

Notes
Article history
The research reported in this issue of the journal was funded by the National Institute for Health and Care Research NIHR Policy Research Programme conducted through the Policy Research Unit in Economic Methods of Evaluation in Health and Social Care Interventions (EEPRU) PR-PRU-1217-20401. The contractual start date was January 2019. The draft manuscript began editorial review in July 2022 and was accepted for publication in October 2023. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HTA editors and publisher have tried to ensure the accuracy of the authors’ manuscript and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this article.
Permissions
Copyright statement
Copyright © 2024 Harnan et al. This work was produced by Harnan et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This is an Open Access publication distributed under the terms of the Creative Commons Attribution CC BY 4.0 licence, which permits unrestricted use, distribution, reproduction and adaptation in any medium and for any purpose provided that it is properly attributed. See: https://creativecommons.org/licenses/by/4.0/. For attribution the title, original author(s), the publication source – NIHR Journals Library, and the DOI of the publication must be cited.
2024 Harnan et al.
Chapter 1 Introduction
This section of the report contains some material reproduced from the study protocol. © NICE 2022. Protocol for the technology evaluation of ceftazidime with avibactam for treating severe aerobic Gram-negative bacterial infections. Available from www.nice.org.uk/about/what-we-do/life-sciences/scientific-advice/models-for-the-evaluation-and-purchase-of-antimicrobials/ceftazidime-with-avibactam#evidence. All rights reserved. Subject to Notice of rights. NICE accepts no responsibility for the use of its content in this product/publication.
Antimicrobial resistance
Antimicrobial (AM) resistance develops when bacteria with mutations that prevent the activity of AMs emerge through selection pressure exerted by the use of AM agents. There are two major genetic processes involved: mutations in the genes native to the organism usually associated with the mechanism of action of the compound; and acquisition of foreign DNA coding for resistance determinants through horizontal gene transfer of plasmids/genes (e.g. transposons). 1,2 The majority of pathogenic microorganisms appear to have the capability to develop resistance to at least some AM agents. Mechanisms of resistance include limiting uptake of a drug by the microbe, modification of a drug target, inactivation of a drug and active efflux of a drug. Resistance to multiple agents can develop via successive mutations, through the dissemination of genes or through a combination of both processes.
The increased mobility of the global population has had the effect of promoting the evolution and movement of antibiotic-resistance genes. For example, very high rates of extended-spectrum beta-lactamase (ESBL) production among Enterobacterales strains in Asian countries has resulted in substantial use of carbapenem antibiotics worldwide, leading to the emergence of plasmid-mediated resistance to carbapenems. 3 These have spread across the globe and between species. Multidrug-resistant (MDR) bacteria can also spread rapidly within both hospitals and community settings, further contributing to increased AM use and heightened resistance,4 and narrowing the choices available for antibiotic treatment.
Gram-negative bacteria pose a significant public health problem due to their increasing levels of resistance to antibiotics. This can lead to severe consequences where infections cannot be treated effectively, or where the increased risk of mortality and morbidity from infection can prevent life-saving procedures such as transplants or other invasive procedures. Enterobacterales account for many Gram-negative infections in humans, including urinary tract infections (UTIs), pneumonia, diarrhoea, meningitis and sepsis, while the non-fermenter Gram-negative bacilli account for the largest share of infections caused by carbapenem-resistant Gram-negative bacteria. 5
Carbapenem resistance is a particular problem in Gram-negative bacteria, since this constitutes the most reliable drug class for treating bacterial infections. There are two main types of carbapenem resistance, and these can be expressed in multiple pathogens:
-
Carbapenemase-mediated carbapenem resistance occurs when the microorganism produces an enzyme (carbapenemase) that hydrolyses carbapenem antibiotics (such as penicillins, cephalosporins, monobactams and carbapenems) and renders them ineffective. There are multiple carbapenemase enzymes, and these are grouped based upon the similarity of their amino acid sequences according to the Ambler classification system as class A, B, C or D. Class A, C and D enzymes have a serine-based hydrolytic mechanism, while class B enzymes are metallo-beta-lactamases (MBL) that contain zinc in the active site. Each class comprises a number of variants, which include:
-
Class A: Klebsiella pneumoniae carbapenemase (KPC), Guiana extended-spectrum beta-lactamase (GES), imipenemase/non-metallocarbapenemase-A (IMI/NMC) and Serratia marcescens enzyme (SME)
-
Class B (MBLs): New Delhi MBL (NDM), Verona integrated-encoded MBL (VIM), imipenemase (IMP), Sao Paulo MBL (SPM) and Germany imipenemase (GIM)
-
Class C: ampicillinase C (AmpC), cephamycinases (CMY)
-
Class D: oxacillinase (OXA)-23, OXA-24, OXA-48, OXA-58 and related enzymes
Carbapenemases are produced by a small but growing number of Enterobacterales strains, especially Escherichia coli and Klebsiella pneumoniae, and some non-fermenter organisms such as Pseudomonas aeruginosa (P. aeruginosa) and Acinetobacter baumannii (A. baumannii). Bacteria producing carbapenemases may cause serious drug-resistant infections, though the profile of resistance is different for each specific variant and is influenced by the pathogen expressing the resistance, and other resistance genes the organism may have. Of the Ambler Class A carbapenemases, the KPC carbapenemases are the most prevalent, found mostly on plasmids in Klebsiella pneumoniae. The class D carbapenemases are frequently detected in A. baumannii. The class B (MBLs) have been detected primarily in P. aeruginosa; however, there are increasing numbers of reports worldwide of this group of beta-lactamases in the Enterobacterales. The main serine-carbapenemases among carbapenemase-producing Enterobacterales (CPE) in the UK are OXA-48 and KPC. The main MBLs in the UK are NDM, VIM and IMP. 6 Specifically, 12.5% of CPE are KPC, 36.5% are OXA-48-like, and 43.2% MBL (mostly NDM) in the UK. 5
-
-
Non-carbapenemase carbapenem resistance occurs through a variety of nonenzymatic mechanisms which include reduced cell membrane permeability to carbapenems through downregulation of porins (membrane proteins that allow carbapenems into the cell), or overexpression of efflux pumps which remove carbapenems from the periplasmic space. Such mechanisms are often considered to produce low-level resistance, and generally more treatment options are available that maintain activity against these mechanisms.
The World Health Organization (WHO) maintains a list of priority pathogens where, due to the development of resistance, new AMs are urgently needed. The pathogens that the WHO deemed ‘critical’ priorities were, at the time of writing, carbapenem-resistant A. baumannii; carbapenem-resistant P. aeruginosa; carbapenem-resistant Enterobacterales (CRE) (where Klebsiella pneumoniae and Escherichia coli account for the large majority of Enterobacterales). These pathogens are typically MDR Gram-negative bacteria that can cause severe infections in secondary care settings, such as pneumonia and bloodstream infections (bacteraemia), that can often be fatal. 7,8
Early, targeted, effective and safe AM treatment is key for the management of patients infected with carbapenemase-producing carbapenem-resistant bacteria; however, reliable AM treatment options remain scarce. Therefore, individual treatment options tailored to susceptibilities of pathogens and severity of infection are the mainstay of clinical practice. 6 Carbapenems are a class of beta-lactams that are often reserved as a last-line treatment option for infections that are resistant to other beta-lactams with a narrower spectrum of action. 9 Carbapenems are considered one of the most reliable drugs for treating bacterial infections,1 therefore the emergence and spread of resistance to these antibiotics are particularly concerning, especially resistance mediated via carbapenemase which renders other treatment options ineffective. This constitutes a major public health problem due to the morbidity and mortality associated with ineffectively treated infections by these bacteria.
New antimicrobials
There is widespread recognition that the pipeline for new AMs is poor, with few AM agents currently in clinical development. A range of policies have been implemented to address this lack of investment; however, these have focuses on ‘push incentives’ that lower the costs of research and development (R&D). In 2015 a joint government and industry antimicrobial-resistance working group was established that highlighted the need for the development of ‘pull mechanisms’ and in particular a more appropriate payment model for new AMs. The payment model should align payment with value, support stewardship goals by delinking payment from drug sale volumes and provide smooth revenue from the point of approval even for AMs which are expected to be subject to strict stewardship and only used as drug-resistance increases.
The National Institute for Health and Care Excellence (NICE), NHS England and NHS Improvement are currently undertaking a project to assess the feasibility of innovative models that pay for AMs based on an evaluation of their value to the NHS as opposed to the volumes used. Following the selection of two products considered to be of high public health importance, this project involves evaluation of the selected products to inform commercial discussions regarding contract value for a period of up to 10 years. The selection process was a formal procurement exercise and aimed to identify one new AM and one existing but ‘nearly new’ AM. The products selected by this process are cefiderocol (Fetcroja), which is manufactured by Shionogi and received its marketing authorisation in April 2020; and ceftazidime with avibactam (Zavicefta), which is manufactured by Pfizer and received its marketing authorisation in June 2016. This report details the evaluation phase of this project for ceftazidime with avibactam (CAZ-AVI).
Ceftazidime-avibactam is a combination AM that consists of ceftazidime and avibactam. Ceftazidime is an established third-generation cephalosporin that inhibits bacterial peptidoglycan cell wall synthesis following binding to penicillin-binding proteins, leading to bacterial cell lysis and death. 10 Avibactam is a non-beta-lactam beta-lactamase inhibitor that protects ceftazidime from hydrolysis by a wide range of serine beta-lactamases. Importantly, the range of inhibition of avibactam includes class A extended-spectrum beta-lactamases and carbapenemases (e.g. Klebsiella pneumoniae carbapenemase), class C beta-lactamases and some class D oxacillinases and carbapenemases. 11 CAZ-AVI is administered by intravenous infusion. CAZ-AVI is not active against MBLs but is active against serine-carbapenemases.
The CAZ-AVI licence permits use in adults and paediatric patients (> 3 months) for complicated intra-abdominal infections (cIAI), complicated UTI (cUTI), hospital-acquired pneumonia, including ventilator-associated pneumonia (HAP/VAP), bacteraemia (adults only) associated with the aforementioned infections and treatment of infections caused by aerobic Gram-negative organisms with limited treatment options.
In a series of in vitro and in vivo studies, CAZ-AVI was shown to be active against ceftazidime-resistant and many carbapenem-resistant clinical isolates of Enterobacterales and Pseudomonas aeruginosa. It has been studied in several clinical trials, compared with either carbapenems or ‘best available’ AM treatment (colistin based or non-colistin based) in adults with HAP, VAP and healthcare-associated pneumonia, bloodstream infection or sepsis, or cUTI. Efficacy has been demonstrated in clinical studies against the following pathogens: Citrobacter freundii, Enterobacter cloacae, Escherichia coli, Klebsiella oxytoca, Klebsiella pneumoniae, Pseudomonas aeruginosa, Proteus mirabilis and Serratia marcescens. In vitro studies have suggested that CAZ-AVI might also be efficacious against Citrobacter koseri, Enterobacter aerogenes, Morganella morganii, Proteus vulgaris and Providencia rettgeri.
Chapter 2 Aims and objectives
This section of the report contains some material reproduced from the study protocol. © NICE 2022. Protocol for the technology evaluation of ceftazidime with avibactam for treating severe aerobic Gram-negative bacterial infections. Available from www.nice.org.uk/about/what-we-do/life-sciences/scientific-advice/models-for-the-evaluation-and-purchase-of-antimicrobials/ceftazidime-with-avibactam#evidence. All rights reserved. Subject to Notice of rights. NICE accepts no responsibility for the use of its content in this product/publication.
The aim of this technology assessment is to assess the value of CAZ-AVI to the NHS in England for the treatment of severe aerobic Gram-negative bacterial infections when used within its licensed indications.
Specific objectives are:
-
To identify two high-value clinical scenarios (HVCSs), within its broad licensed indications, for which CAZ-AVI is expected to have a significant impact on patients’ outcomes in terms of mortality risks and health-related quality of life (HRQoL).
-
To undertake an ‘evidence mapping’ exercise and relevant systematic literature reviews to characterise the available clinical effectiveness evidence.
-
To establish an appropriate decision-analytic model as a framework to quantify the costs and health benefits of the use of CAZ-AVI under various usage scenarios compared with alternative treatments and management strategies (usage scenarios of other available AMs) in the HVCSs. To use the model to estimate costs and health effects at the individual level, but also to aggregate these to a population level in the form of population incremental net health effects (INHEs).
-
Drawing on the systematic reviews, to identify evidence to populate each decision-analytic model in the HVCSs.
-
To use structured expert elicitation as necessary to supplement the available evidence to populate the decision-analytic models at the levels of the individual patient and populations in the HVCSs.
-
To use available evidence and where necessary expert opinion to quantitatively extrapolate estimated population INHEs associated with CAZ-AVI in the HVCSs to other expected uses for the product beyond the HVCSs and within the product’s licensed indications.
A protocol for the study was developed and is available from the study webpage.
Chapter 3 Decision problem
This section of the report contains some material reproduced from the study protocol. © NICE 2022. Protocol for the technology evaluation of ceftazidime with avibactam for treating severe aerobic Gram-negative bacterial infections. Available from www.nice.org.uk/about/what-we-do/life-sciences/scientific-advice/models-for-the-evaluation-and-purchase-of-antimicrobials/ceftazidime-with-avibactam#evidence. All rights reserved. Subject to Notice of rights. NICE accepts no responsibility for the use of its content in this product/publication.
Decision-making context
The overarching purpose of the Health Technology Assessment (HTA) is to inform funding arrangements for CAZ-AVI in England. The drug’s funding will differ from that of drugs evaluated under NICE Technology Appraisals in two important ways. Firstly, the payment for CAZ-AVI will be delinked from usage volumes and, instead, represent a fixed annual payment over the term of the agreement (3 years in the first instance, followed by a potential extension to 10 years). Secondly, in a NICE HTA, the price is proposed by the manufacturer, whereas here the payment will be agreed via commercial discussions between the manufacturer (Pfizer) and NHS England, informed by this evaluation. The role of the evaluation and subsequent NICE Committee deliberations will be to provide guidance on the value of CAZ-AVI to the NHS in England to inform these commercial discussions. This will include providing advice on the preferred usage of CAZ-AVI including the role of stewardship strategies (i.e. policies to ensure appropriate prescribing).
In previous work, the Policy Research Unit in Economic Methods of Evaluation in Health and Social Care Interventions (EEPRU) set out principles for quantitively evaluating the value of a new AM. 12 The starting point for this is to identify the range of ways in which CAZ-AVI can be used and to compare these scenarios to the range of ways in which other comparator AMs can be used (usage scenarios).
Value is defined as the expected impact of each usage scenario on population INHEs; value is defined at the population rather than individual-patient level as payments to the manufacturer will reflect overall value. Population INHEs reflect expected population-level health benefits to patients and the wider population, expected population-level costs borne by (or savings accruing to) the NHS, and a measure of the health opportunity cost of healthcare funds which allows NHS costs to be converted to health foregone. As the purpose of the evaluation work is to inform a value-based payment for CAZ-AVI, the drug acquisition cost for CAZ-AVI is excluded from the calculation of population INHE. The incremental value of CAZ-AVI is the difference between the population net health effect (NHE) associated with a given CAZ-AVI usage scenario and the highest population NHE for clinically relevant usage scenarios that include only comparator AMs. This is shown in Box 1.
Assume a number of strategies are being compared for a given indication. AM(N)i represent strategies using the new AM and AM(E)i are strategies for existing treatments. Table 1 below provides illustrative estimates of the expected per-patient treated costs (column B) and health effects in terms of QALYs per patient (column C), over the relevant time horizon. The costs of the new AM strategies assume zero acquisition cost for the new product. Any indirect effects on others through changes in resistance are assumed to be reflected in the QALYs per patient treated.
Column D shows the expected per-patient NHEs in terms of QALYs. This is calculated as QALY−CostK, where K is the estimate of health opportunity cost, which in this illustration is £15,000 per QALY. Column E details the expected population NHEs in QALYs assuming the potential to benefit 6000 patients over the time horizon of the analysis. AM(N)3 represents the best of the strategies involving the new AM, with an expected population NHE of 54,104 QALYs for the new AM. To calculate the value of the new drug in NHEs, the difference in population NHE between AM(N)3 and the best of the strategies using existing treatments is calculated (54,104–50,400 = 3704 QALYs). This is the population INHE that is the focus of the current assessment as it will inform the value-based payment for the new treatment.
| A | B | C | D | E |
|---|---|---|---|---|
| Strategy | Expected costs, per patient treated | Expected QALYs, per patient treated | Expected net health benefit (QALYs) per patient treated | Expected population net health benefit (QALYs) |
| AM(N)1 | 6800 | 9.0 | 8.547 | 51,280 |
| AM(N)2 | 7000 | 9.3 | 8.833 | 53,000 |
| AM(N)3 | 7240 | 9.5 | 9.017 | 54,104 |
| AM(E)1 | 7500 | 8.9 | 8.400 | 50,400 |
| AM(E)2 | 7800 | 8.5 | 7.980 | 47,880 |
| AM(E)3 | 7600 | 8.4 | 7.893 | 47,360 |
As the population INHEs will inform the value-based payment to the manufacturer, they should reflect the overall value resulting from expected NHS usage. Expected NHS usage, in principle, reflects both the preferred usage specified in NICE guidance and the implications of clinical decisions taken locally.
As documented in Chapter 1, the licensed indication for CAZ-AVI is fairly broad, being available to any patient with limited treatment options, regardless of the site of the infection. In practice, to control the spread of resistance to CAZ-AVI and to preserve its long-term viability as an effective treatment option, CAZ-AVI is expected to be used in a more restricted group of patients than permitted by its licence. Quantifying the health and cost implications of using CAZ-AVI across anticipated NHS usage, even within this restricted population, remains challenging as use is expected across infections which differ in causative organism (pathogen, susceptibility and resistance mechanism), site of the infection, healthcare setting and other underlying features of the health status of the patient.
This evaluation will seek to characterise the value of CAZ-AVI across its range of expected uses using two approaches. Firstly, decision modelling will be used to evaluate quantitatively the value of CAZ-AVI in two scenarios defined by features of the pathogen, site of infection, healthcare setting and other patient characteristics, considered to represent important uses of CAZ-AVI [referred to as the ‘high-value clinical scenarios’ (HVCSs)]. Secondly, we will provide additional information and quantitative estimates to support the NICE Committee in assessing value in the overall population expected to receive CAZ-AVI, including patients who fall outside the HVCSs.
The literature on the economic evaluation of AMs has described a range of elements of value associated with these products that are not relevant to other interventions, and previous work by EEPRU has sought to explain how these elements of value can be quantified in terms of population INHEs. 12 As part of the current report we assess the extent to which these additional elements of value are likely to apply in the context of CAZ-AVI and quantify them where this is feasible and they are expected to be quantitatively important.
The resourcing for this project was equivalent to that of a diagnostic assessment review or multiple technology assessment for NICE, but the levels of analysis extend from the typical focus of those evaluations on a single type of patient for one indication and setting. In this evaluation, we also include population-level health effects now and over time, and across several indications and settings. The objective is to use appropriate analyses of the available evidence at every level, but the detail in those analyses is inevitably constrained by the time and resources available for the project.
High-value clinical scenarios
Pathogen and resistance mechanisms
An important determinant of the efficacy of existing treatment and, therefore, to defining those patients most likely to benefit from CAZ-AVI is the pathogen causing the infection and its mechanism of resistance.
Feedback during the NICE scoping consultation for CAZ-AVI, and subsequent consultation with clinical experts, has emphasised that CAZ-AVI should be prioritised for the treatment of patients with infections with confirmed or suspected carbapenem-resistant Gram-negative bacteria in secondary/tertiary care. Carbapenem-resistant pathogens can be categorised according to two main classes of resistance mechanisms as discussed in Chapter 1: non-carbapenemase carbapenem resistance and carbapenemase-mediated carbapenem resistance. For infections caused by carbapenem-resistant organisms with non-carbapenemase resistance mechanisms, a range of treatment options remains available. Infections caused by carbapenemase-producing pathogens have fewer treatment options. There are two main classes of carbapenemase-producers: serine-carbapenemases and MBLs. The main serine-carbapenemases among CREs in the UK are OXA-48 and KPC. The main MBLs in the UK are NDM, VIM and IMP. CAZ-AVI is not active against MBLs but is active against serine-carbapenemases. 3
Ceftazidime-avibactam is effective in Enterobacterales and Pseudomonas aeruginosa but not A. baumanni. 13 Since carbapenemase are infrequent mechanisms of carbapenem resistance in Pseudomonas aeruginosa, and when there is carbapenemase it is typically MBL, against which CAZ-AVI has no activity, the focus here is on Enterobacteriaceae but not Pseudomonas aeruginosa within the economic modelling. 14,15
Availability of susceptibility data during the course of an infection
Infections in secondary/tertiary care are typically initially treated with empirically chosen antibiotics. At this stage of treatment there is limited information available to inform treatment choice. Indicators of an elevated risk of carbapenem-resistance at this stage include a range of patient- and setting-specific risk factors. Patient-level factors include prior microbiology history, recent history of hospital or long-term care admissions or regular hospital-based treatments, epidemiological links to other carriers, international travel, immunosuppression and recent broad-spectrum antibiotic exposure. Setting-specific factors include being admitted to augmented care or high-risk units and local epidemiology (e.g. previous history of outbreaks). 16
In some hospitals and tertiary care centres, screening for carriage of carbapenem-resistant pathogens is carried out. Routine screening for colonisation with CPEs at the point of admission has recently been recommended by Public Health England (PHE) for specific high-risk patients and healthcare settings. 16 The objective of this screening is primarily to support enhanced infection-control measures, surveillance and outbreak-management efforts. However, information obtained via screening may also support treatment choice, as colonisation with CPE is a risk factor for a CPE infection. Currently, implementation of screening for CPE is variable in the UK despite the PHE guideline,16 and the level and timing of information provided via screening also vary.
At the point an invasive bacterial infection is suspected, where possible, specimens are obtained to support further diagnostic work. Various diagnostic technologies can be used to better understand the causative pathogen and how it may respond to treatment. There are broadly three layers to this:
-
A culture is undertaken to understand the type of pathogen causing the infection.
-
Antimicrobial-susceptibility testing (AST) is conducted to assess the in vitro activity of a range of AMs against the pathogen in question.
-
Gene testing may also be conducted to establish the presence of specific resistance mechanisms.
Cultures are typically available relatively quickly, with AST and gene testing taking longer [typically more than 48 hours, although this depends on local availability of testing technology and laboratory capacity; e.g. centres with access to polymerase chain reaction (PCR) testing may have information much more quickly]. The availability of gene testing also varies geographically. There may be an increase in the use of gene testing in the UK in the future as PHE has recently recommended routine use of molecular or immunochromatographic assays to detect the main carbapenemase producers. 17
Overall, variability in local practice, laboratory capacity and availability of diagnostic technologies means that there is likely to be significant variation in the nature and timing of the information available to inform treatment decisions.
Overview of high-value clinical scenarios
Based on feedback from stakeholders via the NICE scoping consultation and further discussion with clinical experts, EEPRU has identified two HVCSs for use of CAZ-AVI: microbiology-directed treatment and risk-based empiric treatment. We explain these separately here but, in practice, they are often linked in a single patient pathway.
Microbiology-directed treatment refers to the use of CAZ-AVI in individuals with infections caused by a pathogen confirmed to have a specific pathogen and resistance mechanism. This group of patients has undergone susceptibility testing and gene testing to understand specific resistance mechanisms. As this usage of CAZ-AVI will require susceptibility/gene testing to have been undertaken prior to receipt of CAZ-AVI, this clinical scenario will focus predominantly on individuals with severe but non-critical infections at presentation with infection. PICOS for high-value clinical scenarios describes in more detail the specific Population, Intervention, Comparison, Outcomes and Study designs (PICOS) considered for this scenario.
Risk-based empiric treatment refers to use of CAZ-AVI in the empiric setting (ES) for clinically urgent patients with high suspicion (i.e. a high risk) of specific carbapenem resistance based on patient phenotype but for whom information about the pathogen is currently very limited (susceptibility data and gene testing not yet available). Use within this HVCS should be restricted only to those patients in whom microbiology-directed treatment is likely to be considered inappropriate due to the potential delay in time to appropriate therapy. The risk-based empiric treatment HVCS is, therefore, focused on patients who meet two criteria: (1) the infection is considered clinically urgent based on a range of information including infection site and severity, and broader information relating to the health status of the patient; and (2) the patient is considered at elevated risk of a specific type of carbapenem-resistant infection using the type of risk markers described in Availability of susceptibility data during the course of an infection. PICOS for high-value clinical scenarios describes in more detail the PICOS for this scenario.
PICOS for high-value clinical scenarios
Based on feedback from stakeholders via the NICE scoping consultation and further discussion with clinical experts, EEPRU has defined the PICOS for HVCS for the microbiology-directed and risk-based empiric treatment pathways (Table 2). The PICOS refine the NICE scope (which is broad and reflects the licence of CAZ-AVI) to reflect the HVCS.
| Element | Microbiology-directed setting | Risk-based empiric setting |
|---|---|---|
| Population – patients | Where microbiological susceptibility testing and gene testing has been performed | With clinically urgent disease with high risk of an infection caused by a resistant pathogen. Suspicion of infection may be based on knowledge of the local epidemiology where a patient was previously hospitalised, outbreak in the ward where the patient is currently admitted, or previous cultures (taken during the current or previous hospital stays) showing the patient was colonised by an OXA-48 Enterobacterales. |
| Population – pathogen mechanism | Patients with Enterobacterales which have OXA-48 mechanisms of resistance | Infections suspected to be caused by Enterobacterales which have OXA-48 mechanisms of resistance. |
| Population – site of infection | cUTI
|
HAP/VAP. |
| Intervention | CAZ-AVI alone or in combination | CAZ-AVI alone or in combination. |
| Comparators These comparators reflect NHS practice based on clinical advice. The available evidence will determine which of those listed (and possible additional products including combinations) will be formally incorporated into the modelling |
Comparators used in clinical practice in England, as defined by susceptibility testing and/or gene testing and considering infection site and infiltration data. Potential comparators include:
|
Potential comparators in the risk-based empiric HVCS include:
|
If low risk of ESBL and AmpC beta-lactamase suggested by susceptibility testing:
|
||
For HAP/VAP the following comparators may be included also:
|
||
| Outcomes | The outcome measures to be considered include:
|
Same as for microbiology-directed treatment. |
| Study designs | The types of studies and data to be considered include:
|
Same as for microbiology-directed treatment. |
Microbiology-directed treatment
In the microbiology-directed usage scenario, feedback from stakeholders and clinical experts indicated that cUTIs have high prevalence and a slower clinical course than, for example, HAP and VAP. They are also responsible for a high proportion of bloodstream infections (BSI), the reduction of which is a key priority for NHS England (NHSE). cUTI infections were therefore selected as the infection site for the microbiology-directed HVCS, with additional analysis also provided for HAP/VAP in the MDS.
Clinical and stakeholder advice also indicated that CAZ-AVI would be reserved for infections with limited treatment options, where susceptibility is demonstrated. This suggests CAZ-AVI should be reserved to treat infections caused by carbapenemase-producing pathogens. As discussed in High-value clinical scenarios, CAZ-AVI is not active against MBL mechanisms, or against A. baumannii pathogens, and serine carbapenemase mechanisms are not often found in Pseudomonas aeruginosa. The patient group for the HVCS will, therefore, be limited to patients with infections caused by serine Enterobacterales. For this patient group, OXA-48 and KPC resistance mechanisms are most predominant. Patients with pathogens with KPC generally have more treatment options than those with OXA-48 and we therefore focus on OXA-48 in the HVCS.
Ceftazidime-avibactam can be used as a monotherapy but may also be used in combination with other treatments, as indicated by microbiology and gene testing. In clinical practice, alternative treatment options (comparators) would be defined by the results of susceptibility and gene testing.
Risk-based empiric treatment
In the risk-based empiric usage scenario, feedback from stakeholders and clinicians indicated that the most frequent clinically urgent infections are HAP/VAP and BSI. cUTI infections were not considered relevant in this setting since they have a slower clinical course, giving time for AST to be performed. Given the time and resources available for this project, the focus was on the HAP/VAP sites as this was considered the most common indication for empirical antibiotics in high-risk patients such as those in the intensive care units/high-dependency units (ICU/HDU) (whereas patients with BSI are more likely to have had microbiology). Patients will be those who have a high risk of an OXA-48 Enterobacterales. Focusing on this high-risk group was highlighted by the clinical advisors to this project as preferable to considering a broader group of patients with suspected carbapenem resistance, even if deteriorating rapidly on current therapy, as the latter group would be difficult to define and may lead to high levels of prescribing with associated risks of resistance emergence. Three patient characteristics were considered as relevant by our clinical advisors in identifying patients at high risk of an OXA-48 infection: a high rate of OXA-48 Enterobacterales in a healthcare setting where the patient was previously admitted, an outbreak of OXA-48 Enterobacterales in the ward where the patient is currently admitted, or previous cultures (taken during the current or previous hospital stays) showing the patient was colonised by an OXA-48 Enterobacterales. CAZ-AVI may be used as monotherapy in this usage scenario, or may be used in combination with other treatments to provide a broader spectrum of coverage. A range of comparators are relevant in this setting. Once microbiology has confirmed the susceptibility profile and mechanisms of resistance of the pathogen, treatment may be continued or stopped, dosage may be altered or different AMs may be initiated.
Chapter 4 Clinical evidence
The evidence reviews reported within this section focus on the clinical evidence required to inform the patient-level component of the decision-analytic modelling. This includes estimating the comparative effectiveness of treatments, including both efficacy and safety, and the consequences of treatments in terms of long-term clinical outcomes, for both efficacy and safety. Clinical evidence that informs the population-level components of the analysis is described in Chapter 8.
Approaches to estimating comparative effectiveness
Sources of evidence
In comparison to a standard HTA, the data available for evaluating new AMs are less straightforward. This has been discussed in detail in EEPRU’s framework. 12 This is largely because the randomised controlled trial (RCT) evidence is primarily generated for regulatory purposes, to demonstrate safety and efficacy against a range of pathogens. Trials are usually non-inferiority in design (usually with a −10% margin), and the comparators tend to be best available therapy. Patients with extensively drug-resistant infections, such as those with OXA-48 infections, are usually excluded from these trials because it would be unethical to randomise patients to an ineffective comparator treatment, and testing patients to find out which treatments they are susceptible to could introduce critical time delays in treatment of very ill patients. Therefore, trials tend to recruit patients who are expected to be susceptible to the intervention and the comparator, that is, not extensively drug-resistant. The relative treatment effect generated by such trials cannot be generalised to resistant populations, since this would overestimate the efficacy of the comparators, as resistant patients are unlikely to respond as well to best available therapy. In addition, best available therapy may not match clinical practice in England since best practice is highly variable due to local protocols reflecting testing capacities and the microbiological epidemiology in a given area. Regulatory trials also do not tend to address differences in treatment pathways, such as are found between the MDS and risk-based ES, or differences in stewardship protocols, such as rotation of AMs, mixing treatments or combination therapies. For the assessment within the MDS, RCTs and observational studies are required that report outcomes in patients with the confirmed pathogen–mechanism combination of interest, while in the ES patients will only be suspected of having an infection with the pathogen–mechanism combination of interest.
As such, from the outset, EEPRU were aware that additional sources of evidence may be required to fulfil the comparative effectiveness component, since it was unlikely that the RCTs would have been performed in patients with infections caused by the specific pathogen–mechanisms of interest. The next levels of evidence in the evidence hierarchy are non-randomised studies and observational studies. EEPRU’s earlier work12 also highlighted the potential for using susceptibility studies to supplement clinical data. We therefore aimed to identify all these possible sources of evidence in our review (see Review questions). In the next section, a brief description of susceptibility studies is provided, since this study design is one that is not commonly encountered. Following this, a discussion of how the different study designs might be used to produce effectiveness estimates is provided (see Producing comparative efficacy estimates).
Susceptibility studies, PK/PD studies and breakpoints
Susceptibility studies are in vitro studies that report the results of AST. AST is a laboratory method where isolates taken from patients (from infections or during screening) are grown in vitro (cultured), and tested for their susceptibility to various AM treatments. The AM being tested is applied at increasing concentrations to separate cultures of the sampled isolate, and the degree to which microbial growth is inhibited at each concentration is assessed. The lowest concentration at which microbial growth is inhibited is known as the minimum inhibitory concentration, or MIC.
Clinical breakpoints distinguish between isolates where there is a likelihood of treatment success and those where treatment is more likely to fail. 18 If the MIC of a given isolate is at or below the breakpoint, the isolate is judged to be ‘susceptible’. If it is above the breakpoint, the isolate is judged to be ‘resistant’. For some AMs, there is also an intermediate category, which more recently has become ‘susceptible – increased exposure’, indicating that a higher dose of the drug should be used to elicit a response. They may also report the concentration at which 50% of isolates were inhibited (MIC 50), and the concentration at which 90% were inhibited (MIC 90).
The methods for setting breakpoints are not standardised. Currently, they are generally set by considering:19
-
The PK data: how the body affects the drug with respect to absorption, distribution, metabolism and excretion, usually obtained from studies in healthy volunteers.
-
The PD data: how the drug affects the body (efficacy and toxicity) at its site(s) of action, usually obtained from in vitro studies, hollow-fibre studies, animal studies and human studies. These data are used to set PD targets, for example for time above MIC.
-
Mathematical models (e.g. Monte Carlo simulation) to assess the likelihood of achieving the targets suggested by the PD data.
-
Any available clinical data linking treatment to clinical outcomes (e.g. from RCTs or observational studies).
Pharmacokinetic/pharmacodynamic studies are conducted to estimate how much drug will be available at the site of interest, and for what period of time at a given dose. One of its primary uses is by manufacturers and regulatory bodies to decide on the appropriate dose and dose frequency of the drug, such that it is likely to be available at concentrations that are likely to have an effect at the sites of interest.
There are two main organisations that set breakpoints, the Clinical Laboratory Standards Institute (CLSI) in the USA, and the European Committee on Antimicrobial Susceptibility Testing (EUCAST) in Europe. These two organisations use different methodologies to set breakpoints, leading to differences in the breakpoints set both in absolute and in relative terms, between treatments. They also describe different laboratory methods to assess MICs. In addition, many labs may use commercial assays, conducted according to manufacturer’s instructions. Clinical advisors to EEPRU indicated that it was unclear to what extent CLSI, EUCAST and commercial methods would produce the same absolute values, and, in the event that values were different, whether relative values between treatments would also be different (i.e. the difference in absolute values was not consistent across treatments). In the UK, the British Society for Antimicrobial Chemotherapy (BSAC) now recommends use of EUCAST methods and breakpoints.
Susceptibility studies tend to report the proportion S, I and R, or list the number of isolates at each MIC. An example is given in Table 3. Here, for cefepime, the breakpoint is 1 mg/l, and since all isolates had MICs higher than the breakpoint, none were susceptible. For CAZ-AVI, with a breakpoint of 8 mg/l, 90.9% were susceptible, since only one isolate had a MIC above this point.
| Treatment; breakpoint | Number susceptible, cumulative % susceptible | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Drug concentration (mg/l) | ≤ 0.06 | 0.12 | 0.25 | 0.5 | 1 | 2 | 4 | 8 | 16 | 32 | > 32 | Susceptible, % |
| Cefepime (n = 11) | 4 | 3 | 1 | 3 | 0 | |||||||
| BP: 1 mg/l | 36 | 64 | 73 | 100 | ||||||||
| Meropenem (n = 11) | 4 | 3 | 0 | 1 | 3 | 100 | ||||||
| BP: 2 mg/l | 36 | 64 | 64 | 73 | 100 | |||||||
| CAZ-AVI (n = 11) | 1 | 0 | 0 | 1 | 0 | 3 | 5 | 0 | 0 | 0 | 1 | 90.9 |
| BP: 8 mg/l | 9 | 9 | 9 | 18 | 18 | 45 | 91 | 91 | 91 | 91 | 100 | |
Producing comparative efficacy estimates
Three main approaches, relating to the three main types of evidence available, were developed:
-
Approach 1: Review RCTs for any subgroup data relating to the pathogen–mechanisms–sites defined in the HVCSs and use these estimates to inform the model. A network meta-analysis (NMA) would likely be needed to provide estimates for the intervention and comparators, and all these studies would also need to be in the pathogen–mechanism–sites defined in the HVCSs.
-
Approach 2: Construct a network of observational studies relating to the pathogen–mechanism–sites defined in the HVCSs, treated with CAZ-AVI and comparators. Individual patient data (IPD) data would be required for at least one study to adjust for confounders.
-
Approach 3: Use susceptibility studies (see Susceptibility studies, PK/PD studies and breakpoints), that is, those that have tested relevant treatments in OXA-48 Enterobacterales isolates in vitro, to provide estimates of relative treatment effects. Conduct a NMA of susceptibility evidence if necessary, to link the intervention and its comparators. Link in vitro susceptibility to clinical outcomes. Two approaches to linking susceptibility to clinical outcomes were considered:
-
Assume that, for patients who are susceptible to the treatment they are given, clinical outcomes would be similar regardless of the treatment received.
-
Assume that different treatments may result in different outcomes even among those susceptible to the treatment. Use evidence from a NMA of RCTs (in any susceptible pathogen-mechanism, not just those considered within our HVCS) to estimate differences in treatment outcomes among susceptible patients. These relative treatment effects would then be applied to the proportion susceptible to the intervention and comparators, taken from the susceptibility NMA or epidemiological data.
-
Each of these approaches has its own merits and challenges.
In Approach 1, the difficulties with recruiting resistant patients mean subgroup data from RCTs may be underpowered and under-representative of the full spectrum of infections. Where available, however, they could provide estimates with high internal validity (low risk of bias). Equivalent data for comparators from RCTs may be missing in the pathogen–mechanism–sites of interest.
In Approach 2, comparative observational studies are often at high risk of confounding due to imbalances between prognostic and/or predictive factors at baseline, while comparisons across single-arm studies would require advanced synthesis techniques to mitigate any apparent imbalances. Results from such analyses can be prone to a high degree of uncertainty and there may be residual confounding, for example from imbalances in unknown or unobserved confounders. However, such studies may be able to include higher numbers of patients, since the barriers to recruitment described for RCTs are reduced.
In Approach 3, susceptibility studies have the advantage of testing all the treatments in the same sample of isolates, thereby reducing the chance of heterogeneity in patient samples between arms introducing confounding. They also tend to include higher numbers of patients/isolates. However, any given susceptibility study will have its own distribution of susceptibilities for each treatment, which gives rise to the comparative treatment effects as expressed by percentage susceptibility, and this may not match the susceptibility profile of pathogens circulating in the UK, or that are likely to circulate in the future. In addition, susceptibility studies are in vitro, and no clinical outcomes are reported. In order to use this approach in the model, additional evidence requirements would be created since susceptibility can be considered a surrogate endpoint. It would be necessary to link susceptibility to clinical outcomes such as clinical cure, 30-day mortality, 90-day mortality, hospital length of stay (LoS), long-term mortality and recurrence of infections (see questions 4–6 below). As noted above, this approach would assume that, conditional upon susceptibility, clinical outcomes are similar across different AMs. An extension to this approach would be to use evidence from a NMA of RCTs (in broader populations than those considered within our HVCS) to estimate differences in treatment outcomes among susceptible patients regardless of the pathogen–mechanism they are infected by, but dependent on the AM they were treated with. This would assume that relative treatment effects between AMs are generalisable across pathogen mechanisms, so long as patients were susceptible to the treatment they were given. For both approaches, these assumptions would need to be supported by empirical evidence and/or expert opinion.
Review questions
For each approach, a corresponding review question was developed (Table 4). This section briefly states each review question, while sections Review methods to Statistical synthesis describe the PICOS and methods of evidence retrieval for each question. Subsequently, Additional review questions for Approach 3 describes three additional reviews (Reviews 4–6) relating to Approach 3.
| Approach number | Study designs | Review question and number | Analytical approach | Taken forward (with reasons)? | Results |
|---|---|---|---|---|---|
| 1 | RCTs |
|
NMA to estimate comparative efficacy | No, insufficient evidence in patients with OXA-48 infections | See Reviews 1 and 2 |
| 2 | Observational studies |
|
Matched analysis | No, small studies, data not reported specific to the sites of interest; IPD not available | See Reviews 1 and 2 |
| 3 | Susceptibility studies |
|
NMA to estimate comparative efficacy from susceptibility studies; link susceptibility to clinical outcomes | Yes | See Review 3 to Results of the network meta-analysis |
| Any clinical study |
|
See Review questions 4 and 5 | |||
| Any clinical study |
|
To supplement approaches 1–3 | See Review questions 4 and 5 | ||
| RCTs |
|
To supplement approaches 1–3 | See Review questions 6 |
Review 1
Review question: Based on RCT evidence, what is the comparative effectiveness of the intervention and comparators in patients with cUTI or HAP/VAP caused by an OXA-48 Enterobacterales infection?
In addition to recruiting patients infected with the relevant pathogen–mechanism combination, the ideal study would be based on treatment in the UK or a country with a similar demographic and healthcare system, to reduce the impact of other factors on patient outcomes. Only evidence relating to the sites of interest would be relevant, since the risk of mortality and morbidity from infections at other sites is likely to be different.
Review 2
Review question: Based on observational studies, what is the comparative effectiveness of the intervention and comparators in patients with cUTI or HAP/VAP caused by an OXA-48 Enterobacterales infection?
Again, in addition to recruiting patients infected with the relevant pathogen–mechanism combination, the ideal study would include patients in the UK or a country with a similar demographic and healthcare system, and would be in the sites of interest.
Review 3
Review question: What is the comparative effectiveness of the treatment and comparators based on in vitro susceptibility studies?
Because of their in vitro nature, and since clinical experts to EEPRU indicated that the site of the infection the isolate was obtained from was unlikely to affect the susceptibility profile of the infecting pathogen, isolates could be collected from any site.
Table 4 provides a summary of the alternative approaches to estimating comparative efficacy and safety.
Review methods
Since review questions 1–3 were of central importance to estimating the comparative efficacy of treatments, a de novo search from database inception was undertaken to address all three questions. The nature and suitability of the evidence base were unknown but, as already discussed, there was a strong expectation that RCT evidence would not be of high relevance, that is to say, would not have recruited patients with Enterobacterales infections carrying OXA-48. It was also unclear to what extent multiple HVCSs (e.g. including KPC, including BSI) could be addressed in the evaluation (Table 5). Therefore, a map of the available evidence was first constructed to maintain flexibility, and to aid an informed focusing of the inclusion criteria as the project proceeded (Table 6). This methodology has been used elsewhere, and is especially suited to topics such as this where the initial scope is broad. 20,21 The map comprised data extraction of key study characteristics. It was based on systematic literature searches of key bibliographic databases (see Search strategy) supplemented by evidence submitted by experts and stakeholders, including the submission received from Pfizer and data requests to PHE, Pfizer and Shionogi (who were participating in a concurrent EEPRU evaluation of cefiderocol). Evidence was then selected for further consideration according to a balance of relevance with study quality, as recommended in the Decision Support Unit Technical Support Document (TSD) 13. 22 Where preferred sources did not yield data, additional focused searches were employed to ensure studies had not been missed or to fill evidence gaps. Where additional searches still did not yield data, elicitation was performed to fulfil the evidence requirement (see Chapter 5).
| Characteristic | Keyword mappinga | Key characteristics tabulationa | Selection for synthesis |
|---|---|---|---|
| Population | |||
| Patients | Adults or children | Adults | Isolates from adults or children recruited consecutively, purposively, by convenience or as part of another study, e.g. RCT Screened or invasive samples |
| Pathogen–mechanism | MDS: CPE with OXA-48 or OXA-48-like; CPE with KPCb ES: suspected CRE treated empirically |
MDS: CPE with OXA-48 or OXA-48-like ES: suspected CRE treated empirically |
CPE with OXA-48 or OXA-48-like |
| Site of infection | RCTs: any site Observational studies and case-series: cUTI, HAP/VAP or BSIb Susceptibility studies: any site |
RCTs, observational studies and case-series: cUTI, HAP/VAP Susceptibility studies: any site |
Susceptibility studies: any site |
| Setting | MDS or ES | MDS or ES | Any country; UK, Europe, USA, Canada, Australia, Asia and Middle East have highest relevance |
| Intervention | |||
| CAZ-AVI | CAZ-AVI | CAZ-AVI | |
| Comparators | |||
| Any | Any | At least one of: colistin, meropenem, tigecycline, aztreonam, fosfomycin, levofloxacin, ciprofloxacin, gentamicin, amikacin, tobramycin, ceftriaxone, cefepime, ceftazidime | |
| Outcomes | |||
| As listed in PICOS for high-value clinical scenarios | As listed in PICOS for high-value clinical scenarios | In vitro susceptibility reported as proportion susceptible (not including intermediate) according to EUCAST or CLSI criteria Studies only reporting MIC50 and/or MIC90 with range were excluded |
|
| Study designs | |||
| RCT, observational studies, case series, susceptibility, PK/PD | RCT, observational studies, case series, susceptibility, PK/PD | Susceptibility studies where isolates were collected and tested retrospectively or prospectively | |
| Topic | Summary of clinical response |
|---|---|
| Location | Europe, USA, Canada, Australia, the Middle East and Asia have the most relevance since pathogens tend to arrive in the UK from these countries. South America to a lesser extent. |
| Date of recruitment | Studies from 2012 onwards have highest relevance. Likely to observe increases in resistance over time. |
| OXA-48 vs. OXA-48-like | Data relating to either OXA-48 or OXA-48-like isolates should be included, since PHE’s categorisation is OXA-48-like, and since only OXA-163 has a different susceptibility profile and should generally be excluded from the OXA-48-like category. |
| Sampling strategy and outbreaks | Consecutive sampling (which is often associated with studies of outbreaks) not necessarily more generalisable, since outbreaks will reflect a narrow spectrum of pathogens and may therefore underestimate diversity of susceptibility; multicentre studies should be more reflective of the diversity of isolates and should include outbreaks proportionate to their occurrence. |
| Isolates from screening | These are relevant since they will reflect the diversity of susceptibility found. Development of an infection is not dependent on the pathogen or mechanism per se, and so screening samples should be generalisable to infected patients. |
| AST laboratory methodologies | There are differences between EUCAST and CLSI methodologies (see Sources of evidence), and it is unclear whether the two methodologies result in the same distribution of MICs at the same values for a given set of isolates. If the distribution or absolute values differ, the methodologies cannot be considered interchangeable. EEPRU were unable to identify any literature directly comparing the two methodologies for the treatments in the HVCSs and concluded methodologies could not be assumed to be interchangeable. |
| Breakpoints | Expert advice indicated that CLSI and EUCAST breakpoints differ and cannot be assumed to be interchangeable (see Susceptibility studies, PK/PD studies and breakpoints). It is unclear whether studies using EUCAST laboratory methods and breakpoints would return the same % susceptible as studies using CLSI laboratory methods and breakpoints. It cannot be assumed that breakpoints from one guideline can be applied where laboratory methods from the other guideline have been used. |
| PK/PD data | Clinical advisors stated that the methodologies for conducting PK/PD data are not standardised and it is difficult to ascertain whether a study has been conducted well. Since the breakpoints set by EUCAST and CLSI are based on an assessment of the available PK/PD data, and as long as the treatment is known to infiltrate the appropriate site, it is reasonable to assume that susceptibility can be linked directly to clinical outcomes without further explicit consideration of PK/PD evidence. The advisors stated that CAZ-AVI and the comparators for each site penetrate to the sites of interest and it was therefore considered unnecessary to review these data. |
Search strategy
An initial search for studies on CAZ-AVI without study design filters was performed. The first 200 records were reviewed before undertaking searches combined with study design filters (RCTs, observational studies and systematic reviews) and susceptibility-study terms.
To ensure that all susceptibility studies from the UK were identified, a search iteration was conducted. Additional terms were included in the iteration, and these were based on a review of susceptibility studies that were identified by sifting the first 200 citations retrieved by the search without study design filters. The iteration included terms for CAZ/AVI AND a UK filter AND (broader OXA-terms OR AM susceptibility terms).
The following electronic databases were searched from database inception:
-
MEDLINE and Epub Ahead of Print, In-Process, In-Data-Review & Other Non-Indexed Citations, Daily and Versions: Ovid, 1946 to present
-
EMBASE: Ovid, 1980 to present
-
The University of York Centre for Reviews and Dissemination (CRD) platform
-
Database of Abstracts of Reviews of Effects (DARE): CRD, 1994 to 2015
-
Health Technology Assessment Database (HTA): CRD, 1989 to 2018
-
NHS Economic Evaluation Database (NHS EED): CRD, 1972 to 2015.
-
The search strategies are provided in Appendix 1.
In addition to the database searches, the following unpublished data were requested:
-
Public Health England.
Evidence on susceptibility to OXA-48 Enterobacterales for CAZ-AVI and the comparators defined by the HVCS were requested from PHE. This is detailed in Report Supplementary Material 1.
-
data request to Pfizer
-
submitted to NICE on 21 May 2021: request for any data relating to observational studies for which they had access to IPD
-
submitted to NICE on 18 June 2021: request for any OXA-48 Enterobacterales susceptibility data they had access to, for CAZ-AVI and the HVCS comparators.
-
Two surveillance databases were also identified and queried for data that could be included in the review (Antimicrobial Testing Leadership And Surveillance (ATLAS) and SENTRY). 23,24
Keyword mapping, study selection, data extraction and quality assessment
Citations retrieved by the search were uploaded in Endnote [Clarivate Analytics (formerly Thomson Reuters), Philadelphia, PA, USA], deduplicated and considered for inclusion in the review.
Keyword mapping
Citations that met the inclusion criteria listed in Table 5 were tagged in Endnote by one reviewer, according to key study characteristics: treatment (CAZ-AVI); study design (RCT, observational, susceptibility, PK/PD); mechanism (OXA-48, KPC, other); pathogen (Enterobacterales, other) and site (cUTI, HAP/VAP, BSI, other). All potential sources of evidence, including RCTs, observational studies, in vitro studies and national, local or international datasets identified in the grey literature, were included in this stage of mapping.
Key characteristics mapping
A subset of studies that met the inclusion criteria listed in Table 5 were selected for key characteristics tabulation by one reviewer. The full texts of RCT and observational studies identified as being potentially relevant based on their title and abstract were consulted in the first instance, and studies were tabulated and assessed for relevance against the key characteristics mapping criteria, and for relevance to the model. Since an assessment of this map concluded that insufficient relevant in vivo evidence was identified (see Reviews 1 and 2), the next level of evidence (susceptibility studies) was also tabulated.
Key study characteristics tailored to the study designs of interest (e.g. sample size, population, pathogen, mechanism, site, outcomes reported, susceptibility methodology; see Report Supplementary Material 1) were tabulated by one reviewer. Data relating to numeric outcomes were not extracted and quality assessment was not performed at this stage.
Study selection
At the final stage of study selection, only susceptibility studies were considered since other sources did not meet the requirements of the project. The reasons for this decision are detailed in Study selection results (reviews 1–3). The inclusion criteria are listed in Table 5.
Advice was sought from clinical advisors to aid the assessment of the relevance of susceptibility studies to the HVCSs, and to inform the final selection of evidence. Factors including location, date of recruitment, OXA-48 versus OXA-48-like mechanisms, sampling strategy, screening and outbreak populations, and susceptibility testing methodologies were considered, and decisions made (Table 6). At this point, a decision was made not to review the PK/PD data, since these data are reviewed when setting breakpoints, and since clinical advisors to EEPRU stated that since the treatment and comparators penetrate to the sites of interest it was therefore reasonable to link directly between susceptibility and clinical outcomes (Table 5).
Due to time restrictions on the project, only studies reporting susceptibility to both CAZ-AVI and also to any one of the comparators listed in Table 2 were included. This is a pragmatic approach to evidence retrieval, since ideally all susceptibility data relating to all comparators would have been included in the evidence synthesis, but searches to identify this evidence would have been large. No studies reported combinations of AMs, the process for estimating efficacy for combination treatments using the results of the evidence synthesis is described in Clinical parameters – susceptibility evidence. Consequently, studies reporting susceptibility to both CAZ-AVI and also to any one of the comparators listed in Table 2 were included.
Data extraction
Data sources selected for inclusion in the review were data extracted by one reviewer and extractions were checked by a second. The initial key characteristics tabulation was expanded to include numerical outcome data for the susceptibility studies, and data were checked by a second reviewer. Data sources not selected for use in the model or clinical review were tabulated and reasons for their exclusion provided but they were not assessed further.
Quality assessment
Since there is no published quality assessment tool for susceptibility studies, a bespoke set of questions was developed and applied, relating to internal bias and relevance. This tool was developed by consulting two tools developed for the assessment of prevalence studies25,26 (since studies report the prevalence of susceptibility), the risk of bias in non-randomised studies (ROBINS)-1 checklist27 for non-randomised studies (since the studies are comparative, but non-randomised), Cochrane’s risk of bias 2 (RoB2)28 tool [since the network meta-analysis (NMA) will assume the study arms are equivalent to randomised arms of a RCT], and the Newcastle–Ottawa Scale29 (since these are observational studies). Questions from all tools were considered for inclusion, and adapted to the specifics of this review. The tool was reviewed by other members of the reviewing team, but no further validation work was undertaken. The final tool is reported in Appendix 2, Table 36. Risk of bias was assessed using this tool by one reviewer.
Review results
Study selection results (reviews 1–3)
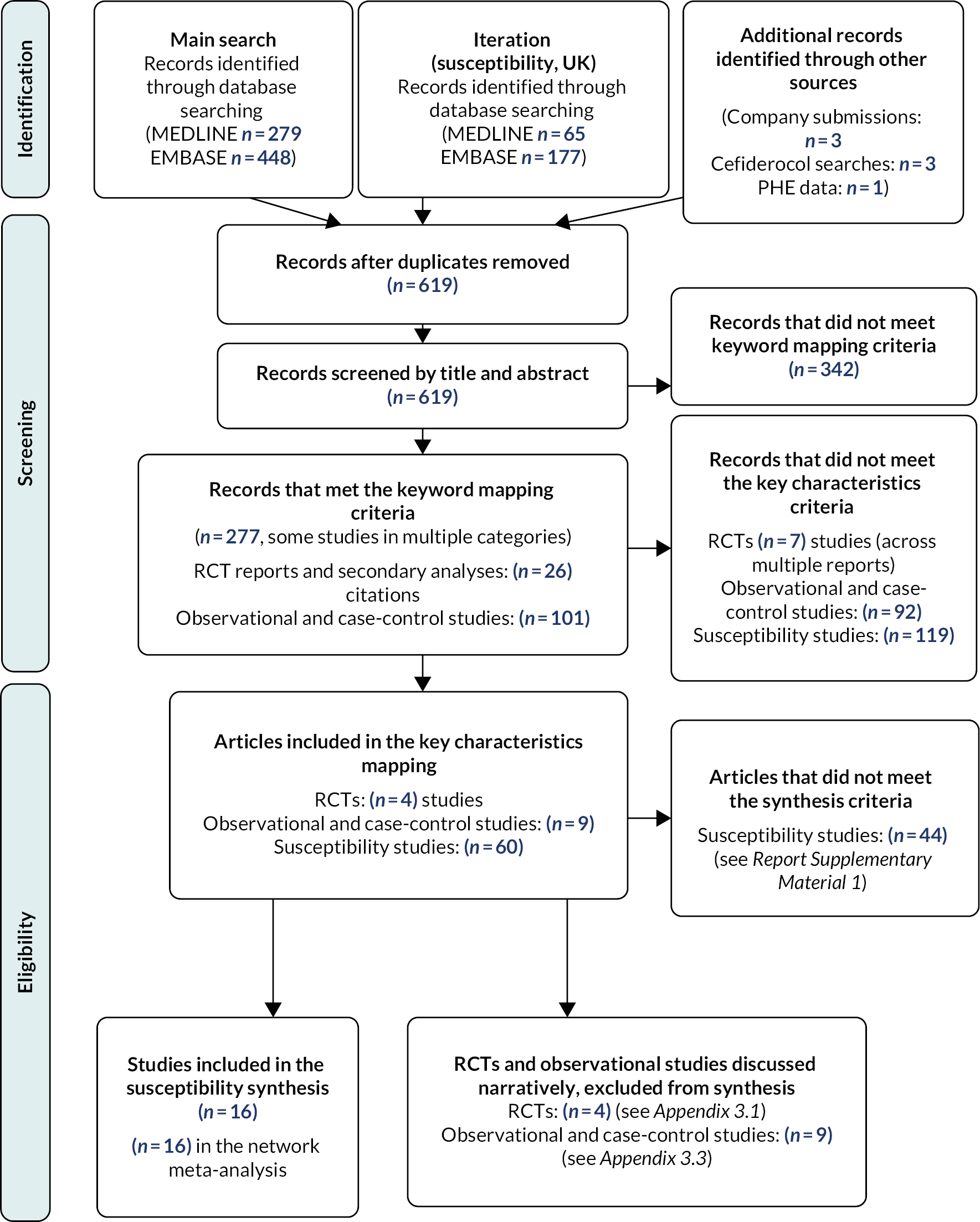
The electronic database searches, following the removal of duplicates, identified 612 records relating to CAZ-AVI. Seven additional records were identified from other sources (Pfizer30 procurement documentation, n = 2; searches for the assessment of cefiderocol, performed by EEPRU, n = 3; data request to Pfizer, n = 1; data request to PHE n = 1), meaning a total of 619 records were assessed. After examination of the titles and abstracts, 277 records met the keyword mapping criteria (Table 5) including 101 observational and case-control studies, 26 reports of RCTs (some reanalyses of the same study) and 179 susceptibility studies (NB, some citations could count in multiple categories, e.g. an observational study that also reported susceptibility), while 342 records were excluded on the basis of their title and abstract. At this point, the decision was made to focus on OXA-48 infections in cUTI and HAP/VAP (i.e. exclude KPC and BSI studies), and not to review PK/PD data (Table 6). Consequently, 7 RCTs (across multiple reports), 92 observational or case-control studies and 119 susceptibility studies were excluded because their title or abstract indicated that they did not meet the inclusion criteria for the key characteristics mapping stage. The full texts of the remaining studies were obtained, and these were tabulated in the key characteristics map. The map included 4 RCTs, 9 observational and case-control studies and 60 susceptibility studies. The RCTs and observational case-control studies were assessed for relevance to the model (see Reviews 1 and 2). Ultimately, it was not possible to use these studies in the modelling and the focus of the review became susceptibility studies. In the final susceptibility synthesis, 16 studies were retained (Table 7). The reasons for exclusion of the 44 other susceptibility studies are provided in Report Supplementary Material 1.
| Study ID, Funding | Country, multisite? Year(s) of recruitment | N, Includes OXA-48-like? | Inclusion criteria/beta-lactamase testing selection criteria | Consecutive sample? | % mero non-susceptible | MBL co-carriage? | Laboratory methods, breakpoints | Source of study | Included in network meta-analyses? |
|---|---|---|---|---|---|---|---|---|---|
| UK studies | |||||||||
| PHE data31 PHE |
UK, multisite 2014-21a |
85 Y |
CPE isolates submitted to PHE AMRHAI with suspected CR tested for CAZ-AVI susceptibility | Unclear | 46% | NR | Unclear | PHE data request | Y: EUCAST; full |
| Livermore 201132 NR |
UK, multisite Unclear, at least 2008 |
19 Unclear |
CPE isolates (all were KP) submitted to PHE AMRHAI with suspected CR | Unclear | 68% | NR | CLSI EUCAST (reviewer-applied) |
EEPRU search | Y, full |
| Non-UK studies (in order of size) | |||||||||
| Confidential information has been removed33 | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
| Kazmierczak 201834 (INFORM) AstraZeneca |
International, multisite 2012–5 |
265b 303c Y |
CPE – CR or ceftazidime-resistant, or positive for ESBL by clavulanic acid testing | No – selected predefined # per species | 73.6% | 0%b 9.01%c |
CLSI CLSI, EUCAST for colistin, US FDA for TIG and CAZ-AVI (≤ 8 mg/l) |
EEPRU search | Y, full |
| Vazquez-Ucha 202135 MSD |
Spain, multisite 2018 |
302b 305c Y |
CPE above meropenem screening cut-off (NR) tested | Unclear (states ‘representative’ sample) | 20.7% | 0%b 0.98% |
EUCAST EUCAST |
EEPRU search | Y: EUCAST; Full; no-MBL (EUCAST) |
| Garcia-Castillo 2018 (iCREST – Spain)36 AstraZeneca + other research bodies |
Spain, multisite 2016 |
164 Unclear |
CPE – screened for CPE using commercial assay | Y | 12.2% | NR | NR EUCAST |
EEPRU search | Y, full |
| Longshaw 2020 (SIDERO-CR 2014–6)37 Shionogi |
European, multisite 2014–6 |
85 Y |
CPE, tested meropenem resistant (> 2 mg/l) | No – selected on susceptibility phenotype and/or species | 87.1% | 9.4% | CLSI EUCAST |
EEPRU search | Y, full |
| Mataraci 202038 Bilimsel Aras¸ tirma Projeleri Birimi |
Turkey, unclear if multisite 2017 |
74 Unclear |
KP, E. coli or E. cloacae – unclear how selected for testing | Unclear | NR | NR | EUCAST EUCAST |
EEPRU search | Y: EUCAST; full |
| Han 202039 NNSFC |
China, multisite 2016–8 |
68 Y |
CPE – resistant to one or more carbapenems, or producing a carbapenemase | Y | 95.6% | 0% | CLSI CLSI, US FDA for TIG |
EEPRU search | Y, full |
| Johnston 202040 Shionogi |
USA and International, multisite 2002–17 |
64 Unclear |
CR E. coli, various criteria to select for testing | No, mix of consecutive and unknown (voluntary submissions to Minnesota DoH) | 24% | NR | CLSI CLSI |
EEPRU search | Y, full |
| Kazmierczak 201941 (SIDERO-WT) Shionogi |
International, multisite 2014 |
32 Y |
CPE, meropenem-resistant or colistin-resistant selected for testing | No – selected predefined # per species | 100% | 15.6% | CLSI CLSI, EUCAST for colistin |
EEPRU search | Y, full |
| Viala 201942 None |
France, single site 2015–7 |
27 Unclear |
CPE – OXA-48, unclear how selected for testing | Y | 40% | NR | NR EUCAST |
EEPRU search | Y, full |
| De la Calle 201943 None |
Spain, single site 2014–6 |
24 Y |
CPE – isolates with reduced susceptibility to carbapenems (EUCAST breakpoint) tested, only included those who received CAZ-AVI | Y | 54.2% | NR | NR EUCAST |
EEPRU search | Y, full |
| Galani 201944 MSD |
Greece, multisite 2014–6 |
19 Y |
KP, carbapenem non-susceptible isolates tested | Y | 100% | 0% | CLSI EUCAST |
EEPRU search | Y, full |
| Sherry 201845 AstraZeneca |
Australia, unclear if multisite 2012–5 |
14 Y |
CPE (E. coli or KP recruited), unclear how selected for testing | No, selected diverse ‘representative’ sample | NR | NR | CLSI CLSI, FDA/EUCAST for CAZ-AVI |
EEPRU search | Y, full |
| Bhagwat 202046 Wockhardt Ltd |
India, multisite 2016–8 |
11b 26c Y |
E. coli with aztreonam-avibactam MICs 1 mg/l | Unclear | 0% | 0%b 57.7%c |
CLSI EUCAST (reviewer-applied) |
EEPRU search | Y, full |
A Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) flow diagram outlining the process of identifying relevant literature is provided in Figure 1.
FIGURE 1.
Preferred Reporting Items for Systematic reviews and Meta-Analyses flow diagram for the CAZ-AVI clinical effectiveness review.
Reviews 1 and 2
The results of review questions 1 and 2 are reported in full in Appendix 3. A brief summary of the findings for each is provided here.
Review 1
Four47–50 RCTs in cUTI and HAP/VAP were identified, but recruited largely carbapenem-susceptible infections and therefore had low relevance to the HVCSs. Two trials47,50 reported a small number of OXA-48 infections (Table 7, n = 3 in each study; see Appendices 3.1 and 3.2, Tables 39 and 40 for further details), but outcome data were not reported for these patients separately. The RCTs indicated that CAZ-AVI was an effective treatment in the sites of interest.
Review 2
Six43,51–55 observational studies (see Appendix 3, Table 41) reporting outcomes for patients with OXA-48 infections treated with CAZ-AVI were identified. However, all reported infections across a range of sites, and in none of these was it possible to separate out patients with cUTI or HAP/VAP. Three observational studies reported outcomes for patients treated on the suspicion of a carbapenem-resistant infection, which may have been relevant to the ES. However, again, no studies reported results for HAP/VAP or cUTI alone and two56,58 reported a mixture of patients treated in the MDS and ES; there was insufficient time to obtain IPD. The studies were of a small sample size and were highly heterogeneous in terms of key characteristics that are prognostic and expected to modify treatment response (e.g. site, pathogen, treatment line), limiting the conclusions that could be drawn from them and increasing the likely uncertainty associated with any synthesis performed.
Approaches 1 and 2 could therefore not be pursued since there was a lack of evidence relating to cUTI and HAP/VAP infections caused by OXA-48s to inform an assessment of comparative effectiveness. Approach 3 was considered the most viable option, and reviews relating to this approach are described in the remainder of this chapter.
Review 3
Studies reporting the susceptibility of OXA-48 Enterobacterales isolates to CAZ-AVI and at least one comparator
Fifty-eight studies that met or potentially met the inclusion criteria on the basis of their abstract were selected from the mapping review. A further two datasets were obtained, one through a data request to PHE (see Report Supplementary Material 1 for details),31 and one through a data request to Pfizer,33 meaning a total of 60 sources were appraised for relevance. After consideration of their full text, 2831–46,53,54,59–68 met the inclusion criteria for the review and 32 studies were excluded (see Report Supplementary Material 1).
Two surveillance databases were also considered for inclusion in the review (ATLAS and SENTRY). 23,24 Both were excluded to avoid double counting, and to avoid underestimation of between-study heterogeneity since published, studies (providing more isolates or more information) drawing from these databases were already included in the review. Full details are provided in Report Supplementary Material 1.
Policy Research Unit in Economic Methods of Evaluation in Health and Social Care Interventions first considered whether any one of the studies met all the requirements of the assessment (ideally consecutive English data from a multisite study reporting outcomes for all relevant comparators, using BSAC/EUCAST breakpoints and laboratory methods), and could fulfil the evidence needs of the project without need of a meta-analysis. The data requested from PHE31 were the most relevant source of evidence since they are derived from English isolates. However, they also had several limitations: isolates have not historically been routinely submitted by testing centres, which may limit how representative these data are of the true distribution of OXA-48 susceptibilities in England. In addition, there is inconsistency in the testing methodologies used by local laboratories (albeit the majority use EUCAST). 69 This presents problems as outlined in Table 6. Finally, not all isolates were tested for each comparator, and a compromise had to be made in conducting the analysis whereby to preserve internal validity only isolates tested among all comparators were included (see Report Supplementary Material 1), which may have introduced selection bias; the PHE data did not report susceptibility for levofloxacin or ceftriaxone. Four other studies32,64,65,67 reported data from the PHE antimicrobial resistance and healthcare-associated infections (AMRHAI) programme, and all were subject to similar limitations. Due to these limitations, EEPRU considered it prudent to review and synthesise in a NMA other available evidence on the susceptibility of OXA-48 Enterobacterales to CAZ-AVI, to supplement the PHE data and to fill evidence gaps for fosfomycin, levofloxacin and ceftriaxone (the PHE data included evidence for fosfomycin, but the numbers were deemed too small to reliably use, with only eight isolates included).
Characteristics of studies entering the network meta-analysis
Of the 2831–46,53,54,59–68 data sources identified, 1253,54,59–68 were excluded from the meta-analysis. The reasons for these exclusions, and a table detailing the characteristics of these studies, can be found in Report Supplementary Material 1. Seven34,59,62–65,67 were excluded to avoid double counting of isolates, three53,54,66 were excluded as they related to outbreaks, and two60,68 were excluded as they reported MIC 50 and MIC 90, but not per cent susceptible. Consequently, between the 28 data sets and the two surveillance databases identified, 1631–46 were eligible for inclusion in the statistical synthesis (see Table 7).
Across the 15 studies that were not academic in confidence,31,32,34–46 sample size ranged from n = 30535 to n = 11 isolates46 [studies with < 10 isolates were excluded from the analysis due to time constraints (see Report Supplementary Material 1 and one study in Appendix 2, Table 38)], with three studies33–35 reporting > 300 isolates. Two31,32 included only isolates submitted to the PHE AMRHAI laboratory because of suspected unusual carbapenem resistance, and were of high relevance to the HVCS. However, one32 of these studies included isolates that were collected at least as long ago as 2008, which is before CAZ-AVI began being investigated, and this diminishes the relevance of this study since resistance in response to use of CAZ-AVI was unlikely to have emerged at this point. Consequently, a modelling scenario was planned using just the more recent PHE data to inform comparator susceptibility, rather than a synthesis of the two English studies, but the older study was retained in the full evidence synthesis analysis (see next paragraph). The remaining 14 studies collected isolates internationally (n = 5),33,34,37,40,41 from multisite locations in a single country (two from Spain,35,36 and one study from each of China,39 Greece44 and India46) from a single site in a single country (one study from each of France42 and Spain43), or were unclear on the number of sites included (one study from each of Turkey38 and Australia45). Expert advice indicated that resistant infections tend to arrive in the UK from around the world, and consequently isolates collected from any location were of relevance to the assessment. All studies were therefore retained in the analysis.
Isolates were generally collected since 2012, with two exceptions: the UK study already noted above32 and an international study which used isolates collected between 2002 and 2017. Expert advice indicated that isolates collected since 2012 were of highest (but not exclusive) relevance, and since the numbers of isolates collected before this period were likely to be small (69 isolates collected between 2002 and 2017,40 and 19 isolates collected at unknown time points32), all studies were retained in the analysis.
Quality assessment of studies entering the meta-analysis
The 16 studies31–46 included in the meta-analysis were assessed for internal and external risk of bias using a bespoke tool developed for this project (see Keyword mapping, study selection, data extraction and quality assessment and Appendix 2). A summary of scores in provided in Table 8. Across these studies, no one study scored well for all risk-of-bias items. There was a high proportion of categories scored ‘unclear’ across the assessment (35/64, 55%), which may reflect the current lack of standardisation around bias assessment and reporting for susceptibility studies. The study that had the lowest overall risk of bias was Vazquez-Ucha 2021,35 which scored low risk for three of the summary items (target population, outcome measurement and missing data) and unclear risk for one (sampling strategy) because it was not clear if the sample was consecutive or representative, and therefore whether it was an unbiased representation of the distribution of susceptibility. The majority of studies scored low risk for two categories overall, but there was no consistency as to which two categories scored well. Outcome measurement scored high risk most often, with 5 out of 16 studies scoring high risk, largely due to studies using laboratory methods from a different guideline than the breakpoints used. Missing data scored low risk most often, with 13 out of 16 studies scoring low risk, since usually all isolates were tested for all treatments. Target population was unclear in 12 out of 16 studies, due to studies not being clear if they included isolates with co-carriage of MBLs, or how they selected isolates for mechanism testing. The strategy for sampling isolates from the population was unclear in 11 studies. Reasons for the scores are provided in Appendix 2, Table 37.
| Study ID | 1. Target population | 2. Sampling strategy | 3. Outcome measurement | 4. Missing data | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Is the target population of the study broadly appropriate to the HVCS? | Were isolates selected based on resistance to comparators? | Was there appropriate inclusion or exclusion of isolates with co-carriage of other significant mechanisms, as per HVCS? | Were all isolates tested for the pathogen–mechanism of interest in a standard way, and does this match the HVCS? | Was the beta-lactamase test appropriate? | Were data collected over an appropriate time period? | Overall judgement | Were isolates sampled from the target population in an appropriate way? | Overall judgement | Was susceptibility measured in an appropriate, standard way? | Does the study demonstrate selective analysis reporting, with respect to S, I and R? | Were S, I and R reported consistently for all treatments? | Overall judgement | Is there a risk of bias from missing data? | Overall judgement | ||
| UK studies | ||||||||||||||||
| PHE data | U | U | U | L | U | L | U | U | U | U | L | L | U | U | U | |
| Livermore 2011 | U | L | U | L | L | U | U | U | U | H | L | L | H | L | L | |
| Non-UK studies (in order of size) | ||||||||||||||||
| Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | |
| Kazmierczak 2018 (INFORM) | L | H | L | L | L | L | H | U | U | U | L | L | U | L | L | |
| Vazquez-Ucha 2021 | L | L | L | L | L | L | L | U | U | L | L | L | L | L | L | |
| Garcia-Castillo 2018 (iCREST – Spain) | L | L | U | L | L | L | U | L | L | U | L | L | U | L | L | |
| Longshaw 2020 (SIDERO-CR 2014-6)44 | L | L | H | L | L | L | H | U | U | H | L | L | H | L | L | |
| Mataraci 2020 | L | U | U | U | L | L | U | U | U | L | L | L | L | L | L | |
| Han 2020 | L | L | L | U | L | L | U | L | L | U | L | L | U | L | L | |
| Johnston 2020 | L | U | U | L | L | U | U | U | U | H | L | L | H | L | L | |
| Kazmierczak 2019 (SIDERO-WT) | L | H | H | L | L | L | H | U | U | U | L | L | U | L | L | |
| Viala 2019 | L | U | U | U | L | L | U | L | L | U | L | L | U | U | U | |
| De la Calle 2019 | L | L | U | L | U | L | U | L | L | U | L | L | U | L | L | |
| Galani 2019 | L | U | U | U | L | L | U | L | L | H | L | L | H | L | L | |
| Sherry 2018 | L | U | U | U | L | L | U | U | U | U | L | L | U | L | L | |
| Bhagwat 2020 | L | U | L | U | L | L | U | U | U | H | L | L | H | U | U | |
Statistical synthesis
Statistical synthesis plan
Α NMA was planned to synthesise all studies identified by the review. Several sources of clinical heterogeneity were identified though the quality assessment and consideration of the study characteristics. As detailed in Table 6, location, whether the sample included screened isolates, and whether the sample included OXA-48 or OXA-48-like isolates were not considered to be important sources of heterogeneity by clinical advisors. This section details the sources of heterogeneity that were considered potentially important by clinical advisors or EEPRU, the reasons why they were considered important, and the sensitivity analyses planned relating to these. A summary of the planned analyses is provided in Table 9. Statistical synthesis plan and Statistical synthesis methods detail the statistical methods used to conduct the NMAsis, Susceptibility data entering the network meta-analysis and Results of the network meta-analysis report which studies entered each analysis, the results of these analyses, and which were used in the decision-analytic model.
| Analysis name | Description | Rationale |
|---|---|---|
| Main analysis | ||
| Full data set | All studies included (n = 16), excluding only the treatment arm for any treatments that were used to select isolates for testing (see first bullet point above). | To include all available evidence |
| Reduced data set | An inconsistency check was conducted and study arms that were inconsistent were removed (n = 16). | To include all available evidence which were consistent |
| Sensitivity analyses | ||
| Unusual inclusion criteria | Subgroup analysis of studies without unusual inclusion criteria (n = 13); meta-regression (n = 16). | To check if studies with unusual inclusion criteria affected the results of the network |
| MBL co-carriage | Only studies that excluded MBL co-carriage (n = 6). | To check if co-carriage of MBLs affected the results of the network |
| Proportion with carbapenem susceptibility | Meta-regression based on % meropenem-susceptible, including studies that reported this covariate (n = 14). | To check if proportion with carbapenem resistance affected the results of the network |
| Consecutive sample recruitment | Meta-regression (n = 16). | To check if consecutive recruitment of samples affected the results of the network |
| EUCAST subgroup | Only studies using EUCAST or BSAC laboratory methods and breakpoints (n = 3). | To check if laboratory methods and breakpoints affected the results of the network |
-
Studies with unusual inclusion criteria: Some studies selected isolates on the basis of resistance to other treatments. Where this included one of the HVCS-defined comparators, this may have affected the comparative efficacy estimates for those treatments. The affected arms (i.e. the treatment arm for the treatment that was used to select isolates for testing) were consequently excluded from all analyses, and an analysis was performed to exclude these studies in case the inclusion criteria affected the relative efficacy of the other treatments they tested.
-
MBL co-carriage: Isolates can co-carry both MBLs and OXA-48s, and those co-carrying MBLs will generally not be susceptible to CAZ-AVI. In the MDS, such isolates would not be treated with CAZ-AVI, and in the ES, where the mechanism-pathogen combination is highly suspected, the same would probably apply. Therefore, studies including isolates with co-carriage of MBLs may report different absolute and potentially relative treatment effects for CAZ-AVI and comparators. A subgroup analysis of studies which excluded MBL co-carriage was therefore planned.
-
Proportion with carbapenem susceptibility: An analysis of both the PHE IPD and the IPD from Vazquez-Ucha et al. indicated that selection of meropenem-resistant isolates may impact on estimates of treatment efficacy for CAZ-AVI. As such, a meta-regression based on the proportion of meropenem non-susceptible isolates per study was planned.
-
Consecutive sample recruitment: Since susceptibility estimates are essentially a prevalence statistic, ideally isolates would have been collected consecutively, or selected to maintain a representative sample through, for example, random sampling. EEPRU considered that although a consecutive sample may over-select for an outbreak and therefore under-represent the diversity of susceptibility, a non-consecutive sample would not be reflective of any real-world population, unless carefully planned to maintain proportionality. A sensitivity analysis was therefore planned to investigate whether sample consecutiveness affected estimates of comparative efficacy.
-
Laboratory methodology and breakpoints used: As detailed in Table 6, it cannot be assumed that all laboratory methods and breakpoints are interchangeable. In England, BSAC guidelines have recommended since 201670 that laboratories should use EUCAST laboratory methods and breakpoints. Therefore, currently in England, studies using EUCAST methods and breakpoints have the highest clinical relevance. However, in their response to EEPRU’s data request, PHE noted that not all English laboratories comply with this guideline, and it is unclear to what extent CLSI and potentially other methods, implemented by commercial assays, may have been included in the PHE data. This is an insurmountable issue with the PHE data, and with respect to this evaluation leaves EEPRU with two main options: (A) include all studies regardless of which methods and breakpoints have been used, since across England there is likely to be a mixture, and (B) only include studies that use EUCAST or BSAC methodologies, since it can be assumed that the majority of centres will comply with BSAC/EUCAST recommendations. Both analyses were therefore planned.
Statistical synthesis methods
A NMA was conducted to determine the relative susceptibility of CAZ-AVI and listed comparators. The data generation process was assumed to follow a binomial likelihood with probabilities modelled using a logit link function. Random-effect (RE) models were assumed to allow for expected between-study heterogeneity in relative effects. Further details of the statistical model are given in Appendix 4.
Potential treatment effect modifiers listed in Statistical synthesis plan were assessed using subgroup analyses and meta-regression. 71 Where appropriate, meta-regressions were performed in preference to subgroup analyses since this provides a test for interactions between the treatment effects and trial-level covariates. Different assumptions can be made about the relationship between the interaction terms for each comparator, and a common interaction for each comparator was assumed. Where this was not considered appropriate, subgroup analyses were presented instead as more complex meta-regression models were ruled out due to the complexity of the network/sparsity of covariate information.
All analyses were conducted in the freely available software package WinBUGS72 and R73 using the R2Winbugsinterface package. Code was modified from NICE TSD 2 example 1c (RE models). 74
Convergence to the target posterior distributions was assessed using the Gelman-Rubin statistic,75 as modified by Brooks and Gelman, for two chains with different initial values. For all outcomes, a burn-in of 80,000 iterations of the Markov chain was used with a further 20,000 iterations retained to estimate parameters using one chain and thinning every 5 iterations.
The absolute goodness of fit was checked by comparing the total residual deviance to the total number of data points included in an analysis. The deviance information criterion (DIC) provides a relative measure of goodness-of-fit that penalises complexity and was used to compare different models for the same likelihood and data. 76 Lower values of DIC are favourable, suggesting a more parsimonious model.
Inconsistency between direct and indirect evidence can arise because of an imbalance in treatment effect modifiers across studies comparing different pairs of treatments. 77 Consistency between direct and indirect evidence can be assessed where there are ‘loops’ of evidence in the network informed by separate, independent trials, so that both direct and indirect estimates are available. Inconsistency was assessed by fitting unrelated mean effect (UME) models, based on code from NICE TSD 4. 77 In the UME model the direct and indirect relative treatment effects are not constrained to be consistent with each other. This is equivalent to having separate, unrelated, meta-analyses for every pairwise contrast and with a common variance parameter in random-effect models. To explore whether the direct and indirect evidence for particular treatment comparisons is inconsistent, the contribution to the posterior mean residual deviance was plotted for the UME model against the NMA model in a deviance contribution plot. 77
Results are presented using the posterior median treatment effects, 95% credible intervals (CrIs) and 95% prediction intervals (PrI). The 95% PrI indicates the extent of between-study heterogeneity by illustrating the range of odds ratios (ORs) that might be expected in a future study. Probabilities of treatment rankings were computed by counting the proportion of iterations of the Markov chain in which each intervention had each rank. Median treatment rankings and the probabilities of each treatment being the best treatment (i.e. ranks the first) are presented.
The estimated between-study standard deviation, τ, for each analysis is also presented. Values below 0.05 are considered to indicate low heterogeneity. Values between 0.05 and 0.5 are considered to indicate moderate heterogeneity. Values between 0.5 and 1.0 are considered to indicate high heterogeneity. Values above 1.0 are considered to indicate extremely high heterogeneity.
In the case of zero events, a continuity correction was applied by adding 1 to the denominator and 0.5 to the numerator as suggested as a solution by the NICE Decision Support Unit. 74
Susceptibility data entering the network meta-analysis
Table 10 presents the susceptibility data from the 16 studies31–46 included in the NMA. Data were available from at least one study for all HVCS comparators, but was particularly sparse for fosfomycin (n = 3 studies)35,43,44 and for ceftriaxone (n = 2 studies). 33,39 Susceptibility to CAZ-AVI was 100% in six studies32,36,39,43–46 and above 90% in a further seven studies. 33–35,40–42,46 The lowest reported susceptibility (60.8%) was from a Turkish study which recruited 74 isolates and used EUCAST lab methods and breakpoints, but which was unclear on a number of other methodological points, including whether isolates co-carried MBLs. Comparators with generally good susceptibility included colistin (9/11 estimates > 60%), tigecycline (6/9 estimates > 60%) and amikacin (5/8 estimates > 60%).
| Study ID, Funding |
NMA | N | % susceptible (number in analysis if different from N) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| C-A | Col | Mer | Tig | Az | Fluoroquinolones | Aminoglycosides | Cephalosporins | |||||||||
| Fos | Levo | Cipro | Gent | Ami | Tob | Ctx | Cefe | CAZ | ||||||||
| PHE data31 | E; Full | 85 | 87.1 | 81.2 | 54.1 | 58.8 | 20.0 | 10.6 | 31.8 | 56.5 | 22.4 | 22.4 | 22.4 | |||
| Livermore 201132 | Full | 19 | 100 | 32 | 57.9 | 57.9 | ||||||||||
| Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | |
| Kazmierczak 201834 (INFORM) |
Full | 303 | 99.3 | 80.2 | 26.4 | 93.7 | 14.2 | 80.2 | ||||||||
| Vazquez-Ucha 202135 | E; Full; MBL |
302 | 98.7 | 88.1 | 79.8 | 11.3 | 47.4 | 6.6 | 36.7 | 79.1 | 33.8 | 12.6 | 9.6 | |||
| Garcia-Castillo, 2018 (iCREST – Spain)36 | Full | 164 | 100 | 87.2 | 87.8 | 66.5 | 23.8 | 14.6 | 0 | |||||||
| Longshaw 2020 (SIDERO-CR 2014–6)37 (SIDERO-CR 2014–6) |
Full | 85 | 88.2 | 67.1 | 12.9 | 1.2 | 1.2 | |||||||||
| Mataraci 202038 | E; Full | 74 | 60.8 | 64.9 | 24.3 | 10.8 | 20.3 | 5.4 | ||||||||
| Han 202039 | Full | 68 | 100 | 4.4 | 100 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||
| Johnston 202040 | Full | 91 | 0 | 76 | 100 | 26 | 52 | 87 | 39 | |||||||
| Kazmierczak 201941 (SIDERO-WT) | Full | 32 | 90.6 | 78.10 | 0 | 3.10 | 12.5 | |||||||||
| Viala 201942 | Full | 27 | 96 | 43 (7) | 86 (7) | 40 (25) | 37 | |||||||||
| De la Calle 201943 | Full | 24 | 100 | 94.1 (17) | 45.8 | 50 (18) | 9.1 (11) | 70.80 | 79.20 | 4.20 | ||||||
| Galani 201944 | Full | 19 | 100 | 42.10 | 0 | 63.20 | 68.40 | 21.10 | ||||||||
| Sherry 201845 | Full | 14 | 100 | 43 | ||||||||||||
| Bhagwat 202046 | Full | 11 | 90.9 | 100 | 0 | |||||||||||
Results of the network meta-analysis
Sixteen studies contributed to the NMA, considering a total of 14 comparators, and the full network diagram is shown in Appendix 4, Figure 16. Nine of the studies contained zero susceptibility counts for one or more of the included comparators and therefore had a continuity correction applied prior to synthesis.
