney S, Salmon P. A randomized controlled trial of group aerobic exercise in primary care patients with persistent, unexplained physical symptoms. Fam Pract 2002;19:665-74. https://doi.org/10.1093/fampra/19.6.665.
- Smith RC, Lyles JS, Gardiner JC, Sirbu C, Hodges A, Collins C, et al. Primary care clinicians treat patients with medically unexplained symptoms: a randomized controlled trial. J Gen Intern Med 2006;21:671-7. https://doi.org/10.1111/j.1525-1497.2006.00460.x.
- Morriss R, Dowrick C, Salmon P, Peters S, Dunn G, Rogers A, et al. Cluster randomised controlled trial of training practices in reattribution for medically unexplained symptoms. Br J Psychiatry 2007;191:536-42. https://doi.org/10.1192/bjp.bp.107.040683.
- Ryan M, Gevirtz R. Biofeedback-based psychophysiological treatment in a primary care setting: an initial feasibility study. Appl Psychophysiol Biofeedback 2004;29:79-93. https://doi.org/10.1023/B:APBI.0000026635.03016.ef.
- Kobeissi L, Mahfoud Z, Khoury B, El Kak F, Ghantous Z, Khawaja M, et al. The Relaxation Exercise and Social Support Trial (RESST): a community-based randomized controlled trial to alleviate medically unexplained vaginal discharge symptoms. BMC Psychiatry 2012;12. https://doi.org/10.1186/1471-244X-12-195.
- Wearden AJ, Dowrick C, Chew-Graham C, Bentall RP, Morriss RK, Peters S, et al. Nurse led, home based self help treatment for patients in primary care with chronic fatigue syndrome: randomised controlled trial. BMJ 2010;340. https://doi.org/10.1136/bmj.c1777.
- Ridsdale L, Godfrey E, Chalder T, Seed P, King M, Wallace P, et al. Fatigue Trialists’ Group . Chronic fatigue in general practice: is counselling as good as cognitive behaviour therapy? A UK randomised trial. Br J Gen Pract 2001;51:19-24.
- Ridsdale L, Darbishire L, Seed PT. Is graded exercise better than cognitive behaviour therapy for fatigue? A UK randomized trial in primary care. Psychol Med 2004;34:37-49. https://doi.org/10.1017/S0033291703001247.
- Chalder T, Wallace P, Wessely S. Self-help treatment of chronic fatigue in the community: a randomized controlled trial. Br J Health Psychol 1997;2:189-97. https://doi.org/10.1111/j.2044-8287.1997.tb00535.x.
- Ridsdale L, Hurley M, King M, McCrone P, Donaldson N. The effect of counselling, graded exercise and usual care for people with chronic fatigue in primary care: a randomized trial. Psychol Med 2012;42:2217-24. https://doi.org/10.1017/S0033291712000256.
- Sumathipala A, Hewege S, Hanwella R, Mann AH. Randomized controlled trial of cognitive behaviour therapy for repeated consultations for medically unexplained complaints: a feasibility study in Sri Lanka. Psychol Med 2000;30:747-57. https://doi.org/10.1017/S0033291799002160.
- Sumathipala A, Siribaddana S, Abeysingha MR, De Silva P, Dewey M, Prince M, et al. Cognitive-behavioural therapy v. structured care for medically unexplained symptoms: randomised controlled trial. Br J Psychiatry 2008;193:51-9. https://doi.org/10.1192/bjp.bp.107.043190.
- Cuesta-Vargas AI, Adams N, Salazar JA, Belles A, Hazañas S, Arroyo-Morales M. Deep water running and general practice in primary care for non-specific low back pain versus general practice alone: randomized controlled trial. Clin Rheumatol 2012;31:1073-8. https://doi.org/10.1007/s10067-012-1977-5.
- Macedo LG, Latimer J, Maher CG, Hodges PW, McAuley JH, Nicholas MK, et al. Effect of motor control exercises versus graded activity in patients with chronic nonspecific low back pain: a randomized controlled trial. Phys Ther 2012;92:363-77. https://doi.org/10.2522/ptj.20110290.
- van der Roer N, van Tulder M, Barendse J, Knol D, van Mechelen W, de Vet H. Intensive group training protocol versus guideline physiotherapy for patients with chronic low back pain: a randomised controlled trial. Eur Spine J 2008;17:1193-200. https://doi.org/10.1007/s00586-008-0718-6.
- Walti P, Kool J, Luomajoki H. Short-term effect on pain and function of neurophysiological education and sensorimotor retraining compared to usual physiotherapy in patients with chronic or recurrent non-specific low back pain, a pilot randomized controlled trial. BMC Musc Dis 2015;16. https://doi.org/10.1186/s12891-015-0533-2.
- Loew TH, Sohn R, Martus P, Tritt K, Rechlin T. Functional relaxation as a somatopsychotherapeutic intervention: a prospective controlled study. Altern Ther Health Med 2000;6:70-5.
- Lansinger B, Larsson E, Persson LC, Carlsson JY. Qigong and exercise therapy in patients with long-term neck pain: a prospective randomized trial. Spine 2007;32:2415-22. https://doi.org/10.1097/BRS.0b013e3181573b4b.
- Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C, Goldenberg DL, et al. The American College of Rheumatology 1990 criteria for the classification of fibromyalgia: report of the Multicenter Criteria Committee. Arthritis Rheum 1990;33:160-72. https://doi.org/10.1002/art.1780330203.
- McBeth J, Prescott G, Scotland G, Lovell K, Keeley P, Hannaford P, et al. Cognitive behavior therapy, exercise, or both for treating chronic widespread pain. Arch Intern Med 2012;172:48-57. https://doi.org/10.1001/archinternmed.2011.555.
- Beasley M, Prescott GJ, Scotland G, McBeth J, Lovell K, Keeley P, et al. Patient-reported improvements in health are maintained 2 years after completing a short course of cognitive behaviour therapy, exercise or both treatments for chronic widespread pain: long-term results from the MUSICIAN randomised controlled trial. RMD Open 2015;1. https://doi.org/10.1136/rmdopen-2014-000026.
- Rothman MG, Ortendahl M, Rosenblad A, Johansson AC. Improved quality of life, working ability, and patient satisfaction after a pretreatment multimodal assessment method in patients with mixed chronic muscular pain: a randomized-controlled study. Clin J Pain 2013;29:195-204. https://doi.org/10.1097/AJP.0b013e318250e544.
- LeFort SM. Randomized Controlled Trial of a Community-Based Nursing Intervention for Those Experiencing Chronic Non-Malignant Pain 2000.
- Kennedy T, Jones R, Darnley S, Seed P, Wessely S, Chalder T. Cognitive behaviour therapy in addition to antispasmodic treatment for irritable bowel syndrome in primary care: randomised controlled trial. BMJ 2005;331. https://doi.org/10.1136/bmj.38545.505764.06.
- Moss-Morris R, McAlpine L, Didsbury LP, Spence MJ. A randomized controlled trial of a cognitive behavioural therapy-based self-management intervention for irritable bowel syndrome in primary care. Psychol Med 2010;40:85-94. https://doi.org/10.1017/S0033291709990195.
- Robinson A, Lee V, Kennedy A, Middleton L, Rogers A, Thompson DG, et al. A randomised controlled trial of self-help interventions in patients with a primary care diagnosis of irritable bowel syndrome. Gut 2006;55:643-8. https://doi.org/10.1136/gut.2004.062901.
- Schaefert R, Kaufmann C, Wild B, Schellberg D, Boelter R, Faber R, et al. Specific collaborative group intervention for patients with medically unexplained symptoms in general practice: a cluster randomized controlled trial. Psychother Psychosom 2013;82:106-19. https://doi.org/10.1159/000343652.
- Marques M, De Gucht V, Leal I, Maes S. Effects of a self-regulation based physical activity program (the ‘4-STEPS’) for unexplained chronic fatigue: a randomized controlled trial. Int J Behav Med 2015;22:187-96. https://doi.org/10.1007/s12529-014-9432-4.
- Schulz KF, Grimes DA. Sample size slippages in randomised trials: exclusions and the lost and wayward. Lancet 2002;359:781-5. https://doi.org/10.1016/S0140-6736(02)07882-0.
- Sutton A, de la Cruz MDCG, Leaviss J, Booth A. Searching for trial protocols: a comparison of methods. Res Synth Meth 2018;9:551-60. https://doi.org/10.1002/jrsm.1281.
- Aiarzaguena JM, Grandes G, Gaminde I, Salazar A, Sánchez A, Ariño J. A randomized controlled clinical trial of a psychosocial and communication intervention carried out by GPs for patients with medically unexplained symptoms. Psychol Med 2007;37:283-94. https://doi.org/10.1017/S0033291706009536.
- Alda M, Luciano JV, Andrés E, Serrano-Blanco A, Rodero B, del Hoyo YL, et al. Effectiveness of cognitive behaviour therapy for the treatment of catastrophisation in patients with fibromyalgia: a randomised controlled trial. Arthritis Res Ther 2011;13. https://doi.org/10.1186/ar3496.
- Luciano JV, Guallar JA, Aguado J, López-Del-Hoyo Y, Olivan B, Magallón R, et al. Effectiveness of group acceptance and commitment therapy for fibromyalgia: a 6-month randomized controlled trial (EFFIGACT study). Pain 2014;155:693-702. https://doi.org/10.1016/j.pain.2013.12.029.
- Luciano JV, Martinez N, Penarrubia-Maria MT. Effectiveness of a psychoeducational treatment program implemented in general practice for fibromyalgia patients: a randomized controlled trial. Clin J Pain 2011;27. https://doi.org/10.1097/AJP.0b013e31820b131c.
- Sañudo B, Galiano D, Carrasco L, Blagojevic M, de Hoyo M, Saxton J. Aerobic exercise versus combined exercise therapy in women with fibromyalgia syndrome: a randomized controlled trial. Arch Phys Med Rehabil 2010;91:1838-43. https://doi.org/10.1016/j.apmr.2010.09.006.
- Zonneveld LN, van Rood YR, Timman R, Kooiman CG, Van’t Spijker A, Busschbach JJ. Effective group training for patients with unexplained physical symptoms: a randomized controlled trial with a non-randomized one-year follow-up. PLOS ONE 2012;7. https://doi.org/10.1371/journal.pone.0042629.
- Smith RC, Gardiner JC, Luo Z, Schooley S, Lamerato L, Rost K. Primary care physicians treat somatization. J Gen Intern Med 2009;24:829-32. https://doi.org/10.1007/s11606-009-0992-y.
- van Ravesteijn H, Lucassen P, Bor H, van Weel C, Speckens A. Mindfulness-based cognitive therapy for patients with medically unexplained symptoms: a randomized controlled trial. Psychother Psychosom 2013;82:299-310. https://doi.org/10.1159/000348588.
- Gili M, Magallón R, López-Navarro E, Roca M, Moreno S, Bauzá N, et al. Health related quality of life changes in somatising patients after individual versus group cognitive behavioural therapy: a randomized clinical trial. J Psychosom Res 2014;76:89-93. https://doi.org/10.1016/j.jpsychores.2013.10.018.
- Pols RG, Battersby MW. Coordinated care in the management of patients with unexplained physical symptoms: depression is a key issue. Med J Aust 2008;188:133-7. https://doi.org/10.5694/j.1326-5377.2008.tb01877.x.
- Rosendal M, Olesen F, Fink P, Toft T, Sokolowski I, Bro F. A randomized controlled trial of brief training in the assessment and treatment of somatization in primary care: effects on patient outcome. Gen Hosp Psychiatry 2007;29:364-73. https://doi.org/10.1016/j.genhosppsych.2007.03.005.
- Schaefert R, Kirsch G, Kaufmann C, Hermann K, Szecsenyi J, Herzog W, et al. New ways in caring for patients with functional syndromes – interdisciplinary group intervention in the primary care setting: a qualitative study. Psychother Psychosom Med Psychol 2013;63:167-75. https://doi.org/10.1055/s-0032-1323790.
- Moreno S, Gili M, Magallón R, Bauzá N, Roca M, Del Hoyo YL, et al. Effectiveness of group versus individual cognitive-behavioral therapy in patients with abridged somatization disorder: a randomized controlled trial. Psychosom Med 2013;75:600-8. https://doi.org/10.1097/PSY.0b013e31829a8904.
- Tummers M, Knoop H, van Dam A, Bleijenberg G. Implementing a minimal intervention for chronic fatigue syndrome in a mental health centre: a randomized controlled trial. Psychol Med 2012;42:2205-15. https://doi.org/10.1017/S0033291712000232.
- Ho RTH, Chan JSM, Wang CW, Lau BW, So KF, Yuen LP, et al. A randomized controlled trial of qigong exercise on fatigue symptoms, functioning, and telomerase activity in persons with chronic fatigue or chronic fatigue syndrome. Annal Behav Med 2012;44:160-70. https://doi.org/10.1007/s12160-012-9381-6.
- Friedberg F, Napoli A, Coronel J, Adamowicz J, Seva V, Caikauskaite I, et al. Chronic fatigue self-management in primary care: a randomized trial. Psychosom Med 2013;75:650-7. https://doi.org/10.1097/PSY.0b013e31829dbed4.
- Moss-Morris R, Sharon C, Tobin R, Baldi JC. A randomized controlled graded exercise trial for chronic fatigue syndrome: outcomes and mechanisms of change. J Health Psychol 2005;10:245-59. https://doi.org/10.1177/1359105305049774.
- Huibers MJ, Beurskens AJ, Van Schayck CP, Bazelmans E, Metsemakers JF, Knottnerus JA, et al. Efficacy of cognitive-behavioural therapy by general practitioners for unexplained fatigue among employees: randomised controlled trial. Br J Psychiatry 2004;184:240-6. https://doi.org/10.1192/bjp.184.3.240.
- Whitehead L, Campion P. Can general practitioners manage chronic fatigue syndrome? A controlled trial. J Chronic Fatigue Syndr 2002;10:55-64. https://doi.org/10.1300/J092v10n01_05.
- Leone SS, Huibers MJ, Kant I, van Amelsvoort LG, van Schayck CP, Bleijenberg G, et al. Long-term efficacy of cognitive-behavioral therapy by general practitioners for fatigue: a 4-year follow-up study. J Psychosom Res 2006;61:601-7. https://doi.org/10.1016/j.jpsychores.2006.04.010.
- Escobar JI, Gara MA, Diaz-Martinez AM, Interian A, Warman M, Allen LA, et al. Effectiveness of a time-limited cognitive behavior therapy type intervention among primary care patients with medically unexplained symptoms. Ann Fam Med 2007;5:328-35. https://doi.org/10.1370/afm.702.
- Burton C, Weller D, Marsden W, Worth A, Sharpe M. A primary care Symptoms Clinic for patients with medically unexplained symptoms: pilot randomised trial. BMJ Open 2012;2. https://doi.org/10.1136/bmjopen-2011-000513.
- Larisch A, Schweickhardt A, Wirsching M, Fritzsche K. Psychosocial interventions for somatizing patients by the general practitioner: a randomized controlled trial. J Psychosom Res 2004;57:507-14. https://doi.org/10.1016/j.jpsychores.2004.04.372.
- Schilte AF, Portegijs PJ, Blankenstein AH, van der Horst HE, Latour MB, van Eijk JT, et al. Randomised controlled trial of disclosure of emotionally important events in somatisation in primary care. BMJ 2001;323. https://doi.org/10.1136/bmj.323.7304.86.
- van der Feltz-Cornelis CM, van Oppen P, Adèr HJ, van Dyck R. Randomised controlled trial of a collaborative care model with psychiatric consultation for persistent medically unexplained symptoms in general practice. Psychother Psychosom 2006;75:282-9. https://doi.org/10.1159/000093949.
- Kashner TM, Rost K, Cohen B, Anderson M, Smith GR. Enhancing the health of somatization disorder patients. Effectiveness of short-term group therapy. Psychosomatics 1995;36:462-70. https://doi.org/10.1016/S0033-3182(95)71627-9.
- Marks I. Behavioural Psychotherapy: Maudsley Pocket Book of Clinical Management. Bristol: Wright; 1986.
- Cohen J. Statistical Power Analysis for the Behavioral Sciences. Hillsdale, NJ: Lawrence Erlbaum Associates, Publishers; 1988.
- Ax S, Gregg VH, Jones D. Chronic fatigue syndrome: sufferers’ evaluation of medical support. J Royal Soc Med 1997;90:250-4. https://doi.org/10.1177/014107689709000505.
- Bayliss K, Goodall M, Chisholm A, Fordham B, Chew-Graham C, Riste L, et al. Overcoming the barriers to the diagnosis and management of chronic fatigue syndrome/ME in primary care: a meta synthesis of qualitative studies. BMC Family Pract 2014;15. https://doi.org/10.1186/1471-2296-15-44.
- Wallace LS, Wexler RK, McDougle L, Miser WF, Haddox JD. Voices that may not otherwise be heard: a qualitative exploration into the perspectives of primary care patients living with chronic pain. J Pain Res 2014;7:291-9. https://doi.org/10.2147/JPR.S62317.
- Deale A, Wessely S. Diagnosis of psychiatric disorder in clinical evaluation of chronic fatigue syndrome. J Royal Soc Med 2000;93:310-12. https://doi.org/10.1177/014107680009300608.
- Raine R, Carter S, Sensky T, Black N. General practitioners’ perceptions of chronic fatigue syndrome and beliefs about its management, compared with irritable bowel syndrome: qualitative study. BMJ 2004;328:1354-7. https://doi.org/10.1136/bmj.38078.503819.EE.
- Glenton C, Colvin CJ, Carlsen B, Swartz A, Lewin S, Noyes J, et al. Barriers and facilitators to the implementation of lay health worker programmes to improve access to maternal and child health: qualitative evidence synthesis. Cochrane Database Syst Rev 2013. https://doi.org/10.1002/14651858.CD010414.
- Rashidian A, Shakibazadeh E, Karimi-Shahanjarini A, Glenton C, Noyes J, Lewin S, et al. Barriers and facilitators to the implementation of doctor-nurse substitution strategies in primary care: qualitative evidence synthesis (Protocol). Cochrane Database Syst Rev 2013;2. https://doi.org/10.1002/14651858.CD010412.
- Colvin CJ, de Heer J, Winterton L, Mellenkamp M, Glenton C, Noyes J, et al. A systematic review of qualitative evidence on barriers and facilitators to the implementation of task-shifting in midwifery services. Midwifery 2013;29:1211-21. https://doi.org/10.1016/j.midw.2013.05.001.
- Munthe-Kaas HM, Hammerstrøm K, Kurtze N, Nordlund KR. Effekt Av Og Erfaringer Med Kontinuitetsfremmende Tiltak I Barnevernsinstitusjoner. Rapport Fra Kunnskapssenteret No. 4–2013 2013.
- Bohren MA, Hunter EC, Munthe-Kaas HM, Souza JP, Vogel JP, Gülmezoglu AM. Facilitators and barriers to facility-based delivery in low- and middle-income countries: a qualitative evidence synthesis. Reprod Health 2014;11. https://doi.org/10.1186/1742-4755-11-71.
- Critical Appraisal Skills Programme . CASP Qualitative Checklist 2018. https://casp-uk.net/wp-content/uploads/2018/03/CASP-Qualitative-Checklist-2018_fillable_form.pdf (accessed 1 June 2019).
- Noyes J, Lewin S, Noyes J, Booth A, Hannes K, Harden A, et al. Supplementary Guidance for Inclusion of Qualitative Research in Cochrane Systematic Reviews of Interventions 2011. http://methods.cochrane.org/qi/supplemental-handbook-guidance (accessed 1 June 2019).
- Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol 2008;8. https://doi.org/10.1186/1471-2288-8-45.
- Noyes J, Popay J, Pearson A, Hannes K, Booth A, Higgins JPT, et al. Cochrane Handbook for Systematic Reviews of Interventions. The Cochrane Collaboration; 2008.
- Peters S, Wearden A, Morriss R, Dowrick CF, Lovell K, Brooks G, et al. Challenges of nurse delivery of psychological interventions for long-term conditions in primary care: a qualitative exploration of the case of chronic fatigue syndrome/myalgic encephalitis. Implement Sci 2011;6. https://doi.org/10.1186/1748-5908-6-132.
- Chew-Graham C, Brooks J, Wearden A, Dowrick C, Peters S. Factors influencing engagement of patients in a novel intervention for CFS/ME: a qualitative study. Prim Health Care Res Dev 2011;12:112-22. https://doi.org/10.1017/S146342361000037X.
- Peters S, Rogers A, Salmon P, Gask L, Dowrick C, Towey M, et al. What do patients choose to tell their doctors? Qualitative analysis of potential barriers to reattributing medically unexplained symptoms. J Gen Int Med 2009;24. https://doi.org/10.1007/s11606-008-0872-x.
- Dowrick C, Gask L, Hughes JG, Charles-Jones H, Hogg JA, Peters S, et al. General practitioners’ views on reattribution for patients with medically unexplained symptoms: a questionnaire and qualitative study. BMC Fam Pract 2008;9. https://doi.org/10.1186/1471-2296-9-46.
- Gerskowitch C, Norman I, Rimes KA. Patients with medically unexplained physical symptoms experience of receiving treatment in a primary-care psychological therapies service: a qualitative study. Cogn Behav Therap 2015;8. https://doi.org/10.1017/S1352465815000235.
- Graham J, Manor O, Wiseman S. Introducing humanistic group counselling for somatisation in a primary care practice: Preliminary findings. Couns Psychother Res 2007;7:220-6. https://doi.org/10.1080/14733140701718420.
- Lewis H. An exploratory study of primary-care therapists’ perceived competence in providing cognitive behavioural therapy to people with medically unexplained symptoms. Cogn Behav Therap 2013;6. https://doi.org/10.1017/S1754470X13000202.
- Morton L, Elliott A, Thomas R, Cleland J, Deary V, Burton C. Developmental study of treatment fidelity, safety and acceptability of a Symptoms Clinic intervention delivered by General Practitioners to patients with multiple medically unexplained symptoms. J Psychosom Res 2016;84:37-43. https://doi.org/10.1016/j.jpsychores.2016.03.008.
- Payne H. The body speaks its mind: the BodyMind Approach for patients with medically unexplained symptoms in primary care in England. Arts Psychoth 2015;42:19-27. https://doi.org/10.1016/j.aip.2014.12.011.
- MacNeela P, Doyle C, O’Gorman D, Ruane N, McGuire BE. Experiences of chronic low back pain: a meta-ethnography of qualitative research. Health Psychol Rev 2015;9:63-82. https://doi.org/10.1080/17437199.2013.840951.
- Harzing AW. Publish or Perish 6.0. London: Harzing.com; 2017.
- Sutton A, de la Cruz MDCG, Booth A, Leaviss J. VP198 efficient retrieval of trial protocols: an empirical study. Int J Technol Assess Health Care 2017;33. https://doi.org/10.1017/S0266462317004251.
- Booth A, Sutton A, Scope A, Leaviss J. OP105 systematically reconstructing trial context-role for CLUSTER searches. Int J Technol Assess Health Care 2017;33. https://doi.org/10.1017/S026646231700174X.
- Morton L, Elliott A, Cleland J, Deary V, Burton C. A taxonomy of explanations in a general practitioner clinic for patients with persistent ‘medically unexplained’ physical symptoms. Patient Educ Counsel 2017;100:224-30. https://doi.org/10.1016/j.pec.2016.08.015.
- Payne H, Brooks SDM. Clinical outcomes from The BodyMind Approach™ in the treatment of patients with medically unexplained symptoms in primary health care in England: practice-based evidence. Arts Psychother 2016;47:55-6. https://doi.org/10.1016/j.aip.2015.12.001.
- Payne H, Warnecke T, Karkou V, Westland G. A comparative analysis of body psychotherapy and dance movement psychotherapy from a European perspective. Body Mov Dance Psychother 2016;11:144-66. https://doi.org/10.1080/17432979.2016.1165291.
- Payne H. Pilot study to evaluate Dance Movement Psychotherapy (the BodyMind Approach) in patients with medically unexplained symptoms: participant and facilitator perceptions and a summary discussion. Body Mov Dance Psychother 2009;4:77-94. https://doi.org/10.1080/17432970902918008.
- Payne H. The BodyMind Approach (BMA) to psychotherapeutic groupwork with patients with medically unexplained symptoms (MUS): a review of the literature, description of approach and methodology for a pilot study. Eur J Psychother Couns 2009;11:287-310. https://doi.org/10.1080/13642530903230392.
- Payne H. Medically unexplained conditions and the bodymind approach. Couns Prim Care Rev 2009;10:6-8.
- Payne H, Stott D. Change in the moving bodymind: quantitative results from a pilot study on the use of the BodyMind approach (BMA) to psychotherapeutic group work with patients with medically unexplained symptoms (MUSs). Couns Psychother Res 2010;10:295-306. https://doi.org/10.1080/14733140903551645.
- Payne H, Fordham R. A Group Bodymind Approach to Medically Unexplained Symptoms: Proof of Concept and Potential Cost Savings 2009.
- Payne H, Eskioglou M, Story J. Medically Unexplained Symptoms: A Holistic BodyMind Approach to Group Therapy for Depression and Anxiety in Primary Care. Newport: East of England Development Agency; 2009.
- Payne H. Psychosomatic conditions in primary care: change within the moving bodymind. E-Motion 2010;20:20-4.
- Payne H. Arts Therapies Conference ‘The Space Between – The Potential For change’. Conference Handbook and Abstract Book. Ottersberg: University of Applied Sciences; 2011.
- Lin Y, Payne H. The BodyMind Approach™, medically unexplained symptoms and personal construct psychology. Body Mov Dance Psychother 2014;9:154-66. https://doi.org/10.1080/17432979.2014.918563.
- Payne H, Payne H, Brooks SD, Brooks SD. Moving on: the BodyMind Approach™ for medically unexplained symptoms. J Pub Ment Health 2017;16:63-71. https://doi.org/10.1108/JPMH-10-2016-0052.
- Payne H, Karkou V, Oliver S, Lycouris S. The Oxford Handbook of Dance and Wellbeing. Oxford: Oxford University Press; 2017.
- Samaritter R, Payne H. Being moved: Kinaesthetic reciprocities in psychotherapeutic interaction and the development of enactive intersubjectivity. Eur Psychother 2016;13.
- Wearden AJ, Riste L, Dowrick C, Chew-Graham C, Bentall RP, Morriss RK, et al. Fatigue Intervention by Nurses Evaluation – the FINE Trial. A randomised controlled trial of nurse led self-help treatment for patients in primary care with chronic fatigue syndrome: study protocol. BMC Med 2006;4. https://doi.org/10.1186/1741-7015-4-9.
- Wearden AJ, Dunn G, Dowrick C, Morriss RK. Depressive symptoms and pragmatic rehabilitation for chronic fatigue syndrome. Br J Psychiatry 2012;201:227-32. https://doi.org/10.1192/bjp.bp.111.107474.
- Wearden AJ, Emsley R. Mediators of the effects on fatigue of pragmatic rehabilitation for chronic fatigue syndrome. J Consult Clin Psychol 2013;81:831-8. https://doi.org/10.1037/a0033561.
- Chew-Graham CA, Cahill G, Dowrick C, Wearden A, Peters S. Using multiple sources of knowledge to reach clinical understanding of chronic fatigue syndrome. Ann Fam Med 2008;6:340-8. https://doi.org/10.1370/afm.867.
- Chew-Graham C, Dixon R, Shaw JW, Smyth N, Lovell K, Peters S. Practice nurses’ views of their role in the management of chronic fatigue syndrome/myalagic encephalitis: a qualitative study. BMC Nurs 2009;8. https://doi.org/10.1186/1472-6955-8-2.
- Chew-Graham C, Dowrick C, Wearden A, Richardson V, Peters S. Making the diagnosis of chronic fatigue syndrome/myalgic encephalitis in primary care: a qualitative study. BMC Fam Pract 2010;11. https://doi.org/10.1186/1471-2296-11-16.
- Wearden AJ, Chew-Graham C. Managing chronic fatigue syndrome in U.K. primary care: challenges and opportunities. Chronic Illn 2006;2:143-53. https://doi.org/10.1177/17423953060020020901.
- Band R, Wearden A, Barrowclough C. Patient outcomes in association with significant other responses to chronic fatigue syndrome: a systematic review of the literature. Clin Psychol 2015;22:29-46. https://doi.org/10.1111/cpsp.12093.
- Hannon K, Peters S, Fisher L, Riste L, Wearden A, Lovell K, et al. Developing resources to support the diagnosis and management of chronic fatigue syndrome/myalgic encephalitis (CFS/ME) in primary care: a qualitative study. BMC Fam Pract 2012;13. https://doi.org/10.1186/1471-2296-13-93.
- Bayliss K, Riste L, Fisher L, Wearden A, Peters S, Lovell K, et al. Diagnosis and management of chronic fatigue syndrome/myalgic encephalitis in black and minority ethnic people: a qualitative study. Prim Health Care Res Dev 2014;15:143-55. https://doi.org/10.1017/S1463423613000145.
- Brooks JM, Daglish J, Wearden AJ. Attributions, distress and behavioural responses in the significant others of people with chronic fatigue syndrome. J Health Psychol 2013;18:1288-95. https://doi.org/10.1177/1359105312464670.
- Brooks J, King N, Wearden A. Couples’ experiences of interacting with outside others in chronic fatigue syndrome: a qualitative study. Chronic Illn 2014;10:5-17. https://doi.org/10.1177/1742395312474478.
- Salmon P, Peters S, Clifford R, Iredale W, Gask L, Rogers A, et al. Why do general practitioners decline training to improve management of medically unexplained symptoms?. J Gen Int Med 2007;22:565-71. https://doi.org/10.1007/s11606-006-0094-z.
- Salmon P, Peters S, Rogers A, Gask L, Clifford R, Iredale W, et al. Peering through the barriers in GPs’ explanations for declining to participate in research: the role of professional autonomy and the economy of time. Fam Pract 2007;24:269-75. https://doi.org/10.1093/fampra/cmm015.
- Morriss R, Dowrick C, Salmon P, Peters S, Rogers A, Dunn G, et al. Turning theory into practice: rationale, feasibility and external validity of an exploratory randomized controlled trial of training family practitioners in reattribution to manage patients with medically unexplained symptoms (the MUST). Gen Hosp Psychiatry 2006;28:343-51. https://doi.org/10.1016/j.genhosppsych.2006.03.012.
- Morriss R, Kai J, Atha C, Avery A, Bayes S, Franklin M, et al. Persistent frequent attenders in primary care: costs, reasons for attendance, organisation of care and potential for cognitive behavioural therapeutic intervention. BMC Fam Pract 2012;13. https://doi.org/10.1186/1471-2296-13-39.
- Salmon P, Wissow L, Carroll J, Ring A, Humphris GM, Davies JC, et al. Doctors’ attachment style and their inclination to propose somatic interventions for medically unexplained symptoms. Gen Hosp Psychiatry 2008;30:104-11. https://doi.org/10.1016/j.genhosppsych.2007.12.002.
- Morriss R, Lindson N, Coupland C, Dex G, Avery A. Estimating the prevalence of medically unexplained symptoms from primary care records. Public Health 2012;126:846-54. https://doi.org/10.1016/j.puhe.2012.05.008.
- Morriss R, Dowrick C, Salmon P, Peters S, Dunn G, Rogers A, et al. ‘Reattribution for medically unexplained symptoms’: authors’ reply. Br J Psychiatry 2008;192. https://doi.org/10.1192/bjp.192.4.315.
- Morriss R, Gask L. Assessment and immediate management of patients with medically unexplained symptoms in primary care and general hospital settings. Found Years 2008;4:59-63. https://doi.org/10.1016/j.mpfou.2008.02.003.
- Salmon P, Ring A, Humphris GM, Davies JC, Dowrick CF. Primary care consultations about medically unexplained symptoms: how do patients indicate what they want?. J Gen Intern Med 2009;24:450-6. https://doi.org/10.1007/s11606-008-0898-0.
- McGowan L, Luker K, Creed F, Chew-Graham CA. ‘How do you explain a pain that can’t be seen?’: the narratives of women with chronic pelvic pain and their disengagement with the diagnostic cycle. Br J Health Psychol 2007;12:261-74. https://doi.org/10.1348/135910706X104076.
- Pawson R, Greenhalgh T, Harvey G, Walshe K. Realist review – a new method of systematic review designed for complex policy interventions. J Health Serv Res Policy 2005;10:21-34. https://doi.org/10.1258/1355819054308530.
- Kendrick E. Impact of Social Support on the Relationship Between Illness Invalidation and Shame Among Individuals with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Norman, OK: University of Oklahoma; 2015.
- Jutel A. Medically unexplained symptoms and the disease label. Social Theory Health 2010;8:229-45. https://doi.org/10.1057/sth.2009.21.
- van der Kar AG. Determinants of Consulting the General Practitioner. Maastricht: Maastricht University; 1992.
- Horton-Salway M. The local production of knowledge: disease labels, identities and category entitlements in ME support group talk. Health 2004;8:351-71. https://doi.org/10.1177/1363459304043474.
- Hoedeman R, Blankenstein AH, van der Feltz-Cornelis CM, Krol B, Stewart R, Groothoff JW. Consultation letters for medically unexplained physical symptoms in primary care. Cochrane Database Syst Rev 2010;12. https://doi.org/10.1002/14651858.CD006524.pub2.
- Sharpe M, Peveler R, Mayou R. The psychological treatment of patients with functional somatic symptoms: a practical guide. J Psychosom Res 1992;36:515-29. https://doi.org/10.1016/0022-3999(92)90037-3.
- Stone L. Managing the consultation with patients with medically unexplained symptoms: a grounded theory study of supervisors and registrars in general practice. BMC Family Pract 2014;15. https://doi.org/10.1186/s12875-014-0192-7.
- Wileman L, May C, Chew-Graham CA. Medically unexplained symptoms and the problem of power in the primary care consultation: a qualitative study. Family Pract 2002;19:178-82. https://doi.org/10.1093/fampra/19.2.178.
- Sobel RK. In the heart, not the head. Chronic fatigue is real. US News World Rep 2000;129.
- Kroenke K, Swindle R. Cognitive-behavioral therapy for somatization and symptom syndromes: a critical review of controlled clinical trials. Psychother Psychosom 2000;69:205-15. https://doi.org/10.1159/000012395.
- Ridd M, Shaw A, Salisbury C. ’Two sides of the coin’ – the value of personal continuity to GPs: a qualitative interview study. Fam Pract 2006;23:461-8. https://doi.org/10.1093/fampra/cml010.
- Royal College of Psychiatrists . Whole-Person Care: From Rhetoric to Reality (Achieving Parity Between Mental and Physical Health) (OP88) 2013.
- Murray AM, Toussaint A, Althaus A, Lowe B. The challenge of diagnosing non-specific, functional, and somatoform disorders: a systematic review of barriers to diagnosis in primary care. J Psychosom Res 2016;80:1-10. https://doi.org/10.1016/j.jpsychores.2015.11.002.
- Johansen ML, Risor MB. What is the problem with medically unexplained symptoms for GPs? A meta-synthesis of qualitative studies. Patient Educ Couns 2017;100:647-54. https://doi.org/10.1016/j.pec.2016.11.015.
- Denz-Penhey H, Murdoch JC. Service delivery for people with chronic fatigue syndrome: a pilot action research study. Fam Pract 1993;10:14-8. https://doi.org/10.1093/fampra/10.1.14.
- National Institute for Health and Care Excellence (NICE) . Guide to the Methods of Technology Appraisal 2013.
- van Ravenzwaaij J, Olde Hartman TC, van Ravesteijn H, Eveleigh R, van Rijswijk E, Lucassen PLBJ. Explanatory models of medically unexplained symptoms: a qualitative analysis of the literature. Ment Health Fam Med 2011;7:223-31.
- Engel CC, Katon W. Commissioned Paper: Unexplained Physical Symptoms in Primary Care and the Community: What Might We Learn for Prevention in the Military? Paper Prepared for the Strategies to Protect the Health of Deployed U.S. Forces: Medical Surveillance, Medical Record Keeping, and Risk Reduction. Washington, DC: Institute of Medicine; 1999.
- van Ravenzwaaij J, Olde Hartman TC, van Ravesteijn H, Eveleigh R, van Rijswijk E, Lucassen PLBJ. Explanatory models of medically unexplained symptoms: a qualitative analysis of the literature. Ment Health Fam Med 2010;7:223-31.
- Hadler NM. If you have to prove you are ill, you can’t get well. The object lesson of fibromyalgia. Spine 1996;21. https://doi.org/10.1097/00007632-199610150-00021.
- Allen A. EU Economies Filter: ISSG Search Filters Resource n.d. https://sites.google.com/a/york.ac.uk/issg-search-filters-resource/other-filters/filters-to-find-studies-of-geographic-locations/eu-economies (accessed 16 May 2017).
- National Institute for Health and Care Excellence (NICE) . Developing NICE Guidelines: The Manual Appendix H 2015.
- Engel GL. The need for a new medical model: a challenge for biomedicine. Science 1977;196:129-36. https://doi.org/10.1126/science.847460.
- O’Dowd H, Gladwell P, Rogers CA, Hollinghurst S, Gregory A. Cognitive behavioural therapy in chronic fatigue syndrome: a randomised controlled trial of an outpatient group programme. Health Technol Assess 2006;10. https://doi.org/10.3310/hta10370.
- Friedberg MW. Group cognitive behavioral treatment improves chronic low back pain in a cost-effective manner. J Clin Outcomes Manage 2010;17:7-9.
- Hill JC, Whitehurst DG, Lewis M, Bryan S, Dunn KM, Foster NE, et al. Comparison of stratified primary care management for low back pain with current best practice (STarT Back): a randomised controlled trial. Lancet 2011;378:1560-71. https://doi.org/10.1016/S0140-6736(11)60937-9.
- Johnson RE, Jones GT, Wiles NJ, Chaddock C, Potter RG, Roberts C, et al. Active exercise, education, and cognitive behavioral therapy for persistent disabling low back pain: a randomized controlled trial. Spine 2007;32:1578-85. https://doi.org/10.1097/BRS.0b013e318074f890.
- Taylor SJ, Carnes D, Homer K, Kahan BC, Hounsome N, Eldridge S, et al. Novel three-day, Community-Based, Nonpharmacological Group Intervention for Chronic Musculoskeletal Pain (COPERS): a randomised clinical trial. PLOS Med 2016;13. https://doi.org/10.1371/journal.pmed.1002040.
- NHS Plymouth . Medically Unexplained Symptoms (MUS): A Whole Systems Approach in Plymouth 2009. www.iapt.nhs.uk/silo/files/medically-unexplained-symptoms-mus-a-wholesystems-approach-in-plymouth.pdf (accessed June 2020).
- McGowan L, Escott D, Luker K, Creed F, Chew-Graham C. Is chronic pelvic pain a comfortable diagnosis for primary care practitioners: a qualitative study. BMC Fam Pract 2010;11. https://doi.org/10.1186/1471-2296-11-7.
- Hoedeman R, Krol B, Blankenstein AH, Koopmans PC, Groothoff JW. Sick-listed employees with severe medically unexplained physical symptoms: burden or routine for the occupational health physician? A cross sectional study. BMC Health Serv Res 2010;10. https://doi.org/10.1186/1472-6963-10-305.
- Geraets JJ, Goossens ME, van Haastregt JC, de Groot IJ, de Bruijn CP, de Bie RA, et al. Implications of process evaluation for clinical effectiveness and clinical practice in a trial on chronic shoulder complaints. Patient Educ Couns 2006;61:117-25. https://doi.org/10.1016/j.pec.2005.02.017.
- Reid S, Whooley D, Crayford T, Hotopf M. Medically unexplained symptoms – GPs’ attitudes towards their cause and management. Family Pract 2001;18:519-23. https://doi.org/10.1093/fampra/18.5.519.
- Shattock L, Williamson H, Caldwell K, Anderson K, Peters S. ‘They’ve just got symptoms without science’: Medical trainees’ acquisition of negative attitudes towards patients with medically unexplained symptoms. Patient Educ Couns 2013;91:249-54. https://doi.org/10.1016/j.pec.2012.12.015.
- Gerhards SA, de Graaf LE, Jacobs LE, Severens JL, Huibers MJ, Arntz A, et al. Economic evaluation of online computerised cognitive-behavioural therapy without support for depression in primary care: randomised trial. Br J Psychiatry 2010;196:310-18. https://doi.org/10.1192/bjp.bp.109.065748.
- Jones R, Barraclough K, Dowrick C. When no diagnostic label is applied. BMJ 2010;340. https://doi.org/10.1136/bmj.c2683.
- Konnopka A, Konig HH, Kaufmann C, Stuhldreher N, Wild B, Szecsenyi J, et al. Cost-effectiveness of a collaborative group intervention for patients with medically unexplained symptoms. J Ment Health Policy Econ 2015;18:S25-6.
- Luciano JV, Sabes-Figuera R, Cardeñosa E, T Peñarrubia-María M, Fernández-Vergel R, García-Campayo J, et al. Cost-utility of a psychoeducational intervention in fibromyalgia patients compared with usual care: an economic evaluation alongside a 12-month randomized controlled trial. Clin J Pain 2013;29:702-11. https://doi.org/10.1097/AJP.0b013e318270f99a.
- Luo Z, Goddeeris J, Gardiner JC, Smith RC. Costs of an intervention for primary care patients with medically unexplained symptoms: a randomized controlled trial. Psychiatr Serv 2007;58:1079-86. https://doi.org/10.1176/ps.2007.58.8.1079.
- Margalit AP, El-Ad A. Costly patients with unexplained medical symptoms: a high-risk population. Patient Educ Couns 2008;70:173-8. https://doi.org/10.1016/j.pec.2007.09.020.
- Meng H, Friedberg F, Castora-Binkley M. Cost-effectiveness of chronic fatigue self-management versus usual care: a pilot randomized controlled trial. BMC Fam Pract 2014;15. https://doi.org/10.1186/s12875-014-0184-7.
- Oliver K, Cronan TA, Walen HR, Tomita M. Effects of social support and education on health care costs for patients with fibromyalgia. J Rheumatol 2001;28:2711-19.
- Salmon P, Sharma N, Valori R, Bellenger N. Patients’ intentions in primary care: relationship to physical and psychological symptoms, and their perception by general practitioners. Social Sci Med 1994;38:585-92. https://doi.org/10.1016/0277-9536(94)90255-0.
- Schade R, Dieleman JP, Sturkenboom MC. Trends in the prescription of antiparkinsonian drugs among patients with Parkinson’s disease in the United Kingdom: a population-based analysis. Mov Disord 2011;26.
- van der Roer N, van Tulder MW, Barendse JM, van Mechelen W, Franken WK, Ooms AC, et al. Cost-effectiveness of an intensive group training protocol compared to physiotherapy guideline care for sub-acute and chronic low back pain: design of a randomised controlled trial with an economic evaluation. BMC Musculoskelet Disord 2004;5. https://doi.org/10.1186/1471-2474-5-45.
- Morriss R, Gask L, Ronalds C, Downes-Grainger E, Thompson H, Leese B, et al. Cost-effectiveness of a new treatment for somatized mental disorder taught to GPs. Fam Pract 1998;15:119-25. https://doi.org/10.1093/fampra/15.2.119.
- Chisholm D, Godfrey E, Ridsdale L, Chalder T, King M, Seed P, et al. Chronic fatigue in general practice: economic evaluation of counselling versus cognitive behaviour therapy. Br J Gen Pract 2001;51:15-8.
- Kennedy TM, Chalder T, McCrone P, Darnley S, Knapp M, Jones RH, et al. Cognitive behavioural therapy in addition to antispasmodic therapy for irritable bowel syndrome in primary care: randomised controlled trial. Health Technol Assess 2006;10. https://doi.org/10.3310/hta10190.
- Hubley S, Uebelacker L, Eaton C. Managing medically unexplained symptoms in primary care: a narrative review and treatment recommendations. Am J Lifestyle Med 2016;10:109-19. https://doi.org/10.1177/1559827614536865.
- McCrone P, Knapp M, Kennedy T, Seed P, Jones R, Darnley S, et al. Cost-effectiveness of cognitive behaviour therapy in addition to mebeverine for irritable bowel syndrome. Eur J Gastroenterol Hepatol 2008;20:255-63. https://doi.org/10.1097/MEG.0b013e3282f2519d.
- McCrone P, Ridsdale L, Darbishire L, Seed P. Cost-effectiveness of cognitive behavioural therapy, graded exercise and usual care for patients with chronic fatigue in primary care. Psychol Med 2004;34:991-9. https://doi.org/10.1017/S0033291704001928.
- Sabes-Figuera R, McCrone P, Hurley M, King M, Donaldson AN, Ridsdale L. Cost-effectiveness of counselling, graded-exercise and usual care for chronic fatigue: evidence from a randomised trial in primary care. BMC Health Serv Res 2012;12. https://doi.org/10.1186/1472-6963-12-264.
- Salmon P, Peters S, Stanley I. Patients’ perceptions of medical explanations for somatisation disorders: qualitative analysis. BMJ 1999;318:372-6. https://doi.org/10.1136/bmj.318.7180.372.
- Richardson G, Epstein D, Chew-Graham C, Dowrick C, Bentall RP, Morriss RK, et al. Cost-effectiveness of supported self-management for CFS/ME patients in primary care. BMC Fam Pract 2013;14. https://doi.org/10.1186/1471-2296-14-12.
- Kirmayer L, Groleau D, Looper K, Dao M. Explaining medically unexplained symptoms. Can J Psychiatr 2004;49:663-71. https://doi.org/10.1177/070674370404901003.
- Fox R, Bendelow G, Carpenter M, Vautier C, Williams S. Gender, Health and Healing: The Public/Private Divide. London: Routledge; 2002.
- Griffiths F, Green E, Tsouroufli M. The nature of medical evidence and its inherent uncertainty for the clinical consultation: qualitative study. BMJ 2005;330. https://doi.org/10.1136/bmj.38336.482720.8F.
- Howman M, Walters K, Rosenthal J, Ajjawi R, Buszewicz M. ‘You kind of want to fix it don’t you?’ Exploring general practice trainees’ experiences of managing patients with medically unexplained symptoms. BMC Med Educ 2016;16. https://doi.org/10.1186/s12909-015-0523-y.
- Wainwright D, Calnan M, O’Neil C, Winterbottom A, Watkins C. When pain in the arm is ‘all in the head’: the management of medically unexplained suffering in primary care. Health Risk Soc 2006;8:71-88. https://doi.org/10.1080/13698570500532512.
- May C, Allison G, Chapple A, Chew-Graham C, Dixon C, Gask L, et al. Framing the doctor-patient relationship in chronic illness: a comparative study of general practitioners’ accounts. Sociol Health Illn 2004;26:135-58. https://doi.org/10.1111/j.1467-9566.2004.00384.x.
- Artus M, Croft P, Lewis M. The use of CAM and conventional treatments among primary care consulters with chronic musculoskeletal pain. BMC Fam Pract 2007;8. https://doi.org/10.1186/1471-2296-8-26.
- Stanley IM, Peters S, Salmon P. A primary care perspective on prevailing assumptions about persistent medically unexplained physical symptoms. Int J Psychiatry Med 2002;32:125-40. https://doi.org/10.2190/AVM3-8GU8-JW70-5RX5.
- Weiland A, Blankenstein AH, Van Saase JL, Van der Molen HT, Jacobs ME, Abels DC, et al. Training medical specialists to communicate better with patients with medically unexplained physical symptoms (MUPS). A randomized, controlled trial. PLOS ONE 2015;10. https://doi.org/10.1371/journal.pone.0138342.
- King M, Davidson O, Taylor F, Haines A, Sharp D, Turner R. Effectiveness of teaching general practitioners skills in brief cognitive behaviour therapy to treat patients with depression: randomised controlled trial. BMJ 2002;324:947-51B. https://doi.org/10.1136/bmj.324.7343.947.
- Yon K, Nettleton S, Walters K, Lamahewa K, Buszewicz M. Junior doctors’ experiences of managing patients with medically unexplained symptoms: a qualitative study. BMJ Open 2015;5. https://doi.org/10.1136/bmjopen-2015-009593.
- van Dessel N, Leone SS, van der Wouden JC, Dekker J, van der Horst HE. The PROSPECTS study: design of a prospective cohort study on prognosis and perpetuating factors of medically unexplained physical symptoms (MUPS). J Psychosom Res 2014;76:200-6. https://doi.org/10.1016/j.jpsychores.2013.12.011.
- Paulson M, Norberg A, Danielson E. Men living with fibromyalgia-type pain: experiences as patients in the Swedish health care system. J Adv Nurs 2002;40:87-95. https://doi.org/10.1046/j.1365-2648.2002.02343.x.
- Toye F, Barker K. Persistent non-specific low back pain and patients’ experience of general practice: a qualitative study. Prim Health Care Res Dev 2012;13:72-84. https://doi.org/10.1017/S1463423611000387.
- Stone L. Blame, shame and hopelessness: medically unexplained symptoms and the ‘heartsink’ experience. Aust Fam Physician 2014;43:191-5.
- Hubley S, Uebelacker LA, Nash J, Eaton CB. Open trial of integrated primary care consultation for medically unexplained symptoms. J Behav Health Serv Res 2017;44:590-601. https://doi.org/10.1007/s11414-016-9528-5.
- Sallinen M, Kukkurainen ML, Peltokallio L. Finally heard, believed and accepted – peer support in the narratives of women with fibromyalgia. Patient Educ Couns 2011;85:e126-30. https://doi.org/10.1016/j.pec.2011.02.011.
- Corbett M, Foster NE, Ong BN. Living with low back pain – stories of hope and despair. Soc Sci Med 2007;65:1584-94. https://doi.org/10.1016/j.socscimed.2007.06.008.
- Larun L, Malterud K. Identity and coping experiences in chronic fatigue syndrome: a synthesis of qualitative studies. Patient Educ Couns 2007;69:20-8. https://doi.org/10.1016/j.pec.2007.06.008.
- Nettleton S. ‘I just want permission to be ill’: towards a sociology of medically unexplained symptoms. Soc Sci Med 2006;62:1167-78. https://doi.org/10.1016/j.socscimed.2005.07.030.
- Anderson VR, Jason LA, Hlavaty LE, Porter N, Cudia J. A review and meta-synthesis of qualitative studies on myalgic encephalomyelitis/chronic fatigue syndrome. Patient Educ Couns 2012;86:147-55. https://doi.org/10.1016/j.pec.2011.04.016.
- Burton C. Beyond somatisation: a review of the understanding and treatment of medically unexplained physical symptoms (MUPS). Br J Gen Pract 2003;53:231-9.
- Drachler Mde L, Leite JC, Hooper L, Hong CS, Pheby D, Nacul L, et al. The expressed needs of people with chronic fatigue syndrome/myalgic encephalomyelitis: a systematic review. BMC Public Health 2009;9. https://doi.org/10.1186/1471-2458-9-458.
- Pinxsterhuis I, Strand EB, Sveen U. Coping with chronic fatigue syndrome: a review and synthesis of qualitative studies. Fatig Biomed Health Behav 2015;3:173-88. https://doi.org/10.1080/21641846.2015.1035519.
- Toye F, Seers K, Allcock N, Briggs M, Carr E, Andrews J, et al. Patients’ experiences of chronic non-malignant musculoskeletal pain: a qualitative systematic review. Br J Gen Pract 2013;63:e829-41. https://doi.org/10.3399/bjgp13X675412.
- Toye F, Seers K, Allcock N, Briggs M, Carr E, Andrews J, et al. A meta-ethnography of patients’ experience of chronic non-malignant musculoskeletal pain. Osteoarthr Cartilage 2013;21:S259-S260. https://doi.org/10.1016/j.joca.2013.02.539.
- Toye F, Seers K, Barker K. A meta-ethnography of patients’ experiences of chronic pelvic pain: struggling to construct chronic pelvic pain as ‘real’. J Adv Nurs 2014;70:2713-27. https://doi.org/10.1111/jan.12485.
- Aiarzaguena JM, Gaminde I, Grandes G, Salazar A, Alonso I, Sánchez A. Somatisation in primary care: experiences of primary care physicians involved in a training program and in a randomised controlled trial. BMC Fam Pract 2009;10. https://doi.org/10.1186/1471-2296-10-73.
- Arnold IA, de Waal MW, Eekhof JA, Assendelft WJ, Spinhoven P, van Hemert AM. Medically unexplained physical symptoms in primary care: a controlled study on the effectiveness of cognitive-behavioral treatment by the family physician. Psychosomatics 2009;50:515-24. https://doi.org/10.1176/appi.psy.50.5.515.
- Blane DN, Williams C, Morrison J, Wilson A, Mercer S. Psychological therapies in primary care: a progress report. Br J Gen Pract 2014;64:556-7. https://doi.org/10.3399/bjgp14X682117.
- Chew-Graham CA. Focus on shared decision-making. Health Expect 2017;20:1181-2. https://doi.org/10.1111/hex.12654.
- den Boeft M, Huisman D, Morton L, Lucassen P, van der Wouden JC, Westerman MJ, et al. Negotiating explanations: doctor-patient communication with patients with medically unexplained symptoms – a qualitative analysis. Fam Pract 2017;34:107-13. https://doi.org/10.1093/fampra/cmw113.
- den Boeft M, Huisman D, van der Wouden JC, Numans ME, van der Horst HE, Lucassen PL, et al. Recognition of patients with medically unexplained physical symptoms by family physicians: results of a focus group study. BMC Fam Pract 2016;17. https://doi.org/10.1186/s12875-016-0451-x.
- den Boeft M, Claassen-van Dessel N, van der Wouden JC. How should we manage adults with persistent unexplained physical symptoms?. BMJ 2017;356. https://doi.org/10.1136/bmj.j268.
- Finset A, Mjaaland TA. The medical consultation viewed as a value chain: a neurobehavioral approach to emotion regulation in doctor–patient interaction. Patient Educ Couns 2009;74:323-30. https://doi.org/10.1016/j.pec.2008.12.007.
- Graugaard PK, Eide H, Finset A. Interaction analysis of physician–patient communication: the influence of trait anxiety on communication and outcome. Patient Educ Couns 2003;49:149-56. https://doi.org/10.1016/S0738-3991(02)00074-5.
- Huibers MJ, Beurskens AJ, Bleijenberg G, van Schayck CP. Psychosocial interventions by general practitioners. Cochrane Database Syst Rev 2007;3. https://doi.org/10.1002/14651858.CD003494.pub2.
- Kromme NMH, Ahaus CTB, Gans ROB, van de Wiel HBM. ‘It just has to click’: internists’ views of: what constitutes productive interactions with chronically ill patients. BMC Health Serv Res 2016;16. https://doi.org/10.1186/s12913-016-1430-6.
- Layard R. The case for psychological treatment centres. BMJ 2006;332:1030-2. https://doi.org/10.1136/bmj.332.7548.1030.
- Malins S, Kai J, Atha C, Avery A, Guo B, James M, et al. Cognitive behaviour therapy for long-term frequent attenders in primary care: a feasibility case series and treatment development study. Br J Gen Pract 2016;66:e729-36. https://doi.org/10.3399/bjgp16X686569.
- McDermott C, Lynch J, Leydon GM. Patients’ hopes and expectations of a specialist chronic fatigue syndrome/ME service: a qualitative study. Fam Pract 2011;28:572-8. https://doi.org/10.1093/fampra/cmr016.
- Picariello F, Ali S, Foubister C, Chalder T. ‘It feels sometimes like my house has burnt down, but I can see the sky’: a qualitative study exploring patients’ views of cognitive behavioural therapy for chronic fatigue syndrome. Br J Health Psychol 2017;22:383-41. https://doi.org/10.1111/bjhp.12235.
- Rask MT, Andersen RS, Bro F, Fink P, Rosendal M. Towards a clinically useful diagnosis for mild-to-moderate conditions of medically unexplained symptoms in general practice: a mixed methods study. BMC Fam Pract 2014;15. https://doi.org/10.1186/1471-2296-15-118.
- Schweickhardt A, Larisch A, Fritzsche K. Differentiation of somatizing patients in primary care: why the effects of treatment are always moderate. J Nerv Ment Dis 2005;193:813-19. https://doi.org/10.1097/01.nmd.0000188975.22144.3d.
- Sirri L, Grandi S, Tossani E. Medically unexplained symptoms and general practitioners: a comprehensive survey about their attitudes, experiences and management strategies. Fam Pract 2017;34:201-5. https://doi.org/10.1093/fampra/cmw130.
- Ziadni MS, Carty JN, Doherty HK, Porcerelli JH, Rapport LJ, Schubiner H, et al. A life-stress, emotional awareness, and expression interview for primary care patients with medically unexplained symptoms: a randomized controlled trial. Health Psychol 2018;37:282-90. https://doi.org/10.1037/hea0000566.
- InterTASC Information Specialists’ Sub-Group . Search Filter Resource n.d. https://sites.google.com/a/york.ac.uk/issg-search-filters-resource/ (accessed 15 May 2017).
- Creed F, Fernandes L, Guthrie E, Palmer S, Ratcliffe J, Read N, et al. The cost-effectiveness of psychotherapy and paroxetine for severe irritable bowel syndrome. Gastroenterology 2003;124:303-17. https://doi.org/10.1053/gast.2003.50055.
- Yardley L, Barker F, Muller I, Turner D, Kirby S, Mullee M, et al. Clinical and cost effectiveness of booklet based vestibular rehabilitation for chronic dizziness in primary care: single blind, parallel group, pragmatic, randomised controlled trial. BMJ 2012;344. https://doi.org/10.1136/bmj.e2237.
- Lamb SE, Hansen Z, Lall R, Castelnuovo E, Withers EJ, Nichols V, et al. Group cognitive behavioural treatment for low-back pain in primary care: a randomised controlled trial and cost-effectiveness analysis. Lancet 2010;375:916-23. https://doi.org/10.1016/S0140-6736(09)62164-4.
- Cherkin DC, Deyo RA, Battié M, Street J, Barlow W. A comparison of physical therapy, chiropractic manipulation, and provision of an educational booklet for the treatment of patients with low back pain. N Engl J Med 1998;339:1021-9. https://doi.org/10.1056/NEJM199810083391502.
- Ritzwoller DP, Crounse L, Shetterly S, Rublee D. The association of comorbidities, utilization and costs for patients identified with low back pain. BMC Musculoskelet Disord 2006;7. https://doi.org/10.1186/1471-2474-7-72.
- Richardson G, Epstein D, Wearden A. PRM23 Cost-effectiveness versus patient acceptability: the exemplar of CFS/ME. Value Health 2012;15. https://doi.org/10.1016/j.jval.2012.08.1487.
- Department of Health and Social Care . NHS Reference Costs 2002 2002.
- Netten A, Curtis L. Unit Costs of Health and Social Care 2003. Canterbury: Personal Social Services Research Unit, University of Kent; 2003.
- Curtis L. Unit Costs of Health and Social Care 2016. Canterbury: PSSRU, University of Kent; 2016.
- Curtis L. Unit Costs of Health and Social Care 2014. Canterbury: PSSRU, University of Kent; 2014.
- van der Roer N, van Tulder M, van Mechelen W, de Vet H. Economic evaluation of an intensive group training protocol compared with usual care physiotherapy in patients with chronic low back pain. Spine 2008;33:445-51. https://doi.org/10.1097/BRS.0b013e318163fa59.
- van Ravesteijn H, Grutters J, olde Hartman T, Lucassen P, Bor H, van Weel C, et al. Mindfulness-based cognitive therapy for patients with medically unexplained symptoms: a cost-effectiveness study. J Psychosom Res 2013;74:197-205. https://doi.org/10.1016/j.jpsychores.2013.01.001.
- LeFort SM, Gray-Donald K, Rowat KM, Jeans ME. Randomized controlled trial of a community-based psychoeducation program for the self-management of chronic pain. Pain 1998;74:297-306. https://doi.org/10.1016/S0304-3959(97)00190-5.
- Smith BJ, McGorm KJ, Weller D, Burton C, Sharpe M. The identification in primary care of patients who have been repeatedly referred to hospital for medically unexplained symptoms: a pilot study. J Psychosom Res 2009;67:207-11. https://doi.org/10.1016/j.jpsychores.2009.01.004.
- Jenkinson C, Layte R. Development and testing of the UK SF-12 (short form health survey). J Health Serv Res Policy 1997;2:14-8. https://doi.org/10.1177/135581969700200105.
- Brazier J, Roberts J, Deverill M. The estimation of a preference-based measure of health from the SF-36. J Health Econ 2002;21:271-92. https://doi.org/10.1016/S0167-6296(01)00130-8.
- Dakin H, Burns R, Yang Y. HERC Database of Mapping Studies, Version 5.0 (past Updated: 16 May 2016) 2016. www.herc.ox.ac.uk/downloads/herc-database-of-mapping-studies (accessed February 2017).
- Dakin HBR, Yang Y. HERC Database of Mapping Studies 2016.
- Kim SH, Kim SO, Lee SI, Jo MW. Deriving a mapping algorithm for converting SF-36 scores to EQ-5D utility score in a Korean population. Health Qual Life Outcomes 2014;12. https://doi.org/10.1186/s12955-014-0145-9.
- Longo M, Cohen D, Hood K, Robling M. Deriving an ‘Enhanced’ EuroQol from SF-36. Health Economists Studying Group Meeting (HESG) 2000.
- Longworth L. Estimating Quality Adjusted Life Years where Health-related Utility Data are Missing. London: Brunel University London; 2007.
- Maund E, Craig D, Suekarran S, Neilson A, Wright K, Brealey S, et al. Management of frozen shoulder: a systematic review and cost-effectiveness analysis. Health Technol Assess 2012;16. https://doi.org/10.3310/hta16110.
- Ara R, Brazier J. Deriving an algorithm to convert the eight mean SF-36 dimension scores into a mean EQ-5D preference-based score from published studies (where patient level data are not available). Value Health 2008;11:1131-43. https://doi.org/10.1111/j.1524-4733.2008.00352.x.
- Rowen D, Brazier J, Roberts J. Mapping SF-36 onto the EQ-5D index: how reliable is the relationship?. Health Qual Life Outcomes 2009;7. https://doi.org/10.1186/1477-7525-7-27.
- Chuang LH, Kind P. Converting the SF-12 into the EQ-5D: an empirical comparison of methodologies. PharmacoEconomics 2009;27:491-505. https://doi.org/10.2165/00019053-200927060-00005.
- Coca Perraillon M, Shih YC, Thisted RA. Predicting the EQ-5D-3L Preference index from the SF-12 health survey in a national US sample: a finite mixture approach. Med Decis Making 2015;35:888-901. https://doi.org/10.1177/0272989X15577362.
- Le QA. Probabilistic mapping of the health status measure SF-12 onto the health utility measure EQ-5D using the US-population-based scoring models. Qual Life Res 2014;23:459-66. https://doi.org/10.1007/s11136-013-0517-3.
- Sullivan PW, Ghushchyan V. Mapping the EQ-5D index from the SF-12: US general population preferences in a nationally representative sample. Med Decis Making 2006;26:401-9. https://doi.org/10.1177/0272989X06290496.
- Zarate V, Chuang L, Kind P. PMC41 mapping SF-12 to EuroQoL EQ-5D preference scores in the Spanish-speaking hispanic community in the United States. Value Health 2008;11. https://doi.org/10.1016/S1098-3015(10)70575-1.
- Conigliani C, Manca A, Tancredi A. Prediction of patient-reported outcome measures via multivariate ordered probit models. J Royal Statistical Soc 2015;178:567-91. https://doi.org/10.1111/rssa.12072.
- Gray AM, Rivero-Arias O, Clarke PM. Estimating the association between SF-12 responses and EQ-5D utility values by response mapping. Med Decis Making 2006;26:18-29. https://doi.org/10.1177/0272989X05284108.
- Rivero-Arias O, Gray A, Ramos-Goñi J. MA2 estimating the association between SF-12 responses to EQ-5D utility values using a response mapping and a parameter uncertainty approach. Value Health 2010;13. https://doi.org/10.1016/S1098-3015(11)71887-3.
- Lawrence WF, Fleishman JA. Predicting EuroQoL EQ-5D preference scores from the SF-12 Health Survey in a nationally representative sample. Med Decis Making 2004;24:160-9. https://doi.org/10.1177/0272989X04264015.
- Franks P, Lubetkin EI, Gold MR, Tancredi DJ, Jia H. Mapping the SF-12 to the EuroQol EQ-5D Index in a national US sample. Med Decis Making 2004;24:247-54. https://doi.org/10.1177/0272989X04265477.
- Franks P, Lubetkin EI, Gold MR, Tancredi DJ. Mapping the SF-12 to preference-based instruments: convergent validity in a low-income, minority population. Med Care 2003;41:1277-83. https://doi.org/10.1097/01.MLR.0000093480.58308.D8.
- Lidbeck J. Group therapy for somatization disorders in primary care: maintenance of treatment goals of short cognitive-behavioural treatment one-and-a-half-year follow-up. Acta Psychiatr Scand 2003;107:449-56. https://doi.org/10.1034/j.1600-0447.2003.00048.x.
- Malouff JM, Thorsteinsson EB, Rooke SE, Bhullar N, Schutte NS. Efficacy of cognitive behavioral therapy for chronic fatigue syndrome: a meta-analysis. Clin Psychol Rev 2008;28:736-45. https://doi.org/10.1016/j.cpr.2007.10.004.
- Kisely SR, Campbell LA, Skerritt P, Yelland MJ. Psychological interventions for symptomatic management of non-specific chest pain in patients with normal coronary anatomy. Cochrane Database Syst Rev 2010;1. https://doi.org/10.1002/14651858.CD004101.pub3.
- Picariello F, Ali S, Moss-Morris R, Chalder T. The most popular terms for medically unexplained symptoms: the views of CFS patients. J Psychosom Res 2015;78:420-6. https://doi.org/10.1016/j.jpsychores.2015.02.013.
- Pajak R, Lackner J, Kamboj SK. A systematic review of minimal-contact psychological treatments for symptom management in irritable bowel syndrome. J Psychosom Res 2013;75:103-12. https://doi.org/10.1016/j.jpsychores.2013.05.007.
- Macedo LG, Smeets RJ, Maher CG, Latimer J, McAuley JH. Graded activity and graded exposure for persistent nonspecific low back pain: a systematic review. Phys Ther 2010;90:860-79. https://doi.org/10.2522/ptj.20090303.
- Action for M.E . M.E. Time to Deliver 2014. www.actionforme.org.uk/uploads/pdfs/me-time-to-deliver-survey-report.pdf (accessed 5 November 2019).
- Rask MT, Rosendal M, Fenger-Grøn M, Bro F, Ørnbøl E, Fink P. Sick leave and work disability in primary care patients with recent-onset multiple medically unexplained symptoms and persistent somatoform disorders: a 10-year follow-up of the FIP study. Gen Hosp Psychiatry 2015;37:53-9. https://doi.org/10.1016/j.genhosppsych.2014.10.007.
- O’Dowd H. ISRCTN Registry n.d. https://doi.org/10.1186/ISRCTN72645894 (accessed 2 May 2019).
- O’Dowd H. WhatdotheyKnow.Com. Results for Trial ID ISRCTN72645894 2016. www.whatdotheyknow.com/request/results_for_trial_id_isrctn72645 (accessed 3 May 2019).
- Duggan C, Parry G, McMurran M, Davidson K, Dennis J. The recording of adverse events from psychological treatments in clinical trials: evidence from a review of NIHR-funded trials. Trials 2014;15. https://doi.org/10.1186/1745-6215-15-335.
- Parry GD, Crawford MJ, Duggan C. Iatrogenic harm from psychological therapies – time to move on. Br J Psychiatry 2016;208:210-12. https://doi.org/10.1192/bjp.bp.115.163618.
- Schwartz D, Lellouch J. Explanatory and pragmatic attitudes in therapeutical trials. J Chronic Dis 1967;20:637-48. https://doi.org/10.1016/0021-9681(67)90041-0.
- Thorpe KE, Zwarenstein M, Oxman AD, Treweek S, Furberg CD, Altman DG, et al. A pragmatic-explanatory continuum indicator summary (PRECIS): a tool to help trial designers. J Clin Epidemiol 2009;62:464-75. https://doi.org/10.1016/j.jclinepi.2008.12.011.
- Lindström I, Öhlund C, Eek C, Wallin L, Peterson LE, Fordyce WE, Nachemson AL. The effect of graded activity on patients with subacute low back pain: a randomized prospective clinical study with an operant-conditioning behavioral approach. Phys Ther 1992;72:279-90. https://doi.org/10.1093/ptj/72.4.279.
- Hodges PW, Richardson CA. Delayed postural contraction of transversus abdominis in low back pain associated with movement of the lower limb. J Spin Disord 1998;11:46-5. https://doi.org/10.1097/00002517-199802000-00008.
- Swedish Council on Technology Assessment in Health Care . Methods of Treating Chronic Pain 2006.
- Salkovoskis PM, Hawton K, Salkovoskis PM, Kirk J, Clark DM. Cognitive Behaviour Therapy for Psychiatric Problems: A Practical Guide. Oxford: Oxford University Press; 1989.
- Gask L, Goldberg D, Porter R, Creed F. The treatment of somatization: evaluation of a teaching package with general practice trainees. J Psychosom Res 1989;33:697-703. https://doi.org/10.1016/0022-3999(89)90085-8.
- Ewing JA. Detecting alcoholism: the CAGE questionnaire. JAMA 1984;252:1905-7. https://doi.org/10.1001/jama.252.14.1905.
- Chalder T, Berelowitz G, Pawlikowska T, Watts L, Wessely S, Wright D, et al. Development of a fatigue scale. J Psychosom Res 1993;37:147-53. https://doi.org/10.1016/0022-3999(93)90081-P.
- Mersky H, Bogduk N. Classification of Chronic Pain. Washington, DC: IASP Press; 1994.
- Drossman DA, Richter JE, Talley NJ, Thompson WG, Corazziari E, Whitehead WE. The Functional Gastrointestinal Disorders: Diagnosis, Pathophysiology and Treatment. McLean, VA: Degnon Associates; 1994.
- Ware JE, Snow KK, Kosinski M. SF-36 Health Survey: Manual and Interpretation Guide, QualityMetric Inc. Lincoln, RI; 1993.
- Robins LN. Composing the CIDI: A Collaboration with the WHO/ADAMHA. St. Louis: Department of Psychiatry Research Seminar; 1988.
- Spitzer RL, Williams JB, Kroenke K, Linzer M, deGruy FV, Hahn SR, et al. Utility of a new procedure for diagnosing mental disorders in primary care. The PRIME-MD 1000 study. JAMA 1994;272:1749-56. https://doi.org/10.1001/jama.1994.03520220043029.
- Brugha TS, Cragg D. The List of Threatening Experiences: the reliability and validity of a brief life events questionnaire. Acta Psychiatr Scand 1990;82:77-81. https://doi.org/10.1111/j.1600-0447.1990.tb01360.x.
- Kressin NR, Spiro A, Skinner KM. Negative affectivity and health-related quality of life. Med Care 2000;38:858-67. https://doi.org/10.1097/00005650-200008000-00009.
- Sullivan MJ, Bishop SR, Pivik J. The pain catastrophizing scale: development and validation. Psychological Assessment 1995;7. https://doi.org/10.1037/1040-3590.7.4.524.
- Hamilton M. Rating depressive patients. J Clin Psychiatry 1980;41:21-4.
- Hamilton M. The assessment of anxiety states by rating. Br J Med Psychol 1959;32:50-5. https://doi.org/10.1111/j.2044-8341.1959.tb00467.x.
- Melzak R. Pain Measurement and Assessment. New York, NY: Raven Press; 1983.
- Burckhardt CS, Clark SR, Bennett RM. The fibromyalgia impact questionnaire: development and validation. J Rheumatol 1991;18:728-33.
- Badia X, Roset M, Montserrat S, Herdman M, Segura A. The Spanish version of EuroQol: a description and its applications. European Quality of Life scale. Med Clin 1999;112:79-85.
- Spitzer RL, Kroenke K, Williams JB. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. Primary Care Evaluation of Mental Disorders. Patient Health Questionnaire. JAMA 1999;282:1737-44. https://doi.org/10.1001/jama.282.18.1737.
- Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med 2006;166:1092-7. https://doi.org/10.1001/archinte.166.10.1092.
- Lewis G, Pelosi AJ, Araya R, Dunn G. Measuring psychiatric disorder in the community: a standardized assessment for use by lay interviewers. Psychol Med 1992;22:465-86. https://doi.org/10.1017/s0033291700030415.
- Goldberg D, Williams P. A User’s Guide to the General Health Questionnaire. Windsor: NFER-NELSON; 1988.
- Stewart AL, Hays R, Ware J. The medical outcomes study short-form general health survey. Medical Care 1988;26:724-35. https://doi.org/10.1097/00005650-198807000-00007.
- Huskisson EC. Measurement of pain. Lancet 1974;304:1127-31. https://doi.org/10.1016/S0140-6736(74)90884-8.
- Kovacs FM, Llobera J, Gil Del Real MT, Abraira V, Gestoso M, Fernández C, et al. Validation of the spanish version of the Roland-Morris questionnaire. Spine 2002;27:538-42. https://doi.org/10.1097/00007632-200203010-00016.
- Luo X, George ML, Kakouras I, Edwards CL, Pietrobon R, Richardson W, et al. Reliability, validity, and responsiveness of the short form 12-item survey (SF-12) in patients with back pain. Spine 2003;28:1739-45. https://doi.org/10.1097/01.BRS.0000083169.58671.96.
- Ware JE, Keller SD, Kosinski M. SF-12: How to Score the SF-12 Physical and Mental Health Summary Scales. Health Institute, New England Medical Center; 1995.
- Beck AT, Steer RA, Brown GK. Manual for the Beck Depression Inventory-II. San Antonio, TX: Psychological Corporation; 1996.
- Woolfolk RL, Allen LA, Tiu JE. New directions in the treatment of somatization. Psychiatric Clinics of North America 2007;30:621-44. https://doi.org/10.1016/j.psc.2007.07.001.
- Lobo A, Campos R, Pérez-Echeverría MJ, Izuzquiza J, García-Campayo J, Saz P, et al. A new interview for the multiaxial assessment of psychiatric morbidity in medical settings. Psychol Med 1993;23:505-10. https://doi.org/10.1017/s0033291700028592.
- Ware JE, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care 1992;30:473-83. https://doi.org/10.1097/00005650-199206000-00002.
- Lam CL, Tse EY, Gandek B. Is the standard SF-12 health survey valid and equivalent for a Chinese population?. Qual Life Res 2005;14:539-47. https://doi.org/10.1007/s11136-004-0704-3.
- Vercoulen JHMM, Alberts M, Bleijenberg G. De checklist individuele spankracht (CIS). Gedragstherapie 1999;32.
- Feinstein AR. Clinimetrics. New Haven, CT: Yale University Press; 1987.
- Derogatis LR, Lipman RS, Covi L. SCL-90: an outpatient psychiatric rating scale – preliminary report. Psychopharmacol Bull 1973;9:13-28.
- Brook RH, Ware JE, Davies-Avery A, Stewart AL, Donald CA, Rogers WH, et al. Overview of adult health status measures fielded in Rand’s Health Insurance Study. Med Care 1979;17:i-131.
- Francis CY, Morris J, Whorwell PJ. The irritable bowel severity scoring system: a simple method of monitoring irritable bowel syndrome and its progress. Aliment Pharmacol Ther 1997;11:395-402. https://doi.org/10.1046/j.1365-2036.1997.142318000.x.
- Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand 1983;67:361-70. https://doi.org/10.1111/j.1600-0447.1983.tb09716.x.
- Mouanoutoua VL, Brown LG. Hopkins Symptom Checklist-25, Hmong version: a screening instrument for psychological distress. J Pers Assess 1995;64:376-83. https://doi.org/10.1207/s15327752jpa6402_16.
- Hosman CMH. Psychosociale problematiek en hulpzoeken Een socialepidemiologische studie t. b. v. de preventive geestelijke gezondheidszorg (Psychosocial problems and help seeking. A social-epidemiological study for the preventive mental health care). Amsterdam: Swets en Zeitlinger; 1983.
- Bridges KR, Sanderman R, Van Sonderen E. An English language version of the social support list: preliminary reliability. Psychological Reports 2002;90:1055-8. https://doi.org/10.2466/pr0.2002.90.3.1055.
- Aaronson NK, Muller M, Cohen PD, Essink-Bot ML, Fekkes M, Sanderman R, et al. Translation, validation, and norming of the Dutch language version of the SF-36 Health Survey in community and chronic disease populations. J Clin Epidemiol 1998;51:1055-68. https://doi.org/10.1016/S0895-4356(98)00097-3.
- Derogatis LR, Cleary PA. Factorial invariance across gender for the primary symptom dimensions of the SCL-90. Br J Soc Clin Psychol 1977;16:347-56. https://doi.org/10.1111/j.2044-8260.1977.tb00241.x.
- Cecile MT, van Wijk G, Kolk AM. Psychometric evaluation of symptom perception related measures. Personality and Individual Differences 1996;20:55-70. https://doi.org/10.1016/0191-8869(95)90023-N.
- Robbins JM, Kirmayer LJ. Attributions of common somatic symptoms. Psychol Med 1991;21:1029-45. https://doi.org/10.1017/S0033291700030026.
- Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: the PANAS scales. J Pers Soc Psychol 1988;54:1063-70. https://doi.org/10.1037//0022-3514.54.6.1063.
- Vernon H, Mior S. The Neck Disability Index: a study of reliability and validity. J Manipulative Physiol Ther 1991;14:409-15. https://doi.org/10.1037/t35122-000.
- Goldberg D, Paul W. A User’s Guide to the General Health Questionnaire. Windsor: Nfer-Nelson; 1991.
- Braden CJ. A test of the Self-Help Model: learned response to chronic illness experience. Nurs Res 1990;39:42-7. https://doi.org/10.1097/00006199-199001000-00009.
- Baker F, Curbow B, Wingard JR. Development of the satisfaction with life domains scale for cancer. J Psychosoc Oncol 1992;10:75-90. https://doi.org/10.1300/J077V10N03_05.
- Melzack R. The short-form McGill pain questionnaire. Pain 1987;30:191-7. https://doi.org/10.1016/0304-3959(87)91074-8.
- Beck AT, Beck RW. Screening depressed patients in family practice. A rapid technic. Postgrad Med 1972;52:81-5. https://doi.org/10.1080/00325481.1972.11713319.
- Jensen MP, Turner JA, Romano JM, Lawler BK. Relationship of pain-specific beliefs to chronic pain adjustment. Pain 1994;57:301-9. https://doi.org/10.1016/0304-3959(94)90005-1.
- Mishel MH. The measurement of uncertainty in illness. Nurs Res 1981;30:258-63. https://doi.org/10.1097/00006199-198109000-00002.
- Lorig K, Chastain RL, Ung E, Shoor S, Holman HR. Development and evaluation of a scale to measure perceived self-efficacy in people with arthritis. Arthritis Rheum 1989;32:37-44. https://doi.org/10.1002/anr.1780320107.
- Rosenbaum M. A schedule for assessing self-control behaviors: preliminary findings. Behavior Therapy 1980;11:109-21. https://doi.org/10.1016/S0005-7894(80)80040-2.
- Göbel H. Paper-pencil tests for retrospective and prospective evaluation of primary headaches on the basis of the IHS criteria. Headache 1994;34:564-8. https://doi.org/10.1111/j.1526-4610.1994.hed3410564.x.
- Rivera J, González T. The Fibromyalgia Impact Questionnaire: a validated Spanish version to assess the health status in women with fibromyalgia. Clin Exp Rheumatol 2004;22:554-60.
- Spielberger CD. State–Trait Anxiety Inventory. The Corsini Encyclopedia of Psychology. Hoboken: John Wiley & Sons, Inc.; 2010.
- McCracken LM, Vowles KE, Eccleston C. Acceptance of chronic pain: component analysis and a revised assessment method. Pain 2004;107:159-66. https://doi.org/10.1016/j.pain.2003.10.012.
- Scrimshaw SV, Maher C. Responsiveness of visual analogue and McGill pain scale measures. J Manipulative Physiol Ther 2001;24:501-4. https://doi.org/10.1067/mmt.2001.118208.
- Pengel LH, Refshauge KM, Maher CG. Responsiveness of pain, disability, and physical impairment outcomes in patients with low back pain. Spine 2004;29:879-83. https://doi.org/10.1097/00007632-200404150-00011.
- Roland M, Morris R. A study of the natural history of low-back pain. Part II: development of guidelines for trials of treatment in primary care. Spine 1983;8:145-50. https://doi.org/10.1097/00007632-198303000-00005.
- Sanson-Fisher RW, Perkins JJ. Adaptation and validation of the SF-36 Health Survey for use in Australia. J Clin Epidemiol 1998;51:961-7. https://doi.org/10.1016/S0895-4356(98)00087-0.
- Borkovec TD, Nau SD. Credibility of analogue therapy rationales. J Behav Ther Experimental Psychiatry 1972;3:257-60. https://doi.org/10.1016/0005-7916(72)90045-6.
- Pengel LH, Refshauge KM, Maher CG, Nicholas MK, Herbert RD, McNair P. Physiotherapist-directed exercise, advice, or both for subacute low back pain: a randomized trial. Ann Intern Med 2007;146:787-96. https://doi.org/10.7326/0003-4819-146-11-200706050-00007.
- Marques M, De Gucht V, Gouveia MJ, Cordeiro A, Leal I, Maes S. Psychometric Properties of the Portuguese Version of the Checklist of Individual Strength (CIS20-P) 2013. https://doi.org/10.5964/pch.v2i1.57.
- Cleeland CS, Ryan KM. Pain assessment: global use of the Brief Pain Inventory. Ann Acad Med Singapore 1994;23:129-38.
- Wendel-Vos GC, Schuit AJ, Saris WH, Kromhout D. Reproducibility and relative validity of the short questionnaire to assess health-enhancing physical activity. J Clin Epidemiol 2003;56:1163-9. https://doi.org/10.1016/S0895-4356(03)00220-8.
- Ware JE, Kosinski M, Turner-Bowker D, Gandek B. Version 2 of the SF-12 Health Survey. Boston, MA: Quality Metric; 2002.
- Derogatis L. Brief Symptom Inventory: Administration, Scoring and Procedures Manual. Minneapolis: National Computer System; 1993.
- Rief W, Hiller W, Geissner E, Fichter MM. Hypochondrie: erfassung und erste klinische ergebnisse. Zeitscrift Fur Klinische Psychologie 1994;23:34-42.
- Beck AT, Steer RA. Beck Depression Inventory Manual. San Antonio, TX: The Psychological Corporation; 1987.
- Franke G. BSI (Brief Symptoms Inventory). Weinheim: Beltz; 2000.
- Rief W, Hiller W. A new approach to the assessment of the treatment effects of somatoform disorders. Psychosomatics 2003;44:492-8. https://doi.org/10.1176/appi.psy.44.6.492.
- Lohaus A, Schmitt GM. Fragebogen zur Erhebung von Kontrolluberzeugungen zu Krankheit und Gesundheit. Gottingen: Hogrefe; 1990.
- Brown GK, Nicassio PM. Development of a questionnaire for the assessment of active and passive coping strategies in chronic pain patients. Pain 1987;31:53-64. https://doi.org/10.1016/0304-3959(87)90006-6.
- Jenkins CD, Stanton BA, Niemcryk SJ, Rose RM. A scale for the estimation of sleep problems in clinical research. J Clin Epidemiol 1988;41:313-21. https://doi.org/10.1016/0895-4356(88)90138-2.
- Roelofs J, Goubert L, Peters ML, Vlaeyen JW, Crombez G. The Tampa Scale for Kinesiophobia: further examination of psychometric properties in patients with chronic low back pain and fibromyalgia. Eur J Pain 2004;8:495-502. https://doi.org/10.1016/j.ejpain.2003.11.016.
- Morriss RK, Gask L. Treatment of patients with somatized mental disorder: effects of reattribution training on outcomes under the direct control of the family doctor. Psychosomatics 2002;43:394-9. https://doi.org/10.1176/appi.psy.43.5.394.
- Moss-Morris R, Weinman J, Petrie K, Horne R, Cameron L, Buick D. The revised illness perception questionnaire (IPQ-R). Psychol Health 2002;17:1-16. https://doi.org/10.1080/08870440290001494.
- Pilowsky I. Dimensions of hypochondriasis. Br J Psychiatry 1967;113:89-93. https://doi.org/10.1192/bjp.113.494.89.
- EuroQoL Group . EuroQoL: a new facility for the measurement of health related quality of life. Health Policy 1990;16:199-208. https://doi.org/10.1016/0168-8510(90)90421-9.
- Fulcher KY, White PD. Randomised controlled trial of graded exercise in patients with the chronic fatigue syndrome. BMJ 1997;314:1647-52. https://doi.org/10.1136/bmj.314.7095.1647.
- Ray C, Weir W, Stewart D, Miller P, Hyde G. Ways of coping with chronic fatigue syndrome: development of an illness management questionnaire. Soc Sci Med 1993;37:385-91. https://doi.org/10.1016/0277-9536(93)90268-9.
- Müller-Lissner S, Koch G, Talley NJ, Drossman D, Rueegg P, Dunger-Baldauf C, et al. Subject’s global assessment of relief: an appropriate method to assess the impact of treatment on irritable bowel syndrome-related symptoms in clinical trials. J Clin Epidemiol 2003;56:310-16. https://doi.org/10.1016/S0895-4356(03)00027-1.
- Mundt JC, Marks IM, Shear MK, Greist JH. The Work and Social Adjustment Scale: a simple measure of impairment in functioning. Br J Psychiatry 2002;180:461-4. https://doi.org/10.1192/bjp.180.5.461.
- Derogatis LR, Lipman RS, Rickels K, Uhlenhuth EH, Covi L. The Hopkins symptom checklist: a self-report symptom inventory. Behav Sci 1971;19:1-15. https://doi.org/10.1002/bs.3830190102.
- Main CJ. The modified somatic perception questionnaire (MSPQ). J Psychosom Res 1983;27:503-14. https://doi.org/10.1016/0022-3999(83)90040-5.
- Ware JE, Snow KK, Kosinski M, Gandek BSF. Health Survey Manual and Interpretation Guide. Boston, MA: The Health Institute, New England Medical Center; 1993.
- Caine TM, Foulds GA, Hope K. Manual of the Hostility and Direction of Hostility Questionnaire. London: University of London Press; 1967.
- Mooney V, Cairns D, Robertson J. A system for evaluating and treating chronic back disability. West J Med 1976;124:370-6.
- Sivik T. Alexithymia and hypersensitivity to touch and palpation. Integr Physiol Behav Sci 1993;28:130-6. https://doi.org/10.1007/BF02691215.
- Sifneos PE. The Schalling-Sifneos personality scale revised. Psychother Psychosom 1986;45:161-5. https://doi.org/10.1159/000287942.
- Weinryb RM, Gustavsson JP, Asberg M, Rössel RJ. The concept of alexithymia: an empirical study using psychodynamic ratings and self-reports. Acta Psychiatr Scand 1992;85:153-62. https://doi.org/10.1111/j.1600-0447.1992.tb01461.x.
- Powell R, Dolan R, Wessely S. Attributions and self-esteem in depression and chronic fatigue syndromes. J Psychosom Res 1990;34:665-73. https://doi.org/10.1016/0022-3999(90)90111-g.
- Dolan P, Gudex C, Kind P, Williams A. A Social Tariff for EuroQol: Results from a UK General Population Study. The University of York, York: Centre for Health Economics; 1995.
- Beck AT, Epstein N, Brown G, Steer RA. An inventory for measuring clinical anxiety: psychometric properties. J Consult Clin Psychol 1988;56. https://doi.org/10.1037/0022-006X.56.6.893.
- Bensoussan A, Talley NJ, Hing M, Menzies R, Guo A, Ngu M. Treatment of irritable bowel syndrome with Chinese herbal medicine: a randomized controlled trial. JAMA 1998;280:1585-9. https://doi.org/10.1001/jama.280.18.1585.
- Patrick DL, Drossman DA, Frederick IO, DiCesare J, Puder KL. Quality of life in persons with irritable bowel syndrome: development and validation of a new measure. Dig Dis Sci 1998;43:400-11. https://doi.org/10.1023/a:1018831127942.
- Ware JE, Kosinski M, Keller S. SF-36 Physical and Mental Health Summary Scales: A User’s Guide. Boston: The Health Institute, New England Medical Center; 1994.
- Bjorner JB, Damsgaard MT, Watt T, Bech P, Rasmussen NK, Kristensen TS, et al. Danish Manual for SF-36. Copenhagen: Lif; 1997.
- Fink P, Ewald H, Jensen J, Sørensen L, Engberg M, Holm M, et al. Screening for somatization and hypochondriasis in primary care and neurological in-patients: a seven-item scale for hypochondriasis and somatization. J Psychosom Res 1999;46:261-73. https://doi.org/10.1016/S0022-3999(98)00092-0.
- Zung WW. A self-rating depression scale. Arch Gen Psychiatr 1965;12:63-70. https://doi.org/10.1001/archpsyc.1965.01720310065008.
- Nyström C, Nyström O. Estimated stress verifies autonomic dysfunction. Lakartidningen 1996;93.
- Fairbank JC, Couper J, Davies JB, O’Brien JP. The Oswestry low back pain disability questionnaire. Physiotherapy 1980;66:271-3.
- Kaplan RM, Ganiats TG, Sieber WJ, Anderson JP. The Quality of Well-Being Scale: critical similarities and differences with SF-36. Int J Qual Health Care 1998;10:509-20. https://doi.org/10.1093/intqhc/10.6.509.
