

Notes
Article history
The research reported in this issue of the journal was funded by the HTA programme as project number 17/70/01. The contractual start date was in April 2018. The draft report began editorial review in June 2019 and was accepted for publication in March 2020. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HTA editors and publisher have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
Niina Kolehmainen is a panel member of the National Institute for Health Research (NIHR) Health Technology Assessment (HTA) Prioritisation Committee for Maternal, Child and Mental Health Care (2018 to present) and was a panel member of the NIHR HTA Maternal, Neonatal and Child Health Topic Identification, Development and Evaluation Panel (2015–18). Jane Noyes was a member of the NIHR Dissemination Centre Advisory Group (2015–20) and was a Trustee of Whizz-Kidz (2005–9) (Whizz-Kidz is a not-for-profit organisation and an NHS provider of wheelchairs for children). Dawn Craig is a member of the NIHR Health Services and Delivery Research Researcher-led Prioritisation Committee (2018 to present) and a member of the Health and Care Research Wales Funding Research for Patient & Public Benefit Committee (2017 to present).
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2020. This work was produced by Bray et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
2020 Queen’s Printer and Controller of HMSO
Chapter 1 Introduction
Background
Non-communicable illness and disability are responsible for most health expenditure in Western countries. Mobility impairment is the leading cause of disability in the UK, accounting for 49% of reported disabilities. 1 Around 8% of children in the UK have a disability, equating to 1.1 million disabled children (aged 0–19 years). Of this number, 19% are estimated to have some form of mobility limitation, which equates to approximately 209,000 UK children with mobility limitations. 1 The ability of public services, including health and social care and education, to improve the life of children with mobility limitations is currently significantly hindered by a lack of effective interventions. 2–6 Patients, policy-makers and health-care providers all agree that improving interventions is an urgent priority. 7,8
One of the most promising interventions is the early provision of powered mobility for very young children (aged < 5 years) with mobility limitations. Early powered mobility interventions enable self-directed movement in children who are limited in their movements or unable to move, and is consequently thought to trigger positive developmental changes, similar to crawling. 9–13 The idea of early powered mobility as an intervention is based on the observation that acquisition of self-directed mobility (e.g. through rolling, crawling, bottom-shuffling) results in a major step change in children’s engagement with the world and, through that, in their perceptual, cognitive, social and physical development. Children with mobility limitations have less self-directed movement than their typically developing peers, with fewer opportunities for exploration of the world around them. 12–16 This places children with mobility limitations at a greater risk of secondary disabilities in terms of life skills (motor, cognitive, social abilities related to daily tasks); general independence and autonomy; and participation in daily life across home, education and leisure. 16,17 These secondary disabilities are hypothesised to be negatively related to a child’s long-term health, development and social integration, as well as having a negative impact on parental physical and mental health, parental productivity and wider society. Early powered mobility could prevent these secondary disabilities by enabling self-directed mobility and exploration, and subsequent developmental benefits.
Powered mobility interventions are complex interventions with several elements and synergistic outcomes and benefits. The use of powered mobility takes place in, and is influenced by, a child’s physical and social environment,11 and the exact features and delivery of the intervention elements varies depending on the child’s age and/or developmental stage and impairments. Provision of powered mobility often involves allied health (e.g. physiotherapy, occupational therapy) and wheelchair services coming together to enable the provision of multifaceted intervention packages. Examples of intervention elements included in such packages are as follows:
-
the powered mobility equipment, for example powered wheelchair, ride-on device or toy car, to enable the child to move around, including any related method of control (e.g. switches)
-
training and other behaviour change techniques, for example goal-setting and self-monitoring, provided to the child and the people around the child to maximise the likelihood that the equipment is used regularly and appropriately
-
adaptations to physical environment, for example ramps and lifts, to enable the physical use of the equipment
-
adaptations to policies and practices, for example safety rules and activity processes, to provide a socially facilitative and safe environment for the use of the equipment
-
maintenance and reviewing, for example maintenance of the equipment and related adaptations and use, in the longer term.
There are currently no agreed standardised descriptions for any of these elements.
Provision of mobility equipment to children is not new. For example, > 60,000 children are registered with NHS posture and mobility services. 18 However, the current provision of powered mobility interventions commonly focuses on children aged ≥ 5 years, with an implicit assumption that most children aged < 5 years do not benefit from it, at least not sufficiently for it to be cost-effective. This assumption may be based on a number of preconceptions about the abilities of very young children to safely use powered mobility, the purpose of powered mobility and the adequacy of other interventions (i.e. buggies and manual wheelchairs) to fulfil the needs of these children.
If the hypotheses about the role of early self-directed mobility in prevention of secondary problems are true, then the current provision may be a missed opportunity to yield the best returns for public resource across the life course. 19 The key remaining question is whether or not early provision of powered mobility is incrementally more effective and cost-effective than later provision (i.e. from the age of 5 years onwards).
There is currently no evidence-based national guidance, or other up-to-date evidence summary, for decision-makers on what is the optimal time point for powered mobility provision for children, how different intervention components relate to cost-effectiveness, how variability in children’s conditions and diagnoses influences effectiveness or what outcomes could be used to monitor benefits of provision. In the absence of guidance or summary, the provision of powered mobility provision is highly variable across services and regions. This further exacerbates the socioeconomic, health and well-being inequalities already experienced by children with mobility limitations and their families.
The aim of this project was to synthesise the existing evidence about the relative benefits and cost-effectiveness of early powered mobility (for children aged < 5 years) compared with later powered mobility (children aged ≥ 5 years) in both the short and long term. We hope to provide health commissioners, wheelchair services, service providers more broadly (both in the NHS and beyond), policy-makers and families with access to timely evidence to facilitate better-informed decisions about how best to use resources to support disabled children and to promote their long-term health and well-being.
From scoping of the literature and from expertise in the team, including the wider project advisory group, an upfront logic model was developed, following published guidance and examples. 20,21 The logic model was developed to provide a simplified representation of the proposed key outcomes and related change processes for powered mobility interventions (Figure 1).
FIGURE 1.
Initial logic model to be used as a framework for the evidence synthesis of the effectiveness and cost-effectiveness of powered mobility for children with mobility limitations. The green box indicates the context and the purple box indicates the moderators.

The literature and expert opinion propose that provision of powered mobility interventions for very young children will reduce the negative effects of mobility limitations by enabling self-directed mobility, which provides opportunities for exploration and the development of a child’s life skills,13,17,22 independence,13,23 autonomy and participation in daily life. 11,24 It is further proposed that these will collectively enhance the child’s long-term health, development and social integration, 11,22,24 and that subsequent developmental gains will reduce a child’s need for parental support14 and reduce related parental stress. 15 A further suggestion, derived from the literature and expert opinion, is that child and parent gains may, together, reduce the burden on public services across health, education and social care.
Chapter 2 Research question and aims
The research question was as follows: is the earlier provision of powered mobility to very young children more cost-effective than currently more common provision to children aged ≥ 5 years?
The aim was to examine and model the relative effectiveness and cost-effectiveness of powered mobility interventions for very young children (aged < 5 years) with mobility limitations, compared with the more common practice of powered mobility provision for children aged ≥ 5 years. To do so, the following of key objectives were defined:
-
to identify and synthesise quantitative, qualitative and mixed-method evidence to determine –
-
the effectiveness and cost-effectiveness of powered mobility interventions for children with mobility limitations, and the wider impacts on health services and society
-
the acceptability, feasibility and anticipated outcomes of relevant interventions from multistakeholder perspectives (children, parents, service providers, commissioners, etc.)
-
the long-term implications of self-directed or independent mobility for very young children (aged < 5 years) compared with older children (aged ≥ 5 years).
-
-
to examine the economic costs and benefits of powered mobility interventions for children by –
-
building tariffs of NHS and non-NHS costs for powered mobility interventions (equipment, training and support, and any other components) for children with mobility limitations using a multiperspective disaggregated cost–consequence framework
-
modelling the relative cost-effectiveness of powered mobility equipment for very young children (aged < 5 years), compared with standard NHS practice (provision of such equipment for children aged ≥ 5 years).
-
Chapter 3 Overall design
Methodology
The Early Mobility and POwered Wheelchair Evidence Review (EMPoWER) study was planned as a mixed-methods evidence synthesis and economic modelling study, incorporating quantitative, qualitative, mixed-methods and economic evidence. The key intended outputs were an overview of the current evidence of powered mobility interventions for children; a logic model of effectiveness and cost-effectiveness for planning and evaluating future interventions and commissioning of services; an economic model, budget impact analysis and value-of information analysis for early powered mobility; and recommendations for powered mobility provision and for future research. To achieve the objectives and deliver the outputs, we planned a number of inter-related research activities:
-
a systematic review of evidence relating to the effectiveness, cost-effectiveness, acceptability, feasibility and anticipated outcomes of paediatric powered mobility interventions, integrating a range of perspectives (children, parents, service providers, commissioners, society)
-
a further second review of available evidence on the long-term implications of self-directed or independent mobility for very young children (aged < 5 years), compared with the implications for older children (aged ≥ 5 years)
-
the development of cost tariffs of NHS and non-NHS costs for powered mobility interventions (equipment, training and support, and any other components) for children with mobility limitations using a multiperspective disaggregated cost–consequence framework
-
an economic model to facilitate a comparison of the relative cost-effectiveness of powered mobility equipment for very young children with standard NHS practice of powered mobility provision for older children
-
an integrative overall synthesis of learnings from across these listed activities in order to develop a new model for assessing the effectiveness and cost-effectiveness of early powered mobility interventions.
Population
The overall study population was children with mobility limitations, defined as limitations in a child’s ability to move around in space. In existing literature, mobility limitations have been described using standardised classification systems [e.g. the Gross Motor Function Classification System (GMFCS)]; codes from the World Health Organization’s International Classification of Functioning, Disability and Health (ICF);25 or clinical observations. Certain medical diagnoses have also been used as indicative proxies for a presence of mobility limitations; for example, a diagnosis of cerebral palsy is indicative of mobility limitations, but it is well recognised that medical diagnoses alone do not provide precise estimates of a child’s capacity for movement. Use of ability-based, as opposed to diagnosis-based, approaches to defining study populations is recommended to reflect the realities of the children and service provision, and thus to support external validity and relevance to the NHS setting. 26,27 In terms of children with mobility limitations, the focus of the present study was on a comparison between children aged < 5 years and children aged ≥ 5 years.
Setting
The settings of interest included any high-income health and social care provision, family contexts and nurseries, education, and communities broadly similar to UK. We anticipated the most common provider setting to be allied health and wheelchair services providing mobility interventions for children, as well as third-sector providers.
The health technology
As a starting point, the intervention of interest, early powered mobility, was defined as consisting of five elements: the powered mobility equipment, adaptations to physical environment, adaptations to policies and practices, training and other behaviour change techniques, and maintenance and reviewing. We anticipated that the review would inform this conceptualisation further, and potentially re-shape it.
Stakeholder involvement
This study contributed to addressing two of the 10 key research questions prioritised by users and providers of children’s neurodisability services in the James Lind Alliance Research Priority Setting Partnership for childhood disability:7
Does appropriate provision of wheelchairs to enable independent mobility for very young children improve their self-efficacy? [Question 1.]
Does the timing and intensity of therapies . . . alter the effectiveness of therapies for infants and young children with neurodisability, including those without specific diagnosis? What is the appropriate age of onset/strategies/dosage/direction of therapy interventions? [Question 4.]
Morris et al. 7
The overall aim was to optimise the relevance, usefulness and potential impact of the study by integrating expertise and insight from expert stakeholders at each stage. Patient and public involvement (PPI) was integrated with and embedded within a wider stakeholder involvement strategy; thus, we refer to stakeholder involvement rather than PPI. We took a comprehensive and ‘real-world’ approach to stakeholder analysis, identifying individuals and organisations with an interest in the study or who could be affected by the study. This included, but was not limited to, service users (i.e. children, young people, and parents). To achieve substantial and meaningful stakeholder involvement, we used a multipronged approach. First, we engaged an expert service user (AG) as a co-investigator from the outset of developing the project. Aimee Grayston has considerable lived experience of using powered mobility in the context of complex mobility and communication limitations, and was already collaborating with two study team members (JM, NK). Her role at the grant application stage was to help develop the up-front logic model (see Figure 1), to advise on the design and projected costs of involvement activities and to respond to selected comments from reviewers. Throughout the study, Aimee Grayston attended study meetings, teleconferences and co-production workshops and engaged in study methods. She guided the wider team’s thinking on the conceptualisation of intervention components, outcomes and the acceptability/feasibility of powered mobility implementation. Her contributions sensitised the team to key ideas and influenced how we conducted the project and revised the logic model. In the end stages of the project, Aimee Grayston developed the plain language summary and provided feedback on the draft report, and will continue to aid in the dissemination of findings.
Second, we convened an international project advisory group consisting of researchers, service providers/managers, service commissioners, policy advisors, commercial directors, representatives of national charitable organisations, and parents of children and young people with mobility limitations (see Appendix 1, Table 39, for a full list of members). We purposefully integrated professional and parent advisors for three reasons: (1) we wanted to centrally embed service user involvement in the wider stakeholder involvement strategy; (2) we were equally as invested in benefiting from professional and service user expertise; and (3) from our prior experiences of PPI in this field, we had learned that many professionals and service users place high value on coming together to share perspectives and experiences. We identified group members on the basis of their wide-ranging expertise in the development, implementation, benefits and costs of powered mobility interventions, and their experience of powered mobility in diverse health service, third-sector and commercial contexts. Appendix 1, Table 39, sets out the particular expertise brought by each individual advisor. We approached the professional advisors directly, and the parent advisors were a combination of existing collaborators of the study team and new collaborators recruited through the charitable organisation Designability.
The advisory group was consulted about a wide range of different topics and we called on it at different time points for different purposes, depending on the fields of expertise of various members. Contact was generally informal, and conducted through e-mails, face-to-face meetings and telephone/video calls. Several specific examples of the advisory group’s involvement are cited throughout this report. The advisors helped to shape the up-front logic model (particularly parents); develop the search strategies; identify key evidence and grey literature; keep up to date with the most recent publications; clarify redundancy and overlap in the literature (particularly researchers, policy advisors and representatives of charitable organisations); and understand and resolve conceptual issues, particularly regarding the long-term implications of self-directed or independent mobility for very young children (particularly researchers). They also helped to inform our understanding and interpretation of the data relating to the feasibility, acceptability, costs and benefits of early powered mobility (particularly parents, service providers/managers and commissioners), and we worked directly with some advisors to identify cost data for the economic analysis (particularly service providers/managers, service commissioners, commercial directors and representatives of charitable organisations). All of this fed directly into how we refined the up-front logic model and the acceptability and clarity of the key messages. The advisors also helped to maintain a public-facing presence for the study in the clinical, research and service user communities, through signposting and discussion on their own social media platforms and at professional conferences. After publication of the report, the group will continue to support the research team by offering potential opportunities for implementation of practice-related recommendations.
Third, we worked with AniMates, a young people’s involvement group that specialises in making artwork to shape and share research28 (Figure 2 presents an example of the artwork the group generated for the EMPoWER project). AniMates comprises young people and artists aged 16–21 years, an interdisciplinary artist and a researcher. AniMates members have experience of living with physical, communication or learning disabilities or of supporting people who live with disabilities. Three members use powered mobility themselves. AniMates enabled the project team to include the views of young powered mobility users and to find creative ways to explain the project and disseminate the findings. Five workshops were held during the project, each facilitated by a member of the research team and an artist. AniMates helped to interpret the emerging results and their relative importance, and challenged the research team’s understanding and assumptions. Their contribution fed into the final logic model and also facilitated creative, engaging dissemination plans.
FIGURE 2.
Artwork produced as part of the EMPoWER workshops.

The research team provided parent and young person advisors with informal training to prepare them for being involved in the study. For parents, this was in the form of accessible written materials explaining key concepts in the study (e.g. cost-effectiveness, systematic review methods) and an extended face-to-face meeting with one researcher to go through the materials, discuss the up-front logic model, and share experiences and ideas about powered mobility interventions. For the young people, informal training was in the form of two workshops, facilitated by a researcher and an artist, exploring the rationale for the study, key concepts, and their roles, rights, and responsibilities as advisors. The contribution of the adult advisors (i.e. the parents and AG) was acknowledged in the form of payments or gift vouchers based on established guidance from INVOLVE. 29 The contribution of young people was similarly acknowledged, based on established guidance about national minimum wage and national living wage rates. 30 Reporting of PPI and stakeholder involvement is summarised in Appendix 2.
Chapter 4 Review 1: a mixed-methods review of the effectiveness, cost-effectiveness, perceived outcomes, acceptability and feasibility of powered mobility
This chapter reports on the first review conducted to explore the effectiveness, cost-effectiveness, acceptability, feasibility and anticipated outcomes of powered mobility interventions, integrating a range of perspectives (children, parents, service providers, commissioners, society, etc.). Therefore, this chapter addresses two of the stated aims; specifically, to determine:
-
the effectiveness and cost-effectiveness of powered mobility interventions for children with mobility limitations, and the wider impacts on health services and society
-
the acceptability, feasibility and anticipated outcomes of relevant interventions from multistakeholder perspectives (children, parents, service providers, commissioners, etc.).
Methods
The initial programme theory in the logic model (see Figure 1) was utilised as a conceptual starting point and was refined throughout the review processes to produce a definitive logic model. The active intervention was provision of powered mobility for children aged < 5 years (i.e. early powered mobility), and the comparator was provision of powered mobility for children aged ≥ 5 years.
Before the review, we anticipated finding limited evidence on effectiveness from formal evaluations such as randomised controlled trials (RCTs), and anticipated that evidence on different types of outcomes (effectiveness, cost-effectiveness) and phenomena of interest (feasibility and acceptability) would be spread across papers. Therefore, we expected to use a mixed-methods review design utilising a variety of synthesis methods. After the search and screening had been completed and the actual body of included papers was known, the specific overall mixed-methods design was decided on.
Processes for searching and for quality appraisal followed the basic principles for conducting effectiveness and cost-effectiveness reviews,31 using additional up-to-date relevant methods and tools, with an explicit protocol registered with PROSPERO as CRD42018096449. 32 With the papers and evidence ultimately identified (see Results: an overview of evidence of powered mobility interventions for children) it was not possible to undertake a meta-analysis. We therefore undertook two types of synthesis to make best use of the available evidence. First, we undertook a convergent data-based, mixed-methods evidence synthesis, using a framework synthesis method, in which textual and numeric data from all included studies (quantitative, qualitative and mixed-methods designs) were analysed and synthesised concurrently in a complementary manner. 33,34 The use of framework synthesis enabled findings from all included studies to be synthesised around common concepts that were derived from the included studies, with regular checking-back to the review question and the initial logic model. We subsequently assessed the certainty of evidence using mixed-methods-specific criteria.
Second, we undertook a separate qualitative evidence synthesis using the Thomas and Harden35 method of thematic synthesis. This method includes three stages: line-by-line coding, development of descriptive themes, and then development of analytical-level themes. The development of analytical-level themes was important to provide new insights that went beyond findings presented in the primary studies. Findings in primary studies were translated and then transformed to look for new patterns and meanings that were not seen in individual primary studies. We subsequently applied the Grading of Recommendations Assessment, Development and Evaluation – Confidence in the Evidence from Reviews of Qualitative research (GRADE-CERQual)35 approach to assess the confidence in synthesised qualitative findings.
The initial logic model evolved during the course of the syntheses as the evidence became known and understood. The service user co-investigator (AG) and the project advisory group were instrumental in the continuous review and critique of the logic model, for example by challenging its assumptions and gaps, and enabling the research team to better understand and convey relationships between powered mobility interventions and outcomes. Care was taken to differentiate between evidence, expert/lay opinion and proposition/conjecture when populating the logic model. We then used the evolving logic model as the framework for integrating the various syntheses and drawing out the relevant evidence to address the original review question and objectives.
The following section reports the search strategy and methods for screening, quality appraisal and general data extraction, which were all undertaken once, but which fed into both synthesis approaches. The two syntheses and approaches to grading the bodies of evidence are then described in more detail, separately, for each synthesis approach.
Search strategy
To identify relevant literature to inform the first review, a search strategy was designed and run in collaboration with an experienced information specialist. The search was designed to prioritise sensitivity over specificity, and was structured according to the facets of ‘children’, ‘powered mobility’ and ‘independent mobility’. For each facet, the search incorporated both thesaurus-controlled subject heading terms and text words or phrases. A full list of search terms is presented in Table 1. For an illustrative example of keywords and a search strategy, see Appendix 3. The searches were not restricted by outcome, disability, activity limitation or medical condition, as these were incorporated at the screening stage, nor by study design, language or publication year.
| Search term | Proximity | Proximal search term |
|---|---|---|
| Facet 1: children | ||
| child(ren) or adolescent (ce) or teen(s)/(ager(s)) or youth(s) or girl(s) or boy(s) p(a)ediatric(s) or juvenile(s) or infant(s) or “young people” or “young person” or “young adult” or “young men” or “young women” or schoolchild(ren) | ||
| Facet 2: powered mobility | ||
|
power(ed) electric(al) motorised (zed) assist(ed) |
within five words of |
(wheel)chair(s) pushchair(s) equipment car(s) scooter(s) toy(s) mobility buggy/ies |
| Facet 3: independent mobility | ||
|
independent(ly) self* autonomous |
within three words of |
Mobile mobility move*/moving walk(ing) crawl(ing) |
The following bibliographic databases were searched in June 2018; searches were updated in early October 2019:
-
Cumulative Index to Nursing and Allied Health Literature (CINAHL) (via EBSCOhost; EBSCO Information Services, Ipswich, MA, USA), 1980 to September 2019
-
MEDLINE (via Ovid®; Wolters Kluwer, Alphen aan den Rijn, the Netherlands), 1946 to September 2019
-
EMBASE™ (Elsevier, Amsterdam, the Netherlands) (via Ovid), 1980 to September 2019
-
Physiotherapy Evidence Database (PEDro), 1999 (inception) to September 2019
-
Occupational Therapy Systematic Evaluation of Evidence (OTSeeker), 2001 (inception) to September 2019
-
Applied Social Sciences Index and Abstracts (ASSIA) (via ProQuest®; ProQuest LLC, Ann Arbor, MI, USA), 1987 to September 2019
-
PsycINFO (via Ovid), 1967 to September 2019
-
Science Citation Index and Social Sciences Citation Index™ (Clarivate Analytics) (via Web of Science™; Clarivate Analytics), 1970 to September 2019
-
Conference Proceedings Citation Index – Science (Clarivate Analytics), and (Clarivate Analytics, Philadelphia, PA, USA) Conference Proceedings Citation Index – Social Science & Humanities (Clarivate Analytics) (via Web of Science), 1990 to September 2019
-
Cochrane Central Register of Controlled Trials (CENTRAL) and Cochrane Database of Systematic Reviews (via the Cochrane Library), 1995 (inception) to September 2019
-
Database of Abstracts of Reviews of Effects (DARE) and NHS Economic Evaluation Database (NHS EED) (via the Cochrane Library), 1994 (inception) to May 2015
-
Health Technology Assessment (HTA) Database (via the Cochrane Library), 1998 (inception) to September 2019.
To reduce publication bias, the electronic searches were supplemented by reference list searching: hand-searching a sample of selected, highly relevant journals (i.e. Clinical Rehabilitation, Archives of Physical Medicine and Rehabilitation and Disability and Rehabilitation: Assistive Technology); searching any highly relevant conference proceedings that were not indexed on the databases listed previously; and identification of relevant grey literature. Grey literature searching included OpenGrey and resources such as government policy documents, third-sector organisation reports and unpublished research, much of which was sourced from within the project advisory group, particularly from the researchers and policy advisors. The project advisory group also directed us to seminal papers.
Screening for inclusion
Papers were included if all of the following criteria were met:
-
The study participants included children with significant mobility limitations with a known risk for the child’s achievement of independent mobility, defined using explicit criteria.
-
The intervention described in the paper involved at least one of the five intervention elements defined in Figure 1 (see also Chapter 1, Background).
-
The outcome (or the ‘phenomenon of interest’) was related to the child, their family, health or social care, or education.
In applying these criteria, ‘mobility limitations’ were defined as impairments in the functions of movement and mobility, including functions of joints, bones, reflexes and muscles; control of voluntary and involuntary movements; gait, muscle tone and power; and joint mobility. Conditions for which movement problems were part of the diagnostic criteria or condition definition (e.g. cerebral palsy) were considered to meet the population criterion; judgements about this were made using explicit rules developed in a previous intervention review in this population (Niina Kolehmainen, Newcastle University, 2018, personal communication) (Table 2). No initial age cut-off point was set for ‘children’ because there is no single agreed cut-off point to use and we wanted to keep the inclusion of evidence broad. Finally, all included papers clearly stated that they either included or did not include children, with no borderline papers present and no specific age cut-off point required.
| Diagnoses and condition groups | Decision | Rationale |
|---|---|---|
|
Always include in the review | Significant movement problems with known risk to independent mobility are part of the diagnostic criteria or condition definition |
|
Included if significant movement problems posing a risk to independent mobility are explicitly mentioned as part of the eligibility criteria or rationale | Although the diagnostic criteria do not necessitate movement problems that are a risk to independent mobility, comorbidity is common |
|
Excluded from the review | Movement problems are not inherently part of the diagnostic criteria or condition definition, or are short term |
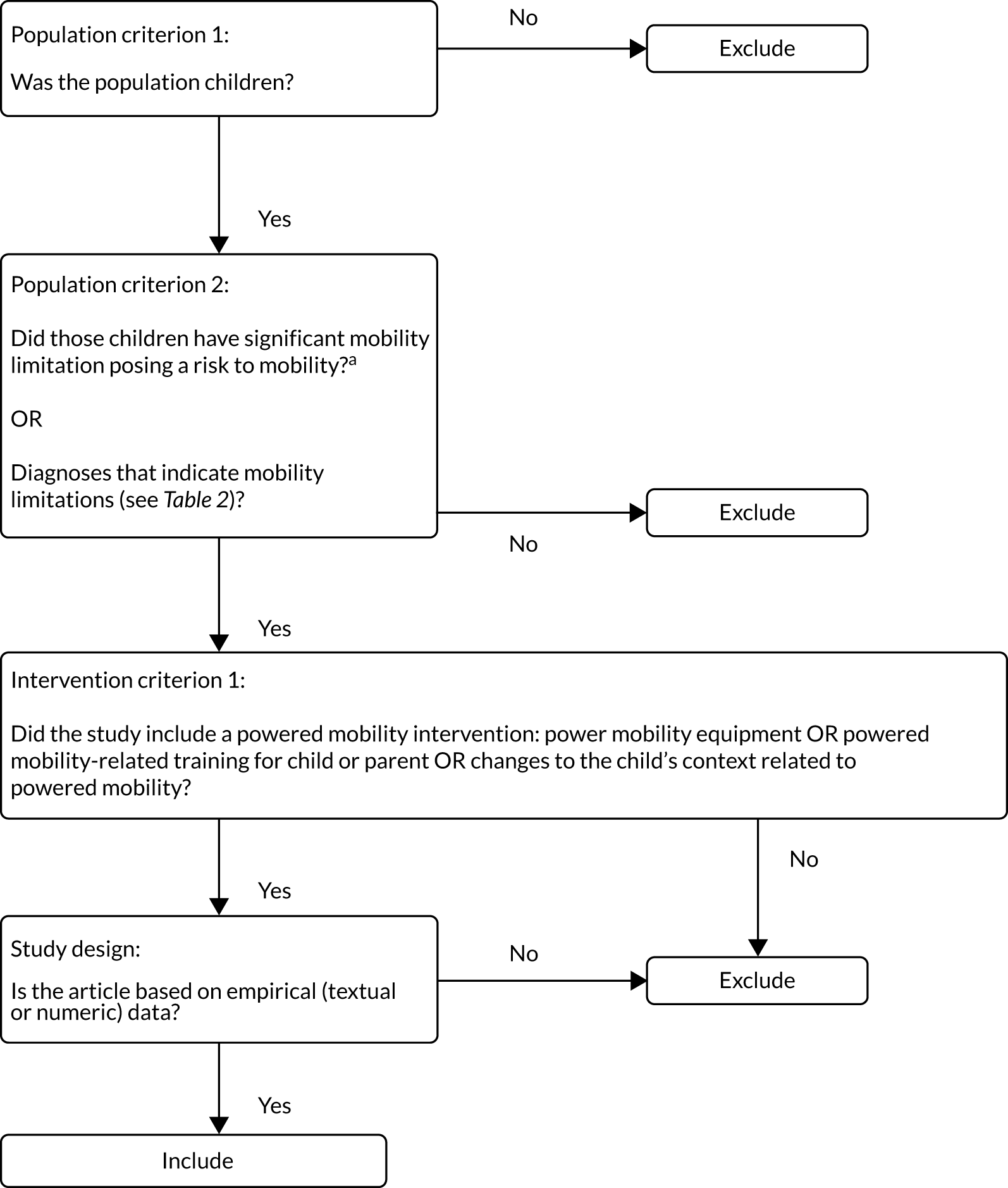
Papers were excluded if it was not possible to identify outcomes (either measured or described qualitatively), if the intervention was solely non-powered mobility (e.g. manual wheelchair) or if the paper was not based on empirical data (e.g. opinion pieces). The self-initiated prone progression crawler36 and a powered standing wheelchair37 were also excluded. Although these could be considered powered mobility interventions in a broad meaning of the word, they were outlier technologies in the scope of the present review. Figure 3 presents the inclusion/exclusion flow chart.
FIGURE 3.
Inclusion/exclusion flow chart used during review 1 screening process. a, Mobility is defined as moving by changing body position or location or by transferring from one place to another; carrying, moving or manipulating objects; walking, running or climbing; and using various forms of transportation.
Although the intention was for the active intervention to be the provision of powered mobility for children aged < 5 years, and for the comparator to be provision for children aged ≥ 5 years, we did not exclude papers on design, comparator or the age of the children in the active intervention at the screening stage, but retained all papers that could broadly inform the review.
Titles and abstracts were screened for inclusion using the software package Rayyan (Qatar Computing Research Institute, Doha, Qatar)38 by two independent reviewers (LTa, JM or NK), of which at least one was a topic expert. Any discrepancies in decisions about eligibility were discussed until a consensus was reached, including a discussion among the wider team, if necessary. All studies judged to be relevant based on title and abstract were retained and obtained as full texts. EndNote version X8 [Clarivate Analytics (formerly Thomson Reuters), Philadelphia, PA, USA] was used to manage literature.
The project advisory group and, in particular, the expert clinicians played a key role in finalising and implementing the inclusion and exclusion criteria, for example by meaningfully defining ‘mobility limitations’ in very young children; by interpreting papers in which mobility limitations were not explicitly reported; and by checking whether or not the reasons for excluding papers, particularly on the basis of population or outcome, were understandable and acceptable.
Quality appraisal of individual studies
Assessment of the methodological strengths and limitations of included studies focused on risk of bias in RCTs, risk of bias and confounding in non-randomised studies and risks to rigour in qualitative studies. The assessments were used to feed into the development and interpretation of results, and to inform sensitivity and subgroup analyses, but were not used to exclude studies owing to the overall limited quality of the evidence.
The assessment consisted of two stages. First, all included studies were classified in design categories based on their design features (as opposed to primary authors’ reported design labels, which are often inconsistently applied). 31 The classification was conducted independently by two reviewers (LTa and JM) using a published algorithm adapted for the purposes of the proposed synthesis,39–41 with disagreements discussed and arbitration from a third reviewer (NK) as required.
Second, the studies were assessed for methodological strengths and limitations within their classified design categories. All included papers were assessed. The approach to the assessment was that of pragmatism, with focus on obtaining a meaningful and informative picture of the quality of the papers, while also being efficient. A range of tools were used, selected on the basis of the study design category. For RCTs, the established Cochrane Collaboration’s tool for assessing risk of bias was used in full, consisting of seven items and options for high, low and unclear risk of bias. 42 For all other quantitative studies, of which the majority were without a comparison group, selected items were used from the Research Triangle Institute (RTI)’s bank of signalling questions for assessing risk of bias, confounding, and precision in non-randomised studies of interventions and exposures. 41 This approach included common items related to sources of threats to validity and precision, including those listed by the Cochrane Collaboration, while allowing them to be used in a way that both differentiated between the studies on quality and was efficient (Table 3). In the original protocol, we had anticipated to use the Risk Of Bias In Non-randomized Studies – of Interventions (ROBINS-I) for non-randomised studies;43 however, using the RTI’s bank of signalling questions had a specific advantage in the present review when considering the particular set of included studies. Namely, it facilitated meaningful consideration of confounding which, based on the designs of the included studies, was likely to be a key quality consideration while also being efficient and consistent. This approach required reviewers to learn only one set of items to quality-assess a large number of papers of various designs.
| Quality appraisal category | Rationale | Proposed RTI items |
|---|---|---|
| Detection bias | An important bias category for differentiating the quality of studies; some studies will have considered this more than others |
|
| Selection bias | Considering the very small sample sizes and the study designs of the included studies, selection bias was an expected issue for most studies; thus, only key items were required to identify selection bias |
|
| Confounding | Owing to the study designs, confounding was expected to be an issue for most studies, especially the studies without controls/comparisons |
|
For qualitative studies, the Critical Appraisal Skills Programme (CASP)44 qualitative tool was used, as recommended in the Cochrane Qualitative and Implementation Methods Group’s guidance. 45 For mixed-method studies, the Mixed Methods Appraisal Tool (MMAT) was used. 46 Grey literature studies were also classified by design, as above, and assessed using the category-appropriate tool. No economic studies were identified and so no tool to quality-assess them was used. Two reviewers (NK and JM) piloted the quality assessment procedures and each included study was independently assessed by two reviewers, with a third reviewer arbitrating disagreements as required to reach consensus and with input from a topic expert. All members of the study were involved in quality assessment.
Data extraction
A bespoke data extraction form was developed based on a previous similar review in this population (Niina Kolehmainen, personal communication), piloted on a small number of included studies and revised as necessary. The following numeric and textual data were extracted from all included papers: the first author; the year of publication; the participants; the country of data collection; verbatim outcome construct/concept(s) targeted or reported by participants (including long-term implications), and any related measure(s); hypothesised change processes (‘mechanism’, ‘process outcomes’) and any related measure(s); relevant cost and economic data, and any related measure(s); and evidence about feasibility and acceptability. For intervention characteristics, we had intended to extract the intervention elements using the Template for Intervention Description and Replication (TIDieR);47 however, owing to reporting limitations in the included studies, this was not possible. We instead used a modified TIDieR-informed template to extract intervention element label(s) verbatim as provided by authors, and key details related to each intervention element. To further inform intervention element descriptions specifically related to very young children, subsets of textual evidence relating to very young powered mobility users were further explored. For these, line-by-line coding was first used to identify data that described any of the intervention elements, and the identified data were then organised thematically. When relevant, the thematic descriptions were further contextualised with visual illustrations (e.g. images of powered mobility equipment or contexts of use).
Throughout, both numeric and textual data were extracted, and the source of the data (e.g. objective measures, participant accounts, author narrative) was recorded. To enable the comparison between the two study groups (children aged < 5 years and children aged ≥ 5 years), both outcomes and intervention data were extracted separately for the two groups when possible.
To extract the data, two independent reviewers (LTa, NK or JM; at least one of whom was a topic expert) read the title, abstract, introduction and methods of the included full texts one at a time; identified the relevant excerpts of text (ranging from a single number or word to strings of numbers and paragraphs) containing information about any of the data aspects above; and copied, verbatim, the extracts from the full texts to a data file. The data extraction was carried out in batches whereby the reviewers independently extracted data for two to five papers and then came together to check consistency. The data extraction process required substantial discussion and interpretation throughout, because of limitations in reporting of the outcomes and related measures, intervention characteristics, and hypothesised change processes.
Mixed-methods framework synthesis of all data
The mixed-methods framework synthesis reviewed and integrated all quantitative, qualitative and mixed-methods evidence to determine the following aims: (aim 1.1) the effectiveness and cost-effectiveness of powered mobility interventions for children with mobility limitations, and the wider impacts to health services and society, and (aim 1.2) the acceptability, feasibility and anticipated outcomes of relevant interventions from multistakeholder perspectives (children, parents, service providers, commissioners, etc.). The included studies provided mainly textual data consisting of brief quotations and original authors’ narrative sentences, supplemented with highly heterogeneous numeric data from non-randomised study designs. Most of the studies covered a mix of textual and numeric evidence across health, feasibility, acceptability and implementation outcomes. It was clear at this stage that a lack of statistical analysis, underpowered studies and poor reporting would hinder the reporting of meaningful numerical and statistical data. Effect sizes, confidence intervals and p-values were not typically (or consistently) reported. Most studies appear to be unpowered to detect a significant difference in any outcome. To avoid vote-counting based on p-values and giving too much weight to the limited numerical findings,48 we opted not to present statistical data for the few studies for which such data were available. Rather, we opted to provide an indication as to whether or not the findings suggested an improvement in the outcome measured, without presenting the extent of that improvement.
We used the identification and development of main concepts relevant to the research question as a key thread and structure to the synthesis: we mapped all data (numeric and textual) against these concepts; identified contrasting, complementary and dissimilar data within and across studies, and interrogated these data in relation to the concepts to further shape them and investigate relationships between the concepts; and extended the coverage and expanded the breadth and range of the inquiry by drawing on one type of data to follow up and extend findings from another. 33,49 We followed the commonly used steps of framework synthesis,34 which mirror the steps of framework analysis. 50
Familiarisation
During the familiarisation stage, all the researchers in the team immersed themselves in, and developed a sense of, the data available from the included papers by reading through a sample of the included papers. Three researchers (LTa, JM and NK) further took the lead in becoming familiar with the data in-depth by repeatedly reading through and discussing selected papers. Louise Tanner familiarised herself in-depth with all the included papers, Jennifer McAnuff familiarised herself in-depth with the papers that had used quantitative designs and Niina Kolehmainen familiarised herself in-depth with the papers that had used qualitative or mixed-methods designs.
The framework
The logic model (see Figure 1) was used as the initial framework and the starting point for organising the data from the included studies. First, textual data from the results sections of the included papers (qualitative, quantitative and mixed methods) were reviewed, compared and contrasted against the concepts in the initial framework. Simultaneously, new issues, codes and themes that emerged from the data were generated and used to shape the concepts, to develop new concepts and to reconfigure the framework. All of the following were considered as data: primary participant quotations, primary author narratives, summary concepts and themes, numbers presented in tables or text, and figures.
Several cycles of concept generation were undertaken; each cycle consisted of the following steps:
-
Two initial researchers (LTa and NK) independently read and coded textual data from qualitative and mixed-methods papers.
-
The same researchers came together to talk through the emerging issues and themes, and relationships between them.
-
The same researchers further agreed key concepts and related content.
-
One of the initial researchers (LTa) summarised the agreed concepts and their content in memos.
-
That researcher (LTa) then systematically sought for any further, related data from the quantitative and mixed-methods papers, and linked these to the memos.
-
The memos were then shared with a third researcher (JM), who independently read them, and critiqued them in relation to the included studies and input from the study expert advisors.
-
The three researchers finally jointly discussed, reviewed and further modified the emerging concepts.
Coding of higher-quality papers was prioritised over that of the lower-quality papers, and data on similar outcomes were coded on a single round.
The three researchers who were primarily involved in the synthesis had, between them, expertise in the study population and context, movement and mobility interventions, mixed-methods synthesis, framework synthesis, and quantitative systematic review and synthesis methods. In addition, both the modified and emerging concepts were shared with the wider research team at fortnightly discussions, for independent critique and input. The concepts were also brought to an AniMates workshop for exploration, discussion, interpretation and brainstorming, with outcomes fed back to the study team. At the workshop, concepts were presented as brief statements, and the AniMates members were encouraged to discuss, debate and share their own experiences related to the concepts. AniMates produced artwork and brief animations about the key concepts that they were most interested in, which, in turn, fed back into the research team’s thinking about the concepts, and later helped to inform the refined logic model. NVivo version 12 (QSR International, Warrington, UK) and Microsoft Word 2016 (Microsoft Corporation, Redmond, WA, USA) were used to facilitate data management and to maintain a transparent audit trail.
Indexing and charting
Once the key concepts had been agreed, the three researchers (LTa, JM and NK) compared the data of all verbatim outcomes and outcome measures against the key concepts, and ‘indexed’ the studies to the concepts. The indexing was based on a combination of the verbatim outcomes stated by the primary study authors and the outcome measures used. Each outcome was indexed independently; all indexing was completed by at least two researchers, and all uncertainties taken to a third researcher for further review and discussion.
Once all the outcomes were indexed, and in line with the latest Cochrane recommendations for reviews for which there are no consistent effect measures or data across studies, we used vote-counting tables based on direction of effect to summarise and present the numeric/semiquantitative data in relation to each outcome concept. 48 We explored options for graphical summaries (e.g. harvest plots),51 but concluded that it was not possible to meaningfully use these, because few studies provided direct, formal evidence about the effectiveness of the intervention. The reasons for the absence of this evidence were various; it was not possible to disentangle these reasons in a manner that supported the construct of harvest plots. For instance, much of the numeric evidence came from studies with a high risk of confounding and/or small sample sizes, or studies with internally conflicting results, making it difficult to place them within the framework that would be used to support harvest plots. In addition, rather than apply one tool to assess bias for all study designs, which is feasible but often lacks sensitivity, we opted to use tools appropriate to study design. This decision introduced an added layer of complexity that would have led to complicated and unclear plots, thus defeating the objective to clearly and succinctly present the findings of the review. Hence, no harvest plots were produced.
Mapping and interpretation
The concepts and the data relating to each concept were shared with the wider research team throughout, and mapped back on to the logic model. In this, the findings from the mixed-methods synthesis were further triangulated and interpreted with the qualitative synthesis findings, and a new framework (in a form of a refined logic model) agreed for evaluating the effectiveness and cost-effectiveness of powered mobility interventions for children (reported in Integrative synthesis: an integrated logic model to inform the future planning for, and evaluation of, the outcomes of powered mobility for children). To aid the interpretation, we assessed the support that the evidence provided for each of the identified concepts. In this, we acknowledged the methodological challenges related to grading bodies of evidence in mixed-methods syntheses, while also appreciating the importance of providing some summary indication of the level of support that the evidence from the present review provides for each of the concepts (for a more detailed discussion, see Appendix 4). In line with the overall logical methodological stance underpinning the mixed-methods synthesis, we adopted a pragmatic approach to grading whereby we engaged with the broad concept of assessing the certainty of a body of evidence52 through a practical set of published mixed-methods-relevant criteria. Specifically, we used the following rating system to provide an overall assessment of the level of support for each concept:
-
strong support – converging evidence from a range of designs; no major gaps
-
moderate support – converging evidence from a range of designs; clear gaps in data or theory
-
low support – converging evidence from a limited pool of designs; clear gaps in data
-
very low support – converging evidence primarily from either qualitative or quantitative designs only; substantial gaps in data
-
inconsistent support – no converging evidence.
This assessment was also informed by the assessment of a range of mixed-methods-specific criteria (Table 4) and supplemented with a criterion for publication bias.
| Concept support criteria | Higher degree of confidence about concept, when | Underpinning scientific principles |
|---|---|---|
| Truth value/bias | The inferences related to an analytical concept remain sensitive to, and clearly reflective of, the numeric and textual data from the primary studies |
Confirmability (qualitative data) and objectivity (quantitative data) Triangulation |
| Explanation credibility | The analytical concept and the related inferences are theoretically and conceptually sounda | Credibility (qualitative data) and validity (quantitative data) |
| Weakness minimisation | The concept is supported by a range of data (numeric and textual) from different study designs | Triangulation |
| Inside–outside | The data related to the concept consists of both subjective (insider) views and objective (outsider) observations |
Credibility (qualitative data) and validity (quantitative data) Triangulation |
| Publication biasb | There is at least one study that shows non-significant, null, or contrasting results | Representativeness |
Qualitative thematic synthesis
Our aim in the qualitative thematic synthesis was to focus specifically on the qualitative evidence and further examine the data to create an understanding of how children, young people, parents, siblings and relevant health-care professionals conceptualise, view and experience powered mobility, from which the factors that influence powered mobility preparation, provision, use and outcomes could be explored.
During the qualitative thematic synthesis, we focused on four key contextual areas related to the processes and outcomes of powered mobility: preparation for powered mobility, provision of powered mobility, use of powered mobility and experience of outcomes related to powered mobility. The specific purpose was to see if further theoretical insights could be developed from the qualitative evidence, and to further explore the differences and similarities between powered mobility provision for children aged < 5 years and children aged ≥ 5 years.
All qualitative evidence (from both qualitative and mixed-methods studies) found in the review was synthesised separately for the qualitative thematic synthesis. In defining relevant stakeholder opinions, data from children and young people who used powered mobility were prioritised. Other key stakeholders included parents, siblings, other family members and professionals involved in powered mobility provision or use (e.g. physiotherapists, occupational therapists, clinicians and teachers).
The Thomas and Harden53 approach to thematic synthesis was used to identify key descriptive themes and to develop further theoretical insights from the published qualitative findings across the body of evidence. This process was undertaken by three members of the research team (NB, JN and Llinos Haf Spencer). Two researchers (NB and Llinos Haf Spencer) used NVivo to independently code the extracted qualitative evidence, and two researchers (NB and JN) synthesised the evidence. The thematic synthesis approach consisted of three stages:
-
line-by-line coding of all qualitative data in the selected studies, including all participant statements, observations and author interpretations (NB and Llinos Haf Spencer)
-
development of descriptive themes by analysing the relationship between common and complimentary codes (NB, JN and Llinos Haf Spencer)
-
generation of analytical themes through constant comparison and discussion of evidence and further refinement of the descriptive themes (NB and JN).
A separate subgroup synthesis was undertaken for qualitative data relating specifically to children aged < 5 years. For this synthesis, we re-examined all of the coded data relating specifically to very young children and developed descriptive themes. The descriptive themes were contextualised with illustrations to visualise the types of powered mobility equipment used by very young children, to show how these conceptually, physically and technically differ from powered mobility equipment used by older children. We also teased out the nuanced differences in anticipated and experienced outcomes between very young children and older children.
Following completion of the primary and subgroup qualitative thematic syntheses, the GRADE-CERQual approach was used to appraise confidence in all of the synthesised qualitative findings. 35 The process consists of assessing four domains: methodological limitations (i.e. concerns about the design or conduct of studies contributing to each finding), relevance (i.e. the applicability of the context of the studies to the review question), coherence (i.e. clarity of support between the study results and each finding) and adequacy of data (richness and quantity of data supporting each finding). Together, these domains contribute to an overall assessment of confidence in the evidence for each finding.
Results: an overview of evidence of powered mobility interventions for children
The first part of this section reports the results from the search and inclusion process, describes the included studies and summarises the descriptions of the health technology as extracted from the included papers. The subsequent two parts report on the findings from the mixed-methods framework synthesis and the qualitative thematic synthesis, including the grading of certainty. The final part presents the revised, integrated logic model for assessing the effectiveness and cost-effectiveness of powered mobility interventions for children aged < 5 and ≥ 5 years.
