Notes
Article history
The research reported in this issue of the journal was funded by the PHR programme as award number NIHR128607. The contractual start date was in July 2020. The draft manuscript began editorial review in September 2022 and was accepted for publication in August 2023. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PHR editors and production house have tried to ensure the accuracy of the authors’ manuscript and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this article.
Permissions
Copyright statement
Copyright © 2024 Blanchard et al. This work was produced by Blanchard et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This is an Open Access publication distributed under the terms of the Creative Commons Attribution CC BY 4.0 licence, which permits unrestricted use, distribution, reproduction and adaptation in any medium and for any purpose provided that it is properly attributed. See: https://creativecommons.org/licenses/by/4.0/. For attribution the title, original author(s), the publication source – NIHR Journals Library, and the DOI of the publication must be cited.
2024 Blanchard et al.
Chapter 1 Background
Description of the problem
This study synthesises the evidence on effectiveness and cost-effectiveness of population interventions to improve diet, as well as understanding policy processes, with a view to informing the most effective responses to unhealthy diets in England. This report details the systematic review of different types (regulatory, voluntary or partnerships) of population interventions to improve diet, and examines effectiveness, cost-effectiveness, and a range of factors influencing effectiveness.
It is difficult to overstate the role that unhealthy diet plays in human ill health, made worse by a strong social gradient in access to healthy foods and in diet-related diseases. 1 Poor diet is now estimated to be responsible for more deaths than any other risk globally. 2 This is also true for England, with diet driving the major chronic diseases currently faced by the population, estimated to be the largest contributor to overall disease and to have the highest impact on the NHS budget. 3,4 Obesity continues to be one of the most challenging long-term population health problems across England, experienced by both adults and children,5,6 and felt more acutely in areas of greater deprivation. 7 Much of this is because high fat, sugar and/or salt (HFSS) foods are often inexpensive, easily accessible, highly promoted and therefore highly consumed. Most of the salt consumed by the English population is already in the foods people purchase. 8 The consumption of free sugars by adults accounts for 16–17% of their total energy intake9more than triple the 5% maximum recommended by the World Health Organization (WHO). 9,10 Intake of free sugars fails to meet the recommendations in all age groups, with unhealthy diet starting at a very young age. Children consume suboptimal fruit, vegetables and fibre and this worsens along the social gradient as with adults. 9 Poor diet during preschool years has been associated with poorer school attainment, and both dietary patterns and diet-related disease have been shown to track from childhood into adulthood. 11
It is in this context that the English government is implementing a range of population interventions to promote diets, which aim to be health-promoting, support physical well-being, and reduce diet-related non-communicable diseases (NCDs), by reducing consumption of energy-dense, nutrient-poor foods, such as free sugars, salt, saturated and trans-fats, and increasing consumption of fruit and vegetables (FV), lean protein and other nutrient-dense foods. Several of these interventions aim to improve population diet by modifying food environments. According to the Food and Agriculture Organization, the food environment refers to food availability and physical access (proximity), economic access (affordability), the promotion, advertising and information about products and health (marketing and information), as well as food quality and safety. 12
The interventions to improve food environments include voluntary reformulation programmes to reduce ingredients like sodium and sugars in foods, alongside regulatory policies, such as the Soft Drinks Industry Levy (SDIL) implemented in 2019. Indeed, population interventions to improve diet can be broadly categorised by ‘governance’ type: (1) regulatory interventions (public regulation with no involvement of private sector actors); (2) public–private partnerships (PPPs) (public and private sector organisations collaborate in the establishment of collective initiatives to improve health) and (3) voluntary approaches (whereby the private sector designs and monitors its own standards of conduct). Though all three types of interventions have demonstrated varying degrees of effectiveness and therefore potential, there are also risks and challenges to all, with studies indicating that they are not yet optimally designed and/or implemented to meet public health goals. 13,14 The authors’ earlier work indicates that a population intervention to improve diet will be most successful if underpinned by clear accountability, monitoring and evaluation processes, as well as a stated public health objective and sufficient political will to sustain it in the face of resistance. Voluntary commitments and PPPs often lack in accountability and oversight mechanisms; moreover, they often do not include the most effective interventions, or well-defined, evidence-based, quantitative targets, which push partners to go beyond ‘business as usual’ and require them to demonstrate progress against the targets, nor do they sufficiently involve the public in the development and monitoring of the interventions. 15
Thus, this evidence synthesis assesses the evidence of effectiveness of such population interventions with a view to informing more effective responses to unhealthy diet in England, and with lessons and implications for the wider world. We reviewed the different types (mandatory, voluntary or partnerships) of population interventions to improve diet, and examine implementation, effectiveness, and cost-effectiveness, and factors influencing effectiveness.
Description of the intervention
Over the past decade, the effectiveness of a range of population interventions to improve diet has been evaluated. Those with most long-term promise are those targeting upstream determinants of poor health, aiming to improve conditions and opportunities, so that the majority of the population can eat healthily. Population interventions can be driven by different types of actors and designed in various ways, ranging from regulatory interventions (where action is required by government and regulated by public authorities), to PPPs (collaborative efforts primarily between private industry and government actors but also including other actors), to voluntary approaches (which are industry-led and without involvement from the public sector). This evidence synthesis will assess the effectiveness of all three types of population interventions, and here below we look at each of these in turn.
Voluntary approaches entail actions by the private sector to create and/or enforce their own initiatives or rules, with no public involvement. Voluntary approaches have been shown to be effective when monitored by arms’ length public health bodies. However, there are also risks and challenges to voluntary agreements, with studies indicating that in their current formats, voluntary agreements to improve diet are usually based on vague commitments, focused on easy but ineffective approaches (such as information sharing), and often hampered by limited monitoring and reporting, generating poor data.
Public–private partnerships Population interventions can be neither entirely regulatory nor voluntary, but with formalised agreements entailing a degree of oversight from a public body, such as a government department of health. These arrangements are most usually referred to as PPPs, involving public and private sector organisations (to varying degrees) in the establishment of collective initiatives to improve health. A PPP in health involves collective work between at least one private for-profit organisation with at least one public (not-for-profit) organisation to jointly share efforts and benefits, with a common commitment to a health outcome. PPPs can be a promising middle option between industry-led voluntary approaches, which are argued to lack sufficient oversight, and regulatory interventions, which can be effective but politically contentious. The rationale for PPPs is that health problems and their solutions should involve all key stakeholders, and that these mechanisms may be cheaper, quicker alternatives to introducing and monitoring legislation, and may help to harness the private sector’s efficiency, cost-saving and expertise to help achieve public health nutrition goals. However, the fundamental purposes of being in PPPs may diverge significantly between the public and private sectors. For public sector partners, PPPs can be a way to supplement funding for research on diet. For private sector partners, PPPs open opportunities to promote their brand and image, and present themselves as legitimate actors in the policy-making processes. While PPPs have had some success in other fields, particularly in the field of environmental policy, some evaluations have shown limited positive impact of PPPs in diet improvement.
A regulatory intervention entails public regulation with no involvement of private actors other than as observers or contributors to consultations. It is an initiative, rule or action by government in which participation is required and there is public sector enforcement. Regulatory population interventions are considered the most effective at meeting objectives but may be politically or commercially unacceptable. Regulatory attempts to reduce consumption of harmful commodities are often met with opposition from producers and marketers of those commodities, and those stakeholders have been shown to use common strategies in resisting the introduction of such upstream regulation.
Reasons for conducting this review
To the best of our knowledge, this is the first comparison of evidence of effectiveness of voluntary, regulatory and partnership approaches to improving diet. It is also the first review that attempts to synthesise evidence to help us understand the theories that underpin these different approaches, and the implementation and monitoring issues that contribute to their impact.
In 2013, we conducted a scoping review of voluntary agreements and their success criteria. The scoping review was an important start but an incomplete exercise, in that it was not a comprehensive, systematic review, and it was not specifically focused on diet. Moreover, and crucially, it only reviewed the evidence of effectiveness of voluntary agreements. Finally, the review was published in 2013, and an update of the latest literature is now warranted. 15
As noted below in the section on the size of the literature, other reviews exist on specific intervention types (e.g. voluntary agreements), and on the effectiveness of interventions to address specific aspects of the diet (e.g. comparisons between regulatory and voluntary approaches to reducing consumption of trans-fatty acids). However, we do not know of any review examining the evidence on the effectiveness of these different intervention approaches to improving diet through the same lens.
It was essential to understand how different policy instruments are meant to work in theory or practice. This evidence synthesis will lead to subcategorisations of approaches, which cut across different governance arrangements: for example, incentive-based mechanisms can be employed in mandatory or partnership arrangements, but be quite different in their construction, that is be driven by different actors and motivated by incentives of a different nature. For example, the SDIL establishes a clearly defined incentive to act (with manufacturers needing to reduce sugar in products by a certain date, at the risk of costing them a certain amount if this is not achieved); the Responsibility Deal (RD) was also an incentive-driven mechanism yet the parameters of that incentive were far less clearly outlined. Thus, we categorise interventions first in terms of governance arrangements to enable an understanding not only of impact of effectiveness, but also the implementation and monitoring issues that contribute to their impact. We believe this to be a major added value of the review. Governance is a key overlooked mechanism in these interventions and reviews of these interventions, and it is a key part of the context, which is rarely discussed. We are confident that studies identified in the systematic review will help to throw light on whether and how governance arrangements have an impact on effectiveness, by understanding what factors relating to interventions, providers, populations and settings affect implementation of such population interventions to improve diet.
Given the range of population interventions to improve diet in England, and the urgent need to resolve the disease burden related to unhealthy diet, it is now essential to understand the effectiveness of different arrangements, levels and types of involvement of the public and/or private sector in improving diet, and what we can learn from the literature about how these could be made more effective at improving diet in England.
Research aims and questions
Aims
To search systematically for, appraise the quality of and synthesise evidence on the effectiveness, cost-effectiveness and policy process of population interventions to improve diet, including regulatory interventions, voluntary approaches and PPPs, and to share the evidence synthesis, and formulate recommendations to improve interventions, with stakeholders with a view to informing more effective responses to unhealthy diet in England.
Research questions
-
How are regulatory interventions, voluntary approaches and PPPs to improve diet assumed to work in theory?
-
What regulatory interventions, voluntary approaches and PPPs to improve diet, and reduce inequalities in diet improvement, have been evaluated?
-
What factors relating to interventions, providers, populations and settings affect implementation of such population interventions to improve diet?
-
Have such population interventions improved process, impact (intermediate and distal) and cost outcomes?
-
Are there any reported unanticipated effects of such population interventions?
-
What is the cost-effectiveness of such population interventions?
-
How can the findings of the evidence review be translated into recommendations for improved interventions?
Chapter 2 Overarching methods
This chapter describes the overarching study design and methods for the series of evidence syntheses, including approaches to the literature search, data extraction and analysis, and a description of the individual evidence syntheses.
Research design overview
This project consists of six distinct evidence syntheses (Table 1) of real-world evaluations of policies aiming to improve population diets by targeting the food environments, published between 2010 and 2020, all of which draw on a common systematic literature search strategy. They consisted of a systematic evidence map of primary research (see Chapter 3), an overview of reviews of the effectiveness of regulatory, voluntary and PPP approaches (see Chapter 4), two systematic reviews of the effectiveness of PPPs (see Chapter 5), and voluntary approaches by private actors (see Chapter 6), a systematic review of the cost-effectiveness of regulatory, voluntary and PPP approaches (see Chapter 7), and a qualitative review of policy process (see Chapter 8).
| Individual outputs | Relevance to research questions and objectives | Report chapter |
|---|---|---|
| Systematic evidence map of regulatory, voluntary and PPP approaches aiming to improve food environments. | Research question 2 Objectives: (1) To map global evidence reports on the breadth, purpose and extent of primary research evaluating the development, implementation, effectiveness and cost-effectiveness of regulatory, voluntary and PPP diet-related policies from both a policy and evaluation perspective; (2) To inform the next stages of the review. |
Chapter 3 |
| Overview of reviews on the effectiveness of regulatory, voluntary and PPP policies to improve food environments. | Research questions 3, 4, 5 Objective: (1) To assess the effectiveness of regulatory, voluntary and PPP diet-related policies; (2) To document how these policies may work (mechanisms of action). |
Chapter 4 |
| Systematic review on the effectiveness of PPPs to improve the food environments. | Research questions 4, 5 Objective: To compare the effectiveness of PPPs targeting the food environment. |
Chapter 5 |
| Systematic review on the effectiveness of voluntary approaches by commercial actors to improve food environments. | Research questions 4, 5 Objective: To compare the effectiveness of voluntary approaches by commercial actors to improve food environments between participants and non-participants, including compliance to the policy guidelines and effects on the food environment, dietary intake and health. |
Chapter 6 |
| Systematic review on the cost-effectiveness of policies to improve food environments. | Research questions 5, 6 Objectives: (1) To assess the cost-effectiveness of regulatory, voluntary and PPP diet-related policies; (2) To identify factors that make some interventions more cost-effective than others. |
Chapter 7 |
| Qualitative systematic review of policy process in regulatory, voluntary and PPP approaches to improve food environments. | Research questions 1, 3, 5 Objectives: (1) To assess factors shaping regulatory, voluntary and PPP diet-related policies, from design to implementation; (2) To advance out understanding of phenomena and mechanisms underpinning the policy process for improving diet, in particular how large food and beverage industries have become legitimate actors in policy interventions to improve diets. |
Chapter 8 |
| Discussion and conclusions. | Research question 7 Objective: To integrate the findings and propose recommendations. |
Chapter 9 |
Eligibility criteria
This series of reviews focuses on ‘real-world’ studies published between 2010 and 2020 and assessing policies promoting healthy food environments. The year of 2010 was chosen for pragmatic reasons: it allowed us to cover the most recent decade fully while limiting the number of records to deal with given the particularly wide scope of topics searched. By food environment, we refer to food availability and physical access (proximity), economic access (affordability), and the promotion, advertising and information about products and health (marketing and information) as defined by the Food and Agriculture Organization,12 with some exceptions listed in Table 2, and we did not consider food quality and safety neither as a topic nor an outcome. Policies had to target the general public, for example, those focusing on athletes, the army, workplaces and other specific groups were excluded. No restriction on language and country was applied. To be considered ‘real-world’, data had to be collected either at least once when the policy was adopted or implemented, or as part of a state or national public consultation. Experiments, simulations and projections were therefore ineligible, unless they were based on ‘real-world’ policy data. Both policies and evaluations had to be conducted at the international, national, or state level. However, assuming that the characteristics of food and drinks offered in supermarket chains or advertised on major TV channels are similar across a region or country, audits of food products, shops and TV adverts could be conducted at any level unless the evaluation specified that they focused on local independent companies or channels.
| Exclusion code | Included | Excluded |
|---|---|---|
| EX 1: Publication date | Between 2010 and 2020 | Before 2010 and after 2020 |
EX 2–3:
|
Policies that …
|
|
|
||
| EX 4: Not general population | The policies aim to improve the health of the general public, including
|
The policy only targets
|
| EX 5: Not real-life policy | Includes data collected
|
|
| Experiments, simulations and projections are included when based on ‘real-world’ policy data defined as above. |
|
|
| EX 6: Local POLICIES |
Policies implemented at the
|
|
| EX 7: Local EVALUATIONS | Evaluations conducted:
|
|
| EX 8: Not evaluation |
|
|
| EX 9: Policy mapping | Studies assessing effectiveness, cost-effectiveness, factors influencing policy development or implementation (including how a policy was covered in media), responses to public consultations. | Studies solely inventorying (‘mapping’) the presence of policies in countries or regions and/or benchmarking their implementation. |
| EX 10: Views of the general public |
|
|
| EX 11: Insufficient focus on governance |
|
Primary research and evidence syntheses of multiple policies that either have unclear governance or do not consider the governance approach in their analysis. |
| EX 12: Overviews of reviews |
|
Overview of reviews (also called umbrella reviews) and other types of evidence syntheses of literature reviews. |
| EX 13 - UK local level and views of the public |
(This was simply to group the following studies about the UK together)
|
|
| Duplicate | Documents that are not identical. | Identical documents (only keep one of them). |
In addition to primary studies, evidence syntheses other than overview of reviews (also called umbrella reviews) were included if they (1) involved a search in at least two bibliographic databases, (2) mentioned the eligibility criteria (3) clearly indicated which studies were included (e.g. in a table or with a series of references at the start of the results section or within each subsection without needing to track down each reference to recreate a full list of included studies manually). Protocols, working papers, dissertations and pre-prints were excluded. Studies and sections of studies assessing the views of the general public outside public consultations were also not considered, as well as studies solely inventorying (‘mapping’) policies or benchmarking their implementation.
Lastly, given the focus of this project on governance, primary research and evidence syntheses of multiple policies that either have unclear governance or do not consider the governance approach in their analysis were excluded. The eligibility criteria are summarised in Table 2 and detailed in Appendix 1 (see Table 24). Note that the criteria were followed in order – that is the papers had to meet criterion 1 before being assessed for criterion 2.
Search strategy
Fourteen databases were searched in November 2020: ABI/INFORM Global, Campbell Collaboration, Cochrane Library, EconLit, EMBASE, Epistemonikos, MEDLINE, PsycInfo, Science Citation Index Expanded, Social Sciences Citation Index, Arts and Humanities Citation Index, Conference Proceedings Citation Index-Science, Conference Proceedings Citation Index-Social Science and Humanities, and Emerging Sources Citation Index. Given the focus of the overarching project on policy governance approaches (i.e. whether policies are regulatory, voluntary or PPPs), the search was structured around the three following ‘blocks’ of terms using various free text and controlled vocabulary for each of them: (regulatory OR PPP OR voluntary) AND policy AND diet. Considering that some terms refer to several of these concepts at once (e.g. taxes are both a policy and generally regulatory), eight different Boolean phrases were conducted and combined at the end (see Appendix 1, Table 24). The search strategy in MEDLINE was tested on a sample of 38 publications that had been identified as potential studies in our funding application (see Appendix 1, Table 24) and was peer-reviewed by a librarian using the Peer Review of Electronic Search Strategies (PRESS) statement. Additionally, we screened the publication lists on the NOURISHING database (https://policydatabase.wcrf.org/) and the Global Food Research Program websites (www.globalfoodresearchprogram.org/); as well as the reference lists of the overviews of reviews retrieved; studies in the systematic reviews of voluntary policy commitments by private actors and of cost-effectiveness, and studies in the evidence syntheses about cost-effectiveness excluded from the overview of reviews.
Data management and screening
Records were uploaded to the Evidence for Policy and Practice Information (EPPI)-Reviewer Web (EPPI-Centre, University College London, UK) for the removal of duplicates, screening, as well as part of the data extractions for the different reviews of the series. Using the eligibility criteria outlined above, a first screening was performed for the overarching project. On top of this, additional screening was performed for each review according to their additional specific eligibility criteria. Details are specified in the methods section of each review. For the overarching project, at least 12% (n = 3346) of titles and abstracts and 33% (n = 637) of eligible full texts were screened by at least two reviewers independently (SR, LB, MJVS, CK, CL). The remaining were screened by one reviewer after reaching a 90% agreement rate. The records excluded because they were ‘not a policy’ were all checked by a second reviewer since disagreements were more common for that criterion. Disagreements were discussed with a third reviewer.
Outputs of literature search
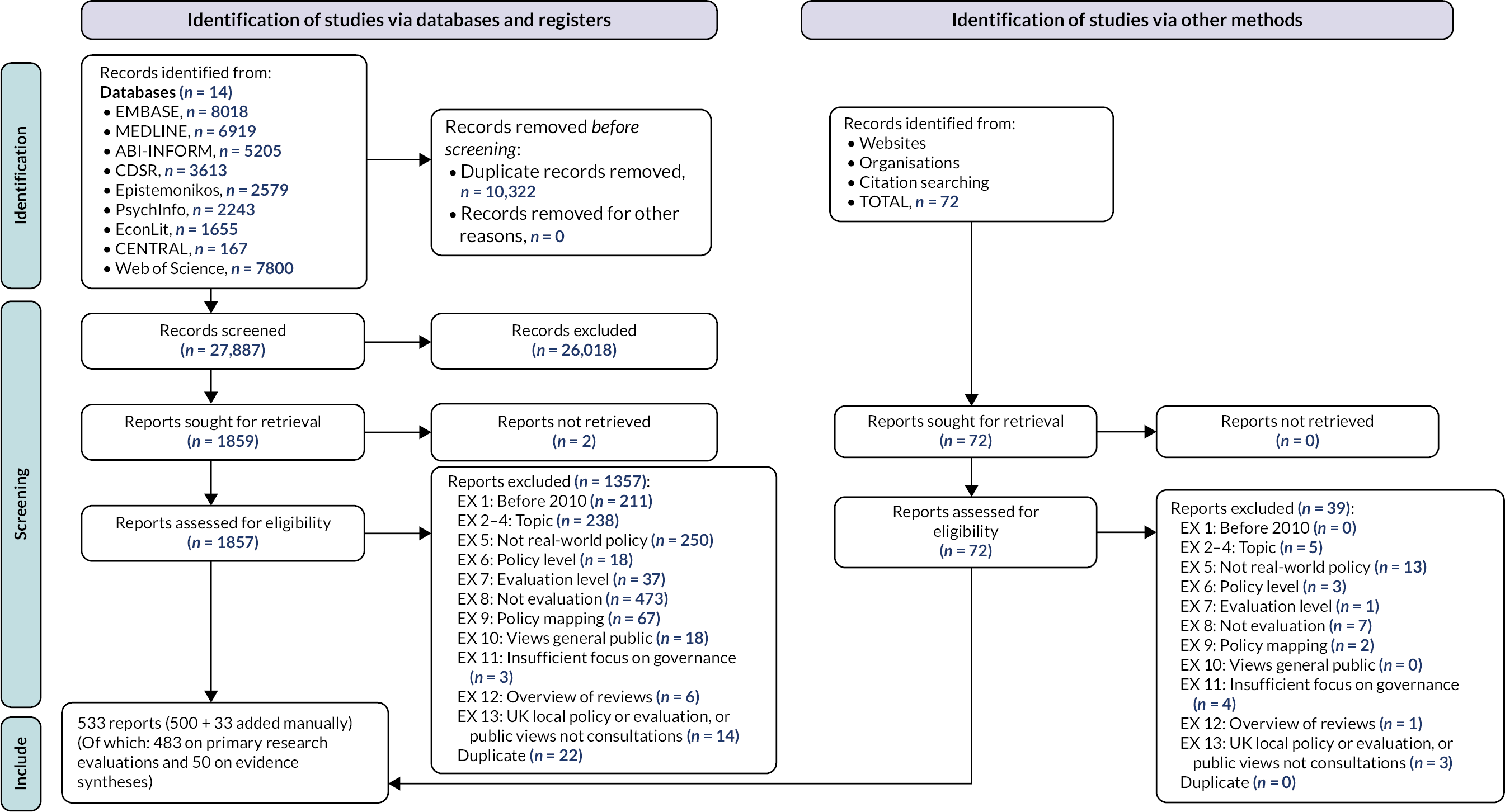
We retrieved 38,209 records from the databases; 27,887 remained after removing duplicates and had their title and abstract screened against the eligibility criteria. Of these, 1859 met the criteria and had their full text screened, resulting in 500 records being included. In parallel, 72 additional full texts were retrieved by screening websites, and reference lists. Of these, 33 met the eligibility criteria, contributing to a total of 533 publications: 483 reporting on primary research evaluations and 50 on evidence syntheses. These became the starting point of all six evidence syntheses. The detail of the selection process for the whole series of reviews is illustrated in Figure 1. The processes and results for each review according to their specific eligibility criteria are presented in the results sections of their respective chapters.