- Alonso J, Prieto L, Antó JM. The Spanish version of the SF-36 Health Survey (the SF-36 health questionnaire): an instrument for measuring clinical results. Med Clin 1995;104:771-6.
- Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatr 1961;4:561-71. https://doi.org/10.1001/archpsyc.1961.01710120031004.
- King S, Wessel J, Bhambhani Y, Maikala R, Sholter D, Maksymowych W. Validity and reliability of the 6 minute walk in persons with fibromyalgia. J Rheumatol 1999;26:2233-7.
- Whaley MH, Brubaker PH, Otto RM, Armstrong LE. Medicine ACoS. ACSM’s Guidelines for Exercise Testing and Prescription. Philadelphia, PA: Lippincott Williams & Wilkins; 2005.
- Bullinger M, Kirchberger I. SF-36. Fragebogen zum Gesundheitszustand. Handanweisung und Fragebogen (SF-36 und SF-12). Gottingen: Hogrefe; 1998.
- Kroenke K, Spitzer RL, Williams JB, Löwe B. The Patient Health Questionnaire Somatic, Anxiety, and Depressive Symptom Scales: a systematic review. Gen Hosp Psychiatry 2010;32:345-59. https://doi.org/10.1016/j.genhosppsych.2010.03.006.
- Löwe B, Gräfe K, Zipfel S, Spitzer RL, Herrmann-Lingen C, Witte S, et al. Detecting panic disorder in medical and psychosomatic outpatients: comparative validation of the Hospital Anxiety and Depression Scale, the Patient Health Questionnaire, a screening question, and physicians’ diagnosis. J Psychosom Res 2003;55:515-19. https://doi.org/10.1016/S0022-3999(03)00072-2.
- Schilte AF, Portegijs PJ, Blankenstein AH, Knottnerus JA. Somatisation in primary care: clinical judgement and standardised measurement compared. Soc Psychiatry Psychiatr Epidemiol 2000;35:276-82. https://doi.org/10.1007/s001270050239.
- Radloff LS. The CES-D scale: a self report depression scale for research in the general population. Appl Psychol Measurement 1977;1:385-401. https://doi.org/10.1177/014662167700100306.
- Smith RC, Lyles JS, Mettler J, Stoffelmayr BE, Van Egeren LF, Marshall AA, et al. The effectiveness of intensive training for residents in interviewing: a randomized, controlled study. Ann Int Med 1998;128:118-26. https://doi.org/10.7326/0003-4819-128-2-199801150-00008.
- Goldberg DP, Blackwell B. Psychiatric illness in general practice. A detailed study using a new method of case identification. Br Med J 1970;1:439-43. https://doi.org/10.1136/bmj.2.5707.439.
- de Silva N, Samarasinghe D. Acceptance of a psychiatric screening questionnaire by general practice attenders. Ceylon Med J 1990;35:105-8.
- Derogatis LR, Melisaratos N. The brief symptom inventory: an introductory report. Psychol Med 1983;13:595-60. https://doi.org/10.1017/S0033291700048017.
- Speckens AE, van Hemert AM, Spinhoven P, Hawton KE, Bolk JH, Rooijmans HG. Cognitive behavioural therapy for medically unexplained physical symptoms: a randomised controlled trial. BMJ 1995;311:1328-32. https://doi.org/10.1136/bmj.311.7016.1328.
- Bergner M, Bobbitt RA, Pollard WE, Martin DP, Gilson BS. The sickness impact profile: validation of a health status measure. Med Care 1976;14:57-6. https://doi.org/10.1097/00005650-197601000-00006.
- Meeuwesen L, Arrindell WA, Huyse FJ. Psychometric qualities of the SCL-90 in outpatients with abdominal or low back pain. Tijdsch Soc Gez 1992;70:123-31.
- Koopmans GT, Meeuwesen L, Huyse FJ, Meiland FJ, Donker JM. Effects of psychiatric consultation on medical consumption in medical outpatients with abdominal pain. Psychosomatics 1995;36:387-99. https://doi.org/10.1016/S0033-3182(95)71648-6.
- Kori SH, Miller RP, Todd DD. Kinesiophobia: a new view of chronic pain behaviour. Pain Management 1990;3:35-42.
- Kraaimat FW, Evers AW. Pain-coping strategies in chronic pain patients: psychometric characteristics of the pain-coping inventory (PCI). In J Behav Med 2003;10:343-63. https://doi.org/10.1207/S15327558IJBM1004_5.
- Nicholas MK. The pain self-efficacy questionnaire: taking pain into account. Eur J Pain 2007;11:153-63. https://doi.org/10.1016/j.ejpain.2005.12.008.
- Hakkaart-van Roijen L, Van Straten A, Donker M, Tiemens B. Manual Trimbos/iMTA Questionnaire for Costs Associated with Psychiatric Illness (TiC-P). Rotterdam: Institute for Medical Technology Assessment, Erasmus University; 2002.
- Baer RA, Smith GT, Lykins E, Button D, Krietemeyer J, Sauer S, et al. Construct validity of the five facet mindfulness questionnaire in meditating and nonmeditating samples. Assessment 2008;15:329-42. https://doi.org/10.1177/1073191107313003.
- Horn KK, Jennings S, Richardson G, Vliet DV, Hefford C, Abbott JH. The patient-specific functional scale: psychometrics, clinimetrics, and application as a clinical outcome measure. J Orthop Sports Phys Ther 2012;42:30-42. https://doi.org/10.2519/jospt.2012.3727.
- Waddell G, Newton M, Henderson I, Somerville D, Main CJ. A Fear-Avoidance Beliefs Questionnaire (FABQ) and the role of fear-avoidance beliefs in chronic low back pain and disability. Pain 1993;52:157-68. https://doi.org/10.1016/0304-3959(93)90127-B.
- Catley MJ, Tabor A, Wand BM, Moseley GL. Assessing tactile acuity in rheumatology and musculoskeletal medicine – how reliable are two-point discrimination tests at the neck, hand, back and foot?. Rheumatology 2013;52:1454-61. https://doi.org/10.1093/rheumatology/ket140.
- Harwood RH, Rogers A, Dickinson E, Ebrahim S. Measuring handicap: the London Handicap Scale, a new outcome measure for chronic disease. Qual Health Care 1994;3:11-6. https://doi.org/10.1136/qshc.3.1.11.
- Arrindell WA, Ettema JHM. Symptom Checklist. Handleiding bij een multidimensionale psychopathologie indicator.[SCL-90. Handbook of a multidimensional psychopathology indicator]. Lisse: Swets & Zeitlinger; 2003.
- Higgins JPT, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011;343. https://doi.org/10.1136/bmj.d5928.
- Netten A, Knight J, Dennett J, Cooley R, Slight A. A Ready Reckoner for Staff Costs in the NHS. Volume II. Methodology. Canterbury: PSSRU, University of Kent; 1998.
- Wortman MS, Lucassen PL, van Ravesteijn HJ, Bor H, Assendelft PJ, Lucas C, et al. Brief multimodal psychosomatic therapy in patients with medically unexplained symptoms: feasibility and treatment effects. Fam Pract 2016;33:346-53. https://doi.org/10.1093/fampra/cmw023.
- Doorn PV, Colla P, Folgering HTM. Een vragenlijst voor hyperventilatieklachten [A questionnaire for hyperventilation syndrome.]. De Psycholoog 1983;18:573-7.
- Ware JE. SF-36 health survey update. Spine 2000;25:3130-9. https://doi.org/10.1097/00007632-200012150-00008.
- Bastien CH, Vallières A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Medicine 2001;2:297-30. https://doi.org/10.1016/S1389-9457(00)00065-4.
- Cowell I, O’Sullivan P, O’Sullivan K, Poyton R, McGregor A, Murtagh G. Perceptions of physiotherapists towards the management of non-specific chronic low back pain from a biopsychosocial perspective: a qualitative study. Musculoskeletal Science and Practice 2018;38:113-19. https://doi.org/10.1016/j.msksp.2018.10.006.
- Arden K, Fatoye F, Yeowell G. Evaluation of a rolling rehabilitation programme for patients with non-specific low back pain in primary care: an observational cohort study. J Eval Clin Pract 2017;23:272-8. https://doi.org/10.1111/jep.12595.
- Balabanovic J, Hayton P. Engaging patients with ‘medically unexplained symptoms’ in psychological therapy: an integrative and transdiagnostic approach. Psychol Psychother 2020;93:347-66. https://doi.org/10.1111/papt.12213.
- Bestall J, Siddiqi N, Heywood-Everett S, Freeman C, Carder P, James M, et al. New models of care: a liaison psychiatry service for medically unexplained symptoms and frequent attenders in primary care. BJPsych Bulletin 2017;41:340-4. https://doi.org/10.1192/pb.bp.116.055731.
- Broughton J, Harris S, Beasant L, Crawley E, Collin SM. Adult patients’ experiences of NHS specialist services for chronic fatigue syndrome (CFS/ME): a qualitative study in England. BMC Health Serv Res 2017;17. https://doi.org/10.1186/s12913-017-2337-6.
- Carlin L, Zhao J, Dubin R, Taenzer P, Sidrak H, Furlan A. Project ECHO telementoring intervention for managing chronic pain in primary care: insights from a qualitative study. Pain Med 2018;19:1140-6. https://doi.org/10.1093/pm/pnx233.
- Carnes D, Mars T, Plunkett A, Nanke L, Abbey H. A mixed methods evaluation of a third wave cognitive behavioural therapy and osteopathic treatment programme for chronic pain in primary care (OsteoMAP). Int J Osteopathic Med 2017;24:12-7. https://doi.org/10.1016/j.ijosm.2017.03.005.
- Casey MB, Smart K, Segurado R, Hearty C, Gopal H, Lowry D, et al. Exercise combined with Acceptance and Commitment Therapy (ExACT) compared to a supervised exercise programme for adults with chronic pain: study protocol for a randomised controlled trial. Trials 2018;19:1-14. https://doi.org/10.1186/s13063-018-2543-5.
- Dresner D, Gergen Barnett K, Resnick K, Laird LD, Gardiner P. Listening to their words: a qualitative analysis of integrative medicine group visits in an urban underserved medical setting. Pain Med 2016;17:1183-91. https://doi.org/10.1093/pm/pnw030.
- Gordon K, Rice H, Allcock N, Bell P, Dunbar M, Gilbert S, et al. Barriers to self-management of chronic pain in primary care: a qualitative focus group study. Br J Gen Pract 2017;67:e209-17. https://doi.org/10.3399/bjgp17X688825.
- Hadi MA, Alldred DP, Briggs M, Marczewski K, Closs SJ. Effectiveness of a community based nurse–pharmacist managed pain clinic: a mixed-methods study. In J Nurs Stud 2016;53:219-27. https://doi.org/10.1016/j.ijnurstu.2015.09.003.
- Hadi MA, Alldred DP, Briggs M, Marczewski K, Closs SJ. ‘Treated as a number, not treated as a person’: a qualitative exploration of the perceived barriers to effective pain management of patients with chronic pain. BMJ Open 2017;7. https://doi.org/10.1136/bmjopen-2017-016454.
- Sibelli A, Moss-Morris R, Chalder T, Bishop FL, Windgassen S, Everitt H. Patients’ perspectives on GP interactions after cognitive behavioural therapy for refractory IBS: a qualitative study in UK primary and secondary care. Br J Gen Pract 2018;68:e654-62. https://doi.org/10.3399/bjgp18X698321.
- Teo M, Mohan B, Oelke ND. Developing and implementing a community–based model of care for fibromyalgia: a feasibility study. Pain Res Manag 2017;2017. https://doi.org/10.1155/2017/4521389.
- Thompson DG, O’Brien S, Kennedy A, Rogers A, Whorwell P, Lovell K, et al. A randomised controlled trial, cost-effectiveness and process evaluation of the implementation of self–management for chronic gastrointestinal disorders in primary care, and linked projects on identification and risk assessment. Programme Grants Appl Res 2018;6. https://doi.org/10.3310/pgfar06010.
- O’Sullivan PB, Caneiro JP, O’Keeffe M, Smith A, Dankaerts W, Fersum K, et al. Cognitive functional therapy: an integrated behavioral approach for the targeted management of disabling low back pain. Phys Ther 2018;98:408-23. https://doi.org/10.1093/ptj/pzy022.
- O’Sullivan P, Dankaerts W, O’Sullivan, K, Fersum K. Grieve’s Modern Musculoskeletal Physiotherapy. Edinburgh: Elsevier; 2015.
- Cowell I, O’Sullivan P, O’Sullivan K, Poyton R, McGregor A, Murtagh G. The perspectives of physiotherapists on managing nonspecific low back pain following a training programme in cognitive functional therapy: a qualitative study. Musculoskeletal Care 2019;17:79-90. https://doi.org/10.1002/msc.1370.
- O’Sullivan P, Caneiro JP, O’Keeffe M, O’Sullivan K. Unraveling the complexity of low back pain. J Orthop Sports Phys Ther 2016;46:932-7. https://doi.org/10.2519/jospt.2016.0609.
- Lee YY, Lin JL. How much does trust really matter? A study of the longitudinal effects of trust and decision-making preferences on diabetic patient outcomes. Patient Education and Counseling 2011;85:406-12. https://doi.org/10.1016/j.pec.2010.12.005.
- Cheng L, Leon V, Liang A, Reiher C, Roberts D, Feldthusen C, et al. Patient-centered care in physical therapy: definition, operationalization, and outcome measures. Physical Therapy Reviews 2016;21:109-23. https://doi.org/10.1080/10833196.2016.1228558.
- Cruz EB, Moore A, Cross V. Clinical reasoning and patient-centred care in musculoskeletal physiotherapy in Portugal – a qualitative study. Man Ther 2012;17:246-50. https://doi.org/10.1016/j.math.2012.02.007.
- Josephson I, Woodward-Kron R, Delany C, Hiller A. Evaluative language in physiotherapy practice: how does it contribute to the therapeutic relationship?. Soc Sci Med 2015;143:128-36. https://doi.org/10.1016/j.socscimed.2015.08.038.
- Mead N, Bower P. Patient-centredness: a conceptual framework and review of the empirical literature. Soc Sci Med 2000;51:1087-110. https://doi.org/10.1016/S0277-9536(00)00098-8.
- Stewart M, Brown JB, Weston WW, McWhinney IR, McWilliam CL, Freeman TR. Patient-centered Medicine – Transforming the Clinical Method. Bourne End: Radcliffe; n.d.
- Overmeer T, Boersma K, Main C, Linton SJ. Do physical therapists change their beliefs, attitudes, knowledge, skills and behaviour after a biopsychosocially orientated university course?. J Eval Clin Pract 2009;15:724-32. https://doi.org/10.1111/j.1365-2753.2008.01089.x.
- Valjakka AL, Salanterä S, Laitila A, Julkunen J, Hagelberg NM. The association between physicians’ attitudes to psychosocial aspects of low back pain and reported clinical behaviour: a complex issue. Scandinavian J Pain 2013;4:25-30. https://doi.org/10.1016/j.sjpain.2012.08.003.
- Foster NE, Delitto A. Embedding psychosocial perspectives within clinical management of low back pain: integration of psychosocially informed management principles into physical therapist practice—challenges and opportunities. Phys Ther 2011;91:790-803. https://doi.org/10.2522/ptj.20100326.
- O’Sullivan P. It’s time for change with the management of non-specific chronic low back pain. Br J Sports Med 2012;46:224-7.
- Sanders T, Foster NE, Bishop A, Ong BN. Biopsychosocial care and the physiotherapy encounter: physiotherapists’ accounts of back pain consultations. BMC Musculoskelet Disord 2013;14. https://doi.org/10.1186/1471-2474-14-65.
- Synnott A, O’Keeffe M, Bunzli S, Dankaerts W, O’Sullivan P, O’Sullivan K. Physiotherapists may stigmatise or feel unprepared to treat people with low back pain and psychosocial factors that influence recovery: a systematic review. J Physiother 2015;61:68-76. https://doi.org/10.1016/j.jphys.2015.02.016.
- Foster NE. Barriers and progress in the treatment of low back pain. BMC Med 2011;9. https://doi.org/10.1186/1741-7015-9-108.
- Bishop FL, Dima AL, Ngui J, Little P, Moss-Morris R, Foster NE, et al. “Lovely pie in the sky plans”: a qualitative study of clinicians’ perspectives on guidelines for managing low back pain in primary care in England. Spine 2015;40:1842-50. https://doi.org/10.1097/BRS.0000000000001215.
- Nielsen M, Keefe FJ, Bennell K, Jull GA. Physical therapist–delivered cognitive-behavioral therapy: a qualitative study of physical therapists’ perceptions and experiences. Phys Ther 2014;94:197-209. https://doi.org/10.2522/ptj.20130047.
- Hill JC, Dunn KM, Lewis M, Mullis R, Main CJ, Foster NE, et al. A primary care back pain screening tool: identifying patient subgroups for initial treatment. Arthritis Care Res 2008;59:632-41. https://doi.org/10.1002/art.23563.
Appendix 1 Literature search strategies
All searches comprised the same population and setting terms, translated for each database, as detailed below. These were combined with search filters to identify systematic reviews, RCTs, qualitative research (UK studies) and economic evaluations, details of which are included below. See Chapter 3 for the search strategy date ranges and dates of searches.
MEDLINE, MEDLINE In-Process & Other Non-Indexed Citations, Epub Ahead of Print, MEDLINE without Revisions via OvidSP
-
medically unexplained symptom*.ti,ab.
-
MUS.ti,ab.
-
medically unexplained physical symptom*.ti,ab.
-
MUPS.ti,ab.
-
(unexplain* adj1 medical*).ti,ab.
-
(unexplain* adj1 (sympt* or problem* or condition* or complain*)).ti,ab.
-
((non specific or nonspecific) adj2 (sympt* or problem* or condition* or complain*)).ti,ab.
-
((unexplain* or inexpl*) and (health* or medical* or physical*) and (sympt* or problem* or condition* or complain*)).ti,ab.
-
unexplained physical symptom*.ti,ab.
-
(Persistent adj2 physical symptom*).ti,ab.
-
distress syndrome.ti,ab.
-
polydistress disorder.ti,ab.
-
medically unexplained syndrome*.ti,ab.
-
or/1-13
-
(functional adj2 (disorder* or syndrome* or symptom* or pain*)).ti,ab.
-
Fibromyalgia/
-
fibromyalgi*.ti,ab.
-
Fatigue Syndrome, Chronic/
-
CFS.ti,ab.
-
(chronic fatigue adj3 (syndrome* or disorder*)).ti,ab.
-
myalgic encephalomyelitis.ti,ab.
-
fatigue syndrome.ti,ab.
-
Colonic Diseases, Functional/
-
Irritable Bowel Syndrome/
-
irritable bowel syndrome*.ti,ab.
-
IBS.ti,ab.
-
Temporomandibular Joint Dysfunction Syndrome/
-
((temporomandibular joint or TMJ) adj2 (disease* or disorder* or dysfunction*)).ti,ab.
-
Myofascial Pain Syndromes/
-
myofascial pain disorder*.ti,ab.
-
Facial Neuralgia/
-
atypical facial pain.ti,ab.
-
facial pain syndrome*.ti,ab.
-
Hyperventilation/
-
hyperventilation.ti,ab.
-
dysfunctional breathing.ti,ab.
-
loin pain h?ematuria syndrome*.ti,ab.
-
Muscle Weakness/
-
functional weakness*.ti,ab.
-
Movement Disorders/
-
movement disorder*.ti,ab.
-
(non-epileptic adj (attack* or seizure*)).ti,ab.
-
Dysmenorrhea/
-
dysmenorrhoea.ti,ab.
-
neurasthen*.ti,ab.
-
Neurasthenia/
-
Multiple Chemical Sensitivity/
-
multiple chemical sensitivity.ti,ab.
-
idiopathic environmental intolerance.ti,ab.
-
Tension-Type Headache/
-
((tension type or idiopathic or psychogenic) adj2 headache*).ti,ab.
-
Neurocirculatory Asthenia/
-
*Asthenia/
-
chronic asthenia.ti,ab.
-
functional atrial arrhythmia.ti,ab.
-
Da Costa’s Syndrome.ti,ab.
-
effort syndrome.ti,ab.
-
functional cardiovascular disease*.ti,ab.
-
subacute asthenia.ti,ab.
-
functional disturbance*.ti,ab.
-
(symptom adj syndrome*).ti,ab.
-
Post-Concussion Syndrome/
-
(post concussi* syndrome* or post-concussi* syndrome*).ti,ab.
-
or/15-63
-
Psychophysiologic Disorders/
-
((psychosomatic or pyschophysiologic) adj (disorder* or syndrome* or symptom*)).ti,ab.
-
briquet syndrome*.ti,ab.
-
Psychosomatic Medicine/
-
psychophysiologic*.ti,ab.
-
psychosomat*.ti,ab.
-
psychogen*.ti,ab.
-
*Somatoform Disorders/
-
somatic symptom*.ti,ab.
-
Somatoform Disorder*.ti,ab.
-
somati?at*.ti,ab.
-
(somatic adj2 syndrome*).ti,ab.
-
*Conversion Disorder/
-
conversion disorder*.ti,ab.
-
subjective health complaint*.ti,ab.
-
cardiac neurosis.ti,ab.
-
or/65-80
-
(Habits/or Tics/or Tic Disorders/) and Cough/
-
(chronic adj2 cough).ti,ab.
-
(habit cough or tic cough).ti,ab.
-
chronic pelvic pain*.ti,ab.
-
chronic widespread pain.ti,ab.
-
((non cardiac or noncardiac or non specific or nonspecific) adj2 chest pain*).ti,ab.
-
NCCP.ti,ab.
-
atypical chest pain*.ti,ab.
-
*Low Back Pain/
-
chronic low back pain*.ti,ab.
-
*chronic pain/
-
(chronic adj2 pain).ti,ab.
-
regional pain.ti,ab.
-
((non ulcer or nonulcer or non-ulcer or functional) adj2 dyspepsia).ti,ab.
-
or/82-95
-
*Sexual Dysfunctions, Psychological/
-
*Vaginismus/
-
(psychological adj2 sexual dysfunction*).ti,ab.
-
vaginismus.ti,ab.
-
psycho-sexual dysfunction*.ti,ab.
-
psychosexual dysfunction*.ti,ab.
-
*Erectile Dysfunction/
-
(impotence or erectile dysfunction).ti,ab.
-
*Vulvodynia/
-
vulvodynia.ti,ab.
-
anorgasmia.ti,ab.
-
or/97-107
-
14 or 64 or 81 or 96 or 108
-
exp Primary Health Care/
-
exp Family Practice/or exp General Practice/
-
PHYSICIANS, FAMILY/
-
FAMILY HEALTHCARE/
-
NURSE PRACTITIONERS/
-
((family or community) adj (medic$or doctor$or physician$or nurs$or health)).ti,ab.
-
((general or family or nurs$) adj1 (practice$or practitioner$)).ti,ab.
-
(primary care or primary healthcare or primary health care or primary health service$or homecare or care in the community).ti,ab.
-
(GP$or generalist$).ti,ab.
-
Occupational Health/
-
(occupational adj (health* or therap*)).ti,ab.
-
or/110-120
-
109 and 121
Search filters
-
To retrieve systematic reviews: Scottish Intercollegiate Guidelines Network (SIGN). Search Filters: Systematic Reviews. URL: www.sign.ac.uk/methodology/filters.html#systematic (accessed 7 April 2017).
-
To retrieve RCTs: SIGN. Search Filters: Randomised Controlled Trials. URL: www.sign.ac.uk/methodology/filters.html#random (accessed 7 April 2017).
-
To retrieve economic evaluations: SIGN. Search Filters: Economic Studies. URL: www.sign.ac.uk/methodology/filters.html#econ (accessed 7 April 2017).
-
To retrieve qualitative research: University of Texas School of Public Health. Search Filters for Various Databases: Ovid MEDLINE – Qualitative studies. URL: http://libguides.sph.uth.tmc.edu/search_filters/ovid_medline_filters (accessed 7 April 2017) combined with (AND) terms to identify UK studies: exp Great Britain/ OR (Britain or british or wales or welsh or Scottish or scots or Scotland or England or English or Birmingham or leeds or London or Liverpool or Manchester or Glasgow or Edinburgh or Cardiff or Belfast or UK or GB or aberdeen).ti,ab,in,hw.
EMBASE (via OvidSP)
-
medically unexplained symptom*.ti,ab.
-
MUS.ti,ab.
-
medically unexplained physical symptom*.ti,ab.
-
MUPS.ti,ab.
-
(unexplain* adj1 medical*).ti,ab.
-
(unexplain* adj1 (sympt* or problem* or condition* or complain*)).ti,ab.
-
((non specific or nonspecific) adj2 (sympt* or problem* or condition* or complain*)).ti,ab.
-
((unexplain* or inexpl*) and (health* or medical* or physical*) and (sympt* or problem* or condition* or complain*)).ti,ab.
-
unexplained physical symptom*.ti,ab.
-
(Persistent adj2 physical symptom*).ti,ab.
-
distress syndrome.ti,ab.
-
polydistress disorder.ti,ab.
-
medically unexplained syndrome*.ti,ab.
-
or/1-13
-
(functional adj2 (disorder* or syndrome* or symptom* or pain*)).ti,ab.
-
fibromyalgia/
-
fibromyalgi*.ti,ab.
-
chronic fatigue syndrome/
-
CFS.ti,ab.
-
(chronic fatigue adj3 (syndrome* or disorder*)).ti,ab.
-
myalgic encephalomyelitis.ti,ab.
-
fatigue syndrome.ti,ab.
-
irritable colon/
-
irritable bowel syndrome*.ti,ab.
-
IBS.ti,ab.
-
temporomandibular joint disorder/
-
((temporomandibular joint or TMJ) adj2 (disease* or disorder* or dysfunction*)).ti,ab.
-
myofascial pain/
-
myofascial pain disorder*.ti,ab.
-
face pain/
-
atypical facial pain.ti,ab.
-
facial pain syndrome*.ti,ab.
-
hyperventilation syndrome/or hyperventilation/
-
hyperventilation.ti,ab.
-
dysfunctional breathing.ti,ab.
-
loin pain h?ematuria syndrome*.ti,ab.
-
muscle weakness/
-
functional weakness*.ti,ab.
-
motor dysfunction/
-
movement disorder*.ti,ab.
-
(non-epileptic adj (attack* or seizure*)).ti,ab.
-
dysmenorrhea/
-
dysmenorrhoea.ti,ab.
-
neurasthenia/
-
neurasthen*.ti,ab.
-
multiple chemical sensitivity/
-
multiple chemical sensitivity.ti,ab.
-
idiopathic environmental intolerance.ti,ab.
-
tension headache/
-
((tension type or idiopathic or psychogenic) adj2 headache*).ti,ab.
-
cardiac anxiety/
-
*asthenia/
-
chronic asthenia.ti,ab.
-
functional atrial arrhythmia.ti,ab.
-
Da Costa’s Syndrome.ti,ab.
-
effort syndrome.ti,ab.
-
functional cardiovascular disease*.ti,ab.
-
subacute asthenia.ti,ab.
-
functional disturbance*.ti,ab.
-
(symptom adj syndrome*).ti,ab.
-
postconcussion syndrome/
-
(post concussi* syndrome* or post-concussi* syndrome*).ti,ab.
-
or/15-62
-
psychosomatic disorder/
-
((psychosomatic or pyschophysiologic) adj (disorder* or syndrome* or symptom*)).ti,ab.
-
briquet syndrome*.ti,ab.
-
psychosomatics/
-
psychophysiologic*.ti,ab.
-
psychosomat*.ti,ab.
-
psychogen*.ti,ab.
-
*somatoform disorder/
-
somatic symptom*.ti,ab.
-
Somatoform Disorder*.ti,ab.
-
somati?at*.ti,ab.
-
(somatic adj2 syndrome*).ti,ab.
-
conversion disorder/
-
conversion disorder*.ti,ab.
-
subjective health complaint*.ti,ab.
-
cardiac neurosis.ti,ab.
-
or/64-79
-
habit/and coughing/
-
tic/and coughing/
-
(chronic adj2 cough).ti,ab.
-
(habit cough or tic cough).ti,ab.
-
chronic pelvic pain*.ti,ab.
-
chronic widespread pain.ti,ab.
-
((non cardiac or noncardiac or non specific or nonspecific) adj2 chest pain*).ti,ab.
-
NCCP.ti,ab.
-
atypical chest pain*.ti,ab.
-
*low back pain/
-
chronic low back pain*.ti,ab.
-
*chronic pain/
-
(chronic adj2 pain).ti,ab.
-
regional pain.ti,ab.
-
((non ulcer or nonulcer or non-ulcer or functional) adj2 dyspepsia).ti,ab.
-
or/81-95
-
psychological aspect/and sexual dysfunction/
-
vaginism/
-
(psychological adj2 sexual dysfunction*).ti,ab.
-
vaginismus.ti,ab.
-
psycho-sexual dysfunction*.ti,ab.
-
psychosexual dysfunction*.ti,ab.
-
*erectile dysfunction/
-
(impotence or erectile dysfunction).ti,ab.
-
vulvodynia.ti,ab.
-
anorgasmia.ti,ab.
-
or/97-106
-
14 or 63 or 80 or 96 or 107
-
exp primary health care/
-
exp general practice/
-
general practitioner/
-
family health/
-
nurse practitioner/
-
((family or community) adj (medic$ or doctor$ or physician$ or nurs$ or health)).ti,ab.
-
((general or family or nurs$) adj1 (practice$ or practitioner$)).ti,ab.
-
(primary care or primary healthcare or primary health care or primary health service$ or homecare or care in the community).ti,ab.
-
(GP$ or generalist$).ti,ab.
-
occupational health/
-
(occupational adj (health* or therap*)).ti,ab.
-
or/109-119
-
108 and 120
-
limit 121 to embase
Search filters
-
To retrieve systematic reviews: Scottish Intercollegiate Guidelines Network (SIGN). Search Filters: Systematic Reviews. URL: www.sign.ac.uk/methodology/filters.html#systematic (accessed 7 April 2017).
-
To retrieve RCTs: SIGN. Search Filters: Randomised Controlled Trials. URL: www.sign.ac.uk/methodology/filters.html#random (accessed 7 April 2017).
-
To retrieve economic evaluations: Canadian Agency for Drugs and Technologies in Health (CADTH). Strings Attached: CADTH’s Database Search Filters: Economic Evaluations/Cost/Economic Models. URL: www.cadth.ca/resources/finding-evidence/strings-attached-cadths-database-search-filters#eco (accessed 7 April 2017).
-
To retrieve qualitative research: McMaster University Health Information Research Unit. Search Strategies for EMBASE in Ovid Syntax: Qualitative (Best Balance of Sensitivity and Specificity). URL: http://hiru.mcmaster.ca/hiru/HIRU_Hedges_EMBASE_Strategies.aspx#Economics (accessed 7 April 2017) combined with (AND) terms to identify UK studies: exp Great Britain/ OR (Britain or british or wales or welsh or Scottish or scots or Scotland or England or English or Birmingham or leeds or London or Liverpool or Manchester or Glasgow or Edinburgh or Cardiff or Belfast or UK or GB or aberdeen).ti,ab,in,hw.
CINAHL (via EBSCOhost)
-
S1 TI medically unexplained symptom* OR AB medically unexplained symptom*
-
S2 TI MUS OR AB MUS
-
S3 TI medically unexplained physical symptom* OR AB medically unexplained physical symptom*
-
S4 TI MUPS OR AB MUPS
-
S5 TI (unexplain* n1 medical*) OR AB (unexplain* n1 medical*)
-
S6 TI ( (unexplain* n1 (sympt* or problem* or condition* or complain*)) ) OR AB ( (unexplain* n1 (sympt* or problem* or condition* or complain*)) )
-
S7 TI ( ((non specific or nonspecific) n2 (sympt* or problem* or condition* or complain*)) ) OR AB ( ((non specific or nonspecific) n2 (sympt* or problem* or condition* or complain*)) )
-
S8 TI ( ((unexplain* or inexpl*) and (health* or medical* or physical*) and (sympt* or problem* or condition* or complain*)) ) OR AB ( ((unexplain* or inexpl*) and (health* or medical* or physical*) and (sympt* or problem* or condition* or complain*)) )
-
S9 TI unexplained physical symptom* OR AB unexplained physical symptom*
-
S10 TI (Persistent n2 physical symptom*) OR AB (Persistent n2 physical symptom*)
-
S11 TI distress syndrome OR AB distress syndrome
-
S12 TI polydistress disorder OR AB polydistress disorder
-
S13 TI medically unexplained syndrome* OR AB medically unexplained syndrome*
-
S14 (MH “Medically Unexplained Symptoms“)
-
S15 S1 OR S2 OR S3 OR S4 OR S5 OR S6 OR S7 OR S8 OR S9 OR S10 OR S11 OR S12 OR S13 OR S14
-
S16 TI ( (functional n2 (disorder* or syndrome* or symptom* or pain*)) ) OR AB ( (functional n2 (disorder* or syndrome* or symptom* or pain*)) )
-
S17 (MH “Fibromyalgia”)
-
S18 TI fibromyalgi* OR AB fibromyalgi*
-
S19 (MH “Fatigue Syndrome, Chronic”)
-
S20 TI CFS OR AB CFS
-
S21 TI ( (chronic fatigue n3 (syndrome* or disorder*)) ) OR AB ( (chronic fatigue n3 (syndrome* or disorder*)) )
-
S22 TI myalgic encephalomyelitis OR AB myalgic encephalomyelitis
-
S23 TI fatigue syndrome OR AB fatigue syndrome
-
S24 (MH “Colonic Diseases, Functional”)
-
S25 (MH “Irritable Bowel Syndrome”)
-
S26 TI irritable bowel syndrome* OR AB irritable bowel syndrome*
-
S27 TI IBS OR AB IBS
-
S28 (MH “Temporomandibular Joint Syndrome”)
-
S29 TI ( ((temporomandibular joint or TMJ) n2 (disease* or disorder* or dysfunction*)) ) OR AB ( ((temporomandibular joint or TMJ) n2 (disease* or disorder* or dysfunction*)) )
-
S30 (MH “Myofascial Pain Syndromes”)
-
S31 TI myofascial pain disorder* OR AB myofascial pain disorder*
-
S32 (MH “Facial Neuralgia”)
-
S33 TI atypical facial pain OR AB atypical facial pain
-
S34 TI facial pain syndrome* OR AB facial pain syndrome*
-
S35 (MH “Hyperventilation”)
-
S36 TI hyperventilation OR AB hyperventilation
-
S37 TI dysfunctional breathing OR AB dysfunctional breathing
-
S38 TI loin pain h?ematuria syndrome* OR AB loin pain h?ematuria syndrome*
-
S39 (MH “Muscle Weakness”)
-
S40 TI functional weakness* OR AB functional weakness*
-
S41 (MH “Movement Disorders”)
-
S42 TI movement disorder* OR AB movement disorder*
-
S43 TI ( (non-epileptic n1 (attack* or seizure*) ) OR AB ( (non-epileptic n1 (attack* or seizure*) )
-
S44 (MH “Dysmenorrhea”)
-
S45 TI dysmenorrhoea OR AB dysmenorrhoea
-
S46 TI neurasthen* OR AB neurasthen*
-
S47 (MH “Multiple Chemical Sensitivity”)
-
S48 TI multiple chemical sensitivity OR AB multiple chemical sensitivity
-
S49 TI idiopathic environmental intolerance OR AB idiopathic environmental intolerance
-
S50 (MH “Tension Headache”)
-
S51 TI ( ((tension type or idiopathic or psychogenic) n2 headache*) ) OR AB ( ((tension type or idiopathic or psychogenic) n2 headache*) )
-
S52 (MM “Asthenia”)
-
S53 TI chronic asthenia OR AB chronic asthenia
-
S54 TI functional atrial arrhythmia OR AB functional atrial arrhythmia
-
S55 TI Da Costa’s Syndrome OR AB Da Costa’s Syndrome
-
S56 TI effort syndrome OR AB effort syndrome
-
S57 TI functional cardiovascular disease* OR AB functional cardiovascular disease*
-
S58 TI subacute asthenia OR AB subacute asthenia
-
S59 TI functional disturbance* OR AB functional disturbance*
-
S60 TI (symptom n1 syndrome*) OR AB (symptom n1 syndrome*)
-
S61 (MH “Postconcussion Syndrome”)
-
S62 TI ( (post concussi* syndrome* or post-concussi* syndrome*) ) OR AB ( (post concussi* syndrome* or post-concussi* syndrome*) )
-
S63 S16 OR S17 OR S18 OR S19 OR S20 OR S21 OR S22 OR S23 OR S24 OR S25 OR S26 OR S27 OR S28 OR S29 OR S30 OR S31 OR S32 OR S33 OR S34 OR S35 OR S36 OR S37 OR S38 OR S39 OR S40 OR S41 OR S42 OR S43 OR S44 OR S45 OR S46 OR S47 OR S48 OR S49 OR S50 OR S51 OR S52 OR S53 OR S54 OR S55 OR S56 OR S57 OR S58 OR S59 OR S60 OR S61 OR S62
-
S64 (MH “Psychophysiologic Disorders”)
-
S65 TI ( ((psychosomatic or pyschophysiologic) n1 (disorder* or syndrome* or symptom*)) ) OR AB ( ((psychosomatic or pyschophysiologic) n1 (disorder* or syndrome* or symptom*)) )
-
S66 TI briquet syndrome* OR AB briquet syndrome*
-
S67 TI psychophysiologic* OR AB psychophysiologic*
-
S68 TI psychosomat* OR AB psychosomat*
-
S69 TI psychogen* OR AB psychogen*
-
S70 (MM “Somatoform Disorders”)
-
S71 TI somatic symptom* OR AB somatic symptom*
-
S72 TI somatoform disorder* OR AB somatoform disorder*
-
S73 TI somati?at* OR AB somati?at*
-
S74 TI (somatic n2 syndrome*) OR AB (somatic n2 syndrome*)
-
S75 TI conversion disorder* OR AB conversion disorder*
-
S76 TI subjective health complaint* OR AB subjective health complaint*
-
S77 TI cardiac neurosis OR AB cardiac neurosis
-
S78 S64 OR S65 OR S66 OR S67 OR S68 OR S69 OR S70 OR S71 OR S72 OR S73 OR S74 OR S75 OR S76 OR S77
-
S79 (MH “Habits”) AND (MH “Cough”)
-
S80 (MH “Tic”) AND (MH “Cough”)
-
S81 TI (chronic n2 cough) OR AB (chronic n2 cough)
-
S82 TI ( (habit cough or tic cough) ) OR AB ( (habit cough or tic cough) )
-
S83 TI chronic pelvic pain* OR AB chronic pelvic pain*
-
S84 TI chronic widespread pain OR AB chronic widespread pain
-
S85 TI ( ((non cardiac or noncardiac or non specific or nonspecific) n2 chest pain*) ) OR AB ( ((non cardiac or noncardiac or non specific or nonspecific) n2 chest pain*) )
-
S86 TI NCCP OR AB NCCP
-
S87 TI atypical chest pain* OR AB atypical chest pain*
-
S88 (MM “Low Back Pain”)
-
S89 TI chronic low back pain* OR AB chronic low back pain*
-
S90 (MM “Chronic Pain”)
-
S91 TI (chronic n2 pain) OR AB (chronic n2 pain)
-
S92 TI regional pain OR AB regional pain
-
S93 TI ( ((non ulcer or nonulcer or non-ulcer or functional) n2 dyspepsia) ) OR AB ( ((non ulcer or nonulcer or non-ulcer or functional) n2 dyspepsia) )
-
S94 S79 OR S80 OR S81 OR S82 OR S83 OR S84 OR S85 OR S86 OR S87 OR S88 OR S89 OR S90 OR S91 OR S92 OR S93
-
S95 (MM “Psychosexual Disorders”)
-
S96 TI (psychological n2 sexual dysfunction*) OR AB (psychological n2 sexual dysfunction*)
-
S97 TI vaginismus OR AB vaginismus
-
S98 TI psycho-sexual dysfunction* OR AB psycho-sexual dysfunction*
-
S99 TI psychosexual dysfunction* OR AB psychosexual dysfunction*
-
S100 (MM “Impotence”)
-
S101 TI ( (impotence or erectile dysfunction) ) OR AB ( (impotence or erectile dysfunction) )
-
S102 TI vulvodynia OR AB vulvodynia
-
S103 TI anorgasmia OR AB anorgasmia
-
S104 S95 OR S96 OR S97 OR S98 OR S99 OR S100 OR S101 OR S102 OR S103
-
S105 S15 OR S63 OR S94 OR S104
-
S106 (MH “Primary Health Care”)
-
S107 (MH “Family Practice”)
-
S108 (MH “Physicians, Family”)
-
S109 (MH “Nurse Practitioners”)
-
S110 TI ( ((family or community) n1 (medic$ or doctor$ or physician$ or nurs$ or health)) ) OR AB ( ((family or community) n1 (medic$ or doctor$ or physician$ or nurs$ or health)) )
-
S111 TI ( ((general or family or nurs$) n1 (practice$ or practitioner$)) ) OR AB ( ((general or family or nurs$) n1 (practice$ or practitioner$)) )
-
S112 TI ( (primary care or primary healthcare or primary health care or primary health service$ or homecare or care in the community) ) OR AB ( (primary care or primary healthcare or primary health care or primary health service$ or homecare or care in the community) )
-
S113 TI ( (GP$ or generalist$) ) OR AB ( (GP$ or generalist$) )
-
S114 (MH “Occupational Health”)
-
S115 TI ( (occupational n1 (health* or therap*)) ) OR AB ( (occupational n1 (health* or therap*)) )
-
S116 S106 OR S107 OR S108 OR S109 OR S110 OR S111 OR S112 OR S113 OR S114 OR S115
-
S117 S105 AND S116
Search filters
-
To retrieve systematic reviews: Scottish Intercollegiate Guidelines Network (SIGN). Search Filters: Systematic Reviews. URL: www.sign.ac.uk/methodology/filters.html#systematic (accessed 7 April 2017).
-
To retrieve RCTs: SIGN. Search Filters: Randomised Controlled Trials. URL: www.sign.ac.uk/methodology/filters.html#random (accessed 7 April 2017).
-
To retrieve economic evaluations: Centre for Reviews and Dissemination (CRD), The University of York. Search strategies: NHS EED. URL: www.crd.york.ac.uk/crdweb/searchstrategies.asp#nhseedcinahl (accessed 7 April 2017).
-
To retrieve Qualitative Research: University of Washington Health Sciences Library. Finding Qualitative Research Articles: CINAHL. URL: http://guides.lib.uw.edu/c.php?g%20=%2099112&p%20=%20642298 (accessed 7 April 2017) combined with (AND) terms to identify UK studies:
-
(MH “Great Britain”) OR (Britain or british or wales or welsh or Scottish or scots or Scotland or England or English or Birmingham or leeds or London or Liverpool or Manchester or Glasgow or Edinburgh or Cardiff or Belfast or UK or GB or aberdeen).
PyscINFO (via OvidSP)
-
medically unexplained symptom*.ti,ab.
-
MUS.ti,ab.
-
medically unexplained physical symptom*.ti,ab.
-
MUPS.ti,ab.
-
(unexplain* adj1 medical*).ti,ab.
-
(unexplain* adj1 (sympt* or problem* or condition* or complain*)).ti,ab.
-
((non specific or nonspecific) adj2 (sympt* or problem* or condition* or complain*)).ti,ab.
-
((unexplain* or inexpl*) and (health* or medical* or physical*) and (sympt* or problem* or condition* or complain*)).ti,ab.
-
unexplained physical symptom*.ti,ab.
-
(Persistent adj2 physical symptom*).ti,ab.
-
distress syndrome.ti,ab.
-
polydistress disorder.ti,ab.
-
medically unexplained syndrome*.ti,ab.
-
or/1-13
-
(functional adj2 (disorder* or syndrome* or symptom* or pain*)).ti,ab.
-
exp Fibromyalgia/
-
fibromyalgi*.ti,ab.
-
Chronic Fatigue Syndrome/
-
CFS.ti,ab.
-
(chronic fatigue adj3 (syndrome* or disorder*)).ti,ab.
-
myalgic encephalomyelitis.ti,ab.
-
fatigue syndrome.ti,ab.
-
Irritable Bowel Syndrome/
-
irritable bowel syndrome*.ti,ab.
-
IBS.ti,ab.
-
((temporomandibular joint or TMJ) adj2 (disease* or disorder* or dysfunction*)).ti,ab.
-
exp Syndromes/and Myofascial Pain/
-
myofascial pain disorder*.ti,ab.
-
atypical facial pain.ti,ab.
-
facial pain syndrome*.ti,ab.
-
Hyperventilation/
-
hyperventilation.ti,ab.
-
dysfunctional breathing.ti,ab.
-
loin pain h?ematuria syndrome*.ti,ab.
-
functional weakness*.ti,ab.
-
Movement Disorders/
-
movement disorder*.ti,ab.
-
(non-epileptic adj (attack* or seizure*)).ti,ab.
-
Dysmenorrhea/
-
dysmenorrhoea.ti,ab.
-
neurasthen*.ti,ab.
-
Neurasthenia/
-
multiple chemical sensitivity.ti,ab.
-
idiopathic environmental intolerance.ti,ab.
-
exp Muscle Contraction Headache/
-
((tension type or idiopathic or psychogenic) adj2 headache*).ti,ab.
-
*Asthenia/
-
chronic asthenia.ti,ab.
-
functional atrial arrhythmia.ti,ab.
-
Da Costa’s Syndrome.ti,ab.
-
effort syndrome.ti,ab.
-
functional cardiovascular disease*.ti,ab.
-
subacute asthenia.ti,ab.
-
functional disturbance*.ti,ab.
-
(symptom adj syndrome*).ti,ab.
-
(post concussi* syndrome* or post-concussi* syndrome*).ti,ab.
-
or/15-56
-
Somatoform Disorders/
-
((psychosomatic or pyschophysiologic) adj (disorder* or syndrome* or symptom*)).ti,ab.
-
briquet syndrome*.ti,ab.
-
Psychosomatic Medicine/
-
psychophysiologic*.ti,ab.
-
psychosomat*.ti,ab.
-
psychogen*.ti,ab.
-
somatic symptom*.ti,ab.
-
Somatoform Disorder*.ti,ab.
-
somati?at*.ti,ab.
-
(somatic adj2 syndrome*).ti,ab.
-
*Conversion Disorder/
-
conversion disorder*.ti,ab.
-
subjective health complaint*.ti,ab.
-
cardiac neurosis.ti,ab.
-
or/58-72
-
(chronic adj2 cough).ti,ab.
-
(habit cough or tic cough).ti,ab.
-
chronic pelvic pain*.ti,ab.
-
chronic widespread pain.ti,ab.
-
((non cardiac or noncardiac or non specific or nonspecific) adj2 chest pain*).ti,ab.
-
NCCP.ti,ab.
-
atypical chest pain*.ti,ab.
-
*Back Pain/
-
chronic low back pain*.ti,ab.
-
*Chronic Pain/
-
(chronic adj2 pain).ti,ab.
-
regional pain.ti,ab.
-
((non ulcer or nonulcer or non-ulcer or functional) adj2 dyspepsia).ti,ab.
-
or/74-86
-
*Sexual Function Disturbances/
-
(psychological adj2 sexual dysfunction*).ti,ab.
-
*Vaginismus/
-
vaginismus.ti,ab.
-
psycho-sexual dysfunction*.ti,ab.
-
psychosexual dysfunction*.ti,ab.
-
*Erectile Dysfunction/
-
(impotence or erectile dysfunction).ti,ab.
-
vulvodynia.ti,ab.
-
anorgasmia.ti,ab.
-
or/88-97
-
14 or 57 or 73 or 87 or 98
-
exp Primary Health Care/
-
exp General Practitioners/
-
Family Physicians/
-
Family Medicine/
-
((family or community) adj (medic$or doctor$or physician$or nurs$or health)).ti,ab.
-
((general or family or nurs$) adj1 (practice$or practitioner$)).ti,ab.
-
(primary care or primary healthcare or primary health care or primary health service$or homecare or care in the community).ti,ab.
-
(GP$or generalist$).ti,ab.
-
Occupational Health/
-
(occupational adj (health* or therap*)).ti,ab.
-
or/100–109
-
99 and 110
Search fiilters
-
To retrieve systematic reviews: The University of Texas School of Public Health. Search Filters for Various Databases: Ovid PsycINFO (Systematic reviews and meta-analyses). URL: http://libguides.sph.uth.tmc.edu/search_filters/ovid_psycinfo_filters (accessed 7 April 2017).
-
To retrieve RCTs: The University of Texas School of Public Health. Search Filters for Various Databases: Ovid PsycINFO (Clinical trials). URL: http://libguides.sph.uth.tmc.edu/search_filters/ovid_psycinfo_filters (accessed 7 April 2017).
-
To retrieve economic evaluations: Centre for Reviews and Dissemination (CRD), The University of York. Search strategies: NHS EED. URL: www.crd.york.ac.uk/crdweb/searchstrategies.asp#nhseedpsycinfo (accessed 7 April 2017).
-
To retrieve qualitative research: The University of Texas School of Public Health. Search Filters for Various Databases: Ovid PsycINFO (Qualitative studies). URL: http://libguides.sph.uth.tmc.edu/search_filters/ovid_psycinfo_filters (accessed 7 April 2017) combined with (AND) terms to identify UK studies: (Britain or british or wales or welsh or Scottish or scots or Scotland or England or English or Birmingham or leeds or London or Liverpool or Manchester or Glasgow or Edinburgh or Cardiff or Belfast or UK or GB or aberdeen).ti,ab,in,hw.
The Cochrane Library (DARE, CDSR, CENTRAL, HTA, NHS EED)
-
medically unexplained symptom*:ti or medically unexplained symptom*:ab
-
MUS:ti or MUS:ab
-
medically unexplained physical symptom*:ti or medically unexplained physical symptom*:ab
-
MUPS:ti or MUPS:ab
-
(unexplain* near/1 medical*):ti or (unexplain* near/1 medical*):ab
-
(unexplain* near/1 (sympt* or problem* or condition* or complain*)):ti or (unexplain* near/1 (sympt* or problem* or condition* or complain*))
-
((non specific or nonspecific) near/2 (sympt* or problem* or condition* or complain*)):ti or ((non specific or nonspecific) near/2 (sympt* or problem* or condition* or complain*)):ab
-
((unexplain* or inexpl*) and (health* or medical* or physical*) and (sympt* or problem* or condition* or complain*)):ti or ((unexplain* or inexpl*) and (health* or medical* or physical*) and (sympt* or problem* or condition* or complain*)):ab
-
unexplained physical symptom*:ti or unexplained physical symptom*:ab
-
(Persistent near/2 physical symptom*):ti or (Persistent near/2 physical symptom*):ab
-
distress syndrome:ti or distress syndrome:ab
-
polydistress disorder:ti or polydistress disorder:ab
-
medically unexplained syndrome*:ti or medically unexplained syndrome*:ab
-
56-#13
-
(functional near/2 (disorder* or syndrome* or symptom* or pain*)):ti or (functional near/2 (disorder* or syndrome* or symptom* or pain*)):ab
-
MeSH descriptor: [Fibromyalgia] explode all trees
-
fibromyalgi*:ti or fibromyalgi*:ab
-
MeSH descriptor: [Fatigue Syndrome, Chronic] explode all trees
-
CFS:ti or CFS:ab
-
(chronic fatigue near/3 (syndrome* or disorder*)):ti or (chronic fatigue near/3 (syndrome* or disorder*)):ab
-
myalgic encephalomyelitis:ti or myalgic encephalomyelitis:ab
-
fatigue syndrome:ti or fatigue syndrome:ab
-
MeSH descriptor: [Colonic Diseases, Functional] explode all trees
-
MeSH descriptor: [Irritable Bowel Syndrome] explode all trees
-
irritable bowel syndrome*:ti or irritable bowel syndrome*:ab
-
IBS:ti or IBS:ab
-
MeSH descriptor: [Temporomandibular Joint Dysfunction Syndrome] explode all trees
-
((temporomandibular joint or TMJ) near/2 (disease* or disorder* or dysfunction*)):ti or ((temporomandibular joint or TMJ) near/2 (disease* or disorder* or dysfunction*)):ab
-
MeSH descriptor: [Myofascial Pain Syndromes] explode all trees
-
myofascial pain disorder*:ti or myofascial pain disorder*:ab
-
MeSH descriptor: [Facial Neuralgia] explode all trees
-
atypical facial pain:ti or atypical facial pain:ab
-
facial pain syndrome*:ti or facial pain syndrome*:ab
-
MeSH descriptor: [Hyperventilation] explode all trees
-
hyperventilation:ti or hyperventilation:ab
-
dysfunctional breathing:ti or dysfunctional breathing:ab
-
loin pain h?ematuria syndrome*:ti or loin pain h?ematuria syndrome*:ab
-
MeSH descriptor: [Muscle Weakness] explode all trees
-
functional weakness*:ti or functional weakness*:ab
-
MeSH descriptor: [Movement Disorders] this term only
-
movement disorder*:ti or movement disorder*:ab
-
(non-epileptic next (attack* or seizure*)):ti or (non-epileptic next (attack* or seizure*)):ab
-
MeSH descriptor: [Dysmenorrhea] explode all trees
-
dysmenorrhoea:ti or dysmenorrhoea:ab
-
neurasthen*:ti or neurasthen*:ab
-
MeSH descriptor: [Neurasthenia] explode all trees
-
MeSH descriptor: [Multiple Chemical Sensitivity] explode all trees
-
multiple chemical sensitivity:ti or multiple chemical sensitivity:ab
-
idiopathic environmental intolerance:ti or idiopathic environmental intolerance:ab
-
MeSH descriptor: [Tension-Type Headache] explode all trees
-
((tension type or idiopathic or psychogenic) near/2 headache*):ti or ((tension type or idiopathic or psychogenic) near/2 headache*):ab
-
MeSH descriptor: [Neurocirculatory Asthenia] explode all trees
-
MeSH descriptor: [Asthenia] explode all trees
-
chronic asthenia:ti or chronic asthenia:ab
-
functional atrial arrhythmia:ti or functional atrial arrhythmia:ab
-
Da Costa’s Syndrome:ti or Da Costa’s Syndrome:ab
-
effort syndrome:ti or effort syndrome:ab
-
functional cardiovascular disease*:ti or functional cardiovascular disease*:ab
-
subacute asthenia:ti or subacute asthenia:ab
-
functional disturbance*:ti or functional disturbance*:ab
-
(symptom next syndrome*):ti or (symptom next syndrome*):ab
-
MeSH descriptor: [Post-Concussion Syndrome] explode all trees
-
(post concussi* syndrome* or post-concussi* syndrome*):ti or (post concussi* syndrome* or post-concussi* syndrome*):ab
-
{or #15-#63}
-
MeSH descriptor: [Psychophysiologic Disorders] explode all trees
-
((psychosomatic or pyschophysiologic) next (disorder* or syndrome* or symptom*)):ti or ((psychosomatic or pyschophysiologic) next (disorder* or syndrome* or symptom*)):ab
-
briquet syndrome*:ti or briquet syndrome*:ab
-
MeSH descriptor: [Psychosomatic Medicine] explode all trees
-
psychophysiologic*:ti or psychophysiologic*:ab
-
psychosomat*:ti or psychosomat*:ab
-
psychogen*:ti or psychogen*:ab
-
MeSH descriptor: [Somatoform Disorders] explode all trees
-
somatic symptom*:ti or somatic symptom*:ab
-
Somatoform Disorder*:ti or Somatoform Disorder*:ab
-
somati?at*:ti or somati?at*:ab
-
(somatic near/2 syndrome*):ti or (somatic near/2 syndrome*):ab
-
MeSH descriptor: [Conversion Disorder] explode all trees
-
conversion disorder*:ti or conversion disorder*:ab
-
subjective health complaint*:ti or subjective health complaint*:ab
-
cardiac neurosis:ti or cardiac neurosis:ab
-
{or #65-#80}
-
MeSH descriptor: [Habits] this term only
-
MeSH descriptor: [Tics] explode all trees
-
MeSH descriptor: [Tic Disorders] explode all trees
-
{or #82-#84}
-
MeSH descriptor: [Cough] this term only
-
#85 and #86
-
(chronic near/2 cough):ti or (chronic near/2 cough):ab
-
(habit cough or tic cough):ti or (habit cough or tic cough):ab
-
chronic pelvic pain*:ti or chronic pelvic pain*:ab
-
chronic widespread pain:ti or chronic widespread pain:ab
-
((non cardiac or noncardiac or non specific or nonspecific) near/2 chest pain*):ti or ((non cardiac or noncardiac or non specific or nonspecific) near/2 chest pain*):ab
-
NCCP:ti or NCCP:ab
-
atypical chest pain*:ti or atypical chest pain*:ab
-
MeSH descriptor: [Low Back Pain] this term only
-
chronic low back pain*:ti or chronic low back pain*:ab
-
MeSH descriptor: [Chronic Pain] this term only
-
(chronic near/2 pain):ti or (chronic near/2 pain):ab
-
regional pain:ti or regional pain:ab
-
((non ulcer or nonulcer or non-ulcer or functional) near/2 dyspepsia):ti ((non ulcer or nonulcer or non-ulcer or functional) near/2 dyspepsia):ab
-
{or #87-#100}
-
MeSH descriptor: [Sexual Dysfunctions, Psychological] this term only
-
(psychological near/2 sexual dysfunction*):ti or (psychological near/2 sexual dysfunction*):ab
-
MeSH descriptor: [Vaginismus] explode all trees
-
vaginismus:ti or vaginismus:ab
-
psycho-sexual dysfunction*:ti or psycho-sexual dysfunction*:ab
-
psychosexual dysfunction*:ti or psychosexual dysfunction*:ab
-
MeSH descriptor: [Erectile Dysfunction] this term only
-
(impotence or erectile dysfunction):ti or (impotence or erectile dysfunction):ab
-
MeSH descriptor: [Vulvodynia] explode all trees
-
vulvodynia:ti or vulvodynia:ab
-
anorgasmia:ti or anorgasmia:ab
-
[or #102-#112]
-
#14 or #64 or #81 or #101 or #113
-
MeSH descriptor: [Primary Health Care] explode all trees
-
MeSH descriptor: [Family Practice] explode all trees
-
MeSH descriptor: [General Practice] explode all trees
-
MeSH descriptor: [Physicians, Family] explode all trees
-
FAMILY HEALTHCARE
-
MeSH descriptor: [Nurse Practitioners] explode all trees
-
((family or community) next (medic* or doctor* or physician* or nurs* or health)):ti or ((family or community) next (medic* or doctor* or physician* or nurs* or health)):ab
-
((general or family or nurs*) next/1 (practice* or practitioner*)):ti or ((general or family or nurs*) next/1 (practice* or practitioner*)):ab
-
(primary care or primary healthcare or primary health care or primary health service* or homecare or care in the community):ti or (primary care or primary healthcare or primary health care or primary health service* or homecare or care in the community):ab
-
(GP* or generalist*):ti or (GP* or generalist*):ab
-
MeSH descriptor: [Occupational Health] explode all trees
-
(occupational next (health* or therap*)):ti or (occupational next (health* or therap*)):ab
-
[or #115-#126]
-
and #127
Search filters
No search filters were applied to the Cochrane Library searches.
Science Citation Index and Social Sciences Citation Index (via Web of Science)
-
TOPIC: (((medically unexplained symptom* or MUS or medically unexplained physical symptom* or MUPS)))
-
TOPIC: ((unexplain*) NEAR/1 (medical* or sympt* or problem* or condition* or complain*))
-
TOPIC: (((non-specific or nonspecific) NEAR/2 (sympt* or problem* or condition* or complain*)))
-
TOPIC: ((unexplain* or inexpl*) and (health* or medical* or physical*) and (sympt* or problem* or condition* or complain*))
-
TOPIC: ((unexplained physical symptom* or (persistent NEAR/2 symptom*) or distress syndrome or polydistress disorder or medically unexplained syndrome*))
-
TOPIC: ((functional) NEAR/2 (disorder* or syndrome* or symptom* or pain*))
-
TOPIC: ((fibromyalgi* or CFS or (fatigue NEAR/3 syndrome* or disorder*) or myalgic encephalomyelitis or irritable bowel syndrome* or IBS))
-
TOPIC: ((temporomandibular or TMJ) NEAR/2 (disease* or disorder* or dysfunction*))
-
TOPIC: ((myofascial pain disorder* or atypical facial pain or facial pain syndrome* or hyperventilation or dysfunctional breathing or loin pain h?ematuria syndrome* or functional weakness* or movement disorder*))
-
TOPIC: ((non-epileptic NEAR attack* or seizure*) or (dysmenorrhoea or neurasthen* or multiple chemical sensitivity or idiopathic environmental intolerance))
-
TOPIC: ((tension or idiopathic or psychogenic) NEAR/2 (headache*))
-
TOPIC: ((chronic asthenia or functional atrial arrhythmia or da costa’s syndrome or effort syndrome or functional cardiovascular disease* or subacute asthenia or functional disturbance* or (symptom NEAR syndrome*)))
-
TOPIC: ((post concussi* syndrome* or post-concussi* syndrome*))
-
TOPIC: ((psychosomatic or pyschophysiologic) NEAR/2 (disorder* or syndrome* or symptom*))
-
TOPIC: ((briquet syndrome* or pyschophysiologic* or psychosomatic* or psychogen* or somatic symptom* or somati?at*))
-
TOPIC: (((somatic NEAR/2 syndrome*) or (conversion disorder* or subjective health complaint* or cardiac neurosis)))
-
TOPIC: ((chronic NEAR/2 cough) or (habit cough or tic cough or chronic pelvic pain* or chronic widespread pain))
-
TOPIC: ((non-cardiac or noncardiac or non-specific or nonspecific) NEAR/2 (chest NEAR pain*))
-
TOPIC: (NCCP or atypical chest pain* or chronic low back pain* or (chronic NEAR/2 pain) or regional pain)
-
TOPIC: ((non-ulcer or nonulcer or functional) NEAR/2 dyspepsia)
-
TOPIC: ((pyschological NEAR/2 sexual NEAR dysfunction*) or vaginismus or psycho-sexual dysfunction* or pyschosexual dysfunction* or impotence or erectile dysfunction or vulvodynia or anorgasmia)
-
#21 OR #20 OR #19 OR #18 OR #17 OR #16 OR #15 OR #14 OR #13 OR #12 OR #11 OR #10 OR #9 OR #8 OR #7 OR #6 OR #5 OR #4 OR #3 OR #2 OR #1
-
TOPIC: ((family or community) NEAR (medic* or doctor* or physician* or nurs* or health))
-
TOPIC: ((general or family or nurs*) NEAR/1 (practice* or practitioner*))
-
TOPIC: ((primary care or primary healthcare or primary health care or primary health service* or homecare or care in the community))
-
TOPIC: (GP or GPs or generalist*)
-
TOPIC: (((occupational) NEAR (health* or therap*)))
-
#27 OR #26 OR #25 OR #24 OR #23
-
#28 AND #22
Search filters
Methodological search filters are not available for Web of Science; therefore, the following terms were combined with the above search strategy using the operator “AND” to identify the specific study types.
-
To retrieve systematic reviews: TI = ((meta analy* or metaanaly* or systematic review*))
-
To retrieve RCTs: TI = (clinical trial* or random* control* trial* or RCT*)
-
To retrieve economic evaluations: TI = ((cost benefit analys* OR health care costs)) OR (budget*) OR ((economic* or cost or costs or costly or costing or price or prices or pricing or pharmacoeconomic* or pharmaco-economic* or expenditure or expenditures or expense or expenses or financial or finance or finances or financed)) OR ((value NEAR/2 (money or monetary))) OR ((decision* NEAR/2 (tree* or analy* or model*)))
-
To retrieve qualitative research: TOPIC = ((((“semi-structured” or semistructured or unstructured or informal or “in-depth” or indepth or “face-to-face” or structured or guide) NEAR/3 (interview* or discussion* or questionnaire*))) or (focus group* or qualitative or ethnograph* or fieldwork or “field work” or “key informant”))] combined with (AND) terms to identify UK studies: TOPIC = ((Britain or british or wales or welsh or Scottish or scots or Scotland or England or English or Birmingham or leeds or London or Liverpool or Manchester or Glasgow or Edinburgh or Cardiff or Belfast or UK or GB or aberdeen)).
Appendix 2 Summary characteristics of included studies
Tables 28–35 show the diagnostic criteria used for individual studies, by condition.