Description of the included studies
Number of studies included
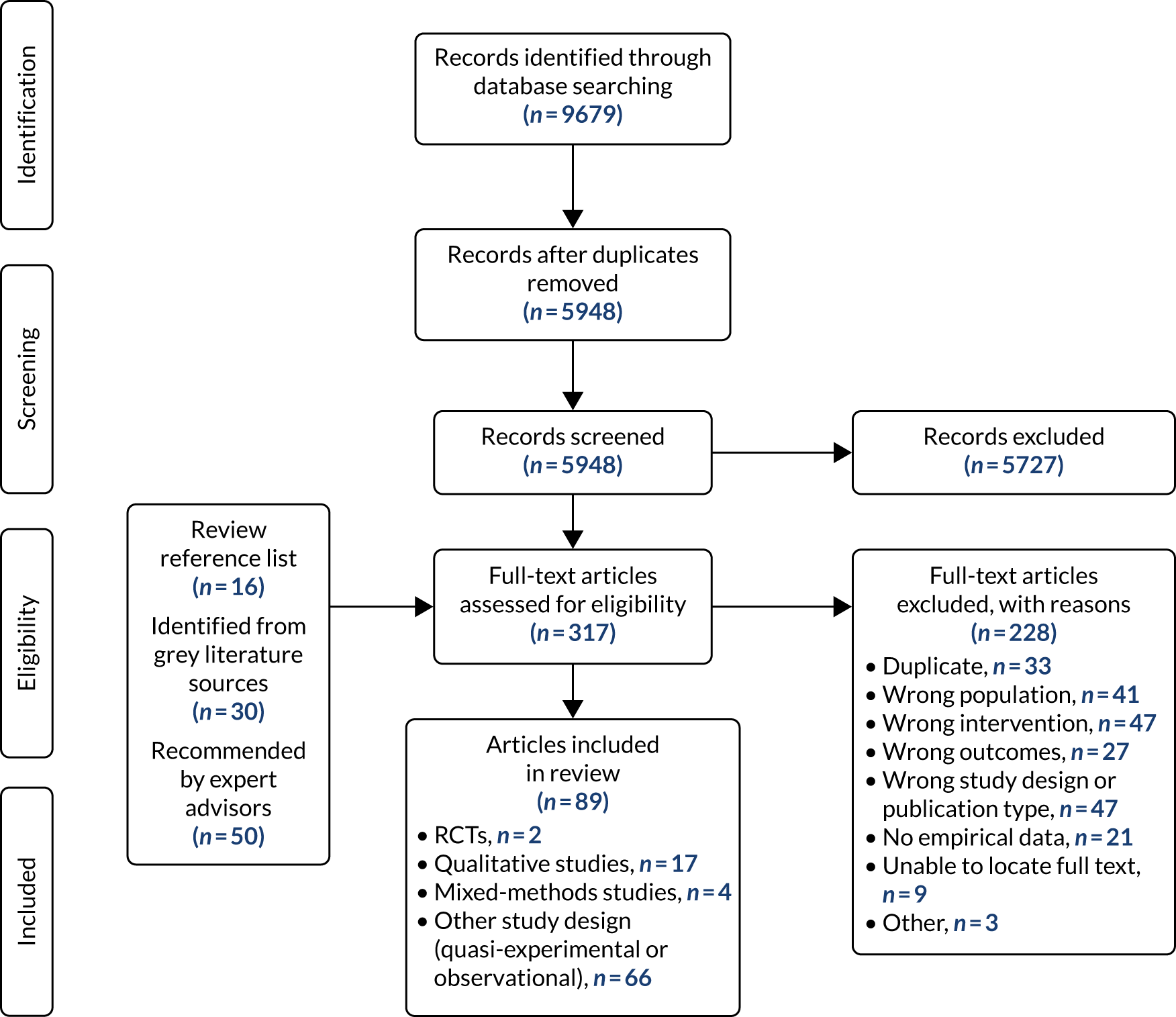
The literature searches of bibliographic databases identified 5948 potentially relevant titles and abstracts, of which 221 were included in full-text screening. A further 16 relevant references were identified from reference lists, 30 were identified from the grey literature and 50 were recommended by expert advisors, resulting in a total of 317 references for full-text screening. Of these, 89 references (covering 89 studies) met the inclusion criteria, and 228 references were excluded. A Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart summarising the study selection process is presented in Figure 4.
FIGURE 4.
The PRISMA flow chart of included and excluded studies.
The list of included studies and associated references is reported in Appendix 5. Reasons for exclusion for a sample of excluded studies are described in Appendix 6, Table 40.
Characteristics of included studies
A full breakdown of included study characteristics is presented in Appendix 7, Table 41. The included studies comprised two RCTs, 18 qualitative studies, three mixed-methods studies and 66 studies of other designs, such as observational and non-randomised trials. Nearly one-third (n = 24) of the studies were single-subject studies, which often consisted of case reports and clinical cases.
The included studies involved an estimated total of 2070 participants. The sample sizes ranged from 1 to 538 participants in individual studies, with a median of five participants. Fourteen studies (16%) had a sample size of ≥ 30 participants, whereas 24 (27%) had only a single participant. One study did not report the number of participants included in the study. 54 The largest study was in children and young people with spina bifida, and reported data for two age groups: children aged 0–15 years (n = 323) and young people aged 16–25 years (n = 215). 55
In terms of the reporting of data specifically for the two age groups of interest, 35 (39%) studies reported data for children aged < 5 years, and 25 (28%) reported data on children aged ≥ 5 years. Twenty-one studies (24%) reported data for children across the age groups; of these, 10 (11% of all included studies) reported separate data for children aged < 5 and ≥ 5 years. The age range was unclear in eight (9%) studies.
Most of the included studies (n = 46) described multiple diagnoses among the characteristics of their participants. One-quarter (n = 22) included solely children with cerebral palsy, three (3%) included solely children with Down syndrome and three (3%) included solely children with spina bifida. About one-third (n = 28) of the studies explicitly stated that they included children with learning/intellectual disabilities; however, because of the lack of standardised reporting, there is uncertainty about the actual number of studies.
Included studies were published between 1971 and 2019. Twelve (13%) were published before 2000, and 58 (65%) from 2010 onwards. Studies were conducted in the USA (n = 46; 52%), the UK (n = 11; 12%), Sweden (n = 6; 7%), Taiwan (n = 4; 4%), Canada (n = 5; 6%), Italy (n = 3; 3%), Japan (n = 3; 3%), Spain (n = 2; 2%) and France, Israel, Australia, Singapore, the Republic of Korea, South Africa, Scotland, Northern Ireland and the Republic of Ireland (n = 1; 1% each).
Quality of included studies
Full, agreed quality assessment scores are provided in Appendix 8, Tables 42–45. For the two RCTs, one study54 was assessed to have a ‘high’ risk of bias as a result of bias arising from the randomisation process. The second14 was assessed as giving rise to ‘some concerns’ about the risk of bias because of missing data and bias in the measurement of the outcome.
In the case of the 66 observational studies, there were substantial concerns about the lack of control for potential confounding, assessed in relation to the limited extent to which study design features had enabled participant characteristics to be balanced or matched between comparison groups. The quality assessment domains that were rated most positively across the observational studies were for attrition and retention rates.
In the case of the qualitative studies, concerns about the recruitment strategy, relationship between researcher and participant and the clarity of stated findings were most prominent. Among the mixed-methods studies, at least one study (albeit not always the same one) fell short on each quality criterion.
Descriptions of the health technology
Of the included studies, 62 (70%) investigated powered mobility equipment, 20 (22%) investigated powered mobility training and seven (8%) investigated a combination of equipment and training. No studies explicitly set out to investigate the effects, feasibility or implementation related to adaptations to physical environment, policies or practices, or maintenance and review. Further overview on the intervention elements evaluated in the studies is provided in Appendix 9, Table 46.
Powered mobility equipment
The powered mobility equipment assessed in the included studies clustered around five broad types. A summary of their key features is provided in Table 5. The main differences between the types related to the equipment size, appearance and controls. Most, but not all, equipment had been used across age groups, disability populations and settings. We found examples of matching the equipment to a child’s development level and desired outcomes, but no single agreed set of principles or prescription criteria emerged.
| Type of powered mobility equipment | Summary description developed from the included studies and expert advisors | Equipment dimensions described to potentially influence uptake, effectiveness and implementation | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Age range | Conditions/populations used for | Locations of use | Physical comfort and appearance | Tyres, tilt mechanisms | Battery, charging | Control, steering | Size, transportability | ||
| Powered wheelchairs, motorised wheelchairs, specialised wheelchair, powered mobility device, EPIOC, SAM system | Full-size powered wheelchairs, and identical scaled-down versions, explicitly designed for use as a mobility aid and tailored for children | 0–81 years | Skeletal dysplasia, above-knee amputations, achondroplasia, arthrogryposis, juvenile rheumatoid arthritis, brain tumour, cerebral palsy, Charcot–Marie–Tooth disease, complete spina bifida without acrania, congenital malformation of limbs, congenital muscular dystrophy, congenital myopathy, Dandy–Walker syndrome, Duchenne muscular dystrophy, failure to thrive, four-extremity limb deficiency, global developmental delay, hydrocephalus, hypoxic brain damage, major postural deficit, multiplex congenita, muscular dystrophy, myelomeningocele, myotonic dystrophy, myotubular myopathy, neurodevelopmental disabilities, neuromuscular disease, orthopaedic disabilities, osteogenesis imperfecta, progeria, quadriplegia of unknown aetiology, rachischisis, spinal muscular atrophy, spina bifida, spinal cord injury, spondyloschisis, stroke, brain tumour, traumatic brain injury, dementia, tetraphocomelia, VATER syndrome | Home, outdoors, laboratory |
|
Problems with tyres and faulty tilt mechanisms reported by EPIOC users | Problems with batteries reported by EPIOC users | Problems with faulty steering reported by EPIOC users | Size can make it difficult for children to join in, participate and access spaces |
| They offer options for support, specialised seating and control systems, and are usually large and heavy | |||||||||
| Examples: P110 Quickie (Sunrise Medical Ltd, Dudley, UK); Everard Turbo chair (Everaids Ltd, Bedford, UK) with a Matrix seat | |||||||||
| Starter powered mobility devices |
Powered wheelchair designed specifically for children aged < 5 years, designed to be safe, compact and manoeuvrable, and to be adjusted to accommodate the child’s growth up to a limited size/weight Explicitly designed for young disabled children; therefore, it has controls that resemble those on a powered wheelchair, but the actual appearance of the device is child-friendly and more akin to a toy |
15–72 months | Cerebral palsy, spinal muscular atrophy, global developmental delay, arthrogryposis, spina bifida | Home and outdoors | Not reported | Not reported | Not reported | Not reported | Size can make it difficult to use device in the home |
| These can be purchased privately, or accessed through loan schemes and certain health services | |||||||||
| Examples: Wizzybug (Designability, Bath, UK), TinyTrax (TinyTrax, Bristol, UK) and Bugzi (MERU, Epsom, UK) | |||||||||
| Smart powered mobility wheelchairs | Standard electric wheelchair chassis to which a computer and a collection of sensors have been added, or a mobile robot base to which a seat has been attached | 10 months to 48 years | Various, cerebral palsy, severe mobility limitations and reduced motor control, severely disabled, traumatic brain injury, severe undifferentiated hypotonia, spastic diplegia | Laboratory, home and outdoors | Not reported | Not reported |
|
Reported options included switch controls, user board buttons, a controlling system that traces electrical tape on the floor, cameras, range finders, speech synthesisers, bumpers, user interfaces, computer vision, haptic guides and force feedback joysticks | Modifications to the home environment, such as installation of ramps to facilitate access, were reported |
| Adaptable to different kinds of wheelchairs (e.g. sports wheelchairs, child wheelchairs, hospital wheelchairs and amphibious wheelchairs) | |||||||||
| Examples: SMART wheelchairs, (SMART Wheelchairs Ltd, King's Lynn, UK) assisted vehicles, AKKA-board, robotic wheelchair, robotic wheelchair trainer | |||||||||
| Ride-on toys and robots | Children’s battery-operated toys, or small robots, specifically modified for the specific needs of an individual child with a disability | 6 months to 5 years | Cerebral palsy, complex developmental delays, Down syndrome, 16p11.2 microdeletion, microcephaly, profound and multiple learning disabilities, physical disability, complex medical needs, developmental delay, Pierre Robin sequence, severe undifferentiated hypotonia |
|
Limited evidence to suggest that some children may find these devices uncomfortable | Not reported | Reported options included 6-V/single-gear small cars and 12-V/dual-gear large cars | Reported options included joysticks mounted on the toy, or weight shift over a balance board | Most are described as small, relatively lightweight and easily transportable |
| Modifications can include large wheels, protective bumpers, adapted seating, customised controls | |||||||||
| Typically used for early movement and active play in early childhood (i.e. < 5 years of age) | |||||||||
| The ride-on toys are commercially available, with adaptations accessed through programmes such as GoBabyGo (Cerebral Palsy Foundation, New York, NY, USA). The robots have limited availability, and are generally restricted to research projects | |||||||||
| Examples: Pioneer (Adept MobileRobots, Amherst, NH, USA), PowerBot (Adept MobileRobots), iRobot Magellan Pro Robot (iRobot Corporation, Bedford, MA, USA), Fisher-Price Mater (Fisher-Price, Inc., East Aurora, NY, USA), PIONEER 3-AT robot (Adept MobileRobots), WeeBot (Adept MobileRobots) | |||||||||
| Powered mobility carts | A seat mounted on a chassis; the seat may be height adjustable. May be specifically constructed for an individual child, and made of various materials | 11 months–14 years | Quadrimembral amputees, multiple limb deficiencies, cerebral palsy, spina bifida, congenital injury of the spine, muscular atrophy, congenital amputations of the arms and legs, cerebral palsy | Laboratory, home and outdoors | Not reported | Not reported | Reported battery options included two 6-V rechargeable gel-cell batteries with 0.5-Ω, 10-W resistor; and a 24-V, 8-Ah lithium ion battery | Reported options included joystick, double-pole, double-throw switch | Removable foam inserts were reportedly used to accommodate child growth over time |
| Example: the CAPP cart | |||||||||
The qualitative thematic synthesis specifically set out to develop an overview of the different types of powered mobility equipment and their conceptualisation, purposes and uses, which, for simplicity, are reported in the following sections and expanded on in Table 5.
Ride-on toys
These interventions are typically battery-operated toys that have been modified for use by a child with a disability. Modifications can include larger wheels, protective bumpers, adapted seating, customised controls, and so on (Figure 5). Although these interventions can vary greatly, depending on the specific needs of the child, they are typically used to give children with mobility limitations a chance to play, socialise and have active control over their own exploration, which, in turn, is thought to facilitate developmental gains. The devices are not commercially available in their adapted form, but can be accessed through programmes such as GoBabyGo. 56,57 Although these devices are relatively simple, the universality of their toy-based design makes them ideal for introducing powered mobility at an early age. 58
FIGURE 5.
Example of adapted ride-on toy. Reproduced with permission from Julie Laurence (2020, personal communication).

Starter powered mobility devices
Starter powered mobility devices are explicitly designed for young disabled children, with controls that resemble those on a larger powered wheelchair. A number of different starter powered mobility devices are now available in the UK, including the Wizzybug (Designability, Bath, UK) (Figure 6), TinyTrax (TinyTrax, Bristol, UK) and Bugzi (MERU, Epsom, UK). Unlike adapted ride-on toys, starter powered mobility devices are registered medical devices and, although customisable, have standardised designs. Similarly to ride-on toys, these interventions are designed to enable children with mobility limitations to experience and enjoy independent mobility, often for the first time. They may also be used as an introduction to powered mobility and as a wheelchair training tool. They are not routinely used as a child’s primary mobility aid, but can be purchased privately or accessed through loan schemes and certain health services. These types of devices are often classed and described as powered wheelchairs, but we believe that they are conceptualised differently to more traditional powered wheelchairs because of their focus on child-centred design.
FIGURE 6.
Example of starter powered mobility device. Reproduced with permission from Designability (Bath, UK).

Powered wheelchairs
Powered wheelchairs for very young children are sometimes scaled-down versions of full-size powered wheelchairs, but can also be specifically designed for children. They are commonly designed to ‘grow’ with the child, and thus can be adapted to meet each child’s needs over time. Therefore, these devices can be used beyond the age of 5 years; weight limit typically defines the upper limit for use, rather than age. They offer more options for support, specialised seating and control systems than starter powered devices, but are usually larger, faster and heavier. Existing models include the Koala Miniflex (Permobil AB, Timrå, Sweden) (Figure 7) and Zippie Salsa M2 (Sunrise Medical Ltd, Dudley, UK). These are typically designed for indoor–outdoor use [i.e. electrically powered indoor–outdoor chairs (EPIOCs)], but some models may also be specifically designed for either indoor or outdoor use.
FIGURE 7.
Example of a powered wheelchair. Reproduced with permission from Permobil AB.

Powered mobility for very young children
There were many similarities in terms of the intervention elements, outcomes and feasibility factors across the age groups, particularly in the prioritisation of autonomy and independence, participation, and social interaction as key outcomes. For example, two studies59,60 found that parents’ primary goals for powered mobility included promotion of independence, autonomy and social inclusion, all of which were noted across studies with older children as well.
Owing to their small sizes and playful, fun designs, ride-on toys60,61 and starter powered mobility devices62 were more common among children aged < 5 years, offering a developmentally appropriate and child-centred approach to introducing powered mobility to very young children. Ride-on toys, in particular, offer a relatively inexpensive and fun way to introduce powered mobility and enable movement, participation, social interaction and independence. 58 From the qualitative studies, utilising developmentally appropriate devices and training was found to be important to ensure that children and families are engaged in the process.
Starter powered mobility devices are not typically designed for children aged > 5 years (because of the child’s size and weight); thus, powered wheelchairs became the predominant powered mobility intervention found in the older age groups.
Powered mobility training
Although some of the included studies reported training elements in detail, 9 of the 27 studies (33%) that included training lacked at least some of the basic information, including information about who delivered the training, how many sessions were provided and how long the sessions lasted (Table 6 presents a summary of the reported training elements). Based on the studies from which information about training was available, the number of sessions ranged from 1 to 64 per participant (estimated median 16 sessions; estimated interquartile range 8–21 sessions), and the session length varied vastly depending on what was described as a session. For example, in one study67 a ‘trial’ lasted for 50 seconds, whereas, in another,74 a session lasted for 30–90 minutes. All studies reported the child as the recipient of the intervention; none reported targeting parents, carers or other people around the child. The training was mainly reported as having been delivered by a researcher and/or a therapy professional, at times with the involvement of parents or carers. Two studies reported using a simulator to deliver the training, and two involved teaching staff in the delivery.
| Study | Number of sessions and frequency | Duration of individual sessions | Who the training was delivered by | Who the training was received by | Targeted outcomes |
|---|---|---|---|---|---|
| aInman et al.54 | Not reported | 2 hours per training session | Not reported; the training scenarios were developed by programmers | Children with orthopaedic impairments |
|
| aInman et al.54 | Not reported | 2 hours per training session | Not reported; the training scenarios were developed by programmers | Children with cerebral palsy or Down syndrome |
|
| Agrawal et al.63 | 10 sessions in pilot study 1; 30 sessions in pilot study 2 (follow-up) provided three times per week over a period of 10–12 weeks |
|
Not reported; caregivers re-located the robot to different positions during the training | Children with cerebral palsy |
|
| Chen et al.64 | 16 sessions in total; four sessions per day conducted over 4 days | The time taken to navigate the training environment varied between trials. The child failed when the travel time reached 600 seconds | The experimenter | Child with spina bifida | To learn navigation and to drive more accurately |
| Hasdai et al.65 | Total number not reported; frequency was twice a week for up to 12 weeks | 30–45 minutes per session | Not reported. Simulator training was used | Children with muscular dystrophy or cerebral palsy | Driving ability and skill involved in operating a powered wheelchair |
| Lynch et al.66 | Total number not reported; the child participated in training three or four times per week from 7 to 12 months of age | In the Open Exploration period, the infant was allowed up to 20 minutes of unrestricted exploration of the training space | The experimenter and the child’s mother | Child with spina bifida |
|
| Marchal-Crespo et al.67 | 12 trials: one without guidance, followed by nine with decreasing level of guidance and two more trials without guidance | 50 seconds per trial | The experimenters | Child with cerebral palsy |
|
| McCourt and Casey68 | One session | 1–1.5 hours per session | Clinical lead occupational therapist | Children with cerebral palsy or Duchenne muscular dystrophy | Ability to safely and competently drive their powered wheelchair outdoors |
| McGarry et al.69 | 16 sessions; two sessions per week for 8 weeks | 1 hour per session | The researcher, a fourth-year occupational therapy (honours) student, with guidance from an experienced occupational therapist | Children with cerebral palsy |
|
| Morère et al.70 | Maximum of 30 sessions; participants would attend at a rate of two sessions per week | 30 minutes per session | Occupational therapist | Children with cerebral palsy | Outdoor driving abilities, including driving behaviour and powered wheelchair control |
| Torkia et al.71 | One session | The simulator testing and subsequent qualitative interview of each participant lasted 30 minutes | Not reported. Simulator training was used | Children; primary diagnoses included muscular dystrophy (n = 6), cerebral palsy (n = 4) and a dual diagnosis of spinal cord injury and stroke (n = 1) | Children’s and adolescents’ overall experiences in using the miWe-CC simulator |
| Ragonesi and Galloway72 | 14 sessions | 35–45 minutes per sessions, depending on the infant’s mood | The experimenter and one or both parents participated in the training | Child with cerebral palsy |
|
| Nilsson et al.73 | The number of training sessions varied between participants. The data were dichotomised for analysis, grouping participants who received < 30 sessions and those who received > 30 sessions; and grouping participants who received training for < 1 year, 1–2 years and > 2 years | The training duration for each trial in the experiments was generally < 15 minutes | At the start of the project, the researcher was the sole trainer; gradually, other trainers were engaged. These included parents, personal assistants, occupational therapists, physical therapists, teachers, teacher assistants and other staff members in the locations where the training took place | Individuals with profound cognitive disabilities and multivariate additional disabilities, or at high risk of developing such conditions | Success or failure to grow consciousness of joystick use |
| Nilsson and Nyberg74 | 42 sessions in total were documented: 20 with one participant and 22 with a second participant. Sessions occurred 1–3 times a week for 4 months | 30–90 minutes per session, depending on the child’s level of alertness and health at the time | The study author provided the training in the clinic; the children’s parents and assistants provided the training at home under supervision from the study author | Two children with profound cognitive disabilities | Children’s behaviours during the training; the target behaviours were reactions to the training, unintentional behaviours and intentional activity in the wheelchair |
| Kenyon et al.75 | Eight sessions; delivered once a week for 8 weeks | 45–60 minutes per session | It was reported that the first author, a paediatric clinical specialist, made decisions regarding whether a joystick or switch should be used | Child with cerebral palsy |
|
| Kenyon et al.76 | 21 sessions; delivered twice weekly over a 12-week period (some sessions cancelled by parents because of inclement weather) | 60 minutes per session | Not reported | Child with cerebral palsy |
|
| Huang and Chen77 | 18 sessions; delivered twice weekly over a 9-week period | The treatment group received 2-hour training sessions using a ride-on car | Occupational therapist | Children with developmental delay, cerebral palsy or Down syndrome |
|
| Huang et al.78 | 18 sessions; delivered twice weekly over a 9-week period | 2 hours per session | Occupational therapist | Children with developmental delay, cerebral palsy, Down syndrome, other |
|
| Huang et al.79,80 | 18 sessions; delivered twice weekly over a 9-week period | 2 hours per session | Occupational therapist | Children with developmental delay or cerebral palsy |
|
| Furumasu et al.81 | Six sessions | 1 hour per session | Physical therapist | Children with arthrogryposis, spinal muscular atrophy, spinal cord injury, other (amputee, osteogenesis imperfecta) |
|
| Zeng et al.82 | There was no set number of trials. The number of trials taken to complete the training tests varied between participants. Tests were considered as failed if the subject could not complete the task in 10 trials | Not reported | Not reported | Individuals with traumatic brain injury |
|
| Ragonesi et al.83 | One ‘training phase’ | ‘Training phase’ lasted 10 days | Therapists and teachers | Child with cerebral palsy |
|
| bNicholson and Bonsall84 | Not applicable | Not applicable | Not applicable | Children with cerebral palsy or spinal muscular atrophy |
|
| Montesano et al.85 | One session | 45–60 minutes per session | School-based therapists and engineers | Individuals with cognitive impairment |
|
| Kenyon et al.86 | 10 sessions for two participants, seven sessions for a third participant; delivered once a week over a 12-week period (12 sessions were scheduled for each participant; however, owing to illness and weather-related issues, some sessions were missed) | 60 minutes per session | Not reported | Children with cerebral palsy |
|
| Logan et al.87 | Between 6 and 64 sessions; delivered over a 12-week period | Session defined as a day when the child drove for at least 20 minutes | Parents and researcher | Children with cerebral palsy, 16p11.2 microdeletion, microcephaly |
|
| Logan et al.88 | Total number not reported; sessions delivered daily over a 12-week period | 5–40 minutes per session | Family and researcher | Child with Down syndrome |
|
In terms of the nature of the training, the techniques described in the papers mainly targeted a child’s skills in driving the powered mobility equipment. From the included papers, five categories of training techniques were identified: (1) graded task, (2) instruction and guidance, (3) feedback, (4) prompts and driving goals and (5) using motivators (Table 7). There was evidence of all the techniques being used across the age groups, from as young as 7 months of age. There was also evidence of the delivery of the techniques through virtual reality or computer simulation scenarios for children as young as 3 years of age.
| Technique | Summary description of the technique as presented in the studies |
|---|---|
| Graded task | Modifying the driving environment, the powered mobility or the driving tasks so that the child was achieving success while also challenged to perform with decreasing levels of support or in increasingly demanding situations |
| The simulation was divided into seven levels of increasing difficulty (. . .)Marchal-Crespo et al.67 | |
| Instruction and guidance | Verbal instruction and physical (e.g. ‘hand-over-hand’) guidance for the child and verbal or written instructions for parents |
| Training included using toys and verbal prompts with hand gestures as well as ‘hand-over-hand’ assistance to move the joystick (. . .)Ragonesi and Galloway72 | |
| Feedback | Verbal, haptic and auditory feedback for the child, and natural consequences, including those taking place during self-directed exploration in controlled and/or natural environments |
| During the entire training program, verbal feedback and natural consequences were used to teach each child that movement and behaviors could have an impact on objects and events in the close vicinityNilsson and Nyberg74 | |
| Prompts and driving goals | Using prompts (people, toys, obstacles, etc.) to indicate driving goals, usually consisting of destinations and driving routes |
| At the start of each trial, he was shown a toy within reaching distance to gain his interest. The experimenter or his mother then moved to the end location and encouraged him to driveLynch et al.66 | |
| Using motivators | Using contextual motivators tailored to the child’s interest to gain and retain their attention and task-engagement |
| The participant also appeared to enjoy interactions with the authors, especially the physical therapist student authors, and was often encouraged to ‘chase’ after a particular student (. . .)Kenyon et al.76 |
Mixed-methods framework synthesis: outcomes, effectiveness and cost-effectiveness
There was no conclusive evidence about the effectiveness or cost-effectiveness of powered mobility in children aged either < 5 or ≥ 5 years. Of the two studies categorised as RCTs, one was a pilot study of early powered mobility provision with 28 children (aged 14–30 months) with various diagnoses. 14 In this study, children in the experimental group received an individually customised powered wheelchair to use for the duration of the study, whereas powered mobility was withheld from the control group for 12 months. The main health outcomes were development [measured using the Battelle Developmental Inventory (BDI)]; mobility, caregiver assistance and self-care [measured using the Pediatric Evaluation of Disability Inventory (PEDI)]; and coping (measured using the Early Coping Inventory); these data were collected at entry and at 12 months. An intention-to-treat analysis showed that the experimental group’s BDI receptive communication and total scores, and PEDI mobility skills, caregiver assistance and self-care caregiver scores, improved significantly more than the control group’s scores. Although the results provide support for early powered mobility interventions, the small sample size limited the power of the study and it is possible that some of the significant results are spurious. The second study54 was a multivariate repeated-measures design with 16 children and young people (aged 4–21 years), conducted to evaluate the effect of a virtual skills training programme in a computer-generated world on the real-world powered mobility skills of children with physical disabilities. All who completed the study (n = 13) showed gains in real-world driving skills; however, the study was assessed as having a high risk of bias, which limited the certainty of the evidence.
Further analysis and synthesis of all extracted data informed the development of six inter-related outcome concepts that were repeatedly described, across papers, as powered mobility outcomes and areas of impact: (1) movement and mobility; (2) learning to drive powered mobility equipment; (3) participation, play and social interactions; (4) self-care; (5) autonomy, independence, choice and control, and freedom; and (6) psychological consequences (including sense of achievement, confidence, motivation and cognitive outcomes). All of these corresponded with, and further advanced, the outcomes in the initial logic model. Furthermore, two clusters of safety outcomes were identified: (1) emotional consequences (positive and negative feelings for the parent or the child) and (2) accidents and pain. Study data charted onto each identified concept are presented in Report Supplementary Material 1.
The following sections report the synthesised numeric and textual data in relation to each of these outcome concepts. For the data that were available, results are presented for both age groups of interest, to enable comparisons. However, overall, across the outcome concepts, we found little evidence to support the hypothesis that the outcomes and impacts of powered mobility were directly related to a child’s biological age, and little evidence that a biological age of 5 years provided a significant cut-off point. Instead, we found evidence that each of the six outcome concepts represented a developmental continuum, and that the impact of powered mobility was commonly considered, by a range of stakeholders, in terms of the ways in which it could progress the child’s performance further along that continuum. This is further illustrated in the outcome concepts described in detail later and summarised in Table 8. Confidence in the findings is discussed at the end of each concept.
Table 8 presents a full list of the papers mapped on to each of the concepts, and a summary of the concepts and their inclusion/exclusion boundaries. Table 9 presents the powered mobility evidence profile from the mixed-methods synthesis.
| The concept (related papers) | Summary description | Included in the concept | Excluded from the concept |
|---|---|---|---|
| Movement and mobility (quantitative studies;12–14,23,58,62,63,66,75–79,86–92,104,111,112,118,119,123,125,168,169 qualitative studies61,99–102,105,109,116) | Whole-body movements, usually play-related movement and activity, or destination-focused mobility |
|
|
| Learning to drive the powered mobility equipment (quantitative studies;13,14,54,58,65–67,69,70,72,75,76,85–88,91–93,106,107,111,113,114,117–119,125,128–130 qualitative studies61,99,102,117) | The stage or process of the child learning to drive the powered mobility equipment | Learning as an important stage or process, separate from the everyday, actual, real-life use. Focuses on acquisition of skills and abilities in a controlled environment or in a formal training context | Movement and mobility in everyday life, fit and physical environment |
| Participation, play and social interactions (quantitative studies;12–15,17,23,58,62,63,75,77–79,83,86,88–98 qualitative studies59–61,99–103) | Children living their everyday lives across activities and contexts |
|
|
| Self-care (quantitative studies;13,17,58,63,86,88,104 qualitative studies60,100,105) | Looking after oneself and directing/making decisions about one’s self-care |
|
|
| Autonomy, independence, choice and control, and freedom (quantitative studies;12,13,58,62,75,76,86,89,91–93,98,106–108 qualitative studies59–61,99–103,105,109,110) | Higher-level values and aspired states related to autonomy, independence, choice and control, and freedom |
|
|
| Psychological outcomes (quantitative studies;14,23,58,66,75,76,79,80,86,91–93,95,106,111–115, qualitative studies60,61,101,116,117) | Sense of achievement and motivation |
|
Objective measured skills, ability and observable competence |
| Cognitive outcomes | Basic cognitive language and communication skills | Social participation, relationships, interactions and friendships | |
| Safety outcomes (quantitative studies;12,15,17,23,76,77,79,82,87,88,91,98,106,112,115,118–121, qualitative studies59–61,74,99–103,109) | Emotional consequences | The child’s and their parents’ emotions and feelings related to powered mobility | Accidents, physical pain, road safety |
| Accidents and pain | Accidents, pain, road safety, traffic, physical discomfort | Any harm that took place during formal training (coded under learning) |
| The outcome concept | Number of studies per design | Combined sample size (n) | Importance of the outcome to children and families as extracted from data | Evidence supporting concept |
|---|---|---|---|---|
| Movement and mobility |
|
812 | Critical | Strong |
| Learning to drive powered mobility |
|
454a | Low | Inconsistent |
| Participation, play and social interactions |
|
469 | Critical | Moderate |
| Self-care |
|
41 | Insufficient evidence | Low |
| Autonomy, independence, choice and control, and freedom |
|
362 | Important, but not critical | Low |
| Sense of achievement, confidence and motivation |
|
728 | Insufficient evidence | Low |
| Cognitive outcomes |
|
673 | Insufficient evidence | Low |
| Positive and negative feelings |
|
366 | Important, but not critical | Low |
| Accidents and pain |
|
397 | Critical | Low |
Movement and mobility
Movement and mobility was the most frequently described outcome of powered mobility, supported by both the textual and numeric data. Descriptions of movement and mobility related to two related dimensions: (1) play-related movement as an integral part of a movement-based activity (e.g. physical play and games) or as an end point itself (e.g. the sensation of spinning) and (2) destination-focused mobility, whereby movement is a means of transfer to a place or a situation.
Play-related movement: selected quotations demonstrating the concept
After a short period of driving in circles after release of guidance, she gave a small smile and later still she laughed with delight. Apparently she enjoyed the activity without being aware of what caused the motion of the chair.
Researcher, Nilsson and Nyberg74
He played baseball this year, so he was able to run the bases in his power chair, which he could never have done beforehand.
Parent, Wiart et al. 102
Enjoying movement for its own sake was also important, particularly for some of the boys who both described and demonstrated their enjoyment of the sensation of movement and speed.
Researcher, Gudgeon and Kirk99
Destination-focused mobility: selected quotations demonstrating the concept
I don’t have to like wait for them and I can get there at my own speed.
Child, Gudgeon and Kirk99
(. . .) he can now go with the others and see what the other people are doing.
Parent, Sonday and Gretschel101
It is this idea that you have one method of walking or moving whereas actually in reality all of us use a different method of moving around and even able bodied children they have (bikes, cars, skateboards. . .).
Professional (clinicians, wheelchair prescribers), Durkin109
One or both of these dimensions of movement and mobility were commonly the primary outcome(s) of powered mobility. Movement and mobility was consistently the first point in the causal chain of hypothesised health outcomes: a key gateway to other health outcomes such as participation, autonomy and freedom, and the stated mechanism that linked these other outcomes to powered mobility. Descriptions of movement and mobility were present in the voices across children, parents, professionals and researchers, as illustrated in the preceding quotations.
We explored both the textual and numeric data for differences in movement and mobility related to age. In textual data, play-related movement was described as a key outcome for all children, from the very youngest powered mobility users101 to teenagers. 59,100,102 Destination-focused mobility appeared to be mediated by a range of factors, including a child’s developmental level and the situational feasibility, with little evidence of a child’s biological age being a directly contributing factor. In the numeric data, most studies indicated that powered mobility had positive effects on children in both age groups (Table 10).
| Study population | Verbatim outcomes (outcome measure) (reference, sample size) | % (n) of studies reporting positive change | Summary codea | ||
|---|---|---|---|---|---|
| Positive change in ‘movement and mobility’ | No change in ‘movement and mobility’ | Negative change in ‘movement and mobility’ | |||
| Study population aged < 5 years |
|
Gross motor skills (BSID) (Lynch et al. ;66 n = 1) Motor skills (BDI fine and gross motor skills subscales, Merrill Palmer Revised fine and gross motor subscales), mobility (PEDI mobility subscale) (Mockler et al. ;111 n = 31) Hip/knee flexion, roll, sit, kick, walk (GMFM-88) (Agrawal et al. ;63 n = 15) Mobility (PEDI mobility subscale), developmental skills (BDI motor subscale) (Jones et al. ;14 n = 28) |
N/A | 77 (16) | ++ |
| Study population aged ≥ 5 years |
|
N/A | N/A | 100 (4) | ++ |
| Study population aged under and over 5 years |
|
Gross motor activities (GMFM) (Bottos et al.;23 n = 29) | N/A | 83.3 (6) | ++ |
In studies of very young children, the most common measure to capture movement and mobility outcomes was the PEDI, especially its mobility scale, which showed improvement in all studies but one (see Table 10). Four studies23,63,66,92 used measures of movement-related skills (e.g. Bayley Scales of Infant Development, Gross Motor Function Measure-88 items), two of which showed improvement. In studies of children aged ≥ 5 years, no two studies used the same measure and none used the PEDI. See Table 10 for verbatim outcomes mapped to the ‘mobility and movement’ concept.
The assessment of certainty for the concept indicated strong support for movement and mobility as a powered mobility outcome (Table 11); this was across the younger and older children, with evidence from both controlled and real-world settings. As for the overall review, there was no formal evidence of effectiveness, but the cumulative support across designs was strong. There was no evidence to make any judgements on cost-effectiveness.
| Concept support criteria | Assessment of support | Level of support |
|---|---|---|
| Truth value/bias | Clear evidence reflected in both numeric and textual data | Strong |
| Explanation credibility | Movement and mobility are established concepts, and efficacy of powered mobility on child’s movement and mobility is directly observable and evidenced in the primary studies. The studies further show feasibility and acceptability of implementation across age range, making this a theoretically sound effectiveness outcome | Strong |
| Weakness minimisation | Supported across different designs (RCTs, observational, qualitative, mixed methods) | Strong |
| Inside–outside | The data cover child, parent, professional and researcher views, and objectively recorded (e.g. video) observations | Strong |
| Publication bias | There are studies that show non-significant results, especially in relation to movement skills (which is theoretically consistent with the intervention hypotheses in this population) | Strong |
| Additional comments | No formal evidence of effectiveness, but the overall cumulative evidence is strong. No evidence to make any judgements on cost-effectiveness | N/A |
Learning to drive the powered mobility equipment
In a chain of powered mobility outcomes, movement and mobility were often implied to emerge after an initial process of learning to acquire the ability to drive powered mobility. Often, although not always, this was learning in a controlled environment before everyday use. The form of the learning process was described differently in different papers, depending on the trainer’s or researcher’s approach to learning. Some studies emphasised emerging skill acquisition through self-directed use (especially those using self-directed exploration; see Powered mobility training), whereas others focused on structured development of skills. Several papers also explicitly drew on both approaches as ways to achieve learning:
Learning to use powered mobility was viewed by all participants as an individualized, cyclical process that occurred over time.
Researcher, Kenyon et al. 61
A lot of children when they first learn to move . . . first need to learn to move and what it is about to move and explore and then driving is much later (. . .).
Professional, Durkin109
The descriptions of the learning process and everyday use could not necessarily be separated from one another by how the activity looked from outside. This was especially true of exploratory play, which was described as both learning and play-related everyday use. Which of these it was viewed to be depended on the purpose of the activity as intended by adults, the child’s developmental stage, the child’s powered mobility competence and preference, and the trainer’s approach to skill acquisition. Although it was common for powered mobility professionals and researchers to conceptualise the initial learning process as a discrete stage, children themselves described continued learning as part of their everyday use of the equipment:
If you crash it tells you how much room you need – how much careful you have to be because it is not that big or it is big.
Child, Durkin109
In terms of differences in learning outcomes by age, there were no differences in the included studies. There was some suggestion that structured learning, targeted through specific techniques, may be particularly important for children with significant cognitive impairments. 74,117 These same papers also demonstrated that it was feasible for children with profound cognitive impairments with added visual impairments and very limited body movements to learn to use powered mobility. All included studies that reported on learning outcomes described positive results, with one study also noting negative results (Table 12). 72 Therefore, there was no scope for assessing the efficacy of specific approaches to supporting children to use powered mobility.
| Study population | Verbatim outcomes (outcome measure) (reference, sample size) | % (n) of studies reporting positive change | Summary codea | ||
|---|---|---|---|---|---|
| Positive change in ‘learning process’ | No change in ‘learning process’ | Negative change in ‘learning process’ | |||
| Study population aged < 5 years |
|
N/A | Increased caregiver mobility time (coding of video footage) (Ragonesi and Galloway;72 n = 1) | 100 (23) | ++/– |
| Study population aged ≥ 5 years |
|
Time to complete a navigation task (on-board monitoring device) (Zeng et al.;82 n = 1 under 18 years) | N/A | 88.9 (9) | ++ |
| Study population aged < and ≥ 5 years |
|
N/A | N/A | 100 (9) | ++ |
The assessment of certainty for the concept indicated inconsistent support for learning to drive powered mobility as a powered mobility intervention outcome (Table 13). A large number of included papers had investigated this outcome, including studies of different designs (although there was no formal evidence of effectiveness). The inconsistent overall rating stemmed largely from the two views of the place of learning in the powered mobility intervention causal chain, and the inconsistent operationalisation of the concept as a possible outcome.
| Concept support criteria | Assessment of support | Level of support |
|---|---|---|
| Truth value/bias | The analytical concept has unclear boundaries, with key elements of the concept described differently in different studies. All aspects of the concept could not be clearly reflected through numeric and textual data from the primary studies | Inconsistent |
| Explanation credibility | The concept of learning skills, or developing an ability to do something, is well established. In the included body of evidence, there was an inconsistent view over the hypothesised role of learning in powered mobility use, and about how central it was as an initial outcome. Some viewed learning as a necessary stage before everyday adoption, whereas others viewed everyday adoption as the most effective way to learn. The elements of powered mobility interventions (primarily the training) proposed to produce the learning outcome were poorly specified on key features | Inconsistent |
| Weakness minimisation | The concept is supported by a range of numeric and textual data from different study designs (RCTs, observational, qualitative, mixed methods) | Strong |
| Inside–outside | The accounts and views between children (insiders) and others (outsiders) diverged, with children viewing learning as ongoing, whereas others (especially professionals) tended to view it as a stage | Inconsistent |
| Publication bias | There is at least one study that reports contrasting results | Strong |
| Additional comments | None | N/A |
Participation, play and social interactions
Participation, play and social interactions formed a prominent cluster of interlinked outcomes in both the textual and numeric data. These outcomes were described as consequences of powered mobility-enabled movement and mobility. Their core focus was children living everyday lives across contexts, including engagement with friends and social interactions, exploration and play, physical activity, and pushing the boundaries of what the children could do and were allowed to do. In the textual data, descriptions of these outcomes were present in the voices across children, parents, professionals and researchers:
I can go shopping (. . .) I can play basketball at my Saturday club all by myself.
Child, Sharma and Morrison98
If she didn’t have the power chair then she’d have to rely on the teacher aide and then the teacher aide’s with her constantly. So that kind of interferes with socialization.
Parent (mother), Wiart et al. 102
(. . .) powered mobility brought major changes in play that was marked by an increase in active play (. . .)
Researcher, Sonday and Gretschel101
She plays hide and seek or sometimes the children runs and she tries to catch them or they sometimes hop onto the back and she gives them a drive.
Parent, Sonday and Gretschel101
[powered mobility allowed] participation in age-appropriate activities within their peer group such as playing in the school’s sports team, shopping, or going out with friends.
Professionals, Pituch et al. 100
(. . .) the importance of participation and how each child’s mobility technology mediated participation, daily activity and interaction with siblings, peers and adults.
Researcher, Feldner et al. 60
In the numeric data, most studies indicated that powered mobility had a positive impact on some of the component skills related to play and social interactions, especially social function (Table 14). There were limited data on the wider concepts of actual everyday participation, play and friendships. We explored, but found little to suggest, substantial variation by age. Although the nature of the activities the children engaged in varied, this variation appeared to be related to their developmental level, powered mobility competence, and environmental factors, rather than biological age.
| Study population | Verbatim outcomes (outcome measure) (reference, sample size) | % (n) of studies reporting positive change | Summary codea | ||
|---|---|---|---|---|---|
| Positive change in ‘participation, play, social interactions’ | No change in ‘participation, play, social interactions’ | Negative change in ‘participation, play, social interactions’ | |||
| Study population aged < 5 years |
|
|
N/A | 77.8 (14) | ++ |
| Study population aged ≥ 5 years |
|
N/A | N/A | 100 (1) | + |
| Study population aged < and ≥ 5 years |
|
N/A | N/A | 100 (5) | ++ |
The assessment of certainty for the concept indicated overall moderate support for participation, play and social interactions as a powered mobility intervention outcome (Table 15). The concept was theoretically sound, including the hypothesised mechanisms linking it to the intervention, and underpinned by data from various designs. However, the overall level was brought down from ‘strong’ by limitations in the numeric data, which focused mainly on the skills underpinning participation, as opposed to the actual doing of it (the dimension emphasised as important in the textual data).
| Concept support criteria | Assessment of support | Level of support |
|---|---|---|
| Truth value/bias | The analytical concept very clearly reflects the textual data from the primary studies, but numeric data are restricted mainly to underlying skills | Low |
| Explanation credibility | The concept of participation (including participation in play and social interactions) is well established, and was expected to emerge as a key outcome of powered mobility (reflected in the pre-review logic model). The included studies provided evidence of two credible hypotheses of mechanisms through which this outcome might link to powered mobility intervention, namely ‘movement and mobility’ and ‘fit’ | Strong |
| Weakness minimisation | The concept is supported by numeric and textual data from different study designs (RCTs, observational, qualitative, mixed methods), but the numeric data focus mainly on the underlying skills. Some of the numeric measures have significant limitations | Moderate |
| Inside–outside | There is substantial convergence in the accounts across all stakeholders, including the child and parent (insider) views and professional and researcher (outsider) views | Strong |
| Publication bias | There are studies that show non-significant results | Strong |
| Additional comments | None | N/A |
Self-care
Self-care emerged initially only from the numeric data, with related textual data identified after a subsequent targeted search; overall data on the concept was limited. In textual data, descriptions of self-care outcomes were brief comments referring to increased ability to undertake basic tasks related to looking after oneself (e.g. eating or drinking), and to decreased need for caregiver assistance. These were in the voices of children, parents and researchers; we found no comments about self-care outcomes from professionals:
(. . .) without it, I could do almost nothing. (. . .) Even eat by myself, I cannot without sitting in my chair.
Child, Pituch et al. 100
(. . .) who would have thought that you could have gotten up and got water [to drink] on your all-terrain vehicle?
Parent, Feldner et al. 60
In turn, [powered mobility] decreased the level of assistance required from caregivers and the need to wait for others’ availability.