FIGURE 1.
PRISMA flow chart representing the selection process for the entire review. Included Science Citation Index Expanded, Social Sciences Citation Index, Arts and Humanities Citation Index, Conference Proceedings Citation Index-Science, Conference Proceedings Citation Index-Social Science and Humanities, and Emerging Sources Citation Index. Adapted from the PRISMA template by Page et al. (2021). 16
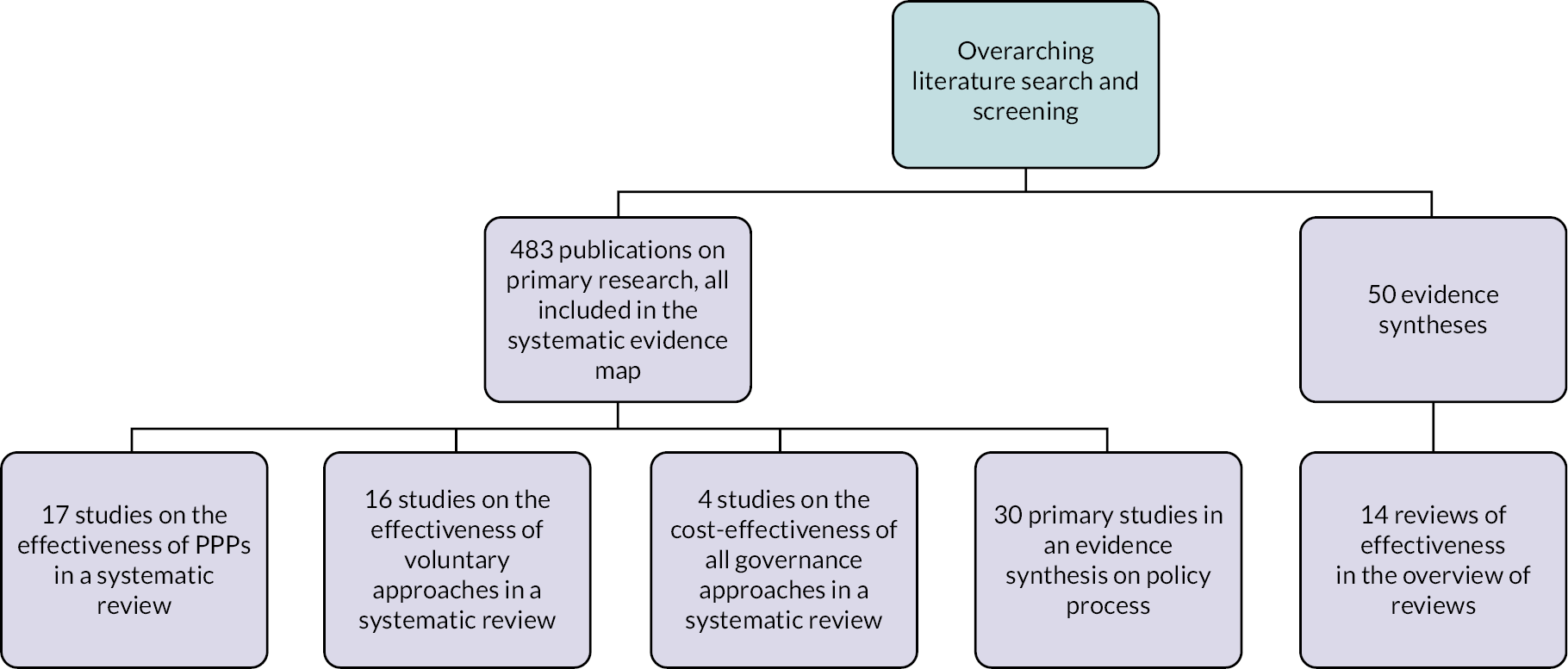
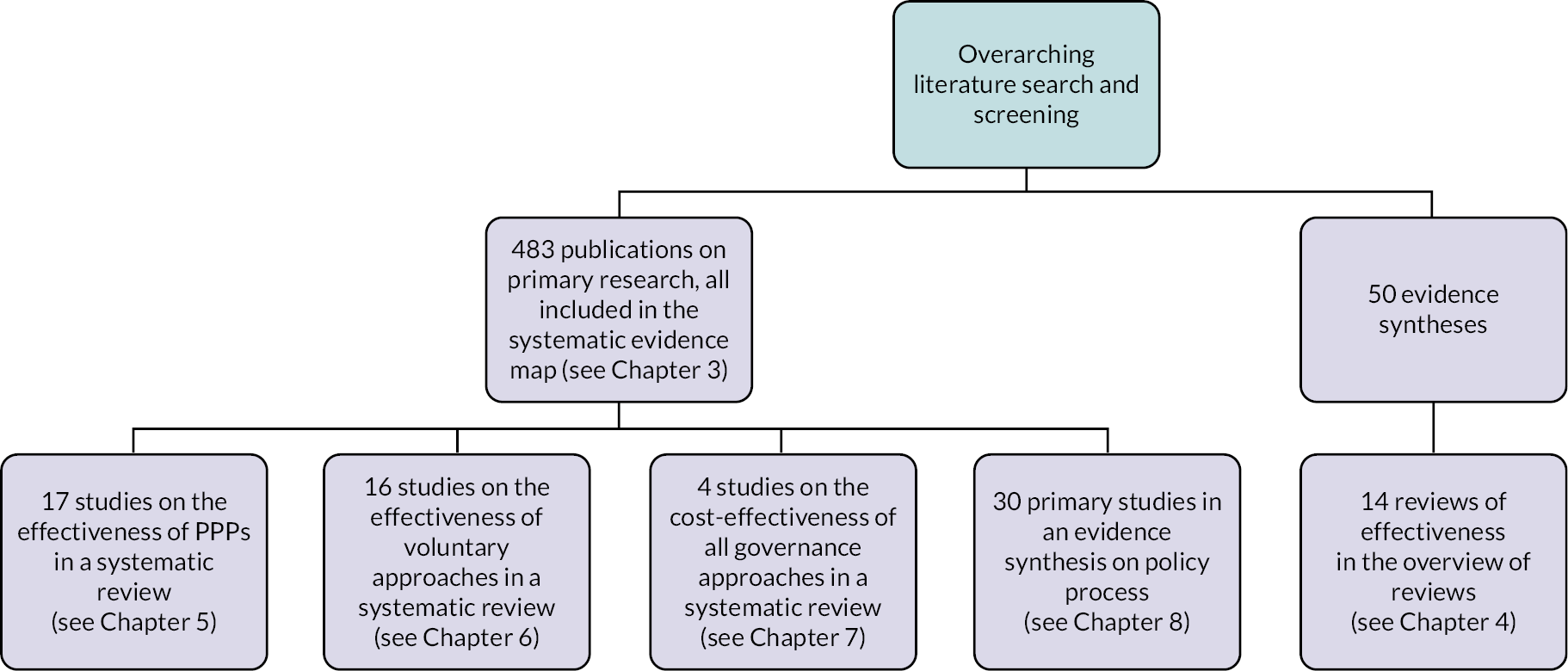
Review outputs’ relationships
Figure 2 illustrates how the different review outputs are related along with the number of studies they include. As explained in Chapter 3, for the systematic evidence map of primary research, given its size, we did link publications reporting on the same studies. Thus, numbers for this output represent publications, not studies. All publications retrieved on primary studies were included in the systematic evidence map, while further screening was applied on the evidence syntheses found for the overview of reviews. Some primary studies and evidence syntheses were also included in additional evidence syntheses specific to a governance approach (e.g. PPP) or study aim (e.g. cost-effectiveness). The systematic reviews in Chapters 5 and 6 addressed gaps in the overview of reviews (see Chapter 4). All evidence syntheses contributed to a systems map.
FIGURE 2.
Relationships between review outputs.
Data extraction
General policy and evaluation characteristics were extracted for all primary studies in the EPPI-Reviewer Web by one reviewer and checked by another (LB, SR, CL). There was one exception: the specific study designs of quantitative studies were extracted by one reviewer (LB) and 10% were checked by a second reviewer (CL), although study designs of studies included in Chapters 5–7 were all further checked by two reviewers separately. Information extraction for each specific review is detailed in their respective chapters. Information was taken at face value unless otherwise specified. A third reviewer was involved to resolve disagreements.
The general policy characteristics extracted included the countries and World Bank regions, the name of the national and international policies (for pragmatic reasons, we did not identify the name of every state policy; instead we grouped them by topic and country regardless of the states), their policy level (international, national, state), the governance approach (regulatory, voluntary, PPP; inspired by a framework by Risse and Börzel17), and policy categories by adapting the ‘NOURIS’ part (which focuses on the food environment) of the NOURISHING framework:18 N-Labelling (excluding health and nutrition claims); O-Specific settings, including schools, child care, health care and leisure; U-Economic tools (which was narrowed down to taxes and price reductions on healthy items); R-Advertising and marketing control; I-Product reformulation by manufacturers; I-Retail and food services environment (excluding those considered under ‘O’ and ‘I’). Subcategories for each policy category were created iteratively. To limit ‘policy noise’, policies had to be the focus of the evaluation, for example, the European Union (EU) pledge (an advertising control policy in the EU) was only captured when specifically evaluated; not every time an advertising control policy was assessed in an EU country. The more we coded publications on governance, the blurrier the line became between voluntary policies and PPPs, and information on the actors involved was scarce. Thus, PPPs became a subcategory of voluntary policies and was joined with two new subcategories: (1) voluntary policies by the private sector (i.e. pledges and self-regulation, in which typically private organisations design their own initiative or their own criteria within an initiative), and (2) voluntary policies by the public or not-for-profit sector. To be qualified as PPPs, policies had to be clearly identified as such or a collaboration between the public and private sectors.
Evaluation characteristics consisted of the publication date; general study aim (e.g. effectiveness, cost-effectiveness, implementation); study design including for quantitative studies the classification of natural experiments by Leatherdale (2019)19 and the presence of a comparison group enabling comparison of either policies, policies versus absence of policies, or participants/products within a policy versus non-participants (NPs)/products; the types of participants and outcomes assessed; and in some of the reviews the health equity dimensions measured as policy outcomes.
The health equity dimensions examined were those from the PROGRESS-Plus framework,20 which stands for Place, Race, Occupation, Gender, Religion and culture, Education, Socioeconomic status (SES) at the individual level, and Social capital. Age and disability were considered for the ‘Plus’. In ‘Place’, in addition to place of residence we included where shops are located. In ‘Age’, we also considered comparisons between media and menus targeting children versus adults, between households with and without children, and data presented for baby and infant products separately. In ‘Education’, we also considered comparison of school characteristics, for example middle versus high schools. Deprivation indices that encompass a range of PROGRESS-Plus dimensions were coded as SES since they generally mostly refer to the latter overall. Health equity domains were searched in each publication by checking figures and tables and searching a list of keywords. A study was considered as exploring an equity dimension when it compared a policy outcome between different groups by the said dimension.
All data extraction categories were non-mutually exclusive, that is a publication could have more than one answer, except for study design.
Study quality appraisal
All studies included in one of the four effectiveness and cost-effectiveness reviews were independently critically appraised by two reviewers (LB, SR, JB, GB, CL) using a tool according to their study design.
The quality of evidence syntheses in the overview of reviews was appraised using the checklist for systematic reviews and meta-analyses by the Scottish Intercollegiate Guidelines Network (SIGN) (see Chapter 4 and Appendix 3, Table 25, for more details).
For the systematic reviews of PPP evaluations (see Chapter 5) and of voluntary approaches (see Chapter 5), study quality was assessed using a modified version of the Newcastle–Ottawa Scale for cross-sectional studies21 (see Appendix 4, Table 26). The use of this tool represents a deviation from the protocol: it was planned to use Risk Of Bias In Non-randomised Studies of Interventions (ROBINS-I),22 but the latter was discarded after trialling it on a few studies. The main challenge was that ROBINS-I was designed for follow-up (cohort) studies of interventions that are assumed to be planned or managed by researchers to some extent. This assumption did not apply well to the policy evaluations that we had, making the questions about cointerventions, classification of interventions and deviations from intended interventions difficult to judge meaningfully. We chose instead the Newcastle–Ottawa Scale, which has been widely used and allows identification of the main weaknesses of studies in a pragmatic manner. We selected a version for cross-sectional studies to match with the study designs included in the reviews. We developed additional guidance for studies of documents and environmental features (and one question focused on vaccines), which is lacking in most tools, and for providing an overall judgement given that the original tool uses a scoring system and this is now discouraged by Cochrane. 23
Our modifications to the tool were tested in an iterative process, during which we conversed and agreed on the items and their interpretation. Like the original Newcastle–Ottawa Scale for cross-sectional studies, the final tool that we used included seven items grouped into three risk domains: (1) selection (including representativeness of sample, sample size, non-response/missing data, and ascertainment of the exposure), (2) comparability of subjects in different outcome groups on the basis of design or analysis and confounding factors controlled and (3) the assessment of the outcome and the statistical analysis. Each item was rated as having a high, moderate or low quality, or insufficient information to judge. The same categories were applied for the overall ratings. Studies that included at least one item rated ‘low’ were attributed an overall low quality. Studies attributed a moderate or unclear quality for the two key domains judged the most important – ascertainment of exposure and statistical tests – could only be rated ‘moderate’ or ‘unclear’ at best overall, respectively. Studies with more than one ‘unclear’ item were attributed an ‘unclear’ quality.
The quality of the cost-effectiveness analyses was assessed with Drummond’s 10-criteria checklist version 2015 (see Chapter 7), while the quality of the studies in the thematic synthesis (see Chapter 8) was appraised using the 10 questions for qualitative studies by the Critical Appraisal Skills Programme (CASP). 24
Data synthesis
This review in essence comprises a number of different reviews, the methods for which are described in respective chapters, and summarised here. The evidence map is descriptive (see Chapter 3), and so data were synthesised narratively using descriptive statistics, and visual maps were produced with EPPI-Mapper (EPPI-Centre, UCL, UK) and Excel. The four effectiveness and cost-effectiveness evidence syntheses (see Chapters 4–7) include quantitative findings, which, based on the initial scope (and confirmed by the subsequent review), were not suitable for statistical pooling techniques, such as meta-analysis. We synthesised findings by adapting narrative synthesis approaches in the three systematic reviews and overview of reviews of effectiveness (see Chapters 5 and 6). 25 For a graphical representation of the summary findings, in the two systematic reviews and the overview of reviews about effectiveness (see Chapters 4–6), we also used the effect direction plot developed by Thomson et al. 26 to represent graphically the summary findings. The effect direction plot displays non-standardised effects across the multiple outcome domains assessed in a review. Studies were grouped by policy and ordered by overall study quality, publication date and study design; with those considered to provide the best and most recent evidence listed first. According to Cochrane’s guidance and the revised guidance for the effect direction plot, the directions of effect are presented independently from statistical significance for domains of outcomes. 26,27 To mark an effect as being positive or negative, at least 70% of the outcomes within the category represented needed to point towards the same direction. When a study compared multiple outcomes between participants and NPs, we split them into categories following those used by the study authors; this was for both increased transparency and for avoiding results to be inconsistent because a wide range of outcomes were considered together. The p-value of each outcome domain was not calculated due to important limitations in the methodology as explained elsewhere27 (studies with conflicting or unclear effects cannot be included). Instead, we used the effect direction plot as a visual tool to present jointly the direction of effect, study quality and indirectness. As for the qualitative review (see Chapter 8), we employed a qualitative synthesis.
Issues with the Grading of Recommendations, Assessment, Development and Evaluation approach
In the three reviews assessing effectiveness (see Chapters 4–6), we had planned that the effect direction plots would have informed assessments with the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach. 28 However, the application of GRADE itself was not possible. In the overview of reviews (see Chapter 4), there were insufficient details in most of the systematic reviews to proceed. In the systematic reviews on private commitments and PPPs (see Chapters 5 and 6), the framework was judged unfit for purpose given the nature of the studies used, and this despite the modifications suggested in the protocol.
The GRADE framework helps determining the level of certainty in the evidence (rated as high, moderate, low, very low) for each outcome. Randomised controlled trials (RCTs) start at the highest certainly level (high) while observational studies start at ‘low’. Certainty in the evidence is then rated down by considering the methodological limitations of the studies (risk of bias), indirectness (applicability and how it represents the research question elements), imprecision [number of events and confidence intervals (CIs)], inconsistency (heterogeneity in results) and likelihood of publication bias. Certainty can also be rated upwards, but this is an exception. As explained in the protocol, we believe that GRADE’s hierarchy of evidence is inappropriate for policy evaluations. It does not reflect the best possible type of evidence that can realistically be obtained for a research question by considering both practical and ethical implications. Thus, in addition to RCTs, we had planned to also attribute a ‘high’ certainty to the following study designs at the start: (1) pre–post time-series analyses and (2) (potentially) cohorts/follow-up studies involving both a comparison group and data collected before and after policy implementation. Eligible comparisons included (1) comparing a policy to either another policy, the absence of a policy, or the same policy but in another location (e.g. different states or countries); (2) comparing participants in a voluntary policy to NPs; (3) comparing products or audience (e.g. TV audience) targeted by the policy to some not targeted by the policy.
However, these modifications did not address the problem. The main issues were that (1) the GRADE framework was developed for specific or narrow research questions while the review included a wide range of heterogeneous interventions and outcomes. The latter is common for policy topics since decision-makers are interested in a range of outcomes, and the policies from which we can learn can be quite different across settings and time. The assessment of publication biases and inconsistency were particularly problematic for this reason; (2) it does little to differentiate levels of certainty in evidence from observational studies. They all are rated as ‘low’ or ‘very low’, and this despite being the best sources that we can sometimes realistically obtain for some policy topics; (3) the exceptions of study designs outlined above were mostly inapplicable to the research questions of the studies included in the systematic reviews in Chapters 5 and 6. Overall, given the nature of the research questions, we could only obtain ‘low’ or ‘very low’ statements no matter what the studies did. We felt that this led to the production of statements on the certainty of evidence that appeared absolute but were in fact uninformative at best, and misleading at worst. It could send the message to decision-makers that there is no good evidence, and that they might as well consider non-evidence-based sources, such as opinions, instead.
Regarding the exceptions outlined in the protocol (i.e. to also attribute a ‘high’ certainty at the start for pre–post time-series analyses and cohorts/follow-up studies involving both a comparison group and data collected before and after policy implementation) (see Appendix 2), they were proven useless because most studies, including all those in Chapter 6, sought to investigate whether a policy had led to improvements in the nutrient content, advertising content or labelling practices. These are outcomes of interest for policies aiming to improve food environments. However, these studies tend to be repeat cross-sectional, not cohort/follow-up studies. They compare the offer of products or adverts available at one point in time to that at another point in time. In this case, examining different products and adverts through time does not represent a methodological weakness. There were also a few document analyses investigating whether a policy was doing what it pretended or was on track. There is currently no guidance for the latter. To avoid producing statements of certainty of evidence that risk misleading decision-makers, a wider discussion about GRADE for policy evaluations in the systematic review community is needed.
Chapter 3 Systematic evidence map of regulatory, voluntary and public–private partnership policies to improve food environments and population diet
Introduction
This chapter reports the systematic evidence map of the included literature, which exposes regional differences in existing across geographical regions, as well as by equity dimension and governance approach.
Evidence map methods
What is a systematic evidence map?
Systematic evidence maps, also known as evidence gap maps, are a type of evidence synthesis and research translation tool that visually presents the breadth of research available on an area using a systematic approach. While they are generally used to produce high-level descriptions and identify gaps in evidence, we believe that they can also be employed from a critical perspective to question practices both in research and in the field. 29 In the present case, examining the characteristics of both the policies that have been evaluated, and of the evaluations themselves, can shed light on the body of evidence that countries have at their disposal to make decisions about policy design and effectiveness. Thus, this systematic map of global evidence reports on the breadth, purpose and extent of primary research evaluating the development, implementation, effectiveness and cost-effectiveness of regulatory, voluntary and PPP diet-related policies from both a policy and evaluation perspective.
