
Notes
Article history
The research reported in this issue of the journal was funded by PGfAR as project number RP-PG-0109-10073. The contractual start date was in January 2011. The final report began editorial review in April 2014 and was accepted for publication in October 2014. As the funder, the PGfAR programme agreed the research questions and study designs in advance with the investigators. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PGfAR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
Dr Yvonne Wren is the director of an independent speech and language therapy provider called ChildSpeech.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2015. This work was produced by Roulstone, et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Introduction and programme overview
Introduction
The focus of this research programme, known as Child Talk, is on speech and language therapist (SLT)-led interventions for preschool children with primary speech and language impairment (PSLI).
Primary speech and language impairment
Primary speech and language impairment is a relatively stable, high-prevalence condition that can persist into adolescence and adulthood and which is associated with a range of negative sequelae. Children with PSLI present with delayed speech and language, which is not associated with any other overt congenital, developmental, neurological or sensory disorders. However, the way that the impairment manifests in any individual varies considerably. Over the years, various terms have been used to refer to this impairment, the most common being specific language impairment. Currently, the Raise Awareness of Language Learning Impairments (RALLI) campaign is promoting awareness of specific language impairment and generating a discussion about agreeing consistency of terminology to avoid confusion. 1 The impairment can be particularly difficult to diagnose during the preschool years because of the wide range of what is considered to be ‘typical development’ in both language and cognition and the absence of conclusive research on the predictors of resolution. Nonetheless, delays that involve only expressive language, the so-called ‘late talkers’, are more likely to resolve before children reach school than difficulties in both receptive and expressive language skills. 2–5
Adult concern begins to consolidate at around the age of 2 years when around 50% of children will be joining words into short phrases and sentences. 6,7 Those considered to be ‘late talkers’ at this age will typically have a vocabulary of < 50 words and will not be joining words. 8 Some children may also find it hard to learn new word meanings, have difficulties understanding what is said to them or show other cognitive difficulties such as problems with attention, symbolic development and memory, despite other aspects of their development proceeding normally. Children who have difficulty with understanding language are thought to have difficulties that are less likely to resolve. 9
The majority of those children whose language is delayed at 2 years will go on to develop functional speech and language, for example they will be able to communicate their needs in everyday situations and be intelligible to strangers. However, they are more likely to have life-long difficulties with language and language-related activities, such as understanding more abstract and inferential language, literacy, social interactions and friendships. 10–16 Prevalence estimates vary, but an accepted rate of PSLI at 6 years is around 7.4%. 17,18 This is higher than for autism, for which a prevalence of 1% is commonly accepted,19,20 and for cleft palate, for which 1 in 700 births is a typically quoted figure. 21,22
Speech and language therapy
Speech and language therapy is the lead profession responsible for diagnosing and managing interventions for these children. This process typically takes place in collaboration with parents, early years practitioners (EYPs), psychologists, paediatricians and health visitors. For this preschool population, speech and language therapy services are primarily funded through the NHS, although there are increasing numbers of SLTs being funded into public health roles by the early years department of local authorities and, for older children, by individual schools.
Preschool children considered at risk for PSLI are typically, and most commonly, identified by EYPs, health visitors and parents themselves and are then referred to speech and language therapy services. Services may be delivered in a range of settings: community clinics, children’s centres, nursery classes and schools and children’s own homes. At this time, 14,016 SLTs are registered with the Health and Care Professions Council23 and it is estimated that approximately 70% of these work with children. 24 There are, however, no national data on the number who work specifically with preschool children or indeed on the spread of pay grades and expertise or the numbers who work with children with different speech and language conditions. A survey by the Royal College of Speech and Language Therapists (RCSLT) is currently under way to help gather some of this information. 25
The process of supporting children with PSLI has changed over the years. Several decades ago the approach was primarily focused on the child. Children were typically brought to a clinic by their parents and, following assessment and identification of the possibility of language impairment, the SLT would carry out interventions directly with the child. Sometimes the parent would observe the SLT working with the child, with the idea of practising the activities at home, but the focus was very much on the child and his or her performance. In recognition that speech and language skills develop in a social context through dialogue between the child and surrounding adults, the emphasis and approach has shifted over the years to focus on the adults’ interactions with the child and on the environment, opportunities and resources available to the child. 26 In most cases, these adults are the child’s parents but it may also be staff who spend time with the child in childcare and nursery settings. The assumption behind this approach is that the child has failed to acquire speech and language in the standard/typical environment and thus needs an environment that is highly adapted and more finely tuned to his or her learning needs. Despite this, the approach, which focuses on the adults’ interactions with the child, does sometimes leave parents with the impression that their interactions with their child are faulty. This increases the adults’ feelings of guilt about the origins of their child’s speech and language impairments. 27 This paradigm shift from the focus on the child to a focus on the environment is widespread throughout services; however, there is still wide variation in how services are delivered and in how interventions are described and configured. 28
What do we know about these interventions/services?
Although speech and language therapy has been found to be effective for some children, a number of systematic and service reviews have identified some limitations of SLT-led interventions for children with PSLI. For example, Law et al. 29 reviewed interventions for children of all ages with PSLI and concluded that the research to date provided evidence of the effectiveness of interventions that target expressive phonology and expressive vocabulary; interventions that target expressive sentence structure may also be effective as long as there is no accompanying receptive language impairment. The evidence to support interventions targeting receptive language impairment was limited both in terms of the volume of research and the synthesised effect sizes for the existing studies. In terms of how interventions could be delivered, no differences were found between interventions delivered in a group and those delivered in one-to-one contexts or between those delivered by therapists and those delivered by parents who had been trained to deliver an intervention. Evidence regarding the ideal frequency and amount of intervention (or ‘dosage’) has also been inconclusive so far. 30 The systematic reviews have identified evidence for the effectiveness of interventions in the short term, that is, for the period of intervention specified in the studies. Although evidence supports early intervention for children who are growing up in socially deprived conditions,31–34 the evidence does not yet extend to long-term follow-up of preschool children with PSLI; thus, the power of interventions to prevent negative sequelae of a speech and language impairment is not known.
A common finding of those attempting to review and synthesise evidence about the effectiveness of any interventions in speech and language therapy services is that the interventions themselves are poorly described. For example, Zeng et al. 30 found that ‘teaching sessions’ that were part of an intervention were rarely described and characteristics of the dosage were not always transparent. Pickstone et al. 35 commented on the variety of terminology and the lack of descriptive detail used to describe interventions. Furthermore, Pickstone et al. 35 concluded that interventions can have differential effects on subgroups of children and/or families and also that the effects of any particular component of an intervention are rarely tested and the effects of individual components are difficult to extract from research using complex interventions. The study by Landry et al. 36 was a noted exception to this. They found a differential effect of mothers’ responsiveness: mothers’ responsive affective behaviours were associated with changes in the children’s behaviour, whereas their responsive language behaviours were associated with changes in the child’s language. This suggests that a targeted responsiveness rather than merely seeking to increase a mother’s general responsiveness to her child might be needed for particular changes to occur in a child’s language.
In 2008 an independent review of services for children and young people with speech, language and communication needs (SLCN) was commissioned by the UK government. 28 The review found that speech and language therapy services in particular were characterised by their variation and were described frequently by families as a ‘postcode lottery’. 28 The Bercow report recommended a programme of research to enhance the evidence base to underpin the design of services. 28 The ensuing research programme, known as the Better Communication Research Programme (BCRP), surveyed practitioners to identify the interventions in common use by SLTs working with children of all ages and with all types of SLCN. It then reviewed the evidence underpinning these interventions and found that, of the 57 interventions that were either in current use or published in the literature, 3% had strong evidence, 56% had moderate evidence and 39% had only indicative evidence. Interestingly, the intervention most commonly cited by practitioners had only indicative evidence, that is, good face validity, and lacked any independent external research evidence. 37
Relationship between the Better Communication Research Programme and Child Talk
The research of the current programme builds, in a number of ways, on the research carried out by the BCRP team described in the previous section. The principal investigator (PI) for this programme was a member of the core team of researchers for the BCRP. The BCRP was a wide-ranging programme covering all ages of children and young people and the full range of SLCN. The current research programme examines a more focused profile of interventions with a particular age group (preschool) and a particular diagnostic category (PSLI). This enables a closer and more detailed examination of both the interventions appropriate to the group and the evidence. The focus on preschool children was important for two main reasons: the difficulties of providing effective and targeted support (as set out earlier) and the policy imperative, which is driving early identification and intervention for children with PSLI.
Policy imperative promoting early identification
The need for early identification and intervention for children with PSLI continues to be a policy priority because of the link between children’s early speech and language skills, their broader well-being and outcomes in later life. 10–13,15,16,38–40 It is argued that poor communication skills in children are a risk factor for their maltreatment and, later, involvement in the criminal justice system. 41,42 To date, there is no proven causative association between PSLI in preschool children and either of these outcomes in childhood and later years, or indeed an indication that SLT-led interventions in early childhood would prevent such outcomes. Nonetheless, UK government policy and initiatives have continued to stress the critical role that speech, language and communication play in a child’s life, health and well-being and to recommend early identification and intervention. 43–45 Before the commencement of the Child Talk research programme, the Better Communication Action Plan46 and Healthy Lives Brighter Futures47 talked about the government’s commitment to a range of improvements. These included early identification and intervention; better information for parents; a reduction in the variability and inequality of services; and increased individualisation of services for children with disabilities, particularly those with SLCN. Over the last 3 years of this research there has been an ongoing emphasis within government and other reports stressing the importance of the link between children’s language and their life chances, alongside a focus on children’s language in relation to the education curricula and training of the workforce. 44,48,49
In summary, PSLI is a high-prevalence condition with the potential to have a negative impact, which has resulted in calls for and expectations of early identification and intervention so that children can benefit from social and educational experiences and to mitigate negative sequelae. The evidence base for early intervention is growing but is underdeveloped, particularly in terms of informing the individualisation of interventions for what is a heterogeneous condition. The social context in which language is acquired adds to the heterogeneity. It is vital to understand how best to shape interventions to best suit the particular needs of each child and his or her family.
Assumptions underpinning an evidence-based framework
The purpose of this research was to investigate whether or not it is possible to develop an evidence-based framework that can support the decision-making of SLTs as they attempt to design and plan interventions that are appropriate to the needs of individual children and their families. Most people are now familiar with the notion of evidence-based practice (EBP) and the seminal definition of Sackett et al. ,50 which suggests that EBP occurs when external research evidence is applied with expertise and in the light of patient preferences; others have also emphasised the role of context in framing EBP. 51 Various barriers to the implementation of EBP have been identified including the time needed to search out research and, in particular, research that is relevant and appropriate to the particular context of an individual patient. 52 There is also a lack of research that attempts to advance our understanding of the process of integration of the three elements.
The emphasis to date, from both research and practice, has been on the systematic research element of EBP rather than on clinical expertise or patient preferences. For example, practitioners are taught how to search out and appraise research and are given advice on how to address the barriers to EBP that have been identified. 53 Despite this emphasis, there has been a number of discussions that have challenged the use of ‘evidence’ to mean only research evidence,54 arguing, for example, that many different kinds of ‘evidence’ are used in clinical decision-making. However, this confuses the idea of systematic research evidence and knowledge. Practitioners draw on various types of knowledge to make their clinical decisions. 55 However, it is suggested that these other types of knowledge are more usefully considered as part of clinical expertise. 56 In this research programme the ‘evidence’ component of EBP is taken to refer only to evidence gained from external, published, systematic research.
Research regarding the nature of clinical expertise and the process of clinical decision-making has rarely been the focus of research or discussion within speech and language therapy. Roulstone56 describes clinical expertise as ‘the skilful and appropriate application of knowledge to the practice situation’ (p. 45). Given the heterogeneous PSLI population, the current dearth of systematic research evidence regarding the individualisation of interventions and the lack of prominence of any particular approach to intervention, the expert practitioner applies and adapts knowledge from a variety of sources (including whatever there is from systematic research). Experts organise their knowledge to be optimally useful to the clinical context in order to retrieve it efficiently when needed. 57 Experts develop ‘theories of practice’ that guide their everyday decisions. 58 Therefore, in developing an evidence-based framework, it is necessary to investigate and understand how everyday practice is framed by practitioners and how the research evidence relates to that practice.
In 1991, The Patient’s Charter stated that patients have the right to a clear explanation about proposed treatments. 59 In the context of EBP, therefore, there is a need to provide patients with information about the evidence so that their choices and preferences can take account of the evidence base. Patients’ preferences exert an important influence on the success of interventions. 56 At the extreme, if patients do not believe in, or understand, an intervention they may not attend appointments or follow through on interventions. Therefore, to develop an evidence-based framework, some conceptualisation is needed of patient views both of the nature of a disorder and of the possible interventions.
In conclusion, an evidence-based framework of speech and language therapy for children with PSLI will take account of clinical expertise and the perspectives of service users so that these can be integrated with evidence from external research.
Aims and objectives
The overarching aim of this research programme was to improve speech and language therapy services for preschool children with PSLI through the development of an evidence-based framework that could inform SLTs’ decision-making and increase the relevance and effectiveness of interventions for individual children and their families.
Definitions of EBP emphasise the relationship between systematic research evidence, clinical expertise and user perspectives (in the case of this research, children and their families). Therefore, to develop an evidence-based framework we proposed to investigate and integrate all three elements. The Child Talk research programme was broadly divided into two phases; the specific aims and objectives for each phase are described in the following sections.
Child Talk phase 1
The first aim of Child Talk was to develop an evidence-based typology of SLT-led interventions for preschool children with PSLI that also incorporated the experiences of families. This typology was developed through several interacting components: a series of surveys of SLT practitioners, parent surveys, case studies, consensus exercises and systematic literature reviews.
Objectives
-
To determine current evidence, practice and user perspectives regarding SLT-led interventions for preschool children with PSLI.
-
To identify how best to engage preschool children in the process of developing appropriate interventions.
-
To develop a model(s) of intervention that can integrate current evidence, professional expertise and family perspectives in ways that allow the intervention to be individualised to children’s and families’ communicative, physical, social and cultural contexts.
Child Talk phase 2
The second aim of Child Talk was to develop a framework and toolkit that could be used to establish effectiveness and cost-effectiveness and which could be used by services nationally to plan services and future evaluations.
Objectives
-
To identify tools that can be developed to ensure the appropriate stratification of interventions and the measurement of outcome.
-
To identify the measures required to develop formal economic assessments of SLT-led interventions and care pathways within speech and language therapy services.
-
To work with the RCSLT to facilitate the national take-up and ownership of the framework.
Research and development and ethics approvals
Research and development (R&D) and ethics approval were obtained in two separate applications (phase 1 and phase 2) before undertaking the research. Ethics approval to undertake phase 1 was given by the National Research Ethics Service Committee – Southmead (reference number 11/SW/0228) and approval for phase 2 was given by the National Research Ethics Service Committee London – Brent (reference number 13/LO/0240) via proportionate review. In addition, both phases underwent ethics review by the University of the West of England and Manchester Metropolitan University. Approval was also given by Barnardo’s Research Ethics Committee, with whom we collaborated to recruit participants into phase 1 of the programme (specifically underserved communities).
Research and development approval for both phase 1 (reference number 2860) and phase 2 (reference number 3048) was given by North Bristol NHS Trust, the lead site and sponsor. The other five case study sites were set up as participant identification centres (PICs); therefore, full R&D approval was not required from these sites. It was decided that these sites should be PICs rather than research sites not only as this was the most appropriate classification for their role on the programme but also to minimise the amount of time that it would take to set up the research programme. It was our experience, however, that there is great variation in the way that R&D offices deal with setting up as a PIC site, with marked differences in their assessment of the risks involved, possibly illustrating differences in their level of experience of operating as PIC sites. In our experience, therefore, it did not expedite the set-up processes.
Both phase 1 (reference number 11461) and phase 2 (reference number 14283) were adopted onto the National Institute for Health Research (NIHR) Clinical Research Network portfolio and by the Medicines for Children Research Network, Paediatrics (Non-Medicines) Specialty Group.
Management and governance arrangements
Steering group
A steering group met every 3 months throughout the programme and was the decision-making group with overall governance of Child Talk. The steering group consisted of a chair, a co-applicant who was not involved in the day-to-day activities of Child Talk, the PI, work package leads and senior members of the research team who submitted progress reports against agreed milestones. In addition the minutes of advisory group meetings were considered and actions discussed.
Advisory group
The advisory group met every 3 months throughout the programme to offer advice and guidance with regard to the development of optimal strategies for the achievement of the programme aims. Membership of the advisory group consisted of:
-
Mary Gale, Speech and Language Therapist Team Leader, North Bristol NHS Trust
-
Davina Evans, Parent Partnership Service, Supportive Parents
-
Beverley Pearce and Duncan Stanaway, Barnardo’s
-
Sally Jaeckle, Service Manager Early Years Services, Bristol City Council
-
Nicola Theobald, Early Years Improvement Officer, Bristol City Council
-
Helen Moylett, Early Years Consultant (formerly the Senior Director, Early Years at National Strategies)
-
Christine Screech, Education Faculty, University of the West of England
-
Karen Evans, Deputy Head of Nursing – Child Health, North Bristol NHS Trust
-
two members of the Child Talk parent panel (rotating membership).
The advisory group was chaired by the PI as agreed by the members of the group. The advisory group kept the research team informed of any external agendas – new policies, programmes or initiatives that might support or have an impact on the relevance of the research programme – and provided support with recruitment strategies and dissemination. The Chair of Council for the RCSLT, Hazel Roddam, contributed to early advisory group discussions on the set up of the research programme. In addition, the principal investigator maintained regular contact with the Chief Executive Officer of the RCSLT, Kamini Gadhok, to discuss study delivery and matters arising from the advisory group.
Expert reference advisors
The PI met individually with expert reference advisors – academic researchers and senior clinicians working in the field of preschool PSLI – who advised on the development of the typology:
-
Dr Catherine Adams, Clinical Senior Lecturer in Speech and Language Therapy, University of Manchester
-
Dr Caroline Bowen, Honorary Associate in Linguistics at Macquarie University, Sydney, Australia, and Honorary Research Fellow in the School of Health Sciences (Speech–Language Pathology) at the University of KwaZulu-Natal, Durban, South Africa
-
Professor James Law, Professor of Speech and Language Sciences, Newcastle University
-
Dr Caroline Pickstone, Honorary Research Associate and Senior Manager, South Yorkshire Comprehensive Local Research Network, Sheffield
-
Professor Sharynne McLeod, Professor of Speech and Language Acquisition, Charles Sturt University, Bathurst, New South Wales, Australia
-
Associate Professor Jane McCormack, Discipline Leader and Lecturer – Speech Pathology, Charles Sturt University, Albany, New South Wales, Australia
-
Dr Kate Crowe, SLT with specific interest in multilingual children with hearing loss, Charles Sturt University, Sydney, New South Wales, Australia
-
Ms Sarah Masso, SLT with specific interests in speech sounds, phonological processing and pre-literacy, Charles Sturt University, Sydney, New South Wales, Australia.
Parent panel
A parent panel was formed to collaborate with the research team on all aspects of the research relating to parents or the public. The parent panel met every 2 months throughout the data collection period (last 2 years) of the research programme.
During the development of the research programme and the set-up phase, third-sector parties Afasic, Supportive Parents and Barnardo’s had been the parent/public representatives and their roles continued throughout the programme as co-applicant (Chief Executive Officer of Afasic) and advisory group members (Barnardo’s and Supportive Parents). During the first year of the programme, and with direction from Afasic, a parent panel was established by advertising in the community for parents of preschool children with PSLI currently accessing speech and language therapy services. It became apparent that we would need to widen the net after receiving little interest from parents. This is possibly because we were looking to engage parents who do not see their child as having an impairment but rather as just being slow to talk and who may not have felt that they had anything useful to offer the team in the long term. Subsequently, the research team advertised for parents of preschool children who may or may not have a communication difficulty. This decision was made because it is the perspective of being a busy parent of a preschool child/children, rather than experience of speech and language therapy services, that is most useful when designing recruitment strategies and materials that are engaging and accessible. From this, we established a panel of 10 parents of whom a core group of four remained until the end of the programme.
At meetings the panel was updated on progress with the research, devised recruitment strategies and developed public-facing materials, such as a recruitment video, advertising, participant information sheets and consent forms. The parent panel also took a lead on running a community-based consultation to determine the key messages for parents arising from Child Talk. Descriptions of the ways in which the panel influenced the delivery of Child Talk are embedded within the chapters of this report. In addition, a description of the impact of involvement on the parents themselves, captured using an arts method, is described in Appendix 7.
Operational project groups
Project groups were formed on an ad hoc basis with members of the research team and relevant co-applicants to plan individual studies and discuss progress. In addition, the co-applicants met annually to discuss progress against programme aims and to consider the data collected as a whole. The role of each co-applicant in the Child Talk programme is described at the end of this report (see Acknowledgements).
Website and logo
The activities of the Child Talk programme were managed through the Bristol Speech and Language Therapy Research Unit website [www.speech-therapy.org.uk (accessed 13 December 2014)], which was used to publicise the research programme and research events, register expressions of interest from potential participants, host electronic surveys and provide a secure area for the parent panel to work on documents and share ideas outside of panel meetings. A Child Talk logo was commissioned from Abigail Beverley, who grew up with a speech and language disorder and is a volunteer with the Afasic Youth Project, specialising in art workshops. The logo provided a clear identity to all of the activities and materials arising from the programme (Figure 1).
FIGURE 1.
Child Talk logo. Reproduced with permission © North Bristol NHS Trust.

Methodology
Methodology overview
The nature of the research programme was exploratory in that it mapped and described current practice and developed a conceptual framework regarding interventions for preschool children with PSLI. The notion of EBP was used to inform the research questions and to shape the study design and the eventual framework. Sackett et al. ,50 some of the original proponents of EBP, suggested that EBP occurs when evidence from external research is applied explicitly, judiciously and conscientiously and in the light of patient preferences. Our research questions covered these three elements of EBP: systematic reviews of the research evidence, investigations of SLTs’ knowledge about the interventions and how they are used with preschool children with PSLI, and investigations of the perspectives of service users or patients, in this case parents and children with or at risk of PSLI, and EYPs. Figure 2 illustrates how the research questions map onto the three elements of the EBP model.
FIGURE 2.
Research questions mapped onto the three elements of the EBP model.
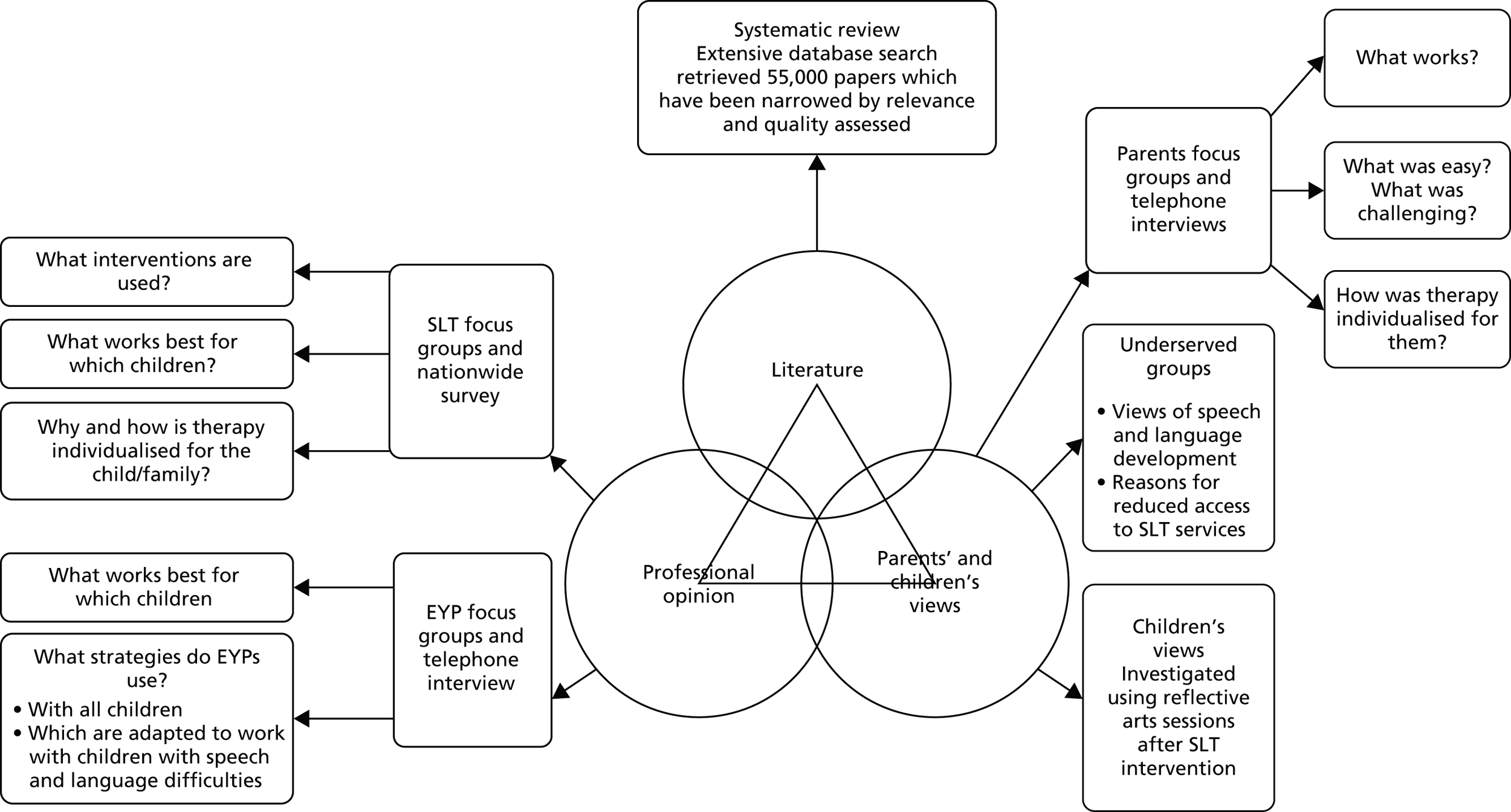
The resulting research programme adopted a multidimensional approach to evidence gathering and synthesis. It encompassed a series of projects that bring together data representing the three key elements of EBP in the development of an evidence-based framework. Our research approach was essentially pragmatic, resulting in a mixed-methods, ‘multiphase’ design60 combining both quantitative and qualitative elements iteratively to enhance our understanding of a complex problem. Within the overall multiphase design, certain elements followed an exploratory sequential process, starting with a qualitative investigation that was built on using quantitative methods. For example, findings from SLT focus groups were further explored and verified using mini-surveys to validate analyses; these were then built on using a national survey. Thus, quantitative methods included surveys and investigated aspects such as the prevalence and patterns of intervention usage, and qualitative data collection methods included focus groups, interviews and reflection to investigate participants’ perspectives and understandings of interventions. Data from quantitative and qualitative studies were analysed separately using analytical approaches of relevance to the nature of the data; therefore, for quantitative data, analysis methods included descriptive and inferential statistics and, for qualitative data, methods included thematic and content analysis and also framework analysis. Interpretation and discussion took place at the end of each element of the research, across phases of the research and, then, in a concluding section at the end of the programme. For example, the findings are reported separately for the thematic analysis of each of the user groups and for the observational study of children’s perspectives; these are then drawn together in a discussion that also relates back to the investigation of the therapists’ perspectives.
The aim of developing a conceptual model or framework has led to an iterative data collection and analytical process in which we have employed processes typically seen in qualitative theory-building methodologies such as grounded theory. 61 These have included theoretical sampling, deviant case analysis and constant comparative analysis. 62
Theoretical sampling is the process of sampling participants, incidents or events on the basis of their relevance to the evolving concepts and/or theory. 61 It was used in two ways in this study: first, in terms of the deliberate sampling of ever-wider and broader groups of participants; second, in terms of developing more detailed and specific research questions and data collection activities. The purpose of theoretical sampling in this study was to better understand the themes and concepts that were identified from each preceding stage of the study; sampling was thus in some part iterative with the analysis (Box 1 provides an example).
The analysis of data from the focus groups with SLTs generated 10 themes that we hypothesised capture the purpose of their interventions. Our analysis provided descriptions of the characteristics of each theme. To develop those themes we needed examples of therapists talking about their interventions in different ways. We therefore asked therapists to provide explanations of each aspect of their work under the headings of the 10 identified themes, as if they were speaking to parents.
In the process of developing the detail of the framework and in establishing the confirmability of findings, we have systematically examined the data for negative instances of the themes (deviant case analysis). Within the iterative process we used negative instances to generate new ‘hypotheses,’ which were then put back to the participants in a new round of questioning (Box 2 provides an example).
The 10 themes were presented to groups of SLTs who were asked to vote on whether or not each theme was essential to their work with preschool children with PSLI. Disagreement was used to stimulate further discussion of the nature of the interventions to generate further understanding of the themes. Additionally, the typology was presented to a small number of academic experts who have developed their own therapy models. As these experts were likely to have a strong pre-existing theory, their perspectives and data provided a strong test of the validity of the themes identified by this research.
Constant comparative analysis was used at each stage of data analysis: themes, categories or groupings that were established at one stage were examined in the light of new data to establish the characteristics and boundaries of themes and categories. This analytical process works iteratively with the theoretical sampling, by which decisions are made about which data should be collected to test and challenge developing themes (Box 3 provides an example).
SLTs’ descriptions of each theme for parents were compared with each other and with the descriptions generated from the focus groups to examine the detailed characteristics of each theme. Descriptions for one theme were also compared with those for similar themes to identify potential overlapping characteristics. To develop those themes we needed examples of therapists talking about their interventions in different ways. We therefore asked therapists to provide explanations of each aspect of their work under the headings of the 10 identified themes, as if they were speaking to parents.
Exploring consensus on the framework
One aspect of EBP is clinical expertise, the expertise of the SLTs in the case of this research programme. Expertise is commonly associated with years of experience. We are also intuitively aware that experience alone is insufficient to guarantee expertise. The research, therefore, needed a way to validate the opinions of SLTs as stemming from a body of knowledge rather than arising from individually held beliefs. 63 Examining levels of consensus about actions to be taken can give an indication of shared knowledge between participants and was thus used as an indicator of a body of expertise. Some cautionary notes are advisable here. First, just because a group of professionals agree about a course of action does not necessarily mean that this is a foolproof approach to take. The history of medicine is riddled with examples in which a consensus approach is later shown to be detrimental to health. On the other hand, lack of consensus does not necessarily indicate inexpert practice; it may be an indicator of a novel response or of a response to a novel case. The aim of this approach was therefore to make the levels of consensus explicit rather than attempting to reach consensus about a particular approach. We also expected the process of investigating consensus to enable us to more thoroughly explore diverse views. A number of ways of defining consensus were used during the course of the study. For example, the qualitative analytical approaches of deviant case analysis and constant comparative analysis by definition focus on instances of disagreement. Various definitions have been used to identify consensus. 63 In this research we have identified 60% agreement as a marker of consensus.
The approach used to investigate consensus on outcome measures used by SLTs (see Chapter 5, Study 5.2: identification of outcome measures for speech and language therapists) followed an iterative process similar to the Delphi process. 64–67 In the Delphi process a series of opinions or views or propositions are generated by a group of experts. These are then subjected to a series of questionnaire rounds whereby participants are asked to rank the statements. The outcomes of those rankings are then analysed and the process iterates to establish a more finely tuned set of statements. In the case of this research, the aim was not necessarily to rule out propositions (such as descriptions of outcomes) but rather to investigate levels of consensus. The process followed was iterative and gave participants information from preceding rounds. Typically, Delphi establishes consensus and priorities with a set group of participants, whereas our participants group was gradually widened to become progressively more inclusive of the profession. Thus, the same participants were not necessarily involved in the successive rounds of data processing. However, they were all SLTs and were considered to be experts in PSLI who had knowledge of the purpose, content and recent findings of the research programme on which their responses were to be based.
The mixed-methods approach pervades the entire programme; thus, each study in this report frequently includes both quantitative and qualitative elements. Furthermore, our data collection events frequently targeted more than one aspect of the framework. For example, data on the identification of outcomes, on the development of the typology and on the exploration of the use of interventions were collected at the same events but are reported in separate sections of this report. Therefore, to avoid repetition, the process of recruitment, data collection and analysis is described in detail in the rest of this chapter and should be used as a reference. The order and context in which these activities were undertaken is described in the study chapters (see Chapters 2–6).
Selection of case study sites
To support the collection of data throughout the research programme and particularly in the first phase, six speech and language therapy services in England were recruited to become case study sites. The process of identifying these sites, to reflect the variety in the current system of service provision, is described in this section.
A literature search was conducted in July 2011 in NHS Evidence to identify factors that are reported to impact on speech and language therapy service provision. No date boundaries were used and the search used key terms suggested by the subject matter expertise of the research team (Box 4).
speech therap* department differences, variety NHS
metropolitan speech therap*
nomics speech therap*
socio-economic speech
bilingual* speech therap*
ethnic* speech therap*
parent identify speech ethnic*
speech demograph*
transient population speech therap*
education* speech therap*
The quality of retrieved papers was assessed using criteria taken from Pennington et al. 68 and the American Speech Hearing Association;69 factors identified as leading to variations between services were divided into seven categories (Table 1). Of these categories, six were mapped onto geographical areas in England to identify speech and language therapy services. From this mapping exercise, six case study sites were chosen, which provided a spread, across the categories; these six sites were invited to become case study sites. It was not possible to use the category ‘service management variation’ in this exercise but this was explored at each of the selected case study sites as part of the economic modelling (see Chapter 6). Three geographical boundaries were used – postcodes, unitary authorities and strategic health authorities – and three main data sources – the Office for National Statistics (ONS), the Department for Education and the early years census (Table 2).
| Categories | Evidence from the literature search |
|---|---|
| Urban, suburban, rural | Urban areas are more likely to have higher ethnic minority populations70–72 |
| Rural areas are more likely to have reduced availability, frequency and choice of services; SLTs in rural areas are more likely to have a consultative role73 | |
| In rural areas SLTs are more likely to have diverse roles; there are fewer specialist therapists74 | |
| In rural areas there is a greater distance between the homes of clients and services; lower availability of public transport has been found to result in lower levels of access73 | |
| Socioeconomic status | Lower SES is associated with a greater need for SLT input, a greater likelihood of speech and language delays75,76 and poor scores on SLT assessments |
| Lower SES households have been found to have different learning environments, with a lower quantity and quality of maternal speech77 | |
| Lower SES individuals are less likely to access SLT services78 | |
| Ethnic minority populations | Ethnic minority populations are associated with not accessing services. Barriers include parental communication, travel and cost, particularly for groups who are new to an area79 |
| Services for ethnic minorities might require more adaptations including providing therapy in more locations to improve access and more time spent working collaboratively with teachers70,71 | |
| Bilingual populations | Speech and language therapy services in areas with high levels of bilingual learners are likely to be required to provide additional training for their SLTs or to have a member of the team who specialises in bilingualism71,80 |
| Additional administration costs and resources may also be needed to meet additional RCSLT guidelines80 | |
| Transience of populations | Transient populations have been shown to have poorer health and are less likely to access health and education services81 |
| This reduced contact with health and education services leads to a reduced likelihood of referral to speech and language therapy services82 | |
| Early years foundation stage | Non-attendance or low attendance at preschool education provision results in lower referral rates to speech and language therapy services82 |
| Poor early years provision may lead to little/no exposure to English before entering preschool education and/or a poor home communication environment may result in language delay83 | |
| Not achieving the early learning goals can impact on later speech and literacy skills84 | |
| Service management variations | Different models of service delivery may be adopted such as consultancy/indirect therapy vs. direct therapy,85 school vs. clinic based86 |
| Services may or may not provide input to secondary school age children87 and vary in their involvement in multidisciplinary team working88 | |
| Formalised protocols vary between services: the time between initial assessment and referral,78 the severity cut-off point,87 prioritisation and discharge criteria and use of special education;85 the composition of staff varies between departments in relation to the number of full-time equivalent staff to meet case load needs and the levels of experience of staff |
| Categories | Data source |
|---|---|
| Ethnic minority populations | ONS-requested data CD – EE1: estimated resident population by ethnic group and sex, mid-2009 (experimental statistics) – ethnic table 2009a |
| Socioeconomic status | ONS-requested data CD – Economic Deprivation Index 2008b |
| Urban, suburban, rural | ONS-requested data CD – 2001 density (number of people per hectare)c |
| Transience of population | Table produced by the Migration Statistics Unit (migstatsunit@ons.gsi.gov.uk) – 1999 numbers to and from each local authority in England and Walesd |
| Bilingual populations | www.education.gov.uk/Sfr09–2010pla (accessed 14 November 2011) |
| Early years foundation stage | www.education.gov.uk/rsgateway/DB/SFR/s000961/sfr28–2010la.xls (accessed 14 November 2011) |
This sampling process aimed to ensure that a range of service types was investigated rather than a representative sample. Therefore, each of the categories was independently ‘sorted’ in Microsoft Excel (2007; Microsoft Corporation, Redmond, WA, USA) and split into groups of equal size. The individual sites within each of these groups were assigned an ordinal ‘group number’ from one to six, with ‘one’ representing ‘low’, for example a low level of ethnic diversity, a low level of socioeconomic deprivation (high income), low level of urban areas (rural), and ‘six’ representing ‘high’, for example a high percentage of pupils scoring well on the early years foundation stage (EYFS), a high percentage of children with English as a second language, a larger percentage of people moving between local authorities. The data were then scrutinised and sites were identified that provided a range of scores on each variable.
Potential sites were approached by the research team through discussions with the speech and language therapy service lead. If a service was not in a position to become a site, the data were re-examined to find a new site with a similar spread of scores. It took three iterations to recruit six sites. Table 3 shows the spread of values for the six sites.
| Case study site | Ethnicity | SES | Urban/rural | EYFS | E2L | Transience | Total |
|---|---|---|---|---|---|---|---|
| 1 | 1 | 1 | 1 | 3 | 1 | 1 | 8 |
| 2 | 6 | 6 | 5 | 2 | 6 | 6 | 31 |
| 3 | 3 | 4 | 1 | 2 | 3 | 1 | 14 |
| 4 | 2 | 5 | 4 | 2 | 1 | 6 | 20 |
| 5 | 4 | 2 | 2 | 1 | 5 | 4 | 18 |
| 6 | 5 | 4 | 6 | 2 | 5 | 6 | 28 |
The six speech and language therapy services recruited as case study sites were used to identify participants for focus groups (SLTs, parents, EYPs), advertise national SLT surveys (alongside other advertising routes) and identify underserved groups and local children’s centres. In addition, information to support the economic modelling of resource use (see Chapter 6) was collected at each site in collaboration with the speech and language therapy service manager.
Focus groups
This section describes the process of recruitment to the SLT, parent and EYP focus groups at each of the case study sites and the methods for data collection and analysis.
Speech and language therapists
At each of the six case study sites, invitations to participate in focus groups were e-mailed to SLTs through the speech and language therapy service leads (Figure 3). Those SLTs who were interested in participating in the study were asked to contact the research team at North Bristol NHS Trust by e-mail. On receipt of expressions of interest, a member of the research team contacted each individual to gain information about his or her case load and experience to determine eligibility: the inclusion criteria were currently practising NHS SLTs with at least 2 years’ experience of working with preschool children with PSLI.
FIGURE 3.
Flow diagram of the recruitment process for SLT focus groups.
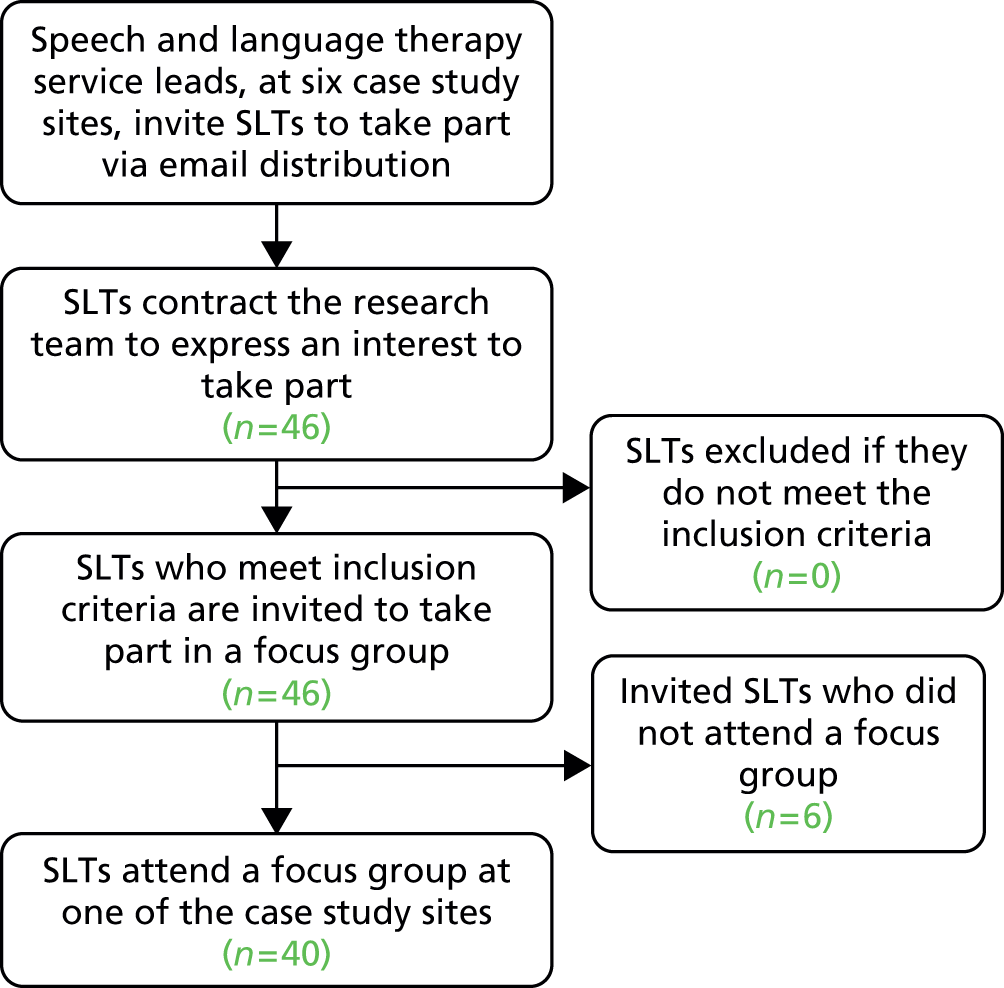
Those who met the inclusion criteria were e-mailed a participant information sheet (which were held in the participants’ local area) and were given the opportunity to ask questions by telephone or e-mail before attending. Nine focus groups were held across the six sites with a total of 40 SLTs. The SLTs who attended had been qualified as an SLT for an average of 14 years (range 2–43 years). They also emanated from a range of different university training courses (Table 4).
| Case study site | Number of focus groups | Number of participants | Average (range) years since qualifying |
|---|---|---|---|
| 1 | 2 | 8 | 5 (2–11) |
| 2 | 2 | 8 | 15 (3–31) |
| 3 | 1 | 8 | 17 (1–32) |
| 4 | 2 | 7 | 12 (3–23) |
| 5 | 1 | 4 | 20 (3–37) |
| 6 | 1 | 5 | 17 (2–43) |
| Total | 9 | 40 | 14 (2–43) |
The nine focus groups, conducted locally on non-NHS sites, lasted between 1 and 1.5 hours. At the start of the focus groups participants were reminded that their contributions were voluntary and that they had the right to withdraw at any time. Consent forms were signed at this point.
The focus group discussions were semistructured, with a topic guide that the moderator followed. An example topic guide is provided in Appendix 8. At the beginning of the focus groups, ground rules for discussion were covered, which included covering the confidential nature of the groups. SLTs were then asked questions about:
-
the interventions that they use with preschool children with PSLI and their components
-
the ways in which they modify their interventions in relation to child, context and family factors
-
the rationales for and purposes of the interventions, including descriptions of how the interventions were thought to cause change.
During the focus groups participants were encouraged to be explicit about their interventions and give detail rather than merely the names of programmes or listing resources. When participants used these, they were encouraged to expand and provide more detail.
At the first focus group fictional vignettes were used; the types of cases that were discussed included the following groups:
-
a child aged between 3 and 4 years with speech impairment/disorder
-
a child aged between 2 and 3 years with receptive and expressive language delay
-
a child aged between 4 and 5 years with social communication problems.
Subsequent to each focus group, audio recordings were transcribed verbatim by a member of the research team. The data were anonymised and participants were given pseudonyms when requested. Thematic and content analysis was conducted using NVivo 9 software (QSR International, Warrington, UK). Issues raised in the earlier groups informed subsequent groups in terms of the questions asked.
Parents
Clinical leads at each case study site were asked to identify children within their service who had received input from the speech and language therapy service, who met the criteria for PSLI and who were aged between 2 years and 5 years 11 months. Invitation letters were sent to the parents of these children by the SLT service on behalf of the research team accompanied by a participant information sheet and an expression of interest slip to be returned in a prepaid addressed envelope to the research team. The invitation letter and participant information sheet were designed in collaboration with the Child Talk parent panel.
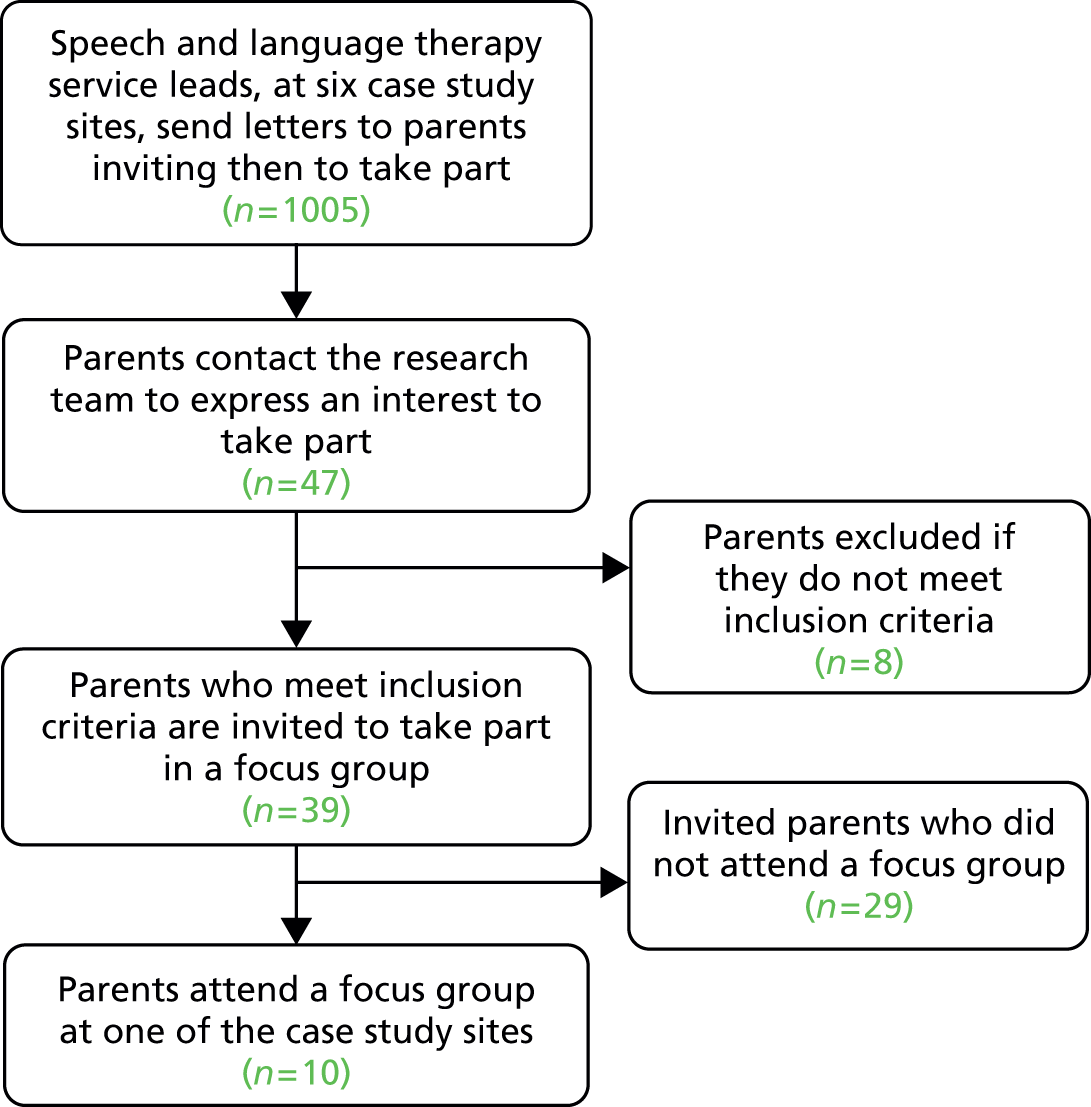
Forty-seven parents expressed an interest in taking part (Figure 4). They were contacted by telephone by a member of the research team and asked a number of screening questions to establish eligibility according to PSLI and age. Parents whose level of spoken English would significantly limit participation in an interview or focus group were excluded. After this process, 39 parents were invited to take part, of whom 10 attended a focus group or an individual face-to-face interview (when only one participant was available to attend). Focus groups did not occur in all case study sites because of the poor take-up of invitations. To boost recruitment rates, possible alternative methods of data collection were discussed with the Child Talk parent panel. Following these discussions, an amendment was submitted to the ethics committee to seek approval to contact the parents who expressed an interest and had been unable to attend the focus groups to ask if they would take part in an audio-recorded telephone interview. As a result, an additional 16 parents were interviewed by telephone by a member of the research team (a qualified SLT).
FIGURE 4.
Flow diagram of the recruitment process for parent focus groups.
The Child Talk parent panel identified lack of childcare as a barrier to participation and suggested that parents might be more likely to attend if offered something additional. In response to this, free play-based arts therapy sessions were set up by the research team and advertised locally for children to attend while parents attended a focus group. In total, 1500 flyers were distributed to advertise these sessions across the locality, and parents who had expressed an interest in taking part in a local focus group but who had been unable to attend were also made aware of the events. Two parents attended these sessions.
Following the various methodologies described above, a total of 28 parents took part in this study across England (10 focus groups, 16 telephone interviews and two play-based sessions). This number was lower than we would have anticipated but it has given an insight into the difficulties of engaging with this population and the lessons that should be learned for future studies (see Chapter 4, Discussion). A summary of the numbers of parents participating in focus groups and interviews is provided in Table 5.
| Case study site | Number of focus group/interview participants | Number of telephone interviewees | Number of arts-based play group participants |
|---|---|---|---|
| 1 | 7 | 6 | 2 |
| 2 | 0 | 0 | NA |
| 3 | 2 | 6 | NA |
| 4 | 0 | 0 | NA |
| 5 | 0 | 4 | NA |
| 6 | 1 | 0 | NA |
| Total | 10 | 16 | 2 |
Informed consent was taken by a member of the research team at the start of the group or interview. The wording of the consent form and participant information sheet was reviewed by the parent panel. Focus groups lasted on average 1 hour 40 minutes whereas individual interviews were typically shorter, lasting between 25 and 50 minutes. Telephone interviews were recorded using an audio-recorder telephone device.
The discussions were semistructured, with a topic guide that the moderator followed (see Appendix 9). At the beginning of the focus groups ground rules for discussion were covered, which included covering the confidential nature of everything that was raised in the groups. Participants in the face-to-face interviews also had the confidentiality process explained to them. Parents were asked questions about:
-
what happened during speech and language therapy sessions, including:
-
activities
-
materials used
-
length of sessions
-
how regularly they were seen
-
advice given
-
targets set
-
-
their understanding of the aim of the activities
-
whether or not any change was seen in their child following SLT intervention and their view on how much of this change was attributable to speech and language therapy
-
whether or not they modified their behaviour/interactions as a result of going to see the SLT
-
if anything was particularly helpful or unhelpful
-
if there was anything about what happened that they would change.
An iterative approach was taken to the focus groups whereby issues raised were followed up in subsequent groups and interviews. Telephone interviews used a semistructured format and followed the topic guide used for the focus groups.
Audio recordings were transcribed verbatim by a member of the research team. All data were anonymised and participants were given pseudonyms when requested.
Early years practitioners
Service managers at each of the six case study sites were asked to identify EYPs who met the inclusion criterion of working directly with preschool children with PSLI. Participants were approached and invited to participate through managers of nurseries and children’s centres in the local area, who distributed the invitation to relevant staff members. In addition, local nurseries and children’s centres were identified through the use of a search engine and government websites.
Early years practitioners who expressed an interest in participating were contacted by a member of the research team. There was no specific inclusion criteria other than that EYPs worked directly with children in an early years venue. Participants were e-mailed an information sheet before attending a focus group and were given the opportunity to ask questions by telephone or e-mail before attending. Twenty-three EYPs expressed an interest in participating in the focus groups (Figure 5), of whom 18 attended from five of the six case study sites (there were difficulties with recruiting within case study site 4). The number of EYPs who attended the focus groups varied between groups (mean 4, range 2–5).
FIGURE 5.
Flow diagram of the recruitment process for EYP focus groups.

Because of the low recruitment levels, ethical approval was sought to invite EYPs who had expressed an interest but who were unable to attend a focus group to take part in an audio-recorded telephone interview. Six EYPs were interviewed by telephone (Table 6).
| Case study site | Number of focus group participants | Number of telephone interviewees |
|---|---|---|
| 1 | 5 | 0 |
| 2 | 4 | 3 |
| 3 | 3 | 0 |
| 4 | 0 | 1 |
| 5 | 4 | 0 |
| 6 | 2 | 2 |
| Total | 18 | 6 |
Focus groups took place at non-NHS sites in each of the selected research sites and typically lasted between 1 and 1.5 hours. At the start of the focus groups, written informed consent was taken by a member of the research team. Telephone interviews were conducted at a time convenient to the participants and typically lasted around 25–35 minutes. Consent was taken verbally by reading each statement and the participant answering ‘yes’ or ‘no’. All participants were offered a copy of their consent form, either by e-mail or by post.
The focus group discussions were semistructured, with a topic guide that the moderator followed (see Appendix 10). At the beginning of the focus groups, ground rules for discussion were covered, which included covering the confidential nature of everything that was raised in the groups. Telephone interviews followed the topic guide used for the focus groups. EYPs were asked questions about:
-
the interventions that they use with preschool children with PSLI and their components
-
the ways in which they modify their interventions in relation to child, context and family factors
-
the rationales for and purposes of the interventions, including descriptions of how the interventions were thought to cause change.
Subsequent to each focus group and telephone interview, audio recordings were transcribed verbatim by a member of the research team. All data were anonymised and participants were given pseudonyms when requested.
Content analysis of data from speech and language therapist, early years practitioner and parent focus groups
After familiarisation with the transcripts, one of the co-applicants who was involved in the focus groups developed a coding framework in NVivo 9. The focus of the content analysis was on description and classification of the interventions. Interventions were classified following the definitions used in Roulstone et al. 89 as follows:
-
activities – specific tasks that are usually targeting impairment
-
strategies – principles, techniques, actions or styles
-
materials or resources – items or published materials used in the delivery of an intervention
-
programmes – published interventions that encompass specific procedures with detailed plans for how to deliver them.
Within these areas, interventions were further classified according to whether their focus was on speech, language or communication. Sections of text (which could be single words, phrases or sentences) were coded by the researchers using the relevant codes. Two members of the research team, who were both SLTs, coded the data. These researchers examined each other’s coding in a validation exercise, in which 20% of the transcript was checked for consistency of the coding technique. Any discrepancies were discussed until a consensus was reached.
For the SLT focus groups, data from the content analysis were used as the basis for the description of current SLT practice (see Chapter 2, Study 2.2: identifying the interventions used by speech and language therapists).
Thematic analysis of data from speech and language therapist, early years practitioner and parent focus groups
Thematic analysis followed the stages set out by Braun and Clarke. 90 The PI and one researcher read and reread the transcripts to familiarise themselves with how therapists talked about their interventions. Both researchers had also been involved with the data collection. The content analysis also supported familiarisation with the data and led to a focusing of the analytical question for the thematic analysis. The transcripts were initially read and coded on paper and then, as codes emerged, a framework was designed in NVivo 9. Additional rounds of coding were carried out directly onto the NVivo 9 framework and codes were adjusted and merged as stronger themes emerged.
For the SLT focus groups the thematic analysis focused on exploring the purposes of SLTs’ work. The thematic analysis, therefore, progressed in terms of analysing and reporting patterns (themes) in relation to the following question, ‘What are the purposes of therapy?’ The themes generated were used as the basis for constructing a typology of SLT-led practice (see Chapter 2, Study 2.1: identifying the themes of speech and language therapy practice).
The focus of the thematic analysis for the EYP focus groups was similar – to explore the purpose and aims of their activities and strategies. For the parent groups the data were analysed slightly differently, with the data being explored in terms of parents’ experiences of therapy.
Each data set was treated as separate initially and coded independently. Finally, however, data from parents and EYPs were examined in the light of the themes emerging from the SLT focus groups to identify synergies and discrepancies.
Cross-tabulation of interventions and themes from the speech and language therapist groups
NVivo 9 has a cross-tabulation function that allows the cross-tabulation of codes. For the SLT groups, each typology theme was cross-tabulated with all 12 intervention codes that were utilised in the NVivo 9 coding (activities, strategies, resources, programmes). This cross-tabulation was designed to help understand which intervention activities and strategies related to the different themes of the typology.
Underserved groups
To identify groups perceived to be underserved, SLT service managers from the six case study sites were asked to identify groups within their geographical areas that they considered fit into one or more of the following categories:
-
groups with poorer attendance rates than other groups in the catchment area
-
groups who were, for other reasons, under-represented on the speech and language therapy services’ PSLI caseloads compared with their representation in the general local population
-
parents/children to whom managers considered that they do not provide appropriate services.
A number of groups were identified by speech and language therapy service managers:
-
carers of looked-after children (children in public care, who are placed with foster carers, in residential homes or with parents or other relatives)
-
people from minority ethnic groups [including specifically the Somali community and refugees and asylum seekers (RAS)]
-
families from areas of low socioeconomic status (SES)
-
travellers or gypsies, defined as those with a cultural tradition of nomadism or living in a caravan, and all other people with a nomadic habit of life, whatever their race or origin. 91
The first three of these groups were selected for inclusion into this study for reasons related to the feasibility of completing data collection within the time frame of this programme. As these were groups perceived to be less likely to be receiving services, recruitment directly through speech and language therapy services or of those currently receiving intervention was unlikely to be successful. It was therefore decided to identify members of the groups selected who were already attending other groups in their local area as a positive strategy for recruitment. Recruitment was therefore targeted to specific groups, as discussed in the following sections.
Carers of looked-after children
Two groups were recruited. Local authority foster care co-ordinators were approached at case study site 1 to identify a group of foster carers who might be interested in taking part. The organiser of one group expressed an interest and approached the carers within the group with the study information sheet to obtain their agreement for the research team to attend their next meeting. Consent was taken by a member of the research team before data collection.
The second group was recruited through a search to identify private foster care agencies. The identified agencies were e-mailed information about the study and one agency, from case study site 3, expressed an interest in participating and facilitated the setting up of a group meeting for the programme. The agency circulated the participant information sheet to attendees before the meeting. Informed consent was obtained by a member of the research before data collection.
Parents from minority ethnic groups
Two groups of parents from minority ethnic groups were accessed, both being recruited from pre-existing parent groups. The group from case study site 1 was a support group for members of a specific ethnic minority group, the Somali community. This group was identified by members of the research team. A researcher attended meetings for a few weeks prior to data collection to establish a relationship with the members. The second group (case study site 2) was accessed through Barnardo’s, who facilitate a group for RAS.
Parents from socioeconomically deprived communities
Two young parent groups were accessed in an area of low SES through case study site 2, with the aid of Barnardo’s who facilitate both groups.
All participants either were requested to have a sufficient grasp of spoken and written English to allow them to understand the participant information sheet and consent form or were provided with translated versions of these documents to allow them to understand them (with some support, if necessary, from facilitators identified by Barnardo’s who were previously known to the participants). For all groups apart from the foster carers, a member of the research team attended one or more meetings of the group, described the study and offered opportunities for questions to be asked about participation in the study. Table 7 provides a summary of the numbers who attended the groups at each case study site.
| Case study site | Looked-after children | Minority ethnic group | Low SES |
|---|---|---|---|
| 1 | One focus group (n = 11) | One focus group (n = 9) | – |
| 2 | – | One focus group (n = 11) | Two focus groups (n = 4 and n = 5) |
| 3 | One focus group (n = 12) | – | – |
| 4 | – | – | – |
| 5 | – | – | – |
| 6 | – | – | – |
| Total | n = 23 | n = 20 | n = 9 |
The focus groups were scheduled to take place during preorganised meeting times and were either to cover the whole session or a designated slot within a longer meeting. All focus groups took place in the groups’ usual meeting places, which were all non-NHS settings. Participants in each group were known to each other. A topic guide was developed (see Appendix 11) covering the participants’ ideas about how children acquire language, signs and causes of language delay and responses to language delay.
Each focus group was facilitated by one of two senior researchers on the team (both SLTs) plus two other researchers from the team and, for two groups, an additional facilitator who was a psychologist specialising in work with black and minority ethnic communities. One of the senior researchers had significant practice and research experience in sub-Saharan Africa.
At the start of each session the researchers were introduced and the purpose of the session was explained. Time was spent describing the study verbally in English, allowing translation to be provided when needed, and assistance in completing the consent forms was given.
The main method of eliciting data was discussion. For one of the minority ethnic groups a fictitious case study was used to stimulate the discussion. The case study (which was aimed at being as culturally inclusive as possible) was read out and then participants split into two groups to discuss it, followed by a whole group discussion. For one of the low SES groups of young parents, role play was used to provoke thoughts about the way that they talk to children; photographs of children in various situations were also shown and participants were encouraged to describe what if any messages the photographs gave about communicating with children, including what about the images was positive and/or negative for speech and language development.
Audio recordings were transcribed verbatim by a member of the research team and all data were anonymised. As English was not the first language of a number of participants, field notes were also kept in case audio recordings were poor. Data analysis was undertaken using an adapted framework analysis92 (Box 5). The data collected from each group of participants were analysed separately. The data analysis software programme NVivo (versions 8–10) was used to support stages 1–4 outlined in Box 5.
The stages in the framework analysis were as follow:
-
Familiarisation. Immersion in the raw data; listing key ideas and recurrent themes.
-
Identifying a thematic framework. This used mainly the a priori issues from the research question and the themes identified in the familiarisation phase. An index was created by creating nodes and subnodes using NVivo 9. As NVivo 9 was used, codes and subcodes with names were used rather than a numbered system. Although the looked-after group was analysed separately, the same initial framework was used.
-
Indexing. In this stage the researcher applies the framework to the data systematically. In this project, however, new themes were added if identified and unlike the original framework the themes were not given numerical codes.
-
Charting. Once all of the data are coded the use of NVivo 9 makes it simpler to carry out the charting phase, that is, to look at the material that has been coded under one code and to consider the whole data set or individual focus groups separately. The material is then summarised and distilled.
-
Mapping and interpretation. At this stage:
-
define concepts, for example the environment
-
map the range and nature of the phenomena – map polarities
-
create typologies
-
fnd associations; provide explanations
-
develop strategies because this is for policy research.
Consensus events
Consensus events were undertaken with SLTs after the focus groups to:
-
determine the level of agreement on the themes of SLT practice (see Chapter 2, Study 2.1: identifying the themes of speech and language therapy practice)
-
determine the level of agreement on how the interventions map onto the themes (see Chapter 2, Study 2.2: identifying interventions used by speech and language therapists)
-
identify the assessment tools most commonly used by SLTs (see Chapter 5, Study 5.1: identification of assessment tools used by speech and language therapists)
-
identify the level of consensus on outcome measures using a modified Delphi process (see Chapter 5, Study 5.2: identification of outcome measures for speech and language therapy).
Consensus activities were undertaken with regional SLT Specific Interest Groups (SIGs) and at two national events.
Specific Interest Groups
Speech and language therapist SIGs and services focusing on preschool and early years populations were identified through a number of sources:
-
local SLTs and the research team’s knowledge of relevant SIGs
-
scanning for SIG advertisements placed in the RCSLT Bulletin magazine over the previous 12 months
-
scanning for advertisements placed by other relevant organisations or groups, for example early years forums, in the RCSLT Bulletin magazine.
Special Interest Group chairs (n = 7), service leads (n = 2) and leaders of other relevant groups and organisations (n = 1) were contacted by e-mail (taken from their adverts) with information about the project. They were invited to express an interest in hosting research events for Child Talk.
Four groups expressed an interest in hosting a research event (Table 8). The organisers of these groups used their normal advertising routes to alert their members to the events. A week before each event the potential participants were sent copies of the information sheet and consent form for information. The potential participants were invited to contact the research office by e-mail or telephone before attending the event if they had any questions regarding the research. Informed consent was taken at the start of the research event by a member of the research team. A total of 66 SLTs took part across the four groups (see Table 9). Of the activities that were undertaken at the four groups, 64 SLTs participated, with two therapists leaving one of the events before the voting activity (see Activity 1: validity of the themes from the speech and language therapists’ perspective).
| Location | Group | n |
|---|---|---|
| A | Internal early years SIG | 16 |
| B | SLTs in children’s centres | 13 |
| C | North-west community clinic SLTs | 18 |
| D | Preschool children SLT continuing professional development day | 19 |
| Total | 66 |
Since these research events took place, the RCSLT have renamed SIGs as Clinical Excellence Networks. We have retained the nomenclature of SIG as the groups were called this at the time of recruitment and data collection.
The data collection activities undertaken at these events are described in the following sections (see Activity 1 to Activity 4); as the activities undertaken varied across the events, the numbers of participants taking part in each activity vary.
Activity 1: validity of the themes from the speech and language therapists’ perspective
The first data collection activities at the SIG events aimed to establish the validity of the themes from the SLTs’ perspective (see Speech and language therapists) and also to explore the relationships between themes. The methods used were quantitative and qualitative. Quantitative data on levels of agreement were collected using a technology called TurningPoint (version 4, Turning Technologies, Belfast, UK). This was used to collect votes digitally and confidentially from each participant and then display the results anonymously for all participants to see. Qualitative data were in the form of discussions following each vote. These data were captured by the research team in the form of field notes and by participants in written form on their tablecloths, flip charts and postcards. These data were collated according to the existing typology themes.
The four data collection activities were as follows:
-
Voting on whether the typology ‘covers everything you do with children with PSLI’ (n = 64). Discussion followed the voting. Participants were encouraged to note anything that they felt was missing from the typology.
-
Voting on the themes: was each one ‘essential’ to their work, ‘desirable’ or ‘never used’ (n = 64). Participants were presented with one theme at a time and asked whether they thought that the theme was ‘essential’, ‘desirable’ or something that they ‘never do’. A short discussion followed each theme.
-
Modelling how the themes related to each other (n = 64). The participants were asked to model/draw how they felt the different themes in the typology related to each other.
-
Participants were asked to describe how they would explain each theme to a parent (n = 37).
At the end of the events the PI examined all of the data collected, summarised the current position and identified ongoing issues that were taken to the national consensus events in the form of a series of challenges or questions for participants to discuss (see National consensus events). Descriptions of the themes were updated to include new data and were presented to the Child Talk parent panel. A ‘teach-back’ process was used with the parent panel to explore the clarity and accessibility of the descriptions for lay people.
Activity 2: mapping interventions onto themes
Using data generated in the cross-tabulation analysis (see Cross-tabulation of interventions and themes from the speech and language therapist groups), therapists were presented with a list of interventions activities and strategies for each theme of the typology. Participating therapists (n = 48) were asked to indicate whether the interventions were ‘essential’, ‘advisory’ or something that they ‘do not use’ for work in that particular theme (see Appendix 12 for an example).
A total of 34 interventions emerged from the focus groups and survey data that had not been associated with any particular theme. These interventions were put onto pieces of card. Each participant (n = 34) was given a set of these cards. They were asked to sort these interventions into the 10 themes when it was possible to do so. Blank cards were also provided for participants to add activities and strategies that had not already been identified in this or the preceding activity.
Activity 3: assessment tools
Activities relating to the assessment tools were undertaken at two of the SIG events, with 16 SLT participants at one event and 13 at the second (29 in total). The activities undertaken at these events were used to validate data from the online survey (see Assessment tool survey), collect additional information about assessment processes used by therapists for PSLI and explore whether length of time in clinical practice influences choice of assessment methods. In addition, the SIG activities identified which assessment processes could be used to inform intervention decisions for the individual typology themes (see Focus groups, Speech and language therapists) and identified any gaps in assessment processes in relation to these themes. Summative content analysis was used to analyse the data from both of the assessment tool activities. 93,94
This activity was based on the lists of commonly used assessments gathered from the online survey (see Assessment tool survey). Participants (n = 29) were split into small groups and provided with a flip chart divided into a grid that included the names of the assessments gathered from the online survey. The definition of PSLI was provided and participants were asked to place a tick against each of the assessments that they used with children with PSLI and to write the names of any other assessments that they used with this group of children at the bottom of the sheet. Participants were then asked to indicate if they used all or part of the assessments and, if only a part, which part they used most frequently.
Participants (n = 29) were provided with forms that each represented one of the themes of the typology and were asked to complete them with a written definition of the theme (see Appendix 13 for an example). They were asked to indicate if they use formal published and/or informal measures to assess each theme. If formal they were asked to name the assessment and to indicate whether they use the complete assessment or only subsections. If they only use subsections they were asked to indicate which. Participants who indicated that they use informal assessment methods were asked to describe what they do in writing on the form.
Activity 4: outcome measures (Delphi round 1)
A modified Delphi technique was used to identify outcomes measures that are used by the speech and language therapy profession and which map onto the typology (see Speech and language therapists). The first stage of this adapted Delphi process was undertaken at SIG events in the form of two activities. In total, 50 SLTs took part in the activities relating to outcome measures across three SIG events (n = 13, n = 18 and n = 19).
Participants were asked an open question – ‘What outcomes do you use, or could you use, in relation to each of the typology themes’ (see Chapter 2, Study 2.1: identifying the themes of speech and language therapy practice) – and were asked to write their responses on Post-it® (3M United Kingdom plc, Bracknell, UK) notes.
Participants were asked to consider if there was a hierarchy to the outcomes that they had generated, for example whether they were short-, medium- or long-term outcomes. They were asked to place the outcomes in ascending order, from short-term to long-term outcomes. Facilitators used prompting questions to elicit further outcomes at differing levels when there were obvious gaps, which were added to the data. The prompts were used to enable the participants to ‘chunk’ information up (to broader higher-order categories) or down (to more specific behaviours).
As many of the ‘outcomes’ had been written as intervention ‘aims’ these were translated into ‘outcomes’ for language consistency. The reworded outcomes were transferred to a Microsoft Excel spreadsheet under the relevant typology theme heading.
The ‘outcomes’ data were examined independently by three members of the research team. Items were removed by consensus that were considered:
-
to be duplications
-
to be irrelevant to the individual theme
-
not to be ‘outcomes’
-
to be too long term.
A small number of outcomes were reallocated to a more appropriate theme following this review of the data.
National consensus events
After the regional SIG events, two national events were held by the research team, one in Leeds and one in London, to assess consensus on the emerging typology and toolkit (assessments and outcomes). These events were open to a range of participants – EYPs, parents and SLTs – including participants who had previously taken part in Child Talk, who were invited to attend by e-mail. In addition, widespread advertising was undertaken in magazines and appropriate publications, on websites and on social media. The parent panel gave suggestions for advertising the event to parents. Anyone interested in taking part in the event was asked to contact the research team to confirm eligibility and register for an event. The inclusion criterion for practitioners (SLTs and EYPs) was experience of working with preschool children with PSLI and that for parents was having a child aged < 7 years and being, or previously being, worried about their child’s talking. Registered participants were sent a participant information sheet and consent form by e-mail at least a week before the consensus event. Informed consent was taken at the start of each consensus event by a member of the research team. Each event lasted a full day and involved a series of exercises suited to the participants’ area of expertise (SLTs, EYPs, and parents). In total, 47 participants attended the event in Leeds (42 SLTs, five EYPs) and 46 participants attended the event in London (44 SLTs, two EYPs). Although seven parents registered to attend, none of them attended on the day. The activities developed for the national events were designed to build on the findings from the SIG event activities (see Specific Interest Groups).
Activity 5: validity of the themes from the speech and language therapists’ perspective
Emerging challenges and specific issues with the typology were brought to the national events for discussion and exploration of consensus. As with the SIG events, quantitative data were generated from voting activities using TurningPoint technology and qualitative data were obtained from discussions with participants and from their written responses.
The issues and challenges discussed related to:
-
the naming of the typology themes
-
the definitions of the typology themes
-
if themes should be merged/expanded
-
whether or not each of the typology themes should be equally weighted or ordered and, if ordered, should this be hierarchical or modular.
Activity 6: intervention vignette
At the start of the national consensus events SLT participants were provided with a booklet and invited to construct a short vignette of a child with PSLI for whom they had provided intervention. This included age, gender, presenting PSLI difficulties, assessments (formal and informal), number of treatment sessions, duration (average) of each treatment session and outcome measures (formal and informal). At the end of the day the participants were asked to reflect back on the child that they had selected and describe what they did with the child (if anything) in relation to each of the typology themes. They were then asked to describe what outcomes they were expecting.
The data from each of the booklets were captured under the headings assessment (formal and informal), typology theme, intervention and outcome measure(s) used. Summative and latent content analysis was used to examine the ‘outcomes’ described for each of the typology themes for similar words and wording and any emerging groupings or domains. 93,94 The ‘outcomes’ were colour coded using highlighter pens when they were deemed to be similar, that is, they could potentially be grouped together, for example ‘attention skills’, ‘attention’, ‘attention aims’, ‘attention levels’ and ‘listening and attention’ were all colour coded the same and categorised together.
Activity 7: outcome measures (Delphi round 2)
Round 2 of the Delphi process usually takes the form of a questionnaire, but in this study further refinement of the data gathered at the SIG events [see Activity 4: outcome measures (Delphi round 1)] was undertaken face to face at the two national consensus events in the form of a ‘card-sorting’ activity.
This activity was designed to sort the outcomes generated for each typology theme into subgroups or categories (outcome domains). Each participant was provided with envelopes relating to the typology themes (randomly assigned) containing cards with individual outcome indicators on them. Participants were asked to sort the outcome indicators from each theme into groups (outcome domains) and to give each domain a label of their own choosing that they felt best described it. They were asked to do this for as many typology themes as possible in the time available.
A summative content approach was used to analyse the data. The data were entered into Microsoft Excel spreadsheets by typology theme, domain labels generated by each participant and the individual outcome indicators that had been grouped within the domains. The data were then resorted by individual outcome indicators (within the typology theme) to see if any similar ‘domains’ emerged across therapists.
The outcome domain labels generated by the SLT participants were reviewed by members of the research team against the following criteria:
-
Is this label conceptually meaningful as a stand-alone outcome domain?
-
Is this label conceptually meaningful both to the typology theme and a number of outcome indicators?
-
Will this be representative as an outcome domain label and be able to capture the individual outcome indicators beneath it?
Consensus was reached by members of the research team (which includes SLTs) on the proposed outcome domain labels for each typology theme.
Surveys
A total of five electronic surveys were undertaken to support data collection. These aimed to:
-
Identify the top three assessment tools commonly used by SLTs (see Chapter 5, Study 5.2: identification of outcome measures for speech and language therapy).
-
Identify the interventions used by SLTs (see Chapter 2, Study 2.2: identifying the interventions used by speech and language therapists). Two separate surveys were developed for this; both sought to identify interventions used by SLTs but the second survey used specific case studies (vignettes).
-
Determine how well parents understand and accept interventions used by SLTs (see Chapter 4, Study 4.2: the perspectives of parents on speech and language therapy).
-
Explore consensus on the top three outcome indictors within the typology themes (see Chapter 5, Study 5.2: identification of outcome measures for speech and language therapy).
All surveys were developed using either Snap Survey (version 11, Snap Survey Ltd, London, UK) or SurveyMonkey® [see www.surveymonkey.com (accessed 15 December 2014)] software, depending on the complexity of the survey, and their development, distribution and analysis are described in detail in the following sections.
Assessment tool survey
A short online survey was developed using Snap Survey software. This survey was designed to gather information on:
-
which three assessments therapists use most frequently with preschool children with PSLI
-
the reasons why these are selected
-
what information the assessments provide to support clinical decision-making.
Appendix 14 provides a screenshot of the online survey. The survey was limited to three assessments to keep the time required to complete it to a minimum and to encourage therapists’ participation. A covering explanatory e-mail and link to the survey was circulated to the 40 SLTs who had participated in the focus groups (see Speech and language therapists) and who had agreed to further involvement in the research programme. Consent for undertaking the survey was implied through completion and submission of survey responses. Of the 40 SLTs invited, 25 took part in the survey.
The first survey question asked participants to identify the three assessments that they use most frequently when working with children with PSLI. The following questions were then asked about the assessments that the SLTs had identified (as free-text boxes):
-
What is your primary reason for selecting this assessment?
-
What information does this assessment provide to support your clinical decision-making?
Summative content analysis was used to analyse the survey data. 93,94
Speech and language therapist intervention surveys
Two surveys were developed, with the first contributing to the development of the second as well as producing data in its own right. The longer second survey was designed to gather more detailed data on the components of interventions and the child, family and contextual factors that might lead to their modification. The focus of the research was on the activities and strategies used rather than on which programmes or resources are used, although, within survey 2, activities and strategies were not explicitly separated.
Intervention survey 1: interventions that speech and language therapists use and the factors that lead them to modify these interventions
The questions focused on SLTs’ reported use of intervention activities and strategies, as well as factors that they reported that led them to adapt their interventions. Appendix 15 provides a list of the questions and response options.
The survey consisted of five items with multiple choice responses plus opportunities to provide further information using free-text responses. SLTs were asked to consider the frequency with which they used interventions and with which children they used them (language delay/disorder, speech delay/disorder or all children).
Lists of intervention activities and strategies provided as response options, as well as factors that led to adaptations, were drawn from their responses. Four SLT researchers reviewed the lists to ensure clarity of terms, agree classification into activity/strategy and ensure that terms were mutually exclusive.
The survey was developed to be distributed online using SurveyMonkey. The survey was piloted by three SLTs and two psychologists. As a result, response options were amended to include response by client group (e.g. speech, language and all children), thus increasing the sensitivity of the data. Additional minor alterations were made to the phrasing of questions and response options. Following this, the survey was checked again by members of the Child Talk team for consistency, formatting and usability.
Intervention survey 2: mapping interventions with a specific preschool child
In this second survey, respondents were asked to base their responses on a specific preschool child (aged from 2 years to 5 years 11 months) with PSLI taken from their own caseload. The decision to use concrete examples is supported by Freeman95 who notes that practitioners are more able to make explicit the knowledge and skills that they use in practice when concrete examples are used.
The survey was designed to gather detailed information on the following:
-
SLTs and their work
-
the interventions delivered for a selected child
-
the child’s speech, language and communication difficulties and other child, family and contextual factors.
Appendix 16 provides a list of the questions asked. The survey utilised predetermined response options, listing interventions and modifying factors. Respondents were, however, also given the option of adding further additional information, using free-text responses. The lists of interventions and modifying factors utilised in survey 1 were further refined. Response options about child characteristics were populated in part by survey data on SLTs’ prioritisation of preschool children. 96 The items and response options were reviewed by two SLTs with experience in survey design and subsequent modifications were made.
Both surveys were disseminated via an e-mail link distributed through a number of sources including the RCSLT SIG leads, Child Talk case study sites, other professional networks and the research team’s professional networks. The survey was also promoted through RCSLT media [Twitter (Twitter, Inc., San Francisco, CA, USA), Facebook (Facebook, Inc., Menlo Park, CA, USA) and LinkedIn (LinkedIn Corporation LAD, Mountain View, CA, USA)]. In addition, an advert for survey 2 was placed in the RCSLT professional magazine Bulletin.
The participant inclusion criteria for both surveys were:
-
qualified SLT
-
working in England
-
experience of working with preschool children (aged from 2 years to 5 years 11 months) with PSLI in the last 12 months.
Screening questions were asked at the start of the surveys to determine eligibility. However, it was not possible for the research team to retrospectively verify that the respondents met the inclusion criteria as the responses were anonymous. Survey 1 received 191 responses and survey 2 received 190 responses.
For survey 1, descriptive statistics were produced using Microsoft Excel. For survey 2, relabelling and categorising of some data was conducted prior to analysis (i.e. free-text responses were categorised and recorded numerically when possible). Data analysis was then carried out using SPSS version 20.0 (IBM Corporation, Armonk, NY, USA). Descriptive statistics and cluster analysis were conducted.
Parent survey
The aim of this parent survey was to obtain the views of parents on the commonly used interventions identified by SLTs (see Chapter 2, Study 2.2: identifying the interventions used by speech and language therapists). Following the challenges with recruitment of parents to the focus groups (see Chapter 4, The perspectives of parents), and in discussion with the Child Talk parent panel, the inclusion criteria for this study were broadened to include any parents who had been worried about their child’s speech and language development. This reflects that fact that parents do not need to have experienced speech and language therapy to be able to feed back on how achievable and/or easy to understand the strategies and activities that SLTs recommend are. It was felt that the inclusion criteria did need to specify that parents needed to have been worried at some time about their child’s speech and/or language development so that they were likely to have experienced similar emotions and therefore be able to relate to parents who had received some degree of speech and language therapy and who had been given these strategies to perform in their home environment. It was also decided that, rather than undertake focus groups, this study would utilise an online survey to elicit parents’ views.
Recruitment took place through the internet, flyers, parent-focused publications and social media. In addition, a recruitment video was developed, scripted and voiced by the parent panel (whiteboard animation), which introduced the Child Talk project and described what parents were being asked to do in a lay and engaging manner. This video was placed on the research unit website [http://speech-therapy.org.uk (accessed 12 January 2015)] and YouTube (YouTube, LLC, San Bruno, CA, USA) [http://youtu.be/fn3ebCd1vc0 (accessed 15 December 2014)] and provided a link to direct parents to the parent survey.
The survey started with a set of nine videos, made by the parent panel and research team, which demonstrated the strategies typically recommended to parents by SLTs and the activities used to model these. The strategies and activities were selected from data provided by SLTs on their current practice from the BCRP’s national survey89 and through content analysis of the Child Talk SLT focus groups (see Chapter 2, Study 2.2: identifying the interventions used by speech and language therapists). The videos included a brief description of the strategies and the rationale behind them followed by a demonstration of the activities and toys that the SLT survey had shown were typically used by SLTs (see Chapter 2, Study 2.2: identifying the interventions used by speech and language therapists). Both the explanation of the strategies and the demonstrations were provided by an experienced SLT [see www.youtube.com/watch?v = 3jM9QZ9nq74 for an example (accessed 23 December 2014)]. Following the video, parents were asked to express their views using a user-friendly rating system (Snap Survey software). The questions were asked to:
-
gain an indication of if parents feel that they understand the rationales behind the strategies
-
investigate if parents would consider it ‘realistic’ or ‘achievable’ to carry out these strategies and, if not, whether this was because of time pressures, not feeling confident to carry them out or other barriers
-
understand how parents might feel about being asked to use these strategies
-
gauge how parents feel about the resources/toys used by SLTs.
Appendix 17 provides a screenshot of the questions and responses for one of the videos. The videos and survey were hosted on the research unit’s website. In addition to parents completing the online survey at home, the research team sought to tap into existing parent groups and organised coffee morning events to allow opportunities for parents to view the videos and rate them in a community setting. This also allowed opportunities for parents who did not have access to the survey to take part. Four groups watched the complete set of videos and completed the survey, including a pre-existing support group for parents of children with SLCN, parents at an event organised by a school and parents at two coffee mornings arranged directly by the research team.
Parents accessing the videos online were not required to respond to all of the videos to submit data and therefore the order of the videos was monitored and adjusted to provide an even response rate to all videos. A total of 56 parents (online and groups) responded to some part of the survey, with at least 28 responding to all of the videos.
Data were entered into SPSS software and descriptive statistics were calculated.
Outcome survey (Delphi round 3)
Delphi round 3 was an online questionnaire, using SurveyMonkey, developed for ranking the outcome indicators within each outcome domain for each typology theme.
The survey was circulated to 109 SLTs who had indicated at the SIG events, at the national consensus events or by e-mail contact with the research team that they would like to be involved further in the research. A covering e-mail and explanation was circulated with the survey. Consent for taking part in the Delphi questionnaire was implied through completion and submission. In total, 79 responses were received.
The themes were split into two groups and participants were randomly assigned to the groups. Within each group the questions were asked in two different orders to account for any participants not completing all questions. This split meant that group 1 respondents were asked to complete 25 ranking questions (totalling 93 individual items to be ranked) and group 2 were asked to complete 32 ranking questions (totalling 101 individual items to be ranked).
The survey asked SLT participants to rank the outcome indicators for each outcome domain. Consensus was reached when > 65% of SLTs ranked a particular outcome indictor in the top three. For outcome domains that had less than three outcome indicators, therapists were asked, ‘Is “X” an acceptable indicator for the outcome “Z”? If “No”, can you suggest any other indicators that could be used to evidence change and/or improvement for the outcome “Z”?’, with responses provided in a free-text box.
Documentary analysis
Case-study audits of the six speech and language therapy services were conducted across England during 2011–12. Interviews with service leads at each site were undertaken to elicit descriptions of how services were organised and what data were available to support analysis of the inputs, outputs and outcomes for each service. Attitudes to measuring short-term outcomes for children and parental satisfaction with services were of particular interest.
Interviews were undertaken by the PI or co-applicant at each study site using a semistructured format agreed by members of the research team. When possible these were completed before the focus groups with SLTs were undertaken (see Speech and language therapists). This allowed the team undertaking the focus groups to understand responses in light of current service delivery pathways and perceived restrictions. Semistructured interviews were undertaken to ensure that previously agreed data were collected. Each interview was audio recorded and, when possible, copies of service documentation were collected. Following each case study audit, the audio recordings were reviewed for data provided verbally and to check which data would be provided by e-mail or post. From this and the subsequent mailings spreadsheets were populated with the documentary evidence, basic data and information from each case study site. Spreadsheets were analysed to ascertain coverage of reporting items required for basic economic evaluation. Reflection was undertaken to build a discussion of the implications of these analyses and these were tested and discussed at a stakeholder event in September 2013.
Assessment tool validity and reliability
To determine the reliability and validity of the formal assessment tools identified by the SLTs, in both the online survey (see Assessment tool survey) and at SIG events (see Specific Interest Groups), the psychometric quality of the tools was assessed using the 11 criteria of Friberg. 97 These were applied to the assessment tools that SLTs had identified as detailed below:
-
the purpose of the assessment tool is identified
-
tester qualifications are explicitly stated
-
testing procedures are sufficiently explained
-
adequate standardisation sample size (> 100) is noted
-
there is a clearly defined standardisation sample [with regard to geographical representation, SES/parent education representation, gender distribution, ethnic background, presence/absence of impairment(s) and age distribution]
-
evidence of item analysis is given
-
measures of central tendency are reported
-
concurrent validity is documented
-
predictive validity is documented
-
test/retest reliability is reported
-
inter-rater reliability is reported.
Items that purported to be screening tools were not included because, as they did not present with any standardisation data at baseline, they were unlikely to meet any of the other psychometric quality criteria.
Systematic review
The systematic review was registered with PROSPERO (reference number CRD42013006369), an international register of prospective systematic reviews.
Search strategy
The Booth and Fry-Smith98 PICO model (population, intervention, comparison, outcome) guided the development of the search strategy. The ‘population’ of interest was defined as preschool children between the ages of 2 years and 5 years 11 months with PSLI. The papers had to include an empirical intervention, although we did not specify the nature of the intervention. A comparison group was not a requirement in the included papers but there had to be at least one outcome measurement of speech or language.
The research team developed the search strategy using previous publications in similar areas,29,35 clinical expertise, information specialist advice and identification of terms used in key papers. The same resources were also used to determine a priori inclusion and exclusion criteria, specify search terms (see Appendix 18) and decide which databases to search. 29,35 The databases were selected to ensure maximum inclusion of published data, unpublished data and conference proceedings. Table 9 provides a summary of the databases searched and the number of studies identified from each database.
| Databasea | Search interface | Search results | Search date |
|---|---|---|---|
| MEDLINE | Ovid | 8374 | 6 December 2011 |
| EMBASE | Ovid | 9663 | 6 December 2011 |
| Cumulative Index to Nursing and Allied Health Literature (CINAHL) | EBSCOhost | 8976 | 2 December 2011 |
| PsycINFO | EBSCOhost | 9107 | 11 January 2011 |
| Cochrane Database of Systematic Reviews (CDSR) | The Cochrane Library | 255 | 13 January 2012 |
| Database of Abstracts of Reviews of Effects (DARE) | The Cochrane Library | 0 | 13 January 2012 |
| NHS Health Technology Assessment database | The Cochrane Library | 0 | 13 January 2012 |
| Cochrane Central Register of Controlled Trials (CENTRAL) | The Cochrane Library | 0 | 13 January 2012 |
| Science Citation Index | Web of Knowledge | 5787 | 13 January 2012 |
| Social Science Citation Index | Web of Knowledge | 0 | 13 January 2012 |
| International Bibliography for the Social Sciences | ProQuest | 0 | 25 November 2011 |
| Applied Social Sciences Index and Abstracts (ASSIA) | ProQuest | 1799 | 25 November 2011 |
| Sociological Abstracts | ProQuest | 3800 | 25 November 2011 |
| Social Services Abstracts | ProQuest | 0 | 25 November 2011 |
| Educational Resource Information Center (ERIC) | ProQuest | 4000 | 26 January 2012 |
| Linguistics and Language Behavior Abstracts | ProQuest | 3006 | 20 January 2012 |
| British Education Index | ProQuest | 464 | 20 January 2012 |
| The Campbell Collaboration | www.campbellcollaboration.org/ | 40 | 13 January 2012 |
| Total | 55,271 | ||
| Duplicates | 21,946 |
To be included, studies had to meet the following requirements:
-
be an empirical evaluation of an intervention, including randomised controlled trials (RCTs), experimental and quasi-experimental studies and case studies, that included multiple baseline or other systematic manipulation of the intervention
-
at least 80% of the sample was required to be within the age range 2 years to 5 years and 11 months at the start of the intervention or at recruitment
-
the intervention had to be led by a SLT (or equivalent profession)
-
language and communication outcomes: at least one of the primary outcome measures of included studies had to address the child’s language (semantic, morphological and/or syntactic aspects), communication (social use of language) or interaction (verbal or non-verbal).
Studies were excluded if they related to:
-
children whose language appeared to be developing typically with no evidence to suggest that their language was ‘at risk’
-
children whose language delays were associated with other developmental or pervasive conditions such as learning difficulties, autism, cleft palate and cerebral palsy
-
social or behavioural outcomes that were not language or communication related.
Search procedure
Subject terms were adapted with similar terms to account for specific variations between database(s) thesauruses. Examples of subject heading terms that were used in different databases are provided in Appendix 19.
No date limit or language restrictions were placed on the reference search. A total of 55,271 references were found across the 18 databases. All search results were downloaded into Reference Manager software (version 11; Thomson ResearchSoft, San Francisco, CA, USA), in which duplicates were removed, leaving 33,325 references.
To assess reliability, two members of the research team independently reviewed the titles of 325 of the papers to screen for relevance, removing animal studies and any others that did not fit the exclusion and inclusion criteria. These authors then reviewed this process and there was 100% consensus. The remaining 33,000 references were shared between these two authors and references were assessed for inclusion at the title level. This process led to the retention of 4574 references, which were divided up for review at the abstract level. This abstract review was undertaken by four members of the research team, including two SLTs, to ensure that at least two people reviewed each manuscript and that one was a SLT. When disagreements occurred the rationale was discussed within the team and consensus was reached. At this point 473 papers were retained and the full papers were reviewed in light of the inclusion and exclusion criteria. Once again, three of the reviewers met and consensus was reached, leading to the final retention of 147 studies. These studies were then quality appraised using one of two tools deemed suitable for each study’s research design/methodology.
Quality appraisal
The quality appraisal tools to be used in the review had to meet certain criteria: they had to be of relevance to the research designs used in the included papers, use a scoring system with a cut-off point indicating an acceptable quality and, preferably, have been used previously in similar content areas. The cut-off point is an indicator of acceptable methodological quality. It is not unusual to undertake a quality appraisal of papers as part of a systematic review process. We aimed for transparency in this process by using quality appraisal tools for which training was available, working to consensus on ratings and operating the same standards for inclusions.
Initial scrutiny of the included papers showed that a range of designs had been used, including RCTs, quasi-experimental group designs and single case experimental designs (SCEDs). A number of quality appraisal tools were considered. Tools from the Critical Appraisal Skills Programme (CASP)99 were considered but could not be used because they either did not have a checklist for single case designs or did not have readily quantifiable criteria. The checklist of Downs and Black100 was also considered and rejected because it is aimed at RCTs and quasi-experimental group designs but is not appropriate for SCEDs. It is considered more valid to use a consistent approach across the study designs.
Finally, two quality appraisal procedures, the Physiotherapy Evidence Database (PEDro)-P scale101 and the SCED scale,102,103 were selected for use in this research. These two tools were adopted by speechBITE, the Australian-based service that evaluates research papers in speech and language therapy across all three methodological types. The PEDro-P scale was designed to appraise the methodological quality of RCTs and non-RCTs. The SCED scale is a parallel tool designed to appraise studies using SCEDs. Scores for the PEDro-P scale range from 0 to 9 whereas scores for the SCED scale range from 0 to 10. The higher the score, the greater the quality of the methodology applied and reported within the study. speechBITE provides online training for the use of these tools, which was undertaken by all reviewing members of the research team.
Of the 100 papers assessed using the PEDro-P scale, scores ranged from 0 to 9, with a mean of 4.2, and of the 47 papers assessed using the SCED scale, scores ranged from 2 to 10, with a mean of 6.8. Previous reviews have used a score of ≥ 6 on these two scales to indicate a high-quality study. 104,105 A score of ≥ 6 was therefore used to determine the studies of acceptably high quality to be retained for inclusion in this work (n = 58).
Data extraction
Data extraction was undertaken on the 58 retained studies (see Chapter 3 for details) and a summary of each was produced detailing the following characteristics:
-
country of origin of the study
-
number of child participants
-
age and gender split of the child participants
-
number of other participants (excluding the research team)
-
demographics of the other participants
-
context/location (e.g. home, clinic, preschool)
-
cultural context
-
study design
-
study focus
-
aim/hypothesis of the intervention
-
description of the intervention
-
whether the intervention was focused on PSLI or whether PSLI was measured as an outcome of a differently focused study
-
intervention type (e.g. parent–child interaction, language enrichment)
-
assessment measures
-
outcome measures
-
who delivered the intervention
-
if the child participants had been diagnosed as having PSLI or were ‘at risk’ of developing PSLI
-
findings/conclusions of the study.
Mapping retained studies onto the Child Talk typology categories
On completion of the data extraction process the studies were reviewed in light of the typology themes identified in Chapter 2 (see Study 2.1: identifying the themes of speech and language therapy practice). Using the definitions of the categories, four members of the research team mapped the studies. This entailed assessing the content of each of the studies, specifically the intervention and outcome measures, and deciding which (if any) of the typology categories were represented by the study. Each study could be represented in more than one theme. Two members of the research team then reviewed the categorisation and reached 100% consensus across all studies.
Synthesis
The synthesis process consisted of two stages. A wide range of characteristics of the studies was extracted. The first were broadly contextual and related to the country, culture and language(s) of the researchers and participants. From this we were able to determine if a diversity of countries was represented in the final data set and if particular interventions or designs were associated with practice in particular countries. The second stage addressed the characteristics of the participants, as age (within the inclusion criterion), gender and diagnosis compared with ‘at risk’ might be associated with particular types of intervention or categories of practice within the typology. The following list gives the factors extracted from the retained papers:
-
evidence of positive change, within each study’s own parameters
-
country of origin/culture
-
size of the sample
-
child participant demographics: age, gender
-
study design
-
what the authors stated the intervention was about
-
who delivered the intervention
-
where the intervention was delivered
-
assessment measures used
-
outcome measures used
-
number of treatment sessions
-
interventions (whole and individual activities and strategies) used in the study mapped against the activities and strategies provided by SLT participants in the Child Talk focus groups and online surveys.
Appendix 20 provides summaries for each paper with regard to the following characteristics: (1) the number of participants, (2) child participant demographics, (3) the context/location of the intervention, (4) the study design, (5) who the intervention was delivered by and (6) the quality rating. Appendix 21 provides summaries for each paper with regard to the following characteristics: (1) assessments used and (2) outcome measures used.
The studies were categorised by typology theme. This consensus was achieved by at least two, but more usually three, members of the research team working independently to map each study against the nine themes. Any disagreements were resolved by discussion. It is worth noting that mapping is dependent on the study authors explicitly stating that they are doing ‘X’ or ‘Y’. This does not mean that the authors of the studies did not undertake activities; some activities might be a part of the assumed procedures of an intervention. However, to ensure rigorous interpretation of the evidence, only those studies that explicitly reported an activity or strategy of relevance to a typology theme were mapped against that theme.
Once the data were synthesised the level of evidence available for each theme was graded A, B or C using the grading scheme formulated by the Clinical Outcomes Group of the NHS Executive. 106 This is outlined in Table 10.
| Level | Type of evidence | Grade | Evidence |
|---|---|---|---|
| I | Evidence obtained from a single RCT or a meta-analysis of RCTs | A | At least one RCT as part of a body of literature of overall good quality and consistency addressing the specific recommendation (evidence level I) without extrapolation |
| IIa | Evidence obtained from at least one well-designed controlled study without randomisation | B | Well-conducted clinical studies but no RCTs on the topic of recommendation (evidence levels II or III); or extrapolated from level I evidence |
| IIb | Evidence obtained from at least one other well-designed quasi-experimental study | ||
| III | Evidence obtained from well-designed non-experimental descriptive studies, such as comparative studies, correlation studies | ||
| IV | Evidence obtained from expert committee reports or opinions and/or clinical experiences of respected authorities | C | Expert committee reports or opinions and/or clinical experiences of respected authorities (evidence level IV). This grading indicates that directly applicable clinical studies of good quality are absent or not readily available |
| GPP | Recommended good practice based on the clinical experience of the NHS Guideline Development Group107 |
An additional step in the analysis of the studies (in relation to the typology themes) was undertaken by mapping the study intervention activities and strategies to those identified by SLTs during focus groups, the online survey and SIGs. This was carried out by SLTs. This allowed identification of aspects of the interventions:
-
undertaken by practitioners and not represented in the literature
-
undertaken by practitioners and represented in the literature
-
represented in the literature but not reported in the other areas of this research programme.
Children’s groups
The original intention had been to conduct investigations in each of the case study sites. However, the logistics of running a series of children’s groups across the UK were considerable and it was decided that, as we would be able to recruit children from a range of backgrounds from within a single city, it was not necessary to do this in each site. We therefore approached three early years settings in Bristol and south Gloucestershire. The settings were identified as having staff who were interested in the research programme (having expressed an interest in taking part in the EYP focus groups) and who served a range of children. The EYPs at each site were asked to identify two groups of four children aged between 2 years and 5 years 11 months. It was asked that the children be of similar age and that they should not be undergoing speech and language therapy, but a child could be included if the EYPs had concerns about his or her speech or language. If the staff had concerns about a child or children, they were asked to group them together. In this way it was hoped that the participation of such children would not be negatively affected by children from the group who were more language or speech proficient. The EYPs identified the children and circulated information sheets and consent forms to the parents. This allowed parents to approach the research team for clarification if required. Parents consenting for their children then returned the completed forms to the EYPs, who held them securely for the research team. All 24 children originally approached were recruited and included in the study.
