

Notes
Article history
The research reported in this issue of the journal was funded by the PHR programme as project number 16/09/13. The contractual start date was in March 2018. The final report began editorial review in January 2022 and was accepted for publication in October 2022. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PHR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Permissions
Copyright statement
Copyright © 2023 Popay et al. This work was produced by Popay et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This is an Open Access publication distributed under the terms of the Creative Commons Attribution CC BY 4.0 licence, which permits unrestricted use, distribution, reproduction and adaptation in any medium and for any purpose provided that it is properly attributed. See: https://creativecommons.org/licenses/by/4.0/. For attribution the title, original author(s), the publication source – NIHR Journals Library, and the DOI of the publication must be cited.
2023 Popay et al.
Chapter 1 Introduction
In 2016 the National Institute for Health and Care Research (NIHR) sought to commission research to address urgent gaps in the evidence on which interventions, using a community engagement approach, are effective in improving health and well-being and reducing health inequalities. The research reported here was funded under that initiative. It was the third phase of the Communities in Control (CiC) study: a longitudinal mixed-methods study that began in 2014 and aimed to evaluate the social and health impacts of England’s largest area-based community empowerment initiative to date – Big Local (BL). Two earlier phases of the CiC study were funded by the NIHR School for Public Health Research (SPHR) (CiC1: 2014–15 and CiC2: 2015–17). 1–3 These earlier phases were the foundation for the phase 3 research reported here (CiC3), enabling the construction of longitudinal qualitative and quantitative data sets and providing early insights into both process and impacts. CiC3 began in March 2018 and was originally to end in May 2021. However, in response to pandemic-related disruptions, described at various points in the report, a short no-cost extension to September 2021 was agreed.
The BL initiative, funded by the then Big Lottery Fund (now the National Lottery Community Fund), was launched in 2010 and began to be implemented in 2011. It was initially due to run for 10 years but has since been extended. The programme gave each of 150 relatively disadvantaged neighbourhoods around England £1M for residents to spend to ‘make their neighbourhood an even better place to live’. 4 Though not an explicit objective, the BL initiative has the potential to influence health outcomes of residents of these neighbourhoods via various pathways. The CiC study has focused on the potential indirect health impacts of communities of place having greater collective control over decisions and actions to improve the areas in which they live, and the direct health impacts of any improvements in the social determinants of health and health equity residents deliver in their neighbourhoods.
Communities in Control (CiC3) has investigated the medium-term social and health impacts of BL on the populations of the 150 areas in England where the programme was implemented and on the most engaged residents in these areas; assessed changes over time in the collective control BL residents had over decisions and actions that aimed to improve social determinants of health in BL areas; explored pathways to any changes in collective control and social and health outcomes identified; and conducted an economic evaluation. We also aimed to draw out policy, practice and research implications for future community engagement strategies.
It is important to note that our research has been significantly impacted by the COVID-19 pandemic. The lives of our respondents and members of our research team have been disrupted by the restrictions imposed by the COVID-19 lockdown and particularly by home working and the closure of schools, nurseries and so forth. While most research staff continued working, their productivity was impacted, affecting the research in ways that are difficult to quantify. Other challenges and delays to the project, partly or wholly due to the pandemic, can be identified. Access to the Office for National Statistics Annual Population Survey (ONS APS) for research on the social and health impacts of BL at the area population level was delayed for almost 2 years, leaving ˂ 2 months to complete the analysis of our primary outcome. This caused severe delays for the economics analyses, which were dependent on the findings from the APS analysis, leading to major redesign of this work. Wave 2 interviews in work package (WP) 3 were halted entirely for 3 months, and when fieldwork began again it was clear that many residents of BL areas would not be able to continue to participate due to disruptions in their lives, severely disrupting recruitment. Notwithstanding these challenges, we believe that the findings described in this report will make a valuable contribution to the development of future public health action with those communities and groups that bear the brunt of social inequalities.
In Chapter 2 we consider the context for the research. This chapter looks in turn at the key underpinning concepts (empowerment, control and community); changes over the past 25 years in policy perspectives on place-based initiatives (PBIs) in which, like BL, community involvement is central; and current evidence on the social and health impacts of these initiatives. The CiC3 study is then described in Chapter 3, including the theoretical framework underpinning the research and our original plans for public involvement. Changes since the research was funded are highlighted, including the impact of the pandemic (the impacts of public involvement are considered in the final chapter). The next six chapters present the main findings. Drawing on a series of interviews with national key informants, Chapter 4 describes how the programme has changed over time and the relationship of BL to the national policy context. Chapter 5 presents the quantitative findings on population-level social and health impacts in BL areas. Quantitative findings on the impacts on the health and well-being of the most engaged residents are presented in Chapter 6. Chapters 7 and 8 draw on our longitudinal qualitative data to explore pathways to changes in collective control in BL communities and to health impacts. Appendix 7 summarises the methods and findings from the earlier phases of the CiC study, some of which are integrated into the report where relevant. Chapter 9 presents findings from our work on the economics of BL. Finally, in Chapter 10 we summarise the main findings from the research and discuss the implications for future policy, practice and research focused on place-based initiatives that aim to ‘empower’ disadvantaged communities to engage in action to reduce social and health inequalities.
Chapter 2 Place-based approaches to address social and health inequalities: concepts, policy and evidence
The conceptual context: empowerment, control and community
Over the past quarter-century, place-based approaches to promote public participation in policy decision-making and empower communities to have more control over their lives have become mainstream, featuring in global, national and local health and social policies (e.g. UN Economic and Social Council 20195). However, the concepts of empowerment, communities and collective control – central to these policies – are subject to multiple and sometimes conflicting interpretations.
Empowerment
Many contemporary understandings of empowerment link it to improvements in individual self-help. For example, in the health field it is linked to personal management of chronic health conditions and/or the adoption of ‘healthier’ behaviours. In contrast, drawing on the work of Freire and Gramsci6,7 and the civil rights and feminist movements of the 1960s and 1970s, others understand empowerment as involving sociopolitical processes that support people bearing the brunt of social injustice to exercise greater collective control over decisions and actions impacting on their lives and health, and in so doing, contributing to greater social equity in society. As Eyben puts it: ‘empowerment happens when individuals and organised groups are able to imagine their world differently and to realise that vision by changing the relations of power that have kept them in poverty, restricted their voice and deprived them of their autonomy’. 8
Like empowerment, ‘control’ is often understood as an individual outcome of successful empowerment. ‘Collective control’, in contrast, is presented as the outcome of successful empowerment at a community or group level, when people act together in their common interest. As we describe in Chapter 7, in the CiC study, the capabilities associated with collective control have been operationalised as different forms of power. 9
Examples of this more political expression of community empowerment find their most radical form in the popular epidemiology examined by Brown,10,11 where people spontaneously and collectively respond to resist a shared threat to their well-being. Brown has studied local people’s resistance to exposure to toxic waste, including, for instance, the action by residents in Woburn, Massachusetts, to try to prove a link between industrial toxins in their water supply and high rates of childhood leukaemia. 10
These different understandings of empowerment sit at the extremes of a continuum along which the significance varies between a focus on individual self-help versus collective action; on changes in personal circumstances/behaviour versus in proximal living and working conditions; of action to increase internal capabilities of individuals/groups to improve their lives versus action on wider political and social change for greater equity.
Elsewhere we have argued that the construct of collective control understood as the outcome of empowerment processes has greater analytical and practical advantage for health policy and practice than the commonly used concept of ‘community empowerment’. 9 In particular, it can help move policy, practice and research beyond the ‘inward gaze’ dominating many contemporary community initiatives, which focuses on developing the internal capabilities of disadvantaged communities in order to better enable them to ‘cope’ with their proximal living circumstances. This inward gaze is embedded, for example, in concepts such as community competencies, capacities, assets, resilience and social capital. Clearly, it is important that people experiencing the brunt of inequalities (however defined) are supported to develop their internal capabilities. It is also important, however, that this inward gaze is complemented by an ‘outward gaze’ aimed at supporting communities to mobilise these capabilities to collectively take more control over the external structures and conditions that drive social, economic and health inequalities. The concept of collective control helps strengthen this outward gaze by placing power and social change at the centre of place-based policy and practice.
Community
The term collective also avoids the ambiguous and contested concept of community. 12 Some 50 years ago, Bell and Newby identified 98 different definitions of community. 13 As Dominelli notes, communities ‘are constantly changing entities with shifting and contested boundaries … because individuals belong to more than one community simultaneously.’14 Communities are self-defined and can be international, national or local. They provide a sense of belonging for ‘members’ sharing an affinity to a particular place, interest or identity but can feel exclusionary to those who do not ‘meet’ the membership criteria. Communities can also be deeply gendered. Women are primarily responsible for constructing the threads that bind local place-based communities together – albeit the relational work they do in these communities is often invisible.
For much of the past 25 years, public policy and practice focused on reducing social and health inequalities in England has been dominated by a focus on place-based communities and particularly people living in the most disadvantaged neighbourhoods. However, as we discuss in the next section, there have also been significant differences in the nature of these policies over time.
The policy context: English place-based community initiatives since 1997
Since the 1960s, numerous PBIs in the UK have aimed to tackle social and geographical inequalities by regenerating disadvantaged areas and improving the lives of the people who live there15–17 (see Box 1 for a timeline of policy developments relevant to community empowerment). These are often collectively referred to as area-based initiatives (ABIs), but in this report we use the more generic term PBIs. Improving health outcomes has not always been a primary focus of these policies, and the role of local government has changed over time, but the active involvement of local people has always been central to how such initiatives are meant to be delivered on the ground, albeit the approaches to community involvement have varied within and between policy initiatives. 18–20
Place-based initiatives gained particular prominence during the Labour administration of 1997–2010. Shortly after the 1997 election, a national strategy for neighbourhood renewal which focused on disadvantaged areas was published; it gave local government the lead role in promoting community empowerment, a role later enshrined in the 2006 Local Government Act. There was also a growing policy emphasis on the role of civil society organisations as partners with local authorities in supporting community empowerment and as providers of publicly funded services. The policy discourse also increasingly emphasised people’s responsibility to contribute to the well-being of their communities alongside their right to receive services and support.
The English place-based New Deal for Communities (NDC) programme, launched in 1998, was a central plank of the Neighbourhood Renewal Strategy. It aimed to reduce the gaps between 39 of the poorest neighbourhoods and the rest of the country in six domains: health, education, worklessness, crime, housing and the community. 21 Each NDC neighbourhood received £50M to achieve outcomes in these domains and had to establish a multisector partnership board to oversee expenditure over 10 years (a longer time period than any previous PBI). Community involvement was central. Residents were a majority on 31 of the 39 NDC partnership boards (in some cases chairing these), which included representatives from the local authority, police, the NHS and civil society agencies. The NDCs had a particular focus on physical regeneration and, driven by central government policy, sought to increase the diversity of local populations through housing improvements. However, implementation varied considerably. Some areas saw large-scale demolition and renewal; others focused on improving existing infrastructure. Despite the community empowerment rhetoric, as with other PBIs during this period, local authorities were accountable for the funds and had considerable influence over the NDC local programmes, while central government set the outcomes to be achieved and became more controlling over time. 21
The Neighbourhood Renewal Action Plan published in 2001 provided funding for community participation in a further 88 neighbourhood renewal areas across England. This plan included the ChangeUp programme (£231M), which supported community associations to access a range of training and support opportunities, and the establishment of community empowerment networks (CENs). These networks of local voluntary, community, faith and social enterprise (VCFSE) agencies were intended to work in partnership with local government in neighbourhood renewal areas to promote community participation in decision-making, though research suggests that at least some local authorities were unwilling to give the CENs a significant community empowerment role. 22 Other initiatives at this time adopted a more targeted focus on health (e.g. Health Action Zones and Healthy Living Centres)23,24 or on particular groups in the community (e.g. Sure Start centres for families with young children). 25
The Conservative/Liberal Democrat coalition government in power from 2010 to 2015 retained a strong policy focus on PBIs in disadvantaged neighbourhoods. However, there was a significant move away from central government involvement and major investment in physical infrastructure. Rather than directly funding or directing community action, the national government’s role shifted to one of creating an enabling environment in which place-based communities could take the initiative for themselves. The leading position of local government was replaced with an even stronger role for civil society organisations in supporting community empowerment and delivering publicly funded services, together with increased involvement of the private sector. 26
The coalition’s initial flagship policy, announced prior to the 2010 election, was the Big Society initiative. Between 2010 and 2012, this comprised a range of measures to encourage people to take an active role in their community and to take more responsibility for local decisions and services in order to achieve ‘fairness and opportunity for all’. 27 In 2011, the Community Organisers programme was launched to recruit and train 500 senior community organisers, to be paid £20,000 for their first year, and 4500 part-time voluntary organisers. 28 These organisers were to help communities, particularly in disadvantaged areas, take advantage of Big Society initiatives established by the 2011 Localism Act that aimed to ‘achieve a substantial and lasting shift in power away from central government and towards local people’. 29 Big Society initiatives included the right to buy public assets for community use and the right to bid to run public services. There was also an emphasis on community members setting up social enterprises that would reinvest their profits back into their business, creating local employment, or into the community to tackle local problems. In 2012 Big Society Capital, a social impact investment initiative, was set up. Run by the four main UK banks – Barclays, HSBC, Lloyds Banking Group and NatWest Group – it used funds from dormant bank accounts to provide loans for social enterprises and community projects.
The Big Society initiative disappeared around 2012. However, together with the Neighbourhood Renewal programme, it fed into a growing debate about the relative merits of supporting civil society organisations and community associations to strengthen community cohesion and deliver publicly funded services, compared with top-down, state-led action. From 2015 onwards, while policies have affirmed the continued importance of PBIs to address social and health inequalities, they have also clearly established the state’s role locally and nationally as less directive and more enabling. This is exemplified in the Civil Society Strategy published in 2018, which continued the emphasis on building a society ‘where people have a sense of control over their future and that of their community’ and on shifting the civil society–state relationship to give greater power and responsibility for service delivery to local people and third-sector organisations. 30
There is considerable literature on the limitations of both the Neighbourhood Renewal and Big Society approaches to place-based community empowerment. Bridle, for example, has argued that there is no evidence that either model led to improvements in volunteering, community action or public services. 31 Additionally, Balazard et al. suggest that between 2010 and 2015, public funding for smaller community associations was reduced, as it was for local government, with most funds going to large civil society organisations and private companies. 32 Other commentators have highlighted problems associated with a lack of funding for ‘social infrastructure’ to support civil society and community action. For example, Wills argued that because the localism agenda failed to provide local structures that enabled common interests to be identified in diverse populations and supported people to mobilise and shift local power dynamics, community empowerment could not be sustained. 33 Additionally, it has been argued that the increasing involvement of civil society organisations in public service delivery has undermined their role in community organising.
The election of a new government in 2019, the UK’s departure from the EU (‘Brexit’) and the COVID-19 pandemic have been accompanied by a reframed policy focus on the ‘levelling up’ of communities. The 2018 Civil Society strategy remains in place. However, in the context of the extensive community mobilisation that was seen during the first COVID-19 pandemic lockdown in England in 2020,34 the Conservative MP Danny Kruger was commissioned to ‘develop proposals to maximise the role of volunteers, community groups, faith groups, charities and social enterprises to contribute effectively to the government’s levelling up agenda’. 35
Published in September 2020, and based on wide consultation with organisations and individuals with experience of place-based/community initiatives, Kruger’s report sets out a series of proposals centred around a new ‘community power’ paradigm. 35 These reflect the broad policy direction embedded in the Big Society initiative and the 2011 Localism Act, but they also address many of the criticisms of previous place-based approaches to reduce social inequalities. For example, it is proposed that while decisions should be devolved to allow residents to ‘make great places “from within” rather than by outside interventions’, small-scale community associations, social enterprises and local groups should be favoured over the large civil society and private sector organisations that have had major roles in the past. 35 Similarly, the role of national and local government as ‘convenors and enablers’, not ‘inhibitors’ of community action is highlighted alongside a call for the central government to invest in renewing and modernising social infrastructure. The report recommends that significant resources be allocated to community associations and local civil society groups (with no strings attached) via a Levelling up Communities Fund (using dormant bank and insurance accounts). A new Community Power Act is proposed to establish a ‘community right to serve’, extending the rights for communities, charities and social enterprises to be involved in the design or delivery of a wide array of public services, and a new national Civil Society Improvement Agency to allocate funds to local organisations to help develop capacity for collective action in communities. Finally, the report argues for a revaluation of social infrastructure and the intangible social benefits of civil society to be included in the Treasury Review of the Green Book and for the development of a new Index of Social Infrastructure that can inform local and national policy-making.
The research context: social and health impacts of place-based community initiatives
Syme termed the theory underpinning policies that aim to empower individuals and/or communities ‘control over one’s destiny’. 36 A number of pathways are embedded in theories linking inequities in ‘control over destiny’ to inequities in health. 37
-
Living in disadvantaged neighbourhoods can produce a sense of collective threat and powerlessness. Over time, these chronic stressors can lead to anxiety, anger or depression – all known to damage mental and physical health. 38
-
Empowerment processes could trigger collective action by residents that successfully challenge local health hazards; for example, by preventing the siting of a toxic waste facility in a neighbourhood. 39,40
-
Members of disadvantaged groups could use their experiential knowledge to identify more appropriate and acceptable ways to address the health risks they face. 37,41–43
-
Participation in collective activities can reduce social isolation and foster greater social connectedness, improving mental and physical health. 39,44–47
-
Individuals participating in collective action can also benefit from an improved sense of self-efficacy and control, which research has linked to better health. 37,48
-
Empowerment processes may lead to increased political understanding and engagement (e.g. increasing voting rates). This could increase public pressure for more accountability in politics and more socially just policies.
High-quality empirical evidence testing these theoretical pathways demonstrates that the level of control an individual has over their life circumstances is a significant determinant of individual-level health outcomes. 49–52 There is also growing evidence on the impact of collective control on population health and on unequal collective control across diverse communities as a determinant of health inequities. For example, research has found positive impacts of collective control by communities on the social determinants of health; for example, social cohesion and environmental improvements. 37,53–56 Evidence for direct impacts of collective control by communities on health outcomes is more limited, but longitudinal studies have reported a positive association with health improvement. Chandlers et al. , for example, found that lower rates of youth suicide among First Nations people in Canada were significantly associated with increased ‘cultural continuity’, measured in terms of the success of land claims, degree of self-government, community control of local services and access to dedicated cultural facilities. 57 Similarly, Baba et al. found significant associations between measures of empowerment, general health and mental health among 4000 adult households in 15 Glasgow neighbourhoods undergoing regeneration. 58
Though limited in number, there are also some high-quality evaluations of the social and health impacts of interventions that aim to increase collective control. Orton et al. , for instance, identified direct health benefits arising from microfinance interventions that increased collective control among women in South Africa, Peru and Bangladesh, including reduced violence against women; reductions in infant mortality that were greater for those in the scheme compared with poor and richer women outside the scheme; and improved nutritional status in children, especially girls. 59 Evaluations of initiatives with a primary focus on community development, mostly small-scale case studies, have also reported positive impacts at individual, community and organisational levels. This has included outcomes for participating individuals such as increased confidence and influence over decision-making,60,61 impacts on social isolation and community connectedness and cohesion,60 and impacts on the capacity for local community organisations and groups to create change. 62,63 Some studies have looked at the effects of community-led initiatives on health outcomes. For example, a survey of communities undergoing regeneration in Glasgow found that residents’ perceptions of their ability to influence decisions where they lived were positively associated with mental health outcomes. 58 Similarly, a study of neighbourhood belonging found moderate associations with well-being stemming from greater social participation and increased feelings of belonging to the neighbourhood. 64
Research also suggests that the potential for PBIs to positively impact on social and health outcomes may be linked to their approach to community involvement. For example, while English policy initiatives such as Health Action Zones, Sure Start centres and Healthy Living centres enabled community members to participate successfully in specific health improvement initiatives and service delivery, evaluations reported there was little community influence over the strategic direction of these initiatives. 20,24,65,66 Factors influencing the degree and nature of collective control by residents in such initiatives are wide-ranging but include the extent to which priorities are conceived to have been ‘top-down’ (e.g. directed by local or national government policies). 67
Approaches to community involvement can also vary across areas within a single programme, producing differential empowerment outcomes and different social and health impacts. For example, in evaluations of regeneration programmes conducted in Scotland and England, despite the presence of engagement processes, lower levels of resident empowerment were observed in neighbourhoods undergoing major redevelopment (e.g. demolition and rebuilding of housing stock) compared to areas with regeneration plans focused on improving existing infrastructure and housing. 68 Similarly, an evaluation of the health equity impacts of the English NDC programme suggests there were greater improvements in mental health/well-being and social cohesion in NDC areas that adopted structures and processes that gave local people significant control over decisions. While few findings were statistically significant, they were consistent with theories about the pathways from empowerment to health and social outcomes. 68 Interestingly, lower levels of empowerment have also been reported when control of social housing has been transferred to resident-led community housing associations. As the quote below highlights, these results point to poor-quality involvement processes but also to a potential mismatch between the nature and scale of the problems facing residents who get involved in decision-making, the degree of control they have over these problems and the level of support they receive:
community engagement processes can be … unable to respond to variations in circumstances faced by communities living in different places. The result is that individual residents may not derive a sense of empowerment from either their participation in, or the ripple effects of, collective community engagement processes. 58
Finally, there is some limited evidence that PBIs that aim to empower local people may have differential impacts depending on the socioeconomic ‘status’ of neighbourhoods, potentially enhancing collective control over decisions in more affluent communities, while undermining capabilities for collective control in more disadvantaged groups. For example, on the basis of an evaluation of four local empowerment initiatives in England, Rolfe concluded that while communities can have control over decisions and actions:
the level of agency in each situation is shaped by community capacity [which] seems to demonstrate a distinct socioeconomic gradient, reinforcing concerns that community participation policies can become regressive, imposing greater risks and responsibilities upon more disadvantaged communities in return for lower levels of power. 69
Conclusion
There is growing evidence supporting the theory that increasing collective control by communities of interest/place over decisions and actions could have positive impacts on their lives and health. However, variations in the type and level of collective control communities are given appear to impact on the potential for positive outcomes, and more disadvantaged communities may be particularly disadvantaged if empowerment processes are not appropriately designed and supportive.
However, it remains the case that, overall, the evidence base on the impact of PBIs on the collective control communities have over decisions and actions, and in turn on social and health outcomes, needs to be strengthened. While a recent non-systematic review highlighted a multitude of studies of community empowerment initiatives reporting positive social and health outcomes, these are generally very small-scale, cover a short time period and rarely include controls or comparators. 70 There is also a lack of attention to health outcomes in many evaluations of interventions aiming to improve neighbourhoods by increasing residents’ collective control over decisions/actions. This is partly because policy-makers, those delivering the intervention, and evaluators do not anticipate health impacts; and partly due to challenges in capturing the impacts on outcomes in complex social initiatives. 71,72
Robust evaluation studies are needed that assess: (1) whether specific community empowerment initiatives actually lead to increased collective control by communities over decisions that impact on their neighbourhood; (2) the factors that enable and/or constrain the development of collective control in communities; and (3) whether initiatives that do enhance collective control can do so in ways that lead to better health-related outcomes and ultimately have the potential to reduce health inequalities. In particular, the studies need to be sensitive to the possibility of negative impacts and to differential impacts across different communities and neighbourhoods. The research reported here aimed to address these questions by evaluating a large community empowerment programme in England, utilising a design that recognised the methodological challenges and built on the latest developments in theory and research on PBIs. 73–75 In the next chapter we describe the Big Local intervention and the CiC study in more detail.
Chapter 3 The Communities in Control study
Introduction
The standard approach to evaluation of social and health interventions is to ask questions about what ‘works’ or ‘does not work’, for whom and in what contexts. The answers to these types of questions, however, while important, are not sufficient when the focus is on complex, socially-embedded, place-based community empowerment interventions like BL, where programme elements vary across place and time, pathways to impact are never linear or predictable and the context varies and is often unstable. As Petticrew argues, in addition to asking ‘what works’, evaluation should also ask ‘what happens’ when an intervention is ‘implemented across a range of contexts, populations and subpopulations, and how have these effects come about?’. 76 This shifts the focus of evaluation towards investigating the chain of events flowing from the introduction of an intervention in a complex, adaptive system and producing evidence that informs decisions about how to make things happen more effectively in the future. 74,77–79
The CiC study adopted this approach to an evaluation of BL and was underpinned by the system-informed theory of change described below. Initially the research was to run for 39 months, but a 4-month extension was granted to deal with some of the disruptions caused by the COVID-19 pandemic.
The Big Local intervention
Background
In 2010, the National Lottery Community Fund (then Big Lottery Fund) announced funding of £271M for the BL programme. The scale of funding allocated, although small compared to government-funded initiatives such as NDC (approximately £2B over 10 years), was the largest ever investment by a non-government funder in a place-based community empowerment programme, and in 2020 remained ‘the biggest ever single-purpose National Lottery-funded endowment’. 80
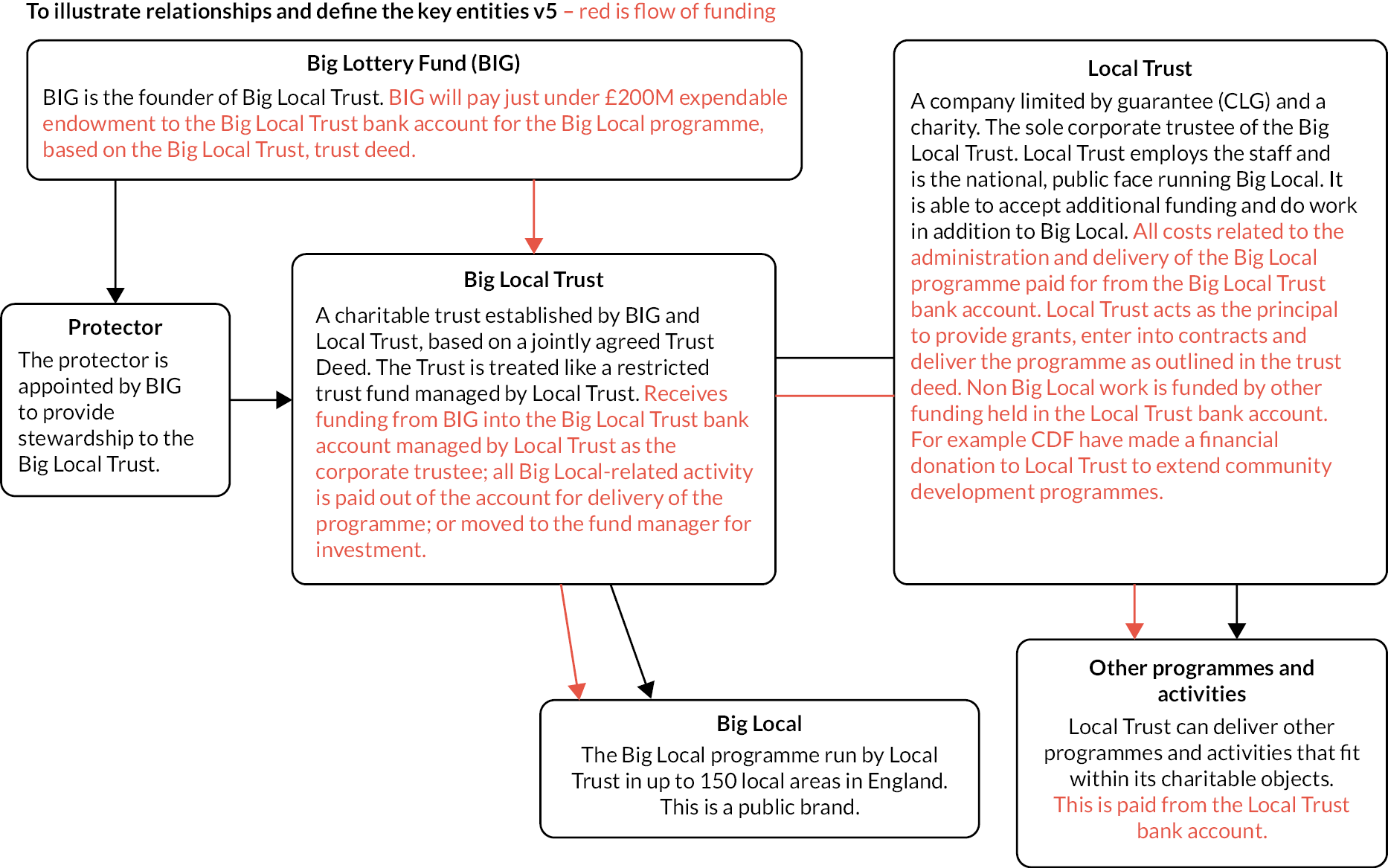
Following a tendering process,81 the Community Development Foundation was appointed to lead a consortium of national organisations to set up a new organisation that would act as the Corporate Trustee for a BL Trust. 82 Consequently, Local Trust (LT) was formed, taking over management of BL from the original consortium in March 2012. Figure 1 outlines the relationship of BL to its key entities: the funder (Big Lottery/National Lottery Community Fund), LT, BL Trust and the legal protector (providing stewardship of the BL Trust). BL Trust was set up as a charitable trust with a jointly agreed trust deed between the National Lottery Community Fund and LT. 83 LT is the sole corporate trustee of the BL Trust. In its role, LT ensures BL is delivered in a way that is in keeping with the trust deed. A key stipulation of the deed was that the total endowment should be committed by a date about 10 years from when the trust was set up, subsequently agreed to be 2026. 83 The trust deed also requires the use of BL funding to be additional to public funding for activities that national/local government is required to provide as part of statutory functions.
FIGURE 1.
Relationship between key BL programme entities. Reproduced with permission of Local Trust.
Selection of areas to be included in the Big Local programme
In total, 150 areas in England were selected for funding in three waves (July 2010, February 2012 and December 2012). The Big Lottery Fund decided on the areas following consultation with local partners (e.g. local authorities). 84 Local areas were selected on the basis that they had historically missed out on lottery and other community funding. 80 Early guidance published in 2010 indicates that the targeted localities were ‘all places where many people face multiple barriers to meeting their needs, and which have not had great success in gaining resources to help’. 81 While all BL areas are relatively disadvantaged, in practice they vary across a range of geographical and demographic characteristics, with local populations ranging from 3000 to 12,000, with most being between 6000 and 7000. There is also considerable variation in the extent to which BL area boundaries are contiguous with pre-existing formal or social boundaries (e.g. a ward or housing estate). 2 Earlier phases of the CiC study found that this influenced the speed and nature of early roll-out of the programme in local areas. 2 This included the ways in which residents were able to engage with other residents and professionals and act collectively to make decisions about how to spend the £1M to improve their neighbourhood. 3
Big Local programme outcomes and framework
The funder set four outcomes for the BL programme, which are listed below. These were intentionally broad, enabling local communities to set their own priorities:81
-
Communities will be better able to identify local needs and take action in response to these.
-
People will have increased skills and confidence so that they continue to identify and respond to needs in the future.
-
The community will make a difference to the needs it prioritises.
-
People will feel that their area is an even better place to live.
Once established, and in consultation with partners, LT developed a programme theory and framework to guide the delivery of BL locally. Central to this was a seven-stage pathway which all areas are expected to move through, albeit iteratively and at their own pace. Although LT no longer refers explicitly to a ‘pathway’ in its guidance for local areas, these key components of the programme framework, shown in Box 2, remain in place.
-
Getting people involved: To spread work about BL and make sure residents know how to get involved.
-
Exploring your BL vision: To understand local aspirations, needs and priorities and develop a shared vision for the area.
-
Forming your BL partnership: To oversee the local programme – guidance says 51% of members must be residents so local community is in majority.
-
Creating a local plan: To describe how BL partnership will improve the neighbourhood, building on identified vision and local priorities. Reviewed and endorsed by LT before funds released to partnership to be managed by a locally trusted organisation (LTO). Plans can change.
-
Delivering your local plan: BL partnerships oversee delivery of actions in the plan, often working with other organisations/groups.
-
Collecting the evidence: To enable BL partnerships to assess and communicate progress and achievements to wider community. LT has produced resources to support partnerships to measure impacts.
-
Reviewing BL plan and partnership: Conduct at least one review when plan is active and submit to LT before submitting new or updated plan requesting further funds. Each BL area also has a BL rep who conducts annual review of partnership.
Initially, each local area received a small grant of £20,000 to consult with residents and produce their plans. Across areas, engagement, consultations and plan development occurred approximately in the first 2 years, before BL partnerships began to draw down the main grant after their initial plans were endorsed by LT. Although there is no formal time frame for expenditure by local areas (e.g. no set date for submission of local plans), all BL partnerships had had their first plan endorsed by 2015. Each area has been allocated approximately £1.1M over time, with an additional £50,000 released to each area in March 2020 to enable BL partnerships to provide additional support to local communities during the pandemic. These additional funds are derived from growth in the BL Trust endowment, which is invested.
National support and management functions for Big Local
Local Trust, and national organisations commissioned by them, provide a range of support for BL partnerships. Firstly, each BL area receives professional support through a BL rep who acts as a ‘critical friend’, helping BL partnerships to develop and deliver their plans. Reps also contribute to a two-way flow of information between LT and the BL partnership; for example, disseminating information about new opportunities (e.g. events, training) as well as updating LT on progress or local issues. Secondly, each BL partnership is required to identify a LTO to manage its funds; these include organisations such as community voluntary services, local civil society organisations, housing associations and parish councils. While not compulsory, many BL partnerships also employ people or organisations to undertake specific tasks (e.g. to run engagement events and/or manage projects). Thirdly, partnerships can secure optional support or expertise such as training and learning opportunities for residents and organisations involved in BL and topic support related to delivering plans (e.g. social investment, managing land assets). Finally, network events are organised nationally and regionally to encourage the exchange of knowledge between BL partnerships and organisations with relevant expertise. We do not have the space in this report to describe the wide range of approaches adopted in BL areas to engage the wider population in the programme – we have written about these elsewhere85 – nor the diverse actions taken to improve the neighbourhoods, which are described on the LT website (https://localtrust.org.uk).
While the broad programme framework described above has remained constant over time, the speed of spend has varied across BL areas. Some are likely to have spent all their funding before 2026; other areas have spent more slowly. Additionally, our fieldwork in this third phase of CiC has identified ways in which programme arrangements have evolved over time, from early stages of set-up to delivering plans and spending money. These changes are explored in more depth in Chapter 4.
The Communities in Control study: theoretical framework
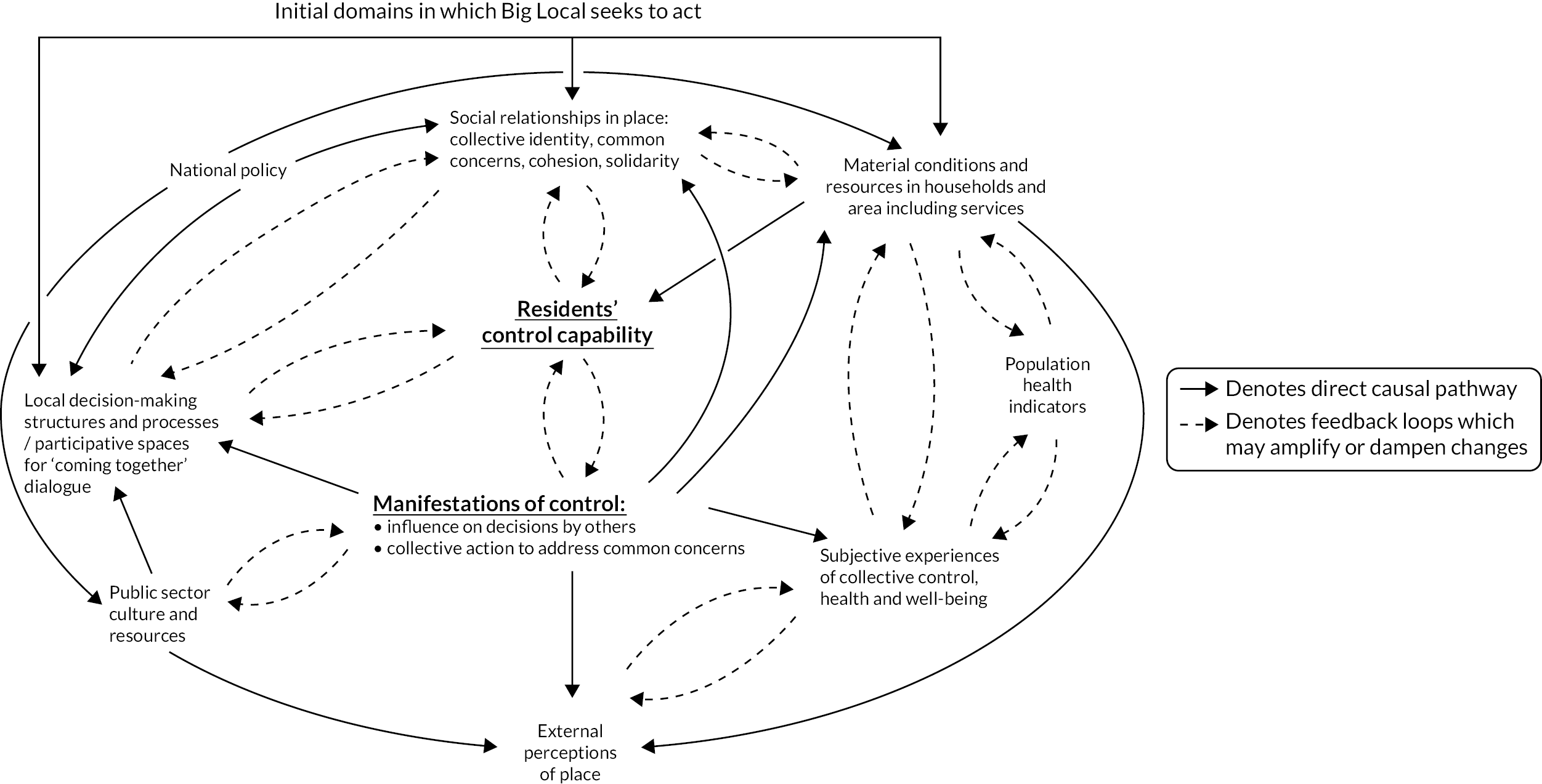
The CiC study is a longitudinal mixed-methods evaluation. Two earlier phases, funded by the NIHR SPHR, ran from 2014 to 2017. During phase 1 we developed a novel theoretical framework for the evaluation, the Collective Control Influence System (CCIS), shown in Figure 2. This diagram depicts the processes and feedback loops that may be triggered by BL, which could enable and/or constrain (in systems language – amplify or dampen) residents’ attempts to improve the conditions in which they live and the pathways that could lead from these improvements to health improvements.
FIGURE 2.
Collective Control Influence System (CCIS).
Our system-informed theory of change starts from the premise that various elements of the BL programme may increase capabilities for collective control among those residents who are most actively engaged. If, in gaining greater collective control, residents are able to act together (with or without others) to prevent or mitigate exposure to health-damaging living and working conditions, then direct health effects may ensue for the active residents and for the wider population, through making their neighbourhood a healthier, better place to live.
The three straight arrows at the top of Figure 2 show the points in the CCIS where the initial impacts of BL would be expected to be felt: on social relationships in place, local decision-making structures and processes, and material resources in households and the environment. Various complex interactions between elements of the system flow from these initial impacts. Proposed direct causal links between different elements of the CCIS are shown with a solid line and arrow, while feedback loops between these are shown with a dotted line.
There may also be indirect health improvements arising from the reduction in social isolation and improvement in mental health that participation in community action can bring about. Finally, increased control may lead indirectly to physical health benefits. Evidence from the work environment shows that employees who experience high job demands but low control over their working conditions are at higher risk of psychosocial stress, which has been linked to physical conditions such as coronary heart disease. Furthermore, exposure to low job control increases with decreasing social position and may have contributed to the observed social inequalities in coronary heart disease incidence. 37 Changes in physical health conditions such as coronary heart disease would only be expected to emerge in the longer term, unlikely in the lifespan of this research. The theory also allows for the possibility that the processes set in train may have negative health impacts, particularly on the residents who are most actively involved. We used this system-informed theory of change, particularly in our analysis of qualitative data, to examine these various processes and to understand how the feedback loops operated in BL areas.
Public involvement in the Communities in Control study
Big Local residents have been involved in the CiC study since it began in 2014. They have contributed to fieldwork design, developing research tools and interpreting findings, particularly but not exclusively in relation to the qualitative research in WP3 described below. We have had regular dialogues with members of BL partnership boards and other residents and workers in our local fieldwork areas. The purpose of these dialogues has been to ensure that local evidence priorities were acknowledged and integrated into the research where possible, that local knowledge of the neighbourhood and of BL informed the fieldwork and that data-gathering methods were acceptable. We have also had regular meetings with LT, the national organisation managing BL, and contributed to their regular engagement events.
Our original plan for ongoing involvement included two or three annual meetings of the BL resident network established in phase 1 of CiC, with other involvement taking place in our fieldwork sites. Members of the network contributed to the original research proposal and the project’s plain English summary, and advised on the ethics approval documentation. Subsequently, they have supported the testing and refining of interview topic guides and contributed to plans for recruitment of respondents and consent processes. BL residents also made a major contribution to the study website (www.communitiesincontrol.uk), including a short video of a CiC public adviser talking about his experience of involvement (https://youtu.be/4auqXfEWbWw). They have also commented on the kinds and formats of outputs to be shared with the BL communities in the future and on the plain English summary for this report. However, following discussions with network members and LT in 2018, we moved away from resident network meetings to activities at a regional and local level. For example, members of our team have worked with BL reps at the regional level to develop and deliver several learning events for BL partnerships in person and online.
The issue of reciprocity emerged as a recurring concern in discussions with members of BL partnerships. This is an ethical issue, with some community members arguing that the research risked ‘taking from’ or ‘gaining from’ the communities studied unless there was an offer of reciprocity. We have endeavoured to meet these reciprocity obligations in various ways. For example, staff have attended and spoken at local stakeholder events, provided advice to partnerships on how to evaluate their work, reviewed funding applications, supported partnerships in their mid-term plan reviews, and identified evidence they could use to show the impact of their work (e.g. the social and health impact of outdoor gyms). Involvement of BL residents in and beyond our fieldwork sites was not possible for much of 2020 and into 2021. Some partnerships put all their time and energies into responding to the needs of their local communities; others stopped meeting, as individuals struggled with their own challenges. However, we were able to support some of the COVID-19 work of partnerships; for example, by providing evidence on the impact of COVID-19 on minority ethnic groups.
Details of our past and future activities aimed at involving BL residents and wider public in interpreting and disseminating our findings are included in Chapter 10.
Communities in Control study: phase 3 study design
From an evaluation perspective, BL is a ‘natural experiment’ in community empowerment. By ‘natural experiment’, we refer to the Medical Research Council’s definition of ‘events, interventions and policies that are not under the control of the researchers, but which are amenable to research using the variation in exposure that they generate to analyse their impact’. 86 No aspect of the BL initiative was under the control of the CiC researchers, but while the function of the programme is standardised, there is considerable variation in the form it has taken across the 150 areas that we have been able to exploit for evaluation purposes. Firstly, there are differences in the social, economic and political contexts in which local programmes are rolled out. These differing contexts could lead to differences in the impact of BL on health and other outcomes. Secondly, the funding can be used flexibly, such as to make social investments, develop projects, award grants or negotiate in-kind support from other organisations (e.g. local authorities). 3 Thirdly, BL plans may include a wide range of actions relevant to local priorities and needs. These include actions to improve the physical and built environment,87 challenge place stigma,88 strengthen social relationships between residents,85,89 and reduce poverty and improve the local economy. 3 As part of planning for sustainability beyond 2026, some BL partnerships have also sought to invest in, or take over management of, assets such as community hubs or public land. Fourthly, while not formally required to do so, the BL partnerships often engage with local public, private and/or third-sector agencies (e.g. NHS organisations and local government) to attain their goals, though the nature and extent of this engagement varies at the local level. Lastly, as there is no fixed BL timescale, there is variation in the pace and scale of roll-out over time. BL areas may also adapt their plans over time, in response to changing local needs.
The objectives of phase 3 of the CiC study were to:
-
investigate longer-term population-level health and social outcomes of BL
-
investigate impacts of BL on health and well-being of engaged residents
-
assess changes in collective control among BL residents and pathways to changes identified
-
illuminate residents’ perspectives on health and well-being impacts and pathways to these
-
conduct an economic evaluation of BL
-
draw out implications for future design and evaluation of PBIs that aim to increase collective control, particularly in disadvantaged communities.
The study comprised four WPs, which are described below.
Work package 1: population-level impacts on health and social outcomes
This WP sought to assess whether the intervention had any positive impacts on social and health outcomes for the populations in BL neighbourhoods. The methods used in this work are described here, and the findings are reported in Chapter 5.