Methods overview
This systematic evidence map used the literature search, eligibility criteria, screening and data extraction strategies detailed in Chapter 2. As a reminder, the data extracted consisted of (1) general policy characteristics, including countries and World Bank regions, policy names, policy levels, governance approaches and policy categories by adapting the ‘NOURIS’ part of the NOURISHING framework:18 N-Labelling, O-Specific settings including schools, child care, health care and leisure, U-Economic tools (narrowed down to taxes and price reductions on healthy items), R-Advertising and marketing control, I-Product reformulation by manufacturers, I-Retail and food services environment; (2) evaluation characteristics, including publication date; general study aim, study design; and for studies assessing policy effectiveness, the types of participants and outcomes assessed and health equity dimensions measured using a generous interpretation of the PROGRESS-Plus framework,20 which stands for Place, Race, Occupation, Gender, Religion and culture, Education, SES at the individual level, and Social capital as well as Age and Disability for the ‘Plus’. A study was considered as exploring an equity dimension when it compared a policy outcome between different groups by the said dimension.
Data were synthesised narratively using descriptive statistics based on the data extraction categories. Visual maps were produced with EPPI-Mapper (EPPI-Centre, UCL, UK) and Excel.
Findings
Included and excluded studies
In addition to the 483 publications reporting on primary studies, the 15 excluded full texts reporting on UK local policies and/or evaluations (see Report Supplementary Material 1, Table S1) (which were part of the 15 UK publications excluded because they were either about the local level or views or the public at the state or national level) were set aside for further analyses. The characteristics of the 483 included publications are described in Report Supplementary Material 2, while those on the local evaluations in the UK and on the excluded publications are listed in Report Supplementary Material 1 (see Table S2). In accordance with Cochrane’s guidance,30 only the characteristics of the full texts excluded for the least apparent reasons are listed, that is because of their policy level (EX 6), evaluation level (EX 7), policy mapping (EX 9), views of the general public (EX 10), evidence synthesis not considering governance (EX 11), UK local policy or evaluation, or public views not consultations, or full texts not obtained (n = 172).
Given the size of this evidence synthesis, we did not attempt at this stage nor for the systematic evidence map of primary research to link publications reporting on the same studies. Thus, the number of ‘includes’ are publications, not studies.
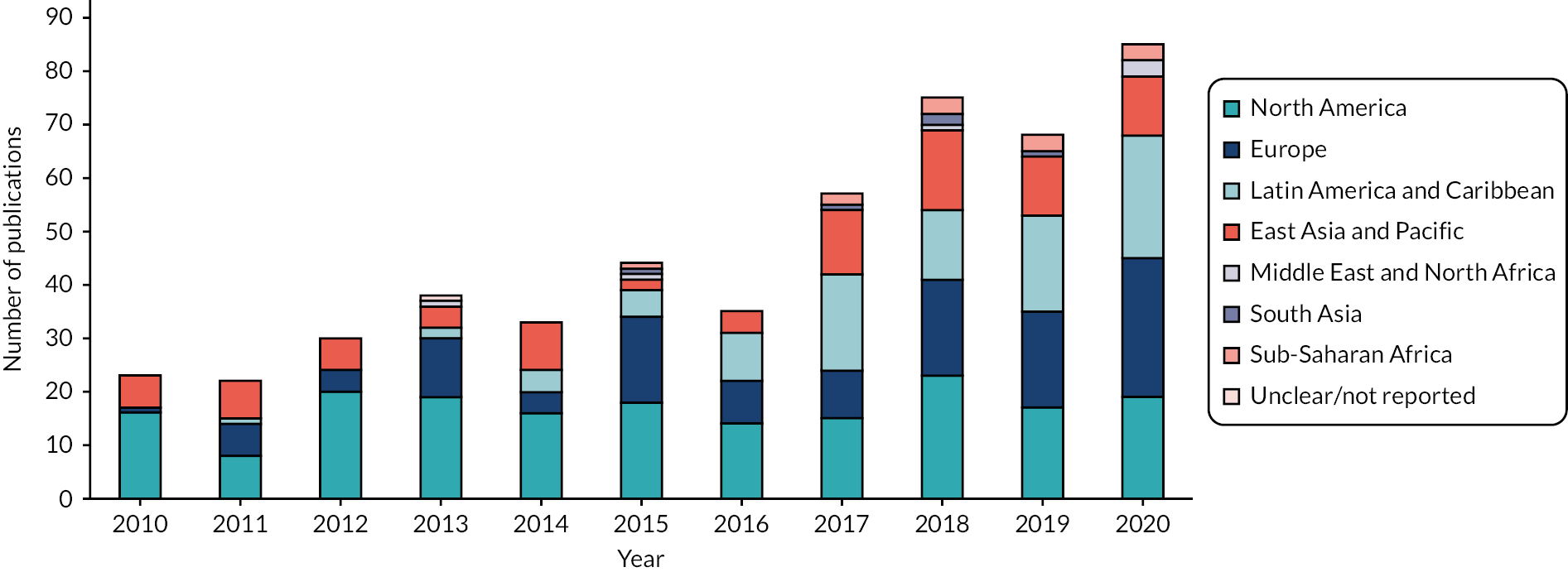
Regional differences across publications
Overall, 70 countries were documented. As shown in Figure 3, there were apparent inequalities in coverage between countries and world regions. The number of evaluations published each year on eligible real-world policies has nearly quadrupled over 11 years, ranging from 23 in 2010 to 85 in 2020 (Figure 4). Studies examining North American countries (38% of publications overall) dominated throughout the period except in 2017 and 2020. The increase in publications worldwide was mainly driven by the World Bank regions of Europe and Central Asia, and of Latin American and the Caribbean (25% and 19% of total publications, respectively), although no Central Asian country was documented and only three studies assessed the Caribbean. East Asia and the Pacific were covered in 18% of total publications. Regarding countries, 30% (n = 146) of publications included the USA, 11% (n = 54) the UK, 11% (n = 51) Australia, 8% (n = 41) Canada, 8% (n = 40) Mexico, 5% (n = 25) Brazil, 4% (n = 19) Chile, 3% (n = 14) France and Spain each, 3% (n = 13) Denmark, and 2% New Zealand and South Africa each (n = 12 and n = 11, respectively). Eighty-one per cent (n = 390) of publications considered these 12 countries alone (without any other country). By contrast, 32 countries were included in only 1 or 2 publications each. While some of these were high-income countries, disparities with and within the least-documented world regions was startling: 12 publications were found about Sub-Saharan Africa (all but 1 about South Africa), 6 about the Middle East and North Africa (4 of which about Saudi Arabia), and 5 about South Asia (all about India). Given that some of these evaluations included multiple countries, the level of details available for some of these countries was particularly limited. One publication had unclear countries and world regions because it assessed companies’ stock markets. 31 Nearly all publications were in English (n = 417), nine were in Spanish, two in Portuguese and one in French.
FIGURE 3.
Number of publications by World Bank world region (n = 482 because it is unclear in one publication). Note: the same publication can include more than one world region (non-mutually exclusive categories).

FIGURE 4.
Number of publications by world region and year (n = 483). Note: since the same publication can include more than one world region (non-mutually exclusive categories), this graph does not reflect the actual total number of publications per year.
Characteristics of policies assessed
The policies examined included 236 national policies (assessed in 73% of publications), 26 groups of state policies (assessed in 26% of publications) and 9 international policies (assessed in 6% of publications). One policy had both a national and a state component. All state policies were implemented in dominant countries (Australia, Brazil, Canada, Spain, the UK and the USA). The five most assessed policies consisted of American state school food standards (n = 37), the Children’s Food and Beverage Advertising Initiative (CFBAI; a national voluntary self-regulation advertising industry code in the USA, n = 21), the Mexican tax on sugar-sweetened beverages (SSBs) (national, n = 19), the UK SDIL (national, n = 14), and various American state SSB taxes (n = 14). Together, these three taxes represented 54% of publications about economic interventions (see below). The three most examined international policies were the Australasian Health Star Rating (HSR) (Australia and New Zealand, n = 11), the EU Pledge (n = 5) and the WHO Code of marketing breastmilk substitutes (n = 5).
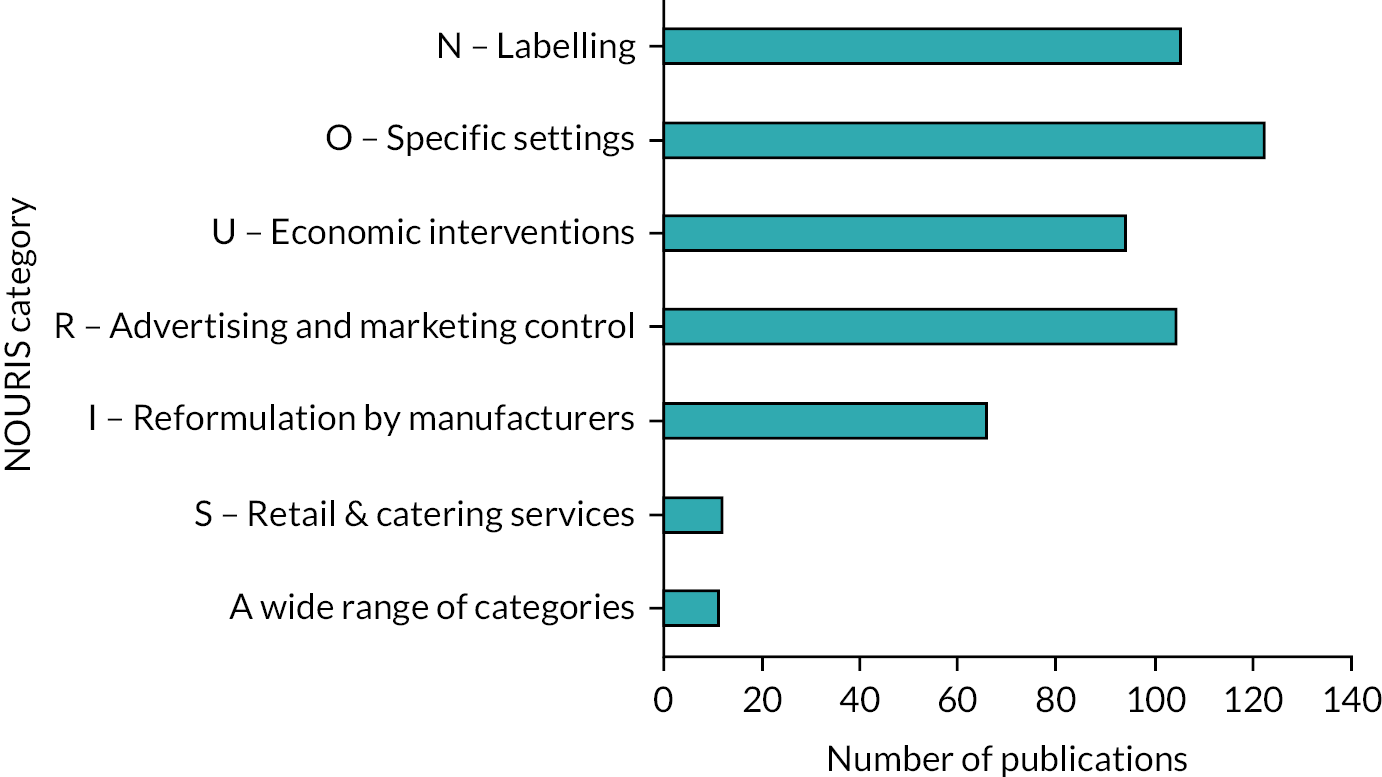
Using the six ‘NOURIS’ categories, as shown in Figure 5, the most assessed policy categories were those specific to school, child care, health care and leisure settings (O, n = 122, 76% of which on schools), followed by labelling [N, n = 105, 39% of which about front-of-packs (FOPs)], advertising and marketing control (R, n = 104, 55% of which about television alone) and economic interventions (U, n = 94, 86% of which about SSB taxes). Evaluations of product reformulation by manufacturers were much less common (I, n = 66, 61% of which about salt) as well as those on the retail and catering sectors (S, n = 12, 83% of which at least aimed to increase the availability of healthy options). Eleven assessed policies that covered a wide range of NOURIS domains (these were grouped separately).
FIGURE 5.
Number of publications by NOURIS category (n = 483). Note: a publication can include more than one policy category (non-mutually exclusive).
Governance arrangements assessed
Sixty per cent (60%, n = 288) of publications reported on at least one regulatory initiative, 43% (n = 209) on at least one voluntary action, and 16 assessed mixed governance policies (e.g. the combined use of regulatory labelling and voluntary limits for trans-fats in Canada) (Figure 6). Evaluations of voluntary policies mainly consisted of those led by the private sector (self-regulation and pledges, n = 97) and actions by the public or not-for-profit sector (n = 90), while a minority has investigated PPPs (n = 31). Most publications on PPPs were about the RD in England, UK (n = 12) or the Australian Food and Health Dialogue (FHD) and/or its updated version, the Healthy Food Partnership (n = 10).
FIGURE 6.
Number of publications by governance mechanism (n = 483). Note: a publication can include more than one governance approach (non-mutually exclusive categories).
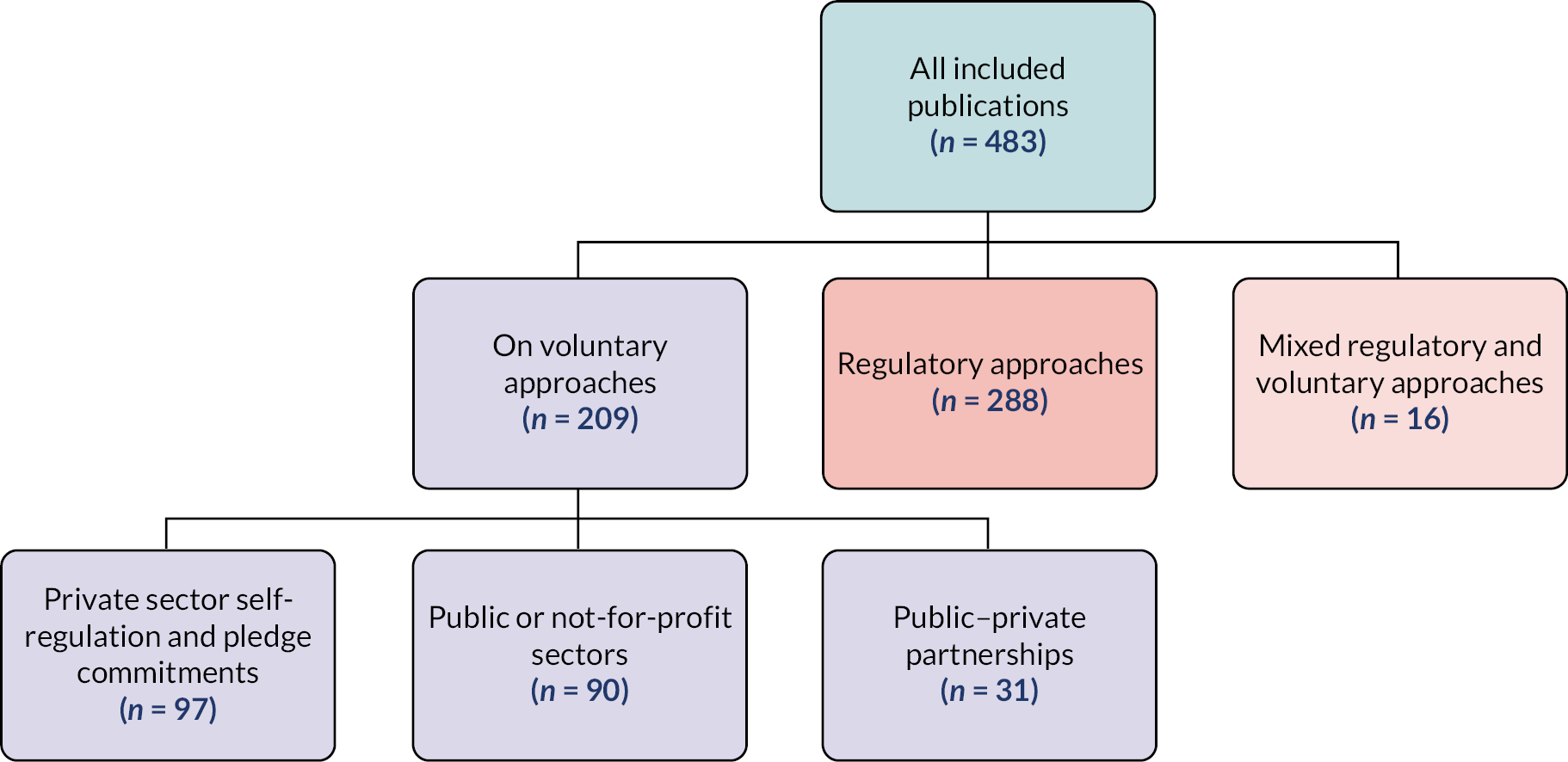
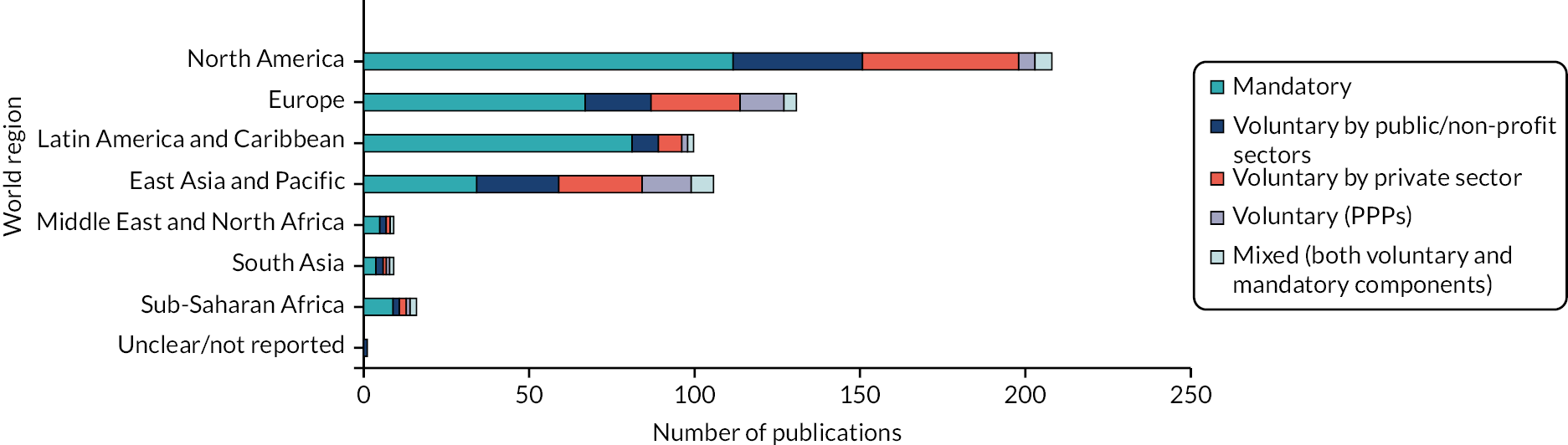
Figure 7 shows the distribution of publication by governance approach and world region. Regulatory approaches represent the majority of publications in all World Bank regions, ranging from 39% in East Asia and the Pacific to 87% in Latin America and Caribbean. East Asia and the Pacific is the region where governance approaches have been assessed the most evenly. Voluntary actions by the private sector were the second most assessed approach in North America and Europe, voluntary actions by the public and not-for-profit sectors were second in Latin America and Caribbean, the Middle-East and North Africa, and South Asia, and the two voluntary categories were equal in East Asia and Pacific and Sub-Saharan Africa, although the sample size in some regions is too small to draw conclusions. As highlighted previously, most PPP evaluations were conducted in Europe (especially the UK) and East Asia and Pacific (especially Australia). There were few evaluations of mixed approaches across all world regions.
FIGURE 7.
Number of publications by world region and governance approach (n = 483). Note: a publication can include more than world region and governance approach (non-mutually exclusive categories).
When combining information on governance approach, world region and policy category together, evaluations about labelling (N) were mainly about regulatory initiatives in North America (especially menu labelling) and Latin America [especially front-of-pack labelling (FOPL)], followed by the voluntary FOP HSR in Australia and New Zealand. Most publications on specific settings (O) evaluated regulatory interventions in schools in North America, then in Europe. Evaluations of economic interventions (U) were mostly concentrated in Latin America, Europe, and the USA, most of which were regulatory since they were taxes. Publications on advertising and marketing control (R) were mainly in North America, followed by East Asia and Pacific and Europe, and were predominantly voluntary actions by the private sector in all three regions. In fact, 53% of evaluations of voluntary approaches by the private sector in this policy category consisted of the CFBAI in the USA; the CFBAI in Canada; the Publicidad, Actividad, Obesidad, Salud code in Spain; and both the Australian Responsible Children’s Marketing and Australian Quick Service Restaurant Industry’s Initiatives (QSRI). Evaluations of product reformulation (I) were about equally distributed across governance approaches in the four dominant world regions, with slightly more PPP evaluations in East Asia and Pacific. The few evaluations of policies targeting the retail and catering sectors or using a wide range of policy categories were only in North America, East Asia and Pacific and Europe, with various distributions of governance approaches. We formulated the hypothesis that evaluations of the least assessed world regions and countries focused on back-of-pack labelling, assuming that it might be the most frequently implemented policy given its simplicity and neutrality. This was not the case: the 18 evaluations covering Africa, the Middle East and South Asia documented a variety of policy areas, which were mainly regulatory (including five on SSB taxes). Similar conclusions were made for the 24 publications that included the 32 least evaluated countries (countries assessed once or twice, in any world region).