As we were seeking to explore what works in terms of the engagement of young children in the activities and resources, it was not considered necessary that the children should have a diagnosis of PSLI. Instead, children exhibited a range of speech and language skills and developmental levels. Details of the children’s backgrounds were kept confidential to the setting, so any existing diagnoses or details of support received from speech and language therapy services were not divulged.
Children were recruited from all three sites approached. These sites were selected to include children with a range of demographic characteristics:
-
site 1: rural (commuter belt), exclusively white Caucasian, high SES
-
site 2: suburban, primarily white Caucasian but with a small number of children with mixed ethnicity or from ethnic minorities, middle SES
-
site 3: city centre, no single ethnic majority, low SES.
The 24 children (16 male) recruited across the three sites were aged between 26 and 48 months (mean 39 months). This resulted in six groups of four children (see Appendix 22). Table 11 displays the ethnic backgrounds of the children who attended the groups.
| Ethnic background | n |
|---|---|
| Asian | 2 |
| Bangladeshi | 1 |
| Black Caribbean | 1 |
| Black Caribbean British | 1 |
| Mixed white and black African | 1 |
| Somalian | 1 |
| White British | 17 |
Activities and strategies were selected from those that emerged from the SLT focus groups (see Speech and language therapists). The SLT interventions for each age group were embedded in activities and with resources that were relevant to the age groups of the child. In all cases the activities were delivered by a qualified SLT. Children were grouped with others from their usual ‘class groups’. Each group of children was seen four times, with a 1-week gap between each session, so that the children could become familiar with the team, the activities and the routine. Typically, sessions lasted approximately an hour with a short food and drink break halfway through the session. This level of contact was similar to that experienced locally by children being seen by a SLT.
Each children’s group was based in a room that was familiar to the children. None of the rooms was directly connected to, or visible from, their usual preschool environment/classroom. This served as a way to separate them from their normal preschool routine and mirror the process of attending a clinic therapy session.
Appendix 23 shows the structure of a typical session and Appendix 24 shows the detailed content of each activity. The first group acted as a pilot to establish working patterns between the members of the research group and to determine ways to introduce the head-mounted cameras (known as Kiddicams in the project) to the group. Although the data from this group were not substantially different from the data from subsequent groups, they were not included in the analysis.
Recording of the children’s groups
A number of methods were used to record data. The drama and movement therapist (DMT) wrote comprehensive field notes and reflections both during and immediately following her observations of the speech and language activities. When she took a more active role in the sessions the notes were made from both her recollections and those of other team members.
All sessions were video recorded with two ‘environmental video cameras’ (Figure 6a). There were also two head-mounted Kiddicams. One was a wide-angle mini waterproof Camcorder 720p [see www.dogcamsport.co.uk/dogcam-bullet-hd-camera-WIDE.html (accessed 15 December 2014)]. This video recorder did not have a monitor; placement was carried out by the research team, who attempted to ensure that it was positioned on a headband (Figure 6b) and captured what the child was looking at.
FIGURE 6.
(a) Environmental video cameras mounted on tripods (‘X’); and (b) wide-angle head-mounted Kiddicam.
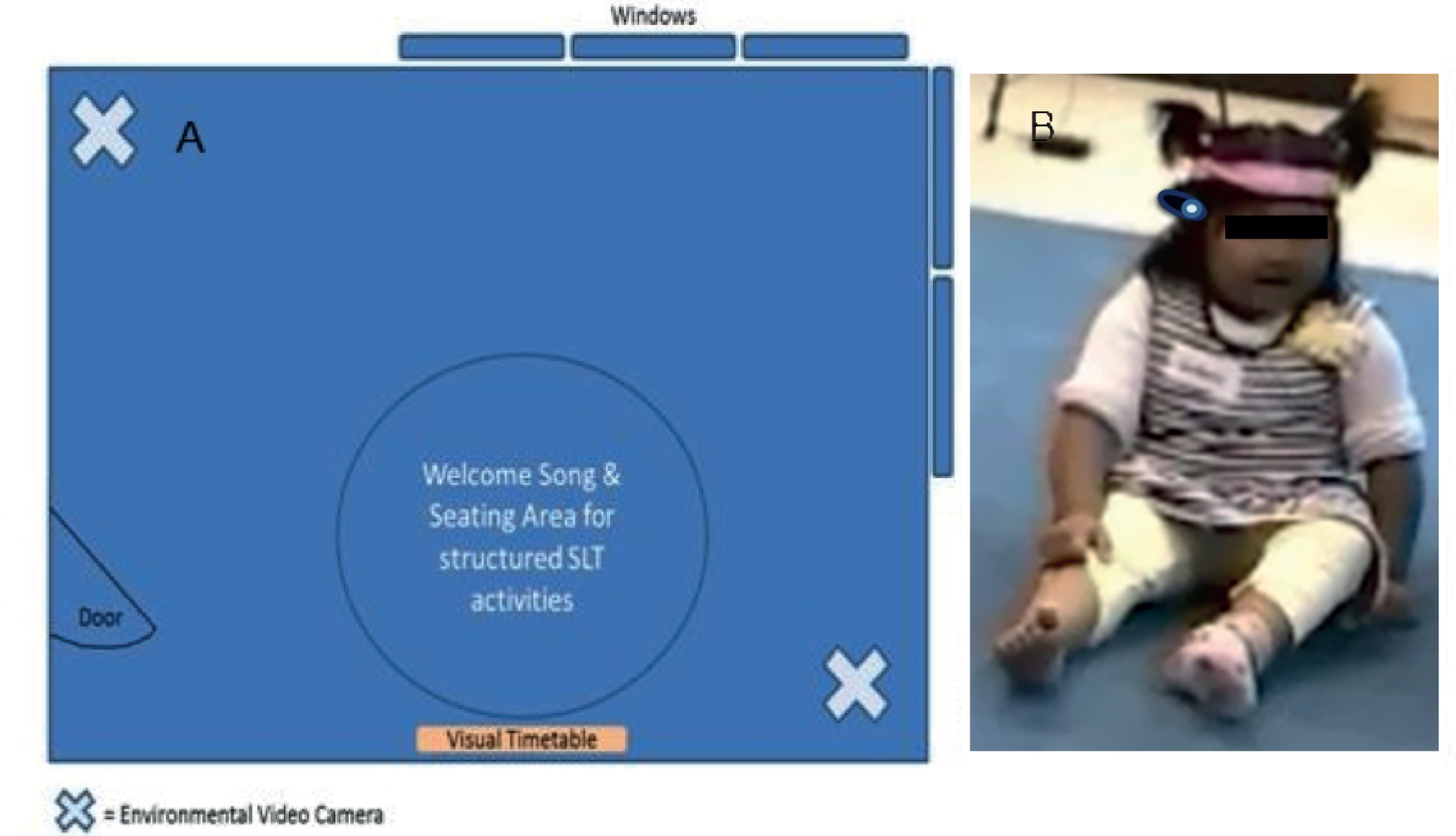
The other Kiddicam was a matchstick camera with a portable digital video recorder [see www.dogcamsport.co.uk/lawmate-ss42-matchstick-camera.html (accessed 15 December 2014)]. The monitor provided with this camera allowed the researchers to adjust the angle of the camera on the headband to ensure that it was pointing in a direction that matched the child’s line of sight. Our intent was to generate video images that capture a child’s-eye view, to gain some insight into the children’s experiences, from their perspective.
Although the children were too young to be able to give informed consent, their assent was considered throughout. The individual activities were explained to the children in suitable language by experienced members of the research team. If they chose to remove themselves from an activity by moving out of the group then the team ensured that they were safe and if appropriate encouraged them to re-engage using similar methods to those that they might use within a nursery setting. If a child continued to display a desire to stop it was taken as a removal of assent and the child was taken back to his or her nursery base. The Kiddicam was introduced to the children by the DMT and the children were asked which of them wanted to wear one of them. When a child volunteered to wear a camera they were assisted by a team member to put it on. If no child volunteered then a member of the research team wore one and opportunities were given between activities for a child to wear it if he or she showed an interest. If a child had been wearing a Kiddicam but wanted to take it off then they were helped with this and other children were offered the opportunity to take over.
Analysis
The principles of the framework analysis approach were used to examine and explore the data. The framework analysis approach was developed by Ritchie and Spencer;109 it is frequently used for large qualitative data sets and allows the analysis to be conducted transparently in a way that can be shared by a number of analysts. This approach was felt to be suitable for this study (see Box 5).
In excess of 72 hours of video data were collected across the groups. One of the researchers attended the majority of the groups (16/24) and reviewed and edited all of the video files. One of the team had extensive experience in framework analysis and intentionally selected 10 sessions as follows: two sessions were selected in which the activities were child led; in two sessions the children were used to a very structured educational setting; two sessions included the youngest children within them; two groups were selected in which the DMT activities took place before the SLT activities; and two groups were selected to allow analysis of, and comment on, changes over the course of the four site visits. Thus, the analysis sampled sessions that varied according to contextual variables that were likely to impact on the children’s experiences of therapy.
-
Each group session was broken down into separate SLT activities and the aims and other variables, such as the materials used for each activity, were recorded in a Microsoft Excel spreadsheet.
-
Two members of the team watched video footage from video cameras on tripods and the Kiddicam cameras simultaneously from each of the 10 group sessions (Figure 7). Each session was an hour in length. Descriptions of what the children were doing and saying in response to the activities, the SLTs and the facilitators were made by the researchers and entered into the Microsoft Excel spreadsheet. The researchers also integrated any field notes from team members (such as the DMT) into the descriptive analysis and this included rich interpretations of children’s perspectives. After describing two groups, the researchers discussed their descriptions to check for consistency and ensure that there was continued consistency in subsequent analyses. A final verifier examined the data set to ensure consistency across researchers.
-
Once all data sets had been coded by the two researchers, the categories were refined and themes generated. Any differences were agreed.
-
Key quotes were extracted from the descriptions of sessions to enable the overall story from the framework set to be told.
-
Biases were reduced by ongoing liaison and meetings between the team members and verification strategies were set in place to ensure trustworthiness. These processes enabled critical review of the analysis.
FIGURE 7.
Multiview Digital Replay System software (University of Nottingham, Nottingham, UK; http://thedrs.sourceforge.net) used to watch and analyse groups (DReSS node, National Centre for e-Social Science, University of Nottingham).

Child Talk phase 1
Aim
To develop an evidence-based typology of SLT-led interventions for preschool children with PSLI that also incorporated the experiences of families.
Objectives
-
To determine current evidence, practice and user perspectives regarding SLT-led interventions for preschool children with PSLI (see Chapters 2–4).
-
To identify how we can best engage preschool children in the process of developing appropriate interventions (see Chapter 4, Study 4.1: the perspectives of preschool children on speech and language therapy).
-
To develop a model(s) of intervention that can integrate current evidence, professional expertise and family perspectives in ways that allow the intervention to be individualised to children’s and families’ communicative, physical, social and cultural contexts (see Chapters 2–4).
Chapter 2 explores the current practice of SLTs with regard to preschool children with PSLI in England in terms of the purpose (themes) of therapy (see Study 2.1: identifying the themes of speech and language therapy practice) and the specific interventions that they use (see Study 2.2: identifying the interventions used by speech and language therapists).
Chapter 3 describes the systematic review undertaken to determine the level of evidence supporting current SLT practice.
Chapter 4 explores users’ perspectives, a methodology for obtaining the views of preschool children (see Study 4.1: the perspectives of preschool children on speech and language therapy), the views of parents about SLTs (see Study 4.2: the perspectives of parents on speech and language therapy), the views of underserved communities about communication and accessing services (see Study 4.3: the perspectives of communities who are undeserved by speech and language therapy services) and the views of EYPs (see Study 4.4: the perspectives of early years practitioners on speech and language therapy).
Chapter 2 The development of a typology of speech and language therapy practice
Introduction
The aim of phase 1 of the Child Talk study is to develop an evidence-based typology of SLT-led interventions for preschool children with PSLI that also incorporates the experiences and views of families. An underpinning assumption of the research programme is that EBP is a three-pronged approach, requiring external systematic evidence, applied appropriately with expertise by therapists and in line with patient preferences. 50,56,69 This chapter reports the findings of an investigation into the reported practice of SLTs and is therefore the main chapter focusing on the clinical expertise element of EBP. The chapter first presents a typology of practice, that is, a set of themes that capture all SLT-led interventions for preschool children with PSLI. Further investigations led to the identification of specific interventions associated with the individual themes of practice. The analysis also identified a number of factors that lead to the modification of interventions. The key factors that may impact on clinical practice and policy and which require further research are drawn together in the discussion section.
The definition of EBP suggests that practice should start with the research evidence base, which is then applied to individual cases. However, practice more commonly starts before explicit research evidence is available and thus precedes research. Therapists are frequently working with children who present with complex impairments that may not necessarily have been described in the research evidence base and are thus having to construct novel combinations of interventions to meet individual child and family needs. Furthermore, as indicated in Chapter 1 (see Introduction), one of the potential barriers to the implementation of EBP is that research does not easily map onto therapists’ existing theories of practice. Therefore, it is helpful to understand and describe existing practice first so that research evidence can be analysed and mapped more closely onto current practice. For this reason, this research programme set out to describe the practice element first.
Descriptions of interventions in research literature vary in the level of detail provided. Indeed, a criticism levelled by reviewers of intervention studies is that it would be difficult to replicate studies because of the dearth of detail about interventions. Nonetheless, the literature does provide suggested models for how interventions might be described. Yoder and Kent110 collected assessment and intervention decision trees that modelled the decision-making process employed by therapists when planning an intervention. One of the decision trees cited in Yoder and Kent110 sets out important factors to consider in planning interventions for children with language impairments, suggesting that therapists should determine linguistic input, the intervention context and the training technique. More recently, McCauley and Fey111 provided a description of seven processes involved in language intervention: the goals, the context, the agent, the dose, the procedures, the ‘goal attack’ strategy and finally the intervention activities. McCauley and Fey111 suggest that using such a model allows practitioners to identify the constituent parts of an intervention and compare and contrast these across interventions. However, these models have not translated into a standard way of reporting interventions in the research literature. An exploration of current practice included in the BCRP89 found that participants referred to more than 150 different interventions, including published interventions, programmes, theories of intervention and training packages. Summarising the literature, Roulstone et al. 89 noted that interventions had been variously described as actions, techniques, activities and procedures that were used to facilitate progress, prevent other problems, modify barriers and facilitate changes to the communication environment.
To provide a description of practice in this study, the aim was to develop a typology of SLT-led interventions. ‘Typology’ in this study is used to denote a systematic description of the characteristics, or components, of practice that are used with preschool children with PSLI. The collection of data and process of analysis have been iterative, whereby the findings from one set of data collected have informed the next. Thus, the detailed structure of the typology evolved as the study progressed. Our starting point was to ask SLTs what they did with preschool children with PSLI. From their descriptions, a thematic analysis generated themes that typified the overall aims of their work. These themes formed the initial structure of the typology; all of the other studies within the research programme gradually converged on this typology, expanding the structure until a final framework was developed that encompassed the work of SLTs with this group of children. The themed descriptions of SLT-led practice do not represent similarly weighted components; some are described in greater detail than others, whereas some have a level of explicitness that is not present in others. As such, this typology can be regarded as only the beginning of a typology of SLT-led practice. However, it provides an initial framework that can be used to generate other hypotheses about practice, and also highlights the gaps in the knowledge and evidence base.
As the one of the objectives of this research programme was to understand the components of interventions, the focus has been on intervention activities and strategies rather than on published programmes or resources. Although resources and materials might be important to the success of an intervention (e.g. in terms of adding motivational value), it is the role that a resource plays in the intervention rather than the resource itself that is important. On the other hand, intervention programmes include a whole range of activities and strategies and thus need some deconstruction to identify the individual components. The definitions used by Roulstone et al. 89 were used in this research programme to differentiate activities and strategies:
-
activities – specific tasks that are usually targeting a specific impairment, for example using minimal pairs activities
-
strategies – general techniques used in interaction with children that might target at the level of impairment, activity or participation and could be used to deliver or support a specific activity such as modelling, for example examples of correct speech or language productions provided for the child.
One of the concerns in focusing on clinical expertise is the issue of how far the practice described is idiosyncratic and how far it is part of a body of knowledge. 63 As suggested in Chapter 1 (see Introduction), the theories of practice that practitioners develop might seem to be particular to each individual practitioner. However, within a knowledge community such as the speech and language therapy community, the knowledge base is built up over time through knowledge sharing, hypothesis formulation and experimentation. Variation in practice is probably inevitable; however, Roulstone112 found that consensus seemed to be present regarding underlying theories but variation in therapists’ practice occurred at the point of implementation of underlying theories and represented procedural interpretations. This research programme determined to investigate levels of consensus as part of the process of describing practice. To some extent, features of practice that give rise to consensus can be viewed as being validated by the profession. Features that vary may be an indication of changing practice, in which innovation is occurring or a particular practice is being phased out. An important caveat, however, is that consensus cannot be equated with efficacy;63 belief systems built up between groups of professionals are no guarantee that the practice concerned is safe, or effective, as some notable medical research has proven recently. An example is Spock’s113 bestselling book, which became a bible for both professionals and parents, advising that babies should sleep on their front. Later empirical studies, however, found that there is a significantly increased risk of sudden infant death syndrome associated with infants sleeping on their abdomens. Examples such as this demonstrate that systematic research is needed to confirm and challenge professional practice.
Objectives
The research presented in this chapter contributes to addressing the following Child Talk objectives:
-
to determine current evidence, practice and user perspectives with regard to SLT-led interventions for preschool children with PSLI
-
to develop a model(s) of intervention that can integrate current evidence, professional expertise and family perspectives in ways that allow the intervention to be individualised to children’s and families’ communicative, physical, social and cultural contexts.
Specifically, this chapter describes the current practice of SLTs for preschool children with PSLI, providing a typology of practice (see Study 2.1: identifying the themes of speech and language therapy practice) and interventions related to it (see Study 2.2: identifying the interventions used by speech and language therapists). Factors that give rise to SLTs’ selection of particular interventions are also described; in particular, the chapter explores the levels of consensus and variation within the profession regarding the use of the interventions by SLTs in practice.
Study 2.1: identifying the themes of speech and language therapy practice
This study aimed to identify the principles and characteristics that are central to therapy for preschool children with PSLI to form a typology of SLT practice. The development of the typology was based on three data sets collected from SLTs in England: focus groups, regional SIG events and national events. Data collection activities were iterative, with findings from earlier activities informing subsequent data collection activities, which went on to refining the themes and exploring consensus and SLTs’ practical application of the typology. The data revealed nine themes that encompass SLTs’ practice and these themes form the basis of the typology.
Research questions
-
Can the key characteristics of SLT-led interventions with preschool children with PSLI be mapped into a coherent theoretical model/framework (typology)?
-
What is the range of opinion, disagreement and consensus around key principles and components and outcomes of SLTs’ practice?
-
Is the typology generated by the research feasible, acceptable and applicable to a national sample of SLTs?
Methodology summary
A summary of the methods is shown in Figure 8; these are described in detail in Chapter 1 (see Methodology overview).
FIGURE 8.
Summary of the methodology used to develop a typology of SLTs’ practice.
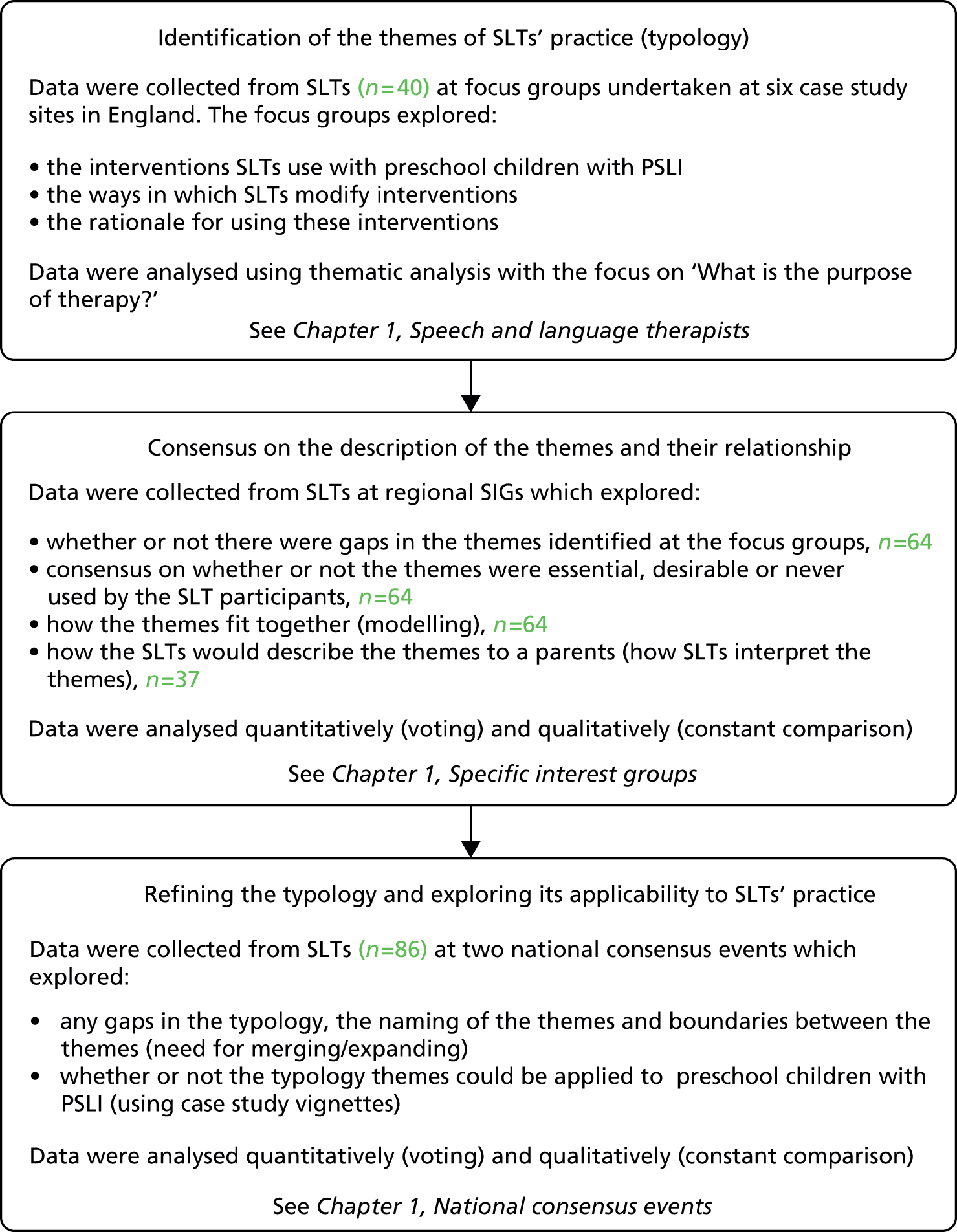
Findings
A thematic analysis of the SLT focus group data initially generated 10 themes that sought to represent therapy aims or what SLTs are trying to achieve through their intervention with preschool children with PSLI. These 10 themes, which formed the first draft of the typology, are shown in Table 12. A more detailed description of the original thematic analysis, with illustrative quotes, can be found in Appendix 25.
| Original theme | Theme label subsequent to SIG and national events |
|---|---|
| Sound awareness | Speech |
| Speech/articulation | |
| Comprehension | Comprehension |
| Structure/content | Expressive language |
| Self-monitoring | Self-monitoring |
| Generalisation | Generalisation |
| Foundation skills | Foundation skills |
| Child participation | Functional communication |
| Empowering/understanding of parents/adults | Adult understanding and empowerment |
| Parent/adult–child interaction | Adult–child interaction |
A number of adjustments were made to the draft typology and the original 10 themes following the SIG and national events using a process of constant comparison Table 12 also summarises the alterations made subsequent to the SIG and national events.
The nine themes and their characteristics that constitute the final typology are shown in Table 13.
| Theme | Characteristics |
|---|---|
| Speech | Therapists described work that increases the accuracy of speech production or articulation, often focusing on specific sound(s). Therapists described a range of activities to work on speech, with work on phonological awareness being integral to this. Phonological awareness activities might include auditory bombardment, syllable counting, discrimination of sounds such as front and back sounds and minimal pairs. Production of speech sounds included activities such as drilling single sounds, working in hierarchy of sound production (C, CV, CVC), cued articulation and blending |
| Comprehension | Therapists described work that aims to improve the children’s understanding of (receptive) language. Interventions in this area might overlap with work that focuses on expressive language, for example vocabulary development. Therapists predominantly described comprehension tasks that focused on following directions and information-carrying word activities |
| Expressive language | Therapists described work that aims to improve the children’s expressive language, in quantity, vocabulary or structure. Therapists reported using a wide range of activities that fit into this category. For instance, work might focus on producing single words, putting words together, other aspects of grammar and morphology or learning new vocabulary, including verbs |
| Self-monitoring | Therapists described work designed to help the children’s awareness of their speech and language difficulties and how they might be able to overcome them. Work that therapists described included some specific strategies for self-monitoring such as token systems as well as more general activities such as discrimination, which aim to encourage children to reflect on their speech and self-correct or repair a communication event |
| Generalisation | Therapists described work to help make speech and language or therapy gains transferable to other situations and environments. Therapists rarely referred to specific activities to enforce generalisation; however, they referred to the importance of parents and other adults working with the child to use activities and strategies in different contexts to encourage generalisation |
| Foundation skills | Therapists described work to practise and improve a range of early skills, many of which might be considered foundations for speech and language development. Activities that therapists reported using to support foundation skills included work on turn taking, play, attention, selective attention and listening; they also described work on non-verbal and social interaction skills |
| Functional communication | Therapists described work focusing on those aspects of communication that help the child’s involvement and participation in life situations; this might be functional language, signing or the use of symbols. A wide range of relevant interventions emerged including materials and resources that help children to access language and ‘make their needs known’, as well as those designed to prepare children or help them cope in life situations |
| Adult understanding and empowerment | Therapists described work that helps parents to understand the nature of their child’s speech and language difficulty, what helps to improve it and why. An important aspect of this is a parent’s or adult’s understanding that he or she is a ‘major tool of change’ (SLT_099). Therapists rarely reported using specific activities or tools to do this but the process of providing explanations for those in regular contact with the child (parent, carer or EYP), either in clinical sessions or training sessions, appeared to be a feature of everyday practice. Therapists referred to ‘changing parent’s perception’ (SLT_106) |
| Adult–child interaction | Therapists described work on the interaction between the parent/adult and the child. All of the changes to adult/parent–child interactions were emphasised in terms of those that encourage speech and language development. These interaction strategies range from things such as sitting and playing with the child or following the child’s lead to commenting on the child’s activities or reducing the number of questions asked of the child. Therapists also referred more generally to the importance of improving the ‘communication environment’ (SLT_095) |
Building consensus on the typology themes
We wanted to explore with SLTs at the SIG and national events whether or not the draft typology was comprehensive and relevant to the work that they do. We also aimed to build consensus over adaptations to the draft typology that would lead to the final typology. The following sections present data that aimed to explore the validity of the draft typology.
Speech and language therapists at SIG events were asked whether they considered the 10 themes in the typology to be essential, desirable or not used in their work with preschool children with PSLI. Table 14 presents the findings of this exercise. Of the 64 therapists who completed this activity, 80% (n = 51) indicated that they thought that the themes covered all aspects of their work with preschool children with PSLI.
| Theme | Essential, n (%) | Desirable, n (%) | Not used, n (%) |
|---|---|---|---|
| Speech/articulation | 36 (56) | 27 (42) | 1 (2) |
| Sound awareness | 40 (63) | 24 (38) | 0 |
| Comprehension | 57 (89) | 6 (9) | 1 (2) |
| Structure/content | 53 (83) | 11 (17) | 0 |
| Self-monitoring | 26 (41) | 32 (50) | 6 (9) |
| Generalisation | 56 (88) | 8 (13) | 0 |
| Child participation | 55 (86) | 9 (14) | 0 |
| Foundation skills | 57 (89) | 7 (11) | 0 |
| Empowering/understanding of parents/adults | 59 (92) | 5 (8) | 0 |
| Parent/adult–child interaction | 59 (92) | 5 (8) | 0 |
The pattern of response was similar across the four events. For seven of the themes, all participants agreed that they would be either essential or desirable to their work. Of the 10 themes, ‘self-monitoring’ and ‘speech’ achieved the lowest level of agreement that these were essential to the work. Some participants provided explanations for not working on certain areas, for example ‘speech’ work was seen as being relevant only with older preschool children and not all SLTs worked with these older children. ‘Self-monitoring’ work was frequently associated in the discussions with ‘speech’ work and therefore similar explanations for its lack of use were given. Despite this, there was general agreement that these two themes were legitimate parts of the SLTs’ practice with preschool children.
Explaining the themes
We next wanted to explore whether or not the initial descriptions of the typology themes were robust, inclusive and able to be accurately interpreted by SLTs. We also required the descriptions of the themes to be understandable by lay audiences. To gauge these factors, participants at the SIGs were asked to describe how they would explain each theme to a parent. To establish SLTs’ ability to accurately interpret the typology themes, descriptions were reviewed for their consistency, that is, the extent to which SLT descriptions were similar to, expanded or were different from the descriptions that we provided.
Thirty-seven participants at SIG events completed explanations of the themes for parents. Of these, 26 provided a description for all 10 themes. For all themes, the majority of participants provided explanations that were consistent (i.e. either the same or expanded) with the given definition. However, some participants wrote explanations that were different in some way for all of the themes except comprehension. These discrepancies consisted of:
-
confusion with/or inclusion of another theme
-
emphasis on a concept not previously included in that theme
-
poor definitions.
Table 15 indicates the numbers of participants who provided written explanations that were very close in content to the original definitions that the team provided (Child Talk definitions), the numbers who expanded on the definitions and the numbers who provided different definitions. Decisions about whether the definitions were the same, expanded or different were made by two members of the research team, who were also qualified SLTs.
| Theme | Expansion of definition, n (%) | Similar definition, n (%) | Different definition, n (%) | Total n |
|---|---|---|---|---|
| Speech/articulation | 13 (46) | 6 (21) | 9 (32) | 28 |
| Sound awareness | 20 (69) | 3 (10) | 6 (21) | 29 |
| Comprehension | 25 (83) | 5 (17) | 0 | 30 |
| Structure/content | 13 (39) | 8 (24) | 12 (36) | 33 |
| Self-monitoring | 9 (29) | 14 (45) | 8 (26) | 31 |
| Generalisation | 15 (45) | 14 (42) | 4 (12) | 33 |
| Foundation skills | 17 (50) | 14 (41) | 3 (9) | 34 |
| Child participation | 9 (35) | 6 (23) | 11 (42) | 26 |
| Empowering/understanding of parents/adults | 9 (32) | 16 (57) | 3 (11) | 28 |
| Parent/adult–child interaction | 13 (45) | 11 (38) | 5 (17) | 29 |
Vignette exercise (final validation)
As a next step we wanted to establish whether SLTs were able to describe their interventions in relation to the typology themes. Participants attending the national events were asked to indicate the interventions used for each theme of the typology for a child from their caseload. Responses were received from 62 participants. The responses of participants were analysed by SLTs from the research team. Responses were explored for consistency of the interventions with the theme descriptions, that is, the extent to which interventions were deemed relevant to that theme. This was used as a form of validation of the themes and their descriptions. This exercise also intended to establish if the typology themes were comprehensive, that is, if SLTs were able to describe all of their work in relation to the themes.
Table 16 reports the number of therapists who provided intervention information in relation to each theme. It also provides information on the number of therapists who explicitly stated that a theme was not applicable to the work that they did with that child. Missing data, that is, when the total number of responses for any theme is < 62, reflect the fact that some SLTs did not provide intervention information or report that the theme was not applicable to their work.
| Themes | Completed intervention information | Reported theme was not applicable, n (%) | Total n | |
|---|---|---|---|---|
| Consistent with theme, n (%) | Inconsistent with theme, n (%) | |||
| Speech/articulation | 38 (62) | 2 (3) | 21 (34) | 61 |
| Sound awareness | 43 (69) | 0 (0) | 19 (31) | 62 |
| Comprehension | 34 (57) | 1 (2) | 25 (42) | 60 |
| Structure/content | 44 (75) | 0 (0) | 15 (25) | 59 |
| Self-monitoring | 31 (51) | 0 (0) | 30 (49) | 61 |
| Generalisation | 42 (69) | 0 (0) | 19 (31) | 61 |
| Foundation skills | 46 (74) | 2 (3) | 14 (23) | 62 |
| Child participation | 40 (66) | 10 (16) | 11 (18) | 61 |
| Empowering/understanding of parents/adults | 60 (97) | 0 (0) | 2 (3) | 62 |
| Parent/adult–child interaction | 51 (88) | 0 (0) | 7 (12) | 58 |
The largest number of responses from SLTs was under the theme of ‘adult understanding and empowerment’ (n = 60). The theme with the least number of responses was ‘self-monitoring’ (n = 31), closely followed by ‘comprehension’ (n = 35). Reasons reported for not working on these areas included that these areas were still being monitored or that they had not been worked on to date with that particular child.
All themes had relevant or consistent interventions reported for them. Most SLTs provided examples of interventions that matched the existing descriptions of the themes. However, the theme ‘participation’ included a relatively large number of intervention activities that were not consistent with the theme (n = 10). These focused on the child’s immediate participation in the session or attendance at clinic, with tasks being based around motivating or engaging the child in the session, for example ‘child chose favourite games or activities at beginning of session’ (B26).
There was a large amount of variance in the level at which therapists worked on ‘adult–child interaction’, although all of the intervention descriptions were consistent with the original theme descriptions. Although some therapists described targeted/detailed work, including programmes such as the Hanen programme [see www.hanen.org (accessed 19 March 2015)], others referred to adult–child interaction as something that they only touched on, for example ‘general advice re parent–child interaction given at initial appointment’ (B36).
Many of the responses for ‘speech’ included interventions that could be categorised under ‘sound awareness’, including phonological awareness and discrimination activities, indicating overlap of these categories. These sound awareness activities were often described alongside speech production activities. Several participants (B13, B29 and A52) also reported the use of minimal pairs, which incorporate aspects of both sound awareness and speech production.
The findings from the vignette activity confirmed that SLTs are able to describe their interventions in relation to the typology themes. Although not all themes were relevant for all of the vignettes used by SLTs, there were no interventions that SLTs reported that they could not describe in relation to at least one of the themes. There were a number of interventions, however, that SLTs reported in relation to several of the themes. Although this might indicate overlap of the themes, it appeared that these interventions were broad (e.g. parent–child interaction, language groups) and were intended to target multiple aspects of the typology at a time.
Refinement of and adaptations to the typology themes
The data gathered from the activities described were reviewed iteratively as data emerged, in terms of emerging challenges, issues and gaps in the typology. At the national events, participants were asked to directly vote on and discuss many of the issues that emerged. Three of the theme changes involved a change of name, with ‘child participation’ becoming ‘functional communication’, ‘structure and content’ becoming ‘expressive language’ and ‘parent/adult–child interaction’ becoming ‘adult–child interaction’. The other change was broader and involved merging the two themes ‘speech’ and ‘sound awareness’. The rationale behind these changes is discussed below.
Data from the SIG events indicated confusion over the theme ‘child participation’, with 42% of participants providing a description that was classified as ‘different’ for this theme. In particular, many participants referred to participation in the session or in therapy rather than to the broader aspects of participating in life events, which was the emphasis in the original theme description. Similarly, at the national events, there were mixed responses: although some therapists felt that ‘participation’ was a label that captured the theme adequately, others indicated a lack of certainty about what it encompassed. Participants used a variety of words and phrases as potential alternatives or to signal their interpretation of the concept of ‘participation’, including ‘functional communication’, ‘engagement’, ‘motivation’ and ‘social use of language’. The predominant term that was used was ‘functional communication’ and thus this term was used in the final typology.
‘Structure and content’ was noted by SLTs to be an unfamiliar phrase and 36% of participants at the national events provided a description that was different from the description that we provided. Adjustments to the term ‘structure and content’ were not discussed at the national events. However, the name of this theme was changed to ‘expressive language’ to be consistent with the phrasing of the theme ‘comprehension’ and to incorporate the use of widely accepted SLT terminology.
The name ‘parent/adult–child interaction’ was changed after a lack of consensus emerged from participants regarding how best to configure this theme and its constituent concepts. A decision was made at the level of the research team to adjust the name of the theme minimally to ‘adult–child interaction’. This distinguishes it from the specific intervention called ‘parent–child interaction therapy’ and includes the broader reference to all adults who interact with the child, that is, in addition to parents.
Two of the original themes ‘sound awareness’ and ‘speech’ were merged into a broader version of the theme ‘speech’, whose new definition incorporates both speech and sound awareness. Responses from SLTs at the SIG events with regard to explaining the themes to parents had indicated that SLTs view these two themes as overlapping. Table 17 shows all items that were taken to vote at the national event and the results. As can be seen, the majority of SLTs felt that the two categories ‘sound awareness’ and ‘speech’ should be merged.
| Question | % of SLTsa | |
|---|---|---|
| Yes | No | |
| Should ‘parent/adult–child interaction’ become ‘communication environment’? | 35 | 65 |
| Should ‘child confidence’ be in the final typology? | 23 | 77 |
| Should basic sound awareness be explicitly included in ‘foundation skills’? | 91 | 10 |
| Should we include speech sounds awareness in the theme ‘speech’ or as a separate theme of ‘speech sound awareness’?a | 71 | 29 |
The description of the characteristics of the theme ‘speech’ with respect to sound awareness was also adjusted to refer exclusively to phonological awareness rather than basic or environmental sound awareness. Although the original description of the sound awareness theme included both speech sound awareness and environmental sound awareness, in the descriptions that SLTs provided for parents at SIG events the majority of participants referred only to speech/sound awareness. Only five of the 29 participants who completed this exercise referred to the more basic skills of identifying and discriminating between environmental sounds. Similarly, in the vignettes activity at the national events only 3 of 62 participants referred to more generic listening activities in the sound awareness theme. Voting at the national events produced > 90% agreement across both sites that more basic aspects of sound awareness were more appropriate to the theme ‘foundation skills’ (see Table 17).
Other challenges to the typology
Three other key challenges to the typology themes emerged from the SIG events:
-
References to children’s emotional well-being or confidence and where this fits in the typology.
-
Many SLTs reported that the training of other adults formed a major part of their interventions (parents and professionals). It was not clear whether this aspect of therapy was a characteristic of ‘parent/adult–child interaction’ or warranted a new theme ‘communication environment’.
-
There was feedback that the themes ‘self-monitoring’ and ‘generalisation’ seemed to overlap.
Discussion of, and voting on, these issues at the national events indicated that no changes to the themes should be made in relation to these three areas. Box 6 provides a summary of the findings from discussions that took place regarding points 1–3 that did not lead to changes in the descriptions of the themes.
Discussions indicated that participants agreed that a child’s well-being could be something that moderated how interventions were delivered. However, it was mostly regarded as an outcome of intervention. Voting indicated that SLTs thought that ‘child confidence’ should not be a separate theme and thus no changes were made to the typology (see Table 17). Concepts of well-being and child confidence already appeared in our data on outcomes (see Chapter 5, Study 5.2: identification of outcome measures for speech and language therapy).
When put to a vote, the majority of the participants indicated that the label for the theme ‘parent–child interaction’ should not be changed to ‘communication environment’ (see Table 17). Participants indicated that they considered that the two terms ‘communication environment’ and ‘parent–child interaction’ were open to a number of other interpretations (such as a particular therapy approach called ‘parent–child interaction’) and should thus be avoided. The decision to use the label ‘adult–child interaction’ therefore encompasses all adults who interact with the child and the process of training those adults.
Participants suggested that self-monitoring is a skill that facilitates generalisation; however, the consensus was that there was a difference between the two and that they should remain as separate themes.
Modelling how the original 10 themes relate to each other
Participants (SLTs, n = 64) at the SIGs were asked to model how the 10 themes from the draft typology related to each other. This task was intended to explore how SLTs perceived the relationship, interaction or overlap between the typology themes. The models produced by participants at the SIG events can be divided into two groups, hierarchical and modular, with some models combining elements of both. In the following sections the two types of models are described separately and examples of relevant models are provided for each.
Hierarchical models
Hierarchical models were presented as lists, pyramids, trees and flow charts and suggested an order to the 10 themes. These orders seemed broadly developmental or progressive, suggesting that some themes were considered more basic or fundamental than others. Examples of these types of models are given in Figures 9 and 10.
FIGURE 9.
Hierarchical tree model representing how the themes might relate to each other.
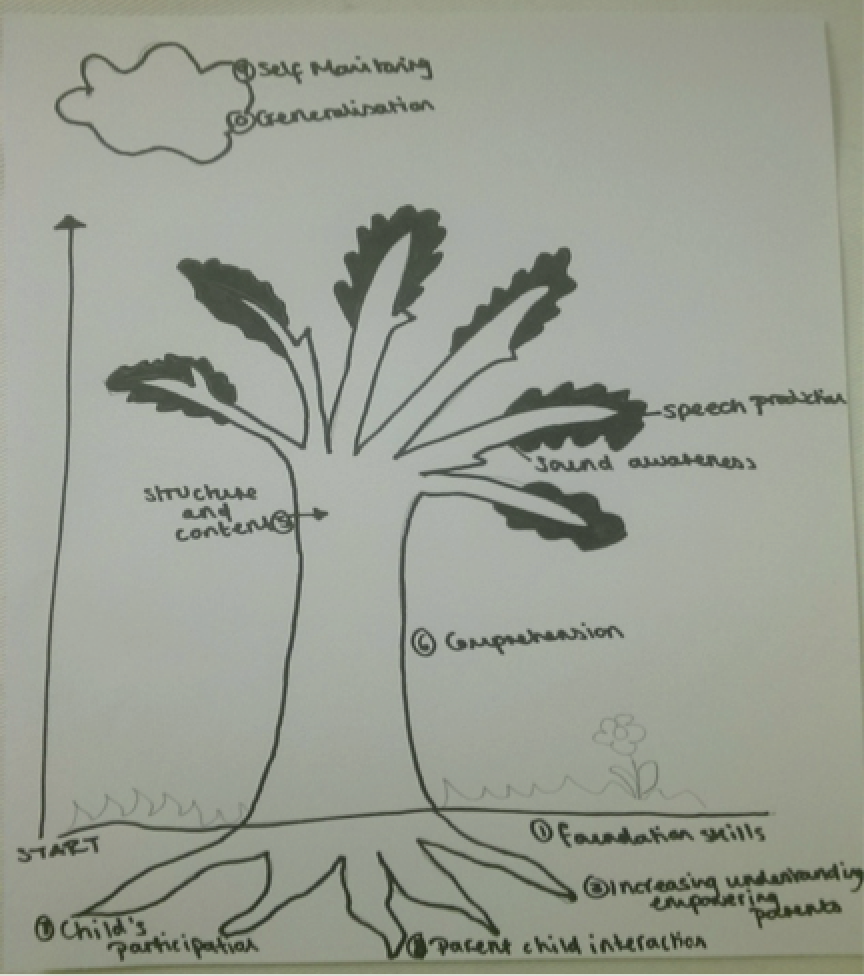
FIGURE 10.
Pyramid model representing how the themes might relate to each other.
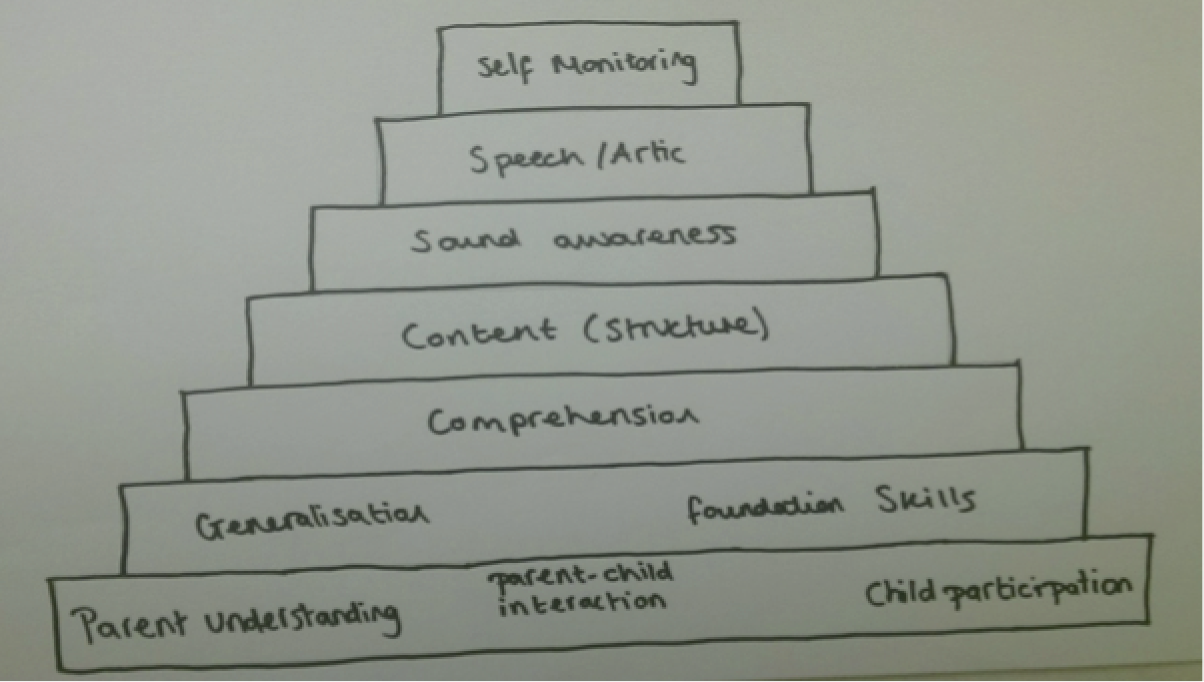
Figure 9 shows a drawing of a tree, which was used to represent a hierarchical structure: at the roots are ‘foundation skills’, ‘parent/adult understanding’, ‘parent–child interaction’ and ‘child participation’, suggesting that these were considered to be underpinning skills; the trunk represents ‘comprehension’ and, further up, ‘structure and content’ of language; these in turn lead to the branches, which represent ‘sound awareness’, and finally the leaves, which represent ‘speech’. A cloud hovering over the tree represents ‘self-monitoring’ and ‘generalisation’, suggesting processes that facilitate growth in the tree.
Figure 10 shows a pyramid, a model used by a number of participants. In this version, the base of the pyramid represents ‘parent understanding’, ‘child participation’ and ‘parent–child interaction’; the next layer represents ‘generalisation’ and ‘foundation skills’, which is followed by ‘comprehension’ and then ‘content’. The layer above this represents ‘sound awareness’ followed by ‘speech’ and finally ‘self-monitoring’. The exact configuration of each pyramid model varied slightly from each other and from the previous tree model but there are clear similarities in both the content and ordered structure of the models (see Figures 9 and 10).
Modular models
Modular models were presented visually as boxes, balloons and Venn diagrams. The themes were then grouped within these, sometimes suggesting orders within a module. Examples are shown in Figures 11 and 12.
FIGURE 11.
Balloon and box modular model representing how the themes might relate to each other.
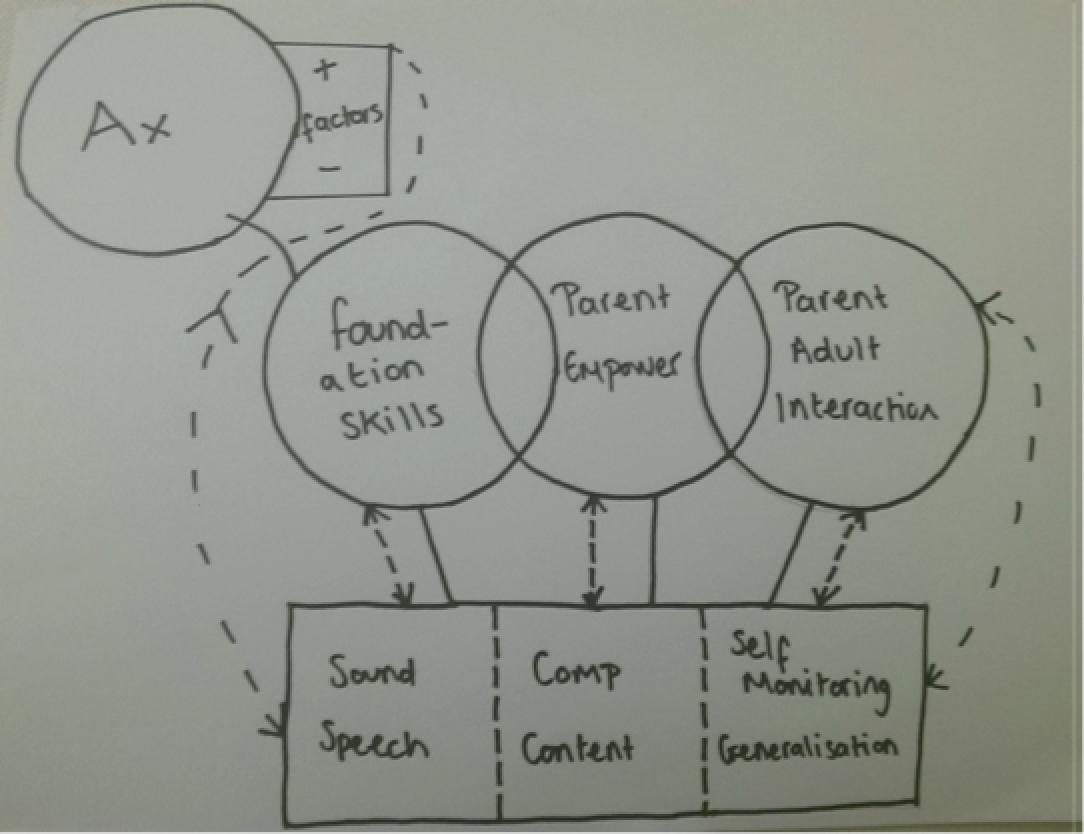
FIGURE 12.
Venn diagram modular model representing how the themes might relate to each other.

Figure 11 shows boxes containing themes – ‘speech’, ‘comprehension’, ‘structure and content’, ‘self-monitoring’ and ‘generalisation’ – with dotted lines between them. Above the box are three balloons, with each balloon representing a different theme: ‘foundation skills’, ‘parent empowerment’ and ‘parent/adult interaction’. Bidirectional arrows connect the balloons and the boxes. The model indicates that assessment drives the selection of relevant themes and that factors such as time and availability, background and age modify these selections.
Figure 12 shows a Venn diagram with overlapping circles representing a speech module and a language module. Within the language module are the themes ‘foundation skills’, ‘comprehension’ and ‘structure and content’; within the speech module are the themes ‘sound awareness’, ‘speech’, ‘self-monitoring’ and ‘generalisation’. There is an implied order within the modules; an arrow from ‘language’ to ‘speech’ further implies an order in which language is tackled before speech. In the overlap of the Venn diagram are the themes ‘parent empowerment’, ‘parent–child interaction’ and ‘child participation’, suggesting that these elements are included in both language and speech modules.
Other differences
The models generated by participants also differed in terms of whether or not themes were represented as distinct stages or as themes that cut across the stages of a hierarchy or the boundaries of a module. Five themes, ‘speech’, ‘structure and content’, ‘comprehension’, ‘sound awareness’ and ‘self-monitoring’, were always represented in a way which suggested that they were seen as a stage in a developmental hierarchy, although the order in which they were represented varied. All of the other themes were represented as cross-cutting themes by at least one participant (or group of participants).
Consensus about modelling the themes
Voting at the national events was used to indicate SLTs’ beliefs about the relationship of the themes to one another (Table 18). Approximately three-quarters of participants felt that the themes were ordered in some way although participants were generally divided on whether a modular or a hierarchical model represented the best fit.
| Question | % of SLTsa | |
|---|---|---|
| Yes | No | |
| Are each of the typology categories equally weighted or ordered? Yes = equally weighted, no = ordered | 24 | 76 |
| If ordered, should it be hierarchical or modular? Yes = hierarchical, no = modular | 49 | 52 |
Final typology of speech and language therapists’ practice with preschool children with primary speech and language impairment
Figure 13 summarises our current understanding of how therapists might combine interventions from the themes to construct an intervention. The figure uses notation from systemic grammar networks. The notation illustrates the choices available and how choices are combined. 114 The following explanation therefore provides a working hypothesis, based on the studies contained in this chapter, of how the themes might be considered in the planning of an intervention.
FIGURE 13.
Working hypothesis of the typology of speech and language therapy for preschool children with PSLI.
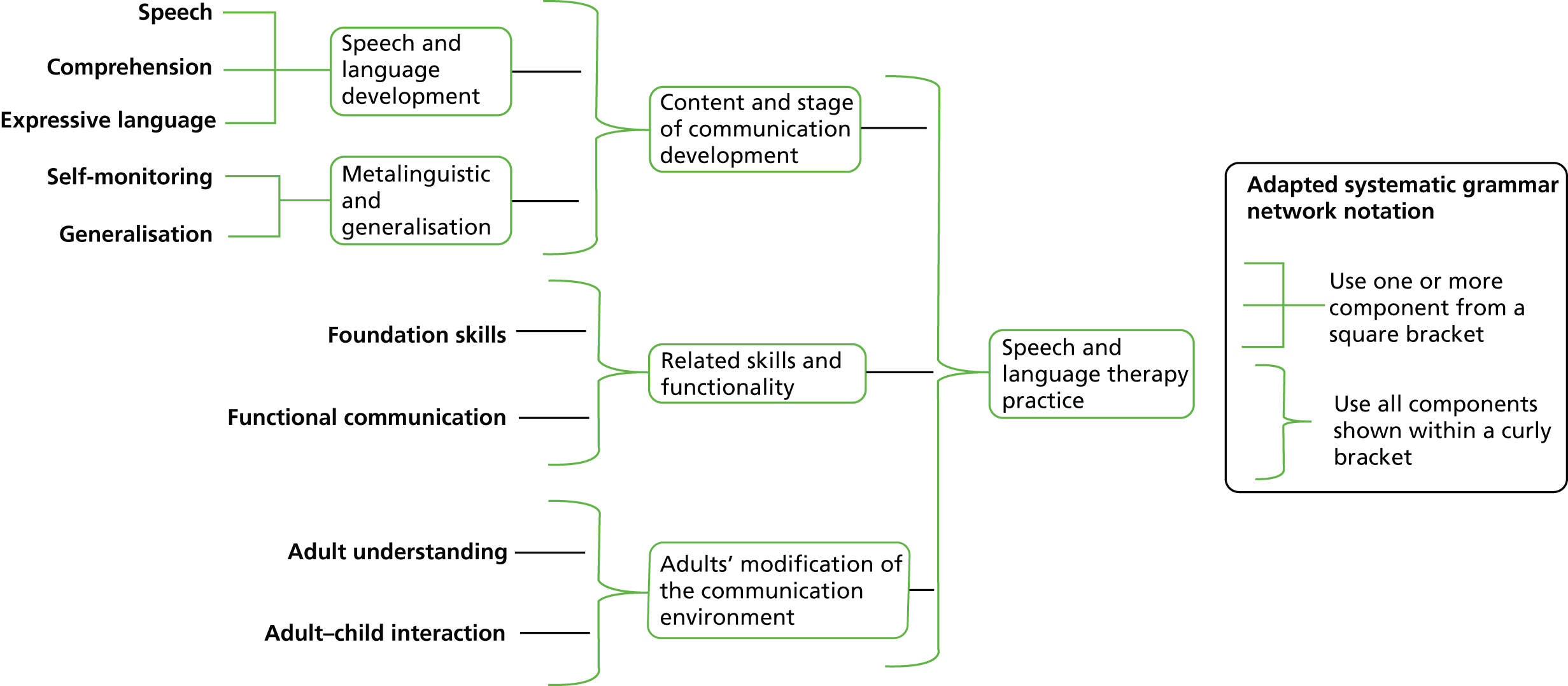
Following assessment, therapists would focus interventions on a particular stage and aspect of a child’s speech and language development (‘speech’, ‘expressive language’ and ‘comprehension’). Depending on the child’s profile, they might choose one or more aspects to focus on. They would, simultaneously, be considering how to support a child’s increasing meta-linguistic or self-monitoring skills and the process of generalisation. The particular focus would depend on the stage of therapy. As well as these ‘content’ areas, therapists would also consider how well the child’s ‘foundation skills’ support their ongoing learning, for example whether or not the child’s attention is sufficient to support learning in the particular content area. They would also consider a child’s ‘functional communication skills’ to ensure that any targets were functionally useful to the child and that he or she had the social communication skills to support functional communication. Finally, therapists would consider what support needs to be in place for adults who are in regular contact with the child, ensuring that they understand the nature of the child’s language learning impairments and are able to interact with the child in a way that supports his or her speech and language development.
Study 2.2: identifying the interventions used by speech and language therapists
This study aimed to identify which intervention components are used by SLTs in England with preschool children with PSLI and which factors might lead SLTs to modify what they do. The identification of interventions and modifying factors was based on several data sets collected from SLTs in England: focus groups, two national electronic surveys, and further exploratory investigations and consensus and validation activities at regional SIG events and national events. The data revealed many ‘activities’ and ‘strategies’ commonly used by SLTs with these children, some of which could be mapped directly onto the typology themes (identified in Study 2.1: identifying the themes of speech and language therapy practice). The data also highlighted the fine-tuning that goes on with respect to how interventions are actually delivered and identify some of the factors that might influence this.
Research questions
-
Which intervention components do SLTs use and consider relevant to preschool children with PSLI?
-
Which factors lead SLTs to adapt or modify their use of intervention components?
-
How do intervention components relate to the developing typology?
Methodology summary
A summary of the methods is shown in Figure 14; the methods are described in detail in Chapter 1 (see Methodology overview).
FIGURE 14.
Summary of the methodology used to identify interventions used by SLTs.
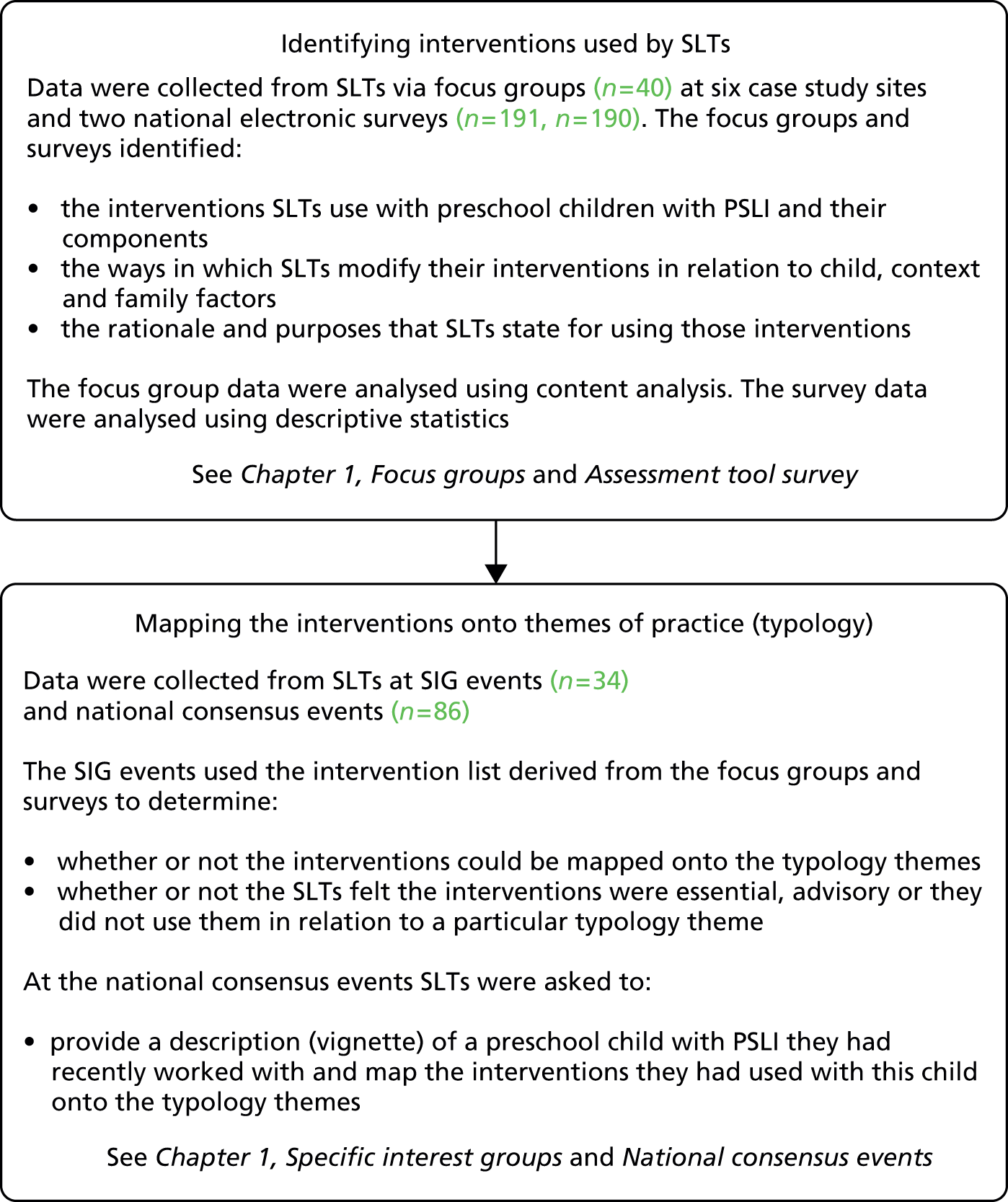
Findings
Data collection was preceded by a review of the findings from a number of previous studies carried out by this group to identify activities and strategies that had already been mentioned by SLTs in connection with children with SLCN. 37,89,96,115 In addition, a selection of published programmes was reviewed to identify activities and strategies that were explicitly mentioned: the Nuffield Centre Dyspraxia Programme (NDP),116 the Derbyshire Language Scheme (DLS),117 the Makaton programme,118 core vocabulary,119 the Hanen programme,120 cued articulation121 and the Metaphon programme. 122 The data were used for later comparison with the interventions presented in the survey to check for comprehensiveness.
A first step in meeting the aim to identify interventions that SLTs use with preschool children with PSLI was conducting focus groups with SLTs.
Content analysis of focus groups
A coding framework was developed by a member of the research team in NVivo 9 software. The framework sought to classify interventions into different categories. The categories were designed to incorporate the different types of disorder within PSLI (e.g. expressive or receptive language, speech, social communication) as well as the different types of intervention (i.e. activities, strategies, programmes or resources). Categories in the framework were not mutually exclusive, so, for example, an intervention might be coded as both an expressive and a receptive language activity. The results of the content analysis are shown in Table 19.
| Categories of interventionsa | Number of interventions coded |
|---|---|
| Generic speech, language and communication activities | 27 |
| Social communication and participation activities | 19 |
| Expressive language activities | 33 |
| Receptive language activities | 43 |
| Speech activities | 90 |
| Materials | 152 |
| Programmes | 121 |
| General speech, language and communication strategies | 123 |
| Language strategies | 150 |
| Speech strategies | 51 |
| Strategies – non-speech, language and communication | 15 |
| Strategies – unsure | 22 |
As shown in Table 19, a large range of interventions was coded. It can be seen that, although participants were encouraged to give detail rather than list programmes or resources, a large number of programmes and materials were coded. Another noteworthy finding is that a large number of strategies for language were coded (n = 150) relative to receptive (n = 43) and expressive (n = 33) language activities. By contrast, speech activities (n = 90) were more commonly coded than speech strategies (n = 51). There were also a large number of strategies (n = 123) that were classified as general speech, language and communication strategies.
Therapy rationale
One of the aims of the focus groups was to explore SLTs’ rationales for therapy. There were 178 references to rationales coded in NVivo 9. These are not going to be reported in full here; however, some noteworthy points are considered. SLTs reported a wide range of rationales for their intervention use, depending on the intervention being delivered. For example, a rationale provided for ‘adult–child interaction’ was ‘to adapt their communication style to then give the child a chance to learn words more effectively’ (SLT_107). In relation to information-carrying word (ICW) activities, by contrast, an example of a rationale provided was ‘you can do verbs and you can do vocabulary development at the same time, as you’ve got a structure you can embed other things in to’ (SLT_025). Thus, rationales showed great variation depending on which particular activity or strategy was being referred to.
Rationales were also provided at a broader level, for example relating to later outcomes [‘importance of language as the foundation of learning and literacy’ (SLT_107)] and evidence of effectiveness [‘I think there’s been some recent evidence that actually it’s pretty strong and robust in terms of being effective intervention’ (SLT_108)].
It was noted that SLTs appeared to find it difficult to provide explicit rationales for their interventions, with many rationales provided in terms of the intervention activity aiming to improve the area that it was targeting, without a clear description of the mechanism of change. Making rationales explicit often involved detailed probing from the facilitator.
Therapy modifications
The focus groups also took a preliminary look at factors that might lead to the individualisation or modification of therapy. Many SLTs talked about the importance of adapting therapy and appeared to find it difficult to describe work in relation to a generic child. Therapists often prefaced their descriptions about the use of an intervention with ‘well it depends’ or ‘depending on . . .’, with ‘depends/depending’ being said 62 times across the focus groups. The following quote from a SLT who attended the focus groups indicates how important the role of adaptations is in planning therapy:
. . . but it’s not one size fits all and you can’t be, that’s not what we‘re about as therapists, now I’m aware that as we’re talking, we’re talking so much about adapting and changing and in professional judgement and those split second judgements that you make and then adapt your own interaction or your own information.
SLT_095
Modifying factors were coded in NVivo 9. Table 20 shows the numbers of factors coded that relate to the child, the family and the context. Examples of commonly raised factors that lead to modifications in relation to these areas are described in more detail in the following three sections.
| Factors leading to modification | Number of factors coded |
|---|---|
| Child factors | 156 |
| Family factors | 141 |
| Context factors | 99 |
Child factors
Factors that were commonly described as important in modifying interventions included the age of the child, the severity and complexity of a child’s difficulties and whether the child had been making progress. Immediate in-session adaptations were also described in terms of the child’s attention and behaviour.
Family factors
A diverse range of factors was raised in relation to adapting therapy for families, including providing therapy that fits around the family lifestyle (e.g. to fit in with a hectic home), managing parents’ needs and preferences, cultural differences and dealing with low levels of engagement or attendance: ‘There’s so many variables about the family, the needs of the family, the place of the family’ (SLT_108).
Context factors
A number of the context factors raised at the focus groups were centred around the influence of the setting and the mode of intervention delivery, for example whether SLTs were working in a clinic or a nursery, in groups, with parents, through assistants or directly with the child. Service constraints was also identified as a theme that ran through the focus groups, with therapists frequently describing time and staffing pressures and issues of access to published programmes that restricted their choice and planning of interventions and thus led to adaptations. It should be noted, however, that service constraint issues were not followed up in subsequent aspects of the research as they are not factors that therapists chose to make adaptations in relation to. They therefore are important to note but are less relevant for making recommendations regarding how and why therapy should be individualised.
The frequency of use of interventions
Interventions and modifying factors identified from the focus group content analysis were used to populate two surveys. Alongside interventions identified from other sources, such as the BCRP,37,89 the two surveys aimed to explore which intervention components SLTs use with preschool children with PSLI, as well as to examine what factors lead SLTs to adapt or modify their use of intervention components. Both surveys utilised predetermined response options. The focus was on components of interventions, that is, activities and strategies, rather than on specific programmes or resources, which are more generalised and may include a range of components within them.
In the first survey SLTs were asked to report the frequency of use of intervention activities and select whether they use them with all preschool children (aged between 2 years and 5 years 11 months) with PSLI, those with primarily language difficulties or those with primarily speech difficulties. They were also asked to select factors that led them to adapt their interventions. In the second survey respondents were asked to base their responses on a specific preschool child with PSLI. In the second survey SLTs were not asked directly about factors that were reported to lead to adaptations; instead, the survey was designed to gather more detailed child, family and contextual information, the purpose being to explore whether or not particular profiles of child/family/context could be linked to particular patterns or individualisation of interventions.
The lists of interventions utilised in survey 1 was refined for survey 2 following the results of that survey and more detailed analysis of the SLT focus groups. Further, to reduce the length of the lists of interventions that SLTs were presented with in survey 2, relevant lists of intervention activities or strategies were presented in relation to the case that they had selected (i.e. speech, language or social communication). These differences mean that, although the surveys are reported together here, there are not matching intervention data for all of the presented interventions. It is also noteworthy that a higher proportion of SLTs would be expected to select interventions in survey 1 than in survey 2, as survey 1 refers to general intervention use whereas in survey 2 responses are based on a specific child.
Participating speech and language therapists
Survey 1 received 191 responses. As participants were not screened for inclusion all participant responses were included in the analysis. Survey 2 received 217 responses; of these, 27 respondents did not meet the inclusion criteria, 17 because they had not worked with a child with PSLI in the last 12 months and 10 because they did not select a preschool child with PSLI. Participants in survey 2 were invited to complete the survey more than once. Ten respondents did so and therefore 180 different SLTs completed the survey.
The number of years since qualifying as a SLT is provided for survey participants in Table 21; the majority had been qualified for > 11 years. For survey 2, more detailed information on the background of the participating SLTs, their work location and the delivery of interventions can be found in Appendix 26.
| Years since qualified | Survey 1 (n = 217), % | Survey 2 (n = 180), % |
|---|---|---|
| 0–2 | 15 | 12 |
| 3–5 | 20 | 21 |
| 6–10 | 23 | 16 |
| 11 + | 43 | 51 |
Child information from survey 2
In survey 1, therapists reported on their general use of interventions. However, in survey 2, therapists reported on interventions that had been used with a particular child from their caseload. The children that they selected were aged between 22 and 72 months, with a mean [standard deviation (SD)] age of 47 (11.0) months. The majority of the children were male (n = 146, 77%).
Approximately half of the SLTs selected a child with primarily speech difficulties (n = 93, 49%) and approximately half selected a child with primarily language difficulties (n = 89, 47%). Those with language difficulties were reported to have either expressive language difficulties (n = 45, 24%) or mixed expressive/receptive language difficulties (n = 44, 23%). Only one respondent selected a child with primarily receptive difficulties. In total, 4% (n = 8) of respondents selected a child with primarily social communication difficulties. Because of the low number of children with primarily social communication difficulties, findings for this group are not reported here.
Other detailed information on the children and their context, including the languages spoken and exposed to, ethnic heritage, preschool childcare provision, medical history, the severity of the PSLI, the effect of PSLI on activity and participation and their behaviour, attention and listening, confidence, awareness, frustration and engagement with therapy, is reported in Appendix 27. Broader contextual and family information was also gathered and is also presented in Appendix 27. These data were extracted to explore whether or not child/family/context factors are related to particular patterns or individualisation of interventions and will be analysed at a later date.
Patterns of intervention use for children with primary speech and language impairment
Descriptive data from both surveys are presented in Table 22. These show the wide variety of interventions in use. From examining the data four key findings emerged in relation to SLTs’ reported use of interventions with preschool children with PSLI:
-
there are differences between intervention activities that SLTs report using for children who have primarily speech delay and intervention activities that SLTs report using for children who have primarily language delay (surveys 1 and 2)
-
strategies are more likely than activities to be reported to be used for all children with PSLI (survey 1)
-
for children with primarily speech difficulties, intervention activities are reported to be more commonly used than strategies, whereas for children with primarily language difficulties the opposite is true, with strategies reported to be more commonly used than activities (survey 2)
-
there is diversity in the responses for some interventions, with about half the sample reporting that they do use particular interventions and half reporting that they do not (survey 1).
| Activities | Speech | Language | ||
|---|---|---|---|---|
| Percentage using intervention always/sometimes with any child with speech impairment (survey 1) (n = 189) | Percentage using intervention with a specified child with speech impairment (survey 2) (n = 93) | Percentage using intervention always/sometimes with any child with language impairment (survey 1) (n = 189) | Percentage using intervention with a specified child with language impairment (survey 2) (n = 93) | |
| ICWs | 1 | NA | 81 | 41 |
| Concepts training | 0 | NA | 73 | NA |
| Basic/key vocabulary | 0 | NA | 69 | 52 |
| Visual timetables | 2 | NA | 48 | 33 |
| Auditory memory activities | 4 | 7 | 48 | 14 |
| Barrier games | 7 | 13 | 47 | 12 |
| What’s in the bag/box | 2 | 30 | 40 | 54 |
| Turn taking | 2 | NA | 35 | 61 |
| Singing hello/goodbye songs | 3 | NA | 35 | NA |
| Core vocabulary | 33 | 24 | 24 | NA |
| Play | NA | 18 | NA | 72 |
| Sharing/reading books | NA | 12 | NA | 69 |
| Attention and listening | NA | 31 | NA | 62 |
| Singing | NA | 8 | NA | 48 |
| Anticipation activities | NA | NA | NA | 33 |
| Sound awareness activities | NA | 70 | NA | 28 |
| Practising key phrases | NA | NA | NA | 19 |
| Working on specific aspects of expressive syntax and/or morphology | NA | NA | NA | 18 |
| Working on semantics and word finding skills | NA | NA | NA | 17 |
| Matching words and objects | NA | NA | NA | 15 |
| Picture sequencing | NA | NA | NA | 11 |
| Work on narrative skills | NA | NA | NA | 6 |
| Phonological awareness | 73 | 48 | 6 | NA |
| Auditory discrimination | 83 | 87 | 6 | NA |
| Minimal pairs | 85 | 57 | 5 | NA |
| Rhyme awareness | 61 | 25 | 4 | NA |
| Focused auditory stimulation | 30 | n/a | 3 | NA |
| Segmentation and blending | 73 | 45 | 3 | NA |
| Auditory bombardment | 47 | 27 | 3 | NA |
| Sequencing sounds | 80 | NA | 3 | NA |
| Maximal oppositions | 45 | 12 | 3 | NA |
| Cued articulation | 47 | 26 | 2 | NA |
| Syllable counting | NA | 65 | NA | NA |
| Drilling speech sounds | NA | 40 | NA | NA |
| Signing | NA | 26 | NA | NA |
| Oromotor work | NA | 28 | NA | NA |
| Cycles approach | NA | 3 | NA | NA |
| Pitch and volume work | NA | 1 | NA | NA |
| Tongue twister | NA | 0 | NA | NA |
These key findings from the survey data are addressed individually in the following section, with supporting data provided in relation to each finding.
Data in Table 22 indicate that SLTs differentiate quite clearly between the intervention activities that are used for children who have primarily speech delay and the intervention activities that are used for those who have primarily language delay. It can be seen that there are a number of intervention activities with relatively high usage for those with primarily speech difficulties but relatively low usage for those with primarily language difficulties. For example, minimal pairs was reported to be used by a large number of participants for those with primarily speech difficulties (survey 1: 85%; survey 2: 57%) but by a relatively low number of participants for those with primarily language difficulties (survey 1: 5%). Similar findings can be found for auditory discrimination activities, with a large number reporting using these activities for those with primarily speech difficulties (survey 1: 83%; survey 2: 87%) and a low number reporting using these activities for those with primarily language difficulties (survey 1: 6%). There are also a number of interventions for which the opposite is true, with relatively high usage reported for those with primarily language difficulties but low usage reported for those with primarily speech difficulties [e.g. ICWs (survey 1): primarily language 81%, primarily speech 1%; basic/key vocabulary (survey 1): primarily language 69%, primarily speech 0%].
Differences between the use of strategies and the use of activities
Table 23 displays intervention activities and Table 24 displays intervention strategies that SLTs reported in survey 1 that they used always/sometimes with ‘all children’. It can be seen that a much higher proportion of SLTs reported using strategies than activities.
| Intervention activities | n | Used always/sometimes with ‘all children’, % |
|---|---|---|
| Turn taking | 185 | 61 |
| What’s in the bag/box | 189 | 52 |
| Visual timetables | 189 | 41 |
| Core vocabulary | 190 | 24 |
| Phonological awareness | 190 | 15 |
| Rhyme awareness | 188 | 13 |
| Auditory discrimination | 190 | 9 |
| Segmentation and blending | 189 | 8 |
| Auditory bombardment | 187 | 8 |
| Minimal pairs | 190 | 4 |
| Sequencing sounds | 190 | 4 |
| Maximal oppositions | 181 | 4 |
| Cued articulation | 188 | 3 |
| Intervention strategies | n | Used always/sometimes with ‘all children’, % |
|---|---|---|
| Using praise | 189 | 97 |
| Modelling | 189 | 96 |
| Making the activity fun | 189 | 96 |
| Reducing distractions | 188 | 93 |
| Going at the child’s pace | 188 | 91 |
| Giving the child time to respond | 188 | 91 |
| Getting on the child’s level | 189 | 88 |
| Scaffolding | 187 | 81 |
| Allowing the child to choose the activity | 188 | 77 |
| Extending | 188 | 65 |
| Providing commentary to the child’s activities | 187 | 63 |
Table 25 displays activities and Table 26 displays strategies that were reported to be used for children with primarily language difficulties. Comparison between the two indicates that higher percentages of SLTs reported using strategies than activities for children with language impairments.
| Intervention activities | n | % of SLTs |
|---|---|---|
| Play | 89 | 72 |
| Sharing/reading books | 89 | 69 |
| Other attention and listening activities | 89 | 62 |
| Turn-taking activities | 89 | 61 |
| What’s in the bag/box activities | 89 | 54 |
| Practising key vocabulary | 89 | 52 |
| Singing | 89 | 48 |
| Extending the number of ICWs that the child uses | 89 | 42 |
| Extending the number of ICWs that the child understands | 89 | 40 |
| Using visual timetables | 89 | 33 |
| Anticipation activities | 89 | 33 |
| Sound awareness activities | 89 | 28 |
| Practising key phrases | 89 | 19 |
| Working on specific aspects of expressive syntax and/or morphology | 89 | 18 |
| Working on semantics and word-finding skills | 89 | 17 |
| Matching words and objects | 89 | 15 |
| Auditory memory activities | 89 | 14 |
| Barrier games | 89 | 12 |
| Picture sequencing | 89 | 11 |
| Other | 89 | 7 |
| Working on narrative skills | 89 | 6 |
| Intervention strategies | n | % of SLTs |
|---|---|---|
| Modelling language constructions for the child | 89 | 83 |
| Extending and expanding language that the child uses | 89 | 81 |
| Reducing the length of the utterances used with the child | 89 | 80 |
| Reducing the complexity of the utterances used with the child | 89 | 79 |
| Giving the child time to respond | 89 | 79 |
| Reducing the number of questions asked of the child | 89 | 74 |
| Providing a commentary on the child’s activities | 89 | 73 |
| Following the child’s lead | 89 | 72 |
| Creating a need for the child to communicate, e.g. giving choices | 89 | 67 |
| Recasting the child’s utterances | 89 | 62 |
| Reducing pressure on the child to speak | 89 | 54 |
| Using gesture | 89 | 44 |
| Signing | 89 | 43 |
| Using visual timetables | 89 | 33 |
| Adopting more varied intonation | 89 | 15 |
Table 27 displays activities and Table 28 displays strategies that were reported to be used for children with primarily speech difficulties. Comparison between the two indicates the opposite pattern, with slightly higher percentages of SLTs reporting using activities than strategies for children with speech impairments.
| Intervention activities | n | % of SLTs |
|---|---|---|
| Auditory discrimination activities | 93 | 87 |
| Practising production of sounds in isolation | 93 | 76 |
| Other sound awareness activities | 93 | 70 |
| Syllable counting activities | 93 | 65 |
| Minimal pairs activities | 93 | 57 |
| Other phonological awareness activities | 93 | 48 |
| Segmentation and blending of phonemes | 93 | 45 |
| Drilling speech sounds | 93 | 40 |
| Other attention and listening activities | 93 | 31 |
| What’s in the bag/box activities | 93 | 30 |
| Oromotor work | 93 | 28 |
| Auditory bombardment | 93 | 27 |
| Cued articulation | 93 | 26 |
| Signing | 93 | 26 |
| Rhyme awareness activities | 93 | 25 |
| Targeted production of specified words/core vocabulary | 93 | 24 |
| Play | 93 | 18 |
| Barrier games | 93 | 13 |
| Maximal opposition activities | 93 | 12 |
| Sharing/reading books | 93 | 12 |
| Singing | 93 | 8 |
| Auditory memory activities | 93 | 7 |
| Other | 93 | 5 |
| Cycles approach | 93 | 3 |
| Pitch and volume work | 93 | 1 |
| Tongue twister | 93 | 0 |
| Intervention strategies | n | % of SLTs |
|---|---|---|
| Adopting a hierarchical approach, e.g. C, CV, CVC | 93 | 74 |
| Emphasising key sounds in the child’s environment | 93 | 46 |
| Supporting sound learning with an action/gesture (other than cued articulation) | 93 | 44 |
| Develop self-monitoring of speech sounds | 93 | 42 |
| Giving the child time to respond | 93 | 26 |
| Reducing pressure on the child to speak | 93 | 25 |
| Using gesture | 93 | 19 |
| Following the child’s lead | 93 | 18 |
| Creating a need to communicate, e.g. providing choices | 93 | 18 |
| Drilling words | 93 | 16 |
| Reducing the number of questions asked of the child | 93 | 16 |
| Reducing dummy use | 93 | 4 |
| Adopting more varied intonation | 93 | 3 |
These findings from both surveys indicate that there are different patterns of intervention use in relation to strategies and activities. The high percentage of SLTs who report that strategies are relevant for ‘all children’ indicates that they are more generalised approaches that are adopted for children with PSLI. Activities, by contrast, are more targeted and specific and thus are less universally applicable to all children. The higher proportion of SLTs reporting using activities than strategies for children with speech delay also indicates that work for speech delay, in particular, is more targeted. Although strategies appear to be important for ‘all children’ they appear to take a more predominant role in therapy for children with language delay.
Interventions with variable use
Interventions could be organised into three groups: (1) those used by a high proportion of therapists; (2) those used by very few therapists; and (3) those used by about half of the sample (40–60%). This last group is interesting as it represents those interventions with the highest variability in use, indicating a lack of consensus regarding their value.
In survey 1, this middle range is particularly interesting to explore as therapists reported on work that they did ‘always or sometimes’ for all children with PSLI. This means that responses should reflect the participating SLTs’ usual practice and thus any differences indicate variability. In survey 2, by contrast, the SLTs were reporting work that they did with a specific child. In this instance it can be expected that many interventions will be used by about half of the therapists, as they may or may not be relevant for that particular child.
Table 29 presents those interventions that were used always/sometimes or occasionally/never by 40–60% of participants according to survey 1. There are four interventions that show this variability in use; all four of these interventions are activities rather than strategies.
| Intervention | n | Used always/sometimes (%) | Used occasionally/never (%) |
|---|---|---|---|
| Auditory bombardment | 187 | 57 | 43 |
| Cued articulation | 188 | 52 | 48 |
| Maximal oppositions | 181 | 51 | 49 |
| Focused auditory stimulation | 183 | 42 | 58 |
Additional responses
In both surveys therapists were able to give additional responses to either provide more detail of their interventions or raise interventions that may not have been covered in the surveys. In survey 1, 122 respondents provided further information about the interventions that they use for preschool children with PSLI. In survey 2, 158 respondents felt that the listed activities and strategies covered all of the interventions that they had used with the specified child. The remaining 17% (n = 32) did not feel that this survey covered all of the interventions that they had used and they therefore listed additional activities and strategies. For details of these responses from both surveys see Appendix 28.
Factors that lead to adaptations of interventions
Both surveys explored factors that are important in the individualisation of therapy. Tables 30–32 indicate the responses obtained from survey 1 in relation to a range of factors that may or may not be influential in modifying the practice of SLTs. Table 30 provides those factors for which there appears to be high consensus that they are influential in modifying practice (> 60% reported that ‘yes’ or ‘usually’ they would adapt their interventions in relation to these factors); Table 31 provides those factors for which there appears to be a lack of consensus that they are influential in modifying practice (40–60% reported that ‘yes’ or ‘usually’ they would adapt their interventions in relation to these factors); and Table 32 provides those factors for which there appears to be high consensus that they are not influential in modifying practice (< 40% reported that ‘yes’ or ‘usually’ they would adapt their interventions in relation to these factors). It can be seen that there are a large number of factors (16/28) for which there is a high level of consensus that they are influential in modifying practice. This indicates that SLTs adapt their interventions in relation to a wide range of factors.
| Factors | n | % Yes | % Usually | % Occasionally | % No |
|---|---|---|---|---|---|
| Severity of the disorder | 189 | 92 | 7 | 1 | 0 |
| Age of the child | 189 | 89 | 8 | 2 | 1 |
| Child’s speech, language and communication diagnosis | 189 | 88 | 8 | 3 | 1 |
| Developmental appropriateness of the intervention | 189 | 88 | 10 | 2 | 1 |
| Level of child’s interest or engagement | 189 | 84 | 12 | 4 | 1 |
| Child’s previous progress | 189 | 80 | 14 | 5 | 1 |
| Child’s level of self-awareness | 189 | 77 | 15 | 8 | 0 |
| Parental understanding | 189 | 73 | 16 | 11 | 1 |
| Poor behaviour | 188 | 63 | 21 | 14 | 2 |
| Resources available | 187 | 62 | 13 | 17 | 8 |
| Parental engagement | 189 | 61 | 22 | 15 | 2 |
| Attendance | 185 | 52 | 17 | 22 | 9 |
| Home environment | 185 | 45 | 19 | 29 | 6 |
| English as an additional language for the child | 189 | 44 | 24 | 24 | 7 |
| Bilingual family | 187 | 40 | 20 | 31 | 9 |
| Parental concern | 188 | 32 | 31 | 35 | 2 |
| Factors | n | % Yes | % Usually | % Occasionally | % No |
|---|---|---|---|---|---|
| Maternal depression | 185 | 30 | 9 | 41 | 20 |
| Culture | 187 | 27 | 16 | 43 | 14 |
| Child’s medical history | 188 | 27 | 15 | 48 | 10 |
| Views of other professionals around the child | 185 | 26 | 24 | 41 | 9 |
| Parental preference | 189 | 26 | 29 | 39 | 6 |
| Factors | n | % Yes | % Usually | % Occasionally | % No |
|---|---|---|---|---|---|
| Religion | 186 | 17 | 6 | 40 | 37 |
| Urban/rural/remote location | 185 | 16 | 4 | 30 | 50 |
| Family SES | 185 | 14 | 7 | 38 | 42 |
| Sociopolitical context | 182 | 7 | 3 | 21 | 69 |
| Ethnicity | 188 | 7 | 5 | 44 | 45 |
| Child’s gender | 189 | 3 | 7 | 41 | 49 |
| Birth order | 186 | 1 | 1 | 14 | 85 |
As with the patterns of variable intervention use, the middle range or 40–60% is interesting as it represents those factors with a lack of consensus in terms of whether or not they are influential in modifying practice, in this case maternal depression, culture, medical history, views of other professionals around the child and parental preference.
Cluster analysis was conducted for survey 2 to explore patterns of individualisation of interventions. Cluster analysis classifies a set of observations into two or more mutually exclusive groups. The purpose is to discover a system of organising groups, in which groups share properties in common. The specific aims of cluster analysis in the present research were to establish whether or not any patterns of intervention emerged. Cluster analysis for both speech and language cases generated two clusters. These clusters appeared to indicate differences in the use of strategies; however, the quality of these clusters was rated as poor and fair. Statistical analysis was then conducted to see if these clusters were related to any child, family or contextual variables (i.e. to see if these factors influenced certain patterns of intervention). The intention was to explore whether or not patterns of intervention were associated with specific variables, which might provide information on the way that SLTs individualise their therapy. Although there were a number of statistically significant findings, the clinical significance of these is questionable, as the quality of the clusters was rated as only fair or poor. Furthermore, a large number of (chi-squared) tests of difference were conducted, increasing the likelihood of false positives. However, the full analysis and significant chi-squared test findings, in relation to child, family and contextual independent variables, are reported in Appendix 29.
Relating intervention components to the developing typology
Having established a wide range of interventions that SLTs report using with preschool children with PSLI, the next step was to explore how they relate to the therapy aims or the typology themes that have emerged. Two key methods for relating intervention components to the typology themes were adopted:
-
focus group cross-tabulations (see Chapter 1, Focus groups)
-
SIG activities: essential/advisory/not used activity and sorting exercise activity (see Chapter 1, Consensus events).
Cross-tabulation
Each typology theme was cross-tabulated with all 12 intervention codes that were utilised in the Nvivo 9 coding categories (activities, strategies, resources, programmes). The result of this cross-tabulation was lists of interventions that were relevant to each theme of the typology.
Special Interest Group activities
Two activities at the SIG days were designed to explore how the emerging intervention components fit with the typology themes. The first activity was designed to assess the validity of the cross-tabulations. Using data generated in the cross-tabulation analysis therapists were asked to indicate whether the interventions were ‘essential’, ‘advisory’ or ‘not used’ in relation to that particular theme.
The second activity explored additional interventions that emerged from the focus groups and survey data that had not been associated with any particular theme. Participants were asked, when possible, to sort these interventions into relevant themes of the typology.
Final collation and analysis
As part of the process of evaluation, it was necessary to collate the various interventions that had emerged from the programme and to examine the validity of their inclusion and association with the typology themes. Using a data-driven process, interventions associated with each theme of the typology were collated. Interventions were added to a typology theme only when there was evidence from one of the data sources that it was associated with that theme. The following data sources were used (in the following order): focus group cross-tabulation of themes and content analysis, card-sorting exercises, survey 1, survey 2 and the national validation check.
In a final checking exercise, any interventions that could be considered to be ‘programmes’ or ‘resources’ were removed. Intervention activities and strategies that were similar were also collapsed. It was not possible to aggregate data across the activities, as the questions all differed slightly in terms of how participants rated or organised their responses and therefore in terms of how the responses can be interpreted. However, by collating the data from the various sources, it was possible to build a picture of the relative popularity of interventions in relation to the typology themes.
The collating exercise produced a list of interventions for each theme of the typology, with the resulting lists varying in length. Table 33 provides a summary of the number of relevant intervention activities and strategies that emerged for each theme. A total of 144 different intervention activities and strategies emerged after removal of duplicates and programmes or resources. The theme ‘speech’ had the largest number of interventions assigned to it (n = 45); however, there were relatively similar numbers across the themes, with seven of the nine themes having between 35 and 45 relevant interventions assigned to them. ‘Generalisation’ (n = 28) and ‘self-monitoring’ (n = 16), in particular, had lower numbers of relevant interventions assigned to them. It should be noted that the interventions were not mutually exclusive, that is, the same intervention could be linked to multiple themes, although it is likely that implementation of an intervention will vary according to the context of the theme.
| Theme | n |
|---|---|
| Speech | 45 |
| Comprehension | 41 |
| Expressive language | 37 |
| Self-monitoring | 16 |
| Generalisation | 28 |
| Foundation skills | 41 |
| Functional communication | 38 |
| Adult understanding and empowerment | 35 |
| Adult–child interaction | 35 |
| Total | 316 |
Table 34 indicates the number of interventions associated with multiple themes. It can be seen that, although most were linked to only one theme (n = 81), many could be linked to multiple themes.
| Number of themes that each intervention spans | Number of interventions |
|---|---|
| 9 | 0 |
| 8 | 2 |
| 7 | 3 |
| 6 | 10 |
| 5 | 6 |
| 4 | 8 |
| 3 | 8 |
| 2 | 26 |
| 1 | 81 |
| Total | 144 |
Strength of associations of interventions with typology theme
Rather than presenting the large amount of data on intervention components, it is more interesting to review the collated data to understand the associations between interventions and typology themes. To evaluate the overall strength of the data supporting the association of an intervention with a theme, the intervention components were rated in relation to whether they appeared to have ‘strong’ or ‘medium’ support from the SIG and national consensus day activities. The strongest indication of a link between an intervention and a theme comes when there is a high level of agreement between participants that an intervention is relevant to a particular theme. For this reason, the following definitions were used to classify a strong or medium association in relation to the SIG data:
-
strong: the intervention was regarded as ‘essential’ to the theme by > 60% of participants or > 60% of participants allocated the intervention to that theme in the sorting exercise
-
medium: the intervention was regarded as essential by 40–60% of participants or was regarded as desirable by > 40% of participants.
The survey data were classified as ‘strong’ when > 60% of SLTs in either survey reported using an intervention and as ‘medium’ when 40–60% in either survey reported using an intervention. As different percentages for use of the interventions were obtained from the two surveys, when differences in classification of the strength of the data occurred between the two surveys, the highest value was taken. This decision was taken as the higher values obtained in survey 1 reflect general use rather than use with a specific child.
In Tables 35–43, the interventions that have been identified for each theme of the typology are presented. The tables present in columns those interventions that have strong and medium evidence from the sorting activities at the SIGs. The rows indicate corresponding survey evidence when applicable. If either there were no survey data available or there was only weak support from survey data the term ‘less support from survey data’ is used. The concepts of strong and medium support described earlier are used throughout.
| Survey data | Sorting activities | |
|---|---|---|
| Strong support from sorting activity | Medium support from sorting activity | |
| Strong support from survey data |
|
|
| Medium support from survey data |
|
|
| Less support from survey data |
|
|
| Survey data | Sorting activities | |
|---|---|---|
| Strong support from sorting activity | Medium support from sorting activity | |
| Strong support from survey data |
|
|
| Medium support from survey data | ||
| Less support from survey data |
|
|
| Survey data | Sorting activities | |
|---|---|---|
| Strong support from sorting activity | Medium support from sorting activity | |
| Strong support from survey data |
|
|
| Medium support from survey data |
|
|
| Less support from survey data |
|
|
| Survey data | Sorting activities | |
|---|---|---|
| Strong support from sorting activity | Medium support from sorting activity | |
| Strong support from survey data |
|
|
| Medium support from survey data |
|
|
| Less support from survey data |
|
|
| Survey data | Sorting activities | |
|---|---|---|
| Strong support from sorting activity | Medium support from sorting activity | |
| Strong support from survey data |
|
|
| Medium support from survey data |
|
|
| Less support from survey data |
|
|
| Survey | Sorting activities | |
|---|---|---|
| Strong support from sorting activity | Medium support from sorting activity | |
| Strong support from survey data |
|
|
| Medium support from survey data |
|
|
| Less support from survey data |
|
|
| Survey | Sorting activities | |
|---|---|---|
| Strong support from sorting activity | Medium support from sorting activity | |
| Strong support from survey data |
|
|
| Medium support from survey data |
|
|
| Less support from survey data |
|
|
| Survey data | Sorting activities | |
|---|---|---|
| Strong support from sorting activity | Medium support from sorting activity | |
| Strong support from survey data |
|
|
| Medium support from survey data |
|
|
| Less support from survey data |
|
|
| Survey data | Sorting activities | |
|---|---|---|
| Strong support from sorting activity | Medium support from sorting activity | |
| Strong support from survey data |
|
|
| Medium support from survey data |
|
|
| Less support from survey data |
|
|
Interventions that had only weak support from the SIG data to link them to a theme are not shown. It is acknowledged, however, that this does not rule them out as being relevant to a theme; it indicates only that they are less likely to be a priority for that theme. For example, for those interventions that spanned multiple themes, SLTs might have instigated a ‘split vote’. Therefore, the activities and strategies that are linked to each theme from the typology are not necessarily a complete list of all of the activities and strategies that could be used for each theme. In addition, one would not expect all activities and strategies to be appropriate for every preschool child with PSLI. Assessment of each child is of course required to identify the most appropriate targets and, hence, the related interventions. Nonetheless, Tables 35–43 provide an overview of the commonly used activities and strategies for each of the themes.
Discussion
The development of a typology of speech and language therapist-led clinical practice
To develop a typology of SLT-led practice we have followed an inductive process. The aim was to examine practice and to identify and describe patterns that capture SLTs’ practice. We did not start with any particular model of or approach to practice but rather aimed to lay open the current practices of therapists. It is important to note, however, that the typology is based on what therapists report that they do rather than on what they might actually do. However, that provides an opportunity to examine how SLTs explain and justify their practice to others and to search for patterns in the way that they do so.
The purposive and theoretical sampling and the iterative nature of the design used in this study adds to our confidence that the findings are comprehensive and robust. In terms of the sample, it is estimated that approximately 70% of the profession registered in England work with children. 24 The RCSLT have been conducting a survey of the profession in the UK but at the moment there are no data on the numbers or the proportion of SLTs in England who work with preschool children with PSLI. It is therefore impossible to comment on how the sample in this study compares with the national picture of those working with, or with expertise in, preschool children with PSLI. However, the design was qualitative and aimed for a purposive/theoretical sample and not a representative one. Sampling was designed to generate participants working with a range of different populations, in different parts of England and in a range of services. Starting first with case study sites, then regional groups with a specific interest in preschool children and finishing with more open national events, the typology has been validated by a progressively widening sample of therapists. Following a qualitative paradigm, we do not make claims about the generalisability of the typology to all SLT-led interventions for preschool children with PSLI. However, it forms a robust hypothesis about the ways that therapists construe their practice with preschool children with PSLI.
This study addressed the following research question: ‘What are the characteristics of SLT-led interventions currently offered to preschool children with PSLI?’ The study investigated the basic purposes of SLTs’ practice in relation to preschool children who have PSLI. The final typology is presented as a list of nine themes. Studies of the application of EBP by SLTs have remarked that their practice reflected what they had learned as undergraduates rather than reflecting the current evidence base. 123 It could similarly be argued that the list of nine themes also reflects topic areas that would be taught and covered during initial training. Nonetheless, levels of consensus reached about the particular descriptions of themes suggests that we have established themes that therapists, from a range of locations and with differing levels of experience, are able to subscribe to and which can cover or include their own ‘theories of practice’. 58 However, where any individual therapist or group of therapists placed the boundaries between themes might vary. Furthermore, each theme was complex and multidimensional and the themes are also combined in complex combinations to form interventions. So, for example, within a theme such as ‘speech’, participants described hierarchical or developmental progressions and also modular components, such as input compared with output processing.
Existing models of intervention refer to different approaches to intervention, for example the didactic approach or environmentally focused approaches or parent-centred approaches. The typology is sufficiently broad to encompass all of these different approaches. Thus, it should be possible to describe any particular intervention for this age group of children who have PSLI by reference to the nine themes of the typology. Validation activities within the study, such as the vignettes described in Study 2.2: identifying the interventions used by speech and language therapists, support this as therapists were able to use the framework to describe their interventions.
However, it is not the case that all nine themes are obligatory in designing an intervention, although it may be that each should be part of the process of assessing a child’s needs. The Medical Research Council guidance on the evaluation of complex interventions requires/encourages practitioners to identify interacting components to be able to systematically identify the active ingredients of any intervention. 124 These active ingredients are typically regarded as the specific techniques used in the intervention and, it is suggested, these enable us to differentiate between interventions. 125,126 However, it is possible to consider active ingredients at different levels of an intervention, from the specific techniques such as modelling or prompting through to higher-order components, such as the themes of the typology developed in this study. 125 The network analysis shown in Figure 13 hypothesises that the particular interpretation and implementation of all nine themes would be driven from the findings of assessments carried out by SLTs. Themes such as ‘adult–child interaction’ and ‘adult understanding’ would be considered as obligatory components of all interventions in some form or another, whereas for themes such as ‘speech’, ‘comprehension’ and ‘expressive language’ an assessment might indicate that there is no identified need to include work on these components.