The Big Local intervention start date
The areas in which the programme was implemented were selected between 2010 and 2012 and received a small grant in the initial period, but most did not start to draw down substantial amounts of money until their plans were approved in 2015. For the analysis of population impacts, we therefore defined 2016 as the start date – that is, the earliest date from which it is plausible that the BL initiative could start to have an impact on population health outcomes. We examined the timing of impacts using alternative start years in the analysis (see below).
Data and sample size
The analysis utilised data from the ONS APS for the years 2011–1990,91 and various secondary sources. The APS is the largest representative household survey in the UK, with a sample size of 320,000. It combines data from four successive quarters of the Labour Force Survey with rolling-year data from the English, Welsh and Scottish Local Labour Force Survey. The sampling frame is the Royal Mail postcode address file and the NHS communal accommodation register, and sampling is stratified to ensure it is representative at the regional level. Where possible, every adult aged 16 and over in a household is interviewed. Where there are other individuals in the household who can answer on behalf of an absent respondent, proxy responses are also collected. Well-being measures (see Outcomes below) are only collected on non-proxy respondents, of which there are approximately 165,000 per year. New respondents in the sample are interviewed face to face, while subsequent interviews are conducted over the telephone where possible.
We used the secure access version of this data set which includes an indicator of the Lower Super Output Area (LSOA) of each respondent. LSOAs are small geographical areas used by the UK’s ONS, each typically containing a population of about 1500 people. This LSOA indicator was used to identify respondents in BL and in comparator areas (see below). This provided a total sample of 26,440 non-proxy respondents in BL areas and 75,580 in comparator areas from 2011 to 2019 (see Appendix 1, Table 13 for annual sample sizes). This was similar to our estimated sample size in our pre-registered protocol of 108,000 respondents over the 9 years. We used simulation methods to investigate the power that this sample would provide across a range of effect sizes, taking into account weights for the study design and using robust clustered standard errors to account for clustering within areas and serial correlation in the data. 92
As Table 1 shows, we would be able to detect an absolute reduction of two percentage points in our primary outcome – the proportion of the population reporting high levels of anxiety – with a power of 83% (at α = 0.05). A two-percentage-point reduction would mean that the proportion of the population reporting high levels of anxiety drops from the estimated baseline level of 21% to 19% in BL areas. For the analysis of secondary outcomes, we used a number of routine data sources to construct a panel of aggregate data for the 880 LSOAs that lie within BL areas and the matched 2640 comparator LSOAs over 9 years (2011–19), providing 31,680 observations for the analysis. These data are based on the total populations and not a sample survey.
| True effect size (risk difference), % | Power (at α = 0.05), % |
|---|---|
| 3 | 99 |
| 2 | 83 |
| 1.5 | 61 |
| 1.2 | 44 |
| 1 | 37 |
| 0.5 | 17 |
Outcomes and control variables
Outcome 1: Our primary outcome was high levels of anxiety self-reported in the APS, measured as the proportion of people reporting a score of > 6 in response to the question ‘Overall, how anxious did you feel yesterday?’, where 0 is ‘not at all anxious’ and 10 is ‘completely anxious’. A threshold of > 6 on the 11-point scale has been identified by the ONS as a measure of high anxiety levels. 93
Outcome 2: The Small Area Mental Health Index (SAMHI) is a composite annual measure of population mental health that we developed for each LSOA in England. The data and methods used to compile the index are available through the open data portal Place-based Longitudinal Data Resource. 94 The SAMHI combines data on mental health from multiple routine sources into a single index, including antidepressant prescribing data from NHS Digital,95 mental health-related hospital attendances as defined below, diagnoses of depression in primary care from the Quality and Outcomes Framework,96 and claims for Incapacity Benefit and Employment Support Allowance for mental illness. 97 Each indicator was individually standardised by rescaling data to have a mean of 0 and a standard deviation of 1 (z-scores). Maximum likelihood factor analysis was used to combine these indicators (by finding appropriate weights) into a single score based on the intercorrelations between all the indicators. The SAMHI is an indicator of poor mental health; a higher score indicates worse population mental health.
Outcome 3: Antidepressant prescribing measured as the average daily quantity of antidepressants prescribed per 1000 population per year using general practitioner (GP) practice prescribing data provided by NHS Digital. 98 This indicator was standardised by rescaling data to have a mean of 0 and standard deviation of 1 (z-scores).
Outcome 4: Mental health-related hospital attendances per 1000 population using Hospital Episode Statistics provided through a data sharing agreement with NHS Digital (DARS-NIC-16656-D9B5T-v3.10). This measure consists of A&E attendances and admitted patient care for alcohol misuse, drug misuse, self-harm, and common mental disorders. Specifically, it includes a count of all admissions with a primary diagnostic ICD-10 code of X60*–X84*, Y10*–Y34*, F00–F99, E244, F10, G312, G621, G721, I426, K292, K70, K852, K860, Q860, R780, T510, T511, T519, X45, X65, Y15, Y90, Y91 but excluding Y33.9*, and Y87*, plus a count of all A&E attendances for self-harm (codes 141–144, 35, 37) in each year for each LSOA, divided by the annual population estimate. This indicator was standardised by rescaling data to have a mean of 0 and standard deviation of 1 (z-scores).
Outcome 5: Recorded crimes and incidents of antisocial behaviour (ASB) per 1000 population for the offence categories violence and sexual offences, burglary, criminal damage and ASB using Open Data from the UK government. 99 The combined indicator was used and additionally each category of crime was analysed separately. These indicators were standardised by rescaling data to have a mean of 0 and standard deviation of 1 (z-scores).
Outcomes 6–8: We also included the three other measures of subjective well-being included in the ONS well-being set – ‘low satisfaction’, ‘low happiness’ and ‘not worthwhile’ – measured as a score of < 7/11 in response to the questions: ‘Overall, how satisfied are you with your life nowadays?’, ‘Overall, how happy did you feel yesterday?’ and ‘Overall, to what extent do you feel that the things you do in your life are worthwhile?’.
In analysis of the APS, we used age and sex plus a number of variables to adjust for potential confounders. Respondents were defined as employed if they reported that they were either an employee or self-employed in the survey week. Socioeconomic status was defined using the National Statistics Socioeconomic Classification (NS-SEC),100 grouped into three categories: (1) higher managerial, administrative and professional occupations; (2) intermediate occupations; and (3) routine and manual occupations or never worked/long-term unemployed. Respondents were defined as coming from a black, Asian or other minority ethnic group if they identified as Asian/Asian British mixed/black/African/Caribbean/black British/Chinese/Arab/multiple ethnic groups/other ethnic group. Education status was defined in three categories based on highest educational qualifications: (1) degree or equivalent, (2) some qualifications but less than a degree, or (3) no qualifications. Marital status was defined as married/civil partnership or other. Respondents were defined as having a disability if they reported a long-standing illness that limited work or other daily activities. We also used survey data on housing tenure. Survey questions related to education and disability are only asked for respondents of working age (aged 16–64) and therefore these variables were only included in analysis limited to this age group.
Matching to define the comparison areas used data on Index of Multiple Deprivation (IMD) 2015 domains of income, health, crime and environment;101 the Community Needs Index 2019 developed by LT;102 the ethnic and age profile of the population using data from the 2011 census; the average distance to the nearest GP practice, hospital and green space, using data from the Access to Healthy Assets and Hazards Index (AHAH),103 the distance to the coast; the ONS area classification based on eight subgroups (affluent England; business, education and heritage centres; countryside living; ethnically diverse metropolitan living; London cosmopolitan; services and industrial legacy; town and country living; and urban settlements);100 and region.
As additional control variables in the LSOA level analysis we used annual estimates of the distance to the nearest GP practice and hospital to account for potential changes in access to health services that might lead to bias in our outcomes that are based on health service utilisation (antidepressant prescribing and mental health-related hospital attendances). To account for potential divergence in the trends in economic conditions in BL and comparator areas, we additionally controlled for the annual unemployment claimant rate using data from the Department for Work and Pensions. 97
Statistical methods
Firstly, we defined our comparator areas based on a set of LSOAs matched with the LSOAs included within BL areas. The entire population of the intervention area (150 BL areas) consists of 880 LSOAs. Each of these intervention LSOAs was matched with three control LSOAs located within England, providing 2640 matched control LSOAs. We used propensity score matching104 to ensure that these comparator areas had similar observed characteristics to the intervention LSOAs in the time period before the start date for the intervention (2011–15). The matching was based on the variables outlined above, along with the prior values of the four secondary outcomes (SAMHI, antidepressant prescribing rate, mental health related hospital admissions, recorded crimes). The nearest neighbour method was used for matching, which selects controls with propensity scores that are closest to that of the intervention LSOAs.
We then used difference-in-differences (DiD) methods105 to compare the change in health and social outcomes in BL areas to those in non-BL areas. The estimate of the effect of the BL programme was therefore calculated as the difference between the change in the outcome in the BL areas and the change in the outcome in the comparator areas. This DiD approach uses a comparison both within and between areas – accounting for secular trends in our outcomes and unobserved time-invariant differences between areas that could confound findings. The primary assumption is that trends in outcomes would have been parallel in the BL and comparator areas in the absence of the BL programme. This is a reasonable assumption as the comparator areas are very similar to the BL areas at baseline and therefore likely to be affected in a similar way as the BL areas by wider national factors such as welfare reforms, austerity measures and economic change.
This involved estimating a regression based on the following formula:
where Yiat is the outcome reported by individual or LSOA i in area a at time t, BLa is a dummy variable taking the value 1 for BL areas and the value 0 for the comparator areas, and AFTERt is a dummy variable taking the value 1 for time periods after 2015. Xiat is a vector of control variables for individual/LSOA i in area a at time t. The coefficient of interest is β3, the coefficient on the interaction term AFTERt∗BLa, sometimes referred to as the DiD parameter. It indicates the change in outcomes in the BL areas relative to the change in outcomes in the comparator areas, that is, the effect of the programme on the outcome. As this interaction term cannot be interpreted as the programme effect in non-linear models, we used linear regression models, even for our binary well-being outcomes, to estimate the DiD parameter. 106 To check the robustness of this approach, we additionally estimated logistic regression models for the binary outcomes and then calculated the contrast of the predicted margins from these models, that is, the equivalent to the interaction term in a linear model. 106
Subgroup and lagged and lead analysis
To investigate differences in effect by sociodemographic conditions, the analysis of our primary outcome using APS data was repeated for subgroups defined by socioeconomic status, ethnicity and for the working-age population (16–64 years). The analysis of our secondary outcomes was repeated for subgroups of BL areas, as the LSOA-level data provided sufficient numbers of observations in each subgroup’s BL area. This subgroup analysis was not possible with the primary outcome, as the APS sample within each BL area was not sufficient.
The analysis of subgroups of BL areas included rematching each subgroup to a comparison group of areas to ensure balance was maintained within subgroups. To investigate whether effects differed according to the scale and type of activity in each BL area, we repeated the analysis including only those BL areas that had spent more than 80% of their grant by 2019/20 (30 BL areas). These areas had progressed furthest with implementation and therefore we might expect that any effects on social and health outcomes would be greatest in these areas. To investigate whether differences in the type of activities in each BL area influenced outcomes, we repeated the analysis for four groups of BL areas defined by the type of activities they prioritised for expenditure. These activities were classified into a fourfold typology based on the determinants of health that they targeted: economic (e.g. money advice, poverty reduction and skills development interventions), social (e.g. arts and culture, community spaces, loneliness interventions), environmental (e.g. community safety, housing and transport interventions) and lifestyle (e.g. sport and physical activity, and health and well-being interventions).
Most BL areas prioritised funding of activities across more than one of these types, and so we replicated our analysis for each group if they had included that activity type in their offer (e.g. environmental interventions). So BL areas could be included in more than one group if they included activities across multiple types in their offer. To understand potential combined effects of the scale and types of activity on outcomes, we repeated the analysis for our four groups of BL areas defined by their type of activity, while also limiting this analysis to those that had spent more than 80% of their grant.
To investigate whether contextual factors influence the effectiveness of the BL programme and potential impacts on social and health outcomes, we repeated the analysis for: (1) three groups of BL areas defined by baseline deprivation using the IMD 2015 income domain score; (2) three groups defined by the proportion of people from ethnic minority groups; and (3) three groups based on the age profile of the population (proportion of people under 16 and over 75).
We also checked the timing of impacts using lags for the 2 years after the BL implementation start date of 2016 and investigated whether impacts happened before this implementation year using leads for the 3 years before this date. Finally, to examine the sensitivity of our models to dichotomising the well-being outcomes, we repeated the analysis for the full scale (0–10) for all four well-being outcomes.
Work package 2: the impact of active engagement with Big Local on health and social outcomes among engaged residents
This WP sought to assess whether the intervention had any positive impacts on health outcomes for the most actively engaged residents in BL neighbourhoods. The methods used in this work are described here, and the findings are reported in Chapter 6.
Data sources
This WP used data from three waves (2016, 2018 and 2020) of a biannual longitudinal survey of those most actively engaged in BL – all BL partnership members in all 150 BL areas. This was conducted by LT. As already noted, BL partnerships have a majority of resident members plus members from local organisations including the local authority, the NHS, and/or faith and other third-sector organisations.
A survey is delivered by the LT every 2 years, online and by post, to all the individuals actively involved as the members of the 150 BL partnerships in England. These include non-residents and residents. We refer to the latter in our reporting as ‘active residents’. The survey was initially developed internally by LT to meet programme and learning requirements of the organisation. However, through our partnership with LT, the CiC research team were able to add additional questions relating to mental well-being, self-rated general health, collective and/individual control, social cohesion and area perception. The BL partnership survey is a repeat cross-sectional survey. Although the survey was conducted in 2014, it was only in 2016 that we were able to insert questions on health, place or experience of collective control. For our purposes, the first-wave survey was therefore in 2016 (baseline, wave 1). Potential respondents were identified using a common sampling frame: all BL partnership members who submitted contact details (over 1200) as part of the annual partnership review carried out by LT were approached via e-mail (for an online questionnaire submission). BL reps were also sent physical copies of questionnaires by post to distribute, to reach as many other partnership members (~400) as possible. This gave a total potential sample of over 1600 partnership members across all 150 BL areas. A total of 862 participants submitted a completed wave 1 questionnaire in 2016, a baseline response rate of over 50%. In 2020 (wave 3), the questionnaire was distributed – online only – to all 1664 current partnership members, and 1018 responses were received, leading to a response of around 61%. These repeated samples provided the basis for a nested cohort, whereby individual records were linked over the three waves (2016, 2018 and 2020). As anticipated in our proposal, the final sample size of the nested cohort was small, with only 217 participants providing linked data over all three waves, and so we also analysed the total responses at each wave using a repeat cross-section design. The repeat cross-sectional survey had samples of n = 862 in wave 1, n = 1011 in wave 2 and n = 1023 at wave 3. Our analytical sample at each wave (comprising those who provided responses across all our variables) was 500, 654 and 636. The analyses also looked separately at resident and non-resident partnership members.
Types of Big Local programmes
Using data provided by LT, we were able to undertake subgroup analyses on the basis of the extent and type of BL activity in each of the 150 BL areas. We used a threefold classification of the amount of funds spent on activities up to 2019/20 – low (spent ˂ 50% of £1M), medium (spent 50–80% of the £1M) and high spend (spent > 80% of the £1M) – and the fourfold typology of activities described earlier. This was based on the determinants of health that BL expenditure targeted: economic (e.g. money advice, poverty reduction and skills development interventions), social (e.g. arts and culture, community spaces, loneliness interventions), environmental (e.g. community safety, housing and transport interventions), and lifestyle (e.g. sport and physical activity, and health and well-being interventions). Most BL areas funded activities across more than one of these groups. In the WP2 analyses, outcomes for partnership members in areas that included a specific expenditure type in their programme plans were compared to those in areas that did not include that specific type but had planned expenditure in any/all of the other three activity groups.
Obtaining and managing the data
Local Trust collated the survey responses and sent them to the research team in an anonymised SPSS (IBM Corporation, Armonk, NY, USA) spreadsheet in October 2018 and October 2020 (we already had baseline data from 2016 from earlier phases of CiC). 107 The anonymised data were uploaded to a shared Box folder which was only accessible to named collaborators. Individual records were linked over the three waves via unique numerical identifiers for the purpose of the nested cohort. The repeat cross-sectional element included area-level data linkage. The data were stored in electronic form on secure university servers and were accessed through password-protected networked PCs and laptops.
Outcome measures
The survey collected data on the characteristics of BL partnership members [demographic data, socioeconomic status (education), perception of individual and collective control and perception of the BL area, levels of participation (number of unpaid hours per week on BL activities) and self-perceived health] using two validated measures: the Short Warwick–Edinburgh Mental Well-being Scale (SWEMWBS) and Census General Health. A copy of the questionnaire is included in the accompanying project documentation.
Our primary outcome was the score from SWEMWBS, which is designed to measure positive mental health states (as opposed to symptoms of mental ill-health such as anxiety and depression). The scale has seven domains, and scores range from 7 to 35, with higher scores indicating higher positive mental well-being. The scale has been validated for the general population. 108 Questions include the degree to which a participant ‘feels useful’ or ‘feels relaxed’, or agrees with the statements ‘I think that I deal with problems well’, ‘I feel close to other people’ and ‘I have been able to make up my mind about things’.
Our secondary outcome was ‘self-rated general health status’ (the census measure), which asks ‘How is your health in general? Would you say it was very good, good, fair, bad, very bad?’ This was recoded with ‘very good’ and ‘good’ coded as ‘good’ and fair, and with ‘bad’ and ‘very bad’ coded as ‘not good health’.
Explanatory variables
Based on our theory of change, engaged residents could be expected to experience improvements in mental well-being and general health as a result of reductions in social isolation as they participate in BL activities, through an improved perception of community, as well as through feeling that they have greater control over decisions that affect their daily lives. At baseline, we therefore examined any association for our two health outcomes with: (1) whether respondents felt able to influence decisions affecting their area, either with others (collective control) or as individuals (individual control); (2) social cohesion around involvement (feels good to know more people in the area, feels more connected, feels more positive about BL area, feels stronger sense of community) and area perception (feels people in the BL area can be trusted, feels people in their BL area are willing to help each other, feels they belong to the area); and (3) hours of involvement among participants. Only the explanatory variables that were significantly statistically associated with our primary outcome at baseline were then included in the follow-up analyses. Typology data on the extent and type of BL activities in different areas were also included in the follow-up analysis to examine whether different levels of expenditure or types of activity were more/less associated with any changes in our primary outcome.
Analysis
We examined whether our primary and secondary health outcome measures changed over time across the three waves using both the repeat cross-sectional and cohort designs.
Baseline analysis
Survey data for 2016 for 862 people involved in the 150 BL areas in England were summarised using descriptive statistics (mean, standard deviation for continuous variables, percentages for categorical variables). Our explanatory factors were then examined for bivariate associations with both the health outcomes, and the initial model included those with p ≤ 0.25. The final parsimonious model retained variables with significant associations – adjusted for age, gender, ethnicity, educational status, resident status and hours volunteered. A random-effects linear model was used to examine the associations between SWEMWBS, demographics and our explanatory variables. Similarly, a generalised estimating equation (GEE) model was used to examine the associations with our secondary outcome of self-rated general health.
We also investigated whether there were differences across a number of predefined groups. Firstly, we investigated health inequalities by analysing whether any health associations at baseline differed by education or gender. Secondly, we investigated any differences in terms of levels of participation in the BL (measured using hours involved) to see whether there was a graded association between participation and our health outcomes. Thirdly, we also examined differences by resident versus non-resident status of BL partnership members.
The SWEMWBS results are presented as mean difference with 95% CIs between the reference category and the comparison group. The self-rated health results are presented as odds ratios with 95% CIs. Where the CIs do not include zero values, this implies a statistically significant positive or negative association.
Follow-up analysis
For the 2018 and 2020 data, we split the sample into a nested cohort (final n = 217 for whom data were available across all three waves) and a three-wave repeat cross-section (n = 500 in wave 1, n = 654 in wave 2 and n = 636 in wave 3). For both our primary and secondary outcomes, we examined associations over time with those variables that were significant at baseline (subjective assessments of collective control, perceptions of community, hours involved, resident status).
For both the nested cohort and cross-sectional analyses, linear mixed-effects models (accounting for the clustering of participants within sites and the repeated measures per participant across the three waves) were utilised to examine changes in the primary SWEMWBS outcome over the three waves. The different waves were treated as categorical variables. Baseline age categories, sex, highest educational qualification, ethnicity and intervention typologies 1 (proportional spend) and 2 (expenditure type) were held as constants, while the other variables (collective control, willingness to help each other, resident status and hours volunteered) were used as time-varying factors. The most parsimonious model was selected using a likelihood ratio test. Likewise, for both sets of analyses, the secondary outcome of self-rated general health was analysed using a GEE model.
For both the cohort and cross-sectional analyses, we also investigated whether there were differences in effects for our primary outcome across a number of predefined groups. Firstly, we investigated potential effects on health inequalities by analysing whether any health effects differed by education or gender (it was not possible to examine inequalities by ethnicity due to low sample sizes). Secondly, we investigated any differences in terms of levels of participation in the BL (measured using hours involved) to see whether there was a graded effect of participation on our health outcomes. Thirdly, we examined differences by resident versus non-resident status of BL members. Finally, for the cohort analysis of the primary outcome, we also investigated differences in effect by area-level variation in BL activities using our two BL intervention typologies (proportional spend and expenditure type).
Constructed comparators
We had originally planned to control for general trends in SWEMWBS, by creating a comparator group using SWEMWBS data from the 2016 and 2018 Health Survey of England (HSE). However, HSE 2018 did not collect SWEMWBS data, and HSE 2020 was not conducted (due to the COVID-19 restrictions). As an alternative, we explored whether the APS variables measuring well-being (used in WP1) could provide a ‘good enough’ comparator. However, there were two problems with this approach. Firstly, the variables used to assess well-being in the APS (ONS4) focused on anxiety (see WP1) were not comparable with the validated SWEMWBS. Secondly, due to COVID-related delays at ONS, the WP1 project team did not receive the APS data until late summer 2021, leaving no time to consider other possible constructed comparators.
Missing data
The cohort analysis we performed utilised a likelihood-based mixed-effects model which assumes that data are missing at random. Missing data rates for the primary outcome were 5% and 11% for the 2018 and 2020 cohort waves, respectively. Missing data rates were tabulated and examined. Only gender predicted missingness and so we adjusted for this in the main models.
Work package 3: understanding pathways to impact
This WP comprised two elements. First, qualitative in-depth interviews were carried out with national BL stakeholders and key informants with expertise in place-based policies. These aimed to identify changes in the BL programme over time and explore the relationship with national policy. Second, as a continuation of our longitudinal qualitative research, we conducted qualitative fieldwork in 15 BL areas. This aimed to assess changes in collective control and perceptions of impacts on health and well-being among actively involved BL residents, identify some of the improvements achieved in the areas, and illuminate pathways to change in both collective control and health. Methods used in this work are described here, and the findings are presented in later chapters.
National fieldwork
The national fieldwork was built upon interviews conducted in 2014 in phase 1 of the CiC study with representatives from national organisations involved in the consortium that established BL. These interviews were completed approximately 2 years into the programme when BL areas were establishing local partnership boards and identifying priorities. In this third phase of CiC, EH conducted 10 further stakeholder interviews over two waves. Participants were identified from programme documentation, advice from LT and the research team’s knowledge and links with national organisations. Participants included stakeholders directly involved in BL nationally and/or with knowledge of the national policy context for places and communities.
The semistructured interviews at each wave shared a common focus on understanding the nature of the BL programme model. Wave 1 interviews (n = 6) were completed in spring 2019. Two of these respondents were also interviewed in 2014. Four further interviews took place 18 months later and included two participants interviewed in wave 1. Three further participants were also approached but either declined to take part or did not respond to the e-mail, despite follow-up reminders. These second-wave interviews also explored perspectives on BL’s position within national policy developments, particularly in the context of the unfolding pandemic. Key organisations (e.g. LT) were represented in the sample during each wave of fieldwork. All participants agreeing to take part were approached by e-mail and provided with an information sheet at least 24 hours in advance of the interview and completed written informed consent before the interview. CiC wave 1 interviews took place face-to-face, and all interviews in wave 2 were conducted virtually via Microsoft Teams® (Microsoft Corporation, Redmond, WA, USA).
Recordings of wave 1 interviews were transcribed by a professional transcriber, with wave 2 interviews transcribed using automated transcription in Microsoft Teams. All transcripts were checked for accuracy, anonymised to remove personal identifiable information, and then uploaded to NVivo 12 (QSR International, Warrington, UK). Analysis combined thematic coding in NVivo with memo writing, drawing out different perspectives on the programme and how it had changed over time and the factors influencing this. Findings from this work are presented in Chapter 4.
Local fieldwork
The local fieldwork was undertaken by researchers based in Newcastle, Sheffield, Lancaster, London, Liverpool and Devon. To support this dispersed team, guidance was produced to facilitate consistent ways of working and ensure that the procedures and processes set out in our Research Ethics application were followed. Methods utilised in this work are described below, and the findings are presented in Chapters 7 and 8.
The qualitative fieldwork focused on:
-
tracking residents’ attempts to exercise collective control over decisions/actions to improve their neighbourhoods – termed critical collective control episodes (CCEs)
-
exploring residents’ subjective perceptions of the impact of their collective action on their health and well-being and that of other residents
-
illuminating the processes operating (within and beyond BL areas) to amplify and/or dampen the impact of these attempts by residents to act collectively and their perceptions of pathways to health impacts at individual and population levels.
We had also planned to collect data on the nature and scale of additional resources (cash or in kind) attracted into BL neighbourhoods, but this was not possible. We were, however, able to obtain some information on this from LT.
The fieldwork was based in a sample of BL areas selected in phase 1 of the CiC study. These are described briefly in Appendix 2. They were identified and recruited through LT, with BL reps facilitating contact with the partnerships in each area. The sites were originally selected on the basis of three criteria: (1) geographical spread across England (NW, NE, SW, Yorkshire and Greater London) and urban/rural split; (2) initial 10 areas selected in 2014 to reflect diversity in local context and population; (3) a further five areas added in 2015 to reflect diversity in the local plans. Data collection for the research reported here comprised two waves of interviews and observations. Efforts were made to follow up with people interviewed in earlier phases of the CiC study, whether still actively involved in BL or not. Unfortunately, 1 of the 15 original fieldwork sites declined to engage in this phase of the research, and in a second area, respondents were unable to participate in the second wave of data collection due to the disruptions of the pandemic.
Observations
We originally planned to undertake observations of two BL partnership meetings to update earlier assessments about the organisation and dynamics of the local partnerships. However, we attended more meetings than anticipated before the pandemic, in order to re-establish and maintain relationships and to have oversight of the partnership work as it developed. Post pandemic we used more diverse methods to keep in touch with sites [joining Zoom meetings (Zoom Video Communications, San Jose, CA, USA), telephone calls with key contacts, following social media, group messaging, etc.]. Success in maintaining contact was dependent upon the local context. Some partnerships had their meetings online and researchers were able to join these and gain some insight into how the pandemic was affecting them and their work, but some partnerships stopped meeting during the first 12 months of the pandemic. Meetings were not recorded. A one-page overview of key concepts developed in earlier phases of the CiC study was used to sensitise researchers when note taking. Field notes were taken but these were not transcribed or coded into NVivo. The notes were shared and used in discussions to contextualise the analyses.
Interviews
The main data collection involved in-depth interviews with key informants in 14 BL areas. We aimed to interview 10 people in each area twice over a 12-month period, that is, 140 interviews in total in each wave of interviews, 280 in total. In practice there was a continuous period of fieldwork. Interviews began in November 2018 and all but two were completed by January 2021 (a final interview was conducted in April 2021 at the respondent’s request). The initial plan was that these would involve two subsamples in each fieldwork area: five members of the BL partnership to obtain a system-wide perspective (e.g. the partnership chair, resident members and other stakeholders such as BL reps, council officers or third-sector reps), and five informants involved in examples of collective action by residents that aimed to improve their neighbourhood (see below). However, it became clear that some respondents combined these two perspectives. In these cases, the interviews covered questions exploring both perspectives. All of the residents interviewed during this third phase of the study were or had been members of a BL partnership in the fieldwork areas. We refer to these as ‘active residents’.
One example of collective action by residents – referred to as CCE – was selected in each fieldwork area. These are detailed in Table 2. They were purposefully sampled to include a diversity of actions (e.g. improving social relationships or physical spaces, or addressing economic issues, and actions involving partnerships with other agencies and activities). The second-wave interviews were to be an opportunity to explore with respondents how the work of the partnership was evolving over time and in particular how these examples of collective control by BL residents were progressing.
| A BL legacy building/community hub |
|---|
| Supporting establishment of social enterprises and developing entrepreneurial skills |
| Establishing and sustaining a local football club for young people |
| Establishing strategic alliance of local VCFSE agencies to work on area improvements |
| New Community Hub outreach programme |
| Asset transfer of library run on voluntary basis |
| Youth motocross venue |
| Establishing the BL partnership as an independent community trust with charitable status |
| Building and running a multiuse games area |
| Purchase and running of a local play-bus |
| Monthly market place for creative civic exchange |
| Supporting growth of social enterprises |
| Developing responsible dog ownership |
| Acquiring and running a community hub |
Where possible, researchers directly approached participants who had been involved in earlier phases of CiC to ask if they would be willing to be interviewed again. Where this was not possible, BL partnership chairs and members were asked to identify other potential interviewees. Potential interviewees were given an information sheet at least 24 hours before the interview and were able to discuss the research with the fieldworker before being asked to give written informed consent. They were also asked to consent to the team approaching them in the future if there were subsequent phases to the evaluation. In the context of the pandemic restrictions, consent from new respondents to the study was obtained remotely. This involved e-mails from the personal accounts of respondents confirming their consent, or verbal consent being taken via an online platform and recorded.
Table 3 provides information on participants recruited, and interviews conducted, over the course of the three phases of the CiC study. As can be seen, in this third phase we obtained 105 first interviews and 66 second interviews (rather than the 140 in each wave as planned). Where respondents combined a strategic view of the BL programme with key roles in the examples of collective action we were tracking, fewer interviews were needed, accounting for some of the reduction in numbers of first interviews. The main reason for the much-reduced number of second interviews was the disruption caused by the pandemic. The total number of respondents interviewed since CiC began in 2014 is 268, including 121 residents and 147 other local key informants such as BL reps, LTO staff and other local stakeholders. There is a small but rich longitudinal data set, with 97 of these respondents being interviewed between two and four times between 2014 and 2020, 57 of whom are residents.
| CiC phase | Total | Residents |
|---|---|---|
| Participants phase 1, single wave | 108 | 49 |
| Participants phase 2, wave 1 | 102 | 66 |
| Participants phase 2, wave 2 | 32 | 18 |
| Participants phase 3, wave 1 | 105 | 58 |
| Participants phase 3, wave 2 | 66 | 30 |
| Participants ALL phases | 268 | 131 |
| Of which repeated participants, any phase | 97 | 57 |
| Total interviews, including repeated | 418 | 223a |
The standard respondent ID provided with illustrative quotations in the findings chapters includes the area reference code, an abbreviation indicating the participant’s primary role (see Table 4) and a unique identifying number followed by the CiC phase and data collection wave in which the data were collected. For example, A1-RPM-1-P3-W1 refers to fieldwork area 1, resident partnership member 1, CiC phase 3, fieldwork wave 1.
| Role abbreviation | Role description |
|---|---|
| RPM | Resident partnership member |
| NRPM | Non-resident partnership member; for example, council officer with voting rights |
| FRPM | Former resident partnership member |
| Chair | Chair of the partnership, usually also resident partnership member |
| BLW | BL worker paid by the partnership |
| Rep | BL rep provided by LT |
| LTO | Locally trusted organisation worker |
| Stakeholder | External stakeholder |
The topic guides for the interviews are included in the accompanying project documentation, along with other fieldwork documentation. They covered respondents’ perception of processes enabling or constraining residents’ attempts to act collectively to improve their area and the impact they felt BL was having in the area, on the local population and on their own health and well-being. Where respondents had been interviewed previously, they were asked about the nature and range of collective activities residents have been involved in since the CiC phase 2 fieldwork in November/December 2016. Respondents involved in delivering a CCE were also asked about their experience of these projects. Two topic guides were produced, but where respondents combined strategic perspectives of BL with experience of CCEs, these were combined. Topic guides were also amended for the second interviews to include questions on the impact of COVID-19 in the area and the BL partnership’s response. Interviews conducted in the first wave were all conducted face to face at a venue chosen by respondents and, with their permission, these were recorded. Following the onset of the pandemic, interviews were conducted and recorded with respondents’ permission online via either Microsoft Teams or Zoom.
Data analysis
Recordings of the first wave of interviews were transcribed by a professional transcriber; most interviews conducted online were transcribed using automated transcription in Microsoft Teams or Zoom. All transcripts were checked for accuracy, anonymised to remove personal identifiable information and uploaded to NVivo-12. All transcripts were coded using a common framework developed collaboratively by the research team, drawing on analysis from previous phases of CiC. Coding also allowed emerging concepts to be captured. Consistency checking was conducted using NVivo’s inter-rater reliability test function. 109
Once all transcripts were coded, detailed longitudinal analyses were conducted to address relevant study objectives. These centred on: (1) the measurement of changes in capabilities required for communities to develop collective control; (2) pathways to collective control and the factors that enabled or constrained the development of these capabilities and their exercise by residents; and (3) residents’ perceptions of pathways to health impacts and the impact of involvement in BL on their own health and well-being. Approaches to these analyses are described below.
Markers of changes in capabilities for collective control
This analysis aimed to assess whether the qualitative markers of capabilities for collective control in BL residents developed in earlier phases of CiC110 were sufficient to capture changes over time, or whether we needed to add a scale or to describe additional markers. These markers are described in Chapter 7. This analysis was based on 48 respondents drawn from across the 14 fieldwork areas and interviewed in the latest phase of CiC and at least one previous phase. We used the framework method111 to undertake a thematic analysis of cross-case data relevant to the original markers, looking initially at first-wave interviews conducted before the pandemic in this latest phase of CiC. We noted evidence of change in capabilities for collective control in respondents’ accounts of progress in local programmes against the existing qualitative markers and looked for data to suggest new empirical markers. The next step involved analysis of CiC phase 2 data from November/December 2016 for the same individuals, to identify the pathways towards any increased capabilities for collective control identified in CiC phase 3 wave 1 data. Lastly, we conceptualised new markers, illustrated with examples, and identified milestones capable of measuring progress towards greater collective control over time in BL and other community empowerment programmes. The findings are reported in Chapter 7.
Pathways to changes in collective control in Big Local communities
This work has involved three related analyses, and the findings are presented in Chapter 7. The first examined the internal dynamics within BL partnerships over time and the potential impact on capabilities for collective control. The second focused on the external dynamics operating to enable and/or constrain BL residents’ attempts to exercise collective control over actions to improve their area. Both drew on longitudinal qualitative data across three time points (2014–15, 2016–17 and 2018–21) in four different fieldwork areas (eight areas in total). The third analysis looked at BL partnership responses to the COVID-19 pandemic.
Partnership dynamics: Four fieldwork areas were purposively selected to enable exploration of the variety of structures and processes within the BL partnership governance spaces witnessed across the areas. Relevant codes were identified from the NVivo analysis frameworks, to enable extraction of data relevant to the broad focus of ‘governance’ for each case study area. Due to the amount of data, this was limited to formal interviews conducted in CiC phases 1 (2014/5) and 3 (2018/21). Guided by the theoretical framework of ‘legitimacy’, extracted data were then reviewed in detail, supplemented by the research team’s knowledge of each area, to capture a longitudinal interpretation of the evolution of the BL partnership governance space since 2014/5.
External dynamics and delivering change: The four fieldwork areas for this analysis were selected to provide diversity in the type of CCE the fieldwork was following and early indications of differences in residents’ capabilities for collective control. All interview transcripts for the four areas across CiC phases 1, 2 and 3 were analysed manually to produce detailed narratives of the development over time of each CCE, with a particular focus on factors shaping progress. The lead researchers for this analysis conducted data collection in two of the four sites. In the other cases, the detailed narratives were shared with the lead researcher of that site for sense-checking and additional details. Cross-case analyses of these detailed narratives identified common themes. Finally, detailed analysis of data from CiC phase 3 for the four case study areas was systematically coded using these common themes and analysed to test and refine the findings emerging from within and cross-case analyses.
Responding to the impact of the COVID-19 pandemic: This is a preliminary piece of work, which is ongoing. The findings presented in this report are based on a targeted keyword search of all interviews conducted following the first lockdown in March 2019 to identify narrative fragments in transcripts relating to the impact of COVID-19 and the BL partnership’s response. These narrative fragments were then subjected to a simple thematic analysis based on emergent coding.
Perceptions of health and well-being impacts
Findings from these two analyses are presented in Chapter 8. The first examined residents’ perceptions of the impacts that BL could have on the health and well-being of local people and the pathways through which these impacts might come about. The second explored residents’ accounts of the impact of involvement in BL on their personal health and well-being, with a particular focus on negative impacts. Both analyses were based on interview data from the two rounds of interviews in 2018–21 in all 14 fieldwork sites. These interviews were all uploaded and coded in NVivo. Codes relevant to an analysis of perceptions of health and well-being were agreed upon after discussion among team researchers. These data were then downloaded into a separate file and subjected to a thematic analysis focused on identifying accounts of pathways to impacts. The second analysis drew on the same subset of coded data and involved a thematic analysis of residents’ accounts of impacts on their health and well-being, focusing in particular on negative impacts. From these accounts we selected four individual residents who had been interviewed at least three times over a 4-year period and utilised data from transcripts and observational notes to produce longitudinal accounts of the diverse impacts of involvement in BL. The production of the vignettes and the thematic analysis also enabled identification of the dominant themes from the wider sample of 15 areas, across the three phases of CiC.
Work package 4: economic evaluation
We evaluated the economic impact of BL by conducting a cost–benefit analysis using the life satisfaction approach to value the benefits of BL. We did not conduct a cost–effectiveness analysis because this requires a single measure of ‘effect’ such as the quality-adjusted life-year (QALY) used in much health care/medical evaluation, which is too narrow for an intervention like BL. The starting point for our cost–benefit analysis was the results produced by WP1 for the subjective well-being measures included in the APS, and specifically the question ‘Overall, how satisfied are you with your life nowadays?’. The life satisfaction approach compares the impact of the intervention or policy of interest to the impact of income on life satisfaction. 112 For example, if an intervention increases life satisfaction by 0.5 on the 0–10 scale and a £5000 increase in income results in a similar 0.5 increase in life satisfaction, the value of the policy to the individual is £5000. Thus, the life satisfaction approach allows us to put a monetary value on the benefits generated by the intervention. We can then compare the benefits with the costs.
The DiD analysis in WP1 found that BL increased life satisfaction on its original 0–10 scale by 0.01 (95% CI –0.057 to 0.077). Although this estimate is not statistically significantly different from zero at conventional levels of significance, we decided to use it for the economic evaluation to at least get an idea of the potential monetary value of BL. WP1 found for the SAMHI that when focusing on the subgroup of BL areas that had spent more than 80% of their grant by 2019/20, the impact estimate increased nearly fivefold and became statistically significant at a significance level of 5%. Unfortunately, the same subgroup analysis was not possible for the subjective well-being measures, as the sample sizes were too small. If we were able to conduct this subgroup analysis, we might find a similar increase in the impact estimate for life satisfaction, which would take the estimate from 0.01 to 0.05. Thus, proceeding with the estimate of 0.01 gives us a conservative indication of the potential benefits of BL.
For our calculations, we followed the procedure described by Dolan et al. 113 We took an estimate of the impact of income on life satisfaction from previous research, specifically that of Sacks et al. ,114 who found that a one-unit increase in log household income increases life satisfaction by between 0.3 and 0.4 standard deviations. We chose the midpoint of this range of estimates (0.35) and, based on the life satisfaction scale in the APS having a standard deviation of 1.90, assumed that a one-unit increase in log household income increases life satisfaction by 0.35 × 1.90 = 0.665. In a robustness test we assumed a larger standard deviation of 2.00, which implies that a one-unit increase in log household income increases life satisfaction by 0.35 × 2.00 = 0.700. A 1% increase in household income is approximately equivalent to a 0.01 increase in log household income. Thus, a 1% increase in household income would result in a 0.01 × 0.665 = 0.00665 increase in life satisfaction. We approximated household income in each BL area by linking the LSOAs that make up a BL area to the Middle Layer Super Output Areas they are part of, for which the ONS provides income estimates. We used the estimates of total annual household income for the financial year ending 2018. At our sample mean of £37,471, a 1% increase in income is £374.71. If a 1% increase in household income increases life satisfaction by 0.00665, then a 0.01 increase in life satisfaction due to BL is equivalent to the increase in life satisfaction achieved by a 0.01/0.00665 = 1.50% increase in household income. Thus, a household with the mean household income would be willing to pay £374.71 × 1.50 = £562.07 per year for BL. In our robustness test, with a standard deviation of 2.00 for the life satisfaction scale, the willingness to pay would be only £374.71 × (0.01/0.00700) = £535.30.
To obtain the willingness to pay per person, we divided the willingness to pay per household by the average household size. We approximated household size in each BL area by using the average household size from the 2011 census for all LSOAs that make up each BL area. At the sample mean of 2.398 persons per household, the willingness to pay for BL for a person in a mean-household-income household would be £562.07/2.398 = £234.39 per year. We calculated the willingness to pay per person for each of the 880 LSOAs that make up the 150 BL areas, so each of these 880 willingness to pay per person values was based on the estimated household income and the average household size in the specific LSOA. We then multiplied the willingness to pay per person value for each LSOA by the number of residents aged 16 and over at the 2011 census to obtain the total willingness to pay in that LSOA. Finally, we summed the total willingness to pay over all the LSOAs that make up a BL area to obtain the total willingness to pay in each of the 150 BL areas.
We then compared the monetised benefits of BL to the cost of BL. In our cost calculations we included the actual payments that each BL area received as well as the value of the time residents and other people have given to BL. The payments are the main BL plan funding plus the funding provided through the Getting People Involved, Getting Started, Creating Plan, Pathway Funding and Marketplace schemes as well as the area admin contribution and any social investment funding.
To obtain the value of the time residents have given to BL, we first extracted information on unpaid hours from the national survey of BL partnership members that LT conducted in 2016, 2018 and 2020. At the end of the questionnaire, respondents are asked ‘How many unpaid hours a week do you spend on BL?’. We multiplied the weekly hours by 52 to obtain an annual value and then summed all the hours reported by all the respondents for each BL area to obtain the total number of unpaid hours for each BL area in 2016, 2018 and 2020. We multiplied the total number of hours by £8.21, which was the national minimum wage in 2019. To extrapolate from the three survey years to years without a survey – that is, 2015, 2017 and 2019 – we simply doubled the value obtained in the previous step. In a robustness test, we tripled the value in an attempt to approximate the value of the time provided between 2011, when the initial BL areas were announced, and 2020.
In a change from our project proposal, we did not examine potential spillover effects of BL on neighbouring communities. Unfortunately, we were given access to the APS so late that it was not possible to conduct this additional analysis. We also were unable to examine in detail the use of additional resources such as premises, reduced-price materials or equipment provision in our 15 fieldwork neighbourhoods. Finally, since WP1 did not identify statistically significant impacts of BL on antidepressant prescribing and mental health-related hospital admissions, we did not calculate the potential cost savings to the NHS.
Conclusion
This chapter has provided details of the methods used in the different WPs that made up this third phase of the CiC study. The results of these different elements are presented in the following chapters. First, Chapter 4 describes the perspectives of national stakeholder interviews on the ways in which the BL programme differed from previous place-based empowerment initiatives, how the programme changed internally, how the external context impacted on the programme, and how its relevance to, and engagement with, the national policy agenda has shifted over time. Quantitative findings on the social and health impacts of the programme on populations in BL areas and on the residents who were most actively engaged in delivering local programmes are presented in Chapters 5 and 6. Chapters 7 and 8 then present findings from the qualitative research conducted in a sample of BL areas. Chapter 7 focuses on barriers and enablers to BL residents developing and exercising collective control over decisions and actions that had potential to improve their neighbourhoods. Residents’ perspectives on the health and well-being impact of the changes they had pursued, and their involvement in delivering these, are explored in Chapter 8. The results of our analysis of the costs and benefits of BL are then described in Chapter 9. Finally, in Chapter 10 we summarise the ‘story’ our findings tell about the social and health impacts of BL 10 years into the programme; identify implications for the future design and evaluation of PBIs that aim to increase collective control, particularly in disadvantaged communities; and outline our plans to involve BL residents and the wider public in interpreting and disseminating our findings in the future.