We explored whether similar trends applied for local policies and/or evaluations using the 15 publications that were excluded because they were about the local level in the UK. One focused on Scotland, another on Wales, and the rest on England. Together, they examined nine different policies in only two categories: specific settings (O, n = 8; six regulatory about schools, two voluntary by the public sector in hospitals) and the retail and catering sector (S, n = 7; three regulatory, two voluntary by the public sector, two voluntary by the private sector). The number is substantial given that only 12 publications were identified for that category in the whole evidence map. This potentially reflects the greater capacity to implement such initiatives at the local level, whereas other policies such as taxes and TV advertising control are easier to establish at a higher level. The local regulatory initiatives in the retail and catering sectors included planning regulations within the healthy weight strategy and takeaway planning restrictions. The voluntary approaches by the private sector consisted of the Change 4 Life programme, the Healthy Catering Commitment in London, and self-regulated checkout policies by some supermarket chains.
Study aims, participants and outcomes assessed
The vast majority of evaluations (n = 389, 81%) assessed the effectiveness of a policy, followed by factors affecting their implementation (n = 67, 14%), factors influencing their development (n = 34, 7%), how a policy was portrayed in the news (n = 11, 2%), responses to public consultations (n = 10, 2%) and cost-effectiveness analyses (n = 4, 1%). The remaining study investigated whether the New Zealand Advertising Standards Authority self-regulation code protects child rights. Only the fifth (n = 25) of the 119 evaluations assessing other aspects than effectiveness covered other countries than the 12 dominant countries (i.e. USA, UK, Australia, Canada, Mexico, Brazil, Chile, France, Spain, Denmark, New Zealand and South Africa). Given that these types of studies aim generally to employ qualitative or mixed methods, unsurprisingly, the latter study designs were also mostly employed in these countries (as well as Fiji). Figure 8 shows the number of publications by governance approach and study aim category. PPPs were those that were the most assessed holistically with 32% of publications assessing factors influencing implementation and 16% assessing policy development. They were followed by regulatory policies (12% on implementation, 9% on development, and representing most studies on media coverage and public consultations). By contrast, policies led by private actors (mainly self-regulations and pledges) were particularly underevaluated on these aspects with only 7% of publications on implementation and one evaluation of policy development.
FIGURE 8.
Number of publications by study aim category and governance approach (n = 483). Note: a publication can include more than one study aim and governance approach (non-mutually exclusive categories). Dark green: ≥ 100 publications; pale green: 75–99; yellow: 50–74; red: 25–49; white: < 5.

Studies assessing effectiveness focused on a wide range of ‘participants’ or samples: out of 389 publications, 43% (n = 166) relied on data collected data via humans only, 57% did not involve humans at all (i.e. they collected data directly on the environment, in the news or documents, n = 182), and 11% (n = 41) involved both. Consequently, the type of outcomes evaluated also varied. Nine per cent (n = 35) have investigated health-related outcomes [e.g. mortality, diseases, disability-adjusted life-years (DALYs), nutritional status and anthropometric]; these were nearly all conducted in the USA, followed to a smaller extent by Denmark (n = 4) and Portugal (n = 3). The other types of outcomes considered included human behaviours (e.g. dietary intake, sales, purchases, advertising viewing and use of labels; 35%, n = 137), environment features (66%, n = 256), policy characteristics or implementation status (6%, n = 22) and other outcomes (2%, n = 9). All policy categories mainly assessed environment features except for U-Economic interventions, which mostly examined human behaviours.
Study designs employed
As explained in Chapter 2, study design was documented for all primary studies. The design of 67% (n = 254) of quantitative studies was further extracted using the classification of natural experiments by Leatherdale19 as well as presence of a comparison group enabling comparison of either policies, policies versus absence of policies, or participants/products within a policy versus NPs/products.
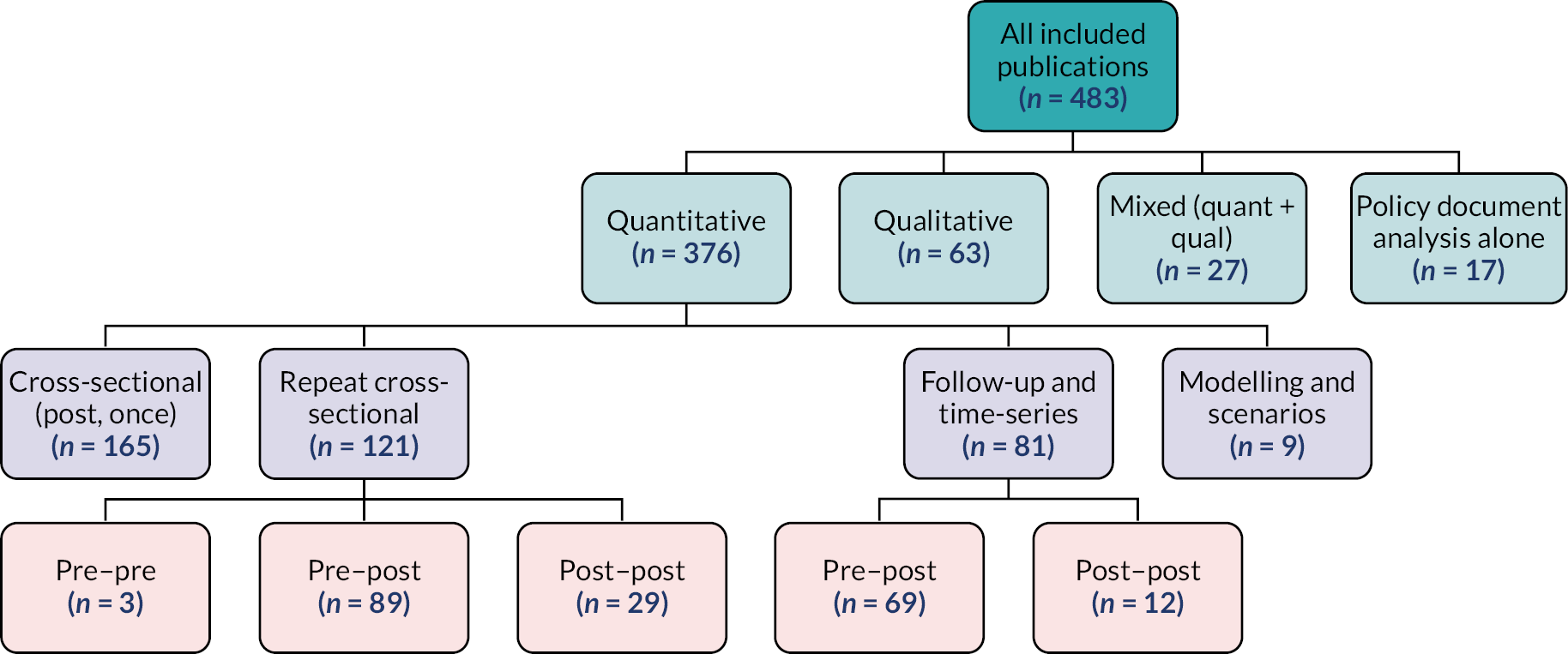
As described in Figure 9 and more detailed in Table 3, 78% (n = 376) of publications employed a quantitative design, 13% (n = 63) a qualitative method and a minority either used both (mixed methods; 6%, n = 27) or analysed policy documents alone (4%, n = 17). Among quantitative studies, most were single post cross-sectional studies (one data collection, 44%, n = 165), followed by repeat cross-sectional studies (32%, n = 121), follow-up and time series (22%, n = 81), and modelling studies and scenarios (n = 9). Note that the label ‘follow-up studies’ was only applied to human participants because non-human ‘participants’, such as products and adverts, are generally not the same through time. Pre–post studies (n = 160) were more common than post–post (n = 41). Three studies focused on the implementation phase alone (i.e. before the official policy implementation date).
FIGURE 9.
Publications by study design (n = 483). Note: a publication can only include one study design (mutually exclusive category).
| Study design | N (%) for the whole map | N (%) for publications only covering the 12 dominating countries (out of n = 390) |
N (%) for publications only covering the USA (out of n = 141) |
N (%) for publications covering other countries than the 12 (out of n = 93) |
|||||
|---|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | N | % | ||
| Quantitative (all) | 376 | 78 | 310 | 79 | 121 | 86 | 66 | 71 | |
| Follow-up studies and time series | (All) | 81 | 17 | 68 | 17 | 22 | 16 | 13 | 14 |
| Pre–post | 69 | 14 | 58 | 15 | 13 | 9 | 11 | 12 | |
| Post–post | 12 | 3 | 10 | 3 | 9 | 6 | 2 | 2 | |
| Repeat cross-sectional | (All) | 121 | 25 | 101 | 26 | 41 | 29 | 20 | 22 |
| Pre–pre | 3 | 1 | 3 | 1 | 1 | 1 | 0 | 0 | |
| Pre–post | 89 | 18 | 74 | 19 | 30 | 21 | 15 | 16 | |
| Post–post | 29 | 6 | 24 | 6 | 10 | 7 | 5 | 5 | |
| Cross-sectional, post, once | 165 | 34 | 134 | 34 | 58 | 41 | 31 | 33 | |
| Modelling and scenarios | 9 | 2 | 7 | 2 | 0 | 0 | 2 | 2 | |
| Qualitative | 63 | 13 | 44 | 11 | 13 | 9 | 19 | 20 | |
| Mixed methods (quantitative and qualitative) | 27 | 6 | 21 | 5 | 4 | 3 | 6 | 6 | |
| Policy document analyses | 17 | 4 | 15 | 4 | 3 | 2 | 2 | 2 | |
| Total | 483 | 100 | 390 | 100 | 141 | 100 | 93 | 100 | |
Table 3 shows the number of publications by study design for the whole map (n = 483), for the publications only focusing on the 12 dominant countries (n = 390, 81% of the map), those focusing only on the USA (n = 141, 29% of the map) and those including other countries than the 12 (n = 93, 19% of the map). According to Leatherdale, the most robust natural experiments are those that include a control (or comparison) group, a pre–post design, as well as time series and follow-up studies. 19 The most used study designs in publications covering only the 12 dominating countries were single cross-sectional studies (34%), followed by repeat cross-sectional studies (26%) and follow-up studies and time series (17%). The same trend was observed for publications on the USA alone, although with a higher proportion of single cross-sectional studies in the American studies (41%). Publications on other countries also had a majority of cross-sectional studies (33% single, 22% repeat) but these were followed by qualitative studies (20%) and then follow-up studies and time series (14%). Quantitative studies in all three categories of publications all tended to use more pre–post designs than post–post. However, nearly all policy analyses, mixed-methods studies, modelling studies and scenarios were about the 12 dominating countries alone. Regarding the use of comparison groups, we documented the number of publications reporting on a quantitative study comparing two policies (or more), a policy versus none, or participants or products targeted by a policy versus some not targeted. Overall for the whole map, 57% of quantitative studies involved such a comparison compared with 60% for the 12 dominating countries alone, 66% for the USA alone and 44% for other countries. Thus, except for pre-post designs, publications focusing only on the 12 dominating countries tend to employ more frequently the most robust quantitative designs or features (i.e. follow-up studies and time series, and comparison groups) compared with publications covering other countries, as well as policy document analyses. However, a smaller proportion of their publications employ qualitative methods. The majority of the publications covering the least documented world regions (i.e. Africa, the Middle East and South Asia) were single cross-sectional or qualitative, although the latter were mainly about South Africa.
Regarding the use of quantitative study design by governance approach, 81% of follow-up studies and time-series analyses, and seven of the nine modelling studies assessed regulatory policies. Very few follow-up studies and time series investigated voluntary policies by the public/not-for-profit or private sectors (7% and 11%, respectively). PPPs were mostly assessed with pre–post cross-sectional studies (n = 6). By policy category, most follow-up studies and time-series analyses, and most modelling studies were employed to evaluate economic interventions. Since these were mainly taxes, it explains why these study designs primarily focused on regulatory interventions.
Health equity as a policy outcome
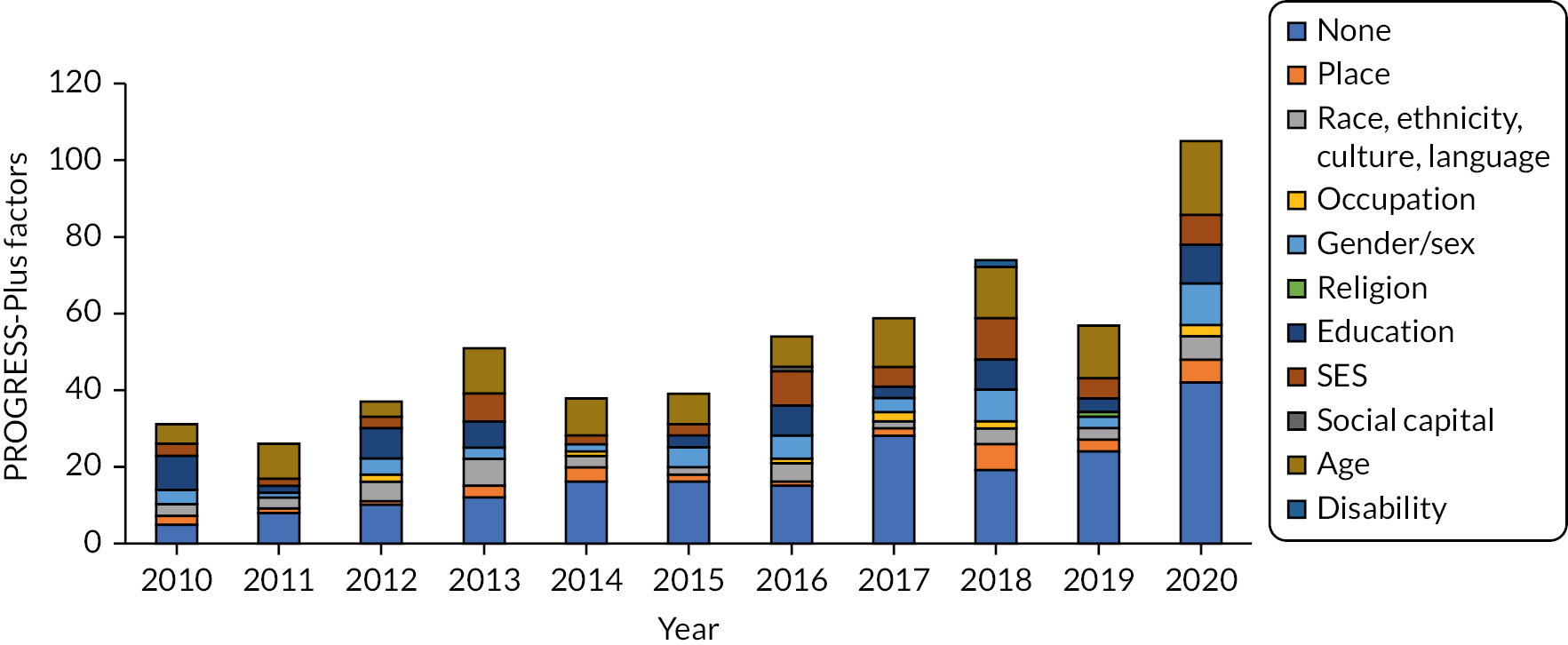
We documented the number of evaluations assessing policy effectiveness comparing a policy outcome between groups by PROGRESS-Plus equity domains. Overall, out of 389 studies used, 50% did not consider any equity domain, 50% assessed at least one, and 21% measured two or more. Age was the most assessed (30%), followed by education (16%, although these mainly related to school characteristics), SES at the individual level (15%), gender/sex (13%), race and culture (11%) and place (8%), whereas only 11 publications considered occupation, and 1 or 2 examined religion, social capital and disability each. This was using a generous interpretation of the PROGRESS-Plus framework, which also considered characteristics of products and places (rather than just humans) and those contributed to higher numbers for age and education. Equity was most frequently considered in the USA (n = 75 with at least one equity dimension), Australia (n = 20), Canada and Mexico (n = 18 each), the UK (n = 17), as well as Chile and France (n = 8 each). Figure 10 illustrates the distribution of publications by year and equity dimension assessed. While the number of quantitative and mixed-methods studies reporting on at least one dimension has increased from 2018, the proportion to the number of studies of effectiveness published per year has reduced, from 72% (n = 13 out of 18) in 2010 to 40% (n = 28 out of 70).
FIGURE 10.
Number of publications comparing policy outcomes by PROGRESS-Plus factors, by publication year. Note: a publication can include more than one health equity dimension (non-mutually exclusive category).
We explored whether evaluations conducted at a smaller scale could capture equity more frequently. In the 15 publications on local policy and/or evaluation in the UK, 8 assessed the effectiveness of a policy. Only four reported on at least one equity dimension: SES (n = 4), place (n = 1), and age (n = 1) representing a similar proportion than for the evidence map, albeit the very small sample size limiting such conclusions.
Conclusions
We found imbalances across the 483 included studies, suggesting that policy evaluations are conducted and published inequitably across the world both in terms of quantity and quality. Though 70 countries were represented overall, 81% of publications focused on only 12 countries (USA, UK, Australia, Canada, Mexico, Brazil, Chile, France, Spain, Denmark, New Zealand and South Africa), and 30% included the USA. Few evaluations were found about Africa, Central and South Asia and the Middle East. Inequities were also detected in the study designs, with the most quantitative robust methods mainly documenting the abovementioned 12 dominant countries. Few publications reported on PPPs (n = 31), and only one assessed the development of voluntary policies led by the public and private sectors each. Using a generous interpretation of the PROGRESS-Plus equity dimensions, we found that not only 50% of publications assessing policy effectiveness did not compare outcomes by any equity domain, but that the proportion of those doing so has decreased over time. Age, education (mainly school characteristics) and SES at individual level were the most frequently assessed dimension, while occupation and education at individual level, religion and culture, social capital and disability were barely considered.
Chapter 4 Overview of reviews of the effectiveness of regulatory, voluntary and public–private partnership policies to improve food environments and population diet
Introduction
This chapter reports the methods and findings of the overview of reviews, including direction of effect stratified by population, and by equity dimension, for regulatory, voluntary and partnership approaches.
Methods
Eligibility criteria and quality appraisal
Fifty initial systematic reviews were identified in the overarching search strategy (see Chapter 2). Additional screening was comprised first, considering only those assessing the effectiveness of interventions. Within these, only the results sections or subgroup analyses containing a majority of studies meeting the project’s eligibility criteria (screened by one reviewer LB) were included. Second, the evidence syntheses without quality or risk-of-bias appraisal were excluded. Third, to limit primary study overlap between systematic reviews, as recommended by Cochrane,32 the ‘most recent, highest quality, “most relevant”, or “most comprehensive” systematic review for groups of overlapping reviews’ were selected.
The quality of each systematic review was assessed using the checklist for systematic reviews and meta-analyses developed by the SIGN with minor modifications, first, excluding systematic reviews without a quality or risk-of-bias appraisal, and second, merging the two lowest of four categories of overall quality proposed by SIGN. 33 The three resulting categories were as follows: ‘high’, ‘acceptable’ and ‘low’. We also added guidance for some of the questions to limit variations in interpretation between reviewers (see Appendix 3, Table 25). Three independent reviewers performed quality appraisal in pairs (LB, SR, CK) in the EPPI-Reviewer Web.
Primary study overlap is a frequent issue in an overview of reviews consisting of having the same primary studies included in multiple systematic reviews. This gives more weight to their findings than those of other primary studies, thus introducing biases, and making data extraction and data synthesis challenging to perform. 32 To overcome this, we employed Cochrane’s approach to ‘all non-overlapping reviews’, and selecting the most recent, highest quality, ‘most relevant’, or ‘most comprehensive’ systematic review for groups of overlapping reviews. The strategy for following this recommendation in the overview of reviews was as follows: First, we extracted general policy and study characteristics for all potentially eligible systematic reviews at this point (see Data extraction for more details). Second, following Cochrane guidance30 we documented primary study overlap in the systematic reviews by creating a matrix and calculating the ‘corrected covered area’. The latter considers the number of publications (including double counting) in evidence syntheses, the number of unique studies, and the number of reviews. 34 Overlaps ranging between 0% and 5% are considered as slight, 6% and 10% as moderate, 11% and 15% as high and more than 15% as very high. Additionally, we documented the number of reviews that overlap with others, the percentage of studies in each review that overlap with others, and the percentage of unique studies that overlap overall. Third, in each group of overlapping reviews, we selected the review that had the highest overall quality (for ‘most robust’), the most recent search date (for ‘most recent’), and that contributed most to the body of research evidence in terms of the number of studies included, topic (NOURISHING policy categories covered) and place (World Bank world regions covered) (for ‘most relevant or comprehensive’). Justifications for the choices were recorded for reasons of transparency. The selection was made by one reviewer (LB).
Data extraction
General review characteristics extracted in a standardised form consisted of which results sections or subgroup analyses were included and excluded, the number of studies included in these analyses, literature search dates in databases, funding, competing interests, and authors’ affiliations. Characteristics of the policies assessed within the selected results sections consisted of countries, policy categories using the NOURISHING framework,18 the types of outcomes assessed, and the equity domains (or effects for population groups that are prone to health inequalities) represented using the PROGRESS-Plus framework. 20 Data were extracted by one reviewer (LB) and a sample verified by another (CK).
The results of the interventions in the eligible results sections were extracted by policy governance approach, type of outcome and equity domain. Some results sections included non-eligible policies. To keep it simple, we extracted information for the whole section; however, results of policies that did not focus on the food environment were disregarded. Given that the results extracted by equity only covered three of the ten domains (gender, SES, age) of PROGRESS-Plus, we also extracted data on equity from the systematic reviews that had been excluded for reducing primary study overlap. This led to the documentation of two additional domains (race and education) as well as additional outcomes within the domains already covered. We also noted that some systematic reviews had assessed their data or drawn conclusions in relation to a hierarchy or ‘level’ of interventions and we documented these instances. Lastly, we briefly documented how the policies work (their mechanisms of action) as described by the review authors (usually as part of their results or discussions).