In conclusion, during the research process we have collected and analysed both quantitative and qualitative data, identified the themes of intervention, refined and developed our understanding of the characteristics of the themes and explored and validated their utility as comprehensive descriptors of practice. Data collection was progressively widened from case study sites to regional groups of specialist SLTs to a more generic national sample (who nonetheless still had a special interest in this group of children). Our participants have come from geographically dispersed locations around England, were working with a range of social communities and had a range of experience both in terms of time and the nature of their preschool caseloads. Thus, the objectives set for this particular study were achieved, that is, to develop a typology of practice that is considered by SLTs to be relevant and comprehensive.
This series of studies, along with the two national surveys, have explored the interventions that SLTs report that they use with children with PSLI, the factors that are associated with modification of interventions and which interventions are associated with the themes of the typology described in Study 2.1: identifying the themes of speech and language therapy practice. As part of the process of developing an evidence-based framework to support SLT-led interventions with these children, the aim was to build a framework that reflects the practice of SLTs. As discussed in previous sections, there are no models of SLTs’ practice that are inclusive of all of the varying approaches to intervention that exist. The risk with this is that current research into the effectiveness of interventions may not map easily onto current practice. By developing our understanding of the way that SLTs frame their practice and their interventions, any gap between research and practice may be lessened.
As with the investigations that led to the typology themes, the design of the surveys used mixed methods, driven primarily by an inductive approach. The questions were exploratory in nature, describing current practice and mapping the range of interventions. No claims can be made about the representativeness of the data based on the sampling methods and sample sizes or about the generalisability of the findings. The quantitative statistical analyses are exploratory in nature, designed not to test existing hypotheses but to better reveal and understand any patterns in the data. As argued earlier in Study 2.1: identifying the themes of speech and language therapy practice, a large amount of data has been generated. Although we do not have a definitive sampling frame, SLT participants came from across England, worked in varying contexts, with differing employers, and had a range of experience, both generally and specifically with children with PSLI. This wide sampling process gives confidence that the findings are robust and comprehensive.
The content analysis of the focus group data, which formed the starting point for this series of studies, confirmed the variety of ways that SLTs describe their interventions. These descriptions are not constructed following any particular structure or framework and interventions are described at different levels, for example as programmes, activities or strategies or merely by referring to the resources that are used. Thus, the type of structure described by McCauley and Fey,127 setting out goals, context, dosage, procedures, strategies, activities and monitoring processes, was not apparent in any coherent way although elements of the model were present. It therefore seems that SLTs could have used a structure such as that suggested by McCauley and Fey127 to describe their interventions, but that they do not do so spontaneously.
Even though the description of interventions focused on activities and strategies and excluded programmes, SLTs managed to generate a large number of different interventions that are used in their everyday practice. There was some overlap with interventions generated in the BCRP. 37,89 However, the focus on activities and strategies used with a particular age group and diagnostic group has resulted in the provision of more detailed data on interventions for these groups of children.
The BCRP was commissioned as part of the Better Communication Action Plan,46 the UK government’s response to the Bercow review of services for children and young people with SLCN. 28 This had recommended a programme of research ‘to enhance the evidence base and inform delivery of better outcomes for children and young people’ (p. 50). The BCRP included a survey study that established the range of programmes used in current practice in the UK across all ages and types of SLCN. 89 Table 44 provides a comparison between the BCRP survey and the Child Talk surveys.
| BCRP survey | Child Talk surveys |
|---|---|
| Reported on children with a range of special education needs | Reported on children with PSLI |
| Reported on children from a wide age range | Reported on children in the age range from 2 years to 5 years 11 months |
| Explored intervention activities, principles and approaches, and programmes | Explored intervention activities and strategies |
| Explored outcomes | Explored what factors lead SLTs to modify or adapt their interventions |
Results from the BCRP are broadly similar to those from the surveys in this research. 89 For example, auditory discrimination was the most commonly reported intervention activity in both. The BCRP explored which programmes SLTs use, finding the DLS to be the most popular. 117 Although the two surveys in this project did not examine the use of published programmes, the DLS can be categorised with the description ‘information-carrying word activities’, which was the most frequently reported intervention activity used with language children in survey 1.
Some interventions showed considerable variation in terms of their use by SLTs. Some of this was clearly related to the diagnostic category of the child. However, it is interesting that the activities showing this variability were all activities targeting children’s speech (auditory bombardment, cued articulation, maximal oppositions and focused auditory stimulation). The lack of consensus regarding the use of some interventions is not surprising given that there are a number of theoretical approaches to any particular impairment in the literature, but no evidence of the superiority of one over another. The case of ‘Jarrod’ in the speech impairment literature was an example: the same child was reviewed by experts with a range of perspectives and all then proposed their particular brand of assessment and intervention. 128 Despite the variation in practice, it was possible to identify some commonly used intervention activities.
There was higher use of intervention strategies than intervention activities across SLTs, irrespective of the type of impairment. It may be that what we have called strategies are closer to what have been called ‘techniques’ elsewhere. 125,126 McCleary et al. 126 explain that techniques may constitute the active ingredients of interventions, which if omitted from an intervention will render that intervention ineffective. The finding in this study that the strategies are likely to be seen as important interventions suggests that SLTs regard them as active ingredients. However, our findings do not allow us to distinguish any strategy or activity that was regarded as exclusive to, or required in, any particular intervention with any particular child or context.
An interesting difference between the two surveys is that, although survey 2 indicates the high proportion of intervention activities in comparison to strategies used with children with speech delay/disorder relative to language delay/disorder, survey 1 suggests that, in fact, many strategies are popular with all children. It may be the case that when SLTs report using interventions for ‘all children’ they are reflecting the fact that many children with PSLI do not present with isolated impairments of either speech or language but rather present with difficulties that often span both domains. Alternatively, it might be that, although the strategies that have emerged are important for all children with PSLI and represent good practice, they are more crucial for children with language delay/disorder. The findings might also in part reflect the design of survey 2, with many of the strategies that are considered relevant only for language children not presented to participants if they had selected that they were reporting on a child with speech delay/disorder.
Modifications of interventions
The studies reported in this chapter also investigated factors that influenced therapists’ selection and modification of interventions. Therapists’ frequent use of ‘it depends’ suggested the constant fine-tuning that goes on with respect to how interventions are actually delivered. This is an expected feature of expert practice whereby the expert practitioner needs to integrate and apply knowledge appropriately from several sources to the needs of an individual child or group of children.
Some factors resulted in divergent responses from SLTs about whether or not they would lead to modifications of their interventions. Some of these differences between therapists may be related to the location or demographics of their clinical work, for example whether or not there is a large presence of bilingual families or different social groups. There are likely to be some geographical areas that are more diverse than others and less exposure to diverse clients may reduce SLTs’ adaptations. For other factors, including the views of other professionals around the child, as well as parent preferences, it is less clear why some SLTs report that they would not make adaptations to their therapy in relation to these factors. How exactly these factors are measured by SLTs and how they influence interventions was also not clear from our findings.
The lack of consensus over whether or not therapists would take parent preferences into account is of particular concern. This is a key feature of EBP: that decisions are made in the light of patient preference. It may be that some practitioners view parent preferences as uninformed by evidence and consider therefore that these views should not affect service decisions. However, The Patient’s Charter declared that patients have the right to information and clear explanations about their condition and about the treatments available. 59 Thus, a lack of parent knowledge should be a trigger to practitioners to ensure that parents are given accessible information about the evidence base and are supported to give their views about their preferences (see Chapter 4).
Further investigation is needed regarding the adaptations that are made in response to the various factors identified within this study, particularly in terms of the impact that such adaptations have on the outcomes for the children. The process by which SLTs identify and measure these factors is also in need of investigation. For example, if parents’ level of engagement is influencing the way that therapists design an intervention, how exactly are they measuring the level of engagement and what levels of engagement trigger changes in their approach?
Another feature of practice that can be related to the literature on expertise is the difficulty that therapists have in explaining the rationale for their choice of intervention and of the factors that lead to modifications. The practice of a novice is characterised by adherence to guidance and rules. With more expert practice, decision-making becomes more tacit and less accessible to explicit scrutiny unless experts are faced with situations in which they have to justify a particular decision. 55,95 Schön129 suggests that, under such circumstances, practitioners ‘turn thought back’ (p. 69) retrospectively to reflect on an action or decision. Freeman95 describes this type of judgement and decision-making as the most difficult to define and articulate (p. 483). Schön130 refers to practitioners knowing ‘more than we can say’ and ‘knowing in action’ (p. 81). Law et al. 9 note that relatively little has been written about this process in speech and language science. The result is that practice knowledge is difficult to define and, perhaps more crucially, difficult to access. It is recognised that there is an ‘inherent problem facing researchers attempting to capture what is, by definition, tacit’ (p. 258). 9 Although the focus groups allowed an engaging environment in which it was hoped that some of the tacit knowledge of SLTs could be tapped, perhaps some of the inherent difficulties in accessing this knowledge were not overcome.
The study found that SLTs could link some of the interventions with the typology themes and we have generated lists of intervention activities and strategies that seemed to be linked strongly to particular themes. In the literature, one would expect to see certain interventions linked with certain conditions. However, as indicated before, these are often described in terms of an approach rather than the specific activities and strategies. McCleary et al. 126 comment that, in such instances, interventions become indistinguishable, both in terms of practitioners attempting to implement them and for researchers attempting to evaluate them. Furthermore, it is clear from the literature that SLTs take an eclectic approach to interventions;131,132 they take the underlying strategies of one programme and apply them in the context of another. Similar comments were apparent in this study.
Issues and challenges
In the descriptions of intervention activities and strategies, the labels and phrases used are not particularly explicit in terms of how to carry out the activities or strategies, for example ‘anticipation activities’ does not specify what this means or what the activities would look like or the particular targets associated with them. Although agreement about the meanings of these interventions was not formally tested, the qualitative data suggest that the content of these kinds of activities forms part of the tacit knowledge of the profession that could be made explicit. In the recordings it was not uncommon to hear noises of agreement as a therapist described an activity; sometimes therapists would explicitly agree that they used a similar activity and then expand on how they might have adapted it.
Comparison of the two speech and language therapist intervention surveys
Drawing direct comparison between the two surveys is difficult because, as described in the methods, the lists of activities and strategies were not identical (additional interventions from other data in the programme of activities, mainly the SLT focus groups, were added into survey 2). Unsurprisingly, higher percentages were reported for all activities and strategies reported on in survey 1 than in survey 2, as survey 1 asked about interventions that SLTs reported using always and sometimes rather than those that they used with a specific child (survey 2). The two surveys have identified some factors that appear to be influential in SLTs’ decision-making about interventions, although opinions are not unanimous. It may be that some factors are relevant only to particular caseloads, or increasing pressures on services put SLTs in a position where they feel unable to adapt their interventions. Alternatively, it may indicate inconsistency in how SLTs approach their practice.
These data present a complex picture: it is apparent that there is a wide variety of interventions being used and of factors that lead to their modification. Unpicking these factors requires more exploration. The present data have been used to feed into the continuing research programme. The present findings confirm that SLTs have a large ‘toolkit’ of interventions, which they vary in relation to a range of child and family factors as well as for pragmatic reasons. The final framework has provided a typology of intervention aims and relevant intervention activities and strategies within these.
The framework of the typology and associated interventions provides a description of themes that can be regarded as key components of an intervention. The data have been subjected to validation with SLTs and this provides evidence that the typology and related interventions form a robust reflection of practice.
Chapter 3 Identifying the evidence base for speech and language therapy practice
Introduction
It is often the case that practitioners have access to, and time to read, only a limited number of papers around their area of interest. This can lead to a slanted view of the published research, with each of the individual papers making claims about ‘what works’ related to the effectiveness of interventions.
Systematic reviews are a way of making sense of the extended body of literature and subsequently making objective judgements across the range of papers. From these they hope to provide a fuller answer about ‘what works’ by providing a map of the areas of uncertainty, the quality and weight of evidence and areas where there is a lack of relevant research.
Systematic reviews of literature on PSLI have concluded that there is evidence to support the effectiveness of interventions for PSLI. However, this evidence base is difficult to interpret in terms of current practice in speech and language therapy. First, the level of evidence varies depending on the aspect of speech and language being considered. Law et al. 29 concluded that interventions targeting children’s sound system or vocabulary were effective whereas there was less evidence to support interventions for receptive language and mixed evidence regarding those for expressive syntax. Interventions used in the literature are not always those found in common practice.
Additional challenges in interpreting findings are that speech and language therapy interventions for PSLI, both in practice and in the literature, lack consensus in how they are described or how the components are characterised. Law et al. 29 differentiate between didactic, naturalistic and hybrid approaches. Pappas and McLeod133 differentiate four approaches: (1) therapist centred; (2) parent as therapist aide; (3) family centred; and (4) family friendly. There are overlaps between these ways of conceptualising SLT-led interventions. However, none provides an overarching analysis of the principles, characteristics and components and associated outcomes that would allow systematic evaluation of their active ingredients and causal mechanisms. Although systematic reviews have attempted to tease out what works for which children in which contexts, the lack of detailed modelling of any intervention means that the evidence base fails to support any specification of interventions for local populations or any particular subgroups of children and families.
The BCRP undertook to identify the ‘best evidence’ for oral language programmes. 37 Law et al. 37 recognised that key to the development of evidence-based interventions for children with SLCN is an awareness of what interventions are already being used. They examined the intervention literature related to children with primary speech and language difficulties and specifically identified interventions from RCTs and included the most recent version of the relevant Cochrane review29 of interventions for children with speech or language delay/disorder. The Child Talk systematic review expands this work by including all study designs but focused on a narrower age range of children with PSLI rather than the more general SLCN category.
As with the BCRP, the Child Talk programme surveyed SLTs (through focus groups, online surveys and SIGs). From this, a typology of practice has been constructed based on evidence collected from, and confirmed by, subject matter experts (SLTs working with children with PSLI). This systematic review described in this chapter has undertaken to review all of the relevant publications related to interventions undertaken with our population of interest. It has then taken a novel step and mapped the papers to the Child Talk typology.
Practitioners may not be aware of evidence related to practice if it is not the main focus of a paper. The Child Talk systematic review aimed to collate all relevant papers and then map the interventions and outcomes against the typology. This means that many papers are represented across multiple themes of the typology as more than one element of practice is considered within the reporting of the intervention and/or outcomes.
To identify the active ingredients of therapy from the perspective of therapists, this systematic review is complemented by a series of focus groups and surveys, which have enabled practitioners to identify the core components of their therapy. This has been developed into a typology of SLT-led practice.
Objectives
The research presented in this chapter contributes to addressing the following Child Talk objectives:
-
to determine current evidence, practice and user perspectives regarding SLT-led interventions for preschool children with PSLI
-
to develop a model(s) of intervention that can integrate current evidence, professional expertise and family perspectives in ways that allow the intervention to be individualised to children’s and families’ communicative, physical, social and cultural contexts.
Specifically, this chapter describes the systematic review undertaken to identify current evidence on speech, language and communication interventions for children with PSLI. The chapter outlines the process of identification, quality appraisal and grading of published evidence and presents how this evidence maps onto the typology of practice developed in Chapter 2 (see Study 2.1: identifying the themes of speech and language therapy practice).
Research questions
-
What is the quality of the published evidence for the effectiveness of SLT interventions for preschool children with PSLI?
-
Which aspects of SLTs’ current practice, as identified in Child Talk, are supported by published evidence and which are not?
Methodology summary
A summary of the methods is provided in Figure 15; a more detailed description is provided in Chapter 1 (see Methodology overview).
FIGURE 15.
Systematic review methodology summary PRISMA flow chart.
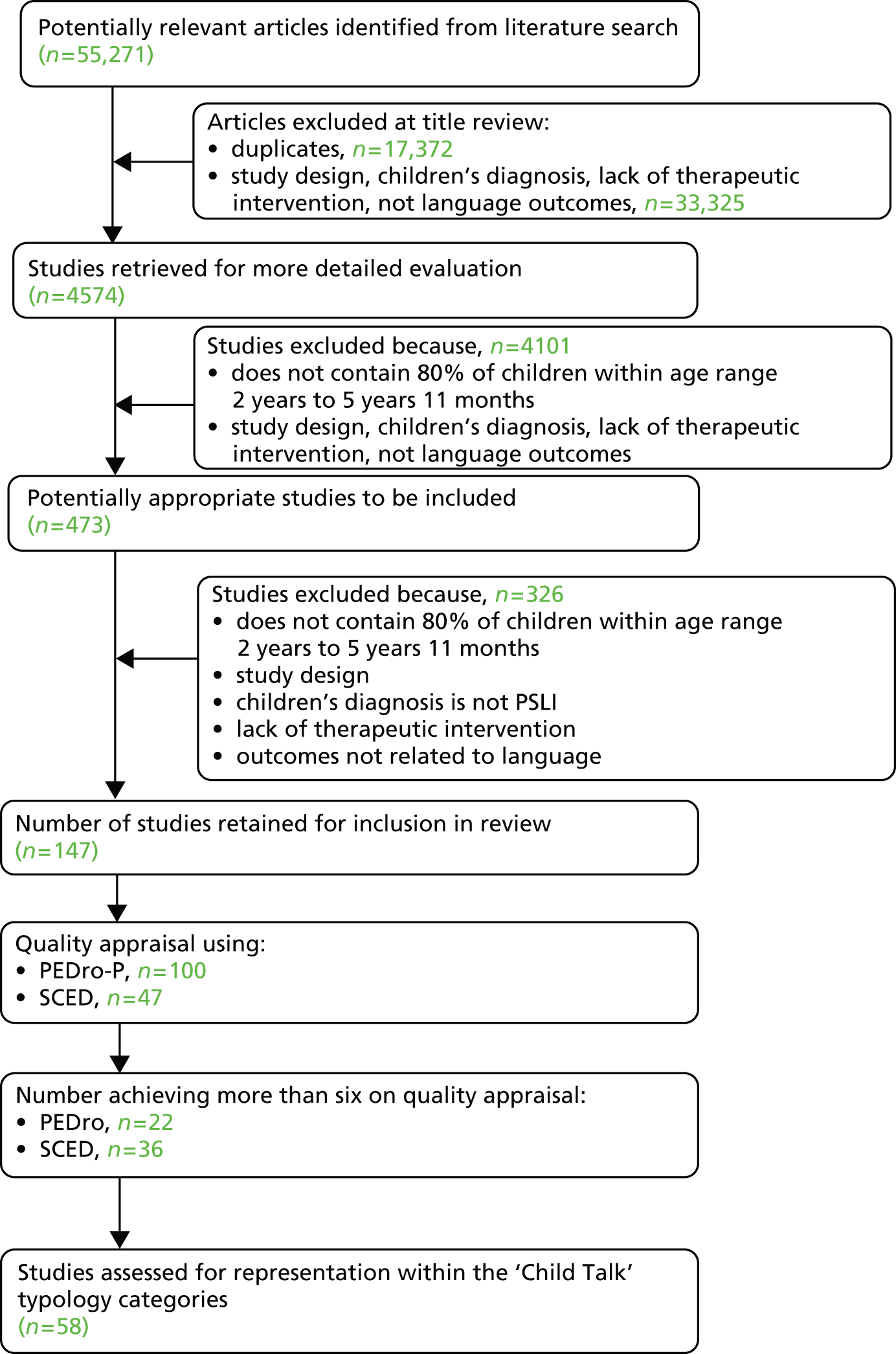
Findings
An extensive search of the published literature was undertaken to find publications reporting interventions used with preschool children with PSLI between the ages of 2 years and 5 years 11 months with at least one outcome measurement of speech or language. As demonstrated in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart (Figure 15), of 55,271 papers retrieved from the initial literature search, 147 studies were identified as being relevant and were included in a quality appraisal. Initial scrutiny of these showed a range of designs, including RCTs, quasi-experimental group designs and SCEDs. In light of this, two quality appraisal tools were used, the PEDro-P scale and the SCED scale, depending on the type of study. Following this quality appraisal 58 studies (56 papers32,70,134–187) were deemed to be of acceptable quality to include in this systematic review and map onto the speech and language therapy typology themes identified in Chapter 2 (see Study 2.1: identifying the themes of speech and language therapy practice).
Mapping the studies onto the typology themes
It was common for studies to address more than one of the typology themes (Table 45), for example ‘speech’ is represented within 33 of the retained studies139–169,171 and five of these studies were also included in the ‘expressive language’ theme,139,154,157,168,169 one in the ‘self-monitoring’ theme,154 17 in the ‘generalisation’ theme,138–140,144–147,149–152,154,157–159,164,167 one in the ‘adult understanding’ theme134 and one in the ‘adult–child interaction’ theme. 143
| Theme | Speech | Comprehension | Expressive language | Self-monitoring | Generalisation | Foundation skills | Functional communication | Adult understanding | Adult–child interaction |
|---|---|---|---|---|---|---|---|---|---|
| Speech | 33 | 0 | 5 | 1 | 17 | 0 | 0 | 1 | 1 |
| Comprehension | 0 | 6 | 5 | 0 | 3 | 0 | 0 | 0 | 2 |
| Expressive language | 5 | 5 | 28 | 1 | 10 | 4 | 5 | 1 | 8 |
| Self-monitoring | 1 | 0 | 1 | 2 | 2 | 1 | 1 | 0 | 0 |
| Generalisation | 17 | 3 | 10 | 2 | 26 | 2 | 2 | 0 | 0 |
| Foundation skills | 0 | 0 | 4 | 1 | 2 | 4 | 3 | 0 | 0 |
| Functional communication | 0 | 0 | 5 | 0 | 2 | 3 | 5 | 0 | 1 |
| Adult understanding and empowerment | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 1 |
| Adult–child interaction | 1 | 2 | 8 | 0 | 0 | 0 | 1 | 1 | 9 |
Table 46 presents the numbers and ages of child participants in the studies by theme. Although the differences are small and there is overlap, studies addressing parent–child interaction and adult understanding tend to be conducted with slightly younger children and those relating to phonology and articulation (speech) tend to be conducted with those at the upper end of the age range.
| Theme | Number of studies in theme | Total number of children in the studies | Mean (median) number of children per study | Mean (range) age (months) |
|---|---|---|---|---|
| Speech | 33 | 542 | 16.4 (4.0) | 51.6 (32.0–66.0) |
| Comprehension | 6 | 135 | 22.5 (27.0) | 40.0 (27.5–50.0) |
| Expressive language | 28 | 923 | 32.9 (18.0) | 43.2 (25.0–66.0) |
| Self-monitoring | 2 | 11 | 5.5 (5.5) | 51.8 (43.0–60.0) |
| Generalisation | 26 | 210 | 8.1 (3.0) | 50.7 (35.0–66.0) |
| Foundation skills | 4 | 59 | 14.7 (7.0) | 44.6 (37.0–60.0) |
| Functional communication | 5 | 82 | 16.4 (6.0) | 48.1 (42.0–54.0) |
| Adult understanding and empowerment | 1 | 4 | – | 57.5 (48.0–67.0) |
| Adult–child interaction | 9 | 1011 | 112.3 (36.0) | 35.9 (25.0–57.5) |
As would be expected, a number of studies fall into two or more categories, demonstrating that the intervention comprises more than one component. Across the nine categories, the largest group of papers was in the ‘speech’ theme [32 papers139–169,171 (33 studies)]. This was followed by ‘expressive language’ with 26 papers70,134,135,137–139,154,157,168–170,173–187 (27 studies), ‘generalisation’ with 24 papers138–140,144–147,149–152,154,157–159,164,167,170,172–174,178,179,187 (24 studies), ‘adult–child interaction’ with nine papers,134,136,137,143,175–177,182 ‘comprehension’ with seven papers,32,169,172–176 ‘functional communication’ with five papers,137,138,170,184,185 ‘foundation skills’ with four papers,70,138,170,185 ‘self-monitoring’ with two papers138,154 and finally ‘adult understanding’ with one paper. 134
In total, 52 of the studies recruited child participants who had a language impairment. 32,70,134,139–176,178–187 Two of the studies recruited children either with a language impairment or who were at risk of developing a language impairment. 32,134 Four studies recruited children ‘at risk’ of language delay/impairment. 135–138
The findings from the systematic review will now be discussed in detail in relation to each typology theme.
Speech
In total, 32 papers139–169,171 (33 studies) are included in this theme, which looks at work that aims to increase the accuracy of speech production or articulation, often focusing on specific sounds.
What was the focus of the studies?
Of the total of 33 studies included in this review, 26 have change in a child’s speech sound system as either their primary or their secondary focus. 140,144–159,161–167,169 For 25 studies, change in the sound system was the primary focus; for the remaining study,139 change in the sound system was an additional focus. Specifically, the primary focus was change in word-finding skills and measurement of change in the speech sound system was carried out as a by-product of the intervention received. 139
Out of the remaining seven studies, one focused on change in prosody of speech rather than the speech sound system, specifically change in the stress pattern of multisyllabic words and sentences. 140 This study observed change in the spoken productions of stress patterns in multisyllabic words and phrases in children with speech and language impairment. Although this is a study of speech production, the focus is on speech prosody rather than the speech sound system and, as a consequence, this study is considered separately to the other 26 studies focusing on children’s speech sound systems.
The focus of the other six studies141–143,160,168,171 was change in a child’s phonological awareness skills following specific intervention targeting phonological awareness. In each study the participants had speech impairment, language impairment or both. In many cases, phonological awareness tasks are used in speech and language therapy intervention with children of preschool age to facilitate improvements in speech or phonological development in particular. These studies, therefore, were focusing on the changes observed in children’s phonological awareness when speech and language skills themselves are impaired. Phonological awareness tasks include activities such as rhyme identification and production, phoneme addition and deletion, phoneme segmentation and phoneme blending. In some cases they also include alphabetical tasks such as letter naming and nonsense word naming.
Country of origin of the papers
Of the 32 papers included, 22 were from the USA,139–159,170 five were from Canada,160–164 three were from Australia165–167 and two were from the UK. 168,169
Design
The most common research design was that of a case series [18 of the studies (in 17 papers139–145,148–150,152–154,158,165–167) employed a case series design]. These case series studies used a combination of multiple baselines, staggered starts and a crossover design. Four studies used a RCT design,157,162,163,168 five used a between-groups method,156,160,161,164,169 one used a single subject multiple baseline design,159 one used an alternating treatment design,147 three were case studies146,151,155 and one used a crossover design with multiple baselines. 171
Size of the sample
By nature of the study designs the sample sizes were typically small. Sample sizes ranged from 1146,151,155 to 159. 169 Ten of the studies had > 10 participants143,157,160–164,168,169,171 but the most common number of participants was two. The total number of children represented in this theme was 542, with a mean of 16.4 (median 4.0).
Child participant demographics
In this category all 33 studies recruited child participants with a language impairment (i.e. none was classed as ‘at risk’).
Not all of the studies reported the gender split of participants. Among the available data there were 170 boys and 62 girls across the studies in this theme. The average age of the participants across all 33 studies was 51.6 months, ranging from 32.0 months to 66.0 months. 141,169
Assessment measures
Speech measures
Measurement of speech in the 26 studies included in the review was carried out for one or more of three prime reasons:
-
to confirm eligibility for participation in the study
-
to identify targets for intervention
-
to measure change in response to intervention (outcome measure).
Clearly, measures are needed for all three reasons at the beginning of a study. In many cases, however, the same measure(s) is used for all three purposes. Further detail is provided in Table 47, which summarises the measures used by each study and whether or not they were used only to confirm eligibility and identify targets or whether they were also used as outcome measures.
| Published assessments | Spontaneous speech sample | Confrontation picture naming | Probe testing |
|---|---|---|---|
| HAPP/APP-R154,161a,162 | 147–149,151,153–155,157,162–164,166,167a | 146,150–152,166,167,169 | 144,145,151,153,155,156,159,161,167 |
| PPA158a | |||
| GFTA144,145,149,153,155,156,159,162–164 | |||
| DEAP165 | |||
| AAPS157 | |||
| PKP/PPKP147,149a,164 |
Measurement of speech output
Measurement of speech output generally consists of two phases: a speech sample collection phase and an analysis phase in which aspects of the sample are inspected on one or more of a number of different dimensions.
Table 47 lists the four approaches to collecting speech samples within the 26 studies that focus on change in the child’s speech sound system. Published assessments were used in a number of cases but often these were used only at the start of the study to confirm eligibility and identify targets.
As an alternative or additional measure, many studies used spontaneous speech samples. These were elicited through conversation, during play activities or while looking at pictures or storybooks. These samples were recorded and later transcribed. In most cases, reliability measures for the transcriptions were reported with point-to-point agreement between two transcribers being carried out. Although some studies used spontaneous speech samples purely for eligibility assessment and target identification, most used them as an outcome measurement.
Some studies used confrontation picture naming as the source of the speech sample. In some cases this was the prime sample used although in other cases it was supplemented with other samples such as published assessments or spontaneous speech samples. When confrontation picture naming was used it was always as an outcome measure, although it may also have been used to check eligibility and identify targets. This type of picture naming task required the child to name a range of pictures, which would enable the entire speech sound system to be sampled.
In contrast, several studies used picture naming as part of a probe-testing protocol. In these cases, specific probe items that related to the child’s targeted phoneme plus sometimes a control phoneme were identified and used to measure change only in these consonants or vowels. Probes were always used as outcome measures and enabled specific phonemes to be measured extensively. Sometimes probe words were elicited by imitation instead of picture naming. In addition, some studies reported measuring stimulability at the pre-intervention stage to confirm eligibility or identify targets.
The second phase of measurement of speech output requires some sort of analysis of the speech sample. There are many possible ways to carry this out depending on the specific area of change that is anticipated as a result of the intervention.
Published assessments contain their own analysis within their protocols. These analyses include process analysis [Hodson Assessment of Phonological Patterns (HAPP), phonological process analysis], phonemic or phonetic inventories (Phonological Knowledge Profile/Productive Phonological Knowledge Profile), percentage phonemes correct, including either or both of percentage consonants correct and percentage vowels correct [Diagnostic Evaluation of Articulation and Phonology (DEAP)] and accuracy of production [Goldman–Fristoe Test of Articulation/Arizona Articulation Proficiency Scale (GFTA/AAPS)].
When spontaneous speech samples, confrontation picture naming or probe lists are used, a number of possible analyses can be carried out, each of which measures levels of accuracy of speech. Box 7 lists these and the studies that have used them. As with Table 47, when the analysis has been used purely to determine eligibility or identify targets this is indicated. In many cases more than one type of analysis has been used on the speech sample as a measure of outcome.
-
Phonetic or phonemic inventory. 144,146–153,155,158,166,167a
-
Percentage phonemes correct (including consonants or vowels). 154,155,157,162–167b
-
Production accuracy of targets or probes. 144–147,149–153,155,156,158,159,164,167,169
-
Inconsistency. 165
-
Intelligibility. 166
-
Acoustic analysis. 155
Only used pre intervention to determine eligibility and/or identify targets for intervention; not used for outcome measurement.
Percentage phonemes correct was calculated on a connected speech sample for all studies listed with the exception of that by McIntosh and Dodd168 in which it was calculated on a single word sample from a picture naming task.
Measurement of speech perception
Although change in speech output was the ultimate goal in all of the 26 studies, three studies were also interested in measuring change in speech perception. This was because the theory behind these interventions linked change in speech output to changes or skills in speech perception. The three studies labelled their speech perception tasks as a word identification test,161 a sound identification test156 and a phonemic perception test. 163 However, all three used the same computer system to measure skill in this area [the Speech Assessment and Interactive Learning System (SAILS) program161] and therefore all three tasks were either the same or very similar. All three studies also measured change in speech output as seen in Table 47.
Measurement of phonological knowledge
Studies that focused exclusively on phonological awareness have not been included in this summary but those studies that measured phonological knowledge or awareness in relation to speech output are included. Two studies looked at this. One considered participants’ phonological knowledge at the pre-intervention stage to describe the participants in each of two groups receiving different interventions. 144 The measure was not repeated post intervention. The other study measured change in phonological awareness pre and post intervention alongside measures of speech output. 163
Measurements used in the study of stress patterns in speech
Eligibility assessment included a published test of single word speech production using picture naming [Bankson–Bernthal Test of Phonology (BBTOP)],194 a published test of language ability [Preschool Language Scale-3 (PLS-3)]195 and collection of a spontaneous speech sample that was recorded, transcribed and analysed in terms of grammatical structure. 195 Speech output using data from the picture naming test was analysed in terms of phonetic inventory, accuracy and processes. Percentage consonants correct was also calculated but it is not clear whether this was calculated on the single word picture naming test or the conversational speech sample.
Outcomes in response to intervention were measured separately using study-specific probes consisting of a total of 26 multisyllabic words and 18 target phrases that would permit the production of the required stress pattern being targeted in the sessions. A subset of the full list of probes was administered repeatedly before intervention, throughout the sessions and at the end of treatment. Picture and object naming stimuli were used to elicit the probes.
Measurements used in the phonological awareness studies
In contrast to the measures used in the speech sound studies, in which assessments used to determine eligibility or target selection were also often used for outcome measurement, assessments in the phonological awareness studies tended to be used for one or other purpose rather than both.
Across all six studies,141–143,160,168,171 measures of language ability (receptive and expressive) and non-verbal cognition were routinely assessed or included as part of the eligibility criteria. Participants either were English monolingual children or used English as their dominant language and they had intact oral musculature structure and function and no known sensory or neurological difficulty. Further assessment was carried out in some of the studies to determine eligibility. Specifically, these assessments were of reading and spelling,142,160 memory,142 phonological awareness142 and speech. 141,168 When these skills were formally assessed for eligibility, a range of published assessments was used. Participants in some of these studies included children with language delay rather than speech delay. In these cases language assessments were used to determine eligibility. This contrasts with the speech sounds system studies in which children with language impairment were excluded. Box 8 summarises those tests used to determine eligibility.
-
Language: Peabody Picture Vocabulary Test,142 Expressive Vocabulary Test,142 Structured Photographic Expressive Language Test (SPELT),141,171 DLS,141 Clinical Evaluation of Language Fundamentals – Preschool,160,168,171 Test of Language Development – Primary, 3rd edn (TOLD-P:3). 143
-
Reading: Test of Early Reading Ability, 2nd edition,142 British Ability Scales – word reading,168 Test of Preschool Early Literacy – Print Knowledge,160 Get Ready to Read. 171
-
Spelling: British Ability Scales – word spelling. 168
-
Phonological awareness: Sound Blending subtest of Woodcock–Johnson III tests – Revised – test of cognitive abilities,142 phonemic analysis subtest of TOLD-P:3. 142
-
Memory: Test of Auditory Perceptual Skills – Numbers Forward (TAPS/NF). 142
-
Visual perception: Test of Visual Perceptual Skills. 141
-
Non-verbal cognition: Kaufman – Assessment Battery for Children,141 British Ability Scales II,168 Kaufman Brief Intelligence Test, 2nd edition,143,160 Standford-Binet. 171
In addition, some study-specific tasks were designed for use in individual trials. Rhyme production and spelling were used in one study142 and in another study a language sample was collected and the mean length of utterance (MLU) calculated. 141
Tasks used for outcome measurement tended to be more specific and to be related to the intervention provided. Those used included subtests from published assessments and study-specific tasks as listed below:
-
study-specific probe measures for rhyming, sound segmentation and sound blending142
-
study-specific probe measures for recognition and production of letter names and sounds, specific to each child141
-
study-specific tasks of phoneme addition and phoneme deletion168
-
Preschool and Primary Inventory of Phonological Awareness (PIPA),196 – subtests of alliteration awareness, phoneme isolation and phoneme segmentation168
-
Test of Preschool Early Literacy (TOPEL),197 subtest of phonological awareness160
-
Dynamic Indicators of Basic Early Literacy Skills (DIBELS)198 subtests of initial sound fluency, letter name fluency, phoneme segmentation fluency, nonsense word fluency160
-
rhyme identification from the Rhyme Individual Growth and Development Indicator171
-
alliteration identification from the Alliteration Individual Growth and Development Indicator171
-
rhyme awareness subtest of the Phonological Awareness Literacy Screening (PALS)143,200 measure.
The common denominator in all of these outcome measures is that change in phonological awareness is measured rather than change in speech output or change in language ability.
Delivery of the interventions
For studies in the area of speech production or articulation there was relatively little variation in who delivered the interventions and where they took place. In all but 5 of the 33 studies, the intervention was delivered by a SLT. In those five studies the intervention was carried out by a combination of SLT and parent,143 a research assistant,163 educators and paraprofessionals160,171 and a graduate student SLT. 144 Twenty-three studies were undertaken in a clinic setting. 146,148,151–159,161–164,168,171–175 One was carried out in the home context,143 one was split between the clinic and preschool169 and another four were carried out purely in a preschool context. 141,154,160,171 The remaining four studies did not state where the intervention was undertaken. 139,159,161,164
Number of treatment sessions
It is difficult to make comparisons across all 33 studies of the number of treatment sessions. The information detailed across the studies is not uniform but overall the interventions were most likely to be delivered either twice a week (seven studies145,146,154–156,165,167) or three times a week (nine studies141,142,147,148,151,152,157,159,171). The duration of an intervention varied from 30 to 60 minutes. The lowest number of sessions delivered was just six,161 with most studies reporting 10–120 sessions. The longest intervention lasted for 9.5 months; in this study a child was seen 67 times. 158 In most of these studies the number of treatment sessions also varied from one child to the next as the intervention was stopped once a child reached 50–90% generalisation on the probes.
Comparison with speech and language therapists’ practice
Table 48 shows the activities and strategies identified by SLTs who participated in the Child Talk focus groups as being ways of working or elements of practice that they use with children with PSLI. It also shows how essential to working on improving speech these interventions are, as rated by SLTs participating in consensus group events (SIG) (see Chapter 1, Methodology overview). Finally, Table 48 shows how many of the studies included in the review used each of these interventions.
| Intervention | SLTs ranking activity/strategy as essential, n (%) | Frequency used in studies |
|---|---|---|
| Building things into a game/making it fun | 46 (98) | 4 |
| Providing feedback | 42 (89) | 7 |
| Adopting a hierarchy (e.g. C, CV, CVC) | 40 (87) | 1 |
| Using repetition | 40 (85) | 4 |
| Making sounds | 37 (79) | 3 |
| Encouraging self-monitoring strategies | 31 (67) | 0 |
| Minimal pairs | 29 (63) | 7 |
| Traditional phonology therapy | 21 (54) | 1 |
| Picking from lots of different areas | 20 (49) | 0 |
| Jolly Phonicsa | 20 (43) | 0 |
| Fishing game | 18 (42) | 0 |
| Cued articulation | 13 (28) | 0 |
| NDP | 9 (19) | 0 |
| Cycles therapy | 7 (17) | 0 |
| Oromotor work | 6 (13) | 0 |
| Metaphon programme | 6 (13) | 0 |
| Maximal pairs | 3 (7) | 2 |
| Gap Houseb | 0 (0) | 0 |
None of the SLTs specifically mentioned use of picture cards or computer-based programmes but these could also have been classed as fun activities and some of the studies that explained the computer-based programmes detailed built-in feedback within the computer games.
Other interventions mentioned in the studies but not by therapists in the research programme were:
-
core vocabulary165
-
giving an auditory model for the student to imitate144–147,149–153,159,164
-
correcting the child’s errors (corrective modelling)144,145,152,157
-
spontaneously saying words containing the target sound147,149–153,159,164
-
contrasting supralaryngeal and laryngeal distinctives153
-
focused stimulation of key words154
-
adult cues, for example descriptions of sounds (long sound, etc.)154
-
broad target recasts157
-
cuing for word retrieval139
-
speech perception training161
-
teaching prosodic patterns (big and little)140
-
auditory bombardment. 140
Evidence of outcomes
Overall, the outcomes were mixed in terms of evidence of positive change. Five studies reported no positive changes/differences between different interventions,143,151,156,158,169 for example it was suggested that minimal pairs treatment was not successful for the children in that study. 158
When positive change was reported, studies found that the following was observed: phonemic expansion,148 greater phonological awareness,142 improved rhyme production,171 increased intelligibility,157,165 improved articulation accuracy,163 greater consistency of word production165 and improved phonemic perception. 163
Success was achieved through a computer-driven speech perception training programme, provided concurrently with sound production training,163 a rhyming module of a phonological training intervention in combination with systematic training in the alphabetic principles,142 a rhyme intervention,171 a maximal opposition approach (two studies),146,147 broad target recast,157 targeting segmental compositions of individual children148 and development of core vocabulary. 165
Comprehension
Seven papers representing seven studies are included within this theme of the typology. 32,169,172–176
What was the focus of the studies?
All seven studies assessed children’s comprehension as an outcome. Five of the seven studies targeted children’s comprehension in addition to other aspects of language. 169,172,173,175,176 Only two studies targeted children’s comprehension specifically. 32,174
Country of origin of the papers
Of the seven papers included in this theme, three were undertaken in the USA32,172,173 and four were undertaken in the UK. 169,174–176
Design
Four studies used a RCT methodology,32,169,174,175 two used a case series design with multiple baselines172,173 and one was a cohort study with pre and post measures. 176
Size of the sample
In total, 294 children were represented by the seven studies in this theme. Study sample size ranged from 2 to 159, with a mean of 22.5 and a median of 30.0.
Child participant demographics
One study recruited children who were either language impaired or at risk of language impairment. 32 The other studies in this category all recruited children who were language impaired. In total, 195 boys and 68 girls were specified as participating in the studies, with an additional 36 children not having their gender reported. The mean age of the children was 40 months (range 27.5–50.0 months).
Assessment measures
Sixteen different measures were used across the studies. Eleven of these measures were used only once and many did not assess comprehension. Of the comprehension measures used, only three were used in more than one study: the Peabody Picture Vocabulary Test (PPVT),201 the Preschool Language Scale (PLS)202 and the Reynell Developmental Language Scales (RDLS). 203
Outcome measures
Twenty-one different outcome measures were used across the studies in this theme; however, only one measure of comprehension (RDLS) was used twice.
Delivery of the interventions
Two interventions in this typology was delivered by a SLT,169,172 two were delivered by both a SLT and parents,174,176 one was delivered by a parent alone following parental training by SLTs,175 one was delivered by trained research assistants32 and one is reported to have been delivered by a clinician but it seems likely that this person was a SLT. 173
A range of settings was used across the studies. One study specifically stated that therapy was undertaken in a community clinic169 and another reported that therapy was undertaken in ‘a clinic’;173 the other studies took place in a Head Start centre,32 the home175 and preschool/nursery and the home,174,176 with one study not specifying the location (given the nature of the study it is likely to have taken place in a clinic setting). 173
Number of treatment sessions
The number of treatment sessions ranged from 8 to 78, with these usually being delivered over a 3- to 6-month period. Studies reported that sessions lasted between 15 and 75 minutes. Comparison between studies that focus on comprehension alone and those that include production is difficult. Comprehension-focused studies included from 30 to 40 comprehension sessions whereas those studies that included a focus on production included fewer sessions (16 sessions of 15 minutes over 8 weeks, i.e. twice a week).
What was the intervention?
The types of intervention varied across studies, for example two studies involved picture activities,172,173 one involved a book-sharing activity,32 two involved a range of games and therapy techniques174,175 and one focused on parent–child interaction. 176 The remaining study was a pragmatic RCT and stated that the children in the therapy group ‘received the one-to-one speech and language therapy routinely offered by the therapist . . . and tailored to their individual needs’ (p. 2). 169
Comparison with speech and language therapists’ practice
Table 49 shows the activities and strategies identified by SLTs who participated in the Child Talk focus groups as being ways of working or elements of practice that they use with children with PSLI. The table also shows how essential to working on children’s comprehension these interventions were judged to be by SLTs participating in consensus group events (see Chapter 1, Methodology overview) and how many of the studies included in the review explicitly mentioned using each of these interventions.
| Intervention | SLTs ranking activity/strategy as essential, n (%) | Frequency used in studies |
|---|---|---|
| Following instructions | 38 (84) | 4 |
| Modelling one word level by labelling things | 36 (80) | 3 |
| Modelling correct choice | 32 (76) | 1 |
| Instructions in play | 34 (76) | 1 |
| Providing choices | 34 (76) | 2 |
| Comprehension games | 30 (73) | 2 |
| Word-level activities | 32 (71) | 2 |
| Gradually building up word levels | 32 (71) | 2 |
| Selecting objects | 30 (70) | 2 |
| Derbyshire activitiesa | 22 (49) | 0 |
| Word categorisation | 19 (43) | 1 |
| Grouping vocabulary | 18 (41) | 0 |
| Turn taking | 17 (40) | 0 |
| Barrier games | 15 (38) | 0 |
| DLS | 16 (36) | 1 |
| Grammatical structures | 14 (32) | 1 |
| Targeting specific speech sounds | 4 (10) | 0 |
Evidence of outcomes
All studies reported improvements in aspects of children’s language. Six of the seven studies saw improvements in comprehension32,169,173–176 and one reported evidence of generalisation from children’s comprehension skills to production skills. 172 Comprehension was seen to improve when the intervention was delivered by parents and also when it was delivered through direct speech and language therapy; between-group differences were found when control groups consisted of ‘no intervention’ but when intervention groups were compared with groups receiving speech and language therapy in a different form then comprehension improvements tended to be comparable in both groups.
Expressive language
In total, 26 papers (27 studies) were included in this theme,70,134,135,137–139,154,157,168–170,173–187 which looked at work that aimed to improve children’s expressive language, in quantity, vocabulary or structure.
What was the focus of the studies?
Although these 27 studies have been grouped together under the theme of ‘expressive language’, the detailed foci of the studies varied. Foci included working on specific aspects of expressive language (e.g. syntax, utterance length, vocabulary) and training parents to support their children’s language development. Of these 27 studies, 25 included interventions to improve expressive language as the primary focus of the study. 70,135,137,139,154,157,169,170,173–187 For two studies,134,168 expressive language was a secondary focus of the study. The following list shows the various expressive language foci:
-
expressive and/or receptive language (10 papers representing 11 studies70,134,135,175,176,177–181)
-
parental intervention for language delay (one study174)
-
phonological awareness (one study168)
-
teaching syntax (one study154)
-
phonology and utterance length (expressive language) (one study157)
-
operant conditioning for non-verbal/minimally verbal children (one study187)
-
language and phonology (one study169)
-
word-finding difficulties (one study139).
Country of origin of the papers
Fifteen papers in this theme were from the USA,134,135,137–139,154,157,170,173,181,183,184,185–187 seven were from the UK,70,168,169,174–176,179 two were from Canada,180,182 one was from Korea178 and one was from Germany. 177
Design
A case series multiple baseline design (n = 5134,139,178,179,183) was the most common study design chosen for the studies that fell into this theme, followed by a RCT design (n = 5157,168,174,175,177). The following study designs were also used: case series (n = 1154), multiple baseline across dyads (n = 4138,170,184,185), single-subject alternating treatment design (n = 1181), pre/post between groups (n = 4135,176,180,182), between groups (n = 370,175,186), case study (n = 1187), between groups, both comparison (n = 2137,169) and between subjects with a crossover treatment design (n = 1173).
Size of the sample
The total number of child participants across all of the studies in this theme was 913. In total, 13 studies had < 10 participants. 134,138,139,154,170,173,178,179,181,183,184,185,187 However, overall, the sample size in this theme was relatively large compared with that in the other categories, with the mean number of children per study being 32.6 (median 15.5 children per study).
Child participant demographics
Of the 27 studies (26 papers), only three studies recruited ‘at-risk’ children,135,137,138 with one study recruiting both children at risk and those with a language impairment. 135 The remaining studies all recruited children with existing language impairment. A number of the studies do not report the gender of the child participants. However, when recorded, there were 257 boys and 154 girls; thus, gender was not provided for 502 participants. The mean age of the child participants was 43.1 months, with a range of 25.0–66.0 months.
Assessment measures
The total number of different assessment measures used across all of the studies in this theme was 71, with 22 of these being identified as appropriate for use as a measure of expressive language.
The three most commonly used assessments that measure expressive language were MLU (n = 10154,157,175,176,178,179,181,182,186), the Preschool Language Scale-3 UK Edition (PLS-3-UK) (n = 8134,138,157,169,170,173,176,185) and the RDLS (n = 470,174,175).
Outcome measures
The total number of different outcome measures used across all of the studies in this theme was 72, with 26 being identified as appropriate for use as a measure of expressive language.
The most commonly used outcome measures to evaluate changes in expressive language were MLU (n = 13138,154,157,170,175,176,178,179,181,182,185,186) and measures of specific expressive language parameters (rate of noun use, number/mean of different words) (n = 8134,135,137,169,173,174,181,182).
Studies that were included in this theme frequently targeted other skills, such as functional communication, speech and generalisation, and frequently measured these other aspects of speech and language too, such as receptive vocabulary using the Peabody Picture Vocabulary Test – Revised (PPVT-R)204 (n = 4134,139,180,183) and the comprehension scale of the RDLS (n = 470,174,175).
Delivery of the interventions
Eleven of the studies stated that a SLT carried out the intervention. 70,139,154,157,168,169,178,180,183,186,187 In four studies it was a combination of a SLT and a parent,174–176,177 in three studies it was a parent alone134,175,182 and in three studies it was a teacher. 170,179,185 Other studies reported that the intervention was carried out by a researcher acting as a teacher,138 EYPs working with parents,137 an assistant SLT184 and graduate student ‘clinicians’181 and that training to teachers was delivered by SLTs,135 with one study stating that the intervention was delivered by a ‘clinician’ but giving no further details. 173 Five of the studies were carried out in a preschool or nursery environment,70,135,178,179,186 five studies were carried out at a child development/Head Start centre,137,138,170,184,185 five were carried out in a speech and language therapy clinic157,168,173,186,187 and a further study was carried out at both a clinic and a preschool. 169 Two studies were carried out within the home environment134,175 and a further three were carried out at both home and at a preschool/nursery. 174–176 Not all of the studies stated where the intervention was carried out.
Number of treatment sessions
There are a large number of studies in this theme and therefore summarising the number of treatment sessions that the children received is not straightforward. In some cases the studies described long-term interventions, for example there was a 3-month programme,181 a 4-month programme182 and one study took place over an entire academic year. 135 At the other extreme a few studies described an intervention taking place over 12 sessions that were delivered twice weekly (e.g. Gallagher and Chiat174). The duration of the sessions varied from 30 to 75 minutes. Finally, some studies described home-based parent training interventions in which the interventions were delivered at least in part by parents (e.g. Gibbard175); these were more individualised in terms of the number and duration of ‘sessions’.
What was the intervention?
This section summarises what took place during the interventions that fall into the ‘expressive language’ theme. Approaches included modelling (n = 9137,169,174,176,177,181,182,184,186), imitation (n = 4173,174,176,178), targeting specific phrases (n = 1138) and sentence recasting (n = 1174).
In terms of materials used during the interventions, the use of picture books or storybooks was commonly mentioned in the studies (n = 6134,135,138,174,177,183), as was a more general use of pictures (often cards) (n = 4154,173,184,187). Toys and play materials were also frequently used (n = 9135,138,169,170,180,182–184,185). These were varied and included dramatic play toys (e.g. kitchen, grocery store and hospital), role-play materials (e.g. clothing, objects) and manipulative toys (e.g. cars, blocks, trains). These items were commonly used for listening tasks and talking tasks and were also used by children to give instructions to other children or to other toys. In some cases the toys were not part of the intervention but were used during the session as a reward.
Parents were also commonly involved in the interventions described (n = 7134,137,174–176,177,182). Examples of how parents were involved included encouraging sharing of picture books,177 introducing parents to language modelling techniques176 and assignment of home practices. 174,183 Feedback was sometimes given to parents through home visits and/or by using videotapes of the child and mother during free play. 176
Reinforcement was frequently integrated into the interventions. Positive reinforcement was given in the form of verbal praise (n = 5138,154,178,186,187), correct responses were reinforced with the stimulus requested (n = 1;187 tokens were given for correct responses with tokens being able to be redeemed for a reward such as ‘playtime’) and, as indicated above, in some studies toys and games were available after the children had performed the therapy task. 173,187 Negative reinforcement was also used (n = 2178,187), for example inappropriate responses were punished continuously by presenting the verbal stimulus ‘no!’ and concurrently withdrawing the stimulus picture for a brief period and avoiding eye contact187 and by partial responses and a request to the child to repeat. 178
Comparison with speech and language therapists’ practice
Table 50 provides details of the strategies and activities mentioned by the SLTs who participated in the Child Talk focus groups in relation to work that aims to improve the children’s expressive language, in quantity, vocabulary or structure. The table also provides the percentage of SLTs ranking each intervention as essential and how many of the studies included in the review explicitly mentioned using each intervention.
| Intervention | SLTs ranking activity/strategy as essential, n (%) | Frequency used in studies |
|---|---|---|
| Encouraging the child | 44 (96) | 8 |
| Extending phrases | 43 (93) | 1 |
| Modelling | 41 (89) | 9 |
| Building things in to play | 41 (89) | 13 |
| Providing choices | 38 (83) | 0 |
| Expressive language games | 34 (77) | 2 |
| Holding the child’s attention and making language the important bit | 28 (67) | 1 |
| Word-level activities | 29 (63) | 1 |
| Improving parent–child interaction | 29 (63) | 1 |
| Using words in different contexts | 27 (59) | 1 |
| Singing, doing action songs | 23 (50) | 0 |
| Grouping vocabulary | 23 (50) | 0 |
| Selecting objects | 21 (49) | 0 |
| Building anticipation | 18 (41) | 0 |
| Turn taking | 17 (40) | 1 |
| Sentence Buildera | 15 (33) | 0 |
| Following instructions | 13 (31) | 4 |
| Having themed weeks, e.g. certain vocabulary | 12 (27) | 3 |
| DLS | 12 (27) | 1 |
| Small world activities | 11 (26) | 0 |
Evidence of outcomes
Overall, the studies that looked at work that aimed to improve children’s expressive language, in quantity, vocabulary or structure, report fairly positive outcomes. As the studies had varied aims, comparison is difficult (e.g. some of the studies aimed to examine differences between different types of interventions), but overall only three of the studies reported no improvement in language for the child participants. 135,169,183
In summary, despite numerous different approaches to intervention, the interventions when grouped together led to a reduction in word-finding substitution,139 an increase in social communication behaviour,138 an increase in the use of verbal behaviours and target vocabulary words,138 improved expressive language skills,175 an increased amount of child talk during play,185 an increase in the number of requests and descriptive talk and an increase in the complexity and diversity of language. 185
In terms of working with parents, the studies demonstrated mixed outcomes. Successful outcomes were achieved through increasing the number of interactions between a mother and her child, which in turn led to increases in the child’s vocabulary and grammatical complexity. 182
Some studies reported that not all of the participants benefited from the intervention. As the sample sizes were generally small this could mean that, for example, two out of three children showed improvement (e.g. Hart and Gonzalez154).
In some studies a comparison was made between two different approaches to therapy, for example in one study significantly more children improved in a ‘phonological awareness’ group than in a ‘language stimulation’ group. 168
Self–monitoring
Only two studies were represented in this theme. 138,154 Both of these studies contained elements that required the child to self-monitor, although this was not explicitly the main aim of the interventions, nor is it commented on or used as a justification (or mode of action) for the interventions. Both of these studies are included in the ‘expressive language’ and ‘speech’ themes.
With only two studies, and with the difference in the use of assessment and outcome measures between the two studies, comparisons between the interventions and assessments of their success were difficult.
Country of origin of the papers
Both papers representing this aspect of the typology were undertaken in the USA.
Design
One study consisted of three case studies154 and the other used a between-group study design with four dyads. 138
Size of the sample
The total number of child participants across the two studies was only 11 (eight in one study138 and three in the other154).
Child participant demographics
It should be noted that, although the studies in this category all recruited children with a language impairment, one study recruited children who were at risk of impairment. 138 The gender split was not detailed in either of the studies. The average age of the participants across both studies was 51.8 months, ranging from 43 months to 60 months.
Assessment measures
Five different assessment measures were used in this typology, with each one used only once; none of them measured self-monitoring:
Outcome measures
Nine different outcome measures were used in this typology, with each one used only once; none of them measured self-monitoring:
Delivery of the interventions
One of the studies described interventions undertaken by a researcher acting as the teacher138 and the other study was undertaken by SLTs. 154
Both studies were conducted in preschool settings. One was reported as being a Head Start centre, suggesting that this study was undertaken in an economically deprived area. 138
Number of treatment sessions
In the study by Stanton-Chapman et al. 138 there were 12 individual treatment sessions, delivered twice weekly for 30 minutes. In the study by Hart and Gonzalez, three to four 20-minute sessions were delivered per week. 154 The first dyad had 16 sessions, the second had 14 sessions and the third had 12 sessions. 154 With only two studies represented in this theme of the typology, a comparison of the number of treatment sessions delivered across studies is of limited value.
Comparison with speech and language therapists’ practice
Interventions (whole and individual activities and strategies) used in the studies were mapped against the activities and strategies provided by SLT participants from the Child Talk focus groups and online surveys. Table 51 shows which interventions were ranked as essential within consensus group events (SIGs) and how many of the studies used each of these interventions.
| Intervention | SLTs ranking activity/strategy as essential, n (%) | Frequency used in studies |
|---|---|---|
| Using reward systems, e.g. tokens for correct production | 31 (67) | 0 |
| Providing something visual | 29 (63) | 2 |
| Self-monitoring using minimal pairs | 24 (52) | 1 |
| Articulation placement cues | 23 (50) | 0 |
| Cued articulation | 15 (33) | 1 |
| Talking about loud sounds and quiet sounds | 12 (26) | 0 |
| Syllable counting | 10 (22) | 0 |
| Rhyming | 6 (13) | 0 |
| Metaphon programme | 5 (11) | 0 |
In addition to the interventions in Table 51, the two studies used other activities and strategies:
Evidence of outcomes
There is preliminary support for the effectiveness of communication-centred approaches in facilitating change in children’s phonological system. 154 However, neither study provided any theory or suggestion of how self-monitoring helps this to happen. Peer-directed interventions were generally effective in increasing social communication behaviours of children who had fewer social interactions at baseline. 138 Because of the different aims of the studies included in this theme (i.e. phonology, social interaction), it is not possible to draw conclusions as to the effectiveness of self-monitoring.
Generalisation
In total, 24 papers (24 studies) are included in the typology theme ‘generalisation’. 138–140,144–147,149–152,154,157–159,164,167,170,172–174,178,179,187 These studies contain a facet that looks at generalisation as defined by the typology. However, only 12 studies have ‘generalisation’ as the main focus. 138–140,146,152,157–159,170,172,178,187 These studies, at least in part, aimed to investigate gains in therapy sessions that were transferable to outside of the therapy environment. Thus, this theme does not stand alone, with all included studies also being included in another theme.
What was the focus of the studies?
Although each of these studies included ‘generalisation’ in the research design, the overall focus of each of the studies was more varied. The 12 studies with a main focus on generalisation are detailed below:
-
Comprehension treatment using cards. 172
-
Effects of a multicomponent intervention, implemented in a play context, which aimed to improve children’s social–communicative interactions. 170
-
Maximal oppositions. 146
-
Acquisition of word-initial three-element clusters. 152
-
Intervention to learn the correct use of three pronouns and the verb form ‘are’. 187 The target behaviours were trained individually and positively reinforced when correctly used, or modelled, with children punished for inappropriate responses.
-
An intervention with two parts: (1) a script-based intervention in which individualised targeted semantic constructions were trained and (2) generalisation of semantic changes. 178
-
Investigation of the effects of a multicomponent intervention strategy to increase peer-directed social communication. 138
-
Treatment designed to facilitate both sentence length and speech intelligibility. 157
-
Investigation of how phonological information contributes to the effectiveness of treatment. 139
-
Minimal pairs treatment. 158
-
Articulation – effectiveness of treatment with repeated probes. 159
-
The effect of a prosodic intervention on children’s metrical patterns. 140
Country of origin of the papers
The dominance of research based in the USA in relation to encouraging generalisation is striking. Of the 24 studies included in this typology, 20 were from the USA,138–140,144–147,149–152,154,157–159,170,172,173,179,187 one was from Australia,168 one was from South Korea,178 one was from the UK174 and one was from Canada. 164
Design
Fourteen studies used a case series design (including multiple baseline, staggered start, multiple baseline; single subject design with staggered baseline; multiple baseline alternating crossover design). 138–140,144,145,150,152,154,158,167,170,172,178,179 Case studies were used three times (using an AB design or multiple baselines). 146,151,187 Other designs included RCTs,157,174 alternating treatments,147 an across-subject staggered multiple baseline design,149 a between-group design,164 a single subject multiple baseline design159 and between subjects with a crossover treatment design (including multiple baseline measures). 173
Size of the sample
In total, 204 children were represented across the 24 studies. Only three studies had > 10 participants, with 24 participants,174 48 participants164 and 52 participants. 157 The mean number of children per study was 8.5, with a median of 3.5 per study.
Child participant demographics
It should be noted that, although the studies in this category all recruited children with a language impairment, one study also recruited children who were at risk of impairment. 138 Four of the studies did not provide information that could be used to identify the gender of the participants. Of the remaining studies, there were 73 male and 23 female participants. The age range of children across the studies was 35.0–66.0 months, with an average age of 50.8 months.
Assessment measures
Across the 24 studies, 53 different assessment measures were used. The most frequently used assessment measures relevant to generalisation were MLU, used seven times,140,147,157,167,172,178,179 and percentage consonants correct, used four times. 140,144,157,167
Outcome measures
Seventy-seven different outcome measures were used across the 24 studies, with 71 being used in only one study. The majority of the outcomes reported across the studies were not relevant to generalisation. The only two outcome measures used four or more times were MLU157,170,172,178,179 and percentage consonants correct,144,157,164,167 and when used pre and post intervention these are appropriate measures to evaluate ‘generalisation’.
Delivery of the interventions
In 18 of the 24 studies the intervention was delivered by SLTs;139,140,145–147,149–152,154,157–159,164,167,172,178,187 of the other studies two were delivered by teachers,170,179 one by a clinician,192 one by a graduate student SLT,144 one by a combination of SLT and parent174 and one by a researcher acting as a teacher. 138 The studies were undertaken in a range of settings: a clinic (n = 14140,144–147,149–152,157,158,167,173,187), home and preschool,174 a special language preschool,179 a preschool154,178 and a Head Start centre. 138,170 In four studies it was not stated where the intervention took place. 139,159,164,172
Number of treatment sessions
In this typology it was most common for an intervention to be delivered three times a week (n = 7147,151,152,157,159,173,178), followed by twice weekly (n = 4144,146,154,167). Interventions lasted between 25 and 60 minutes. There were generally between 12 and 46 sessions, which took place over 6–24 weeks (although in one study the intervention took place over 9.5 months for one child158).
Comparison with speech and language therapists’ practice
Table 52 shows the activities and strategies that were identified by SLTs who participated in the Child Talk focus groups in connection with the theme of ‘generalisation’. The table also provides the percentage of SLTs ranking each intervention as essential and how many of the studies included in the review explicitly mentioned using each intervention.
| Intervention | SLTs ranking activity/strategy as essential, n (%) | Frequency used in studies |
|---|---|---|
| Making it functional and meaningful | 44 (96) | 0 |
| Explaining to parents | 43 (96) | 1 |
| Providing lots of opportunities | 41 (91) | 0 |
| Practising in lots of different contexts | 40 (89) | 0 |
| Repetition | 37 (86) | 1 |
| Working at the phrase level | 34 (81) | 2 |
| Doing activities within play | 35 (78) | 1 |
| Self-monitoring activities/strategies | 33 (73) | 0 |
| Consistency | 27 (63) | 0 |
| Using something visual | 24 (55) | 0 |
| Picture description | 23 (52) | 5 |
| Carried phrases | 21 (49) | 0 |
| Using tokens | 14 (33) | 1 |
| Minimal pair therapy | 9 (20) | 1 |
| Auditory bombardment | 4 (9) | 0 |
| Using posters with the target sound | 3 (7) | 0 |
| Metaphon programme | 2 (5) | 0 |
| Tongue twisters | 1 (2) | 0 |
Evidence of outcomes
In relation to EBP, generalisation is most frequently a secondary focus within the published studies. The 12 studies in this theme whose primary focus was generalisation showed mixed results:
-
The results of one study indicated generalisation of preposition–object phrases not only to untreated two-word combinations but also to comprehension of four-word phrases. In addition, there was also some generalisation of production of two-and four-word structures. 172
-
In one study, children learned the three-element clusters but were unable to generalise them. 152
-
Generalisation of trained responses to untrained stimuli was obtained for each of four target ‘linguistic behaviours’ (she, him, he, are). 187
-
Script-based training was effective at increasing all participants’ use of semantic relation skills and generalising acquired semantic relation skills across non-trained scripts and pictures. All participants maintained increased semantic relation performance across the 3-week maintenance assessment period. 178
-
The results of one study suggested that broad target recasts facilitate speech intelligibility of only the most developmentally immature speech producers. However, there was no support for this being transferred into speech outside the clinic or home setting. 157
-
Phonologically based treatment resulted in a reduction of both phonological word-finding substitutions and semantic word-finding substitutions. Generalisation effects were not as powerful as the authors had hoped; however, no phonological errors occurred during post-treatment testing. 139
-
Two subjects met the various performance criteria at each step of the treatment intervention but they did not generalise modified speech sounds production of treated phonemes to untreated words or to untreated phonemes. 158
-
In one study an intervention was generally effective in increasing the social communication behaviours of children who had fewer social interactions during baseline conditions. Specifically, the intervention increased the use of verbal behaviours, social communication skills and target vocabulary words in unstructured play with peer partners. 138
-
How often a list of targeted treatment words (probe lists) was administered did not have an effect on the extent of generalisation or the occurrence of a practice effect. 159
-
Generalisation probes were structured to evaluate the use of specific grammatical forms and syllabic shapes over the course of up to 30 sessions. The results indicate that the intervention procedures facilitated change in children’s productions of w-S stress patterns in untrained multisyllabic words, although less so in untrained phrases. 140
As indicated above, the 24 studies included in this theme represented a wide range of primary foci of intervention. Accordingly, a wide range of interventions and assessment measures was used. These, and the outcome measures, relate to the focus of the intervention rather than to generalisation.
Foundation skills
A very limited number of studies in the systematic review were represented in the ‘foundation skills’ theme of the typology (n = 470,138,170,185). Three of these had a main focus on foundation skills. 138,170,185 There is little uniformity to these studies, each of which included a small number of children/families. The interventions represented in the studies were diverse and as such no patterns of treatment and effect could be drawn across the studies. The variation in the assessment and outcome measures used across studies also makes comparisons between the interventions and assessments of their success difficult.
What was the focus of the studies?
Of the three studies focused on ‘foundations skills’, two focused on an adult supporting the children to organise play (including assigning roles, identifying and naming toys to be used), play in dyads and self-evaluation with the support of an adult. 170,185 Impact on the children’s social communication was measured by the amount and complexity of language used and the amount of time spent on each type of play;170,185 one study aimed to increase peer-directed social communication. 170 This was particularly related to initiations, responding appropriately to other’s initiations/questions or actions, appropriately obtaining a peer’s attention and maintaining a social interaction (turn taking). 138
Country of origin of the papers
Of the four papers included in this typology theme, three were from the USA138,170,185 and one was from the UK. 70
Design
One study used a between-group study design. 70 The most common research design was that of a multiple baseline case series using dyads. 138,170,185
Size of the sample
Fifty-nine children were represented by the four studies, with a minimum of 6 children and a maximum of 39 children across the studies (mean 14.8, median 7.0).
Child participant demographics
It should be noted that, although the studies in this category all recruited children with a language impairment, one study also recruited children who were at risk of impairment. 138 Of the 59 children, 37 were male. The ages of the children ranged between 37 and 60 months, with an average of 44.6 months.
Assessment measures
Eight different measures were used across the studies in this theme; however, only two were directly relevant to the theme:
-
peer language behaviour code138,170,185 – subdivided into:
-
measuring communication behaviours = descriptive (peer-directed comments, play organiser statements and acknowledgement responses) and request utterances (information requests, yes/no questions, action and stop action requests and clarification requests)185
-
Outcome measures
Twelve different outcome measures were used across the four studies in this theme. Eight measures were used only once. Two were used more than once and were directly relevant to the theme of ‘foundation skills’ (child communication measures, peer play code). A social validation scale (which was a teacher rating scale for impressions of verbal engagement during play) was used in one study. 170
Delivery of the interventions
Three of the studies described interventions undertaken by teachers (with research experience). 138,170,185 One study was undertaken by SLTs. 70 In three of the four studies the interventions were carried out in Head Start centres138,170,185 and in the final study the intervention was carried out in a preschool nursery. 70
Number of treatment sessions
As the number of studies in this theme was small, it is possible to detail the number of treatment sessions for each study. In the study by Barratt et al. ,70 children were randomised to a weekly or an intensive intervention. The weekly intervention was delivered once a week for 40 minutes for up to 24 sessions, whereas the intensive intervention was delivered on 4 days a week for 40 minutes for up to 24 sessions. In the study by Stanton-Chapman et al. ,138 intervention sessions were conducted on 5 days per week and lasted for 25 minutes (with a total of 20 sessions). The studies by Craig-Unkefer and Kaiser170,185 included 20-minute interventions three to four times per week, with the first dyad having 16 interventions, the second having 14 and the third having 12.
What was the intervention
Interventions (whole and individual activities and strategies) used in the study were mapped against the activities and strategies reported by SLT participants from the Child Talk focus groups and online surveys.
Comparison with speech and language therapists’ practice
Table 53 shows the activities and strategies identified by SLTs who participated in the Child Talk focus groups that targeted children’s foundation skills. The table also provides the percentage of SLTs ranking each intervention as essential and how many of the studies included in the review explicitly mentioned using each intervention.
| Intervention | SLTs ranking activity/strategy as essential, n (%) | Frequency used in studies |
|---|---|---|
| Explaining to parents importance of early skills | 47 (100) | 0 |
| Laying foundation skills | 40 (98) | 0 |
| Advice to parents | 44 (94) | 1 |
| Maintaining child’s attention | 42 (91) | 3 |
| Optimising the environment | 42 (89) | 0 |
| Attention and listening activities | 41 (89) | 2 |
| Turn taking | 41 (87) | 1 |
| Not putting pressure on the child | 32 (71) | 1 |
| Taking time for the adult and the child to sit together | 32 (70) | 0 |
| Building anticipation/excitement | 33 (69) | 0 |
| Playing language games | 18 (40) | 4 |
| Hanen programme | 14 (31) | 0 |
| Table-top activities | 13 (30) | 1 |
| Snack time | 11 (28) | 0 |
| Auditory memory activities | 12 (27) | 0 |
| Using interactive stories | 11 (26) | 0 |
| Parent workshop | 9 (20) | 0 |
| Thinking about where in the mouth sounds are made | 4 (9) | 0 |
| Using workstations | 2 (5) | 0 |
| Cued articulation | 1 (2) | 0 |
| Metaphon programme | 1 (2) | 0 |
Intervention activities or strategies mentioned within studies in the review but not by therapists in focus groups include:
Evidence of outcomes
Most of the studies appear to indicate that the treatments were successful but, again, overall, the studies report fairly low levels of specific intervention success. Peer-directed interventions were generally effective at increasing social communication behaviours of children who had fewer social interactions at baseline. Modelling of interaction to a mother increased verbal interaction with her child and suggested increased utterances in response from her child. Play–plan–report therapy increased social communication behaviours. The four studies represented in this theme are also included in other themes. As such, they are very diverse, with few common elements for any conclusions to be drawn. Two aspects of SLT-recommended interventions – maintaining attention and playing language games – were well represented within the four studies and showed positive change following the interventions. 138,170,185 Again, book reading is included in the research studies but was not mentioned by therapists in focus groups.
Functional communication
Five studies were included in this theme of the typology,137,138,170,184,185 with two having a primary focus on ‘functional communication’. 138,184 This theme also included studies that focused primarily on language and skills or assistive materials/resources that help the child’s involvement and participation in life situations.
Country of origin of the papers
All five of the studies representing this area of the typology were undertaken in the USA.
Design
Four of the studies used a case series design, often with multiple baselines. 138,170,184,185 The other study used a between-group design. 137
Size of the sample
The five studies representing this area of the typology included a total of 82 children. The number of children included ranged from 5 to 57, with a mean of 16.4 and a median of 6.0.
Child participant demographics
Two studies recruited children who were ‘at risk’137,138 whereas the other studies all recruited children with language delay. One study did not specify the gender split of the children involved. 137 The other studies included a total of 11 boys and 14 girls. One study simply stated that the children were 5 years of age and gave no other details. 137 The other studies included children aged between 42.0 and 54.0 months (average 48.1 months).
Assessment measures
Seven different assessments were used across the five studies. However, only two – the Child Behavior Checklist/2–3 (CBCL/2–3)209 and the SSRS207 – could be identified to be relevant to functional communication.
Outcome measures
Across the five studies 19 outcome measures were identified. Fifteen of these were used once and the majority were not relevant to the theme of functional communication. However, child communication measures and the peer play code were used in two studies170,185 and can be argued to measure functional elements of communication.
Delivery of the intervention
There was no consistency across the studies in relation to who delivered the intervention. In one study the intervention was delivered by a combination of early years professionals and parents,137 whereas in another an assistant SLT delivered the intervention. 184 One study used a researcher to act as a teacher138 and the final two studies used the children’s preschool teachers. 170,185 Four of the interventions were undertaken in Head Start centres138,170,184,185 and one was undertaken in a child development centre. 137
Number of treatment sessions
In the longest study in this typology, children received the intervention for 5 days a week for 50 weeks a year from 6 months to kindergarten (although age was not specified), with the parents of these children receiving home visits every 1.5 weeks as well as monthly group meetings. 137 The remaining four studies carried out interventions lasting between 7 and 25 minutes, delivered three to five times per week, for a total of 12–23 sessions. 138,170,184,185
What was the intervention?
In addition to the interventions mapped in Table 54 to the typology theme, the included studies used other activities and strategies:
| Intervention | SLTs ranking activity/strategy as essential, n (%) | Frequency used in studies |
|---|---|---|
| Modelling | 40 (87) | 1 |
| Accepting other ways to communicate, e.g. pointing | 36 (84) | 0 |
| Using functional vocabulary | 37 (82) | 1 |
| Using short non-ambiguous sentences | 37 (80) | 0 |
| Play | 36 (80) | 1 |
| Encouraging adults to use explicit language | 34 (77) | 0 |
| Making things visual | 32 (74) | 0 |
| Using visual cues | 31 (72) | 0 |
| Defining expectations | 25 (56) | 0 |
| Helping child to prepare for situations | 24 (55) | 0 |
| Preparing the child | 22 (51) | 0 |
| Signing | 21 (46) | 0 |
| Using visual timetables | 20 (44) | 0 |
| Makaton programme | 20 (44) | 0 |
| Using now and next boards | 18 (39) | 0 |
| Using symbols for choices | 17 (38) | 0 |
| Small language groups with a social focus | 17 (38) | 0 |
| Using photobooks/symbol books | 16 (36) | 2 |
| Naming emotions | 11 (25) | 0 |
| Signalonga | 10 (23) | 0 |
| Social stories | 9 (20) | 0 |
| Reasoning work | 5 (9) | 1 |
Comparison with speech and language therapists’ practice
Table 54 shows interventions that were identified as being used to have a positive impact on children’s functional communication skills. The table also provides the percentage of SLTs ranking each intervention as essential and how many of the studies included in the review explicitly mentioned using each intervention.
Evidence of outcomes
In the studies in this theme there seemed to be only limited concordance between the approaches used in the studies and those recommended by SLTs.
The findings suggest that the interventions were generally effective in increasing children’s social communication. Specifically, the interventions increased the use of verbal behaviours, social communication skills and target vocabulary words138 and results in improvements in preschoolers’ generation of personal narratives. 184 The findings of Craig-Unkefer et al. 170,185 suggest that the interventions increased the amount of child talk during play and the number of requests and descriptive talk. However, although the studies report successful outcomes, their methodologies are too diverse for a grading of the evidence.
Adult understanding
Only one study is included in this theme of the typology. 134 This typology theme focuses on studies that aim to help parents to understand the nature of their child’s speech and language difficulty, what helps to improve it and why. It focuses on the acquisition of knowledge and understanding, not the teaching/learning of skills.
What was the focus of the studies?
The sole study is a PhD thesis and investigates whether low educational-level migrant mothers can be effectively trained to implement dialogic reading techniques, and what effects the mothers’ implementation of dialogic reading techniques have on the oral language production of migrant preschool children. One element of this thesis looks at the level of understanding, in relation to dialogic reading, of the parents before and after undertaking training.
Country of origin of the paper
The study was based in the USA.
Design
The study used a case series with staggered starts and multiple baselines.
Size of the sample and child participant demographics
Only four children (two boys and two girls) are represented in this typology theme. They were recruited from a mixture of at-risk children and those with a diagnosed language delay. The children were aged between 4.0 and 5.7 years.
Assessment measures
None of the assessment measures used in the study were relevant to measuring the knowledge and understanding of adults/parents regarding preschool language delay.
Outcome measures
In relation to the theme of ‘adult understanding’, parents underwent training in dialogic reading and had to score 100% on an assessment tool designed specifically for the project. Another measure used in this study was social validity questionnaires. These targeted the importance, effectiveness and practicality of the intervention and thus examined parents’ perspectives of the intervention rather than specifically their understanding of the intervention; they are thus only of partial relevance to the typology theme.
Delivery of intervention
The study was undertaken in the homes of patients.
Number of treatment sessions
The number of sessions administered ranged from 5 to 11. The lengths of the sessions were comparatively long, with 3-hour and 2-hour sessions in some cases. These sessions were delivered over periods of between 3 and 6 months. The scale of the interventions varied from two instruction sessions followed by a mother being observed on six occasions, up to one home visit made every 1.5 weeks from age 3 months to elementary school (approximately 200 sessions over 5 years).
What was the intervention?
The intervention in this theme focused on increasing parent knowledge about preschool language delay. This was carried out through an educational programme with parents and book reading. 134
Comparison with speech and language therapists’ practice
Table 55 shows interventions that SLTs identified as being used to enhance adult understanding. The table also provides the percentage of SLTs ranking each intervention as essential and how many of the studies included in the review explicitly mentioned using each intervention.
| Intervention | SLTs ranking activity/strategy as essential, n (%) | Frequency used in study |
|---|---|---|
| Explaining activities to parents and their purpose | 42 (95) | 1 |
| Practising strategies with parents | 44 (94) | 0 |
| Being positive about the child | 43 (93) | 0 |
| Explaining things that help communication | 42 (91) | 0 |
| Explaining that language/vocabulary needs to be functional | 40 (87) | 0 |
| Explaining the importance of working on input first | 36 (82) | 0 |
| Providing opportunities to practise strategies | 37 (79) | 0 |
| Developing play experience with parents | 33 (75) | 1 |
| Providing games that parents are able to take home | 31 (66) | 1 |
| Providing information prior to groups | 30 (64) | 0 |
| Talking about communication styles | 29 (62) | 1 |
| Pointing out good/bad strategies as you work with parents | 28 (60) | 1 |
| Parent–child interaction | 28 (60) | 1 |
| Providing instructions in play | 21 (49) | 0 |
| Showing video footage | 15 (32) | 0 |
| Parent workshops/groups | 12 (26) | 0 |
| Getting parents to make things with the child, e.g. collage | 3 (7) | 0 |
Evidence of outcomes
The study undertook parent training sessions, with two assessments of parents’ understanding of dialogic reading. Parents who did not obtain a score of 88% at the end of the course were given an additional coaching session and subsequently gained 100% when reassessed. Although apparently successful at changing parents’ interactions and parenting styles, the small number of parents included (n = 4) and the lack of reporting of data showing the levels of pre-training understanding mean that there is insufficient information relating to increases in adult knowledge and understanding to make any judgements about the effectiveness of the intervention in improving child language development.
Adult–child interaction
Eight papers (nine studies) were included in this theme of the typology. 134,136,137,143,175–177,182 This typology includes activities and strategies that aim to improve the quality of the exchanges between the parent/adult and the child.
What was the focus of the studies?
The majority of the studies included in this theme had a primary focus on the treatment of expressive language delay, with the others looking at expressive and receptive language delay. None of the included studies specifically focused on the success of adult–child interactions.
Country of origin of the papers
One study was undertaken in Germany,177 four were undertaken in the USA,134,136,137,143 one with Spanish-speaking families,134 one was carried out in Canada182 and three were carried out in the UK. 175,176
Design
Three of the studies within this theme were RCTs. 175,177 Two studies used a pre-test/post-test design (allocation to groups: random, location),176,182 two were case series with multiple baselines134,143 and two used a between-group design. 136,137
Size of the sample
The nine studies in this theme included 1011 children, with a mean number of children per study of 112.3 (median 36.0, range 4–731).
Child participant demographics
Two studies recruited children who were at risk. 136,137 One study recruited both children at risk and those who had been diagnosed with a language delay. 134 The other studies recruited children with a diagnosed delay/impairment. Several studies did not report on the gender split of the participants but among those that did 450 boys and 383 girls were investigated. 134,137,176,177 The ages of the children ranged from 24 to 58 months.
Assessment measures
Thirty-one measures were used across the nine studies. These assessed various levels of the children’s abilities. Lunkenheimer et al. 136 undertook four observational measures of parenting in the home. They focused on parent involvement using the Home Observation for Measurement of the Environment (HOME) Inventory,210 the two subscales of the Relationship Process Code (RPC) (positive reinforcement and engagement interaction)211 and proactive parenting using the Coder Impressions Inventory. 212
Outcome measures
These studies used multiple outcome measures; however, very few measures were related to adult–child interaction. Six studies used language samples of children and mothers,134,136,143,175,176,182 often using Systematic Analysis of Language Transcript (SALT) to support coding,143,182 and thus looked only at the child’s output and not at the adult–child interaction. Another measure asked mothers to complete a satisfaction questionnaire that assessed whether they/their child enjoyed participating in the intervention and whether they thought that it had helped their child. 143
Delivery of the interventions
Parents were instructed to enhance their child’s speech and language learning in a number of ways. Four studies used the Hanen programme or a modified version of the Hanen programme. 175,176,182 Buschmann et al. 177 taught parents how to promote interaction and undertake language modelling using the Heidelberg Parent-based Language Intervention. 213 Roberts et al. 137 undertook parent interaction interventions from when the child was 3 months old until the child started elementary school. These interactions ‘educated’ the family in learning games, child management and parent problem-solving. The other three studies undertook short-term assessments and education, with one study providing feedback on parent–child interactions from the pre-intervention assessment. 136 The other two studies taught strategies such as modelling, pausing and praise. 134,143 Only one study assessed the understanding of the techniques taught to the parents. 134
The interventions for the children were delivered in a number of ways. In four of the studies the intervention was delivered by SLTs working with parents. 175,176,177 In a further three it was reported that parents delivered the intervention134,175,182 and in a further one it was reported that the intervention was facilitated by parents and EYPs. 137 In the final study it was reported that the intervention was delivered by a ‘family/consultant’ dyad, but this is not clear. 136 The interventions were delivered in children’s homes and nursery settings.
Number of treatment sessions
The interventions varied in length from approximately 2–3 months for parent training programmes to a whole academic year for preschool programmes. Sessions lasted from 10–15 minutes for a home reading programme up to 2.25 hours for group sessions.
Comparison with speech and language therapists’ practice
Table 56 shows interventions that SLTs identified as being used to have a positive impact on adult–child interactions. The table also provides the percentage of SLTs ranking each intervention as essential and how many of the studies included in the review explicitly mentioned using each intervention.
| Intervention | SLTs ranking activity/strategy as essential, n (%) | Frequency used in studies |
|---|---|---|
| Modelling | 45 (96) | 3 |
| Commenting | 44 (96) | 1 |
| Simplifying language | 44 (94) | 0 |
| Reducing language/questions | 44 (94) | 0 |
| Practising strategies | 44 (94) | 1 |
| Following the child’s lead | 44 (94) | 0 |
| Extending | 44 (94) | 1 |
| Repetition | 43 (93) | 2 |
| Play experience | 43 (93) | 1 |
| Joining in play (parent) | 43 (93) | 0 |
| Being on the same level | 43 (93) | 0 |
| Utilising opportunities | 41 (89) | 0 |
| Providing choices | 41 (89) | 0 |
| Waiting | 39 (87) | 2 |
| Improving the communication environment | 39 (83) | 1 |
| Advice to parents on play | 36 (80) | 2 |
| Talking tips | 37 (79) | 1 |
| OWLing | 30 (67) | 0 |
| Ready, steady, go activities | 24 (53) | 0 |
| Free and directed play | 22 (49) | 1 |
| Watching videos of interactions with parents | 21 (48) | 1 |
| Parent–child interaction | 19 (48) | 2 |
| Vocabulary activities | 20 (44) | 1 |
| Putting things in a bag and describing them | 20 (43) | 0 |
| Emphasising sounds/talking about sounds | 20 (43) | 1 |
| Picking a limited number of words and using them in different contexts | 16 (37) | 2 |
| Videoing parents | 16 (34) | 4 |
| Work on word levels | 15 (33) | 0 |
| Hanen programme | 14 (31) | 2 |
| Cloze statementsa | 6 (14) | 0 |
In addition to the interventions mapped in Table 56 to the typology theme, the included studies used other activities and strategies:
Evidence of outcomes
The review found some evidence that interventions can be effective in their intended goals of modifying the behaviour of parents in their child’s environment,134,136,176,182 although one study found that parental language support actually declined over the course of the intervention. 143 The case series, which examined book reading, focused on the process of change throughout the interventions. 134,143 The evidence for the effectiveness of these interventions was varied and came from studies with small sample sizes.
The heterogeneity of the included studies, particularly in terms of intervention type and study design, prevents clear conclusions from being drawn about the effectiveness of adult-based interventions. However, the review findings suggest that, overall, involvement in these early preschool interventions can lead to language gains for children with, or at risk of, PSLI.
There was some evidence that environmental approaches to speech and language therapy can have comparable results to those of individually delivered clinic sessions, but that particular approaches may be best suited to children according to their profiles of language delay. 175,176 Around 75% of children who had taken part in interventions were shown to make significant continued language improvements in two studies that carried out 12-month follow-up assessments;176,177 in one study these children were shown to ‘catch up’ to age-appropriate levels of language. 177 However, it is important to draw attention to the fact that a quarter of these children therefore had persisting difficulties with language despite intervention. Furthermore, not all children were found to make equivalent gains as a result of intervention. 175
Discussion
As can be seen from the PRISMA flow diagram (see Figure 15), this systematic review has been a substantial undertaking. Of the 55,271 papers originally identified, 4574 were retrieved for detailed examination. This careful process, involving two reviewers per paper, identified 473 studies that appeared appropriate for the review, of which only 147 met the inclusion and exclusion criteria. Reliability procedures are described in Chapter 1 (see Methodology overview).
All team members involved in quality appraisal undertook the PEDro-P training programme [see www.pedro.org.au/english/tutorial/pedro-scale-training-program/ (accessed 7 January 2015)] and appraisal was undertaken by a minimum of two raters, including at least one SLT. Mapping these studies against the typology was undertaken independently by a minimum of two, but typically three, raters and any disagreements were resolved by discussion to consensus.
The end of this process was a perhaps surprisingly small number of studies (n = 58), suggesting a dearth of high-quality, well-reported intervention studies in this vitally important research area. The distribution of studies across the typology was not even, with more studies in the categories of ‘speech’ (n = 33)’ and ‘expressive language’ (n = 28). In contrast to this attention to expression or output, few studies were concerned with comprehension of language. The category of ‘adult–child interaction’ could be viewed as the less visible aspects of language. Interestingly, the two largest categories address the expressive nature of speech or language. A relatively high proportion of these quality-appraised studies include consideration of the ‘generalisation’ of intervention targets.
The proportions of studies that met the quality appraisal criteria were not equal across the two key research design types – group design compared with SCED. A far higher proportion of the latter (SCED) were scored at ≥ 6 on the SCED scale than group designs assessed through PEDro-P. It is unclear whether this is because SCED studies are better designed and reported or because the SCED scale is less rigorous. A paper by the authors of the SCED scale describes a revision to the earlier scale,103 but the new scale is not yet available.
The included research comes from a variety of countries – the USA, the UK, Canada, Australia, South Korea, Germany and New Zealand – with well over half of the studies being conducted in North America. Although some of the North American papers do include children who speak languages other than English, there is a clear Anglophone bias in the review. Cross-language differences in terminology and the nature of abstracting systems are both likely to have contributed to this outcome.
Speech
In speech and language therapy literature this theme could be argued to sit under the umbrella of speech sound disorder (SSD). This is also referred to as speech impairment, speech delay and other related terms within the field of SLCN. Yet in spite of this, consensus has not been reached regarding how SSD should be classified. It is clear that the group of children described as having SSD is heterogeneous and that there is significant variation in the presentation of their difficulties. Some classification systems have been proposed, the most well-known of which is that of Shriberg et al. ,214 which is based on aetiology, and Dodd’s215 classification based on surface presentation of speech. Although a classification of one or other type of SSD using these systems would lead a clinician down a particular path with regard to intervention approaches, it is more difficult to match existing intervention studies to these classifications. This is because the interventions themselves have arisen from a number of differing theories about speech development and/or have selected a specific sample of children within the broad category of SSD whose needs warrant a particular approach to intervention. In the Child Talk programme we were able to distinguish three groups within the theme. These were speech output, phonological awareness and stress patterns.
This overarching theme was represented by the greatest number of studies (n = 33). Twenty-six focused on speech output, six focused on phonological awareness and one, which stood out as being different from all the others, focused on stress patterns. This split is interesting in that it provides a challenge for the interpretation of evidence.
The studies designated as focusing on speech output were of sufficient quality and number to suggest an evidence grading of A. To a lesser extent the evidence for phonological awareness could be argued to be approaching grade A as it does contain one RCT. However, in general, only a small number of children were represented (n = 110) across the six studies. No evidence rating can be made for stress patterns.
As mentioned, although there is a significant body of work theorising and modelling the relationships within SSD, consensus has not been reached regarding how SSD should be classified and further work and refinement needs to be undertaken with the studies identified as residing in this theme of the typology.
Comprehension
Only two studies exclusively addressed comprehension. In another four studies, comprehension was targeted in conjunction with other aspects of language. Three studies were RCTs, two were multiple baseline studies and one was a cohort study. The mean number of participants per study was 22.5.
The assessment and outcome measures included vocabulary measures and more general tests of language development. A diversity of intervention approaches was used including the Hanen programme, direct training by SLTs using picture materials, a scripted intervention based on shared book reading and a play-based intervention delivered by parents.
The small number of studies means that it is not feasible to assess concordance between approaches used in these studies and those recommended by SLTs. Five of the six studies had positive outcomes, with one reporting, additionally, generalisation to language production. The small number of studies and their diversity of approach necessitates caution, but the findings suggest that successful interventions for comprehension are available. Further research is needed in this underevaluated area; therefore, it is possible to evaluate this theme only as grade C evidence.
Expressive language
Differences in terminology pose some challenges in synthesising the findings from the 28 papers (29 studies) in this theme. Included studies aimed to improve children’s expressive language, in quantity, vocabulary or structure, both length and complexity. This diversity is reflected in the assessments used, which included MLU, standardised vocabulary assessments and more general language assessments.
Although more than half of the studies involved a multiple baseline design, there were also five RCTs and the mean number of participants per study was quite large (30.9). Typically, interventions were delivered by SLTs in a wide range of settings (preschool, child development centre, clinics and the home).
Modelling was the intervention approach used in half of the studies, and toys and role-play materials predominate in the materials used. One-third of the studies explicitly involved parent participation.
Only four of the studies, not including any of the RCTs, did not report positive outcomes, although some showed progress for only some participants. The weight of evidence, however, suggests that intervention using modelling by SLTs to improve expressive language is approaching grade A. More detailed analysis is needed to give more specific recommendations.
Self-monitoring
Only two studies are represented in this theme, both of which were included in other categories. One is a phonological intervention. The other involves play and social interaction. No conclusions can be drawn from the data reported.
Generalisation
The studies included in this theme represented a wide range of primary foci of intervention. Accordingly, a wide range of interventions and assessment measures were used. These, and the outcome measures, relate to the focus of the intervention rather than to generalisation.
Effectiveness across the included studies was variable but, as this relates to the primary focus of the intervention rather than generalisation, conclusions cannot be drawn and grading of the evidence cannot be carried out.
Foundation skills
The studies in this theme were all included in other categories. As such, they are very diverse, with too few common elements for any conclusions to be drawn.
Two aspects of SLT-recommended interventions – maintaining attention and playing language games – were well represented within the four studies. Book reading was included in the studies but was not mentioned by SLTs in the focus groups or online surveys. The incorporation of laying foundation skills into other interventions means that it does not make sense to grade the weight of supporting evidence.
Functional communication
All five studies included in this theme were also included in the theme ‘expressive language’. Studies targeted social communication/social interaction, narrative skills or more general aspects of children’s language development.
Four of the studies used a multiple baseline design and one used a group design. There were no RCTs. Assessment and outcome measures included standardised language and communication assessments, an assessment of play and more informal measures of behaviour and social skills.
Although the numbers included are very small, there seemed to be only limited concordance between the approaches used in these studies and those recommended by SLTs. The studies report successful outcomes but are too diverse for grading of the evidence.
Adult understanding
Only one study was retained in the systematic review that had any element of work involved with improving ‘adult understanding’. Its focus on low educational-level migrant mothers makes this small study very limited and it is not appropriate to grade the weight of supporting evidence.
Adult–child interaction
As might be expected, all nine studies included in this theme involved some form of training for parents and/or day-care staff. Two studies used the Hanen programme, one involved a book-reading intervention and another used a more general training programme.
Three of the studies were RCTs, two used a pre-test/post-test design (allocation to groups: random, location), two were case series with multiple baselines and two used a between-group design.
Although the number of studies is not large, the activities used, with the notable exception of book-sharing activities, are in the main included among those recommended by SLTs.
The studies report short-term positive outcomes. However, the designs used mean that it is difficult to exclude the possibility that progress was attributable in part to maturation and, in general, there is a need for longer-term follow-up. The variety in study design and the focus of at least two of the studies on adult interactions mean that the evidence could be allocated an A grade.
Limitations
Terminological differences, relating to both intervention approaches and study designs, across time and countries, represent a challenge for synthesising the data, especially when there were few studies to draw on.
In general, there is a need for additional and more robust research of interventions for children with PSLI, especially in the areas of comprehension of language, increasing participation or parent/adult–child interaction. To achieve this, greater attention to both the quality of study design and reporting is required.
Ultimately, the important questions that we sought to answer in this review were:
-
if there is robust evidence for speech, language and communication interventions for preschool children with PSLI
-
if speech and language therapy practice was supported by/conformed to the existing evidence
-
what aspects of practice were not supported by robust evidence, that is, when SLTs were using interventions for which there is no evidence
-
where robust evidence was not being implemented as speech and language therapy practice, that is, when robust evidence for an intervention exists but the intervention is not used in practice.
Because of methodological and reporting limitations, the quantity of robust research that can be drawn on is modest in all categories. However, using the grading system described in Chapter 1, the weight of evidence for interventions that use speech and language therapy modelling to increase expressive language approached grade A. Studies reporting on interventions with a focus on speech were also graded highly, with speech perception studies reaching grade A and phonological awareness studies being graded as B.
In relation to the typology theme ‘adult–child interaction’, there is a growing body of evidence suggesting that interventions with these aims are a worthwhile adjunct to other interventions. There is insufficient research to draw conclusions relating to the theme ‘comprehension’, but the positive outcomes of the studies included suggest that effective interventions for comprehension do exist. Further research is urgently needed in this area. In all other areas, there are too few studies for a grading to be considered.
The extent of concordance between SLTs’ reported practice and intervention approaches supported by evidence is discussed when there are sufficient studies to make this feasible. There is insufficient evidence to match back from the extensive detail on speech and language therapy practice to the evidence base. However, most interventions with robust evidence are being used by SLTs in practice. The exception to this would seem to be shared reading activities. There is a need for evidence of this type of intervention to be disseminated to SLTs.
Chapter 4 User perspectives on speech and language therapy
Introduction
The standard definition of EBP, as described in Chapter 1, suggests that EBP requires the integration of systematic research evidence with clincial expertise in the light of patient values. In the context of this research programme, the ‘patients’ are preschool children with PSLI. Parents and carers are prominent in the children’s day-to-day lives, particularly preschool children, mediating the children’s interactions with services such as speech and language therapy. Parents’ roles in supporting their child’s development makes them key to the process of delivering many interventions and thus their perspectives, as well as their child’s, are important to the notion of EBP. As many children are cared for during the day by carers other than their parents, EYPs have also been included in this study. To ensure that we explored the views of a range of the population, parents from populations that are considered to be underserved by speech and language therapy were also included in the study. The studies described in this chapter include qualitative studies of the perspectives of preschool children, parents (this includes both parents of children attending speech and language therapy and parents from underserved communities who are not necessarily currently accessing services) and EYPs. A survey of parents’ views of the strategies and activities undertaken by SLTs is also included. The chapter is completed by an analysis of parents’ and EYPs’ perspectives in the light of the themes of the typology presented in Chapter 2 (see Study 2.1: identifying the themes of speech and language therapy practice).
Children
Traditionally, childhood and children’s lives have been explored solely through the views and understandings of their adult caretakers (e.g. parents, grandparents, guardians, teachers), who claim to speak for children. This renders the child as an object and excludes him or her from the research process. This view is being challenged by researchers and practitioners who see children as possessing distinctive cognitive and social developmental characteristics that researchers, wishing to use child informants, must consider during the research design and methodology. It is also important to note that children’s perspectives are often different from those of their parents and the professionals who support them and therefore listening to and valuing children’s perspectives is important for identifying therapeutic goals and for the delivery of engaging speech and language therapy. Increasingly, researchers and practitioners acknowledge children’s rights to be heard and believe that their voice should be valued in its own right.
Listening to the voices of preschool children can be challenging, particularly if they have a potential speech and language need. The speech, language and cognitive skills of preschool children are such that their ability to reflect on past events is still developing, as are their abilities to communicate their experiences through more traditional verbal and non-verbal methods. 216–218 The perspectives of primary and secondary school-aged children with PSLI on their experiences at home and at school and their aspirations have been elicited through arts-based interviews, play-based methods and questionnaires. 219–223 The views of primary school-aged children with PSLI on school-based SLT sessions were elicited through interviews with visual support and have informed the content and method of SLT delivery for this age group. 224
Few studies have explored the perspectives of preschool children with PSLI225 and none has investigated their perspectives on speech and language therapy specifically. Researchers have had some success listening to young children’s voices through arts-based and play-based methods,221,222 but they have also found inconsistencies in children’s voices over time. Observation of children’s body language and behaviour has proved a successful method by which to explore young children’s perspectives. 226,227
In this study we were interested in examining preschool children’s engagement in, and response to, speech and language therapy interventions, using arts-based activities as a way of accessing their perspectives. In this study ‘engagement’ was considered to include children’s persistence in attempting or repeating actions and vocalisations and their attention to, and participation in, activities. 228 Given that the target population of this study was preschool children, there are limits regarding the level of participation in the research that it is possible to achieve. However, it is important not to assume that we cannot access these children’s views.