Chapter 4 Changes to the Big Local programme and positioning in relation to national policy: findings from national fieldwork
Introduction
Based on interviews with national stakeholders involved in managing and delivering the programme, this chapter begins by briefly setting the context for the early years of BL – highlighting how the programme sought to be different from previous PBIs. Next, we outline key developments since the time the programme was initially rolled out when the CiC study began. In particular, we highlight internal changes to support and management functions within Local Trust (LT) following a change of chief executive in 2017. Alongside this, the increasing external interest in the BL model is documented; this is explained, in part, by the shifting perspectives on places and communities in national policy, but also by LT’s more proactive focus on external policy engagement. Finally, the chapter reports on the ways in which major ‘shocks’ – including austerity, welfare reform, the EU referendum and most recently the COVID-19 pandemic – are perceived to have a bearing on the programme. Where quotes are used, the reference cites the phase of the CiC study when national interviews took place (CiC1 or CiC3) and the wave of fieldwork in CiC3 (wave 1 or 2) as well as the unique participant identifier (e.g. Nat-Interview-12; see Table 4).
Context: learning from the past
In 2014, national informants spoke of their aspiration to build on learning from the ‘plethora’ of past policy initiatives pre-dating BL, such as NDC. Particularly emphasised in how BL differed was its perceived independence compared to government-funded initiatives. Independence was defined with respect to the funding source (Lottery not government), the establishment of a new organisation at ‘arm’s length’ from the funder (LT) and allocation of funds to resident-led partnerships (rather than local authorities). Combined, these elements were understood to enable the programme to develop at its own pace, viewed as critical in supporting resident-led change. As this participant explained, such independence meant a lesser likelihood of top-down ‘interference’ when progress was perceived to be slow.
In most cases the first sign of something going wrong and the government … or the local authority stepped in or usually both … because … they just couldn’t bear any form of scandal or failure or whatever. The difference with Big Local is that the Big Lottery Fund have set this up, so they are not government.
CiC1-Nat-Interview-11
Participants also emphasised the perceived benefits of BL’s ‘non-political’ status meaning it was less likely to be knocked off course by election cycles, with some participants disassociating the programme from concurrent policy developments.
… of course, there are political things, there’s bound to be I imagine somewhere, but I’ve not seen any, for example, political interference in what we do, I’ve not seen that at all. I like the way that the … funding model is not associated [with] election cycle.
CiC1-Nat-Interview-01
Big Society was kicking off at the same time but actually the thinking about that was that we didn’t want to be attached to that in any way … I think definitely [respondent X] wanted the programme [Big Local] to go under the radar, in terms of Big Society because we wanted to kind of test it first and also it wasn’t, it’s non-political.
CiC1-Nat-Interview-10
In part, this emphasis on being ‘non-political’ was an effort, as the above participant observes, to protect the programme (and residents involved) from unwanted external scrutiny. But, as the quote below illustrates, participants also stressed perceived differences between the underlying philosophies of Big Society and BL. In particular, funding to support resident-led change was seen as a defining feature of the BL programme, particularly when the political motivation for Big Society was being questioned in the context of austerity measures.
I think Cameron lost out on that one [Big Society] because it was a view that you are cutting back so you want people to do things for free … But with Big Local ’cause we had money attached we were able to say ‘yeah we can do this’ and we can say to a community ‘what do you want to do, how do you want to spend it?’
CiC1-Nat-Interview-04
Overview of national-level developments
In the previous chapters we outlined the key BL model functioning at a national and local level. By 2017, a number of developments were influencing changes in this model. Internally, these included a change in LT’s leadership, a more proactive organisational focus on external policy engagement, and evolving support and management arrangements, as partnerships moved along the BL pathway to deliver plans and spend money. Externally, BL had gained more visibility compared to the early years of the programme, and learning from BL was increasingly influencing policy spaces for places and communities. Finally, participants also reflected on wider contextual influences on BL in the social, economic and political environment during this period.
Internal developments: Big Local support and management functions
In interviews conducted in 2019, informants connected to LT highlighted key developments in the programme centrally. While these changes involved substantive remodelling of BL’s support and management, those interviewed also emphasised that the programme’s ‘fundamentals’ remained unchanged:
the fundamentals are still there in terms of how Big Local areas engage with the Big Local programme, you know … long-term … resident-led, non-judgemental, light-touch support from reps. [however], nearly all of the delivery architecture, the structures that support that have been reviewed and changed over the last 24 months.
CiC3-Nat-Interview-13-W1
Three key changes to delivery architecture are outlined below.
Increased breadth of support opportunities
Since BL’s inception, the range of support opportunities for partnerships has expanded considerably. For example, the need for more specialist support for partnerships was highlighted where BL plans were addressing complex issues, such as efforts to secure land or buildings as assets. Another approach described was the increasing use of clusters of BL areas with similar interest around a specific theme, enabling learning to be shared, or for partnerships to access expertise from national organisations on an issue of shared concern (e.g. knife crime, climate change).
… they [BL partnerships] have been asking for more help and more specialist help to go with what they want to do and now for instance we have them thinking about legacy, because what we hope is that the improvement is sustainable.
CiC3-Nat-Interview-11-W1
Negotiated support offer
In the early years of BL, all support opportunities were largely available for any BL partnership to apply for. In recent years, support has shifted to a more negotiated position between BL partnerships and national stakeholders. While the needs are still driven by local areas, key players including LT and BL reps are now more involved in agreeing on the nature of support provided. In some cases, there is also an expectation that BL partnerships contribute to the costs of support to encourage local ownership of the support received. Support has also been increasingly targeted when spending has slowed due to internal problems (e.g. conflicts between BL partnership members) or where a BL partnership is perceived to have lost impetus or direction. This has resulted in a more bespoke support model for some areas.
it’s always the area’s choice if they want to take up an offer. But sometimes they are being targeted … I think the benefit … [areas] are more likely to get the right support that the area actually needs at that particular moment and can make the best of it. I guess it might feel slightly different to areas than it would be before … if you put your hand up and put yourself forward then you would get it.
CiC3-Nat-Interview-12-W1
Performance management and learning
Finally, the role of LT has expanded. In the early years of BL, LT functioned with a small team, with support arrangements such as the management of BL reps contracted to external organisations. Since 2017, LT has increasingly managed key functions, with the pool of BL reps brought ‘in house’. The internal capacity of LT has increased, providing greater opportunity for staff to engage directly with BL partnerships at the local level. This has been accompanied by the implementation of more comprehensive systems for capturing information on progress and learning across all 150 areas, as well as support for BL partnerships to measure and evaluate change. Also in 2018, LT agreed on an amendment to the original trust deed that has allowed them to invest more significantly in research and learning as part of efforts to support dissemination from the programme.
We started to increase the extent to which we … have capacity to manage the programme, ... invest quite a lot in developing management information. Not so much to performance-manage BL areas but to ensure that as an organisation we understand what’s happening across the whole programme and can then look at BL areas and their individual needs in the context of what is happening in every other area.
CiC3-Nat-Interview-13-W1
External developments: relationship of Big Local to the national policy context
Developments in places’ and communities’ policy
Reflecting on the decade since BL was launched, participants pointed to a changing focus on place and communities within the English policy landscape. This was firstly explained in relation to the localism agenda pursued by the coalition government since 2010. While this agenda emphasised a changing relationship between national and local government, it also had salience for initiatives such as BL to the extent that localism emphasised communities taking control, and Brexit reinforced this:
I mean I think Big Local came at a very particular political moment when [Cabinet Minister] wanted to devolve a lot and part of that was bypassing local authorities … I think the Brexit vote did shift policy interest into place. It sort of became fashionable … to start talking about place as mattering and communities as mattering … actually, I think it’s the Brexit vote that sharpened that …
CiC3-Nat-Interview-17-W2
However, participants also highlighted practical and ideological issues linked to these developments. For example, one participant expressed uncertainty as to the extent to which localism policies – such as neighbourhood rights and asset transfers – had genuinely reached or benefited local communities. Other participants suggested there was ambiguity in the framing of key concepts such as ‘left-behind’ neighbourhoods – a term increasingly used within national policy rhetoric following the EU vote. Participants suggested this context presented a window for learning from programmes like BL to more proactively inform developments within the unfolding public policy landscape.
Growing policy-focused work in Local Trust
Since 2017, LT’s work to more proactively influence policy developments has been evident in a range of ways, including establishing a new policy team and encouraging the transfer of learning from BL to other national organisations. As noted already, a revision to the trust deed has also enabled greater investment in ‘telling the story of BL’ with a view to disseminating lessons more widely.
Respondents were asked about the ways in which BL was perceived to be contributing to the development of thinking and policy at the national level. There were frequent comments on this increased external profile compared to BL’s early years, which had been largely concerned with the internal organisation and delivery of the programme. As one participant, involved in BL and interviewed in 2014 and then again in 2019, observed: ‘there is a lot more learning and sharing and everything going on’ (CiC3-Nat-Interview-02-W1).
One example of policy influence is LT’s involvement in establishing a new alliance campaigning for a Community Wealth Fund. The aim of the alliance is to dedicate dormant assets (from stocks, shares, bonds, insurance and pension policies) to create a new, independent endowment. It has generated considerable interest, with 400 members now signed up. There is also evidence of political interest in the idea, illustrated, for example, by the proposal for a Levelling Up Communities Fund in MP Danny Kruger’s Levelling Up Our Communities Review (September 2020),35 which shares similarities with the Community Wealth Fund. The work LT commissioned in 2019 on the nature and geography of ‘left-behind’ neighbourhoods, and specifically the paucity of social infrastructure in these areas, is another notable example of policy influence. 102 Following the dissemination of the report, they were appointed as secretariat for an all-party parliamentary group for left-behind neighbourhoods in 2020.
External factors influencing Big Local
Finally, participants identified a number of factors external to the programme which they felt had potential to shape BL and in turn residents’ capabilities for collective control.
Austerity and welfare changes
Austerity and welfare changes were highlighted as having a significant impact on residents in BL areas; this was a finding observed across the different waves of fieldwork. Firstly, in a context of deepening public sector cuts, there was growing evidence of BL partnerships supplementing or supporting services previously delivered by local councils.
At first a huge number of areas would have said … ‘Oh we are not going into supplementing sort of like services that the local authority should be providing’. But as time has gone on and with austerity, they have found that they are doing that – they are providing youth services for example and they have realised that really if they didn’t do it then … it wouldn’t be happening at all.
CiC3-Nat-Interview-12-W1
Others suggested that changes to welfare systems were impacting resident engagement in BL:
One of our research partners … did some research into the impact of welfare reform in some of the Big Local areas – so massive increase in use of food banks, lots of people being displaced through the bedroom tax and people being too distracted by all of that to want to participate and get involved.
CiC1-Nat-Interview-10-W2
Such factors were perceived as also having a bearing on residents’ sense of collective control. The following participant observed that while BL funding enabled residents to exercise some control over external factors shaping living conditions in their areas, this could simultaneously be disempowering, changing the dynamic between residents involved in the BL partnership and those in receipt of BL support.
[T]hat feels sometimes and comes across as a … bit of the like Lady Bountiful kind of, oh no let’s provide some food …. That’s not the sort of relationship that you want … residents on partnerships to have with the wider community, to feel that there is this sort of, like, this powerful group of people who can then bestow you know the means of life to another person who is in the community. That really wasn’t in the plan.
CiC3-Nat-Interview-12-W1
EU referendum and Brexit
A second major development has been the EU referendum, followed by the UK’s departure from the EU. Different views were expressed on its significance for local areas during the study time frame. Participants largely spoke of its heightening political attention to places where a majority of the local population had voted to leave. At the time of the interviews, however, the UK’s imminent departure from the EU was not viewed as a particularly prominent issue for local partnerships. Nevertheless, one participant suggested that some BL areas could be disproportionately impacted by the economic consequences of Brexit:
I think stuff like that [job losses] will impact. But when you go out and visit them [BL areas] at the moment, [I] don’t sense that’s something that people have on their mind.
CiC3-Nat-Interview-13-W2
The COVID-19 pandemic
The final wave of interviews was conducted a number of months into the pandemic when events were still unfolding and the longer-term effects were relatively unclear. Participants reflected on the ways in which communities involved in BL had proactively responded to the pandemic, a theme also covered in Chapter 7. In light of the need for all funds to be spent by 2026, some concern was expressed about the effects of the pandemic on the rate of expenditure, particularly in areas already struggling prior to the pandemic.
when there were issues before COVID happened, COVID only made those issues worse …. The partnerships just weren’t doing anything, weren’t making decisions at all, and in some of those areas it’s been difficult … so we will have to have a look.
CiC3-Nat-Interview-12-W2
Conclusion
In this chapter, we have explored the ways in which the BL programme has changed over time. Internally, in recent years there has been greater investment in research, learning and programme management within LT and more active engagement between national and local programme functions, as well as more targeted support provided to local areas. Alongside this, informants provided insight into key shifts in the policy context throughout BL’s life course, as well as the ways in which the programme as a whole is attracting more visible policy and national interest. Finally, the findings reported here help illuminate the wider context in which BL operates. While national interviewees were uncertain about the longer-term implications of Brexit and COVID-19, a consistent theme across all waves of fieldwork was the potential negative impact of austerity and welfare changes on residents’ engagement with the programme itself, for their ability to control decisions and actions impacting on their lives and on their well-being. We will return to these issues in the final chapter of the report.
Chapter 5 Population-level impacts of Big Local on health and social outcomes
Introduction
As described in Chapter 3, our theory of the change in population health outcomes that could happen when BL is implemented starts from the premise that if residents develop the capabilities for greater collective control over decisions and actions, they can use these to prevent or mitigate exposure to health-damaging conditions. Direct positive health effects may derive from these actions making the neighbourhood a healthier, better place to live. Indirect health improvements may also arise from the reduction in social isolation and improvement in mental health that participation in community action can produce. Finally, having increased control may lead indirectly to health benefits for individuals, albeit that this pathway is more likely to operate on residents who are actively engaged in BL. While in theory there could be positive impacts on physical health outcomes, these would only emerge in the much longer term. Positive impacts on mental health and well-being, in contrast, could be seen in a shorter time frame. This chapter presents results from our investigation into these potential health and social impacts of BL at the population health level. In the next chapter, our findings on the health impact of BL on actively engaged residents are presented.
Details of the outcome and control measures used and analytical approach are provided in Chapter 3. In summary, the analysis looked at changes from 2011 to 2019 in BL populations and populations in matched comparison areas for a primary outcome – self-reported anxiety – and a number of secondary outcomes: the SAMHI, antidepressant prescribing, mental health-related hospital admissions, three measures of subjective well-being (low satisfaction with life, low levels of happiness, and feeling things are not worthwhile) and recorded crimes and ASB. All of the outcome measures are scaled so that a higher level is more adverse, that is, an increase in the SAMHI is a deterioration in mental health in the population. The potential impacts on population subgroups defined in terms of age, sex, employment status, socioeconomic status, ethnicity, educational qualifications, marital status and disability were also considered. Finally, the analysis considered impacts in subgroups of BL areas on the basis of the types of activities they prioritised and the level of expenditure overall by 2019/20.
The characteristics of Big Local areas and matched comparison areas
The characteristics of the BL and matched comparison areas are shown in Table 5. Broadly, they are very similar across a wide range of characteristics.
| Measure | BL areas | Comparator areas |
|---|---|---|
| SAMHI (2015) (mean) | 0.22 | 0.24 |
| Antidepressant prescribing (2015, mean z-score) | 0.04 | 0.06 |
| Mental health-related hospital admissions (2015, mean z-score) | 0.42 | 0.43 |
| All crimes and ASB (2015, mean z-score) | 0.39 | 0.42 |
| Criminal damage (2015, mean z-score) | 0.60 | 0.63 |
| ASB (2015, mean z-score) | 0.35 | 0.38 |
| Violent crimes (2015, mean z-score) | 0.25 | 0.27 |
| Burglary (2015, mean z-score) | 0.20 | 0.22 |
| Income score of the indices of deprivation (2015) | 0.24 | 0.25 |
| Crime score of the indices of deprivation (2015) | 0.57 | 0.57 |
| Environment score of the indices of deprivation (2015) | 0.26 | 0.26 |
| Health score of the indices of deprivation (2015) | 0.68 | 0.67 |
| Proportion of population white ethnicity (2011 census), % | 79 | 80 |
| Proportion of population black ethnicity (2011 census), % | 10 | 9 |
| Proportion of population Asian ethnicity (2011 census), % | 7 | 7 |
| Proportion of the population aged under 16, % | 21 | 21 |
| Proportion of the population aged over 75, % | 6 | 6 |
| Community Needs Index (2019) | 83.9 | 83.6 |
| Average distance to nearest GP practice (km) | 1.1 | 1.1 |
| Average distance to nearest A&E (km) | 5.2 | 5.4 |
| Average distance to nearest green space (km) | 0.5 | 0.5 |
| Average distance to the coast (km) | 48.3 | 47.4 |
FIGURE 3.
Map showing the location of the BL areas and the comparison areas.
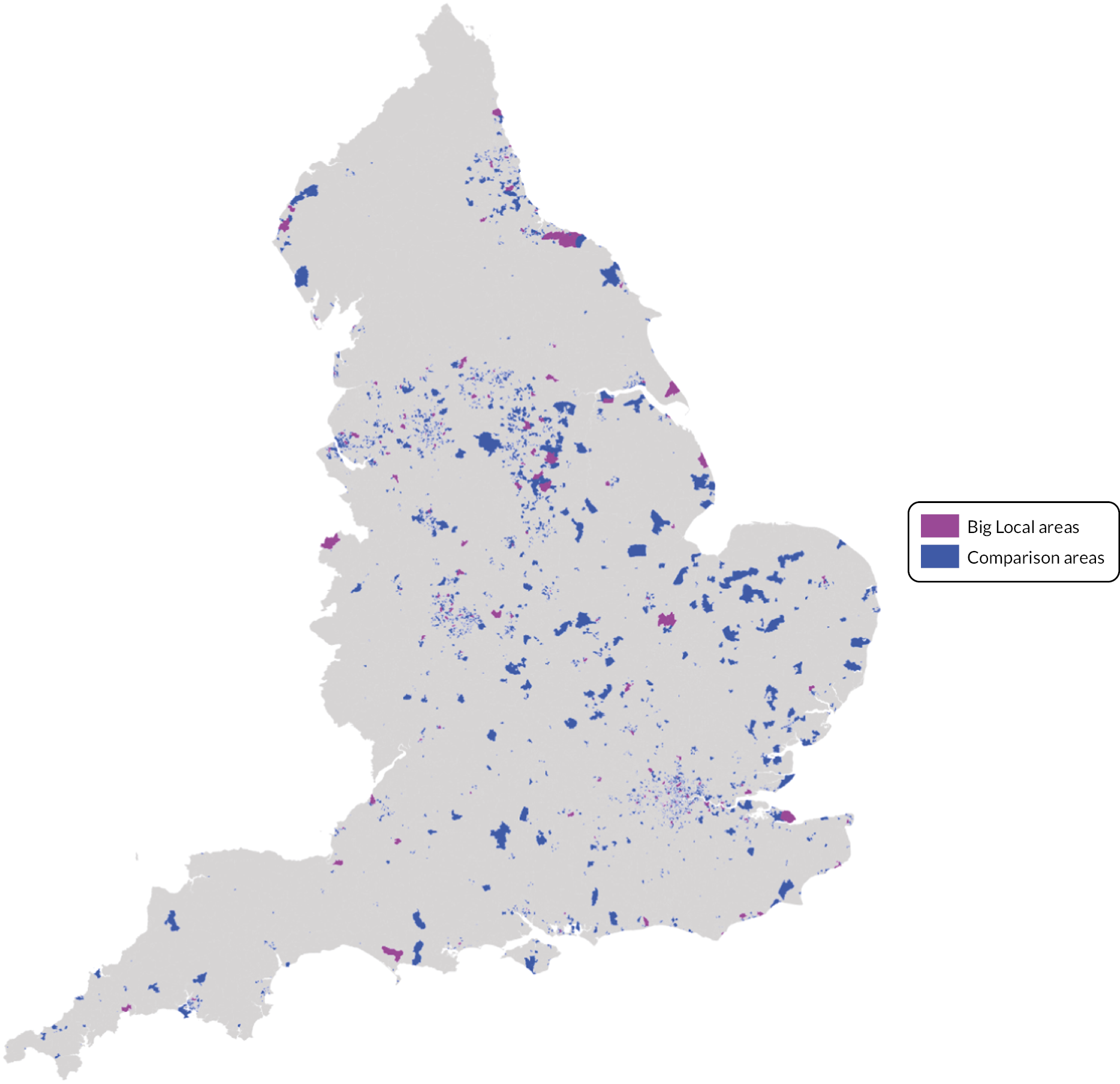
Trends in each of the outcomes in the BL and comparison areas before and after the BL programme plans began to be fully implemented, from 2015–16, are shown in Figure 4. These indicate that the trends in each outcome in the BL and comparison areas were very similar before the start of BL, and for most outcomes remained so after BL plans began to be implemented. However, there was a slightly greater decline in the BL areas compared to the comparison areas for ‘feeling that things are not worthwhile’, and ‘all crimes’ increased to a lesser extent in the BL areas compared to the comparison areas.
FIGURE 4.
Trends from 2011 to 2019 in each of the outcomes in the BL and comparison areas before and after the intervention: (a) high anxiety, (b) low satisfaction, (c) low happiness, (d) not worthwhile, (e) SAMHI, (f) antidepressant prescribing, (g) mental health-related hospital admissions and (h) all crimes.

Table 6 shows the DiD parameter for each of the outcomes. For the majority of outcomes, there was no noticeable effect of the BL interventions, including for our primary outcome: high anxiety. The analysis suggests that the intervention was associated with a reduction in the proportion of people with a low ‘worthwhile’ score (–1.3%, 95% CI –2.8% to 0.2%, p = 0.097), although this is not significant at the 5% level. This is the equivalent to one fewer person out of every 100 in the BL areas reporting a low ‘worthwhile’ score due to the BL intervention. There was also some evidence of a reduction in burglaries associated with the intervention; however, the effect size is very small (0.054 of a standard deviation, 95% CI –0.1 to –0.009, p = 0.019). Our main results remained similar when using the full scale of our well-being outcomes (0–10), rather than dichotomising these outcomes (see Appendix 3, Table 25).
| Outcomea | Estimate (95% CI) | p-value | Units |
|---|---|---|---|
| High anxiety (%) | –0.8% (–2.4%, 0.7%) | 0.288 | 100,752 |
| Low satisfaction (%)a | –0.4% (–1.9%, 1.2%) | 0.624 | 100,958 |
| Low happiness (%)a | 0.5% (–1.2%, 2.2%) | 0.538 | 100,920 |
| Not worthwhile (%)a | –1.3% (–2.8%, 0.2%) | 0.097 | 100,531 |
| SAMHI | –0.011 (–0.040, 0.019) | 0.472 | 3,520 |
| Antidepressant prescribing | 0.005 (–0.025, 0.035) | 0.743 | 3,520 |
| Mental health-related hospital admissions | –0.007 (–0.046, 0.032) | 0.734 | 3,520 |
| All crimes | –0.023 (–0.055, 0.008) | 0.145 | 3,520 |
| Criminal damage | –0.014 (–0.061, 0.034) | 0.579 | 3,520 |
| ASB | –0.029 (–0.071, 0.012) | 0.169 | 3,520 |
| Violent crimes | 0.001 (–0.052, 0.054) | 0.967 | 3,520 |
| Burglary | –0.054 (–0.100, –0.009) | 0.019 | 3,520 |
Subgroup analysis
The full set of subgroup analyses is given in Appendix 3. There was some suggestion that the BL intervention may have had a beneficial effect on reducing anxiety in higher socioeconomic groups, in that people from higher socioeconomic groups experienced a greater reduction in anxiety in BL areas than their counterparts in the comparison areas, though this indication was not statistically significant at the 5% level (see Appendix 3, Table 15). There were no noticeable differences in effect of the intervention on the well-being measures when analysed by any other population subgroup.
When the analysis was limited to the group of BL areas that had spent more than 80% of their grant by 2019/20, the intervention was associated with a small improvement in the composite measure of population mental health (SAMHI), with the SAMHI score reducing by 0.05 in BL areas compared to the matched comparison areas (–0.053, 95% CI –0.103 to –0.002, p < 0.042), indicating an improvement in mental health. The reduction in burglaries associated with the intervention was also larger when the analysis was limited to this group of BL areas (–0.154, 95% CI –0.254 to –0.555, p = 0.002) (see Appendix 3, Table 16).
Effects did not differ substantially when we analysed the data by subgroups of BL areas defined by the type of activity they prioritised – social, economic, environmental or lifestyle (see Appendix 3, Table 17). When limiting this analysis to those that had also spent more than 80% of their grant, there was a greater reduction in crimes in those areas that had focused on environmental activities. This was driven mainly by a reduction in burglaries and, to a lesser extent, ASB. There was a greater improvement in mental health as measured by the SAMHI in those places that had spent more than 80% of their grant and prioritised social activities (see Appendix 3, Table 18). There were no marked differences in effect on any secondary outcome based on the level of deprivation, ethnic composition, or age profile of the BL areas (see Appendix 3, Tables 19–22). There is some evidence that the intervention could have had some effect on reducing levels of anxiety after 2017 (see Appendix 3, Tables 23–25). The association of the intervention with a reduction in burglaries does not seem to have been particularly sensitive to the year we set as the start date for the intervention.
Conclusion
Overall, the evidence for population-level social or health impacts from BL is very limited. In terms of our primary outcome, there is some weak evidence that BL was associated with reduced anxiety after 2017. There is also some weak evidence that BL increased the number of people reporting that things in their life were worthwhile. There is also evidence that BL may have reduced burglaries, although this effect is very small. Where BL areas had progressed more with implementation (i.e. had spent > 80% of the grant by 2019/20), there appears to have been an impact on improving mental health, particularly where these areas had prioritised social activities. There was also evidence that where the higher-spending areas focused on environmental activities, there was a greater reduction in burglaries and, to a lesser extent, ASB.
Notwithstanding the limitations discussed in the final chapter, the approach we have taken is robust to many sources of bias and sufficiently powered to identify a modest impact on our outcomes of the overall programme. It suggests some possible emerging beneficial impacts on the outcomes measured, occurring in those BL areas that had progressed to the greatest extent. These findings will be considered in more detail in the final chapter.
Chapter 6 Assessing the impact of Big Local on health and social outcomes in engaged residents
Introduction
As we saw in the previous chapter, there is very limited evidence for BL improving social and health outcomes at the population level, but what of those residents most actively involved as members of BL partnerships? Based on our theory of change, these residents could be expected to experience improvements in mental well-being and general health as a result of reductions in social isolation as they participate in BL activities, through an improved perception of community, as well as through feeling that they have greater control over decisions that affect their daily lives. In order to explore these potential pathways, we utilised data from three waves of the biannual survey of BL partnership members conducted by LT (2016, 2018 and 2020). These data include both resident (> 70% of sample) and non-resident BL partnership members (< 30% of sample). The analysis used both a repeat cross-sectional design and a nested cohort design across three waves and examined outcomes for the sample as a whole and by residential status.
The outcomes were a measure of positive mental health states (the SWEMWBS) and the 2011 census measure of self-rated general health status. The analysis examined changes in these outcome measures over time and the association with whether respondents felt able to influence decisions affecting their area with others (collective control); a measure of social cohesion (people in the area willing to help); and hours of involvement. The analysis also examined whether different levels of expenditure or types of activity prioritised in a BL area were more/less associated with any changes in SWEMWBS. We also conducted subgroup analysis by education and gender. More details of the outcome measures and analytical approach are provided in Chapter 3.
Repeat cross-sectional analysis
Main analysis
Table 7 provides the descriptive statistics for respondent characteristics and the health and explanatory outcomes for the repeat cross-sectional study across all three waves of the survey (2016, 2018 and 2020). The mean mental well-being score was 24.2 (± 4.2) at baseline, rising to 24.7 (± 4.1) at wave 2 and falling to 23.8 (± 4.2) at wave 3 (see further information in Appendix 4, Table 26). The proportions reporting good self-rated health were 74.35%, 68.9% and 70.2% at waves 1, 2 and 3 respectively.
| Variable | Categories | 2016, % (n) | 2018, % (n) | 2020, % (n) |
|---|---|---|---|---|
| Age | ≤ 64 years | 73.5 (622) | 69.0 (660) | 68.9 (641) |
| ≥ 65 years | 26.5 (224) | 31.0 (297) | 31.1 (290) | |
| Sex | Female | 56.9 (472) | 53.0 (536) | 63.8 (624) |
| Male | 43.1 (358) | 42.3 (393) | 36.2 (354) | |
| Ethnicity | Ethnic minority | 9.2 (75) | 11.6 (108) | 13.7 (133) |
| White | 90.8 (742) | 88.4 (820) | 86.3 (836) | |
| Highest education | No degree | 56.2 (434) | 58.3 (524) | 58.3 (490) |
| Degree | 43.8 (338) | 41.7 (375) | 41.7 (350) | |
| Willing to help each other | Agree | 85.5 (645) | 81.7 (773) | 89.8 (823) |
| Disagree | 14.5 (109) | 18.3 (173) | 10.2 (93) | |
| Collectively can influence area decisions | Agree | 87.1 (736) | 86.5 (851) | 86.2 (771) |
| Neither | 9.3 (179) | 10.2 (100) | 11.2 (100) | |
| Disagree | 3.6 (30) | 3.4 (33) | 2.6 (23) | |
| Resident | No | 31.1 (266) | 26.3 (253) | 28.4 (283) |
| Yes | 68.9 (590) | 73.7 (709) | 71.6 (713) | |
| Hours volunteered | Mean ± SD | 5.7 ± 6.7 (662) | 6.6 ± 9.5 (823) | 6.2 ± 8.6 (750) |
| Mental well-being | Mean ± SD | 24.2 ± 4.2 (787) | 24.7 ± 4.1 (921) | 23.8 ± 4.2 (841) |
| Self-rated general health | Good | 74.3 (620) | 68.9 (654) | 70.2 (616) |
| Not good | 25.7 (214) | 31.1 (295) | 29.8 (261) |
In the analysis, we included the two explanatory factors that were significantly associated with our health outcomes at baseline: ‘willing to help’ and ‘collective control’. 107 We also included resident status and hours volunteered. Across all three waves, over 80% agreed that people in the area are willing to help each other, and over 80% of respondents agreed that they have collective control over decisions in their area. Residents of BL areas made up 70% of the participants, and the average number of hours volunteered per week on BL activities was around six.
The final fully adjusted parsimonious model in Table 8 shows the associations between our explanatory factors and our primary outcome of mental well-being among the BL partnership members (split by resident status). The results show that compared to baseline mental well-being score in 2016 (20.20, 95% CI 18.18 to 22.21), there was no overall significant change in the mental well-being of participants or resident participants at wave 2 in 2018 (22.32, 95% CI 20.49 to 24.15) or wave 3 in 2020 (19.67, 95% CI 17.35 to 21.99) (see further information in Appendix 4, Table 27). However, those who perceived that people in the area were willing to help each other had a significantly higher mental well-being score at wave 3 (1.1, 95% CI 0.59 to 1.67). Similarly, those who agreed that collectively they can influence decisions in the area had a higher mental well-being score at wave 3 (3.4, 95% CI 1.5 to 5.2). Results were similar for resident and non-resident members of the BL partnerships.
| Variables | Categories | 2016 | 2018 follow-up | 2020 follow-up | |||
|---|---|---|---|---|---|---|---|
| All (n = 500) | Resident (n = 340) | All (n = 654) | Resident (n = 486) | All (n = 636) | Resident (n = 463) | ||
| Intercept | 20.20 (95% CI 18.18 to 22.21) | 19.61 (95% CI 17.20 to 22.01) | 22.32 (95% CI 20.49 to 24.15) | 21.19 (95% CI 19.12 to 23.27) | 19.67 (95% CI 17.35 to 21.99) | 19.55 (95% CI 17.15 to 21.95) | |
| Sex | Female | 0.07 (95% CI –0.61 to 0.75) |
–0.12 (95% CI –0.95 to 0.71) |
–0.47 (95% CI –0.16 to 0.12) |
–0.52 (95% CI –1.21 to 0.16) |
–0.22 (95% CI –0.86 to 0.42) |
–0.06 (95% CI –0.81 to 0.69) |
| Male | Ref | Ref | Ref | ||||
| Education | Have degree | –0.40 (95% CI –1.0 to 0.29) |
–0.02 (95% CI –0.87 to 0.82) |
0.08
(95% CI 0.03 to 1.58) |
0.11 (95% CI –0.59 to 0.81) |
–0.04 (95% CI –0.69 to 0.60) |
0.01 (95% CI –0.77 to 0.79) |
| No degree | Ref | Ref | Ref | Ref | Ref | Ref | |
| People in their BL are willing to help each other | Agree |
1.77
(95% CI 0.75 to 2.78) |
1.66
(95% CI 0.54 to 2.78) |
0.80
(95% CI 0.03 to 1.58) |
0.84 (95% CI –0.02 to 1.71) |
1.19
(95% CI 0.13 to 2.24) |
1.09 (95% CI –0.11 to 2.28) |
| Disagree | Ref | Ref | Ref | Ref | Ref | Ref | |
| Collective involvement can influence decisions in area | Agree |
3.06
(95% CI 1.23 to 4.90) |
3.72
(95% CI 1.59 to 5.85) |
2.19
(95% CI 0.57 to 3.81) |
3.04
(95% CI 1.20 to 4.88) |
3.82
(95% CI 1.60 to 6.04) |
3.83
(95% CI 1.55 to 6.10) |
| Neither | 0.40 (95% CI –1.76 to 2.56) |
1.11 (95% CI –1.39 to 3.62) |
–0.02 (95% CI –1.87 to 1.83) |
0.75 (95% CI –1.38 to 2.88) |
1.98 (95% CI –0.40 to 4.36) |
1.67 (95% CI –0.83 to 4.17) |
|
| Disagree | Ref | Ref | Ref | Ref | Ref | Ref | |
Subgroup analysis by education level
The subgroup analysis by education level also found that there was no significant difference in 2018 or 2020 in mental well-being by education level (see Appendix 4, Table 28). However, participants with a degree who felt that people in the area were willing to help had a two-unit higher mental well-being score in 2020 (2.10, 95% CI 0.28 to 3.91), while those in the lower educational group who agreed that they had collective control had a 2- to 4-unit higher mental well-being score in 2018 and 2020 than those who did not (no degree = 4.65, 95% CI 1.92 to 7.38).
Subgroup analysis by gender
The subgroup analysis by gender found no significant difference in 2018 or 2020 in mental well-being for men or women (see Appendix 4, Table 27). However, more highly educated women had a slightly higher mental well-being score in 2020 (30.52, 95% CI 0.26 to 1.03) (Appendix 4, Table 28) compared to lower educated women in 2020. For women who agreed that people in the area were willing to help, their mental well-being score was higher in 2016 (2.55, 95% CI 1.01 to 4.10), but not in 2018 or 2020, than for women who did not agree. Likewise, the mental well-being score among women agreeing that they had collective control was higher across all three waves compared to women who did not agree. There was no association for men between agreeing that people in the area were willing to help and mental well-being score. For men, those agreeing that they had collective control had higher mental well-being scores in both 2018 (3.96, 95% CI 1.44 to 6.48) and 2020 (5.79, 95% CI 2.34 to 9.08).
Self-reported general health
For the secondary outcome of self-reported general health, analysis of the repeat cross-sectional sample used a GEE model (adjusted for age, sex, ethnicity, educational qualifications, number of hours volunteered). This showed that over the study period, there was no significant change in good health in 2018 or 2020 (see Appendix 4, Table 29). This did not differ by resident status.
Nested cohort
Main analysis
Table 9 summarises the descriptive statistics for the demographic, health and explanatory factors of the 217 survey respondents who responded across all three waves. There was a higher proportion of women than men, and those aged 65 or over were the largest age group (33.3%). Most of these respondents were white (91.5%), while only 8.5% were from black and minority ethnic groups. Regarding educational status, a sizeable minority (37.8%) had one or more degrees. The vast majority of participants were residents of the BL area (e.g. 76.7% at wave 3), and the average hours volunteered per week were > 7.
| Variable | Categories | 2016, % (n) | 2018, % (n) | 2020, % (n) |
|---|---|---|---|---|
| Age | ≥ 65 years | 33.3 (72) | ||
| Sex | Female | 56.0 (121) | ||
| Male | 44.0 (95) | |||
| Ethnicity | Ethnic minority | 8.5 (18) | ||
| White | 91.5 (194) | |||
| Highest education | No degree | 62.2 (125) | ||
| Degree | 37.8 (76) | |||
| Willing to help each other | Agree | 88.4 (176) | 78.7 (155) | 89.4 (178) |
| Disagree | 11.6 (23) | 21.3 (42) | 10.6 (21) | |
| Collectively can influence area decisions | Agree | 90.2 (193) | 87.9 (189) | 85.9 (177) |
| Neither | 8.4 (18) | 10.2 (22) | 11.2 (23) | |
| Disagree | 1.4 (3) | 1.9 (4) | 2.9 (6) | |
| Resident | No | 20.3 (44) | 21.7 (46) | 23.3 (50) |
| Yes | 79.7 (173) | 78.3 (166) | 76.7 (165) | |
| Hours volunteered | Mean ± SD (n) | 7.2 ± 7.4 (183) | 8.4 ± 9.4 (202) | 7.7 ± 7.8 (182) |
| Mental well-being | Mean ± SD | 24. 5 ± 4.5 (199) | 25.0 ± 4.0 (205) | 23.9 ± 4.0 (193) |
| Self-rated general health | Good | 75.1 (157) | 71.6 (149) | 70.9 (144) |
| Not good | 24.9 (52) | 28.4 (59) | 29.1 (59) |
The mean mental well-being score was 24.5 (± 4.5) at baseline, 25.0 (± 4.0) at wave 2 and 23.9 (± 4.0) at wave 3. Over 70% of the participants reported that their general health was ‘good’ or ‘very good’ across all three waves. Across all three waves, the vast majority (> 78%) agreed that people in the area are willing to help each other and a very high proportion of respondents agreed that they have collective control over decisions in their area (e.g. 85.9% at wave 3).
Table 10 shows the final fully adjusted parsimonious model showing the associations between our explanatory factors and our primary outcome of mental well-being among the BL partnership members.
| Variables | Categories | Estimate | CI: lower | CI: upper | p-value |
|---|---|---|---|---|---|
| Intercept | 20.310 | 17.718 | 22.926 | < 0.0001 | |
| Time | 2020 | 0.062 | –1.409 | 1.533 | 0.934 |
| 2018 | 1.456 | 0.139 | 2.769 | 0.030 | |
| 2016 | Ref | ||||
| Age groups | ≤ 29 years | –2.447 | –6.447 | 1.554 | 0.230 |
| 30–44 years | –1.400 | –2.840 | 0.039 | 0.057 | |
| 45–64 years | –0.927 | –1.816 | –0.038 | 0.041 | |
| 65 and above | Ref | ||||
| Gender | Female | –0.210 | –1.122 | 0.703 | 0.639 |
| Male | Ref | ||||
| Ethnicity | Non-white | 0.380 | –1.236 | 1.997 | 0.632 |
| White | Ref | ||||
| Highest education | No degree | 0.213 | –0.686 | 1.112 | 0.642 |
| One or more degrees | Ref | ||||
| Residents are willing to help | Agree | 1.091 | 0.187 | 1.996 | 0.018 |
| Disagree | Ref | ||||
| Collectively can influence area decisions | Agree | 3.363 | 1.512 | 5.213 | < 0.001 |
| Neither | 1.397 | –0.644 | 3.437 | 0.179 | |
| Disagree | Ref | ||||
| Resident | Resident | 0.831 | –0.668 | 2.350 | 0.282 |
| Non-resident | Ref | ||||
| Time × resident | 2020 vs. 2016 diff | –1.566 | –3.224 | 0.091 | 0.060 |
| 2018 vs. 2016 diff | –1.530 | –2.991 | –0.068 | 0.037 | |
| Baseline difference | Ref | ||||
| Hours volunteered | 0.075 | 0.033 | 0.118 | 0.001 |
The results show that compared to baseline status in 2016, there was a 1.46 (95% CI 0.14 to 2.77) unit increase in mental well-being at wave 2 in 2018 but there was no statisticsally significant difference in 2020 (0.06, 95% CI –1.41 to 1.53). Respondents who perceived that people in the area are willing to help each other had a significantly higher mental well-being score (1.09, 95% CI 0.19 to 2.0). Similarly, those who agreed that collectively they can influence decisions in the area had a higher mental well-being score (3.36, 95% CI 1.51 to 5.21). Hours volunteered also had a small positive association with mental well-being (0.08, 95% CI 0.03 to 0.12). However, there was no significant association between mental well-being and resident status.
Big Local intervention typologies
For the nested cohort analysis, we also examined associations with the two BL intervention typologies: spend (low, medium, high) and type (environment/social/economic/lifestyle). The amount of spend in the BL area had no association with mental well-being (see Appendix 4, Table 30: high –1.45, 95% CI –3.25 to 0.35; medium –0.97, 95% CI –2.56 to 0.63; low = reference). In terms of the type of activities prioritised in an area (see Appendix 4, Table 31), only the environmental activity type was significantly associated with mental well-being (1.15, 95% CI 0.10 to 2.20).
Subgroup analysis by education
The subgroup analysis by education found that there was no significant difference in 2018 or 2020 in mental well-being for those without a degree-level education (see Appendix 4, Table 32). However, for those with one or more degrees (see Appendix 4, Table 33), there was an increase (1.99, 95% CI 0.14 to 3.84) in mental well-being in 2018, but no significant difference in 2020. In both educational groups, those with higher hours volunteered had a very small increase in mental well-being (no degree = 0.06, 95% CI 0.01 to 0.11; degree = 0.11, 95% CI 0.04 to 0.18). Likewise, in both educational groups, those participants who agreed that they had collective control had a higher mental well-being score than those who did not (no degree = 2.77, 95% CI 0.38 to 5.17; degree = 2.71, 95% CI 0.02 to 5.41). Mental well-being scores for residents with a degree were higher (2.29, 95% CI 0.22 to 4.36) than for non-residents with a degree.
Subgroup analysis by gender
The subgroup analysis by gender found that there was no significant difference in 2018 or 2020 in mental well-being for women (see Appendix 4, Table 34). Men had a significant increase of > 2 units (2.41, 95% CI 0.55 to 4.28) in mental well-being score in 2018 but not 2020 (see Appendix 4, Table 35). The mental well-being score among men agreeing that they had collective control was much higher (4.91, 95% CI 2.36 to 7.46) than men who did not agree, while for female participants, mental well-being score was significantly higher (1.64, 95% CI 0.48 to 2.79) among those who agreed that people in the area are willing to help each other compared to women who did not agree. For both male (0.20, 95% CI 0.12 to 0.28) and female (0.02, 95% CI –0.02 to 0.07) participants, there was a small positive association between hours volunteered and mental well-being score.
For the secondary outcome of self-rated health, analysis of the nested cohort sample used a GEE model (adjusted for age, sex, ethnicity, educational qualifications and number of hours volunteered). This showed that over the study period, there was no significant change in the odds of respondents reporting not good health in 2018 (OR 0.63, 95% CI 0.17 to 2.29) or 2020 (OR 0.53, 95% CI 0.14 to 1.47) (see Appendix 4, Table 36). This did not differ by resident status.
Conclusion
Analysis of the nested cohort – but not the repeat cross-sectional survey – found that there was a statisticlly significant increase in mental well-being in 2018 but that this was no longer present by 2020. This suggests that being involved in BL had a positive impact on the well-being of participants in the medium term (2018) but not over the longer term (2020). However, the 2020 survey was delivered in summer 2020, during the COVID-19 pandemic when the mental well-being of the whole country had declined. 115 This may account for why the 2018 improvement in mental well-being among BL participants was not maintained in 2020.
The impact of the COVID-19 pandemic is an extremely important – and unforeseeable – issue in our trend data as the bias it creates potentially affects both the outcomes and all of the explanatory variables (control, willingness, hours of volunteering, the implementation of the different types of BL intervention). It is therefore very difficult to interpret the 2020 survey data.
However, across all waves – even in the 2020 COVID-19 data point – residents who perceived that people in the area are willing to help each other and those who agreed that collectively they can influence decisions in the area had a significantly higher mental well-being score. Hours volunteered also had a small positive association with increased mental well-being in both the nested cohort and the repeated cross-sectional analyses, for both men and women and for groups with both high and lower education levels.