A summary of the key NMA results is presented in Appendix 4, Table 42. The NMA results informing the decision-analytic model are presented in detail below (i.e. the reduced data set and EUCAST subgroup). Additional results supporting the described analysis choices are presented in Appendix 4.3, Figures 19–29 and Table 43.
Network meta-analysis including all studies
The analysis including the full data from all 16 studies indicated an extremely high amount of heterogeneity, with the between-study standard deviation (SD) estimated to be 1.99 (95% CrI 1.64 to 2.44). Results from the UME model suggested possible inconsistency in the network. Although the DIC of the UME model was substantially higher than the NMA model, suggesting a poorer model fit, the between-study SD was smaller. Inconsistency was therefore explored further by inspecting the deviance contribution plot (see Appendix 4.4, Figure 30). Two data points were highlighted as having substantially lower deviance contributions under the UME model: the tigecycline arm of Han 202039 and the colistin arm of Johnston. 40 The NMA model was re-fitted on a reduced data set with these two inconsistent observations removed. No further inconsistency was detected following the removal of these data points (see Appendix 4.3, Figure 31).
Sixteen studies contributed to the NMA using reduced data, considering a total of 14 comparators, and the full network diagram is shown in Appendix 4.2, Figure 17. Nine of the studies32,36,43–45,78–81 contained zero susceptibility counts for one or more of the included comparators and therefore had a continuity correction applied prior to synthesis.
The relative susceptibility for each comparator relative to colistin is shown in Figure 2. The model fitted the data well, with a total residual deviance of 109.9, which was close to the number of data points included in the analysis of 109. The between-study SD was 1.56 (95% CrI 1.28 to 1.93), which, while still indicating extremely high heterogeneity, offers a noticeable reduction compared to the full analysis including the inconsistent data points. CAZ-AVI was associated with a statistically significant higher susceptibility relative to colistin (OR 7.24, 95% CrI 2.58 to 20.94) with probability 100% of being the most effective treatment; median rank 1. The remainder of the treatments were associated with lower susceptibility than colistin (OR < 1) although this was not statistically significant for tigecycline or amikacin based on the 95% CrI. For all comparators the extremely high between-study SD results in wide 95% PrI.
FIGURE 2.
Forest plot of OR vs. colistin for reduced data set, NMA model.
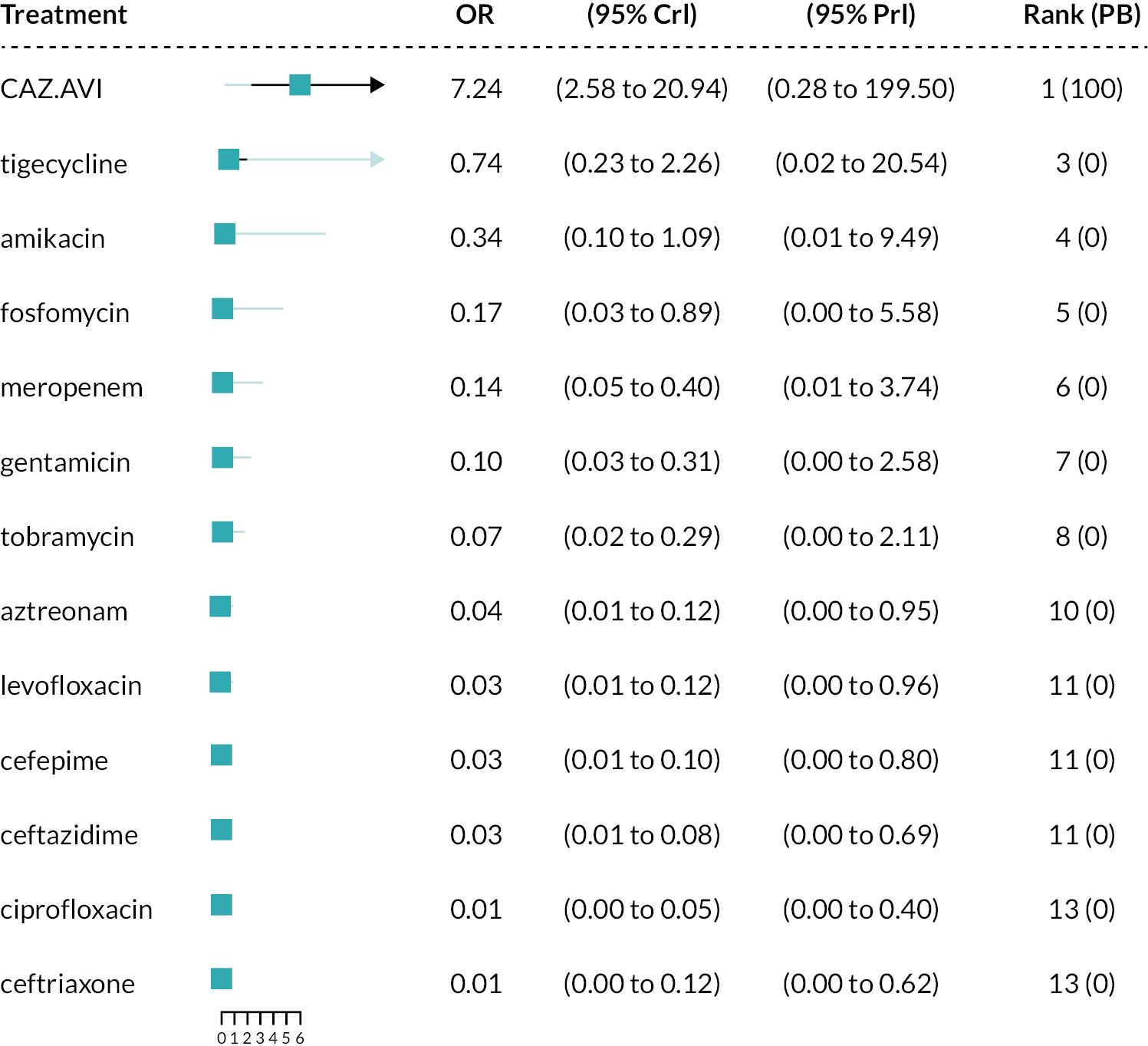
Selection of the reduced data set (with inconsistent observations removed) was based on the statistical identification of inconsistency in the network. Inclusion of these observations resulted in extremely high heterogeneity and unfeasibly large uncertainty estimates for the relative effects. No data extraction errors or reasons to exclude the entire studies (rather than individual arms) based on the inclusion/exclusion criteria were identified. The planned meta-regression and subgroup analyses were therefore conducted using both the full dataset as planned (in an attempt to explain the identified inconsistency shown in Appendix 4.3) and the reduced dataset. The conclusions of the analyses were consistent between using the full dataset and reduced dataset. The reduced data set was selected for use in the decision-analytic model scenario analyses.
Sensitivity analyses
The meta-regression and/or subgroup analysis investigating the potential sources of heterogeneity due to studies with unusual inclusion criteria, MBL co-carriage, proportion with carbapenem susceptibility, consecutive sample recruitment and laboratory methodology and breakpoints used shows that (1) there was no evidence to suggest that the relative treatment effects differ according to the identified unusual inclusion criteria; (2) there was no conclusive evidence that co-carriage of MBLs has a statistically significant effect on the resulting relative effects, but the estimated OR versus colistin was increased compared to the model with all studies included, and the heterogeneity SD was decreased; (3) there was no evidence to suggest that the relative treatment effects differ according to the proportion with carbapenem susceptibility; (4) there was no conclusive evidence that laboratory methodology and breakpoints used had a statistically significant effect on the resulting relative effects, but the estimated OR versus colistin was decreased compared to the model with all studies included (see details of the results below) and the heterogeneity SD was decreased.
Based on the findings from the sensitivity analyses, for the cost-effectiveness modelling, it was decided to use the EUCAST subgroup results in the base case and to include a scenario analysis based on studies which recruited 0% MBL co-carriage and used EUCAST methods and breakpoints to inform the relative effectiveness on susceptibility (see Sources of evidence for details of further sensitivity analyses undertaken for the cost-effectiveness modelling). This resulted in one study being selected (Vazquez-Ucha 2021)35 for this scenario analysis – see Table 10 for the evidence used. The details of the sensitivity analysis relating to laboratory methods and breakpoints (which produced the EUCAST subgroup analysis) are described next, while the details of the other sensitivity analyses, including the MBL co-carriage analysis, are reported in Appendix 4.2.
Network meta-analysis using EUCAST subgroup
Six studies33,34,39–41,45 used CLSI breakpoints and methodologies, two35,38 used EUCAST or BSAC breakpoints and methodologies, three32,37,44 used CLSI methods, but EUCAST breakpoints, one46 used CLSI methods and EEPRU applied EUCAST breakpoints and three36,42,43 did not report one or both elements. As already noted, it was unclear what methods were used by the submitting laboratories in the PHE data;31 it was assumed that the majority would comply with BSAC recommendations and use EUCAST methods and breakpoints.
A subgroup analysis containing only the two EUCAST and one PHE study was performed. The network diagram for this subgroup of studies is shown in Appendix 4, Figure 18. The susceptibility to each comparator relative to colistin is shown in Appendix 4.2, Figure 3. The model fitted the data well, with a total residual deviance of 28.21, which was close to the number of data points included in the analysis of 28. The between-study SD was 0.98 (95% CrI 0.62 to 1.63), indicating high, but noticeably reduced, heterogeneity compared to the analysis including all 16 studies.
FIGURE 3.
Forest plot of OR vs. colistin for EUCAST studies subgroup.
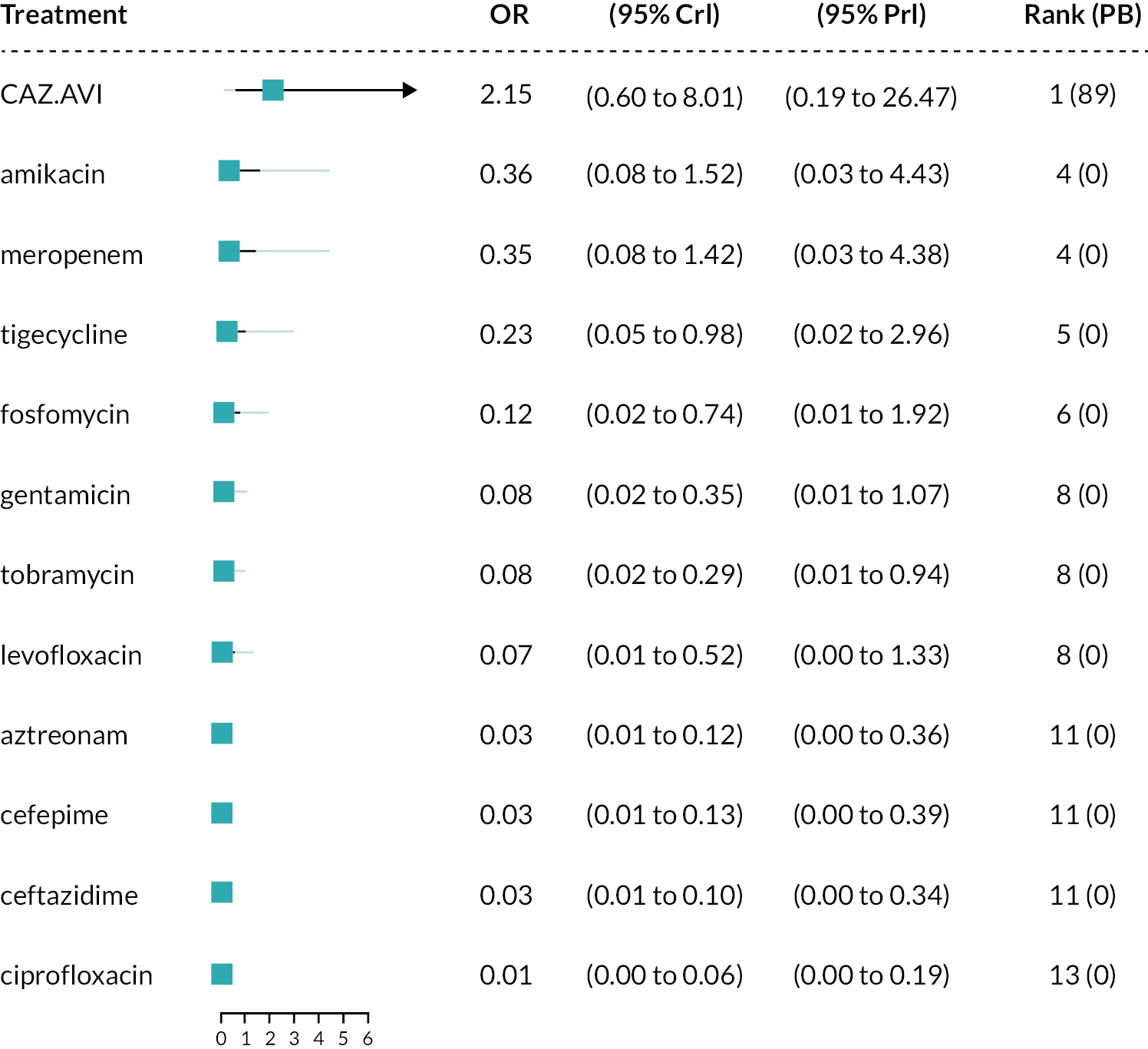
Ceftazidime-avibactam was associated with a higher susceptibility relative to colistin (OR 2.15, 95% CrI 0.60 to 8.01); however, the magnitude of the point estimate is lower than that of the full analysis and the result is not statistically significant. The remainder of the treatments were associated with lower susceptibility than colistin (OR < 1) although this was not statistically significant for amikacin or meropenem based on the 95% CrI.
Additional review questions for Approach 3
Review questions 4–6 were defined in order to supply estimates to populate the decision-analytic model. This section describes the rationale for and requirements of each additional question, while Review questions 4 and 5 and Review question 6 describe the methods and results for each question. The approach to evidence identification and selection differed for each of these three questions, due to their perceived importance to the model, time constraints and the availability of existing reviews.
Additional questions generated by Approach 3 were:
Review 4. What is the link between in vitro susceptibility and clinical outcomes from the published literature, in the sites of relevance, in patients according to their susceptibility to the treatment they were given?
As described above in Susceptibility studies, PK/PD studies and breakpoints, susceptibility studies do not report clinical outcomes; therefore, it was necessary to establish the link between susceptibility in vitro and clinical outcomes. Two approaches to evidencing this link were proposed:
-
Assume that clinical outcomes do not differ according to the specific antibiotic used or the specific pathogen–mechanism causing the infection, conditional upon susceptibility to that antibiotic. This assumption was validated by our clinical experts.
-
Assume that different treatments may result in different outcomes, conditional on susceptibility to the antibiotic given.
In both approaches, studies should have tested the susceptibility of a patient to the treatment they were given, and reported clinical outcomes for those susceptible or not in cUTI and HAP/VAP separately. In approach (b) data on effectiveness conditional upon susceptibility would be required for the intervention and comparators, and would need to comprise a viable NMA. Initial scoping work based on a previous systematic review [reported as part of Shionogi’s application to European Network for Health Technology Assessment (EUNETHTA) (Project PTJA11)]82 indicated that the RCTs in the HVCS sites provided poor coverage of the comparators of interest. Clinical advisors were also supportive of approach (a), and consequently approach (b) was not pursued further.
Review 5. What is the long-term risk of mortality (and other outcomes) for patients with carbapenem-resistant cUTI or HAP/VAP?
This question became necessary since review question 4 did not identify any studies that reported long-term clinical outcomes. The question was widened to include any carbapenem-resistant infections.
Review 6. What are the important safety implications of CAZ-AVI?
This question was required to inform the modelling of important adverse events (AEs).
Review questions 4 and 5
The methods and results for review questions 4 and 5 are presented in Appendix 5. Review 4 (link between susceptibility and clinical outcomes) identified three studies in patients with HAP/VAP conducted solely in the ES. The inclusion criteria are listed in Appendix 5, Table 44. No useful evidence relating to the MDS was identified. The inclusion criteria are listed in Appendix 5, Table 45. Review 5 (link between susceptibility and long-term clinical outcomes) did not identify any relevant literature.
Review question 6
What are the important safety implications of CAZ-AVI?
Methods
A comprehensive review of the safety of comparators was not possible within the timeframe of this evaluation. AEs included in the model for the intervention and comparators are described in Modelling direct patient net health effects in HVCS. Clinical advisors to EEPRU indicated that CAZ-AVI is predominantly a safe treatment, but that colistin and aminoglycosides have significant AEs relating to acute kidney injury (AKI). Another key AE related to antibiotic use is the emergence of C. difficile in a patient’s digestive tract, which can lead to diarrhoea and serious damage to the colon. EEPRU conducted a review of the RCT trial evidence for CAZ-AVI to establish whether it supported the clinical view that CAZ-AVI is a safe treatment. EEPRU were especially interested in establishing safety comparative to toxic alternatives (colistin and aminoglycosides) and the other ‘safer’ treatments used in the HVCSs.
Rates of serious treatment-related AEs, nephrotoxicity AEs and C. difficile infections were extracted from the included RCT publications and/or their ClinicalTrials.gov NCT record. Only RCTs relating to the sites of interest were reviewed, due to time and resource constraints. Only RCTs were considered as these give comparative data. In the absence of nephrotoxicity events, other kidney and renal AEs were extracted. The data were then synthesised narratively for any important safety signals.
Results
The extracted AE data in the RCTs for CAZ-AVI are presented in Table 11.
| Author (date) Acronym | AE | Intervention | Comparator |
|---|---|---|---|
| Carmeli et al. (2016)47 REPRISE (NCT01644643) cUTI |
Serious treatment-related AE (total safety pop) n (%) | CAZ-AVI 7/152 (4.61%) | Best available therapy 5/153 (3.27%) |
| Nephrotoxicity n (%) | Renal failure 0/152 (0%) |
Renal failure 1/153 (0.66%) |
|
| C. diff infection n (%) | NR | NR | |
| Any other AEs of concerna (name, n/N and %) | Infections and infestations Incision site infection 0/152 (0.00%) Oral herpes 0/152 (0.00%) Orchitis 0/152 (0.00%) Respiratory-tract infection viral 0/152 (0.00%) Respiratory, thoracic and mediastinal disorders Acute respiratory failure 0/152 (0.00%) Pneumonia aspiration 0/152 (0.00%) Pulmonary embolism 0/152 (0.00%) Respiratory failure 0/152 (0.00%) |
Infections and infestations Incision site infection 0/153 (0.00%) Oral herpes 0/153 (0.00%) Orchitis 0/153 (0.00%) Respiratory-tract infection viral 0/153 (0.00%) Respiratory, thoracic and mediastinal disorders Acute respiratory failure 1/153 (0.65%) Pneumonia aspiration 1/153 (0.65%) Pulmonary embolism 1/153 (0.65%) Respiratory failure 0/153 (0.00%) |
|
| Wagenlehner et al. (2016)50 RECAPTURE 1 & 2 (NCT01595438 and NCT01599806) cUTI |
Serious treatment-related AE (total safety pop) n (%) | CAZ-AVI 21/511 (4.1%) |
Doripenem 12/509 (2.4%) |
| Nephrotoxicity n (%) | NCT01595438 and NCT01599806 CAZ-AVI Calculus ureteric 1/511 (0.20%) Hydronephrosis 1/511 (0.20%) Nephrolithiasis 3/511 (0.59%) Renal failure chronic 0/511 (0.00%) Renal impairment 1/511 (0.20%) |
NCT01595438 and NCT01599806 Doripenem Calculus ureteric 0/509 (0.00%) Hydronephrosis 0/509 (0.00%) Nephrolithiasis 0/509 (0.00%) Renal failure chronic 1/509 (0.20%) Renal impairment 0/509 (0.00%) |
|
| C. diff infection n (%) | CAZ-AVI 2/511 (0.4%) |
Doripenem 0/509 (0%) |
|
| Any other category that is important (name, n/N and %) | Infections and infestations Abdominal abscess 1/511 (0.20%) Appendicitis 0/511 (0.00%) Cellulitis 1/511 (0.20%) Chronic hepatitis C 1/511 (0.20%) C. diff colitis 1/511 (0.20%) Diverticulitis 1/511 (0.20%) Gastroenteritis 1/511 (0.20%) Orchitis 0/511 (0.00%) Pneumonia 0/511 (0.00%) Urinary tract infection 0/511 (0.00%) Respiratory, thoracic and mediastinal disorders Acute pulmonary oedema 0/511 (0.00%) Hyperventilation 1/511 (0.20%) |
Infections and infestations Abdominal abscess 0/509 (0.00%) Appendicitis 1/509 (0.20%) Cellulitis 0/509 (0.00%) Chronic hepatitis C 0/509 (0.00%) C. diffi colitis 0/509 (0.00%) Diverticulitis 0/509 (0.00%) Gastroenteritis 0/509 (0.00%) Orchitis 1/509 (0.20%) Pneumonia/509 (0.20%) Urinary tract infection 1/509 (0.20%) Respiratory, thoracic and mediastinal disorders Acute pulmonary oedema 1/509 (0.20%) Hyperventilation 0/509 (0.00%) |
|
| Vázquez et al (2012)49 (NCT00690378) cUTI |
Serious treatment-related AE (total safety pop) n (%) | CAZ-AVI 6/68 (8.82%) |
Imipenem-cilastatin 2/67 (2.99%) |
| Nephrotoxicity n (%) | Rénal failure acute 1/68 (1.47%) Renal impairment 1/68 (1.47%) |
Renal failure acute 0/67 (0.00%) Renal impairment 0/67 (0.00%) |
|
| C. diff infection n (%) | NR | NR | |
| Any other category that is important (name, n/N and %) | Infections and infestations Urosepsis 0/68 (0%) |
Infections and infestations Urosepsis 0/67 (0%) |
|
| Torres et al. (2018)48 REPROVE (NCT01808092) VAP |
Serious treatment-related AE (total safety pop) n (%) | CAZ-AVI 75/405 (19%) |
Meropenem 54/403 (13%) |
| Nephrotoxicity n (%) | NCT01808092 CAZ-AVI Acute kidney injury 2/405 (0.49%) Renal failure 1/405 (0.25%) Renal impairment 0/405 (0.00%) |
NCT01808092 Meropenem Acute kidney injury 1/403 (0.25%) Renal failure 0/403 (0.00%) Renal impairment 1/403 (0.25%) |
|
| C. diff infection n (%) | NR | NR | |
| Any other category that is important (name, n/N and %) | Infections and infestations Urinary tract infection 11/405 (2.72%) Respiratory, thoracic and mediastinal disorders Pleural effusion 9/405 (2.22%) |
Infections and infestations Urinary tract infection 14/403 (3.47%) Respiratory, thoracic and mediastinal disorders Pleural effusion 7/403 (1.74%) |
As described in Review 1, there were three RCTs in cUTI47,49,50 and one in VAP. 48 Statistical comparisons were not reported for AE rates in any of the trials.
The proportion of patients with serious adverse events (SAEs) was numerically similar or slightly higher when compared to best available therapy (4.61% and 3.27%),47 doripenem (4.1% and 2.4%)50 and meropenem (19% and 13%),48 and appeared numerically higher when compared to imipenem-cilastatin (8.82% and 2.99%). 49 However, doripenem and imipenem-cilastatin are not comparators within the HVCSs.
Among renal AEs, rates were very low, and were in some studies a little higher in CAZ-AVI arms (see RECAPTURE 1 and 2 and REPROVE in Table 11), whereas in one trial they were lower (see REPRISE in Table 11). 47 This may be due to the small proportion of patients in the best available therapy arm who received colistin or aminoglycosides (3.6%).
Only one study reported C. difficile rates. Again, the event rates were extremely low, with one event (0.4%) in the CAZ-AVI arm, and zero in the doripenem arm. 50
Event rates were generally low for other AEs in both arms.
Overall, no strong signal for additional AEs to be included in the modelling were identified. The data appeared to bear out the clinical view that CAZ-AVI is a largely safe treatment with no or extremely little effect on renal AEs or on the emergence of C. difficile when used to treat infections at the sites of interest.
Overview and critique of evidence in Pfizer’s submission to NICE
In their submission, Pfizer include evidence on CAZ-AVI from RCTs, non-RCTs and real-world evidence. Pfizer’s modelling took a different approach (see Review of manufacturer’s model for CAZ-AVI) and included a wider population than EEPRU’s, and their evidence requirements were therefore wider. No systematic review methodology is reported to support the clinical section of their submission, and it is therefore unclear to what extent the evidence submitted is comprehensive with respect to their wider scope.
Policy Research Unit in Economic Methods of Evaluation in Health and Social Care Interventions checked that the evidence submitted by Pfizer that was relevant to the HVCSs was captured by their own systematic searches and found that all relevant studies were present, unless unpublished. Some RCTs cited by Pfizer were not considered relevant to the EEPRU HVCSs, since they were in the wrong site or the wrong population. For example, several RCTs were not relevant since they recruited patients with intra-abdominal infections,83,84 or were conducted in children (unpublished ANDI20 trial). RCTs47,48,50 in the correct site and population were included in EEPRU’s review, as was one phase 2 study that did not feature in Pfizer’s submission, but met EEPRU’s selection criteria. 49 Of the six54,55,85–88 observational studies discussed by Pfizer, only two reported a subgroup of data relating to OXA-48s,54,55 and both were included in EEPRU’s review (see Review 2). The four85–88 remaining were considered as sources of evidence for Review 4 (link between susceptibility and clinical outcomes), and one87 was included as part of that review since the other three were based on the sites outside the HVCS85,86 or mixed sites. 88 The real-world data56 discussed in Pfizer’s submission was also included in EEPRU’s review.
Discussion and conclusions
There are evidential challenges when evaluating the use of new AMs to treat infections caused by MDR pathogens. RCTs are of generally low relevance as they tend not to recruit patients with MDR pathogens. Therefore, relative treatment effects between the intervention and comparator cannot be generalised to MDR pathogens, as this may overestimate the efficacy of the comparator.
Since it was anticipated that RCTs were unlikely to be the primary source of evidence, three approaches to estimating comparative efficacy between the intervention and comparators were considered. In Approaches 1 and 2, RCTs and observational studies (respectively), with data for patients with HAP/VAP or cUTI infections caused by OXA-48 Enterobacterales, could be used to construct a NMA to compare the intervention and comparators. In Approach 3, in vitro susceptibility studies could be used to indicate the proportion of OXA-48 Enterobacterales that are susceptible to treatment; additional evidence would be required to link susceptibility to clinical outcomes in cUTI and HAP/VAP.
Approaches 1 and 2 were not pursued since insufficient evidence from RCTs and observational studies was identified during the mapping review. The key limitation of the RCTs was that they included small numbers of OXA-48 infections (n = 3 in each of two RCTs) and did not report these data separately. The key limitation of the observational data were that they were not reported separately for the sites of interest (cUTI and HAP/VAP) and there was insufficient time to obtain IPD.
In Approach 3, relatively large samples of OXA-48 Enterobacterales isolates obtained from a range of clinical sites of infection were available from several in vitro susceptibility studies and susceptibility (unlike clinical outcomes) was expected to generalise across sites. Therefore, a NMA of susceptibility studies was conducted. This included English-specific susceptibility evidence provided by PHE. Sixteen studies met the inclusion criteria and were synthesised. A series of sensitivity analyses was conducted to ascertain the impact of several sources of clinical heterogeneity, including inclusion criteria (use of resistance to a comparator to select study sample); co-carriage of MBLs; the proportion who were carbapenem sensitive; whether the sample was recruited consecutively and what laboratory methods and breakpoints were used to assess susceptibility.
After consistency checks (which resulted in two study arms being removed), and otherwise using the full analysis set (all available studies), CAZ-AVI was associated with a statistically significantly higher susceptibility relative to colistin (OR 7.24, 95% CrI 2.58 to 20.94). The remainder of the treatments were associated with lower susceptibility than colistin (OR < 1). Heterogeneity was extremely high (SD 1.56, 95% CrI 1.28 to 1.93). A sensitivity analysis including only studies where no isolates co-carried both MBL and OXA-48 resistance mechanisms (n = 6 studies) decreased heterogeneity (SD 1.38, 95% CrI 0.95 to.06). It also produced a very high OR for CAZ-AVI versus colistin, but with a large amount of uncertainty (OR 35.83, 95% Cr 7.91 to 165.60). Another sensitivity analysis, including only studies that used EUCAST laboratory methods and breakpoints (n = 3 studies), reduced the heterogeneity further to SD 0.98 (95% CrI 0.62 to 1.65). CAZ-AVI was associated with a higher susceptibility relative to colistin (OR 2.15, 95% CrI 0.60, 8.01); however, the magnitude of the point estimate was lower than that using the full analysis set (OR 7.24, 95% CrI 2.58 to 20.94) and the result is not statistically significant.
Networks used in the economic evaluation
The EUCAST network was selected as the base-case analysis to inform the economic evaluation since heterogeneity was lower and there was a clinical rationale to support restricting to studies that had used EUCAST laboratory methods and breakpoints as these are more commonly used in England. A scenario analysis was planned to include the result from the full analysis set. A further scenario was planned restricting to studies with no-MBLs and that had used EUCAST laboratory methods and breakpoints, which left one study (Vazquez-Ucha et al. ). 35 This study did not report an estimate for tigecycline, but was the study with the lowest risk of bias as judged by the bespoke risk-of-bias tool developed for this evaluation. A further scenario analysis was planned using the PHE data alone, due to its high relevance to the evaluation.
Three additional clinical reviews were conducted to support Approach 3. In Review 4, evidence relating to the link between in vitro susceptibility and clinical outcomes in the sites of relevance was sought, since susceptibility studies do not report clinical outcomes. In Review 5, evidence relating to the long-term risk of mortality (and other clinical outcomes such as hospital LoS) for patients with carbapenem-resistant cUTI or HAP/VAP was sought, since no evidence relating to long-term outcomes was identified by Review 4. In Review 6, the important safety implications of CAZ-AVI, as reported by RCTs conducted in the sites of interest, were reviewed. Clinical advisors indicated that colistin and aminoglycosides (comparators in the HVCSs) increase the risk of AKI, but that CAZ-AVI did not. C. difficile infections were highlighted in the NICE scope as a potential consequence of treatment with broad-spectrum antibiotics. Data were sought relating to AKI or related AEs, to C. difficile rates, and to any other serious AEs reported in the literature.
Review 4 (link between susceptibility and clinical outcomes) identified two studies that reported mortality or hospital LoS conditional on susceptibility to empiric treatment and were selected for use in the model for the ES. No useful evidence relating to the MDS was identified. Review 5 (link between susceptibility and long-term clinical outcomes) did not identify any relevant literature, but an unpublished study (CARBAR)57 was submitted by Shionogi during the parallel appraisal of CAZ-AVI that contained useful data. Review 6 indicated that CAZ-AVI does not appear to increase the risk of AKI, C. difficile, or any other serious AEs, compared to non-toxic comparators (i.e. comparators that were not colistin or an aminoglycoside). No study reported a comparison of CAZ-AVI exclusively to colistin or aminoglycosides. Event rates were generally very low or zero.
Strengths
The clinical review was conducted using a mapping approach based on robust systematic searches to capture relevant literature. This allowed EEPRU to focus resources from a relatively early stage on a viable approach to deriving clinical efficacy estimates, while still conducting a comprehensive search despite a paucity of high-quality evidence. Data extractions were checked by a second reviewer to ensure data integrity, and statistical analyses were performed using standard NMA approaches. At all stages of the clinical review, clinical advisors were consulted where there was uncertainty, and the resulting methods of synthesis have attempted to account for clinical sources of heterogeneity where feasible. Susceptibility studies, while not reporting clinical outcomes, have the advantage of testing all the treatments in the same sample of isolates, thereby reducing the chance of heterogeneity in patient samples between arms introducing confounding. They also tend to include a higher number of patients/isolates compared to RCTs and observational studies.
Limitations
There are limitations to the clinical review, largely due to the availability of evidence and time available to conduct the evaluation.
A lack of availability of relevant RCT or observational evidence has meant that in vitro susceptibility, which can be considered, at best, a surrogate outcome, has been relied upon. A link was then made between susceptibility and clinical outcomes using published data and expert elicitation. No pre-specified criteria for judging the suitability of the surrogate or the linking evidence were applied. The data available to evidence the link between susceptibility and clinical outcomes were sparse and were not specifically for the pathogen–mechanism of interest. For the MDS, expert elicitation was used to derive the link between susceptibility and clinical outcomes (see Chapter 6).
Other limitations relate to the review methods applied in this evaluation. Because this was the first evaluation of this type commissioned by NICE, and because EEPRU could not foresee the evidence and synthesis requirements at the inception of the project, no registration with the International Prospective Register of Systematic Reviews (PROSPERO) was performed. The statistical analysis plan was made in response to the available data, rather than being formulated a priori, since the types of heterogeneity that would be encountered and their importance were largely unknown at the project outset. Due to time constraints, many stages of the review process were done by only one reviewer, which introduces a risk of inaccuracy. Data were checked by a second reviewer for the susceptibility review, but study selection and risk-of-bias assessment were conducted by only one. Since there was no suitable risk-of-bias tool available, EEPRU created a bespoke tool. This was done by consulting other available tools, but no face validity checks were performed by experts in susceptibility testing, and no other validation of the tool has been undertaken. This could be an area of future research. To allow for this, risk-of-bias scores were not used in the statistical synthesis to weight studies, subgroup studies or exclude studies, and instead aspects of clinical heterogeneity were considered in sensitivity analyses individually.
In terms of the statistical synthesis, there were also some limitations introduced by time constraints. The review only included studies that reported data for CAZ-AVI and at least one comparator, whereas ideally all susceptibility evidence for all comparators would have been sought to construct the network, regardless of whether CAZ-AVI had also been tested.
There were also some limitations introduced by problems inherent to susceptibility testing, and clinical practice in England. Setting clinical breakpoints is a subjective process conducted by relevant experts taking in to account a range of evidence, which may have been generated differently for different comparators. Therefore, any given breakpoint may not reflect the true activity of a treatment in clinical practice, and the extent to which it does may vary between treatments. Breakpoints also change over time, as pathogens increasingly acquire resistance. EEPRU were not able to resolve whether it is better to use breakpoints contemporaneous to the sample collection date, or apply current breakpoints to the available data (where data allowed), and for pragmatic reasons used data as reported in the published reports. Laboratory methods of susceptibility testing recommended by EUCAST and CLSI have also changed over time, and before 2016 BSAC had its own set of methods, which may have affected the estimates of susceptibility derived before and since then, as practice did not change immediately. As noted in Statistical synthesis plan, PHE data were a mixture of BSAC, CLSI and EUCAST methods, which will potentially affect the estimates of susceptibility derived. Clinical advisors also noted that in vitro susceptibility to meropenem in particular does not always indicate how well a patient will respond to this treatment in clinical practice.
Conclusions
Susceptibility estimates have been used to estimate the clinical effectiveness of CAZ-AVI and its comparators in the HVCSs. Several sensitivity analyses were conducted as part of the NMA. In the majority of the analyses CAZ-AVI had higher susceptibility relative to colistin, but this was not always statistically significant. Heterogeneity in all analyses was high, but was lower in some. Relevant base-case and scenario analyses for the model were selected based on heterogeneity and clinical rationales. These included a network of studies which used EUCAST laboratory methods and breakpoints, a consideration of all the studies in the network (removing two arms with large inconsistency), one study that reported no MBL co-carriage and used EUCAST laboratory methods and breakpoints, and using the PHE data alone. There was no signal that CAZ-AVI was associated with an increase in AKI or C. difficile infections compared to other non-toxic treatments.
Chapter 5 Structured expert elicitation
As detailed in Appendix 5, it is assumed that clinical outcomes would be similar regardless of the treatment received, conditional upon susceptibility. Review 4 did not identify any studies that informed clinical outcomes in HAP/VAP and cUTI patients conditional upon susceptibility, following microbiology-directed treatment. In the absence of empiric evidence, outcomes were informed by eliciting judgements of individuals who have expertise on the subject matter.
Methods
A structured elicitation process was used to improve accountability and transparency. Specifically, the reference methods developed at York as part of the Medical Research Council (MRC) elicitation work89 were employed. The full elicitation protocol is presented in Report Supplementary Material 2.
Approach to elicitation
Clinical experts were recruited to take part in the elicitation exercise, and their beliefs were elicited individually and remotely using an application developed in R, SHINY package. 90
Experts were trained in the approach to elicitation prior to the task, using an online training webinar (slides are presented in Report Supplementary Material 2). Experts were asked to express their uncertainty about the outcomes of interest using a histogram (chips and bins approach). 91 This approach has been shown to work well for experts not trained in probabilities and statistics. 89
Once experts were individually asked to express their beliefs, these were then aggregated using linear opinion pooling. First, a probability distribution was fitted to each expert’s beliefs from the histogram and then these were pooled, assuming that each expert contributed equally to the group overall distribution.
This overall distribution was then relayed back to the experts, and they were given the opportunity to revise their own beliefs on the histograms they previously completed.
Expert recruitment
Experts recruited to take part in the elicitation exercise included medical consultants, ICU consultants, pulmonary consultants and microbiologists. The literature suggests that around 10 experts should be included in an individual elicitation, and that recruitment should strive for a representative sample. 89 To this end we sought to recruit experts from across the UK using our clinical leads. We approached experts directly and asked for their participation. Experts who agreed to participate were invited to attend a training webinar. The majority of experts attended this session, with a few choosing to view the pre-recorded slides instead. Experts’ identities were known to the modelling team; however, in aggregating, feeding back and reporting, all experts’ identities were anonymised.
Parameters elicited
The elicitation was conducted to inform outcomes in HAP, VAP and cUTIs caused by carbapenem-resistant Gram-negative bacteria of interest, following microbiology-directed treatment. The elicitation exercise was used to inform outcomes in two distinct reports where the pathogens of interest included Enterobacterales OXA-48, MBL Enterobacterales or MBL Pseudomonas aeruginosa.
For each of the three sites of infections, we elicited outcomes depending on whether the infectious pathogen is susceptible to treatment. Therefore, outcomes only depend on whether a patient is susceptible to treatment or not, and not to the specific treatment given. The outcomes of interest were 30-day mortality, LoS in hospital, and the type of ward these patients would stay on in hospital.
As background information we presented several related studies to experts (see Report Supplementary Material 2 for details).
Results
Completion rate
Eleven experts agreed to take part in the elicitation task and took part in the training. Only five provided usable data (see Appendix 6).
Group summaries and use in the modelling
Pooled summaries for each elicited quantity are shown in Appendix 6. The group summaries on 30-day mortality (see Appendix 6.3, Figures 32, 34 and 36) indicate that survival is the lowest for VAP patients and highest for cUTI patients and that susceptibility to treatment increases the probability of survival, for all three sites of infection. The group summaries on LoS (see Appendix 6.3, Figures 33, 35 and 37) indicate that the LoS is the shortest in patients with cUTIs and the longest for patients with VAP. For all three sites of infection, susceptibility to treatment decreased the LoS. The group summaries for the proportion of time spent on different types of wards (see Appendix 6.3, Tables 46–48) indicate that patients with VAP spend the most time in ICU and the least time on general medical wards, followed by HAP, then cUTIs. Furthermore, patients who are susceptible to treatment are expected to spend more time on the general medical ward and less on ICU and HDU, for all three sites of infection.
In the model, outcomes of HAP and VAP were modelled together, and so experts’ responses were pooled. When pooling, outcomes for HAP and VAP were weighted by their relative occurrence in Tumbarello et al. (2013): 0.283 (28/99) for HAP and 0.617 (71/99) for VAP. Tumbarello was chosen as the study where participants were the most representative of patients in the HVCSs that reported the proportion of patients with HAP that was ventilator-associated.
The pooled results for expert beliefs are shown in Figure 4 and summarised in Table 12.
| ICU | HDU | General medical ward | |
|---|---|---|---|
| HAP/VAP, susceptible | 49.90 | 14.94 | 35.16 |
| HAP/VAP, not susceptible | 58.92 | 17.21 | 23.86 |
| cUTI, susceptible | 15.00 | 17.00 | 68.00 |
| cUTI, not susceptible | 23.33 | 18.33 | 58.33 |
FIGURE 4.
Survival and LoS by susceptibility. (a) Thirty-day survival with HAP/VAP combined. (b) Expected LoS with HAP/VAP combined. cUTI, complicated urinary tract infection; HAP/VAP, hospital-acquired pneumonia or ventilator-associated pneumonia; P, proportion.
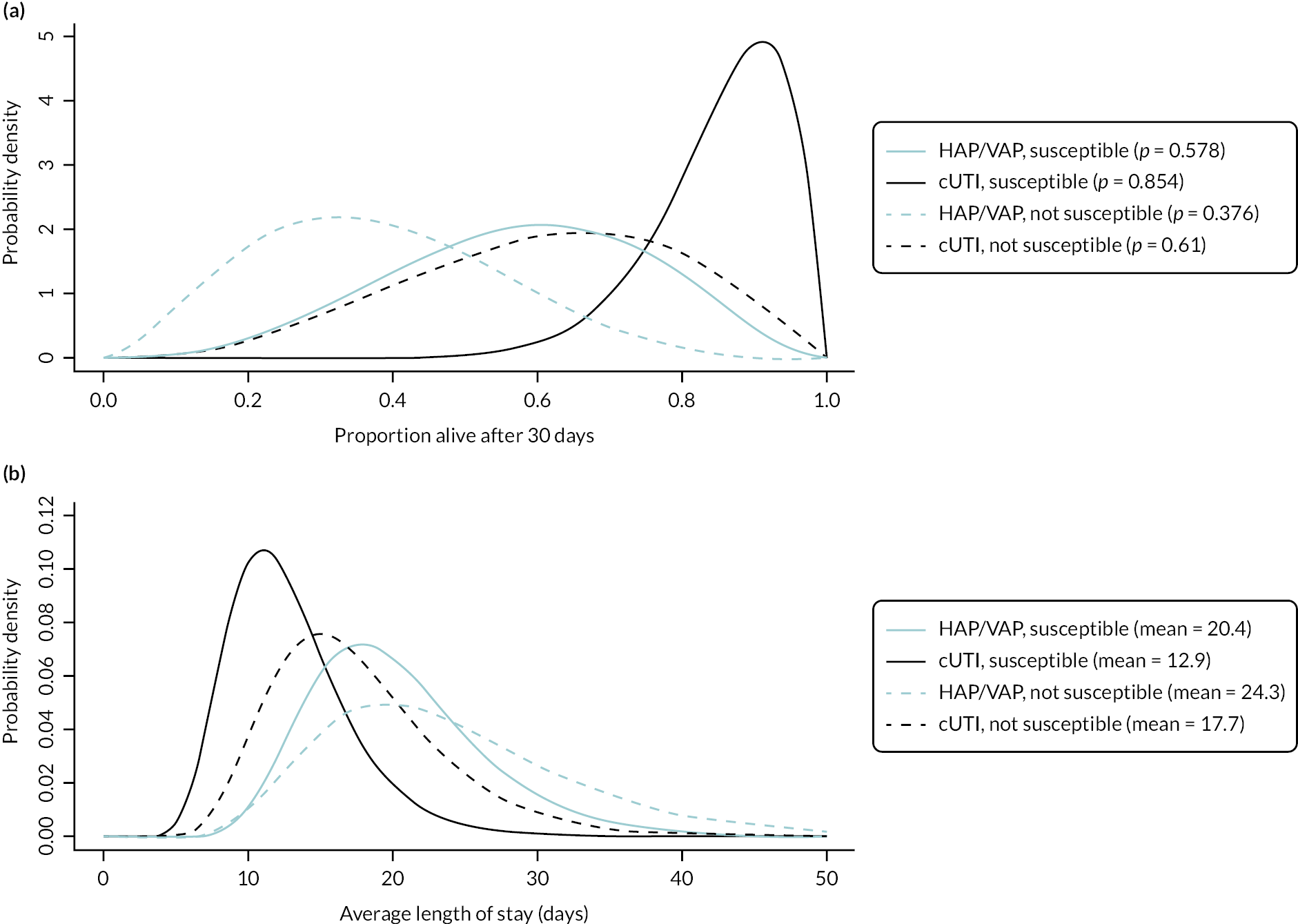
Validation of experts’ estimates
We explored alternative sources of evidence to inform LoS in the model, in order to validate the elicitation results. This suggested that the LoS elicited from the experts is broadly comparable to the estimates within the literature; for further details, see Appendix 6.
Chapter 6 Existing economic evidence
Assessment of existing cost-effectiveness evidence and modelling approaches
A series of reviews of existing cost-effectiveness evidence and modelling approaches was conducted:
-
A review of existing cost-effectiveness evidence for CAZ-AVI with a focus on studies that include decision-analytic models. The aims were to establish the existence of potentially policy-relevant models to guide NICE and NHS decisions, and to identify relevant analytical methods and data sources.
-
A review of existing approaches to modelling the existence of resistant pathogens in the target population, currently and over time. The aim of this review was to identify methods that could be adopted for this purpose in EEPRU’s modelling.
-
A review of existing cost-effectiveness models in HAP/VAP to understand modelling approaches and data sources.
-
A review of existing cost-effectiveness models in cUTI. Again, the purpose was to understand modelling approaches and data sources.
Each review involved searches of bibliographic databases using standardised search terms, selection of studies based on explicit inclusion criteria and data extraction using an agreed template. Details of each review are provided in Report Supplementary Material 3. Here the key results of each review are outlined.
Review 1: existing cost-effectiveness evidence for CAZ-AVI
A total of 89 potentially relevant papers or abstracts were identified for the review. When the various levels of screening were complete, five studies were included. 13,92–95 All studies considered costs and benefits at a patient level with no attempt to aggregate across the licensed CAZ-AVI indications likely to represent the product’s expected population. All studies had relatively short-term time horizons (3–5 years) and no attempt was made to consider the value of CAZ-AVI as resistance to the new and existing therapies increases over time. Three analyses made assumptions (rather than drawing on evidence) about the proportions of patients with resistant infection in the relevant population, and the impact of resistance on clinical parameters. 13,92,93 The other two studies drew on evidence from observational studies to quantify the impact of resistance on relevant parameters in the modelling. 94,95 The wider set of sources of value for novel antibiotics mentioned in Decision-making context was not considered in any of the studies. None of the analyses related to clinical practice or evidence from the UK. As such, their relevance to this evaluation of CAZ-AVI is very limited.
Review 2: review of existing approaches for resistance modelling
Nine studies were included in this review. Note that this includes the five papers already identified from Review 1. As discussed under Review 1, the five studies looking at the cost-effectiveness of CAZ-AVI provided limited insights regarding how to reflect resistance in the modelling and no attempt was made to consider the implications of changes in resistance over time. The additional four studies in this review provided some indications of how resistance could be captured. One study assessed the appropriateness of alternative empiric therapies based on susceptibility data from a specific Taiwanese hospital. 96 Another looked at procalcitonin-guided antibiotic stewardship and estimated the correlation between the percentage reduction in days of antibiotic use resulting from the procalcitonin-guided test and antibiotic resistance. 97
The other two studies in this review attempted to deal with resistance through mechanistic infectious disease modelling. One used hypothetical data for illustrative purposes. 98 The other (which is a key source for the model detailed in the CAZ-AVI manufacturer’s submission – see Review of manufacturer’s model for CAZ-AVI) used the combination of a dynamic transmission model and a treatment pathway model as a generic framework to evaluate antibiotics for different indications and pathogens. 99 In principle, such a model could be capable of quantifying not just the direct health effects of a new antibiotic, but also the indirect impacts via any reduction in transmission of relevant pathogens. It could also reflect changes in resistance over time in response to different stewardship strategies and the introduction of new AMs. However, whether the model can achieve this in practice will inevitably depend on the available evidence and the assumptions necessary to address the evidence gaps.
Review 3: existing cost-effectiveness models in HAP/VAP
This review used an earlier systematic review100 to extract information on the characteristics of three relevant studies including target population, modelling assumptions, model structure and key evidence. 101–103 All of these studies included standard cost-effectiveness models and did not consider the impact of alternative therapies on resistance patterns over time. One study attempted to include transmission rates in the modelling but this was not extrapolated to estimate population-level health effects. 103 As a UK study, one study provided some potentially useful evidence sources for the current evaluation. 101
Review 4: existing cost-effectiveness models in cUTI
One study was identified104 in addition to the models in cUTI identified in Reviews 1 and 2. 93,95,96,99,105 As for Review 3, the UK-based studies provided some insights on evidence sources. The additional study104 was US-based and used micro-simulation to track patients, allowing for treatment switching as microbiological information becomes available. A surveillance dataset was used to sample isolates and to determine susceptibility to different treatments. This use of susceptibility data rather than standard in vivo evidence from RCTs and other designs is novel and has the potential to address modelling challenges.
Review of manufacturer’s model for CAZ-AVI
To support this assessment, CAZ-AVI’s manufacturer submitted a model to evaluate the value of CAZ-AVI. Appendix 7 provides an overview and critique of the company’s submitted model. As shall be seen, there were high-level concerns about the relevance of the company’s model and evaluation. In addition, for some areas, there was a lack of transparency on the processes that are driving the economic results. Because of these issues, EEPRU has not provided a detailed critique of the company’s submitted model and evaluation, but focuses on a description of the model and its results (see Appendices 7.1–7.4, including Tables 49–51 and Figures 38–42), areas of inconsistency (see Appendix 7.5, Table 52), and other concerns with the model (see Appendix 7.6).
In summary, EEPRU notes that the company has submitted a dynamic cohort-based model to analyse the NMB associated with the introduction of CAZ-AVI. The model considers changing the pattern of use of existing AMs in an infectious environment with a constant number of patients but changing proportions that are susceptible, colonised and infected. Pathogens may be resistant or sensitive to treatment. The base-case NMB estimate was £598,779,222 (at a cost-effectiveness threshold of £30,000/QALY) for the three indications cUTI, cIAI and HAP/VAP combined in the population of England over a 10-year time horizon.
There is concern that the population considered in the model diverges from the guidance provided by clinical advisors to EEPRU, where usage of CAZ-AVI would be restricted to patients who are suspected of having a carbapenem-resistant infection. The broader use of CAZ-AVI in the company’s model will contribute to an increased population NMB estimate. In addition, the model assumes that treatment can completely eradicate patients of colonisation with a sensitive or resistant pathogen. This also diverges from the clinical advice given to EEPRU.
Single use of CAZ-AVI compared to a single comparator could be expected to generate broadly similar rates of mortality given the broadly similar efficacy and baseline resistance of CAZ-AVI and alternative treatments. Therefore, the large NMB may be accounted for by the dynamic aspects of the model such as the diversification stewardship strategy and the company’s approach to the decision problem, with no microbiology-directed tested treatment sequence, and a three-line treatment sequence with CAZ-AVI compared to a two-line comparator. The company has not provided an account of the processes driving the large health benefits in the model.
Chapter 7 Methods for EEPRU quantitative assessment of value
Overview of EEPRU approach
This section of the report contains some material reproduced from the study protocol. © NICE 2022. Protocol for the technology evaluation of ceftazidime with avibactam for treating severe aerobic Gram-negative bacterial infections. Available from www.nice.org.uk/about/what-we-do/life-sciences/scientific-advice/models-for-the-evaluation-and-purchase-of-antimicrobials/ceftazidime-with-avibactam#evidence. All rights reserved. Subject to Notice of rights. NICE accepts no responsibility for the use of its content in this product/publication.
The quantitative economic analysis developed for this appraisal comprises three components: an assessment of the INHEs of introducing CAZ-AVI within the HVCSs at the patient level; an assessment of INHEs within the HVCSs at the population level and an assessment of how population-level INHEs within the HVCSs might appropriately be rescaled to reflect expected usage across the NHS. An overview of each component is provided below, and the methods for each component are described in the following sections. In line with the NICE Reference Case, the model perspective is the NHS and Personal and Social Services, health benefits are expressed in terms of quality-adjusted life-years (QALYs) and both costs and QALYs are discounted at a rate of 3.5% per annum.
The patient-level component of the model is structured similarly to models developed as part of other NICE programmes, and characterises the likely comparative effectiveness of CAZ-AVI and existing AM usage scenarios; also the impact of CAZ-AVI and existing AM usage scenarios on costs, HRQoL and mortality over the lifetime of the patient.
The population-level component aggregates the patient-level predictions to the population-level accounting for the size of, and growth over time in, the eligible patient population in England within each HVCS. This component also reflects how resistance is likely to develop to CAZ-AVI and existing AMs over time. The previous EEPRU framework outlined two broad approaches to modelling this: mechanistic dynamic transmission modelling, which attempts to explain the way in which susceptible and resistant pathogens spread through the population; and statistical forecasting models, which predict the number of people with infections with specific resistance profiles without explicitly modelling the underlying mechanistic processes of pathogen transmission and resistance acquisition. 12 We considered both approaches but ultimately used a forecast-based approach, for reasons detailed below.
The use of a transmission model was considered but not pursued on three grounds. Firstly, developing a mechanistic transmission model that characterises the spread of carbapenem-resistant organisms, with an adequate level of detail to model the introduction of CAZ-AVI, and that is appropriately calibrated to historical epidemiological data, was not considered feasible within the time and resources available for this 9-month project. Secondly, our clinical advisors considered that the direction and magnitude of the effects of the new treatments on transmission were uncertain and not well evidenced (see Additional elements of value relevant to AMs). Thirdly, advice during our previous EEPRU work12 indicated that transmission modelling in AMR is an evolving science where the degree of parameter and structural uncertainty can lead to instability in model predictions and that, although there is no guarantee that a forecast-based approach will offer more certain or robust predictions, it should offer greater transparency. The company submitted a transmission model which we review in detail in Review of manufacturer’s model for CAZ-AVI. This highlighted some of the challenges of developing and communicating these types of models in a way that allows appropriate levels of scrutiny of their outputs.
The final quantitative assessment performed is to rescale the population INHEs observed in the HVCSs to reflect expected usage. This part of the quantitative assessment takes a very pragmatic approach seeking to identify the range of clinical scenarios in which CAZ-AVI is expected to be used, enumerate the corresponding population sizes using the best available evidence, and rescale the population INHEs estimated for the HVCS accordingly.
The literature on the economic evaluation of AMs has described a range of elements of value associated with these products that are not relevant to and therefore do not feature in evaluations of other drugs and health technologies. 12,106 Following presentation of the quantitative assessments of value, we therefore discuss whether these additional elements of value might be delivered via use of CAZ-AVI, the extent to which they are captured by our quantitative assessments, and where they are not captured whether they are likely to substantively modify the estimates of value presented (see Additional elements of value relevant to AMs).
Modelling direct patient net health effects in HVCS
Relationship with decision problem
Population
The patient populations modelled align with the decision problem outlined in Chapter 4. These are summarised in Table 13.
| Site | Pathogen | Mechanism | Setting |
|---|---|---|---|
| HAP/VAP | Enterobacterales | OXA-48 | Microbiology directed |
| HAP/VAP | Enterobacterales | OXA-48 | Risk-based empiric treatment |
| cUTI | Enterobacterales | OXA-48 | Microbiology directed |
Intervention
Ceftazidime-avibactam is considered as monotherapy only due to a lack of in vivo or in vitro evidence about how it performs in combination with other agents. The clinical advisors confirmed that monotherapy was more likely to be used in practice.
Comparators
A wide range of drugs is considered relevant in the HVCS, and different drugs were considered relevant depending on the site, pathogen, mechanism and setting. The full list of comparators is provided in PICOS for high-value clinical scenarios. Due to the paucity of data available to inform the comparative effectiveness assessment (see Chapter 5), and our reliance on in vitro susceptibility data to inform comparative effectiveness, it was possible to take a simplified approach to modelling these comparators rather than conducting a fully incremental analysis of all available AM options as is typically recommended in economic evaluation. The approach taken is documented in the following section.
Model structure
The model structure differs according to the setting (MDS or ES) but not the site, pathogen or mechanism of resistance. We describe the structure for the MDS first as it is more straightforward and forms part of the ES model structure.
Due to the paucity of in vivo data relevant to the modelled HVCS (see Review results), we have assumed that differences across treatments in in vitro susceptibility are predictive of in vivo clinical outcomes. This was considered reasonable by the clinical advisors to this project, and evidence relating to treatment susceptibility as a surrogate for clinical outcomes is reviewed in Review questions 4 and 5. We link susceptibility to time in hospital and mortality. We do not model the development of infection sequalae such as sepsis. This would have required a range of additional evidence including the rate of development of sepsis, how this relates to susceptibility to the treatment administered, and mortality and hospitalisation outcomes conditional upon whether a patient developed sepsis. Given the sparsity of evidence available, including these additional parameters was not considered appropriate. We would, however, expect 30-day mortality and hospitalisation outcomes to implicitly reflect the possibility that patients will develop additional complications including sepsis. Repeat infection following discharge was also not explicitly modelled (though will be implicitly reflected in the mortality data) as this was considered unlikely to be a significant driver of population INHEs in the HVCS.
As well as differences in effectiveness, we model differences in treatment safety. We focus on nephrotoxicity and, in particular, the occurrence of AKI. This was considered to have the most significant implications for the modelling in terms of driving treatment choices (with clinicians keen to avoid highly nephrotoxic comparator drugs), and influencing INHEs as CAZ-AVI is expected to be associated with lower rates of nephrotoxicity than some comparators.
Ototoxicity was raised by our clinical advisors as a safety concern associated with use of aminoglycosides. This was not modelled as it was expected that significant hearing impairment associated with aminoglycosides would be rare in this patient group. 107 Reduced rates of Clostridium difficile infection were highlighted by a number of stakeholders as a potential benefit of the new drugs. This was not included in the modelling as rates of clostridium difficile are very low108 (see Review question 6).
Model structure for microbiology-directed setting
In the MDS, each patient’s susceptibility to available treatment options is known, and treatment can be tailored accordingly. Based on feedback from our clinical advisors, the two main reasons for initiating treatment with CAZ-AVI (provided patients are susceptible to it) within the MDS HVCS would be that patients are either: (1) not susceptible to any other available treatment options (i.e. patients are completely MDR to relevant existing treatment options) or (2) the only other treatments to which they are susceptible carry an elevated risk of nephrotoxicity. We include colistin and aminoglycosides within the category of nephrotoxic drugs as our clinical advisors indicated that they are likely to be associated with elevated levels of nephrotoxicity. To reflect these considerations, patients within the MDS are divided into three categories based on their susceptibility to existing therapies and, within each category, further subdivided according to their susceptibility to CAZ-AVI.
Table 14 shows these subgroups, how they determine treatment choice under existing care, and how that would change if CAZ-AVI was to become available to this patient group. The groups for which a switch to CAZ-AVI is expected are highlighted in bold.
| Susceptibility to existing drugs | Susceptibility to CAZ-AVI | Therapy under existing care | Therapy with new drug available |
|---|---|---|---|
| Susceptible to one or more non-colistin/aminoglycosides option | Susceptible | Non-colistin/amino | Non-colistin/amino |
| Resistant | Non-colistin/amino | Non-colistin/amino | |
| Susceptible only to colistin or aminoglycosides | Susceptible | Colistin/amino-based | CAZ-AVI |
| Resistant | Colistin/amino-based | Colistin/amino-based | |
| Not susceptible to any available treatment options | Susceptible | Multidrug salvage | CAZ-AVI |
| Resistant | Multidrug salvage | Multidrug salvage |
In the group of patients who are susceptible only to colistin or an aminoglycoside, and susceptible to CAZ-AVI, CAZ-AVI offers a safety advantage. In the group of patients who are not susceptible to any available treatment options and, in the absence of the new treatments under evaluation, would receive multidrug salvage therapy, CAZ-AVI offers a safety and efficacy advantage. This is because, for many patients, multidrug salvage therapy would be expected to include a colistin or aminoglycoside component. Throughout the modelling, isolates classed as intermediate-resistant are grouped with those which are resistant as patients infected with intermediate-resistant and resistant pathogens are expected to experience similar outcomes in the HVCS based on feedback from EEPRU’s clinical advisors, and much of the data relating mortality and hospitalisation to susceptibility follow this grouping. Our clinical advisors noted that it may be possible to overcome intermediate resistance via higher dosing, but also considered that it would be difficult to evidence this within the model. Given the diverse range of data sources informing susceptibility and the link between susceptibility and outcomes, and the level of reporting within these studies, it was not feasible to explore the implications of differential outcomes between intermediate-resistant and resistant patients.
In the MDS the model is, therefore, driven by the proportion of individuals within each category of ‘susceptibility to existing drugs’ and the proportion of individuals susceptible to CAZ-AVI. This is based on susceptibility data as documented in Clinical parameters – susceptibility evidence. The comparison made within the model is between the overall MDS cohort who receive tailored therapy with the new drug available (column four of Table 14) and the overall MDS cohort who receive tailored therapy under existing treatment options only (column 3 of Table 14).
Importantly, the fact that the susceptibility profile is known prior to initiation of treatment in the MDS, alongside the assumption that susceptibility is the sole predictor of treatment effectiveness, means that we do not need to model each individual treatment option within the MDS. For example, it is not relevant (to clinical outcomes) whether a patient is susceptible to fosfomycin or aztreonam, as susceptibility to these treatments would be assumed to result in the same outcomes. Although there are differences in the costs of therapies, these are modest in relation to other costs such as that of hospitalisations which may include periods in the ICU/HDU. In practice, patients may receive a combination of agents, but this is not modelled explicitly due to a lack of evidence. The clinical advisors considered it reasonable to assume that, in the MDS, patients susceptible to a single AM within a multi-agent regimen perform as well as those susceptible to all components of that regimen (i.e. it does not matter if you are susceptible to drug A, drug B or drug A and B as long as you are susceptible to one of the agents received).
Following receipt of treatment in the MDS, patients are modelled to experience one of four alternative 30-day outcomes which determine their long-term outcomes (Figure 5). A decision tree is used to determine the distribution of patients across these categories at 30 days. This is as shown in (Figure 6). Probabilities highlighted in bold differ by treatment in this figure. In the MDS we only model one line of treatment explicitly, though hospitalisation and mortality evidence will reflect the fact that some patients entering the MDS receive multiple lines of therapy.
FIGURE 5.
Thirty-day outcomes in the MDS.
FIGURE 6.
Decision tree used to calculate impact of AKIs on 30-day outcomes in MDS.
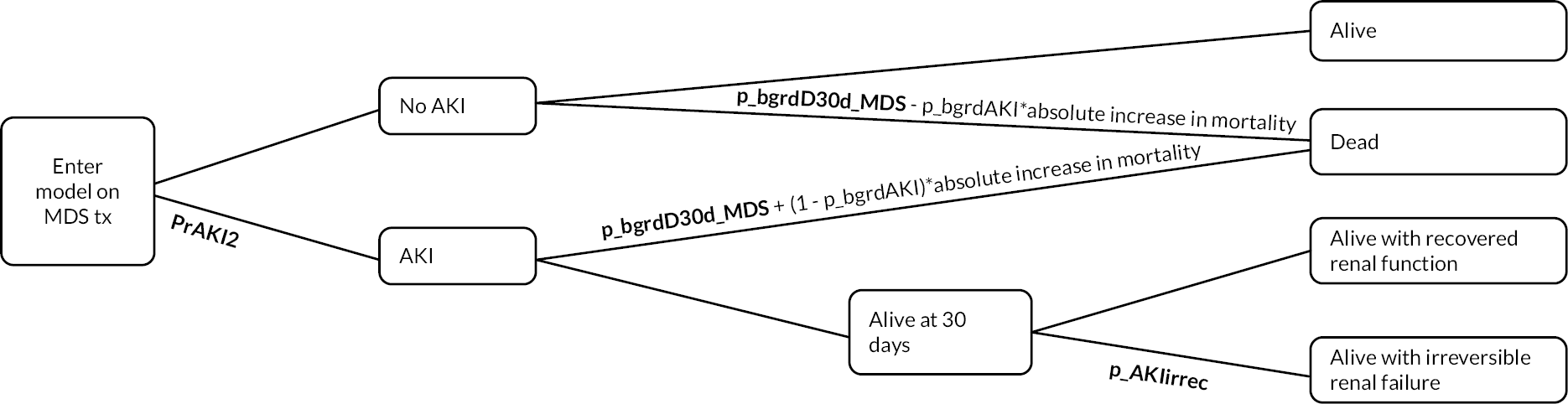
All patients face a risk of death due to their infection and comorbidities (p_bgrdD30d_MDS). The risk differs according to whether patients have received a treatment to which they are susceptible or not. In the MDS, given that treatments are tailored according to patients’ known susceptibility profiles, only patients infected with a fully MDR infection (who receive multidrug salvage treatment) are expected to face the elevated risk of death of those non-susceptible to treatment. The efficacy advantage of CAZ-AVI is, therefore, driven by the proportion of people who switch from ‘multidrug salvage’ to CAZ-AVI in Table 14 as these patients switch from experiencing the mortality of non-susceptible patients to experiencing the mortality of susceptible patients.
In addition, patients face differing drug-related risks of experiencing an AKI. Patients who experience an AKI face an elevated risk of death compared to those who do not. When modelling the effect of AKI on mortality, we account for the fact that the available mortality data already reflect both the underlying risk of AKI associated with currently available non-colistin/aminoglycoside AMs and the background risk of AKI associated with patients underlying comorbidities and infection (Figure 6). Patients who experience an AKI and survive until 30 days face a risk of adverse long-term outcomes according to whether they have (1) recovered their renal function or (2) suffered irreversible renal failure, that is, developed chronic kidney disease (CKD).
At 30 days, patients who are discharged alive without renal dysfunction are assigned a comorbidity-adjusted QALY outcome estimated using an alive-dead area-under-the-curve approach. This is independent of the assigned treatment, as patients alive at 30 days without a history of AKI are assumed to experience similar outcomes regardless of the treatment they received for their infection.
Patients discharged with recovered renal function face the same HRQoL outcomes, but they face an additional risk of progressing to CKD and elevated mortality. Patients discharged with CKD or who develop CKD face further elevated mortality, reduced HRQoL and additional healthcare costs. The experience of the two groups of patients with a history of AKI is modelled as a semi-Markov process (with transition probabilities dependent on time in model) for all transitions, as shown in Figure 7.
FIGURE 7.
Markov model used to calculate post-30-day outcomes in patients with recovered renal function and irreversible renal failure.
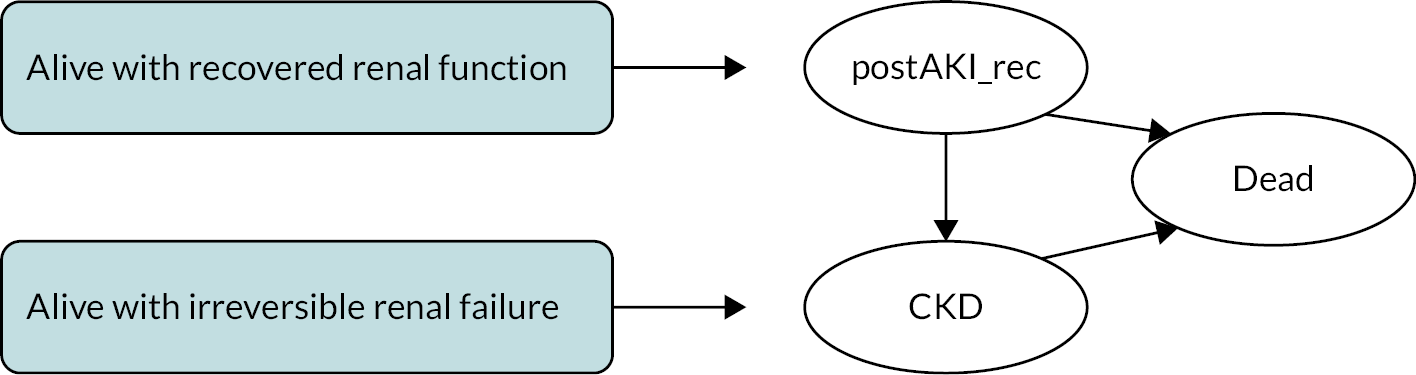
Model structure for the risk-based empiric setting
The approach taken in the ES is similar to that taken in the MDS in terms of the possible 30-day outcomes patients can experience and the long-term implications of these outcomes. However, the decision tree describing differences across comparators in the first 30 days is more complex for two reasons. Firstly, there is a need to model outcomes both in those correctly identified as having the pathogen–mechanism combination suspected, as well as in those who were labelled as high-risk but in fact have a different causative pathogen or mechanism. Secondly, there is a need to model both the ES phase of treatment and progression of some patients to the MDS for further treatment.
Unlike in the MDS, in the ES the susceptibility of patients to treatments provided is unknown at the time of initiating empiric treatment. It is, therefore, necessary to model the probability of susceptibility to individual treatment combinations as this determines clinical outcomes and, in particular, the need for further treatment. Since, as documented in PICOS for high-value clinical scenarios, there are a number of feasible treatment combinations for these patients, to simplify the modelling we compare empiric use of CAZ-AVI in the ES to two alternative treatment options:
-
the non-colistin or aminoglycoside-based treatment combination with the current highest estimated susceptibility in the UK population
-
the colistin or aminoglycoside-based treatment combination with the current highest estimated susceptibility in the UK population.
When considering possible treatment pathways in the ES, the following possible pathways are relevant (shorthand labels E1, E2nca etc. are used in the results section):
-
E1: empiric use of CAZ-AVI followed by existing treatments in the MDS.
-
E2nca: empiric treatment using non-colistin or aminoglycoside-based existing therapies followed by existing therapies in the MDS.
-
E2ca: empiric treatment using colistin or aminoglycoside-based existing therapies followed by existing therapies in the MDS.
-
E3nca: empiric treatment using non-colistin or aminoglycoside-based existing therapies followed by CAZ-AVI use if indicated in the MDS.
-
E3ca: empiric treatment using colistin or aminoglycoside-based existing therapies followed by CAZ-AVI use if indicated in the MDS.
Repeated usage of CAZ-AVI in the MDS for patients who fail CAZ-AVI in the ES was not modelled as this was not considered to represent a priority use for CAZ-AVI.
Thirty-day outcomes in the ES are determined by a decision tree which comprises three subcomponents:
-
the risk of carrying the pathogen–mechanism of concern
-
outcomes at the point at which patients are assessed for MDS treatment, that is, at around 3–5 days when susceptibility results report
-
30-day outcomes following MDS assessment.
Each of these is considered in more detail below.
-
Risks of carrying the pathogen–mechanism of concern
Patients may or may not have the suspected pathogen–mechanism of concern. We assume that patients who do not have the pathogen–mechanism of interest experience the same effectiveness outcomes regardless of the choice of empiric treatment (though safety differs), as our clinical advisors confirmed that these patients represented a broadly susceptible population (rather than a population enriched with pathogens carrying other resistance mechanisms) and that for this reason effectiveness is likely to be similar across all empiric treatment options considered. For simplicity we assume that patients who have a different pathogen–mechanism experience the susceptibility associated with colistin/aminoglycoside-based therapy in people with the pathogen–mechanism of interest regardless of the choice of treatment. Colistin/aminoglycoside-based therapy was chosen as more representative of outcomes across susceptible patients as this treatment class showed robust and high susceptibility across subgroups and scenarios. The structure of this element of the ES model is presented in Figure 8.
FIGURE 8.
First component of 30-day outcomes model for ES: risk of carrying pathogen–mechanism of concern.
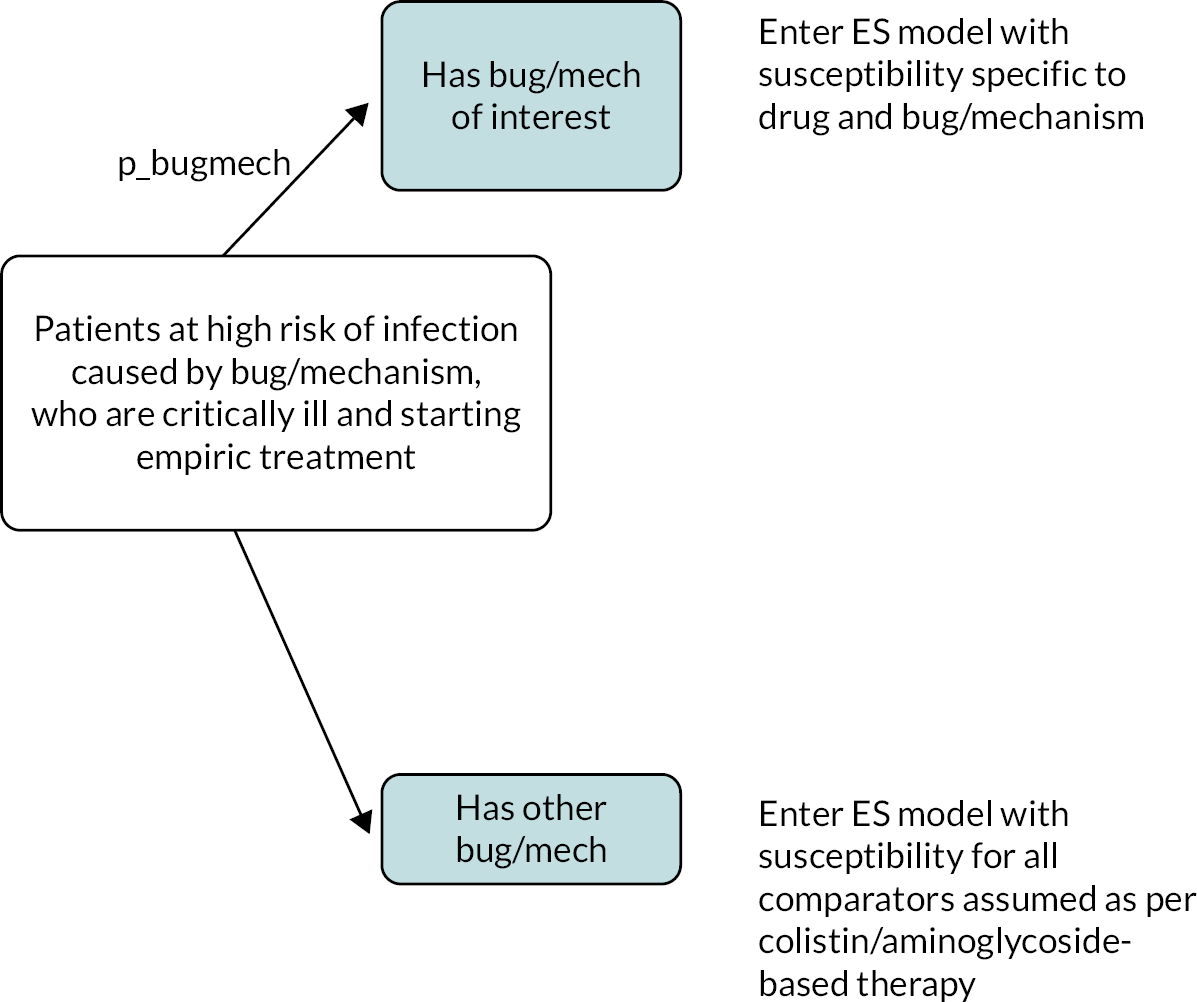
-
Outcomes at the point at which patients are assessed for MD treatment
At initiation of empiric treatment patients are classified by the model as susceptible or non-susceptible to their empiric therapy (Figure 9). As in the MDS, susceptibility is the driver of differences in effectiveness across treatments. Note that we are able to model differences in susceptibility across treatments used in the ES dependent on whether a patient is susceptible or non-susceptible, even though clinicians will not observe this information until patients enter the MDS.
FIGURE 9.
Second component of 30-day outcomes model for ES: outcomes at the point at which patients are assessed for MD treatment. Note that mortality (p_bgrd_Dst_S and p_bgrdDst_nonS) is also adjusted to reflected differences in mortality due to AKI, in the same way as shown in Figure 10, but this is not shown for parsimony.
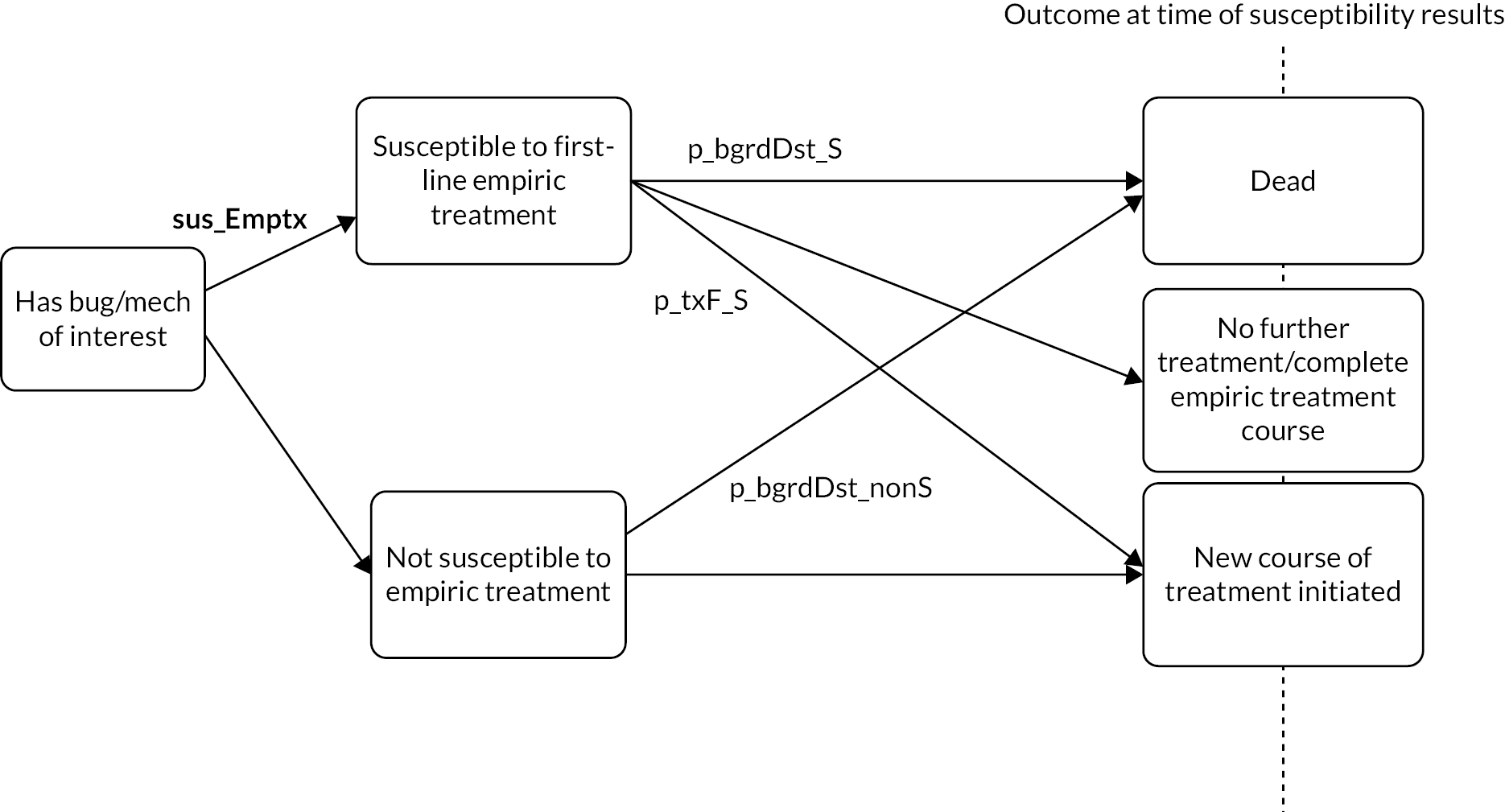
At the point at which patients’ microbiology results become available, patients may have died, may require initiation of a new AM treatment (e.g. due to lack of efficacy) or may complete their course of empiric treatment (Figure 9). The probability of these three outcomes depends on whether patients were susceptible to their empiric treatment or not, but not directly on the choice of specific treatment. Patients who have received empirically a treatment to which they are later found not to be susceptible are all assumed to require further treatment in the MDS, provided they survive until microbiology results are available. This assumption is based on evidence presented in Tumbarello et al. 2013, which found that all patients who received inappropriate empiric treatment and survived until their microbiology results were received switched to appropriate therapy (further details on Tumbarello are provided in Clinical parameters – AKI risk and subsequent outcomes). 109
-
Thirty-day outcomes following assessment for MD treatment
People who survive until the time point of assessment for MD treatment enter the third part of the decision tree which is shown in Figure 10. Those requiring no further treatment face a risk of dying between this point and 30 days, which depends on whether they experienced an AKI. Those surviving to 30 days face the possibility of entering the (1) alive, (2) alive with recovered renal function or (3) alive with irreversible renal failure health states described in Figure 10. While patients may experience an AKI following empiric treatment, clinicians confirmed that in this patient group, where treatment options are limited, the AKI alone would not typically trigger a treatment switch, provided the treatment was effective.
FIGURE 10.
Third component of 30-day outcomes model for ES: 30-day outcomes following assessment for MDS treatment.