One of the central questions of the Child Talk programme was ‘How can we best engage preschool children in the process of developing appropriate interventions?’ The research programme therefore aimed to explore the perspectives of preschool children, aged from 2 years to 5 years 11 months, on the types of activities and strategies that they are likely to experience if referred for speech and language therapy. The purpose of this was to gain insight into their feelings, attitudes, experiences and perceptions in relation to SLTs’ activities. As this kind of investigation with this age of child with a speech and language impairment has not been widely carried out, we set out to develop innovative methods, tools and skills to investigate whether or not it was possible to record preschool children’s ‘views’ of SLT activities. Typically, when SLTs observe children in sessions they are trying to determine whether or not the interventions are effecting changes in children’s communicative behaviour. The interventions are designed, for example, to improve children’s attention and listening or the amount and complexity of vocalisation or communication. SLTs are alert to signs that children are engaged and motivated and will modify interventions to facilitate engagement. In contrast, the observations in this research aimed to understand the activities from the child’s perspective. We are not therefore asking the question, ‘Does the activity increase or decrease the child’s attention or improve their vocalisation or other aspects of their communication or development in general?’. That is, this is not an evaluative study of the success of the interventions but a study of the children’s perspectives of those interventions. Hence, the aim of this study was to identify how we can best engage preschool children in the process of developing appropriate interventions.
Parents
Although parents’ involvement in speech and language therapy has been an accepted part of practice for some decades now, parents’ perspectives on therapy have not been widely investigated until more recently. 223 Their perspectives have been investigated alongside child language data as part of an evaluation of intervention,27,169,176 and their perspectives on issues such as the nature of their child’s language development,229 their expectations for the future233 and outcomes that are valued160 are beginning to appear in the literature. Before 2000, the majority of research that has included parents, particularly with respect to preschool children, tended to focus on changes that parents were able to make to their own speech and language in response to training. Not only is there a dearth of research examining parents’ perspectives but also our understanding of how to integrate parent perspectives into clinical decision-making is under-researched. 56
As indicated above, the Child Talk research programme has taken a position that the perspectives of parents must be included in the development of an evidence-based framework. Within the programme, parents have played an important role in a number of ways: the chief executive of a national parent organisation joined the applicant team in the development of the original research proposal; local parent panel representatives have been included on the advisory group and a parent panel was established to advise and work with the research team throughout the programme. The work of the parent panel is reported in Chapter 1 (see Management and governance arrangements). Here, the focus is on the perspectives of families with preschool children. The focus of this study was to understand the perspectives of parents in relation to their experiences of SLT and their perceptions of typical SLT activities and strategies.
Underserved groups
In addition to parents who have attended speech and language therapy services, the research programme deliberately targeted a number of groups who were considered by managers to be ‘underserved’ by their services. In determining the perspectives of parents on speech and language therapy services, it was considered important to include those who may have experienced barriers to receiving equitable services so that, when planning future services, their perspectives may be recognised. Wylie et al. 231 comment that the term ‘medically underserved’ can refer both to people or groups with insufficient services and to those who experience barriers to accessing services. We have chosen to use the term ‘underserved’ rather than ‘hard to reach’ or ‘non-engaging’.
However, it can be difficult to define or identify populations who are underserved as these groups are heterogeneous as well as being part of diverse communities, cultures and language groups. 232 McAllister et al. 233 state that both stakeholders and communities may hold different views regarding who is underserved by services. Data are limited about the particular groups who are underserved by speech and language therapy services, although there is evidence of disproportionality in the representation of certain social and ethnic groups who are identified in the education system in England as having SLCN. 234 Similar investigations of under-/over-representation of children from diverse social groups within speech and language therapy services have not been carried out.
Previous research in the field of cross-cultural competence and communication disability suggests that service users may not all share the same perceptions of disabilities, levels of willingness to engage with services or preferences about the types of services that they want. 235,236 Additionally, community members may not all share the same explanatory models and levels of knowledge regarding the specific impairment/disability in question: causes, norms, interventions. 229 This is important because it is assumed that attitudes, beliefs and explanatory models may impact on engagement with services. Data on these issues are limited, particularly for groups who may be underserved by speech and language therapy services. Explorations of these influencing factors were the driving force for this study.
The aim of this study was to describe the beliefs about development, delay or disorder of speech and language as well as the reported practices and community responses to supporting children’s language development and difficulties of speech and language. These responses are of particular interest, coming from a number of groups perceived by speech and language therapy service professional leads to be underserved by services.
Early years practitioners
The term ‘early years practitioner’ is used inclusively in this study to refer to all practitioners who work in early years and childcare contexts, including nurseries, nursery classes, reception classes, children’s centres and child-minding settings. Typically, the term is used to refer to practitioners who have an Early Years Educator (or equivalent) qualification, although we did not require our participants to present evidence of this.
It is the case that > 90% of children in the UK now spend a proportion of their time in some kind of preschool setting. This has increased since the government introduced subsidised places that guarantee all preschool children a place in a preschool setting. Thus, as explained earlier, in terms of the adults who interact with speech and language therapy services with regard to the management of children with PSLI, EYPs play a key role. Research has linked the quality of childcare more broadly, and the quality of the interactions in childcare settings more specifically, with children’s language development. This relationship has been emphasised in the training of EYPs and in policy for workforce development for the childcare sector. 48 However, little is known about EYP perspectives on support for children with PSLI. Therefore, the aim of this study was to investigate the perspectives of EYPs on interventions for children with PSLI.
Objectives
The research presented in this chapter contributes to addressing the following Child Talk objectives:
-
to determine current evidence, practice and user perspectives regarding SLT-led interventions for preschool children with PSLI
-
to identify how we can best engage preschool children in the process of developing appropriate interventions
-
to develop a model(s) of intervention that can integrate current evidence, professional expertise and family perspectives in ways that allow the intervention to be individualised to children’s and families’ communicative, physical, social and cultural contexts.
Specifically, this chapter describes a methodology for gaining the perspectives of preschool children on SLT-led sessions and commonly used interventions (see Study 4.1: the perspectives of preschool children on speech and language therapist-led interventions), the views of parents on speech and language therapy through direct experience and also more general views on the acceptability of activities and strategies used by SLTs (see Study 4.2: the perspectives of parents on speech and language therapy), the views of underserved communities on communication development and accessing speech and language therapy services (see Study 4.3: the perspectives of communities who are underserved by speech and language therapy services) and the perspectives of EYPs on speech and language interventions in an early years setting (see Study 4.4: the perspectives of early years practitioners on speech and language therapy).
Study 4.1: the perspectives of preschool children on speech and language therapist-led interventions
This study aimed to develop a methodology for exploring the perspectives of preschool children on activities that are commonly used by SLTs. An observational methodology was developed that utilised the filming of preschool children during a series of therapy sessions with field cameras and matchstick cameras worn by the children and researcher field notes. Following each therapy session a play session was undertaken with a DMT to gain further insight into the engagement of the children. A framework was developed to analyse the data based on body movement, vocalisation and visual attention of the children during these sessions. The data revealed the dynamic nature of children’s perspectives and factors that may influence the levels of interaction (‘ebb and flow’) observed in the children throughout the series of therapy sessions.
Research questions
-
What methodology could be employed to gain the perspectives of preschool children on SLT-led interventions?
-
How do children experience the different approaches used by SLTs and how acceptable are they?
-
What factors influence whether or not children access, engage with and/or actively participate in SLT services?
Methodology summary
A summary of the methods is provided in Figure 16; the methods are described in detail in Chapter 1 (see Methodology overview).
FIGURE 16.
Summary of the methodology used to gain the perspectives of preschool children.
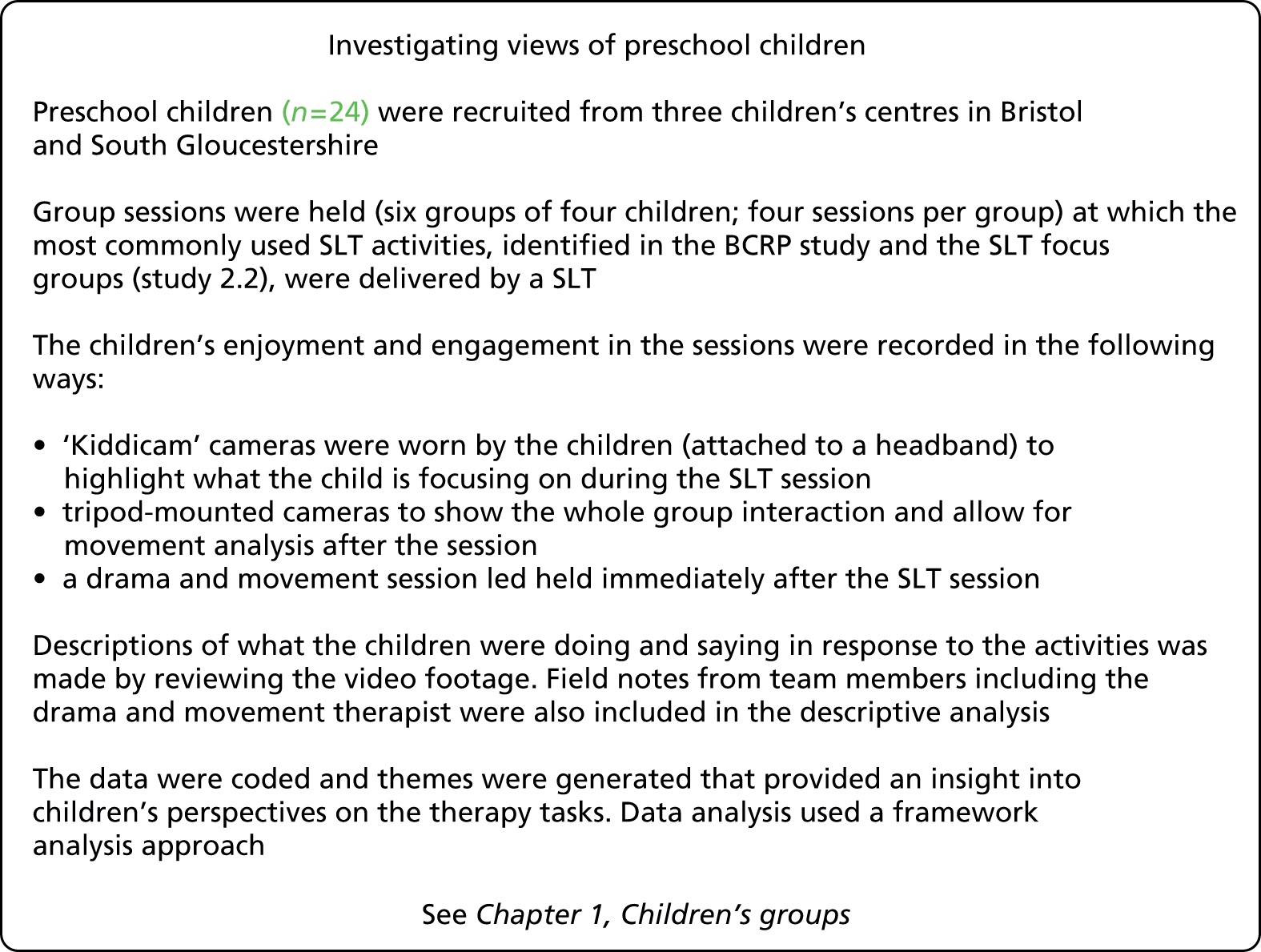
Findings
A multimethod approach based on the Mosaic approach237 was chosen for this stream of the work as this was felt to be flexible and would enable the voices of preschool children to be heard. Elements of the Mosiac approach were adapted:
-
to include preschool children’s and practitioners’ ways of talking to children and how they interpreted reactions
-
to ensure that our methods could be applied in a variety of early childhood settings
-
to be focused on the aim but grounded in the children’s lived experiences in a fun, flexible format
-
to produce a framework for listening to the child that had the potential both to be used as an evaluative tool and to become embedded into early years practice.
The aim was to deliver a range of activities and strategies for children to experience so that we could observe their behaviour across a range of intervention situations. In particular, activities were selected that provided both structured and unstructured contexts, picture and object materials and familiar and unfamiliar resources. The SLT activities were embedded in a context or in games or used resources relevant to the age group or development of the child. Table 57 highlights typical activities and their aims. The sessions were delivered by a SLT supported by a DMT.
| Children’s groups | Purpose of the intervention | Task variables |
|---|---|---|
| Communication skills group (age 2–3 years) | Good looking/attending, good listening, good turn taking, understanding emotions, pretend play | Familiar/unfamiliar objects, familiar/unfamiliar pictures |
| Language skills group (age 3–4 years) | Following child’s lead in play, waiting, expanding and adding words, naming items, Derbyshire language scheme, introduce ‘who’ and ‘where’ | Structured/unstructured, familiar/unfamiliar objects, familiar/unfamiliar pictures, culturally relevant (multiethnicities) |
| Speech sound group (age 4–5 years) | Rhyme, syllable clapping, individual sound identification, sound identification in words, introduction to blending | Structured/unstructured, familiar/unfamiliar objects, familiar/unfamiliar pictures, culturally relevant (multiethnicities) |
Initially, four themes (body language, vocalisations, attention and engagement) were generated after the familiarisation stage of analysis (see Chapter 1, Methodology overview), which provided insight into the children’s perspectives on the therapy tasks. These were revised down to three during the charting and indexing stages, which then became the basis of the thematic framework. The theme of ‘attention’ was revised to ‘visual attention’ as it was often difficult for the researcher to ascertain other aspects of children’s attention, such as if they were listening. Visual attention provided a more accurate reflection of the researcher’s analysis. The theme of ‘engagement’ was taken out of the thematic framework as it was considered that this was actually a higher-order theme that included all of the others. So, for example, analysis of children’s body language, vocalisations and visual attention enables us to give voice to the children’s levels of engagement. This final stage of analysis is the interpretive stage of framework analysis and seeks to link the objective observation of children’s behaviour through interpretation to a view of the children’s engagement and their perspectives. The link between the thematic framework, which is based on observations of children’s behaviours, and the interpretive analysis is shown in Figure 17.
FIGURE 17.
Framework developed for exploring children’s perspectives.
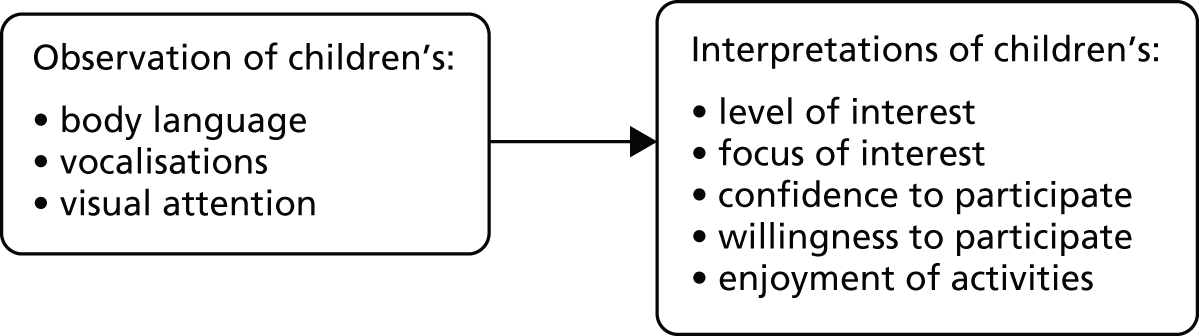
In the next sections the characteristics of the child’s body language, vocalisations and visual attention are described along with the interpretations regarding how they link to children’s perspectives on the therapy activities. Examples from the analysis are presented but all names have been changed to protect confidentiality. Examples are also provided from researcher field notes.
Body language
Body language included any position or movement of the body that communicated something about the child’s participation, including the position and orientation of their body, movements associated with the expression of emotions, general body activity and movement and also fidgeting. Different aspects of the child’s body language gave insight into the child’s perspective.
Table 58 displays the different aspects of body language that were explored.
| Categories | Subcategories |
|---|---|
| Body position | Orientation |
| Openness of the body | |
| Extensions | |
| Proximity to object, group or activity | |
| Emotional expression | Facial expressions |
| Whole body movements | |
| Body activity/movement | Size of movement |
| Strength of movement | |
| Completion of movement | |
| Fidgeting | Handling objects |
| Repetitive movements |
Children’s body position, such as their orientation towards an activity or the openness of their body, spoke about their willingness and confidence to participate. For example, often early on within sessions children’s bodies were more closed in, their shoulders hunched over, legs tucked in or heads low. Children were watching and listening to the SLT or activity, but were cautious.
This contrasted with other occasions when children were sat up with their legs stretched out in front of them, or leaning back on their hands, suggesting that they were more relaxed. Sometimes they extended a part of their body towards an object, demonstrating their curiosity in an object and wish to touch it. Children’s proximity to objects or other children also spoke about their wish to touch that object or have their turn. For example, one child stood right next to a toy whilst another child played with it. Their close proximity to the toy suggested that they were guarding it, wanting it for themselves.
Children expressed emotion through facial expressions and their body movements. Children frequently smiled during SLT activities, particularly as they became more familiar with the therapist and activities and were more confident and relaxed. They often expressed excitement and enjoyment through body movements, such as clapping their hands or bouncing on to their knees or emphasising specific movements.
The size, strength and completeness of children’s body movements gave some indication of their confidence to participate. Body language often became more confident and energetic during activities in which participation was simultaneous, rather than in turn-taking activities, within unstructured (child-led) sessions. Children were often more vocal during active, simultaneous activities, sometimes giggling and laughing and initiating vocalisations, as highlighted in the following quotes:
Shakera is rolling on the floor. Lottie [facilitator] lies down on the floor. Then Tajo lies down and giggles.
General play, site 2, session 4
Jazz then plays with a cup and shows Naomi. Jazz says something to Naomi and then tells her ‘I’m getting dressed up’. Naomi repeats more clearly ‘you’re getting dressed up’. Jazz says again ‘I’m getting dressed up’.
Miniature world, site 2, session 2
He [Tajo] echoes Sam [facilitator] saying ‘taller’ and gestures with his arms. He is confident in his movements as he puts the bricks on one by one and smiles when they come down.
Bricks, site 2, session 4
Children fidgeting was common throughout all activities in which they were watching or listening to another person. Children fidgeted with their clothes or their fingers or a specific object, sometimes for no apparent reason. Sometimes children appeared to be listening while fidgeting; at other times they seemed distracted or disengaged.
Some (but not all) children who were initially reluctant or cautious in their body language responses became more confident in repeated sessions of the same activities or as they began to be more familiar with the adult facilitators. There were also different responses between the specific focused activities and the physical, more active play. Within most groups, one of the children displayed body language indicating their discomfort with and withdrawal from more physical activities, which the majority of children enjoyed. For example, one child during the musical instrument and more active session appeared to be ‘deliberately not taking part’ and ‘was reluctant to take part in the running’, whereas the other three enjoyed the experience. During most of the physical activities this particular child also had limited eye contact with the adult facilitator.
Vocalisation
Children’s perspectives were evident through the quality of vocalisations, the number and type of child-initiated vocalisations and their responses to other vocalisations, as well as through non-verbal vocalisations, such as giggling or screaming. Often children’s vocalisations demonstrated their seeking interaction and relationships with the SLT or facilitators and went alongside making eye contact with them.
Table 59 displays the different aspects of vocalisation that were explored.
| Categories | Subcategories |
|---|---|
| Quality | Loudness |
| Speed | |
| Child initiated | Questions |
| Communicating wants and needs | |
| Commenting | |
| Declaring ability | |
| Responses to SLT or facilitator | Completeness of response |
| Repetitions | |
| Expressing support | |
| Non-verbal | Expressing emotion |
| Expressing needs | |
| Commenting |
The quality of vocalisations, in terms of loudness and speed, provided another indicator of children’s confidence to participate. Children were initially quite quiet during structured SLT activities. As children became more familiar with activities and with the SLT, they responded more quickly. For example, some children gently mouthed the words of the ‘hello song’. They wished to participate in the song but were unsure or unconfident. Other children sang along:
All children sat quietly while each was sung the ‘hello song’, none joined in with the words or actions. John asked ‘what’s that there’ about something behind Lydia. Saul then joined in with the actions for the song when sung for Lottie and Sam and Lydia. Giles joined in with signing on the last one for Lydia, quite loudly.
Site 1, session 3
Children often initiated vocalisations to gain the SLT’s or another facilitator’s attention. Some children asked questions or commented on what was happening. Children also initiated vocalisations to communicate their wants and needs. For example children said the names of objects that they wished to touch or, if they needed help fixing their camera, they made a vocalisation to attract the facilitator’s or the SLT’s attention. There was a marked difference between structured and unstructured groups in terms of the range and quantity of vocalisations. Within the unstructured groups there were many more child-initiated vocalisations, particularly children commenting on what they were doing. Their vocalisations and making of eye contact with the SLT or facilitators suggested that they wished to interact with them and tell them about the activity that they were engaged with.
When the preschool children were given an activity, they responded in a variety of ways. Some did not appear to understand and did not speak at all (John not moving; Tajo upset; Jade sucking her finger; Christopher sitting outside of the circle). It then needed considerable skill to coax them to the activity or even to join in with the others. Others were full of ‘chatter’ and in some cases would sing (Lotte, Natasha):
When challenged to talk Christopher put his chin on his chest and did not look at the person asking him to speak.
Putting things in tube, site 3, session 4
Saul speaks confidently and loudly; ‘a pig’, ‘oink oink’, ‘it’s a chicken’, ‘ba ba’, ‘moos’, ‘cow’, ‘horsey horsey’, ‘ney ney’.
Animal noises, site 1, session 3
When they sing to Sam, Terry bounces his head a little with the rhythm of the song and is louder and more confident singing the words, he looks around a little more. Natasha doesn’t join in at all, but looks at Emily and Sam and the songs are sung to them. Emily asks Terry to take the picture off the timetable. He takes a while to respond and then shuffles on his bottom to the timetable, stands up and takes the picture and gives it to Emily. He then puts his hand in his mouth and runs back to his seat – his facial expression is one of uncertainty/self-consciousness, head still slightly bent down.
Hello song, site 2, session 1
Visual attention
Visual attention refers to the direction and movement of children’s visual gaze and included children watching the SLT and other children, making eye contact, focusing on objects and also looking away. Observation of children’s visual gaze was assisted by analysing video footage from the Kiddicam. Table 60 displays the different aspects of visual attention that were explored.
| Categories | Subcategories |
|---|---|
| Watching SLT | Watching talking |
| Watching movements | |
| Making eye contact | During activities |
| Before speaking | |
| Watching other children | Turn taking |
| General monitoring | |
| Focus on objects | |
| Looking away from activity | Looking down |
| General monitoring | |
| At another specific object or activity | |
| Switching attention | Between eye contact and object |
| Between another and own activity |
Children spent a lot of time watching the SLT, particularly in the structured groups. They watched her face while she was speaking and also her body movements as she brought objects and toys out within activities. Their focus on her suggested that they were listening and were interested in what she was saying and doing. At times, children’s visual focus switched to focus on objects that were involved in the activity. For example, during the musical instruments activity children’s visual attention was directed more at the instruments whereas, during the activity in which children were listening to animal noises, children’s visual attention was directed at the SLT’s face.
Children would also spend time switching attention between the SLT’s face and objects within activities. This was more notable within the unstructured sessions in which children played with different objects independently. Children’s switching of attention between objects and faces and making eye contact with the SLT or facilitators suggested that they sought the SLT’s affirmation, reassurance and shared participation in play.
Children also watched other children. Children directed their visual attention towards other children a lot during turn-taking activities in structured groups. This also occurred within unstructured groups. Children would move to watch another child in the room more closely as they played and interacted with a facilitator or the SLT. Children would also glance around the room to monitor what other children were doing. These observations in the unstructured groups suggest that children were curious about the activities of other children and wished to be a part of those activities. Some would stare at the other children as if seeking their cues from them.
On occasion, children spent time looking away from a group activity. Sometimes their visual attention was caught by something specific and at other times children would glance around the room, as if monitoring if anything else of interest was occurring. Many children lost slight concentration and had to be brought back to the activity. On the other hand, children were rarely distracted for long and some children appeared attentive throughout (Lottie) whereas a few showed evidence of less attention in the activities, although they were happy to be there:
All attentive, except for John . . . distracted by other things in room.
Magic, site 1, session 3
Terry needed his attention to be taken to the black fabric and away from the one that he had selected. At this he looked at Sam and Pascale, it appeared that he was looking for reassurance. Mitchell and Natasha both laid down and watched Terry being swung back and forth.
Warm-up, site 2, session 1
During the ball rolling activity all of the children seemed to display good looking. Mitchell moved into the middle of the circle, indicating a real desire to engage in the activity. The turn taking element to this game seemed to help Mitchell retain his focus. The game developed into more throwing than rolling, with both Mitchell and Terry throwing the ball. Lydia then allowed the game to move into more free play with the children rolling it to anyone in the circle. This seemed to suggest a high level of focus and engagement.
Facilitator field notes, site 2, session 3
A few children also attempted to gain attention through physical contact (Mitchell running around) rather than by speech. In these situations the noise that the child made was noticeably loud and may have even been misinterpreted as aggression if the facilitator had not swiftly acted to regain attention.
Structured and unstructured activities
The initial choice of therapy activities and the framework method also allowed an analysis of issues relating to the structure of the groups and how this subsequently impacted on the groups’ engagement with adult facilitators as well as other children. In unstructured (child-led) activities, children’s body language showed relaxed movements and there was much louder vocalisation, suggesting that the children were more confident in these contexts. However, there was also less turn taking, active listening and attending and more interruptions, fidgeting and watching of other children than in structured groups. Conversely, in structured groups more active listening and watching what the adult was doing and saying was observed. The familiarity of the activity was also influential, leading to body language and vocalisations associated with confidence.
The three themes of body language, vocalisations and visual attention provided a useful framework for observing and interpreting children’s perspectives. In general, children’s experiences of speech and language therapy were positive. The majority of children were attentive and engaged in all of the activities. Children’s engagement and enjoyment ebbed and flowed throughout the sessions and individual children responded in different ways to the various activities. Children tended to be more relaxed, confident and expressive when participating in activities simultaneously with other children than in turn-taking activities, although as the turn-taking activities became more familiar to children their confidence and enjoyment of these increased.
Study 4.2: the perspectives of parents on speech and language therapy
This study aimed to explore parents’ views of speech and language therapy and the activities that SLTs commonly use with children. The views of parents of preschool children who have received speech and language therapy were explored using three data sets: (1) focus groups; (2) telephone interviews; and (3) play-based group sessions. The data revealed key themes that describe parents’ experiences of therapy, their role and their perceptions of the effectiveness of intervention. The themes that emerged from these discussions are described along with a description of how the parents’ perspectives map onto the typology themes (identified in Chapter 2, Study 2.1: identifying the themes of speech and language therapy practice). In addition, the views of parents who are concerned about their preschool child’s talking were gathered, using a national online survey of the acceptability and feasibility of the activities that SLTs commonly use and whether parents understood the rationales behind the activities.
Research questions
In terms of understanding parents’ direct experiences of speech and language therapy with their child with PSLI, the research questions were:
-
What were parents’ experiences and understandings of the SLT-led interventions offered to their child?
-
What were parents’ perceptions of the changes occurring in their child and their views on what had contributed to those changes?
In terms of understanding parents’ views on the parent strategies and activities recommended by SLTs for preschool children with PSLI, the research questions were:
-
Do parents feel that they understand the intervention strategies used by SLTs?
-
Do parents consider the strategies as appropriate for their child and feasible to implement?
Methodology summary
A summary of the methods is shown in Figure 18; the methods are described in detail in Chapter 1 (see Methodology overview).
FIGURE 18.
Summary of the methodology used to gain the perspectives of parents.
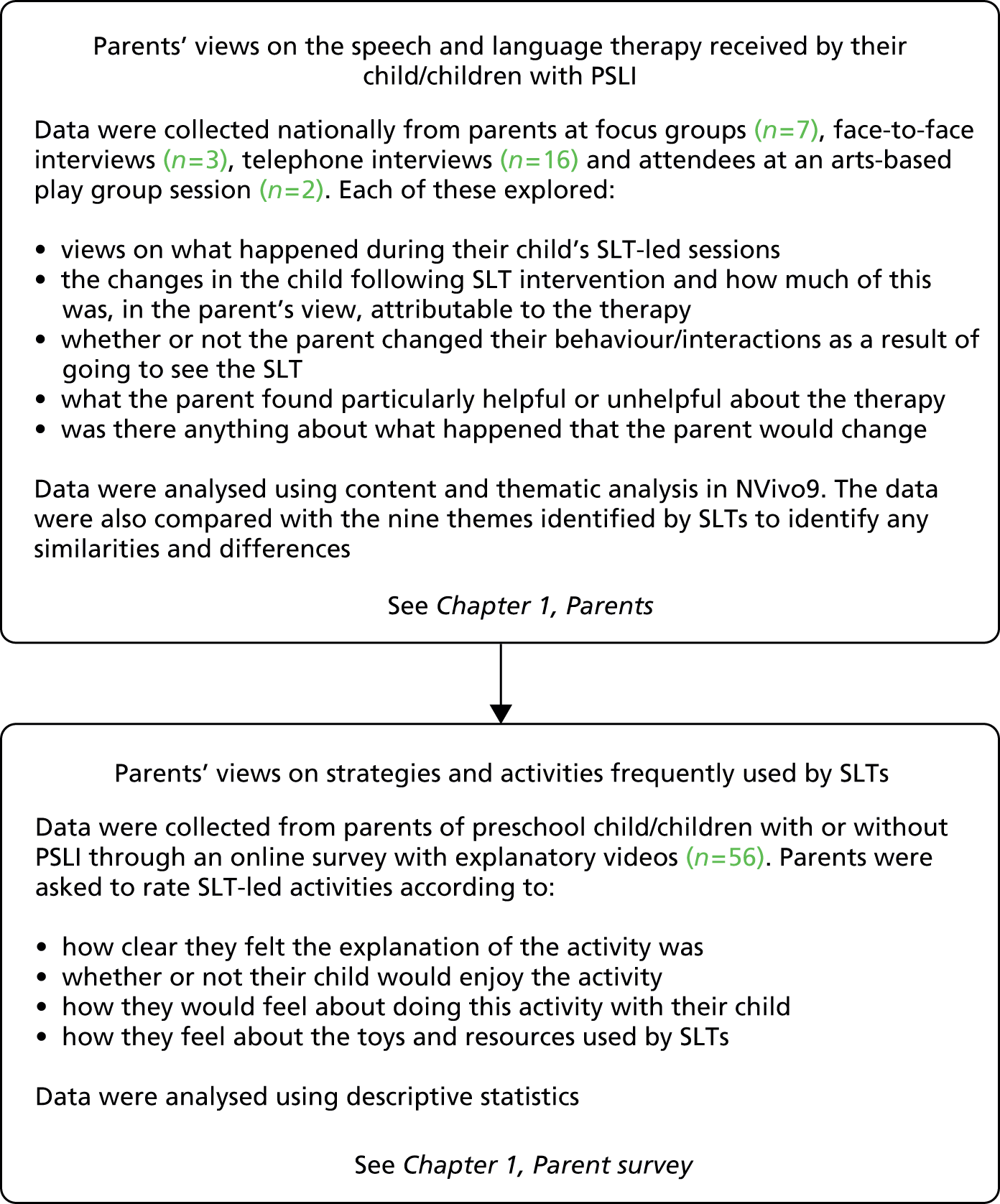
Findings
Parents’ views on the speech and language therapy received by their children
The themes and main characteristics that were identified from the parent data are shown in Table 61. Each theme is presented below with illustrative quotes.
| Theme | Characteristics |
|---|---|
| Enlightening | Realisation and acceptance |
| Learning about my child’s communication | |
| Learning about me interacting with my child | |
| Reassuring | My child’s prospects |
| My role in my child’s speech and language development | |
| Uncertainty | Rationale for therapy activities |
| Future support for my child | |
| Passive | |
| Anxiety | |
| My responsibility | An additional pressure |
| Guilt and failure | |
| Empowering | |
| Fun and engaging | Games |
| SLT–child relationship | |
| Familiarity | |
| Skill | |
| Fear of judgement (stigma) | On my child |
| On me as a parent | |
| Low expectation of services | Lucky to have support |
| Burden to services | |
| Seeing my child improve | Specific sounds |
| Saying more | |
| Others understand more | |
| Joining in | |
| Friends | |
| Confidence to speak | |
| Less frustrated | |
| Better behaviour |
Enlightening
For many parents, interaction with SLT services was enlightening in different ways. Some parents found answers to questions that they had been asking in terms of their child’s diagnosis. For some parents, engaging with SLT services was threatening to their ideas about their child, and over time parents came to realise and accept that their child had communication difficulties that may impact on his or her life in different ways as he or she grows older and which require support:
And it is being a parent thinking ‘speech and language’ is going to sort him out, and I think I did think that.
umhum.
You know ‘he is going to be able to talk’ and obviously it isn’t that, it’s not how it works, it is there to enable and help as far as possible. and whether he would have done that without, I don’t think he would have done, I don’t think he would have done it as quickly and as confidently, I think it has given him that confidence. It has given us the confidence as well. To sort of work with him and he has a habit of whispering, if he is not sure he whispers and he would do that quite a lot at the beginning of a session but then, I think it was him understanding that if he would try then it is a two way thing as it were and actually it is quite nice to have a conversation and you can ask for something rather than just going ‘aaaaaa’. Then I think it was a confidence thing definitely.
So this change in your perception of going from a position where you originally felt that speech therapy was going to solve everything to a position where you are now. How did that come about, tell me, talk me through that sort of process?
Well I think that was a hope of ours that that was going to be the case. Obviously in our heart of hearts in reality that wasn’t going to be the case. But it has, I think it is just acceptance as well from our point of view that, of where he is at and where he is against his peers. But I think it was more of an acceptance thing.
. . . it was like oh my god we’ve got to, you know this is like going to be a massive part of his development that is missing. I mean I don’t know whether I just sort of thought merrily it would all happen [laughs] it’ll be fine! Um but that was really, but I really, I really appreciated that honesty, that I mean they were really supportive, and I’ve always felt that I’ve been able to just ask them something at the end of the group.
PAR_TELL_521
Some parents also described learning about their child and themselves, in terms of their interacting with their child, through observation and video feedback work they had done in parent–child interaction therapy specifically and also through watching the SLT interact with their child in therapy sessions and noting strategies that the SLT used that supported their child’s communication:
Can you put the carrot in the cup so make sure she understood what on, under, behind and all that kind of thing was, that was quite good.
Yeah.
And quite informative actually because I didn’t realise how much she didn’t know. It was really helpful actually, about how as a parent becoming over involved in play, about sitting back and letting your child, cos the child can’t hear and you’re talking about another toy, like look at the dolly, and they’re looking at something else, it’s just quite confusing. And just quite simple stuff that I was probably doing anyhow, but it just sort of crystallised, it was very helpful, those four sessions and the speech therapist.
That was helpful with speech therapist video work, because you could see how you were doing it. And she gave quite positive feedback, which is good because it’s always nice to hear that. But I think the four sessions before at the nursery with speech therapist helped with that. I don’t think the role-play was as good. . . . And seeing films of speech therapists work with other mums, and how not to do it and helpful things, it’s a very effective tool, role-play and to slow down your child you know just . . . let him lead the play instead of me leading the play, and I’d never thought of that before.
PAR_371
. . . from a parental perspective it took, it felt like she, you know it could have been achieved, it could have been achieved forcefully but obviously that wasn’t the way to get him to say it and in actual fact her pace was exactly right because he does now say, he’s now says them both fine and it must have been giving him the space to do it at his own pace I think really.
PAR_TELL_518
Reassuring
Many parents found their contact with speech and language therapy services reassuring. Parents sought and received reassurance from SLTs about their child’s prospects. Some parents looked for clues about the seriousness of their child’s condition from the ways that SLTs talked about their child and the amount of support provided. Another parent described being explicitly reassured by SLTs through comparison between their child and other children whose difficulties were perceived as worse. Some parents sought reassurance about their role in their child’s speech and language development and whether or not they were doing enough:
So I guess the sort of slightly laid-back attitude gave me reassurance that they weren’t worried.
PAR_TELL_518
She was very positive, what was helpful from her was she was very nice, um very positive and kept saying she sees children a lot worse.
PAR_371
it’s just nice to get the professional advice and just feeling I’m doing ok, right things.
PAR_TELL_519
Uncertainty
Many parents expressed uncertainty about why SLTs were doing specific activities with their child or uncertainty over the reason for focusing on one aspect of speech and language over another. Within the research interview some parents questioned what SLTs were doing and had alternative opinions about the needs of their child, but they did not articulate their questions or opinions to the SLT at the time of therapy. In this respect, parents were passive in the intervention process and put themselves in the hands of the expert SLT, which they then later questioned:
I did but I didn’t personally, I mean obviously I don’t, I’ve not studied speech therapy and studied the method to how it’s done, from someone not knowing anything about it, just as a parent, it did seem like there was more important things to concentrate on than her using the word the . . . but like I say I don’t understand the grounding behind it I guess and the reason for doing it in that particular way.
What would you have thought was more valuable or important to work on?
Getting her to say the words that she is saying correctly.
Yeah, I mean she had a whole range of, she looked to have a whole range of toys and games in the room but I must admit most of the time we went there we ended up doing the same things, I don’t know whether there was some reasoning behind that or I don’t know.
PAR_546
you don’t know what to believe, yer, its not really clear whether our way is the right way or why we have it this way and what has informed that judgement.
PAR_020
So of all the things that the speech therapists have done and said to you, what, could you pick out one or two things that have been the most helpful messages or advice that they have given to you, in terms of understanding R’s difficulties or the kind of therapy they have provided, explanations they have given?
No, I don’t . . . they have[n’t] given much feedback there really. Because you don’t really . . . he goes in and does what he is supposed to do and then come out.
OK.
There isn’t that much communication.
So that is a lack really.
Yer.
What about in terms of your?
But then it is up to me to like listen to what they are doing or to ask.
yeah but nothing seems to, it seems to be getting better but I’m anxious to see her again, to see what else we can do, because at the moment it’s not very clear.
PAR_371
Parents were also uncertain about the support that their child would receive in the future, both from speech and language therapy services and also within nursery and later at school. Parents were concerned in terms of their child’s experience of, and participation in, nursery and/or school and perceived support as important for both of these. Uncertainty about future support for their child was a source of anxiety for parents. For one parent, uncertainty about the quantity and regularity of SLT support was a source of anxiety and a reason why she had sought support from a private SLT. The private SLT provided her with stability in terms of the quantity and timing of therapy that her child would receive for the coming year, whereas the quantity and timing of support provided by the NHS speech and language therapy service was unclear:
So I don’t like that I don’t know whether that’s the preschool playgroup or whether that’s the speech therapist that need to make the contact. I don’t know who contacts who but I’m happy I’ve said to both parties you know I’m happy for you to work together.
PAR_TELL_515
So, and he’s just started a new nursery cos we’ve moved, and I do worry about little peer groups, with other children and, yeah, I’m just worried, very worried for school.
PAR_371
My responsibility
Many parents talked about their role in, and responsibility for, their child’s speech and language development. This was often in the form of homework activities that the SLT had given parents to do with their child at home. There were many mixed emotions associated with parents’ perceptions of responsibility, from feeling empowered to help and wishing to know what more they could do to feeling guilty:
it’s more trying to get him to talk and then obviously if he’s saying sand and I say oh what sound does that start with, is it a ‘s’ or a ‘f’, you know that kind of thing.
Yeah, do you think you would have done that if you hadn’t been to the speech therapist or would you have made.
I probably wouldn’t have been as confident to do it so.
it’s advice you’re given and you think oh that, you know that’s really good advice. Yeah we definitely changed the way we do things, definitely.
PAR_TELL_516
erm, I think stuff like accepting, accepting all his communication speech, that was very helpful. In like terms of, the whole thing of taking the burden of not understanding. But onto my shoulders rather than his.
PAR_TELL_521
we were in the car, and because I was getting more response from her, ‘xxxxxxx look at that’ and she’d say what it was, and it made me think ?? but it made me get him involved more. And I do more, since that I’m very conscious, I’ll say to both the boys now in the car xxxxx is at school, he jokes to me now he’s older he’s four, and I’ll say, ‘and look xxx too’ so I’m getting them both involved. Because I was so focused with my daughter.
PAR_371
I suppose the one thing that stuck in my mind is to not interrogate him and ask him lots of questions . . . because it would bombard him. Which seems like common sense, but sometimes having it suggested reinforces it a little bit. So that has really helped me think about how I discuss things with [child] and also allowing him to kind of take the lead on some things.
PAR_020
Many parents perceived the responsibility of spending more time with their child as an additional pressure on their already busy lives. They wanted to be able to spend more time but often found it difficult to achieve in practice or, when they did, their child did not respond to them as the SLT had suggested. This pressure was also a reminder to parents that their child was different from other ‘normal’ children:
We were given a programme to kind of reinforce the messages at home, etc. and I think if I am perfectly honest, I found that quite stressful, because you are very conscious that it was something, whilst there was no pressure put on by the therapist, I mean there still isn’t now, but there is still that kind of added. It’s something else you feel you should be doing, even if the child isn’t necessarily receptive to it.
PAR_046
and the stress of it all and him not wanting to do it and yer, I suppose it felt like another, and it did feel like another activity, no I think you are right as we had had physiotherapy and had the stuff that they had sent us in terms of his cognitive, yer, you are probably right, it felt like something else to do that most other people don’t have to do if that makes sense.
PAR_046
I think for me it was just the time you know, the time doing it, I just thought it, for me ‘cause I’ve got three children and I work . . . it’s a busy life all the time, I just thought I haven’t got hours and hours to be sat down doing all these things with R all the time.
PAR_546
No I think, I mean she obviously gave us all the sheets to practise at home and we could go through every single sound and he could do it at the time, but it’s just obviously he’s doing it at home but when it came to do it should I say performing he wasn’t really interested in doing it so again this is why I was more interested in having maybe speech and language at home or maybe in a school to be a familiar environment for him.
PAR_TELL_517
And the pre I mean for the first sort of six months I was doing it every day and then she kind of went to the preschool which was quite good for me because I just found that being R’s mother she didn’t really want to . . . co-operate with me, she just, she’d just like to have a tantrum or you know like they do with their mums, they just play them up.
PAR_546
The responsibility that parents described was sometimes associated with feelings of guilt and failure. Parents described their own failures to give attention to their child and to be patient and recognised the impact that this may have on their child in terms of their child’s frustration and behaviour:
So does he often get frustrated with you these days? If he is not able to get his message across?
Yer, he can easily [child interrupts] but, not all the time, maybe a couple of times a week.
Right.
But I suppose it depends what mood I am in as well.
Yes.
Like if you can’t get tea and like get things done you are not as patient are you.
You are not dropping everything to concentrate exactly on what he says.
Yer, so that could be sometimes he gets frustrated because of me.
Yes.
And perhaps I don’t have as much time as what I should have with him. So sometimes it is maybe my fault as well but . . .
I’m not doing enough of it. So I feel guilty a lot of the time. It’s about how I feel guilty, that I’m not doing enough with him.
PAR_371
Fun and engaging
Parents tended to talk about speech and language therapy in terms of the games and activities that SLTs showed them and which they did with their child. Parents talked less about the aims of activities and, when probed on this, parents were often uncertain about the SLTs’ rationale for activities, as described above. The child-friendly, fun elements of games and activities were talked about with animation by parents and many parents noted the efforts that SLTs made to engage their child at an appropriate level, establish a good relationship and make activities fun and unpressurised. Occasionally, parents described instances in which a SLT had not engaged their child appropriately, but in general parents celebrated this aspect of SLTs’ work:
yeah, so work on all different letters all the way through, but very much, and this is why I wanted to show this, cos I’ve been so impressed, is this sound, the talking was, it was so embedded in the games that the children were playing, that they didn’t feel pressurised by it.
PAR_TELL_521
Yeah, yeah I do, he, well most importantly he really enjoyed going there . . . and he really enjoyed he really enjoyed playing the games and he never it was never he never felt like he was there because he couldn’t do something.
PAR_TELL_518
Sorry, little games as well, like have you ever heard of the game hanging monkeys.
No.
Basically it’s on a magnet thing and you have to roll the dice and then roll a hang a monkey and after a while the magnet gets too heavy and falls off, well to make it a bit more fun she said well every time you get one right you can hang an extra monkey on the tree and obviously make it a bit more fun for him.
Yeah.
Just little things like that made it more interesting.
Yes I think so, as I say you know she’s enjoyed it.
Yeah great.
She sees it as something fun to do so I think if nothing else we’ve got that out of it.
A good relationship between the SLT and the child and the fun and engaging nature of speech and language therapy activities were important to parents and were often linked by parents with the SLT’s familiarity with a child and his or her skill in understanding a child’s communication and attention needs:
. . . yeah because obviously, being that bit younger, she, I remember the game with the bag, so she used it. And the speech therapist was, cos she’s changed now because this particular one went on maternity leave, but she was really really lovely, she really spoke to [daughter] she really connected with [daughter] and [daughter] didn’t feel at any point that she was being pushed. Because [daughter] went through a bit of a defensive phase where she knew she was being pushed, and if she couldn’t do it she would just stop talking. If you kept pushing and pushing her she would just not talk at all, so she did have a very good way of making her, engaging with her, she’d sit down and she would talk to her.
PAR_TELL_596
I would have liked to have like seen him maybe progress a bit more like I say I don’t think the techniques that she had it was totally well successful, if suppose, like I say she didn’t really vary it a great deal you maybe she was getting bored of the fact that he wasn’t really answering the questions and he didn’t want to co-operate.
PAR_TELL_517
absolutely [L: yeah] yes definitely and he gets on so well with the speech therapist he’s seeing, they get on so well together, I think that gives him confidence as well.
PAR_TELL_516
I think really, it’s getting the children comfortable, familiarising them with the situation, and I think as well again like I say, I think the fact that they would do a similar activity with different toys to start off the session each time, built his trust in the group to speak.
PAR_TELL_521
Fear of judgement (stigma)
Several parents were fearful of others’ reactions to their child attending speech and language therapy services and any associated diagnoses that their child might receive, meaning that their child would be viewed by others as having low intelligence. These parents emphasised that their child was otherwise bright and able and had difficulty only with his or her speech and language. One parent was concerned that her child’s referral to speech and language therapy services was a judgement about her as a parent. For these parents, engagement with speech and language therapy services was negatively impacting on the identity of their child and their family:
I don’t want them judging her intelligence.
No.
Because her intelligence is fine it’s . . .
Yeah.
Just being able to say the words.
Low expectations of services
When asked about their satisfaction with speech and language therapy services, many parents talked about the additional support that they would like or the resources that they thought could be better, but in the same breath they described themselves as fortunate to be receiving support and were accepting of inadequacies. Parents often mentioned the resource implications of the support that they received. In this sense they perceived themselves and their child as a ‘burden on the state’. They did not have high expectations for speech and language therapy services and were grateful for the support that they received:
And were you kind of happy with the frequency of therapy and the kind of resources available and amount of time.
Well to be honest I was sort of grateful to be receiving it at all really.
Well, I don’t know if, I don’t know if more frequent, seen more frequently would help, once a week does feel like it’s quite a long time between each appointment.
Yeah.
I’m just thinking he’s on this reading recovery scheme at school at the moment which I’m wondering, makes me wonder if he’s on that, if that’s if it’s a result of having had speech therapy but he’s seen every day for that.
Like I say I think the following sessions did benefit him a bit more, I know it’s probably a bit more financially well quite more expensive for the NHS.
PAR_TELL_517
Seeing my child improve
Parents talked about the improvements that they had seen in their child’s speech and language, particularly in terms of their child interacting with others more, being able to make specific sounds, being more confident to speak, joining in at home and at nursery, playing with friends and showing fewer signs of frustration or difficult behaviour, as well as others being able to better understand what their child says. Some parents linked improvements directly to SLT activities and other parents found it difficult to know whether the improvements that they were seeing in their child would have happened in the absence of therapy:
hm, yeah. I think he’s quite clear compared to how he was.
PAR_371
He’s interacting better with other children, other adults can understand him when he asks for things.
That’s great.
He just seems a happier more sociable child now.
Because she can talk now and you can understand her.
Yeah.
Half the words aren’t perhaps that clear, people don’t have a problem with understanding her now so for her to socially she’s now making friends and got a good little group of friends whereas before when she was at preschool before she had the speech therapy sessions she wasn’t really doing that she was quite sort of . . .
Yeah.
Other than the friends we had in our own circle she wasn’t making any sort of external friends by herself.
It’s it’s getting a lot better, I think being at school helps that, he still struggles to form sentences, we’re probably looking sort of up until probably six months ago it was two three words, it’s probably moved on a little bit now sort of, he’s starting to put sentences together but you know he wouldn’t say ‘please can I have a drink of water, mummy?’ or something like that he’d just say ‘water, mummy’ and that kind of thing. His speech is getting a lot clearer, he’s still in terms of his pronunciation, his blending of sounds, sometimes it’s quite hard to understand what he’s saying, particularly out of context and then that can make him frustrated.
PAR_046
Yes, yeah definitely I think, I really think the speech therapy’s been vital to that. Like I say being able to make those letter sounds, because he refers to the signs that he makes in speech therapy, if he’s not getting the sound right. so that really helps me. Like if he’s trying to say something he like a ‘d’ he does like a drum, so I know that’s what he wants to, but he can’t get his mouth around it. Or, or sometimes when he’s, like when he really learnt to say ‘knee’ cos for him he just couldn’t do the first sound at all, even when he’d progressed from ‘dadada’, he could do ‘eee’ but not ‘neee’ and making those initial letter sounds, that has definitely come from speech therapy.
PAR_TELL_521
Absolutely, he’s so much more confident with his, in himself, and so many words all the time, and sometimes he’ll come out with words, and you’ll think ‘oh did you just say so and so’? You know improving what he’s saying all of the time.
PAR_TELL_516
I mean this time last year to what he is now there’s such a huge difference in him you know myself and the family can see you know it’s amazing and you know obviously that’s not all through speech and language it’s just that he, maybe the fact that his hearing cleared up as well.
PAR_TELL_517
Some parents described how changes in their child’s communication and/or strategies that the SLT had taught them to help with communication had helped their relationship with their child and their own frustration with their child:
Just I didn’t force to like, I used to get, feel frustrated when she cannot say thank you, just one word say thank you, my friend and I felt like I felt parents should and yeah so I kind of asked her why can you not say thank you for food and it’s not polite, not nice and I just stopped saying these things.
Yeah.
And said if you don’t want to say it you don’t have to say it and . . .
Took the pressure off.
So, yeah.
In general, parents spoke positively about their SLTs and the intervention that their child had received. Parents appreciated the relationship that SLTs built with their child and the way that they engaged their child in speech and language activities that were fun and held their child’s attention. But there were many anxieties and uncertainties about the kind of progress that their child was making, about the potential stigma associated with the impairment and receiving speech and language therapy and about what was actually happening in therapy sessions.
Parent views on strategies and activities frequently used by speech and language therapists
To obtain the views of parents on commonly used SLT-led activities, the research team worked in collaboration with the parent panel to produce videos of a SLT undertaking these activities with a child. Each video was followed by three survey questions asking whether parents understood the activity and the acceptability of it. The research team organised four ‘coffee mornings’, which took place in a range of locations. One was at a pre-existing support group meeting for parents of children with SLCN, another was facilitated by a school, which organised the event for parents, and two further coffee mornings were arranged directly by the research team. A further 43 parents responded to the online survey, which was advertised via a recruitment video: a whiteboard animation designed and voiced by the parent panel. Across the groups a total of 57 parents responded to some part of the survey, with at least 28 parents responding to all of the videos. It was not necessary for parents to have had direct experience of speech and language therapy for them to take part as we were asking for their views on the activities and how acceptable they would be to them and their child. However, we did target recruitment at parents who were ‘worried’ about their child’s talking as this feeling of ‘concern’ might impact on how they felt about activities compared with parents who had no concerns at all. The number of survey responses for each video is provided in Table 62.
| SLT activity | Coffee mornings | Online survey | Total |
|---|---|---|---|
| Auditory discrimination | 27 | 29 | 56 |
| Child’s levela | 14 | 43 | 57 |
| Commenting | 15 | 34 | 49 |
| Concepts | 15 | 28 | 43 |
| Eye contact | 16 | 23 | 39 |
| Praise | 12 | 22 | 34 |
| Repetition | 12 | 18 | 30 |
| Turn taking | 12 | 16 | 28 |
| Waiting | 12 | 17 | 29 |
As indicated, not all of the 57 respondents watched all nine videos. Furthermore, not all respondents answered all three questions that related to each video. Responses to the three questions are provided in Appendix 30. Overwhelmingly, respondents indicated that they understood the explanations given, that the activity or strategy was feasible and that they and their child would be happy to carry out the activity. There were no statistically significant differences in parents’ responses across the different therapy activities (r = 0.774, p < 0.024). Therefore, data have been collapsed into the three main questions rather than presenting the survey responses for each activity individually (Figure 19).
FIGURE 19.
Parents’ views about the acceptability of the speech and language therapy activities: collated responses from parents (n = 57) to survey questions regarding nine SLT activities.
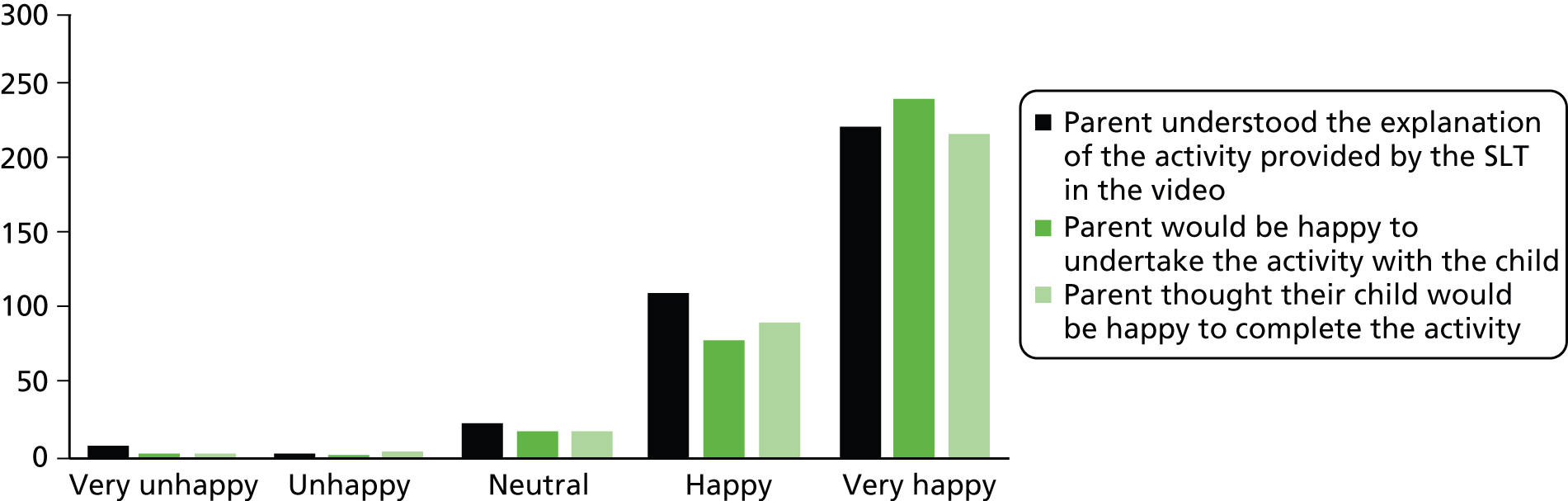
Thus, of the 57 parents who responded, the activities posed no particular problems for the majority. However, a small number found the explanations unhelpful, were unsure that their child would enjoy the activities and felt that they would not be able to carry out the activities with their child.
Study 4.3: the perspectives of communities who are underserved by speech and language therapy services
This study aimed to explore the views of communities who were perceived by speech and language therapy services to be ‘underserved’ by their service. The communities identified included carers of looked-after children, minority ethnic groups and families of low SES. The views of these communities on speech and language development and engagement with services were explored using focus groups that were held with established parent groups and which were accessed with the support of Barnardo’s. A thematic framework was used to analyse the data, which revealed themes, both within and between the communities. The data suggest that, although parents were confident about how to support children’s language development, they were less informed about the nature of speech and language impairments and the function of speech and language therapy.
Research questions
-
What are the beliefs about development, delay and disorders of speech and language of people from groups who are perceived by speech and language therapy service professional leads to be underserved?
-
What are the reported practices of these people with respect to the development, delay and disorder of speech and language in their children?
Methodology summary
A summary of the methods is provided in Figure 20; the methods are described in detail in Chapter 1 (see Methodology overview).
FIGURE 20.
Methodology summary for the underserved groups.
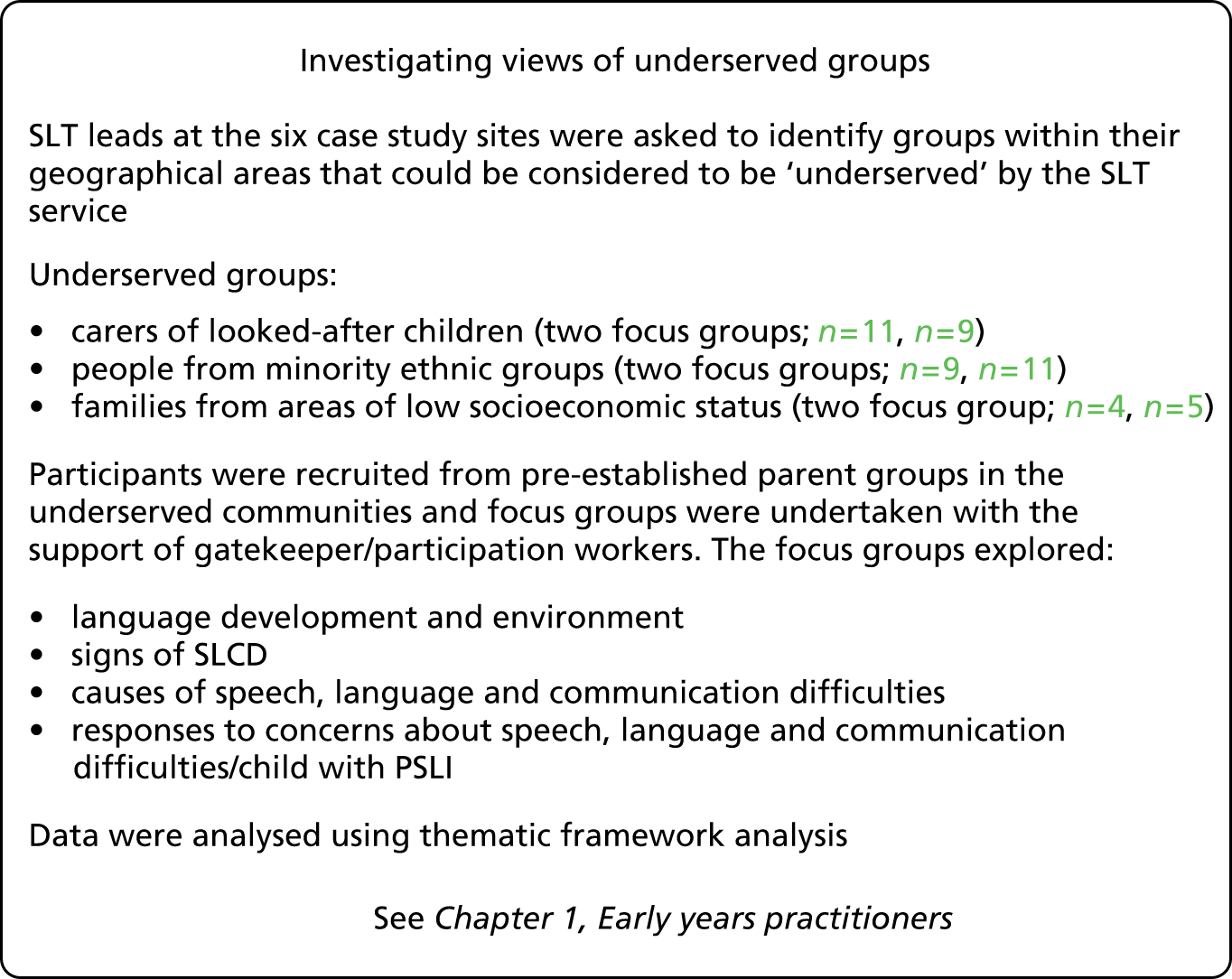
Findings
Following the familiarisation stage of the analysis, and using the a priori issues from the research questions, a thematic framework was developed. Data were charted using this framework and the characteristics of each theme were identified. The findings are presented for each focus group separately. A final stage of analysis looked across the groups with regard to each of the main themes.
Carers of looked-after children
Two focus groups were held with carers of looked-after children. Participants in the first group were part of a local authority group based in the north-east of England (n = 11; one male, 10 female) and participants in the second group were engaged with an independent fostering agency in the south-west of England (n = 12; two male, 10 female). The length of experience of fostering ranged from 18 months to 8.5 years (mean 4.3 years). A number of the carers also had their own biological children. The report of the discussion from this group is presented in terms of the key themes identified in the group discussion.
Language development and environment
The carers described the children who they cared for as typically receiving little language input before being placed with foster carers, children who had been previously discouraged from speaking and/or who tend to regress when they have contact with their birth parents. The carers described the strategies that they use to facilitate children’s language development. Their ideas were not novel, for example start early, keep talking, singing, don’t criticise and encourage socialisation and engagement. They described the efforts that they made to try and support the development of social/pragmatic communication skills with children who have lacked previous opportunities to develop important communicative functions, for example learning to argue, contradict and interact:
They don’t get the opportunity to develop that skill, um not necessarily a debating skill but a conversational skill where it can be safe to disagree.
F1078
It is not clear if the carers see this as a speech and language difficulty per se. Hence, there is an overlap between actions that facilitate language development and their responses to what they consider to be speech and language concerns. They emphasised how quickly children progress when they are with adults who talk to them and provide one-to-one input.
Signs of speech, language and communication difficulties
The signs that the carers mentioned seemed to reflect their experiences of children who had been taken into care, for example a lack of attempts to communicate or adults not engaging with children:
It’s just not natural human behaviour for a small child not to want to babble.
F1078
Causes of speech, language and communication difficulties
Similarly, when giving their views on the causes of speech, language and communication difficulties, these seemed to reflect their experiences of children who had lived in atypical environments, for example children who are neglected, lack adult input, lack experiences, have a reduced need to communicate and have a lack of language input. They considered that previous discouragement from speaking impacts negatively on children’s language development:
There are a lot children who are fostered, I think a lot of it’s the same, either they’ve been ignored, nobody asking their opinion, nobody’s wanted their opinion. And all these signals come from every different direction.
F1083
Responses to concerns about speech, language and communication difficulties
The carers frequently described children whose language environment before being taken into care was less than optimal. As already mentioned, when they described supporting these children’s language they did not always describe a clear difference between what they provided for children with delayed language and what they provided for all children coming into their care. They described ‘talking all the time’, discouraging others from talking for the child, using picture cards and games, reading and singing.
There seemed to be a lack of agreement about whether help would be sought sooner if the child had other difficulties or if the speech/language delay was an isolated concern. Some also described supporting children without accessing support from speech and language therapy services:
For me it would only be something that I couldn’t deal with so if it was a child stuttering or stammering and tell them to slow down and listen no matter how long it takes. I haven’t had a need to go seek other professional help.
F1083
Other issues
Carers made suggestions including speedier access to speech and language therapy, assessment in the home, awareness of previous experiences and consideration of the gender of the SLT:
Even the difference between a male therapist and a female therapist could make a huge difference.
F1083
In their view some professionals lack understanding of looked-after children’s possible experiences and speech and language challenges.
Carers described working to facilitate the language development of the children in their care. They seemed to recognise specific types of difficulties that children might experience based on their previous, less than optimal environment.
It is possible that carers have different views on what constitutes a significant enough problem to merit involvement from SLTs, with their views being tempered by their knowledge that looked-after children have previously experienced environments that may not have been conducive to language development and that they may well ‘catch up’ when they are in a more positive environment.
Minority ethnic groups
Three focus groups were held with two different minority ethnic groups. The first was a support group for the Somali community based in south-west England (n = 9; all female). The research team met with this group twice to collect data. The second was a group for RAS based in north-west England, which was accessed through Barnardo’s (n = 11; all female). All of the participants were first-generation immigrants to the UK of African descent, some of whom were refugees or asylum seekers (it was not considered appropriate to collect specific data regarding their status/background).
These were group discussions and, in two of the groups, not all participants spoke or understood English fluently. In these cases other group members acted as informal translators and appeared to summarise the group discussion in response to specific questions posed by the interviewers. It was therefore difficult to capture consensus compared with diversity.
Somali support group
Ideas about typical speech and language development (ages and stages) revealed a range of views, for example that first words emerge between the ages of 6 months and 1 year. Aspects of typical communicative environments for young babies were described and included eating with children, keeping the child close to the mother, children talking to each other, lots of eye contact, singing and talking to babies and using actions to support spoken language. Television was viewed as a positive aspect of the communication environment:
Mum is start talking to the baby cause the baby doesn’t understand, that’s how it develops.
EM0101
The group described and appeared to agree on two types of causes, which appear to be broadly intrinsic and environmental. There was specific description of the apparently high incidence of autism among this community.
Agents that were mentioned as possible causes of speech, language and communication difficulties included injections, air pollution, global warming (because of wars), the English weather, learning two languages and a lack of organic, fresh food:
She believe that the problem we have with children speech is that, children that can’t talk, is because of the war, the food we eat, and the weather.
EM0102
It was mentioned that the reason for a particular child being affected by one of these agents was because of ‘God testing’ parents by giving them a child with a disability; also mentioned was the possibility that having a child with a disability was a punishment for sins. However, the group members agreed that mothers’ behaviour did not cause PSLI and no sense of guilt was expressed:
That is right no guilt, it comes from God and you just try your best and then if it doesn’t work then that is it. We always think that anything comes to us, if you are sick or your child is sick, or anything happen in your life, you have to accept because you don’t, we don’t question.
EM0202
When talking about children with speech and language difficulties there were few signs that were agreed on, although the participants mentioned frustration, lack of concentration and deafness. The age at which lack of speech would elicit concern varied from 6 months to 2 years, with comments also relating to experience of family members who started to talk much later:
Then you can start worrying, but then again we are in denial because they say that your grandfather didn’t talk until he was 6 years old.
EM0101
Responses included both medical and non-medical approaches. Typically, a mother may take her child to the general practitioner or health visitor. The child may also be taken to the mosque at the same time as or before being taken to the health-care practitioner. At the mosque the parent may receive instructions from the imam, passages from the Qor’an may be read over the child or over water/honey that is then given to the child or the child may be prayed over. Neighbours will be consulted about their experiences and advice sought:
We have a saying that ‘100 people will advise you when you are sick’.
EM0202
In response to specific questions, participants agreed that cutting of the lingual frenulum occurred and that honey that has been blessed by the imam may be given to the child to ‘taste’. This group also reported that they might consult doctors outside the UK. One person described being told that a tablet could be given to a non-speaking child as a cure/treatment. There did not seem to be agreement about if a child would be hidden from other community members if he or she had communication difficulties or if the mother would be in denial about the child’s difficulties. To help a child with a disability (they did not always specify PSLI) they suggested that:
She will always support him and bring him what he wants and so for example he is playing with a toy and it rolls away, she will always support him in getting what he wants.
EM0102
Suggestions for supporting language comprehension when a child has difficulties included signing and using body language.
This group also described the things that would encourage families to feel positive about health-care professionals in general (and they were asked if these would apply to SLTs). This included the use of appropriate body language (facial expression, shaking your hand), taking care to ask families for their views and parents feeling that the health-care professional is the expert and that is the reason for consulting him/her. However, they also felt that health-care professionals did not spend sufficient time assessing a child.
Refugee/asylum seeker group
At this focus group a fictitious case study was used to stimulate discussion (see Appendix 31). The group divided into two groups for discussion. Most of the women spoke English reasonably fluently but the facilitators felt that a small number struggled to understand fully.
The participants considered the following to be important in facilitating language development: reading with, and talking to, a child, telling stories, imitation, not using ‘baby talk’, interacting with small babies, singing, a big garden, trips out and providing toys. There were mixed views about the impact of television:
It’s due to us as parents to encourage talking to the children, to prompt them to start talking early, things like reading them books, telling them stories. Even, even, they say children don’t really understand, but it’s not like when you spend time with them like reading the books or anything, it’s not like it’s a waste of time. They still do pick up a few things.
EM03
Intrinsic factors were mentioned, such as genetic causes, prematurity, inability to lift the tongue, laziness, being a ‘slow learner’ and prenatal maternal alcohol consumption.
In terms of environmental factors there was some discussion about the social context of this community in the UK, for example small, fractured families; stressed, withdrawn, isolated or depressed mothers who may not talk to their children a great deal; tension at home; exposure to multiple languages; and bewitchment:
. . . it could be like the mother’s depressed and the mother is not even having time to spend time to read to her, to spend time to, to help her with anything at all so probably could be an issue.
EM03
One participant reported on a traditional view that if a child cries for its mother ‘ma ma ma ma’ it means that there is something wrong but if it cries for its father ‘da da da’ then there no significant problem.
Parents would be concerned if the child was not talking (even when at nursery), was not making any sounds or did not understand language. The point at which they would be concerned varied and there was some suggestion that communicative behaviours that would be a cause for concern in the UK would not be in the participants’ countries of birth.
One participant suggested that time should be spent with a child before identifying a concern and that parents should watch and try to help their child. Participants also mentioned talking to their own mother, a ‘spiritual man’ or a pastor. There were varying views about whether or not to seek advice from a doctor, partly related to whether or not the difficulty arose in their country of origin, where they report that it is more likely that people will wait for a child to mature. They also reported that lack of speech may not be given priority as is it not seen as a ‘sickness’. Isolation was considered to have a detrimental effect on help seeking for this community in the UK, together with a limited understanding of UK services, which may limit interactions with and responses to services:
We don’t know how this country runs, we don’t know anywhere where to get advice, you don’t know whom to ask it.
EM03
In terms of specific interventions, participants suggested saying words for the child to repeat. One participant described how her own grandmother told her to stop stammering and hit her. Another participant reported that stammering is not viewed as a serious problem.
There appeared to be varied knowledge of and degrees of trust of professionals among this group.
Summary of the data from minority ethnic groups
These two groups of women from minority ethics groups, all of whom were African and many of whom were RAS, gave a range of views about speech and language development, delay and interventions. They provided some previously unreported ideas about the causes of language delay, such as global warming and prenatal maternal stress.
Their responses to concerns about speech, language and communication included professional, religious and community responses as well as direct intervention with their child. Lack of confidence in professionals and/or lack of awareness of professionals’ roles may be significant. Views about television were not unanimous and positive views may in part be linked to mothers’ perceived lack of proficiency in English.
The responses of these two groups of women from minority ethnic groups suggest that there may be some translation issues. Additionally, as only two small groups of participants were included, these data should be treated with caution; however, this may indicate an area that merits further investigation.
Families from areas of low socioeconomic status
Two focus group were held (n = 4 and n = 5) with parents from an established group for young mothers in an area of low SES in the north-west of England. This group was accessed through, and is run by, Barnardo’s. All participants were mothers of children aged between 6 months and 2.5 years and so unsurprisingly the discussion focused more on younger children. One parent reported having training in childcare.
Language development and environment
The groups did not add any novel ideas about language development that have not been reported elsewhere in previous research. The participants described a number of positive influences including imitation and repetition (by the child). Talking to and reading to their child (including bedtime stories) was emphasised. Not asking questions was mentioned as something that they had been told by a SLT. Adults viewed using exaggerated intonation positively:
The way you say things helps ‘em remember the words.
LSES1
Fathers were considered to sometimes lack appropriate interaction with young children and babies:
He just reads the story like he’s reading the paper.
LSES1 06
One group talked much more explicitly about play. Some considered that playing alone had positive benefits. Singing was discussed by one group:
If you’re singing the nursery rhymes, they’re learning the words in a happy way.
LSES2 662
Swearing in front of children, regional accents and non-standard pronunciation of words were considered by some to be negative influences and some participants had strong views about these.
Television occupied a significant part of the discussion in both groups, with explanations given by participants about why they generally view television positively, with some qualification about appropriate programmes and the positives of exposure to new vocabulary:
Not everyday words that we’d say ‘oh look that’s a flamingo’, cos you’re not going to say flamingo at home are you.
LSES1 05
There was a range of views about bilingualism and whether children should learn English before starting school and English or their home/family language first.
Causes of speech, language and communication difficulties
These included both environmental factors and factors intrinsic to the child. Intrinsic factors included hearing loss, lisp and cleft palate, other disabilities and ‘psychological difficulties’ (the child is ‘excited’ or ‘mad’) that may result in what appeared to the mothers to be non-fluency. Environmental factors such as ‘baby talk’ were discussed, with members of one group considering this to be a negative influence, although they were not clear if they considered it to be causative of speech and language delay:
I’m not saying it’s wrong but I don’t want xxxx being taught I don’t like it.
LSES2 662
Participants in both groups mentioned the negative impact of dummies (pacifiers/soothers):
If you try and say S with your mouth shut, or something in your mouth, you can’t do it.
LSES1 04
Lack of parental language input was considered to be negative:
I think some mums just don’t realise how like, how it can affect a child if you don’t speak to them from a young age.
LSES1 03
Responses to a child with primary speech and language impairment
One comment, which was not repeated by others but which is pertinent to the ‘adult–child interaction’ approach, was:
I’d think to meself if the child hasn’t picked up as much I’d like now then there’s, then there’s it’s not gunna make much difference if I try a bit more cos I’ve been doing everything that I feel that’s right.
LSES2 663
Participants reported a range of help-seeking responses. These included seeking advice from their mother and friends and professionals, such as a health visitor, SLT or doctor. Three people in one group mentioned that it is important to talk to someone who knows the mother and the child (a member of the family or a friend initially) and that professionals need to spend time with the child before making a judgement and that they should not make assumptions about what the mother is already doing:
. . . knows me and knows xxxxx, so they know like that I’m doing everything right and xxxxx’s still not talking.
LSES1 06
They also talked about the need for early referral compared with a ‘wait and see’ approach and their concerns about being judged by authorities. The more general strategies that they suggested included exposing their child to other children and spending time with their child, including one-to-one time:
. . . introduce ‘em to other children but not children who are slow at speaking . . . so they can play with them, cos I think kids interact with kids better than adults.
LSES1 06
The participants described a small number of specific activities/responses, such as ensuring that they make eye contact with their child to improve attention, using facial expressions to emphasise meaning, repeating a mispronounced word correctly and telling a child to slow down or complete a sentence if a child is non-fluent. There was some discussion about swallowing difficulties, but it has not been documented here. The views of young mothers from one area of low socioeconomic status suggest a level of observation, analysis and justification/explanation regarding language that makes sense to them. They gave reasoned descriptions about language development, influenced by their own experiences, their own mothers, study and the input of professionals. They demonstrated a range of levels of knowledge and views. Their ideas about language development, causes of delay and support for language development have also been described elsewhere. The view that professionals should not make quick judgements about a child, although based on limited knowledge, is important.
Themes emerging across the underserved groups
As described in the methods (see Chapter 1, Methodology overview), following framework analysis procedures the data were examined across groups within each theme. The following themes were identified.
I’m doing my best
Participants in all three underserved groups had ideas about how language develops and how that process is facilitated. They presented themselves as competent language facilitators. Some of them had been exposed to professional advice about facilitating language development and they talked easily about strategies that they consider to support language development (singing, reading, talking, etc.), including some that are viewed negatively by, or that are at least controversial for, professionals (e.g. television viewing). Participants also described some controversial issues, with varying levels of awareness and engagement in discussion about these (e.g. the impact of bilingualism on language development). They also commented on the competence of others, apparently regarding some other people as less competent, for example some fathers and biological mothers (in the case of looked-after children). Views varied, which suggests that professionals should not make assumptions about individual parents’ beliefs and practices.
Speculation about causes of speech and language difficulties
Participants varied in their recognition of speech and language difficulties and had a range of ideas about causes, probably from a range of sources and often, unsurprisingly, related to their own experiences. Some descriptions of causes do not appear to have been previously reported in the literature and merit further investigation. Even among members of individual groups views were not homogeneous, and so again these data suggest that professionals should not make assumptions about the beliefs of any individual or community and that beliefs about causes of speech and language difficulties should be discussed and explored with every family.
Who can help
Patterns for seeking help varied, as did the point at which/reasons why people reported that they would seek help. Sources of help included mothers, friends, spiritual/religious leaders, general practitioners and community members. Many of the participants seemed to be unaware of speech and language therapy and reported that they would rely on the sources of support used for other challenges in life. Investigation of the knowledge, skills and responses of those to whom participants would go to seek help in relation to concerns about communication development would be worth pursuing.
Get to know me and my child
Parents and carers suggested that they wanted professionals to take time to get to know them, their child and their context (e.g. understanding about looked-after children and their experiences) in a non-judgemental way.
Finally, it’s different if you are not from the UK. A number of responses, for example around television and help-seeking behaviour, may well be influenced by participants being unfamiliar with the UK health-care system and not speaking English as a first language.
Study 4.4: the perspectives of early years practitioners on speech and language therapy
This study aimed to explore EYPs’ views of speech and language therapy and how they modified their practice after working with SLTs. The identification of interventions and modifying factors was based on two data sets collected from workers in early years settings in England: focus groups and telephone interviews. The data revealed EYPs’ perspectives on their role and practice, typically described in relation to universal provision to all children within their setting rather than those children with speech and language difficulties. The themes that emerged from these discussions are described along with a description of how EYPs’ perspectives map onto the typology themes (identified in Chapter 2, Study 2.1: identifying the themes of speech and language therapy practice).
Research questions
-
How do EYPs understand the effectiveness of interventions that they deliver?
-
Which intervention components do EYPs use and consider relevant to preschool children with PSLI?
-
Which factors lead EYPs to adapt or modify their use of interventions?
Methodology summary
A summary of the methods is provided in Figure 21; methods are described in detail in Chapter 1 (see Methodology overview).
FIGURE 21.
Summary of the methodology used to gain the perspectives of EYPs.

Findings
We have referred to these participants as EYPs; this term is meant to include a range of practitioners who are working with children during their early years and our participants varied in the specific role that they fulfilled, for example our sample included managers and special education needs co-ordinators as well as practitioners with a particular interest in speech and language. Their use of terminology therefore varied, for example words such as speech, language and talking were used interchangeably.
These participants discussed their work with children with enthusiasm and gave many practical examples of activities that they used. Typically, they described their practice in terms of universal provision and good practice for all of the children in their care rather than specifying their practice with children with particular difficulties with speech and language. It seemed that activities that they had perhaps learned in the context of a particular child with speech and language difficulties had been applied to all children as an example of good practice. The following areas of their work were identified from a thematic analysis of data collected in the focus groups.
Maintaining attention/motivating the child
The EYPs discussed using a range of activities that aimed to be motivating and would engage the children. The discussion around children’s attention appeared to have a slightly different emphasis from that of SLTs, with less focus on improving attention per se. Instead, EYPs referred to attention in terms of having games and activities that are sufficiently motivating and engaging:
it keeps them motivated doesn’t it [group: yes].
EYP_010
. . . making it exciting, making them want, if you can, gotta be something that they’re really gunna enjoy, and it’s gunna grab their attention because . . .
EYP_008
Bags and bubbles: a repertoire of activities
The EYP described many ‘universal interventions’, particularly in ‘circle time’, that aimed to promote basic communication skills, or foundation skills such as turn taking, sitting still and listening activities. They described their repertoires, including rhyming games, singing, massaging, baby signing, treasure basket and using bubbles:
. . . yeah, there’s sort of very clear expectations around sort of specific things so you know, sitting, looking, listening [general group agreement] and lots of specific praise, and that sort of stuff, and just really simple activities, like it might just be a what’s in the box kind of, sing a song and they all take a turn to look what’s in the box and that sort of stuff.
EYP_006
‘Communication all the time in all the rooms’
As well as the specific activities mentioned above, EYPs emphasised the ongoing adaptations that they made to the children’s communication environment, with an emphasis on ‘continual provision’. In this context the focus was also on supporting the parent to make similar changes at home:
Well it is all the time, communication is all the time in all the rooms. We have baby room, we have pre-two, preschool, it is in every theme that we do. You know talking to the children all the time. The adult lead and child initiated activities always talking to each other.
EYP_092
. . . if dummies were in we’d ask parents to remove dummies, TV would be turned off for background noise, and we’d just do things like maybe making playdough, or painting or go for a walk, and just talking about the environment, and what was around them. And just anything really to try and get some get some words bless them, and try and develop their . . .
EYP_545
Dealing with all the issues
The EYPs described their holistic approach to the child and family in terms of examining and assisting with issues not directly related to speech and language therapy, such as family violence and the child’s behaviour. Some EYPs also referred to the inter-relationship between these factors as well, for example EYPs reported that those with attachment issues appeared to be more likely to have SLT difficulties. Links were also drawn between behavioural difficulties and speech and language difficulties:
I think it’s always worth emphasising isn’t about that emotional side of things because a lot of the children I work with have got you know really significant emotional difficulties for a huge amount of reasons, whether their um parents are you know drug or alcohol addicts or they, yeah that under stimulation they’ve bin in the care system . . . for me an attachment, . . . the the long-term affects of that . . . wanna get a bit more understanding about that early attachment and that early experiences.
EYP_006
Helping routines or transitions
The EYPs emphasised the importance of routines, as well as strategies that they had in place to assist with these, such as visual timetables and the Picture Exchange Communication System [see www.pecs-unitedkingdom.com (accessed 19 March 2015)]. The nurseries appeared to adhere to the same structure or daily routine so that children knew what to expect. EYPs also talked about assisting transitions between activities (such as with a song or bell) and more broadly transition to preschool as the children get older:
We use things like, when it’s tidy up time, we use a tambourine, so that that signals it’s tidy up time. So we use visual and audio aids um.
EYP_522
Increasing the child’s confidence or self-esteem
Many EYPs described an underlying purpose to activities or that many activities were designed to increase the child’s confidence or self-esteem, especially when the child was shy or withdrawn. EYPs discussed the importance, more generally, of ensuring that children were comfortable or relaxed and some EYPs referred to the importance of building a relationship with the children:
There are lots of activities based around talking and gaining the children’s confidence as well, in order to have a conversation, initiate one, ask questions, show an interest in toys.
EYP_092
Observation
Observation of the children was seen as a key role to monitor their progress. Participants talked about a process of ‘getting to the bottom’ of a delay in a child’s speech and language development to identify if there was a need to refer for external support and ‘work out what’s going on’. This process included discussion with parents about worries/concerns to determine whether the child’s behaviour was typical of behaviour at home (particularly if the child was shy):
Well we kind, there’s a bit of everybody’s really, we sort of observe, let them settle in for six weeks, I wouldn’t be assessing the child in the first week I think it’s a bit early to be honest, because they’ve got to be comfortable. And just, three year observations and then we, we go from there. And if you’re not worried about anything else apart from speech, we would start working one to one with them.
EYP_010
Improving participation and interactions with other children
The EYPs reported using signing/the Makaton programme to allow children to make their needs known. They also talked about a range of activities that encourage all children to be involved, as well as interact with one another, for example ‘circle time’ and ‘show and tell’:
They’re also, I’m trying to socialise them in that everybody is included, and it doesn’t matter whether or not what your language is or what state you’re in or things anything like that, we’re all friends together.
EYP_042
Delivering speech and language therapists’ suggestions
The EYPs described delivering specific programmes and activities as requested by SLTs. They also described adopting more general strategies that SLTs had advised them to use. Specific speech or language targets were likely to come from SLTs:
It might be that speech and language therapist is able to identify something else that’s going on in addition to the speech and language . . . But I think really it’s getting a professional assessment on that child’s abilities, so that’s obviously we know at what point we’re able to step in assist that child, support their development, their language, their vocabulary and knowing we’re going about it in the appropriate way and we’ve got a realistic understanding of what their abilities are.
EYP_526
Supporting parents
The EYPs appear to have a broader role in supporting parents than SLTs; however, there are many overlapping features. As well as their role in improving parent understanding and interactions between parents and children, EYPs also discussed the importance of building relationships with parents and finding out about their context, family structures and culture. They described a range of strategies and events that encouraged parents to engage more with services and activities to help their child:
What we do is, we invite them in and they have a drink and a biscuit, and then like the last one we did, we did ‘Owl Baby’, so they listened to the story of the Owl Baby, and we had a story sack, and we did a little display on the wall anyway, and they all made their own little owls. It’s just a way of getting the parents in and getting them to communicate with us really.
EYP 530
Summary
When asked to talk about their work with children with PSLI, EYPs mainly talked in terms of good practice for every child. Their work focused on the child in the context of the preschool setting and preparation for transition to school. There was also a key emphasis on the child’s broader context and the support that was offered to families.
The typology and perspectives of parents and early years practitioners
In a final analysis of the data from parents (see Study 4.2: the perspectives of parents on speech and language therapy) and EYPs (see Study 4.4: the perspectives of early years practices on speech and language therapy), data were mapped onto the typology themes, that is, the transcripts from parents and EYPs were reviewed to identify what if anything resonated with the thematic analysis of the SLT transcripts from Study 2.1: identifying the themes of speech and language therapy practice (see Chapter 2). In the following sections the themes from the typology are presented along with examples from the parent and EYP transcripts that are consistent with these themes.
Speech
Work targeting speech sounds was discussed in detail by parents. Parents described both input (sound awareness) and output (production) work:
. . . he had the letter sounds on the cards and then he like she’d pick up a chair and she’d say to [child] what is this, it’s a chair what sound do we need a ch, a s or a k and he’d have to choose what sound it was.
PAR_TEL_517
. . . she was saying to me that we just need to get him making as many sounds as possible, the more sounds he makes the sooner those sounds will turn into wards, words. They are the precursor of the words.
PAR_020
Parents varied in whether or not they could remember which sounds in particular were being targeted. They tended to describe activities including naming specific games:
. . . sounds stuck underneath the ducks and rollercoaster type marble runs with sounds sort of attached to those and or taking it in turns in that way with whose ball reached the bottom of the run first and what else did they do, lots of games sort of snap activities and sort of practising those sounds.
PAR_TEL_518
. . . a monkey game in which again he really enjoyed so, she’d say the word, he’d say the word and then put the monkey on if he got it correctly.
PAR_TEL_603
Several parents described the progression of therapy, which reflected the hierarchical structures that therapists had reported:
There’s a lot more sentences and things now, but to start with it was him using a sound in repeating words and we would write a list of words that he used beginning with that sound or ending with that sound, and she would make a sheet of pictures to do with those words, if he repeated them, it would be playing a game at the same time, . . . So it was all playing, and getting him to talk. And some listening games as well, so he would have to sort out what she said, and put it in the right pile for the right sound.
PAR_TEL_602
As before, indicators of therapy success were functional, often based on the child’s ability to be understood by unfamiliar listeners and the impact of this on their social interactions:
Half the words aren’t perhaps that clear, people don’t have a problem with understanding her now so for her to socially she’s now making friends and got a good little group of friends whereas before when she was at preschool before she had the speech therapy sessions she wasn’t really doing that she was quite sort of, other than the friends we had in our own circle she wasn’t making any sort of external friends by herself.
PAR_TEL_515
. . . now people understand, are understanding more, better, yeah, so he’s becoming more confident and this I feel, whether it’s his age and he’s getting more confident in general, but I feel that that’s as a result of this therapy.
PAR_TEL_598
He’s interacting better with other children, other adults can understand him when he asks for things.
PAR_TEL_514
Early years practitioners rarely commented on direct speech sound work for individual children, although they did report on whole-class sound awareness work, including rhyme, sound discrimination or formal sound programmes used by the nursery. Several commented that speech sounds was something that was targeted from reception onwards:
I also work on phonology as well as in groups but only in listening . . . listening to lots of rhyme, lots of singing lots of rhyme.
EYP_008
. . . they might just have the key worker doing ‘letters and sounds’ or they might have the speech and language therapist they might be in a separate room, doing some strategies in there.
EYP_201
. . . some of it’s not always completely a hundred percent spot on with her phonics and stuff, but that will come in reception to be perfectly honest with you.
EYP_010
One EYP referred to a child having one-to-one work on input using a sound bag:
. . . basically we’ve got a bag with a kind of a little kind of bag within that. We’ve got, um just some pictures of objects and kind of associated words. So for example, the suggestions [the SLT] gave us were to have one object with the picture sound only. So a snake to emphasize the ‘s’ sound a rabbit or a toy fish to emphasize the ‘f’ sound. And then it becomes a little bit more involved, so like a camera, so when it clicks you say ‘c’. And I think these are, I think some of these can be generic, but these are the ones they want us to focus on.
EYP_TEL_526
Both EYPs and parents discussed using the strategy of modelling back correct production:
. . . we model back the correct way of saying it, so we just give them a clear adult model of what they’ve said rather than saying you don’t say it like that or, trying to sort of make them say it fifty times to you in the right way, it’s just about repeating what they say back, so if they say ‘it’s a tat’ you say ‘oh yes it’s a cat, it’s a black cat’.
EYP_043
. . . [try] not to say ‘no you don’t say it like that’, but just to repeat the words, how it should be said so that she was hearing it how it should sound.
PAR_TEL_531
Comprehension
Parents and EYPs typically referred to targeting ‘language’ and distinctions between expressive language and receptive language were not particularly explicit. Nonetheless, both parents and EYPs described ways that they adapted their communication to support the child’s understanding of language:
Sort of telling her what you‘ve done so she can understand it and sort of take it on board, and just to repeat everything she says.
PAR_TEL_586
. . . it was all about breaking down instructions, making things a bit simpler for him.
PAR_TEL_599
Early years practitioners also named specific resources and activities such as visual aids, objects of reference, songs and routine:
. . . we use a visual timetable for each session that we’re doing, so we show all the children the next sort of stage of what we’re going to do next.
EYP_042
I use lots of props, especially you know during story telling as well. We use lots of props and visual aids . . . [L: when you use them, those props and objects and things?] . . . I think it helps them to understand the story better, so they can follow it. And for children whose concentration is quite, their listening and attention is quite poor. I think it helps them to keep a focus and visualise a bit better than reading it from the book.
EYP_TEL_522
Most parents referred to strategies and activities broadly targeting understanding of language. A small number of parents did refer to specific receptive language goals:
The other thing she’d put is that he struggled with the ‘he/she’, and she gave me some pictures to work on trying, to try and sort that out. [child]’s not yet following any instructions which include before and after. So again there was all things there that we had to practise at home, and the teachers would practise at school, to try and get him to understand before and after.
PAR_TEL_599
. . . she concentrated on things that are big and things that are small.
PAR_TEL_516
Expressive language
Parents described goals such as having a ‘more rounded vocabulary’, targeting ‘key words’, use of verbs and ‘working on he/she’. These would be categorised under ‘expressive language’ in the typology:
. . . a lot of it was focusing on getting her to try and say linking words like ‘the’ and ‘is’ and ‘and’ because she was just missing some of those words out.
PAR_TEL_515
. . . matching the cards and the dogs jumping and that was the use of verbs certainly in the second sessions was quite, it was something he wasn’t tending to do at that point, he wasn’t, obviously to make a sentence to encourage him to use jumping or you know verb generally. Action verbs rather than anything else.
PAR_TEL_046
Both parents and EYPs referred to adult targets such as ‘giving more rounded descriptions’, ‘adding an extra word’ and ‘emphasising things more’. These adult targets were tied to specific child targets that mirrored the SLT descriptions that were categorised under the typology theme ‘expressive language’:
. . . always add another word, so if he was to say to you ‘red car’ you would say ‘a little red car’. And that was the sentence structure that has always been the main strategy that of always adding an extra word. Even now I still find that I am a bit of a parrot, I think it just that way it has developed, because things are not always clear what he says, I repeat it back to him and I think it is just the way it has kind of developed.
PAR_TEL_046
. . . you do things with simple words simple vocabulary, repetition, and then um, listening for the child’s response, repeating that then perhaps what they’ve said. Um . . . it’s this kind of interaction to children, following their line of interest, depending on what they talk to you about or volunteer, and following that up.
EYP_TEL_526
Self-monitoring
Neither EYPs nor parents referred to self-monitoring explicitly. However, there were occasional examples from both EYPs and parents of activities that SLTs had referred to as targeting self-monitoring. Neither group explained the rationale behind these activities and so it is not clear whether or not they understood the link to self-monitoring. Both parents and EYPs referred to activities such as mirroring back errors to encourage the child to correct them:
It’s just a matter of, just constantly picking her up, she’ll come, every now and then she still drops it, she’ll still letters, but if you remind her she’ll pick it back up again. [L: ok. So d’you just give her the correct way to say it, or do you ask her to say it again with?] Yeah, if it’s something really silly like she’ll say something like ‘oh yeah I want some oast’, just out of lazy, it’s not lazy cos that’s not right, it’s not lazy it’s habit I think, I’ll say to her ‘what’s oast?’ and then she’ll go ‘toast’ and cos then she’ll realise what I’ve said, but it’s just she says something like a sentence, I’ll repeat the sentence but emphasise the words she didn’t pick up on, so ‘I’m going to go TO THE toilet’ and get her to pick up on that. I give back the sign that they are mispronouncing and I emphasise it and just give it back, but I also work on phonology as well as in groups but only only in listening the listening all the time.
EYP_008
Generalisation
Most parents talked about being given resources and activities by the SLT to work on at home but described these in terms of practice rather than ‘generalisation’ activities:
I’m sitting with him and showing him pictures of things with ‘s’ on the end and we’re practising them. And the sort of words the speech therapists get you to practise are more common words that he would use in conversations.
PAR_TEL_599
. . . she gave us things to take home, so when we got onto the words stage, it would be like a sound or word lotto.
PAR_TEL_603
I was always told things to focus on and if I asked for advice I was given it. And I was also given like sheets with different sounds and things to work on with him at home.
PAR_TEL_597
Similarly, EYPs referred to the importance of practice and use of the strategies in the home environment but there was no mention of transfer of skills:
. . . [parents are] aware the targets and we give them ideas of how they can support that with the home.
EYP_007
. . . some of the sounds he was able to do, some he wasn’t so we practised twice a day.
EYP_TEL_519
Foundation skills
Aspects of the interventions described by both parents and EYPs can be equated to those identified within the ‘foundation skills’ theme from the typology. Parents and EYPs talked about targeting eye contact and ‘face-to-face contact’, play, listening, attending and taking turns, all of which are included within the SLT theme of ‘foundation skills’:
. . . it really is really important to get their attention and things, if you haven’t got that, even if you’re modelling, you could be talking nineteen to the dozen and they’re not taking a single word in.
EYP_008
. . . they’d make animal sounds for animals, and he would have to pick out which farm animal it was. And he’d have to concentrate on listening because listening is a type of problem for children you know for speech, always focus and listen.
PAR_TELL_597
Parents perceived ‘play’ to be a large part of what SLTs did. Some specifically linked play to development of the foundations skills:
He’d say the odd thing, but she helped me with playing with him, and getting him to light up.
PAR_020
Early years practitioners also referred to play, typically describing it as a vehicle to work on a range of skills:
. . . [they] choose which one they want to play with, and then just gradually over time increase the amount of time they’re spending on any one activity, so maybe start off at three or four minutes, and then gradually help by using lots of ‘ohhh,’ you know ‘what’s happening now?’, ‘oh my goodness!’, and kind of grabbing their attention back in.
EYP_009
. . . they’re learning through play anyway . . . These things are probably happening without you actually physically sitting them down and, like now we’re going to do this. Just talking to them all the time anyway, instructions and they learn from their peers anyway.
EYP_TEL_530
Parents often referred to play as a means of making activities fun and referred to their child’s enjoyment of and engagement in sessions as an important factor to them:
. . . they often get out toys like pop up pirate as well and so, play games around that so if she gets the sound right then she gets to put a sword in the pirate sort of thing. Or little things like that, so that’s good cos it keeps her interest in it, because four year olds get fed up eventually.
PAR_TEL_596
The focus of EYPs tended to relate foundation skills to children’s overall development and classroom inclusion whereas SLTs and parents referred to them in the context of speech and language development specifically:
. . . yeah, I think attention is also very important because you you look at a group, mean I know you probably have the same situation, but we make sure that every child has a chance to participate in that group at some stage because you’ll always get the overriding dominant child, but in their way in their own way, so it really is really important to get their attention.
EYP_008
Parents and EYPs both referred to ways that adults could support development of foundation skills, including activities and strategies to engage the child’s attention and reducing the pressure on the child:
. . . she asked me to basically try not to do so much for him so that rather than just get his coat and pick it off the peg and put it on him, ask him to get the coat, and put it on himself.
PAR_TEL_599
I suppose it’s more face to face contact it’s getting him to look at you when you’re talking to him not sort of looking away and just hoping he’d listen to you, getting his full attention.
PAR_TEL_514
. . . sitting back and giving him ten seconds to answer. ’Cos you don’t get an instant response you just carry on going.
PAR_TEL_599
Functional communication
Parents and EYPs referred to resources to support children’s functional communication that mirrored those discussed by the SLTs, including the Makaton programme, symbols and flash cards to allow children to communicate fully:
. . . the other thing the speech therapist did was she did a little tiny bit of Makaton with her, sort of like the language for ‘more’, showed her how to say more, but said the word with it. Just to help her communicate with me, because obviously there was that communication, sort of frustration for her . . . it’s not that she’s teaching her sign language, she’s just helping [child] communicate with us whilst learning her words.
PAR_TEL_596
. . . we try to use [symbols] in most of our sessions that we deliver, find it’s helpful for parents as well if you’re wanting children to wash their hands, and the parents are, wanting the parents to help them, you show them that sign, and if they’ve got English as a second language they know that symbol that you’re expecting them to wash their hands, so it’s good for that as well. So we do that in all of our sessions, right across the board yeah.
EYP_044
Early years practitioners typically referred to developing functional communication strategies to facilitate a child’s inclusion in classroom activities such as participating in group time:
I pick the Makaton up with the sing and sign up a bit more cos I do quite a lot, I don’t have the, so many of the sort of have a wide ranging age come to they’re up to four, and they’re universal so it’s my groups and a special list, but I do do quite a lot of Makaton signing with the singing and things like that. Parachute games sort of, and that really gets them going and we, we sing some songs over the parachute and we try to hit the ceiling with the balls and you know, ‘look where’s it gone?’ you know that kind of thing, can you go find them all, can you go and find them all, where are they that kind of thing. Just because it does, they love it when they’re little, but they like to continue with it and I sit them all in a circle as well, and make them introduce themselves to each other and everybody in the group, you know adults do it as well, so you have your a toy and you say your name and you pass it onto the next person, say your name, pass it on, pass it on, pass it on, so that everyone feels included even though they might not necessarily be saying something themselves because if the children are too young to say their own names and the parents can say it, you know they sort of go ‘and what’s your name?’ ‘it’s so and so’ whatever, and we do that.
EYP_042
Parents and SLTs tended to refer to functional communication at a more individual level, such as the child being able to have successful interactions with other individuals and form friendships:
. . . he’s got loads of friends, we were worried that children wouldn’t be able to understand him but he’s got loads of friends and they all seem to play really well together and really happily.
PAR_011
. . . [SLT provided] flash cards so if she needed something and rather than she have to speak up in front of everyone she can just show the flash card to the teacher first. It’s just took all the pressure off from her.
PAR_TEL_519
. . . her friends help as well, as well her friends obviously like ‘cos she has like a little group of friends and she’ll sit down with them to do certain things like you said so she doesn’t just feel isolated and she’s got to do certain exercises and umm they help her, because they live so close they actually come round to see her and just do stuff with her anyway, so yeh that’s [S: So friends and other children is really important?] yeh definitely.