In terms of our subgroup analysis, there were some differences in results between our study designs. For the cohort, among those with no degree, there was no significant change in mental well-being score in 2018 or 2020, but there was a significant improvement among those who had one or more degrees. In both study designs, ‘collective control’ and ‘willing to help’ in the area had positive associations with mental well-being. In the repeat cross-section, in the lower education group, those residents who agreed that they had collective control had a higher mental well-being score in 2018 and 2020 than those who did not, but this association was not significant in the more highly educated group. However, residents with a degree who felt that people in the area were willing to help had a higher score in 2020. In the cohort, the positive association with collective control was present for both educational groups. Together, these results suggest that the health benefits of BL participation – especially for less well-educated residents – may depend on whether they felt a sense of collective control.
The results in terms of gender were similarly mixed across the two study designs. In the repeat cross-section, there was no significant difference in 2018 or 2020 in mental well-being for men or women. However, more highly educated women had a small significant increase in mental well-being score in 2020. Collective control was positively associated with higher mental well-being scores for women and – especially – men. Feeling that people in the area were willing to help was positively associated with mental well-being score for women but not for men. In the cohort analysis, there was no significant difference in mental well-being over time for women, but men in the cohort had a significant increase in the short term only (2018).
The amount of BL budget spent had no impact on the well-being scores of respondents; and of the different types of BL activity, only the environmental interventions had a significant, positive association with well-being. Our secondary outcome of self-rated health did not change in either study design over the time period.
Limitations
This analysis is subject to a number of important limitations. Firstly, the sample is small, which restricts statistical power. Secondly, the survey population is skewed towards highly educated people, white people and older age groups. This is unsurprising given the evidence that shows how people from more disadvantaged social backgrounds or those with poor health are less likely to participate in volunteering activities,116 but it does further limit generalisability. Thirdly, the study relies on self-reported outcomes, which may limit the precision and reliability of our findings. However, there is evidence that shows a strong association between self-reported health and more objective outcomes such as mortality. 117 Fourthly, our nested cohort analysis assumed that data were missing at random, which might not be the case (although in our examination only sex predicted missingness, so we adjusted for this in the main models). Fifthly, the study had no control group, and this restricts our ability to conclude that the changes observed were related to participation in BL. Our study can therefore only assess correlation between participation, collective control and so on, and mental well-being – it cannot establish causation. Finally, the impact of the COVID-19 pandemic is an extremely important – and unforeseeable – issue in our trend data as the bias it creates potentially affects both the outcome and all the explanatory variables (control, willingness, hours of volunteering). It is therefore very difficult to interpret the 2020 survey data. Indeed, other research has suggested that the pandemic and the associated restrictions negatively impacted on mental well-being. 115
Chapter 7 Exploring pathways to increased collective control among Big Local residents: findings from local qualitative fieldwork
Introduction
One of the core challenges for the CiC study has been how to theorise and ‘measure’ collective (population or group) control. In this chapter we describe how we have theorised the development of collective control, discuss our work on qualitative markers of changes in collective control, and present findings on the barriers to, and enablers of, the development and exercise of collective control by residents in BL areas. These findings are based on qualitative research conducted in a 10% purposive sample of 150 BL areas. The analyses included data from the three phases of the CiC study (2014–15, 2015–17 and 2018–21) and built on findings from the earlier phases of the study. More details of data collection and analysis are provided in Chapter 3.
This chapter has three sections. First the CiC power frameworks are described. These define the capabilities needed to exercise collective control over decisions and actions and the barriers that can constrain the development of these capabilities as different forms of power. Our ongoing work updating a set of qualitative markers of growing collective control, initially constructed from analysis of CiC phase 1 data, is also described. 110 The second section examines pathways through which residents developed and sought to exercise capabilities for collective control, and the enablers and barriers they encountered along the way. Finally, we present preliminary findings exploring how BL partnerships’ responses to the impacts of the COVID-19 pandemic in their areas were shaped by the interaction between local context and capabilities for collective control.
Collective control and power
The Communities in Control power frameworks
In phases 1 and 2 of the CiC study, we produced two frameworks to aid in the operationalisation of the concept of collective control and the barriers to its development. Their development is described in more detail elsewhere. 9 The frameworks are adapted from the work of others, drawing on learning from earlier phases of CiC and a systematic literature review of theories by Whitehead et al. 37
The emancipatory power framework (EPF) shown in Box 3 comprises a power lens through which capabilities for collective control, and changes in these, can be understood and assessed. It draws upon the concepts of ‘power within’, ‘power with’ and ‘power to’ (previously developed and applied at the individual level)118–121 and theoretical literature on empowerment. 122–125 However, much of the framing in this literature is instrumental, focusing on the ‘ingredients’ needed to achieve more effective empowerment, or focused at the level of individuals. The CiC EPF is distinguished by its focus on collective capabilities,126 developed within and by communities to exercise greater collective control.
Power within: Foundational capabilities internal to a community (e.g. recognition of shared interest)
Power with: Capabilities required to build alliances and act with others to achieve common goals
Power to: Capabilities required to achieved change including establishing structures, procedures and opportunities for collective decisions and actions and the outcomes of these
‘Power within’ refers to collective capabilities internal to a community, including recognition of shared values and interests. ‘Power with’ refers to the power emerging when a community acts with other agencies or communities to achieve common ends. ‘Power to’ refers to collective capabilities associated with implementation of community action. Interactions between the EPF dimensions are non-linear, although development and exercise of ‘power to’ and ‘power with’, initially at least, require some degree of ‘power within’, and changes in one power domain will feed back into others. These dimensions reflect an understanding of power as generative, expansive and ‘non-dominating’, emanating from relationships with others. 127
The CiC limiting power framework shown in Box 4 is adapted from a typology developed by Barnett and Duvall in 2005. 128 It identifies four forms of power that can be used to restrict the development and exercise of collective control by disadvantaged communities of interest/place. Importantly, these forms of power are not always used illegitimately, and individuals/groups in these communities can use them to exercise ‘control’ over others in the same community.
Compulsory power: Direct and visible, exercised, for example, by formal instruments of the state (e.g. police, government departments and legislation)
Institutional power: Less visible, exercised through organisational rules, procedures and norms (e.g. controlling information put into the public domain, restricting who is involved in decision-making)
Structural power: Invisible, works through systematic bias embedded in social institutions that generate and sustain social hierarchies of class, gender, ethnicity and so on that influence distribution of resources, opportunities and social status
Productive power: Invisible, operates through diffuse social discourses and practices that legitimise some forms of knowledge and marginalise others, which in turn shapes meanings of different social identities
‘Compulsory power’ is direct and visible: it can involve physical, psychological or economic force. ‘Institutional power’ is less visible, exercised through organisational rules, procedures and norms. ‘Structural power’ works invisibly through institutions such as the law, the labour market and education, creating and sustaining hierarchical structures (e.g. social class, gender/sexuality and race/ethnicity) through which resources, opportunities and social status are distributed. ‘Productive power’, in contrast, operates through social discourses and practices, with institutions (e.g. the media, politics, law, medicine, and education) legitimising some forms of knowledge/discourse while marginalising others. From the perspective of this research, ‘place stigma’ is one of the most relevant consequences of the illegitimate exercise of the productive form of power.
Assessing changes in capabilities for collective control
If the concept of collective control capabilities, understood as different forms of power, is to be of benefit to health research policy and practice, ways to identify and measure these capabilities at the level of the collective are needed. Collective impacts/outcomes, however, by their very nature, cannot be captured adequately by simply aggregating measures of psychological empowerment of individuals in a community or group. 56,129 We need measures that capture the dynamics of interactions within and between the collective, on the principle that the whole is greater than the sum of its parts. 130 In a recent review, Laverack and Pratley also confirmed that ‘standard quantitative indicators are insufficient to measure the complexity of the concept’ and advocate combining these with some form of rapid qualitative assessment. 131 In phases 1 and 2 of the CiC study, we took up the challenge and identified qualitative markers of changes in the different forms of power as they occurred in the first three years of BL. In this third phase of CiC, we have begun to elaborate further on these markers based on our most recent qualitative research in these neighbourhoods. This part of our analysis has been severely disrupted by impacts of the pandemic on our research team and is still ongoing, but our analysis of phase 2 and 3 primary data has both begun to reveal new empirical markers against the three dimensions of the power framework and has led to the addition of milestones marking the evolution of collective control capabilities through three main programme stages: initial implementation, development and bedding in. We thus adapted and extended our initial qualitative markers to become ‘progress markers’. The original markers of collective control capabilities are illustrated in Box 5, together with examples of the newly identified progress markers (depicted in emboldened text).
-
Drawing together existing skill and expertise across the community (implementation stage) moving to developing perspective, the ability to prioritise and put community needs first (developmental stage) and finally to developing qualities such as emotional resilience and professional persona (bedding-in stage).
-
Increasing sense of group efficacy and confidence in ability to act together (implementation stage) moving to evolving as a partnership and gaining autonomy (bedding-in stage).
-
Visible expressions of ‘shared values, interests’ and common identity (e.g. valuing collective ownership of decision/actions; agreeing formal group name, logo, web presence and recognisable community hub).
-
Developing new collective knowledge, skill and ‘know-how’ to address local issues.
-
Recognition by activists of the need for breath and depth of participation of wider community.
-
Arrival at shared vision for area improvements and negotiated priorities.
-
Recognition of potential benefits of working with other institutions or groups towards common goals.
-
Identifying opportunities to develop relationships and/or work with others.
-
Establishing new (or positively reshaping previously acrimonious) relationships with other institutions.
-
Inviting local non-governmental organisations, local government staff, local politicians and/or local businesses to participate in partnership meetings or sit on advisory boards.
-
Formation of new governance structures with relatively stable membership, procedural ‘rules’, regular meeting times and recognisable physical locations for decision-making.
-
Establishment of organisational practices; legal, financial and governance frameworks.
-
An ‘opening out’ of opportunities beyond formal governance spaces for the wider community to participate in developing shared narratives and to contribute to shared decision-making on action.
-
Examples of improvements in local social, cultural and/or economic conditions resulting from direct collective action by residents or their influence on decisions of others.
Taking the example of the dimension ‘power within’, a BL partnership might progress from ‘drawing together existing skills and expertise’ in the initial implementation stage of a community empowerment programme to meeting the milestone ‘developing perspective, the ability to prioritise and put community needs first’ in the developmental stage and finally to ‘developing qualities such as emotional resilience and a professional persona’ (which could be individual or collective) in the bedding-in stage. In another example in the ‘power within’ column, a BL partnership might be seen to progress from ‘increasing group efficacy and confidence’ during implementation to ‘evolving as a partnership and gaining autonomy’ as the programme is bedded in.
Pathways to collective control
Our research has illuminated different dimensions of the complex pathways BL residents traverse in seeking to develop and exercise collective control over decisions and actions that aim to improve their neighbourhood and the lives of local people. In this section, we consider these pathways from three perspectives. First, we consider the impact of internal dynamics in the governance space associated with BL partnerships. Second, we adopted a wider lens exploring the pathways BL residents followed as they attempted to deliver changes in the area, and the barriers and enablers they encountered along the way. These findings are based on longitudinal analyses of the qualitative interviews in four case study areas – eight in total. As described in Chapter 3, these interviews explored perceptions of processes enabling or constraining residents’ attempts to act collectively to improve their area and the impact they felt BL was having in the area, on the local population and on their own health and well-being. Third, we look at how the BL partnerships in our 14 fieldwork areas responded to the COVID-19 pandemic. This analysis involved qualitative interviews from the second wave when respondents were specifically asked about the impact of COVID-19 on the work of the BL partnership. Details of the methods used in these analyses are provided in Chapter 3.
The internal dynamics of Big Local partnerships
In phase 1 of the CiC study, we examined how BL partnerships emerged as governance spaces in the early stages of the programme. 132 We described the ways in which residents initially began working as a group brought together by the BL rep and/or other local stakeholders, with the expectation of having a 51% resident majority. These earlier findings revealed how residents began ‘taking charge’, reflecting growing power within the BL partnership and how the initial setting-up of governance structures, such as a code of conduct and constitutions, helped BL partnerships develop power with others by constructing themselves as a legitimate forum with which external, professional stakeholders can engage. 132
We have continued to explore how BL partnerships evolved as governance spaces since those early years as they navigated internal and external issues arising from the implementation of their plans in local areas. In this recent analysis, we have used Connelly’s framing of ‘legitimacy’ – a ‘property constructed in and through specific processes of governance’133 – to consider how partnership members sought to transfer their emerging ‘power within’ into ‘authority’ recognised by external stakeholders. 133 The analysis considers two types of legitimacy: process (or input) legitimacy – gained through how the process of decision-making is defined – and substantive (or output) legitimacy – gained through the outcomes of the decision-making process. 134 In large part this analysis has focused on governance, understood as structures and processes that enable partnership members to make decisions about how the BL money would be spent, determine who will act on behalf of BL, and be accountable to the local population and the national oversight organisation (LT) for delivering improvements in the area. However, it is also important to recognise that these governance spaces were also the location for a great deal of relational work by partnership members that moved beyond the work required for the practising of governance.
Four cross-cutting themes reflect different dynamics of the enactment of governance and can be argued to have shaped the development of capabilities for collective control in BL partnerships and contributed to external perceptions of their legitimacy: (1) representation and the movement of actors through the governance space; (2) mechanisms and tools of governance; (3) external expectations for governance; and (4) memories and legacies of governance.
Representation and engagement
The status and eligibility of actors in the BL partnership governance spaces have been negotiated and sometimes challenged from the earliest phases of the initiative, shaping how residents are involved and represented in decision-making. An important context for these dynamics was the ongoing difficulties experienced by BL partnerships in recruiting and maintaining members from among local residents, with a sense of fatigue developing in some areas as the initiative continued:
Some of them are getting, you know, they’ve been on it 10 years and 10 years of their life and it’s time that they’re retired so to speak. They feel they have done their bit, which they certainly have, so let it run its course.
A8-RPM-P3-W2
A more stable partnership membership over time appeared to accompany more informality of decision-making structures and a lack of explicit challenges to the internal governance arrangements. However, a ‘tightly knit’ group in A7 and the sense in A8 that the partnership had reached something of a ‘stalemate’, with a lack of interest among wider residents to join after most work had been completed, could suggest limited attempts to engage more widely with the community. This was highlighted as a concern by the BL rep in A8. Initially noting that the partnership had been reluctant to involve residents until they had something to ‘show’ for their work, he later described ‘founder’s syndrome’ as limiting engagement efforts:
New people came in, with good ideas, some of them had been tried before, but [the partnership] were very dismissive and not intentionally maybe, but they’d say, oh we’ve tried that; our people, they don’t want to do that. People very quickly, the new blood, either didn’t stay or shut up.
A8-Rep-P3-W2
On one hand, the stability of these partnerships suggests a strong, if informal, set of internal relationships. Yet the limited opportunity for wider involvement potentially undermines the input legitimacy of the partnership, where members are expected to act with, for and on behalf of wider resident groups.
In BL partnerships with more turbulent internal relationships and more disruption to membership over time, there were more explicit challenges to input legitimacy, and shifting debates about who was eligible to contribute to decision-making. In A4, these debates moved over time from challenging non-residents’ eligibility to contribute, to challenging members’ capacity to represent the needs of local residents, reflecting an insider/outsider divide among partnership members. The ousting of several long-standing partnership members following tension around this debate was seen by remaining members to establish a new kind of eligibility for involvement:
At this stage where we are like halfway through the project and we’ve got to make some big decisions and spend a lot of money, that we can be a bit more selective and bring in people that are focused on our aims rather than just wanting to be in a local group, that [are] actually in line, that they fit. So I think we’re happier now to maybe headhunt one or two people but also put out an invite, but be selective.
A4-RPM-14-P3-W2
Here, ongoing challenges around internal legitimacy were felt to have constrained the group’s ability to progress. Amid concerns that the BL was seen as a ‘a waste of time’ by the wider community, this was used as justification to reshape what partnership members must offer at a later stage in the process, effectively narrowing its representativeness. In other areas, challenges to a partnership’s legitimacy as representative of the wider community resulted in different responses. In A3, for example, concerns about the lack of representation in the partnership of the substantial non-white ethnic population had been identified by the BL rep at an early stage, but without much action.
We have this core of white, middle-aged people … They’re in a community where there are more non-white people than there are white people … [The partnership have] … looked at that data as part of the writing of the last plan. So they know it, they’re not ignorant of it.
A3-Rep-P3-W2
However, following accusations of racism against a partnership member, LT intervened. This prompted the partnership to take action to widen the structure and processes of engagement, including creating a multifaith group to support involvement and submission of grant applications from different local communities.
Mechanisms and tools of governance
The evolution and use of structures and tools of governance over time impacted on relationships among partnership members, the flow of projects and activities delivered by the partnerships and attempts to establish legitimacy of their operations. Examples of these mechanisms are shown in Box 6.
-
Codes of conduct or constitutions for the group’s structure and operation
-
Terms of reference or criteria for membership
-
Processes for managing conflicts of interest or other disputes
-
Establishing subgroups and hierarchies of decision-making and accountability
-
Seeking formal, legal status, for example as community interest organisation (CIO) or community interest company (CIC), to give more authority and capacity for decision-making
-
Communications processes for maintaining transparency of decision-making
Many BL partnerships set up multilayer structures for decision-making, with one or more subgroups focused on a particular area of decision-making (such as communications or events). These networks of decision-making spaces were established fairly early and had potential to widen the impact on capabilities for collective control in the local population. However, in some areas they were short-lived, dissolving or petering out. For instance, in A8, a temporary pause on giving out small grants, while the partnership developed a new plan, resulted in the dissolution of the small grants subgroup and decisions on subsequent requests for small grants being made by the main partnership. In contrast, the A8 events subgroup continued to organise local activities. At monthly partnership meetings, they would inform the rest of the partnership what would be happening regarding local events, rather than open up discussion or invite inputs to decision-making:
The events team were very decisive and confident in stating their decisions about upcoming events and what they’ll do for the gala next year – there was little sense of hesitancy or questioning.
Observation of partnership meeting in A8, 2 September 2019
In other areas, the subgroup structure appeared to contribute to and/or magnify challenges to authority for decision-making within partnerships. In A4 this was observed early on, where a subgroup structure – agreed to make decision-making in full partnership meetings more efficient – was undermined by a lack of trust between members, leading to further discussion of the subgroup’s decisions at the main partnership meeting. A few years later, only one subgroup remained, described by the rep as a ‘hotbed of falling out’ (A4-Rep-P3-W1) as it reflected a division between those who saw themselves as long-standing residents of the area and those perceived to be more recent ‘incomers’. When the subgroup stopped meeting formally due to the departure of a few members, and COVID-19 restrictions, the BL partnership chair decided to take more ‘executive decisions’ without the formal agreement of the wider partnership, in the interests of ‘getting things done’.
These shifts in the status and role of partnership subgroups reflect changes in the nature of decision-making work, as well as the dynamics within subgroups and between them and the main partnership. In some cases, over time, subgroup members gained greater confidence in their authority to make decisions and take action, and a growing sense of legitimacy in doing so: increasing power within, with and to. In other cases, relationships between the main partnership and its subgroups’ members seemed to lack the trust needed for the formal devolution of power to be enacted effectively, potentially weakening the internal legitimacy of governance structures and undermining the wider development of collective control capabilities.
Over time the tools of governance, such as codes of conduct and other regulations that all BL partnerships were expected to establish, were applied in different ways. Some partnerships employed the tools when difficulties arose around decision-making or the eligibility of people to contribute was questioned. For example, in A4, the partnership’s rules were used to challenge the authority of the then chair, who was perceived to be stalling the annual elections. Codes of governance were also revisited, and in some cases rewritten, following a significant challenge or disruption within the partnership. In A15, problems with a project prompted an attempt among the members to take more control over the process of deciding and overseeing how money was to be spent. The LTO worker supporting the partnership described how she used governance tools to work:
with them with looking at their values, looking at their code of conduct, looking at their constitution and how they wanted to operate … [it] was almost like let’s analyse what things are problems for you, what things are upsetting people, because there was a lot of upset at the time.
A15-LTO-P3-W1
Reviewing and revising codes of conduct could also serve to distance current members from practices or relationships that might be perceived as illegitimate or inappropriate. In A4, for example, following the departure of two long-standing partnership members after a period of tension, the rep noted that:
The first thing we did then when everything had been settled is we looked at the governance stuff, and we didn’t just look at the process for a breach of code of conduct; we looked at the whole governance picture. We [re]wrote the constitution.
A4-Rep-P3-W2
External expectations about Big Local partnerships’ legitimacy
Big Local partnerships responded to external expectations about their legitimacy in different ways, reflecting in part their perspectives on how their authority and control was best maintained. Some partnerships sought to align themselves with external governance structures by becoming ‘incorporated’, or formally constituted as a CIO or CIC. In A10, the partnership decided to establish a CIO in addition to the main partnership, to be ‘in control’ (A10-RPM-3-P3-W1) and to function independently as an organisation that could hold responsibility for financial and staffing management. Those involved described feeling the need to establish a group as a ‘legal entity’, to create a formal ‘identity’ that was perceived to be lacking (A10-NRPM-2-P3-W1).
The pursuit of CIO or CIC status was similarly argued by members of partnerships in other BL areas to reflect their need to have more control over the management of their finances, ability to employ workers, and opportunity to apply for external funding, particularly when other stakeholders were perceived to be constraining their actions. In A10 and A9, frustration with the LTO was identified as one influencing factor leading the partnerships to establish themselves as a CIO. However, in A9, this process began only a year after the approval of their first plan, shaped by expectations of other external stakeholders, including the BL rep, who argued that:
Yeah, I would sow that seed … because I think that if they are going to be a legal entity and be sustainable and really become a major actor, you know, on the regeneration scene, I think they have to become … an organisation … Otherwise, there is nothing they can do in their own name.
A9-Rep-P1
Taking on an externally recognised governance form, such as a CIO, can give rise to a range of new governance challenges. In A10, over time considerable tensions emerged among CIO trustees, partnership members and other stakeholders about the relationship between the two governance spaces and concerns that the overlapping membership of the CIO and the BL partnership was concentrating power and creating conflicts of interest. As the rep noted:
Three big players, influential people, are on both [the CIO and the partnership] … I said: ‘... you need to get some boundaries and some definition again because you’ve got so many conflicts of interest’.
A10-Rep 2-P3-W1
Eventually, LT formally intervened, the partnership was restructured and the CIO disbanded. With formal support from external stakeholders, the partnership has reverted to a resident-led decision-making steering group but with new external requirements dictated by the LTO, including the expectation that its procurement policies will be followed to the letter. While partnership members recognised the importance of doing things ‘correctly’, there were also new tensions, as the BL partnership chair explained:
Absolutely we have to follow their requirements in terms of procurement … unfortunately it just caused a bit of frustration with those projects that we thought we were going to go ahead with but we’re just going to have to put on ice for a few months until we’ve got the process in place.
A10-RPM/Chair-P3-W2
Reflecting back on this difficult time, stakeholders such as employed workers highlighted a lack of understanding among partnership members of the ‘legal requirements’ of being a CIO, and the ‘real responsibility’ it requires of trustees. The failure of this process was perceived to have put the whole partnership ‘at risk’ due to the stress it created.
In contrast, some partnerships developed ad hoc forms of alignment with external governance processes, seeking external approval of activities for the purposes of achieving a particular outcome. For example, partnership members involved in planning, designing and overseeing the build of a large new community building in A8 described significant processes of negotiating a wide range of different administrative, financial and legal requirements stipulated by external stakeholders, such as the council. Under the project management of one partnership member, the community building was completed and has been considered a very successful outcome of the BL, but has left the partnership unchanged in its internal structure and decision-making processes.
Memories and legacies of governance
Shared memories of previous ‘poor’ governance in a partnership could lead members to reject particular ways of doing governance and to enhance their legitimacy with explicit or implicit reference to the governance memories. In A15, for example, members shared narratives about the ‘bullying’ ways of a previous chair, who had stepped down from the post. As this member explained, her readiness to take on the role of vice chair, including her ‘good governance’ skills, was assessed against these memories:
Basically, last year I was thinking of taking up vice chair, but … I was told that I did not have the confidence to speak up in meetings. So [outgoing chair] goes, do you really think that you will be able to take on people like the ex-chair and that, vocally in a meeting and I’m like, no. So, she says well leave it for a year and then see how you get on.
A15-RPM-3-P3-W1
Area A4 presents a more extreme example of the power of memories of ‘disruption’ in earlier phases. There was a prominent narrative of the partnership having had ‘long-running problems’ and members who ‘aren’t used to things going well’ (A4-RPM-11-P3-W2). The legacies of this shared governance memory became apparent when the longest-standing partnership members, who complained about a potential conflict of interest in the appointment of a paid worker, were accused of being ‘disruptive’ by more recent ‘incomers’. As the dispute escalated, the shared memory of ‘disruption’ became an act of governance to justify the pushing out of these members. As the rep noted: ‘it was clear that they were intent on being disruptive’ (A4-Rep-P3-W2).
In other areas, memories of governance had more positive and productive influences on governance processes. In A7, for example, despite the lack of a formal plan for the continuation of BL, previous successful ways of working contributed to optimism for the future. This partnership member’s lack of concern about any uncertainty around how the BL will continue illustrates this:
I don’t know, yes, I mean it’s never say never. I mean if we had a project going or something we, yes there may be opportunities but yes I really don’t know at the moment, but hopefully there will be yes, some, it won’t just sort of end, there’ll be, it’ll go on in one way or another.
LS2-RPM-10-P3-W2
External dynamics: relationships in delivering of change
The previous section focused on the internal dynamics of the BL partnership governance spaces. Here we adopt a wider ‘external’ lens that focuses on residents’ experience of being involved in significant attempts to deliver improvements in their neighbourhood and how the barriers and enablers they encountered along the way impacted on the exercise of collective control. As described in Chapter 3, these findings are based on thematic analysis of qualitative and observational data within and across four case study areas.
The beginning: developing power within the partnership
Partnerships needed some measure of ‘power within’ before they could embark on larger change initiatives. The dynamics of BL governance spaces described in the previous section could create significant barriers to partnerships deciding on the actions they would prioritise, and while some partnerships were able to work through these differences, others had to do much more relational work to build a consensus around the plan. Once a plan was endorsed, however, all the BL partnerships in our fieldwork areas set about implementing a range of initiatives that aimed to improve their areas and the lives of local people.
Ready to act
Most partnerships started with small pieces of work, including the early consultation on their plans. Distributing small grants and running events such as festivals and community clean-ups contributed to improving material and social conditions in the area and created ‘sense-making’ spaces,89 where the wider community could find out about BL, share stories about the place and establish new social connections. They also enabled residents on BL partnerships to learn new skills and to gain experience and a sense of achievement, which all contributed to increasing confidence in their collective capabilities.
They did an event and it went well. There were a few hiccups but like I said, there’s going to be, you’re only just learning to work together, it’s a new board, you know, it happens and you’ve just got to take the good with the bad. Just keep smiling and keep persevering with it ... Then we did another event that went a lot more smoother and connections have definitely improved.
A15-RPM-9-P3-W1
Receiving positive feedback from the community also contributed to growing power within the partnerships and fuelled their motivation to continue and try new things.
When we first started working in the park, people would come and say, it’s never gonna work; they’re never going to do anything; you’re never gonna have anything … I hear less of that now.
A15-RPM-5-P3-W1
Reaching a stage in their journey where they were working better together meant that partnerships were able to make collective decisions about more challenging priorities and projects.
It has led to a group of people who are much more confident than 9 months ago. Who have a real sense of ownership that it is a, much more of a resident-led partnership than it was, say a year ago. It just shows residents given the chance through good old-fashioned community work and facilitation, can take the initiative, can get in there even without a lot of relevant skills and experience, can take the lead and do.
A13-Rep-1-P3-W1
However, in the process of getting to this point, residents could experience external support in both positive and negative ways.
Power with or the exercise of power over Big Local partnerships
The support received from external agents locally, such as an employed worker, the BL rep, the LTO and the local authority, or from LT and other national organisations, could contribute significantly to a partnership’s confidence in its ability to act collectively for the common good. In some areas, the BL rep was very hands-on while the LTO took a back seat, or vice versa, or workers in a local statutory or third-sector agency were seconded to support the partnership. This BL rep reflected on the progress since a worker was appointed:
Employing her has pulled a lot of things together with her background experience and her contacts and just her, how she deals with people, XX Big Local has jumped big steps.
A14-RPM-3-P3-W1
However, in some areas, members of resident partnerships’ felt that rather than supporting them to develop and execute their own ideas and plans, individuals in supporting roles were pursuing their own agendas. For example, this resident commented on the controlling behaviour of an individual from their LTO:
We’re supposed to be project managing … We are the board and it’s supposed to be board-led but he used to come round and say, no we’re doing it this way, my way, or no way.
A13-RPM-2-P3-W1
People in support roles often commented on the difficulties they experienced trying to balance being supportive versus directive. Some were aware that if external agents exerted too much influence, residents would not gain the capabilities they needed to take collective control of decisions and actions in the future. As this BL rep noted:
I think that as it currently stands, unless there are some real community development opportunities and practice delivered by the new worker, supported by the board and understood by the board, they will come to the end of this programme and everything will go back to how it was.
A1-Rep-52-P3-W2
Big Local partnerships could and did resist attempts by support staff to exercise power over them, where possible drawing on the institutional power provided by governance structures and reflecting their growing ‘power within’. One partnership, for example, decided not to renew the LTO’s contract. Following negotiations, a different contract was agreed limiting the power of key individuals, as explained by this resident member:
Well, first of all we fired them, but then they’ve come back, but they’ve come back with stipulations.
A13-RPM-2-P3-W1
Addressing the big issues: merging power with others
Our earlier research demonstrated that the first step in developing the capabilities needed to collaborate effectively – power with – was for BL partnerships to recognise that they could achieve more by combining time, energy and resources with others to address shared issues. This often started with an appreciation that a desired outcome was contingent upon the actions of others in the system. This rep explained how a partnership moved from trying to get others to act, to working with others:
It came about initially [because] there was a major … incident. The chair … organised a meeting with the police crime commissioner and senior police people and council people and so on, which was basically along the lines of you’ve got to do something about this …. [the] LTO then was looking for what could the partnership do that would be a kind of positive initiative given the need on the estate and would be in line with BL.
A15-Rep-1-P3-W1
Often the motivation for BL partnerships to work with external organisations was instrumental: a means of achieving a community priority. For example, in one area the partnership wanted to be represented on the steering group of a local community centre. In exchange for funding, they were seeking to collaborate with a local charity in order to have more influence over the outcome, as the LTO worker explained:
… if we had given them the money, we could easily have worked within those parameters to try and effect change. It’s hard to effect change if you’re on the outside. If you were a partner, a proactive partner, you could do it.
A13-LTO-3-P3-W1
Managing conflict in external relations
Developing the capabilities needed to establish and sustain external relationships – power with – required BL partnership members to engage with tensions embedded in the history of relationships within and between local people and local organisations. Sometimes these problematic relationships operated at an individual level:
There’s also bad blood between one of our councillors and our chair and that’s a family history from the area that she resides in.
A13-RPM-17-P3-W1
More often, the difficulties resided in residents’ past experience of the staff of local organisations such as the local council, a housing association or a local charity. As this resident noted:
It’s that constant paternalistic control over everything that goes on in the area.
A1-RPM-1-P3-W1
A significant source of tension in some partnerships, particularly in the early stages of BL, was resident members feeling that something had been forced upon them and/or that residents’ views had been ignored. This resident, for example, in an area where the BL partnership had wanted to have greater involvement with the running of a local community centre, noted that:
Everybody fell out with [local charity]. They got themselves a really bad name from the negotiations and the way they started running the centre.
A13-RPM-3-P3-W1
However, external stakeholders in the same area felt that resident members of the partnership had unrealistic expectations and lacked understanding of processes and procedures.
There were all sorts of things that they thought were OK in that centre; so they would have birthday parties with alcohol and all sorts of stuff going on …. We don’t operate like that … as a big organisation you’ve got to look at things like safeguarding policies and procedures.
A13-Stakeholder-5-P3-W1
Relationships could also be strained when the partnership felt that an external agency, whose support they needed, was acting unreasonably. For example, members could be frustrated by what they perceived as unnecessary red tape:
Their general behaviour just seemed like they didn’t want to know anything about the community development side, it was purely business … we were in there as a powerful group of people asking for a twig in a forest and these guys wouldn’t give it to us.
A14-RPM-5-P3-W2
At times, partnership members and/or the workers they employed felt that they were subject to greater scrutiny compared to other organisations. This is illustrated in this description of a conversation with a staff member of a company employed by the partnership to undertake work on a property owned by a housing association:
He phoned me a week later and he said, I’m not happy. I’m going to kick off. He said the housing association are standing in your way. He said they are putting barriers up that just aren’t meant to be there.
A15; Worker-01-P3-W1
Partnership members, and/or the workers they employed, frequently complained that external agencies only entered relationships with them because they wanted to access the BL funds.
They only seem to want us if they want some cash. Because they think it’s easy money, don’t they, but actually, it’s not what we’re about ….
A15; BLW-01-P3-W1
Resisting pressure from external agencies
For some BL partnerships, developing the ‘power within’ needed to stand up to larger organisations was a key turning point in the pathway to having collective control over decisions and actions that would benefit the community. There were several examples in the fieldwork sites where BL partnerships walked away from negotiations with external agencies because they felt they were not being treated respectfully or said no to requests to fund a particular project. In A15, the BL worker described how employees from the local council informed BL partnership members that they expected them to match-fund a project when the bid had already been submitted without consultation. She said:
So, they’ve already applied for this bid … we want Big Local to match the other year but they’ve not come to us first. They did that in a meeting, that wasn’t even about Big Local …. So, you’ve already applied but you should have come to us before you were applying; it was really unprofessional.
A15-BLW-P3-W1
Reflecting on the same situation, this resident explains how their resistance to this pressure caused tension in relations between the partnership and the council staff.
They got mad at us because we said no that we would not give Big Local funding for it because we had not been consulted along the way and we had not committed ourselves to help pay for it. They got really upset over that but we are working on solving that one.
A15-RPM-5-P3-W1
As the quotes illustrate, external agencies appeared to be surprised by these decisions and while partnership members realised that they may have to return to the negotiations, they also recognised that they would have greater ‘power within’ when they did this:
We had the power to say no; I don’t think they actually expected us to say no.
A13-RPM-3-P3-W1
In one case, after several attempts to work collaboratively to develop a community space, the BL partnership withdrew from the discussions as they felt the conditions being proposed were not in their best interests. However, rather than giving up the project, they set up their own independent social enterprise, eventually opening a community hub grounded in and valued by the local community.
So we found another shop; it’s bigger, cheaper, it already had everything in it.
A13-RPM-19-P3-W2
We have published findings from earlier phases of CiC on the symbolic power of the £1M each BL area had to spend. 3 There are many examples across the 150 BL areas demonstrating that BL residents simply having the money shifted the traditional balance of power away from professionals in favour of BL partnerships. The partnerships recognise their increased ‘power to’ act and the experience contributes to a growing sense of confidence, increasing ‘power within’. Describing a situation where the partnership resisted attempts by a local councillor to ‘infiltrate the group’, one resident member said:
I was almost clapping on my doorstep for my community that they’re able to do this. So, there are a lot of things that are not going to float with people now and it’s almost nice to see.
A14- RPM-5-P3-W2
Renegotiating relationships and power to act
Over time, there appeared to be a growing recognition by BL partnerships and other agencies that they had to collaborate if they were to improve the lives of local people. Local agencies had to work with the partnership if they wanted to access their funds, and the partnership had to work with local agencies to achieve their objectives for the area. This led to adaptive attitudes and behaviours on all sides, as this quote illustrates:
So, we are now trying to rebuild that, which I feel, touch wood, is going quite well, because at the last meeting the three people that threw accusations were actually very nice and they didn’t throw any accusations and they actually deal with us in a nice manner. So, fingers crossed.
A15-RPM-4-P3-W1
Not all of the resident members of BL partnership involved in this research felt that their work had made a significant contribution to improving the area, but for some, like this resident, the impacts were direct and positive:
My personal view is that it has been exceedingly beneficial. The number of issues we’ve had with … has certainly reduced …. The police have said that the … has reduced. So they are seeing some change and I can only assume that it’s because of, or as a result of, the [project].
A15-RPM-3-P3-W1
Whatever the ultimate outcomes, residents involved in the journey towards achieving change were developing new knowledge, skills and social connections. In some cases, a partnership’s experience of success increased their collective ambitions to have a greater impact on the area and local people in the future:
The idea that we’ve got is that we become a CIC; we take over the asset of the land. … We would then rent it out to [project]. So that would give us a small income … then we would be using that money to fund [other things] …. That would generate its own income to be able to buy further equipment and pay whatever nominal charges we have to.
A15-RPM-3-P3-W1
Responding to COVID-19
Big Local partnerships’ responses to the challenges presented by COVID-19 varied. Some areas were extremely active in providing local humanitarian support and adapting existing activities in light of the restrictions, while other partnerships, as one rep describes, were ‘almost dormant’ (A1-Rep-P3-W2). In this final section we present preliminary findings on these diverse responses to the impact of the COVID-19 pandemic and how they illuminate the complex interaction between local context and the degree of collective control achieved 10 years into the programme.
Moving online
The main factor constraining partnership work was the implications of the national lockdown for face-to-face meetings. Some partnerships did not connect online at all as they were not comfortable engaging with online meeting platforms. This was particularly evident during the early stages of the pandemic.
We’ve not had a lot of contact with each other through COVID. So, a lot of people … are from the era where Zoom calling is not for them.
A8-RPM-14-P3-W2
Some paid workers responsible for supporting the partnership were furloughed by their employing organisation; for example, staff paid for by the BL partnership but employed through the LTO, which further exacerbated difficulties. Those partnerships that did meet online still experienced disruption as both partnership members and employed staff adjusted to new ways of working:
Working from home … slowed everything down massively because it wasn’t the norm.
A5-RPM-15-P3-W2
Having the Zoom meeting while trying to put them [children] to bed is enough to drive anyone crazy.
A7-RPM-4-P3-W2
However, after an initial period of adjustment, some BL partnerships reported positive changes to group dynamics when using online meeting platforms. For example, one BL paid worker suggested in positive terms that online meetings had allowed the partnership to ‘have that connection, the face to face without being face to face’ (A12-BLW-18-P3-W2), while a BL rep argued that pre-existing relationship problems ‘were actually easier to deal with over Zoom’ (A5-Rep-P3-W2).
An unexpected outcome where partnerships had embraced social media as a communication tool was an increased awareness of BL work in the wider community. This may have been because people were generally spending more time online during lockdown and because partnerships were engaging in these different forms of communication – for example, Facebook (Meta Platforms, Inc., Menlo Park, CA, USA) and Slack (Slack Technologies, LLC, San Francisco, CA, USA) for outreach and WhatsApp (Meta Platforms, Inc.) groups for informal communication between partnership members.
We are seeing a real boost online this year. It might be the amount of page likes; the amount of people coming; it’s like people posting on our page and things like that. People are definitely aware of who we are and what My [BL name] is about.
A5-RPM-15-P3-W2
Restricting activity
A particular disappointment for many partnership members and local people was the cancellation of planned events, such as festivals and excursions. Prior to COVID-19, such events could be central elements of partnership work, providing fun activities and connecting local people, as well as giving BL partnerships visibility in the community.
I have people asking when are the trips and I said forget it. We’re not looking at anything properly now till next year.
A13-RPM-2-P3-W2
Other planned projects were impacted by disruptions in partner organisations. One LTO worker describes the implications for building work that was due to commence at the beginning of the first lockdown:
Everything went on standstill. It took builders a long time to provide all the documents that the housing association needed …. They then furloughed all their staff so we didn’t have many people that we could deal with at the builders.
A15-LTO-P3-W2
There were also areas of work that were seen to be not amenable to online working. Outreach youth work was highlighted in this context, because of a mismatch between the type of online platforms BL partnerships and youth workers had access to and those that young people were most likely to use. This BL worker describes the difficulties faced by a colleague in an outreach role:
The raison d’être of his job was about face-to-face contact with young people and he can’t do that as much. He’s doing a bit of it but it has to be socially distanced and properly managed. So, he’s doing a lot of online stuff and the ones that are classified as hard to reach are even more difficult to reach because they’ll do Instagram or TikTok but they won’t do Zoom or come into a Teams meeting run by Microsoft if we paid them.
A11-BLW-P3-W2
Adapting activity and shifting perspectives
While mainstream BL work was extremely limited by the COVID-19 restrictions, some BL partnerships ‘really jumped into action’ (A8-RPM-P3-W2). Galvanised by the crisis, they started to contribute to humanitarian support for people who were shielding or otherwise struggling with basic needs.
They set up from the Hub and started making food isolation packs for the elderly and vulnerable residents and then delivered them out in the village and they were receiving referrals also from the borough council as well and taking out emergency supplies to people that were continuing to contact them directly.
A8-LTO- P3-W2
Some partnerships approached organisations they were funding in order to maximise the local response. As this BL worker explained:
I got in touch with all of the grant-funded recipients to say, ‘Do you need to repurpose?’ or, ‘What are your struggles?’ That’s allowed groups to be able to react to COVID with existing funding that they’d already allocated.
A12-BLW-18-P3-W2
Some saw opportunities for creativity in online formats where people ‘battered out different ideas’ (A5-RPM-15-P3-W2). Here, a resident partnership member describes how they adapted a planned activity to work virtually:
Let’s think of a way of doing it during COVID. So now it’s all online and it’s like a downloadable PDF pack, there’s a video tutorial and then people have got to send in their submissions to us.
A5- RPM-15-P3-W2
There was some criticism that these reactions were putting in place lots of short-term projects that might reduce the funding available for longer-term initiatives, as this BL rep noted:
They’ve invested heavily in their food bank, but not in a very sustainable way … it will mean diverting a lot of resources from their other activities to one or two key activities …. It could be that it shortens the life of Big Local, because money will be going through faster.
A7-Rep-P3-W2
However, there was evidence that these COVID-19 responses were generating increased knowledge among BL partnership members about local needs and problems of inequality in the community. As one BL rep put it, ‘COVID has sharpened their awareness of what they already knew’ (A5-Rep-P3-W2). And, as this resident partnership member illustrates, some understood that these issues required a long-term approach:
We found out through COVID that people do need these things now through COVID, and after COVID when we’ve finished here … they will still have some support.
A13-RPM-2-P3-W2
Readiness to respond and ability to adapt
The readiness of BL partnerships to respond to COVID-19 and their ability to adapt were influenced by many factors, but the extent to which they had developed collective capabilities prior to the pandemic appeared to be important, as this BL rep highlighted:
Everything stopped but then we used this as a base for what we did. Our background from Big Local helped us form this coronavirus response straight away.
A8-LTO-P3-W2
Observations showed that prior to and during the early stages of the pandemic, this partnership remained fairly stable as a group and was well supported by the LTO, with the same chair leading, although many of the actions fell to a few active members. The partnership had invested around half of their budget into the building of a new community centre, which it was suggested had contributed to greater social connectivity and a sense of pride in place, and enabled them to mobilise and provide a direct response.
In another area, the BL rep described how BL partnership members had been through a tense period prior, but were strong enough to draw a line under the dispute, move on and adapt their work to the COVID-19 response:
They seemed to have managed to work through it. And if you attend any of the meetings, you’ll find that they’re still fairly merry … They were very focused, particularly as this coincided with the start of COVID …. It made it all very immediate, I mean important that we were able to carry on, and so people pulled together, I think, on that basis.
A7-Rep-2-P3-W2
Longitudinal observational data suggest that this partnership was generally well functioning, with committed members and a good relationship with their support workers, who were also considered to be good at their job. Prior to the pandemic, the partnership had been particularly successful with the activities they delivered directly, with support from the paid worker. Success in these endeavours likely contributed to confidence in their ability to respond to COVID-19, with the worker encouraging a radical switch in focus so that the partnership helped deliver a large food bank initiative and additional support to community members.
In some partnerships, success in supporting their local community triggered a positive feedback loop whereby the members grew in confidence through the work they were doing. For example, this BL rep reported that the partnership chair had said:
‘this is the making of us; this is what we’re here for’ … he really ties what happened over COVID with what Big Local is in essence.
A8-Rep-P3-W2
The rep went on to describe how they were also attracting new partnership members and volunteers, while this resident partnership member described how their work in the community was contributing to wider reach within the community.
Through doing the meals, the isolation packs for pensioners, we picked up some more because they didn’t know about it and they get talking.
A8-RPM-2-P3-W2
Some partnerships that had achieved success in their response to the crisis were also benefiting from improved relationships with partner organisations, as this BL rep noted:
I think their impact has perhaps been bigger, and you know, in a shorter period, and more widely recognised, and valued as a result, and so I think they’ve brokered some more relationships, and some more respect, you know, with councillors, etc.