| First author and year of publication | Condition | Intervention | Intervention description | Grouping |
|---|---|---|---|---|
| Aiarzaguena, 2007136 | MUS/somatoform | Psychosocial intervention |
|
GP – reattribution (modified) |
| Goldberg reattribution technique | Active control. GPs were trained to emphasise a link between symptoms and emotions based on Goldberg’s reattribution technique | GP – reattribution | ||
| Alda, 2011137 | Pain – multisite (fibromyalgia) | CBT | Cognitive restructuring, which focuses on reducing pain-specific dysfunctional cognitions (primarily PC), and coping, which focuses on teaching cognitive and behavioural coping strategies | CBTHI |
| Recommended pharmacological treatment | Treatment with pregabalin (300–600 mg per day) and duloxetine (60–120 mg per day) was administered to patients with major depressive disorder | ME | ||
| GP treatment as usual | Control group. However, the treatment recommended in the guide that they received matched that of the recommended pharmacological intervention | UC | ||
| Burton, 2012157 | MUS/somatoform | Primary care symptoms clinic | Structured set of consultations with a specially trained GP with specialist interest in MUS. GP explores acceptable explanation for symptoms in terms of biological mechanisms rather than psychological cause | GP-MM |
| Usual care | Usual primary care alone | UC | ||
| Chalder, 1997114 | Chronic fatigue | Self-help intervention | A booklet suggesting that fatigue may be associated both with doing too much and with doing too little, and the emphasis being on achieving a balance between the two. A section on how to improve sleep. Basic cognitive techniques such as identifying and challenging unhelpful thoughts | GSH |
| No treatment | Control group | UC | ||
| Cuesta-Vargas, 2012118 | Pain – single site (back) | DWR plus general practice | During DWR axial compression on the lumbar spine is minimised compared with exercising on a motor-driven treadmill or shallow-water running. DWR guarantees predominantly aerobic exercise while at the same time improving mobility, strength and MUS/somatoform endurance associated with reduced pain and physical disability | MM (sport + Education) |
| General practice | Booklet and verbal presentation | GSH | ||
| Escobar, 2007156 | MUS/somatoform | CBT-type intervention plus a consultation letter | Time-limited CBT-type intervention expressly designed for patients with somatisation problems. The intervention focuses on the reduction of physical distress and somatic preoccupation through training in relaxation techniques, activity regulation, facilitation of emotional awareness, cognitive restructuring and interpersonal communication | CBTHI |
| Usual clinical care from their PCP plus a consultation letter (control condition) | Control group | UC+ (letter) | ||
| Friedberg, 2013151 | Chronic fatigue | Fatigue self-management | Based on cognitive–behavioural treatment programme | CBTLI |
| Attention control | To control for therapist attention, homework assignments, and other non-specific effects | RSSE | ||
| Usual care | Control condition | UC | ||
| Gili 2014/Moreno, 2013144,148 | MUS/somatoform | Individual CBT | The CBT intervention is structured as follows:
|
CBTHI |
| Group CBT | Identical to intervention 1 in a group format | CBTHI | ||
| GP usual care improved with Smith’s norms | Control group | UC+ (letter) | ||
| Ho, 2012150 | Chronic fatigue | Qigong training | Education and exercise. Introduction to the basic theories of traditional Chinese medicine or educational session on the physiology of mind–body connections (30–40 minutes), followed by mindful meditation for relaxation and mind concentration and then gentle movement or body stretching in standing postures to facilitate a harmonious flow of qi along the energy channels (20 minutes). Followed by 1 hour’s qigong exercise | RSSE |
| Waiting list control | Control condition. Participants assigned to the control group were advised to undertake normal activities but were asked to refrain from joining any outside qigong training class | UC | ||
| Huibers, 2004/Leone, 2006153,155 | Chronic fatigue | CBT | The goals of the intervention were to diminish fatigue and other complaints, establish work resumption and other personal goals, and to establish self-perceived recovery | GP-CBT |
| GP usual care | Control group | UC | ||
| Kashner, 1995161 | MUS/somatoform disorder | Group therapy | Develop a source of peer support, share methods of coping with physical problems, enable patients to increase their ability to perceive and express emotion, and enjoy the experience of participating in the group | RSSE |
| Psychiatric consultation letter | Control group – standard consultation liaison | UC+ (letter) | ||
| Kennedy, 2005129 | IBS | CBT plus 270 mg of mebeverine × 3 per day | Based on Lang’s three systems model (which explains how cognitive, behavioural and emotional or physiological responses are linked and how changes in one system may cause a change in another). Therapy included education about the nature of IBS, behavioural techniques aimed at improving bowel habits, cognitive techniques to address unhelpful thoughts related to the syndrome, and techniques to reduce symptom focusing, manage stress and prevent relapse | MM (CBTLI + ME) |
| 270 mg of mebeverine × 3 per day | Control group | ME | ||
| Kobeissi, 2012110 | MUS/somatoform (MUVD) | Relaxation exercise and social support (RESST trial) | Psychosocial component (social support, problem-solving and venting) and relaxation exercises (including visual guided imagery exercises, stretching and progressive MUS/somatoform relaxation). Aims to reduce the burden of MUVD by focusing on common mental disorders | RSSE |
| Usual care, treat later | Control group. Offered treatment after intervention completed | UC | ||
| Kocken, 2008103 | MUS/somatoform | Counselling, information transfer and facilitation of communication between GP and patient by migrant health educator | Counselling with help from the migrant health educator. The intervention protocol comprised the following phases of patient support:
|
OP |
| Usual care (GP without help of migrant health educator) | Control group | UC | ||
| Kolk, 2004104 | MUS/somatoform | Psychological intervention | Depending on the therapist orientation a cognitive– behavioural, client-centred or eclectic therapy was provided, thereby reflecting usual treatment practice | OP |
| Usual care | Control group, usual care with no psychological therapy element | UC | ||
| Lansinger, 2007123 | Pain single site (neck) | Qigong | Qigong was performed according to medical qigong and was conducted in groups of 10–15 participants. Each qigong session started with information about the philosophy of medical qigong, followed by selected qigong exercises according to the Biyun method | RSSE |
| Exercise therapy | Exercise therapy was performed according to an individually adjusted training programme. The resistance was between 30% and 70% of a person’s maximal voluntary capacity, and for each exercise between one and three sets of 10 to 30 repetitions were performed. The amount of resistance and the number of repetitions started at a pain-free level and were gradually increased throughout the treatment period | SES | ||
| Larisch, 2004158 | MUS/somatoform | PPC and reattribution | Whether additional training in reattribution could improve the treatment results of somatising patients compared with PPC alone | GP – reattribution |
| Usual care (PPC) | Control group (PPC alone) | UC | ||
| LeFort, 1998128 | Pain multisite (mixed) | Community-based psychoeducation programme for the self-management of chronic pain | Designed to maximise discussion and group problem-solving, encourage individual participation and experimentation with various cognitive/behavioural self-management techniques, and facilitate mutual support | GSH |
| Waiting list | 3-month waiting list control group | UC | ||
| Loew, 2000122 | Pain single site (headache) | Elements of functional relaxation and usual treatment with analgesics | Concentration of body perception while moving the joints of the skeleton smoothly and simultaneously breathing out | RSSE |
| Alternative intervention technique and usual treatment with analgesics | Control | RSSE | ||
| Luciano, 2011139 | Pain multisite (fibromyalgia) | Psychoeducational programme plus usual care | Based on education about the illness and autogenic relaxation training. The educative part of the programme (five sessions) included information about typical symptoms, usual course, comorbid medical conditions, potential causes of the illness, the influence of psychosocial factors on pain, current pharmacological and non-pharmacological treatments, the benefits of regular exercise, and the typical barriers to behaviour change. The autogenic training (four sessions), especially recommended for immediate physical and mental relaxation, pain relief and stress reduction | MM (GSH + RSSE) |
| Usual care | Control group | UC | ||
| Luciano, 2014138 | Pain multisite (fibromyalgia) | Group ACT | Specific exercises and topics with the ACT practice and training including mindfulness practice | CBTHI |
| Recommended pharmaceutical therapy | 30–600 mg per day of pregabalin. Those with depression also received 60–120 mg per day of duloxetine | ME | ||
| Waiting list | Control group. No active treatment | UC | ||
| Macedo, 2012119 | Pain single site (back) | CBT-based GA | Based on the treatment programme reported by Lindström et al.379 A primary goal of the programme was to increase activity tolerance by performing individualised and submaximal exercises, in addition to ignoring illness behaviours and reinforcing wellness behaviours. Cognitive–behavioural principles were used to help the participants overcome the natural anxiety associated with pain and activities | GA |
| Motor control exercises | Based on the treatment programme reported by Hodges and Richardson.380 A primary goal was to enable the patient to regain control and co-ordination of the spine and pelvis using principles of motor learning such as segmentation and simplification. Based on assessment of the individual participant’s motor control impairments and treatment goals | GA | ||
| Margalit, 2008268 | MUS/somatoform | Short-term family therapy in ambulatory care | Advice and recommendations about lifestyle changes (e.g. tobacco use, body weight, relaxation techniques and exercise), basic psychotherapy (i.e. awareness of defence mechanisms and empathy), patient empowerment in self-monitoring of medical regimens (e.g. diabetes, blood pressure), involvement of the family and, if appropriate, further diagnostic tests, consultations and change in medication. The intervention tools consisted of various therapeutic methods (CBT, hypnosis, family/systems therapy, etc.) in a ‘tailor-made’ manner | OP |
| Usual care | NR | UC | ||
| Marques, 2015133 | Chronic fatigue | 4-STEPS to control your fatigue | A brief SR-based intervention to promote physical activity in chronic fatigue patients. Structured around the SR phases of goal pursuit (goal selection and setting, active goal pursuit and goal attainment, maintenance and disengagement) | GA |
| Enhanced standard care | Control group. In addition to standard medical care, patients assigned to the control condition received a flyer with information about the general health benefits of physical activity and current physical activity guidelines for adults and set a personal physical activity goal for the upcoming months | GSH | ||
| Martin, 200799 | MUS/somatoform | CBT | With only one treatment session and the recruitment of subjects from primary care practices, the treatment was tailored to the needs of primary care management of somatisation. Psychophysiological explanation of symptoms, relaxation, the importance of cognitions, activity instead of avoidance behaviours, treatment options and health-care utilisation | CBTLI |
| Waiting list | Control group | UC | ||
| McBeth, 2012125/Beasley, 2015126 | Pain multisite (widespread) | Telephone CBT | Therapists conducted a patient-centred assessment, developed a shared understanding and formulation of the current problem, and identified two or three patient-defined goals. Patients received a self-management CBT manual: Managing Chronic Widespread Pain | CBTHI |
| Exercise | Leisure facility- and gym-based exercise programme consistent with the American College of Sport Medicine’s guidelines for improving cardiorespiratory fitness | SES | ||
| Combined | Telephone CBT and exercise protocols as above | MM | ||
| Treatment as usual | Usual care from their family physician | UC | ||
| McLeod, 1997105 | MUS/somatoform | Ways to wellness (behavioural medicine intervention) | A general behavioural medicine intervention developed to address the needs of primary care patients with un diagnosable complaints related to mood | OP |
| Waiting list for 2 months, then received behavioural intervention treatment | Control group | UC | ||
| Morriss, 2007108 | MUS/somatoform | Reattribution | Feeling understood: elicit physical symptoms, psychosocial problems, mood state, beliefs held by patient about their problem, relevant physical examination and investigations. Broadening the agenda. Summarise physical and psychosocial findings. Negotiate these findings with patient. Making the link: give explanation relating physical symptom to psychosocial problems of lifestyle because of link in time or physiology. Negotiating further treatment: arrange follow-up or treatment of symptoms, psychosocial problems or mental disorder | GP – reattribution |
| Treatment as usual | Control group | UC | ||
| Moss-Morris, 2005152 | Chronic fatigue | GET | The rationale behind the graded exercise programme was explained using an adapted version of the cognitive–behavioural model of CFS. The model focused on the downwards spiral of activity reduction, physical deconditioning and symptoms | GA |
| Standard care | Control group. Standard medical care from their CFS specialist | UC | ||
| Moss-Morris, 2010130 | IBS | Cognitive–behavioural self-management programme plus treatment as usual | Focuses on changing cognitive and behavioural responses to IBS symptoms, reducing stress and anxiety levels, and altering unhelpful beliefs associated with perfectionism | CBTLI |
| Treatment as usual | Control group | UC | ||
| Peters, 2002106 | MUS/somatoform | Group aerobic exercise | Exercise presented as a way of keeping the body conditioned so better able to cope with the strains put on it by everyday life | SES |
| Stretching | Active control group consisting of group activity, contact with therapist and mastery of physical skills | RSSE | ||
| Pols, 2008145 | MUS/somatoform | Co-ordinated care | Patient self-management, using a patient-derived ‘problems and goals approach’ integrated with medical and community care. Patients’ services and medication use were monitored, with associated Medicare Benefits Scheme and Pharmaceutical Benefits Scheme information being fed back to GPs on a monthly basis on CD-ROM. Active listening, examination of the affected part being complained of, reassurance that no further investigations or referrals were required, and positive encouragement for living effectively despite ongoing symptoms | MM (self-management + medication + CBT) |
| Standard treatment | Control group | UC | ||
| Posse, 200496 | MUS/somatoform | Jungian psychotherapy and usual care | Non-verbal communication in the form of dreams, pictures, myths and fairy tales. These approaches can be the link to the verbally non-communicating alexithymic patient’s world and psyche | OP |
| Usual care and waiting list | Control | UC | ||
| Ridsdale, 2001112 | Chronic fatigue | CBT | Based on a model of understanding fatigue that makes a distinction between precipitating and perpetuating factors. Perpetuating factors were the focus of the intervention | CBTHI |
| Counselling | Active control group | OP | ||
| Ridsdale, 2004113 | Chronic fatigue | CBT | Based on a model that distinguishes between precipitating and perpetuating factors, with the perpetuating factors becoming the focus of the intervention | CBTLI |
| GET | GET is structured and supervised activity management that aims for a gradual but progressive increase in aerobic activities, usually walking | GA | ||
| Ridsdale, 2012115 | Chronic fatigue | GET | Supervised exercise, adapted to each patient’s current physical capacity, that is gradually increasing in duration according to a protocol designed for patients with CFS | GA |
| Counselling | Rogerian client-centred counselling. Non-directive format that encouraged the patient to talk through difficulties, and reflect on their experiences and thoughts so as to understand themselves better, to arrive at alternative understandings, to uncover the links between current distress and past experience, and to provide the conditions for growth and healing | OP | ||
| Usual care with CBT booklet | Control group received usual care treatment from their family doctors. To encourage practice and patient participation, this was coupled with a booklet describing causes of fatigue and providing self-help techniques based on CBT principles | GSH | ||
| Rief, 2006102 | MUS/somatoform | MUS management training package for GPs | ‘The Training Package: How to Manage Patients With Unexplained Physical Symptoms’. Information on the diagnosis of somatoform disorders, anxiety disorders and depression was provided. Topics included how to communicate with these patients, when to start and when to stop medical examinations, how to handle the organic health beliefs of the patients, their need for reassurance, and their avoidance of physical activity | GP-MM |
| No training package | Control group | UC | ||
| Robinson, 2006131 | IBS | Self-help guidebook plus group meetings | Focus group meetings with other IBS patients who described the information they required to help them cope with their symptoms better. The guidebook contained information about lifestyle, diet, and pharmacological and alternative therapies, and was based on up-to-date evidence and patients’ own anecdotal experiences | GSH |
| Self-guidebook plus one group meeting | The guidebook plus a one-off self-help group meeting (8–12 patients). Patients shared their experiences of living with their functional bowel symptoms and described approaches that helped them to manage their illness | MM (RSSE + GSH) | ||
| Usual care | Control group | UC | ||
| Rosendal, 2007146 | MUS/somatoform | The extended reattribution and management model | Intervention comprised a multifaceted educational programme on the assessment, treatment and management of MUPS (the TERM model) | GP – MUS management |
| Control FPs were only informed about the definitions of somatisation in writing and during meetings with the project leader | Control group | UC | ||
| Rothman, 2013127 | Pain multisite | Multimodal assessment and reattribution/rehabilitation | MM assessment followed principles for MM teamwork according to the Swedish Guidelines for rehabilitation complemented with the concepts of motivational interviewing and psychosomatic integrated assessment.381 Avoidance of arguing with the patient about the causes of pain and instead try to understand and encourage patient’s own reflections concerning factors that might influence their perceptions and experiences of pain. MM treatment reflected patients’ own preferences and could be multidisciplinary group therapy, individual multidisciplinary therapy or referral back for conventional treatment | GP – multidisciplinary assessment + motivational interview + psychotherapy |
| Conventional assessment and multidisciplinary pain management or unidisciplinary treatment from the GP or associated staff | Assessment followed conventional, actual applied medical principles for patients with chronic pain. GP determined how the continuing investigation should be performed. Treatment options were conventional multidisciplinary pain management or unidisciplinary treatment from the GP or associated staff. Addressed physical symptoms, function and/or psychosocial problems and could include pain management, treatment by a physiotherapist or psychologist, or medical treatment by the GP | UC+ (multidisciplinary assessment + choice of treatment) | ||
| Ryan, 2004109 | MUS/somatoform (mixed) | Biofeedback, progressive relaxation training, breathing retraining, problem-solving | Aimed at cultivated low arousal in general and thus used traditional modalities such as finger temperature training and forehead EMG. Heart rate variability feedback was also used as a core technique for all of the protocols | OP |
| No treatment | Control group | UC | ||
| Sañudo, 2010140 | Pain – multisite (fibromyalgia) | Aerobic exercise | Slow walks, easy movements of progressive intensity. Including continuous walking with arm movements and jogging; interval training | SES |
| Combined exercise | Combined aerobic exercise and resistance exercise, MUS/somatoform strengthening exercises, flexibility exercises | SES | ||
| Usual care | Control group, continued their normal daily activities during the intervention period, which did not include structured exercise | UC | ||
| Schade, 2011272 | MUS/somatoform | BFI | BFI was designed by the two authors as a new way of implementing family counselling with somatoform patients. BFI integrates the main concepts of brief systemic therapy into a broader, co-operation-based approach adapted to the Chilean social and cultural environment. The goal of BFI is that patients activate their personal and interpersonal resources to handle and improve their problems and function autonomously again | OP |
| Treatment as usual. Varying mixture of interventions, from direct advice giving to Rogerian active listening, history taking, and home visits | Control group | UC | ||
| Schaefert, 2013147 | MUS/somatoform | Collaborative group intervention | Psychodynamically based therapy embedding cognitive–behavioural elements into the framework. Aimed to empower interpersonal factors through group work and build strong therapeutic relationships between group members. Build understanding of interaction between biopsychosocial illness factors, physical and mental stabilisation, and strengthening self-functioning | MM (GP – MUS Management + OP) |
| GP training in diagnosis and management of MUS/somatoform | Control group, aimed at building a sustainable working alliance between patient and GP | GP – MUS management | ||
| Schilte, 2001159 | MUS/somatoform | Usual care + disclosure intervention | Use of emotional expression techniques. The disclosure doctor asked open questions about family life, health, work situation and childhood. Evocative interview style, using non-directive consultation techniques, such as open questions, reflection of emotions, inquiry on vague or unclear statements, and summarising. The disclosure doctor showed sincere interest in the patient’s story | GP – OP |
| Usual care | An extra control group to test for contamination of the effect of the trial as a whole. No intervention (data not presented) | N/A | ||
| Usual care | Control group | UC | ||
| Smith, 1995100 (Linked to Kashner, 1995161) | MUS/somatoform | Psychiatric consultation intervention | Psychiatric letter told the physician that the patient met criteria for somatisation syndrome. Recommended regularly scheduled brief appointments with the PCP for the patient, and to avoid as-needed appointments. Avoid hospitalisation, diagnostic procedures, surgery and laboratory evaluations unless clearly indicated. Physician encouraged not to tell the patient that the disorder was ‘all in your head’ but was instead encouraged to view the development of symptoms as an unconscious process | UC+ |
| Usual care | Control group | UC | ||
| Smith, 2006107 | MUS/somatoform | A behaviourally defined patient-centred intervention | A behaviourally defined, five-step patient-centred method to establish a positive patient–provider relationship and communicate effectively and a three-step patient-centred method to inform and motivate patients specifically about treatment. NPs used a collaborative stepped-care method. Treatment included antidepressants, reduction/elimination of controlled substance medications that were ineffective, exercise, relaxation training, physical therapy and comorbid organic disease management | MM |
| Usual care | Control group | UC | ||
| Smith, 2009142 | MUS/somatoform | Primary care management | CBT in the context of a behaviourally defined, evidence-based patient-centred method to maximise communication and the provider–patient relationship. See Smith et al.107 – delivered for this study by PCPs not NPs | MM (GP-CBT + medication) |
| Usual care | Control group | UC | ||
| Sumathipala, 2000116 | MUS/somatoform | CBT | The intervention aimed to ‘contain’ the patient at the level of detection in primary care, by offering structured regular visits to one professional carer, thereby hoping to reduce unstructured visits to different practitioners and co-ordinating the care. The treatment was based on the principles of CBT, using modifications of that described by Salkovoskis et al.382 and Sharpe et al.234 and Goldberg et al.’s45 reattribution technique | CBTLI |
| Standard clinical care | Control group | UC | ||
| Sumathipala, 2008117 | MUS/somatoform | CBT | Intervention aimed to contain the patient’s help-seeking behaviour by offering structured regular visits to one HP. Treatment based on principles of CBT and reattribution technique | MM (GP-MM + CBTLI) |
| Structured care | Active control. The same as intervention apart from no CBT component | GP-MM | ||
| Toft, 201097 | MUS/somatoform | TERM model | Treatment model developed for GPs and based on both the original reattribution model and principles from cognitive therapy, called TERM model. The model provides GPs with both theoretical knowledge about FSSs and the practical skills necessary for the assessment and treatment of functional somatic symptoms (MUS) patients | GP-MM |
| UC | Control group | UC | ||
| Tummers, 2012149 | Chronic fatigue | Minimal guided self-instruction intervention | Based on the protocol of CBT for CFS. Precipitating (triggering) and perpetuating (maintaining) factors are explained and individualised. Fatigue-related cognitions are challenged and patients encouraged to develop a sense of control over their symptoms. Patients learn to reduce the focus on fatigue and gradually increase their physical activity | CBTLI |
| Waiting list control | Control group | UC | ||
| van der Feltz-Cornelis, 2006160 | MUS/somatoform | Collaborative care model | Consultation with a psychiatrist plus MUS management based on techniques by Gask et al.383 – CBT techniques based on reattribution | MM (reattribution + collaborative care) |
| Training in MUS case management | MUS management based on techniques by Gask et al.383 – CBT techniques based on reattribution | GP reattribution | ||
| van der Roer, 2008120 | Pain – single site (back) | Intensive group training | Combines exercise therapy, back school and behavioural principles. Operant-conditioning behavioural principles based on baseline functional capacity | MM (sport + education + behavioural programme) |
| Guideline physiotherapy | Physiotherapy | SES | ||
| van Ravesteijn, 2013143 | MUS/somatoform | MBCT | Based on MBCT format for depression. Formal meditation exercises such as body scan, sitting meditation and mindful movement. Cultivate awareness of everyday activities. Cognitive techniques, such as psychoeducation, monitoring and scheduling of activities, identification of negative automatic thoughts and relapse prevention planning | OP |
| Enhanced usual care | Control group. Offered MBCT after treatment phase of trial complete | UC+ | ||
| Walti, 2015121 | Pain – single site (back) | MM treatment | MM treatment includes:
|
MM (education + sport + sensory discrimination) |
| Usual physiotherapy treatment | Control | SES | ||
| Wearden, 2010111 | Chronic fatigue | Pragmatic rehabilitation | A programme of graded return to activity is designed collaboratively by the patient and the therapist on the basis of a physiological dysregulation model of CFS/myalgic encephalomyelitis | GA |
| Supportive listening | A listening therapy based on non-directive counselling in which the therapist aims to provide an empathic and validating environment in which the patient can discuss his or her concerns and work towards resolution of whichever problems the patient wishes to prioritise | OP | ||
| GP care as usual | GPs were asked to manage their cases as they saw fit, but not to refer for systematic psychological therapies for CFS/myalgic encephalomyelitis during the 18-week treatment period | UC | ||
| Whitehead, 2002154 | Chronic fatigue | Management package for GPs | Management package to train GPs in the diagnosis and management of CFS. To provide GPs with the skills necessary to make a diagnosis of CFS and to manage patients with CFS in primary care | GP-MM |
| Usual care | GPs encouraged to treat patients as usual, which included referrals to secondary care | UC | ||
| Zonneveld, 2012141 | MUS/somatoform | CBT | CBT based on the consequences model. Psychological and social factors that are commonly labelled as causes, are labelled as consequences of UPS. The objective of the consequences model is to alleviate symptoms. The model was tailored to primary care patients | CBTHI |
| Waiting list | Control group | UC |
| First author and year of publication | Condition | Diagnostic criteria | Diagnosis by |
|---|---|---|---|
| Aiarzaguena, 2007136 | MUS/somatoform | Abridged somatisation disorder (Escobar et al.98) – lifetime six or more medically unexplained symptoms for females, four or more for males, including one in the past year | GP |
| Burton, 2012157 | MUS/somatoform | A score of ≥ 10 on the PHQ-14 | GPs |
| Escobar, 2007156 | MUS/somatoform | Abridged somatisation disorder (Escobar et al.98) – lifetime six or more MUS for females, four or more for males, including one in the past year | PCP and psychologists |
| Gili, 2014/Moreno, 2013144,148 | MUS/somatoform | Abridged somatisation disorder (Escobar et al.98) | GPs and researchers |
| Kashner, 1995161 | MUS/somatoform | Somatisation disorder meeting DSM-III-R criteria | Research psychiatrist |
| Kocken, 2008103 | MUS/somatoform | Symptoms rated by GPs as psychosomatic in origin | GPs |
| Kolk, 2004104 | MUS/somatoform | GP confirmed medically unexplained nature of patient symptoms | GP and researchers |
| Larisch, 2004158 | MUS/somatoform | Four somatoform symptoms for men or six for women, GHQ cut-off point of 2 +. Screen positive on SOMS-2 and GHQ-12 | GPs and researchers |
| Margalit, 2008268 | MUS/somatoform | Highest costing patients with no apparent reason or diagnosis for high annual cost of care | Community clinic data |
| Martin, 200799 | MUS/somatoform | Two or more MUS within past 6 months | GP and researchers |
| McCleod, 1997105 | MUS/somatoform | PCPs had recognised that emotional status may have been related to their patients’ symptoms | PCPs |
| Morriss, 2007108 | MUS/somatoform | > 3 months’ physical symptoms not explained by physical pathology | GP and independent GP |
| Peters, 2002106 | MUS/somatoform | Duration of unexplained complaints of at least 12 months and unexplained after specialist investigation | GP and researchers |
| Pols, 2008145 | MUS/somatoform | Diagnosis of somatisation including unexplained physical symptoms as part of anxiety, chronic benign pain or somatoform disorder. Checked by CIDI interview against ICD-10 criteria | GP and researchers |
| Rief, 2006102 | MUS/somatoform | Multiple unexplained symptoms | GP and researchers |
| Rosendal, 2007146 | MUS/somatoform | Positive score on SCL-SOM or Whiteley Index-7. Cut-off points of 3/4 for SCL-SOM and of 1/2 for Whiteley Index-7 | Family physicians |
| Schade, 2011272 | MUS/somatoform | Diagnosis of somatoform disorder, diagnostic criteria no described | NR |
| Schaefert, 2013147 | MUS/somatoform | At least mild somatic severity on PHQ-15, represented by a cut-off point of 5; or relevant health anxiety on Whitely Index-7 | GP and consultation with psychosomatic specialist if necessary |
| Schilte, 2001159 | MUS/somatoform | 15 contacts or more with the doctor in the past 3 years, plus five or more somatisation symptoms (Somatisation Questionnaire, based on DSM-III-R) | NR |
| Smith, 1995100 | MUS/somatoform | Lifetime history of 6–12 unexplained medical symptoms. Meeting DSM-III-R diagnostic criteria for somatisation disorder | Research psychiatrist |
| Smith, 2006107 | MUS/somatoform | Having no documented organic disease to explain symptoms of at least 6 months’ duration | Research team |
| Smith, 2009142 | MUS/somatoform | At least 8 yearly visits for 2 previous years. ICD-9 diagnosis codes suggesting MUS used to identify patients | Research team |
| Sumathipala, 2000116 | MUS/somatoform | Five or more symptoms meeting the definition of unexplained | PCP and research team |
| Sumathipala, 2008117 | MUS/somatoform | Five or more symptoms meeting the definition of unexplained during past 6 months | Trial physician |
| Toft, 201097 | MUS/somatoform | Functional somatic/MUS. Scoring ≥ 2 on dichotomised Whiteley Index-7, SCL-8 or CAGE,384 or ≥ 4 on dichotomised SCL-SOM identified by SCAN interview. Three groups:
|
GP and psychiatrist |
| van der Feltz-Cornelis, 2006160 | MUS/somatoform | Serious persistent MUS: Symptoms remain unexplained after specialist diagnostic examination and continuing patient requests for further diagnostic testing. Meeting ICD-10 somatoform disorder criteria and Whiteley Index threshold | GP |
| van Ravesteijn, 2013143 | MUS/somatoform | Physical symptoms for at least 6 months not fully explained by a physical disease or substance abuse. Symptoms causing functional impairment. Confirmed with MINI interview and somatoform disorders section on DSM-IV structured clinical interview | GP and trainee psychiatrist |
| Zonneveld, 2012141 | MUS/somatoform | Undifferentiated somatoform disorder or chronic pain disorder according to DSM-IV | GP and researchers |
| First author and year of publication | Condition | Diagnostic criteria | Diagnosis by |
|---|---|---|---|
| Kobeissi, 2012110 | MUVD | Symptom-reporting questionnaire, laboratory tests, physical examination | Gynaecologists |
| First author and year of publication | Condition | Diagnostic criteria | Diagnosis by |
|---|---|---|---|
| Ryan, 2004109 | Mixed functional disorders | Any functional disorder: IBS, fibromyalgia, CFS, myofascial pain, anxiety with somatic features, or non-cardiac chest pain. Confirmed no underlying organic cause of pain | Physician and research team |
| First author and year of publication | Condition | Diagnostic/inclusion criteria | Diagnosis by |
|---|---|---|---|
| Chalder, 1997114 | Chronic fatigue | Chronic fatigue, scoring ≥ 4 on the Chalder Fatigue Scale.385 Not CFS | GP and research nurse |
| Friedberg, 2013151 | Chronic fatigue | US CDC criteria for CFS6 | PCP and researcher |
| Ho, 2012150 | Chronic fatigue | US CDC criteria for CFS6 | NR |
| Huibers, 2004/Leone, 2006153,155 | Chronic fatigue | A score of 35 or more on the fatigue subscale of the Dutch Checklist Individual Strength | Researcher |
| Marques, 2015133 | Chronic fatigue | CDC criteria for idiopathic chronic fatigue6 | Researcher |
| Moss-Morris, 2005152 | Chronic fatigue | US CDC criteria for CFS6 | Specialist GP |
| Ridsdale, 2001112 | Chronic fatigue | US CDC criteria for CFS6 or Chalder Fatigue Scale score of ≥ 4385 | Researcher |
| Ridsdale, 2004113 | Chronic fatigue | > 3 months unexplained fatigue. Met either US CDC criteria for CFS6 or Chalder Fatigue Scale score of ≥ 4385 | Researcher |
| Ridsdale, 2012115 | Chronic fatigue | > 3 months’ fatigue. Excluded if scored < 4 on the Chalder Fatigue Scale385 | GP |
| Tummers, 2012149 | Chronic fatigue | US CDC criteria for CFS6 | GP and research team and psychiatric nurse |
| Wearden, 2010111 | Chronic fatigue | Oxford criteria for CFS/ME (Chalder Fatigue Scale) | GP and research team |
| Whitehead, 2002154 | Chronic fatigue | US CDC criteria for CFS6 | GP |
| First author and year of publication | Condition | Diagnostic criteria | Diagnosis by |
|---|---|---|---|
| Cuesta-Vargas, 2012118 | Back pain | > 3 months’ non-specific chronic low back pain without radiation to lower limbs | GP |
| Lansinger, 2007123 | Neck pain | > 3 months’ non-specific chronic neck pain | Physiotherapist |
| Loew, 2000122 | Headache | Subgroup 2 but not 3–13 of IHS criteria. Pain > 1 year. Exclusion of organic disease | NR |
| Macedo, 2012119 | Back pain | Chronic non-specific low back pain > 3 months’ duration, with or without leg pain | NR |
| van der Roer, 2008120 | Back pain | Non-specific chronic low back pain | Physiotherapist |
| Walti, 2015121 | Back pain | Non-specific chronic low back pain | NR |
| First author and year of publication | Condition | Diagnostic criteria | Diagnosis by |
|---|---|---|---|
| LeFort, 1998128 | Mixed chronic pain | Chronic idiopathic pain lasting longer than expected healing time (> 3–6 months)386 | HPs and researchers |
| Rothman, 2013127 | Mixed chronic pain | Pain classified into chronic generalised or chronic regional pain according to ACR. Organic explanations for pain ruled out | GP |
| McBeth, 2012125 | Mixed chronic pain | Chronic widespread pain, classified according to the definition used in the ACR criteria for fibromyalgia | Research nurse |
| First author and year of publication | Condition | Diagnostic criteria | Diagnosis by |
|---|---|---|---|
| Alda, 2011137 | Fibromyalgia | 1990 ACR diagnostic criteria for fibromyalgia124 | Primary care doctors |
| Luciano, 2011139 | Fibromyalgia | 1990 ACR diagnostic criteria for fibromyalgia124 | GP and rheumatologist |
| Luciano, 2014138 | Fibromyalgia | 1990 ACR diagnostic criteria for fibromyalgia124 | Rheumatologists, GPs and researcher |
| Sañudo, 2010140 | Fibromyalgia | 1990 ACR diagnostic criteria for fibromyalgia124 | NR |
| First author and year of publication | Condition | Diagnostic criteria/inclusion criteria | Diagnosis by |
|---|---|---|---|
| Kennedy, 2005129 | IBS | Rome I diagnostic criteria387 | GP and research nurse |
| Moss-Morris, 2010130 | IBS | Rome I or Rome II diagnostic criteria387 | GP |
| Robinson, 2006131 | IBS | Functional gastrointestinal symptoms diagnosed as IBS, but not necessarily fulfilling Rome II criteria387 | GP or specialist |
| First author and year of publication | Condition | Primary outcomes | Secondary outcomes |
|---|---|---|---|
| Aiarzaguena, 2007136 | MUS/somatoform | HRQoL – Medical Outcomes Study – 36-item (SF-36)388 |
Symptoms – number of active explained and unexplained symptoms in the past year reported at CIDI interview389 Mental disorders – primary care evaluation of mental disorders390 Stressful life events391 Negative affect – negative affectivity scale392 |
| Alda, 2011137 | Chronic pain – multisite (fibromyalgia) | Pain catastrophisation – Pain Catastrophisation Scale (Spanish version393) |
Depression – HAM-D394 Anxiety – HAM-A395 Pain – VAS396 Global function – Fibromyalgia Impact Scale397 Quality of life – EQ-5D (Spanish version398) |
| Burton, 2012157 | MUS/somatoform | Acceptability – Client Satisfaction Questionnaire; Physical Symptoms – PHQ-14;9 health status (Medical Outcomes Short Form (SF-12); depression – PHQ-9;399 anxiety – General Anxiety Disorder 7 Questionnaire;400 and patient global impression of change | |
| Chalder, 1997114 | Chronic fatigue |
Psychiatric morbidity – Revised Clinical Interview Scale401 Fatigue – The Fatigue Scale (11-item)385 |
HRQoL – GHQ 12402 Physical functioning –Medical Outcome Study physical functioning subscale403 |
| Cuesta-Vargas, 2012118 | Chronic pain – single site (back pain) | Pain – 100-mm VAS;404 Disability – RMDQ (Spanish version;405 General Health, physical and mental – SF-12 (Spanish version, adapted from SF-36 for people with back pain406) | |
| Escobar, 2007156 | MUS/somatoform disorder | Global rating of severity of symptoms – Clinical Global Impressions Scale (study specific) |
Physical functioning – Medical Outcomes Study (MOS-10)407 Anxiety – HAM-A395 Depression – HAM-D394 Symptoms – Severity of Current Symptoms 0–100 VAS Severity of somatic complaints – PHQ-15399 |
| Friedberg, 2013151 | Chronic fatigue | Fatigue – Fatigue Severity Scale |
Physical function – SF-36 physical function subscale Depression – BDI – second edition408 Anxiety – BAI Activities, symptoms and stress ratings – web diary |
| Gili, 2014/Moreno, 2013144,148 | MUS/somatoform disorder | Somatic symptoms – SOMS;10 Severity of somatic symptoms – VAS;409 Psychiatric morbidity – SPPI;410 Anxiety – HAM-A;395 and depression – Hamilton Depression Rating Scale;394 HRQoL – SF-36411 | |
| Ho, 2012150 | Chronic fatigue | Fatigue – Chalder’s Fatigue Scale (14-item385); physical and mental functioning – SF-12 (Chinese version412) and telomerase activity – TeloTAGG telomerase PCR ELISA (F. Hoffman-La Roche Ltd, Basel, Switzerland) | |
| Huibers, 2004/Leone, 2006153,155 | Chronic fatigue |
Fatigue – fatigue subscale of the CIS413 Absenteeism – self-reported work-resumption/number of sick days Clinical recovery – CIS score of ≤ 34 and return to work |
Global perceived effect – 7-point scale414 Physical functioning – SF-36411 Psychological distress – Symptom Checklist 90415 |
| Kashner, 1995161 | MUS/somatoform disorder | Health status – RAND;416 and health-care utilisation – medical and billing records | |
| Kennedy, 2005129 | IBS | Symptom severity – IBS Severity Score417 |
Anxiety and Depression – Hospital Anxiety and Depression Scale418 Impact – Work and Social Adjustment Scale162 |
| Kobeissi, 2012110 | MUVD | MUVD – one item |
Common Mental Disorder – Hopkins Symptom Checklist 25419 Somatisation – Scale for Assessment of Somatic Symptoms |
| Kocken, 2008103 | MUS/somatoform disorder | Perceived stressful situations – 14 items adapted from biographical problem inventory list (BIOPRO);420 social support – Social Support List;421 general health – SF-36 (Dutch version422); Perceived pain – SF-36 (Dutch version422); and mental health – SCL-90 psychological discomfort415 | |
| Kolk, 2004104 | MUS/somatoform disorder | MUPS – Symptom Checklist 90 Somatisation Scale psychological symptoms – Symptom Checklist 90 Anxiety and Depression;423 registered unexplained symptoms; GP consultations; tendency to selective attention to the body – The Somatic Awareness Questionnaire;424 tendency to somatic and psychological attribution – Symptom Interpretation Questionnaire;425 and negative affectivity – Positive and Negative Affectivity Scale426 | |
| Lansinger, 2007123 | Chronic pain – single site (neck pain) | Pain intensity – VAS; pain over 1 week – pain diary; disability – Neck Disability Index;427 grip strength – Grippit; and cervical range of motion – Myrin goniometer | |
| Larisch, 2004158 | MUS/somatoform disorder | MUPS – SOMS-7;10 general health – GHQ;428 HRQoL – 12-item short form of the SF-36;388 anxiety and depression – Hospital Anxiety and Depression Scale;418 doctor visits; and medication use | |
| LeFort, 1998128 | Chronic pain | Self-help – Inventory of Adult Role Behaviours;429 life satisfaction – Satisfaction with Life Domains Scale;430 HRQoL – SF-36;388 pain quality – The Pain Rating Index of the Short-Form McGill Pain Questionnaire;431 depression – BDI;432 perceived level of disability – disability subscale of the Survey of Pain Attitudes;433 severity of pain – VAS; dependency – single item 100-mm VAS; Uncertainty – Mishel’s Uncertainty in Illness Scale;434 enabling skill – Self-Efficacy Scale;435 and resourcefulness – 100-mm VAS version of Self Control Schedule436 | |
| Loew, 2000122 | Chronic pain – single site | Pain – German Headache Diary (German version of ASTRA headache diary437) | |
| Luciano, 2011139 | Chronic pain – multisite (fibromyalgia) | Functional status – FIQ (Spanish version438); and anxiety – the State–Trait Anxiety Inventory (Spanish version439) | |
| Luciano, 2014138 | Chronic pain – multisite (fibromyalgia) | Impact – FIQ397 |
Pain catastrophising – Pain Catastrophisation Scale393 Anxiety – Hospital Anxiety and Depression Scale418 Depression – Hospital Anxiety and Depression Scale418 Chronic pain acceptance – Chronic Pain Acceptance Questionnaire440 Pain – 100-mm VAS HRQoL – EQ-5D398 |
| Macedo, 2012119 | Chronic pain – single site (back pain) |
Pain intensity over past week – 0–10 NRS441 Function – 0–10 Patient-Specific Functional Scale442 |
Global impression of change – Global Perceived Effect Scale442 Disability – RMDQ443 Quality of life – SF-36444 Recovery defined as a pain-free period that lasted 1 month Credibility of treatment445 Therapist ratings446 Adherence to home exercises |
| Margalit, 2008268 | MUS/somatoform disorder | Health-care utilisation with associated costs – medical records | |
| Marques, 2015133 | Chronic fatigue | Fatigue severity – Checklist of Individual Strength (Portuguese version447); fatigue impact – Brief Pain Inventory;448 physical activity – Short Questionnaire to Assess Health-Enhancing Physical Activity449 plus pedometer plus goal progress VAS; HRQoL – SF-12;450 somatic distress – Patient Health Questionnaire-15;9 and psychological distress – Brief Symptom Inventory Depression and Anxiety subscales451 | |
| Martin, 200799 | MUS/somatoform disorder |
Health-care utilisation – structured interview, patient-reported GP and specialist visits Somatoform symptoms – Brief Symptom Inventory454 and SOMS-7455 |
Hypochondriacal anxiety and concern – Whiteley Index452 Depression – BDI453 Health-related locus of control – Self-Report Questionnaire456 |
| McBeth, 2012125/Beasley, 2015126 | Chronic pain | Clinical Global Impression Score – change since entering trial |
Fatigue Scale385 Vanderbildt Pain Management Inventory457 GHQ The Sleep Scale458 Tampa Scale for Kinesiophobia459 SF-36411 |
| McLeod, 1997105 | MUS/somatoform disorder | Somatisation – Symptom Checklist-90 Revised;423 depression – Symptom Checklist-90 Revised;423 and anxiety – Symptom Checklist-90 Revised423 | |
| Morriss, 2007108 | MUS/somatoform disorder | Overall proportion of GP consultation that was consistent with the Goldberg Reattribution Model – audio-taped transcripts of GP–patient consultations |
Satisfaction with GP communication – Patient Satisfaction Questionnaire460 Patient’s symptom beliefs – Revised Illness Perception Questionnaire461 Anxiety – Hospital Anxiety Scale418 % caseness Depression – Hospital Depression Scale418 % caseness Health anxiety – Whiteley Index462 Quality of Life – EQ-5D463 Prescriptions, investigations, health contacts – patient records |
| Moss-Morris, 2005152 | Chronic fatigue | Global rating of improvement – single item464 |
CFS-related impairment – The Fatigue Scale (14-item385) Physical functioning – physical functioning subscale of SF-36 Physiological assessments Illness beliefs – The Illness Perception Questionnaire-Revised461 Symptom focusing – Illness Management Questionnaire – symptoms subscale465 |
| Moss-Morris, 2010130 | IBS |
Subject’s Global Assessment of Relief466 Irritable Bowel Severity Scoring System417 |
Work and Social Adjustment Scale467 Hospital Anxiety and Depression Scale418 Acceptability of treatment – three questions Engagement and adherence – quantity of homework completed 0–10 |
| Peters, 2002106 | MUS/somatoform disorder | Clinical data: symptoms (number and type), number of doctor consultations, number of referrals to secondary care, number of prescriptions – medical records/GP report; emotional state – Hospital Anxiety and Depression scale;418 somatisation – Hopkins Symptom Checklist468 and Modified Somatic Perception Questionnaire;469 and perceived disability – Health Outcomes Questionnaire (SF-36)470 | |
| Pols, 2008145 | MUS/somatoform disorder | Depression – BDI, second edition;408 anxiety – State–Trait Anxiety Inventory;439 hostility – Hostility and Direction of Hostility Questionnaire;471 and HRQoL – SF-36 | |
| Posse, 200496 | MUS/somatoform disorder | Somatisation – Patient Pain Drawing Test472 and Symptom List;473 alexithymia – Schalling Sifneos Personality scale474 and personality traits – Karolinska Scale of Personality475 | |
| Ridsdale, 2001112 | Chronic fatigue | Fatigue – The Fatigue Questionnaire (11-item385); Anxiety and Depression – Hospital Anxiety and Depression Rating;418 attribution – attributions scale;476 social adjustment – MOS-SF;411 general health – MOS-SFGHS;411 and satisfaction with therapy – 10-item questionnaires | |
| Ridsdale, 2004113 | Chronic fatigue | Fatigue – The Fatigue Scale385 |
Anxiety and Depression – Hospital Anxiety and Depression Scale418 Functional impairment – WASA (cited as Ware et al. 411) Illness attributions – attributions scale476 Step test |
| Ridsdale, 2012115 | Chronic fatigue | Fatigue – The Fatigue Questionnaire385 |
Anxiety and Depression – Hospital Anxiety and Depression Scale418 Functional impairment – Work and Social Adjustment Scale (cited as Ware et al. 411) Patient satisfaction with treatment – seven-category questionnaire HRQoL – EQ-5D477 |
| Rief, 2006102 | MUS/somatoform | Health-care use, past 6 months – structured interview and GP records |
Symptoms – Screening for Somatoform Disorders (SOMS)10 Health anxiety – Whiteley Index462 Depression – BDI453 Anxiety – BAI478 |
| Robinson, 2006131 | IBS |
Number of primary care consultations Clinical Global Impression Score – Severity and Improvement |
Hospital consultation rates Quality of life – IBS QOL480 |
| Rosendal, 2007146 | MUS/somatoform disorder | Quality of life – Medical Outcomes Study 36-Item Short-Form;482 disability days – one item from WHO’s Disability Assessment Schedule (WHO-DAS); illness worry and conviction – Whiteley Index-7;483 somatisation – Hopkins Symptom Checklist (SCL-SOM);415 mental Illness – Hopkins Symptom Checklist (SCL-8)415 | |
| Rothman, 2013127 | Chronic pain | Pain intensity during past week (VAS); Depression – Zung Self-Rating Depression scale;484 Stress – The Stress and Crisis Inventory-93;485 quality of life – SF-36, Swedish version;393 disability – ODI;486 work ability; and patient satisfaction (study-specific questionnaire) | |
| Ryan, 2004109 | MUS/somatoform disorder (mixed) | Specific referral symptoms – symptom log 1–10 scale; overall functioning – quality of well-being measure;487 costs – medical records | |
| Sañudo, 2010140 | Chronic pain – multisite (fibromyalgia) | Impact – Fibromyalgia Impact Scale (Spanish version438) |
HRQoL – SF-36 (Spanish version488) Depression – BDI489 Aerobic capacity – 6-minute walk test490 Hand grip strength – hand dynometer491 Range of motion – manual goniometer |
| Schade, 2011272 | MUS/somatoform disorder | Health-care visits – number of visits to the primary health-care team in relation to psychosomatic complaints; medical tests – number of medical analyses taken; and medications – number of prescribed medications taken | |
| Schaefert, 2013147 | MUS/somatoform disorder | Quality of life – SF-36492 |
Somatic symptom severity – PHQ-15 somatic symptom severity scale493 Depressive symptoms – PHQ-9 depressive symptom severity scale493 Generalised anxiety – PHQ anxiety493 Panic – 5-item PHQ panic module494 Health anxiety – 7-item Whitely Index483 |
| Schilte, 2001159 | MUS/somatoform disorder | Use of medical services – number of GP and health-care professional visits; subjective health – combined score of seven items of 0–100; sick leave – weeks off in previous 6 months; severity of symptoms – Symptom checklist-90 somatisation, depression, anxiety and agoraphobia subscales;423 quality of life (patient rated) – 0–100 VAS; and somatisation (doctor rated) – five-point Likert Scale495 | |
| Smith, 1995100 | MUS/somatoform disorder |
Health status – RAND Health Status Measures416 Days in bed during last month |
Health-care utilisation – charges from medical and billing records |
| Smith, 2006107 | MUS/somatoform disorder | HRQoL – SF-36;481 depression – Center for Epidemiological Studies Depression Scale (CES-D);496 anxiety – Spielberger State Anxiety Scale (SSAS);439 and antidepressant and controlled substance use – medical records | |
| Smith, 2009142 | MUS/somatoform disorder | HRQoL – SF-36;481 depression – Center for Epidemiological Studies Depression Scale (CES-D);496 anxiety – Spielberger State Anxiety Scale (SSAS);439 physical symptom evaluation – Patient Health Questionnaire-15;9 and satisfaction with the patient–provider relationship (SQ-1)497 | |
| Sumathipala, 2000116 | MUS/somatoform disorder | Level of distress/psychiatric morbidity – GHQ-30498 (Sri Lankan version499); symptom score – Bradford Somatic Inventory;11 and satisfaction – VAS 0–5 (patient and carer reports); health-care visits – diary | |
| Sumathipala, 2008117 | MUS/somatoform disorder | Psychological morbidity – GHQ-30498 |
Number of symptoms, patient-reported – Bradford Somatic Inventory11 Health-care visits (patient initiated) |
| Toft, 201097 | MUS/somatoform disorder | Physical functioning – SF-36 physical functioning subscale |
Mental and social functioning, perceived health, vitality and pain – SF-36 subscales Somatic symptoms – SCL-SOM Health anxiety – Whitely-7 Index |
| Tummers, 2012149 | Chronic fatigue |
Fatigue severity – CIS fatigue severity subscale413 Disabilities – SF-36 physical functioning and social functioning subscales403 |
Psychological distress – Brief Symptom Inventory (BSI)500 |
| van der Feltz-Cornelis, 2006160 | MUS/somatoform |
Physical well-being – severity and number of MUS501 Psychological symptoms – Symptom Checklist-90-Revised503 |
General functioning – sickness impact profile, household, work and recreational activities and social interaction subscales502 Health-care use – scale ‘Visits to Doctors and Other Health Care Professionals’504 |
| van der Roer, 2008120 | Chronic pain – single site (back pain) |
Functional status – RMDQ443 Pain Intensity – 11-point NRS Global Perceived Effect – 6-point scale Work absenteeism – HLQ508 |
Fear of movement/reinjury – 17-item Tampa Scale505 Pain coping strategies – Pain Coping Inventory506 Self-efficacy beliefs – Pain Self-Efficacy Questionnaire507 |
| van Ravesteijn, 2013143 | MUS/somatoform disorder | General Health Status – EQ-5D VAS463 |
Mental and physical functioning – Medical Outcomes Study 36-item Short-Form (SF-36)519 Physical and mental symptoms – Patient Health Questionnaire (PHQ) scale for somatisation399 Depression – PHQ-9399 Health anxiety – Whiteley Index462 Mindfulness skills – Five-Facet Mindfulness Questionnaire509 |
| Walti, 2015121 | Chronic pain – single site (back pain) | Mean pain intensity over the past 7 days – NRS 0–10 |
Disability – RMDQ443 Patient-specific disability – PSFS510 Fear avoidance beliefs – Fear Avoidance Beliefs Questionnaire511 Catastrophising thoughts – Pain Catastrophising Scale393 Movement control impairment – six movement control tests Sensory acuity of the lower back – TPD threshold512 Sick leave during past 7 days Analgesic intake past 7 days |
| Wearden, 2010111 | Chronic fatigue |
Physical functioning – SF-36 physical functioning subscale411 Fatigue – Fatigue Scale (11-item)385 |
Anxiety and depression – Hospital Anxiety and Depression Scales418 Sleep problems – Sleep Scale458 Costs |
| Whitehead, 2002154 | Chronic fatigue | Health status – London Handicap Scale;513 fatigue – The Fatigue Scale (11-item);385 and, anxiety and depression – Hospital Anxiety and Depression Scale418 | |
| Zonneveld, 2012141 | MUS/somatoform disorder | Functional health and well-being, component summaries – Medical Outcomes Short Form General Health Survey (SF-36)388 |
Functional health and well-being, individual scales – Medical Outcomes Short Form General Health Survey (SF-36)388 Psychological problems and psychopathological symptoms – Revised 90-Item Symptom Checklist (SCL-90)514 |
| First author and year of publication | Condition | Pain | Fatigue | Bowel symptoms | Somatisation | Generic physical symptoms | Emotional distress | Anxiety | Depression | Physical functioning | Impact |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Aiarzaguena, 2007136 | MUS/somatoform | SF-36 BP | ✗ | ✗ | ✗ | ✗ | SF-36 MH | ✗ | ✗ | SF-36 PF | ✗ |
| Alda, 2011137 | Pain-MS (fibromyalgia) | VAS | ✗ | ✗ | ✗ | ✗ | ✗ | HARS | HAM-D | ✗ | FIQ total |
| Burton, 2012157 | MUS/somatoform | ✗ | ✗ | ✗ | PHQ-14 | ✗ | SF-12-MCS | GAD-7 | PHQ-9 | SF-12-PCS | ✗ |
| Chalder, 1997114 | Chronic fatigue | ✗ | CFQ | ✗ | ✗ | ✗ | GHQ-12 | ✗ | ✗ | SF-36 PF | ✗ |
| Cuesta-Vargas, 2012118 | Pain-SS (back) | VAS | ✗ | ✗ | ✗ | ✗ | SF-12 – MH | ✗ | ✗ | SF-12 PF | 24-RMDQ |
| Escobar, 2007156 | MUS/somatoform | ✗ | ✗ | ✗ | PHQ-15 | Severity – VAS | ✗ | HAM-A | HAM-D | MOS-10 PF | ✗ |
| Friedberg, 2013151 | Chronic fatigue | ✗ | FSS | ✗ | ✗ | ✗ | ✗ | BAI | BDI | SF-36 PF | ✗ |
| Gili, 2014/Moreno, 2013144,148 | MUS/somatoform | SF-36 BP | ✗ | ✗ | SOMS | ✗ | SF-36 – MH | HAM-A | HAM-D | SF-36 PF | ✗ |
| Ho, 2012150 | Chronic fatigue | ✗ | CFQ | ✗ | ✗ | ✗ | SF-12 – MH | ✗ | ✗ | SF-12 PF | ✗ |
| Huibers, 2004/Leone, 2006153,155 | Chronic fatigue | ✗ | CIS | ✗ | ✗ | ✗ | SCL-90 | ✗ | ✗ | SF-36 PF | ✗ |
| Kashner, 1995161 | MUS/somatoform | ✗ | ✗ | ✗ | ✗ | ✗ | RAND – MH | ✗ | ✗ | RAND – PF | ✗ |
| Kennedy, 2005129 | IBS | ✗ | ✗ | IBS-SSS | ✗ | ✗ | HADS total | HADS-Ab | HADS-Db | ✗ | WASA – FI |
| Kobeissi, 2012110 | MUVD | ✗ | ✗ | ✗ | SASS | ✗ | ✗ | HSCL-25-A | HSCL-25-D | ✗ | ✗ |
| Kocken, 2008103 | MUS/somatoform | SF-36 1 item | ✗ | ✗ | ✗ | ✗ | SCL-90 | ✗ | ✗ | ✗ | Restriction of daily activities |
| Kolk, 2004104 | MUS/somatoform | ✗ | ✗ | ✗ | SCL-90 | Unexplained symptoms | ✗ | SCL-90-A | SCL-90-D | ✗ | ✗ |
| Lansinger, 2007123 | Pain-SS (neck) | VAS | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | NDI |
| Larisch, 2004158 | MUS/somatoform | ✗ | ✗ | ✗ | SOMS-7 | ✗ | SF-12 MH | HADS-A | HADS-D | SF-12 PF | ✗ |
| LeFort, 1998128 | Pain-MS | Pain severity – VAS | ✗ | ✗ | ✗ | ✗ | SF-36 MH | ✗ | BDI | SF-36 PF | SOPA-D |
| Loew, 2000122 | Pain-SS | Days | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ |
| Luciano, 2011139 | Pain-MS (fibromyalgia) | FIQ P | FIQ GF | ✗ | ✗ | ✗ | ✗ | FIQ-A | FIQ-D | FIQ PF | FIQ total |
| Luciano, 2014138 | Pain-MS (fibromyalgia) | VAS | ✗ | ✗ | ✗ | ✗ | ✗ | HADS-A | HADS-D | ✗ | FIQ total |
| Macedo, 2012119 | Pain-SS (back) | NRS | ✗ | ✗ | ✗ | ✗ | SF-36 MH | ✗ | ✗ | SF-36 PF | RMDQ-24 |
| Margalit, 2008268a | MUS/somatoform | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ |
| Marques, 2015133 | Chronic fatigue | ✗ | CIS20-P | ✗ | PHQ-15 | ✗ | SF-12 MH | BSI-A | BSI-D | SF-12 PF | ✗ |
| Martin, 200799 | MUS/somatoform | ✗ | ✗ | ✗ | SOMS-7 | ✗ | ✗ | ✗ | BDI | ✗ | ✗ |
| McBeth, 2012125/Beasley, 2015126 | Pain-MS | SF-36 BP | CFQ | ✗ | ✗ | ✗ | SF-36 MH | ✗ | ✗ | SF-36 PF | ✗ |
| McLeod, 1997105 | MUS/somatoform | ✗ | ✗ | ✗ | SCL-90-R | ✗ | ✗ | SCL-90-R A | SCL-90-R D | ✗ | ✗ |
| Morriss, 2007108 | MUS/somatoform | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | HADS-A | HADS-D | ✗ | ✗ |
| Moss-Morris, 2005152 | Chronic fatigue | ✗ | CFQ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | SF-36 PF | ✗ |
| Moss-Morris, 2010130 | IBS | ✗ | ✗ | IBS-SSS | ✗ | ✗ | ✗ | HADS-A | HADS-D | ✗ | WSAS |
| Peters, 2002106 | MUS/somatoform | SF-36 BP | ✗ | ✗ | HSCL | ✗ | SF-36 MH | HADS-A | HADS-D | SF-36 PF | ✗ |
| Pols, 2008145 | MUS/somatoform | SF-36 | ✗ | ✗ | ✗ | ✗ | SF-36 MH | STAI | BDI-II | SF-36 PF | ✗ |
| Posse, 200496 | MUS/somatoform | ✗ | ✗ | ✗ | ✗ | Symptom list | ✗ | Somatic anxiety | ✗ | ✗ | ✗ |
| Ridsdale, 2001112 | Chronic fatigue | ✗ | CFQ | ✗ | ✗ | ✗ | ✗ | HADS-A | HADS-D | ✗ | MOS-SF SA |
| Ridsdale, 2004113 | Chronic fatigue | ✗ | CFQ | ✗ | ✗ | ✗ | ✗ | HAD-A | HAD-D | ✗ | WASA |
| Ridsdale, 2012115 | Chronic fatigue | ✗ | CFQ | ✗ | ✗ | ✗ | ✗ | HADS-A | HADS-D | ✗ | WASA |
| Rief, 2006102 | MUS/somatoform | ✗ | ✗ | ✗ | SOMS | ✗ | ✗ | BAI | BDI | ✗ | ✗ |
| Robinson, 2006131 | IBS | ✗ | ✗ | CGIS | ✗ | ✗ | SF-36 MH | ✗ | ✗ | SF-36 PF | ✗ |
| Rosendal, 2007146 | MUS/somatoform | SF-36 BP | ✗ | ✗ | SCL-90 | ✗ | SF-36 MH | ✗ | ✗ | SF-36 PF | WHO-DAS |
| Rothman, 2013127 | Pain-MS | VAS | ✗ | ✗ | ✗ | ✗ | ✗ | SCI-93 | Zung | SF-36 PF | ODI |
| Ryan, 2004109 | MUS/somatoform | ✗ | ✗ | ✗ | ✗ | Symptom log | ✗ | ✗ | ✗ | ✗ | ✗ |
| Sañudo, 2010140 | Pain-MS (fibromyalgia) | SF-36 Pain | ✗ | ✗ | ✗ | ✗ | SF-36 MH | ✗ | BDI | SF-36 PF | FIQ Total |
| Schade, 2011272 | MUS/somatoform | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ |
| Schaefert, 2013147 | MUS/somatoform | SF-36-Pain | ✗ | ✗ | PHQ-15 | ✗ | SF-36 MH | ✗ | PHQ-9 | SF-36 PF | ✗ |
| Schilte, 2001159 | MUS/somatoform | ✗ | ✗ | ✗ | SCL-90 | ✗ | ✗ | SCL-90-A | SCL-90-D | ✗ | SCL-90 Total |
| Smith, 1995100 | MUS/somatoform | ✗ | ✗ | ✗ | ✗ | ✗ | RAND MH | ✗ | ✗ | RAND PF | ✗ |
| Smith, 2006107 | MUS/somatoform | ✗ | ✗ | ✗ | PSC | ✗ | SF-36 MH | SSAS | CES-D | SF-36 PF | ✗ |
| Smith, 2009142 | MUS/somatoform | SF-36 | ✗ | ✗ | PHQ-15 | ✗ | SF-36 MH | SSAS | CES-D | SF-36 PF | ✗ |
| Sumathipala, 2000116 | MUS/somatoform | ✗ | ✗ | ✗ | Bradford Somatic Inventory | ✗ | GHQ-30 | ✗ | ✗ | ✗ | ✗ |
| Sumathipala, 2008117 | MUS/somatoform | ✗ | ✗ | ✗ | Bradford Somatic Inventory | ✗ | GHQ-30 | ✗ | ✗ | ✗ | ✗ |
| Toft, 201097 | MUS/somatoform | ✗ | ✗ | ✗ | SCL – SOM | ✗ | SF-36 MH | ✗ | ✗ | SF-36 PF | ✗ |
| Tummers, 2012149 | Chronic fatigue | ✗ | CIS | ✗ | ✗ | ✗ | ✗ | Bradford Somatic Inventory | ✗ | SF-36 PF | ✗ |
| van der Feltz-Cornelis, 2006160 | MUS/somatoform | ✗ | ✗ | ✗ | ✗ | Speckens | SIP P | ✗ | ✗ | ✗ | SIP total |
| van der Roer, 2008120 | Pain-SS (back) | NRS | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | RMDQ |
| van Ravesteijn, 2013143 | MUS/somatoform | SF-36 BP | ✗ | ✗ | PHQ-15 | ✗ | SF-36 MH | ✗ | PHQ-9 | SF-36 PF | ✗ |
| Walti, 2015121 | Pain-SS (back) | NRS | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | RMDQ |
| Wearden, 2010111 | Chronic fatigue | ✗ | CFQ | ✗ | ✗ | ✗ | ✗ | HADS-A | HADS-D | SF-36 PF | ✗ |
| Whitehead, 2002154 | Chronic fatigue | ✗ | CFQ | ✗ | ✗ | ✗ | ✗ | HADS | HADS | ✗ | LHS |
| Zonneveld, 2012141 | MUS/somatoform | SF-36 BP | ✗ | ✗ | SCL-90-R S | ✗ | SF-36 MH | SCL-90-R-A | SCL-90-R-D | SF-36 PF | SCL-90-R G |
| First author and year of publication | Baseline | End of treatment (duration, months) | Short term (time since end of treatment, months) | Long term (time since end of treatment, months) |
|---|---|---|---|---|
| Aiarzaguena, 2007136 | Y | 8 | 4 | |
| Alda, 2011137 | Y | 2.76 | 6 | |
| Burton, 2012157 | Y | 2.76b | ||
| Chalder, 1997114 | Y | 3b | ||
| Cuesta-Vargas, 2012118 | Y | 4 | 2 | 8 |
| Escobar, 2007156 | Y | 3 | 6 | |
| Friedberg, 2013151 | Y | 3 | 12 | |
| Gili, 2014/Moreno, 2013144,148 | Y | 2.3 | 12 | |
| Ho, 2012150 | Y | 1.15 | 2.85 | |
| aHuibers, 2004153 | Y | 4 | 12 | |
| Kashner, 1995161 | N | 4 | 8 | |
| Kennedy, 2005129 | Y | 1.38 | 3 | 12 |
| Kobeissi, 2012110 | Y | 1.38 | 4.5 | |
| Kocken, 2008103 | Y | 12 | ||
| Kolk, 2008104 | Y | 6 | 6 | |
| Lansinger, 2007123 | Y | 3 | 12 | |
| Larisch, 2004158 | Y | 3 | 3 | 9 |
| LeFort, 1998128 | Y | 1.38 | ||
| Loew, 2000122 | Y | 1.97 | ||
| Luciano, 2011139 | Y | 2 | ||
| Luciano, 2014138 | Y | 3 | 3 | |
| Macedo, 2012119 | Y | 2 | 4 | 10 |
| Marques, 2015133 | Y | 2.76 | ||
| Martin, 200799 | Y | 0.92 | 6 | |
| McBeth, 2012125/Beasley, 2015126 | Y | 6 | 3 | |
| McLeod, 1997105 | Y | 1.6 | 6 | |
| Morriss, 2007108 | Y | 3 | ||
| Moss-Morris, 2005152 | Y | 2.76 | 6 | |
| Moss-Morris, 2010130 | Y | 2 | 3 | 6 |
| Peters, 2002106 | Y | 2.3 | 6 | |
| Pols, 2008145 | Y | 12 | ||
| Posse, 200496 | Y | 6 | ||
| Ridsdale, 2001112 | Y | 3 | 3 | |
| Ridsdale, 2004113 | Y | 3 | 2.5 | |
| Ridsdale, 2012115 | Y | 2 | 10 | |
| Rief, 2006102 | Y | 0.92b | 6b | |
| Robinson, 2006131 | Y | 12 | ||
| Rosendal, 2007146 | Y | 3b | 12b | |
| Rothman, 2013127 | Y | 15 | ||
| Ryan, 2004109 | Y | 15 | ||
| Sañudo, 2010140 | Y | 5.52 | ||
| Schaefert, 2013132 | Y | 3 | 9 | |
| Schilte, 2001159 | Y | 24 | ||
| Smith, 1995100 | Y | 12b | ||
| Smith, 2006107 | Y | 12 | ||
| Smith, 2009142 | Y | 12 | ||
| Sumathipala, 2000116 | Y | 3 | ||
| Sumathipala, 2008117 | Y | 3 | 3 | 9 |
| Toft, 201097 | Y | 3b | 24b | |
| Tummers, 2012149 | Y | 6 | ||
| van der Feltz-Cornelis, 2006160 | Y | 1.38b | 6b | |
| van der Roer, 2008120 | Y | 2.99 | 6 | 12 |
| van Ravesteijn, 2013143 | Y | 3 | 9 | |
| Walti, 2015121 | Y | 0.92 | ||
| Wearden, 2010111 | Y | 4.6 | 12 | |
| Whitehead, 2002154 | Y | 6b | 12b | |
| Zonneveld, 2012141 | Y | 2.99 | 12 |
| First author and year of publication | Condition | Setting | Setting: referral | Setting: assessment | Setting: intervention | Setting: outcome assessment |
|---|---|---|---|---|---|---|
| Aiarzaguena, 2007136 | MUS/somatoform | Primary care | Recruited by GP | GP and home | GP practices | Home interview |
| Alda, 2011137 | Pain–MS (fibromyalgia) | Primary care | Recruited by doctors working in primary care | NR | At the health centre | Research team |
| Burton, 2012157 | MUS/somatoform | Primary care specialist clinic | GP practices | GPs and researcher | At the treatment centre | Researcher team |
| Chalder, 1997114 | Chronic fatigue | Primary care | GP | GP and research nurse | Self-help booklet | NR |
| Cuesta-Vargas, 2012118 | Pain–SS (back) | Adjunct to GP care | PCPs | Primary care practices | Health centre | In clinic |
| Escobar, 2007156 | MUS/somatoform | Primary care | Eight physicians performed the initial evaluations and referred patients to the research team | Research team | Two university-based primary care clinics | Research team |
| Friedberg, 2013151 | Chronic fatigue | Primary care and home based | Stony Brook family medicine/primary care practice | Stony Brook practice | Guided sessions in primary care setting, with home-based self-management | Face-to-face follow-up assessments |
| Moreno, 2013/Gili, 2014144,148 | MUS/somatoform | Primary care | Primary health-care centres | NR | Primary care | NR |
| Ho, 2012150 | Chronic fatigue | Community based | Community recruitment | Web-based screening | Group and home based | NR |
| Huibers, 2004/Leone, 2006153,155 | Chronic fatigue | Primary care | Occupational health service | Research centre | GP practices but outside normal hours | Research centre |
| Kashner, 1995161 | MUS/somatoform | Primary care | PCPs | Home based | NR | Home based |
| Kennedy, 2005129 | IBS | General practice | GP | GP/study nurse | Not explicitly reported | Not explicitly reported |
| Kobeissi, 2012110 | MUS/somatoform | Community based | Schools, factories, gynaecology clinics, satellite networks | Research team | Local facilities | Research team |
| Kocken, 2008103 | MUS/somatoform | General practice | Doctors’ practices | NR | General practices | NR |
| Kolk, 2004104 | MUS/somatoform | NR | Recruited via general practices and advertisements in local newspapers | Research team first and then confirmed by GP | Therapist referred regularly to the subject’s GP | Research team |
| Lansinger, 2007123 | Pain–SS (neck) | Primary care physiotherapy departments | Newspaper advertisements | NR | Physiotherapy departments in primary care | NR |
| Larisch, 2004158 | MUS/somatoform | General practice | GP | GPs | General practice | NR |
| LeFort, 1998128 | Pain–MS (mixed) | Community based | Referred from pain clinic, community HP, or self-referred | Research team | A range of community settings | Research team |
| Loew, 2000122 | Pain–SS (headache) | Primary care, ambulatory private practice | GP | NR | NR | NR |
| Luciano, 2011139 | Pain–MS (fibromyalgia) | General practice | GPs at these centres refer those patients who are suspected of having FM to the Viladecans Hospital Rheumatology Unit | Screened through an initial telephonic interview by researchers | Three general practices | NR |
| Luciano, 2014138 | Pain–MS (fibromyalgia) | Primary health-care centres | Primary health-care centres | GP | Group sessions with home-based tasks | NR |
| Macedo, 2012119 | Pain–MS (back) | Primary care | Primary care, outpatient clinic | NR | Private clinical practices or at the university clinic | Telephone |
| Margalit, 2008268 | MUS/somatoform | Primary care clinic | Referred/offered the treatment by their PCP | Research team | A multidisciplinary primary care clinic | Primary care clinic |
| Marques, 2015133 | Chronic fatigue | Four primary health-care centres and one private practice | Patients from the health-care centres were referred by their medical doctor | In the health-care centre, inclusion and exclusion criteria were checked by the research team using self-report measures based on the CDC criteria | Health-care institutions (four public primary care centres and one private practice) and in the Portuguese Fibromyalgia and Chronic Fatigue Syndrome Patient Association | Not explicitly reported |
| Martin, 200799 | MUS/somatoform | Aim is to design primary care intervention | Recruited in primary care practices | Research team | An outpatient treatment centre with GP support | Four trained and supervised research assistants |
| McBeth, 2012125/Beasley, 2015126 | Pain–MS (widespread) | Home-based/community settings to primary care patients | Primary care patients from general practices | Research team telephone interview or postal questionnaire | Telephone delivered or leisure centre/gym based | Research team telephone interview or postal questionnaire |
| McLeod, 1997105 | MUS/somatoform | Primary care as adjunctive treatment | Large health maintenance organisation | Primary care | Primary care | NR |
| Morriss, 2007108 | MUS/somatoform | Primary care | Recruited by a researcher in a surgery waiting room | NR | GP practices | NR |
| Moss-Morris, 2005152 | Chronic fatigue | Mainly home-based intervention with general practice consultation | Recruited from a specialist CFS private general practice | Assessed by the specialist GP | Mostly home-based exercises with some face-to-face contact with researchers | Not explicitly reported |
| Moss-Morris, 2010130 | IBS | Primary care and home based | Referred from previous IBS trial | Assessment by GP | Home based | Research team |
| Peters, 2002106 | MUS/somatoform | Primary care | Referred by GP | Research team | University gymnasium and home based | Primary care |
| Pols, 2008145 | MUS/somatoform | Primary care | Recruited by participating GPs | GPs and research team | GP practices | Service co-ordinators |
| Posse, 200496 | MUS/somatoform | Primary care | Primary care | NR | NR | NR |
| Ridsdale, 2001112 | Chronic fatigue | Primary care | 10 general practices collaborated in recruiting patients to the trial | Assessment of the patients was undertaken at their doctor’s practice by one of the authors | Not explicitly reported | Questionnaire given to patient by therapist at the end of treatment, follow-up questionnaire by post |
| Ridsdale, 2004113 | Chronic fatigue | Primary care | Recruited from 22 general practices | NR | Treatment was offered on the premises of each patient’s doctor in primary care. Homework exercises | NR |
| Ridsdale, 2012115 | Chronic fatigue | Primary care and home based | Recruited from general practices | GP assessed patients for eligibility and referred to researcher | Face-to-face sessions at their local primary care practice with homework | Follow-up questionnaires sent by post and analysed by researchers |
| Rief, 2006102 | MUS/somatoform | Primary care | GP practices | Research team | GP practices | Telephone – research team |
| Robinson, 2006131 | IBS | Primary care and home based | Primary care centres | GP and research team | Self-help booklet or self-help book plus group meeting | NR |
| Rosendal, 2007146 | MUS/somatoform | Primary care | Primary care | Waiting room | Routine practice | Postal questionnaires |
| Rothman, 2013127 | Pain–MS | Psychosomatic clinic | Referral from GP | NR | Psychosomatic clinic or GP | NR |
| Ryan, 2004109 | MUS/somatoform | HMOs | Recruited from a local HMO | Research team | Within a HMO medical group, only sites that hosted family and internal medicine specialists | Research team |
| Sañudo, 2010140 | Fibromyalgia | Unclear | Recruited from physician practices and local FMS support groups | Research team | Unclear | Research team |
| Schade, 2011272 | MUS/somatoform | Family health centres. These centres are in charge of primary health care | Primary care | NR | Family counselling implemented in primary care | N/A |
| Schaefert, 2013147 | MUS/somatoform | GP practices | Recruited by GPs in consultation with psychosomatic specialist when necessary | Specifically trained GP | GP practices | |
| Schilte, 2001159 | MUS/somatoform | Patient’s home and primary care | Postal questionnaire | NR | GP practice and patient’s home for disclosure intervention | NR |
| Smith, 1995100 | MUS/somatoform | Primary care | PCPs | Home-based by research team | Primary care practice | Home based by research team |
| Smith, 2006107 | MUS/somatoform | Primary care | Primary care chart review | Chart rater in primary care | HMOs | NR |
| Smith, 2009142 | MUS/somatoform | Primary care | Henry Ford Health System | Research team | Henry Ford Health System | Research team |
| Sumathipala, 2000116 | MUS/somatoform | Primary care outpatient clinic | Referred from primary care clinician | Research team | A general outpatient clinic that provided primary care, where patients initiated their own visits, without prior appointments | Research team |
| Sumathipala, 2008117 | MUS/somatoform | Primary care outpatient clinic | Patients screened at clinic | Research team | Primary care outpatient clinic | Primary care outpatient clinic |
| Toft, 201097 | MUS/somatoform | Primary care | GP practices | GP and psychiatrists | GP practices | Postal questionnaire |
| Tummers, 2012149 | Chronic fatigue | Community-based mental health centre | Referred by a GP or consultant | GP, research team, CFS expert, psychiatric nurse | Mostly home-based activities but based at a community mental health centre | Not explicitly reported |
| van der Feltz-Cornelis, 2006160 | MUS/somatoform | Primary care | GPs at each general practice | GPs | Psychiatrist visits the GP practice | Research team |
| van der Roer, 2008120 | Pain–SS (back) | Primary physiotherapy care setting | Referred by participating physiotherapists | Local research centres | Local research centres | Local research centres |
| van Ravesteijn, 2013143 | MUS/somatoform | Primary care patients with home-based intervention | Frequently attending primary care patients from participating GP practices | GPs assessed patient’s for inclusion criteria | Group intervention setting unclear. Home-based practice | Research team |
| Walti, 2015121 | Pain–SS (back) | Primary care physiotherapy centre | GP practice | NR | Primary care physiotherapy centre | NR |
| Wearden, 2010111 | Chronic fatigue | Primary care patients with home-based intervention | GPs referred | Patients were assessed at home by a researcher after referral | In patients’ homes | Assessments were performed by trained researchers |
| Whitehead, 2002154 | Chronic fatigue | Primary care | GP referral | GP with research team assistance | GP practice | Research team |
| Zonneveld, 2012141 | MUS/somatoform | Primary care | GPs referred to research team | Research team | Local medical settings | Research team |
| First author and year of publication | Intervention 1 | I/G | Intervention 2 (control) | I/G | Intervention 3 (where applicable) | I/G |
|---|---|---|---|---|---|---|
| Aiarzaguena, 2007136 | GP intervention – reattribution (modified) | I | GP intervention – reattribution | I | ||
| Alda, 2011137 | CBT high intensity | G | UC | Medication | ||
| Burton, 2012157 | GP-MM | I | UC | I | ||
| Chalder, 1997114 | Guided self-help | I | UC | |||
| Cuesta-Vargas, 2012118 | Multimodal (sport + education) | I | Guided self-help | I | ||
| Escobar, 2007156 | CBT high intensity | I | UC+ (letter) | |||
| Friedberg, 2013151 | CBT low intensity | I | UC | Relaxation/stretching/social support/emotional support | I | |
| Gili 2014/Moreno, 2013144,148 | CBT high intensity – individual | I | UC+ (letter) | CBT high intensity – group | G | |
| Ho, 2012150 | Relaxation/stretching/social support/emotional support | G | UC | |||
| Huibers, 2004/Leone, 2006153,155 | GP – CBT | I | UC | |||
| Kashner, 1995161 | UC+ (letter) | Relaxation/stretching/social support/emotional support | G | |||
| Kennedy, 2005129 | Multimodal (CBT low intensity + medication) | I | Medication | |||
| Kobeissi, 2012110 | Relaxation/stretching/social support/emotional support | G | UC | |||
| Kocken, 2008103 | Other psychotherapy | G | UC | |||
| Kolk, 2004104 | Other psychotherapy | I | UC | |||
| Lansinger, 2007123 | Relaxation/stretching/social support/emotional support | G | SES | I | ||
| Larisch, 2004158 | GP intervention – reattribution (modified) | I | UC | |||
| LeFort, 1988128 | Guided self-help | G | UC | |||
| Loew, 2000122 | Relaxation/stretching/social support/emotional support | G | Relaxation/stretching/social support/emotional support | G | ||
| Luciano, 2011139 | Multimodal | G | UC | |||
| Luciano, 2014138 | CBT – high intensity | G | Medication | |||
| Macedo, 2012119 | Graded activity | I | Graded activity | I | ||
| Margalit, 2008268 | Other psychotherapy | I | UC | |||
| Marques, 2015133 | Graded activity | I | Guided self-help | |||
| Martin, 200799 | CBT – low intensity | G | UC | |||
| McBeth, 2012125/Beasley, 2015126 | CBT – high Intensity | I | Exercise + fourth group of UC | Multimodal (CBT + exercise) | I | |
| McLeod, 1997105 | Other psychotherapy | G | UC | |||
| Morriss, 2007108 | GP intervention – reattribution | I | UC | |||
| Moss-Morris, 2005152 | Graded activity | I | UC | |||
| Moss-Morris, 2010130 | CBT low intensity | I | UC | |||
| Peters, 2002106 | SES | G | Relaxation/stretching/social support/emotional support | G | ||
| Pols, 2008145 | Multimodal (self-management + medication + CBT) | I | UC | |||
| Posse, 200496 | Other psychotherapy | UC | ||||
| Ridsdale, 2001112 | CBT high intensity | I | Other psychotherapy | I | ||
| Ridsdale, 2004113 | CBT low intensity | I | Graded activity | I | ||
| Ridsdale, 2012115 | Graded exercise | I | Guided self-help | OP | I | |
| Rief, 2006102 | GP intervention – MUS management | I | UC | |||
| Robinson, 2006131 | Guided self-help | I | UC | Multimodal | G | |
| Rosendal, 2007146 | GP intervention – MUS management | I | UC | |||
| Rothman, 2013127 | GP intervention – multidisciplinary assessment + motivational interview + psychotherapy | I/G | UC+ (multidisciplinary assessment + choice of treatment) | I/G | ||
| Ryan, 2004109 | Other psychotherapy | I | UC | |||
| Sañudo, 2010140 | SES | I | UC | SES | I | |
| Schade, 2011272 | Other psychotherapy | I | UC | |||
| Schaefert, 2013147 | Multimodal (GP intervention – MUS management + other psychotherapy) | G | GP intervention – MUS management | I | ||
| Schilte, 2001159 | GP intervention – other psychotherapy | I | UC | |||
| Smith, 1995100 | UC+ (letter) | UC | ||||
| Smith, 2006107 | Multimodal | I | UC | |||
| Smith, 2009142 | Multimodal (GP intervention CBT + Medication) | I | UC | |||
| Sumathipala, 2000116 | CBT low intensity | I | UC | |||
| Sumathipala, 2008117 | Multimodal (GP-CBT + GP intervention – MUS management) | I | GP intervention – MUS management | |||
| Toft, 201097 | GP intervention – MUS management | I | UC | |||
| Tummers, 2012149 | CBT low intensity | I | UC | |||
| van der Feltz-Cornelis, 2006160 | Multimodal (reattribution + collaborative care) | I | GP intervention – reattribution | |||
| van der Roer, 2008120 | Multimodal (sport + education + behavioural programme) | G | SES | I | ||
| van Ravesteijn, 2013143 | Other psychotherapy | G | UC+ | |||
| Walti, 2015121 | Multimodal (education + sport + sensory discrimination) | I | SES | I | ||
| Wearden, 2010111 | Graded activity | I | UC | OP | I | |
| Whitehead, 2002154 | GP intervention – MUS management | I | UC | |||
| Zonneveld, 2012141 | CBT high intensity | G | UC |
| First author and year of publication | Condition | Total number | Arms | Interventions | Assessment points |
|---|---|---|---|---|---|
| Aiarzaguena, 2007136 | MUS | Clusters of four patients attended by 39 GPs. 156 patients | 2 | GP-re vs. GP-re | Baseline, 3 months (when both study groups had completed five sessions), after 8 months (when the intervention was finished), and 12 months after enrolment |
| Alda, 2011137 | Fibromyalgia | 169 randomised | 3 | CBTHI vs. ME vs. UC | Baseline, end of treatment, 6-month follow-up |
| Burton, 2012157 | MUS/somatoform | 32 randomised | 2 | GP-MM vs. UC | Baseline, 12 weeks |
| Chalder, 1997114 | Chronic fatigue | 150 randomised | 2 | GSH vs. UC | Baseline, 3 months |
| Cuesta-Vargas, 2012118 | Chronic pain – single site | 58 patients | 2 | MM vs. GSH | Pre intervention (baseline), post intervention 4 months, post intervention 6 months, 1-year follow-up |
| Escobar, 2007156 | MUS | 172 randomised | 2 | CBTHI vs. UC+ | Screening, baseline (1 to 2 weeks later), end of treatment (approximately 3 months after baseline), 6-month follow-up |
| Friedberg, 2013151 | Chronic fatigue | 111 randomised | 3 | CBTLI vs. RSSE vs. UC | Baseline and 3 months and 12 months post treatment |
| Moreno, 2013/Gili, 2014144,148 | Somatoform disorder | 168 patients randomised, from 21 primary health-care centres | 3 | CBTHI vs. CBTHI vs. UC+ | Baseline, post treatment, 6 and 12 months |
| Ho, 2012150 | Chronic fatigue | 64 randomised | 2 | RSSE vs. UC | Baseline, 5 weeks after, 4 months after |
| Huibers, 2004/Leone, 2006153,155 | Chronic fatigue | 151 randomised | 2 | GP-CBT vs. UC | Data collected on four occasions: baseline, end of the treatment period (4 months) and at two follow-up points (i.e. 8 months and 12 months). Leone 2006155 is 4-year follow-up |
| Kashner, 1995161 (follow-on study to Smith, 1995100) | Somatoform disorder | 70 randomised | 2 | RSSE vs. UC+ | Data collected every 4 months |
| Kennedy, 2005129 | IBS | 149 randomised | 2 | MM vs. ME | Baseline, 6 weeks after randomisation, 3 months, 6 months, 12 months after completion of therapy |
| Kobeissi, 2012110 | Single MUS | 271 randomised | 2 | RSSE vs. UC | Baseline, 1.5 months, 6 months |
| Kocken, 2008103 | Somatoform disorder | 104 randomised | 2 | OP vs. UC | Baseline and post treatment |
| Kolk, 2004104 | MUS | 106 randomised | 2 | OP vs. UC | Baseline, 6 months (end of treatment), 12 months (end of follow-up) |
| Lansinger, 2007123 | Neck pain | 122 randomised | 2 | RSSE vs. SES | Baseline, end of treatment, 6- and 12-month follow-up |
| Larisch, 2004158 | Somatoform disorder | 42 GPs randomised; 127 patients | 2 | GP-re vs. UC | Baseline, 3-, 6- and 12-month follow-up |
| LeFort, 1998128 | Chronic pain | 110 randomised | 2 | GSH vs. UC | Baseline, 12 weeks (3 months post treatment) |
| Loew, 2000122 | Single chronic pain | 54 patients | 2 | RSSE vs. RSSE | 60 days pre treatment, 60 days post treatment |
| Luciano, 2011139 | Fibromyalgia | 108 randomised | 2 | MM vs. UC | Baseline, post treatment |
| Luciano, 2014138 | Fibromyalgia | 156 randomised | 3 | CBTHI vs. ME vs. UC | Baseline, end of treatment, 3 months, 6 months |
| Macedo, 2012119 | Back pain | 172 patients | 2 | GA vs. GA | Baseline, 2, 6 and 12 months post intervention |
| Margalit, 2008268 | MUS | 42 randomised | 2 | OP vs. UC | Baseline, one and 2 years after randomisation, 3 years, 5 years |
| Marques, 2015133 | Chronic fatigue | 99 randomised | 2 | GA vs. GSH | Baseline and 12 weeks later (post treatment) |
| Martin, 200799 | MUS | 140 randomised | 2 | CBTLI vs. UC | Baseline, 4 weeks, 6 months later |
| McBeth, 2012125/Beasley, 2015126 | Chronic pain | 442 randomised | 4 | CBTHI vs. SES vs. MM vs. UC | Baseline, 6 months (post treatment), 9 months, 2 years |
| McLeod, 1997105 | Somatoform disorder | 96 randomised | 2 | OP vs. UC | 1 week prior, 1 week post treatment, 6-month follow-up |
| Morriss, 2007108 | MUS | 16 GP practices randomised, with 74 GPs and 141 patients | 2 | GP-re vs. UC | Baseline, 1- and 3-month follow-up |
| Moss-Morris, 2005152 | Chronic fatigue | 49 randomised | 2 | GA vs. UC | End of treatment at 12 weeks and at 6-month follow-up |
| Moss-Morris, 2010130 | IBS | 64 randomised | 2 | CBTLI vs. UC | Baseline (pre treatment), post treatment (2 months) and 3 and 6 months post treatment |
| Peters, 2002106 | MUS | 228 randomised | 2 | SES vs. RSSE | Baseline (T1 randomisation), T2 start of programme, T3 mid-programme, T4 end of programme, T5 6-month follow-up |
| Pols, 2008145 | MUS | 133 randomised | 2 | MM vs. UC | Baseline, 12 months |
| Posse, 200496 | Somatoform disorder | 10 | 2 | OP vs. UC | Baseline and 6-month follow-up |
| Ridsdale, 2001112 | Chronic fatigue | 160 randomised | 2 | CBTHI vs. OP | Baseline, 3 months (completion of treatment), 6 months |
| Ridsdale, 2004113 | Chronic fatigue | 123 randomised | 2 | CBTLI vs. GA | Baseline, 3 months, 8 months from baseline. Mean of the two periods used as primary outcome |
| Ridsdale, 2012115 | Chronic fatigue | 222 randomised | 3 | GA vs. OP vs. GSH | Baseline, 3 and 12 months |
| Rief, 2006102 | Somatoform disorder | 26 GPs, 295 patients | 2 | GP-MM vs. UC | Baseline, 6-month follow-up |
| Robinson, 2006131 | IBS | 420 randomised | 3 | GSH vs. MM vs. UC | Baseline, 12-month follow-up |
| Rosendal, 2007146 | Somatoform disorder | 27 practices randomised, 22 GPs, 506 patients | 2 | GP-MM vs. UC | Baseline, 3-month follow-up, 12-month follow-up |
| Rothman, 2013127 | Chronic pain | 220 randomised | 2 | GP-O vs. UC+ | Baseline, 15-month follow-up |
| Ryan, 2004109 | Mixed MUS | 70 randomised | 2 | OP vs. UC | Pre-treatment phase (6 months prior to treatment, T1), 8-week treatment phase (T2), 6 months post treatment (T3) |
| Sañudo, 2010140 | Fibromyalgia | 64 randomised | 3 | SES vs. SES vs. UC | Baseline and 24 weeks (immediately post treatment) |
| Schade, 2011272 | Somatoform disorder | 256 patients, 102 professionals | 2 | OP vs. UC | 6 months pre treatment, 6 months post treatment, 1-year follow-up |
| Schaefert, 2013147 | MUS | 39 GPs randomised, 328 patients | 2 | MM vs. GP-MM | Baseline, 6 months (3 months after 3 month intervention phase), 12 months (9 months after intervention phase) |
| Schilte, 2001159 | Somatoform disorder | 161 patients | 2 | GP-OP vs. UC | Baseline, 6, 12 and 24 months |
| Smith, 1995100 (see Kashner, 1995161 for post 1 year) | MUS | 56 patients | 2 | UC+ vs. UC | Baseline, then every 4 months until 1 year crossover |
| Smith, 2006107 | MUS | 206 randomised | 2 | MM vs. UC | Baseline, 12 months |
| Smith, 2009142 | MUS | 30 randomised | 2 | MM vs. UC | Baseline and 12 months |
| Sumathipala, 2000116 | MUS | 68 randomised | 2 | CBTLI vs. UC | Baseline and 3 months (end of treatment) |
| Sumathipala, 2008117 | MUS | 150 randomised | 2 | MM vs. GP-MM | Baseline and 3, 6 and 12 months post baseline |
| Toft, 201097 | MUS | 40 GPs randomised. 524 patients included | 2 | GP-MM vs. UC | Baseline and 3-, 12- and 24-month follow-up |
| Tummers, 2012149 | Chronic fatigue | 123 randomised | 2 | CBTLI vs. UC | Baseline and 6-month post-baseline assessment |
| van der Feltz-Cornelis, 2006160 | MUS | 36 general practices, 81 patients | 2 | MM vs. GP-re | Baseline, 6 weeks and 6 months |
| van der Roer, 2008120 | Back pain | 114 randomised | 2 | MM vs. SES | Baseline and 6, 13, 26 and 52 weeks after randomisation |
| van Ravesteijn, 2013143 | MUS | 125 randomised | 2 | OP vs. UC+ | Baseline, end of treatment (3 months from baseline), 9 months after treatment (12 months from baseline) |
| Walti, 2015121 | Back pain | 28 patients | 2 | MM vs. SES | Baseline, 12 weeks after baseline |
| Wearden, 2010111 | Chronic fatigue | 296 randomised | 3 | GA vs. OP vs. UC | Baseline, week 20 (completion of treatment), 70 weeks (1 year post treatment completion) |
| Whitehead, 2002154 | CFS | 65 randomised | 2 | GP-MM vs. UC | Baseline and 6- and 12-month follow-up |
| Zonneveld, 2012141 | MUS | 162 randomised | 2 | CBTHI vs. UC | Baseline, end of treatment (13 weeks), 1-year follow-up |
| First author and year of publication | Condition | Intervention 1 delivery: duration of sessions | Intervention 3 delivery: duration of sessions | Intervention 2 delivery: duration of sessions |
|---|---|---|---|---|
| Aiarzaguena, 2007136 | MUS | 30 minutes × 6 sessions | N/A | 30 minutes × 6 sessions |
| Alda, 2011137 | Fibromyalgia | 90 minutes × 10 sessions | N/A | N/A |
| Burton, 2012157 | MUS | 1 session × 1 hour duration + 3 sessions × 20 minutes | N/A | N/A |
| Chalder, 1997114 | Chronic fatigue | 1 × 10–15 minutes | N/A | N/A |
| Cuesta-Vargas, 2012118 | Back pain | 30-minute sessions of DWR. Educational session of 1 hour | N/A | Educational session of 1 hour |
| Escobar, 2007156 | MUS | 9 × 50-minute sessions, (range, 45–60 minutes), 1 × 90-minute session | N/A | N/A |
| Friedberg, 2013151 | Chronic fatigue | Up to 60 minutes | N/A | N/A |
| Huibers, 2004/Leone, 2006153,155 | Chronic fatigue | 30 minutes | N/A | N/A |
| Kashner, 1995161 | Somatoform disorder | NR | N/A | N/A |
| Kennedy, 2005129 | IBS | 50 minutes | N/A | N/A |
| Kobeissi, 2012110 | Single MUS | 75 minutes (psychosocial component), 30 minutes relaxation sessions | N/A | N/A |
| Kocken, 2008103 | Somatoform disorder | NR | N/A | NR |
| Kolk, 2004104 | MUS | 1-hour sessions | N/A | N/A |
| Lansinger, 2007123 | Neck pain | 1 hour | N/A | 1 hour |
| Larisch, 2004158 | Somatoform disorder | 20 minutes planned, but in practice shorter duration | N/A | 20 minutes planned, but in practice shorter duration |
| LeFort, 1998128 | Chronic pain | 2 hours per week | N/A | N/A |
| Loew, 2000122 | Single chronic pain | 45-minute introduction to eFR | N/A | 45-minute introduction to UIR |
| Luciano, 2011139 | Fibromyalgia | 2-hour sessions | N/A | N/A |
| Luciano, 2014138 | Fibromyalgia | 8 × 2.5 hour sessions plus 10–15 minutes daily homework | N/A | N/A |
| Macedo, 2012119 | Back pain | 1 hour, recommended 30 minutes extra per week at home in the first month and 1 hour extra per week at home in the second month | N/A | 1 hour, recommended 30 minutes extra per week at home in the first month and 1 hour extra per week at home in the second month |
| Margalit, 2008268 | MUS | Duration of initial encounters NR. Follow-up sessions 30 minutes | N/A | N/A |
| Marques, 2015133 | Chronic fatigue | Up to 60 minutes | N/A | NR |
| Martin, 200799 | MUS | 3–4 hours | N/A | N/A |
| McBeth, 2012125/Beasley, 2015126 | Chronic pain | 30–45 minutes | 20–60 minutes | N/A Group 4 combined CBT and exercise |
| McLeod, 1997105 | Somatoform disorder | NR | N/A | NR |
| Moreno, 2013/Gili, 2014144,148 | Somatoform disorder | 1 hour | 2 hours | NR |
| Morriss, 2007108 | MUS | N/A for patients | N/A | N/A |
| Moss-Morris, 2005152 | Chronic fatigue | Two 1-hour face-to-face individual motivational interviewing sessions and two brief SR-based telephone counselling sessions | N/A | N/A |
| Moss-Morris, 2010130 | IBS | 1 × 1 hour face to face with health psychologist, 2 × 1-hour telephone sessions | N/A | N/A |
| Peters, 2002106 | MUS | 1 hour supervised with three times per week 20 minutes’ homework | N/A | 1 hour supervised with 3 times per week 20 minutes’ homework |
| Pols, 2008145 | MUS | NR | N/A | N/A |
| Posse, 200496 | Somatoform disorder | NR | N/A | NR |
| Ridsdale, 2001112 | Chronic fatigue | Initial 1 hour interview for goal-setting. Home-based exercise starting at 10–15 minutes four or five times a week. Increases generally involved duration increases of 3–5 minutes per week. The final goal was for each participant to be exercising for approximately 30 minutes for 5 days per week | N/A | N/A |
| Ridsdale, 2004113 | Chronic fatigue | 6 × 1-hour sessions | N/A | 6 × 1-hour sessions |
| Ridsdale, 2012115 | Chronic fatigue | 6 × 45-minute sessions over 12 weeks | N/A | 6 × 45-minute sessions over 12 weeks |
| Rief, 2006102 | MUS | Not specified – dependent on patient | N/A | N/A |
| Robinson, 2006131 | IBS | Several group sessions and self-help | 1 x session and self-help | N/A |
| Rosendal, 2007146 | Somatoform disorder | NR | N/A | NR |
| Rothman, 2013127 | Chronic pain | Not specified – dependent on individual | N/A | Not specified – dependent on individual |
| Ryan, 2004109 | Mixed MUS | 1-hour weekly sessions | N/A | N/A |
| Sañudo, 2010140 | Fibromyalgia | Two sessions per week of 45–60 minutes’ duration | Two sessions per week of 45 to 60 minutes’ duration | N/A |
| Schade, 2011272 | Somatoform disorder | First session 1 hour, subsequent sessions between 30 and 45 minutes | NR | First session 1 hour, subsequent sessions between 30 and 45 minutes |