Data synthesis
As expected, a high degree of heterogeneity was observed among the primary studies and systematic reviews in terms of types of policies and outcomes evaluated. We adapted the effect direction plot developed by Thomson et al. 26 and Boon et al. 27 to visually display non-standardised effects by governance approach, type of outcome and quality rating, but at the review level rather than primary study level. We classified the direction of effect by type of governance approaches compared (regulatory vs. voluntary, regulatory alone, or voluntary alone). Direction of effect was documented independently from statistical significance, consulting primary studies when not reported in the systematic reviews where necessary. The same approach was applied to reporting the number of studies and total participants by outcome. We had planned to assess the level of certainty in the evidence for each outcome using the GRADE framework but information available was insufficient. Thus, as a compromise, the effect direction plot was also used to present jointly the direction of effect, review quality and indirectness.
Findings
Included studies
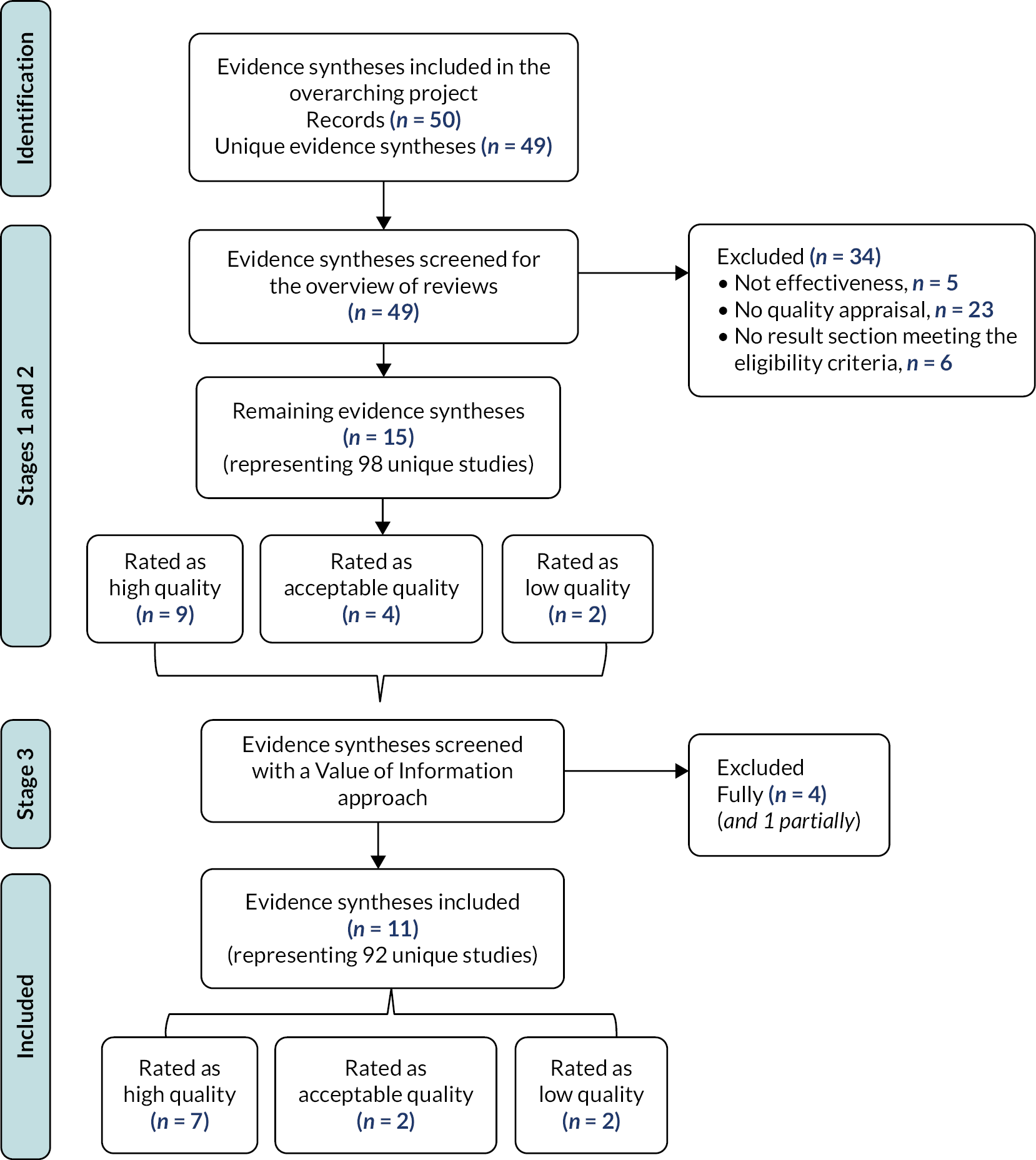
As outlined in Figure 11, of the 50 (49 unique) evidence syntheses identified in the overarching search, 5 were excluded as they did not evaluate the effectiveness of policies, 23 for not appraising study quality and 6 for not including a results section meeting the eligibility criteria. This left 15 systematic reviews, which were assessed for primary study overlap. Nine were rated high quality (including three Cochrane reports), four as acceptable and two as low. The assessment of primary study overlap and selection of reviews in each overlapping group of reviews is presented in Appendix 5, Tables 27 and 28. The latter process led to the full exclusion of 4 additional reviews35–38 (2 of high quality, 2 of acceptable quality) and of 1 results section in an additional review39 leaving 11 reviews in the overview of reviews (see Appendix 5, Table 30). However, as explained in the methods, three of the reviews35,36,38 excluded because of primary study overlap were used to document effects on specific population groups (equity). The excluded evidence syntheses along with the justifications are listed in the Report Supplementary Material 1. For the sake of transparency, the latter also lists the five publications representing four systematic reviews that were excluded as part of the screening for the overarching project (see Chapter 2) because of an insufficient focus on governance (i.e. governance was either not documented or documented but not considered in the analysis).
FIGURE 11.
PRISMA flow chart representing the selection process. Adapted from the PRISMA template by Page et al. (2021). 16
Primary study overlap
Calculations for the corrected covered area, which is the current recommended method to measure primary study overlap, suggests that before excluding reviews for reducing primary study overlap, overlap was already ‘slight’ (1.3% overlap). However, 9 of the 15 reviews overlapped with other reviews: 5 with 1 other review, 3 with 2 other reviews, and 1 with 3. Among these nine overlapping reviews, six had 80% or more of their studies included in other reviews; three of which overlapped at 100%. Overall, the 15 reviews included 98 unique primary studies, 17 of which overlapped once (i.e. it was included in 1 other review), and one twice (i.e. it was included in 2 other reviews). The detail of primary study overlap is presented in Appendix 5, Tables 27–29.
By excluding reviews to limit primary study overlap, overlap fell down to 0 with 92 unique primary studies and 11 reviews remaining. Among the primary studies excluded, 18 were included in other included reviews, whereas 6 (6%) did not. Yet, excluding the latter six had little impact since one did not assess policies, another one was not an evaluation, and four assessed SSB taxes (two in the USA, one in France and one in Mexico) – a topic that is well covered by other systematic reviews included in the overview.
Quality appraisal of systematic reviews
Table 4 presents the results for the quality appraisal. Seven were rated high quality (++), two acceptable (+) and two low (−). The main reason for attributing low ratings was inappropriate synthesis methods (in addition to inappropriate or lack of use of quality or risk-of-bias assessment). The main reason for attributing ‘acceptable’ ratings was inappropriate or lack of use of quality or risk-of-bias assessment. Other common issues related to not listing the excluded studies (n = 7) and not reporting competing interests in the included studies (n = 6). Most assessments of publication bias were rated as ‘not applicable’ due to the absence of meta-analysis in the selected results sections.
| Lead author (year) |
Section(s) of synthesis in systematic reviews included and excluded from the data extraction and data synthesis in the overview of reviews | Dates searched | N studies included Type of synthesis |
Countries | Categories of eligible policies | Types of outcomes measured | Funding reported | Declaration of competing interests |
|---|---|---|---|---|---|---|---|---|
| Dodd (2020)40 High (++) |
Included: Findings from real-world evaluation of impact Excluded: Findings from modelling studies, findings from experimental studies, perceptions of taxation of high-salt foods |
January 2000–October 2019 | N = 4 (out of 18) Narrative |
FIJ, HUN, MEX, TONG | U-Salt taxes (on salt in non-essential foods and imports of salty foods) | Consumer behaviour (dietary intake, sales); economy (imports, government revenue) |
No funding | Declared industry and non-industry competing interests (e.g. Novartis) |
| Hillier-Brown (2017)41 High (++) |
Included: Changing pre-packed children’s meals, voluntary calorie labelling | January 1993–October 2015 | N = 2 (out of 30) Narrative |
USA | N-Menu Labelling S-Retail and food services (children’s meal content; TV promotions) |
Consumer behaviour (sales/purchase, use of labels) | Non-industry funding | None declared |
| Excluded: Trans-fat law (local), price increases for unhealthy choices (trial), calorie labelling law ×2 (local), Incentives (rewards) (trial), price reductions for healthier choices (experiment), signposting ×2 (trials, local), personalised receipts (not envt), Award schemes (local), telemarketing (not envt). | ||||||||
| Lhachimi (2020)42 High (++) |
Included All |
Until October 2019a | N = 2 (out of 2) Narrative |
DEN | U-Saturated fat tax | Health (overweight and obesity); consumer behaviour (dietary intake based on sales) |
Non-industry funding | Declaration of non-industry interests only |
| Croker (2020)43 High (++) |
Included: Interrupted-time-series studies Excluded: Experimental studies |
January 2017–April 2019 | N = 3 (out of 14) Narrative |
CHL, ECU, UK | N-FOP labelling | Consumer behaviour (sales/purchases, dietary intake); food envt (nutritional composition) |
Non-industry funding | None declared |
| Pfinder (2020)44 High (++) |
All | Until September 2019 | N = 1 (out of 1) Narrative |
HUN | U-tax on non-essential food (focus on sugar) | Consumer behaviour (dietary intake based on sales, expenditures)b | Non-industry funding | Declaration of non-industry interests only |
| Teng (2019)45 High (++) |
Included All |
Until June 2018 | N = 18 (out of 18); 15 of which in a meta-analysis | CHL, FIN, FRA, HUN, MEX, SPA, USA | U-Tax on SSBs and non-essential foods | Consumer behaviour (intake, purchases/sales) | Non-industry funding | Declaration of non-industry interests only |
| von Philipsborn (2019, 2020)46,47 High (++) |
Included: A.2 Nutritional rating score shelf labels, E.1 Voluntary industry initiatives. Excluded: The rest (A.1, A.3, A.4, B.1, B.2, B.3, B.4, B.5, C.1, C.2, C.3, F.1, F.2, F.3, F.4, F.5, G.1, G.2, G.3, G.4, H.1, H.2) (trials and/or local level) |
Until January 2018 | 8 (out of 58) Meta-analysis (C.1) Narrative (A.2, E.1) |
AUS, CAN, UK, USA | N-Labelling (on-shelf); U-Price increase on SSBs in shops, leisure centres and restaurants; I-Reformulation (industry pledges) Focus on SSBs |
Consumer behaviour (intake, purchases/sales); economy (industry revenue) |
Non-industry funding | Declaration of industry interests, including the food industry (Nestlé, Danone, Weight Watchers) |
| Downs (2017)48 Acceptable (+) |
Included: Real-world policies Excluded: Modelling studies |
1990–August 2017 | N = 23 (out of 32) Narrative |
BRA, CAN, CR, DEN, IRAN, KOR, MEX, NET, USA, Americas (partly not specified) | N-trans-fat labelling; I-Trans-fat reformulation/limits/ban by manufacturers; S-Retail and food services (trans-fat reformulation/limits/ban) |
Health (heart diseases and mortality, trans-fat in body); consumer behaviour (dietary intake); food envt (nutritional composition) |
Non-industry funding | None declared |
| Sisnowski (2017)39 Acceptable (+) |
Included: Nutritional labelling of products |
January 2004–October 2015 | N = 1 (out of 36) Narrative |
AUS | N-Back-of-pack labelling | Food envt (nutrition composition, price) | Non-industry funding | None declared |
| Excluded: Menu labelling (local), subsidies for healthy foods, procurement standards for public institutions (local), improvement of food infrastructure (mainly local); taxation (excluded due to primary study overlap) |
||||||||
| Rincón-Gallardo (2020)49 Low (−) |
Included: All |
January 2000–February 2020 | N = 15 (out of 15) Narrative |
AUS, CAN, UK, USA | N-Menu labelling | Food envt (availability, nutrition composition) | NR except publication costs | None declared |
| Hyseni (2017b)50 Low (−) |
Included: Multicomponent interventions Excluded: Dietary counselling in school based and worksite interventions, Dietary counselling at community level, Nutrition labelling (RCT), Media campaigns, Reformulation, Labelling, Taxes |
30 October 2015 | N = 15 (out of 70) Narrative |
AUS, CHI, DEN, FIN, FRA, ICE, IRE, JAP, KOR, LIT, MONG, SLOV, TKY, UK, USA, VIET, Unclear (75 countries) | N-Salt labelling (FOP, BOP); I-salt reformulation by manufacturers |
Health (heart diseases and mortality); consumer behaviour (dietary intake) |
Non-industry funding | None declared |
Characteristics of included systematic reviews
Table 4 describes the general characteristics of the systematic reviews included. The number of eligible studies per review ranged from 1 to 23. One conducted their search in databases in 2020, four in 2019, while the oldest were in 2015 (n = 3). None reported on PPPs. Twenty-eight countries were covered overall, all of which were high or upper-middle income countries according to the World Bank with the exception of Iran, Mongolia and Vietnam. The most assessed countries consisted of the USA (n = 6 systematic reviews), Australia (n = 4), as well as Canada, Denmark, Hungary, Mexico and the UK (n = 3 each). All focused on the general population. In terms of real-world policy topics assessed, seven evaluated labelling schemes (on front and back of packages, shelves and menus), five assessed economic interventions (taxes on salt, saturated fat, SSBs/non-essential foods), three included product reformulation initiatives, and two focused on the retail and catering sector. None considered initiatives in schools, nurseries, health care or leisure settings, nor advertising and marketing control. Three focused on SSBs or sugar, two on fat, and two on salt. Regarding the outcomes evaluated, nine investigated effects on consumer behaviour (e.g. dietary intake, purchases/sales), four (on the food environment (e.g. nutrition composition, price), three on health (e.g. heart diseases, obesity), and two on the economy (imports, governments’ and food industry’s revenue). Two conducted meta-analyses. None of the included systematic reviews reported industry funding though one author in the review by Dodd et al. 40 had been a paid consultant for the Novartis Foundation and Midway Corporation; and the systematic review by von Philipsborn et al. 46 was partly funded by the Danone Research Center to the National Institute of Public Health, Cuernavaca, Mexico, and two authors have received grants from the latter of the British Nutrition Society.
Quality and characteristics of systematic reviews and results sections excluded to reduce primary study overlap
Four systematic reviews35–37,50 were fully excluded to reduce primary study overlap, two of which were rated as high quality, and two as acceptable. Patterns in quality appraisal was similar to those included in the overview. Details of the quality appraisal is presented in Appendix 5, Table 30. The additional systematic review,39 which had a results section excluded to reduce overlap had an acceptable quality (Table 5). The five reviews and results section included between three and eight studies and covered the USA (n = 4), Denmark (n = 2), as well as in Canada, Costa Rica, France, Hungary and Mexico (n = 1 each). Four assessed different types of taxes (SSBs, sugar, saturated fat and restaurants), and another examined trans-fats relating to labelling, reformulation, and the retailing and catering sector. All assessed consumer behaviours, four assessed health outcomes, three the food environment and one economic impacts. Thus, apart from a few health and economic outcomes, excluding these to reduce primary study overlap appears not to have affected the scope of the studies included, but also reduced the overemphasis on the USA and on taxation that would have been present otherwise.
| Lead author (year) | 1.1 | 1.2 | 1.3 | 1.4 | 1.5 | 1.6 | 1.7 | 1.8 | 1.9 | 1.10 | 1.11 | 1.12a | 1.12b | Overall rating |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Croker (2020)43 | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | N/A | Yes | No | High (++) |
| Dodd (2020)40 | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | N/A | Yes | No | High (++) |
| Downs (2017)48 | No | Yes | Yes | Yes | Yes | No | Yes | Yes | No | Yes | N/A | Yes | No | Acceptable (+) |
| Hillier-Brown (2017)41 | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | N/A | Yes | Yes | High (++) |
| Hyseni (2017b)38 | No | Yes | Yes | Yes | Yes | No | Yes | Yes | No | No | N/A | Yes | No | Low (−) |
| Lhachimi (2020)42 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | N/A | Yes | Yes | High (++) |
| Pfinder (2020)44 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | N/A | N/A | Yes | Yes | High (++) |
| Rincón-Gallardo (2020)49 | No | Yes | Yes | ? | Yes | No | Yes | Yes | No | No | N/A | Yes | ? | Low (−) |
| Sisnowski (2017)39,a | Yes | Yes | No | No | Yes | No | Yes | Yes | No | Yes | N/A | Yes | No | Acceptable (+) |
| Teng (2019)45 | Yes | Yes | No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | No | High (++) |
| von Philipsborn (2019, 2020)46,47 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High (++) |
Direction of effects by governance approach for the general population
Table 6 describes the directions of effects of interventions categorised by types of governance approaches and their comparison, and types of outcomes. The first column describes 25 groups of outcomes grouped into consumer behaviours (n = 15), the food environment (n = 5), health (n = 3) and the economy (n = 2). The next three columns describe three categories of governance approaches that were assessed or compared: regulatory versus voluntary, regulatory alone and voluntary alone. As mentioned earlier, no review assessed PPPs. In each of these cells, the direction of the arrow indicates whether results were overall positive (or desired), negative (or undesired) or mixed. In the column comparing regulatory to voluntary actions, a larger triangle indicates a larger effect compared to the other governance approach. Twelve (48%) categories of outcomes only included regulatory interventions, five (20%) only voluntary actions and eight (32%) both.
| Key outcomes reported | Direction of effect (or association) by comparison of governance approaches (k = N studies, n = N participants; colour/signs = quality) | Policies and governance approaches (countries) | ||
|---|---|---|---|---|
| Regulation (R) vs. voluntary (V) | Regulatory alone | Voluntary alone | ||
| Health | ||||
| Heart diseases and mortality | R▲, V▲ diverse measures of MI, stroke and mortality rates k = 3, n = 10,337; (+) |
Trans-fat policies:48 V self-regulated limits (Costa Rica), R trans-fat limits or ban in restaurants (NYC, USA) | ||
| RV▲, V▲ stroke and CHD mortality k = 3, (−) |
Salt policies:50 V reformulation + R label + campaigns (Finland), V reformulation + V label + campaigns (Japan, UK) | |||
| Behaviours | ||||
| Dietary intake of unhealthy foods or nutrients | ◄► salt intake k = 2, n = 883 individuals + 1395 households; (++) |
Taxes on salt reduction in40 non-essential food (Hungary); imported instant noodles (Tonga) | ||
| R▲, V▲ trans-fat intake k = 4, n = 34,031; (+) |
Trans-fat reduction policies: R ban (Denmark), R labelling + V limits (Canada), V self-regulated limits (Costa Rica, the Netherlands)48 | |||
| R▲, V▲ trans-fat in plasma serum and breastmilk k = 5, n = 3869; (+) |
Trans-fat policies:48 R labelling + V limits (Canada), self-regulated limits (Costa Rica), R labelling (USA) | |||
| RV▲, V▲ salt intake k = 7; (−) |
Salt policies: V reformulation + R label + campaigns (Finland), V reformulation + V label + campaigns (China, Japan, UK) V bread reformulation + campaigns (France)50 |
|||
| ▲ total and sat fat intake (via sales tax) k = 2; 2000 households + 1293 supermarkets; (++) |
Tax on saturated fat42 (Denmark) | |||
| ▲ difference in mean intake of taxed vs. untaxed sugar-added food k = 1, n = 40,210 households; (++) |
Tax on non-essential food (Hungary)44 | |||
| Purchases and sales of healthy or unhealthy foods | R▲, V▲ range of food and SSBs purchaseda k = 3; (++) |
FOP labels: R warning (Chile), R traffic lights (Ecuador), V Guideline Daily Amount (UK)43 | ||
| ▲ purchases of taxed food k = 1, (++) |
Tax on non-essential food (Mexico)40 | |||
| ▲ Total energy, SSBs and healthier option purchases k = 1, n = 30 chain restaurants; (++) |
V change in sides sold with children’s meals in three fast-food chains + TV promotions about healthier beverages (USA)41 | |||
| ◄► % customers choosing lowest-energy option k = 1, n = 30 restaurants; (++) | V change in sides sold with children’s meals in three fast-food chains + TV promotions about healthier beverages (USA)41 | |||
| ▲ purchases of energy, fat, sodium and carbohydrates in main meals k = 1, n = 6 restaurants and ~16,000 main meals; (++) |
V menu-labelling in restaurants (USA)41 | |||
| ◄► sales of minced beef, cream, sour cream k = 2; 2000 households + 1293 supermarkets; (++) |
Tax on total and saturated fat (Denmark)42 | |||
| ▲ sales of least healthy SSBs and beverages k = 2, n = 442 stores; (++) |
V self-regulation on-shelf Guiding Star labelling (Canada and USA)46 | |||
| ◄► SSBs sold/purchased (k = 3, n = 61,126 households + 17 companies) (++) |
V self-regulation/pledges:46 HWCF Market Place Pledge (by manufacturers about calorie) and Walmart’s Healthier Food Initiative (USA) | |||
| ▲ difference in mean expenditure on taxed vs. untaxed sugar-added food k = 1, n = 40,210 households; (++) |
Tax on non-essential food (Hungary).44 | |||
| Intake, sales and purchases combined | ▲ SSBs intake/sales/purchases k = 15, n = 539,952; (++) |
SSB taxes (Chile, France, Mexico, Spain, USA)45 | ||
| Use of labels | Noticing and using nutrient menu labels k = 1, n = 6 non-chain restaurants and ~16,000 main meals V▲ |
V nutrient menu-labelling in restaurants (USA)41 | ||
| Food environment | ||||
| Food and drinks nutrition content | ▲ soft drink sugar content k = 1; (++) |
R traffic light FOP label (Ecuador)43 | ||
| R▲, V▲ trans-fat content k = 8, n = 13,123 products + 6969 purchases; (+) |
Trans-fat policies:48 R ban (Denmark, NYC), R labelling + V limits (Canada), R labelling (USA, Korea), V self-regulated limits (Costa Rica, Netherlands) | |||
| R▲, V◄► calorie content k = 11, n = 678 restaurant chains; (−) |
Calorie menu labelling:49 R (Australia, Canada, USA), V (UK)a | |||
| Price | ▲ price of high- and low- fat food k = 2; 2000 households + 1293 supermarkets; (++) |
Tax on saturated fat (Denmark)42 | ||
| Labelling adequacy/compliance | ▼ nutrient content k = 1; 350 product labels matching nutrition content; (+) |
R back-of-pack labelling (Australia)39 | ||
| Economy | ||||
| Government revenue | ▲ tax gain for govt k = 1; (++) |
Tax on non-essential food (Mexico)40 | ||
| Food imports | ▼ volume of instant noodles imported k = 1, n = N/A (imports data); (++) |
Tax on imported instant noodles (Tonga) and MSG (Fiji)40 | ||
Both regulatory and voluntary
Eight outcome categories measuring both regulatory and voluntary approaches were reported in four systematic reviews: two of low quality, one acceptable and one high. Information mainly relied on cross-sectional (single and repeat) and follow-up studies. The policies assessed were in 13 countries across 4 World Bank world regions: Australia, Canada, Chile, China, Costa Rica, Denmark, Ecuador, Finland, Japan, Republic of Korea, the Netherlands, the UK and the USA. Two groups of outcomes measured health, four consumer behaviour and two the food environment. Overall, they suggest positive effects for both governance approaches, except for calorie menu labelling, which was only positive for regulations. Few regulatory and voluntary policies could be directly compared due to the high heterogeneity in the measurement methods. Among those that could be, a larger arrow in the effect direction plot indicates a greater effect size. This includes interventions for reducing trans-fats in the food supply and diet: regulatory bans appear to be the most promising (based on one acceptable quality review). 48
Regarding effects on health, Downs et al. (acceptable quality)48 found that in Costa Rica, following self-regulatory trans-fat targets, the concentration of trans-fat in subcutaneous adipose tissue had reduced sufficiently not to be associated with increased risk of myocardial infarction anymore. In the USA, only 3 years after the local trans-fat ban (or regulatory restrictions) in restaurants in New York City, and using hospital admissions data, cardiovascular disease (CVD) mortality rates had declined by 4.5%, with a greater reduction in stroke in young people than in the normal trend. Regarding salt, according to Hyseni et al. 50 (low quality), in Finland about 30 years after implementing both regulatory labelling and voluntary reformulation, stroke and coronary heart disease (CHD) mortality had fallen by over 60–75%. A similar reduction in stroke mortality was noted in Japan, where voluntary labelling, voluntary reformulation and awareness campaigns had been implemented. In England, the voluntary salt targets were associated with a fall in stroke mortality from 128/1,000,000 in 2003 to 82/1,000,000 in 2011 (36% reduction, p < 0.001).