Researcher, Pituch et al. 100
In the numeric data, self-care outcomes were assessed mainly in very young children, with all studies using the PEDI (Table 16). The results were mixed, but reported an overall consistent message that, although powered mobility may not directly change children’s skills in self-care, it may reduce the need for caregiver assistance by enabling a child’s sense of independence and control.
| Study population | Verbatim outcomes (outcome measure) (reference, sample size) | % (n) of studies reporting positive change | Summary codea | ||
|---|---|---|---|---|---|
| Positive change in ‘self-care’ | No change in ‘self-care’ | Negative change in ‘self-care’ | |||
| Study population aged < 5 years |
|
N/A | 42.9 (3) | ?? | |
| Study population aged ≥ 5 years | N/A | Self-care (WeeFIM) (Kornafel et al.;104 n = 1) | N/A | 0 (0) | 0 |
The assessment of certainty for the concept indicated overall low support for self-care as a powered mobility intervention outcome (Table 17); this reflected the overall limited data available for this concept. Furthermore, owing to the limited data, we were not able to explore variation by age.
| Concept support criteria | Assessment of support | Level of support |
|---|---|---|
| Truth value/bias | Both numeric and textual data clearly reflected the analytical concept, but these data were limited in breadth. Numeric data were absent for a part of the study population (children aged ≥ 5 years) | Low |
| Explanation credibility | The concept of self-care is well established in practice, although published evidence and theories are limited. The included studies provide some early hypotheses about how self-care might be influenced by powered mobility interventions; these require further investigation, which may also result in refinement of the concept | Low |
| Weakness minimisation | The concept was supported by limited numeric and textual data from a small pool of study designs (observational, qualitative) | Low |
| Inside–outside | The concept was reflected in child and parent (insider) views and in researcher (outsider) observations, but not in professionals’ (outsider) views | Moderate |
| Publication bias | There is at least one study that shows non-significant, null or contrasting results | Strong |
| Additional comments | None | N/A |
Autonomy, independence, choice and control, and freedom
Autonomy, independence, choice and control, and freedom were a broad cluster of concepts that emerged primarily from the textual data, and were repeatedly represented in the voices across children, parents, professionals and researchers. They were often articulated and framed through specific incidents of movement, mobility, participation and self-care that the different stakeholders attended to as observable manifestations of the abstract, desirable states of being autonomous, independent and free, and having choices, controls and self-expression:
Going through the door, getting outside. That’s very cool – I mean, talk about freedom (. . .) that is an entrance to his own world. There are no limitations on that.
Parent, Durkin109
It’s given her far more freedom, independence. To go out with friends, she doesn’t need someone.
Parent, Evans et al. 59
Learning to use a power mobility device also altered how children were able to express themselves.
Researcher, Kenyon et al. 61
Analysis of interview responses revealed that nine young people and their families (50%) mentioned increased independence as a result of the EPIOC.
Researcher, Evans et al. 59
We explored the data for differences between the age groups. In the textual data, there was variation in the nature of activities and decisions in which the children expressed their autonomy, freedom, choice and control, and independence; this nature appeared to relate to the children’s developmental stage. Yet, the descriptions of the actual abstract concepts remained consistent across age groups. One specific, repeated example of this was children, across ages, using powered mobility to express their autonomy, choice and control by defying demands and expressing anger or disagreement. This included, for example, deliberately driving away or crashing into objects or people, and was often, but not always, interpreted by parents, professionals and researchers as positive and as developmentally appropriate self-expression:
I think the best picture I have of him is driving away from me. I get tears every time I see it because he’s on his own and he’s able to get somewhere by himself without any help.
Parent, Wiart et al. 102
So it’s quite interesting to see there is a personality now whereas before, you didn’t realize was quite a little naughty streak and someone who actually wanted to go quite fast.
Professional (occupational therapist), Sonday and Gretschel101
Running over people’s toes, hitting walls, (. . .) purposely being naughty because (it) is developmentally appropriate to be . . . naughty (. . .).
Professional, Kenyon et al. 61
Numeric data related to this concept cluster focused mainly on two aspects within the broad cluster: (1) children’s increased self-initiation (as a manifestation of control, choice and independence) and (2) reduced caregiver assistance (as a manifestation of independence) (Table 18). Of these, the latter overlapped with the self-care data.
| Study population | Verbatim outcomes (outcome measure) (reference, sample size) | % (n) of studies reporting positive change | Summary codea | ||
|---|---|---|---|---|---|
| Positive change in ‘autonomy, independence, choice and control, freedom’ | No change in ‘autonomy, independence, choice and control, freedom’ | Negative change in ‘autonomy, independence, choice and control, freedom’ | |||
| Study population aged < 5 years |
|
Responsibility (PEDI-CAT responsibility subscale) (Kenyon et al.;75 n = 1) | N/A | 83 (5) | ++ |
| Study population aged ≥ 5 years |
|
N/A | N/A | 100 (3) | ++ |
| Study population aged < and ≥ 5 years |
|
N/A | N/A | 100 (4) | ++ |
The assessment of certainty for the concept indicated overall low support for autonomy, independence, choice and control, and freedom as powered mobility intervention outcomes (Table 19). Although the textual evidence was rich and converging, the theoretical focus and linking of the concepts was limited, as was the scope of the numeric data.
| Concept support criteria | Assessment of support | Level of support |
|---|---|---|
| Truth value/bias | The analytical concept clearly reflects the textual data; the numeric data relate to a narrower segment of the overall concept | Low |
| Explanation credibility | This is an elaborate cluster of several inter-related and overlapping concepts that are broadly recognisable, but that, in their current format in the included evidence, lack clear, specific links to wider theories and evidence | Very low |
| Weakness minimisation | The data supporting the concept come from a range of study designs (observational, qualitative, mixed methods), but include limited experimental data | Moderate |
| Inside–outside | The data consisted of child and parent (insider) views, and professionals’ and researchers’ (outsider) views and observations | Strong |
| Publication bias | There was at least one study that showed non-significant results | Strong |
| Additional comments | None | N/A |
Psychological outcomes: sense of achievement, confidence, motivation and cognitive outcomes
Psychological outcomes of powered mobility for children were reported in relation to sense of achievement; a child’s confidence and beliefs about capabilities, motivation and identity; and cognitive outcomes including alertness, language, communication and understanding. In textual data, descriptions of these concepts were present in the voices of parents, professionals and researchers, but not in the voices of the children themselves. The descriptions for sense of achievement, confidence and motivation were easier to find than descriptions of cognitive outcomes:
And she realized then: ‘I thought initially I can’t do it, but I tried and I can’.
Parent, Sonday and Gretschel101
[Researcher:] The family noted pride and self-efficacy (. . .) Teresa [parent] narrated, ‘He had just driven and a bunch of people were telling him how amazing he was and that was his response. That smile was just, like, proud.’ When Sam [child] described the photo, he narrated, ‘I drive. In the gym, I’m happy’.
Researcher, parent and child, Kenyon et al. 60
Observed effects judged to be the result of the training included increased wakefulness and alertness, (. . .) John sometimes arrived at the training sessions asleep or acting very tired, but as he was being positioned in the powered wheelchair, he would straighten up and look around.
Researcher, Nilsson and Nyberg74
The numeric data for achievement, motivation and confidence suggested a consistently positive impact across age groups (Table 20). The achievement data were from measures that require families to uniquely generate items, limiting the interpretation of this finding. The motivation data were based on mastery motivation. The cognitive outcome measurement emphasised language and communication skills, and the data suggested a positive impact (Table 21). There were insufficient data to draw conclusions about differences in responses in the psychological outcomes based on age.
| Study population | Verbatim outcomes (outcome measure) (reference, sample size) | % (n) of studies reporting positive change | Summary codea | ||
|---|---|---|---|---|---|
| Positive change in ‘achievement, motivation and confidence’ | No change in ‘achievement, motivation and confidence’ | Negative change in ‘achievement, motivation and confidence’ | |||
| Study population aged < 5 years |
|
N/A | N/A | 100 (6) | ++ |
| Study population aged < and ≥ 5 years | N/A | N/A | 100 (3) | ++ | |
| Study population | Verbatim outcomes (outcome measure) (reference, sample size) | % (n) of studies reporting positive change | Summary codea | ||
|---|---|---|---|---|---|
| Positive change in ‘cognitive outcomes’ | No change in ‘cognitive outcomes’ | Negative change in ‘cognitive outcomes’ | |||
| Study population aged < 5 years |
|
N/A | 85.7 (6) | ++ | |
| Study population aged ≥ 5 years | Health-related quality of life (CPCHILD) (Kenyon et al.;76 n = 1) | N/A | N/A | 100 (1/1) | + |
| Study population aged < and ≥ 5 years |
|
Intellectual development (Leiter International Performance Scale Performance IQ score, Peabody Developmental Verbal Scale Verbal IQ score) (Bottos et al.;23 n = 29) | N/A | 75 (3) | ++ |
The assessment of certainty for the concept indicated overall low support for achievement, motivation and confidence as powered mobility intervention outcomes (Table 22), and indicated moderate support for cognitive outcomes as an outcome (Table 23). For achievement, motivation and confidence, the overall rating was low, primarily because of the limited data and the lack of a clear theory about linking these outcomes to powered mobility interventions in the included studies. Although the data were assessed as being more supportive of the cognitive outcomes, it is worth emphasising that there was no direct, high-quality evidence of effectiveness.
| Concept support criteria | Assessment of support | Level of support |
|---|---|---|
| Truth value/bias | The analytical concept reflected the underpinning numeric and textual data, but overall data were limited | Low |
| Explanation credibility | The concepts of confidence, achievement and motivation are well established and sound; the evidence to support their linkage to powered mobility intervention in the present review was limited | Low |
| Weakness minimisation | The concept was supported by limited numeric and textual data from a small pool of study designs (observational, qualitative). Outcome measurement in several of the studies had significant limitations | Very low |
| Inside–outside | The data consisted primarily of parent (insider) and professional (outsider) views and researcher (outsider) observations | Moderate |
| Publication bias | There was a lack of contrasting results | Low |
| Additional comments | None | N/A |
| Concept support criteria | Assessment of support | Level of support |
|---|---|---|
| Truth value/bias | The analytical concept clearly reflects the numeric data from the primary studies; examples in textual data are limited | Low |
| Explanation credibility | Potential impact of self-directed movement on cognitive development is an established hypothesis. The concept, as it was synthesised and presented in much of the primary studies, covered a number of subcategories of cognition (e.g. language, attention), which could plausibly be differentially affected by a use of powered mobility; this was not further explored | Moderate |
| Weakness minimisation | The concept is supported by a range of numeric and textual data from different study designs (RCT, observational, qualitative). The contribution from qualitative designs was limited | Moderate |
| Inside–outside | The data related to the concept consists of mainly outsider views and observations. For this concept, the requirement of insider (child) voice was assessed as being of lesser importance, and potentially something that is not feasible to gain in younger children; it was noted that the data included detailed, direct observations explicitly designed to capture cognitive engagement from the child perspective | Moderate |
| Publication bias | There was at least one study that showed non-significant results | Strong |
| Additional comments | Although there was consistent and cumulative evidence of possible impact on at least some cognitive outcomes, the size of these effects and the precise aspect of cognitive function remains to be clarified | N/A |
Safety outcomes: emotional consequences, accidents and pain
The included studies did not include straightforward negative safety outcomes. Instead, the information relevant to safety outcomes was more nuanced, akin to considerations about benefits and risks of powered mobility interventions. The data clustered around two themes: (1) emotional consequences and (2) accidents and pain.
Emotional consequences of powered mobility for the parent and child
Child and parent feelings were frequently reported to change as a result of powered mobility intervention. For parents, both negative feelings (anxiety, distress, sadness) and positive feelings (relief, happiness, joy) were reported. These feelings were not necessarily mutually exclusive, but could coincide within a parent for the same event, as well as two parents feeling the opposite way about the same event. One common example of a trigger for emotions in parents was the initial proposal for, and prescription of, powered mobility by professionals. The emotional consequences varied; negative feelings were reported in several papers:
The power wheelchair was the really big step, although when we first started talking wheelchairs and they had said, ‘Oh, possibly a power wheelchair’, I got my back up, thinking going in a manual wheelchair was hard enough.
Parent, Wiart et al. 102
When the idea of a power chair was presented (. . .) that actually was a great source of relief for me and it was a good thing.
Parent, Wiart et al. 102
As children progressed to try the powered mobility equipment, to learn to use it and to actually use it, parents were described to often report more positive emotions. These were often reported to relate to parents observing their child gaining control, freedom, independence and self-expression (see Autonomy, independence, choice and control, and freedom) in everyday situations:
For example, Sam set his own mobility agenda (. . .) He tells me ‘No, mommy, I want to go here’ . . . to even be able to talk back to me – it makes me want to cry, in a good way.
Parent, Feldner et al. 60
The process of learning to use powered mobility was recognized as an emotionally charged undertaking for all those involved. Some parents expressed joy or excitement at seeing their child use a power mobility device. Other parents expressed a mix of emotions.
Researcher, Kenyon et al. 61
For emotional consequences on the children, there was some evidence about a trajectory of feelings related to learning to drive powered mobility:
Participants reported that children learning to use a power mobility device may experience a wide range of emotions from excitement and joy, to pride in being able to move and do for themselves, to frustration, anxiety, and despair.
Researcher, Kenyon et al. 61
However, most data related to everyday situations that the children experienced. One example was the experience of fear and worry related to road traffic, even in older children, who may have been expected to feel safe in such situations:
(. . .) he wouldn’t have any chance at all if someone was to hit him. He doesn’t feel safe to go up the road. He goes out with someone with him, but he’s sixteen years old. He should really feel alright to go out by himself.
Parent, Evans et al. 59
Similar data were identified in relation to general worries and fears about any accidents that might result in the child losing control of the powered mobility equipment:
I just said ‘I’m not doing this on me own’ because if it skids I’m gonna be really scared.
Child, Gudgeon and Kirk99
Further triggers of negative emotions in children described in the data were other people and their actions, and problems in fit between the child and the child’s environment. These could frustrate and upset children using powered mobility:
You feel quite frustrated you’re just sitting there and next minute this person walks right in front of you (. . .) like ‘Did you not see me sat there?’ you know what I mean, it’s frustrating.
Child, Gudgeon and Kirk99
Liam was particularly frustrated and upset at the time of the interview as he had been unable to go on the bus to swimming with his classmates as his EPIOC could not be transported and he described the whole experience as ‘crap’ (. . .).
Researcher, Gudgeon and Kirk99
In the numeric data, feelings were mainly operationalised through parenting stress and child enjoyment (Table 24). For both of these, positive impact was consistently reported for very young children and from mixed-age studies. There was only one relevant study12 for children aged ≥ 5 years, and that reported no effect.
| Study population | Verbatim outcomes (outcome measure) (reference, sample size) | % (n) of studies reporting positive change | Summary codea | ||
|---|---|---|---|---|---|
| Positive change in ‘safety outcomes: emotional consequences’ | No change in ‘safety outcomes: emotional consequences’ | Negative change in ‘safety outcomes: emotional consequences’ | |||
| Study population aged < 5 years |
|
N/A | N/A | 100 (6) | ++ |
| Study population aged ≥ 5 years | Affect (number of observations for which positive affect was recorded for each child, percentages of moments for which positive affect was recorded for each child) (Deitz et al.;12 n = 2) | N/A | 66.6 (2) | ? | |
| Study population aged < and ≥ 5 years |
|
N/A | Enjoyment (frequency count of positive/negative facial expressions) (Logan et al.;118 n = 3) | 100 (7) | ++ |
The assessment of certainty for the concept indicated overall low support for emotional consequences as powered mobility intervention outcomes (Table 25). It was noted that the textual data supporting this concept were rich in detail, and converged around similar themes; however, further theory development of these themes was limited, as were numeric data. It was also noted that the data underpinning the emotional consequences concept were, at least in part, overlapping with the autonomy, independence, choice and control, and freedom concept cluster, and that the boundaries or processes through which these concepts connected were not clear.
| Concept support criteria | Assessment of support | Level of support |
|---|---|---|
| Truth value/bias | The analytical concept reflects the textual data; the numeric data relate to a narrower segment of the overall concept | Low |
| Explanation credibility | The concept mirrors an existing theory and evidence-based concepts (e.g. affect, feeling, emotion), but in the present data there was little explicit linkage of these concepts or bodies of knowledge, and limited unpicking of the mechanisms that may link emotions to the intervention | Low |
| Weakness minimisation | The data supporting the concept come from a range of designs (observational, qualitative) across a number of studies | Moderate |
| Inside–outside | The data related to the concept consisted of child and parent (insider) views and researcher (outsider) observations | Moderate |
| Publication bias | There is at least one study with contrasting results | Strong |
| Additional comments | It was noted that some of the textual data supporting this concept were particularly rich in detail, and consistent from across a number of studies. Data linked to this concept were, at least in part, the same as data linked to the autonomy concept cluster | N/A |
Accidents and pain
The data in the review included descriptions of accidents and pain resulting from the use of powered mobility equipment. The accidents related mainly to the child losing control of the equipment. This could be an accident due to the environment not being a good fit for the child’s use of the equipment or due to the human factors in the environment (Table 26):
Erm I crushed Oliver and Elliot at school once because my arm got stuck and then I flied forward into them.
Child, Gudgeon and Kirk99
Especially when he’s driving with his chin, which is how he drives. He’s not actually gripping the control with his hand. His head flies off and he loses control of the chair if the terrain is rough.
Parent, Evans et al. 59
| Study population | Summary outcomes |
|---|---|
| Study population aged < 5 years | Safety (reported by authors):119 the power of the cart is sufficient to move the child, but not sufficient to cause injury to family members, furniture or the child himself. The large wheel spacing and low centre of gravity make tipping over unlikely |
| Accidents during powered wheelchair use (questionnaire prepared by the study authors):112 30% of facilities reported that accidents were present during powered wheelchair use, 61% reported that accidents were absent and 9% were unknown. Specific details of the accidents were collisions with indoor obstacles (reported by 18.2% of facilities), collisions with outdoor objects (reported by 9.1%), collisions with people (reported by 9.1%), falls from the wheelchair (reported by 27.3%), falls related to uneven surfaces (reported by 18.2%); running into a ditch on a public road (9.1%); and other (9.1%). There was no significant increase in the number of facilities that experienced an accident during powered wheelchair use, despite increased demands by children to have more time to use powered wheelchairs in some facilities | |
| Study population aged ≥ 5 years | Number of collisions (supervisor observations):130 the number of collisions decreased when the child used the mid-wheel drive chair to perform all three tasks. Collisions while moving through a doorway decreased from six to one; while manoeuvring through three cones, collisions decreased from five to two; and while manoeuvring in the hallways, collisions decreased from six to two |
| Number of collisions (supervisor observations):85 there were six collisions that required the intervention of the supervisor to free or unblock the wheelchair. Three of them were due to system failures, and the rest were due to the sensory capabilities of the robot | |
| Study population aged < and ≥ 5 years | Accidents (parent questionnaire):106 when parents were asked if their child had ever had an accident in the equipment, 39 said no and 18 said yes. The variety of comments from those who said yes included a range of accidents and injuries, including trapped fingers, falling off kerbs, broken bones, damage to furniture and buildings, tipping and so on |
| Accidents/incidents (parent report):95 three incidents happened in more than 1 year. None of the children was hurt in the incidents | |
| Safety (questionnaire administered to intervention recipients):91 the Smart Wheelchair described as a safe learning environment for physically, cognitively and perceptually impaired children |
The percentage of children reported to have experienced accidents during real-world use was similar in very young and older children (30% and 31.5%, respectively), and the descriptive examples were also similar. No data were found to substantiate the concerns about traffic-related risks (see Emotional consequences of powered mobility for the parent and child).
Beyond accidents, there was also evidence in the textual data that powered mobility equipment could cause pain and discomfort to the child; one commonly mentioned reason was sitting in the equipment for a long time:
Analysis of the ‘in-depth’ interviews indicated that 38 (59%) users described ways in which they felt their pain was influenced by their EPIOC and 19 (30%) reported pain or discomfort aggravated by sitting.
Researcher, Frank et al. 131
Due to certain school policies where children are left in wheelchairs all day long, she is bound to experience pain and discomfort and yes, she does complain of it sometimes. Juddering happens just going along the road because of so many holes in the pavement.
Parent, Evans et al. 59
The assessment of certainty for the concept indicated low support for accidents and pain as powered mobility intervention outcomes (Table 27). Although the nature of accidents and pain were well described, the prevalence data came from a limited pool of studies, and, within those studies, came mainly from parents.
| Concept support criteria | Assessment of support | Level of support |
|---|---|---|
| Truth value/bias | The analytical concept clearly reflected both the numeric and textual data from the primary studies | Strong |
| Explanation credibility | Both aspects of the concept (accidents and pain) are clearly articulated and operationalised for measurement. Mechanisms through which they may relate to powered mobility interventions are described | Strong |
| Weakness minimisation | The concept is supported by data from a limited pool of studies of different designs (observational, qualitative) | Low |
| Inside–outside | The data related to the concept consist mainly of parent reports | Low |
| Publication bias | Several studies reported accidents. It is unclear whether or not absence of reports of no accidents constitutes publication bias | Moderate |
| Additional comment | Some of the accident data included in the studies came from experimental studies; however, the primary focus of assessment of certainty in the present review relates to the data from pragmatic studies reporting accidents resulting from everyday real-world use | N/A |
Mixed-methods framework synthesis: factors associated with feasibility and acceptability
In addition to the six outcome concepts and two safety concepts, three further concepts were identified in relation to feasibility and acceptability of powered mobility (Table 28): (1) ‘fit’ and opportunities for everyday use, (2) social environment and (3) physical environment. These were often reported as being inextricably linked to the outcomes, processes and contexts of powered mobility use, and to the issues of acceptability and feasibility. Table 29 presents the powered mobility evidence profile from the mixed-methods synthesis.
| The concept (related papers) | Summary description | Included in the concept | Excluded from the concept |
|---|---|---|---|
| ‘Fit’ and opportunities for everyday use (quantitative studies;55,83,96,98,132 qualitative studies59–61,71,99–103,109) | The fit as a dynamic ‘coming-together’ of the child, powered mobility equipment, and the child’s everyday social, physical and policy environment |
|
|
| Opportunities to use powered mobility in everyday situations |
|
Excludes the actualisations of the possibilities, for instance the actual use of powered mobility (coded under ‘movement and mobility’) and the subsequent outcomes (coded under ‘participation, freedom, etc.’) | |
| Social environment (quantitative studies;91,96,98 qualitative studies59,61,99,101,102) | Characteristics and actions of other people, social rules and norms, policies and practices that either shape or are shaped by the child’s use of powered mobility |
|
Excludes professionals and service provision, and emotions of other people (coded under ‘emotional consequences’) |
| Physical environment (quantitative studies;91,106,132 qualitative studies59–61,99,100,102) | Built and natural physical surroundings and spaces that shape a child’s use of powered mobility |
|
Excludes social environment; see row above |
| The outcome concept | Number of studies per design | Number of participants across studies | Evidence about the importance of the outcome | Overall quality of evidence |
|---|---|---|---|---|
| ‘Fit’ and opportunities for everyday use |
|
797 | Critical | Low |
| Social environment |
|
111 | Insufficient evidence | Very low |
| Physical environment |
|
216 | Insufficient evidence | Very low |
‘Fit’ and opportunities for everyday use
The concept of ‘fit’ was explicitly labelled and articulated in only one qualitative paper;99 others implied this concept and illustrated it in examples:
Using an EPIOC was an experience which required active involvement from [the child] as they worked to balance, or achieve an adequate fit, between their own abilities, desires and needs; those of their parents and friends; the demands of the environment; and the capabilities and limitations of the EPIOC itself.
Researcher, Gudgeon and Kirk99
As a synthesised concept across the included data, fit can be described as a coming-together of three elements: (1) the child, (2) the equipment and (3) the child’s social, physical and policy environments. Fit is dynamic in that it changes with any of the three elements, and it is a spectrum, that is there are degrees of better and worse fit. Achieving a sufficiently good fit was repeatedly described as a necessary condition for a child’s use of powered mobility, and as something that a child needed to seek to constantly negotiate:
It depends, say err if it’s like a test and there’s a massive space I’ll probably go in (to the classroom in the equipment) (. . .) but say it’s a small one I’ll just maybe like drive into the doorway and leave it there.
Child, Gudgeon and Kirk99
Restrictions in fit were reported to translate to suboptimal powered mobility use and outcomes, and an increased likelihood of negative emotional consequences. In contrast, a good fit had the potential to transform a child’s movement, mobility and participation:
He just sailed on into the camp meeting area where registration was, and he was going around (. . .) chatting with everybody. I was just blown away, because I had never, ever understood that David had the capacity nor would have the opportunity to do something like that.
Parent, Sonday and Gretschel101
Good fit required psychological, social and physical compatibility. The psychological compatibility was described in terms of the child’s self-identity; the social compatibility was described in terms of the way others viewed the child. In this, using powered mobility in everyday life required both the child and those around the child to develop a new sense of what the child is like and what the child can do and actually does in everyday life. From this reframing, a new ‘integrated self’ of the child emerged, both in the child’s own mind and in the eyes of others:
The children perceived that the ‘self’ that existed before they had (the powered mobility) did not adequately fit the environment, and hence they were prevented from fulfilling their needs and desires. In contrast, using (powered mobility) was seen as allowing a new self to emerge, one that integrated their body and (powered mobility).
Researcher, Gudgeon and Kirk99
It (powered wheelchair) changed his peers’ attitudes toward him because they saw that he could do something on his own and that he could actually think on his own.
Parent, Wiart et al. 102
You start to see your child in a different light and they start to see themselves in that light (. . .).
Parent, Kenyon et al. 61
Furthermore, this change in the perceptions about the child was often described to be a catalyst for more opportunities for the child to use the powered mobility and to actualise further positive outcomes in terms of participation and independence:
Learning to use a power mobility device often changed the way that the participants and others perceived a child (. . .) Such changes in how a child was perceived often led to increased opportunities for social interaction and participation and expanded the child’s growing sense of independence and responsibility.
Researcher Kenyon et al. 61
He can go out and wander around the playground with the kids, do everything within his ability that the other kids do, and they don’t look at him as, ‘Oh, God, we have to push the wheelchair’. (. . .) They look at him as a whole person.
Parent (mother), Wiart et al. 102
Numeric data on fit and opportunities were very limited (Table 30), and an overall impression from the data was that fit was a concept emerging from the child and parent narratives, but was less well recognised in professional and researcher narratives. In professional narratives, the focus of fit was often limited to adapting the powered mobility equipment set-up to the point where the child was able to drive it, with limited evidence of broader consideration of fit in the wider sense of compatibility between the child, the equipment and their everyday environment:
Several participants described the individualized nature of equipment needs as a ‘Catch-22’ in which proper equipment and set-up were necessary to enable a child to use a power mobility device, but a child needed to actually use the power mobility device to discover what equipment and set-up were needed (. . .).
Researcher, Kenyon et al. 61
| Study population | Verbatim outcomes (outcome measure) (reference, sample size) | % (n) of studies reporting positive change | Summary codea | ||
|---|---|---|---|---|---|
| Positive change in ‘fit’ and opportunities for ‘everyday use’ | No change in ‘fit’ and opportunities for ‘everyday use’ | Negative change in ‘fit’ and opportunities for ‘everyday use’ | |||
| Study population aged < 5 years | N/A | Cost of assistive technology [Cost (US$) of assistive technology purchases per annum] (Bamer et al.;55 n = 538) | 66.7 (2) | + | |
| Study population aged ≥ 5 years | N/A | N/A | 100 (2) | + | |
Both the numeric and textual data suggested that it was possible to achieve a good fit in very young children, as well as across age groups, but that this required careful consideration of a child’s wider social and physical environment. The evidence related to these is further summarised in the next two sections on social and physical environment. The assessment of certainty for the concept indicated overall low support for ‘fit’ and opportunities for everyday use (Table 31); the key limitations were the small pool of data and the lack of theory integration.
| Concept support criteria | Assessment of support | Level of support |
|---|---|---|
| Truth value/bias | The analytical concept clearly reflects the textual data from the primary studies; numeric data are limited | Low |
| Explanation credibility | The analytical concept is theoretically novel in the field, and was explicitly discussed mainly in just one study. More broadly, the concept mirrors biopsychosocial frameworks of disability and functioning (e.g. by the WHO), which position everyday functioning as a successful coming-together of the person, the health condition and related interventions, and the wider environment. As presented in this review and the included data, the concept lacks clarity and is not directly measurable | Low |
| Weakness minimisation | The concept is supported by data from a limited pool of studies of different designs (observational, qualitative) | Low |
| Inside-outside | The data related to the concept consisted of child (insider) and parent and researcher (outsider) views, and researcher (outsider) observations | Moderate |
| Publication bias | Rated one step down from strong, as the interaction between the person and their environment is widely discussed among the research community; this was not reflected in the included publications related to this concept | Moderate |
| Additional comments | None | N/A |
Social environment: the people and policies around the child
Previous sections have already illustrated ways in which people and policies around the child can shape their powered mobility use and outcomes (e.g. see concepts in Emotional consequences of powered mobility for the parent and child and ‘Fit’ and opportunities for everyday use). As a specific concept, social environment mainly emerged from, and was supported by, textual data (Table 32 presents a summary of the quantitative findings).
| Study population | Verbatim outcomes (outcome measure) (reference, sample size) | % (n) of studies reporting positive change | Summary codea | ||
|---|---|---|---|---|---|
| Positive change in ‘social environment’ | No change in ‘social environment’ | Negative change in ‘social environment’ | |||
| Study population aged < 5 years | Socialisation in the classroom, defined as the amount of time the child spent interacting with peers and teachers in the classroom (coding from video footage) (Ragonesi et al.;96 n = 1) | N/A | N/A | 100 (1) | + |
| Study population aged ≥ 5 years | Parent feelings (quotations from participants) (Sharma and Morrison;98 n = 35) | N/A | Feasibility issues (quotations from participants) (Sharma and Morrison;98 n = 35) | 50 (1) | ? |
Broadly, the social environment concept covered two dimensions. The first dimension was the people and social structures (informal policies, rules, practices) as shapers of children’s use of powered mobility, their user experiences, and the related outcomes. These influences could be negative or positive:
The power that adults have to override the children’s autonomy by disabling their powered mobility equipment – switching the equipment off or by turning down the speed – was clear (. . .).
Researcher, Durkin109
Rocky explained how another child had caused a crash: ‘Sometimes people touch (the EPIOC) ‘cos there was somebody called Oscar and he drove my chair . . . once he made me go head first into the wall, head forwards (. . .)’.
Researcher and child, Gudgeon and Kirk99
Due to certain school policies where children are left in wheelchairs all day long, she is bound to experience pain and discomfort and yes, she does complain of it sometimes.
Parent, Evans et al. 59
The second dimension was the reciprocal impact of children’s powered mobility use on other people and social structures. Common examples were the perceptions that a child’s powered mobility use can make things easier for others, and has the power to fundamentally change how children with disabilities are perceived:
The children also perceived that these gains in independence were beneficial in reducing the need for others to help them. In fact Farrah indicated that this was her main reason for using her EPIOC (. . .).
Researcher, Gudgeon and Kirk99
His mother perceived the identification of her family’s needs and the opportunity of her community members to assist in meeting these needs as a positive step toward a better understanding of disability issues and a step toward interdependence in her community.
Researcher, Wiart et al. 102
The assessment of certainty for the concept indicated overall very low support for social environment (Table 33), due to limitations in the volume and diversity of data, and lack of clear links to theory.
| Concept support criteria | Assessment of support | Level of support |
|---|---|---|
| Truth value/bias | The analytical concept clearly reflects textual data from the primary studies; there are a lack of numeric data | Very low |
| Explanation credibility | The role of social environment as a factor in intervention feasibility and acceptability is well established; however, the consideration of that idea in the included studies was very limited | Very low |
| Weakness minimisation | The concept was supported from a small pool of qualitative studies | Very low |
| Inside–outside | The data related to the concept consists of child (insider) and parent (outsider) views, but no objective observations | Very low |
| Publication bias | Rated down because the importance of social environment in implementation of powered mobility interventions is widely discussed among the research community (e.g. conference presentations); this was not reflected in the included publications related to this concept | Low |
| Additional comments | None | N/A |
Physical environment
Similarly to social environment, the concept of physical environment had very limited dedicated data and has already been illustrated in previous sections (e.g. see the concepts Accidents and pain and ‘Fit’ and opportunities for everyday use); furthermore, the data underpinning it were largely textual (Table 34).
| Study population | Verbatim outcomes (outcome measure) (reference, sample size) | % (n) of studies reporting positive change | Summary codea | ||
|---|---|---|---|---|---|
| Positive change in ‘physical environment’ | No change in ‘physical environment’ | Negative change in ‘physical environment’ | |||
| Study population aged < 5 years | Home affordances (Affordance in the Home Environment for Motor Development – Toddler version – Chinese version) (Huang et al.;80 n = 3) | N/A | N/A | 100 (1) | + |
| Study population aged ≥ 5 years | Pain or discomfort related to the intervention (questionnaire) (Frank et al.;131 n = 74) | N/A | N/A | 100 (1) | + |
| Study population aged < and ≥ 5 years | N/A | N/A | 100 (2) | + | |
The features of the physical environment described in the data included access, built spaces and other built features (especially kerbs and potholes), natural environment and the impact of weather (especially issues related to ice and mud), and road safety and traffic. The data originated primarily from children’s and parents’ voices, and focused largely (although not exclusively) on descriptions of physical environment as a barrier.
The assessment of certainty for the concept indicated overall very low support for physical environment (Table 35) due to limitations in the volume and diversity of data, and lack of clear links to theory.
| Concept support criteria | Assessment of support | Level of support |
|---|---|---|
| Truth value/bias | The analytical concept reflects textual data from the primary studies; there are a lack of numeric data | Very low |
| Explanation credibility | The role of physical environment as a factor in intervention feasibility and acceptability is well established; however, the consideration of that idea in the included studies was very limited | Very low |
| Weakness minimisation | The concept was supported from a small pool of studies of different designs (observational, qualitative) | Low |
| Inside–outside | The data related to the concept consists of child (insider) and parent (outsider) views, but no objective observations | Very low |
| Publication bias | Rated down because the importance of social environment in implementation of powered mobility interventions is widely discussed among the research community (e.g. conference presentations); this was not reflected in the included publications related to this concept | Low |
| Additional comments | None | N/A |
Qualitative thematic synthesis: preparation, provision, use and expectations
From the separate synthesis of all qualitative evidence from the qualitative studies and relevant mixed-methods studies (n = 21), 17 descriptive themes were developed, comprising 60 subthemes. These were mapped onto four care processes and outcome contexts (Table 36).
| Context: care processes and outcomes | Descriptive themes | Subthemes | Studies contributing to subthemes |
|---|---|---|---|
| Preparation | Preparing for powered mobility | Education and information for parents and children | Pritchard-Wiart et al.,58 Feldner et al.,60 Durkin109 and Berry et al.133 |
| Skill preparation | Pritchard-Wiart et al.,58 Evans and Baines,62 Torkia et al.,71 Durkin109 and Currier et al.105 | ||
| Emotional journey for parents and children | Feldner et al.,60 Kenyon et al.,61 McGarry et al.,69 Pituch et al.,100 Wiart et al.,102 Feldner,116 Cerruti and Biondi103 and Cronin134 | ||
| Conceptualising intervention | Defining aims and goals | Evans and Baines,62 Nilsson and Nyberg74 and Cerruti and Biondi103 | |
| Change in intervention conceptualisation over time | Pritchard-Wiart et al.,58 Kenyon et al.,61 McGarry et al.,69 Wiart et al.102 and Cerruti and Biondi103 | ||
| Provision | Assessment | Consulting stakeholders throughout provision process | Kenyon et al.,61 Pituch et al.100 and Berry et al.133 |
| Conflict between therapist and caregiver | Durkin,109 Wiart et al.,102 and Berry et al.133 | ||
| Providing information and choice | Evans et al.59 and Durkin109 | ||
| Defining eligibility | Evans et al.59 and Durkin109 | ||
| Impact of bureaucracy on provision | Evans et al.,59 Pituch et al.100 and Feldner116 | ||
| Variance in assessment and provision between different services | Feldner et al.,60 Pituch et al.,100 and Feldner116 | ||
| Training and skill development | Experiential learning through use and play | Kenyon et al.,61 Evans and Baines,62 Durkin,109 Pituch et al.,100 Currier et al.105 and Nilsson et al.117 | |
| Importance of time to develop skills and reveal potential | Pritchard-Wiart et al.,58 Kenyon et al.,61 Evans and Baines,62 Nilsson and Nyberg,74 Durkin,109 Sonday and Gretschel,101 Currier et al.,105 Jonasson110 and Berry et al.133 | ||
| Defining learning continuums | Kenyon et al.,61 Evans and Baines62 and Durkin109 | ||
| Use | Accessibility | Accessibility of public spaces | Evans et al.,59 Feldner et al.,60 Kenyon et al.,61 Gudgeon and Kirk,99 Pituch et al.,100 Wiart et al.,102 Feldner116 and Berry et al.133 |
| Terrain | Pritchard-Wiart et al.,58 Evans et al.,59 Feldner et al.,60 Kenyon et al.,61 Gudgeon and Kirk,99 Pituch et al.100 and Berry et al.133 | ||
| Accessibility of home environments | Pritchard-Wiart et al.,58 Kenyon et al.,61 Evans and Baines,62 Gudgeon and Kirk,99 Pituch et al.,100 Wiart et al.102 and Berry et al.133 | ||
| Usability | Size, weight and manoeuvrability of device | Pritchard-Wiart et al.,58 Evans et al.,59 Feldner et al.,60 Kenyon et al.,61 Gudgeon and Kirk,99 Pituch et al.,100 Wiart et al.,102 Feldner,116 Cerruti and Biondi103 and Berry et al.133 | |
| Logistics of transporting device | Evans et al.,59 Kenyon et al.,61 Gudgeon and Kirk,99 Pituch et al.,100 Wiart et al.,102 Cerruti and Biondi103 and Berry et al.133 | ||
| Support from school/nursery to use device | Kenyon et al.,61 Evans and Baines,62 Durkin,109 Gudgeon and Kirk,99 Pituch et al.100 and Berry et al.133 | ||
| Appearance of device | Pritchard-Wiart et al.,58 Evans et al.59 and Gudgeon and Kirk99 | ||
| Integration | Achieving fit between child, device and environment | Kenyon et al.,61 Gudgeon and Kirk99 and Pituch et al.100 | |
| Device becomes child’s ‘legs’ | Evans et al.,59 Gudgeon and Kirk,99 Pituch et al.100 and Berry et al.133 | ||
| Safety | Concerns about safety to child and others | Evans et al.,59 Kenyon et al.,61 Evans and Baines62 Durkin,109 Gudgeon and Kirk,99 Pituch et al.100 and Berry et al.133 | |
| Balancing perceived and actual risks | Evans and Baines,62 and Gudgeon and Kirk99 | ||
| Adverse weather conditions | Kenyon et al.,61 Evans and Baines62 and Pituch et al.100 | ||
| Accidents affect confidence | Evans et al.,59 and Gudgeon and Kirk99 | ||
| Postural support and seating | Postural support and seating | Evans et al.,59 Feldner116 and Berry et al.133 | |
| Maintenance and review | Adapting device as child grows | Evans et al.,59 Frank et al.131 and Berry et al.133 | |
| Ongoing review and maintenance | Evans et al.59 Pituch et al.100 and Berry et al.133 | ||
| Poor maintenance affects use and outcomes | Evans et al.59 Feldner,116 Frank et al.131 and Berry et al.133 | ||
| Outcomes (anticipated and experienced) | Independence | Independence and autonomy | Pritchard-Wiart et al.,58 Evans et al.,59 Feldner et al.,60 Kenyon et al.,61 Evans and Baines,62 McGarry et al.,69 Gudgeon and Kirk,99 Pituch et al.,100 Sonday and Gretschel,101 Wiart et al.,102 Currier et al.,105 Feldner,116 Cerruti and Biondi,103 Jonasson110 and Cronin134 |
| Freedom | Evans et al.,59 Feldner et al.,60 Pituch et al.,100 Sonday and Gretschel,101 Wiart et al.,102 Currier et al.105 and Feldner116 | ||
| Self-efficacy | Evans et al.,59 Feldner et al.,60 Kenyon et al.,61 Evans and Baines,62 McGarry et al.,69 Gudgeon and Kirk,99 Pituch et al.,100 Sonday and Gretschel,101 Wiart et al.,102 Currier et al.,105 Feldner,116 Jonasson110 and Cronin134 | ||
| Self | Self-expression through movement and choice | Feldner et al.,60 Kenyon et al.,61 Durkin109 and Jonasson110 | |
| Disobedience and risky behaviours | Feldner et al.,60 Kenyon et al.,61 Durkin,109 Feldner116 and Cerruti and Biondi103 | ||
| Confidence and esteem | McGarry et al.,69 Gudgeon and Kirk99 and Feldner116 | ||
| Agency over body | Feldner et al.,60 Kenyon et al.,61 Gudgeon and Kirk99 and Feldner116 | ||
| Device becomes negative symbol | Kenyon et al.61 and Wiart et al.102 | ||
| Participation | Taking part in valued activities | Evans et al.,59 Feldner et al.,60 Kenyon et al.,61 Evans and Baines,62 McGarry et al.,69 Gudgeon and Kirk,99 Pituch et al.,100 Sonday and Gretschel,101 Wiart et al.,102 Cerruti and Biondi103 and Cronin134 | |
| Facilitating age-appropriate play | Pritchard-Wiart et al.,58 Evans et al.,59 Feldner et al.,60 Evans and Baines,62 McGarry et al.,69 Durkin,109 Sonday and Gretschel,101 Wiart et al.102 and Feldner116 | ||
| Broadening horizons | Feldner et al.,60 Pituch et al.,100 Sonday and Gretschel,101 Wiart et al.102 and Currier et al.105 | ||
| Frustration resulting from restriction | Gudgeon and Kirk99 and Pituch et al.100 | ||
| Exploratory behaviour | Feldner et al.,60 Evans and Baines,62 Sonday and Gretschel,101 Wiart et al.102 and Feldner116 | ||
| Social | Social interaction | Pritchard-Wiart et al.,58 Evans et al.,59 Feldner et al.,60 Kenyon et al.,61 Evans and Baines,62 McGarry et al.,69 Gudgeon and Kirk,99 Pituch et al.,100 Sonday and Gretschel,101 Wiart et al.,102 Currier et al.,105 Feldner,116 Cerruti and Biondi103 and Cronin134 | |
| Acceptance among peers | Wiart et al.,102 Feldner116 and Cerruti and Biondi103 | ||
| Emotions | Fun and joy | Feldner et al.,60 Kenyon et al.,61 Evans and Baines,62 McGarry et al.,69 Nilsson and Nyberg,74 Durkin,109 Pituch et al.,100 Sonday and Gretschel,101 Wiart et al.,102 Feldner,116 Cerruti and Biondi103 and Jonasson110 | |
| Joy of movement | Pritchard-Wiart et al.,58 Feldner et al.,60 Kenyon et al.,61 Evans and Baines,62 McGarry et al.,69 Nilsson and Nyberg,74 Kirk,99 Pituch et al.,100 Wiart et al.,102 Currier et al.,105 Feldner116 and Jonasson110 | ||
| Improving frustration and positive affect | Evans and Baines,62 McGarry et al.69 and Feldner116 | ||
| Development | Emotional development | Durkin109 and Jonasson110 | |
| Communication | Pritchard-Wiart et al.,58 McGarry et al.,69 Currier et al.105 and Jonasson110 | ||
| Learning cause and effect | Pritchard-Wiart et al.,58 Evans and Baines,62 McGarry et al.,69 Nilsson and Nyberg,74 Currier et al.105 and Nilsson et al.117 | ||
| Initiative and motivation | Pritchard-Wiart et al.,58 McGarry et al.,69 Sonday and Gretschel101 and Currier et al.105 | ||
| Interaction and attention to stimuli | McGarry et al.,69 Nilsson and Nyberg74 and Nilsson et al.117 | ||
| Impact on others | Reduce burden on parent/family | Evans et al.,59 Evans and Baines,62 Pituch et al.,100 Wiart et al.,102 Jonasson110 and Berry et al.133 | |
| Sharing in child’s joy and accomplishment | Evans et al.,59 Feldner et al.,60 Kenyon et al.,61 Evans and Baines62 McGarry et al.,69 Wiart et al.,102 Currier et al.,105 Cerruti and Biondi103 and Jonasson110 | ||
| Changing other’s expectations for child | Kenyon et al.,61 McGarry et al.,69 Pituch et al.,100 Sonday and Gretschel,101 Wiart et al.,102 Currier et al.105 and Feldner116 | ||
| Family togetherness | Evans and Baines62 | ||
| Parental independence | Evans et al.,59 Evans and Baines62 and Jonasson110 | ||
| Parental loss of control | Kenyon et al.,61 Evans and Baines62 and Cerruti and Biondi103 |
From the 17 descriptive themes, five analytical themes were developed, which moved beyond the descriptive themes to provide new theoretical insights not seen in individual primary studies. These were as follows:
-
children’s and parents’ emotional journeys towards acceptance of powered mobility
-
experiential learning and play to support a continuum of powered mobility skill development
-
the importance of parent and therapist time and support to realise the full potential of powered mobility
-
fit between the child, device and environment influences the child’s sense of self and identity
-
children’s independence, freedom and self-expression as key outcomes of powered mobility.
In the following sections, we focus on reporting the analytical-level themes relating to the feasibility, acceptability and anticipated outcomes of powered mobility. Quotations are taken directly from papers and are used as illustrative examples for the analytical themes. For each quotation, relevant study information is presented for context, including the respondent (i.e. child, parent, therapist), child condition/diagnosis, child age and relevant type of powered mobility device. For cases for which the specific information about the respondent was not recorded, we present the study sample details instead.
Children’s and parents’ emotional journeys towards acceptance of powered mobility
The experiences of children and families concerning the proposal and acceptance of powered mobility varied greatly, on a broad spectrum, from very positive to very negative. 60,61,69,100,102,103,116,134 One mother of a boy with cerebral palsy described seeing her son use powered mobility for the first time at age 5 years as the ‘best and worst day of her life’ owing to the contrast between the child’s joy and her own beliefs about powered mobility as a symbol of disability. 61 Some parents expressed reluctance in seeking and accepting powered mobility;69,103 conversely, physiotherapists could also be a source of hesitation. 102 The children in the studies had a wide range of diagnoses and mobility needs; some children had deteriorating life-limiting conditions, whereas others did not, which created different contexts towards acceptance of powered mobility. For some parents, the transition to powered mobility was traumatic, uncertain or difficult to accept,61,102,103,134 and prompted an often emotional re-evaluation of their expectations and hopes for their child:61,100,102,134
I was still thinking, ‘Okay, maybe one of these days, he’ll get up and he’ll walk, and we don’t need this.’ Then going into a power wheelchair, it was kind of a realization that ‘No, he isn’t going to be able to walk,’ (. . .) So it was a little tough.