A7-Rep-P3-W2
Limited readiness
Not all partnerships were in the same position at the start of the pandemic. Some appeared to have not yet developed sufficient ‘power within’ to respond to the COVID-19 crisis. As one LTO representative reflected:
They could have made a decision to really take the bull by the horns as it were, yeah, do things similar to other partnership area, but they didn’t have enough depth in the partnership in my opinion …. I think they made the right decision really because it’s intense, it’s resource intense if you’re leading on something. You know, if they decided to do some kind of food-related project or if they wanted to support digital on a big scale, they would have found that very challenging.
A4-LTO-12-P3-W2
The LTO rep went on to suggest that the problem was related to the internal dynamics in the partnership: ‘[It] doesn’t feel connected does it? It doesn’t feel like the relationships are there’ (A4-LTO-12-P3-W2). Our longitudinal data reveal that this BL partnership had experienced considerable challenges since the beginning of the programme. They struggled to agree direction and how best to spend the money. There was high turnover in partnership members, and distinct factions among those that remained. In response to COVID-19 restrictions, the partnership struggled to meet online and provided little direct support in the neighbourhood but, as the LTO rep noted:
They put up a good part of £10,000 in emergency funding, which is fair play to them …. So they didn’t completely inject themselves; they put more money into the system and offered more help indirectly via us.
A4-LTO-12-P3-W2
Existing governance arrangements could also limit BL partnerships’ response. In one area, a BL worker revealed that the partnership’s terms of reference required decisions to be made face-to-face. Proposals were put forward to amend the terms of reference to facilitate online decision-making, but the decision could not be ratified at a face-to-face meeting. Thus, the board were caught in a closed loop, unable to progress:
Our structures aren’t flexible enough; one of the proposals from the residents was that they should be allowed to submit their views by proxy or write it down …. they were told they couldn’t have the proposal ratified or approved because we couldn’t have a meeting.
A11-BLW-1-P3-W2
The worker had previously described a ‘resistance to change’ among particular partnership members, suggesting that the previous reliance on governance arrangements to manage challenging internal dynamics was ‘extraordinarily frustrating. At the time when we were needed most, we were appearing to do the least’ (A11-BLW-1-P3-W2).
A further factor limiting the ability of partnerships to contribute to the local humanitarian response was not having their own premises from which to operate; in part, this was a reflection of the progress that had been made in delivering BL plans. For example, this LTO rep explained that the partnership:
didn’t have a space, we couldn’t activate like a community hub in response to the COVID-19 like some of the other Big Locals have been doing …. If it had been another 12 months down the line they might have been able to do that. We would be a bit more established with the activities in the Hub.
A15-LTO-P3-W2
The COVID-19 pandemic was also adversely affecting the personal lives of BL partnership members. Reflecting on the recent loss of several partnership members, this BL rep said he ‘would connect all of them leaving to some degree to COVID’ (A5-Rep-P3-W2). Inevitably, this was causing instability and undermining the BL partnership’s power to act.
Conclusion
In this chapter we have described how we are developing our earlier work on a qualitative approach to measuring the capabilities for collective control over decisions and actions emerging in communities involved in place-based empowerment initiatives. In particular, we have presented preliminary work identifying markers of the progress communities make in developing these capabilities over time.
We have also described some of the pathways through which these capabilities can be developed and the barriers and enablers communities experience along the way. These findings reveal how the dynamics in a BL partnership could influence the development and exercise of residents’ collective control over decisions and actions to improve BL areas. Responses to inevitable tensions in BL partnerships over who had a legitimate ‘right’ to contribute to decision-making and how decisions should be made can either increase or decrease the diversity of BL partnership members, in turn enabling or limiting the development of capabilities for collective control in the wider BL community. Some BL partnerships used governance tools (e.g. constitutions and codes of conduct) as technologies for reflection and dialogue at points of potential crisis, enabling them to further develop ‘power within’ and to identify and address enduring problems. Alternatively, these tools could be used by some BL residents to exercise power over others. Our findings also highlight the potential for programmes like BL to be in tension with established legal governance principles. Seeking formal incorporation as a CIC, for example, was one response, but failure to meet external requirements proved highly disruptive. In some cases, external intervention led to a reconfiguration of the partnership, which could limit the scope for collective control by residents.
As BL partnership members moved beyond the partnership governance space, seeking to implement their plans by developing power with others and exercising their power to act, they had to overcome other challenges. The scale and complexity of the relational work required to deliver their plans are evident from our findings, as too are the pivotal but sometimes problematic role of support workers and the wider social infrastructure in the community, voluntary and faith (CVF) and public sectors. The final section of this chapter described the diversity in responses by BL partnerships to the impact of COVID-19 on local people. Some partnerships were extremely active, while others were able to do little collectively, reflecting the complex interaction between local context and the degree of collective control BL partnerships had achieved 10 years into the programme.
Chapter 8 Pathways to health and social impacts: findings from Big Local residents’ narratives
Introduction
Earlier chapters have explored the quantitative evidence on positive social and health impacts for BL residents and for populations in the 150 BL areas. We will consider these again in the next and final chapters. In this chapter, we explore the pathways to social and health outcomes at both the population and individual levels that are embedded in residents’ narratives about their experience of BL. The first part of the chapter focuses on residents’ accounts of pathways to positive outcomes, particularly those operating indirectly through the actions that BL delivered locally. These findings are based on analysis of qualitative data collected in 2018/20 from 58 active residents involved in the BL partnerships in our fieldwork areas. The second part of the chapter shifts attention to consider an often neglected issue in the evaluation of community empowerment initiatives: narratives of negative impacts on individual health and well-being from the residents who are most actively involved. These findings are based on thematic analysis of a subsample of the 57 longitudinal qualitative interviews from phases 1 (2014/15) and 3 (2018/21) of the CiC study.
Residents’ perspectives on pathways to positive social and health impacts
Residents with experience as members of BL partnerships were asked about the various initiatives that they had sought to deliver over the years to improve their area, what impacts they judged them to have had (if any), and how they thought that impact came about. Residents described positive impacts through various pathways described below, operating at both the individual and population levels, highlighting dampening and amplifying processes along these pathways.
Social environment pathways
The most prominent pathways to improved health and well-being embedded in residents’ narratives were related to the improvements in the social environment. There were two linked themes: one describing individual benefits, the other collective benefits.
The first pathway led from activities that sought to reduce social isolation and encourage social interaction, leading to improvements in mental health at the personal level. As this resident partnership member explained, some of their activities brought people together and got them talking and making friends. This participation then, in turn, led on to better mental health:
It’s a social thing … so you can come along and you do an activity but you’re also talking to people, relating to people, getting to know people. So, to me it’s the same sort of thing. So, like the choir, it is a social thing as well as an activity … I think people are engaged. I think they feel better.
A10-RPM-8-P3-W1
There were many descriptions of BL activities that started off with a specific practical purpose but evolved into more general social interaction and support. A self-management course set up by and for people with chronic illness, for instance, led participants on to further activities and friendships. Potentially, as one resident suggested, this could feed back into improvements in people’s living conditions by giving them confidence to do new things in their lives:
Yeah, so we funded a course for people to manage chronic illness and the feedback we got was that this was a massive thing for the people who went, that it had changed how they saw themselves; it changed how they felt; that they were better able to cope with the chronic illness …. Actually, it had been life changing for people …. When you … increase people’s capacity … to cope you give them an opportunity to do other stuff … because they have the resilience that they need to be able to undertake new stuff and for me that’s really powerful.
A4-RPM-9-P3-W1
The ripple effect of people getting to know each other was a recurring theme, as was the recognition that although the BL activities might not be able to change the wider conditions of life for residents, they had value at the personal level. The sentiments expressed by this resident echo those of others:
For me, the stuff that Big Local does that has a lot of value is actually more of the quieter stuff. For instance, I’m involved in the open-door mental health group that they run there, but Big Local kept going after the funding was pulled by providing Mind with a space to run that group. By connecting with Big Local, I’ve been able to do some volunteering sessions with them … information sessions, using my knowledge as a clinical psychologist for the people in the group, which I think people have found really useful and which wouldn’t have happened if Big Local hadn’t been able to coordinate that. It’s those things, I think, which actually make a difference at ground level, despite what’s happening at a larger, strategic level.
A2-RPM-30-P3-W1
The second pathway described by residents highlighted improvements operating at the collective level. These activities included bringing people together to fix problems that they identified as important and, in so doing, building trust and helping people get to know each other in their day-to-day lives, which in turn made them feel safer in the neighbourhood and improved community perceptions of well-being:
Big Local bringing people together to fix their own problems … people feel safer, there’s less crime, all that kind of stuff, that contributes to your well-being.
A7-RPM-9-P3-W1
Many of the residents mentioned the importance of creating friendly social environments, including establishing community hubs/centres, and creating spaces for people to gather and enjoy each other’s company, to create common interest, paying attention to the cultural environment:
I think it was a trigger to get people together. A lot of groups seem to have the same problem whereas (another BL area) for instance they’ve spent all their [BL money] … They bought a run-down old community centre and they done it up so they have a big space to do stuff.
A10-RPM-8-P3-W1
There were compelling examples of activities aiming to increase social participation/mutual support benefiting a group as well as individuals. For example, this resident partnership member gave the example of a successful group of single mothers supporting each other, facilitated by BL providing space and a creche for their children:
So, there are projects which have benefited people individually and the community, but with minute amounts of [financial] support, almost no support probably … [the success] is off the back of the hard work that the single mothers are putting in, not the hard work that the Local Trusted Organisation is putting in or Big Local.
A2-RPM-22-P3-W1
Health promotion pathways: less a purpose, more a vehicle to bring community together
There was a category of initiatives in BL areas that, superficially, could be characterised as health promotion: promoting healthier lifestyles, predominantly encouraging people to become more physically active, as a pathway to better health outcomes. On the whole, however, they did not originate with the aim of improving health as such, nor was success judged by BL partnership members in terms of changes in individual lifestyle, but rather in terms of the impact that the initiatives had on wider social relationships in the community.
Many of these activities grew out of a desire to do something for young people in the area, to make them a priority for action. The ideas generated often involved some form of physical activity, such as football clubs, skateboard parks and multisports areas. The motivation was not so much that the youngsters were unfit, but rather that there was little for them in the area and they were neglected and as a consequence just ‘hanging about’ or getting into trouble:
It’s getting the youngsters from doing illegal motorbikes around the estate, it’s getting them off the road and into a trained environment where they’re learning consequences, they’re learning how to maintain the bikes, how to ride safely and … it’s rough riding, which gives them a lot more pleasure …. They know that if they get into problems or into trouble, they’re going to lose that privilege of being able to ride. So, it’s all about consequences and this kind of thing. So that is the project for [this area’s] Big Local. It is the big one.
A15-RPM-3-P3-W1
Football clubs of one form or another had been set up in several fieldwork areas, in response to the priorities expressed by the local community. Perceptions of impacts of these initiatives were invariably positive, spreading beyond the immediate participants to the effects on families and the wider community. Residents described wider impacts of the football initiatives in terms of camaraderie, involvement, friendliness, participation, and ‘getting everyone together’. Such engagement was seen as a valuable achievement in itself, adding to community well-being:
Well, the football club … it’s probably our biggest success story so far. We’ve got hundreds and hundreds involved, we’ve got teams from like toddler group just having training sessions and then teams for under-sevens all the way up to adult men and I think they did start a women’s team as well …. They’ve got a lot of the teams winning different tournaments, getting top of their like, kind of, leagues, moving up the table and stuff. So, the amount of people we’ve engaged through that project has been phenomenal, really big …. Yeah, yeah. Yeah, they’ve all got their qualifications for coaching, I mean they’re all still volunteers but they’ve all got that and a lot of them have done the referee course and a lot of them are parents to children that are in the teams as well, so it’s just them investing in their children and having time together and yeah, I think it’s been a really all-round good.
A7-RPM-4-P3-W1
Economic environment pathways
Residents’ accounts highlighted several potential economic pathways to health impacts. Some were centred around enhancing food security, suggesting that tackling food poverty would lead to improved access to food and a more nutritious diet, especially for children from low-income households, which in turn would lead to improved health and development.
A very diverse array of food security initiatives was described, supported by BL and provided by residents. They included breakfast clubs and schemes to provide free midday meals for children in the school holidays, community breakfasts, lunch clubs for older people, help with distribution of donated food from supermarkets, food clubs for people sanctioned under Universal Credit, and community gardens. One user of a food club, for example, who had joined the BL partnership, explained the multiple benefits it had had:
I suppose actually if I hadn’t gone to [X] I wouldn’t have known about the sustainability food project that runs at Food Club … and I now go to that, which has benefited our nutrition and our finances because we have a fixed income. I’ve not got my pension yet. All I have is PIP so we have quite a limited income and by going to the food club we’re eating better than we would perhaps otherwise and I wouldn’t have known about that if it weren’t for X.
A4-RPM-9-P3-W1
Organisers of food projects for schoolchildren in the six-week summer holidays described the benefits for the children and the positive impact of them as they witnessed first-hand the difference this initiative was making to the local children:
We recognised that we got a lot of kids in the area who are [receiving] free school meals and during the summer holidays they weren’t going to get any. So we set up with a local school chef and six weeks feeding these kids, so we had to give them breakfast and had the YMCA come in and get them doing various activities … then they come back and have lunch … it was such an uplifting thing.
A10-RPM-8-P3-W1
Some BL initiatives took a direct approach to reducing poverty, supporting people to claim the welfare benefits to which they were entitled and thereby raising their standard of living. Examples of such initiatives provided by resident members of partnerships included the setting up of welfare advice sessions, some in collaboration with the local Citizens Advice; practical advice with filling in forms for Universal Credit offered at a community hub set up by BL; and the formation of credit unions for mutual financial support:
There was another [welfare benefit] one as well, this Universal Credit that people have been struggling with and we talked to people about it and we said, you know, need any help come in. It takes me and [name of another resident] about 2–3 hours to go through it all and it’s hard work for us, but that’s another thing we’ve got on. Any information they want, they can come in here and we’ll put them to right.
A13-RPM-4-P3-W1
Resident members of BL partnerships also described how they made attempts to respond to the clearly expressed need to do something about the low employment rates in many areas: ‘they need jobs, they need training’ (A3-RPM-5-P3-W1). Boosting employment was seen by some as a way of not only increasing individual incomes and security and hence improving mental health, but also benefiting the local economy and collective perceptions of the area, which would increase overall well-being.
Residents described initiating many work-related schemes, including job clubs, skills updating, support for people to gain heavy goods vehicle (HGV) driving licences and imaginative small grant schemes for start-up businesses, such as hairdressers. However, although these schemes benefited individuals, they struggled to have a wider impact. Indeed, as these quotes illustrate, some of these schemes got into difficulty getting off the ground as economic conditions worsened or national welfare reforms created additional barriers to helping local people and support from public services reduced:
The HGV one’s been really successful. Not obviously on as big a scale as some things that we’ve done, because I think we’ve had about five people pass, but for those people, their families and their lives, that’s made a big difference because they either were not working or were in, like, lower paid employment and now they have a skill that they can use and earn decent money from and it’s been really popular, really popular. We do provide quite a lot of free training courses in all different things and we’ve always had some kind of job club going on in the last couple of years but we’re running it ourselves now, so …
A7-RPM-4-P3-W1
What we try to do is we give grants to start new businesses, we’ve started three this year and that’s not a lot but it’s three more than there were last year. I think that helps.
A15-RPM-5-P3-W1
Physical environment pathways
Though there were many references to BL initiatives that aimed to improve the physical environment, the impacts identified were often envisaged as essentially involving a social environment pathway to enhanced health and well-being. So, for example, residents on BL partnerships explained the rationale for improving street lighting in terms of people being able to walk the streets and take exercise safely; community walks and pocket parks were seen as helping people to socialise as well as engage in physical activity; community transport schemes were perceived as encouraging social inclusion and befriending; and the provision of music and arts facilities was described as ‘feeding the soul’.
Talking about a community transport scheme, for example, this resident explained how the driver of the bus bought by the BL scheme saw one of her important roles as to be a befriending service for her older, socially isolated passengers. The BL partnership took this idea further and saw other opportunities to make the most of their vehicle, and now offer a diabetes transport service for people who have difficulty accessing services locally:
[X] is our driver and she does befriending stuff, so the bus itself was always a plinth; it was always a way of getting somewhere that we could go and branch out and offer loads of more things … the NHS doesn’t provide the diabetes transport service as far as I’m aware locally. So we have invented a transport service for befriending and elderly, so over-60s and over-70s and stuff like that, but we … have got a diabetes group that have difficulty getting around and stuff and they’ve got difficulty accessing buses so we brought the bus to them.
A14-RPM-5-P3-W1
A distinctly different rationale for some BL initiatives on the physical environment aimed to improve the aesthetics of the local area. One line of reasoning was that pleasing surroundings and opportunities to interact with nature improve the way people think about themselves, their neighbours and the area as ‘a better place to live’. Many residents commented favourably on the impact of even small-scale schemes to brighten up streets with flower planters:
Yeah, they’ve got more pride in the area then, yeah. Also, I remember when we were planting one of the planters down the road, this man and he said he couldn’t get out, he couldn’t walk very far but he could walk up to the planters and see them and he said he quite enjoyed it, which was nice, you know, someone coming up and appreciating what you were doing.
A10-RPM-19-P1-W1
Other partnerships, however, had found it difficult to implement schemes such as window boxes on balconies, where outside contractors had been commissioned to carry out the installation and there was little or no sign of what they had done. Tree-planting schemes also did not always pan out as hoped, running into difficulties with vandalism and ASB. Some BL partnerships were working with local councils to find a way round these setbacks:
We’ve had 420 trees delivered to plant … there was originally a tree line up the hill, and there’s been big gaps occurred. So we were going to fill in the gaps with some of these trees. But because of the antisocial behaviour I was concerned that those trees aren’t going to last very long, because three apple trees we planted as start of an orchard, didn’t last very long. They were broken off, so I was concerned that these trees would have the same sort of treatment. We had a meeting with the council last Friday … and they said the same thing that we do. So they’ve had suggestions that we plant throughout the area down along the school precincts and other areas like that. So that’s what we’re looking at now.
A10-RPM-8-P3-W1
Reducing place-based stigma pathways
Residents’ accounts highlighted a final, more intangible, place-based pathway to health impacts, relatively neglected in public health policy and practice. This pathway operated through an area’s reputation and the stigma that might have become associated with it over the years. As a PBI, BL has the potential to alleviate stigma through action to improve social, physical and economic conditions in areas, as well as by promoting more positive portrayals of areas and residents living in these areas. Conversely, as a targeted initiative, the programme could conceivably risk stigmatising areas in receipt of funding as well.
Our findings suggest that while there may have been an initial risk when the programme was launched that it would create or exacerbate place stigma, there is less evidence of this affecting BL residents and areas negatively over time. For example, our earlier research in phase 2 of CiC on coverage of BL in the media found that more negative coverage mainly featured around the time when the initiative was launched. 88 While coverage typically presented BL as a positive development, this coverage sometimes dwelled on why areas were targeted for funding, citing areas as ‘needy’ or ‘deprived’. Largely, however, more negative associations of targeting were balanced through a focus in the programme that promoted a more positive emphasis (e.g. making areas even better places to live) and that emphasised the assets of the area and the residents living there.
Over time, our findings also suggest that resident-led partnerships have aspired to regenerate a vibrant identity for their area, and in some localities have actively promoted good news stories in local media, challenging negative external perceptions of neighbourhoods. 88 Some BL initiatives aimed to improve the aesthetics of the neighbourhood partly to reduce stigma. As this resident partnership member described, while they cannot say for sure that this strategy will definitely improve the area’s reputation, they are optimistic about the reaction so far:
Yeah, definitely, and even the things [like] the Christmas event … make us become quite renowned and I don’t know whether it will kind of make people think more fondly of [A14] but it’s definitely going to give people good things to say about the area, like they’ve put on a good event and they have good services. … So, might kind of encourage people to find when they’re looking for their place to live, whether that be private rented, social rent or purchasing, you know, these things that we’re working on that would hit the scales in [A14]’s favour and people will be investing in the area.
A14-RPM-4-P3-W1
The resident-led ethos of BL has also led to greater visibility of residents participating in civic activity, helping to challenge portrayals of communities as being disengaged or lacking pride in where they live. By improving a sense of pride in the area, this may have also contributed to improving residents’ internal perceptions and attachment to their neighbourhood. Some BL resident partnership members talked enthusiastically about their desire to create more of a buzz about the place by holding events that people want to get involved with and talk about. As this resident explained, these events were intended to make residents feel better about the area as a place to live, but potentially also to shift the outside narrative towards a more positive idea of the place:
Yes, and a sense of hopefulness about the area … I think there’s a wider reputation of [A2] being quite a depleted place. For instance, where I used to work, I’d talk about going into [A2] to meet people and people in the office would say, ‘Oh, but you’re never getting out of there. Everyone moves so slowly. There’s no sense of urgency there at all,’ like, ‘You’ve got e-mail in [A2]?’ So it’s really got a reputation as being somewhere with almost no excitement and oomph to it … Sometimes, I do get the sense that people don’t have an awful lot of hope about what could be achieved. So I do think there’s something about Big Local bringing that in general and that that does, maybe, have a significant impact on those feelings of well-being because there’s plenty of life.
A2-RPM-30-P3-W1
The potential negative impacts of community-led place-based intervention
As the previous section illustrates, many of the residents and other stakeholders interviewed since the CiC study began in 2014 have highlighted positive impacts of BL activities on their neighbourhood, on the well-being of the local population, and on their own well-being. However, there were also accounts of negative impacts on health and well-being from residents actively involved in the BL partnerships – impacts that were on occasion also observed by researchers. In this section we consider some of the recurring themes in these accounts, based on thematic analysis of a subset of the 57 longitudinal qualitative interviews from 2015–17 and 2018–21. Brief vignettes of accounts of impacts over time on their health and well-being from four resident members of BL partnerships are also provided in Appendix 5 to illustrate the complexity of these experiences.
Partnership dynamics
The complex dynamics in BL partnerships were described earlier. These clearly changed over time, but the conflicts and tensions that emerged could cause visible distress during meetings. These tensions could be episodic or ongoing. As one resident partnership member noted: ‘As far as the relationships within the partnership are concerned, I think some of them are quite strained …’ (A10-RPM-7- P1-W2). However, as the quotes below illustrate, while ongoing conflict could have significant negative effects, BL partnerships could develop the competencies required to work through very difficult interpersonal dynamics:
The negative was when the board was divided …. Just grinding me down, yeah. It was just like the same thing over and over; the same argument, and it was, like, draining.
A13-RPM-2-P3-W1
Some people want to be dictating to us … and if you say anything, you’re wrong. And I feel that you can’t say what you want to say, because you know, they don’t like it and then it’s all hell to lose. But, yeah, sometimes I go to the meetings and I sit there and think to myself, what am I doing here? I’m wasting my time here.
A6-RPM-4-P3-W1
It’s a lot less fractious, isn’t it. It’s not stomach churning on a Monday when you’ve got to get ready to go to the meeting …
A4-RPM-5-P3-W1
The burden of responsibilities
As time passed and BL areas progressed, tasks and responsibilities changed, and the sense of obligation could become more burdensome for some residents:
We have become more structured in … what we are trying to achieve. But that has brought with it more work … this is an anxiety for me, we haven’t really got the Environment and Play theme off the ground properly yet, and that is partly because I have been extremely busy … I feel a bit of an obligation to lead … I have got some expertise in leading things … other people haven’t and so I kind of feel a bit of an obligation to the group.
A3-RPM-14-P3-W1
As residents became more invested in BL and embedded in the initiative, they could feel somewhat trapped in their roles in what was often a small core group. These residents reflected on their experience:
It created a lot of stress but to a large extent you could say I could just walk away, and that stress would go, except I could never just walk away.
A3-RPM-2-P3-W1
I felt invested in them as a group. I felt like I was maybe letting them down because they didn’t have people to do things and so to lose a person … I felt, I just felt bad about it.
A6-FRPM-25-P3-W1
The burden of responsibility as a resident member of the BL partnership could be exacerbated when on occasion it was necessary for them to take on things that they had no experience of, or training in. They often felt an obligation to do this, but it could require more commitment than they anticipated. The longer they had been involved in the partnership, it seemed, the greater their sense of obligation:
That month that he [paid worker] was off was very, very hard – very, very hard … because it was myself and [BL worker] morning and evening really propping her up … because she was still learning … I didn’t expect to do being a volunteer, is managing all this HR … it was too much … for me … to put that level of commitment in and that level of worry and thoughts and pretty much pulling things along.
A6-RPM-3-P3-W1
In some BL areas, the employment of staff meant more rather than fewer responsibilities for resident partnership members, sometimes without systems and human resources at hand to provide guidance and support. There were examples of problems or particular needs arising with paid staff that residents were not equipped to manage, a situation described vividly here:
I went through a period about 18 months ago where I was kind of completely frazzled by the whole thing … as the partnerships mature, they take on more responsibility and one of the areas where we took on that responsibility was employing people … So we were dealing with those two people with very complicated health issues, yet as a partnership board we had no legal constitution; we had no [human resources] procedures to speak of; we delegated all of that to [name] and that caused a lot of kind of strain.
A5-RPM-2-P3-W1
This resident went on to describe the impact on him of an ‘exit conversation’ with one employee with cancer who had been undergoing treatment and was under enormous pressure:
His reflection was that we were completely incapable and unequipped to deal with that well for him …. I went through quite a long time of kind of beating myself up about that, really, and thinking … have we made the situation worse?
A5-RPM-2-P3-W1
The burdens of volunteering
The challenges of being a volunteer member of the BL partnership were commonly described as burdensome and stressful, often in the context of ‘too few people’ being actively involved: ‘I do wonder … I’ve been saying “how do we get more people involved to take the stress off?”’ (A14-Stakeholder-P2-W1). For some resident partnership members in paid employment, the stress of making time to volunteer and feeling obliged to continue in key roles was exacerbated when they were criticised by others on the partnership. As one vice chair resident noted:
Where you’ve only got a couple of key people doing a lot of work, you expect people’s sympathy or empathy … and people are having to fit it around full-time work, but you don’t get that, it’s like, oh why hasn’t this been done … there needs to be like more understanding.
A14-RPM-4-P2-W1
There were other examples of residents feeling frustrated by being underappreciated. One resident (heading a communications subgroup) who had been enthusiastic during the interview in phase 1 of the CiC study in 2014 had left the partnership a year later. In her interview after she left, she used the metaphor of a minefield to explain how difficult it was when her expertise and knowledge were ignored and others with no experience dominated discussions and decisions:
I thought they wanted someone with my skills and expertise … [and say] ‘We’ve got an expert here, let’s work with this expert to achieve an objective’ … on paper I’m responsible but in reality, I’ve got people walking all over this minefield and it’s blowing up in my face … I couldn’t stand the frustration … It was like … I can devote my time to this, or I can pull out before it gets too traumatic … So that was it.
A10-RPM-7-P1
The stress and anxiety of voluntary membership of BL partnerships and the relentless nature of the responsibilities could also spill over into everyday life:
I get frustrated sometimes because we’re retired and I have never worked so hard in all my life. It consumes us many times seven days a week and there’s no turn off, it doesn’t stop … it never stops. We get home and it’s hitting us in our e-mails, on Facebook, on everywhere, it’s just constant. So it is tiring at times.
A15-RPM5-P3-W1
My quality of life [sighs] … I do get very stressed out with it sometimes. The frustration that it’s not being, the money’s not being spent properly frustrates me terrible.
A6-RPM4-P3-W1
Some residents also described how the voluntary work for the BL partnership encroached on their employment. While this was fine in the short term, when combined with the tensions and conflicts of partnership dynamics it could become too burdensome and lead to residents resigning. For this resident, trying to deal with conflict on the partnership and the obligations of daily life proved too much:
I’ve stepped back … there were bitter conflicts … my sister, although we work very closely together, I felt like I was arguing with her and I thought I’m not falling out with my sister over it. I was working full time, overseeing that, applying for grants and trying to get on top of it. It was getting a bit overpowering and I was short-tempered … when I thought I was going to lose my sister over it, that were it … I’m fed up with arguing and I weren’t going to fall out, that was it. It is stressful – my husband, he got a few ear bashings …. The upsetting part was that’s cost a friendship.
A8-RPM1-P3-W1
Organising large-scale events could be particularly stressful. This resident, organising an event they felt was not a success, in the context of an already overstretched daily life with caring responsibilities, decided to leave the partnership:
The gala I found very stressful this year because it were down to me to organise it all. It didn’t turn out … then you just think … all this hassle; you’ve got your mum and dad who are getting older and poorly. Two sisters who are disabled. So, your family comes first. That’s why … what I said is I’ll step back.
A8-RPM2-P3-W1
And this resident member of a different partnership expressed similar sentiments:
It can be quite stressful … organising events, there’s always something that will go wrong at the last minute, no matter what you do! … And obviously I have a job, I have a family, so trying to organise events and projects, time restraints is an issue.
A7-PM4-P3-W1
The pressure of leadership
The difficulties associated with problematic internal dynamics in partnerships could be amplified for those with particular governance responsibility. As this partnership chair commented: ‘I wouldn’t wish the chair on anybody …. it’s very stressful’ (A14-RPM/Chair2-P2-W1). This chair stayed until the project she was leading had been successfully completed and then left. She was replaced by a resident who had been vice chair, who described how the partnership dynamics had made her role more difficult and extended into her home life:
They’ve kept me as chair … I got attacked by this person, to say, ‘You’ve let the ball slip … You basically have not done what you were supposed to be doing. How dare you?’ … I find that people are quick to attack … That’s one of the things that I struggle with, getting attacked …. As chair you have to be very robust, you have to have a thick skin. [Also] as a chair you never get a thank you … this was affecting my home life, my kids … when you’re a chair they just expect you to get on with it.
A6-RPM3-P3-W1
In another area, the new chair described the situation after taking over from the previous chair and the BL rep leaving due to tensions and conflict between partnership members:
Things have been hard … the dynamics of the group … ‘chaos and the mess’ … It’s walking a minefield, trying to get the balance … It’s a matter of spinning plates – being chair – working out how to move forward and out of the chaos … People dynamics are a huge issue. We need resilience. It’s much harder than I thought it would be.
A10-RPM2-Chair-P2-W2
The experience of a vice chair in yet another area illustrates the enormous burden large projects can create for residents who agree to lead them. This project involved drawn-out negotiations over a lease for a community hub. Observational notes (A14-P2-W1) reveal how the vice chair was repeatedly verbally attacked by other partnership members, including the chair, and was visibly distressed. The impact was commented upon by others at interview: ‘The vice chair … is really down at the moment and he was going to give it all up, he … is on a knife edge’ (A14-RPM-1-P2-W1). The BL rep reaffirmed this: ‘The vice chair, who works and has been off sick, he has only just come back this week, and there was stress on him mentally. He was feeling the partnership was difficult’ (A14-Rep1-P2-W1). Similarly, a local stakeholder who attends partnership meetings commented: ‘When I say I hope vice chair isn’t broken by this, I fear that the kind of stresses and the strain he’s been under could actually do him harm … he’s having a really hard time’ (A14-Stakeholder-P2-W1).
The vice chair subsequently left the partnership, and in his last interview in 2019 he reflected on his experiences:
Yeah, it’s been very much up and down … I was … diagnosed with depression before I got involved with Big Local … I didn’t know whether the work that I was doing in Big Local was making me more depressed … not being well in my mind because I was trying to deal with things that I hadn’t dealt with before and was in situations which I had no knowledge of and you know how that makes you feel in terms of maybe feeling a bit inadequate.
A14-RPM4-P3-W1
While some resident members of BL partnerships decided to resign, others ‘stepped back’ as a temporary respite – sometimes on multiple occasions, as this resident partnership member highlights:
You can definitely get burnt out. The resident who runs [name of project], we’ve worked together for a very long time now since the beginning. She’s burnt out several times; she has had to step away for a few months. I have burnt out once or maybe twice now.
A14-RPM5-P3-W1
However, alongside their reports of significant negative impacts, some residents also described positive benefits from their involvement in BL. The vice chair in A14, who felt that BL had triggered his depression, also noted that without his experience in BL he may well not have decided to enrol in higher education. Similarly, this resident partnership member noted that she had learnt a lot from her negative experience:
I’m feeling better having kind of taken a step back from everything, was involved for about five years … it gets to a point where … it’s not easy any more … More than likely Big Local did affect my health in a negative way but I don’t blame Big Local for that. If anything, I am happy that it happened because I am now more self-aware about … what triggers my kind of bad days and a bit more aware on what I can take on and I feel a bit happier with kind of like saying no to certain things. It’s kind of like I’ve taken a step back from lots of different things and then at the time they may have affected my mental health negatively but I’m also glad that I was a part of them.
A14-RPM4-P3-W1
Conclusion
In this chapter, we have reported on BL residents’ perceptions of the health and well-being impacts of involvement in BL and the improvements BL partnerships have delivered. Residents made frequent references to positive impacts at individual and collective levels, typically expressed in terms of mental well-being. Varied pathways were identified. Improvements in social connectivity and cohesion were the most prominent, but pathways via improvements in the physical environment and material living standards were also identified. However, alongside these very positive accounts there were also accounts of negative impacts on individual resident members of BL partnerships, most often arising from problematic relationship dynamics and/or the burden of responsibility associated with membership of the partnership. This could be particularly acute where residents had leadership roles. A frequent response from residents experiencing difficulties was the decision to ‘step back’ from their partnership role; sometimes this was temporary and on other occasions permanent. This response reflects the complex relationships many had with BL. Despite sometimes significant negative impacts, they would often also stress positive benefits of their involvement.
Chapter 9 The economics of Big Local: a cost–benefit analysis
Introduction
Our economic evaluation has involved a cost–benefit analysis, not a cost–effectiveness analysis. Cost–effectiveness analysis requires a single measure of ‘effect’ such as the QALY typically used in evaluating health care and medical interventions. This is too narrow for an intervention like BL. In a cost–benefit analysis the ‘effects’ of an intervention are measured in monetary form, which enables the inclusion of broad-ranging outcomes. If the monetised benefits of BL exceed the costs, it means that the BL programme provides a positive net benefit. Providing information on the costs, benefits and the net benefits of interventions like BL is useful for decision-makers who have to prioritise expenditure from a given budget.
Our cost–benefit analysis used the life satisfaction approach to value the benefits of BL. This approach compares the impact of the intervention or policy of interest on life satisfaction to the impact of an increase in income on life satisfaction. 112 The methods used in this analysis are described in detail in Chapter 3. The starting point was the finding reported in Chapter 5 that BL increased life satisfaction on a scale of 0–10 by 0.01 (95% CI –0.057 to 0.077). There are likely to be multiple pathways through which BL might be expected to have improved life satisfaction for residents. One pathway highlighted by residents, for example, was BL activities that brought people together to fix problems they identified as important and in so doing built trust, helped people get to know each other and built mutual support. This in turn was reported to have made residents feel safer in the neighbourhood, developed greater cohesion, and improved community perceptions of well-being. Although the estimated 0.01 increase in life satisfaction is not statistically significantly different from zero at conventional levels of significance, we decided to use it for the economic evaluation to at least get an idea of the potential monetary value of BL. However, as we discuss later, there is considerable uncertainty around the findings.
Results
Table 11 presents descriptive statistics of the estimated benefits, costs and resulting net benefits in each of the 150 BL areas. The benefit estimates are derived by essentially comparing the estimated impact of BL on life satisfaction to the impact of an increase in annual household income on life satisfaction; thus the benefit estimates can be interpreted as annual benefits. Since the WP1 estimation of the impact of BL is based on a 4-year intervention period (2016–19), the total benefits would be four times the annual benefits. Table 11 presents as ‘net benefits A’ the more conservative estimate that compares the annual benefits to the total cost of BL and as ‘net benefits B’ an estimate that uses four times the annual benefits.
| Annual benefits | Total cost | Net benefits A: annual benefits – total cost | Net benefits B: total benefits – total cost | |
|---|---|---|---|---|
| Mean | £1,800,114 | £806,180 | £993,934 | £6,394,276 |
| Standard deviation | £975,225 | £237,407 | £1,036,747 | £3,942,470 |
| 5th percentile | £659,610 | £440,628 | –£337,793 | £1,807,622 |
| 25th percentile | £1,079,556 | £634,397 | £328,030 | £3,570,758 |
| 50th percentile | £1,607,710 | £785,771 | £825,969 | £5,653,500 |
| 75th percentile | £2,235,639 | £961,234 | £1,516,104 | £8,194,042 |
| 95th percentile | £3,607,118 | £1,270,504 | £2,895,103 | £13,716,455 |
| Total over all 150 BL areas | £270,017,100 | £120,927,000 | £149,090,100 | £959,141,400 |
We can see that the benefits and costs, and the resulting net benefits, vary across the 150 BL areas. In some areas the net benefits are negative, but in the vast majority of areas they are positive. On average, the net benefits are nearly £1M according to the conservative estimate A, and £6.4M for estimate B. Summing over all 150 BL areas, the total net benefits are nearly £150M according to the conservative estimate and nearly £1B when we assume the annual benefits are accrued in each year of the intervention period.
Table 12 explores the reasons for the variation in benefits, costs and net benefits across the 150 BL areas by presenting descriptive statistics on the variables that we used in our cost–benefit calculations for all 150 BL areas, the 38 BL areas for which we obtained net benefit A estimates that are at or below the 25th percentile of the distribution of net benefit estimates, and the 38 BL areas whose net benefit A estimates are at or above the 75th percentile. Table 12 shows that the small or even negative net benefits below the 25th percentile are driven by both lower annual benefits and higher total cost.
| All 150 BL areas | BL areas with net benefits A ≤ 25th percentile | BL areas with net benefits A ≥ 75th percentile | |
|---|---|---|---|
| Annual benefits | £1,800,114 | £892,806 | £3,116,958 |
| Average household income | £37,099 | £34,625 | £42,148 |
| Average household size | 2.40 persons | 2.45 persons | 2.41 persons |
| Number of residents aged 16 and over | 7516 | 4215 | 11,818 |
| Total cost | £806,180 | £965,969 | £715,924 |
| Payments received by BL areas | £727,250 | £881,742 | £641,275 |
| Value of unpaid hours provided by partnership members | £78,930 | £84,227 | £74,648 |
| Observations | 150 | 38 | 38 |
The lower benefits are due to these areas having lower household incomes and larger household sizes. The relationship between benefits, household income and household size is due to the mechanics of our cost–benefit calculations. Recall that we calculate the willingness to pay for BL per person in each of the 880 LSOAs that make up the 150 BL areas by dividing a 1.50% increase in average household income by the average household size because the results from WP1 suggest that the impact of BL on life satisfaction is equivalent to the increase in life satisfaction achieved by a 1.50% increase in household income. Thus, mechanically we will obtain a lower willingness to pay per person in areas with lower average income and larger average household size.
As an example, we can calculate the willingness to pay per person using the mean values for average household income and average household size reported in Table 12. Using the mean values for BL areas with net benefits A below the 25th percentile, we obtain a willingness to pay per person of (£346.25 × 1.50)/2.45 = £211.99, while with the mean values for areas with net benefits A above the 75th percentile, we obtain a willingness to pay per person of (£421.48 × 1.50)/2.41 = £262.33. Additionally, the number of residents aged 16 and over tends to be smaller in areas with net benefits A below the 25th percentile, so the lower willingness to pay per person is multiplied by a smaller number of residents when we calculate the total willingness to pay in these areas. Continuing our two examples, we would obtain annual benefits of £211.99 × 4215 = £893,538 for our calculation with the mean values for areas with net benefits A below the 25th percentile, versus £262.33 × 11,818 = £3,100,216 for areas with net benefits A above the 75th percentile.
We assessed the robustness of our estimates to changes in the assumptions underlying our calculations. For the benefits calculation, we assumed that the standard deviation in the life satisfaction scale is 2.00 rather than 1.90, which results in a smaller willingness to pay for BL, that is, a more conservative estimate of the annual benefits. For the costs, we included not only the actual payments to each of the BL areas but also BL plan funding that has been committed but not yet distributed. Additionally, we tripled the value of the unpaid hours that we obtained from the 2016, 2018 and 2020 surveys instead of only doubling it. The results are in Appendix 6, Table 37. The estimates for ‘net benefits A’ are our most conservative estimates of the net benefits of BL. On average, they are £641,553 per BL area, resulting in a total net benefit of £96M. In some areas, our most conservative estimates suggest negative net benefits. At the 25th percentile the costs exceed the benefits by £105,890, while at the 5th percentile the loss is £590,511. However, even with negative net benefits in 45 out of the 150 BL areas, the total net benefit across all 150 BL areas is still in the millions. The estimates for ‘net benefits B’ are positive in all 150 BL areas, with the total being £866M.
In an additional robustness test, we used a different measure for our cost calculation. Instead of basing it on the payments that each BL area received, we used the sum of the total expenditure reported by LT in each of its annual reports for the years 2012–20. Appendix 6, Table 38 lists the total expenditures from all nine reports. We see that annual expenditure gradually increased until it reached around £30M per year in 2017. The sum over all 9 years is £174,575,189. The tripled value of unpaid hours provided by partnership members is £17,759,250, so the most conservative estimate of the total cost of BL is £192,334,439. Using our most conservative estimate of the benefits of BL of £256,516,200 from Appendix 6, Table 37, we obtain a net benefit estimate of £64,181,761. Adjusting the expenditure values for the earlier years for inflation might increase the total cost estimate but it is unlikely to change the overall net benefit from a positive number to a negative number.
Finally, we explored the sensitivity of our results to the size of the estimate of the impact of BL on life satisfaction. As discussed above, the WP1 estimate of 0.01 (95% CI –0.057 to 0.077) is not statistically significantly different from zero but potentially is an underestimate because the estimation sample includes BL areas that have spent more than 80% of their grant as well as BL areas that have spent as little as 30% or 40% of their grant. We might see a bigger impact of BL once it is fully developed in all BL areas. Nevertheless, we explored a worst-case scenario that assumes that the estimate of 0.01 is an overestimate. Appendix 6, Table 39 presents the total net benefits over all 150 BL areas for successively smaller estimates of the impact of BL on life satisfaction. Row 1 repeats our main results based on the impact estimate of 0.01 for reference, while rows 2–9 go through 0.009, 0.008, 0.007 and so on until 0.001, which would be only one-tenth of our actual impact estimate. We see that for ‘net benefit A’, which uses only the annual value of the benefits, the net benefit is positive until 0.005 and becomes negative when the impact estimate takes values of 0.004 or lower. For ‘net benefit B’, which assumes that the annual benefit is accrued over the whole 4-year intervention period, the net benefit becomes negative only at the lowest impact value of 0.001. Appendix 6, Table 40 repeats this analysis using the more conservative assumptions for the benefit and cost calculations from the robustness test in Appendix 6, Table 38; that is, the standard deviation of the life satisfaction scale is assumed to be 2.00 rather than 1.90 and the costs include committed but not yet distributed BL plan funding and triple the value of the unpaid hours from the three survey years. The value of ‘net benefit A’ becomes negative for impact estimates of 0.006 or lower, while the value of ‘net benefit B’ only becomes negative for 0.001.
Conclusion
In summary, the overall net benefit of BL is positive in nearly all of our scenarios. Only if the life satisfaction impact of BL is much lower than our current estimate as reported in Chapter 5 does the overall net benefit become negative. However, it is more likely that our current life satisfaction impact estimate is an underestimate. Using the current impact estimate of 0.01, our most conservative net benefit estimate is £64M (£256M − 192M). This estimate translates to a benefit–cost ratio of 1.3. Alternatively, we can translate our estimate into a rate of return on the original investment. BL Trust was established with a National Lottery grant of £196,873,499. Thus, the rate of return on the original investment is 30% (£256M/£196M).
Chapter 10 Discussion and conclusions
Introduction
This report presents findings from the third phase of an evaluation of BL, a place-based community empowerment initiative launched in 2010, implemented in 150 neighbourhoods across England from 2011, and due to end in 2026. This third phase of the CiC study was commissioned in response to a call in 2016 by the NIHR Public Health Research Programme (PHRP) for research to address urgent gaps in the evidence on which interventions, using a community engagement approach, are effective in improving health and well-being and reducing health inequalities.
We identified that the most glaring gaps were in relation to community empowerment initiatives. In theory these have great potential for reducing health inequalities. First, they could increase the collective control communities in disadvantaged places have over decisions and actions that impact on members’ lives, and research has shown that having greater control is associated with improved health. Second, communities can exercise their enhanced collective control in ways that improve the social, economic and environmental determinants of health inequalities in neighbourhoods, which in turn could improve the health of the local population. To study these processes, we were able to take advantage of the BL programme: a rare example of an experiment in community empowerment.
In Chapter 2 we reviewed the existing evidence on the potential health impacts of communities having collective control over decisions and actions that impact on members’ lives. We concluded that while the evidence base is growing, more research on the nature of, and pathways to, these impacts is needed. We also highlighted evidence that positive social and health impacts are shaped by the type and level of collective control communities have, and that the conditions and resources communities need to develop and exercise collective control are unequally distributed. This raises the possibility that PBIs that aim to empower communities could be ‘imposing greater risks and responsibilities upon more disadvantaged communities in return for lower levels of power’. 69 In this context, there is a particular need for evidence on the differential impacts and experience of these PBIs and how these inequalities in impact can be avoided.