| Schaefert, 2013147 | MUS | 10 × 90-minute sessions plus two booster meetings ‘of equal length’ 3 and 9 months after group phase | N/A | N/A |
| Schilte, 2001159 | Somatoform disorder | First meeting 2 hours, second meeting 1 hour, third meeting (where applicable) 30 minutes to 1 hour | NR | First meeting 2 hours, second meeting 1 hour, third meeting (where applicable) 30 minutes to 1 hour |
| Smith, 1995100 | MUS | Regular consultations every 4–6 weeks but duration not specified | N/A | N/A |
| Smith, 2006107 | MUS | 12 × 20-minute visits were scheduled but additional visits could occur. Telephone contact (5–10 minutes) was scheduled between visits | N/A | N/A |
| Smith, 2009142 | MUS | Mean number of encounters (minutes per encounter) encounter: office visits – 7 (38.3); scheduled phone – 3 (20.5); after-hours phone – 3 (14.7); co-ordination of care – 1 (20) | N/A | N/A |
| Sumathipala, 2000116 | MUS | 6 × 30-minute sessions | N/A | N/A |
| Sumathipala, 2008117 | MUS | 3 × 30-minute sessions over 3 weeks, 3 × optional fortnightly follow-up sessions | N/A | 3 × 30-minute sessions over 3 weeks, 3 × optional fortnightly follow-up sessions |
| Toft, 201097 | MUS | NR | N/A | NR |
| Tummers, 2012149 | Chronic fatigue | 30-minute sessions with physiotherapists plus daily home-based exercise tailored 5–30 minutes per day | 50-minute sessions with counsellors | N/A |
| van der Feltz-Cornelis, 2006160 | MUS | NR | N/A | NR |
| van der Roer, 2008120 | Back pain | NR | N/A | NR |
| van Ravesteijn, 2013143 | MUS | 8 × 2.5-hour group sessions. Home practice 6 days per week for 45 minutes per day | N/A | N/A |
| Walti, 2015121 | Back pain | 30-minute physiotherapy sessions. Home assignments to be performed for 30 minutes | N/A | 30-minute physiotherapy sessions. Home assignments to be performed for 30 minutes |
| Wearden, 2010111 | Chronic fatigue | 90-minute home visit on week 1; 1-hour home visits on weeks 2, 4, 10 and 19; and 30-minute telephone calls on weeks 3, 6, 8, 12, and 15 | 90-minute home visit on week 1; 1-hour home visits on weeks 2, 4, 10, and 19; and 30-minute telephone calls on weeks 3, 6, 8, 12, and 15 | N/A |
| Whitehead, 2002154 | Chronic fatigue | 10 minutes on average | N/A | 10 minutes on average |
| Zonneveld, 2012141 | MUS | 13 × 2-hour group sessions | N/A | N/A |
| First author and year of publication | Condition | Intervention 1 delivery: number of sessions | Intervention 3 delivery: number of sessions | Intervention 2 delivery: number of sessions | Intervention 1 delivery: time period | Intervention 3 delivery: time period | Intervention 2 delivery: time period |
|---|---|---|---|---|---|---|---|
| Aiarzaguena, 2007136 | MUS | 6 sessions | N/A | 6 sessions | 8 months | N/A | 8 months |
| Alda, 2011137 | Fibromyalgia | 10 sessions | 6 months | 6 months | 10–12 weeks | 6 months | 6 months |
| Burton, 2012157 | MUS | N/A | N/A | ||||
| Chalder, 1997114 | Chronic fatigue | 1 session with nurse then self-help | N/A | N/A | 3 months | N/A | 3 months |
| Cuesta-Vargas, 2012118 | Back pain | 3 sessions per week for 15 weeks. A lower limit of training compliance was set to 80% of the training sessions. 1 educational session | N/A | 1 educational session | 4 months | N/A | N/A |
| Escobar, 2007156 | MUS | 10 sessions | N/A | N/A | 3 months | N/A | 3 months |
| Friedberg, 2013151 | Chronic fatigue | 2 sessions | 2 sessions | None | 3 month self-management period | Face-to-face sessions were 2 weeks apart, homework diaries were for 3 months’ duration | N/A |
| Huibers, 2004/Leone, 2006153,155 | Chronic fatigue | 5–7 sessions | N/A | N/A | Over the course of 4 months | N/A | N/A |
| Kashner, 1995161 | Somatoform disorder | 8 sessions every other week | N/A | 4 months | N/A | ||
| Kennedy, 2005129 | IBS | 6 sessions | N/A | N/A | 6 weeks | N/A | > 6 weeks (patients already on drug) |
| Kobeissi, 2012110 | Single MUS | 12 sessions | N/A | Telephone call every 2 weeks | 6 weeks | N/A | 6 weeks |
| Kocken, 2008103 | Somatoform disorder | Average 3.2 counselling sessions per patient, 2.1 sessions with GP and health educator, 6.3 education group sessions | N/A | NR | Mean duration 12 months | N/A | NR |
| Kolk, 2004104 | MUS | Once per week or every 2 weeks | N/A | N/A | Maximum 12 weeks | N/A | N/A |
| Lansinger, 2007123 | Neck pain | 10 to 12 sessions, 1 or 2 times per week | N/A | 10 to 12 sessions, 1 or 2 times per week | 3 months | N/A | 3 months |
| Larisch, 2004158 | Somatoform disorder | 6 sessions every other week | N/A | 6 sessions every other week | 3 months | N/A | 3 months |
| LeFort, 1998128 | Chronic pain | 6 sessions | N/A | N/A | 6 weeks | N/A | 6 weeks |
| Loew, 2000122 | Single chronic pain | 1 session | N/A | 1 session | NR | N/A | NR |
| Luciano, 2011139 | Fibromyalgia | 9 sessions | N/A | N/A | Sessions delivered over a 2-month period (1 afternoon session per week) | N/A | N/A |
| Luciano, 2014138 | Fibromyalgia | 8 sessions | N/A | N/A | N/A | ||
| Macedo, 2012119 | Back pain | 14 sessions; 12 initial, twice a week for the first 4 weeks and once a week for the remaining 4 weeks. Plus 2 booster sessions | N/A | 14 sessions; 12 initial, twice a week for the first 4 weeks and once a week for the remaining 4 weeks. Plus 2 booster sessions | 8 weeks (initial sessions), 1 booster session at 4 months following randomisation, 1 booster session at 10 months following randomisation | N/A | 8 weeks (initial sessions), 1 booster session at 4 months following randomisation, 1 booster session at 10 months following randomisation |
| Margalit, 2008268 | MUS | 3–28 (mean: 7.3) encounters over a period of 1.5–12 months. Follow-up once per week | N/A | N/A | 1.5–12 months | N/A | 12 months |
| Marques, 2015133 | Chronic fatigue | Two 1-hour face-to-face individual motivational interviewing sessions and two brief SR-based telephone counselling sessions | N/A | N/A | 12-week intervention period | N/A | 12 weeks |
| Martin, 200799 | MUS | 1 session | N/A | N/A | 1 session only | N/A | Unclear – presume 4 weeks |
| McBeth, 2012125/Beasley, 2015126 | Chronic pain | 7 weekly sessions (each 30–45 minutes), and 1 session 3 months and 1 session 6 months after randomisation | 3–5 days per week |
N/A Group 4 combined CBT and exercise |
6 months | 6 months |
6 months Group 4 6 months |
| McLeod, 1997105 | Somatoform disorder | 6 sessions, 1 per week. Plus daily homework assignments | N/A | 6 sessions, 1 per week. Plus daily homework assignments | 6 weeks | N/A | After 2 months’ wait, 6 weeks |
| Moreno, 2013/Gili, 2014144,148 | Somatoform disorder | 10 per week | 10 per week | NR | NR | NR | NR |
| Morriss, 2007108 | MUS | N/A for patients | N/A | N/A | N/A for patients | N/A | N/A for patients |
| Moss-Morris, 2005152 | Chronic fatigue | One initial meeting followed by 12 weekly meetings. Exercises were 4/5 times per week for 12 weeks | N/A | N/A | 12 weeks | N/A | 12 weeks |
| Moss-Morris, 2010130 | IBS | 7 chapters of self-help manual, 1 face-to-face session, 2 telephone sessions | N/A | N/A | 7 to 8 weeks | N/A | 7 to 8 weeks |
| Peters, 2002106 | MUS | 2 sessions per week for 20 sessions supervised plus 3 times per week for 10 weeks homework | N/A | 2 sessions per week for 20 sessions supervised plus 3 times per week for 10 weeks homework | 10 weeks | N/A | 10 weeks |
| Pols, 2008145 | MUS | 4- to 6-weekly appointments | N/A | N/A | 12-month care plan that was reviewed quarterly | N/A | N/A |
| Posse, 200496 | Somatoform disorder | One per week | N/A | NR | 6 months | N/A | NR |
| Ridsdale, 2001112 | Chronic fatigue | 6 sessions | N/A | 6 sessions | 3 months | N/A | 3 months |
| Ridsdale, 2004113 | Chronic fatigue | 6 sessions | N/A | 6 sessions | 12 weeks | N/A | 12 weeks |
| Ridsdale, 2012115 | Chronic fatigue | 8 sessions at 2-week intervals | 8 sessions at 2-week intervals | None | 16 weeks | 16 weeks | 16 weeks |
| Rief, 2006102 | MUS | 1-day training for GPs | N/A | N/A | 1-day training for GPs | N/A | N/A |
| Robinson, 2006131 | IBS | Several group sessions | 1 session | N/A | NR | NR | N/A |
| Rosendal, 2007146 | Somatoform disorder | NR | N/A | NR | NR | N/A | NR |
| Rothman, 2013127 | Chronic pain | Not specified – dependent on individual | N/A | Not specified – dependent on individual | Not specified – dependent on individual | N/A | Not specified – dependent on individual |
| Ryan, 2004109 | Mixed MUS | 8 sessions followed by monthly optional maintenance sessions | N/A | N/A | 8 weeks plus follow-up visits | N/A | 8 weeks |
| Sañudo, 2010140 | Fibromyalgia | 2 sessions per week | 2 sessions per week | N/A | 24 weeks | 24 weeks | 24 weeks |
| Schade, 2011272 | Somatoform disorder | NR | N/A | NR | NR | N/A | NR |
| Schaefert, 2013147 | MUS | 10 weekly sessions | N/A | N/A | 10 weeks group sessions, plus 2 booster sessions at 3 and 9 months later | N/A | 12 months |
| Schilte, 2001159 | Somatoform disorder | 2 disclosure meetings and an additional third meeting if the patient agreed | N/A | NR | First meeting within 2 weeks after inclusion, second meeting 1 week later, third meeting (where applicable) another week later | N/A | NR |
| Smith, 1995100 | MUS | Regular scheduled meeting perhaps every 4–6 weeks | N/A | N/A | 12 months | N/A | 12 months |
| Smith, 2006107 | MUS | 12 face-to-face sessions minimum plus telephone contact | N/A | N/A | 12 months | N/A | 12 months |
| Smith, 2009142 | MUS | 7 visits with the PCP (and 3 with the CM who also made eight scheduled phone calls) | N/A | N/A | 12 months | N/A | 12 months |
| Sumathipala, 2000116 | MUS | 6 sessions | N/A | N/A | 3 months | N/A | 3 months |
| Sumathipala, 2008117 | MUS | 6 sessions | N/A | 6 sessions | 10 weeks | N/A | 10 weeks |
| Toft, 201097 | MUS | Not specified | N/A | N/A | 2 years | N/A | 2 years |
| Tummers, 2012149 | Chronic Fatigue | Week-by-week programme | N/A | N/A | Minimum 20 weeks | N/A | N/A |
| van der Feltz-Cornelis, 2006160 | MUS | No specified number of sessions | N/A | No specified number of sessions | 6 months | N/A | 6 months |
| van der Roer, 2008120 | Back Pain | 10 individual sessions and 20 group sessions | N/A | Number of sessions at the discretion of physiotherapist. Mean number of sessions was 13 | Unclear | N/A | Unclear |
| van Ravesteijn, 2013143 | MUS | 8 group sessions, 48 home exercise sessions | N/A | N/A | 8 weeks | N/A | 8 weeks |
| Walti, 2015121 | Back pain | 1 or 2 sessions per week (maximum of 16 sessions) plus 1 home session 5 days per week | N/A | 1 or 2 sessions per week (maximum of 16 sessions) plus 1 home session 5 days per week | 8 weeks | N/A | 8 weeks |
| Wearden, 2010111 | Chronic fatigue | 10 sessions | 10 sessions | N/A | 18 weeks | 18 weeks | 18 weeks |
| Whitehead, 2002154 | Chronic fatigue | Weekly or biweekly visits over 12-month study period | N/A | N/A | 12 months | N/A | 12 months |
| Zonneveld, 2012141 | MUS | 13 weekly sessions | N/A | N/A | 13 weeks | N/A | 13 weeks |
| First author and year of publication | Condition | Intervention 1 provider: position | Intervention 3 provider: position | Intervention 2 provider: position | Intervention 1 provider: time spent on delivery | Intervention 23 provider: time spent on delivery | Intervention 2 provider: time spent on delivery |
|---|---|---|---|---|---|---|---|
| Aiarzaguena, 2007136 | MUS | GP | N/A | GP | Six sessions of 30 minutes’ duration | N/A | Six sessions of 30 minutes’ duration |
| Alda, 2011137 | Fibromyalgia | Trained therapists | 2 × psychiatrists | Family doctors | 10 × 90 minutes | NR | 1 × per month for 6 months |
| Burton, 2012157 | MUS | Specialist GP | N/A | GP | 120 minutes | N/A | NR |
| Chalder, 1997114 | Chronic fatigue | Nurse | N/A | NR | 10–15 minutes | N/A | N/A |
| Cuesta-Vargas, 2012118 | Back pain | A physiotherapist supervised both the technique and the intensity of exercise and controlled and supervised the sessions including the exercise workloads | N/A | GP | Three 30-minute sessions per week for 15 weeks. Plus 1-hour education session | N/A | 1 hour in education session |
| Escobar, 2007156 | MUS | 4 doctoral-level psychologists and 4 psychology doctoral candidates | N/A | GP | 9 × 50 minutes and 1 × 90-minutes session | N/A | N/A |
| Friedberg, 2013151 | Chronic fatigue | Nurse | Nurse therapist | N/A | Up to 2 hours | NR | N/A |
| Huibers, 2004/Leone, 2006153,155 | Chronic fatigue | GP | N/A | GP | 150 minutes | N/A | NR |
| Kashner, 1995161 | Somatoform disorder | Family doctor | N/A | Family doctor | Regular schedules meetings | N/A | N/A |
| Kennedy, 2005129 | IBS | 4 general practice nurses | N/A | Unclear – GP prescription | 6 × 50-minute sessions at weekly intervals of face-to-face contact | N/A | N/A |
| Kobeissi, 2012110 | Single MUS | 5 × clinical psychologists and physical trainers | N/A | Clinical psychologist | 12 × 75 minutes clinical psychologist, 12 × 30 minutes physical trainer | N/A | 3 × telephone calls |
| Kocken, 2008103 | Somatoform disorder | Health educators and GP | GP | NR | NR | ||
| Kolk, 2004104 | MUS | 15 psychologists qualified as therapists | N/A | GP | 1-hour sessions, once a week, or every 2 weeks, with a maximum of 12 sessions | N/A | N/A |
| Lansinger, 2007123 | Neck pain | Physiotherapists | N/A | Physiotherapists | 10–12 × 1-hour sessions | N/A | 10–12 × 1-hour sessions |
| Larisch, 2004158 | Somatoform disorder | GP | N/A | GP | Six 20-minute sessions every other week for 3 months | N/A | Six 20-minute sessions every other week for 3 months |
| LeFort, 1998128 | Chronic pain | The author | N/A | N/A | 6 × 2-hour sessions | N/A | N/A |
| Loew, 2000122 | Single chronic pain | Experienced eFR therapists | N/A | Experienced eFR therapists | 1 hour | N/A | 1 hour |
| Luciano, 2011139 | Fibromyalgia | Speakers included 4 GPs and 1 rheumatologist (educative training), and a clinical psychologist (autogenic training) | N/A | GPs | 9 × 2-hour sessions | N/A | N/A |
| Luciano, 2014138 | Fibromyalgia | Clinical psychologist | Clinicians supervised by GP | N/A | 8 × 2.5 hours | N/A | N/A |
| Macedo, 2012119 | Back pain | Physical therapists | N/A | Physical therapists | Fourteen 1-hour sessions per patient for 8 weeks | N/A | Fourteen 1-hour sessions per patient for 8 weeks |
| Margalit, 2008268 | MUS | A primary care team with expertise in the biopsychosocial approach | N/A | PCP | 3–28 (mean: 7.3) encounters over a period of 1.5–12 months. Follow-up lasting 30 minutes once per week | N/A | NR |
| Marques, 2015133 | Chronic fatigue | Health psychologist | N/A | N/A | 4 hours | N/A | N/A |
| Martin, 200799 | MUS | A clinical psychologist and a medical specialist for psychotherapeutic medicine | N/A | GP | 3–4 hours | N/A | N/A |
| McBeth, 2012125/Beasley, 2015126 | Chronic pain | 4 therapists accredited by the British Association for Behaviour and Cognitive Psychotherapies | Fitness instructor |
Family physician Group 4 combination of CBT and exercise |
Initial assessment (45–60 minutes), 7 × weekly sessions (30–45 minutes), 1 session 3 months and 1 session 6 months post randomisation | 6 x monthly 20–60 minutes sessions |
N/A Group 4 combination CBT and exercise |
| McLeod, 1997105 | Somatoform disorder | Led by trained leaders including physicians, nurses, social workers, and psychologists | N/A | Led by trained leaders including physicians, nurses, social workers, and psychologists | 1 weekly session for 6 weeks | N/A | After 2 months, 1 weekly session for 6 weeks |
| Moreno, 2013/Gili, 2014144,148 | Somatoform disorder | 2 psychologists | 2 psychologists | GPs | 10 weekly 1-hour sessions | 10 weekly 2-hour sessions | NR |
| Morriss, 2007108 | MUS | 3 nurses and a psychologist (health facilitators) with professional experience in primary care or liaison psychiatry but not reattribution therapy | N/A | GP | NR | N/A | N/A |
| Moss-Morris, 2005152 | Chronic fatigue | Researcher | N/A | GP | 12 hours | N/A | NR |
| Moss-Morris, 2010130 | IBS | Health psychologist | N/A | N/A | 1-hour face to face and 2 × 1-hour telephone sessions | N/A | N/A |
| Peters, 2002106 | MUS | 1 of 2 physiotherapists | N/A | 1 of 2 physiotherapists | 20 × 1-hour sessions | N/A | 20 × 1-hour sessions |
| Pols, 2008145 | MUS | GP | N/A | GP | 4–6 weekly appointments | N/A | N/A |
| Posse, 200496 | Somatoform disorder | Author and diploma candidate under the supervision of training analysts | N/A | GP | 1 hour per patient per week for 6 months | N/A | NR |
| Ridsdale, 2001112 | Chronic fatigue | 3 qualified CBT therapists | N/A | Three qualified counsellors | 6 × 1-hour sessions | N/A | 6 × 1-hour sessions |
| Ridsdale, 2004113 | Chronic fatigue | 6 cognitive–behaviour therapists | N/A | Five physiotherapists | 6 × 45-minute sessions | N/A | 6 × 45-minute sessions |
| Ridsdale, 2012115 | Chronic fatigue | 8 registered physiotherapists | 8 British Association for Counselling and Psychotherapy-registered therapists | Usual care with GP | 8 × 30-minute sessions plus 2 telephone calls as follow-up | 8 × 50 minute sessions plus 2 telephone calls as follow-up | N/A |
| Rief, 2006102 | MUS | GP | N/A | GP | NR | N/A | NR |
| Robinson, 2006131 | IBS | NR | Trial co-ordinator | PCP | NR | NR | N/A |
| Rosendal, 2007146 | Somatoform disorder | Family physician | N/A | Family physician | NR | N/A | NR |
| Rothman, 2013127 | Chronic pain | Multidisciplinary – GP, physiotherapist, psychologist | N/A | Multidisciplinary – GP, physiotherapist, psychologist | NR – depended on patient | N/A | NR – depended on patient |
| Ryan, 2004109 | Mixed MUS | 4 × clinical or health psychology graduate students | N/A | N/A | 8 × 1-hour sessions | N/A | N/A |
| Sañudo, 2010140 | Fibromyalgia | NR | NR | Family physician | 2 × 45–60 minutes per week for 24 weeks | 2 × 45–60 minutes per week for 24 weeks | N/A |
| Schade, 2011272 | Somatoform disorder | The professionals had different professional backgrounds (family doctors, general medical practitioners, psychologists, physiotherapists, social workers, nurses, birth assistants and dentists) | N/A | GPs and other professionals | NR | N/A | NR |
| Schaefert, 2013147 | MUS | GP | N/A | GP | 10 × 90-minute sessions plus 2 booster sessions | N/A | N/A |
| Schilte, 2001159 | Somatoform disorder | Disclosure doctor in the first and second meetings. Both disclosure doctor and GP together in third meeting (where applicable) | N/A | GP | 3 hours (in some cases an additional 30 minutes to 1 hour) | N/A | NR |
| Smith, 1995100 | MUS | Family doctor + psychiatrist | N/A | N/A | Regular schedules meetings, perhaps every 4–6 weeks | N/A | N/A |
| Smith, 2006107 | MUS | 4 nurse practitioners | N/A | NR | Minimum 12 × 20 minutes face to face with additional telephone contacts | N/A | N/A |
| Smith, 2009142 | MUS | 4 PCPs and 1 experienced case manager | N/A | GP | 7 visits with the PCP (and 3 with the CM who also made eight scheduled telephone calls). Mean number of encounters (minutes per encounter): office visits – 7 (38.3); scheduled telephone calls – 3 (20.5); after-hours telephone calls – 3 (14.7); co-ordination of care – 1 (20) | N/A | N/A |
| Sumathipala, 2000116 | MUS | A psychiatrist trained in CBT | N/A | Their own primary care provider although they may have consulted with a number of practitioners over the study period | 6 × 30-minute sessions | N/A | N/A |
| Sumathipala, 2008117 | MUS | 8 × PCPs | N/A | 3 × PCPs | 6 × 30-minute sessions | N/A | 6 × 30-minute sessions |
| Toft, 201097 | MUS | GPs | N/A | GPs | Not specified | N/A | N/A |
| Tummers, 2012149 | Chronic fatigue | 8 psychiatric nurses | N/A | N/A | NR but fortnightly e-mail contact | N/A | N/A |
| van der Feltz-Cornelis, 2006160 | MUS | N/A | N/A | ||||
| van der Roer, 2008120 | Back pain | 105 primary care physiotherapists | N/A | 105 primary care physiotherapists | Unclear but 30 sessions | N/A | Unclear but mean 13 sessions |
| van Ravesteijn, 2013143 | MUS | 2 × mindfulness trainers | N/A | GP | 8 × 2.5-hour sessions | N/A | N/A |
| Walti, 2015121 | Back pain | Physiotherapist A | N/A | Physiotherapist B | 30 minutes once or twice per week for 8 weeks per patient | N/A | 30 minutes once or twice per week for 8 weeks per patient |
| Wearden, 2010111 | Chronic fatigue | 3 registered, adult specialty, general nurses | 3 registered, adult specialty, general nurses | GP | 90-minute home visit on week 1; 1-hour home visits on weeks 2, 4, 10 and 19; and 30-minute telephone calls on weeks 3, 6, 8, 12 and 15 | 90-minute home visit on week 1; 1-hour home visits on weeks 2, 4, 10 and 19; and 30-minute telephone calls on weeks 3, 6, 8, 12 and 15 | N/A |
| Whitehead, 2002154 | Chronic fatigue | GPs | N/A | GPs | 10 minute biweekly sessions over 12 months | N/A | 10-minute biweekly sessions over 12 months |
| Zonneveld, 2012141 | MUS | 6 psychologists | N/A | NR | 13 × 2-hour sessions | N/A | N/A |
Narrative synthesis of results
| First author and year of publication | Condition | Interventions Scale | Results summary |
|---|---|---|---|
| Cuesta-Vargas, 2012118 | Pain single site |
MM vs. GSH VAS |
DWR+GP intervention group significantly better than GP group alone at all time points |
| Macedo, 2012119 | Pain single site |
GA vs. GA NRS |
No significant or clinically important differences between groups at any time point |
| van der Roer, 2008120 | Pain single site |
MM vs. SES NRS |
Significantly lower pain intensity for MM group at 26 weeks. No significant difference at 1 year |
| Walti, 2015121 | Pain single site |
MM vs. SES NRS |
Mean pain decreased significantly more in MM group |
| LeFort, 1998128 | Pain multisite |
GSH vs. UC VAS |
Intervention group showed reduced pain problem severity compared with control group |
| Alda, 2011137 | Pain multisite |
CBTHI vs. ME vs. UC VAS |
No significant differences in pain between groups at the end of treatment. Greater reduction in pain for RPT group compared with TAU group at 6-month follow-up |
| Luciano, 2014138 | Pain multisite |
CBTHI vs. ME vs. UC VAS |
ACT was more effective than medication and waiting list in subjective pain reduction |
| Luciano, 2011139 | Pain multisite |
MM vs. UC FIQ – Pain Subscale |
Psychoeducation group showed less pain than usual-care group at follow-up |
| Sañudo, 2010140 | Pain multisite |
SES vs. SES vs. UC SF-36 Pain |
Significant improvement from baseline only for combined exercise group at 24 weeks. No improvement for usual-care group |
| Aiarzaguena, 2007136 | MUS/somatoform |
GP-re vs. GP-re SF-36 Pain |
Both groups showed an improvement in bodily pain at 12-month follow-up. Modified reattribution group showed significantly greater improvement than standard reattribution group |
| Peters, 2002106 | MUS/somatoform |
SES vs. RSSE SF-36 Pain |
No significant change over time or between groups |
| Gili, 2014/Moreno, 2013144,148 | MUS/somatoform |
CBTHI vs. CBTHI vs. UC+ SF-36 Pain |
Individual CBT group showed greater improvement in pain compared with group at follow-up and at 6 months. Group CBT was no more effective than TAU at any time point |
| Rothman, 2013127 | Pain multisite |
GP-O vs. UC+ VAS |
No significant difference in pain intensity between groups |
| Loew, 2000122 | Pain single site |
RSSE vs. RSSE Pain days |
Functional relaxation group showed greater reduction of intense pain; medium pain; and significantly fewer total pain days than the placebo relaxation technique |
| Rosendal, 2007146 | MUS/somatoform |
GP-MM vs. UC SF-36 Pain |
Significantly greater improvement in pain in control group than in intervention group. Significance disappeared after controlling for multiple comparisons |
| van Ravesteijn, 2013143 | MUS/somatoform |
OP vs. UC+ SF-36 Pain |
No significant differences between groups at any time point. Within-group analyses showed significant improvement in bodily pain in MBCT group at 9-month follow-up but not in the enhanced usual-care group |
| Zonneveld, 2012141 | MUS/somatoform |
CBTHI vs. UC SF-36 Pain |
Significantly better improvement in bodily pain in the intervention group than in the control group |
| McBeth, 2012125/Beasley, 2015126 | Pain multisite |
CBTHI vs. SES vs. MM vs. UC SF-36 Pain |
Summaries not given. Means show trends towards 6 months TAU being the lowest, then exercise, then combined and then TCBT. 9 months pain lowest then exercise and combined, then TCBT |
| Lansinger, 2007123 | Pain single site |
RSSE vs. SES VAS |
No significant differences in average neck pain in past week between groups at any time point but both groups improved from baseline to end of treatment and at 6 and 12 months |
| Pols, 2008145 | MUS/somatoform |
MM vs. UC SF-36 Pain |
No significant improvement |
| Kocken, 2008103 | MUS/somatoform |
OP vs. UC SF-36 (1 pain item) |
Significant improvement for intervention group on SF-36 (1 item measured) |
| Schaefert, 2013132 | MUS/somatoform |
MM vs. GP-MM SF-36 Pain |
No significant improvement |
| Smith, 2009142 | MUS/somatoform |
MM vs. UC SF-36 Pain |
Significance not reported |
| First author and year of publication | Condition | Interventions scale | Results summary |
|---|---|---|---|
| Ho, 2012150 | Chronic fatigue |
RSSE vs. UC The Fatigue Scale |
Total fatigue score was significantly improved at 5 weeks and 4 months for both the qigong group and the waiting list group |
| Friedberg, 2013151 | Chronic fatigue |
CBTLI vs. RSSE vs. UC Fatigue Severity Scale |
Changes in Fatigue Severity Scale scores from baseline to 12 months were unrelated to diagnostic group. Significantly greater improvement in fatigue for CBT group compared with support or usual-care groups. Only CBT group showed significant within-group improvement in fatigue |
| Huibers, 2004/Leone, 2006153,155 | Chronic fatigue |
GP-CBT vs. UC CIS – Fatigue Severity Subscale |
No significant difference between CBT and usual-care groups at any point including 4 years’ follow-up |
| Marques, 2015133 | Chronic fatigue |
GA vs. GSH CIS20-P Total Fatigue severity |
Significant effect of GA intervention on fatigue severity after controlling for the effects of covariates |
| Moss-Morris, 2005152 | Chronic fatigue |
GA vs. UC 14-item Fatigue Scale |
GA group scored lower on total fatigue at 12 weeks’ follow-up compared with usual-care group after controlling for age and baseline differences. Effect persisted at 6 months |
| Ridsdale, 2001112 | Chronic fatigue |
CBTHI vs. OP 11-item Fatigue Questionnaire |
Fatigue scores fell in both groups. Analyses showed a non-significant trend in favour of counselling at 6-month follow-up |
| Ridsdale, 2004113 | Chronic fatigue |
CBTLI vs. GA 11-item Fatigue Questionnaire |
Significant fall in fatigue in both groups for average follow-up time. A small difference between groups favoured CBT over GA. This pattern was replicated when analysing data only from patients who completed all six sessions |
| Ridsdale, 2012115 | Chronic fatigue |
GA vs. OP vs. GSH 11-item Fatigue Questionnaire |
Significant improvement in fatigue score at 6 and 12 months for all three groups, with no significant difference between groups |
| Tummers, 2012149 | Chronic fatigue |
CBTLI vs. UC CIS – Fatigue Severity Subscale |
Significantly greater decrease in fatigue severity for patients in the CBT group |
| Wearden, 2010111 | Chronic fatigue |
GA vs. OP vs. UC The Fatigue Scale |
Patients in GA group had significantly improved fatigue compared with UC group at 20 weeks but no longer significant at 70 weeks. No significant effect for OP intervention at either time point |
| Luciano, 2011139 | Pain multisite |
MM vs. RSSE FIQ – Fatigue Subscale |
Psychoeducation group showed less general fatigue than usual-care group at follow-up |
| Whitehead, 2002154 | Chronic fatigue |
GP-MM vs. UC The Fatigue Scale |
Fatigue fell in both groups but no significant difference between groups at 6 or 12 months. Fatigue remained abnormally high in both groups |
| Chalder, 1997114 | Chronic fatigue |
GSH vs. UC Fatigue Questionnaire |
Total fatigue scores fell in both groups. Patients in the intervention group were less fatigued over average of all time points than control group when pre-intervention fatigue was controlled for |
| McBeth, 2012125/Beasley, 2015126 | Pain multisite |
CBTHI vs. SES vs. MM vs. UC CFQ |
Improvements observed but not significant after adjusting for multiple comparisons |
| First author and year of publication | Condition | Interventions scale | Results summary |
|---|---|---|---|
| Kennedy, 2005129 | IBS |
MM vs. ME IBS-SSS |
CBT plus medication had a beneficial summary effect over medication alone. Benefits of CBT declined over time. No significant effect by 12 months after treatment |
| Moss-Morris, 2010130 | IBS |
CBTLI vs. UC IBS-SSS |
No difference at the end of treatment. 3- and 6-month follow-ups favoured SM group over TAU |
| Robinson, 2006131 | IBS |
GSH vs. MM vs. UC CGIS – Severity of Symptoms |
Neither guidebook nor self-help group intervention had an effect on scores on the severity subscale of the CGIS over 1 year compared with controls |
| First author and year of publication | Condition | Interventions scale | Results summary |
|---|---|---|---|
| Peters, 2002106 | MUS/somatoform |
SES vs. RSSE HSCL – somatisation |
Significant decline in somatisation (HSCL) over time, from start of treatment to 6-month follow-up, but was not significant at mid-programme or end of programme. No significant difference between groups |
| Zonneveld, 2012141 | MUS/somatoform |
CBTHI vs. UC SCL-90-S |
Significantly better improvement in SCL-90-S for the intervention group compared with the control group |
| Kobeissi, 2012110 | MUVD |
RSSE vs. UC SASS – somatisation |
Small reduction favours intervention, not significant |
| Larisch, 2004158 | MUS/somatoform |
GP-re vs. UC SOMS-7 |
Significant improvement of symptoms in the intervention group compared with the control group at 3 months. This effect was lost after controlling for confounders and baseline variables. At 6 months this effect was significant even after controlling for confounding factors |
| McLeod, 1997105 | MUS/somatoform |
OP vs. UC SCL-90-S |
Significantly greater decrease in somatisation for the intervention group compared with the waiting list group |
| Rosendal, 2007146 | MUS/somatoform |
GP-MM vs. UC SCL-90-S |
No significant difference between groups |
| Schilte, 2001159 | MUS/somatoform |
GP-OP vs. UC SCL-90-S |
No significant difference between groups at any time point |
| Toft, 201097 | MUS/somatoform |
GP-MM vs. UC SCL SOM |
Patients in GP MUS management group meeting criteria for SD or somatisation disorder showed a smaller improvement in symptoms than patients in the usual-care group |
| Rief, 2006102 | MUS/somatoform |
GP-MM vs. UC SOMS |
Significant reduction in somatoform symptoms for patients in the trained GP group compared with the untrained GP group for the SSI interview, but no difference between groups on the SOMS |
| Martin, 200799 | MUS/somatoform |
CBTLI vs. UC SOMS-7/Bradford Somatic Inventory |
Significant reduction in number of symptoms in both groups on SOMS-7. For Bradford Somatic Inventory severity of symptoms, CBT group showed a greater reduction than control group. No improvement in severity for the control group |
| Gili, 2014/Moreno, 2013144,148 | MUS/somatoform |
CBTHI vs. CBTHI vs. UC+ SOMS |
CBT groups showed greater improvement at the end of treatment than TAU. Individual CBT was more effective than group CBT. Effects remained but decreased over 6 and 12 months’ follow-up |
| Kolk, 2004104 | MUS/somatoform |
OP vs. UC SCL-90-S |
No significant difference between intervention groups, although a positive main effect for time from baseline to end of treatment and follow-up was found |
| Escobar, 2007156 | MUS/somatoform |
CBTHI vs. UC+ PHQ-15 – somatic complaints |
Significant improvement in physical symptoms for the intervention group compared with the control at the end of treatment and at 6-month follow-up |
| Schaefert, 2013147 | MUS/somatoform |
MM vs. GP-MM PHQ-15 – somatic complaints |
Significantly greater increase in somatic symptom severity for MM group compared with GP-MM group at 6 months was no longer significant at 12 months |
| Smith, 2009142 | MUS/somatoform |
MM vs. UC PHQ-15 – somatic complaints |
Significant effect for the intervention on the PHQ-15 over time. Trend towards greater improvement for the intervention compared with controls but not significant |
| Sumathipala, 2000116 | MUS/somatoform |
CBTLI vs. UC Bradford Somatic Inventory somatic symptoms |
Significantly greater reduction in Bradford Somatic Inventory score for the intervention group compared with the control group |
| Sumathipala, 2008117 | MUS/somatoform |
MM vs. GP-MM Bradford Somatic Inventory – somatic symptoms |
No significant difference in change in Bradford Somatic Inventory between intervention and control group, although both groups improved over time |
| van Ravesteijn, 2013143 | MUS/somatoform |
OP vs. UC+ PHQ-15 – somatic complaints |
No significant differences between groups at either time point. Within-group analyses showed improvement for the MBCT group at the end of treatment and at 9 months’ follow-up, whereas the enhanced usual-care group did not show improvement |
| Marques, 2015133 | Chronic fatigue |
GA vs. GSH PHQ-15 – somatic complaints |
Intervention showed no significant effect |
| Burton, 2012157 | MUS/somatoform |
GP-MM vs. UC PHQ-14 |
Difference favours symptoms clinic over usual care. No measures of significance given due to small sample size |
| Smith, 2006107 | MUS/somatoform |
MM vs. UC PSC |
PSC findings not reported |
| First author and year of publication | Condition | Interventions scale | Results summary |
|---|---|---|---|
| Cuesta-Vargas, 2012118 | Pain single site |
MM vs. GSH SF-12-MH |
DWR + GP intervention group significantly better than GP group alone at all time points |
| Macedo, 2012119 | Pain single site |
GA vs. GA SF-36-MCS |
No significant or clinically important differences between groups at any time point |
| Ho, 2012150 | Chronic fatigue |
RSSE vs. UC SF-12-MH |
Mental functioning was significantly improved at 5 weeks and 4 months for the qigong group but not in the waiting list group |
| Huibers, 2004/Leone, 2006153,155 | Chronic fatigue |
GP-CBT SCL-90 |
No significant difference between CBT and usual-care groups at any point including 4-year follow-up |
| Marques, 2015133 | Chronic fatigue |
GA vs. GSH SF-12-MH |
Significant time-by-group interaction after controlling for covariates in favour of intervention group |
| LeFort, 1998128 | Pain multisite |
GSH vs. UC SF-36-MH |
Positive trend to improvement for intervention group compared with controls |
| Aiarzaguena, 2007136 | MUS/somatoform |
GP-re vs. GP-re SF-36-MH |
Both groups showed an improvement in mental health at 12-month follow-up. Modified reattribution group showed a greater improvement than standard reattribution group; this effect almost reached significance |
| Peters, 2002106 | MUS/somatoform |
SES vs. RSSE SF-36-MH |
Mental health (SF-36) significantly improved over time from start of treatment to 6-month follow-up, with significance at end of programme. No significant difference between groups |
| Pols, 2008145 | MUS/somatoform |
MM vs. UC SF-36-MH |
Almost significant trend towards greater improvement for intervention group for mental health subscale compared with controls at 12 months |
| Smith, 2009142 | MUS/somatoform |
MM vs. UC SF-36-MCS |
Significant effect for the intervention on the SF-36 MCS over time. Trend towards greater improvement for the intervention compared with controls but not significant |
| Sumathipala, 2008117 | MUS/somatoform |
MM vs. GP-MM GHQ-30 – Psychological Morbidity |
No significant difference in change in emotional distress between intervention and control group, although both groups improved over time |
| van Ravesteijn, 2013143 | MUS/somatoform |
OP vs. UC+ SF-36-MH |
Significantly greater improvement in MCS but not MH subscale at the end of treatment for MBCT group only. At 9-month follow-up, within group analyses for MCS and MH subscale showed significantly improved scores for both groups |
| Zonneveld, 2012141 | MUS/somatoform |
CBT-HI SF-36-MH |
No significant differences for mental health between groups, nor for the MCS |
| Gili, 2014/Moreno, 2013144,148 | MUS/somatoform |
CBTHI vs. CBTHI vs. UC+ SF-36-MH |
Individual CBT showed greater improvement in mental health than TAU at 6- and 12-month follow-up. No other significant differences between groups |
| Kocken, 2008103 | MUS/somatoform |
OP vs. UC SCL-90 Anxiety and Depression |
Significant improvement in mental health compared with control group |
| Larisch, 2004158 | MUS/somatoform |
GP-re vs. UC SF-12 |
No significant differences between groups |
| Rosendal, 2007146 | MUS/somatoform |
GP-MM vs. UC SF-36-MH |
No significant difference between groups |
| Schaefert, 2013147 | MUS/somatoform |
MM vs. GP-MM SF-36-MCS |
Significantly greater increase in mental component summary for MM group compared with GP-MM group, significant for per-protocol analysis at 6 and 12 months, only at 12 months for ITT analysis |
| Smith, 1995100 | MUS/somatoform |
UC+ vs. UC RAND MHI |
No statistical differences between groups |
| Toft, 201097 | MUS/somatoform |
GP-MM vs. UC SF-36-MH |
No significant differences between intervention groups for any diagnostic subgroups |
| van der Feltz-Cornelis, 2006160 | MUS/somatoform |
MM vs. GP-re SIP |
No significant difference between groups for SCL-90 psychological symptoms. Note that no means were reported because of a lack of significance |
| Robinson, 2006131 | IBS |
GSH vs. MM vs. UC SF-36 – MH |
No significant effect for guidebook on mental health, although difference favoured guidebook |
| Kashner, 1995161 | MUS/somatoform |
RSSE vs. UC+ RAND MHI |
Significant improvement in mental health for therapy group compared with UC group. Trend towards patients who attended one or more sessions showing greater improvement but not statistically significant. The more sessions attended, the greater the improvement in mental health |
| McBeth, 2012125 | Pain multisite |
CBTHI vs. SES vs. MM vs. UC SF-36-MCS |
Summaries not given. The means show trends towards 6 months’ TAU being the lowest, then combined, then TCBT, then exercise highest. 9 months’ TAU is the lowest, then combined, then exercise then TCBT |
| Sumathipala, 2000116 | MUS/somatoform |
CBTLI vs. UC GHQ-30 |
Significantly greater reduction in level of distress for intervention group compared with control group |
| Chalder, 1997114 | Chronic fatigue |
GSH vs. UC GHQ-12 |
The self-help group slightly improved, whereas the control group deteriorated |
| Kennedy, 2005129 | IBS |
MM vs. ME HADS total |
Summary effect of CBT over 1 year was significant reduction in HADS score |
| Sañudo, 2010140 | Pain multisite |
SES vs. SES vs. UC SF-36-MH |
Significant improvement from baseline only for combined exercise group at 24 weeks. No improvement for usual-care group |
| Burton, 2012157 | MUS/somatoform |
GP-MM vs. UC SF-12-MCS |
No measures of statistical significance included as a result of the small sample size |
| Smith, 2006107 | MUS/somatoform |
MM vs. UC SF-36-MH |
Findings not reported |
| First author and year of publication | Condition | Interventions scale | Results summary |
|---|---|---|---|
| Friedberg, 2013151 | Chronic fatigue |
CBTLI vs. RSSE vs. UC BAI |
No significant differences for change in anxiety change by time, treatment group, or diagnostic group and no significant interactions between any of the above factors |
| Marques, 2015133 | Chronic fatigue |
GA vs. GSH BSI – Anxiety |
Intervention showed no significant effect |
| Ridsdale, 2001112 | Chronic fatigue |
CBTHI vs. OP HADS-A |
No significant differences between groups |
| Ridsdale, 2004113 | Chronic fatigue |
CBTLI vs. GA HADS-A |
Anxiety scores fell in both groups following treatment. Anxiety scores were significantly lower for CBT group compared with GA group |
| Ridsdale, 2012115 | Chronic fatigue |
GA vs. OP vs. GSH HADS-A |
Reduction in anxiety at 6 months of similar magnitude for all three groups |
| Wearden, 2010111 | Chronic fatigue |
GA vs. OP vs. UC HADS-A |
No significant effect for OP intervention |
| Alda, 2011137 | Pain multisite |
CBTHI vs. ME vs. UC HARS |
Equal significant reduction in anxiety at the end of treatment and at 6-month follow-up for CBT and RPT groups compared with TAU |
| Luciano, 2014138 | Pain multisite |
CBTHI vs. ME vs. UC HADS-A |
ACT more effective than medication and waiting list in reduction in anxiety short and long term |
| Luciano, 2011139 | Pain multisite |
MM vs. UC FIQ – Anxiety Subscale |
Psychoeducation group showed lower anxiety than usual-care group at follow-up |
| Moss-Morris, 2010130 | IBS |
CBTLI vs. UC HADS-A |
Small group-by-time interaction. No between groups differences. Within-groups significant reduction in anxiety from baseline to 6 months’ follow-up for SM, none for TAU |
| Escobar, 2007156 | MUS/somatoform |
CBTHI vs. UC+ HAM-A |
No significant difference between groups at either time point |
| Kolk, 2004104 | MUS/somatoform |
OP vs. UC SCL-90 – Anxiety |
No significant difference between intervention groups. Although a positive main effect for time from baseline to end of treatment was found |
| Morriss, 2007108 | MUS/somatoform |
GP-re vs. UC HADS-A % caseness |
No significant difference between groups for anxiety caseness |
| Peters, 2002106 | MUS/somatoform |
SES vs. RSSE HADS-A |
Significant decline in anxiety from start of treatment to 6-month follow-up. This decline was significant from mid-programme. No significant difference between groups |
| Smith, 2009142 | MUS/somatoform |
MM vs. UC SSAS |
No significant effects |
| Zonneveld, 2012141 | MUS/somatoform |
CBTHI vs. UC SCL-90A |
No significant differences between groups for anxiety |
| Kobeissi, 2012110 | MUVD |
RSSE vs. UC HSCL-25 – Anxiety |
Marginal reduction for intervention, not significant |
| Gili, 2014/Moreno, 2013144,148 | MUS/somatoform |
CBTHI vs. CBTHI vs. UC+ HAM-A |
Individual CBT group had more improved anxiety than group CBT or TAU at the end of treatment. By 12 months, only group CBT had maintained improvement |
| Larisch, 2004158 | MUS/somatoform |
GP-re vs. UC HADS-A |
Significant improvement in anxiety in the intervention group compared with the control group at 3 months. This effect was lost after controlling for confounders and baseline variables |
| McLeod, 1997105 | MUS/somatoform |
OP vs. UC SCL-90 Anxiety |
Significantly greater decrease in anxiety for the intervention group compared with the waiting list group |
| Schilte, 2001159 | MUS/somatoform |
GP-OP vs. UC SCL-90 Anxiety |
No significant difference between groups at any time point |
| Posse, 200496 | MUS/somatoform |
OP vs. UC Somatic Anxiety |
No significant change after therapy |
| Rothman, 2013127 | Pain multisite |
GP-O vs. UC+ SCI-93 Stress |
No significant difference between groups for perceived stress |
| Rief, 2006102 | MUS/somatoform |
GP-MM vs. UC BAI |
Significant improvement in anxiety for the patients in the trained GP group compared with those in the untrained GP group |
| Whitehead, 2002154 | Chronic fatigue |
GP-MM vs. UC HAD |
No significant differences between groups at any time point |
| Pols, 2008145 | MUS/somatoform |
MM vs. UC STAI |
Significant improvement in anxiety at 12 months for intervention group |
| Burton, 2012157 | MUS/somatoform |
GP-MM vs. UC GAD-7 |
No measures of statistical significance included due to small sample size |
| Tummers, 2012149 | Chronic fatigue |
CBTLI vs. UC BSI |
No significant difference between groups |
| Smith, 2006107 | MUS/somatoform |
MM vs. UC SSAS |
Findings not reported |
| Kennedy, 2005129 | IBS |
MM vs. ME HADS |
Summary effect of CBT over 1 year was a significant reduction in HADS anxiety and depression |
| First author and year of publication | Condition | Interventions scale | Results summary |
|---|---|---|---|
| Friedberg, 2013151 | Chronic fatigue |
CBTLI vs. RSSE vs. UC BDI |
No significant differences for change in depression by time, treatment group, or diagnostic group and no significant interactions between any of the above factors |
| Marques, 2015133 | Chronic fatigue |
GA vs. GSH BSI – Depression |
Intervention showed no significant effect |
| Ridsdale, 2001112 | Chronic fatigue |
CBTHI vs. OP HADS–D |
No significant differences between groups |
| Ridsdale, 2004113 | Chronic fatigue |
CBTLI vs. GA HADS–D |
Depression scores fell in both groups following treatment. No significant difference between groups |
| Ridsdale, 2012115 | Chronic fatigue |
GA vs. OP vs. GSH HADS–D |
Reduction in depression at 6 months of similar magnitude for all three groups |
| Wearden, 2010111 | Chronic fatigue |
GA vs. OP vs. UC HADS–D |
Patients in GA group had significantly improved depression. No significant effect for OP intervention |
| LeFort, 1998128 | Pain multisite |
GSH vs. UC BDI |
No significant difference between groups |
| Alda, 2011137 | Pain multisite |
CBTHI vs. ME vs. UC HAM-D |
No significant differences between the groups at the end of treatment. Significantly greater reduction in depression at 6-month follow-up for the CBT group than in the TAU group |
| Luciano, 2014138 | Pain multisite |
CBTHI vs. ME vs. UC HADS–D |
ACT more effective than medication and waiting list in reduction of depression |
| Luciano, 2011139 | Pain multisite |
MM vs. UC FIQ – Depression Subscale |
Psychoeducation group were less depressed than usual-care group at follow-up |
| Sañudo, 2010140 | Pain multisite |
SES vs. SES vs. UC BDI |
Significant improvement from baseline for both exercise groups at 24 weeks. No improvement for usual-care group |
| Moss-Morris, 2010130 | IBS |
CBTLI HADS |
No significant group-by-time interaction |
| Escobar, 2007156 | MUS/somatoform |
CBTHI vs. UC+ HAM-D |
Significant improvement in depression for the intervention group compared with the control group at the end of treatment. This effect was no longer significant at 6-month follow-up |
| Kolk, 2004104 | MUS/somatoform |
OP vs. UC SCL-90 – Depression |
No significant difference between intervention groups. Although a positive main effect for time from baseline to end of treatment was found |
| Martin, 200799 | MUS/somatoform |
CBTLI vs. UC BDI |
Both groups showed a significant reduction in depression at follow-up. No significant difference between groups |
| Morriss, 2007108 | MUS/somatoform |
GP-re vs. UC HADS–D % caseness |
No significant difference between groups for depression caseness |
| Peters, 2002106 | MUS/somatoform |
SES vs. RSSE HADS-D |
Significant decline in depression from start of treatment to 6-month follow-up. This decline was significant from mid-programme |
| Smith, 2009142 | MUS/somatoform |
MM vs. UC CES-D |
Significant effect for the intervention on the CES-D over time and compared with the control group |
| van Ravesteijn, 2013143 | MUS/somatoform |
OP vs. UC+ PHQ-9 |
No significant differences between groups at either time point. The enhanced usual-care group showed improvement in depressive symptoms at the 9-month follow-up, whereas the MBCT group did not |
| Zonneveld, 2012141 | MUS/somatoform |
CBTHI vs. UC SCL-90 Depression |
No significant differences between groups for depression |
| Kobeissi, 2012110 | MUVD |
RSSE vs. UC HSCL-25 – Depression |
Marginal reduction for intervention, not significant |
| Gili, 2014/Moreno, 2013144,148 | MUS/somatoform |
CBTHI vs. CBTHI vs. UC+ HAM-D |
Individual CBT group had more improved depressive symptoms than group CBT or TAU at the end of treatment. Individual CBT group more improved than TAU at 6 months. No differences at 12-month follow-up |
| Larisch, 2004158 | MUS/somatoform |
GP-re vs. UC HADS-D |
Significant improvement in depression in the intervention group compared with the control group at 3 months. This effect was lost after controlling for confounders and baseline variables |
| McLeod, 1997105 | MUS/somatoform |
OP vs. UC SCL-90 Depression |
Significantly greater decrease in depression for the intervention group than in the waiting list group |
| Schilte, 2001159 | MUS/somatoform |
GP-OP vs. UC SCL-90 Depression |
No significant difference between groups at any time point |
| Rothman, 2013127 | Pain multisite |
GP-O vs. UC+ Zung |
No significant difference between groups for depression |
| Rief, 2006102 | MUS/somatoform |
GP-MM vs. UC BDI |
Both groups showed a significant reduction in symptoms over time, but there was no significant difference between groups |
| Whitehead, 2002154 | CFS |
GP-MM vs. UC HADS |
No significant differences between groups at any time point |
| Pols, 2008145 | MUS/somatoform |
MM vs. UC BDI-II |
Significant improvement in depression for intervention group at 12 months |
| Schaefert, 2013147 | MUS/somatoform |
MM vs. GP-MUS PHQ-9 |
No significant differences between groups |
| Smith, 2006107 | MUS/somatoform |
MM vs. UC CES-D |
Significant improvement in depression score from baseline to the 12-month follow-up for the intervention group but not the UC group |
| Burton, 2012157 | MUS/somatoform | PHQ-12 | No measures of statistical significance included as a result of the small sample size |
| First author and year of publication | Condition | Interventions scale | Results summary |
|---|---|---|---|
| Cuesta-Vargas, 2012118 | Pain single site |
MM vs. GSH SF-12-PF |
DWR+GP intervention group significantly better than GP group alone at all time points |
| Macedo, 2012119 | Pain single site |
GA vs. GA SF-36-PCS |
No significant or clinically important differences between groups at any time point |
| Friedberg, 2013151 | Chronic fatigue |
CBTLI vs. RSSE vs. UC SF-36-PF |
No significant differences for change in physical function by time, treatment group or diagnostic group and no significant interactions between any of the above factors |
| Ho, 2012150 | Chronic fatigue |
RSSE vs. UC SF-12-PF |
Physical functioning did not improve in either qigong or waiting list groups |
| Huibers, 2004/Leone, 2006153,155 | Chronic fatigue |
GP-CBT SF-36-PF |
No significant difference between CBT and usual-care groups at any point including at the 4-year follow-up |
| Marques, 2015133 | Chronic fatigue |
GA vs. GSH SF-12-PF |
Significant group by time interaction after controlling for the effect of covariates |
| Moss-Morris, 2005152 | Chronic fatigue |
GA vs. UC SF-36-PF |
No significant differences between groups at either the 12-week or 6-month follow-up |
| Tummers, 2012149 | Chronic fatigue |
CBTLI vs. UC SF-36-PF |
No significant difference between groups for physical functioning |
| Wearden, 2010111 | Chronic fatigue |
GA vs. OP vs. UC SF-36-PF |
Patients in OP group had significantly worse physical functioning than UC group at 20 weeks. No significant difference for GA group compared with UC at 20 or 70 weeks |
| LeFort, 1998128 | Pain multisite |
GSH vs. UC SF-36-PF |
No significant difference between groups |
| Luciano, 2011139 | Pain multisite |
MM vs. UC FIQ – PF |
Psychoeducation group showed less physical impairment than usual-care group at follow-up |
| Aiarzaguena, 2007136 | MUS/somatoform |
GP-re vs. GP-re SF-36-PF |
Both groups showed an improvement in physical functioning at 12-month follow-up. Modified reattribution group showed significantly greater improvement than standard reattribution group |
| Escobar, 2007156 | MUS/somatoform |
CBTHI vs. UC+ MOS-10 PF |
No significant difference at either time point |
| Peters, 2002106 | MUS/somatoform |
SES vs. RSSE SF-36-PF |
No change for physical function |
| Pols, 2008145 | MUS/somatoform |
MM vs. UC SF-36-PF |
No significant difference between groups at 12 months in physical functioning subscale or physical component summary |
| Smith, 2009142 | MUS/somatoform |
MM vs. UC SF-36-PCS |
No significant effects |
| van Ravesteijn, 2013143 | MUS/somatoform |
OP vs. UC+ SF-36-PF |
No significant difference between groups for physical functioning at the end of treatment. Significant within-group improvement at 9-month follow-up for MBCT group but not for enhanced usual-care group, but only for PCS not for PF subscale |
| Zonneveld, 2012141 | MUS/somatoform |
CBTHI vs. UC SF-36-PF |
No significant differences between groups for physical functioning subscale, although PCS was significant in favour of intervention group |
| Gili, 2014/Moreno, 2013144,148 | MUS/somatoform |
CBTHI vs. CBTHI vs. UC+ SF-36-PF |
Individual CBT group showed greater improvement in physical functioning than group CBT or TAU at all time points. No improvement for group CBT compared with TAU at any time point |
| Larisch, 2004158 | MUS/somatoform | GP-re vs. UC SF-12-PF | Significant improvement in physical functioning in the intervention group compared with the control group at 3 months. This effect was lost after controlling for confounders and baseline variables |
| Rosendal, 2007146 | MUS/somatoform |
GP-MM vs. UC SF-36-PF |
No significant difference between groups |
| Schaefert, 2013147 | MUS/somatoform |
MM vs. GP-MM SF-36-PCS |
Increase in physical functioning in both groups at 12 months. No significant difference in physical component summary between groups |
| Smith, 1995100 | MUS/somatoform |
UC+ vs. UC RAND – PFI |
Patients in psychiatric consultation group reported significantly greater physical functioning compared with usual-care group during the year after the intervention |
| Chalder, 1997114 | Chronic fatigue |
GSH vs. UC MOS – PF |
Physical functioning was slightly improved in the self-help group but deteriorated in the control group |
| Toft, 201097 | MUS/somatoform |
GP-MM vs. UC SF-36-PF |
Patients meeting diagnostic criteria for SD (ICD-10) had greater improvement in physical functioning compared with controls, but only at 3-month follow-up. No statistically significant improvement for patients with somatisation disorder or those with subthreshold SD |
| Robinson, 2006131 | IBS |
GSH vs. MM SF-36-PF |
No significant effect for guidebook on physical function, although difference favoured guidebook |
| Kashner, 1995161 | MUS/somatoform |
RSSE vs. UC+ RAND – PFI |
Significant improvement in physical functioning for therapy group compared with UC group. Trend towards patients who attended one or more sessions showing greater improvement but not statistically significant |
| McBeth, 2012125/Beasley, 2015126 | Pain multisite |
CBTHI vs. SES vs. MM vs. UC SF-36-PCS |
Summaries not given. The means show a trend towards 6 months, with TAU being the lowest, exercise, TCBT, then combined highest. 9 months’ TAU being the lowest, TCBT, exercise, then combined |
| Rothman, 2013127 | Pain multisite | GP-O vs. UC+ | Significant improvement in physical function for the multimodal group |
| Sañudo, 2010140 | Pain multisite |
SES vs. SES vs. UC SF-36-PF |
Significant improvement from baseline for both exercise groups at 24 weeks. No improvement for usual-care group |
| Burton, 2012157 | MUS/somatoform |
GP-MM vs. UC SF-12-PCS |
No measures of statistical significance included as a result of the small sample size |
| Smith, 2006107 | MUS/somatoform |
MM vs. UC SF-36-PF |
No significant improvement for physical functioning |
| First author and year of publication | Condition | Interventions scale | Results summary |
|---|---|---|---|
| Aiarzaguena, 2007136 | MUS/somatoform | GP – reattribution (modified) vs. GP intervention – reattribution | 76% of patients in the ‘modified’ reattribution group attended all six standardised sessions, compared with 91% in the reattribution group |
| Larisch, 2004158 | MUS/somatoform | GP – reattribution (modified) vs. UC | Reattribution group received a mean 4.8/6 sessions during the 3-month treatment period. Usual-care group received a mean 4.6/6 sessions of care |
| Morriss, 2007108 | MUS/somatoform | GP – reattribution vs. UC | All eligible GPs completed the training. 91% attended all three sessions. 22/27 practitioners felt confident or very confident about dealing with patients with MUS after training. 5/27 were uncertain or unchanged in their confidence. Non-significant trend towards increased patient satisfaction measures for intervention group compared with controls |
| Rief, 2006102 | MUS/somatoform | GP – MUS management UC | GP satisfaction ratings were similar across items. For the key item ‘how relevant was the workshop for your everyday practice in your GP office’ 48% said extremely relevant, 39% said highly relevant, 9% said partially relevant and 4% said low relevance and 0% said very low relevance |
| Rosendal, 2007146 | MUS/somatoform | GP – MUS management vs. UC | Practice level: three practices dropped out before the intervention. Another three practices were excluded as a result of low levels of patient inclusion. Patient level: 15% of eligible patients refused to participate. No significant difference between groups on patients’ satisfaction with care (‘Very satisfied with doctor–patient relationship’ 39.1% intervention group compared with 36.5% control group. ‘Very satisfied with medical-technical care’ 29.0% intervention group, 24.7% control group. ‘Very satisfied with information and support’ 36.8% intervention group, 30.6% control group) |
| Toft, 201097 | MUS/somatoform | GP – MUS management vs. UC | 412/2197 potential participants refused to participate. No reasons given |
| Whitehead, 2002154 | CF | GP intervention – MUS management vs. UC | Follow-up data obtained for 18/26 patients (69%) in the intervention group and 28/39 (72%) in the control group at 6 months and 9/26 (35%) in the intervention group and 21/39 (54%) in the control group at 12 months. In the intervention group, 5/26 (19%) patients used the diaries for ≤ 1 month, a further 5/26 (19%) stopped using the diaries at 3 months. 8/26 (31%) used the diaries for ≥ 8 months. 4/26 (15%) used the diaries for ≥ 12 months. Reasons for discontinuation included regaining full or a satisfactory level of health, feeling no need for the diaries, or feeling no benefit from the diaries |
| Huibers, 2004/Leone, 2006153,155 | CF | GP – CBT vs. UC | 5/76 participants allocated to CBT refused treatment immediately. 51/71 remaining participants completed the intervention according to protocol. The mean number of sessions attended was 5.3 |
| Schilte, 2001159 | MUS/somatoform | GP intervention – other psychotherapy vs. UC | 35/362 potential participants declined to take part. 77/81 patients in the disclosure group completed the two meetings with the disclosure doctor. 22/81 attended an additional joint consultation with their own doctor. 30 out of the 55 remaining participants did not disclose important information at the meetings, 11/55 did not want to share the disclosed information with their own doctor, 9/55 had already disclosed the information, 5/55 gave no reason for not attending the additional meeting. 47/77 disclosure group participants disclosed emotionally important events. 55/77 judged the intervention to be positive. One patient criticised the disclosure intervention, refusing to discuss her disclosure again |
| Rothman, 2013127 | Pain-MS | GP – multidisciplinaryassessment + motivational interview + psychotherapy vs. UC | Patient satisfaction with their assessment was significantly higher in the multimodal group |
| Burton, 2012157 | MUS/somatoform | GP-MM vs. UC | 8/11 patients responding to the client satisfaction questionnaire reported the intervention helped them deal with their problems more effectively. Patients appreciated the time and explanatory approach |
| First author and year of publication | Condition | Interventions scale | Results summary |
|---|---|---|---|
| Alda, 2011137 | Pain-MS | CBT high intensity vs. UC | 16/218 eligible patients decided not to participate. No reasons given |
| Escobar, 2007156 | MUS/somatoform | CBT high intensity vs. UC+ | 244/416 eligible patients were not enrolled. Reasons included patient declining to participate, being unable to make regular visits, having severe psychiatric problems or having medical explanations for their symptoms |
| Gili, 2014/Moreno, 2013144,148 | MUS/somatoform | CBT high intensity – individual vs. CBT high intensity group vs. UC+ | 53/518 potential participants refused to participate. 18/152 participants dropped out of the study of whom three were randomised to individual CBT, one to group CBT and 14 to TAU. Reasons included family problems, moving away and onset of new medical problems |
| Luciano, 2014138 | Pain-MS | CBT – high intensity vs. medication | 20 participants dropped out of the study, six in ACT group, eight in medication group and six in waiting list group |
| McBeth, 2012125/Beasley, 2015126 | Pain-MS | CBT – high intensity vs. multimodal vs. SES vs. UC | 157/224 (70.1%) of TCBT group completed at least six therapy sessions. 65/130 (50%) of the exercise group reached the compliance threshold of at least two sessions per week. 21/130 (16.2%) did not attend any sessions on their own |
| Ridsdale, 2001112 | CF | CBT high intensity vs. other psychotherapy | 51/80 (64%) patients in the counselling group completed all six therapy sessions. 55/80 (69%) patients in the CBT group completed all six therapy sessions. Reasons for not completing included not tired any more, too busy, did not find the intervention useful. 26/54 non-completers across both groups had no therapy. CBT group were significantly more satisfied with the process of therapy than the counselling group |
| Zonneveld, 2012141 | MUS/somatoform | CBT high intensity vs. UC | Participants in the intervention group attended a mean 11/20 sessions. The minimum number of attended sessions was six |
| Friedberg, 2013151 | CF | CBT low intensity vs. UC | Among FSM participants, 30/37 (81%) completed the two-session intervention and 3 months’ follow-up, and 19/37 (51%) completed the 12 months’ follow-up. Among AC participants, 31/38 (82%) completed the two-session intervention and 3 months’ follow-up, and 22 (58%) completed the 12 months’ follow-up. Among UC participants, 28/36 participants (78%) completed the two-session intervention and 3 months’ follow-up and 18 (47%) completed the 12 months’ follow-up. Reasons given not specified by intervention group |
| Martin, 200799 | MUS/somatoform | CBT low intensity vs. UC | Total drop-out rate was 15%, no significant difference in drop-out rates between groups (n = 10 in the CBT group, n = 11 in the control group). Ratings of satisfaction for CBT participants were 96% would recommend to a friend; 96% thought the intervention should be offered more; 94% felt understood by the therapist; and 92% rated the intervention as a promising strategy for the management of their symptoms |
| Moss-Morris, 2010130 | CF | CBT low intensity vs. UC | Adherence: 24/30 (80%) in self-management group returned homework sheets. Mean 6.94/10 sheets completed. Acceptability: 21/30 (70%) rated self-management treatment as much better or better than other treatment they had received. 18/30 (60%) rated SM as highly or very effective. 27/30 (90%) enjoyed the SM treatment |
| Ridsdale, 2004113 | CF | CBT low intensity vs. GA | Participants in the intervention groups attended an average of 4.6 out of a possible six sessions. Reasons for non-completion included 13/120 (11%) too busy, 8/120 (7%) lack of faith in therapy, 4/120 (3%) feeling better. Significantly more patients completed all six sessions in the CBT group (45/63, 71%) compared with the GET group (36/60, 60%). seven patients allocated to GET group did not start treatment. More patients cited lack of faith in therapy as a reason for not starting or not completing treatment in the GET group than in the CBT group |
| Sumathipala, 2000116 | MUS/somatoform | CBT low intensity vs. UC | Number of referrals to the study varied by doctor (range 7–43 referrals). 4/80 eligible patients declined to consent, 8/80 eligible patients did not attend baseline assessment. 34/34 CBT group participants attended at least one session. 29/34 (85%) attended two or more sessions. 22/34 attended three or more sessions. Drop-out rates in the CBT group were 15% between session one and two and 21% between second and third session. Drop-out rate at 3-month follow-up was 30% for the CBT group compared with 38% for the control group. Two patients were diagnosed with physical illnesses and did not complete the follow-up at 3 months. These patients reported that they ‘felt they did not have the type of illness we think’ (i.e. having a psychological basis). Satisfaction was higher at follow-up in the intervention group. Dissatisfaction was higher in the control group at follow-up |
| Tummers, 2012149 | CF | CBT low intensity vs. UC | 19/142 patients (13%) refused to take part for a number of reasons including preference for face-to-face contact, experiencing remission of symptoms, having no faith in the treatment or preferring a different treatment |
| First author and year of publication | Intervention group | Condition | Satisfaction, acceptability or adherence |
|---|---|---|---|
| Ho, 2012150 | Relaxation/stretching/social support/emotional support vs. UC | CF | 27/35 (81.8%) of participants completed the qigong intervention. 25/35 (80.6%) of participants dropped out of the waiting list group |
| Kashner, 1995161 | Relaxation/stretching/social support/emotional support vs. UC | MUS/somatoform | 20/44 participants in the group therapy group participated in one or more sessions. Mean number of sessions attended was 2.2. 4/44 attended one or two sessions. 5/44 attended three or four sessions. 5/44 attended five or six sessions. 6/44 attended seven or eight sessions |
| Kobeissi, 2012110 | Relaxation/stretching/social support/emotional support vs. UC | MUVD | 49/75 (65%) participants in the intervention group attended at least six sessions |
| Lansinger, 2007123 | Relaxation/stretching/social support/emotional support vs. SES | Pain-SS | During the intervention period: 12/60 withdrawals in qigong group; 6/62 withdrawals in exercise group |
| Loew, 2000122 | Relaxation/stretching/social support/emotional support vs. relaxation/stretching/social support/emotional support | Pain-SS | Not reported |
| First author and year of publication | Intervention group | Condition | Satisfaction, acceptability or adherence |
|---|---|---|---|
| Chalder, 1997114 | GSH vs. UC | CF | 11/70 (16%) dropouts in self-help intervention group, 14/80 (18%) dropouts in the control group. 50/70 (71%) of participants in the intervention group said they had read the booklet and, of these, 42/50 (84%) said they found it helpful |
| LeFort, 1988128 | GSH vs. UC | Pain-MS | 5/57 participants considered to be dropouts. n = 1 admitted to hospital for acute illness, n = 1 discovered ineligible after randomisation, n = 3 attended one or no classes and declined to complete questionnaire. 3/53 dropouts in control group could not be contacted at follow-up |
| First author and year of publication | Intervention group | Condition | Satisfaction, acceptability or adherence |
|---|---|---|---|
| Cuesta-Vargas, 2012118 | Multimodal (sport + education) vs. guided self-help | Pain-SS | 17.2% drop-out rate across both interventions. DWR + GP group 25/29 completers; GP alone 24/29 completers |
| Kennedy, 2005129 | Multimodal (CBT low intensity + medication) vs. medication | IBS | Fewer than half of patients were considered to have completed CBT. 14% declined therapy or dropped out. Reasons for non-attendance included no time off work or child care commitments |
| Pols, 2008145 | Multimodal (self-management + medication + CBT) vs. UC | MUS/somatoform | 35/420 (8.3%) eligible GPs approached for the study enrolled potential participants. Not all eligible patients were referred. 17/320 eligible patients were referred in one particular GP practice. 18/89 intervention patients in the intervention group dropped out before completing initial assessments, followed by a further 22 dropouts. 25/89 intervention group patients were referred to and attended CBT. 15/89 were referred to CBT but did not attend. 13/35 control patients dropped out |
| Luciano, 2011139 | Relaxation/stretching/social support/emotional support vs. UC | Pain-MS | 7/108 (6.5%) drop-out rate in the psychoeducation group. 14/108 (13%) drop-out rate in usual-care group. Reasons for dropouts not specified by intervention group |
| Schaefert, 2013147 | Multimodal (GP intervention – MUS management + other psychotherapy) vs. GP – MUS management | MUS/somatoform | More decliners in the GP-MM group than in the MM group. No difference in reasons given between groups. Reasons included reservations about the treatment (MM 29%, GP-MM 22%); lack of time (MM 22%, GP-MM 20%); lack of interest (MM 9%, GP-MM 18%); other reasons including organic disease, language barrier, low degree of suffering (MM 18%, GP-MM 9%); no reason (MM 22%, GP-MM 32%) |
| Smith, 2006107 | Multimodal vs. UC | MUS/somatoform | 200/208 (97%) participants (98/101 intervention group, 102/105 control group) completed the study |
| Smith, 2009142 | Multimodal (GP intervention CBT + medication) vs. UC | MUS/somatoform | 44/82 eligible patients agreed to take part, of whom 30 patients were included in the study |
| Sumathipala, 2008117 | Multimodal (GP-CBT + GP – MUS management) vs. GP – MUS management | MUS/somatoform | 64/75 (85%) participants in each group completed all three mandatory sessions. Low uptake of optional sessions. Significantly more participants from the structured care group (37%) attended all six sessions, compared with 20% of the CBT + structured care group |
| van der Feltz-Cornelis 2006160 | Multimodal (reattribution + collaborative care) vs. GP – reattribution | MUS/somatoform | Compliance with collaborative care model as reported by the patient was 93.2%. Compliance as reported by the GP was 91.2% |
| van der Roer, 2008120 | Multimodal (sport + education + behavioural programme) vs. strength/endurance/sport | Pain-SS | MM group 12/60 discontinued protocol, reasons were n = 3 no time, n = 5 no reason, n = 1 patient fell ill, n = 3 intervention not helping. SES group 13/54 discontinued protocol, reasons were n = 3 no time, n = 5 no reason, n = 1 patient fell ill, n = 2 intervention not helping, n = 2 patient moved away |
| Walti, 2015121 | Multimodal (education + sport + sensory discrimination) vs. strength/endurance/sport | Pain-SS | 3/14 from MM group and 3/14 from SES did not complete 8 weeks of programme participation. Reasons included MM group: no aid for home training, problems with home training interface, inappropriate and misleading use of home training interface. SES group: exacerbation of pain, no time for home training, reason unknown |
| First author and year of publication | Intervention group | Condition | Satisfaction, acceptability or adherence |
|---|---|---|---|
| Kocken, 2008103 | Other psychotherapy vs. UC | MUS/somatoform | 104/139 eligible patients agreed to participate |
| Kolk, 2004104 | Other psychotherapy vs. UC | MUS/somatoform | 3/83 intervention group patients withdrew from the study or were excluded due to lack of outcome data. 77/80 entered treatment. The mean number of sessions attended was 9.2 out of a possible 12. 17/80 stopped treatment after ≥ 1 sessions. 30/80 completed all 12 sessions. 30/80 completed 8–11 sessions (considered completion). 43% received CBT, 36% received eclectic therapy, 21% received client-centred therapy. 5/23 control group patients withdrew from the study. 17% of the control group found psychological therapy elsewhere |
| Margalit, 2008268 | Other psychotherapy vs. UC | MUS/somatoform | Not reported |
| McLeod, 1997105 | Other psychotherapy vs. UC | MUS/somatoform | 34/130 eligible participants declined to attend a group because of scheduling difficulties. 3/130 declined to be studied. 13/51 (25%) dropped out of the intervention group. 1/45 (2%) dropped out of the waiting list group |
| Posse, 200496 | Other psychotherapy vs. UC | MUS/somatoform | All patients attended all sessions |
| Ryan, 2004109 | Other psychotherapy vs. UC | MUS/somatoform | 20/40 patients allocated to other psychotherapy group refused to participate or dropped out after commencement of treatment. Reasons given included lack of interest, conflicts of time, reduction in symptoms, or started treatment but felt it was not helping their symptoms |
| Schade, 2011272 | Other psychotherapy vs. UC | MUS/somatoform | Not reported |
| van Ravesteijn, 2013341 | Other psychotherapy vs. UC+ | MUS/somatoform | 500/685 (73%) eligible participants were not interested in taking part. A further 10 declined to participate after initial interview because of lack of time. four participants (8%) who started MBCT did not complete four or more sessions |
| First author and year of publication | Intervention group | Condition | Satisfaction, acceptability or adherence |
|---|---|---|---|
| Macedo, 2012119 | GA vs. GA | Pain-SS | For the initial 8-week intervention period, both groups attended a mean 10.3 (SD 3.6) of the planned 12 sessions. For the two booster treatment sessions and home programme: 43% in GA group attended the 4-month booster session and 31.4% attended the 10-month booster session. For the motor control group, attendance was 50% and then 25.6%. For home exercises, GA vs. MCE: all the time 23% vs. 15%; most of the time 44% vs. 42%; some of the time 19% vs. 26%; a little of the time 6% vs. 5%; none of the time 5% vs. 1%. No significant difference between groups for credibility |
| Marques, 2015133 | GA vs. GSH | CF | 5/49 participants in intervention group discontinued due to lack of time |
| Moss-Morris, 2005152 | GA vs. UC | CF | 68% of GA group rated the intervention as ‘effective’ or ‘highly effective’. 68% rated the intervention as ‘better’ or ‘very much better’ than previously received interventions |
| Ridsdale, 2012115 | GA vs. other psychotherapy vs. GSH | CF | Mean 5.8 out of a possible eight sessions were attended by GET group participants. Mean 5.9 out of 8 sessions were attended by OP group participants. Half of all participants reported they were dissatisfied with care at 6 months. There was no significant difference between the three intervention groups. Regression analyses showed positive association between duration of fatigue and dissatisfaction. Dissatisfaction increased in UC+ group between 6 and 12 months. Satisfaction increased between 6 and 12 months in the GA and OP groups |
| First author and year of publication | Intervention group | Condition | Satisfaction, acceptability or adherence |
|---|---|---|---|
| Peters, 2002106 | SES vs. RSSE | MUS/somatoform | No significant difference in expectations of benefit between aerobic or stretching groups. 177/228 (78%) patients who were randomised attended a first training session. No significant difference in level of attendance between groups. Median sessions attended overall was 11 – 95 patients attended 10 or more sessions and 61 attended 15 or more sessions. 88/177 (50%) of those who began either intervention completed the homework diary – 42 in the stretching group and 46 in the aerobic group. No differences in level of homework task completion between groups |
| Sañudo, 2010140 | SES vs. SES vs. UC | Pain-MS | 4/22 participants from aerobic exercise group dropped out: n = 2 illness, n = 1 work commitments, n = 1 unable to exercise. 4/21 participants from combined exercise group dropped out: n = 1 work commitments, n = 2 illness, n = 1 family problems. Compliance: participants in aerobic exercise group attended on average 43/48 (89%) sessions. Participants in combined exercise group attended on average 41/48 (86%) of sessions |
| First author and year of publication | Intervention group | Condition | Satisfaction, acceptability or adherence |
|---|---|---|---|
| Smith, 1995100 | UC vs. UC+ | MUS/somatoform | All patients agreed to participate in the study |
| First author and year of publication | Intervention group | Condition group | Health-care utilisation |
|---|---|---|---|
| Larisch, 2004158 | GP – reattribution (modified) vs. UC | MUS/somatoform | Greater but non-significant reduction in number of visits to the doctor at 6-month follow-up for the intervention group compared with the controls group. Intervention group 54.2% reduction (mean 7.1–3.3 visits) compared with controls 26.6% reduction (mean 7.2 to 5.3 visits) |
| Morriss, 2007108 | GP – reattribution vs. UC | MUS/somatoform | No significant difference between groups in use of health-care resources |
| Rief, 2006102 | GP – MUS management UC | MUS/somatoform | Significant time by intervention group difference in doctor visits. Patients of GPs who had received the training showed a significant reduction in doctor visits compared with those in the untrained GP group |
| Huibers, 2004/Leone, 2006153,155 | GP – CBT vs. UC | Chronic fatigue | CBT group: mean 4.2 visits to the regular GP during the intervention period. Control group: mean 3.5 visits |
| Schilte, 2001159 | GP intervention – other psychotherapy vs. UC | MUS/somatoform | No significant effect for disclosure intervention on health-care utilisation |
| First author and year of publication | Intervention group | Condition group | Health-care utilisation |
|---|---|---|---|
| Ridsdale, 2001112 | CBT high intensity vs. other psychotherapy | Chronic fatigue | Mean GP consultations reduced from 4.2 before therapy to 3.1 after therapy, with no significant difference between the groups |
| Martin, 200799 | CBT low intensity vs. UC | MUS/somatoform | Both groups showed a significant reduction in GP and medical specialist visits over time. There was a significantly greater reduction in health-care visits for CBT group compared with control group. The difference in reduction was significant for GP visits but not medical specialist visits or psychotherapist visits |
| Moss-Morris, 2010130 | CBT low intensity vs. UC | Chronic fatigue | During 2-month intervention period. SM group: 4/30 (13.8%) saw a GP compared with 8/33 (26.3%) in TAU group. One patient in each group saw a specialist for IBS symptoms (3.6% SM and 3.4% TAU) |
| Ridsdale, 2004113 | CBT low intensity vs. GA | Chronic fatigue | Frequency of doctor consultations per year declined in both groups following treatment. No significant difference between groups |
| Sumathipala, 2000116 | CBT low intensity vs. UC | MUS/somatoform | Significantly fewer doctor visits during the 3-month period following baseline assessment for the CBT group compared with the control group for completers and intention-to-treat analyses |
| First author and year of publication | Intervention group | Condition group | Health-care utilisation |
|---|---|---|---|
| Kashner, 1995161 | Relaxation/stretching/social support/emotional support vs. UC | MUS/somatoform | Almost significantly greater decrease in costs of medical treatments for year following treatment for therapy group compared with UC group |
| Robinson, 2006131 | Guided self-help vs. multimodal vs. UC | IBS | Primary care visits declined in all three groups. Guidebook group patients saw significantly greater decline. Estimated effect of guidebook was to reduce GP visits by mean 1.56 visits, or 60% reduction compared with no guidebook. No significant impact of self-help group on GP visits. For hospital visits, number of visits was significantly lower for guidebook group than no guidebook. 40% reduction compared with no guidebook. No additional effect for self-help group |
| First author and year of publication | Intervention group | Condition group | Health-care utilisation |
|---|---|---|---|
| Kashner, 1995161 | Relaxation/stretching/support/stress relief/education vs. UC | MUS/somatoform | Greater decrease in costs of medical treatments for year following treatment for therapy group compared with UC group almost significant |
| Robinson, 2006131 | GSH vs. multimodal vs. UC | IBS | Primary care visits declined in all three groups. Guidebook group patients saw significantly greater decline. Estimated effect of guidebook was to reduce GP visits by mean 1.56 visits, or 60% reduction compared with no guidebook. No significant impact of self-help group on GP visits. For hospital visits, number of visits was significantly lower for guidebook group than no guidebook. 40% reduction compared with no guidebook. No additional effect for self-help group |
| First author and year of publication | Intervention group | Condition group | Health-care utilisation |
|---|---|---|---|
| Pols, 2008145 | Multimodal (self-management + medication + CBT) vs. UC | MUS/somatoform | No reduction in hospitalisation |
| Schaefert, 2013132 | Multimodal (GP intervention – MUS management + other psychotherapy) vs. GP – MUS management | MUS/somatoform | Decrease in number of visits to the GP in both groups, but only significant for the MM group. No significant difference between groups |
| Sumathipala, 2008117 | Multimodal (GP-CBT + GP – MUS management) vs. GP – MUS management | MUS/somatoform | No significant difference between groups in patient-reported consultations at 3 months |
| van der Feltz-Cornelis, 2006160 | Multimodal (reattribution + collaborative care) vs. GP – reattribution | MUS/somatoform | Significant and consistent decrease in health-care service use in both health care and general practice settings for the collaborative care model group |
| van der Roer, 2008120 | Multimodal (sport + education + behavioural programme) vs. SES | Chronic pain – single site | Detailed cost analysis in van der Roer et al.120 |
| First author and year of publication | Intervention group | Condition group | Health-care utilisation |
|---|---|---|---|
| Kolk, 2004104 | Other psychotherapy vs. UC | MUS/somatoform | No interaction effect of time by intervention group for number of GP consultations. No significant effect for intervention group. Both groups showed a significant reduction in consultations over time |
| Margalit, 2008268 | Other psychotherapy vs. UC | MUS/somatoform | No significant change in health-care utilisation over 2 years for the usual-care group. Statistically significant decline in consultant visits, emergency ward visits and hospital days for the intervention group compared with controls |
| Ryan, 2004109 | Other psychotherapy vs. UC | MUS/somatoform | Data only reported as health-care utilisation costs. Both groups showed cost reduction over time |
| van Ravesteijn, 2013341 | Other psychotherapy vs. UC+ | MUS/somatoform | No significant difference between groups in health-care utilisation during the 12-month study period. The median number of health-care contacts was 26 (range 0–129) in the MBCT group and 22 (range 0–166) in the usual-care group |
| First author and year of publication | Intervention group | Condition group | Health-care utilisation |
|---|---|---|---|
| Wearden, 2010111 | GA vs. UC | Chronic fatigue | Median GP visits during 18-week treatment period: UC group 3 (range 0–16), pragmatic rehabilitation group 2 (range 0–14), supportive listening group 3 (range 0–23). Median visits to practice nurses: UC group 0 (range 0–22), pragmatic rehabilitation 0 (range 0–4), supportive listening 0 (range 0–5) |
| First author and year of publication | Intervention group | Condition group | Health-care utilisation |
|---|---|---|---|
| Peters, 2002106 | Strength/endurance/sport vs. relaxation/stretching/social support/emotional support | MUS/somatoform | No significant differences between groups in health-care utilisation. Significant decrease for both groups in GP consultations and number of secondary care contacts at 6-month follow-up |
| First author and year of publication | Intervention group | Condition group | Health-care utilisation |
|---|---|---|---|
| Smith, 1995100 | UC vs. UC+ | MUS/somatoform | No patient in either group had frequency of visits to the referring physician at the rate recommended by the psychiatrist during the first year of study. Consultation letter patients had more visits (mean 2.1 visits) than usual-care group (mean 2.1 visits). Consultation letter patients had 0.5 fewer hospital days, 0.7 more ED visits, and 0.2 more outpatient visits than usual-care group. No statistical significance for any of these outcomes |
| First author and year of publication | Intervention group | Condition group | Adverse events |
|---|---|---|---|
| Huibers, 2004/Leone, 2006153,155 | GP – CBT vs. UC | Chronic fatigue | No adverse events reported that were attributable to CBT |
| First author and year of publication | Intervention group | Condition group | Health-care utilisation |
|---|---|---|---|
| Alda, 2011137 | CBT high intensity vs. UC | Chronic pain – multisite | |
| Gili, 2014/Moreno, 2013144,148 | CBT high intensity – individual vs. CBT high intensity group vs. UC+ | MUS/somatoform | 16/168 patients across intervention groups were withdrawn due to adverse events. Individual CBT group n = 6, group CBT n = 6, TAU n = 4. Exact nature of events not specified |
| Luciano, 2014138 | CBT – high intensity vs. medication | Chronic pain – multisite | No severe adverse events in ACT group. In the medication group 25% had nausea, 23.1% dry mouth, 21.2% drowsiness, 19.2% constipation, 21.2% headache, 21.2% fatigue |
| McBeth, 2012125/Beasley, 2015126 | CBT – high intensity vs. multimodal vs. SES vs. UC | Chronic pain – multisite | Two deaths recorded. Causes of death were metastatic cancer and pancreatic cancer. No adverse reactions to the interventions |
| Zonneveld, 2012141 | CBT high intensity vs. UC | MUS/somatoform | One adverse event was reported. One patient reported rumination about the death of a loved one, which was tiring |
| Martin, 200799 | CBT low-intensity vs. UC | MUS/somatoform | No formal assessment of side effects. No adverse events were spontaneously reported |
| Ridsdale, 2004113 | CBT low intensity vs. GA | Chronic fatigue | Adverse events not specifically reported. Two patients died before outcome: one had bronchopneumonia, the other committed suicide. This patient had a history of depression, although baseline depression score was not particularly high. This patient was in the CBT group and received 4/6 sessions of CBT before being referred back to the doctor |
| Sumathipala, 2000116 | CBT low intensity vs. UC | MUS/somatoform | Not reported but no physical disorders were detected for any participant who attended the 3-month follow-up assessment |
| Tummers, 2012149 | CBT low intensity vs. UC | Chronic fatigue | Adverse events not explicitly reported, but 12 patients, equally distributed between intervention and control groups, were found to have received an incorrect diagnosis of CFS. Of these, 4/12 had a possible somatic explanation for their fatigue (e.g. brain damage), and 8/12 seemed to have a psychiatric disorder |
| First author and year of publication | Intervention group | Condition group | Health-care utilisation |
|---|---|---|---|
| Cuesta-Vargas, 2012118 | Multimodal (sport + education) vs. guided self-help relief/education | Chronic pain – single site | One participant dropped out of GSH group as a result of increased pain |
| Kennedy, 2005129 | Multimodal (CBT low intensity + medication) vs. medication | IBS | No significant harms reported |
| van der Roer, 2008120 | Multimodal (sport + education + behavioural programme) vs. SES | Chronic pain – single site | No serious adverse events in either group |
| First author and year of publication | Intervention group | Condition group | Health-care utilisation |
|---|---|---|---|
| Margalit, 2008268 | Other psychotherapy vs. UC | MUS/somatoform | Not reported as adverse events but mortality rate at 5 years was 6/21 in the intervention group and 17/21 in the usual-care group. Note that population is patients with general medical problem confounded by psychological problems, with unexplained high costs due to symptoms that were medically unexplained. |
| First author and year of publication | Intervention group | Condition group | Health-care utilisation |
|---|---|---|---|
| Macedo, 2012119 | GA vs. GA | Chronic pain – single site | Mild adverse events reported in both groups. 17 adverse events in GA vs. 19 in motor control. n = 27 exacerbation of pain; n = 7 increase in pain in pre-existing conditions; n = 1 shin splints; n = 1 hip bursitis |
| Wearden, 2010111 | GA vs. UC | Chronic fatigue | Four events considered unrelated to the interventions were recorded during the trial period: one herpes simplex infection, one attempted suicide, one bleeding peptic ulcer and one recurrence of cancer |
Appendix 3 Quality assessment: Higgins’ risk-of-bias tool515
Summary tables


Individual risk-of-bias assessments
| Aiarzaguena 2007136 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Cluster randomised by the study epidemiologist | Unknown risk of bias. Randomisation method not described |
| Allocation concealment | GPs unaware of randomisation sequence. Recruitment of patients was performed before assignment of GPs to the study groups performed by the epidemiologist of the research team | Low risk of bias. Adequate allocation concealment |
| Performance bias | ||
| NR | Unknown risk of bias. No description of blinding of patients | |
| Detection bias | ||
| Patients completed the outcome measure with the help of an interviewer blind to the study group | Low risk of detection bias due to blinding of outcome assessment | |
| Attrition bias | ||
| 4/74 dropouts in active control group by end of study compared with 1/72 dropouts in intervention group | Low risk of bias. Similar rates of dropout between groups | |
| Reporting bias | ||
| SF-36 reported as primary outcome in protocol. No secondary outcomes listed in protocol | Low risk of bias. Primary reported outcome is SF-36 | |
| Alda 2011137 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Randomised, parallel-group, controlled trial in which patients were randomly assigned to one of three study arms (ratio 1 : 1 : 1). Computer-generated random number sequence, stratified by presence of comorbidities | Low risk of bias, adequate randomisation |
| Allocation concealment | Central telephone allocation sequence performed by researcher unconnected to study and concealed until interventions were assigned | Low risk of bias, adequate randomisation |
| Performance bias | ||
| Patients and therapists not blinded due to nature of interventions | High risk of bias due to lack of blinding | |
| Detection bias | ||
| Evaluators were blinded to participants’ treatment group assignments | Low risk of bias, adequate blinding of outcome assessment | |
| Attrition bias | ||
| 83.9% completed the study, comprising 85.9% in CBT group, 82.1% in RPT group and 83.6% in the treatment-as-usual group | Low risk of bias. Similar rates of attrition in each group | |
| Reporting bias | ||
| Outcomes in protocol are reported in the study paper, with the addition of EQ-5D data | Unclear risk of bias. EQ-5D outcome is not stated in protocol | |
| Burton 2012157 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Randomisation by automated telephone system using block allocation with variable block size | Low risk of bias. Adequate method of randomisation |
| Allocation concealment | Automated telephone system | Low risk of bias. Adequate method of allocation concealment |
| Performance bias | ||
| Patients were not blinded to allocation | High risk of bias. No blinding of patients or providers | |
| Detection bias | ||
| Follow-up assessments conducted by an investigator with no involvement in the trial | Unclear risk of bias. Unclear whether the investigator was aware of allocation | |
| Attrition bias | ||
| 15/16 participants in usual care completed follow-up compared with 11/16 in symptoms clinic | High risk of bias. > 20% attrition in intervention group | |
| Reporting bias | ||
| Outcomes stated in protocol reported in study paper | Low risk of bias. Outcomes reported as per protocol | |
| Chalder 1997114 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Computer-generated randomisation sequence | Low risk of bias. Adequate randomisation procedure |
| Allocation concealment | No description of allocation concealment strategy | Unclear risk of bias |
| Performance bias | ||
| No blinding described, but unlikely due to nature of intervention vs. usual care | High risk of bias. Patients not blinded | |
| Detection bias | ||
| NR | Unclear risk of bias. Outcome assessor not described | |
| Attrition bias | ||
| 11 dropouts in the intervention group and 14 dropouts in the control group | Low risk of bias. Similar proportion of dropout between groups | |
| Reporting bias | ||
| Protocol not located | ||
| Cuesta-Vargas 2012118 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Computer generated random sequence generation | Low risk of bias. Adequate randomisation procedure |
| Allocation concealment | Sealed, sequentially numbered envelopes | Low risk of bias. Adequate allocation concealment |
| Performance bias | ||
| Study described as single blind | Unclear risk of bias. Unclear whether patients in the exercise group would be aware that theirs was the active intervention | |