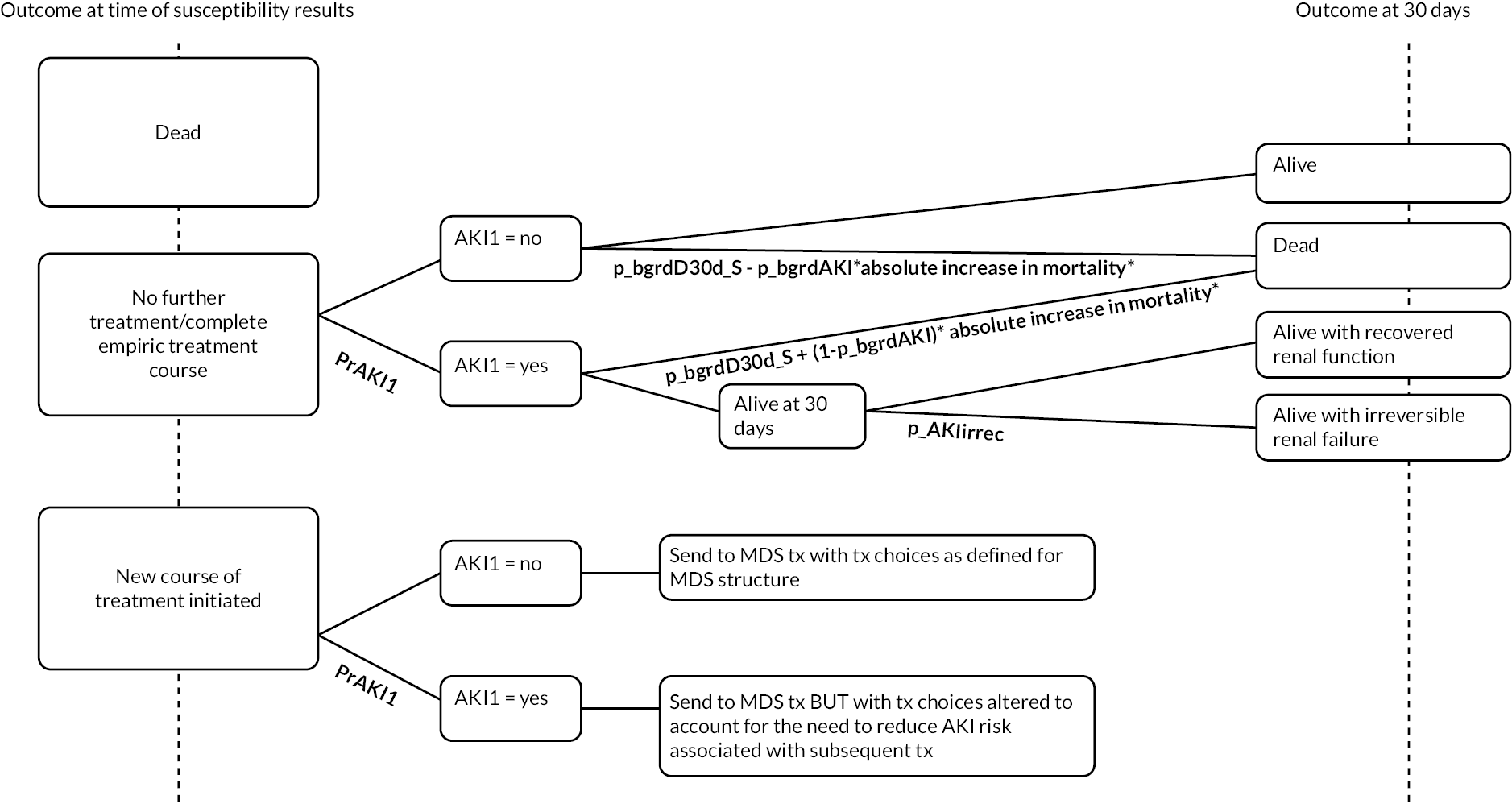
Patients who require further treatment enter the MDS component of the model. Their outcomes depend on whether they experienced an AKI following first-line treatment (i.e. this is ‘remembered’ within the model) as this determines both their outcomes (patients who experience an AKI experience elevated mortality and the implications of reversible or irreversible kidney damage) and their choice of treatment in the MDS. Our clinical advisors informed us that patients requiring further treatment in the MDS who experienced an AKI following treatment in the ES are unlikely to receive colistin- or aminoglycoside-based treatment in the MDS. Patients who fit this profile, and are only susceptible to colistin or aminoglycoside-based treatment, are, therefore, assumed to receive multidrug salvage therapy in the MDS, or the new drug if available. For these patients, multidrug salvage therapy is assumed not to include colistin or an aminoglycoside. Instead, they are assumed to receive the outcomes of multidrug salvage therapy without elevated risk of AKI.
In the absence of evidence to support more detailed modelling, we assume that a patient’s susceptibility to treatment is the same in the ES and MDS. In reality, patients entering the MDS who were already assessed as having a high risk of carrying a highly resistant pathogen in the ES are likely to receive aggressive treatments in the ES which may change their resistance profile in the MDS. The nature of the effects on individual resistance are hard to predict as they are influenced by the treatment received in the ES, the effectiveness of this treatment and the development of acquired resistance. These are not, therefore, considered within the model.
Sources of evidence
Identification of evidence
Susceptibility evidence and evidence linking susceptibility to mortality and hospitalisation were obtained via the systematic reviews and structured expert elicitation described in Chapters 5 and 6. Other key clinical parameters were obtained from existing systematic reviews where possible, otherwise clinical parameters were obtained from existing UK cost-effectiveness models. HRQOL weights (utilities) were obtained from a systematic review (described below) and cost parameters via targeted searches.
Clinical parameters – susceptibility evidence
The susceptibility data used in the model base case analysis are summarised in Table 15. These represent the mean values of the samples used in the probabilistic sensitivity analysis, along with 95% percentile-based confidence intervals. Five key susceptibility parameters inform the model. One parameter describes susceptibility to CAZ-AVI in the MDS and ES. Two parameters describe susceptibility to colistin/aminoglycoside-based therapy and to non-colistin/aminoglycoside-based therapy in the ES. Two parameters describe the number of individuals in each category of susceptibility in the MDS as shown in Table 14 (namely susceptible to a non-colistin/aminoglycoside AM, susceptible only to a colistin/aminoglycoside AM).
| Pathogen–mechanism subgroup | Description | Value | 95% CI |
|---|---|---|---|
| Enterobacterales/OXA-48 | Proportion of isolates susceptible to one or more non-colistin/aminoglycosides option | 65% | 55% to 75% |
| Enterobacterales/OXA-48 | Proportion of isolates susceptible only to colistin or aminoglycosides | 35% | 25% to 45% |
| Enterobacterales/OXA-48 | Proportion of isolates susceptible to CAZ-AVI | 92% | 77% to 98% |
| Enterobacterales/OXA-48 | Proportion of isolates susceptible to the most effective non-colistin/aminoglycoside-based empiric treatment | 35% | 7% to 79% |
| Enterobacterales/OXA-48 | Proportion of isolates susceptible to the most effective colistin/aminoglycoside-based empiric treatment | 94% | 88% to 98% |
Susceptibility to existing drugs is obtained from both the analysis of PHE data and the NMA, as described in Statistical synthesis. These analyses can be combined to provide evidence on absolute rates of susceptibility to AMs for the HVCSs. This evidence required further adjustment before it could be used in the economic model, with different adjustments for the ES and MDS. The methods employed to obtain estimates for these two settings are discussed in turn, with further details provided in Appendix 8 and Appendix 8, Table 53. Of note, while evidence on susceptibility to meropenem was available, this was not used in the economic modelling. This is because clinical advice was that, for meropenem, susceptibility among carbapenem-producing pathogens was not a good surrogate predictor of clinical outcomes. This reflects advice in the literature. 67,110 Hence, while meropenem is included as a comparator in the PICOS, it is assumed to have zero efficacy in the economic modelling (and so not actively modelled).
Susceptibility is estimated to be specific to the pathogen–mechanism subgroup of interest but is assumed to generalise across sites and settings. This was considered a reasonable assumption by our clinical advisors and preferable to further subgrouping the susceptibility data given the small sample sizes available to inform these parameter estimates for the HVCSs. Due to this assumption, there was one deviation from the PICOS, with tigecycline used for both sites (cUTI and HAP/VAP). In the PICOS, tigecycline was only included for HAP/VAP.
Susceptibility for antimicrobials used in the empiric setting
Clinical advice, as reflected in the PICO, was that combination treatment was frequently used in the ES. Hence evidence on absolute susceptibilities for individual drugs needed to be converted to evidence on overall susceptibility to combination treatments, to identify the most effective combination treatments. This requires information on conditional susceptibility (e.g. for combination treatment of AM ‘X’ and AM ‘Y’, evidence is required on the susceptibility to AM ‘Y’ conditional on being resistant to AM ‘X’). For use in the model, the most effective ES treatment which did not include colistin or an aminoglycoside was considered, as well as the most effective ES which did. A discussion of the available evidence on conditional susceptibility is provided in Appendix 7.
For the base-case analysis, evidence on absolute susceptibilities for combination treatments and monotherapies was obtained from the NMA based on EUCAST studies (see Statistical synthesis) applied to the absolute colistin susceptibility from the PHE data (colistin was chosen as the reference AM as it appeared in the majority of studies, and susceptibility to this AM was relatively constant over time as illustrated by an analysis of PHE data; see Report Supplementary Material 3). Where the NMA provided evidence for multiple AMs within the same class (such as aminoglycosides), the most effective AM was used. The assumption of independence of absolute susceptibilities was relaxed in scenario analyses, as detailed in Appendix 8.
There are two main approaches for defining breakpoints for susceptibility evidence (which in turn affect relative and absolute rates of susceptibility): EUCAST and CLSI (see Susceptibility studies, PK/PD studies and breakpoints). The former was judged to be of the most relevance to the UK; hence evidence from studies using EUCAST breakpoints was used in the base case. A scenario analysis included all studies regardless of breakpoint (with the exclusion of selected arms based on their inconsistency with the overall evidence base, as detailed in Statistical synthesis).
Another scenario analysis used only evidence from PHE, as this represents UK-specific evidence. As there was insufficient evidence for fosfomycin in the PHE data, this scenario assumes that fosfomycin is not used. A further analysis was restricted to the EUCAST studies for which co-carriage of MBL was not present (due to a concern that CAZ-AVI would not be used where co-carriage is known). This only left the study by Vasquez-Ucha et al. 35 This study does not have evidence for tigecycline, so it was assumed that this AM is not used in this scenario.
For the PSA (which was performed for the base-case analysis only), two sources of uncertainty were considered:
-
uncertainty in the ORs obtained from the NMA posterior distribution
-
uncertainty in the absolute susceptibility of colistin (to which ORs are applied), obtained from PHE data and modelled using a beta distribution.
Susceptibility for antimicrobials used in the microbiology-directed setting
When microbiology test results are available it is assumed that patients will receive an AM to which they are susceptible (if they are susceptible to an AM). It was further assumed that, given their toxicity, use of either colistin or an aminoglycoside would be reserved for when a patient was not susceptible to any other relevant AMs. Hence, for use in the economic model, it was necessary to convert absolute susceptibility evidence for each AM into the proportion of patients falling into each of the following mutually exclusive groups:
-
susceptible to an AM that is not colistin or an aminoglycoside
-
susceptible only to colistin or an aminoglycoside
-
not susceptible to any available treatment options.
The AMs contributing to the first susceptibility grouping are:
-
aztreonam
-
cephalosporins
-
fluoroquinolones
-
fosfomycin
-
tigecycline.
In the ES, for the base-case analysis susceptibility to a given AM was assumed independent of susceptibility to any other AM. This assumption could also be used to derive the proportion in each susceptibility group for the MDS. A discussion of the appropriateness of this assumption is provided in Appendix 8. This suggested that, in the MDS, the assumption of independence did not hold. Instead, evidence from PHE was used to estimate the bias arising when assuming independence to derive the proportion in each susceptibility group. This bias was then used to adjust estimates of the proportion in each susceptibility group obtained from the NMA using an assumption of independence of susceptibilities. Scenario analyses that only used isolate-level data from either PHE or Vasquez-Ucha et al. to directly estimate the MDS groupings were also considered. 35 Due to a lack of evidence, these scenarios assume that fosfomycin and tigecycline are not used, respectively.
For the PSA, two primary sources of uncertainty were considered:
-
Uncertainty in the ORs obtained from the NMA posterior distribution.
-
Uncertainty in the scaling factor used. This in turn had two components: variation in the true proportions in each susceptibility group from the PHE data (modelled using a Dirichlet distribution), and variation in the absolute susceptibility to each AM in the PHE data (modelled using a beta distribution).
Overview of options for including susceptibility data in the economic model
A base case and four scenarios were used when generating susceptibility probabilities for use in the economic model (for both CAZ-AVI and the comparators).
-
In the base-case analysis, the NMA of EUCAST studies was used assuming susceptibility to a given AM was independent of susceptibility to any other AM.
-
In Scenario 1 (S1), the NMA of EUCAST studies was used assuming susceptibility to a given AM was not independent of susceptibility to any other AM.
-
In Scenario 2 (S2), the NMA including all studies regardless of breakpoints, but excluding specific arms due to inconsistency was used.
-
In Scenario 3 (S3), PHE isolate level data were used (excludes fosfomycin).
-
In Scenario 4 (S4), Vazquez-Ucha et al. isolate-level data (excludes tigecycline) were used.
The susceptibility probabilities used in each analysis are shown in Table 16. CAZ-AVI susceptibility is 88–99% across scenarios for both the ES and MDS. In the ES CAZ-AVI is associated with similar susceptibility to the best available colistin or aminoglycoside-based therapies, which across scenarios is 89–97%. The best available non-colistin or aminoglycoside-based therapy is associated with lower and more variable susceptibility across scenarios of 7–35%. In the MDS, scenarios 1 to 3 indicate that 65–73% of patients will be susceptible to a non-colistin/aminoglycoside-based treatment, and 27–35% only to a colistin/aminoglycoside-based treatment. Scenario 4 indicates poorer susceptibility, with 44% susceptible only to a colistin/aminoglycoside-based treatment. This is primarily due to the exclusion of tigecycline in this scenario due to a lack of evidence.
| Base case | S1 | S2 | S3 | S4 | |
|---|---|---|---|---|---|
| Empiric treatment setting | |||||
| Susceptibility to the most effective non-colistin/aminoglycoside | 35% | 35% | 18% | 23% | 7% |
| Most effective non-colistin/aminoglycoside | Levofloxacin | Levofloxacin | Levofloxacin | Ciprofloxacin | Ciprofloxacin |
| Susceptibility to the most effective colistin/aminoglycoside | 94% | 93% | 97% | 94% | 89% |
| Most effective colistin/aminoglycoside | Colistin + tigecycline | Colistin + tigecycline | Colistin + tigecycline | Colistin + tigecycline | Amikacin + fosfomycin |
| Microbiology-directed setting | |||||
| Susceptibility to a non-colistin/aminoglycoside | 65% | 65% | 73% | 65% | 55% |
| Susceptibility to colistin/aminoglycoside | 35% | 35% | 27% | 35% | 44% |
| Susceptibility to CAZ-AVI % | 92% | 92% | 97% | 88% | 99% |
Furthermore, NICE’s consultation and Committee deliberations indicated that, in terms of existing therapies (i.e. in a world without CAZ-AVI), there is a proportion of patients who would not receive colistin/aminoglycosides, even if they were susceptible, and no other effective therapy was available. This would be due to a patient’s high clinical risk of renal toxicity. For such patients, it can be assumed that they would only receive salvage therapy. The size of this subgroup of patients with an absolute contraindication to colistin/aminoglycosides was considered small by EEPRU’s clinical advisors. However, on request from NICE, a separate scenario was run where a proportion of patients who, without CAZ-AVI, were only susceptible to colistin received multidrug salvage therapy. Considering the lack of empiric evidence, the NICE Committee suggested the plausible range for the proportion of patients to be 20–40%. Details of the methods are provided in Appendix 9.3, Table 63.
Clinical parameters – linking susceptibility to 30-day outcomes in the MDS
The remaining clinical evidence predicting 30-day outcomes in the MDS is presented in Table 17. Thirty-day mortality differs across comparators via two mechanisms in the MDS. Thirty-day mortality does not differ in the MDS setting if infections are susceptible to existing treatments because patients will be treated with the correct AM, though it does differ if patients have infections resistant to existing options but susceptible to CAZ-AVI, as their recovery will be more likely if they take CAZ-AVI. In addition, patients’ mortality risk varies according to the AKI-rate associated with the AM used.
| Site | Parameter name | Description | Value | Uncertainty (measure) | Source |
|---|---|---|---|---|---|
| cUTI | p_bgrdS30d_MDS_S | 30-day survival in cUTI patients receiving a treatment to which they are susceptible | 0.854 | Beta (12.10, 2.07) 95% CI (0.636 to 0.979) |
Structured expert elicitation |
| cUTI | p_bgrdS30d_MDS_nonS | 30-day survival in cUTI patients receiving a treatment to which they are resistant | 0.610 | Beta (3.55, 2.27) 95% CI (0.227 to 0.923) |
Structured expert elicitation |
| HAP/VAP | p_bgrdS30d_MDS_S | 30-day survival in HAP/VAP patients receiving a treatment to which they are susceptible | 0.578 | Beta (3.99, 2.91) 95% CI (0.226 to 0.888) |
Structured expert elicitation |
| HAP/VAP | p_bgrdS30d_MDS_nonS | 30-day survival in HAP/VAP patients receiving a treatment to which they are resistant | 0.376 | Beta (2.71, 4.51) 95% CI (0.090 to 0.726) |
Structured expert elicitation |
| All | p_AKI_ca | Risk of AKI in patients receiving colistin or an aminoglycoside | 0.45 | 95% CI (0.41 to 0.49) | Sisay 2021111 |
| All | OR_AKI_ca | Elevation in risk of AKI associated with colistin or aminoglycosides compared to other less nephrotoxic therapies | 1.81 | 95% CI (1.13 to 2.92) | Chien 2020112 |
| All | OR_AKI_death | Odds ratio of mortality for AKI compared to no AKI | 5.11 | 95% CI (4.23 to 6.17) | Kerr 2014113 |
| HAP/VAP | p_AKIirrec | Proportion of individuals who experience an AKI who have ESRD | 0.003 | 0.002 | Sisay 2021111 |
| cUTI | p_AKIirrec | Proportion of individuals who experience an AKI who have ESRD | 0.001 | 0.002 |
As documented in Review questions 4 and 5, several studies have explored the link between whether patients have been administered a treatment to which they are susceptible and their 30-day mortality outcomes in the infection sites of interest for the HVCSs. However, these studies have focused on the empiric setting and none was available relating specifically to the MDS where outcomes are expected to differ substantively. Patients in the MDS who receive an inappropriate drug are much more likely to be MDR than patients receiving inappropriate treatment in the ES and are more likely to be in critical state that reduces the possibility of further treatment.
This data gap is perhaps unsurprising as multidrug resistance (including to colistin) remains rare and it may, therefore, be difficult to recruit or include sufficient patients in this setting. Given the absence of data to inform this important parameter, a structured expert elicitation exercise was conducted. The methods and results of the expert elicitation are described in Chapter 6. These estimates were elicited separately for cUTI, HAP and VAP as these infection sites are expected to have quite different mortality rates. Separate estimates were not produced by causative pathogen–mechanism. This is because, among those receiving a treatment to which they are susceptible, outcomes are expected to be similar across the pathogen–mechanism combinations relevant to the CAZ-AVI HVCSs. Similarly, among patients receiving multidrug salvage therapy due to multidrug resistance, outcomes are expected to be similar across the pathogen–mechanism combinations relevant to the CAZ-AVI HVCSs.
Clinical parameters – AKI risk and subsequent outcomes
Rates of nephrotoxic-drug-induced AKI and their implications are assumed to generalise across sites, pathogens and mechanisms in the absence of subgroup-specific data. The evidence from the CAZ-AVI RCTs did not provide any meaningful evidence on the safety implications of aminoglycoside/colistin use (see Results) and these data were not considered by our advisors to be generalisable to the highly comorbid patients who tend to acquire carbapenem-resistant infections. These parameters were therefore obtained from existing systematic reviews where possible or, if not available, from UK-specific sources.
Several recent systematic reviews and meta-analyses estimated the pooled cumulative incidence of AKI in patients treated with colistin or polymyxins B111,112,114,115 and two of these reported differences in the rates of AKI between colistin- or polymyxin B-based therapy and other agents. 112,114 The absolute risk of an AKI and the likelihood that an AKI resulted in irrecoverable kidney damage was derived from Sisay et al. 2021111 as this study had the most recent searches, included a broad range of study designs and was restricted to studies using the Risk Injury Failure Loss end-stage renal disease (ESRD) (RIFLE) criteria. The difference between colistin- (or polymyxin B, a similar drug from the same class) based therapy and other agents was obtained from Chien et al. 2020112 as this review made some attempt to control for confounding. Chien et al. 2020112 included both RCTs and comparative cohort studies but excluded studies considered poor quality as assessed by the Newcastle-Ottawa scale (in particular the authors state that only cohort studies of parallel design with patients of comparable clinical characteristics were included). Alternative sources for these parameters are explored as scenario analyses.
The excess death from AKI was derived by comparing in-hospital mortality rates in the UK for individuals who experienced an AKI as defined by the Acute Kidney Injury Network (AKIN) criteria and individuals without AKI using the East Kent Hospitals University NHS Foundation Trust (EKHUFT) dataset from Kerr et al. 2014. 113 The latter gathers admission records from three inpatient hospitals in the South of England. The analysis of the EKHUFT dataset was deemed more appropriate than that obtained using the HES dataset as EKHUFT includes older and more comorbid patients who are, therefore, more similar to our patient population, and is more likely to include all AKIs than the HES dataset.
The impact of AKI on mortality was estimated by the authors adjusting for a range of covariates including history of hospital admission, comorbidities and primary diagnosis. We assumed the relative increase in mortality associated with AKI observed in the Kerr et al. analysis113 applied to the baseline risk of mortality in our HVCS despite the patients within our HVCS exhibiting a much higher baseline mortality risk. AKI is more prevalent in patients with poor prognosis; although Kerr et al. attempted to adjust for these factors the elevated mortality estimated was considered high by expert advisors. 113 A scenario analysis was, therefore, run whereby the excess mortality associated with AKI was halved from the reported value.
Clinical evidence – linking susceptibility to 30-day outcomes in the ES
The evidence informing the decision tree predicting 30-day outcomes in the ES is presented in Table 18. The mechanisms database described in Appendix 1 was searched to identify papers providing quantitative estimates of the risk of carrying the pathogen–mechanism of interest among patients with specific characteristics. This was supplemented by papers known to the study team. Two searches were conducted. The first was to identify UK-specific studies. This had two concepts; the first was to identify ‘risk’ studies (any field containing any of ‘risk’, ‘prevalence’, ‘incidence’, ‘character*’, or ‘outbreak’), returning 1696 studies. The second concept was for UK studies [abstract contains any of (‘United Kingdom’, ‘Great Britain’, ‘England’, ‘UK’, ‘NHS’, ‘Trust’, ‘London’, ‘*Shire’)], returning 119 studies. Combining both concepts provided 61 studies for the first search. The second search was expanded to identify non-UK risk models and returned 51 studies based on their title containing ‘Risk’. No risk models were identified from either search. Indeed, even in the wider population of patients at risk of a carbapenem-resistant infection, there is a paucity of UK data available to estimate the risk of having a carbapenem-resistant infection among patients with relevant risk factors. 117
| Pathogen/mechanism subgroup | Parameter name | Description | Value | Uncertainty (measure) | Source |
|---|---|---|---|---|---|
| Entero-bacterales/OXA-48 | p_bug_mech_EOXA | Proportion of people in ES who have the suspected pathogen–mechanism | 0.20 | 97 (n) | PHE SGSSa |
| All | p_bgrdDst_S | Proportion of patients who received a treatment to which they are susceptible who are dead at the point MDS results become available (assumed to be at 5 days based on CARBAR study) | 0.03 | 0.02 (se) | Tumbarello 2013109 |
| All | p_bgrdDst_nonS | Proportion of patients who received a treatment to which they are not susceptible who are dead at the point MDS results become available (assumed to be at 5 days based on CARBAR study) | 0.11 | 0.04 (se) | Tumbarello 2013109 |
| All | prtxF_S | Proportion of patients who received a treatment to which they are susceptible who require further treatment | 0.07 | 0.02 (se) | APEKS-NP 116 |
| All | p_bgrdD30d_S | Proportion of patients who survive to MDS assessment and do not require further treatment who die by 30 days | 0.32 | 0.06 (se) | Tumbarello 2013109 susceptible cohort |
The probability that a patient entering the ES who actually has the suspected pathogen–mechanism was obtained from the Second Generation Surveillance System (SGSS) data supplied by PHE as shown in Table 18 (for further discussion, see Quantitative extrapolation to expected usage). These data provide the number of tests for a given mechanism of resistance and the proportion of those tests that returned a positive result. These data are unlikely solely to reflect the ES HVCS of focus in the current analysis. For example, testing may be conducted due to a suspicion in the lab rather than at the level of the treating clinician (e.g. a lab finding of carbapenem non-susceptibility might trigger a test), some tests may be run following treatment failure or may be run in the ES but at a lower level of suspicion than considered in our HVCS.
Given these uncertainties in the available data, we also conducted a survey of the mailing list of the BSAC. This survey asked microbiologists and infectious disease specialists how many times they saw patients who would fall into our ES HVCS of interest, and the proportion of those who had the pathogen–mechanism of interest. A survey was used in preference to the structured expert elicitation as this parameter was expected to vary according to local epidemiology and history of outbreaks of resistant infections and it was not considered realistic that the expert elicitation exercise could include enough experts to adequately reflect this geographical heterogeneity. Unfortunately, the response to the survey was low, with only nine experts providing usable responses. On average these experts reported that, of the OXA-48 Enterobacterales HAP/VAP seen where there was a high suspicion of the mechanism of interest, 57% of patients would be confirmed as having the mechanism. These values are used in a sensitivity analysis. Given the high level of uncertainty around this parameter, sensitivity analysis results are shown for a wide range of alternative values.
Mortality at the time of assessment for entry to the MDS conditional upon susceptibility status, and 30-day mortality among patients not requiring further treatment, was obtained from Tumbarello et al. 2013. 109 This study was conducted in 110 ICU patients with confirmed Pseudomonas aeruginosa pneumonia in a hospital in Italy and compared 30-day mortality in patients who were susceptible to initial empiric treatment and those who were not. Surviving patients who were not susceptible to empiric treatment were switched to definitive therapy, on average ~62 hours after symptom onset. Tumbarello 2013109 was chosen as it reported a relatively high incidence of MDR strains in infecting organisms (42/110) compared to the other studies identified in the review and was the only study reporting Kaplan–Meier curves (see Review question 6 for details). No UK studies were identified.
The probability of requiring further treatment for susceptible patients was taken from the CAZ-AVI arm of the APEKS-NP study. 116 Within the studies included in the CAZ-AVI mappings, this was identified as the only study representing a predominantly empirically treated susceptible population of HAP/VAP patients that also reported subsequent treatment rates.
Clinical evidence – long-term mortality
All patients surviving to 30 days face an ongoing mortality risk based on the CARBAR57 and Merrick118 studies. Both studies included UK patients with infections caused by carbapenem-resistant organisms and were, therefore, considered relevant in terms of capturing the highly comorbid nature of patients who acquire these infections. Searches were conducted as described in Appendix 1, but did not identify any further evidence of relevance. A targeted search indicated a lack of data on long-term outcomes in both HAP/VAP and cUTI. It also seemed unlikely that outcomes in all-comer HAP/VAP and cUTI patients would reflect those of MDR patients who tend to have developed MDR infections as a result of multiple contacts with the health systems, reflecting a wide range of comorbidities. We therefore chose to focus our review of long-term mortality on patients with resistant infections.
CARBAR57 was used to inform mortality in the base case as it included more geographically diverse patients, had a longer follow-up (2 years compared to 1 year in Merrick) and provided continuous survival estimates over time (i.e. Kaplan–Meier curves). Merrick118 reported all-cause mortality at 1 year of 31%, which is similar to the 1-year mortality in CARBAR of 34%.
Kaplan–Meier curves from CARBAR were digitised and we used a published algorithm to recover pseudo-individual patient data from the Kaplan–Meier curve for analysis. We fitted parametric survival models to these data to facilitate extrapolation beyond the observed data. Data from 30 days onwards were used as these were of most relevance to the model. We followed guidance from the NICE Technical Support119 document and fitted a range of parametric survival models: exponential, Weibull, Gompertz, log-logistic, log-normal and generalised gamma. Model fit was assessed according to Akaike’s Information Criteria (AIC), log-cumulative hazard plots, hazard plots and visual assessment of the concordance between model predictions and Kaplan–Meier plots. No specific external data were identified to support validation of long-term predictions, so probabilities of death predicted by each model were compared to general population mortality over 20 years to assess plausibility. A summary of these assessments is provided in Appendix 8, Table 54. Overall, the Weibull, log-logistic and log-normal models were all considered plausible candidates and in the absence of further evidence log-normal was selected to offer a middle ground with the Weibull and log-logistic trialled in scenario analyses. Mortality is restricted so that it too remains above that in the general population within the model.
In addition, patients alive with recovered renal function face an elevated risk of death and a risk of developing irreversible renal failure (CKD). 120 Patients alive with irreversible renal failure face the elevated risk of death of CKD patients.
A recent body of evidence, with which our group of experts agreed, suggests that AKI and CKD are closely linked and interconnected, whereby CKD is a risk factor for experiencing subsequent AKI and AKI is a promoter or instigator of CKD. It was, therefore, considered important to capture the fact that AKI is not a ‘self-limited process’ and that patients with recovered renal function post-AKI are at risk of adverse renal outcomes and of developing CKD.
In our literature searches to identify evidence of the impact of AKI on the development of CKD and on long-term survival, we looked for studies that would control for the confounding impact of comorbidities as stringently as possible as we aimed to estimate the causal effect of AKI on subsequent outcomes. The US study by Bucaloiu 2012120 was selected as it compared outcomes of patients with hospital-associated AKI (with recovered renal function) against a non-AKI patient population matched for a wide range of relevant clinical and demographic characteristics. A total of 1610 patients with AKI and 3652 without were followed up from 90 days post discharge to approximately 6 years. A limitation of this study is that the propensity score matching process excluded the most comorbid patients due to a lack of sufficiently closely matching controls, and the study excluded patients with impaired kidney function prior to hospitalisation. This evidence was used to inform the increased risk of death and the increased risk of developing CKD in patients with recovered renal function after an AKI. Relevant parameters are shown in Table 19.
| Site | Pathogen/mechanism subgroup | Parameter name | Description | Value | Uncertainty (measure) | Source |
|---|---|---|---|---|---|---|
| All | All | TPnoAKItoCKD | 1-year absolute probability of experiencing CKD in non-AKI patients Approach to computation: baseline risk of CKD development in non-AKI: 1218 events over a median follow-up of 4.3 years in 3652 individuals [= 1218/(4.3 × 3652)] |
0.078 | SE for baseline risk assumed 10% of mean | Bucaloiu 2012120 (note that these probabilities are assumed to apply from the second cycle onwards as Bucaloiu measured outcomes from 90 days post discharge) |
| All | All | TPAKItoCKD | 1-year absolute probability of experiencing CKD in post-AKI patients with recovered renal function Approach to computation: baseline risk of CKD development in non-AKI (0.078) multiplied by adjusted HR 1.91 (95% CI 1.75 to 2.09) |
0.143 | SE around HR of CKD development: 0.087, SE for baseline risk assumed 10% of mean | |
| All | All | AKIodeath | 1-year probability of death in post-AKI patients with recovered renal function Derived by multiplying the mortality from CARBAR by the HR of excess death adjusted for de novo CKD development from Bucaloiu 2012: 1.18 (95% CI 0.95 to 1.46) |
1.18 × mortality rate in non-AKI | SE 0.119 for HR | |
| All | All | TPCKDtodeath | 1-year probability of death in CKD patients Derived by multiplying AKI mortality by the HR of excess death in CKD patients compared to AKI patients in Bucaloiu 2012: 3.65 (95% CI 2.42 to 5.52) |
3.65 × mortality rate in AKI | SE 0.783 for HR |
There are several limitations to the approach taken to reflect the long-term implications of AKI within the model:
-
The CARBAR data will have included patients who experienced AKI and, therefore, including additional mortality risk associated with AKI, and CKD development is likely to exaggerate mortality risk in the model.
-
The risk of CKD development is likely to be higher than estimated from Bucaloiu120 in the highly comorbid patient group considered within the HVCS.
-
The hazard ratios on mortality are applied multiplicatively despite the much higher baseline risk of death in the patient population considered within the HVCS.
Scenarios are explored to address each of these assumptions in turn:
-
CARBAR mortality rate reduced by 10% reflecting an assumed AKI rate of 20% and an assumed excess mortality associated with AKI of 1.48 (95% CI 1.19 to 1.82) based on Bucaloiu 2012. 120
-
Patients in HVCS face double risk of CKD compared to patients in Bucaloiu 2012.
-
Patients in HVCS face absolute increase in mortality risk observed in Bucaloiu 2012.
-
All of the above applied simultaneously.
We did not account for life-years accrued within the first 30 days in the model as these were expected to have a marginal effect on the model results.
Health-related quality of life
The HRQoL implications of the infection are not modelled as these are expected to be short-lived and, therefore, are not expected to impact substantively on the model results. However, to quality adjust the life expectancy estimates accurately, we did consider it important to reflect the underlying comorbidities of the patients within the HVCS. We did not identify any relevant utility data from existing models, most of which assumed that post-infection patients would return to the HRQoL of the general population. Therefore, we conducted a review of utility studies that provide evidence according to the Charlson Comorbidity Index (CCI). The CCI is a summary score of comorbidity based on 17 included comorbidities. The comorbidities considered in the CCI have been selected and then weighted based on their ability to predict 1-year mortality among hospitalised patients. Importantly, the CCI is reported within the CARBAR study for patients with infections caused by carbapenem-resistant organisms, allowing utility values presented by CCI score to be re-weighted to reflect the CCI scores in a population similar to that included in our HVCSs.
The methods for this review are described in Report Supplementary Material 3. This identified two studies reporting utilities by CCI in the general population. Both studies were based on large national surveys in France and Germany and estimated the SF-6D based on the SF-36 and SF-12, respectively. 121,122 The French study was chosen in preference to the German study as the latter controlled for several variables likely to be associated with CCI (pain level, socio-demographic variables and health behaviours). Utility values by CCI score are reported in Appendix 8, Table 55. These are weighted by the distribution of CCI scores observed in CARBAR, also shown in Appendix 8, Table 55; these reflect UK general population valuations. This produced an overall weighted utility score of 0.66 for the CARBAR population based on their comorbidities; this is intended to reflect their long-term HRQoL rather than the immediate impact of infection. This was used to compute a multiplicative reduction in HRQoL associated with comorbidities by comparing the CARBAR population to the general population (assumed to have a CCI score of 0). General population HRQoL was derived from a regression model estimated by Ara and Brazier 2010123 using Health Survey for England (HSE) survey data for the years 2003 and 2006 (n = 26,679). This produced a baseline utility value of 0.73 for all patients. This resulted in a utility-multiplier of 0.66/0.73 = 0.90. This was then applied to the age- and gender-specific EQ-5D HRQoL weights of the general UK population based on Ara and Brazier. 123
Patients who have recovered their renal function post AKI are not expected to experience further reductions in HRQoL (disutility) unless they develop CKD. The HRQoL decrement applied to the CKD patients is computed using pooled estimates from a systematic review and meta-analysis by Wyld et al. (2011). 124 The authors reported HRQoL decrements of 0.02 (−0.04, 0.09) for those in CKD pre-treatment and of 0.11 (0.08, 0.15) for those with CKD in dialysis, where the latter were estimated to represent 2% of the diagnosed CKD population based on UK data. 125 These were applied to the baseline utility value of 0.73 such that the utility of those with CKD pre-treatment was 0.71 and the utility of those with CKD in dialysis was 0.62.
Resource use and costs
The model includes costs relating to hospital stay, infection control during hospitalisation, AKI-related costs during hospitalisation, long-term costs associated with CKD and costs relating to use of existing AMs. The purchase price of CAZ-AVI is not included in the costings as the objective of the value assessment is to inform the payment for CAZ-AVI. Costs relating to testing (for pathogen, resistance mechanism or AM susceptibility) were not included as, in the HVCS populations, these tests were expected to be conducted to the same degree regardless of the introduction of CAZ-AVI.
An important cost driver in the model is time spent in hospital. Data on time in hospital for patients according to their treatment pathway and outcomes are presented in Table 20. As for 30-day mortality, we did not identify any studies in the MDS linking treatment susceptibility to duration or type of hospitalisation. This was, therefore, elicited as part of the structured expert elicitation exercise. LoS and the proportion of time spent in ICU or HDU were estimated conditional upon susceptibility for patients with cUTI and HAP/VAP separately. In the base case, all patients in the ES were assumed to spend 5 days in hospital prior to receipt of their microbiology results, the median wait reported in CARBAR. 57
| Site | Parameter name | Description | Value | Uncertainty (measure) | Source (costing year) |
|---|---|---|---|---|---|
| cUTI | los_MDS_S | LoS following treatment in the MDS for cUTI patients who received a treatment to which they are susceptible (days) | 12.9 | Lnorm (2.507, 0.321) 95% CI (6.54 to 23.02) |
Structured expert elicitation |
| cUTI | los_MDS_nonS | LoS following treatment in the MDS for cUTI patients who received a treatment to which they are not susceptible (days) | 17.7 | Lnorm (2.817, 0.334) 95% CI (8.68 to 32.2) |
Structured expert elicitation |
| cUTI | p_ICU_MDS_S | Proportion of time in hospital in ICU for cUTI patients who received a treatment to which they are susceptible | 0.150 | NAa | Structured expert elicitation |
| cUTI | P_ICU_MDS_nonS | Proportion of time in hospital in ICU for cUTI patients who received a treatment to which they are not susceptible | 0.233 | NAa | Structured expert elicitation |
| cUTI | p_HDU_MDS_S | Proportion of time in hospital in HDU for cUTI patients who received a treatment to which they are susceptible | 0.170 | NAa | Structured expert elicitation |
| cUTI | p_HDU_MDS_nonS | Proportion of time in hospital in HDU for cUTI patients who received a treatment to which they are not susceptible | 0.183 | NAa | Structured expert elicitation |
| HAP/VAP | los_prior_ast | Time from empiric treatment initiation to receiving microbiology results (days) | 5b | NA | CARBAR57 |
| HAP/VAP | los_txsucc1 | Relative reduction in LoS for patients not requiring further treatment | 0.503 | NA | Muscedere 2012126 |
| HAP/VAP | LoS_ES_success | LoS in empiric setting for patients not requiring further treatment (days) | 12.8 | Assume uncertainty as for LoS HAPVAP_MDS_S, with fixed time to MDS (5 days) and relative reduction in LoS (0.503) | Derived from structured expert elicitation and Muscedere 2012126 |
| HAP/VAP | p_ICU_tx_succ1 | Proportion of time in ICU following receipt of empiric treatment for patients not requiring further treatment | 0.300c | NAa | Derived from Muscedere 2012126 |
| HAP/VAP | los_MDS_S | LoS following treatment in the MDS for HAP/VAP patients who received a treatment to which they are susceptible (days) | 20.4 | Lnorm (2.971, 0.298) 95% CI (10.88 to 34.97) |
Structured expert elicitation |
| HAP/VAP | los_MDS_nonS | LoS following treatment in the MDS for HAP/VAP patients who received a treatment to which they are not susceptible (days) | 24.3 | Lnorm (3.118, 0.380) 95% CI (10.73 to 47.63) |
Structured expert elicitation |
| HAP/VAP | p_ICU_MDS_S | Proportion of time in hospital in ICU for HAP/VAP patients who received a treatment to which they are susceptible | 0.499 | NAa | Structured expert elicitation |
| HAP/VAP | P_ICU_MDS_nonS | Proportion of time in hospital in ICU for HAP/VAP patients who received a treatment to which they are not susceptible | 0.589 | NAa | Structured expert elicitation |
| HAP/VAP | p_HDU_MDS_S | Proportion of time in hospital in HDU for HAP/VAP patients who received a treatment to which they are susceptible | 0.149 | NAa | Structured expert elicitation |
| HAP/VAP | p_HDU_MDS_nonS | Proportion of time in hospital in HDU for HAP/VAP patients who received a treatment to which they are not susceptible | 0.172 | NAa | Structured expert elicitation |
| All | c_AKI | Increase in in-hospital cost associated with experiencing an AKI | £5138 | (4724 – 5548) | Kolhe 2014127 (2008 prices updated to 2019) |
| cUTI | c_genward | Unit cost per day for cUTI patient on general ward | £687.08 | NA | NHS reference costs |
| HAP/VAP | c_genward | Unit cost per day for HAP/VAP patient on general ward | £870.51 | NA | NHS reference costs |
| All | c_ICU | Unit cost per day for person in ICU | £1689.09 | NA | Derived from NHS reference costs and CARBAR |
| All | c_HDU | Unit cost per day for HDU | £1299.67 | NA | NHS reference costs |
| All | c_Isolation | Daily cost of isolation | £21.96 | NA | Knight 2018128 |
The LoS for patients successfully treated in the ES was estimated from the LoS in patients who are susceptible to treatment in the MDS based on structured expert elicitation, the time to receiving MDS from CARBAR57 and the relative reduction in the LoS associated with receiving appropriate empiric treatment from Muscedere 2012. 126 The proportion of time spent in the ICU for patients who received a treatment to which they are susceptible and who did not require further treatment was derived from Muscedere 2012. 126 The study was conducted in 350 adult ICU patients with VAP (any pathogen and resistance profile) in Canada who received empiric treatment with meropenem or meropenem + ciprofloxacin. The study reported hospital and ICU LoS in patients who were susceptible to their empiric treatment and those who were not. Muscedere126 was chosen as it was the only study identified in the review in Review question 6 that reported LoS conditional upon AM susceptibility in patients with HAP/VAP. The LoS reported by Muscedere 2012 was skewed. The mean LoS was derived by fitting a log-normal distribution to the reported median and interquartile range. The derived mean LoS in patients who received appropriate and inappropriate treatment (43.1 days and 85.7 days, respectively) were used to derive the relative reduction in the LoS associated with receiving appropriate treatment. The derived mean LoS and stay in ICU were used to derive the proportion of hospital stay that was spent in ICU.
The additional hospitalisation costs associated with in-hospital AKI are informed by estimates derived from Kolhe et al. 2014. 127 This study used the NHS costing system’s relative value units that capture cost information associated with several cost items including LoS on wards, drugs, physiotherapy, radiology and medical staff costs. Unit costs were obtained from standard sources and in consultation with those suggested in the manufacturer submissions. Where necessary, costs were adjusted to 2019/20 prices using standard sources. 129 The daily cost of cUTIs treated on general medical wards was derived from the weighted average cost of non-elective short-stay for kidney or urinary tract infections with/without interventions (LA04H to LA04S). The daily cost of HAP/VAP treated on general medical wards was derived from the cost of non-elective short-stay bronchopneumonia with or without interventions (DZ23H to DZ23N). The daily cost of ICU was assumed to be the weighted average cost of non-specific, general adult critical care (CCU01) with zero to six organs supported (XC01Z to XC07Z), assuming that ventilation cost is reflected in the organ support costs. The daily cost of HDU was assumed to be the weighted average cost of medical adult patients in critical care (CCU03) with zero to six organs supported (XC01Z to XC07Z). Weighting was based on the overall volume of each type of organ support reported for the NHS. The daily cost of isolation was derived from Knight et al. 2018128 and included the cost of gloves, aprons and infectious waste stream. We assumed that all patients would be subject to isolation measures as they are either highly suspected of having or confirmed to have a MDR infection. One-off costs of stock disposal are not included as these are assumed to apply equally to all patients.
Following discharge, patients’ long-term costs are determined by their health state. Patients alive without a history of AKI, or with recovered renal function, experience no further costs. Patients with irreversible renal failure (i.e. CKD) face a weighted average cost that reflects the CKD-severity distribution in England and requirement for dialysis. Kerr et al. 2012125 estimated the annual per-patient NHS expenditure on CKD direct care, dialysis and transplants. The mean annual cost of direct CKD care per patient not on dialysis (that is antihypertensive drugs, primary care tests and consultations, nephrology consultations and cost due to excess incidence of cardiovascular events) was estimated at £278, while the annual cost of CKD-related care for a patient on dialysis was estimated at £31,933. As for HRQoL, 2% of the diagnosed CKD population were estimated to be receiving dialysis based on UK data. 125 The clinical advisors to EEPRU for this project indicated that this may be an overestimate but use of a lower value is unlikely to substantively change the results of the modelling. Our clinical advisors expected that, in the highly comorbid group considered within the HVCSs, transplantation would be rare, so the costs of transplantation were not included in the CKD cost estimates. This results in a weighted average cost of CKD of £911 per annum in 2019/20 prices.
We did not include differential rates of discharge to long-term care facilities in the base-case analysis as no evidence was found comparing UK usage of care among those with and without AKI that adjusted for differences between patients with and without AKI. US data suggest that AKI is associated with an elevated risk of discharge to long-term care even with adjustment for other predictive factors. Liangos et al. [Liangos O, Wald R, O’Bell JW, Price L, Pereira BJ, Jaber BL. Epidemiology and outcomes of acute renal failure in hospitalized patients: a national survey. Clin J Am Soc Nephrol 2006;1(1):43–51] found that 8.9% of patients without AKI will be discharged to long-term care and this is elevated to 17.8% in those with an AKI [reflecting an adjusted OR of 2.2 (95% CI 2.1, 2.2)]. We combine this with information on the costs of long-term care and model a scenario based on this. We use a weekly cost of £1049 (average of private-sector nursing home and local-authority own-provision residential care for older people129) and apply this for the lifetime of the patient. This is likely to be an overestimate as some patients may be discharged from long-term care and the full cost of this care may not fall on the NHS/PSS budgets.
We did not include the cost of end-of-life or palliative care as this was considered unlikely to substantively influence model outcomes.
Drug acquisition costs were based on the cost of the daily dose derived from published sources,92,130 the daily doses reported by WHO Collaboration Centre for Drug Statistics Methodology12 and the treatment duration derived from published literature. 94,95,105,130 When more than one formulation or pack size was available, we based costs on the largest pack size and IV formulations. When the treatment duration was provided as a range, we used the longest duration, to reflect the high severity of infections. When more than one AM was available for treatment in a particular setting (e.g. colistin or aminoglycosides for the treatment of HAP/VAP in MDS), the most expensive treatment was chosen to reflect that often combination or higher doses of therapy may be used. In the ES, patients who require a treatment switch following availability of their susceptibility results are assumed to receive 5 days of treatment, whereas those who do not require a treatment switch receive the full course.
The unit cost of all comparators is shown in Appendix 8, Table 56. The drug acquisition costs used in the model are summarised in Table 21.
| Colistin/aminoglycoside-based treatment in ES | nca-based ES | Colistin/aminoglycoside-based treatment in MDS | nca-based MDS | Salvage | |
|---|---|---|---|---|---|
| OXA-48 Enterobacterales | Full course: £452.10 (colistin + tigecycline) Five days: £187.50 |
Full course: £10.57 (ciprofloxacin) Five days: £7.55 |
£232.30 (amikacin) | £280.00 (cefepime) | £397.78 |
Drug administration costs were assumed to be included in the cost of hospital stay, where patients are assumed to be treated.
Model outputs and uncertainty analysis
Per-patient lifetime costs, QALYs and NHEs are presented for each subgroup described in Table 14. For the subgroups of patients eligible for treatment in the MDS, incremental results are presented for the comparison of the overall MDS cohort who receive tailored therapy with the new drug available to the overall cohort who receive tailored therapy under existing treatment options only. For patients eligible for treatment in the ES, incremental results are presented for the pathway including CAZ-AVI as an empiric treatment, and the pathway including CAZ-AVI as a MDS treatment, each compared to the treatment pathways including only existing AMs. These estimates represent the INHEs offered by CAZ-AVI over and above existing therapeutic options.
Calculation of NHEs requires a measure of health opportunity cost to convert additional healthcare costs (or savings) to health foregone (or accrued). We present estimates of NHEs using a measure of health opportunity cost of £20,000/QALY as specified in the NICE scope for this evaluation136 with scenarios presented using £15,000 to reflect empirical estimates of health opportunity cost used by the Department of Health and Social Care137 and £30,000/QALY to reflect the upper bound of the approval norm used by NICE in its technology appraisal process. 138
Results are presented using the base-case assumptions and data sources outlined above. In addition, a series of scenarios is generated to address uncertain assumptions and reflect alternative plausible evidence sources. Parameter uncertainty is quantified using probabilistic sensitivity analysis (PSA). Results of the PSA are presented as distributions of INHEs.
Modelling direct population net health effects in HVCS
Two key drivers of estimates of population INHEs are the size of the affected population and the efficacy of AMs in this population. Both drivers are expected to vary over time. Increasing rates of resistance to carbapenems (due to an OXA-48 mechanism) will increase the population that could benefit from treatment with a newer AM. For CAZ-AVI, and potentially for the comparators, it is anticipated that resistance will change over time, with some of this change driven by changes in rates of AM use. The focus of this section is to describe the methods used to obtain quantitative estimates of changes in the affected population and AM efficacy over time. These estimates are used to generate predictions of the total population INHEs for CAZ-AVI over 20 years. This time horizon was chosen pragmatically to explore the long-term value of CAZ-AVI while avoiding additional uncertainties associated with very long-term population-level predictions.
There are four main aims of this section:
-
Predict how the number of people in each HVCS will change in the future.
-
Predict how rates of resistance to existing AMs will change within the HVCS in the future if CAZ-AVI is not used (‘current practice’ scenario).
-
Predict how resistance will increase over time for CAZ-AVI.
-
Predict the impact, if any, on resistance of reducing current levels of AM use due to the introduction of CAZ-AVI.
There is a degree of overlap in the above aims. For example, aims 2–4 each involve the prediction of how resistance to an AM will change over time. In addition, for aims 1 and 2, the evidence sources were time-series data for the HVCSs. These time series were made available by PHE and these were analysed using time-series methods. For aims 3 and 4, a range of potential evidence sources was considered. These sources included the published literature and publicly available surveillance data, and in general were for a population that was more broadly defined than the HVCS. Evidence for a broader patient population was considered as it included evidence on both AM use and AM resistance and so allowed for an estimate of how these two factors interact (this evidence was not available for the population of interest). As there are distinct modelling challenges associated with each aim, they are discussed in turn. A brief overview is presented here, with more details provided in Appendix 8.6.
Predicting the future sizes of the HVCS
The objective of this analysis was to statistically model changes in the number of patients within the HVCS over time, to inform a quantitative forecast of the number of patients presenting in the HVCS over the next 20 years.
Data on the number of infections over time for the mechanisms of interest were provided as a time series by PHE. One population was included: CPE with an OXA-48 mechanism.
Data were supplied for invasive infections which are predominantly infections where the specimen sample relates to a BSI or cerebrospinal fluid infection. It was assumed that, for each pathogen–mechanism of interest, the trends in population size for invasive infections generalise to the HVCS. This was considered reasonable by the clinical advisors to the project. The small number of invasive infections made it challenging to reliably identify if there was a trend in the growth of the HVCS. As such, this analysis is supplemented by a secondary analysis which looks at trends in the number of screening isolates. These isolates are from screening specimen sites. Screening samples were broadly categorised as samples from swabs, wounds and the lower gastrointestinal tract. This includes potential infections as well as isolates from people who don’t have infections but may be colonised by a MDR pathogen. These screening isolates were only used to confirm or refute the potential presence of a trend rather than inform the growth estimates as they may be influenced by screening policy changes over time which may not feed through to changes in identified infections. Data on both invasive infections and screening isolates were obtained from the AMRHAI national reference laboratory. These data were provided by PHE as monthly counts and are available from 2004 to April 2021. During 2018, guidance on which samples should be sent to AMRHAI changed, and charges were introduced. This led to a gradual ‘artificial’ decrease in referrals. Further detail on the nature of this dataset is provided in Report Supplementary Material 1.
Due to small numbers, data on invasive infections were aggregated to quarterly for analyses and restricted to October 2012 onwards. The last observations used were for March 2018 (inclusive), as after this point the observed numbers decreased. For screening isolates numbers were larger so monthly data were used. For these, the first observation was set to be the first time point for which there were no future months with zero counts (June 2013).
Time-series (state-space exponential smoothing) models were used to forecast the isolate data. For the invasive isolates the use of other time-series models was also considered. Further details on the models considered and the justification and implementation of the state-space models are provided in Appendix 8.6. Three state-space models were considered. These varied with regard to the assumptions made about any long-term trends in the growth of the HCVS:
-
No growth (no trend).
-
Growth in the short term that in the long term changes to no growth (a ‘damped trend’ model; the degree of dampening is estimated from the data and influences how quickly the growth tends to zero).
-
Persistent growth (trend that is not damped).
Within-sample goodness of fit statistics for the three models and the two datasets are provided in Appendix 8.5, Table 57. Estimates of population growth are provided in Figure 11. Figure 11 shows the change in population size over time for both the dataset of invasive infections and the screening isolates.
FIGURE 11.
Change in population size over time (top panel = invasive isolates, bottom = screening isolates). OXA, number of isolates with Enterobacterales OXA-48.
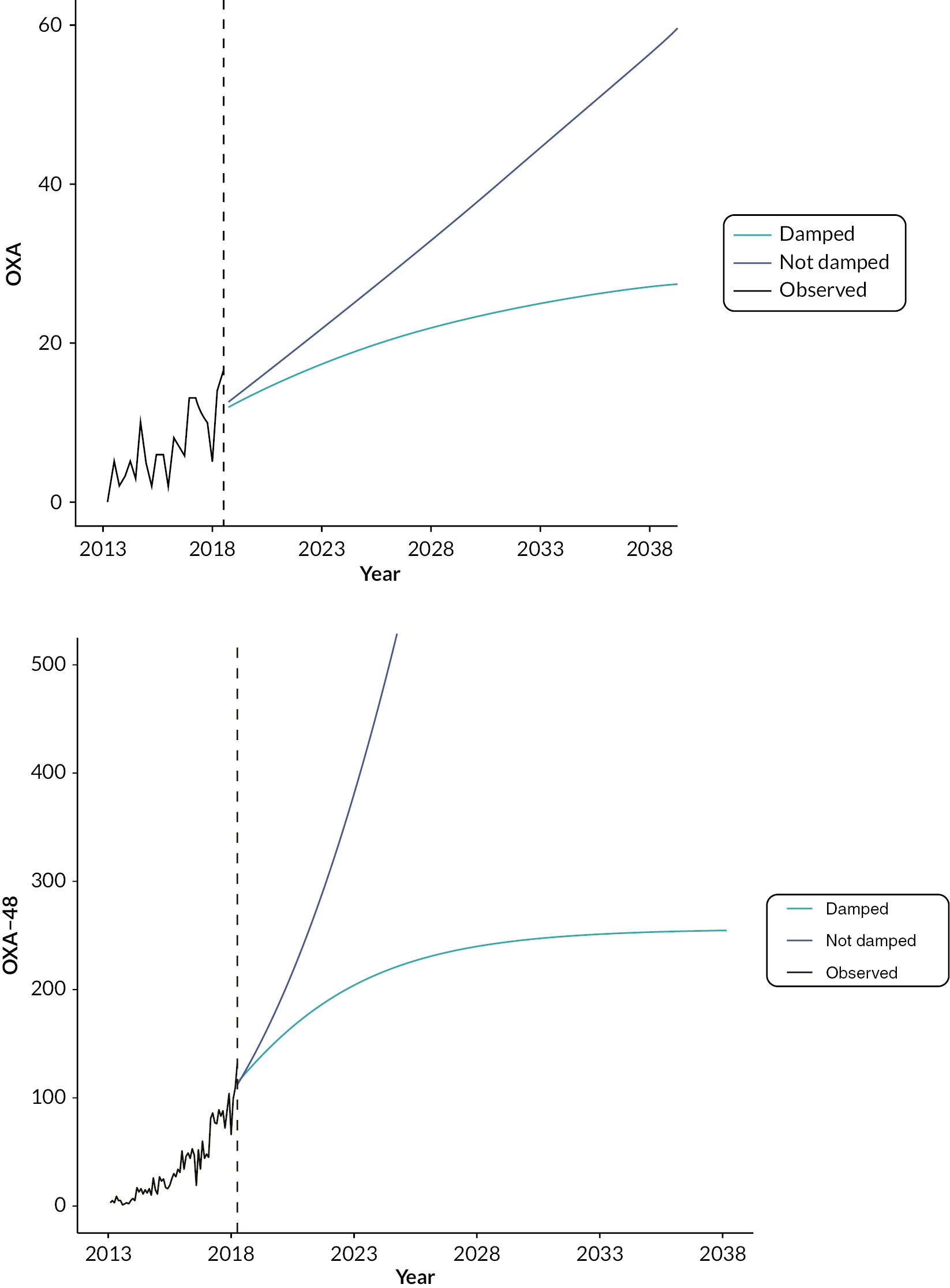
Table 57 (for which comparisons should only be made within columns) shows that for both isolate types, the model with a persistent trend provides the best within-sample fit. However, the difference between values is relatively small, while the differences in extrapolations are very large. The largest population growth was estimated for the screening isolates with a non-damped trend and the smallest (non-constant) population growth was for the invasive isolates with a damped trend model. For the screening isolates it is unclear if long-term increases in the mechanism reflect genuine increases or the results of increased testing. It is also unclear if any genuine increases would persist into the future. As long-term estimates were very sensitive to the choice of model, and there were few statistical grounds to choose between the two models, both the damped trend and trend models for invasive isolates were considered within the decision-analytic modelling.
Details on how the estimates of future change in the HVCS were used in the economic model are provided in Appendix 8.6.
Predicting future rates of resistance for current practice
The objective of this analysis was to characterise historical changes in resistance to existing AMs among patients with OXA-48 Enterobacterales to inform a quantitative forecast of how resistance might change in the future.
This analysis used time-series data provided by PHE, obtained from the same evidence sources as described in the previous subsection (i.e. the AMRHAI national reference unit). Analyses were restricted to comparators used in the economic model. Resulting data were available for:
-
aminoglycosides (gentamicin, amikacin, tobramycin)
-
aztreonam
-
cephalosporins (cefotaxime, ceftazidime, cefepime)
-
ciprofloxacin
-
colistin
-
tigecycline.
For AM classes with evidence from multiple AMs, the most resistant result was retained in the supplied data. It is not expected that retaining the least resistant result would have a noticeable impact on estimates of resistance over time. As already described, isolates that were reported as ‘intermediate’ resistant were assumed to represent resistant isolates for the purpose of this analysis. Hence any tested isolate was either categorised as ‘susceptible’ or ‘resistant’ for this analysis. Combining ‘intermediate’ and ‘resistant’ categories was based on advice from clinical advisors. It is, however, noted that current EUCAST guidance is to combine ‘intermediate’ and ‘susceptible’ when only two categories are used. 139 The methods used to generate forecasts are broadly the same as those considered in the previous section, and are discussed in more detail in Appendix 8.6, Table 58. Due to the sparsity of the available evidence trends in the resistance (or susceptibility) to comparator AMs were not incorporated into the decision-analytic model.
Predicting future resistance trajectories for CAZ-AVI
The time-series data on susceptibility provided by PHE (as detailed in the previous subsection) include CAZ-AVI. Hence, one approach is to use the forecasts from the previous subsection as inputs to the economic model. However, the economic modelling explores different scenarios of CAZ-AVI use, such as in the ES or MDS. As CAZ-AVI has high rates of susceptibility in the HVCSs (and a good safety profile), then without penalising drug use the scenarios with the highest levels of CAZ-AVI would provide the greatest health benefits. A disadvantage of increased AM use is the potential for increased levels of resistance, which would decrease the future effectiveness of CAZ-AVI. There is a large body of evidence demonstrating a relationship between AM use (and prescribing) and the development of AM resistance. 140–142 However, this relationship has been shown to vary by both type of AM and geographical setting and, in some situations, there is no apparent relationship. 141,143,144 Hence there is uncertainty about the relationship between CAZ-AVI use (in the economic model) and subsequent changes in rates of resistance.
Evidence on trends in CAZ-AVI resistance for the UK in the HVCSs is available from PHE but there is no corresponding evidence on CAZ-AVI use for this population. These data also did not suggest that there was any trend in resistance to CAZ-AVI over time. Data sources are available for other AMs and other patient populations (henceforth referred to as ‘external AM use-resistance data’) which include both use and resistance, but their relevance to CAZ-AVI in this HVCS is unclear.
Two approaches were used to identify external AM use-resistance data that may inform the use-resistance association. First, the entire database of studies that were used during the reviewing process (for both CAZ-AVI and cefiderocol) was searched. Studies were filtered to include those which included ‘use’, ‘usage’, ‘volume’ or ‘consumption’ and these were searched for any relevant evidence. In addition, to identify any English studies (which may use evidence from PHE, or the online portal ‘fingertips’) a Web of Science search was conducted with the terms ‘(antimicrobial* OR antibiotic* OR resistant*) AND (fingertip OR “Public health England”)’. These searches were complemented by any studies that were identified via other reviewing activities or already known to the study team. As a result, three studies were identified that, while not using data in the public domain, provided information on a use-resistance relationship. 145–147 Details of these studies are provided in Appendix 8.6, Table 59. These existing studies informed the de novo analyses reported here by suggesting that ARIMA models would be suitable time-series models for capturing use-resistance associations, with a lag of 1 year between use and resistance when using annual data.
In addition, several studies used publicly available surveillance data. 143,148–152 These data were re-analysed for this project to identify potentially useful associations. For this project there were two types of data that were of interest:
-
English data on AM use and AM resistance, from the ‘AMR local indicators profile’;153
-
European data on AM use and AM resistance from the European Antimicrobial Resistance Surveillance Network (EARS-Net) and European Surveillance of Antimicrobial Consumption Network (ESAC-Net), respectively. 154,155 These are available as annual data.
Further details on these evidence sources are provided in Appendix 8.6, Table 60 and Report Supplementary Material 3. For CAZ-AVI, increases in resistance will be from a low starting point. Observed trajectories for external evidence which also showed an increase from a low starting point were only identified for the European data, so these were used in subsequent analyses.
Thirty countries from the European Union contribute data to EARS-Net on AM resistance for up to eight pathogens. 156 These data were further filtered based on the following criteria:
-
Pathogen is included in the HVCS (Escherichia coli as a CPE).
-
Data were available for both AM use and AM resistance (cephalosporins of all types, and carbapenems).
-
Countries with at least 5000 isolates were tested, baseline resistance (average over the first 3 years of available data) was less than 3% (CPE), with at least 10 years of observations for carbapenems and 15 years of observations for cephalosporins (these did not have to be consecutive).
This resulted in the following 16 pathogen–drug–country combinations:
-
Escherichia coli, carbapenems: France, Greece, Netherlands, Norway.
-
Escherichia coli, cephalosporins: Bulgaria, Croatia, Estonia, Finland, France, Greece, Ireland, Luxembourg, Malta, Norway, Slovenia, Sweden.
For these countries, ARIMA models were used to estimate the impact of increasing AM use [defined daily doses (DDDs) per 1000 inhabitants per day] in a given year on resistance to that AM in the following year. Of the 16 combinations considered:
-
Half provided a significant association (8/16; Escherichia coli = 2/4 for carbapenems and 6/12 for cephalosporins).
-
Of the eight significant associations, four were positive associations (increasing use led to an increase in resistance), while four were negative (decreasing use led to an increase in resistance). All of the negative associations were for Escherichia coli cephalosporins.
Hence this analysis resulted in up to four significant positive associations that could be used to link increases in AM use to AM resistance in the economic model. Increases in AM use are driven by increases in the eligible population over time.
Projections of expected usage for CAZ-AVI from Chapter 8 were linked to these estimates of the relationship between usage and resistance to predict emergence of resistance to CAZ-AVI over time. Even under more extreme usage predictions and the strongest associations between usage and resistance emergence this predicted modest absolute increases in resistance of ˂ 1% over 20 years (see Report Supplementary Material 3 for more details). EEPRU considered that this may represent an underestimate of the potential for resistance emergence for two reasons. Firstly, the spread of MDR infections is influenced by international travel and the ‘importation’ of MDR pathogens. Resistance emergence may, therefore, be influenced by CAZ-AVI usage outside the UK which is not accounted for in these projections.
Secondly, the relationships between usage and resistance characterised in the available data reflect all tested isolates in the community and hospital settings. Resistance emergence may be much higher within the HVCSs where usage will be concentrated. For this reason, EEPRU has conducted a range of scenario analyses to characterise the potential emergence of resistance to CAZ-AVI. These were informed by considering the absolute increases in resistance for the drug–pathogen combinations and countries discussed above, where there was a statistically significant increase (see Report Supplementary Material 3 for more details). The highest absolute increase in resistance (an annual absolute increase of 1.65%, leading to a projected 20-year increase of 33%) was used to bound these analyses. The second largest increase was 0.95% per year (19% over 20 years). Based on these considerations, EEPRU ran analyses with resistance emergence reaching 1%, 5%, 10% and 30% at 20 years. It is noted that the upper scenario may be very extreme.
Of note, this analysis was focused on datasets which demonstrated an increase in resistance over time. Hence any significant associations between AM use and decreasing resistance were not explored. As an alternative to an ARIMA model, a dynamic differential equations model was also developed. This was designed to incorporate AM use and resistance, as well as the spontaneous loss or gain of resistance over time as well as the impact of deaths. Details of this model are provided in Report Supplementary Material 3; when evaluated in a simulation study it was shown to provide biased parameter estimates. This was potentially due to the non-identifiability of the model (due to the number of potential AM drivers considered), so this model was not considered further.
As a face-validity check of the estimates of AM use employed in the model, these were compared to hospital inpatient drug use as reported in the 2019/20 ESPAUR report. 5 This provided an estimate of 2.4 DDD/1000 inhabitants for all AMs used in an inpatient setting. Drug use during the first year of the economic model for both CAZ-AVI and cefiderocol (combining results from both evaluations) for the sites cUTI, IAI, HAP/VAP and BSI (all four in CPE, Pseudomonas and Stenotrophomonas) was estimated to be 0.00018 DDD/1000 inhabitants, hence representing 0.01% of all hospital inpatient AM use. This estimate, as an upper bound on the potential use of both cefiderocol and CAZ-AVI, was felt by the modelling team to have face validity.
Predicting the impact of reduced drug use on resistance
Introducing CAZ-AVI (compared with the situation when it is not available) may lead to a reduced use of comparator AMs. As the economic model includes an association between increased use of CAZ-AVI and increased resistance (as described in the previous subsection), then intuitively a decrease in AM use would be expected to lead to a decrease in resistance. However, AM use in the population of interest is only one of a multitude of potential drivers for increases in AM resistance. Other potential drivers include the number of invasive procedures, AM use in other countries, environmental factors, and AM use in animals. 157,158 The existing evidence on the effect of reduced AM use on AM resistance is mixed,159 with findings including no decrease, a decrease and even an increase in AM resistance. 160–162 Hence, while the introduction of a new AM is expected to lead to an increase in resistance over time, reducing AM use has less predictable effects on resistance. Due to the heterogeneity in the existing literature and the lack of evidence for the population and AMs of interest, it was assumed that reductions in use of existing AMs did not lead to reductions in resistance over time.
Extrapolation from HVCS to expected usage
An important part of understanding the value of CAZ-AVI is understanding the range of patients in whom it is expected to be used. This is also relevant in understanding how resistance to CAZ-AVI is likely to emerge over time (as higher usage is likely to contribute to higher resistance). To inform this assessment we provide a qualitative description of the range of ways (outside of the HVCS) that CAZ-AVI is expected to be used. This is informed by discussions with our clinical advisors, the manufacturer submission for CAZ-AVI, and input by other stakeholders during the NICE process to identify patient groups in whom CAZ-AVI may offer significant improvements in HRQoL and mortality compared to existing therapies.
Following this, for those areas of usage considered by the clinical advisors and study team to be most significant in terms of population size and potential impact on INHEs, we have quantified the likely size of the populations who would receive CAZ-AVI. This is based on data from PHE, where available, and supplemented by data from the literature and expert opinion where necessary. These estimates are then used to rescale the population INHEs from the HVCS.
Areas of expected usage
Infection sites and patient characteristics
Outside of the HVCSs, the following infection sites were considered to be most important in driving expected usage and INHEs: BSI and intrabdominal infections (IAI). Our clinical advisors emphasised the importance of CAZ-AVI in treating BSIs. The incremental value of CAZ-AVI (and AMs in general) in IAI is less clear as the quality of surgical procedures used to manage IAI was considered more important than the choice of AM and identifying MDR infections is more challenging. The clinical advisors also emphasised the importance of CAZ-AVI in treating patients who are immunocompromised (e.g. haematology, transplant), patients with cystic fibrosis and patients with burn injuries, who are predisposed to acquiring resistant infections. In immunocompromised patients, BSIs are of particular concern, while in patients with cystic fibrosis, chronic respiratory infections are of particular concern. Patients with a higher propensity for renal complications and those with renal impairment may receive more significant benefits from CAZ-AVI, as renal complications may rule out or increase the toxicity of agents that remain effective in treating MDR infections (i.e. colistin, aminoglycosides). Other sites of infection discussed by the manufacturer were skin and soft tissue, bone and joint and meningitis. The clinical advisors considered that MDR infections at these sites would be very rare.
Multidrug-resistant pathogens/mechanisms
Outside of the HVCSs the following pathogen–mechanism combinations were discussed as relevant areas for usage for CAZ/AVI:
-
non-MBL pseudomonas
-
pathogens with other serine carbapenemases (e.g. KPC) or non-carbapenemase causes of carbapenem resistance (e.g. porin and efflux pump mechanisms).
Our clinical advisors considered that, in both of these pathogen–mechanism combinations, patients had available other treatment options and that they were not, therefore, a priority area of usage for CAZ-AVI. The exception to this was infections that were MDR due to multiple types of carbapenem resistance (e.g. serine, porin and efflux pump) in whom CAZ-AVI may represent an important treatment option.
Empiric usage
During these evaluations there was substantial debate about the appropriate definition of the ES. Stakeholders were broadly aligned that the risk-based ES should be driven by the severity of the clinical scenario rather than the site of infection alone.
The manufacturer and the clinical advisors to this project presented differing perspectives on how to define a patient as at high risk of carbapenem resistance for the purposes of identifying patients who might appropriately receive risk-based empiric treatment with CAZ-AVI. As documented throughout this report, the clinical advisors to this project considered that it was appropriate to restrict usage in the ES to patients with a high risk of an infection caused by OXA-48 Enterobacterales where this high risk was based on one of three factors:
-
the patient was previously hospitalised in a healthcare setting with high prevalence of CPE with OXA-48
-
there had been an outbreak of infection with CPE with OXA-48 on a ward where the patient has stayed during their current admission
-
previous cultures (taken during the current or previous hospital stays) show that the patient was previously colonised/infected by CPE with OXA-48.
This view was based on the desire to restrict usage to those in whom benefit was most significant, thus controlling the emergence of resistance; the clinical advisors also expressed concerns that a broader definition could lead to stewardship challenges.
The manufacturer considered a broader definition of patients at high risk of a drug-resistant infection. This included patients at risk of resistance due to ‘previous admission to ICU, longer admission times, critical illness, use of invasive devices and prior antibiotic therapy including cephalosporin, carbapenem or fluoroquinolone use’ and:
symptoms or signs starting more than 5 days after hospital admission, relevant comorbidity such as severe lung disease or immunosuppression, recent use of broad-spectrum antibiotics, colonisation with multi-drug-resistant bacteria, and recent contact with a health or social care setting before current admission.
No evidence was presented quantifying the likelihood that patients with these characteristics have a MDR infection, which is likely to reflect the paucity of evidence available. 117
The clinical advisors considered that usage under a broader suspicion of resistance should only be considered in exceptional cases. The appropriateness of a wider definition of empiric usage is, in principle, a question that could be addressed empirically, by assessing the health benefits of a more inclusive definition, against the health costs of treating more patients who do not have a resistant infection with CAZ-AVI and therefore contributing to higher levels of long-term resistance. This trade-off was not addressed quantitively by EEPRU or the manufacturer, largely reflecting the difficulties in accurately quantifying the long-term implications of different levels of usage for the emergence of resistance to CAZ-AVI.
Quantitative extrapolation to expected usage
Current population sizes
The aim was to estimate the number of infections in the HVCS and other important areas of expected usage. Based on feedback from our clinical advisors, the majority of CAZ-AVI use in HAP/VAP and BSIs was expected to be in the ES, and the majority of CAZ-AVI use in cUTI and IAI was expected to be in the MDS. We therefore set out to estimate the number of patients with the following characteristics:
-
HAP/VAP and BSIs with suspected infection caused by OXA48, according to the criteria outlined in PICOS for high-value clinical scenarios
-
cUTIs and IAIs caused by OXA48, as confirmed by resistance mechanism testing.
The current population size was derived from SGSS data (AMR module) supplied by PHE. SGSS is a national database of laboratory data provided by approximately 98% of hospital microbiology laboratories in England. 5 It contains resistance mechanism and antibiotic susceptibility testing for all submitted isolates. We analyse data for the period between October 2020 and April 2021 as from October 2020 reporting of acquired carbapenemase-producing Gram-negative bacteria by laboratories become mandatory.
The SGSS dataset includes anonymised patient ID, specimen type, species, referral location, laboratory, resistance mechanism tested and mechanism results. The site of infection was not available directly; instead it was inferred from the specimen types.
Clinical advisors to the project highlighted that there is considerable uncertainty in the categorisation of infection sites according to the specimen type. To reflect this uncertainty we explored two separate classifications in scenario analyses, as shown in Table 22. The classification in Scenario 1 was derived by PHE, based on a set of specimens that map directly to infection sites. The scenario excluded all specimens from female patients in cUTIs except nephrostomy specimens, and all sputum samples. The sputum samples were removed following a clinical review (discussed in more detail in ESPAUR report 20215) because a large number of sputum samples are considered to be contaminants without further evidence of clinical infection. The clinical advisors to EEPRU considered this classification to be conservative and derived a broader classification in Scenario 2 with guidance from clinical advisors. Scenario 2 included sputum samples, and urine samples from both male and female patients where the medical requestor is ‘acute’ care, as a proxy for hospitalised patients. The scenario is likely to capture other relevant infections excluded from Scenario 1 but may include some specimens that do not relate to the infection types of interest.
| HAP/VAP | cUTIs | BSIs | IAIs | |
|---|---|---|---|---|
| Specimen types in scenario I1 | Lower respiratory tract (bronchial) | Urine/kidney specimens from all male patients, irrespective of setting (urine, CSU, MSU, urinary catheter, suprapubic aspirate, bladder, kidney, urethra, urine/kidney, spa, ureter, urethral swab, EMU, ileal/bladder conduit, perinephric, first void, pus associated kidney/urinary tract); nephrostomy specimens in male and female patients |
Blood samples (blood, plasma, dried blood spot, haematoma, cord blood, fetal blood) | Wound specimens (surgical and traumatic wounds) |
| Additional specimen types in scenario I2 | Lower respiratory tract (alveolar lavage, trachea, BAL, chest, lung, lower respiratory tract, tracheal aspirate), sputum (sputum, endotracheal secretions, endotracheal aspirate, endotracheal tube, induced sputum), swab (lung swab) | Urine/kidney specimens in scenario 1 in all hospitaliseda patients (both male and female), upper genital tract in male and female hospitaliseda patients | Heart/heart valve (heart, heart valve, mitral valve), intra-vascular line (TIP-NOS, arterial line/tip, Hickman line, CVP line tip, aortic valve, Venflon, aorta, haemodialysis access, arterio-venous shunt), pacemaker, catheter swab, aortic tissue, heart valve prosthesis (cardiac prosthesis, heart valve prosthesis), vascular graft (vascular graft), liver/bile (bile, gall bladder), hip tissue, hip swab, skin/wound (pressure sore), bone (bone, bone/joint, vertebra), bone marrow, bone pin/plate (prosthesis pin, bone pin/plate, prosthesis plate), joint prosthesis (artificial joint), intervertebral disc (intervertebral disc), IUCD, peritoneum, foreign body, implant NOS, CSF shunt (ventriculo-atrial valve), bone biopsy sample | None |
In the dataset, repeated entries were only removed if they were directly repeated for the same patient, species, specimen, referral location, laboratory, mechanism, and mechanism results. However, it is possible that reported numbers included multiple entries from the same infectious episode if multiple specimen samples were analysed (e.g. on different days).
The number of specimens tested for OXA48 was used to approximate the population size in ES. This reflects an assumption that all of the mechanism testing conducted was initiated following high suspicion of that resistance mechanism by the treating clinicians for the reasons specified in PICOS for high-value clinical scenarios. The number of isolates confirmed to have the resistance mechanism was used to approximate the population size in the MDS. The derived population sizes are shown in Table 23. The specimen types included did not impact on the number of BSIs and IAIs.
| HAP/VAP (tested) | cUTIs (confirmed positive) | BSIs (tested) | IAIs (confirmed positive) | |
|---|---|---|---|---|
| Scenario P1 | 24 | 82 | 161 | 36 |
| Scenario P2 | 166 | 132 | 161 | 36 |
It should be noted that the sum of population sizes for individual infection sites may overestimate the total population size, if the same infection presents at multiple sites. For example, BSIs are often sequelae of other infections. If a BSI develops from HAP/VAP following unsuccessful treatment with CAZ-AVI, it would likely be treated with an alternative AM, despite having the resistance mechanism of interest.
The estimates in Table 23 are associated with considerable uncertainty due to uncertainty in the completeness of the SGSS dataset (labs may not submit all specimens to SGSS), uncertainty in how accurately specimen types represent the infection sites of interest, uncertainty about whether all tested patients would fall within the defined target population for empiric treatment, and the potential double counting of samples from the same infectious episode.
To provide an alternative estimate of the population size, we conducted a survey (mentioned in Clinical evidence – linking susceptibility to 30-day outcomes in the ES) about the number of HAP/VAP infections eligible for treatment in the ES. The survey targeted infectious disease specialists and collected information about the participants’ place of work (number of hospital beds, and the number of other infectious disease specialists), and the number of suspected and confirmed HAP/VAP infections caused by CPE OXA48 they encountered per annum. The survey was disseminated to infectious disease consultants and microbiologists who were members of the BSAC, to clinical advisors to the project, and to experts recommended by the clinical advisors. The infection numbers were scaled to country-level estimates using the number of hospital beds per infectious disease specialist (derived from the survey responses) and the unweighted average number of hospital beds in England for four quarters in 2020/1. 163
In total, 25 participants started the survey, of whom nine provided information required to estimate the total number of patients eligible for treatment in ES in England. The estimates varied considerably between experts (with responses implying 0 to 13,422 suspected and 0 to 6711 confirmed infections in England). The weighted average (5099 suspected and 2922 confirmed infections) was considered to be implausibly high by clinical advisors to the project, possibly because of higher survey take-up among experts who are more likely to encounter the infections of interest, and these estimates were not therefore taken forward to the decision-analytic modelling.
The population size over 20 years was derived by applying the year-on-year population growth detailed in Chapter 8 to the current annual population size (Table 23). The population size estimates are used to rescale the estimates of patient-level INHEs and are presented in Appendix 9.1, Figure 43. Four scenarios are used to model the eligible population over time. Scenario P1G1 is the most conservative, as it uses the conservative baseline number of infections (scenario P1 in Table 23), and the population growth derived from a time-series model with a damped trend (see Predicting the future sizes of the HVCS for details). Scenario P2G2 is the least conservative, as it uses the larger baseline number of infections (scenario P2 in Table 23), and the population growth derived from a time series without a damped trend (see Predicting the future sizes of the HVCS for details). The difference between the scenarios is largely driven by the assumptions about long-term growth in infection numbers. When using the model with a damped trend, the total population size across all sites of infection increased from between 303 and 495 (P1G1 and P2G1) in year 1 to between 377 and 615 in year 20. The model with the non-damped trend increased the total population size substantially, from between 303 and 495 (P1G2 and P2G2) in year 1 to between 1340 and 11,053 in year 20.
In addition, we derive estimates of expected total drug usage for CAZ-AVI as these influence some of the scenarios relating to resistance emergence (see Modelling direct population net health effects in HVCS). Expected usage of CAZ-AVI was derived by adjusting the population size for the proportion eligible for treatment with CAZ-AVI. In ES, all infections were assumed to be eligible for empiric treatment. In MDS, infections confirmed to have the relevant resistance mechanisms were adjusted for the mean proportion of patients who were not susceptible to non-colistin/aminoglycoside-based treatments, but were susceptible to CAZ-AVI, as described in Model structure for microbiology-directed setting. When deriving expected usage, susceptibility was assumed to be static over time for simplicity, as susceptibility changes over time were expected to have a small impact on usage.
The total expected usage over 20 years is shown in Table 24.
| HAP/VAP | cUTI | BSI | IAI | |
|---|---|---|---|---|
| Scenario P1G1 | 576 | 588 | 3866 | 257 |
| Scenario P1G2 | 1279 | 1306 | 8586 | 571 |
| Scenario P2G1 | 3990 | 943 | 3866 | 257 |
| Scenario P2G2 | 8860 | 2095 | 8586 | 571 |
Extrapolation of INHEs between populations
Population-level INHEs were derived by multiplying patient-level INHEs by the population size. Patient-level INHE, derived from the model described in Modelling direct patient net health effects in HVCS, was conditional on the site and the treatment setting (ES or MDS). Patient-level INHEs for cUTIs in the MDS and for HAP/VAP in the ES were estimated by the model. Patient-level INHEs in BSI and IAIs were assumed to be the same as in HAP/VAP and cUTIs, respectively, based on feedback from our clinical advisors. BSI and HAP/VAP are both severe infections where CAZ-AVI is expected to be used predominantly empirically. Although the consequences of IAIs can be more severe than the consequences of cUTI as they are very difficult to treat (requiring a combination of ABs and surgery), on the other hand the benefits of CAZ-AVI may be smaller due to the complexity of treating these infections and the lesser role of AMs compared to other treatment modalities in their management.
Population-level INHEs in years 1–20 were discounted at an annual rate of 3.5% to account for the delayed start of treatment.
Probabilistic analysis
The parameters included in the probabilistic analysis were chosen pragmatically. The analysis incorporated uncertainty in the patient-level INHE (as described in Modelling direct patient net health effects in HVCS) and uncertainty in the population growth. The probabilistic analysis did not reflect uncertainty in the current population size, instead this was explored in scenario analyses outlined above. Expected usage and the link between this and resistance was not made probabilistic for simplicity and due to the challenges in characterising with any accuracy the uncertainty around emergence of resistance; again this was explored via scenario analyses outlined in Modelling direct population net health effects in HVCS.
Additional elements of value for new AMs
The literature on the economic evaluation of AMs has described the different sources of value associated with these products. 12,106 In EEPRU’s earlier work on evaluation methods12 the principles by which each of these ‘elements of value’ can be reflected in models focused on estimating the impact of new products on population NHEs were discussed.
In Additional elements of value relevant to AMs, we present a summary of how the different elements of value are conceptualised in the literature, within the manufacturer submission and how they are understood by our clinical advisory group. We summarise the extent to which each element of value is reflected in the quantitative assessments of value for the HVCSs, or quantitative evidence presented in the manufacturer submission. For each element of value for which a quantitative assessment was not conducted we provide a discussion of the extent to which that element of value is likely to be quantitively important in influencing the assessment of population INHEs for CAZ-AVI. This is based on evidence from the literature, evidence presented in the manufacturer submission and the views of our clinical advisors.
Validation
To ensure the appropriateness of the decision problem, scope of the decision model, model structure and evidence used, we consulted extensively with microbiologists and clinicians involved in treating serious drug-resistant infections, and, in related research, those with expertise in transmission modelling and those with expertise in specific types of evidence. Given the complexity of the appraisal and the multiple components of the work this required approximately 10 separate calls on different aspects of the work.
A technical validation of the data analyses, synthesis and decision-analytic modelling conducted by EEPRU was conducted. This comprised a review of the code by a second reviewer.