PAR_014
Adult understanding
Parents typically reported that they understood what the therapist was aiming to achieve. They usually talked about what they had observed as opposed to recounting how the therapist helped them to understand the rationale behind the goals and activities. SLTs referred to parental understanding as an important step in the therapy process. Parents did not specify whether they had understood the therapy aims without direct questioning and often just stated that they understood rather than elaborating on this further. Some examples of parents’ descriptions of what the therapist was aiming to do include:
. . . understanding that speech is, speech is for some children is a very gradual thing.
PAR_TEL_521
. . . they was just trying to get him to pronounce his ‘S’ words better.
PAR_TEL_514
. . . a lot of it was just trying to get him in to ask and talk, and ask me for objects.
PAR_TEL_599
Parents did refer to individual incidents in which it had been difficult to understand the point of activities:
Trying to understand why we were doing them was difficult, sort of why is saying what the child is doing beneficial instead of saying why is he doing that to try and get him to explain his thoughts umm, because obviously as adults we’re encouraged to explain our thoughts and we’ve got the vocabulary to do it obviously that was, in my mind, you had to build up the vocabulary not realising that actually getting him to realise ‘put a car on head’ is picking up the language, so that was difficult for my point of view, to get to terms with that side of . . .
PAR_011
Early years practitioners also talked about the importance of parental understanding:
I think, sometimes parents don’t really understand how important it is to just talk through experiences, so at the end of the day, you know, what did you do, um, and that, all that sort of information is just gone, and now onto the next thing, so they don’t really get to talk, and live experiences, and therefore the sort of whole, the whole speech just doesn’t thrive.
EYP_009
Early years practitioners also referred to working with SLTs or receiving SLT training to extending their knowledge of speech and language difficulties:
I guess the most recent advice. The little girl who I have mentioned before with the sensory activities. I was trying to get her to come, because she would go without saying anything all morning, and I was trying so hard, I was asking her questions and saying ‘oh you have got a teddy bear’ and what have you got and trying to get her to say it back to me and I said to the speech and language therapist ‘I am really not getting anywhere, she is not engaging with me’, well she is engaging but she is looking at me and smiling, but I was getting absolutely nowhere, but they said to me ‘well don’t focus on trying to get any language out, just put the language in and give her play opportunities’, so I stepped back and she played and I followed her round.
EYP_009
Adult–child interaction
Most parents talked about interaction strategies that they had heard about in speech and language therapy sessions, including the process of being videoed, with therapists giving them strategies or information:
. . . we just played on the floor with all the different toys she had and she watched me interact with him, and she watched how he responded to me, and she just gave me advice on, you know, you need to be giving him time to, to speak and to ask questions himself rather than me asking the questions then answering it for him.
PAR_TEL_598
. . . it was the video process to begin with and then the video process was repeated and then, then it kind, then she, the speech therapist has been to his nursery and chatted with them and introduced a few targets for them to do and its kind of been kind of maybe every few months we’ve had discussions.
PAR_TEL_020
One EYP referred to specific training received from SLTs using video reflection techniques:
We’ve done the ‘ACT’ [Adult–Child interaction Therapy] as well as practitioners so we’ve done the parent child interaction filming stuff for parents which has had a massive impact but also as members of staff as practitioners or key workers for specific children we’ve done that with the therapists as well and that’s really powerful.
So the therapists are working with you as a practitioner to look at your interaction with the children is that what?
So, and you, I’ve done it the context of one of those children, and that’s who I’ve done my um you know activity with, while I’ve been filmed and then you obviously review it.
And what sort of things came out of the review?
Well um how much you’re . . .
Sort of personal but um general strategies what sort of things?
All those sorts of things really about how often you’re commenting how often you’re um asking questions, how often you’re directing, and those sorts of things, and you literally tally how, yourself on how, have you done it. You sort of tally yourself on as you’re watching yourself on video and you revisit that a few times, and its really powerful actually and it really does get you out of bad habits and things you don’t know you do, you realise you do, I think it’s great.
As well as describing the strategies they used most, EYPs viewed themselves as having a role in modelling strategies to parents:
So the modelling for parents, what sort of things are you trying to model there? You talked a little bit about turn taking, what other things are you trying to model and why?
All types of play, the importance of play . . . it is role modelling you getting down on the floor, maybe starting off that play and then trying to bring, if they are not confident to do so, bring them into that play. So we are role modelling from probably the minute we walk in the centre in the morning.
Speech and language have been great, they’ve been quite proactive in terms of well making us aware of what kind of, you know what we can do. Or what children can do at such an early age, so they’ve promoted early communication, which has been good for us, because we can then share that with parents, so it’s about informing us so that we can empower parents and say yeah it’s great that you follow your child round and you talk as appropriate with your child, and you follow the lead, and you know things around the dummies, and that sort of stuff.
EYP_TEL_601
An examination of the parent and EYP data revealed descriptions of interventions that can be seen to mirror those discussed by the SLTs and to cover all of the themes of the typology. However, they were not always linked explicitly to the same issues as described by the SLTs.
Discussion
This chapter has presented the findings from an investigation into the perspectives of users on interventions for preschool children with PSLI. This was in recognition of the need to take account of patient preferences in developing EBP. In the case of this research, ‘users’ included children, parents and EYPs. Before discussing the findings it is useful first to examine how these findings may be interpreted and the implications for the development of an evidence-based framework.
In the context of making evidence-based decisions regarding an individual case, ideally the clinical expert would discuss with parents (and other adults involved in a child’s care) the nature of the child’s difficulties; the intervention(s) that might be appropriate; the evidence that underpins the intervention(s); and details of possible alternatives and the associated evidence. The decision about the most appropriate intervention would then be made jointly by the clinician and the user on the basis of the evidence and paying due regard to the preferences of the user. In this context the clinician has the opportunity to discuss alternatives with the user.
However, in developing a framework, one cannot include the full range of possible user preferences. In this case the user perspectives can only inform the clinician about the range of preferences or perspectives that were identified through the research. Similarly, for a clinician working with an individual child and family, one can ensure that he or she is informed about the options and the associated evidence relevant to that particular situation. However, when investigating perspectives within this research it would have been inappropriate to attempt to inform participants about all of the research evidence. Therefore, it is important to consider the sense in which our participants can be considered to be ‘informed’.
The preferred participants in this study were those who have had first-hand experience of SLT-led interventions, that is, children and parents. As reported in Study 4.2: the perspectives of parents on speech and language therapy, the recruitment of parents was a major challenge in this research. Recruitment was therefore broadened to include parents who were, or who had been, concerned about their child’s speech and language development. The inclusion of parents from underserved communities takes a further step away from parents who are informed about interventions, but it provided perspectives from a wider range of the population. Finally, the inclusion of EYPs provided additional insights into the perspectives of those working in one of the main contexts in which SLT-led interventions are delivered.
The perspectives of preschool children
The study of children’s perspectives aimed to provide evidence of children’s engagement in SLT activities. The observation of children’s behaviour proved a valuable method for understanding the perspectives of preschool children for whom the use of reflective interviews or arts-based methods may not have been appropriate. With the preschool age group, particularly for those at risk of speech and language difficulties, emphasising verbal responses or reflection on past events would have been challenging. In contrast, observing children’s body language, vocalisations and visual attention in the moment allowed a more direct understanding of children’s perspectives on specific activities. Using observation methods has also revealed the dynamic nature of children’s perspectives, as children interacted with different activities and people within SLT sessions and their interest, excitement, confidence and enjoyment ebbed and flowed over time and through activities. Individuals’ changing perspectives over time may not have been revealed so explicitly using more traditional reflective interview or arts-based methods.
This study adds to a growing body of work investigating the perspectives of children and young people with speech and language impairments and provides new information about preschool children’s perspectives on speech and language therapy in particular. 219,221,223–225,238 In general, preschool children within the study echoed the perspectives of primary school-aged children with PSLI and found the therapy activities enjoyable and engaging, although there were some instances in which individuals expressed discomfort with, or disinterest in, specific activities. 224 Although evidence of disengagement seemed to be related to the responses of individual children at particular times, there were some patterns that were predictable. For example, children relaxed and engaged more as their familiarity with the therapist and activities increased and, although structured activities supported children’s attention, they behaved in a more tentative way and were less vocal than in activities in which they took a lead in the activity.
It was also noted that, as the children became more familiar to those observing their behaviour, the observers felt better able to interpret their perspectives. There was discussion about whether or not to involve children’s parents in the observation and interpretation of children’s behaviour, as parents are often most familiar with the way that children express themselves through their body language and vocalisations, but it proved too ethically and practically challenging within the context of this study. The involvement of parents in observing and assisting with the interpretation of children’s behaviour in research studies may be worthy of consideration in the future.
It is important that, in the planning of therapy sessions, consideration is given to the amount of time needed to engage preschool children, particularly at the start of therapy and in the initial assessment and diagnosis process. Children are often familiar with a relatively small number of adults and communication contexts. There were notable differences in the levels of engagement of the children when they first encountered therapists or new activities and contexts. Thus, even when the SLT assessment process asks parents to interact with their child rather than the therapist interacting directly, a preschool child is likely to be less engaged when an unfamiliar adult is present. Parents also commented on the need to ‘get to know my child’ and not make diagnostic judgements on the basis of a child’s performance in an unfamiliar context. Although this has been common knowledge for many years and is written into guidance about the monitoring and assessment of preschool children,239,240 the current pressure on services is leading to a reduction in the time allocated to the first assessment, with 45 minutes being allocated to see the child, make the next appointment and write up notes following a diagnosis. Some services use home visits for the first assessment of newly referred preschool children, but this is clearly costly in terms of therapist time and travel, particularly in rural areas. An investigation into the costs and benefits of assessments in different contexts is needed to determine the optimum process and outcomes.
In summary, using the three themes of body language, vocalisations and visual attention, a rich description of the young children emerged, which enabled analysis and interpretation of preschool children’s perspectives in terms of their level of interest, confidence and willingness to participate, their enjoyment of activities and their relationships with SLTs and other adults and children. Thus, the framework of the subthemes of body language, vocalisations and visual attention could be useful for SLTs but would require further testing.
The perspectives of parents
Parents’ views about therapy, both in the interviews and in the survey of activities, were generally positive. This reflects the findings of other research and consultations in which parents are commonly satisfied with therapy once they have gained access. 28 It is also likely that there is a relationship between parents’ levels of satisfaction and their views of the therapists’ success in engaging their child. So, for example, parents talked about the fun and games that therapists provided for their child and that they wanted the therapist to get to know their child. It is likely that this gives parents confidence in the skills of the therapist and in the decisions that are made.
Despite these positive views, there was clearly some anxiety and uncertainty surrounding the process of attending speech and language therapy, which reflects Glogowska and Campbell,27,241 who found that the process was seen as stressful and stigmatising. In this study parents talked about their concerns that their child would be regarded as having a learning disability because of their language delay. Some parents were unclear about the rationale underpinning some interventions and did not regard activities as feasible for them to carry out.
Parents seem aware of the pressures on NHS therapists’ time and expressed the view that they were ‘lucky’ to have access to therapy. This seemed to cast parents in a passive role in which they may be concerned to challenge and ask questions. When interviewed, some parents expressed uncertainty about the point of particular strategies or about their effectiveness, but they did not appear to have discussed this with their therapist. This does not mean that therapists had not attempted explanations but it may mean that they had not repeated explanations, delivered them in an accessible fashion or checked parents’ understanding. Two doctoral research projects carried out as part of this research programme may shed some light on this process (see Appendix 32). Davies documents developments in role conceptions that parents have as they progress through therapy whereas Blackwell focuses on adult–child Interactions in the development of language.
As indicated above and elsewhere in this report (see Study 4.2: the perspectives of parents on speech and language therapy), in this study recruitment of parents of preschool children with PSLI who are attending or who have recently attended speech and language therapy was challenging. Despite the efforts of the research team, with the support of the parent panel and SLTs in local case study sites, the numbers recruited were disappointingly low. Discussion among the research team and with our partners has generated some explanations. The recruitment rates in our study were compared, first, with those in projects such as that by Hunt et al. ,239,240 who worked with families of children undergoing palliative care. In that study parents were turned away as levels of interest were so high. Second, the recruitment rates in our study were compared with those in studies such as that by Dockrell et al. ,242 which included families in which the children were at school, or those in the national consultation of parents of children with a range of SLCN. 28 Comparison with these other, higher-recruiting studies suggests that the explanation for our low recruitment rates may lie in the nature and stage of the condition of PSLI in preschool children. In these other studies either the children have a highly salient and emotive diagnosis such as cancer or the parents have been living with a diagnosis of speech and language impairment or autism spectrum disorder for a number of years and are aware of the impact of that disorder on their child’s educational and social life. In contrast, the parents of preschool children with PSLI have often not received a diagnosis, or perhaps not one that they understand or recognise. Furthermore, the received wisdom among their peers and advisers may well be that the child will grow out of the speech and language delay; this in turn may mean that these parents do not identify themselves with research into an impaired population in the longer term. These ideas are speculative but need further research and evaluation if recruitment to studies of children during their preschool years is to be successful.
The perspectives of underserved communities
The data presented in this project aimed to extend the range of parents’ views, ideas and reported practices to those groups who are not always proportionately represented in SLT caseloads. Therefore, the ideas generated indicate areas worthy of investigation in further research with the same or different groups. They also indicate topics that SLTs may consider trying to address when working with families from underserved communities. No claims are made about the representativeness of the populations or the data.
Carers of looked-after children
As the project progressed it became clear that the carers of looked-after children seemed to be underserved in different ways from the other two underserved groups. The carers of looked-after children appear to be underserved because of SLTs’ limited experience and knowledge about this group of children and the challenges of providing a responsive service. These carers were knowledgeable and engaged and in some ways could be considered to be acting as ‘providers’ of services to the children in their care. In one focus group participants described professionals responding to them differently depending on whether they were seeking services as a biological parent or whether they were seeking services in their capacity as the carer of a looked-after child – in the latter case they reported being treated more like another professional. The finding that carers did not distinguish between children whose difficulties may be a result of their previous environment and those who have a ‘non-reversible’ communication difficulty is of interest. Questions arise about how carers make judgements about previous linguistic environments and accurately identify persistent and more complex difficulties; in this respect their skill level and experience may be important. Carers’ requests for knowledgeable and speedy speech and language therapy services should be considered. Concerns over the gender of the SLT and the possible impact on a child should also be considered by speech and language therapy services.
Ethnic minority and refugee/asylum-seeker groups
The data from these groups suggest that SLTs cannot make assumptions about what constitutes a typical language environment, typical beliefs and typical language socialisation practices for a community or individual family. For example, one of the minority ethnic groups reported that eye contact is encouraged with young children, which is different from what is often reported anecdotally for non-white communities in the UK. Partly because of challenges in translation, ideas expressed about causes of PSLI, such as global warming and pollution, were not fully explored and merit further research.
Some of the ideas expressed regarding the causes of communication disability fit with the findings of Kuenzli,243 who, in a study of the Somali community’s experiences of autism (carried out by professionals in Minnesota, USA), stated that parents talked about causes such as diet, immunisations, events in Somalia and factors related to immigration. She also reported in her study that professionals said that language delay was often the reason why Somali families sought services. This may suggest that parents may be more likely to engage with services in relation to language delay than other issues, which may in turn have implications for the roles that SLTs can adopt.
Groups/individuals may have ideas about the causes of language delay with which UK SLTs are unfamiliar. It is therefore important for SLTs and other professionals to find ways to allow people to express their beliefs about causes and intervention so that they can be discussed in a non-judgemental way and so that SLTs can provide evidence to support their views. Finding ways to ask questions openly can be a challenge. Experience from this small set of interviews suggests that, if interviewers are able to demonstrate some cultural knowledge of the topics in question (e.g. perceived causes of language delay), this may signal familiarity to the participants and they may be more open to sharing ideas that they may realise are not typically spoken about in the UK.
It is important for professionals and parents to ensure shared understanding of terms. For example, in the case of one of the minority ethnic groups, autism was discussed at length, which led the researchers to speculate if some groups think that autism is the sole cause of communication disability and/or if autism could be the only term used to describe non-speaking children that the participants were familiar with.
Participants’ descriptions of seeking help from religious leaders are worthy of further investigation, to better understand religious figures’ understanding of communication disability and the advice that they give and to determine whether or not any discussion/training with these groups would be beneficial. Similarly, the reliance on other forms of community support and advice may suggest the need for community education about speech and language therapy and speech/language development and difficulties. Parental guilt may not be a universal response, in contrast to Glogowska and Campbell’s27 data from England.
Participants’ suggestions about how SLTs may improve their work with families may indicate that SLTs need to ensure that they have a clearer idea about what families expect and want (particularly in relation to collaborative approaches to intervention) and what families are already trying (in accordance with the findings of Marshall et al. 229). This suggests the need for all SLTs to continually develop their cultural competence.
Low socioeconomic status groups
This group’s comment, that parents may not be aware of the impact of language input on the child, is supported by the findings of Marshall and Lewis. 117 Participants’ views about how some fathers interact with children may suggest a need to investigate further, such as whether or not interventions to influence some fathers’ practices may be beneficial. Comments regarding television and professionals taking time are discussed below. Raising awareness of the impact of regional accents and ‘baby talk’ would also be useful.
There were several themes that were common to more than one underserved group. All three underserved groups discussed television, with mixed views. The evidence (particularly about different types of programmes244 and the effect for different families and children245–247) is unclear regarding the impact of television. This therefore merits further investigation so that appropriate advice is given to families, particularly in homes where the adults are not proficient in English and where the effect of watching television may be differential.
Spending time with a child before making judgements about their speech and language skills was mentioned by the RAS group as well as by one of the low SES groups. This has implications for the way in which assessments and referrals are carried out, as increases in time spent on assessment may be valued by families. This is particularly significant in a time of health cuts, which may result in less time being available for each child.
There appears to be a range of levels of knowledge and awareness about speech and language, with some participants articulating knowledge that appeared to have been explicitly taught by professionals. This is worthy of further investigation as information was not available about who had received input about child language development, who had imparted this information and, furthermore, whether or not this knowledge is translated into parents’ practice with their children.
Each group of low SES and RAS participants produced some ideas that are consistent with previous research and some unique perspectives. This suggests that it is worth continuing to investigate the perspectives of underserved groups. The diversity of opinion within each group indicates the need to ask each family individually about their explanatory ideas, beliefs and practices.
Thought should be given to developing ways of increasing culturally competent practice among professionals. This should include, first, the best ways to elicit explanatory models from families, especially when they may differ markedly from mainstream British views; second, determining the most positive ways to address families’ views and ideas when they are considered to conflict with research evidence and best practice for supporting children’s speech and language development; and, third, if such culturally competent practice is used, determining what, if any, impact it has on families’ views about and engagement with services and on child language outcomes.
Of interest are issues that have been raised in other studies but which were not evident in these underserved groups. For example, the SES of an area and poverty per se were not mentioned. 229 None of the participants mentioned links between language development and literacy and there was no mention of auditory problems.
The themes identified in this data set provide the impetus to investigate some of these issues with a wider range of groups living in the UK and for SLTs to explicitly take account of them when assessing and working with families and children with PSLI.
Challenges of data collection with user groups
Identifying community gatekeepers and participants was challenging. The research team employed multiple techniques to recruit participants. These included ‘cold e-mailing’ to foster agencies, attending a meeting organised by the target groups to introduce the project and identification of potential groups by the project advisory group. These methods resulted in limited engagement and so additionally a snowballing process was used to contact potential groups.
Working with gatekeepers and non-governmental organisations was slow, particularly as some members of the underserved groups identified were vulnerable and so gatekeepers were careful and thorough in establishing contact and giving permission for researchers to talk to group members. The process of recruitment was time-consuming as many participants were unfamiliar with participation in research and had limited (English) literacy and, in some cases, limited verbal skills in English.
There was a lack of control over venues. To help build a good working alliance with the research participants, undertaking focus groups in settings with which they were familiar was considered to be desirable. However, aspects of some of those venues were less than ideal, for example some venues were acoustically poor, which affected the quality of the interview recordings.
As well as for recruitment, English being an additional language for some participants was a challenge during data collection. The groups’ key worker facilitators rejected the use of an external translator and so other group members were relied on to translate. Key workers facilitated translation in both directions (to and from the participants) and often needed the research team to clarify terms. Additionally, it seemed that translations were not verbatim for all contributions but were instead perhaps a summary or consensus view reached by the group before a translation was offered. The two-way translation and the cultural diversity in styles of group discussion and responding impacted on our access to the range of views that may exist within a group. There are thus challenges to credibility and transferability and interpretation when the researchers cannot follow idea development and check group agreement. 248
Researchers were often asked questions by participants during the focus groups. These questions revealed cultural differences and misconceptions that the research team had been unaware of, such as knowledge and beliefs about the aetiology of disorders and expectations of British health care. Also, information was often requested from the researchers, responses to which, whenever possible, were deferred until after the end of data collection. A careful balance had to be found between developing and maintaining a respectful, open and honest working alliance with the group, but not colouring the participants’ interactions and responses.
The practicalities of researching with underserved groups mean that when planning future research greater amounts of time and resources need to be built into grant applications. Researchers’ familiarity with the background of the communities being interviewed can benefit the interview process.
In conclusion, this data set has revealed both previously reported and new beliefs and practices with regard to language development, delay and intervention among parents of underserved groups in the UK. The data reveal the breadth of views and suggest the need for further data and for SLTs to be aware of the potential range of views, beliefs and practices that their clients may have. Challenges to data collection should be heeded in future research and the impact of more culturally aware and competent practice evaluated.
The perspectives of early years practitioners
The discussions with EYPs revealed an emphasis on universal provision, a consideration of the whole child and preparation of the child for the school environment. Although EYPs talked about how they supported SLTs in the delivery of interventions for specific children with PSLI, the emphasis in their discussions was on the need to develop good practice regarding language and communication for all children. Ideas from SLTs for particular children were frequently applied as good practice for larger groups of children or in ‘circle time’. For children who have PSLI, the provision of a quality environment provides an essential context in which the more specialised and individualised targets can perhaps be more successfully implemented. However, it does beg the question of how far the suggestions being given by SLTs to EYPs are generic good practice or universal strategies and how far they need to be tailored to the needs of a specific child and, furthermore, how far a universal strategy is enough to bring about change for a child with PSLI. More detailed evaluation is needed of the outcomes for these children in relation to whether or not they have received universal or targeted provision.
When EYPs talked about the speech, language and communication skills of the children in their care, they related them to the children’s growing confidence, their success as communicators and, in particular, how this would be a preparation for school. In this way it seems that EYPs see the power of speech and language in bringing about changes in a child’s performance in other aspects of life. This is similar to the findings of Roulstone et al. 223 with respect to the valued outcomes of parents of children with SLCN. These parents valued communication in as far as it facilitated increases in their child’s independence and social inclusion.
Mapping parents’ and early years practitioners’ perspectives onto the typology
Parents and EYPs were not asked directly about the typology as it was under development at the same time as the interviews with users took place. However, following thematic analyses to identify the salient perspectives of parents and EYPs, analysis was carried out to explore how far parents and EYPs talked about interventions in ways that reflected the themes of the SLTs’ typology. When analysed in this way, all of the elements of the typology were evident in the parent and EYP data. Apart from the different themes that emerged, the main difference between the data sets was in the explicitness of the underlying rationales. As discussed earlier, parents were often uncertain about the underlying rationale of an activity and none ever posed a question about the research evidence to support a particular approach. Thus, it would seem that parents who were participants in this study could not be seen as ‘informed’ in the sense of being informed or enquiring about levels of evidence, although they are clearly informed about the role of parents dealing with children’s emerging speech and language. To move to a point where parents are informed about the choices available to them, a number of changes would be needed. First, accessible summaries of research evidence are needed. The What Works website, developed as an outcome of the BCRP, is an example of this [see www.gov.uk/government/publications/what-works-interventions-for-children-and-young-people-with-speech-language-and-communication-needs (accessed 14 January 2015)]. Although it is targeted mainly at practitioners, it is nonetheless accessible to a wider audience to allow them to explore the level of evidence associated with different intervention programmes. The website planned for this research programme will supplement and complement the What Works website. However, it would also be appropriate for speech and language therapy services to provide accessible summaries of the evidence to support interventions that are offered within any particular service.
When developing care pathways and service specifications, introducing parent panels to discuss and inform the combination of interventions on offer would contribute to ensuring acceptability of services for parents. Such parent panels could also support the development of the accessible evidence summaries mentioned above. However, recruitment to such panels is likely to be challenging and having flexible ideas about the constituencies from which one draws to compose such panels is needed.
In summary, the data sets collected from a range of users, drawing on a number of data collection methods, have provided new information about user perspectives, suggested topics that merit further investigation, both in research and when working with individual users, and tested out novel ideas on how to gain information about users’ perspectives, particularly in relation to the challenges of seeking the perspectives of preschool children.
Child Talk phase 2
Aim
To develop a framework and toolkit that can be used to establish effectiveness and cost-effectiveness and that can be used by services nationally to plan services and future evaluations.
Objectives
-
To identify tools can be developed to ensure the appropriate stratification of interventions and the measurement of outcomes (see Chapter 5).
-
To identify the measures required to develop formal economic assessments of SLT-led interventions and care pathways within services (see Chapter 6).
-
To work with the RCSLT to facilitate the national take-up and ownership of the framework (see Chapter 7).
Chapter 5 focuses on the development of a toolkit to support the typology framework developed in phase 1. Specifically, the work in this chapter identifies the formal and informal assessment tools used by SLTs with preschool children with PSLI (see Study 5.1: identification of assessment tools used by speech and language therapists) and explores the outcome measures linked to the typology themes (see Study 5.2: identification of outcome measures for speech and language therapy).
Chapter 6 assesses the ability of speech and language therapy services to collect and report information that could be used to evaluate the cost-effectiveness of SLT practice and support decision-makers in commissioning services.
Chapter 7 describes the development of a website to host the intervention framework, which is accessible to practitioners and parents.
Chapter 5 Identifying a toolkit for assessment and outcome measurement
Introduction
The preceding three chapters have described SLT-led interventions from the perspective of SLTs, linked with the evidence from systematic research in relation to their effectiveness. The perspectives of children and parents have also been made explicit. The next set of studies, described in this chapter, reports and appraises the tools that are currently used for targeted assessment and measurement of outcomes. The aim was to identify tools that can be used to help target interventions within the typology to meet individual child and family needs and measure the subsequent outcomes.
This chapter is organised into two sections: the first reports findings on the assessment processes used by SLTs to decide whether or not a particular aspect of intervention is appropriate; the second reports on the outcomes that are linked to the typology themes described in Chapter 2 (see Study 2.1: identifying the themes of speech and language therapy practice). Recommendations are made regarding the types of assessment, measurement and evaluation processes that are needed for the future. Before the findings are reported, a brief introduction is provided outlining the issues surrounding assessment and measurement of outcomes.
Assessment
Assessment is the process of collecting reliable and valid information and integrating and interpreting it to form a sound basis for all clinical judgements and decision-making. 249 It is stated in Communicating Quality 3,250 the standards and guidance manual for UK SLTs, that ‘All intervention is delivered on the basis of on-going assessment and review of progress with the individual (and/or carer as appropriate) as measured against targeted outcomes’ (p. 35).
This highlights the strong, dynamic inter-relationship that should exist between assessment of need, intervention and subsequent outcomes. SLTs are required to conduct thorough assessments to ensure provision of the most appropriate intervention matched to identified need. 165,251,252 In terms of Child Talk, clarification is needed about which assessment processes can help determine which themes from the typology should be included in an intervention.
A number of studies have explored the assessment procedures used by therapists working with children with communication difficulties and what influences the choices they make253,254 and, in particular, what formal (standardised) or informal (non-standardised) assessments are used and how uniform the practice is across the profession. 253,255,256 Internationally, a high proportion of therapists report using informal, self-designed assessments. 253,254,257,258 Each method of assessment has its own strengths and limitations and, ideally, the determination of the most appropriate intervention should be made on the basis of information collected using a number of processes. 250 Formal assessment measures are usually norm-referenced and standardised, enabling children’s scores to be compared with data from typically developing (TD), same-aged peers. However, published assessments may lack a professional evidence base and independent verification of concurrent and construct validities because of the high costs and time involved. 259 On the other hand, informal measures have not undergone a standardisation process. These measures tend to be developed for a specific population or investigative purpose and do not have their own normative data. Findings from these so-called ‘informal’ assessments are interpreted by therapists with reference to therapists’ knowledge about functional or developmental norms or with reference to other relevant theories about speech and language development and impairment gained through training, from the literature and from experience. 260 Limbrick et al. 253 acknowledge that, although many informal therapist-generated measures lack scientific rigour, positive features include being user-friendly and appropriate for the intended population and context.
Although there is an acknowledgement in professional literature that different methods are needed to provide a comprehensive picture of a child and his or her family, there is wide variation in the exact combinations of assessment processes that are used in any particular instance. Studies have found that, although there are similarities in the parameters assessed, therapists differ in their choice of procedure,63,254 and this seems to be related to clinicians’ beliefs and theoretical perspectives. 261 In line with UK findings, the choice appeared to be influenced primarily by financial constraints although factors such as validity and reliability, versatility, efficiency, ease of administration and familiarity are also important. 132
Outcomes
Context of speech and language service provision in England
There has been a significant change over the past 10 years in the information required from providers of education, health and social care, not only about what services are offered but also about how well they are delivered and with what outcomes. This information is necessary not only for quality assurance and the evaluation of services, but also, most importantly for service users and the public, so that all can make informed choices about their care. 262–264 In the UK, health-care provision is now based on a model of commissioning services that is measured against the NHS Outcomes Framework. 264–267 The quality of provision is judged against three broad indicators: (1) safety, (2) importantly for this research programme, the effectiveness of the treatment and care provided and (3) patient (service user) experience, measured by both clinical and patient-reported outcomes. Thus, in developing a framework of interventions for preschool children with PSLI, it is crucial to show the links between the interventions and the outcomes. Either on its own is insufficient,268 although when interventions are complex, involving large teams and multiple contexts, identifying the outcome of any particular contribution to an intervention is challenging. 269
In the context of health care, outcomes should reflect change resulting from therapeutic interventions and should represent a key aspect of assessing the effectiveness of care. 270 They have been defined as ‘a predicted measure of change that demonstrates a valid and significant therapeutic impact following an agreed intervention’271 (p. 3).
Outcome measurement seeks to capture the benefits of interventions in ‘real-world’ conditions, particularly functional (positive) change for the individual client. 272 However, the development of ‘functional outcomes’ for speech and language therapy that are consistent, psychometrically sound and clinically meaningful has been both problematic and long awaited. 255,273,274 Over the last 20 years there has been significant investment in terms of time and finance to develop robust outcome measurement systems in speech and language therapy, notably the Therapy Outcome Measures (TOMs)275–277 and the American Speech–Language–Hearing Association (ASHA) National Outcomes Measurement System (NOMS). 255 Although both are widely used, there is by no means universal take-up of either system. Indeed, recent surveys suggest that it is not even clear to many practitioners what constitutes an outcome measure. 89 Roulstone et al. 89 found that only one-third or 33% of therapists working in England were delivering any outcome data to their manager and, of those, under half referred to systems that used criterion-based measures such as checklists or standardised (norm-referenced) tests.
Various sources provide recommendations regarding the domains that can be related to interventions for speech and language impairments. For example, in Communicating Quality 3250 it is suggested that the outcomes from speech and language therapy that contribute to health, educational and psychosocial benefits will include:
-
diagnosis of communication and/or swallowing disorders
-
maintenance of optimal communication and/or swallowing abilities
-
improvement in the speech, language and communication abilities of individuals
-
improved use of existing function
-
reduction of communication anxiety and avoidance
-
improvement in interaction and effective social communication
-
increased awareness of others about communication and/or improved communication environment
-
greater opportunities for communication.
The Commissioning Support Programme (CSP)273 suggests three types of outcomes from speech and language service provision that commissioners should consider:
-
the users’ reported experiences of services that they have received (patient-reported outcome measures)
-
the achievement of therapy or intervention goals
-
the directly measured impact of services on users’ speech, language and communication skills, attainment and well-being.
From the BCRP223 a number of outcome themes were identified as important by, and for, children:
-
time for fun and laughter, both in terms of social activities and in relationships with teachers and family
-
feeling supported and listened to
-
dealing with emotions, particularly feelings of frustration, anger and sadness
-
improving other people’s behaviour towards them in terms of listening more and interrupting less, teasing and shouting.
Parents in the study identified, and understood, the vital role of successful communication in supporting their children to achieve the ‘fundamental outcomes’ of physical and emotional well-being and staying safe, but the two key outcomes were for their children to achieve independence and social inclusion.
Although there are a number of tools available for the measurement of outcomes, there are also considered to be gaps in relation to certain groups. For example, a lack of available resources to demonstrate change and development of communication skills for individuals who use augmentative and alternative communication (AAC) prompted a review of outcome measurement tools by a multidisciplinary group of members of Communication Matters. 278 They reviewed 23 measures applicable across the lifespan including those addressing quality of life, functional abilities, goal attainment, functional health and well-being, self-image and self-esteem, self-perception, occupational performance, environmental technologies and communicative competencies. They provide readers with a comprehensive overview and thorough description of each measure including the focus, administrative procedures and psychometric qualities and whether or not it is an assessment or a measurement tool, if it is based on a specific framework, whether or not data can be aggregated and the appropriateness for AAC. Following the study of parents’ and children’s perspectives on outcomes, Roulstone et al. 223 reviewed 27 self-report instruments to identify those that measured the outcomes of interest to parents and children. A critical appraisal of those instruments identified nine measures of quality of life, functional communication and socioemotional functioning that were considered to be relevant and robust.
Therefore, there are a number of potential measures available; however, the direct link between particular interventions and their related outcomes has not been identified.
The purpose of this study is to explore and achieve consensus on what are the best ‘outcomes’ and ‘outcome measures’ for interventions for preschool children with PSLI. This phase of the research programme has focused on outcomes specifically related to interventions in the typology framework.
Objective
The research presented in this chapter contributes to addressing the following Child Talk objective:
-
to identify tools that can be developed to ensure the appropriate stratification of interventions and the measurement of outcomes.
Specifically, this chapter describes the work undertaken to identify the formal and informal assessment tools used by SLTs with preschool children with PSLI that can be mapped onto the typology (see Study 5.1: identification of assessment tools used by speech and language therapists) and explores the outcome measures (indicators) and outcome categories (domains) that can be linked to the typology themes (see Study 5.2: identification of outcome measures for speech and language therapy).
Study 5.1: identification of assessment tools used by speech and language therapists
In this study we investigated the methods of assessment used by SLTs in England with preschool children with PSLI. The identification of assessment tools was based on three data sets collected from SLTs: (1) an online survey; (2) activities at regional SIG events; and (3) activities at national events. Data collection activities were iterative with findings from earlier activities informing subsequent data collection. The data include the results of a comprehensive search of the assessment tools currently available and in use along with indications of the reliability and validity of the standardised assessments identified. The assessments identified, both formal and informal, were mapped directly onto the typology themes (identified in Chapter 2, Study 2.1: identifying the themes of speech and language therapy practice), which highlighted where there are gaps and a possible need for new assessment tools to be developed or existing tools to be adapted.
Research questions
-
What combination of measurement tools best identifies appropriate intervention components and allows measurement of outcomes for preschool children with PSLI?
-
What existing measurement tools are appropriate or could be adapted to be used with the intervention approaches identified in the typology/guidelines?
-
How valid and reliable are these measures in assessing the child, their family and the environment and the interventions applied?
-
What parameters require the development of additional tools and how should these be measured?
Methodology summary
A summary of the methods is provided in Figure 22; the methods are described in detail in Chapter 1 (see Methodology overview).
FIGURE 22.
Summary of the methodology used to identify assessments used by SLTs.
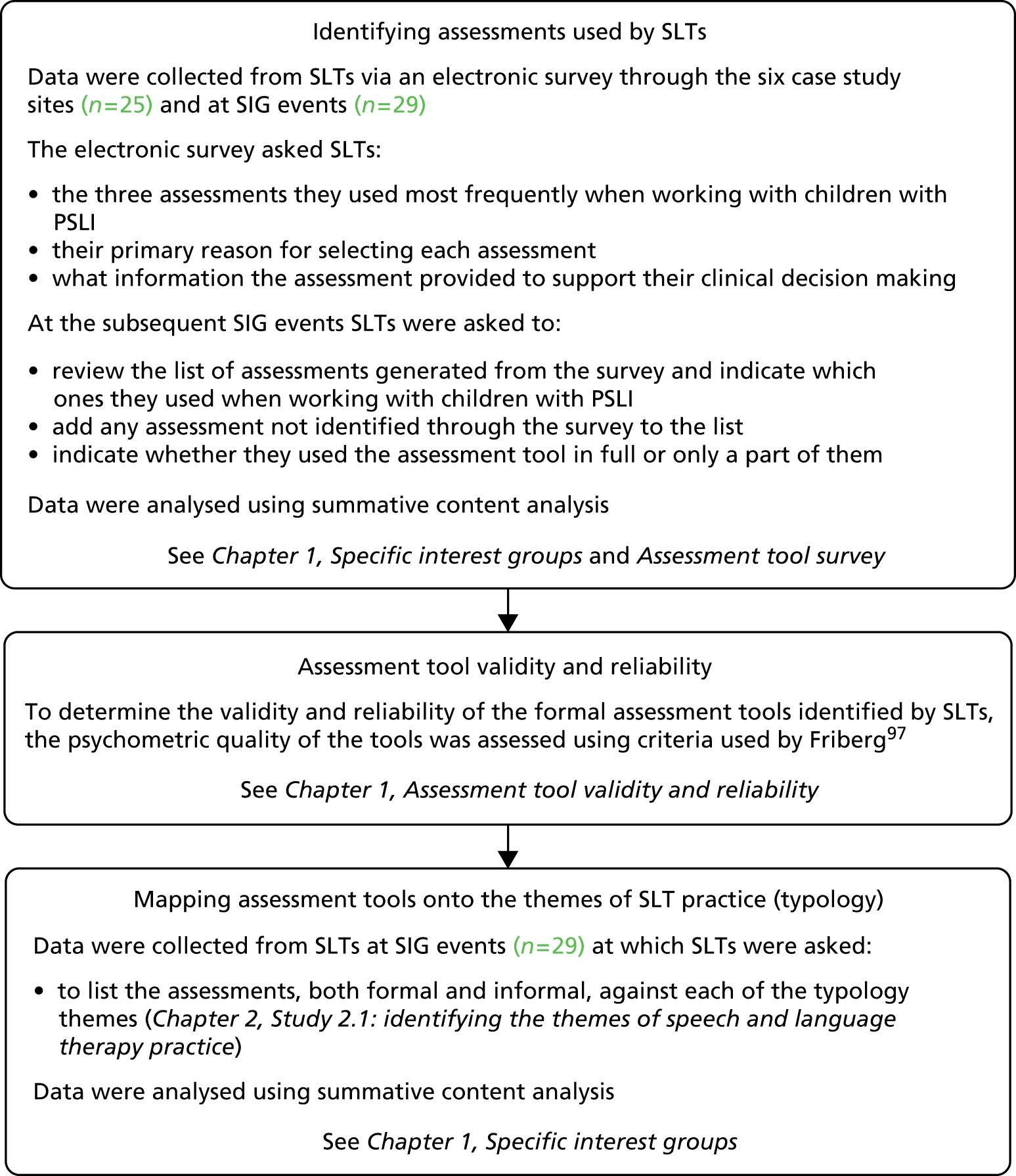
Findings
Formal assessment tools commonly used by speech and language therapists
The online survey (n = 25 participants), which asked for the top three assessments used by SLTs with preschool children with PSLI, identified 11 formal (published) assessment tools. The SIG activities (n = 29 participants) identified a further 16 assessment tools bringing the total to 27. All therapists indicated that they frequently use only subsections of the assessments identified and very rarely complete the whole assessment. Figure 23 provides a summary of the assessment tools used by SLTs with preschool children.
FIGURE 23.
Assessment tools used by SLTs. STAP is believed to be same as STASS and RWF is a subset of RAPT. Therefore, discounting STAP and RWF, Table 63 lists the top seven assessments. BBCS, Bracken Basic Concept Scale; BLADES, Bristol Language Development Scales; BPVS, British Picture Vocabulary Scale; CELF, Clinical Evaluation of Language Fundamentals; EAT, Edinburgh Articulation Test; PSA, Phonological Screening Assessment; RAPT, Renfrew Action Picture Test; RWF, Renfrew Word Finding Vocabulary Test; SPELT-P2, Structured Phonographic Expressive Language Test-Preschool 2; STAP, South Tyneside Assessment of Phonology; STASS, South Tyneside Assessment of Syntactic Structures; TALC, Test of Language Comprehension; TOPA-2+, Test of Phonological Awareness Second Edition: PLUS; TROG, Test for Reception of Grammar.
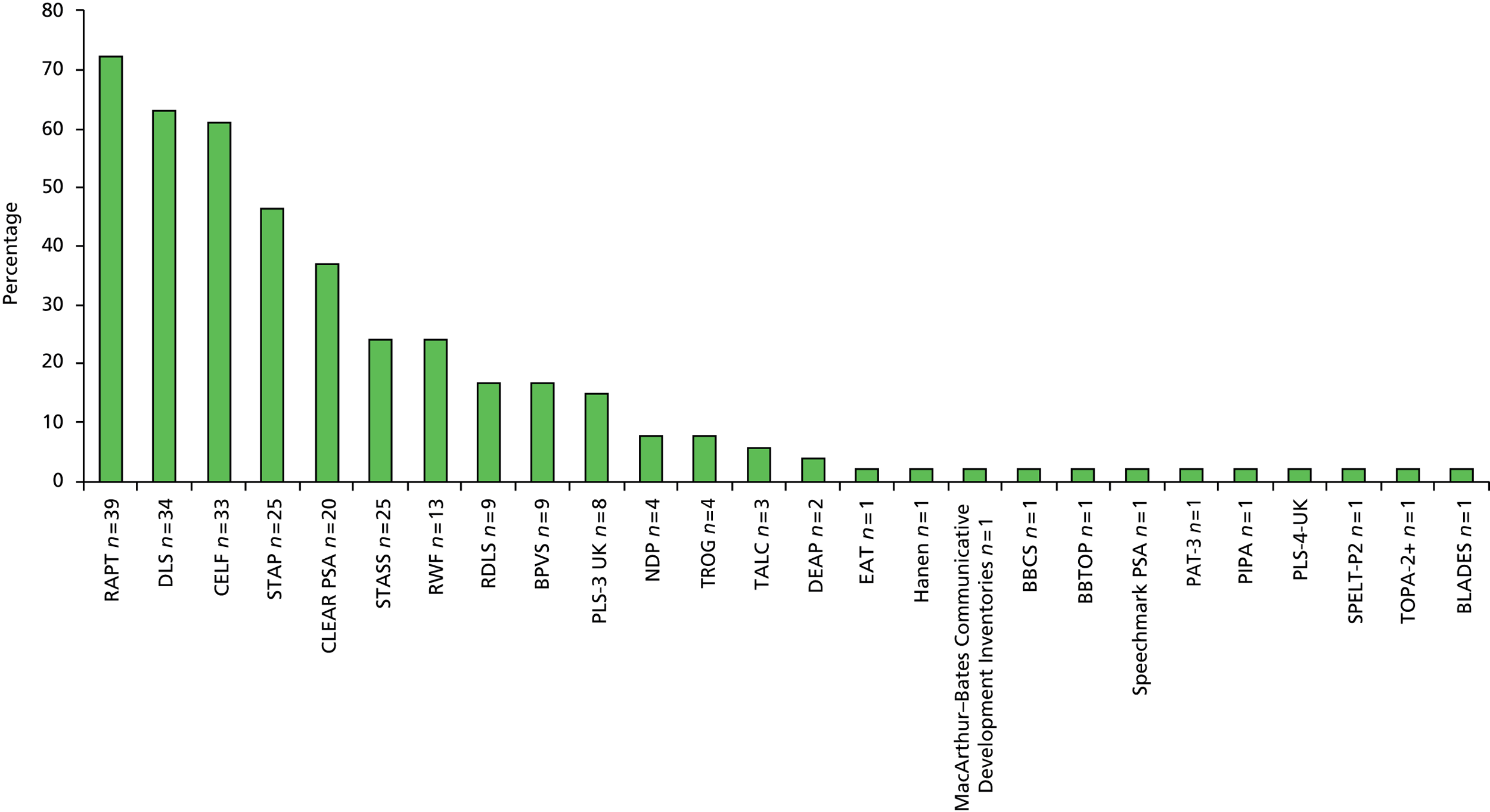
Rationale behind speech and language therapists’ decisions to use these assessment tools
The reasons outlined for the selection of different assessments by individual respondents in the survey can be found in Appendix 33. Information derived from a summative content analysis of the data for the top seven formal assessments is provided in Table 63.
| Assessment | Primary reasons for selection | Information provided to support clinical decision-making |
|---|---|---|
| RAPT | Standardised and easy to score; quick and easy to administer for screening expressive language; culturally diverse; availability | Age-equivalent and standardised score information helps identification of delay/disorder; highlights areas of expressive language and grammar requiring therapy; gives an indication of comprehension difficulties and the need for more in-depth assessment |
| CELF | Standardised – provides percentile scores; breadth and depth of detailed information for receptive and expressive language; stimulating materials to hold attention; ease of use and availability | Profile identifies strengths and difficulties to target therapy; standardised scores allow comparison with other standardised assessments; helps differentiation of delay and disorder; expressive/receptive comparison and measure of attention and listening |
| DLS Rapid Screening Test | Quick screen for receptive and expressive language; ease of adaptation for children with very early language development; can be adapted easily into activities for therapy | Provides comprehension levels: ICWs; provides information about functional vocabulary and concepts; ability to listen to short instructions and follow adult-led task; helps target setting in therapy and the provision of advice to others |
| STAP | Quick comprehensive screen of phonological profile; easy vocabulary for assessment of speech profile; availability | Identifies patterns of errors to target therapy; identifies phonological processes used and delay or disorder, and severity |
| CLEAR PSA | Quick to administer, clear layout; easy to share information with parents; accessible, familiar, colourful pictures | Identifies sounds missing/incorrect in word initial, word medial and word final positions; error patterns easily seen; helps identify if speech sound development is delayed/disordered and in need of intervention; identifies therapy targets |
| PLS-3 | The only assessment readily available in clinic; quick to administer | Overview of comprehension and expression of early language skills; standardised score; allows for comparisons with same-age peers |
| RDLS | Standardised in UK with age norms; quick to administer; easy to explain to parents; friendly materials: toys, real objects and pictures | Information about receptive and expressive language levels; provides information about ICWs, concept development and verbal reasoning |
Influence of the number of years in practice
The assessments that SLTs reported using were examined to see whether there were any apparent trends or differences in relation to the number of years in practice. However, it was clear from the data that SLTs across the span of years in practice made similar choices about which assessments to use. In light of this, the data were pooled. Table 64 provides details about the time that SLTs had been working with children with PSLI.
| No. of years of working with children with PSLI, n | ||||
|---|---|---|---|---|
| 0–2 | 2–5 | 5–15 | 15+ | Total |
| 4 | 5 | 12 | 8 | 29 |
Validity and reliability of the formal assessment tools
Therapists reported using standardised assessments and we know from previous research that they place particular emphasis on the findings from these to determine eligibility for services and to plan intervention. 279 However, it is also known that assessments are not always as ‘standardised’ as therapists may assume in relation to psychometric criteria. 97,280–282 The reliability and validity of the standardised assessment tools identified by the SLTs, in both the online survey and at SIG events, were assessed using the 11 criteria of Friberg. 97 These 11 criteria were applied to 15 of the assessment tools identified in this study. Items that purported to be screening tools such as the Derbyshire Rapid Screening Test were not included as it was already known that they did not have any normative or standardised data. A summarised version is shown in Table 65.
| Tool | Main purpose identified | Tester qualifications explicitly stated | Test procedure sufficiently explained | Standardisation size adequate | Demographics of standardised sample provided | Evidence of item analysis provided | Measures of central tendency reported | Concurrent validity documented | Predictive validity documented | Test/retest reliability reported | Inter-rater reliability reported |
|---|---|---|---|---|---|---|---|---|---|---|---|
| DLS | ++ | + | ++ | – | + | – | – | – | – | – | – |
| CELF-3 | ++ | ++ | ++ | ++ | ++ | ++ | ++ | – | – | + | – |
| RWF | ++ | – | ++ | ++ | + | – | ++ | – | + | + | – |
| RAPT | ++ | ++ | ++ | ++ | + | – | ++ | – | + | + | + |
| RBS | ++ | ++ | ++ | ++ | + | – | ++ | – | – | – | – |
| STASS | ++ | ++ | ++ | ++ | + | – | – | – | – | – | – |
| STAP | ++a | ++a | ++a | ++a | +a | +a | +a | +a | +a | +a | +a |
| TALC | ++ | – | ++ | – | – | – | – | – | – | – | – |
| CELF-4 | ++ | ++ | ++ | ++ | ++ | ++ | ++ | ++ | ++ | ++ | ++ |
| DEAP | ++ | ++ | ++ | ++ | ++ | – | – | ++ | – | + | ++ |
| RDLS-III | ++ | ++ | ++ | ++ | ++ | – | ++ | ++ | – | – | – |
| PLS-4 | ++ | ++ | ++ | ++ | ++ | ++ | ++ | + | – | ++ | ++ |
This process has demonstrated that there is variability with regard to meeting the strict psychometric standards applied to the different measures, with only the Clinical Evaluation of Language Fundamentals-4 (CELF-4) complying with all. Therapists employ a wide range of methods to assess children, including formal (published) assessments, and as outlined above not all are standardised or have measures of validity and reliability. There are certainly a number of reliable and valid measures available, and being used, for the assessment of children, but, given the variability in use of subscales and variability among the measures themselves, the more knowledgeable therapists need to be about the theoretical basis, psychometric properties and clinical impact of each assessment. 259
Informal assessments
The online survey and SIG event activities identified a number of ‘informal’ assessment procedures that had been developed by therapists themselves or which were based on methods of observation. In total, 28% of therapists reported using informal assessment methods to supplement the information gathered from published assessments, with nine information-gathering methods emerging from the descriptive data collected:
-
observation
-
parent verbal report
-
parent written report/questionnaires
-
videoing
-
audio recording
-
language/speech sampling in context
-
play
-
own or departmental screening tool
-
other speech- and language-eliciting activities including picture description, books and posting games.
Assessments identified for individual typology themes
Therapists were asked to map the formal published and informal assessment methods that they employed to gather data against each of the typology themes. Initially, 10 themes of SLT practice were identified from SLT focus groups and these were used in the SIG activities. However, subsequently, two of the themes were combined – ‘sound awareness’ and ‘speech/articulation’ – as described in Study 2.1: identifying the themes of speech and language therapy practice. The assessments mapped by participants against each of the subsequent nine themes are displayed in Table 66.
| Typology theme | Informal assessment methods | Formal assessment tools | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Observation | Parent report verbal | Parent report/questionnaires | Videoing | Audio recording | Language/speech sample | Play | Own/departmental screen | Other eliciting activities | Standardised norms data | Non-standardised norms data | |
| Speech | ✗ | ✗ | ✗ | ✗ | ✗ | BBTOP, DEAP, PAT, EAT, PIPA | STAP, NDP, CLEAR PSA, Speechmark PSA | ||||
| Comprehension | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | CELF, PLS-4, RDLS, BPVS, TROG | DLS (RST) | |||
| Expressive language | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | RAPT, RBS, RDLS, RWF, BLADES, SPELT | STASS | |||
| Self-monitoring | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | |||||
| Generalisation | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | RAPT | CLEAR PSA, Hanen | ||
| Foundation skills | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | PLS-4, PIPA | ||||
| Functional communication | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | CELF, RAPT | DLS | ||
| Adult understanding and empowerment | ✗ | ✗ | ✗ | ✗ | ✗ | ||||||
| Adult–child interaction | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | |||||
The three typology themes for which no formal assessment measures were identified were ‘ability to self-monitor’, ‘adult understanding’ and ‘adult–child interaction’. Four measures were identified for ‘functional use of language’ but only the Pragmatics Profile and CELF are designed to gather information about this. Therapists are possibly making subjective judgements about how the child participates and engages with the assessment process generally when administering the Renfrew Action Picture Test (RAPT) and DLS. Therapists report using a minimum of four informal assessment, or data-gathering, methods to supplement more formal assessment measures for all nine typology themes. Interestingly, therapists reported routinely using observation and adult/parent report to provide information about children’s functional communication and to support their clinical decision-making for all of the typology themes. It also highlights the importance that therapists place on adult/parental knowledge of their child’s communication in daily activities and reflects the ‘performance’ aspect of the World Health Organization (WHO) International Classification of Functioning, Disability and Health (ICF) – children and youth version. 283
For themes for which no formal assessments are reportedly used – ‘self-monitoring’, ‘adult understanding’ and ‘adult–child interaction’ – therapists are filling the gap with information gathered from a minimum of five different methods of informal data collection. Therapists did not report using any published formal measures to assess a child’s family or the environment. Despite this, therapists gather information and make decisions about these dimensions to determine the need for intervention focused on ‘adult understanding’ and ‘adult–child interaction’, but the methods are neither standardised nor reliable.
Study 5.2: identification of outcome measures for speech and language therapy
This study investigated which outcome measures could be linked to the typology themes (identified in Chapter 2, Study 2.1: identifying the themes of speech and language therapy practice) and examined consensus on the ranking of these by SLTs in England using a modified Delphi technique. The identification of outcomes, consensus building and validation were based on several data sets collected from SLTs in England: activities at regional SIG events, national events and a national electronic survey. An iterative process was used to identify SLTs’ views on grouping these identified outcome measures under the typology themes. The data were analysed to reveal outcome domains (categories) for each typology theme as well as specific outcome indicators (measures) within each domain. The outcome indictors were ranked by SLTs in terms of their relevance to the outcome domains and the level of consensus determined.
Research questions
-
What is the range of opinion, disagreement and consensus around key principles and components and outcomes of SLTs’ practice?
-
What combination of measurement tools best allows measurement of outcomes for preschool children with PSLI?
-
What outcomes or combinations of outcomes are considered to be priorities for service development and delivery?
Methodology summary
A summary of the methods is provided in Figure 24; the methods are described in detail in Chapter 1 (see Methodology overview).
FIGURE 24.
Summary of the methodology used to identify outcome measures for speech and language therapy.
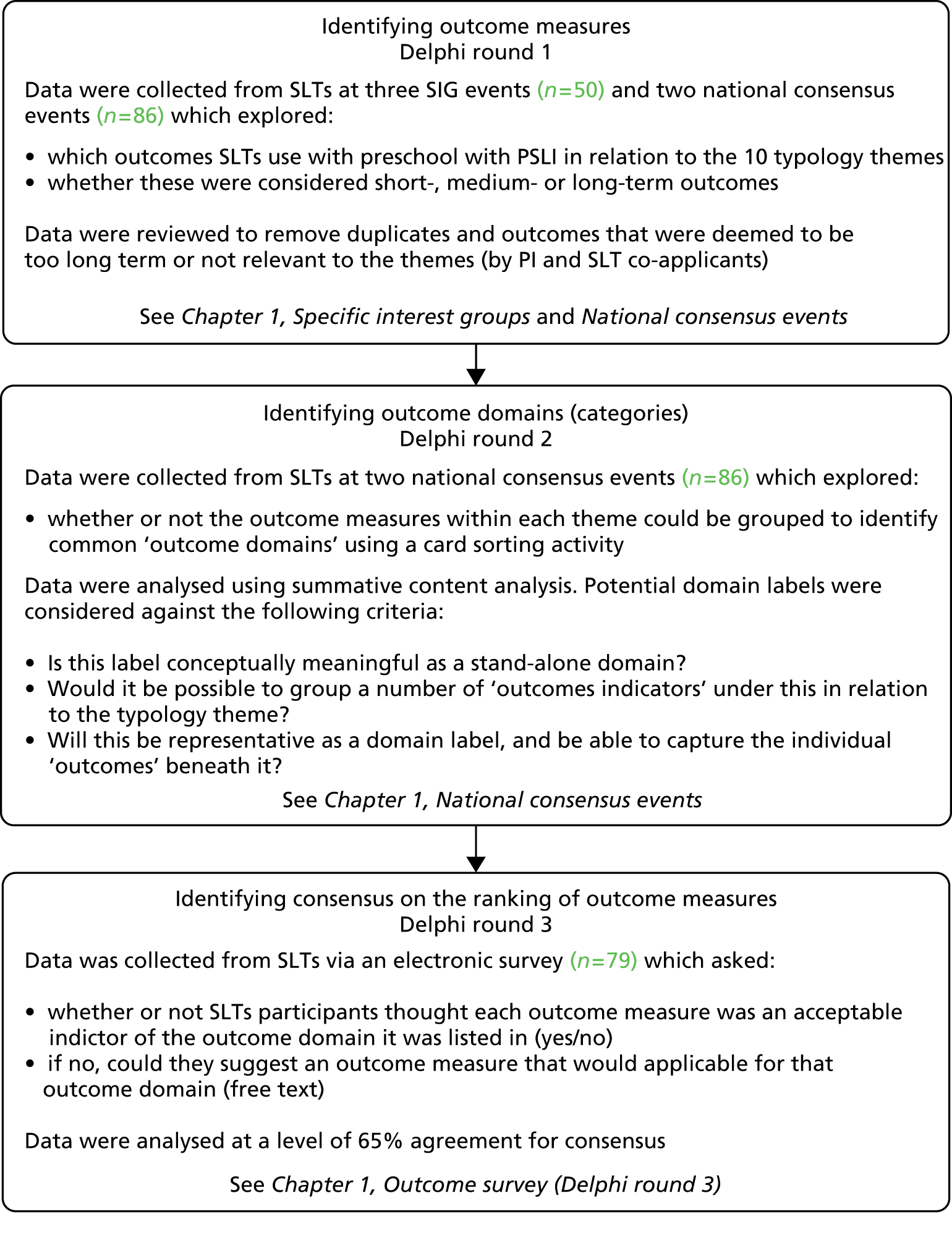
Findings
This study used a modified Delphi methodology. All participants were SLTs and were considered to be experts in PSLI with knowledge of the purpose, content and recent findings of the research programme on which their responses were based. The Delphi technique is an iterative process and therefore (with the exception of round 1) a summary of the feedback/findings from the previous rounds was presented for further consideration in the subsequent rounds, for refinement and evaluation by the participants. 65,66,284 Traditionally, the Delphi technique uses the same participants in each round; however, those participating in the current Delphi process were not necessarily involved in the successive rounds of data processing.
Delphi round 1: data generation and gathering
The first round of a Delphi methodology generates qualitative data and ideas. An inclusive approach was adopted, allowing participants the freedom to respond to open-ended questions using three activities and methods of data elicitation and collection. The outcome measures that SLTs use in relation to the typology themes were collected from SLTs at SIG and national consensus events. The number of outcomes identified for each typology theme varied widely, as shown in Table 67.
| Typology theme | Number of outcomes |
|---|---|
| Speech/articulation | 18 |
| Sound awareness | 8 |
| Comprehension | 15 |
| Structure/content | 23 |
| Self-monitoring | 11 |
| Generalisation | 26 |
| Foundation skills | 18 |
| Child participation | 16 |
| Empowering/understanding of parents/adults | 25 |
| Parent/adult–child interaction | 34 |
As many of the ‘outcomes’ had been written using terminology that was more consistent with intervention ‘aims’, these were translated into ‘outcomes’ for language consistency, that is, to describe the manifesting behaviour, impact or functional change resulting from intervention. Using the WHO International Classification of Functioning, Disability and Health (ICF) terms, it could be argued that many of the ‘outcomes’ were in fact ‘outputs’, ‘intermediate outcomes’ or ‘clinically derived outcomes’, in terms of the immediate results of intervention relating to the ‘body and function’ and ‘impairment level’. 274,283,285 For example, some SLTs reported more direct, short-term outcomes, such as ‘80% accuracy in discriminating minimal/maximal pairs’, whereas others reported outcomes that were high level and longer term, such as ‘increased participation in society’.
The data showed that for each typology theme there appeared to be subgroups or categories emerging. For example, within the theme ‘foundation skills’ six subgroups or categories emerged:
-
listening and attention
-
turn taking
-
eye contact
-
basic sound awareness (symbolic level)
-
co-operation
-
play.
After discussion within the research team, it was proposed that the emerging subgroup or category labels be classified as ‘outcome domains’ and the underpinning individual outcomes be classified as ‘outcome indicators’, as this would be more meaningful in terms of comparability with the NHS Outcomes Framework263 and better represent the different levels: short-, medium- and long-term outcomes.
Delphi round 2: data refinement
Round 2 of the Delphi methodology usually takes the form of a questionnaire, but in this study further refinement of the data set was undertaken face-to-face with SLTs at national consensus events using a card-sorting activity (see Chapter 1, Methodology overview). SLTs were asked to group ‘outcome indicators’ for each typology theme and were then asked to give each group a name of their choosing to best describe that group (outcome domain). The number of therapists who completed the card-sorting activity for each typology theme is shown in Table 68.
| Speech/articulation | Sound awarenessa | Comprehension | Structure/content | Self -monitoring | Generalisation | Foundation skills | Child participation | Empowering/understanding of parents/adults | Parent/adult–child interaction | |
|---|---|---|---|---|---|---|---|---|---|---|
| n | 42 | 39 | 42 | 35 | 41 | 38 | 38 | 33 | 41 | 40 |
The data were then examined by the research team to identify any similarities in the grouping of outcome indicators or labelling of outcome domains between SLTs within each theme. For example, the outcome indicator ‘able to make friends and go to birthday parties’ in the typology theme ‘participation’ was assigned to 27 different participant-generated outcome domain labels, eight of which are shown in Table 69.
| Outcome indicator | Outcome domains |
|---|---|
| Able to make friends and go to birthday parties | Broader outcome Social/educational/behavioural Communication End of episode of care aims Fulfilling function Functional and holistic Functional applied gains Generalising social and learning skills |
The research team identified that all eight of the outcome domains and outcome indicators for the typology theme ‘sound awareness’ appeared to relate more meaningfully to either ‘foundation skills’ or ‘speech’. This finding supported the decision by the research team to subsume this theme into ‘foundation skills’ or ‘speech’ during the development of the typology (see Chapter 2, Study 2.1: identifying the themes of speech and language therapy practice). The data were therefore re-examined under nine typology themes rather than under the original 10 themes.
It was agreed by consensus using a latent content analysis approach within the research team that 15 higher-level outcome domains emerged from the data across all of the typology themes (Figure 25). Some outcome domains appeared more frequently, being more generic, and others were more specific to an individual typology theme, such as ‘intelligibility’. The frequency with which outcome domains occur across the nine typology themes is shown in Table 70.
FIGURE 25.
The outcome domains identified as underpinning each of the typology themes.
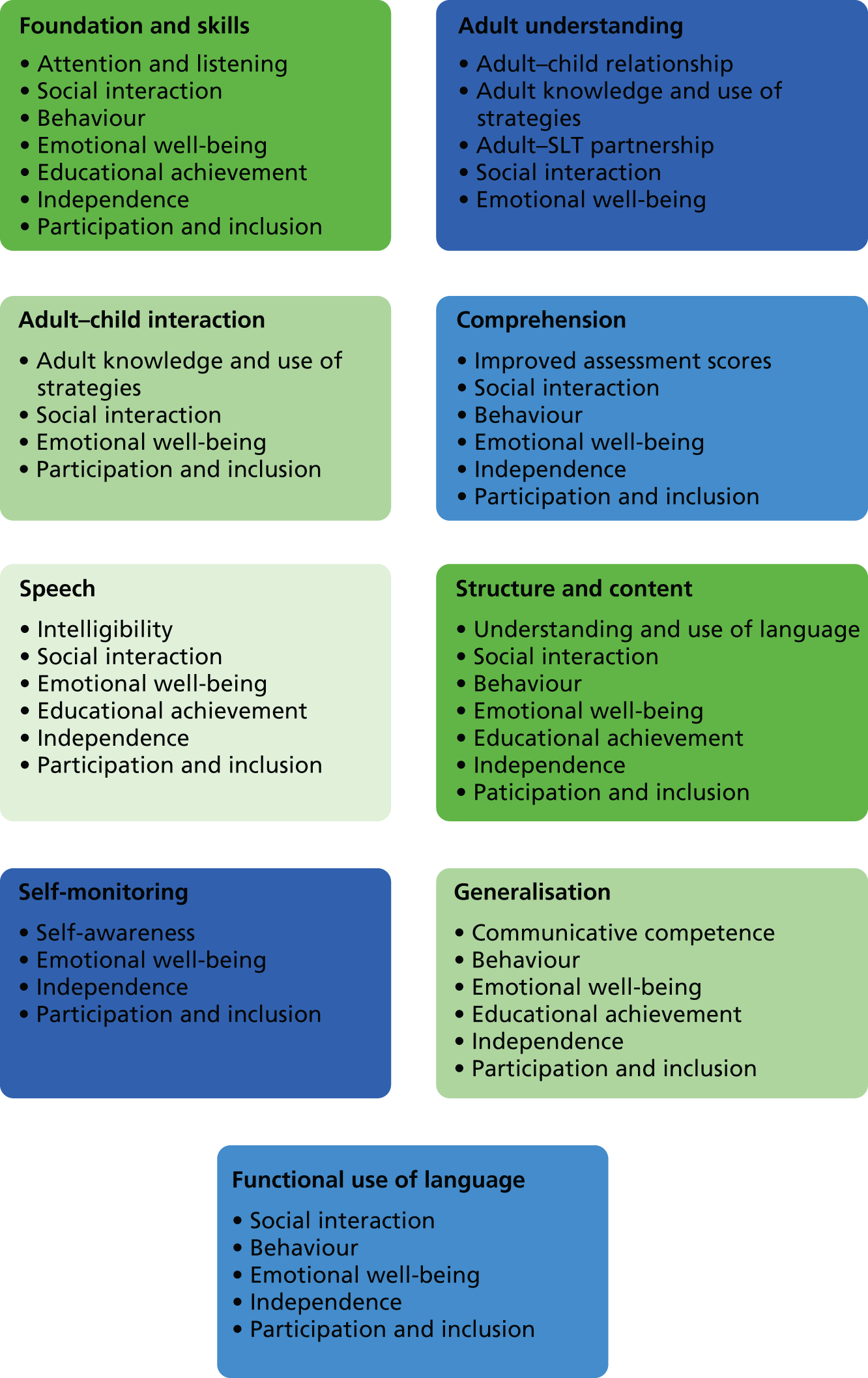
| Outcome domain | Number of typology themes |
|---|---|
| Emotional well-being | 9 |
| Participation and inclusion | 8 |
| Social interaction | 7 |
| Independence | 7 |
| Behaviour | 5 |
| Educational achievement | 4 |
| Adult knowledge and use of strategies | 2 |
| Attention and listening | 1 |
| Adult–child relationship | 1 |
| Understanding and use of language | 1 |
| Intelligibility | 1 |
| Self-awareness | 1 |
| Communicative competence | 1 |
| Adult–SLT partnership | 1 |
| Improved assessment scores | 1 |
The outcome indicators underpinning each of the outcome domains can be found in Appendix 34. The proposed outcome domains and outcome indicators were taken to the Child Talk parent panel to review their terminology to ensure that the wording was accessible to non-SLTs. Following this exercise, the wording of a number of the descriptions was changed in line with parents’ comments, for example ‘adults feel potent and aware of agency in child’s education’ was changed to ‘adults realise their role and importance in helping’.
Delphi round 3: data ranking
Delphi round 3 was designed using data from Delphi round 2 to provide an opportunity for SLTs to identify items with high consensus and to investigate SLTs’ views on the relative importance of items by ranking or ordering the data. Round 3 used an online questionnaire, developed so that SLTs could rank the top three outcome indicators within each outcome domain for each typology theme.
In total, 79 (72%) of the 109 therapists who were contacted responded to the survey. This is believed to be an acceptable number of respondents to have provided a representative pooling of judgements, given that the approximate size of a typical Delphi panel is generally < 50286 and the majority of Delphi studies have used between 15 and 20 respondents. 284
This Delphi round sought to identify consensus on the top three outcome indictors for each outcome domain. The level of ‘consensus’ was set at 65% agreement; this had been agreed at an earlier RCSLT event focused on outcomes. In line with recommendations, the number of outcome indicators that reached 65% consensus was identified and these were then ranked from highest to lowest. 65–67 The full results for those outcome domains with more than three outcome indicators can be found in Appendix 35. The level of consensus for outcome indicators within each outcome domain was tabulated (for each typology theme). An example is provided in Table 71 for the typology theme ‘foundation skills’ and the outcome domain ‘attention and listening’.
| Outcome indicators | % of SLTs placing the outcome indicator in the top three |
|---|---|
| Able to switch attention from activity to adult instruction with strategies (e.g. call name) (joint attention) | 95 |
| Able to switch attention without support (joint attention) | 92 |
| Age-appropriate attention | 84 |
| Basic sound awareness (symbolic level) | 16a |
| Percentage increase in correct identification of different sounds | 8a |
| Able to clap number of syllables | 5a |
The final number of outcome indicators that reached consensus for each typology theme is shown in Table 72.
| Typology theme | Outcome domain | Outcome indicators reaching consensus, n |
|---|---|---|
| Speech | Intelligibility | 0 |
| Social interaction | 3 | |
| Participation and inclusion | 3 | |
| Comprehension | Improved assessment scores | 2 |
| Participation and inclusion | 1 | |
| Expressive language | Understanding and use of language | 2 |
| Emotional well-being | 3 | |
| Participation and inclusion | 2 | |
| Self-monitoring | Self-awareness | 2 |
| Independence | 1 | |
| Participation and inclusion | 3 | |
| Generalisation | Communicative competence | 3 |
| Emotional well-being | 2 | |
| Participation and inclusion | 2 | |
| Foundation skills | Attention and listening | 4 |
| Social interaction | 2 | |
| Functional communication | Social interaction | 2 |
| Participation and inclusion | 2 | |
| Adult understanding and empowerment | Adult–child relationship | 3 |
| Adult knowledge and use of strategies | 1 | |
| Adult–SLT partnership | 2 | |
| Adult–child interaction | Adult knowledge and use of strategies | 3 |
| Social interaction | 2 | |
| Emotional well-being | 1 | |
| Participation and inclusion | 3 |
A number of other outcome indicators were very close to consensus, with three being placed in the top three by 62% of participants and one being placed in the top three by 64% of participants. For the typology theme ‘speech’, the outcome domain ‘intelligibility’ had no outcome indicators that reached consensus. There were eight outcome indicators for this domain, seven of which were ranked in the top three by between 30% and 45% of participants. This suggests that participants felt that there was a large range of outcome indicators that were relevant to this domain.
Although some indicators did not reach consensus with SLTs, it may be that service users, adults and parents feel that they are important and highly relevant. For example, ‘spontaneous development of ideas by adults’ under the domain ‘adult knowledge and use of strategies’ did not reach consensus but was commented on by a father at an earlier meeting as a good example of how levels of understanding change. The father now felt able to, and understood why he should, talk to his son about where the car was and use other positional vocabulary when doing the shopping or when out in the park.
For outcome domains that had only two or three outcome indicators, consensus regarding the top three would always be reached. However, clear preferences emerged in the rankings. These need to be considered alongside the additional suggested outcome indicators generated from the free-text responses. Table 73 provides the ordered responses for typology themes with outcome domains having two or three outcome indicators.
| Typology theme | Outcome domain | Rank | Outcome indicators |
|---|---|---|---|
| Foundation skills | Behaviour | 1 | Increased level of co-operation at home and in setting |
| 2 | Reduction in challenging behaviour | ||
| 3 | Improved behaviour displayed at home and in setting | ||
| Emotional well-being | 1 | Reduced levels of adult and child frustration | |
| 2 | Happier home environment | ||
| Participation and inclusion | 1 | Increased participation in group activities | |
| 2 | Increased inclusion in educational environment | ||
| 3 | Increased inclusion in education | ||
| Adult understanding and empowerment | Social interaction | 1 | Adult and child engage in co-operative play |
| 2 | Increase in child’s output/words utterances | ||
| Emotional well-being | 1 | Increase in child’s confidence | |
| 2 | Reduced levels of adult stress and anxiety | ||
| 3 | Increased levels of adult confidence | ||
| Comprehension | Social interaction | 1 | Improved range of social play, role play, co-operative play |
| 2 | Increased incidences of initiation of play | ||
| 3 | Improved use of appropriate expressive language | ||
| Emotional well-being | 1 | Increase in child’s confidence | |
| 2 | Increased quality of family life | ||
| Speech | Emotional well-being | 1 | Increased self-esteem and confidence in talking to others |
| 2 | Reduced levels of anxiety, frustration and stress | ||
| 3 | Reduced levels of adult stress and anxiety | ||
| Educational achievement | 1 | Has necessary skills to support literacy in year 1 | |
| 2 | Reduced levels of staff concern regarding child’s ability to learn | ||
| Behaviour | 1 | Reduction in challenging behaviour | |
| 2 | Improved behaviour in setting | ||
| Educational achievement | 1 | Improved narrative ability | |
| 2 | Improved literacy skills |
Free-text responses
The outcome domains for which SLTs made additional suggestions for outcome indicators were behaviour, educational achievement, emotional well-being, independence and social interaction (see Appendix 36 for the free-text responses). The free-text responses were initially grouped under emerging categories within the typology themes and then across outcome domains. For example, ‘behaviour’ had free-text responses across the typology themes of ‘comprehension’, ‘structure and content’, ‘functional communication’ and ‘generalisation’. Categories emerged relating to reduced negative emotions, positive participation and co-operation, but not all responses fitted into broader categories. Content analysis identified duplications and, when meanings were very similar, they were collapsed. A number of very pertinent indicators were suggested, some of which had already been identified as outcome indicators in other outcome domains. Because of the large number of indicators that have emerged it will be necessary to undertake further Delphi rounds to determine which outcome indicators are most relevant for each of the typology themes and outcome domains. An expert panel will need to consider safeguarding against an unmanageable number of items having to be considered and the excessive amount of time that this will take. 66
There is still extensive work to be undertaken in this area, which is outside the scope of this programme. Ideally, the next step will be two further Delphi rounds to agree by consensus which of these free-text responses as well as ranked responses from the last round will be selected as core outcome indicators. Once this has been completed measures can be identified that can be used to collect the evidence in a valid, reliable and transparent way. The future success of the outcomes work will depend on a core set of outcome indicators for each outcome domain being available that are sensitive to change, valid, reliable, universally applied, easily identifiable and transparent. This will require a further dedicated piece of development work, with tight parameters, to identify current, or create appropriate, measurement tools for these new indicators.
Discussion
The need to demonstrate what works in terms of the outcomes of speech and language therapy is not a new phenomenon. 274 Following the Bercow review,28 the CSP produced a set of documents designed to support joint commissioning and an appreciation of the perspectives of children and young people and their parents. Three documents are now available on the website of the Communication Trust [see www.thecommunicationtrust.org.uk/commissioners/slcn-commissioning-tools (accessed 30 March 2015)]. Despite this, there is still a lack of consistency in the way that services are commissioned and provided and in how the subsequent outcomes are measured. Surveys have also shown that the SLT profession is not currently collecting, or required to report, any consistent information nationally relating to the outcomes of intervention. 287 This is compounded further by the lack of inclusion in the NHS Outcomes Framework263 of any outcomes pertinent to children with SLCN and of the services that they require. This is particularly concerning given that one of the three main purposes of the NHS Outcomes Framework is ‘to provide an accountability mechanism between the Secretary of State for Health and the NHS Commissioning Board [now NHS England 2014] for the effective spend of some £95bn of public money’ (p. 4). 263
Without recognition, or appropriate evidence, of the contribution that speech and language therapy makes to the lives, and life chances, of children and families, resource allocation is likely to diminish. This is particularly relevant as the commissioning of all public services, including education and health, is now in an era of ‘value-based’ care. 288 In addition, given the current and future economic position of public services funding, the main driver for all commissioners is ‘maximising value for patients: that is, achieving the best outcomes at the lowest cost’ (p. 51). 288
Porter and Lee288 acknowledge the challenge of the change involved in moving to outcomes-driven provision, given decades of entrenched practices. They urge for changes to come from within the professions because, ultimately, value will be determined by how therapy is practised.
This chapter has explored what is currently known about the current, and potential, measurement tools and outcomes linked to the typology themes for children with PSLI. The research first considered what combinations of measurement tools best identify appropriate interventions, in relation to the typology themes. Published, norm-referenced assessments are considered essential diagnostic tools and should have standardised administrative, scoring and interpretative procedures with established validity, reliability and applicability for specified populations, in this case children with PSLI. 259,289 However, diagnosis is not the only purpose of assessment. Therapists need to draw on a range of information sources to support their clinical decision-making, including what to prioritise when a number of aspects require intervention (specifically in this research, which typology themes to target), how to track progress, how to determine when intervention is no longer required and how to measure outcomes. Some of the influencing factors are ‘child based’, such as developmental level and profile, ability to engage, learning style and preferences and level of severity of the presenting difficulty. These features would be the focus of assessment for the majority of the typology themes (including ‘speech’, ‘expressive language’, ‘comprehension’, ‘functional communication’, ‘foundation skills’, ‘self-monitoring’ and ‘generalisation’). Other factors can be considered as ‘environmental’, including the level of understanding of significant adults and their ability to support, adapt and ‘scaffold’ the child’s learning and provide opportunities for communication. These would be investigated mainly with respect to the typology themes of ‘adult understanding’ and ‘adult–child interaction’. It is acknowledged that, optimally, therapists should incorporate data from both quantitative and qualitative sources to fully examine the abilities of any child97 and provide a holistic picture. WHO283 suggests that comparing ‘capacity’ and ‘performance’ can provide useful information about how the environment can be adapted to improve an individual’s performance in functional activities. A dynamic assessment approach involves evaluating a child’s ability to perform activities when provided with additional cues or ‘scaffolding’, that is, when the linguistic context is modified. This dynamic assessment process can reveal a child’s ‘learning potential’ and capacity for change at an individual or an environmental level but may be difficult to carry out in a reliable and valid way. 250 It also provides valuable information about which strategies will best help a child to achieve and facilitate the transfer, or generalisation, of skills to other environments. 290 This approach is particularly valuable for SLTs who focus much of their intervention on enhancing the child’s communication environment by supporting parents and significant others to help the child progress. However, therapists report a limited number of assessments that provide evidence of children’s communication performance in everyday environments. 132,253,291–293
In terms of which assessments or methodologies were found to be routinely employed to identify therapy aims, practice is not consistent across services or therapists. We found that therapists use mixed methods of data collection to provide information about children’s communication in both ideal (capacity) and functional (performance) contexts. 283 This included nine naturalistic or informal methods of data collection that were used to determine how children performed functionally day-to-day and to determine the level of knowledge and understanding of significant adults in their communication environments, either at home or in a care setting. These methods yielded information relating mainly to six of the typology themes: ‘foundation skills’, ‘adult understanding’, ‘adult–child interaction’, ‘self-monitoring’, ‘generalisation’ and ‘functional use of language’. Standardised and norm-referenced assessments were used to gather information particularly about a child’s developmental level and the characteristics, or profile, of the presenting communication difficulty or impairment, such as its severity. The use of standardised assessments tended to focus mainly on three typology themes – ‘comprehension’, ‘speech’ and ‘expression’ – although these assessments were also used to a lesser degree in relation to ‘foundation skills’ and ‘functional use of language’. Without exception, for all typology themes, naturalistic or informal data were used to supplement formal assessment findings to determine children’s needs and to measure the outcomes of intervention, which is in line with earlier findings. 253 However, of the standardised measures in common use, only the CELF-4 met all of the psychometric quality standards as specified by Friberg. 97 In addition, therapists reported administering only subsections of assessments that they felt were relevant to a particular area and they rarely completed the whole of an assessment. This affects the sensitivity (accurately identifying the presence of impairment) and specificity (accurately identifying the absence of impairment) of the assessment findings and potentially leads to over- or underdiagnosis. As a result, some children may not receive early or appropriate intervention that could optimise their outcomes. 294 Alternatively, some children may receive intervention that may not necessarily be required and therefore resources may not be being targeted as effectively as possible. It also raises questions about validity and how the findings are used to determine need, eligibility, intervention, evaluation of outcomes and comparison across services. 97,253,258,259 Therapists using assessments in this way are not necessarily using the standardised scores; rather, they seem to be using the assessments as a way of standardising the sampling context and as such the assessments supplement other informal assessment processes. This too has the potential to undermine the reliability of the results across children.
The research programme also considered the measurement of outcomes for preschool children with PSLI. To capture outcomes that are relevant to all stakeholders, including children, families, therapists, commissioners and quality assurance agencies, outcome measures need to be multidimensional and multilevel. 274,295,296 This will include qualitative and quantitative data that are valid, reliable, sensitive to change, specific, comparable and understandable and which have a particular focus on functional changes for the individual child and family. 274 One tool would be unable to capture data for all purposes; hence, the NHS Outcomes Framework outcome domains are underpinned by a range of indicators, which, when the data are aggregated, will provide evidence of how well the overarching outcome has been met at the individual, family, service, community, society and national levels. 263
A large number of standardised measurement tools exist that can provide information pre and post intervention about children’s communication (capacity) in ideal conditions, particularly at the ‘impairment’ level. However, in this study we found that therapists consistently reported that intervention across the typology themes can impact on much wider aspects of children’s lives. Fifteen outcome domains emerged from the nine themes. Some are common across a number of typology themes, such as emotional well-being (all), participation and inclusion, social interaction, behaviour and educational achievement. However, others are specific to an intervention or to a typology theme; these are adult–SLT partnership, adult knowledge and use of strategies, adult–child relationship, attention and listening, communicative competence, intelligibility, self-awareness, and understanding and use of language. We therefore have a picture of the PSLI intervention typology contributing to a range of outcomes impacting on the child and his or her family, eight of which are typology theme specific.
Findings from the BCRP223 identified two overarching outcomes that parents wanted for their children: to be able to achieve independence and social inclusion. Therapists in this study believe that their interventions do impact on these two outcome domains. Children in the BCRP were concerned about emotional well-being and social interactions; these outcomes were also identified in this study, demonstrating a high level of consensus between service users and therapists on desired outcomes. However, as already highlighted, measurement and data gathering practices are inconsistent and currently focus predominantly on the presenting area of difficulty, for example sound production, and/or hypothetically contributory factors, such as styles of ‘adult–child interaction’. As it is now necessary to be able to demonstrate the wider impact of SLT-led intervention, the desired outcomes must have a starting point at the beginning of intervention to demonstrate change over time. This requires measurement tools and specific outcome indicators that are reliable and valid to provide appropriate supporting evidence.
A review of existing tools was undertaken to identify any that might be relevant to the measurement of outcomes related to the typology themes. As already indicated, a number of formal measurement tools were identified in the study that are appropriate and which are frequently used to identify the need for intervention at the impairment level for individual typology themes, including ‘comprehension’, ‘speech’, ‘foundation skills’ and ‘expression’. However, in line with international consensus, there were felt to be few reliable measures to assess children’s performance, that is, functional use of speech and language in their everyday context rather than ‘capacity’ under controlled or ‘ideal’ test conditions. 297 Of particular note was the lack of common valid and reliable tools to specifically identify the need for intervention in PSLI for the themes of ‘adult understanding’, ‘adult–child interaction’ and, to a lesser degree, ‘generalisation’ and ‘functional use of language’.
Tools appear to be particularly lacking for measuring specific outcomes related to outcome domains. So, for example, therapists reported that interventions would impact on outcome domains but no mechanism or tool was available to measure the outcomes. This included outcome domains such as adult–child relationship, adult knowledge and use of strategies, adult–therapist relationship, behaviour, emotional well-being, communicative competence, independence, intelligibility, participation and inclusion, self-awareness and social interaction. In terms of measuring outcomes in relation to the adult–child relationship and adult knowledge and use of strategies, a new common tool is needed that is of relevance to PSLI. In some areas, tools are available. For example, there are a number of useful tools in existence for intelligibility including the Intelligibility in Context Scale258 and the Children’s Speech Intelligibility Measure (CSIM). 298 The adoption of a common measure requires further consensus work. Many of the other domains are encompassed in the WHO International Classification of Functioning, Disability and Health (ICF) – children and youth version, which is known to be both valid and reliable. 283 There are two tools based on this that have been developed to capture information specifically in relation to communication. They are the TOMs275 and the Focus on the Outcomes of Communication Under Six (FOCUS) measure,299 either of which would be appropriate. Again, further consensus work is required with the profession. In relation to the adaptation of existing tools, this would require a considerable amount of resources to achieve agreed content, reliability and validity.
Further consideration was given to the principles that should govern further tool selection and use. A combination of core quantitative and qualitative valid and reliable measures is considered to be a priority for service development and delivery to capture consistent data that are specific, allow accurate diagnosis of the presenting or potential difficulty, highlight the relevant typology theme(s) and provide a baseline from which to measure progress and achievement of desired outcomes. A core combination of measurement tools should ideally identify:
-
relevant information from parents and significant others (adults) who know the child well
-
relevant information about the child and his or her environment – including the level of support for the planned intervention
-
information about the impact of the presenting PSLI on the child’s current day-to-day functioning and participation and academic achievement
-
diagnostic information about the severity of the presenting difficulty and the potential for change
-
which typology theme requires intervention
-
when progress is adequate and further intervention is not necessary
-
appropriate measurable outcomes.
This would provide the basis of a core national data set to allow monitoring of progress, comparison of intervention approaches and provision of information to service users, commissioners and researchers.
In summary, the study has identified a number of measurement tools and methodologies that therapists might use to focus intervention on the nine typology themes and measure outcomes, mainly at the impairment level. Fifteen outcome domains have been identified that link to the typology themes, eight of which are theme specific. There is a need for a core set of current and, additionally, valid and reliable measures to focus intervention appropriately on the typology themes. These should also provide evidence-based outcome indicators, particularly in relation to the functional ‘real-life’ impact of interventions.
Chapter 6 Economic evaluation of speech and language therapist-led intervention
Introduction
In preschool children specifically, specialist speech and language therapy services have been charged over the last decade with meeting the needs of the local population and improving services to prevent future problems as well as achieving best value for money in the allocation of NHS resources. 28 A 2008 review of service provision for children and young people (aged 0–19 years) with SLCN reported that the current system for providing support was routinely described by families as a ‘postcode lottery’. 28 This review highlighted the inconsistencies found in the way that different areas commission and deliver services to children with SLCN, indicating that geographical variation in the effectiveness and cost-effectiveness of speech and language therapy services for preschool children is a potential issue. 28
It is important for speech and language therapy services to be able to contribute the information and evidence required by commissioners and policy-makers to reduce the ‘high variability and a lack of equity’ in speech and language therapy services for preschool children. 28
This study aimed to collect information held by speech and language therapy services in six case study areas regarding:
-
Where referrals originate and at what age and the response times, to identify criteria for initial assessment, eligibility for speech and language therapy services and criteria used to diagnose PSLI.
-
SLT management pathways for referral, processes for establishing management plans, intervention aims, locations and use of multidisciplinary agencies and/or other staff. Also of interest were intervention descriptions, dose/intensity and time frames of interventions, modes of intervention delivery (individual direct/indirect and group) and interaction processes between SLTs and parents/carers in the course of delivery.
-
Understanding of systems used for the continuity of management, discharge, review and transfer as they relate to service efficiency and outcome measures applied.
Summaries of the research evidence for effectiveness and cost-effectiveness have demonstrated that different speech and language therapy services have different impacts on patient outcomes and discharge patients at different points in their intervention pathway. 29,35,300,301
Recent work by Law et al. 37 identifies that very little is known about the range of speech and language therapy care packages provided across the NHS and notes the small number of both partial and full economic evaluations in this area. In addition, how these packages can be described in terms of resource use, staff interaction with parents, how children access complex speech and language therapy interventions and the implications (and costs) for parents of being involved in home therapy are highlighted as areas in urgent need of attention. 37,302
Another challenge is evaluating the interventions. Speech and language therapy interventions are complex and can be identified by five main criteria:
-
several interacting components
-
number and difficulty of behaviours (functioning) required of those delivering and those receiving an intervention
-
multiple outcomes of interest
-
degree of flexibility and tailoring of an intervention
-
groups or organisational levels targeted by an intervention. 124
The causal pathways by which speech and language therapy interventions might reduce the risk of difficulties in reading and writing and their association with behavioural difficulties are understood to some extent as short-term outcomes. However, speech and language therapy interventions occur at the same time as other changes in child development and the child’s environment and it can be difficult to assess any causal association with improvements in long-term outcomes (such as mental health, social isolation and employment prospects) using simple before and after studies. RCTs can assess causal association, but measuring long-term outcomes is a struggle because of the expense of following children prospectively over a long period of time. Consequently, there are many potential barriers to the conduct of robust economic evaluations for commissioning services and monitoring performance.
Recent high-quality research identified four information gaps for costing speech and language therapy pathways and packages of care. 302 The authors of this report concluded that:
-
There was insufficient detail about therapists – how staff mix is used to deliver speech therapy interventions.
-
There was insufficient information about service users – for example the use of group rather than individual delivery mechanisms for interventions, which has implications for ‘dose’ and/or intervention intensity.
-
Description of the full scope of speech and language therapy activities other than intervention delivery was lacking. For example, preparation time for delivery, travel time and administration connected with delivery, time spent in consultation with the parent/carer and time to write up notes afterwards are all part of the actual costs to an organisation of providing speech and language therapy interventions.
-
Costs to parents/carers are not included – parents have an important role in terms of reinforcement, practice and support and may need to take time off work or other activities. There are out-of-pocket expenses for travelling to treatment centres and subsistence costs that should also be considered.
Beecham et al. 302 conclude that assumptions about any of these four areas made to plug the information gap would have a marked effect on the estimated cost of an intervention during economic analysis, increasing uncertainty in estimates of cost-effectiveness.
There is a dearth of evidence to indicate which short-term outcomes and impacts matter to children and parents, but there is some research evidence and user accounts of the system to build on. 303 There is also work from the BCRP that investigated outcomes valued by parents and children and which concluded that these outcomes are not routinely measured yet in either research or practice and neither do we have well-articulated theories about the causal pathways between changes in children’s speech and language and the kind of social and functional outcomes that are of importance to parents.
Objective
The research presented in this chapter addresses the following Child Talk objective:
-
to identify the measures required to develop formal economic assessments of SLT-led interventions and care pathways within services.
Specifically, this chapter describes the level of basic activity data being routinely reported and collected by speech and language therapy services and explores the feasibility of undertaking a comparative economic analysis looking at cost per referral by area.
Research questions
-
What resources are utilised in the delivery of individualised SLT-led interventions across geographical settings and with differing levels of engagement from children, families and carers?
-
To what extent are speech and language therapy services routinely collecting and reporting basic activity data to support economic evaluation of cost per referral by geographical area?
Methodology summary
A summary of the methods is provided in Figure 26; the methods are described in detail in Chapter 1 (see Methodology overview).
FIGURE 26.
Summary of the methodology used to Identifying resource use by speech and language therapy services.
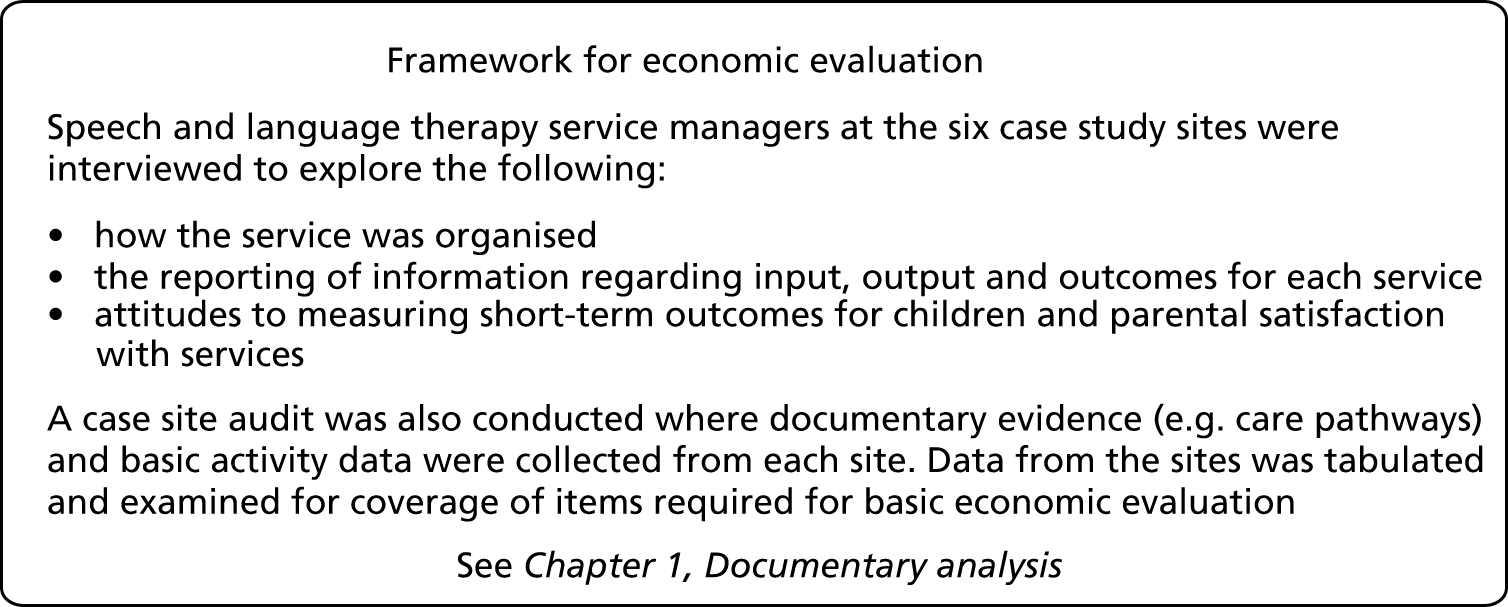
Findings
This study explored the reporting of resources that are utilised in the delivery of care pathways by SLTs to preschool children with PSLI. Documentary analysis was undertaken across the six case study sites in England to assess the extent to which speech and language therapy services are currently collecting data on resource use. In addition, the ability of speech and language therapy services to collect and report information that might be used by decision-makers in commissioning services was explored. The data revealed variation in routine recording of data relating to care pathways, resource use and outcome measures.
Across case study sites, the capture and reporting of the basic data needed for costing service delivery varied in coverage and level of detail. There are problems caused by frequently changing and evolving pathways and sites with more than one pathway in operation. All case study sites recorded data for most of the variables in Table 74 at an individual service user level, usually in the notes. Sites were not able to access data aggregated at a service level for preschool children with speech and language needs. There was very little available in terms of systems and processes to support routine data collection and management. Most case study sites were able to report the number of patients treated, the number of referrals and their current caseload. However, very few data were available regarding the severity of speech and language impairment across the caseload (i.e. proportions of mild, moderate and severe cases), which has implications for resource intensity. Case study sites did not appear to routinely record the full range of resources used in the process of care in terms of staff activity, staff working in teams with a different skill mix and staff interaction with parents/carers to support home activities related to speech and language therapy. Basic descriptions of the frequency, duration and intensity of typical care packages and staff activity associated with care pathways (e.g. number of assessments, use of groups and one-to-one delivery) were lacking. Table 74 illustrates the variables that could and could not be provided by case study sites at the service level per annum.
| Data item | Site 1 | Site 2 | Site 3 | Site 4 | Site 5 | Site 6 |
|---|---|---|---|---|---|---|
| Preschool population (age 0–4 years) 2011 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Details of staff working with preschool children with PSLI exclusively | ✓ | ✗ | ✓ | ✓ | ✓ | ✓ |
| Number of staff (whole-time equivalent) and band | ✓ | ✗ | 2 SLTs, 1 SLT assistant, students | 4 Band 6, 2 Band 5, 0.6 Band 7 | Band unspecified | 2 Band 4, 3.8 Band 5, 10.2 Band 6, 1.8 Band 7 |
| Number of PSLI referrals 2011 | ✓ | 1730 | 900 | 900 | 450 | 1822 |
| By referral source | ✓ | ✗ | ✗ | ✓ | ✓ | ✗ |
| By age | ✓ | ✗ | ✗ | ✗ | ✗ | ✗ |
| By level/severity of PSLI | ✓ | ✗ | ✗ | ✗ | ✗ | ✗ |
| Current caseload | ✓ | ✗ | ✗ | 900 | 569 | 1822 |
| By referral source | ✓ | ✗ | ✗ | ✗ | ✗ | ✗ |
| By age | ✓ | ✗ | ✗ | ✗ | ✗ | ✗ |
| By level/severity of PSLI | ✓ | ✗ | ✗ | ✗ | ✗ | ✗ |
| By associated condition | ✓ | ✗ | ✗ | ✗ | ✓ | ✗ |
| First assessment (1A) | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| By setting (clinic, home) | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| By professional | ✓ SLT | ✗ | ✓ SLT | ✓ SLT | ✓ SLT | ✓ SLT |
| By duration (minutes) | 45–60 | 45 | 45 | 45 | 45 | 45 |
| By severity level (used to decide setting for 1A) | ✓ | ✗ | ✗ | ✗ | ✗ | ✗ |
| Others present | ✓ | ✗ | ✗ | ✗ | Parent/carer | ✗ |
| Severity of impairment across caseload | ✓ | ✗ | ✗ | ✗ | Mild 5%, moderate 25%, severe 70% | ✗ |
| Details about care pathways | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Parental satisfaction | ✗ | ✗ | ✗ | ✗ | ✓ Parent–child interaction self-evaluation, group feedback sheets | ✓ Survey designed by Ipsos MORI for trust-wide use on PDA |
| Parental rating | ✗ | ✗ | ✗ | ✗ | ✓ Parent–child interaction sheets | ✓ Designed by Ipsos MORI for trust-wide use on PDA |
| Outcome measures | ✓ Goal attainment scales304 | ✗ Have used TOMs,275 EKOS,305 site developing Outcomes Framework on functioning and capabilities | ✗ Provide discharge numbers and associated codes | ✗ Provide discharge numbers and associated codes | ✓ Malcomess Care Aims306 | ✓ EKOS |
Matching care pathways to preschool children depends on accurate data concerning the level of severity of the speech and language impairment. Although it is apparent that these category labels are generated to decide whether a clinic or home setting is more appropriate to undertake the first assessment, they were not recorded routinely at a service level in five of the six case study sites (see Table 74). Although descriptions of care packages and care pathways matched to severity level were provided by most sites (Table 75), they are not adequate for costing within economic evaluation because it is unclear how many children proceed down each arm of the pathway in any given year. When care pathways relate to severity of PSLI it would be possible to audit to collect routine data and it may be the case that most speech and language therapy services see cases of moderate and severe PSLI. Conducting an audit to populate a database that might be interrogated for economic evaluation is something that services might consider.
| Case study site | Description of care pathways |
|---|---|
| 1 | Care pathways relate to severity of PSLI. There are two care pathways for preschool children: (1) language delay – up to four sessions of parent–child interaction followed by joint target setting three times per year in early years setting; talking tips, Hanen parent groups; (2) phonology delay – package of listening activities, up to three sessions; severe cases include one-to-one weekly or fortnightly therapy, up to six sessions |
| 2 | There are two care pathways, with parent workshops being used across some parts of the city. Parents attend these after referral, before the first appointment, to discuss any concerns. Also, adult and toddler groups run by non-SLTs and SLTs or learning disability workers may offer a slot called ‘play and say’. Chatterbox groups are parent–child interaction based and are for the core caseload; they are run by children’s centre SLTs. The care pathways include trying not to review more than once. Pathway 2 (persistent) includes speech and language therapy based on the Hanen programme |
| 3 | First stage for most children is either a parent language group for children using single words or less or a listening group. Children with more complex/severe impairments or those who have family or environmental complications are offered individual sessions. Language group is based on the Hanen programme and consists of three sessions. A centralised service is made possible by the city base. Critical mass is always an issue and therefore groups do not always run throughout the year. Model of intervention is seen as eclectic (open to additional ideas and new approaches) to the existing framework |
| 4 | No description of pathways available |
| 5 | Five pathways identified: Children’s Centre 0–3 years service-level agreement; core service community clinic for mild to moderate severity; core service preschool; specific language impairment/school-aged specific language impairment; Early Support Programme/Common Assessment Framework |
| 6 | Currently in state of transition. Was a unified profession, now moving to five multidisciplinary teams. These will consist of three healthy child pathways (team includes SLT, health visitor, school nurse), one complex needs pathway (team may include specialised SLT, community SLT, psychologist, occupational therapist, specialist nurses) and one learning disabilities and development team (team may include SLT, psychologist, community nurse, mental health) |
Speech and language therapy services do not appear to be collecting (or are at the time of writing are unable to tell us) the levels of activity by type (e.g. initial assessment, clinic visit, home visit) and patient type (PSLI/other) that would allow them to allocate costs (directly or indirectly) to patients and to estimate unit costs for client groups (e.g. all children with severe PSLI) or patient encounters (e.g. home visit for therapy).