| Detection bias | ||
| No description of blinding of outcome assessors | Unclear risk of bias. Described as single-blind but unclear whether patients or outcome assessors were blind | |
| Attrition bias | ||
| Similar rates of dropout between groups | Low risk of bias. No significant rates of dropout or differences between groups | |
| Reporting bias | ||
| All outcomes stated in protocol reported in study paper | Low risk of bias. All outcomes reported as per protocol | |
| Escobar 2007156 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Computer-generated random number sequence for patient allocation | Low risk of bias. Adequate randomisation sequence |
| Allocation concealment | NR | Unclear risk of bias. No reporting of allocation concealment |
| Performance bias | ||
| Not described | High risk of bias. Patients in intervention group unlikely to be able to be blinded due to nature of intervention | |
| Detection bias | ||
| Outcome assessors blinded to study group | Low risk of bias. Adequate blinding of outcome assessment | |
| Attrition bias | ||
| 12/87 dropped out of intervention group compared with 21/85 who dropped out of control group | High risk of bias. > 20% drop-out rate in control group | |
| Reporting bias | ||
| All outcomes stated in protocol are reported in the study paper. Physical functioning is reported in the study paper but not in the protocol | Low risk of bias. All outcomes reported as per protocol with the additional of MOS-10 | |
| Friedberg 2013151 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Computer-generated block randomisation schedule | Low risk of bias. Adequate randomisation procedure |
| Allocation concealment | Randomisation performed by project team. Nurse interventionist sent allocation by project team | Low risk of bias. Adequate allocation concealment |
| Performance bias | ||
| No blinding of patients described | Unclear risk of bias. Unlikely that patients in control group were unaware of a lack of intervention, although the two active intervention groups may have been | |
| Detection bias | ||
| Outcome assessors blinded to treatment condition | Low risk of bias. Adequate blinding of outcome assessors | |
| Attrition bias | ||
| For the intervention group, 51% completed the 12-month follow-up. For the active control group, 58% completed the 12-month follow-up. For the UC group, 47% completed the 12-month follow-up | High risk of bias. > 20% dropouts in all group at follow-up. However, similar drop-out rates between groups, no significant difference in baseline measures for dropouts | |
| Reporting bias | ||
| Unclear whether secondary outcome of Global Impression of Change (GIC) relates to the diary. No scale reported for this outcome in the protocol and no outcome described as GIC in the study paper | Unclear risk of bias. Unclear whether global impression of change outcome is reported | |
| Moreno 2013/Gili 2014144,148 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Computer-generated random number sequence used | Low risk of bias. Adequate randomisation method |
| Allocation concealment | Allocation was carried out by personnel not involved in the study | Low risk of bias |
| Performance bias | ||
| Patients did not know which condition they were allocated to. GPs were blinded to condition | Low risk of bias. Patients and GPs were blinded | |
| Detection bias | ||
| NR | Unclear risk. No description of blinding of outcome assessors | |
| Attrition bias | ||
| 47/56 CBT individual, 57/64 CBT group, and 30/48 TAU completed final follow-up | High risk of bias. < 20% attrition in both intervention arms, although > 20% in TAU group | |
| Reporting bias | ||
| All outcomes from protocol reported in study papers | Low risk of bias. All outcomes reported as per protocol | |
| Ho 2012150 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Computer-generated list of random numbers | Low risk of bias. Adequate randomisation procedure |
| Allocation concealment | Participants were assigned a study order number before randomisation | Low risk of bias. Adequate allocation concealment method |
| Performance bias | ||
| Blinding participants not possible due to the nature of intervention | High risk of bias. No blinding of participants | |
| Detection bias | ||
| Group allocation blinded for laboratory technicians | Low risk of bias. Adequate blinding of outcome assessors | |
| Attrition bias | ||
| 81.8% completers in intervention group. 80.6% in the control group completed the programme | Low risk of bias. < 20% drop-out rates and similar between groups | |
| Reporting bias | ||
| Protocol not located | ||
| Huibers 2004/Leone 2006153,155 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Computer-generated list | Low risk of bias. Adequate randomisation procedure |
| Allocation concealment | Sealed opaque envelopes prepared by non-study personnel | Low risk of bias. Adequate allocation concealment |
| Performance bias | ||
| Patients unaware of randomisation procedure and existence of other group | Unclear risk of bias. Unclear whether participants would guess they were in the active intervention group | |
| Detection bias | ||
| Researchers and GPs were not blind to treatment allocation | High risk of bias. No blinding of outcome assessors | |
| Attrition bias | ||
| 70/76 intervention group participants completed final follow-up compared with 68/75 control participants | Low risk of bias. < 20% and similar drop-out rates between groups | |
| Reporting bias | ||
| All outcomes reported in protocol are reported in the study papers | Low risk of bias. Outcome reporting as per protocol | |
| Kashner 1995161 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Stratified randomisation by distance from practice | Unclear risk of bias. Randomisation procedure not described |
| Allocation concealment | NR | Unclear risk of bias. No allocation concealment method reported |
| Performance bias | ||
| NR | Unclear risk of bias. No blinding reported | |
| Detection bias | ||
| Outcome assessment by research assistant who was unaware of group allocation | Low risk of bias. Adequate blinding of outcome assessment | |
| Attrition bias | ||
| No comparison of attrition between groups | Unclear risk of bias | |
| Reporting bias | ||
| Protocol not located | ||
| Kennedy 2005129 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Random numbers in blocks of four generated from random number tables | Low risk of bias. Adequate randomisation procedure |
| Allocation concealment | Planned allocation concealment involved non-study personnel keeping allocation details. However, on occasion, the research nurse became aware of the allocation | High risk of bias. Intervention nurse aware of allocation for some participants |
| Performance bias | ||
| NR | Unclear risk of bias. No blinding of patients reported | |
| Detection bias | ||
| NR | Unclear risk of bias. No blinding of outcome assessors reported | |
| Attrition bias | ||
| Fewer than half of patients completed therapy. 41% declined therapy or dropped out | High risk of bias. High drop-out rate from intervention group | |
| Reporting bias | ||
| No distinction between primary and secondary outcomes in protocol | Unclear risk of bias, no distinction between primary and secondary outcomes | |
| Kobeissi 2012110 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Randomisation by computer-generated allocation schedule | Low risk of bias. Adequate randomisation method |
| Allocation concealment | Remote allocation by telephone was planned but actually took place in the field. Computerised allocation conducted | Low risk of bias. Adequate allocation concealment |
| Performance bias | ||
| Blinding of allocation was not feasible due to the nature of the intervention | ||
| Detection bias | ||
| Blinding of outcome assessors not described | Unclear risk of bias. No description of outcomes assessors | |
| Attrition bias | ||
| 10/99 in the intervention group lost to follow-up. 16/97 in the control group lost to follow-up | Low risk of bias. < 20% and similar rates of attrition in both groups | |
| Reporting bias | ||
| Protocol not located | ||
| Kocken 2008103 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Blocked randomisation procedure used. No further details | Unclear risk of bias. No description of randomisation method |
| Allocation concealment | No description of allocation concealment | Unclear risk of bias. Allocation concealment not known |
| Performance bias | ||
| No description of blinding of patients | High risk of bias. Blinding unlikely due to nature of interventions | |
| Detection bias | ||
| No description of blinding of outcome assessors | Unclear risk of bias. Blinding of outcome assessors unclear | |
| Attrition bias | ||
| 8 dropouts in intervention group compared with 8 lost to follow-up in control group | Low risk of bias. Similar dropouts in each group | |
| Reporting bias | ||
| All outcomes reported from protocol | Low risk of bias. Outcomes reported as per protocol | |
| Kolk 2004104 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Randomisation code generated from randomisation table | Low risk of bias. Adequate randomisation method |
| Allocation concealment | Sealed envelopes with sequence numbers | Low risk of bias. Adequate method of allocation concealment |
| Performance bias | ||
| Participants blind to allocation until pre test | High risk of bias. Nature of intervention did not enable blinding throughout the intervention | |
| Detection bias | ||
| NR | Unclear risk of bias. No description of blinding of outcome assessor | |
| Attrition bias | ||
| 55/83 in intervention group remained at long-term follow-up. 13/23 in control group remained after follow-up | High risk of bias. > 20% loss to follow-up in both groups | |
| Reporting bias | ||
| Protocol not located | ||
| Lansinger 2007123 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Block randomisation, no further description of method | Unclear risk of bias. Insufficient description of randomisation method |
| Allocation concealment | Sealed enveloped technique used | Low risk of bias. Adequate method of allocation concealment |
| Performance bias | ||
| Blinding not possible due to nature of intervention | High risk of bias. No blinding of groups allocation | |
| Detection bias | ||
| No blinding of outcome assessors | High risk of bias. No blinding of outcome assessors | |
| Attrition bias | ||
| 12 participants in the qigong group and five in the exercise group refused to participate after allocation. 46/72 qigong completed follow-up, 54/67 exercise group completed follow-up | High risk of bias. High drop-out rate for qigong group | |
| Reporting bias | ||
| Protocol not located | ||
| Larisch 2004158 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Cluster randomised using table of random numbers | Low risk of bias. Adequate randomisation method |
| Allocation concealment | Randomisation by statistician blinded to the GPs | Low risk of bias. Adequate allocation concealment |
| Performance bias | ||
| Patients unaware of the allocation of their GP | Low risk of bias. Blinding of patients | |
| Detection bias | ||
| NR | Unclear risk of bias. Blinding of outcome assessor not described | |
| Attrition bias | ||
| 44/70 patients in intervention group remained at final follow-up compared with 34/64 in control group | High risk of bias. > 20% drop-out rates in both groups | |
| Reporting bias | ||
| Protocol not located | ||
| LeFort 1998128 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Stratified block randomisation | Low risk of bias. Adequate randomisation method |
| Allocation concealment | Opaque, sealed, numbered envelopes | Low risk of bias. Adequate allocation concealment method |
| Performance bias | ||
| Not possible to blind participants due to nature of intervention | High risk of bias. No blinding of participants | |
| Detection bias | ||
| Research assistant blinded to treatment allocation conducted post-treatment assessments | Low risk of bias. Blinded outcome assessors | |
| Attrition bias | ||
| Low and equal rate of attrition in both groups | Low risk of bias. Both groups demonstrated low dropout | |
| Reporting bias | ||
| Protocol not located | ||
| Loew 2000122 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | ‘Randomly controlled’ but no description of randomisation method | Unclear risk of bias. No description of randomisation method |
| Allocation concealment | No description of allocation concealment method | Unclear risk of bias. No description of allocation concealment |
| Performance bias | ||
| Patients told they were in one of two different relaxation technique groups | Low risk of bias. Blinding was conducted | |
| Detection bias | ||
| NR | Unclear risk of bias. No description of blinding of outcome assessors | |
| Attrition bias | ||
| 24/27 intervention group completed diaries. 12/27 in the control group completed diaries | High risk of bias. > 20% drop-out rate in control group | |
| Reporting bias | ||
| Protocol not located | ||
| Luciano 2011139 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Computer-generated randomisation list | Low risk of bias. Adequate randomisation method |
| Allocation concealment | NR | Unclear risk of bias. No reported methods of allocation concealment |
| Performance bias | ||
| Blinding of participants not possible due to nature of intervention and control | High risk of bias. No blinding of participants | |
| Detection bias | ||
| Outcome assessment by research assistant blind to group allocation | Low risk of bias. Blind outcome assessment | |
| Attrition bias | ||
| 6.5% drop-out rate in intervention group compared with 13% in the control group | Low risk of bias. < 20% drop-out rate in each group | |
| Reporting bias | ||
| Primary outcome as stated in protocol. Study paper also included STAI anxiety | Low risk of bias. All primary outcomes as stated in protocol | |
| Luciano 2014138 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Computer-generated randomisation list. Randomisation stratified by comorbid depression | Low risk of bias. Adequate randomisation method |
| Allocation concealment | Randomisation sequence concealed by researcher not involved in the study | Low risk of bias. Adequate allocation concealment |
| Performance bias | ||
| Participants not blinded to treatment allocation due to nature of intervention | High risk of bias. No blinding of participants possible | |
| Detection bias | ||
| Outcome assessors blind to allocation groups | Low risk of bias. Blind outcome assessment | |
| Attrition bias | ||
| Similar rates of attrition across intervention groups | Low risk of bias. Low drop-out rates for all groups | |
| Reporting bias | ||
| All outcomes stated in protocol reported in the study paper | Low risk of bias. All outcomes reported as per protocol | |
| Macedo 2012119 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Computer-generated randomisation sequence | Low risk of bias. Adequate randomisation method |
| Allocation concealment | Allocations concealed in numbered, opaque, sealed envelopes by a researcher not involved in the study | Low risk of bias. Adequate method of allocation concealment |
| Performance bias | ||
| NR | Unclear risk of bias. No reporting of participant blinding | |
| Detection bias | ||
| Outcomes measured by blinded assessors | Low risk of bias. Blind outcome assessment | |
| Attrition bias | ||
| Good adherence to treatment during intervention period but adherence reduced for booster sessions. 6/86 in GA group were lost to follow-up compared with 11/86 in the motor control group | Low risk of bias. < 20% drop-out rate in each group | |
| Reporting bias | ||
| All outcomes outlined in protocol reported in study paper | Low risk of bias. All outcomes reported as per protocol | |
| Margalit 2008268 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Assignment to groups by odd or even numbers on list | Moderate risk of bias. Method of randomisation not robust |
| Allocation concealment | NR | Unclear risk of bias. No description of allocation concealment |
| Performance bias | ||
| NR | Unclear risk of bias. Blinding of participants unclear | |
| Detection bias | ||
| NR | Unclear risk of bias. Blinding of outcome assessors not reported | |
| Attrition bias | ||
| NR | Unclear risk of bias. Drop-out numbers by group unclear | |
| Reporting bias | ||
| Protocol not located | ||
| Marques 2015133 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Computer-generated randomisation sequence | Low risk of bias. Adequate randomisation method |
| Allocation concealment | Randomisation and allocation undertaken by an external researcher | Low risk of bias. Adequate allocation concealment method |
| Performance bias | ||
| No blinding of patients or intervention providers | High risk of bias. Group allocation known to patients and intervention providers | |
| Detection bias | ||
| No blinding of outcome assessors | High risk of bias. Group allocation known to outcome assessors | |
| Attrition bias | ||
| Attrition to the trial was > 20% | High risk of bias. High attrition rate | |
| Reporting bias | ||
| All outcomes stated in protocol reported in the study paper | Low risk of bias. All outcomes as stated in study protocol | |
| Martin 200799 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Randomisation based on predefined list of binary variables, using blocking procedures to ensure sample sizes were comparable | Low risk of bias. Adequate randomisation method |
| Allocation concealment | Assignment to groups undertaken by study assistants | Low risk of bias. External group allocation |
| Performance bias | ||
| NR | High risk of bias. Blinding likely not possible due to nature of intervention | |
| Detection bias | ||
| NR | Unclear risk of bias. Blinding of outcome assessors not reported | |
| Attrition bias | ||
| 59/70 participants remained in the study at final follow-up for both groups | Low risk of bias. < 20% equal drop-out rates for both groups | |
| Reporting bias | ||
| Protocol not located | ||
| McBeth 2012125/Beasley 2015126 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Electronic individual randomisation | Low risk of bias. Adequate randomisation method |
| Allocation concealment | NR | Unclear risk of bias. No reporting on allocation concealment method |
| Performance bias | ||
| Patients and therapists were not blinded to group allocation | High risk of bias. No blinding for both participants and intervention providers | |
| Detection bias | ||
| Outcome assessors were blind to group allocation | Low risk of bias. Blind outcome assessors | |
| Attrition bias | ||
| High follow-up rate. Twice as many lost to follow-up in telephone CBT group | Moderate risk of bias. Unequal drop-out rate for one group | |
| Reporting bias | ||
| Outcomes reported in protocol however no specific measures given | Unclear risk of bias. No measures specified | |
| McLeod 1997105 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Randomisation by table of random numbers | Low risk of bias. Adequate randomisation sequence |
| Allocation concealment | NR | Unclear risk of bias. No reporting of allocation concealment |
| Performance bias | ||
| No blinding of participants reported | High risk of bias. Blinding not possible due to nature of the interventions | |
| Detection bias | ||
| NR | Unclear risk of bias. Unclear whether outcome assessors were blind to group allocation | |
| Attrition bias | ||
| 13 participants dropped out of treatment group compared with one in the control group | High risk of bias. High attrition in intervention group compared with control group | |
| Reporting bias | ||
| Protocol not located | ||
| Morriss 2007108 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Cluster randomised. Randomisation by computer-generated sequence | Low risk. Adequate randomisation procedure |
| Allocation concealment | Group allocation communicated by telephone | Low risk. Adequate allocation concealment method |
| Performance bias | ||
| NR | Unclear risk of bias. Unclear whether participants were blind | |
| Detection bias | ||
| NR | Unclear risk of bias. Unclear whether outcome assessors were blind | |
| Attrition bias | ||
| High rates of follow-up, no attrition bias | Low risk of bias. Low attrition | |
| Reporting bias | ||
| All outcomes stated in protocol reported in study paper, with the addition of EQ-5D QoL | Low risk of bias. All outcomes stated as per protocol with the addition of HRQoL from EQ-5D | |
| Moss-Morris 2005152 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Randomisation by computer-generated random numbers | Low risk. Adequate randomisation sequence |
| Allocation concealment | Sealed opaque envelopes distributed by independent administrator | Low risk. Adequate allocation concealment |
| Performance bias | ||
| NR | Unclear risk. Patient blinding not reported | |
| Detection bias | ||
| Testing conducted by a research assistant blind to intervention group | Low risk. Blinding of outcome assessment | |
| Attrition bias | ||
| 3 participants in each group lost to follow-up | Low risk. Low attrition rates in both groups | |
| Reporting bias | ||
| Protocol not located | Unclear risk of bias | |
| Moss-Morris 2010130 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | The words control or treatment were placed in sealed opaque envelopes by an administrator. Envelopes were ordered using a computer-generated random sequence | Low risk of bias. Adequate randomisation method |
| Allocation concealment | Sealed envelopes distributed by a different administrator | Low risk of bias. Adequate allocation concealment method |
| Performance bias | ||
| Participants not blinded | High risk of bias. No blinding of participants due to nature of intervention and control | |
| Detection bias | ||
| Research assistant who assessed outcomes was blind to group allocation | Low risk of bias. Blind outcome assessment | |
| Attrition bias | ||
| 26/31 returned the 8-month follow-up questionnaires in the intervention group compared with 26/33 in the control group | Low risk of bias. Low and similar attrition rates in each group | |
| Reporting bias | ||
| Retrospective protocol registration | Unclear risk of bias | |
| Peters 2002106 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Randomised trial but method of randomisation not reported | Unclear risk of bias. Randomisation method not reported |
| Allocation concealment | NR | Unclear risk of bias. Method of allocation concealment not reported |
| Performance bias | ||
| Participants were blinded to the hypothesis and to the nature of the other intervention | Low risk of bias. Participants blinded | |
| Detection bias | ||
| Researchers and intervention providers were not blinded to group allocation | High risk of bias | |
| Attrition bias | ||
| Long-term attrition by group not reported | Unclear risk of bias. Dropouts at last follow-up not reported by group | |
| Reporting bias | ||
| Protocol not located | ||
| Pols 2008145 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Random number allocation | Low risk of bias. Adequate randomisation method |
| Allocation concealment | Allocation group provided to the research officer by telephone | Low risk of bias. Adequate method of allocation concealment |
| Performance bias | ||
| GPs not blinded to allocation group. Blinding of participants not reported | Unclear risk of bias. Participant blinding not reported | |
| Detection bias | ||
| Local evaluation team blinded to allocation group | Low risk of bias. Blind outcome assessment | |
| Attrition bias | ||
| 42/89 intervention group participants assessed at follow-up compared with 22/44 control participants | High risk of bias. > 20% attrition at longest follow-up in both groups | |
| Reporting bias | ||
| Protocol not located | ||
| Posse 200496 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Patients randomly assigned to treatment groups | Unclear risk of bias. No description of randomisation method reported |
| Allocation concealment | NR | Unclear risk of bias. No description allocation concealment |
| Performance bias | ||
| Blinding of participants not possible due to nature of intervention | High risk of bias. No blinding of participants | |
| Detection bias | ||
| NR | Unclear risk of bias. Blinding of outcome assessment not reported | |
| Attrition bias | ||
| No dropouts in either group | Low risk of bias. No attrition | |
| Reporting bias | ||
| Protocol not located | ||
| Ridsdale 2001112 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Randomisation in blocks of 10 by computer-generated random number combinations | Low risk of bias. Adequate randomisation method |
| Allocation concealment | Opaque sealed envelopes bearing sequential ID numbers | Low risk of bias. Adequate allocation concealment method |
| Performance bias | ||
| NR | Unclear risk of bias. Blinding of participants not reported | |
| Detection bias | ||
| NR | Unclear risk of bias. Blinding of outcome assessment not reported | |
| Attrition bias | ||
| 81% of participants in the counselling group vs. 80% in the CBT group completed the final follow-up | Low risk of bias. ≤ 20% attrition in both groups | |
| Reporting bias | ||
| Protocol not located | ||
| Ridsdale 2004113 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Stratified and blocked (size 10) randomisation to four sets of random combinations | Low risk of bias. Adequate randomisation method |
| Allocation concealment | Allocation concealed in four series of consecutive, opaque, sealed envelopes | Low risk of bias. Adequate method of allocation concealment |
| Performance bias | ||
| NR | Unclear risk of bias. Blinding of participants unclear | |
| Detection bias | ||
| NR | Unclear risk of bias. Blinding of outcome assessors unclear | |
| Attrition bias | ||
| 94% (CBT), 97% (GET) and 93% (TAU) of participants completed the last follow-up | Low risk of bias. Low attrition across all groups | |
| Reporting bias | ||
| Protocol not located | ||
| Ridsdale 2012115 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Block randomisation prepared by a statistician | Low risk of bias. Adequate randomisation method |
| Allocation concealment | Opaque sealed envelopes bearing sequential ID numbers | Low risk of bias. Adequate allocation concealment method |
| Performance bias | ||
| NR | Unclear risk of bias. Blinding of participants not reported | |
| Detection bias | ||
| NR | Unclear risk of bias. Blinding of outcome assessor not reported | |
| Attrition bias | ||
| 73% of graded exercise group assessed at longest follow-up compared with 85% of counselling group | High risk of bias. Higher rate of dropouts and > 20% for graded exercise group than counselling group | |
| Reporting bias | ||
| All outcomes from protocol reported with the exception of illness attributions | Low risk of bias. All outcomes reported as per protocol apart from illness attributions. Judged low risk of bias as this is not a relevant outcome in our review | |
| Rief 2006102 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Cluster randomised. Method not described | Unclear risk of bias. Method of randomisation not described |
| Allocation concealment | NR | Unclear risk of bias. No allocation concealment method reported |
| Performance bias | ||
| NR | Unclear risk of bias. Blinding of participants not reported | |
| Detection bias | ||
| NR | Unclear risk of bias. Blinding of outcome assessor not reported | |
| Attrition bias | ||
| NR | Unclear reporting of dropouts by group | |
| Reporting bias | ||
| Protocol not located | ||
| Robinson 2006131 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Randomisation based on minimisation | Low risk of bias. Adequate randomisation method |
| Allocation concealment | Central telephone randomisation system | Low risk of bias. Adequate method of allocation concealment |
| Performance bias | ||
| NR | Unclear risk. Blinding of participants not reported | |
| Detection bias | ||
| NR | Unclear risk. Blinding of participants not reported | |
| Attrition bias | ||
| Similar attrition across groups by longest follow-up | Low risk of bias. Low attrition across groups | |
| Reporting bias | ||
| Protocol not located | ||
| Rosendal 2007146 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Cluster randomisation. Non-transparent lots containing code numbers | Low risk of bias. Adequate method of randomisation |
| Allocation concealment | A person not involved in the study performed the randomisation | Low risk of bias. Adequate method of allocation concealment |
| Performance bias | ||
| It was not possible to blind GPs, but their patients were blind | Low risk of bias. Patients unaware of group allocation | |
| Detection bias | ||
| NR | Unclear risk of bias. Blinding of outcome assessor unclear | |
| Attrition bias | ||
| 65% response rate at 12-month follow-up for the intervention group compared with 74% for the control group | High risk of bias. > 20% attrition for both groups at follow-up | |
| Reporting bias | ||
| Protocol not located | ||
| Rothman 2013127 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Block randomisation by computer-generated list | Low risk of bias. Adequate randomisation method |
| Allocation concealment | Closed envelopes | Low risk of bias. Adequate allocation concealment method |
| Performance bias | ||
| NR | Unclear risk of bias. Blinding of participants not reported | |
| Detection bias | ||
| NR | Unclear risk of bias. Blinding of outcome assessors not reported | |
| Attrition bias | ||
| 8/99 participants in the intervention group and 17/108 participants in the control group did not complete the 15-month follow-up | Low risk of bias. < 20% attrition in both groups | |
| Reporting bias | ||
| Protocol not located | ||
| Ryan 2004109 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Participants were randomised but method is not described | Unclear risk of bias. No description of randomisation method |
| Allocation concealment | NR | Unclear risk of bias. No description of method of allocation concealment |
| Performance bias | ||
| NR | Unclear risk of bias. Blinding of participants not reported | |
| Detection bias | ||
| NR | Unclear risk of bias. Blinding of outcome assessor not reported | |
| Attrition bias | ||
| 21/40 intervention group participants dropped out before treatment or refused to participate | High risk of bias. > 20% drop-out rate in intervention group | |
| Reporting bias | ||
| Protocol not located | ||
| Sañudo 2010140 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Randomisation by computer-generated random number sequence | Low risk of bias. Adequate randomisation method |
| Allocation concealment | Randomisation by personnel not directly involved in the recruitment or assessment of patients. Randomisation list kept at a separate location in a locked cabinet | Low risk of bias. Adequate method of allocation concealment |
| Performance bias | ||
| NR | Unclear risk of bias. Blinding of participants not reported | |
| Detection bias | ||
| Outcome assessment performed by personnel who were unaware of group allocation | Low risk of bias. Outcomes assessor blinded | |
| Attrition bias | ||
| Four participants from each exercise group dropped out of the study. One participant from the control group dropped out of the study | Low risk of bias. Low attrition in both intervention groups, although marginally higher than control group | |
| Reporting bias | ||
| All outcomes stated in the protocol are reported in the study paper, but there are differences in whether outcomes are stated as primary or secondary. SF-36 and physical fitness measures are stated as primary outcomes in the protocol but as secondary outcomes in the paper | Unclear risk of bias. All outcomes reported but differences in reporting as primary/secondary | |
| Schade 2011272 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Participants randomised but no description of method given | Unclear risk of bias. No method of randomisation given |
| Allocation concealment | NR | Unclear risk of bias. No method of allocation concealment given |
| Performance bias | ||
| No blinding due to the nature of the interventions | High risk of bias. No blinding of participants | |
| Detection bias | ||
| Outcome assessors were blind to the study conditions | Low risk of bias. Adequate allocation concealment | |
| Attrition bias | ||
| NR | Unclear risk of bias. No reporting of drop-out rates | |
| Reporting bias | ||
| Protocol not located | ||
| Schaefert 2013132 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Cluster randomised. Exact method not described, although was performed by a statistician | Low risk of bias. Statistical method of randomisation |
| Allocation concealment | Blinded randomisation at a research centre | Low risk of bias. Adequate randomisation method |
| Performance bias | ||
| NR | Unclear risk of bias. Participant blinding not reporting | |
| Detection bias | ||
| Outcomes assessed by blinded research assistants | Low risk of bias. Blinded outcome assessment | |
| Attrition bias | ||
| Attendance at intervention sessions dropped to 56% by final booster session. Questionnaire completion significantly higher in the intervention group than with controls | High risk of bias. > 20% did not complete intervention and significant difference in completion of follow-up questionnaires between group (lower completion for control group) | |
| Reporting bias | ||
| Protocol not located | ||
| Schilte 2001159 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Randomised sequence performed. Exact method not specified | Unclear risk of bias. Unspecified randomisation technique |
| Allocation concealment | An independent person performed the randomisation. Opaque, sealed numbered envelopes used | Low risk of bias. Adequate allocation concealment |
| Performance bias | ||
| GPs knew which patients received the intervention, but not which patients were controls. Unclear whether patients were blinded | Moderate risk of bias. Unblinded GPs and unclear about patient blinding | |
| Detection bias | ||
| NR | Unclear risk of bias. Outcome assessment not reported | |
| Attrition bias | ||
| 70/81 participants in the intervention group remained at follow-up compared with 67/80 in the control group | Low risk of bias. < 20% attrition and similar between groups | |
| Reporting bias | ||
| Protocol not located | ||
| Smith 1995100 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Randomised trial with one-way crossover. Related to Kashner 1995.161 Randomisation method not reported | Unclear risk of bias. Randomisation method not reported |
| Allocation concealment | NR | Unclear risk of bias. Allocation concealment method not reported |
| Performance bias | ||
| NR | Unclear risk of bias. No reporting of patient blinding | |
| Detection bias | ||
| NR | Unclear risk of bias. No reporting of blinding of outcome assessor | |
| Attrition bias | ||
| 96% of participants completed all four follow-ups | Low risk of bias. Low attrition | |
| Reporting bias | ||
| Protocol not located | ||
| Smith 2006107 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Randomisation sequence by computerised random number generator | Low risk of bias. Adequate randomisation method |
| Allocation concealment | Randomisation by statistician with no patient knowledge | Low risk of bias. Adequate allocation concealment method |
| Performance bias | ||
| Patients and intervention providers not blinded | High risk of bias. No blinding of participants | |
| Detection bias | ||
| Outcome assessors were blinded | Low risk of bias. Blinded outcome assessment | |
| Attrition bias | ||
| 98/101 participants in the intervention condition completed all follow-ups compared with 102 out of 105 in control group | Low risk of bias. Low attrition and similar between groups | |
| Reporting bias | ||
| Protocol not located | ||
| Smith 2009142 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Random number generator used | Low risk of bias. Adequate method of randomisation |
| Allocation concealment | NR | Unclear risk of bias. No reporting of allocation concealment |
| Performance bias | ||
| NR | Unclear risk of bias. No reporting of participant blinding | |
| Detection bias | ||
| NR | Unclear risk of bias. No reporting of outcome assessor blinding | |
| Attrition bias | ||
| No dropouts in either group, although small sample of 15 in each group | Low risk of bias. No attrition | |
| Reporting bias | ||
| Protocol not located | ||
| Sumathipala 2008117 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Randomisation by permuted block design, with block size of four. Randomisation codes generated by a statistician | Low risk of bias. Adequate randomisation method |
| Allocation concealment | An independent epidemiologist executed the random allocation | Low risk of bias. Adequate allocation concealment method |
| Performance bias | ||
| Patients could not be blinded due to the nature of the intervention | High risk of bias. No blinding of patients | |
| Detection bias | ||
| The study physician and all research assistants were blinded to the group allocation | Low risk of bias. Blinded outcome assessors | |
| Attrition bias | ||
| 5/75 lost to follow-up in intervention group. 8/75 lost to follow-up in control group | Low risk of bias. Low attrition and similar between groups | |
| Reporting bias | ||
| Protocol not located | ||
| Sumathipala 2000116 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Random numbers generated from a calculator | Low risk of bias. Adequate randomisation method |
| Allocation concealment | Independent epidemiologist performed the randomisation. Sealed opaque envelopes bearing sequential registration numbers used | Low risk of bias. Adequate allocation concealment method |
| Performance bias | ||
| Patients not blinded due to nature of intervention | High risk of bias. Patients not blinded | |
| Detection bias | ||
| Non-clinical research assistant remained blind to group allocation throughout the study | Low risk of bias. Blinded outcome assessment | |
| Attrition bias | ||
| 4/12 patients who attended either one or two sessions, were present at follow-up. Considerable drop-out rates from both treatment and follow-up | High risk of bias. > 20% attrition | |
| Reporting bias | ||
| Protocol not located | ||
| Toft 201097 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Cluster randomised, stratified by number of GPs in the practice and block-randomised by drawing lots | Low risk of bias. Adequate randomisation method |
| Allocation concealment | A neutral party performed the randomisation | Low risk of bias. Adequate method of allocation concealment |
| Performance bias | ||
| Patients not informed about assignment of their GP to either the intervention or control group | Low risk of bias. Patients were blinded | |
| Detection bias | ||
| Interviewers were blinded to group allocation | Low risk of bias. Blinded outcome assessment | |
| Attrition bias | ||
| Attrition not reported | Unclear risk of bias. Attrition not discussed | |
| Reporting bias | ||
| Protocol not located | ||
| Tummers 2012149 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Computer-generated randomisation | Low risk of bias. Adequate randomisation method |
| Allocation concealment | A statistical advisor, independent of the study, prepared numbered and sealed envelopes | Low risk of bias. Adequate allocation concealment method |
| Performance bias | ||
| Blinding of patients not possible due to nature of interventions | High risk of bias. No blinding of patients | |
| Detection bias | ||
| NR | Unclear risk of bias. Blinding of outcome assessor not reported | |
| Attrition bias | ||
| 55/62 in intervention group completed follow-up assessment compared with 56/61 in control group | Low risk of bias. < 20% attrition and similar between groups | |
| Reporting bias | ||
| All outcomes stated in protocol reported in study paper | Low risk of bias. All outcomes reported as per protocol | |
| van der Feltz-Cornelis 2006160 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Cluster randomised. Method not described | Unclear risk of bias. No description of randomisation method |
| Allocation concealment | Randomisation conducted by a research assistant | Low risk of bias. Allocation conducted independently of the practices |
| Performance bias | ||
| Practices not informed about group allocation until 6 weeks after first patient included, although interventions not blinded | Moderate risk of bias. Patients and practices blinded to intervention group for 6 weeks | |
| Detection bias | ||
| Research assistant was not aware of the treatment allocation | Low risk of bias. Blinded outcome assessment | |
| Attrition bias | ||
| None lost to follow-up in either group | Low risk of bias. Low attrition | |
| Reporting bias | ||
| All outcomes outlined in protocol are reported in the study paper | Low risk of bias. Outcomes reported as per protocol | |
| van der Roer 2008120 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Randomisation lists generated using series of random numbers | Low risk of bias. Adequate randomisation sequence |
| Allocation concealment | Prepared opaque, sealed envelopes | Low risk of bias. Adequate allocation concealment |
| Performance bias | ||
| Patients and physiotherapist could not be blinded due to the nature of the interventions | High risk of bias. No blinding of patients and practitioners | |
| Detection bias | ||
| NR | Unclear risk of bias. Blinding of outcome assessor not reported | |
| Attrition bias | ||
| Number of patients lost to follow-up similar in both groups indicating non-selective dropout | Low risk of bias. Similar attrition in both groups | |
| Reporting bias | ||
| All primary and secondary outcomes reported in protocol are reported in the paper | Low risk of bias. All outcomes reported as per protocol | |
| van Ravesteijn 2013143 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Computer-generated permuted-block randomisation table with a block size of 20 | Low risk of bias. Adequate randomisation method |
| Allocation concealment | Research assistant blinded to the interview data performed the randomisation | Low risk of bias. Adequate allocation concealment |
| Performance bias | ||
| NR | Unclear risk of bias. No reporting of whether patients were blinded | |
| Detection bias | ||
| NR | Unclear risk of bias. No reporting of blinding of outcome assessor | |
| Attrition bias | ||
| 12/49 mindfulness group dropped out of treatment with additional four participants lost to follow-up. 1/55 control group received intervention due to strong preference, with an additional six particpants lost to follow-up | High risk of bias. > 20% attrition from intervention group and deviation from the protocol in control group | |
| Reporting bias | ||
| Protocol not located | ||
| Walti 2015121 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Electronically generated randomisation list | Low risk of bias. Adequate randomisation method |
| Allocation concealment | Allocation stated as concealed | Low risk of bias. Explicit allocation concealment, although method not described |
| Performance bias | ||
| Patients not blinded | High risk of bias. Patients not blinded | |
| Detection bias | ||
| Outcome assessments conducted by independent physiotherapist blinded to the group assignment | Low risk of bias. Blinded outcome assessment | |
| Attrition bias | ||
| Six patients dropped out of treatment (three each from the MMT and UPT groups). All patients, except one, in the UPT attended post-therapy outcome assessment | Low risk of bias. Low attrition and comparable between groups | |
| Reporting bias | ||
| All outcomes stated in protocol are reported in the study paper | Low risk of bias. All outcomes reported as per protocol | |
| Wearden 2010111 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Computer-generated randomised permuted blocks | Low risk of bias. Adequate randomisation method |
| Allocation concealment | Random allocation was e-mailed to the trial manager | Low risk of bias. Adequate random sequence generation |
| Performance bias | ||
| Patients not blinded to allocation | High risk of bias. No blinding of patients | |
| Detection bias | ||
| Assessments by trained researchers blind to treatment allocation | Low risk of bias. Blinded outcome assessment | |
| Attrition bias | ||
| Low drop-out rates and high rates of follow-up | Low risk of bias. Low attrition | |
| Reporting bias | ||
| Protocol reports ‘time to take 20 steps, (or number of steps taken, if this is not achieved) and maximum heart rate reached on a step-test’ as a secondary outcome. This is not reported in the study paper | Unclear risk of bias. No report of number of steps fatigue secondary outcome outlined in protocol | |
| Whitehead 2002154 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Cluster randomised. Randomisation method not described | Unclear risk of bias. No description of method of randomisation |
| Allocation concealment | NR | Unclear risk of bias. No description of allocation concealment |
| Performance bias | ||
| NR | Unclear risk of bias. Blinding of patients or practices not reported | |
| Detection bias | ||
| NR | Unclear risk of bias. Blinding of outcome assessors not reported | |
| Attrition bias | ||
| 18/26 participants in the intervention group and 28/39 in the control group provided data at first follow-up. Data from 9/26 and 21/39 at last follow-up | High risk of bias. High attrition in both groups | |
| Reporting bias | ||
| Protocol not located | ||
| Zonneveld 2012141 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Computer-generated randomisation list | Low risk of bias. Adequate randomisation method |
| Allocation concealment | Allocation concealed for patients and assessors due to randomisation list generated after assessment for eligibility and enrolment | Low risk of bias. Adequate allocation concealment |
| Performance bias | ||
| Patients and trainers not blinded due to nature of the interventions | High risk of bias. No blinding of patients and trainers | |
| Detection bias | ||
| NR | Unclear risk of bias. No reporting of blinding of outcome assessor | |
| Attrition bias | ||
| 23/84 dropped out of intervention group. 6/78 dropped out of control group | High risk of bias. > 20% attrition in intervention group | |
| Reporting bias | ||
| All outcomes stated in protocol are reported in study paper | Low risk of bias. All outcomes reported as per protocol | |
A 20% attrition rate was taken as the cut-off point for low risk of bias. 134
Appendix 4 Table of excluded studies with rationale
| Citation | Reason for exclusion |
|---|---|
| Brealey S, Burton K, Coulton S, Farrin A, Garratt A, Harvey E, et al. UK Back pain Exercise And Manipulation (UK BEAM) trial – national randomised trial of physical treatments for back pain in primary care: objectives, design and interventions [ISRCTN32683578]. BMC Health Serv Res 2003;3:16. https://doi.org/10.1186/1472-6963-3-16 | Population not all meeting inclusion for unexplained |
| van Erp RM, Huijnen IP, Verbunt JA, Smeets RJ. A biopsychosocial primary care intervention (Back on Track) versus primary care as usual in a subgroup of people with chronic low back pain: protocol for a randomised, controlled trial. J Physiother 2015;61:155. https://doi.org/10.1016/j.jphys.2015.03.003 | Population not all meeting inclusion for unexplained |
| Arnold IA, de Waal MW, Eekhof JA, Assendelft WJ, Spinhoven P, van Hemert AM. Medically unexplained physical symptoms in primary care: a controlled study on the effectiveness of cognitive-behavioral treatment by the family physician. Psychosomatics 2009;50:515–24. https://doi.org/10.1176/appi.psy.50.5.515 | Not a RCT |
| Senlöf P, Denison E, Lindberg P. Long-term follow-up of tailored behavioural treatment and exercise based physical therapy in persistent musculoskeletal pain: a randomized controlled trial in primary care. Eur J Pain 2009;13:1080–8. https://doi.org/10.1016/j.ejpain.2009.01.010 | Population not all meeting inclusion for unexplained |
| Basler HD. Follow-up results of a cognitive-behavioural treatment for chronic pain in a primary care setting. Pychol Health 1990;4:293–304 | Population not all meeting inclusion criteria for unexplained |
| Becker N, Sjøgren P, Bech P, Olsen AK, Eriksen J. Treatment outcome of chronic non-malignant pain patients managed in a danish multidisciplinary pain centre compared to general practice: a randomised controlled trial. Pain 2000;84:203–11 | Not in a primary care setting, the intervention is in a pain centre |
| Becker N, Sjogren P, Olsen A. Behandlingsresultater ved kroniske, non-maligne smertetilstande hos patienter, behandlet i et dansk, tvaerfagligt smertecenter sammenlignet med almen praksis. Ugeskr Laeger 2001;163:3078–82 | Not in a primary care setting |
| Bernal Cercós A, Fusté Vallverdú R, Urbieta Solana R, Montesinos Molina I. Tratamiento de relajación en pacientes con trastornos de ansiedad y somatoformes en atención primaria. Aten Primaria 1995;15:499–504 | Population have anxiety or somatoform disorders |
| Best M, Lange M, Karpinski N, Hessel A, Söpper-Terborg B, Sieling W, Petermann F. [Psychosomatic rehabilitation: effects of pre-treatment counselling under the statutory pension insurance scheme.] Rehabilitation 2009;48:283–7. https://doi.org/10.1055/s-0029-1239544 | Outcomes not appropriate |
| Bonetti F, Curti M, Curti S, Ferrari C, Mattioli S, Mugnai R, et al. Effectiveness of a global posture reeducation program for patients with low back pain. Physiotherapy 2011;97:eS1001 | Conference abstract |
| Carmody TP, Duncan CL, Huggins J, Solkowitz SN, Lee SK, Reyes N, et al. Telephone-delivered cognitive-behavioral therapy for pain management among older military veterans: a randomized trial. Psychol Serv 2013;10:265–75. https://doi.org/10.1037/a0030944 | Population is military veterans |
| Chalder T, Godfrey E, Ridsdale L, King M, Wessely S. Predictors of outcome in a fatigued population in primary care following a randomized controlled trial. Psychol Med 2003;33:283–7 | Appropriate outcomes are in Ridsdale et al.112 |
| Chelimsky TC, Fischer RL, Levin JB, Cheren MI, Marsh SK, Janata JW. The primary practice physician program for chronic pain (© 4PCP): outcomes of a primary physician-pain specialist collaboration for community-based training and support. Clin J Pain 2013;29:1036–43. https://doi.org/10.1097/AJP.0b013e3182851584 | No patient outcomes for any controls |
| Christensen SS, Frostholm L, Ørnbøl E, Schröder A. Changes in illness perceptions mediated the effect of cognitive behavioural therapy in severe functional somatic syndromes. J Psychosom Res 2015;78:363–70. https://doi.org/10.1016/j.jpsychores.2014.12.005 | Outcomes not appropriate |
| Da Costa D, Abrahamowicz M, Lowensteyn I, Bernatsky S, Dritsa M, Fitzcharles MA, Dobkin PL. A randomized clinical trial of an individualized home-based exercise programme for women with fibromyalgia. Rheumatology 2005;44:1422–7 | Setting is not primary care |
| Cuesta-Vargas AI, Adams N. A pragmatic community-based intervention of multimodal physiotherapy plus deep water running (DWR) for fibromyalgia syndrome: a pilot study. Clin Rheumatol 2011;30:1455–62. https://doi.org/10.1007/s10067-011-1825-z | Non-randomised pilot clinical trial |
| Darbishire L, Seed P, Ridsdale L. Predictors of outcome following treatment for chronic fatigue. Br J Psychiatry 2005;186:350–1 | Outcomes – predictors of successful outcome |
| Del Pozo-Cruz B, Adsuar JC, Parraca J, Del Pozo-Cruz J, Moreno A, Gusi N. A web-based intervention to improve and prevent low back pain among office workers: a randomized controlled trial. Arch Prev Riesgos Labor 2013;16:138 | Pain is subacute |
| del Pozo-Cruz B, del Pozo-Cruz J, Adsuar JC, Parraca J, Gusi N. Reanalysis of a tailored web-based exercise programme for office workers with sub-acute low back pain: assessing the stage of change in behaviour. Psychol Health Med 2013;18:687–97. https://doi.org/10.1080/13548506.2013.765019 | Pain is subacute |
| Dobbin A, Dobbin J, Ross SC, Graham C, Ford MJ. Randomised controlled trial of brief intervention with biofeedback and hypnotherapy in patients with refractory irritable bowel syndrome. J R Coll Physicians Edinb 2013;43:15–23. https://doi.org/10.4997/JRCPE.2013.104 | Setting not primary care |
| Domenech J, Baños R, Peñalver L, Garcia-Palacios A, Herrero R, Ezzedine A, et al. Design considerations of a randomized clinical trial on a cognitive behavioural intervention using communication and information technologies for managing chronic low back pain. BMC Musculoskelet Disord 2013;14:142. https://doi.org/10.1186/1471-2474-14-142 | Study design paper |
| Egan S, Saper R. (Predictors of adherence to treatment for chronic low back pain in a 12-week RCT comparing yoga, physical therapy, and education. J Altern Complement Med 2014;20:A56 | Conference abstract |
| van Eijk-Hustings Y, Kroese M, Tan F, Boonen A, Bessems-Beks M, Landewé R. Challenges in demonstrating the effectiveness of multidisciplinary treatment on quality of life, participation and health care utilisation in patients with fibromyalgia: a randomised controlled trial. Clin Rheumatol 2013;32:199–209. https://doi.org/10.1007/s10067-012-2100-7 | Setting is not primary care |
| Enezei HH, Alam MK. Variation in the efficacy of two different treatment modalities used for myofacial pain dysfunction syndrome: clinical trial. Int Med J 2015;22:410–12 | Not in a primary care setting |
| Escobar JI, Gara M, Alex I, Allen L, Diaz-Martinez A, Warman M. Treatment of patients presenting with unexplained physical symptoms in primary care. Neuropsychopharmacology 2004;29(Suppl. 1):S101 | Conference abstract |
| Everitt H, Landau S, Little P, Bishop FL, McCrone P, O’Reilly G, et al. Assessing Cognitive behavioural Therapy in Irritable Bowel (ACTIB): protocol for a randomised controlled trial of clinical-effectiveness and cost-effectiveness of therapist delivered cognitive behavioural therapy and web-based self-management in irritable bowel syndrome in adults. BMJ Open 2015;5:e008622. https://doi.org/10.1136/bmjopen-2015-008622 | Protocol only |
| Everitt H, Moss-Morris R, Sibelli A, Tapp L, Coleman N, Yardley L, et al. Management of irritable bowel syndrome in primary care: the results of an exploratory randomised controlled trial of mebeverine, methylcellulose, placebo and a self-management website. BMC Gastroenterol 2013;13:68. https://doi.org/10.1186/1471-230X-13-68 | Insufficient primary care involvement. Invitation letter from practices |
| Faas A, Chavannes AW, van Eijk JT, Gubbels JW. A randomized, placebo-controlled trial of exercise therapy in patients with acute low back pain. Spine 1993;18:1388–95 | Pain is acute |
| Falcão DM, Sales L, Leite JR, Feldman D, Valim V, Natour J. Cognitive behavioral therapy for the treatment of fibromyalgia syndrome: a randomized controlled trial. J Musculoskelet Pain 2008;16:133–40 | Not in a primary care setting |
| Moshkani Farahani D, Tavallaie SA, Ahmadi K, Fathi Ashtiani A. Comparison of neurofeedback and transcutaneous electrical nerve stimulation efficacy on treatment of primary headaches: a randomized controlled clinical trial. Iran Red Crescent Med J 2014;16:e17799. https://doi.org/10.5812/ircmj.17799 | Setting not primary care |
| Farnam A, Somi MH, Farhang S, Mahdavi N, Ali Besharat M. The therapeutic effect of adding emotional awareness training to standard medical treatment for irritable bowel syndrome: a randomized clinical trial. J Psychiatr Pract 2014;20:3–11. https://doi.org/10.1097/01.pra.0000442934.38704.3a | Setting not primary care |
| Fernandez C, Perez M, Amigo I, Linares A. Stress and contingency management in the treatment of irritable bowel syndrome. Stress Health 1998;14:31–42 | Not in a primary care setting |
| Fjorback L, Schroder A, Ornbol E, Rehfeld E, Arendt M, Fink P. Mindfulness therapy for bodily distress syndrome – a randomized controlled trial. J Psychosom Res 2011;70:292–3 | Conference abstract |
| Fernández R, Peñarubia MT, Luciano JV, Blanco ME, Jiménez M, Montesano A, et al. Effectiveness of a psycho-educational program for improving quality of life of fibromyalgia patients. BMC Musculoskelet Disord 2008;9:2 | Protocol |
| Vibe Fersum K, O’Sullivan P, Skouen JS, Smith A, Kvåle A. Efficacy of classification-based cognitive functional therapy in patients with non-specific chronic low back pain: a randomized controlled trial. Eur J Pain 2013;17:916–28. https://doi.org/10.1002/j.1532-2149.2012.00252.x | Setting is not primary care |
| Fink P, Rosendal M, Toft T. Assessment and treatment of functional disorders in general practice: the extended reattribution and management model – an advanced educational program for nonpsychiatric doctors. Psychosomatics 2002;43:93–131 | No study data, description of a treatment programme |
| French SD, McKenzie JE, O’Connor DA, Grimshaw JM, Mortimer D, Francis JJ, et al. Evaluation of a theory-informed implementation intervention for the management of acute low back pain in general medical practice: the IMPLEMENT cluster randomised trial. PLOS ONE 2013;8:e65471. https://doi.org/10.1371/journal.pone.0065471 | Pain is acute |
| Ben Salah Frih Z, Fendri Y, Jellad A, Boudoukhane S, Rejeb N. Efficacy and treatment compliance of a home-based rehabilitation programme for chronic low back pain: a randomized, controlled study. Ann Phys Rehabil Med 2009;52:485–96. https://doi.org/10.1016/j.rehab.2009.04.002 | Setting not primary care – referral from outpatient service |
| Gale G, Nussbaum D, Rothbart P, Hann B, Leung V, Kanetz G. A randomized treatment study to compare the efficacy of repeated nerve blocks with cognitive therapy for control of chronic head and neck pain. Pain Res Manage 2002;7:185–9 | Insufficient primary care involvement |
| García-Campayo J, Arevalo E, Claraco LM, Alda M, Lopez del Hoyo Y. A prevention programme for somatoform disorders is effective for affective disorders. J Affect Disord 2010;122:124–32. https://doi.org/10.1016/j.jad.2009.06.031 | Prevention study |
| García-Campayo J, Serrano-Blanco A, Rodero B, Magallón R, Alda M, Andrés E, et al. Effectiveness of the psychological and pharmacological treatment of catastrophization in patients with fibromyalgia: a randomized controlled trial. Trials 2009;10:24. https://doi.org/10.1186/1745-6215-10-24 | Protocol |
| Gawriołek K, Azer SS, Gawriołek M, Piotrowski PR. Mandibular function after myorelaxation therapy in temporomandibular disorders. Adv Med Sci 2015;60:6–12. https://doi.org/10.1016/j.advms.2014.05.002 | Not a RCT |
| Gaylord SA, Whitehead WE, Coble RS, Faurot KR, Palsson OS, Garland EL, et al. Mindfulness for irritable bowel syndrome: protocol development for a controlled clinical trial. BMC Complement Altern Med 2009;9:24. https://doi.org/10.1186/1472-6882-9-24 | Protocol and recruitment data only |
| Genç A, Sağıroğlu E. Fibromiyalji tedavisinde iki farklı egzersiz programının karşılaştırılması | Not in a primary care setting |
| Geraets JJ, Goossens ME, van Haastregt JC, de Groot IJ, de Bruijn CP, de Bie RA, et al. Implications of process evaluation for clinical effectiveness and clinical practice in a trial on chronic shoulder complaints. Patient Educ Couns 2006;61:117–25 | Outcomes not appropriate |
| Geraghty AW, Kirby S, Essery R, Little P, Bronstein A, Turner D, et al. Internet-based vestibular rehabilitation for adults aged 50 years and over: a protocol for a randomised controlled trial. BMJ Open 2014;4:e005871. https://doi.org/10.1136/bmjopen-2014-005871 | Protocol only |
| Gilbert JR, Taylor DW, Hildebrand A, Evans C. Clinical trial of common treatments for low back pain in family practice. Br Med J 1985;291:791–4 | Pain is acute |
| Godfrey E, Chalder T, Ridsdale L, Seed P, Ogden J. Investigating the active ingredients of cognitive behaviour therapy and counselling for patients with chronic fatigue in primary care: developing a new process measure to assess treatment fidelity and predict outcome. Br J Clin Psychol 2007;46:253–72 | Trial data are in Ridsdale113 |
| Goldstein LH, Chalder T, Chigwedere C, Khondoker MR, Moriarty J, Toone BK, Mellers JD. Cognitive-behavioral therapy for psychogenic nonepileptic seizures: a pilot RCT. Neurology 2010;74:1986–94. https://doi.org/10.1212/WNL.0b013e3181e39658 | Setting not primary care |
| Goldstein LH, Mellers JD, Landau S, Stone J, Carson A, Medford N, et al. COgnitive behavioural therapy vs standardised medical care for adults with Dissociative non-Epileptic Seizures (CODES): a multicentre randomised controlled trial protocol. BMC Neurol 2015;15:98. https://doi.org/10.1186/s12883-015-0350-0 | Study protocol |
| Greene B, Blanchard EB. Cognitive therapy for irritable bowel syndrome. J Consult Clin Psychol 1994;62:576–82 | Not in a primary care setting |
| Griffiths C, Dziedzic K, Waterfield J, Sim J. Effectiveness of specific neck stabilization exercises or a general neck exercise program for chronic neck disorders: a randomized controlled trial. J Rheumatol 2009;36:390–7. https://doi.org/10.3899/jrheum.080376 | Intervention is posture correction implies pain is explained |
| Grundmann O, Yoon SL. Mind-body therapies for functional bowel disorders – a review of recent clinical trials. Eur J Integr Med 2013;5:296–307 | Review |
| Guenter D, Angeles R, Bullock L, McCarthy L, Bauer M, Wolfson M, Chacon M. Living everyday above-and-beyond pain (LEAP): Design of an RCT evaluating an interprofessional cognitive-behavioral group therapy in primary care. Pain Res Manage 2011;16:118 | Conference abstract |
| Haldorsen EM, Kronholm K, Skouen JS, Ursin H. Multimodal cognitive behavioral treatment of patients sicklisted for musculoskeletal pain: a randomized controlled study. Scand J Rheumatol 1998;27:16–25 | Pain is less than 12 weeks’ duration |
| Hammerich AS, Maluf KS. Effects of biofeedback on stress-evoked activation of the upper trapezius muscle in subjects with chronic neck pain. 2008 Combined Sections Meeting. Nashville, TN, USA, February 6–9, 2008. J Orthop Sports Phys Ther 2008;38:A23–24 | Conference abstract |
| Hansen Z, Daykin A, Lamb SE. A cognitive-behavioural programme for the management of low back pain in primary care: a description and justification of the intervention used in the Back Skills Training Trial (BeST; ISRCTN 54717854). Physiotherapy 2010;96:87–94. https://doi.org/10.1016/j.physio.2009.09.008 | Description of trial design only |
| Hassink-Franke LJ, van Weel-Baumgarten EM, Wierda E, Engelen MW, Beek MM, Bor HH, et al. Effectiveness of problem-solving treatment by general practice registrars for patients with emotional symptoms. J Prim Health Care 2011;3:181–9 | Population not meeting the inclusion criteria for MUS |
| Hay EM, Mullis R, Lewis M, Vohora K, Main CJ, Watson P, et al. Comparison of physical treatments versus a brief pain-management programme for back pain in primary care: a randomised clinical trial in physiotherapy practice. Lancet 2005;365:2024–30 | Pain not greater than 3 months |
| Hayes S, Hogan M, Dowd H, Doherty E, O’Higgins S, Nic Gabhainn S, et al. Comparing the clinical-effectiveness and cost-effectiveness of an internet-delivered acceptance and commitment therapy (ACT) intervention with a waiting list control among adults with chronic pain: study protocol for a randomised controlled trial. BMJ Open 2014;4:e005092. https://doi.org/10.1136/bmjopen-2014-005092 | Protocol only |
| Heitkemper MM, Jarrett ME, Levy RL, Cain KC, Burr RL, Feld A, et al. Self-management for women with irritable bowel syndrome. Clin Gastroenterol Hepatol 2004;2:585–96 | Insufficient primary care involvement |
| Hildebrandt VH, Proper KI, van den Berg R, Douwes M, van den Heuvel SG, van Buuren S. [Cesar therapy is temporarily more effective in patients with chronic low back pain than the standard treatment by family practitioner: randomized, controlled and blinded clinical trial with 1 year follow-up.] Ned Tijdschr Geneeskd 2000;144:2258–64 | Intervention is posture correction implies pain is explained |
| Hill J, Dunn KM, Lewis M, Mason E, Vohora K, Main C, et al. A randomised trial of targeted treatment for low back pain compared with current best practice: the start back trial [ISRCTN37113406]. Physiotherapy 2011;97:eS485–6 | Conference abstract |
| Hill JC, Whitehurst DG, Lewis M. Risk-stratified primary care management of low back pain reduced disability. Ann Int Med 2012;156:JC2–7 | Population not meeting inclusion criteria for unexplained |
| Hofmann J, Peters S, Geidl W, Hentschke C, Pfeifer K. Effects of behavioural exercise therapy on the effectiveness of a multidisciplinary rehabilitation for chronic non-specific low back pain: study protocol for a randomised controlled trial. BMC Musculoskelet Disord 2013;14:89. https://doi.org/10.1186/1471-2474-14-89 | Population is inpatients |
| Hofmann SG. Review: cognitive behavioural interventions may be effective for chronic fatigue syndrome and chronic back pain. Evid Based Ment Health 2003;6:55 | Commentary |
| van der Horst HE, Schellevis FG, Eijk J. How effective is patient education and counseling for patients with ‘irritable bowel syndrome’ in general practice? Ned Tijdschr Geneeskd 1998;142:1417. Retrieved from http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/834/CN-00267834/frame.html | Conference abstract |
| Hoving JL, de Vet HCW, Koes BW, van Mameren H, Deville W, van der Windt D, et al. Manual therapy, physical therapy, or continued care by the general practitioner for patients with neck pain – long-term results from a pragmatic randomized clinical trial. Clin J Pain 2006;22:370–7. https://doi.org/10.1097/01.ajp.0000180185.79382.3f | Duration of pain is not greater than 3 months |
| Huibers M, Beurskens A, Van Schayck C, Bazelmans E, Metsemakers J, Knottnerus A, Bleijenberg G. [Efficacy of cognitive behavioral therapy by general practitioners for unexplained fatigue among employees.] Huisarts Wet 2005;48:267–72 | Dutch version of Huibers et al.153 |
| Hurley M, Walsh NE, Jessep S. Clinical effectiveness and costs of an integrated rehabilitation programme compared with outpatient physiotherapy for chronic knee pain. Arthr Rheumat 2012;64:S1026. Retrieved from http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/235/CN-01008235/frame.html | Conference abstract |
| Hutting N, Bart Staal J, Engels JA, Heerkens YF, Detaille SI, Nijhuis-van der Sanden MWG. Effect evaluation of a self-management programme for employees with complaints of the arm, neck or shoulder: a randomised controlled trial. Occup Environ Med 2015;72:852–61 | Insufficient primary care involvement |
| Hutting N, Staal JB, Heerkens YF, Engels JA, Nijhuis-van der Sanden MW. A self-management program for employees with complaints of the arm, neck, or shoulder (CANS): study protocol for a randomized controlled trial. Trials 2013;14:258. https://doi.org/10.1186/1745-6215-14-258 | Protocol only |
| Janse A, Worm-Smeitink M, Bussel-Lagarde J, Bleijenberg G, Nikolaus S, Knoop H. Testing the efficacy of web-based cognitive behavioural therapy for adult patients with chronic fatigue syndrome (CBIT): study protocol for a randomized controlled trial. BMC Neurol 2015;15:137. https://doi.org/10.1186/s12883-015-0392-3 | Protocol only |
| Jarrett ME, Cain KC, Burr RL, Hertig VL, Rosen SN, Heitkemper MM. Comprehensive self-management for irritable bowel syndrome: randomized trial of in-person vs. combined in-person and telephone sessions. Am J Gastroenterol 2009;104:3004–14. https://doi.org/10.1038/ajg.2009.479 | Setting is not primary care |
| Jellema P, van der Horst HE, Vlaeyen JW, Stalman WA, Bouter LM, van der Windt DA. Predictors of outcome in patients with (sub)acute low back pain differ across treatment groups. Spine 2006;31:1699–705. https://doi.org/10.1097/01.brs.0000224179.04964.aa | Pain not greater than 3 months |
| Jellema P, van der Roer N, van der Windt DA, van Tulder MW, van der Horst HE, Stalman WA, Bouter LM. Low back pain in general practice: cost-effectiveness of a minimal psychosocial intervention versus usual care. Eur Spine J 2007;16:1812–21. https://doi.org/10.1007/s00586-007-0439-2 | Pain is subacute |
| Jellema P, van der Horst HE, Vlaeyen JW, Stalman WA, Bouter LM, van der Windt DA. Predictors of outcome in patients with (sub)acute low back pain differ across treatment groups. Spine 2006;31:1699–705. https://doi.org/10.1097/01.brs.0000224179.04964.aa | Pain is subacute |
| Jellema P, van der Windt DA, van der Horst HE, Blankenstein AH, Bouter LM, Stalman WA. Why is a treatment aimed at psychosocial factors not effective in patients with (sub)acute low back pain? Pain 2005;118:350–9 | Pain is subacute |
| Jellema P, van der Windt DA, van der Horst HE, Stalman WA, Bouter LM. Prediction of an unfavourable course of low back pain in general practice: comparison of four instruments. Br J Gen Pract 2007;57:15–22 | Pain is subacute |
| Jellema P, van der Windt DAW, van der Horst HE, Twisk JWR, Stalman WAB, Bouter LM. Should treatment of (sub)acute low back pain be aimed at psychosocial prognostic factors? Cluster randomised clinical trial in general practice. BMJ 2005;331:84–7. https://doi.org/10.1136/bmj.38495.686736.E0 | Pain is subacute |
| Jensen CE, Riis A, Pedersen KM, Jensen MB, Petersen KD. Study protocol of an economic evaluation of an extended implementation strategy for the treatment of low back pain in general practice: a cluster randomised controlled trial. Implement Sci 2014;9:140. https://doi.org/10.1186/s13012-014-0140-x | Protocol only |
| Johnson RE, Jones GT, Wiles NJ, Chaddock C, Potter RG, Roberts C, et al. Active exercise, education, and cognitive behavioural therapy for persistent disabling low back pain. Spine 2007;32:1578–85 | Pain not unexplained |
| Jones GT, Mertens K, Macfarlane GJ, Palmer KT, Coggon D, Walker-Bone K, et al. Maintained physical activity and physiotherapy in the management of distal upper limb pain - a protocol for a randomised controlled trial (the arm pain trial). BMC Musculoskelet Disord 2014;15:71. https://doi.org/10.1186/1471-2474-15-71 | Protocol only |
| Jones M, Koloski N, Boyce P, Talley NJ. Pathways connecting cognitive behavioral therapy and change in bowel symptoms of IBS. J Psychosom Res 2011;70:278–85. https://doi.org/10.1016/j.jpsychores.2010.10.004 | Setting not primary care |
| Jonsbu E, Dammen T, Morken G, Moum T, Martinsen EW. Short-term cognitive behavioral therapy for non-cardiac chest pain and benign palpitations: a randomized controlled trial. J Psychosom Res 2011;70:117–23. https://doi.org/10.1016/j.jpsychores.2010.09.013 | Setting not primary care |
| Jonsbu E, Martinsen EW, Morken G, Moum T, Dammen T. Change and impact of illness perceptions among patients with non-cardiac chest pain or benign palpitations following three sessions of CBT. Behav Cogn Psychother 2013;41:398–407. https://doi.org/10.1017/S1352465813000179 | Outcomes not appropriate |
| Kaleth AS, Saha CK, Jensen MP, Slaven JE, Ang DC. Effect of moderate to vigorous physical activity on long-term clinical outcomes and pain severity in fibromyalgia. Arthritis Care Res 2013;65:1211–18. https://doi.org/10.1002/acr.21980 | Insufficient primary care involvement |
| Kalmatayeva Z, Zholamanova A. Cost-effectiveness analysis of psychotherapy in treatment of essential hypertension in primary care. Arch Psychiatry Psychother 2014;16:57–64 | Population not unexplained |
| Katsamanis M, Lehrer PM, Escobar JI, Gara MA, Kotay A, Liu R. Psychophysiologic treatment for patients with medically unexplained symptoms: a randomized controlled trial. Psychosomatics 2011;52:218–29. https://doi.org/10.1016/j.psym.2011.01.015 | Setting not primary care |
| Kemani MK, Olsson GL, Lekander M, Hesser H, Andersson E, Wicksell RK. Efficacy and cost-effectiveness of acceptance and commitment therapy and applied relaxation for longstanding pain: a randomized controlled trial. Clin J Pain 2015;31:1004–16. https://doi.org/10.1097/AJP.0000000000000203 | Includes tertiary care |
| Knox CR, Lall R, Hansen Z, Lamb SE. Treatment compliance and effectiveness of a cognitive behavioural intervention for low back pain: a complier average causal effect approach to the BeST data set. BMC Musculoskelet Disord 2014;15:17. https://doi.org/10.1186/1471-2474-15-17 | Pain is not greater than 3 months |
| Kristjansdottir OB, Fors EA, Eide E, Finset A, Dulmen S, Wigers SH, Eide H. The effect of web-based diaries and situational feedback on catastrophizing in women with chronic widespread pain – a randomized trial. Eur J Pain Suppl 2011;5:259–60 | Conference abstract |
| Kristjánsdóttir OB, Fors EA, Eide E, Finset A, Stensrud TL, van Dulmen S, et al. A smartphone-based intervention with diaries and therapist-feedback to reduce catastrophizing and increase functioning in women with chronic widespread pain: randomized controlled trial. J Med Internet Res 2013;15:e5. https://doi.org/10.2196/jmir.2249 | Setting not primary care |
| Kroenke K, Swindle R. Cognitive-behavioral therapy for somatization and symptom syndromes: a critical review of controlled clinical trials. Psychother Psychosom 2000;69:205–15 | Systematic review |
| Lahmann C, Henningsen P, Dieterich M, Radziej K, Schmid G. Tailored care for somatoform vertigo/dizziness: study protocol for a randomised controlled trial evaluating integrative group psychotherapy. J Neurol 2015;262:1867–75. https://doi.org/10.1007/s00415-015-7784-6 | Protocol only |
| Lamb SE, Hansen Z, Lall R, Castelnuova E, Withers E, Nichols V, Potter R. Group cognitive behavioral intervention in primary care in low back pain: a randomized, controlled study and analysis of cost-effectiveness. Osteopath Med 2010;11:24–6 | Pain is subacute |
| Lamb SE, Mistry D, Lall R, Hansen Z, Evans D, Withers EJ, Underwood MR, Back Skills Training Trial Group. Group cognitive behavioural interventions for low back pain in primary care: extended follow-up of the Back Skills Training Trial (ISRCTN54717854). Pain 2012;153:494–501. https://doi.org/10.1016/j.pain.2011.11.016 | Pain is subacute |
| Lang E, Liebig K, Kastner S, Neundörfer B, Heuschmann P. Multidisciplinary rehabilitation versus usual care for chronic low back pain in the community: effects on quality of life. Spine J 2003;3:270–6 | Study design – non randomised trial |
| Leonhardt C, Keller S, Chenot JF, Luckmann J, Basler HD, Wegscheider K, et al. TTM-based motivational counselling does not increase physical activity of low back pain patients in a primary care setting – a cluster-randomized controlled trial. Patient Educ Couns 2008;70:50–60 | Pain includes acute |
| Lin J, Luking M, Ebert DD, Buhrman M, Andersson G, Baumeister H. Effectiveness and cost-effectiveness of a guided and unguided internet-based acceptance and commitment therapy for chronic pain: study protocol for a three-armed randomised controlled trial. Internet Interv 2015;2:7–16 | Heterogeneous pain population not necessarily unexplained |
| Litt MD, Porto FB. Determinants of pain treatment response and nonresponse: identification of TMD patient subgroups. J Pain 2013;14:1502–13. https://doi.org/10.1016/j.jpain.2013.07.017 | Setting not primary care |
| Ljótsson B, Andersson G, Andersson E, Hedman E, Lindfors P, Andréewitch S, et al. Acceptability, effectiveness, and cost-effectiveness of internet-based exposure treatment for irritable bowel syndrome in a clinical sample: a randomized controlled trial. BMC Gastroenterol 2011;11:110. https://doi.org/10.1186/1471-230X-11-110 | Setting not primary care |
| Lofvander MB. Cognitive-behavioural treatment of chronic pain in primary care: a three-year follow-up. Eur J Gen Pract 2002;8:151–8 | Not a RCT |
| López-García-Franco A, del-Cura-González MI, Caballero-Martinez L, Sanz-Cuesta T, Díaz-García MI, Rodriguez-Monje MT, et al. Effectiveness of a cognitive behavioral intervention in patients with medically unexplained symptoms: cluster randomized trial. BMC Fam Pract 2012;13:35. https://doi.org/10.1186/1471-2296-13-35 | Protocol only |
| Luciano JV, D’Amico F, Cerdà-Lafont M, Peñarrubia-María MT, Knapp M, Cuesta-Vargas AI, et al. Cost-utility of cognitive behavioral therapy versus U.S. Food and Drug Administration recommended drugs and usual care in the treatment of patients with fibromyalgia: an economic evaluation alongside a 6-month randomized controlled trial. Arthritis Res Ther 2014;16:451. https://doi.org/10.1186/s13075-014-0451-y | Cost-utility |
| Luciano JV, Sabes-Figuera R, Cardeñosa E, T Peñarrubia-María M, Fernández-Vergel R, García-Campayo J, et al. Cost-utility of a psychoeducational intervention in fibromyalgia patients compared with usual care: an economic evaluation alongside a 12-month randomized controlled trial. Clin J Pain 2013;29:702–11. https://doi.org/10.1097/AJP.0b013e318270f99a | Outcomes are costs |
| Luo Z, Goddeeris J, Gardiner JC, Smith RC. Costs of an intervention for primary care patients with medically unexplained symptoms: a randomized controlled trial. Psychiatr Serv 2007;58:1079–86 | Costs data |
| Macfarlane GJ, Beasley M, Keeley P, Lovell K, Hannaford P, Symmons DPM, et al. A randomised controlled trial (RCT) of telephone delivered cognitive behaviour therapy (TCBT) and exercise in the management of chronic widespread pain (CWP): Identifying long-term outcome and who benefits from which treatment. Arthritis Rheum 2013;65:S1221 | Conference abstract |
| Machado LA, Azevedo DC, Capanema MB, Neto TN, Cerceau DM. Client-centered therapy vs exercise therapy for chronic low back pain: a pilot randomized controlled trial in Brazil. Pain Med 2007;8:251–8 | Not in a primary care setting |
| Magallón R, Gili M, Moreno S, Bauzá N, García-Campayo J, Roca M, et al. Cognitive-behaviour therapy for patients with Abridged Somatization Disorder (SSI 4,6) in primary care: a randomized, controlled study. BMC Psychiatry 2008;8:47. https://doi.org/10.1186/1471-244X-8-47 | Protocol |
| Mannerkorpi K, Nyberg B, Ahlmén M, Ekdahl C. Pool exercise combined with an education program for patients with fibromyalgia syndrome. A prospective, randomized study. J Rheumatol 2000;27:2473–81 | Not in a primary care setting |
| Marques M, De Gucht V, Maes S, Leal I. Protocol for the ‘four steps to control your fatigue (4-STEPS)’ randomised controlled trial: a self-regulation based physical activity intervention for patients with unexplained chronic fatigue. BMC Public Health 2012;12:202. https://doi.org/10.1186/1471-2458-12-202 | Protocol only |
| Mårtensson L, Marklund B, Fridlund B. Evaluation of a biopsychosocial rehabilitation programme in primary healthcare for chronic pain patients. Scand J Occup Ther 1999;6:157–65 | Not a RCT |
| Martins MR, Gritti CC, dos Santos Junior R, de Araújo MC, Dias LC, Foss MH, et al. Randomized controlled trial of a therapeutic intervention group in patients with fibromyalgia syndrome. Rev Bras Reumatol 2014;54:179–84 | Setting is secondary care |
| Mason E, Hill JC, Lewis M, Dunn KM, Hay EM. Does targeted treatment for low back pain improve patient satisfaction and better meet expectations compared to current best care? Physiotherapy 2011;97:eS757–8 | Conference abstract |
| McCracken LM, Sato A, Taylor GJ. A trial of a brief group-based form of acceptance and commitment therapy (ACT) for chronic pain in general practice: pilot outcome and process results. J Pain 2013;14:1398–406. https://doi.org/10.1016/j.jpain.2013.06.011 | Population not meeting inclusion criteria for unexplained |
| McCracken LM, Sato A, Wainwright D, House W, Taylor GJ. A feasibility study of brief group-based acceptance and commitment therapy for chronic pain in general practice: recruitment, attendance, and patient views. Prim Health Care Res Dev 2014;15:312–23. https://doi.org/10.1017/S1463423613000273 | Population not meeting inclusion criteria for unexplained |
| McCrone P, Knapp M, Kennedy T, Seed P, Jones R, Darnley S, Chalder T. Cost-effectiveness of cognitive behaviour therapy in addition to mebeverine for irritable bowel syndrome. Eur J Gastroenterol Hepatol 2008;20:255–63. https://doi.org/10.1097/MEG.0b013e3282f2519d | Cost-effectiveness from Kennedy et al.129 |
| McCrone P, Ridsdale L, Darbishire L, Seed P. Cost-effectiveness of cognitive behavioural therapy, graded exercise and usual care for patients with chronic fatigue in primary care. Psychol Med 2004;34:991–9 | Cost-effectiveness from Ridsdale et al.113 |
| McDonough SM, Tully MA, Boyd A, O’Connor SR, Kerr DP, O’Neill SM, et al. Pedometer-driven walking for chronic low back pain: a feasibility randomized controlled trial. Clin J Pain 2013;29:972–81. https://doi.org/10.1097/AJP.0b013e31827f9d81 | Not in a primary care setting, referral to hospital lists |
| Meijer EM, Sluiter JK, Heyma A, Sadiraj K, Frings-Dresen MH. Cost-effectiveness of multidisciplinary treatment in sick-listed patients with upper extremity musculoskeletal disorders: a randomized, controlled trial with one-year follow-up. Int Arch Occup Environ Health 2006;79:654–64. https://doi.org/10.1007/s00420-006-0098-3 | Setting is not primary care |
| Meng H, Friedberg F, Castora-Binkley M. Cost-effectiveness of chronic fatigue self-management versus usual care: a pilot randomized controlled trial. BMC Fam Pract 2014;15:184. https://doi.org/10.1186/s12875-014-0184-7 | Costs from Friedberg et al.151 |
| Menzel NN, Robinson ME. Back pain in direct patient care providers: early intervention with cognitive behavioral therapy. Pain Manag Nurs 2006;7:53–63 | Setting not primary care |
| Miller J, MacDermid JC, Walton DM, Richardson J. Chronic pain self-management support with pain science education and exercise (COMMENCE): study protocol for a randomized controlled trial. Trials 2015;16:462. https://doi.org/10.1186/s13063-015-0994-5 | Protocol only |
| Milosavljevic S, Clay L, Bath B, Trask C, Penz E, Stewart S, et al. Walking away from back pain: one step at a time - a community-based randomised controlled trial. BMC Public Health 2015;15:144. https://doi.org/10.1186/s12889-015-1496-9 | Protocol only |
| Moffett JK, Torgerson D, Bell-Syer S, Jackson D, Llewlyn-Phillips H, Farrin A, Barber J. Randomised controlled trial of exercise for low back pain: clinical outcomes, costs, and preferences. BMJ 1999;319:279–83 | Pain is not greater than 3 months |
| Mongini F, Evangelista A, Milani C, Ferrero L, Ciccone G, Ugolini A, et al. An educational and physical program to reduce headache, neck/shoulder pain in a working community: a cluster-randomized controlled trial. PLOS ONE 2012;7:e29637. https://doi.org/10.1371/journal.pone.0029637 | Not in a primary care setting |
| Monticone M, Ferrante S, Rocca B, Baiardi P, Farra FD, Foti C. Effect of a long-lasting multidisciplinary program on disability and fear-avoidance behaviors in patients with chronic low back pain: results of a randomized controlled trial. Clin J Pain 2013;29:929–38. https://doi.org/10.1097/AJP.0b013e31827fef7e | Not in a primary care setting |
| Moore JE, Von Korff M, Cherkin D, Saunders K, Lorig K. A randomized trial of a cognitive-behavioral program for enhancing back pain self care in a primary care setting. Pain 2000;88:145–53 | Pain not unexplained |
| Moreno S, Gili M, Magallon R, Bauza N, Roca M, del Hoyo YL, Garcia-Campayo J. Effectiveness of group versus individual cognitive-behavioral therapy in patients with abridged somatization disorder: a randomized controlled trial. Erratum. Psychosom Med 2014;76:399 | Conference abstract |
| Morriss R. Specific psychosocial interventions for somatizing patients by the general practitioner: a randomised controlled trial. J Psychosom Res 2004;57:515–16 | Commentary |
| Morriss R, Gask L, Dowrick C, Dunn G, Peters S, Ring A, et al. Randomized trial of reattribution on psychosocial talk between doctors and patients with medically unexplained symptoms. Psychol Med 2010;40:325–33. https://doi.org/10.1017/S0033291709990353 | Outcomes not appropriate for quantitative review |
| Moseley GL, Nicholas MK, Hodges PW. A randomized controlled trial of intensive neurophysiology education in chronic low back pain. Clin J Pain 2004;20:324–30 | Setting is not primary care |
| Moss-Morris R, Chilcot J. Changes in illness-related cognitions rather than distress mediate improvements in ibs symptoms and disability following a brief cognitive behavioural therapy intervention. Psychosom Med 2013;75:A-37 | Mediator analysis from Moss-Morris et al.130 |
| Mourad G, Stromberg A, Johansson P, Jaarsma T. Internet-based cognitive behavioural therapy in patients with non-cardiac chest pain-design of a randomized controlled pilot study. Europ J Cardiovasc Nursi 2014;13:S67–8 | Conference abstract |
| Mullally WJ, Hall K, Goldstein R. Efficacy of biofeedback in the treatment of migraine and tension type headaches. Pain Physician 2009;12:1005–11 | Population is migraine |
| Mulet M, Decker KL, Look JO, Lenton PA, Schiffman EL. A randomised clinical trial assessing the efficacy of adding 6 × 6 exercises to self-care for the treatment of masticatory myofascial pain. J Orofacial Pain 2007;21:318 | Population not meeting the inclusion for unexplained |
| NCT. Effectiveness of a Cognitive Behavioral Intervention in Patients With Symptoms Somatization, as Measure Quality of Life, Front the Clinical Practice Usual Action in Primary Health Care. A Controlled Clinical Trial With Parallel Groups. 2011. http://clinicaltrials.gov/show/NCT01484223 | Protocol only |
| Nevedal DC, Wang C, Oberleitner L, Schwartz S, Williams AM. Effects of an individually tailored web-based chronic pain management program on pain severity, psychological health, and functioning. J Med Internet Res 2013;15:e201. https://doi.org/10.2196/jmir.2296 | Study design – not a RCT |
| Nicassio PM, Radojevic V, Weisman MH, Schuman C, Kim J, Schoenfeld-Smith K, Krall T. A comparison of behavioral and educational interventions for fibromyalgia. J Rheumatol 1997;24:2000–7 | Not in a primary care setting |
| Nørregaard J, Lykkegaard JJ, Mehlsen J, Danneskiold-Samsøe B. Exercise training in treatment of fibromyalgia. J Musculoskelet Pain 1997;5:71–9 | Secondary care referrals |
| O’Dowd H, Gladwell P, Rogers CA, Hollinghurst S, Gregory A. Cognitive behavioural therapy in chronic fatigue syndrome: a randomised controlled trial of an outpatient group programme. Health Technol Assess 2006;10(37) | Not in a primary care setting |
| Oliver K, Cronan TA, Walen HR, Tomita M. Effects of social support and education on health care costs for patients with fibromyalgia. J Rheumatol 2001;28:2711–19 | Outcomes not appropriate |
| Overmeer T, Boersma K, Denison E, Linton SJ. Does teaching physical therapists to deliver a biopsychosocial treatment program result in better patient outcomes? A randomized controlled trial. Phys Ther 2011;91:804–19. https://doi.org/10.2522/ptj.20100079 | Duration of pain not necessarily more than 3 months |
| Palsson OS. Should we incorporate psychological care into the management of IBS? Gastroenterol Hepatol 2006;3:474 | Commentary |
| Payne A, Blanchard EB. A controlled comparison of cognitive therapy and self-help support groups in the treatment of irritable bowel syndrome. J Consult Clin Psychol 1995;63:779–86 | Not a primary care setting |
| Payne H. Pilot study to evaluate dance movement psychotherapy (the BodyMind approach) in patients with medically unexplained symptoms: participant and facilitator perceptions and a summary discussion. Body Mov Dance Psychother 2009;4:77–94 | Study design – not a RCT |
| Perry J, Green A, Singh S, Watson P. A preliminary investigation into the magnitude of effect of lumbar extension exercises and a segmental rotatory manipulation on sympathetic nervous system activity. Man Ther 2011;16:190–5. https://doi.org/10.1016/j.math.2010.10.008 | Thesis |
| Poleshuck EL, Gamble SA, Bellenger K, Lu N, Tu X, Sörensen S, et al. Randomized controlled trial of interpersonal psychotherapy versus enhanced treatment as usual for women with co-occurring depression and pelvic pain. J Psychosom Res 2014;77:264–72. https://doi.org/10.1016/j.jpsychores.2014.07.016 | Population must meet criteria for major depression |
| Puder RS. Age analysis of cognitive-behavioral group therapy for chronic pain outpatients. Psychol Aging 1988;3:204–7 | Not a primary care setting |
| Rasmussen-Barr E, Nilsson-Wikmar L, Arvidsson I. Stabilizing training compared with manual treatment in sub-acute and chronic low-back pain. Man Ther 2003;8:233–41 | Duration of pain is not greater than 3 months |
| Reme SE, Kennedy T, Jones R, Darnley S, Chalder T. Predictors of treatment outcome after cognitive behavior therapy and antispasmodic treatment for patients with irritable bowel syndrome in primary care. J Psychosom Res 2010;68:385–8. https://doi.org/10.1016/j.jpsychores.2010.01.003 | Predictors of outcomes from Kennedy 2005 |
| Ringström G, Störsrud S, Posserud I, Lundqvist S, Westman B, Simrén M. Structured patient education is superior to written information in the management of patients with irritable bowel syndrome: a randomized controlled study. Eur J Gastroenterol Hepatol 2010;22:420–8. https://doi.org/10.1097/MEG.0b013e3283333b61 | Not a primary care setting |
| Roberts L, Little P, Chapman J, Cantrell T, Pickering R, Langridge J. The back home trial: general practitioner-supported leaflets may change back pain behavior. Spine 2002;27:1821–8 | Pain is acute |
| Rooks DS, Gautam S, Romeling M, Cross ML, Stratigakis D, Evans B, et al. Group exercise, education, and combination self-management in women with fibromyalgia: a randomized trial. Arch Intern Med 2007;167:2192–200 | Insufficient primary care involvement – recruitment from multiple sources |
| Rossignol M, Abenhaim L, Séguin P, Neveu A, Collet JP, Ducruet T, Shapiro S. Coordination of primary health care for back pain. A randomized controlled trial. Spine 2000;25:251–8 | Pain is not greater than 3 months |
| Saarijärvi S. A controlled study of couple therapy in chronic low back pain patients. Effects on marital satisfaction, psychological distress and health attitudes. J Psychosom Res 1991;35:265–72 | Population not meeting inclusion criteria for unexplained |
| Sabes-Figuera R, McCrone P, Hurley M, King M, Donaldson AN, Ridsdale L. The hidden cost of chronic fatigue to patients and their families. BMC Health Serv Res 2010;10:56. https://doi.org/10.1186/1472-6963-10-56 | Costs data from Ridsdale et al.115 |
| Salmon P, Humphris GM, Ring A, Davies JC, Dowrick CF. Primary care consultations about medically unexplained symptoms: patient presentations and doctor responses that influence the probability of somatic intervention. Psychosom Med 2007;69:571–7 | Outcomes not appropriate for quantitative review |
| Saner J, Kool J, de Bie RA, Sieben JM, Luomajoki H. Movement control exercise versus general exercise to reduce disability in patients with low back pain and movement control impairment. A randomised controlled trial. BMC Musculoskelet Disord 2011;12:207. https://doi.org/10.1186/1471-2474-12-207 | Protocol |
| Sattel H, Kittner A, Henningsen P. A brief psychodynamic-interpersonal psychotherapy for patients with multisomatoform disorder (PISO) – one size fits all? Psychother Psychosom Med Psychol 2011;61:A070 | Conference abstract |
| Sattel H, Lahmann C, Gündel H, Guthrie E, Kruse J, Noll-Hussong M, et al. Brief psychodynamic interpersonal psychotherapy for patients with multisomatoform disorder: randomised controlled trial. Br J Psychiatry 2012;200:60–7. https://doi.org/10.1192/bjp.bp.111.093526 | |
| Schaller A, Froboese I. Movement coaching: study protocol of a randomized controlled trial evaluating effects on physical activity and participation in low back pain patients. BMC Musculoskelet Disord 2014;15:391. https://doi.org/10.1186/1471-2474-15-391 | Protocol |
| Schiltenwolf M, Buchner M, Heindl B, von Reumont J, Müller A, Eich W. Comparison of a biopsychosocial therapy (BT) with a conventional biomedical therapy (MT) of subacute low back pain in the first episode of sick leave: a randomized controlled trial. Eur Spine J 2006;15:1083–92. https://doi.org/10.1007/s00586-005-0008-5 | Pain is subacute |
| Schröder A, Rehfeld E, Ornbøl E, Sharpe M, Licht RW, Fink P. Cognitive-behavioural group treatment for a range of functional somatic syndromes: randomised trial. Br J Psychiatry 2012;200:499–507. https://doi.org/10.1192/bjp.bp.111.098681 | Setting is not primary care |
| Seferlis T, Németh G, Carlsson AM, Gillström P. Conservative treatment in patients sick-listed for acute low-back pain: a prospective randomised study with 12 months’ follow-up. Eur Spine J 1998;7:461–70 | Pain is acute |