Chapter 8 Results of quantification of value
Direct patient net health effects in HVCS
OXA-48 empiric setting HAP/VAP
The base-case results are shown in Table 25 for patients correctly suspected as having OXA-48 Enterobacterales, those wrongly suspected of having OXA-48 Enterobacterales, and in the average patient suspected to have OXA-48 Enterobacterales in the ES (whose outcomes are a weighted average of those with and without OXA-48 Enterobacterales).
| Comparator treatment strategies in the empiric setting | Incremental results | ||||||
|---|---|---|---|---|---|---|---|
| E1 | E2nca | E2ca | E3nca | E3ca | E1-E2nca | E1-E2ca | |
| Patients with OXA-48 Enterobacterales | |||||||
| Summary of in-hospital outcomes (proportions) across both lines of treatment available | |||||||
| Death | 0.361 | 0.463 | 0.409 | 0.450 | 0.407 | −0.102 | −0.049 |
| Survival no AKI | 0.514 | 0.403 | 0.423 | 0.417 | 0.425 | 0.111 | 0.090 |
| Survival AKI | 0.125 | 0.135 | 0.167 | 0.133 | 0.168 | −0.009 | −0.042 |
| Survival CKD | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 |
| Economic outcomes (all discounted) | |||||||
| Treatment costs | £39 | £177 | £440 | £125 | £430 | −£138 | −£402 |
| AKI costs hospital | £1735 | £2356 | £2318 | £2256 | £2305 | −£621 | −£583 |
| Other costs hospital | £17,543 | £26,651 | £16,803 | £26,289 | £16,694 | −£9108 | £739 |
| Long-term costs | £601 | £510 | £563 | £521 | £566 | £91 | £37 |
| Total costs | £19,917 | £29,694 | £20,125 | £29,191 | £19,996 | −£9776 | −£208 |
| Life-years | 2.75 | 2.29 | 2.49 | 2.34 | 2.51 | 0.468 | 0.26 |
| QALYs | 1.93 | 1.61 | 1.75 | 1.65 | 1.76 | 0.329 | 0.182 |
| Per-person NHE (QALYs) | 0.94 | 0.12 | 0.75 | 0.19 | 0.76 | 0.818 | 0.193 |
| Patients without OXA-48 Enterobacterales | |||||||
| Summary of in-hospital outcomes (proportions) across both lines of treatment available | |||||||
| Death | 0.357 | 0.357 | 0.409 | 0.357 | 0.409 | 0.000 | −0.052 |
| Survival no AKI | 0.517 | 0.517 | 0.423 | 0.517 | 0.423 | 0.000 | 0.094 |
| Survival AKI | 0.125 | 0.125 | 0.167 | 0.125 | 0.167 | 0.000 | −0.042 |
| Survival CKD | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 |
| Economic outcomes (all discounted) | |||||||
| Treatment costs | £34 | £44 | £440 | £44 | £440 | −£10 | −£406 |
| AKI costs hospital | £1714 | £1714 | £2318 | £1714 | £2318 | £0 | −£604 |
| Other costs hospital | £17,213 | £17,213 | £16,803 | £17,213 | £16,803 | £0 | £409 |
| Long-term costs | £604 | £604 | £563 | £604 | £563 | £0 | £40 |
| Total costs | £19,564 | £19,574 | £20,125 | £19,574 | £20,125 | −£10 | −£561 |
| Life-years | 2.768 | 2.768 | 2.493 | 2.768 | 2.493 | 0.000 | 0.275 |
| QALYs | 1.945 | 1.945 | 1.752 | 1.945 | 1.752 | 0.000 | 0.193 |
| Per-person NHE (QALYs) | 0.967 | 0.966 | 0.746 | 0.966 | 0.746 | 0.001 | 0.221 |
| All patients presenting in the ES | |||||||
| Total costs | £19,634 | £21,575 | £20,125 | £21,476 | £20,100 | −£1941 | −£491 |
| QALYs | 1.943 | 1.878 | 1.752 | 1.886 | 1.754 | 0.065 | 0.191 |
| Per-person NHE (QALYs) | 0.961 | 0.799 | 0.746 | 0.812 | 0.749 | 0.163 | 0.215 |
Ceftazidime-avibactam is associated with similar susceptibility to colistin/aminoglycoside-based therapy but improved safety in both individuals with and without OXA-48 Enterobacterales. The per-patient INHE is, therefore, similar in patients with OXA-48 Enterobacterales, without OXA-48 Enterobacterales and the average ES patient at 0.16–0.22 QALYs. The safety advantage delivers a small cost saving as cost savings associated with reduced rates of AKI are offset by longer time spent in hospital for patients receiving CAZ-AVI, which is a result of the slightly higher susceptibility to colistin (94% compared to 92% for CAZ-AVI) and the fact that preventing AKIs lowers early in-hospital mortality, thus prolonging hospital stay. The safety advantage delivers a substantive QALY gain due to the reduced mortality associated with AKI in the short and long term.
Among patients with OXA-48 Enterobacterales, CAZ-AVI is associated with improved susceptibility and comparable safety to non-colistin/aminoglycoside-based therapy. The large difference in susceptibility between these comparators (92% vs. 35%) drives a large per-patient INHE of 0.82 QALYs in this group. This reflects both the QALY gain associated with the higher susceptibility (0.40) and the substantive cost saving associated with a reduced LoS (£9108). In patients without OXA-48 Enterobacterales, CAZ-AVI and non-colistin/aminoglycoside-based therapy offer similar susceptibility and safety.
In the average ES patient suspected of having OXA-48 Enterobacterales, use of CAZ-AVI in the ES is associated with a per-patient INHE gain of 0.22 QALYs compared to colistin/aminoglycoside-based therapy and of 0.16 QALYs compared to non-colistin or aminoglycoside-based therapy.
Restricting use of CAZ-AVI to patients who fail empiric treatment and require treatment in the MDS is associated with a small increase in INHE benefit compared to existing therapies. This is attributable to several factors. Many patients can be treated effectively in the ES with existing treatment or die prior to reaching the MDS (i.e. not all patients progress to the MDS); many patients do not have OXA-48 Enterobacterales and are not, therefore, eligible to receive CAZ-AVI in the MDS, and among those with OXA-48 Enterobacterales the majority (68%) are susceptible to a non-colistin-based treatment option and, therefore, do not receive CAZ-AVI in the model when they reach the MDS.
There is a large degree of parameter uncertainty around the incremental per-patient INHEs of CAZ-AVI. The distribution of per-patient INHEs is shown in Figure 12. This reflects uncertainty in the probability a patient has OXA-48 Enterobacterales, the relative susceptibility of these treatment options, their safety and the benefits of avoided AKIs.
FIGURE 12.
Distribution of per-patient INHEs of CAZ-AVI in OXA-48 HAP/VAP ES compared to (a) non-colistin/aminoglycoside-based therapy and (b) colistin/aminoglycoside-based therapy (2000 simulations). NHE, net health effects.
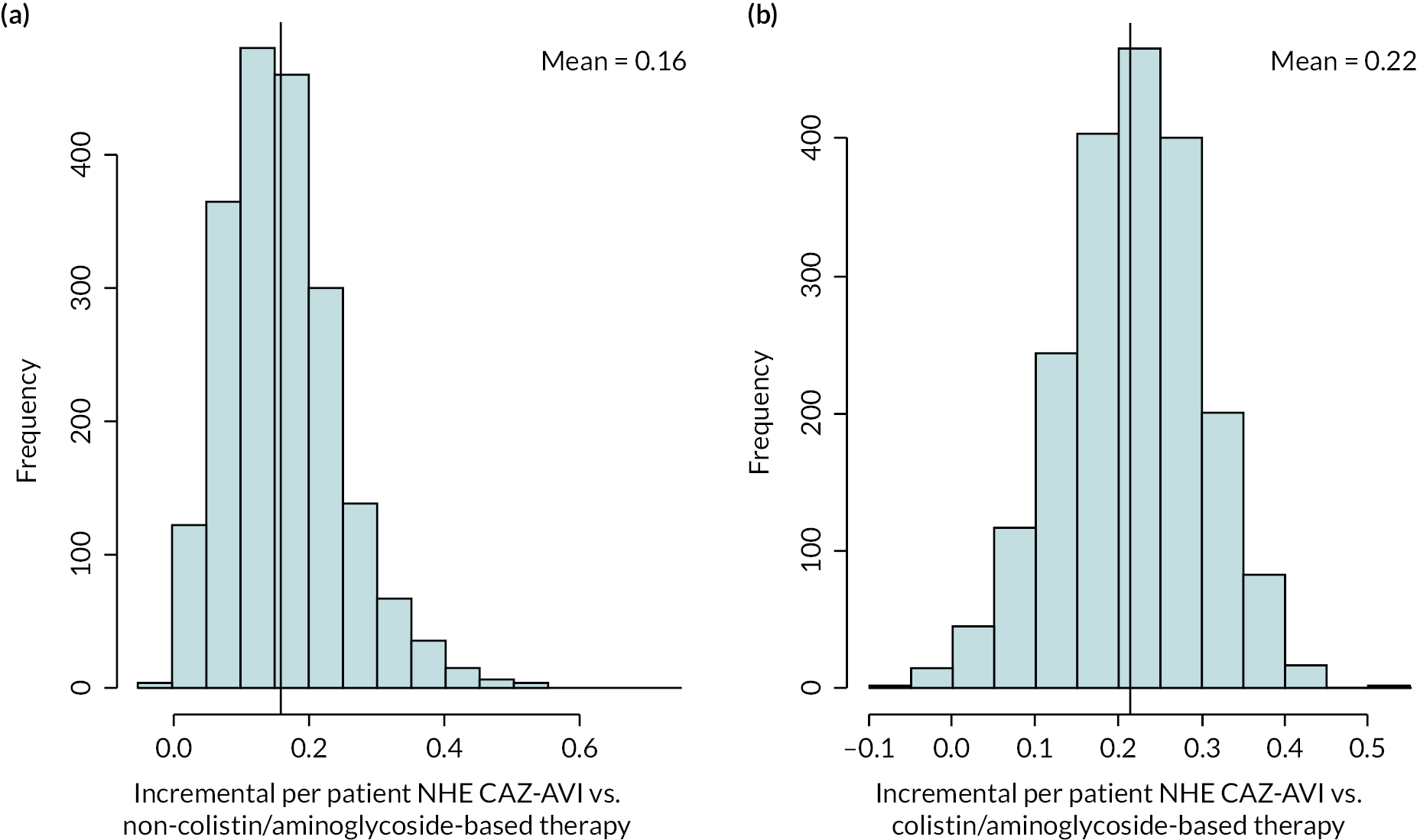
Scenario analyses that modified the deterministic base case INHE by more than 10% (and three scenario analyses requested by NICE marked by *) are shown in Table 26. The main areas of uncertainty relate to the probability an individual has OXA-48 Enterobacterales, the susceptibility scenarios and long-term survival following discharge from hospital.
| Scenario name | Base-case value/assumption | Scenario value/assumption | Best existing treatment | Patient-level INHE of CAZ-AVI |
|---|---|---|---|---|
| Base case | – | – | Non-colistin/amino-based | 0.159 |
| p_bug_survey | Probability patient has OXA-48 Enterobacterales is 0.20 | Probability patient has MBL Enterobacterales is 0.57 based on BSAC survey data | Colistin/amino-based | 0.222 |
| p_bug_0 | Probability patient has OXA-48 Enterobacterales is 0.20 | Probability patient has OXA-48 Enterobacterales is 0.00 | Non-colistin/amino-based | 0.001 |
| p_bug_10 | Probability patient has OXA-48 Enterobacterales is 0.20 | Probability patient has OXA-48 Enterobacterales is 0.10 | Non-colistin/amino-based | 0.082 |
| p_bug_30 | Probability patient has OXA-48 Enterobacterales is 0.20 | Probability patient has OXA-48 Enterobacterales is 0.30 | Colistin/amino-based | 0.230 |
| p_bug_40 | Probability patient has OXA-48 Enterobacterales is 0.20 | Probability patient has OXA-48 Enterobacterales is 0.40 | Colistin/amino-based | 0.227 |
| p_bug_50 | Probability patient has OXA-48 Enterobacterales is 0.20 | Probability patient has OXA-48 Enterobacterales is 0.50 | Colistin/amino-based | 0.225 |
| p_bug_60 | Probability patient has OXA-48 Enterobacterales is 0.20 | Probability patient has OXA-48 Enterobacterales is 0.60 | Colistin/amino-based | 0.222 |
| p_bug_70 | Probability patient has OXA-48 Enterobacterales is 0.20 | Probability patient has OXA-48 Enterobacterales is 0.70 | Colistin/amino-based | 0.219 |
| p_bug_80 | Probability patient has OXA-48 Enterobacterales is 0.20 | Probability patient has OXA-48 Enterobacterales is 0.80 | Colistin/amino-based | 0.216 |
| p_bug_90 | Probability patient has OXA-48 Enterobacterales is 0.20 | Probability patient has OXA-48 Enterobacterales is 0.90 | Colistin/amino-based | 0.213 |
| p_bug_100 | Probability patient has OXA-48 Enterobacterales is 0.20 | Probability patient has OXA-48 Enterobacterales is 1.00 | Colistin/amino-based | 0.210 |
| S2 | Susceptibility based on network meta-analysis of EUCAST studies | Network meta-analysis: include all studies regardless of breakpoints, excluding specific arms due to inconsistency | Colistin/amino-based | 0.217 |
| S3 | Susceptibility based on network meta-analysis of EUCAST studies | Susceptibility based on PHE isolate-level data (excludes fosfomycin) | Non-colistin/amino-based | 0.180 |
| S4 | Susceptibility based on network meta-analysis of EUCAST studies | Susceptibility based on Vazquez-Ucha et al. isolate-level data (excludes tigecycline) | Colistin/amino-based | 0.263 |
| Weibull | Log-normal model fit to CARBAR survival data | Weibull model fit to CARBAR survival data | Non-colistin/amino-based | 0.135 |
| thresh15* | Cost-effectiveness threshold £20,000 | Cost-effectiveness threshold £15,000 | Non-colistin/amino-based | 0.191 |
| thresh30* | Cost-effectiveness threshold £20,000 | Cost-effectiveness threshold £30,000 | Non-colistin/amino-based | 0.128 |
| dr1.5* | Discount rate for costs and benefits 3.5% | Discount rate for costs and benefits 1.5% | Non-colistin/amino-based | 0.168 |
When the probability of having OXA-48 Enterobacterales is low, the preferred existing treatment option is to use non-colistin/aminoglycoside-based therapy and the efficacy and safety advantage of CAZ-AVI are reduced. This results in per-patient INHEs of 0.00 and 0.08 QALYs when the probability of having OXA-48 Enterobacterales is 0 and 0.10, respectively.
When susceptibility was informed using the all-studies NMA (scenario S2), PHE isolate-level data (scenario S3) or the Vazquez-Ucha study (scenario S4) in place of the EUCAST NMA, the per-patient INHE increased to 0.18–0.26 QALYs, reflecting the decrease in susceptibility to non-colistin/aminoglycoside-based treatment under these scenarios. The increase in the patient-level INHE was particularly high in scenarios S2 and S4 where susceptibility to CAZ-AVI also increased from 92% to 97% and 99%. In these scenarios, the substantial reduction in susceptibility to non-colistin/aminoglycoside-based treatments (from 35% to 18% and 7%), along with the increase in susceptibility to colistin/aminoglycosides in scenario S2, meant that colistin/aminoglycosides became the best existing treatment.
The results were also sensitive to the parametric survival model used to predict long-term survival post-discharge. Use of the Weibull model reduced the per-patient INHE gain to 0.14 QALYs.
The patient-level INHEs are lower as the cost-effectiveness threshold is increased. In the base case increasing the cost-effectiveness threshold reduces the amount of health generated by the cost savings generated by CAZ-AVI. Using a lower discount rate of 1.5% for costs and health outcomes increases the patient-level INHEs to 0.17 QALYs.
OXA-48 microbiology-directed setting HAP/VAP and cUTI
The probabilistic base-case results are shown in Table 27 for patients with confirmed OXA-48 Enterobacterales in the MDS who have HAP/VAP or cUTI. The advantages of CAZ-AVI are smaller in the MDS as once susceptibility results are known, many patients (65%) can be treated with a non-colistin/aminoglycoside-based option to which they are susceptible and do not receive CAZ-AVI. The per-patient INHEs associated with CAZ-AVI are driven by avoided safety issues related to use of colistin and aminoglycosides in those susceptible to these agents (35% of the MDS cohort). Overall, the per-patient INHEs associated with using CAZ-AVI in the MDS are 0.07 QALYs for HAP/VAP and for cUTI.
| MDS pathway with CAZ-AVI | MDS pathway without CAZ-AVI | Incremental values | |
|---|---|---|---|
| HAP/VAP | |||
| Summary of in-hospital outcomes (proportions) across both lines of treatment available | |||
| Death | 0.373 | 0.388 | –0.014 |
| Survival no AKI | 0.497 | 0.466 | 0.030 |
| Survival AKI | 0.130 | 0.146 | –0.016 |
| Survival CKD | 0.000 | 0.000 | 0.000 |
| Economic outcomes (all discounted) | |||
| Treatment costs | £189 | £264 | –£74 |
| AKI costs hospital | £1673 | £1884 | –£211 |
| Other costs hospital | £34,723 | £34,737 | –£15 |
| Long-term costs | £591 | £580 | £10 |
| Total costs | £37,176 | £37,465 | –£289 |
| Life-years | 2.691 | 2.611 | 0.08 |
| QALYs | 1.891 | 1.835 | 0.056 |
| Per-person NHE | 0.032 | –0.038 | 0.071 |
| cUTI | |||
| Summary of in-hospital outcomes (proportions) across both lines of treatment available | |||
| Death | 0.125 | 0.136 | –0.011 |
| Survival no AKI | 0.646 | 0.607 | 0.039 |
| Survival AKI | 0.228 | 0.257 | –0.028 |
| Survival CKD | 0.000 | 0.000 | 0.000 |
| Economic outcomes (all discounted) | |||
| Treatment costs | £189 | £264 | –£74 |
| AKI costs hospital | £1673 | £1884 | –£211 |
| Other costs hospital | £17,344 | £17,355 | –£11 |
| Long-term costs | £831 | £825 | £5 |
| Total costs | £20,037 | £20,328 | –£291 |
| Life-years | 3.713 | 3.636 | 0.077 |
| QALYs | 2.609 | 2.555 | 0.054 |
| Per-person NHE | 1.607 | 1.539 | 0.069 |
There is a moderate degree of uncertainty around the per-patient INHEs of CAZ-AVI compared to the existing treatment options. The distribution of per-patient INHEs is shown in Figure 13.
FIGURE 13.
Distribution of INHEs of introducing CAZ-AVI in to the MDS compared to existing therapies: (a) OXA-48 Enterobacterales HAP/VAP and (b) OXA-48 Enterobacterales cUTI (2000 simulations). MDS, microbiology-directed setting; NHE, net health effects.
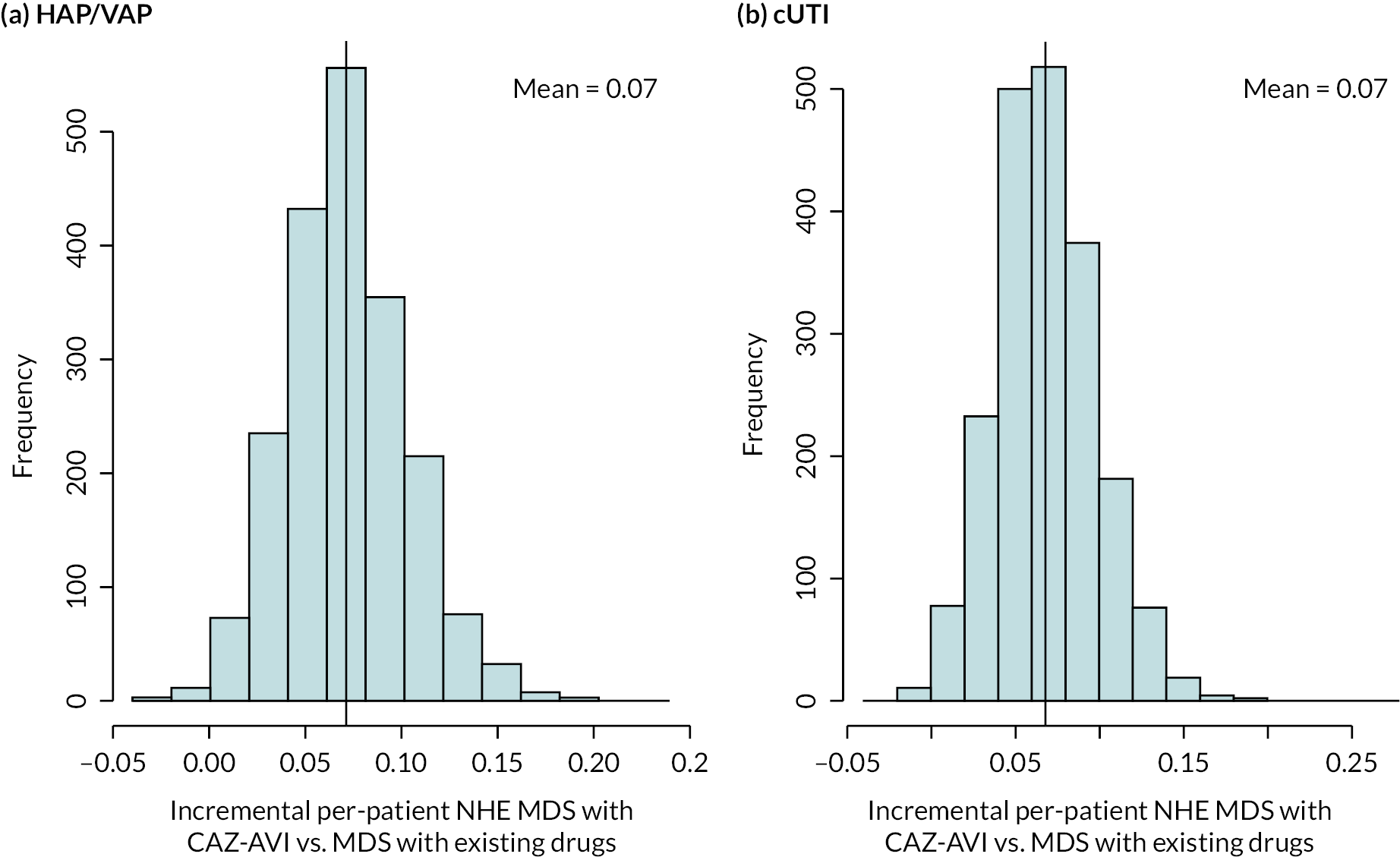
Scenario analyses that modified the deterministic base case INHE by more than 10% (and three scenario analyses requested by NICE marked by *) are shown in Table 28. The main areas of uncertainty relate to the susceptibility scenarios, the impact of colistin/aminoglycoside-based therapy on AKI risk and its long-term implications, and long-term survival following discharge from hospital.
| Scenario name | Base-case value/assumption | Scenario value/assumption | INHE per patient: HAP/VAP | INHE per patient: cUTI |
|---|---|---|---|---|
| Base case | – | – | 0.080 | 0.078 |
| S2 | Susceptibility based on network meta-analysis of EUCAST studies | Network meta-analysis: include all studies regardless of breakpoints, excluding specific arms due to inconsistency | 0.066 | 0.065 |
| S4 | Susceptibility based on network meta-analysis of EUCAST studies | Susceptibility based on Vazquez-Ucha et al. isolate-level data | 0.119 | 0.116 |
| p_AKI_Chien | Probability of AKI with colistin/aminoglycoside therapy based on Sisay 2021 (0.45) | Probability of AKI with colistin/aminoglycoside therapy based on Chien (0.32) | 0.066 | 0.064 |
| OR_AKI_Wagenlehner | Odds ratio comparing AKI for colistin/aminoglycoside-based therapy to non-colistin/aminoglycoside-based therapy from all studies analysis in Chien 2020 (1.81) | Odds ratio comparing AKI for colistin/aminoglycoside-based therapy to non-colistin/aminoglycoside-based therapy from all studies analysis in Wagenlehner 2021 (2.23) | 0.103 | 0.100 |
| OR_AKI_ChienRIFLE | Odds ratio comparing AKI for colistin/aminoglycoside-based therapy to non-colistin/aminoglycoside-based therapy from all studies analysis in Chien 2020 (1.81) | Odds ratio comparing AKI for colistin/aminoglycoside-based therapy to non-colistin/aminoglycoside-based therapy from RIFLE criteria studies analysis in Chien 2020 (1.61) | 0.067 | 0.065 |
| OR_AKI_death_halved | Odds ratio of mortality for AKI compared to no AKI derived from Kerr (2014) (5.11) | Odds ratio of mortality for AKI compared to no AKI halved (2.56) | 0.063 | 0.060 |
| double.ckd.risk | Risk of CKD as observed in Bucaloiu 2012 | Risk of CKD doubled to reflect potential higher propensity for CKD in HVCS | 0.070 | 0.068 |
| abs.increase | Odds ratios on mortality associated with nephrotoxicity from Bucaloiu 2012 are applied multiplicatively to underlying risk in HVCS | Absolute risk increases in Bucaloiu 2012 are assumed to apply | INHE changed by < 10% | INHE changed by < 10% |
| all.aki.lt | Base case assumptions with respect to long-term effects of AKI | Applying a range of alternative assumptions to model the long-term effects of AKI | INHE changed by < 10% | INHE changed by < 10% |
| Weibull | Log-normal model fit to CARBAR survival data | Weibull model fit to CARBAR survival data | 0.055 | 0.054 |
| loglogistic | Log-normal model fit to CARBAR survival data | Log-logistic model fit to CARBAR survival data | 0.070 | 0.068 |
| lt.care | No costs of long-term care | Costs of discharge to long-term care included | INHE changed by < 10% | 0.091 |
| thresh15* | Cost-effectiveness threshold £20,000 | Cost-effectiveness threshold £15,000 | 0.085 | 0.083 |
| thresh30* | Cost-effectiveness threshold £20,000 | Cost-effectiveness threshold £30,000 | 0.075 | 0.072 |
| dr1.5* | Discount rate for costs and benefits 3.5% | Discount rate for costs and benefits 1.5% | 0.090 | 0.089 |
In both HAP/VAP and cUTI when the NMA of susceptibility data included all studies regardless of breakpoints (S2), the patient-level INHEs were lower at 0.07 QALYs for both HAP/VAP and cUTIs. In this scenario although susceptibility to CAZ-AVI is higher the proportion susceptible to a non-colistin/aminoglycoside-based treatment is also higher so a smaller proportion of individuals receive CAZ-AVI in the model. The patient-level INHEs were higher when using the Vazquez-Ucha data (S4) to inform susceptibility at 0.12 QALYs for both HAP/VAP and cUTI. This reflects the higher proportion of individuals who are only susceptible to a colistin/aminoglycoside-based therapy in this scenario and who are therefore eligible to receive CAZ-AVI within the model (though we note that this is largely driven by the fact that tigecycline is not available in this scenario).
Using the Wagenlehner 2021 meta-analysis to inform the effect of colistin/aminoglycoside-based therapy on AKI risk rather than the Chien meta-analysis also increased the INHEs to 0.10 QALYs in HAP/VAP and cUTI. Similar effects were observed for HAP/VAP when exploring alternative assumptions about the long-term implications of AKIs. Reduced within-hospital mortality from AKI decreased the INHE to 0.06 for HAP/VAP and cUTI as this reduces the safety advantage of CAZ-AVI.
Using a Weibull model to inform long-term mortality reduced the patient-level INHEs to 0.05 QALYs in HAP/VAP and cUTI.
Direct population net health effects in HVCS and broader areas of expected usage
Figure 14 shows the population INHE over 20 years, derived using alternative assumptions about the population size (based on different categorisation of specimen types), population growth (derived with different models for the population growth predictions) and resistance emergence (reaching 1%, 10% and 30% at 20 years; 5% scenario not shown for parsimony). Population INHE declines year on year in scenarios where the discount rate exceeds the rate of population growth in all period; rises and then declines in scenarios where the population growth rate exceeds the discount rate in earlier periods but then falls below the discount rate in later periods; and rises year on year in scenarios where the rate of population growth exceeds the discount rate. Table 29 shows the total discounted population INHE aggregated over the 20 year period.
FIGURE 14.
Population INHE (QALYs) over 20 years based on two population size scenarios. P1, baseline population based on PHE categorisation of infection sites; P2, baseline population based on clinical advisors’ categorisation of infection sites; G1, damped growth rate; G2, growth rate not damped; R1, 1% resistance after 20 years; R2, 10% resistance after 20 years; R3, 30% resistance after 20 years. (a) PHE categorisation. (b) Expert-guided categorisation of specimen types.
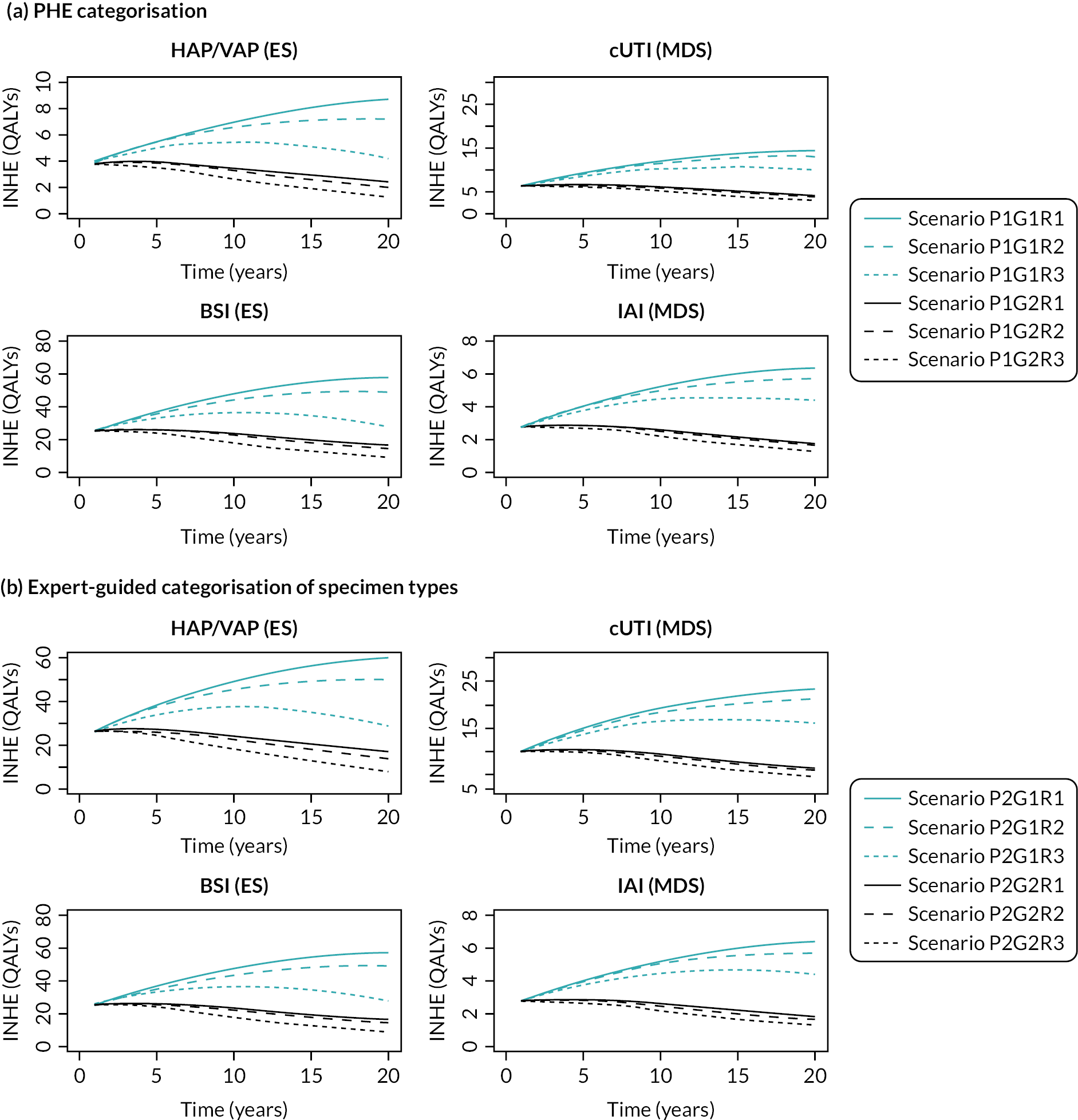
| Baseline population | Population growth rate | Change in resistance, % | HAP/VAP | cUTI | BSI | IAI | Total |
|---|---|---|---|---|---|---|---|
| PHE categorisation of infection sites (scenario P1) |
Model with damped effect (scenario G1) |
1 (R1) | 66 | 112 | 446 | 49 | 673 |
| 5 (R2) | 64 | 109 | 432 | 48 | 653 | ||
| 10 (R3) | 61 | 107 | 414 | 47 | 630 | ||
| 30 (R4) | 51 | 95 | 343 | 42 | 531 | ||
| Model without damped effect (scenario G2) |
1 (R1) | 137 | 231 | 921 | 101 | 1390 | |
| 5 (R2) | 132 | 225 | 885 | 98 | 1340 | ||
| 10 (R3) | 125 | 218 | 839 | 95 | 1277 | ||
| 30 (R4) | 98 | 189 | 656 | 83 | 1026 | ||
| Clinical advisors’ categorisation of infection sites (scenario P2) |
Model with damped effect (scenario G1) |
1 (R1) | 460 | 179 | 446 | 49 | 1134 |
| 5 (R2) | 446 | 175 | 432 | 48 | 1101 | ||
| 10 (R3) | 427 | 171 | 414 | 47 | 1059 | ||
| 30 (R4) | 354 | 153 | 343 | 42 | 892 | ||
| Model without damped effect (scenario G2) |
1 (R1) | 950 | 370 | 921 | 101 | 2342 | |
| 5 (R2) | 913 | 361 | 885 | 98 | 2257 | ||
| 10 (R3) | 866 | 349 | 839 | 95 | 2149 | ||
| 30 (R4) | 677 | 303 | 656 | 83 | 1719 |
Hospital-acquired pneumonia/VAP and BSIs are the key drivers of population-level benefit consistently across all scenarios due to the population size. The impact of the population size is evident when comparing results across different scenarios, where different categorisations of specimen types (which determine the baseline number of infections) have the greatest impact, changing the total 20-year population INHE from between 531 and 1390 to between 892 and 2342 QALYs. Population growth impacts population-level INHE to a greater extent than resistance, as shown by the red and black lines which represent different population growth scenarios diverging more than the solid and dashed lines which represent different resistance scenarios. Resistance between 1% and 10% results in similar total INHE.
We also estimated how much of the value of CAZ-AVI accrues to patients initiating treatment in the first 10 years of use, as this is the period of the contract for the delinked payment. Full results are presented in Appendix 9.2, Table 61. Across scenarios relating to baseline population, population growth and resistance emergence, the proportion of value that accrues in the first 10 years of use is 41–65%. With the exception of the scenarios examining very high rates of emergence to resistance, the proportion of value accruing in the first 10 years is less than might be expected for other pharmaceuticals. For a pharmaceutical where population size is expected to be stable over time we would expect 59% of the value to accrue in the first 10 years.
Following a request from NICE, we also assessed the impact on the population-level results of using a 1.5% discount rate. These results reflect an assumption of zero emergence of resistance to CAZ-AVI and are intended to give an indication of the broad effect of a lower discount rate. Across the scenarios relating to population size and population growth the 20-year population-level INHE ranged from 866 to 3136 when using a 1.5% discount rate. This indicates a substantive increase compared to the results observed using a 3.5% discount rate.
There is a large degree of uncertainty around the population-level INHEs of CAZ-AVI. The distribution of population INHEs for two population size scenarios (P1G1, P2G2) under a scenario of no resistance emergence to CAZ-AVI is shown in Figure 15. The distribution of population INHE reflects the patient-level INHE parameter uncertainty discussed in OXA-48 empiric setting HAP/VAP and OXA-48 microbiology-directed setting HAP/VAP and cUTI, as well as uncertainty in the rate of population growth over time. The difference in dispersion (range) between two histograms indicates the uncertainty in population growth between the two scenarios.
FIGURE 15.
Distribution of total population INHEs of CAZ-AVI (2000 simulations). P1G1, baseline population (point estimate) based on PHE categorisation of infection sites, growth rate damped (uncertain); P2G2, baseline population (point estimate) based on clinical advisors’ categorisation of infection sites, growth rate not damped (uncertain); CrI, credible interval.
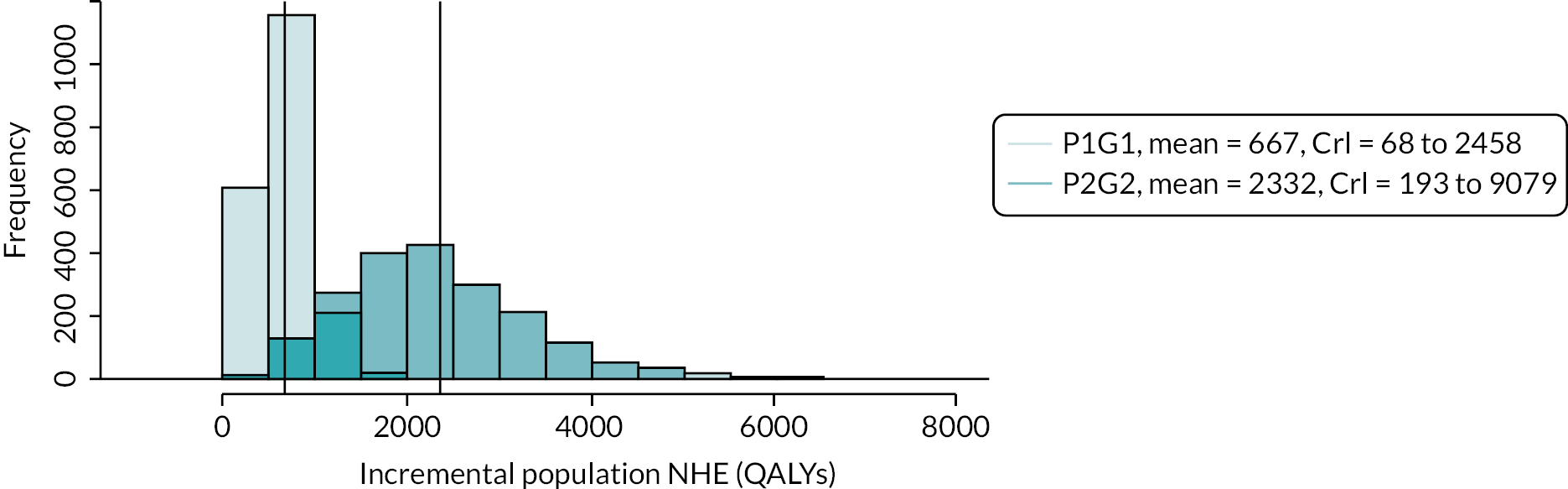
An additional scenario presented in Appendix 9.3 was provided to reflect the population-level benefit when a proportion of patients (20–40%) who, despite being susceptible to colistin/aminoglycosides, would instead be given salvage therapy due to the risk of colistin/aminoglycoside toxicity, in the absence of CAZ-AVI. The results of this scenario are presented in detail in Appendix 9.3, Table 62. Population-level INHE (see Appendix 3, Table 64 and Figure 44) increased from a base case range of 629–2211 QALYs to 1035–3833 QALYs if 20% of patients who are susceptible to colistin/aminoglycosides do not receive these treatments due to toxicity concerns. This increases to 1441–5456 if the proportion of patients increases to 40%.
These expected population-level INHEs may overestimate the total INHE for several reasons. Firstly, the 20–40% proportion of patients who would not be given colistin/aminoglycosides because of toxicity fears in the absence of CAZ-AVI is high compared to the assessment of the clinical advisors consulted by EEPRU. Secondly, the scenario assumes that outcomes in patients who can and cannot take colistin/aminoglycosides are comparable when, in practice, patients who cannot take colistin may have poorer prognoses than patients who can. Thirdly, the scenario assumes patients would be contraindicated to colistin and aminoglycosides, but clinical advisors to EEPRU (and consultation comments from the British Infection Association) suggested that most of the concern is about colistin.
Finally, the scenario results represent the benefit in HVCSs when, in the ES, all patients with suspected OXA-48 infection are treated with colistin/aminoglycosides. In the EEPRU base case, the empiric treatment with non-colistin/glycoside therapy had a higher patient-level net benefit (and lower incremental benefit of CAZ-AVI) than treatment with colistin/glycosides, suggesting that, without CAZ-AVI, non-aminoglycosides are the preferred empiric treatment.
Results showing the combined effect of uncertainty at the patient and population level are presented in Appendix 9.5, Table 65.
Additional elements of value relevant to AMs
Conceptualisation of additional elements of value
The conceptualisation of each additional element of value and how these additional elements of value may influence the INHEs associated with CAZ-AVI are presented in Table 30. These reflect the different viewpoints on the additional elements of value found in the literature, presented by the manufacturer, and discussed by the clinical advisors and other stakeholders in this project.
| Element of value | What this represents | Specific pathways to INHEsa |
|---|---|---|
| Enablement value | Impact on population health from additional medical procedures being possible as a result of CAZ-AVI being available to manage otherwise resistant infections with few alternative treatment options. |
|
| Diversity value | Impact on population health over time as a result of CAZ-AVI being available and adding to the range of treatments currently available. This can result in a reduction in selection pressure on and resistance to other available treatments, hence retaining their effectiveness for longer. |
|
| Insurance value | Insurance value is presented in the literature in different ways.12 One relates to the impact on population health over time as a result of CAZ-AVI being ‘held back’ in reserve until resistance to existing treatments effectively eliminates the latter as options. Resistance to CAZ-AVI would be limited due to being used less. A second meaning is that CAZ-AVI would ameliorate a potentially catastrophic situation where multidrug resistance becomes so widespread that CAZ-AVI is the only option across a large number of clinical scenarios. This is a low-probability but high-consequence outcome. |
|
| Transmission value | The impact on population health over time as a result of CAZ-AVI reducing the rate of transmission of a given pathogen from patients treated with that product to other individuals, potentially reducing the rate of resistant infections. |
|
| Spectrum value | Benefits of CAZ-AVI replacing broad-spectrum AMs and the problems associated with their over-use: potential collateral damage to the human microbiome resulting in a greater chance of developing resistance to AMs used in the future. |
|
The manufacturer also discussed productivity and fiscal benefits associated with the use of CAZ-AVI. These are not considered within the NICE reference case, and it is not clear why AMs would be considered differently with respect to these effects.
Importance and quantification of additional elements of value
Enablement value
Improved treatment of pre- and post-operative MDR infections is included within our HVCS and expected usage projections. There is some uncertainty as to whether the full benefits of treatment of pre-operative infections are reflected within our analysis. We assume that all patients who are alive at 30 days experience the same survival. If, however, the speed of resolution of an infection influences whether a procedure or treatment can go ahead, then it is possible that 30-day survival is longer for patients whose infection resolves more quickly as they may be more likely to receive procedures. The magnitude of this effect is uncertain due to uncertainties about the number of patients who experience infections pre-operatively, the impact of infection duration on the likelihood that operations will go ahead, and the implications of operations not going ahead (which will depend on the type of procedure, and whether the procedure is not conducted at all or delayed).
Enablement value may be also realised if the risk of MDR infection and clinicians’ ability to treat a MDR infection influences a decision about whether to bring a patient in for a procedure. An example of this scenario was provided by our clinical advisory group, whereby if a MDR infection is known to be circulating in a haematology unit, certain patients may not receive planned procedures or treatments. This is particularly likely to apply for patients in whom existing antibiotics for MDR infections are not an option. Here, the specific example of myeloma patients was highlighted as myeloma patients are predisposed to renal impairment, which rules out key effective treatments for MDR infections such as colistin. There is uncertainty with respect to the number of patients who would be affected as this would depend on both the number of patients whose treatment would be impacted by an outbreak and the frequency of outbreaks in key units such as haematology. There is also uncertainty about the consequences for patients not receiving planned therapy, as this will depend on the nature of the procedure/treatment and whether therapy is not received at all or delayed. These effects are not captured within the EEPRU modelling or any quantitative assessments submitted by the manufacturer.
A related way in which enablement value may be realised is if the availability of effective treatments for MDR infections allows wards to be kept open in the face of outbreaks. EEPRU considers it unlikely that CAZ-AVI would have this effect as most patients with drug-resistant infections do have alternative (albeit more toxic) treatment options – namely colistin. These effects are not captured within the EEPRU modelling or any quantitative assessments submitted by the manufacturer.
A final way in which enablement value may be realised is by use of CAZ-AVI freeing up healthcare resources. For example, use of CAZ-AVI may reduce time in hospital (alleviating pressure on beds), including time in the ICU/HDU. This may be particularly important where patients with MDR infections consume additional resources and staff time due to the need for additional infection-control procedures, including isolation measures. Any freed-up resources can then provide care for other patients within the hospital. To the extent possible, the impact of CAZ-AVI on resource use has been captured in the EEPRU modelling. When calculating the INHEs of CAZ-AVI we have translated cost savings to health benefits using standard measures of health opportunity cost (which allow monetary savings in healthcare resources to be translated to health gains across the NHS).
Diversity value
Our clinical advisors indicated that, within the HVCS, diverse prescribing strategies (e.g. randomly allocating patients with similar clinical indications to different treatments) were unlikely to be appropriate given the lack of safe and effective alternative treatments. They were not supportive of the use of CAZ-AVI in broader populations as part of a diverse prescribing strategy due to the desire to reduce emergence of resistance to CAZ-AVI and concerns that the evidence for diverse prescribing was uncertain. This is in contrast to the views of the manufacturer, who emphasised the potential for CAZ-AVI to be used alongside other therapeutic options in patients at high risk of a resistant infection. Diverse prescribing strategies were not, therefore, included in our quantitative assessments of population INHEs. Diverse prescribing strategies were included in the quantitative modelling presented by the manufacturer. However, as presented in Review of manufacturer’s model for CAZ-AVI, EEPRU has concerns about the extent to which that modelling appropriately reflected likely uses of CAZ-AVI within the NHS, the conceptualisation of the model and the lack of clarity about what was driving the model results. No information was presented by the manufacturer on the extent to which diversity value was driving the model results.
There is uncertainty about how reduced use of existing agents (e.g. colistin) due to availability of the CAZ-AVI will contribute to the emergence of resistance to these drugs. Due to these uncertainties this was not reflected in the EEPRU modelling. If reduced use of existing agents reduces resistance to existing drugs within areas of expected usage for CAZ-AVI this will reduce the INHEs associated with CAZ-AVI; however, if resistance reduces outside areas of expected usage for CAZ-AVI this will increase the INHEs associated with CAZ-AVI. Given the potential for these countervailing effects, and the wide range of factors driving resistance to existing drugs, this is not expected to have a large impact on INHEs. Again, this was captured within the manufacturer’s quantitative modelling but the same caveats apply.
Insurance value
The scenarios modelled can be considered to reflect this form of insurance value as they involve heavily restricting usage to preserve long-term effectiveness.
It is generally agreed that the value of CAZ-AVI will depend on the trajectory of emergence of MDR infections over time. Within the HVCS we have used statistical forecasting methods and explored uncertainty around these to understand the possibility that CAZ-AVI results in the avoidance of significant/catastrophic health losses. This is presented as distributions of population INHEs to inform the committee’s deliberations about whether avoidance of these extreme events should be considered differentially to other forms of health losses.
There is uncertainty around whether these distributions adequately reflect the uncertainty around high-consequence/low-probability outcomes. There are several reasons why this may not fully quantify longer-term benefits:
-
We may see higher levels of resistance to existing drugs within the areas of expected usage over time.
-
We may see MDR pathogens, against which the new drugs are effective, emerge that are currently rare or even unknown.
-
We may see pathogens that are currently treatable with existing therapies (and are not, therefore, included in the areas of expected usage) become resistant.
If one or more of these factors emerge, they would be expected to occur in the long term and quite possibly beyond 20 years.
Conducting quantitative modelling of these effects is unavoidably highly speculative. However, on request from the NICE committee, EEPRU developed an additional scenario to explore the magnitude of these effects. The scenario aimed to assess the effect on INHEs of CAZ-AVI in the case of emergence of multiresistant pathogens against which CAZ-AVI l is the only effective treatment and, in that product’s absence, clinicians would be forced to use multidrug salvage therapy. A simple Excel tool was developed to explore the potential magnitude of these effects informed by parameters obtained from the NICE Committee. This showed an additional benefit of 0.8–58.4 QALYs, which is low relative to other expected benefits of CAZ-AVI as estimated by the main analysis (896–3559 QALYs). This reflects the low likelihood of the emergence of a highly resistant strain and the low number of individuals affected by the strain in the medium term. Further details of the methods and results of this additional analysis are presented in Appendix 9.5, Tables 66–68.
Transmission value
Our clinical advisors indicated that the direction of effect of introduction of CAZ-AVI on transmission was uncertain, but that overall, the magnitude of effect was expected to be small. This reflects the fact that introducing a new effective drug for the treatment of MDR infections has a number of countervailing effects. If the drugs reduce time in hospital this is expected to reduce transmission. However, among MDR patients with poor prognosis, more effective treatments may, feasibly, increase time spent in hospital by reducing mortality. In addition, where use of the new drugs reduces mortality this will increase the number of people returning colonised to the community as CAZ-AVI was considered unlikely to eradicate colonisation by the clinical advisors to this project. This may contribute to increased transmission in the community or via further hospitalisations in this highly comorbid population.
The key drivers of transmission of OXA-48 Enterobacterales, are broad and driven by transmission in populations beyond the HVCS (e.g. colonised individuals in the community and in the hospital, and importation of drug resistance from abroad), making this a challenging area to model. Given the views of our clinical advisors that this would not be a key driver of population INHE and these modelling challenges we did not attempt to quantify transmission value using transmission modelling.
To support the committee in its decision-making, we do, however, provide a summary of the impact of each drug on time in hospital and time alive post discharge. Briefly, CAZ-AVI led to a short reduction in the hospital LoS of 0–1.1 days, and increased the length of life by up to 33 days (0.05–0.09 years). We note that time post discharge is likely to include further periods spent in hospital given the patient population though we did not quantify these.
A number of advisors discussed the substantial impact of outbreaks of MDR infections in terms of disrupting healthcare provision and incurring large costs due to the need for more extensive infection-control measures. However, no evidence was provided that CAZ-AVI would substantially impact on the likelihood of an outbreak or its spread. The possibility of outbreaks leading to large numbers of cases and the additional potential value of CAZ-AVI as a treatment in this scenario are discussed under insurance value.
Transmission effects were included in the quantitative modelling presented by the manufacturer. However, as presented in Review of manufacturer’s model for CAZ-AVI, EEPRU has concerns about the extent to which that modelling appropriately reflected likely uses of CAZ-AVI within the NHS, the conceptualisation of the model, and the lack of clarity about what was driving the model results. No information was presented by the manufacturer on the extent to which transmission value was driving the model results.
Spectrum value
Our clinical advisors and other stakeholders did not consider spectrum value to be a significant consideration for CAZ-AVI, which has a broad spectrum of activity. Therefore, this was not considered in our quantitative assessments of population INHE.
Summary
Table 31 summarises where EEPRU has been able to quantify the additional elements of value and, for those elements where this has not been feasible, provides an indication of their likely importance. Overall, EEPRU considers that the main areas of uncertainty are enablement value, transmission value and insurance value. EEPRU considers it unlikely that transmission value is a significant driver of population INHE, though this remains an area of uncertainty. EEPRU considers that it is possible that, by treating pre-operative infections and offering the possibility of an effective low-toxicity option for treating MDR infections, CAZ-AVI will facilitate additional or at least more prompt receipt of required treatments/procedures for certain groups. EEPRU considers that the magnitude of these population INHEs remains highly uncertain.
| Element of value | Specific pathways to INHEs | Quantified in HVCS? EEPRU assessment of importance if not quantified. |
|---|---|---|
| Enablement value |
|
Quantified in HVCS and extrapolation to expected usage |
|
Partially quantified in HVCS and extrapolation to expected usage (area of uncertainty) | |
|
Potential significant driver of population INHEs (area of uncertainty) | |
|
Unlikely to be significant driver of population INHEs | |
|
Quantified in HVCS, and in an additional scenario | |
| Diversity value |
|
Diverse prescribing not considered appropriate for CAZ-AVI |
|
Unlikely to be significant driver of population INHEs | |
| Insurance value |
|
Quantified in HVCS |
|
Quantified in HVCS (though no differential valuation applied) | |
| Transmission value |
|
Unlikely to be significant driver of population INHEs (area of uncertainty) |
| Spectrum value |
|
Unlikely to be significant driver of population INHEs |
Chapter 9 Discussion and conclusion
Table 32 summarises the patient-level INHEs for CAZ-AVI in the HVCS. The benefits of CAZ-AVI are driven by similar susceptibility but improved safety compared to colistin/aminoglycoside-based treatments, and, in the ES, by higher susceptibility than non-colistin/aminoglycoside-based treatment. The two most significant sources of uncertainty relate to the ES and are (1) the preferred source of susceptibility evidence and (2) the proportion of patients in the ES who are suspected of having OXA-48 Enterobacterales who are later confirmed to have this resistant pathogen. Using the results of the susceptibility evidence synthesis that included all studies regardless of breakpoints (EUCAST or CLSI) and using the single Vazquez-Ucha study to inform susceptibility increased the patient-level INHEs from 0.016 up to 0.22 and 0.26 QALYs, respectively, as susceptibility to CAZ-AVI relative to comparators is higher in these scenarios. Conversely, if the proportion of individuals suspected to have an infection caused by OXA-48 Enterobacterales who are confirmed to have this pathogen–mechanism falls to 10% the patient-level INHEs fall to 0.08 QALYs.
| Empiric setting HAP/VAP | Microbiology-directed setting HAP/VAP | Microbiology-directed setting cUTI | |
|---|---|---|---|
| OXA-48 Enterobacterales | 0.16 (0.00–0.26) | 0.08 (0.05–0.12) | 0.08 (0.05–0.12) |
In addition to these uncertainties, the modelling approach makes a number of important assumptions which were not amenable to sensitivity analysis or scenario testing within the scope of this project: (1) patients with intermediate resistance are assumed to respond as per those with resistant infections; (2) patients receiving multi-AM regimens perform as well if they are susceptible to one component, two components or more components of the regimen; (3) the use of meropenem in OXA-48 Enterobacterales confers no clinical benefit; (4) patients’ AM susceptibility remains stable between the empiric and MDS; and (5) patients who are suspected to have OXA-48 Enterobacterales who have another pathogen–mechanism are broadly susceptible and experience the same outcomes regardless of the choice of empiric treatment. We also did not account for uncertainties relating to the availability or usage of other agents in the future – for example, since the current project was completed, evidence has emerged that supports a role for CAZ-AVI combined with aztreonam in MBL Enterobacterales,164,165 widening the potential usage of CAZ-AVI.
Due to the scope of work required to produce the population-level estimates of INHE, comprehensive reviews were not possible for all parameters, and it is possible that additional evidence was missed. In particular, we were reliant on existing systematic reviews and meta-analyses to quantify the safety implications of alternative treatments. A preferred approach would have been to conduct a de novo systematic review and synthesis tailored to the current decision problem; however, this was not feasible. There were limitations to the evidence underpinning the model and, in particular, the surrogacy relationships between susceptibility and mortality/hospitalisation were informed by a combination of evidence of associations at the individual patient level, and structured expert elicitation.
Policy Research Unit in Economic Methods of Evaluation in Health and Social Care Interventions were unable to select a base case for the population-level results. Population-level results are, therefore, presented for two different approaches to estimating current OXA-48 Enterobacterales infection numbers (based on different methods to classify infections from clinical specimen sites), two alternative approaches to forecasting increases in infections over time (based on whether observed trends are assumed to persist indefinitely or not), and three different trajectories with respect to resistance emergence (1%, 5% and 10% at 20 years). These results are summarised in Table 33.
| Baseline population | Population growth rate | Predicted patients initiating CAZ-AVI over 20 years | Range of population INHEs across resistance scenarios 1%, 5% and 10% at 20 years (base-case assumptions used for patient-level model) |
|---|---|---|---|
| PHE categorisation of infection sites | Model with damped trends | 5287 | 531–673 |
| Model with persistent trends | 11,742 | 1026–1390 | |
| Clinical advisors’ categorisation of infection sites | Model with damped trends | 9056 | 892–1134 |
| Model with persistent trends | 20,112 | 1719–2342 |
Table 33 shows that assumptions about baseline population size and growth are strong drivers of population INHEs, which vary from 531 to 2342 QALYs depending on the scenario. The results are particularly sensitive to the assumption about which clinical specimen sites are indicative of HAP/VAP, with the more conservative definition provided by PHE indicating 24 suspected OXA-48 HAP/VAP infections per annum, and the broader definition provided by our clinical advisors indicating 166 suspected OXA-48 HAP/VAP infections per annum.
Departures from the base-case assumptions in the patient-level model also had substantive effects on population INHEs, as did the additional scenario where, without CAZ-AVI, a proportion of patients cannot take colistin and other aminoglycoside treatments and, therefore, without the new drug, would receive multidrug salvage therapy.
The population size estimates used to generate the estimates of population INHEs are subject to considerable uncertainties relating to the completeness of the national data, how accurately specimen types represent the infection sites of interest, whether all tested patients would fall within the HVCS population for empiric treatment, the potential double counting of samples from the same infectious episode, and inherent uncertainties in forecasting population size over time.
In addition, estimates of population INHEs were generated using a number of strong assumptions about how evidence can be generalised between settings. Namely, that patient-level INHEs of CAZ-AVI in patients with BSI can be approximated based on outcomes in HAP/VAP patients, and that the patient-level INHE of CAZ-AVI in patients with intra-abdominal infections can be proxied by that in patients with cUTIs. These assumptions were based on discussions with clinical experts.
Table 34 summarises where EEPRU has been able to quantify the additional elements of value and, for those elements where this has not been feasible, provides an indication of their likely importance. Overall, EEPRU considers that the main areas of uncertainty are enablement value and transmission value. EEPRU considers it unlikely that transmission value is a significant driver of population INHE, though this remains an area of uncertainty. EEPRU considers that it is possible that, by treating pre-operative infections and offering the possibility of an effective low-toxicity option for treating MDR infections, CAZ-AVI will facilitate additional or at least more prompt receipt of required treatments/procedures for certain groups. EEPRU considers that the magnitude of these population INHEs remains highly uncertain.
| Element of value | Summary of importance in modifying quantitative estimates of population INHEs |
|---|---|
| Enablement value | Benefits of improved treatment of post-operative infections quantified Benefits of improved treatment of pre-operative infections partially quantifieda Benefits of increasing number of procedures that can go ahead not quantifieda Benefits of keeping wards open during MDR infection outbreaks unlikely to be a significant driver of population INHEs Benefits of reduced use of hospital resources quantified |
| Diversity value | Unlikely to be a significant driver of population INHEs |
| Insurance value | Benefit in HVCSs quantified. Benefit in novel, hypothetical outbreaks highly uncertain. |
| Transmission value | Unlikely to be a significant driver of population INHEsa |
| Spectrum value | Unlikely to be a significant driver of population INHEs |
Equality, diversity and inclusion: we sought to identify data sources that were representative of the patients within the HVCSs, and used nationally representative data wherever possible. This research emphasised the high level of comorbidities among people with drug-resistant infections; further work should ensure that research in these populations reflects these comorbidities.
Patient and public involvement: there was no patient or public involvement for this research.
Conclusion
The quantitative assessment of value in this report indicates that CAZ-AVI is associated with a base-case population INHE across its areas of expected usage of 531–2342 QALYs over 20 years. These quantitative assessments of value were informed by a series of interlinked decision-analytic models informed by evidence collated via systematic reviews of the literature and evidence synthesis, additional national data provided by PHE, structured expert elicitation and, where necessary, assumptions informed by clinical opinion.
This work has provided quantitative estimates of the value of CAZ-AVI within its areas of expected usage within the NHS. The results indicate that the maximum amount the NHS could pay for CAZ-AVI was £11 million to £47 million if the health lost as a result of making these payments rather than funding other NHS services is not to exceed the health benefits of using this antimicrobial. The high level of uncertainty could be addressed via further research (see Chapter 10). An important question is whether this and other post-approval evidence should inform adjustments to payments. Although this would better align payments with value delivered to the NHS, it would add additional uncertainty to payments to manufacturers in a context where investment conditions are already considered unfavourable. Further research is required to assess the potential costs and benefits of conditional reimbursement in this context. A broader and important question is ‘what would represent the ‘optimal’ scope of usage for CAZ-AVI?’ Further methodological and quantitative work is required to address this question.
Chapter 10 Recommendations for future research
Our recommendations for further research (in priority order) are:
-
Data linkage studies linking patient-level clinical, prescribing and laboratory data
Evaluations of new AMs, and indeed of many anti-AMR interventions, would benefit from linked national-level clinical, prescribing and laboratory (microbiology) data. This would facilitate improved estimates of the relationship between in vitro susceptibility to an antimicrobial treatment and relevant outcomes in people with MDR infections. It would also provide improved estimates of the patterns of resistance across the UK to identify likely areas of expected usage, the number of patients with specific types of MDR infections, and emerging threats.
-
Post-approval routine randomisation to assess clinical effectiveness
The reliance on in vitro susceptibility evidence (linked to other data sources) to infer clinical effectiveness and safety is a major source of uncertainty in the current evaluation. The lack of relevant clinical data for cefiderocol in MDR infections is problematic not only within the current evaluation which was designed to inform payment, but also for clinicians who need to trade-off the risks and benefits of alternative therapeutic choices. The use of post-approval routine randomisation (e.g. using novel trial designs166) should be supported to improve the evidence base informing AM choice for MDR infections.
-
Improved methods for the conduct, review and synthesis of susceptibility studies
Susceptibility study conduct, reporting and appraisal could be improved by the development of reporting guidelines (similar to those provided by PRISMA and CONSORT) and quality-assessment tools. To inform appropriate choices when synthesising susceptibility evidence, further research is warranted to assess the comparability of different laboratory methods and clinical breakpoints, and the appropriateness of applying newer breakpoints to historical data.
-
Methods to quantify the enablement benefits of new antimicrobials
An important potential benefit of new antibiotics is in ensuring that patients’ infections are managed so that planned medical procedures and treatments unrelated to these infections can go ahead. Data collection [e.g. data from the UK Antimicrobial Registry (UKAR) on occurrence of procedures following CAZ-AVI] and decision models should be developed to assess the magnitude of these benefits.
-
Methods for quantifying the benefits and costs associated with different usage scenarios
An important question is: how extensively should new antimicrobials be used? More extensive use may deliver benefits to a wider set of patients in the short term but will be associated with higher levels of resistance emergence over time. Further work is required to quantify the nature of these trade-offs; this requires decision modelling and further clinical and epidemiological research to quantify the relationship between AM usage and resistance emergence.
-
Methods for quantifying the benefits and costs of conditional reimbursement
Post-approval evidence is likely to improve estimates of the value of new antimicrobials. In principle this could inform revisions to payment levels over time. Further research is required to assess the appropriate design of conditional reimbursement approaches for AMs, and whether the benefits of aligning payment with value exceed the disadvantages in terms of exposing manufacturers to additional revenue risk and potentially discouraging investment in AM development.
Additional information
Contributions of authors
Sue Harnan (https://orcid.org/0000-0002-9318-9206) (Senior Research Fellow) was responsible for the day-to-day management of the systematic review of clinical efficacy data, designed and conducted the systematic review of clinical efficacy data and was responsible for drafting the clinical efficacy review sections of the report, including the discussion.
Ben Kearns (https://orcid.org/0000-0001-7730-668X) (Research Fellow) designed and conducted the economic modelling for the population-level component of the model and was responsible for drafting these sections of the report.
Alison Scope (https://orcid.org/0000-0003-1604-1758) (Research Fellow) contributed to the design and conduct of the systematic review of clinical efficacy, drafted some of the clinical review sections of the report and reviewed other sections of the clinical review.
Laetitia Schmitt (https://orcid.org/0000-0003-1052-488X) (Research Fellow) designed and conducted the economic modelling for patient-level outcomes.
Dina Jankovic (https://orcid.org/0000-0002-9311-1409) (Research Fellow) conducted the expert elicitation, the literature searches that informed the structure of the patient-level economic model with Laetitia Schmitt and Claire Rothery, conducted modelling of population-level outcomes, drafted the relevant sections of the report and performed model validation.
Jean Hamilton (https://orcid.org/0000-0003-3326-9842) (Research Fellow) designed and conducted the network meta-analysis and was responsible for drafting those sections of the report.
Tushar Srivastava (https://orcid.org/0000-0002-5961-9348) (Research Associate) contributed to literature searches for the economic modelling and the analyses for the population-level component.
Harry Hill (https://orcid.org/0000-0002-0908-5595) (Research Fellow) contributed to analyses for the population-level component.
Chu Chang Ku (https://orcid.org/0000-0002-4719-117X) (Research Associate) contributed to modelling for both the patient-level and population-level components.
Shijie Ren (https://orcid.org/0000-0003-3568-7124) (Senior Research Fellow) designed and conducted the network meta-analysis and was responsible for drafting those sections of the report.
Claire Rothery (https://orcid.org/0000-0002-7759-4084) (Senior Research Fellow) designed the literature searches that informed the model structure and provided support with scoping of the project and drafting of the report.
Laura Bojke (https://orcid.org/0000-0001-7921-9109) (Professor) led the design and conduct of the expert elicitation and was responsible for drafting those sections of the report.
Mark Sculpher (https://orcid.org/0000-0003-3746-9913) (Professor) was jointly responsible for the day-to-day management of the project and development of the work elements. He was responsible for drafting specific report sections.
Beth Woods (https://orcid.org/0000-0002-7669-9415) (Senior Research Fellow) was jointly responsible for the day-to-day management of the project and development of the work elements. She led the design of the economic model and conducted modelling for the patient-level and extrapolation components of the model and was responsible for drafting these sections of the report, as well as the discussion.
Acknowledgements
The views expressed are those of the authors and not necessarily those of the NHS, the National Institute for Health and Care Research, the Department of Health and Social Care or its arm’s-length bodies, or other UK government departments. We are grateful for the support of our clinical advisors: Professors David Jenkins, William Hope, Philip Howard, Colm Leonard, Mark Wilcox, and Drs Alan Ashworth and Andrew Bentley. Thanks for modelling advice to Professor Mark Jit and Dr Gwen Knight; and for comments on drafts we thank Professor Allan Wailoo, Dr James Fotheringham, Professor Simon Dixon, Rita Neves De Faria and Professor Stephen Palmer. We are also grateful for support from Sarah Gerver and Rebecca Guy at UK Health Security Agency (formerly Public Health England). Finally, we thank Marrissa Martyn-St-James, Kath Devlin, Kay Fountain, Tim Glover, Ruth Helstrip, Liz Mclintock, Donna Davis, Steph Richards and Alex Rollinger for their support in developing this report. Any errors are the responsibility of the authors.
Data-sharing statement
The only primary data collection for this study related to the expert elicitation; ethics approval for this element of the study does not permit data sharing. All queries should be sent to the corresponding author.
Ethics statement
Ethics approval for the expert elicitation exercise was granted from the University of York Department of Health Sciences Research Governance committee (reference number: HSRGC/2021/448/G; date of approval: 14 May 2021). No other activities required primary data collection, so no further ethics approval was required.
Information governance statement
The University of York is committed to handling all personal information in line with the UK Data Protection Act (2018) and the General Data Protection Regulation (EU GDPR) 2016/679. Under the Data Protection legislation, the University of York is the Data Controller, and you can find out more about how we handle personal data, including how to exercise your individual rights and the contact details for our Data Protection Officer, here: www.york.ac.uk/records-management/dp/.
Disclosure of interests
Full disclosure of interests: Completed ICMJE forms for all authors, including all related interests, are available in the toolkit on the NIHR Journals Library report publication page at https://doi.org/10.3310/YAPL9347.
Primary conflicts of interest: All authors declare funding for the current work from the National Institute for Health and Care Research (NIHR) Policy Research Programme, conducted through the Policy Research Unit in Economic Methods of Evaluation in Health and Social Care Interventions, PR-PRU-1217-20401. Beth Woods sits on the Board of the York Health Economics Consortium, a private sector company (role not remunerated). Beth Woods sits on the HTA Clinical Evaluation and Trials Committee 2020–4. Claire Rothery sits on the HTA Commissioning Committee 2021–5. Laura Bojke sat on the NICE Technology Appraisals committee B 2019–22. Laura Bojke is a member of the HS&DR Committee, NIHR 2019 to present. Mark Sculpher has been a paid consultant to various life sciences companies, none relating to antimicrobials.
Disclaimers
This article presents independent research funded by the National Institute for Health and Care Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, the HTA programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, the HTA programme or the Department of Health and Social Care.
References
- Hawkey PM, Warren RE, Livermore DM, McNulty CAM, Enoch DA, Otter JA, et al. Treatment of infections caused by multidrug-resistant Gram-negative bacteria: report of the British Society for Antimicrobial Chemotherapy/Healthcare Infection Society/British Infection Association Joint working party. J Antimicrob Chemother 2018;73:iii2-78.
- Munita JM, Arias CA. Virulence Mechanisms of Bacterial Pathogens. New York: John Wiley & Sons; 2016.
- Hawkey PM. Multidrug-resistant Gram-negative bacteria: a product of globalization. J Hosp Infect 2015;89:241-7.
- McNulty CAM, Boyle P, Nichols T, Clappison P, Davey P. Don’t wear me out: the public’s knowledge of and attitudes to antibiotic use. J Antimicrob Chemother 2007;59:727-38.
- Public Health England . English Surveillance Programme for Antimicrobial Utilisation and Resistance (ESPAUR) Report 2019 to 2020 2020.
- Hughes S, Gilchrist M, Heard K, Hamilton R, Sneddon J. Treating infections caused by carbapenemase-producing Enterobacterales (CPE): a pragmatic approach to antimicrobial stewardship on behalf of the UKCPA Pharmacy Infection Network (PIN). JAC-Antimicrobial Resistance 2020;2.
- World Health Organization . WHO Publishes List of Bacteria for Which New Antibiotics Are Urgently Needed 2017.
- World Health Organization . Global Priority List of Antibiotic-Resistant Bacteria to Guide Research, Discovery, and Development of New Antibiotics 2017.
- Tan X, Kim HS, Baugh K, Huang Y, Kadiyala N, Wences M, et al. Therapeutic options for metallo-β-lactamase-producing Enterobacterales. Infect Drug Resist 2021;14:125-42.
- Medicines.org.uk . Zavicefta 2 g 0.5 G Powder for Concentrate for Solution for Infusion – Summary of Product Characteristics (SPC) – (eMC) 2021. www.medicines.org.uk/emc/medicine/33061 (accessed 30 July 2024).
- European Medicines Agency . European Public Assessment Reports – Zavicefta – EMEA H C 004027 – II 0015 2021. www.ema.europa.eu/en/medicines/human/EPAR/zavicefta (accessed 30 July 2024).
- Rothery C, Woods B, Schmitt L, Claxton K, Palmer S, Sculpher M. Framework for Value Assessment of New Pharmaceuticals: Implications of alternative funding arrangements for NICE Appraisal. EEPRU; 2018.
- Pogue JM, Bonomo RA, Kaye KS. Ceftazidime/avibactam, meropenem/vaborbactam, or both? Clinical and formulary considerations. Clin Infect Dis 2019;68:519-24.
- Schäfer E, Malecki M, Tellez-Castillo CJ, Pfennigwerth N, Marlinghaus L, Higgins PG, et al. Molecular surveillance of carbapenemase-producing Pseudomonas aeruginosa at three medical centres in Cologne, Germany. Antimicrob Resist Infect Contr 2019;8:1-7.
- Tamma PD, Hsu AJ. Defining the role of novel β-lactam agents that target carbapenem-resistant Gram-negative organisms. J Pediatric Infect Dis Soc 2019;8:251-60.
- Public Health England . Framework of Actions to Contain Carbapenemase-Producing Enterobacterales 2020.
- Public Health England . UK Standards for Microbiology Investigations: Detection of Bacteria With Carbapenem-Hydrolysing β-Lactamases (Carbapenemases) 2020.
- Turnidge J, David L. Paterson Setting and Revising Antibacterial Susceptibility Breakpoints n.d. www.ncbi.nlm.nih.gov/pmc/articles/PMC1932754/ (accessed 15 August 2023).
- European Committee on Antimicrobial Susceptibility Testing . Setting Breakpoints for New Antimicrobial Agents, EUCAST SOP 1.3 2019. http://www.eucast.org/www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/EUCAST_SOPs/EUCAST_SOP_1.3_Setting_breakpoints_new_agents_20191023.pdf (accessed 30 July 2024).
- Harnan SE, Cooper K, Jones SL, Jones E. Pruning and prioritising: a case study of a pragmatic method for managing a rapid systematic review with limited resources. Evidence &Amp; Policy 2015;11:589-601.
- Uttley L, Whiteman BL, Woods HB, Harnan S, Philips ST, Cree IA. Early Cancer Detection Consortium . Building the evidence base of blood-based biomarkers for early detection of cancer: a rapid systematic mapping review. EBioMed 2016;10:164-73.
- Kaltenthaler E, Tappenden P, Paisley S, Squires H. NICE DSU Technical Support Document 13: Identifying and Reviewing Evidence to Inform the Conceptualisation and Population of Cost-Effectiveness Models. Sheffield: Decision Support Unit, ScHARR, University of Sheffield; 2011.
- Pfizer Inc . Antimicrobial Testing Leadership and Surveillance (ATLAS) n.d. https://atlas-surveillance.com/#/login (accessed 30 July 2024).
- Element . SENTRY Microbiology Visualization Platform (MVP) n.d. https://sentry-mvp.jmilabs.com/ (accessed 30 July 2024).
- Hoy D, Brooks P, Woolf A, Blyth F, March L, Bain C, et al. Assessing risk of bias in prevalence studies: modification of an existing tool and evidence of interrater agreement. J Clin Epidemiol 2012;65:934-9.
- Munn Z, Moola S, Lisy K, Riitano D, Tufanaru C. JBI Manual for Evidence Synthesis. JBI; 2020.
- Hinneburg I. ROBINS-1: a tool for asssessing risk of bias in non-randomised studies of interventions. Med Monatsschr Pharm 2017;40:175-7.
- Sterne JA, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 2019;366:1-8.
- Peterson J, Welch V, Losos M, Tugwell P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Ottawa: Ottawa Hospital Research Institute; 2011.
- Pfizer . Evidence Submission to NICE. Ceftazidime With Avibactam for Treating Severe Aerobic Gram-Negative Bacterial Infections 2021.
- Public Health England . OXA-48 Isolates 2021.
- Livermore DM, Mushtaq S, Warner M, Zhang J, Maharjan S, Doumith M, et al. Activities of NXL104 combinations with ceftazidime and aztreonam against carbapenemase-producing Enterobacteriaceae. Antimicrob Agents Chemother 2011;55:390-4.
- Deshpande L. North Liberty, IA: NICE; 2021.
- Kazmierczak KM, Bradford PA, Stone GG, de Jonge BLM, Sahm DF. In vitro activity of ceftazidime-avibactam and aztreonam-avibactam against OXA-48-carrying Enterobacteriaceae isolated as part of the International Network for Optimal Resistance Monitoring (INFORM) Global Surveillance Program from 2012 to 2015. Antimicrob Agents Chemother 2018;62.
- Vazquez-Ucha JC, Seoane-Estevez A, Rodino-Janeiro BK, González-Bardanca M, Conde-Pérez K, Martínez-Guitián M, et al. Activity of imipenem/relebactam against a Spanish nationwide collection of carbapenemase-producing Enterobacterales. J Antimicrob Chemother 2021;76:1498-510.
- Garcia-Castillo M, Garcia-Fernandez S, Gomez-Gil R, Pitart C, Oviaño M, Gracia-Ahufinger I, et al. iCREST Study Group . Activity of ceftazidime-avibactam against carbapenemase-producing Enterobacteriaceae from urine specimens obtained during the infection-carbapenem resistance evaluation surveillance trial (iCREST) in Spain. Int J Antimicrob Agents 2018;51:511-5.
- Longshaw C, Manissero D, Tsuji M, Echols R, Yamano Y. In vitro activity of the siderophore cephalosporin, cefiderocol, against molecularly characterized, carbapenem-non-susceptible Gram-negative bacteria from Europe. JAC: Antimicrob Resist 2020;2.
- Mataraci Kara E, Yilmaz M, Istanbullu Tosun A, Ozbek Celik B. Evaluation of the synergy of ceftazidime/avibactam in combination with colistin, doripenem, levofloxacin, tigecycline, and tobramycin against OXA-48 producing Enterobacterales. J Chemother 2020;32:171-8.
- Han R, Shi Q, Wu S, Yin D, Peng M, Dong D, et al. China Antimicrobial Surveillance Network (CHINET) Study Group . Dissemination of carbapenemases (KPC, NDM, OXA-48, IMP, and VIM) among carbapenem-resistant Enterobacteriaceae isolated from adult and children patients in China. Front Cell Infect Microbiol 2020;10.
- Soares MO, Bojke L, Dumville J, Iglesias C, Cullum N, Claxton K. Methods to elicit experts’ beliefs over uncertain quantities: application to a cost effectiveness transition model of negative pressure wound therapy for severe pressure ulceration. Stat Med 2011;30:2363-80. https://doi.org/10.1002/sim.4288.
- Kazmierczak KM, Tsuji M, Wise MG, Hackel M, Yamano Y, Echols R, et al. In vitro activity of cefiderocol, a siderophore cephalosporin, against a recent collection of clinically relevant carbapenem-non-susceptible Gram-negative bacilli, including serine carbapenemase- and metallo-beta-lactamase-producing isolates (SIDERO-WT-2014 Study). Int J Antimicrob Agents 2019;53:177-84.
- Viala B, Zaidi FZ, Bastide M, Dumont Y, Le Moing V, Jean-Pierre H, et al. Assessment of the in vitro activities of ceftolozane/tazobactam and ceftazidime/avibactam in a collection of beta-lactam-resistant Enterobacteriaceae and Pseudomonas aeruginosa clinical isolates at Montpellier University Hospital, France. Microb Drug Resist 2019;25:1325-9.
- De la Calle C, Rodriguez O, Morata L, Marco F, Cardozo C, García-Vidal C, et al. Clinical characteristics and prognosis of infections caused by OXA-48 carbapenemase-producing Enterobacteriaceae in patients treated with ceftazidime-avibactam. Int J Antimicrob Agents 2019;53:520-4.
- Galani I, Souli M, Nafplioti K, Adamou P, Karaiskos I, Giamarellou H, et al. Study Collaborators . In vitro activity of imipenem-relebactam against non-MBL carbapenemase-producing Klebsiella pneumoniae isolated in Greek hospitals in 2015–2016. Eur J Clin Microbiol Infect Dis 2019;38:1143-50.
- Sherry NL, Baines SL, Howden BP. Ceftazidime/avibactam susceptibility by three different susceptibility testing methods in carbapenemase-producing Gram-negative bacteria from Australia. Int J Antimicrob Agents 2018;52:82-5.
- Bhagwat SS, Hariharan P, Joshi PR, Palwe SR, Shrivastava R, Patel MV, et al. Activity of cefepime/zidebactam against MDR Escherichia coli isolates harbouring a novel mechanism of resistance based on four-amino-acid inserts in PBP3. J Antimicrob Chemother 2020;75:3563-7.
- Carmeli Y, Armstrong J, Laud PJ, Newell P, Stone G, Wardman A, et al. Ceftazidime-avibactam or best available therapy in patients with ceftazidime-resistant Enterobacteriaceae and Pseudomonas aeruginosa complicated urinary tract infections or complicated intra-abdominal infections (REPRISE): a randomised, pathogen-directed, phase 3 study. Lancet Infect Dis 2016;16:661-73.
- Torres A, Zhong N, Pachl J, Timsit J-F, Kollef M, Chen Z, et al. Ceftazidime-avibactam versus meropenem in nosocomial pneumonia, including ventilator-associated pneumonia (REPROVE): a randomised, double-blind, phase 3 non-inferiority trial. Lancet Infect Dis 2018;18:285-95.
- Vazquez JA, Gonzalez Patzan LD, Stricklin D, Duttaroy DD, Kreidly Z, Lipka J, et al. Efficacy and safety of ceftazidime-avibactam versus imipenem-cilastatin in the treatment of complicated urinary tract infections, including acute pyelonephritis, in hospitalized adults: results of a prospective, investigator-blinded, randomized study. Curr Med Res Opin 2012;28:1921-31.
- Wagenlehner FM, Sobel JD, Newell P, Armstrong J, Huang X, Stone GG, et al. Ceftazidime-avibactam versus doripenem for the treatment of complicated urinary tract infections, including acute pyelonephritis: RECAPTURE, a Phase 3 randomized trial program. Clin Infect Dis 2016;63:754-62.
- Alraddadi BM, Saeedi M, Qutub M, Alshukairi A, Hassanien A, Wali G. Efficacy of ceftazidime-avibactam in the treatment of infections due to carbapenem-resistant Enterobacteriaceae. BMC Infect Dis 2019;19.
- Katchanov J, Asar L, Klupp EM, Both A, Rothe C, König C, et al. Carbapenem-resistant Gram-negative pathogens in a German university medical center: prevalence, clinical implications and the role of novel beta-lactam/beta-lactamase inhibitor combinations. PLOS ONE 2018;13.
- Lim FH, Modha DE, Collins E, Westmoreland D, Ashton C, Jenkins DR. An outbreak of two strains of OXA-48 producing Klebsiella pneumoniae in a teaching hospital. Infect Prev Pract 2020;2.
- Sousa A, Perez-Rodriguez MT, Soto A, Rodríguez L, Pérez-Landeiro A, Martínez-Lamas L, et al. Effectiveness of ceftazidime/avibactam as salvage therapy for treatment of infections due to OXA-48 carbapenemase-producing Enterobacteriaceae. J Antimicrob Chemother 2018;73:3170-5.
- Temkin E, Torre-Cisneros J, Beovic B, Benito N, Giannella M, Gilarranz R, et al. Ceftazidime-avibactam as salvage therapy for infections caused by carbapenem-resistant organisms. Antimicrob Agents Chemother 2017;61.
- Nwankwo L, Butt Z, Schelenz S. Experience of ceftazidime/avibactam in a UK tertiary cardiopulmonary specialist center. Expert Rev Anti Infect Ther 2021;19:101-8.
- OPEN VIE Ltd . UK Draft Study Report: CARBAR – A Retrospective Study to Evaluate the Epidemiology, Standard of Care, Outcomes and Resource Use Associated With Patients Who Have or Are at Risk Of, Infection With Carbapenem Non-Susceptible Gram-Negative Organisms of Interest (Enterobacterales, Pseudomonas spp., Stenotrophomonas Spp. And Acinetobacter spp.) 2020.
- Karaiskos I, Daikos GL, Gkoufa A, Adamis G, Stefos A, Symbardi S, et al. Hellenic Ceftazidime/Avibactam Registry Study Group . Ceftazidime/avibactam in the era of carbapenemase-producing Klebsiella pneumoniae: experience from a national registry study. J Antimicrob Chemother 2021;76:775-83.