Regarding effects on consumer behaviours, although both regulatory and voluntary approaches appear to be effective, in Downs et al. 48 (acceptable quality) the Danish trans-fat ban (regulatory) was shown as most effective to reduce trans-fat intake since it had eliminated trans-fat from the food supply. By contrast, in Costa Rica and the Netherlands (self-regulated trans-fat limits), consumption reduced by −38% and −20%, respectively. In Canada and the USA, which both employed mandatory labelling and voluntary reformulation, trans-fat concentrations reduced by −54% to −58% in plasma serum (Canada and USA) and by −30% to −74% in breastmilk (Canada) (reported as a proxy for consumption). Hyseni et al. 50 (low quality) found that all voluntary and mixed-approach salt policies reduced salt intake, although none assessed were purely regulatory. Effect size in Finland (mixed approach) and Japan (voluntary) was similar (−4 g/day and −3.9 g/day, respectively) while it was lower in the UK (voluntary, −1.4 g/day). They explained part of the success of the UK with the ‘degree of political pressure [that was] applied to the food industry and [the] regular, independent monitoring’. Lastly, in Croker et al. 43 (high quality), the effect of FOP labels was measured using analyses of sales or purchase data for the regulatory warning label in Chile (fruit juices, breakfast cereals, chocolate, candies and cookies), the regulatory traffic lights in Ecuador (SSBs) and the voluntary Guideline Daily Amounts that was in place before the traffic lights in the UK (calories from biscuits, breakfast cereals and SSBs). We could not directly compare governance approaches, but both had some positive effects.
As for the food environment, Downs et al. 48 (acceptable quality) reported clear impacts for trans-fat policies on product content with the regulatory ban in Denmark leading to complete elimination of trans-fats in the food supply. Rincón-Gallardo et al. 49 (low quality) examined 11 studies on menu calorie labelling policies in restaurants in the USA (regulatory, n = 8 studies), Australia (regulatory, n = 2) and the UK (voluntary, n = 1). All eight American studies showed a positive effect on menu calorie content whereas this was mixed in Australia (it had reduced in some food items and increased in others) and the UK (menus contained 45% less fat and 60% less salt but calorie, fat, sugar and sodium increased in some menu categories). Given that all positive results are about the same country, it is unclear whether this is due to differences in country contexts or policy processes. Rincón-Gallardo49 has noted the challenges of implementing regulatory menu labelling at the subnational level (e.g. state), as this was the case in Australia: it can create different regulations for the same restaurant chains to implement in different regions, including definitions of what constitutes a ‘chain’.
Regulatory approaches alone
The 12 outcome categories measured for regulatory approaches alone were reported in 6 systematic reviews (for 10 countries across 3 World Bank world regions: Australia, Denmark, Ecuador, Fiji, France, Hungary, Mexico, Spain, Tonga and the USA). Seven groups of outcomes were about consumer behaviours, three about the food environment, and two about economic outcomes (none on health). Eight showed positive effects, two showed mixed effects (salt intake and high-fat food sales) and two negative effects (labelling compliance and food imports). All came from high-quality systematic reviews except labelling compliance, which was from a review rated acceptable. Although effects for regulatory approaches might appear mixed overall, this might be due to the type of policy and outcome assessed. For instance, one negative result was the very low compliance in relation to back-of-pack labels in Australia. However, this has more to do with policy implementation than direct effects on the environment like affordability, availability or accessibility. Regarding taxes, as suggested below, those on SSBs and sugary food appear promising. Evaluations of taxes relating to salt suggest a lack of effectiveness but this might have more to do with the narrow focus of some of the taxes: one of the three taxes assessed was only on imported instant noodles (in Tonga) and another on monosodium glutamate (MSG) sold in bag (in Fiji). Evidence on the effectiveness of a tax on saturated fat is limited by the limited experience worldwide (Denmark only) as well as number and scope of evaluations. On the one hand, according to Dodd et al. 40 (high quality), in Mexico and using panel household data before and 2 years after the tax implementation, the tax on non-essential foods was associated with a 6% reduction in purchases of taxed foods (all categories). 40 In their meta-analysis, Teng et al. 45 (high quality) showed that the equivalent of a 10% SSB tax in Chile, France, Mexico, Spain and the USA corresponded with an average reduction in beverage purchases and dietary intake of 10.0% (95% CI −5.0% to −14.7%, n = 17 studies), although with high heterogeneity (I2 = 97%). The largest impacts were for the highest taxes, that is an ad valorem equivalent rate of 33.3% in Philadelphia (USA), 21.9% in Berkeley (USA) and 11.4% in Catalonia (Spain). There was also a non-significant 1.9% increase in total untaxed beverage consumption (95% CI −2.1% to 6.1%, n = 6 studies in France, Mexico, Spain and the USA). Using a single interrupted time series, Pfinder et al. 44 (high quality) suggested that the Hungarian tax on non-essential food led to a reduced intake and expenditure on taxed sugar-added food compared to untaxed ones. On the other hand, using sales data from two interrupted time series by the same authors, Lhachimi et al. 42 (high quality) showed varied effects for the Danish tax on saturated fat intake and sales of high-fat foods – although this might be due to the limited sample of foods assessed (minced beef, cream, sour cream in one study; and butter, butter blends, margarine and oils in the other). In the first study, total fat intake declined by about 41.8 g per week per person (p < 0.001); in the second, sales reduced by 4.2% for minced beef and 5.8% for cream but increased by 0.5% for sour cream sales42 As for salt, effects on dietary intake based on surveys conducted before and after tax implementation were also mixed in Hungary and Tonga, although the taxes and outcomes assessed were quite different. 40 In Hungary, the proportion of adults consuming taxed salty snacks increased from 69% to 71%, but among people consuming salty snacks or condiments, 16% and 11%, respectively, either reduced intake or changed for a cheaper brand. Only 5% of salty snack eaters reported selecting healthier options. In Tonga, 70% of people surveyed reported not having changed their consumption of instant noodles after a tax on imported instant noodles. The review authors reported that people had substituted imported noodles with noodles produced locally.
For the food environment, according to an interrupted time series reported in Croker et al. 43 (high quality), the regulatory traffic light labels in Ecuador encouraged product reformulation for soft drinks: mean sugar content decreased by 0.93 g per 100 ml. The interrupted time series in Denmark mentioned above (high quality) also mention that the tax on saturated fat was passed on to consumers for selected high-fat products, sometimes at higher rates than the tax itself, while prices for the low-fat options of these products reduced (p < 0.001, no precision estimate). On the other hand, Sisnowki et al. 39 (acceptable quality) documented a cross-sectional study assessing whether back-of-pack labels of 350 products in Australia matched their actual nutrition content. Only 7% of products were 100% compliant.
As for economic outcomes, Dodd et al. 40 (high quality) reported that the tax on non-essential foods in Hungary contributed to 30% of tax revenue gain. On the other hand, import taxes on instant noodles in Tonga or MSG sold in bags in Fiji did not refrain imports of such products. Imports of instant noodles in Tonga drastically declined in the first year following the tax (from 2,083,000 kg in 2014–5 to 439,000 kg in 2016–7 but doubled to reach 806,000 kg in 2017–8, despite the tax also doubling during that time. In Fiji, MSG imports rose from < 50,000 kg in 2011 to 200,000 kg in 2013.
Voluntary approaches alone
The five groups of outcomes measured for voluntary approaches come from two high-quality systematic reviews. All policies were from the private sector, about the USA (and one also about Canada) and investigated purchases and sales in either the retail or restaurant sectors. Four showed positive effects and one mixed effects. Overall, limited data from the USA suggested positive effects on consumer awareness of the policy itself for labelling initiatives in supermarkets and restaurants (based on two studies); positive effects on sales of SSBs, healthy food and beverages options, and/or nutrients in restaurants following on-self labelling in supermarkets (one study), calorie menu labelling (one study), and changing defaults in children’s meals (one study); and mixed effects on sales of SSBs (measured as volume and calorie sold) in large retail chains (three studies).
In the retail sector, von Philipsborn et al. 46 found variable effectiveness in relation to SSB sales from three studies by the same team in the USA (n = 61,126 households + 17 companies) for assessing industry-led pledge-based programmes to improve the food supply: the Healthy Weight Commitment Foundation (HWCF) Market Place Pledge by food and drinks manufacturers, and the Healthier Food Initiative at Walmart’s. A controlled before–after study by Ng et al. 51 found that energy sold from SSBs from companies participating (P) in the healthy weight commitment (HWC) decreased by −14 kcal per capita/day versus −3 kcal for non-participating companies (no precision estimates); an interrupted time series also by Ng et al. and on the same pledge found that it did not decrease as much as anticipated (p < 0.001, shown visually only); another interrupted time series by Taillie et al. 52 on the Healthier Food Initiative at Walmart’s reported that the percentage volume of SSB purchased at Walmart decreased more than expected (p < 0.01, shown visually only). Certainty in the evidence was rated as very low. The same systematic review also included on an interrupted time series in the USA and a controlled-before-after study in Canada evaluating the Guiding Star, a commercially driven voluntary shelf-labelling scheme for supermarkets. They found that sales of SSBs or all beverages with zero stars (the least healthy) decreased (by −27.3% after 16 months in the USA for SSBs, no absolute numbers available for all beverages in Canada). Six months after implementation, a ‘modest’ proportion of clients ‘were aware of, understood, and trusted’ the system, and there was a strong support for supermarket labelling schemes. Certainty in the evidence was rated low.
In restaurants, Hillier-Brown et al. 41 reported on two cross-sectional studies on two different initiatives. The first one analysed transactions from 30 fast-food chain-owned restaurants to evaluate voluntary changes in children’s meals. The chains had also promoted healthier beverage options on television. Improvements were noted in the total energy, SSBs and options purchased, but the proportion of customers buying the lowest-energy option did not change. The second study assessed the effects of a voluntary menu labelling for calories, fat, sodium and carbohydrates in six non-chain restaurants on the purchases of the latter nutrients from about 16,000 mains. They found a significant decrease of purchases of energy, fat and sodium but no change for carbohydrates. A survey suggested that 71% of customers had noticed the labels, and about a fifth reported that the labels made them choose mains that contained a lower content in energy or fat.
Direction of effects for specific population groups (equity)
This section reports findings for specific population groups using the PROGRESS-Plus equity dimensions. Data come from seven systematic reviews: four of high quality, two acceptable and one low. Four of them44,45,49,50 were included in the whole overview of reviews, while three35,36,38 had previously been excluded to reduce primary study overlap. Table 7 illustrates the directions of effect stratified by PROGRESS-Plus dimension while the specific results extracted for each review are presented in the Report Supplementary Material 2. Only two policies, in two different reviews, were not regulatory. Both provided information on gender. The direction of the arrow indicates whether results were overall positive (or desired), negative (or undesired) or mixed while its size reflects the sample size. Most policies were American state SSB taxes, and most results relied on a single policy, although some evaluations had large sample sizes. Only 5 out of 10 dimensions were documented. SES was the most frequently documented. No information was found about place, religion, occupation, social capital and disability. Effects were generally positive for the population groups evaluated for race/ethnicity and gender, and mixed for SES, education and age.
| Equity domains | Direction of effect (or association) by comparison of governance approaches (k = N studies, n = N participants; quality) | Governance approaches and policies (countries) |
|---|---|---|
| Place | NR | |
| Race, ethnicity, culture, language | △ for non-Hispanic white adults (trans-fat in blood) (k = 1, n = 229–292 in 2000–9); (++) |
R trans-fat limits and M labels (USA)38 |
| ▲ for African American (SSB intake); (k = 1, n = 7300); (+) | R State SSB taxes (USA)36 | |
| Unclear (BMI); (+) | R State SSB taxes (USA)36 | |
| Occupation | NR | |
| Gender | ▲ for women (BMI); (k = 2, n = 4,658,255); (+) | R Tax on SSBs and fast-food restaurants (USA)36 |
| Mixed governance: ▲ for men and women (salt intake); (k = 1, n = 1206–909 in 1979–2002); (−) |
R salt labelling + V reformulation + media campaign (Finland)50 | |
| Voluntary: ▲ for men and women (salt intake); (k = 1, n = NR in 2006–10); (−) |
V salt targets + V FOP logo + education (Denmark)50 | |
| Religion | NR | |
| Education | ◄► BMI (k = 2, n = 2,863,095); (++) |
SSB taxes (USA)36 |
| SES | ▲ for low-income (purchases of taxed foods) (k = 1, n = 6089 households); (++) |
R Tax on non-essential food (Mexico)45 |
| ▲ for low-income (intake of taxed sugar-added foods (k = 1, n ~ 10,000 households); (++) |
R Tax on non-essential food (Hungary)45 | |
| ◄► (SSB/calorie intake) (k = 2, n = 9953 households + 7300 children); (++) |
SSB taxes (Mexico, USA)45 | |
| ◄► (purchases/sales SSBs) (k = 6, n = 96,884 households + 284,464 sales in Spain); (++) |
SSB taxes (Chile, Mexico, Spain)45 | |
| ▲ households in lowest income quartile (likely for the consumption of unprocessed sugar or sugar-added food) (k = 1, n = 40,210 households; (++) |
Tax on non-essential foods (Hungary)44 | |
| ◄► (k = 2; n = 2,716,288 participants); (++) | SSB taxes (USA)35 | |
| Social capital | NR | |
| Age | ▲ adult vs. children (declined in both; SSB intake) (k = 5, n unclear); (++) |
SSB taxes (USA)45 |
| ▲ for middle-aged and older (BMI); (k = 1, n = 2,709,422); (+) | State SSB taxes (USA)36 | |
| ▲ for children low-income (SSB intake); (k = 1, n = 7414); (+) | SSB state taxes (USA)36 | |
| ◅▻ children’s menus (calorie and other nutrients) (k = 3, n = 291 restaurants); (+) |
R calorie menu labelling (Australia, USA)49 | |
| Disability | NR | |
Race/ethnicity was analysed in two systematic reviews. According to Hyseni et al. 38 (high quality), following the introduction of regulatory labelling and voluntary limits for trans-fats in the USA, trans-fat concentrations in blood samples of white (non-Hispanic) adults (n = 229) fell by about 56% over 9 years (reduced by 24.3 µmol/l; 95% CI 19.6 to 29.0). Alagiyawanna et al. 36 (acceptable quality) reported one study that found an association between American state taxes on SSBs and soft drink consumption among African American children and adolescents (direction of effect presumably positive), and in another study that effects on body mass index (BMI) varied by race and ethnicity (no details).
Gender was documented in two systematic reviews. In Alagiyawanna et al. 36 (acceptable quality), two studies found a negative association between state taxes on SSBs and fast-food restaurants and women’s BMI. One (n = 1,948,833) recorded a reduction of 0.55 kg/m2, (p < 0.05) while effect size and precision estimates were not provided for the other. Hyseni et al. 50 (low quality) noted a reduction in salt intake in both men and women between the introduction of regulatory salt labelling and voluntary limits in Finland in 1987 and 2007 [reduced from 13 to 8.3 g/day in men, and from 11 to 7 g/day in women (n ~ 1000 individuals)]. A similar trend was observed for the voluntary salt labelling and limits in Denmark between 2006 and 2010: reduced from 10.7 to 9.9 g/day in men, and from 7.5 to 7.0 g/day in women (sample size not reported).
Education was only documented in the review by Backholer et al. 35 (high quality). The review found contradictory results from two studies on American state SSB taxes. One found no relationship between variations in taxes and BMI in adolescents by level of parental education; the other reported a significant reduction in BMI following a 1% increase in SSB tax rate among both adults who had a high-school diploma (0.0031 kg/m2) or a college diploma (0.0076 kg/m2).
Socioeconomic status was documented in three high-quality systematic reviews. Teng et al. 45 reported that effects of taxes on non-essential food in both Mexico (on purchases of taxed food) and Hungary (on consumption of taxed sugar-added food) were greatest in low-socioeconomic households. Impact of SSB taxes on SSB and calorie intake was mixed in Mexico and the USA, and were mixed as well for purchases and sales of SSBs in Mexico, the USA and Spain (n = 6 studies). Pfinder et al. 44 reported that the Hungarian Tax on non-essential food was most effective in the lowest income quartile (likely for the consumption of unprocessed sugar or sugar-added food). Backholer et al. 35 mentioned, on the one hand, no association between variations in American state SSB taxes and BMI in children from low-income families and on the other hand, a significant BMI reduction in both low-income (0.015 kg/m2) and high-income adults (0.008 kg/m2).
Age was documented in three systematic reviews. In a meta-analysis, Teng et al. 45 (high quality) compared the effect of American state SSB taxes on SSB intake between children and adults and found no statistical difference (it reduced by 6.4% in adults and by 7.7% in children, p = 0.91, five studies in the USA). In Alagiyawanna et al. 36 (acceptable quality), one study found that American state SSB taxes had a greater effect on BMI in middle-age and older people, while in another children from low-income families consumed 0.142 SSB less by week following a 1% increase in a SSB tax rate (statistically significant but arguably negligible). Lastly, in Rincón-Gallardo et al. ,49 effects from three studies (n = 291 restaurants) were inconsistent on whether regulatory menu labelling improve the nutrition composition of children’s menus. The first study, in the USA, found that mean calorie content of new items was lower than in the previous menus. In a second American study, mean energy content had reduced in quick-service chains by 40 calories and increased in upscale restaurants by 46 calories (no precision estimates). The third study, in Australia, found that mean energy, saturated fat, sodium and sugar had reduced by serving for some menus but had increased in others (no precision estimate).
Direction of effects by intervention level
Four systematic reviews of various quality ratings assessed different types of policy interventions and/or commented on their effectiveness by considering the level of restriction of choice or degree of structural change. Hillier-Brown et al. 41 (high quality) used the Nuffield intervention ladder53 to analyse policies aiming to improve takeaway meals. They found that policies restricting choices or manipulating price were more effective than those only providing information or enabling choice. They suggested that ‘the level of intrusiveness’ played a greater role than the type of policy itself. Downs et al. 48 (acceptable quality) came to similar conclusions for trans-fats policies. They found that limits, and particularly bans, were the most effective for reducing trans-fat levels in the food supply and diet while labelling had a lesser impact and was uneven across product categories. Hyseni et al. 38 (low quality) employed the upstream versus downstream classification, or population versus targeted interventions to assess salt-related policies. They concluded that ‘comprehensive multicomponent strategies involving upstream population-wide policies (regulation, regulatory reformulation and food labelling)’ had a much greater impact than downstream interventions targeting individuals (e.g. dietary counselling, media campaigns alone). They did not differentiate intervention levels within the ‘upstream’ category but highlighted the potential of combining interventions, such as labelling with salt targets. Lastly, Sisnowski et al. 39 (acceptable quality) concluded that regulations applied in isolation could improve the food environment and other distal outcomes but not dietary intake so far; yet they mentioned the promising results of taxation, which were published after their systematic review. Like Hyseni et al. ,50 they recommended combining interventions.