Capture of care outcomes (e.g. goal attainment) and parental satisfaction using measurement tools devised for that purpose was patchy across case study sites, with three of six case study sites currently not collecting data of this nature. Child well-being outcomes are not routinely measured and none of the case study sites collects more long-term outcome information such as educational progression or attainment. The following outcome measures were mentioned: TOMs,275 the East Kent Outcomes System,305 goal attainment scales and Malcomess Care Aims. 306
These outcome measures have been mentioned in previous surveys of the profession [BCRP89 and the completed RCSLT survey; see www.rcslt.org/news/events/past_events_docs/anja_lowit_report (accessed 11 March 2015)]. Some case study sites asked about parental satisfaction with services but none was measuring outcomes at the time of our documentary analysis. Some respondents referred to process and output variables, but the concept of ‘outcome’ is not considered routinely or collected under a systematic process.
Discussion
This documentary analysis has demonstrated that NHS speech and language therapy systems for collecting the required data, describing care pathways sufficiently and mapping the activities and interactions associated with care pathways and reporting patient-level data to support the conduct of economic evaluation are in their infancy. Spending resources efficiently is a policy imperative for all public sector organisations. Expectations and pressures around how services are collecting and reporting data to demonstrate performance for commissioning have grown under conditions of economic austerity. Making a case to justify receipt of future scarce public sector resources is therefore an important priority.
Beecham et al. ,302 in stating the requirements for full economic evaluation of speech and language interventions per se, note that accurate estimation of the costs of intervention is one of the first steps in this process. The findings of this programme of research support these conclusions, but it is important to explain how this programme can move economic evaluation in this area forward.
First, there are challenges in evaluating the impact of SLTs delivering complex interventions in complex environments. Describing and mapping the activity associated with a care pathway that incorporates the stages of referral (from different sources) and assessment (undertaken in different settings including clinics, hospital and the home and in different ways depending on the age of a child) is a challenge. Matching children to speech and language therapy appropriate to their needs and delivering therapy to individuals and groups depends on a range of factors. Delivery of standard packages (which vary by region according to a range of factors), interacting with parents and involving them in supporting the outcomes of speech and language therapy and assessing and measuring progress and outcomes requires that data are routinely collected, recorded and managed. These data should not languish within patient notes; they should be cleaned, processed and managed so that they can be accessed, analysed and reported to decision-makers.
A number of key variables should be routinely collected and recorded. The items in italics are the key inputs to economic analysis. Services should aim to record data that can be used to estimate the cost of referral (based on the proportions of cases referred from different sources), initial assessment (based on the proportions of assessments by location), service delivery (based on the description of the care pathways for children with PSLI) and interactions with parents/carers, children with PSLI, schools and the environment (based on assumptions about the proportions of children with differing levels of severity that are present in the caseload relative to the proportions expected from known prevalence rates). Resource utilisation will include the skill mix of therapists and their banding, locations for assessment and delivery of therapy and the frequency and duration of delivery across cases. Direct and indirect overheads for staff and delivery locations are also important cost items. 302
One of the aims of the documentary analysis was to preliminarily compare differences in resource use per referral by case study site based on the data in Table 74. However, it was decided that there would not be much value in attempting to do this and it might provide a false sense of accuracy. This is a limitation of this part of the study.
Our current visualisation of the relationship between resource inputs to complex environmental interventions for preschool children and the contingent child and parent/carer outcomes arising is that it is mediated and moderated by a range of individual child, family/carer, physical environmental and social environmental factors. Stratifying children according to ‘severity’ of need is an important element of developing and planning the allocation of resources. Services need to collect information that will enable description of the range and delivery costs (high, medium, low) of care currently offered to children with PSLI of differing severity (severe, moderate and mild cases). Resource inputs by staff and other resources are required to make diagnostic assessments and match complex interventions with preschool children’s speech and language needs. There are further resource inputs required to engage preschool children with PSLI needs and their parents/guardians in ‘underserved’ families or settings, to maintain them on long-term programmes, as well as adapt their environments as part of intervention. Parental/carer costs also need to be recorded.
All of these elements of the complex intervention consume resources and modify or mediate outcomes and these associations will need to be described and captured by service providers to populate a database to enable economic evaluation. Each service needs to collect and manage data to be able to demonstrate the range of resource utilisation. Reporting of short-term outcomes is poor and this needs to be addressed quickly if economic evaluation for commissioning is to become a reality.
A useful starting point for data collection is to record the following items routinely:
-
the number of referrals per annum and the percentage split between mild–moderate and severe PSLI cases seen per annum
-
a basic description of each typical care package by severity of PSLI case
-
the frequency and duration of ‘typical care pathways’ relative to the degree of impairment at referral, assessment and service delivery
-
the number and staff band of professionals involved in delivering these typical packages and a brief description detailing staff, service user and parent/carer interactions and costs, including out-of-pocket expenses
-
the location of delivery of each typical care package, for example hospital, children’s centre
-
the mode of delivery to the service user: individual or group based
-
a description of how the speech and language therapy package works in terms of interactions with parents and supporting work at home to tease out pathways
-
outcome and impact measurement – more widespread application of tools to report on communication skills outcomes, goal attainment and longer-term educational attainment.
There principles are laid out in the NHS Costing Manual,307 for costing, and by the Commissioning Support Programme,308 for measuring outcomes that might be considered. All of these recommendations require that appropriate data and narrative are routinely collected, recorded and managed in an accessible system that is flexible and which can respond to frequently changing and evolving pathways and sites with more than one pathway in operation.
From a research perspective, this data set would be required for future evaluations of the cost-effectiveness of the intervention framework developed in the Child Talk programme and appropriate mechanisms would need to be developed to capture these data prospectively.
Chapter 7 Development of a website to host the intervention framework
An intervention framework has been developed that sets out the purpose of speech and language therapy for preschool children with PSLI, along with the underpinning interventions, outcomes and assessment tools. In addition, the research evidence from an extensive systematic review has been mapped onto the framework along with user perspectives. To support the uptake and use of this framework it is being developed into an interactive website, designed in a way that will be accessible to SLTs, EYPs and members of the public.
The work presented in this chapter addresses the following Child Talk objective:
-
to work with the RCSLT to facilitate the national take-up and ownership of the framework.
The RCSLT has been very supportive of this research programme throughout. The PI regularly discussed aspects of the programme delivery and aims with the Chief Executive Officer of the RCSLT, who also attended, and presented at, the mid-programme co-applicant meeting. More recently, the research team has discussed with the RCSLT how the intervention framework developed through the Child Talk programme could be presented. The intervention framework will be presented as a freely accessible website with a link from the Bristol Speech and Language Therapy Research Unit (BSLTRU) [see www.speech-therapy.org.uk (accessed 11 March 2015)].
Where does Child Talk fit with other websites supporting evidence-based practice?
Over the last few years there has been an increase in the number of websites that support EBP by SLTs (Table 76):
-
Communication Trust – What Works
-
Speech Pathology Australia – SpeechBITE
-
ASHA – Evidence Maps.
| Website | Age group and specialty covered | Levels at which interventions are covered | Level of evidence scrutiny | Inclusion of family perspectives |
|---|---|---|---|---|
| ASHA – Evidence Maps [http://.ncemaps.org (accessed 11 March 2015)] | Covers very specialist groups; nothing yet on PSLI and nothing specifically with preschool children | Each evidence map breaks ‘intervention’ down into various different sections, but there is no explanation about how these are derived | Provides summaries of the level of evidence behind relevant clinical guidelines and grades any research evidence provided based on the hierarchy of evidence; no sign of quality appraisal of articles | If there are relevant papers these are referenced and reviewed |
| Speech Pathology Australia – SpeechBITE [www.speechbite.com (accessed 15 January 2015)] | Covers intervention studies across the scope of speech pathology practice. Can search for studies about children aged < 2 years, children aged < 5 years or ‘children’. A search for ‘under 5 developmental language impairment’ yielded 116 results | Can search according to targets (language impairment is a target not a condition under the database). Refining the previous search by ‘language therapy’ delivered 96 papers | Papers are quality appraised using PEDro | No |
| Communication Trust – What Works [www.thecommunicationtrust.org.uk/whatworks (accessed 11 March 2015)] | Covers children with SLCN. Searching for ‘preschool intervention’ yielded 45 results | Covers mostly programmes but also some strategies; based on previous survey of current practice from the BCRP | Grades the level of evidence according to the evidence hierarchy, but no quality appraisal of the research papers | No |
| Child Talk [www.speech-therapy.org.uk (accessed 11 March 2015)] | Focused on preschool children with PSLI | Nine themes of intervention plus activities and strategies commonly used by SLTs | All levels of evidence included but only studies of robust quality are included (score of ≥ 6 on PEDro) | Children’s and parents’ views included |
The framework developed by the Child Talk programme differs on a number of parameters (see Table 76). The Child Talk programme focuses on a relatively narrow client group, preschool children with PSLI, and this group is not covered by the Evidence Maps website. Although the other sites include a number of interventions and research papers appropriate for this client group, SpeechBITE does not sort interventions according to current practice, making it more difficult for practitioners to find research that maps onto their practice, and What Works focuses mostly on programmes and although it does include some strategies it does not analyse the components of interventions.
The Child Talk programme builds on the work carried out by the BCRP, from which the What Works website was developed. The What Works website is hosted by the Communication Trust and is highly accessible; however, it only includes those interventions that have research evidence and the robustness of the studies is not appraised. The Child Talk programme provides an analysis of current practice based on a series of consensus exercises with SLTs and provides information about the research supporting that practice. Furthermore, this is set in the context of a broader framework which indicates the outcomes that are expected for each component of intervention and whether or not the delivery of that outcome is supported by evidence.
Chapter 8 Discussion and conclusions
The evidence-based framework and its application
The main output from this research is an evidence-based framework of SLT-led interventions for preschool children with PSLI. The framework is based on the practice of SLTs, the professional group who have responsibility for managing children with PSLI. It includes evidence from systematic reviews of research and considers the perspectives of significant users.
There is an accompanying consideration of measurement processes, including the assessments used to identify appropriate interventions and the outcome domains of relevance to the framework as well as the data needed for the economic evaluation of services. The central concept of the framework is the typology of therapy, as presented in Figure 27. This figure presents the nine themes of the typology and the hypothesised relationships between them that were derived from discussions between SLTs in focus groups and refined through a number of exploratory workshops. The findings suggest that these nine themes provide a high-level overview that is inclusive of all practice of SLTs with preschool children with PSLI. Although some components of the typology are applicable to all children in this group, others, such as ‘speech’, ‘expressive language’ and ‘comprehension’, are used only when appropriate for the particular needs of an individual child, thus supporting the concept of individualised care.
FIGURE 27.
Working hypothesis of the typology of speech and language therapy for preschool children with PSLI.
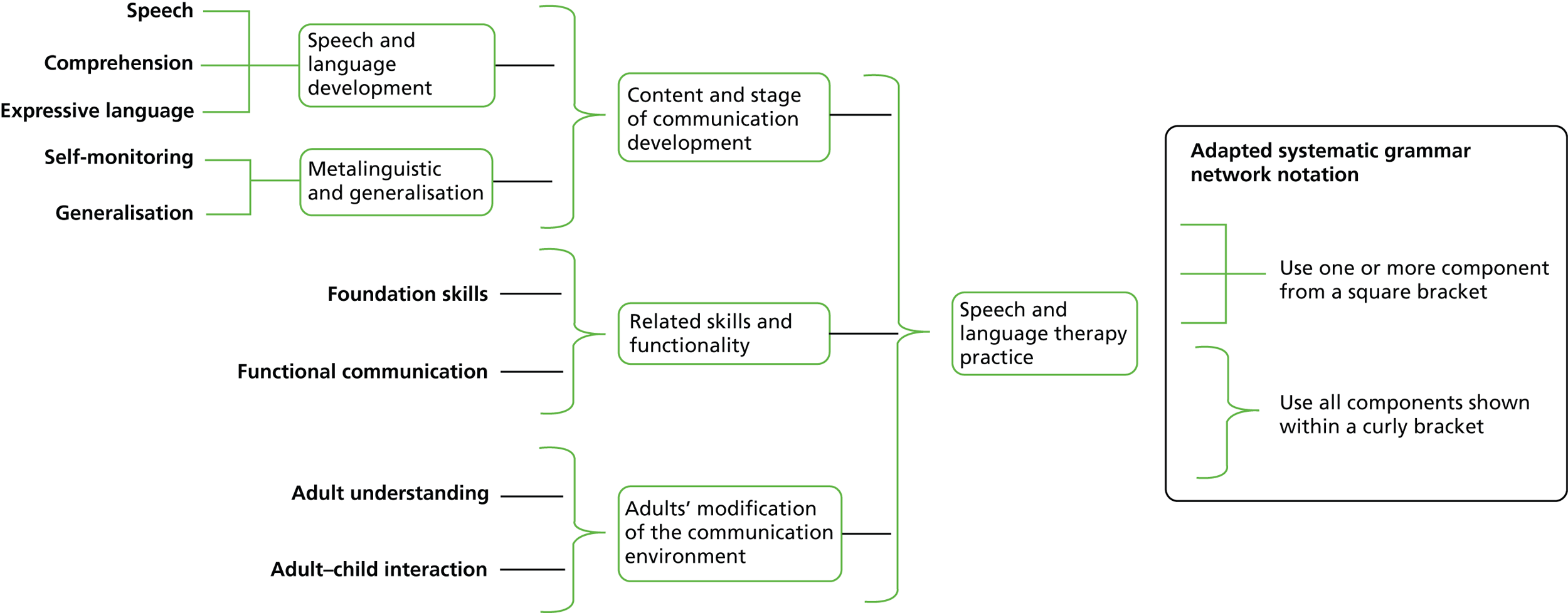
The practice of SLTs was further explored through national surveys, which produced additional information about the use of particular intervention activities and strategies. It was possible to link interventions to each theme of the typology, although this was more straightforward for some themes than for others, depending on how easy it was for therapists to make such knowledge explicit. The research also identified a number of factors that influence SLTs’ selection of interventions. However, it was not possible to identify particularly subtle patterns of how interventions are adapted and targeted for individual children and their families because of the wide heterogeneity of the child population and the range of interventions that SLTs have knowledge of. This detailed knowledge that therapists use during their online decision-making seems to be available to therapists in a tacit form that was not amenable to explication and documentation within the research.
A wide-ranging series of systematic reviews of intervention research was completed, which, once the evidence had been appraised, synthesised the level of evidence that is currently available for each theme of the typology. Similar to previous systematic reviews,17 the areas of practice most strongly supported by research evidence are those relating to ‘expressive language’ and ‘speech,’ with particular components such as modelling being supported by grade A evidence. A further two themes of the typology (‘comprehension’ and ‘adult–child understanding’) include studies that show some promise in that a number of interventions are beginning to accrue research evidence. It is also the case that the interventions that are supported by evidence do appear in current use. However, the other five themes had very weak evidence, either because the research does not address the area of the theme closely enough or the evidence is insufficiently robust.
The third component of EBP concerns the preferences of service users. The study has generated a wealth of data about the views of a wide range of parents regarding their perspectives on speech and language therapy and on the process of children’s developing language. Observations of children’s body language, vocalisations and attention have also provided insights into their perspectives on therapy activities. SLTs who implement EBP must be able to consider how the evidence might be applied in ways that are acceptable to children and their parents. When taken together, the data from the children, the parents and the EYPs in this study provide a rich source of insights that can be used to sensitise therapists to potential perspectives of children and their families. For example, many parents and their children expressed uncertainty, anxiety and even fear in connection with speech and language therapy. Some parents from underserved communities were unfamiliar with the role of SLTs. Others expressed some passivity in their responses and had not questioned aspects of intervention, or of services, that had puzzled or challenged them.
The perspectives of these parents suggest that EBP is not always implemented effectively, as EBP requires parents (and children) who are knowledgeable about the choices that are available to them and empowered to make evidence-informed choices. There is a certain irony in this, given that one of the themes of the typology is that of increasing adult understanding and feelings of empowerment, so that they feel confident in their role supporting their child’s communication. It seems possible that therapists view the idea of empowerment in a restricted way in that they wish parents to feel that they have a role to play in implementing the therapists’ suggestions, rather than the parents themselves being empowered to make informed choices. Parents being empowered to make choices requires SLTs to provide transparent and accessible information about the evidence base as it relates to the interventions that are widely available and those that are more specifically offered by a particular service in relation to the individual needs of the child and family.
To facilitate the implementation of the evidence-based framework, the aim was also to identify appropriate measurement tools that could support the selection of appropriate interventions and measure the subsequent outcomes. Despite a plethora of assessment tools being available, there seems to be a focus on the screening and diagnostic process for the typology themes of ‘speech’, ‘expressive language’ and ‘comprehension’ and, to a lesser extent, ‘functional communication’. Other aspects addressed in practice such as the communication environment are less well served by published materials. In addition, therapists reported the use of informal, naturalistic and observational methods of data collection. For this kind of assessment, therapists are reliant on their theoretical and experiential knowledge to interpret the observations meaningfully (Box 9).
-
12 formal/published assessments are frequently used.
-
Nine informal naturalistic information-gathering methods are used.
-
DLS.
-
CELF-3 and CELF-4.
-
RWF.
-
RAPT.
-
Renfrew Bus Story.
-
STASS.
-
STAP.
-
TALC.
-
CLEAR PSA.
-
DEAP.
-
RDLS-III.
-
PLS-3 and PLS-4.
-
Observation.
-
Adult/parent verbal report.
-
Adult/parent written report and questionnaires.
-
Video.
-
Audio recording.
-
Language/speech sampling in context.
-
Play.
-
Own or departmental screen.
-
Other speech- and language-eliciting activities including picture description, books, posting games.
CELF-3, Clinical Evaluation of Language Fundamentals-3; PLS-4, Preschool Language Scale-4; PSA, Phonological Screening Assessment; RDLS-III, Reynell Developmental Language Scales – III; RWF, Renfrew Word Finding Vocabulary Test; STAP, South Tyneside Assessment of Phonology; STASS, South Tyneside Assessment of Syntactic Structures; TALC, Test of Abstract Language Comprehension.
As an initial step towards developing a process to measure the impact of intervention for PSLI the research programme has identified outcome domains for each of the nine themes of the typology. Some of the outcome domains are common across the themes (e.g. ‘social interaction’), whereas eight are specific to only one theme, such as ‘intelligibility’, which is an outcome domain for the theme of ‘speech’ alone. For some domains it has been possible to identify existing measures or outcome indicators that, although not currently in common usage, could provide appropriate evidence of impact. For other domains there is a need to develop new measures or approaches to measurement processes. In particular, the perspective or conceptualisation of assessment or measurement of adults’ engagement needs adjusting to become a participatory process that is carried out in partnership with parents. So, for example, for the themes of ‘adult understanding’ or ‘adult–child interaction’, it would be inappropriate to see this as a process whereby the SLT ‘assessed’ the parent. Rather, the process should be a participatory and collaborative one whereby the underlying aims are discussed transparently between parent and therapist. Box 10 provides a summary of the outcome domains identified.
15 outcome domains – some generic across typology themes, others theme specific.
Outcome domains common across typology themes (frequency of occurrence)-
Emotional well-being (9).
-
Participation and inclusion (8).
-
Social interaction (7).
-
Independence (7).
-
Behaviour (5).
-
Educational achievement (4).
-
Adult knowledge and use of strategies (2).
-
Attention and listening.
-
Adult–child relationship.
-
Understanding and use of language.
-
Intelligibility.
-
Self-awareness.
-
Communicative competence.
-
Improved assessment scores.
-
Adult–SLT relationship.
Underpinned with clinical-level outcome indicators requiring further refinement and consensus.
When developing the evidence-based framework, a number of validation exercises were conducted. At the national events, for example, SLT participants were asked to give an example of a preschool child with PSLI with whom they had recently worked. They were then asked to show, for each theme of the typology, what assessments and interventions they had used and what outcomes they were aiming for (see Chapter 1, Methodology overview, for a description of the methods and Chapter 2, Study 2.1: identifying the themes of speech and language therapy practice, and Chapter 5, Study 5.1: identification of assessment tools used by speech and language therapists and Study 5.2: identification of outcome measures for speech and language therapy, for a summary of the findings). These descriptions provide useful summaries that illustrate the use of the framework in describing interventions. The case studies in Figures 28–31 are taken from these descriptions and are provided here as examples. Table 77 shows that all of the themes were used at least once in the four example case studies. The application of the framework by therapists to their current caseloads confirmed that the typology was comprehensive and allowed therapists to represent their interventions for a range of children. Furthermore, they add weight to the hypothesis illustrated in the systemic grammar network diagram (see Figure 27).
FIGURE 28.
Case study A described using the intervention framework.
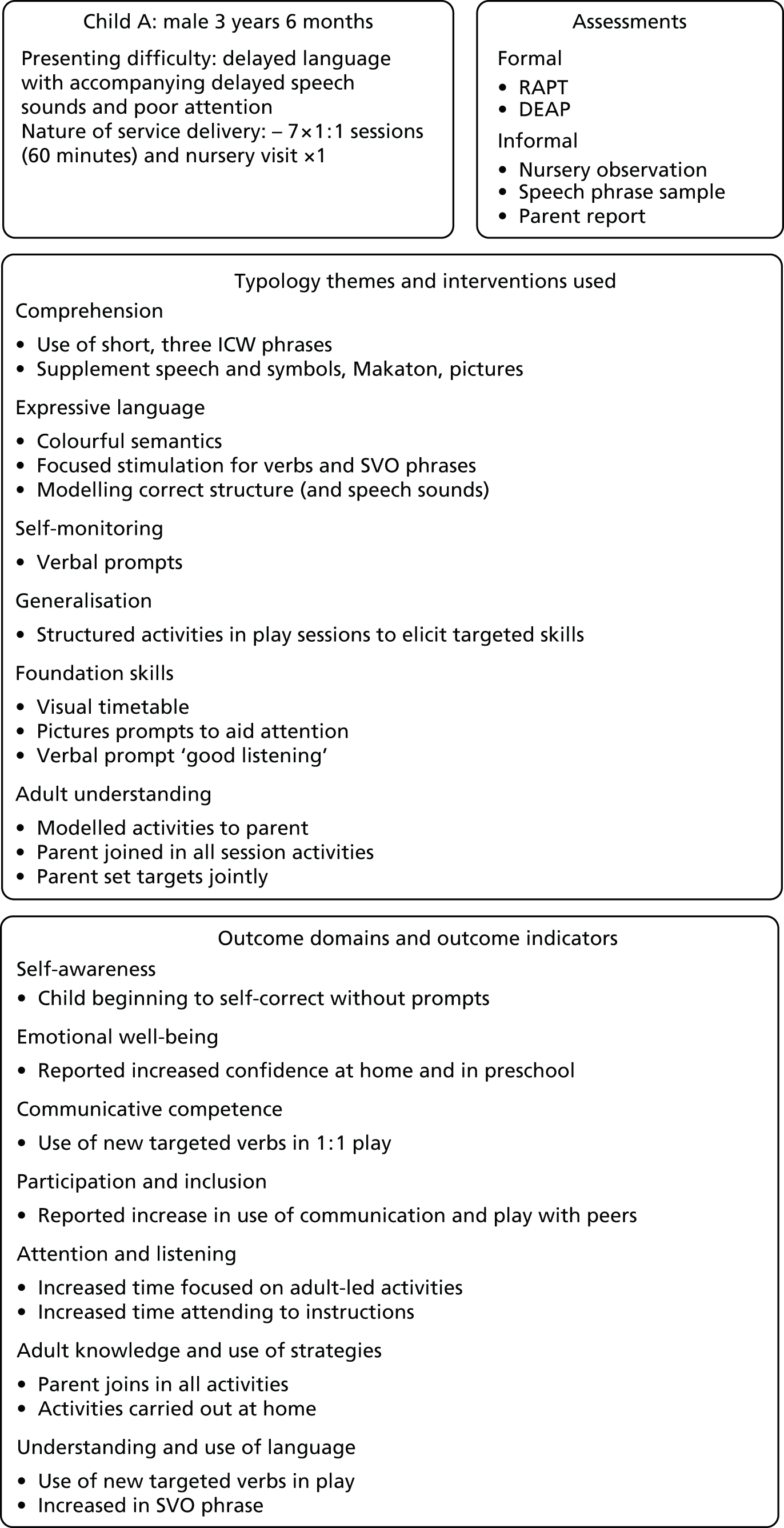
FIGURE 29.
Case study B described using the intervention framework. CELF, Clinical Evaluation of Language Fundamentals; STAP, South Tyneside Assessment of Phonology; STASS, South Tyneside Assessment of Syntactic Structures.
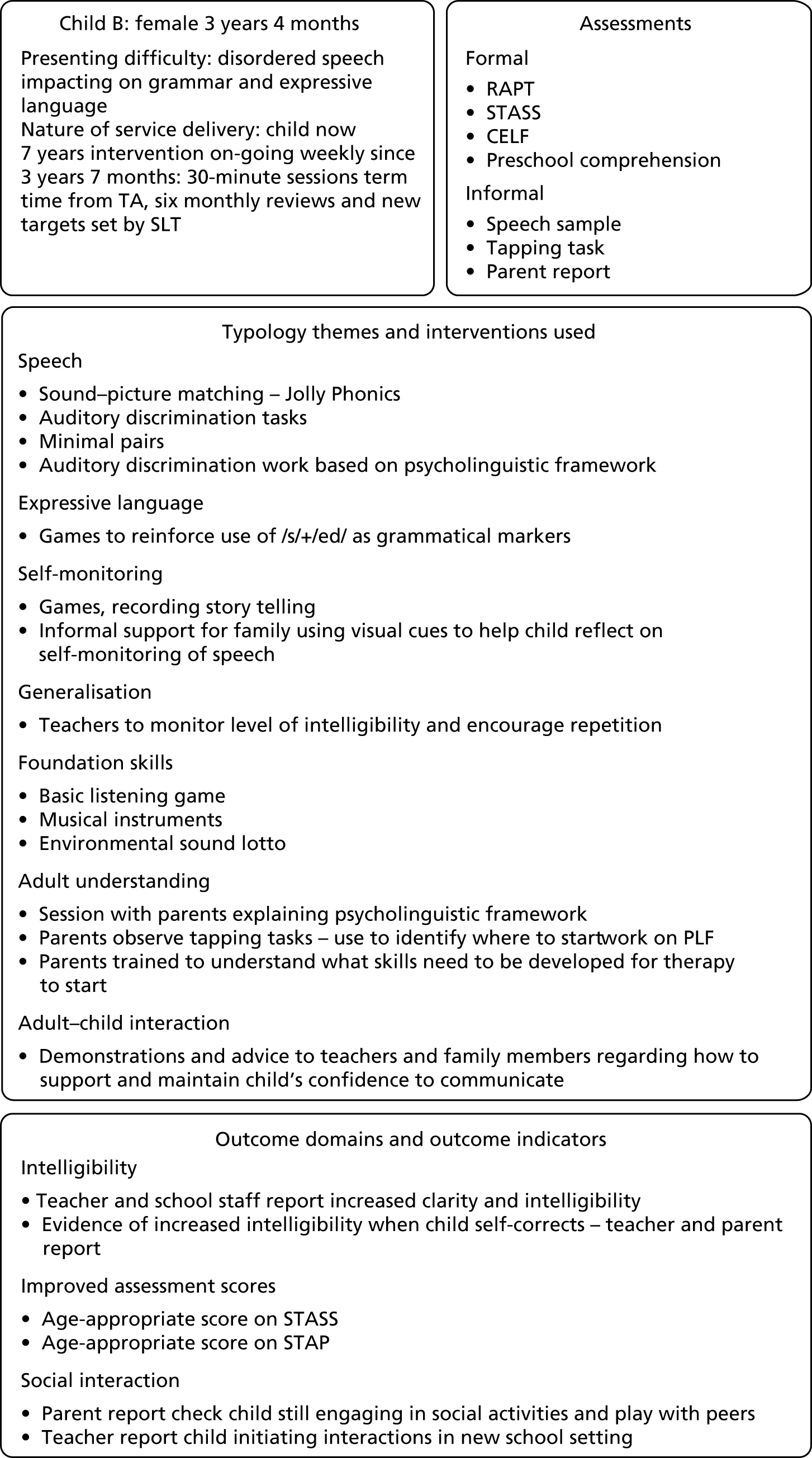
FIGURE 30.
Case study C described using the intervention framework.

FIGURE 31.
Case study D described using the intervention framework.
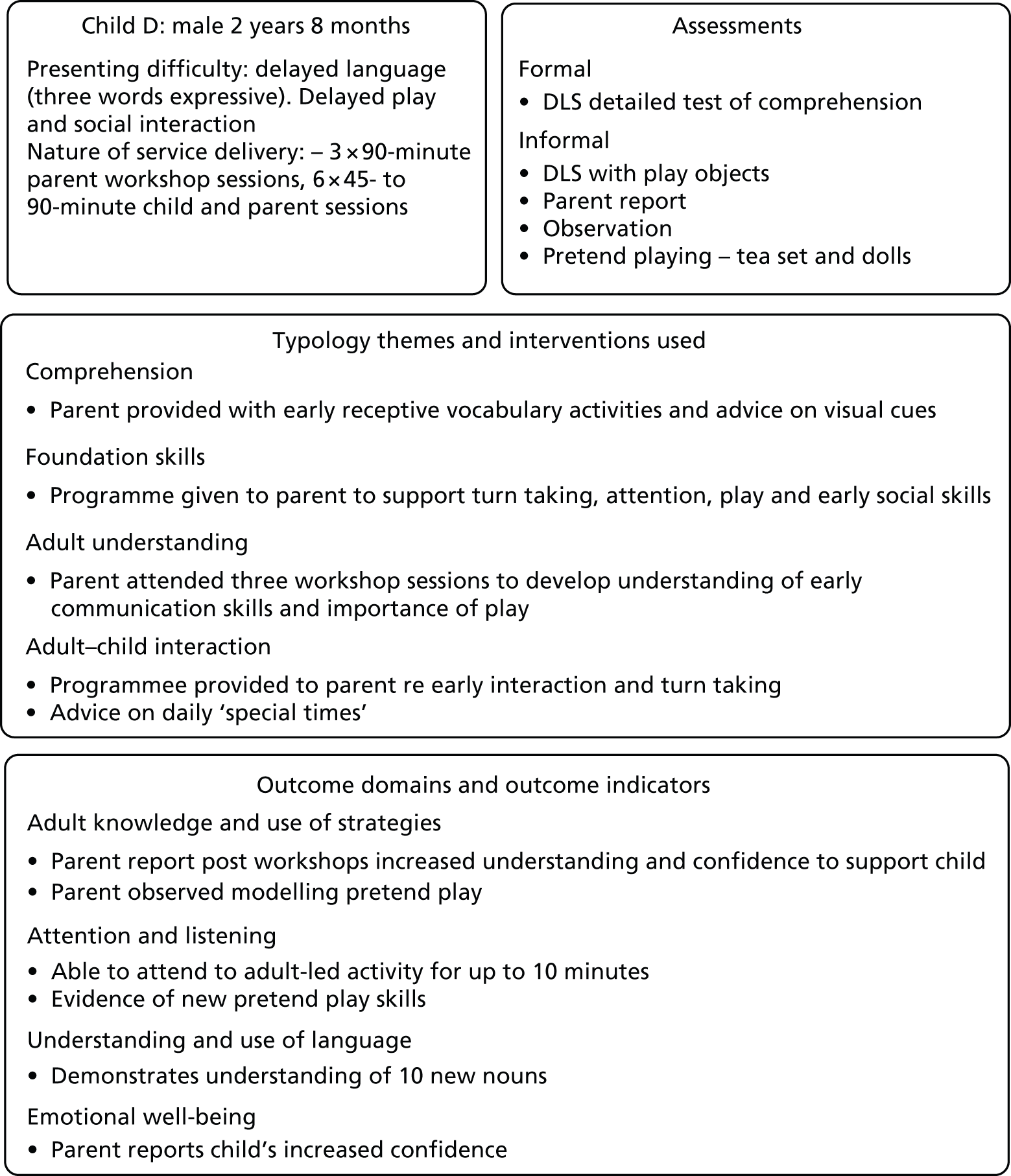
| Typology theme | Child A | Child B | Child C | Child D |
|---|---|---|---|---|
| Speech | ✗ | |||
| Comprehension | ✗ | ✗ | ✗ | |
| Expressive language | ✗ | ✗ | ✗ | |
| Self-monitoring | ✗ | ✗ | ✗ | |
| Generalisation | ✗ | ✗ | ✗ | |
| Foundation skills | ✗ | ✗ | ✗ | ✗ |
| Functional communication | ✗ | |||
| Adult understanding and empowerment | ✗ | ✗ | ✗ | ✗ |
| Adult–child interaction | ✗ | ✗ | ✗ |
Ongoing challenges to evidence-based practice
The purpose of developing an evidence-based framework has been to improve speech and language therapy services for preschool children with PSLI. Rather than rolling out mass interventions, the purpose was to design a framework that can support the decision-making of SLTs so that they can put together interventions that are more tailored to the individual needs of a child and his or her family. Typically, the approach in the literature to supporting EBP has been to support practitioners to identify their research questions, to search the literature and to critically appraise the studies that they identify. 53 Practitioners identify the clinical area that they wish to improve and seek out evidence to inform the changes that can be made on the basis of research evidence. These early attempts to support practitioners were met with some resistance, with practitioners finding it difficult to find the time or to access and interpret the research. 309 In part, the process of systematic reviewing was a response to this, an attempt to assist practitioners in dealing with the large volume of research studies. Although EBP is now more widely acknowledged as evidence of the maturity of the profession and research evidence is viewed positively, there are still challenges to its universal implementation. A 2012 review, examining EBP in speech and language therapy, identified issues to do with the way that research evidence is both generated and used in practice. 309 One of the suggestions from the review is that SLTs do not necessarily find EBP problematic; rather, they find it irrelevant in that the research is not tied closely into practice.
Findings from this research suggest that this is indeed a difficulty, as it was not possible to neatly juxtapose research evidence to the therapy typology. For some of the themes, for example ‘speech’, the level of associated theory and research was considerable, with unresolved competing theoretical positions. In comparison to this plethora of theory, practitioners’ perspectives are relatively simple, a view suggested by Joffe and Pring,132 who found that SLTs would focus on only one aspect of a child’s presenting problem rather than a more in-depth analysis of the whole picture.
The language of intervention
There has been some attempt in the theoretical literature to provide models for describing interventions. However, these are not used routinely to describe interventions in either practice or research contexts. Indeed, descriptions provided in both contexts contain much tacit information that often defies attempts to surface it to a more explicit level. The result was that, in this research, it was not always possible to map important aspects of practice against research evidence – in either direction: descriptions of interventions from therapists were not uniform or consistent; therapists found it challenging to surface their underlying rationale; and reviews of intervention literature did not map easily onto the typology.
Theories of practice compared with research theories
In this research, participating therapists were encouraged to describe components of their interventions to uncover the detail of practice. As in previous studies, we found that the theoretical frameworks used in the literature are not commonly cited as discrete entities or approaches that practitioners follow slavishly. Rather, SLTs take an eclectic approach that brings together elements from different theories, different approaches or research studies. 89,131,132 Some see this as the pragmatism of practitioners who are simplifying complex material. 309 How far this works against the evidence supporting the effects of any particular approach and how far it is an example of EBP whereby the practitioner is skilfully and appropriately applying research to a particular context is not known. Therefore, it is not clear whether in fact therapists are doing a good job of individualising the interventions within the context of a heterogeneous caseload and producing stratified speech and language therapy or whether they are undermining the effects of a targeted approach.
Detailed analysis of the problem
A related issue that emerges from a number of the studies is the level of investigation that is carried out before a period of intervention. Although therapists may indeed be attempting to individualise their interventions, it seems as though they are attempting to do so on the basis of relatively superficial information. The use of formal or standardised assessments with preschool children as the sole source of data would be seen as problematic as formal assessments are less reliable the younger the child. This is a reflection of their likely inhibited responses in novel contexts. The behaviours of the children in our observational study reinforced this: children’s body postures became more relaxed and their vocalisations increased and became noisier as they became more familiar with people, objects and activities. The parents too expressed their concerns that sufficient time should be spent getting to know their child before judgements were made. Therefore, it is not unreasonable that therapists are using a balance of formal and informal assessments. However, with standardised assessments, therapists frequently used only a part of the assessment, or screening rather than diagnostic assessments were applied. Areas of work that were considered to be essential to an effective intervention, such as ‘adult understanding’ or ‘adult–child interaction’, were characterised by underspecified assessment processes. Some therapists also commented on the short times allocated for initial assessments. Although some therapists reported that they carried out observations of children in nursery settings or at home, this was not typical; thus, most assessments are taking place in contexts that are not particularly child friendly.
Conclusion
In conclusion, the practice of SLTs has been examined to form the basis of an evidence-based framework. The framework summarises the work of therapists under nine themes. Relevant assessments, interventions and outcome domains and evidence of the effects of interventions have been identified for each of the nine themes although the level of detail that we have been able to construct for each theme varies. Areas of tacit knowledge, underspecified processes and a patchy evidence base have contributed to this variability in the detail of the framework. The framework should be viewed mainly as descriptive and as a support for the decision-making process of therapists as they select and deliver interventions and measure the outcomes. It should also support discussions between SLTs, users of their services and those who commission the services. At this stage it is not meant to be prescriptive. However, with further research to establish the impact of using the framework on guiding and structuring services, it may evolve to act as a benchmark against which speech and language therapy services can be compared.
Chapter 9 Implications and research recommendations
This final chapter considers the implications for commissioners of speech and language therapy services, for speech and language therapy practice and for parents. It concludes with recommendations for future research. In considering the various implications it is important to bear in mind the strengths and limitations of the research programme. Each component study has highlighted issues that were specific to that study. However, some have particular relevance to the overall interpretation of the findings. Those are discussed in the following section before proceeding to a discussion of the implications and research recommendations.
Strengths and limitations of the research programme
The design of this research programme took a multiphase mixed-method approach, pragmatically reflecting the complexity of the research questions. Within the overall design, a series of studies iteratively explored components of speech and language therapy practice, following a model of EBP that includes clinical expertise, patient experience and systematic research evidence, to develop a framework that makes explicit each of those components. Although exploratory in nature, the a priori use of the evidence-based model to drive the questions, the selection of participants and the nature of the studies themselves is one of the unique features and strengths of the programme. The use of mixed methods followed an exploratory sequential process whereby quantitative methods were used to explore hypotheses and test levels of consensus that emerged from the qualitative data. The exploratory sequential process was not used within every set of studies, so, for example, the findings from the observational studies of children could have been tested within the same data set by examining frequency counts of certain behaviours in response to different therapy tasks. However, this approach had not been planned at the outset and would have been extremely time intensive. It is hoped to carry out such quantitative testing of the data in some follow-up analyses. Despite this, the iterative and cumulative process that has been followed in the programme as a whole means that the credibility and value of the overall framework have been tested and found to be sound.
A key challenge to the validity of any research programme lies in the success of the sampling process. As highlighted in previous chapters, the research programme is qualitative and exploratory. Therefore, the approach has always been to sample a range of participants rather than a representative sample. In each participant group, the aim has always been to identify participants from varying constituencies and with varying experiences who are therefore likely to bring varying perspectives, enabling the research to uncover a range of views. In terms of the SLTs, the participants whose data formed the foundation of the final framework, a wide range of professionals were recruited who were experienced in delivering interventions with preschool children with PSLI. The recruitment strategy was successful in reaching the planned numbers. However, data on the number of SLTs who work specifically with preschool children with PSLI and their range of qualifications and places of work are not available nationally and so it is not possible to know how well the sample that was achieved has covered the range of possible working practices. Nevertheless, the sample did include therapists from across England, working in services with very different demographics. We are therefore confident that the sample has included key perspectives from the profession. As the perspectives of the therapists provided the themes that formed the central concepts of the framework, we can be confident that the framework will be meaningful and have validity for the profession.
The story was somewhat different for other participant groups, in particular the parent participants and more specifically the parents of preschool children who are currently accessing or who have recently accessed speech and language therapy services. Despite major recruitment drives, the support and problem-solving of our parent panel and support from Afasic, the numbers recruited were disappointingly low. The reasons why this might have occurred are discussed in Chapter 4. In summary, we hypothesise that it may have something to do with the perceptions of these parents regarding the nature of their child’s developmental status and their identification with the notion of language impairment; this may relate to a relatively low-profile diagnostic process and diagnostic label that is largely misunderstood and to some extent stigmatised and associated with learning disability. These conclusions are, however, speculative and further investigation of how to engage these parents in research is needed. The recruitment of a broader sample including parents who have expressed concern (but who have not necessarily accessed therapy services) and also parents from groups who are commonly regarded as underserved by therapy services has increased not only the sample size but also the breadth of experience that we were able to examine. Thus, although the sample was still relatively small, there was a rich data set to examine, which has provided new insights into parent perspectives on therapy services.
One of the strengths of the programme is that it included a study of preschool children’s perspectives. This study has provided a rich data set presenting the perspectives of young children, whose voices are often absent from a consideration of interventions. The sample did not focus exclusively on children with diagnosed speech and language impairment, which could suggest that the findings from this study do not reflect how children with PSLI would behave in the same context. However, it did include those who were perceived by their EYPs to have speech and language delay. The participants also came from a range of preschool age groups and from a range of social backgrounds and thus provide insights into how a range of children at risk of PSLI behave when exposed to speech and language therapy activities. It was particularly challenging to set up this study for a number of reasons. It was felt that direct observation of large numbers of children undertaking therapy would be intrusive and that recruitment under such circumstances would be problematic. The behaviours of young children are particularly vulnerable to disruption when they are being observed by strangers; the use of cameras that capture the entirety of the interactions is also potentially intrusive for the adults involved. By using contexts with which the children were already familiar and working with the children over several weeks, we can be more confident that we are seeing the reactions of the children to the interventions activities rather than their more general responses to the context and people alone.
Each study is in itself relatively small. However, the iterative and cumulative nature of the research results in a strong final picture in which the inductive analyses have been validated by successive data collection rounds. Nonetheless, caution must be exercised in making claims about the generalisability of the findings and the primary conclusions should be regarded as descriptive of current practice and the current perspectives of the participants and of the links to the literature rather than predictive of the whole of practice in this field. With those caveats in mind, the implications of the research will now be considered.
Implications of the research programme
Implications for commissioners
Services for preschool children with PSLI are now largely commissioned by local clinical commissioning groups although there are some examples of joint commissioning with local authorities. There is little direct commissioning of targeted services for this group by early years settings.
The nine themes of the therapy typology provide an outline of the range of work that is encompassed by SLTs working with preschool children with PSLI. Commissioners could therefore expect services to describe explicitly how and what services/interventions are delivered for each theme. The framework also provides an outline of outcome domains associated with each theme. Thus, commissioners could use the framework to specify the kind of outcomes that they would expect to see reported for each of the themes. Furthermore, a discussion of these outcome domains with parent representatives on commissioning panels might enable commissioners to focus services. For example, by identifying which outcomes are particularly valued by parents, commissioners could then require speech and language therapy services to provide interventions that specifically address those outcomes.
Issues raised about the depth of assessment are likely to be of particular concern for commissioners. The suggestion that more time is needed for any aspect of a service in a time of austerity is not likely to be popular. However, it may be that services would be able to show increased efficiency if, with more detailed assessment, they were able to deliver more finely tuned interventions, prevent the use of inappropriate interventions and improve clinical outcomes and parent satisfaction.
The framework presented here along with others such as the What Works website developed as part of the BCRP (see Chapter 7) will support services to select interventions with the best available evidence. However, because of the heterogeneity of speech and language impairments and the diverse populations who access services, therapists will need to provide differing combinations and adaptations of interventions to meet the varying needs of individuals and their families. There should therefore be an expectation of differentiated care pathways to meet the needs of diverse groups. Data on service outcomes, informed by the findings from this study regarding relevant outcome domains, could help to monitor the impact of such differentiations. In addition, a focus on critical appraisal skills as part of continuing professional development for existing SLTs would enhance the profession’s ability to review and interpret research evidence in relation to practice. Critical appraisal is now part of SLT basic training but the process of integrating research evidence into practice remains a challenge.
Implications for practice
The framework presented here will have applications for individual SLTs, both those who are employed and commissioned directly through the NHS and those who are employed independently of the NHS, and for services. It will also be of relevance to the profession at a national level and for those who train SLTs.
The finding of this study is that, in both research and practice, descriptions of interventions lack consistency and detail. The detail of what interventions consist of and how they are delivered often forms part of the tacit knowledge of the profession and interventions are described in ways that lack transparency for non-professionals and for those in training. For parents in particular, the rationale for an intervention is not always clear. If the language used is unclear then there may be misunderstandings, a lack of consistency between therapists and inappropriate assumptions made. Finding a shared language and consistent ways of talking about interventions would increase the transparency of interventions, support partnership with others and facilitate the deconstruction of interventions into components that can be separated and evaluated. Making the descriptions of interventions more transparent alongside the levels of evidence would also help to inform parents in their choices. Developing consistency in the way that SLTs describe their interventions could also be addressed within the initial training process. The Child Talk framework could provide an outline starting place for this process.
The study has found variability in the way that children are assessed in terms of the assessment measures that are used. This makes it potentially confusing for parents who move between professionals and also makes it difficult for service outcomes to be compared. Indeed, the ongoing lack of data collection regarding outcomes is of particular concern, as services are in no position to show the impact of changes or cuts in funding. Furthermore, it renders the evaluation of cost-effectiveness impossible (see Chapter 6).
This study provides a set of outcome domains that have been reached by consensus between SLTs. This is a strong basis on which to build a core data set of assessments and outcomes that could be used to benchmark services and for national evaluations of outcomes. Clinical Evaluation Networks (formally known as SIGs) that specialise in therapy for preschool are in a prime position to undertake this kind of follow-up activity and, indeed, many members of these groups have been participants in this research process.
The observation study that was part of this research programme provided detailed accounts of children’s perspectives on therapy activities. Most therapists see engagement with the children as part of their role and expertise: it is the skill that allows them to identify interaction strategies that will lead to change in the child. However, the voices of preschool children are often absent in service planning or indeed in individual therapy planning; we tend to defer to their parents. Use of themes generated through the observation study could help to explore a child’s perspective on the process of intervention.
Implications for parents
This research programme explored the views of parents of preschool children who have received speech and language therapy and their views were generally positive. However, the research highlighted that some parents can feel that their role in therapy is passive and they are afraid to challenge or ask questions, rather than feeling that they have an active role in supporting their child’s speech and language development. This emphasises the need for more readily available information on speech and language therapy services in terms of how and when to access these services, how the services fit within the NHS, the demonstrable difference that these services can make and the important role of parents in the delivery of interventions, to facilitate the empowerment of parents. Routes for distributing this information should be widespread and should include parent groups, early years settings and child health services. Third-sector organisations also have a crucial role to play in supporting parents to access information. Increasing collaborations between speech and language therapy services and national and local organisations to support the development of accessible information would be helpful.
Implications for research
In the final stage of this research programme we undertook a small public consultation regarding possible future research directions. This took place at a local nursery and soft-play area and included 73 parents. It involved giving parents a list of five possible areas of research that were related to the findings of the research programme and asking them to prioritise these areas. The five areas were prioritised as follows:
-
investigation of the kinds of information that help parents to understand when and if their child needs help with their speech and language development
-
evaluations of the effectiveness of speech and language therapy interventions
-
an investigation of the support needed by other professionals, such as EYPs, to work effectively with children with PSLI
-
examination of the impact of new technology on children’s patterns of language development
-
examining differences in how services are organised, their effects and their cost-effectiveness.
The context in which the questions were posed to parents required that the examples were given in brief with simple suggestions rather than with lengthy and detailed discussions. Nevertheless, they provide insight into the interests of parents. Interestingly, although the consultation was set in a public place, the proportion of participants who had experience of speech and language therapy was high at 37%, and a further 18% (who did not have experience of speech and language therapy) had concerns about their child’s talking.
Research recommendations
The research recommendations arising from the Child Talk programme are presented in this section, reflecting the priorities of the parents:
-
An investigation of how best to recruit and engage parents of children with language impairment in the preschool years and the wider family in both research and service evaluation and development. The challenge of recruiting and engaging with parents and, through them, with their children is fundamental to all future research and service delivery in this area. This is particularly important for the creation of services that deliver outcomes of value to the families themselves. Parents in our survey indicated that a high priority for them is the need for information about speech and language impairments.
-
A programme of studies to evaluate the effectiveness of interventions in under-researched typology themes: adult–child interaction, developing parents’ understanding, children’s comprehension and the generalisation of skills into functional contexts. These studies should include how best to differentiate services, particularly to meet the needs of diverse groups. The systematic reviews have identified particular aspects of the work of SLTs in which the evidence base is poor. Evidence is also lacking about how the differentiation of existing interventions impacts on outcomes. Parents in our consultation exercise indicated that information about which interventions work is their second priority.
-
The development of assessment processes that can be used consistently and objectively and in partnership with parents, particularly to enable the identification of interventions appropriate for adult–child interaction, adult understanding and self-monitoring. This area of research may be combined with the previous recommendation regarding the investigation of effectiveness: if research targets the evaluation of interventions then valid and acceptable ways of assessing eligibility and measuring outcomes are also needed. This area of research was not one rated by our parent survey.
-
An evaluation of the effectiveness and cost-effectiveness of services that adopt the evidence-based framework compared with the effectiveness and cost-effectiveness of services that are not using the framework. In particular, the research should consider how the specification of outcome domains can drive the development and subsequent commissioning of services. Having developed a descriptive evidence-based framework, the next logical step is to evaluate the impact on services of using the framework. Comparative research should examine how services adopt and adapt their practices to take account of the framework and subsequently the impact on the children and families who access the services. The current national context of outcomes-based commissioning requires urgent consideration of how an emphasis on outcomes can drive service development.
Acknowledgements
This report presents independent research commissioned by the NIHR. The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NIHR Central Commissioning Facility (CCF), the Programme Grants for Applied Research programme or the Department of Health. The views and opinions expressed by the interviewees in this publication are those of the interviewees and do not necessarily reflect those of the authors, the NHS, the NIHR CCF, the Programme Grants for Applied Research programme or the Department of Health.
The research reported here was made possible through the participation and support of a number of individuals, groups and organisations. We are grateful for the support of all our participants and those who facilitated our engagement with the participants, without whom this research would not have happened:
-
to the young children from preschool settings around Bristol who participated in group activities and to their early years settings for facilitating those groups and to their parents for volunteering their consent
-
to parents who participated in interviews and focus groups and to the women who invited us into their groups to talk to them
-
to the SLTs and EYPs who shared their knowledge with us and to their managers for facilitating our contact with them and who also described their services.
We would also like to acknowledge the support from our parent panel, advisory group and expert advisors. The time that you gave to the research programme and your willingness to share your thoughts, expertise, knowledge and networks have been much appreciated and have contributed significantly to our thinking and progress with the research.
We are pleased to acknowledge here the contribution of a number of researchers who have worked with us on the projects and whose specialisms brought new insights and skills into the team: Lottie Jamieson who facilitated dramatherapy sessions with the children; Dr Iyabo Fatimilehin who supported the focus groups with women refugees and asylum seekers; Sue Caton who supported the systematic reviewing of a large bank of research literature; and Kevin Rowley who provided statistical support for the analysis of the national surveys.
We could not have completed the research without the efforts and enthusiasm of the larger research team at the BSLTRU and the team at Manchester Metropolitan University, including Elizabeth Lewis, Anna Blackwell, Karen Davies, Mary Kisanga, Ruth Cornish, Julie Ward, Julia McCleary and Fay Smith. This team supported the research endeavour in terms of data collection and data management processes, transcriptions and analysis, proofreading and reference checking, administrating and supporting our parent panel and advisory group, developing our web presence, supporting our IT needs and many other tasks that have ensured the smooth running of the research.
We would also like to thank Jenny Costley for her support in the financial management of the programme and Abigail Beverley for the design of the Child Talk logo. Finally, we are grateful for the support of the NIHR Programme Grants for Applied Research programme.
Contribution of authors
Sue E Roulstone (Professor of Speech and Language Therapy) (PI) was the overall lead on the design, methodology, data collection and data analysis for all work packages and led the writing, revision and approval of the final report. She was a member of the steering and advisory groups.
Julie E Marshall (Senior Research Fellow) (co-applicant) led the SLT survey and the underserved groups work packages and contributed to the writing, revision and approval of the final report. She was a member of the steering and advisory groups.
Gaye G Powell (Independent Consultant Speech and Language Therapist) (co-applicant) led the assessment and outcome work packages and contributed to the writing, revision and approval of the final report. She was a member of the steering and advisory groups.
Juliet Goldbart (Professor of Developmental Disabilities) (co-applicant) led the systematic review work package and contributed to the writing, revision and approval of the final report.
Yvonne E Wren (Research Fellow) (co-applicant) made substantial contributions to the design and methodology of the programme and contributed to the revision and approval of the final report. She was a member of the steering and advisory groups.
Jane Coad (Professor in Children and Family Nursing) (co-applicant) led the children’s work package and contributed to the writing, revision and approval of the final report.
Norma Daykin (Professor of Arts in Health) (co-applicant) made contributions to methodological design and interpretation of the data (from the observational children’s study, from the adapted Delphi study and from the study of underserved communities) and contributed to the revision and approval of the final report.
Jane E Powell (Professor of Public Health Economics) (co-applicant) co-led the economic evaluation work package and contributed to the writing, revision and approval of the final report.
Linda Lascelles (Chief Executive Officer, Afasic) (co-applicant) contributed to the formation of the parent panel and integration into the programme, advised on the capture and interpretation of parent perspectives and contributed to the revision and approval of the final report.
William Hollingworth (Professor of Health Economics) (co-applicant) co-led the economic evaluation work package and contributed to the revision and approval of the final report.
Alan Emond (Professor of Community Child Health) (co-applicant) contributed to the interpretation of data for all phases of the programme and to the revision and approval of the final report. He was the chair of the steering group.
Tim J Peters (Professor of Primary Care Health Services Research) (co-applicant) contributed to the overall design of the programme and interpretation of the SLT survey data and made substantial contributions to the revision and approval of the final report.
Jon I Pollock (Associate Professor of Epidemiology) (co-applicant) contributed to the overall design and methodology of the programme and made substantial contributions to the revision and approval of the final report.
Cres Fernandes (Head of Statistics at GL Assessment) (co-applicant) led on the determination of the validity and reliability of the assessment and outcome measures and contributed to the revision and approval of the final report.
Jenny Moultrie (Head of Profession, Children’s Speech and Language Therapy) (co-applicant) contributed to the design, methodology and interpretation of the data related to aspects of speech and language therapy services and practice and contributed to the revision and approval of the final report.
Sam A Harding (Senior Research Assistant) made a substantial contribution to data collection and analysis for the systematic review, underserved groups and children’s group work packages and contributed to the writing, revision and approval of the final report. She was a member of the steering and advisory groups.
Lydia Morgan (Research Assistant) made a substantial contribution to data collection and analysis for the SLT typology and intervention work packages and contributed to the writing, revision and approval of the final report.
Helen F Hambly (Research Assistant) made a substantial contribution to data collection and analysis for the children’s group work package and subsections of the systematic review and contributed to the writing, revision and approval of the final report.
Naomi K Parker (Research Assistant) made a substantial contribution to data collection and analysis for the EYP and parent perspective work packages and contributed to the writing, revision and approval of the final report.
Rebecca A Coad (Research Programme Manager) had oversight of the set-up and delivery of all work packages against programme milestones and made a substantial contribution to the writing, revision and approval of the final report. She was a member of the steering and advisory groups.
Publications
Roulstone S, Harding S. Defining communication disability in underserved communities in response to the World Report on Disability. Int J Speech Lang Pathol 2013;15:27–31.
Blackwell AKM, Harding SA, Babayigit S, Roulstone S. Characteristics of parent–child interactions: a systematic review of studies comparing children with primary language impairment and their typically developing peers [published online ahead of print 8 August 2014]. Communication Disord Q 2014. doi:10.1177/1525740114540202.
Roulstone S. Exploring the relationship between client perspectives, clinical expertise and research evidence. Int J Speech Lang Pathol 2015;17:211–21.
Data sharing statement
All available data can be obtained from the corresponding author.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, CCF, NETSCC, PGfAR or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the PGfAR programme or the Department of Health.
References
- YouTube . RALLIcampaign n.d. www.youtube.com/user/RALLIcampaign (accessed 20 March 2014).
- Bishop DV, Holt G, Line E, McDonald D, McDonald S, Watt H. Parental phonological memory contributes to prediction of outcome of late talkers from 20 months to 4 years: a longitudinal study of precursors of specific language impairment. J Neurodev Disord 2012;4. http://dx.doi.org/10.1186/1866-1955-4-3.
- Paul R, Roth FP. Characterizing and predicting outcomes of communication delays in infants and toddlers: implications for clinical practice. Lang Speech Hear Serv Sch 2011;42:331-40. http://dx.doi.org/10.1044/0161-1461(2010/09-0067).
- Thal DJ, Tobias S. Communicative gestures in children with delayed onset of oral expressive vocabulary. J Speech Hear Res 1992;35:1281-9. http://dx.doi.org/10.1044/jshr.3506.1289.
- Thal D, Tobias S, Morrison D. Language and gesture in late talkers: a 1-year follow-up. J Speech Hear Res 1991;34:604-12. http://dx.doi.org/10.1044/jshr.3403.604.
- Bates E, Dale PS, Thal DJ. Individual Differences and their Implications for Theories of Language Development. Handbook of Child Language. Oxford: Basil Blackwell; 1995.
- Reilly S, Bavin EL, Bretherton L, Conway L, Eadie P, Cini E, et al. The Early Language in Victoria Study (ELVS): a prospective, longitudinal study of communication skills and expressive vocabulary development at 8, 12 and 24 months. Int J Speech Lang Pathol 2009;11:344-57. http://dx.doi.org/10.1080/17549500903147560.
- Rescorla L. The Language Development Survey: a screening tool for delayed language in toddlers. J Speech Hear Disord 1989;54:587-99. http://dx.doi.org/10.1044/jshd.5404.587.
- Law J, Campbell C, Roulstone S, Adams C, Boyle J. Mapping practice onto theory: the speech and language practitioner’s construction of receptive language impairment. Int J Lang Commun Disord 2008;43:245-63. http://dx.doi.org/10.1080/13682820701489717.
- Aram DM, Ekelman BL, Nation JE. Preschoolers with language disorders: 10 years later. J Speech Hear Res 1984;27:232-44. http://dx.doi.org/10.1044/jshr.2702.244.
- Beitchman JH, Jiang H, Koyama E, Johnson CJ, Escobar M, Atkinson L, et al. Models and determinants of vocabulary growth from kindergarten to adulthood. J Child Psychol Psychiatry 2008;49:626-34. http://dx.doi.org/10.1111/j.1469-7610.2008.01878.x.
- Conti-Ramsden G, Mok PLH, Pickles A, Durkin K. Adolescents with a history of specific language impairment (SLI): strengths and difficulties in social, emotional and behavioral functioning. Res Dev Disabil 2013;34:4161-9. http://dx.doi.org/10.1016/j.ridd.2013.08.043.
- Mok PLH, Pickles A, Durkin K, Conti-Ramsden G. Longitudinal trajectories of peer relations in children with specific language impairment. J Child Psychol Psychiatry 2014;55:516-27. http://dx.doi.org/10.1111/jcpp.12190.
- Scarborough HS, Dobrich W. Development of children with early language delay. J Speech Hear Res 1990;33:70-83. http://dx.doi.org/10.1044/jshr.3301.70.
- Stothard SE, Snowling MJ, Bishop DVM, Chipchase BB, Kaplan CA. Language-impaired preschoolers: a follow-up into adolescence. J Speech Lang Hear Res 1998;41:407-18. http://dx.doi.org/10.1044/jslhr.4102.407.
- Whitehouse AJO, Robinson M, Zubrick SR. Late talking and the risk for psychosocial problems during childhood and adolescence. Pediatrics 2011;128:e324-32. http://dx.doi.org/10.1542/peds.2010-2782.
- Law J, Boyle J, Harris F, Harkness A, Nye C. Screening for primary speech and language delay: a systematic review of the literature. Int J Lang Commun Disord 2010;33:21-3. http://dx.doi.org/10.3109/13682829809179388.
- Tomblin JB, Records NL, Buckwalter P, Zhang X, Smith E, O’Brien M. Prevalence of specific language impairment in kindergarten children. J Speech Lang Hear Res 1997;40:1245-60. http://dx.doi.org/10.1044/jslhr.4006.1245.
- Baird G, Simonoff E, Pickles A, Chandler S, Loucas T, Meldrum D, et al. Prevalence of disorders of the autism spectrum in a population cohort of children in South Thames: the Special Needs and Autism Project (SNAP). Lancet 2006;368:210-15. http://dx.doi.org/10.1016/S0140-6736(06)69041-7.
- Williams E, Thomas K, Sidebotham H, Emond A. Prevalence and characteristics of autistic spectrum disorders in the ALSPAC cohort. Dev Med Child Neurol 2008;50:672-7. http://dx.doi.org/10.1111/j.1469-8749.2008.03042.x.
- Watson A, Sell D, Grunwell P. Management of Cleft Lip and Palate. London: Wiley-Blackwell; 2001.
- Watson A, Watson A, Sell D, Grunwell P. Management of Cleft Lip and Palate. Hoboken, NJ: Wiley-Blackwell; 2001.
- Health & Care Professions Council . Professions n.d. www.hpc-uk.org/aboutregistration/professions/index.asp?id = 13 (accessed 4 March 2014).
- Gascoigne M. Supporting Children with Speech, Language and Communication Needs within Integrated Children’s Services: Position Paper. London: Royal College of Speech and Language Therapists; 2006.
- Gadhok K. Looking ahead to 2014. Bulletin 2014.
- Glogowska M. Parents’ beliefs and ideas about children’s early speech and language difficulties. Int J Lang Commun Disord 1998;33:538-43. http://dx.doi.org/10.3109/13682829809179482.
- Glogowska M, Campbell R. Parents’ views of surveillance for early speech and language difficulties. Child Soc 2004;18:266-77.
- Bercow J. The Bercow Report. London: Department for Education; 2008.
- Law J, Garrett Z, Nye C. Speech and language therapy interventions for children with primary speech and language delay or disorder. Cochrane Database Syst Rev 2010;5.
- Zeng B, Law J, Lindsay G. Characterizing optimal intervention intensity: the relationship between dosage and effect size in interventions for children with developmental speech and language difficulties. Int J Speech Lang Pathol 2012;14:471-7. http://dx.doi.org/10.3109/17549507.2012.720281.
- Love JM, Kisker EE, Ross C, Constantine J, Boller K, Chazan-Cohen R, et al. The effectiveness of Early Head Start for 3-year-old children and their parents: lessons for policy and programs. Dev Psychol 2005;41:885-901. http://dx.doi.org/10.1037/0012-1649.41.6.885.
- Van Kleeck A, Vander Woude J, Hammett L. Fostering literal and inferential language skills in Head Start preschoolers with language impairment using scripted book-sharing discussions. Am J Speech Lang Pathol 2006;15:85-9. http://dx.doi.org/10.1044/1058-0360(2006/009).
- Wasik BA, Bond MA, Hindman A. The effects of a language and literacy intervention on Head Start children and teachers. J Educ Psychol 2006;98:63-74. http://dx.doi.org/10.1037/0022-0663.98.1.63.
- Whitehurst G, Epstein J, Angell A, Payne A, Crone DA, Fischel J. Outcomes of an emergent literacy intervention in Head Start. J Educ Psychol 1994;86:542-55. http://dx.doi.org/10.1037/0022-0663.86.4.542.
- Pickstone C, Goldbart J, Marshall M, Rees A, Roulstone S. A systematic review of environmental interventions to improve child language outcomes for children with or at risk of primary language impairment. J Res Spec Educ Needs 2009;9:66-79. http://dx.doi.org/10.1111/j.1471-3802.2009.01119.x.
- Landry SH, Smith KE, Swank PR. Responsive parenting: establishing early foundations for social, communication, and independent problem-solving skills. Dev Psychol 2006;42:627-42. http://dx.doi.org/10.1037/0012-1649.42.4.627.
- Law J, Lee W, Roulstone S, Wren Y, Lindsay G. What Works: Interventions for Children and Young People with Speech, Language and Communication Needs. London: Department for Education; 2012.
- Conti-Ramsden G, St Clair MC, Pickles A, Durkin K. Developmental trajectories of verbal and nonverbal skills in individuals with a history of specific language impairment: from childhood to adolescence. J Speech Lang Hear Res 2012;55:1716-35. http://dx.doi.org/10.1044/1092-4388(2012/10-0182).
- Rescorla L. Age 17 language and reading outcomes in late-talking toddlers: support for a dimensional perspective on language delay. J Speech Lang Hear Res 2009;52:16-30. http://dx.doi.org/10.1044/1092-4388(2008/07-0171).
- St Clair MC, Pickles A, Durkin K, Conti-Ramsden G. A longitudinal study of behavioral, emotional and social difficulties in individuals with a history of specific language impairment (SLI). J Commun Disord 2011;44:186-99. http://dx.doi.org/10.1016/j.jcomdis.2010.09.004.
- Sullivan PM, Knutson JF. Maltreatment and disabilities: a population-based epidemiological study. Child Abuse Negl 2000;24:1257-73. http://dx.doi.org/10.1016/S0145-2134(00)00190-3.
- Snow PC, Powell MB. Oral language competence in incarcerated young offenders: links with offending severity. Int J Speech Lang Pathol 2011;13:480-9. http://dx.doi.org/10.3109/17549507.2011.578661.
- Allen G. Early Intervention: The Next Steps. London: Department for Work and Pensions; 2011.
- Field F. The Foundation Years: Preventing Poor Children Becoming Poor Adults. London: Cabinet Office; 2010.
- Tickell C. The Early Years: Foundations for Life, Health and Learning. London: Department for Education; 2011.
- Better Communication: An Action Plan to Improve Services for Children and Young People with Speech, Language and Communication Needs. London: Department for Children, Schools and Families; 2008.
- Healthy Lives, Brighter Futures – the Strategy for Children and Young People’s Health. London: Department of Health; 2009.
- Nutbrown C. Nutbrown Review Reports. London: Department for Education; 2012.
- The Links Between Speech, Language and Communication Needs and Social Disadvantage. London: Houses of Parliament; 2013.
- Sackett DL, Rosenberg WM, Gray JA, Haynes RB, Richardson WS. Evidence based medicine: what it is and what it isn’t. BMJ 1996;312:71-2. http://dx.doi.org/10.1136/bmj.312.7023.71.
- Foster AM, Worrall LE, Rose ML, O’Halloran R. Turning the tide: putting acute aphasia management back on the agenda through evidence-based practice. Aphasiology 2013;27:420-43. http://dx.doi.org/10.1080/02687038.2013.770818.
- Grol R, Wensing M. What drives change? Barriers to and incentives for achieving evidence-based practice. Med J Aust 2004;180:S57-60.
- Greenhalgh T. How to Read a Paper: The Basics of Evidence-Based Medicine. Hoboken, NJ: Wiley-Blackwell; 2010.
- Rycroft-Malone J, Seers K, Titchen A, Harvey G, Kitson A, McCormack B. What counts as evidence in evidence-based practice?. J Adv Nurs 2004;47:81-90. http://dx.doi.org/10.1111/j.1365-2648.2004.03068.x.
- Higgs J, Titchen A. Practice Knowledge and Expertise in the Health Professions. Oxford: Butterworth-Heinemann; 2001.
- Roulstone S. Evidence, expertise, and patient preference in speech-language pathology. Int J Speech Lang Pathol 2011;13:43-8. http://dx.doi.org/10.3109/17549507.2010.491130.
- Boschuizen HPA, Schmidt HG, Higgs J, Jones MA. Clinical Reasoning in the Health Professions. Oxford: Butterworth Heinemann; 2000.
- Argyris C, Schon D. Theory in Practice: Increasing Professional Effectiveness. San Francisco, CA: Jossey-Bass; 1974.
- The Patients Charter. London: Department of Health; 1997.
- Creswell JW, Clark VLP. Designing and Conducting Mixed Methods Research. London: Sage Publications; 2011.
- Strauss AL, Corbin JM. Basics of Qualitative Research: Grounded Theory Procedures and Techniques. Thousand Oaks, CA: Sage Publications; 1990.
- Silverman D. Interpreting Qualitative Data: Methods for Analyzing Talk, Text and Interaction. London: Sage Publications; 2006.
- Roulstone S. Consensus and variation between speech and language therapists in the assessment and selection of preschool children for intervention: a body of knowledge or idiosyncratic decisions?. Int J Lang Commun Disord 2001;36:329-48. http://dx.doi.org/10.1080/13682820010019928.
- Dalkey N, Helmer O. An experimental application of the Delphi method to the use of experts. Manag Sci 1963;9:458-67. http://dx.doi.org/10.1287/mnsc.9.3.458.
- Hsu C, Sandford BA. The Delphi technique: making sense of consensus practical assessment. Res Eval 2007;12:1-8.
- Keeney S, McKenna H, Hasson F. The Delphi Technique in Nursing and Health Research. New York: John Wiley; 2010.
- Rayens MK, Hahn EJ. Building consensus using the policy Delphi method. Policy Polit Nurs Pract 2000;1:308-15. http://dx.doi.org/10.1177/152715440000100409.
- Pennington L, Goldbart J, Marshall J. Speech and language therapy to improve the communication skills of children with cerebral palsy. Cochrane Database Syst Rev 2004;2.
- Dollaghan C. Evidence-Based Practice: Myths and Realities. The ASHA Leader 2004. www.asha.org/publications/leader/2004/040413/f040413a1.htm#2 (accessed 28 October 2013).
- Barratt J, Littlejohns P, Thompson J. Trial of intensive compared with weekly speech therapy in preschool children. Arch Child 1992;67:106-8. http://dx.doi.org/10.1136/adc.67.1.106.
- Winter K. Speech and language therapy provision for bilingual children: aspects of the current service. Int J Lang Commun Disord 1999;34:85-98. http://dx.doi.org/10.1080/136828299247658.
- Wilson L, Lincoln M, Onslow M. Availability, access, and quality of care: inequities in rural speech pathology services for children and a model for redress. Int J Speech Lang Pathol 2002;4:9-22. http://dx.doi.org/10.1080/14417040210001669191.
- O’Callaghan AM, McAllister L, Wilson L. Barriers to accessing rural paediatric speech pathology services: health care consumers’ perspectives. Aust J Rural Health 2005;13:162-71. http://dx.doi.org/10.1111/j.1440-1854.2005.00686.x.
- Sheppard L. Work practices of rural and remote physiotherapists. Aust J Rural Health 2001;9:84-90. http://dx.doi.org/10.1046/j.1440-1584.2001.00340.x.
- Locke A, Ginsborg J, Peers I. Development and disadvantage: implications for the early years and beyond. Int J Lang Commun Disord 2002;37:3-15. http://dx.doi.org/10.1080/13682820110089911.
- Lundberg I, Larsman P, Strid A. Development of phonological awareness during the preschool year: the influence of gender and socio-economic status. Read Writ 2010;25:305-20. http://dx.doi.org/10.1007/s11145-010-9269-4.
- Dollaghan CA, Campbell TF, Paradise JL, Feldman HM, Janosky JE, Pitcairn DN, et al. Maternal education and measures of early speech and language. J Speech Lang Hear Res 1999;42:1432-43. http://dx.doi.org/10.1044/jslhr.4206.1432.
- Paradice R, Adewusi A. ‘It’s a continuous fight isn’t it?’: parents’ views of the educational provision for children with speech and language difficulties. Child Lang Teach Ther 2002;18:257-88. http://dx.doi.org/10.1191/0265659002ct238oA.
- Engaging Effectively with Black and Minority Ethnic Parents in Children’s and Parental Services. London: Department for Children, Schools and Families; 2007.
- Mennen I, Stansfield J, Johnston S. Speech and Language Therapy Services for Bilingual Children in England and Scotland: A Tale of Three Cities n.d.:1578-96.
- Cleemput PV, Parry G. Health status of gypsy travellers. J Public Health 2001;23:129-34. http://dx.doi.org/10.1093/pubmed/23.2.129.
- Enderby P, Petheram B. An analysis of referrals to speech and language therapy in 11 centres, 1987–95. Int J Lang Commun Disord 2000;35:137-46. http://dx.doi.org/10.1080/136828200247304.
- Shevell M, Ashwal S, Donley D, Flint J, Gingold M, Hirtz D, et al. Practice parameter: evaluation of the child with global developmental delay: report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society. Neurology 2003;60:367-80. http://dx.doi.org/10.1212/01.WNL.0000031431.81555.16.
- Gillon GT. Phonological Awareness: From Research to Practice. New York: Guilford Press; 2004.
- Dockrell JE, Lindsay G, Letchford B, Mackie C. Educational provision for children with specific speech and language difficulties: perspectives of speech and language therapy service managers. Int J Lang Commun Disord 2006;41:423-40. http://dx.doi.org/10.1080/13682820500442073.
- McCartney E. Scoping and hoping: the provision of speech and language therapy services for children with special educational needs. Br J Spec Educ 1999;26:196-200. http://dx.doi.org/10.1111/1467-8527.00138.
- McCartney E. Include us out? Speech and language therapists’ prioritization in mainstream schools. Child Lang Teach Ther 2000;16:165-80. http://dx.doi.org/10.1191/026565900677051146.
- Williams G, Laungani P. Analysis of teamwork in an NHS community trust: an empirical study. J Interprof Care 1999;13:19-28. http://dx.doi.org/10.3109/13561829909025532.
- Roulstone S, Wren Y, Bakopoulou I, Goodlad S, Lindsay G. Exploring Interventions for Children and Young People with Speech, Language and Communication Needs: a Study of Practice. London: Department for Education; 2012.
- Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol 2006;3:77-101. http://dx.doi.org/10.1191/1478088706qp063oa.
- South West Regional Assembly . Gypsy and Traveller Additional Pitch Requirements Consultation – Frequently Asked Questions 2014. www.southwest-ra.gov.uk/nqcontent.cfm?a_id = 3182&tt = swra (accessed 21 February 2014).
- Ritchie J, Spencer L, O’Connor W, Ritchie J, Lewis J. Qualitative Research Practice: A Guide for Social Science Students and Researchers. London: Sage Publications; 2003.
- Hsieh-Fang H, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res 2005;15:1277-88. http://dx.doi.org/10.1177/1049732305276687.
- Potter WJ, Levine-Donnerstein D. Rethinking validity and reliability in content analysis. J Appl Commun Res 1999;27:258-84. http://dx.doi.org/10.1080/00909889909365539.
- Freeman M. SLT talk and practice knowledge: a response to Ferguson and Armstrong. Int J Lang Commun Disord 2004;39:481-6.
- Hambly H, Roulstone S. How Do Therapists Prioritise Pre-School Children for Speech and Language Therapy? A Survey of Therapists’ Treatment Decisions n.d.
- Friberg JC. Considerations for test selection: how do validity and reliability impact diagnostic decisions?. Child Lang Teach Ther 2010;26:77-92. http://dx.doi.org/10.1177/0265659009349972.
- Booth A, Fry-Smith A. Developing a Research Question. Systematic Reviews in the Social Sciences. Oxford: Blackwell; 2004.
- Public Health Resources Unit England . Critical Appraisal Skills Programme (CASP) – Making Sense of Evidence: 10 Questions to Help You Make Sense of Qualitative Research 2006. www.phru.nhs.uk/Doc_Links/Qualitative%20Appraisal%20Tool.pdf (accessed 19 January 2015).
- Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health 1998;52:377-84. http://dx.doi.org/10.1136/jech.52.6.377.
- Murray E, Power E, Togher L, McCabe P, Munro N, Smith K. The reliability of methodological ratings for speechBITE using the PEDro-P scale. Int J Lang Commun Disord 2013;48:297-306. http://dx.doi.org/10.1111/1460-6984.12007.
- Perdices M, Tate RL. Single-subject designs as a tool for evidence-based clinical practice: are they unrecognised and undervalued?. Neuropsychol Rehabil 2009;19:904-27. http://dx.doi.org/10.1080/09602010903040691.
- Tate RL, McDonald S, Perdices M, Togher L, Schultz R, Savage S. Rating the methodological quality of single-subject designs and n-of-1 trials: introducing the single-case experimental design (SCED) scale. Neuropsychol Rehabil 2008;18:385-401. http://dx.doi.org/10.1080/09602010802009201.
- Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther 2003;83:713-21.
- Camarinos J, Marinko L. Effectiveness of manual physical therapy for painful shoulder conditions: a systematic review. J Man Manip Ther 2009;17:206-15. http://dx.doi.org/10.1179/106698109791352076.
- Mann T. Clinical Guidelines Using Clinical Guidelines to Improve Patient Care within the NHS. London: Crown Copyright; 1996.
- National Institute for Health and Care Excellence . The Guideline Development Group (GDG) n.d. http://publications.nice.org.uk/how-nice-clinical-guidelines-are-developed-an-overview-for-stakeholders-the-public-and-the-nhs-pmg6f/the-guideline-development-group-gdg (accessed 12 January 2015).
- Eccles M, Mason J. How to develop cost-conscious guidelines. Health Technol Assess 2001;5. http://dx.doi.org/10.3310/hta5160.
- Ritchie J, Spencer L, Bryman A, Burgess B. Analyzing Qualitative Data. London: Routledge; 1994.
- Yoder DE, Kent RD. Decision Making in Speech–Language Pathology. Philadelphia, PA: BC Decker; 1988.
- McCauley RJ, Fey ME, McCauley RJ, Fey ME. Treatment of Language Disorders in Children. Baltimore, MD: Brookes; 2006.
- Roulstone S. The Child, the Process and the Expertise: Identification of Priority Children from Preschool Referrals to Speech and Language Therapy 1995.
- Spock B. Baby and Child Care. New York: Pocket Books; 1957.
- Roulstone S. What’s driving you? A template which underpins the assessment of preschool children by speech and language therapists. Eur J Disord Commun 1997;32:299-316. http://dx.doi.org/10.3109/13682829709017897.
- Marshall J, Lewis E. ‘It’s the way you talk to them.’ The child’s environment: early years practitioners’ perceptions of its influence on speech and language development, its assessment and environment targeted interventions [published online ahead of print 29 December 2013]. Child Lang Teach Ther 2013. http://clt.sagepub.com/content/early/2013/12/26/0265659013516331 (accessed 19 February 2014).
- Connery V. The Nuffield Dyspraxia Programme. London: Miracle Factory; 1992.
- Knowles W, Masidlover M. Derbyshire Language Scheme. Nottingham: Ripley Education Office; 1982.
- Walker M, Armfield A. What is the Makaton vocabulary?. Spec Educ Forward Trends 1981;8:19-20.
- Dodd B, Holm A, Crosbie S, McIntosh B. A core vocabulary approach for management of inconsistent speech disorder. Int J Speech Lang Pathol 2006;8:220-30. http://dx.doi.org/10.1080/14417040600738177.
- Pepper J, Weitzman E. It Takes Two to Talk: a Practical Guide for Parents of Children with Language Delays. Toronto, ON: Hanen Centre; 2004.
- Passy J. Cued Articulation. Howthorn, VIC: ACER; 1990.
- Dean E, Howell J, Waters D, Reid J. Metaphon: a metalinguistic approach to the treatment of phonological disorder in children. Clin Linguist Phon 1995;9:1-19. http://dx.doi.org/10.3109/02699209508985318.
- Stephens D, Upton D. Speech and language therapists’ understanding and adoption of evidence-based practice. Int J Ther Rehabil 2012;19:328-34. http://dx.doi.org/10.12968/ijtr.2012.19.6.328.
- Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ 2008;337. http://dx.doi.org/10.1136/bmj.a1655.
- Abraham C, Michie S. A taxonomy of behaviour change techniques used in interventions. Health Psychol 2008;27:379-87. http://dx.doi.org/10.1037/0278-6133.27.3.379.
- McCleary N, Duncan EM, Stewart F, Francis JJ. Active ingredients are reported more often for pharmacologic than non-pharmacologic interventions: an illustrative review of reporting practices in titles and abstracts. Trials 2013;14. http://dx.doi.org/10.1186/1745-6215-14-146.
- McCauley RJ, Fey ME. Treatment of Language Disorders in Children. Baltimore, MD: Paul H Brookes; 2006.
- Baker E. Management of speech impairment in children: the journey so far and the road ahead. Int J Speech Lang Pathol 2006;8:156-63. http://dx.doi.org/10.1080/14417040600701951.
- Schön DA, Dowie J, Elstein A. Professional Judgement A Reader in Clinical Decision Making. Cambridge University Press; 1988.
- Schön DA. The Reflective Practitioner: How Professionals Think in Action. New York, NY: Basic Books; 1983.
- Roulstone S, Wren Y. Investigation of theoretical models and therapy activities: phonological difficulties. Int J Lang Commun Disord 2001;36:441-6. http://dx.doi.org/10.3109/13682820109177926.
- Joffe V, Pring T. Children with phonological problems: a survey of clinical practice. Int J Lang Commun Disord 2008;43:154-64. http://dx.doi.org/10.1080/13682820701660259.
- Pappas NW, McLeod S. Working with Families in Speech–Language Pathology. Plymouth: Plural Publishing; 2008.
- Tardaguila-Harth JM. Assessing the Effects of Dialogic Reading on the Oral Language Skills of Migrant Preschoolers at Risk for Reading Difficulties. Gainesville, FL: University of Florida; 2007.
- Justice LM, Mashburn A, Pence KL, Wiggins A. Experimental evaluation of a preschool language curriculum: influence on children’s expressive language skills. J Speech Lang Hear Res 2008;51:983-1001. http://dx.doi.org/10.1044/1092-4388(2008/072).
- Lunkenheimer ES, Dishion TJ, Shaw DS, Connell AM, Gardner F, Wilson MN, et al. Collateral benefits of the family check-up on early childhood school readiness: indirect effects of parents’ positive behavior support. Dev Psychol 2008;44:1737-52. http://dx.doi.org/10.1037/a0013858.
- Roberts JE, Rabinowitch S, Bryant DM, Burchinal MR, Koch MA, Ramey CT. Language skills of children with different preschool experiences. J Speech Hear Res 1989;32:773-86. http://dx.doi.org/10.1044/jshr.3204.773.
- Stanton-Chapman TL, Kaiser AP, Vijay P, Chapman C. A multicomponent intervention to increase peer-directed communication in Head Start children. J Early Interv 2008;30:188-212. http://dx.doi.org/10.1177/1053815108318746.
- McGregor KK. Use of phonological information in a word-finding treatment for children. J Speech Hear Res 1994;37:1381-93. http://dx.doi.org/10.1044/jshr.3706.1381.
- Shea RL, Tyler AA. The effectiveness of a prosodic intervention on children’s metrical patterns. Child Lang Teach Ther 2001;17:55-76. http://dx.doi.org/10.1191/026565901668193508.
- Lafferty AE, Gray S, Wilcox MJ. Teaching alphabetic knowledge to pre-school children with developmental language delay and with typical language development. Child Lang Teach Ther 2005;21:263-77. http://dx.doi.org/10.1191/0265659005ct292oa.
- Roth FP, Troia GA, Worthington CK, Dow KA. Promoting awareness of sounds in speech: an initial report of an early intervention program for children with speech and language impairments. Appl Psycholinguist 2002;23:535-65. http://dx.doi.org/10.1017/S0142716402004034.
- Skibbe LE, Justice LM, Bowles RP. Implementation processes associated with a home-based phonological awareness intervention for children with specific language impairment. Int J Speech Lang Pathol 2011;13:110-24. http://dx.doi.org/10.3109/17549507.2011.524246.
- Forrest K, Elbert M, Dinnsen D. The effect of substitution patterns on phonological treatment outcomes. Clin Linguist Phon 2000;14:519-31. http://dx.doi.org/10.1080/026992000750020341.
- Forrest K, Elbert M. Treatment for phonologically disordered children with variable substitution patterns. Clin Linguist Phon 2001;15:41-5. http://dx.doi.org/10.3109/02699200109167628.
- Gierut JA. Maximal opposition approach to phonological treatment. J Speech Hear Disord 1989;54:9-19. http://dx.doi.org/10.1044/jshd.5401.09.
- Gierut JA. Differential learning of phonological oppositions. J Speech Hear Res 1990;33:540-9. http://dx.doi.org/10.1044/jshr.3303.540.
- Gierut JA. An experimental test of phonemic cyclicity. J Child Lang 1996;23:81-102. http://dx.doi.org/10.1017/S0305000900010102.
- Gierut JA, Morrisette ML, Hughes MT, Rowland S. Phonological treatment efficacy and developmental norms. Lang Speech Hear Serv Sch 1996;27:215-30. http://dx.doi.org/10.1044/0161-1461.2703.215.
- Gierut JA, Champion AH. Interacting error patterns and their resistance to treatment. Clin Linguist Phon 1999;13:421-31. http://dx.doi.org/10.1080/026992099298960.
- Gierut JA, Champion AH. Ingressive substitutions: typical or atypical phonological pattern?. Clin Linguist Phon 2000;14:603-17. http://dx.doi.org/10.1080/026992000750048134.
- Gierut JA, Champion AH. Syllable onsets II: three-element clusters in phonological treatment. J Speech Lang Hear Res 2001;44:886-904. http://dx.doi.org/10.1044/1092-4388(2001/071).
- Gierut JA, Morrisette ML. Triggering a principle of phonemic acquisition. Clin Linguist Phon 1996;10:15-30. http://dx.doi.org/10.3109/02699209608985159.
- Hart S, Gonzalez L. The effectiveness of using communication-centered intervention to facilitate phonological learning in young children. Commun Disord Q 2010;32:13-25. http://dx.doi.org/10.1177/1525740109333966.
- Robb MP, Bleile KM, Yee SSL. A phonetic analysis of vowel errors during the course of treatment. Clin Linguist Phon 1999;13:309-21. http://dx.doi.org/10.1080/026992099299103.
- Wolfe V, Presley C, Mesaris J. The importance of sound identification training in phonological intervention. Am J Speech Lang Pathol 2003;12:282-8. http://dx.doi.org/10.1044/1058-0360(2003/074).
- Yoder P, Camarata S, Gardner E. Treatment effects on speech intelligibility and length of utterance in children with specific language and intelligibility impairments. J Early Interv 2005;28:34-49. http://dx.doi.org/10.1177/105381510502800105.
- Saben CB, Ingham JC. The effects of minimal pairs treatment on the speech-sound production of two children with phonologic disorders. J Speech Hear Res 1991;34:1023-40. http://dx.doi.org/10.1044/jshr.3405.1023.
- Winner M, Elbert M. Evaluating the treatment effect of repeated probes. J Speech Hear Disord 1988;53:211-18. http://dx.doi.org/10.1044/jshd.5302.211.
- Hund-Reid C. Effectiveness of phonological awareness intervention for kindergarten children with moderate to severe language impairment. Can J Speech Lang Pathol Audiol 2009;37:6-25.
- Rvachew S. Speech perception training can facilitate sound production learning. J Speech Hear Res 1994;37:347-57. http://dx.doi.org/10.1044/jshr.3702.347.
- Almost D, Rosenbaum P. Effectiveness of speech intervention for phonological disorders: a randomized controlled trial. Dev Med Child Neurol 1998;40:319-25.
- Rvachew S, Nowak M, Cloutier G. Effect of phonemic perception training on the speech production and phonological awareness skills of children with expressive phonological delay. Am J Speech Lang Pathol 2004;13:250-63. http://dx.doi.org/10.1044/1058-0360(2004/026).
- Rvachew S, Nowak M. The effect of target-selection strategy on phonological learning. J Speech Lang Hear Res 2001;44:610-23. http://dx.doi.org/10.1044/1092-4388(2001/050).
- McIntosh B, Dodd B. Evaluation of Core Vocabulary intervention for treatment of inconsistent phonological disorder: three treatment case studies. Child Lang Teach Ther 2008;24:307-27. http://dx.doi.org/10.1177/0265659007096295.
- Dodd B, Iacano T. Phonological disorders in children: changes in phonological process use during treatment. Br J Disord Commun 1989;24:333-52. http://dx.doi.org/10.3109/13682828909019894.
- Baker E, McLeod S. Evidence-based management of phonological impairment in children. Child Lang Teach Ther 2004;20:261-85. http://dx.doi.org/10.1191/0265659004ct275oa.
- Hesketh A, Dima E, Nelson V. Teaching phoneme awareness to pre-literate children with speech disorder: a randomized controlled trial. Int J Lang Commun Disord 2007;42:251-71. http://dx.doi.org/10.1080/13682820600940141.
- Glogowska M, Roulstone S, Enderby P, Peters TJ. Randomised controlled trial of community based speech and language therapy in preschool children. BMJ 2000;321. http://dx.doi.org/10.1136/bmj.321.7266.923.
- Craig-Unkefer LA, Kaiser AP. Increasing peer-directed social-communication skills of children enrolled in Head Start. J Early Interv 2003;25:229-47. http://dx.doi.org/10.1177/105381510302500401.
- Ziolkowski RA, Goldstein H. Effects of an embedded phonological awareness intervention during repeated book reading on preschool children with language delays. J Early Interv 2008;31:67-90. http://dx.doi.org/10.1177/1053815108324808.
- Bunce BH, Ruder KF, Ruder CC. Using the miniature linguistic system in teaching syntax: two case studies. J Speech Hear Disord 1985;50:247-53. http://dx.doi.org/10.1044/jshd.5003.247.
- Connell PJ. Acquisition of semantic role by language-disordered children: differences between production and comprehension. J Speech Hear Res 1986;29:366-74. http://dx.doi.org/10.1044/jshr.2903.366.
- Gallagher AL, Chiat S. Evaluation of speech and language therapy interventions for pre-school children with specific language impairment: a comparison of outcomes following specialist intensive, nursery-based and no intervention. Int J Lang Comm Dis 2009;44:616-38. http://dx.doi.org/10.1080/13682820802276658.
- Gibbard D. Parental-based intervention with pre-school language-delayed children. Eur J Disord Commun 1994;29:131-50. http://dx.doi.org/10.3109/13682829409041488.
- Baxendale J, Hesketh A. Comparison of the effectiveness of the Hanen Parent Programme and traditional clinic therapy. Int J Lang Commun Disord 2003;38:397-415. http://dx.doi.org/10.1080/1368282031000121651.
- Buschmann A, Jooss B, Rupp A, Feldhusen F, Pietz J, Philippi H. Parent based language intervention for 2-year-old children with specific expressive language delay: a randomised controlled trial. Arch Dis Child 2009;94:110-16. http://dx.doi.org/10.1136/adc.2008.141572.
- Kim Y-T, Yang Y-S, Hwang B. Generalization effects of script-based intervention on language expression of preschool children with language disorders. Educ Train Ment Retard Dev Disabil 2001;36:411-23.
- Warren SF, McQuarter RJ, Rogers-Warren AK. The effects of mands and models on the speech of unresponsive language-delayed preschool children. J Speech Hear Disord 1984;49:43-52. http://dx.doi.org/10.1044/jshd.4901.43.
- Washington KN. Exploring the Impact of Two Direct Treatment Programs for the Remediation of Expressive Grammar Deficits in Preschool and Kindergarten Children with Specific Language Impairment. London, ON: University of Western Ontario; 2007.
- Weismer SE, Murray-Branch J, Miller JF. Comparison of two methods for promoting productive vocabulary in late talkers. J Speech Hear Res 1993;36:1037-50. http://dx.doi.org/10.1044/jshr.3605.1037.
- Girolametto L, Pearce PS, Weitzman E. Interactive focused stimulation for toddlers with expressive vocabulary delays. J Speech Hear Res 1996;39:1274-83. http://dx.doi.org/10.1044/jshr.3906.1274.
- Olswang LB, Coggins TE. The effects of adult behaviours on increasing language delayed children’s production of early relational meanings. Int J Lang Commun Disord 1984;19:15-34. http://dx.doi.org/10.3109/13682828409019833.
- Spencer TD, Slocum TA. The effect of a narrative intervention on story retelling and personal story generation skills of preschoolers with risk factors and narrative language delays. J Early Interv 2010;32:178-99. http://dx.doi.org/10.1177/1053815110379124.
- Craig-Unkefer LA, Kaiser AP. Improving the social communication skills of at-risk preschool children in a play context. Top Early Child Spec Educ 2002;22:3-13. http://dx.doi.org/10.1177/027112140202200101.
- Yoder PJ, Molfese D, Gardner E. Initial mean length of utterance predicts the relative efficacy of two grammatical treatments in preschoolers with specific language impairment. J Speech Lang Hear Res 2011;54:1170-81. http://dx.doi.org/10.1044/1092-4388(2010/09-0246).
- Hegde MN, Gierut J. The operant training and generalization of pronouns and a verb form in a language delayed child. J Commun Disord 1979;12:23-34. http://dx.doi.org/10.1016/0021-9924(79)90018-2.
- Barker Fudala J. Arizona Articulation Proficiency Scale. Torrance, CA: WPS Publishing; 2014.
- Dodd B, Zhu H, Crosbie S, Holm A, Ozanne A. Diagnostic Evaluation of Articulation and Phonology (DEAP). London: Psychology Corporation; 2002.
- Goldman R, Fristoe M. Goldman–Fristoe Test of Articulation. Circle Pines, MN: American Guidance Service; 1986.
- Hodson BW. Hodson Assessment of Phonological Patterns. Austin, TX: Pro-Ed; 2004.
- Weiner FF. Phonological process analysis. Int J Rehabil Res 1979;2. http://dx.doi.org/10.1097/00004356-197912000-00034.
- Robertson C, Salter W. The Phonological Awareness Profile. Austin, TX: Linguisystems Inc.; 1995.
- Bankson N, Bernthal J. Bankson–Bernthal Test of Phonology (BBTOP). Dallas, TX: ASHA; n.d.
- Zimmerman I, Pond R, Boucher J, Steiner V. Preschool Language Scale-3 UK Edition (PLS-3 UK) 1997. www.pearsonclinical.co.uk/AlliedHealth/Generic/PreschoolLanguageScale-3UKEdition%28PLS-3UK%29/PreschoolLanguageScale-3UKEdition%28PLS-3UK%29.aspx (accessed 8 January 2014).
- Ozanne A, Dodd B, McIntosh B, Crosbie S, Teitzel T. Preschool and Primary Inventory of Phonological Awareness (PIPA). London: Pearson Clinical; 2000.
- Lonigan CJ, Phillips BM. Research-Based Instructional Strategies for Promoting Children’s Early Literacy Skills 2007. www.literacyencyclopedia.ca/index.php?fa = items.show&topicId = 224 (accessed 19 January 2015).
- Good RHI, Gruba J, Kaminski RA. Best Practices in Using Dynamic Indicators of Basic Early Literacy Skills (DIBELS) in an Outcomes-Driven Model. Best Practices in School Psychology IV: Vol. 1. Bethesda, MD: National Association of School Psychologists; 2001.
- MacLean M, Bryant PE, Bradley L. Rhymes, nursery rhymes and reading in childhood. Palmer Q 1987;33:255-82.
- Invernizzi M, Sullivan A, Swank L, Meier J. PALS Pre-K: Phonological Awareness Literacy Screening for Preschoolers. Charlotteville, VA: University Printing Services; 2004.
- Dunn L, Dunn L. Peabody Picture Vocabulary Test. Circle Pines, MN: American Guidance Service; 1997.
- Zimmerman IL, Steiner VG, Evatt RL. Preschool Language Scale. Columbus, OH: Charles E. Merrill; 1969.
- Reynell J, Curwen M. Manual for the Reynell Developmental Language Scales (Revised). Windsor: NFERNelson; 1983.
- Dunn L, Dunn L. Peabody Picture Vocabulary Test – Revised. Circle Pines, MN: American Guidance Service; 1981.
- Achenbach TM. Guide for the Caregiver Teacher Report Form for Ages 2–5. Burlington, VT: University of Vermont, Department of Psychiatry; 1997.
- Zimmerman I, Steiner V, Pond R. Preschool Language Scale – Fourth Edition (PLS-4UK). St Antionio, TX: Psychological Corporation; 2002.
- Gresham FM, Elliot SN. Social Skills Rating System Manual. Circle Pines, MN: American Guidance Service; 1990.
- Stanton-Chapman TL, Kaiser AP, Viajay P, Craig-Unkefe L. The Peer Language and Behaviour Code. Nashville, TN: Vanderbilt University; 2003.
- Achenbach TM. A Manual for the Child Behavior Checklist – 2–3. Burlington, VT: University of Vermont, Department of Psychiatry; 1992.
- Caldwell, Bradley . HOME Inventory n.d. http://fhdri.clas.asu.edu/home/index.html (accessed 7 January 2014).
- Jabson J, Dishion TJ, Gardner F, Burton J. Relationship Process Code v-2.0 Training Manual: A System for Coding Relationship Interactions. Eugene, OR: University of Oregon, Child and Family Center; 2004.
- Rains C. Coder Impressions Inventory – Original and Addendum 2003. www.fasttrackproject.org/techrept/c/cii/cii3tech.pdf (accessed 29 July 2015).
- Buschmann A. Handbook of Heidelberg Parent-Based Language Intervention. Munich: Elsevier Urban & Fischer Bei Elsevier; 2008.
- Shriberg LD, Fourakis M, Hall SD, Karlsson HB, Lohmeier HL, McSweeny JL, et al. Extensions to the speech disorders classification system (SDCS). Clin Linguist Phon 2010;24:795-824. http://dx.doi.org/10.3109/02699206.2010.503006.
- Dodd B. Procedures for Classification of Sub-Groups of Speech Disorder. Differential Diagnosis and Treatment of Children with Speech Disorder. San Diego, CA: Singular Publishing Group; 1995.
- Boehm AE, Weinberg RA. The Classroom Observer: Developing Observation Skills in Early Childhood Settings. New York: Teachers College Press; 1997.