- de Jonge BL, Karlowsky JA, Kazmierczak KM, Biedenbach DJ, Sahm DF, Nichols WW. In vitro susceptibility to ceftazidime-avibactam of carbapenem-nonsusceptible Enterobacteriaceae isolates collected during the INFORM Global Surveillance Study (2012 to 2014). Antimicrob Agents Chemother 2016;60:3163-9.
- Dobias J, Denervaud-Tendon V, Poirel L, Nordmann P. Activity of the novel siderophore cephalosporin cefiderocol against multidrug-resistant Gram-negative pathogens. Eur J Clin Microbiol Infect Dis 2017;36:2319-27.
- Galani I, Karaiskos I, Karantani I, Papoutsaki V, Maraki S, Papaioannou V, et al. Study Collaborators . Epidemiology and resistance phenotypes of carbapenemase-producing Klebsiella pneumoniae in Greece, 2014 to 2016. Euro Surveill 2018;23.
- Karlowsky JA, Kazmierczak KM, Bouchillon SK, de Jonge BLM, Stone GG, Sahm DF. In vitro activity of ceftazidime-avibactam against clinical isolates of Enterobacteriaceae and Pseudomonas aeruginosa collected in Asia-Pacific countries: results from the INFORM Global Surveillance Program, 2012 to 2015. Antimicrob Agents Chemother 2018;62.
- Karlowsky JA, Kazmierczak KM, Bouchillon SK, de Jonge BLM, Stone GG, Sahm DF. In vitro activity of ceftazidime-avibactam against clinical isolates of Enterobacteriaceae and Pseudomonas aeruginosa collected in Latin American countries: results from the INFORM Global Surveillance Program, 2012 to 2015. Antimicrob Agents Chemother 2019;63.
- Livermore DM, Meunier D, Hopkins KL, Doumith M, Hill R, Pike R, et al. Activity of ceftazidime/avibactam against problem Enterobacteriaceae and Pseudomonas aeruginosa in the UK, 2015–16. J Antimicrob Chemother 2018;73:648-57.
- Livermore DM, Mushtaq S, Warner M, Vickers A, Woodford N. In vitro activity of cefepime/zidebactam (WCK 5222) against Gram-negative bacteria. J Antimicrob Chemother 2017;72:1373-85.
- Mavroidi A, Katsiari M, Likousi S, Palla E, Roussou Z, Nikolaou C, et al. Changing characteristics and in vitro susceptibility to ceftazidime/avibactam of bloodstream extensively drug-resistant Klebsiella pneumoniae from a Greek intensive care unit. Microb Drug Resist 2020;26:28-37.
- Mushtaq S, Garello P, Vickers A, Woodford N, Livermore DM. Activity of cefepime/zidebactam (WCK 5222) against ‘problem’ antibiotic-resistant Gram-negative bacteria sent to a national reference laboratory. J Antimicrob Chemother 2021;76:1511-22.
- Delgado-Valverde M, Del Carmen Conejo M, Serrano L, Fernandez-Cuenca F, Pascual A. Activity of cefiderocol against high-risk clones of multidrug-resistant Enterobacterales, Acinetobacter baumannii, Pseudomonas aeruginosa and Stenotrophomonas maltophilia. J Antimicrob Chemother 2020;75:1840-9.
- Public Health England . English Surveillance Programme for Antimicrobial Utilisation and Resistance (ESPAUR) Report 2018 to 2019 2020.
- Brown DFJ, Wootton M, Howe RA. Antimicrobial susceptibility testing breakpoints and methods from BSAC to EUCAST. J Antimicrob Chemother 2015;71:3-5.
- Dias S, Sutton AJ, Welton NJ, Ades AE. NICE DSU Technical Support Document 3: Heterogeneity: Subgroups, Meta-Regression, Bias and Bias-Adjustment 2011. www.nicedsu.org.uk (accessed 15 August 2023).
- Lunn DJ, Thomas A, Best N, Spiegelhalter D. WinBUGS – a Bayesian modelling framework: concepts, structure, and extensibility. Stat Comput 2000;10:325-37.
- Dias SWNJ, Sutton AJ, Ades AE. NICE Technical Support Document 2. A Generalised Linear Modelling Framework for Pairwise and Network Meta-Analysis of Randomised Controlled Trials. London: National Institute for Health and Care Excellence; 2011.
- Dias S, Welton NJ, Sutton AJ, Ades A. NICE DSU Technical Support Document 2: A Generalised Linear Modelling Framework for Pairwise and Network Meta-Analysis of Randomised Controlled Trials. London: National Institute for Health and Care Excellence (NICE); 2014.
- Brooks SG, Gelman A. General methods for monitoring convergence of iterative simulation. J Comput Graph Statist 2021;7:434-55.
- Spiegelhalter DJ, Best NG, Carlin BP, Linde AVD. Bayesian measures of model complexity and fit. J R Statist Soc: Ser B (Statist Methodol) 2002;64:583-639.
- Dias S, Welton NJ, Sutton AJ, Caldwell DM, Lu G, Ades AE. NICE DSU Technical Support Document 4: Inconsistency in Networks of Evidence Based on Randomised Controlled Trials 2011. www.nicedsu.org.uk (accessed April 2014).
- Kazmierczak KM, Tsuji M, Wise M, Hackel M, Yamano Y, Echols R, et al. In vitro activity of cefiderocol, a siderophore cephalosporin, against a recent collection of clinically relevant carbapenem-non-susceptible Gram-negative bacilli, including serine carbapenemase- and metallo-β-lactamase-producing isolates (SIDERO-WT-2014 Study). Int J Antimicrob Agents 2019;53:177-84.
- Bhagwat SS, Hariharan P, Joshi PR, Palwe SR, Shrivastava R, Patel MV, et al. Activity of cefepime/zidebactam against MDR Escherichia coli isolates harbouring a novel mechanism of resistance based on four-amino-acid inserts in PBP3. J Antimicrob Chemother 2020;75:3563-7.
- Han R, Shi Q, Wu S, Yin D, Peng M, Dong D, et al. China Antimicrobial Surveillance Network (CHINET) Study Group . Dissemination of carbapenemases (KPC, NDM, OXA-48, IMP, and VIM) among carbapenem-resistant Enterobacteriaceae isolated from adult and children patients in China. Front Cell Infect Microbiol 2020;10.
- Johnston BD, Thuras P, Porter SB, Anacker M, VonBank B, Snippes Vagnone P, et al. Activity of cefiderocol, ceftazidime-avibactam, and eravacycline against carbapenem-resistant Escherichia coli isolates from the United States and international sites in relation to clonal background, resistance genes, coresistance, and region. Antimicrob Agents Chemother 2020;64:e00797-20.
- EUnetHTA PTJA11. Authoring Team . Cefiderocol (Fetcroja®) for the Treatment of Infections Due to Aerobic Gram-Negative Organisms in Adults With Limited Treatment Options 2020. www.eunethta.eu (accessed 30 July 2024).
- Mazuski JE, Gasink LB, Armstrong J, Broadhurst H, Stone GG, Rank D, et al. Efficacy and safety of ceftazidime-avibactam plus metronidazole versus meropenem in the treatment of complicated intra-abdominal infection: results from a randomized, controlled, double-blind, phase 3 program. Clin Infect Dis 2016;62:1380-9.
- Qin X, Tran BG, Kim MJ, Wang L, Nguyen DA, Chen Q, et al. A randomised, double-blind, phase 3 study comparing the efficacy and safety of ceftazidime/avibactam plus metronidazole versus meropenem for complicated intra-abdominal infections in hospitalised adults in Asia. Int J Antimicrob Agents 2017;49:579-88.
- Caston JJ, Lacort-Peralta I, Martin-Davila P, Loeches B, Tabares S, Temkin L, et al. Clinical efficacy of ceftazidime/avibactam versus other active agents for the treatment of bacteremia due to carbapenemase-producing Enterobacteriaceae in hematologic patients. Int J Infect Dis 2017;59:118-23.
- Shields RK, Nguyen MH, Chen L, Press EG, Potoski BA, Marini RV, et al. Ceftazidime-avibactam is superior to other treatment regimens against carbapenem-resistant Klebsiella pneumoniae bacteremia. Antimicrob Agents Chemother 2017;61.
- Tumbarello M, Trecarichi EM, Corona A, De Rosa FG, Bassetti M, Mussini C, et al. Efficacy of ceftazidime-avibactam salvage therapy in patients with infections caused by Klebsiella pneumoniae carbapenemase-producing K. pneumoniae. Clin Infect Dis 2019;68:355-64.
- van Duin D, Lok JJ, Earley M, Cober E, Richter SS, Perez F, et al. Antibacterial Resistance Leadership Group . Colistin versus ceftazidime-avibactam in the treatment of infections due to carbapenem-resistant Enterobacteriaceae. Clin Infect Dis 2018;66:163-71.
- Bojke L, Soares MO, Claxton K, Colson A, Fox A, Jackson C, et al. Developing a reference protocol for structured expert elicitation in health-care decision-making: a mixed-methods study. Health Technol Assess 2021;25:1-124.
- Chang W, Cheng J, Allaire J, Xie Y, McPherson J. Shiny: Web Application Framework for R 2020.
- O’Hagan A, Buck CE, Daneshkhah A, Eiser JR, Garthwaite PH, Jenkinson DJ, et al. Uncertain Judgements: Eliciting Experts’ Probabilities. Chichester: John Wiley & Sons; 2006.
- Tichy E, Torres A, Bassetti M, Kongnakorn T, Di Virgilio R, Irani P, et al. Cost-effectiveness comparison of ceftazidime/avibactam versus meropenem in the empirical treatment of hospital-acquired pneumonia, including ventilator-associated pneumonia, in Italy. Clin Ther 2020;42:802-17.
- Kongnakorn T, Wagenlehner F, Falcone M, Tichy E, Di Virgilio R, Baillon-Plot N, et al. Cost-effectiveness analysis of ceftazidime/avibactam compared to imipenem as empirical treatment for complicated urinary tract infections. Int J Antimicrob Agents 2019;54:633-41.
- Simon MS, Sfeir MM, Calfee DP, Satlin MJ. Cost-effectiveness of ceftazidime-avibactam for treatment of carbapenem-resistant Enterobacteriaceae bacteremia and pneumonia. Antimicrob Agents Chemother 2019;63.
- Nguyen CP, Dan Do TN, Bruggemann R, Ten Oever J, Kolwijck E, Adang EMM, et al. Clinical cure rate and cost-effectiveness of carbapenem-sparing beta-lactams vs meropenem for Gram-negative infections: a systematic review, meta-analysis, and cost-effectiveness analysis. Int J Antimicrob Agents 2019;54:790-7.
- Chen GJ, Pan SC, Foo J, Morel C, Chen WT, Wang JT. Comparing ceftolozane/tazobactam versus piperacillin/tazobactam as empiric therapy for complicated urinary tract infection in Taiwan: a cost-utility model focusing on Gram-negative bacteria. J Microbiol Immunol Infect 2019;52:807-15.
- Mewes JC, Pulia MS, Mansour MK, Broyles MR, Nguyen HB, Steuten LM. The cost impact of PCT-guided antibiotic stewardship versus usual care for hospitalised patients with suspected sepsis or lower respiratory tract infections in the US: a health economic model analysis. PLOS ONE 2019;14.
- Nelson RE, Ray W, Rubin MA, Schweizer M. Evaluating the cost-effectiveness of decolonization for prevention of MRSA infections using a dynamic transmission model. Antimicrobial Resistance and Infection Control Conference: 5th International Conference on Prevention and Infection Control. ICPIC 2019;8.
- Gordon J, Darlington O, McEwan P, Lumley M, Taie A, Hicks M, et al. Estimating the value of new antimicrobials in the context of antimicrobial resistance: development and application of a dynamic disease transmission model. PharmacoEcon 2020;38:857-69.
- Wagner AP, Enne VI, Livermore, Craig DM, Turner JV. DAINHALE Study Group . Review of health economic models exploring and evaluating treatment and management of hospital-acquired pneumonia and ventilator-associated pneumonia. J Hosp Infect 2020;106:745-56.
- Edwards SJ, Wordsworth S, Clarke MJ. Treating pneumonia in critical care in the United Kingdom following failure of initial antibiotic: a cost-utility analysis comparing meropenem with piperacillin/tazobactam. Eur J Health Econ 2012;13:181-92.
- Grau S, Alvarez-lerma F, Del castillo A, Neipp R, Rubio-terrés C. Cost-effectiveness analysis of the treatment of ventilator-associated pneumonia with linezolid or vancomycin in Spain. J Chemother 2005;17:203-11.
- Kongnakorn T, Mwamburi M, Merchant S, Akhras K, Caro JJ, Nathwani D. Economic evaluation of doripenem for the treatment of nosocomial pneumonia in the US: discrete event simulation. Curr Med Res Opin 2010;26:17-24.
- Kauf TL, Prabhu VS, Medic G, Borse RH, Miller B, Gaultney J, et al. Cost-effectiveness of ceftolozane/tazobactam compared with piperacillin/tazobactam as empiric therapy based on the in-vitro surveillance of bacterial isolates in the United States for the treatment of complicated urinary tract infections. BMC Infect Dis 2017;17.
- Lopes S, Franceschini M, Han Y, Green W, Dymond A, Gill A. Economic evaluation of cefiderocol for the treatment of carbapenem resistant infections in the United States n.d.
- Schaffer SK, West P, Towse A, Henshall C, Mestre-Ferrandiz J, Masterton R, et al. Assessing the Value of New Antibiotics: Additional Elements of Value for Health Technology Assessment Decisions. London: Office of Health Economics; 2017.
- Aminoglycosides (Gentamicin, Amikacin, Tobramycin, and Neomycin): Increased Risk of Deafness in Patients With Mitochondrial Mutations. GOV.UK 2021. www.gov.uk/drug-safety-update/aminoglycosides-gentamicin-amikacin-tobramycin-and-neomycin-increased-risk-of-deafness-in-patients-with-mitochondrial-mutations (accessed 15 August 2023).
- Pfizer Ltd . National Institute of Health and Care Excellence, Antimicrobial Health Technology Evaluation: Ceftazidime With Avibactam for Treating Severe Aerobic Gram-Negative Bacterial Infections. Company Evidence Submission, Document A. 2021. www.nice.org.uk/guidance/hte1/documents/agenda-5 (accessed 30 July 2024).
- Tumbarello M, De Pascale G, Trecarichi EM, Spanu T, Antonicelli F, Maviglia R, et al. Clinical outcomes of Pseudomonas aeruginosa pneumonia in intensive care unit patients. Intensive Care Med 2013;39:682-92.
- Livermore DM, Nicolau DP, Hopkins KL, Meunier D. Carbapenem-resistant Enterobacterales, carbapenem resistant organisms, carbapenemase-producing Enterobacterales, and carbapenemase-producing organisms: terminology past its “sell-by date” in an era of new antibiotics and regional carbapenemase epidemiology. Clin Infect Dis 2020;71:1776-82.
- Sisay M, Hagos B, Edessa D, Tadiwos Y, Mekuria AN. Polymyxin-induced nephrotoxicity and its predictors: a systematic review and meta-analysis of studies conducted using RIFLE criteria of acute kidney injury. Pharmacol Res 2021;163.
- Chien H-T, Lin Y-C, Sheu C-C, Hsieh K-P, Chang J-S. Is colistin-associated acute kidney injury clinically important in adults? A systematic review and meta-analysis. Int J Antimicrob Agents 2020;55.
- Kerr M, Bedford M, Matthews B, O’Donoghue D. The economic impact of acute kidney injury in England. Nephrol Dial Transplant 2014;29:1362-8.
- Wagenlehner F, Lucenteforte E, Pea F, Soriano A, Tavoschi L, Steele VR, et al. Systematic review on estimated rates of nephrotoxicity and neurotoxicity in patients treated with polymyxins. Clin Microbiol Infect 2021;27:671-86.
- Oliota AF, Penteado ST, Tonin FS, Fernandez-Llimos F, Sanches AC. Nephrotoxicity prevalence in patients treated with polymyxins: a systematic review with meta-analysis of observational studies. Diagn Microbiol Infect Dis 2019;94:41-9.
- Wunderink RG, Matsunaga Y, Ariyasu M, Clevenbergh P, Echols R, Kaye KS, et al. Cefiderocol versus high-dose, extended-infusion meropenem for the treatment of Gram-negative nosocomial pneumonia (APEKS-NP): a randomised, double-blind, phase 3, non-inferiority trial. Lancet Infect Dis 2021;21:213-25.
- Palacios-Baena ZR, Giannella M, Manissero D, Rodríguez-Baño J, Viale P, Lopes S, et al. Risk factors for carbapenem-resistant Gram-negative bacterial infections: a systematic review. Clin Microbiol Infect 2020;27:228-35.
- Merrick B, Tan MKI, Bisnauthsing K, Goldenberg SD. Healthcare resource use in hospitalized patients with carbapenem-resistant Gram-negative infections. J Hosp Infect 2021;110:7-14.
- Latimer N. NICE DSU Technical Support Document 14: Survival Analysis for Economic Evaluations alongside Clinical Trials – Extrapolation with Patient-Level Data. London: NICE Decision Support Unit; 2011.
- Bucaloiu ID, Kirchner HL, Norfolk ER, Hartle JE, II, Perkins RM. Increased risk of death and de novo chronic kidney disease following reversible acute kidney injury. Kidney Int 2012;81:477-85.
- Hadjiat Y, Serrie A, Treves R, Chomier B, Geranton L, Billon S. Pain associated with health and economic burden in France: results from recent National Health and Wellness Survey data. ClinicoEconomics Outcomes Res 2018;10:53-65.
- Langley PC. The societal burden of pain in Germany: health-related quality-of-life, health status and direct medical costs. J Med Econ 2012;15:1201-15.
- Ara R, Brazier JE. Populating an economic model with health state utility values: moving toward better practice. Value Health 2010;13:509-18.
- Wyld M, Morton RL, Hayen A, Howard K, Webster AC. A systematic review and meta-analysis of utility-based quality of life in chronic kidney disease treatments. PLOS Med 2012;9.
- Kerr M, Bray B, Medcalf J, O’Donoghue DJ, Matthews B. Estimating the financial cost of chronic kidney disease to the NHS in England. Nephrol Dial Transplant 2012;27:iii73-80.
- Muscedere JG, Shorr AF, Jiang X, Day A, Heyland DK. Canadian Critical Care Trials Group . The adequacy of timely empiric antibiotic therapy for ventilator-associated pneumonia: an important determinant of outcome. J Crit Care 2012;27:322.e7-e14.
- Kolhe NV, Eldehni MT, Selby NM, McIntyre CW. The reimbursement and cost of acute kidney injury: a UK hospital perspective. Nephron Clin Pract 2014;126:51-6.
- Knight GM, Costelloe C, Deeny SR, Moore LSP, Hopkins S, Johnson AP, et al. Quantifying where human acquisition of antibiotic resistance occurs: a mathematical modelling study. BMC Med 2018;16.
- Curtis L, Burns A. Unit Costs of Health & Social Care. Kent: PSSRU, University of Kent; 2020.
- Kongnakorn T, Eckmann C, Bassetti M, Tichy E, Di Virgilio R, Baillon-Plot N, et al. Cost-effectiveness analysis comparing ceftazidime/avibactam (CAZ-AVI) as empirical treatment comparing to ceftolozane/tazobactam and to meropenem for complicated intra-abdominal infection (cIAI). Antimicrob Resist Infect Control 2019;8.
- British National Formulary . BNF: British National Formulary – NICE 2021. https://bnf.nice.org.uk/ (accessed 15 August 2023).
- Kallel H, Hergafi L, Bahloul M, Hakim A, Dammak H, Chelly H, et al. Safety and efficacy of colistin compared with imipenem in the treatment of ventilator-associated pneumonia: a matched case-control study. Intensive Care Med 2007;33:1162-7.
- Department of Health and Social Care . Drugs and Pharmaceutical Electronic Market Information Tool (eMIT) 2021. www.gov.uk/government/publications/drugs-and-pharmaceutical-electronic-market-information-emit (accessed 30 July 2024).
- World Health Organization . WHO Collaboration Centre for Drug Statistics Methodology 2021. https://atcddd.fhi.no/ (accessed 30 July 2024).
- Renascience Pharma Ltd . Renapime 1g Powder for Solution for Injection Infusion: SmPC n.d. www.medicines.org.uk/emc/product/9671/smpc#gref.
- Antimicrobial Health Technology Evaluation: Ceftazidime With Avibactam for Treating Severe Aerobic Gram-Negative Bacterial Infections: Final Scope 2021. www.nice.org.uk/about/what-we-do/life-sciences/scientific-advice/models-for-the-evaluation-and-purchase-of-antimicrobials/ceftazidime-with-avibactam (accessed 17 October 2021).
- Department of Health and Social Care . Impact Assessment 9553: 2018 Statutory Scheme – Branded Medicines Pricing 2018.
- Guide to the Methods of Technology Appraisal 2013 2013. www.nice.org.uk/process/pmg9/chapter/foreword (accessed 10 March 2017).
- New S, I and R Definitions 2021. www.eucast.org/newsiandr/ (accessed 15 August 2023).
- Costelloe C, Metcalfe C, Lovering A, Mant D, Hay AD. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: systematic review and meta-analysis. BMJ 2010;340.
- Bell BG, Schellevis F, Stobberingh E, Goossens H, Pringle M. A systematic review and meta-analysis of the effects of antibiotic consumption on antibiotic resistance. BMC Infect Dis 2014;14:1-25.
- Bakhit M, Hoffmann T, Scott AM, Beller E, Rathbone J, Del Mar C. Resistance decay in individuals after antibiotic exposure in primary care: a systematic review and meta-analysis. BMC Med 2018;16:1-19.
- Jeffrey B, Aanensen DM, Croucher NJ, Bhatt S. Predicting the future distribution of antibiotic resistance using time series forecasting and geospatial modelling. Wellcome Open Res 2020;5.
- Organisation for Economic Co-operation and Development . Stemming the Superbug Tide: Just a Few Dollars More 2019. www.oecd.org/health/stemming-the-superbug-tide-9789264307599-en.htm (accessed 15 August 2023).
- Ortiz-Brizuela E, Caro-Vega Y, Bobadilla-del-Valle M, Leal-Vega F, Criollo-Mora E, López Luis BA, et al. The influence of hospital antimicrobial use on carbapenem-non-susceptible Enterobacterales incidence rates according to their mechanism of resistance: a time-series analysis. J Hosp Infect 2020;105:757-65.
- Gharbi M, Moore LS, Gilchrist M, Thomas CP, Bamford K, Brannigan ET, et al. Forecasting carbapenem resistance from antimicrobial consumption surveillance: lessons learnt from an OXA-48-producing Klebsiella pneumoniae outbreak in a west London renal unit. Int J Antimicrob Agents 2015;46:150-6.
- Berger P, Pascal L, Sartor C, Delorme J, Monge P, Ragon CP, et al. Generalized additive model demonstrates fluoroquinolone use/resistance relationships for Staphylococcus aureus. Eur J Epidemiol 2004;19:453-60.
- McDonnell L, Armstrong D, Ashworth M, Dregan A, Malik U, White P. National disparities in the relationship between antimicrobial resistance and antimicrobial consumption in Europe: an observational study in 29 countries. J Antimicrob Chemother 2017;72:3199-204.
- Pouwels KB, Freeman R, Muller-Pebody B, Rooney G, Henderson KL, Robotham JV, et al. Association between use of different antibiotics and trimethoprim resistance: going beyond the obvious crude association. J Antimicrob Chemother 2018;73:1700-7.
- Colson AR, Megiddo I, Alvarez-Uria G, Gandra S, Bedford T, Morton A, et al. Quantifying uncertainty about future antimicrobial resistance: comparing structured expert judgment and statistical forecasting methods. PLOS ONE 2019;14.
- Durham L, Ge M, Cuccia A, Quinn J. Modeling antibiotic resistance to project future rates: quinolone resistance in Escherichia coli. Eur J Clin Microbiol Infect Dis 2010;29:353-6.
- Goossens H, Ferech M, Vander Stichele R, Elseviers M, Group EP. Outpatient antibiotic use in Europe and association with resistance: a cross-national database study. Lancet 2005;365:579-87.
- Johnson AP, Muller-Pebody B, Budd E, Ashiru-Oredope D, Ladenheim D, Hain D, et al. Improving feedback of surveillance data on antimicrobial consumption, resistance and stewardship in England: putting the data at your fingertips. J Antimicrob Chemother 2017;72:953-6.
- European Centre for Disease Prevention and Control . European Surveillance of Antimicrobial Consumption Network (ESAC-Net) 2021. www.ecdc.europa.eu/en/about-us/partnerships-and-networks/disease-and-laboratory-networks/esac-net (accessed 15 August 2023).
- European Centre for Disease Prevention and Control . European Antimicrobial Resistance Surveillance Network (EARS-Net) 2021. www.ecdc.europa.eu/en/about-us/partnerships-and-networks/disease-and-laboratory-networks/ears-net (accessed 15 August 2023).
- European Centre for Disease Prevention and Control . Antimicrobial Resistance in the EU EEA (EARS-Net) – Annual Epidemiological Report for 2019 2020. www.ecdc.europa.eu/en/publications-data/surveillance-antimicrobial-resistance-europe-2019 (accessed 15 August 2023).
- Morel CM, Alm RA, Årdal C, Bandera A, Bruno GM, Carrara E, et al. A one health framework to estimate the cost of antimicrobial resistance. Antimicrob Resist Infect Control 2020;9:1-14.
- Chatterjee A, Modarai M, Naylor NR, Boyd SE, Atun R, Barlow J, et al. Quantifying drivers of antibiotic resistance in humans: a systematic review. Lancet Infect Dis 2018;18:e368-78.
- Schuts EC, Boyd A, Muller AE, Mouton JW, Prins JM. The effect of antibiotic restriction programs on prevalence of antimicrobial resistance: a systematic review and meta-analysis. Open Forum Infect Dis 2021;8.
- Holmes AH, Moore LS, Sundsfjord A, Steinbakk M, Regmi S, Karkey A, et al. Understanding the mechanisms and drivers of antimicrobial resistance. Lancet 2016;387:176-87.
- Enne VI, Livermore DM, Stephens P, Hall LM. Persistence of sulphonamide resistance in Escherichia coli in the UK despite national prescribing restriction. Lancet 2001;357:1325-8.
- Nasrin D, Collignon PJ, Roberts L, Wilson EJ, Pilotto LS, Douglas RM. Effect of betalactam antibiotic use in children on pneumococcal resistance to penicillin: prospective cohort study. BMJ 2002;324:28-30.
- NHS England . Bed Availability and Occupancy Data – Overnight n.d. www.england.nhs.uk/statistics/statistical-work-areas/bed-availability-and-occupancy/bed-data-overnight/ (accessed 15 August 2023).
- Paul M, Carrara E, Retamar P, Tängdén T, Bitterman R, Bonomo RA, et al. European Society of Clinical Microbiology and Infectious Diseases (ESCMID) guidelines for the treatment of infections caused by multidrug-resistant Gram-negative bacilli (endorsed by European Society of Intensive Care Medicine). Clin Microbiol Infect 2022;28:521-47.
- Infectious Diseases Society of America . Antimicrobial-Resistant Treatment Guidance: Gram-Negative Bacterial Infections 2022. www.idsociety.org/practice-guideline/amr-guidance/#null (accessed 24 March 2022).
- Walker AS, White IR, Turner RM, Hsu LY, Yeo TW, White NJ, et al. Personalised randomised controlled trial designs-a new paradigm to define optimal treatments for carbapenem-resistant infections. Lancet Infect Dis 2021;21:e175-81.
- Ayiku L, Levay P, Hudson T, Craven J, Barrett E, Finnegan A, et al. The MEDLINE UK filter: development and validation of a geographic search filter to retrieve research about the UK from OVID MEDLINE. Health Info Libr J 2017;34:200-16.
- Ayiku L, Levay P, Hudson T, Craven J, Finnegan A, Adams R, et al. The EMBASE UK filter: validation of a geographic search filter to retrieve research about the UK from OVID EMBASE. Health Info Libr J 2019;36:121-33.
- Harnan SE, Tappenden P, Essat M, Gomersall T, Minton J, Wong R, et al. Measurement of exhaled nitric oxide concentration in asthma: a systematic review and economic evaluation of NIOX MINO, NIOX VERO and NObreath. Health Technol Assess 2015;19:1-330.
- Montori VM, Wilczynski NL, Morgan D, Haynes RB, Hedges T. Optimal search strategies for retrieving systematic reviews from MEDLINE: analytical survey. BMJ 2005;330.
- The National Institute for Health and Care Excellence . Diabetic Foot Infection: Antimicrobial Prescribing 2019.
- Li L, Smith HE, Atun R, Tudor Car L. Search strategies to identify observational studies in MEDLINE and EMBASE. Cochrane Database Syst Rev 2019;3.
- Bassetti M, Rello J, Blasi F, Goossens H, Sotgiu G, Tavoschi L, et al. A systematic review on the impact of appropriate versus inappropriate initial antibiotic therapy on the outcomes of patients with severe bacterial infections. Int J Antimicrob Agents 2020;56.
- Arber M, Garcia S, Veale T, Edwards M, Shaw A, Glanville JM. Performance of Ovid MEDLINE search filters to identify health state utility studies. Int J Technol Assess Health Care 2017;33:472-80.
- Zasowski EJ, Bassetti M, Blasi F, Goossens H, Rello J, Sotgiu G, et al. A systematic review of the effect of delayed appropriate antibiotic treatment on the outcomes of patients with severe bacterial infections. Chest 2020;158:929-38.
- Muscedere JG, Shorr AF, Jiang X, Day A, Heyland DK. Group CCCT . The adequacy of timely empiric antibiotic therapy for ventilator-associated pneumonia: an important determinant of outcome. J Crit Care 2012;27:322.e7-e14.
- Herkel T, Uvizl R, Doubravska L, Adamus M, Gabrhelik T, Htoutou Sedlakova M, et al. Epidemiology of hospital-acquired pneumonia: results of a Central European multicenter, prospective, observational study compared with data from the European region. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub 2016;160:448-55.
- Tumbarello M, De Pascale G, Trecarichi EM, De Martino S, Bello G, Maviglia R, et al. Effect of aerosolized colistin as adjunctive treatment on the outcomes of microbiologically documented ventilator-associated pneumonia caused by colistin-only susceptible Gram-negative bacteria. Chest 2013;144:1768-75.
- Pena C, Gómez-Zorrilla S, Oriol I, Tubau F, Dominguez MA, Pujol M, et al. Impact of multidrug resistance on Pseudomonas aeruginosa ventilator-associated pneumonia outcome: predictors of early and crude mortality. Eur J Clin Microbiol Infect Dis 2013;32:413-20.
- Amaral AC, Holder MW. Timing of antimicrobial therapy after identification of ventilator-associated condition is not associated with mortality in patients with ventilator-associated pneumonia: a cohort study. PLOS ONE 2014;9.
- Abdul-Mutakabbir JC, Alosaimy S, Morrisette T, Kebriaei R, Rybak MJ. Cefiderocol: a novel siderophore cephalosporin against multidrug-resistant Gram-negative pathogens. Pharmacotherapy 2020;40:1228-47.
- Hyndman RJ, Athanasopoulos G. Forecasting: Principles and Practice. OTexts; 2018.
- Liboschik T, Fokianos K, Fried R. An R package for analysis of count time series following generalized linear models. J Statist Software 2017;82:1-51.
- Aliabadi S, Anyanwu P, Beech E, Jauneikaite E, Wilson P, Hope R, et al. Effect of antibiotic stewardship interventions in primary care on antimicrobial resistance of Escherichia coli bacteraemia in England (2013–18): a quasi-experimental, ecological, data linkage study. Lancet Infect Dis 2021;21:1689-700.
- Kearns B, Stevenson MD, Triantafyllopoulos K, Manca A. Generalized linear models for flexible parametric modeling of the hazard function. Med Decis Making 2019;39:867-78.
- AMR Local Indicators 2021. https://fingertips.phe.org.uk/profile/amr-local-indicators (accessed 15 August 2023).
- UK Health Security Agency . Escherichia Coli (E. Coli): Guidance, Data and Analysis 2017. www.gov.uk/government/collections/escherichia-coli-e-coli-guidance-data-and-analysis (accessed 30 July 2024).
- Sharland M, Pulcini C, Harbarth S, Zeng M, Gandra S, Mathur S, et al. 21st WHO Expert Committee on Selection and Use of Essential Medicines . Classifying antibiotics in the WHO Essential Medicines List for optimal use—be AWaRe. Lancet Infect Dis 2018;18:18-20.
- OpenPrescribing.net . Bennett Institute for Applied Data Science, University of Oxford 2024. https://openprescribing.net/ (accessed 15 August 2023).
- Davey P, Brown E, Charani E, Fenelon L, Gould IM, Holmes A, et al. Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Syst Rev 2013;2.
- Bhattacharya A, Hopkins S, Sallis A, Budd EL, Ashiru-Oredope D. A process evaluation of the UK-wide Antibiotic Guardian campaign: developing engagement on antimicrobial resistance. J Pub Health 2017;39:e40-7.
- McKenzie E, Gardner Jr ES. Damped trend exponential smoothing: a modelling viewpoint. Int J Forecast 2010;26:661-5.
- Spicknall IH, Foxman B, Marrs CF, Eisenberg JN. A modeling framework for the evolution and spread of antibiotic resistance: literature review and model categorization. Am J Epidemiol 2013;178:508-20.
Appendix 1 Search strategies
A1.1 Clinical searches
Number of records retrieved
| Search | Resultsa | |||
|---|---|---|---|---|
| MEDLINE | EMBASE | CRD | WoS-CPCI | |
| Clinical: sampling search (1–200 records) | 738 | 1524 | 0 | NS |
| Clinical: RCTs and observational | 222 | 358 | NS | NS |
| Clinical: CAZ/AVI susceptibility studies search | 57 | 90 | NS | NS |
| Clinical: first iteration of the susceptibility searches | 65 | 179 | NS | NS |
| CEA models | 16 | 56 | 0 | 14 |
A1.2 CAZ/AVI
A1.2.1 Sampling search (first 1–200 records)
Term group(s): CAZ/AVI AND filter
Filters: Exclusions filter (MEDLINE, EMBASE)
Limits: None
A total of 2214 records were retrieved and 1478 are unique. Only the first 200 records were reviewed to inform the antibiotic susceptibility studies searches (2.3).
Ovid MEDLINE(R) and Epub Ahead of Print, In-Process, In-Data-Review & Other Non-Indexed Citations, Daily and Versions(R) 1946 to 17 March 2021 (searched via the Ovid SP platform)
17 March 2021
| # | Searches | Results |
|---|---|---|
| 1 | ceftazidime.mp. | 10,237 |
| 2 | Ceftazidime/ | 4055 |
| 3 | 1 or 2 | 10,237 |
| 4 | avibactam.mp. | 974 |
| 5 | 3 and 4 | 797 |
| 6 | ceftazidime-avibactam.mp. | 718 |
| 7 | zavicefta.mp. | 2 |
| 8 | avycaz.mp. | 9 |
| 9 | (ctz-avi or caz-avi).mp. | 65 |
| 10 | or/5–9 | 800 |
| 11 | Letter/ | 1,127,089 |
| 12 | Historical article/ | 362,579 |
| 13 | 11 or 12 | 1,482,068 |
| 14 | exp Animals/ | 23,901,218 |
| 15 | Humans/ | 19,100,537 |
| 16 | 14 not (14 and 15) | 4,800,681 |
| 17 | 13 or 16 | 6,235,842 |
| 18 | 10 not 17 | 738 |
EMBASE 1974 to 16 March 2021 (searched via the Ovid SP platform)
17 March 2021
| # | Searches | Results |
|---|---|---|
| 1 | ceftazidime.mp. | 45,294 |
| 2 | ceftazidime/ | 43,140 |
| 3 | 1 or 2 | 45,294 |
| 4 | avibactam.mp. | 1916 |
| 5 | 3 and 4 | 1630 |
| 6 | ceftazidime-avibactam.mp. | 973 |
| 7 | zavicefta.mp. | 18 |
| 8 | avycaz.mp. | 61 |
| 9 | (ctz-avi or caz-avi).mp. | 161 |
| 10 | or/5–9 | 1639 |
| 11 | Abstract report/ or letter/ | 1,192,921 |
| 12 | editorial.pt. | 688,595 |
| 13 | animal/ | 1,511,248 |
| 14 | human/ | 22,017,643 |
| 15 | 13 not (13 and 14) | 1,106,807 |
| 16 | 11 or 12 or 15 | 2,971,223 |
| 17 | 10 not 16 | 1524 |
CRD database (searched via the University of York CRD platform)
1 March 2021
| # | Searches | Results |
|---|---|---|
| 1 | (ceftazidime) | 49 |
| 2 | MeSH DESCRIPTOR Ceftazidime EXPLODE ALL TREES | 12 |
| 3 | #1 OR #2 | 49 |
| 4 | (avibactam) | 0 |
| 5 | #3 AND #4 | 0 |
| 6 | (ceftazidime-avibactam) | 0 |
| 7 | (zavicefta) | 0 |
| 8 | (avycaz) | 0 |
| 9 | ((ctz-avi or caz-avi)) | 0 |
| 10 | #5 OR #6 OR #7 OR #8 OR #9 | 0 |
A1.2.2 CAZ/AVI RCTs, observational, susceptibility studies search
Term group(s): CAZ-AVI AND filters OR focused OXA-48/antimicrobial susceptibility search terms
Filters: RCTs, observational studies filter
Limits: None
Ovid MEDLINE(R) and Epub Ahead of Print, In-Process, In-Data-Review & Other Non-Indexed Citations, Daily and Versions(R) 1946 to 21 April 2021 (searched via the Ovid SP platform)
29 March 2021 and 22 April 2021
| # | Searches | Results |
|---|---|---|
| 1 | ceftazidime.mp. | 10,296 |
| 2 | Ceftazidime/ | 4067 |
| 3 | 1 or 2 | 10,296 |
| 4 | avibactam.mp. | 997 |
| 5 | 3 and 4 | 815 |
| 6 | ceftazidime-avibactam.mp. | 736 |
| 7 | zavicefta.mp. | 2 |
| 8 | avycaz.mp. | 9 |
| 9 | (ctz-avi or caz-avi).mp. | 67 |
| 10 | or/5–9 | 818 |
| 11 | Randomized Controlled Trial.pt. | 527,450 |
| 12 | Controlled Clinical Trial.pt. | 94,123 |
| 13 | Clinical Trial.pt. | 528,337 |
| 14 | exp Clinical Trials as Topic/ | 355,534 |
| 15 | Placebos/ | 35,440 |
| 16 | Random Allocation/ | 105,128 |
| 17 | Double-Blind Method/ | 163,610 |
| 18 | Single-Blind Method/ | 30,020 |
| 19 | Cross-Over Studies/ | 49,955 |
| 20 | ((random$ or control$ or clinical$) adj3 (trial$ or stud$)).tw. | 1,326,053 |
| 21 | (random$ adj3 allocat$).tw. | 38,558 |
| 22 | placebo$.tw. | 224,234 |
| 23 | ((singl$ or doubl$ or trebl$ or tripl$) adj (blind$ or mask$)).tw. | 179,495 |
| 24 | (crossover$ or (cross adj over$)).tw. | 90,299 |
| 25 | or/11–24 | 2,133,174 |
| 26 | animals/ not humans/ | 4,781,769 |
| 27 | 25 not 26 | 2,002,497 |
| 28 | Observational Studies as Topic/ | 6139 |
| 29 | Observational Study/ | 96,666 |
| 30 | Epidemiologic Studies/ | 8624 |
| 31 | exp Case-Control Studies/ | 1,160,431 |
| 32 | exp Cohort Studies/ | 2,116,863 |
| 33 | Cross-Sectional Studies/ | 360,619 |
| 34 | Controlled Before-After Studies/ | 604 |
| 35 | Historically Controlled Study/ | 197 |
| 36 | Interrupted Time Series Analysis/ | 1190 |
| 37 | Comparative Study.pt. | 1,887,768 |
| 38 | case control$.tw. | 136,555 |
| 39 | case series.tw. | 82,265 |
| 40 | (cohort adj (study or studies)).tw. | 232,629 |
| 41 | cohort analy$.tw. | 8972 |
| 42 | (follow up adj (study or studies)).tw. | 50,946 |
| 43 | (observational adj (study or studies)).tw. | 120,378 |
| 44 | longitudinal.tw. | 263,982 |
| 45 | prospective.tw. | 606,748 |
| 46 | retrospective.tw. | 584,947 |
| 47 | cross sectional.tw. | 391,367 |
| 48 | or/28–47 | 4,885,385 |
| 49 | (“phase 3” or “phase three”).tw. | 16,551 |
| 50 | 25 or 48 or 49 | 6,204,759 |
| 51 | 10 and 50 | 222 |
| 52 | (oxa-48 or “oxa 48” or oxacillinase-48 or “oxacillinase 48”).tw. | 1210 |
| 53 | (antibiotic* or antimicrob* or anti-microb* or antibact* or anti-bacter* or “in vitro”).tw. | 1,750,265 |
| 54 | (susceptib* or “minimum inhibitory concentration” or sensitiv* or resistan* or activ* or isolate or isolates).tw. | 7,084,782 |
| 55 | 53 and 54 | 945,882 |
| 56 | 10 and 52 and 55 | 57 |
| 57 | 51 or 56 | 261 |
EMBASE 1974 to 21 April 2021 (searched via the Ovid SP platform)
29 March 2021 and 22 April 2021
| # | Searches | Results |
|---|---|---|
| 1 | ceftazidime.mp. | 44,756 |
| 2 | ceftazidime/ | 42,587 |
| 3 | 1 or 2 | 44,756 |
| 4 | avibactam.mp. | 1875 |
| 5 | avibactam/ | 738 |
| 6 | 4 or 5 | 1875 |
| 7 | 3 and 6 | 1596 |
| 8 | ceftazidime-avibactam.mp. | 1025 |
| 9 | zavicefta.mp. | 16 |
| 10 | avycaz.mp. | 60 |
| 11 | (ctz-avi or caz-avi).mp. | 177 |
| 12 | or/7–11 | 1606 |
| 13 | Randomization/ | 92,650 |
| 14 | Placebo/ | 370,211 |
| 15 | Double Blind Procedure/ | 185,230 |
| 16 | Single Blind Procedure/ | 42,836 |
| 17 | Crossover Procedure/ | 66,963 |
| 18 | ((random$ or control$ or clinical$) adj3 (trial$ or stud$)).tw. | 1,860,752 |
| 19 | (random$ adj3 allocat$).tw. | 48,808 |
| 20 | placebo$.tw. | 328,545 |
| 21 | ((singl$ or doubl$ or trebl$ or tripl$) adj (blind$ or mask$)).tw. | 253,412 |
| 22 | (crossover$ or (cross adj over$)).tw. | 113,308 |
| 23 | or/13–22 | 2,287,059 |
| 24 | nonhuman/ not human/ | 4,849,224 |
| 25 | 23 not 24 | 2,188,317 |
| 26 | Clinical study/ | 154,534 |
| 27 | Case control study/ | 169,380 |
| 28 | Family study/ | 25,397 |
| 29 | Longitudinal study/ | 151,121 |
| 30 | Retrospective study/ | 1,057,830 |
| 31 | comparative study/ | 867,060 |
| 32 | Prospective study/ | 682,380 |
| 33 | Randomized controlled trials/ | 200,667 |
| 34 | 32 not 33 | 674,399 |
| 35 | Cohort analysis/ | 687,697 |
| 36 | cohort analy$.tw. | 14,572 |
| 37 | (Cohort adj (study or studies)).tw. | 342,114 |
| 38 | (Case control$ adj (study or studies)).tw. | 147,652 |
| 39 | (follow up adj (study or studies)).tw. | 66,592 |
| 40 | (observational adj (study or studies)).tw. | 190,068 |
| 41 | (epidemiologic$ adj (study or studies)).tw. | 111,957 |
| 42 | (cross sectional adj (study or studies)).tw. | 251,201 |
| 43 | case series.tw. | 115,673 |
| 44 | prospective.tw. | 927,526 |
| 45 | retrospective.tw. | 980,960 |
| 46 | or/26–31,34–45 | 4,350,379 |
| 47 | (“phase 3” or “phase three”).tw. | 43,241 |
| 48 | 25 or 46 or 47 | 5,859,476 |
| 49 | 12 and 48 | 358 |
| 50 | (oxa-48 or “oxa 48” or oxacillinase-48 or “oxacillinase 48”).tw. | 1508 |
| 51 | (antibiotic* or antimicrob* or anti-microb* or antibact* or anti-bacter* or “in vitro”).tw. | 2,208,761 |
| 52 | (susceptib* or “minimum inhibitory concentration” or sensitiv* or resistan* or activ* or isolate or isolates).tw. | 8,842,097 |
| 53 | 51 and 52 | 1,221,015 |
| 54 | 12 and 50 and 53 | 90 |
| 55 | 49 or 54 | 424 |
A1.2.3 First iteration of the susceptibility searches
Term group(s): CAZ/AVI AND UK filter AND (broader OXA-48 [statements 11 and 12] OR antimicrobial susceptibility [statement 27])
Filters: UK
Limits: None
Ovid MEDLINE(R) and Epub Ahead of Print, In-Process, In-Data-Review & Other Non-Indexed Citations, Daily and Versions(R) 1946 to 11 May 2021 (searched via the Ovid SP platform)
12 May 2021
| # | Searches | Results |
|---|---|---|
| 1 | ceftazidime.mp. | 10,338 |
| 2 | Ceftazidime/ | 4079 |
| 3 | 1 or 2 | 10,338 |
| 4 | avibactam.mp. | 1015 |
| 5 | 3 and 4 | 831 |
| 6 | ceftazidime-avibactam.mp. | 749 |
| 7 | zavicefta.mp. | 2 |
| 8 | avycaz.mp. | 9 |
| 9 | (ctz-avi or caz-avi).mp. | 68 |
| 10 | or/5–9 | 834 |
| 11 | (oxa-48* or “oxa 48*” or oxacillinase-48* or “oxacillinase 48*”).tw. | 1233 |
| 12 | (blaoxa-48* or “blaoxa 48*”).tw. | 509 |
| 13 | 11 or 12 | 1569 |
| 14 | exp Great Britain/ | 373,468 |
| 15 | (national health service* or nhs*).ti,ab,in. | 218,667 |
| 16 | (english not ((published or publication* or translat* or written or language* or speak* or literature or citation*) adj5 english)).ti,ab. | 40,422 |
| 17 | (gb or “g.b.” or britain* or (british* not “british columbia”) or uk or “u.k.” or united kingdom* or (england* not “new england”) or northern ireland* or northern irish* or scotland* or scottish* or ((wales or “south wales”) not “new south wales”) or welsh*).ti,ab,jw,in. | 2,176,325 |
| 18 | (bath or “bath’s” or ((birmingham not alabama*) or (“birmingham’s” not alabama*) or bradford or “bradford’s” or brighton or “brighton’s” or bristol or “bristol’s” or carlisle* or “carlisle’s” or (cambridge not (massachusetts* or boston* or harvard*)) or (“cambridge’s” not (massachusetts* or boston* or harvard*)) or (canterbury not zealand*) or (“canterbury’s” not zealand*) or chelmsford or “chelmsford’s” or chester or “chester’s” or chichester or “chichester’s” or coventry or “coventry’s” or derby or “derby’s” or (durham not (carolina* or nc)) or (“durham’s” not (carolina* or nc)) or ely or “ely’s” or exeter or “exeter’s” or gloucester or “gloucester’s” or hereford or “hereford’s” or hull or “hull’s” or lancaster or “lancaster’s” or leeds* or leicester or “leicester’s” or (lincoln not nebraska*) or (“lincoln’s” not nebraska*) or (liverpool not (new south wales* or nsw)) or (“liverpool’s” not (new south wales* or nsw)) or ((london not (ontario* or ont or toronto*)) or (“london’s” not (ontario* or ont or toronto*)) or manchester or “manchester’s” or (newcastle not (new south wales* or nsw)) or (“newcastle’s” not (new south wales* or nsw)) or norwich or “norwich’s” or nottingham or “nottingham’s” or oxford or “oxford’s” or peterborough or “peterborough’s” or plymouth or “plymouth’s” or portsmouth or “portsmouth’s” or preston or “preston’s” or ripon or “ripon’s” or salford or “salford’s” or salisbury or “salisbury’s” or sheffield or “sheffield’s” or southampton or “southampton’s” or st albans or stoke or “stoke’s” or sunderland or “sunderland’s” or truro or “truro’s” or wakefield or “wakefield’s” or wells or westminster or “westminster’s” or winchester or “winchester’s” or wolverhampton or “wolverhampton’s” or (worcester not (massachusetts* or boston* or harvard*)) or (“worcester’s” not (massachusetts* or boston* or harvard*)) or (york not (“new york*” or ny or ontario* or ont or toronto*)) or (“york’s” not (“new york*” or ny or ontario* or ont or toronto*))))).ti,ab,in. | 1,504,740 |
| 19 | (bangor or “bangor’s” or cardiff or “cardiff’s” or newport or “newport’s” or st asaph or “st asaph’s” or st davids or swansea or “swansea’s”).ti,ab,in. | 59,745 |
| 20 | (aberdeen or “aberdeen’s” or dundee or “dundee’s” or edinburgh or “edinburgh’s” or glasgow or “glasgow’s” or inverness or (perth not australia*) or (“perth’s” not australia*) or stirling or “stirling’s”).ti,ab,in. | 222,632 |
| 21 | (armagh or “armagh’s” or belfast or “belfast’s” or lisburn or “lisburn’s” or londonderry or “londonderry’s” or derry or “derry’s” or newry or “newry’s”).ti,ab,in. | 28,291 |
| 22 | or/14–21 | 2,735,913 |
| 23 | (exp africa/ or exp americas/ or exp antarctic regions/ or exp arctic regions/ or exp asia/ or exp oceania/) not (exp great britain/ or europe/) | 2,999,329 |
| 24 | 22 not 23 | 2,603,545 |
| 25 | 10 and 13 | 91 |
| 26 | 24 and 25 | 8 |
| 27 | (susceptib* or inhibit* or mic or mics or isolat* or in-vitro or “in vitro” or activ*).tw. | 7,765,079 |
| 28 | 10 and 27 | 689 |
| 29 | 24 and 28 | 65 |
EMBASE 1974 to 11 May 2021 (searched via the Ovid SP platform)
12 May 2021
| # | Searches | Results |
|---|---|---|
| 1 | ceftazidime.mp. | 46,493 |
| 2 | ceftazidime/ | 44,258 |
| 3 | 1 or 2 | 46,493 |
| 4 | avibactam.mp. | 2029 |
| 5 | avibactam/ | 775 |
| 6 | 4 or 5 | 2029 |
| 7 | 3 and 6 | 1740 |
| 8 | ceftazidime-avibactam.mp. | 1031 |
| 9 | zavicefta.mp. | 18 |
| 10 | avycaz.mp. | 65 |
| 11 | (ctz-avi or caz-avi).mp. | 178 |
| 12 | or/7–11 | 1749 |
| 13 | (oxa-48* or “oxa 48*” or oxacillinase-48* or “oxacillinase 48*”).tw. | 1521 |
| 14 | (blaoxa-48* or “blaoxa 48*”).tw. | 818 |
| 15 | 13 or 14 | 2042 |
| 16 | United Kingdom/ | 396,661 |
| 17 | (english not ((published or publication* or translat* or written or language* or speak* or literature or citation*) adj5 english)).ti,ab. | 48,166 |
| 18 | (gb or “g.b.” or britain* or (british* not “british columbia”) or uk or “u.k.” or united kingdom* or (england* not “new england”) or northern ireland* or northern irish* or scotland* or scottish* or ((wales or “south wales”) not “new south wales”) or welsh*).ti,ab,jx,in,ad. | 3,375,725 |
| 19 | (bath or “bath’s” or ((birmingham not alabama*) or (“birmingham’s” not alabama*) or bradford or “bradford’s” or brighton or “brighton’s” or bristol or “bristol’s” or carlisle* or “carlisle’s” or (cambridge not (massachusetts* or boston* or harvard*)) or (“cambridge’s” not (massachusetts* or boston* or harvard*)) or (canterbury not zealand*) or (“canterbury’s” not zealand*) or chelmsford or “chelmsford’s” or chester or “chester’s” or chichester or “chichester’s” or coventry or “coventry’s” or derby or “derby’s” or (durham not (carolina* or nc)) or (“durham’s” not (carolina* or nc)) or ely or “ely’s” or exeter or “exeter’s” or gloucester or “gloucester’s” or hereford or “hereford’s” or hull or “hull’s” or lancaster or “lancaster’s” or leeds* or leicester or “leicester’s” or (lincoln not nebraska*) or (“lincoln’s” not nebraska*) or (liverpool not (new south wales* or nsw)) or (“liverpool’s” not (new south wales* or nsw)) or ((london not (ontario* or ont or toronto*)) or (“london’s” not (ontario* or ont or toronto*)) or manchester or “manchester’s” or (newcastle not (new south wales* or nsw)) or (“newcastle’s” not (new south wales* or nsw)) or norwich or “norwich’s” or nottingham or “nottingham’s” or oxford or “oxford’s” or peterborough or “peterborough’s” or plymouth or “plymouth’s” or portsmouth or “portsmouth’s” or preston or “preston’s” or ripon or “ripon’s” or salford or “salford’s” or salisbury or “salisbury’s” or sheffield or “sheffield’s” or southampton or “southampton’s” or st albans or stoke or “stoke’s” or sunderland or “sunderland’s” or truro or “truro’s” or wakefield or “wakefield’s” or wells or westminster or “westminster’s” or winchester or “winchester’s” or wolverhampton or “wolverhampton’s” or (worcester not (massachusetts* or boston* or harvard*)) or (“worcester’s” not (massachusetts* or boston* or harvard*)) or (york not (“new york*” or ny or ontario* or ont or toronto*)) or (“york’s” not (“new york*” or ny or ontario* or ont or toronto*))))).ti,ab,in,ad. | 2,611,006 |
| 20 | (bangor or “bangor’s” or cardiff or “cardiff’s” or newport or “newport’s” or st asaph or “st asaph’s” or st davids or swansea or “swansea’s”).ti,ab,in,ad. | 106,769 |
| 21 | (aberdeen or “aberdeen’s” or dundee or “dundee’s” or edinburgh or “edinburgh’s” or glasgow or “glasgow’s” or inverness or (perth not australia*) or (“perth’s” not australia*) or stirling or “stirling’s”).ti,ab,in,ad. | 359,669 |
| 22 | (armagh or “armagh’s” or belfast or “belfast’s” or lisburn or “lisburn’s” or londonderry or “londonderry’s” or derry or “derry’s” or newry or “newry’s”).ti,ab,in,ad. | 48,772 |
| 23 | or/16–22 | 4,091,713 |
| 24 | (exp “arctic and antarctic”/ or exp oceanic regions/ or exp western hemisphere/ or exp africa/ or exp asia/) not (united kingdom/ or europe/) | 3,115,003 |
| 25 | 23 not 24 | 3,8745,23 |
| 26 | 12 and 15 and 25 | 25 |
| 27 | (susceptib* or inhibit* or mic or mics or isolat* or in-vitro or “in vitro” or activ*).tw. | 9,609,593 |
| 28 | 12 and 27 | 1268 |
| 29 | 12 and 25 and 28 | 177 |
A1.3 CAZ/AVI CEA models
Term group(s): CAZ/AVI AND filters
Filters: Economic (MEDLINE, EMBASE), Exclusion (EMBASE)
Limits: None
Ovid MEDLINE(R) and Epub Ahead of Print, In-Process, In-Data-Review & Other Non-Indexed Citations, Daily and Versions(R) 1946 to 26 February 2021 (searched via the Ovid SP platform)
1st March 2021
| # | Searches | Results |
|---|---|---|
| 1 | ceftazidime.mp. | 10,210 |
| 2 | Ceftazidime/ | 4047 |
| 3 | 1 or 2 | 10,210 |
| 4 | avibactam.mp. | 964 |
| 5 | 3 and 4 | 789 |
| 6 | ceftazidime-avibactam.mp. | 711 |
| 7 | zavicefta.mp. | 2 |
| 8 | avycaz.mp. | 8 |
| 9 | (ctz-avi or caz-avi).mp. | 65 |
| 10 | or/5–9 | 792 |
| 11 | exp “Costs and Cost Analysis”/ | 242,835 |
| 12 | Economics/ | 27,294 |
| 13 | exp Economics, Hospital/ | 24,969 |
| 14 | exp Economics, Medical/ | 14,242 |
| 15 | Economics, Nursing/ | 4002 |
| 16 | exp models, economic/ | 15,443 |
| 17 | Economics, Pharmaceutical/ | 2971 |
| 18 | exp “Fees and Charges”/ | 30,592 |
| 19 | exp Budgets/ | 13,800 |
| 20 | budget*.tw. | 30,546 |
| 21 | ec.fs. | 431,631 |
| 22 | cost*.ti. | 125,579 |
| 23 | (cost* adj2 (effective* or utilit* or benefit* or minimi*)).ab. | 157,179 |
| 24 | (economic* or pharmacoeconomic* or pharmaco-economic*).ti. | 50,939 |
| 25 | (price* or pricing*).tw. | 42,703 |
| 26 | (financial or finance or finances or financed).tw. | 97,358 |
| 27 | (fee or fees).tw. | 18,704 |
| 28 | (value adj2 (money or monetary)).tw. | 2515 |
| 29 | quality-adjusted life years/ | 12,949 |
| 30 | (qaly or qalys).af. | 11,325 |
| 31 | (quality adjusted life year or quality adjusted life years).af. | 19,387 |
| 32 | or/11–31 | 801,858 |
| 33 | 10 and 32 | 16 |
EMBASE 1974 to 26 February 2021 (searched via the Ovid SP platform)
1st March 2021
| # | Searches | Results |
|---|---|---|
| 1 | ceftazidime.mp. | 45,327 |
| 2 | ceftazidime/ | 43,189 |
| 3 | 1 or 2 | 45,327 |
| 4 | avibactam.mp. | 1893 |
| 5 | 3 and 4 | 1609 |
| 6 | ceftazidime-avibactam.mp. | 955 |
| 7 | zavicefta.mp. | 18 |
| 8 | avycaz.mp. | 62 |
| 9 | (ctz-avi or caz-avi).mp. | 156 |
| 10 | or/5–9 | 1618 |
| 11 | “cost benefit analysis”/ | 87,111 |
| 12 | “cost effectiveness analysis”/ | 158,540 |
| 13 | economics/ | 241,957 |
| 14 | health economics/ | 33,700 |
| 15 | pharmacoeconomics/ | 7505 |
| 16 | fee/ | 14,329 |
| 17 | budget/ | 30,564 |
| 18 | budget$.tw. | 40,639 |
| 19 | cost$.ti. | 168,111 |
| 20 | (cost$ adj2 (effective$ or utilit$ or benefit$ or minimi$)).ab. | 218,259 |
| 21 | (economic$ or pharmacoeconomic$ or pharmaco-economic$).ti. | 64,563 |
| 22 | (price$ or pricing$).tw. | 60,859 |
| 23 | (financial or finance or finances or financed).tw. | 135,326 |
| 24 | (fee or fees).tw. | 25,728 |
| 25 | (value adj2 (money or monetary)).tw. | 3455 |
| 26 | health care quality/ | 247,699 |
| 27 | quality adjusted life year/ | 28,517 |
| 28 | (qaly or qalys).tw. | 21,188 |
| 29 | (quality adjusted life year or quality adjusted life years).tw. | 20,472 |
| 30 | or/11–29 | 1,102,354 |
| 31 | letter.pt. | 1,185,036 |
| 32 | editorial.pt. | 691,062 |
| 33 | historical article.pt. | 0 |
| 34 | or/31–33 | 1,876,098 |
| 35 | 30 not 34 | 1,021,484 |
| 36 | animals/ | 1,253,461 |
| 37 | humans/ | 13,458,185 |
| 38 | 36 not (36 and 37) | 965,742 |
| 39 | 35 not 38 | 1,010,813 |
| 40 | 10 and 39 | 56 |
CRD database (searched via the University of York CRD platform)
1 March 2021
| # | Searches | Results |
|---|---|---|
| 1 | (ceftazidime) | 49 |
| 2 | (avibactam) | 0 |
| 3 | (ceftazidime-avibactam) | 0 |
| 4 | (zavicefta) | 0 |
| 5 | (avycaz) | 0 |
| 6 | ((ctz-avi or caz-avi)) | 0 |
Web of Science – Conference proceedings index (searched via the Clarivate Analytics platform)
1 March 2021
| # | Searches | Results |
|---|---|---|
| 1 | TOPIC: (ceftazidime) | 9711 |
| 2 | TOPIC: (avibactam) | 1167 |
| 3 | #2 AND #1 | 984 |
| 4 | TOPIC: (ceftazidime-avibactam) | 919 |
| 5 | TOPIC: (zavicefta) | 2 |
| 6 | TOPIC: (avycaz) | 6 |
| 7 | TOPIC: ((ctz-avi or caz-avi)) | 59 |
| # 8 | #7 OR #6 OR #5 OR #4 OR #3 | 14 |
A1.4 Non-clinical evidence
Systematic searches were conducted from March until July 2021 to identify non-clinical evidence for relating to the evaluation.
The following electronic databases were searched from database inception:
-
MEDLINE and Epub Ahead of Print, In-Process, In-Data-Review & Other Non-Indexed Citations, Daily and Versions: Ovid, 1946 to Present
-
EMBASE: Ovid, 1980 to present
-
The University of York Centre for Reviews and Dissemination (CRD) platform
-
Database of Abstracts of Reviews of Effects (DARE): CRD, 1994 to 2015
-
Health Technology Assessment Database (HTA): CRD, 1989 to 2018
-
NHS Economic Evaluation Database (NHS EED): CRD, 1972 to 2015
-
| # | Search | Resultsa | ||
|---|---|---|---|---|
| MEDLINE | EMBASE | CRD | ||
| 1. | AMR models search | 26 | 67 | 2 |
| 2. | OXA-48 MBL search for dredging | 2507 | 3047 | 0 |
| 3. | Outcomes search: long-term outcomes | 23 | 72 | 0 |
| 4. | Outcomes search: medium outcomes | 562 | NS | NS |
| 5. | Utilities search | 367 | NS | NS |
A1.4.1 Focused AMR models search
Term group(s): Focused antimicrobial resistance AND modelling AND filter
Filters: Pragmatic and unvalidated economic filter (MEDLINE, EMBASE)
Limits: 2011–present, English language
Ovid MEDLINE(R) and Epub Ahead of Print, In-Process, In-Data-Review & Other Non-Indexed Citations, Daily and Versions(R) 1946 to 31 March 2021 (searched via the Ovid SP platform)
1 April 2021
| # | Searches | Results |
|---|---|---|
| 1 | ((antimicrobial or antibiotic or antibacterial) and resistan*).mp. | 148,175 |
| 2 | (model* or “population dynamic*” or simulat*).ti. | 718,508 |
| 3 | 1 and 2 | 2671 |
| 4 | limit 3 to yr=“2011 -Current” | 1901 |
| 5 | limit 4 to english language | 1884 |
| 6 | Cost-benefit analysis/ | 83,842 |
| 7 | Economic value of life/ | 5741 |
| 8 | Quality-adjusted life years/ | 13,042 |
| 9 | exp models, economic/ | 15,508 |
| 10 | cost utilit$.tw. | 4939 |
| 11 | cost benefit$.tw. | 11,329 |
| 12 | cost minim$.tw. | 1563 |
| 13 | cost effect$.tw. | 143,618 |
| 14 | economic evaluation$.tw. | 12,455 |
| 15 | or/6–14 | 213,673 |
| 16 | 5 and 15 | 26 |
EMBASE 1974 to 31 March 2021 (searched via the Ovid SP platform)
1 April 2021
| # | Searches | Results |
|---|---|---|
| 1 | ((antimicrobial or antibiotic or antibacterial) and resistan*).mp. | 298,764 |
| 2 | (model* or “population dynamic*” or simulat*).ti. | 863,662 |
| 3 | 1 and 2 | 4531 |
| 4 | limit 3 to yr=“2011 -Current” | 3042 |
| 5 | “cost benefit analysis”/ | 86,983 |
| 6 | Economic value of life/ | 145,299 |
| 7 | quality adjusted life year/ | 28,664 |
| 8 | exp economic model/ | 2513 |
| 9 | cost utilit$.tw. | 7843 |
| 10 | cost benefit$.tw. | 15,750 |
| 11 | cost minim$.tw. | 2664 |
| 12 | cost effect$.tw. | 198,907 |
| 13 | economic evaluation$.tw. | 17,713 |
| 14 | (“quality adjusted life year*” or qaly or qalys).tw. | 26,170 |
| 15 | or/5–14 | 433,603 |
| 16 | 4 and 15 | 67 |
CRD database (searched via the University of York CRD platform)
1 April 2021
| # | Searches | Results |
|---|---|---|
| 1 | (((antimicrobial or antibiotic or antibacterial) and resistan*)) | 459 |
| 2 | ((model* or “population dynamic*” or simulat*)):TI | 1554 |
| 3 | #1 AND #2 | 8 |
| 5 | (#3) FROM 2011 TO 2021 | 2 |
A1.4.2 Broad OXA-48 MBL search for database dredging
Term group(s): Mechanisms (OXA-48, NDM, VIM, IMP) AND Germ (enterobacteria, E. coli, K. pneumonia, P. aeruginosa) AND filters
Filters: Reviews, RCTs, observational studies filter (MEDLINE, EMBASE)
Limits: None
Ovid MEDLINE(R) and Epub Ahead of Print, In-Process, In-Data-Review & Other Non-Indexed Citations, Daily and Versions(R) 1946 to 29 March 2021 (searched via the Ovid SP platform)
7 April 2021
| # | Searches | Results |
|---|---|---|
| 1 | (oxa-48 or “oxa 48” or oxacillinase-48 or “oxacillinase 48”).tw. | 1202 |
| 2 | ((“new delhi” or ndm or “verona integrated-encoded” or vim or imipenemase or imp) and (mbl or “metallo-beta-lactamase” or “metallo beta lactamase”)).tw. | 1867 |
| 3 | 1 or 2 | 2969 |
| 4 | Enterobacteriaceae/ | 19,296 |
| 5 | Escherichia coli/ | 271,295 |
| 6 | Klebsiella pneumoniae/ | 14,859 |
| 7 | Pseudomonas aeruginosa/ | 43,940 |
| 8 | (enterobact* or enterobacteriaceae or “escherichia coli” or “e. coli” or “klebsiella pneumoniae” or “k. pneumoniae” or “pseudomonas aeruginosa” or “p. aeruginosa”).tw. | 399,190 |
| 9 | or/4–8 | 495,144 |
| 10 | 3 and 9 | 2507 |
| 11 | (MEDLINE or systematic review).tw. or meta analysis.pt. | 312,794 |
| 12 | Randomized Controlled Trial.pt. | 526,445 |
| 13 | Controlled Clinical Trial.pt. | 94,120 |
| 14 | Clinical Trial.pt. | 528,138 |
| 15 | exp Clinical Trials as Topic/ | 354,862 |
| 16 | Placebos/ | 35,413 |
| 17 | Random Allocation/ | 105,006 |
| 18 | Double-Blind Method/ | 163,341 |
| 19 | Single-Blind Method/ | 29,950 |
| 20 | Cross-Over Studies/ | 49,836 |
| 21 | ((random$ or control$ or clinical$) adj3 (trial$ or stud$)).tw. | 1,322,185 |
| 22 | (random$ adj3 allocat$).tw. | 38,452 |
| 23 | placebo$.tw. | 223,839 |
| 24 | ((singl$ or doubl$ or trebl$ or tripl$) adj (blind$ or mask$)).tw. | 179,179 |
| 25 | (crossover$ or (cross adj over$)).tw. | 90,152 |
| 26 | (“phase 3” or “phase three”).tw. | 16,453 |
| 27 | or/12–26 | 2,134,299 |
| 28 | animals/ not humans/ | 4,776,462 |
| 29 | 27 not 28 | 2,002,988 |
| 30 | Observational Studies as Topic/ | 6077 |
| 31 | Observational Study/ | 95,871 |
| 32 | Epidemiologic Studies/ | 8608 |
| 33 | exp Case-Control Studies/ | 1,155,597 |
| 34 | exp Cohort Studies/ | 2,110,104 |
| 35 | Cross-Sectional Studies/ | 359,015 |
| 36 | Controlled Before-After Studies/ | 605 |
| 37 | Historically Controlled Study/ | 196 |
| 38 | Interrupted Time Series Analysis/ | 1184 |
| 39 | Comparative Study.pt. | 1,886,769 |
| 40 | case control$.tw. | 136,201 |
| 41 | case series.tw. | 81,917 |
| 42 | (cohort adj (study or studies)).tw. | 231,371 |
| 43 | cohort analy$.tw. | 8925 |
| 44 | (follow up adj (study or studies)).tw. | 50,873 |
| 45 | (observational adj (study or studies)).tw. | 119,734 |
| 46 | longitudinal.tw. | 263,046 |
| 47 | prospective.tw. | 604,957 |
| 48 | retrospective.tw. | 582,233 |
| 49 | or/30–48 | 4,760,829 |
| 50 | 10 and 11 | 11 |
| 51 | 10 and 29 | 80 |
| 52 | 10 and 49 | 311 |
EMBASE 1974 to 6 April 2021 (searched via the Ovid SP platform)
7 April 2021
| # | Searches | Results |
|---|---|---|
| 1 | (oxa-48 or “oxa 48” or oxacillinase-48 or “oxacillinase 48”).tw. | 1483 |
| 2 | ((“new delhi” or ndm or “verona integrated-encoded” or vim or imipenemase or imp) and (mbl or “metallo-beta-lactamase” or “metallo beta lactamase”)).tw. | 2156 |
| 3 | 1 or 2 | 3502 |
| 4 | Enterobacteriaceae/ | 24,817 |
| 5 | Escherichia coli/ | 355,829 |
| 6 | Klebsiella pneumoniae/ | 44,139 |
| 7 | Pseudomonas aeruginosa/ | 102,141 |
| 8 | (enterobact* or enterobacteriaceae or “escherichia coli” or “e. coli” or “klebsiella pneumoniae” or “k. pneumoniae” or “pseudomonas aeruginosa” or “p. aeruginosa”).tw. | 446,239 |
| 9 | or/4–8 | 573,320 |
| 10 | 3 and 9 | 3045 |
| 11 | (meta-analysis or systematic review).tw. | 352,331 |
| 12 | Randomization/ | 90,999 |
| 13 | Placebo/ | 367,151 |
| 14 | Double Blind Procedure/ | 183,893 |
| 15 | Single Blind Procedure/ | 42,628 |
| 16 | Crossover Procedure/ | 66,858 |
| 17 | ((random$ or control$ or clinical$) adj3 (trial$ or stud$)).tw. | 184,6260 |
| 18 | (random$ adj3 allocat$).tw. | 48,159 |
| 19 | placebo$.tw. | 325,978 |
| 20 | ((singl$ or doubl$ or trebl$ or tripl$) adj (blind$ or mask$)).tw. | 251,245 |
| 21 | (crossover$ or (cross adj over$)).tw. | 112,515 |
| 22 | or/12–21 | 2,272,133 |
| 23 | nonhuman/ not human/ | 4,810,057 |
| 24 | 22 not 23 | 2,173,105 |
| 25 | Clinical study/ | 157,356 |
| 26 | Case control study/ | 171,323 |
| 27 | Family study/ | 26,257 |
| 28 | Longitudinal study/ | 153,994 |
| 29 | Retrospective study/ | 1,061,177 |
| 30 | comparative study/ | 895,931 |
| 31 | Prospective study/ | 678,405 |
| 32 | Randomized controlled trials/ | 201,238 |
| 33 | 31 not 32 | 670,835 |
| 34 | Cohort analysis/ | 693,427 |
| 35 | cohort analy$.tw. | 14,434 |
| 36 | (Cohort adj (study or studies)).tw. | 338,607 |
| 37 | (Case control$ adj (study or studies)).tw. | 146,583 |
| 38 | (follow up adj (study or studies)).tw. | 66,194 |
| 39 | (observational adj (study or studies)).tw. | 188,213 |
| 40 | (epidemiologic$ adj (study or studies)).tw. | 111,182 |
| 41 | (cross sectional adj (study or studies)).tw. | 248,198 |
| 42 | case series.tw. | 114,881 |
| 43 | prospective.tw. | 921,226 |
| 44 | retrospective.tw. | 972,633 |
| 45 | or/25–30,33–44 | 4,373,011 |
| 46 | 10 and 11 | 13 |
| 47 | 10 and 24 | 80 |
| 48 | 10 and 45 | 382 |
CRD database (searched via the University of York CRD platform)
30 March 2021
| # | Searches | Results |
|---|---|---|
| 1 | ((oxa-48 or “oxa 48” or oxacillinase-48 or “oxacillinase 48”)) | 0 |
| 2 | (((“new delhi” or ndm or “verona integrated-encoded” or vim or imipenemase or imp) and (mbl or “metallo-beta-lactamase” or “metallo beta lactamase”))) | 0 |
A1.4.3 Focused long-term outcomes search
Term group(s): (Carbapenem resistance OR mechanisms) AND (sites [UTI/HAPVAP]) AND filters
Filters: UK (MEDLINE, EMBASE), Europe (unvalidated)
Limits: 2010–present, English language
Ovid MEDLINE(R) and Epub Ahead of Print, In-Process, In-Data-Review & Other Non-Indexed Citations, Daily and Versions(R) 1946 to 10 June 2021 (searched via the Ovid SP platform)
11 June 2021
| # | Searches | Results |
|---|---|---|
| 1 | (carbapenem-resistan* or “carbapenem resistan*” or carbapenemase).tw. | 10,189 |
| 2 | (carbapenem* and (non-susceptib* or “non susceptib*” or nonsusceptib*)).tw. | 674 |
| 3 | (oxa-48* or “oxa 48*” or oxacillinase-48* or “oxacillinase 48*” or blaoxa-48* or “blaoxa 48*”).tw. | 1595 |
| 4 | ((“new delhi” or ndm or “verona integrated-encoded” or vim or imipenemase or imp) and (mbl or “metallo-beta-lactamase” or “metallo beta lactamase”)).tw. | 1900 |
| 5 | or/1–4 | 11,737 |
| 6 | (cohort* or longitudinal or prospective or retrospective or follow-up or “follow up” or long-term or “long term” or year).tw. | 4,211,288 |
| 7 | (mortality or death* or survival).tw. | 2,271,430 |
| 8 | Urinary Tract Infections/ | 39,976 |
| 9 | urinary tract infection*.tw. | 42,419 |
| 10 | (uti or utis or cuti or cutis).tw. | 17,460 |
| 11 | exp Pneumonia/ | 178,125 |
| 12 | pneumon*.tw. | 202,270 |
| 13 | exp Intensive Care Units/ | 91,189 |
| 14 | ((hospital* or ventilator* or icu or intensive care) adj3 (acquired or associat*)).tw. | 49,009 |
| 15 | Pneumonia, Ventilator-Associated/ | 3704 |
| 16 | (hap or vap).tw. | 10,159 |
| 17 | (11 or 12) and (13 or 14) | 17,397 |
| 18 | 8 or 9 or 10 or 15 or 16 or 17 | 91,038 |
| 19 | 5 and 6 and 7 and 18 | 160 |
| 20 | limit 19 to english language | 154 |
| 21 | limit 20 to yr=“2010 -Current” | 146 |
| 22 | exp Great Britain/ | 374,892 |
| 23 | (national health service* or nhs*).ti,ab,in. | 220,908 |
| 24 | (english not ((published or publication* or translat* or written or language* or speak* or literature or citation*) adj5 english)).ti,ab. | 40,760 |
| 25 | (gb or “g.b.” or britain* or (british* not “british columbia”) or uk or “u.k.” or united kingdom* or (england* not “new england”) or northern ireland* or northern irish* or scotland* or scottish* or ((wales or “south wales”) not “new south wales”) or welsh*).ti,ab,jw,in. | 2,187,630 |
| 26 | (bath or “bath’s” or ((birmingham not alabama*) or (“birmingham’s” not alabama*) or bradford or “bradford’s” or brighton or “brighton’s” or bristol or “bristol’s” or carlisle* or “carlisle’s” or (cambridge not (massachusetts* or boston* or harvard*)) or (“cambridge’s” not (massachusetts* or boston* or harvard*)) or (canterbury not zealand*) or (“canterbury’s” not zealand*) or chelmsford or “chelmsford’s” or chester or “chester’s” or chichester or “chichester’s” or coventry or “coventry’s” or derby or “derby’s” or (durham not (carolina* or nc)) or (“durham’s” not (carolina* or nc)) or ely or “ely’s” or exeter or “exeter’s” or gloucester or “gloucester’s” or hereford or “hereford’s” or hull or “hull’s” or lancaster or “lancaster’s” or leeds* or leicester or “leicester’s” or (lincoln not nebraska*) or (“lincoln’s” not nebraska*) or (liverpool not (new south wales* or nsw)) or (“liverpool’s” not (new south wales* or nsw)) or ((london not (ontario* or ont or toronto*)) or (“london’s” not (ontario* or ont or toronto*)) or manchester or “manchester’s” or (newcastle not (new south wales* or nsw)) or (“newcastle’s” not (new south wales* or nsw)) or norwich or “norwich’s” or nottingham or “nottingham’s” or oxford or “oxford’s” or peterborough or “peterborough’s” or plymouth or “plymouth’s” or portsmouth or “portsmouth’s” or preston or “preston’s” or ripon or “ripon’s” or salford or “salford’s” or salisbury or “salisbury’s” or sheffield or “sheffield’s” or southampton or “southampton’s” or st albans or stoke or “stoke’s” or sunderland or “sunderland’s” or truro or “truro’s” or wakefield or “wakefield’s” or wells or westminster or “westminster’s” or winchester or “winchester’s” or wolverhampton or “wolverhampton’s” or (worcester not (massachusetts* or boston* or harvard*)) or (“worcester’s” not (massachusetts* or boston* or harvard*)) or (york not (“new york*” or ny or ontario* or ont or toronto*)) or (“york’s” not (“new york*” or ny or ontario* or ont or toronto*))))).ti,ab,in. | 1,514,463 |
| 27 | (bangor or “bangor’s” or cardiff or “cardiff’s” or newport or “newport’s” or st asaph or “st asaph’s” or st davids or swansea or “swansea’s”).ti,ab,in. | 60,165 |
| 28 | (aberdeen or “aberdeen’s” or dundee or “dundee’s” or edinburgh or “edinburgh’s” or glasgow or “glasgow’s” or inverness or (perth not australia*) or (“perth’s” not australia*) or stirling or “stirling’s”).ti,ab,in. | 223,983 |
| 29 | (armagh or “armagh’s” or belfast or “belfast’s” or lisburn or “lisburn’s” or londonderry or “londonderry’s” or derry or “derry’s” or newry or “newry’s”).ti,ab,in. | 28,507 |
| 30 | or/22–29 | 2,749,551 |
| 31 | (exp africa/ or exp americas/ or exp antarctic regions/ or exp arctic regions/ or exp asia/ or exp oceania/) not (exp great britain/ or europe/) | 3,021,384 |
| 32 | 30 not 31 | 2,615,096 |
| 33 | 21 and 32 | 10 |
| 34 | (europe* or austria* or belgium* or “czech republic*” or france* or paris* or germany* or berlin* or ireland* or greece* or athens* or hungary* or italy* or rome* or netherlands* or luxembourg* or poland* or portugal* or scandinav* or denmark* or estonia* or finland* or iceland* or norway* or sweden* or “slovak republic*” or slovenia* or spain* or switzerland* or turkey* or israel*).ti,ab,tw. | 905,468 |
| 35 | 21 and 34 | 17 |
| 36 | 33 or 35 | 23 |
EMBASE 1974 to 10 June 2021 (searched via the Ovid SP platform)
11 June 2021
| # | Searches | Results |
|---|---|---|
| 1 | (carbapenem-resistan* or “carbapenem resistan*” or carbapenemase).tw. | 13,503 |
| 2 | (carbapenem* and (non-susceptib* or “non susceptib*” or nonsusceptib*)).tw. | 1006 |
| 3 | (oxa-48* or “oxa 48*” or oxacillinase-48* or “oxacillinase 48*” or blaoxa-48* or “blaoxa 48*”).tw. | 2084 |
| 4 | ((“new delhi” or ndm or “verona integrated-encoded” or vim or imipenemase or imp) and (mbl or “metallo-beta-lactamase” or “metallo beta lactamase”)).tw. | 2210 |
| 5 | or/1–4 | 15,369 |
| 6 | (cohort* or longitudinal or prospective or retrospective or follow-up or “follow up” or long-term or “long term” or year).tw. | 6,159,657 |
| 7 | (mortality or death* or survival).tw. | 3,257,266 |
| 8 | urinary tract infection/ | 108,436 |
| 9 | urinary tract infection*.tw. | 63,504 |
| 10 | (uti or utis or cuti or cutis).tw. | 29,713 |
| 11 | exp pneumonia/ | 330,487 |
| 12 | pneumon*.tw. | 280,722 |
| 13 | exp intensive care unit/ | 217,620 |
| 14 | ((hospital* or ventilator* or icu or intensive care) adj3 (acquired or associat*)).tw. | 75,142 |
| 15 | ventilator associated pneumonia/ | 11,398 |
| 16 | (hap or vap).tw. | 14,412 |
| 17 | (11 or 12) and (13 or 14) | 37,422 |
| 18 | 8 or 9 or 10 or 15 or 16 or 17 | 175,174 |
| 19 | 5 and 6 and 7 and 18 | 413 |
| 20 | limit 19 to english language | 400 |
| 21 | limit 20 to yr=“2010 -Current” | 386 |
| 22 | United Kingdom/ | 391,825 |
| 23 | (english not ((published or publication* or translat* or written or language* or speak* or literature or citation*) adj5 english)).ti,ab. | 48,212 |
| 24 | (gb or “g.b.” or britain* or (british* not “british columbia”) or uk or “u.k.” or united kingdom* or (england* not “new england”) or northern ireland* or northern irish* or scotland* or scottish* or ((wales or “south wales”) not “new south wales”) or welsh*).ti,ab,jx,in,ad. | 3,336,942 |
| 25 | (bath or “bath’s” or ((birmingham not alabama*) or (“birmingham’s” not alabama*) or bradford or “bradford’s” or brighton or “brighton’s” or bristol or “bristol’s” or carlisle* or “carlisle’s” or (cambridge not (massachusetts* or boston* or harvard*)) or (“cambridge’s” not (massachusetts* or boston* or harvard*)) or (canterbury not zealand*) or (“canterbury’s” not zealand*) or chelmsford or “chelmsford’s” or chester or “chester’s” or chichester or “chichester’s” or coventry or “coventry’s” or derby or “derby’s” or (durham not (carolina* or nc)) or (“durham’s” not (carolina* or nc)) or ely or “ely’s” or exeter or “exeter’s” or gloucester or “gloucester’s” or hereford or “hereford’s” or hull or “hull’s” or lancaster or “lancaster’s” or leeds* or leicester or “leicester’s” or (lincoln not nebraska*) or (“lincoln’s” not nebraska*) or (liverpool not (new south wales* or nsw)) or (“liverpool’s” not (new south wales* or nsw)) or ((london not (ontario* or ont or toronto*)) or (“london’s” not (ontario* or ont or toronto*)) or manchester or “manchester’s” or (newcastle not (new south wales* or nsw)) or (“newcastle’s” not (new south wales* or nsw)) or norwich or “norwich’s” or nottingham or “nottingham’s” or oxford or “oxford’s” or peterborough or “peterborough’s” or plymouth or “plymouth’s” or portsmouth or “portsmouth’s” or preston or “preston’s” or ripon or “ripon’s” or salford or “salford’s” or salisbury or “salisbury’s” or sheffield or “sheffield’s” or southampton or “southampton’s” or st albans or stoke or “stoke’s” or sunderland or “sunderland’s” or truro or “truro’s” or wakefield or “wakefield’s” or wells or westminster or “westminster’s” or winchester or “winchester’s” or wolverhampton or “wolverhampton’s” or (worcester not (massachusetts* or boston* or harvard*)) or (“worcester’s” not (massachusetts* or boston* or harvard*)) or (york not (“new york*” or ny or ontario* or ont or toronto*)) or (“york’s” not (“new york*” or ny or ontario* or ont or toronto*))))).ti,ab,in,ad. | 2,582,812 |
| 26 | (bangor or “bangor’s” or cardiff or “cardiff’s” or newport or “newport’s” or st asaph or “st asaph’s” or st davids or swansea or “swansea’s”).ti,ab,in,ad. | 105,817 |
| 27 | (aberdeen or “aberdeen’s” or dundee or “dundee’s” or edinburgh or “edinburgh’s” or glasgow or “glasgow’s” or inverness or (perth not australia*) or (“perth’s” not australia*) or stirling or “stirling’s”).ti,ab,in,ad. | 355,745 |
| 28 | (armagh or “armagh’s” or belfast or “belfast’s” or lisburn or “lisburn’s” or londonderry or “londonderry’s” or derry or “derry’s” or newry or “newry’s”).ti,ab,in,ad. | 48,430 |
| 29 | or/22–28 | 4,048,950 |
| 30 | (exp “arctic and antarctic”/ or exp oceanic regions/ or exp western hemisphere/ or exp africa/ or exp asia/) not (united kingdom/ or europe/) | 3,102,680 |
| 31 | 29 not 30 | 3,833,270 |
| 32 | 21 and 31 | 25 |
| 33 | (europe* or austria* or belgium* or “czech republic*” or france* or paris* or germany* or berlin* or ireland* or greece* or athens* or hungary* or italy* or rome* or netherlands* or luxembourg* or poland* or portugal* or scandinav* or denmark* or estonia* or finland* or iceland* or norway* or sweden* or “slovak republic*” or slovenia* or spain* or switzerland* or turkey* or israel*).ti,ab,tw. | 1,633,082 |
| 34 | 21 and 33 | 52 |
| 35 | 32 or 34 | 72 |
CRD database (searched via the University of York CRD platform)
11 June 2021
| # | Searches | Results |
|---|---|---|
| 1 | ((carbapenem-resistan* or “carbapenem resistan*” or carbapenemase)) | 5 |
| 2 | ((carbapenem* and (non-susceptib* or “non susceptib*” or nonsusceptib*))) | 0 |
| 3 | ((oxa-48* or “oxa 48*” or oxacillinase-48* or “oxacillinase 48*” or blaoxa-48* or “blaoxa 48*”)) | 0 |
| 4 | (((“new delhi” or ndm or “verona integrated-encoded” or vim or imipenemase or imp) and (mbl or “metallo-beta-lactamase” or “metallo beta lactamase”))) | 0 |
| 5 | ((cohort* or longitudinal or prospective or retrospective or follow-up or “follow up” or long-term or “long term” or year)) | 29,687 |
| 6 | ((mortality or death* or survival)) | 16,968 |
| 7 | #1 AND #5 AND #6 | 0 |
A1.4.4 Focused medium outcomes search
Search terms adapted from Bassetti et al. (2021): Sites (UTI/HAPVAP) AND (inappropriate OR appropriate antibiotics)/susceptibility AND hospitalisation AND filter
Filters: UK
Limits: MEDLINE only, 2007–present
Ovid MEDLINE(R) and Epub Ahead of Print, In-Process, In-Data-Review & Other Non-Indexed Citations, Daily and Versions(R) 1946 to June 30, 2021 (searched via the Ovid SP platform)
1 July 2021
| # | Searches | Results |
|---|---|---|
| 1 | urinary tract infection/ | 40,171 |
| 2 | urinary tract infection*.tw. | 42,550 |
| 3 | (uti or utis or cuti or cutis).tw. | 17,530 |
| 4 | exp pneumonia/ | 182,723 |
| 5 | pneumon*.tw. | 202,985 |
| 6 | exp intensive care unit/ | 91,779 |
| 7 | ((hospital* or ventilator* or icu or intensive care) adj3 (acquired or associat*)).tw. | 49,262 |
| 8 | ventilator associated pneumonia/ | 3730 |
| 9 | (hap or vap).tw. | 10,187 |
| 10 | (4 or 5) and (6 or 7) | 17,538 |
| 11 | 1 or 2 or 3 or 8 or 9 or 10 | 91,372 |
| 12 | ((inappropriat$ or inadequat$ or ineffectiv$ or discordan$ or incorrect$ or appropriat$ or adequate$ or concordan$) and (antibiotic$ or anti-biotic$ or antimicrobial$ or anti-microbial$ or antibacterial$ or anti-bacterial$ or bacteriocid$ or antimycobacterial$ or anti-mycobacterial$)).ti. | 1302 |
| 13 | ((inappropriat$ or inadequat$ or ineffectiv$ or discordan$ or incorrect$ or appropriat$ or adequate$ or concordan$) adj3 (antibiotic$ or anti-biotic$ or antimicrobial$ or anti-microbial$ or antibacterial$ or anti-bacterial$ or bacteriocid$ or antimycobacterial$ or anti-mycobacterial$)).ab,kf. | 16,750 |
| 14 | 12 or 13 | 17,382 |
| 15 | exp Hospitalization/ | 259,764 |
| 16 | exp Hospitals/ or exp Hospital Units/ | 395,569 |
| 17 | (hospital$ or inhospital$).ti,ab,kf,hw. | 1,709,507 |
| 18 | secondary care/ or tertiary healthcare/ or ((secondary or tertiary) adj (care or healthcare or health care)).ti,ab,kf. | 61,580 |
| 19 | (ward or wards or infirmary or infirmaries).ti,ab,kf. | 67,375 |
| 20 | (inpatient$ or in-patient).ti,ab,kf. | 184,282 |
| 21 | (ER or ERs or emergency room$1 or emergency department$1 or ED or EDs or casualty department$1 or “accident and emergency” or “A&E” or “A & E” or triage).ti,ab,kf. | 316,488 |
| 22 | (admission$1 or admitted$1 or readmission$1 or readmitted$1).ti,ab,kf. | 424,729 |
| 23 | (nosocomial or healthcare associated or health care associated or ventilator associated).ti,ab,kf. | 45,058 |
| 24 | exp Critical Care/ | 61,100 |
| 25 | exp Intensive Care Units/ | 91,779 |
| 26 | (acute care or critical care or critically ill or critical illness$).ti,ab,kf. | 106,880 |
| 27 | (high dependency adj2 (care or unit$1)).ti,ab,kf. | 955 |
| 28 | intensive care.ti,ab,kf. | 161,143 |
| 29 | intensive therapy unit$1.ti,ab,kf. | 646 |
| 30 | recovery room$.ti,ab,kf. | 3442 |
| 31 | (ITU or ICU or CCU or CICU or CITU or HDU or ITUs or ICUs or CCUs or CICUs or CITUs or HDUs).ti,ab,kf. | 71,336 |
| 32 | (level 2 care or level 3 care or level two care or level three care).ti,ab,kf. | 41 |
| 33 | or/15–32 | 2,397,151 |
| 34 | 11 and 14 and 33 | 1226 |
| 35 | limit 34 to yr=“2007 -Current” | 889 |
| 36 | exp Great Britain/ | 375,996 |
| 37 | (national health service* or nhs*).ti,ab,in. | 222,142 |
| 38 | (english not ((published or publication* or translat* or written or language* or speak* or literature or citation*) adj5 english)).ti,ab. | 40,948 |
| 39 | (gb or “g.b.” or britain* or (british* not “british columbia”) or uk or “u.k.” or united kingdom* or (england* not “new england”) or northern ireland* or northern irish* or scotland* or scottish* or ((wales or “south wales”) not “new south wales”) or welsh*).ti,ab,jw,in. | 2,194,256 |
| 40 | (bath or “bath’s” or ((birmingham not alabama*) or (“birmingham’s” not alabama*) or bradford or “bradford’s” or brighton or “brighton’s” or bristol or “bristol’s” or carlisle* or “carlisle’s” or (cambridge not (massachusetts* or boston* or harvard*)) or (“cambridge’s” not (massachusetts* or boston* or harvard*)) or (canterbury not zealand*) or (“canterbury’s” not zealand*) or chelmsford or “chelmsford’s” or chester or “chester’s” or chichester or “chichester’s” or coventry or “coventry’s” or derby or “derby’s” or (durham not (carolina* or nc)) or (“durham’s” not (carolina* or nc)) or ely or “ely’s” or exeter or “exeter’s” or gloucester or “gloucester’s” or hereford or “hereford’s” or hull or “hull’s” or lancaster or “lancaster’s” or leeds* or leicester or “leicester’s” or (lincoln not nebraska*) or (“lincoln’s” not nebraska*) or (liverpool not (new south wales* or nsw)) or (“liverpool’s” not (new south wales* or nsw)) or ((london not (ontario* or ont or toronto*)) or (“london’s” not (ontario* or ont or toronto*)) or manchester or “manchester’s” or (newcastle not (new south wales* or nsw)) or (“newcastle’s” not (new south wales* or nsw)) or norwich or “norwich’s” or nottingham or “nottingham’s” or oxford or “oxford’s” or peterborough or “peterborough’s” or plymouth or “plymouth’s” or portsmouth or “portsmouth’s” or preston or “preston’s” or ripon or “ripon’s” or salford or “salford’s” or salisbury or “salisbury’s” or sheffield or “sheffield’s” or southampton or “southampton’s” or st albans or stoke or “stoke’s” or sunderland or “sunderland’s” or truro or “truro’s” or wakefield or “wakefield’s” or wells or westminster or “westminster’s” or winchester or “winchester’s” or wolverhampton or “wolverhampton’s” or (worcester not (massachusetts* or boston* or harvard*)) or (“worcester’s” not (massachusetts* or boston* or harvard*)) or (york not (“new york*” or ny or ontario* or ont or toronto*)) or (“york’s” not (“new york*” or ny or ontario* or ont or toronto*))))).ti,ab,in. | 1,520,233 |
| 41 | (bangor or “bangor’s” or cardiff or “cardiff’s” or newport or “newport’s” or st asaph or “st asaph’s” or st davids or swansea or “swansea’s”).ti,ab,in. | 60,441 |
| 42 | (aberdeen or “aberdeen’s” or dundee or “dundee’s” or edinburgh or “edinburgh’s” or glasgow or “glasgow’s” or inverness or (perth not australia*) or (“perth’s” not australia*) or stirling or “stirling’s”).ti,ab,in. | 224,761 |
| 43 | (armagh or “armagh’s” or belfast or “belfast’s” or lisburn or “lisburn’s” or londonderry or “londonderry’s” or derry or “derry’s” or newry or “newry’s”).ti,ab,in. | 28,660 |
| 44 | or/36–43 | 2,757,556 |
| 45 | (exp africa/ or exp americas/ or exp antarctic regions/ or exp arctic regions/ or exp asia/ or exp oceania/) not (exp great britain/ or europe/) | 3,038,160 |
| 46 | 45 not 44 | 2,902,099 |
| 47 | 35 and 46 | 172 |
| 48 | (susceptib$ and (antibiotic$ or anti-biotic$ or antimicrobial$ or anti-microbial$ or antibacterial$ or anti-bacterial$ or bacteriocid$ or antimycobacterial$ or anti-mycobacterial$)).ti. | 10,075 |
| 49 | (susceptib$ adj3 (antibiotic$ or anti-biotic$ or antimicrobial$ or anti-microbial$ or antibacterial$ or anti-bacterial$ or bacteriocid$ or antimycobacterial$ or anti-mycobacterial$)).ab,kf. | 27,690 |
| 50 | 48 or 49 | 32,247 |
| 51 | 11 and 33 and 50 | 1563 |
| 52 | 46 and 51 | 520 |
| 53 | limit 52 to yr=“2007 -Current” | 425 |
A1.4.5 Utilities search: Charlson Comorbidity Index
Search terms: Charlson Comorbidity Index and utility filter
Filters: Health State Utility Value filter by Arber et al. (2017)
Limits: MEDLINE, English language
Ovid MEDLINE(R) and Epub Ahead of Print, In-Process, In-Data-Review & Other Non-Indexed Citations, Daily and Versions(R) 1946 to 12 July 2021
13 July 2021
| # | Searches | Results |
|---|---|---|
| 1 | Quality-Adjusted Life Years/ | 13,500 |
| 2 | Value of Life/ | 5752 |
| 3 | (qaly* or qald* or qale* or qtime*).ti,ab,kf. | 12,063 |
| 4 | (quality adjusted or adjusted life year*).ti,ab,kf. | 18,964 |
| 5 | disability adjusted life.ti,ab,kf. | 3946 |
| 6 | daly*1.ti,ab,kf. | 3468 |
| 7 | ((index adj3 wellbeing) or (quality adj3 wellbeing) or qwb).ti,ab,kf. | 868 |
| 8 | (multiattribute* or multi attribute*).ti,ab,kf. | 1013 |
| 9 | (utility adj3 (score*1 or scoring or valu* or measur* or evaluat* or scale*1 or instrument*1 or weight or weights or weighting or information or data or unit or units or health* or life or estimat* or elicit* or disease* or mean or cost* or expenditure*1 or gain or gains or loss or losses or lost or analysis or index* or indices or overall or reported or calculat* or range* or increment* or state or states or status)).ti,ab,kf. | 37,081 |
| 10 | utility.ab./freq=2 | 19,465 |
| 11 | utilities.ti,ab,kf. | 7876 |
| 12 | disutili*.ti,ab,kf. | 515 |
| 13 | (HSUV or HSUVs).ti,ab,kf. | 84 |
| 14 | health*1 year*1 equivalent*1.ti,ab,kf. | 40 |
| 15 | (hye or hyes).ti,ab,kf. | 75 |
| 16 | (hui or hui1 or hui2 or hui3).ti,ab,kf. | 1679 |
| 17 | (illness state*1 or health state*1).ti,ab,kf. | 7144 |
| 18 | (euro qual or euro qual5d or euro qol5d or eq-5d or eq5-d or eq5d or euroqual or euroqol or euroqual5d or euroqol5d).ti,ab,kf. | 12,834 |
| 19 | (eq-sdq or eqsdq).ti,ab,kf. | 1 |
| 20 | (short form* or shortform*).ti,ab,kf. | 37,135 |
| 21 | (sf36* or sf 36* or sf thirtysix or sf thirty six).ti,ab,kf. | 23,718 |
| 22 | (sf6 or sf 6 or sf6d or sf 6d or sf six or sfsix or sf8 or sf 8 or sf eight or sfeight).ti,ab,kf. | 3519 |
| 23 | (sf12 or sf 12 or sf twelve or sftwelve).ti,ab,kf. | 5294 |
| 24 | (sf16 or sf 16 or sf sixteen or sfsixteen).ti,ab,kf. | 30 |
| 25 | (sf20 or sf 20 or sf twenty or sftwenty).ti,ab,kf. | 344 |
| 26 | (15D or 15-D or 15 dimension).ti,ab,kf. | 5601 |
| 27 | (standard gamble* or sg).ti,ab,kf. | 11,912 |
| 28 | (time trade off*1 or time tradeoff*1 or tto or timetradeoff*1).ti,ab,kf. | 2046 |
| 29 | or/1–28 | 160,013 |
| 30 | (“charlson comorbidity index” or “charlson index” or (cci and (comorbid* or “co morbid*” or multimorbid* or “multi morbid*”))).mp. | 8444 |
| 31 | 29 and 30 | 387 |
| 32 | limit 31 to english language | 368 |
Appendix 2 Risk-of-bias assessment tool and scores
A2.1 The bespoke risk-of-bias assessment tool
| Questions | Score Low risk Unclear risk High risk |
|---|---|
|
|
Is the target population of the study broadly appropriate to the HVCS? Consider:
|
|
Were isolates selected based on resistance to comparators?