| Seferlis T, Németh G, Carlsson AM. Prediction of functional disability, recurrences, and chronicity after 1 year in 180 patients who required sick leave for acute low-back pain. J Spinal Disord 2000;13:470–7 | Pain is acute |
| Semrau J, Hentschke C, Buchmann J, Meng K, Vogel H, Faller H, et al. Long-term effects of interprofessional biopsychosocial rehabilitation for adults with chronic non-specific low back pain: a multicentre, quasi-experimental study. PLOS ONE 2015;10:e0118609. https://doi.org/10.1371/journal.pone.0118609 | Study design – not a RCT |
| Sencan S, Ak S, Karan A, Muslumanoglu L, Ozcan E, Berker E. A study to compare the therapeutic efficacy of aerobic exercise and paroxetine in fibromyalgia syndrome. J Back Musculoskelet Rehabil 2004;17:57–61 | Not in a primary care setting |
| Sharpe M, Hawton K, Simkin S, Surawy C, Hackmann A, Klimes I, et al. Cognitive behaviour therapy for the chronic fatigue syndrome: a randomized controlled trial. BMJ 1996;312:22–6 | Setting is secondary care (hospitals) |
| Sharpe M, Walker J, Williams C, Stone J, Cavanagh J, Murray G, et al. Guided self-help for functional (psychogenic) symptoms: a randomized controlled efficacy trial. Neurology 2011;77:564–72. https://doi.org/10.1212/WNL.0b013e318228c0c7 | Setting not primary care |
| Sheeran L, van Deursen R, Caterson B, Sparkes V. Classification-guided versus generalized postural intervention in subgroups of nonspecific chronic low back pain: a pragmatic randomized controlled study. Spine 2013;38:1613–25. https://doi.org/10.1097/BRS.0b013e31829e049b | Not in a primary care setting |
| Sheeran L, van Deursen R, Caterson B, Sparkes V. Classification-guided versus generalized postural intervention in subgroups of nonspecific chronic low back pain: a pragmatic randomized controlled study. Spine 2013;38:1613–25. https://doi.org/10.1097/BRS.0b013e31829e049b | Intervention is posture correction |
| Sherman KJ, Cherkin DC, Erro J, Miglioretti DL, Deyo RA. Comparing yoga, exercise, and a self-care book for chronic low back pain: a randomized, controlled trial. Ann Intern Med 2005;143:849–56 | Population not meeting the inclusion criteria for medically unexplained |
| Shpaner M, Kelly C, Lieberman G, Perelman H, Davis M, Keefe FJ, Naylor MR. Unlearning chronic pain: a randomized controlled trial to investigate changes in intrinsic brain connectivity following cognitive behavioral therapy. Neuroimage Clin 2014;5:365–76. https://doi.org/10.1016/j.nicl.2014.07.008 | Population not meeting the inclusion criteria for medically unexplained |
| Siemonsma PC, Stuive I, Roorda LD, Vollebregt JA, Walker MF, Lankhorst GJ, Lettinga AT. Cognitive treatment of illness perceptions in patients with chronic low back pain: a randomized controlled trial. Phys Ther 2013;93:435–48. https://doi.org/10.2522/ptj.20110150 | Setting is not primary care |
| Simon D, Kriston L, von Wolff A, Buchholz A, Vietor C, Hecke T, et al. Effectiveness of a web-based, individually tailored decision aid for depression or acute low back pain: a randomized controlled trial. Patient Educ Couns 2012;87:360–8. https://doi.org/10.1016/j.pec.2011.10.009 | Pain is acute |
| Sjögren T, Nissinen KJ, Järvenpää SK, Ojanen MT, Vanharanta H, Mälkiä EA. Effects of a workplace physical exercise intervention on the intensity of headache and neck and shoulder symptoms and upper extremity muscular strength of office workers: a cluster randomized controlled cross-over trial. Pain 2005;116:119–28 | Setting is not primary care |
| Skouen JS, Grasdal A, Haldorsen EM. Return to work after comparing outpatient multidisciplinary treatment programs versus treatment in general practice for patients with chronic widespread pain. Eur J Pain 2006;10:145–52 | Insufficient primary care involvement |
| Skouen JS, Grasdal AL, Haldorsen EM, Ursin H. Relative cost-effectiveness of extensive and light multidisciplinary treatment programs versus treatment as usual for patients with chronic low back pain on long-term sick leave: randomized controlled study. Spine 2002;27:901–9 | Setting is not primary care |
| Slade SC, Molloy E, Keating JL. People with non-specific chronic low back pain who have participated in exercise programs have preferences about exercise: a qualitative study. Aust J Physiother 2009;55:115–21 | Protocol |
| Slater H, Davies SJ, Parsons R, Quintner JL, Schug SA. A policy-into-practice intervention to increase the uptake of evidence-based management of low back pain in primary care: a prospective cohort study. PLOS ONE 2012;7:e38037. https://doi.org/10.1371/journal.pone.0038037 | Study design – not a RCT |
| Sleptsova M, Woessmer B, Grossman P, Langewitz W. Culturally sensitive group therapy for Turkish patients suffering from chronic pain: a randomised controlled intervention trial. Swiss Med Wkly 2013;143:w13875. https://doi.org/10.4414/smw.2013.13875 | Insufficient primary care involvement |
| Smith RC, Gardiner JC, Lyles JS, Sirbu C, Dwamena FC, Hodges A, et al. Exploration of DSM-IV criteria in primary care patients with medically unexplained symptoms. Psychosom Med 2005;67:123–9 | Summary of Smith et al.107 |
| Soares JJ, Grossi G. A randomized, controlled comparison of educational and behavioural interventions for women with fibromyalgia. Scand J Occup Ther 2002;9:35–45 | Insufficient primary care involvement |
| Söderberg E. No differences for acupuncture, physical training and relaxation training in the treatment effects of patients with chronic tension-type headache. Focus Altern Complement Ther 2007;12:109–110 | Acupuncture not behavioural intervention |
| Speckens A, Van Hemert A, Spinhoven P, Hawton K, Bolk J, Rooijmans H. Gunstige effecten van cognitieve gedragstherapie voor onverklaarde lichamelijke klachten; een gerandomiseerd onderzoek. Tijdschr Psychiatr 1996;140;1227–32 | Hospital setting |
| Speckens AE, van Hemert AM, Spinhoven P, Hawton KE, Bolk JH, Rooijmans HG. Cognitive behavioural therapy for medically unexplained physical symptoms: a randomised controlled trial. BMJ 1995;311:1328–32 | Setting is not primary care |
| Staal JB, Hlobil H, Twisk JW, Smid T, Koke ArJ, van Mechelen W. Graded activity for low back pain in occupational health care: a randomized, controlled trial. Ann Intern Med 2004;140:77–84 | Pain is not greater than 3 months |
| Storheim K, Brox JI, Holm I, Koller AK, Bø K. Intensive group training versus cognitive intervention in sub-acute low back pain: short-term results of a single-blind randomized controlled trial. J Rehabil Med 2003;35:132–40 | Pain is subacute |
| Thorn BE, Day MA, Burns J, Kuhajda MC, Gaskins SW, Sweeney K, et al. Randomised trial of group cognitive behavioural therapy compared with a pain education control for low literacy rural people with chronic pain. Pain 2011;152:2710–20 | Population not meeting inclusion criteria for unexplained |
| Tkachuk GA. Controlled Trial of a Multicomponent Cognitive-behavioral Group Treatment for Irritable Bowel Syndrome. 2002. URL: https://mspace.lib.umanitoba.ca/handle/1993/2088 (accessed 5 November 2019) | Dissertation |
| Tschuschke V, Weber R, Horn E, Kiencke P, Tress W. Psychodynamic short-term outpatient group therapy with patients suffering from somatoform disorders. Z Psychiatr Psychol Und Psychother 2007;55:87–95 | Not in a primary care setting |
| Turner JA, Mancl L, Aaron LA. Short- and long-term efficacy of brief cognitive-behavioral therapy for patients with chronic temporomandibular disorder pain: a randomized, controlled trial. Pain 2006;121:181–94 | Setting is not primary care |
| Underwood M, Mistry D, Lall R, Lamb S. Predicting response to a cognitive-behavioral approach to treating low back pain: secondary analysis of the BeST data set. Arthritis Care Res 2011;63:1271–9. https://doi.org/10.1002/acr.20518 | Pain duration not greater than 3 months |
| Valenzuela-Pascual F, Molina F, Corbi F, Blanco-Blanco J, Gil RM, Soler-Gonzalez J. The influence of a biopsychosocial educational internet-based intervention on pain, dysfunction, quality of life, and pain cognition in chronic low back pain patients in primary care: a mixed methods approach. BMC Med Inform Decis Mak 2015;15:97. https://doi.org/10.1186/s12911-015-0220-0 | Protocol |
| Valim V, Oliveira L, Suda A, Silva L, de Assis M, Barros Neto T, et al. Aerobic fitness effects in fibromyalgia. J Rheumatol 2003;30:1060–9 | Not in a primary care setting |
| van den Hout JH, Vlaeyen JW, Heuts PH, Zijlema JH, Wijnen JA. Secondary prevention of work-related disability in nonspecific low back pain: does problem-solving therapy help? A randomized clinical trial. Clin J Pain 2003;19:87–96 | Pain not greater than 3 months |
| van der Roer N, Boos N, van Tulder MW. Economic evaluations: a new avenue of outcome assessment in spinal disorders. Eur Spine J 2006;15(Suppl. 1):109–17. https://doi.org/10.1007/s00586-005-1052-x | Outcomes not appropriate |
| van der Roer N, Ostelo RW, Bekkering GE, van Tulder MW, de Vet HC. Minimal clinically important change for pain intensity, functional status, and general health status in patients with nonspecific low back pain. Spine 2006;31:578–82. https://doi.org/10.1097/01.brs.0000201293.57439.47 | Outcomes not appropriate |
| van Erp RMA, Huijnen IPJ, Köke AJA, Abbink FE, den Hollander M, Smeets RJEM. Development and content of the biopsychosocial primary care intervention ‘Back on Track’ for a subgroup of people with chronic low back pain. Physiotherapy 2017;103:160–6 | Study protocol |
| van Erp RM, Huijnen IP, Verbunt JA, Smeets RJ. A biopsychosocial primary care intervention (Back on Track) versus primary care as usual in a subgroup of people with chronic low back pain: protocol for a randomised, controlled trial. J Physiother 2015;61:155. https://doi.org/10.1016/j.jphys.2015.03.003 | Conference abstract |
| van Santen M, Bolwijn P, Landewé R, Verstappen F, Bakker C, Hidding A, et al. High or low intensity aerobic fitness training in fibromyalgia: does it matter? J Rheumatol 2002;29:582–7 | Not in a primary care setting |
| van Wilgen CP, Bloten H, Oeseburg B. Results of a multidisciplinary program for patients with fibromyalgia implemented in the primary care. Disabil Rehabil 2007;29:1207–13 | Study design – non-controlled treatment study |
| Verkerk K, Luijsterburg PA, Heymans MW, Ronchetti I, Pool-Goudzwaard AL, Miedema HS, Koes BW. Prognosis and course of pain in patients with chronic non-specific low back pain: a 1-year follow-up cohort study. Eur J Pain 2015;19:1101–10. https://doi.org/10.1002/ejp.633 | Study design – not a RCT |
| Verstappen FT, van Santen-Hoeuftt HMS, Bolwijn PH, van der Linden S, Kuipers H. Effects of a group activity program for fibromyalgia patients on physical fitness and well being. J Musculoskelet Pain 1997;5:17–28 | Not in a primary care setting – outpatient clinics at general hospital |
| Von Korff M, Balderson BH, Saunders K, Miglioretti DL, Lin EH, Berry S, et al. A trial of an activating intervention for chronic back pain in primary care and physical therapy settings. Pain 2005;113:323–30 | Population inclusion based on severity not duration |
| Von Korff M, Moore JE, Lorig K, Cherkin DC, Saunders K, González VM, et al. A randomized trial of a lay person-led self-management group intervention for back pain patients in primary care. Spine 1998;23:2608–15 | Population not meeting inclusion for unexplained symptoms |
| Vonk F, Verhagen AP, Twisk JW, Köke AJ, Luiten MW, Koes BW. Effectiveness of a behaviour graded activity program versus conventional exercise for chronic neck pain patients. Eur J Pain 2009;13:533–41. https://doi.org/10.1016/j.ejpain.2008.06.008 | Setting is not primary care |
| Vos-Vromans DC, Smeets RJ, Rijnders LJ, Gorrissen RR, Pont M, Köke AJ, et al. Cognitive behavioural therapy versus multidisciplinary rehabilitation treatment for patients with chronic fatigue syndrome: study protocol for a randomised controlled trial (FatiGo). Trials 2012;13:71. https://doi.org/10.1186/1745-6215-13-71 | Setting is secondary care |
| Weiland A, Blankenstein AH, Van Saase JL, van der Molen HT, Jacobs ME, Abels DC, et al. Training medical specialists to communicate better with patients with Medically Unexplained Physical Symptoms (MUPS). A randomized, controlled trial. PLOS ONE 2015;10:e0138342. https://doi.org/10.1371/journal.pone.0138342 | Setting is not primary care |
| Williams DA, Cary MA, Groner KH, Chaplin W, Glazer LJ, Rodriguez AM, Clauw DJ. Improving physical functional status in patients with fibromyalgia: a brief cognitive behavioral intervention. J Rheumatol 2002;29:1280–6 | Setting is not primary care |
| Williams DA, Kuper D, Segar M, Mohan N, Sheth M, Clauw DJ. Internet-enhanced management of fibromyalgia: a randomized controlled trial. Pain 2010;151:694–702. https://doi.org/10.1016/j.pain.2010.08.034 | Setting is not primary care |
| Wilson M, Roll JM, Corbett C, Barbosa-Leiker C. Empowering patients with persistent pain using an internet-based self-management program. Pain Manag Nurs 2015;16:503–14. https://doi.org/10.1016/j.pmn.2014.09.009 | Patients not meeting inclusion criteria for unexplained symptoms |
| Yardley L, Barker F, Muller I, Turner D, Kirby S, Mullee M, et al. Clinical and cost effectiveness of booklet based vestibular rehabilitation for chronic dizziness in primary care: single blind, parallel group, pragmatic, randomised controlled trial. BMJ 2012;344:e2237. https://doi.org/10.1136/bmj.e2237 | Patients not meeting inclusion criteria for unexplained symptoms |
| Zaby A, Heider J, Schröder A. Warten, Entspannung oder Verhaltenstherapie. Z Klin Psychol Psychother 2008;37:15–23 | Not all from primary care |
| Zonneveld LN, van ‘t Spijker A, Passchier J, van Busschbach JJ, Duivenvoorden HJ. The effectiveness of a training for patients with unexplained physical symptoms: protocol of a cognitive behavioral group training and randomized controlled trial. BMC Public Health 2009;9:251. https://doi.org/10.1186/1471-2458-9-251 | Protocol only |
Appendix 5 Raw data from individual studies by outcome
| Data for the outcome pain | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| First author and year of publication | Intervention 1 | Control 1 | ||||||||
| Intervention code | Time point 1 – mean (SD/SE) | Time point 2 – mean (SD/SE) | Time point 3 – mean (SD/SE) | Time point 4 – mean (SD/SE) | Intervention code | Time point 1 – mean (SD/SE) | Time point 2 – mean (SD/SE) | Time point 3 – mean (SD/SE) | Time point 4 – mean (SD/SE) | |
| Cuesta-Vargas, 2012118 | MM | 67.9 (17.1) | 18 (10.3) | 20 (8.9) | 10 (8.1) | GSH | 62.7 (17.1) | 32.9 (18.9) | 34.3 (7.8) | 36 (15.1) |
| Macedo, 2012119 | GA | 6.1 (2.1) | 4.1 (2.5) | 4.1 (2.7) | 3.7 (2.6) | GA | 6.1 (1.9) | 4.1 (2.5) | 4.1 (2.5) | 3.7 (2.7) |
| van der Roer, 2008120 | MM | 6.2 | 4.4 | 4.1 | 3.9 | SES | 5.9 | 4.9 | 4.8 | 4.6 |
| Walti, 2015121 | MM | 4.86 (1.61) | SES | 4.64 (1.82) | ||||||
| LeFort, 1998128 | GSH | 72.67 (18.44) | 60.98 (21.26) | UC | 73.02 (17.61) | 71.22 (15.83) | ||||
| aAlda, 2011137 | CBTHI | 64.2 (10.78) | 36.88 (8.29) | 40.68 (10.93) | UC | 64.72 (10.44) | 38.68 (7.48) | 44.34 (8.56) | ||
| aLuciano, 2014138 | CBTHI | 65.43 (18.34) | 48.07 (10.5) | 49.58 (10.98) | UC | 64.04 (18.72) | 64.28 (15.76) | 64.36 (15.34) | ||
| Luciano, 2011139 | MM | 7.37 (1.86) | 6.34 (2.35) | UC | 7.37 (2.1) | 7.7 (2.03) | ||||
| Sañudo, 2010140 | SES | Only graphical data available for SF-36 pain | UC | |||||||
| Aiarzaguena, 2007136 | GPRE | 43.6 (24.4) | GPRE | 46.2 (25.2) | ||||||
| Peters, 2002106 | SES | 37.83 (2.92) | 43.3 (4.04) | 43.65 (3.48) | RSSE | 37.39 (2.92) | 40.93 (3.62) | 42.59 (3.74) | ||
| Pols, 2008145 | MM | Mean difference from T1 at T2 0.82 at T3 4.64 | UC | |||||||
| Smith, 2009142 | MM | 45.8 | 51.8 | UC | 43.8 | 39.9 | ||||
| aGili, 2014/Moreno, 2013144,148 | CBTHI | 27.91 (18.5) | 28.26 (21.97) | 38.44 (28.87) | UC+ | 28.67 (14.46) | 33.54 (20.34) | 31.13 (24.22) | ||
| Kocken, 2008103 | OP | 1.89 (1.74) | 2.46 (1.84) | UC | 1.75 (0.69) | 1.86 (0.83) | ||||
| Rothman, 2013127 | GP-O | 69.5 (59–80) | 60 (30–81) | UC+ | 74.5 (60–81) | 65.5 (38–80) | ||||
| Loew, 2000122 | RSSE | 11.4 (8) | 5.8 (4) | RSSE | 11.7 (7.2) | 10.1 (4.9) | ||||
| Rosendal, 2007146 | GP-MM | 49.6 (46.8 to 52.4) | 5 (2.9 to 7.0) | 6.5 (3.8 to 9.3) | UC | 48 (44.8 to 51.1) | 8.2 (4.6 to 11.8) | 10.5 (8.5 to 12.5) | ||
| van Ravesteijn, 2013143 | OP | 48.8 (18.5) | 53.1 (18.6) | 56.2 (23.6) | UC+ | 54.2 (19.5) | 57.8 (20.5) | 59.3 (22.1) | ||
| Zonneveld, 2012141 | CBTHI | Intercepts and model estimates given | UC | |||||||
| a,bMcBeth, 2012125/Beasley, 2015126 | CBTHI | 61.3 (23.6) | 62.1 (22.3) | UC | 53.5 (21.3) | 56.2 (19.9) | ||||
| Lansinger, 2007123 | RSSE | 50 (20 to 100) | 41 (2 to 81) | 35 (0 to 87) | SES | 56 (20 to 97) | 26 (0 to 84) | 30 (0 to 91) | ||
| Schaefert, 2013132 | MM | 50.34 (25.92) | 51.27 (22.48) | 51.04 (25.74) | GP-MM | 44.99 (23.64) | 50.01 (24.63) | 51.27 (25.68) | ||
| Data for the outcome fatigue | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Study author and date | Intervention 1 | Control 1 | ||||||||
| Intervention code | Time point 1 – mean (SD/SE) | Time point 2 – mean (SD/SE) | Time point 3 – mean (SD/SE) | Time point 4 – mean (SD/SE) | Intervention code | Time point 1 – mean (SD/SE) | Time point 2 – mean (SD/SE) | Time point 3 – mean (SD/SE) | Time point 4 – mean (SD/SE) | |
| Ho, 2012150 | RSSE | 39.9 (6.3) | 26.3 (10.9) | 21.6 (10.4) | UC | 39.7 (6.1) | 34.8 (8) | 32.1 (8.8) | ||
| aFriedberg, 2013151 | CBTLI | 5.400 (0.160) | 4.940 (0.190) | 4.190 (0.260) | UC | 5.720 (0.160) | 5.450 (0.190) | 5.310 (0.320) | ||
| Huibers, 2004/Leone, 2006153,155 | GP-CBT | 48.8 (5.3) | 38.2 (12.7) | 35.5 (12.9) | UC | 48.5 (7.1) | 39.8 (13.7) | 33.9 (13.8) | ||
| Marques, 2015133 | GA | 98.4 (16.43) | 93.73 (22.37) | GSH | 103.54 (19.07) | 106.76 (20.32) | ||||
| Moss-Morris, 2005152 | GA | 24.45 (8.79) | 13.91 (10.88) | UC | 25.35 (8.05) | 24.41 (9.69) | ||||
| aRidsdale, 2001112 | CBTHI | 22.4 (5.1) | 14 | 15 (8.5) | OP | 24.2 (4.8) | 15.6 | 15.6 (8) | ||
| Ridsdale, 2004113 | CBTLI | 25.3 (4.7) | 13.3 (8.8) | 14.8 (7.9) | GA | 24.7 (5.5) | 15.1 (9) | 15.3 (9.4) | ||
| Ridsdale, 2012115 | GA | 24.8 (4.9) | 14.6 (8.5) | 14.5 (7.7) | GSH | 23.4 (4.5) | 15.3 (8) | 13.8 (7.7) | ||
| Tummers, 2012149 | CBTLI | 51 (5.3) | 39.6 (14.1) | UC | 51.6 (5.5) | 48.3 (8.1) | ||||
| aWearden, 2010111 | GA | 10.49 (1.12) | 8.39 (3.67) | 8.72 (3.65) | UC | 10.34 (1.17) | 9.32 (3.18) | 9.48 (2.71) | ||
| Luciano, 2011139 | MM | 8.18 (1.83) | 7.06 (2.41) | UC | 8.13 (1.89) | 7.8 (2.17) | ||||
| Whitehead, 2002154 | GP-MM | 25.58 | 21.89 | 19.11 | UC | 24.26 | 20.04 | 19.57 | ||
| Chalder, 1997114 | GSH | 7.04 (6.35–7.73) | 3.2 (2.25–4.15) | UC | 6.89 (6.35–7.43) | 4.89 (3.88–5.90) | ||||
| a,bMcBeth, 2012125/Beasley, 2015126 | CBTHI | 19.9 (6.3) | 15.9 (7.7) | 16 (6.9) | 17.8 (6.6) | UC | 19.4 (5.9) | 18.4 (7) | 18.6 (7) | 19.1 (7.3) |
| Data for the outcome physical functioning | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| First author and year of publication | Intervention 1 | Control 1 | ||||||||
| Intervention code | Time point 1 – mean (SD/SE) | Time point 2 – mean (SD/SE) | Time point 3 – mean (SD/SE) | Time point 4 – mean (SD/SE) | Intervention code | Time point 1 – mean (SD/SE) | Time point 2 – mean (SD/SE) | Time point 3 – mean (SD/SE) | Time point 4 – mean (SD/SE) | |
| Cuesta-Vargas, 2012118 | MM | 32.9 (5.8) | 47 (8.5) | 52.6 (8.6) | 57.6 (6.8) | GSH | 34.3 (6.8) | 39.3 (4.6) | 37.6 (6.5) | 40.3 (2.9) |
| Macedo, 2012119 | GA | 43.8 (10.3) | 51.6 (13.4) | 51.2 (13.8) | 53.3 (14) | GA | 43.9 (10.8) | 51.6 (12) | 52.6 (13) | 53.8 (12.7) |
| aFriedberg, 2013151 | CBTLI | 68.49 (4.06) | 74.82 (4.01) | 66.3 (4.89) | UC | 59.77 (4.02) | 64.92 (3.67) | 56.44 (4.21) | ||
| Ho, 2012150 | RSSE | 36.9 (7.2) | 38.4 (6.1) | 40.1 (6.9) | UC | 35.7 (7.1) | 37.5 (8.1) | 37.8 (5.6) | ||
| Huibers, 2004/Leone, 2006153,155 | GP-CBT | 56.8 (25) | 65.2 (25.8) | 70.1 (24.7) | UC | 67.1 (22) | 72.5 (19.1) | 77.4 (20.9) | ||
| Marques, 2015133 | GA | 38.22 (17.78) | 43.33 (21.87) | GSH | 31.3 (18.9) | 28.15 (21.43) | ||||
| Moss-Morris, 2005152 | GA | 53.1 (18.39) | 69.05 (21.94) | UC | 45.65 (21.07) | 55 (22.94) | ||||
| Tummers, 2012149 | CBTLI | 50 (22) | 65.4 (24.9) | UC | 51.6 (22.6) | 59.3 (22.9) | ||||
| aWearden, 2010111 | GA | 29.84 (17.86) | 39.94 (25.21) | 43.27 (27.38) | UC | 29.8 (19.63) | 40.27 (26.45) | 39.83 (27.77) | ||
| LeFort, 1998128 | GSH | 41.68 (24.7) | 44.64 (25.07) | UC | 38.41 (20.22) | 38.3 (21.63) | ||||
| Luciano, 2011139 | MM | 3.31 (2.27) | 2.44 (2.51) | UC | 2.8 (2.4) | 3.22 (2.79) | ||||
| Aiarzaguena, 2007136 | GPRE | 73.2 (23.2) | GPRE | 70.5 (25.1) | ||||||
| Escobar, 2007156 | CBTHI | 63.28 (2.67) | 72.19 (2.95) | 73.22 (3.36) | UC+ | 61.41 (2.71) | 69.71 (2.95) | 69.41 (3.45) | ||
| Peters, 2002106 | GSH | 49.38 (2.66) | 57.88 (3.66) | 57.66 (6.15) | SES | 49.06 (3.11) | 54.67 (3.92) | 52.73 (3.73) | ||
| Pols, 2008145 | MM | MD_b I1 4.06; I2 –2.32 | UC | |||||||
| Smith, 2009142 | MM | 38.2 | 38 | UC | 32.6 | 33.6 | ||||
| Smith, 2006107 | MM | 37.4 (10.2) | UC | 35.5 (10.5) | ||||||
| van Ravesteijn, 2013143 | OP | 65.2 (22.9) | 68.4 (24.8) | 69.1 (27.8) | UC+ | 70.3 (23) | 71.3 (24.9) | 73.4 (22.6) | ||
| Zonneveld, 2012141 | CBTHI | Intercepts and model estimates given | UC | |||||||
| aGili, 2014/Moreno, 2013144,148 | CBTHI | 51.28 (29.82) | 56.86 (27.2)1 | 61.28 (25.35) | UC+ | 44.17 (26.97) | 52.08 (29.45) | 50.63 (22.71) | ||
| Larisch, 2004158 | GPRE | 41.4 (8.2) | 2.8 (0.7) | 2.7 (1.6) | 3.8 (2) | UC | 43 (11) | –0.8 (–1.2) | 1.2 (–0.4) | 0.5 (–0.7) |
| Rosendal, 2007146 | GP-MM | 80 (95% CI 61.1 to 95) | UC | 84.2 (95% CI 65 to 95) | ||||||
| Schaefert, 2013132 | MM | 71.96 (22.95) | 78.34 (21.32) | 78.17 (23.36) | GP-MM | 69.77 (25.12) | 73.01 (25.95) | 75.12 (23.7) | ||
| Smith, 1995100 | UC+ | 33.3 (35.1) | UC | 26.4 (28.8) | ||||||
| Chalder, 1997114 | GSH | 74 (95% CI 66 to 88) | 76.1 (95% CI 68 to 84) | UC | 70 (95% CI 62 to 77) | 66.6 (95% CI 58 to 75) | ||||
| Toft, 201097 | GP-MM | 85 (60.0 to 95.0) | UC | 95 (80.0 to 100) | ||||||
| Robinson, 2006131 | RSSE | No significant associations between guidebook and score on SF-36 dimension of PF, but trend favoured guidebook: PF 2.85 (95% CI –1.03 to 6.72) | UC | |||||||
| Kashner, 1995161 | UC+ | Intervention 1 difference from I3: 3.36 – This is RSSSE vs. UC+. These intervention group names look back to front – RSSSE is experimental group, UC+ is control | RSSE | |||||||
| a,bMcBeth, 2012125 | CBTHI | 38.9 (8.4) | 41.5 (11) | 40.8 (11.2) | UC | 37.4 (8.2) | 39.9 (10.1) | 39.6 (10.5) | ||
| Burton, 2012157 | GP-MM | 33.7 | 38.8 | UC | 35 (35.3) | |||||
| Data for the outcome somatisation | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| First author and year of publication | Intervention 1 | Control 1 | ||||||||
| Intervention code | Time point 1 – mean (SD/SE) | Time point 2 – mean (SD/SE) | Time point 3 – mean (SD/SE) | Time point 4 – mean (SD/SE) | Intervention code | Time point 1 – mean (SD/SE) | Time point 2 – mean (SD/SE) | Time point 3 – mean (SD/SE) | Time point 4 – mean (SD/SE) | |
| Peters, 2002106 | SES | 23.31 (0.83) | 21.3 (1) | 20.81 (0.92) | RSSE | 21.98 (0.78) | 20.8 (1.07) | 21.45 (0.88) | ||
| Zonneveld, 2012141 | CBTHI | No means given for outcomes, data presented for intercept, time, time by training, training vs. waitlist. Training vs. wait group post treatment – Cohen’s d = 0.23. The 1-year follow-up was not randomised – waiting list patients crossed over therefore cannot use these data: Cohen’s d post training –0.38, 3 months –0.45, 1 year –0.36 | UC | |||||||
| Kobeissi, 2012110 | RSSE | Short term MD_I3 –0.81 (95% CI –4.90 to 3.27) | UC | |||||||
| Larisch, 2004158 | GPRE | 14.8 (8.3) | –2.8 (–0.1) | –0.4 (1.9) | –0.7 (3.1) | UC | 12.3 (9.8) | 1.5 (0) | 0.8 (1.2) | 1.6 (0.6) |
| McLeod, 1997105 | OP | 60.3 (8.8) | 53.2 (10.9) | 53 (12.2) | UC | 58.4 (11.7) | 58.6 (12.9) | NR | ||
| Rosendal, 2007146 | GP-MM | 2.3 (median 25th–75th percentiles 1.9 to 2.6) | –0.2 (95% CI –0.2 to –0.1) | –0.2 (95% CI –0.2 to –0.1) | UC | 2.3 (2.0 to 26) | –0.2 (95% CI –0.3 to –0.2) | –0.2 (95% CI –0.3 to –0.2) | ||
| Schilte, 2001159 | GP-OP | 20 (median 16 to 25) | 0 (median –6 to 5) | UC | 22 | Median 17 to 27 | 0 (median –5 to 5) | |||
| Toft, 201097 | GP-MM | 26 (21 to 30) | UC | 25 (21 to 31) | ||||||
| Rief, 2006102 | GP-MM | 15.5 (8.2) | 15.4 (8.2) | 15.3 (9.5) | UC | 13.8 (8.2) | 13.2 (7.5) | 13.7 (8.2) | ||
| Martin, 200799 | CBTLI | 9.5 (8.2) | 7.2 (8) | 7.8 (7.1) | UC | 7.2 (5.7) | 6.3 (5.9) | 6.4 (4.9) | ||
| aGili, 2014/Moreno, 2013144,148 | CBTHI | 22.17 (19.08 to 25.27) | 14.17 (11.97 to 16.37) | 20.86 (16.94 to 24.78) | UC+ | 21.26 (18.01 to 24.51) | 19.47 (17.06 to 21.88) | 29.02 (24.77 to 33.28) | ||
| Kolk, 2004104 | OP | 27.77 (8.8) | 21.09 (7.6) | 19.9 (7.4) | UC | 25.19 (5.6) | 22.19 (6.9) | 21 (7.1) | ||
| Escobar, 2007156 | CBTHI | 14.17 (0.58) | 9.32 (0.67) | 9.11 (0.59) | UC+ | 13.98 (0.59) | 11.5 (0.66) | 10.91 (0.62) | ||
| Martin, 200799 | CBTLI | 0.79 (0.75) | 0.59 (0.55) | 0.59 (0.59) | UC | 0.6 (0.61) | 0.5 (0.5) | 0.61 (0.63) | ||
| Schaefert, 2013132 | MM | 12.56 (4.73) | 9.47 (4.71) | 9.55 (5.12) | GP-MM | 12.66 (4.89) | 11.42 (5.44) | 10.57 (5.1) | ||
| Smith, 2009142 | MM | 27.9 | 24.8 | UC | 27.5 | 26.8 | ||||
| Sumathipala, 2000116 | CBTLI | 16.2 (5.5) | 13.2 (95% CI 11.3 to 15.1) | UC | 18.9 (6.6) | 15.6 (95% CI 13.6 to 17.5) | ||||
| Sumathipala, 2008117 | MM | 19.9 (9.6) | 12.4 (9.6) | 11.5 (9) | 11.1 (8.7) | GP-MM | 18.6 (9) | 12.4 (8.9) | 11.8 (8.9) | 11 (9.1) |
| van Ravesteijn, 2013143 | OP | 12.6 (4.68) | 10.9 (4.9) | 11 (5.44) | UC+ | 12.7 (5.15) | 12.6 (6.1) | 11.8 (5.46) | ||
| Marques, 2015133 | GA | 14.02 (4.04) | 13.05 (4.72) | GSH | 16.2 (4.47) | 15.76 (4.48) | ||||
| Burton, 2012157 | GP-MM | 15 | 11.7 | UC | 14.6 | 12.4 | ||||
| Data for the outcome bowel | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| First author and year of publication | Intervention 1 | Control 1 | ||||||||
| Intervention code | Time point 1 – mean (SD/SE) | Time point 2 – mean (SD/SE) | Time point 3 – mean (SD/SE) | Time point 4 – mean (SD/SE) | Intervention code | Time point 1 – mean (SD/SE) | Time point 2 – mean (SD/SE) | Time point 3 – mean (SD/SE) | Time point 4 – mean (SD/SE) | |
| Kennedy, 2005129 | MM | 295.5 (75.7) | ME | 310.2 (84.9) | ||||||
| Moss-Morris, 2010130 | CBTLI | 228.5 (83.8) | 156.7 (81.9) | 135.4 (73.3) | 119.4 (81.7) | UC | 222.8 (80.7) | 195 (82.9) | 190.5 (89.4) | 193.3 (92.3) |
| aRobinson, 2006131 | MM | 3.23 (0.98) | 4.03 (1.33) | UC | 3.29 (0.88) | 3.93 (1.31) | ||||
| Data for the outcome emotional distress | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| First author and year of publication | Intervention 1 | Control 1 | ||||||||
| Intervention code | Time point 1 – mean (SD/SE) | Time point 2 – mean (SD/SE) | Time point 3 – mean (SD/SE) | Time point 4 – mean (SD/SE) | Intervention code | Time point 1 – mean (SD/SE) | Time point 2 – mean (SD/SE) | Time point 3 – mean (SD/SE) | Time point 4 – mean (SD/SE) | |
| Cuesta-Vargas, 2012118 | MM | 34.6 (9.2) | 56.7 (6.1) | 57.6 (6.5) | 60.9 (6.4) | GSH | 37.2 (10.4) | 44.7 (10.7) | 43.5 (12.5) | 39.2 (13.7) |
| Macedo, 2012119 | GA | 54.7 (11.5) | 55.8 (13) | 56.9 (11.8) | 58.2 (10.8) | GA | 52.9 (10.5) | 56 (10.9) | 54.9 (10.4) | 57 (10.1) |
| Ho, 2012150 | RSSE | 32.5 (10.7) | 43.8 (6.9) | 42.7 (7.2) | UC | 33.5 (9.6) | 34.6 (9.6) | 35.7 (9.5) | ||
| Huibers, 2004/Leone, 2006153,155 | GP-CBT | 175 (42) | 156 (42) | 152 (51) | UC | 190 (57) | 163 (55) | 153 (62) | ||
| Marques, 2015133 | GA | 41.57 (16.12) | 46.85 (19.71) | GSH | 37.59 (17.62) | 36.79 (19.15) | ||||
| LeFort, 1998128 | GSH | 60.46 (19.67) | 68.15 (18.37) | UC | 58.08 (19.27) | 60.84 (19.93) | ||||
| Aiarzaguena, 2007136 | GPRE | 50.1 (21.6) | GPRE | 50.3 (20.2) | ||||||
| Peters, 2002106 | RSSE | 48.42 (2.39) | 60.35 (3.15) | 55.02 (2.49) | SES | 52.61 (2.6) | 61.26 (2.6) | 57.16 (2.38) | ||
| Pols, 2008145 | MM | UC | ||||||||
| Smith, 2009142 | MM | 35.7 | 47.9 | UC | 46.6 | 46.1 | ||||
| Smith, 2006107 | MM | 46.5 (11.6) | UC | 48.6 (11.9) | ||||||
| Sumathipala, 2008117 | MM | 14.9 (9.4) | 5.5 (7.7) | 6.2 (8.3) | 5.6 (8) | GP-MM | 14.7 (9.4) | 6.1 (8.3) | 7.2 (9.7) | 5.7 (9.5) |
| van Ravesteijn, 2013143 | OP | 66 (19.1) | 67.9 (19.6) | 66.9 (20.1) | UC+ | 59.7 (20.5) | 61.2 (18.2) | 66.6 (17.9) | ||
| Zonneveld, 2012141 | CBTHI | UC | ||||||||
| aGili, 2014/Moreno, 2013144,148 | CBTHI | 47.91 (16.37) | 47.44 (16.53) | 51.16 (21.37) | UC+ | 40.5 (18.99) | 53 (22.26) | 42.67 (20.69) | ||
| Kocken, 2008103 | OP | 228 (70.9) | 211 (65.2) | UC | 244 (61.8) | 245 (72.1) | ||||
| Larisch, 2004158 | GPRE | 37.6 (9.6) | 1 (1.6) | 1.5 (2.2) | 2.2 (5.2) | UC | 41 (10.3) | –1.6 (2.3) | –0.5 (1.5) | 4.3 (3.6) |
| Rosendal, 2007146 | GP-MM | 65.6 (63.4 to 67.8) | UC | 67 (64.4 to 69.5) | ||||||
| Schaefert, 2013132 | MM | 55.76 (18.68) | 63.34 (18) | 64.25 (18.89) | GP-MM | 53.86 (21.2) | 56.14 (20.57) | 58.03 (21.99) | ||
| Smith, 1995100 | UC+ | 52.7 (18.9) | UC | 54.7 (25.5) | ||||||
| Sumathipala, 2000116 distress only | CBTLI | 12.1 (8.6) | 6.3 (4.1 to 8.5) | UC | 11 (6.7) | 10.4 (8.1 to 12.7) | ||||
| Toft, 201097 | GP-MM | 62.5 (20.4) | UC | 61.6 (21.5) | ||||||
| van der Feltz-Cornelis, 2006160 | MM | 20.9 (16.9) | 15.3 (16.3) | 10.8 (13.9) | GPRE | 23.3 (21.6) | 29.4 (22.8) | 26.8 (21.7) | ||
| Robinson, 2006131 | GSH | UC | ||||||||
| Kashner, 1995161 | UC+ | RSSE | ||||||||
| a,bMcBeth, 2012125 | CBTHI | 43.6 (10.9) | 46.3 (9.9) | 47 (10.2) | UC | 42.5 (10.6) | 43.4 (10.2) | 43.4 (11) | ||
| Kennedy,129 2005 | MM | 16.6 (6.4) | ME | 18.1 (7.4) | ||||||
| Chalder, 1997114 | GSH | 6.27 (CI 5.27 to 7.27) | 3.06 (CI 2.06 to 4.07) | UC | 5.92 (CI 5.04 to 6.80) | 4.31 (CI 3.33 to 5.29) | ||||
| Burton, 2012157 | GP-MM | 45.8 | 56.7 (6.1) | 57.6 (6.5) | 60.9 (6.4) | UC | 41.2 | 45.2 | ||
| Data for the outcome anxiety | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| First author and year of publication | Intervention 1 | Control 1 | ||||||||
| Intervention code | Time point 1 – mean (SD/SE) | Time point 2 – mean (SD/SE) | Time point 3 – mean (SD/SE) | Time point 4 – mean (SD/SE) | Intervention code | Time point 1 – mean (SD/SE) | Time point 2 – mean (SD/SE) | Time point 3 – mean (SD/SE) | Time point 4 – mean (SD/SE) | |
| aFriedberg, 2013151 | CBTLI | 11.97 (1.47) | 10.98 (1.6) | 12.02 (1.89) | UC | 14.99 (1.46) | 14.5 (1.65) | 14.39 (2.23) | ||
| Marques, 2015133 | GA | 1.63 (0.77) | 1.44 (0.79) | GSH | 1.66 (0.79) | 1.64 (0.81) | ||||
| Ridsdale, 2001112 not ITT | CBTHI | 8.8 (4.5) | 7.9 (4) | OP | 10.6 (4.2) | 8.9 (4.2) | ||||
| Ridsdale, 2004113 | CBTLI | 10.4 (4.4) | 7.9 (4.4) | 8.5 (4.2) | GA | 10.4 (4.7) | 9.3 (4.8) | 9.8 (5.3) | ||
| aRidsdale, 2012115 | GA | 9.3 (4.4) | 8.2 (4) | GSH | 9.1 (4.3) | 9.4 (4) | ||||
| Tummers, 2012149 | CBTLI | 1.02 (0.64) | 0.77 (0.68) | UC | 1.02 (0.61) | 0.86 (0.55) | ||||
| aWearden, 2010111 | GA | 11.02 (4.77) | 9.04 (4.51) | 9.54 (4.7) | UC | 9.65 (5.06) | 8.63 (5.06) | 8.89 (5.4) | ||
| aAlda, 2011137 | CBTHI | 10.84 (4.27) | 7.09 (2.96) | 7.25 (3.02) | UC | 9.5 (2.98) | 7.4 (2.18) | 7.58 (2.07) | ||
| aLuciano, 2014138 | CBTHI | 12.67 (4.36) | 8.28 (2.38) | 8.73 (2.04) | UC | 12.4 (4.31) | 11.36 (3.8) | 12.15 (4.2) | ||
| Luciano, 2011139 | MM | 7.94 (2.22) | 6.07 (3.19) | UC | 7.45 (2.42) | 7.14 (2.61) | ||||
| Moss-Morris, 2010130 | CBTLI | 9.1 (3.8) | 8.7 (4.4) | 7 (2.9) | 7.5 (3.8) | UC | 6.9 (4.3) | 6.6 (4.7) | 6.7 (4.5) | 6.4 (4.1) |
| Escobar, 2007156 | CBTHI | 20.46 (0.75) | 15.89 (1.08) | 14.85 (0.94) | UC+ | 20.99 (0.76) | 18.47 (1.07) | 17.58 (1) | ||
| Kolk, 2004104 | OP | 22.55 (9.1) | 15.51 (5.4) | 15.39 (5.7) | UC | 20.44 (8.1) | 15.44 (5.8) | 13.56 (4.2) | ||
| Martin, 200799 | CBTLI | 6.5 (3.8) | 5.9 (4.1) | 5.4 (3.3) | UC | 5.7 (3.2) | 5.5 (3.6) | 5.5 (3.2) | ||
| bMorriss, 2007108 | GPRE | 31 (47%) | UC | 27 (36%) | ||||||
| Peters, 2002106 | SES | 10.33 (0.52) | 8.6 (0.58) | 9.15 (0.59) | RSSE | 10.14 (0.5) | 8.49 (0.64) | 9.37 (0.58) | ||
| Smith, 2009142 | MM | 47.3 | 46.8 (MD_b –0.45 95% CI –4.6 to 3.7) | UC | 47.6 | 47.8 (MD_b 0.12 95% CI –3.5 to 3.7) | ||||
| Zonneveld, 2012141 | CBTHI | Only estimates of intercepts given | UC | |||||||
| Kobeissi, 2012110 | RSSE | 2.5 (0.4) | UC | 2.4 (0.4) | ||||||
| aGili, 2014/Moreno, 2013144,148 | CBTHI | 20.18 (17.69 to 22.68) | 11.47 (9.45 to 13.49) | 9.28 (7.28 to 11.27) | UC+ | 17.84 (15.04 to 20.64) | 13.07 (10.93 to 15.22) | 16.22 (13.91 to 18.53) | ||
| Larisch, 2004158 | GPRE | 9.3 (3.9) | –1.1 (0.4) | –0.9 (0.8) | –0.8 (0.7) | UC | 7.7 (4.2) | 0.3 (0.2) | –0.3 (0.6) | –0.3 (0.7) |
| McLeod, 1997105 | OP | 62.9 (11.9) | 56.8 (12.5) | 54.9 (15.5) | UC | 63 (9.2) | 60.9 (12.8) | NR | ||
| Schilte, 2001159 | GP-OP | 15 (9 to 23) | –2 (median –5 to 2) | UC | 17 (10 to 31) | 0 (median –5 to 3) | ||||
| Posse, 200496 | OP | 53.8 (14) | 53 (10.2) | UC | 55 (10.7) | 58.3 (10.6) | ||||
| Rothman, 2013127 | GP-O | 60.45 to 79 | 56 (38 to 75) | UC+ | 54.5 (33 to 76) | 51 (33 to 76) | ||||
| Rief, 2006102 | GP-MM | 14.4 (10.3) | 14 (11.1) | 11.8 (10.6) | UC | 11.8 (10) | 10.2 (8.6) | 11.5 (9.2) | ||
| Burton, 2012157 | GP-MM | 6.5 | 5.9 | UC | 5.4 | 5.2 | ||||
| Data for the outcome depression | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| First author and year of publication | Intervention 1 | Control 1 | ||||||||
| Intervention code | Time point 1 – mean (SD/SE) | Time point 2 – mean (SD/SE) | Time point 3 – mean (SD/SE) | Time point 4 – mean (SD/SE) | Intervention code | Time point 1 – mean (SD/SE) | Time point 2 – mean (SD/SE) | Time point 3 – mean (SD/SE) | Time point 4 – mean (SD/SE) | |
| aFriedberg, 2013151 | CBTLI | 17.1 (1.45) | 13.52 (1.64) | 14.89 (1.86) | UC | 18.31 (1.44) | 16.17 (1.83) | 14.03 (1.86) | ||
| Marques, 2015133 | GA | 1.49 (0.88) | 1.55 (0.95) | GSH | 1.55 (0.95) | 1.91 (0.93) | ||||
| Ridsdale, 2001112 not ITT | CBTHI | 7.3 (4.1) | 6.3 (4.3) | OP | 7.8 (3.5) | 6.2 (4.1) | ||||
| Ridsdale, 2004113 | CBTLI | 8.1 (3.2) | 5.8 (3.8) | 6.6 (4.3) | GA | 8.4 (4) | 6.6 (4.6) | 6.8 (4.9) | ||
| aRidsdale, 2012115 | GA | 8.4 (3.8) | 6.5 (4.3) | GSH | 7.4 (5.7) | 6.2 (4.3) | ||||
| aWearden, 2010111 | GA | 9.67 (4.08) | 7.28 (4.02) | 7.88 (4.45) | UC | 9.26 (4.25) | 8.48 (4.47) | 8.06 (4.75) | ||
| LeFort, 1998128 | GSH | 7.67 (4.91) | 6.83 (5.63) | UC | 7.48 (4.63) | 7.68 (4.75) | ||||
| aAlda, 2011137 | CBTHI | 14.47 (3.93) | 7.78 (2.46) | 7.91 (2.5) | UC | 14.09 (4.64) | 8.17 (2.25) | 8.57 (2.47) | ||
| aLuciano, 2014138 | CBTHI | 8 (2.88) | 5.41 (1.36) | 5.84 (1.6) | UC | 9.23 (3.56) | 9.34 (2.63) | 9.32 (3.04) | ||
| Luciano, 2011139 | MM | 7.42 (3.02) | 5.24 (3.54) | UC | 6.82 (3.11) | 6.45 (3.09) | ||||
| Sañudo, 2010140 | SES | 28 (4) | UC | 31 (3) | ||||||
| Moss-Morris, 2010130 | CBTLI | 3.9 (3.4) | 3.9 (3.42) | 2.9 (2.5) | 2.9 (2.4) | UC | 4.1 (3.1) | 3.8 (3.2) | 3.8 (3.5) | 4 (3.7) |
| Escobar, 2007156 | CBTHI | 18.25 (0.64) | 12.85 (0.85) | 12.88 (0.88) | UC+ | 17.41 (0.65) | 14.6 (0.84) | 14.29 (0.93) | ||
| Kolk, 2004104 | OP | 38.9 (11.9) | 26.93 (10.2) | 25.93 (9.6) | UC | 34.56 (9.1) | 25.94 (10.8) | 23.12 (6.4) | ||
| Martin, 200799 | CBTLI | 15.9 (9.6) | 13.7 (9.1) | 14.2 (9.5) | UC | 13.2 (6.4) | 12.5 (7.4) | 11.9 (7.5) | ||
| bMorriss, 2007108 | GPRE | 18 (27%) | UC | 21 (28%) | ||||||
| Peters, 2002106 | SES | 9.22 (0.49) | 7.38 (0.61) | 7.75 (0.58) | RSSE | 9.14 (0.41) | 7.49 (0.52) | 8.44 (0.56) | ||
| Smith, 2009142 | MM | 26.3 | 15.7 (MD_b –10.6 95% CI –20.8 to –0.41) | UC | 18.3 | 22.9 (MD_b 4.6 95% CI –4.0 to 13.2) | ||||
| van Ravesteijn, 2013143 | OP | 8.5 (5.11) | 7.61 (5.92) | 7.26 (5.61) | UC+ | 8.77 (5.44) | 7.87 (5.35) | 7.66 (5.33) | ||
| Zonneveld, 2012141 | CBTHI | Only estimates of intercepts given | UC | |||||||
| Kobeissi, 2012110 | RSSE | 2.5 (0.4) | UC | 2.4 (0.4) | ||||||
| aGili, 2014/Moreno, 2013144,148 | CBTHI | 14.12 (12.44 to 15.8) | 11.22 (9.46 to 12.98) | 8.1 (6.2 to 10.01) | UC+ | 13.43 (11.55 to 15.32) | 10.87 (9 to 12.74) | 13.41 (11.19 to 15.63) | ||
| Larisch, 2004158 | GPRE | 7.9 (4.5) | –1.2 (–0.3) | –0.7 (0.1) | –0.8 (0) | UC | 6.3 (3.5) | 0.5 (1.1) | –0.4 (0.9) | –0.2 (0.7) |
| McLeod, 1997105 | OP | 64.5 (16.8) | 57.2 (15.3) | 56.5 (13.1) | UC | 66.5 (11.7) | 66.8 (18.3) | NR | ||
| Schilte, 2001159 | GP-OP | 22 (13 to 33) | –2 (median –8 to 4) | UC | 22 (15 to 35) | –2 (median –10 to 5) | ||||
| Rothman, 2013127 | GP-O | 3 (2 to 3) | 2 (2 to 3) | UC+ | 2 (1 to 3) | 2 (2 to 3) | ||||
| Rief, 2006102 | GP-MM | 13.9 (9.1) | 13.6 (9.5) | 11.8 (9.5) | UC | 12.5 (8.4) | 12.2 (9.3) | 11.8 (8.1) | ||
| Burton, 2012157 | GP-MM | 9.2 | 8.4 | UC | 7.8 | 6.7 | ||||
| Schaefert, 2013132 | MM | 8.89 (5.11) | 6.68 (4.82) | 6.29 (4.5)8 | GP-MM | 9.76 (5.54) | 8.12 (4.2) | 7.98 (5.25) | ||
| Data for the outcome generic physical symptoms | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| First author and year of publication | Intervention 1 | Control 1 | ||||||||
| Intervention code | Time point 1 – mean (SD/SE) | Time point 2 – mean (SD/SE) | Time point 3 – mean (SD/SE) | Time point 4 – mean (SD/SE) | Intervention code | Time point 1 – mean (SD/SE) | Time point 2 – mean (SD/SE) | Time point 3 – mean (SD/SE) | Time point 4 – mean (SD/SE) | |
| aMoreno, 2013148 | CBTHI | 92.06 (95% CI 79.02 to 105.1) | 41.52 (95% CI 32.69 to 50.35) | 67.84 (95% CI 61.03 to 74.65) | UC+ | 71.48 (95% CI 57.78 to 85.19) | 59.98 (95% CI 50.44 to 69.51) | 67.7 (95% CI 60.42 to 74.98) | ||
| van der Feltz-Cornelis, 2006160 | MM | 3.53 (0.6) | 2.49 (0.77) | 2.15 (0.77) | GPRE | 3.43 (0.51) | 3.38 (0.81) | 3.44 (0.62) | ||
| Ryan, 2004109 | OP | 8.11 (0.85) | 2.73 (0.98) | UC | ||||||
| Aiarzaguena, 2007136 | GPRE | Assessed but no data reported | GPRE | |||||||
| Posse, 200496 | OP | 13.6 (6.3) | 13.2 (6.3) | UC | 13.6 (3.6) | 13 (2.8) | ||||
| Escobar, 2007156 | CBTHI | 42.34 (1.94) | 23.47 (1.77) | 23.72 (1.67) | UC+ | 39.62 (1.97) | 27.94 (1.75) | 25.25 (1.77) | ||
| Kolk, 2004104 | OP | 4.39 (4.2) | 2.98 (4.7) | 1.95 (3.5) | UC | 2.731.9 | 1.67 (2.1) | 0.87 (1.2) | ||
| Data for the outcome impact | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| First author and year of publication | Intervention 1 | Control 1 | ||||||||
| Intervention code | Time point 1 – mean (SD/SE) | Time point 2 – mean (SD/SE) | Time point 3 – mean (SD/SE) | Time point 4 – mean (SD/SE) | Intervention code | Time point 1 – mean (SD/SE) | Time point 2 – mean (SD/SE) | Time point 3 – mean (SD/SE) | Time point 4 – mean (SD/SE) | |
| van der Roer, 2008120 | MM | 11.6 | 7.9 | 7.4 | 6.7 | SES | 12.1 | 7.5 | 7.7 | 7.1 |
| Walti, 2015121 | MM | 10.21 (4.44) | SES | 11.21 (3.95) | ||||||
| Ridsdale, 2004113 | CBTLI | 5.1 (1.8) | 4.1 (1.9) | GA | 4.6 (2.2) | 4.1 (2.4) | ||||
| aRidsdale, 2012115 | GA | 4.5 (1.9) | 3.9 (1.9) | GSH | 4.4 (2) | 3.7 (2.3) | ||||
| aAlda, 2011137 | CBTHI | 65.91 (10.85) | 46.21 (9.18) | 48.8 (9.11) | UC | 64.48 (10.5) | 48.64 (6.77) | 53.26 (7.54) | ||
| aLuciano, 2014138 | CBTHI | 68.2 (8.96) | 48.7 (6.91) | 49.49 (8.77) | UC | 65.87 (7.63) | 67.68 (9.23) | 67.45 (9.15) | ||
| aSañudo, 2010140 | SES | 60.9 (3.4) | UC | 60.5 (3.8) | ||||||
| Kennedy, 2005129 | MM | 15.3 (8.7) | ME | 15.1 (8.4) | ||||||
| Moss-Morris, 2010130 | CBTLI | 3.7 (6.7) | 4.3 (6.2) | 4.7 (6.6) | UC | –1.2 (5.7) | –0.7 (5.5) | –0.72 (5.3) | ||
| Rothman, 2013127 | GP-O | 40 (28–50) | 36 (22–49) | UC+ | 38 (28 to 50) | 38 (28–50) | ||||
| Whitehead, 2002154 | GP-MM | 58.25 | 65.03 | 59.2 | UC | 62.77 | 63.52 | 65.62 | ||
| van der Feltz-Cornelis, 2006160 | MM | GPRE | ||||||||
| Lansinger, 2007123 | RSSE | 26 (6 to 60) | 24 (2 to 68) | 22 (0 to 54) | SES | 22 (8 to 52) | 17 (2 to 52) | 18 (0 to 52) | ||
| Macedo, 2012119 | GA | 11.2 (5.3) | 8 (6.5) | 8.6 (6.8) | 8 (6.9) | GA | 11.4 (4.8) | 7.5 (6.4) | 8 (7.1) | 7.4 (6.7) |
| Cuesta-Vargas, 2012118 | MM | 7.1 (2.2) | 2.7 (1.8) | 2.1 (1.3) | 1.3 (1.2) | GSH | 8.2 (2.2) | 5.1 (3.9) | 5 (3.2) | 3.8 (3.6) |
| Ridsdale, 2001112 | CBTHI | 4.9 (1.8) | 3.7 (2.2) | OP | 4.9 (1.7) | 3.5 (2.2) | ||||
| Kocken, 2008103 | OP | 2.48 (1.15) | 3.2 (1.36) | UC | 1.95 (1.08) | 2.45 (1.4) | ||||
| LeFort, 1998128 | GSH | 2.51 (0.84) | 2.29 (0.78) | UC | 2.29 (0.76) | 2.81 (0.72) | ||||
| Luciano, 2011139 | MM | 58.9 (12.9) | 46.87 (16.77) | UC | 55.97 (14.01) | 54.72 (15.95) | ||||
Appendix 6 Table of excluded studies from the qualitative review
| Number | Reference | Reason |
|---|---|---|
| 1 | Arnold IA, Speckens AE, van Hemert AM. Medically unexplained physical symptoms: the feasibility of group cognitive-behavioural therapy in primary care. J Psychosom Res 2004;57:517–20 | Does not include data about a specific intervention |
| 2 | Artus M, Croft P, Lewis M. The use of CAM and conventional treatments among primary care consulters with chronic musculoskeletal pain. BMC Fam Pract 2007;8:26 | No qualitative data reported |
| 3 | Austrian JS, Kerns RD, Reid MC. Perceived barriers to trying self-management approaches for chronic pain in older persons. J Am Geriatr Soc 2005;53:856–61 | Non-UK |
| 4 | Beattie A, Shaw A, Yardley L, Little P, Sharp D. Participating in and delivering the ATEAM trial (Alexander technique lessons, exercise, and massage) interventions for chronic back pain: a qualitative study of professional perspectives. Complement Ther Med 2010;18:119–27. https://doi.org/10.1016/j.ctim.2010.05.037 | Population did not fit the inclusion criteria |
| 5 | Brown CA. Occupational therapists’ beliefs regarding treatment options for people with chronic pain. Br J Occup Ther 2002;65:398–404 | No qualitative data reported |
| 6 | Brown CA. The beliefs of people with chronic pain in relation to ‘important’ treatment components. Eur J Pain 2004;8:325–33. https://doi.org/10.1016/j.ejpain.2003.10.005 | No qualitative data reported |
| 7/8 |
Calnan M, Wainwright D, O’Neill C, Winterbottom A, Watkins C. Evaluating health-care: the perspectives of sufferers with upper limb pain. Health Expect 2005;8:149–60 Calnan M, Wainwright D, O’Neill C, Winterbottom A, Watkins C. Making sense of aches and pains. Fam Pract 2006;23:91–105 |
Population did not fit the inclusion criteria |
| 9 | Carnes D, Homer K, Underwood M, Pincus T, Rahman A, Taylor SJ. Pain management for chronic musculoskeletal conditions: the development of an evidence-based and theory-informed pain self-management course. BMJ Open 2013;3:e003534. https://doi.org/10.1136/bmjopen-2013-003534 | Population did not fit the inclusion criteria |
| 10 | Chew-Graham C, Dixon R, Shaw JW, Smyth N, Lovell K, Peters S. Practice Nurses’ views of their role in the management of Chronic Fatigue Syndrome/Myalagic Encephalitis: a qualitative study. BMC Nurs 2009;8:2. https://doi.org/10.1186/1472-6955-8-2 | Does not include data about a specific intervention |
| 11 | Cooper K, Smith BH, Hancock E. Patients’ perceptions of self-management of chronic low back pain: evidence for enhancing patient education and support. Physiotherapy 2009;95:43–50. https://doi.org/10.1016/j.physio.2008.08.005 | Population did not fit the inclusion criteria |
| 12 | Hadi MA, Alldred DP, Briggs M, Marczewski K, Closs SJ. Effectiveness of a community based nurse-pharmacist managed pain clinic: a mixed-methods study. Int J Nurs Stud 2016;53:219–27. https://doi.org/10.1016/j.ijnurstu.2015.09.003 | Population did not fit the inclusion criteria |
| 13 | Harris J, Williams T, Hart O, Hanson C, Johnstone G, Muthana A, Nield C. Using health trainers to promote self-management of chronic pain: can it work? Br J Pain 2014;8:27–33. https://doi.org/10.1177/2049463713511956 | Population did not fit the inclusion criteria |
| 14 | Lamb SE, Lall R, Hansen Z, Withers EJ, Griffiths FE, Szczepura A, et al. Design considerations in a clinical trial of a cognitive behavioural intervention for the management of low back pain in primary care: Back Skills Training Trial. BMC Musculoskelet Disord 2007;8:14 | No qualitative data reported |
| 15 | Lamb SE, Lall R, Hansen Z, Castelnuovo E, Withers EJ, Nichols V, et al. A multicentred randomised controlled trial of a primary care-based cognitive behavioural programme for low back pain. The Back Skills Training (BeST) trial. Health Technol Assess 2010;14(41). https://doi.org/10.3310/hta14410 | Population did not fit the inclusion criteria |
| 16 | MacKichan F, Paterson C, Britten N. GP support for self-care: the views of people experiencing long-term back pain. Fam Pract 2013;30:212–18. https://doi.org/10.1093/fampra/cms062 | Population did not fit the inclusion criteria |
| 17 | Masterton G. Training practices in reattribution for medically unexplained symptoms. J R Coll Physicians Edinb 2008;38:39 | Opinion piece |
| 18 | McCracken LM, Sato A, Wainwright D, House W, Taylor GJ. A feasibility study of brief group-based acceptance and commitment therapy for chronic pain in general practice: recruitment, attendance, and patient views. Prim Health Care Res Dev 2014;15:312–23. https://doi.org/10.1017/S1463423613000273 | Population did not fit the inclusion criteria |
| 19 | McCrae N, Correa A, Chan T, Jones S, de Lusignan S. Long-term conditions and medically-unexplained symptoms: feasibility of cognitive behavioural interventions within the improving access to Psychological Therapies Programme. J Ment Health 2015;24:379–84. https://doi.org/10.3109/09638237.2015.1022254 | Population did not fit the inclusion criteria |
| 20 | Morriss R, Dowrick C, Salmon P, Peters S, Rogers A, Dunn G, et al. Turning theory into practice: rationale, feasibility and external validity of an exploratory randomized controlled trial of training family practitioners in reattribution to manage patients with medically unexplained symptoms (the MUST). Gen Hosp Psychiatry 2006;28:343–51 | No qualitative data reported |
| 21 | Morriss RK, Gask L, Ronalds C, Downes-Grainger E, Thompson H, Goldberg D. Clinical and patient satisfaction outcomes of a new treatment for somatized mental disorder taught to general practitioners. Br J Gen Pract 1999;49:263–7 | No qualitative data reported |
| 22 | Payne H, Brooks SDM. Clinical outcomes from The BodyMind ApproachTM in the treatment of patients with medically unexplained symptoms in primary health care in England: practice-based evidence. Arts Psychother 2016;47:55–65 | No qualitative data reported |
| 23 | Peters S, Goldthorpe J, McElroy C, King E, Javidi H, Tickle M, Aggarwal VR. Managing chronic orofacial pain: a qualitative study of patients’, doctors’, and dentists’ experiences. Br J Health Psychol 2015;20:777–91. https://doi.org/10.1111/bjhp.12141 | Does not include data about a specific intervention |
| 24 | Ruecroft G. Development of a self-management tool in the chronic pain service. Pract Dev Health Care 2004;3:143–56 | Does not include data about a specific intervention |
| 25 | Sumathipala A, Siribaddana S, Hewege S, Sumathipala K, Prince M, Mann A. Understanding the explanatory model of the patient on their medically unexplained symptoms and its implication on treatment development research: a Sri Lanka Study. BMC Psychiatry 2008;8:54. https://doi.org/10.1186/1471-244X-8-54 | Non-UK |
| 26 | Underwood MR, Harding G, Klaber Moffett J, UK BEAM trial team. Patient perceptions of physical therapy within a trial for back pain treatments (UK BEAM) [ISRCTN32683578]. Rheumatology 2006;45:751–6 | Population did not fit the inclusion criteria |
| 27 | van Hooff ML, Ter Avest W, Horsting PP, O’Dowd J, de Kleuver M, van Lankveld W, van Limbeek J. A short, intensive cognitive behavioral pain management program reduces health-care use in patients with chronic low back pain: two-year follow-up results of a prospective cohort. Eur Spine J 2012;21:1257–64. https://doi.org/10.1007/s00586-011-2091-0 | No qualitative data reported (non-UK) |
| 28 | Walsh N, Cramp F, Palmer S, Pollock J, Hampson L, Gooberman-Hill R, et al. Exercise and self-management for people with chronic knee, hip or lower back pain: a cluster randomised controlled trial of clinical and cost-effectiveness. Study protocol. Physiotherapy 2013;99:352–7. https://doi.org/10.1016/j.physio.2012.09.002 | No qualitative data reported |
| 29 | Wearden AJ, Riste L, Dowrick C, Chew-Graham C, Bentall RP, Morriss RK, et al. Fatigue Intervention by Nurses Evaluation – the FINE Trial. A randomised controlled trial of nurse led self-help treatment for patients in primary care with chronic fatigue syndrome: study protocol. BMC Med 2006;4:9 | No qualitative data reported |
| 30 | Whitehead L, Campion P. Can general practitioners manage Chronic Fatigue Syndrome? A controlled trial. J Chronic Fatig Syndr 2002;10:55–64 | No qualitative data reported |
| 31 | Wilkinson P, Mynors-Wallis L. Problem-solving therapy in the treatment of unexplained physical symptoms in primary care: a preliminary study. J Psychosom Res 1994;38:591–8 | No qualitative data reported |
| 32 | Williams A, Wiggers J, O’Brien KM, Wolfenden L, Yoong S, Campbell E, et al. A randomised controlled trial of a lifestyle behavioural intervention for patients with low back pain, who are overweight or obese: study protocol. BMC Musculoskelet Disord 2016;17:70. https://doi.org/10.1186/s12891-016-0922-1 | No qualitative data reported |
Appendix 7 Excluded studies for the review of cost-effectiveness studies
| Citation | Reason for exclusion |
|---|---|
| Akehurst RL, Brazier JE, Mathers N, O’Keefe C, Kaltenthaler E, Morgan A, et al. Health-related quality of life and cost impact of irritable bowel syndrome in a UK primary care setting. PharmacoEconomics 2002;20:455–62 | Costing analysis |
| Annemans L, Wessely S, Spaepen E, Caekelbergh K, Caubère JP, Le Lay K, Taïeb C. Health economic consequences related to the diagnosis of fibromyalgia syndrome. Arthritis Rheum 2008;58:895–902. https://doi.org/10.1002/art.23265 | Costing analysis |
| Bermingham SL, Cohen A, Hague J, Parsonage M. The cost of somatisation among the working-age population in England for the year 2008–2009. Ment Health Fam Med 2010;7:71–84 | Costing analysis |
| Bromley JS, Turner A. A proactive and acceptable clinic solution for patients with medically unexplained symptoms. Psychiatr Bull 2014;38:307–8. https://doi.org/10.1192/pb.38.6.307a | Costing analysis |
| Burton C, McGorm K, Richardson G, Weller D, Sharpe M. Healthcare costs incurred by patients repeatedly referred to secondary medical care with medically unexplained symptoms: a cost of illness study. J Psychosom Res 2012;72:242–7. https://doi.org/10.1016/j.jpsychores.2011.12.009 | Costing analysis |
| Canavan C, West J, Card T. Review article: the economic impact of the irritable bowel syndrome. Aliment Pharmacol Ther 2014;40:1023–34. https://doi.org/10.1111/apt.12938 | Costing analysis |
| Cherkin DC, Deyo RA, Battié M, Street J, Barlow W. A comparison of physical therapy, chiropractic manipulation, and provision of an educational booklet for the treatment of patients with low back pain. N Engl J Med 1998;339:1021–9. https://doi.org/10.1056/NEJM199810083391502 | Non-UK |
| Chisholm D, Godfrey E, Ridsdale L, Chalder T, King M, Seed P, et al. Chronic fatigue in general practice: economic evaluation of counselling versus cognitive behaviour therapy. Br J Gen Pract 2001;51:15–18 | Cost–consequence study |
| Creed F, Fernades L, Guthrie E, Sivagnanam S, Louon A, Barbezat G. Both psychotherapy and paroxetine are cost-effective for the treatment of severe irritable bowel syndrome. Evid Based Healthc 2003;7:151–3 | Not primary care |
| Creed F, Fernandes L, Guthrie E, Palmer S, Ratcliffe J, Read N, et al. The cost-effectiveness of psychotherapy and paroxetine for severe irritable bowel syndrome. Gastroenterology 2003;124:303–17. https://doi.org/10.1053/gast.2003.50055 | Not primary care |
| Friedberg MW. Group cognitive behavioral treatment improves chronic low back pain in a cost-effective manner. J Clin Outcomes Manage 2010;17:7–9 | Not MUS |
| Geraets JJ, Goossens ME, de Bruijn CP, de Groot IJ, Köke AJ, Pelt RA, et al. Cost-effectiveness of a graded exercise therapy program for patients with chronic shoulder complaints. Int J Technol Assess Health Care 2006;22:76–83 | Non-UK |
| Gerhards SA, de Graaf LE, Jacobs LE, Severens JL, Huibers MJ, Arntz A, et al. Economic evaluation of online computerised cognitive-behavioural therapy without support for depression in primary care: randomised trial. Br J Psychiatry 2010;196:310–18. https://doi.org/10.1192/bjp.bp.109.065748 | Non-UK |
| Greig E, Gore S, Staveley K, Phillips I, Benneyworth R, Matull R, et al. Delivering cost effective management for irritable bowel syndrome (IBS) across Somerset. Gut 2015;64:A192–3 | Costing analysis |
| Gudleski GD, Li X, Ma C, Dunlap LJ, Baweja V, Satchidanand N, et al. Modeling health care utilization in irritable bowel syndrome patients: distinguishing factors that influence the decision to consult a doctor from those that influence frequency of doctor visits. Gastroenterology 2014;146:S224 | Costing analysis |
| Hill JC, Whitehurst DG, Lewis M, Bryan S, Dunn KM, Foster NE, et al. Comparison of stratified primary care management for low back pain with current best practice (STarT Back): a randomised controlled trial. Lancet 2011;378:1560–71. https://doi.org/10.1016/S0140-6736(11)60937-9 | Not MUS |
| Hong J, Reed C, Happich M, Novick D. Cost of treating chronic lower back pain (CLBP) in patients consulting primary care physicians in the UK. Eur J Pain Suppl 2011;5:125 | Costing analysis |
| Hong J, Reed C, Novick D, Happich M. Costs associated with treatment of chronic low back pain: an analysis of the UK General Practice Research Database. Spine 2013;38:75–82. https://doi.org/10.1097/BRS.0b013e318276450f | Costing analysis |
| Hong J, Reed C, Novick D, Lenox-Smith A, Happich M. Healthcare costs before and after diagnosis of depression in patients with unexplained pain: a retrospective cohort study using the United Kingdom general practice research database. Int J Neuropsychopharmacol 2012;15:232 | Costing analysis |
| Houghton LA, Heyman DJ, Whorwell PJ. Symptomatology, quality of life and economic features of irritable bowel syndrome – the effect of hypnotherapy. Aliment Pharmacol Ther 1996;10:91–5 | Costing analysis |
| Johnson RE, Jones GT, Wiles NJ, Chaddock C, Potter RG, Roberts C, et al. Active exercise, education, and cognitive behavioral therapy for persistent disabling low back pain: a randomized controlled trial. Spine 2007;32:1578–85. https://doi.org/10.1097/BRS.0b013e318074f890 | Not MUS |
| Juniper M, Le TK, Mladsi D. The epidemiology, economic burden, and pharmacological treatment of chronic low back pain in France, Germany, Italy, Spain and the UK: a literature-based review. Expert Opin Pharmacother 2009;10:2581–92. https://doi.org/10.1517/14656560903304063 | Costing analysis |
| Kennedy TM, Chalder T, McCrone P, Darnley S, Knapp M, Jones RH, Wessely S. Cognitive behavioural therapy in addition to antispasmodic therapy for irritable bowel syndrome in primary care: randomised controlled trial. Health Technol Assess 2006;10(19) | Cost–consequence study |
| Konnopka A, Konig HH, Kaufmann C, Stuhldreher N, Wild B, Szecsenyi J, et al. Cost-effectiveness of a Collaborative Group Intervention for Patients with Medically Unexplained Symptoms. J Ment Health Policy Econ 2015;18:S25–S6 | Non-UK |
| Lamb SE, Hansen Z, Lall R, Castelnuovo E, Withers EJ, Nichols V, et al. Group cognitive behavioural treatment for low-back pain in primary care: a randomised controlled trial and cost-effectiveness analysis. Lancet 2010;375:916–23. https://doi.org/10.1016/S0140-6736(09)62164-4 | Not MUS |
| Lamotte M, Maugars Y, Le Lay K, Taieb C. Health economic comparison of outpatient management of fibromyalgia before and after diagnosis in five European countries. Value Health 2009;12:A438 | Costing analysis |
| Le TK, Roskell N, Mladsi D, Mitra D, Shannon P, Wilson AG, et al. Database analysis to estimate medical and pharmacotherapy resource utilization and costs of fibromyalgia prior to and following diagnosis in the United Kingdom primary care setting. Pain Med 2009;10:274 | Costing analysis |
| Luciano JV, D’Amico F, Cerdà-Lafont M, Peñarrubia-María MT, Knapp M, Cuesta-Vargas AI, et al. Cost-utility of cognitive behavioral therapy versus U.S. Food and Drug Administration recommended drugs and usual care in the treatment of patients with fibromyalgia: an economic evaluation alongside a 6-month randomized controlled trial. Arthritis Res Ther 2014;16:451. https://doi.org/10.1186/s13075-014-0451-y | Non-UK |
| Luciano JV, Sabes-Figuera R, Cardeñosa E, T Peñarrubia-María M, Fernández-Vergel R, García-Campayo J, et al. Cost-utility of a psychoeducational intervention in fibromyalgia patients compared with usual care: an economic evaluation alongside a 12-month randomized controlled trial. Clin J Pain 2013;29:702–11. https://doi.org/10.1097/AJP.0b013e318270f99a | Non-UK |
| Luo Z, Goddeeris J, Gardiner JC, Smith RC. Costs of an intervention for primary care patients with medically unexplained symptoms: a randomized controlled trial. Psychiatr Serv 2007;58:1079–86 | Non-UK |
| Maetzel A, Li L. The economic burden of low back pain: a review of studies published between 1996 and 2001. Best Pract Res Clin Rheumatol 2002;16:23–30. https://doi.org/10.1053/berh.2001.0204 | Costing analysis |
| Margalit AP, El-Ad A. Costly patients with unexplained medical symptoms: a high-risk population. Patient Educ Couns 2008;70:173–8 | Non-UK |
| Maxion-Bergemann S, Thielecke F, Abel F, Bergemann R. Costs of irritable bowel syndrome in the UK and US. PharmacoEconomics 2006;24:21–37 | Costing analysis |
| McCrone P, Darbishire L, Ridsdale L, Seed P. The economic cost of chronic fatigue and chronic fatigue syndrome in UK primary care. Psychol Med 2003;33:253–61 | Costing analysis |
| McCrone P, Darbishire L, Ridsdale L, Seed P, Brage S, Raine R. Chronic fatigue has high, but mainly hidden, costs. Evid Based Healthc 2003;7:196–7 | Costing analysis |
| McCrone P, Knapp M, Kennedy T, Seed P, Jones R, Darnley S, Chalder T. Cost-effectiveness of cognitive behaviour therapy in addition to mebeverine for irritable bowel syndrome. Eur J Gastroenterol Hepatol 2008;20:255–63. https://doi.org/10.1097/MEG.0b013e3282f2519d | Cost–consequence study |
| McCrone P, Ridsdale L, Darbishire L, Seed P. Cost-effectiveness of cognitive behavioural therapy, graded exercise and usual care for patients with chronic fatigue in primary care. Psychol Med 2004;34:991–9 | Cost–consequence study |
| Meng H, Friedberg F, Castora-Binkley M. Cost-effectiveness of chronic fatigue self-management versus usual care: a pilot randomized controlled trial. BMC Fam Pract 2014;15:184. https://doi.org/10.1186/s12875-014-0184-7 | Non-UK |
| Morriss R, Gask L, Ronalds C, Downes-Grainger E, Thompson H, Leese B, Goldberg D. Cost-effectiveness of a new treatment for somatized mental disorder taught to GPs. Fam Pract 1998;15:119–25. https://doi.org/10.1093/fampra/15.2.119 | Not behavioural intervention |
| Murray-Thomas T, Dedman D, Canavan C, West J, Card T. Utilisation and costs of inpatient and outpatient services among patients with irritable bowel syndrome – a study using the clinical practice research datalink (CPRD). Value Health 2013;16:A495–6 | Costing analysis |
| O’Dowd H, Gladwell P, Rogers CA, Hollinghurst S, Gregory A. Cognitive behavioural therapy in chronic fatigue syndrome: a randomised controlled trial of an outpatient group programme. Health Technol Assess 2006;10(37) | Not primary care |
| Oliver K, Cronan TA, Walen HR, Tomita M. Effects of social support and education on health care costs for patients with fibromyalgia. J Rheumatol 2001;28:2711–19 | Non-UK |
| Parsons S, Symmons DPM. The burden of musculoskeletal conditions. Medicine 2010;38:126–8 | Costing analysis |
| Radhakrishnan M, Hammond G, Jones PB, Watson A, McMillan-Shields F, Lafortune L. Cost of improving Access to Psychological Therapies (IAPT) programme: an analysis of cost of session, treatment and recovery in selected primary care trusts in the East of England region. Behav Res Ther 2013;51:37–45. https://doi.org/10.1016/j.brat.2012.10.001 | Costing analysis |
| Reid S, Wessely S, Crayford T, Hotopf M. Frequent attenders with medically unexplained symptoms: service use and costs in secondary care. Br J Psychiatry 2002;180:248–53 | Costing analysis |
| Ridsdale L, Godfrey E, Chalder T, Seed P, King M, Wallace P, Wessely S, Fatigue Trialists’ Group. Chronic fatigue in general practice: is counselling as good as cognitive behaviour therapy? A UK randomised trial. Br J Gen Pract 2001;51:19–24 | Clinical paper with economic paper included in cost–consequence analysis |
| Ritzwoller DP, Crounse L, Shetterly S, Rublee D. The association of comorbidities, utilization and costs for patients identified with low back pain. BMC Musculoskelet Disord 2006;7:72 | Non-UK |
| Robinson A, Lee V, Kennedy A, Middleton L, Rogers A, Thompson DG, Reeves D. A randomised controlled trial of self-help interventions in patients with a primary care diagnosis of irritable bowel syndrome. Gut 2006;55:643–8 | Cost–consequence study |
| Ryan M, Gevirtz R. Biofeedback-based psychophysiological treatment in a primary care setting: an initial feasibility study. Appl Psychophysiol Biofeedback 2004;29:79–93 | Non-UK |
| Sabes-Figuera R, McCrone P, Hurley M, King M, Donaldson AN, Ridsdale L. The hidden cost of chronic fatigue to patients and their families. BMC Health Serv Res 2010;10:56. https://doi.org/10.1186/1472-6963-10-56 | Costing analysis |
| Sabes-Figuera R, McCrone P, Hurley M, King M, Donaldson AN, Ridsdale L. Cost-effectiveness of counselling, graded-exercise and usual care for chronic fatigue: evidence from a randomised trial in primary care. BMC Health Serv Res 2012;12:264. https://doi.org/10.1186/1472-6963-12-264 | Cost–consequence study |
| Schade N, Torres P, Beyebach M. Cost-efficiency of a brief family intervention for somatoform patients in primary care. Fam Syst Health 2011;29:197–205. https://doi.org/10.1037/a0024563 | Non-UK |
| Simrén M, Brazier J, Coremans G, Dapoigny M, Müller-Lissner SA, Pace F, et al. Quality of life and illness costs in irritable bowel syndrome. Digestion 2004;69:254–61. https://doi.org/10.1159/000079846 | Costing analysis |
| Soubieres A, Wilson P, Poullis A, Wilkins J, Rance M. Burden of irritable bowel syndrome in an increasingly cost-aware National Health Service. Frontline Gastroenterol 2015;6:246–51. https://doi.org/10.1136/flgastro-2014-100542 | Costing analysis |
| Soubieres A, Wilson P, Poullis A, Wilkins J, Rance M. The cost of irritable bowel syndrome (IBS) in England. Value Health 2014;17:A365. https://doi.org/10.1016/j.jval.2014.08.813 | Costing analysis |
| Spaeth M. Epidemiology, costs, and the economic burden of fibromyalgia. Arthritis Res Ther 2009;11:117. https://doi.org/10.1186/ar2715 | Costing analysis |
| Taylor SJ, Carnes D, Homer K, Kahan BC, Hounsome N, Eldridge S, et al. Novel three-day, community-based, nonpharmacological group intervention for chronic musculoskeletal pain (COPERS): a randomised clinical trial. PLOS Med 2016;13:e1002040. https://doi.org/10.1371/journal.pmed.1002040 | Not MUS |
| van der Roer N, van Tulder MW, Barendse JM, van Mechelen W, Franken WK, Ooms AC, de Vet HC. Cost-effectiveness of an intensive group training protocol compared to physiotherapy guideline care for sub-acute and chronic low back pain: design of a randomised controlled trial with an economic evaluation. BMC Musculoskelet Disord 2004;5:45 | Non UK |
| Wilson P, Poullis A, Wilkins J, Rance M. The costs of irritable bowel syndrome (IBS) in an increasingly cost aware NHS. Gut 2014;63:A194 | Costing analysis |
| Yardley L, Barker F, Muller I, Turner D, Kirby S, Mullee M, et al. Clinical and cost effectiveness of booklet based vestibular rehabilitation for chronic dizziness in primary care: single blind, parallel group, pragmatic, randomised controlled trial. BMJ 2012;344:e2237. https://doi.org/10.1136/bmj.e2237 | Not MUS |
| Yiannakou Y, Eugenicos M, Sanders DS, Emmanuel A, Whorwell P, Butt F, et al. Economic and quality-of-life burden of moderate-to-severe irritable bowel syndrome with constipation (IBS-C) in the UK: the IBIS-C study. Gut 2015;64:A33–4 | Costing analysis |
Appendix 8 Applicability and quality of cost-effectiveness studies
| First author, year: Richardson 2013282 (clinical paper Wearden 2010111) | Population: CFS/ME | Intervention vs. comparator: pragmatic rehabilitation vs. supportive listening vs. treatment as usual |
|---|---|---|
| Element | ||
| Section 1: Applicability. This checklist should be used first to filter out irrelevant studies | Yes/partly/no/unclear/NA | Comments |
| 1.1 Is the study population appropriate for the review question? | Yes | Clinical paper met criteria for inclusion in clinical review |
| 1.2 Are the interventions appropriate for the review question? | Yes | Clinical paper met criteria for inclusion in clinical review |
| 1.3 Is the system in which the study was conducted sufficiently similar to the current UK context? | Yes | UK NHS |
| 1.4 Are the perspectives clearly stated and are they appropriate for the review question? | Yes | NHS and PSS |
| 1.5 Are all direct effects on individuals included, and are all other effects included where they are material? | Yes | QALYs accrued by patients |
| 1.6 Are all future costs and outcomes discounted appropriately? | Yes | Discounting at 3.5% for both costs and QALYs over 70-week horizon |
| 1.7 Is QALY used as an outcome, and was it derived using NICE’s preferred methods? If not, describe rationale and outcomes used in line with analytical perspectives taken (item 1.4 above) | Yes | QALYs derived from EQ-5D |
| 1.8 Are costs and outcomes from other sectors fully and appropriately measured and valued? | Yes | Costs to patient and family including lost working days also reported but not included in CE |
| 1.9 Overall judgement: directly applicable/partially applicable/not applicable There is no need to use section 2 of the checklist if the study is considered ‘not applicable’ | Directly applicable | |
| Section 2: Study limitations (the level of methodological quality). This checklist should be used once it has been decided that the study is sufficiently applicable to the context of the guideline | Yes/partly/no/unclear/NA | Comments |
| 2.1 Does the model structure adequately reflect the nature of the topic under evaluation? | NA | Trial-based evaluation |
| 2.2 Is the time horizon sufficiently long to reflect all important differences in costs and outcomes? | No | 70-week time horizon inadequate in a chronic condition |
| 2.3 Are all important and relevant outcomes included? | Yes | |
| 2.4 Are the estimates of baseline outcomes from the best available source? | Yes | Trial-based analysis |
| 2.5 Are the estimates of relative intervention effects from the best available source? | Yes | Trial-based analysis |
| 2.6 Are all important and relevant costs included? | Partly | Relevant aspects of health service resource use are captured. Not all relevant social care services captured but discussed as limitation |
| 2.7 Are the estimates of resource use from the best available source? | Partly | Self-reporting of resource use is not ideal |
| 2.8 Are the unit costs of resources from the best available source? | Yes | Standard unit cost sources, e.g. PSSRU337/NHS Reference Costs336 |
| 2.9 Is an appropriate incremental analysis presented or can it be calculated from the data? | Yes | |
| 2.10 Are all important parameters whose values are uncertain subjected to appropriate sensitivity analysis? | Yes | Boot-strapping used to generate CEAC. Sensitivity analysis on complete-case data |
| 2.11 Is there any potential conflict of interest? | No | |
| 2.12 Overall assessment: minor limitations/potentially serious limitations/very serious limitations | Minor limitations | |
| First author, year: Beasley, 2015126 (short-term follow-up in McBeth 2012125) | Population: chronic pain | Intervention vs. comparator: CBT vs. exercise vs. CBT with exercise vs. treatment as usual |
|---|---|---|
| Element | ||
| Section 1: Applicability (relevance to specific review questions and the NICE reference case as described in section 7.5) This checklist should be used first to filter out irrelevant studies | Yes/partly/no/unclear/NA | Comments |
| 1.1 Is the study population appropriate for the review question? | Yes | Met criteria for inclusion in clinical review |
| 1.2 Are the interventions appropriate for the review question? | Yes | Met criteria for inclusion in clinical review |
| 1.3 Is the system in which the study was conducted sufficiently similar to the current UK context? | Yes | UK (presumed NHS) |
| 1.4 Are the perspectives clearly stated and are they appropriate for the review question? | Yes | Perspective not clearly stated but approach taken is consistent with NHS perspective |
| 1.5 Are all direct effects on individuals included, and are all other effects included where they are material? | Yes | QALYs accrued by patients |
| 1.6 Are all future costs and outcomes discounted appropriately? | Yes | Discounting at 3.5% |
| 1.7 Is QALY used as an outcome, and was it derived using NICE’s preferred methods? If not, describe rationale and outcomes used in line with analytical perspectives taken (item 1.4 above). | Yes | QALYs derived from EQ-5D |
| 1.8 Are costs and outcomes from other sectors fully and appropriately measured and valued? | No | None included |
| 1.9 Overall judgement: directly applicable/partially applicable/not applicable There is no need to use section 2 of the checklist if the study is considered ‘not applicable’. | Directly applicable | |
| Section 2: study limitations (the level of methodological quality) This checklist should be used once it has been decided that the study is sufficiently applicable to the context of the guideline | Yes/partly/no/unclear/NA | Comments |
| 2.1 Does the model structure adequately reflect the nature of the topic under evaluation? | NA | Within-trial analysis |
| 2.2 Is the time horizon sufficiently long to reflect all important differences in costs and outcomes? | Yes | 2-year time horizon reported by Beasley et al.126 |
| 2.3 Are all important and relevant outcomes included? | Yes | |
| 2.4 Are the estimates of baseline outcomes from the best available source? | Yes | Within-trial analysis |
| 2.5 Are the estimates of relative intervention effects from the best available source? | Yes | Within-trial analysis |
| 2.6 Are all important and relevant costs included? | Yes | |
| 2.7 Are the estimates of resource use from the best available source? | Partly | Self-reporting of resource use is not ideal |
| 2.8 Are the unit costs of resources from the best available source? | Yes | Standard sources of unit costs (e.g. PSSRU337 and NHS Reference Costs336) |
| 2.9 Is an appropriate incremental analysis presented or can it be calculated from the data? | Yes | |
| 2.10 Are all important parameters whose values are uncertain subjected to appropriate sensitivity analysis? | Yes | Bootstrapping used to produce CEACs. Sensitivity analysis conducted on missing data |
| 2.11 Is there any potential conflict of interest? | No | |
| 2.12 Overall assessment: minor limitations/potentially serious limitations/very serious limitations | Minor limitations | |
Appendix 9 Applicability and quality of cost–consequence studies
| First author, year: McCrone, 2004279 (clinical paper is Ridsdale 2004113) | Population: chronic fatigue | Intervention vs. comparator: GA vs. CBT (plus a non-randomised comparison with usual care with self-help booklet) |
|---|---|---|
| Element | ||
| Section 1: applicability (relevance to specific review questions and the NICE reference case as described in section 7.5). This checklist should be used first to filter out irrelevant studies | Yes/partly/no/unclear/NA | Comments |
| 1.1 Is the study population appropriate for the review question? | Yes | Clinical paper met inclusion criteria for clinical effectiveness |
| 1.2 Are the interventions appropriate for the review question? | Yes | Clinical paper met inclusion criteria for clinical effectiveness |
| 1.3 Is the system in which the study was conducted sufficiently similar to the current UK context? | Yes | General practices in UK (presumed to be NHS) |
| 1.4 Are the perspectives clearly stated and are they appropriate for the review question? | Partly | Perspective described as ‘broad’ but reports both health-care costs and societal costs borne by caregivers. Costs for complementary therapy are included but it is not clear if these costs are borne by the patient or the health service |
| 1.5 Are all direct effects on individuals included, and are all other effects included where they are material? | NA | Benefits not reported as QALYs so focusing on cost outcomes only here |
| 1.6 Are all future costs and outcomes discounted appropriately? | Yes | No discounting as 8-month time frame |
| 1.7 Is QALY used as an outcome, and was it derived using NICE’s preferred methods? If not, describe rationale and outcomes used in line with analytical perspectives taken (item 1.4 above) | NA | Benefits not reported as QALYs so focusing on cost outcomes only here |
| 1.8 Are costs and outcomes from other sectors fully and appropriately measured and valued? | Partly | Informal carer hours valued using commercial cost for public sector care |
| 1.9 Overall judgement: directly applicable/partially applicable/not applicable There is no need to use section 2 of the checklist if the study is considered ‘not applicable’ | Partially applicable | Health service costs not reported separately from costs of informal care |
| Section 2: study limitations (the level of methodological quality). This checklist should be used once it has been decided that the study is sufficiently applicable to the context of the guideline | Yes/partly/no/unclear/NA | Comments |
| 2.1 Does the model structure adequately reflect the nature of the topic under evaluation? | NA | Within-trial analysis |
| 2.2 Is the time horizon sufficiently long to reflect all important differences in costs and outcomes? | No | 8 months is not a sufficient time horizon for a chronic condition |
| 2.3 Are all important and relevant outcomes included? | NA | Benefits not reported as QALYs so focusing on cost outcomes only here |
| 2.4 Are the estimates of baseline outcomes from the best available source? | Partly | Within-trial analysis is a good source for comparison between GA and CBT but non-randomised comparison with usual care with self-help booklet is potentially biased |
| 2.5 Are the estimates of relative intervention effects from the best available source? | Partly | Within-trial analysis is a good source for comparison between GA and CBT but non-randomised comparison with usual care with self-help booklet is potentially biased |
| 2.6 Are all important and relevant costs included? | Yes | |
| 2.7 Are the estimates of resource use from the best available source? | Partly | Patient-reported data are not ideal |
| 2.8 Are the unit costs of resources from the best available source? | Cites standard sources (e.g. PSSRU unit costs337 and NHS Reference Costs336). Cost of booklet is described as being nominal | |
| 2.9 Is an appropriate incremental analysis presented or can it be calculated from the data? | NA | Benefits not reported as QALYs so focusing on cost outcomes only here |
| 2.10 Are all important parameters whose values are uncertain subjected to appropriate sensitivity analysis? | Bootstrapping used to estimate uncertainty around incremental costs. Sensitivity analyses were reported | |
| 2.11 Is there any potential conflict of interest? | Yes | |
| 2.12 Overall assessment: minor limitations/potentially serious limitations/very serious limitations | Potentially serious limitations for the comparison against 3. Minor limitations for 1 vs. 2 | The non-randomised comparison against usual care with self-help booklet is potentially biased |
| First author, year: Kennedy, 2005129 | Population: IBS | Intervention vs. comparator: CBTLI plus mediation vs. medication alone |
|---|---|---|
| Element | ||
| Section 1: applicability (relevance to specific review questions and the NICE reference case as described in section 7.5). This checklist should be used first to filter out irrelevant studies. | Yes/partly/no/unclear/NA | Comments |
| 1.1 Is the study population appropriate for the review question? | Yes | Clinical paper met inclusion criteria for clinical effectiveness |
| 1.2 Are the interventions appropriate for the review question? | Yes | Clinical paper met inclusion criteria for clinical effectiveness |
| 1.3 Is the system in which the study was conducted sufficiently similar to the current UK context? | Yes | General practices in UK (presumed to be NHS) |
| 1.4 Are the perspectives clearly stated and are they appropriate for the review question? | Unclear | Perspective not explicitly stated but health service costs reported separately from societal costs. Health service costs included alternative/complementary therapies |
| 1.5 Are all direct effects on individuals included, and are all other effects included where they are material? | NA | Benefits not reported as QALYs so focusing on cost outcomes only here |
| 1.6 Are all future costs and outcomes discounted appropriately? | Yes | Outcomes were not discounted as time horizon was 12 months |
| 1.7 Is QALY used as an outcome, and was it derived using NICE’s preferred methods? If not, describe rationale and outcomes used in line with analytical perspectives taken (item 1.4 above) | NA | Benefits not reported as QALYs so focusing on cost outcomes only here |
| 1.8 Are costs and outcomes from other sectors fully and appropriately measured and valued? | Yes | Lost employment included but health service costs also reported separately |
| 1.9 Overall judgement: directly applicable/partially applicable/not applicable. There is no need to use section 2 of the checklist if the study is considered ‘not applicable’ | Directly applicable | For outcome of health service costs |
| Section 2: study limitations (the level of methodological quality). This checklist should be used once it has been decided that the study is sufficiently applicable to the context of the guideline | Yes/partly/no/unclear/NA | Comments |
| 2.1 Does the model structure adequately reflect the nature of the topic under evaluation? | NA | Within-trial analysis |
| 2.2 Is the time horizon sufficiently long to reflect all important differences in costs and outcomes? | No | 12 months is not a sufficient time horizon for a chronic condition |
| 2.3 Are all important and relevant outcomes included? | NA | Benefits not reported as QALYs so focusing on cost outcomes only here |
| 2.4 Are the estimates of baseline outcomes from the best available source? | Yes | Within-trial analysis |
| 2.5 Are the estimates of relative intervention effects from the best available source? | Yes | Within-trial analysis |
| 2.6 Are all important and relevant costs included? | Yes | Intervention costs reported separately from costs of service use and total costs not reported |
| 2.7 Are the estimates of resource use from the best available source? | Partly | Patient-reported data are not ideal |
| 2.8 Are the unit costs of resources from the best available source? | Partly | Standard unit cost sources are cited (e.g. PSSRU). Production costs estimated for lost employment |
| 2.9 Is an appropriate incremental analysis presented or can it be calculated from the data? | NA | Benefits not reported as QALYs so focusing on cost outcomes only here |
| 2.10 Are all important parameters whose values are uncertain subjected to appropriate sensitivity analysis? | Yes | Bootstrapping used to estimate uncertainty. Sensitivity analysis on treatment costs reported in McCrone et al.278 |
| 2.11 Is there any potential conflict of interest? | Yes | Authors declared the following conflict of interest: RH Jones has been a consultant in companies with a therapeutic interest in IBS. These are Solvay Healthcare, Boots, Novartis and Glaxo |
| 2.12 Overall assessment: minor limitations/potentially serious limitations/very serious limitations | Minor limitations | |
| First author, year: Sabes-Figuera, 2012280 (clinical paper is Ridsdale 2012115) | Population: chronic fatigue | Intervention vs. comparator: GA vs. counselling (other psychotherapy) vs. usual care plus a self-help booklet (GSH) |
|---|---|---|
| Element | ||
| Section 1: applicability (relevance to specific review questions and the NICE reference case as described in section 7.5). This checklist should be used first to filter out irrelevant studies | Yes/partly/no/unclear/NA | Comments |
| 1.1 Is the study population appropriate for the review question? | Yes | Clinical paper met inclusion criteria for clinical effectiveness |
| 1.2 Are the interventions appropriate for the review question? | Yes | Clinical paper met inclusion criteria for clinical effectiveness |
| 1.3 Is the system in which the study was conducted sufficiently similar to the current UK context? | Yes | General practices in UK (presumed to be NHS) |
| 1.4 Are the perspectives clearly stated and are they appropriate for the review question? | Perspective is described as health service. Costs for alternative therapy are included but it is not clear if these costs are usually borne by the patient or the health service | |
| 1.5 Are all direct effects on individuals included, and are all other effects included where they are material? | NA | Benefits not reported as QALYs so focusing on cost outcomes only here |
| 1.6 Are all future costs and outcomes discounted appropriately? | Yes | No discounting as 6-month time frame |
| 1.7 Is QALY used as an outcome, and was it derived using NICE’s preferred methods? If not, describe rationale and outcomes used in line with analytical perspectives taken (item 1.4 above) | NA | Benefits not reported as QALYs so focusing on cost outcomes only here |
| 1.8 Are costs and outcomes from other sectors fully and appropriately measured and valued? | Partly | Informal carer hours valued using commercial cost for public sector carer, but full salary costs used to value sick days rather than friction costs methods |
| 1.9 Overall judgement: directly applicable/partially applicable/not applicable There is no need to use section 2 of the checklist if the study is considered ‘not applicable’ | Directly applicable | For outcome of health service costs |
| Section 2: study limitations (the level of methodological quality). This checklist should be used once it has been decided that the study is sufficiently applicable to the context of the guideline | Yes/partly/no/unclear/NA | Comments |
| 2.1 Does the model structure adequately reflect the nature of the topic under evaluation? | NA | Within-trial analysis |
| 2.2 Is the time horizon sufficiently long to reflect all important differences in costs and outcomes? | No | 6 months is not a sufficient time horizon for a chronic condition |
| 2.3 Are all important and relevant outcomes included? | NA | Benefits not reported as QALYs so focusing on cost outcomes only here |
| 2.4 Are the estimates of baseline outcomes from the best available source? | Yes | Within-trial analysis |
| 2.5 Are the estimates of relative intervention effects from the best available source? | Yes | Within-trial analysis |
| 2.6 Are all important and relevant costs included? | Yes | |
| 2.7 Are the estimates of resource use from the best available source? | Partly | Patient-reported data are not ideal |
| 2.8 Are the unit costs of resources from the best available source? | Yes | Cites standard sources, e.g. PSSRU unit costs337 and NHS Reference Costs.336 Cost of booklet is described as being nominal |
| 2.9 Is an appropriate incremental analysis presented or can it be calculated from the data? | NA | Benefits not reported as QALYs so focusing on cost outcomes only here |
| 2.10 Are all important parameters whose values are uncertain subjected to appropriate sensitivity analysis? | Yes | Bootstrapping used to estimate uncertainty around incremental costs |
| 2.11 Is there any potential conflict of interest? | No | |
| 2.12 Overall assessment: minor limitations/potentially serious limitations/very serious limitations | Minor limitations | |
| First author, year: Chisholm, 2001275 (clinical paper is Ridsdale 2001112) | Population: chronic fatigue | Intervention vs. comparator: counselling vs. CBT |
|---|---|---|
| Element | ||
| Section 1: applicability (relevance to specific review questions and the NICE reference case as described in section 7.5). This checklist should be used first to filter out irrelevant studies | Yes/partly/no/unclear/NA | Comments |
| 1.1 Is the study population appropriate for the review question? | Yes | Clinical paper met inclusion criteria for clinical effectiveness |
| 1.2 Are the interventions appropriate for the review question? | Yes | Clinical paper met inclusion criteria for clinical effectiveness |
| 1.3 Is the system in which the study was conducted sufficiently similar to the current UK context? | Yes | General practices in UK (presumed to be NHS) |
| 1.4 Are the perspectives clearly stated and are they appropriate for the review question? | Unclear | Perspective not clearly stated but reports both health-care costs and societal costs borne by caregivers. Costs for alternative therapy are included but it is not clear if these costs are borne by the patient or the health service |
| 1.5 Are all direct effects on individuals included, and are all other effects included where they are material? | NA | Benefits not reported as QALYs so focusing on cost outcomes only here |
| 1.6 Are all future costs and outcomes discounted appropriately? | Yes | No discounting as 6-month time frame |
| 1.7 Is QALY used as an outcome, and was it derived using NICE’s preferred methods? If not, describe rationale and outcomes used in line with analytical perspectives taken (item 1.4 above) | NA | Benefits not reported as QALYs so focusing on cost outcomes only here |
| 1.8 Are costs and outcomes from other sectors fully and appropriately measured and valued? | Partly | Informal carer hours valued using commercial cost for public sector carer, but full salary costs used to value sick days rather than friction costs methods |
| 1.9 Overall judgement: directly applicable/partially applicable/not applicable. There is no need to use section 2 of the checklist if the study is considered ‘not applicable’ | Directly applicable | For outcome of health service costs |
| Section 2: study limitations (the level of methodological quality). This checklist should be used once it has been decided that the study is sufficiently applicable to the context of the guideline | Yes/partly/no/unclear/NA | Comments |
| 2.1 Does the model structure adequately reflect the nature of the topic under evaluation? | NA | Within-trial analysis |
| 2.2 Is the time horizon sufficiently long to reflect all important differences in costs and outcomes? | No | 6 months is not a sufficient time horizon for a chronic condition |
| 2.3 Are all important and relevant outcomes included? | NA | Benefits not reported as QALYs so focusing on cost outcomes only here |
| 2.4 Are the estimates of baseline outcomes from the best available source? | Yes | Within-trial analysis |
| 2.5 Are the estimates of relative intervention effects from the best available source? | Yes | Within-trial analysis |
| 2.6 Are all important and relevant costs included? | Yes | |
| 2.7 Are the estimates of resource use from the best available source? | Partly | Patient-reported data are not ideal |
| 2.8 Are the unit costs of resources from the best available source? | Unclear | Source described as NHS Ready Reckoner, which is published by PSSRU516 |
| 2.9 Is an appropriate incremental analysis presented or can it be calculated from the data? | NA | Benefits not reported as QALYs so focusing on cost outcomes only here |
| 2.10 Are all important parameters whose values are uncertain subjected to appropriate sensitivity analysis? | Yes | Bootstrapping used to estimate uncertainty around incremental costs and some sensitivity analysis reported |
| 2.11 Is there any potential conflict of interest? | Unclear | Not reported |
| 2.12 Overall assessment: minor limitations/potentially serious limitations/very serious limitations | Minor limitations | |
| First author, year: Robinson, 2006131 | Population: IBS | Intervention vs. comparator: self-help guidebook (GSH) vs. self-help group in addition to guidebook vs. usual care (MM = GSH + RSSE) |
|---|---|---|
| Element | ||
| Section 1: applicability (relevance to specific review questions and the NICE reference case as described in section 7.5). This checklist should be used first to filter out irrelevant studies | Yes/partly/no/unclear/NA | Comments |
| 1.1 Is the study population appropriate for the review question? | Yes | Clinical paper met inclusion criteria for clinical effectiveness |
| 1.2 Are the interventions appropriate for the review question? | Yes | Clinical paper met inclusion criteria for clinical effectiveness |
| 1.3 Is the system in which the study was conducted sufficiently similar to the current UK context? | Yes | UK study |
| 1.4 Are the perspectives clearly stated and are they appropriate for the review question? | Yes | NHS perspective |
| 1.5 Are all direct effects on individuals included, and are all other effects included where they are material? | NA | Benefits not reported as QALYs so focusing on cost outcomes only here |
| 1.6 Are all future costs and outcomes discounted appropriately? | Yes | No discounting applied as 1-year time horizon |
| 1.7 Is QALY used as an outcome, and was it derived using NICE’s preferred methods? If not, describe rationale and outcomes used in line with analytical perspectives taken (item 1.4 above) | NA | Benefits not reported as QALYs so focusing on cost outcomes only here |
| 1.8 Are costs and outcomes from other sectors fully and appropriately measured and valued? | No | Cost analysis limited to NHS costs |
| 1.9 Overall judgement: directly applicable/partially applicable/not applicable. There is no need to use section 2 of the checklist if the study is considered ‘not applicable’ | Directly applicable | For outcome of health service costs |
| Section 2: study limitations (the level of methodological quality). This checklist should be used once it has been decided that the study is sufficiently applicable to the context of the guideline | Yes/partly/no/unclear/NA | Comments |
| 2.1 Does the model structure adequately reflect the nature of the topic under evaluation? | NA | Within-trial analysis |
| 2.2 Is the time horizon sufficiently long to reflect all important differences in costs and outcomes? | No | 1 year is not a sufficient time horizon for a chronic condition |
| 2.3 Are all important and relevant outcomes included? | NA | Benefits not reported as QALYs so focusing on cost outcomes only here |
| 2.4 Are the estimates of baseline outcomes from the best available source? | Yes | Within-trial analysis |
| 2.5 Are the estimates of relative intervention effects from the best available source? | Yes | Within-trial analysis |
| 2.6 Are all important and relevant costs included? | Partly | Secondary care consultations were included but inpatient care was not. Intervention costs do not appear to have been included |
| 2.7 Are the estimates of resource use from the best available source? | Partly | Primary care resource use from GP records but secondary care resources use from patient self-report which is not ideal |
| 2.8 Are the unit costs of resources from the best available source? | Yes | Cites standard sources, e.g. PSSRU unit costs337 and NHS Reference Costs.336 Cost of self-help guidebook is not provided |
| 2.9 Is an appropriate incremental analysis presented or can it be calculated from the data? | NA | Benefits not reported as QALYs so focusing on cost outcomes only here |
| 2.10 Are all important parameters whose values are uncertain subjected to appropriate sensitivity analysis? | Partly | Bootstrapping was used to estimate uncertainty around incremental costs and a secondary analysis adjusting for missing data were conducted in addition to the primary analysis |
| 2.11 Is there any potential conflict of interest? | None | |
| 2.12 Overall assessment: minor limitations/potentially serious limitations/very serious limitations | Potentially serious limitations | |
Appendix 10 Costing analysis assumptions
General assumptions for costing interventions applied across all studies.