Our CiC study has spanned 7 years. It offers an unparalleled opportunity to learn from the BL experience for future community empowerment initiatives, focusing on the effects on health and well-being and on reducing health inequalities. In this final chapter, we summarise the ‘story’ our research tells about the social and health impacts of BL 10 years into the programme, the pathways to these impacts, and the barriers and enablers along the way. We focus here mainly on findings from the third phase of the CiC study, but reference is made to findings from the two earlier phases. These are also summarised in Appendix 7. Second, we identify some implications for future policy and practice that aim to increase collective control, particularly in disadvantaged communities, and for research intended to evaluate interventions. Third, we describe past activities and future plans to involve BL residents, the wider public and practitioners involved in community empowerment initiatives in interpreting and disseminating our findings. Finally, we offer some brief concluding comments.
The Communities in Control story
Communities in Control is a longitudinal mixed-methods evaluation of the population- and individual-level social and health impacts of BL and an investigation into the chain of events flowing from the introduction of this intervention into local systems that shape these impacts. 74,77–79 An equity lens was integrated throughout the research process.
The BL programme was launched in 2010 and runs until 2026. It has involved 150 relatively disadvantaged, but diverse, communities of place around England. They each received around £1M to enable residents to decide on, and deliver, action to improve their neighbourhoods. The programme is managed by a BL partnership board in each area, often chaired by a resident, with at least 51% resident members. There is considerable variation in the local context, in the use of the funds, in the type and timing of actions delivered and in the alliances BL partnerships have established to implement their plans.
FIGURE 2A.
Collective Control Influence System.

The CiC theoretical framework adopts a systems perspective. It depicts the processes and feedback loops that our theory of change hypothesised could enable or constrain the development of capabilities for collective control among BL residents and their attempts to exercise these to improve the conditions in which they live. The theory, described in more detail in Chapter 3 and Appendix 7, postulates that these improvements could in turn improve social and health outcomes at the population and individual levels. Informed by this system-focused theory of change, our analyses have sought to understand how these processes operated in BL areas.
Pursuing improvements in a hostile context
In assessing the potential social and health impacts of BL, it is important to remember that the programme was implemented from 2010, the beginning of a decade of unprecedented cuts in public sector finances. These cuts have been shown to have been deepest in the most disadvantaged areas of the country and to have resulted in the devastation of many local public services. 135–137 Additionally, by the end of 2018, all parts of the UK had introduced Universal Credit for unemployed and economically inactive people, which has had negative mental health impacts on those in receipt of this benefit. 138,139 These policies are likely to have created a disempowering environment, particularly for populations in the relatively disadvantaged areas in which BL was implemented. The often extraordinary commitment residents made to deliver improvements in their areas, utilising the opportunities afforded by BL, are all the more impressive when seen against this hostile backdrop of worsening economic conditions, cuts to public services and restricted eligibility for welfare benefits. This was a recurrent theme in the account of the BL experience given by residents and by local and national stakeholders. The impact of these policies on communities has also been referenced in research commissioned by LT. 102 As the programme moved into the later stages, BL residents also had to face the challenges imposed by the COVID-19 pandemic (see Chapter 7) which, like austerity, have hit the most disadvantaged neighbourhoods of England the hardest. 115,140,141
Big Local’s impact on residents’ capabilities for collective control over decisions and actions
Local dynamics
Despite the difficult context, the qualitative markers we constructed reveal increasing capabilities for collective control – defined as different types of power – over time among residents who were most active in the programme (see Chapter 7). Residents in all our fieldwork sites reported growing confidence in their individual and collective ability to act together to improve the area (power within); greater understanding of the need for alliances to deliver improvements, together with enhanced skills in forging and sustaining external relationships (power with); and in all these areas, meaningful improvements in important social determinants of health inequalities were delivered (power to act). However, there was variation across BL areas and, as we discuss later, the experience of participation in BL was not universally positive.
Big Local partnerships are a key ‘space’ in which residents can develop capabilities for collective control. These partnerships provide the formal governance framework in each BL area. Partnership members make decisions about how the BL money is spent and determine who will act on behalf of BL, and they are accountable to the local population and the national oversight organisation (LT) for delivering improvements in the area. Our findings suggest that the capacity to establish, enact and maintain inclusive, equitable and effective governance processes varied across BL areas. As a result, the dynamics of these BL governance spaces could operate to exclude some groups in the local population and undermine the development of collective control capabilities among residents on the partnership and in the wider community. External expectations that BL partnerships would adopt systems of governance comparable to those of legally constituted agencies also created problems. Attempts by BL partnerships to meet these expectations could cause significant disruption and undermine progress made by residents towards greater collective control. Our findings in this sphere, combined with previous research, raise important questions about the assumption that devolving greater power to community organisations will necessarily increase the democratic legitimacy of governance structures and increase a community’s ability to exercise greater control over decisions and actions locally. 133,134
Beyond the formal governance role, as BL partnerships moved to develop and implement their plans, they had to create power within the local community, that is, the recognition of common interest, mutual trust, knowledge and skills that are prerequisites for collective action. They also had to develop power with others and their own power to act. The scale and complexity of the relational work residents had to do in order to develop these capabilities is vividly illustrated in the accounts presented in Chapter 7, as too is the pivotal role of support workers and the wider infrastructure provided by the VCFSE and public sectors, notably local government.
Without input from BL support workers, other professionals and local organisations, the achievements in some BL areas would have been seriously compromised. On the other hand, these same actors could behave in ways that undermined the development and exercise of collective control capabilities by BL residents. Partnerships had different levels and types of capabilities at different points in time and therefore required different types and levels of external input, albeit that this was not always a linear development process. Those in support roles (including workers paid for by BL partnerships) and representatives of external agencies inevitably made judgements about the capabilities a BL partnership had to deliver improvements locally. Their actions, shaped by these judgements, could be experienced by residents as paternalistic, patronising and/or controlling.
In the interviews, some BL workers reflected on the difficulties they experienced striking the right balance between ‘support’ and ‘direction’. But this language is at odds with the aspirations expressed by many BL residents to be treated as equal partners in decision-making and action for change, based on their democratic right to participate and their ‘lived experience’ expertise. There was also a balance to be struck between delivering tangible improvement in the area and doing this in ways that increased sustainable collective control capabilities in the community. In this context, the understandable desire to help deliver the BL plan led some support workers to encourage BL partnerships to fund projects that could be demonstrated to improve the neighbourhood but had little, if any, potential to enhance the partnership’s collective control over decisions and actions. This dilemma is illustrated by the involvement over time of some BL partnerships in more complex, potentially more impactful, projects, including the transfer of local assets (e.g. local library) into community control. These projects could adversely affect confidence levels – power within – as partnerships had to negotiate with local authorities and/or deal with situations without knowledge of legal processes. As one national stakeholder put it: ‘when you start looking at it, you just see how everything is stacked up against keeping communities in control of assets, really’ (CiC3-Nat-Interview-12).
National dynamics
Although not funded by government, BL is a nationally funded programme, with procedures and regulations decided centrally by LT. In this context, LT has needed to negotiate what Warr defines as a ‘paradoxical space’ between ‘top-down’ and ‘bottom-up’ requirements. 142 Since 2017, major changes have been made to BL’s management and support functions nationally. There is no evidence that these have diluted the programme’s resident-led ethos, but they have resulted in increased involvement of LT in decisions about what support would be received by BL partnerships and which areas would be targeted for additional support. Alongside this, there has been greater investment in information collected by LT about local areas through research, evaluation and performance management, and a growing focus on the need to ensure that BL partnerships have used the funds available to their areas by the 2026 deadline.
These changes could suggest that BL has moved towards a more ‘top-down’ model to the extent that the national function is intervening in local delivery. We had planned to explore whether these changes had influenced residents’ experiences of the programme in our local fieldwork but were unable to do this due to pandemic-related fieldwork challenges. We can therefore only hypothesise about the influence of these national programme changes on levels of collective control among BL residents.
On the one hand, residents could construe the increased involvement of LT in local decisions and the performance management arrangements as ‘interference’ or ‘bureaucracy’ that constrains their control over decisions. In the qualitative fieldwork, there was certainly some questioning by residents and other local stakeholders about whose perspective should be given priority when considering how BL’s impact is measured. There was also pushback from some against what was perceived to be LT’s heavy emphasis on achieving financial sustainability. For this resident partnership member, for example, this could mean other important aspects of sustainability being neglected:
[Local Trust] makes a big deal of sustainability – financial sustainability and financial legacy, but … personal satisfaction is a legacy, and cultural legacy, and changing people’s ways of doing things, and learning … there is a type of personal legacy as well – Big Local tend to put all the emphasis on financial legacies. And it has got to be a balance … when you put a project on, it is not necessarily for financial reasons, it is more for cultural and art and music and personal satisfaction.
A3-RPM5-P3-W1
Looking ahead to the final years of the programme, it is also possible that LT could become increasingly interventionist locally, particularly in BL areas that continue to spend slowly.
On the other hand, national stakeholders argued that the negotiated and tailored nature of support now offered to BL areas meant that it was more likely to be relevant and appropriate to local needs, compared to the ‘one size fits all’ model perceived to characterise earlier years of the programme. Where LT had intervened, this was typically stated to be in areas where the BL partnerships were experiencing significant conflict, resulting in relationships becoming ‘dysfunctional’ and local programme delivery coming to a halt. Therefore, LT perceived their intervening in these areas to be a positive and necessary step – enabling collective control by supporting BL partnerships to work through entrenched problems and stressors that were disempowering.
Big Local’s impacts on social and health outcomes
The CiC study has sought to assess the impact on health and well-being outcomes and their social determinants at two levels – among the populations of BL areas and among the residents most active in the programme – and both quantitatively and qualitatively. The quantitative research on the impact on active residents utilised data from the LT survey of partnership members only. In earlier phases of CiC, the qualitative research included residents engaged in a range of BL-sponsored activities, but in the third phase, resource constraints meant residents’ interviews were restricted to members of the BL partnerships. CiC has also explored the possible pathways to health and well-being impacts identified.
The numbers
Given the hostile social and economic environment in which the BL programme has been running – most recently including the impacts of a global pandemic – it is notable that our analysis of impacts on BL populations found tentative evidence that the initiative was associated with reduced anxiety in populations in BL areas after 2017 and an increased number of people in these areas reporting that things in their life were worthwhile. Additionally, for those areas that had made most progress implementing their plans – having spent more than 80% of their grant by 2019–20 – the BL programme was associated with a small improvement in our multidimensional measure of population mental health (SAMHI) compared to the matched comparison areas without the BL programme. This improvement in mental health was greater in BL areas that had spent more than 80% of their grant and prioritised social activities, while the reduction in burglaries was also larger when the analysis was limited to these BL areas and greater still in those in this group that had focused on environmental activities.
There was also evidence of an improvement in mental well-being among residents involved in BL partnerships between 2016 and 2018 (in the nested cohort only). Though this improvement was no longer present by 2020, interpretation of data from this year was complicated by the COVID-19 pandemic. Partnership members who perceived that people in the area are willing to help each other, and those who agreed that collectively they can influence decisions in the area, had higher well-being scores. Importantly, however, we also found some evidence that these benefits were unequally distributed by education and gender. For example, in the nested cohort of residents, the mental well-being of those with higher educational qualifications (a proxy for higher socioeconomic status) improved between 2018 and 2020, but it did not improve in the same period for those with no degree. There was also some suggestion in the nested cohort data that (at least up to 2018) men were more likely than women to report improvements in mental well-being. Inequalities in the distribution of positive outcomes from initiatives aiming to build social trust within communities and engage people in collective action have also been reported in previous research – with residents from higher socioeconomic backgrounds having greater benefits. 143
The narratives: pathways to positive health and well-being
Reinforcing the tentative evidence for positive quantifiable health and well-being benefits at the population level, many residents and other stakeholders participating in the qualitative fieldwork highlighted positive impacts of the area improvements they had delivered and described the pathways through which these were achieved (see Chapter 8). These impacts were typically expressed in terms of improved mental well-being.
The importance of initiatives that brought local people together and improved the social environment was a particularly prominent theme in narratives about pathways to better mental health. More details of these activities can be found on the BL website https://localtrust.org.uk/big-local/ and publications from earlier phases of CiC. 85 This was evident at the personal level, where activities that sought to reduce social isolation and encourage social interaction were perceived to have enhanced the well-being of people who took part. Impacts were also perceived as operating at the collective level through initiatives bringing people together to fix problems they identified as important and in so doing building trust, helping people get to know each other and building mutual support. This in turn made them feel safer in the neighbourhood, developed greater cohesion and improved community perceptions of well-being. There were also compelling examples of initiatives to improve the physical environment, often involving a central focus on increasing social participation, leading to improvements in mental well-being at individual and group levels. These accounts are supported by our quantitative findings that members in BL partnerships that had made most progress with implementation and had prioritised expenditure on improvements in physical and/or social environments were more likely to report better mental health and reduced burglaries.
Mental well-being impacts through pathways in the economic environment were less commonly described, as these initiatives were rarer in our fieldwork areas. However, the few accounts we received suggested that these initiatives were highly valued and were perceived to improve mental health. These included initiatives to provide new skills that enhanced employment opportunities, hence leading to increased household incomes. There were also initiatives tackling food poverty, improving access to free or subsidised meals for children and providing a more nutritious, affordable diet for low-income families. These initiatives were also experienced as positively ‘uplifting’ for residents who helped to deliver them.
Influencing area reputation and stigma were less tangible goals, but they elicited thoughtful strategies to essentially influence the social environment, including putting on high-profile events that drew people into the area to see for themselves how vibrant the place could be, as well as giving local organisers and residents something to be proud of and to participate in.
The narratives: unintended negative consequences
It is rare for research to report negative impacts of community initiatives on community members, perhaps partly because studies do not attempt to look for these. In CiC the frequent positive accounts of BL were paralleled by frequent accounts of negative experience, and in some instances individuals reported both positive and negative impacts on their own health and well-being. Negative impacts were also observed on occasion by researchers. Though we cannot estimate how common it was for residents to have negative experiences, some described chronic problems, while for others the experience was short-lived and linked to a specific piece of work.
Negative impacts were frequently associated with problematic relationship dynamics within partnerships and the responsibilities associated with partnership membership. The latter included the scale and complexity of a project an individual was leading, as well as specific issues, such as problems arising when staff were employed by the BL partnership. All resident members of BL partnerships are volunteers, and there was frequent reference to the time commitment being too great, partly because of the shortage of residents willing to volunteer to join the partnership and/or take on other work. For some, partnership work spilled over into private lives and/or paid employment. Less tangibly, residents would link the stress they experienced to their sense of responsibility for, and commitment to, BL. They did not feel they could walk away. Influences on levels of collective control and experience of stress are complex, but it is plausible that our findings of more educated residents reporting higher control and well-being by 2020, while less educated residents did not, and women being less likely to report mental health improvement up to 2018 compared to men, could reflect the differential impacts of cuts in public services and reduced access. These impacts hit those on lower incomes and less secure employment and women hardest, leading to more stress and a reduced sense of control.
The economics of Big Local
Our evaluation of the economic impact of BL (see Chapter 9) involved a cost–benefit analysis, not a cost–effectiveness analysis. As noted earlier, the latter requires a single measure of ‘effect’ such as the QALY typically used in evaluating health care and medical interventions. Instead, we used the life satisfaction approach to value the benefits of BL, this approach involves findings from BL residents’ responses to the question ‘Overall, how satisfied are you with your life nowadays?’. The costs of the programme included the funds each BL area received, as well as the value of the time residents and other people have given to BL. Our benefit estimates might seem very large. The reason is that a small difference at the individual level becomes a large difference at the aggregate level. On average, we estimated that the 0.01 increase in life satisfaction on the 0–10 scale is equivalent to an income increase of £234. Once we apply this small increase to the whole BL population of approximately 1.1 million, we get to an aggregate value of approximately £260M per year. We realise that this figure is the best-case scenario. We also acknowledge that the original life satisfaction finding was not statistically significant in conventional terms. We therefore undertook an extensive sensitivity analysis. In summary, though there is much uncertainty around the estimates, the overall net benefit of BL was positive in nearly all of our scenarios. Our most conservative net benefit estimate is £64M. This estimate translates to a 30% rate of return on the original National Lottery grant of £196,873,499.
Implications for policy and practice for place-based community empowerment initiatives
As noted earlier, the longitudinal nature of our research, spanning 7 years, offers an unparalleled opportunity to learn from the BL experience for future community empowerment initiatives. In particular, our evaluation provides insights into what helps or hinders the development of the capabilities communities need in order to exercise collective control over decisions and actions that improve their lives in ways that have potential to improve health.
Our findings are particularly timely. There are growing calls for local initiatives that are more truly empowering for communities, particularly those communities bearing the brunt of growing social and economic inequalities. These include calls for a new ‘community paradigm’ that includes key elements of the BL model. 35,70 The government proposals for Levelling-Up policies in England are expected to extend current initiatives, devolving more decision-making down to local people via place-based empowerment initiatives, opening up more opportunities for community control of local services and giving them direct control over financial resources to implement their decisions, supported by the VCFSE sector, with a ‘soft’ enabling role for local government.
On the basis of our findings (and other research, reviewed in Chapter 2), we recommend that those involved nationally and locally in shaping future place-based community empowerment initiatives to address social and health inequalities should consider the following questions:
-
What processes can be put in place to more effectively share formal responsibility equally with local communities, rather than expecting local people to shoulder the burden of responsibility for delivering improvements? Our study supports other research in highlighting that while communities are uniquely able to take the lead in defining and prioritising issues for action and designing solutions in place-based empowerment initiatives, the responsibility of leading and delivering neighbourhood improvements can take a heavy toll on the well-being of community members, particularly those individuals and groups experiencing the greatest burden of poverty, stigma and discrimination.
-
How can future community-based initiatives nurture the different forms of power communities required in order to exercise greater collective control over actions and decisions, while navigating a wider system of increased scrutiny that could entail community groups having more formal responsibility for meeting higher externally determined standards for accountability and legitimacy? As our research and other studies suggest, a framework of ‘bottom-up community’ and ‘top-down government’ legitimacy, embedded in programmes like BL, may not always align and the resulting conflict may undermine the empowerment potential of these local initiatives. 144,145
-
Can practices in the public and VCFSE sectors be redesigned to support more authentic co-production and collaborative practice with communities of place and interest. The success of PBIs depends on organisational and professional cultures that prioritise working as equal partners with communities of place and interest; that give equivalent value to the expertise derived from lived experience as to knowledge from professional experience and research; and that understand that even the most disadvantaged communities have capacities that can be ‘released’ rather than ‘built’. But our study, like other research, has shown that the behaviour of local agencies and practitioners can be far from collaborative and that co-production can involve costs for all involved, including community members. 146
-
Can investment in local infrastructure be increased to develop and sustain smaller-scale community associations and organisations that can emerge from and work with local communities of place (also prioritised in the research reviewed by Kruger)35? Careful targeting of this investment locally is crucial if the social and health benefits BL-type empowerment initiatives can deliver are to reach all members of a community and, importantly, are to be distributed equitably across different communities.
-
Can training and development opportunities be developed to improve the capabilities and knowledge of practitioners who are, or could be, involved in PBIs that aim to empower communities? This is particularly important for initiatives involving more socially and economically disadvantaged communities, when the risk of interventions being experienced as patronising or stigmatising may be greatest. Of particular value would be opportunities for practitioners to:
-
explore the benefits of understanding capabilities for collective control as the different forms of power that communities require to exercise greater collective control over decisions and actions
-
consider the potential to shift the focus from mapping and activating a community’s assets to mapping local power dynamics to understand the capabilities for control communities already have and those that could be nurtured, and to reveal the forms of power limiting a community’s capabilities to develop and exercise collective control
-
reflect on the importance of language and how the way communities are described may stigmatise and disempower and may not reflect how a community sees itself. In addition to practitioners directly involved in place-based community initiatives, these development opportunities would also be relevant to general practitioners and other clinical health professionals, social workers, housing officers, etc.
-
Recommendations for future research evaluating community empowerment initiatives
The CiC study is an ambitious attempt to assess the social and health impacts of a community empowerment initiative at a population and individual level and to explore pathways to these impacts. Not surprisingly, the study has a number of limitations. Perhaps the most important is the impact of the COVID-19 pandemic. As already noted, it can be expected to have impacted significantly on both explanatory and outcome measures in our analysis of individual impacts. The pandemic also severely delayed the analysis of our primary outcome in WP1 as we did not get access to the APS data until a few weeks before the formal end of the study. This also prevented us from constructing comparators for the analysis of impacts on active residents. Our qualitative fieldwork was halted for around 2 months at a critical time; when it resumed, progress was very slow, partly due to difficulties organising interviews with people living in neighbourhoods most severely affected by the pandemic and partly due to the impacts on the lives of research team members, many of whom were caring for young children at home. Efforts to broaden our national sample to include external perspectives on BL were also unsuccessful, due in large part to the demands of the pandemic on the individuals we approached. Another important limitation of the third phase of CiC was the restricted reach we had into the wider communities in BL areas. The quantitative analysis of social and health impacts on ‘active’ residents was also restricted to secondary data from involved residents, as members of the BL partnerships and resources did not allow us to extend our qualitative interviews with residents involved in BL activities beyond partnership membership. Although we have been able to look at impacts on the populations of BL areas as a whole using national data sources (see Chapter 5), this means that we have been unable to explore what, if any, impacts there were on individual residents beyond the partnership or the ‘reach’ of BL activities through the eyes of the wider communities.
Obviously, research may not be able to be pandemic-proofed, but our study, and its limitations, highlights important implications for future evaluations of place-based community empowerment initiatives. These are summarised in Box 7 and discussed in more detail below.
-
Be conducted over a long time frame, including a cohort of community members, and having matched comparator areas.
-
Be sufficiently powered to detect small but important effects at both population and individual levels, and within and between areas if relevant.
-
Combine secondary data sources with collection of new data more sensitive to potential impacts of specific programmes.
-
Integrate an equity lens across the research process to ensure a focus on potential differential positive and negative impacts across social groups.
-
Combine quantitative components with longitudinal qualitative components to enable a more dynamic understanding of experiences, context and changes over time.
Our research suggests that funders of health-related research should consider increasing their investment in applied evaluations of place-based community empowerment initiatives and methodological research to further develop the approaches and instruments needed to progress this field.
This research was commissioned by the NIHR PHRP in order to help fill gaps in the evidence on which interventions, using a community engagement approach, are effective in improving health and well-being and reducing health inequalities. The research reported here suggests that place-based interventions that aim to give disadvantaged communities greater collective control over decisions and actions impacting on their lives can positively impact on social drivers of health inequalities and on individual and population health. Distinctive features of the BL programme were the scale of funding over which communities were given control and the long time frame over which the programme has run. And although there are uncertainties around the estimates, our economic analysis suggests these types of interventions can provide a positive rate of return on investment. However, as we have also acknowledged, there are important limitations to the CiC study. Given this, and given the possibility that initiatives like BL will form part of any future strategy to reduce health inequalities, NIHR and other funders of health-related research should consider increasing their investment in applied evaluations of place-based community empowerment initiatives and methodological research to further develop the approaches and instruments needed to progress this field. Specific recommendations for future research based on our experience with CiC are listed below.
-
Future evaluations of place-based community empowerment initiatives should integrate an equity lens into the research questions, design, analysis and dissemination. This must include a focus on potential differential positive and negative impacts across social groups, including data on socioeconomic status, gender and ethnicity.
Our research found evidence that individual benefits of the BL initiatives were unequally distributed by education and gender – for example, the mental well-being of residents with higher educational qualifications (a proxy for higher socioeconomic status) improved between 2018 and 2020, but this was not the case for those with no degree. The secondary data sources we used did not include data on other dimensions of inequality, including ethnicity.
-
Evaluations of the social and health impacts of community empowerment initiatives need to be conducted over a long time frame, include a cohort of community members and have matched comparator areas.
It is likely that it takes time for interventions such as BL to have an effect on health and social outcomes. As most BL areas did not start to draw down substantial amounts of money until their plans were approved around 2015, our analysis took 2016 as the starting point, giving 4 years of follow-up. This may not have been sufficient to observe substantial effects, particularly given many areas had not completed all planned activities by 2020. The nested cohort we had access to in the LT partnership survey to explore impacts on engaged residents was valuable. However, it was small, which restricted statistical power, and limited to resident members of BL partnerships, excluding members of the wider population. Additionally, due to changes in the APS, we were unable to construct comparators for our analysis of the impact on individual residents and hence had no control for the study. This restricted our ability to conclude that the changes observed in active residents were related to participation in BL.
-
Evaluations need to be sufficiently powered to detect small but important effects at both population and individual level, within and between areas in initiatives implemented in multiple neighbourhoods.
Our analysis was not sufficiently powered to detect very small effects and, while we were able to explore potential differences in impacts across broad groups of BL areas, our analysis did not have sufficient power to analyse effects for populations within each BL area or subgroups within BL areas. Analysis that was able to take account of significant variations in local programmes could have provided important information on pathways to positive impacts.
-
The obvious benefits of secondary data sources should be combined with collection of new data more sensitive to potential impacts of programmes like BL. This would enable samples to be constructed to reflect relevant theories of change and development of bespoke quantitative measures of population and individual outcomes and samples.
Our population and individual outcomes were all derived from secondary data sources and may not be a good match for BL activities. The measures we used will also be affected by response bias in the case of the well-being measures, and variations in access to services and changes in reporting for our other outcomes. Additionally, the survey of partnership members was skewed towards more highly educated older residents with very good or good health at baseline. Finally, as discussed above, collecting data from the wider community rather than restricting the sample of the residents most actively involved in place-based community initiatives would provide important additional insights into the reach and impacts of these initiatives.
-
Future evaluations of place-based community empowerment initiatives should combine quantitative components with longitudinal qualitative components incorporating ethnographic methods, to enable a more dynamic understanding of experiences, context and changes to be captured over time.
From a systems perspective, initiatives such as BL present challenges in how to combine evaluation of change at the individual and population level with evaluation of the collective and community-level changes that happen in between. Methods such as social network analysis could be used to investigate the ways in which interventions shape changes in relationships, resources and interactions within systems. 79 In a multisite study, in-depth longitudinal qualitative research will have considerable financial and time implications given the intensity of work required in implementing such approaches but, despite many uncertainties, our estimates of the economics of BL suggest these types of interventions could provide good value for money. Given this, further high-quality evidence to provide a firmer foundation for the design and delivery of these initiatives would be valuable. Shiell and Hawe argue that this evidence base cannot rely on individual self-reported measures in surveys to meaningfully capture changes in community empowerment and control, as these ‘confuse properties of individuals with the properties of the setting in which they live’. 130
-
Methodological research could include a review of the scope for extending current routine and national survey data sources to include measures that could be used in evaluation of community empowerment initiatives. Further work on qualitative markers of progress in developing capabilities for collective control would also be valuable.
Kruger also argues for a revaluation of social infrastructure and the intangible social benefits of civil society to be included in the Treasury Review of the Green Book and for the development of a new Index of Social Infrastructure that can inform local and national policy making. 35
Public and practitioner involvement in interpreting and disseminating our findings
As described in Chapter 3, we engaged residents and workers in BL areas beyond our fieldwork sites in a variety of ways to contribute to sense-checking and interpreting preliminary findings from different parts of the research. However, in the final 20 months, COVID-19 restrictions on social engagement and more general disruptions in people’s lives (including members of the research team) severely limited these activities. To date, we have:
-
discussed the research findings with young people participating in a BL initiative aimed at that age group
-
run a half-day workshop attended by members of our resident network and other stakeholders from three BL partnership boards, providing basic training in qualitative data analysis followed by exploration of preliminary data emerging from the first wave of fieldwork in 2019
-
run two further workshops with residents and other BL stakeholders to explore preliminary quantitative findings on the impact of BL on residents most actively involved and the qualitative findings on factors enabling and/or constraining residents’ action to improve their neighbourhoods
-
presented our findings at a national BL Connects conference in November 2021 and run a ‘market stall’ to engage people in discussions about the implication of some of our findings.
In the future, we hope to run further workshops with residents of disadvantaged areas where community-led PBIs are under way to develop more accessible outputs based on research findings from the CiC study and other initiatives.
We will work proactively with a range of organisations to ensure our research outputs are relevant and accessible to community activists and professional practitioners involved in designing, delivering or evaluating place-based community empowerment initiatives. This will include working with the Local Government Organisation, the new Office for Health Improvement and Disparities and regional network. In particular, we will maintain our links with LT, the organisation overseeing the BL programme, and seek to contribute to their work with the all-party parliamentary group for ‘left-behind’ neighbourhoods, which aims to develop practical policy solutions that help build community confidence and capacity to deliver improved social and economic outcomes for local residents. 147
Conclusion
By evaluating BL as a natural policy experiment in community empowerment, our findings help to address a key gap in evidence of the impacts of purposeful attempts to develop capabilities for collective control among residents of relatively disadvantaged places and the ways this is exercised to improve the conditions in which they live. Informed by our systems-focused theoretical framework and combining longitudinal quantitative assessments of impacts at population and individual levels with qualitative exploration of subjective experiences, we have woven a narrative argument concerning the likelihood that the BL community empowerment initiative will have long-term positive social and health impacts at a population and individual level. However, the story is complex. Overall, our findings suggest that capabilities for collective control among BL residents actively involved in the programme had increased over time and they had exercised this control to deliver demonstrable improvements in their neighbourhoods. We were unable to explore whether BL programme dynamics at a national level were impacting on capability for collective control at a local level, but traversing the paradoxical space between the national and the local will be a challenge for any large-scale community empowerment initiative like BL.
It is clear that increases in capabilities for collective control in BL populations did not have a linear trajectory and progress varied across BL partnerships. Despite this diversity, all the partnerships in our fieldwork sites had delivered substantial improvements in their area. Though the quantitative evidence for social and health impacts in BL populations and among engaged residents is tentative, the lived experience of resident members of BL partnerships illuminates logical pathways to health and well-being impacts through social environmental and material improvements. There is also evidence for negative impacts of varying degrees and the suggestion that positive impacts may be socially patterned, with residents with lower educational qualifications (a proxy for lower socioeconomic status), and particularly women, faring less well. Though there are considerable uncertainties around the estimates, our cost–benefit work also suggests that BL provides good value for money.
Countervailing conditions – including COVID-19, as well as austerity measures and welfare changes that have disproportionally impacted those experiencing the greatest economic disadvantage – are likely to have influenced our findings. There were also limitations in the data and resources we had available to measure the outcomes of an emergent complex initiative, with more innovative evaluation methods also needed that are sensitive to the systems-wide effects of PBIs at the community/collective level, beyond individual- and population-level measures.
The current social, political and economic context provides a paradoxical climate for achieving conditions that enable communities of place or interest to have greater control over decisions affecting their lives. BL’s success – compared to previous initiatives – in empowering communities to take action is likely to be an important legacy of its funding, as evidenced by the growing policy and national interest in the programme. Initiatives such as BL that are genuinely committed to resident-led ‘control’ involve an element of risk in the ways that such funding is organised, as well as in decisions taken about how and when to assist communities and/or intervene. As one of our national interview participants observed in the first phase of CiC, part of the reason past initiatives ‘failed’ was not because people designing and implementing such programmes were ‘not thoughtful’; it was because ‘being resident led is hard’ (CiC1-Nat-Interview-05). Successful community empowerment initiatives require a commitment within the VCFSE and public sectors to listen and act on lay knowledge, a recognition of the vital role of local small grassroots organisations in reaching and working with local people, and an acknowledgement of the limits of community action alone. BL has demonstrated that to do this well requires a significant investment of resources, flexibility in how funds are used and long-term equal partnerships with communities. Our research has also highlighted the need for investment to be carefully targeted to ensure that the benefits of empowerment are equally distributed within and between communities. While place-based empowerment initiatives have a role to contribute to tackling inequalities, this is only possible when they and their evaluations are designed with equity at their heart to ensure that groups and individuals who feel they already have least control over their circumstances are not disadvantaged further.
Acknowledgements
This study was funded by the NIHR PHRP (16/09/13). We are very grateful to everyone in our local fieldwork sites and other local stakeholders for the diverse support they have provided in all phases of the CiC study. The BL reps and staff of BL’s LTOs were a significant source of support in many sites. We would also like to thank those BL residents, including members of our Residents Advisory Network, who contributed to the design of the study, advised on aspects of the qualitative fieldwork, joined in conversations about our preliminary findings and most recently this report. We are particularly grateful to Thomas Marshall, Michael Tye and Stephen Colghan, long-standing members of the resident network, who made significant contributes to the CiC website; and Elaine Samson, chair of Shadsworth with Whitebirk BL partnership, and Mohammed Khan from Blackburn with Darwen Healthy Living, who spoke about our research at a King’s Fund conference and contributed to the plain English summary for this report. We look forward to continued engagement with members and support workers from BL partnerships. We would like to thank our Advisory Group members for their support (Emeritus Professor Ken Judge, chair; Professor John Frank; Professor Alan Shiell; Professor Penny Hawe; Professor David Hunter, Dr Mel Sorotkin and Richard Wilson). Unfortunately, due to disruptions caused by the COVID-19 pandemic we were unable to meet with the Advisory Group in the latter stages of the research but hope to do this in the future to report on the final outcomes. We also extend our thanks to LT, whose staff have provided invaluable support, advice and data throughout this and earlier phases of the CiC study. Particular thanks go to Jayne Humm, Head of Research and Learning, and to Jeremy Yung and Lucy Terry, senior researchers.
Contributions of authors
Jennie Popay (https://orcid.org/0000-0001-9234-908X) (Professor of Sociology & Public Health) is the principal investigator on the CiC study; led, with other senior members of the team, the design of the study and writing of the grant application; chaired the Project Management Group providing high-level support for the research; co-led WP3 (qualitative fieldwork), contributed to all analyses and writing up of qualitative data; commented on all analyses from other WPs; and led writing of the report.
Emma Halliday (https://orcid.org/0000-0002-2216-9259) (Senior Research Fellow) co-applicant, contributed to the design of the CiC study overall and writing of grant application, member of the Project Management Group providing high-level support for the research; supported public involvement; member of the WP3 team providing input to all aspects of the work; undertook the qualitative research with national stakeholders and analysis and write-up of these data; commented on all other qualitative analyses; contributed to writing the report.
Rebecca Mead (https://orcid.org/0000-0002-1954-5276) (Senior Research Associate) supported the management of the CiC Project Management Group and WP3 team; member of the WP3 team; supported public involvement; led on production of WP3 instruments; managed the development and maintenance of the NVivo qualitative database and oversaw uploading of qualitative data from all WP3 fieldwork sites; led on qualitative fieldwork in two local sites in the north-west; co-led analyses of qualitative data on pathways to increased collective control; contributed to all qualitative data collection and analysis; and contributed to writing the report.
Anne Townsend (https://orcid.org/0000-0001-8114-752X) (Senior Research Associate) contributed to design of fieldwork instruments for WP3 and led fieldwork in two local sites in the south-west; assisted with the development and maintenance of the NVivo qualitative database and uploading of qualitative data from all sites; co-led analyses of qualitative data on pathways to increased collective control and residents’ perceptions of impacts on well-being; contributed to all qualitative data collection and analysis; and contributed to writing the report.
Nasima Akhter (https://orcid.org/0000-0002-5424-1593) (Assistant Professor Research) undertook analysis of survey data for WP2; co-led the write-up of these analyses.
Clare Bambra (https://orcid.org/0000-0002-1294-6851) (Professor Public Health) co-applicant; contributed to design of the CiC study and grant application; member of the Project Management Group providing high-level support for the research; led WP2 impact on engaged residents; designed data analysis approach and oversaw all analyses for WP2; managed WP3 fieldwork in the north-east; and contributed to writing the report.
Ben Barr (https://orcid.org/0000-0002-4208-9475) (Professor Applied Public Health) co-applicant, contributed to design of the CiC study and grant application; member of the Project Management Group providing high-level support for the research; led WP1 population social and health impacts; led design of data analysis approach and contributed to all analyses for WP1; contributed to writing the report.
Rachel Anderson de Cuevas (https://orcid.org/0000-0001-7790-5332) (Research Associate) member of WP3 team; contributed to design of fieldwork instruments, conducted qualitative fieldwork in two local sites in the north-west; assisted with the development and maintenance of the NVivo qualitative database; led analysis of qualitative data on markers.
Konstantinos Daras (https://orcid.org/0000-0002-4573-4628) (Research Associate) member of the WP1 team; managed data access process and contributed to all analyses for WP1; contributed to writing the report.
Matt Egan (https://orcid.org/0000-0002-4040-200X) (Professor Public Health) co-applicant, contributed to design of the CiC study and grant application; member of the Project Management Group, WP 1 population social and health impacts team and WP3 qualitative research team; oversaw and conducted qualitative fieldwork in three local sites in the south-east; contributed to collection and analyses of all qualitative data; commented on analyses from other WPs; and contributed to writing of the report.
Katja Gravenhorst (https://orcid.org/0000-0001-9618-8260) (Research Fellow) member of the WP3 team; conducted qualitative fieldwork in three local sites in the south-east; contributed to design of fieldwork instruments; contributed to analysis of qualitative data on governance; and commented on the report.
Katharina Janke (https://orcid.org/0000-0003-0205-2958) (Lecturer, Health Economics) co-applicant, contributed to design of the CiC study and grant application; member of the Project Management Group providing high-level support for the research and WP1 team; led WP4 economics of BL and conducted all analyses for this WP; commented on WP1 analysis and contributed to writing of the report.
Adetayo Safiriyu Kasim (https://orcid.org/0000-0002-0411-3059) (Honorary Professor Statistics) co-designed data analysis approach and oversaw all analyses for WP2 impact on engaged residents; supported write-up of analyses.
Victoria McGowan (https://orcid.org/0000-0002-4743-9120) (Research Associate) member of WP2 and WP3 teams; WP2 supported data collection and write-up of analyses; WP3 contributed to design of fieldwork instruments; conducted qualitative fieldwork in three local sites in North-East; contributed to analysis of qualitative data; commented on the report.
Ruth Ponsford (https://orcid.org/0000-0003-2612-0249) (Assistant Professor) co-applicant, contributed to design of the CiC study and grant application; member of WP3 research team; supported fieldwork in three local sites in the south-east; contributed to analysis of qualitative data on markers of collective control; commented on the report.
Joanna Reynolds (https://orcid.org/0000-0002-2650-6750) (Senior Research Fellow) member of WP3 team; contributed to design of fieldwork instruments; conducted qualitative fieldwork in two local sites in Yorkshire; led analysis of qualitative data on governance; contributed to other qualitative data analyses; contributed to writing the report.
Margaret Whitehead (https://orcid.org/0000-0001-5614-6576) (Professor Public Health) co-applicant; contributed to design of CiC study and the grant application; member of the Project Management Group providing high-level support for the research; member of the WP1 team; co-led WP3 (qualitative fieldwork); oversaw fieldwork in two north-west sites; led analyses of qualitative data on pathways to health impacts; oversaw analysis of qualitative data on markers of collective control; commented on data analyses in all other WPs; contributed to writing the report.
Data-sharing statements
This project made extensive use of secondary data sources and collected new empirical qualitative data, but it is unlikely to be made available in its entirety in the future due to particular conditions that were agreed with local fieldwork sites and LT. Additionally, all available qualitative data arising from interviews and observations in the CiC study are being retained for the exclusive use of the CiC team until the publication of major outputs and potentially until after a fourth phase of the research. However, access to some anonymised data may be granted in the future; please contact the corresponding author, Professor Popay, for any additional information or queries.
Ethics approval
Ethical approval was obtained from Lancaster University Faculty of Health and Medicine Ethics Committee on 5 July 2018 (Reference: FHMREC17092). The partner universities accepted the requirements set out in Lancaster University’s approval (University of Liverpool Ref. 3870; London School of Hygiene and Tropical Medicine Ref. 15996; University of Newcastle Ref. 6823/2018). There was a subsequent amendment to take account of pandemic-related changes to recruitment and consent processes for the qualitative fieldwork, on 18 August 2020 (FHMREC19141).
Disclaimers
This report presents independent research funded by the National Institute for Health and Care Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, the PHR programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, the PHR programme or the Department of Health and Social Care.
References
- NIHR SPHR . Communities in Control n.d. https://communitiesincontrol.uk/ (accessed 10 December 2021).
- Orton L, Halliday E, Collins M, Egan M, Lewis S, Ponsford R, et al. Putting context centre stage: evidence from a systems evaluation of an area based empowerment initiative in England. Crit Publ Health 2017;27:477-89. https://doi.org/10.1080/09581596.2016.1250868.
- Townsend A, Abraham C, Barnes A, Collins M, Halliday E, Lewis S, et al. ‘I realised it weren’t about spending the money – it’s about doing something together’: the role of money in a community empowerment initiative and the implications for health and wellbeing. Soc Sci Med 2020;260. https://doi.org/10.1016/j.socscimed.2020.113176.
- Local Trust . Creating Lasting Change: Big Local 2012.
- UN Economic and Social Council . Empowering People and Ensuring Inclusiveness and Equality, Report of the Secretary-General 2019.
- Alinsky S. Rules for Radicals. New York, NY: Vintage Books; 1971.
- Ledwith M. Community work as critical pedagogy: re‐envisioning Freire and Gramsci. Commun Develop J 2001;36:171-82. https://doi.org/10.1093/cdj/36.3.171.
- Eyben R. Supporting Pathways of Women’s Empowerment: A Brief Guide for International Development Organisations. Policy Paper. Brighton: Institute of Development Studies; 2011.
- Popay J, Whitehead M, Ponsford R, Egan M, Mead R. Power, control, communities and health inequalities I: theories, concepts and analytical frameworks. Health Promot Int 2020;36:1253-63. https://doi.org/10.1093/heapro/daaa133.
- Brown P. Popular epidemiology and toxic waste contamination: lay and professional ways of knowing. J Health Soc Behav 1992;33:267-81.
- Brown P. Toxic Exposures. New York, NY: Columbia University Press; 2007.
- Reynolds J, Egan M, Renedo A, Petticrew M. Conceptualising the ‘community’ as a recipient of money: a critical literature review, and implications for health and inequalities. Soc Sci Med 2015;143:88-97. https://doi.org/10.1016/j.socscimed.2015.08.049.
- Bell C, Newby H. Community Studies: An Introduction to the Sociology of the Local Community. London: Routledge; 1971.
- Dominelli L. Women and Community Action: Local and Global Perspectives. Bristol: University of Bristol, Policy Press; 2019.
- Thomson H. A dose of realism for healthy urban policy: lessons from area-based initiatives in the UK. J Epidemiol Commun Health 2008;62:932-6. https://doi.org/10.1136/jech.2007.068775.
- McCartney G, Hearty W, Taulbut M, Mitchell R, Dryden R, Collins C. Regeneration and health: a structured, rapid literature review. Publ Health 2017;148:69-87. https://doi.org/10.1016/j.puhe.2017.02.022.
- Crowley L, Balaram B, Lee N. People or Place? Urban Policy in the Age of Austerity. Lancaster: Lancaster University, Work Foundation; 2012.
- Gustafsson U, Driver S. Parents, power and public participation: Sure Start, an experiment in New Labour governance. Soc Pol Admin 2005;39:528-43. https://doi.org/10.1111/j.1467-9515.2005.00454.x.
- Lawless P, Pearson S. Outcomes from community engagement in urban regeneration: evidence from England’s New Deal for Communities programme. Plan Theor Pract 2012;13:509-27. https://doi.org/10.1080/14649357.2012.728003.
- Sullivan H, Judge K, Sewel K. ‘In the eye of the beholder’: perceptions of local impact in English Health Action Zones. Soc Sci Med 2004;59:1603-12. https://doi.org/10.1016/j.socscimed.2004.02.013.
- Lawless P, Foden M, Wilson I, Beatty C. Understanding area-based regeneration: the New Deal for Communities programme in England. Urban Stud 2010;47:257-75. https://doi.org/10.1177/0042098009348324.
- Scott H. Empathy in Healthcare Settings. London: University of London; 2011.
- Bauld L, Judge K, Barnes M, Benzeval M, Mackenzie M, Sullivan H. Promoting social change: the experience of Health Action Zones in England. J Soc Pol 2005;34:427-45. https://doi.org/10.1017/S0047279405008858.
- Hills D, Elliot E, Kowarzik U, McGregor E, Miller P, Rugkasa J, et al. The Evaluation of the Big Lottery Fund Healthy Living Centres Programme. London: Tavistock Institute and Bridge Consortium; 2007.