Parent of a child with cerebral palsy or myelomeningocele, aged 10–18 years, powered wheelchair users, Wiart et al. 102 Specific characteristics of the individual being quoted are not reported in the paper
Some parents held on to the hope that their child would one day walk, and therefore saw powered mobility as a ‘last resort’;61,102 thus, the offer or provision of powered mobility symbolised a significant change in their life and a powerful symbol of loss or change. 61,100,102 This appeared to be particularly relevant for children with higher skills and abilities, for instance one parent of a child with Duchenne muscular dystrophy stated that their child’s transition to powered mobility at age 7 years was a negative symbol of the child’s reduced independence:61
He . . . caught on (quickly to driving a power wheelchair but) . . . for him, I think (driving a power wheelchair is) a degenerative ability . . . I think his obstacles (to using a power mobility device) are (going to) come.
Father of a 13-year-old male with Duchenne muscular dystrophy, powered mobility device user from age 7 years, Kenyon et al. 61
Interestingly, one parent described using a powered ride-on toy to avoid or postpone their child needing a wheelchair. 116 The process of adjustment to powered mobility can be a source of conflict between parents and therapists/clinicians, resulting from different levels of knowledge and expectations for the child. 102,109,133 The emotional journey for the child and family is an important part of the provision process and should be seen as a key factor for (either a facilitator of or barrier to) intervention effectiveness, particularly for children who need prolonged support and facilitation to get the most out of their powered mobility:
Viewpoints of parents and therapists often varied (. . .) One informant sarcastically told the interviewer: ‘I think that they’re (the footstraps are) useless . . . But then I am not a professional. All I am is her mother and all I have been doing is just watching her and helping her at night . . .
Berry et al. 133 (Parents of children with cerebral palsy, myelomeningocele or other diagnosis, aged 5–23 years, powered wheelchair users)
Children need emotional and practical support through this journey, as the transition to powered mobility can be stressful and full of uncertainty. This requires support from parents and other institutions (i.e. school, social services) to promote confidence and engagement with the learning and provision process, and to let children know that their opinion is valid:
Parent 4 noted that the process of learning powered mobility was very emotional for her child: ‘how are people going to treat me? . . . Will I be able to do it? . . . What if I get stuck?’ There are so many (emotions).
Parent of 7-year-old male with cerebral palsy, powered mobility device user from age 3 years, Berry et al. 133
The development of skills helps children to take agency over the process and motivates continued engagement and ownership. 61,74,105,109 Likewise, parental observation of the child’s development and achievement is emotionally rewarding and vindicates the decision to progress with powered mobility:69,105
I’ve always been very hesitant about a motorised wheelchair for lots of different reasons, but seeing her do this and that she is able to do it, I think has changed my view of the whole thing.
Mother of 6-year-old female with spastic diplegia involving both spasticity and dystonia, smart-wheelchair user69
This emotionally charged experience requires early support from services to help families make the transition. This can be facilitated by early provision of information about what powered mobility may offer, and early education, assessment and training for parents/children to promote better understanding of each child’s long-term potential through powered mobility. 58,102,133
Experiential learning and play to support a continuum of powered mobility skill development
The learning of powered mobility is not initially about learning to drive; there is an important distinction between the process of learning movement and driving a powered mobility device. Children must first understand the concept of movement, then the relationship between their movement and the movement of their device. 61,62,109 They can then begin to understand the relationship between their movement and the space/environment around them:
The developmental learning process now needs to be viewed as a continuum from understanding the concept of movement, understanding how the machine works, through to using the machine as part of attaining a desired lifestyle.
Durkin109 [Children with cerebral palsy or hypoxic brain damage (and their clinicians/therapists), aged 5–12 years, powered wheelchair users]
The learning process in and of itself can have benefits for children, such as encouraging response to stimuli and developing a sense of cause/effect. 58,62,69,74,101,105,117 The act of practising and training helps children to refine their skills and begin to integrate the device into their own sense of movement and space:
After a few sessions she started to look intensely at her hand when it was placed on the joystick. Both children seemed to react more to external stimuli and to show more interest in persons and objects in their vicinity.
Researcher observations of children with profound cognitive disabilities, aged 4–5 years, powered wheelchair users, Nilsson and Nyberg74
Experiential learning is key to developing mobility skills, and requires real-world use of aids and time to develop skills. 61,62,100,105,109,117 Bumping, crashing and receiving feedback on movement can help children to understand the relationship between their movement and the world around them. 109 During the introduction of powered mobility and training, the process should be framed as an opportunity for children to play, explore and engage in fun activities at their own pace. 61,69,101,109 Adult conceptualisations of movement should be avoided, and training should not be focused on teaching children how to ‘drive’. 109 As noted by Durkin,109 very young children benefit from powered mobility interventions that are framed as toys and opportunities to play, thus highlighting the importance of chronologically and developmentally age-appropriate interventions:
When the powered wheelchair appearance was changed by producing a front facade of a well-known children’s character the parents responded very positively which encouraged the children (. . .) As the 12- to 18-month-old children approached 18 months they became more reluctant to enter the powered wheelchair for play.
Durkin109 [Children with cerebral palsy or hypoxic brain damage (and their clinicians/therapists), aged 5–12 years, powered wheelchair users]
Although continuums of skill development are specific to each child, children tend to follow a trajectory of, first, understanding cause and effect and the concept of movement; second, developing purposeful movement; third, gaining basic control of powered mobility (i.e. directional movement and stopping); fourth, developing spatial awareness; and, finally, utilising powered mobility to facilitate lifestyle goals. 61,62,109 It is important that, as part of a powered mobility intervention, the development of mobility and driving skills is started at a very early stage of the process, for instance as a preparatory stage. The development of controlled, safe movement was described as the first stage towards promoting long-term independence and autonomy:
Spinning and experiencing the joy of movement were identified as common first steps. Understanding cause and effect, developing a sense of purposeful movement, driving in the real world, and responding to multiple attentional demands were identified as some of the quintessential points in learning.
Kenyon et al. 61 (Parents and therapists of children with arthrogryposis multiplex congenita, acquired brain injury, cerebral palsy or Duchenne muscular dystrophy; the mean age at powered mobility device use commencement was 3 years)
An important omission is the evaluation of young children’s readiness for powered mobility; a standard approach to assessing readiness for powered mobility in young children is not apparent from the existing qualitative evidence.
The importance of parent and therapist time and support to realise the full potential of powered mobility
The powered mobility needs and abilities of each child are highly variable, and it can take time for them to be revealed. 58,61,62,74,101,109,110,133 Early promotion of skill development and individually tailored interventions can help children to achieve their full potential. It is therefore important that children are given adequate time to learn and practise powered mobility:
We have to give of our time, believe in their ability and really see that this is happening for that person. If we don’t put this effort into the kids they will quit driving eventually. Abilities may therefore be lost (. . .).
Jonasson110 [Parents and therapists of ‘severely disabled’ children, age not specified, smart powered wheelchair users (AKKA-board)]
The relationship between a child’s abilities, impairments and potential to benefit from powered mobility may not be apparent until after powered mobility has already been introduced. 58,74,109 Therefore, powered mobility loan or trial schemes could help to identify children who may benefit from powered mobility, but who would have otherwise been overlooked:
John was, in the beginning, assessed as having a better potential for driving than Anna. The results, however, clearly showed us how wrong this assessment had been. It was Anna who had the greater potential, but that potential was masked by her restricted ability to move her arms and hands.
Researcher observations of children with profound cognitive disabilities, aged 4–5 years, powered wheelchair users, Nilsson and Nyberg74
Because of the high degree of variance between children in terms of their chronological and developmental age, abilities, needs and potential to benefit, ‘there’s no recipe’61 to guide provision; therefore, individualised approaches to assessment, provision and training are required. 61,100,133 This, in turn, requires a commitment of time and co-operation from clinicians/therapists, parents and other key stakeholders to ensure that the intervention meets the unique needs of each child:
I think (that) some people strive to have (a recipe to teach children how to use a power mobility device), but (a recipe) doesn’t work . . . (the recipe is) . . . whatever works (for each) individual . . . Parents and therapists recognized the importance of involving all stakeholders (. . .).
Occupational therapist of children with arthrogryposis multiplex congenita, acquired brain injury, cerebral palsy or Duchenne muscular dystrophy (mean age at powered mobility device use commencement was 3 years), Kenyon et al. 61
Strict eligibility criteria may be counterproductive, and clinicians/therapists should instead be given adequate time to conceptualise the intervention as a means to promote a better lifestyle for the child and their family, rather than solely as a means to mobilise the child:99,109
Clinicians should be given time to assess the children and problem-solve in a more holistic way, which is led from the perspective of giving the child and family a ‘lifestyle’ rather than just a piece of mobility equipment.
Durkin109 [Children with cerebral palsy or hypoxic brain damage (and their clinicians/therapists), aged 5–12 years, powered wheelchair users]
Both clinicians and parents can act as facilitators of a child’s development of mobility and independence, rather than as directors or supervisors. Durkin109 defined this role as being a ‘responsive partner’; children should be allowed to direct their exploration and skill development, with careful and subtle encouragement/support from responsive partners, to allow children to develop at their own pace and under their own volition:
The children gave clear messages about how they liked to learn the skills for powered mobility; the importance of exploring and being able to do things on their own; not being watched; learning in a ‘cool’ way; taking the lead in how they played and learnt.
Durkin109 [Children with cerebral palsy or hypoxic brain damage(and their clinicians/therapists), aged 5–12 years, powered wheelchair users]
The support and advocacy of institutions around the child is key to ensuring that the intervention can be optimised. For instance, schools can play an important role in supporting children to use and learn powered mobility. 61,62,99,100,109 Without this support, sceptical or risk-averse institutions can detrimentally affect the powered mobility intervention, and thus affect a child’s potential. To maximise the effectiveness of interventions, physical and attitudinal adaptation may be required, and influential institutions need to be educated about safety and potential benefits. This could form part of the intervention, through a holistic approach to assessment, provision and training. Evans and Baines62 found that interventions for very young children failed when schools and parents did not fully engage from the outset:
He was happy to try it but lack of fine motor skills and dystonia meant his usage remained limited to large flat grassed areas . . .
Parent of a child with cerebral palsy, spinal muscular atrophy, global developmental delay, arthrogryposis, spina bifida, aged 15–72 months, starter powered mobility device users, Evans and Baines. 62 Specific characteristics of the individual being quoted are not reported in the paper
Unfortunately critical school staff did not support the use of Wizzybug and did not follow through with regular use of it to help her master these skills.
Parent of a child with cerebral palsy, spinal muscular atrophy, global developmental delay, arthrogryposis, spina bifida, aged 15–72 months, starter powered mobility device users, Evans and Baines,62 Specific characteristics of the individual being quoted are not reported in the paper
Fit between the child, device and environment influences the child’s sense of self and identity
Powered mobility devices were conceptualised by some parents133 and children59,99,100 as being a child’s ‘legs’. This integration of self and device illustrates a process of adaptation that allows a child’s ‘new self’ to emerge as a result of powered mobility and independent movement. 99 This is an important concept for therapists and clinicians to take account of, as powered mobility can become integral to the child as they become increasingly independent and able to engage with the world around them on their own terms:
Children perceived that the ‘self’ that existed before they had an EPIOC did not adequately fit the environment, and hence they were prevented from fulfilling their needs and desires. In contrast using an EPIOC was seen as allowing a new self to emerge, one that integrated their body and EPIOC.
Gudgeon and Kirk99 [Children with cerebral palsy, muscular dystrophy, spinal muscular atrophy or brain tumour (or their parents), aged 7–16 years, powered wheelchair users]
One of the key barriers to powered mobility use is access. This is particularly relevant in public spaces, which are often poorly designed for powered mobility use. 59–61,99,100,102,116,133 Access can also be an issue in home settings, owing to issues of space and adaptation. 58,61,62,99,100,102,133 Restricted access impedes children’s opportunities to participate in activities59–61,99,100,102,116,133 and to integrate powered mobility into daily life. 99,100 Powered mobility interventions can attempt to actively address these barriers by taking into account the home and public environment in which the child exists:
(. . .) children’s increased sense of liberty was dependent upon and directly limited by environmental obstacles: ‘life when you have an electric wheelchair is still a lot more complicated, due to society, not necessarily because of the wheelchair’ (. . .) Mothers identified various obstacles in the community, notably architectural barriers.
Pituch et al. 100 (Parents of children with skeletal dysplasia, osteogenesis imperfecta, spinal muscular atrophy, arthrogryposis or cerebral palsy, aged 12–18 years, powered wheelchair users)
The logistical issues of transporting powered mobility devices adds another layer of complexity, as a result of the size and weight of such devices. 59,61,99,100,102,103,133 In some circumstances, families may be deterred from using powered mobility outside common settings (such as home and school) because of practical or financial barriers to transportation:61
Most young people did transport their EPIOCs. However, nearly all said that the chair was heavy and cumbersome to take in the family vehicle, thus limiting the chair’s use away from home.
Evans et al. 59 [Children with muscular dystrophy, cerebral palsy or other diagnoses (or their parents), aged 10–18 years, EPIOC users]
Poor fit between the child, device and environment is a major barrier to participation, which, in turn, causes frustration, isolation and affects mood and self-efficacy. 59,99,100,133 Furthermore, poor fit can lead to reduced safety and to risks of harm to the child and people around the child. 59,61,62,100 This requires children and parents to be continually alert and vigilant, particularly in public spaces. The negative experience of accidents/injury can have a detrimental impact on the confidence of children, leading to fear, anxiety or a reluctance to use powered mobility:59,99
Even minor mishaps may affect children’s confidence in the chairs. Many young people said they did not always feel safe in the chair.
Evans et al. 59 [Children with muscular dystrophy, cerebral palsy or other diagnoses (or their parents), aged 10–18 years, EPIOC users]
In contrast, minor bumps and crashes can also be a positive learning experience, and can help children to refine physical driving skills. 109 A balance is needed between encouraging regular use of powered mobility and managing potential safety concerns. For some children, their sense of safety may be too limited to allow unsupervised use of powered mobility,59,109 but this does not mean that they cannot benefit from supervised powered mobility use. Furthermore a child’s initial inability to adequately control a powered mobility device does not indicate an inability to benefit from powered mobility or to develop control at a later date:74
Sometimes an individual’s ability and potential are difficult to assess because of his or her profound disabilities. In such cases ‘driving to learn’ may help to make the underlying potential more apparent. The training may reveal previously unrecognized abilities and determine an individual’s full potential.
Researcher observations of children with profound cognitive disabilities, aged 4–5 years, powered wheelchair users, Nilsson and Nyberg74
The interface between the child, device and environment is complex and multifaceted,61 and is also observed in dynamics between the child and wider society, for instance in the perceived stigma of powered mobility100 and other mobility aids. 58 The appearance of powered mobility devices is also important to children,59,99 highlighting the relationship between device and identity. Ongoing review and follow-up can ensure that devices are fit for purpose as a child grows, and as their needs change. 59,131,133 This requires close monitoring of children and devices, timely maintenance and a sensitivity for the child’s sense of self and emerging personality.
Children’s independence, freedom and self-expression as key outcomes of powered mobility
Independence was identified as an important powered mobility outcome in most studies,58–62,69,99–103,105,110,116,134 and was related, to some extent, with many other outcomes. For instance, independence was related to social participation58–62,69,99–103,105,116,134 and increased opportunities for play58–60,62,69,101,102,105,116 and exploration. 58,60,62,101,102,116 The experience of independent movement for children who would not be otherwise mobile or independent can have a profound impact on a child and their family. Powered mobility is perceived to broaden a child’s horizons as they begin to find new ways to interact with the world in age-appropriate ways:60,100–102,105,116
While Linda’s reluctance to consider a wheelchair for Jamie reflects similar perceptions describing early responses to wheelchair use in the literature, both mothers also share the view that wheelchair and ride-on car function in ‘opening up his world’ so Sam and Jamie can play with siblings and peers more independently.
Feldner et al. 60 (Parents of children with cerebral palsy, aged 4–5 years, powered wheelchair and ride-on toy users)
Freedom was also an important outcome across the age range. 59,60,100–102,105,116 The concept of freedom related to a child’s ability to control their chair, and the suitability of the environment to allow free movement and exploration, linking to the need to integrate child, device and environment. In younger age groups, caregiver vigilance is still required and may even increase when a child starts using powered mobility. However, child freedom can also spill over into positive impacts to the family and carers through the sharing of joy, reduced caring burden and more free time:62,133
Another parent reported: ‘. . . it allows her the freedom to go where she wants . . .’. Many parents used the word ‘freedom’ in describing what they liked the best about the chair. Freedom for the child helped to ‘free up’ time for the caregiver.
Berry et al. 133 (Parents of children with cerebral palsy, myelomeningocele or other diagnosis, aged 5–23 years, powered wheelchair users)
The wider family may begin to feel a sense of leading a ‘normal family life’62 as they begin to engage in more activities that involve the whole family in fun and play, thus facilitating a sense of family togetherness. 62 Conversely, some parents felt a sense of losing control as a result of their child’s newfound independence:61,62,103
I think it also means losing control as a parent . . . because now things can be run over in your house . . . it was a change to know that it was now happening in our lives . . .
Mother of an 8-year-old male with cerebral palsy, powered mobility device user from age 5 years, Kenyon et al. 61
Self-expression through movement and behaviour can be an indicator of growing agency and self-efficacy. 60,61,109,110,116 The development of independent movement can create a positive feedback loop of growing confidence and motivation, which encourages the child to continue to develop and push the boundaries of their world. 60 This relates to the growing sense of self and integration of powered mobility and body. Children use their powered mobility devices to express themselves and to communicate through movement,58,61,105,109,110 for instance moving away from tasks they do not want to do. They may also engage in risky behaviours and become disobedient as a means of pushing the boundaries of their world and expressing their newfound autonomy. 60,61,103,109,116 Although disobedience can be negative, it may also be indicative of a child participating in typical age-appropriate behaviour, and learning to makes choices and exert control. Therefore, a balance must be struck between encouraging age-appropriate behaviour and maintaining safety:
He tells me ‘No, mommy, I want to go here’ . . . to even be able to talk back to me – it makes me want to cry, in a good way.
Mother of 5-year-old male with cerebral palsy, powered wheelchair user, Feldner et al. 60
It appeared that it was the act of directing their own mobility agenda that brought forward the changes in agency (. . .)
Researcher, Feldner et al. 60
Synthesis of findings specifically relating to powered mobility for very young children
Seven studies referred specifically to children aged < 5 years and presented findings in such a way as to allow subgroup analysis of qualitative evidence;58,60–62,74,105,116 four studies were related to ride-on toys;58,60,61,116 three were related to powered wheelchairs;61,74,105 and one was related to starter powered mobility devices. 62
Very young children varied in their ability to control such devices; some children use these interventions as a means to promote independence and autonomy,60–62,105 some use them to understand cause/effect and response to stimuli58,62,74,105 and others use them to prepare for future powered mobility use,58,62,105 although these were not always mutually exclusive. Early provision of powered mobility was described as an important factor in promoting better outcomes:
They need to be able to keep up to their age, and at one we’re walking, we’re exploring different things, so it’s really no different. It’s just a different way of doing it (. . .) It made us say ‘absolutely he needs power mobility, right now! We can’t waste time (. . .)’.
Mother of 13-month-old male with arthrogryposis multiplex and hypotonia, ride-on toy user, Pritchard-Wiart et al. 58
The underlying conditions of the children and their related abilities appear to govern the purpose and potential of these interventions. This is an important distinction, as children can benefit from using powered mobility devices even if the ultimate goal is not for them to be used completely autonomously, or as a means to be fully independent in their movement. 74 Parents may seek early powered mobility as a means to achieving benefits for the child in the future, which also links to parents’ expectations and hopes:
When he gets older, he’s going to have a better life because of the chair – because he has that independence. When he goes to school, he won’t just be sitting in that chair; he’ll be on the same level that children who can walk are on.
Parent or grandparent of a child with cerebral palsy, myotubular myopathy or tetraphocomelia, aged 2–3 years, powered wheelchair user, Currier et al. 105 Specific characteristics of the individual being quoted are not reported in the paper
The perception of powered mobility devices designed specifically for very young children is also of importance. For instance, the universality of ride-on toys and their close resemblance to age-appropriate toys means that children are not seen as ‘different’ when using them. 58 This also speaks to the stigmatising experience that mobility aid users report. Ride-on toys may therefore be more acceptable to parents and children, with some families even pushing back the need for a wheelchair as a result of ride-on toy use. 58 Ride-on toys and starter powered mobility devices may provide a gentler introduction to powered mobility that is more in tune with parental expectations:
It was kind of neat to give him the opportunity to have a toy that other typical kids in the neighbourhood have . . . and I liked that it didn’t look obvious, as far as a tool for [children with] special needs, it was more subtle.
Mother of 50-month-old male with cerebral palsy, ride-on toy user, Pritchard-Wiart et al. 58
Across all seven studies, it appeared that most very young children gain enjoyment and benefit from their powered mobility devices. It is of note that some starter powered mobility devices were returned unused;62 reasons included the limited motor skills of the child, concerns about safety, poor access to the home, progression to walking rather than powered mobility and lack of parental time to facilitate use of the powered mobility. Likewise, some ride-on car users lost interest in the device over time or progressed to crawling instead. 58 Some negative outcomes of early powered mobility were noted from the parents’ perspective, including parental feelings of loss of control of their child61,62 and concerns about safety when the child used the powered mobility. 60–62 Conversely, parents also expressed that they were able to share in their child’s joy60–62,105,116 and that their expectations for their child improved. 61,105
Summary of findings and GRADE-CERQual assessment
In the final stage of the thematic synthesis, we compared and contrasted the analytical themes to better understand the relationships between the themes and to develop a cohesive summary of the thematic synthesis findings. Subsequently, we developed key findings arising from the qualitative data relating to (1) the acceptance of powered mobility, (2) developing powered mobility skills and competency, (3) using powered mobility safely, (4) anticipated and experienced outcomes from powered mobility and (5) the overall benefit of powered mobility. Further description is provided in Table 37. For each of these key findings, we applied the GRADE-CERQual approach to assess overall confidence in the evidence supporting the findings (see Table 37). Full details of the GRADE-CERQual assessment are provided in Appendix 10, Table 47.
| Findings | GRADE-CERQual assessment of confidence in the evidence | Explanation of GRADE-CERQual assessment |
|---|---|---|
| 1. Acceptance of powered mobility | ||
| 1.1. Parents experienced both positive and negative emotions about their child transitioning to powered mobility. Although there was no clear difference in parental acceptance of powered mobility across the age range, parents of children with deteriorating conditions had more difficulty accepting powered mobility. In this specific context, powered mobility can be perceived as a negative symbol of a child’s deteriorating condition and increasing disability, and thus affect initial parental acceptance | High confidence | Eight studies with moderate methodological limitations.60,61,69,100,102,103,116,134 Minor concerns about coherence. No or very minor concerns about adequacy and relevance |
| 1.2. Children did not commonly report issues with the acceptance of powered mobility, regardless of age, although very young children were seen to prefer toy-based interventions over powered wheelchairs. The process of learning to optimally use powered mobility can be stressful for older children | Low confidence | Two studies with minor methodological limitations.61,109 Minor concerns about coherence and relevance. Serious concerns about adequacy |
| 2. Developing powered mobility skills and competency | ||
| 2.1. Early introduction of powered mobility to very young children helped facilitate their development of powered mobility skills through playing and learning to use the powered mobility device. The same principle applied to older children, whereby early introduction of powered mobility provided a longer time frame to develop optimal skills and competency in using their powered mobility device. Early introduction of powered mobility promoted future powered mobility use and the attainment of children’s lifestyle goals | Moderate confidence | Five studies with minor methodological limitations.9,61,62,105,109 Minor concerns about coherence. Moderate concerns about adequacy due to limited data. No or very minor concerns about relevance |
| 2.2. Regardless of age, children needed time and support to master powered mobility and benefited when they had the right device, an environment that was compatible for using the device freely and the motivation of those around them to facilitate use. Frequently, elements of the interface between child, device and environment are missing or inadequate | High confidence | Twelve studies with moderate methodological limitations.58,61,62,74,99-101,105,109,110,116,133 No or very minor concerns about coherence and adequacy. Minor concerns about relevance |
| 2.3. Children benefit from learning to use powered mobility through play and experiential learning. A child’s potential to benefit from powered mobility may not become apparent until after powered mobility use. Powered mobility for very young children is conceptualised differently, as the primary purpose is to facilitate play and learning powered mobility skills through play | High confidence | Seven studies with minor methodological limitations.58,61,62,100,105,109,117 Minor concerns about coherence and adequacy. No or very minor concerns about relevance |
| 3. Using powered mobility safely | ||
| 3.1. Children’s understanding and experience of safety in relation to powered mobility was different from that of their parents and therapists. Therapists and some parents were generally more risk averse than, especially older, children desired. Some children across the age range were frightened by bumps and accidents when using their powered mobility, whereas others learned from the experience. The conceptualisation of safety was mediated by a child’s past experiences of accidents/injury and their age, level of development and cognitive abilities | Moderate confidence | Four studies with minor methodological limitations.59,61,99,109 Moderate concerns about coherence and adequacy. Minor concerns about relevance |
| 3.2. Safety concerns from parents and professionals were heightened when the child lacked an understanding of powered mobility safety owing to cognitive ability or young age. Some children had little concern for or an awareness of their safety when using their powered mobility. When a child lacked powered mobility safety awareness, parental concerns about safety were used as a reason for stopping their child from using and benefiting from their powered mobility device (especially in very young children). This decision to stop their child using their powered mobility was also connected to the requirement of parents (or other responsible adults) to be available to supervise children when using their powered mobility | Low confidence | Three studies with minor methodological limitations.59,61,62 Moderate concerns about coherence. Serious concerns about adequacy due to limited, thin data. No or very minor concerns about relevance |
| 3.3. Children can engage in risky or disobedient behaviours while using powered mobility. This behaviour was typically age appropriate and indicative of a child asserting control over their actions and behaviours, but may also put the child and other people at risk. The right balance must be achieved between facilitating a child’s independent movement and maintaining safety, but this did not always appear to happen | Moderate confidence | Seven studies with minor methodological limitations.60–62,99,103,109,116 Minor concerns about coherence. Moderate concerns about adequacy. No or very minor concerns about relevance |
| 4. Anticipated and experienced outcomes from powered mobility | ||
| 4.1. A core set of anticipated and experienced outcomes overlapped across the age range, with independent mobility and a greater degree of independence as the predominant outcomes. Independent mobility and a greater degree of independence were linked to other key anticipated and experienced outcomes such as social participation, freedom and self-efficacy. A child’s potential for independent mobility and increased independence using powered mobility were determined by their chronological and developmental age, and mediated by parental beliefs and attitudes towards powered mobility use and acceptance. There were subtle age-related differences in anticipated and experienced outcomes, particularly relating to parents’ and children’s desire for fun and enjoyment as outcomes in their own right for very young children | High confidence | Fifteen studies with moderate methodological limitations.58–62,69,99–103,105,110,116,134 No or very minor concerns about coherence, adequacy and relevance |
| 4.2. Although independent mobility and a greater degree of independence were key outcomes of powered mobility, not all children will achieve sufficient powered mobility control to become independent. For very young children and children with cognitive impairments, powered mobility can also be used to achieve developmental outcomes. Ability to achieve independent movement should not therefore be used as an explicit eligibility criteria for powered mobility provision | High confidence | Eight studies with moderate methodological limitations.58,62,69,74,101,109,110,117 No or very minor concerns about coherence, adequacy and relevance |
| 4.3. Parents experienced both positive and negative outcomes associated with their child’s increased mobility and associated independence. Parents share in their child’s joy of being able to move independently, but may also experience a sense of losing control over the child | High confidence | Ten studies with moderate methodological limitations.59–62,69,102,103,105,110,116 No or very minor concerns about coherence, adequacy and relevance |
| 5. Overall benefit of powered mobility | ||
| 5.1. Although intended and experienced outcomes of powered mobility are conceptualised differently (with some overlap) before and after the age of 5 years, there was little discernible difference in the potential for children across the age range to benefit from powered mobility. Irrespective of age, earlier introduction of powered mobility has the potential to provide children with a longer time frame to potentially become skilled and competent in optimal powered mobility use, and therefore maximise their potential to benefit from it | High confidence | Sixteen studies with moderate methodological limitations.58–62,69,99–103,105,109,110,116,134 No or very minor concerns about coherence, adequacy and relevance |
Chapter 5 Review 2: review of the long-term consequences of independent mobility
The original aim of review 2 was to identify and synthesise quantitative, qualitative and mixed-method evidence to determine the long-term implications of self-directed or independent mobility for very young children (< 5 years), compared with older children (≥ 5 years).
To meet this aim, we developed and applied a search strategy to identify any studies that have investigated consequences of independent movement. Two broad facets were used to explore searching: (1) ‘independent mobility’ and (2) ‘children or young people’. We defined independent movement to include crawling, cruising, etc., and to include any related outcomes.
The search resulted in > 47,000 potential papers. We had initially planned to screen these for inclusion/exclusion using an artificial intelligence algorithm; however, hand-screening of a proportion of the titles and abstracts identified no relevant papers to begin to develop an algorithm. We subsequently did a targeted search for economic studies looking at children with autism, Down syndrome, attention deficit hyperactivity disorder or cerebral palsy to inform the economic modelling. Although conditions such as autism and attention deficit hyperactivity disorder are not normally associated with mobility impairments and wheelchair use, some very young children with these conditions are provided with adapted buggies from an early age for a variety of reasons, including safety and posture. Therefore, these conditions were included in the search in case any broadly relevant economic data could be identified. This did not result in relevant papers. From this, we approached a targeted sample of our advisory group to search for any example papers that could be used as key texts to inform a further search and/or a development of an algorithm, but again we were not able to identify any.
Therefore, at this point, it has not been possible to systematically identify research studies related to the long-term benefits of independent mobility, and we are not able to confirm that such studies even exist outside the powered mobility field. This was reported to the funder during the study, and it was agreed that continuing with the review 2 was not feasible or of sufficient benefit.
From the review 1 search and screening, we have papers that scope the implementation and consequences of powered mobility over time; and we have used these, as well as the overall logic model of linked outcomes from review 1, as a starting point for understanding the potential long-term consequences of independent mobility resulting from powered mobility.
Chapter 6 Economic analysis: development of tariff of costs for paediatric powered mobility and a budget impact analysis for increased powered mobility provision for very young children
This chapter reports on a budget impact analysis to estimate the costs associated with different scenarios of paediatric powered mobility provision in the UK. As part of this analysis, a tariff of costs associated with paediatric powered mobility provision was developed.
The original objectives of the economic analysis were the development of:
-
cost tariffs of NHS and non-NHS costs for powered mobility interventions (i.e. equipment, training and support, and any other components) for children with mobility limitations using a multiperspective disaggregated cost–consequence framework
-
an economic model to facilitate a comparison of the relative cost-effectiveness of powered mobility equipment for very young children (< 5 years), compared with standard NHS practice (≥ 5 years).
After the completion of data extraction in review 1, it became apparent that there was very limited conclusive quantitative effectiveness evidence and no cost-effectiveness evidence. Hence, there were insufficient published data to allow a robust synthesis of cost-effectiveness evidence and the subsequent development of an economic model. In addition, no further relevant health economic or cost-effectiveness evidence was identified from further targeted searching.
As an alternative to the economic modelling of cost-effectiveness, we focused on costs and modelled different scenarios of providing increased access to powered mobility for children aged < 5 years with mobility limitations. We developed three hypothetical scenarios of service provision mapped on to the intervention elements outlined in the refined logic model. We aimed to illustrate the costs of early powered mobility, and the potential budget impact of increased powered mobility provision for very young children.
For the budget impact analysis, we established the costs of current provision of powered mobility to very young children (i.e. the base case), and the impact of making such provision available to all children who could potentially benefit. Provision to all by the NHS would inevitably lead to increased costs, due to a number of factors, as highlighted in the assumptions below; however, this increased cost should be considered in the light of the potential benefits to the children, as detailed in the syntheses, and additional cost implications for other services in the NHS. The conduct and reporting of the budget impact analysis follows the International Society for Pharmacoeconomics and Outcomes Research’s good-practice guidance. 135
Design and methods
The collection of primary economic data was not within the scope of this evidence synthesis project. To generate cost data, we liaised with a number of different organisations and individuals both within and beyond our project advisory group, including NHS Posture and Mobility Services; the National Wheelchair Managers Forum; charitable organisations such as Whizz-Kidz, Designability and the Medical Engineering Resource Unit (MERU) of Queen Elizabeth’s Foundation for Disabled People; and various wheelchair manufacturers.
Data were also obtained from publicly available sources and publications. UK government data sets and related websites [e.g. Office for National Statistics (ONS), Department for Work and Pensions, Motability] were consulted to inform population calculations, allowances and grants available to people with disabilities and their carers. 136–138 NHS data sets were used to inform numbers of users and input to costings. 18,139–142 Published reference sources, published research and a freedom-of-information request were used to further inform aspects of the powered mobility costs, including staffing and equipment, and for costings of local authority spend on housing adaptations.
The studies included in the systematic review were screened for any cost or resource use information that could inform the analysis. Further targeted searching was carried out in an attempt to locate economic and cost-effectiveness data using the terms ‘children’ and ‘condition’ and an economic evaluation filter, whereby ‘condition’ referred to a list of conditions known to restrict children’s mobility, and the economic evaluation filter was the narrow filter from the Canadian Agency for Drugs and Technologies in Health. 143 No further relevant economic or cost-effectiveness evidence was found from this targeted search, for either very young or older children.
In addition, detailed information on costs and resources used in the provision of powered mobility and training of children accessing assisted mobility options was obtained from personal communications with a number of NHS providers and third-sector organisations, including members of the project advisory group. [Advisory group personal communication: Amanda Allard, Council for Disabled Children; Rae Baines, Designability; Sara Crombie, Sussex Community NHS Foundation Trust; James C (Cole) Galloway, University of Delaware; Simon Halsey, TinyTrax; Susan Hillman, Newcastle upon Tyne Hospitals NHS Foundation Trust; and Krys Jarvis, Shropshire Community Health NHS Trust. Other personal communication: Ruth Everard, DragonMobility Ltd (Cambridge, UK); Roy Wild and colleagues, Go Kids Go!; Invacare Ltd (Bridgend, UK); Paula Jackson, Samantha Sterling and colleagues, Leeds Wheelchair Centre; Press and Public Relations Department, Motability UK; and Nicky Ellis, North East Essex Wheelchair Service. All personal communication took place in 2019.] Personal experiences of the pathway to obtaining their child’s assisted mobility interventions were obtained from telephone discussions with the parent members of the project advisory group. These discussions focused on what the parents had to do to get powered mobility (e.g. appointments, travel, communication, out-of-pocket expenses), so that the costs could be estimated.
Data were obtained for 2018/19 whenever possible. We originally planned to inflate any earlier cost data not covered by recent publications using the Bank of England inflation calculator;144 however, this proved unnecessary as we did not need to inflate any cost data. All of the relevant cost data were synthesised into a tariff of NHS and non-NHS costs relating to paediatric powered mobility provision, which was subsequently used to inform the budget impact analysis (see Report Supplementary Material 2 for the budget impact analysis model).
Because the literature did not provide any data on the long-term impacts of powered mobility, a long time horizon could not be used. The calculations presented therefore relate only to the cost for very young children. From communication with various wheelchair services, we assume that wheelchairs are often refurbished and used by multiple patients over the life of the device; thus, it was important to adjust costs accordingly. We therefore assumed that a powered wheelchair or starter powered mobility device for a child would be useable for 5 years, and used by two consecutive children during that time.
It is anticipated that the budget impact analysis will be most relevant to the UK NHS setting, and, owing to the availability of data sets, specifically the NHS in England. The initial approach was to take a broader societal perspective; thus, cost implications for social care providers and for the families of children requiring powered mobility are presented when available, or the expected impact of increased provision is discussed in general terms.
Patient population
For the budget impact analysis, the target population was assumed to be all children aged < 5 years with a mobility problem sufficient for referral to NHS Wheelchair or Posture and Mobility Services. In current practice, some children who could benefit from powered mobility do not receive it, as they do not meet the criteria for provision. The aim of the budget impact analysis was to examine hypothetical scenarios in which more children are referred and more children receive powered mobility.
Medical diagnoses alone cannot be used to adequately estimate a child’s capacity for movement; therefore, underlying diagnoses, conditions and diseases were not used to define the patient population. Rather, the anticipated aim was to explore paediatric powered mobility provision from a service level. Furthermore, from the systematic review, insufficient evidence was identified to support separate economic analyses for individual diagnoses. We therefore focused more generally on the provision of powered mobility to very young children. Likewise, there was very little long-term evidence to allow evaluation over time.
There is no national data set on provision of mobility equipment by age; therefore, we could not easily determine the exact number of children (across all ages) who currently receive powered mobility. Estimations of the total current population provided with powered mobility, and of the total population of very young children who could potentially benefit from powered mobility, were therefore based on available data from the NHS and ONS.
The quarterly National Wheelchair Data Collection requests top-line data from each Clinical Commissioning Group (CCG) in England, including the number of adults and children registered with and referred to wheelchair services. In the financial year 2018/19, at least 60,000 children aged up to 18 years were registered with wheelchair services. 18,139–141 This is potentially an underestimate, as the data for a number of CCGs are not presented. According to ONS population data for England, approximately 24% of children aged 1–17 years were aged 1–4 years;138 applying this to the NHS data suggests that some 14,400 children aged < 5 years are currently registered with wheelchair services.
The national data collection reports 9200 new referrals of children aged 0–17 years to wheelchair services and up to 23,900 re-referrals annually. It is likely that children aged < 5 years will account for a disproportionately large number of new referrals, given that many mobility issues associated with conditions present from birth will be first noticed in this time. Anecdotal evidence from discussion with expert advisors suggests that the figure is about 80% of child referrals, suggesting that around 7300 children aged < 5 years are referred per year. Data were reported from only 182 of the 195 CCGs (93%), so it is possible that up to 7900 children are being referred nationally, which we have used as a maximum value in our calculations.
According to the NHS reference costs, of the 17,299 wheelchairs issued to children aged 0–18 years in 2017/18, 3591 were powered wheelchairs, accounting for 20.8% of wheelchairs issued. 142 Applying the proportion of children aged < 5 years to those aged < 18 years from national statistics, as noted above (24%), would suggest that almost 900 powered wheelchairs were supplied to this age group; this is likely to be an overestimate given the restrictions noted. Personal communication with a small number of individual NHS services and with manufacturers suggests that, on average, annual provision of powered mobility for very young children is likely to be in single figures per service (Susan Hillman; Krys Jarvis; Paula Jackson, Samantha Sterlin and colleagues; Nicky Ellis; Simon Halsey; and Ruth Everard, personal communication). Assuming that each of the 195 CCGs supplies around two very young children with a powered mobility intervention each year, this would put the figure at somewhere closer to 400.
In addition, data from the suppliers of Wizzybug145 and Bugzi146 indicate that around 200 starter powered mobility devices were loaned to children aged ≤ 4 years in 2018. We also know that a small number of families purchase powered mobility equipment privately for their very young children. There is no way to accurately calculate how many families are doing so, but we estimate that 25 families obtain powered mobility through private purchase each year. Thus, the base-case assumption is that only 625 children aged < 5 years are receiving some form of powered mobility through the NHS or elsewhere.
The calculations here are, necessarily, based on assumptions, but they do suggest that the number of children who could potentially benefit from some form of powered mobility provision before the age of 5 years is, conservatively, at least double that of the current provision; however, realistically, this could be as high as three or four times the current provision level.
Powered mobility provision: current practice
Although powered mobility provision is not always explicitly restricted by age, very young children often fail to meet the necessary criteria and are thus ineligible by default. Individual protocols for provision of powered mobility vary from service to service, but assessment of suitability is usually influenced by considerations of ability, safety in use, supervisory elements and a child’s environment. An NHS Wheelchair Service powered mobility provision process flow chart can be seen in Appendix 11, Figure 9.
There are some differences between provision for very young children and older children. Very young children who currently use powered mobility devices are likely to be from a limited or self-selecting group (i.e. their parents sought out powered mobility or they happened to live in an area where powered mobility was an option offered to them through the NHS), as there is not yet universal provision of powered mobility for children aged < 5 years. Conversely, older children are able to access powered mobility as part of routine NHS practice. Given the limitations in accessing such provision for the very young, it is possible that those very young children who are currently in receipt of a powered mobility are not representative of the wider population of very young children who could potentially benefit from such interventions.
In most cases, budgetary constraints mean that only one mobility aid is provided to each child by the NHS. As very young children are usually perceived to require a specialised buggy or manual/assistant-propelled wheelchair more urgently, services are commonly financially unable to support powered mobility for very young children. A number of third-sector organisations provide financial assistance to families seeking powered mobility, and families may be directed, or identify themselves, to such organisations, thus shifting cost and resource to the third sector. Alternatively, the NHS voucher scheme allows families to obtain a voucher to the value of the equipment prescribed by the NHS, in order to top up with other funds for another item. This is being superseded by the introduction of Personal Wheelchair Budgets, as part of the personalised health budgets, aiming to give people with long-term health conditions and disabilities more choice and control over the money spent on meeting their health and well-being needs. 147 A small number of NHS services work in partnership with the third sector to offer enhanced access to powered mobility.
Intervention mix
Aside from the actual device, powered mobility interventions also include referral, assessment, fitting, training, repair and review. The following aspects were considered in the development of the tariff of costs and the budget impact analysis: the cost of the mobility equipment itself; the accessories/modifications required; resources used in repair and maintenance; the cost of any training delivered; adaptations to the home, transport and school environment; and any service staff time or other human resource required.
At present, a significant amount of provision of equipment and training is carried out by the third sector. These costs are also discussed, with a view to costing the impact on NHS or other central resources should they take on a more comprehensive approach to the provision of powered mobility for very young children.
Items for which costs were not anticipated to be affected by the type of equipment provided are also discussed.
Uncertainty analyses
The findings from the evidence review and the lack of detailed data available on the provision of wheelchairs means that there is a high level of structural uncertainty in the costing analysis presented here on current and projected provision of powered mobility to very young children. We attempted to account for this by including broad minimum/maximum cost ranges. Further investigation into the resources used in the provision of mobility equipment to this age group and the long-term implications are needed to make a more robust model. The interactive model underlying the budget impact analysis is presented in Report Supplementary Material 2.
Tariff of costs for children’s powered mobility
All relevant costs are summarised in the tariff of costs, presented in Appendix 12, Tables 48–50. The data, estimates and assumptions underpinning the cost estimates are presented in the following sections for each cost category, and the cost ranges used in the analysis are stated.
Powered mobility equipment
The systematic review and discussions with the project advisory group identified a number of ways in which powered mobility devices can be defined (see Table 5 for further information). For the purpose of this economic analysis, we focused on interventions that are currently supplied by the NHS (i.e. starter powered mobility devices and powered wheelchairs).
In addition, we included adapted ride-on toys in our analyses. Such devices are in use outside the UK, notably in the USA and Canada, and were the subject of a relatively large number of the studies identified in review 1. Although they represent a promising, low-cost approach to powered mobility provision, they are currently considered to be outside the remit of NHS practice as they do not meet the classification for medical devices. The adaptation of ride-on toys fitted with harnesses, supportive seating and/or controls through schemes such as GoBabyGo56,57 can allow very young children with mobility limitations to have relatively inexpensive experiences of independent mobility. These devices could be a future route for NHS powered mobility provision, and thus have been included in a sensitivity analysis.
Other options described in the literature have not been considered to be relevant to the NHS in the immediate future, and so are not covered in the scenario analyses presented here. This includes models and robots designed for specific research, the manufacture of which would need to be scaled up and undergo medical device assessment before use could be routinely endorsed by the NHS.
Powered wheelchairs
The price of powered wheelchairs varies widely according the features required to address individual clinical need. In addition, NHS and other providers serving the NHS will be offered discounted prices that are lower than the publicly available list price. Although, in general, powered wheelchairs are more expensive than manual wheelchairs or buggies, the actual prices paid and the relative differential between powered and manual equipment varies widely in the limited national data available; therefore, it is possible to suggest only an approximate average cost.
The NHS reference costs for children’s ‘high need’ powered wheelchairs increased over a 5-year period from £377 in 2012/14, to £1760 in 2016/17. The most recent published figures for 2017/18 state a unit cost of £656 for the basic cost of a ‘high need’ powered wheelchair for children. This is more than double the cost of ‘low need’ (£266) and > 60% higher than ‘medium need’ (£394), but only slightly higher than the cost of a ‘high need’ manual wheelchair (£646). In addition, ‘specialist modification costs without supply’ are stated to be £139. 142
The Unit Costs of Health and Social Care 2018148 does not distinguish between provision for adults and children, but cites a capital cost of £1528 for a powered wheelchair, annuitised to £338 over 5 years. This is more than five times the cost for a self- or attendant-propelled manual wheelchair. Combined with maintenance revenue costs of £129, the unit cost rises to £467 per annum over 5 years. The authors of these unit costs148 cite one commercial site where costs range from £100 to £1300 for self- or attendant-propelled manual wheelchairs, and from £1000 to £5000 for powered wheelchairs.
From discussions with contacts within the NHS and the project advisory group (predominantly service providers/managers, service commissioners, commercial directors and representatives of national charitable organisations), and from reviewing the equipment cited in publications identified in the evidence review, we ascertained that the prices for powered wheelchairs for very young children are higher, ranging from £1800 to £8500. Based on the cost of chairs cited by NHS contacts and manufacturers’ list prices, our best estimate for the average cost of a powered wheelchair in this age range is £3939 (range £1800–8500). We assumed that these devices would be used by two children over the life of the chair; the cost per child is thus £1970 (range £900–4250). This is similar to the figures presented in the report Developing a Wheelchair Tariff Pilot Programme. 149
Starter powered mobility devices
Starter powered mobility devices, such as the Wizzybug145 and Bugzi,146 are generally aimed at children up to the age of 5 years (or weight limit of 25 kg). Other items aimed at this younger age group offer the potential for continued use after the age of 5 years, such as the TinyTrax, with a ‘grow with me’ design, and the SnapDragon (Dragonmobility Ltd). 150
These devices are not generally funded directly by the NHS, and are usually provided by loan through the third sector, either directly from the organisation or referred to by (or in collaboration) with therapists in the NHS. Families often obtain funding by application to other third-sector organisations for support, or fund the loan themselves. Manufacturers and other third-sector sites provide links to potential sources of funding. Families may privately fund the purchase entirely, although this is not thought to happen regularly.
Some professionals actively direct families to loan schemes or make them available to children through their own service. The current refundable deposit fees for Bugzi and the Wizzybug loans are between £100 and £200. The devices are loaned until the child no longer requires them, and are then returned for refurbishment for future loan. Capital costs of the items are between £3500 and £5000. Costs of provision and maintenance are often met by the supplying charity; however, in some cases, there will be extra associated costs, such as transport to the assessment/for collection and for maintenance. Based on these costs, our best estimate for the average cost of a starter powered mobility device is £4250 (range £3500–5000). Assuming that these devices would be used by two children over the life of the device, the cost per child is £2125 (range £1750–2500).