- Baker E, McLeod S. Evidence-based practice for children with speech sound disorders: part 1 narrative review. Lang Speech Hear Serv Sch 2011;42:102-39. http://dx.doi.org/10.1044/0161-1461(2010/09-0075).
- Garbarino J, Stott FM, Institute E. What Children Can Tell Us: Eliciting, Interpreting, and Evaluating Critical Information from Children. San Francisco, CA: Jossey-Bass; 1992.
- Simkin Z, Conti-Ramsden G. ‘I went to a language unit’: adolescents’ views on specialist educational provision and their language difficulties. Child Lang Teach Ther 2009;25:103-21. http://dx.doi.org/10.1177/0265659008098663.
- Coad J, Hambly H, Roulstone S, McLeod S. Listening to Children and Young People with Speech, Language and Communication Needs. Surrey: J&R Press; 2011.
- McLeod S, McCormack J, McAllister L, Harrison L, Holliday E, Roulstone S, et al. Listening to Children and Young People with Speech, Language and Communication Needs. Surrey: J&R Press; 2011.
- Lawford J, Volavka N, Eiser C. A generic measure of quality of life for children aged 3–8 years: results of two preliminary studies. Pediatr Rehabil 2001;4:197-20. http://dx.doi.org/10.1080/13638490210124033.
- Roulstone S, Coad J, Ayre A, Hambley H, Lindsay G. The Preferred Outcomes of Children with Speech, Language and Communication Needs and their Parents. London: Department for Education; 2012.
- Owen R, Hayett L, Roulstone S. Children’s views of speech and language therapy in school: consulting children with communication difficulties. Child Lang Teach Ther 2004;20:55-73. http://dx.doi.org/10.1191/0265659004ct263oa.
- McCormack J, McLeod S, McAllister L, Harrison LJ. My speech problem, your listening problem, and my frustration: the experience of living with childhood speech impairment. Lang Speech Hear Serv Sch 2010;41:379-92. http://dx.doi.org/10.1044/0161-1461(2009/08-0129).
- McKechnie L. Ethnographic observation of preschool children. Libr Inf Sci Res 2000;22:61-76. http://dx.doi.org/10.1016/S0740-8188(99)00040-7.
- Press F, Bradley BS, Goodfellow J, Harrison L, McLeod S, Sumsion J, et al. Listening to Children and Young People with Speech, Language and Communication Needs. Surrey: J&R Press; 2011.
- Mahoney G, Wheeden CA. The effect of teacher style on interactive engagement of preschool-aged children with special learning needs. Early Child Res Q 1999;14:51-68. http://dx.doi.org/10.1016/S0885-2006(99)80004-0.
- Marshall J, Goldbart J, Phillips J. Parents’ and speech and language therapists’ explanatory models of language development, language delay and intervention. Int J Lang Commun Disord 2007;42:533-55. http://dx.doi.org/10.1080/13682820601053753.
- Conti-Ramsden G, Botting N, Durkin K. Parental perspectives during the transition to adulthood of adolescents with a history of specific language impairment (SLI). J Speech Lang Hear Res 2008;51:84-96. http://dx.doi.org/10.1044/1092-4388(2008/006).
- Wylie K, McAllister L, Davidson B, Marshall J. Changing practice: implications of the World Report on Disability for responding to communication disability in under-served populations. Int J Speech Lang Pathol 2013;15:1-13. http://dx.doi.org/10.3109/17549507.2012.745164.
- Roulstone S, Harding S. Defining communication disability in under-served communities in response to the World Report on Disability. Int J Speech Lang Pathol 2013;15:27-31. http://dx.doi.org/10.3109/17549507.2012.727870.
- McAllister L, Wylie K, Davidson B, Marshall J. The World Report on Disability: an impetus to reconceptualize services for people with communication disability. Int J Speech Lang Pathol 2013;15:118-26. http://dx.doi.org/10.3109/17549507.2012.757804.
- Strand S, Lindsay G. Ethnic Disproportionality in the Identification of Speech, Language and Communication Needs (SLCN) and Autism Spectrum Disorders (ASD). London: Department for Education; 2012.
- Marshall J. Critical reflections on the cultural influences in identification and habilitation of children with speech and language difficulties. Int J Disabil Dev Educ 2000;47:355-69. http://dx.doi.org/10.1080/713671154.
- Marshall J. International and cross-cultural issues: six key challenges for our professions. Folia Phoniatr Logop 2003;55:329-36. http://dx.doi.org/10.1159/000073257.
- Clark A, Moss P. Listening to Young Children: the Mosaic Approach. London: National Children’s Bureau; 2001.
- Markham C, Dean T. Parents’ and professionals’ perceptions of quality of life in children with speech and language difficulty. Int J Lang Commun Disord 2006;41:189-212. http://dx.doi.org/10.1080/13682820500221485.
- Hunt A, Coad J, West E, Hex N, Staniszewska S, Hacking S, et al. The Big Study for Life-Limited Children and their Families. Bristol: Together for Short Lives; 2013.
- Coad J. Breathing Matters – Improving Care with a Training Needs Analysis of Ventilated Children, Young People, Families and Professionals. London: Department of Health; 2013.
- Glogowska M, Campbell RM. Investigating parental views of involvement in pre-school speech and language therapy. Int J Lang Commun Disord 2000;35:391-405. http://dx.doi.org/10.1080/136828200410645.
- Dockrell J, Lindsay G, Law J, Roulstone S. Supporting children with speech, language and communication needs: an overview of the results of the Better Communication Research Programme. Int J Lang Commun Disord 2014;49:534-55. http://dx.doi.org/10.1111/1460-6984.12089.
- Kuenzli J. The Somali Community’s Experiences With Autism: An Exploratory Study. Master of Social Work Clinical Research Papers 2012. http://sophia.stkate.edu/msw_papers/50 (accessed 19 January 2015).
- Linebarger D, Walker D. Infants’ and toddlers’ television watching and language outcomes. Am Behav Sci 2005;48:624-45. http://dx.doi.org/10.1177/0002764204271505.
- Christakis DA, Gilkerson J, Richards JA, Zimmerman FJ, Garrison MM, Xu D, et al. Audible television and decreased adult words, infant vocalizations, and conversational turns: a population-based study. Arch Pediatr Adolesc Med 2009;163:554-8. http://dx.doi.org/10.1001/archpediatrics.2009.61.
- Zimmerman FJ, Gilkerson J, Richards JA, Christakis DA, Xu D, Gray S, et al. Teaching by listening: the importance of adult–child conversations to language development. Pediatrics 2009;124:342-9. http://dx.doi.org/10.1542/peds.2008-2267.
- Wright JC, Huston AC, Murphy KC, St. Peters M, Piñon M, Scantlin R, et al. The relations of early television viewing to school readiness and vocabulary of children from low-income families: the early window project. Child Dev 2001;72:1347-66. http://dx.doi.org/10.1111/1467-8624.t01-1-00352.
- Lincoln YS, Guba EG. Naturalistic Inquiry. London: Sage Publications; 1985.
- Shipley K, McAfee J. Assessment in Speech–Language Pathology: A Resource Manual. Andover: Cengage Learning; 2008.
- Communicating Quality 3. London: RCSLT; 2006.
- Stow C, Dodd B. Providing an equitable service to bilingual children in the UK: a review. Int J Lang Commun Disord 2003;38:351-77. http://dx.doi.org/10.1080/1368282031000156888.
- Baker E, Bernhardt B. From hindsight to foresight: working around barriers to success in phonological intervention. Child Lang Teach Ther 2004;20:287-318. http://dx.doi.org/10.1191/0265659004ct276oa.
- Limbrick N, McCormack J, McLeod S. Designs and decisions: the creation of informal measures for assessing speech production in children. Int J Speech Lang Pathol 2013;15:296-311. http://dx.doi.org/10.3109/17549507.2013.770552.
- Skahan SM, Watson M, Lof GL. Speech-language pathologists’ assessment practices for children with suspected speech sound disorders: results of a national survey. Am J Speech Lang Pathol 2007;16:246-59. http://dx.doi.org/10.1044/1058-0360(2007/029).
- Mullen R. Evidence for whom?: ASHA’s National Outcomes Measurement System. J Commun Disord 2004;37:413-17. http://dx.doi.org/10.1016/j.jcomdis.2004.04.004.
- Mullen R, Schooling T. The National Outcomes Measurement System for pediatric speech–language pathology. Lang Speech Hear Serv Sch 2009;41:44-60. http://dx.doi.org/10.1044/0161-1461(2009/08-0051).
- Priester GH, Post WJ, Goorhuis-Brouwer SM. Problems in speech sound production in young children. An inventory study of the opinions of speech therapists. Int J Pediatr Otorhinolaryngol 2009;73:1100-4. http://dx.doi.org/10.1016/j.ijporl.2009.04.014.
- Williams CJ, McLeod S. Speech–language pathologists’ assessment and intervention practices with multilingual children. Int J Speech Lang Pathol 2012;14:292-305. http://dx.doi.org/10.3109/17549507.2011.636071.
- Hoffman LM, Frome Loeb D, Brandel J, Gillam RB. Concurrent and construct validity of oral language measures with school-age children with specific language impairment. J Speech Lang Hear Res 2011;54:1597-608. http://dx.doi.org/10.1044/1092-4388(2011/10-0213).
- Bernthal JE, Bankson NW, Flipsen P. Articulation and Phonological Disorders: Speech Sound Disorders in Children. Boston, MA: Pearson Education; 2012.
- Hoffman P, Norris J. Phonological assessment as an integral part of language assessment. Am J Speech Lang Pathol 2002;11:230-5. http://dx.doi.org/10.1044/1058-0360(2002/024).
- The NHS Outcomes Framework 2011/12. London: Department of Health; 2011.
- The NHS Outcomes Framework 2013/14. London: Department of Health; 2013.
- The NHS Outcomes Framework 2014/15. London: Department of Health; 2014.
- Quality and Outcomes Framework – 2011/12. London: Health & Social Care Information Centre; 2012.
- Quality and Outcomes Framework – 2012/13. London: Health & Social Care Information Centre; 2013.
- Everyone Counts: Planning for Patients 2013/14. London: NHS; 2013.
- Lezzoni L. Risk Adjustment for Measuring Health Outcomes. Ann Arbor, MI: Health Administration Press; 1994.
- Survey of Health Care Consumers Global Report: Key Findings, Strategic Implications. Washington, DC: Deloitte Development LL; 2011.
- John A. Therapy outcome measures: where are we now?. Int J Speech Lang Pathol 2011;13:36-42. http://dx.doi.org/10.3109/17549507.2010.497562.
- Perigo G, Callaghan S. Commissioning for Outcomes: A Resource Guide for Commissioners of Health and Social Care 2011. www.fadelibrary.org.uk/wp/downloads/?did = 306 (accessed 19 January 2015).
- Olswang LB, Rodriguez B, Timler G. Recommending intervention for toddlers with specific language learning difficulties. Am J Speech Lang Pathol 1998;7:23-32. http://dx.doi.org/10.1044/1058-0360.0701.23.
- Commissioning Support Programme . Speech &Amp; Communication Needs – the Commissioning Support Community 2011. www.commissioningsupport.org.uk/resource-bank/childrens-health/speech--communication-needs.html (accessed 28 March 2014).
- Frattali C. Measuring Outcomes in Speech–Language Pathology. New York: Thieme-Stratton Corp; 1998.
- Enderby P, John A, Petheram B. Therapy Outcome Measures for Rehabilitation Professionals: Speech and Language Therapy, Physiotherapy, Occupational Therapy. Chichester: John Wiley; 2006.
- Perry A, Morris M, Unsworth C, Duckett S, Skeat J, Dodd K, et al. Therapy outcome measures for allied health practitioners in Australia: the AusTOMs. Int J Qual Health Care 2004;16:285-91. http://dx.doi.org/10.1093/intqhc/mzh059.
- Enderby PM, John A. Therapy outcome measures in speech and language therapy. Int J Lang Commun Disord 1999;34:417-30. http://dx.doi.org/10.1080/136828299247360.
- Shining a Light on Augmentative and Alternative Communication. Edinburgh: Communication Matters; 2012.
- Roulstone S, Peters TJ, Glogowska M, Enderby P. Predictors and outcomes of speech and language therapists’ treatment decisions. Int J Speech Lang Pathol 2008;10:146-55. http://dx.doi.org/10.1080/17549500801894362.
- McCauley RJ, Swisher L. Use and misuse of norm-referenced tests in clinical assessment: a hypothetical case. J Speech Hear Disord 1984;49:338-48. http://dx.doi.org/10.1044/jshd.4904.338.
- Plante E, Vance R. Selection of preschool language tests: a data-based approach. Lang Speech Hear Serv Sch 1994;25:15-24. http://dx.doi.org/10.1044/0161-1461.2501.15.
- Plante E, Vance R. Diagnostic accuracy of two tests of pre-school language. Am J Speech Lang Pathol 1995;4:70-6. http://dx.doi.org/10.1044/1058-0360.0402.70.
- International Classification of Functioning, Disability and Health (ICF). Geneva: WHO; 2001.
- Ludwig B. Predicting the future: have you considered using the Delphi methodology?. J Ext 1997;35:1-4.
- Rosen A, Proctor EK. Distinctions between treatment outcomes and their implications for treatment evaluation. J Consult Clin Psychol 1981;49:418-25. http://dx.doi.org/10.1037/0022-006X.49.3.418.
- Witkin BR, Altschuld J. Planning and Conducting Needs Assessments: A Practical Guide. Thousand Oaks, CA: Sage Publications; 1995.
- RCSLT Outcomes Survey Report. Birmingham: RCSLT; 2013.
- Porter ME, Lee TH. The Strategy That Will Fix Health Care. Harvard Business Review 2013. http://hbr.org/2013/10/the-strategy-that-will-fix-health-care/ar/1 (accessed 19 January 2015).
- Hannus S, Kauppila T, Pitkäniemi J, Launonen K. Use of language tests when identifying specific language impairment in primary health care. Folia Phoniatr Logop 2013;65:40-6. http://dx.doi.org/10.1159/000350318.
- Law J, Camilleri B. Dynamic assessment and its application to children with speech and language learning difficulties. Int J Speech Lang Pathol 2007;9:271-2. http://dx.doi.org/10.1080/14417040701516522.
- Baker E, Munro N. An Overview of Resources for Assessing Toddlers’ Productions of Polysyllables. Peer Review Abstr ACQ 2011;13. www.speechpathologyaustralia.org.au/index.php?option=com_content&view=article&id=1047 (accessed 8 January 2014).
- Khan LM. The sixth view: assessing preschoolers’ articulation and phonology from the trenches. Am J Speech Lang Pathol 2002;11:250-4. http://dx.doi.org/10.1044/1058-0360(2002/027).
- Tyler AA, Tolbert L. Speech–language assessment in the clinical setting. Am J Speech Lang Pathol 2002;11:215-20. http://dx.doi.org/10.1044/1058-0360(2002/022).
- Nelson HD, Nygren P, Walker M, Panoscha R. Screening for speech and language delay in preschool children: systematic evidence review for the US Preventive Services Task Force. Pediatrics 2006;117:e298-319. http://dx.doi.org/10.1542/peds.2005-1467.
- Donabedian A. The Definition of Quality and Approaches to its Assessment. Chicago, IL: Health Administration Press; 1980.
- Donabedian A. The Methods and Findings of Quality Assessment and Monitoring: an Illustrated Analysis. Chicago, IL: Health Administration Press; 1985.
- Eadie TL, Yorkston KM, Klasner ER, Dudgeon BJ, Deitz JC, Baylor CR, et al. Measuring communicative participation: a review of self-report instruments in speech–language pathology. Am J Speech Lang Pathol 2006;15:307-20. http://dx.doi.org/10.1044/1058-0360(2006/030).
- Wilcox K, Morris S. Children’s Speech Intelligibility Measure (CSIM). London: Pearson Clinical; 1999.
- Thomas-Stonell NL, Oddson B, Robertson B, Rosenbaum PL. Development of the FOCUS (Focus on the Outcomes of Communication Under Six), a communication outcome measure for preschool children. Dev Med Child Neurol 2010;52:47-53. http://dx.doi.org/10.1111/j.1469-8749.2009.03410.x.
- Moran P, Ghate D, van der Merwe A. What Works in Parenting Support? A Review of the International Evidence. Nottingham: Department for Education and Skills; 2004.
- Cajkler W, Tennant G, Tiknaz Y, Sage R, Tucker S, Taylor C. A Systematic Literature Review on How Training and Professional Development Activities Impact on Teaching Assistants’ Classroom Practice (1988–2006). London: EPPI-Centre, Social Science Research Unit; 2007.
- Beecham J, Law J, Zeng B, Lindsay G. Costing children’s speech, language and communication interventions. Int J Lang Commun Disord 2012;47:477-86. http://dx.doi.org/10.1111/j.1460-6984.2012.00157.x.
- Markham C, van Laar D, Gibbard D, Dean T. Children with speech, language and communication needs: their perceptions of their quality of life. Int J Lang Commun Disord 2009;44:748-68. http://dx.doi.org/10.1080/13682820802359892.
- Kiresuk TJ, Sherman RE. Goal attainment scaling: a general method for evaluating comprehensive community mental health programs. Community Ment Health J 1968;4:443-53. http://dx.doi.org/10.1007/BF01530764.
- Johnson M, Elias A. East Kent Outcome System for Speech and Language Therapy 2002.
- Malcomess K. The Care Aims Model. Speech and Language Therapy: Issues in Professional Practice. London: Wiley-Blackwell; 2005.
- NHS Costing Manual. London: Department of Health; 2012.
- Commissioning Support Programme . Speech, Language and Communication Needs: Evaluating Outcomes Tool 2011. www.thecommunicationtrust.org.uk/media/12886/slcn_tools_evaluating-outcomes_1_.pdf (accessed 13 January 2014).
- McCurtin A, Roddam H. Evidence-based practice: SLTs under siege or opportunity for growth? The use and nature of research evidence in the profession. Int J Lang Commun Disord 2012;47:11-26. http://dx.doi.org/10.1111/j.1460-6984.2011.00074.x.
- Nippold MA, Hesketh LJ, Duthie JK, Mansfield TC. Conversational versus expository discourse: a study of syntactic development in children, adolescents, and adults. J Speech Lang Hear Res 2005;48:1048-64. http://dx.doi.org/10.1044/1092-4388(2005/073).
- Bates E, Bretherton I, Snyder L. From First Words to Grammar: Individual Differences and Dissociable Mechanisms. Cambridge: Cambridge University Press; 1988.
- Royal College of Speech and Language Therapists . Communicating Quality. Guidance on Best Practice in Service Organisation and Provision 2006.
- Ferguson A, Worrall L, Davidson B. Talk about goals for aphasia therapy. J Interact Res Commun Disord 2010;1:95-118. http://dx.doi.org/10.1558/jircd.v1i1.95.
- Dixon-Woods M, Agarwal S, Jones D, Young B, Sutton A. Synthesising qualitative and quantitative evidence: a review of possible methods. J Health Serv Res Policy 2005;10:45-53. http://dx.doi.org/10.1258/1355819052801804.
- Dixon-Woods M, Cavers D, Agarwal S, Annandale E, Arthur A, Harvey J, et al. Conducting a critical interpretative synthesis of the literature on access to healthcare by vulnerable groups. BMC Med Res Methodol 2006;6. http://dx.doi.org/10.1186/1471-2288-6-35.
- Torraco RJ. Writing integrative literature reviews: guidelines and examples. Hum Res Dev Rev 2005;4:356-67. http://dx.doi.org/10.1177/1534484305278283.
- Kaiser A, Hancock T. Teaching parents new skills to support their young children’s development. Infant Young Child 2003;16:9-21. http://dx.doi.org/10.1097/00001163-200301000-00003.
- Roberts MY, Kaiser AP. The effectiveness of parent-implemented language interventions: a meta-analysis. Am J Speech Lang Pathol 2011;20:180-99. http://dx.doi.org/10.1044/1058-0360(2011/10-0055).
- Lindsay G, Dockrell JE, Law J, Roulstone S. Better Communication Research Programme: 2nd Interim Report. London: Department for Education; 2011.
- Westerlund M. Expressive vocabulary in 18-month-old children in relation to demographic factors, mother and child characteristics, communication style and shared reading. Child Care Health Dev 2008;34:257-66. http://dx.doi.org/10.1111/j.1365-2214.2007.00801.x.
- Girolametto L, Bonifacio S, Visini C, Weitzman E, Zocconi E, Pearce PS. Mother-child interactions in Canada and Italy: linguistic responsiveness to late-talking toddlers. Int J Lang Commun Disord 2002;37:153-71. http://dx.doi.org/10.1080/13682820110116794.
- Bowen C, Cupples L. The role of families in optimising phonological therapy outcomes. Child Lang Teach Ther 2004;20:245-60. http://dx.doi.org/10.1191/0265659004ct274oa.
- Fourie R, Crowley N, Olivera A. A qualitative exploration of therapeutic relationships from the perspective of six children receiving speech-language therapy. Topics Lang Disord 2011;31:310-24. http://dx.doi.org/10.1097/TLD.0b013e3182353f00.
- Rannard A, Lyons C, Glenn S. Parent concerns and professional responses: the case of specific language impairment. Br J Gen Pract 2005;55:710-14.
- Band S, Lindsay G, Law J, Soloff N, Peacey N, Gascoigne M, et al. Are health and education talking to each other? Perceptions of parents of children with speech and language needs. Eur J Special Needs Educ 2002;17:211-27. http://dx.doi.org/10.1080/08856250210162121.
- Beresford B, Rabiee P, Sloper P. Priorities and Perceptions of Disabled Children and Young People and their Parents Regarding Outcomes from Support Services. York: Social Policy Research Unit; 2007.
- Davis H, Meltzer L. Working with Parents in Partnership. London: Department for Education and Skills; 2007.
- Attride-Stirling J. Thematic networks: an analytic tool for qualitative research. Qual Res 2001;1:385-40. http://dx.doi.org/10.1177/146879410100100307.
- Vosniadou S. International Handbook of Research on Conceptual Change. New York: Routledge; 2013.
- Vygotsky LS. Mind in Society. Cambridge MA: Harvard University Press; 1978.
- Whitehurst GJ, Novak G, Zorn GA. Delayed speech studied in the home. Dev Psychol 1972;7:169-77. http://dx.doi.org/10.1037/h0033078.
- Zimmerman IL, Steiner VG, Pond RE. PLS-3: Preschool Language Scale-3. San Antonio, TX: Psychological Corporation; 1992.
- Bayley N. Bayley Scales of Infant Development. San Antonio, TX: Psychological Corporation, Harcourt Brace and Company; 1993.
- Fenson L, Marchman VA, Thal DJ, Dale PS, Reznick JS, Bates E. MacArthur–Bates Communicative Development Inventories: User’s Guide and Technical Manual. Baltimore, MA: Paul H. Brookes Publishing; 2007.
- LENA Research Foundation . Automatic Language Assessment in Three Easy Steps 2011. www.lenafoundation.org/ProSystem/Overview.aspx (accessed 10 February 2015).
- Thorpe KJ, Bell P. The Thorpe Interaction Measure: A Standard Measure to Assess Parent’s Behaviour at a Picture Book With Their Child n.d.
- Thorpe K, Rutter M, Greenwood R. Twins as a natural experiment to study the causes of mild language delay: II: family interaction risk factors. J Child Psychol Psychiatry 2003;44:342-55. http://dx.doi.org/10.1111/1469-7610.00126.
- Oller DK, Niyogi P, Gray S, Richards JA, Gilkerson J, Xu D, et al. Automated vocal analysis of naturalistic recordings from children with autism, language delay, and typical development. Proc Natl Acad Sci 2010;107:13354-9. http://dx.doi.org/10.1073/pnas.1003882107.
- Xu D, Yapanel U, Gray S, Gilkerson J, Richards JA, Hansen J. Signal Processing for Young Child Speech Language Development n.d.
- Paul R. Clinical implications of the natural history of slow expressive language development. Am J Speech Lang Pathol 1996;5:5-21. http://dx.doi.org/10.1044/1058-0360.0502.05.
Appendix 1 Glossary of speech and language therapist-led activities
| Anticipation activities | Engaging activities, possibly specifically tailored to the child’s individual interests, to capture the child’s attention. A pause is then inserted before the activity’s climax, which may also be supported by an excited expression/vocalisation from the adult to indicate that an exciting event is about to occur. This pause allows an opportunity for eye contact, shared enjoyment, request vocalisations and early sequencing development, e.g. before blowing bubbles |
| Auditory bombardment | In phonological therapy, this process refers to repeatedly presenting target phonemes to an individual, either in isolation or with repetition of words containing the target sound |
| Barrier games | Activities that involve two or more participants working towards the same goal using only verbal instructions. A physical barrier is used to separate the participants. There is a ‘speaker’ and a ‘listener’. The speaker gives the listener instructions to follow from behind the barrier such as a description of an image that the listener must reproduce. This activity provides opportunities for children to develop their receptive language (listening to instructions) and expressive language (giving instructions) |
| Fishing game | Commonly used game within therapy sessions in which the child chooses an item to practise (sound, word, etc.), commonly displayed on a card |
| Focused auditory stimulation | See Auditory bombardment |
| Free and directed play | Free play involves the child having no restrictions on what or how he or she chooses to play. This can be done independently but the adult can choose to follow the child’s choices and partake in his or her play while not influencing his or her choices. In directed play the adult selects the object or toy to play with or specifies how the toy is to be played with |
| ICW(s) | In an instruction or command the ICW is the important word that will allow the child to carry out a given instruction. For example, if the child was presented with a car and a doll and told ‘show me dolly’, dolly would be the ICW |
| Maximal oppositions (activities) | A set of words that differ by one phoneme. The phonemes differ in more than one element of production (place of articulation, manner of articulation and phonation), e.g. the first letter in the following words: ‘seat’ (/si:t/), ‘beat’ (/bi:t/), feet (/fi:t/) and wheat (/wi:t/), which vary by place (alveolar, bilabial, labiodental, labial-velar), manner (fricative and stop) and phonation (voiced and voiceless) |
| Maximal pairs (activities) | As Maximal oppositions but use of a pair of words as opposed to a set |
| Minimal pairs | A pair of words that are the same but which have one phoneme that differs by only one feature, either place, manner or phonation, e.g. pay (/peɪ/) and bay (/beɪ/), which differ by voicing only |
| Narrative | The child’s ability to retell stories or events. Asking a child to retell a story can be used to assess his or her language abilities and measure use of specific grammatical forms |
| Oromotor work | Activities to develop oral movement accuracy, speed and strength |
| Picture sequencing | Placing pictures in the correct order |
| Pitch and volume work | Work to target the highness or lowness of voice tone and use of appropriate loudness of voice |
| Segmentation of phonemes | The process of breaking a word down into the individual sounds that it consists of, e.g. table as ‘t’ ‘ay’ ‘b’ ‘l’ |
| Sequencing sounds | An individual’s ability to arrange sounds in a required order, e.g. to form a word |
| Social stories | A therapy tool typically used for individuals on the autistic spectrum and who therefore have difficulties with social interactions. Social stories provide an opportunity to detail and explain factors that contribute to effective communication to support these individuals in interactions |
| Sound awareness | Activities that aim to improve children’s listening and perception of sounds as well as their understanding of how these are important for speech and language. Therapists reported using a wide range of sound awareness activities; these included listening to environmental sounds such as musical instruments, auditory bombardment, rhyming, syllable counting and activities focusing on discrimination of sounds such as front and back sounds and minimal pairs |
| Tongue twisters | A group of words with similar consonant sounds that are difficult to articulate rapidly, e.g. Peter Piper picked a peck of pickled pepper |
| Turn taking | In which an individual participates in an activity for a set amount of time before stopping to allow another to complete the activity. This may be a turn at rolling a ball or a conversational turn. It requires looking, listening and social awareness skills. It is an important skill in communication |
| What’s in the bag/box | A game in which items are placed in a bag/box and are then revealed by the adult or the child pulling the items out. It can be used to promote either receptive language (by the adult naming an item as it is revealed) or expressive language (in which the child is encouraged to name the item) or both |
Appendix 2 Glossary of speech and language therapist-led interventions
| Adult/parent–child interaction | The parent/adult is supported by the SLT to reflect on his or her interaction with the child and to understand the child’s communication needs and which strategies would be beneficial to support him or her. Reflection on interaction style is often achieved through the use of video analysis |
| Adult understanding | The adult/s working with the child (parent, EYP) having the necessary knowledge relating to the purpose of, and how to implement, the therapy strategies and activities |
| Cycles therapy/approach | In phonological therapy, this is the process of addressing several targeted sounds within the same pattern of error in a rotating approach over several cycles or training periods |
| Foundation skills | Work to practise and improve a range of early skills that are considered to be foundations for speech and language development. Activities that therapists reported using to support foundation skills included work on turn taking, play, attention and listening |
| Functional communication/functional use of language | Getting one’s message across in practical, everyday situations. An example of functional communication may be teaching a child to use a sign for ‘toilet’ in order to request this and therefore increase their independence at nursery |
| Generalisation | Making speech and language or therapy gains transferable to other situations and environments. SLTs rarely referred to specific activities to enforce generalisation (with the exception of self-monitoring activities for speech); however, they referred to the importance of parents and other adults working with the child to use activities and strategies in different contexts to encourage generalisation |
| Mands | Mands is derived from the word command and in therapy it refers to making a request. Before a mand is made a therapist will use a deprivation or aversive technique, e.g. holding up a toy and not giving it to the child until he or she uses the right mand to request the toy |
| Principle of laryngeal–supralaryngeal cyclicity | Laryngeal sounds are sounds that are produced in the larynx, e.g. ‘H’; supralaryngeal sounds are produced above the larynx. Cyclicity is a process whereby distinctions are added to an inventory in alternation (in this principle laryngeal and supralaryngeal sounds are addressed in a cycle that is alternated) |
Appendix 3 Glossary of speech and language therapist-led programmes
| Core vocabulary | May be used to refer to either (1) commonly used words that aid in communication and the learning of language or (2) a specific technique for children with inconsistent phonological disorder in which the children are taught specific words (core vocabulary) identified by them/their parent as important to them until they produce the words in the same way each time |
| Gap House programme | A therapy programme involving the use of pictures representing individual phonemes that are arranged to support the child in sounding out the word phonetically (how it sounds) as opposed to how it is spelled, e.g. crocodile as ‘k’ ‘r’ ‘o’ ‘k’ ‘er’ ‘d’ ‘eye’ ‘l’ |
| Hanen programmes | Programmes developed by the Hanen Centre in Canada. These programmes help parents and educators to take on the primary role of promoting the social, language and literacy skills of young children |
| Makaton programme | A language programme that uses signs and symbols alongside spoken words to aid communication. In speech it is used within spoken word order |
Appendix 4 Glossary of speech and language therapist-led strategies
| Adopting a hierarchy approach (e.g. C, CV, CVC) | A strategy for teaching targeted speech sounds beginning with the sound (consonant, C) in isolation, producing with a vowel (V), moving into more complex word structures (CVC, CVCV, etc.) up to phrase and sentence levels and eventually to use in conversational speech |
| Adopting more varied intonation | Therapy to target the appropriate stress patterns within the English language. May also include specific intonation markers such as rising intonation to indicate a question |
| Chunking | The process of grouping words into phrases. Can also refer to grouping individual numbers of letters to assist memory |
| Cloze | An intervention whereby the child is asked to insert words that have been deleted in a text. This kind of test evaluates reading comprehension. A therapist may also omit a word from a common rhyme/story for the child to complete it to encourage expressive language |
| Drilling words | Continual repetition of target words to practise accurate production |
| Milieu language teaching | This is a conversation-based teaching technique that uses a child’s interest and a naturalistic environment to elicit communicative responses from the child |
| Modelling | Demonstrating what is to be carried out |
| Recasting the child’s utterance | Repeating the child’s phrase or sentence back with the errors corrected |
| Scaffolding | Adults providing support for the child that promotes the development of speech or language |
| Sentence recasting | Repeating back an erroneous sentence with the error corrected but the sentence meaning not being altered |
| Signing | Communicating by using visual gestures and signs |
| Visual timetables | A series of pictures representing a task or routine that is to be carried out within a given time frame |
Appendix 5 Glossary of study design
| Before-and-after study | An evaluation study that assess children before a given intervention and immediately afterwards. No comparison group is used |
| Case study | A type of study giving a description of the exploratory or explanatory analysis of people, groups or situations. This type of study is conducted over a period of time |
| Cluster analysis | A statistical technique for assigning a set of individual people or other items to groups called clusters on the basis of one or more measurements of the individuals, so that people within the same cluster are in some sense closer or more similar to one another than to individuals in another cluster |
| Content analysis | Analysing the content of text data by looking at it objectively and systematically, counting incidences and reporting on descriptions and classifications |
| Delphi | A forecasting research method that involves sending out several rounds of questionnaires to an expert panel. Results are collected anonymously and shared with the panel and members of the panel are then allowed to change their responses. The aim is to reach consensus |
| Documentary analysis | A research method that involves analytically reading or reviewing documents to provide evidence/support for facts stated in research. Analysis of documents can be qualitative or quantitative |
| Effectiveness | Evaluation of intervention in practice, which follows on from efficacy study. This answers the question, ‘does the intervention work under real-life conditions?’ |
| Efficacy | Evaluation of an intervention in controlled and optimal conditions, with the highest level of staffing, best equipment, etc. This answers the question, ‘can the intervention work compared with nothing or with an alternative intervention?’ |
| Framework analysis | A qualitative research method that uses a thematic framework to classify and organise data. Through use of an iterative process, themes, concepts and categories arise that are further subdivided into subthemes or topics |
| Level of evidence | The confidence level for the effectiveness of an intervention. This can be reported as being strong, moderate or indicative |
| Multiple baseline design | A research design involving the measurement of multiple participants, settings or conditions. The baseline refers to the pre-intervention condition. At some point in the study an intervention is applied and measurements taken before and after the study are evaluated |
| Outcome | The measure used to assess change following intervention |
| RCT | A study whereby participants are randomly allocated to a treatment. A RCT is considered to be the best-quality design for a study of effectiveness or efficacy |
| Thematic analysis | The process of pinpointing, examining and recording patterns and themes within qualitative data |
Appendix 6 Glossary of general processes and terms
| Anglophone | English-speaking person |
| Articulation | Physically producing speech sounds through shaping of the airflow by the articulators (lips, tongue, jaw and soft palate) and where appropriate additional voicing through the larynx |
| Auditory discrimination | The ability to recognise and distinguish between speech sounds |
| Auditory memory | The ability to hear information, process it and retain it |
| Autism spectrum disorders | Term used to describe and diagnose a range of developmental conditions with common features primarily affecting social communication skills and interaction and with restricted, repetitive behaviours |
| Blending of phonemes | Blending is the process of taking individual sounds and combining them to make a word |
| Commissioner(s) | Those purchasing services within health, education or charitable sectors for children with SLCN |
| Communication | The process of relaying information, which can include thoughts and messages. Communication can be delivered by speech, writing, body language, hand gestures and symbols |
| Complex needs | Children who have a number of different health, social and development needs at the same time. These children commonly have SLCN |
| Comprehension | The child’s ability to understand what is said by others. Often assessed in formal language tests in which the child has to rely on his or her understanding of the words/sentences used and not the context in which they are said |
| Concept | A concept is an abstract word that can relate to physical appearance, positioning, order, time, etc. Addition of concept words often changes the meaning of the sentence and the child will need to understand these to follow an instruction. e.g. big/little, hard/soft, above/below or before/after. Concepts in the following sentence are shown in italics: ‘Jonny carried all the big books except the old ones’ |
| Diagnosis | The process of identifying a disease/medical condition |
| Dyspraxia | A developmental co-ordination disorder that affects basic and fine motor co-ordination |
| Expressive language | The ability to express thoughts as words/sentences. This can be spoken or written |
| Fricative | Consonant speech sounds that are made by constricting a passageway and forcing breath through it, creating a disrupted release. Fricatives used in English include ‘s’, ‘z, ‘f’, ‘v’, ‘sh’, ‘j’, ‘ch’ and ‘s’, e.g. in vision, measure |
| Inference | Term used to describe what a child understands from what has been said. If a child has difficulty with inference it suggests that he or she has difficulty distinguishing between what has been said and what the speaker actually means |
| Input | A term used to describe what is said to a child by a therapist/parent. Input can be an intervention (e.g. listening and discrimination tasks) and is monitored through output |
| Intelligibility | A way of rating how easy it is to understand someone’s speech. This can be achieved by informal judgement or through formal calculations of intelligibility such as the number of individual sounds or words identifiable to the listener |
| Intervention | Support given to children with SLCN above what they would normally receive in the class or home environment |
| Key/basic vocabulary | Words considered to be important for the child to understand and use to have the most impact on their communicative ability |
| Key phrases | A combination of key words |
| Key sounds | Specific sounds targeted within therapy or sounds that have greatest impact on the child’s intelligibility |
| Manner of articulation | How the articulators (tongue, lips, palate and jaw) are configured to produce a speech sound, e.g. close proximity results in fricative sound production whereas complete closure results in a stopped sound |
| Morphology | The means of describing the structure of words. Words can be subdivided into morphemes – the smallest unit of meaning, e.g. root words (e.g. ‘walk) – and the use of tense markers such as ‘ing’ to show present tense |
| Non-ambient ingressive substitution pattern | A substitution pattern involving production of a click (a type of consonant) for sounds with a hissing effect, e.g. ‘s’, ‘sh’ (sibilants). Clicks are ingressive sounds as the airstream flows inward through the mouth or nose |
| Phoneme | A unit of sound that, when combined with other units, forms words |
| Phonological awareness | An awareness of the sound structure of spoken words. Awareness can be tested in sound segmentation, rhyme and alliteration tasks. Phonological awareness is an indicator of reading ability |
| Phonology | The speech sounds made in any language |
| Place of articulation | The location of an articulator’s contact within the vocal tract when producing a speech sound, e.g. the tongue tip being used to touch the alveolar ridge |
| Practitioner | A professional who provides intervention, carries out assessment and in some cases teaches |
| PSLI | Term used to describe children whose speech and/or language difficulties occur in the absence of other physical or cognitive difficulties |
| Programme | An intervention that has been systematised |
| Prosodic | In linguistics this refers to the rhythm, pitch, loudness and tempo of speech |
| Receptive language | Understanding of written or spoken language |
| Rhyme awareness | Awareness of word endings sharing the same sounds. It relates to their endings sounding alike when spoken, not necessarily when written, e.g. ‘bite’ (/bait/) and might (/mait/) rhyme when spoken even though their spellings differ |
| Self-monitoring | An individual’s ability to listen to his or her own speech and/or language and judge whether or not it was produced correctly |
| Semantics | The meaning associated with a given word or combination of words |
| Session | A term used to define a specific period of intervention, e.g. the period when a teaching assistant or SLT works with a given group of children within school |
| Sonority Sequencing Principle | This is a principle that examines the structure of syllables in a language in terms of sonority (peak of loudness). In this principle, at the centre of a syllable there is a nucleus that is usually a vowel; at this vowel point there is a sonority peak and this is followed by consonants that progressively decrease in level of sonority |
| Special educational needs | This term is used to refer to children whose learning difficulties of any sort make it harder for them to learn than most children of their own age |
| Specific language impairment | Term applied to children who have difficulties acquiring language but who do not have difficulties in other areas (general developmental delays, severe hearing loss, etc.) |
| Speech | The vocalisation of language consisting of phonemes combined to form words with a commonly acknowledged meaning |
| SLCN | An umbrella term used to describe children with speech and language difficulties regardless of origin or presenting features |
| SLT | A practitioner with the primary responsibility for assessing a child with SLCN and providing intervention |
| Strings of jargon | Use of nonsense words that do not have a defined meaning. Children with language difficulties may insert jargon words into their language or produce continual jargon words, forming strings of jargon |
| Syllable | A unit of sound consisting of a vowel and which may or may not include a consonant. Words can be subdivided into syllables, e.g. computer: ‘com’, ‘pu’, ‘ter’ |
| Syntactic | Relating to the rules of syntax |
| Syntax | In linguistics this is the arrangement of words in a sentence. Each language follows rules that determine which word orders within a sentence are acceptable |
| Target | The specific aim of activity within an intervention programme. The target is usually prespecified and measured as part of the evaluation of the intervention |
| Utterances | Vocal expression – this can be a single word or a combination of words |
| Word finding | The ability to recall words that have previously been learnt and stored in the lexicon. Retrieval difficulties can be linked to poor storage of phonological and semantic representations or can be a result of a specific disorder or brain injury |
| Word-initial three-element clusters | Clusters are two or three consonants within a word that are not separated by a vowel. An example of a word-initial (i.e. occurring at the start of the word) three-element cluster is ‘spring’ |
Appendix 7 Child Talk parent panel
The parent panel was proactive in making sure that all participant literature was written in plain English and contained all of the practical information about the research that a parent would need. It was active in designing promotional materials to aid recruitment, such as flyers and a recruitment video (whiteboard animation) [see www.speech-therapy.org.uk/child-talk-what-works-whiteboard-video (accessed 19 January 2015)].
Two panel members participated in the advisory board meetings, which meant that they had an input into the management strategy and implementation of the programme. The parent panel was an active partner with the research team and details about its involvement are embedded throughout the report. Further detail on the specific activities of the panel is provided in the following section.
Contribution of the parent panel to the Child Talk programme
Research design
Contributions
-
Reviewed wording of parent consent forms.
-
Reviewed parents’ web resources page.
-
Reviewed wording, content and design of the parent online survey, for example made suggestions to improve clarity, reduce repetitiveness.
-
Reviewed content of the questionnaire of one of the Child Talk PhD students.
-
Helped design the national consensus events parent recruitment strategy, for example selecting appropriate times that avoid school pick-up, using text reminders, reminding parents that travel costs are covered.
-
Designed, scripted and provided the voiceover for an animated recruitment video. The panel had many suggestions for improvements to the animation video, such as the need for more perspective with the main characters clearly set in front of a park scene/the child being more clearly isolated and the need to show the child’s speech as broken/to show their frustration.
-
Designed and took part in SLT activity modelling videos.
-
Helped to decide the participant group for phase 2.
-
Developed a strategy for recruiting parents through the community, for example advertising through doctors’ surgeries, children’s centres, Netmums, flyer drops at public venues (libraries, swimming pools, etc.) and leaflets for book bags, providing free play sessions or a free crèche at groups, speaking to parents on the telephone and engaging parents during the summer holidays.
-
Designed parent adverts and flyers, including providing advice on using colours and starting with a question/hooking parents in.
-
Designed and reviewed parent information sheets and gave feedback on keeping writing concise and the use of texts to remind parents of the time/date of groups
Outputs
-
Recruitment video: https://youtu.be/fn3ebCd1vc0 (accessed 23 April 2015).
-
SLT videos and survey: www.youtube.com/user/BristolSLTRU (accessed 19 January 2015).
-
Patient information sheets and consent forms.
-
Adverts and flyers.
-
Numbers of parents recruited.
Research delivery
Contributions
-
Practice sessions for the research assistants undertaking telephone interviews; feedback included being explicit about recording and anonymity, taking details of the child’s age to deliver appropriate childcare and being clear that there are no required future commitments but opportunities for involvement if the participant wishes.
-
Attendance at national consensus event.
-
Attendance at co-applicant meeting.
-
Distribution of flyers and adverts to parents.
-
Designed poster for co-applicant meeting.
Outputs
-
Numbers of flyers distributed.
-
Feedback from SLTs on having parent panel member present – validity of research.
-
Feedback from research assistants on interview practice.
-
Contribution of parents to co-applicant meeting (input into new research questions).
-
Parent poster for co-applicant meeting.
Research analysis/research recommendations
Contribution
-
Lay description of themes of SLT-led interventions.
-
Interpreting the research findings to develop key messages for parents.
-
Discussion of research findings; topics raised included if the theme ‘participation’ is an outcome not an aim of therapy and suggestions for future research, including determining whether sites that collect data for economic analysis are more diligent in other areas.
-
Development of the intervention framework website including a range of feedback and suggestions:
-
need to clarify aims, that is, present research findings or something that would help (or both)
-
parents will be interested in the tool and making it accessible but will not want information about how it was developed
-
need to inform parents of the importance of the early years
-
a website map to avoid frustration if users click on the wrong area
-
would like to see case studies of other children with those difficulties
-
videos of therapy types, including a link to the typology, would be interesting for parents
-
information on what SLTs do, where to go to get help and services available and case studies of parents saying how speech and language therapy helped.
-
Outputs
-
Accessible intervention framework website (website in development; please check www.speech-therapy.org.uk for updates).
-
Key messages for parents.
Dissemination
Contributions
-
Designed research poster for the INVOLVE conference (Nottingham, November 2012).
-
Prepared research summary for research participants.
-
Wrote the plain English summary for the final report.
-
Contributed to reporting of public–patient involvement (PPI) in the final report.
-
Strategy for dissemination of research findings to parents and the public:
-
SLTs to act as a link to make information available for parents
-
leaflet before seeing the therapist for the first appointment so know where the tools are on the web
-
expect this information to be available at general practices, nurseries, from health visitors
-
Afasic, the RCSLT and the Communication Trust to signpost the website.
-
Outputs
-
Research poster presented at the INVOLVE conference.
-
Final report with embedded PPI.
Other activities
-
Being part of the advisory group.
-
Contribution to new research ideas.
-
Logo design.
-
Identifying ideas for training for future panels:
-
using social media
-
what is research? – how is it set up?, how do you get funding?
-
different types and methodologies of studies
-
what are the different levels of evidence?
-
Impact on the parents
The research team tried a variety of methods to capture the panel’s experiences, including questionnaires and the use of a blog. After discussions with the panel and with the support of Afasic, it was decided that informal discussion and drawing would be more effective for collecting the qualitative data. Members of the panel were asked at the start, middle and end of the programme to draw pictures representing how they felt at various stages in the research programme and to attach speech bubbles to express their feelings at those points. The questions included the following themes: What motivated you to become involved in Child Talk?, How did you feel (at the first meeting, after a year, at the end)?, What is your role on the programme?, Were there any particular activities that you have enjoyed?, What have you gained from the experience?, What would you like to do next?
In relation to the question, ‘Were there any particular activities that you have enjoyed?’, one parent noted the following regarding the distribution of recruitment adverts in the local community: ‘This is what I am doing, I feel involved, passionate excited by explaining it to others, feeling I’m part of it’.
The parents were all motivated by a combination of personal and professional reasons. Two of the parents work in a nursery and they feel that their knowledge base about speech and language has increased and they believe that this has improved their ability to identify children’s communication difficulties. One member felt that being part of the programme would help her to network with professionals and would be a useful aid to returning to work as a primary school teacher. She has achieved this goal. Another member wanted to gain useful experiences for his CV and has valued learning about speech and language therapy and research.
All of the parents indicated that they valued being part of a research project that will improve outcomes for children, although they felt frustrated about the difficulties in recruiting other parents to participate in the study. The following quote from a panel member indicates why she felt that her role on the panel was important:
It has been a really interesting process to go from the beginning a bit mind blowing to start with as there was a lot going on . . . Because, it just made me feel that we were helping to extend research to reach other parents; as I think early intervention for children is so important, it such an obvious one that is just not being met.
All of the panel members said that they have learnt a lot about research processes and that they are now actively interested in research and how the evidence is put into practice. On a personal level they enjoyed learning that their opinions were important and that their input did make a difference to the programme.
The panel agreed that it was important to consult other parents on future research topics arising from the Child Talk programme. One panel member consulted all of the parents attending the nursery where she works and the panel led a consultation with parents in a public soft-play facility to decide on the ordering and prioritisation of research questions arising from the Child Talk programme. Three of the panel members are planning to carry on working with the research team to disseminate the results and to design the Child Talk website. They have also agreed to be mentors for new panel members and collaborate on future research projects.
Impact on the research unit
The research team has been inspired by the ideas of the parent panel and believes that its input has greatly enhanced the implementation and delivery of the parent-focused strands of the Child Talk programme. The panel was a useful resource for the research team to try out ideas and techniques, for example members of the research team practised their interview technique before undertaking telephone interviews with the study participants. The PhD students consulted with the panel on how to design their studies and develop their recruitment strategies. The dialogue process between the panel and the researchers has helped them to clarify ideas and formulate ways of clearly expressing the research findings. This included writing an abstract and producing a poster for the INVOLVE conference in Nottingham (Coad R. Parent Involvement, Making it Meaningful. INVOLVE conference, Nottingham, UK, November 2012).
The parent involvement journey has resulted in a culture change in the BSLTRU. A public involvement and engagement strategy has subsequently been developed that sets out our vision to embed PPI in all aspects of the research unit’s activities at all levels (strategic, operational and project specific). From this, a 3-year delivery plan has been developed with supporting documentation including a tool for evaluating the impact of PPI. The vision is to embed public involvement into the heart of the research unit’s operational and strategic activities to ensure that all of the projects are relevant to people who have speech and language difficulties.
Appendix 8 Example topic guide for the speech and language therapist focus groups
S etting ground rules.
Introductions.
As stated in the information sheet, during this focus group we will ask you about:
-
the interventions you use
-
how and why you think they work
-
what does not work well and
-
if/how you adapt them based on family/child/contextual factors.
It may be slightly different from the information that you were first sent, as each group builds on the previous one. We will not be asking you to discuss specific real cases but will use examples to prompt further discussion. Your responses will help us to design a questionnaire that will be sent to SLTs in England, to discover the range of ways in which they work and their reasons for their decisions, and also to develop a model of intervention.
There are NO RIGHT answers and this is not a test of your knowledge. You may recall that the purpose of this phase of our research is to describe the range of practice that SLTs use and the child and contextual factors that influence decision-making.
Define significant terminology
To help us make the most of your valuable time and expertise, we have already provided you with some ‘working definitions’ and given you a more detailed idea of what we plan to discuss.
A reminder:
-
Children with primary speech and language impairment (PSLI): A preschool child who has (in the last 6 months) been identified, by a SLT, as having a significant language impairment. The child may or may not have co-existing speech impairments. There is no indication that the child possesses other neurological, sensory or developmental conditions including hearing impairment, autism and learning difficulties that might account for the language impairment.
-
Intervention: Those actions, techniques, activities and procedures that are used to facilitate progress, prevent other problems, modify barriers and facilitate changes to the communication environment.
-
Outcomes (for the child): The effects of the intervention, that is, the change that you expect to see in the child by the end of the intervention.
-
Mechanism (of change): The explanation of how the intervention that is provided causes the communication outcome you intended, for example (the explanatory steps) how a suggestion to a parent to spend some time each day with the television switched off leads to an improvement in the child’s speech, language and communication skills.
First of all I just want to find out how you think about what interventions you use with these children with PSLI and we are really interested in the components, not just the name of a programme. We aim to do this in two ways today.
Describe your favourite intervention
Treat this as an expository task. 310
-
What is your favourite intervention for preschool children?
-
Why is [x] your favourite intervention?
-
I’m not too familiar with [x] so I would like you to tell me all about it. For example, tell me what the goals are and how deliver it. Tell me everything you can think of about [x] so that a therapist who has never done it before will know how to use it.
-
Now I would like you to tell me what a SLT should do in order to deliver it in the most effective way possible (or if you delivered it in the most perfect way, what would it look like).
-
In other words, what are the key components of that intervention that every SLT should know?
-
What are the things that are likely to make you adapt or change it and why?
-
(If appropriate) how does it differ from what would be offered by early years practitioners?
Describe your most typical child with primary speech and language impairment
-
Jointly create a vignette of a most typical child.
-
What would you do to support this child/family? Again, think about components.
-
What’s the one thing that you would say is a central component?
As they reply, the observer records on a flip chart (and tries to categorise, e.g. activities, strategies and targets/goals).
-
Do you always do all of these things? If not, what might lead you to do something different?
-
Discuss the factors and influences that might result in the modification of intervention activities, strategies and targets.
-
Discuss how intervention/targets might be modified.
Additional probes
-
How would it differ from what an early years practitioner might do with this child before referring to you?
-
What would you do after the period of assessment and initial advice (i.e. after parent–child interaction)?
-
What is it about the intervention that makes it effective?
-
When does it not work?
-
For children with PSLI, what do you see as the likely cause of their problems?
-
How does that impact on what you decide to do with a child?
Appendix 9 Topic guide for parent focus groups
S etting ground rules.
Introductions.
As we explained in the information sheet, we want to understand your views as parents on what speech and language therapists do with your children. This is part of a larger project to try and improve how services are targeted for individual children and their families. Before we go any further, it would be helpful if we all knew just a little bit about each other, so I’m going to ask you all just to say your name and the name and age of your child and just something brief about their speech and language.
Question 1: The first thing I’d like us to discuss is what happens when you take your child to the speech and language therapist
Probes:
-
What sort of activities do you do (together, separately)?
-
Tell me about a typical session – how long does it last, what do you do, what sorts of toys, games, activities do you use, what do you do during the session, what does your child do, what do the therapists do, were you given suggestions of things to do at home?
-
For anything that they offer ask – what do you thing the therapist was trying to achieve? Did it work?
-
Did you understand everything that went on?
-
Any views about:
-
the advice you were given, the amount of time required, location, materials used
-
targets that were set, planning for what happened, review/discharge
-
frequency, amount of time required, resources available (toys, games, handouts, leaflets).
-
Question 2: What sort of changes have you seen in your child since you started seeing the speech and language therapist?
Probes:
-
How far were the changes the result of what the therapists did or the result of what you or others did?
-
Did you change what you were doing with your child as a result of going to see the speech and language therapist?
Question 3: Was there anything that the therapist did or said that was particularly helpful? Or not helpful?
Question 4: If you could change anything about what happened what would it be?
Appendix 10 Topic guide for early years practitioner focus groups
S etting ground rules.
Introductions.
As stated in the information sheet, during this focus group we will ask you about your experiences of children with speech and language difficulties.
We are going to refer to them as children with PSLI (and we’ll define that in a bit).
Specifically we are interested in:
-
how you support children with PSLI and
-
your experiences and perceptions of speech and language interventions (we will be asking how effective you think different types of intervention or methods are).
We will not be asking you to discuss specific cases but, if you have examples, we need you to remember about confidentiality for the children and families you refer to. We will use ‘true to life’ examples to prompt further discussion.
-
Additionally we would like to gain insight into the factors that you think encourage and discourage parents accessing speech and language services for their children.
(For focus group 2 and later: if/how you adapt them based on family/child/contextual factors.)
Your responses will help us to understand how EYPs and SLTs work together to help young children.
Before we start, please all say your name for the tape.
Define significant terminology.
Just to make sure we are all talking about the same kinds of children:
-
Specify age range: 2 years to 5 years 11 months.
-
Children with primary speech and language impairment (PSLI): what do you understand by this? What sorts of terms do you use to describe children with speech, language and communication needs. (As they describe people, gradually refine so that we have an agreed definition of PSLI.)
Discuss interventions for children with PSLI.
There are NO RIGHT answers and this is not a test of your knowledge. You may recall that the purpose of this phase of our research is to describe how EYPs work together with SLTs to support young children with PSLI.
We want to identify the typical way that you work with SLTs to support children with PSLI.
Give me an example of a PSLI child that you have worked with, together with the SLT, during this last term (obtain descriptions of age, family, context, speech language and communication).
-
Describe the main intervention that you have used? What did you do (when, how often, resources) and why?
-
What are you trying to achieve?
-
Would anyone else do this kind of thing?
-
What might you do differently and why?
-
What do you think works particularly well and why?
-
What is less successful and why?
If time:
-
How do the parents who you work with respond to interventions
-
What involvement with SLT?
-
What promotes good collaboration between parents and SLTs?
-
What kinds of issues cause problems and what sorts of solutions have they found?
Appendix 11 Topic guide for underserved focus groups
The topic guide for all sessions covered the following topics, although methods used to elicit contributions and whether all topics were covered varied between groups.
-
(How do children learn to talk?) What are the important influences in children learning to talk?
-
If a child has difficulties learning to talk:
-
How can you tell/what are the signs when a child is having difficulties?
-
At what age would you worry about a child not talking?
-
What reasons do people give for children having difficulties learning to talk? (they themselves, family members, spouses, the older generation and other people in their community here and in their home community)
-
-
Reponses (they themselves, family members, spouses, the older generation and other people in their community here and in their home community) to a child having difficulties learning to talk.
Additional topics (or topics that were probed further) for the carers of looked-after children were:
-
experiences of speech and language therapy
-
barriers to speech and language therapy.
Appendix 12 Example of ‘essential’, ‘advisory’ and ‘do not use’ activity at the Specific Interest Group events
Typology theme ‘fostering understanding’
| Intervention | Essential | Desirable | Do not use it | Comments |
|---|---|---|---|---|
| Talk about communication styles | □ | □ | □ | |
| Showing video footage | □ | □ | □ | |
| Providing opportunities to practise strategies | □ | □ | □ | |
| Providing instructions in play | □ | □ | □ | |
| Providing information prior to groups | □ | □ | □ | |
| Providing games that parents are able to take home | □ | □ | □ | |
| Practising strategies with parents | □ | □ | □ | |
| Pointing out good/bad strategies as you are working with them | □ | □ | □ | |
| Parent workshops/groups | □ | □ | □ | |
| Parent–child interaction | □ | □ | □ | |
| Getting parents to make things with the child, e.g. collage | □ | □ | □ | |
| Explaining things that help communication | □ | □ | □ | |
| Explaining the importance of working on input first | □ | □ | □ | |
| Explaining that language/vocabulary needs to be functional | □ | □ | □ |
| Intervention | Essential | Desirable | Do not use it | Comments |
|---|---|---|---|---|
| Developing play experience with the parent | □ | □ | □ | |
| Being positive about the child | □ | □ | □ | |
| Other (please specify) | □ | □ | □ | |
| Other (please specify) | □ | □ | □ |
Appendix 13 Example of the assessment activity for typology themes at the Specific Interest Group events
| Formal | Informal | Goal | Which formal assessment(s)? | All or part of assessment | Which part most? | If informal, what do you do? |
|---|---|---|---|---|---|---|
| □ | □ | Comprehension | All □ Part □ | |||
| Definition: Working directly with the child to increase their understanding of spoken language | ||||||
Appendix 14 Screenshot of the speech and language therapist assessment tool survey
Appendix 15 Questions in the speech and language therapist intervention survey 1
The following questions were addressed in survey 1:
-
How often do you use the following activities with preschool children with PSLI?
The activities listed were:
-
turn taking
-
singing hello/goodbye songs
-
what’s in the bag/box
-
barrier games
-
auditory memory activities
-
visual timetables
-
information-carrying words
-
concepts training
-
basic vocabulary
-
sequencing sounds
-
minimal pairs
-
maximal oppositions
-
auditory discrimination
-
rhyme awareness
-
cued articulation
-
phonological awareness
-
core vocabulary
-
auditory bombardment
-
focused auditory stimulation
-
segmentation and blending
-
other (please specify in free text box).
-
-
How often do you use the following strategies with preschool children with PSLI?
The strategies listed were:
-
providing a daily routine or structure
-
making intervention activities functional
-
increasing/improving eye contact
-
getting on the child’s level
-
going at the child’s pace
-
allowing the child to choose the activity
-
making the activity fun
-
creating trust
-
using praise
-
role reversal
-
reducing distractions
-
modelling
-
scaffolding
-
extending
-
chunking
-
providing commentary to child’s activities
-
repeated practice
-
making activities structured
-
having clear expectations
-
using singing or music
-
reducing the pressure on child to speak
-
giving the child time to respond
-
reducing questions.
-
-
Would you adapt your interventions in relation to the following factors?
Factors listed were:
-
age of the child
-
child’s speech, language and communication diagnosis
-
the severity of the disorder
-
child’s previous progress
-
developmental appropriateness of the intervention
-
child’s gender
-
child’s medical history
-
poor behaviour
-
English as an additional language for the child
-
bilingual family
-
level of child’s interest or engagement
-
child’s level of self-awareness
-
birth order
-
ethnicity
-
maternal depression
-
paternal engagement
-
parental understanding
-
parental preference
-
parent concern
-
culture
-
religion
-
attendance
-
views of other professionals around the child
-
family socioeconomic status
-
urban/rural/remote location
-
resources available
-
home environment
-
sociopolitical context
-
please list any other factors that might lead you to adapt your intervention (in the free text box).
-
-
Please tell is us about a common intervention that you use with preschool children with PSLI, how you might adapt it and why (free-text response).
-
How many years have you been qualified?
Possible response options were:
-
0–2 years
-
3–5 years
-
6–10 years
-
11–20 years
-
20+ years.
-
For questions 1–2 the response options were always with all children, always with language delay/disorder, sometimes with language delay/disorder, rarely with language delay/disorder, always with speech delay/disorder, rarely with speech delay/disorder, sometimes with all children and never.
For question 3 the response options were yes/usually/occasionally/no.
Appendix 16 Questions in the speech and language therapist intervention survey 2
Thank you for agreeing to complete this questionnaire. We are using the results of this questionnaire to help us identify which interventions speech and language therapists (SLTs) use with preschool children (aged 2 years to 5 years 11 months) with primary speech and language impairment (PSLI) and what kinds of factors might lead them to modify their interventions. Through collecting data from lots of SLTs we are hoping to build a picture of practice for preschool children with different background and context factors.
All of your responses will need to be based on a child from your recent caseload. There is an opportunity to complete the questions for more than one child. We will provide space at the end for you to add any comments on issues that we have omitted or where your responses do not fit any of the options. We are interested in the components of interventions and therefore we have not listed programmes or resources. The options provided should cover most if not all components of relevant programmes.
The questions are split into five sections and the whole questionnaire should take you 20 minutes to complete in total. In this survey we are interested in your work with preschool children (aged 2 years to 5 years 11 months) with PSLI. We know that this is not a term that you may use in your everyday work but we hope that you will recognise the description of PSLI given here:
A preschool child who has been identified, by a speech and language therapist, as having a significant language and/or speech impairment. There is no indication that the child possesses other neurological, sensory or developmental conditions including, hearing impairment, autism and learning difficulties that might account for the language impairment.
Section 1: questions about you
-
Have you worked with children with PSLI in the last 12 months?
-
Where do you work primarily?
-
How many years since you qualified as a SLT?
-
How many years of experience do you have working with children with PSLI?
-
What is your NHS band (If non-NHS, equivalent if you know)?
-
Who is your main employer?
-
In what location(s) do you work? (tick all that apply)
Section 2: questions about a child on your caseload
In order to answer the rest of the questions in this survey, we need you to think of a child on your caseload who has PSLI and who was aged between 2 years and 5 years 11 months when you last saw them. The child should be someone who you have seen for intervention and who has either completed an episode of care or been discharged within the last 6 months. The remainder of this survey relates to this child. Keep this child in mind as you answer the next four sections.
The child (characteristics)
-
What age was this child when you last saw them?
-
How would you describe the primary nature of the child’s difficulties?
-
Is the child a boy or a girl?
The intervention delivered for this child
-
How was the intervention delivered for this child? How frequently do you have contact with the child or the family or other caregivers (e.g. nursery staff)?
-
Roughly how many times have you or the other agent of therapy provided intervention for this child in total?
-
Where was the intervention delivered for this child?
The child (presentation)
These questions are all specifically related to the child you have in mind.
-
Did this child have medical history such as low birth weight, birth trauma, syndrome, etc. that impacted on their speech and language development or intervention?
-
Did the child speak English as an additional language?
The following questions refer to how the child presented at the beginning of the intervention:
-
How did you rate the severity of the child’s PSLI?
-
How did you rate the effect of the PSLI on the child’s activity and participation?
-
How did you rate the child’s behaviour?
-
How did you rate the child’s attention and listening skills?
-
How did you rate the child’s confidence?
-
How aware was the child of his/her difficulties?
-
How frustrated did the child appear to be by their PSLI?
The following question refers to how the child presented during the intervention:
-
How engaged was the child with intervention?
Please tick any of the following that were important factors in selecting the intervention/s to be used with this child. Select as many as you wish.
Section 3: family factors
These questions are all related to the child’s family.
-
How would you describe the child’s ethnic heritage?
-
Were you aware of the family’s religious beliefs/practices impacting on (your choice of) SLT intervention?
-
Were you aware of the primary caregiver/s having mental health difficulties that impacted on (your choice of) SLT intervention?
-
Was there a family history of unclear speech or slow language development?
-
How many siblings/half-siblings did the child have?
-
Were you aware of any family cultural factors that impacted on (your choice of) SLT intervention?
The following questions refer to how the parents presented at the beginning of the intervention:
-
How did you rate the parents’ understanding of what was required of them in the intervention?
-
How did you rate the parents’ understanding of their child’s difficulties?
-
How did you rate the parents’ interaction skills with their child?
-
How concerned were the parents about the child’s PSLI?
-
Did the parents have strong preferences for the type of intervention the child should have?
The following questions refer to how parents presented during the intervention:
-
What was the parents’ attendance at appointments like?
-
How engaged were the parents with intervention?
Section 4: context factors
These questions are all about the environment beyond the family to which the child is exposed.
-
Please give an estimate of the predominant socioeconomic status of your caseload?
-
How would you classify the community type?
-
Was the child receiving some sort of preschool childcare provision?
-
Number of (half-day) sessions per week.
Section 5: intervention
-
Which of these interventions did you use with this child on your caseload/or did you encourage parents or other adults to do? (Please tick all that apply)
-
What other specific intervention activities or strategies did you use with the child? (Remember, we are interested in the intervention activities and not programmes. For example, if you used ‘Hanen’ or a Hanen-type approach, identify the components of Hanen such as encouraging parents to follow their child’s lead, rather than simply stating Hanen.)
Closing questions
-
Is this the first time you have completed this survey?
-
How many times have you completed this survey before?
-
Would you like to add any comments on issues we have omitted or is there anything you feel you have not been able to express in this survey?
Appendix 17 Screenshot of the parent survey

Appendix 18 Example search strategy for the systematic literature review
EMBASE (via Ovid)
Searched: inception to 30 September 2011.
URL: gateway.ovid.com.
Date of search: 1 October 2011.
-
exp Pediatrics/
-
exp CHILD/
-
exp INFANT/
-
child$.mp. [mp=title, original title, abstract, name of substance word, subject heading word]
-
infant$.mp. [mp=title, original title, abstract, name of substance word, subject heading word]
-
(paediatric$ or pediatric$).mp. [mp=title, original title, abstract, name of substance word, subject heading word]
-
toddler$.mp. [mp=title, original title, abstract, name of substance word, subject heading word]
-
boy$.ti,ab.
-
girl$.ti,ab.
-
(school child$ or schoolchildren$).ti,ab.
-
(pre school$ or preschool$).ti,ab.
-
or/1-11
-
speech disorder$.ti,ab.
-
speech intelligibility$.ti,ab.
-
speech therap$.ti,ab.
-
language therap$.ti,ab.
-
speech development.ti,ab.
-
speech delay.ti,ab.
-
language disorder$.ti,ab.
-
language development disorder$.ti,ab.
-
sign language$.ti,ab.
-
child$ language.ti,ab.
-
language therap$.ti,ab.
-
language development.ti,ab.
-
language delay.ti,ab.
-
nonverbal communication.ti,ab.
-
non verbal communication.ti,ab.
-
communication development.ti,ab.
-
exp Speech Disorders/
-
speech Intelligibility/
-
“rehabilitation of speech and language disorders”/ or language therapy/ or speech therapy/
-
Language Development Disorders/
-
Language Disorders/
-
Sign Language/
-
Child Language/
-
Language Development/
-
exp Nonverbal Communication/
-
Communication Disorders/
-
maternal responsiveness.tw.
-
directiveness.tw.
-
maternal interactive styles.tw.
-
compliance.tw.
-
maternal personality.tw.
-
child temperament.tw.
-
or/13-44
-
exp Mental Retardation/
-
exp child development disorders, pervasive/ or asperger syndrome/
-
Cleft Palate/ or Cleft Lip/
-
Otitis Media with Effusion/
-
exp Hearing Loss/
-
exp Blindness/
-
Stuttering/
-
Aphonia/
-
exp Pain/
-
Crying/
-
exp Analgesia/
-
Reading/
-
exp Dyslexia/
-
Cerebral Palsy/
-
(alternative and augmentative communication).mp. [mp=title, original title, abstract, name of substance word, subject heading word]
-
“alternative and augmentative communication”.mp. [mp=title, original title, abstract, name of substance word, subject heading word]
-
exp aged/
-
geriatrics/
-
or/46-63
-
(12 and 45) not 64
-
randomized controlled trial.pt.
-
controlled clinical trial.pt.
-
randomized controlled trials/
-
random allocation/
-
double blind method/
-
single blind method/
-
clinical trial.pt.
-
exp clinical trials/
-
(clin$ adj25 trial$).tw.
-
((singl$ or doubl$ or trebl$ or tripl$) adj25 (blind$ or mask$)).tw.
-
placebos/
-
placebo$.tw.
-
random$.tw.
-
research design/
-
“comparative study”/
-
exp evaluation studies/
-
follow-up studies/
-
prospective studies/
-
(control$ or prospectiv$ or volunteer$).tw.
-
(control$ or prospectiv$ or volunteer$).tw.
-
or/66-85
-
“animal”/
-
“human”/
-
87 not 88
-
86 not 89
Appendix 19 Subject headings used in the systematic literature review
| Subject headings | ERIC | CINAHL | ASSIA | Social Services Abstracts |
|---|---|---|---|---|
| 29. exp Speech Disorders/ | NA | Speech disorders | NA | NA |
| 30. Speech Intelligibility/ | NA | Speech intelligibility | NA | NA |
| 31. ‘rehabilitation of speech and language disorders’/or language therapy/or speech therapy/ | Speech therapy | Rehabilitation speech and language, speech therapy | Speech therapy, speech and language therapy | NA |
| 32. Language Development Disorders/ | NA | Language therapy | Language development | NA |
| 33. Language Disorders/ | NA | Language disorders | Language disordered preschool children, language disordered young children, language disordered children, language development, language disorders | Language disorders |
| 34. Sign Language/ | NA | Sign language | British sign language OR American sign language | NA |
| 35. Child Language/ | Child language | NA | NA | NA |
| 36. Language Development/ | Language acquisition | Language development | NA | Language acquisition |
| 37. exp Nonverbal Communication/ | NA | Nonverbal communication | Nonverbal communication skills, body language, emblematic gestures or facial expressions, frowns, gestures, nonverbal communication OR smiles | Manual communication |
| 38. Communication Disorders | Communication disorders | Communication disorders | Communication disorders | NA |
Appendix 20 The properties of papers in the systematic literature review
| Reference | Number of child participants | Child participant demographics (age and gender) | Context/location (e.g. home, clinic, preschool) | Study design | Delivered by | PEDro consensus | SCED consensus |
|---|---|---|---|---|---|---|---|
| Almost 1998161 | 30 | Experimental group (n = 13): 12 boys, 1 girl; age range 2 years 9 months–5 years 1 month (mean 3 years 7 months) Delayed treatment group (n = 13): 9 boys, 4 girls; age range 2 years 9 months–4 years 3 months (mean 3 years 5 months) |
Clinic | RCT (crossover design) | SLT | 9 | |
| Baker 2004167 | 2 | 2 boys aged 4 years 9 months and 4 years 4 months | Clinic | Case series | SLT | 7 | |
| Barratt 199270 | 42 | Intensive group (n = 18): 12 boys, 6 girls; age range 3 years 1 month–3 years 6 months (mean 3 years 4 months) Weekly group (n = 21): 15 boys, 6 girls; age range 3 years 2 months–3 years 7 months (mean 3 years 5 months) |
Nursery | Between groups | SLT | 6 | |
| Baxendale 2003176 | 37 | Experimental group (Hanen) (n = 19): 14 boys, 5 girls; age range 2 years 5 months–3 years (mean 2 years 7 months) Control (clinical) group (n = 18): 16 boys, 2 girls; age range 2 years 5 months–3 years 5 months (mean 2 years 10 months) |
Nursery/home | Pre/post between groups | SLT/parent | 6 | |
| Bunce 1985172 | 2 | 2 boys aged 4 years 1 month and 3 years 11 months | Language intervention preschool | Case series | SLT | 6 | |
| Buschmann 2009177 | 83 | PSLI groups: experimental group (n = 24), waiting group (n = 23): age range 2 years–2 years 3 months (mean 2 years 1 month) (gender split not given) TD group (n = 36): mean age 2 years 1 month |
Children’s hospital | RCT | SLT/parents | 7 | |
| Connell 1986173 | 6 | Age range 2 years 8 months–3 years 2 months (gender not specified) | Clinic/therapy room | Between subjects with a crossover treatment design (including multiple baseline measures) | Clinician | 6 | |
| Craig-Unkefer 2002185 | 6 | Three boy/girl dyads. Age range of all children 3 years 5 months–3 years 11 months | Head Start centre | Case series (three dyads), multiple baseline across dyads | Teachers/educationalists | 10 | |
| Craig-Unkefer 2003170 | 6 | Three boy/girl dyads. Age range of all children 3 years 1 month–3 years 11 months | Head Start centre | Case series (three dyads), multiple baseline across dyads | Teachers/educationalists | 10 | |
| Dodd 1989166 | 7 | 4 boys, 3 girls; age range 3 years–4 years 9 months (mean 3 years 8 months) | University clinic | Within subjects | SLT | 6 | |
| Forrest 2000144 | 10 | 8 boys, 2 girls; age range 3 years 4 months–4 years 6 months (mean 4 years 4 months) years | Clinic | Case series, single subject design with staggered baseline | Graduate student SLT | 8 | |
| Forrest 2001145 | 4 | 4 boys; age range 4 years 11 months–5 years 3 months | Clinic | Case series, multiple baseline | SLT | 6 | |
| Gallagher 2009174 | 24 | 18 boys, 6 girls; age range 3 years 9 months–5 years (mean 3 years 10 months) | Home and preschool | RCT | SLT/parent | 7 | |
| Gibbard 1994175 (study 1) | 36 | Experimental group: 12 boys, 6 girls; age range 2 years 5 months–3 years 3 months (mean 2 years 1 months) years Control group: 13 boys, 5 girls; age range 2 years 3 months–3 years 3 months (mean 2 years 8 months) |
Home | RCT | Parents | 7 | |
| Gibbard 1994175 (study 2) | 25 | Individual group: 7 boys, 1 girl; age range 2 years 3 months–3 years 3 months (mean 2 years 8 months) Parent–child interaction experimental: 6 boys, 3 girls; age range 2 years 5 months–3 years (mean 2 years 8 months) Parent–child interaction control group: 6 boys, 2 girls; age range 2 years 5 months–2 years 11 months (mean 2 years 7 months) |
Home and preschool | Between groups | SLT and mothers | 7 | |
| Gierut 1989146 | 1 | Boy aged 4 years 7 months | Clinic | Case study | SLT | 8 | |
| Gierut 1990147 | 3 | 3 boys; age range 4 years 1 month–4 years 10 months (mean 4 years 5 months) | Clinic | Alternating treatment design, multiple baseline, staggered start | SLT | 9 | |
| Gierut 1996148 | 7 | Age range 3 years 4 months–5 years 8 months; gender not specified | Clinic | Case series, multiple baseline, staggered start | SLT | 6 | |
| Gierut 1996149 | 3 | 3 girls; age range 3 years 7 months–5 years 6 months | Clinic | Case series, multiple baseline, alternating crossover design | SLT | 7 | |
| Gierut 1996149 | 6 | 5 boys, 1 girl; age range 3 years 5 months–5 years 6 months | Clinic | Case series, multiple baseline | SLT | 7 | |
| Gierut 1996153 | 2 | Two children aged 3 years 11 months and 5 years 2 months; no gender specified | Clinic | Case series, multiple baseline, staggered start | SLT | 6 | |
| Gierut 1999150 | 2 | 2 boys aged 4 years and 4 years 8 months | Clinic | Case series, multiple baseline, staggered start | SLT | 6 | |
| Gierut 2000151 | 1 | Boy aged 4 years 5 months | Clinic | Case study (ABAa) | SLT | 6 | |
| Gierut 2001152 | 8 | 6 boys, 2 girls; age range 3 years 4 months–3 years 3 months (mean 4 years 11 months) | Clinic | Case series, multiple baseline design, staggered start | SLT | 9 | |
| Girolametto 1996182 | 25 | Experimental group (n = 12): age range 2 year 1 month–2 years 11 months (mean 2 years 5 months) Control group (n = 13): age range 1 year 11 months–2 years 10 months (mean 2 years 5 months) |
– | Pre/post between groups | Parents | 9 | |
| Glogowska 2000169 | 159 | Therapy (n = 71): mean age 2 years 8 months Watchful waiting (n = 88): mean age 2 years 8 months |
Clinic and preschool | Between groups, observational | SLT | 8 | |
| Hart 2010154 | 3 | 3 boys; age range 3 years 7 months–4 years 11 months | Preschool | Case series, longitudinal | SLT | 8 | |
| Hegde 1979187 | 1 | Boy aged 4 years 9 months | Clinic | Case study, multiple baseline | SLT | 6 | |
| Hesketh 2007168 | 42 | Phoneme awareness group (n = 22): age range 4 years–4 years 7 months (mean 4 years 3 months) Language stimulation group (n = 20): age range 4 years–4 years 7 months (mean 4 years 3 months) Gender not specified |
Clinic | RCT | SLT | 6 | |
| Hund-Reid 2009160 | 30 | Experimental group (n = 22): 16 boys, 6 girls; mean age 5 years 6 months Control group (n = 8): 6 boys, 2 girls; mean age 5 years 5 months |
Preschool | Between groups | Teachers, occupational therapists, physical therapists, SLTs, educational assistants | 8 | |
| Justice 2008135 | 196 | 102 boys and 94 girls; 143 (73%) white, 36 (18%) black, 8 (4%) Hispanic, 6 (3%) unspecified, 3 information unavailable; 97% had English as a first language Age range 4 years–4 years 11 months at start of the study (mean 4 years 5 months) |
Three public preschools serving children deemed at risk | Between groups, pre/post study | Training to teachers delivered by SLTs | 6 | |
| Kim 2001178 | 4 | 3 boys, 1 girl; age range 5 years 2 months–5 years 10 months | Preschool | Case series, multiple baseline, staggered start | SLT | 9 | |
| Lafferty 2005141 | 4 | Language delay: 1 boy, 1 girl; TD 2 boys; age range 3 years 7 months–4 years 10 months | Preschool | Case series, multiple baseline, staggered start | SLT | 8 | |
| Lunkenheimer 2008136 | 731 | 51% boys; age range 2 years–2 years 11 months (mean 2 years 6 months) | Home | RCT | Clinician | 8 | |
| McGregor 1994139 | 2 | 2 boys aged 5 years and 4 years 9 months | – | Case series, multiple baseline design | SLT | 8 | |
| McIntosh 2008165 | 3 | 3 boys aged 3 years, 3 years 9 months and 4 years 2 months years | Clinic | Case series | SLT | 6 | |
| Olswang 1984183 | 2 | Boy aged 2 years 7 months, girl aged 3 years | University clinic | Case series, multiple baseline | SLT | 6 | |
| Robb 1999155 | 1 | Girl aged 4 years | Clinic | Case study | SLT | 6 | |
| Roberts 1989137 | 57 | Day care and parent group (n = 13), parent education group (n = 24), control group (n = 20) | Child development centre | Between groups | EYPs/parents | 7 | |
| Roth 2002142 | 8 | 5 boys, 3 girls; age range 4 years–6 years (mean 4 years 6 months) | University clinic | Case series, multiple baseline | SLT | 8 | |
| Rvachew 1994161 | 27 | 21 boys and 6 girls were split into three groups. Group 1, correct and incorrect pronunciation (n = 10): mean age 4 years 5 months; group 2, correct/correct pronunciation (n = 9): mean age 4 years 6 months; group 3, unrelated (n = 8): mean age 4 years 4 months | Clinic | Between groups | SLT | 6 | |
| Rvachew 2001164 | 48 | Early group (n = 24): mean age 4 years 3 months; later group (n = 24) mean age 4 years 1 month; no gender splits provided | – | Between groups | SLT | 6 | |
| Rvachew 2004163 | 34 | Experimental group (n = 17): 12 boys, 5 females; mean age 4 years 5 months Control group (n = 17): 12 boys, 5 girls; mean age 4 years 2 months |
Clinic | RCT | Research assistant | 6 | |
| Saben 1991158 | 2 | Boy aged 4 years 4 months and girl aged 3 years 9 months | Clinic | Case series, multiple baseline | SLT | 8 | |
| Shea 2001140 | 2 | Aged 3 years 1 month and 3 years 7 months; gender split not provided | Clinic | Case series, multiple baseline, staggered | SLT | 7 | |
| Skibbe 2011143 | 13 | 9 boys, 4 girls; age range 4 years 1 month–4 years 10 months (mean 4 years 5 months) | Home | Case series, multiple baseline | SLT/parent | 6 | |
| Spencer 2010184 | 5 | 1 boy and 4 girls; age range 4 years 3 months–5 years 1 month (mean 4 years 6 months) | Head Start centre | Multiple baseline across participants | Assistant SLT | 6 | |
| Stanton-Chapman 2008138 | 8 | 4 boys and 4 girls; age range 3 years 9 months–5 years (6 children had PSLI and 2 children were included because their teachers had concerns about their language; 3 children met criteria for having problem behaviour) | Head Start centre | Multiple baseline across dyads | Researcher acting as teacher | 10 | |
| Tardaguila-Harth 2007134 | 4 | 2 boys, 2 girls; age range 4 years–5 years 7 months | Home | Case series, staggered start, multiple baseline design | Parent | 9 | |
| Van Kleeck 200632 | 30 | 17 boys, 13 girls; experimental group (n = 15), control group (n = 15); age range 3 years 10 months–5 years (mean 4 years 2 months) | Head Start preschool | RCT | Trained research assistants | 7 | |
| Warren 1984179 | 3 | Boy aged 2 years 11 months and 2 girls aged 3 years 7 months and 2 years 3 months | Special preschool for children with additional language needs | Case series, multiple baseline | Teachers | 7 | |
| Washington 2007180 | 23 | 18 boys, 5 girls; age range 3 years 6 months–4 years 11 months (mean 4 years 3 months) | Clinic or home | Pre/post test | SLT | 6 | |
| Weismer 1993181 | 3 | 2 boys, 1 girl; age range 2 years–2 years 4 months | Playroom in laboratory | Case series, single subject alternating treatment design | Graduate student clinicians | 9 | |
| Winner 1988159 | 4 | Girl aged 3 years 10 months and 3 boys aged 4 years 3 months–5 years 8 months | None stated | Single subject, multiple baseline | SLT | 7 | |
| Wolfe 2003156 | 9 | 7 boys, 2 girls; age range 3 years 5 months–4 years 7 months Perception group (n = 4): 3 boys, 1 girl; age range 3 years 11 months–4 years 7 months Production group (n = 5): 4 boys, 1 girl; age range 3 years 5 months–4 years 2 months |
Clinic | Between groups | SLT | 6 | |
| Yoder 2005157 | 52 | Experimental group (n = 26): mean age 3 years 7 months; no gender split reported Control group (n = 26): mean age 3 years 7 months; no gender split reported |
Clinic | RCT | SLT | 7 | |
| Yoder 2011186 | 57 | Broad target recast group (n = 30): age range 2 years 6 months–5 years (mean 3 years 6 months) Milieu language teaching (n = 27): age range 2 years 6 months–5 years (mean 3 years 6 months) Gender split not provided |
Preschool for children with specific language impairment | Between groups | SLT | 8 | |
| Ziolkowski 2008171 | 13 | 5 boys, 8 girls; age range 4 years 2 months–5 years 4 months (mean 4 years 8 months) | Preschool | Crossover design with multiple baseline | Educators and paraprofessionals | 9 |
Appendix 21 Assessment and outcome measures used in the systematic literature review
| Reference | Assessment measures | Outcome measures |
|---|---|---|
| Almost 1998162 | APP-R, GFTA | APP-R, GFTA, PCC, MLU |
| Baker 2004167 | PCC, CELF-P, MLU, WPPSI-R | Initial/s/consonant cluster reduction, PCC, generalisation probes |
| Barratt 199270 | RDLS | RDLS |
| Baxendale 2003176 | PLS-3-UK, MLU, proportional number of utterances of parent and child, parental language-modelling techniques | PLS-3-UK, MLU, proportional number of utterances of parent and child, parental language-modelling techniques |
| Bunce 1985172 | PPVT, MLU | MLU, percentage correct scores on probes |
| Buschmann 2009177 | ELFRA-2 (the German version of the MacArthur Communication Development Inventories), SETK-2, SETK 3–5, Mental scale of the Bayley Scales of Infant Development – 2nd edn, Netherlands version, Mental Development Index | ELFRA-2 (the German version of the MacArthur Communication Development Inventories) SETK-2, SETK 3–5, encoding semantic information, plural forming |
| Connell 1986173 | PPVT, PLS | Number of correct responses to comprehension probes, number of correct responses to production probes, noun–verb–noun sentence percentage correct |
| Craig-Unkefer 2002185 | PLS-3, CBCL/2–3 | Child communication measures, lexical diversity, MLU, Peer Play Code |
| Craig-Unkefer 2003170 | PLS-3, SSRS | Child communication measures, lexical diversity, MLU, Peer Play Code |
| Dodd 1989166 | Test for Reception of Grammar, Test for Auditory Comprehension of Language, PCC | PCC, number of consonant phonemes, missing phonemes, relative influence on unintelligibility |
| Forrest 2000144 | CELF-P, PPVT-R, GFTA, 306-item probe, PCC, percentage of correct underlying representations, variable substitutes, consistent substitutes | PCC, percentage of correct underlying representations, variable substitutes, consistent substitutes |
| Forrest 2001145 | CELF-P, PPVT-R, GFTA | Sound omitted from inventory, treatment target, generalisation probe |
| Gallagher 2009174 | RDLS-III, RAPT, RWFT, WPPSI, BPVS, TEA-Ch | RDLS-III, RAPT, RWFT, TEA-Ch, comprehension of grammar, comprehension of vocabulary, expressive language, expressive grammar, expressive vocabulary |
| Gibbard 1994175 (study 1) | Denver Developmental Screening Test, McCarthy Scales of Children’s Abilities, RDLS, MLU, RAPT, DLS Picture Test | Denver Developmental Screening Test, McCarthy Scales of Children’s Abilities, RDLS, MLU, RAPT, DLS Picture Test |
| Gibbard 1994175 (study 2) | RDLS, MLU, RAPT, DLS Picture Test | RDLS, MLU, RAPT, DLS Picture Test |
| Gierut 1989146 | GFTA, PLS – Revised, phonemic awareness | Phonemic awareness – word-initial sounds, non-occurring word-initial sounds, percentage accurate production of 21 word-initial sounds |
| Gierut 1990147 | GFTA, TOLD-P:2, PPVT-R, MLU, Leiter International Performance Scale (Arthur Adaptation) | Picture-naming tasks, percentage accuracy on probe production, change in excluded but treated sounds, change in comparison sounds, change in excluded but untreated sounds |
| Gierut 1996148 | None given | Percentage mean probe accuracy |
| Gierut 1996149 | TOLD-P:2, TELD, GFTA | Percentage probe accuracy |
| Gierut 1996153 | GFTA, PPVT, percentage mean probe accuracy | Percentage mean probe accuracy, percentage final probe accuracy, phonemic inventory, phonemic redundancies |
| Gierut 1999150 | GFTA, receptive and expressive language | Change in chain shift pattern, place distinction, phonemic contrast, phonetic accuracy, percentage accuracy of production |
| Gierut 1999151 | GFTA, receptive and expressive language | Percentage accuracy, percentage probe accuracy, percentage ingressive use, word-initial egressive, word-initial ingressive, post-vocalic egressive, post-vocalic ingressive |
| Gierut 2001152 | GFTA, receptive and expressive language, production accuracy, percentage accuracy of production | Production accuracy, percentage accuracy of production, phonemic inventory, phonemic clusters |
| Girolametto 1996182 | Stanford–Binet Intelligence Scale, Developmental Profile – II, age-equivalent score on Symbolic Play Test, Sequenced Inventory of Communication Development, MacArthur Communication Development Inventories, phonetic inventory, utterances, words per minute, MLU, target words used, focused targets | MacArthur Communication Development Inventories, phonetic inventory, utterances, words per minute, MLU, target words used, focused targets, number of different words, number of different target words, number of different control words, diversity of target |
| Glogowska 2000169 | PLS, percentage error rate, Bristol Language Scale, Vineland Adaptive Behaviour Scales, symbolic play, TOMs | Percentage error rate, Bristol Language Scale, Vineland Adaptive Behaviour Scales, symbolic play, TOMs, phonology error rate, auditory comprehension, expressive language, phonology error rate |
| Hart 2010154 | PLS-4, HAPP, 3rd edn | PLS-4, HAPP, 3rd edn, TOMPD |
| Hegde 1979187 | PPVT | Percentage response correct |
| Hesketh 200777 | Edinburgh Articulation Test, CELF, British Ability Scales II, phoneme addition or deletion tasks, PCC, PIPA, Renfrew Bus Story, Metaphon screening assessment | Phoneme addition or deletion tasks, PCC, PIPA, Renfrew Bus Story, Metaphon screening assessment |
| Hund-Reid 2009160 | CELF-P-2, K-BIT2, TOPEL, DIBELS | TOPEL, DIBELS, initial sound fluency, letter-naming fluency, phonemic segmentation fluency, nonsense word fluency |
| Justice 2008135 | Teacher use of language stimulation teaching; child: gender, SES, preschool attendance | Expressive language skill (percentage complex utterances, rate of noun use, number of different words, upper bound index, Renfrew Bus Story |
| Kim 2001178 | PPVT, Preschool Receptive and Expressive Language Scale, MLU, correct responses on the script intervention | MLU, correct responses on the script intervention, percentage of correct semantic relations to training items, percentage of correct semantic relations to generalisation items |
| Lafferty 2005141 | Kaufmann Assessment Battery for children, GFTA-2, SPELT-P, RDLS, Test of Visual Perception Skills, MLU | MLU, number of correct probe responses |
| Lunkenheimer 2008136 | Demographic questionnaire, positive behaviour support questionnaire, parent involvement: Infant/Toddler HOME Inventory, RPC, Coder Impression Inventory, Fluharty-2, CBQ | Demographic questionnaire, positive behaviour support questionnaire, parent involvement: Infant/Toddler HOME Inventory, RPC, Coder Impression Inventory, Fluharty-2, CBQ |
| McGregor 1994139 | PPVT-R, Expressive One-Word Picture Vocabulary Test, sound mimicry subtest of the Goldman–Fristoe–Woodcock Auditory Skills Test Battery | PPVT-R, Expressive One-Word Picture Vocabulary Test, sound mimicry subtest of the Goldman–Fristoe–Woodcock Auditory Skills Test Battery, number of errors on confrontation naming probes, numbers of semantic substitutions, phonological substitutions, no response and self-corrections |
| McIntosh 2008165 | DEAP, PCC, percentage vowels correct, percentage phonemes correct, single words versus connected speech agreement | DEAP, PCC, percentage vowels correct, percentage phonemes correct, single words versus connected speech agreement |
| Olswang 1984183 | PPVT, SICD, Boyd Developmental Progress Scale, Ordinal Scales of Psychological Development, number of spontaneous imitations and number of spontaneous productions | PPVT, SICD, Boyd Developmental Progress Scale, Ordinal Scales of Psychological Development, number of spontaneous imitations and number of spontaneous productions |
| Robb 1999155 | PPVT-R, morphological analysis of 100 utterances, single-word picture-naming task | Morphological analysis of 100 utterances, single-word picture-naming task, PCC, percentage vowels correct, primary vowel substitutions |
| Roberts 1989137 | WPPSI, Woodcock-Johnson Psycho-Educational Battery | Mean number of words per communication, mean number of dependent clauses per communication, total number of different words, total number of different conjunctions, total number of different pronouns, number of complete and intelligible communication units, total number of words, responsiveness |
| Roth 2002142 | PPVT-III, GFTA, Expressive Vocabulary Test, Test of Early Reading Ability, 2nd edn, TAPS/NF, sound blending subtest of the Woodcock–Johnson Psychoeducational Battery – Revised, phonemic analysis subtest of TOLD-P:3 | PCC, accuracy of production (blending, segmentation, rhyming) |
| Rvachew 1994161 | RDLS, computerised analysis of phonological processes | RDLS, computerised analysis of phonological processes |
| Rvachew 2001164 | GFTA, PPKP | GFTA, PPKP, PCC |
| Rvachew 2004163 | GFTA-2, PPVT-III, DSS, PCC | Number of errors and raw data of GFTA-2, PPVT-III, DSS, PCC, phonemic perception, articulation (single word), articulation (conversation), phonological awareness, SAILS program |
| Saben 1991158 | Test of Auditory Comprehension of Language, PPVT-III, TELD, SPELT-II | Speech sounds over time (fricatives, affricatives, nasals, liquids, velars, initial voiceless sounds, clusters), generalisation of productions |
| Shea 2001140 | BBTOP, PLS-3, MLU, PCC, generalisation probes to examine all phases of the therapy sequence and untrained stimuli- assessed children’s productions of w-S stress patterns in untrained words and phrases and multisyllabic words | Generalisation probes to examine all phases of the therapy sequence and untrained stimuli; children’s productions of w-S stress patterns in untrained words and phrases and multisyllabic words |
| Skibbe 2011143 | TOLD-P:3, K-BIT, Wide Range Achievement Test, 3rd edn | PALS Pre-K |
| Spencer 2010184 | Renfrew Bus Story | Narrative retell and personal story generation |
| Stanton-Chapman 2008138 | SSRS, child behaviour checklist (CTRF), PLS-3 | Peer Language and Behaviour Code, MLU, use of target vocabulary, use of child’s name, relatedness, turn taking |
| Tardaguila-Harth 2007134 | PLS-4 Spanish edn, PPVT-R, parent use of PEER Steps (prompt, evaluate, expand, repeat), CROWD/FRASE (English/Spanish versions of acronym to summarise types of prompt that the adult has been trained to use – Completion prompts, Recall prompts, Open-ended prompts, Why prompts and Distancing prompts), child’s oral language production (range of nouns, verbs and ‘others’) | PLS-4 Spanish edn, PPVT-R, parent use of PEER Steps (prompt, evaluate, expand, repeat), CROWD/FRASE (English/Spanish versions of acronym to summarise types of prompt that the adult has been trained to use – Completion prompts, Recall prompts, Open-ended prompts, Why prompts and Distancing prompts), child’s oral language production (range of nouns, verbs and ‘others’) |
| van Kleeck 200632 | SPELT-II, cognitive ability using the Columbia Mental Maternity Scale, PLAI, PPVT-III | PLAI, PPVT-III |
| Warren 1984179 | Verbalisations following mands, total verbalisations, non-obligatory speech, percentage score for child’s ‘responsiveness’, MLU, PPVT, Houston Test for Language Development | Verbalisations following mands, total verbalisations, non-obligatory speech, percentage score for child’s ‘responsiveness’, MLU, mean number of verbalisations per observation, rate of total child verbalisation, non-obligatory verbalisations, percentage child responses |
| Washington 2007180 | K-BIT2, PPVT-IIIB, CELF-P, SPELT-P, Developmental Sentence Scoring | PPVT-IIIB, CELF-P, SPELT-P, Developmental Sentence Scoring |
| Weismer 1993181 | ELI, MacArthur Communicative Development Inventory Toddler Form, Bayley Scale of Infant Development, Stanford–Binet Intelligence Scale, Symbolic Play Test, Sequenced Inventory of Communication Development – Revised, MLU, PCC | ELI (Bates et al.311), MacArthur Communicative Development Inventory Toddler Form, Bayley Scale of Infant Development, Stanford–Binet Intelligence Scale, Symbolic Play Test, Sequenced Inventory of Communication Development – Revised, MLU, PCC, number of different words, correct productions |
| Winner 1988159 | GFTA, PPVT-R | Percentage correct scores on speech sample and probe list; compared by frequent probe, infrequent probe, spontaneous speech sample and target sound |
| Wolfe 2003156 | GFTA, PLS-3 | Articulatory improvement using ‘production probes’ (spontaneous picture naming, scored correct vs. incorrect) and ‘perception probes’ (SAILS program) |
| Yoder 2005157 | MLU, PCC, PLS-3, Leiter International Performance Scale – Revised, AAPS, Oral Speech Mechanism Screening Exam – Revised | MLU, PCC, AAPS |
| Yoder 2011186 | IPSyn, MLU, GFTA-2, expressive language, non-verbal cognition | IPSyn, MLU |
| Ziolkowski 2008171 | Stanford–Binet Intelligence Scale, 4th edn, SPELT-III, CELF-P, Get Ready to Read! screening tool, bead memory, pattern analysis | Rhyming IGDI, Alliteration IGDI, Initial Sound Fluency subtest of DIBELS, 6th edn |
Appendix 22 Characteristics of the children in the children’s groups
| Psedonymn | Age (months) | Gender | Ethnicity | Sole/birth order |
|---|---|---|---|---|
| Harry | 39 | Male | White British | 4/4 |
| Ted | 41 | Male | White British | 2/3 |
| Jade | 28 | Female | White British | Sole |
| Christopher | 26 | Male | White British | 2/2 |
| Natasha | 26 | Female | White British | 3/3 |
| Michael | 29 | Male | White British | 1/2 |
| Terry | 41 | Male | White British | 2/3 |
| Malcolm | 44 | Male | White British | 2/3 |
| Alton | 30 | Male | Black Caribbean, British | 1/2 |
| Lilly-Anne | 30 | Female | White British | 2/2 |
| Shakera | 40 | Female | Black African, Somalian | Sole |
| Jazz | 47 | Female | Bangladeshi, British | Sole |
| Tajo | 34 | Male | Black Caribbean, British | Sole |
| Bow | 38 | Female | White British | Sole |
| Arend | 45 | Male | Asian, British | 2/2 |
| Rob | 45 | Male | Asian, British | 3/3 |
| Sara | 36 | Female | White British | Sole |
| John | 36 | Male | White British | Sole |
| Saul | 36 | Male | White British | 3/3 |
| Giles | 36 | Male | White British | 2/2 |
| Ella | 36 | Female | White British | 2/2 |
| Charlotte | 48 | Female | White British | 3/3 |
| Sally | 48 | Female | White British | 2/2 |
| Rich | 48 | Male | White British | 2/3 |
Appendix 23 Structure of a typical children’s group session
Activity 1: the ‘Hello’ song
Children sat in a circle on the floor with one facilitator at the front leading the ‘Hello’ song. The other facilitators sat among the children on the floor. The facilitator went round in a circle singing ‘hello’ to all of the children and facilitators. All of the facilitators joined in and encouraged the children to sing along as well.
Activity 2: camera magic
Children were introduced to the cameras as if they became magic when the light was on. The facilitator rubbed her hands together as if creating magic and the children were encouraged to join in. Facilitators then helped attach the cameras to the children’s heads. This became a routine at the beginning of each session with which the children became familiar.
Activity 3: timetable
Using visual symbols on a board, the lead facilitator talked though the timetable for the session and encouraged children to listen.
Activities 4–6: speech and language therapist activities
Speech and language therapist activities were predominantly facilitator directed, sedentary and quiet and involved turn-taking activities with children watching and waiting. Children were encouraged to listen to verbal instruction alongside visual demonstration and physically interact with objects and toys and sometimes make verbal expressions.
Listening and attention
These activities involved children sitting in a circle and taking turns to hold or play with toys or other objects, such as taking it in turns to roll a ball or play a musical instrument.
Developing language, building language
These activities often involved waiting and listening skills such as turn taking but they also encouraged the expression and development of speech, language and sign, for example a ‘nonsense rhyme’ about a monster and a postbox to identify what food the monster wants to eat.