-
For CBT interventions, the published unit cost for CBT is applied regardless of the individual delivering the intervention because the unit cost for CBT reflects an average across a range of professionals (specialty doctor, clinical psychologist and mental health nurse).
-
For other psychological interventions, the unit cost for CBT has been applied as the default where the therapy has been provided by a mix of health-care professionals (e.g. ‘primary care staff’) or where it has not been possible to identify a more specific unit cost for the health-care professional who is reported to have delivered the intervention.
-
For exercise-based interventions, the unit cost for physiotherapists has been applied when the intervention is delivered by non-health-care professionals (e.g. fitness instruction).
-
For hospital-based staff (e.g. consultant medical and psychiatric specialists), we have assumed that the ratio of direct to indirect time is the same as the ratio for GPs (1 : 0.61, i.e. every hour spent with a patient requires an additional 37 minutes (60 × 0.61) spent on activities that are not face-to-face contact time with patients.
-
Unit costs including qualification costs have been chosen where these are available.
-
For interventions delivered to groups:
-
We have assumed that any patient who attended at least one session would incur the cost of the full course of sessions as their place in the group would not be given to someone else. Therefore, the cost per patient is calculated using the number of patients who attended one or more sessions.
-
If the number attending one or more sessions is not reported, then we assume that all patients allocated to the intervention attended one or more sessions.
-
Where the number of groups has not been reported, this has been estimated based on the reported group size, and if this is not reported we have assumed one group.
-
-
For interventions delivered to individuals:
-
We have assumed that planned sessions that are not attended incur the full cost as missed or cancelled sessions cannot always be used by another patient and, therefore, we have used the number of planned sessions to estimate the cost rather than the mean number of sessions attended per patient.
-
In studies where the number of sessions was not specified, or was patient led (e.g. one or two sessions per week), we have used the mean number of sessions attended.
-
-
If neither the actual nor the intended duration of the sessions is reported (and could not be obtained following requests to the corresponding author), then we have recorded the cost as not estimable.
-
Where data on session number and duration are reported in several papers, we have used the paper reporting the longest follow-up and where data are reported differently in the clinical and economic papers, we have used the data from the economic papers.
-
Interventions that consist of training health-care professionals to manage patients with MUS in a particular way (i.e. the GP interventions) are costed based on the duration of time the health-care professionals committed to attending the training, but the cost of the trainer’s time is not included.
-
For interventions directed towards the individual with MUS, the costs of training health-care professionals to deliver interventions (e.g. training CBT therapists to deliver CBT or physiotherapists to deliver exercise sessions) has been excluded as qualification and ongoing training costs are already incorporated in the unit costs for health-care professionals.
-
For GP interventions, studies have been categorised according to the combination of the following elements:
-
GP training
-
interventions delivered to individual patients
-
interventions delivered to groups of patients.
-
Decisions regarding costing or categorisation of individual studies:
-
Kennedy 2005129 – medication was given in both arms as part of usual care and has therefore not been costed.
-
Larisch 2004158 – patients in both the intervention and the comparator arm (usual care) received six sessions of 20 minutes with the GP. These are not costed into the GP intervention as they were provided in both arms and the cost of the GP intervention is estimated relative to usual care.
-
Rothman 2013127 – both the intervention and the control arm have been costed as different forms of GP intervention. Multimodal assessment arm has been included under GP interventions delivered to individuals but in fact some patients in the multimodel assessment arm received group therapy. Cost could not be determined in either arm because of a lack of information on duration of sessions.
-
Sumathipala 2008101 – both arms received a structured GP intervention and the intervention arm received additional CBT elements not provided in the comparator arm. The intervention arm is categorised as a GP intervention with training for GPs (five sessions plus additional supervisory sessions) and individual delivery of CBT but the training element could not be costed because of a lack of information on session duration. Comparator arm is costed as a GP MUS management intervention with individual intervention with patients but no specific training for GPs.
-
van Ravesteijn 2013143 – control arm described as ‘enhanced usual care’ and categorised as usual care plus. The authors describe that patients in both trial arms received a psychiatric interview and their GP was informed of the results of that interview, which may have influenced future care. However, no other details are provided on how usual care was enhanced so we have assumed no additional cost for enhanced usual care.
Appendix 11 Tables of intervention and comparator costs
| First author and year of publication | Session facilitator | Face to face (F) or distance (D) | Number of sessions | Duration of sessions (minutes) | Unit cost | Cost per patient |
|---|---|---|---|---|---|---|
| Friedberg, 2013151 | Nurse with CBT training | F | 2.00 | 60 | CBT | £211.64 |
| Kennedy, 2005129 | Nurse therapists (trained in IBS-specific CBT) | F | 6.00 | 50 | CBT | £529.09 |
| Moss-Morris, 2010130 | Psychologist | Mix of F and D | 3.00 | 60 | CBT | £317.45 |
| Ridsdale, 2004113 | CBT therapists | F | 6.00 | 45 | CBT | £476.18 |
| Sumathipala, 2000116 | Psychiatrist trained in CBT | F | 6.00 | 30 | CBT | £317.45 |
| Tummers, 2012149 | Psychiatric nurses trained in CBT | D | 13.00a | NR | CBT | NE |
| First author and year of publication | Session facilitator | Number of sessions | Duration of sessions (minutes) | Total individuals started | Number of groups | Unit cost | Cost per patient |
|---|---|---|---|---|---|---|---|
| Martin, 200799 | Licensed CBT professionalsa | 1 | 210 | 60 | 20b | CBT | £123.45 |
| First author and year of publication | Session facilitator | Face to face (F) or distance (D) | Number of sessions | Duration of sessions (minutes) | Unit cost | Cost per patient |
|---|---|---|---|---|---|---|
| Escobar, 2007156 | Psychologist | F | 10.00 | 54a | CBT | £952.36 |
| Gili, 2014144 | Psychologist | F | 10.00 | 60 | CBT | £1058.18 |
| McBeth, 2012125 | Psychotherapist | D | 10 | 35b | CBT | £612.27 |
| Ridsdale, 2001112 | CBT therapist | F | 6 | 60 | CBT | £634.91 |
| First author and year of publication | Session facilitator | Number of sessions | Duration of sessions (minutes) | Total individuals started | Number of groups | Unit cost | Cost per patient |
|---|---|---|---|---|---|---|---|
| Alda, 2011137 | CBT therapist | 9 | 90 | 57 | 8a | CBT | £200.50 |
| Gili, 2014 (group arm)144 | Psychologist | 10 | 120 | 64 | 7b | CBT | £231.48 |
| Luciano, 2014138 | Clinical psychologist | 8 | 150 | 51 | 4c | CBT | £165.99 |
| Zonneveld, 2012141 | Psychologist | 13 | 120 | 145d | 20 | CBT | £379.49 |
| First author and year of publication | Session facilitator | Face to face (F) or distance (D) | Number of sessions | Duration of sessions (minutes) | Unit cost | Cost per patient |
|---|---|---|---|---|---|---|
| Kolk, 2004104 | Psychologists qualified as therapists | F | 12 | 60 | CBTa | £1269.82 |
| Margalit, 2008268 | Multidisciplinary primary care team | F | 7.3b | 30 | CBT | £386.24 |
| Posse, 200496 | Psychotherapist | F | 26 | 60 | CBT | £2751.27 |
| Ridsdale, 2001112 | Qualified counsellors | F | 6 | 50 | Counsellor | £255.59 |
| Ridsdale, 2012115 | Counsellors | Mixed | 10 | 50 | Counsellor | £511.19 |
| Ryan, 2004109 | Clinical or health psychology graduate students | F | 8 | 60 | CBT | £846.55 |
| Schade, 2011272 | Primary care staff | F | 2.86c | 45d | CBT | £226.98 |
| Wearden, 2010 (supportive listening)111 | General nurses | Mixed | 10a | 48e | Nurse (GP) | £412.80 |
| First author and year of publication | Session facilitator | Number of sessions | Duration of sessions (minutes) | Total individuals started | Number of groups | Unit cost | Cost per patient |
|---|---|---|---|---|---|---|---|
| Kocken, 2008103 | Migrant health worker | 10.63a | 84b | 48 | NR | CBTc | £289.81 |
| McLeod, 1997105 | Physicians, social workers and psychologists | 6 | NR | 51 | 3 | CBTd | NE |
| van Ravesteijn, 2013143 | Mindfulness trainers | 8 | 150 | 53 | 5 | Mindfulness trainer | £165.89 |
| First author and year of publication | Session facilitator | Face to face (F) or distance (D) | Number of sessions | Duration of sessions (minutes) | Unit cost | Cost per patient |
|---|---|---|---|---|---|---|
| Macedo, 2012 (GA)119 | Physical therapists | F | 14 | 60 | Physiotherapist | £863.10 |
| Macedo, 2012 (motor control)119 | Physical therapists | F | 14 | 60 | Physiotherapist | £863.10 |
| Marques, 2015133 | Health psychologista | F and D | 4.00 | 60 | Clinical psychologist | £564.35 |
| Moss-Morris, 2005152 | Health psychologist | F | 12.00 | 60 | Clinical psychologist | £1693.05 |
| Ridsdale, 2004113 | Physiotherapist | F | 6 | 45 | Physiotherapist | £277.43 |
| Ridsdale, 2012115 | Physiotherapist | F | 10 | 32b | Physiotherapist | £323.66 |
| Wearden, 2010111 | General nurses | F and D | 10 | 41c | Nurse (GP) | £412.80 |
| First author and year of publication | Session facilitator | Face to face (F) or distance (D) | Number of sessions | Duration of sessions (minutes) | Unit cost | Cost per patient |
|---|---|---|---|---|---|---|
| Lansinger, 2007123 | Physiotherapist | F | 11a | 60 | Physiotherapist | £678.15 |
| McBeth, 2012125 | Fitness instructor | F | 7 | 87b | Physiotherapist | £628.59 |
| Sañudo, 2010 (aerobic)140 | NR | F | 48.00 | 53c | Physiotherapist | £2589.30 |
| Sañudo, 2010 (combined)140 | NR | F | 48.00 | 53c | Physiotherapist | £2589.30 |
| van der Roer, 2008340 | Physiotherapist | F | 13.00d | 60e | Physiotherapist | £801.45 |
| Walti, 2015121 | Physiotherapist | F | 8.00d | 30 | Physiotherapist | £246.60 |
| First author and year of publication | Session facilitator | Number of sessions | Duration of sessions (minutes) | Total individuals started | Number of groups | Unit cost | Cost per patient |
|---|---|---|---|---|---|---|---|
| Peters, 2002106 | Physiotherapist | 20 | 60 | 87 | 9 | Physiotherapist | £127.55 |
| First author and year of publication | Session facilitator | Face to face (F) or distance (D) | Number of sessions | Duration of sessions (minutes) | Unit cost | Cost per patient |
|---|---|---|---|---|---|---|
| Friedberg, 2013151 | Nurse therapist with CBT training | F | 2.00 | 60a | CBT | £211.64 |
| First author and year of publication | Session facilitator | Number of sessions | Duration of sessions (minutes) | Total individuals started | Number of groups | Unit cost | Cost per patient |
|---|---|---|---|---|---|---|---|
| Ho, 2012150 | qigong Master | 10 | 120 | 33 | 1a | Physiotherapist | £37.36 |
| Kashner, 1995161 | ‘Masters-level clinicians’ | 8 | 120 | 20 | 4b | CBTc | £338.62 |
| Kobeissi, 2012110 | Clinical psychologists, social workers and physical trainers | 12 | 105d | 99 | 10 | Clinical psychologist, social workers and physiotherapist | £346.18 |
| Lansinger, 2007123 | Physiotherapist | 12 | 60 | 60 | 5e | Physiotherapist | £61.65 |
| Loew, 2000122 (eFR technique) | ‘Therapists’ | 1 | 45 | 27 | 7e | Physiotherapist | £11.99 |
| Loew, 2000 (UIR technique)122 | ‘Therapists’ | 1 | 45 | 27 | 7e | Physiotherapist | £11.99 |
| Peters, 2002 (stretch)106 | Physiotherapist | 20 | 60 | 90 | 9 | Physiotherapist | £123.30 |
| First author and year of publication | Session facilitator | Face to face (F) or distance (D) | Number of sessions | Duration of sessions (minutes) | Unit cost | Cost per patient |
|---|---|---|---|---|---|---|
| Chalder, 1997114 | GP nurse | F | 1.00 | 12.5a | Nurse (GP) | £10.75 |
| Cuesta-Vargas, 2012118 | GPb | F | 2.00 | 60 | GP (treat) | £468.00 |
| First author and year of publication | Session facilitator | Number of sessions | Duration of sessions (minutes) | Total individuals started | Number of groups | Unit cost | Cost per patient |
|---|---|---|---|---|---|---|---|
| LeFort, 1998342 | Nurse delivered | 6 | 120 | 52 | 6 | Nurse (GP) | £142.89 |
| First author and year of publication | Session facilitator | Number of sessions | Duration of sessions (minutes) | Total individuals started | Number of groups | Unit cost | Cost per patient |
|---|---|---|---|---|---|---|---|
| Luciano, 2011139 | GPs, clinical psychologist and rheumatologist | 9 | 120 | 98 | 6a | GP (treat), clinical psychologist and medical consultant | £193.06 |
| Robinson, 2006131 | Trial co-ordinator | 1 | 120 | 59 | 7a | Nurse (GP) | £12.24b |
| van der Roer, 2008340 | Physiotherapist | 30 | 68c | 50 | NR | Physiotherapist | £2088.06 |
| First author and year of publication | Session facilitator | Face to face (F) or distance (D) | Number of sessions | Duration of sessions (minutes) | Unit cost | Cost per patient |
|---|---|---|---|---|---|---|
| Cuesta-Vargas, 2012118 | Physiotherapist for exercise and GP for education | F | 47 | 31a | Physiotherapist and GP (treat) | £1855.13 |
| McBeth, 2012125 | CBT therapist and fitness instructor | F | 17 | 56b | CBT and physiotherapist | £1221.18 |
| Pols, 2008145 | GP and service co-ordinator | F | 10c | 10 | GP (treat) | £390.00 |
| Smith, 2004107 | Nurse practitioners | F + D | 24 | 28d | Nurse Practitioners | £892.43 |
| Walti, 2015121 | Physiotherapist | F | 8.6e | 30 | Physiotherapist | £258.00 |
| First author and year of publication | Number of GPs allocated | Number of training sessions | Duration of sessions (minutes) | Number of patients | Unit cost | Cost per patient |
|---|---|---|---|---|---|---|
| Reattribution | ||||||
| Larisch, 2004a (modified reattribution)158 | 20 | 2 | 360b | 73 | GP (train) | £483.29 |
| Morriss, 2007108 | 34 | 3 | 120 | 66 | GP (train) | £454.36 |
| van der Feltz-Cornelis, 2006160 | 18 | 6 | 180 | 58c | GP (train) | £821.17 |
| MUS management | ||||||
| Rief, 2006102 | 12 | 1 | 420 | 46 | GP (train) | £268.43 |
| Rosendal, 2007146 | 22 | 7 | 214b | 506 | GP (train) | £159.78 |
| Schaefert, 2013147 | 17 | 4 | 233 | 145 | GP (train) | £289.06 |
| Toft, 201097 | 20 | 7 | 214b | 218 | GP (train) | £337.16 |
| First author and year of publication | GP training | GP contact with patients | Unit cost | Cost per patient | ||||
|---|---|---|---|---|---|---|---|---|
| Number allocated | Number of sessions | Duration of sessions (minutes) | Session facilitators | Number of sessions | Duration of sessions (minutes) | |||
| Reattribution | ||||||||
| Aiarzaguena, 2007136 | 20 | 1 | 180 | GP | 6.00 | 29a | GP (train and treat) | £792.75 |
| Aiarzaguena, 2007 (modified reattribution)136 | 19 | 5 | 240 | GP | 6.00 | 34a | GP (train and treat) | £1534.50 |
| CBT | ||||||||
| Huibers, 2004153 | 9 | 4 | 210 | GP | 5.30 | 33 | GP (train and treat) | £939.36 |
| Other psychotherapy | ||||||||
| Schilte, 2001159 | 3 | NR | NR | GPs with training on disclosureb | 3c | 69d | GP (treat) | £802.29b |
| MUS management | ||||||||
| Whitehead 2002154 | 31 | 1 | 60 | GP | 9.60e | 10 | GP (train and treat) | £549.76 |
| Multimodal | ||||||||
| Smith, 2009 (CBT and pharmacological)343 | 4 | 6 | 240 | GP and case managerf | 14.00 | 28.12143 | GP and CBT (train and treat) | £2560.63 |
| Sumathipala, 2008 (CBT, reattribution and MUS management)101 | 3 | 5 | NRg | GP | 4.27 | 30 | GP (treat) | £499.59g |
| van der Feltz-Cornelis, 2006 (collaborative care plus reattribution)160 | 18 | 6 | 180 | GP and psychiatrist | 1.00 | 60 | GP (train and treat), psychiatrist | £1277.35 |
| First author and year of publication | GP training | GP contact with patients | Unit cost | Cost per patient | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Number of GPs | Number of sessions | Duration of sessions (minutes) | Session facilitators | Number of sessions | Duration of sessions (minutes) | Total individuals started | Number of groups | |||
| Multimodal | ||||||||||
| Schaefert, 2013132 (collaborative group care + MUS management)147 | 18 | 8 | 240 | GPs and physician specialists in psychosomatic medicine | 12 | 90 | 179 | 18 | GP (train and treat) and consultant psychiatrist | £1298.74 |
| First author and year of publication | Session facilitator | Face to face (F) or distance (D) | Number of sessions | Duration of sessions (minutes) | Unit cost | Cost per patient |
|---|---|---|---|---|---|---|
| Multimodal assessment and treatment | ||||||
| Rothman, 2013 (intervention)127 | Multidisciplinary assessment and treatment | F | 26.35a | NR | NE | NE |
| Conventional assessment and treatment | ||||||
| Rothman, 2013 (control)127 | Uni- or multidisciplinary | F | 26.56a | NR | NE | NE |
| MUS management | ||||||
| Burton, 2012157 | Specially trained GP with special interestb | F | 4 | 30 | GP | £468.00 |
| Sumathipala, 2008101 | PCPs | F | 4.64 | 30 | GP (treat) | £542.88 |
| First author and year of publication | Drugs and doses | Unit cost | Study period | Cost over study period |
|---|---|---|---|---|
| Alda, 2011137 |
Pregabalin (300 to 600 mg per day) and duloxetine (60 to 120 mg per day) (All were prescribed pregabalin but only 50% were prescribed duloxetine) |
£64.40 for 56 × pregabalin 300-mg capsules £2.37 for 28 × duloxetine 60-mg gastro resistant capsules |
6 months | £217.60 |
| Luciano, 2014138 |
Pregabalin (300 to 600 mg per day) and duloxetine (60 to 120 mg per day) (All were prescribed pregabalin but only 26.9% were prescribed duloxetine) |
£64.40 for 56 × pregabalin 300-mg capsules £2.37 for 28 × duloxetine 60-mg gastro resistant capsules |
6 months | £214.03 |
Appendix 12 Standardised mean differences for individual studies and for significant intervention groups
| Outcome | End of treatment | Short term | Long term | |||
|---|---|---|---|---|---|---|
| Significant intervention | SMD (95% CrI) | Significant intervention | SMD (95% CrI) | Significant intervention | SMD (95% CrI) | |
| Physical symptoms | ||||||
| Pain | CBTHI | 0.55 (0.28 to 0.87) | CBTHI | 0.73 (0.10 to 1.39) | GSH | –2.27 (–3.30 to –1.23 |
| MM | 0.48 (0.11 to 0.84) | |||||
| Fatigue | RSSEa | 0.87 (0.20 to 1.55) | CBTLI | 0.62 (0.11 to 1.14) | CBTLI | 0.64 (0.05 to 1.20) |
| CBTLIa | 0.72 (0.27 to 1.21) | |||||
| MM | 0.52 (0.14 to 0.92) | RSSE | 0.51 (0.06 to 1.00) | |||
| GA | 0.51 (0.14 to 0.93) | |||||
| Bowel | No NMA | No NMA | CBTLIa | 0.84 (0.17 to 1.52) | ||
| Somatisation | No significant effects | No significant effects | No significant effects | |||
| Generic physical symptoms | No significant effects | No NMA | No NMA | |||
| Physical functioning and impact | ||||||
| Physical functioning | MM | 0.33 (0.09 to 0.59) | MM | 0.78 (0.23 to 1.40) | No significant effects | |
| GSHa | –0.73 (–1.18 to –0.29) | |||||
| Impact | CBTHIa | 1.30 (0.58 to 2.00) | CBTHIa | 2.21 (1.28 to 3.14) | CBTLIa | –0.91 (–1.58 to –0.24) |
| GSH | –1.10 (–2.08 to –0.07) | |||||
| Emotional distress | ||||||
| Anxiety | CBTHI | 0.52 (0.06 to 0.96) | CBTHI | 0.74 (0.14 to 1.37) | No significant effects | |
| Depression | CBTHI | 0.80 (0.26 to 1.38) | CBTHIa | 0.93 (0.37 to 1.52) | No significant effects | |
| Emotional distress | CBTHI | 0.61 (0.04 to 0.71) | RSSE | 0.82 (0.02 to 1.65) | GSHa | –1.44 (–2.60 to –0.30) |
| OP | 0.60 (0.13 to 1.05) | |||||
| RSSEa | 0.65 (0.23 to 1.21) | MM | 0.43 (0.04 to 0.91) | |||
| SES | 0.49 (0.13 to 0.94) | |||||
| GSHa | –1.03 (–1.83 to –0.14) | |||||
| First author and year of publication | Condition | Number | Intervention groups | End of treatment SMD (SE) | Short-term SMD (SE) | Long-term SMD (SE) |
|---|---|---|---|---|---|---|
| Marques, 2015133 | Chronic fatigue | 99 | GSH vs. GA | 0.25 (0.20) | NR | NR |
| Ridsdale, 2004113 | Chronic fatigue | 123 | CBTLI vs. GA | –0.30 (0.18) | –0.27 (0.18) | NR |
| Tummers, 2012149 | Chronic fatigue | 123 | UC vs. CBTLI | 0.15 (0.18) | NR | NR |
| Luciano, 2011139 | Pain multisite | 108 | UC vs. MM | 0.37 (0.14) | NR | NR |
| Moss-Morris, 2010130 | IBS | 64 | UC vs. CBTLI | –0.46 (0.25) | –0.08 (0.25) | –0.28 (0.25) |
| Escobar, 2007156 | MUS/somatoform | 172 | UC+ vs. CBTHI | 0.26 (0.15) | NR | 0.30 (0.15) |
| Kolk, 2004104 | MUS/somatoform | 106 | UC vs. OP | –0.01 (0.23) | NR | –0.34 (0.24) |
| Gili, 2014/Moreno, 2013144,148 | MUS/somatoform | 168 | UC+ vs. CBTHI | 0.50 (0.17) | NR | 0.90 (0.18) |
| Larisch, 2004158 | MUS/somatoform | 127 | UC vs. GPRE | –0.05 (0.18) | –0.21 (0.18) | –0.23 (0.18) |
| McLeod, 1997105 | MUS/somatoform | 96 | UC vs. OP | 0.32 (0.20) | NR | NR |
| Posse, 200496 | MUS/somatoform | 10 | UC vs. OP | 0.46 (0.58) | NR | NR |
| Wearden, 2010111 | Chronic fatigue | 296 | UC vs. OP | –0.18 (0.14) | NR | –0.14 (0.14) |
| UC vs. GA | –0.09 (0.14) | NR | –0.13 (0.14) | |||
| Alda, 2011137 | Pain multisite | 169 | UC vs. CBTHI | 0.19 (0.19) | NR | NR |
| UC vs. ME | 0.13 (0.19) | NR | NR | |||
| Luciano, 2014138 | Pain multisite | 156 | UC vs. CBTHI | 0.97 (0.21) | NR | |
| UC vs. ME | 0.73 (0.20) | NR | ||||
| Ridsdale, 2001112 | Chronic fatigue | 160 | CBTHI vs. OP | NR | –0.24 (0.16) | NR |
| Rief, 2006102 | MUS/somatoform | 295 | UC vs. GP-MM | NR | –0.39 (0.14) | –0.03 (0.14) |
| Burton, 2012157 | MUS/somatoform | 32 | UC vs. GP-MM | NR | 0.02 (0.35) | NR |
| Friedberg, 2013151 | Chronic fatigue | 111 | UC vs. CBTLI | NR | 0.35 (0.23) | 0.19 (0.23) |
| UC vs. RSSE | NR | 0.00 (0.23) | 0.04 (0.23) | |||
| Ridsdale, 2012115 | Chronic fatigue | 222 | OP vs. GSH | NR | –0.05 (0.16) | NR |
| OP vs. GA | NR | 0.25 (0.17) | NR | |||
| Schilte, 2001159 | MUS/somatoform | 161 | UC vs. GP-OP | NR | NR | 0.18 (0.16) |
| Rothman, 2013127 | Pain multisite | 220 | UC+ vs. GP-O | NR | NR | –0.10 (0.14) |
| Alda, 2011137 | Pain multisite | 169 | UC vs. CBTHI | NR | NR | 0.13 (0.19) |
| UC vs. ME | NR | NR | 0.08 (0.19) |
| Study | Condition | Number | Intervention groups | End of treatment SMD (SE) | Short-term SMD (SE) | Long-term SMD (SE) |
|---|---|---|---|---|---|---|
| Moss-Morris, 2010130 | IBS | 64 | UC vs. CBTLI | NR | NR | 0.84 (0.26) |
| Robinson, 2006131 | IBS | 420 | UC vs. GSH | NR | NR | 0.16 (0.12) |
| Study | Condition | Number | Intervention groups | End of treatment SMD (SE) | Short-term SMD (SE) | Long-term SMD (SE) |
|---|---|---|---|---|---|---|
| Ridsdale, 2004113 | Chronic fatigue | 123 | CBTLI vs. GA | –0.19 (0.18) | –0.04 (0.18) | NR |
| Luciano, 2011139 | Pain multisite | 108 | UC vs. MM | 0.36 (0.14) | NR | |
| Moss-Morris, 2010130 | IBS | 64 | UC vs. CBTLI | –0.03 (0.25) | 0.29 (0.25) | 0.35 (0.25) |
| Escobar, 2007156 | MUS/somatoform | 172 | UC+ vs. CBTHI | 0.22 (0.15) | NR | 0.17 (0.15) |
| Kolk, 2004104 | MUS/somatoform | 106 | UC vs. OP | –0.10 (0.23) | NR | –0.31 (0.23) |
| Gili, 2014/Moreno, 2013144,148 | MUS/somatoform | 168 | UC+ vs. CBTHI | 0.29 (0.17) | NR | 0.80 (0.18) |
| Martin, 200799 | MUS/somatoform | 140 | UC vs. CBTLI | –0.14 (0.17) | NR | –0.27 (0.17) |
| van Ravesteijn, 2013143 | MUS/somatoform | 125 | UC+ vs. OP | 0.05 (0.18) | NR | 0.07 (0.18) |
| Larisch, 2004158 | MUS/somatoform | 127 | UC vs. GPRE | 0.02 (0.18) | –0.29 (0.18) | –0.23 (0.18) |
| McLeod, 1997105 | MUS/somatoform | 96 | UC vs. OP | 0.57 (0.21) | NR | NR |
| Wearden, 2010111 | Chronic fatigue | 296 | UC vs. OP | –0.09 (0.14) | NR | –0.13 (0.14) |
| UC vs. GA | 0.28 (0.14) | NR | 0.04 (0.14) | |||
| Alda, 2011137 | Pain multisite | 169 | UC vs. CBTHI | 0.16 (0.19) | NR | NR |
| UC vs. ME | 0.09 (0.19) | NR | NR | |||
| Luciano, 2014138 | Pain multisite | 156 | UC vs. CBTHI | 1.85 (0.23) | NR | |
| UC vs. ME | 0.74 (0.20) | NR | ||||
| Ridsdale, 2001112 | Chronic fatigue | 160 | CBTHI vs. OP | NR | 0.02 (0.16) | NR |
| Rief, 2006102 | MUS/somatoform | 295 | UC vs. GP-MM | NR | –0.15 (0.14) | 0 (0.14) |
| Burton, 2012157 | MUS/somatoform | 32 | UC vs. GP-MM | NR | –0.18 (0.35) | NR |
| Friedberg, 2013151 | Chronic fatigue | 111 | UC vs. CBTLI | NR | 0.25 (0.23) | –0.08 (0.23) |
| UC vs. RSSE | NR | –0.02 (0.23) | –0.05 (0.23) | |||
| Ridsdale, 2012115 | Chronic fatigue | 222 | OP vs. GSH | NR | 0.16 (0.16) | NR |
| OP vs. GA | NR | 0.09 (0.16) | NR | |||
| Schilte, 2001159 | MUS/somatoform | 161 | UC vs. GP-OP | NR | NR | –0.03 (0.16) |
| Rothman, 2013127 | Pain multisite | 220 | UC+ vs. GP-O | NR | NR | 0 (0.15) |
| LeFort, 1998128 | Pain multisite | 110 | UC vs. GSH | NR | 0.16 (0.19) | NR |
| Kobeissi, 2012110 | MUVD | 271 | UC vs. RSSE | NR | 0.10 (0.12) | NR |
| Schaefert, 2013132 | MUS/somatoform | 328 | GP-MM vs. MM | NR | 0.30 (0.11) | 0.34 (0.11) |
| Smith, 2009142 | MUS/somatoform | 30 | UC vs. MM | NR | NR | 0.79 (0.37) |
| Study | Condition | Number | Intervention groups | End of treatment SMD (SE) | Short-term SMD (SE) | Long-term SMD (SE) |
|---|---|---|---|---|---|---|
| Cuesta-Vargas, 2011 | Pains singles site | 58 | GSH vs. MM | 1.36 (0.29) | 1.40 (0.29) | 2.00 (0.32) |
| Ho, 2012150 | Chronic fatigue | 64 | UC vs. RSSE | 1.09 (0.25) | 0.82 (0.25) | NR |
| LeFort, 1998128 | Pain multisite | 110 | UC vs. GSH | NR | 0.38 (0.19) | NR |
| Huibers, 2004/Leone, 2006153,155 | Chronic fatigue | 151 | UC vs. GP-CBT | 0.14 (0.16) | NR | 0.02 (0.16) |
| Marques, 2015133 | Chronic fatigue | 99 | GSH vs. GA | 0.51 (0.20) | NR | NR |
| Peters, 2002106 | MUS/somatoform | 228 | RSSE vs. SES | 0.02 (0.13) | NR | NR |
| Sumathipala, 2008117 | MUS/somatoform | 150 | GP-MM vs. MM | 0.08 (0.16) | 0.11 (0.16) | 0.01 (0.16) |
| van Ravesteijn, 2013143 | MUS/somatoform | 68 | UC+ vs. OP | 0.35 (0.18) | NR | 0.02 (0.18) |
| Zonneveld, 2012141 | MUS/somatoform | 162 | UC vs. CBTHI | 0.44 (0.16) | NR | NR |
| Gili, 2014/Moreno, 2013144,148 | MUS/somatoform | 168 | UC+ vs. CBTHI | –0.06 (0.17) | NR | 0.61 (0.17) |
| Kocken, 2008103 | MUS/somatoform | 104 | UC + OP | 0.49 (0.20) | NR | NR |
| Larisch, 2004158 | MUS/somatoform | 127 | UC vs. GPRE | –0.15 (0.18) | –0.12 (0.18) | –0.38 (0.18) |
| Rosendal, 2007146 | MUS/somatoform | 506 | UC vs. GP-MM | NR | –0.10 (0.07) | NR |
| Schaefert, 2013132 | MUS/somatoform | 328 | GP-MM vs. MM | NR | 0.38 (0.11) | 0.31 (0.11) |
| van der Feltz-Cornelis 2006160 | MUS/somatoform | 81 | GPRE vs. MM | NR | 0.76 (0.25) | 0.96 (0.26) |
| Kennedy, 2005129 | IBS | 149 | ME vs. MM | 0.43 (0.17) | 0.49 (0.17) | 0.41 (0.16) |
| Chalder, 1997114 | Chronic fatigue | 150 | UC vs. GSH | NR | 0.28 (0.16) | NR |
| Sumathipala, 2000116 | MUS/somatoform | 68 | UC vs. CBTLI | 0.61 (0.25) | NR | NR |
| McBeth, 2012125 | Pain multisite | 442 | UC vs. CBTHI | 0.29 (0.14) | 0.34 (0.14) | NR |
| UC vs. SES | 0.31 (0.14) | 0.23 (0.14) | NR | |||
| UC vs. MM | 0.25 (0.14) | 0.19 (0.13) | NR | |||
| Burton, 2012157 | MUS/somatoform | 32 | UC vs. GP-MM | NR | –0.35 (0.16) | NR |
| Fatigue | ||||||
|---|---|---|---|---|---|---|
| Study | Condition | Number | Intervention groups | End of treatment SMD (SE) | Short-term SMD (SE) | Long-term SMD (SE) |
| Ho, 2012150 | Chronic fatigue | 64 | UC vs. RSSE | 0.88 (0.25) | 1.08 (0.25) | NR |
| Huibers, 2004/Leone, 2006153,155 | Chronic fatigue | 151 | UC vs. GP-CBT | 0.12 (0.16) | NR | –0.12 (0.16) |
| Marques, 2015133 | Chronic fatigue | 99 | GSH vs. GA | 0.60 (0.20) | NR | NR |
| Moss-Morris, 2005152 | Chronic fatigue | 49 | UC vs. GA | 1.00 (0.30) | NR | NR |
| Ridsdale, 2004113 | Chronic fatigue | 123 | CBTLI vs. GA | –0.20 (0.18) | –0.06 (0.18) | NR |
| Tummers, 2012149 | Chronic fatigue | 123 | UC vs. CBTLI | 0.75 (0.19) | NR | NR |
| Chalder, 1997114 | Chronic fatigue | 150 | UC vs. GSH | NR | 0.39 (0.16) | NR |
| Luciano, 2011139 | Pain multisite | 108 | UC vs. MM | 0.32 (0.14) | NR | NR |
| McBeth, 2012125 | Pain multisite | 442 | UC vs. CBTHI | 0.34 (0.14) | 0.37 (0.14) | 0.19 (0.13) |
| UC vs. SES | 0.43 (0.14) | 0.40 (0.14) | 0.20 (0.14) | |||
| UC vs. MM | 0.72 (0.14) | 0.51 (0.14) | 0.21 (0.13) | |||
| Wearden, 2010111 | Chronic fatigue | 296 | UC vs. OP | –0.12 (0.14) | NR | 0.03 (0.14) |
| UC vs. GA | 0.27 (0.14) | NR | 0.24 (0.14) | |||
| Ridsdale, 2001112 | Chronic fatigue | 160 | CBTHI vs. OP | NR | 0.07 (0.16) | NR |
| Friedberg, 2013151 | Chronic fatigue | 111 | UC vs. CBTLI | NR | 0.43 (0.23) | 0.62 (0.23) |
| UC vs. RSSE | NR | 0.05 (0.23) | 0.08 (0.23) | |||
| Ridsdale, 2012115 | Chronic fatigue | 222 | OP vs. GSH | NR | 0.11 (0.16) | 0.17 (0.16) |
| OP vs. GA | NR | 0.19 (0.16) | 0.09 (0.16) | |||
| Study | Condition | Number | Intervention groups | End of treatment SMD (SE) | Short-term SMD (SE) | Long-term SMD (SE) |
|---|---|---|---|---|---|---|
| Kolk, 2004104 | MUS/somatoform | 106 | UC vs. OP | –0.30 (0.24) | NR | NR |
| Posse, 200496 | MUS/somatoform | 10 | UC vs. OP | –0.04 (0.57) | NR | NR |
| Study | Condition | Number | Intervention groups | End of treatment SMD (SE) | Short-term SMD (SE) | Long-term SMD (SE) |
|---|---|---|---|---|---|---|
| Walti, 2015121 | Pain single site | 28 | SES vs. MM | –0.41 (0.37) | NR | NR |
| Sañudo, 2010140 | Pain multisite | 64 | UC vs. SES | –0.48 (0.26) | NR | NR |
| Kennedy, 2005129 | IBS | 149 | ME vs. MM | –0.4 (0.17) | –0.46 (0.17) | –0.26 (0.17) |
| Ridsdale, 2004113 | Chronic fatigue | 123 | CBTLI vs. GA | NR | 0 (0.18) | NR |
| Luciano, 2011139 | Pain multisite | 108 | UC vs. MM | 0.48 (0.14) | NR | NR |
| Moss-Morris, 2010130 | IBS | 64 | UC vs. CBTLI | –0.78 (0.26) | –0.84 (0.26) | –0.90 (0.26) |
| Kocken, 2008103 | MUS/somatoform | 104 | UC + OP | 0.54 (0.20) | NR | NR |
| Cuesta-Vargas, 2012118 | Pain single site | 58 | GSH vs. MM | 0.78 (0.27) | 1.17 (0.28) | 0.92 (0.27) |
| LeFort, 1998128 | Pain multisite | 110 | UC vs. GSH | NR | 0.69 (0.20) | NR |
| Alda, 2011137 | Pain multisite | 169 | UC vs. CBTHI | –0.28 (0.19) | NR | 0.05 (0.19) |
| UC vs. ME | 0.30 (0.19) | NR | 0.53 (0.19) | |||
| Luciano, 2014138 | Pain multisite | 156 | UC vs. CBTHI | NR | ||
| UC vs. ME | NR | |||||
| Ridsdale, 2012115 | Chronic fatigue | 222 | OP vs. GSH | NR | 0.23 (0.16) | NR |
| OP vs. GA | NR | 0.15 (0.16) | NR |
| Study | Condition | Number | Intervention groups | End of treatment SMD (SE) | Short-term SMD (SE) | Long-term SMD (SE) |
|---|---|---|---|---|---|---|
| Cuesta-Vargas, 2012118 | Pain single site | 58 | GSH vs. MM | 0.97 (0.27) | 1.69 (0.30) | 2.12 (0.32) |
| LeFort, 1998128 | Pain multisite | 110 | UC vs. GSH | NR | 0.54 (0.19) | NR |
| Rosendal, 2007146 | MUS/somatoform | 506 | UC vs. GP-MM | NR | –0.11 (0.07) | –0.15 (0.07) |
| Schaefert, 2013132 | MUS/somatoform | 328 | GP-MM vs. MM | NR | 0.05 (0.11) | –0.01 (0.11) |
| Rothman, 2013127 | Pain multisite | 220 | UC+ vs. GP-O | NR | NR | 0.12 (0.14) |
| Walti, 2015121 | Pain single site | 28 | SES vs. MM | –0.40 (0.37) | NR | |
| van Ravesteijn, 2013143 | MUS/somatoform | 125 | UC+ vs. OP | –0.24 (0.18) | NR | –0.13 (0.18) |
| Zonneveld, 2012141 | MUS/somatoform | 162 | UC vs. CBTHI | 0.51 (0.16) | NR | NR |
| Peters, 2002106 | MUS/somatoform | 228 | RSSE vs. SES | 0.06 (0.13) | NR | NR |
| Luciano, 2011139 | Pain multisite | 108 | UC vs. MM | 0.62 (0.14) | NR | NR |
| Gili, 2014/Moreno, 2013144,148 | MUS/somatoform | 168 | UC+ vs. CBTHI | 0.21 (0.17) | NR | 0.37 (0.17) |
| Alda, 2011137 | Pain multisite | 169 | UC vs. CBTHI | 0.17 (0.19) | NR | 0.41 (0.19) |
| UC vs. ME | 0.23 (0.19) | NR | 0.37 (0.19) | |||
| Luciano, 2014138 | Pain multisite | 156 | UC vs. CBTHI | NR | ||
| UC vs. ME | NR | |||||
| McBeth, 2012125 | Pain multisite | 442 | UC vs. CBTHI | 0.35 (0.14) | 0.28 (0.14) | NR |
| UC vs. SES | 0.20 (0.14) | 0.19 (0.14) | NR | |||
| UC vs. MM | 0.34 (0.14) | 0.17 (0.13) | NR |
| Study | Condition | Number | Intervention groups | End of treatment SMD (SE) | Short-term SMD (SE) | Long-term SMD (SE) |
|---|---|---|---|---|---|---|
| Marques, 2015133 | Chronic fatigue | 99 | GSH vs. GA | 0.70 (0.21) | NR | NR |
| Cuesta-Vargas, 2012118 | Pain single site | 58 | GSH vs. MM | 1.11 (0.28) | 1.94 (0.31) | 3.27 (0.40) |
| Ho, 2012150 | Chronic fatigue | 64 | UC vs. RSSE | 0.12 (0.24) | 0.36 (0.24) | NR |
| LeFort, 1998128 | Pain multisite | 110 | UC vs. GSH | NR | 0.27 (0.19) | NR |
| Huibers, 2004/Leone, 2006153,155 | Chronic fatigue | 151 | UC vs. GP-CBT | –0.32 (0.16) | NR | –0.32 (0.16) |
| Rosendal, 2007146 | MUS/somatoform | 506 | UC vs. GP-MM | NR | 0.01 (0.07) | –0.01 (0.07) |
| Schaefert, 2013132 | MUS/somatoform | 328 | GP-MM vs. MM | NR | 0.23 (0.11) | 0.13 (0.11) |
| Chalder, 1997114 | Chronic fatigue | 150 | UC vs. GSH | NR | 0.26 (0.16) | NR |
| Tummers, 2012149 | Chronic fatigue | 123 | UC vs. CBTLI | 0.25 (0.18) | NR | NR |
| Luciano, 2011139 | Pain multisite | 108 | UC vs. MM | 0.29 (0.14) | NR | NR |
| van Ravesteijn, 2013143 | MUS/somatoform | 125 | UC+ vs. OP | –0.16 (0.18) | NR | –0.17 (0.18) |
| Zonneveld, 2012141 | MUS/somatoform | 162 | UC vs. CBTHI | 0.39 (0.16) | NR | NR |
| Peters, 2002106 | MUS/somatoform | 228 | RSSE vs. SES | –0.08 (0.13) | NR | –0.09 (0.13) |
| Escobar, 2007156 | MUS/somatoform | 172 | UC+ vs. CBTHI | 0.09 (0.15) | NR | 0.12 (0.15) |
| Gili, 2014/Moreno, 2013144,148 | MUS/somatoform | 168 | UC+ vs. CBTHI | 0.61 (0.17) | NR | 0.83 (0.18) |
| Larisch, 2004158 | MUS/somatoform | 127 | UC vs. GPRE | 0.21 (0.18) | –0.01 (0.18) | 0.17 (0.18) |
| Smith, 2009142 | MUS/somatoform | 30 | UC vs. MM | NR | NR | 0.53 (0.36) |
| Smith, 2006107 | MUS/somatoform | 206 | UC vs. MM | NR | NR | 0.32 (0.14) |
| Wearden, 2010111 | Chronic fatigue | 296 | UC vs. OP | –0.28 (0.14) | NR | –0.15 (0.14) |
| UC vs. GA | –0.01 (0.14) | NR | 0.12 (0.14) | |||
| McBeth, 2012125 | Pain multisite | 442 | UC vs. CBTHI | 0.15 (0.13) | 0.11 (0.13) | NR |
| UC vs. SES | 0.03 (0.13) | 0.23 (0.14) | NR | |||
| UC vs. MM | 0.32 (0.13) | 0.31 (0.14) | NR | |||
| Burton, 2012157 | MUS/somatoform | 32 | UC vs. GP-MM | NR | 0.61 (0.35) | NR |
| Friedberg, 2013151 | Chronic fatigue | 111 | UC vs. CBTLI | NR | 0.42 (0.23) | 0.35 (0.23) |
| UC vs. RSSE | NR | 0.09 (0.23) | 0.36 (0.23) |
| Study | Condition | Number | Intervention groups | End of treatment SMD (SE) | Short-term SMD (SE) | Long-term SMD (SE) |
|---|---|---|---|---|---|---|
| Zonneveld, 2012141 | MUS/somatoform | 162 | UC vs. CBTHI | 0.23 (0.16) | NR | NR |
| Peters, 2002106 | MUS/somatoform | 228 | RSSE vs. SES | 0.01 (0.13) | NR | NR |
| Kobeissi, 2012110 | MUVD | 271 | UC vs. RSSE | 0.05 (0.12) | NR | NR |
| van Ravesteijn, 2013143 | MUS/somatoform | 125 | UC+ vs. OP | 0.31 (0.18) | NR | 0.15 (0.18) |
| Martin, 200799 | MUS/somatoform | 140 | UC vs. CBTLI | –0.13 (0.17) | NR | –0.23 (0.17) |
| Sumathipala, 2000116 | MUS/somatoform | 68 | UC vs. CBTLI | 0.41 (0.24) | NR | NR |
| Escobar, 2007156 | MUS/somatoform | 172 | UC+ vs. CBTHI | 0.35 (0.15) | NR | 0.32 (0.15) |
| Kolk, 2004104 | MUS/somatoform | 106 | UC vs. OP | 0.15 (0.23) | NR | 0.15 (0.23) |
| Gili, 2014/Moreno, 2013144,148 | MUS/somatoform | 168 | UC+ vs. CBTHI | 0.77 (0.18) | NR | 0.66 (0.17) |
| Larisch, 2004158 | MUS/somatoform | 127 | UC vs. GPRE | 0.20 (0.18) | –0.12 (0.18) | –0.02 (0.18) |
| McLeod, 1997105 | MUS/somatoform | 96 | UC vs. OP | 0.45 (0.21) | NR | NR |
| Sumathipala, 2008117 | MUS/somatoform | 150 | GP-MM vs. MM | NR | 0.03 (0.16) | –0.01 (0.16) |
| Rosendal, 2007146 | MUS/somatoform | 506 | UC vs. GP-MM | NR | 0 (0.07) | 0 (0.07) |
| Schaefert, 2013132 | MUS/somatoform | 328 | GP-MM vs. MM | NR | 0.39 (0.11) | 0.20 (0.11) |
| Rief, 2006102 | MUS/somatoform | 295 | UC vs. GP-MM | NR | –0.28 (0.14) | –0.18 (0.14) |
| Burton, 2012157 | MUS/somatoform | 32 | UC vs. GP-MM | NR | 0.28 (0.35) | |
| Schilte, 2001159 | MUS/somatoform | 161 | UC vs. GP-OP | NR | NR | 0 (0.16) |
Appendix 13 Inconsistency check for network meta-analysis
Figures 75–84 show the contributions to the deviance for both consistency model and inconsistency model. When the points are close to the line of equality, it suggests that there is no evidence to suggest inconsistency in the network. The number next to the point indicates the study where potential inconsistency may exist.
Pain
FIGURE 75.
Individual data points’ posterior mean deviance contributions for the consistency model and the inconsistency model along with the line of equality: (a) post treatment; (b) short term; and (c) long term. Note: at short term, 1 is for Cuesta-Vargas et al. 118 comparing guided self-help with multimodal; 5 is for Luciano et al. 138 comparing usual care with medication and CBTHI.
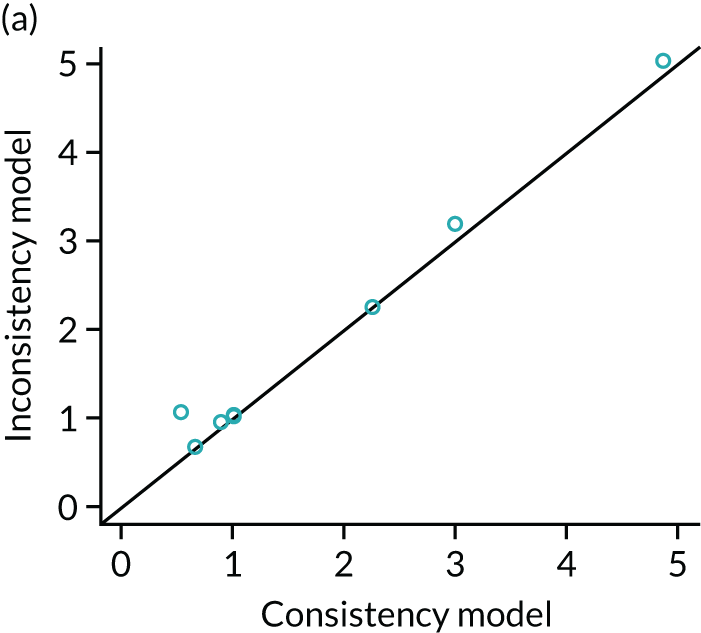
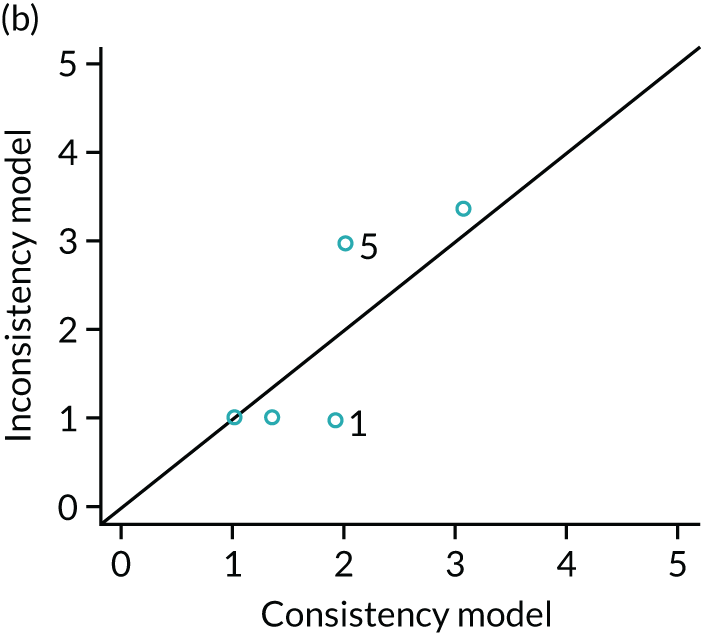
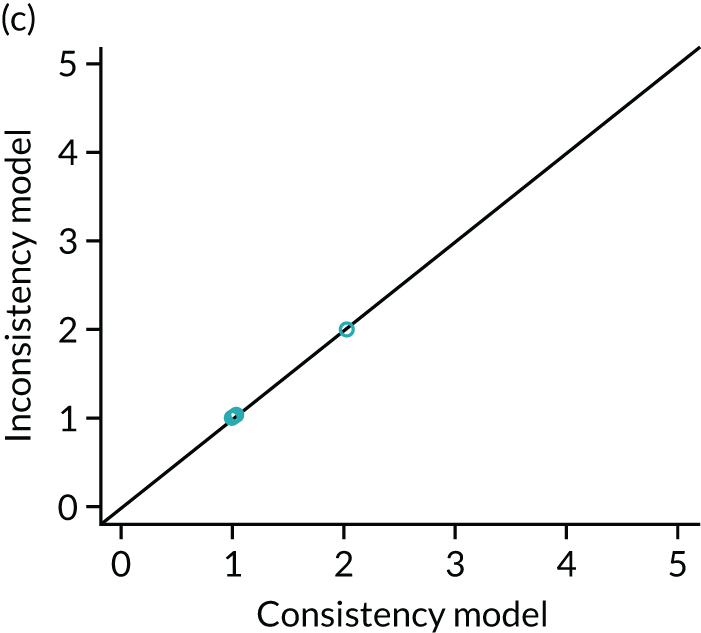
Fatigue
FIGURE 76.
Individual data points’ posterior mean deviance contributions for the consistency model and the inconsistency model along with the line of equality: (a) post treatment; (b) short term; and (c) long term. Note: at short term, 1 is for Ho et al. 150 comparing usual care with RSSE.

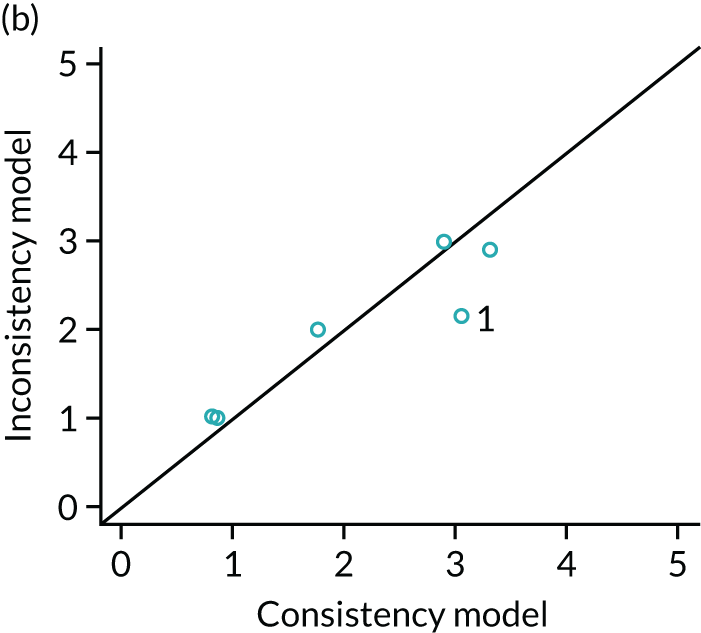
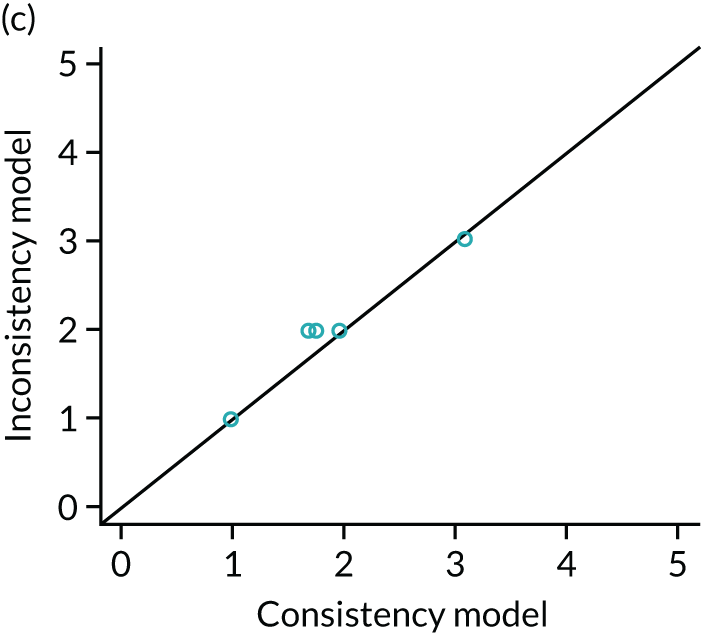
Bowel symptoms
FIGURE 77.
Individual data points’ posterior mean deviance contributions for the consistency model and the inconsistency model along with the line of equality: long term.

Somatisation
FIGURE 78.
Individual data points’ posterior mean deviance contributions for the consistency model and the inconsistency model along with the line of equality: (a) post treatment; (b) short term; and (c) long term.
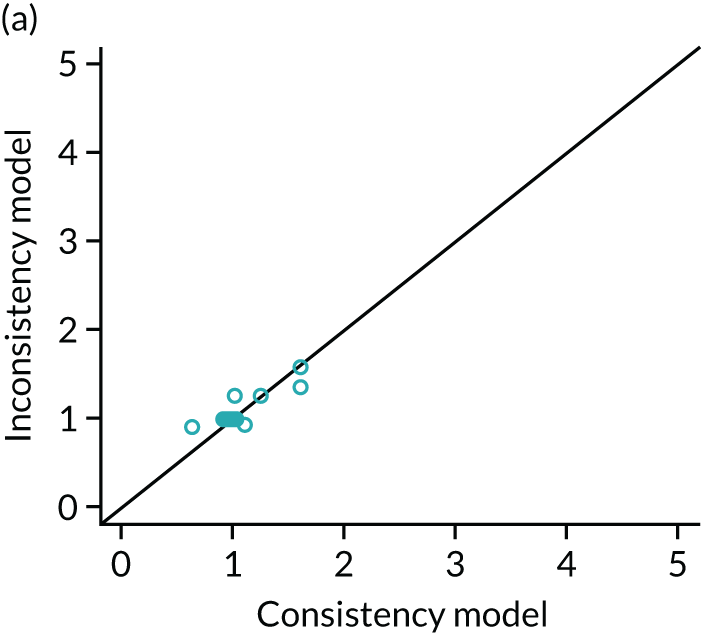


Generic physical symptoms
FIGURE 79.
Individual data points’ posterior mean deviance contributions for the consistency model and the inconsistency model along with the line of equality: post treatment.

Physical functioning
FIGURE 80.
Individual data points’ posterior mean deviance contributions for the consistency model and the inconsistency model along with the line of equality: (a) post treatment; (b) short term; and (c) long term. Note: at short term, 1 is for Cuesta-Vargas et al. 118 comparing guided self-help with multimodal; 8 is for Burton et al. 157 comparing usual care with GP MUS management.
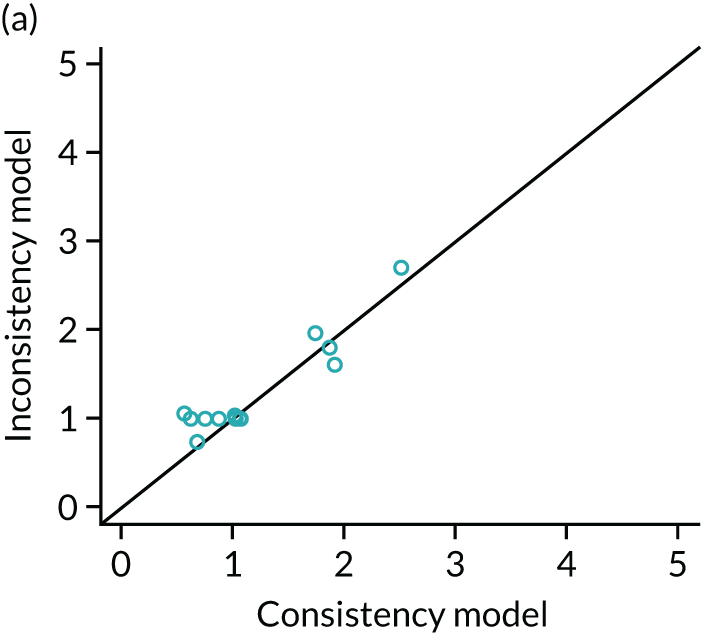

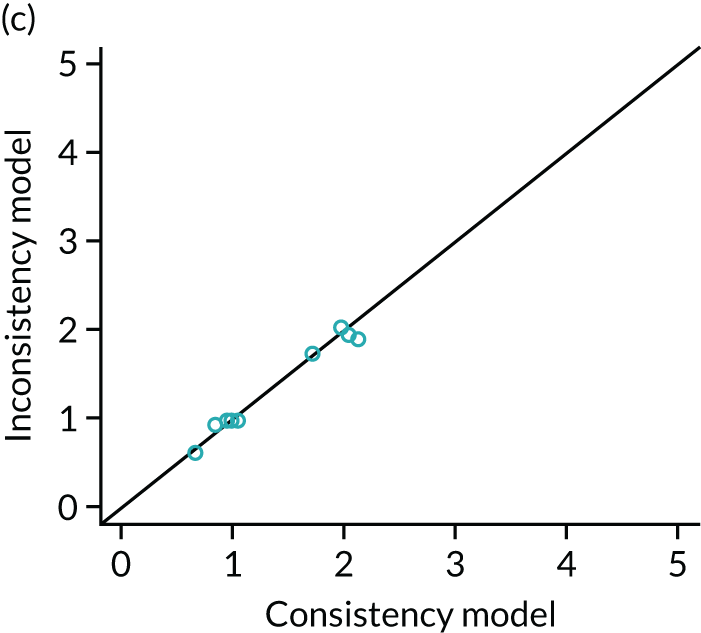
Impact
FIGURE 81.
Individual data points’ posterior mean deviance contributions for the consistency model and the inconsistency model along with the line of equality: (a) post treatment; (b) short term; and (c) long term. Note: at short term, 4 is for Cuesta-Vargas et al. 118 comparing guided self-help with multimodal.
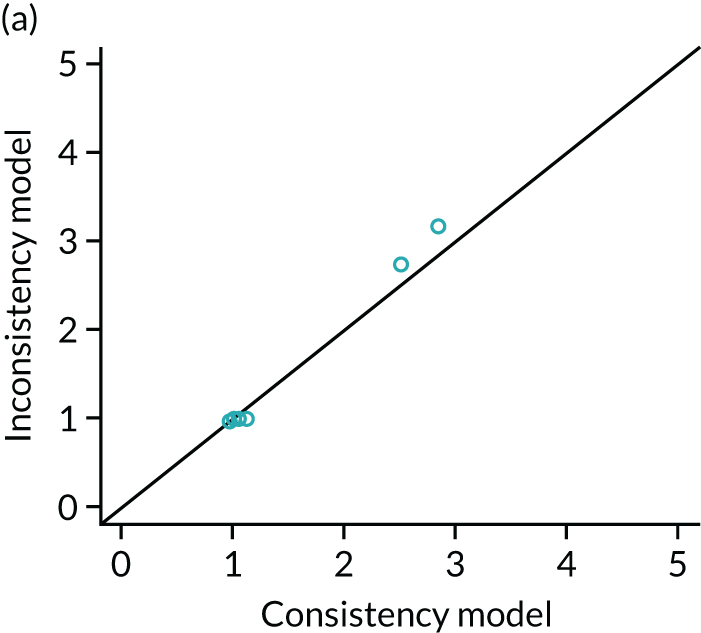


Emotional distress
FIGURE 82.
Individual data points’ posterior mean deviance contributions for the consistency model and the inconsistency model along with the line of equality: (a) post treatment; (b) short term; and (c) long term. Note: at post treatment, 2 is for Ho et al. 150 comparing usual care with RSSE; at short term 1 is for Cuesta-Vargas et al. 118 comparing guided self-help with multimodal.

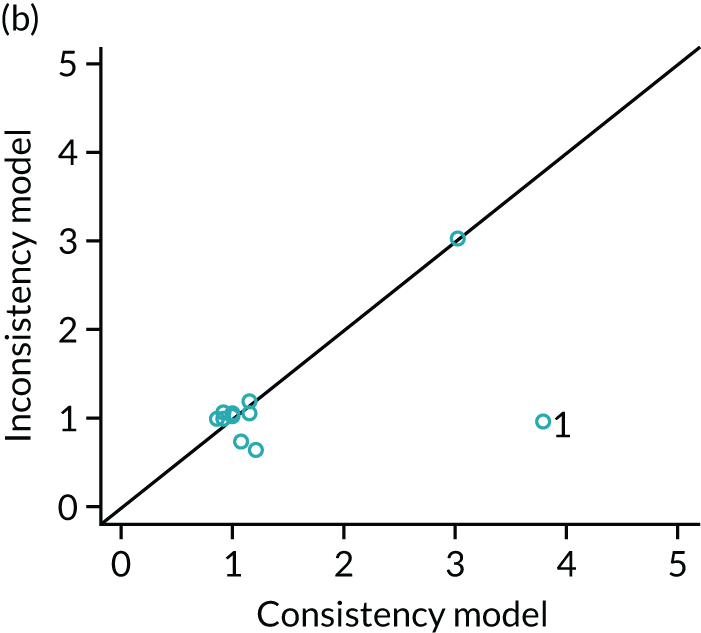
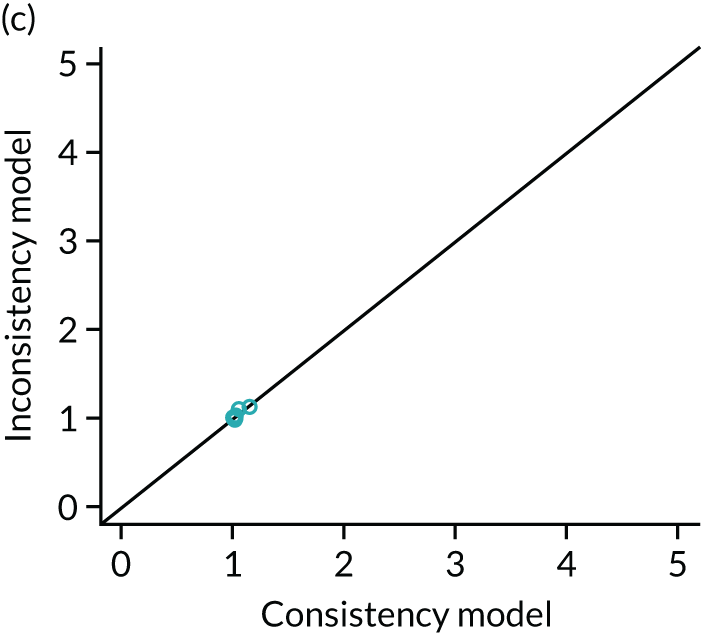
Anxiety
FIGURE 83.
Individual data points’ posterior mean deviance contributions for the consistency model and the inconsistency model along with the line of equality: (a) post treatment; (b) short term; and (c) long term.
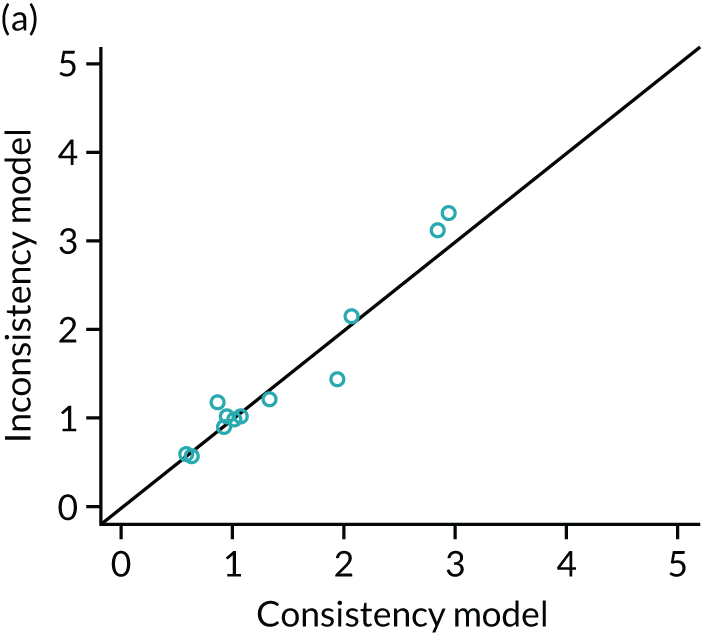
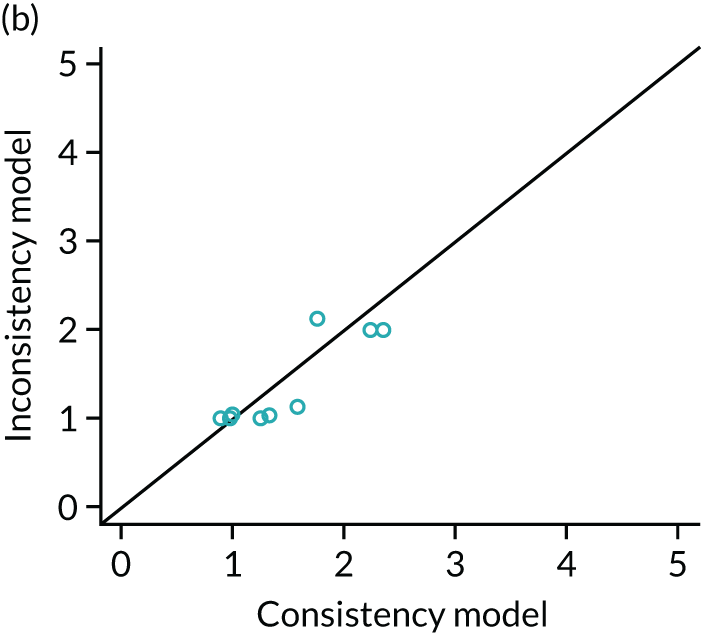
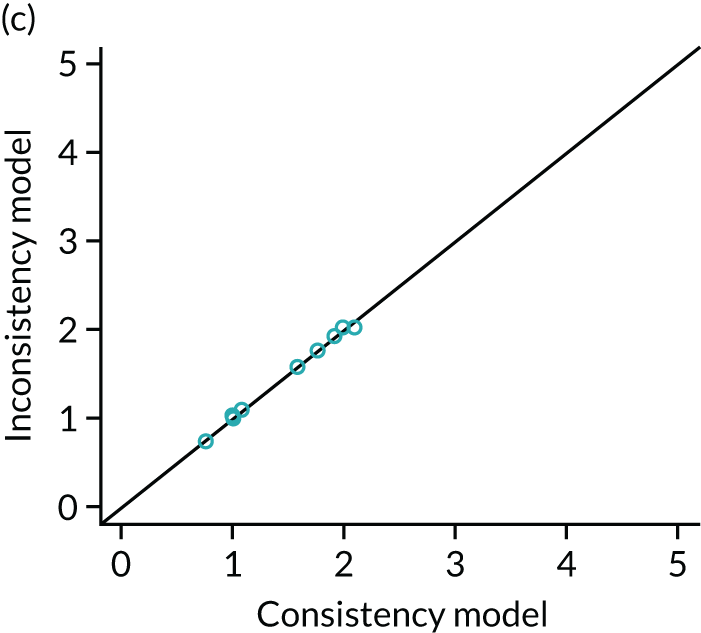
Depression
FIGURE 84.
Individual data points’ posterior mean deviance contributions for the consistency model and the inconsistency model along with the line of equality: (a) post treatment, (b) short term; and (c) long term. Note: at short term 12 is Luciano et al. 138 comparing usual care with medication and CBTHI.

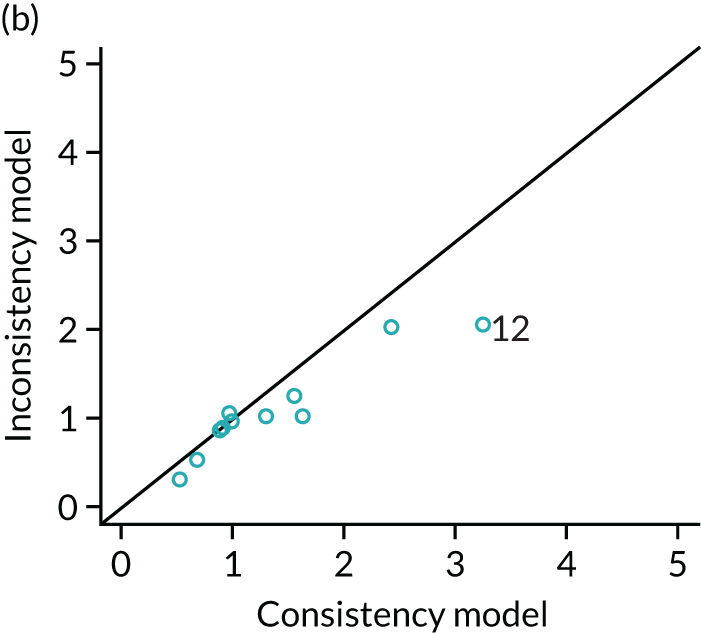
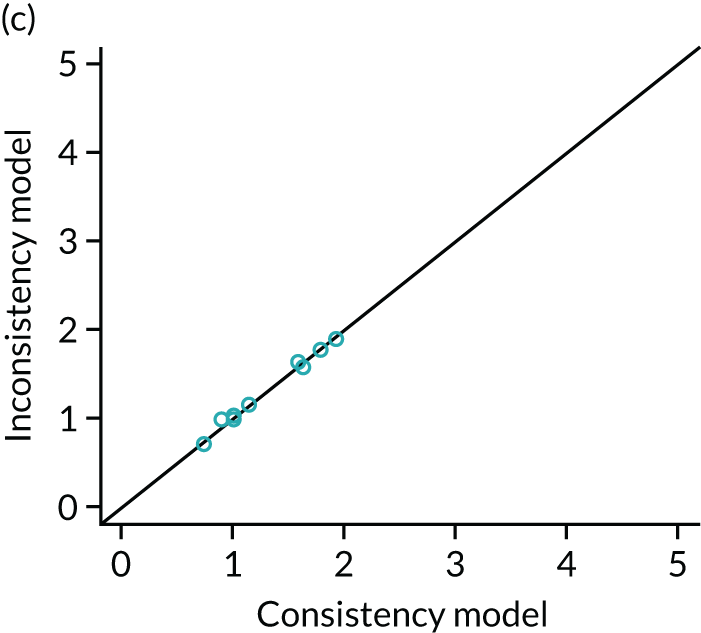
Appendix 14 Update of the review
An update of all the searches was conducted in order to identify new studies published since the original searches. This appendix describes the updated search strategies for each review: clinical effectiveness, qualitative and cost-effectiveness. The realist synthesis was also updated. All results are presented in this appendix as a narrative synthesis. No additional statistical analyses have been undertaken.
Update search strategies
Clinical effectiveness
An updated search was carried out in February 2019 on the same databases as the original search, excluding DARE, which is no longer updated (from April 2015). The search strategies and search filters from the original searches were used. Searches were limited to November 2015 onwards when possible.
Qualitative
An updated search was carried out in February 2019 on the same databases as the original search. The search strategies and search filters from the original searches were used. Searches were limited to July 2016 onwards when possible.
Economic
An update search was run in March 2019 on the same databases as the original search, excluding NHS Economic Evaluation Database, which is no longer updated (from April 2015). The search strategies and search filters from the original searches were used. Searches were limited to August 2016 onwards when possible.
Full details of these amendments are detailed below for each database.
MEDLINE
-
Clinical Effectiveness: AND (2015 11* or 2015 12* or 2016* or 2017* or 2018* or 2019*).dt
-
Qualitative: (2016 07* or 2016 08* or 2016 09* or 2016 10* or 2016 11* or 2016 12* or 2017* or 2018* or 2019*).dt.
-
Economic: (2016 08* or 2016 09* or 2016 10* or 2016 11* or 2016 12* or 2017* or 2018* or 2019*).dt
EMBASE
-
Clinical Effectiveness: AND (2015 11* or 2015 12* or 2016* or 2017* or 2018* or 2019*).dc.
-
Qualitative: (2016 07* or 2016 08* or 2016 09* or 2016 10* or 2016 11* or 2016 12* or 2017* or 2018* or 2019*).dc.
-
Economic: (2016 08* or 2016 09* or 2016 10* or 2016 11* or 2016 12* or 2017* or 2018* or 2019*).dc
CINAHL
-
Clinical Effectiveness: Limiters – Published Date: 11 January 2015–31 December 2019
-
Qualitative: Limiters – Published Date: 7 January 2016–31 December 2019
-
Economic: Limiters – Published Date: 8 January 2016–31 December 2019
PsycINFO
-
Clinical Effectiveness: limit to yr=“2015 -Current”
-
Qualitative: limit 115 to yr=“2016 -Current”
-
Economic: limit 141 to yr=“2016 -Current”
Cochrane
Clinical effectiveness:
-
Note that #75 was edited to (somatisation or somatization):ti,ab because of database changes (the original #75 when re-run retrieved over 1 million records).
-
CDSR: the Cochrane Library publication date between November 2015 and February 2019.
-
CENTRAL: publication year from 2015 to 2019, in Trials.
-
Note that the HTA database was searched via the CRD website at: https://www.crd.york.ac.uk/CRDWeb/ because it was no longer accessible via the Cochrane Library. Limits applied: * WHERE LPD FROM 01/11/2015 TO 07/03/2019 (note the HTA database has not been updated since 31/03/2018).
Web of Science
-
Clinical Effectiveness: Indexes=SCI-EXPANDED, SSCI Timespan=2015-2019.
-
Qualitative: Indexes=SCI-EXPANDED, SSCI Timespan=2016-2019.
-
Economic: Timespan: 2016-2019. Indexes: SCI-EXPANDED, SSCI.
Update of clinical effectiveness studies
This section provides an overview of the clinical effectiveness literature published since the original searches were performed. In addition, new evidence on the effectiveness of behavioural interventions for MUS is outlined. The review methods applied were consistent with those reported in Chapter 3, with the exception that only a narrative synthesis of newly included studies is presented. No additional statistical analyses have been conducted. A second reviewer (AS) has checked data extractions and quality assessments for included studies. The results of the review update are presented below.
Results
A total of 3192 unique citations were identified in the searches. There were 132 remaining after the title and abstract sift, and these citations were considered at full-paper sift for the clinical effectiveness review update. Figure 85 shows the flow chart of studies included in the clinical effectiveness review update. The sifting process resulted in the inclusion of two published studies328,517 and one unpublished study. 373,374 Details of studies excluded at full-paper sift together with reasons are shown in Table 127. All data from O’Dowd373,374 are taken from the protocol registered on the ISRCTN trial registry, with outcome data retrieved from an additional file uploaded to the registry on 27 March 2019. Data were accessed on 2 May 2019. Further information was obtained from a previous freedom of information request published in 2016. Although only three new studies were identified, several potentially relevant protocols have been registered since the original searches. No published studies of any of the functional somatic syndromes were identified, although the O’Dowd373,374 study is in a population of patients with chronic fatigue. Reasons for exclusion of these studies were often that, although the focus of the study was a behavioural intervention, these were conducted in secondary care settings. Many studies of chronic pain were identified; however, none is included as they did not meet the inclusion criteria for ‘unexplained’. Eligibility criteria for studies of behavioural interventions for chronic pain often specified persistence/duration of pain, but did not exclude by cause (other than severe pathology/cancer). The three included studies were relatively small. Larger-scale studies were identified but these tended to be cohort studies rather than randomised controlled trials.
FIGURE 85.
The 2009 PRISMA flow diagram: updated clinical effectiveness review.
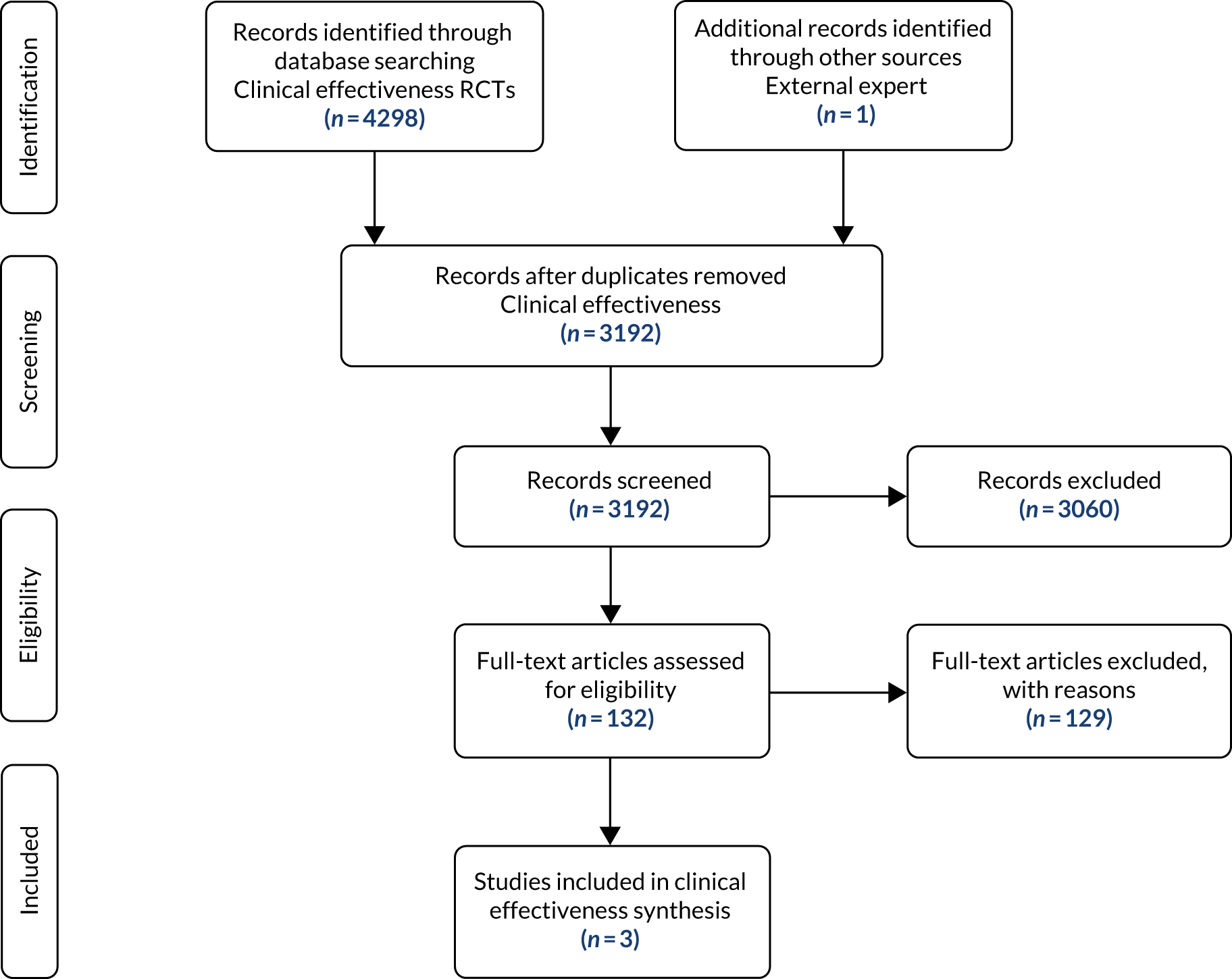
Two of the three studies were randomised controlled trials of populations of patients with ‘MUS’,328,517 and the remaining study373,374 was for patients with unexplained fatigue, randomising a total of 161 participants. Wortman517 was a pilot feasibility study of a brief multimodal psychosomatic therapy delivered by physiotherapists and exercise therapists in primary care. Ziadni et al. 328 was a trial of a life stress, emotional awareness and expression interview for primary care patients. In both studies, the interventions were compared with usual care. Tables 108–117 present the study characteristics of the two trials. Although both studies were of patients with ‘MUS’, diagnostic criteria were different between studies. Wortman et al. 517 required participants to consult with their primary care physician more than once with one of a specified range of symptoms where a cause could not be found, whereas Ziadni et al. 328 required a score of > 10 on the PHQ-15 with no known cause of the symptoms identified. The behavioural intervention delivered in the trial by Ziadni et al. 328 was a one-off 90-minute interview, whereas the trial by Wortman et al. 517 delivered the intervention over a maximum of nine 45-minute sessions. The unpublished study by O’Dowd373,374 investigated the feasibility and acceptability of an early intervention based on the principles of cognitive–behavioural therapy and graded exercise for primary care patients with fatigue of duration 1–4 months. Eligible patients were identified by their GP. The intervention included a 1-hour appointment with a fatigue specialist, an information booklet and three 20-minute telephone support sessions, and was compared with standard care by a GP.
| First author and year of publication | Condition | Intervention | Intervention description | Grouping |
|---|---|---|---|---|
| Wortman, 2016517 | MUS/SD | Brief multimodal psychosomatic therapy | Multicomponent approach focusing on the combination of physical, psychological and behavioural symptoms of stress in order to reduce bodily symptoms and to empower patients to assert control over factors that affect their health. Consists of (1) psychoeducation, (2) relaxation therapy and mindfulness, (3) cognitive–behavioural approaches and (4) activation therapy | MM |
| Usual care | Usual care provided by the GP and other HPs | UC | ||
| Ziadni, 2018328 | MUS/SD | Life stress, emotional awareness and expression interview | An interview aimed to help patients with MUS to:
|
OP |
| Treatment as usual | ‘Delayed interview’: treatment as usual until follow-up measures complete, then offered the intervention | UC | ||
| O’Dowd, unpublished373,374 | Unexplained fatigue | Early intervention | A package of advice and support that could be offered early, for patients with a short history of fatigue (1–4 months). The intervention was based on the principles of CBT and graded exercise | Uncleara |
| Standard care | Standard care by a GP | UC |
| First author and year of publication | Condition | Diagnostic criteria | Diagnosis by |
|---|---|---|---|
| Wortman, 2016517 | MUS/SD | Patients consulting their practice more than once for one or more of the following where no organic pathology could be found: stomach/abdominal pain, back/neck/shoulder pain, pain in arms/legs/joints, headache, chest pain, dizziness, fainting spells, palpitations of the heart, shortness of breath, nausea/indigestion, feeling tired and sleeping disorders | GP |
| Ziadni, 2018328 | MUS/SD | Patients scoring > 10 (moderate) on the PHQ-15, with exclusion of disease or injury that might account for elevated somatic symptoms | Primary care clinicians + study researcher |
| O’Dowd, unpublished373,374 | Unexplained fatigue | Patients presenting with an unexplained primary complaint of fatigue, as a new episode, lasting > 1 month but < 4 months. Score of > 4 on the Chalder Fatigue Scale | GP + trial manager |
| First author and year of publication | Condition | Primary outcomes | Secondary outcomes |
|---|---|---|---|
| Wortman, 2016517 | MUS/SD |
Patient satisfaction with received therapy: five-point Likert scale (dissatisfied to very satisfied) Perceived symptom severity: VAS range 0–10 where 10 represents most severe symptoms Distress: self-rated symptoms of distress, depression, anxiety and somatisation – Four-Dimensional Symptom Questionnaire Hyperventilation: Nijmegen Hyperventilation List (NHL)518 Physical and mental health status and quality of life: SF-36519 |
|
| Ziadni, 2018328 | MUS/SD |
Pain severity: Brief Pain Inventory – Short Form448 Pain interference: Brief Pain Inventory – Short Form448 |
Sleep problems: Insomnia Severity Index520 Psychological symptoms: Brief Symptom Inventory500 |
| O’Dowd, unpublished373,374 | Unexplained fatigue | Recruitment, adherence and follow-up | Chalder Fatigue Score;385 pain VAS; physical Function (SF-36); anxiety (HADS); depression (HADS); EQ-5D-5L; hours missed from work because of health problems in the past 7 days; health problems affected productivity while working in the past 7 daysa |
| First author and year of publication | Condition | Pain | Fatigue | Bowel symptoms | Somatisation | Generic physical symptoms | Emotional distress | Anxiety | Depression | Physical functioning | Impact |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Wortman, 2016517 | MUS/SD | ✗ | ✗ | ✗ | 4DSQ | Symptom severity (VAS) | 4DSQ and SF-36 | 4DSQ | 4DSQ | SF-36 | ✗ |
| Ziadni, 2018328 | MUS/SD | BPI-SF | ✗ | ✗ | ✗ | ✗ | BSI | ✗ | ✗ | ✗ | ✗ |
| O’Dowd, unpublished373,374 | Unexplained fatigue | VAS | CFS | ✗ | ✗ | ✗ | ✗ | HADS | HADS | SF-36 | ✗ |
| First author and year of publication | Baseline | End of treatment (duration, months) | Short term (time since end of treatment, months) | Long term (time since end of treatment, months) |
|---|---|---|---|---|
| Wortman, 2016517 | Y | 3 | 6 | 12 |
| Ziadni, 2018328 | Y | 1.38 | ||
| O’Dowd, unpublished373,374 | Unclear | 3 | 6 |
| First author and year of publication | Condition | Setting | Setting: referral | Setting: assessment | Setting: intervention | Setting: outcome assessment |
|---|---|---|---|---|---|---|
| Wortman, 2016517 | MUS/SD | Primary care | Recruited by GPs (six practices) | NR | NR | NR |
| Ziadni, 2018328 | MUS/SD | Primary care | Family medicine clinic | Primary care clinic | Primary care clinic | Home-based online questionnaires |
| O’Dowd, unpublished373,374 | Unexplained fatigue | Primary care | GP practices | GP practices | Unclear setting for 1-hour appointment with fatigue specialist. 20-minute support sessions by telephone | NR |
| First author and year of publication | Condition | Total n | Arms | Interventions | Assessment points |
|---|---|---|---|---|---|
| Wortman, 2016517 | MUS/SD | 42 randomised | 2 | MM vs. UC | Baseline, end of intervention (3 months), 6 months, 12 months |
| Ziadni, 2018328 | MUS/SD | 75 randomised | 2 | OP vs. UC | Baseline, 6 weeks |
| O’Dowd, unpublished373,374 | Unexplained fatigue | 44 randomised | 2 | EI vs. UCa | 3 months and 6 monthsb |
| First author and year of publication | Condition | Intervention 1 delivery: duration of sessions | Intervention 3 delivery: duration of sessions | Intervention 2 delivery: duration of sessions |
|---|---|---|---|---|
| Wortman, 2016517 | MUS/SD | 45 minutes | N/A | N/A |
| Ziadni, 2018328 | MUS/SD | 90 minutes | N/A | N/A |
| O’Dowd, unpublished373,374 | Unexplained fatigue | 1 hour + 3 × 20 minutes | N/A | N/A |
| First author and year of publication | Condition | Intervention 1 delivery: number of sessions | Intervention 3 delivery: number of sessions | Intervention 2 delivery: number of sessions | Intervention 1 delivery: time period | Intervention 3 delivery: time period | Intervention 2 delivery: time period |
|---|---|---|---|---|---|---|---|
| Wortman, 2016517 | MUS/SD | 9 sessions | N/A | N/A | 3 months | N/A | 3 months |
| Ziadni, 2018328 | MUS/SD | 1 session | N/A | N/A | Within 1 week of baseline assessments | N/A | N/A |
| O’Dowd, unpublished373,374 | Unexplained fatigue | 1 + 3 telephone support sessions | N/A | N/A | NR | N/A | N/A |
| First author and year of publication | Condition | Intervention 1 provider: position | Intervention 3 provider: position | Intervention 2 provider: position | Intervention 1 provider: time spent on delivery | Intervention 3 provider: time spent on delivery | Intervention 2 provider: time spent on delivery |
|---|---|---|---|---|---|---|---|
| Wortman, 2016517 | MUS/SD | Physiotherapists and exercise therapists | N/A | GP | 9 × 45 minutes | N/A | N/A |
| Ziadni, 2018328 | MUS/SD | Doctoral students in clinical psychology | N/A | Family clinic physician | 90 minutes | N/A | N/A |
| O’Dowd, unpublished373,374 | Unexplained fatigue | Fatigue specialist | N/A | GP | 1 hour + 3 × 20 minutes | N/A | N/A |
Tables 118–126 report the outcomes measured in the three trials, with their associated means/SDs across follow-up time points. Ziadni et al. 328 and Wortman et al. 517 measured emotional distress. Both studies reported significant improvements for participants receiving the behavioural interventions compared with usual care. For other outcomes, Ziadni et al. 328 and O’Dowd373,374 measured pain; Wortman et al. 517 and O’Dowd373,374 measured anxiety, depression and physical functioning; whereas Wortman et al. 517 was the only study to measure symptom severity and somatisation. Ziadni et al. 328 reported significant improvements for both pain and emotional distress. Wortman et al. ,517 although not powered to detect treatment effects, reported the potential for their intervention to achieve significant improvements in symptoms. Only Wortman et al. 517 measured patient satisfaction, reporting that 81% of patients were very satisfied with treatment; however, two patients were dissatisfied and disappointed with the treatment.
| Pain | |||||
|---|---|---|---|---|---|
| First author and year of publication | Intervention group | Baseline mean/SD | Time 1 mean/SD | Time 2 mean/SD | Summary |
| Wortman, 2016517 | Outcome not measured | ||||
| Ziadni, 2018328 |
OP UC |
4.91 (2.17)a 4.82 (2.24)a |
4.12 (2.46)a 4.95 (1.83)a |
NR | Patients in interview condition (OP) had a significantly lower-pain severity at follow-up than treatment as usual (UC), with a medium to large between-condition effect |
| O’Dowd, unpublished373,374 |
EI UC |
NR |
22.1 (8.5 to 35.7)b 18.9 (5.8 to 31.9)b |
NR | Baseline data not reported. Pain was no different between the two groups at the end of the study |
| Somatisation | |||||
|---|---|---|---|---|---|
| First author and year of publication | Intervention group | Baseline mean/SD | Time 1 mean/SD | Time 2 mean/SD | Summary |
| Wortman, 2016517 |
MM UC |
11.7 (6.5) 10.9 (6.9) |
8.5 (8.3) 10.1 (6.3) |
7.5 (7.5) 11.5 (7.4) |
Significant improvement in somatisation at each time point for brief multimodal psychosomatic therapy group compared with usual care group |
| Ziadni, 2018328 | Outcome not measured | ||||
| O’Dowd, unpublished373,374 | Outcome not measured | ||||
| Fatigue | |||||
|---|---|---|---|---|---|
| First author and year of publication | Intervention group | Baseline mean/SD | Time 1 mean/SD | Time 2 mean/SD | Summary |
| O’Dowd, unpublished373,374 |
EI UC |
NR |
12.3 (9.3, 15.3) 14.7 (10.6, 18.9) |
NR | Baseline data not reported. Fatigue was no different between the two groups at the end of the study |
| Wortman, 2016517 | Outcome not measured | ||||
| Ziadni, 2018328 | Outcome not measured | ||||
| Generic physical symptoms | |||||
|---|---|---|---|---|---|
| First author and year of publication | Intervention group | Baseline mean/SD | Time 1 mean/SD | Time 2 mean/SD | Summary |
| Wortman, 2016517 |
MM UC |
5.9 (2.4) 5.3 (2.9) |
3.9 (3.0) 4.9 (2.6) |
3.1 (2.5) 5.0 (2.4) |
Significant improvement in somatisation at each time point for brief multimodal psychosomatic therapy group compared with the usual care group |
| Ziadni, 2018328 | Outcome not measured | ||||
| O’Dowd, unpublished373,374 | Outcome not measured | ||||
| Emotional distressa | |||||
|---|---|---|---|---|---|
| First author and year of publication | Intervention group | Baseline mean/SD | Time 1 mean/SD | Time 2 mean/SD | Summary |
| Wortman, 2016517 |
MM UC |
49.2 (11.3) 50.7 (10.3) |
51.8 (8.3) 48.6 (11.7) |
50.7 (8.4) 49.5 (10.1) |
Significance not reported, low effect size |
| Ziadni, 2018328 |
OP UC |
1.27 (0.83)b 1.27 (0.85)b |
0.87 (0.87)b 1.29 (0.70)b |
Patients in interview condition (OP) had significantly less psychological symptoms at follow-up than treatment as usual (UC), with a medium between-condition effect | |
| O’Dowd, unpublished373,374 | Outcome not measured | ||||
| Anxiety | |||||
|---|---|---|---|---|---|
| First author and year of publication | Intervention group | Baseline mean/SD | Time 1 mean/SD | Time 2 mean/SD | Summary |
| Wortman, 2016517 |
MM UC |
3.3 (3.6) 2.4 (4.3) |
2.4 (3.9) 2.4 (3.6) |
2.6 (4.4) 2.8 (4.7) |
Significance not reported, low effect size |
| O’Dowd, unpublished373,374 |
EI UC |
NR |
7.8 (5.4, 10.3) 7.8 (4.9, 10.6) |
NR | Baseline data not reported. No difference between groups at the end of the study |
| Ziadni, 2018328 | Outcome not measured | ||||
| Depression | |||||
|---|---|---|---|---|---|
| First author and year of publication | Intervention group | Baseline mean/SD | Time 1 mean/SD | Time 2 mean/SD | Summary |
| Wortman, 2016517 |
MM UC |
1.9 (3.4) 0.9 (1.6) |
1.4 (2.3) 0.9 (1.7) |
0.9 (1.8) 0.6 (1.4) |
Significance not reported, low effect size |
| O’Dowd, unpublished373,374 |
EI UC |
NR |
4.9 (3.0, 6.9) 4.6 (2.9, 6.2) |
NR | Baseline data not reported. No difference between groups at the end of the study |
| Ziadni, 2018328 | Outcome not measured | ||||
| Physical functioning | |||||
|---|---|---|---|---|---|
| First author and year of publication | Intervention group | Baseline mean/SD | Time 1 mean/SD | Time 2 mean/SD | Summary |
| Wortman, 2016517 |
MM UC |
51.6 (9.0) 48.5 (10.2) |
49.6 (10.4) 50.3 (10.1) |
51.9 (9.1) 48.5 (10.2) |
Significance not reported, low effect size |
| O’Dowd, unpublished373,374 |
EI UC |
NR |
76.8 (65.1, 88.4) 84.4 (72.4, 96.3) |
NR | NR |
| Ziadni, 2018328 | Outcome not measured | ||||
| Acceptability | ||
|---|---|---|
| First author and year of publication | Intervention group | Summary |
| Wortman, 2016517 | MM vs. UC |
16/82 of those screened for eligibility declined to participate. In MM group, 16/20 received intervention and completed first follow-up (2/4 withdrew consent after allocation, of whom 1/4 withdrew because of psychological symptoms, and 1/4 withdrew as a result of physical disease explaining their symptoms). In the UC care group, 2/22 withdrew consent after allocation because of ‘too much MUS complaints’, 2/22 were deviations from protocol and received MM. No further loss to follow-up In the MM group, 81% of patients were very satisfied with treatment and reported that it had helped them deal with their problems more effectively. One patient had a neutral opinion. Two patients were dissatisfied and disappointed with the treatment and continued to seek an explanation for their symptoms |
| Ziadni, 2018328 | OP vs. UC | 12.9% of eligible patients were not interested or able to participate in the study. 2/49 patients randomised to the interview intervention did not respond to scheduling requests and did not receive an interview. 6/49 in OP group were lost to follow-up, 2/26 in UC group were lost to follow-up |
| O’Dowd, unpublished373,374 | EI vs. UC | 11/90 of those assessed for eligibility declined to participate. 9/28 of those randomised were lost to follow-up, of whom two gave reasons: both reasons were ‘not accepting of the therapeutic model’ |
Risk of bias
Risk of bias in the included studies was explored using the Cochrane risk-of-bias tool. 87 Individual risk-of-bias summaries are presented in Update of the cost-effectiveness review. As the O’Dowd373,374 study is unpublished, study information was obtained from what was available publicly, and this was insufficient to complete most of the risk-of-bias tool, although a high risk of bias was found for attrition, with a 32% attrition rate. For the remaining trials, neither study blinded participants to the treatment nor reported assessor blinding. Wortman et al. 517 reported an attrition rate of 20%, which represented a high risk of bias. Both studies demonstrated adequate randomisation procedures.