Ride-on powered toys
A number of researchers have explored building equipment to give very young children some experience of mobility through self-builds, using carts, robots and adaptations of ride-on car toys. The materials costs are relatively low in comparison with commercially available powered mobility equipment; however, the items are often bespoke for the child, so the amount of engineer resource may vary significantly according to need and the complexity of the build. The GoBabyGo scheme utilises students’ science, technology, engineering and mathematics (STEM) projects and estimates costs of the toy and adaptations as US$500. 56 Our best estimate for the average cost of an adapted ride-on powered toy is, therefore, £410 (range £310–510), based on the assumption that these devices would be useable by only one child, and the similar provision of engineering resource, using STEM students or voluntary resource.
Staff time and activities
The NHS reference costs for 2017/18142 include separate unit costs for a number of activities relevant to the provision and maintenance of wheelchairs to children up to the age of 18 years, primarily associated with staff costs (i.e. physiotherapists, occupational therapists, engineers and administrative staff). Unit costs are presented for assessment (unit cost £368), modification/customisation (unit cost £139), review (unit cost £232) and repair/maintenance (unit cost £214). In the budget impact analysis, these have been combined into two costs: one for assessment, modification and provision and one for review, repair and maintenance. Costs for assessment, modification and provision are one-off costs, occurring only once for each child, whereas costs for review, repair and maintenance occur on an annual basis, assuming that reviews and subsequent maintenance are carried out annually. Therefore, our best estimate of the additional staff cost to provide a powered wheelchair is £507 per child (range £368–936). Our best estimate of the additional cost to review and maintain a powered wheelchair is £446 per year, and, assuming each child receives three reviews/maintenances during their use of the device, this equates to a best estimate of £1338 (range £1017–1365) per child.
The staff costs of assessment, provision, review and maintenance for starter powered mobility devices, such as Wizzybug and Bugzi, are typically met by the provider organisation, and are thus assumed to be included as overheads in the cost of the device. Therefore, for the purpose of this analysis, we have not included separate staff costs for third-sector staff activities.
Accessories, modification and customisation
The level of need for accessories and modifications varies widely according to a child’s needs and clinical circumstances. Some users will require additional items and adaptations such as seating and other support, seatbelts or harnesses and bags or carriers for other essential medical equipment. These may be relatively standard or require bespoke manufacture for an individual user.
In terms of modification and customisation, the national schedule of reference costs for wheelchair services includes just over 1000 units of activity for children, described as ‘Equipment, Specialist Modification Without Supply’ in 2017–18, at a unit cost of £139. Over 4500 units of activity were described as ‘Specialised Complex Wheelchair Services’, at a unit cost of £429. Neither of these was categorised further. 142
The NHS reference costs assume a unit cost of £143 for a review of substantial accessories. 142 Manufacturers may include the cost of harnesses, certain seating, headrests, armrests, etc., in their list price, but there may be a need for bespoke specialised supportive seating as well. It has been assumed that these would be similar for a powered and a non-powered mobility device. Other additional costs associated with powered mobility equipment include attendant or dual controls, plus additional batteries and charging equipment, both of which may run into several hundreds of pounds.
Owing to the large variance in children’s needs for accessories, modification and customisation, it is difficult to apply a single cost for these aspects of the intervention. Based on previously reported data on the proportion of paediatric wheelchair intervention costs associated with accessories, modification and customisation,151 we have used a multiplier rate of 23% to the base cost of powered mobility devices and 6% to the base cost of starter powered mobility devices to predict the cost of accessories, modification and customisation (excluding staff costs).
Training
The studies identified in the systematic review were reviewed for information on any training provided to children aged < 5 years. There was a wide variation in the duration of training interventions and settings. The number of attendances and total duration of interventions delivered in this way also varied, with some lasting several months. 74,117 Several studies describe provision of an initial single session or guidance provided to the caregiver, for example Evans and Baines’s62 description of the training provided to families on receipt of the Wizzybug and training provided by Mockler et al. 111 to parents of users of powered wheelchairs, in a manner presumed similar to the NHS. There was no consensus on the optimum duration/number of training sessions.
Provision of training for use of powered mobility varied widely among the NHS services contacted. Some level of training will be achieved through any trial undertaken as part of the assessment of suitability of provision of powered mobility, but this has not been costed as such for the purposes of this section of the report, to avoid double-counting. Training is also delivered by the therapists at a clinic, at home or in school, usually at the point where the equipment is provided, which may be at the provider site or at the user’s home or school. It is usually limited to showing how the controls work and observing the chair in use, lasting up to 1 hour, but could take much longer for children with cognitive impairments. Again, this has not been costed separately to avoid double-counting. Provision of training for use of the starter powered mobility devices is limited to handover, during which the charity or the partner organisation’s therapist will provide caregivers with bespoke advice on learning through play. 62 Thus, training that we believe to be part of assessment/provision has not been costed separately.
More formal training sessions are provided by a number of third-sector organisations; for example, the NHS web page How to Care for a Disabled Child152 specifically refers to Whizz-Kidz153 and Go Kids Go!154 as providing free training services. Go Kids Go! provides workshops aimed at children aged > 2 years using manual and/or powered wheelchairs. Family members may also attend and some workshops are aimed at school groups, including non-users of wheelchairs. In 2017, training was delivered to almost 300 children with disabilities and > 2000 beneficiaries in total, including the children themselves, family members, school attendees and health and education professionals. 155 This is one area for which the costs of powered mobility provision may be less than for a non-powered wheelchair; without balancing training (users of self-propelled manual chairs require training on balancing skills to manage uneven surfaces, kerbs etc.; powered chairs are more stable and so this element of training is not required), training sessions may be reduced from 5 to 3 hours. The overall cost of running a workshop is in the region of £2000, requiring trained professionals to run the session, and often additional support from technicians and volunteer wheelchair mentors. According to Roy Wild of Go Kids Go! (personal communication), the cost per user is around £450 (estimated range £350–550), including overheads; thus, we have used this as our unit cost for training. We have also assumed that 10% of powered mobility users access this training.
Adaptations to housing, community facilities and transport
Powered wheelchairs are generally larger and heavier than manual wheelchairs; therefore, greater and/or further adaptations to housing, community facilities and transport may be required. For example, doorway widths may need to be further adjusted. In 2003, work from Canada surveying users of powered wheelchairs found that 50% experienced barriers to use in the house, 62% found physical barriers in the workplace or at school and 56% experienced barriers in community buildings. 132 Although half of those surveyed had received a wheelchair before the age of 5 years, no information is presented detailing when these issues first arose. As it is probable that, in recent years, more housing and community facilities are being designed to be accessible, information on the costs of modifications are included in the analysis.
Housing
Families with a disabled child may be able to access funding from their local authority for up to £30,000 in England to adapt the home. 147 The mean grant provided is £7500 (this value includes adults, as adaptations for wheelchair use are standard and unrelated to age of user). 156 The number of families accessing these grants is unknown, but is likely to be a small proportion; we have therefore assumed that 10% of children would receive funding for housing modifications before the age of 5 years, factoring in that some homes would not need to be adapted.
Costs calculated for relevant housing modifications were taken from the Personal Social Services Research Unit’s Unit Costs of Health and Social Care 2018. 148 Assuming that an entrance requires a ramp (at a cost of £906 per ramp), a doorway widened (at a cost of £667 per door) and path (at a cost of £153 per path) installed, and that each child would require two entrances to be adapted, the total cost equates to £3452 (range £1726–7500) per child, which we have used for our unit cost.
Community facilities
Adaptations may be required to community buildings likely to be visited by children who might benefit from powered mobility outside the home, for example schools, recreation centres, community centres and places of worship. No specific information was found about the associated costs of community adaptation in the systematic review. Although it is assumed that the costs of providing adaptations to accommodate a powered mobility device in such spaces would be the same as for housing, as most new community buildings are already built with accessibility in mind, and many older buildings will have adaptations already in place. It is anticipated that the number of new adaptations specifically for a child using powered mobility would be small; therefore, these costs are not included in the analysis.
Transport
There are no current data on the proportion of families requiring different or adapted vehicles because of their child’s disability, nor of the relative requirement for this based on use of a powered versus a manual mobility device. However, transport is recognised as causing issues throughout the review data. In the Canadian survey,132 > 70% of respondents cited difficulty transporting their powered wheelchair. In 2003, the organisation Whizz-Kidz published findings from a postal survey106 among families of children aged < 7 years who had been provided with powered wheelchairs; 61% said that they transported the child in the car, using a four-point strap and/or ratchet clamps. The Motability Scheme in the UK allows parents or carers of children aged ≥ 3 years to use their mobility allowance to lease a car or wheelchair-accessible vehicle. 137 Data obtained from personal communication with Motability UK (Press and Public Relations Department, Motability UK, 2019) indicate that, in the financial year 2018/19, 120 grants for these were made in relation to children aged < 5 years, which is < 10% of the grants awarded to all children aged < 18 years. This might be expected to increase should a greater number of this age group be given access to powered mobility options suitable for use outside the home.
Motability grant values averaged £2706 in 2018, so this has been used for our best estimate (range £2435–2977). 157 We have assumed that 10% of children will receive Motability grants. Families may need to top up this funding, but the exact levels involved have not been determined for this report. Similarly, we acknowledge that there will be additional travel and associated increased costs, such as fuel and depreciation of vehicles, for travel to appointments, training, etc., but insufficient data are available to quantify this.
In terms of transport to school, local authorities are responsible for the provision of free transport in appropriate circumstances, including to children with disabilities that affect their ability to walk. Legally, transport is required to be provided for eligible children only from the age of compulsory education (5 years),158 although many authorities provide transport for eligible children from the commencement of the school year in which the child attains the age of 5 years and starts full-time education, which is more commonly at age 4 years. Provision of powered mobility suitable for indoor and outdoor use to very young children, as opposed to waiting until they reach the age of 5 years, may increase the need for provision by an extra year per child, but, because of the lack of corroborating data, we have not included this cost in the analysis.
Human resource
The human resource costs of powered mobility interventions are significant, as already highlighted by the staff costs (see Staff time and activities) and cost of home adaptations (see Housing). 148,159 As noted above, for assessments, provision, review and maintenance, we have used the costs suggested in the NHS reference costs, which have incorporated relevant staff resource.
The potential impact on wider society in terms of the caregiver and the wider family, and on those involved in provision of early-years schooling, has been considered; minimal evidence of reduced need for support in school was found in the literature or in consultation with our advisors; therefore, human resource costs associated with education have not been included.
Likewise, there was no evidence on the impact of powered mobility provision on parent/family productivity; therefore, these costs have also been excluded from the analysis. Although we appreciate that, in reality, there are likely to be financial implications for families, there are insufficient data to accurately calculate this at present.
Areas of no impact
There was no evidence of impact on a child’s medical diagnosis; therefore, we have not assumed any differences in need for, or type of, medical interventions including medication or surgery, nor of any staff or other resources related to these. Although changes in children’s behaviour/independence levels may affect some other areas with cost implications, it was not possible to determine the probable impact from the literature; the evidence does not allow us to quantify by how much or in what time frame any benefits may be realised.
Defining powered mobility provision scenarios for the budget impact analysis
To estimate the change in costs associated with increased powered mobility provision, a base-case (i.e. current provision) scenario was defined and a further three hypothetical scenarios were developed (see Box 1). The costs associated with individual provision do not vary between scenarios because the budget impact analysis is based on changes to the number of referrals and powered mobility devices provided. The assumptions regarding population and resources are presented in the next section. The analysis model, based on our estimations of minimum, best-estimate and maximum levels for population, equipment and resources required, is presented in Report Supplementary Material 2. In the analyses, it has been assumed that all referred children receiving mobility equipment from NHS services will receive a buggy or assisted/manual wheelchair and that the provision of powered mobility will be an additional cost.
Base-case assumptions
Population
-
A total of 7300 children aged < 5 years are referred to NHS Wheelchair Services.
-
Of these, 400 are assessed for a powered mobility device and receive it.
-
-
An additional 225 children receive a starter powered mobility device from the third sector or privately outside NHS services.
Mobility equipment
-
Powered mobility device costs are based on the assumption that each device will last for 5 years and be used by two children during that time, assuming that each device is refurbished and then reused once (refurbishment costs are included in repair/maintenance costs).
-
NHS provision is based on current NHS practice. Specific powered mobility device models are likely to vary, and may include some starter powered mobility devices: best estimate £3939 per device (range £1800–8500), equating to a cost per child of £1970 (range £900–4250).
-
Third-sector provision is based on reported costs from manufacturers. Specific devices include Wizzybug145 and Bugzi:146 best estimate £4250 per device (range £3500–5000), equating to a cost per child of £2125 (range £1750–2500).
-
Powered wheelchair costs and starter powered mobility device costs are multiplied by 23% and 6%, respectively, for each child, to account for customisation and modification.
Resources used in assessment, provision, handover and maintenance of powered mobility
-
One-off staff costs associated with the assessment, provision and customisation of powered mobility are included in the analysis: £507 (range £368–936) per child.
-
It is assumed that each child receives three reviews/maintenances during their use of the device: £1338 (range £1017–1365) per child, with lower maintenance frequency for less complex needs.
-
For third-sector provision, it is assumed that all costs associated with assessment, provision, review and maintenance are included as overheads in the cost of each device.
Training
-
Families of children requiring training for all wheelchair types are directed to further wheelchair training, provided by third-sector organisations such as Go Kids Go! or Whizz-Kidz, with 10% of children attending this training: £450 per child (range £350–550).
Housing and transport
-
It is assumed that 10% of families receive adaptations to the home associated with powered mobility provision: £3452 per child receiving adaptation (range £1726–7500).
-
It is assumed that 10% of families apply for a Motability grant to adapt their car for a powered mobility device: £2706 per child receiving adaptation (range £2435–2977).
Alternative service scenario assumptions
The three alternative service scenarios used to estimate the costs associated with increased powered mobility provision for very young children are defined in Box 1.
-
The number of children aged < 5 years referred to NHS Wheelchair Services remains unchanged (n = 7300); however, all 7300 children are offered assessment for an appropriate powered mobility option. Although the volume of assessments increases, there are no changes to NHS resources used in referral, handover, review or maintenance for each child.
-
As a result of increased assessments, more children are offered powered mobility – in this scenario we have assumed that the number of children who receive powered mobility doubles, to 800. The types of interventions offered by the NHS do not change; thus, the cost of equipment per child remains the same.
-
Third-sector/private provision also increases, as more children are assessed for powered mobility by the NHS, but then seek such equipment elsewhere, either because of refusal or unmet need. For uniformity, third-sector/private provision also doubles, to 450.
-
Although this scenario would have implications on staff numbers, training and clinic space, we have assumed that current NHS and third-sector provision of equipment, training and staff resource can expand to meet demand.
-
The number of children aged < 5 years referred to NHS Wheelchair Services increases by 10%, to 8000. All children are still offered a powered mobility assessment. Although the volume of assessments increases, there are no changes to NHS resources used in referral, handover, review or maintenance for each child.
-
The number of children who receive powered mobility consequently increases by 10%, to 880. The types of interventions offered by the NHS do not change; thus, the cost of equipment per child remains the same.
-
Third-sector provision also increases, as more children are assessed for powered mobility but then seek such equipment elsewhere because of refusal or unmet need. For uniformity, third-sector provision also increases by 10%, to 495.
-
As scenario B, but the NHS takes on the costs currently assumed by the third sector; therefore, the number of very young children receiving powered mobility through the NHS increases to 1375.
-
The proportion of children receiving powered wheelchairs and starter powered mobility devices remains the same.
-
The NHS resource costs are unchanged from scenario B, assuming that the third-sector maintenance costs are included in the transferred provision.
-
The NHS also takes on the cost of formally training each child to use powered mobility: £450 per child, with 50% of children accessing training.
Results: budget impact analysis
The data presented in the tariff of costs in Appendix 12 and the assumptions stated in Box 1 were used to estimate the current cost of provision of powered mobility options by the NHS, additional costs due to housing and vehicle adaptation, and the cost of provision of equipment and training by the third sector. See Report Supplementary Material 2 for the budget impact analysis model. Table 38 summarises the findings.
| NHS provision of powered mobility (£) | Adaptations to home and/or vehiclea (£) | Third-sector provision of powered mobility and trainingb (£) | Overall combined cost | NHS spend as % of reported wheelchair service spendc | NHS spend as % of estimated wheelchair service spendd | |
|---|---|---|---|---|---|---|
| Estimated cost per child | 4720 | 6200 | 2830 | |||
| Base case | 1.89M | 0.38M | 0.56M | 2.84M | 1.75 | 1.46 |
| Scenario A | 3.78M | 0.77M | 1.13M | 5.67M | 3.50 | 2.93 |
| Scenario B | 4.15M | 0.85M | 1.24M | 6.24M | 3.85 | 3.22 |
| Scenario C | 5.64M | 0.85M | N/A | 6.49M | 5.22 | 4.37 |
Based on the results from the budget impact analysis, we predict that the NHS CCG spend on the provision of powered mobility to very young children is currently around £1.9M annually, which is < 2% of the overall reported CCG spend on wheelchair services. This is based on an assumption that 400 very young children are provided with powered mobility each year. Based on our analysis, the third sector spends > £0.5M on powered mobility provision to a further 225 children, and provision of some training in this age group. Although it appears that the costs of provision per child are lower for the third sector than for the NHS, this is largely driven by the lower costs of the equipment provided, as we have assumed that the NHS currently provides powered wheelchairs with additional servicing costs, whereas we have assumed that the third sector largely provides starter mobility devices for which these costs are included. A further £0.4M is spent on adaptations to support powered mobility through funding from public services and the third sector.
To estimate the cost of increasing supply and demand for powered mobility, we modelled hypothetical increases to powered mobility provision. In scenario A, the number of children provided with powered mobility was doubled in both NHS and third-sector provision, to illustrate the change in cost associated with a more open approach to early powered mobility provision, and based on current numbers of children referred for mobility equipment. The cost to NHS services increased to £3.8M, and the cost to the third sector increased to £1.1M.
In scenario B, we modelled a situation in which more children are also referred for powered mobility, as well as increased provision, increasing costs to £4.2M and £1.2M for NHS and third-sector providers, respectively. In the final scenario, scenario C, we developed a hypothetical situation whereby the NHS takes on all early powered mobility provision, and therefore covers all costs associated with third-sector provision. Although this is highly speculative, at present the third sector is relied on to fill the gap in early powered mobility provision, and, given the potential health and developmental benefits of early powered mobility, there is an argument that the NHS, or other centralised funding, should be responsible for supporting all provision. We therefore undertook scenario C to estimate the associated cost implications of shifting all costs for powered mobility provision to the NHS. The results indicated that NHS costs would increase to £5.6M (including an additional increase in standardised provision of powered mobility training).
Of the 195 CCGs covered by the National Wheelchair data collection, 131 reported annual spend on wheelchair services,18,139–141 indicating a total spend of > £108M. Assuming that the mean spend for each CCG providing data can be assigned to those CCGs that did not, the total figure could be in the region of £129M. The results indicate that even if the NHS were to double provision of powered mobility for very young children, and to take on responsibility for all third-sector provision, the costs would remain relatively low, in relation to the overall budget for wheelchair services, at between 4.3% and 5.2% of reported CCG costs.
Factoring in all relevant public sector and third-sector costs, the cost of an early powered mobility intervention is likely to fall below £10,000 per child. This cost could be reduced through bulk purchasing, increased repair/maintenance and subsequent reuse of individual devices. In the highest-cost scenario, the potential cost to the NHS exceeds £10M, but it is of note that this is based on the worst-case scenario for all variables, and is therefore unlikely.
Despite the speculative nature of this analysis, the results indicate that powered mobility provision for very young children could feasibly be increased without major increases to budget. Furthermore, the results could be used to inform budget allocation to support increased provision.
Outside the UK, particularly in North America, there is interest in provision of adapted ride-on toys to provide a powered mobility experience. Currently, we do not believe that access to this kind of intervention is being provided by the NHS, and have little evidence of bespoke adaptations being made outside this. However, if the NHS were to adopt a scheme like GoBabyGo in the USA, where student resource is used to adapt the vehicles, the costs are estimated to be in the region of £410 per vehicle. If every very young child with mobility needs referred to wheelchair services was offered access to such a device, the potential cost would be £3M per year (range £2.9M–3.2M). It is likely that this kind of intervention would not be suitable for all children because of their differing needs and abilities, which would reduce this cost. However, if the adaptations were to be taken on by the NHS, costs of engineer resource would need also to be taken into consideration.
In addition to the lack of conclusive data from the systematic review on the probable positive and negative influences of early powered mobility on costs, the nationally available NHS sources lack detail on the provision by age, in terms of both patient numbers and equipment costs. The scope of this project was not to undertake primary data collection for the purposes of an economic analysis. We have therefore used published NHS costs when available, supplemented by discussion with members of the project advisory group (specifically service providers/managers, service commissioners, commercial directors and representatives of national charitable organisations). Feedback suggests that the costs of equipment cited in the reference sources are likely to be underestimated, and thus the costs of service provision may also be inaccurate. However, although we have attempted to cost equipment more realistically, we have used NHS data on resource use, as we identified a wide variety of approaches used locally across CCGs and services contacted. These include the following:
-
differences in protocols for provision of early powered mobility that affect access, even if not categorically setting an age threshold
-
the number of CCGs supported by a wheelchair/posture and mobility service
-
use of centralisation of some aspects, for example engineering across multiple services
-
the level of contracting out to non-NHS providers
-
the level of collaboration with third-sector providers
-
the choice of powered mobility equipment provided and the variation in contract prices for equipment
-
the type and level of professional and support staff involved at different stages of provision.
There were no robust economic data on the impact on users’ families identified from the systematic review. In particular, there was no detail on the level of funding outside the NHS through top-ups to funding accessed by vouchers or personalised wheelchair budgets, or by third-sector grants. In addition, we know that individuals may fully fund the purchase of new or second-hand equipment, but the extent of this is unknown. Based on this, we acknowledge, but have not attempted to cost, this aspect.
We have not incorporated any costs associated with initial referral, which may increase from scenario B onwards. We are aware of significant staff and carer time and resource use to make a case for provision for exceptional cases, but the number is unknown; thus, we could not incorporate such cost in the analysis.
A further significant consideration is the general capacity for increasing the resource allocated to increased provision. Increased staff resource would require re-allocation and/or recruitment and training of additional staff. Our calculations have not considered any costs of new assessment equipment or new/extended buildings to accommodate increased clinics.
Scenario C makes a hypothetical transition from no collaboration with third sector to the NHS assuming all costs of provision by the third sector. However, in reality there is some collaboration now, which is likely to grow. We do not intend to imply that there is no role for the third sector in the future, only that the costs related to the provision of equipment should be covered elsewhere. For the purposes of this review, we have assumed that this is the NHS, but it could come from other central funds.
We did not attempt to make assumptions about future developments, which are likely to affect this field. It is likely that technological advances will be introduced, and therefore costs will change. In addition, the roll-out of personalised wheelchair budgets, replacing the current voucher scheme, may also affect the range of items provided and associated costs.
The awareness of and interest in the importance of early powered mobility is growing. Earlier provision of powered mobility is unlikely to change the number of children with mobility needs being referred to the NHS; however, the interaction with the service, the provision of powered mobility and associated need for adaptations, reviews and repairs will occur earlier in their lives, bringing the costs forward. The result may be that more children are referred earlier, and that more children meet the criteria for early powered mobility earlier.
We found that the most recent reference costs were far lower than the costs of powered wheelchairs reported by the CCGs we contacted, and we found a variation in the protocols and activities associated with the provision of early powered mobility. These issues were also noted in the report149 on the work carried out by Deloitte (London, UK) in the development of a wheelchair tariff generally, not just for this specific group of users. Further work is needed to determine, in more detail, the extent and cost of provision of mobility equipment and the supporting services.
Chapter 7 Integrative synthesis: an integrated logic model to inform the future planning for, and evaluation of, the outcomes of powered mobility for children
The final resulting logic model (Figure 8) presents, in a single figure, the key hypotheses about powered mobility outcomes resulting from an overarching synthesis of the components of this work. The logic model provides a key set of powered mobility outcomes that those planning and commissioning powered mobility equipment may wish to consider. It also provides information about the direction of the outcomes and the overall evidence base, across different study designs and types, underpinning those outcomes. It provides a framework for future research and service evaluations of powered mobility outcome interventions, including a clear map of the current evidence gaps. The following section provides a brief, narrative overview of our overarching synthesis and logic model.
FIGURE 8.
An integrated logic model to inform the future planning for, and evaluation of, the outcomes of powered mobility for children. Solid arrows linking concepts represent hypotheses that were developed based on consistent evidence across different study types. Dotted arrows linking concepts represent tentative hypotheses implied in selected studies but with a limited evidence base across study types. Arrows above the lines signify whether the hypothesised relationship is positive (arrows up), negative (arrows down), mixed (one arrow down and one up) or uncertain (a question mark). The stated level of support (inconsistent, very low, low, moderate or strong) for each concept refers to the overall range and depth of evidence across different types of studies for each concept.

The identified evidence focused on two intervention elements: the powered mobility equipment and training for the child to learn to drive that equipment. There was strong evidence from a range of study designs, clinical populations, and ages of children to suggest that powered mobility equipment is generally a feasible and acceptable intervention. Evidence from qualitative studies further contextualised feasibility and acceptability, for example by exploring how parents of children with degenerative conditions could express the negative inevitability of their child’s degenerative condition towards the need for powered mobility, which shaped their conceptualisation of acceptability. Likewise, some parents of very young children preferred ride-on toys to powered wheelchairs because of the former’s resemblance to the types of toys a child would usually play with in young childhood; thus, they were not perceived to stigmatise their child in the same way as a wheelchair.
The evidence across studies further indicated that powered mobility equipment can have a positive impact on a child’s movement and mobility, and that movement and mobility as an outcome consisted of two inter-related dimensions: (1) play-related movement, whereby a child was doing ‘movement for movement’s sake’, and which included a range of age-appropriate and developmentally appropriate experiences, exploration and enjoyment of movement-based play and physical activities, and (2) destination-focused mobility, whereby a child moved to get from A to B for a purpose of doing something else at destination B. Although the specific play-related movement activities varied based on a child’s age and developmental level, the core concept of movement for its own sake as an important powered mobility outcome was present across the age groups. The overall synthesis did not support a hypothesis that play-related movement is important only for younger children, or that its primary function is the learning of movement skills. There was some evidence to suggest that destination-focused movement may become increasingly important as children grow older and ascertain increasing control and independence over where they go, when and with whom.
Although there is no conclusive evidence of effectiveness, it is clear that powered mobility equipment is a good way to enable children to move around (for play and physical activity) and to get to places. When considering the outcomes of powered mobility, both of these (moving for play and moving to get to places) are important.
There was evidence that powered mobility training can enable children to learn to drive powered mobility equipment, but this evidence was inconsistent, in that training was not equally effective for all children (especially for children with cognitive impairments), and in that there were two contrasting ways to hypothesise the place of learning in powered mobility intervention outcomes. One was that learning to drive powered mobility equipment was a prerequisite for powered mobility use, for the movement and mobility outcomes, and for all other subsequent outcomes. The other was that learning to drive the equipment was the result, an outcome, of using powered mobility in movement and mobility. There was evidence to support both perspectives. There is little doubt that learning to use powered mobility equipment is a relevant outcome. However, how and when the learning can be enabled in the most cost-effective way remains a key question, and is a recommendation for future research.
Early introduction of powered mobility can facilitate children to develop powered mobility skills through playing and learning to use the powered mobility devices. Regardless of age, children need time and support to master powered mobility, and benefit when the device, environment and motivation of those around them are optimised. Powered mobility training need not be seen solely as a formal activity, as children benefit from simply using such devices and developing skill through experience.
Beyond movement and mobility, outcomes related to participation (including play and social interactions) and autonomy (including choice, control, freedom and independence) were consistently presented in the data as being highly valued. There was evidence to link participation outcomes to powered mobility, mainly from textual data, with quantitative outcome measurement lagging behind the narrative conceptualisation. Autonomy, as a more abstract term, remained more elusive. It was often described and illustrated through everyday movement and participation examples, but corresponding quantitative data were limited.
Outcomes related broadly to participation and autonomy are likely to be important; further research is needed to capture them meaningfully and to evaluate the effectiveness and cost-effectiveness on them. In health economics research, these types of outcomes are typically understood through the evaluation of health-related quality of life or capability, and, in turn, the relationship between incremental cost and incremental benefit can be evaluated to determine cost-effectiveness. For such young children, the use of standard health economics outcomes measures (such as the EuroQol-5 Dimensions) is likely to be difficult, as few are validated for this age group. Likewise, the variance in impairments, abilities and prognoses is likely to introduce confounding variables without tight control of the sampled population. Given the small number of children aged < 5 years who use or could benefit from using powered mobility, this poses great difficulty in the assessment of cost-effectiveness. One solution is to monetise all costs and benefits, and to use a long time horizon to evaluate impacts to public service expenditure over time, assuming that early provision of powered mobility has health and developmental benefits in the future. At present, there is essentially no evidence to support this analysis; thus, additional research is needed to identify a core set of outcomes that can be evaluated reliably to determine effectiveness and cost-effectiveness. The budget impact analysis demonstrated that, even with greatly increased provision, NHS costs for early powered mobility provision would still remain a small proportion of overall wheelchair service costs, but the relationship between these costs and children’s outcomes is still unknown.
The issue of risk and safety in relation to early powered mobility has often been used as a barrier to acceptability and feasibility of earlier provision. This concern is not just expressed by wheelchair services, but also by parents, who may initially be reluctant to accept powered mobility. This reluctance can also be related to the symbolic nature of powered mobility, as parents may see these devices as a negative symbol of disability. Therefore, parents need to be supported and educated on the potential benefits; likewise, guidance is needed to support wheelchair services to make balanced judgements about potential risks and harms. Very young children clearly need to be supervised in any early powered mobility, but this is the same for all young children, and thus should be approached in a developmentally appropriate manner. There was limited overall evidence about accidents and pain as powered mobility intervention outcomes; the nature of accidents and pain were well described, but the prevalence data came from a limited pool of studies.
In terms of key factors influencing feasibility and acceptability of initial uptake, as well as sustainable, long-term implementation, the ‘fit’ between the child, the equipment and the child’s everyday environment (physical and social) was identified as critical. A good fit could make the powered mobility use sustainable and positive, and spiral into many new participation and development opportunities for the child. A poor fit could result in the child not using the equipment, accidents to the child and people around them, the child feeling negative, and the child missing out on participation and opportunities. Evidence underpinning ‘fit’ as an implementation concept came mainly from the textual data. Fit between the child, the equipment and their social and physical environment is likely to be critical for feasibility, acceptability and optimum effectiveness, and is thus a priority concept for further primary research.
Overall, this research found little evidence to suggest that 5 years of age is a meaningful or evidence-based cut-off point for powered mobility provision. Although few studies explored this explicitly, the implied view from the evidence appeared to be that powered mobility provision use was shaped by a child’s developmental and cognitive profiles, not by their age. However, these considerations were often not made explicit, or were not consistent across the studies, and it was not possible to identify a uniform protocol of what powered mobility intervention elements to provide to which children, when and how. It would be a clinically valuable piece of work to seek to develop a national consensus protocol, and jointly identify the remaining key uncertainties and areas of equipoise.
The final logic model (see Figure 8) provides an overview of powered mobility outcomes and information about the direction of the outcomes and the overall evidence base. It is worth explicitly restating that we were unable to find conclusive evidence of the effectiveness or cost-effectiveness of powered mobility interventions, and that the description of the evidence base refers to the different types of evidence from across studies. The logic model should be read as a proposal for hypotheses from this review, as opposed to a statement of evidence of effects. In the model, solid arrows mean hypotheses that were developed based on consistent evidence across different study types. Dotted arrows mean tentative hypotheses implied in selected studies, but with limited evidence base across study types. Three of the concepts are not explicitly linked to the interventions, as we were not able to identify clear evidence about hypothesised causal chains linking them to the intervention. Arrows above the lines mean that the hypothesised relationship is positive (arrows up), negative (arrows down), mixed (one arrow down and one up) or uncertain (a question mark). Finally, as there is currently no established method for formally grading the certainty of mixed-methods synthesis findings, we were not able to provide such a formal grade for the overall synthesised concepts. Instead, the stated level of support (from strong to very low) refers to the overall range and depth of evidence across different types of studies that we were able to find for that concept. This is inevitably subjective and should be treated with caution. See also Chapter 8, Strengths and weaknesses, where the methodological limitations of the approach used to determine the stated level of support are further discussed.
Chapter 8 Discussion
The aim of this research was to assess whether or not earlier provision of powered mobility to very young children is more cost-effective than provision to children aged ≥ 5 years. This was not achievable because of the lack of published conclusive effectiveness evidence and non-existent cost-effectiveness evidence. For this reason, we re-evaluated the data we had, and subsequently felt that a different approach to evaluating effectiveness and performing economic analysis might be achievable. We therefore conducted two syntheses of the evidence, making use of the wide variety of evidence types, and conducted a budget impact analysis to identify the additional costs associated with increasing powered mobility provision for very young children.
Main findings
The main findings from this review are as follows. There are no formal, randomised, sufficiently powered evaluations of effectiveness of powered mobility on any outcomes in children aged either < 5 or ≥ 5 years. There were no economic data to allow us to determine the cost-effectiveness of powered mobility interventions for children; therefore, we are unable to make any definitive statements about the potential economic impacts of early powered mobility. It was also not possible to answer the question about the long-term implications of self-directed or independent mobility for very young children (as previously defined) compared with older children (≥ 5 years), again because of a lack of evidence.
However, the review identified an abundance of evidence, across age and diagnostic groups, that showed that powered mobility provision for children is feasible and acceptable. We further assessed the overall body of evidence to suggest, with strong certainty, that powered mobility may have a positive impact on children’s movement and mobility across the age groups. In this, movement and mobility consisted of two dimensions: (1) ‘movement for movement’s sake’, such as play-related movement; and (2) destination-focused mobility whereby a child moved to get from A to B. Although the direction of this effect was consistent, it was not possible to assess the size of a potential effect because of heterogeneity of the studies that contributed to this finding.
From descriptive and qualitative evidence, four further potential powered mobility outcomes were identified: (1) participation, play and social interaction; (2) autonomy, independence, choice and control, and freedom; (3) self-care; and (4) psychological outcomes. Evidence of effectiveness on all of these was scarce, with assessment of certainty ranging from low to moderate. The main focus of intervention descriptions to date has been on the powered mobility equipment and training; little was found about intervention elements targeting the wider context.
The main reported powered mobility safety events related to accidents and pain for the child, and parent and child feelings about the intervention and its consequences. The evidence about the frequency of these events was limited. Overall, the evidence suggested that a relevant lens for considering the safety of powered mobility may be that of a universal need for parents to balance the degree of risk and independence as they seek to support their child’s development and growth.
The factors and processes that underpin acceptability, uptake and use of powered mobility included the ‘fit’ between a child’s characteristics, the powered mobility equipment and the context (physical and social). The integration of self, device and environment appears to influence a child’s potential to benefit from powered mobility, but is not necessarily related to a child’s age. This is an important consideration in the conceptualisation of these interventions and in encouraging children to use powered mobility devices. When powered mobility interventions are presented as a means for play and moving for movement’s sake, children may be more engaged and thus more likely to use the device routinely. This could also be helpful for parents who are learning to adjust to their child’s need for powered mobility and trying to support skill development at home.
For the specific comparison of powered mobility for very young children and children aged ≥ 5 years, the systematic review found, overall, little evidence to suggest a difference based on chronological age. There was some indication that developmental level, cognitive abilities or a child’s size may influence the types of equipment that are suitable for a child and, for example, the training that a child may benefit from. The review found that formal powered mobility training is a potentially expensive intervention component, with equipoise over its format and delivery, its hypothesised importance to actual powered mobility uptake, and its effects.
Based on the results from the budget impact analysis, we predict that NHS spend on the provision of powered mobility to very young children is currently around £1.9M annually, which is < 2% of the overall reported CCG spend on NHS Wheelchair Services. We estimate that this figure could rise to up to £5.64M per annum with increased provision and integration of third-sector provision. We estimate that current NHS provision of early powered mobility covers only a limited proportion (50% at most) of very young children who could benefit from early powered mobility, with third-sector providers filling the gap in provision.
We developed a tariff of both NHS and non-NHS costs associated with powered mobility interventions for children. Owing to the lack of published evidence, it was necessary to derive the data from many different sources. The project advisory board and various NHS Wheelchair Services and providers were instrumental in identifying unit costs for the tariff. For assessing the costs and benefits, there is an overall lack of disaggregated data relating to very young powered mobility users, which makes it difficult to assess the costs and benefits for very young children, compared with older children. Further work is now needed to collect national data of paediatric wheelchair provision by age group and type of wheelchair.
Strengths and weaknesses
A key strength of this study was the synthesis of diverse types of evidence and perspectives. Including a wide variety of research types in our synthesis allowed a broad examination of the topic area, and allowed us to include the views and experiences of various key stakeholders. A focus on only quantitative evidence would have been of limited benefit, as there were few robust quantitative data to determine the effectiveness or cost-effectiveness of early powered mobility. The qualitative evidence was key to shaping our conceptualisations of the outcomes of powered mobility and determining the various factors that can influence feasibility and acceptability. The triangulation of different types of evidence allowed us to determine our confidence in the emerging concepts, and to highlight the gaps in evidence. Stakeholder involvement was also embedded in this project from the outset, which enabled us to optimise the relevance, usefulness and potential impact of the study by integrating expertise and insight from service users and providers at each stage. Stakeholder input will also enable us to develop dissemination materials that are engaging and relevant to a wide variety of audiences.
The primary limitation of this study relates to the lack of published evidence from formal, appropriately powered evaluations of effectiveness and cost-effectiveness, which meant that we were not able to answer our original research question. We utilised a wide range of established methods to attempt to configure the evidence in relation to the research question, pragmatically re-evaluating our approaches and adopting alternative methods to examine the data and persevere with our analyses. We feel that the resulting findings and syntheses offer various novel and useful insights into the potential effectiveness and economic costs of early powered mobility, and the priorities for future research.
The original intention was to develop an economic model to examine the long-term cost-effectiveness of early powered mobility. However, after the completion of the reviews, it became apparent that there were insufficient published data to develop a robust economic model. We had also intended to implement a value-of-information analysis as part of the model outputs. We intended to use this analysis to quantify the expected gain in net benefit from obtaining further information to inform any decisions. As highlighted throughout the report, there is uncertainty in both the provision pathway of early powered mobility provision and the quantification of the benefits that might be realised in very young children. Given these uncertainties, and the many areas where there was no, or very limited, evidence, we determined that it was not feasible to conduct the planned value-of-information analysis.
We accept that, with the budget impact analysis, many assumptions had to be made, but, whenever possible, the assumptions were based on evidence or expert advice, and we have been explicit about all sources of the data we used. One of the keys issues we experienced was in identifying the population of children who currently use powered mobility across the age range, and the number of children who could potentially benefit if early provision was standardised across the NHS. The published national data sets do not detail information by age for wheelchair provision; therefore, we had to extrapolate from population data to achieve our goal. This was a common issue, as the reporting of population and cost data in this area is quite limited. In several circumstances, we triangulated several sources of evidence to generate the costs. For this reason, we have presented wide ranges in costs as part of a simple sensitivity analysis to show the potential variance in our best estimates.
As wheelchair services and providers move towards use of electronic data management systems, it should become more feasible to collate data on types and cost of provision by age for use in future evaluations.
We also feel that it is important to comment further on the limitations in the approach used to make judgements about the level of support for the mixed-methods findings. As discussed in Appendix 4, there are no tools for assessing certainty or confidence in integrated quantitative and qualitative findings. A common approach is to undertake method-specific reviews and use method-specific tools such as Grading of Recommendations Assessment, Development and Evaluation (GRADE) and GRADE-CERQual, the assessments of which are brought together in an integrative framework such as the Developing and Evaluating Communication Strategies to Support Informed Decisions and Practice Based on Evidence (DECIDE) framework. In the current mixed-methods synthesis, there were few trials, but there were diverse sources of other types of evidence, which were considered useful. Using established approaches would not have allowed a full assessment of the evidence, so an integrative mixed-methods framework synthesis was used. In the absence of a validated tool to assess confidence in integrated findings, we developed an approach to assessing support for each concept. See for Appendix 4 for details of the approach, and see Table 11 for a worked example.
This approach was not developed using the extensive process used for the development of GRADE or GRADE-CERQual, and, as previously noted, the assessments must be interpreted with caution. Application of our approach also produced some methodological issues that are worthy of further discussion. The premise of the approach is that different types of evidence are considered uniquely useful for answering research questions. This includes acknowledgement that some types of data are more suited for answering some questions than others. For example, questions of effect are more usefully addressed by quantitative evidence, whereas questions about feasibility and acceptability benefit from qualitative evidence, although it is acknowledged that information about both issues can be found in other study types. One example of when the application of the approach produced a potential difference in interpretation relates to the assessment of feasibility and acceptability evidence in the interpretive evidence synthesis of the qualitative data. When GRADE-CERQual was applied, findings concerning these phenomena were assessed to be of high or moderate confidence. In contrast, in the mixed-methods synthesis, the absence of quantitative evidence regarding feasibility and acceptability was considered a limitation, and the evidence base was subsequently rated lower.
Overall, the approach presented in this report to assessing the level of support for mixed-method integrated quantitative and qualitative findings should be considered a useful first step to facilitate methodological debate on how best to do this. The approach used requires further development and refinement using an agreed consensus-based development method and further testing before it can be considered a validated approach.
Strengths and weaknesses in relation to other studies
Three seminal evidence syntheses have been conducted in this context: Bray et al. 160 synthesised evidence about the effectiveness, cost-effectiveness, barriers to/facilitators of provision, and current policy guidelines relating to paediatric wheelchair provision; Livingstone and Field10,11 synthesised evidence about the impact of paediatric powered mobility use10 and child/family user experiences. 11 No Cochrane reviews have been published in this area of research. Across the previous syntheses, it was consistently reported that powered mobility for children with mobility limitations may promote a range of beneficial outcomes, such as child-initiated movement, independent movement, social interaction, engagement in meaningful experiences and play, developmental attainment, reduced need for caregiver assistance and reduced parental stress. These effects have been found in younger children as well as in older children, and are, in turn, believed to affect the attainment of development milestones in early childhood and longer-term development. 22 However, the supporting evidence for these outcomes is often underpowered or of limited quality.
Although the existing syntheses offer a comprehensive picture of the literature at completion, they are limited in that they are now out of date. Furthermore, none of these syntheses attempted to explore the incremental benefits and costs of providing powered mobility for very young children, compared with later provision, and none summarised the evidence in the form of a causal, intervention-focused logic model that could be used to guide NHS planning and provision. In this respect, this study has numerous strengths over the previous syntheses, not least because the scope of this synthesis was broader and focused specifically on examining early powered mobility. However, one key issue is that we are still no closer to understanding the incremental benefits and costs of early powered mobility compared with later provision, because of the distinct lack of appropriate evidence. That being said, we now have a better understanding of the impact of age on a child’s potential to benefit from powered mobility, and the likely arbitrariness of using the age of 5 years as a strict criterion for powered mobility provision.
This topic was prioritised by the users and providers of children’s neurodisability services. Specifically, two of the 10 key questions prioritised in the recent James Lind Alliance Priority Setting Partnership for childhood neurodisability were as follows:7
Does appropriate provision of wheelchairs to enable independent mobility for very young children improve their self-efficacy? [Question 1.]
Does the timing and intensity of therapies . . . alter the effectiveness of therapies for infants and young children with neurodisability, including those without specific diagnosis? What is the appropriate age of onset/strategies/dosage/direction of therapy interventions? [Question 4.]
Morris et al. 8
Although we have not been able to directly answer these questions because of the lack of conclusive evidence, we believe that the synthesised findings provide new insights into the topics posed by these questions, and we now have a clearer picture of how best to focus future research.
Meaning of the study
The evidence supported two key, distinct ways of conceptualising the primary powered mobility outcome, movement and mobility. The first was ‘movement for movement’s sake’ (e.g. play, exploring, acting on the environment, autonomy, misbehaving, cognition and learning). This is relevant to all children, regardless of physical or cognitive ability, and appears to be the primary function of adapted ride-on cars and starter powered mobility devices. In this, two further outcome chains are implied: (1) developmental benefits achieved through movement and (2) preparing children for becoming powered wheelchair users. Of these, the former is relevant to all children, whereas the latter can be difficult to prospectively judge in terms of which children this applies to.
The second was destination-focused mobility (i.e. getting from A to B, a key mechanism of participating at home, in education, in the community). This is essentially the conceptualised purpose of adult powered wheelchairs, and, although our review did find evidence of the importance of this dimension for children, this was only one of the two dimensions, and not always the most important one, especially for the very youngest children. These two conceptualisations of powered mobility outcomes suggest that the provision of early powered mobility should not be considered through the same framework as provision of adult powered mobility, nor should it be treated as a stepping stone to powered wheelchair use. Instead, a key criterion for provision should include the potential of powered mobility to enable a child to move – for movement for movement’s sake or for a child to go from A to B – to promote a child’s development, play, exploration and independence.
We further conclude from this review that age-based provision is not the key factor in paediatric powered mobility provision. What appears to be coming from the evidence is that there are few data to support the restriction of powered mobility provision by age. Instead, the focus should be on providing powered mobility interventions in a developmentally appropriate manner, and focusing on ‘movement for movement’s sake’ in the first instance and establishing good ‘fit’ between the child, their powered mobility device and the social/physical environment they inhabit. Therefore, comparing powered mobility effectiveness and cost-effectiveness before and after the age of 5 years may not be informative, as these interventions are likely to have different aims, purposes and conceptualisations. Furthermore, this is not simply a case of age appropriateness, as the focus should be on developmental appropriateness, regardless of age, because of the wide variation in the needs of children who use powered mobility.
In the context of NHS expenditure, it is apparent that significantly increasing the provision of powered mobility would, relatively speaking, not be a major economic expense. If we think of powered mobility interventions like orphan drugs (as they are relatively high cost and for a small population), we can see that powered mobility is a comparatively inexpensive way of improving long-term outcomes for children with disabilities. We believe that the number of children in England aged < 5 years who are likely to benefit from powered mobility in any year could be as high as 7000, for an intervention costing the NHS < £5000 per child.