Break
Activities 7–10: drama and arts-based activities
These had a more active format with the children moving from the floor to standing up and moving around the room. The facilitator sometimes directed children, sometimes guided them and sometimes followed their leads. Activities involved more simultaneous participation. Children were encouraged to copy and follow movements and were rarely expected to express themselves verbally.
Activity 7: creating a safe space, exploring movement qualities and assessing mood
These activities aimed to create a safe space for children to express themselves and explore movements and for the facilitator to assess mood. Children were invited to choose a coloured cloth from a basket. Each child’s cloth was spread out on the floor and children were encouraged to move in different ways on the cloth following the facilitator’s lead. Children also took it in turns to do something imaginative or movement based with their cloth, such as using it as a magic carpet or pulling it in different directions. This cloth play aimed to provide distance from ‘self’ to become less self-conscious and more confident in their choice of behaviours.
Activities 8–10: Kitty Kite
Children were encouraged to sit on the floor and Kitty Kite, a large yellow kite with a face, was flown into the room and said ‘hello’ to the children. Kitty Kite provided children with a transition from the here and now to an imaginary space. Following Kitty Kite, ‘the main event’ would take place, such as a story or a drawing activity. After the main event, children were encouraged to run around the room following Kitty. Kitty then said goodbye to the children and was flown out of the room. In this way Kitty provided a final transition back to the real world of the children.
Activity 9: the main event
The main event was either a story or a drawing activity. Stories such as The Three Little Pigs were enacted by the facilitator and children were encouraged to join in with actions and words in the story. The stories were linked to earlier SLT activities, such as expression of animal noises. The drawing activity involved colouring in stick men and then playing with them. The facilitator used the activity to explore children’s emotions.
Appendix 24 Detailed content of activities in the children’s groups
| Activity | Aims/rational |
|---|---|
| ‘Hello’ song | Settle the children |
| Visual timetable | Provide the children with a routine for the session |
| Miniature world/DLS games | Develop imaginative play; develop listening skills; model and expand language; assess word levels |
| Click Clack Track | Good turn taking during activities; develop waiting skills |
| Ball rolling with ‘ready steady go’ or ‘fast and slow’ | Introduce ‘where’ and ‘who’ Makaton signs; turn taking during activities; develop waiting skills; encourage good eye contact |
| Hide and seek in the den | Introduce ‘where’ Makaton sign; turn taking during activities; develop waiting skills |
| Lion (soft toy) ‘on’ head | Introduce ‘where’ Makaton sign |
| Bubbles | Develop attention; waiting and turn-taking skills; elicit ‘bubbles’; basic vocabulary |
| Bricks | Model and expand language; shared attention |
| Tea party | Develop imaginative play; develop listening skills; model and expand language; commenting |
| Play activities | Shared attention and enjoyment; adult modelling play and language; expanding on language used by the children; commenting |
| Musical instruments | Develop listening skills; turn taking |
| Listening to animal noises (wearing a mask or running to a mask or soft toy when hearing the sound) | Develop listening skills |
| Matching objects to gesture, ‘feely’ bag, name objects | Basic vocabulary; naming objects/pictures; turn taking |
| Putting things in a tube | Modelling basic vocabulary |
| Push down and let go train | Turn taking; attempting to elicit ‘go’ |
| ‘Simple Simon Says’ | Looking and attention skills; introduction of ‘what’ Makaton sign |
| Parachute game | Turn-taking skills; listening skills |
| Shopping games based on DLS | Turn-taking skills; develop waiting skills |
| Emotions story | Understand emotions |
| Nonsense rhyme – food names, children’s names and soft toys | Detect nonsense rhyme |
| Syllable clapping (identification) | Identify the number of syllables in a word |
| Using initial sounds /p/, /k/ /m/ /d/ and /f/ matching sound symbol picture, gesture and object with first sound of words | Identify and discriminate initial sounds |
| Real rhyme detection | Detect a rhyme |
| Robot talking | Blend a segmented word |
| Who game | Practising ‘who’ with Makaton sign |
| Where game | Practising ‘where’ with Makaton sign and encouraging expressive language at the three-word level |
| ‘If You’re Happy and You Know It’ song | Learn about emotions |
Appendix 25 First draft of the typology with illustrative quotes
Foundation skills
Work to practise and improve a range of early skills that are considered to be foundations for speech and language development.
Activities that therapists reported using to support foundation skills included work on turn taking, play, attention and listening.
We might see nothing in terms of the increase in terms of their language levels but if we see an improvement in their attention and listening skills we know we’ve put that building block in that will eventually lead to . . .
SLT_095
For me it’s an exception to work with children below four on speech sound difficulties rather than a rule because of attention so I would be very much looking at is there attention able to support successful intervention below four.
SLT_002
. . . work around the kind of listening skills so their attention and listening erm their eye contact, their anticipation, so it’s looking very much at those early pre-verbal skills and assessing those at that initial appointment and determining whether or not we feel they’re at a level in order to access what we’re offering.
SLT_098
Sound awareness
Activities that aim to improve children’s listening and perception of sounds as well as their understanding of how these are important for speech and language.
Therapists reported using a wide range of sound awareness activities; these included listening to environmental sounds such as musical instruments, auditory bombardment, rhyming, syllable counting and activities focusing on discrimination of sounds such as front and back sounds and minimal pairs.
I might do auditory bombardment games, so um where they listen to the words all beginning with or all end in the same sound again and again and again. I might get them listening to minimal pairs.
SLT_001
. . . to increase their awareness of sounds and knowing like with the syllable counting and compound words knowing that words are made up of different parts and thinking about which sounds fit in to the word.
SLT_005
Parent or adult understanding/empowering parents
Helping parents to understand the nature of their child’s speech and language difficulty, what helps to improve it and why, an important aspect of this being parents’ or adults’ understanding that they are a vehicle for change.
SLTs rarely reported using specific activities or tools to do this; rather, explanation appeared to be a feature of everyday practice.
It’s about changing a parent’s perception of what [therapy group] is about isn’t it and helping the parents to take on board the fact that they have some input in to changing or supporting, developing this child’s language.
SLT_106
They have to accept that there is a problem, they have to accept that it is not the child being lazy, it is a difficulty that they have got and they have to accept that they are the major tool of change and they have to, sometimes they will do that, sometimes they won’t do the work. So they have to listen and actually do the work.
SLT_099
Parent/adult–child interaction
Work on interaction between the parent/adult and the child.
Speech and language therapists described a range of strategies or aspects of interaction that they might work on depending on the preferences and needs of the parents or adults involved. These interaction strategies ranged from things such as sitting and playing with the child or following the child’s lead to commenting on the child’s activities or reducing the number of questions asked of the child.
Very often we are looking at how we’re improving their communication environment so that we can get the best environment for them to be in to encourage their language to develop and that’s very much our role in doing that whether it’s working with parents either individually at home which we don’t do a huge amount of, or in groups or whether that’s working within settings to improve the quality of the interactions that are in the setting.
SLT_095
. . . usually go through the checklist where we look at good umm good communication I guess where we talk about do you wait for your child to to respond umm do you use too much language there’s lots of things and we tend to just look at a couple of those and have a feel for what the parents think is good interaction, and then what I might do then is umm set up a situation where we do some play umm to have go at thinking about some of those things.
SLT_019
Structure or content of language
Work that aims to improve the children’s expressive language, in quantity, vocabulary or structure.
Speech and language therapists described a wide range of activities that fit into this category. For instance, work might focus on producing single words, putting words together or learning new vocabulary, including verbs.
. . . think I’m just identifying opportunities in the day for them to target certain vocabulary or to target, sometimes its grammar it might be, but to be honest for most of my preschoolers it’s still at the stage of vocabulary.
SLT_017
If they are at the right level for information-carrying words than maybe a concept target and then some form of expressive language target, whether that is increasing single words or putting two words together or SVO [subject, verb, object] depending on the level.
SLT_063
Comprehension
Work that aims to improve the children’s receptive language.
Interventions in this area might overlap with work that focuses on the structure or content of language, for example vocabulary development. SLTs predominantly described comprehension tasks that focused on following directions and word-level activities.
Can they relate two objects together, can they gradually build up to things like can you brush dollies hair, give me the key, the spoon and the cup, can you put the spoon under the plate, so building up the different levels of language that the child can understand.
SLT_063
. . . a bed, a chair, a table or umm fridge/sink and some people and ask the child to do some actions with them, make the man jump on the table, make the boy hide under the table, so one one hand I’m checking their ability to follow that kind of instruction and we’re also feeding in the verb because I find an awful lot of my children know nouns, but don’t seem to have come very far with verbs and build up language in that way, and using very short sentences.
SLT_061
. . . target their vocabulary at that time or target that activity that they are doing and so if they’re doing the sing time they could do action songs, if we’re targeting verbs think of a time in the day that they can model lots of action words.
SLT_017
Participation
Focusing on language and skills or assistive materials/resources that help the child’s involvement and participation in life situations.
Speech and language therapists described a wide range of relevant interventions including materials and resources that help children to access language as well as those designed to prepare the child or help them cope in life situations.
Visuals and ‘now and next’ boards to help them to understand what’s coming next and what’s expected of them. And sometimes that fits in with the rewards system so it might be now story time but next you get to choose or do free play or whatever it might be, effectively facilitating the children like that and I think a lot of those things enable you to facilitate you getting interaction or play or facilitating strategies within a classroom that are then going to make life more predictable and easier.
A lot of those things enable you to facilitate you getting interaction or play or facilitating strategies within a classroom that are then going to make life more predictable and easier.
SLT_002
. . . to have the visual support to help them to understand the words and to link that umm or for expressive language to enable them to actually participate and to make a choice or to make their needs known because often, especially in nursery, they’re the child that is not getting their needs met or not being able to communicate.
SLT_017
Speech
Increasing the accuracy of speech production or articulation, often focusing on specific sound(s).
Speech and language therapists described a range of activities to work on speech, in particular drilling single sounds, working in hierarchy of sound production (consonant, consonant–vowel, consonant–vowel–consonant; C, CV, CVC), using minimal pairs, cued articulation and blending.
I always start with single sound production and lots of repetition of the single sounds so I usually do it so we play it alongside a game, pop up pirate or buckaroo or something on the table at the same time and you roll the dice and see how many times you each have to say the certain sound and then we get up to consonant and vowel together and then we’re looking at a minimal pair, preferably a CV minimal pair if there is one to start with and then other minimal pairs then I’d move up to single word level and then I do phrase level like blue or big or colours or sizes in front of the word and then up to sentence level.
SLT_002
We all do the same thing, so if it’s at CV level, I just have bunch of consonants on the one side and vowels on the other so if the child picks up the saw so /s/ is the consonant and the vowel, and blend them together and put them into the barrel and same with the fishing game, and like you know for blend or clusters then I try to sort of you know sometimes I try to use a train like a you know, put them together /cl/.
SLT_064
Self-monitoring
Activities or strategies that are designed to help the child’s awareness of their speech and language difficulties and how they might be able to overcome them.
Self-monitoring was raised most commonly in relation to speech disorder. Activities that SLTs described included some specific strategies for self-monitoring such as token systems as well as more general activities such as discrimination and cued articulation, which aimed to encourage children to reflect on their speech.
I would only do the kind of tongue twisters self-monitoring stages if they were really able in that age group, but I tend to use kind of tokens cause that’s the self-monitoring bit, is the bit that I always find is quite a big lip to get over.
SLT_002
Getting them to think, again laying some foundations so if they’re voicing later on we can say ‘oh do you remember that was our quiet sound’ or ‘that was our long sound’ or ‘that was our back sound’ and then back it up with cued articulation especially for ‘k’ and ‘g’.
SLT_001
Generalisation
Making speech and language or therapy gains transferable to other situations and environments.
Speech and language therapists rarely referred to specific activities to enforce generalisation (with the exception of self-monitoring activities for speech); however, they referred to the importance of parents and other adults working with the child to use activities and strategies in different contexts to encourage generalisation.
. . . shared target that then is going to give the child lots and lots of opportunities to learn that whatever it is, vocabulary, or the grammar and so a lot of it is probably repetition and the other the thing is to try and generalise it into lots of different contexts so that it is functional and meaningful and motivating.
SLT_017
. . . reinforcement and carry over at home, to get, to get, otherwise they’re just not going to move forward so it’s getting that carry over isn’t it.
SLT_103
Appendix 26 Detailed background information on speech and language therapists participating in intervention survey 2
Table 78 provides information on the areas where SLTs worked and Table 79 provides information on their years of experience working with children with PSLI.
| Location worked | n | % of respondents |
|---|---|---|
| North East England | 30 | 17 |
| North West England | 19 | 11 |
| Yorkshire and the Humber | 7 | 4 |
| East Midlands | 14 | 8 |
| West Midlands | 16 | 9 |
| East of England | 9 | 5 |
| London | 21 | 12 |
| South East England | 22 | 12 |
| South West England | 41 | 23 |
| Other | 1 | 0.5 |
| Years of experience | % of respondents |
|---|---|
| 0–2 | 11 |
| 3–10 | 41 |
| 11–20 | 30 |
| 21+ | 17 |
With regard to banding, the largest proportion of respondents were in band 6 (38%), followed by band 7 (23%) and band 5 (22%). Most of the SLTs who responded were employed by the NHS (92%); the remaining SLTs worked independently or were employed elsewhere. SLTs reported working in a range of locations and it was evident that most worked across several locations. The majority worked in community clinics (71%), schools (64%), nursery classes attached to schools (53%) and other preschool settings (53%).
Delivery of intervention
The most commonly cited way that SLTs reported working with their chosen case was to ‘give parents or carers verbal advice’ (85%), but many SLTs reported more than one mode of delivery. A large proportion reported both ‘demonstrating activities with the child for others to carry out’ (78%) as well as ‘working directly with the child individually’ (70%), indicating that most SLTs used a combination of approaches with the child. Of the 9% who reported that they worked in ‘other ways’, 3% reported that an SLT assistant worked with the child and 3% reported that they adopted parent–child interaction.
Most SLTs reported that they had contact with the child, family or other caregiver weekly (51%); the next most common response was monthly (14%), with others reporting that they had termly (9%) or fortnightly (7%) contact.
Speech and language therapists reported a range of times over which they or another agent of therapy provided intervention. Most reported > 10 sessions (34% reported > 20 sessions, 23% reported 11–20 sessions ); 3% of respondents had only seen the child/other caregiver once.
The majority of SLTs reported that intervention took place in a clinic (49%); other popular locations included schools (26%), the home (28%) and education nurseries (24%).
The predominant SES of the SLTs’ caseloads was unskilled workers (36%), followed by skilled workers (32%), predominantly unemployed (17%) and predominantly professional (15%). The majority of SLTs reported working in either urban (42%) or suburban (38%) areas, with 21% working in rural communities.
Appendix 27 Detailed information regarding child and family factors reported by speech and language therapists in survey 2
Child factors
In total, 5% of SLTs reported that the child who they were working with had a medical history that impacted on his or her speech and language development or intervention. This included premature birth and prolonged periods in hospital.
A total of 14% of SLTs reported that the child who they were working with spoke English as an additional language; 15% reported that the child came from a bi/multilingual family. Languages cited included Punjabi (most common), Bengali, Urdu, Gujarati, Polish, Hungarian, Mandarin, Arabic, French, Japanese, Tigrinya, Sylheti, Somali and Turkish.
The majority of SLTs described children with ‘white ethnic’ heritage (81%), with the second biggest reported group being of mixed background (5%). A significant proportion of SLTs reported on a child of Asian descent (2% Indian, 2% Pakistani, 2% Bangladeshi, 2% any other Asian background) or African descent (2%).
A relatively large number of SLTs reported that the child who they were involved with had no siblings (19%); however, most of the children had one sibling (53%), many had two siblings (20%) and relatively few had three (6%), four (2%) or five (1%) siblings.
Most SLTs (52%) reported that the PSLI had a ‘moderate’ effect on the child’s activity and participation; however, a significant proportion felt that it had a severe effect (28%), with less feeling that it had a mild effect (11%) or a very severe effect (10%).
The majority of SLTs reported that the child’s behaviour was ‘good’ (56%), a large proportion described it as ‘moderate’ (30%), 12% described it as poor and only 2% reported that it was very poor. The child’s attention and listening skills were commonly described as good (36%) or moderate (37%), with some SLTs reporting that they were poor (20%) and a few describing them as very poor (6%). SLTs most frequently reported the child’s confidence to be ‘moderate’ (39%); however, there was a spread across the categories, with 29% reporting it to be good, 22% reporting it to be poor and 10% reporting it to be very poor.
Speech and language therapists reported that the children with PSLI had a variety of levels of awareness of their difficulties, with most reporting that they were ‘somewhat’ aware (35%), 29% reporting that they were a little aware, 19% reporting that they were very aware and 17% reporting that they were not at all aware. SLTs also reported that the children experienced a variety of levels of frustration, with a similar number reporting that the child with PSLI was a ‘little’ (37%) or ‘somewhat’ (37%) frustrated, with fewer reporting that the child was ‘very’ frustrated (11%) or not at all frustrated (15%).
The majority of SLTs reported that the child who they were working with was very engaged with intervention (50%), with 42% reporting that the child was ‘somewhat’ engaged and 9% reporting that the child was only a ‘little’ engaged.
Speech and language therapists reported that most children (69%) were receiving some sort of preschool childcare provision. Of those receiving childcare provision, most were in some form of nursery (45% were in state nursery, 20% were in a nursery attached to a school, 15% were in an independent nursery and 10% were in another nursery or preschool setting). A total of 5% of children were in a local authority children’s centre and 1% had a child minder. Of those who were receiving childcare provision, most (76%) received between 3 and 6 half-day sessions a week, 16% received < 3 half-day sessions a week and 8% received ≥ 7 half-day sessions a week.
Family and parent factors
In total, 26% of SLTs reported that there was a family history of unclear speech or slow language development.
The majority of SLTs rated the parents’ understanding of what was required of them in intervention as good (46%) or average (39%), with 10% feeling that it was poor and 2% feeling that it was very poor. Similar ratings were found for parent’s understanding of their child’s difficulties, with most reporting it to be good (47%) or average (41%), 11% feeling that it was poor and 2% feeling that it was very poor.
The majority of SLTs (51%) reported that the parents’ interaction skills with their child were good, with 34% reporting that they were average, 12% reporting that they were poor and 3% reporting that they were very poor.
Most SLTs (60%) reported that parents were very concerned about their child with PSLI, 33% reported that parents were somewhat concerned, 6% reported that parents were a little concerned and 1% reported that parents were not at all concerned. By contrast, SLTs reported that parents did not appear to have strong preferences for the type of intervention that their child received. In total, 37% reported that parents did ‘not at all’ have a preference, 22% reported that parents had a ‘little’ preference, 20% reported that parents ‘somewhat’ had a preference and 7% reported that parents ‘very much’ had a preference. However, 14% of SLTs reported that they did not provide a choice of interventions to parents.
In total, 67% of SLTs reported that parents attended most appointments but a significant proportion (26%) reported that parents missed or cancelled one or two appointments and 5% reported that parents missed or cancelled a lot of appointments. The majority of SLTs (61%) reported that parents were very engaged with intervention, with 28% reporting that parents were ‘somewhat’ engaged, 10% reporting that they were a ‘little’ engaged and 2% reporting that they were ‘not at all’ engaged.
Appendix 28 Additional responses from speech and language therapists in intervention surveys 1 and 2
Survey 1
In survey 1, 122 respondents provided further information about the interventions that they use for preschool children with PSLI. Of these, 46 included a parent–child interaction-type approach. This was not listed in the survey as it describes a broad approach or programme rather than components of intervention. A number of participants described interventions that were included in the lists presented to them, for example 19 referred to ICW activities, 12 described work on auditory discrimination or phonological awareness including minimal pairs, three described ‘what’s in the bag/box’ activities and two described vocabulary work. A number of participants also referred to method of delivery, with six reporting that they held language or early communication groups. Other relevant interventions listed included symbolic play and building subject verb object sentences.
Survey 2
In survey 2, 83% of respondents (n = 158) felt that the listed interventions and strategies covered all of the interventions that they had used with the child. The remaining 17% (n = 32), who did not feel that the survey covered all of the interventions that they had used, listed interventions and strategies.
Many of the interventions were considered by the research team to be synonymous with interventions already listed. Additional interventions provided included listing resources and programmes, which were excluded as it was components that were of interest.
However, several strategies were mentioned that had not been listed in the survey. These included ‘waiting for child to initiate communication’ (n = 1), ‘positioning face-to-face/same eye level’ (n = 2), waiting for the child to make eye contact before the adult speaks (n = 1), observe, wait and listen (OWLing, n = 1) and using a multisensory approach to learning sounds (n = 1). Other interventions raised included using communication books/passports (n = 3) and using symbols (n = 1). Two SLTs reported building up phrases and the MLU as well as practising carrier phrases (e.g. ‘I found the . . .’).
Appendix 29 Full statistical analysis of data from intervention survey 2
To determine (1) whether or not any groups of interventions clustered together and (2) whether or not any identified clusters were related to any child, family or contextual variables, two-step cluster analysis with dichotomous variables was carried out. Cases were divided according to how SLTs classified each child’s primary impairment. The data on children with primarily social communication (n = 8) were then excluded as there were only a small number of responses that fell into this group. Cluster analysis for speech cases and then language cases was conducted in relation to responses to the intervention (activities and strategies) items.
To compare cluster membership with child, family or contextual variables (used as evaluation fields), t-tests and chi-squared tests were carried out. For any evaluation field (child, family or contextual variables) in which the values were continuous, a t-test was carried out. For evaluation fields using nominal data, the responses were checked to see if they satisfied the requirements for a chi-squared test. When appropriate, chi-squared tests of independence were performed to examine the relationship between cluster membership and any child, family or contextual variable. The responses on the child, family and contextual independent variables (used as evaluation fields) were mainly closed items with a choice of four responses; responses were therefore often collapsed into dichotomous responses.
Speech cases
In total, 93 respondents reported on a child with primarily speech problems. Two-step cluster analysis using dichotomous variables generated two clusters (ratio 2.88; cluster quality fair). One of the clusters was associated with the use of a number of additional strategies such as giving the child time to respond, reducing pressure on the child to speak and following the child’s lead (predictor values 0.91–1.0). Creating a need to communicate, reducing the number of questions asked of the child and using gesture, play and signing showed less marked differences (predictor values 0.44–0.66). The cluster that used additional strategies has been tentatively labelled the ‘additional strategies cluster’ and the cluster that did not has been labelled the ‘limited strategies cluster’.
Chi-squared tests of independence were performed to examine the relationship between cluster membership and child, family and contextual variables. The cluster ratio was high (groups were of uneven size) and so, for many of the evaluation fields (child, family and contextual variables) of interest, further analysis was not possible. In total, there were 46 child, family and contextual variables; of these, it was possible to conduct only 19 chi-squared tests. Of those that could be tested, only significant results (p < 0.05) are reported here. A significant relationship was found between cases in the additional strategies cluster and the following factors:
-
the SLT’s view was that the child’s difficulties resulted in severe/very severe effects on participation {χ2 [degrees of freedom (df) = 1, n = 93] = 9.78, p = 0.002}
-
the SLT’s view was that the child had poor or very poor confidence [χ2 (df = 1, n = 93) = 10.01, p = 0.002]
-
if parents were judged to be somewhat or a little concerned [χ2 (df = 1, n = 93) = 4.67, p = 0.03]
-
if the SLT reported that the child’s inability to communicate ideas was an important factor in his or her selection of interventions [χ2 (df = 1, n = 93) = 6.53, p = 0.011]
-
if the SLT reported that the child saying very little was an important factor in his or her selection of interventions [χ2 (1, n = 93) = 7.79, p = 0.005]
-
if the SLT reported that the child having vowel distortions was an important factor in his or her selection of interventions [χ2 (1, n = 93) = 6.69, p = 0.010].
Language cases
In total, 89 respondents reported on a child with primarily expressive language difficulties, primarily receptive language difficulties or mixed expressive/receptive language difficulties. Two-step cluster analysis using dichotomous variables was performed and this generated two clusters (ratio 1.02; cluster quality poor). The findings related to these two clusters are reported here. Interpretation should, however, be cautious as the quality of the clusters was rated as ‘poor’. One of these two clusters was associated with use of a number of additional strategies (tentatively labelled the ’additional strategies cluster’) compared with the other cluster (labelled the ‘limited strategies cluster’).
The ‘additional strategies cluster’ was associated with the use of (two) additional strategies: following the child’s lead (predictor value 1.00) and play (predictor value 0.86). A number of other strategies showed less marked differences, including reducing questions to the child, reducing the complexity of utterances to the child, using gesture, creating a need for the child to communicate, singing and adopting more varied intonation (predictor values ranged from 0.46 to 0.64). The ‘additional strategies cluster’ was not associated with any additional activities except ‘What’s in the bag/ box activities’ (predictor value 0.52).
An independent-samples t-test was conducted to compare age in months between the additional strategies cluster and the limited strategies cluster. There was a significant difference in age between the limited strategies cluster (mean 46.7 months, SD 12.38 months) and the additional strategies cluster [mean 41.36 months, SD 10.134 months; t(87) = 2.23, p = 0.028], with additional strategies being associated with younger children.
Chi-squared tests of independence were performed to examine the relationship between cluster membership and other child, family and contextual variables. In total there were 46 child, family and contextual variables and, of these, it was possible to conduct 37 chi-squared tests. Of those that could be tested, only significant results (p < 0.05) are reported here. A significant relationship was found between the additional strategies cluster and the following factors:
-
the SLT’s view was that the child’s difficulties resulted in severe/very severe effects on participation [χ2 (df = 1, n = 89) = 6.08, p = 0.014]
-
if the SLT reported that there is no evidence that the child joins words [χ2 (df = 1, n = 89) = 5.183, p = 0.023]
-
if the SLT reported that the child uses strings of jargon [χ2 (df = 1, n = 89) = 5.121, p = 0.024]
-
if the SLT reported that the child is able to select objects only at the single word level in context [χ2 (df = 1, n = 89) = 4.788, p = 0.029]
-
if the SLT reported that the child cannot cope with complex commands in play situations [χ2 (df = 1, n = 89) = 4.209, p = 0.04].
Appendix 30 Responses to the parent survey
| Strategy/activity | Not really, n (%) | Parts of it, n (%) | Kind of, n (%) | Clear, n (%) | Very clear, n (%) |
|---|---|---|---|---|---|
| Auditory discrimination | 1 (1.8) | 6 (10.7) | 16 (28.6) | 33 (58.9) | |
| Child’s levela | 5 (8.8) | 12 (21.1) | 40 (70.2) | ||
| Commenting | 1 (2.0) | 4 (8.2) | 16 (32.7) | 28 (57.1) | |
| Concepts | 2 (4.7) | 1 (2.3) | 14 (32.6) | 26 (60.5) | |
| Eye contact | 1 (2.6) | 3 (7.7) | 13 (33.3) | 22 (56.4) | |
| Specific praise | 1 (2.9) | 11 (32.4) | 22 (64.7) | ||
| Repetition | 8 (26.7) | 22 (73.3) | |||
| Turn taking | 1 (3.6) | 9 (32.1) | 18 (64.3) | ||
| Waiting | 1 (3.4) | 3 (10.3) | 12 (41.4) | 13 (44.8) |
| Strategy/activity | Very unhappy n (%) | Unhappy n (%) | Neutral n (%) | Happy n (%) | Very happy n (%) |
|---|---|---|---|---|---|
| Auditory discrimination | 1 (2.1) | 5 (10.6) | 16 (34.0) | 25 (53.2) | |
| Child’s levela | 2 (3.9) | 10 (19.6) | 39 (76.5) | ||
| Commenting | 1 (2.2) | 2 (4.4) | 14 (31.1) | 28 (62.2) | |
| Concepts | 3 (7.9) | 10 (26.3) | 25 (65.8) | ||
| Eye contact | 1 (2.9) | 1 (2.9) | 10 (28.6) | 23 (65.7) | |
| Specific praise | 1 (3.1) | 5 (15.6) | 26 (81.3) | ||
| Repetition | 6 (20.7) | 23 (79.3) | |||
| Turn taking | 1 (3.7) | 1 (3.7) | 11 (40.7) | 14 (51.9) | |
| Waiting | 3 (11.1) | 8 (29.6) | 16 (59.3) |
| Strategy/activity | Very unhappy n (%) | Unhappy n (%) | Neutral n (%) | Happy n (%) | Very happy n (%) |
|---|---|---|---|---|---|
| Auditory discrimination | 1 (1.9) | 5 (9.3) | 15 (27.8) | 33 (61.1) | |
| Child’s levela | 2 (4.0) | 9 (18.0) | 39 (78.0) | ||
| Commenting | 1 (2.2) | 2 (4.4) | 14 (31.1) | 28 (62.2) | |
| Concepts | 1 (2.6) | 9 (23.1) | 29 (74.4) | ||
| Eye contact | 1 (2.8) | 7 (19.4) | 28 (77.8) | ||
| Specific praise | 1 (3.1) | 5 (15.6) | 26 (81.3) | ||
| Repetition | 4 (13.8) | 25 (86.2) | |||
| Turn taking | 1 (3.7) | 7 (25.9) | 19 (70.4) | ||
| Waiting | 3 (11.1) | 8 (29.6) | 16 (59.3) |
Appendix 31 Fictitious case study for the asylum seekers group
Hello, my name is Marian. I am 30 years old. I came to Britain 5 years ago and have lived in Manchester since then. I came with my husband and my daughter Ana, who is now 8 years old. When we arrived I was pregnant with my son Adam, who is now 4 years old, and later I had my daughter, Sara, who is now 2.5 years old.
My husband left me 2 years ago and now lives in Bolton. He comes to visit us every month and spends some time with the children. I miss my mother a lot. She is still living back home and I have not seen her since I left. We talk on the phone at least once a week but there are times when she does not have credit and I cannot help her. I pray that God will provide for her.
Back home I qualified and worked as a nurse but I have not been allowed to work since I came to this country. I take my daughter Sara to the mother and toddler group in the children’s centre and we go to a group for asylum seekers every 2 weeks.
We live in a small flat with two bedrooms and there is no garden. I got some toys for the children from a charity.
I am worried about Sara because she does not talk at all. She makes a few sounds and points at things, but her brother and sister were talking much more by her age.
Appendix 32 The Child Talk programme PhD project reports
Parents’ and speech and language therapists’ roles in intervention for preschool children with speech and language needs
Karen Davies, Manchester Metropolitan University, Manchester, UK
(Karen Davies was awarded her PhD in 2015 for her thesis: Karen ED. Parents’ and Speech and Language Therapists’ Roles in Intervention for Pre-School Children with Speech and Language Needs. PhD thesis. Manchester: Manchester Metropolitan University; 2015.)
Preschool children with PSLI form a significant part of SLTs’ workload in the community. The process of assessment through to intervention often relies on parents and therapists working closely together, assuming a variety of roles over an intervention period. Currently, there is limited research exploring the nature of roles and the conceptions of roles that participants have in the field of speech and language therapy. This study provides an original contribution to knowledge by exploring the role conception of parents of preschool children with PSLI and their SLTs, using both qualitative and quantitative research methods. Furthermore, a longitudinal design provided the opportunity to investigate any changes in parents’ conceptions of their role over time, giving a unique perspective on the association between therapy intervention and changes in conception. The evidence from the study is discussed with reference to conceptual change theory.
Background
The principle of partnership with clients has been encouraged in speech and language therapy practice,312 but a tension may exist between principle and practice, with research identifying a mismatch between the desired outcomes expressed by service users and goals set by professionals. 235,241,313 This may suggest that the relationship between user and professional is not necessarily one of partnership, characterised by mutual understanding of each other’s roles and goals agreed through negotiation. At the current time little research has explored the conceptions that SLTs and parents have of their respective roles in speech and language intervention. Little is known about how these conceptions relate to the nature of the partnership or if conceptions change as intervention progresses.
A literature review was conducted to evaluate the research on the theory and practice of roles in the parent–professional partnership, with specific reference to support for children with speech and language needs. A systematic approach to the literature was undertaken using the principles of critical interpretive synthesis,314,315 designed specifically to combine the findings of theoretical and empirical reports from a wide range of sources. 316
It is widely believed that parents and carers play a central role in supporting speech, language and communication development in young children. 317,318 This is reflected in a number of recent policy developments in England, most notably the introduction of parenting programmes to support parenting skills, including communication. Practitioners such as SLTs believe that parents’ roles may be particularly important for those children who are acquiring language more slowly than their peers. Intervention for children with speech and language needs frequently uses either (1) a parent education model intended to promote change in parents’ interaction style with their children319 or (2) a parent-as-aide model, with parents implementing home activities. 139 A typical intervention used for preschool children with PSLI uses coaching to enable parents to support speech and language development in a child’s usual social context. A number of studies evaluating intervention based on coaching parents have reported positive outcomes for parents in supporting language learning and for children in language development. 318,320,321 Parents-as-aides conceptualises parents as assuming an active role in supporting implementation of therapy objectives. In this instance, SLTs often provide home activities for parents to reinforce learning that has taken place during therapist-led intervention with the child. 139,322 Little is known about parents’ and therapists’ conceptions of their own and each other’s roles during either approach. Moreover, the part that relationship building plays in encouraging a shared understanding of roles and responsibilities between parents and professionals has rarely been explored in speech and language therapy. 323 The evidence from a small number of studies of parents’ views suggests that parents may feel excluded from the team(s) supporting their child with speech and language needs. 28,324,325 However, it is difficult to generalise from these studies to the wider context of speech and language therapy or evaluate the changes that may be taking place as a result of increasing awareness of partnership and co-working. 326,327
Research aims
To explore parents’ and SLTs’ conceptions of their respective roles in intervention for preschool children with PSLI and to understand the features that contribute to changing conceptions and their influence on children’s outcomes.
Research questions
-
What is the range of parents’ and SLTs’ conceptions of their own and each other’s roles in different phases of intervention?
-
To what extent are parents’/SLTs’ conceptions of their roles associated with behavioural outcomes such as attendance or shared goal setting?
-
In what ways are parents’/SLTs’ conceptions of their roles associated with personal background and experience or service design/constraints?
-
Do parents’/SLTs’ conceptions change during different phases of intervention and what factors influence this?
-
In what ways and to what extent do SLTs promote conceptual change across the different phases of intervention and how is this associated with particular behaviours?
Methods
A two-phase exploratory study was designed using a mixed-methods approach to explore parents’ and SLTs’ conceptions of their respective roles in intervention. Study 1 was a longitudinal qualitative study exploring parents’ and SLTs’ conceptions of their roles and possible association with behaviours such as attendance at appointments and participation in intervention in four typical NHS services in England. Data collection was undertaken using semistructured interviews of parent–SLT dyads. Each parent was interviewed three times over a 30-week period. The interviews were analysed for initial themes using thematic network analysis328 to identify basic, organising and global themes. A second-level analysis used framework analysis92 to track any changes in parents’ conception of roles. A total of seventeen parents were recruited from twenty parents who were invited to participate. There were two mother and father pairs who were interviewed together and these have been analysed as one set of views. In total, 12 SLTs agreed to participate. Three SLTs were interviewed about more than one parent and child. A total of eight parents participated in the follow-up interviews, five in the second and third interviews and an additional three in the second interviews only. Five SLTs completed the second interviews. Study 2 was a quantitative cross-sectional survey of a larger sample of parents and SLTs to examine the generalisability of the findings to a wider range of therapeutic contexts. A questionnaire was designed using the initial findings from the qualitative study. In total, 51 parents and 62 SLTs completed the questionnaires, which were analysed to identify the frequency of different role conceptions and behaviours of parents and SLTs, and any association between these conceptions and behaviours and the variation in SLT practice.
Initial results
The thematic networks from the phase 1 study suggested that, before involvement with speech and language therapy, many parents’ conceptions of their own and the SLT’s role were vaguely formulated. They were seeking clear and unambiguous advice from a professional who was trained and experienced in speech and language development. They were seeking both reassurance and clarity about any actions that were required. Their concept of acting as partners was also vaguely formulated and only occasionally articulated, but they frequently expressed readiness to participate in intervention. This readiness was described in terms of learning how to help and doing activities with their children. Even at the outset of involvement in speech and language therapy, a number of parents referred to teaching their child. Although the parents in the study showed their willingness to be involved in intervention through attending speech and language therapy and co-operating with the process, there was clear evidence that they had accomplished considerably more than this by the time they met the SLT in the first assessment. The majority perceived themselves as active advocates for their children, frequently negotiating a pathway to find specialist advice that they sensed to be confusing, daunting or discouraging. Two additional roles were derived from the data: a learner/teacher role and an adult with responsibility role. The latter specifically relates to responsibility for supporting speech and language learning.
A small subset of eight parents participated in follow-up during intervention in the longitudinal study. These parents showed considerable variation in their conception of roles at the outset of involvement in intervention. However, after participating in speech and language therapy they referred more frequently to teaching and facilitating roles and the use of specific techniques that they had learned through co-working with the SLT. This suggests a process of change in parents’ conceptions and reported behaviour as intervention progressed. Moreover, the pattern of changes observed in these parents could be described as showing three different trajectories of role conception for parents in the study. On the basis of the sample studied in this research, it may be helpful to describe these three trajectories of role conception to illustrate the way that some parents participate in intervention. Nonetheless, it is important to exercise caution in interpreting these as discreet categories given the small numbers in the study. They should not be regarded as illustrating a ‘type’ of parent that belongs to a specific category, but more as a cluster of features that might be indicative of parents’ motivation and capacity to assume specific roles.
The first trajectory is change that signified a fundamental modification in understanding and behaviour, with parents describing changes in understanding their role and becoming the agents of change. The second trajectory is characterised by parents as helpers, adjusting what they do, but not displaying a significant shift in their thinking. The third trajectory is typified by little evidence of change in behaviour, despite expressing a better knowledge of their child’s speech and language needs. Evidence from current conceptual change theory329 suggests that people’s understanding is as likely to grow progressively and change gradually as involve a sudden change in conceptualisation. It is difficult to verify if this is the case in these data as parents were at different stages of intervention and the interviews represented a snapshot of their views at one distinct point. It is possible that further changes could take place as time progressed beyond the limits of the longitudinal study.
Speech and language therapists described their own role as that of assessor and adviser, intending to help parents set realistic goals, acquire specific strategies to support their child and adapt their approach to facilitating speech and language development. SLTs described a careful interplay between themselves and parents, often referring to evaluating parents’ concerns, reactions and circumstances and then adjusting their advice and expectations. This evaluation included adapting the recommendations and type of intervention offered according to parents’ contexts. Even when therapists used service care pathways and guidance documents, they talked of allowing their judgement to over-ride their usual practice. Moreover, some SLTs referred to the frustration of not being able to be as flexible as they perceived the situation required. SLTs also emphasised the importance of a relationship that is open and direct about the child’s needs and the options available – options that the service can offer and options that the parents can contribute.
A cross-sectional survey using parent and SLT questionnaires is currently under way. This was designed using the findings from the qualitative study to inform the questions for the survey. A total of 17 parents were recruited from 20 parents who were invited to participate. Two mother and father pairs were interviewed together and have been analysed as one set of views. In total, 12 SLTs agreed to participate. Three SLTs were interviewed about more than one parent and child.
Discussion: outcomes without relationships?
Parents’ roles in supporting their children with PSLI appear to be those of advocacy, learner/teacher and adult with responsibility for supporting their child’s speech and language learning. Parents in this study most confidently described their role as one of advocacy. They described other roles of teaching and taking the responsibility for supporting their child less distinctly. Significantly, they had few preconceived ideas about speech and language therapy or their own support role unless their older children had needed support. However, they were not uncritical users of support. They both expected expert advice and made judgements about the quality of what they received. On the other hand, SLTs described their own role with clarity, referring to assessment, advice giving and education. There was a clear coaching role, aiming to enable parents to change their understanding and behaviour to support their children’s language learning. This is consistent with one of the findings from the full research programme and presented in the Child Talk What Works typology of interventions for children with PSLI. Nevertheless, SLTs do not directly refer to parents as learners, suggesting that this may be an underdeveloped conception of parents’ roles by SLTs. A key role for SLTs within a partnership is enabling parents to assume new roles themselves as primary agents of change in supporting their child’s speech and language development. Rather than presenting a mismatch of expectations between parents and SLTs, there appeared to be marked equilibrium between parents’ advocacy role and readiness to support and SLTs’ education role. This may be best conceptualised as parent and SLT roles that offer complementary functions, activated by explicit discussion and negotiation, as part of decision-making about intervention. The quality of the relationship between parents and SLTs was reported by study participants to be important in facilitating negotiation. Thus, the parent–SLT partnership should be considered an essential element of evidence-based interventions in clinical practice. Visualising intervention alone, without reference to skilled facilitation by SLTs and parents, may be somewhat misleading. The Child Talk What Works programme of research has devised a detailed typology of interventions for preschool children with PSLI, based on a review of empirical evidence and professional consensus. To use an intervention typology of this nature, practitioners need to understand their own and parents’ perception of roles and the impact of roles on the outcomes of intervention. Professional expertise is therefore required to apply the evidence appropriately, but equally important are skills in negotiating roles and supporting conceptual change in parents to enable them to become equal participants in achieving intervention outcomes.
Profiles of disordered language acquisition
Anna Blackwell, University of the West of England, Bristol, UK
(This thesis is due to be submitted in the autumn of 2015.)
Background
This study was undertaken as part of the ongoing PhD studentship carried out at the University of the West of England, Bristol, and funded through the research programme. This exploratory study of the early language development of children with PSLI was developed independently but was intended to complement the research programme goals. A review of the literature demonstrated an abundance of research on language development in the TD population. Themes emerged from this regarding the rate and style of early vocabulary development and the external factors that influence language growth, in particular parent–child interaction. However, the research with a language-delayed population was more limited.
The Child Talk typology identified nine categories that SLTs may address when planning intervention approaches for preschool children with PSLI. These included adult–child interaction, in particular parent–child interaction, which is the focus of this PhD study. The importance of parent–child interaction for understanding and facilitating child language development is based on the social interactionist perspective, which suggests that children learn language from their interactions with others, particularly parents. Vygotsky330 proposed that children are able to learn language in their ‘zone of proximal development’ (the gap between their own language skills and those of more skilled interaction partners) as parents provide linguistic scaffolding appropriate to their abilities, stimulating language growth. The relationship between parent–child interaction and child language development is understood to be reciprocal. However, because of the limited language skills of children with language delay it is possible that their interactions are less facilitative for language learning than those of TD children. Interventions therefore aim to optimise parent language input to provide increased opportunities for language learning.
Previous research has shown parent–child interaction to be a common intervention target, particularly during the earlier preschool stage. In a UK survey of > 500 SLTs, 73% reported parent–child interaction as an outcome target of therapy with children aged 2–3 years, whereas targets for older school-age children focused on child-related factors such as attention and listening skills. 90 These approaches are derived from factors positively related to TD language. 35 Research has suggested that the communicative environment of children with delayed language is different from that of TD peers in terms of the language input that they receive or interactions that they partake in, which may impact on their language development. 331
Systematic reviews of the literature have suggested that speech and language therapy interventions that include parents could have beneficial effects103 but that methodological limitations restrict the evaluation of findings. 35 Speech and language therapy interventions that target parent–child interaction have had mixed results and studies often do not report parental language outcomes necessary for identifying the mechanisms of change. A multifactorial approach is necessary, which aims to understand the complex nature of language development and relationships between parent and child language use.
Aim and research questions
To address these issues this PhD project aimed to examine the course of language development of young preschool children (26–41 months at study entry) with PSLI. Children were recruited at the one-word stage of language production to examine vocabulary growth during the period of change to more complex language. These data were used to identify children’s developmental trajectories and the role of their natural language environment, focusing on parent–child interaction. The objective was to develop the foundations for theoretical understanding of delayed language acquisition.
The research questions were:
-
How does the vocabulary of children with primary language impairment change over time?
-
How does parent–child interaction and child language input change over time?
-
How are these factors related?
Methodology
Method
A case study design was used to collect detailed data on child and parent language use. To first establish the feasibility and practicality of the proposed methods, a pilot study was carried out with two TD preschool children. For the full-scale study, four preschool children with language delay (all male) and their families were recruited as case studies. Parents were provided with information about the study and they gave consent on behalf of themselves and their children. Initial baseline data collection sessions included case histories and language and developmental assessments. The children had expressive language > 1.25 SDs below the mean, with scores ranging from 71 to 80 on the PLS-3. 332 All children had age-appropriate cognitive skills, assessed using the Bayley Scales of Infant Development – 2nd edition. 333
Data collection
A mixed-methods approach was used to collect information on children’s language growth and their communicative environment. Data were collected at four time points at 3-month intervals over 9 months. Parents completed checklists of words that their child used to track their language development using the MacArthur–Bates Communicative Development Inventories. 334 To develop a picture of how children spend their time, parents filled out diary records of their child’s daily activities. The Language Environment Analysis (LENA) system335 was used to collect up to 16-hour recordings of children in their natural environment at home, without researcher presence. This uses a small audio recorder worn by the child in a specialised vest. Parents were also videoed during picture book reading interaction with their child, which was coded using the Thorpe Interaction Measure (TIM). 336,337 At the end of the study period, semistructured interviews were carried out with parents to get their perspectives on how the language use and interactions of their child had changed over the 9 months and the impact of this.
Data analysis
Communicative Development Inventory reports were scored manually and changing language production was plotted graphically. The information from the diaries was presented pictorially as well as being used to assist with analysis of the all-day LENA recordings. The audio LENA data were analysed using LENA Pro software version 3.10 (LENA Research Foundation, Boulder, CO, USA),338,339 which produced frequency counts for adult words, child vocalisations and conversational turns in 5-minute, hourly or daily sections. Summary data for these variables were obtained. The audio from 5-minute samples with high-frequency conversational turn counts was played back and transcribed for detailed coding and analysis of child and parent language use. The videos of the book-sharing sessions were transcribed and coded using an extended version of the TIM, which was used to look at parent warmth, control and cognitive scaffolding (teaching style) in the Avon Longitudinal Study of Parents and Children. 337 The interviews were transcribed and analysed using thematic analysis.
Systematic review
As part of this project a systematic review was carried out that examined studies that used naturalistic observations of parent–child interaction, to better understand the complex relationship between children’s communicative environment and their language development. The aim of this review was to identify whether or not there are differences in the characteristics of parent–child interaction with preschool children between those who have language delay and their TD peers. The review found issues across studies with the criteria used to define language delay, discrepancies in the severity of delay, presence of receptive delay and the level of study detail. However, it suggested that differences in the characteristics of parent–child interaction between children with language delay and TD peers are limited. Furthermore, differences found were generally attributed to behavioural differences in children rather than parents.
Methodological considerations were highlighted regarding the use of matched groups and case–control designs. Many studies measured parent and child language at the same time point, which made it difficult to identify the direction of the relationship. This review suggested a need for longitudinal studies that examine the dynamics of change in child and parent language behaviour over time.
Initial results
The main aim of the study was to explore the changing dynamics of parent and child language over the course of the study. Some preliminary data are presented here. At the first data collection time point vocabulary size ranged from 23 to 137 words across cases. The children then demonstrated relatively stable rates of vocabulary growth, although those with the largest vocabulary size at the first time point did not necessarily show the highest rate of growth. Child B had the third smallest vocabulary size, 63 words, at the first time point but by the third time point had the largest, with 471 words. This child had a baseline receptive language (comprehension) score 1.6 SDs above the mean and was the youngest at the start of the study (26 months). Although it is not possible to generalise from this small sample, these salient markers are consistent with the literature, which suggests that age and receptive language ability are important factors when considering the likelihood of persistent delay. 2,3,5,340
Vocabularies were divided into different types of words: naming words, verbs and adjectives and closed class words (e.g. pronouns, prepositions and connecting words). The largest proportion (> 50%) of children’s vocabularies was naming words at each time point. For some children the proportion of naming words increased while the proportion of other types of words decreased whereas the reverse was true for others, as shown in Table 83.
| Word type | Child A (%) | Child B (%) | Child C (%) | Child D (%) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| t1 | t2 | t3 | t1 | t2 | t3 | t1 | t2 | t3 | t1 | t2 | t3 | |
| Naming words | 67 | 60 | 55 | 50 | 70 | 63 | 62 | 64 | 66 | 54 | 58 | |
| Verbs and adjectives | 15 | 19 | 25 | 32 | 23 | 27 | 26 | 25 | 27 | 23 | 21 | |
| Closed class | 18 | 21 | 20 | 18 | 7 | 10 | 13 | 11 | 8 | 23 | 21 | |
Children’s communicative environment and parent–child interactions were assessed using the LENA system, from whole-day recordings at home, and the TIM, during picture book-reading sessions. Preliminary data suggest that there was substantial variation in the language environment of the four children. During waking hours, the number of adult words that children were exposed to (average per hour) ranged from 468 to 1429 words. Conversational turns between the child and adults ranged from 25 to 100 and child vocalisations ranged from 111 to 394. The TIM findings (Table 84) outline the frequency of teaching techniques used by parents. Although these data are currently incomplete, some parents appear to demonstrate a stable trend in teaching style across time whereas others display a changing style, which includes decreased labelling at later time points.
| Teaching style | Child A | Child B | Child C | Child D | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| t1 | t2 | t3 | t1 | t2 | t3 | t1 | t2 | t3 | t1 | t2 | t3 | |
| Labelling | 21 | 24 | 26 | 27 | 18 | 21 | 4 | 0 | 21 | 13 | ||
| Short elaboration | 28 | 30 | 33 | 49 | 31 | 22 | 31 | 22 | 14 | 24 | ||
| Long elaboration | 1 | 1 | 14 | 18 | 1 | 11 | 15 | 14 | 9 | 3 | ||
| Concept structuring | 0 | 1 | 0 | 2 | 4 | 0 | 4 | 1 | 0 | 1 | ||
| Linking | 1 | 2 | 6 | 11 | 1 | 5 | 10 | 1 | 8 | 9 | ||
| Child involvement – language | 0 | 0 | 2 | 1 | 7 | 0 | 0 | 1 | 1 | 0 | ||
| Child involvement – activity | 0 | 0 | 2 | 0 | 0 | 1 | 0 | 0 | 1 | 2 | ||
| Total | 51 | 58 | 83 | 108 | 62 | 60 | 64 | 39 | 54 | 52 | ||
Discussion
The findings from this PhD study will contribute towards the Child Talk programme, particularly with regard to informing the next steps following completion of the programme. Together, the Child Talk and PhD systematic reviews have established a lack of robust evidence for the effectiveness of parent–child interaction interventions and for understanding the relationship between parent–child interaction and delayed language development. The review findings will inform future research questions, appropriate designs and methodological considerations necessary to explore parent–child interaction. The interviews carried out as part of this project established parents’ perspectives on their child’s language development and their experiences of having a child with language delay, including the support that their child had received. This will be important for feeding into the research programme’s findings on parents’ views of interventions and will add to the knowledge about parents’ understanding of activities involved in speech and language therapy, outlined in the Child Talk typology. The project will provide a detailed description of the developmental trajectories of children with PSLI in the context of their communicative environments, and specifically of the relationship between parent and child language use. These findings will identify key features that should be addressed in future research with language-delayed populations, regarding both assessment and outcomes of interest related directly to the child or to their broader environment.
Ethical approval codes
-
Research Ethics Committee reference number: 12/SW/0142.
-
R&D reference: 2862.
-
University of the West of England application number: HLS/12/08/91.
Appendix 33 Rationale behind speech and language therapists’ decisions to use assessment tools
| Assessment | Reason for use |
|---|---|
| CELF-P | Detailed information on wide range of language skills |
| CELF-P | Overview but also more in-depth of many areas |
| CELF-P | Standardised measure of language function |
| CELF-P | I particularly use the receptive language subtests and for children who are in reception. I think the stimulus material is good and the information collected is helpful |
| CELF-P | More detailed language assessment for children who have the necessary attention and listening skills to complete it |
| CELF-P | A thorough assessment of comprehension and easy to maintain attention |
| CELF-P | Gives a standardised assessment of receptive and expressive language. Particularly useful for children who have language impairment and for whom I am deciding which area of language to target through intervention |
| CELF-P | Useful indication of aspects of language development. Gives standardised scores. Easy to use |
| CELF-P | It is available in my clinic and it is a broad-spectrum assessment |
| CELF-P | Child-friendly and gives standard score |
| CELF-P | Good overview assessment of receptive and expressive language |
| CELF-P-2 | Good pictures |
| CELF-P | Detailed assessment of the child’s comprehension. Gives percentile scores |
| CELF-P | It is standardised and gives a lot of information about conceptual development |
| CLEAR Phonological Screening Assessment | The way the assessment is designed |
| CLEAR Phonological Screening Assessment | Sound assessment structured as one page per sound so you can see quickly which ones are missing/incorrect |
| CLEAR Phonological Screening Assessment | It’s quick to administer |
| CLEAR Phonological Screening Assessment | Colourful pictures |
| CLEAR Phonological Screening Assessment | I like the record form and feel this is easy to evaluate and share with parents |
| CLEAR Phonological Screening Assessment | Accessible phonology assessment for younger children (i.e. coloured cards with familiar pictures) |
| CLEAR Phonological Screening Assessment | Quick to administer |
| CLEAR Phonological screening assessment | Quick screen and starting point |
| DLS | Can be adapted easily into activities for therapy |
| DLS | Provides concrete areas can work on |
| DLS | I use both the rapid screen and sometimes the full Derbyshire assessment. I like the fact that it can be just object based for the younger children and it also uses functional items. It is good for children who are younger and need more play-based assessments |
| DLS | Quick screen of comprehension and quick way to get some expressive language samples |
| DLS | Informally used to screen understanding of preschool children. Can be adapted and varied depending on child and can be easily simplified or made more difficult |
| DLS – Picture Test | Gives a quick and easy measure of language comprehension and expressing in terms others can understand |
| DLS – Picture Test | Gives an idea for younger children of their level of language understanding |
| DLS – Rapid Screening Test | For children with very early language development |
| DLS – Rapid Screening Test | The RST [Rapid Screening Test] gives information about the child’s Verbal Language Comprehension score from a quick and simple to administer assessment |
| Edinburgh Articulation test | I know it well. Despite its age |
| Informal | Observation in classroom highlights needs that formal assessments don’t show |
| Informal play assessment | More suitable to younger children |
| Informal assessment of play and interaction | Gives information about child’s play stage |
| Informal receptive language assessment | Age appropriate and does not put too much demand on the child |
| Phonological awareness batteries – home devised | To gain a detailed assessment of a child’s phonological processing level |
| PLS-3 | It is the only one readily available to me in my clinic! |
| PLS-3 – Receptive Scale | Quick to administer |
| Quick screening tool | If speech is primary concern – as a first step |
| RAPT | Again availability and ease and speed of administering |
| RAPT | Good expressive language screen. Can sometimes be difficult to tell whether a child has expressive language difficulties or just using age-appropriate errors |
| RAPT | Quick and easy to use |
| RAPT | As a quick screening tool as first step if language is primary concern |
| RAPT | It is very user-friendly |
| RAPT | Flexible |
| RAPT | Quick and easy to administer |
| RAPT | I feel that it is a quick accessible assessment for most children aged 3.5 years and above that provides me with some good information about their vocabulary and sentence structure. It is fairly culturally diverse as well |
| RAPT | Quick |
| RAPT | It is a quick standardised screening of expressive language |
| RAPT | It is a quick and handy way to look at expressive language |
| RAPT | Quick to administer |
| RAPT | Quick |
| RAPT | Quick and simple. Easy to evaluate and mark |
| RAPT | Provides surprising range of data for such a short assessment. Rather old but children still respond positively and find it easy to co-operate |
| RAPT | Quick to administer |
| RDLS | Age norms for child’s language levels |
| RDLS | Uses real objects as well as pictures. Simple to explain assessment results to parents. Can identify clear areas to target and easily formulate activities for children. Quick to administer |
| RDLS | Quick |
| RDLS – Verbal Comprehension | It is standardised rigorously and on British subjects (as opposed to American). It gives information about ICWs and concept development and verbal reasoning and is user-friendly having toys and pictures |
| RDLS – Verbal Comprehension | The only real assessment available to check comprehension levels in young children |
| Renfrew Word Finding Vocabulary Test | It is the most helpful in determining if there is a specific word-finding difficulty |
| STAP | It gives a comprehensive screen of a child’s phonology |
| STAP | Assess child’s speech |
| STAP | A good corpus of words to sample sounds in all positions and a very user-friendly phonological analysis sheet |
| STAP | Used within department |
| STAP | Easy to use – child-friendly |
| STAP | Quick |
| STAP | Quick |
| STAP | Easy vocabulary for children and provides a quick profile of speech |
| STAP | Quick to administer and gives a phonological profile of the child |
| STASS | Screening assessment of expressive language/connected speech sound sample |
| STASS | Quick way to assess grammar and information provided by child |
| STASS | Provides a good language sample and is attractive to children |
| Test of Abstract Language Comprehension | Good general screen of comprehension if child is working beyond play-based information-carrying words and concepts |
Appendix 34 List of outcome indicators underlying the outcome domains within each typology theme
Attention and listening.
Social interaction.
Behaviour.
Emotional well-being.
Educational achievement.
Independence.
Participation and inclusion.
| Outcome domains | Outcome indicators (intervention level) | Source |
|---|---|---|
| Attention and listening | Age-appropriate attention | V |
| Basic sound awareness (symbolic level) | V | |
| Able to switch attention from activity to adult instruction with strategies (e.g. call name) (joint attention) | L | |
| Able to switch attention without support (joint attention) | L | |
| Able to clap number of syllables | L | |
| % increase in correctly identifying different sounds | V | |
| Social interaction | Increased eye contact | V |
| Improved social communication skills | L | |
| Able to take turns with an adult in structured activity | V | |
| Able to initiate turn taking with a peer | L | |
| Age-appropriate play | V | |
| Behaviour | Increased level of co-operation at home and in setting | L |
| Reduction in temper tantrums/challenging behaviour | L | |
| Improved behaviour displayed at home and in setting | L | |
| Emotional well-being | Reduced levels of child and adult frustration | L |
| Happier home environment | L | |
| Educational achievement | Improved educational achievement | L |
| Independence | Able to await turn in a small group without adult support | L |
| Participation and inclusion | Increased inclusion in education | L |
| Increased participation in group activities | V | |
| Increased inclusion in educational environment | V |
Adult–child relationship.
Adult knowledge and use of strategies.
Adult–SLT partnership.
Social interaction.
Emotional well-being.
| Outcome domains | Outcome indicators (intervention level) | Source |
|---|---|---|
| Adult–child relationship | Improved adult–child attachment | L |
| Adults able to value their role in helping the child | L | |
| Adult acceptance of child’s difficulty | L | |
| Adults report enjoyment of child’s company | L | |
| Adult knowledge and use of strategies | Effective carry-over of skills by adults | VL |
| Appropriate adult use of specific praise | L | |
| Able to explain tasks to others | L | |
| Spontaneous development of ideas by adults | L | |
| Adults feel potent and aware of agency in child’s education | L | |
| Adults able to cue child appropriately | L | |
| Adults able to use the same language and examples as SLTs | L | |
| Increased awareness of own communication by adults | L | |
| Increased frequency of therapy carry-over and more progress | VL | |
| Adult–SLT partnership | Increased frequency of therapy carry-over and more progress | L |
| Conversations between adults and therapists reflect a partnership | L | |
| Adults view SLT as supportive rather than critical | L | |
| Appropriate adult engagement with service | L | |
| Good appointment attendance | L | |
| Adult engagement with intervention process | L | |
| Social interaction | Increase in child’s output/words/utterances | V |
| Adult and child engage in co-operative play | L | |
| Emotional well-being | Increase in child’s confidence | V |
| Increased levels of adult confidence | VL | |
| Reduced levels of adult stress and anxiety | V |
Adult knowledge and use of strategies.
Social interaction.
Emotional well-being.
Participation and inclusion.
| Outcome domains | Outcome indicators (intervention level) | Source |
|---|---|---|
| Adult knowledge and use of strategies | Increased communication-friendly environment (language support strategies) | V |
| Adults able to identify their own goals to work on | V | |
| Adults remove background noise and distraction | L | |
| Improved attention and listening | L | |
| Child experiences a positive communication environment | L | |
| Adults able to adopt interaction strategies | L | |
| Social interaction | Appropriate adult and child turn taking | V |
| Adults follow child’s lead in conversation and play | L | |
| Increased use of concrete language by adults | L | |
| Improved turn taking | V | |
| Increased communicative initiations by child | V | |
| Increase in child’s output/words/utterances | L | |
| Improved joint attention | L | |
| Child’s language is age appropriate | L | |
| Emotional well-being | Increased levels of adult confidence | VL |
| Increased adult confidence in supporting child (self-report) | V | |
| Increased adult understanding | V | |
| Adult confidence to try at home | L | |
| Reduced levels of adult stress and anxiety | V | |
| Increase in child’s confidence | V | |
| Reduced levels of child’s frustration | V | |
| Child has increased happiness | V | |
| Participation and inclusion | Increased access to the curriculum | V |
| Increased ability to follow instructions in setting | L | |
| Increased confidence in communicating with unfamiliar adults | L | |
| Increased participation in conversation | V |
Improved assessment scores.
Social interaction.
Behaviour.
Emotional well-being.
Independence.
Participation and inclusion.
| Outcome domains | Outcome indicators (intervention level) | Source |
|---|---|---|
| Improved assessment scores | Improved standardised assessment scores | VL |
| Improved DLS word level | VL | |
| Increased understanding of ICWs, vocabulary and concepts | VL | |
| Increased ability to follow instructions | V | |
| Increased understanding of questions | V | |
| Social interaction | Improved use of appropriate expressive language | L |
| Increased incidences of initiation of play | L | |
| Improved range of social play: role play and co-operative play | L | |
| Behaviour | Improved behaviour | L |
| Emotional well-being | Increase in child’s confidence | V |
| Improved quality of family life | L | |
| Independence | Reduced level of support required by child to join in | L |
| Participation and inclusion | Increased understanding of consequences, e.g. road safety | L |
| Increased ability to follow instructions in setting | L | |
| Ability to follow comments, commands and simple questions in setting | V | |
| Increased participation in group activities | V | |
| Increase in number of friendships | L | |
| Improved understanding of routines | L |
Intelligibility.
Social interaction.
Emotional well-being.
Educational achievement.
Independence.
Participation and inclusion.
| Outcome domains | Outcome indicators (intervention level) | Source |
|---|---|---|
| Intelligibility | Comparing sounds used at baseline at reassessment in word-initial and word-final positions | V |
| Target sounds accurately produced at all levels | V | |
| Production of target sound at sound, word and sentence level | V | |
| Improved consistency of production | L | |
| Increased phoneme production (range and number) | V | |
| Improved discrimination skills | V | |
| Age-appropriate use of speech sounds | V | |
| Clear intelligible speech | L | |
| Social interaction | Increased use of vocabulary | V |
| Improved attempts at core vocabulary | V | |
| Improved social skills | L | |
| Improved peer interaction | L | |
| Emotional well-being | Increased self-esteem and confidence in talking to others | L |
| Reduced levels of frustration, anxiety and stress | L | |
| Reduced levels of adult stress and anxiety | L | |
| Educational achievement | Has necessary skills to support literacy in Year 1, e.g. use of Jolly Phonics, familiarity with sound grapheme | L |
| Reduced levels of staff concern regarding child’s ability to learn | L | |
| Independence | Reduced level of support needed in setting | L |
| Participation and inclusion | Increased participation in curriculum | L |
| Reduction in likelihood of teasing and being identified as different | L | |
| Increased intelligibility to familiar and unfamiliar listeners | L | |
| Able to communicate effectively with peers and adults | L |
Understanding and use of language.
Social interaction.
Behaviour.
Emotional well-being.
Educational achievement.
Independence.
Participation and inclusion.
| Outcome domains | Outcome indicators (intervention level) | Source |
|---|---|---|
| Understanding and use of language | Improved standardised assessment scores | V |
| Increased use of grammatical structures | V | |
| Improved understanding of language | L | |
| Increased vocabulary – knowledge and use | VL | |
| Improved imitation skills | V | |
| Able to present information clearly | L | |
| Social interaction | Increase in child’s output/words/utterances | V |
| Behaviour | Improved behaviour in setting | L |
| Reduction in temper tantrums/challenging behaviour | L | |
| Emotional well-being | Improved emotional well-being | L |
| Increase in child’s confidence | L | |
| Decreased adult stress and anxiety | L | |
| Increased levels of happiness | L | |
| Educational achievement | Improved narrative ability | L |
| Improved literacy skills | L | |
| Independence | Increased level of independence | L |
| Participation and inclusion | Improved access to education | L |
| Increased access to the curriculum | V | |
| Increased setting attendance | L | |
| Speaks with more people | L | |
| Increased number of friendships | L | |
| Increased play with others in setting and home | L | |
| Able to communicate effectively in and outside home | L |
Self-awareness.
Emotional well-being.
Independence.
Participation and inclusion.
| Outcome domains | Outcome indicators (intervention level) | Source |
|---|---|---|
| Self-awareness | Evidence of increased self-correction | V |
| Able to identify errors in others’ speech and language | V | |
| Recognises incidences of error production and attempts to self-correct | V | |
| Increased intelligibility | L | |
| Emotional well-being | Increase in child’s confidence | V |
| Independence | Increased independent learning | L |
| Able to seek clarification independently | L | |
| Engagement in active learning and self-help | L | |
| Reduced level of prompting required | V | |
| Able to recognise own difficulties and self-correct independently | L | |
| Reduced level of support needed in setting | L | |
| Participation and inclusion | Increased levels of confidence in class participation | L |
| Able to sustain relationships | L | |
| Increased setting attendance | L | |
| Able to act appropriately in a number of settings | L | |
| Improved negotiation skills | L |
Communicative competence.
Behaviour.
Emotional well-being.
Educational achievement.
Independence.
Participation and inclusion.
| Outcome domains | Outcome Indicators (intervention level) | Source |
|---|---|---|
| Communicative competence | Improved attention in home and setting | V |
| Increased use of complex language | L | |
| Child able to request novel items outside of session | L | |
| Evidence of wider use of intervention target (beyond therapy session) | L | |
| Transfer and impact of skills beyond intervention target focus | L | |
| Behaviour | Reduction in temper tantrums/challenging behaviour | L |
| Emotional well-being | Increase in child’s confidence | L |
| Reduced levels of frustration | L | |
| Reduced levels of anxiety | L | |
| Able to gain pleasure from communication | L | |
| Educational achievement | Improved literacy skills | L |
| Independence | Able to communicate basic needs | L |
| Participation and inclusion | Increased access to the curriculum | V |
| Increased participation at home and in setting | V | |
| Increased participation in all aspects of child’s life | L | |
| Increased number of friendships | L | |
| Able to be understood by adults and peers | L | |
| Increased intelligibility to unfamiliar listeners | L | |
| Child able to request novel items outside of session | L | |
| Increased motivation to communicate | L | |
| Increased participation | L |
Social interaction.
Behaviour.
Emotional well-being.
Independence.
Participation and inclusion.
| Outcome domains | Outcome indicators (intervention level) | Source |
|---|---|---|
| Social interaction | Increased levels of initiation and response | V |
| Able to request clarification | L | |
| Increased levels of interaction | V | |
| Improved turn taking | L | |
| Increased number of communication functions and frequency of use | L | |
| Behaviour | Reduction in temper tantrums/challenging behaviour | L |
| Emotional well-being | Increase in child’s confidence | V |
| Improved quality of family life | L | |
| Independence | Able to communicate basic needs | L |
| Participation and inclusion | Increased communicative ability in a variety of settings | L |
| Increased confidence and willingness to engage with others | V | |
| Able to social network and make friends | L | |
| Able to participate in conversations to share information | L | |
| Able to make friends and go to birthday parties | L | |
| Increased access to the curriculum | L |
Appendix 35 Delphi consensus data for outcome domains with more than three outcome indicators
| Typology theme | Outcome domain | Indicators | % of SLTs placing the outcome indicator in the top three |
|---|---|---|---|
| 1. Speech | Intelligibility | Comparing sounds used at baseline at reassessment in word-initial and word-final positions | 44 |
| Improved consistency of production | 44 | ||
| Clear intelligible speech | 44 | ||
| Increased phoneme production (range and number) | 42 | ||
| Age-appropriate use of speech sounds | 39 | ||
| Target sounds accurately produced at all levels | 31 | ||
| Improved discrimination skills | 31 | ||
| Production of target sound at sound, word and sentence level | 25 | ||
| Social interaction | Improved peer interaction | 89 | |
| Improved social skills | 83 | ||
| Increased use of vocabulary | 69 | ||
| Improved attempts at core vocabulary | 58 | ||
| Participation and inclusion | Able to communicate effectively with peers and adults | 97 | |
| Increased intelligibility to familiar and unfamiliar listeners | 89 | ||
| Increased participation in curriculum | 69 | ||
| Reduction in likelihood of teasing and being identified as different | 44 | ||
| 2. Comprehension | Improved assessment scores | Increased understanding of ICWs, vocabulary and concepts | 89 |
| Increased ability to follow instructions | 76 | ||
| Increased understanding of questions | 49 | ||
| Improved standardised assessment scores | 43 | ||
| Improved DLS word level | 43 | ||
| Participation and inclusion | Increased participation in group activities | 81 | |
| Ability to follow comments, commands and simple questions in setting | 62 | ||
| Improved understanding of routines | 57 | ||
| Increase in number of friendships | 49 | ||
| Increased ability to follow instructions in setting | 38 | ||
| Increased understanding of consequences, e.g. road safety | 14 | ||
| 3. Expressive language (structure and content) | Understanding and use of language | Improved understanding of language | 94 |
| Increased vocabulary – knowledge and use | 89 | ||
| Improved standardised assessment scores | 43 | ||
| Increased use of grammatical structures | 40 | ||
| Able to present information clearly | 23 | ||
| Improved imitation skills | 11 | ||
| Emotional well-being | Increase in child’s confidence | 100 | |
| Improved emotional well-being | 83 | ||
| Increased levels of happiness | 74 | ||
| Decreased adult stress and anxiety | 43 | ||
| Participation and inclusion | Able to communicate effectively in and outside home | 74 | |
| Increased play with others in setting and home | 66 | ||
| Speaks with more people | 49 | ||
| Increased number of friendships | 40 | ||
| Increased access to the curriculum | 34 | ||
| Improved access to education | 20 | ||
| Increased setting attendance | 17 | ||
| 4. Self-monitoring | Self-awareness | Evidence of increased self-correction | 100 |
| Recognises incidences of error production and attempts to self-correct | 100 | ||
| Able to identify errors in others’ speech and language | 56 | ||
| Increased intelligibility | 44 | ||
| Independence | Engagement in active learning and self-help | 69 | |
| Able to seek clarification independently | 61 | ||
| Able to recognise own difficulties and self-correct independently | 56 | ||
| Increased independent learning | 47 | ||
| Reduced level of prompting required | 44 | ||
| Reduced level of support needed in setting | 22 | ||
| Participation and inclusion | Increased levels of confidence in class participation | 97 | |
| Able to sustain relationships | 86 | ||
| Able to act appropriately in a number of settings | 75 | ||
| Increased setting attendance | 22 | ||
| Improved negotiation skills | 19 | ||
| 5. Generalisation | Communicative competence | Evidence of wider use of intervention target (beyond therapy session) | 94 |
| Transfer and impact of skills beyond intervention target focus | 69 | ||
| Improved attention in home and setting | 67 | ||
| Child able to request novel items outside of session | 50 | ||
| Increased use of complex language | 19 | ||
| Emotional well-being | Increase in child’s confidence | 92 | |
| Reduced levels of frustration | 86 | ||
| Reduced levels of anxiety | 64 | ||
| Able to gain pleasure from communication | 58 | ||
| Participation and inclusion | Increased participation at home and in setting | 81 | |
| Increased motivation to communicate | 67 | ||
| Increased participation in all aspects of child’s life | 44 | ||
| Increased participation | 39 | ||
| Increased access to the curriculum | 22 | ||
| Able to be understood by adults and peers | 19 | ||
| Increased number of friendships | 14 | ||
| Child able to request novel items outside of session | 8 | ||
| Increased intelligibility to unfamiliar listeners | 6 | ||
| 6. Foundation skills | Attention and listening | Able to switch attention from activity to adult instruction with strategies (e.g. call name) (joint attention) | 95 |
| Able to switch attention without support (joint attention) | 92 | ||
| Age-appropriate attention | 84 | ||
| Basic sound awareness (symbolic level) | 16 | ||
| Percentage increase in correctly identifying different sounds | 8 | ||
| Able to clap number of syllables | 5 | ||
| Social interaction | Able to initiate turn taking with a peer | 76 | |
| Able to take turns with an adult in structured activity | 70 | ||
| Improved social communication skills | 62 | ||
| Increased eye contact | 54 | ||
| Age-appropriate play | 38 | ||
| 7. Functional communication | Social interaction | Increased levels of initiation and response | 97 |
| Increased levels of interaction | 84 | ||
| Increased number of communication functions and frequency of use | 61 | ||
| Improved turn taking | 37 | ||
| Able to request clarification | 21 | ||
| Participation and inclusion | Increased confidence and willingness to engage with others | 100 | |
| Increased communicative ability in a variety of settings | 97 | ||
| Able to participate in conversations to share information | 42 | ||
| Increased access to the curriculum | 29 | ||
| Able to social network and make friends | 24 | ||
| Able to make friends and go to birthday parties | 8 | ||
| 8. Adult understanding and empowerment | Adult–child relationship | Adults able to value their role in helping the child | 91 |
| Adult acceptance of child’s difficulty | 82 | ||
| Improved adult–child attachment | 71 | ||
| Adults report enjoyment of child’s company | 56 | ||
| Adult knowledge and use of strategies | Increased awareness of own communication by adults | 71 | |
| Appropriate adult use of specific praise | 50 | ||
| Adults feel potent and aware of agency in child’s education | 47 | ||
| Effective carry-over of skills by adults | 44 | ||
| Increased frequency of therapy carry-over and more progress | 32 | ||
| Adults able to cue child appropriately | 26 | ||
| Spontaneous development of ideas by adults | 12 | ||
| Spontaneous development of ideas by adults | 9 | ||
| Able to explain tasks to others | 6 | ||
| Adults able to use the same language and examples as SLTs | 3 | ||
| Adult–SLT partnership | Conversations between adults and therapists reflect a partnership | 68 | |
| Adult engagement with intervention process | 68 | ||
| Adults view SLT as supportive rather than critical | 59 | ||
| Increased frequency of therapy carry-over and more progress | 41 | ||
| Appropriate adult engagement with service | 32 | ||
| Good appointment attendance | 32 | ||
| 9. Adult–child interaction | Adult knowledge and use of strategies | Adults able to adopt interaction strategies | 78 |
| Increased communication-friendly environment (language support strategies) | 73 | ||
| Child experiences a positive communication environment | 73 | ||
| Adults able to identify their own goals to work on | 32 | ||
| Adults remove background noise and distraction | 27 | ||
| Improved attention and listening | 16 | ||
| Social interaction | Adults follow child’s lead in conversation and play | 73 | |
| Increased communicative initiations by child | 70 | ||
| Improved joint attention | 62 | ||
| Appropriate adult and child turn taking | 38 | ||
| Improved turn taking | 19 | ||
| Increased use of concrete language by adults | 16 | ||
| Increase in child’s output/words/utterances | 16 | ||
| Child’s language is age appropriate | 5 | ||
| Emotional well-being | Reduced levels of child’s frustration | 68 | |
| Increase in child’s confidence | 46 | ||
| Increased adult confidence in supporting child (self-report) | 43 | ||
| Increased adult understanding | 35 |
Appendix 36 Free-text responses to the Delphi survey
| Outcome domains | Additional suggested outcome indicators from Delphi round 3 for domains for which only one indicator was provided in the survey |
|---|---|
| Behaviour | Improved behaviours include increased co-operation and attention and reduction of undesirable behaviours and incidents, e.g. aggressionIncreased participation in group situationsIncrease in co-operative play with peersReduction in negative emotionsChild can communicate with adults and peers leading to a reduction in frustration and increased co-operationPositive outcomes, e.g. following instructions, helpful behaviour, follows routineIncrease in positive behaviours and interactionsUse a positive outcome measureDevelopmentally appropriate behaviours demonstratedAble to communicate needs to adults and peers, showing reduced frustration and unwanted behavioursParent report, scale of concernReduced impact of behaviour difficulties allowing for increased participation in activities for daily living and family activitiesReduced frustrationImproved self-regulation skillsIncrease in co-operative learningAble to reason and negotiate rather than use behaviour from communicationReduced need for support to conform to expected behaviourInclude examples of ‘improved behaviour’ |
| Educational achievement | Level of participation in classConfidence to participate fully in class oral workChanges in assessment scores/measurementsAge-appropriate literacy levels, e.g. ‘p’ scoresProgress markers for communication in EYFS and National Curriculum expected levelsAchieving at a level consistent with global learning levelEvery Child a Talker monitoring toolGreater than expected progress compared to past levelsImproved ability to follow and use a narrativeSustained attention (e.g. to stories); task completion; independent learningAbility to learn the routine of school, engage in large groups/small groups, interact with others, learn and retain informationBenchmark against, e.g. faster progress through ‘p’ levels/achievement of IEP [Individual Education Plan] objectives |
| Emotional well-being | Child self-rating on a scale at baseline and again after therapy around well-beingChild confident to participate in activities within and out of settingChild more likely to leave parent independently to interact with others.Joins in class discussionsParent rating, teacher rating, child self-rating if old enoughAble to express/control emotions appropriatelyPositive interactions:Plays and interacts happily with adults and peersChild talks more to peers or adultsIncreased confidence in interaction and less anxietyIncreased participation in activities with othersReduction in child anxiety/anxiety behavioursLevel of resilience |
| Independence | Asking for help:Can communicate difficulties as and when they occur so that others can support more appropriatelyAn ability to use strategies to self-manage any difficulty including asking for help/clarificationAble to communicate needs to peers and adultsSelf-help:Able to meet own needs through more independent social communicationAble to use a range of communicative functionsAbility to initiate interaction:Child able to initiate communication/verbal interaction without adult or other visual promptsChild’s ability to use strategies and function at a similar level to peers in a supportive environmentAble to indicate a choice, comment and make requestsEffectiveness of communication, e.g. how well they use the skills they haveAble to separate from parent and take active part in activities (one-to-one and group) without parentAble to participate in an activity without adult supportChild able to participate in an activity with less adult supportAble to carry out specific, appropriate tasks independently after initial demonstration/support from adultNeed descriptive indicators related to attention, initiating, play, asking questionsDemonstrates more independence in self-help skillsDecreased need to rely on others to help communicate needsDecreased need to follow others to follow directionsBefore and after measures of what is needed to help child join a specific activity |
| Social interaction | Increased initiation and responding to interactionIncrease in frequency of communicative attemptsChild initiates interaction with adults and/or peersChild uses language for social as well as functional purposesIncreased eye contact, turn taking, shared play with adults, shared play with peersIncrease in turn taking, respect for turns, social register use, proximity, improved understanding and use of facial expressions and gestureIncrease in range of people with whom child communicatesSustains interaction for more turnsAbility to interact across a range of settingsIncrease in number of meaningful interactions, either verbal or non-verbal, child has with adults and peersIncreased engagement with peersIncrease in shared interaction, ability to sustain and initiate communication with othersMore confident communicator and participator in conversationsUse of language, e.g. turn taking, conversation repair, co-operative playAdult change:Adult using appropriate linguistic level and modelsAdult uses opportunities that arise to support child to develop greater range of language functions (e.g. request, greet, initiate, question) |
Appendix 37 The Child Talk programme research protocols: phase 1 and phase 2
Appendix 38 Publications and engagement and dissemination activities
Publications
Roulstone S, Harding S. Defining communication disability in under-served communities in response to the World Report on Disability. Int J Speech Lang Pathol 2013;15:27–31.
Engagement activities
Afasic newsletter
| Activity type | A magazine, newsletter or online publication |
| Presentation type | Paper presentation |
| Geographical reach | National |
| Primary audience | Public/other audiences |
| Activity years | 2013 |
| Result description | Parker N (and Child Talk – What Works team). News from the Child Talk – What Works Programme and How You Can Get Involved. Afasic newsletter, Spring 2013 Afasic is a parent-led organisation that helps children and young people with speech and language impairments and their families. It provides information and training for parents – and professionals – and produces a range of publications. Members meet in local groups in many areas of the UK. In excess of 2000 people receive the Afasic newsletter |
| Impact description | The article in the newsletter prompted a group organiser to promote the parent survey to its attendees and facilitated them to complete the survey by providing access to online computers. The information was also sent on to local SLTs and EYPs leading to a number of SLTs expressing an interest in participating in the Delphi study and obtaining a copy of the final report |
Royal College of Speech and Language Therapists Bulletin
| Activity type | A magazine, newsletter or online publication |
| Presentation type | Paper presentation |
| Geographical reach | National |
| Primary audience | Health professionals |
| Activity years | 2013 |
| Result description | Morgan L, Marshall J, Harding S, Roulstone S. Why Do SLTs Adapt the Therapy They Provide? Bulletin, October 2013 Bulletin is the RCSLT monthly magazine and is circulated to all members of the RCSLT. At present there are approximately 11,500 SLTs in the UK |
| Impact description | It is expected that circulation of the article in Bulletin will have raised awareness of the research programme |
INVOLVE conference
| Activity type | Scientific meeting (conference/symposium, etc.) |
| Presentation type | Poster presentation |
| Geographical reach | National |
| Primary audience | Public/other audiences |
| Activity years | 2012 |
| Result description | Coad R. Parent Involvement, Making it Meaningful. INVOLVE conference, Nottingham, UK, November 2012 (external, national) INVOLVE holds a national conference every other year to bring together people with a common interest in public involvement in NHS, public health and social care research. This includes members of the public, service users, researchers, research commissioners and representatives of voluntary sector organisations. The aim of the INVOLVE conference is to encourage the sharing of knowledge and learning |
| Impact description | General discussion during the poster session around good practice for PPI |
North Bristol NHS Trust research day
| Activity type | A talk or presentation |
| Presentation type | Paper presentation |
| Geographical reach | Local |
| Primary audience | Other academic audiences (collaborators, peers, etc.) |
| Activity years | 2012 |
| Result description | Coad R. Parent Involvement and Partnership. North Bristol NHS Trust research day, Bristol, UK, November 2012 (internal) |
| Impact description | To support the parent panel established for the Child Talk programme, terms of reference, a payment policy and other tools were developed and presented at this meeting. These have now been picked up by the Research & Innovation office at North Bristol NHS Trust and are used as a template for researchers setting up PPI panels in other areas of the trust |
Birmingham City University seminar
| Activity type | Scientific meeting (conference/symposium, etc.) |
| Presentation type | Keynote/invited speaker |
| Geographical reach | Regional |
| Primary audience | Health professionals |
| Activity years | 2012 |
| Result description | Harding S. Child Talk – What Works Overview. Birmingham City University Seminar, 7 November 2012 The Department of Speech and Language Therapy and Rehabilitation at Birmingham City University hold an ongoing seminar series. The regional speech and language therapy departments are invited, as are individual therapists and service leads. In addition, the SLT course cohorts and other allied health-care professionals/course attendees/lecturers are invited. Approximately 300 people attended the event |
| Impact description | A few of the therapists approached the Child Talk – What Works team to express an interest in taking part in the research. Additionally, more people requested a copy of the final project report when it is published. There was also an increase in the number of people visiting the research unit’s website and joining the Facebook page and Twitter account |
Afasic presentation
| Activity Type | Scientific meeting (conference/symposium, etc.) |
| Presentation type | Keynote/invited speaker |
| Geographical reach | National |
| Primary audience | Public/other audiences |
| Activity years | 2012 |
| Result description | Coad R, Harding S. Child Talk – What Works Programme Overview. Afasic, Bristol, UK, December 2012 Afasic is a parent-led organisation that helps children and young people with speech and language impairments and their families. It provides information and training for parents – and professionals – and produces a range of publications. Members meet in local groups in many areas of the UK. It has in excess of 2000 members. Approximately 100 people attended this event and approximately 30 people attended the Child Talk – What Works presentation (parallel sessions) |
| Impact description | General discussion following the presentation |
Bristol Centre for Linguistics (University of the West of England seminar series)
| Activity type | A talk or presentation |
| Presentation type | Paper presentation |
| Geographical reach | Local |
| Primary audience | Health professionals |
| Activity years | 2013 |
| Result description | Blackwell A. Characteristics of Parent–Child Interactions Which Influence the Vocabulary Development of Preschool Children with Impaired Language: a Systematic Review, February 2013 (internal) |
| Impact description | General discussion following the presentation |
Afasic presentation
| Activity type | Scientific meeting (conference/symposium, etc.) |
| Presentation type | Keynote/invited speaker |
| Geographical reach | National |
| Primary audience | Public/other audiences |
| Activity years | 2013 |
| Result description | Coad R, Harding S. Child Talk – What Works Programme Overview. Afasic, London, UK, March 2013 Afasic is a parent-led organisation that helps children and young people with speech and language impairments and their families. It provides information and training for parents – and professionals – and produces a range of publications. Members meet in local groups in many areas of the UK. It has in excess of 2000 members. Approximately 150 people attended this event and 30 people attended the Child Talk – What Works presentation (parallel sessions) |
| Impact description | Several SLTs contacted the research unit following the event to ask for more information on the research programme and how they could get involved |
Bristol Research in Practice Annual Symposium
| Activity type | Scientific meeting (conference/symposium, etc.) |
| Presentation type | Paper presentation |
| Geographical reach | Local |
| Primary audience | Health professionals |
| Activity years | 2013 |
| Result description | Blackwell A. Characteristics of Parent–Child Interactions: a Systematic Review of Studies Comparing Children with Primary Language Impairment (PLI) and Their Typically Developing Peers. Bristol Research in Practice Annual Symposium, May 2013 (internal) This local symposium is particularly aimed at nurses, midwives, allied health professionals, health-care scientists and clinical psychologists. It provides an opportunity for local researchers to present their work and situate it within current practice. It is also a networking opportunity. Approximately 260 people attended the event |
| Impact description | General discussion following the presentation |
Child Language Seminar, Manchester
| Activity type | Scientific meeting (conference/symposium, etc.) |
| Presentation type | Paper presentation |
| Geographical reach | International |
| Primary audience | Health professionals |
| Activity years | 2013 |
| Result description | Roulstone S, Morgan L, Parker N, Marshall J. Intervention for Preschool Children with Primary Speech and Language Impairments (PSLI): Therapists’ Perspectives on the Components/Goals/Purposes of Therapy. Child Language Seminar, Manchester, June 2013 (external) The Child Language Seminar is an interdisciplinary conference with a long tradition that attracts a diverse international audience of linguists, psychologists and speech–language therapists and provides a forum for research on language acquisition and developmental language disorders. Approximately 200 people attended the event |
| Impact description | General discussion following the presentation |
Research Institute for Health and Social Change, Manchester Metropolitan University
| Activity type | Scientific meeting (conference/symposium, etc.) |
| Presentation type | Paper presentation |
| Geographical reach | Regional |
| Primary audience | Other academic audiences (collaborators, peers, etc.) |
| Activity years | 2013 |
| Result description | Parker N, Harding S, Marshall J, Roulstone S. Listening to Parents – Improving Speech and Language Therapy Provision for Pre-School Children with Primary Speech and Language Impairment. Research Institute for Health and Social Change, Manchester Metropolitan University, 4–5 July 2013 (external) The Research Institute for Health and Social Change hosts an annual conference giving undergraduates, postgraduates and early years researchers the opportunity to present the research that they are currently undertaking to their peers. Manchester Metropolitan University provides a speech and language course and some members of the audience were from that discipline, with others from areas such as psychology, occupational therapy, and physiotherapy. Approximately 200 people attended the event |
| Impact description | General discussion following the presentation |
International Association of Logopedics and Phoniatrics (IALP) World Congress
| Activity type | Scientific meeting (conference/symposium, etc.) |
| Presentation type | Paper presentation |
| Geographical reach | International |
| Primary audience | Other academic audiences (collaborators, peers, etc.) |
| Activity years | 2013 |
| Result description | Harding S, Coad J, Hambly H, Morgan L, Parker N, Roulstone S. Preschool Children’s Engagement in Speech and Language Therapy. IALP 29th World Congress, Turin, Italy, August 2013 Roulstone S, Morgan L, Parker N, Marshall J. Identifying Components of Interventions for Preschool Children with Primary Speech and Language Difficulties. IALP 29th World Congress, Turin, Italy, August 2013 Marshall J, Morgan L, Ward J, Roulstone S. Interventions for Preschool Children with Primary Speech and Language Impairment: What Speech and Language Therapists Do and What Influences Them. IALP 29th World Congress, Turin, Italy, August 2013 Harding S, Goldbart J, Morgan L, Parker N, Lewis E, Marshall J, Roulstone S. A Systematic Review of the Interventions Used with Preschool Children with Primary Speech and Language Impairment. IALP 29th World Congress, Turin, Italy, August 2013 Wren Y, Harding S, Goldbart J, Morgan L, Parker N, Lewis E, Marshall J, Roulstone S. A Systematic Review of the Interventions to Improve Preschool Children’s Phonological Awareness and Speech Output. IALP 29th World Congress, Turin, Italy, August 2013 Approximately 2000 people attended the event |
| Impact description | A number of therapists requested a copy of the final project report when it is ready. There was also an increase in the number of people visiting the website and the joining the Facebook page and Twitter account in the week after the conference |
Talk to your Baby conference
| Activity type | Scientific meeting (conference/symposium, etc.) |
| Presentation type | Keynote/invited speaker |
| Geographical reach | National |
| Primary audience | Other academic audiences (collaborators, peers, etc.) |
| Activity years | 2013 |
| Result description | Hambly H. Child Talk: The Perspectives of Pre-School Children. Talk to your Baby conference, London, UK, 25 November 2013 (external) Approximately 150 people attended the event. The audience consisted of the heads of children’s services, early years and childcare services and Sure Start children’s centres, EYFS consultants, children’s centre teachers and EYPs and parenting/family support teams |
| Impact description | Following on from the conference, News and Online Editor Catherine Grant from Nursery World [see www.nurseryworld.co.uk/ (accessed 21 January 2015)] contacted the research team to produce an article about the research. Several attendees have also e-mailed requesting documentation about parent–child interaction and empowerment and a copy of the final programme report |
Health visitor conference
| Activity type | Participation in an activity, workshop or similar |
| Presentation type | Workshop facilitator |
| Geographical reach | Local |
| Primary audience | Health professionals |
| Activity years | 2013 |
| Result description | Morgan L, Blackwell A. What Can Health Visitors Learn from Child Talk – What Works. Health visitor conference, Bristol, UK, 6 November 2013 (external, local) Approximately 70 people attended the event |
| Impact description | Information about the website resources was disseminated as well as more general information about the research unit and Child Talk – What Works. In the week following this event there was an 18% increase in the number of website visits and also Twitter followers. Additionally, a number of telephone calls were received seeking additional information and requesting a copy of the final project report |
Child Language Seminar, Manchester
| Activity type | Scientific meeting (conference/symposium, etc.) |
| Presentation type | Poster presentation |
| Geographical reach | International |
| Primary audience | Health professionals |
| Activity years | 2013 |
| Result description | Roulstone S, Goldbart J, Harding S, Morgan L, Parker N, Lewis E, Marshall J. A Systematic Review of the Interventions Used with Preschool Children with Primary Speech and Language Impairment. Child Language Seminar, Manchester, UK, June 2013 Roulstone S, Harding S, Coad J, Hambly H, Morgan L, Parker N. Preschool Children’s Engagement in Speech and Language Therapy. Child Language Seminar, Manchester, UK, June 2013 Lewis E, Morgan L, Marshall J, Ward J, Roulstone S. Modification of Speech and Language Therapy Interventions for Preschool Children with PSLI. Child Language Seminar, Manchester, UK, June 2013 Parker N, Lewis E, Morgan L, Harding S, Marshall J, Roulstone S. Descriptions of Interventions for Preschool Children with Primary Speech and Language Impairment: A Comparative Content Analysis. Child Language Seminar, Manchester, UK, June 2013 The Child Language Seminar is an interdisciplinary conference with a long tradition that attracts a diverse international audience of linguists, psychologists and speech–language therapists and provides a forum for research on language acquisition and developmental language disorders. Approximately 200 people attended the event |
| Impact description | General discussion during the poster session |
CogDev conference, Reading
| Activity type | Scientific meeting (conference/symposium, etc.) |
| Presentation type | Poster presentation |
| Geographical reach | International |
| Primary audience | Health professionals |
| Activity years | 2013 |
| Result description | Blackwell A. Characteristics of Parent–Child Interactions: A Systematic Review of Studies Comparing Children with Primary Language Impairment (PLI) and Their Typically Developing Peers. Joint Annual Conference of the British Psychological Society Developmental and Cognitive Sections (CogDev), Reading, UK, September 2013 Blackwell A. Methodological Considerations When Using Technology for Automated Vocal Analysis (LENA) with Young Children. Joint Annual Conference of the British Psychological Society Developmental and Cognitive Sections (CogDev), Reading, UK, September 2013 CogDev 2013 attracted many of the leaders in cognitive and developmental psychology from the UK and Europe. The theme of the conference was the relationship between cognition and development and the related fields |
| Impact description | General discussion during the poster session |
Glossary
See Appendices 1–6 for additional glossaries of activities, interventions, programmes, strategies, study designs and general processes and terms respectively.
- Activity/activities
- Specific tasks that are usually targeting impairment.
- Adult–child interaction (typology theme)
- Work on the interaction between the parent/adult and the child. All of the changes to the parent/adult–child interaction were emphasised in terms of those that encourage speech and language development. These interaction strategies range from activities such as sitting and playing with the child or following the child’s lead to commenting on the child’s activities or reducing the number of questions used in interactions with a child.
- Adult understanding and empowerment (typology theme)
- Work that helps parent to understand the nature of their child’s speech and language difficulty, what helps to improve it and why. An important aspect of this is a parent’s or adult’s understanding that he or she is a ‘major tool of change’.
- Assessment
- The activity/tool used by speech and language therapists to evaluate a child’s speech and language and identify any areas of difficulty.
- Comprehension (typology theme)
- Work that aims to improve the child’s understanding of (receptive) language.
- Content analysis
- Analysing the content of text data by looking at it objectively and systematically, counting incidences and reporting on descriptions and classifications.
- Documentary analysis
- A research method that involves analytically reading or reviewing documents to provide evidence/support for facts stated in research. Analysis of documents can be qualitative or quantitative.
- Expressive language (typology theme)
- Work that aims to improve the child’s expressive language (the ability to express thoughts as words/sentences – can be spoken or written) in terms of quantity, vocabulary or structure.
- Foundation skills (typology theme)
- Work to practise and improve a range of early skills, many of which might be considered foundations for speech and language development.
- Functional communication/functional use of language (typology theme)
- Work focused on aspects of communication that help the child’s involvement and participation in life situations; this might be functional language, signing or the use of symbols.
- Generalisation (typology theme)
- Work to help make speech and language or therapy gains transferable to other situations and environments.
- Intervention
- Support given to children with speech, language and communication needs above what they would normally receive in the class or home environment.
- Materials
- Items or published materials used in the delivery of an intervention (also resources).
- Outcome
- The measure used to assess change following an intervention.
- Preschool
- Children aged between 2 years and 5 years 11 months (using the international average age for starting school).
- Primary speech and language impairment
- Term used to describe children whose speech and/or language difficulties occur in the absence of other overt physical or cognitive difficulties.
- Programme
- An intervention that encompasses specific procedures with detailed plans for how to deliver the intervention.
- Resources
- Items or published materials used in the delivery of an intervention (also materials).
- Self-monitoring (typology theme)
- Work designed to increase the child’s awareness of his or her speech and language difficulties and how he or she might be able to overcome them.
- Speech (typology theme)
- Work that increases the accuracy of speech production or articulation, often focusing on specific sound(s).
- Speech and language therapist
- A practitioner with the primary responsibility for assessing a child with speech, language and communication needs and providing intervention.
- Speech, language and communication needs
- An umbrella term used to describe children with speech and language difficulties regardless of origin or presenting features.
- Strategies
- General things used in interactions with children that might target at the level of impairment, activity or participation.
- Thematic analysis
- The process of pinpointing, examining and recording patterns and themes within qualitative data.
- Typology
- A systematic description of the characteristics or components of speech and language therapy practice.
List of abbreviations
- AAC
- augmentative and alternative communication
- AAPS
- Arizona Articulation Proficiency Scale
- ASHA
- American Speech–Language–Hearing Association
- BBTOP
- Bankson–Bernthal Test of Phonology
- BCRP
- Better Communication Research Programme
- C
- consonant
- CBCL/2–3
- Child Behavior Checklist 2–3
- CCF
- Central Commissioning Facility
- CELF-4
- Clinical Evaluation of Language Fundamentals-4
- CSP
- Commissioning Support Programme
- CTRF
- Caregiver Teacher Report Form
- CV
- consonant–vowel
- CVC
- consonant–vowel–consonant
- DEAP
- Diagnostic Evaluation of Articulation and Phonology
- df
- degrees of freedom
- DIBELS
- Dynamic Indicators of Basic Early Literacy Skills
- DLS
- Derbyshire Language Scheme
- DMT
- drama and movement therapist
- EBP
- evidence-based practice
- EYFS
- early years foundation stage
- EYP
- early years practitioner/professional
- GFTA
- Goldman–Fristoe Test of Articulation
- HAPP
- Hodson Assessment of Phonological Patterns
- HOME
- Home Observation for Measurement of the Environment
- ICW
- information-carrying word
- LENA
- Language Environment Analysis
- MLU
- mean length of utterance
- NDP
- Nuffield Centre Dyspraxia Programme
- NIHR
- National Institute for Health Research
- ONS
- Office for National Statistics
- PALS
- Phonological Awareness Literacy Screening
- PEDro
- Physiotherapy Evidence Database
- PI
- principal investigator
- PIC
- participant identification centre
- PIPA
- Preschool and Primary Inventory of Phonological Awareness
- PLS
- Preschool Language Scale
- PLS-3
- Preschool Language Scale-3
- PLS-3-UK
- Preschool Language Scale-3 UK Edition
- PLS-4-UK
- Preschool Language Scale-4 UK Edition
- PPI
- public–patient involvement
- PPVT
- Peabody Picture Vocabulary Test
- PPVT-R
- Peabody Picture Vocabulary Test – Revised
- PRISMA
- Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- PSLI
- primary speech and language impairment
- R&D
- research and development
- RAPT
- Renfrew Action Picture Test
- RAS
- refugees and asylum seekers
- RCSLT
- Royal College of Speech and Language Therapists
- RCT
- randomised controlled trial
- RDLS
- Reynell Developmental Language Scales
- RPC
- Relationship Process Code
- SAILS
- Speech Assessment and Interactive Learning System
- SCED
- single case experimental design
- SD
- standard deviation
- SES
- socioeconomic status
- SIG
- Specific Interest Group
- SLCN
- speech, language and communication needs
- SLT
- speech and language therapist
- SSD
- speech sound disorder
- SSRS
- Social Skills Rating System
- TAPS/NF
- Test of Auditory Perceptual Skills – Numbers Forward
- TD
- typically developing
- TIM
- Thorpe Interaction Measure
- TOLD-P:3
- Test of Language Development – Primary, 3rd edn
- TOM
- Therapy Outcome Measure
- TOMPD
- total occurrences of major phonological deviations
- TOPEL
- Test of Preschool Early Literacy
- WHO
- World Health Organization