- Belsky J, Melhuish E, Barnes J, Leyland AH, Romaniuk H. Effects of Sure Start local programmes on children and families: early findings from a quasi-experimental, cross sectional study. BMJ 2006;332. https://doi.org/10.1136/bmj.38853.451748.2F.
- Slocock C. A Shared Society? The Independence of the Voluntary Sector. London: Civil Exchange; 2017.
- Cabinet Office . Building the Big Society 2010.
- Wiggins K. 2011. www.thirdsector.co.uk/locality-wins-15m-community-organisers-programme/finance/article/1055870 (accessed 14 November 2021).
- Department of Communities and Local Government . Plain English Guide to the Localism Act 2011.
- Department for Digital Culture Media & Sport OfCS . Civil Society Strategy: Building a Future That Works for Everyone 2018.
- Brindle D. A History of the Volunteer: How Active Citizenship Became the Big Society 2015. www.theguardian.com/voluntary-sector-network/2015/jun/01/a-history-of-the-volunteer-how-active-citizenship-became-the-big-society (accessed 10 December 2021).
- Balazard H, Fisher R, Scott M. The ‘Big Society’ in the United Kingdom: privatisation or democratisation of public services. Revue Franc d’Admin Publ 2017;163:507-20. https://doi.org/10.3917/rfap.163.0507.
- Wills J. Locating Localism: Statecraft, Citizenship and Democracy. Bristol: Policy Press; 2016.
- South J, Stansfield J, Amlôt R, Weston D. Sustaining and strengthening community resilience throughout the COVID-19 pandemic and beyond. Persp Publ Health 2020;140:305-8. https://doi.org/10.1177/1757913920949582.
- Kruger D. Levelling Up Our Communities: Proposals for a New Social Covenant – A Report for Government by Danny Kruger MP 2020.
- Syme SL. Personal Control and Health. Oxford: John Wiley & Sons; 1989.
- Whitehead M, Pennington A, Orton L, Nayak S, Petticrew M, Sowden A, et al. How could differences in ‘control over destiny’ lead to socio-economic inequalities in health? A synthesis of theories and pathways in the living environment. Health Place 2016;39:51-6. https://doi.org/10.1016/j.healthplace.2016.02.002.
- Ross CE. Collective threat, trust, and the sense of personal control. J Health Soc Behav 2011;52:287-96. https://doi.org/10.1177/0022146511404558.
- Popay J. International Health and Development: Investing in Assets of Individuals, Communities and Organisations. New York, NY: Springer; 2010.
- De Vos P, De Ceukelaire W, Malaise G, Pérez D, Lefèvre P, Van der Stuyft P. Health through people’s empowerment: a rights-based approach to participation. Health Hum Rights 2009;11:23-35. https://eresearch.qmu.ac.uk/handle/20.500.12289/9921 (accessed 12 November 2021).
- Popay J, Williams G. Public health research and lay knowledge. Soc Sci Med 1996;42:759-68. https://doi.org/10.1016/0277-9536(95)00341-X.
- Picken C, Popay J, Staley K. Developing a model to enhance the capacity of statutory organisations to engage with lay communities. J Health Serv Res Pol 2002;7:34-42. https://doi.org/10.1258/1355819021927656.
- Wallerstein N. Empowerment to reduce health disparities. Scand J Publ Health 2002;30:72-7. https://doi.org/10.1177/14034948020300031201.
- Bernard P, Charafeddine R, Frohlich KL, Daniel M, Kestens Y, Potvin L. Health inequalities and place: a theoretical conception of neighbourhood. Soc Sci Med 2007;65:1839-52. https://doi.org/10.1016/j.socscimed.2007.05.037.
- Oakley A. Social Support and Motherhood: The Natural History of a Research Project. Bristol: Bristol University Press; 1992.
- Reblin M, Uchino BN. Social and emotional support and its implication for health. Curr Opin Psychiatry 2008;21:201-5. https://doi.org/10.1097/YCO.0b013e3282f3ad89.
- White H, Saran A, Polack S, Kuper H. Rapid Evidence Assessment of What Works to Improve Social Inclusion and Empowerment for People with Disabilities in Low- and Middle-income Countries. London: International Centre for Evidence in Disability, London School of Hygiene and Tropical Medicine, and Campbell Collaboration; 2018.
- Zimmerman MA, Rappaport J. Citizen participation, perceived control, and psychological empowerment. Am J Community Psychol 1988;16:725-50. https://doi.org/10.1007/BF00930023.
- Bosma H, Marmot MG, Hemingway H, Nicholson AC, Brunner E, Stansfeld SA. Low job control and risk of coronary heart disease in Whitehall II (prospective cohort) study. BMJ 1997;314:558-65. https://doi.org/10.1136/bmj.314.7080.558.
- Orton LC, Pennington A, Nayak S, Sowden A, Petticrew M, White M, et al. What is the evidence that differences in ‘control over destiny’ lead to socioeconomic inequalities in health? A theory-led systematic review of high-quality longitudinal studies on pathways in the living environment. J Epidemiol Community Health 2019;73:929-34. https://doi.org/10.1136/jech-2019-212565.
- Siegrist J, Marmot M. Health inequalities and the psychosocial environment: two scientific challenges. Soc Sci Med 2004;58:1463-73. https://doi.org/10.1016/S0277-9536(03)00349-6.
- Woodall J, Raine G, South J, Warwick-Booth L. Empowerment and Health and Well-Being: Evidence Review. Leeds: Leeds Metropolitan University: Centre for Health Promotion Research; 2010.
- Laverack G. Improving health outcomes through community empowerment: a review of the literature. J Health Popul Nutr 2006;24.
- Milton B, Attree P, French B, Povall S, Whitehead M, Popay J. The impact of community engagement on health and social outcomes: a systematic review. Commun Develop J 2012;47:316-34. https://doi.org/10.1093/cdj/bsr043.
- Pennington A, Orton L, Nayak S, Ring A, Petticrew M, Sowden A, et al. The health impacts of women’s low control in their living environment: a theory-based systematic review of observational studies in societies with profound gender discrimination. Health &Amp; Place 2018;51:1-10. https://doi.org/10.1016/j.healthplace.2018.02.001.
- Wallerstein N. What Is the Evidence on Effectiveness of Empowerment to Improve Health? Health Evidence Network Report 2006.
- Chandler MJ, Lalonde CE. Cultural continuity as a protective factor against suicide in First Nations youth. Horizons 2008;10:68-72.
- Baba C, Kearns A, McIntosh E, Tannahill C, Lewsey J. Is empowerment a route to improving mental health and wellbeing in an urban regeneration (UR) context?. Urban Stud 2017;54:1619-37. https://doi.org/10.1177/0042098016632435.
- Orton L, Pennington A, Nayak S, Sowden A, White M, Whitehead M. Group-based microfinance for collective empowerment: a systematic review of health impacts. Bull World Health Organ 2016;94:694-70. https://doi.org/10.2471/blt.15.168252.
- Ecorys . Active Communities Programme Evaluation 2020.
- Sender H, Khor Z, Carlisle B. National Empowerment Partnership: Final Evaluation Report 2011.
- Pearmain D, Hatamian A, Khor Z. Grassroots Grants: Final Evaluation Report 2011.
- Sally Downing consulting with Alison Millward Associates BSP . Evaluation of the Fair Share Initiative. Report on End of Phase 2 of Evaluation 2007.
- Elliott J, Gale CR, Parsons S, Kuh D. Neighbourhood cohesion and mental wellbeing among older adults: a mixed methods approach. Soc Sci Med 2014;107:44-51. https://doi.org/10.1016/j.socscimed.2014.02.027.
- Myers P, Barnes J, Brodie I. Partnership Working in Sure Start Local Programmes: Early Findings From Local Programme Evaluations. NESS Synthesis Report No. 1 2004.
- Stern E, Platt S, Boydell L, Popay J, Williams G, Petticrew M, et al. The Evaluation of the Big Lottery Fund Healthy Living Centres, Third Annual Report of the Bridge Consortium 2005.
- Wright JSF, Parry J, Mathers J, Jones S, Orford J. Assessing the participatory potential of Britain’s New Deal for Communities. Pol Stud 2006;27:347-61. https://doi.org/10.1080/01442870601010051.
- Popay J, Whitehead M, Carr-Hill R, Dibben C, Dixon P, Halliday E, et al. The impact on health inequalities of approaches to community engagement in the New Deal for Communities regeneration initiative: a mixed-methods evaluation. Publ Health Res 2015;3:1167-46. https://doi.org/10.3310/phr03120.
- Rolfe S. Governance and governmentality in community participation: the shifting sands of power, responsibility and risk. Soc Pol Soc 2018;17:579-98. https://doi.org/10.1017/S1474746417000410.
- Pollard G, Studdert J, Tiratelli L. Community Power: The Evidence; New Local in Partnership with Local Trust. London: New Local; 2021.
- South J, Button D, Quick A, Bagnall A-M, Trigwell J, Woodward J, et al. Complexity and community context: learning from the evaluation design of a national community empowerment programme. Int J Environ Res Public Health 2020;17. https://doi.org/10.3390/ijerph17010091.
- South J, Phillips G. Evaluating community engagement as part of the public health system. J Epidemiol Community Health 2014;68:692-6. https://doi.org/10.1136/jech-2013-203742.
- Krieger N. Proximal, distal, and the politics of causation: what’s level got to do with it?. Am J Public Health 2008;98:221-30. https://doi.org/10.2105/AJPH.2007.111278.
- Diez Roux AV. Complex systems thinking and current impasses in health disparities research. Am J Public Health 2011;101:1627-34. https://doi.org/10.2105/AJPH.2011.300149.
- Hawe P. Lessons from complex interventions to improve health. Annu Rev Public Health 2015;36:307-23. https://doi.org/10.1146/annurev-publhealth-031912-114421.
- Petticrew M. Time to rethink the systematic review catechism? Moving from ‘what works’ to ‘what happens’. Syst Rev 2015;4. https://doi.org/10.1186/s13643-015-0027-1.
- Angeles RN, Dolovich L, Kaczorowski J, Thabane L. Developing a theoretical framework for complex community-based interventions. Health Promot Pract 2014;15:100-8. https://doi.org/10.1177/1524839913483469.
- Egan M, Penney T, Anderson de Cuevas R, Er V, Orton L, White M, et al. NIHR SPHR Guidance on Systems Approaches to Local Public Health Evaluation – Part 2: What to Consider When Planning a Systems Evaluation. Technical Report 2019.
- Hawe P, Shiell A, Riley T. Theorising interventions as events in systems. Am J Community Psychol 2009;43:267-76. https://doi.org/10.1007/s10464-009-9229-9.
- Local Trust . Big Local Trust. Annual Report and Financial Statements for 1 April 2019 to 31 March 2020. Submitted by Local Trust As the Corporate Trustee for Big Local 2020.
- Big Lottery Fund . A Guide for Organisations Wanting to Apply to Run the Big Local Trust: Programme Guide 2010.
- James D, Jochum V, Kane D, Curtis A, Ockenden N, Johnston L, et al. Big Local: The Early Years. Evaluation Report 2014.
- Big Local Trust . TRUST DEED. Establishing a Charity Called Big Local Trust. Dated 13 February 2021. Big Lottery Fund and Local Trust. Conformed Copy, 05 June 2013 2013.
- Big Lottery Fund . Question and Answers for the Big Local Trust 2011.
- Lewis S, Bambra C, Barnes A, Collins M, Egan M, Halliday E, et al. Reframing ‘participation’ and ‘inclusion’ in public health policy and practice to address health inequalities: evidence from a major resident-led neighbourhood improvement initiative. Health &Amp; Social Care in the Community 2019;27:199-206. https://doi.org/10.1111/hsc.12640.
- Medical Research Council . Using Natural Experiments to Evaluate Population Health Interventions: Guidance for Producers and Users of Evidence 2011.
- Egan M, Abba K, Barnes A, Collins M, McGowan V, Ponsford R, et al. Building collective control and improving health through a place-based community empowerment initiative: qualitative evidence from communities seeking agency over their built environment. Crit Publ Health 2021;31:268-79. https://doi.org/10.1080/09581596.2020.1851654.
- Halliday E, Collins M, Egan M, Ponsford R, Scott C, Popay J. A ‘strategy of resistance?’ How can a place-based empowerment programme influence local media portrayals of neighbourhoods and what are the implications for tackling health inequalities?. Health Place 2020;63. https://doi.org/10.1016/j.healthplace.2020.102353.
- Powell K, Barnes A, Anderson de Cuevas R, Bambra C, Halliday E, Lewis S, et al. Power, control, communities and health inequalities III: participatory spaces – an English case. Health Promot Int 2020;36:1264-74. https://doi.org/10.1093/heapro/daaa059.
- Office For National Statistics SSD . Annual Population Survey, 2004: Secure Access Annual Population Survey, 2004–2019: Secure Access 2020. https://doi.org/10.5255/UKDA-SN-6721-14.
- Office For National Statistics SSD . APS; Personal Well-Being; Subjective Well-Being Annual Population Survey, 2004: Secure Access Annual Population Survey: Well-Being, April 2011 – March 2015: Secure Access 2016. https://doi.org/10.5255/UKDA-SN-7961-1.
- Feiveson AH. Power by simulation. Stata J 2002;2:107-24. https://doi.org/10.1177/1536867x0200200201.
- Office for National Statistics . Personal and Economic Well-Being: What Matters Most to Our Life Satisfaction? 2019. www.ons.gov.uk/releases/howsatisfiedareyouwithyourlife (accessed 11 November 2021).
- Place-Based Longitudinal Data Resource . Small Area Mental Health Index (SAMHI) – Place-Based Longitudinal Data Resource n.d. https://pldr.org/dataset/2noyv/small-area-mental-health-index-samhi (accessed 12 November 2021).
- NHS Digital . Practice Level Prescribing Data n.d. https://digital.nhs.uk/data-and-information/publications/statistical/practice-level-prescribing-data (accessed 12 November 2021).
- NHS Digital . Quality and Outcomes Framework, Achievement, Prevalence and Exceptions Data 2018–19 [PAS] n.d. https://digital.nhs.uk/data-and-information/publications/statistical/quality-and-outcomes-framework-achievement-prevalence-and-exceptions-data/2018-19-pas (accessed 12 November 2021).
- Office for National Statistics . NOMIS: Official Labour Market Statistics n.d. www.nomisweb.co.uk/ (accessed 12 November 2021).
- Place-based Longitudinal Data Resource . Prescribing Indicators: Antidepressants (P_1_07) – Place-Based Longitudinal Data Resource n.d. https://pldr.org/dataset/emyye/prescribing-indicators-antidepressants-p107 (accessed 12 November 2021).
- Data Police UK . About | data.police.Uk n.d. https://data.police.uk/about/ (accessed 12 November 2021).
- Office for National Statistics . About the Area Classifications 2011. www.ons.gov.uk/methodology/geography/geographicalproducts/areaclassifications/2011areaclassifications/abouttheareaclassifications (accessed 12 November 2021).
- Ministry of Housing CLG . English Indices of Deprivation 2015 2015.
- Local Trust . Left Behind? Understanding Communities on the Edge 2019.
- Place-based Longitudinal Data Resource . AHAH Version 2 (Access to Healthy Assets and Hazards) – Place-Based Longitudinal Data Resource n.d. https://pldr.org/dataset/2z9yv/ahah-version-2-access-to-healthy-assets-and-hazards (accessed 12 November 2021).
- Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multiv Behav Res 2011;46:399-424. https://doi.org/10.1080/00273171.2011.568786.
- Donald SG, Lang K. Inference with difference-in-differences and other panel data. Rev Econ Stat 2007;89:221-33. https://doi.org/10.1162/rest.89.2.221.
- Puhani PA. The treatment effect, the cross difference, and the interaction term in nonlinear ‘difference-in-differences’ models. Econ Letters 2012;115:85-7. https://doi.org/10.1016/j.econlet.2011.11.025.
- McGowan VJ, Akhter N, Halliday E, Popay J, Kasim A, Bambra C. Collective control, social cohesion and health and well-being: baseline survey results from the Communities in Control study in England. J Publ Health 2021;44:378-86. https://doi.org/10.1093/pubmed/fdaa227.
- Ng Fat L, Scholes S, Boniface S, Mindell J, Stewart-Brown S. Evaluating and establishing national norms for mental wellbeing using the short Warwick–Edinburgh Mental Well-being Scale (SWEMWBS): findings from the Health Survey for England. Qual Life Res 2017;26:1129-44. https://doi.org/10.1007/s11136-016-1454-8.
- Woolf NH, Silver C. Qualitative Analysis Using NVivo. Milton: Routledge; 2017.
- Ponsford R, Collins M, Egan M, Halliday E, Lewis S, Orton L, et al. Power, control, communities and health inequalities – part II: measuring shifts in power. Health Promot Int 2020;36:1290-9. https://doi.org/10.1093/heapro/daaa019.
- Ritchie J, Lewis J. Qualitative Research Practice. London: Sage; 2003.
- Fujiwara D, Campbell R. Valuation Techniques for Social Cost–Benefit Analysis: Stated Preference, Revealed Preference and Subjective Well-being Approaches: A Discussion of the Current Issues. London: HM Treasury; 2011.
- Dolan P, Kavetsos G, Krekel C, Mavridis D, Metcalfe R, Senik C, et al. Quantifying the intangible impact of the Olympics using subjective well-being data. J Public Econ 2019;177. https://doi.org/10.1016/j.jpubeco.2019.07.002.
- Sacks DW, Stevenson B, Wolfers J. Subjective Well-Being, Income, Economic Development and Growth 2010. www.nber.org/papers/w16441.
- Bambra C, Munford L. COVID-19 and the Northern Powerhouse. Tackling Inequalities for UK Health and Productivity. Newcastle: Northern Health Science Alliance; n.d.
- McMunn A, Nazroo J, Wahrendorf M, Breeze E, Zaninotto P. Participation in socially-productive activities, reciprocity and wellbeing in later life: baseline results in England. Age Soc 2009;29:765-82. https://doi.org/10.1017/S0144686X08008350.
- Norman P, Bambra C. Incapacity or unemployment? The utility of an administrative data source as an updatable indicator of population health. Populat Space Place 2007;13:333-52. https://doi.org/https://doi.org/10.1002/psp.458.
- Townsend J, Zapata E, Rowlands J, Alberti P, Mercado M. Women and Power: Fighting Patriarchies and Poverty. London; New York, NY: Zen Books; 1999.
- Starhawk . Truth or Dare: Encounters With Power, Authority, and Mystery 1987.
- Allen A. Rethinking power. Hypatia 1998;13:21-40. https://doi.org/10.1111/j.1527-2001.1998.tb01350.x.
- Allen A. Feminist Perspectives on Power 2005. https://plato.stanford.edu/entries/feminist-power/ (accessed 10 December 2021).
- Cyril S, Smith BJ, Renzaho AMN. Systematic review of empowerment measures in health promotion. Health Promot Int 2015;31:809-26. https://doi.org/10.1093/heapro/dav059.
- Laverack G, Wallerstein N. Measuring community empowerment: a fresh look at organizational domains. Health Promot Int 2001;16:179-85. https://doi.org/10.1093/heapro/16.2.179.
- Lindacher V, Curbach J, Warrelmann B, Brandstetter S, Loss J. Evaluation of empowerment in health promotion interventions: a systematic review. Eval Health Profess 2018;41:351-92. https://doi.org/10.1177/0163278716688065.
- Rifkin SB. A framework linking community empowerment and health equity: it is a matter of CHOICE. J Health Popul Nutr 2003;21:168-80.
- Sen A. The possibility of social choice. Amer Econ Rev 1999;89:349-78. https://doi.org/10.1257/aer.89.3.349.
- Rowlands J. Questioning Empowerment: Working with Women in Honduras. Oxford: Oxfam; 1997.
- Barnett M, Duvall R. Power in international politics. Int Organ 2005;59:39-75. https://doi.org/10.1017/S0020818305050010.
- Lawson L, Kearns A. Rethinking the purpose of community empowerment in neighbourhood regeneration: the need for policy clarity. Local Econ 2014;29:65-81. https://doi.org/10.1177/0269094213519307.
- Shiell A, Hawe P. Health promotion community development and the tyranny of individualism. Health Econ 1996;5:241-7. https://doi.org/0.1002/(SICI)1099-1050(199605)5:3<241::AID-HEC197>3.0.CO;2-G.
- Laverack G, Pratley P. What Quantitative and Qualitative Methods Have Been Developed to Measure Community Empowerment at a National Level. Copenhagen: Copenhagen World Health Organization, Regional Office for Europe; 2018.
- Powell K, Barnes A, Anderson de Cuevas R, Bambra C, Halliday E, Lewis S, et al. Power, control, communities and health inequalities III: participatory spaces – an English case. Health Promot Int 2020;36:1264-74. https://doi.org/10.1093/heapro/daaa059.
- Connelly S. Constructing legitimacy in the new community governance. Urban Stud 2010;48:929-46. https://doi.org/10.1177/0042098010366744.
- Cowie P, Davoudi S. Reconsidering Localism. London: Routledge; 2015.
- Barr B, Kinderman P, Whitehead M. Trends in mental health inequalities in England during a period of recession, austerity and welfare reform 2004 to 2013. Social Science &Amp; Medicine 2015;147:324-31. https://doi.org/https://doi.org/10.1016/j.socscimed.2015.11.009.
- Taylor-Robinson D, Gosling R, Harrison D, Khan M, Barr B. Austerity measures hit the sickest hardest. BMJ 2013;347. https://doi.org/10.1136/bmj.f4208.
- Alexiou A, Fahy K, Mason K, Bennett D, Brown H, Bambra C, et al. Local government funding and life expectancy in England: a longitudinal ecological study. Lancet Publ Health 2021;6:e641-7. https://doi.org/https://doi.org/10.1016/S2468-2667(21)00110-9.
- Cheetham M, Moffatt S, Addison M, Wiseman A. Impact of universal credit in North East England: a qualitative study of claimants and support staff. BMJ Open 2019;9. https://doi.org/10.1136/bmjopen-2019-029611.
- Wickham S, Bentley L, Rose T, Whitehead M, Taylor-Robinson D, Barr B. Effects on mental health of a UK welfare reform, Universal Credit: a longitudinal controlled study. Lancet Publ Health 2020;5:e157-64. https://doi.org/10.1016/S2468-2667(20)30026-8.
- Daras K, Alexiou A, Rose TC, Buchan I, Taylor-Robinson D, Barr B. How does vulnerability to COVID-19 vary between communities in England? Developing a Small Area Vulnerability Index (SAVI). J Epidemiol Community Health 2021;75:729-34. https://doi.org/10.1136/jech-2020-215227.
- Bambra C, Riordan R, Ford J, Matthews F. The COVID-19 pandemic and health inequalities. J Epidemiol Community Health 2020;74:964-8. https://doi.org/10.1136/jech-2020-214401.
- Warr DJ, Mann R, Kelaher M. ‘A lot of the things we do … people wouldn’t recognise as health promotion’: addressing health inequalities in settings of neighbourhood disadvantage. Crit Publ Health 2013;23:95-109. https://doi.org/10.1080/09581596.2012.739681.
- Portes A. Social capital: Its origins and applications in contemporary society. Annual Review of Sociology 1998;24:1-24. https://doi.org/10.1146/annurev.soc.24.1.1.
- Bénit-Gbaffou C, Katsaura O. Community leadership and the construction of political legitimacy: unpacking Bourdieu’s ‘political capital’ in post-apartheid Johannesburg. Int J Urban Reg Res 2014;38:1807-32. https://doi.org/https://doi.org/10.1111/1468-2427.12166.
- Baum F. Cracking the nut of health equity: top down and bottom up pressure for action on the social determinants of health. Promot Educ 2007;14:90-5. https://doi.org/10.1177/10253823070140022002.
- Wilton C. Coproduction and partnership with people and communities. BMJ Leader 2021;5:79-82. https://doi.org/10.1136/leader-2020-000424.
- All-Party Parliamentary Group for ‘Left Behind’ Neighbourhoods . A Cross-Party Voice at Westminster Speaking Up for ‘Left Behind’ Neighbourhoods 2021. www.appg-leftbehindneighbourhoods.org.uk/ (accessed 2 January 2022).
Appendix 1 Office for National Statistics annual population health survey descriptive statistics
| Sample size | |||
|---|---|---|---|
| All areas | BL areas | Comparator areas | |
| 2011 | 13,896 | 3696 | 10,200 |
| 2012 | 13,616 | 3614 | 10,002 |
| 2013 | 11,943 | 3090 | 8853 |
| 2014 | 11,668 | 3036 | 8632 |
| 2015 | 11,213 | 2887 | 8326 |
| 2016 | 10,442 | 2694 | 7748 |
| 2017 | 10,401 | 2620 | 7781 |
| 2018 | 9710 | 2446 | 7264 |
| 2019 | 9131 | 2357 | 6774 |
| Total | 102,020 | 26,440 | 75,580 |
| Variable | Missing | % |
|---|---|---|
| Anxiety | 1151 | 1.1 |
| Happiness | 981 | 1.0 |
| Worthwhile | 1370 | 1.3 |
| Satisfaction | 943 | 0.9 |
| 0% economic activity | 0 | 0 |
| Socioeconomic status | 0 | 0 |
| Ethnicity | 82 | 0.1 |
| Education statusa | 4166 | 4.1 |
| Marital status | 0 | 0 |
| Housing tenure | 57 | 0.1 |
| Disabilitya | 4921 | 4.8 |
Appendix 2 Qualitative fieldwork sites
A1, in the north-east, is a large estate, with mixed housing, and a main road running along one edge. Formerly social housing for well-paid blue-collar workers in the town’s now declined industries, it has a predominantly white British population. It is seen as a good place to live, with large public green spaces, children’s play areas, and a mix of local shops, previously regarded as the heart of the community, now rather run-down. The BL partnership has a small number of residents and is dominated by a councillor. Recently membership has declined. They have experienced some conflict leading to upheaval with a change of rep, paid support and chairs. They continue to need extensive support. BL priorities were to improve community spaces, including activities for children; provide young people with employment support; and improve local transportation. A multiuse games area was developed, a joint venture with the council. The bus service and the asset transfer/community building were unsuccessful. A local organisation was commissioned to deliver projects; for example, a youth club. The small grants scheme is ongoing, providing funds to local community organisations. The partnership continues to be disempowered and to need support.
A2, in the north-east, covers a postindustrial town and includes a mix of terraced houses and flats. A main road divides the area. Population is around 4500, mainly white British with a minority Muslim population. Good community resources are available but there are some access issues. The BL partnership has a large, broadly stable, membership of roughly 20–25 individuals with around five or fewer residents, with no agency association. Most noticeable investment has been in the physical environment, linked to apprenticeships for young people to support employment, and work with local schools on small-scale gardening projects; this involves working with local organisations to develop three gateway features that sit at the entrance to the BL area. A fourth feature has stalled due to council permissions. A youth project aimed to bring young people into BL. A youth-focused charity was commissioned to provide the service with a high level of success.
A3, in the north-west, covers a large, densely populated inner-city area, across two wards separated by a busy road, with a large Asian/British Asian population and a sizeable Eastern European population. It is a former industrial centre, in decline. There are high levels of crime and ASB. An established resident-led community organisation with close ties to the city council initially received the BL award. Priorities included developing local skills and job opportunities; enhancing green space and play facilities; creating social and recreational opportunities for the community; improving the image and environmental features; and addressing financial exclusion. The programme has funded a successful affordable loan scheme for residents and businesses. In 2020, the BL programme and host community organisation separated by mutual agreement. BL then created themed stakeholder groups of local agencies to address priority areas such as health and well-being, environment and play, and employment. A model of buying in staff time from external organisations for project delivery was used, including buying in services from the council. An example of longer-term action on environmental improvement and health was a land swap (with a housing developer) and development of a pocket park. The process to agree the land swap was long and drawn out, involving a lot of hard work, but injecting a sense of pride.
A4, selected for BL in 2012, is located in a seaside town in the north-west of England. It was previously at the heart of the town’s tourist trade, now declined. It has some shops and many vacant premises. Housing is primarily privately rented flats and maisonettes. A prevalence of poor-quality houses of multiple occupancy means that population density is very high and there is limited access to green spaces. The partnership is strongly connected to the impacts of austerity measures. Multiple applications for funding from local agencies hampered plan delivery together with anxiety around spending money, match-funding and decision-making. Across three phases, A4 struggled to make progress, with a high turnover of members and substantial disagreements, including concerns around the power of the chair. By phase three a new LTO and BL rep were in place, and new members had been recruited. The focus shifted from enterprise, young people, housing, and festivals to community, health and well-being, enterprise and economy, and place. There was a move from grant-giving to a focus on partnership-building seeking opportunities to match-fund, for example, with the council renovation of a local park. By the end of phase 3, however, LT had expressed concern about the limited amount of spending that had taken place. The shift in approach was also not welcomed equally by all partners, with ‘original’ members feeling sidelined in the decision-making process, animosity building, and some of these members subsequently being asked to leave or voluntarily leaving.
A5 is a predominantly residential, densely populated, inner-city area in the north-west of England with a population of 14,000, largely white British, and comprising five housing estates separated by main roads. House ownership is low. The BL programme began in 2014, prioritising: a community hub; increasing community spaces; providing grant awards for individuals and groups; partnership with residents and other organisations; strengthening programme capacity through paid employees and supporting volunteers; community consultation and evidence. The board has developed its independence. Initially the residents felt that the council was attempting to take over and made it clear the initiative was resident led. The Hub, a leased building, became a focal point for local activity. Allotments, and greening of the environment and strengthening community ties were priorities, as well as promoting responsible dog ownership as a method of cleaning up the local environment and reducing dog bites. The partnership has run an annual show in partnership with several local organisations. Two part-time support workers are employed. More recently, the partnership became part of a funded project in partnership with the city council’s neighbourhood engagement team and local university. Partnership members have been trained as community researchers. The partnership runs a small grant awards scheme via their LTO (a major voluntary sector organisation in the city) for voluntary projects, community enterprise and business start-ups.
A6 is a ward in an outer east London borough; it has a diverse ethnic and socioeconomic population with distinct subcommunities, mixed housing, a large park and easy access to green spaces in the county. A busy main road with limited shopping facilities runs through the middle of the ward, and a busy road runs alongside. It has a reputation for youth and gang crime, which has improved recently. During fieldwork, the area was being gentrified with new amenities, potentially benefiting longer-term residents. BL priorities for the area included improving ‘communications’ with residents, intergenerational working and increasing access to green spaces, and community spaces. The partnership appeared to be independent, with no LTO, resistant to engaging with other organisations and suspicious of involvement with the local council. Caution around spending the money was linked to differences around how projects should be delivered; they struggled to progress, and their attempts to do so became a source of tension. Key members left, with a reduction in representation from the ward’s most disadvantaged subarea. Another challenge for this partnership has been in hiring and managing staff, which has resulted in several members of staff staying with the partnership only briefly and a lot of effort and stress resulting from this. There has been involvement with other organisations to deliver projects; for example, youth services, art projects and collaborations for community events. The partnership has been involved in protracted negotiations to support the purchase of a community hall at risk of being sold off to private developers, and these were still ongoing in 2020.
A7 is an outer south-east London borough with good mainline train links, although it is isolated and ‘village-like’. A number of industrial units, many out of use, surround the residential homes. It is a run-down, white working-class area with a reputation for high crime and troubled families. Relationships with the council are fractious. There has been recent rapid change, with several major housing redevelopments and changes in the ethnic and socioeconomic profile. There are few shops and amenities. The priorities are community safety, community hubs and activities, green spaces, and the local economy. A partnership board, a youth forum, specific subgroups and a stakeholder board of local organisations make them well placed to deliver a wide range of projects. The partnership appears to be well functioning, with committed members. Early points of contention have escalated in more recent years. For example, a paid employee who was also a local community activist was a major strength, but they were perhaps too dominant. The LTO role being transferred to another organisation that BL had worked with in the past was a tense period for the partnership, but it was strong enough to move forward, emphasising capacity building and providing training opportunities. They have been successful with the programmes and initiatives they have directly delivered, in large part driven by the paid employee; less successful with the larger, more strategic projects, such as getting a community hub.
A8 is a former coal mining village in the north of England. There has been some regeneration, including new housing. It is perceived as isolated geographically, being surrounded by fields with motorways nearby. There are well-established social networks. The population is mainly white British. Houses in areas are somewhat dilapidated, particularly the privately rented. The area has many material assets (i.e. social clubs, community buildings) which provide social spaces for residents. The building of a new community centre (the ‘Hub’) on the site of an old cricket pavilion was a major BL project and investment. This provided opportunities for community activities and connections – for example, a youth club and more engagement between some youth and residents; increased sports, fitness and leisure classes; and a resource for elderly, isolated people in the village – but there are some tensions around the hub, with concerns that it is taking away custom from other facilities. There is increased awareness of BL work and partnership, with local environmental actions, involvement and engagement of more residents, and connection between some partnership members and the borough council. The partnership is broadly stable. Three young people (aged around 12/13) joined the partnership just before phase 3 started, supported by the youth worker. The partnership is well supported by their LTO. They contract another employee to support them.
A9 is a former coal mining area in the north of England, comprising three distinct estates separated by a dual carriageway. The population is mainly white British. There is a high street with shop fronts showing some decline. The BL partnership comprises older members. A project manager who was key to delivery through phase 1 and 2 left in 2017 and was replaced. The overarching priority is improving and making safe the local environment. The partnership has focused on one underused area on the edge of the BL boundary, but reports that progress is slow. Their attempt to improve the shop frontages was thwarted by cost and complex issues of the land and property ownership. They have successfully taken over running of the local library, which has changed to a busy space acting as a community hub, with events and employment support services. There has been some work with local agencies to deliver youth activities, including development of a local space into a skate park, completed in late 2019. It has proved difficult to keep contact with A9, and no interviews or further observations were conducted during phase 3 of our research.
A10 was selected for BL in 2011. It is a small, distinct, compact area of a small town in the south-west of England with around 8000 residents. It lies on the outskirts of the town centre, close to a large coastal town, and 20 miles south of a major city, and is considered a commuter belt. It is situated in a wider rural area, with pockets of green space and mixed housing association and private ownership. It is not considered disadvantaged by the residents or media representations. Lacking in community resources, the priorities of BL were to connect people, create more community space, support older people and young families/people and so improve health and well-being. Development of the hub was the main project. This acted as a community resource in response to their main goals and is a visible success where activities and events take place and support staff are based. The BL process has been stressful for some residents and support staff, with tensions and conflict leading to major upheaval within the partnership. Very few partnership members were residents. The partnership effectively started again in 2019–20 with a new chair, key members and support staff. There had been a lot of stress overall for the partnership members, as well as the now ex-support staff. The LTO is now also taking a more central role, acting as support and emphasising governance measures.
A11 is in London, with good transport connections to the city. It is diverse, with high levels of inequality and mixed housing, and high population density. Less than half the population is white English, while black, Asian, and ‘other white’ communities are well represented. The partnership is run through an executive with extensive experience in community organising. They have taken a system-level approach and delayed spending money while focusing on building a strategic alliance across relevant organisations to pool resources and expertise and build capacity to address common issues in the local area. Themes include: youth development, volunteers support, organisational capacity building, intergenerational connections, transitions and mental health support. The strategy aimed to connect and extend existing local community services and projects, develop new programmes, leverage funding and share the learning across London and the UK. There have been some objections around how this supported existing organisations that already had their own income streams. They employ a worker who delivers smaller community activities and events through a small community chest, funding initiatives in phase 3 such as intergenerational work and improving green spaces and social isolation. The partnership seems stable but has had a change of chair.
A12 is in an ex-coal mining area in the north-east, comprising six contiguous villages with distinct identities in a semi-rural setting. Having been a centre for shopping for a wider population, it suffered decline, but more recently the high street has been rejuvenated, with massive charitable investments outside the BL boundary having had a large economic impact. Within the partnership, small grant schemes funded projects to improve social factors, isolation and green spaces/environment. Subgroups have focused on particular priorities; for example, crime and community safety, health and well-being, intergenerational connections, employment and training, children and young people. Within the partnership there have been difficulties and disagreements about the LTO’s structure and responsibilities, and tension over the original LTO refusing to enact board requests. An apprenticeship scheme with an external organisation was halted, due to breach of contract. They continue to award grants to organisations – for example, a youth and the arts charity – to help deliver projects, and continue to make environmental changes including allotment development, litter picking, landscaping.
A13 was selected for BL in 2011. With a population of around 8500, this ward on the outskirts of a postindustrial town in the north-west is divided into seven distinct residential areas. With mixed housing, a large proportion being social, the local housing association is influential. Housing and the local environment are seen as neglected, and there is gang activity. BL priorities include: building a stronger sense of community; reducing crime and ASB; support for financial management; building pride in the environment; education and employment; local job opportunities; and helping people to live healthier lives. The partnership has experienced difficulties, reflecting community divisions, and exacerbated by board membership, some of whom are representatives/activists from key organisations in each of the main areas. Relationships have also been difficult between the partnership and the LTO and an external organisation, with conflict based around issues of power and control. There are suggestions that the board has not been supported adequately through phase 1 and 2. With changes including a new chair, new rep and new partnership structure, this has improved in phase 3. BL has made significant investments in community assets, young people and youth workers, and apprenticeships. Community clean-ups, improvements and events meant the physical environment has improved, and there are signs of increased pride within the area and an increasingly cohesive community.
A14 is a fringe estate with around 7500 residents. It is in a rural setting, four miles north of a coastal city in the south-west. Described by residents as ‘run-down’, it is very disadvantaged, with poor health indicators and high levels of deprivation. There is a small central green space, with local amenities – a café, supermarket, small shops – but very limited leisure or social facilities. It has a somewhat negative reputation in the media, with frequent reports of ASB and substance misuse. The BL priorities were to create a community hub, develop more green spaces for exercise and leisure, improve services for older and younger people, bring people together to share skills and interests, create social enterprise opportunities, build confidence and increase employment. The partnership has been fairly stable over time, although has experienced tensions and conflict within and with external agencies, but has remained a core group, employing a support worker, and working through difficulties with support. They no longer plan a community hub, as community spaces have increased over time, including a health and well-being hub.
A15 is a 1960s housing estate, built for miners, in the north of England; it joined BL in 2010. It has a mostly white British population. With the decline of mining, it became increasingly run-down, with negative news stories, drug use, and a reputation for ASB. It has poor public transport. It is set among green and brownfield sites, with motorways and visible industry close by. Prior to BL, there was some investment in the infrastructure. There is some friction between BL and the local housing association. There were low levels of resident involvement at the start of BL, and subsequent disagreements meant progress stalled, with a lack of governance around spending. A new structure was formulated, and also a new board and LTO. The residents actively involved made up the ‘board’, and the wider ‘partnership’ includes other stakeholders. BL priorities include economic and employment, social enterprise, and a more positive image for the estate. There is a crossover with another community organisation; for example, membership and some identity issues. Consequently, the board acquired their own ‘hub’. Key activities include community events and local park improvements. They are funding a youth initiative, involving asset transfer of a plot of land, that they hope to develop as a motocross track and community space. There has been good LTO support. Since phase 3 the board has decreased in size, and a significant division has developed between the LTO worker and key members of the board. Overall, there seems reasonable group rapport.