Unanswered questions and future research
The two key unanswered questions are whether or not early powered mobility is more cost-effective than powered mobility from the age of 5 years on, and what the optimal age is at which to provide powered mobility. In terms of unanswered questions and future research, four main conclusions could be drawn. First, there is unlikely to be equipoise about the impact of powered mobility on movement and mobility in any age group, and benefits of a formal large-scale evaluation are likely to be limited. Second, powered mobility training is a potentially expensive component of this intervention, which could be provided more formally by the NHS and for which there seems to be a genuine equipoise. Although we were not able to identify one established training intervention protocol in the literature, there was evidence of emerging stability of key components and tailoring to specific populations (e.g. children with cognitive impairments), which could be built on with a view to a formal evaluation of cost-effectiveness of different training protocols. In this, no formal training may be a control group option, especially for children without cognitive impairments. Third, there is currently limited published large-scale evidence of the impact of powered mobility on all outcomes (including safety outcomes) other than movement and mobility. This is regardless of the children’s age. Non-randomised designs could be considered for evaluating these impacts to enable parents, commissioners and providers to better understand the consequences of the intervention. The findings from the present review provide a framework for outcomes that such an evaluation may consider. Fourth, optimising powered mobility use and impact is likely to require a good fit between a child, their powered mobility equipment, and the wider context. To date, investigations of, and interventions for targeting, the context have so far been very limited, and further research to specifically investigate the fit could greatly enhance the impact of powered mobility interventions.
Broadly, priorities for future research should focus on:
-
developing, implementing, evaluating and comparing different protocols, programmes and training packages for introducing and implementing early powered mobility at home, in education, in the community and so on
-
evaluating different delivery models and care pathways for early powered mobility, including the most efficient way to commission/deliver early powered mobility in UK health systems, taking into account personalised wheelchair budgets and the different organisations and sectors involved in provision
-
developing detailed and age-related national data sets on the provision/uptake of mobility equipment and related adaptations
-
examining different conceptualisations of mobility and movement, in particular the concept of ‘movement for movement’s sake’, and the potential benefits of structuring early powered mobility provision around this concept
-
identifying and quantifying the developmental benefits brought about by early powered mobility and independent mobility in early childhood
-
examining the long-term health, psychosocial, developmental and economic benefits of early powered mobility.
Collection and availability of such information will be essential for future work in this area, particularly with regard to establishing the effectiveness and cost-effectiveness of early powered mobility.
Conclusion and recommendations
Provision of independent mobility options, including powered mobility, should start as early as is feasible, and interventions should be tailored to each child’s current and future developmental and cognitive abilities. The relationship between a child’s abilities, impairments and potential to benefit from powered mobility may not be apparent until after powered mobility has been introduced. Therefore, the use of strict age- and skill-related eligibility criteria for powered mobility may exclude children who may otherwise have benefited from early powered mobility. Early powered mobility interventions should be developmentally appropriate and focus on ‘movement for movement’s sake’ in the first instance. Therefore, comparing powered mobility before and after the age of 5 years may be of little benefit, as these interventions are likely to have different aims, purposes and conceptualisations. Likewise, the use of the age of 5 years as a comparative cut-off point appears to be of limited benefit because of the wide variance in the needs and abilities of young children with mobility limitations. The physical and social environment around a child is also an important factor in achieving the best ‘fit’ between a child and powered mobility, and should be explicitly optimised as part of any powered mobility intervention.
Acknowledgements
We would like to acknowledge Dr Llinos Haf Spencer, who supported the conduct of the qualitative thematic synthesis, and Lucy Barker (interdisciplinary artist and creative producer), who jointly led the stakeholder involvement activities related to young people’s engagement with the project and findings (https://lucy-barker.co.uk/about/; accessed 8 August 2020).
We would like to acknowledge the support of AniMates, a group of young people, artists, and researchers who make artwork about research projects. AniMates members have experience of living with disability or supporting people who live with disability. They helped to interpret the study findings and create artwork to support dissemination (www.facebook.com/animatesleeds; accessed 8 August 2020).
We would like to acknowledge the support we received from the members of the project advisory group: Dr Tim Adlam, Ms Amanda Allard, Ms Rae Baines, Dr Johan Borg, Ms Catharine Brown, Dr Sarah Crombie, Mr Lambert Felix, Professor James C (Cole) Galloway, Dr Jenny Gibson, Dr Rosie Gowran, Mr Simon Halsey, Professor Nigel Harris, Ms Susan Hillman, Ms Claire Holdcroft, Ms Amanda Hopkin, Ms Krys Jarvis, Ms Maria Kemeys, Dr Lisa Kenyon, Ms Roslyn Livingstone, Dr Sam Logan, Dr Jane Mischenko, Dr Chris Morris, Dr Lisbeth Nilsson, Mr Alex Ball, Ms Lisa Bazin, Ms Liz Golborne, Dr Karen Rispin, Ms Lauren Rosen, Ms Sarah Vines and Ms Sarah Wallace. See Appendix 1 for further details.
A number of organisations and manufacturers provided assistance in identifying information relevant to the economic analysis:
-
Ruth Everard, DragonMobility Ltd
-
Roy Wild and colleagues, Go Kids Go!
-
Invacare Ltd
-
Paula Jackson and colleagues, Leeds Wheelchair Centre
-
Sophia Nunn, Motability UK
-
Nicky Ellis, North East Essex Wheelchair Service
-
Kate El Bizanti, Queen Elizabeth’s Foundation for Disabled People
-
Dr Sally Payne, Royal College of Occupational Therapists
-
Sophie Thomson, William Merritt Disabled Living Centre.
Current approved protocol version: 1.1 (PROSPERO ID: CRD42018096449).
Contributions of authors
Nathan Bray (https://orcid.org/0000-0001-7646-5435) (Lecturer in Healthcare Improvement) was the chief investigator, led the qualitative thematic synthesis and contributed to the economic analysis.
Niina Kolehmainen (https://orcid.org/0000-0002-9229-9913) (Senior Clinical Lecturer and Honorary Consultant Allied Health Professional) was a co-applicant and led the conduct of the systematic reviews and mixed-methods framework synthesis.
Jennifer McAnuff (https://orcid.org/0000-0002-1636-0049) (Research Fellow) was a co-applicant, jointly led stakeholder involvement activities and supported the conduct of the systematic reviews and mixed-methods framework synthesis.
Louise Tanner (https://orcid.org/0000-0003-2340-8677) (Research Associate) supported the conduct of the systematic reviews and mixed-methods framework synthesis.
Lorna Tuersley (https://orcid.org/0000-0003-1780-258X) (Research Programme Support Officer) led the economic analysis.
Fiona Beyer (https://orcid.org/0000-0002-6396-3467) (Senior Research Associate) supported the conduct of the systematic reviews and mixed-methods framework synthesis.
Aimee Grayston (https://orcid.org/0000-0001-6820-7727) (Service User Co-investigator and student) was a co-applicant, and contributed experiential knowledge that guided the study design, conduct and dissemination.
Dor Wilson (https://orcid.org/0000-0002-3034-001X) (Research Associate) supported the conduct of the systematic reviews.
Rhiannon Tudor Edwards (https://orcid.org/0000-0003-4748-5730) (Professor of Health Economics and Co-Director of the Centre for Health Economics and Medicines Evaluation) was a co-applicant and oversaw and contributed to the economic analysis.
Jane Noyes (https://orcid.org/0000-0003-4238-5984) (Professor of Health and Social Services Research and Child Health) was a co-applicant and oversaw and contributed to the qualitative thematic synthesis.
Dawn Craig (https://orcid.org/0000-0002-5808-0096) (Professor of Practice in Evidence Synthesis) was a co-applicant and oversaw and contributed to the economic analysis and mixed-methods framework synthesis.
All authors contributed to the conduct of the overall project, interpretation of findings and to drafting, revising and approving the final report. All co-applicants were involved in conceiving and designing the project.
Data-sharing statement
This is an evidence synthesis project; therefore, no new data were generated. Further information can be obtained from the corresponding author.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HTA programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HTA programme or the Department of Health and Social Care.
References
- Department for Work and Pensions . Family Resources Survey: Financial Year 2017 18 n.d. www.gov.uk/government/statistics/family-resources-survey-financial-year-201718 (accessed 28 October 2019).
- Novak I, McIntyre S, Morgan C, Campbell L, Dark L, Morton N, et al. A systematic review of interventions for children with cerebral palsy: state of the evidence. Dev Med Child Neurol 2013;55:885-910. https://doi.org/10.1111/dmcn.12246.
- Scianni A, Butler JM, Ada L, Teixeira-Salmela LF. Muscle strengthening is not effective in children and adolescents with cerebral palsy: a systematic review. Aust J Physiother 2009;55:81-7. https://doi.org/10.1016/S0004-9514(09)70037-6.
- McPherson AC, Keith R, Swift JA. Obesity prevention for children with physical disabilities: a scoping review of physical activity and nutrition interventions. Disabil Rehabil 2014;36:1573-87. https://doi.org/10.3109/09638288.2013.863391.
- Tatla SK, Sauve K, Virji-Babul N, Holsti L, Butler C, Van Der Loos HF. Evidence for outcomes of motivational rehabilitation interventions for children and adolescents with cerebral palsy: an American Academy for Cerebral Palsy and Developmental Medicine systematic review. Dev Med Child Neurol 2013;55:593-601. https://doi.org/10.1111/dmcn.12147.
- Barton EE, Reichow B, Schnitz A, Smith IC, Sherlock D. A systematic review of sensory-based treatments for children with disabilities. Res Dev Disabil 2015;37:64-80. https://doi.org/10.1016/j.ridd.2014.11.006.
- Morris C, Simkiss D, Busk M, Morris M, Allard A, Denness J, et al. Setting research priorities to improve the health of children and young people with neurodisability: a British Academy of Childhood Disability-James Lind Alliance Research Priority Setting Partnership. BMJ Open 2015;5. https://doi.org/10.1136/bmjopen-2014-006233.
- Morris C, Janssens A, Allard A, Thompson Coon J, Shilling V, Tomlinson R. Informing the NHS Outcomes Framework: what outcomes of NHS care should be measured for children with neurodisability?. Health Serv Deliv Res 2014;2. https://doi.org/10.3310/hsdr02150.
- Uchiyama I, Anderson DI, Campos JJ, Witherington D, Frankel CB, Lejeune L, et al. Locomotor experience affects self and emotion. Dev Psychol 2008;44:1225-31. https://doi.org/10.1037/a0013224.
- Livingstone R, Field D. Systematic review of power mobility outcomes for infants, children and adolescents with mobility limitations. Clin Rehabil 2014;28:954-64. https://doi.org/10.1177/0269215514531262.
- Livingstone R, Field D. The child and family experience of power mobility: a qualitative synthesis. Dev Med Child Neurol 2015;57:317-27. https://doi.org/10.1111/dmcn.12633.
- Deitz J, Swinth Y, White O. Powered mobility and preschoolers with complex developmental delays. Am J Occup Ther 2002;56:86-9. https://doi.org/10.5014/ajot.56.1.86.
- Jones MA, McEwen IR, Hansen L. Use of power mobility for a young child with spinal muscular atrophy. Phys Ther 2003;83:253-62. https://doi.org/10.1093/ptj/83.3.253.
- Jones MA, McEwen IR, Neas BR. Effects of power wheelchairs on the development and function of young children with severe motor impairments. Pediatr Phys Ther 2012;24:131-40. https://doi.org/10.1097/PEP.0b013e31824c5fdc.
- Tefft D, Guerette P, Furumasu J. The impact of early powered mobility on parental stress, negative emotions, and family social interactions. Phys Occup Ther Pediatr 2011;31:4-15. https://doi.org/10.3109/01942638.2010.529005.
- Tefft D, Guerette P, Furumasu J. Cognitive predictors of young children’s readiness for powered mobility. Dev Med Child Neurol 1999;41:665-70. https://doi.org/10.1017/s0012162299001371.
- Huang HH, Ragonesi CB, Stoner T, Peffley T, Galloway JC. Modified toy cars for mobility and socialization: case report of a child with cerebral palsy. Pediatr Phys Ther 2014;26:76-84. https://doi.org/10.1097/PEP.0000000000000001.
- NHS Digital . Wheelchair Services: Operational Data Collection – Quarter 1 Dataset (April–June 2018) n.d. www.england.nhs.uk/publication/wheelchair-services-operational-data-collection-quarter-1-dataset-april-june-2018/ (accessed 28 October 2019).
- Edwards R, Bryning L, Lloyd-Williams H. Exploring the case for investing in early years in Wales: a broad evidence review. Lancet 2016;388. https://doi.org/10.1016/S0140-6736(16)32283-8.
- Anderson LM, Petticrew M, Rehfuess E, Armstrong R, Ueffing E, Baker P, et al. Using logic models to capture complexity in systematic reviews. Res Synth Methods 2011;2:33-42. https://doi.org/10.1002/jrsm.32.
- Kneale D, Thomas J, Harris K. Developing and optimising the use of logic models in systematic reviews: exploring practice and good practice in the use of programme theory in reviews. PLOS ONE 2015;10. https://doi.org/10.1371/journal.pone.0142187.
- Logan SW, Schreiber M, Lobo M, Pritchard B, George L, Galloway JC. Real-world performance: physical activity, play, and object-related behaviors of toddlers with and without disabilities. Pediatr Phys Ther 2015;27:433-41. https://doi.org/10.1097/PEP.0000000000000181.
- Bottos M, Bolcati C, Sciuto L, Ruggeri C, Feliciangeli A. Powered wheelchairs and independence in young children with tetraplegia. Dev Med Child Neurol 2001;43:769-77. https://doi.org/10.1017/s0012162201001402.
- Furumasu J, Tefft D, Guerette P. The Impact of Early Powered Mobility on Young Children’s Play and Psychosocial Skills n.d.
- World Health Organization . International Classification of Functioning, Disability and Health (ICF) 2001.
- Stein RE, Jessop DJ. A noncategorical approach to chronic childhood illness. Public Health Rep 1982;97:354-62.
- Varni JW, Seid M, Rode CA. The PedsQL™: measurement model for the pediatric quality of life inventory. Med Care 1999;37:126-39. https://doi.org/10.1097/00005650-199902000-00003.
- NIHR INVOLVE . Welcome to INVOLVE 2019. www.invo.org.uk/ (accessed 30 October 2019).
- Hayes H, Buckland S, Tarpey M. Briefing Notes for Researchers: Public Involvement in NHS, Public Health and Social Care Research 2012. www.invo.org.uk/wp-content/uploads/2014/11/9938_INVOLVE_Briefing_Notes_WEB.pdf (accessed 30 October 2019).
- Gov.uk . National Minimum Wage and National Living Wage Rates 2019. www.gov.uk/national-minimum-wage-rates (accessed 30 October 2019).
- Centre for Reviews and Dissemination . Systematic Reviews – CRD’s Guidance for Undertaking Systematic Reviews in Healthcare 2009.
- Bray N, Beyer FR, Craig D, Grayston A, Tudor-Edwards R, McAnuff J, et al. Early Mobility and POwered Wheelchair Evidence Review (EMPoWER): Cost-Effectiveness of Earlier Provision of Powered Mobility Interventions for Children With Mobility Limitations; A Systematic Review 2018. www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=96449 (accessed 30 October 2019).
- Hong QN, Pluye P, Bujold M, Wassef M. Convergent and sequential synthesis designs: implications for conducting and reporting systematic reviews of qualitative and quantitative evidence. Syst Rev 2017;6. https://doi.org/10.1186/s13643-017-0454-2.
- Brunton G, Thomas J, O’Mara-Eves A, Jamal F, Oliver S, Kavanagh J. Narratives of community engagement: a systematic review-derived conceptual framework for public health interventions. BMC Public Health 2017;17. https://doi.org/10.1186/s12889-017-4958-4.
- Lewin S, Glenton C, Munthe-Kaas H, Carlsen B, Colvin CJ, Gülmezoglu M, et al. Using qualitative evidence in decision making for health and social interventions: an approach to assess confidence in findings from qualitative evidence syntheses (GRADE-CERQual). PLOS Med 2015;12. https://doi.org/10.1371/journal.pmed.1001895.
- Kolobe THA, Fagg AH. Robot reinforcement and error-based movement learning in infants with and without cerebral palsy. Phys Ther 2019;99:677-88. https://doi.org/10.1093/ptj/pzz043.
- Vorster N, Evans K, Murphy N, Kava M, Cairns A, Clarke D, et al. Powered standing wheelchairs promote independence, health and community involvement in adolescents with Duchenne muscular dystrophy. Neuromuscul Disord 2019;29:221-30. https://doi.org/10.1016/j.nmd.2019.01.010.
- Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev 2016;5. https://doi.org/10.1186/s13643-016-0384-4.
- Seo HJ, Kim SY, Lee YJ, Jang BH, Park JE, Sheen SS, et al. A newly developed tool for classifying study designs in systematic reviews of interventions and exposures showed substantial reliability and validity. J Clin Epidemiol 2016;70:200-5. https://doi.org/10.1016/j.jclinepi.2015.09.013.
- Hartling L, Bond K, Santaguida PL, Viswanathan M, Dryden DM. Testing a tool for the classification of study designs in systematic reviews of interventions and exposures showed moderate reliability and low accuracy. J Clin Epidemiol 2011;64:861-71. https://doi.org/10.1016/j.jclinepi.2011.01.010.
- Viswanathan M, Berkman ND, Dryden DM, Hartling L. Assessing Risk of Bias and confounding in Observational Studies of Interventions or Exposures: Further Development of the RTI Item Bank. Rockville, MD: Agency for Healthcare Research and Quality; 2013.
- Higgins JPT, Savović J, Page MJ, Elbers RG, Sterne JAC, Higgins JPT, et al. Cochrane Handbook for Systematic Reviews of Interventions. London: The Cochrane Collaboration; 2019.
- Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016;355. https://doi.org/10.1136/bmj.i4919.
- Critical Appraisal Skills Programme . CASP Checklists 2018. https://casp-uk.net/casp-tools-checklists/ (accessed 22 May 2018).
- Noyes J, Booth A, Flemming K, Garside R, Harden A, Lewin S, et al. Cochrane Qualitative and Implementation Methods Group guidance series – paper 3: methods for assessing methodological limitations, data extraction and synthesis, and confidence in synthesized qualitative findings. J Clin Epidemiol 2018;97:49-58. https://doi.org/10.1016/j.jclinepi.2017.06.020.
- Pace R, Pluye P, Bartlett G, Macaulay AC, Salsberg J, Jagosh J, et al. Testing the reliability and efficiency of the pilot Mixed Methods Appraisal Tool (MMAT) for systematic mixed studies review. Int J Nurs Stud 2012;49:47-53. https://doi.org/10.1016/j.ijnurstu.2011.07.002.
- Hoffmann TC, Glasziou PP, Boutron I, Milne R, Perera R, Moher D, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014;348. https://doi.org/10.1136/bmj.g1687.
- McKenzie JE, Brennan SE, Higgins JPT, Thomas J, Chandler J, Cumpston M, et al. Cochrane Handbook for Systematic Reviews of Interventions. London: The Cochrane Collaboration; 2019.
- Teddlie C, Tashakkori A. Foundations of Mixed Methods Research: Integrating Quantitative and Qualitative Approaches in the Social and Behavioral Sciences. Thousand Oaks, CA: SAGE Publications, Inc.; 2009.
- Richie J, Spencer L, Bryman A, Burgess RG. Analyzing Qualitative Data. London: Routledge; 1994.
- Ogilvie D, Fayter D, Petticrew M, Sowden A, Thomas S, Whitehead M, et al. The harvest plot: a method for synthesising evidence about the differential effects of interventions. BMC Med Res Methodol 2008;8. https://doi.org/10.1186/1471-2288-8-8.
- Schünemann H, Brożek J, Guyatt G, Oxman Andrew D. Handbook for Grading the Quality of Evidence and the Strength of Recommendations Using the GRADE Approach. Updated October 2013 n.d. https://gdt.gradepro.org/app/handbook/handbook.html (accessed 26 February 2020).
- Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol 2008;8. https://doi.org/10.1186/1471-2288-8-45.
- Inman DP, Loge K, Cram A, Peterson M. Learning to drive a wheelchair in virtual reality. J Spec Educ Technol 2011;26:21-34. https://doi.org/10.1177/016264341102600303.
- Bamer AM, Connell FA, Dudgeon BJ, Johnson KL. Frequency of purchase and associated costs of assistive technology for Washington State Medicaid program enrollees with spina bifida by age. Disabil Health J 2010;3:155-61. https://doi.org/10.1016/j.dhjo.2009.10.009.
- University of Delaware . GoBabyGo! 2019. https://sites.udel.edu/gobabygo/ (accessed 30 October 2019).
- Galloway JC, Ryu JC, Agrawal SK. Babies driving robots: self-generated mobility in very young infants. Intell Serv Robot 2008;1:123-34. https://doi.org/10.1007/s11370-007-0011-2.
- Pritchard-Wiart L, Bragg E, Thompson-Hodgetts S. The Young Movers Project: a case series describing modified toy car use as an early movement option for young children with mobility limitations. Phys Occup Ther Pediatr 2019;39:598-613. https://doi.org/10.1080/01942638.2019.1585403.
- Evans S, Neophytou C, de Souza L, Frank AO. Young people’s experiences using electric powered indoor–outdoor wheelchairs (EPIOCs): potential for enhancing users’ development?. Disabil Rehabil 2007;29:1281-94. https://doi.org/10.1080/09638280600964406.
- Feldner HA, Logan SW, Galloway JC. Mobility in pictures: a participatory photovoice narrative study exploring powered mobility provision for children and families. Disabil Rehabil Assist Technol 2019;14:301-11. https://doi.org/10.1080/17483107.2018.1447606.
- Kenyon LK, Mortenson WB, Miller WC. ‘Power in Mobility’: parent and therapist perspectives of the experiences of children learning to use powered mobility. Dev Med Child Neurol 2018;60:1012-17. https://doi.org/10.1111/dmcn.13906.
- Evans N, Baines R. Trends, goals and outcomes for children and families using early powered mobility in a charitable loan scheme. J Enabling Technol 2017;11:138-47. https://doi.org/10.1108/JET-08-2017-0032.
- Agrawal SK, Kang J, Chen X, Kim MJ, Lee Y, Kong SW, et al. Robot-enhanced mobility training of children with cerebral palsy: short-term and long-term pilot studies. IEEE Syst J 2016;10:1098-106. https://doi.org/10.1109/JSYST.2014.2368455.
- Chen X, Ragonesi C, Galloway JC, Agrawal SK. Training toddlers seated on mobile robots to drive indoors amidst obstacles. IEEE Trans Neural Syst Rehabil Eng 2011;19:271-9. https://doi.org/10.1109/TNSRE.2011.2114370.
- Hasdai A, Jessel AS, Weiss PL. Use of a computer simulator for training children with disabilities in the operation of a powered wheelchair. Am J Occup Ther 1998;52:215-20. https://doi.org/10.5014/ajot.52.3.215.
- Lynch A, Ryu JC, Agrawal S, Galloway JC. Power mobility training for a 7-month-old infant with spina bifida. Pediatr Phys Ther 2009;21:362-8. https://doi.org/10.1097/PEP.0b013e3181bfae4c.
- Marchal-Crespo L, Furumasu J, Reinkensmeyer DJ. A robotic wheelchair trainer: design overview and a feasibility study. J Neuroeng Rehabil 2010;7. https://doi.org/10.1186/1743-0003-7-40.
- McCourt E, Casey J. Electrically powered indoor/outdoor chair performance for children aged 7 to 9 years. Br J Occup Ther 2016;79:584-90. https://doi.org/10.1177/0308022616636405.
- McGarry S, Moir L, Girdler S. The Smart Wheelchair: is it an appropriate mobility training tool for children with physical disabilities?. Disabil Rehabil Assist Technol 2012;7:372-80. https://doi.org/10.3109/17483107.2011.637283.
- Morère Y, Bourhis G, Cosnuau K, Guilmois G, Rumilly E, Blangy E. ViEW: a wheelchair simulator for driving analysis [published online ahead of print August 7 2018]. Assist Technol 2018. https://doi.org/10.1080/10400435.2018.1503204.
- Torkia C, Ryan SE, Reid D, Boissy P, Lemay M, Routhier F, et al. Virtual community centre for power wheelchair training: experience of children and clinicians. Disabil Rehabil Assist Technol 2019;14:46-55. https://doi.org/10.1080/17483107.2017.1392622.
- Ragonesi CB, Galloway JC. Short-term, early intensive power mobility training: case report of an infant at risk for cerebral palsy. Pediatr Phys Ther 2012;24:141-8. https://doi.org/10.1097/PEP.0b013e31824c764b.
- Nilsson L, Nyberg P, Eklund M. Training characteristics important for growing consciousness of joystick-use in people with profound cognitive disabilities. Int J Ther Rehabil 2010;17:588-95. https://doi.org/10.12968/ijtr.2010.17.11.79539.
- Nilsson LM, Nyberg PJ. Driving to learn: a new concept for training children with profound cognitive disabilities in a powered wheelchair. Am J Occup Ther 2003;57:229-33. https://doi.org/10.5014/ajot.57.2.229.
- Kenyon LK, Farris JP, Aldrich NJ, Rhodes S. Does power mobility training impact a child’s mastery motivation and spectrum of EEG activity? An exploratory project. Disabil Rehabil Assist Technol 2018;13:665-73. https://doi.org/10.1080/17483107.2017.1369587.
- Kenyon LK, Farris J, Brockway K, Hannum N, Proctor K. Promoting self-exploration and function through an individualized power mobility training program. Pediatr Phys Ther 2015;27:200-6. https://doi.org/10.1097/PEP.0000000000000129.
- Huang HH, Chen CL. The use of modified ride-on cars to maximize mobility and improve socialization – a group design. Res Dev Disabil 2017;61:172-80. https://doi.org/10.1016/j.ridd.2017.01.002.
- Huang HH, Chen YM, Huang HW. Ride-on car training for behavioral changes in mobility and socialization among young children with disabilities. Pediatr Phys Ther 2017;29:207-13. https://doi.org/10.1097/PEP.0000000000000426.
- Huang HH, Chen YM, Huang HW, Shih MK, Hsieh YH, Chen CL. Modified ride-on cars and young children with disabilities: effects of combining mobility and social training. Front Pediatr 2017;5. https://doi.org/10.3389/fped.2017.00299.
- Huang HH, Huang HW, Chen YM, Hsieh YH, Shih MK, Chen CL. Modified ride-on cars and mastery motivation in young children with disabilities: effects of environmental modifications. Res Dev Disabil 2018;83:37-46. https://doi.org/10.1016/j.ridd.2018.08.001.
- Furumasu J, Guerette P, Tefft D. The development of a powered wheelchair mobility program for young children. Technol Disabil 1996;5:41-8. https://doi.org/10.3233/TAD-1996-5106.
- Zeng Q, Burdet E, Teo CL. Evaluation of a collaborative wheelchair system in cerebral palsy and traumatic brain injury users. Neurorehabil Neural Repair 2009;23:494-50. https://doi.org/10.1177/1545968308323692.
- Ragonesi CB, Chen X, Agrawal S, Galloway JC. Power mobility and socialization in preschool: follow-up case study of a child with cerebral palsy. Pediatr Phys Ther 2011;23:399-406. https://doi.org/10.1097/PEP.0b013e318235266a.
- Nicholson J, Bonsall M. Powered mobility for children under five years of age in England. Br J Occup Ther 2002;65:291-3. https://doi.org/10.1177/030802260206500608.
- Montesano L, Díaz M, Bhaskar S, Minguez J. Towards an intelligent wheelchair system for users with cerebral palsy. IEEE Trans Neural Syst Rehabil Eng 2010;18:193-202. https://doi.org/10.1109/TNSRE.2009.2039592.
- Kenyon LK, Farris JP, Gallagher C, Hammond L, Webster LM, Aldrich NJ. Power mobility training for young children with multiple, severe impairments: a case series. Phys Occup Ther Pediatr 2017;37:19-34. https://doi.org/10.3109/01942638.2015.1108380.
- Logan SW, Hospodar CM, Feldner HA, Huang HH, Galloway JC. Modified ride-on car use by young children with disabilities. Pediatr Phys Ther 2018;30:50-6. https://doi.org/10.1097/PEP.0000000000000468.
- Logan SW, Huang HH, Stahlin K, Galloway JC. Modified ride-on car for mobility and socialization: single-case study of an infant with Down syndrome. Pediatr Phys Ther 2014;26:418-26. https://doi.org/10.1097/PEP.0000000000000070.
- Butler C. Effects of powered mobility on self-initiated behaviors of very young children with locomotor disability. Dev Med Child Neurol 1986;28:325-32. https://doi.org/10.1111/j.1469-8749.1986.tb03881.x.
- Logan SW, Lobo MA, Feldner HA, Schreiber M, MacDonald M, Winden HN, et al. Power-Up: exploration and play in a novel modified ride-on car for standing. Pediatr Phys Ther 2017;29:30-7. https://doi.org/10.1097/PEP.0000000000000336.
- Odor J, Watson M. Learning Through Smart Wheelchairs: A Formative Evaluation of the Effective Use of the CALL Centre’s Smart Wheelchairs As Part of Children’s Emerging Mobility, Communication, Education, and Personal Development. Final Report 1994. www.callscotland.org.uk/Common-Assets/ckfinder/userfiles/files/Learning%20Through%20Smart%20Wheelchairs%20complete.pdf (accessed 6 July 2020).
- Stokes M, Cook E, Sanders C, Coker-Bolt P. The case for early power mobility: developmental outcomes for a toddler born with a rare neuromuscular disorder. Technol Special Interest Section Q 2014;24:1-3.
- Weinstein ML, Lloyd M, finch KA, Laszacs AD. Underappreciated challenges to pediatric powered mobility – ways to address them as illustrated by a case report. Assist Technol 2018;30:74-6. https://doi.org/10.1080/10400435.2016.1257520.
- Dennis CW, Stansfeld S, Larin HM. Effect of Providing Powered Mobility on Infants’ Social Behavior and Vocalization: Two Case Studies n.d.
- Paulsson K, Christoffersen M. Psychosocial Aspects of Technical Aids: How Does Independent Mobility Affect the Psychosocial and Intellectual Development of Children With Physical Disabilities? n.d.
- Ragonesi CB, Chen X, Agrawal S, Galloway JC. Power mobility and socialization in preschool: a case study of a child with cerebral palsy. Pediatr Phys Ther 2010;22:322-9. https://doi.org/10.1097/PEP.0b013e3181eab240.
- Ross SM, Catena M, Twardzik E, Hospodar C, Cook E, Ayyagari A, et al. Feasibility of a modified ride-on car intervention on play behaviors during an inclusive playgroup. Phys Occup Ther Pediatr 2018;38:493-509. https://doi.org/10.1080/01942638.2017.1400491.
- Sharma N, Morrison J. Don’t Push Me Around! Disabled Children’s Experiences of Wheelchair Services in the UK 2007. www.whizz-kidz.org.uk/uploads/general/Support_us/Trusts__statutory_and_lottery/dont_push_me_around_report.pdf (accessed 26 February 2020).
- Gudgeon S, Kirk S. Living with a powered wheelchair: exploring children’s and young people’s experiences. Disabil Rehabil Assist Technol 2015;10:118-25. https://doi.org/10.3109/17483107.2013.870609.
- Pituch E, Rushton PW, Ngo M, Heales J, Poulin Arguin A. Powerful or powerless? Children’s, parents’, and occupational therapists’ perceptions of powered mobility. Phys Occup Ther Pediatr 2018;39:1-16. https://doi.org/10.1080/01942638.2018.1496964.
- Sonday A, Gretschel P. Empowered to play: a case study describing the impact of powered mobility on the exploratory play of disabled children. Occup Ther Int 2016;23:11-8. https://doi.org/10.1002/oti.1395.
- Wiart L, Darrah J, Hollis V, Cook A, May L. Mothers’ perceptions of their children’s use of powered mobility. Phys Occup Ther Pediatr 2004;24:3-21. https://doi.org/10.1300/J006v24n04_02.
- Cerruti M, Biondi R. Timely insertion of electronic wheelchair in overall rehabilitation plan for cerebral palsy in young children: investigation on the opinion of parents. Sci Riabil 2010;12:14-23.
- Kornafel T, Tsao EY, Sabelhaus E, Surges L, Apkon SD. Physical and occupational therapy for a teenager with acute flaccid myelitis: a case report. Phys Occup Ther Pediatr 2017;37:485-59. https://doi.org/10.1080/01942638.2016.1255289.
- Currier BA, Jones MA, DeGrace BW. Experiences of families with young power wheelchair users. J Early Interv 2019;41:125-40. https://doi.org/10.1177/1053815118819204.
- Home AM, Ham R. Provision of powered mobility equipment to young children: the Whizz-Kidz experience. Int J Ther Rehabil 2003;10:511-7. https://doi.org/10.12968/bjtr.2003.10.11.13462.
- Kakimoto A, Suzuki S, Sekiguchi Y. Development of a cart for independent mobility assistance for non-ambulatory children. Conf Proc IEEE Eng Med Biol Soc n.d.;2009:7273-6. https://doi.org/10.1109/IEMBS.2009.5334838.
- Gehant BA. Evaluation of the CAPP cart. Artif Limbs 1971;15:16-24.
- Durkin J. Discovering powered mobility skills with children: ‘responsive partners’ in learning. Int J Ther Rehabil 2009;16:331-41. https://doi.org/10.12968/ijtr.2009.16.6.42436.
- Jonasson M. The AKKA-board – performing mobility, disability and innovation. Disabil Soc 2014;29:47-90. https://doi.org/10.1080/09687599.2013.823079.
- Mockler SR, McEwen IR, Jones MA. Retrospective analysis of predictors of proficient power mobility in young children with severe motor impairments. Arch Phys Med Rehabil 2017;98:2034-41. https://doi.org/10.1016/j.apmr.2017.05.028.
- Uyama S, Hanaki K. Current status of the utilization of powered wheelchair in preschool children with locomotive disability in Japan. Phys Ther Res 2016;19:13-2. https://doi.org/10.1298/ptr.E9888.
- Lovett S. Discrimination learning in multiply handicapped children using an electromechanical car. Adv Behav Res Ther 1988;10:39-52. https://doi.org/10.1016/0146-6402(88)90010-0.
- Omori K, Sugimoto Y, Kitayama I, Ohnabe H, Collins DM. Selected Papers from the Japanese Conference on the Advancement of Assistive and Rehabilitation Technology. Amsterdam: IOS Press; 2011.
- Douglas J, Ryan M. A preschool severely disabled boy and his powered wheelchair: a case study. Child Care Health Dev 1987;13:303-9. https://doi.org/10.1111/j.1365-2214.1987.tb00547.x.
- Feldner H. Impacts of early powered mobility provision on disability identity: a case study. Rehabil Psychol 2019;64:130-45. https://doi.org/10.1037/rep0000259.
- Nilsson L, Eklund M, Nyberg P, Thulesius H. Driving to learn in a powered wheelchair: the process of learning joystick use in people with profound cognitive disabilities. Am J Occup Ther 2011;65:652-60. https://doi.org/10.5014/ajot.2011.001750.
- Logan SW, Feldner HA, Galloway JC, Huang HH. Modified ride-on car use by children with complex medical needs. Pediatr Phys Ther 2016;28:100-7. https://doi.org/10.1097/PEP.0000000000000210.
- Zazula JL, Foulds RA. Mobility device for a child with phocomelia. Arch Phys Med Rehabil 1983;64:137-9.
- Ceres R, Pons JL, Calderon L, Jimenez AR, Azevedo L. A robotic vehicle for disabled children. IEEE Eng Med Biol Mag 2005;24:55-63. https://doi.org/10.1109/MEMB.2005.1549731.
- Logan SW, Catena MA, Sabet A, Hospodar CM, Yohn H, Govindan A, et al. Standing tall: feasibility of a modified ride-on car that encourages standing. Pediatr Phys Ther 2019;31:E6-E13. https://doi.org/10.1097/PEP.0000000000000568.
- Flodin E. Interactive design – the desire for autonomous upright mobility: a longitudinal case study. Technol Disabil 2007;19:213-24. https://doi.org/10.3233/TAD-2007-19407.
- Smania N, Gandolfi M, Marconi V, Calanca A, Geroin C, Piazza S, et al. Applicability of a new robotic walking aid in a patient with cerebral palsy. Eur J Phys Rehabil Med 2012;48:147-53.
- Guerette P, Furumasu J, Tefft D. The positive effects of early powered mobility on children’s psychosocial and play skills. Assist Technol 2013;25:39-50. https://doi.org/10.1080/10400435.2012.685824.
- Pope PM, Bowes CE, Booth E. Postural control in sitting the SAM system: evaluation of use over three years. Dev Med Child Neurol 1994;36:241-52. https://doi.org/10.1111/j.1469-8749.1994.tb11837.x.
- Butler C, Okamoto GA, McKay TM. Motorized wheelchair driving by disabled children. Arch Phys Med Rehabil 1984;65:95-7.
- Dunaway S, Montes J, O’Hagen J, Sproule DM, Vivo DC, Kaufmann P. Independent mobility after early introduction of a power wheelchair in spinal muscular atrophy. J Child Neurol 2013;28:576-82. https://doi.org/10.1177/0883073812449383.
- Schoepflin ZR, Chen X, Ragonesi CB, Galloway JC, Agrawal SK. Design of a novel mobility device controlled by the feet motion of a standing child: a feasibility study. Med Biol Eng Comput 2011;49:1225-31. https://doi.org/10.1007/s11517-011-0820-5.
- Larin HM, Dennis CW, Stansfield S. Development of robotic mobility for infants: rationale and outcomes. Physiotherapy 2012;98:230-7. https://doi.org/10.1016/j.physio.2012.06.005.
- Huhn K, Guarrera-Bowlby P, Deutsch JE. The clinical decision-making process of prescribing power mobility for a child with cerebral palsy. Pediatr Phys Ther 2007;19:254-60. https://doi.org/10.1097/PEP.0b013e31812c65cc.
- Frank AO, De Souza LH, Frank JL, Neophytou C. The pain experiences of powered wheelchair users. Disabil Rehabil 2012;34:770-8. https://doi.org/10.3109/09638288.2011.619620.
- Wiart L, Darrah J, Cook A, Hollis V, May L. Evaluation of powered mobility use in home and community environments. Phys Occup Ther Pediatr 2003;23:59-75. https://doi.org/10.1080/J006v23n02_05.
- Berry ET, McLaurin SE, Sparling JW. Parent/caregiver perspectives on the use of power wheelchairs. Pediatr Phys Ther 1996;8:146-50. https://doi.org/10.1097/00001577-199608040-00002.
- Cronin S. Exploring the Lived Experiences of Children With Specialised Wheelchair and Seating Needs from a Family Perspective 2012.
- Sullivan SD, Mauskopf JA, Augustovski F, Jaime Caro J, Lee KM, Minchin M, et al. Budget impact analysis-principles of good practice: report of the ISPOR 2012 Budget Impact Analysis Good Practice II Task Force. Value Health 2014;17:5-14. https://doi.org/10.1016/j.jval.2013.08.2291.
- Department for Work and Pensions . Family Resources Survey 2017 18 n.d. www.gov.uk/government/statistics/family-resources-survey-financial-year-201718 (accessed 30 October 2019).
- Motability . What Age Can I First Receive the Mobility Allowance? n.d. www.motability.org.uk/contact/faqs/what-age-can-i-receive-the-mobility-allowance (accessed 30 October 2019).
- Office for National Statistics . United Kingdom Population Mid-Year Estimate 2019. www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/timeseries/ukpop/pop (accessed 30 October 2019).
- NHS Digital . Wheelchair Services: Operational Data Collection – Quarter 4 Dataset 2017 18 (January–March 2018) n.d. www.england.nhs.uk/publication/wheelchair-services-operational-data-collection-quarter-4-dataset-2017-18-january-march-2018/ (accessed 30 October 2019).
- NHS Digital . Wheelchair Services: Operational Data Collection – Quarter 2 Dataset (July–September 2018) n.d. www.england.nhs.uk/publication/wheelchair-services-operational-data-collection-quarter-2-dataset-july-september-2018/ (accessed 30 October 2019).
- NHS Digital . Wheelchair Services: Operational Data Collection – Quarter 3 Dataset (October–December 2018) n.d. www.england.nhs.uk/publication/wheelchair-services-operational-data-collection-quarter-3-dataset-october-december-2018/ (accessed 30 October 2019).
- NHS Improvement . Reference Costs 2018. https://improvement.nhs.uk/resources/reference-costs/ (accessed 30 October 2019).
- Canadian Agency for Drugs and Technology in Health . Strings Attached: CADTH’s Database of Search Filters 2016. www.cadth.ca/resources/finding-evidence/strings-attached-cadths-database-search-filters (accessed 22 October 2018).
- Bank of England . Inflation Calculator 2019. www.bankofengland.co.uk/monetary-policy/inflation/inflation-calculator (accessed 30 October 2019).
- Designability . Wizzybug Loan Scheme: Information Sheet 2019. https://designability.org.uk/wp-content/uploads/2017/11/FRM-011-Wizzybug-Loan-Scheme-Information-Sheet-3.0-6th-November-2017.pdf (accessed 30 October 2019).
- MERU . Bugzi Loan Scheme – Bugzi Deposit 2019. https://meru.org.uk/product/bugzi-loan-scheme-bugzi-deposit/ (accessed 30 October 2019).
- NHS England . Personal Wheelchair Budgets 2019. www.england.nhs.uk/personal-health-budgets/personal-wheelchair-budgets/ (accessed 30 October 2019).
- Curtis L, Burns A. Unit Costs of Health and Social Care 2018 n.d. www.pssru.ac.uk/project-pages/unit-costs/unit-costs-2018/ (accessed 30 October 2019).
- NHS England . Developing a Wheelchair Tariff Pilot Programme 2016. www.england.nhs.uk/wp-content/uploads/2016/07/rep-deve-wheelchair-tariffs.pdf (accessed 30 October 2019).
- Dragonmobility . SnapDragon 2019. www.dragonmobility.com/snapdragon.php (accessed 30 October 2019).
- Bray N. More Than Mobility: Applying Health Economics to Wheelchair Interventions for Disabled Children 2016.
- NHS UK . How to Care for a Disabled Child 2019. www.nhs.uk/conditions/social-care-and-support-guide/caring-for-children-and-young-people/how-to-care-for-a-disabled-child/ (accessed 30 October 2019).
- Whizz-Kids . Wheelchair Skills Training 2019. www.whizz-kidz.org.uk/get-our-help/young-people/wheelchair-skills-training (accessed 30 October 2019).
- Go Kids Go! . Wheelchairs Skills Workshops 2019. https://go-kids-go.org.uk/go-kids-go-workshops.php (accessed 30 October 2019).
- Go Kids Go! . Report of the Trustees and Unaudited Financial Statements for the Year Ended 31 January 2018 for Go Kids Go! Association of Wheelchair Children 2018. https://go-kids-go.org.uk/PDFS/2018%20Accounts.pdf (accessed 30 October 2019).
- Equality and Human Rights Commission . Housing and Disabled People. A Toolkit for Local Authorities in England: Adaptations 2018. www.equalityhumanrights.com/sites/default/files/housing-and-disabled-people-local-authorities-toolkit-england-adaptations.pdf (accessed 30 October 2019).
- Motability . Charitable Grants 2019. www.motability.org.uk/grants/ (accessed 30 October 2019).
- Department for Education . Home to School Travel and Transport Guidance. Statutory Guidance for Local Authorities 2014. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/575323/Home_to_school_travel_and_transport_guidance.pdf (accessed 30 October 2019).
- Curtis L, Beecham J. A survey of local authorities and Home Improvement Agencies: identifying the hidden costs of providing a home adaptations service. Br J Occup Ther 2018;81:633-40. https://doi.org/10.1177/0308022618771534.
- Bray N, Noyes J, Edwards RT, Harris N. Wheelchair interventions, services and provision for disabled children: a mixed-method systematic review and conceptual framework. BMC Health Serv Res 2014;14. https://doi.org/10.1186/1472-6963-14-309.
- Staniszewska S, Brett J, Simera I, Seers K, Mockford C, Goodlad S, et al. GRIPP2 reporting checklists: tools to improve reporting of patient and public involvement in research. BMJ 2017;358. https://doi.org/10.1136/bmj.j3453.
- Creswell JW, Plano Clark VL, Gutmann ML, Hanson WE, Tashakkori A, Teddlie C. Handbook of Mixed Methods in Social and Behavioral Research. Thousand Oaks, CA: SAGE Publications, Inc.; 2003.
- Noyes J, Booth A, Moore G, Flemming K, Tunçalp Ö, Shakibazadeh E. Synthesising quantitative and qualitative evidence to inform guidelines on complex interventions: clarifying the purposes, designs and outlining some methods. BMJ Glob Health 2019;4. https://doi.org/10.1136/bmjgh-2018-000893.
- Heyvaert M, Hannes K, Onghena P. Using Mixed Methods Research Synthesis for Literature Reviews. Thousand Oaks, CA: SAGE Publications, Inc.; 2016.
- Fetters MD, Molina-Azorin JF. The Journal of Mixed Methods Research starts a new decade: the mixed methods research integration trilogy and its dimensions. J Mixed Methods Res 2017;11:291-307. https://doi.org/10.1177/1558689817714066.
- Movsisyan A, Dennis J, Rehfuess E, Grant S, Montgomery P. Rating the quality of a body of evidence on the effectiveness of health and social interventions: a systematic review and mapping of evidence domains. Res Synth Methods 2018;9:224-42. https://doi.org/10.1002/jrsm.1290.
- Johnson SD, Tilley N, Bowers KJ. Introducing EMMIE: an evidence rating scale to encourage mixed-method crime prevention synthesis reviews. J Exp Criminol 2015;11:459-73. https://doi.org/10.1007/s11292-015-9238-7.
- Cooper RA, Tolerico M, Kaminski BA, Spaeth D, Ding D, Cooper R. Quantifying wheelchair activity of children: a pilot study. Am J Phys Med Rehabil 2008;87:977-83. https://doi.org/10.1097/PHM.0b013e31818dfe74.
- Huang HH, Galloway JC. Modified ride-on toy cars for early power mobility: a technical report. Pediatr Phys Ther 2012;24:149-54. https://doi.org/10.1097/PEP.0b013e31824d73f9.
- Furumasu J. Powered mobility readiness: a case study. Directions 2015;6:42-6. https://nrrts.org/wp-content/uploads/2019/06/DIRECTIONS_2015.6_RehabCaseStudy.pdf (accessed 1 November 2019).
- Andrich R, Salatino C, Converti RM, Saruggia M. Cost-effectiveness of powered wheelchairs: findings of a study. Stud Health Technol Inform 2015;217:84-91.
- Barnard AM, Nelson NG, Xiang H, McKenzie LB. Pediatric mobility aid-related injuries treated in US emergency departments from 1991 to 2008. Pediatrics 2010;125:1200-7. https://doi.org/10.1542/peds.2009-3286.
- Bartonek A, Saraste H, Danielsson A. Health-related quality of life and ambulation in children with myelomeningocele in a Swedish population. Acta Paediatr 2012;101:953-6. https://doi.org/10.1111/j.1651-2227.2012.02742.x.
- Bloemen MA, Verschuren O, van Mechelen C, Borst HE, de Leeuw AJ, van der Hoef M, et al. Personal and environmental factors to consider when aiming to improve participation in physical activity in children with spina bifida: a qualitative study. BMC Neurol 2015;15. https://doi.org/10.1186/s12883-015-0265-9.