To explore the policies assessed in the overview of reviews further, we classified them by intervention levels and identified those with several components using the Nuffield intervention ladder. 53 However, since this project focused on interventions modifying the food environment, we did not document education programmes and public campaigns. As shown in Figure 12, most of the interventions assessed eliminated choice (by eliminating a nutrient or reducing its level), guided choices through disincentives (taxation) or provided information (labelling). One guided choice by changing the default (sides offered in children’s meals) while pledges by the retail sector encompassed several levels, from labelling to eliminating choice (reformulation).
FIGURE 12.
Types of policies assessed in the systematic reviews by governance approach and intervention level using the Nuffield intervention ladder. Black and grey: the Nuffield Intervention ladder. 53 Blue: regulatory. Green: voluntary. Orange: mixed (both regulatory and voluntary components). Line with ‘+’ sign: multicomponent intervention.
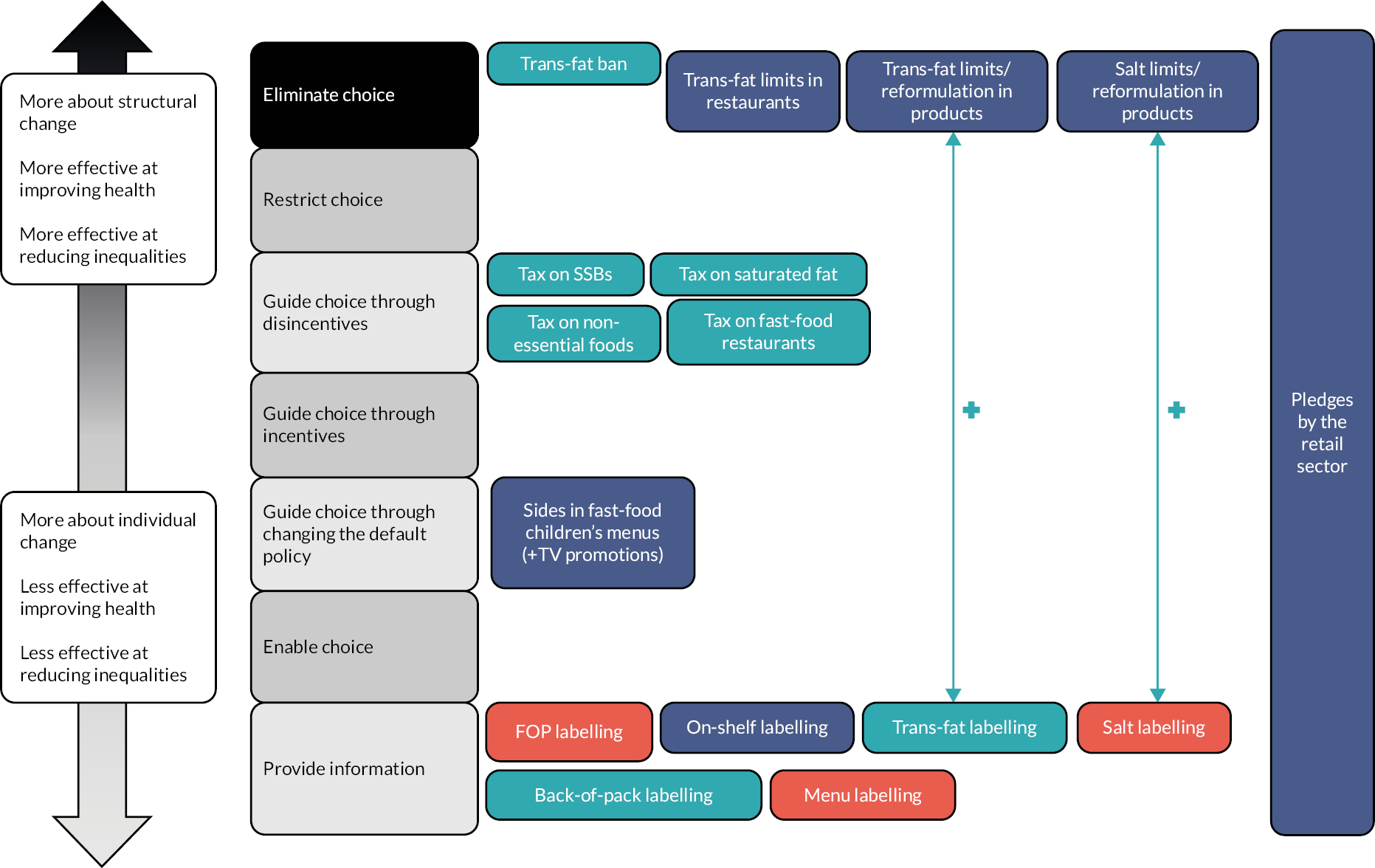
Furthermore, while some limited evidence suggests that it can help the public to make informed choices, has the support from the population, and can encourage food reformulation, Downs et al. and Hyseni et al. 38,48 highlighted that they are likely to increase inequalities for two reasons; (1) products can continue to contain a high amount of salt, sugar and fat, and low fibres, FV, especially cheaper options, so people from low SES are more likely to continue to consume them; (2) whether labels are regulatory or voluntary, customers need to understand and use them, which requires a certain health literacy level. By completely eliminating trans-fats, bans were identified as not only the most effective approach for reducing trans-fat consumption but also the most equitable. Therefore, the level of intervention, or extent of structural changes involved, potentially plays a role in both policy effectiveness and the reduction of inequalities. Yet, structural interventions also have their own challenges politically. Sisnowski et al. 39 mentioned that government policies can be softened to ‘appease industry and political opponents’, for instance, by bringing the focus on individual behaviours or reducing the extent of structural changes involved, thus misaligning them with public health recommendations.
Conclusions
Overall, the results suggest that, except for salt and saturated fat-related taxes, for which evidence is limited to few real-world initiatives including some with particularly narrow scopes, most regulatory approaches designed to improve health, consumer behaviour (e.g. food intake, purchases), and food environment outcomes were evaluated as effective. These mainly consisted of trans-fat bans, taxes on SSBs and non-essential foods (except for salt intake), and FOPL. Effects for voluntary approaches by public and private actors were also generally positive for salt and trans-fat reformulation (but regulatory trans-fat bans were more promising). Effects of labelling on products and supermarket shelves, and of changing defaults in children’s menus in restaurants were also generally positive, although limited to one or two studies each, mainly from the USA. Results for voluntary menu labelling and multicomponent commitments by large retail chains were mixed. The findings stratified by PROGRESS-Plus categories indicate a lack of reporting of outcomes in systematic reviews for population groups that are prone to health inequalities: overall, evidence on equity is patchy, incomplete, mainly inconsistent, and largely relies on single studies (although some evaluations had large samples) rather than aggregated bodies of evidence.
Chapter 5 Systematic review on the effectiveness of public–private partnerships to improve food environments and population diet
Introduction
This systematic review reports the evidence of effectiveness of PPPs to improve food environments and population diet, complementing the overview of reviews (see Chapter 4), which did not report on PPPs.
Methods
Literature search and eligibility criteria
This systematic review used the primary studies from the systematic evidence map that assessed the effectiveness of a PPP (see Chapter 3, Figure 8). To be considered as such, policies had to either be clearly labelled as a PPP or involve collaboration between at least one public and one private actor. Studies of any design (including document analyses) were considered if they assessed effects on the food environment, human behaviour or health, or the economy; or if they assessed the content or progress of the policy itself. Results had to be provided for PPPs separately, that is those aggregated with findings for other governance approaches were excluded.
Data extraction
In addition to the policy and evaluation characteristics extracted for the systematic evidence map (see Chapter 2), in a standardised extraction form we documented the following information: policy and study objectives, the policy leader and other main actors involved, implementation and data collection dates, study design, samples’ characteristics, results about effects including policy content, project or adherence as well as effect size and precision estimates, and potential competing interests of study authors using information from the declaration of competing interests, funding sources and authors’ affiliations. Data were extracted by one reviewer (CK, GB) and checked by another (CK, GB, JB, LB).
Study quality appraisal
Study quality was assessed using a modified version of the Newcastle–Ottawa Scale for cross-sectional studies. Studies were rated on seven domains and rated overall as having a low, moderate, high or unclear quality. Each item was assessed by one reviewer and checked by two others (JB, GB, LB). Disagreements were discussed until reaching consensus. Details about the tool are provided in Chapter 2 and Appendix 4, Table 26. This includes specifications for the document analyses. For appraising the representativeness of the sample, we considered whether the literature search was comprehensive; for the sample size justification, we considered the variety of information sources used taking into account the study aim; we considered the ‘analytical methods’ rather than ‘statistical tests’ only; questions relating to ascertainment of exposure and confounders were deemed non-applicable (because the documents were about the policies themselves, and there is currently no guidance for assessing confounders for such studies including if this is relevant). For studies involving human participants, both the original question about non-response and the modified guidance about missing data were applied. For appraising ascertainment to exposure, when participation status in a policy was unclear in a study, we compared the number of participants in the policy in general to those mentioned in the study in order to get a sense of whether participation status was up to date and likely to have remained relatively stable during the study or not.
Data synthesis
Due to high heterogeneity in the outcomes assessed, data were synthesised narratively by considering the general direction of effect by type of participants (human, environment, documents) and policy as well as overall study quality.
Findings
Of the 18 primary studies assessing the effectiveness of a PPP, 1 was excluded for not focusing on PPPs separately, leaving 17 studies in the systematic review.
Public–private partnership characteristics
Seven PPPs implemented in four countries between 2007 and 2016 were assessed (Table 8). Nine of the studies were about the FHD in Australia. Two of these also assessed the Australian Division of World Action on Salt and Health (AWASH) voluntary programme, including one together with the New Zealand Heart Foundation (NZHF) voluntary programme (the three policies overlapped in time). 54,55 Four studies evaluated the Public Health RD in England, UK,13,56–58 and another four investigated PPPs in the USA (the HWC twice,51,59 Choose Healthy Now (CHN)60 and the Strong4Life School Nutrition Program61). All studies in Australia and New Zealand (n = 9) focused on salt reformulation, two of which also assessed interventions to improve sugar, fat, fibres, fruit, vegetables content and portion size. In the other countries, the policy categories based on the NOURISHING framework ranged from menu and on-shelf labelling to food reformulation (calories or fat), the retail and catering sectors, and schools.
| PPP name | Policy categories assessed | PPP description and objectives | Implement. (I) and Eval. I years | PPP lead and partners |
|---|---|---|---|---|
| Australia (AUS) | ||||
| The AWASH voluntary programme (AWASH)54,55 | I-Reformulation by manufacturers (salt) | To reduce average population salt intake by 30% by 2025. | I: 2007 E: 2007–10 |
Lead: AWASH (NGO); Partners: NGOs, health and medical and food industry organisations |
| FHD54,55,62–68 | I-Reformulation by manufacturers (salt in all studies, other nutrients and food groups in two studies) | To act on food innovation through a voluntary reformulation programme on packaged foods, consumer education and portion standardisation in order to reduce the saturated fat, added sugar, sodium and energy content, and increase the fruit, vegetable, fibre and wholegrain content of foods in order to make ‘healthier’ food choices more accessible to Australians.63 | I: 2009 E: 2007–10 |
Lead: AUS government; Partners: Food industry, public health groups |
| New Zealand | ||||
| NZHF voluntary programme54 | I-Reformulation by manufacturers (salt) | To engage the industry for reducing sodium content in bread. Information on targets is not available anymore. | I: 2007 E: 2007–10 |
Lead: NZHF (NGO); Partners: Food industry (no further details) |
| UK | ||||
| The Public Health RD, England, UK13,56–58 | 12-Reformulation by manufacturers (fat); N-Labelling (menu/on-shelf); A wide range of categories |
The RD invited voluntary agreements across four ‘networks’ (food, alcohol, health at work and physical activity). | I: 2011 E: 2000–18 |
Lead: English Department of Healthb (government); Partners: Commercial actors (n majority), NGOs |
| USA | ||||
| CHN60 | S-Retail and catering sectors | To improve the healthfulness of snacks and drinks in convenience stores and snack shops. CHN nutritional criteria developed in collaboration with the Hawaii State Department of Health. | I: 2016 E: 2018 |
Lead: Hawaii State Department of Health; Partners: Convenience stores and snack shops |
| HWC51,59 | I-Reformulation by manufacturers (calories) | Compared to 2007, to collectively sell 1 trillion fewer calories in the USA by 2012 and 1.5 trillion fewer by 2015 to help reduce obesity (especially childhood obesity. | I: 2008 E: 2000–12 |
Lead: HWCF; Partners: 16 food companies |
| Strong4Life School Nutrition Program61 | O-Specific settings (schools) | To increase school meal participation and consumption of healthier foods in Georgia school cafeterias by better equipping school nutrition managers and staff members with skills and resources to make positive and visible changes in the cafeteria. Strategy includes sell, taste, visibility, convenience and price. | I: 2012 E: 2015 |
Lead: Governor of Georgia; Partners: Children’s Healthcare of Atlanta (a large paediatric clinical care providers) and schools |
Study characteristics
Two studies were cross-sectional,57,60 10 were repeat cross-sectional (7 pre–post,51,54,58,59,61–63 3 post–post55,64,65), 1 a time-series analysis59 and 5 were policy document analyses. 13,56,66–68 Five had humans as study participants (directly or by using purchases or sales data),13,56,66–68 six assessed food items, one assessed display of calorie labelling and five assessed documents. The human studies were about the USA and the UK, the studies of products were about Australia and New Zealand, the study of labelling practices was about the UK, and the policy document analyses were about Australia and the UK. All policies were assessed between 2 and 8 years after their introduction, giving time for the participants to implement the changes. Sample size of participant groups ranged from 16 restaurant chains (sample size can be especially small when studies used the number of companies as a unit of analysis, which is limited) to more than 2500 products. All studies of food products focused on salt content and were from Australia (with one on New Zealand as well). Two studies involving humans assessed the purchases and sales of calories, one trans-fat intake, and two looked at awareness, belief and/or self-efficacy relating to the policy. Two of the five document investigated achievements while the remaining three focused on the policy process, for instance whether the PPP encouraged participants to do more than what they were already doing, whether the actions they commit on are likely to be effective based on evidence, and whether they document progress and make it a priority.
Quality appraisal
Nine of the 17 studies were rated as having a low quality overall, 3 as moderate, 3 as high and 2 as unclear (Tables 9–11). Six of the nine studies about Australia were given a ‘low’ rating, whereas the three studies rated ‘high’ were policy document analyses. The main reason for an overall low quality was the lack of control group (which was not applicable to document analyses), which highly increased the risk of bias. Two studies involving humans only included people exposed to the PPP, and five studies of humans or products combined data for both PPP participants and NPs together, making it difficult to determine whether the effect was due to the PPP or not. Nevertheless, of the latter five, three were about the FHD in Australia, where a high proportion of products on the market were part of the PPP. For instance, Trevena et al. (2014)62,64 noted that about 95% of the market share of processed meats, 85% of pasta sauces, 80% of bread products and 60% of breakfast cereals were from participants in the FHD. Changes (or lack of changes) in these products overall are likely to be at least partly due to changes (or lack of) in participating products in the PPP.
| Author (date) | Selection | Comparability | Outcome | Overall rating | |||||
|---|---|---|---|---|---|---|---|---|---|
| Representativeness of sample size | Sample size justification | Non-response | Missing data | Ascertainment of exposure | Confounders | Assessment of outcome | Statistical methods | ||
| Beckelman et al. (2020)60 | Low (−) | Low (−) | Low (−) | Unclear (?) | High (++) (all exposed) | Low (−) (P only) | Low (−) | High (++) | Low (−) |
| Hutchinson et al. (2018)58 | High (++) | Low (−) | Unclear (?) | Unclear (?) | N/A (P and NP combined) | Low (−) (P and NP combined) | High (++) | High (++) | Low (−) |
| Ng et al. (2014)59 | High (++) | High (++) | Unclear (?) | Moderate (+) | High (++) | Moderate (+) | High (++) | High (++) | Moderate (+) |
| Ng et al. (2014)51 | High (++) | High (++) | Unclear (?) | High (++) | High (++) | Moderate (+) | High (++) | High (++) | Moderate (+) |
| Rajbhandari-Thapa et al. (2017)61 | High (++) | Low (−) | Low (−) | Low (−) | High (++) (all exposed) | Low (−) (P only) | Low (−) | High (++) | Low (−) |
| Author (date) | Selection | Comparability | Outcome | Overall rating | ||||
|---|---|---|---|---|---|---|---|---|
| Representativeness of sample size | Sample size | Missing data | Ascertainment of exposure | Confounders | Assessment of outcome | Statistical methods | ||
| Christoforou et al. (2013)55 | Moderate (+) | Unclear (?) | Unclear (?) | N/A (P and NP combined) | Low (−) (P and NP combined) | Low (−) | High (++) | Low (−) |
| Dunford et al. (2011)54 | Low (−) | Unclear (?) | Unclear (?) | N/A (P and NP combined) | Low (−) (P and NP combined) | Low (−) | High (++) | Low (−) |
| Levi et al. (2018)63 | Moderate (+) | High | Unclear (?) | Unclear (?) | Moderate (+) | High | High (++) | Unclear (?) |
| Sparks et al. (2018)65 | Moderate (+) | Unclear (?) | Unclear (?) | N/A (P and NP combined) | Low (−) (P and NP combined) | Low (−) | High (++) | Low (−) |
| Trevena et al. (2014)62 | Moderate (+) | Unclear (?) | High (++) | N/A (P and NP combined) | Low (−) (P and NP combined) | Low (−) | High (++) | Low (−) |
| Trevena et al. (2014)64 | Moderate (+) | Unclear (?) | High (++) | High (++) (all exposed) | Moderate (+)a | High (++) | High (++) | Moderate (+) |
| Robinson et al. (2019)69 | Moderate (+) | Unclear (?) | Unclear (?) | High (++) | Moderate (+) | Moderate (+) | Unclear (?) | Unclear (?) |
| Author (date) | Selection | Outcome | Overall rating | |||
|---|---|---|---|---|---|---|
| Search strategy | Variety of information sourcesa | Missing data | Assessment of outcome | Analytical methods | ||
| Elliot et al. (2014)66 | Low (−) | High (++) | Unclear (?) | Low (−) | Moderate (+) | Low (−) |
| Jones et al. (2016)67 | High (++) | High (++) | High (++) | Low (−) | Moderate (+) | Low (−) |
| Lindberg et al. (2017)68 | High (++) | High (++) | Unclear (?) | High (++) | High (++) | High (++) |
| Knai et al. (2015)56 | High (++) | High (++) | High (++) | High (++) | High (++) | High (++) |
| Knai et al. (2017)13 | High (++) | High (++) | Unclear (?) | High (++) | High (++) | High (++) |
Furthermore, justifications for sample size in studies of humans and products, and of information on non-responders in human studies were mostly judged as non-appropriate or not reported (unclear). Only seven studies reported information on missing data and how they were dealt with. Eight did not report on the number of people collecting or verifying data independently, contributing to a low quality for assessment of outcomes since such information missing likely means that only one person was involved. Quality of the analytical methods was generally rated high. All policy document analyses were judged to have sufficiently diverse sources of information.