Discussion
Three additional trials were identified in the update of clinical effectiveness. Two showed positive results for behavioural interventions,328,517 with the remaining study showing no positive results for clinical outcomes. 373,374 Some issues that were identified in the original review were raised again; for example, there was wide variation in the number of eligible patients identified by individual GPs in Wortman et al. 517 As a result of a lack of potentially eligible participants being identified, the recruitment of additional GPs was needed for the study. In addition, the possibility of misdiagnosis was raised, with one patient in the intervention group in Wortman et al. 517 discontinuing the study because of a physical disease being identified that explained the symptoms experienced. This issue was previously identified as a concern for both patients and GPs in the original review. A lack of standardised reporting of adverse events means that drawing conclusions on the type and nature of adverse events associated with these behavioural interventions is not possible. The O’Dowd373,374 study did record adverse events, with no expected adverse events recorded and one unexpected adverse event (an accident and emergency admission for cardiac symptoms). Finally, a high rate of attrition was seen in two of the studies, which suggests that these types of interventions are unacceptable to some patients.
Tables 118–126 show means, SDs and narrative summary for each outcome.
Risk-of-bias assessments for each study
| Wortman 2016517 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Computer-generated permuted block randomisation table | Low risk of bias, adequate randomisation |
| Allocation concealment | Research assistant responsible for randomisation not aware of health status of patient. ID numbers for patients only matched with corresponding name after randomisation | Low risk of bias, adequate allocation concealment |
| Performance bias | ||
| No blinding of patients or GPs | High risk of bias, no blinding of patients or providers | |
| Detection bias | ||
| Blinding of outcome assessors not described | Unclear risk of bias | |
| Attrition bias | ||
| In the intervention group, 4/20 did not complete the study compared with 2/22 in the UC group. ITT analyses conducted | High risk of bias. 20% attrition in intervention group | |
| Reporting bias | ||
| All outcomes in protocol reported in study paper | Low risk of bias | |
| Ziadni 2018328 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | Computer-based randomisation scheme | Low risk of bias |
| Allocation concealment | Research assistant opened a sealed envelope at allocation | Low risk of bias, sealed envelope methods employed |
| Performance bias | ||
| No blinding of patients | High risk of bias, no blinding possible | |
| Detection bias | ||
| Blinding of outcome assessor not described | Unclear risk of bias | |
| Attrition bias | ||
| 6/49 lost to follow-up in OP group. ITT analysis conducted | Low risk of bias, attrition < 20% | |
| Reporting bias | ||
| Primary outcome reported as Symptom Interpretation Questionnaire in protocol, but as pain severity and interference in study paper. Not all secondary outcomes reported in study paper | High risk of bias. Not all outcomes described in protocol reported | |
| O’Dowd unpublished373,374 | ||
|---|---|---|
| Domain | Support for judgement | Reviewer judgement |
| Selection bias | ||
| Random sequence generation | NR | Unclear risk of bias |
| Allocation concealment | NR | Unclear risk of bias |
| Performance bias | ||
| NR | Unclear risk of bias | |
| Detection bias | ||
| NR | Unclear risk of bias | |
| Attrition bias | ||
| 9/28 in the intervention group lost to follow-up | High risk of bias. Attrition > 20% | |
| Reporting bias | ||
| Secondary outcomes not described in the protocol | Unclear risk of bias. Unknown secondary outcomes in protocol | |
| Yamato TP, Maher CG, Saragiotto BT, Hancock MJ, Ostelo RW, Cabral CM, et al. Pilates for low back pain. São Paulo Med J 2016;134:366 | Review |
| TelePain: improving primary care pain management. Conference: 36th Annual Scientific Meeting of the American Pain Society, USA, 2017. J Pain 2017;18(Suppl. 1):S67–8 | Conference abstract only |
| Champagne R, Ronzi Y, Roche-Leboucher G, Begue C, Dubus V, Bontoux L, et al. Effectiveness of an outpatient rehabilitation program with multidisciplinary approach on return to work for patients with non-specific chronic lombal pain. Annals of Physical and Rehabilitation Medicine 2018;61:e16 | Conference abstract only |
| Abbott A, Schröder K, Enthoven P, Nilsen P, Öberg B. Effectiveness of implementing a best practice primary healthcare model for low back pain (BetterBack) compared with current routine care in the Swedish context: an internal pilot study informed protocol for an effectiveness-implementation hybrid type 2 trial. BMJ Open 2018;8:e019906. https://doi.org/10.1136/bmjopen-2017-019906 | Protocol only |
| Adamse C, Dekker-Van Weering MG, van Etten-Jamaludin FS, Stuiver MM. The effectiveness of exercise-based telemedicine on pain, physical activity and quality of life in the treatment of chronic pain: a systematic review. J Telemed Telecare 2018;24:511–26. https://doi.org/10.1177/1357633X17716576 | Review |
| Alda M, Luciano JV, Andrés E, Serrano-Blanco A, Rodero B, del Hoyo YL, et al. Effectiveness of cognitive behaviour therapy for the treatment of catastrophisation in patients with fibromyalgia: a randomised controlled trial. Arthritis Res Ther 2011;13:R173. https://doi.org/10.1186/ar3496 | Included in original review |
| Amirova A, Cropley M and Theadom A. The effectiveness of the Mitchell method relaxation technique for the treatment of fibromyalgia symptoms: a three-arm randomized controlled trial. Int J Stress Manage 2017;24:86–106. https://doi.org/10.1037/str0000017 | Not primary care |
| Amorim AB, Pappas E, Simic M, Ferreira ML, Jennings M, Tiedemann A, et al. Integrating Mobile-health, health coaching, and physical activity to reduce the burden of chronic low back pain trial (IMPACT): a pilot randomised controlled trial. BMC Musculoskelet Disord 2019;20:71. https://doi.org/10.1186/s12891-019-2454-y | Not primary care |
| Andersen LL, Persson R, Jakobsen MD, Sundstrup E. Psychosocial effects of workplace physical exercise among workers with chronic pain: randomized controlled trial. Medicine 2017;96:e5709. https://doi.org/10.1097/MD.0000000000005709 | Does not meet criteria for unexplained symptoms |
| Andersen LN, Juul-Kristensen B, Sørensen TL, Herborg LG, Roessler KK, Søgaard K. efficacy of tailored physical activity or chronic pain self-management programme on return to work for sick-listed citizens: a 3-month randomised controlled trial. Scand J Public Health 2015;43:694–703. https://doi.org/10.1177/1403494815591687 | Protocol only |
| Angelovski A, Sattel H, Henningsen P, Sack M. Heart rate variability predicts therapy outcome in pain-predominant multisomatoform disorder. J Psychosom Res 2016;83:16–21. https://doi.org/10.1016/j.jpsychores.2016.02.003 | Not primary care |
| Aragonès E, López-Cortacans G, Caballero A, Piñol JL, Sánchez-Rodríguez E, Rambla C, et al. Evaluation of a multicomponent programme for the management of musculoskeletal pain and depression in primary care: a cluster-randomised clinical trial (the DROP study). BMC Psychiatry 2016;16:69. https://doi.org/10.1186/s12888-016-0772-2 | Protocol only |
| Azevedo DC, Van Dillen LR, Santos Hde O, Oliveira DR, Ferreira PH, Costa LO. Movement system impairment-based classification versus general exercise for chronic low back pain: protocol of a randomized controlled trial. Phys Ther 2015;95:1287–94. https://doi.org/10.2522/ptj.20140555 | Protocol only |
| Baird E, Williams ACC, Hearn L, Amris K. Interventions for treating persistent pain in survivors of torture. Cochrane Database Syst Rev 2017;8:CD012051. https://doi.org/10.1002/14651858.CD012051.pub2 | Review |
| Baumueller E, Winkelmann A, Irnich D, Weigl M. Electromyogram biofeedback in patients with fibromyalgia: a randomized controlled trial. Complement Med Res 2017;24:33–9. https://doi.org/10.1159/000454692 | Not primary care |
| Ben-Ami N, Chodick G, Mirovsky Y, Pincus T, Shapiro Y. Increasing recreational physical activity in patients with chronic low back pain: a pragmatic controlled clinical trial. J Orthop Sports Phys Ther 2017;47:57–66. https://doi.org/10.2519/jospt.2017.7057 | Not primary care |
| Ben-Ami N, Shapiro Y, Pincus T. Outcomes in distressed patients with chronic low back pain: subgroup analysis of a clinical trial. J Orthop Sports Phys Ther 2018;48:491–5. https://doi.org/10.2519/jospt.2018.7670 | Not primary care |
| Beneciuk JM, George SZ. Pragmatic implementation of a stratified primary care model for low back pain management in outpatient physical therapy settings: two-phase, sequential preliminary study. Phys Ther 2015;95:1120–34. https://doi.org/10.2522/ptj.20140418 | Does not meet criteria for unexplained symptoms |
| Bennell KL, Nelligan R, Dobson F, Rini C, Keefe F, Kasza J, et al. Effectiveness of an internet-delivered exercise and pain-coping skills training intervention for persons with chronic knee pain: a randomized trial. Ann Intern Med 2017;166:453–62. https://doi.org/10.7326/M16-1714 | Paper not available |
| Bier JD, Sandee-Geurts JJW, Ostelo RWJG, Koes BW, Verhagen AP. Can primary care for back and/or neck pain in the Netherlands benefit from stratification for risk groups according to the STarT back tool classification? Arch Phys Med Rehabil 2018;99:65–71 | Not a RCT |
| Brage, K., Ris, I., Falla, D., Søgaard, K., & Juul-Kristensen, B. (2015). Pain education combined with neck- and aerobic training is more effective at relieving chronic neck pain than pain education alone – a preliminary randomized controlled trial. Man Ther 20:686–93 | Not primary care |
| Bramberg EB, Bergstrom G, Jensen I, Hagberg J, Kwak L. Effects of yoga, strength training and advice on back pain: a randomized controlled trial. BMC Musculoskelet Disord 2017;18 | Not primary care |
| Braschinsky M, Haldre S, Kals M, Arge M, Saar B, Niibek M, Steiner TJ. Structured education to improve primary-care management of headache: how long do the benefits last? A follow-up observational study. Eur J Neurol 2018;25:497–502 | Does not meet criteria for unexplained symptoms |
| Braunger C, Kubiak N, Müller G, von Wietersheim J, Oster J. Effectiveness of telephone and face-to-face aftercare conversations following inpatient psychosomatic rehabilitation. Die Rehabil 54:290–6 | Not primary care |
| Calner T, Nordin C, Eriksson MK, Nyberg L, Gard G, Michaelson P. Effects of a self-guided, web-based activity programme for patients with persistent musculoskeletal pain in primary healthcare: a randomized controlled trial. Eur J Pain 2017;21:1110–20 | Does not meet criteria for unexplained symptoms |
| Canaway A, Pincus T, Underwood M, Shapiro Y, Chodick G, Ben-Ami N. Is an enhanced behaviour change intervention cost-effective compared with physiotherapy for patients with chronic low back pain? Results from a multicentre trial in Israel. BMJ Open 2018;8:e019928 | Does not meet criteria for unexplained symptoms |
| Cano-Garcia FJ, Gonzalez-Ortega MD, Sanduvete-Chaves S, Chacon-Moscoso S, Moreno-Borrego R. Evaluation of a psychological intervention for patients with chronic pain in primary care. Front Psychol 2017;8:435 | Not a RCT |
| Caravaca JMR, Martínez AC, Fuentes MCC. Es el masaje efectivo para reducir el dolor lumbar ocupacional de las enfermeras? Evidentia 2017;14:22 | Not a behavioural intervention |
| Carnes D, Mars T, Plunkett A, Nanke L, Abbey H. A mixed methods evaluation of a third wave cognitive behavioural therapy and osteopathic treatment programme for chronic pain in primary care (OsteoMAP). Int J Ostopath Med 2017;24:12–17. https://doi.org/10.1016/j.ijosm.2017.03.005 | Not a RCT |
| Cherkin D, Balderson B, Brewer G, Cook A, Talbert Estlin K, Evers SC, et al. Evaluation of a risk-stratification strategy to improve primary care for low back pain: the MATCH cluster randomized trial protocol. BMC Musculoskelet Disord 2016;17:1–11. https://doi.org/10.1186/s12891-016-1219-0 | Protocol only |
| Cherkin D, Balderson B, Wellman R, Hsu C, Sherman KJ, Evers SC, et al. Effect of low back pain risk-stratification strategy on patient outcomes and care processes: the MATCH randomized trial in primary care. J Gen Int Med 2018;33:1324–36 | Not a behavioural intervention |
| Cherkin DC, Sherman KJ, Balderson BH, Cook AJ, Anderson ML, Hawkes RJ, Turner JA. Effect of mindfulness-based stress reduction vs cognitive behavioral therapy or usual care on back pain and functional limitations in adults with chronic low back pain: a randomized clinical trial. JAMA 2016;315:240–9. https://doi.org/10.1001/jama.2016.2323 | Possibly include – check setting is primary care |
| Christensen SS, Frostholm L, Ornbol E, Schroder A. Changes in illness perceptions mediated the effect of cognitive behavioural therapy in severe functional somatic syndromes. J Psychosom Res 2015;78:363–70. https://doi.org/10.1016/j.jpsychores.2014.12.005 | Not primary care |
| Cuesta-Vargas AI, White M, Gonzalez-Sanchez M, Kuisma R. The optimal frequency of aquatic physiotherapy for individuals with chronic musculoskeletal pain: a randomised controlled trial. Disabil Rehab 2015;37:311-318. https://doi.org/10.3109/09638288.2014.918191 | Not all patients meet criteria for unexplained symptoms |
| Damush TM, Kroenke K, Bair MJ, Wu J, Tu W, Krebs EE, Poleshuck E. Pain self-management training increases self-efficacy, self-management behaviours and pain and depression outcomes. Eur J Pain 2016;20:1070–8. https://doi.org/10.1002/ejp.830 | Does not meet criteria for unexplained symptoms |
| Daulat A. A pragmatic randomized controlled trial to compare a novel group physiotherapy programme with a standard group exercise programme for managing chronic low back pain in primary care. Int Musculoskelet Med 2016;38:97–108. https://doi.org/10.1080/17536146.2016.1261234 | Paper not available |
| Davis K, Sargent L, Menzies V. Community-based care of the fibromyalgia patient: strategies to promote self-management. Home Healthc Now 2017;35:364–72. https://doi.org/10.1097/NHH.0000000000000570 | Review |
| den Hollander M, Goossens M, de Jong J, Ruijgrok J, Oosterhof J, Onghena P, Vlaeyen JWS. Expose or protect? A randomized controlled trial of exposure in vivo vs pain-contingent treatment as usual in patients with complex regional pain syndrome type 1. Pain 2016;157:2318–29. https://doi.org/10.1097/j.pain.0000000000000651 | Not primary care |
| den Hollander M, Heijnders N, De Jong JR, Vlaeyen JWS, Smeets R, Goossens M. Exposure in vivo versus pain-contingent physical therapy in complex regional pain syndrome type 1: a cost-effectiveness analysis. Int J Technol Assess Health Care 2018;34:400–9. https://doi.org/10.1017/s0266462318000429 | Tertiary care rehabilitation centre |
| Devasahayam, A J, Ho DRY, Leung EYS, Goh MR, Koh P. The effects of a novel pilates exercise prescription method on people with non-specific unilateral musculoskeletal pain: a randomised pilot trial. Proceedings of Singapore Healthcare 2016;25:201–6 | Not primary care |
| Domingo-Esteban S and Navas-Cámara FJ. [Posibles beneficios de la pinza rodada en el dolor y la incapacidad en la lumbalgia inespecífica crónica.] Fisioterapia 2017;39:60–7. https://doi.org/10.1016/j.ft.2016.09.001 | Not a behavioural intervention |
| Drane DL, LaRoche SM, Ganesh GA, Teagarden D, Loring DW. A standardized diagnostic approach and ongoing feedback improves outcome in psychogenic nonepileptic seizures. Epilepsy Behav 2016;54:34–9. https://doi.org/10.1016/j.yebeh.2015.10.026 | Not primary care |
| Dunleavy K, Kava K, Goldberg A, Malek MH, Talley SA, Tutag-Lehr V, Hildreth J. Comparative effectiveness of Pilates and yoga group exercise interventions for chronic mechanical neck pain: quasi-randomised parallel controlled study. Physiotherapy 2016;102:236–42. https://doi.org/10.1016/j.physio.2015.06.002 | Not a RCT |
| Eaton LH, Langford DJ, Meins AR, Rue T, Tauben DJ, Doorenbos AZ. Use of self-management interventions for chronic pain management: a comparison between rural and nonrural residents. Pain Manag Nurs 2018;19:8–13. | Does not meet criteria for unexplained symptoms |
| Elder CR, Debar LL, Ritenbaugh C, Rumptz MH, Patterson C, Bonifay A, et al. Health care systems support to enhance patient-centered care: lessons from a primary care-based chronic pain management initiative. Perm J 2017;21:16–101. https://doi.org/10.7812/TPP/16-101 | Outcomes not relevant |
| Ford AC, Lacy BE, Talley NJ. Irritable bowel syndrome. N Engl J Med 2017;376:2566–78. https://doi.org/10.1056/NEJMra1607547 | Review |
| Ford JJ, Hahne AJ, Surkitt LD, Chan AY, Richards MC, Slater SL, et al. Individualised physiotherapy as an adjunct to guideline-based advice for low back disorders in primary care: a randomised controlled trial. Br J Sports Med 2016;50:237–45. https://doi.org/10.1136/bjsports-2015-095058 | Pain duration includes subacute |
| Frederiksen P, Indahl A, Andersen LL, Burton K, Hertzum-Larsen R, Bendix T. Can group-based reassuring information alter low back pain behavior? A cluster-randomized controlled trial. PLOS ONE 2017;12:e0172003. https://doi.org/10.1371/journal.pone.0172003 | Intervention is for prevention |
| French SD, Green SE, Francis JJ, Buchbinder R, O’Connor DA, Grimshaw JM, Michie S. Evaluation of the fidelity of an interactive face-to-face educational intervention to improve general practitioner management of back pain. BMJ Open 2015;5:e007886. https://doi.org/10.1136/bmjopen-2015-007886 | Pain is acute |
| Frostholm L, Hornemann C, Ørnbøl E, Fink P, Mehlsen M. Using illness perceptions to cluster chronic pain patients: results from a trial on the chronic pain self-management program. Clin J Pain 2018;34:991–9. https://doi.org/10.1097/AJP.0000000000000627 | Not primary care |
| Gannon J, Atkinson JH, Chircop-Rollick T, D’Andrea J, Garfin S, Patel S, et al. Telehealth therapy effects of nurses and mental health professionals from 2 randomized controlled trials for chronic back pain. Clin J Pain 2019;35:295–303. https://doi.org/10.1097/AJP.0000000000000678 | Does not meet criteria for unexplained symptoms |
| Garcia AN, Costa L, Hancock MJ, Souza FS, Gomes G, Almeida MO, Costa LOP. McKenzie Method of Mechanical Diagnosis and Therapy was slightly more effective than placebo for pain, but not for disability, in patients with chronic non-specific low back pain: a randomised placebo controlled trial with short and longer term follow-up. Br J Sports Med 2018;52:594–600. https://doi.org/10.1136/bjsports-2016-097327 | Not primary care |
| Geraghty AW, Stanford R, Little P, Roberts L, Foster NE, Hill JC, et al. Using an internet intervention to support self-management of low back pain in primary care: protocol for a randomised controlled feasibility trial (SupportBack). BMJ Open 2015;5:e009524. https://doi.org/10.1136/bmjopen-2015-009524 | Protocol only |
| Goossens ME, de Kinderen RJ, Leeuw M, de Jong JR, Ruijgrok J, Evers SM, Vlaeyen JW. Is exposure in vivo cost-effective for chronic low back pain? A trial-based economic evaluation. BMC Health Serv Res 2015;15:549. https://doi.org/10.1186/s12913-015-1212-6 | Not primary care |
| Hahne AJ, Ford JJ, Richards MC, Surkitt LD, Chan AYP, Slater SL, Taylor NF. Who benefits most from individualized physiotherapy or advice for low back disorders? A preplanned effect modifier analysis of a randomized controlled trial. Spine 2017;42:E1215–E1224. https://doi.org/10.1097/BRS.0000000000002148 | Paper not available |
| Heapy AA, Higgins DM, Goulet JL, LaChappelle KM, Driscoll MA, Czlapinski RA, et al. Interactive voice response-based self-management for chronic back pain: the COPES noninferiority randomized trial. JAMA Intern Med 2017;177:765–73. https://doi.org/10.1001/jamainternmed.2017.0223 | Not primary care |
| Herman PM, Anderson ML, Sherman KJ, Balderson BH, Turner JA, Cherkin DC. Cost-effectiveness of mindfulness-based stress reduction versus cognitive behavioral therapy or usual care among adults with chronic low-back pain. Spine 2017;42:1511–20. https://doi.org/10.1097/brs.0000000000002344 | Cost paper from excluded Cherkin |
| Hutting N, Staal JB, Engels JA, Heerkens YF, Detaille SI, Nijhuis-van der Sanden MWG. (2015). Effect evaluation of a self-management programme for employees with complaints of the arm, neck or shoulder: a randomised controlled trial. Occupational and Environmental Medicine 2015;72:852–61. https://doi.org/10.1136/oemed-2015-103089 | Not primary care |
| Jakobsen MD, Sundstrup E, Brandt M, Andersen LL. Effect of physical exercise on musculoskeletal pain in multiple body regions among healthcare workers: secondary analysis of a cluster randomized controlled trial. Musculoskelet Sci Pract 2018;34:89–96. | Does not meet criteria for unexplained symptoms |
| Jakobsen MD, Sundstrup E, Brandt M, Jay K, Aagaard P, Andersen LL. Physical exercise at the workplace prevents deterioration of work ability among healthcare workers: cluster randomized controlled trial. BMC Public Health 2015;15:1174. https://doi.org/10.1186/s12889-015-2448-0 | Intervention is workplace prevention |
| Jakobsen MD, Sundstrup E, Brandt M, Jay K, Aagaard P, Andersen LL. Physical exercise at the workplace reduces perceived physical exertion during healthcare work: cluster randomized controlled trial. Scand J Public Health 2015;43:713–20. https://doi.org/10.1177/1403494815590936 | Intervention is workplace prevention |
| Janse A, Wiborg JF, Bleijenberg G, Tummers M, Knoop H. The efficacy of guided self-instruction for patients with idiopathic chronic fatigue: a randomized controlled trial. J Consult Clin Psychol 2016;84:377–88. https://doi.org/10.1037/ccp0000085 | No primary care involvement |
| Janse A, Worm-Smeitink M, Bussel-Lagarde J, Bleijenberg G, Nikolaus S, Knoop H. Testing the efficacy of web-based cognitive behavioural therapy for adult patients with chronic fatigue syndrome (CBIT): study protocol for a randomized controlled trial. BMC Neurol 2015;15:137. https://doi.org/10.1186/s12883-015-0392-3 | Protocol only |
| Jarrett ME, Cain KC, Barney PG, Burr RL, Naliboff BD, Shulman R, et al. Balance of autonomic nervous system predicts who benefits from a self-management intervention program for irritable bowel syndrome. J Neurogastroenterol Motil 2016;22:102–11. https://doi.org/10.5056/jnm15067 | Not primary care |
| Jeitler M, Brunnhuber S, Meier L, Lüdtke R, Büssing A, Kessler C, Michalsen A. Effectiveness of jyoti meditation for patients with chronic neck pain and psychological distress – a randomized controlled clinical trial. J Pain 2015;16:77–86. https://doi.org/10.1016/j.jpain.2014.10.009 | Not primary care |
| Jensen CE, Riis A, Petersen KD, Jensen MB, Pedersen KM. Economic evaluation of an implementation strategy for the management of low back pain in general practice. Pain 2017;158:891–9. https://doi.org/10.1097/j.pain.0000000000000851 | Not a behavioural intervention |
| Jones GT, Jones EA, Beasley MJ, Macfarlane GJ. Investigating generalizability of results from a randomized controlled trial of the management of chronic widespread pain: the MUSICIAN study. Pain 2017;158:96–102. https://doi.org/10.1097/j.pain.0000000000000732 | Include – is related to McBeth and Beasley trial |
| Kaleth AS, Slaven JE, Ang DC. Obesity moderates the effects of motivational interviewing treatment outcomes in fibromyalgia. Clin J Pain 2018;34:76–81. https://doi.org/10.1097/AJP.0000000000000500 | Not primary care, specialty referrals |
| Kanzler K, Robinson P, Munante M, Lopez E, McGeary D, Potter J, et al. Evaluating act for chronic pain in integrated primary care with a population health-driven RCT. Annals of Behavioral Medicine 2018;52:S188 | Paper not available |
| Kanzler KE, Robinson P, Munante M, McGeary D, Potter J, Lopez E, et al. Early findings from a real-world RCT: acceptance and commitment therapy (ACT) for persistent pain in an integrated primary care setting. J Clin Transl Sci 2018;2(Suppl. 1):81 | Conference abstract only |
| Kemani MK, Olsson GL, Lekander M, Hesser H, Andersson E, Wicksell RK. Efficacy and cost-effectiveness of acceptance and commitment therapy and applied relaxation for longstanding pain: a randomized controlled trial. Clin J Pain 2015;31:1004–16. https://doi.org/10.1097/AJP.0000000000000203 | Not primary care |
| Kolu P, Tokola K, Kankaanpää M, Suni J. Evaluation of the effects of physical activity, cardiorespiratory condition, and neuromuscular fitness on direct healthcare costs and sickness-related absence among nursing personnel with recurrent nonspecific low back pain. Spine 2017;42:854–62. https://doi.org/10.1097/BRS.0000000000001922 | Not a RCT |
| Konnopka A, König HH, Kaufmann C, Egger N, Wild B, Szecsenyi J, et al. Cost-utility of a specific collaborative group intervention for patients with functional somatic syndromes. J Psychosom Res 2016;90:43–50 | Costs paper from Schaefer trial |
| Lami MJ, Martinez MP, Miro E, Sanchez AI, Prados G, Caliz R, et al. Efficacy of combined cognitive-behavioral therapy for insomnia and pain in patients with fibromyalgia: a randomized controlled trial. Cogn Ther Res 2018;42:63–79. https://doi.org/10.1007/s10608-017-9875-4 | Not primary care |
| Lin IB, Coffin J, O’Sullivan PB. Using theory to improve low back pain care in Australian Aboriginal primary care: a mixed method single cohort pilot study. BMC Fam Pract 2016;17:44. https://doi.org/10.1186/s12875-016-0441-z | Not a RCT |
| Lin J, Paganini S, Sander L, Lüking M, Ebert DD, Buhrman M, et al. An internet-based intervention for chronic pain. Dtsch Arztebl Int 2017;114:681–8. https://doi.org/10.3238/arztebl.2017.0681 | Not primary care |
| Lin J, Faust B, Ebert DD, Krämer L, Baumeister H. A web-based acceptance-facilitating intervention for identifying patients’ acceptance, uptake, and adherence of internet- and mobile-based pain interventions: randomized controlled trial. J Med Internet Res 2018;20:e244. https://doi.org/10.2196/jmir.9925 | Not primary care |
| Løchting I, Storheim K, Werner EL, Småstuen Cvancarova M, Grotle M. Evaluation of individualized quality of life and illness perceptions in low back pain. A patient education cluster randomized controlled trial. Patient Educ Couns 2016;99:1992–8 | Includes sub-acute |
| Löwe B, Piontek K, Daubmann A, Härter M, Wegscheider K, König HH, Shedden-Mora M. Effectiveness of a stepped, collaborative, and coordinated health care network for somatoform disorders (Sofu-Net): a controlled cluster cohort study. Psychosom Med 2017;79:1016–24. https://doi.org/10.1097/PSY.0000000000000491 | Paper unavailable |
| Luciano JV, D’Amico F, Cerdà-Lafont M, Peñarrubia-María MT, Knapp M, Cuesta-Vargas AI, et al. Cost-utility of cognitive behavioral therapy versus U.S. Food and Drug Administration recommended drugs and usual care in the treatment of patients with fibromyalgia: an economic evaluation alongside a 6-month randomized controlled trial. Arthritis Res Ther 2014;16:451. https://doi.org/10.1186/s13075-014-0451-y | Already included in original review |
| Luciano JV, D’Amico F, Feliu-Soler A, McCracken LM, Aguado J, Peñarrubia-María MT, et al. Cost-utility of group acceptance and commitment therapy for fibromyalgia versus recommended drugs: an economic analysis alongside a 6-month randomized controlled trial conducted in Spain (EFFIGACT Study). J Pain 2017;18:868–80 | Costs from included trial |
| Mansell G, Hill JC, Main C, Vowles KE, van der Windt D. Exploring what factors mediate treatment effect: example of the STarT back study high-risk intervention. J Pain 2016;17:1237–45 | Pain is any duration |
| Mansell G, Storheim K, Løchting I, Werner EL, Grotle M. Identification of indirect effects in a cognitive patient education (COPE) intervention for low back pain. Phys Ther 2017;97:1138–46. https://doi.org/10.1093/ptj/pzx091 | Outcomes are mediators only |
| Marques M, De Gucht V, Leal I, Maes S. Effects of a self-regulation based physical activity program (the ‘4-STEPS’) for unexplained chronic fatigue: a randomized controlled trial. Int J Behav Med 2015;22:187–96. https://doi.org/10.1007/s12529-014-9432-4 | Already included in original review |
| McCrae N, Correa A, Chan T, Jones S, de Lusignan S. Long-term conditions and medically-unexplained symptoms: feasibility of cognitive behavioural interventions within the improving access to Psychological Therapies Programme. J Ment Health 2015;24:379–84. https://doi.org/10.3109/09638237.2015.1022254 | Not a RCT |
| Mehlsen M, Hegaard L, Ørnbøl E, Jensen JS, Fink P, Frostholm L. The effect of a lay-led, group-based self-management program for patients with chronic pain: a randomized controlled trial of the Danish version of the Chronic Pain Self-Management Programme. Pain 2017;158:1437–45. https://doi.org/10.1097/j.pain.0000000000000931 | Does not meet criteria for unexplained symptoms |
| Meng H, Friedberg F. Cost-utility of home-based fatigue self-management versus usual care for the treatment of chronic fatigue syndrome. Fatigue 2017;5:202–14. https://doi.org/10.1080/21641846.2017.1343171 | Costs |
| Meng K, Peters S, Faller H. Effectiveness of a standardized back school program for patients with chronic low back pain after implementation in routine rehabilitation care. Patient Educ Couns 2017;100:1161–8 | Not primary care |
| Michalsen A, Kunz N, Jeitler M, Brunnhuber S, Meier L, Lüdtke R, et al. Effectiveness of focused meditation for patients with chronic low back pain – a randomized controlled clinical trial. Complement Ther Med 2016;26:79–84. https://doi.org/10.1016/j.ctim.2016.03.010 | Not primary care |
| Murphy SE, Blake C, Power CK, Fullen BM. Comparison of a stratified group intervention (STarT Back) with usual group care in patients with low back pain: a non-randomized controlled trial. Spine 2016;41:645–52. https://doi.org/10.1097/BRS.0000000000001305 | Not a RCT |
| Newton-Cross P, Howell A, Dewar J, Chasey R. ‘Moving forwards with fibromyalgia’: preliminary feedback from patients attending primary care based education seminars and workshops. The Chartered Society of Physiotherapy UK Conference 2018, Birmingham, UK, 19–20 October 2018. Physiotherapy 2019;105:e173–4. https://doi.org/10.1016/j.physio.2018.11.180 | Not a RCT |
| Nøst TH, Steinsbekk A, Bratås O, Grønning K. Effect of an easily accessible chronic pain self-managment intervention in public primary care. Pain Practice 2018;18:69 | Conference abstract only |
| Nøst TH, Steinsbekk A, Bratås O, Grønning K. Short-term effect of a chronic pain self-management intervention delivered by an easily accessible primary healthcare service: a randomised controlled trial. BMJ Open 2018;8:e023017. https://doi.org/10.1136/bmjopen-2018-023017 | Does not meet criteria for unexplained symptoms |
| Nost TH, Steinsbekk A, Bratas O, Gronning K. Short-term effect of a chronic pain self-management intervention delivered by an easily accessible primary healthcare service: a randomised controlled trial. BMJ Open 2018;8(12). https://doi.org/10.1136/bmjopen-2018-023017 | Does not meet criteria for unexplained symptoms |
| Nøst TH, Steinsbekk A, Bratås O, Grønning K. Expectations, effect and experiences of an easily accessible self-management intervention for people with chronic pain: study protocol for a randomised controlled trial with embedded qualitative study. Trials 2016;17:325. https://doi.org/10.1186/s13063-016-1462-6 | Protocol only |
| Nøst TH, Steinsbekk A, Bratås O, Grønning K. Twelve-month effect of chronic pain self-management intervention delivered in an easily accessible primary healthcare service – a randomised controlled trial. BMC Health Serv Res 2018;18:1012. https://doi.org/10.1186/s12913-018-3843-x | Does not meet criteria for unexplained symptoms |
| Otto J, Linden M. Regeneration orientation is better than resistance orientation in behaviour activation. Results from an intervention study with psychosomatic patients. Psychiatr Danub 2017;29:201–6. https://doi.org/10.24869/psyd.2017.201 | Not primary care |
| Patti A, Bianco A, Paoli A, Messina G, Montalto MA, Bellafiore M, et al. Pain perception and stabilometric parameters in people with chronic low back pain after a pilates exercise program: a randomized controlled trial. Medicine 2016;95:e2414. https://doi.org/10.1097/MD.0000000000002414 | Not primary care |
| Peters ML, Smeets E, Feijge M, van Breukelen G, Andersson G, Buhrman M, Linton SJ. Happy despite pain: a randomized controlled trial of an 8-week internet-delivered positive psychology intervention for enhancing well-being in patients with chronic pain. Clin J Pain 2017;33:962–75. https://doi.org/10.1097/AJP.0000000000000494 | Not primary care |
| Phattharasupharerk S, Purepong N, Eksakulkla S, Siriphorn A. Effects of Qigong practice in office workers with chronic non-specific low back pain: a randomized control trial. J Bodywork Move Ther 2019;23:375–81. | Not primary care |
| Pinxsterhuis I, Sandvik L, Strand EB, Bautz-Holter E, Sveen U. Effectiveness of a group-based self-management program for people with chronic fatigue syndrome: a randomized controlled trial. Clin Rehabil 2017;31:93–103. https://doi.org/10.1177/0269215515621362 | Not primary care |
| Pleizier M, de Haan RJ, Vermeulen M. Management of patients with functional neurological symptoms: a single-centre randomised controlled trial. J Neurol Neurosurg Psychiatry 2017;88:430–6. https://doi.org/10.1136/jnnp-2015-312889 | Not primary care |
| Pringsheim T and Edwards M. Functional movement disorders. Neurol Clin Pract 2017;7:141–7. https://doi.org/10.1212/cpj.0000000000000350 | Review |
| Reme SE, Tveito TH, Harris A, Lie SA, Grasdal A, Indahl A, et al. Cognitive interventions and nutritional supplements (The CINS Trial): a randomized controlled, multicenter trial comparing a brief intervention with additional cognitive behavioral therapy, seal oil, and soy oil for sick-listed low back pain patients. Spine 2016;41:1557–64. https://doi.org/10.1097/BRS.0000000000001596 | Does not meet criteria for unexplained symptoms |
| Rhon DI, Miller RB, Fritz JM. Effectiveness and downstream healthcare utilization for patients that received early physical therapy versus usual care for low back pain: a randomized clinical trial. Spine 2018;43:1313–21. https://doi.org/10.1097/BRS.0000000000002619 | Population is miltary service personnel |
| Richmond H. Using a CBT approach to manage low back pain. Nurs Times 2016;112:12–14 | Population is subacute |
| Rutledge T, Atkinson JH, Chircop-Rollick T, D’Andrea J, Garfin S, Patel S, et al. Randomized controlled trial of telephone-delivered cognitive behavioral therapy versus supportive care for chronic back pain. Clin J Pain 2018;34:322–7. https://doi.org/10.1097/AJP.0000000000000555 | Population is military veterans |
| Rutledge T, Atkinson, JH, Holloway R, Chircop-Rollick T, D’Andrea J, Garfin SR, et al. Randomized controlled trial of nurse-delivered cognitive-behavioral therapy versus supportive psychotherapy telehealth interventions for chronic back pain. J Pain 2018;19:1033–9 | Does not meet criteria for unexplained symptoms |
| Salaffi F, Ciapetti A, Gasparini S, Atzeni F, Sarzi-Puttini P, Baroni M. Web/internet-based telemonitoring of a randomised controlled trial evaluating the time-integrated effects of a 24-week multicomponent intervention on key health outcomes in patients with fibromyalgia. Clin Exper Rheumatol 2015;33:S93–S101 | Not primary care |
| Salvat I, Zaldivar P, Monterde S, Montull S, Miralles I, Castel A. Functional status, physical activity level, and exercise regularity in patients with fibromyalgia after Multidisciplinary treatment: retrospective analysis of a randomized controlled trial. Rheumatol Int 2017;37:377–87. https://doi.org/10.1007/s00296-016-3597-x | Not primary care |
| Saper RB, Lemaster C, Delitto A, Sherman KJ, Herman PM, Sadikova E, et al. Yoga, physical therapy, or education for chronic low back pain: a randomized noninferiority trial. Ann Intern Med 2017;167:85–94. https://doi.org/10.7326/M16-2579 | Not primary care |
| Scott EL, Kroenke K, Wu J, Yu Z. Beneficial effects of improvement in depression, pain catastrophizing, and anxiety on pain outcomes: a 12-month longitudinal analysis. J Pain 2016;17:215–22. https://doi.org/10.1016/j.jpain.2015.10.011 | Does not meet criteria for unexplained symptoms |
| Scott W, Chilcot J, Guildford B, Daly-Eichenhardt A, McCracken LM. Feasibility randomized-controlled trial of online acceptance and commitment therapy for patients with complex chronic pain in the United Kingdom. Eur J Pain 2018;22:1473–84. https://doi.org/10.1002/ejp.1236 | Not primary care |
| Seferiadis A, Ohlin P, Billhult A, Gunnarsson R. Basic body awareness therapy or exercise therapy for the treatment of chronic whiplash associated disorders: a randomized comparative clinical trial. Disabil Rehabil 2016;38:442–51. https://doi.org/10.3109/09638288.2015.1044036 | Does not meet criteria for unexplained symptoms |
| Sullivan M, Langford DJ, Davies PS, Tran C, Vilardaga R, Cheung G, et al. A controlled pilot trial of paintracker self-manager, a web-based platform combined with patient coaching, to support patients’ self-management of chronic pain. J Pain 2018;19:996–1005 | Setting is pain specialty clinic |
| Suman A, Schaafsma FG, van de Ven PM, Slottje P, Buchbinder R, van Tulder MW, Anema JR. Effectiveness of a multifaceted implementation strategy compared to usual care on low back pain guideline adherence among general practitioners. BMC Health Serv Res 2018;18:358. https://doi.org/10.1186/s12913-018-3166-y | Outcomes are measures of guideline adherence |
| Taylor SJ, Carnes D, Homer K, Kahan BC, Hounsome N, Eldridge S, et al. Novel three-day, community-based, nonpharmacological group intervention for chronic musculoskeletal pain (COPERS): a randomised clinical trial. PLOS Med 2016;13:e1002040. https://doi.org/10.1371/journal.pmed.1002040 | Population includes mixed causes of pain (e.g. osteoarthritis) |
| Thorn BE, Eyer JC, Van Dyke BP, Torres CA, Burns JW, Kim M, et al. Literacy-adapted cognitive behavioral therapy versus education for chronic pain at low-income clinics: a randomized controlled trial. Ann Intern Med 2018;168:471–80. https://doi.org/10.7326/M17-0972 | Does not meet criteria for unexplained symptoms |
| Bartz PT, Vieira A, Noll M, Candotti CT. Effectiveness of the back school program for the performance of activities of daily living in users of a basic health unit in Porto Alegre, Brazil. J Phys Ther Sci 2016;28:2581–6. https://doi.org/10.1589/jpts.28.2581s | Does not meet criteria for unexplained symptoms |
| Turner B, Yin Z, Bobadilla R, Rodriguez N, Liang Y, Winkler P, Simmonds M. Randomized trial of multimodality chronic pain care for primary care patients in clinic versus in community: preliminary results. J Pain 2017;18:S62 | Conference abstract only |
| Turner BJ, Liang Y, Simmonds MJ, Rodriguez N, Bobadilla R, Yin Z. Randomized trial of chronic pain self-management program in the community or clinic for low-income primary care patients. J Gen Intern Med 2018;33:668–77. https://doi.org/10.1007/s11606-017-4244-2 | Does not meet criteria for unexplained symptoms |
| van Ravesteijn H. [Mindfulness-based cognitive therapy for patients with somatoform disorders.] Tijdschr Psychiatr 2016;58:198–206 | Study already included in original review |
| Verbrugghe J, Agten A, Stevens S, Eijnde BO, Vandenabeele F, Timmermans A. Effects of high intensity training on pain, disability, exercise capacity and muscle strength in persons with nonspecific chronic low back pain: preliminary RCT results. Ann Phys Rehabil Med 2018;61:e17. https://doi.org/10.1016/j.rehab.2018.05.036 | Conference abstract only |
| Villafañe JH, Perucchini D, Cleland JA, Barbieri C, de Lima E Sá Resende F, Negrini S. The effectiveness of a cognitive behavioral exercise approach (CBEA) compared to usual care in patients with a whiplash associated disorder: a quasi-experimental clinical trial. J Back Musculoskelet Rehabil 2017;30:943–50. https://doi.org/10.3233/BMR-140162 | Not a RCT |
| Vogler CN, Sattovia S, Salazar LY, Leung TI, Botchway A. Assessing outcomes of educational videos in group visits for patients with chronic pain at an academic primary care clinic. Postgrad Med 2017;129:524–30. https://doi.org/10.1080/00325481.2017.1324228 | Not a RCT |
| Vos-Vromans DC, Smeets RJ, Huijnen IP, Köke AJ, Hitters WM, Rijnders LJ, et al. Multidisciplinary rehabilitation treatment versus cognitive behavioural therapy for patients with chronic fatigue syndrome: a randomized controlled trial. J Intern Med 2016;279:268–82 | Not primary care |
| Wälti P, Kool J, Luomajoki H. Short-term effect on pain and function of neurophysiological education and sensorimotor retraining compared to usual physiotherapy in patients with chronic or recurrent non-specific low back pain, a pilot randomized controlled trial. BMC Musculoskelet Disord 2015;16:83. https://doi.org/10.1186/s12891-015-0533-2 | Already included in original review |
| Weiland A, Blankenstein AH, Van Saase JL, Van der Molen HT, Jacobs ME, Abels DC, et al. Training medical specialists to communicate better with patients with medically unexplained physical symptoms (MUPS). A randomized, controlled trial. PLOS ONE 2015;10:e0138342. https://doi.org/10.1371/journal.pone.0138342 | Not primary care |
| Woodman J, Ballard K, Hewitt C, MacPherson H. Self-efficacy and self-care-related outcomes following Alexander Technique lessons for people with chronic neck pain in the ATLAS randomised, controlled trial. Eur J Integr Med 2018;17:64–71. https://doi.org/10.1016/j.eujim.2017.11.006 | Intervention designed to address underlying causes |
Update of the qualitative review: the acceptability of primary care or community-based behaviour modification interventions for medically unexplained symptoms – qualitative systematic review: update
This section provides an overview of the qualitative literature published since the original searches were performed. The new evidence for patients’ and HPs’ perspectives on the acceptability, relative benefits and potential harms of primary care- or community-based behaviour modification interventions for MUS is outlined here. The review methods applied were the same as those documented in Chapter 4, and a second reviewer (AB) checked the data extractions and completed independent quality assessment for each paper as in the original review. The results of the review update are presented below.
Results of the qualitative review update
Included studies: qualitative review
From the 384 citations identified during the initial searches, 16 remained after the title and abstract sift; these citations were considered at full-paper sift for the qualitative review update. Figure 86 shows the flow chart of studies included in the qualitative review. The sifting process resulted in the inclusion of one study (two citations) at full paper. 521 This study examined HPs’ perspectives of an intervention, there were no new studies relating to patients’ perspectives. Details of studies excluded at full-paper sift together with reasons are shown in Table 128. Both of the full papers that were included were published in 2018.
FIGURE 86.
The PRISMA flow diagram: updated qualitative review.

| Author (year) | Reason for exclusion at full-paper sift |
|---|---|
| Arden (2017)522 | Does not include qualitative data |
| Balabanovic (2020)523 | Does not include data about a specific intervention |
| Bestall (2017)524 | Population does not fit the inclusion criteria |
| Broughton (2017)525 | The study was not conducted in primary care |
| Carlin (2018)526 | Population does not fit the inclusion criteria |
| Carnes (2017)527 | Population does not fit the inclusion criteria |
| Casey (2018)528 | Population does not fit the inclusion criteria |
| Dresner (2016)529 | Population does not fit the inclusion criteria |
| Gordon (2017)530 | Population does not fit the inclusion criteria |
| Hadi (2016)531 | Population does not fit the inclusion criteria |
| Hadi (2017)532 | Population does not fit the inclusion criteria |
| Sibelli (2018)533 | The study was not conducted in primary care |
| Teo (2017)534 | The study was not conducted in the UK |
| Thompson (2018)535 | Mixed population |
| First author and year of publication | Sample (contributing qualitative data) | Population being treated as described in the study | Data collection | Intervention | Age | Sex |
|---|---|---|---|---|---|---|
| Cowell et al.521 | 10 physiotherapists | Non-specific chronic low back pain | Semistructured interview | CFT | Not reported (number of years working in MSK range from 3 years to > 14 years) | Seven male, three female |
| First author and year of publication | Population being treated as described in the study | Intervention | Intervention provider | Intervention setting | Intervention duration | Individual or group |
|---|---|---|---|---|---|---|
| Cowell et al.521 | Non-specific chronic low back pain | CFT | Physiotherapists | Not reported other than primary care | Not reported as report of HPs being trained in the intervention | Individual |
Study respondents
The included study assessed HPs’ attitudes to the intervention. The study contained qualitative data from 10 physiotherapists following a training programme in cognitive functional therapy (CFT) for the management of non-specific chronic low back pain.
Respondent characteristics
There were seven male physiotherapists and three female physiotherapists. The physiotherapists were in band 5–7 and had been working in the area of musculoskeletal disorders for between 3 years and > 14 years.
Study setting
The intervention took place in a primary care department in the North East London Foundation Trust.
Intervention description and facilitators
Physiotherapists were trained to deliver CFT. CFT is a biopsychosocially orientated behavioural intervention for lower back pain. 536 A multidimensional clinical reasoning framework (MDCRF) underpins CFT,536 and adopting this approach successfully requires physiotherapists to develop skills across these broad domains. 537
Quality of the included studies
As described in Chapter 4, we have used an adaptation of the CASP assessment of study quality for qualitative studies to assess the included studies. Studies were assessed in terms of the extent to which they met each of the seven CASP requirements. If the study met all seven requirements it was assessed as high quality, if it met six of the criteria it was assessed as moderate quality and if it met five or fewer of the criteria it was assessed as low quality. Overall, the study was categorised as being of moderate quality; however, both reviewers highlighted issues relating to reflexivity, given that the lead author was both the intervention trainer and the interviewer in the study.
| Question | Cowell et al.521,538 | |
|---|---|---|
| 1 | Is the study qualitative research or does it provide qualitative data? | Yes |
| 2 | Are the study context and aims clearly described? | Yes |
| 3 | Is there evidence of research reflexivity? | Reflexivity is mentioned in the methods but not obviously applied in the analysis |
| 4 | Are the sampling methods clearly described and appropriate for the research question? | Yes |
| 5 | Are the methods of data collection clearly described and appropriate to the research question? | Yes |
| 6 | Is the method of analysis clearly described and appropriate to the research question? | Yes |
| 7 | Are the claims made supported by sufficient evidence (i.e. did the data provide sufficient depth, detail and richness)? | Yes |
Certainty of the review findings: the Confidence in the Evidence from Reviews of Qualitative research assessment
As the review update identified only one new study, it was not possible to complete the CERQual assessment across the update studies; however, we have highlighted where the new study corresponds to the findings reported in the original review, and the implications for CERQual have been considered.
Qualitative synthesis: evidence from Cowell et al.521,538
The evidence from the one new study on health yielded 11 findings overall, and corresponded to six findings identified in the original review. The findings in the form of meta-themes, together with subthemes, are presented in Table 132.
Of the findings identified in the new study, six corresponded to existing findings. These six findings are presented in Table 132. The original CERQual assessment is presented in Table 133. With the addition of the new study the implications are that the CERQual assessment would be strengthened for these findings. As the new study is rated as moderate quality, it included thick data the study represents a different context with a different intervention and different facilitators and the data were coherent across the studies.
| Meta-theme: finding | Subtheme |
|---|---|
| Positive factors relating to behavioural modification interventions as reported by HPs/What did you gain from being trained to deliver and/or delivering a behavioural modification intervention? | |
| Supervision and training | Supervision was helpful |
| Learning about integration of factors across multiple domains, linking psychological factors and mechanical pain | |
| Communication | Improved communication skills, effective communication and active listening |
| Challenging perspectives | |
| Increased confidence | Increased confidence in ability to help patients |
| Increased confidence in identifying and addressing psychosocial factors | |
| Ability to address sensitive issues | |
| Improved relationships | Ability to build a patient– therapist relationship |
| Engaging patients to self-manage | |
| Empowering patients | Developing patient awareness |
| Enhanced patients’ confidence | |
| Benefits to patients | Individualised care, collaboratively agreeing treatment goals |
| Quick results | |
| What did not help or was detrimental to the patients or the delivery of the intervention? | |
| Complexity of approach | Not an easy approach presenting challenges of having to consider and target pain drivers across broad domains extending their traditional scope of practice beyond just physical factors |
| HP lacked confidence | Lack of confidence in addressing psychological factors |
| Lack of training in effective communication | |
| Factors reported as important, wanted or expected for training in and delivery of behavioural modification interventions | |
| More (clinical) experience | Requires real-life observation |
| Requires clinical experience to develop competency and confidence | |
| Requires ongoing support | |
| Barriers: from the perspective of HPs, why patients did not want behavioural interventions or could not engage with them or barriers to delivery of the intervention | |
| Resource constraints | Time constraints |
| Patient beliefs | Patients with rigid biomedical beliefs and expectations for passive treatment were, at times, difficult to engage in the approach |
| Meta theme | CERQual assessment of confidence in the evidence | Explanation CERQual assessment |
|---|---|---|
| Positive factors relating to behavioural modification interventions as reported by HPs/What did you gain from being trained to deliver and/or delivering a behavioural modification intervention? | ||
| Training and supervision was useful | Moderate confidence | Two studies, both of moderate quality, both including thick data. Evidence came from different intervention types with different facilitators. Coherent data across the studies |
| Extended knowledge and skill of the HP | High confidence | Three studies, one of high quality, two of moderate quality. All three included thick data. Evidence came from different intervention types with different facilitators. Coherent data across the studies |
| What did not help or was detrimental to the patients or the delivery of the intervention? | ||
| When HPs felt that they were novices or did not have the required skill levels | High confidence | Two studies, one of high quality, one of moderate quality, both including thick data. Evidence came from different intervention types with different facilitators. Coherent data across the studies |
| Barriers: from the perspective of HPs, why patients did not want behavioural interventionsor could not engage with them or barriers to delivery of the intervention | ||
| Resource constraints | Moderate confidence | Three studies, all of moderate quality, both including thick data. Evidence came from different intervention types with different facilitators. Coherent data across the studies |
| Patient beliefs | High confidence | Three studies, one of high quality, two of moderate quality. All three including thick data. Evidence came from different intervention types with different facilitators. Coherent data across the studies |
| Factors reported as important, wanted or expected for training in and delivery of behavioural modification interventions | ||
| More training and supervision required | Moderate confidence | Two studies, one of high quality, one of moderate quality. Both including thick data. Evidence came from different intervention types with different facilitators. Coherent data across the studies |
Synthesis of evidence
The evidence from the one new study health yielded 11 findings overall, and corresponded to six findings identified in the original review. The evidence from the new study is described below.
Factors identified as being helpful for being trained in the intervention
Supervision and training
Physiotherapists reported that supervision and learning were important to being successfully trained in the intervention. They reported that the CFT training programme taught integration of factors across multiple domains, linking psychosocial factors and mechanical pain presentations:
Before, I’d tend to separate things, not intentionally, but tend to be, ‘Oh well, this is what’s going on mechanically and then this is what’s going on with their life’, but then not necessarily making the link between the two, and I think that’s what CFT does.
P09
Communication
The physiotherapists reported improved communication skills, and were more prepared to actively listen to their patients, which helped to facilitate patient disclosure and improved their ability to identify problems:
Communication with the patients has changed quite a bit from before the training to after, and you have to be able to communicate well and listen well for this concept to work effectively. The biggest shift for me, personally, is that change in communication, which just allows me then, probably, to identify more drivers.
P09
Improvement in communication skills also included the HPs developing the ability to challenge perspectives without jeopardising the patient–therapist relationship.
Increased confidence
Health professionals reported that by taking part in the training their confidence in their ability to help patients had increased, as had their ability to identify and address psychosocial factors. They also felt more able to address sensitive issues:
Rather than me being scared about asking the questions, which, again, is probably a change from before to after training, just in terms of confidence.
P09
Improved relationships leading to patient empowerment
Physiotherapists reported improved abilities to build good patient–therapist relationships, and this was reported to help engaged patients to self-manage, by giving patients confidence and empowering them to take personal control:
I think the therapist–patient relationship is really key in any scenario, otherwise they’re going to be unlikely to engage in what you’re going to try to get them to do.
P09
Specifically the intervention used ‘. . . behavioural experiments to demonstrate less painful ways to move during provocative tasks’,539 the physiotherapists were able to highlight discrepancies between what patients believed and their pain response:
So, if you can show that you can modify their symptoms for the better, then you change their belief system; it gives you the right to go there and it changes the patient’s belief, which changes their behaviour.
P02
Benefits to patients
Health professionals emphasised specific benefits to patients including individualised care, including collaboratively agreeing treatment goals:
I think it’s just got to be really, really patient specific. I think you need to sit and spend your time listening to all the factors involved in that particular patient’s back pain to find an approach that’s tailored to them and then I think you’ve really got to get them on board to buy into whatever the best approach you feel is for them.
P03
Health professionals also felt that the intervention could deliver quick results for the patients, providing them with hope for change:
They see changes really very quickly because of those behavioural experiments. So, as a result of that, I’ve seen patients generally much happier, and for the first time in years often seeing a glimmer of hope.
P05
Factors identified as unhelpful or difficult for health professionals
Complexity
Physiotherapists found the complexity of approach challenging. They:
. . . highlighted the challenges of having to consider and target pain drivers across broad domains. This required that physiotherapists extend their traditional scope of practice beyond just physical factors: I don’t think it’s an easy approach to use. It is complex because there’s so much involved in it and within it but, it’s certainly the way forward, for most physiotherapy.
P09
Health professional lacked confidence
Physiotherapists reported that they lacked confidence in addressing psychological factors, and felt that, although effective communication was highly important, there was a lack of specific training in effective communication. Specifically, HPs reported a lack of confidence in exploring emotional distress (high levels of anxiety and depressed mood). The physiotherapists felt uncomfortable in this domain such that they often avoided sensitive issues:
It’s easy to go into an avoidance mode I think, and then skip past it and move onto something else. I think the concern is you go in and then you’re out of your depth.
P10
Factors reported as required for successful training in the intervention
More clinical experience
Physiotherapists reported that they needed more real-life observation and more clinical experience, together with ongoing support in delivering the intervention. They felt that this would build confidence and competency:
There was a sense that just attending large CFT workshops, which included a traditional didactic lecture format and masterclass observation, although providing inspiration, was insufficient to develop an in-depth understanding of the clinical reasoning processes that underpinned CFT: real-life observation of a clinician and a patient . . . and you watch things unfold and you feel inspired but you don’t really know how he [the educator] has got to where he’s got to. The course [formal training] allows some analysis of that, and some breakdown.
P05
Factors identified as barriers to successful training in the intervention
Resource constraints
The physiotherapists felt that a lack of time represented the biggest service constraint to effective implementation.
Patient beliefs
A further barrier reported by physiotherapists was around patient beliefs. The study reported that patients with rigid biomedical beliefs and expectations for passive treatment were ‘difficult’ to engage in the approach; however, they reported that developing competence in the approach made it easier to develop relationships to overcome contrasting beliefs.
Discussion of the qualitative review update
This review presents an update to the qualitative review presented in Chapter 4. One new study was identified that presented HPs’ perspectives on the acceptability, relative benefits and potential harms of primary care or community-based behaviour modification interventions for medically unexplained symptoms. The new study was rated as of moderate quality. The new study provided 11 findings, corresponding to six findings presented in the original review, and added weight to the confidence in those findings. The five additional findings were largely related to the specific intervention and sample described in the study, which was quite different from the studies included in the original review.
The evidence from HPs described important facilitators. They reported that they found being trained in the intervention helped them to develop their own knowledge and skills, thus improving their confidence, helped them develop effective communication skills, and develop patient–therapist relationships. Other important facilitators were training and supervision for the interventions, and HPs reported that they would benefit from more clinical experience to improve their competency. HPs also reported that they felt the intervention provided specific benefits to patients by providing individualised, collaborative care and that the intervention could potentially provide quick results.
Barriers to potential successful delivery of the intervention were time constraints, HPs’ lack of confidence in their own skills and abilities to deliver the intervention (given the complexity of the intervention) and to address psychosocial factors, and patient beliefs that went against some aspects of the intervention.
Limitations
A limitation of this study was that it did not include any data from patients. The study reported a training programme and, therefore, it appears that the intervention had not yet been rolled out to patients; therefore, it is unclear how acceptable and beneficial the intervention may be in the patients’ view. Furthermore, patient beliefs are raised as a potential barrier to successful intervention. However, without patient data it is unclear whether or not HP beliefs would be implicated in this; for example, it may be that for people who don’t respond to treatment or who find the intervention unacceptable being labelled ’difficult’ affects the therapeutic alliance. Reflexivity may also represent a limitation due to potential bias as the lead author and interviewer was also the intervention trainer.
Update of the realist synthesis: the contribution of contextual factors to the success or failure of behaviour modification interventions for medically unexplained symptoms – realist synthesis
Following the update search for qualitative research studies (see Qualitative systematic review update methods), which retrieved one additional eligible study reported in two related papers,521,538 the review team revisited the eight original programme theory component statements (see Box 1) to determine which of these, if any, might have been modified by findings from the additional study. These papers focused on the perceptions of physiotherapists in primary care in England about adopting a biopsychosocial approach to managing patients with non-specific chronic low back pain521 and the perceptions of the same sample on the impact of a formal training programme in CFT.
In line with realist synthesis methods, verbatim data from the participants and author observations from the Discussion sections of the two papers were mapped against an eight-item framework based on the previously generated programme theory components from the main review (programme theories 1–8). Particular attention was focused on findings not explained within this prior framework.
Findings
Overall, the two papers521,538 supported the previous findings from the realist synthesis although contributed more detailed perspectives from a professional group (physiotherapists) that was not previously the focus of the included studies. Unsurprisingly, the emphasis on breaking the destructive diagnostic cycle (programme theory 6) was less prominent in this sample as patients will typically have already entered the treatment pathway. Similarly, the need to focus on symptoms, not labels (programme theory 2), was correspondingly muted given that physiotherapists typically handle the mechanical aspects of the condition in this way as part of their routine care. However, the authors observed a tension between being seen to be doing something (in order to sustain the patient–therapist relationship) and a consequent burden on health service utilisation. 521 Physiotherapists in the sample described the perceived pressure from patients to request scans in order to provide reassurance for those holding catastrophic beliefs about their pain disorder:
They need that reassurance that actually, there isn’t anything going on . . . until they’ve been given that all clear you can’t actually move them forward no matter how hard you try . . .
P04
Prominent emphases within the data included the centrality of the professional–patient relationship (programme theory 3), the need for a contextually sensitive (‘individualised’) therapeutic response (programme theory 4) and the need for congruity between patient and professional cognitive models (programme theory 5). These aspects emerge as substantive components of the training programme described in the second paper. 538 An interesting aspect of the therapeutic relationship was the implication that physiotherapists were prepared to make early concessions from what they considered to be the optimal evidence-based treatment in order to secure patient trust, which would prove advantageous in the long run:
. . . it was seen as a way of placating the patient to protect the therapeutic relationship.
Cowell et al. 521
It also provided a context for developing patient insight into their disorder:
If their expectation is that they’re going to have manual therapy, and that gives me buy in for them to make sure that they trust me, I can get them to believe in the concept, get them moving, then what harm does it do?
P02521
Use of the biopsychosocial model was central to both papers and was seen as a mechanism by which individualised care could be recognised and delivered, to the benefit not only of this patient group but patients in general. “The inadequacy of a ‘one-size-fits-all’ treatment approach”521 emerges from both papers and offers justification for an approach that requires full exploration of the patient’s psychosocial circumstances; however, communication proved particularly challenging when the patient persisted with a biomedical-only model of their own condition:
It’s my back, what do you mean it’s got anything to do with relaxation or it’s in my head . . . some people find that difficult.
P03521
As a consequence of this emphasis, both papers placed great importance on the ‘potential dissonance between patients’ and physiotherapists’ attitudes and beliefs’. 521 In both papers, the perceived response to this ‘was having effective communication skills to develop patient insight and challenge patient perspectives’. 521
Where these papers specifically contributed to the synthesis was in making explicit justifications for the likely success of programme theory components; for example, the benefits of maintaining a professional–patient relationship, based on trust, are described in starkly pragmatic terms: ‘facilitating patient disclosure, providing opportunities to reconcile patient unhelpful beliefs and enhancing adherence’. Furthermore, it was evident from several observations and verbatim extracts that much of the therapist resistance to exploring a biopsychosocial model of the condition (programme theory 7) was based on the therapists’ own discomfort and lack of training in the use of this model rather than simply from anticipating a negative patient response. This helps to explain the ambiguity in professional attitudes detected in the original synthesis data exploring this programme theory component.
Interpretation
It should be recognised that both these additional papers521,538 were framed within the biopsychosocial model and it is, therefore, not surprising that they have largely confirmed the findings from the original realist synthesis. At the same time, it is helpful to step outside the research domain most commonly inhabited by GPs to explore the views of an additional professional group with a different perspective and different prior training. One undercurrent from the original realist synthesis emerges more strongly in both the additional papers, namely the constraints of time within a typical NHS setting. Nevertheless, it is encouraging to see that physiotherapists were prepared to be innovative in creating time opportunities in recognition that time spent in building up a positive professional–patient relationship and in constructive communication holds the potential to achieve future benefit in terms of both patient and health service outcomes. 538
Further value of these ‘sibling papers’ derives from the fact that, as a needs assessment and training programme paper respectively, the papers present a coherent response to the issues previously identified from the programme theory. This coherence has helped us to examine the extent to which specific training programme components match or resonate with the specific needs identified from each of the programme theory components, strengthening our own analysis.
Finally, it is useful to report that supporting recent literature evoked by the discussion sections of these supplementary papers confirms the overall direction of our previous interpretation. For example:
the themes/sub-themes identified in this study reflect some of the key dimensions suggested to underpin this model of care: acknowledging a BPS perspective, sharing information, considering the individual needs of patients and prioritising the therapeutic relationship.
Cowell et al. 521
Acknowledging that this observation reflects the subjective editorialising by the authors within a biopsychosocial framework, rather than the objective evidentiary basis of the programme, this nevertheless confirms that our previous analysis resonates with studies that lie beyond our initial inclusion set and which reflect contemporary academic and practitioner views. We continue to conclude, with this study data, that:
being afforded the necessary time to develop a trusting patient–therapist relationship, and acquiring broader competencies, particularly in communication skills, are worth exploring in the successful delivery of such an approach.
Cowell et al. 521
Following the update search for qualitative research studies, which retrieved one additional eligible study reported in two related papers, the review team revisited the eight original programme theory component statements to determine which of these, if any, might have been modified by findings from the additional study.
Cowell et al.521
One of the key vehicles identified for managing potential dissonance between patients’ and physiotherapists’ attitudes and beliefs was having effective communication skills to develop patient insight and challenge patient perspectives. This was not always a straightforward process, and required competency to conduct an effective patient-centred consultation that was capable of nurturing trust between practitioner and patient and enhance patient disclosure. 540
Opportunities for early follow-up treatment were also seen as important to nurture a trusting relationship, promote active coping strategies, build self-efficacy and promote behaviour change; however, this was difficult to support in primary care, and consequently patients were at risk of defaulting to biomedical beliefs and treatment expectations and were thereby difficult to engage.
Although a clear overall definition on patient-centred care has yet to be established in physiotherapy,541,542 the themes/subthemes identified in this study reflect some of the key dimensions suggested to underpin this model of care: acknowledging a biopsychosocial perspective, sharing information, considering the individual needs of patients and prioritising the therapeutic relationship. 542–545
The inadequacy of a ’one-size-fits-all’ treatment approach was reflected in the physiotherapists’ concerted efforts to individualise management and consider each patient’s unique biopsychosocial profile; however, studies have highlighted discrepancies between health-care practitioners’ psychosocial awareness and incorporating such perspectives into practice. 546,547
The physiotherapists in this study reflected on the learning challenges required to develop competencies across the wider dimensions reflected in a biopsychosocial model of care. 548,549 They highlighted a lack of confidence in addressing psychological factors, often avoiding sensitive topics, as it felt intrusive and beyond their realm of expertise. This lack of confidence has been reported in other studies,550,551 and has been attributed to inadequacies in undergraduate-level training and a lack of available professional development training. 551,552
Another key barrier to implementing a broader biopsychosocial approach was the perceived lack of time allocated within primary care, a theme echoed in recent studies. 553,554 It has been demonstrated that patients at high risk of a poor outcome have higher levels of emotional distress555 and require longer appointments to explore these issues. 254 The physiotherapists felt that unravelling the complexity of persistent pain presentations could not be done appropriately in the short time available.
A shared consensus with patients on the underlying cause of the pain and appropriate management, as well as treatment goals, appears central to maintaining a productive working relationship. These data suggest that being afforded the necessary time to develop a trusting patient–therapist relationship and acquiring broader competencies, particularly in communication skills, are worth exploring in the successful delivery of such an approach.
Themes and subthemes
-
Recognising the need to assess and manage non-specific chronic low back pain from a biopsychosocial perspective
-
multidimensional nature of non-specific chronic low back pain
-
limitations of a biomedical model.
-
-
Challenge of addressing psychological factors
-
reconciling patient perspectives
-
confidence
-
time.
-
-
Engaging patients to self-manage their non-specific chronic low back pain
-
patient–therapist relationship
-
effective communication
-
individualised care
-
modifying pain-related functional behaviours.
-
Themes and subthemes
-
A challenging learning journey
-
requires formal training
-
requires clinical experience.
-
-
Enhanced confidence: ‘making the hard stuff easier’
-
identifying and addressing psychosocial factors
-
addressing sensitive issues.
-
-
Change in professional practice
-
communication practice.
-
-
Enhanced comprehension, by physiotherapist and patient
-
importance of developing patient awareness
-
influence of psychosocial factors
-
importance of therapeutic relationship.
-
-
‘This seems great, but there are obstacles to applying this . . .’
-
better outcomes
-
application to wider patient populations
-
time constraints
-
difficulty to engage patients with biomedical beliefs.
-
Update of the cost-effectiveness review
This section provides an overview of the searches for cost-effectiveness studies published since the original searches were performed. The review methods applied were consistent with those reported in Chapter 6. Results of the updated searches are presented below.
Results
A total of 726 unique citations were retrieved in the updated cost-effectiveness search. There were 698 citations excluded at the title and abstract stage, with 28 full papers retrieved for further scrutiny. No studies were found to meet the inclusion criteria; therefore, there are no new included studies of cost-effectiveness. Table 134 presents a list of all studies excluded at full-paper stage with reasons.
FIGURE 87.
The PRISMA flow diagram: cost-effectiveness review.

| Paper | Reason for exclusion |
|---|---|
| Abhulimen S, Hirsch A. Quantifying the economic impact of a digital self-care behavioral health platform on Missouri Medicaid expenditures. J Med Econ 2018;21:1084–90. https://doi.org/10.1080/13696998.2018.1510834 | Non-UK |
| Basu S, Landon BE, Williams JW, Bitton A, Song ZR, Phillips RS. Behavioral health integration into primary care: a microsimulation of financial implications for practices. J Gen Intern Med 2017;32:1330–41. https://doi.org/10.1007/s11606-017-4177-9 | Does not meet review criteria for MUS |
| Bestall J, Siddiqi N, Heywood-Everett S, Freeman C, Carder P, James, M, et al. New models of care: a liaison psychiatry service for medically unexplained symptoms and frequent attenders in primary care. Psychiatrist 2017:41:340–4 | Not a cost-effectiveness study |
| Bromley JS, Turner A. A proactive and acceptable clinic solution for patients with medically unexplained symptoms. Psychiatr Bull 2014;38:307–8 | Not a cost-effectiveness study |
| Buono JL, Carson RT, Flores NM. Health-related quality of life, work productivity, and indirect costs among patients with irritable bowel syndrome with diarrhea. Health Qual Life Out 2017;15:35 | Not a cost-effectiveness study |
| Canaway A, Pincus T, Underwood M, Shapiro Y, Chodick G, Ben-Ami N. Is an enhanced behaviour change intervention cost-effective compared with physiotherapy for patients with chronic low back pain? Results from a multicentre trial in Israel. BMJ Open 2018;8(4). https://doi.org/10.1136/bmjopen-2017-019928 | Does not meet criteria for MUS |
| Cano-Garcia FJ, Gonzalez-Ortega MD, Sanduvete-Chaves S, Chacon-Moscoso S, Moreno-Borrego R. Evaluation of a psychological intervention for patients with chronic pain in primary care. Front Psychol 2017;8:435 | Non-UK |
| Clare A, MacNeil S, Bunton T, Jarrett S. ’The Doctor doesn’t need to see you now’: reduction in general practice appointments following group pain management. Br J Pain 2019;13:121–9. https://doi.org/ 10.1177/2049463718812501 | Paper not available |
| Collin SM, Bakken IJ, Nazareth I, Crawley E, White PD. Health care resource use by patients before and after a diagnosis of chronic fatigue syndrome (CFS/ME): a clinical practice research datalink study. BMC Fam Pract 2017;18:1–13. https://doi.org/10.1186/s12875-017-0635-z | Not a cost-effectiveness study |
| Cooper, A, Abbass A, Town J. Implementing a psychotherapy service for medically unexplained symptoms in a primary care setting. J Clin Med 2017;6:109 | Non-UK |
| Fink P, Rask MT, Rosendal M, Ornbol E. (2016). Long-term outcome of Bodily Distress Syndrome (BDS) on sick leave, healthcare costs and work disability in primary care patients. A ten-year follow-up study. J Psychosom Res 2016;85:65. https://doi.org/10.1016/j.jpsychores.2016.03.158 | Non-UK |
| Frogner BK, Harwood K, Andrilla CHA, Schwartz M, Pines JM. Physical therapy as the first point of care to treat low back pain: an instrumental variables approach to estimate impact on opioid prescription, health care utilization, and costs. Health Serv Res 2018;53:4629–46 | Non-UK |
| Görge M, Ziehm J, Farin E. Health-care utilization of patients with chronic back pain before and after rehabilitation. BMC Health Serv Res 2017;17:1–10. https://doi.org/10.1186/s12913-017-2757-3 | Not primary care |
| Grochtdreis T, Brettschneider C, Shedden-Mora M, Piontek K, Konig HH, Lowe B. (2018). Cost-effectiveness analysis of a stepped, collaborative and coordinated health care network for patients with somatoform disorders (Sofu-Net). J Ment Health Policy Econ 2018;21:59–69 | Not a behavioural intervention |
| Herrick LM, Spalding WM, Saito YA, Moriarty J, Schleck C. A case-control comparison of direct healthcare-provider medical costs of chronic idiopathic constipation and irritable bowel syndrome with constipation in a community-based cohort. J Med Econ 2017;20:273–79 | Non-UK |
| Kolu P, Tokola K, Kankaanpää M, Suni M. Evaluation of the effects of physical activity, cardiorespiratory condition, and neuromuscular fitness on direct healthcare costs and sickness-related absence among nursing personnel with recurrent nonspecific low back pain. Spine 2017;42:854–62 | Non-UK |
| Konnopka A, König HH, Kaufmann C, Egger N, Wild B, Szecsenyi J, et al. Cost-utility of a specific collaborative group intervention for patients with functional somatic syndromes. J Psychosom Res 2016;90:43–50. https://doi.org/10.1016/j.jpsychores.2016.09.001 | Costs from the Schaefert et al. trial, not UK |
| Lamsal R, Stalke CA, Cait CA, Riemer M, Horton S. Cost-effectiveness analysis of single-session walk-in counselling. J Ment Health 2018;27:560–66. https://doi.org/10.1080/09638237.2017.1340619 | Non-UK |
| Luciano JV, D’Amico F, Feliu-Soler A, McCracken LM, Aguado J, Penarrubia-Maria MT, et al. Cost-utility of group acceptance and commitment therapy for fibromyalgia versus recommended drugs: an economic analysis alongside a 6-month randomized controlled trial conducted in Spain (EFFIGACT study). J Pain 2017;18:868–880 | Costs from the Luciano et al. trial, not UK |
| Meng H, Friedberg F. Cost-utility of home-based fatigue self-management versus usual care for the treatment of chronic fatigue syndrome. Fatigue 2017;5:202–14 | Does not meet review criteria for primary care |
| Rask MT, Ørnbøl E, Rosendal M, Fink P. Long-term outcome of bodily distress syndrome in primary care: a follow-up study on health care costs, work disability, and self-rated health. Psychosom Med 2017;79:345–57 | Non-UK |
| Röhricht F, Zammit I, Papadopoulos N. Novel primary care treatment package for patients with medically unexplained symptoms: a cohort intervention study. BJGP Open 2018;1(4) | Not a comparative study |
| Shea JA, Adejare A, Volpp KG, Troxel AB, Finnerty D, Hoffer K, et al. Patient’s views of a behavioral intervention including financial incentives. Am J Manag Care 2017;23:366–71 | Does not meet review criteria for MUS |
| van Eijk-Hustings Y, Kroese M, Creemers A, Landewe R, Boonen A. Resource utilisation and direct costs in patients with recently diagnosed fibromyalgia who are offered one of three different interventions in a randomised pragmatic trial. Clin Rheumatol 2016;35:1307–15. https://doi.org/10.1007/s10067-015-3067-y | Does not meet review criteria for primary care |
| van Ravesteijn H. Mindfulness-based cognitive therapy for patients with somatoform disorders. Tijdschri Psychiatr 2016;58:198–206 | Non-UK |
| Wenger HC, Cifu AS. Treatment of low back pain. JAMA 2017;318:743–4 | Acute |
| Williams A, van Dongen JM, Kamper SJ, O’Brien KM, Wolfenden L, Yoong SL, et al. Economic evaluation of a healthy lifestyle intervention for chronic low back pain: a randomized controlled trial. Eur J Pain 2019;23:621–34. https://doi.org/10.1002/ejp.1334 | Does not meet review criteria for MUS |
| Wortman MSH, Lokkerbol J, van der Wouden JC, Visser B, van der Horst HE, Hartman TCO. Cost-effectiveness of interventions for medically unexplained symptoms: a systematic review. PLOS ONE 2018;13. https://doi.org/10.1371/journal.pone.0205278 | Systematic review, includes secondary care |
List of abbreviations
- ACR
- American College of Rheumatology
- ACT
- acceptance and commitment therapy
- BAI
- Beck Anxiety Inventory
- BDI
- Beck Depression Inventory
- BSI
- Brief Symptom Inventory
- CASP
- Critical Appraisal Skills Programme
- CBT
- cognitive–behavioural therapy
- CBTHI
- high-intensity cognitive–behavioural therapy
- CBTLI
- low-intensity cognitive–behavioural therapy
- CDC
- Centers for Disease Control and Prevention
- CDSR
- Cochrane Database of Systematic Reviews
- CEAC
- cost-effectiveness acceptability curve
- CENTRAL
- Cochrane Central Register of Controlled Trials
- CERQual
- Confidence in the Evidence from Reviews of Qualitative research
- CFS
- chronic fatigue syndrome
- CFT
- cognitive functional therapy
- CGIS
- Clinical Global Impression Scale
- CI
- confidence interval
- CINAHL
- Cumulative Index to Nursing and Allied Health Literature
- CIS
- Checklist of Individual Strength
- CRD
- Centre for Reviews and Dissemination
- CrI
- credible interval
- DARE
- Database of Abstracts of Reviews of Effects
- DIC
- deviance information criterion
- DSM
- Diagnostic and Statistical Manual of Mental Disorders
- EQ-5D
- EuroQol-5 Dimensions
- FINE
- Fatigue Intervention by Nurses Evaluation
- FIQ
- Fibromyalgia Impact Questionnaire
- FSS
- functional somatic syndrome
- GA
- graded activity
- GET
- graded exercise therapy
- GHQ
- General Health Questionnaire
- GP
- general practitioner
- HADS-A
- Hospital Anxiety and Depression Scale – Anxiety
- HADS-D
- Hospital Anxiety and Depression Scale – Depression
- HAM-A
- Hamilton Anxiety Rating Scale
- HAM-D
- Hamilton Rating Scale for Depression
- HERC
- Health Economic Research Centre
- HP
- health professional
- HRQoL
- health-related quality of life
- HTA
- Health Technology Assessment
- IAPT
- Improving Access to Psychological Therapies
- IBS
- irritable bowel syndrome
- ICD
- International Classification of Diseases
- ICER
- incremental cost-effectiveness ratio
- IQR
- interquartile range
- MBSR
- mindfulness-based stress reduction
- MCS
- mental component summary
- MeSH
- medical subject heading
- MM
- multimodal
- MOS
- Medical Outcomes Survey
- MUPS
- medically unexplained physical symptoms
- MUS
- medically unexplained symptoms
- MUSICIAN
- Managing Unexplained Symptoms (chronic widespread pain) In primary Care: Involving traditional and Accessible New approaches
- NHS EED
- NHS Economic Evaluation Database
- NICE
- National Institute for Health and Care Excellence
- NIHR
- National Institute for Health Research
- NMA
- network meta-analysis
- NRS
- numerical rating scale
- ODI
- Oswestry Disability Index
- OLS
- ordinary least squares
- PCP
- primary care physician
- PCS
- physical component summary
- PHQ
- Patient Health Questionnaire
- PPI
- patient and public involvement
- PRECIS
- PRagmatic Explanatory Continuum Indicator Summary
- PrI
- prediction interval
- PRISMA
- Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- PSSRU
- Personal Social Services Research Unit
- QALY
- quality-adjusted life-year
- RCT
- randomised controlled trial
- RMDQ
- Roland–Morris Disability Questionnaire
- RSSE
- relaxation/stretching/social support/emotional support
- SASS
- Scale for Assessment of Somatic Symptoms
- ScHARR
- School of Health and Related Research
- SCL-90
- Symptom Checklist-90
- SCL-90-A
- Symptom Checklist-90 – Anxiety
- SCL-90-D
- Symptom Checklist-90 – Depression
- SCL-90-G
- Symptom Checklist-90 – Global Wellness
- SCL-90-S
- Symptom Checklist-90 – Somatisation
- SD
- standard deviation
- SE
- standard error
- SES
- strength/endurance/sport
- SF-12
- Short Form questionnaire-12 items
- SF-36
- Short Form questionnaire-36 items
- SF-6D
- Short Form questionnaire-6 Dimensions
- SIP
- sickness impact profile
- SMD
- standardised mean difference
- SOMS
- Screening for Somatoform Symptoms
- TIDieR
- Template for Intervention Description and Replication
- VAS
- visual analogue scale