- Butler C. Measuring participation for children with mobility limitations: a modified Delphi survey for those who use power mobility. Dev Med Child Neurol 2015;57. https://doi.org/10.1111/dmcn.12648.
- Douglas J, Reeson B, Ryan M. Computer microtechnology for a severely disabled preschool child. Child Care Health Dev 1988;14:93-104. https://doi.org/10.1111/j.1365-2214.1988.tb00566.x.
- Ekiz T, Özbudak Demir S, Sümer HG, Özgirgin N. Wheelchair appropriateness in children with cerebral palsy: a single center experience. J Back Musculoskelet Rehabil 2017;30:825-8. https://doi.org/10.3233/BMR-150522.
- Field DA, Miller WC, Ryan SE, Jarus T, Abundo A. Measuring participation for children and youth with power mobility needs: a systematic review of potential health measurement tools. Arch Phys Med Rehabil 2016;97:462-77. https://doi.org/10.1016/j.apmr.2015.08.428.
- Sanders DA. Non-model-based control of a wheeled vehicle pulling two trailers to provide early powered mobility and driving experiences. IEEE Trans Neural Syst Rehabil Eng 2018;26:96-104. https://doi.org/10.1109/TNSRE.2017.2726443.
- Motability . Making a Difference: Information for Advisors and Professionals n.d. www.motability.org.uk/Motability_Professional_Guide.pdf (accessed 6 July 2020).
Appendix 1 List of project advisory group members
| Name | Position | Expertise | Department | Organisation |
|---|---|---|---|---|
| Dr Tim Adlam | Clinical Scientist, Associate Professor of Global Disability Innovation, Principal Engineer with Designability | Design, implementation and evaluation of early powered mobility in low- and middle-income countries | Global Disability Innovation Hub | University College London, London, UK |
| Ms Amanda Allard | Assistant Director for Health | Health policy implementation; children and young people’s involvement in decision-making | Not applicable | Council for Disabled Children, London, UK |
| Ms Rae Baines | Senior Children’s Occupational Therapist | Implementation of early powered mobility | Not applicable | Designability, Bath, UK |
| Dr Johan Borg | Postdoctoral Fellow | Equitable provision and outcomes of assistive technology; socioeconomic impacts of disability | School of Medicine and Global Health | Lund University, Lund, Sweden |
| Ms Catharine Brown | Chief Executive of Designability | Technical and strategic development and implementation of early powered mobility | Not applicable | Designability, Bath, UK |
| Dr Sarah Crombie | Professional Lead Physiotherapist | Implementation of powered mobility with children and young people of all ages | Chailey Heritage Clinical Services | Sussex Community NHS Trust, Brighton, UK |
| Mr Lambert Felix | Systematic Reviewer, Physiotherapist | Physiotherapy management of long-term conditions; rehabilitation medicine | Nuffield Department of Orthopaedics, Rheumatology and Musculoskeletal Sciences | University of Oxford, Oxford, UK |
| Professor James C (Cole) Galloway | Director of the Paediatric Mobility Laboratory and Design Studio, Physical Therapist | Design, implementation, and evaluation of early powered mobility; founder of the GoBabyGo programme operating in 70 locations worldwide | Department of Physical Therapy | University of Delaware, Newark, DE, USA |
| Dr Jenny Gibson | Lecturer in Psychology and Education, Speech and Language Therapist | Allied health interventions and early years development in the context of childhood disability | Faculty of Education | University of Cambridge, Cambridge, UK |
| Dr Rosie Gowran | Lecturer in Occupational Therapy | Development of sustainable wheelchair and seating assistive technology provision | School of Allied Health | University of Limerick, Limerick, Republic of Ireland |
| Mr Simon Halsey | Director | Technical, strategic and commercial development and implementation of early powered mobility | Not applicable | TinyTrax, Bristol, UK |
| Professor Nigel Harris | Director of Innovation and Growth | Technical and strategic development and implementation of early powered mobility | West of England Academic Health Science Network | Academic Health Science Network, Bristol, UK |
| Ms Susan Hillman | Head of Rehabilitation Engineering and Aids for Living, Clinical Scientist, Trustee of the Posture and Mobility Group | Implementation of powered mobility across the lifespan | Department of Rehabilitation Engineering and Aids for Living | Newcastle upon Tyne Hospitals NHS Foundation Trust, Newcastle upon Tyne, UK |
| Ms Claire Holdcroft | Outreach Worker, Occupational Therapist | Implementation of powered mobility with children and young people affected by spinal muscular atrophy | Not applicable | Spinal Muscular Atrophy UK, Stratford-upon-Avon, UK |
| Ms Amanda Hopkin | Case Manager, Occupational Therapist | Implementation of powered mobility with children and young people of all ages | Not applicable | Social Return, Durham, UK |
| Ms Krys Jarvis | Service Manager, Chairperson of the NHS National Wheelchair Managers’ Forum | Implementation of powered mobility across the lifespan | Shropshire Wheelchair and Posture Service | Shropshire Community Health NHS Trust, Shrewsbury, UK |
| Ms Maria Kemeys | Business Development Officer | Design and production of bespoke assistive technology for children and young people with mobility limitations | Cerebra Innovation Centre | Cerebra, Carmarthen, UK |
| Dr Lisa Kenyon | Associate Professor, Physical Therapist | Development, implementation, and evaluation of powered mobility | Department of Physical Therapy | Grand Valley State University, Allendale, MI, USA |
| Ms Roslyn Livingstone | Occupational Therapist, Clinical Instructor, Researcher | Development, implementation, and evaluation of early powered mobility | Faculty of Medicine | University of British Colombia, Vancouver, BC, Canada |
| Dr Sam Logan | Assistant Professor | Development, implementation, and evaluation of low-technology early powered mobility | College of Public Health and Human Sciences | Oregon State University, Corvallis, OR, USA |
| Dr Jane Mischenko | Lead Commissioner of Children and Maternity Services | NHS commissioning for children and young people with mobility limitations | Not applicable | NHS Leeds South and East Clinical Commissioning Group, Leeds, UK |
| Dr Chris Morris | Senior Research Fellow in Child Health | Identification, prioritisation and measurement of health outcomes in childhood neurodisability | Peninsula Cerebra Research Unit | University of Exeter, Exeter, UK |
| Dr Lisbeth Nilsson | Occupational Therapist, Researcher | Implementation of powered mobility for people with cognitive impairments across the lifespan | Not applicable | Driving to Learn, Lund, Sweden |
| Ms Lisa Bazin and Mr Alex Ball | Parents, founders of A Very Special Journey campaign | Lived experience of early powered mobility. Their 3-year-old son has spinal muscular atrophy (type 2) and received powered mobility aged 21 months | Not applicable | Not applicable (UK) |
| Liz Golborne | Parent | Lived experience of early powered mobility. Her 18-year-old daughter has cerebral palsy and complex communication needs, and received powered mobility aged ≈ 4 years | Not applicable | Not applicable (UK) |
| Dr Karen Rispin | Associate Professor of Biology | Implementation and evaluation of powered mobility in low-income countries | Department of Biology and Kinesiology | LeTourneau University, Longview, TX, US |
| Ms Lauren Rosen | Physiotherapist, Strategic Leader within RESNA | Implementation of early powered mobility, development of national guidance on powered mobility for children and young people | Motion Analysis Centre | St Joseph’s Children’s Hospital and University of South Florida, Tampa, FL, USA |
| Ms Sarah Vines | Head of Mobility Services | Implementation of early powered mobility | QEF Mobility Services | QEF, Leatherhead, UK |
| Ms Sarah Wallace | Senior Mobility Therapist, Occupational Therapist | Implementation of early powered mobility | North West Assistive Technology Team | Whizz-Kidz, London, UK |
Appendix 2 Reporting summary for patient, public and stakeholder involvement
We used the Guidance for Reporting Involvement of Patients and the Public 2 (GRIPP2) (short-form) reporting checklist161 to summarise reporting of patient, public and stakeholder involvement. Results are summarised as follows:
-
Report the aim of PPI in the study – reported in Chapter 3, Stakeholder involvement.
-
Provide a clear description of the methods used for PPI in the study – reported in Chapter 3, Stakeholder involvement.
-
Outcomes – report the results of PPI in the study, including both positive and negative outcomes: the aspects of the study to which parents and young people contributed are reported in Chapter 3, Stakeholder involvement, and throughout Chapter 4, Methods. There are no negative effects to report. We are not yet able to report the results of the young people’s involvement in dissemination, as these activities are currently under way.
-
Outcomes – comment on the extent to which PPI influenced the study overall. Describe positive and negative effects – reported in Chapter 8, Strengths and weaknesses, and Strengths and weaknesses in relation to other studies, and throughout Chapter 3, Stakeholder involvement, and Chapter 4, Methods. There are no negative effects to describe.
-
Comment critically on the study, reflecting on the things that went well and those that did not, so others can learn from this experience – we report the involvement of PPI positively throughout Chapter 3, Stakeholder involvement, Chapter 4, Methods, and Chapter 8, Strengths and weaknesses, and Strengths and weaknesses in relation to other studies; there are no negative effects to report. We anticipate being able to comment more critically on the involvement of the young person’s group in disseminating findings; however, this work is currently in progress and will primarily be undertaken following the publication of this report. We intend to include commentary on this aspect of the study in a future publication.
Appendix 3 Illustrative example of keywords and search strategy for review 1
MEDLINE (via Ovid)
Date range searched: 1946 to June 2018.
Date searched: June 2018; updated in October 2019.
Search strategy
-
wheelchair.mp. or exp Wheelchairs/
-
((power* or motoris* or assist*) adj5 (mobility* or locomotion or wheelchair* or pushchair* or buggy or equipment or scooter* or toy* or car)).mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms]
-
((independent* or ‘self directed’ or self* or autonomous or functional*) adj3 (mobil* or move* or limit* or mov* or walk* or crawl*)).ti,ab.
-
(child* or infant* or toddler or paediatric* or teen* or adolescen* or young adult* or youth* or juvenile* or young pe* or young men or young women).mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms]
-
1 or 2 or 3
-
4 and 5
-
limit 6 to (“newborn infant (birth to 1 month)” or “infant (1 to 23 months)” or “preschool child (2 to 5 years)” or “child (6 to 12 years)” or “adolescent (13 to 18 years)” or “young adult (19 to 24 years)”
Appendix 4 Rationale for the chosen approach to assessing the certainty in the body of evidence in the integrated mixed-methods evidence synthesis
Important general methodological considerations related to assessing certainty of a body of evidence in mixed-methods reviews
-
Mixed-methods reviews start with review questions that can be answered only through a combination of qualitative and quantitative information. A well-established principle of mixed-methods research is that mixed methods should be used only when the research question demands inclusion of both qualitative and quantitative data. 49,162 Therefore, from the outset, the assumption in mixed-methods reviews is that the relevant body of evidence needs to include both qualitative and quantitative information.
-
The principle of ‘mixing’ is key to the rigour and credibility of findings in mixed-methods reviews. That is, the straddling across the qualitative and quantitative, and bringing together methods and data from both (in contrast to conducting qualitative and quantitative research separately in a single study), underpins the methodological rigour and credibility of findings in mixed-methods studies, including mixed-methods reviews. To enable this, there is an abundance of published, converging literature on the principles to guide mixing. 49,163–165
-
The synthesis is a key stage of mixing. Considering the importance of mixing (see point 2), the synthesis stage that brings together qualitative and quantitative data is key to the production of mixed-methods review findings. Arguably, the most robust, credible findings are the combined, mixed findings that provide the most complete body of evidence relevant to the research question (keeping in mind that a mixed-methods review starts on the premise that the review question can be answered only by such mixed evidence; see point 1). Therefore, there is an argument that it is the combined, mixed findings that should be graded.
-
The stated meaning of assessing (or ‘grading’) the certainty of a body of evidence is based on the review question and methodology. The concept of assessing, or grading, the certainty of a body of evidence originally comes from systematic reviews of RCTs, which seek to answer questions about effectiveness of interventions on predefined outcomes. In that context, the established meaning of grading refers to the assessment of confidence in how close the effect estimate is to that of the true effect. 52 The desire to apply the concept of grading to qualitative questions and syntheses has subsequently resulted in an adoption of a revised meaning for qualitative reviews. In them, grading refers to an assessment of the extent to which a review finding is a reasonable representation of the phenomenon of interest. Both GRADE and GRADE-CERQual were designed for a decision-making process whereby quantitative and qualitative reviews are conducted separately and then their findings and assessments of certainty (quantitative) and confidence (qualitative) are presented together in an evidence to decision framework.
-
There are published, converging principles for assessing the certainty of the findings from mixed-methods studies, but no agreed meaning of grading a body of evidence. The published principles related to assessing certainty of the findings from mixed-methods studies focus on the quality of the method and data obtained, and the credibility of the inferences and interpretations resulting from mixing the qualitative and quantitative data. 49 For the purposes of grading certainty in mixed-methods reviews, we summarise these as ‘confidence that the identified concepts, variables and/or relationships are true’, where ‘true’ is understood through dimensions of validity.
-
There is a lack of grading tools for bodies of evidence in mixed-methods reviews. A recent review found that, of the 17 systems for rating bodies of evidence identified, only one was developed with mixed-methods reviews in mind,166 and that system167 focused on improving and rating the quality of the reviews themselves, rather than grading the evidence. To overcome this issue, many decision-making contexts conduct method-specific quantitative and qualitative reviews separately, and then bring the findings together in an evidence to decision framework. However, it can be argued that this reduces the benefit of using a mixed-methods approach, in which the integration and mixing are viewed as the fundamental strengths (see points 1 and 2).
-
There is no consensus on whether or not to grade bodies of evidence in reviews that are mixed methods from the outset and that aim to combine quantitative and qualitative evidence using a common rubric. In summary, in the present mixed-methods review, we acknowledged the various methodological considerations and challenges to grading bodies of evidence in reviews that are mixed methods from the outset, as opposed to method-specific reviews that are subsequently brought together. On balance, we felt that it was important to provide some summary indication of the level of support that the evidence from the current mixed-methods review (that was mixed from the outset) provides for each of the concepts identified, while stopping short of claiming that we applied a validated approach to do so. The following section describes the pragmatic approach that we used to make judgements about the level of support for the mixed-method findings.
Approach to assessing certainty of the body of evidence in the present mixed-methods review
We ultimately adopted a pragmatic approach to grading. We specifically came up with an initial typology of levels of support that the evidence provided for concepts identified in the mixed-methods framework synthesis. As a result, we have provided an overall assessment about the level of support for each concept. Our approach to assessing level of support for each concept is detailed in Box 2. This assessment was informed by the application of the mixed-methods-specific criteria (see Table 4). To the mixed-methods-specific criteria we also added a criterion for publication bias. In addition, to maximise the transparency of the assessment, for each concept we noted any additional important methodological considerations related to the quality of the underpinning studies.
Strong support: converging evidence from a range of designs; no major gaps.
Moderate support: converging evidence from a range of designs; clear gaps in data or theory.
Low support: converging evidence from a limited pool of designs; clear gaps in data.
Very low support: converging evidence primarily from either qualitative or quantitative designs only; substantial gaps in data.
Inconsistent support: no converging evidence.
Having used this approach in the current review, we outline our experiences and observations in Chapter 8, Strengths and weaknesses, and make some recommendations about the need for further methodological research to develop a validated approach.
Appendix 5 List of included studies
Agrawal SK, Kang J, Chen X, Kim MJ, Lee Y, Kong SW, et al. Robot-enhanced mobility training of children with cerebral palsy: short-term and long-term pilot studies. IEEE Syst J 2016;10:1098–106. 63
Bamer AM, Connell FA, Dudgeon BJ, Johnson KL. Frequency of purchase and associated costs of assistive technology for Washington State Medicaid program enrollees with spina bifida by age. Disabil Health J 2010;3:155–61. 55
Berry ET, McLaurin SE, Sparling JW. Parent/caregiver perspectives on the use of power wheelchairs. Pediatr Phys Ther 1996;8:146–50. 133
Bottos M, Bolcati C, Sciuto L, Ruggeri C, Feliciangeli A. Powered wheelchairs and independence in young children with tetraplegia. Dev Med Child Neurol 2001;43:769–77. 23
Butler C. Effects of powered mobility on self-initiated behaviors of very young children with locomotor disability. Dev Med Child Neurol 1986;28:325–32. 89
Butler C, Okamoto GA, McKay TM. Motorized wheelchair driving by disabled children. Arch Phys Med Rehabil 1984;65:95–7. 126
Ceres R, Pons JL, Calderon L, Jimenez AR, Azevedo L. A robotic vehicle for disabled children. IEEE Eng Med Biol Mag 2005;24:55–63. 120
Cerruti M, Biondi R. Timely insertion of electronic wheelchair in overall rehabilitation plan for cerebral palsy in young children: investigation on the opinion of parents. Sci Riabil 2010;12:14–23. 103
Chen X, Ragonesi C, Galloway JC, Agrawal SK. Training toddlers seated on mobile robots to drive indoors amidst obstacles. IEEE Trans Neural Syst Rehabil Eng 2011;19:271–9. 64
Cooper RA, Tolerico M, Kaminski BA, Spaeth D, Ding D, Cooper R. Quantifying wheelchair activity of children: a pilot study. Am J Phys Med Rehabil 2008;87:977–83. 168
Cronin S. Exploring the Lived Experiences of Children with Specialised Wheelchair and Seating Needs from a Family Perspective. PhD thesis. Limerick: University of Limerick; 2012. 134
Currier BA, Jones MA, DeGrace BW. Experiences of families with young power wheelchair users. J Early Interv 2019;41:125–40. 105
Deitz J, Swinth Y, White O. Powered mobility and preschoolers with complex developmental delays. Am J Occup Ther 2002;56:86–96. 12
Dennis CW, Stansfeld S, Larin HM. Effect of Providing Powered Mobility on Infants’ Social Behavior and Vocalization: Two Case Studies. Paper presented at the Rehabilitation Engineering and Assistive Technology Society of North America (RESNA) annual conference, New Orleans, LA, 26–30 June 2017. 94
Douglas J, Ryan M. A preschool severely disabled boy and his powered wheelchair: a case study. Child Care Health Dev 1987;13:303–9. 115
Dunaway S, Montes J, O’Hagen J, Sproule DM, Vivo DC, Kaufmann P. Independent mobility after early introduction of a power wheelchair in spinal muscular atrophy. J Child Neurol 2013;28:576–82. 127
Durkin J. Discovering powered mobility skills with children: ‘Responsive partners’ in learning. Int J Ther Rehabil 2009;16:331–41. 109
Evans N, Baines R. Trends, goals and outcomes for children and families using early powered mobility in a charitable loan scheme. J Enabling Technol 2017;11:138–47. 62
Evans S, Neophytou C, de Souza L, Frank AO. Young people’s experiences using electric powered indoor–outdoor wheelchairs (EPIOCs): potential for enhancing users’ development? Disabil Rehabil 2007;29:1281–94. 59
Feldner H. Impacts of early powered mobility provision on disability identity: a case study. Rehabil Psychol 2019;64:130–45. 116
Feldner HA, Logan SW, Galloway JC. Mobility in pictures: a participatory photovoice narrative study exploring powered mobility provision for children and families. Disabil Rehabil Assist Technol 2019;14:301–11. 60
Flodin E. Interactive design – the desire for autonomous upright mobility: a longitudinal case study. Technol Disabil 2007;19:213–24. 122
Frank AO, De Souza LH, Frank JL, Neophytou C. The pain experiences of powered wheelchair users. Disabil Rehabil 2012;34:770–8. 131
Furumasu J, Guerette P, Tefft D. The development of a powered wheelchair mobility program for young children. Technol Disabil 1996;5:41–8. 81
Galloway JC, Ryu JC, Agrawal SK. Babies driving robots: self-generated mobility in very young infants. Intell Serv Robot 2008;1:123–34. 57
Gehant BA. Evaluation of the CAPP cart. Artif Limbs 1971;15:16–24. 108
Gudgeon S, Kirk S. Living with a powered wheelchair: exploring children’s and young people’s experiences. Disabil Rehabil Assist Technol 2015;10:118–25. 99
Guerette P, Furumasu J, Tefft D. The positive effects of early powered mobility on children’s psychosocial and play skills. Assist Technol 2013;25:39–50. 124
Hasdai A, Jessel AS, Weiss PL. Use of a computer simulator for training children with disabilities in the operation of a powered wheelchair. Am J Occup Ther 1998;52:215–20. 65
Home AM, Ham R. Provision of powered mobility equipment to young children: the Whizz-Kidz experience. Int J Ther Rehabil 2003;10:511–7. 106
Huang HH, Chen CL. The use of modified ride-on cars to maximize mobility and improve socialization – a group design. Res Dev Disabil 2017;61:172–80. 77
Huang HH, Galloway JC. Modified ride-on toy cars for early power mobility: a technical report. Pediatr Phys Ther 2012;24:149–54. 169
Huang HH, Ragonesi CB, Stoner T, Peffley T, Galloway JC. Modified toy cars for mobility and socialization: case report of a child with cerebral palsy. Pediatr Phys Ther 2014;26:76–84. 17
Huang HH, Chen YM, Huang HW. Ride-on car training for behavioral changes in mobility and socialization among young children with disabilities. Pediatr Phys Ther 2017;29:207–13. 78
Huang HH, Chen YM, Huang HW, Shih MK, Hsieh YH, Chen CL. Modified ride-on cars and young children with disabilities: effects of combining mobility and social training. Front Pediatr 2017;5:299. 79
Huang HH, Huang HW, Chen YM, Hsieh YH, Shih MK, Chen CL. Modified ride-on cars and mastery motivation in young children with disabilities: effects of environmental modifications. Res Dev Disabil 2018;83:37–46. 80
Huhn K, Guarrera-Bowlby P, Deutsch JE. The clinical decision-making process of prescribing power mobility for a child with cerebral palsy. Pediatr Phys Ther 2007;19:254–60. 130
Inman DP, Loge K, Cram A, Peterson M. Learning to drive a wheelchair in virtual reality. J Spec Educ Technol 2011;26:21–34. 54
Jonasson M. The AKKA-board – performing mobility, disability and innovation. Disabil Soc 2014;29:477–90. 110
Jones MA, McEwen IR, Hansen L. Use of power mobility for a young child with spinal muscular atrophy. Phys Ther 2003;83:253–62. 13
Jones MA, McEwen IR, Neas BR. Effects of power wheelchairs on the development and function of young children with severe motor impairments. Pediatr Phys Ther 2012;24:131–40. 14
Kakimoto A, Suzuki S, Sekiguchi Y. Development of a cart for independent mobility assistance for non-ambulatory children. Conf Proc IEEE Eng Med Biol Soc 2009;2009:7273–6. 107
Kenyon LK, Farris J, Brockway K, Hannum N, Proctor K. Promoting self-exploration and function through an individualized power mobility training program. Pediatr Phys Ther 2015;27:200–6. 76
Kenyon LK, Farris JP, Aldrich NJ, Rhodes S. Does power mobility training impact a child’s mastery motivation and spectrum of EEG activity? An exploratory project. Disabil Rehabil Assist Technol 2018;13:665–73. 75
Kenyon LK, Farris JP, Gallagher C, Hammond L, Webster LM, Aldrich NJ. Power mobility training for young children with multiple, severe impairments: a case series. Phys Occup Ther Pediatr 2017;37:19–34. 86
Kenyon LK, Mortenson WB, Miller WC. ‘Power in Mobility’: parent and therapist perspectives of the experiences of children learning to use powered mobility. Dev Med Child Neurol 2018;60:1012–17. 61
Kornafel T, Tsao EY, Sabelhaus E, Surges L, Apkon SD. Physical and occupational therapy for a teenager with acute flaccid myelitis: a case report. Phys Occup Ther Pediatr 2017;37:485–595. 104
Larin HM, Dennis CW, Stansfield S. Development of robotic mobility for infants: rationale and outcomes. Physiotherapy 2012;98:230–7. 129
Logan SW, Catena MA, Sabet A, Hospodar CM, Yohn H, Govindan A, Galloway JC. Standing tall: feasibility of a modified ride-on car that encourages standing. Pediatr Phys Ther 2019;31:E6–E13. 121
Logan SW, Feldner HA, Galloway JC, Huang HH. Modified ride-on car use by children with complex medical needs. Pediatr Phys Ther 2016;28:100–7. 118
Logan SW, Hospodar CM, Feldner HA, Huang HH, Galloway JC. Modified ride-on car use by young children with disabilities. Pediatr Phys Ther 2018;30:50–6. 87
Logan SW, Huang HH, Stahlin K, Galloway JC. Modified ride-on car for mobility and socialization: single-case study of an infant with Down syndrome. Pediatr Phys Ther 2014;26:418–26. 88
Logan SW, Lobo MA, Feldner HA, Schreiber M, MacDonald M, Winden HN, et al. Power-Up: exploration and play in a novel modified ride-on car for standing. Pediatr Phys Ther 2017;29:30–7. 90
Lovett S. Discrimination learning in multiply handicapped children using an electromechanical car. Adv Behav Res Ther 1988;10:39–52. 113
Lynch A, Ryu JC, Agrawal S, Galloway JC. Power mobility training for a 7-month-old infant with spina bifida. Pediatr Phys Ther 2009;21:362–8. 66
Marchal-Crespo L, Furumasu J, Reinkensmeyer DJ. A robotic wheelchair trainer: design overview and a feasibility study. J Neuroeng Rehabil 2010;7:40. 67
McCourt E, Casey J. Electrically powered indoor/outdoor chair performance for children aged 7 to 9 years. Br J Occup Ther 2016;79:584–90. 68
McGarry S, Moir L, Girdler S. The Smart Wheelchair: is it an appropriate mobility training tool for children with physical disabilities? Disabil Rehabil Assist Technol 2012;7:372-80. 69
Mockler SR, McEwen IR, Jones MA. Retrospective analysis of predictors of proficient power mobility in young children with severe motor impairments. Arch Phys Med Rehabil 2017;98:2034–41. 111
Montesano L, Díaz M, Bhaskar S, Minguez J. Towards an intelligent wheelchair system for users with cerebral palsy. IEEE Trans Neural Syst Rehabil Eng 2010;18:193–202. 85
Morère Y, Bourhis G, Cosnuau K, Guilmois G, Rumilly E, Blangy E. ViEW: a wheelchair simulator for driving analysis [published online ahead of print August 7 2018]. Assist Technol 2018. 70
Nicholson J, Bonsall M. Powered mobility for children under five years of age in England. Br J Occup Ther 2002;65:291–3. 84
Nilsson L, Eklund M, Nyberg P, Thulesius H. Driving to learn in a powered wheelchair: the process of learning joystick use in people with profound cognitive disabilities. Am J Occup Ther 2011;65:652–60. 117
Nilsson L, Nyberg P, Eklund M. Training characteristics important for growing consciousness of joystick-use in people with profound cognitive disabilities. Int J Ther Rehabil 2010;17:588–95. 73
Nilsson LM, Nyberg PJ. Driving to learn: a new concept for training children with profound cognitive disabilities in a powered wheelchair. Am J Occup Ther 2003;57:229–33. 74
Odor J, Watson M. Learning Through Smart Wheelchairs: A Formative Evaluation of the Effective Use of the CALL Centre’s Smart Wheelchairs as Part of Children’s Emerging Mobility, Communication, Education, and Personal Development. Final Report. 1994. URL: www.callscotland.org.uk/Common-Assets/ckfinder/userfiles/files/Learning%20Through%20Smart%20Wheelchairs%20complete.pdf (accessed 6 July 2020). 91
Omori K, Sugimoto Y, Kitayama I. Development of Power Wheelchair with Support Functions for Learning how to Operate – Trial at a School for Children with Physical or Developmental Disabilities. In Ohnabe H, Collins DM, editors. Selected Papers from the Japanese Conference on the Advancement of Assistive and Rehabilitation Technology. Amsterdam: IOS Press; 2011. pp. 67–71. 114
Paulsson K, Christoffersen M. Psychosocial Aspects of Technical Aids: How does Independent Mobility Affect the Psychosocial and Intellectual Development of Children with Physical Disabilities? Paper presented at the 2nd International Conference of the Rehabilitation Engineering Society of North America; Ottawa, ON, 17–22 June 1984. 95
Pituch E, Rushton PW, Ngo M, Heales J, Poulin Arguin A. Powerful or powerless? Children’s, parents’, and occupational therapists’ perceptions of powered mobility. Phys Occup Ther Pediatr 2018;39(3):1–16. 100
Pope PM, Bowes CE, Booth E. Postural control in sitting the SAM system: evaluation of use over three years. Dev Med Child Neurol 1994;36:241–52. 125
Pritchard-Wiart L, Bragg E, Thompson-Hodgetts S. The Young Movers Project: a case series describing modified toy car use as an early movement option for young children with mobility limitations. Phys Occup Ther Pediatr 2019;39:598–613. 58
Ragonesi CB, Chen X, Agrawal S, Galloway JC. Power mobility and socialization in preschool: a case study of a child with cerebral palsy. Pediatr Phys Ther 2010;22:322–9. 96
Ragonesi CB, Chen X, Agrawal S, Galloway JC. Power mobility and socialization in preschool: follow-up case study of a child with cerebral palsy. Pediatr Phys Ther 2011;23:399–406. 83
Ragonesi CB, Galloway JC. Short-term, early intensive power mobility training: case report of an infant at risk for cerebral palsy. Pediatr Phys Ther 2012;24:141–8. 72
Ross SM, Catena M, Twardzik E, Hospodar C, Cook E, Ayyagari A, et al. Feasibility of a modified ride-on car intervention on play behaviors during an inclusive playgroup. Phys Occup Ther Pediatr 2018;38:493–509. 97
Schoepflin ZR, Chen X, Ragonesi CB, Galloway JC, Agrawal SK. Design of a novel mobility device controlled by the feet motion of a standing child: a feasibility study. Med Biol Eng Comput 2011;49:1225–31. 128
Sharma N, Morrison J. Don’t Push Me Around! Disabled Children’s Experiences of Wheelchair Services in the UK. London: Whizz-Kids; 2007. URL: www.whizz-kidz.org.uk/uploads/general/Support_us/Trusts__statutory_and_lottery/dont_push_me_around_report.pdf (accessed 26 February 2020). 98
Smania N, Gandolfi M, Marconi V, Calanca A, Geroin C, Piazza S, et al. Applicability of a new robotic walking aid in a patient with cerebral palsy. Case report. Eur J Phys Rehabil Med 2012;48:147–53. 123
Sonday A, Gretschel P. Empowered to play: a case study describing the impact of powered mobility on the exploratory play of disabled children. Occup Ther Int 2016;23:11–18. 101
Stokes M, Cook E, Sanders C, Coker-Bolt P. The case for early power mobility: developmental outcomes for a toddler born with a rare neuromuscular disorder. Technol Special Interest Section Q 2014;24:1–3. 92
Tefft D, Guerette P, Furumasu J. The impact of early powered mobility on parental stress, negative emotions, and family social interactions. Phys Occup Ther Pediatr 2011;31:4–15. 15
Furumasu J. Powered mobility readiness: a case study. Directions, 2015;6:42–6. URL: https://nrrts.org/wp-content/uploads/2019/06/DIRECTIONS_2015.6_RehabCaseStudy.pdf (accessed 1 November 2019). 170
Torkia C, Ryan SE, Reid D, Boissy P, Lemay M, Routhier F, et al. Virtual community centre for power wheelchair training: experience of children and clinicians. Disabil Rehabil Assist Technol 2019;14:46–55. 71
Uyama S, Hanaki K. Current status of the utilization of powered wheelchair in preschool children with locomotive disability in Japan. Phys Ther Res 2016;19:13–23. 112
Weinstein ML, Lloyd M, Finch KA, Laszacs AD. Underappreciated challenges to pediatric powered mobility – ways to address them as illustrated by a case report. Assist Technol 2018;30:74–6. 93
Wiart L, Darrah J, Cook A, Hollis V, May L. Evaluation of powered mobility use in home and community environments. Phys Occup Ther Pediatr 2003;23:59–75. 132
Wiart L, Darrah J, Hollis V, Cook A, May L. Mothers’ perceptions of their children’s use of powered mobility. Phys Occup Ther Pediatr 2004;24:3–21. 102
Zazula JL, Foulds RA. Mobility device for a child with phocomelia. Arch Phys Med Rehabil 1983;64:137–9. 119
Zeng Q, Burdet E, Teo CL. Evaluation of a collaborative wheelchair system in cerebral palsy and traumatic brain injury users. Neurorehabil Neural Repair 2009;23:494–504. 82
Appendix 6 Sample of excluded studies and reasons for exclusion
| Study | Reason for exclusion |
|---|---|
| Andrich 2015171 | Wrong population |
| Barnard 2010172 | Wrong intervention. No outcomes |
| Bartonek 2012173 | No empirical data. No outcomes |
| Bloeman 2015174 | No powered mobility intervention. Wrong intervention |
| Bray 2014160 | Wrong study design |
| Butler 2015175 | Wrong publication type |
| Douglas 1988176 | Duplicate of Douglas and Ryan.115 No outcomes |
| Ekiz 2017177 | Wrong intervention. No outcomes |
| Field 2016178 | Wrong study design. No outcomes. Wrong intervention |
| Sanders 2018179 | No empirical data. No outcomes |
Appendix 7 Characteristics of included studies
| Study | Year of publication | Country | Study design classification | Description of non-comparative aspects | Health condition(s) | GMFCS level | Sample size (n) | Age | Gender | Intervention |
|---|---|---|---|---|---|---|---|---|---|---|
| Agrawal et al.63 | 2016 | The Republic of Korea | Non-randomised controlled trial | N/A | Cerebral palsy | II–III | 15 (n = 5 children in the short-term experiment; n = 5 children plus n = 5 controls in the long-term experiment) | Short-term experimental study: 18.6 ± 5.28 months; longer experimental study: 14.4 ± 2.33 months; control group in longer study were 28.8 ± 5.88 months | Not specified | Training sessions to drive two mobile robots, namely the PIONEER AT (Adept MobileRobots) and PowerBot (Adept MobileRobots), with identical conventional joysticks |
| Bamer et al.55 | 2010 | USA | Non-comparative study | Secondary data analysis of electronic claims and eligibility records of persons covered by the Medicaid program over a 4-year period (2001–4) who had at least one service with a coded diagnosis of spina bifida | Spina bifida | N/A | 0–15 years: n = 323; 16–25 years: n = 215 | 0–15, 16–25, and ≥ 26 years | Mixed; numbers not specified | Powered wheelchairs |
| Berry et al.133 | 1996 | USA | Non-comparative study | Mixed methods – interviews and descriptive statistics | Cerebral palsy, myelomeningocele, Charcot–Marie–Tooth disease, VATER syndrome | N/A (study preceded GMFCS) | 36 | 5–23 years | 18 male, 18 female | Powered wheelchairs |
| Bottos et al.23 | 2001 | Italy | Before-and-after study | N/A | Cerebral palsy | Assume IV/V | 29 | 3–8 years | 15 males, 14 females | Powered wheelchairs |
| Butler89 | 1986 | USA | Interrupted time series | N/A | Myelomeningocele, spastic quadriplegic cerebral palsy, congenital malformation of limbs, arthrogryposis multiplex congenita and osteogenesis imperfecta | N/A (study preceded GMFCS) | 6 | 23–38 months | Mixed; number of males and females not specified | Motorised wheelchair |
| Butler et al.126 | 1984 | USA | Non-comparative study | Data from daily records made by parents | Myelomeningocele, cerebral palsy, arthogryposis multiplex congenita, osteogenesis imperfecta, spinal muscular atrophy, four-extremity limb deficiency, quadriplegia of unknown aetiology | N/A (study preceded GMFCS) | 13 | 20–37 months | 6 females; 7 males | Motorised wheelchairs |
| Ceres et al.120 | 2005 | Spain | Before-and-after study | N/A | Severe mobility limitations and reduced motor control | Not specified | 5 | 3–7 years | Not specified | Assisted vehicle for disabled children: PALMA |
| Cerruti and Biondi103 | 2010 | Italy | Non-comparative study | Online structured interview/survey | Cerebral palsy | Not specified | 4 | 6–10 years | Not specified | Powered wheelchair |
| Chen et al.64 | 2011 | USA | Before-and-after study | N/A | Spina bifida | Not specified | 1 | 2 years | Male | Force-feedback on the joystick that trains the children to navigate while avoiding obstacles |
| Cooper et al.168 | 2008 | USA | Non-concurrent cohort study | N/A | Muscular dystrophy, cerebral palsy, spina bifida, spinal cord injury | Not specified | 9 | 8–16 years | 5 males, 4 females | Powered wheelchair |
| Currier et al.105 | 2019 | USA | Non-comparative study | Qualitative, grounded theory approach | Cerebral palsy; myotubular myopathy; tetraphocomelia | Not specified | 8 | 2 years and 2 months to 3 years and 6 months | 3 male, 5 female | Powered wheelchair |
| Deitz et al.12 | 2002 | USA | Before-and-after study | N/A | Cerebral palsy (spastic quadriplegia), complex developmental delays | (Assume IV-V) | 2 | 5 years | 1 male, 1 female | Powered mobility riding toy (battery-operated ride-on car) |
| Dennis et al.94 | 2017 | USA | Before-and-after study | N/A | Severe undifferentiated hypotonia, and spastic diplegia cerebral palsy | 4 for one child, not specified for the other | 2 | 10 months and 22 months | Female | The WeeBot: a robotic mobility device assembled from commercially available components: a wheeled, aluminium frame is attached to a PIONEER 3DX (Adept MobileRobots) mobile robot. Attached to this frame is a Nintendo® Wii™ Balance Board (Nintendo Co., Ltd, Kyoto, Japan) with an infant seat mounted on top of it |
| Douglas and Ryan115 | 1987 | England, UK | Non-comparative study | Clinical case study | Spinal cord injury (C4) at age 1 year | Not specified | 1 | 4.5 years | Male | Powered wheelchair |
| Dunaway et al.127 | 2013 | USA | Non-comparative study | Descriptive intervention study | Spinal muscular atrophy type I–II, congenital muscular dystrophy | Not specified | 6 | 16–23 months at initial wheelchair evaluation, 24–34 months at wheelchair delivery | 5 male, 1 female | Powered wheelchair |
| Durkin109 | 2009 | England, UK | Non-comparative study | Qualitative, observation and focus groups, grounded theory approach | Cerebral palsy, hypoxic brain damage (CYP observations) | III-V (CYP observations) | CYP focus groups n = 7, professional focus groups n = 22, CYP observations n = 11 | CYP focus groups: 9–12 years, CYP observations: 5–10 years | CYP focus groups: 3 male, 4 female; CYP observations: 5 female, 6 male | Powered wheelchair with three types of operational mode: freedrive, electronic track guidance system and systems collision avoidance device |
| Evans and Baines62 | 2017 | England, UK | Non-comparative study | Mixed methods, descriptive statistics and thematic analysis | Cerebral palsy, spinal muscular atrophy, global developmental delay, arthrogryposis, spina bifida | Not specified | 90 | 15–72 months | 51 male, 39 female | Wizzybug |
| Evans et al.59 | 2007 | England, UK | Non-comparative study | Qualitative, telephone questionnaire and interview | Muscular dystrophy, cerebral palsy, other | Not specified | 13 | 10–18 years | 13 male, 5 female | EPIOC |
| Feldner et al.60 | 2019 | USA | Non-comparative study | Qualitative, ethnographic case study, photovoice | Cerebral palsy | Not specified | 2 | 4 and 5 years | Male | Powered wheelchair and modified powered ride-on toy car |
| Feldner116 | 2019 | USA | Non-comparative study | Qualitative, grounded theory approach | Quadriplegic cerebral palsy | Not specified | 2 | 4 and 5 years | Male | Powered wheelchair; adapted mobility toy |
| Flodin122 | 2007 | Sweden | Non-comparative study | Longitudinal case study | Spinal muscular atrophy type II | Not specified | 1 | 13 months at start of study | Female | Motorised walking aid |
| Frank et al.131 | 2012 | England, UK | Non-comparative study | Qualitative – telephone interviews | Muscular dystrophy, cerebral palsy, spina bifida | Not specified | 64 | 10–81 years | 32 male, 32 female | Powered wheelchairs |
| Furumasu et al.81 | 1996 | USA | Non-comparative study | Other; development of battery to assess wheelchair skills | Arthrogryposis, spinal muscular atrophy, spinal cord injury, other (e.g. amputee) | Not specified | 24 | 18–36 months | Not specified | Powered mobility skills/training programme |
| Furumasu170 | 2015 | USA | Non-comparative study | Case studies | Cerebral palsy | Not specified | 2 | 3.5 years (child 1); 7–17 years (child 2) | 1 male, 1 female | Powered wheelchair |
| Galloway et al.57 | 2008 | USA | Non-comparative | Descriptive intervention study | Down syndrome | Not specified | 1 | 14 months | Male | Joystick-controlled mobile robot with cart |
| Gehant108 | 1971 | USA | Non-comparative study | Quantitative, descriptive intervention study | Quadrimembral amputees | Not specified | 11 | 6–14 years | 4 male, 7 female | Motorised ‘CAPP cart’, powered by a 12-V battery, travels at a constant speed of 1.5 mph, controlled by a chin-controlled lever |
| Cronin134 | 2012 | Republic of Ireland | Non-comparative study | Qualitative study, data obtained using semistructured interviews, interpretive phenomenological approach was used | Cerebral palsy-spastic diplegia; cerebral palsy – spastic quadriplegia, DiGeorge syndrome; osteogenesis imperfecta | Not specified | 5 (parents of three young persons with mobility limitations) | 13–18 years (children with mobility limitations whose parents were interviewed) | Not specified | Specialised wheelchair and specialised seating |
| Gudgeon and Kirk99 | 2015 | England, UK | Non-comparative study | Qualitative: semistructured interviews, interpretative phenomenological analysis | Cerebral palsy, muscular dystrophy, spinal muscular atrophy, brain tumour | Not specified | 9 | 7–16 years | 7 male, 2 female | Powered wheelchair |
| Guerette et al.124 | 2013 | USA | Before-and-after study | N/A | Cerebral palsy, arthrogryposis, congenital muscular dystrophy, osteogenesis imperfect, spinal muscular atrophy, spinal cord injury | Not specified | 23 | 18 months–6 years | Not specified | Powered wheelchair |
| Hasdai et al.65 | 1998 | Israel | Controlled before-and-after study | N/A | Muscular dystrophy, cerebral palsy | Not specified | 22 | 7–22 years | 9 male, 13 female | Computer simulator driving programme |
| Home and Ham106 | 2003 | England, UK | Non-comparative study | Retrospective survey with 24 open-ended questions | Cerebral palsy, spinal muscular atrophy | Not specified | 331 families contacted; 61 questionnaires returned; 57 were included | < 7 years (most common age for issue of the powered wheelchair was 4 years) | 33 (58%) male | Powered wheelchair |
| Huang and Chen77 | 2017 | Taiwan | Non-randomised | N/A | Developmental delay, cerebral palsy, Down syndrome | Not specified | 20 | 1–3 years | 10 male, 10 female | Training to drive a modified, powered toy car |
| Huang et al.78 | 2017 | Taiwan | Before-and-after study | N/A | Developmental delay, cerebral palsy, Down syndrome, other | Not specified | 10 | 1–3 years; mean age 21.0 months (standard deviation 8.78 months) | 6 female, 4 male | Ride-on car training for 9 weeks, (2 hours per session, two sessions per week) |
| Huang and Galloway169 | 2012 | USA | Non-comparative study | Clinical case study | Cerebral palsy | IV | 1 | 28 months | Female | Modified ride-on toy car |
| Huang et al.80 | 2018 | Taiwan | Non-randomised controlled trial | N/A | Developmental delay; cerebral palsy; others | Not reported | 15 (treatment group); 14 (control group) | 1–3 years | 7 males and 8 females in the treatment group; 5 males and 9 females in the control group | Modified ride-on cars and social interaction training programme |
| Huang et al.17 | 2014 | Taiwan | Before-and-after study | N/A | Cerebral palsy | IV | 1 | 21 months | Male | Modified powered toy car |
| Huang et al.79 | 2017 | Taiwan | Non-randomised controlled trial | N/A | Developmental delay, cerebral palsy | Not specified | 29 (n = 15 in the treatment group, n = 14 in the control group) | 1–3 years | 12 male, 17 female | 2-hour ride-on car training sessions twice per week, for a total of 9 weeks, in the hospital environment |
| Huhn et al.130 | 2007 | USA | Before-and-after study | N/A | Cerebral palsy | V | 1 | 9 years | Female | Powered wheelchair; mid-wheel and rear-wheel drive |
| aInman et al.54 | 2011 | USA | Controlled before-and-after study | N/A | Orthopaedic impairments | Not specified | Not specified | 3–15 years | Not specified | Mobility training platform and virtual training scenarios |
| aInman et al.54 | 2011 | USA | RCT | N/A | Cerebral palsy, Down syndrome | Not specified | 13 (subjects who completed the trial) | 4–20 years | 7 female, 6 male | Virtual reality training motorised wheelchair training programme |
| Jonasson110 | 2014 | Sweden | Non-comparative study | Qualitative, interviews | Severely disabled (specific medical conditions were not specified) | Not specified | Eight interviews, including three mothers of children with an AKKA-board in their homes | Not specified | Not specified | AKKA-board: a mobility device classified as an electric wheelchair that can be prescribed as an aid for severely disabled individuals offering mobility |
| Jones et al.13 | 2003 | USA | Before-and-after study | N/A | Spinal muscular atrophy (type II) | Not specified | 1 | 20 months at receipt of the intervention | Female | Powered wheelchair |
| Jones et al.14 | 2012 | USA | RCT | N/A | Cerebral palsy, achondroplasia, Dandy–Walker syndrome, myotubular myopathy, congenital myopathy, hydrocephalus, myotonic dystrophy, failure to thrive, tetraphocomelia, progeria, arthrogryposis | IV–V | 28 | 14–30 months | 15 female, 13 male | Powered wheelchair |
| Kakimoto et al.107 | 2009 | Japan | Non-comparative study | Description of prototype and evaluation of usefulness through tests by a boy and a girl with combined cerebral palsy | Cerebral palsy | IV–V | 2 | 4 and 8 years | 1 male, 1 female | Cart for mobility assistance: battery operated, joystick operated; a prototype cart for independent mobility assistance that allows users to get on while sitting in a chair with seating and positioning system |