|
|
Was there appropriate inclusion or exclusion of isolates with co-carriage of other significant mechanisms, as per HVCS?
|
|
Were all isolates tested for the pathogen–mechanism of interest in a standard way, and does this match the HVCS?
|
|
Was the beta-lactamase test appropriate?
|
|
Were data collected over an appropriate time period? Consider:
|
|
Target population overall judgement
|
|
|
|
Were isolates sampled from the target population in an appropriate way?
|
|
NB
|
|
| Sampling strategy overall judgement If any item scores high risk or unclear risk, the overall judgement should be high or unclear risk, respectively. If all items score low risk, the overall judgement should be low risk. |
|
|
|
Was susceptibility measured in an appropriate, standard way? Consider:
|
|
Does the study demonstrate selective analysis reporting, with respect to S, I and R?
|
|
Were S, I and R reported consistently for all treatments?
|
|
Outcome measurement overall judgement
|
|
|
|
| Is there a risk of bias from missing data? Were all isolates tested for all treatments? Where this isn’t the case, is it likely that missingness was associated with treatment outcome? Where some isolates were not tested for some treatments, and reasons were not provided, score unclear risk of bias. Where some isolates were not tested for some treatments, and the reasons for this were due to expected susceptibility, score high risk of bias. |
|
Missing data overall judgement
|
A2.2 Risk-of-bias scores with reasons
| Study ID | 1. Target population | 2. Sampling strategy | 3. Outcome measurement | 4. Missing data | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Is the target population of the study broadly appropriate to the HVCS? | Were isolates selected based on resistance to comparators? | Was there appropriate inclusion or exclusion of isolates with co-carriage of other significant mechanisms, as per HVCS? | Were all isolates tested for the pathogen-mechanism of interest in a standard way, and does this match the HVCS? | Was the beta-lactamase test appropriate? | Were data collected over an appropriate time period? | Target population overall judgement | Were isolates sampled from the target population in an appropriate way? | Sampling strategy: overall judgement | Was susceptibility measured in an appropriate, standard way? | Does the study demonstrate selective analysis reporting, with respect to S, I and R? | Were S, I and R reported consistently for all treatments? | Outcome measurement: overall judgement | Is there a risk of bias from missing data? | Missing data: overall judgement | |
| UK studies | |||||||||||||||
| PHE data | Unclear – not clear if outbreaks will be over-represented | Unclear – isolates submitted to PHE for suspected carbapenemases, unclear how this judged | Unclear – not clear if MBLs were included | Low risk – all isolates were tested for beta-lactamases | Unclear what methodology used? | Low risk – 2014 to 2021 | Unclear risk | Unclear – unclear if all isolates that met PHE criteria for submission were submitted since submission was voluntary | Unclear risk | Unclear – PHE do not have access to the methods of susceptibility testing by each lab | Low risk | Low risk | Unclear risk | Unclear – the analysis excluded isolates not tested for all treatments, but it was not clear why some isolates were not tested | Unclear risk |
| Livermore 2011 | Unclear – not clear if outbreaks will be over-represented | Low risk – submitted due to carbapenem resistance | Unclear – not clear if MBLs were included | Low risk – all isolates were tested for beta-lactamases | Low risk – PCR | Unclear – dates of recruitment not fully reported | Unclear risk | Unclear – unclear if all isolates that met PHE criteria for submission were submitted since submission was voluntary | Unclear risk | High risk – EUCAST and CLSI not interchangeable (clinical opinion) | Low risk | Low risk | High risk | Low risk | Low risk |
| Non-UK studies (in order of size) | |||||||||||||||
| Kazmierczak 2018 (INFORM) |
Low risk | High risk – some isolates selected on basis of ceftazidime resistance | Low risk – data without MBL co-carriage reported | Low risk – methodology likely to capture all beta-lactamases since it includes CR | Low risk – PCR | Low risk – 2012 to 2015 | High risk | Unclear – selected on basis of predefined # per species – unclear if this would produce a representative sample | Unclear risk | Unclear risk – used CLSI, EUCAST for colistin, FDA for tigecycline and CAZ-AVI as no breakpoints from CLSI, unclear if CLSI equivalent to EUCAST | Low risk | Low risk | Unclear risk | Low risk | Low risk |
| Vazquez-Ucha 2021 | Low risk | Low risk – screening threshold for CR | Low risk – data without MBL co-carriage reported | Low risk – methodology likely to capture all beta-lactamases since used screening cut-off | Low risk – whole genome sequencing | Low risk – 2018 | Low risk | Unclear – not clear if consecutive or what ‘representative’ means | Unclear risk | Low risk – EUCAST for both methods and breakpoints | Low risk | Low risk | Low risk | Low risk | Low risk |
| Garcia-Castillo 2018 (iCREST – Spain) | Low risk | Low risk – consecutive, then screened for CPE using commercial assay | Unclear | Low risk – consecutive, then screened for CPE using commercial assay | Low risk – used molecular characterisation, and whole genome sequencing | Low risk – 2016 | Unclear risk | Low risk – consecutive | Low risk | Unclear – lab method not reported | Low risk | Low risk | Unclear risk | Low risk | Low risk |
| Longshaw 2020 (SIDERO-CR 2014–16)33 | Low risk | Low risk – meropenem non-susceptible | High risk – includes MBLs | Low risk – all meropenem non-susceptible tested | Low risk – PCR | Low risk – 2014 to 2016 | High risk | Unclear – selected from surveillance collection based on AST or species, unclear if the sample will therefore be representative | Unclear risk | High risk – EUCAST and CLSI not interchangeable (clinical opinion) | Low risk | Low risk | High risk | Low risk | Low risk |
| Mataraci 2020 | Low risk | Unclear – not reported | Unclear – not reported | Unclear – not reported | Low risk – PCR | Low risk – 2017 | Unclear risk | Unclear – not reported | Unclear risk | Low risk – EUCAST for both methods and breakpoints | Low risk | Low risk | Low risk | Low risk | Low risk |
| Han 2020 | Low risk | Low risk – not selected on resistance to comparators | Low risk – none co-carried MBLs | Unclear – unclear how isolates were selected for genetic testing | Low risk – PCR | Low risk – 2016 to 2018 | Unclear risk | Low risk – consecutive | Low risk | Unclear risk – used CLSI, FDA for Tigecycline, unclear if CLSI equivalent to EUCAST | Low risk | Low risk | Unclear risk | Low risk | Low risk |
| Johnston 2020 | Low risk | Unclear – not clear how some isolates selected | Unclear – not reported | Low risk – all CR tested | Low risk – PCR | Unclear risk – 2002–2017 | Unclear risk | Unclear – some isolates submitted voluntarily which may skew population | Unclear risk | High risk – EUCAST and CLSI not interchangeable (clinical opinion) | Low risk | Low risk | High risk | Low risk | Low risk |
| Kazmierczak 2019 (SIDERO-WT) | Low risk | High risk – may overselect for colistin-resistant isolates | High risk – includes MBLs | Low risk – methodology likely to capture all beta-lactamases since it includes CR | Low risk – PCR | Low risk – 2014 | High risk | Unclear – selected on basis of predefined # per species – unclear if this would produce a representative sample | Unclear risk | Unclear – CLSI lab, CLSI breakpoints, EUCAST for colistin (no breakpoint from CLSI), unclear if CLSI equivalent to EUCAST | Low risk | Low risk | Unclear risk | Low risk | Low risk |
| Viala 2019 | Low risk | Unclear risk – unclear how selected for study | Unclear – not reported | Unclear risk – unclear how selected for testing | Low risk – PCR | Low risk – 2015 to 2014 | Unclear risk | Low risk – consecutive | Low risk | Unclear – lab method not reported | Low risk | Low risk | Unclear risk | Unclear risk – missing data for high proportion of isolates for 3 comparators | Unclear risk |
| De la Calle 2019 | Low risk | Low risk – meropenem non-susceptible | Unclear – not reported | Low risk – methodology likely to capture all beta-lactamases since it includes CR | Unclear risk – some isolates only tested using rapid immunochromatographic test | Low risk – 2014 to 2016 | Unclear risk | Low risk – consecutive | Low risk | Unclear – lab method not EUCAST | Low risk | Low risk | Unclear risk | Low risk | Low risk |
| Galani 2019 | Low risk | Unclear – unclear how isolates were selected | Unclear – not reported | Unclear risk – unclear how selected for testing | Low risk – whole genome sequencing | Low risk – 2014 to 2016 | Unclear risk | Low risk – consecutive | low risk | High risk – EUCAST and CLSI not interchangeable (clinical opinion) | Low risk | Low risk | High risk | Low risk | Low risk |
| Sherry 2018 | Low risk | Unclear – unclear how isolates were selected | Unclear – not reported | Unclear risk – unclear how selected for testing | Low risk – PCR | Low risk – 2012 to 2015 | Unclear risk | Unclear – not reported | Unclear risk | Unclear risk – used CLSI, FDA for CAZ-AVI, unclear if CLSI equivalent to EUCAST | Low risk | Low risk | Unclear risk | Low risk | Low risk |
| Bhagwat 2020 | Low risk | Unclear risk – isolates selected on basis of aztreonam-avibactam resistance, not clear if this will affect susceptibility | Low risk – data without MBL co-carriage reported | Unclear risk – unclear how selected for testing | Low risk – whole genome sequencing | Low risk – 2017 to 2018 | Unclear risk | Unclear – not clear how isolates were chosen for inclusion | Unclear risk | High risk – EUCAST and CLSI not interchangeable (clinical opinion) | Low risk | Low risk | High risk | Unclear risk – missing data for high proportion of isolates for 3 comparators | Unclear risk |
| Study ID, Funding | Country, multisite? Year(s) of recruitment |
N, Includes OXA-48-like? | Inclusion criteria/beta-lactamase testing selection criteria | Consecutive sample? | % mero non-susceptible | MBL co-carriage? | Laboratory methods, Breakpoints | Source of study | Included in network meta-analyses? |
|---|---|---|---|---|---|---|---|---|---|
| Excluded from meta-analysis (reported MIC 50 and MIC 90 but not % susceptible) | |||||||||
| Dobias 201760 Shionogi |
International | 154 Y |
CPE, unclear how selected for testing | No, selected for ‘most widespread and broad spectrum resistance’ | NR | NR | CLSI CLSI |
EEPRU search | N, only reported MIC 50/90 |
| Delgado-Valverde 202068 Shionogi |
Spain | 57 Unclear |
KP, ESBL and/or carbapenemase producer, unclear how selected for testing | No, selected on various criteria | NR | 1.8% | CLSI CLSI |
EEPRU search | N, only reported MIC 50/90 |
| UK studies excluded from meta-analysis due to overlap with PHE data | |||||||||
| Livermore 201864 PHE & MSD |
UK (PHE), 1%, International, multisite 2015–6 |
333 Y |
CPE isolates submitted to PHE AMRHAI with suspected CR | Unclear | NR | NR | BSAC EUCAST |
EEPRU search | N, overlap with PHE dataset |
| Mushtaq 202167 Wockhardt Ltd |
UK (PHE), multisite 2015–6 |
250a 274b Y |
CPE isolates submitted to PHE AMRHAI with suspected CR | Unclear | 27.2% | 0%a 8.75%b |
BSAC EUCAST |
EEPRU search | N, overlap with PHE dataset |
| Livermore 2017a65 Wockhardt Ltd |
UK (PHE), multisite NR |
15 Y |
CPE [isolates submitted to PHE AMRHAI with suspected CR + resistance surveys (unclear how selected for testing)] | Unclear | 86.7% | NR | CLSI EUCAST |
EEPRU search | N, overlap with PHE dataset |
| Studies excluded to avoid double counting of isolates | |||||||||
| de Jonge 2016 (INFORM)59 AstraZeneca |
International, multisite 2012–6 |
134 Y |
CPE, meropenem non-susceptible tested | Assume same as Kazmierczak 201834 | 100% | 0% | CLSI CLSI, EUCAST col, FDA TIG, CAZ-AVI |
EEPRU search | N, overlap with Kazmierczak 201834 |
| Karlowsky 2019 (INFORM Latin America)63 | Latin America, multisite 2012–15 |
14 Y |
CPE – CR or ceftazidime-resistant, or positive for ESBL by clavulanic acid testing | No – Selected predefined # per species | 14.3% | Unclear | EEPRU search | ||
| Karlowsky 2018 (INFORM Asia-Pacific)62 | Asia-Pacific | Data extraction not performed as n < 10. Reported here as relates to INFORM study. | EEPRU search | N, overlap with Kazmierczak 201834 N<10 |
|||||
| Galani 201861 | Greece, multisite 2014–6 |
14 Y |
CR KP, non-susceptible to any carbapenem were tested | Y | 100% | 0% | CLSI EUCAST |
EEPRU search | |
| Outbreaks | |||||||||
| Lim 202053 NR |
UK, single-site 2018 |
60 Unclear |
KP OXA-48 outbreak, then all medical wards were screened (not all screened were KP) | Y | 10% | NR | EUCAST EUCAST |
EEPRU search | N, outbreak study |
| Sousa 201854 Internal hospital funding |
Spain, single-site 2016–7 |
57 Unclear |
KP outbreak | Y | 98% | NR | CLSI CLSI |
EEPRU search | N, outbreak study |
| Mavroidi 202066 | Greece, single-site 2014–6 |
23 Unclear |
KP outbreak, then retrospective screening of frozen isolates and testing of colistin-resistant isolates | Y | 0% | 0% | CLSI CLSI, EUCAST for colistin and TIG |
EEPRU search | N, outbreak study |
Appendix 3 Reviews 1 and 2 results
A3.1 Review 1: RCTs in HAP/VAP and/or cUTI
Based on RCT evidence, what is the comparative effectiveness of the intervention and comparators in patients with cUTI or HAP/VAP caused by an OXA-48 Enterobacterales infection?
Of the studies included in the key characteristics mapping, four47–50 were RCTs (three phase III,47,48,50 one phase II49) reporting outcomes for adult patients with cUTI47,49,50 or HAP/VAP48 who had been treated with CAZ-AVI (see Appendix 3, Table 39). Three47,48,50 recruited patients with infections caused by Enterobacterales or Pseudomonas aeruginosa, and one49 recruited patients with any Gram-negative organism. The comparator in the four trials varied, including best available therapy [meropenem, imipenem, doripenem, colistin and (for cIAI) tigecycline],47 doripenem,50 meropenem48 and imipenem-cilastatin. 49 All trials aimed to recruit patients who were expected to be responsive to the study treatments, based on the treating physician’s judgement or known susceptibility. Consequently, all trials recruited largely carbapenem-susceptible infections and therefore had low relevance to the HVCSs. Two trials47,50 reported a small number of OXA-48 infections (Table 39, n = 3 in each study), but outcome data were not reported for these patients separately.
Although the RCTs have low relevance to the HVCSs due to the low numbers of OXA-48 or carbapenem-resistant infections, it is important to establish that CAZ-AVI is an effective treatment in the sites of interest (HAP/VAP and cUTI). The four trials47–50 at these sites reported similar or non-inferior efficacy (Table 39) between CAZ-AVI and comparator arms, as determined by the primary outcome measure (clinical cure,47,48 patient-reported symptomatic resolution,50 or microbiological response49). In the interest of brevity, and to allow a more detailed consideration of the evidence that is used in the EEPRU CE model, more detail about the clinical outcomes of these studies is not reported here, but can be found in the company submission108 sections: REPROVE in Section 3.1.1 (outcomes reported in Tables 12 and 13), RECAPTURE 1 and 2 reported in Section 3.3.1 (outcomes reported in Tables 33 and 34), REPRISE reported in Section 3.3.2 (outcomes for REPRISE reported in Table 37). Vazquez et al. 2012 was not listed in the company submission,108 but is detailed in Table 40 of this report. Outcomes for RCTs are not included in this review because they were performed in the sites outside the HVCS and are also available from the company submission. 108 The safety of CAZ-AVI is addressed by Review 6 in the main report.
| Author, year, study acronym | Country; study design | Key Inclusion criteria | Site of infection, Pathogens, OXA-48 (N) | Intervention, comparator (N randomised) | Limitations in terms of HVCSs | Data for R4?a | Primary outcome |
|---|---|---|---|---|---|---|---|
| HAP/VAP | |||||||
| Torres et al. (2018)48 REPROVE (NCT01808092) N = 879 |
Multicentre; multinational; phase III RCT | GNOs not likely to be CAZ-AVI or meropenem resistant: (suspected CPE excluded at baseline) | HAP/VAP Enterobacterales and PA OXA-48: N = 0 |
CAZ-AVI (n = 409) Meropenem (n = 408) |
Suspected CPE (and therefore OXA-48) excluded at baseline | None | CC at ToC CAZ-AVI: 245/356 (68.8%) Mero: 270/370 (73.0%) Difference: 4–4.2% (95% CI 10.8 to 2.5%) |
| cUTI | |||||||
| Carmeli et al. (2016)47 REPRISE (NCT01644643) N = 333 |
Multicentre; multinational; phase III RCT | 18–80 years with cUTI or IAI, ceftazidime-resistant | cUTI or cIAI Enterobacterales and PA OXA-48: N=3 |
CAZ-AVI (n = 165) BATb (n = 168) |
Only 3 OXA-48 infections | None | CC at ToC CAZ-AVI 140/154 (91%; 95% CI 85·6 to 94·7) BAT: 135/148 (91%; 85·9 to 95·0) Difference NR |
| Wagenlehner et al. (2016)50 RECAPTURE 1 and 2 (NCT01595438 and NCT01599806) N = 1033 |
Multicentre; multinational; phase III RCT | cUTI and for whom study drugs were considered appropriate empiric therapy | cUTI Enterobacterales and PA OXA-48: N = 3 |
CAZ-AVI (n = 516) DPM (n = 517) |
Only 3 OXA-48 infections | None | Patient-reported symptomatic resolution CAZ-AVI: 276/393 (70.2%) DPM 276/417 (66.2%) Difference: 4% (95% CI −2.39 to 10.42%) |
| Vazquez et al. (2012)49 (NCT00690378) N = 137 |
Multicentre; multinational; phase II RCT | GNOs likely to be susceptible to study drugs; excluded known CRO | cUTI GNOs OXA-48: N = 0 |
CAZ-AVI (N = 69) Imi-cil (N = 68) |
Known CR infections excluded at baseline; zero OXA-48 infections | None | Microbiological responseCAZ-AVI: 19/27 (70.4%) Imi-cil: 25/35 (71.4%) Difference: −1.1% (95% CI −27.2 to 25.0%) |
A3.2 Summary of results for the phase II study (Vazquez et al. 2012)49 not included in the Pfizer company submission
| Outcomes | Results |
|---|---|
| Efficacy results – primary endpoint |
|
| Efficacy results – key secondary endpoint(s) | ME population
|
CE population
|
|
Microbiological and clinical responses
|
|
MITT population
|
|
| Safety results |
|
| Conclusion(s) | CAZ/AVI and BAT led to the same proportion of patients achieving an overall clinical cure at the test-of-cure visit in the mMITT population (91% in both groups). The efficacy and safety of CAZ-AVI may be similar to that of imipenem–cilastatin for the treatment of cUTI in adults, including those with ceftazidime-non-susceptible pathogens. |
A3.3 Review 2: observational studies
Based on observational studies, what is the comparative effectiveness of the intervention and comparators in patients with cUTI or HAP/VAP caused by an OXA-48 Enterobacterales infection?
Since the RCTs did not recruit or report outcomes for subgroups of patients with OXA-48 infections and were largely in patients susceptible to carbapenems, Approach 2 was considered.
Of the studies included in the key characteristics mapping, nine43,51–58 were observational or case-control studies, reporting treatment with CAZ-AVI.
Of the nine observational studies43,51–58 (Table 41), six43,51–55 reported outcomes for patients with OXA-48 infections. However, all reported infections across a range of sites, and in none of these was it possible to separate out patients with cUTI or HAP/VAP. In addition, five did not report comparator data, and as such it would have been necessary to obtain patient-level data from at least one study in order to perform any (adjusted) form of synthesis; given the timescales of the project it was thought unlikely this could be achieved. A question was raised with the company regarding whether they had conducted or would be conducting their own adjusted comparison, and whether they had access to the relevant IPD data (submitted to NICE on 21 May 2021, see Report Supplementary Material 1), but the company were unable to help. Additionally, all studies were of a small sample size, limiting the conclusions that could be drawn from them due to the possibility of chance imbalances at baseline biasing results, and increasing the likely uncertainty associated with any synthesis performed.
The three remaining studies56–58 treated a wider selection of pathogens, which may have had relevance to the ES, where patients were treated on the suspicion of a carbapenem-resistant infection. However, again, no studies reported results for HAP/VAP or cUTI alone and two56,58 reported a mixture of patients treated in the MDS and ES. One (CARBAR)57 only reported data for three patients treated with CAZ-AVI. It was therefore concluded that observational studies would not be able to fulfil the evidential requirements of an economic model.
| Author, year | Country | Site of infection | Intervention comparator |
Pathogen–mechanism | Sample size | Outcomes | Reason for exclusion |
|---|---|---|---|---|---|---|---|
| Studies reporting all or a subgroup of OXA-48 infections treated with CAZ-AVI | |||||||
| De la Calle et al. 201943 | Spain | Any/mixed | CAZ-AVI; mono and combination No comparator arm |
OXA-48 Enterobacterales | 23 | 30-day and 90-day mortality 8.3% and 20.8%, respectively Clinical cure at 30 days 62.5% of episodes |
Mixed infection sites; no comparator arm; small number of patients |
| Sousa et al. 201854 | Spain | Any/mixed (mortality by site) | CAZ-AVI; mono and combination No comparator arm |
OXA-48 Enterobacterales | 57 | 14- and 30-day all-cause mortality 14% and 22%, respectively Clinical cure 77% Microbiological cure 65% |
Mixed infection sites; no comparator arm; small number of patients |
| Temkin et al. 201755 | Europe; Australia | Any/mixed | CAZ-AVI; mono and combination No comparator arm |
OXA-48 Enterobacterales | 38 | All-cause in-hospital mortality 39.5% (95% CI 24.0 to 56.6%). Clinical and/or microbiological cure 73.7% (95% CI 56.9 to 86.6%) |
Mixed infection sites; no comparator arm; small number of patients |
| Lim 202053 | UK | Screening, and 6 clinical isolates (4 urine, 1 blood, 1 pus) | CAZ-AVI No comparator arm |
KP OXA-48 | 4 | Antibiotic susceptibility results for the OXAKp isolates 100% for CAZ-AVI appearing sensitive on disc diffusion testing (EUCAST methodology) |
Mixed infection sites; no comparator arm; small number of patients |
| Alraddadi et al. 201951 | Saudi Arabia | Mixed; BSI; HAP; cUTI; cIAI; soft-tissue infection | CAZ-AVI Various comparatorsa |
CRE OXA-48 | CAZ-AVI n = 8 Comparator n = 19 |
Complete remission CAZ-AVI: 80% (8/10) Comparator: 53.6% (15/28) P = 0.14 Clinical cure without relapse or death within 30 days CAZ-AVI: 40% (4/10) Comparator: 39% (11/28) P > 0.99 Other outcomes not extracted |
Mixed infection sites; small number of patients |
| Katchanov 201852 | Germany | Any | CAZ-AVI No comparator arm |
KP OXA-48 | 5 | In-hospital mortality 100% |
Mixed infection sites; small number of patients |
| Studies recruiting wider populations potentially applicable to the ES, treated with CAZ-AVI | |||||||
| Nwankwo 202156 | UK | Respiratory diseases not limited to HAP/VAP | CAZ-AVI No comparator arm |
NR (various) | 28 | Susceptibility 56% susceptibility (15/27 isolates) of MDR organisms |
Not limited to HAP/VAP; mixture of MDS and ES treatment; unclear if any patients had OXA-48; outcomes reported for whole cohort |
| CARBAR (Shionogi submission)57 | UK | Any/mixed | CAZ-AVI Various comparators |
CRE, CR Pseudomonas spp., CR Stenotrophomonas spp. and CR Acinetobacter spp. | 157 | Mortality 51% (76/148) In-hospital mortality 26% (n = 39/148) Microbial cure 89% (33/37) |
Mixed infection sites; only 3 patients were treated with CAZ-AVI, mechanism not reported |
| Karaiskos 202158 | Greece | Any | CAZ-AVI No comparator arm for the OXA-48 patients |
KP OXA-48 KP KPC |
147 OXA-48 (n = 7, 5%) |
14- and 28-day all-cause mortality 9% and 20%, respectively Microbiological eradication 37.4% (55/147) |
Mixed population of MDS and ES patients; not reported by site |
Appendix 4 Susceptibility synthesis methods and sensitivity analysis results
A4.1 Statistical model for the network meta-analysis
The data are presented as the total number of susceptible rik out of the total number of isolates, nik for patients arm k of study i. The data generation process is assumed to follow a binomial likelihood such that
where pik represents the probability of an event in arm k of trial i. The probabilities are modelled on the logit scale as
where the µik are trial-specific baselines, representing the log-odds of response in the baseline treatment. The trial-specific treatment effects, δi,1k, are log-odds ratios of response for the treatment in arm k, relative to the baseline treatment.
For the random-effects model, the trial-specific treatment effects, δi,1k, are assumed to arise from a common random-effects distribution
where dti1tik represents the mean effect of the treatment in arm k of study i,tik, compared to the treatment in arm 1 of study i,ti1 and τ2 represents the between-study variance in treatment effects (heterogeneity), which is assumed to be the same for all treatments.
The model was completed by specifying prior distributions for the parameters. Where there were sufficient sample data, conventional non-informative prior distributions were used:
-
trial specific baseline, μi~N(0,1002)
-
treatment effects relative to reference treatment, d1k~N(0,1002)
-
between-study standard deviation of treatment effects, τ~U(0,3).
A4.2 Network diagrams and Model FIT statistics
FIGURE 16.
Network diagram of all studies contributing to the NMA.
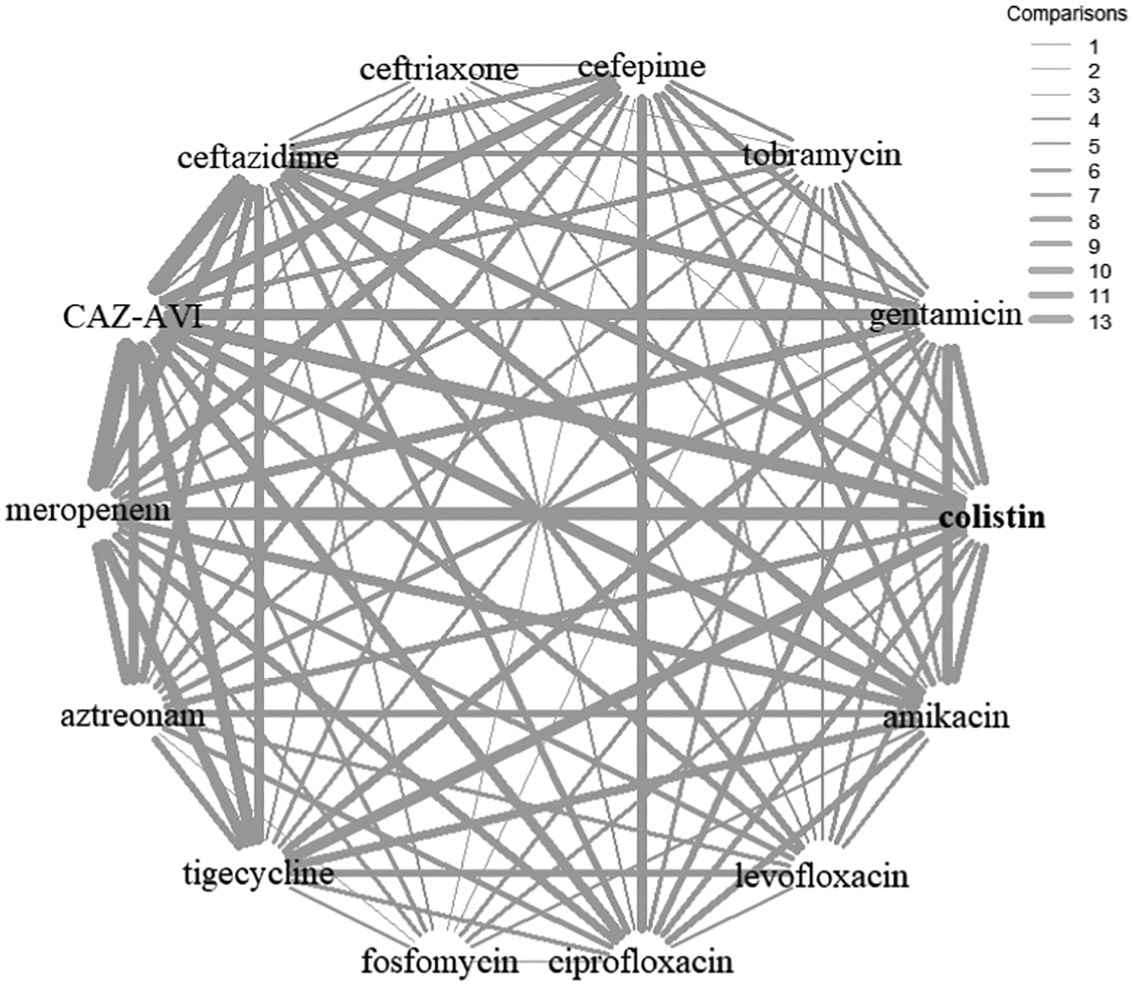
| Model descriptiona | Studies | Absolute model fit | Model comparison | Heterogeneity | |
|---|---|---|---|---|---|
| DP | TRD | DIC | SD (95 % CrI) | ||
| Main analyses | |||||
| Full data set, NMA model | 16 | 111 | 110.9 | 616.82 | 1.99 (1.64 to 2.44) |
| Full data set, UME model | 111 | 120.8 | 626.05 | 1.71 (1.38 to 2.14) | |
| Reduced data set,b NMA model | 109 | 109.9 | 608.14 | 1.56 (1.28 to 1.93) | |
| Reduced data set,b UME model | 109 | 131.5 | 629.31 | 1.38 (1.08 to 1.78) | |
| Sensitivity analyses c | |||||
| Unusual inclusion criteria, MR model | 16 | 109 | 109.3 | 607.41 | 1.57 (1.28 to 1.95) |
| Unusual inclusion criteria subgroup | 13 | 96 | 95.42 | 537.45 | 1.51 (1.22 to 1.89) |
| MBL co-carriage, subgroupd | 6 | 49 | 50.8 | 287.398 | 1.38 (0.95 to 2.06) |
| Carbapenem susceptibility, MR model | 14 | 101 | 101.7 | 563.03 | 1.56 (1.26 to 1.96) |
| Consecutive samples. MR model | 16 | 109 | 109.4 | 607.63 | 1.57 (1.28 to 1.95) |
| EUCAST, subgroup | 3 | 28 | 28.21 | 189.39 | 0.98 (0.62 to 1.65) |
FIGURE 17.
Network diagram using reduced dataset contributing to the NMA.
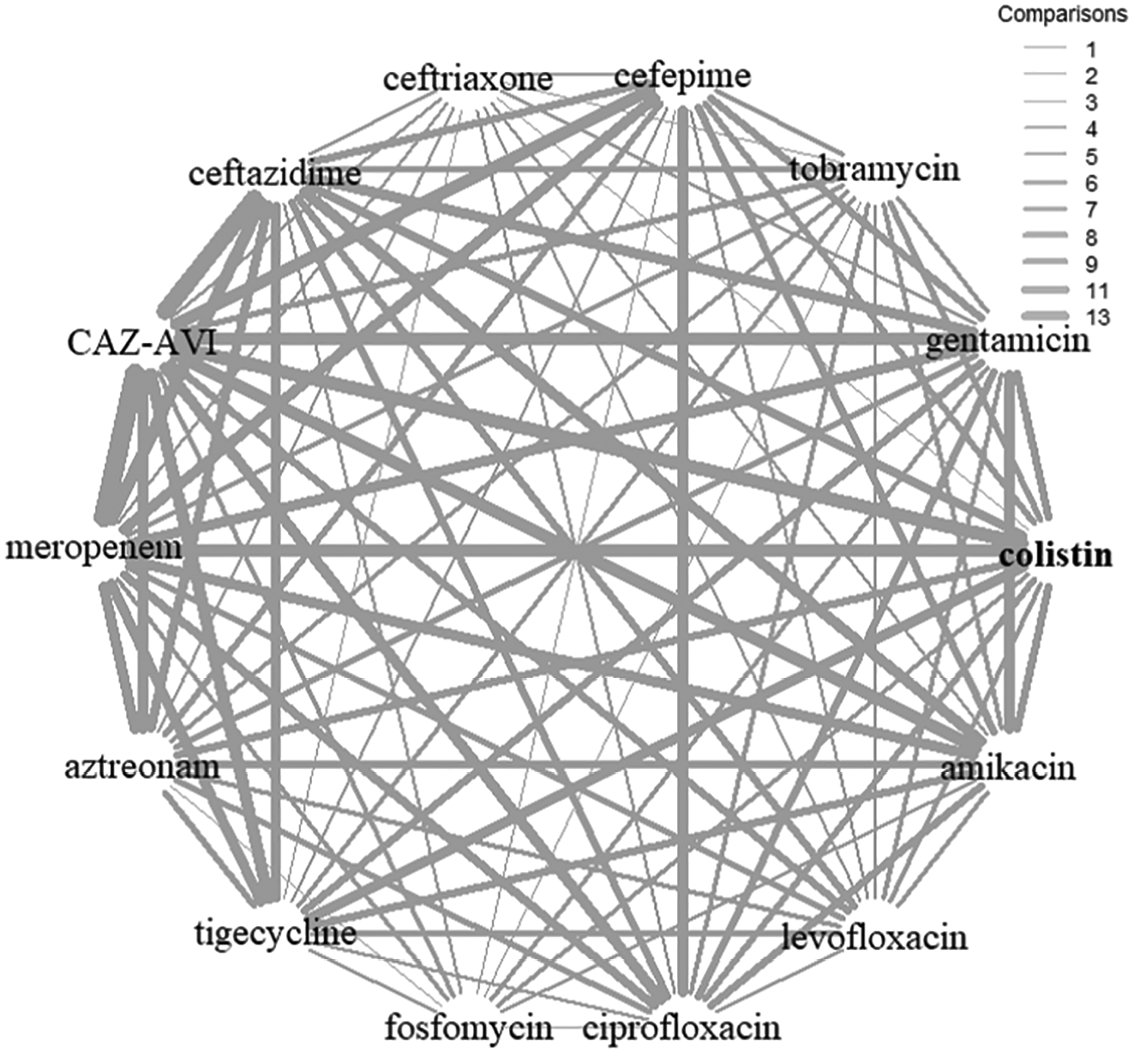
FIGURE 18.
Network diagram studies contributing to the NMA restricted to EUCAST breakpoints.
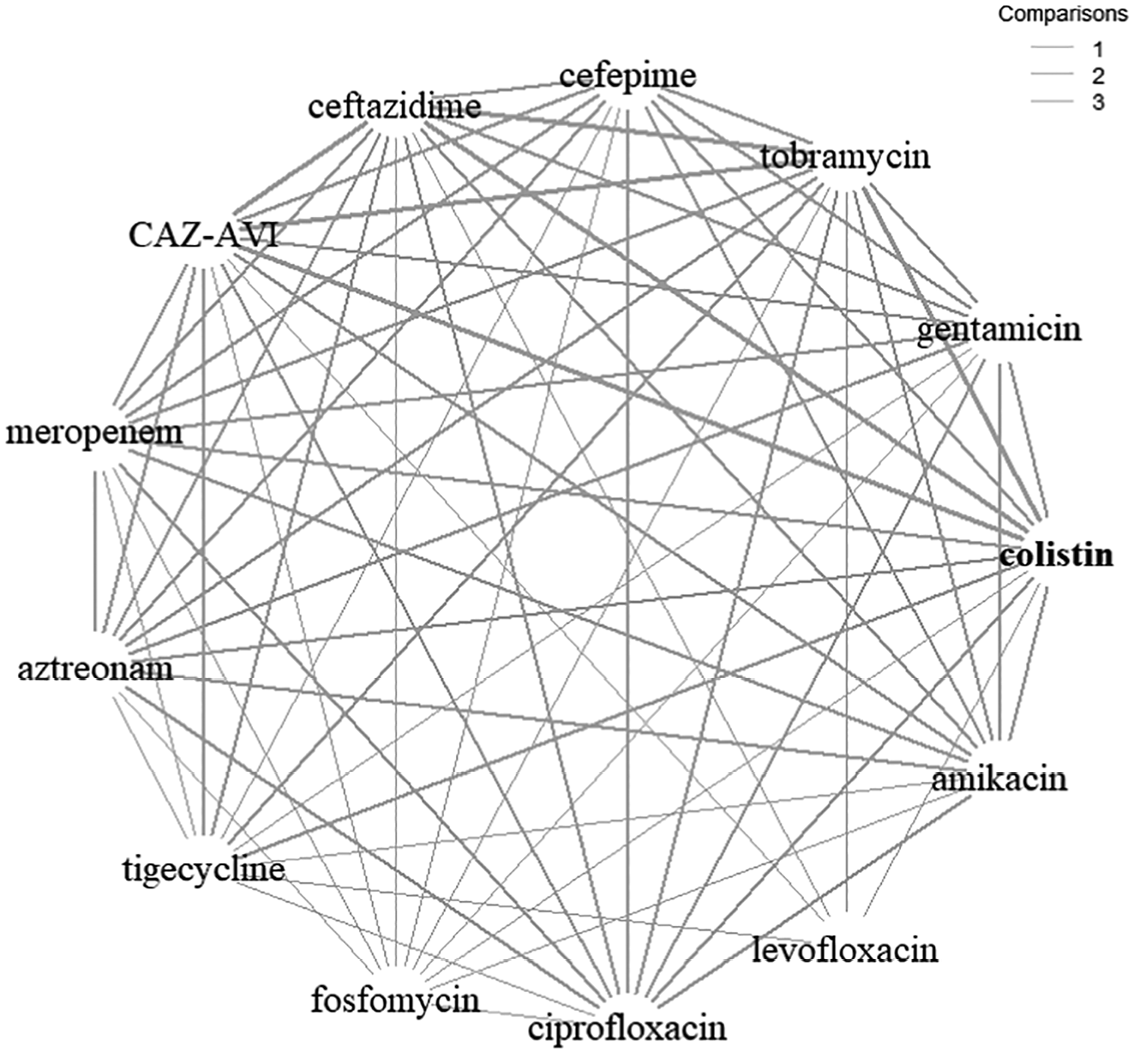
A4.3 Studies with unusual inclusion criteria
The methods of recruitment of isolates and identification of OXA-48 carriage were not always well reported,32,33,36,38,42,45 but generally isolates were selected for the more resource-intensive beta-lactamase testing through some form of screening process. In five studies,35,37,39,40,43,44 this was by identification of carbapenem resistance or non-susceptibility, probably through AST, though this wasn’t always clear. Resistance to other treatments was used to select isolates for beta-lactamase testing in three cases (ceftazidime resistance,34 meropenem or colistin resistance,41 aztreonam-avibactam resistance46). In the NMA, the affected ceftazidime (along with the cefepime arm, since this is also a cephalosporin) and colistin arms were removed from the analysis altogether, since these relate to comparator treatments.
A meta-regression model (Figure 19) was fitted with a covariate indicating whether the study had unusual inclusion criteria. 34,41,46 Compared to the standard NMA model, the meta-regression model provided a similar fit to the data based on the DIC and did not reduce the estimated between-study SD (1.57, 95% CrI 1.28 to 1.95). The coefficient from the meta-regression was not statistically significant (0.81, 95% CrI −1.75 to 3.40). There was therefore no evidence to suggest that the relative treatment effects differ according to the identified unusual inclusion criteria.
FIGURE 19.
Forest plot of OR vs. colistin for reduced dataset, meta-regression model for unusual inclusion criteria. CrI, credible interval; OR, odds ratio; PB, probability being the best treatment; PrI, prediction interval.
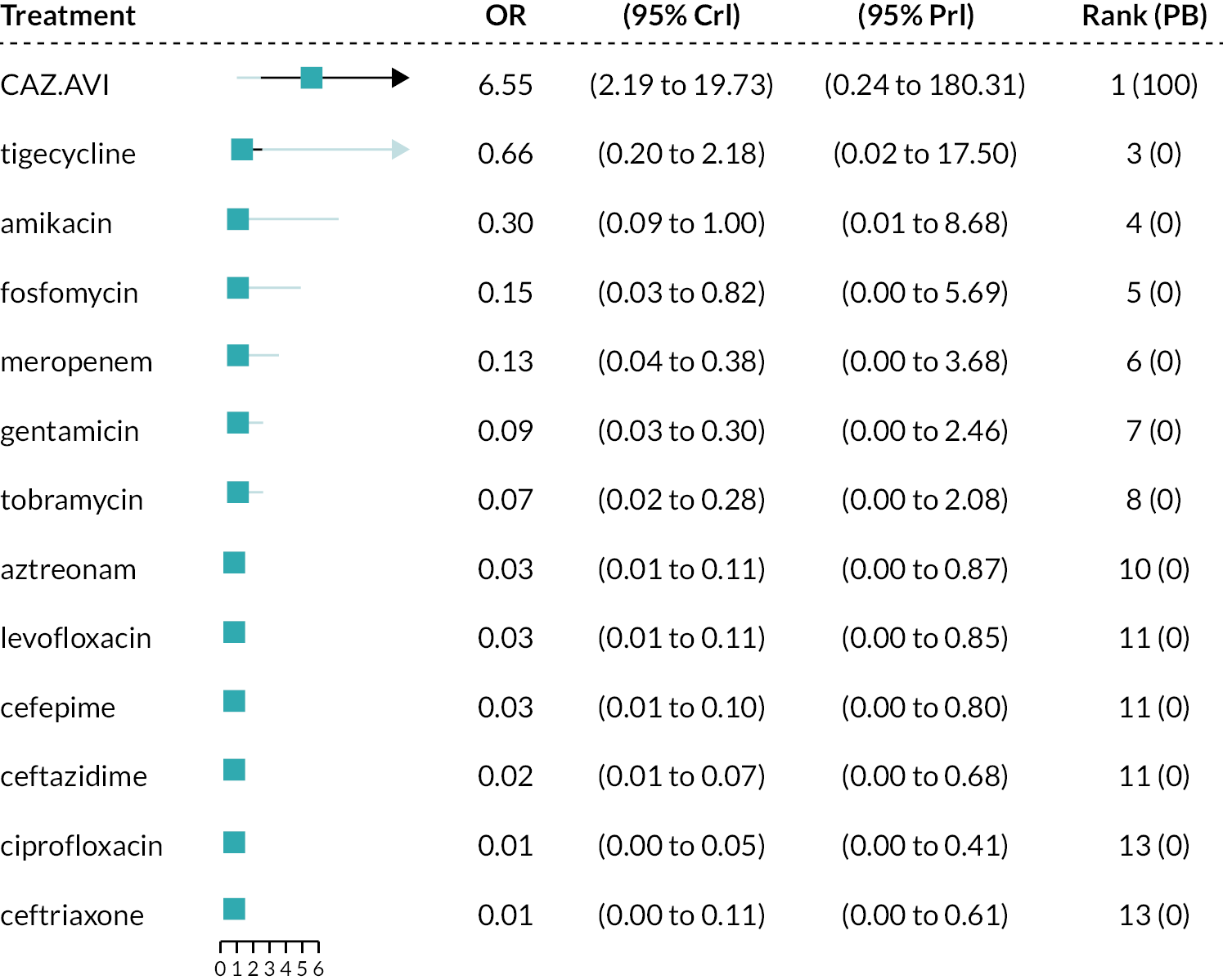
A subgroup analysis (Figure 20) was performed excluding the studies that had unusual inclusion criteria. 34,41,46 The between-study SD was 1.51 (95% CrI 1.21 to 1.89) which was similar to the base-case NMA. CAZ-AVI was associated with a statistically significant higher susceptibility relative to colistin (OR 6.57, 95% CrI 2.23 to 20.30) with probability 100% of being the most effective treatment; median rank 1. The remainder of the treatments were associated with lower susceptibility than colistin (OR < 1) although this was not statistically significant for tigecycline based on the 95% CrI. For all comparators, the extremely high between-study SD results in wide 95% PrI.
FIGURE 20.
Forest plot of OR vs. colistin for reduced dataset, subgroup analysis for unusual inclusion criteria. CrI, credible interval; OR, odds ratio; PB, probability being the best treatment PrI, prediction interval.
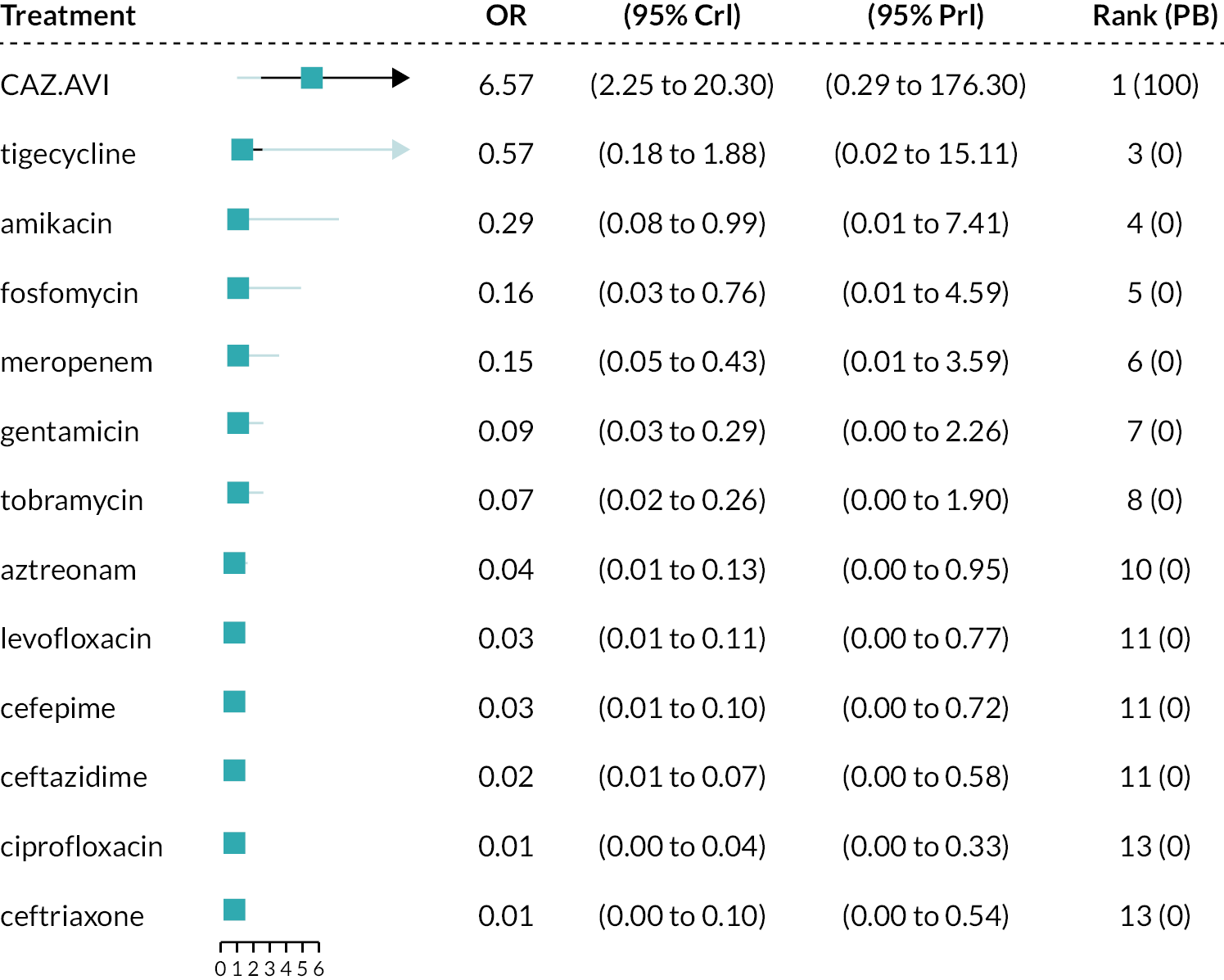
Metallo-beta-lactamases co-carriage
The majority of studies (eight)31,32,36,38,40,42,43,45 did not state whether isolates with MBL co-carriage were included. Two studies reported data both with and without MBL co-carriage34,46 and the IPD for one study35 was reanalysed by EEPRU to exclude MBL co-carriage. Two studies37,41 included isolates with MBL co-carriage and reported that 9.4%37 and 15.6%41 of isolates co-carried MBLs. Two studies39,44 excluded isolates co-carrying MBLs from the analysis.
A subgroup analysis (Figure 21) was performed including just the six studies that provided data with no co-carriage of MBLs. A meta-regression model was not considered appropriate in this instance since the direction of the interaction effect may differ for alternative comparators.
FIGURE 21.
Forest plot of OR vs. colistin for reduced dataset, NMA model for MBL co-carriage subgroup. CrI, credible interval; OR, odds ratio; PB, probability being the best treatment; PrI, prediction interval.
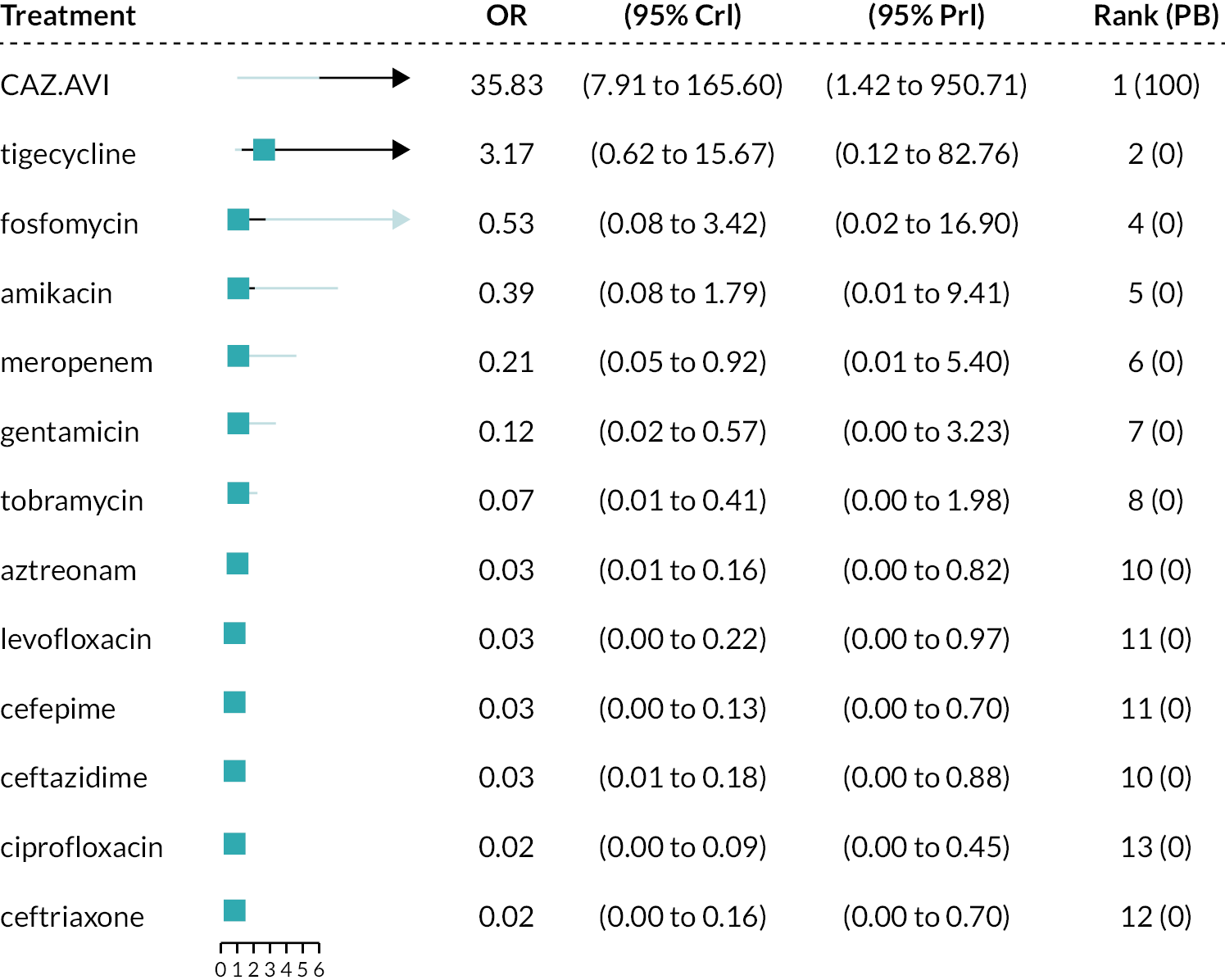
The estimated between-study SD was slightly reduced (1.38, 95% CrI 0.95 to 2.06) compared to the standard NMA model, but with wider CrI and still classed as extremely high. Estimated OR versus colistin were increased compared to the model with all studies included; however, there was a large amount of uncertainty. Although the analysis did not provide conclusive evidence that co-carriage of MBLs has a statistically significant effect on the resulting relative effects, the analysis further highlights the heterogeneity in treatment effects and, since there was a good clinical rationale to support this analysis, a scenario analysis based on co-carriage of MBLs was planned in the modelling. Since it was also concluded that restricting to studies using EUCAST methods and breakpoints was the preferred approach (see Results of the network meta-analysis), this left only one study (Vazquez-Ucha et al. 2021)15 that both reported data with 0% MBLs and used EUCAST methods and breakpoints. A scenario analysis within the cost-effectiveness analysis based on this one study was therefore planned.
Proportion with carbapenem susceptibility
To investigate the impact of the proportion of carbapenem non-susceptible isolates on CAZ-AVI susceptibility, the % non-susceptible to meropenem was extracted for each study as this was the most frequently reported statistic.
A meta-regression was performed (Figure 22) including a covariate indicating the proportion of non-susceptible isolates for each study. Two studies did not provide information on carbapenem susceptibility and so were not included in the analysis. 38,45 For the remaining 14 studies, the percentage non-susceptible ranged from 0%46 to 100%,41,44 with mean 53.3% non-susceptible.
FIGURE 22.
Forest plot of OR vs. colistin for reduced dataset, meta-regression model for carbapenem susceptibility. CrI, credible interval; OR, odds ratio; PB, probability being the best treatment; PrI, prediction interval.
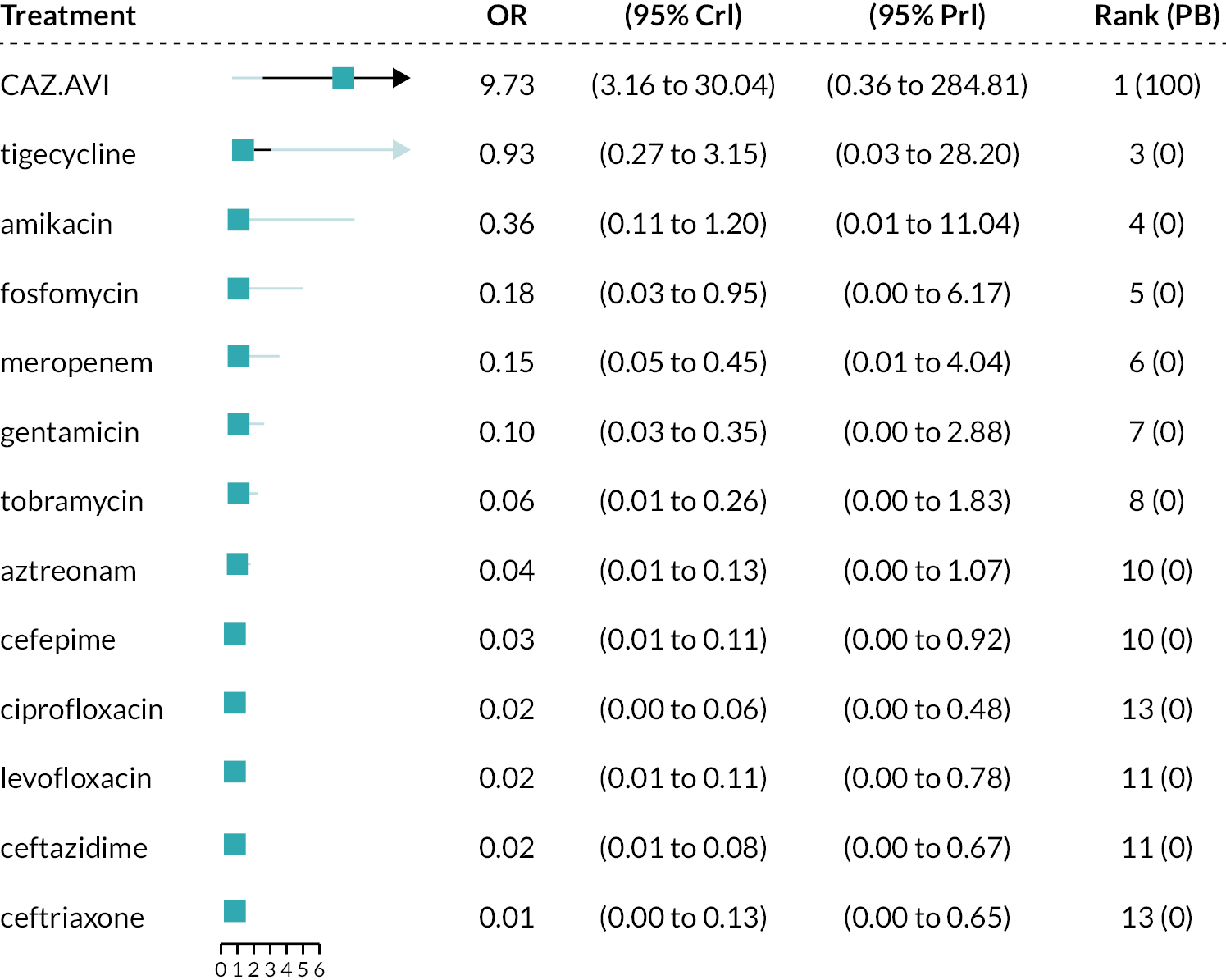
The meta-regression model did not reduce the estimated between-study SD (1.56, 95% CrI 1.26 to 1.96) compared to the standard NMA model. The coefficient from the meta-regression was 0.30 (95% CrI −2.60 to 3.24), which is close to zero and not statistically significant. There was therefore no evidence to suggest that the relative treatment effects differ according to the proportion with carbapenem susceptibility.
Consecutive sample recruitment
Five studies36,39,42–44 selected consecutive isolates, while the remainder were either unclear31–33,35,38,46 how isolates were selected, or used specific criteria to do so. 34,37,40,41,45 A meta-regression model was conducted (Figure 23) comparing those studies with consecutive samples (the reference category) to those where sampling was either non-consecutive or unclear.
FIGURE 23.
Forest plot of OR vs. colistin for reduced dataset, meta-regression model for consecutive samples. CrI, credible interval; OR, odds ratio; PB, probability being the best treatment; PrI, prediction interval.
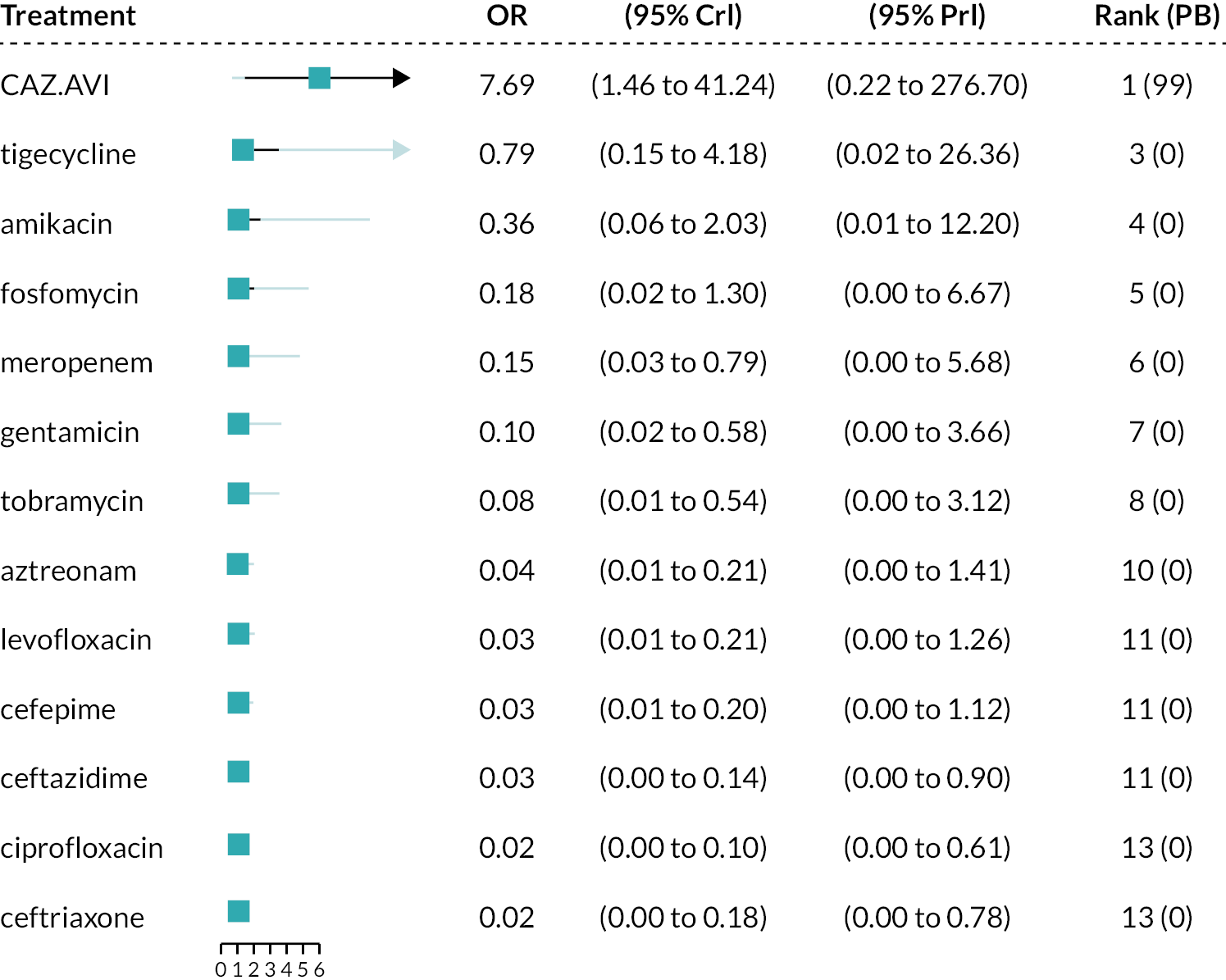
Compared to the standard NMA model, the meta-regression model provided a similar fit to the data based on the DIC and did not reduce the estimated between-study SD (1.57, 95% CrI 1.28 to 1.95). The coefficient from the meta-regression was not statistically significant (−0.10, 95% CrI −1.93 to 1.75). There was therefore no evidence to suggest that the relative treatment effects differ according to method of sample recruitment.
Network meta-analysis results with full dataset
The conclusions of the sensitivity analyses using the full data (Table 43 and Figures 29–34) were consistent with the analyses using the reduced data.
| Model description | Studies | Absolute model fit | Model comparison | Heterogeneity | Meta-regression coefficient | |
|---|---|---|---|---|---|---|
| DP | TRD | DIC | SD (95 % CrI) | |||
| Sensitivity analyses using full data | ||||||
| Unusual inclusion criteria, meta-regression model | 16 | 111 | 110.3 | 616.57 | 2.01 (1.66, 2.46) | 0.05 (−3.16,3.49) |
| Unusual inclusion criteria subgroup | 13 | 98 | 96.96 | 547.13 | 2.01 (1.64, 2.50) | NR |
| MBL co-carriage, subgroup | 6 | 50 | 50.53 | 291.30 | 1.74 (1.22, 2.53) | NR |
| Carbapenem susceptibility, meta-regression model | 14 | 103 | 102.5 | 571.95 | 2.02 (1.65, 2.50) | −1.60 (−5.15,1.94) |
| Consecutive samples. meta-regression model | 16 | 111 | 110.9 | 617.301 | 2.00 (1.65, 2.46) | 0.91 (−1.20,3.28) |
FIGURE 24.
Forest plot of OR vs. colistin for full data, NMA model. CrI, credible interval; OR, odds ratio; PB, probability being the best treatment; PrI, prediction interval.
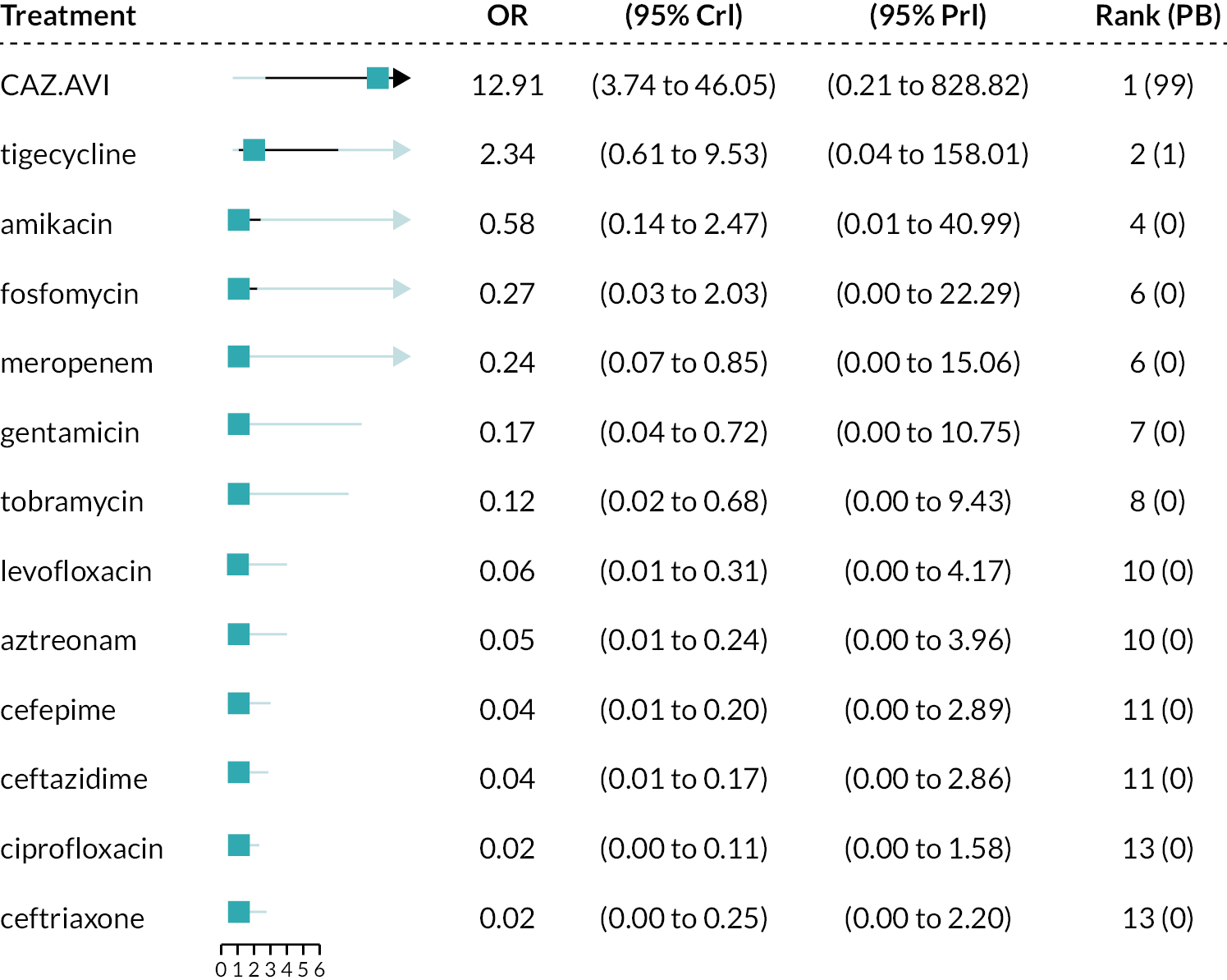
FIGURE 25.