Appendix 3 Subgroup, lead and lagged analyses: work package 1
Analysis of subgroups of Annual Population Survey respondents
| Subgroup | Primary outcome: high anxiety (%) | Observations | ||
|---|---|---|---|---|
| Estimate, % | LCI/UCI, % | p-value | ||
| Socioeconomic status | ||||
| Higher managerial, administrative and professional occupations | –3.5 | –8.4/1.5 | 0.173 | 7367 |
| Intermediate occupations | –0.8 | –3.1/1.4 | 0.465 | 42,020 |
| Routine and manual occupations | –0.5 | –2.8/1.8 | 0.671 | 51,365 |
| Age group (years) | ||||
| 16–39 | –0.8 | –3.2/1.6 | 0.517 | 37,392 |
| 40–64 | –1.1 | –3.2/1 | 0.315 | 49,475 |
| 16–64a | –1 | –2.6/0.6 | 0.230 | 86,369 |
| Ethnicity | ||||
| Ethnic minority | –1.3 | –5.1/2.4 | 0.494 | 14,878 |
Analysis of subgroups of Big Local areas
| Outcome | All BL areas (N = 880 LSOAs) | > 80% spending BL areas (N = 112 LSOAs) | ||||||
|---|---|---|---|---|---|---|---|---|
| Estimate | LCI | UCI | p-value | Estimate | LCI | UCI | p-value | |
| SAMHI | –0.005 | –0.035 | 0.024 | 0.725 | –0.094 | –0.144 | –0.044 | 0.000 |
| Antidepressant prescribing | 0.019 | –0.012 | 0.049 | 0.225 | –0.032 | –0.092 | 0.029 | 0.308 |
| Mental health-related hospital admissions | –0.016 | –0.055 | 0.024 | 0.438 | 0.028 | –0.061 | 0.117 | 0.534 |
| All crimes | –0.017 | –0.051 | 0.017 | 0.321 | –0.086 | –0.174 | 0.001 | 0.052 |
| Criminal damage | –0.029 | –0.076 | 0.018 | 0.228 | –0.018 | –0.123 | 0.088 | 0.742 |
| ASB | –0.008 | –0.048 | 0.032 | 0.696 | –0.087 | –0.193 | 0.019 | 0.106 |
| Violent crimes | –0.053 | –0.098 | –0.008 | 0.021 | –0.136 | –0.228 | –0.045 | 0.003 |
| Burglary | –0.001 | –0.038 | 0.037 | 0.979 | 0.019 | –0.044 | 0.083 | 0.547 |
| Observations | 3,520 | 448 | ||||||
| Outcome | Economic (N = 694 LSOAs) | Environmental (N = 630 LSOAs) | Social (N = 694 LSOAs) | Lifestyle (N = 503 LSOAs) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Estimate | LCI/UCI | p-value | Estimate | LCI/UCI | p-value | Estimate | LCI/UCI | p-value | Estimate | LCI/UCI | p-value | |
| SAMHI | –0.024 | –0.056/0.009 | 0.151 | 0.017 | –0.018/0.052 | 0.331 | 0.011 | –0.022/0.044 | 0.52 | 0.006 | –0.034/0.046 | 0.768 |
| Antidepressant prescribing | –0.003 | –0.037/0.030 | 0.838 | 0.032 | –0.004/0.069 | 0.079 | 0.027 | –0.007/0.062 | 0.116 | 0.014 | –0.025/0.053 | 0.475 |
| Mental health-related hospital admissions | 0.003 | –0.041/0.047 | 0.900 | –0.016 | –0.061/0.03 | 0.506 | –0.011 | –0.056/0.034 | 0.646 | 0.014 | –0.039/0.068 | 0.600 |
| All crimes | –0.037 | –0.076/0.001 | 0.059 | –0.031 | –0.068/0.007 | 0.108 | –0.031 | –0.066/0.004 | 0.086 | –0.013 | –0.054/0.029 | 0.553 |
| Criminal damage | –0.018 | –0.072/0.037 | 0.523 | –0.033 | –0.092/0.025 | 0.263 | –0.036 | –0.089/0.017 | 0.178 | –0.003 | –0.066/0.059 | 0.921 |
| ASB | –0.031 | –0.077/0.015 | 0.186 | –0.02 | –0.063/0.023 | 0.353 | –0.023 | –0.065/0.018 | 0.273 | –0.004 | –0.052/0.043 | 0.858 |
| Violent crimes | –0.076 | –0.125/–0.026 | 0.003 | –0.074 | –0.129/–0.018 | 0.009 | –0.072 | –0.124/–0.02 | 0.006 | –0.062 | –0.119/–0.005 | 0.034 |
| Burglary | –0.020 | –0.060/0.020 | 0.321 | –0.011 | –0.056/0.034 | 0.62 | 0.024 | –0.017/0.065 | 0.243 | –0.025 | –0.064/0.015 | 0.227 |
| Observations | 2776 | 2520 | 2776 | 2012 | ||||||||
| Outcome | Economic (N = 379 LSOAs) | Environmental (N = 336 LSOAs) | Social (N = 405 LSOAs) | Lifestyle (N = 306 LSOAs) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Estimate | LCI/UCI | p-value | Estimate | LCI/UCI | p-value | Estimate | LCI/UCI | p-value | Estimate | LCI/UCI | p-value | |
| SAMHI | –0.049 | –0.105/0.006 | 0.083 | –0.063 | –0.124/–0.002 | 0.042 | –0.092 | –0.148/–0.037 | 0.001 | –0.029 | –0.113/0.055 | 0.496 |
| Antidepressant prescribing | –0.005 | –0.071/0.061 | 0.889 | –0.014 | –0.088/0.059 | 0.706 | –0.030 | –0.094/0.034 | 0.358 | –0.004 | –0.097/0.089 | 0.933 |
| Mental health-related hospital admissions | 0.011 | –0.081/0.104 | 0.812 | –0.003 | –0.096/0.090 | 0.949 | –0.005 | –0.101/0.09 | 0.915 | 0.136 | –0.014/0.285 | 0.076 |
| All crimes | –0.042 | –0.134/0.051 | 0.377 | –0.135 | –0.230/–0.039 | 0.006 | –0.094 | –0.183/–0.006 | 0.036 | –0.042 | –0.160/0.077 | 0.491 |
| Criminal damage | –0.008 | –0.116/0.101 | 0.889 | –0.050 | –0.160/0.060 | 0.377 | –0.088 | –0.202/0.026 | 0.131 | –0.005 | –0.127/0.116 | 0.930 |
| ASB | –0.038 | –0.150/0.074 | 0.509 | –0.128 | –0.243/–0.014 | 0.028 | –0.090 | –0.193/0.014 | 0.091 | –0.043 | –0.188/0.102 | 0.562 |
| Violent crimes | –0.108 | –0.208/–0.008 | 0.034 | –0.207 | –0.318/–0.096 | 0.000 | –0.081 | –0.183/0.021 | 0.121 | –0.033 | –0.143/0.077 | 0.554 |
| Burglary | 0.034 | –0.038/0.105 | 0.355 | –0.022 | –0.105/0.061 | 0.599 | –0.004 | –0.069/0.062 | 0.913 | –0.045 | –0.138/0.048 | 0.346 |
| Observations | 1516 | 1344 | 1620 | 1224 | ||||||||
| Outcome | 1st tercile (least deprived) | 2nd tercile (average) | 3rd tercile (most deprived) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Estimate | LCI/UCI | p-value | Estimate | LCI/UCI | p-value | Estimate | LCI/UCI | p-value | |
| SAMHI | –0.001 | –0.046/0.044 | 0.976 | –0.041 | –0.088/0.007 | 0.091 | 0.021 | –0.036/0.079 | 0.465 |
| Antidepressant prescribing | 0.003 | –0.047/0.053 | 0.908 | –0.018 | –0.069/0.033 | 0.491 | 0.024 | –0.032/0.080 | 0.401 |
| Mental health-related hospital admissions | 0.021 | –0.033/0.075 | 0.452 | –0.051 | –0.116/0.013 | 0.119 | 0.025 | –0.049/0.100 | 0.504 |
| All crimes | –0.023 | –0.060/0.014 | 0.228 | –0.010 | –0.074/0.054 | 0.757 | –0.081 | –0.143/–0.020 | 0.010 |
| Criminal damage | 0.009 | –0.050/0.068 | 0.774 | –0.017 | –0.088/0.055 | 0.645 | –0.035 | –0.132/0.062 | 0.484 |
| ASB | –0.013 | –0.056/0.030 | 0.553 | 0.000 | –0.080/0.079 | 0.991 | –0.085 | –0.154/–0.016 | 0.016 |
| Violent crimes | –0.096 | –0.169/–0.023 | 0.010 | –0.054 | –0.126/0.018 | 0.139 | –0.091 | –0.179/–0.003 | 0.042 |
| Burglary | –0.045 | –0.098/0.008 | 0.098 | –0.014 | –0.081/0.052 | 0.671 | 0.035 | –0.029/0.100 | 0.284 |
| Observations | 1104 | 1240 | 1176 | ||||||
| Outcome | 1st tercile (high proportion) | 2nd tercile (average) | 3rd tercile (low proportion) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Estimate | LCI/UCI | p-value | Estimate | LCI/UCI | p-value | Estimate | LCI/UCI | p-value | |
| SAMHI | –0.035 | –0.067/–0.003 | 0.032 | –0.011 | –0.058/0.036 | 0.651 | 0.000 | –0.039/0.038 | 0.993 |
| Antidepressant prescribing | –0.018 | –0.047/0.010 | 0.211 | –0.018 | –0.059/0.022 | 0.373 | 0.028 | –0.009/0.066 | 0.139 |
| Mental health-related hospital admissions | –0.015 | –0.072/0.043 | 0.617 | 0.012 | –0.066/0.090 | 0.765 | 0.052 | –0.017/0.120 | 0.138 |
| All crimes | –0.032 | –0.077/0.014 | 0.176 | –0.022 | –0.093/0.049 | 0.541 | 0.000 | –0.048/0.048 | 0.994 |
| Criminal damage | –0.010 | –0.079/0.060 | 0.782 | 0.017 | –0.078/0.112 | 0.728 | –0.018 | –0.101/0.065 | 0.674 |
| ASB | –0.028 | –0.084/0.029 | 0.339 | –0.020 | –0.104/0.064 | 0.644 | 0.010 | –0.045/0.064 | 0.730 |
| Violent crimes | –0.054 | –0.135/0.026 | 0.184 | –0.061 | –0.149/0.026 | 0.170 | –0.047 | –0.114/0.020 | 0.168 |
| Burglary | –0.030 | –0.129/0.068 | 0.545 | –0.033 | –0.088/0.022 | 0.237 | 0.005 | –0.015/0.025 | 0.607 |
| Observations | 1164 | 1068 | 1288 | ||||||
| Outcome | 1st tercile (low proportion) | 2nd tercile (average) | 3rd tercile (high proportion) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Estimate | LCI/UCI | p-value | Estimate | LCI/UCI | p-value | Estimate | LCI/UCI | p-value | ||
| SAMHI | 0.010 | –0.038/0.057 | 0.693 | –0.003 | –0.057/0.052 | 0.925 | –0.029 | –0.083/0.024 | 0.281 | |
| Antidepressant prescribing | 0.024 | –0.029/0.076 | 0.380 | 0.011 | –0.044/0.067 | 0.687 | –0.021 | –0.068/0.027 | 0.400 | |
| Mental health-related hospital admissions | 0.020 | –0.049/0.089 | 0.570 | 0.006 | –0.065/0.077 | 0.873 | –0.003 | –0.068/0.062 | 0.924 | |
| All crimes | –0.035 | –0.095/0.025 | 0.255 | –0.027 | –0.081/0.027 | 0.331 | –0.047 | –0.094/0.001 | 0.056 | |
| Criminal damage | –0.045 | –0.131/0.041 | 0.306 | –0.014 | –0.093/0.065 | 0.731 | –0.022 | –0.100/0.056 | 0.587 | |
| ASB | –0.034 | –0.110/0.042 | 0.382 | –0.020 | –0.082/0.042 | 0.532 | –0.043 | –0.094/0.008 | 0.099 | |
| Violent crimes | –0.004 | –0.092/0.084 | 0.927 | –0.062 | –0.138/0.014 | 0.112 | –0.076 | –0.146/–0.007 | 0.031 | |
| Burglary | –0.006 | –0.082/0.069 | 0.868 | –0.030 | –0.092/0.032 | 0.337 | –0.006 | –0.055/0.043 | 0.815 | |
| Observations | 1184 | 1156 | 1180 | |||||||
| Outcome | 1st tercile (low proportion) | 2nd tercile (average) | 3rd tercile (high proportion) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Estimate | LCI/UCI | p-value | Estimate | LCI/UCI | p-value | Estimate | LCI/UCI | p-value | |
| SAMHI | –0.027 | –0.079/0.025 | 0.310 | 0.039 | –0.016/0.093 | 0.163 | 0.002 | –0.040/0.045 | 0.918 |
| Antidepressant prescribing | 0.003 | –0.047/0.053 | 0.915 | 0.040 | –0.012/0.092 | 0.130 | 0.028 | –0.017/0.073 | 0.217 |
| Mental health-related hospital admissions | –0.046 | –0.108/0.016 | 0.143 | 0.031 | –0.047/0.109 | 0.442 | 0.012 | –0.057/0.080 | 0.736 |
| All crimes | –0.039 | –0.094/0.017 | 0.170 | –0.035 | –0.089/0.019 | 0.208 | –0.040 | –0.091/0.011 | 0.123 |
| Criminal damage | –0.034 | –0.117/0.049 | 0.426 | 0.007 | –0.081/0.096 | 0.873 | –0.021 | –0.095/0.052 | 0.572 |
| ASB | –0.029 | –0.095/0.037 | 0.387 | –0.041 | –0.105/0.023 | 0.208 | –0.041 | –0.101/0.019 | 0.182 |
| Violent crimes | –0.065 | –0.145/0.015 | 0.112 | –0.066 | –0.150/0.018 | 0.122 | –0.049 | –0.118/0.019 | 0.158 |
| Burglary | –0.046 | –0.129/0.038 | 0.282 | 0.071 | 0.016/0.126 | 0.012 | 0.025 | –0.012/0.061 | 0.186 |
| Observations | 1200 | 1076 | 1244 | ||||||
Analysis setting the intervention start date earlier or later than 2016
| Outcome | 1 year before (2015) | 2 years before (2014) | 3 years before (2013) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Estimate | LCI/UCI | p-value | Estimate | LCI/UCI | p-value | Estimate | LCI/UCI | p-value | |
| High anxiety (%) | –1.3% | –2.8%/0.2% | 0.101 | –0.8% | –2.3%/0.8% | 0.321 | –0.3% | –2%/1.4% | 0.756 |
| SAMHI | –0.017 | –0.047/0.012 | 0.250 | –0.010 | –0.041/0.021 | 0.521 | 0.013 | –0.017/0.044 | 0.398 |
| Antidepressant prescribing | –0.001 | –0.031/0.029 | 0.930 | 0.000 | –0.031/0.031 | 0.993 | 0.007 | –0.024/0.038 | 0.663 |
| Mental health-related hospital admissions | –0.010 | –0.051/0.030 | 0.617 | 0.003 | –0.040/0.046 | 0.896 | –0.035 | –0.079/0.008 | 0.111 |
| All crimes | –0.037 | –0.068/–0.006 | 0.019 | –0.024 | –0.058/0.010 | 0.165 | –0.053 | –0.088/–0.018 | 0.003 |
| Criminal damage | –0.040 | –0.089/0.008 | 0.106 | –0.035 | –0.087/0.016 | 0.180 | –0.074 | –0.128/–0.019 | 0.008 |
| ASB | –0.028 | –0.064/0.008 | 0.131 | –0.013 | –0.052/0.026 | 0.522 | –0.038 | –0.079/0.002 | 0.063 |
| Violent crimes | –0.068 | –0.114/–0.021 | 0.004 | –0.058 | –0.108/–0.009 | 0.022 | –0.076 | –0.130/–0.022 | 0.006 |
| Burglary | –0.017 | –0.052/0.018 | 0.341 | –0.028 | –0.067/0.011 | 0.153 | –0.038 | –0.079/0.004 | 0.074 |
| Observations | 3520 | 3520 | 3520 | ||||||
| Outcome | 1 year after (2017) | 2 years after (2018) | ||||||
|---|---|---|---|---|---|---|---|---|
| Estimate | LCI | UCI | p-value | Estimate | LCI | UCI | p-value | |
| High anxiety (%) | –1.3% | –2.9% | 0.4% | 0.130 | –1.7% | –3.6% | 0.2% | 0.082 |
| SAMHI | –0.016 | –0.045 | 0.013 | 0.278 | –0.002 | –0.030 | 0.027 | 0.897 |
| Antidepressant prescribing | 0.004 | –0.026 | 0.033 | 0.804 | 0.020 | –0.009 | 0.049 | 0.171 |
| Mental health-related hospital admissions | –0.018 | –0.059 | 0.024 | 0.412 | –0.019 | –0.064 | 0.026 | 0.409 |
| All crimes | –0.017 | –0.052 | 0.017 | 0.326 | –0.025 | –0.061 | 0.011 | 0.176 |
| Criminal damage | –0.053 | –0.099 | –0.007 | 0.025 | –0.049 | –0.093 | –0.004 | 0.032 |
| ASB | 0.002 | –0.041 | 0.044 | 0.931 | –0.016 | –0.058 | 0.027 | 0.467 |
| Violent crimes | –0.067 | –0.113 | –0.021 | 0.004 | –0.025 | –0.071 | 0.021 | 0.282 |
| Burglary | –0.048 | –0.103 | 0.008 | 0.094 | –0.027 | –0.069 | 0.015 | 0.208 |
| Observations | 3520 | 3520 | ||||||
Comparison between analysis using dichotomised well-being outcomes and full-scale well-being outcomes
| Outcome | Dichotomised scale (0–1) | Full scale (0–10) | ||||||
|---|---|---|---|---|---|---|---|---|
| Estimate | LCI/UCI | p-value | Outcome | Estimate | LCI/UCI | p-value | Observations | |
| High anxiety (%) | –0.8% | –2.4%/0.7% | 0.288 | Anxiety | –0.015 | –0.125/0.094 | 0.781 | 100,752 |
| Low satisfaction (%) | –0.4% | –1.9%/1.2% | 0.624 | Satisfaction | 0.010 | –0.057/0.077 | 0.767 | 100,958 |
| Low happiness (%) | 0.5% | –1.2%/2.2% | 0.538 | Happiness | –0.036 | –0.119/0.047 | 0.393 | 100,920 |
| Not worthwhile (%) | –1.3% | –2.8%/0.2% | 0.097 | Worthwhile | 0.045 | –0.021/0.112 | 0.182 | 100,531 |
Appendix 4 Impact on engaged residents, additional tables: work package 2
| Variables | Categories | Estimate | LCI | UCI | p-value |
|---|---|---|---|---|---|
| Intercept | 20.928 | 19.595 | 22.926 | < 0.0001 | |
| Time | 2020 | –0.267 | –1.103 | 0.569 | 0.092 |
| 2018 | 0.723 | –0.118 | 1.569 | 0.532 | |
| 2016 | Ref | ||||
| Age groups | ≤ 29 years | 0.214 | –0.720 | 1.148 | 0.653 |
| 30–44 years | –0.728 | –1.292 | –0.163 | 0.012 | |
| 45–64 years | –0.470 | –0.909 | –0.031 | 0.036 | |
| ≥ 65 years | Ref | ||||
| Gender | Female | –0.183 | –0.552 | 0.187 | 0.333 |
| Male | Ref | ||||
| Ethnicity | Non-white | 0.951 | 0.339 | 1.563 | 0.002 |
| White | Ref | ||||
| Highest education | No degree | 0.092 | –0.286 | 0.469 | 0.634 |
| One or more degrees | Ref | ||||
| Collectively can influence area decisions | Agree | 3.363 | 1.512 | 5.213 | < 0.001 |
| Neither | 1.397 | –0.644 | 3.437 | 0.179 | |
| Disagree | Ref | ||||
| Residents are willing to help | Agree | 1.126 | 0.585 | 1.667 | < 0.001 |
| Disagree | Ref | ||||
| Resident | Resident | –0.092 | –0.829 | 0.645 | 0.827 |
| Non-resident | Ref | ||||
| Time × resident | 2020 vs. 2016 diff | –0.456 | –1.449 | 0.537 | 0.368 |
| 2018 vs. 2016 diff | –0.594 | –1.588 | 0.400 | 0.241 | |
| Baseline difference | Ref | ||||
| Hours volunteered | 0.049 | 0.026 | 0.072 | < 0.001 |
| Female | Male | ||||||
|---|---|---|---|---|---|---|---|
| 2016 (n = 260) | 2018 (n = 671) | 2020 (n = 395) | 2016 (n = 216) | 2018 (n = 287) | 2020 (n = 254) | ||
| Intercept | 20.61 (95% CI 17.09 to 24.13) | 22.06 (95% CI 20.27 to 23.86) | 21.30 (95% CI 18.10 to 24.51) | 20.37 (95% CI 18.02 to 22.72) | 20.63 (95% CI 17.88 to 23.39) | 18.14 (95% CI 14.89 to 21.39) | |
| Education | Have degree | –0.60 (95% CI –1.63 to 0.42) | 0.03 (95% CI –0.56 to 0.63) | 0.52 (95% CI 0.26 to 1.03) | −0.33 (95% CI −1.25 to 0.60) | 0.60 (95% CI –1.50 to 0.29) | –0.26 (95% CI –1.40 to 0.87) |
| No degree | Ref | Ref | Ref | Ref | Ref | Ref | |
| People are willing to help | Agree | 2.55 (95% CI 1.01 to 4.10) | 0.93 (95% CI 0.16 to 1.71) | 0.96 (95% CI –0.27 to 2.20) | 1.12 (95% CI −0.21 to 2.45) | 0.24 (95% CI –0.49 to 1.47) | 1.42 (95% CI –0.54 to 3.38) |
| Disagree | Ref | Ref | Ref | Ref | Ref | Ref | |
| Collective control can influence area | Agree | 2.15 (95% CI –1.28 to 5.58) | 2.07 (95% CI 0.47 to 3.68) | 1.80 (95% CI –1.32 to 4.92) | 3.35 (95% CI 1.30 to 5.40) | 3.96 (95% CI 1.44 to 6.48) | 5.79 (95% CI 2.34 to 9.08) |
| Neither | –0.88 (95% CI –4.77 to 3.01) | –0.09 (95% CI –1.94 to 1.75) | 0.41 (95% CI –2.87 to 3.68) | 0.95 (95% CI –1.53 to 3.44) | 1.06 (95% CI –1.81 to 3.93) | 2.99 (95% CI –0.73 to 6.71) | |
| Disagree | Ref | Ref | Ref | Ref | Ref | ||
| No degree | Have degree | ||||||
|---|---|---|---|---|---|---|---|
| 2016 (n = 265) |
2018 (n = 368) |
2020 (n = 370) |
2016 (n = 211) |
2018 (n = 368) |
2020 (n = 266) |
||
| Intercept | 20.59 (95% CI 18.02 to 23.16) | 22.19 (95% CI 19.72 to 24.67) | 19.62 (95% CI 16.94 to 22.29) | 19.75 (95% CI 16.48 to 23.02) | 22.28 (95% CI 19.64 to 24.92) | 19.20 (95% CI 14.91 to 23.49) | |
| Gender | Female | 0.15 (95% CI –0.80 to 1.09) |
–0.86 (95% CI –1.65 to –0.08) |
–0.51 (95% CI –1.35 to 0.33) |
–0.02 (95% CI –1.02 to 0.98) |
0.07 (95% CI –0.83 to 0.98) |
0.19 (95% CI –0.80 to 1.18) |
| Male | Ref | Ref | Ref | Ref | Ref | Ref | |
| People are willing to help | Agree |
1.90
(95% CI 0.58 to 3.23) |
0.59 (95% CI –0.40 to 1.57) |
0.72 (95% CI –0.60 to 2.04) |
1.35 (95% CI –0.33 to 3.02) |
1.01 (95% CI –0.24 to 2.26) |
2.10
(95% CI 0.28 to 3.91) |
| Disagree | Ref | Ref | Ref | Ref | Ref | Ref | |
| Collective control can influence area | Agree |
2.66
(95% CI 0.24 to 5.08) |
2.56
(95% CI 0.31 to 4.81) |
4.65
(95% CI 1.92 to 7.38) |
3.41
(95% CI 0.53 to 6.28) |
1.81 (95% CI –0.54 to 4.17) |
2.59 (95% CI –1.36 to 6.54) |
| Neither | 0.11 (95% CI –2.67 to 2.90) |
0.46 (95% CI –2.09 to 3.01) |
3.08
(95% CI 0.08 to 6.08) |
0.21 (95% CI –3.36 to 2.90) |
–0.57 (95% CI –3.21 to 2.16) |
0.64 (95% CI –3.47 to 4.75) |
|
| Disagree | Ref | Ref | Ref | Ref | Ref | Ref | |
| Variables | Category | Odds ratio (CIs) |
|---|---|---|
| Time | 2020 | 0.85 (95% CI 0.46 to 1.55) |
| 2018 | 0.84 (95% CI 0.46 to 1.51) | |
| 2016 | Ref | |
| Resident | Yes | 0.66 (95% CI 0.40 to 1.09) |
| No | Ref | |
| Time × resident | 2020 (res vs. non) | 0.84 (95% CI 0.41 to 1.87) |
| 2018 (res vs. non) | 0.87 (95% CI 0.44 to 1.74) | |
| 2016 (res vs. non-res) | Ref |
| Variables | Categories | Estimate |
|---|---|---|
| Intercept | 21.10 (95% CI 18.18 to 24.02) | |
| Time | 2020 | 0.05 (95% CI –1.42 to 1.52) |
| 2018 | 1.44 (95% CI 0.13 to 2.76) | |
| 2016 | Ref | |
| Age groups | ≤ 29 years | –2.52 (95% CI –6.53 to 1.49) |
| 30–44 years | –1.43 (95% CI –2.87 to 0.01) | |
| 45–64 years | –0.91 (95% CI –1.80 to –0.01) | |
| 65 and above | Ref | |
| Gender | Female | –0.27 (95% CI –1.19 to 0.65) |
| Male | Ref | |
| Ethnicity | Non-white | 0.36 (95% CI –1.26 to 1.98) |
| White | Ref | |
| Highest education | No degree | 0.18 (95% CI –0.72 to 1.09) |
| One or more degrees | Ref | |
| Collectively can influence area decisions | Agree | 3.52 (95% CI 1.67 to 5.38) |
| Neither | 1.58 (95% CI –0.47 to 3.63) | |
| Disagree | Ref | |
| Residents are willing to help | Agree | 1.10 (95% CI 0.19 to 2.00) |
| Disagree | Ref | |
| Type of spend | High | –1.45 (95% CI –3.25 to 0.35) |
| Medium | –0.97 (95% CI –2.56 to 0.63) | |
| Low | Ref | |
| Resident | Resident | 0.90 (95% CI –0.62 to 2.42) |
| Non-resident | Ref | |
| Time × resident | 2020 vs. 2016 diff | –1.55 (95% CI –3.21 to 0.10) |
| 2018 vs. 2016 diff | –1.51 (95% CI –2.98 to –0.05) | |
| Baseline difference | Ref | |
| Hours volunteered | 0.08 (95% CI 0.03 to 0.12) |
| Variables | Categories | Estimate |
|---|---|---|
| Intercept | 20.60 (95% CI 17.49 to 23.72) | |
| Time | 2020 | 0.15 (95% CI –1.33 to 1.63) |
| 2018 | 1.50 (95% CI 0.18 to 2.82) | |
| 2016 | Ref | |
| Gender | Female | –0.14 (95% CI –1.04 to 0.77) |
| Male | Ref | |
| Ethnicity | Non-white | 0.22 (95% CI –1.37 to 1.81) |
| White | Ref | |
| Highest education | No degree | 0.20 (95% CI –0.70 to 1.09) |
| One or more degrees | Ref | |
| Collectively can influence area decisions | Agree | 3.34 (95% CI 1.49 to 5.19) |
| Neither | 1.36 (95% CI –0.69 to 3.40) | |
| Disagree | Ref | |
| Residents are willing to help | Agree | 1.10 (95% CI 0.19 to 2.00) |
| Disagree | Ref | |
| Economic intervention | Yes | –0.97 (95% CI –2.10 to 0.16) |
| No | Ref | |
| Social intervention | Yes | 0.14 (95% CI –1.10 to 1.37) |
| No | Ref | |
| Environmental intervention | Yes | 1.15 (95% CI 0.10 to 2.20) |
| No | Ref | |
| Lifestyle intervention | Yes | –0.67 (95% CI –1.62 to 0.27) |
| No | Ref | |
| Resident | Resident | 0.90 (95% CI –0.62 to 2.420 |
| Non-resident | Ref | |
| Time × resident | 2020 vs. 2016 diff | –1.67 (95% CI –3.34 to 0.00) |
| 2018 vs. 2016 diff | –1.58 (95% CI –3.05 to –0.12) | |
| Baseline difference | Ref | |
| Hours volunteered | 0.08 (95% CI 0.03 to 0.12) |
| Variables | Categories | Estimate | LCI | UCI | p-value |
|---|---|---|---|---|---|
| Intercept | 22.437 | 19.090 | 25.785 | 0.000 | |
| Time | 2020 | –0.189 | –2.458 | 2.080 | 0.870 |
| 2018 | 1.018 | –0.998 | 3.033 | 0.320 | |
| 2016 | Ref | ||||
| Age groups | ≤ 29 years | –4.875 | –9.071 | –0.679 | 0.023 |
| 30–44 years | –1.766 | –3.865 | 0.333 | 0.099 | |
| 45–64 years | –1.461 | –2.575 | –0.346 | 0.010 | |
| ≥ 65 years | Ref | ||||
| Ethnicity | Non-white | 2.045 | –0.333 | 4.423 | 0.091 |
| White | Ref | ||||
| Gender | Female | –0.034 | –1.143 | 1.075 | 0.952 |
| Male | Ref | ||||
| Willing to help each other | Agree | 0.968 | –0.158 | 2.094 | 0.091 |
| Disagree | Ref | ||||
| Collectively can influence area decisions | Neither | 0.410 | –2.261 | 3.081 | 0.762 |
| Agree | 2.772 | 0.378 | 5.166 | 0.024 | |
| Disagree | Ref | ||||
| Resident | Resident | –0.185 | –2.406 | 2.035 | 0.869 |
| Non-resident | Ref | ||||
| Time × resident | 2018 diff vs. 2016 diff | –0.990 | –3.241 | 1.262 | 0.387 |
| 2020 diff vs. 2016 diff | –1.654 | –4.221 | 0.912 | 0.205 | |
| 2016 diff (res vs. non-res) | Ref | ||||
| Hours volunteered | 0.063 | 0.011 | 0.114 | 0.017 |
| Variables | Categories | Estimate | LCI | UCI | p-value |
|---|---|---|---|---|---|
| Intercept | 19.063 | 14.962 | 23.163 | 0.000 | |
| Time | 2020 | 0.471 | –1.382 | 2.323 | 0.616 |
| 2018 | 1.990 | 0.141 | 3.840 | 0.035 | |
| 2016 | Ref | ||||
| ≤ 29 years | 8.235 | –0.409 | 16.879 | 0.062 | |
| Age groups | 30–44 years | –1.012 | –3.076 | 1.052 | 0.333 |
| 45–64 years | –0.200 | –1.648 | 1.247 | 0.784 | |
| ≥ 65 years | Ref | ||||
| Non-white | –1.508 | –3.716 | 0.701 | 0.179 | |
| Ethnicity | White | Ref | |||
| Female | –0.243 | –1.728 | 1.242 | 0.746 | |
| Gender | Male | Ref | |||
| Agree | 1.350 | –0.142 | 2.842 | 0.076 | |
| Willing to help each other | Disagree | Ref | |||
| Neither | 1.392 | –1.436 | 4.220 | 0.332 | |
| Collectively can influence area decisions | Agree | 2.713 | 0.017 | 5.410 | 0.049 |
| Disagree | Ref | ||||
| Resident | Resident | 2.289 | 0.215 | 4.363 | 0.031 |
| Non-resident | Ref | ||||
| Time × resident | 2018 diff vs. 2016 diff | –2.289 | –4.336 | –0.241 | 0.029 |
| 2020 diff vs. 2016 diff | –1.380 | –3.455 | 0.695 | 0.190 | |
| 2016 diff (res vs. non-res) | Ref | ||||
| Hours volunteered | 0.110 | 0.036 | 0.183 | 0.004 |
| Variables | Categories | Estimate | LCI | UCI | p-value |
|---|---|---|---|---|---|
| Intercept | 22.228 | 18.666 | 25.790 | < 0.001 | |
| Time | 2018 | 0.086 | –1.802 | 1.974 | 0.929 |
| 2020 | –0.659 | –2.735 | 1.416 | 0.531 | |
| 2016 | Ref | ||||
| Age groups | ≤ 29 years | N/A | |||
| 30–44 years | –1.904 | –3.722 | –0.086 | 0.040 | |
| 45–64 years | –1.567 | –2.721 | –0.413 | 0.008 | |
| ≥ 65 years | Ref | ||||
| Ethnicity | Non-white | –0.480 | –2.573 | 1.613 | 0.651 |
| White | Ref | ||||
| Highest education | No degree | 0.508 | –0.633 | 1.649 | 0.381 |
| One or more degrees | Ref | ||||
| Willing to help each other | Agree | 1.635 | 0.480 | 2.790 | 0.006 |
| Disagree | Ref | ||||
| Collectively can influence area decisions | Agree | 1.403 | –1.321 | 4.127 | 0.311 |
| Neither | 0.524 | –2.419 | 3.468 | 0.725 | |
| Disagree | Ref | ||||
| Resident | Resident | 1.003 | –1.074 | 3.079 | 0.342 |
| Non-resident | Ref | ||||
| Time × resident | 2018 diff vs. 2016 diff | –0.295 | –2.375 | 1.785 | 0.780 |
| 2020 diff vs. 2016 diff | –1.048 | –3.397 | 1.301 | 0.380 | |
| 2016 diff (res vs. non-res) | Ref | ||||
| Hours volunteered | 0.024 | –0.023 | 0.072 | 0.308 | |
| Variables | Categories | Estimate | LCI | UCI | p-value |
|---|---|---|---|---|---|
| Intercept | 17.371 | 13.541 | 21.200 | 0.000 | |
| Time | 2020 | 0.847 | –1.256 | 2.950 | 0.427 |
| 2018 | 2.412 | 0.547 | 4.277 | 0.012 | |
| 2016 | Ref | ||||
| Age groups | ≤ 29 years | –2.712 | –6.555 | 1.130 | 0.165 |
| 30–44 years | –0.863 | –3.119 | 1.393 | 0.450 | |
| 45–64 years | –0.222 | –1.459 | 1.016 | 0.723 | |
| ≥ 65 years | Ref | ||||
| Ethnicity | Non-white | 0.792 | –1.488 | 3.073 | 0.493 |
| White | Ref | ||||
| Highest education | No degree | –0.033 | –1.301 | 1.234 | 0.959 |
| One or more degrees | Ref | ||||
| Willing to help each other | Agree | 1.326 | –0.057 | 2.708 | 0.060 |
| Disagree | Ref | ||||
| Collectively can influence area decisions | Agree | 4.909 | 2.356 | 7.463 | < 0.001 |
| Neither | 2.048 | –0.812 | 4.907 | 0.159 | |
| Disagree | Ref | ||||
| Resident | Resident | 0.849 | –1.329 | 3.027 | 0.442 |
| Non-resident | Ref | ||||
| Time × resident | 2018 diff vs. 2016 diff | –2.214 | –4.319 | –0.110 | 0.039 |
| 2020 diff vs. 2016 diff | –2.263 | –4.616 | 0.090 | 0.059 | |
| 2016 diff (res vs. non-res) | Ref | ||||
| Hours volunteered | 0.198 | 0.119 | 0.276 | < 0.001 |
| Variables | Category | Odds ratio (CIs) |
|---|---|---|
| Time | 2020 | 0.53 (0.14 to 1.47) |
| 2018 | 0.63 (0.17 to 2.29) | |
| 2016 | Ref | |
| Resident | Yes | 0.37 (0.09 to 1.47) |
| No | Ref | |
| Time × resident | 2020 (res vs. non) | 1.68 (0.39 to 7.26) |
| 2018 (res vs. non) | 1.50 (0.37 to 6.04) | |
| 2016 (res vs. non) | Ref |
Appendix 5 Brief vignettes of residents’ accounts of the impact of their involvement
Resident partnership member SW2-RPM-5
I had a conflict but now there’s a lot of people stepped back and we’ve sort of empowered ourselves … going to meetings … running stuff on our own without anyone telling us how to do it. It’s incredible, it feels great. … You can definitely get burnt out … I have burnt out once or maybe twice now but at the same time it’s like it’s incredibly, I don’t know
SW2-RPM-5-P3-W1
This resident partnership member was interviewed repeatedly over several years, phases 2–3, and four waves of interviews. This is a male in his late 20s with self-reported diagnosed health conditions which impact his interaction with others. He is a resident. He is unemployed, is a relative newcomer to the area (moved here before BL) and displays great enthusiasm for equality, community empowerment, and the BL initiative and is actively working to make the area a better place to live for residents, through his role and the green projects he drives/is involved in. This involves collaborating with external organisations (school, council) which he describes as confidence and skill building to better equip him with skills. As a key and very active resident, his confidence has grown over time, and he describes his new/developing capacity to talk and liaise with professionals and learn skills as a new way of being. He is reflective of the new spaces he acts in and how he is required to, and does, change his behaviour. Part of his changing self-perception is the way he describes being perceived by others. More recently (phase 3), he has been given the opportunity to work, in a formal setting and capacity, alongside his volunteer role for BL. He describes how this gives him a sense of self and purpose, and confidence that he is perceived differently as not just a volunteer. It is this ‘through the eyes of others’, which is confidence building. He describes being empowered, changing his behaviour and learning the skills to be in formal spaces. This is through his paid role, his projects and how he develops them for community participation. There have been times when his health conditions have manifested, and he has stepped back, but these appear to have been brief. The main BL partnership support worker emphasised how there is a need to support residents who take part in BL and similar interventions, in terms of their mental health, and the need for herself and the partnership members, staff and residents to be supportive of those with mental health diagnoses or conditions, which may be exacerbated by the stresses of being a partnership member.
Resident partnership member L2-RPM-5
I’m not stressed out anymore. It was the first thing I had ever volunteered for in a community and I will not volunteer for any community activity ever again.
L2-RPM-5
A resident for 20 years and retired teacher, this member was interviewed three times between 2016 and 2020 (along with her partner). She initially described negative aspects: ‘it’s quite difficult to pin anybody down on doing anything’. Partnership dynamics had been difficult for 2 years before they started pulling together. She described personal benefits of networking and being more connected in the community (2016). By 2018, there had been more problems, and she reflected how the partnership had come through fractious times; but now, she no longer dreaded meetings: ‘There’s no chairs being hurled across the room any more … it was really horrible’. Also, volunteering was time-consuming, especially with ongoing conflicts being a constant within the partnership. She felt worried and had endured sleepless nights. She then had sciatica, hip surgery and bereavements and was left feeling low. She stepped back from BL for a few months. By 2020 she had been voted off the partnership; things had become heated. She had been shouted at in a meeting, felt threatened and communicated a sense of injustice, describing a ‘kangaroo court’. Her experience had been negative, exacerbated by a lack of support from LT. Overall, it has been ‘a nightmare …. I feel a lot better now I’m not going.’
Resident partnership member SW1-RPM-1
I suppose in the end that [the second episode of major conflict on the partnership] give me the opportunity of resigning, all this what’s blown up. So I got out. No more. Not running around after every Tom, Dick and Harry any more. I’m 71, I’m retired; I shouldn’t be belting around like that. I enjoy doing it, don’t get me wrong, I enjoy doing it a lot. It gives me something to do, kept me occupied.
SW1-RPM-11-P3-W1
Interviewed repeatedly over several years, this member is a white working-class manual worker and a resident partnership member. Retired, he lived alone and had recently moved to the area at the start of BL. He lived very close to the BL hub, where activities and meetings are held and staff are based. He was embedded in the BL structure and network in a range of ways. Over time, he expressed enthusiasm about BL and the meaning it held for him. He regularly attended meetings, volunteered alongside paid workers, met with council officials and acted in a ‘caretaker role’ for the hub building. This gave him a social network, daily life structure, community responsibility and visibility. He occupied a significant role in the partnership and among residents in the wider community, who used the hub for regular activities and events. He expressed at the interview how this was positive for his mental health and well-being, as he described it explicitly as ‘meaningful occupation’ which provided him with a network of relationships within the partnership and looser networks in the wider community. Over time, he was impacted by the tensions in and subsequent restructuring of the partnership. Although during this period he described being unhappy with these issues, which he found stressful, he remained supportive of BL and continued in his pivotal role, and the stressful episode and its impact on him subsided. When the cycle repeated itself, however, with more conflict and tension with a new group of key partnership residents and staff, he was unable to continue as a partnership member. He described the cumulative impact of the sequential tensions and conflict, which was significant enough for him to give up his valued role when on balance, the experience had become negative and outweighed the positive well-being benefits felt earlier on in the initiative. This was diluted by his tendency to still attend the hub and meetings but to distance himself from any key role.
SW1-RPM-4
Sometimes I’ve been depressed … feel a bit down and then pull myself up again. But apart from that no; I can see a future … I can see things ahead for these teenagers … They are our tomorrow.
SW1-RPM-4-P3-W1
RPM4 was interviewed three times across phases 2–3 (2016–20). She is female, resident for 52 years, 72 years old, well known and active in her subarea of BL, with a paid role in a community organisation, running its community centre which pre-dated BL. She was vice chair of BL in 2016 and chair by 2017, leaving by 2020 to focus on her community organisation role. She had intended to resign earlier due to partnership dynamics: ‘I had lost my confidence … I didn’t think I was in control …’ Partnership members were at ‘loggerheads’ and she felt ‘I just can’t hack it any more’. She also described limited teamwork and ongoing challenges with LTO workers, one of whom tried to dominate. However, she remained as chair due to partnership requests. Over time, things improved: ‘It’s going great; I am going places and I’m seeing people … teamwork is working.’ In her last interview, she described continued issues with LTO … but she would ‘not be manipulated’ and would ‘take the flak’. In her third interview, she reflected ‘I’m a fighter … if it stressed me out, I’ve still fought through it … It’s a hard job.’ But she felt it was a ‘satisfying job’ due to the differences they had made and her increased confidence.
Appendix 6 The economics of Big Local
| Annual benefits with standard deviation in life satisfaction scale = 2.00 | Total cost based on actual payments and committed funding and triple unpaid hours value | Net benefits A: annual benefits – total cost | Net benefits B: total benefits – total cost |
|
|---|---|---|---|---|
| Mean | £1,710,108 | £1,068,555 | £641,553 | £5,771,878 |
| Standard deviation | £926,464 | £236,871 | £989,764 | £3,748,365 |
| 5th percentile | £626,630 | £632,145 | –£590,511 | £1,407,068 |
| 25th percentile | £1,025,578 | £909,544 | –£105,890 | £2,964,367 |
| 50th percentile | £1,527,324 | £1,091,060 | £444,486 | £4,989,716 |
| 75th percentile | £2,123,857 | £1,226,757 | £1,181,029 | £7,579,942 |
| 95th percentile | £3,426,762 | £1,438,999 | £2,482,632 | £12,940,535 |
| Total over all 150 BL areas | £256,516,200 | £160,283,250 | £96,232,950 | £865,781,550 |
| Period ended | Total expenditure |
|---|---|
| March 2012 | £43,530 |
| March 2013 | £6,348,487 |
| March 2014 | £10,668,071 |
| March 2015 | £16,381,350 |
| March 2016 | £21,906,751 |
| March 2017 | £34,676,000 |
| March 2018 | £30,313,000 |
| March 2019 | £32,778,000 |
| March 2020 | £21,460,000 |
| Total over all years | £174,575,189 |
| Value of impact of BL on life satisfaction | Annual benefits: total over all 150 BL areas | Total cost: total over all 150 BL areas | Total net benefits A: annual benefits – total cost | Total net benefits B: total benefits – total cost |
|---|---|---|---|---|
| 0.010 | £270,017,100 | £120,927,000 | £149,090,100 | £959,141,400 |
| 0.009 | £243,015,450 | £120,927,000 | £122,088,450 | £851,134,800 |
| 0.008 | £216,013,650 | £120,927,000 | £95,086,650 | £743,127,600 |
| 0.007 | £189,012,000 | £120,927,000 | £68,085,000 | £635,121,000 |
| 0.006 | £162,010,200 | £120,927,000 | £41,083,200 | £527,113,800 |
| 0.005 | £135,008,550 | £120,927,000 | £14,081,550 | £419,107,200 |
| 0.004 | £108,006,750 | £120,927,000 | –£12,920,250 | £311,100,000 |
| 0.003 | £81,005,100 | £120,927,000 | –£39,921,900 | £203,093,400 |
| 0.002 | £54,003,300 | £120,927,000 | –£66,923,700 | £95,086,200 |
| 0.001 | £27,006,650 | £120,927,000 | –£93,925,350 | –£12,900,400 |
| Value of impact of BL on life satisfaction | Annual benefits with standard deviation in life satisfaction scale = 2.00: total over all 150 BL areas | Total cost based on actual payments and committed funding and triple unpaid hours value: total over all 150 BL areas | Total net benefits A: annual benefits – total cost | Total net benefits B: total benefits – total cost |
|---|---|---|---|---|
| 0.010 | £256,516,200 | £160,283,250 | £96,232,950 | £865,781,550 |
| 0.009 | £230,864,700 | £160,283,250 | £70,581,450 | £763,175,550 |
| 0.008 | £205,213,050 | £160,283,250 | £44,929,800 | £660,568,950 |
| 0.007 | £179,561,400 | £160,283,250 | £19,278,150 | £557,962,350 |
| 0.006 | £153,909,750 | £160,283,250 | –£6,373,500 | £455,355,750 |
| 0.005 | £128,258,100 | £160,283,250 | –£32,025,150 | £352,749,150 |
| 0.004 | £102,606,450 | £160,283,250 | –£57,676,800 | £250,142,550 |
| 0.003 | £76,954,800 | £160,283,250 | –£83,328,450 | £147,535,950 |
| 0.002 | £51,303,150 | £160,283,250 | –£108,980,100 | £44,929,350 |
| 0.001 | £25,651,500 | £160,283,250 | –£134,631,750 | –£57,677,250 |
Appendix 7 Phases 1 and 2 of the Communities in Control study: a longitudinal evaluation of the Big Local community empowerment initiative
The CiC study is a multiphase investigation of the health and social impacts arising from the BL community empowerment programme and the processes that enable and/or constrain these impacts. The first two phases of the study were funded by the NIHR SPHR. Phase 1 comprised a process evaluation and assessment of options for an outcome evaluation (2013–15; BL years 3–5). Phase 2, 2016–17 (BL years 6–7), involved the development of intervention and context typologies and assessment of short-term health and social outcomes. Phase 3 was funded by the NIHR PHRP and ran from 2018 to 2021.
During phase 1 we began to develop geographically linked data sets covering each BL area, including a limited range of variables from the census. These data sets were used to explore different ways of characterising and measuring local ‘context’. In addition, analyses of qualitative data contributed to important conceptual clarification about the effects of local context on the nature and delivery of the BL intervention. Four types of participative spaces associated with BL were identified: the partnership space, the resident space, the project space and the event space. We began to identify critical processes that can amplify or dampen the positive potential of these spaces. We identified markers of capability for, and the exercise of, collective control by BL residents: increases in connections with other organisations and evidence of attracting resources/matched funding.
Phase 1 findings also illuminated ways in which processes of inclusion and exclusion operated among different subgroups within BL populations and pointed to the potential for different approaches to participation to impact differentially on the experience of collective control among these subgroups. Finally, findings from phase 1 highlighted the diverse ways in which the money given to the BL communities under the initiative can ‘work’ as a mechanism for supporting and sustaining residents’ collective control of decisions and/or actions that can improve their neighbourhood. Negative aspects were also identified, including tensions around how the money should be used, who has entitlement and the practicalities of the day-to-day governance of the money.
Significant findings from phase 2 included: (1) confirming the most appropriate approach to conceptualise and measure local ‘context’ in BL areas using secondary data analysis; (2) piloting a national survey of health and control among BL engaged residents; (3) Identifying different types of local programmes for use in subsequent quantitative analyses; (4) construction and early testing of hypotheses relating to pathways to impact and processes in neighbourhoods that amplify and/or dampen capabilities for collective control; and (5) initial insight into the impact of BL activities on the built environment, social relationships between residents, and area reputations, including media portrayals.
More information about findings from phases 1 and 2 of the CiC study can be found on the project website (https://communitiesincontrol.uk). The CiC project page on the website of the NHR SPHR also has a number of SPHR briefings on findings from these earlier phases. (https://sphr.nihr.ac.uk/research/health-inequalities-research-programme-communities-in-control-study-overview/).
List of abbreviations
- APS
- Annual Population Survey
- ASB
- antisocial behaviour
- BL
- Big Local
- CCE
- collective control episode
- CCIS
- Collective Control Influence System
- CEN
- community empowerment network
- CiC
- Communities in Control (study)
- CIC
- community interest company
- CIO
- community interest organisation
- CVF
- community, voluntary and faith
- CVFSE
- community, voluntary, faith and social enterprise
- DiD
- difference-in-differences
- EPF
- emancipatory power framework
- GEE
- generalised estimating equation
- GP
- general practitioner
- HSE
- Health Survey of England
- IMD
- Index of Multiple Deprivation
- LSOA
- Lower Super Output Area
- LT
- Local Trust
- LTO
- locally trusted organisation
- NDC
- New Deal for Communities
- NIHR
- National Institute for Health and Care Research
- NS-SEC
- National Statistics Socioeconomic Classification
- ONS
- Office for National Statistics
- PBI
- place-based initiative
- PHRP
- Public Health Research Programme
- QALY
- quality-adjusted life-year
- SAMHI
- Small Area Mental Health Index
- SPHR
- School for Public Health Research
- SWEMWBS
- Short Warwick–Edinburgh Mental Well-being Scale
- VCFSE
- voluntary, community, faith and social enterprise
- WP
- work package