| Kenyon et al.75 | 2017 | USA | Before-and-after study | N/A | Cerebral palsy | V | 1 | 3 years, 2 months | Female | Power mobility training (motorised platform) |
| Kenyon et al.61 | 2018 | USA | Non-comparative study | Qualitative: focus groups and one-to-one interviews | Arthrogryposis multiplex congenita, acquired brain injury, cerebral palsy, Duchenne muscular dystrophy | Not specified | 33 (parents and therapists) | 6 months–7 years (children’s age at starting to use powered mobility devices) | Not specified | Powered mobility device |
| Kenyon et al.86 | 2017 | USA | Before-and-after study | N/A | Cerebral palsy | III–V | 3 | 17 months, 2 years, 5 months, and 3 years, 5 months | 2 male, 1 female | Powered mobility device, powered mobility trainer platform |
| Kenyon76 | 2015 | USA | Before-and-after study | N/A | Cerebral palsy | V | 1 | 18 years | Female | Powered wheelchair training platform |
| Kornafel et al.104 | 2017 | USA | Non-comparative study | Case report | Acute flaccid myelitis | Not specified | 1 | 13 years | Male | Powered wheelchair |
| Larin et al.129 | 2012 | USA | Non-comparative study | Description of children’s capability to control the WeeBot | Cerebral palsy; Down syndrome | IV | 3 | 15 months and 7 months | Male | Infants were seated over a PIONEER 3-DX mobile robot. Some used a Nintendo Wii Balance Board (the WeeBot) to control movement, others used a modified joystick |
| Logan et al.88 | 2014 | USA | Before-and-after study | N/A | Down syndrome | Not specified | 1 | 13 months | Female | Modified ride-on car, education, and training |
| Logan et al.90 | 2017 | USA | Non-comparative study | Case description | Physical disability | Not specified | 1 | 4.5 years | Male | Novel modified ride-on car for standing: modified 12-V, Fisher-Price Power Wheels Kawasaki (US$251.99) that travelled at two speeds forward, 2.5 and 5 mph, and one speed in reverse, 2.5 mph. A small activation switch |
| Logan et al.118 | 2016 | USA | Before-and-after study (with caveat that the children did engage with the intervention at baseline) | N/A | Complex medical needs (diagnoses not specified) | Not specified | 3 | 6 months, 19 months, 5 years 10 months | 2 female, 1 male | Ride-on car |
| Logan et al.87 | 2018 | USA | Before-and-after study | N/A | Cerebral palsy, 16p11.2 microdeletion, microcephaly | III | 3 | 12–29 months | 2 female, 1 male | Modified ride-on car, education, and training |
| Logan et al.121 | 2019 | USA | Interrupted time series | N/A | Down syndrome | Not specified | 4 | The infants began the study at ages (months:days): 7:12, 7:19, 9:7; adjusted age 8:20 for prematurity, and 7:19 | 1 female, 3 male | Ride-on car that was modified to have a seated mode and a standing mode |
| Lovett113 | 1988 | England, UK | Before-and-after study | N/A | Profound and multiple learning disabilities (‘Nonambulatory, profoundly mentally retarded’113) | Not specified | 4 | 3.1–13.4 | 1 female, 3 male | Microelectronic battery-operated car built on a standard go-kart frame onto which an infant safety seat has been attached, and discriminative cues |
| Lynch et al.66 | 2009 | USA | Before-and-after study | N/A | Spina bifida | Not specified | 1 | 7 months | Male | Powered mobility training |
| Marchal-Crespo et al.67 | 2010 | USA | Controlled before-and-after study | N/A | Cerebral palsy | Not specified | 1 | 8 years | Female | Robotic wheelchair trainer that steers itself along a course marked by a line on the floor using computer vision, haptically guiding the driver’s hand in appropriate steering motions using a force feedback joystick |
| McCourt and Casey68 | 2016 | Northern Ireland, UK | Non-comparative study | Descriptive intervention study | Cerebral palsy, Duchenne muscular dystrophy | Not specified | 3 | 7–9 years | 2 male, 1 female | EPIOC training/testing; exposure (time in years) to having an EPIC |
| McGarry et al.69 | 2012 | Australia | Before-and-after study | Mixed-methods component | Cerebral palsy | V | 4 | 4–14 years | 2 male, 2 female | 16 session Smart Wheelchair mobility training programme (an augmentative mobility aid equipped with specialised sensors and a computerised control system) |
| Mockler et al.111 | 2017 | USA | Nested case–control study | Secondary analysis of data from intervention groups in two previous RCTs | Motor impairments that prevented independent mobility (diagnoses not specified) | Not specified | 31 | 14–31 months at baseline | Not specified | Children practised manoeuvring individually customised powered wheelchairs for 12 months in natural environments |
| Montesano et al.85 | 2010 | Spain | Non-comparative study | Case series (descriptive intervention study) | Cerebral palsy | Not specified | 4 | 11–16 years | 3 male, 1 female | Intelligent wheelchair (that allows the user to select arbitrary local destinations through a tactile screen interface, and incorporates an automatic navigation system that drives the vehicle, avoiding obstacles even in unknown and dynamic scenarios) and training |
| Morère et al.70 | 2018 | France | Non-RCT | N/A | Cerebral palsy | II–IV | 12 | 8–24 years | 8 male, 4 female | Wheelchair simulator: a virtual environment designed specifically for the purpose of this study and was modelled to accurately reflect the real outdoor environment of the rehabilitation centre. Simulations were conducted using ViEW (Virtual Electrical Wheelchair), a 3D wheelchair simulator designed in laboratory |
| Nicholson and Bonsall84 | 2002 | England, UK | Non-comparative study | Survey of wheelchair services in England | Cerebral palsy, spinal muscular atrophy | Not specified | 139 contacted, 97 replied | < 5 years | Not specified | Powered wheelchairs for indoor–outdoor use, and training |
| Nilsson et al.73 | 2010 | Sweden | Nested case–control study | N/A | Profound cognitive disabilities and multivariate additional disabilities, or high risk of developing this condition (diagnoses not specified) | Not specified | 45 | 12 months–52 years; five of the participants who were included in the training programme were aged between 1 and 6 years, two were between 7 and 20 years, and one was aged 35 years | 20 female, 25 male | Powered wheelchair training |
| Nilsson et al.117 | 2011 | Sweden | Non-comparative study | Qualitative, grounded theory approach with constant comparative analysis | Profound cognitive disabilities (n = 45); lesser degrees of cognitive disability (n = 64), including learning disability, neurodevelopmental disabilities, stroke, brain tumour, traumatic brain injury, or dementia | Not specified | 45 (a further n = 64 with lesser degree of cognitive disability aged 16 months–86 years) | The age at inclusion was between 1 and 52 years, distributed as follows: 14 preschool children (1–6 years), 18 schoolchildren (7–20 years) and 13 adults (21–52 years) | Not specified | Joystick-operated powered wheelchair |
| Nilsson and Nyberg74 | 2003 | Sweden | Non-comparative study | Qualitative case studies using constant comparative analysis of video-recordings, field notes, and in-depth interviews | Profound cognitive disabilities (diagnoses not specified) | Not specified | 2 | 4 and 5 years | 1 male, 1 female | Intensive training in powered wheelchair |
| Odor and Watson91 | 1994 | Scotland, UK | Non-comparative study | Case studies | Various (diagnoses not specified) | Not specified | 13 | The main group (n = 10) were aged from 3.5 to 15 years | 2 female, 11 male | Smart wheelchair |
| Omori et al.114 | 2011 | Japan | Non-comparative study | Case summaries | Athetoid cerebral palsy; physical disabilities | Not specified | 2 | 1 first grader and 1 fourth grader | Female | Powered wheelchair with adapted support functions |
| Paulsson and Christoffersen95 | 1986 | Sweden | Before-and-after study | N/A | Spina bifida, congenital injury of the spine, muscular atrophy, congenital amputations of the arms and legs, cerebral palsy | Not specified | 12 | 2.5–5 years | Not specified | Electric go-karts |
| Pituch et al.100 | 2018 | Canada | Non-comparative study | Semistructured qualitative interviews | Skeletal dysplasia, osteogenesis imperfecta, spinal muscular atrophy, arthrogryposis, cerebral palsy | Not specified | 18: children (n = 6), parents (n = 2), rehabilitation centre occupational therapists (n = 4), and special needs school-based occupational therapists (n = 6) | Children were aged 12–18 years | 4 male, 5 female (children) | Powered wheelchairs |
| Pope et al.125 | 1994 | England, UK | Uncontrolled before-and-after study | N/A | Major postural deficit | Not specified | 9 | Not specified | Not specified | SAM system |
| Pritchard-Wiart et al.58 | 2019 | Canada | Non-comparative study | Mixed-methods case series | Cerebral palsy (n = 4) and arthrogryposis and hypotonia (n = 1) | III, IV and V | 5 | 13–58 months | 4 male, 1 female | Modified toy car |
| Ragonesi et al.96 | 2010 | USA | Controlled before-and-after study (socialisation outcome only; non-comparative study for mobility outcome) | N/A | Cerebral palsy | III | 1 | 3 years | Male | Robot-enhanced mobility device – UD2 (University of Delaware) |
| Ragonesi et al.83 | 2011 | USA | Controlled before-and-after study (socialisation outcome only); before-after study for mobility outcome | N/A | Cerebral palsy | III | 1 | 3 years | Male | Short-term, adult-directed power mobility and socialisation training; UD2 device also provided |
| Ragonesi and Galloway72 | 2012 | USA | Non-comparative study | Descriptive intervention study | Cerebral palsy | Not specified | 1 | 11 months | Female | Short-term intensive power mobility training |
| Ross et al.97 | 2018 | USA | Before-and-after study | N/A – multiple single subjects repeated measures | Spastic triplegia cerebral palsy; hypotonic cerebral palsy; Dandy–Walker syndrome; Down syndrome; hemiplegic cerebral palsy; diplegic cerebral palsy | Not specified | 5 | 15.8–20.2 months | 1 female, 4 males | Ride-on car |
| Schoepflin et al.128 | 2011 | USA | Non-comparative study | Descriptive intervention study | Cerebral palsy | I–V | 1 | 49 months | Male | Bio-driven mobile assistive device that is controlled and driven by moving feet |
| Sharma and Morrison98 | 2007 | England, UK | Non-comparative study | Case studies and survey | Various (diagnoses not specified) | Not specified | 35 completed questionnaires were returned | 22 months to 14 years | Not specified | Powered wheelchair |
| Smania et al.123 | 2012 | Italy | Before-and-after study | N/A | Cerebral palsy | Not specified | 1 | 11 years | 1 male | Robotic walking aid |
| Sonday and Gretschel101 | 2016 | South Africa | Non-comparative study | Qualitative case study | Cerebral palsy, spinal muscular atrophy | Not specified | 2 | 8 and 9 years (both received the intervention at 2 years) | 1 male, 1 female | Powered wheelchair |
| Stokes et al.92 | 2014 | USA | Before-and-after study | N/A | Pierre Robin sequence | Not specified | 1 | 22 months | Male | Adapted ride-on toy |
| Tefft et al.15 | 2011 | USA | Before-and-after study | N/A | Cerebral palsy, orthopaedic disabilities (arthrogryposis, spinal muscular atrophy, spinal cord injury, or osteogenesis imperfecta) | Not specified | Parents of 23 children with disabilities | Average age of children with cerebral palsy was 47.0 months (SD 11.1 months); average age of children with orthopaedic disabilities was 30.1 months (SD 6.0 months) | Not specified | Powered wheelchair |
| Torkia et al.71 | 2017 | Canada | Non-comparative study | Qualitative research design with structured interviews was used | Muscular dystrophy (n = 6), cerebral palsy (n = 4), and a dual diagnosis of spinal cord injury and stroke (n = 1) | Not specified | 15 clinicians and 11 children | Children were aged between 10 and 18 years | Not specified | miWe-CC simulator |
| Uyama and Hanaki112 | 2016 | Japan | Non-comparative study | Cross-sectional questionnaire survey | Cerebral palsy, spondyloschisis, neuromuscular disease, arthropy | Not specified | 318 facilities | Not specified | Not specified | Powered wheelchair |
| aWeinstein et al.93 | 2018 | USA | Non-comparative study | Case summary | Rachischisis, complete spina bifida without acrania, and Chiari malformation type II with severe hydrocephalus | V | 1 | 2 years and 10 months | Male | Powered wheelchair |
| aWeinstein et al.93 | 2018 | USA | Non-comparative study | Case report | Rachischisis (cervical-level spina bifida) | V | 1 | 2 years and 10 months | Male | Powered wheelchair |
| Wiart et al.132 | 2003 | Canada | Non-comparative study | Questionnaire survey | Cerebral palsy, bilateral, above-knee amputations, arthrogryposis, juvenile rheumatoid arthritis, osteogenesis imperfecta, spina bifida, tetraplegia due to spinal cord injury, traumatic brain injury, and non-progressive syndromes | Not specified | 66 families | Mean age when wheelchair received: 7 years (SD 4.3 years) | 40 male, 26 female | Powered wheelchair |
| Wiart et al.102 | 2004 | Canada | Non-comparative study | Qualitative (phenomenological approach, interviews) | Cerebral palsy; myelomeningocele | Not specified | 5 | 10–18 years | 3 male, 2 female | Powered wheelchair |
| Zazula and Foulds119 | 1983 | USA | Non-comparative study | Case summary | Multiple limb deficiencies | Not specified | 1 | 11 months | Male | Electric cart |
| Zeng et al.82 | 2009 | Singapore | Non-comparative study | Case report | Traumatic brain injury | Not specified | 1 (5 in total, but only 1 was < 18 years) | 16–48 years (note that only one participant was aged < 18 years) | 4 male, 1 female | Collaborative Wheelchair Assistant (CWA; National University of Singapore), a robotic wheelchair that lets the user control the speed and provides guiding assistance along virtual paths programmed in software; also training |
Appendix 8 Quality appraisal results
| Study | Randomisation process | Deviations from the intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported result | Overall |
|---|---|---|---|---|---|---|
| Jones et al.14 | Low | No agreement between reviewers | Some concerns | Some concerns | No agreement between reviewers | Some concerns |
| Inman et al.54 | High | Some concerns | Low | Low | Some concerns | High |
| Study | Outcome assessor blinded? | Valid and reliable measures for inclusion/exclusion criteria? | Valid and reliable measures for exposure/intervention? | Valid and reliable measures for participant health benefits and harms? | Attrition/retention reported? | Inclusion/exclusion criteria and recruitment strategy clearly reported? | Valid and reliable measures to assess confounding? | Any attempt to balance the allocation between the groups or match groups? |
|---|---|---|---|---|---|---|---|---|
| Ceres et al.120 | No or cannot determine | No or cannot determine | No or cannot determine | No or cannot determine | No | Partially yes | No | N/A |
| Chen et al.64 | No or cannot determine | N/A | Yes | Partially yes | N/A | Partially yes | No | N/A |
| Cooper et al.168 | No | Partially yes | Yes | Partially yes | Partially yes | Partially yes | Yes | N/A |
| Deitz et al.12 | Yes | N/A | Partially yes | Partially yes | Yes | Partially yes | Partially yes | N/A |
| Furumasu170 | No or cannot determine | No or cannot determine | No or cannot determine | No or cannot determine | N/A | No | No | N/A |
| Douglas and Ryan115 | No or cannot determine | N/A | No | No | N/A | N/A | No | N/A |
| Dunaway et al.127 | No or cannot determine | No or cannot determine | Partially yes | Partially yes | Yes | Partially yes | Partially yes | N/A |
| Flodin122 | N/A | N/A | No or cannot determine | No or cannot determine | N/A | N/A | No or cannot determine | N/A |
| Furumasu et al.81 | No or cannot determine | No or cannot determine | Partially yes | Partially yes | No | No | No or cannot determine | N/A |
| Galloway et al.57 | No | No or cannot determine | Yes | Yes | N/A | Partially yes | No or cannot determine | N/A |
| Gehant108 | No or cannot determine | Partially yes | No or cannot determine | No or cannot determine | Yes | Partially yes | Partially yes | N/A |
| Guerette et al.124 | No | Partially yes | Partially yes | Partially yes | Yes | Partially yes | Partially yes | N/A |
| Hasdai et al.65 | Partially yes | Partially yes | Partially yes | Partially yes | No or cannot determine | Partially yes | Partially yes | Partially yes |
| Home and Ham106 | No | Partially yes | No or cannot determine | No or cannot determine | Yes | Partially yes | No | N/A |
| Huang et al.17 | No | N/A | Partially yes | Partially yes | N/A | Partially yes | No | N/A |
| Huang and Galloway169 | N/A | N/A | N/A | No or cannot determine | N/A | No | No or cannot determine | N/A |
| Huang and Chen77 | Yes | Yes | No or cannot determine | Partially yes | Partially yes | Partially yes | No or cannot determine | No |
| Huang et al.78 | No or cannot determine | Partially yes | No or cannot determine | Yes | Partially yes | Partially yes | Partially yes | No |
| Huang et al.79,80 (same study) | No or cannot determine | Partially yes | Yes | Partially yes | N/A | Partially yes | No or cannot determine | N/A |
| Huhn et al.130 | N/A | N/A | No or cannot determine | Partially yes | N/A | N/A | No or cannot determine | N/A |
| Inman et al.54 | N/A | Yes | Partially yes | N/A | No | Partially yes | N/A | N/A |
| Jones et al.13 | N/A | N/A | No or cannot determine | Yes | N/A | N/A | No | N/A |
| Kakimoto et al.107 | No or cannot determine | No or cannot determine | No or cannot determine | No or cannot determine | N/A | Partially yes | No or cannot determine | N/A |
| Kenyon et al.76 | N/A | N/A | No or cannot determine | Yes | N/A | N/A | No | N/A |
| Kenyon et al.86 | No or cannot determine | Partially yes | No or cannot determine | Yes | No or cannot determine | Partially yes | No or cannot determine | N/A |
| Kenyon et al.75 | No or cannot determine | Partially yes | No or cannot determine | Yes | Yes | Partially yes | No or cannot determine | N/A |
| Kornafel et al.104 | N/A | N/A | No | Partially yes | N/A | N/A | Partially yes | N/A |
| Larin et al.129 | No or cannot determine | No or cannot determine | No or cannot determine | No or cannot determine | N/A | No or cannot determine | No or cannot determine | N/A |
| Logan et al.88 | No or cannot determine | Partially yes | Partially yes | Partially yes | N/A | Partially yes | No | N/A |
| Logan et al.87 | Partially yes | No or cannot determine | Partially yes | Partially yes | No or cannot determine | No or cannot determine | No | N/A |
| Logan et al.118 | No or cannot determine | No or cannot determine | Yes | Partially yes | Yes | No or cannot determine | No | N/A |
| Logan et al.121 | No or cannot determine | Partially yes | Partially yes | Partially yes | Partially yes | No or cannot determine | No | N/A |
| Agrawal et al.63 | Yes | Yes | No or cannot determine | Yes | Yes | Yes | No or cannot determine | Partially yes |
| Bamer et al.55 | N/A | Yes | N/A | N/A | N/A | Partially yes | No or cannot determine | N/A |
| Dennis et al.94 | No or cannot determine | No or cannot determine | Partially yes | Partially yes | Yes | No or cannot determine | No or cannot determine | N/A |
| Butler89 | No or cannot determine | No or cannot determine | Partially yes | Partially yes | Yes | No or cannot determine | No or cannot determine | N/A |
| Bottos et al.23 | No or cannot determine | No or cannot determine | No or cannot determine | Yes | Yes | No or cannot determine | No or cannot determine | N/A |
| Butler et al.126 | No or cannot determine | No or cannot determine | Partially yes | Partially yes | Yes | No or cannot determine | No or cannot determine | N/A |
| Paulsson and Christoffersen95 | No or cannot determine | No or cannot determine | No or cannot determine | No or cannot determine | Yes | No or cannot determine | No or cannot determine | N/A |
| Logan et al.90 | No or cannot determine | N/A | No or cannot determine | Partially yes | Yes | Partially yes | No or cannot determine | N/A |
| Lovett113 | No or cannot determine | No or cannot determine | Partially yes | No | Yes | No or cannot determine | No or cannot determine | N/A |
| Lynch et al.66 | No | N/A | Yes | Yes | N/A | N/A | No or cannot determine | N/A |
| Marchal-Crespo et al.67 | No or cannot determine | No or cannot determine | No or cannot determine | No or cannot determine | Yes | No or cannot determine | No or cannot determine | No |
| McCourt and Casey68 | Yes | No or cannot determine | No or cannot determine | Partially yes | N/A | Yes | No or cannot determine | N/A |
| Mockler et al.111 | N/A | N/A | Partially yes | Yes | N/A | Yes | Yes | N/A |
| Montesano et al.85 | No or cannot determine | No or cannot determine | Partially yes | Partially yes | Yes | Yes | No or cannot determine | N/A |
| Morère et al.70 | No or cannot determine | Yes | Partially yes | No | Yes | Partially yes | No or cannot determine | No |
| Nicholson and Bonsall84 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
| Nilsson and Nyberg74 | No or cannot determine | No or cannot determine | No or cannot determine | No | Yes | Partially yes | No or cannot determine | N/A |
| Odor and Watson91 | No or cannot determine | No or cannot determine | No or cannot determine | Partially yes | Yes | No or cannot determine | No or cannot determine | N/A |
| Omori et al.114 | No | N/A | No | No | N/A | No or cannot determine | No or cannot determine | N/A |
| Pope et al.125 | N/A | Yes | Partially yes | Partially yes | Yes | Partially yes | No or cannot determine | N/A |
| Ragonesi et al.96 | No | N/A | Partially yes | Partially yes | N/A | N/A | N/A | N/A |
| Ragonesi et al.83 | No | N/A | Partially yes | Partially yes | N/A | N/A | No or cannot determine | N/A |
| Ragonesi and Galloway72 | No | N/A | Partially yes | No or cannot determine | N/A | N/A | No or cannot determine | N/A |
| Ross et al.97 | No | Yes | Yes | Yes | Yes | Partially yes | Partially yes | No |
| Schoepflin et al.128 | No or cannot determine | No or cannot determine | No or cannot determine | Partially yes | Yes | No or cannot determine | No or cannot determine | N/A |
| Sharma and Morrison98 | No or cannot determine | No or cannot determine | N/A | N/A | No | Partially yes | N/A | N/A |
| Smania et al.123 | No | N/A | No or cannot determine | Yes | N/A | Partially yes | N/A | N/A |
| Stokes et al.92 | No | N/A | No or cannot determine | Yes | N/A | N/A | N/A | N/A |
| Tefft et al.15 | No or cannot determine | Partially yes | Yes | Yes | Yes | Partially yes | No or cannot determine | N/A |
| Uyama and Hanaki112 | N/A | No or cannot determine | Partially yes | Partially yes | Yes | Partially yes | N/A | N/A |
| Weinstein et al.93 | N/A | N/A | No or cannot determine | No or cannot determine | N/A | N/A | N/A | N/A |
| Wiart et al.132 | N/A | Partially yes | Yes | No | Yes | Partially yes | N/A | N/A |
| Zazula and Foulds119 | No | N/A | Partially yes | No | N/A | N/A | N/A | N/A |
| Zeng et al.82 | No or cannot determine | No or cannot determine | No or cannot determine | Partially yes | Yes | No or cannot determine | No or cannot determine | N/A |
| Study | Clear statement of aims? | Qualitative methodology appropriate? | Research design appropriate? | Recruitment strategy appropriate? | Data collected in a way that addressed the issue? | Researcher–participant relationship considered? | Ethics issues considered? | Data analysis rigorous? | Clear statement of findings? |
|---|---|---|---|---|---|---|---|---|---|
| Currier et al.105 | Yes | Yes | Unclear | Unclear | Yes | No | Unclear | Yes | No |
| Evans et al.59 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Pituch et al.100 | Yes | Yes | Yes | Yes | Yes | Cannot tell | Yes | Yes | Yes |
| Nilsson et al.117 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No |
| Nilsson and Nyberg74 | Yes | Yes | Yes | Cannot tell | Yes | Cannot tell | No | Yes | Yes |
| Kenyon et al.61 | Yes | Yes | Yes | Yes | Yes | Cannot tell | Yes | Yes | Yes |
| Jonasson110 | Yes | Yes | Cannot tell | Cannot tell | Cannot tell | No | Cannot tell | Cannot tell | Yes |
| Gudgeon and Kirk99 | Yes | Yes | Yes | Yes | Yes | Cannot tell | Yes | Yes | Yes |
| Wiart et al.102 | Yes | Yes | Yes | Cannot tell | Yes | No | Yes | Yes | Yes |
| Frank et al.131 | Yes | Yes | Cannot tell | Yes | No | Yes | Yes | Cannot tell | Yes |
| Feldner116 | Yes | Yes | Yes | Cannot tell | Yes | Cannot tell | Yes | No | Cannot tell |
| Feldner et al.60 | Yes | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes |
| Durkin109 | Yes | Yes | Yes | Yes | Yes | Cannot tell | Yes | Yes | Yes |
| Cronin134 | Yes | Yes | Yes | Yes | Yes | Cannot tell | Yes | Yes | Yes |
| Berry et al.133 | Yes | Yes | Yes | Cannot tell | Cannot tell | Cannot tell | No | Cannot tell | Yes |
| Torkia et al.71 | Yes | Yes | Yes | Cannot tell | Yes | No | Yes | Cannot tell | Yes |
| Sonday and Gretschel101 | Yes | Yes | Yes | Cannot tell | Yes | Cannot tell | Cannot tell | Cannot tell | Cannot tell |
| Cerruti and Biondi103 (in Italian; could not appraise) | – | – | – | – | – | – | – | – | – |
| Study | Screening questions | Qualitative | Quantitative | Mixed methods | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 1.1 | 1.2 | 1.3 | 1.4 | 4.1 | 4.2 | 4.3 | 4.4 | 5.1 | 5.2 | 5.3 | |
| Evans et al.59 | Yes | Yes | Yes | Yes | Cannot tell | No | No | Yes | Yes | Yes | Yes | Yes | No | No |
| McGarry et al.69 | Yes | Yes | Yes | Yes | Yes | Yes | No | No | No | No | N/A | Yes | Yes | Yes |
| Pritchard-Wiart et al.58 | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Unclear | Unclear | Yes | Yes | No | No |
Appendix 9 Number of included studies by intervention element
| Intervention element | Number of studies | Intervention description | Studies |
|---|---|---|---|
| Powered mobility equipment for the child | 62 | Powered wheelchairs, motorised wheelchairs, assisted vehicle, ride-on toy, ride-on car, WeeBot, EPIOC, powered ride-on toy, motorised walking aid, mobile robot, motorised CAPP cart, specialised wheelchair, AKKA-board, cart for mobility assistance, powered mobility device, mobile robot, battery-operated car, Smart wheelchair, electrical go-karts, SAM system, robot-enhanced mobility device, robotic walking aid, ride-on toy, electric cart | Deitz et al.,12 Jone et al.,13 Jones et al.,14 Tefft et al.,15 Huang et al.,17 Bottos et al.,23 Bamer et al.,55 Galloway et al.,57 Pritchard-Wiart et al.,58 Evans et al.,59 Feldner et al.,60 Kenyon et al.,61 Evans and Baines,62 Furumasu et al.,81 Logan et al.,87 Butler,89 Cooper et al.,168 Huang and Galloway,169 Kornafel et al.,104 Logan et al.,90,118 Mockler et al.,111 Odor and Watson,91 Pope et al.,125 Smania et al.,123 Stokes et al.,92 Uyama and Hanaki,112 Zazula and Foulds,119 Durkin,109 Gudgeon and Kirk,99 Pituch et al.,100 Sonday and Gretschel,101 Wiart et al.,102 Currier et al.,105 Feldner,116 Home and Ham,106 Huhn et al.,130 Kakimoto et al.,107 Lovett,113 Omori et al.,114 Schoepflin et al.,128 Weinstein et al.,93 Larin et al.,129 Nilsson et al.,117 Ragonesi et al.,96 Ross et al.,97 Sharma and Morrison,98 Cerruti and Biondi,103 Gehant,108 Jonasson,110 Douglas and Ryan,115 Ceres et al.,120 Flodin,122 Guerette et al.,124 Butler et al.,126 Dunaway et al.,127 Frank et al.,131 Wiart et al.,132 Berry et al.133 and Cronin134 |
| Adaptations to physical environment (e.g. ramps, lifts) | 0 | N/A | N/A |
| Adaptations to policies and practices (e.g. nurseries, leisure centres) | 0 | N/A | N/A |
| Training for the child and people around the child in the use of the equipment | 20 | Training sessions to drive mobile robots, force-feedback on the joystick that trains the children to navigate while avoiding obstacles, powered mobility skills/training programme, computer simulator driving programme, training to drive a modified, powered toy car, ride-on car training for 9 weeks (2 hours per session, two sessions per week), ride-on car training sessions, mobility training platform and virtual training scenarios, power wheelchair training platform, power mobility training, robotic wheelchair trainer, wheelchair simulator, powered wheelchair training, miWe-CC simulator | Inman et al.,54 Agrawal et al.,63 Chen et al.,64 Hasdai et al.,65 Lynch et al.,66 Marchal-Crespo et al.,67 McCourt and Casey,68 McGarry et al.,69 Morère et al.,70 Torkia et al.,71 Ragonesi and Galloway,72 Nilsson et al.,73 Nilsson and Nyberg,74 Kenyon et al.,75,76 Huang and Chen,77 Huang et al.78,79 and Furumasu et al.81 |
| Maintenance and review including of the equipment | 0 | N/A | N/A |
| Equipment and training | 7 | As above | Zeng et al.,82 Ragonesi et al.,83 Nicholson and Bonsall,84 Montesano et al.,85 Kenyon et al.86 and Logan et al.87,88 |
Appendix 10 The GRADE-CERQual assessment of confidence in the qualitative thematic synthesis findings
| Findinga | Studies contributing to findings | Methodological limitations | Coherence | Adequacy | Relevance | GRADE-CERQual assessment of confidence in the evidence | Explanation of GRADE-CERQUAL assessment |
|---|---|---|---|---|---|---|---|
| 1.1: Acceptance of powered mobility – parents | Feldner et al.,60 Kenyon et al.,61 McGarry et al.,69 Pituch et al.,100 Wiart et al.,102 Feldner,116 Cerruti and Biondi,103 and Cronin134 | Moderate methodological limitations
|
Minor concerns about coherence: some concerns about the fit between the data from the primary studies and the review findings | No or very minor concerns about adequacy: eight studies, which, together, offer rich data | No or very minor concerns about relevance: four studies included data relating to very young children; and all studies were from high-income settings | High confidence | Eight studies with moderate methodological limitations. Minor concerns about coherence. No or very minor concerns about adequacy and relevance |
| 1.2: Acceptance of powered mobility – children | Kenyon et al.61 and Durkin109 | Minor methodological limitations: neither study clearly reported researcher–participant relationship | Minor concerns about coherence: some concerns about the fit between the data from the primary studies and the review findings | Serious concerns about adequacy: only two studies, which, together, offer thin data | Minor concerns about relevance: both studies included data relating to very young children; and both studies were from high-income settings. One study reported data relating to typically developing children | Low confidence | Two studies with minor methodological limitations. Minor concerns about coherence and relevance. Serious concerns about adequacy |
| 2.1: Developing powered mobility skills and competency – early introduction | Pritchard-Wiart et al.,58 Kenyon et al.,61 Evans and Baines,62 Durkin109 and Currier et al.105 | Minor methodological limitations:
|
Minor concerns about coherence: some concerns about the fit between the data from the primary studies and the review findings | Moderate concerns about adequacy: five studies, which, together, offer rich data | No or very minor concerns about relevance: four studies included data relating to very young children; and all studies were from high-income settings | Moderate confidence | Five studies with minor methodological limitations. Minor concerns about coherence. Moderate concerns about adequacy due to limited data. No or very minor concerns about relevance |
| 2.2: Developing powered mobility skills and competency – time and support | Pritchard-Wiart et al.,58 Kenyon et al.,61 Evans and Baines,62 Nilsson and Nyberg,74 Durkin,109 Gudgeon and Kirk,99 Pituch et al.,100 Sonday and Gretschel,101 Currier et al.,105 Feldner,116 Jonasson110 and Berry et al.133 | Moderate methodological limitations:
|
No or very minor concerns about coherence | No or very minor concerns about adequacy: 12 studies, which, together, offer rich data | Minor concerns about relevance: six studies included data relating to very young children and one study was from an upper middle-income country. One study reported data relating to typically developing children | High confidence | Twelve studies with moderate methodological limitations. No or very minor concerns about coherence and adequacy. Minor concerns about relevance |
| 2.3: Developing powered mobility skills and competency – play and experiential learning | Pritchard-Wiart et al.,58 Kenyon et al.,61 Evans and Baines,62 Durkin,109 Pituch et al.,100 Currier et al.105 and Nilsson et al.117 | Minor methodological limitations:
|
Minor concerns about coherence: some concerns about the fit between the data from the primary studies and the review findings | Minor concerns about adequacy: seven studies, which, together, offer moderately rich data | No or very minor concerns about relevance: five studies included data relating to very young children; and all studies were from high-income settings | High confidence | Seven studies with minor methodological limitations. Minor concerns about coherence and adequacy. No or very minor concerns about relevance |
| 3.1: Using powered mobility safely – conceptualising safety | Evans et al.,59 Kenyon et al.,61 Durkin109 and Gudgeon and Kirk99 | Minor methodological limitations:
|
Moderate concerns about coherence: some concerns about the fit between the data from the primary studies and the review findings | Moderate concerns about adequacy: four studies, which, together, offer moderately thin data | Minor concerns about relevance: one study included data relating to very young children; and all studies were from high-income settings | Moderate confidence | Four studies with minor methodological limitations. Moderate concerns about coherence and adequacy. Minor concerns about relevance |
| 3.2: Using powered mobility safely – cognitive ability | Evans et al.,59 Kenyon et al.61 and Evans and Baines62 | Minor methodological limitations:
|
Moderate concerns about coherence: some concerns about the fit between the data from the primary studies and the review findings | Serious concerns about adequacy: three studies, which, together, offer thin data | No or very minor concerns about relevance: two studies included data relating to very young children; and all studies were from high-income settings | Low confidence | Three studies with minor methodological limitations. Moderate concerns about coherence. Serious concerns about adequacy due to limited, thin data. No or very minor concerns about relevance |
| 3.3: Using powered mobility safely – risky and disobedient behaviour | Feldner et al.,60 Kenyon et al.,61 Evans and Baines,62 Durkin,109 Gudgeon and Kirk,99 Feldner116 and Cerruti and Biondi103 | Minor methodological limitations:
|
Minor concerns about coherence: some concerns about the fit between the data from the primary studies and the review findings | Moderate concerns about adequacy: seven studies, which, together, offer thin data | No or very minor concerns about relevance: four studies included data relating to very young children; and all studies were from high-income settings | Moderate confidence | Seven studies with minor methodological limitations. Minors concerns about coherence. Moderate concerns about adequacy. No or very minor concerns about relevance |
| 4.1: Anticipated and experienced outcomes from powered mobility – independent movement and independence | Pritchard-Wiart et al.,58 Evans et al.,59 Feldner et al.,60 Kenyon et al.,61 Evans and Baines,62 McGarry et al.,69 Gudgeon and Kirk,99 Pituch et al.,100 Sonday and Gretschel,101 Wiart et al.,102 Currier et al.,105 Feldner,116 Cerruti and Biondi,103 Jonasson110 and Cronin134 | Moderate to serious methodological limitations:
|
No or very minor concerns about coherence | No or very minor concerns about adequacy: 15 studies, which, together, offer rich data | No or very minor concerns about relevance: seven studies included data relating to very young children; and one study was from an upper middle-income country | High confidence | 15 studies with moderate methodological limitations. No or very minor concerns about coherence, adequacy and relevance |
| 4.2: Anticipated and experienced outcomes from powered mobility – developmental benefits | Pritchard-Wiart et al.,58 Evans and Baines,62 McGarry et al.,69 Nilsson and Nyberg,74 Durkin,109 Sonday and Gretschel,101 Nilsson et al.117 and Jonasson110 | Moderate to serious methodological limitations:
|
No or very minor concerns about coherence | No or very minor concerns about adequacy: eight studies, which, together, offer rich data | No or very minor concerns about relevance: four studies included data relating to very young children; and one study was from an upper middle-income country | High confidence | Eight studies with moderate methodological limitations. No or very minor concerns about coherence, adequacy and relevance |
| 4.3: Anticipated and experienced outcomes from powered mobility – parent outcomes | Evans et al.,59 Feldner et al.,60 Kenyon et al.,61 Evans and Baines,62 McGarry et al.,69 Wiart et al.,102 Currier et al.,105 Feldner,116 Cerruti and Biondi103 and Jonasson110 | Moderate to serious methodological limitations:
|
No or very minor concerns about coherence | No or very minor concerns about adequacy: 10 studies, which, together, offer rich data | No or very minor concerns about relevance: six studies included data relating to very young children; and one study was from an upper middle-income country | High confidence | Ten studies with moderate methodological limitations. No or very minor concerns about coherence, adequacy and relevance |
| 5.1: Overall benefit of powered mobility | Pritchard-Wiart et al.,58 Evans et al.,59 Feldner et al.,60 Kenyon et al.,61 Evans and Baines,62 McGarry et al.,69 Durkin,109 Gudgeon and Kirk,99 Pituch et al.,100 Sonday and Gretschel,101 Wiart et al.,102 Currier et al.,105 Feldner,116 Cerruti and Biondi,103 Jonasson110 and Cronin134 | Moderate to serious methodological limitations:
|
No or very minor concerns about coherence | No or very minor concerns about adequacy: 16 studies, which, together, offer rich data | No or very minor concerns about relevance: seven studies included data relating to very young children; and one study was from an upper middle-income country | High confidence | Sixteen studies with moderate methodological limitations. No or very minor concerns about coherence, adequacy and relevance |
Appendix 11 Example of the powered mobility provision process for an NHS Wheelchair Service
FIGURE 9.
Example of the powered mobility provision process for an NHS Wheelchair Service. Reproduced with permission from Leeds Wheelchair Service, Leeds Teaching Hospitals NHS Trust, Leeds, UK.

Appendix 12 Tariff of costs associated with early powered mobility provision
| Item | Source | Year | 2018 cost (£) | Comment | Reference |
|---|---|---|---|---|---|
| Mean cost of powered wheelchair | Manufacturers/suppliers | 2019 | 3939 | Costs of powered wheelchairs referred to by services, users, literature | Various, see Powered wheelchair individual model costs section of this table for specific models |
| Highest-cost powered wheelchair cited by NHS/literature | Supplier (Better Mobility, Chesham, UK) | 2019 | 8500 | Koala Miniflex (Permobil AB) list price | www.bettermobility.co.uk/catalog/product.php?CI_ID=3080 (accessed 30 October 2019) |
| Lowest-cost powered wheelchair cited by NHS contacts | NHS Wheelchair Service manager | 2018 | 1800 | Lowest-cost powered wheelchair, referred to by NHS contacts and provided to very young children | Krys Jarvis, Shropshire Community Health NHS Trust, 2018, personal communication |
| Add-on cost for seating and accessories for powered wheelchair | Estimation from previous research | 2016 | Add 23% | Costs vary by individual need | Bray151 |
| Mean cost of starter powered mobility device (designed for children aged < 5 years) | Manufacturers (MERU and Designability) | 2019 | 4250 | Maintenance included, cost derived from two models: Wizzybug (Designability) and Bugzi (MERU). Range £3500–5000 | Personal communication:
|
| Cost of starter powered mobility device loan | Manufacturers (MERU and Designability) | 2019 | 100–200 | Item is loaned for refundable deposit of £100–200 |
|
| Add-on cost for seating and accessories for starter powered mobility device | Estimation from previous research | 2016 | Add 6% | Costs vary by individual need | Bray151 |
| Estimated cost of adapted ride-on toy | GoBabyGo and retailers [Amazon (Amazon.com Inc., Bellevue, WA, USA) and fisher-Price] | 2019 | 410 |
|
|
| Powered wheelchair individual model costs | |||||
| Invicta (RMS, Sittingbourne, UK) | NHS Wheelchair Service manager | 2019 | 1800 | Price may vary, depending on service | Krys Jarvis, personal communication |
| Zippie Salsa (Sunrise Medical, Brierley Hill, UK) | NHS Wheelchair Service manager | 2019 | 2500 | Price varied, depending on source | Personal communication: anonymous representative for AJM Healthcare (Hailsham, UK) and Derbyshire Wheelchair Service (Derby, UK), 2019 |
| Stakeholder representative | 3100 | Personal communication: anonymous patient representative from project advisory group, 2019 | |||
| Wheelchair supplier | 4835 | www.bettermobility.co.uk/catalog/product.php?CI_ID=2175 (accessed 30 October 2019) | |||
| Esprit Action 4NG Junior (Invacare Ltd) | Manufacturer (Invacare) | 2019 | 1980 | Price may vary, depending on service | Peter Hubbard, Invacare Ltd, 2019, personal communication |
| Koala Miniflex (Permobil AB) | Supplier (Better Mobility) | 2019 | 8500 | Price may vary, depending on supplier | www.bettermobility.co.uk/catalog/product.php?CI_ID=3080 (accessed 30 October 2019) |
| Sparky Paediatric (Pride Mobility Products Ltd, Bicester, UK) | Supplier (Complete Care Shop, Preston, UK) | 2019 | 3150 | Price may vary, depending on supplier | www.completecareshop.co.uk/wheelchairs/quantum-power-wheelchairs/sparky-paediatric-power-wheelchair-view-large?gclid=CjwKCAjwuqfoBRAEEiwAZErCsvGA4rm4SuxxUGtcEmtozUX_vyFRN6rJOWL99Ie9KT3LgW55Mzgg6xoCePgQAvD_BwE (accessed 30 October 2019) |
| Skippi (Ottobock, Egham, UK) | Supplier (Better Mobility) | 2019 | 4455 | Price may vary, depending on supplier | www.bettermobility.co.uk/catalog/product.php?CI_ID=2395 (accessed 30 October 2019) |
| Salsa 2 Mini (Sunrise Medical) | Supplier (Better Mobility) | 2019 | 5565 | Price may vary, depending on supplier | www.bettermobility.co.uk/catalog/product.php?CI_ID=2662 (accessed 30 October 2019) |
| K300 PS Junior (Permobil AB) | Supplier (Better Mobility) | 2019 | 6881 | Price may vary, depending on supplier | www.bettermobility.co.uk/catalog/product.php?CI_ID=3082 (accessed 30 October 2019) |
| Models not stated | NHS Disablement Service Centre manager | 2019 | 2600 | Cost represents the average cost of paediatric powered wheelchairs supplied by this centre. Includes equipment, overheads and engineering costs | Susan Hillman, Newcastle upon Tyne Hospitals NHS Foundation Trust, 2019, personal communication |
| Item | Source | Date | 2018 costs (£) | Comment | Reference |
|---|---|---|---|---|---|
| Ramp to door | Unit Costs of Health and Social Care 2018 148 | 2018 | 334 | Materials (author annuitised 10 years at 3.5%) | Curtis and Burns, 2019148 |
| Ramp to door | Unit Costs of Health and Social Care 2018 148 | 2018 | 232 | Staff costs NHS | Curtis and Burns, 2019148 |
| Ramp to door | Unit Costs of Health and Social Care 2018 148 | 2018 | 340 | Staff costs HIA | Curtis and Burns, 2019148 |
| Path to door | Unit Costs of Health and Social Care 2018 148 | 2018 | 0 | Materials (author annuitised 10 years at 3.5%) | Curtis and Burns, 2019148 |
| Path to door | Unit Costs of Health and Social Care 2018 148 | 2018 | 126 | Staff costs NHS | Curtis and Burns, 2019148 |
| Path to door | Unit Costs of Health and Social Care 2018 148 | 2018 | 27 | Staff costs HIA | Curtis and Burns, 2019148 |
| Door widening | Unit Costs of Health and Social Care 2018 148 | 2018 | 104 | Materials (author annuitised 10 years at 3.5%) | Curtis and Burns, 2019148 |
| Door widening | Unit Costs of Health and Social Care 2018 148 | 2018 | 290 | Staff costs NHS | Curtis and Burns, 2019148 |
| Door widening | Unit Costs of Health and Social Care 2018 148 | 2018 | 241 | Staff costs HIA | Curtis and Burns, 2019148 |
| 1 × ramp, path, widening (all costs) | N/A | 2018 | 1726 | Minimum cost of housing adaptation, based on data from Unit Costs of Health and Social Care 2018148 | N/A |
| 2 × ramp, path, widening (all costs) | N/A | 2018 | 3452 | Best estimate of cost of housing adaptation, based on data from Unit Costs of Health and Social Care 2018148 | N/A |
| Average cost of Disabled Facilities Grant | Equality and Human Rights Commission156 | 2018 | 7500 | No annuitisation, as we assume this includes staff cost | Equality and Human Rights Commission, 2018156 |
| Mean Motability grant | Mot Living Ability | 2018 | 2706 | Calculated from Motability website, which states that in the previous year Motability provided £23M in charitable grants to 8500 customers180 | Motability, 2019157 |
| Item | Source | Year | 2018 cost (£) | Comment | Reference |
|---|---|---|---|---|---|
| Assessment | NHS Improvement | 2018 | 368 | Unit cost reference: WC04 | NHS Improvement, 2018142 |
| Specialist modification without supply | NHS Improvement | 2018 | 139 | Unit cost reference: WC14 | NHS Improvement, 2018142 |
| Specialised complex wheelchair services | NHS Improvement | 2018 | 429 | Unit cost reference: WC13 | NHS Improvement, 2018142 |
| Repair and maintenance | NHS Improvement | 2018 | 214 | Unit cost reference: WC10 | NHS Improvement, 2018142 |
| Review | NHS Improvement | 2018 | 232 | Unit cost reference: WC11 | NHS Improvement, 2018142 |
| Review of substantial accessories | NHS Improvement | 2018 | 143 | Unit cost reference: WC12 | NHS Improvement, 2018142 |
| Training workshop | Go Kids Go! | 2019 | 450 | Average cost per child attending training workshop | Roy Wild and colleagues, Go Kids Go! 2019, personal communication |
List of abbreviations
- BDI
- Battelle Developmental Inventory
- CASP
- Critical Appraisal Skills Programme
- CCG
- Clinical Commissioning Group
- EMPoWER
- Early Mobility and POwered Wheelchair Evidence Review
- EPIOC
- electrically powered indoor–outdoor chair
- GMFCS
- Gross Motor Function Classification System
- GRADE
- Grading of Recommendations Assessment, Development and Evaluation
- GRADE-CERQual
- Grading of Recommendations Assessment, Development and Evaluation – Confidence in the Evidence from Reviews of Qualitative research
- MERU
- Medical Engineering Resource Unit
- MMAT
- Mixed Methods Appraisal Tool
- ONS
- Office for National Statistics
- PEDI
- Pediatric Evaluation of Disability Inventory
- PPI
- patient and public involvement
- PRISMA
- Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- RCT
- randomised controlled trial
- RTI
- Research Triangle Institute
- STEM
- science, technology, engineering and mathematics
- TIDieR
- Template for Intervention Description and Replication
Notes
Supplementary material can be found on the NIHR Journals Library report page (https://doi.org/10.3310/hta24500).
Supplementary material has been provided by the authors to support the report and any files provided at submission will have been seen by peer reviewers, but not extensively reviewed. Any supplementary material provided at a later stage in the process may not have been peer reviewed.