Forest plot of OR vs. colistin for full dataset, meta-regression model for unusual inclusion criteria. CrI, credible interval; OR, odds ratio; PB, probability being the best treatment; PrI, prediction interval.
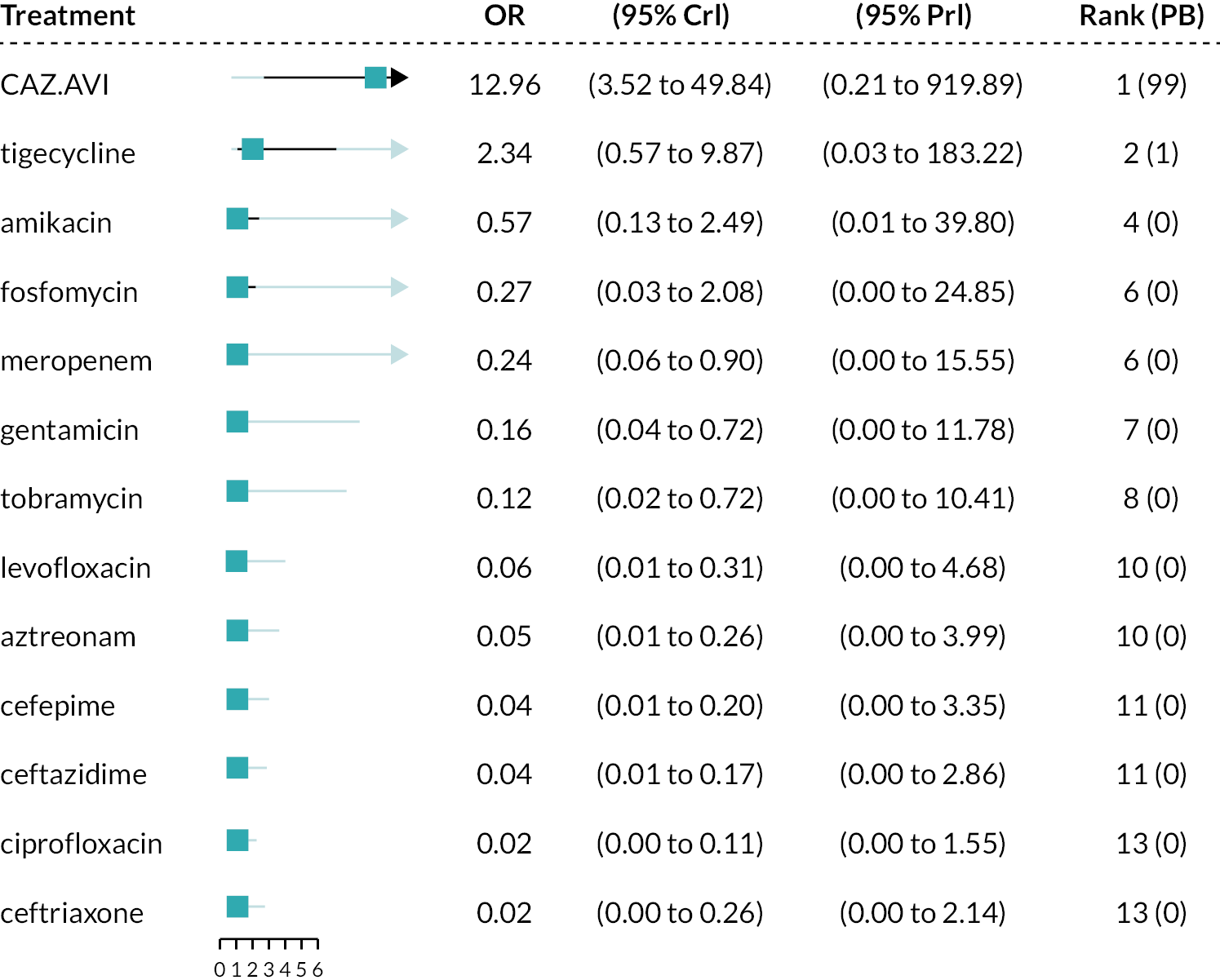
FIGURE 26.
Forest plot of OR vs. colistin for full dataset, subgroup analysis for unusual inclusion criteria. CrI, credible interval; OR, odds ratio; PB, probability being the best treatment; PrI, prediction interval.
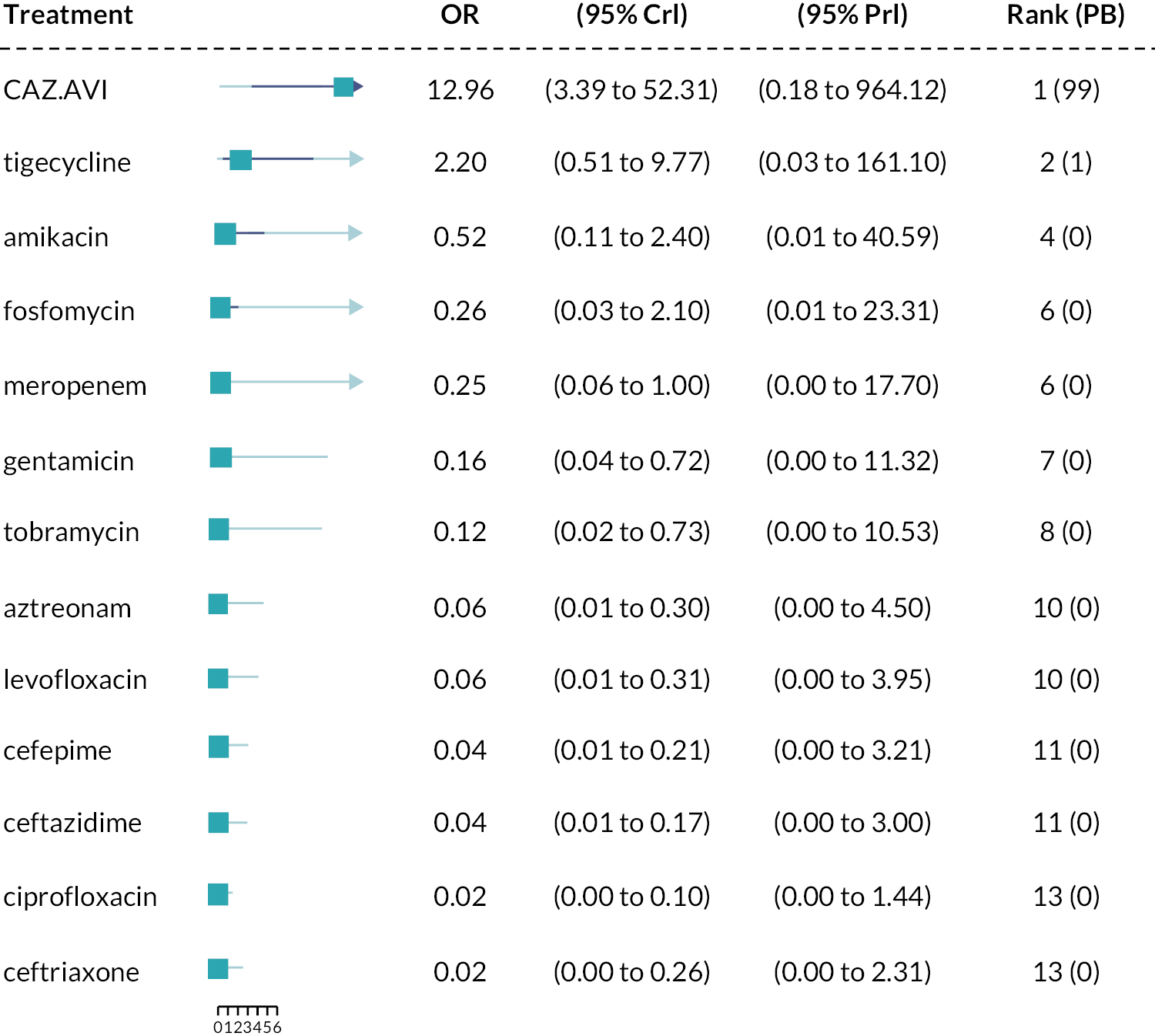
FIGURE 27.
Forest plot of OR vs. colistin for full dataset, NMA model for MBL co-carriage subgroup. CrI, credible interval; OR, odds ratio; PB, probability being the best treatment; PrI, prediction interval.
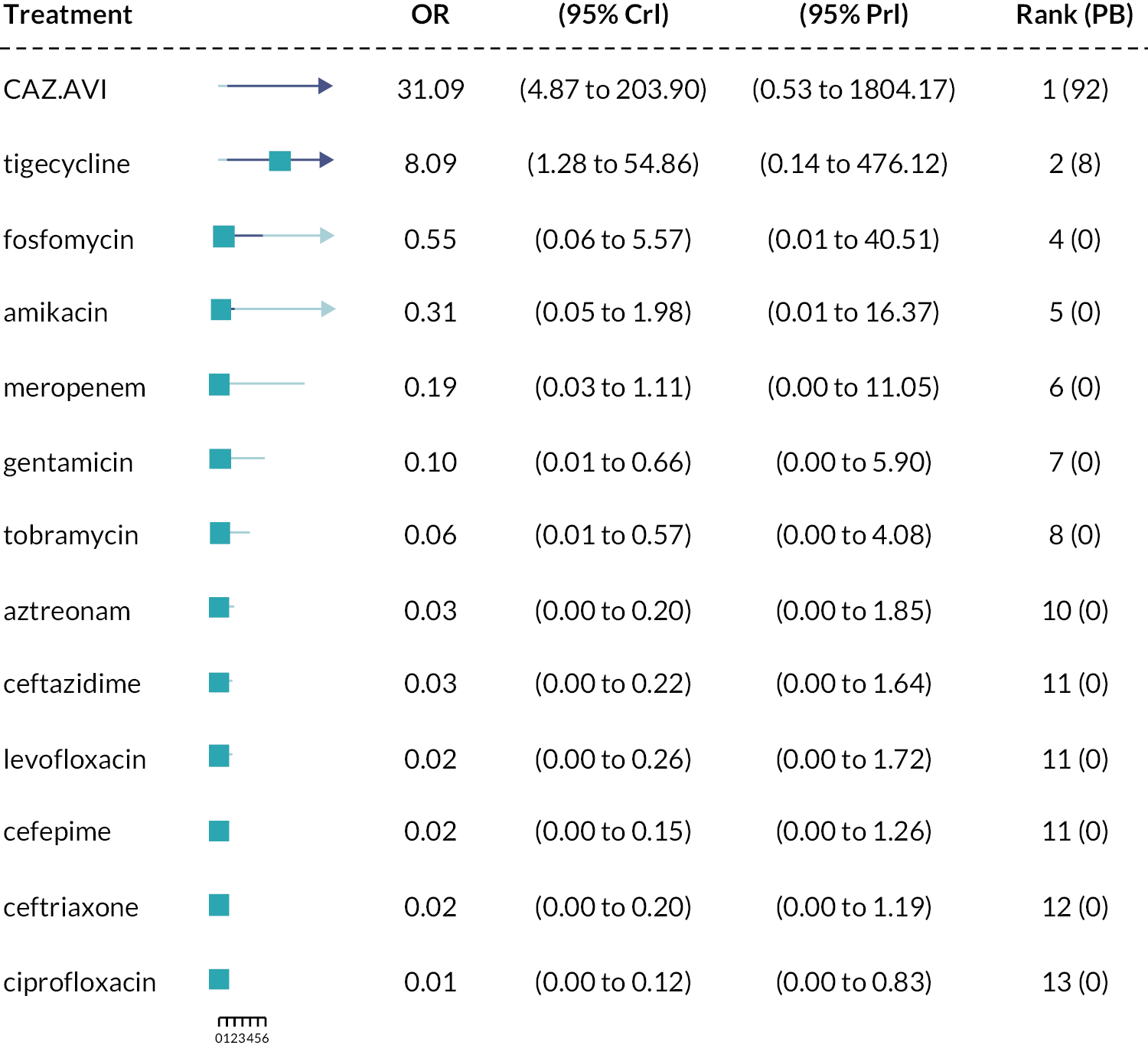
FIGURE 28.
Forest plot of OR vs. colistin for full dataset, meta-regression model for carbapenem susceptibility. CrI, credible interval; OR, odds ratio; PB, probability being the best treatment; PrI, prediction interval.
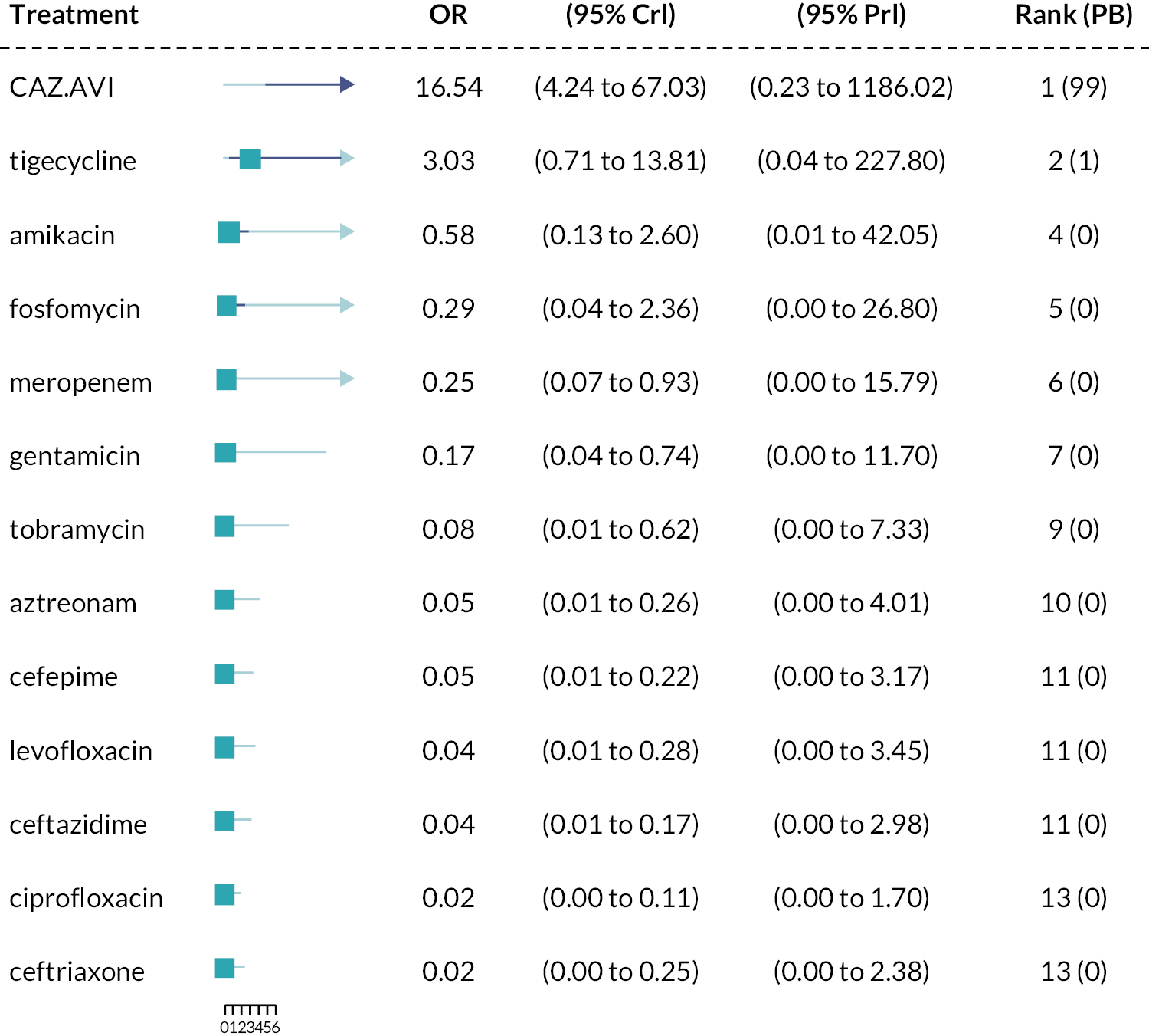
FIGURE 29.
Forest plot of OR vs. colistin for full dataset, meta-regression model for consecutive samples. CrI, credible interval; OR, odds ratio; PB, probability being the best treatment; PrI, prediction interval.
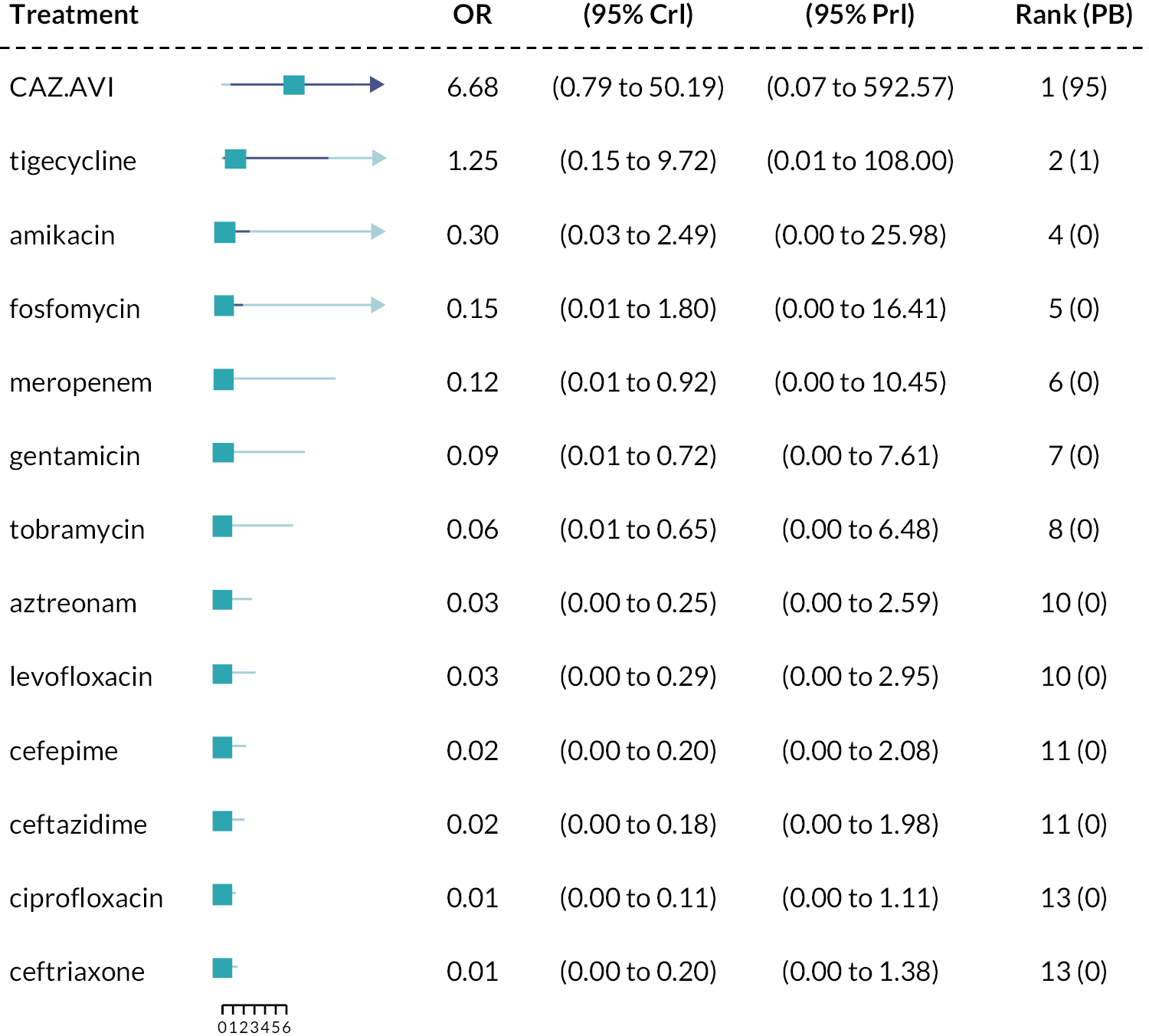
A4.4 Inconsistency checks
FIGURE 30.
Deviance contribution plot for the full data analysis.
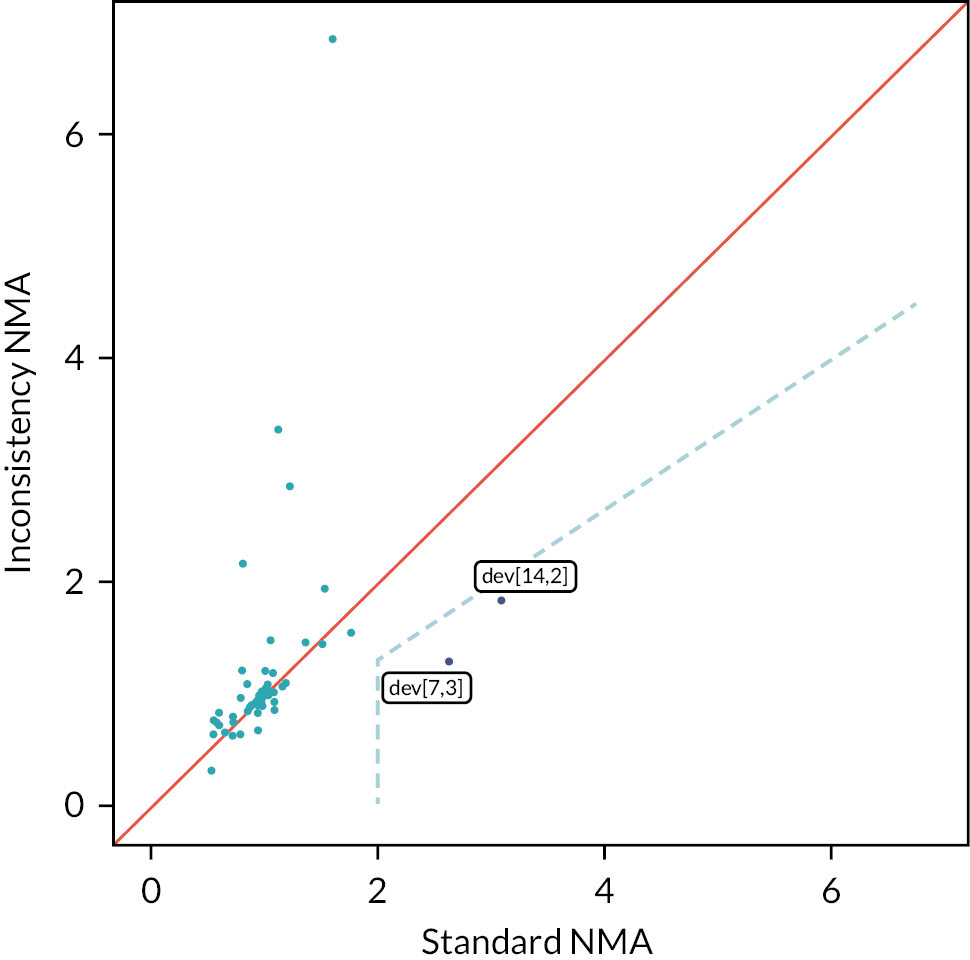
FIGURE 31.
Deviance contribution plot for the reduced data analysis.
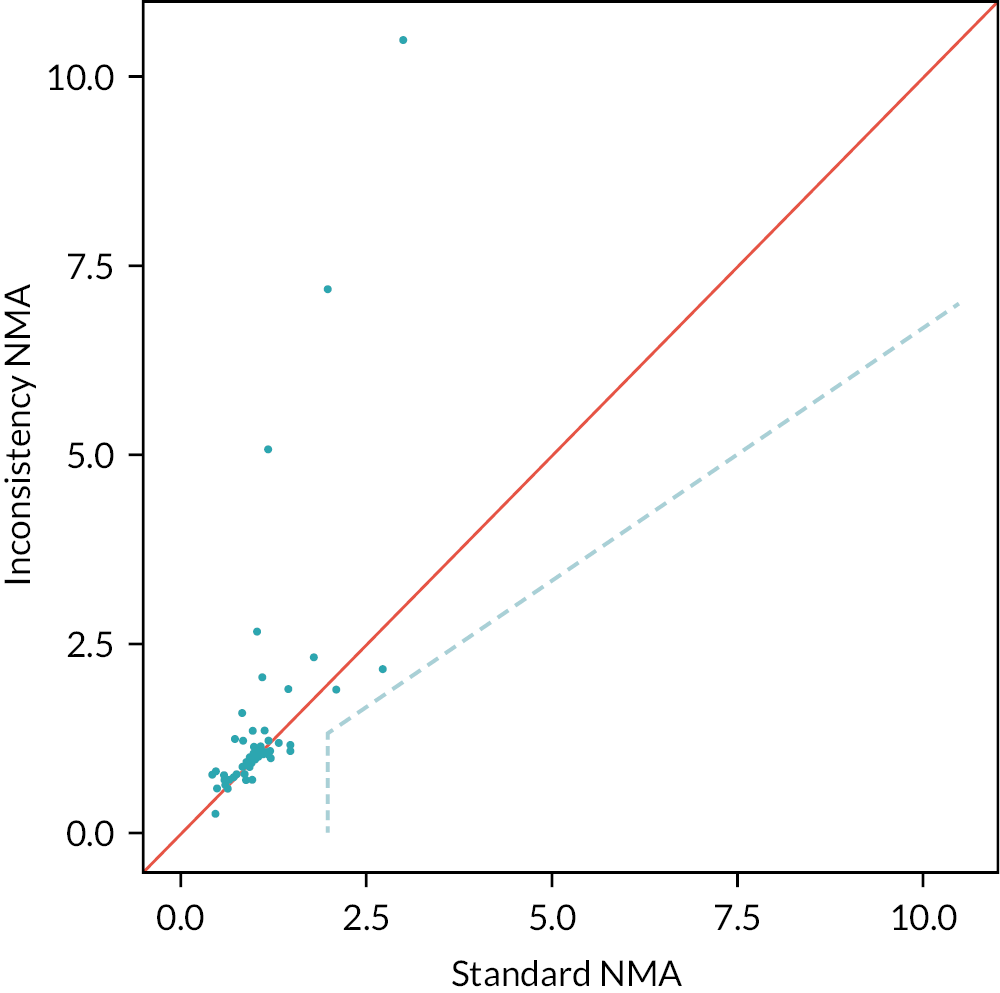
Appendix 5 Methods and results for reviews 4 and 5
A5.1 Review question 4
A5.1.1 Methods
As detailed in Additional review questions for Approach 3, of the two proposed approaches, only approach (a) was taken forward. In this approach, it is assumed that clinical outcomes would be similar regardless of the treatment received, conditional upon susceptibility. This review included studies of any design linking susceptibility (to any antibiotic) to clinical outcomes in cUTI or HAP/VAP caused by any pathogen–mechanism (Table 44). Three approaches were used to identify evidence relating to this question.
-
A systematic review update of Bassetti et al. 2020173
-
Searching and screening of additional databases and review of studies included within Bassetti et al. 2020173
-
Review of the RCTs identified in Review 1 for any subgroup data
-
Bassetti et al. 2020173 systematically reviewed the impact of appropriate and inappropriate antibacterial therapy on clinical outcomes of patients with severe bacterial infections, where appropriate therapy was defined as treatment with an antibiotic the isolate was susceptible to. The review was assessed for quality and relevance (see Report Supplementary Material 1, Section 4) and was judged to be of good quality and suitable for updating. The original review covered the period from 2007 (to ensure clinical practices were contemporary) and the searches were performed in 2018. For the update, given resource and time constraints the search strategy was restricted to terms relating to the UK (since clinical practice may differ in other countries) and the sites of interest (cUTI, HAP/VAP), and to remove terms relating to treatment delay, which were included in Bassetti et al. 2020173 to address a separate review question (the effect of delayed appropriate antibiotic therapy) addressed in Zasowski et al. 2020. 175 The adapted search strategy was run from 2007 to June 2021, to capture any new studies, as well as any studies the adapted strategy identified that were missed by the previous review (between 2007 and 2018). It was further noted that the original search strategy did not include search terms relating to susceptibility, and therefore an additional search, using this search term, was conducted to capture any additional studies from 2007 onwards. The search strategies are presented in Appendix 1 and were run in Ovid MEDLINE and Epub Ahead of Print, In-Process, In-Data-Review & Other Non-Indexed Citations, Daily and Versions: Ovid, 1946 to Present. Studies included in the original review and citations identified by the search strategy were assessed for relevance against pre-specified inclusion criteria listed in Table 44.
-
In addition to the update of Bassetti et al. ,173 a number of other approaches were taken to identify relevant studies (more detail is provided in Report Supplementary Material 1, High-value clinical scenarios):
-
A large database (3172 references) was created, based on search terms for the mechanisms of resistance relevant to the two concurrent EEPRU evaluations relating to CAZ-AVI and cefiderocol (namely MLB, NDM, VIM and IMP). This database was then searched using a series of keywords and phrases to identify relevant studies. The search strategy is presented in Appendix 1.4.2.
-
Screening, citation searching and reference checking of studies retrieved by a search for cost-effectiveness models (66 references) (see Assessment of existing cost-effectiveness evidence and modelling approaches).
-
Keyword search of the Endnote library provided by Shionogi as part of the EEPRU evaluation of cefiderocol (1261 references).
-
Screening the list of key references provided by Shionogi as part of the EEPRU evaluation of cefiderocol (45 references).
-
Keyword search of references provided by Pfizer as part of the EEPRU evaluation of CAZ-AVI (299 references).
-
Screening the studies included in two systematic review articles provided by Shionogi as part of the EEPRU evaluation of cefiderocol (Zasowski et al. , 2020;175 Bassetti et al. , 2020). 173
-
-
In addition to the two previous approaches, the RCTs identified for the intervention were examined for any additional data relating to this question (see Appendix 3.1, Table 39).
| Item | Inclusion criteria | Exclusion criteria |
|---|---|---|
| Population | cUTI or HAP/VAP Any infective pathogen |
Other sites |
| Exposure | Treatment with any antibiotic that the isolate is susceptible to | Treatment with an antibiotic that the isolate has intermediate susceptibility to |
| Comparison | Treatment with any antibiotic that the isolate is not susceptible to (resistant or intermediate/increased exposure) | No comparison provided |
| Outcomes | Mortality, hospitalisation, length of stay (LoS), bloodstream infections (BSI) or other subsequent infections, health-related quality of life (HRQoL) | Short-term outcomes such as clinical cure |
| Setting | MDS or ES UK studies |
Not UK (only applied to search update) |
| Study design | Experimental or observational studies that assessed susceptibility to treatment prospectively or retrospectively | Published prior to 2010 |
5.1.2 Results
1. Systematic review update of Bassetti et al. (2020)
The searches for the systematic review update yielded 172 citations; the screening process did not result in any studies that met the inclusion criteria.
2. Searching and screening additional databases
Eight studies were extracted in total, of which four and five studies reported outcomes in patients with cUTIs and HAP/VAP, respectively. None of the studies were conducted in the UK. None of the studies on patients with cUTIs included patients who received microbiology-directed treatment. In studies on patients with HAP/VAP, three studies only included patients on empiric treatment 176–178, one study179 included patients on both microbiology-directed and empiric treatment (it did not report outcomes conditional on this factor), and one study180 did not report whether treatment was microbiology-directed or empiric. Of the three studies conducted in ES, one176 reported ICU mortality, hospital mortality, mechanical ventilation, LoS and ICU LoS, one study177 reported 30-day mortality only and one178 reported Kaplan–Meier curves for 30-day mortality.
3. Review of RCTs
No data were identified relating to variation in clinical outcomes according to susceptibility (see Appendix 3.1, Table 39).
5.2 Review question 5
What is the long-term risk of mortality (and other outcomes) for patients with carbapenem-resistant cUTI or HAP/VAP?
5.2.1 Methods
The previous reviews did not identify any long-term mortality data. Given the paucity of data in this area, the scope of this review question was widened to include any carbapenem-resistant infections treated with any treatment, under the assumption these data could be generalised to OXA-48 Enterobacterales infections. A focused search was conducted to identify UK studies reporting long-term (> 3 months) mortality and other outcomes such as hospitalisation, subsequent infection, costs and AEs for patients with carbapenem-resistant [including multidrug-resistant (MDR) and extensively drug-resistant (XDR)] cUTI or HAP/VAP. The search strategy comprised terms for (Carbapenem Resistance OR mechanisms) AND [sites (UTI/HAPVAP)] AND filters. The search scope was limited using terms for the UK, and the search was run from 2010 to ensure clinical practices were contemporary. Since no UK studies were identified, the search was expanded to include studies from Europe. The search strategy is presented in Appendix 1.4.2. The inclusion criteria for this review are reported in Table 45. Studies were assessed for eligibility against the inclusion criteria by one reviewer.
| Item | Inclusion criteria | Exclusion criteria |
|---|---|---|
| Population | CR, XDR or MDR cUTI or HAP/VAP infections | Infections at sites other than cUTI or HAP/VAP |
| Exposure | Any treatment or no treatment | |
| Outcomes | Mortality measured more than 3 months after treatment Other long-term outcomes such as hospitalisations, subsequent infections, costs, AEs |
Outcomes measured at or before 3 months after treatment |
| Setting | UK, expand to Europe if no UK studies | |
| Study design | Experimental or observational studies or datasets | Studies published prior to 2010 |
5.2.2 Results
The electronic database searches, following the removal of duplicates, identified 76 records relating to long-term outcomes for patients with carbapenem-resistant cUTI or HAP/VAP. After examination of the title and abstracts, 76 records were excluded because they did not meet the inclusion criteria.
Appendix 6 Structured expert elicitation
A6.1 Description of elicited parameters
We required outcomes for patients with hospital-acquired pneumonia (HAP), ventilator-associated pneumonia (VAP), and complicated urinary tract infections (cUTIs) caused by carbapenem-resistant Gram-negative bacteria. We were only interested in outcomes following microbiology-directed treatment for patients with an infection caused by Enterobacterales with an OXA-48 or MBL resistance mechanism, or Pseudomonas with a MBL resistance mechanism.
Outcomes were elicited depending on whether the infectious pathogen is susceptible to treatment. Therefore, outcomes only depend on whether a patient is susceptible to treatment or not, and not to the specific treatment given. The outcomes we were interested in were 30-day mortality, LoS in hospital, and the type of ward these patients would stay on in hospital.
As background information we provided experts with several related studies. In these studies, infecting pathogens were not confirmed to be susceptible to the antibiotics administered (cefiderocol or CAZ-AVI); however, in our assessment, they are likely to have been susceptible.
For HAP, VAP and cUTI, both for susceptible and not-susceptible patients, the following questions were asked of experts:
-
Question 1. In this patient population, what proportion of patients will still be alive 30 days after starting microbiology-directed treatment?
-
Question 2. In the patient population described at the top of the page, what will be the average LoS?
-
Question 3. In the patient population described at the top of the page, what proportion of hospital stay would be spent on each of the following wards? This number should represent the average for all such patients, regardless of their outcome.
A6.2 Protocol for elicitation
The following sections describe the details of the elicitation exercise, according to the elements as described in the MRC elicitation guidance.
A6.2.1 Selecting the quantities (preparation and design stage)
The choice of quantity considered the following three objectives:40 fitness for purpose; directly observable and homogeneity in the quantities elicited. Eliciting the same summaries throughout will reduce the burden of training (Soares M, Claxton K, Schulpher M. Health opportunity costs in the NHS: assessing the implications of uncertainty using elicitation methods with experts. Universities of Sheffield and York; 2017).
For question 1 the quantities elicited relate to the proportion of patients with an event at a certain time. Question 2 relates to a continuous outcome, LoS, which, in principle, can take values up to ∞. Question 3 relates to the proportionate split of LoS between the three types of ward – general ward, HDU and ICU. As the total proportion must sum to 100, these quantities were not elicited with uncertainty, and instead a mean proportion was elicited.
A6.2.2 Methods to encode judgements (preparation and design stage)
Either the Chips and Bins method or a Bisection method have been shown to work equally well in healthcare elicitation. The Chips and Bins approach, however, is viewed as less complex and easier to complete by healthcare professionals, and so this method is used here.
Experts were first asked to express the range for their beliefs: the minimum, which is the value such that the experts believe that there is a 1% probability that the proportion is less than that value, and the maximum, a value such that the experts believe that there is a 1% probability that the proportion is more than that value. Grids were then generated based on this range and experts were asked to place ‘chips’ on this grid to represent their beliefs.
A6.2.3 Validation (preparation and design stage)
At the end of each task, experts were given a qualitative summary of their responses. If experts felt that these did not represent their views they were encouraged to revise their responses. Experts also had an opportunity to revise their responses following the feedback round (see below).
A6.2.4 Selecting experts (preparation and design stage)
The models developed for this project span across HAP, VAP and cUTI and also relate to likely outcomes depending on susceptibility to treatment. Therefore, there are multiple types of experts relevant for this task. Here we have included hospital consultants, microbiologists and pharmacists as experts. As part of the task, experts were asked to identify which of these disciplines they worked in. Experts were not expected to have any normative skills. Experts were recruited using recommendation from peers.
A6.3 Pilot exercise (preparation and design stage)
The wording of the questions was piloted for clarity and adequacy. The draft exercise was sent to a lead clinician and feedback sought. Following feedback, the questions were modified, specifically the wording of the questions.
A6.3.1 Training and preparation for experts (preparation and design stage)
A narrated PowerPoint training session was delivered to experts prior to the task (see Report Supplementary Material 2). The training session described the objectives of the elicitation exercise, clarified concepts such as uncertainty, familiarised the experts with the quantities elicited, described and explained the impact of bias and heuristics, and trained experts on the methods of elicitation used. A recorded version of the training slides was also sent to the experts following the session and also key details from this were repeated in the task itself.
Experts were also reminded throughout the SEE that they were to elicit uncertainty on their estimate rather than thinking about variability across this heterogeneous group of patients.
A6.3.2 Level of elicitation (elicitation stage)
Each expert elicited their judgements individually without interaction with other experts. Eliciting judgements individually reduced the risk of estimates being biased by a subset of experts. In the SEE elicitation literature, there are concerns that experts may not feel confident in eliciting judgements individually; however, the experts in this SEE process elicited their beliefs on a condition that they encounter regularly in general practice. Concerns regarding individual-level elicitation and lower confidence among experts generally arise when dealing with problems/technologies or conditions that are new or unknown to the experts.
A6.3.3 Mode of administration (elicitation stage)
The elicitation exercise was administered via an application in SHINY. The task was delivered remotely, due to restrictions on face-to-face meetings. Experts were offered the opportunity to complete the exercise remotely alongside one of the team. E-mail contacts were given to provide any support needed.
A6.3.4 Feedback to experts and revision (elicitation stage)
Once experts expressed their beliefs and completed each question, they were presented with graphical feedback of what their estimates looked like. Experts were able to see how the grid looked once they have placed all of their chips on it. In addition, once experts had completed the grid, a summary of their answers was relayed to them. This provided the following information.
Your answers imply that (example quantities given):
-
There is a 17% probability that the proportion of patients is between 19% and 20%.
-
There is a 50% probability that the proportion of patients is between 20% and 21%.
-
There is a 33% probability that the proportion of patients is between 21% and 22%.
Following the individual elicitation beliefs were then aggregated using linear opinion pooling. This overall distribution was then relayed back to experts and they were given the opportunity to revise their own beliefs on the histograms they previously completed. This approach has been shown to generate less biased parameters when the quantities elicited are unknown to the experts. Following this revision, experts’ beliefs were aggregated using the same approach, linear opinion pooling, and the final parameter values were determined.
A6.3.5 Opportunity for interaction (elicitation stage)
Given the individual level of elicitation that was chosen, there was no opportunity for interaction between the experts. The revision stage was done remotely so experts did not interact with each other.
A6.3.6 Feedback from experts on process (elicitation stage)
Qualitative feedback on the elicitation process was collected from the experts, including rationales for their responses. This was collected during the task using free-text boxes. This form of validation helps to highlight whether experts understood the task and responded as well as they could.
A6.3.7 If/how to aggregate (aggregation, analysis and post elicitation)
As an individual level of elicitation was chosen, mathematical aggregation was applied to generate the distributions, specifically linear opinion pooling using equal weighting of experts. First a probability distribution was fitted to each expert’s beliefs from the histogram and then these were pooled, assuming that each expert contributed equally to the group overall distribution.
This overall distribution was then relayed back to experts and they were given the opportunity to revise their own beliefs. Following this revision, experts’ beliefs were aggregated using the same approach, linear opinion pooling, and the final parameter values were determined.
A6.3.8 Fit to distribution (aggregation, analysis and post elicitation)
A beta distribution was fitted to experts’ distributions for question 1 as these relate to proportions. For question 2, a log-normal distribution was fitted. Question 3 only asked for point estimates so no fitting was required.
A6.3.9 Data protection and anonymity (aggregation, analysis and post elicitation)
Experts were asked to give their opinions individually (not in groups). The information provided, including personal details, is kept anonymous and confidential, stored securely and only accessed by those carrying out the study.
A6.4 Results
Eleven experts agreed to take part in the elicitation task and took part in the training. Of these 11, 9 experts attempted the task. The experts included medical consultants (n = 2), microbiologists (n = 5), ICU consultants (n = 1) and pulmonary consultants (n = 1). Seven experts completed the task, while two terminated it before answering all questions. Responses from the two experts who terminated the task before answering all questions were included in the analysis for all outcomes where they provided an estimate for both susceptible and not susceptible populations. Following the elicitation task, experts were sent group summaries and asked if they would like to revise their responses. Only two experts stated that they reviewed the group summaries, and one adjusted their initial responses in light of group summaries.
Two experts indicated that the probability of survival was lower in patients who were susceptible to treatment than those who were not susceptible, for two sites of infection. This was judged to be implausible, and so the two experts were removed from the sample in the base case. Ultimately, five experts’ judgements were therefore included within the analysis.
A6.4.1 Group summaries – base case
The group summaries on 30-day mortality (Figure 32) indicate that survival is the lowest for VAP patients and highest for cUTI patients, and that susceptibility to treatment increases the probability of survival, for all three sites of infection. The group summaries on LoS (Figure 33) indicate that the LoS is the shortest in patients with cUTIs and the longest for patients with VAP. For all three sites of infection, susceptibility to treatment decreased the LoS.
FIGURE 32.
Thirty-day survival. cUTI, complicated urinary tract infection; HAP, hospital-acquired pneumonia; P, proportion; VAP, ventilator-associated pneumonia.
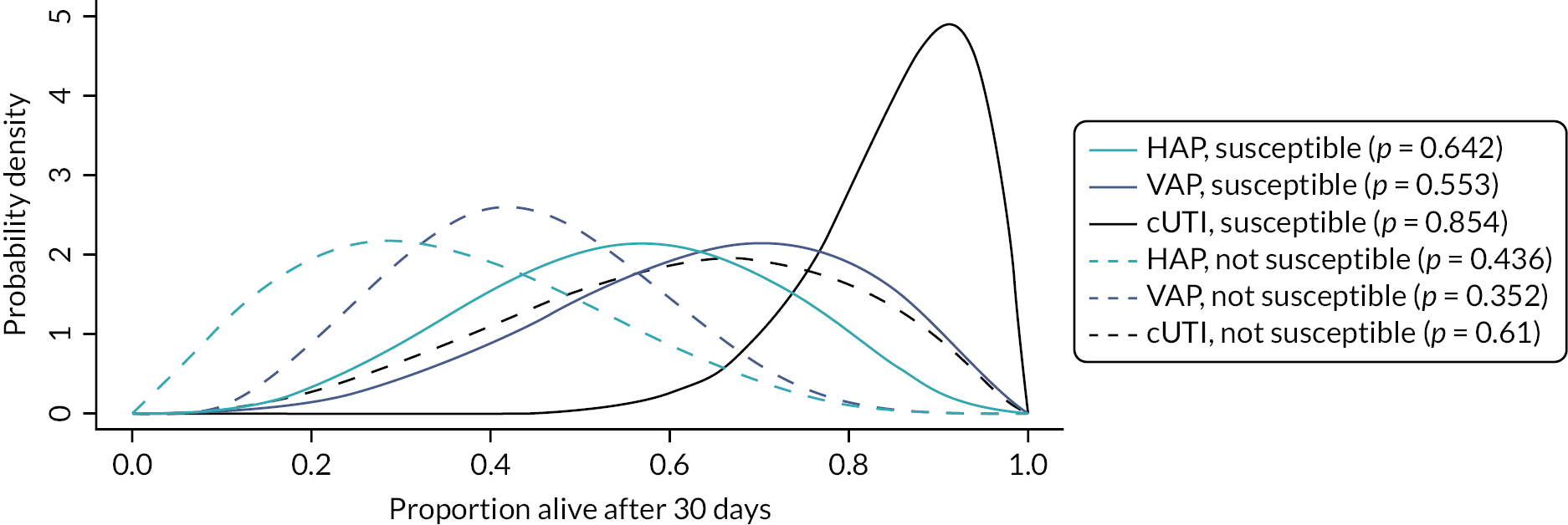
FIGURE 33.
Expected LoS. cUTI, complicated urinary tract infection; HAP, hospital-acquired pneumonia; VAP, ventilator-associated pneumonia.
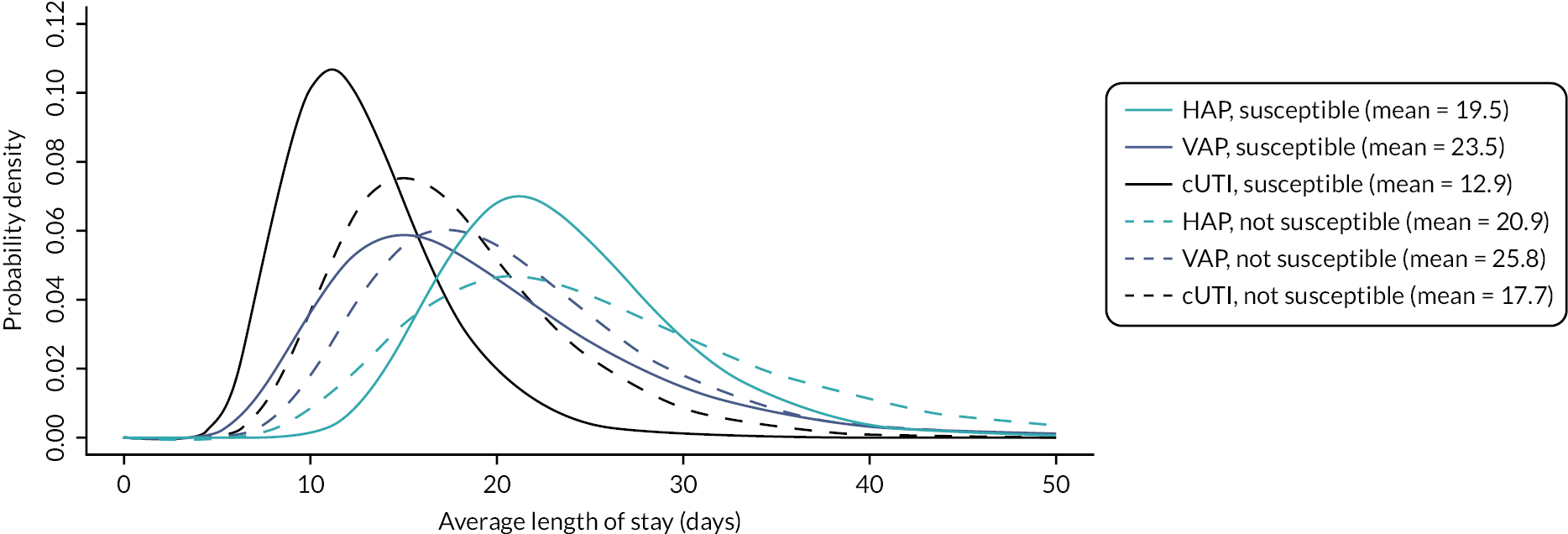
The group summaries about the proportion of time spent on different types of wards are shown in Table 46. The summaries indicate that patients with VAP spend the most time in ICU and the least time on general medical wards, followed by HAP, then cUTIs. Furthermore, patients who are susceptible to treatment are expected to spend more time on the general medical ward and less on ICU and HDU, for all three sites of infection.
| ICU | HDU | General medical ward | |
|---|---|---|---|
| HAP, susceptible | 24.3 | 19.0 | 56.7 |
| VAP, susceptible | 60.0 | 13.3 | 26.7 |
| cUTI, susceptible | 15.0 | 17.0 | 68.0 |
| HAP, not susceptible | 39.3 | 20.7 | 40.0 |
| VAP, not susceptible | 66.7 | 15.8 | 17.5 |
| cUTI, not susceptible | 23.3 | 18.3 | 58.3 |
In the model, outcomes of HAP and VAP were modelled together, and so experts’ priors on outcomes were pooled. When pooling the priors, outcomes for HAP and VAP were weighted by their relative occurrence in Tumbarello et al. (2013): 0.283 (28/99) for HAP and 0.617 (71/99) for VAP. Tumbarello was chosen as the study where participants were the most representative of patients in our HVCS, and that reported the proportion of patients with hospital-acquired pneumonia that was ventilator-associated.
The pooled priors are shown in Figures 34 and 35 and Table 47.
FIGURE 34.
Thirty-day survival with HAP/VAP combined. cUTI, complicated urinary tract infection; HAP/VAP, hospital-acquired pneumonia or ventilator-associated pneumonia; P, proportion.
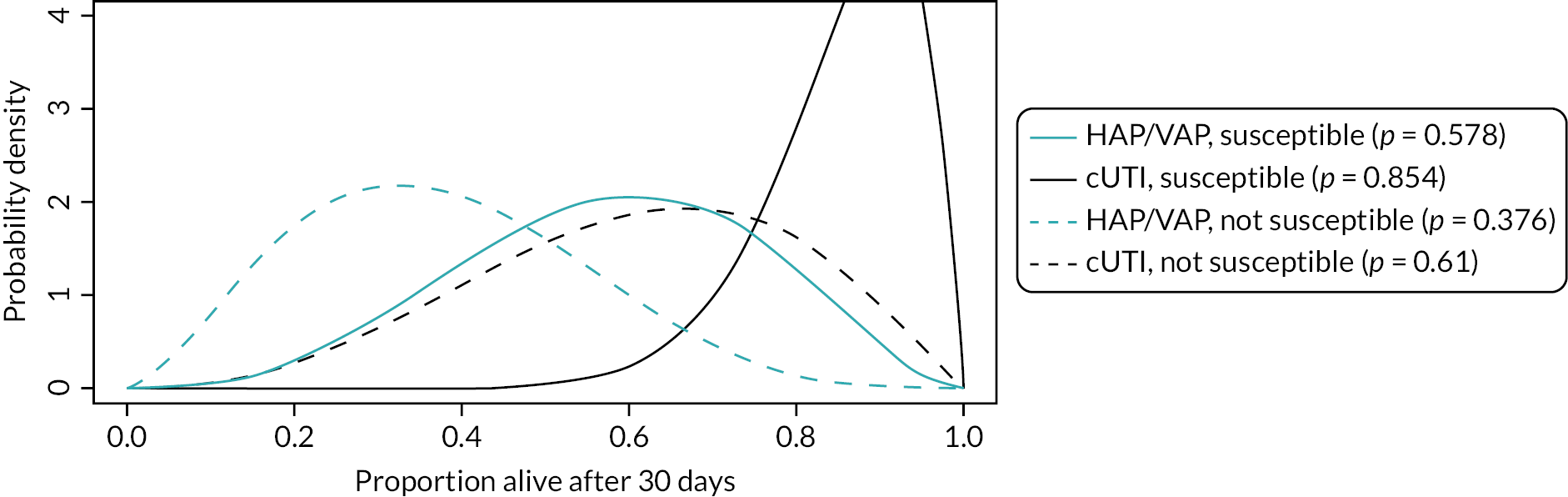
FIGURE 35.
Expected LoS with HAP/VAP combined. cUTI, complicated urinary tract infection; HAP/VAP, hospital-acquired pneumonia or ventilator-associated pneumonia.
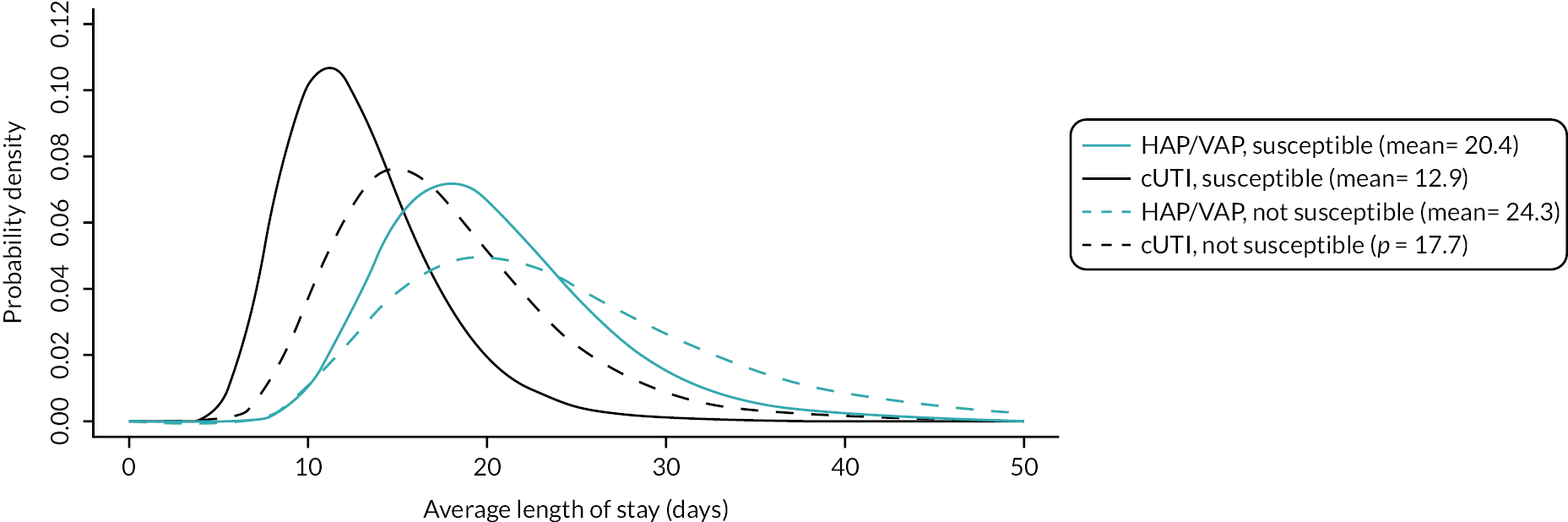
| ICU | HDU | General medical ward | |
|---|---|---|---|
| HAP/VAP, susceptible | 49.90 | 14.94 | 35.16 |
| cUTI, susceptible | 15.00 | 17.00 | 68.00 |
| HAP/VAP, not susceptible | 58.92 | 17.21 | 23.86 |
| cUTI, not susceptible | 23.33 | 18.33 | 58.33 |
A6.4.2 Group summaries – all experts included
Results with all priors, including those that indicated that survival would be lower in susceptible patients, are shown in Figures 36 and 37, and Table 48. Overall, the priors indicate the same relative differences between outcomes and sites of infection.
FIGURE 36.
Thirty-day mortality – all experts. cUTI, complicated urinary tract infection; HAP, hospital-acquired pneumonia; P, proportion; VAP, ventilator-associated pneumonia.
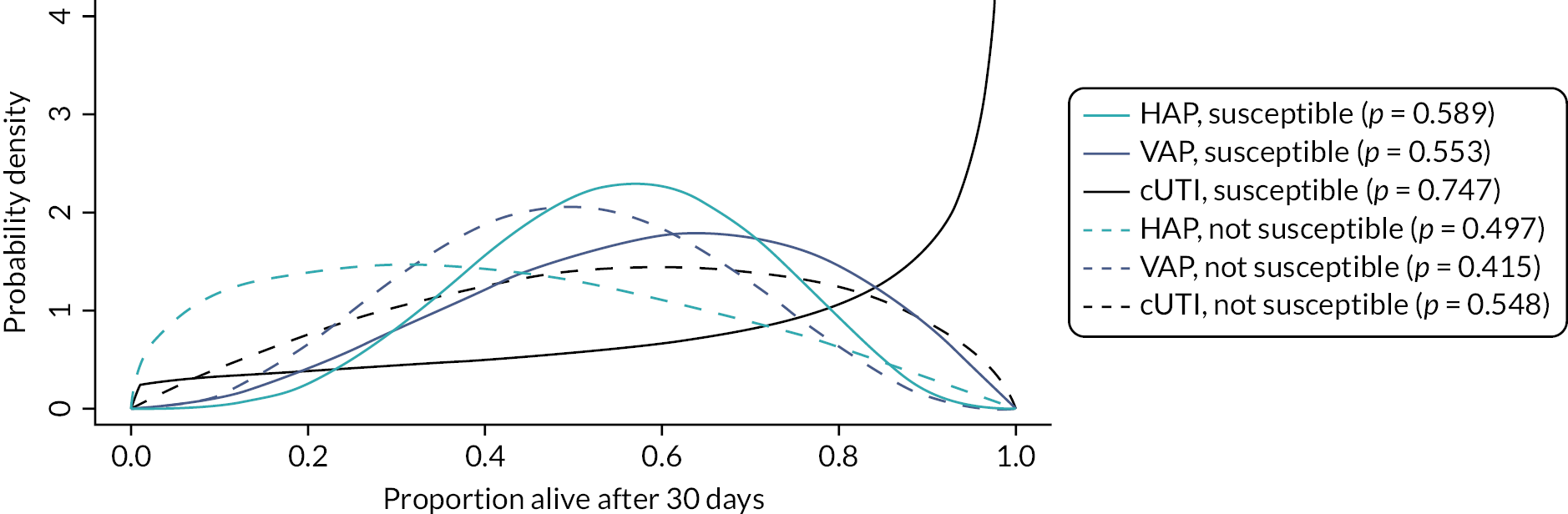
FIGURE 37.
Expected LoS – all experts. cUTI, complicated urinary tract infection; HAP, hospital-acquired pneumonia; VAP, ventilator-associated pneumonia.
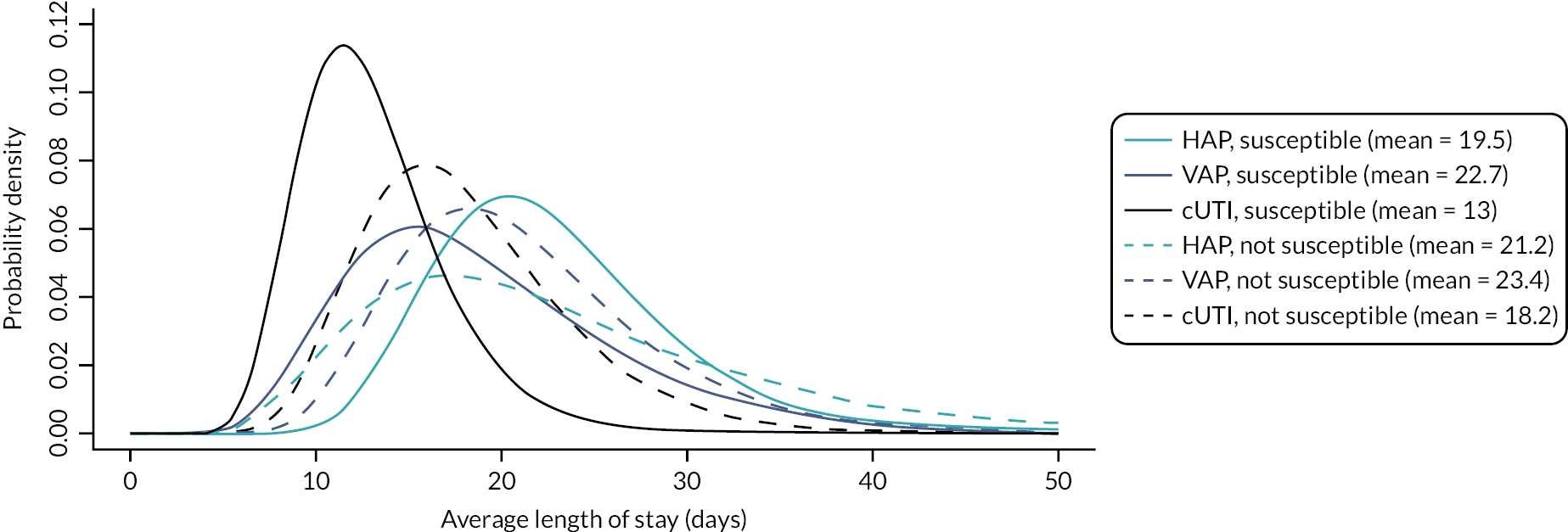
| ICU | HDU | General medical ward | |
|---|---|---|---|
| HAP, susceptible | 23.56 | 21.22 | 55.22 |
| VAP, susceptible | 62.86 | 14.29 | 22.86 |
| cUTI, susceptible | 13.57 | 16.00 | 70.43 |
| HAP, not susceptible | 36.00 | 22.00 | 42.00 |
| VAP, not susceptible | 68.57 | 16.43 | 15.00 |
| cUTI, not susceptible | 21.43 | 18.57 | 60.00 |
A6.5 Validation of experts’ estimates
We explored alternative sources of evidence to inform LoS in the model, in order to validate the elicitation results. In particular, we considered two UK-based studies that reported LoS in patients with carbapenem-resistant organisms – CARBAR181 and Merrick,118 and the study by Muscedere126 that was used to derive the relative reduction in the LoS associated with appropriate empiric therapy in the ES (further detail provided in Sources of evidence).
The mean LoS in CARBAR181 was 47.2 days. The median LoS in Muscedere126 in patients who received appropriate and inappropriate empiric treatment was 27.9 and 42.2 days, respectively. This was estimated to equate to a mean LoS of 43.1 days and 85.7 days, respectively (further detail provided in Sources of evidence). The LoS in both studies was considerably longer than experts’ estimates (~20 and ~24 days from the start of microbiology-directed treatment in susceptible and resistant patients, respectively). However, the LoS in both studies was measured from hospital admission, rather than from the start of microbiology-directed treatment following infection onset.
CARBAR reported that the average time between hospitalisation and infection was 8 days (median) for all patients, 16.8 days (mean) time for infections diagnosed from sputum samples and 13.9 days for UTI-related samples. In addition, the median time between infection onset and microbiology-directed treatment in CARBAR was 5 days. Assuming that 13 (8 + 5) to 21.8 (16.8 + 5) days passed between admission and administration of microbiology-directed treatment, the LoS from the start of microbiology-directed treatment in CARBAR (25.4–34.2 days) was comparable to experts’ estimates. Muscedere did not report the time between admission and infection onset, and so could not be directly compared to experts’ estimates. In Merrick118, the median LoS after infections caused by carbapenem-resistant organisms was 24 days, comparable to the mean estimates from experts. The authors did not report the mean.
Appendix 7 Manufacturer economic model for CAZ-AVI
To support this assessment, the CAZ-AVI’s manufacturer submitted a model to evaluate the value of CAZ-AVI. This section provides an overview of the company’s submitted model. As shall be seen, there were high-level concerns about the relevance of the company’s submitted model and evaluation. In addition, for some areas, there was a lack of transparency on the processes that are driving the economic results. Because of these issues, this section does not provide a detailed critique of the company’s submitted model and evaluation.
The company’s submitted economic model considers CAZ-AVI as an additional treatment line for patients with three types of infections (cIAI, cUTI and HAP/VAP) caused by three Gram-negative bacterial species (E. coli, K. pneumoniae and Pseudomonas aeruginosa) for 1000 patients in a single hospital. The comparator treatment is meropenem and either piperacillin/tazobactam (for cIAI or cUTI) or colistin (for HAP/VAP). The hospital is modelled as an infectious environment, with the transmission of infection occurring at a constant proportion of the infected population. Consequently, patients’ exposure to up to three AMs (when CAZ-AVI is used) is influenced by treatment efficacy and the prevalence of AMR in the infected population.
This section begins with an overview of the decision problem considered in the evaluation, followed by details of the submitted model structure (including its processes and results), followed by a discussion of areas where there was a lack of transparency in the model description and an explanation of the most substantive issues identified. It finishes with an overview of other issues of concern with the submitted model.
A7.1 Summary of the company’s model
A summary of the model, including key elements of the decision problem (population, intervention, comparison and outcomes), is provided in Table 49 and Figure 38.
The economic model’s estimate of the cost-effectiveness of CAZ-AVI accounts for the efficacy of CAZ-AVI and diversification strategies to prevent the development of AMR across all available treatment lines. The model is based on a multistate disease transmission model which estimates the incidence and prevalence of bacterial infections within a single hospital infectious environment. Infections are caused by transmission from patient interactions, and environmental exposure. The multistate disease transmission module is linked to a decision-tree treatment pathway module to determine the health economic impact of empiric usage of CAZ-AVI in all patients with cIAI, cUTI and HAP/VAP. The model has a three-line strategy when examining the introduction of CAZ-AVI and a two-line strategy examining the comparators. The model has a diversity-based strategy, where multiple AMs are used in the same line of the treatment pathway. The baseline diversity strategy means that patients are distributed evenly between each of the following treatment sequences in the CAZ-AVI arm:
-
Treatment A → Treatment B → Treatment C
-
Treatment B → Treatment A → Treatment C
-
Treatment C → Treatment A → Treatment B
For example, the treatment lines for HAP/VAP when CAZ-AVI is introduced as an additional line are:
-
colistin → meropenem → CAZ-AVI
-
meropenem → colistin → CAZ-AVI
-
CAZ-AVI → colistin → meropenem
The comparator line is without CAZ-AVI, and the treatment line is a sequence of two antibiotics:
-
colistin → meropenem
-
meropenem → colistin
| Element | Description |
|---|---|
| Setting | 1000 patients in a single hospital with an infectious environment. It was assumed that the number of admissions and discharges are equal in each cycle (i.e. the total number of patients modelled in the infectious environment is constant). Results are scaled-up to reflect 93,432 beds being occupied over a 10-year horizon |
| Patients | Alive patients can be in one of three main health states: susceptible (not colonised or infected with a pathogen of interest); infected with a pathogen of interest; and colonised (but not infected). For infected and colonised patients, a distinction is made between if the pathogen is sensitive or resistant |
| Treatment pathways for HVCSs | Mainly risk-based empiric treatment pathways: 20% receive directed treatment (i.e. microbiological susceptibility testing has been performed) and 80% have empiric treatment (i.e. the pathogen and susceptibility profile of the infection are not yet known). It is unclear how ‘risk-based’ is defined |
| Pathogen–mechanism | The economic analysis considers infection with three Gram-negative bacterial species across each indication: •Escherichia coli •Klebsiella pneumoniae •Pseudomonas aeruginosa |
| Site of infection | Patients with the following common healthcare-associated infections: •cIAI •cUTI •HAP/VAP |
| Intervention | CAZ-AVI as an additional treatment line (in combination with comparators) |
| Comparators | Meropenem and either piperacillin/tazobactam (for cIAI or cUTI) or colistin (for HAP/VAP) used in sequence |
| Outcomes | The economic analysis outputs were expressed in population NMB, with the effectiveness input measured in QALYs (and an assumed willingness to pay of £30,000 per QALY), to inform the potential annual value, estimated both over the full-time horizon of the economic model and the potential 10-year contract period. In addition, the following outcomes are considered: •Number of deaths •Number of infections •Number of patients eligible for CAZ-AVI •LYs/QALYs lost due to infection |
| Elements of value as set out in the Evaluation Framework | Diversity value and transmission value are included in the modelled analysis. Both insurance and enablement value are only reflected in the modelled analysis to a very limited capacity |
| Study designs | The types of studies and data used to parametrise to the model are: •RCTs •Observational studies •National and international datasets |
The model has a time horizon of 10 years with monthly cycles. The transmission model pathway structure is outlined in. During each model cycle, patients may move between discrete health states representing the following states: susceptible, colonised, infected health states or death. Susceptible is the absence of infection and pathogen, colonised patients have a pathogen without clinical symptoms of infection and infected individuals carry the pathogen and have symptomatic infection. The colonised and infected health states are subdivided according to whether pathogen is sensitive or resistant to specific antibiotics. Colonised or infected with a sensitive pathogen means there is no resistance to any of the modelled treatments, while colonisation or infected with a resistant pathogen means resistance to either one, two or three of the modelled treatments.
FIGURE 38.
Diagram of the transmission pathway structure (from Figure 13 of the company submission).
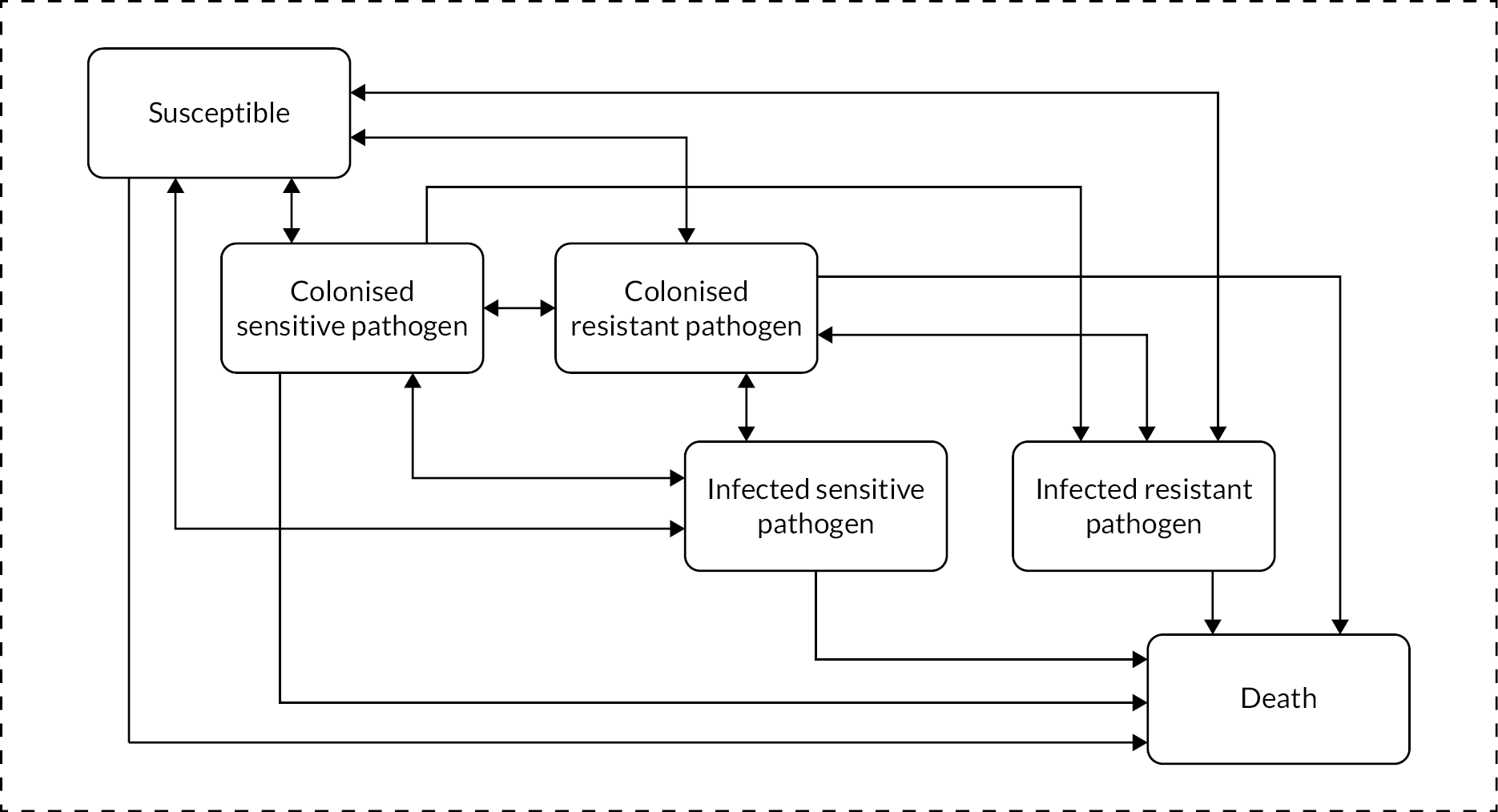
A7.2 Pathways to health effect in the model
Health effects are the main drivers of cost-effectiveness results and are generated in the model from baseline resistance and treatment efficacy inputs. These inputs are summarised in Table 50 for CAZ-AVI and comparator treatments. There are five pathways to health effect, all of which are influenced by the efficacy of, and baseline resistance to, the treatments. With greater efficacy and a lower level of baseline resistance the following health effects can occur:
-
Direct patient benefits – clinical efficacy: it is more likely an infection will be cured without the need for any further treatment. This lowers the period of exposure to infection-related mortality, as patients in the infected health state incur a daily probability of mortality.
-
Indirect patient benefits – additional treatment: it is less likely that the patient will be exposed to the assumption of immediate mortality from treatment failure across all lines; patients who have exhausted all available antibiotic treatment options and fail to clear the infection naturally are assumed to die 3 days after their last available line of treatment.
-
Population-level benefits – infection transmission: a shorter period of infection resulting in fewer person-to-person transmissions of infections and a reduction in infection mortality.
-
Population-level benefits – diversification and resistance development. It is more likely an infection will be cured without the need for any further treatment. This reduces the selection pressure that would otherwise benefit resistance-giving mutations (since each additional treatment exerts its own selection pressure). The reduced selection pressure results in lower resistance levels and consequently infections are cured more often and more quickly, resulting in less mortality. In addition, a shorter period of infection means a greater chance of clearing pathogens naturally, resulting in lower resistance levels. This is because when infections are cleared patients move to colonised or susceptible, and colonised patients then have an opportunity to clear pathogens naturally. In contrast patients who remain infected are assumed to be subject only to the efficacy of the treatment.
| Type of model input | Infection and pathogen | Piperacillin/tazobactam, % | Meropenem, % | Colistin, % | CAZ-AVI, % |
|---|---|---|---|---|---|
| Baseline resistance | E. coli | 8.89 | 0.09 | 1.06 | 0.57 |
| K. pneumoniae | 14.62 | 0.87 | 3.15 | 5.31 | |
| P. aeruginosa | 6.57 | 6.87 | 1.22 | 3.79 | |
| Efficacy | In cUTI – E. coli | 91.6 | 71.9 | – | 78.4 |
| In cUTI – K. pneumoniae | 91.6 | 62.5 | – | 75.0 | |
| In cUTI – P. aeruginosa | 91.6 | 75.0 | – | 66.7 | |
| In cIAI – E, coli | 82.4 | 87.4 | – | 80.4 | |
| In cIAI – K. pneumoniae | 82.4 | 75.5 | – | 78.4 | |
| In cIAI – P. aeruginosa | 82.4 | 94.4 | – | 85.7 | |
| In HAP/VAP – E. coli | – | 80.0 | 75.0 | 76.5 | |
| In HAP/VAP – K. pneumoniae | – | 74.6 | 75.0% | 62.7 | |
| In HAP/VAP – P. aeruginosa | – | 38.3 | 75.0 | 37.9 |
A7.3 Detailed explanation of model structure
Patients who are susceptible or colonised may or may not become infected or colonised at the end of a cycle, as illustrated in Figure 39. Susceptible or colonised patients who are infected (at the end of a given cycle) move to the infected state at the start of the next cycle and will receive all lines of treatment within a single cycle. The spread and treatment of infection within the hospital environment is illustrated in Figure 39, and the pathway from first line of treatment is illustrated in Figure 40. Only infected patients receive active treatment.
FIGURE 39.
Overview of transmission in the infectious environment (from Figure 4 of the company submission Appendix K).
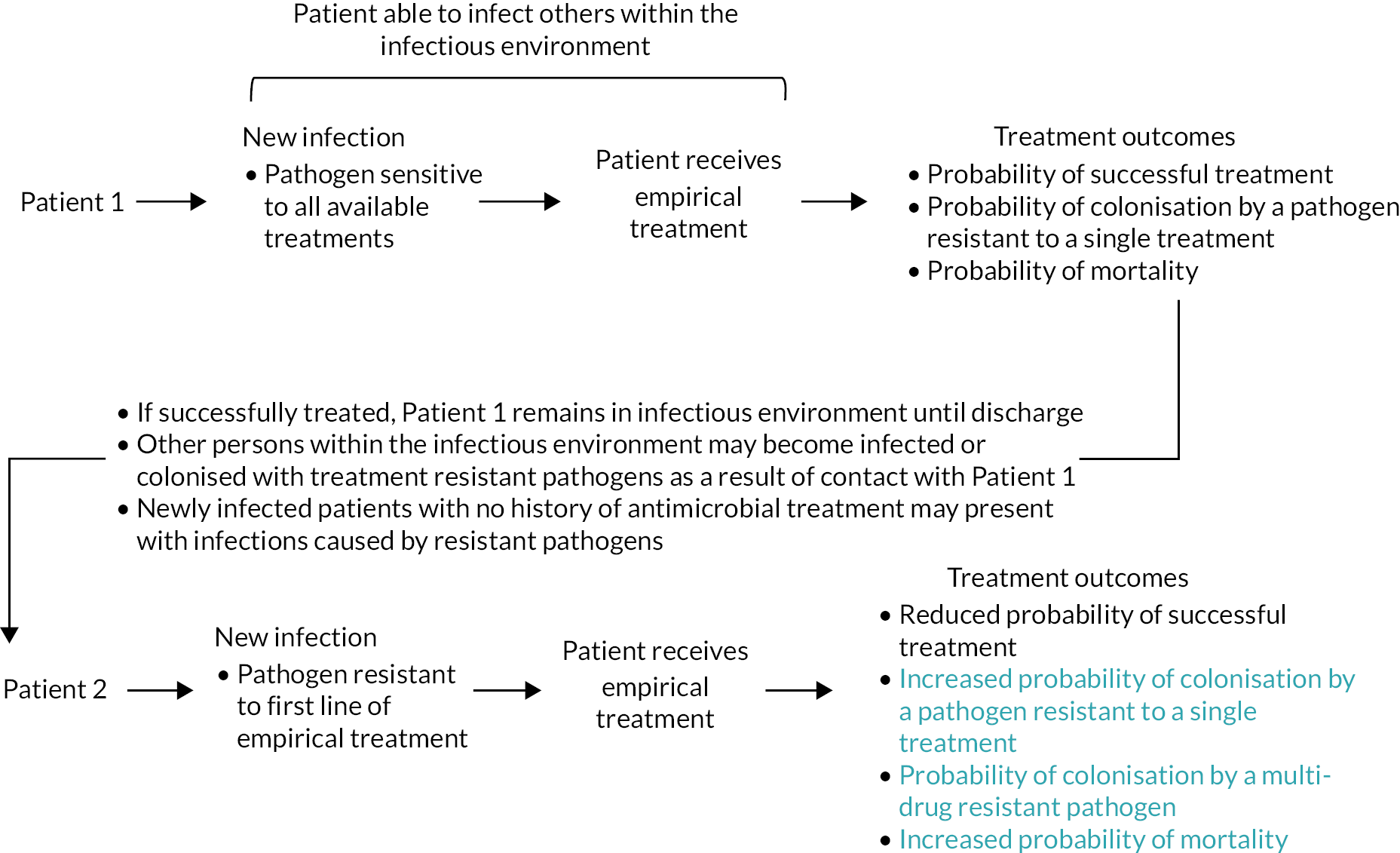
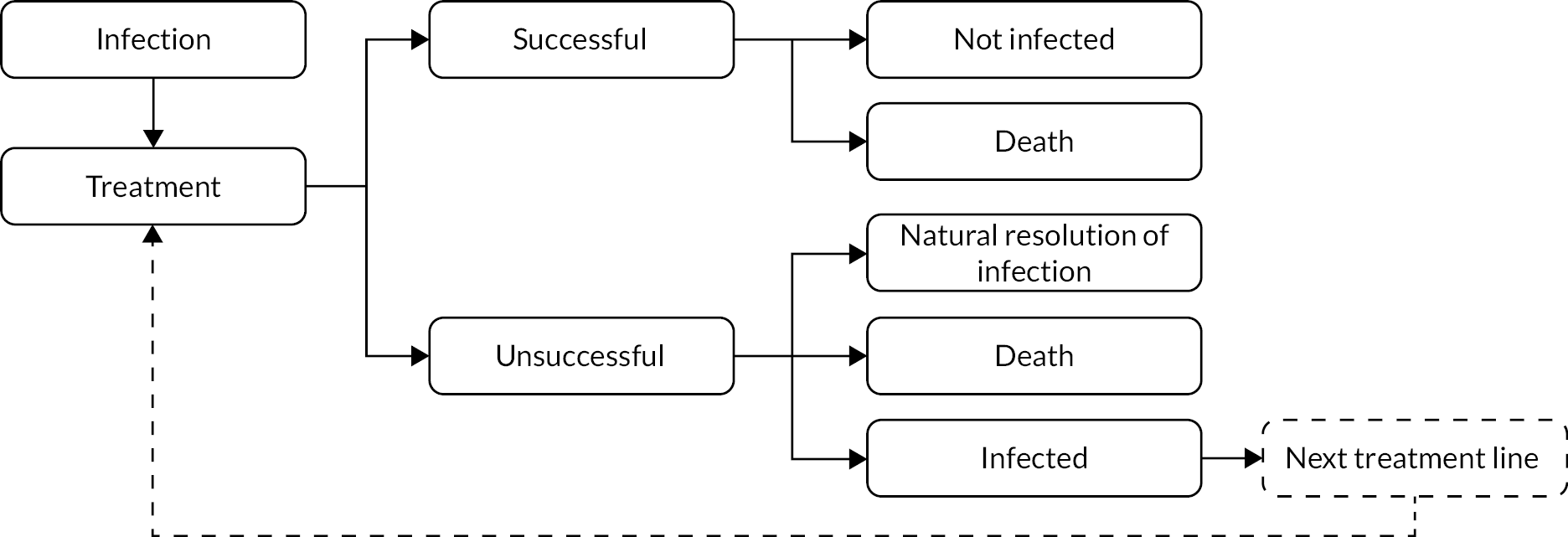
There are two pathways to the spread of infections and colonisations in a cycle. A susceptible patient may become infected or gain a pathogen (without infection) from direct transmission from patients who are infected or colonised, respectively, and this probability increases with the number of infected or colonised patients within the hospital. Colonised patients can become infected via direct contact with patients with the same strain (sensitive or resistant) of bacteria, and this probability of infection rises with the number of infected patients within the hospital. A constant proportion of colonised patients will also become infected from environmental exposure (with the proportion varying by type of pathogen). This represents spontaneous infection development in colonised patients from causes other than person-to-person transmission. In the absence of treatment, resistance in colonised patients is gradually lost at a fixed rate over time, which represents the pathogen being outcompeted by sensitive pathogens. As colonised patients do not receive AMs this is the only process by which they can be cleared of a resistant pathogen. There is no gradual loss of resistance in infected patients.
Infection may be viewed as a temporary state, as patients do not remain in it for more than one cycle (Figure 38). Clinical success is accounted for as clearance of symptoms of an infection, which may or may not result in the patient no longer being colonised by pathogen. If the infection is not cleared, the patient will move to the next line of treatment to which they may be sensitive, and any resistant pathogens will be retained. Infected patients who are resistant to their current antibiotic treatment regimen or have exhausted all treatment options have a probability of naturally clearing their infection and pathogen while receiving treatment. Infected patients for whom the last available line of treatment was unsuccessful are assumed to die. These patients are replaced in the next cycle by new admissions who are in the susceptible or colonised state. Hence the number of individuals in the hospital remains constant (at 1000) and all infections are acquired within the hospital environment from person-to-person transmission rather than from admissions.
A7.4 Overview of economic results
The economic results show the effect of adding CAZ-AVI as an additional treatment line to form a three-line diversified treatment strategy compared to a non-diversified two-line treatment strategy made up of existing drugs. The base-case analysis is shown in Table 51. The introduction of CAZ-AVI had the greatest clinical benefits when used for treating HAP/VAP. When a weighted analysis was performed, combining results from all pathogens for each indication, the net monetary benefit (NMB) estimate was £598,779,222 over a 10-year time horizon at a cost per QALY threshold of £30,000.
| Infection | Treatment | QALYs lost due to infection | Incremental costs (£) | Incremental QALYs saved via infections avoided | NMB at cost per QALY threshold of £30,000 |
|---|---|---|---|---|---|
| cUTI | CAZ-AVI | 3392 | 9034.97 | 5529 | £156,835,028 |
| No CAZ-AVI | 8921 | ||||
| cIAI | CAZ-AVI | 1687 | 827.25 | 4747 | £141,582,748 |
| No CAZ-AVI | 6434 | ||||
| HAP/VAP | CAZ-AVI | 10,090 | 5968.55 | 10,211 | £300,361,446 |
| No CAZ-AVI | 20,302 | ||||
| All indications above combined | CAZ-AVI | 15,169 | 15830.78 | 20,487 | £598,779,222 |
| No CAZ-AVI | 35,657 |
A probabilistic sensitivity analysis was not conducted due to limited uncertainty information for parameters. Scenario analyses were conducted by altering the following base-case values by ± 10%: baseline resistance; infection incidence; treatment efficacy; treatment/hospital duration; rate of death; costs; utilities; inputs related to Clostridium difficile infections; inputs related to disease transmission parameters; patients with known resistance status (i.e. directed treatment).
In addition, a scenario explored the impact of varying the discount rate on costs and benefits at 1.5% and 5%. The results are presented in a Tornado diagram (Figure 41). The major influences on NMB were treatment efficacy, discounting, utility, life expectancy and the transmission and clearance rate.
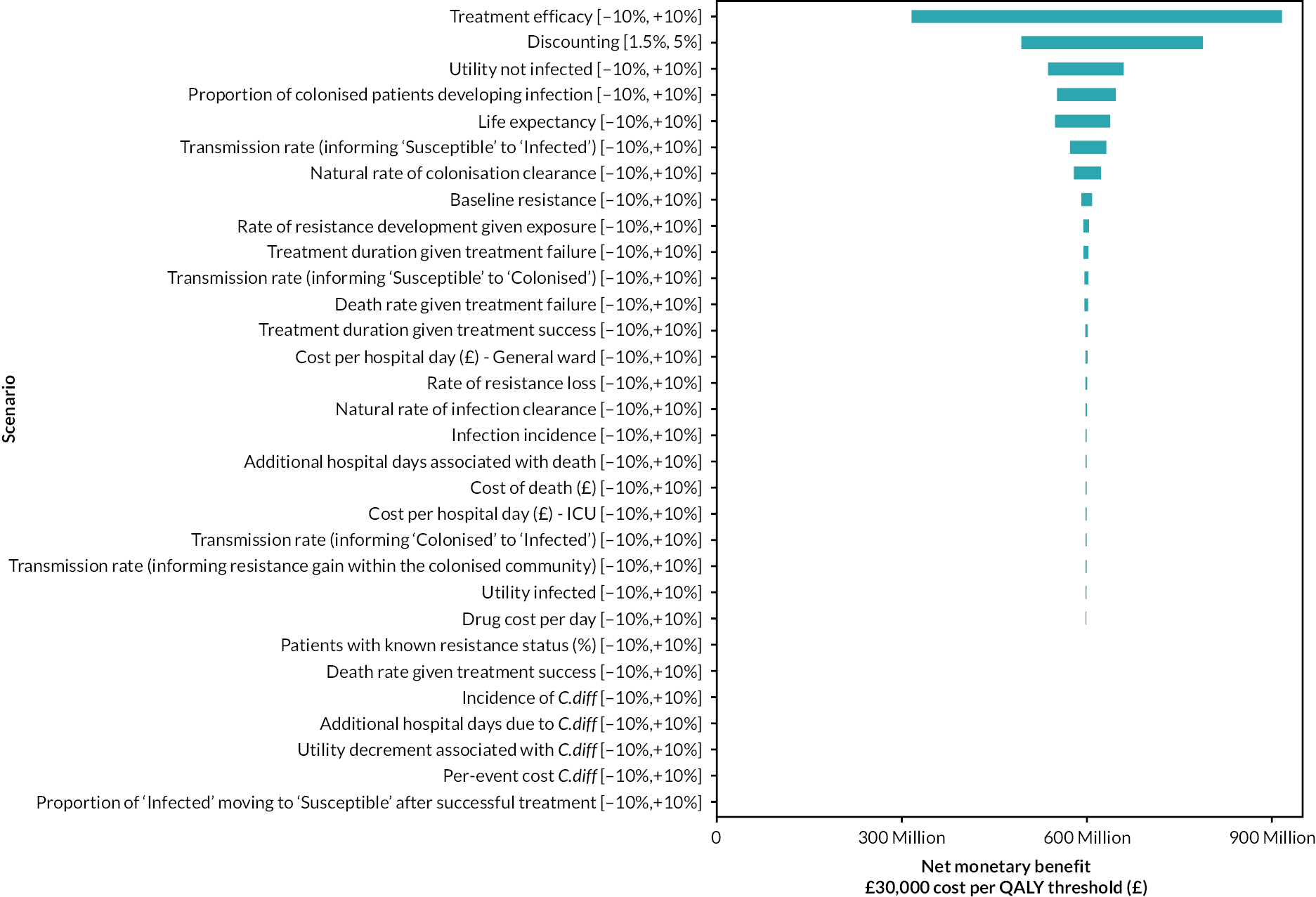
The following scenario analysis analyses were also considered: varying the baseline resistance by ± 20%; varying the percentage of patients receiving targeted treatment to 15% and 25%; applying a 3-year time horizon. The results are presented in Figure 42 and show minor variation across the scenarios, with the results most sensitive to the 3-year time horizon scenario.
FIGURE 42.
Annual NMB outcomes based on the uncertainty analysis on key model parameters (from Figure 16 of the company submission).
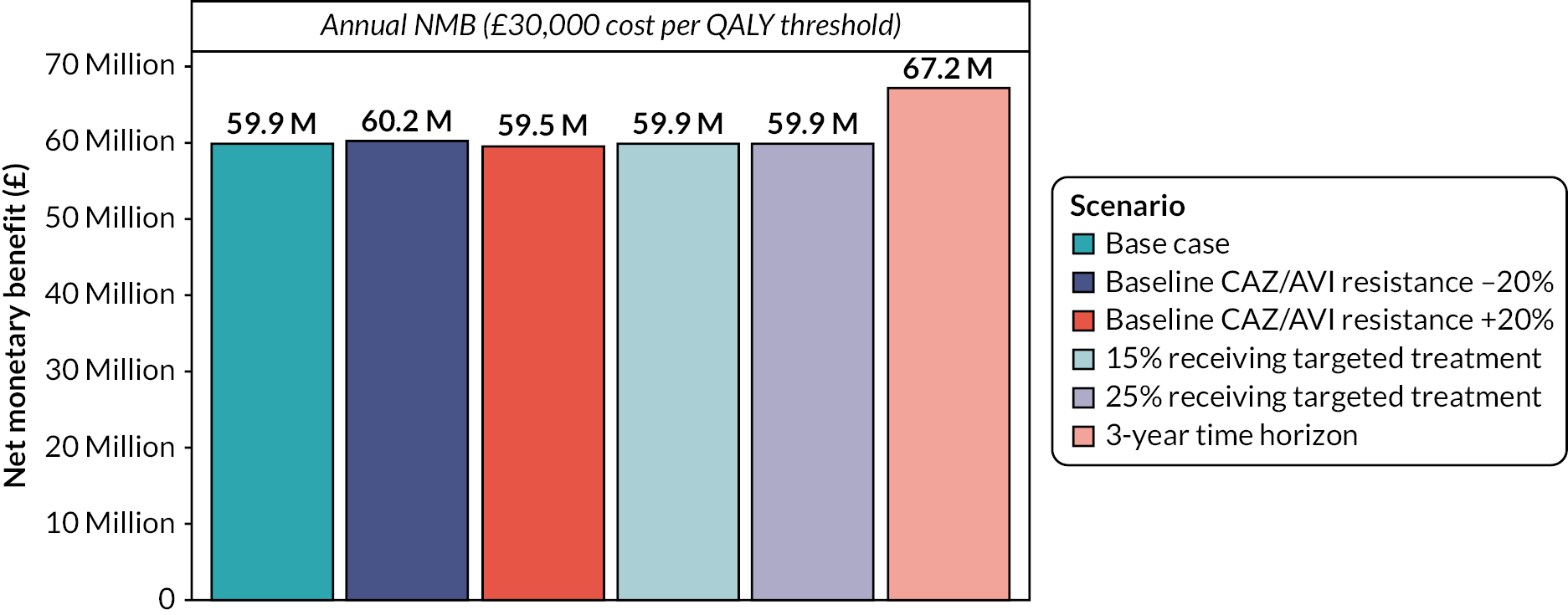
A7.5 Areas of inconsistency or lack of clarity in the company submission
There were some key processes of the company’s submitted model which was difficult to understand based on the submitted documentation. The following are key aspects of the model that were not transparent from the description provided in the submission:
-
During the treatment pathway, a patient with an infection and sensitive pathogen may develop resistance from treatment and become infected with a resistant pathogen. Such changes are not represented in the model. The model structure necessitates the full treatment pathway (Figure 40) to be completed before there is a movement to a different health state (Figure 38).
-
The model assumptions appear to be inconsistent regarding the transmission of resistant pathogens between colonised patients. The company submission states that ‘Patients may not move directly between different colonised health states’ (p. 182). This appears to contradict the model schematic.
-
There is a transition from infected with a sensitive pathogen to colonised with a sensitive pathogen. The submission does not explain the mechanism of this transition.
-
The description of treatment success is ambiguous in places: ‘after a patient is successfully treated, they may return to the susceptible or colonised health states’ (p. 160) is in contrast to a suggestion that the pathogen is always eliminated: ‘The proportion of infections cleared, denoted by the symbol φ, corresponds to the likelihood that a patient has been successfully treated, resulting in the patient no longer being infected or colonised by the pathogen’ (p. 11, Appendix K).
-
The model can allow treatment cycling to examine the impact of different stewardship strategies. The approach to treatment cycling adopted in the model is explained in detail in the submission. However, it appears that all results are presented without any form of treatment cycling because cycling is not mentioned in the company’s results section. Therefore, it is unclear why different approaches to treatment cycling were outlined.
Issues identified by the review group with the company’s model
A detailed discussion of key concerns is followed by a brief overview of other issues with the model.
-
The company’s interpretation of the population considered likely to receive CAZ-AVI and the setting in which it would be received
In comparison to the PICOS developed for this assessment (Table 2), the analyses submitted by the company capture a broader population of all patients with certain (cIAI, cUTI and HAP/VAP) hospital infections. Use in this population creates the risk of rapid emergence of resistance to CAZ-AVI and the treatment becoming obsolete.
The model assumes that on presentation, 20% of patients have known resistance and receive directed treatment rather than empirical treatment, meaning that they will not receive an antibiotic to which the infectious pathogen is resistant. Directed treatment in the model probably represents the proportion of first-line treatment that is informed by microbiology testing. Based on clinical advice EEPRU considers that a more plausible model assumption is that most patients receive microbiology-directed treatment at the second line (i.e. patients receive empiric treatment followed by microbiology-directed treatment where needed). The expected effect of this assumption in the model could be to reduce the level of infection and resistance in the hospital due to patients receiving an appropriate treatment by at least the second treatment line, resulting in lower infection-related mortality, which in turn reduces the health gains that can be attributable to the addition of CAZ-AVI. This approach (which corresponds to the modelling approach used by EEPRU) would also mean that only two treatment lines need modelling, again reducing the modelled benefits of CAZ-AVI which arise by virtue of it resulting in a third treatment line.
For those patients who receive first-line directed treatment, the model does not account for a delay of 3–5 days for the test results to be produced during which a patient may die from infection and incur hospital costs due to bed occupancy. Further, no evidence is provided for the assumed 20% rate of directed testing. The clinical advisors to EEPRU believe that the rates of testing vary greatly across the UK. The variation in microbiology-directed testing rates may be due to variation across hospital in type of infection. Alternatively, delaying treatment to wait for test results may not be considered an option when an infection is life threating. For this reason, it is preferable that the economic model considers a wide range of different rates for directed testing.
Modelling assumptions concerning eradication of colonisation
A potentially important assumption within the model is that there can be complete eradication of colonisation with any pathogen (sensitive or resistant), and that treatment increases the likelihood of this occurring. The clinical advisors to EEPRU believe that complete eradication is unlikely to happen as there will always be a reservoir of the pathogen remaining in the gut. The influence on results of introducing this alternative assumption into the model is difficult to know due to the dynamic-transmission aspects of the model. However, if it is assumed that discharged patients are prone to developing the same pathogen again (and that this can lead to further infections) the result will be a lower population health benefit from treatment, including from the introduction of CAZ-AVI.
Issues with absence of information on the key drivers of net monetary benefit
The base-case NMB estimate, at a cost per QALY threshold of £30,000, was £598,779,222 for the three indications cUTI, cIAI and HAP/VAP combined, in the population of England, over a 10-year time horizon. These results are shown in Table 50. The magnitude of the NMB is likely to be driven by additional health gains (QALYs) with the use of CAZ-AVI as the incremental costs are comparably small in the absence of CAZ-AVI acquisition costs. The incremental QALY gains are likely to be driven by differences in mortality rather than changes in utility during infection because the duration of disutility due to an infection is short: the duration of treatment is assumed to be 2 days for unsuccessful treatment and less than 10 days for successful treatment, while mortality occurs 3 days after the final unsuccessful treatment. If the NMB of CAZ-AVI is driven by differences in mortality from infection, it is unclear how these results were obtained. This is because CAZ-AVI is never the most effective treatment option, and any improvements in efficacy over comparators are modest (see Table 49). Similarly, CAZ-AVI never has the lowest rates of baseline resistance, and values are generally very similar to those for meropenem and colistin (see Table 49). This lack of clarity is compounded as the company’s submission does not go to reasonable lengths to provide a detailed analysis of what is driving this outcome.
The company presents a range of sensitivity analyses of changes in key parameter values and the NMB results are found to be most sensitive to treatment efficacy, as shown in Figure 41. However, absent from the sensitivity analysis is information on the relative contribution to incremental QALYs from treatment-related causes that are most likely to be driving mortality and hence the NMB results. The company submission is not transparent on how much of the improvement in mortality with CAZ-AVI is due to static effects in the model (direct patient benefits from the relative clinical efficacy of CAZ-AVI) and how much is due to the different dynamic aspects of the model that influence population-level benefits such as the health benefits from reduced infection transmission and from diversity strategies. To validate the plausibility of the economic results, information is needed on the QALYs gained in each distinct pathway of treatment effect on mortality. A potential explanation for the large NMB attributable to CAZ-AVI may be the specification of the comparators in the decision problem, as discussed next.
Implications of a two-line comparator treatment sequence
The comparators used in the company submission are shown in Table 52. This suggests that the company’s model applies a two-line sequence as the comparator (it is unclear if a treatment could be used twice). A clear justification for choice of comparators is not provided in the company’s submission. In addition, the assumption of a two-line comparator sequence is not supported by evidence as several antibiotics are likely to be effective in the non-resistance enriched patient population considered by the model. For example, the EEPRU’s PICOS in Table 2 lists several AMs. The inclusion of one of these would allow for treatment sequences with three (or more) treatments in the company’s model.
| Intervention | Indication | ||
|---|---|---|---|
| cIAI | cUTI | HAP/VAP | |
| Piperacillin/tazobactam (Pip/Taz) | ✓ | ✓ | ✗ |
| Colistin | ✗ | ✗ | ✓ |
| Meropenem | ✓ | ✓ | ✓ |
| CAZ-AVI | ✓ | ✓ | ✓ |
Patients who have exhausted all available antibiotic treatment options and fail to clear the infection naturally are assumed to die after 3 days. Hence the addition of any drug to a treatment sequence is expected to generate an advantage when compared to a two-line sequence. Further, it is unclear if person-to-person transmission of resistance is greater in two-line treatment lines compared to a three-line sequence in the company’s model. A difference would be due to the reduced benefit from diversification: there is less opportunity in a two-line sequence for infected patients to move to the colonised state before exhausting available treatments, and patients are assumed to gradually lose resistance at a fixed rate over time only when in a colonised state.
As previously noted, clinical advisors to EEPRU suggest that microbiological testing is appropriate for the infections considered. The company considers a broadly empiric strategy for all treatment lines; this will enhance the relative benefits of a three-line treatment sequence compared to a two-line comparator sequence.
Further sources of concern in the NMB calculation
There is uncertainty in the appropriateness of the population size used in the NMB calculations, which is not fully justified. The company submission states that the population level in England was ‘based on 2019 overnight hospital bed occupancy where it was assumed 93,432 beds in England are constantly occupied in the general and acute wards’ (p. 159) and that approximately 3100 patients per annum over a 10-year period were used (p. 16). The sources and calculations used to establish the overall population size are not clearly stated. If the population size is unreasonably large, this will magnify the NMB of CAZ-AVI. Further, as previously noted, the submitted analyses consider an indication for CAZ-AVI that is broader than that expected by the clinical advisors to EEPRU. An increase in patient numbers receiving CAZ-AVI will contribute to health gains associated with the CAZ-AVI arm and hence NMB.
The model appears to have overestimated the health losses of patients from mortality, which is expected to advantage the per-patient NMB of introducing CAZ-AVI. This is because the corresponding QALY decrement was derived by comparing the health utility and life expectancy of infected patients to the general population. A more accurate comparison would be to people who are in contact with the health system and at high risk of infection; such patients are likely to have a worse quality of life and life expectancy than the general population. Furthermore, it is unclear if discounting was applied to each additional year of expected survival of non-infected patients. The choice of a cost-effectiveness threshold of £30,000 is also not justified.
A7.6 Other concerns with the model
The following are additional limitations of the model:
-
All transition parameters were established from calibration to infection incidence and resistance development time-series data reported by PHE and Fingertips. Model calibration is conducted with reference to national resistance and incidence data in all settings. Calibration to the subset of data available from hospital settings (acute trusts) is more appropriate given that the model simulates a hospital environment and the greater use of antibiotics in hospital environments means the rates of resistance are typically higher than in the community.
-
The model requires evidence for a large number of parameters to allow the prediction of outcomes. As such, a significant number of data-related assumptions was required to produce the published outcomes. There do not appear to be any formal structured expert elicitation exercises to reduce this reliance on assumptions. This is a concern as there is no validation of the model outcomes to additional data sources. This may be because of the limited range of data sources on resistance and incidence. Validation of the model could assess the extent it can predict historical time trends outside the range of years used in calibration (i.e. prior to 2013 and after the year 2018) from the same data sources.
-
The model assumes that AM use drives resistance. The reverse may also hold; for example due to considerations of AM stewardship, known resistance may lead to reduced use of an AM. Therefore, it is preferable if calibration is to data that include the rate of consumption of antibiotics in hospitals to allow the model to construct a more complete picture of the ecological forces that drive the spread of antibiotic resistance.
-
The output of the model does not include any estimate of uncertainty from a probabilistic sensitivity analysis.
-
The base-case NMB estimates appear to be for a scenario without any treatment cycling. However, the benefits of treatment cycling may already be accounted for in the results because the rate of resistance data used in calibration to determine key transmission parameters in the model will include any cycling behaviour between antibiotics that has taken place in England.
Appendix 8 Further detail on methods for economic evaluation
A8.1 Incorporating susceptibility evidence into the economic model
Evidence on conditional susceptibilities
In general, the review of susceptibility studies described in Chapter 5 (and subsequent NMA) provided evidence on absolute susceptibility to a given AM (or in statistical language, the marginal susceptibility). To use evidence on susceptibility in the economic modelling, information on conditional susceptibility is required. This required evidence takes two different forms depending on the treatment setting. In the ES many treatments are combinations of two AMs. For this, evidence is required on the susceptibility to one AM in the combination treatment, conditional on being resistant to the other AM in the combination (so collectively this evidence allows for a derivation of overall susceptibility to the combination treatment). In the MDS interest lies in the proportion of patients who are susceptible to at least one AM in a given group (where the groupings are one of ‘colistin or an aminoglycoside’, ‘a different AM’ or ‘no AMs’). Here the required evidence is again for susceptibility to an AM given resistance to other AMs, but now this resistance could be to multiple AMs. These two settings are discussed in turn, followed by a discussion of issues specific to CAZ-AVI.
The evidence used to inform estimates and assumptions about conditional susceptibilities was obtained from two primary sources. The first was the review of susceptibility studies described in Chapter 5 (approach 3). The second was de novo data requests, as described in Report Supplementary Material 1.
Empiric setting
Two options were considered:
-
Assume independence of absolute susceptibilities when determining overall susceptibility to combination treatments. Under this assumption, the susceptibility of a given isolate to a given AM is the same irrespective of what other AMs the isolate is susceptible to. With this assumption, to obtain overall susceptibility to two AMs, the following equation is used:
Overall susceptibility = susceptibility to AM1 + (1 − susceptibility to AM1) × susceptibility to AM2
In other words, it is assumed that those not susceptible to AM1 have the same susceptibility to AM2 as the whole sample.
-
Use observed evidence on overall susceptibility. This includes evidence on conditional susceptibility (susceptibility to an AM given resistance to another AM). Isolate-level data were available from two sources: a de novo data request from PHE, and supplementary material from Vazquez-Ucha et al. 35 Under this second approach, ‘susceptibility to AM2’ becomes ‘susceptibility to AM2 given resistance to AM1’.
The second approach will provide more nuanced estimates of overall susceptibility to combination treatments by accounting for cross-resistance. However, it is restricted to AM combinations for which there is evidence and is reliant on smaller samples of susceptibility data. In particular, the NMA of susceptibility evidence described in the main text does not provide any evidence on overall or conditional susceptibility. In contrast, the first approach may be used with the NMA results and any other studies. The key assumption of the first approach is that of independence of absolute susceptibility. To assess the credibility of this assumption, analyses of the isolate-level data were performed.
Of the empiric combinations included in the PICOS, data from PHE included colistin with tigecycline. Among those who were resistant to colistin, susceptibility to tigecycline was 59%, compared to an absolute tigecycline susceptibility of 64% in the whole data set. Among those who were resistant to tigecycline, susceptibility to colistin was 82%, compared to an absolute colistin susceptibility of 85% in the whole data set. A two-sided z-test for a difference in proportions was not significant for either comparison, supporting the assumption of independence. The other combination treatment in the ES is fosfomycin with an aminoglycoside. The PHE data had very small numbers for fosfomycin (eight isolates), so were not used to examine combination treatment. Evidence on fosfomycin and aminoglycosides (amikacin, gentamicin and tobramycin) is available from Vazquez-Ucha et al. 35 and summarised in Table 53. This also suggests that, for the combination of treatments included in the PICO, an assumption of independence is tenable, since susceptibilities for all treatments were very similar in the absolute compared to the conditional groups.
| Drug | Absolute susceptibility | Conditional susceptibility | |||
|---|---|---|---|---|---|
| Isolates | Susceptibility, % | Isolates | Susceptibility, % | Resistant to | |
| Amikacin | 302 | 79 | 159 | 79 | Fosfomycin |
| Gentamicin | 302 | 37 | 159 | 38 | Fosfomycin |
| Tobramycin | 302 | 34 | 159 | 31 | Fosfomycin |
| Fosfomycin | 302 | 47 | 63 | 48 | Amikacin |
| Fosfomycin | 302 | 47 | 191 | 48 | Gentamicin |
| Fosfomycin | 302 | 47 | 200 | 45 | Tobramycin |
Microbiology-directed setting
In the MDS (for which it is assumed that individuals will receive any AM to which they are susceptible), one approach would be to also assume independence of susceptibilities when deriving susceptibility groups (susceptible to a non-colistin/aminoglycoside AM, susceptible to only colistin or an aminoglycoside, and not susceptible to any AM). The appropriateness of this assumption for the first group was checked using data from PHE (which includes all the comparators apart from fosfomycin) and Vazquez-Ucha et al. (which includes all the comparators apart from tigecycline). 35 Applying an assumption of independence to the PHE data resulted in 87% of patients being susceptible to a non-colistin/aminoglycoside AM. The real value from PHE is 68%, suggesting that in this instance the assumption of independence does not hold. Similarly, applying an assumption of independence to the Vazquez-Ucha et al. data resulted in 62% of patients being susceptible to a non-colistin/aminoglycoside AM, compared with a true value of 55%. Hence the assumption of independence was not employed when deriving susceptibility for the groups. Instead, the PHE data were used to calculate the likely overestimate when assuming independence. Hence, given the above numbers, the true value is likely to be 68/87 = 78% of the value obtained when assuming independence. As the NMA evidence does not capture dependencies among AMs, these estimates were first combined to obtain susceptibility groups assuming independence. The scaling factor from the PHE data was then applied to adjust for the likely overestimate due to assuming independence. The same method was used to derive adjusted values for the second susceptibility group (with the third susceptibility group obtained by noting that the sum across the three groups had to sum to 100%).
Ceftazidime-avibactam
Isolate-level data from PHE and Vazquez-Ucha et al. can provide some insight into these questions. Based on PHE data, the overall susceptibility to CAZ-AVI is 87.6%, while among patients resistant to all non-toxic AMs it is 86.8%. Susceptibility values from Vazquez-Ucha et al. are 97.7% and 97.0%, respectively. Fewer than five people were resistant to all AMs for both evidence sources, so susceptibility to CAZ-AVI in this subgroup could not be calculated. This suggests that, while there may be a very small decrease in susceptibility, as a simplifying assumption it is acceptable to assume that susceptibility to CAZ-AVI is independent of resistance to other AMs.
Scenario analyses for susceptibility evidence
For the base-case analysis it was assumed that conditional susceptibilities were the same as absolute susceptibilities. This assumption was relaxed in the following scenario analyses:
-
Scaling conditional susceptibility: with this scaling factor informed by PHE data, where available. For example, if in the PHE data the conditional susceptibility to tigecycline among isolates that were resistant to colistin was 10% lower than the absolute susceptibility to tigecycline, then the absolute susceptibility to tigecycline obtained from the NMA was reduced by 10% to obtain the conditional susceptibility.
-
Use of PHE data for both the absolute and conditional susceptibilities.
-
Use of data from Vazquez-Ucha et al. for both the absolute and conditional susceptibilities. 35
For the last two scenarios, conditional susceptibilities were obtained directly from the evidence used (PHE or Vazquez-Ucha et al. ) and hence not assumed to be the same as the absolute susceptibilities. The PHE data did not include fosfomycin, while the Vazquez-Ucha et al. data did not include tigecycline. 35 Hence for the scenarios which used these evidence sources, it was assumed that the drugs without data were not used.
A8.2 Parametric survival modelling of CARBAR
Table 54 summarises the assessment of internal and external validity of the parametric survival analysis of all-cause mortality from CARBAR.
| Distribution | AIC | Visual assessment of fit | Comparison with external data and assessment of face validity |
|---|---|---|---|
| Exponential | 953 | Poor | No convergence with general population mortality |
| Weibull | 935 | Moderate | Converges towards general population mortality but annual probability of death always greater |
| Gompertz | 952 | Poor | Converges with general population mortality at 9 years |
| Log-logistic | 938 | Moderate | Converges with general population mortality at 15 years |
| Log-normal | 953 | Moderate | Converges with general population mortality at 13 years |
| Generalised gamma | 933 | Poor | Rapidly accelerating mortality and divergence with general population mortality |
A8.3 HRQoL weights by comorbidity level
Table 55 shows SF-6D utilities by CCI, and the distribution of people within each CCI score within the CARBAR study.
| CCI score | SF-6D score 121 | Proportion of people within each CCI score (CARBAR), % |
|---|---|---|
| CCI 0 | 0.729 | 20 |
| CCI 1–2 | 0.667 | 31 |
| CCI 3–4 | 0.621 | 21 |
| CCI 5+ | 0.615 | 28 |
A8.4 Drug acquisition costs
Table 56 shows the drug costs used in the model.
| AM | Price | Daily dose | Cost per day, £ | Cost per course of treatment (treatment duration in days), £ | Cost per 5 days of treatment, £ |
|---|---|---|---|---|---|
| Colistimethate sodium | £18.00 (10 × 1 MU vial)131 | 9 MU | 16.20 | 153.9 (9.5 days132) | 81.00 |
| Aminoglycosides (gentamicin) | £10.97 (20 × 360 mg/120 ml solution for infusion bags)133 | 0.24 g134 | 10.97 | 76.79 (maximum IV treatment 7 days131) | 54.85 |
| Aminoglycosides (amikacin) | £38.72 (5 × 500 mg/2 ml vials)133 | maximum dose 1.5 g134 | 23.23 | 232.30 (10 days131) | 116.15 |
| Aminoglycosides (tobramycin) | £10.69 (1 × 240 mg/6 ml solution for injection vials)133 | 0.24 g134 | 10.69 | 74.83 (maximum treatment 7 days131) | 53.45 |
| Tigecycline | £106.52 (10 × 50 mg vials)133 | 0.1 g134 | 21.30 | 298.20 (14 days131) | 106.5 |
| Fosfomycin | £4.86 (1 × 3 g sachet)131 | 3 g (1 sachet)131 | 4.86 | 9.66 (2 doses1) | 9.66 |
| Fluoroquinolones (ciprofloxacin) |
£5.02 (10 × 400 mg/200 ml infusion)133 | 1.2 g134 | 1.51 | 10.57 (7 days131) | 7.55 |
| Fluoroquinolones (levofloxacin) |
£20.95 (10 × 500 mg/100 ml infusion bags)133 | 0.5 g134 | 2.10 | 29.40 (14 days131) | 10.5 |
| Cephalosporins (cefepime) | £70.00 (10 × 1 g vial)131 | 4 g134 | 28.00 | 280.00 (10 days135) | 140.00 |
| Cephalosporins (ceftriaxone) | £5.25 (10 × 1 g vial)133 | 4 g134 | 2.10 | 29.40 (14 days 131) | 10.5 |
| Aztreonam | £18.82 (2 g powder for solution for injection)131 | 4 g134 | 37.64 | 263.48 (7 days, assumed) | 188.2 |
A8.5 Goodness of fit of forecast models
Table 57 shows the goodness-of-fit statistics (AIC, for which lower values indicate better fit) for the alternative forecasting models.
| Model | Invasive isolates | Screening isolates |
|---|---|---|
| No trend | 120.80 | 307.09 |
| Damped trend | 118.62 | 308.54 |
| Trend | 115.31 | 302.18 |
A8.6 Further details on modelling direct population net health effects in HVCS
Predicting the future sizes of the HVCS
Time-series data were provided by PHE. This included evidence on changes over time in both invasive infection isolates and screening isolates. Neither isolate type (invasive infections and screening) is the same as the isolate type included in the HVCS (all infections). Of the two types available, the invasive infections were the most similar to all infections, so were the primary focus of analyses. Screening isolates were considered in secondary analyses. Data were supplied from the Reference Laboratory provided by the AMRHAI national reference unit, with data available until April 2021. Further details on the analyses of invasive infections and screening isolates are provided in the subsequent subsections.
Time-series models
Time-series methods were used to generate future predictions of the population size. Three classes of model were considered:
-
Exponential smoothing (state-space) models. 182 This models variation in the data via variation in latent (unobserved) states representing a level (average) and trend. For extrapolations, predictions of these states are informed by all the available data, with more weight given to more recent observations and less weight given to older observations. The weight given to older observations decreases based on an exponential function, with the amount of decay estimated from the data. Use of this model assumes that extrapolations of (the logarithm of) the population follow a linear model. An alternative assumption is that the trend in the linear model is successively ‘damped’ over time so that eventually it becomes zero, and extrapolations become constant. This dampening can help to avoid forecasts becoming too large. Hence three exponential smoothing models were considered; a trend model, a damped-trend model, and a model with no trend.
-
Autoregressive integrated moving average (ARIMA) models. 182 These model the autocorrelations in the data. Unlike exponential smoothing models, ARIMA models do not incorporate a trend. Instead, they assume that after differencing the data (calculating the differences between observations; this is potentially repeated multiple times), there is no trend.
-
Generalised linear models for count time-series data. 183 Poisson and negative binomial models were considered, with a logarithmic link for both. Hence for both models it is assumed that the logarithm of the counts follows a linear model. These models may be viewed as extending standard regression models to account for correlations among observations.
All models were fitted in R version 4.0.2, using the ‘forecast’ package for both exponential smoothing and ARIMA models, and the ‘tscount’ package for the generalised linear models. 182,183 The exponential smoothing and ARIMA models are for Gaussian (normally distributed) outcomes. Count data are not normally distributed, and due to the small numbers involved in the analysis the normal distribution would not be a good approximation. Instead, the logarithm of the data was taken prior to fitting the exponential smoothing and ARIMA models.
Point estimates from the three model types were generally very similar, as were model diagnostics (which included visual goodness of fit, statistical significance of the autocorrelation function, the distribution of residuals, and the Ljung–Box test). Initially none of the models identified a trend in the time series, with forecasts being set to either the last observed value or an average of the observed data. As such, subsequent analyses focused on exponential smoothing models, for the following reasons:
-
the ability to specify models that include a trend (in contrast to ARIMA models which do not have an explicit trend parameter)
-
having analytical formulae to express uncertainty in forecasts (which was not available for the generalised linear models).
Exponential smoothing models with both damped and undamped additive trends were considered. The error type (additive or multiplicative) was chosen by the fitting software (based on model goodness-of-fit), as was a Box–Cox transformation.
Incorporating forecasts in the economic model
To incorporate the extrapolations within the economic model, these were converted into year-on-year relative changes. That is, the relative change in year ‘t’ was calculated as the forecast in year ‘t+1’ divided by the forecast in year ‘t’. For PSA, forecasts were obtained using the following process:
-
Obtain the mean and standard deviation, both on the log-scale, at each time point. For example, to obtain forecasts for 20 years, 20 pairs of mean and standard deviation are obtained.
-
Use these values to sample a value from a log-normal distribution. Hence for a 20-year forecast, for a single iteration of the PSA, 20 samples are obtained: one for each year where each year has its own unique mean and standard deviation.
Within a single iteration of the PSA the same random number was used for sampling. Different random numbers were used across PSA iterations. This ensured that trends in forecast were retained in the PSA.
Predicting future rates of resistance for current practice
Two options were considered for which data to use:
-
Forecast counts of both ‘susceptible’ (or ‘resistant’) as well as the denominator (susceptible plus resistant) and use the outputs from these forecasts to estimate future percentages of susceptibility or resistance. To reduce the noise in the data, forecasts would focus on the numerator for which there are the highest counts (e.g. for drugs to which isolates are mainly susceptible, the forecast would be counts of susceptible isolates).
-
Forecast the percentage susceptible (or resistant) directly.
An advantage of the first approach is that the data to be forecast (counts) are of the same type as the data forecast in the previous section, so the models of that section can also be considered. The main disadvantage of the first approach is that it ignores any correlations among the numerator and denominator, whereas by definition these are correlated. The second approach removes the need to consider correlations but has the main limitation it ignores evidence on the denominator (number of tests), which varies over time. As such, the second approach will give equal weight to each time point, even if some are based on a larger number of tests.
Prior to generating forecasts, exploratory modelling of the susceptibility data was undertaken to visually assess if there was likely to be a trend in the available data. Due to the typically small numbers and high variation observed in the susceptibility data, a visual approach to identifying a trend was taken in preference to significance testing. A Poisson generalised additive model was used, with the number of susceptible tests as the outcome and the number of tests as the offset (so allowing for a derivation of the susceptibility rate). This statistical approach is consistent with a recent publication of susceptibility data, with a further improvement to make the statistical model more flexible and so less prone to model misspecification (by using a generalised additive model instead of a generalised linear model). 184,185
Graphs for each AM are provided in Report Supplementary Material 3. Table 58 provides an overview of any trends in susceptibility using data from PHE. To add additional context, information on any trends in AM prescribing in secondary care in the time period 2015–9 (obtained from the ESPAUR report) is also included.
| Antimicrobial | Trends in susceptibility (PHE data) | Trends in prescribing (ESPAUR report) |
|---|---|---|
| Aminoglycosides | No trend | Increase of 10.7% and 22.3% in inpatient and outpatient wards, respectively (2015–9, statistical significance not stated) |
| Aztreonam | Decreasing susceptibility | No evidence provided |
| Cephalosporins | No trend | Significant increase in third-, fourth- and fifth-generation cephalosporins |
| Ciprofloxacin | Decreasing susceptibility from 2015 | No evidence of change (statistical significance not stated) |
| Colistin | Potential decreasing susceptibility, but due to uncertainty data are also consistent with no trend | Increase from 15.8 to 25.2 defined daily doses per 1000 admissions (2015–9, statistical significance not stated) |
| Tigecycline | Potential decreasing susceptibility, but due to uncertainty data are also consistent with no trend | Significant increase in tetracyclines |
| CAZ-AVI | No trend | Increase from 0.1 to 0.5 defined daily doses per 1000 admissions (2016–9, statistical significance not stated) |
In summary, there was evidence of decreasing susceptibility for aztreonam and ciprofloxacin. For colistin and tigecycline it was unclear if susceptibility was decreasing over time or not. For the remaining three AMs there was no evidence of a trend. Any interpretation of trends in susceptibility over time is confounded by changes to EUCAST breakpoints for defining susceptibility. For example, for both ciprofloxacin and tigecycline the breakpoints at which a susceptible isolate becomes intermediate-resistant (and at which an intermediate-resistant isolate becomes resistant) changed during the period of interest; in 2017 for ciprofloxacin and 2019 for tigecycline. Because of this, and the large uncertainty in the susceptibility data (due to both small numbers and being restricted to invasive infections), it was decided that for the base-case analysis no trend would be used.
Predicting future resistance trajectories for CAZ-AVI
Supporting evidence
An overview of the studies identified via literature searches is provided in Table 59.
| Study | Design | Population | Antimicrobials | Association |
|---|---|---|---|---|
| Ortiz-Brizuela 2020145 | ARIMA models with lags between 1 and 12 months | Carbapenem-non-susceptible Enterobacterales treated in a hospital setting in Mexico City between July 2013 and December 2018, N = 451 | Resistance for three populations: carbapenem-non-susceptible Enterobacterales, CPE, and OXA-232 CPE. Evaluated for 17 AMs (DDD per 100 hospital patient days) | For each population a positive association was only found for piperacilline-tazobactam at a 6-month lag |
| Gharbi 2015146 | ARIMA models. Considered multiple yearly lags (not stated) | An outbreak of Klebsiella pneumoniae with OXA-48 in a London renal unit, January 2008 to April 2010, N = 13 | Meropenem consumption (DDD per 100 occupied bed days) | One-year lag had the largest correlation, with a coefficient from the ARIMA model of 1.07 (95% CI 0.10 to 2.05) |
| Berger 2004147 | Generalised additive model. Tested monthly lags | Staphylococcus aureus treated in hospitals in France, July 1997 to June 2000, N = 1116 | Fluoroquinolone (DDD per 1000 days of hospitalisation) | The best fit was with a 4-month lag. Increasing use from the 25th to 75th percentile had a relative risk of 1.27 (95% CI 1.13 to 1.42) |
While these studies were not used to estimate the link between AM use and AM resistance, they informed the approach to subsequent analysis. Two model types were used to assess the relationship between use and resistance: ARIMA models and generalised additive models. Of these, only the former are time-series models in the sense that they can capture autocorrelations within the data. Hence this model type was retained for the de novo analyses reported here. With regard to the time lag to use, findings from the studies in Table 59 suggest that for monthly data a lag of 4–6 months would be appropriate, while for annual data a 1-year lag should be used.
When performing a de novo analysis, two types of publicly available evidence were available:
-
English data on AM use and AM resistance, from the ‘AMR local indicators profile’153
-
European data on AM use and AM resistance from EARS-Net and ESAC-Net, respectively. 154,155
The England-specific data are made publicly available by PHE via the Fingertips database. 186 Data on resistance are available for Escherichia coli bacteraemia for four AMs: gentamicin, ciproflaxacin, piperacillin/tazobactam and cephalosporins. Reporting of Escherichia coli has been mandatory for NHS acute trusts since June 2011, and Fingertips provides quarterly data since the last quarter of 2015. 187 Data on AM use cover both primary and secondary care. For primary care, data are available for both the total number of AM prescriptions and the total number of prescriptions of broad-spectrum AMs, defined as cephalosporins, fluoroquinolones and co-amoxiclav. Secondary care AM use is available for the total number of AM prescriptions, the number of carbapenems prescriptions and the number of prescriptions for each of the World Health Organization’s access, watch, reserve categories. 188 An alternative data source for AM prescriptions is OpenPrescribing.net. 189 This provides information on primary care prescriptions for the last 5 years in England. This source does not include secondary care prescriptions but does include some of the drugs that are included in the Fingertips resistance data (gentamicin, ciproflaxin and piperacillin/tazobactam).
Thirty countries from the European Union contribute data to EARS-Net on AM resistance for up to eight pathogens. 156 The analyses reported here focused on two pathogens that overlapped with those in the HVCS: Escherichia coli and Klebsiella pneumoniae (as Enterobacterales). There was initially no restriction on the time periods, countries or AMs considered. The AMs for which resistance data are available are Escherichia coli (aminoglycosides, aminopenicillins, carbapenems, fluoroquinolones and cephalosporins) and Klebsiella pneumoniae (aminoglycosides, carbapenems, fluoroquinolones and cephalosporins).
Data on AM consumption (DDDs per 1000 inhabitants per day) were obtained from ESAC-Net, which provides use in both the community and hospitals. 154 Data are drawn from a variety of sources; for example, AM use in acute hospitals is based on a point-prevalence survey, while both sales and reimbursement data could contribute to overall estimates of use. DDDs were developed by the World Health Organization Collaborating Centre for Drug Statistics Methodology and are the average maintenance dose per day for a drug when used in its main adult indication. There were two AMs for which surveillance data on both consumption and resistance were available: cephalosporins and carbapenems; hence analyses were restricted to these. Data for cephalosporins included first-, second-, third- and fourth-generation cephalosporins, as well as ‘other cephalosporins and penems’.
The general aim was to identify trajectories of resistance to existing AMs, and to assess the association with AM use. This would then provide a set of potential use-resistance trajectories which could then be applied to CAZ-AVI, for which levels of use would be estimated from the economic model. A two-stage approach was employed. In the first stage, resistance trajectories were visualised to identify any trajectories for which resistance started at a low level (as baseline resistance to CAZ-AVI was estimated to be 92% in Sources of evidence). Trajectories were retained even if there was no apparent trend in resistance over time. This was because existing evidence suggested that for some AMs there may be no association between use and resistance. 143 Within the England-specific data there were no clear examples of when resistance increased from a low baseline. Hence subsequent analyses were restricted to the European surveillance data.
A visual inspection of the two Enterobacterales pathogens showed that low initial levels of resistance were more common for Escherichia coli than for Klebsiella pneumoniae, hence only the former was retained. For Escherichia coli, an initial filter was applied to only retain countries for which at least 5000 isolates were tested, and baseline resistance (average over the first 3 years of available data) was ˂ 3%. As a result 27 countries were retained. After visually examining plots of AM use and AM resistance for these countries, it was decided to further filter the list of countries by restricting the evidence for carbapenems to countries with at least 10 non-zero observations for both AM use and AM resistance. For cephalosporins at least 15 non-zero observations were required, due to the large list of retained countries. This resulted in the following 16 pathogen–drug–country combinations:
-
Carbapenems: France, Greece, Netherlands, Norway.
-
Cephalosporins: Bulgaria, Croatia, Estonia, Finland, France, Greece, Ireland, Luxembourg, Malta, Norway, Slovenia, Sweden.
For these countries, time-series models were used to assess the association between drug use in 1 year and resistance in the following year. This was achieved by fitting ARIMA models for which resistance over time was the outcome, and the lagged time series of drug use was the predictor. The regression coefficient for this predictor provides inferences: if it is significantly different from zero this suggests that there is an association between AM use and resistance, with positive coefficients indicating that an increase (decrease) in use will lead to an increase (decrease) in resistance in the following year. Conversely, a negative coefficient indicates that an increase (decrease) in use will lead to a decrease (increase) in resistance in the following year. An overview of the coefficients for each retained country is provided in Table 60. Corresponding graphs are provided in Report Supplementary Material 3.
| Country | Coefficient (standard error) | Interpretation |
|---|---|---|
| Escherichia coli , carbapenems | ||
| France | 1.07 (0.32) | Significant: increase in use → increase in resistance |
| Greece | 7.06 (0.71) | Significant: increase in use → increase in resistance |
| Netherlands | −5.5 (3.25) | Not significant |
| Norway | −1.21 (0.91) | Not significant |
| Escherichia coli , cephalosporins | ||
| Bulgaria | 5.78 (1.16) | Significant increase in use → increase in resistance |
| Croatia | 0.69 (0.76) | Not significant |
| Estonia | 10.11 (1.59) | Significant increase in use → increase in resistance |
| Finland | −0.88 (1.62) | Not significant |
| France | −1.11 (0.64) | Not significant |
| Greece | 0.18 (0.67) | Not significant |
| Ireland | −2.03 (1.59) | Not significant |
| Luxembourg | −2.08 (0.93) | Significant: decrease in use → increase in resistance |
| Malta | 1.31 (0.77) | Not significant |
| Norway | −27.69 (2.27) | Significant: decrease in use → increase in resistance |
| Slovenia | −11.29 (3.71) | Significant: decrease in use → increase in resistance |
| Sweden | −12.63 (2.01) | Significant: decrease in use → increase in resistance |
In summary, of the 16 combinations considered:
-
Half provided a significant association (8/16; Escherichia coli = 2/4 for carbapenems and 6/12 for cephalosporins).
-
Of the eight significant associations, four were positive associations (increasing use led to an increase in resistance), while four were negative (decreasing use led to an increase in resistance). All of the negative associations were for Escherichia cephalosporins.
Of note, this analysis was focused on datasets which demonstrated an increase in resistance over time. Hence any significant associations between AM use and decreasing resistance were not explored.
Based on this we decided to explore three associations between increasing AM use and resistance:
-
no association
-
a weak positive association
-
a strong positive association.
There were four significant positive associations from the Escherichia coli analyses, ranging from 1.07 (France, carbapenems) to 10.11 (Estonia, cephalosporins). Hence these values were used to represent weak and strong associations for the CPE population, respectively.
Use-resistance association: statistical models considered
Time-series model
An ARIMA time-series model was used because, in contrast to exponential smoothing models, software exists to fit models that include covariate effects. This provides the time-series version of a linear regression for which the outcome is the rate of resistance, and the dependent variable is AM use over time. 182
An advantage of using time-series methods (in preference to regression models) is that they capture autocorrelations among the data. That is, observations closer together in time are likely to be more similar than observations further apart in time. Incorporating this temporal structure is of particular importance when producing estimates of future values (extrapolations). In general, the further into the future predictions are required, the more uncertain they will be. This extrapolation uncertainty is accommodated by time-series models, but not standard regression models.
A key property of time-series methods is that predictions of the future assume that trends observed in the historical data will continue into the future. External factors may alter these trends and hence lead to inaccurate forecasts. For example, an increased use or effectiveness of antimicrobial stewardship strategies/campaigns may lead to a reduced rate of resistance gain. 190 This may apply to both the AMs evaluated here and existing AMs such as carbapenems. UK examples of stewardship campaigns include the ‘Antibiotic Guardians’ and the Quality premium. 184,191 Use of a damped-trend model can partly mitigate this, as it successively reduces the extrapolated trend as the extrapolated time horizon increases. There is also empirical evidence from the literature that long-term forecasts from a time-series model with a damped trend will generally outperform similar models without a damped trend. 192
Differential equation model
A de novo model was developed to link the rate of change in AM resistance to AM use and other factors: natural mutations leading to resistance, loss of resistance (reflecting ‘fitness’ cost) and deaths among people with a resistant infection. This model was developed to provide a more comprehensive quantification of the differing potential drivers of AM resistance. Model conceptualisation was informed by an existing review-based modelling framework. 193 Report Supplementary Material 3 provides details on the model specification.
Due to the relatively large number of parameters in the model, there was a danger that some of the parameters may lack identifiability (cannot be estimated from the available data). To explore this possibility, a simulation study was conducted. This study (reported in Report Supplementary Material 3) had two objectives: firstly to identify the sample size required and secondly to quantify any bias in parameter estimates. This suggested that approximately 15 observations were required, and that while estimates of rates of natural resistance gain and loss were unbiased, there was a persistent underestimation of the effect of AM use on AM resistance. Due to this bias, the differential equation model was not pursued further.
Model of no association
The sensitivity analysis exploring no relationship between AM use and resistance was motivated by existing literature demonstrating no, or very weak, association in certain settings. 143,144 This is likely to be because there are many drivers of resistance beyond AM use. This includes use in other populations (including other countries) as well as natural mutations. Hence it may be that relative to these other drivers, use in the populations of interest plays a minimal role, so does not need to be explicitly modelled.
Appendix 9 Additional results from economic evaluation
A9.1 Predicted population size over time
Figure 43 shows the base-case scenarios for population size over time by pathogen and infection site.
FIGURE 43.
Population size over time. P1G1, baseline population based on PHE categorisation of infection sites, damped growth rate; P1G2, baseline population based on PHE categorisation of infection sites, growth rate not damped; P2G1, baseline population based on clinical advisors’ categorisation of infection sites, damped growth rate; P2G2, baseline population based on clinical advisors’ categorisation of infection sites, growth rate not damped. Green/blue solid line, P1G1; green/blue dashed line, P1G2; red solid line, scenario P2G1; red dashed line, scenario P2G2.
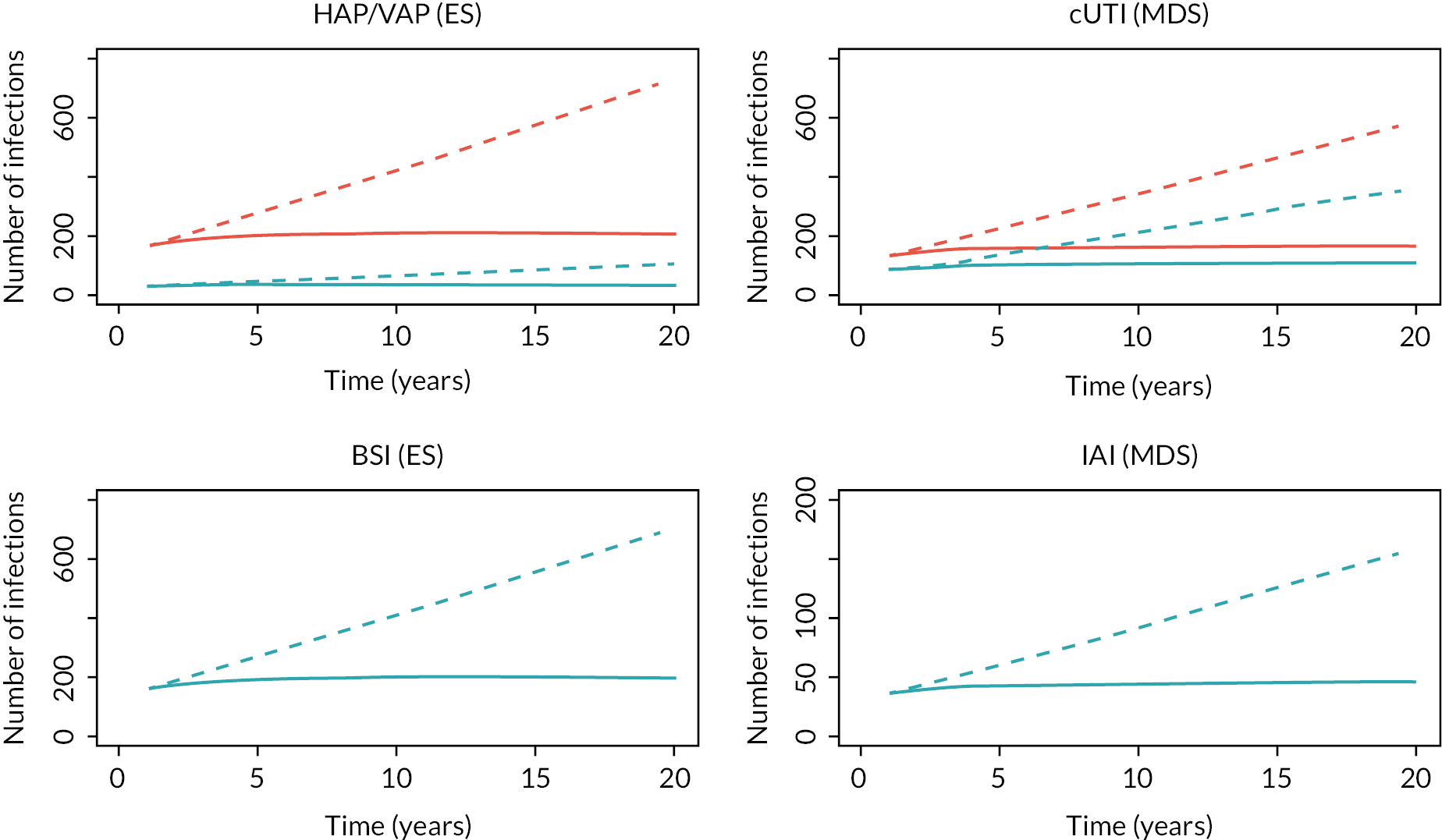
A9.2 Total population INHE across the first 10 years of usage
| Baseline population | Population growth rate | Change in resistance | HAP/VAP | cUTI | BSI | IAI | Total | Proportion of 20-year INHE (%) |
|---|---|---|---|---|---|---|---|---|
| PHE categorisation of infection sites (scenario P1) | Model with damped effect (scenario G1) | 1% (R1) | 38 | 63 | 254 | 28 | 383 | 56.9 |
| 5% (R2) | 37 | 63 | 250 | 27 | 377 | 57.7 | ||
| 10% (R3) | 36 | 62 | 245 | 27 | 370 | 58.7 | ||
| 30% (R4) | 33 | 59 | 224 | 26 | 342 | 64.4 | ||
| Model without damped effect (scenario G2) | 1% (R1) | 56 | 94 | 377 | 41 | 568 | 40.9 | |
| 5% (R2) | 55 | 93 | 370 | 41 | 559 | 41.7 | ||
| 10% (R3) | 54 | 92 | 362 | 40 | 548 | 42.9 | ||
| 30% (R4) | 49 | 86 | 327 | 38 | 500 | 48.7 | ||
| Clinical advisors’ categorisation of infection sites (scenario P2) | Model with damped effect (scenario G1) | 1% (R1) | 262 | 102 | 254 | 28 | 646 | 57.0 |
| 5% (R2) | 258 | 101 | 250 | 27 | 636 | 57.8 | ||
| 10% (R3) | 253 | 100 | 245 | 27 | 625 | 59.0 | ||
| 30% (R4) | 232 | 94 | 224 | 26 | 576 | 64.6 | ||
| Model without damped effect (scenario G2) | 1% (R1) | 389 | 151 | 377 | 41 | 958 | 40.9 | |
| 5% (R2) | 382 | 150 | 370 | 41 | 943 | 41.8 | ||
| 10% (R3) | 373 | 147 | 362 | 40 | 922 | 42.9 | ||
| 30% (R4) | 337 | 139 | 327 | 38 | 841 | 48.9 |
A9.3 Additional scenario: contraindications to colistin and aminoglycosides
A9.3.1 Background
The analysis in the EEPRU base case was based on a proportion of patients being resistant to existing therapies other than colistin/aminoglycosides. In this case it was assumed that, in the absence of CAZ-AVI, colistin/aminoglycosides would be administered to patients. The negative health effects and additional costs of renal toxicity associated with these products were explicitly modelled in assessing the patient-level INHEs of CAZ-AVI compared with existing therapies. Based on the results of the NMA of EUCAST studies (Clinical parameters – susceptibility evidence), 65% of patients shown to have OXA-48 in the ES were resistant to existing therapies other than colistin/aminoglycosides. In the MDS, 35% of patients were resistant to existing therapies other than colistin/aminoglycosides.
Consultees have indicated that, in terms of existing therapies (i.e. in world without CAZ-AVI), there is a proportion of patients who would not receive colistin/aminoglycosides even if no other effective therapy was available. This would be due to a patient’s high clinical risk of renal toxicity. For such patients it can be assumed that they would only receive salvage therapy. The size of this subgroup of patients contraindicated to colistin/aminoglycosides was considered small by EEPRU’s clinical advisors. The Committee has requested a scenario which considers the magnitude of population-level INHEs for this subgroup using the Committee’s assumptions about the size of the cohort as a proportion of those estimated for the HVCSs.
A9.3.2 Methods
The scenario aimed to reflect the benefit of CAZ-AVI in patients who cannot take colistin and other aminoglycoside treatments and, therefore, without the new drug, would receive multidrug salvage therapy.
A9.3.2.1 Patient-level benefit
For this scenario, the patient-level INHEs in those who can take colistin (the EEPRU base case) and those who cannot are shown in Table 62. In the ES (HAP/VAP and BSIs), the incremental patient-level benefit of CAZ-AVI was derived by combining the EEPRU base case and Scenario 1 above. In patients who were treated empirically and who were later confirmed to have an infection caused by OXA-48 (20% of patients, Table 18), outcomes were derived from Scenario 1 above, assuming that, without CAZ-AVI, all patients received ineffective empiric treatment. The incremental benefit of CAZ-AVI in this subgroup was 2.2 QALYs per person. In patients who were treated empirically and who were later confirmed not to have an infection caused by OXA-48 (80% of the sample), outcomes with colistin and with salvage therapy were assumed to be the same (0.221 QALYs in Table 25).
| ESa | MDSb | |
|---|---|---|
| Base case | 0.215 | 0.069 |
| New scenario | 0.622 | 1.032 |
In the MDS (cUTI and IAI, as discussed in Section Quantitative extrapolation to expected usage), without CAZ-AVI, patients who cannot take colistin/aminoglycosides were assumed to receive multidrug salvage therapy. The incremental benefit of CAZ-AVI was derived in Scenario 1 above (1.032 for cUTIs in Table 62).
A9.3.2.2 Population-level benefit
The population-level benefit was derived from the updated patient-level INHE and the extrapolation parameters shown in Table 63.
| User defined parameter | Base case (range) |
|---|---|
| Probability of event (emergence of highly resistant strains) | 100% |
| Time of event (from now) | 0 years |
| The number of patients affected in the first year | See Table 23 |
| The annual growth in the number of infections (from baseline) | 1.2% or 17.1% |
| Analysis time horizon (years) | 20 |
| Population annual discount rate | 3.5% |
The initial population size was site- and setting-specific, derived as described in the Section Quantitative extrapolation to expected usage. Two different scenarios for the initial population size were explored derived from different classifications of specimen samples in SGSS dataset (Scenarios P1 and P2 in Table 23). The population growth rate was assumed to be the same across all sites of infection and settings. It was approximated using the population size in year 1 and year 20 (shown in Figure 43), assuming a constant rate of increase between those two time points. Two scenarios for the population growth rate were explored derived assuming damped and non-damped population growth trends (Scenarios G1 and G2 in Figure 43) – these correspond to 1.2% and 17.1% annual increase on baseline in the Excel tool.
The overall benefit was derived by averaging the total INHE from the base case and the new scenario, weighted by the proportion of the total treated population who are susceptible to colistin/aminoglycosides but would be given salvage therapy due to colistin/aminoglycoside toxicity.
Considering the lack of empiric evidence, the NICE Committee suggested a plausible range (20–40%) for the proportion of patients who, despite being susceptible to colistin/aminoglycosides, would instead be given salvage therapy due to colistin/aminoglycoside toxicity, in the absence of CAZ-AVI.
In the ES (HAP/VAP and BSIs), this represents 20–40% of the total treated population when colistin/aminoglycosides are used empirically.
In the MDS (cUTI and IAI), the scenario is assumed to be applicable to 20–40% of the patients who were not susceptible to non-colistin/aminoglycoside therapy (100–65% = 35% of the sample, as per Table 16), assuming that all such patients would be considered for colistin/aminoglycoside therapy. Therefore, the proportion of the total sample in the MDS who would be in this subgroup was between 7% (= 0.2*35%) and 14% (= 0.4*35%).
A9.3.3 Results
Figure 44 shows how the total expected INHE changes with the proportion of patients who cannot take colistin, compared to the EEPRU base case. In summary, reflecting the outcomes of patients who cannot take colistin/aminoglycosides increases the benefit of CAZ-AVI, and the benefit increases with the proportion of such patients. The absolute increase in INHE in this scenario increases with the population size, as shown by the orange solid and dashed lines (representing a scenario with a higher patient population) diverging more than the blue solid and dashed lines.
FIGURE 44.
Change in total population-level INHE with varying proportion of patients who cannot take colistin, derived from different assumptions about the population size. P1G1, baseline population (point estimate) based on PHE categorisation of infection sites, growth rate damped; P2G2, baseline population (point estimate) based on clinical advisors’ categorisation of infection sites, growth rate not damped.
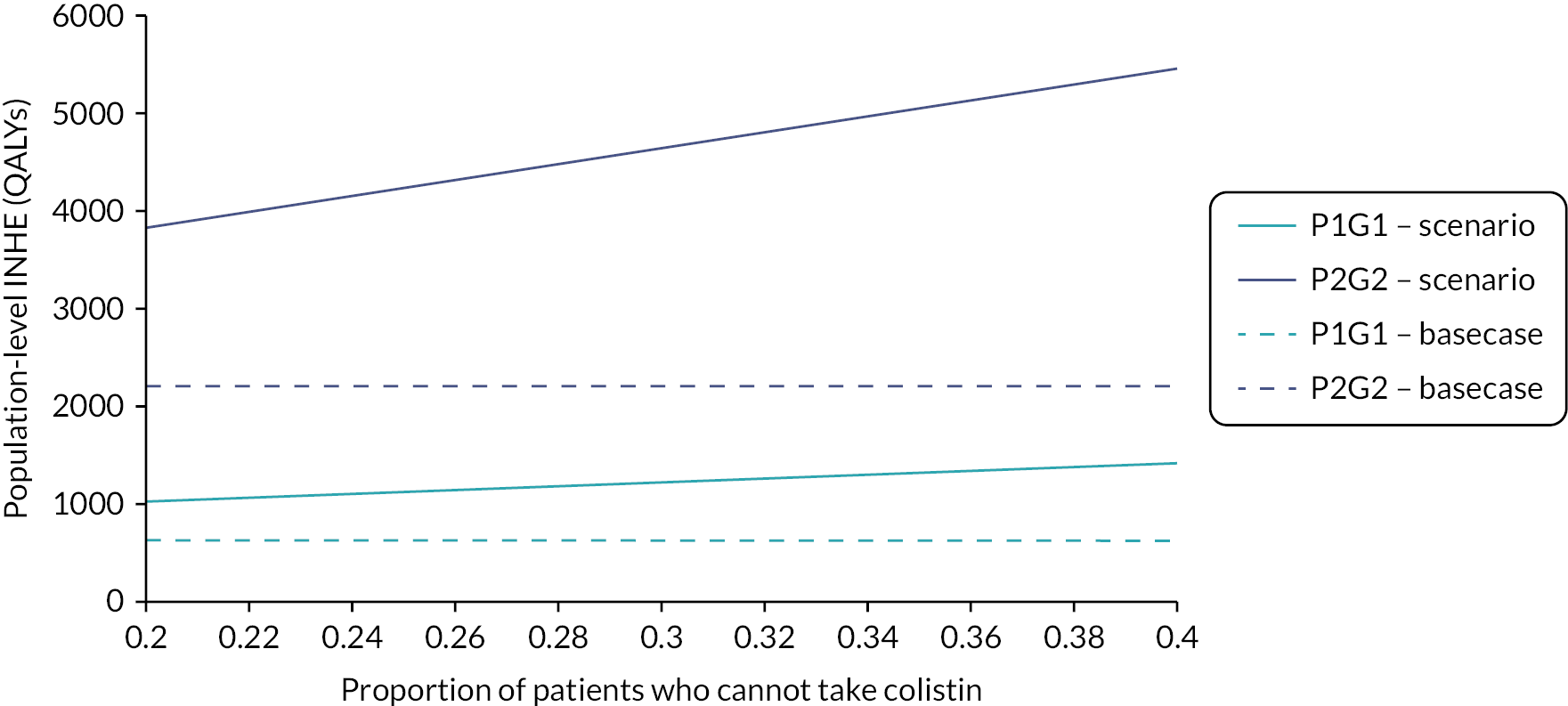
Table 64 shows the breakdown of the population-level INHE for each site of infection for a range of proportions of patients who cannot take colistin/aminoglycosides, compared to the EEPRU base case. The change in INHE compared to the base case is higher in the MDS (cUTI and IAI) than the ES (HAP/VAP and BSI) because the patient-level benefit of CAZ-AVI in patients who cannot take colistin is higher in the MDS than the ES (shown in Table 64).
| Proportion of susceptible patients who cannot take colistin/aminoglycosides, % | HAP/VAPa | cUTIa | BSIa | IAIa | Totala |
|---|---|---|---|---|---|
| 0 (base case)b | 66–946 | 83–274 | 444–916 | 36–75 | 629–2211 |
| 20 | 102–1546 | 174–619 | 683–1499 | 76–169 | 1035–3833 |
| 40 | 137–2147 | 265–965 | 922–2081 | 116–263 | 1441–5456 |
These expected population-level INHEs may overestimate the total INHE for several reasons. Firstly, the 20–40% proportion of patients who would not be given colistin/aminoglycosides because of toxicity fears in the absence of CAZ-AVI is high compared to the assessment of the clinical advisors consulted by EEPRU. Secondly, the scenario assumes that outcomes in patients who can and cannot take colistin/aminoglycosides are comparable when, in practice, patients who cannot take colistin may have poorer prognoses than patients who can. Thirdly, the scenario assumes patients would be contraindicated to colistin and aminoglycosides, but clinical advisors to EEPRU (and consultation comments from the British Infection Association) suggested that most of the concern is about colistin.
Finally, the scenario results in Table 64 represent the benefit in HVCSs when, in the ES, all patients with suspected OXA-48 infection are treated with colistin/aminoglycosides. In the EEPRU base case, the empiric treatment with non-colistin/glycoside therapy had a higher patient-level net benefit (and lower incremental benefit of CAZ-AVI) than treatment with colistin/glycosides, suggesting that, without CAZ-AVI, non-aminoglycosides are the preferred empiric treatment. The base-case results in the EEPRU report and in Table 64 reflect this lower incremental benefit of CAZ-AVI achieved when only non-colistin/aminoglycosides are used as first-line empiric treatment.
The benefit of CAZ-AVI generated in patients who are susceptible to, but who cannot take, colistin in the ES is likely to be lower than the estimates in Table 64 if empiric treatment does not include colistin/aminoglycosides. This is because it would only apply to between 6% and 12% of the total sample of patients in this setting [20–40% of the 13% (0.2 × 65%) who have the infection but are not susceptible to the empiric treatment with non-aminoglycosides]. The benefit in this subpopulation could not be quantified as EEPRU did not explicitly model the second line of treatment in the ES. The lower bound of the estimate, assuming no added benefit of CAZ-AVI when suspected OXA-48 infections are treated with non-colistin/aminoglycosides in the ES, leads to 760–2651 QALYs if 20% of susceptible patients cannot take colistin/aminoglycosides, and 891–3090 QALYs if that proportion is 40%.
A9.4 Combined effect of uncertainties at the patient and population level
Patient-level scenario analyses that modified the total base-case population-level INHE by more than 10% are shown in Table 65. The results are presented as the range based on most and least conservative assumptions about the population size (scenarios P1G1 and P2G2 in Figure 43) and assuming zero resistance emergence. The scenarios assume that, where applicable, the same assumptions apply across populations, for example, if a certain assumption is considered more appropriate for HAP/VAP ES patients, it is also considered more appropriate for BSI ES patients.
| Scenario name | Base-case value/assumption | Scenario value/assumption | HAP/VAP (ES) | cUTI (MDS) | BSI (ES) | IAI (MDS) | Total |
|---|---|---|---|---|---|---|---|
| Base case | – | – | 67–960 | 112–372 | 449–930 | 49–102 | 677–2364 |
| p_bug_survey | Probability patient has OXA-48 Enterobacterales is 0.20 | Probability patient has OXA-48 Enterobacterales is 0.57 based on BSAC survey data | 93–1338 | 112–372 | 627–1297 | 49–102 | 881–3109 |
| p_bug_10 | Probability patient has OXA-48 Enterobacterales in ES is 0.20 | Probability patient has OXA-48 Enterobacterales is 0.10 | 34–493 | 112–372 | 231–478 | 49–102 | 426–1445 |
| p_bug_30 | Probability patient has OXA-48 Enterobacterales in ES is 0.20 | Probability patient has OXA-48 Enterobacterales is 0.30 | 97–1386 | 112–372 | 649–1343 | 49–102 | 907–3203 |
| p_bug_40 | Probability patient has OXA-48 Enterobacterales in ES is 0.20 | Probability patient has OXA-48 Enterobacterales is 0.40 | 95–1368 | 112–372 | 641–1326 | 49–102 | 897–3168 |
| p_bug_50 | Probability patient has OXA-48 Enterobacterales in ES is 0.20 | Probability patient has OXA-48 Enterobacterales is 0.50 | 94–1351 | 112–372 | 633–1309 | 49–102 | 888–3134 |
| p_bug_60 | Probability patient has OXA-48 Enterobacterales in ES is 0.20 | Probability patient has OXA-48 Enterobacterales is 0.60 | 93–1333 | 112–372 | 624–1292 | 49–102 | 878–3099 |
| p_bug_70 | Probability patient has OXA-48 Enterobacterales in ES is 0.20 | Probability patient has OXA-48 Enterobacterales is 0.70 | 92–1316 | 112–372 | 616–1275 | 49–102 | 869–3065 |
| p_bug_80 | Probability patient has OXA-48 Enterobacterales in ES is 0.20 | Probability patient has OXA-48 Enterobacterales is 0.80 | 91–1299 | 112–372 | 608–1258 | 49–102 | 860–3031 |
| p_bug_90 | Probability patient has OXA-48 Enterobacterales in ES is 0.20 | Probability patient has OXA-48 Enterobacterales is 0.90 | 89–1281 | 112–372 | 600–1241 | 49–102 | 850–2996 |
| S2 | Susceptibility based on network meta-analysis of EUCAST studies | Susceptibility based on network meta-analysis of all studies regardless of breakpoints (excludes inconsistent arms) | 91–1308 | 93–309 | 613–1268 | 41–84 | 838–2969 |
| S3 | Susceptibility based on network meta-analysis of EUCAST studies | Susceptibility based on PHE isolate-level data | 76–1084 | 111–368 | 508–1051 | 48–100 | 743–2603 |
| S4 | Susceptibility based on network meta-analysis of EUCAST studies | Susceptibility based on Vazquez-Ucha et al. isolate-level data | 110–1584 | 167–554 | 742–1535 | 73–151 | 1092–3824 |
| abs.increase | Odds ratios on mortality associated with nephrotoxicity from Bucaloiu 2012 are applied multiplicatively to underlying risk in HVCS | Absolute risk increases in Bucaloiu 2012 are assumed to apply | 71–1023 | 105–347 | 479–992 | 46–95 | 701–2457 |
| all.aki.lt | Base-case assumptions with respect to long-term effects of AKI | Applying a range of alternative assumptions to model the long-term effects of AKI | 72–1027 | 104–347 | 481–995 | 46–95 | 703–2464 |
| Weibull | Log-normal model fit to CARBAR survival data | Weibull model fit to CARBAR survival data | 57–812 | 77–257 | 380–787 | 34–70 | 548–1926 |
| OR_AKI_death_halved | Odds ratio of mortality for AKI compared to no AKI derived from Kerr (2014) (5.11) | Odds ratio of mortality for AKI compared to no AKI halved (2.56) | 64–923 | 87–288 | 432–894 | 38–79 | 621–2184 |
Population growth impacts population-level INHE to a greater extent than scenarios in the patient-level model, as the variation in the total INHE across different population size scenarios of 896 to 3559 QALYs (the base-case range in Table 65) is more substantial than the variation across different rows in the table (e.g. 419 to 1647 QALYs in the more conservative scenario about the population size).
The main areas of uncertainty relate to the probability that a patient has MBL, the susceptibility scenarios, the impact of colistin/aminoglycoside-based therapy on AKI risk and long-term mortality post hospital discharge. These were the most impactful scenarios in patient-level results for MBL Enterobacterales in ES (see OXA-48 empiric setting HAP/VAP), the setting with the greatest population size.
A9.5 Additional analysis to reflect insurance value
The patient-level benefit was derived by adapting the model. Specifically, we assumed that, in patients with these new highly resistant infections, existing therapies are no longer effective. In this model, this was achieved by setting the susceptibility for all comparators to zero. Under this illustrative scenario, no safety differences are assumed as it is expected that, if treatments become completely ineffective, no treatment or only safe antimicrobials will be used. Furthermore, the susceptibility for CAZ-AVI is set to 90% (an estimate broadly reflecting the susceptibility across different scenarios in the report), and maintained at this level over the long term, although we note that this is likely to overestimate INHEs as susceptibility to CAZ-AVI may be expected to wane over time.
In the ES, we assume everyone gets CAZ-AVI or non-colistin/aminoglycosides (comparator), then 5 days later they move into the MDS, and switch to the treatment they are susceptible to. For both CAZ-AVI and the comparator, 80% of the patients are assumed not to have the target MDR infection (as in the base-case modelling) and these patients receive something else. When CAZ-AVI is available, the 20% who do have that target infection receive either CAZ-AVI (for 90% who are susceptible) or salvage therapy (for the 10% not susceptible to CAZ-AVI). When CAZ-AVI is not available, 100% of patients receive salvage therapy (the comparator).
In MDS we assume 90% CAZ-AVI/10% salvage therapy (when CAZ-AVI is available) or 100% salvage therapy (comparator).
The results represent the lifetime patient-level INHE of CAZ-AVI relative to multidrug salvage therapy expressed in QALYs.
To derive population-level benefits, patient-level INHE is multiplied by the expected population size over the relevant time horizon and the probability of this scenario occurring. The patient-level INHE is assumed to remain constant over time. The population size is increased over time at a constant rate relative to baseline. Population benefits over time are discounted to reflect the delay in benefits received. Note that the relevant population here is not the same as the expected population in the main EEPRU report as these are assumed to be entirely different pathogens.
The hypothetical nature of the scenario means that there is no formal evidence to inform the extrapolation parameters and, as result, the parameter ranges were provided by the Committee. However, given the highly speculative nature of the analysis, EEPRU provided a flexible Excel-based tool, with user-defined parameters, to support Committee deliberations in assessing the potential additional long-term health effects that may result from CAZ-AVI usage.
The modifiable parameters in the Excel tool included the six extrapolation parameters: the probability of emergence of the highly resistant strains; the time of the first event; the number of patients affected in the first year; the annual growth rate in the number of infections (constant, relative to baseline); the analysis time horizon; and the discount rate.
In addition, the user could specify the site of infection and treatment setting reflected in the results (HAP/VAP ES, HAP/VAP MDS and cUTI microbiology-directed setting), or an alternative patient-level INHE reflecting the impact of these highly resistant infections in an alternative population.
The parameter estimates to use in the model were sought from the Committee (Table 66).
| User-defined parameter | Base case (range) |
|---|---|
| Probability of event (emergence of highly resistant strains) | 1% (0.5–5%) |
| Time of first event (from now) | 10 years (5–15 years) |
| The number of patients affected in the first year | 25 individuals (25–100) |
| The annual growth in the number of infections (from baseline) | 20% (3–30%) |
| Analysis time horizon (years) | 50 (20–50) |
| Population discount rate | 3.5% |
The patient-level INHEs in the base case and as used in this additional scenario, expressed in QALYs per patient, are shown in Table 67. In summary, assuming all specific existing treatment options have zero effectiveness increases the patient-level INHE for all sites and settings. The increase is greatest in the MDS, as all patients benefit from the treatment with CAZ-AVI, compared to the ES where only 20% of people have the suspected pathogen–mechanism (as per Table 18).
| HAP/VAP, ES | HAP/VAP, MDS | cUTIs, MDS | |
|---|---|---|---|
| Base case | 0.163 compared to non-colistin/aminoglycosides 0.215 compared to colistin/aminoglycosides |
0.071 | 0.069 |
| New scenario | 0.395 | 1.031 | 1.032 |
The population-level INHE (assuming patient-level benefit in cUTIs – the site with the highest patient-level INHE) is shown in Table 68 for a range of population-related scenarios. Overall, the benefit is relatively low (between 0.8 and 58.4 QALYs) compared to the benefit in EEPRU base case (between 629 and 2211 QALYs).
| Value/assumption in base case | Value/assumption in sensitivity analyses | Total number of patients | Total INHE (QALYs) conditional on event occurring | Expected INHE (QALYs) |
|---|---|---|---|---|
| Base case, parameter values shown in Table 66 | 4720 | 1460 | 14.6 | |
| Probability of event = 1% | Probability of event = 0.5% | 4720 | 1460 | 7.3 |
| Probability of event = 1% | Probability of event = 5% | 4720 | 1460 | 73.0 |
| Event occurs in 10 years | Event occurs in 5 years | 6195 | 2180 | 21.8 |
| Event occurs in 10 years | Event occurs in 15 years | 3245 | 870 | 8.7 |
| Number of patients in year 1 = 25 | Number of patients in year 1 = 100 | 18,880 | 5839 | 58.4 |
| Population growth = 20% | Population growth = 3% | 1388 | 452 | 4.5 |
| Population growth = 20% | Population growth = 30% | 6680 | 2053 | 20.5 |
| Analysis time horizon = 50 years | Analysis time horizon = 20 years | 145 | 79 | 0.8 |
List of abbreviations
- AE
- adverse event
- AIC
- Akaike’s information criteria
- AKI
- acute kidney injury
- AM
- antimicrobial
- AmpC
- ampicillinase C
- AMRHAI
- antimicrobial resistance and healthcare-associated infections
- AST
- antimicrobial susceptibility testing
- ATLAS
- Antimicrobial Testing Leadership And Surveillance
- AWARE
- European Surveillance of Antimicrobial Consumption Network
- BSAC
- British Society for Antimicrobial Chemotherapy
- BSI
- bloodstream infections
- CAZ-AVI
- ceftazidime-avibactam
- CCI
- Charlson comorbidity index
- cIAI
- complicated intra-abdominal infections
- CKD
- chronic kidney disease
- CLSI
- Clinical Laboratory Standards Institute
- CMY
- cephamyacinases
- CPE
- carbapenemase-producing Enterobacterales
- CRD
- Centre for Reviews and Dissemination
- CRE
- carbapenem-resistant Enterobacterales
- CrI
- credible intervals
- cUTI
- complicated UTI
- DDD
- defined daily dose
- DIC
- deviance information criterion
- EARS-Net
- European Antimicrobial Resistance Surveillance Network
- EEPRU
- Policy Research Unit in Economic Methods of Evaluation in Health and Social Care Interventions
- EKHUFT
- East Kent Hospitals University NHS Foundation Trust
- ERS
- electronic reporting system
- ES
- empiric setting
- ESAC-Net
- European Surveillance of Antimicrobial Consumption Network
- ESBL
- extended-spectrum beta-lactamase
- ESPAUR
- English Surveillance Programme for Antimicrobial Utilisation and Resistance
- ESRD
- end-stage renal disease
- EUCAST
- European Committee on Antimicrobial Susceptibility Testing
- EUNETHTA
- European Network for Health Technology Assessment
- GES
- Guiana extended-spectrum beta-lactamase
- GIM
- Germany imipenemase
- HAP
- hospital-acquired pneumonia
- HDU
- high-dependency units
- HRQoL
- health-related quality of life
- HSE
- Health Survey for England
- HTA
- Health Technology Assessment
- HVCS
- high-value clinical scenario
- ICU
- intensive care unit
- IMI/NMC
- imipenemase/non-metallocarbapenemase-A
- IMP
- imipenemase
- INFORM
- International Network for Optimal Resistance Monitoring
- INHE
- incremental net health effects
- IPD
- individual patient data
- KPC
- Klebsiella pneumoniae carbapenemase
- LoS
- length of stay
- MBL
- metallo-beta-lactamases
- MCMC
- Markov chain Monte Carlo
- MDR
- multidrug-resistant
- MDS
- microbiology-directed setting
- MIC
- minimum inhibitory concentration
- MIC 50
- minimum inhibitory concentration 50%
- MIC 90
- minimum inhibitory concentration 90%
- MRC
- Medical Research Council
- NDM
- New Delhi metallo-beta-lactamase
- NHE
- net health effects
- NHSE
- NHS England
- NICE
- National Institute for Health and Care Excellence
- NMA
- network meta-analysis
- NMC
- non-metallocarbapenemase-A
- OR
- odds ratios
- OXA-48
- oxacillinase-48
- PA
- Pseudomonas aeruginosa
- PCR
- polymerase chain reaction
- PD
- pharmacodynamic
- PHE
- Public Health England
- PICOS
- population, intervention, comparator, outcome, study design
- PK
- pharmacokinetic
- PRISMA
- Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- PrI
- prediction intervals
- PROSPERO
- international prospective register of systematic reviews
- QALY
- quality-adjusted life-year
- R&D
- research and development
- RCT
- randomised controlled trials
- RE
- random effects
- SAE
- serious adverse event
- SD
- standard deviation
- SGSS
- second-generation surveillance system
- SME
- Serratia marcescens enzyme
- SPM
- Sao Paulo MBL
- TEST
- Tigecycline Evaluation Surveillance Trial
- TSD
- technical support document
- UME
- unrelated mean effects
- UTI
- urinary tract infections
- VAP
- ventilator-associated pneumonia
- VIM
- Verona integrated-encoded metallo-beta-lactamase
- WHO
- World Health Organization
- XDR
- extensively drug resistant
Notes
Supplementary material can be found on the NIHR Journals Library report page (https://doi.org/10.3310/YAPL9347).
Supplementary material has been provided by the authors to support the report and any files provided at submission will have been seen by peer reviewers, but not extensively reviewed. Any supplementary material provided at a later stage in the process may not have been peer reviewed.