Effects of public–private partnerships
Table 12 presents a summary of the study characteristics and key findings. Six studies assessed changes in salt content in Australia, all relating to the FHD and AWASH programme, which took place concomitantly. Findings pointed towards no or mixed effects overall, with four studies (three of low quality, one moderate) showing mixed or no effects, and two studies on the FHD (one low and one unclear quality) showed improvements overall. On the one hand, Levi et al. (2018)63 (unclear study quality) found that sodium levels in soups had fallen by 6% between 2011 and 2014. Sparks et al. (2018)65 (low quality) assessed sodium levels in processed meats between 2010 and 2017. They reported an 11% reduction in median sodium levels in the processed meats that had a salt target versus no change in those without a target. However, by category of products they reported mixed results with significant reductions in bacon, ham/cured meat and wet savoury pasties (p < 0.001, p = 0.012 and p = 0.006, respectively) and significant no change in emulsified luncheon meats (p = 0.363 and dry savoury pasties (p = 0.111). On the other hand, Dunford et al. (2011)54 (low quality) found that while the proportion of breads meeting the national salt target increased from 29% in 2007 to 50% in 2010, the mean sodium content did not change (434 mg/100 g in 2007 vs. 435 mg/100 g in 2010). Trevena et al. (2014)62 (low quality) noted no significant difference in the mean sodium content of pasta sauces (451 mg/100 g in 2008 vs. 423 mg/100 g in 2011; p = 0.016), cautioning the need to reformulate sauce products well beyond the FHD commitment. Another study by the same authors64 (moderate quality) examined breads, ready-to-eat breakfast cereals and processed meats. They reported significant reductions of sodium in bread (unlike Dunford et al. ) and breakfast products, and some reduction in processed meats, though with no apparent difference between participating brands, calling into question whether the partnership drove the reduction. Christoforou et al. (2013)55 (low quality) set out to report on changes in sodium levels in the ready meal market between 2008 and 2011. They concluded that the voluntary efforts of industry to reduce sodium levels of these foods over 4 years yielded a reduction of less than 1%. They ascribed this to the lack of co-ordination across industry and a failure of the Australian government to take leadership in improving the quality of the food supply.
| Lead author (year) PPP; study quality |
Study aim | Study design (data collection dates) |
Sample and data sources | Outcomes assessed | Results | Reported competing interests |
|---|---|---|---|---|---|---|
| Australia and New Zealand ( n = 9) | ||||||
| Dunford et al. (2011)54 NZHF and AWASH voluntary programmes Low (−) |
To define the effectiveness of recent efforts by AWASH, and the NZHF to reduce Na levels in breads in AUS and NZ. | Repeat cross-sectional (pre–post) (2007 and 2010) |
Packaged sliced bread labels (n = 157 in 2007, n = 167 in 2010) sold in AUS and NZ supermarkets. | Mean sodium (Na) content per 100 g, compared overall, by bread type, by manufacturer, and between nations. | From 2007 to 2010, the mean Na content of bread products in AUS did not change: 434 mg/100 g in 2007 vs. 435 mg/100 g in 2010; 7% reduction in NZ: 469 mg/100 g and 439 mg/100 g. The proportion of AUS breads meeting the national target increased from 29% in 2007 to 50% in 2010; the proportion of NZ breads meeting the national target increased from 49% in 2007 to 90% in 2010. Differences between the results achieved by different companies. |
Authors affiliated to AWASH |
| Christoforou et al. (2013)55 AWASH programme and FHD Low (−) |
To define changes in sodium levels within the ready meal market in AUS between 2008 and 2011. | Repeat cross-sectional (post–post) (2008, 2009, 2010, 2011) |
Ready meal products: n = 107 (2008), 313 (2009), 219 (2010), 265 (2011). Labels collected from two major and three smaller stores (together control 96% of AUS grocery market). |
Mean Na content per 100 g. Compared overall, by ready meal type, and by manufacturer. |
From 2008 to 2011, overall Na content of ready meal products was largely unchanged (279 → 277 mg) The proportion of AUS ready meals meeting the AWASH target fell slightly over the study period (59–57%) Differences between the results achieved by different companies. |
Authors affiliated to AWASH |
| Trevena et al. (2014)62 FHD Low (−) |
To assess the change in Na content of AUS pasta sauces between 2008 and 2011. (FHD) To project the mean Na content of products in 2014, comparing to the 2012 UK Na target for pasta sauce (330 mg/100 g). |
Repeat cross-sectional (post–post) (2008 and 2011) |
Pasta sauces sold in five supermarkets in Sydney, AUS (124 pasta sauces in 2008 and 187 in 2011). |
Mean Na content. Manufacturers grouped by type according to % volume share in 2009 (supermarket own label; leading manufacturers; other manufacturers). Na content assessed from product labels. |
Mean Na content was not sig different between 2008 and 2011 (451 mg/100 g vs. 423 mg/100 g; p = 0.16). Projected means exceeded 2012 UK target. Scenario 1: 381 mg/100 g; scenario 2: 375 mg/100 g. 22% reduction needed from 2011 levels to meet target. |
Authors affiliated to AWASH |
| Trevena et al. (2014)64 FHD Moderate (+) |
To assess Na reduction targets for breads, ready-to-eat breakfast cereals and processed meats, and quantify the magnitude of any changes in Na content and to explore whether changes differed by manufacturer or product category. (FHD) | Repeat cross-sectional (post–post) (July and September, 2010–3) |
Packaged foods in AUS supermarkets (n = 1849 in total); bread products, n = 885; breakfast cereals, n = 532; bacon/ham/cured meat, n = 387; emulsified meat, n = 45; bread: 2010, P (FHD participant) products, n = 145 (84%); 2013, P products, n = 177 (66%); bacon/ham/cured meat: 2010, P, n = 83, (92%); 2013, P, n = 98 (88%); emulsified meat: 2010, P, n = 9 (69%); 2013, n = 7 (64%); breakfast cereals; 2010, P, n = 86 (70%); 2013, n = 107 (67%). Data from product labels. |
Mean Na content. Products included bread products; value added products; ready-to-eat breakfast cereals; and processed meats (bacon/ham/cured meat and emulsified meat). |
Mean Na content of bread products and breakfast cereals sig reduced from 454 to 415 mg/100 g and 316 to 237 mg/100 g (p < 0.001), respectively. Sig increase in bread products reaching target (42–67%) (p < 0.005). Smaller but still sig reduction in Na in cured meats, bacon, ham (1215–1114 mg/100 g, p = 0.001). No apparent difference in Na reductions between P and P brands. |
Authors affiliated to AWASH |
| Elliot et al. (2014)66 FHD Low (−) |
To evaluate whether the FHD, is having an impact on reducing premature death and disability caused by unhealthy diet in AUS. | Policy document analysis adoption, (October 2009 to September 2013) |
Data on processed foods obtained from a food composition database. Data from the FHD website, media releases, communiqués and e-newsletters. |
Assessment of the FHD achievements (goals, targets, actions and health outcomes) by adopting the RE-AIM framework (reach, efficacy, implementation and maintenance. Na, saturated fat, added sugar, energy, fibre, whole grains, fruit/vegetable content, portion size. |
Data available to evaluate the FHD was limited. Several reports on achievements were missing. None of the targets were due to have been met by September 2013. Eight product categories had set Na targets. One product category had saturated fat targets, and only two product categories had portion size targets set. Engagement of relevant companies across product categories ranges from 60% to 100%. |
Authors affiliated to AWASH |
| Jones et al. (2016)67 FHD Low (−) |
To evaluate FHD over 6 years and to use the findings to develop recommendations for the success of the new HFP. | Policy document analysis (October 2013–November 2015) |
137 areas of possible FHD action. Data from FHD website, media releases, communiqués, e-newsletters, materials released under freedom-of-info, and Parliamentary Hansard. |
Assessment of the FHD (goals, targets, actions and health outcomes) by adopting the RE-AIM framework (reach, efficacy, adoption, implementation and maintenance). | Limited data is available to assess achievements. Not info about progress towards milestones published since October 2011. | No competing interests declared |
| Lindberg et al. (2017)68 FHD High (++) |
To explore if Australia’s largest food manufacturers positive (nutrition) changes to their product portfolios as disclosed in their public policies, priorities, and communications; To assess if salt reduction a priority for processed food manufacturers. | Policy document analysis (2010–May 2017) |
Grey literature by 33 Australian food manufacturers producing product lines of relevance to salt-reduction included. | Evidence of priority and progress for the FHD salt targets. | All (n = 33) manufacturers state nutrition and healthy eating as part of their policies, protocols and priorities. Many (n = 16) manufacturers provide no evidence or documentation of reducing salt in their products. Half of the sample (n = 17) describe some salt reduction activities, but the scale and efficacy of these changes is unclear. |
No competing interests declared |
| Levi et al. (2018)63 FHD Unclear (?) |
To examine the food industry’s progress and compliance with the FHD Na reduction targets for soup. | Repeat cross-sectional (pre–post) (between August and December in 2011, 2012, 2013, 2014) |
1153 dry, canned and chilled soups from the same four grocery retail stores in Sydney, Australia. [Products in PPP in 2014: 68 (77%) dry and 125 (59%) wet soups from 5 companies; Products not in PPP in 2014: 20 dry and 87 wet]. N companies (NR) Nutrition info from the George Institute Branded Food Composition Database. |
Na content of ‘wet and condensed’ and of ‘dry’ soups ‘as consumed’. | 6% reduction in Na levels in soups overall from 2011 to 2014 (p = 0.002). Sig reductions in Na observed in P products (p < 0.05). Not observed for NP products. In 2014, 67% of dry soups and 75% of wet soups met the Na reduction targets. In 2014, the number of dry soups from P that met the targets compared to when they entered the market sig increased (p = < 0.001). The same pattern was not witnessed with NP (some non-sig reductions were noted). For wet products, there was no sig change in the proportion of manufacturers meeting the target between 2011 and 2014 by participation status. |
No competing interests declared |
| Sparks et al. (2018)65 FHD Low (−) |
To assess the median Na sodium levels of 2510 processed meat products, including bacon and sausages, available in major Australian supermarkets in 2010, 2013, 2015 and 2017, and assessed changes over time. |
Repeat cross-sectional (post–post) (2010, 2013, 2015 and 2017) |
2510 processed meat products in four major supermarkets in Australia 2010: 181 (43%) P; 2017: 236 (35%) P. Nutrition data from the Australian FoodSwitch database. |
Na content of processed meat, of which five product categories have targets (P): bacon, ham/cured meat products, emulsified luncheon meats, wet savoury pasties and dry savoury pasties. | Median Na of P processed meats reduced by 11% (p < 0.001) vs. no change in NP (median difference 6%, p = 0.450). It was 1010 mg/100 g in 2010 vs. 898 mg/100 g in 2017 for P and 765 mg/100 g in 2010 vs. and 717 mg/100 g in 2017 for all processed meat. A higher proportion of bacon, ham/cured meat products and wet savoury pasties met the targets between 2010 and 2017 (p < 0.001, p = 0.012 and p = 0.006, respectively) while there were no change for emulsified luncheon meats (p = 0.363 and dry savoury pasties (p = 0.111). |
Declared affiliations with WHO Collaborating Centre on Population Salt Reduction |
| UK ( n = 4) | ||||||
| Knai et al. (2015)56 Public Health RD High (++) |
To analyse the evidence of the effectiveness of the specific interventions in the RD pledges and the likelihood that the pledges have brought about actions among organisations that would not otherwise have taken place. |
Policy document analysis (synthesis of RD website reports using evidence on effectiveness from an overview of reviews) (At implementation: 2011 and post-impl.: 2015) |
Six RD pledges, 17 evidence reviews. Comparative analysis of published progress reports and publicly available data on RD website. |
Likely effectiveness and added value of pledges. Explored changes over time, and compared to what was originally set out in delivery plans. |
Progress reports were very inconsistently provided on the RD website and mostly unavailable. The most common intervention in the salt reduction pledge involved reformulation activities (46%). Reformulation of recipes and menus was the most commonly listed intervention in the calorie reduction pledge (64%). Some of the RD food interventions could be effective, if fully implemented. Most interventions reported by organisations seemed either clearly (37%) or possibly (37%) already underway. |
No competing interests declared. Funding: NIHR Policy Research Unit |
| Knai et al. (2017)13 Public Health RD High (++) |
To evaluate the Public Health RD effectiveness at encouraging signatory organisations to remove artificially produced TFAs from their products. | Policy document analysis (2015) |
Publicly available data in the progress reports of the signatory organisations to the pledge confirming non-use of TFAs (n = 90). | Compared progress reports against what had been originally set by organisations in their delivery plans. |
91% of the signatory organisations (n = 82) had already removed TFAs or had removal of TFAs underway before the RD started. 9% (n = 11) signatory organisations signed up to part 2 of the pledge (pledging artificial TFA removal). Five were not in a position to reformulate food products at the point of manufacture, some reported replacing products. |
No competing interests declared. Funding: NIHR Policy Research Program |
| Hutchinson et al. (2018)58 Public Health RD Low (−) |
To explore whether voluntary reformulation results in different intakes of TFAs among socioeconomic groups. |
Repeat cross-sectional (pre–post) (pre-reformulation: 2000–1 vs. postreformulation: 2010–1 to 2011–2) |
UK adults aged 19–64 years from the UK National Diet and Nutrition Surveys (NDNS) Pre-reformulation: n = 1724; Postreformulation: n = 848 Food intake collected by 7-day weighed records pre-ref and 4-day diaries postref. |
TFA intake pre- and postvoluntary reformulation with comparisons between high and low TFA consumers. | Pre-ref 57% of adults exceeded the WHO TFA intake limit, compared with 2.5% postref. Pre-ref: high TFA intake associated with lower income, lower education and long-term illness; Artificial TFA’s prominent. Postref: people with higher incomes 2.5–3.3 times more likely to be top 10% consumers; ruminant TFAs prominent. |
Affiliation to WHO Funding: WHO |
| Robinson et al. (2019)57 Public Health RD Unclear (?) |
Threefold aims: 1.To examine the proportion of major UK restaurant (fast-food and full-service) and takeaway chains that provide kcal info at point of choice and if current practices comply with the RD rec. 2.To examine the adequateness of kcal labelling practises among eligible chains that also signed the RD (2011) kcal labelling pledge. 3.To explore how common it was for chains not to provide instore kcal info but have info available on their websites. |
Cross-sectional (post, once) August 2018 |
Food and beverage items from 104 large chains (16 P; 88 NP) Full-service restaurant chains (n = 58) Takeaway or fast-food chains (n = 22) Coffee shops (n = 20) Supermarket chains (n = 4) Verified by contacting companies, reviewing websites and conducting some physical audits. |
Presence of calorie labelling and adherence to policy guidelines. | Of the 104 chains, 18 displayed calorie labelling in stores: 12 (67%) of participants, and 6 (7%) of NPs. None fulfilled all seven recommended labelling criteria. Only one P and two NP chains provided calorie labelling for all items sold. 43/86 (50%) of the chains that did not provide in store kcal labelling had product kcal info on their websites or were able to provide this info on request. |
Declared prior funding from American Beverage Association and Unilever; Affiliations: university and NR |
| USA ( n = 4) | ||||||
| Ng et al. (2014) sales51 HWCF Moderate (+) |
To evaluate the HWCF companies’ collective change in total calorie sales between 2007 and 2012 and to identify which food and beverage categories were major sources of the reductions or increases in calories sold. | Time-series analysis (pre–post) (2007 and 2012) |
Calories sold from consumer packaged goods sales data from mass merchandisers and convenience stores (2012 only + nutrition info from Nielsen Scantrak data, Nutrition Fact Label data from Gladson, Mintel GNPD, Datamonitor PLA). | Calories in food and beverages sold. | Total calories sold by the HWCF companies fell from 60.4 trillion in 2007 to 54 trillion in 2012 – a decrease of 6.4 trillion calories (or –10.6%) over the 5-year pledge period. CPG caloric sales (all brands) fell from 1548 to 1449 kcal/capita/day between 2007 and 2012. With an average decline of 78 kcal/capita/day from P brands and an average of 22 kcal from NP brands. Absolute caloric sales from retailers’ private label products essentially did not change. Reductions from HWCF brands came primarily from sweets and snacks (21 kcal); grain products (17 kcal) such as RTE cereal and granolas; fats and oils; sauces and condiments (15 kcal); beverages (14 kcal), particularly carbonated soft drinks (7 kcal); and shelf-stable FV drinks/juices (5 kcal). |
Declared prior funding from Nestlé, Kraft and Gerber Foods |
| Ng et al. (2014) purchases59 HWCF Moderate (+) |
To assess the total CPG calories purchased per capita per day by households. To compare HWCF name-brand products with non-HWCF name-brand products and private label products, and using a counterfactual based on pre-pledge trends, see if the HWCF contributed to a reduction in calories purchased. | Repeat cross-sectional (pre–post) (2000–12) |
CPG purchase data (food and beverages) Nutrition info from Nielsen Homescan data, Nutrition Fact Label data from Gladson, Mintel GNPD, Datamonitor PLA. |
Calories purchased per capita per day by households. | Unadjusted annualised caloric sales of CPG declined faster in the post pledge (2008–12) period than pre-pledge (2000–7). Private labels saw sig declines postpledge. HWCF products saw the greatest absolute and relative declines in calories. The rate was statistically steeper postpledge. Non-HWCF calorie declines across private label products slowed postpledge, not sig. A sig (p < 0.001) reduction in CPG calories between 2007 and 2012 of −206 kcal/capita/day, −96 kcal from HWCF products, −63 kcal from non-HWCF and −47 from private labels. Postpledge reductions were greater than pre-pledge trends (counterfactual). |
Declared prior funding by Nestlé’s Water USA received a gift from Kraft and Gerber Foods to cofund a national dietary survey |
| Rajbhandari-Thapa (2017)61 Strong4Life School Nutrition Program Low (−) |
To assess the effect of the Strong4Life School Nutrition Program on (1) participant knowledge of evidence-based strategies for improving school cafeteria and student school meal practices and self-confidence in their ability to make changes, (2) the school cafeteria environment and (3) National School Lunch Program participation. | Repeat cross-sectional (pre–post): Strong4Life School Nutrition Program 90-minute training session (2018) |
Follow-up questionnaire with 842 participants (managers and staff). | Changes in participant knowledge, beliefs, and self-efficacy. | Significant improvements were noted in Ps for: •knowledge of improving taste perception by using appealing menu names (from 78% to 95%, p < 0.001). •understanding that food selection is influenced by location in the lunch line (from 78% to 95%, p < 0.001) •self-perceived capacity to modify the cafeteria environment (from 91% to 96%, p < 0.001). Participation in school lunch in the month following training did not change. |
Funding: Strong4Life Program at Children’s Healthcare of Atlanta. Authors were employed by Children’s Healthcare of Atlanta’s Strong4Life Program |
| Beckelman (2020)60 CHN Low (−) |
To describe the efforts of the Hawaii State Department of Health to scale up the CHN program through partnerships with two convenience store chains at a statewide level. | Cross-sectional (2015) |
Adults > 18 years living in Hawaii (n = 162); exit store survey and Hawaii Behavioral Risk Factor Surveillance System, a statewide random digit−dial telephone survey. | Awareness of CHN and influence: exit surveys with convenience store customers > 18 years | Store survey exit: convenience and price were the most influencing factors, followed by health and nutrition. Nearly half of Ps (n = 162; 46.3%) recalled seeing a CHN sign in the store when shown an example. Sign recall did not differ by age, gender, and ethnicity. Among those who recalled seeing a sign (n = 75), 13.3% said that it influenced their purchases. Telephone survey: one-third (34.8%) said having seen or heard a CHN campaign advertisement, especially native Hawaiian and other Pacific Islanders, who had a higher recall rate (43.6%) |
None reported |
In Australia again, three studies assessed potential achievements or the policy process of the FHD using documents. Elliot et al. (2014)66 (low quality) assessed whether the FHD was reducing premature death and disability but found that the data available were limited, with several reports on achievements missing, concluding that the current voluntary approach to preventing diet-related ill health is insufficient. Jones et al. (2016)67 (low quality) evaluated the FHD over 6 years (from October 2019 to September 2013) but found limited data to assess achievements,67 much like Elliot et al. (2014). They found that no information about milestones had been published since October 2011. They concluded that strong government leadership, adequate funding, clear targets and timelines, management of conflict of interest, comprehensive monitoring and evaluation, and a plan for responsive regulation in the event of missed milestones will be required to ensure that the new partnership set out as a continuity of the FHD, the Healthy Food Partnership, achieves its public health goals. 66 This echoes the studies on the Public Health RD (England, UK) below. 56 Lindberg et al. (2017)68 (high quality) set out to understand whether salt reduction was a priority for processed food manufacturers in Australia. They reported that manufacturers did not appear to be making significant and comprehensive positive (nutrition) changes in relation to salt. This included 16 of the 33 manufacturers assessed not providing evidence of reducing salt in their products.
For New Zealand, Dunford et al. (2011) (low quality) reported an estimated 7% reduction of mean sodium content in bread products compared to none in Australia, highlighting important disparities between company efforts. The authors felt that this indicated lack of government leadership, non-governmental organisations (NGOs) lack authority and resources, and a renewed need for committed leadership from the government. 54
Four studies evaluated the Public Health RD in England, UK. As part of the RD evaluation covering alcohol, food, physical activity and health at work, Knai et al. (2015)56 (high quality) reported on the effectiveness of the food pledges using policy documents. Much like Elliot et al. (2014) and Jones et al. (2016) in Australia, they found that the lack of data reported by participating food industries made the evaluation challenging. They reported an overall lack of additionality of the RD, as most of the reported actions were already underway (meaning that the PPP had had little added value). They also found that the majority of the food pledges propose interventions that favour information provision, awareness raising and communication with consumers, which may have limited effect. Another study by Knai et al. (2017) (high quality) focused specifically on the RD’s trans-fat reduction pledges. Based on progress reports from 2015, the pledges appeared to have had negligible impact on reducing artificial trans-fats from England’s food supply beyond pre-2011 levels. 13 The authors concluded that the most effective strategies to improve diet are not reflected in the RD food pledges, and that there was paucity and heterogeneity of organisations’ progress reports. Hutchinson et al. (2018)58 (low quality) assessed whether the RD resulted in different intakes of trans-fatty acids (TFA) across different socioeconomic groups before (2000–11) and after the PPP (2010–2). They reported that voluntary reformulation had had some effect in reducing TFA of many UK products, when comparing data from the National Diet and Nutrition Surveys before and after the RD implementation. However, the surveys only include a small variety of popular foods and brands from large retailers, which may mask TFA differences between foods consumed by different population groups. High TFA consumption was associated with socio-economic disadvantage pre-RD, but post results were less clear regarding inequalities. Finally, Robinson et al. (2019)57 (unclear quality) studied calorie labelling practices in the UK eating out of home sector in 2018 and whether they were aligned with the RD pledges. They found that it was rare for eating out and takeaway chains to provide in store kcal labelling and when labelling is provided it does not meet recommended labelling practices.
Four studies from the United States. Two of these, both by Ng et al. 201451,59 (moderate quality), evaluated the impact of the HWC on total calories sales and calories purchased. They both reported successes, including over 10% fall in calories sold over the 5-year pledge period among participating companies, though absolute caloric sales from retailers’ private label products essentially did not change. As with the RD evaluation findings, the additionality of the HWC, that is whether there was added value from signing up to it to motivate change (e.g. reformulation), was questioned, and was reported as potentially relating to factors beyond the pledges such as changes in consumer demands, or economic factors. Moreover, it should be noted that 13 of the 16 signatories also belong to the CFBAI, which is another self-regulated voluntary pledge by the industry. Two other American partnerships were evaluated: Rajbhandari-Thapa (2017)61 (low quality) evaluated the Strong4Life School Nutrition Program. They found that the programme’s training increased school nutrition manager and staff member knowledge of the Strong4Life Smart Serving Strategies, as well as their beliefs, self-efficacy, and confidence in their ability to make positive behavioural and environmental changes in the school cafeteria. Beckelman (2020)60 (low quality) assessed the Hawaii State Department of Health’s work to scale up the CHN programme through partnerships with two convenience store chains at a statewide level. The programme was considered a mutually beneficial partnership, with leadership buy-in, support for implementation, and a need to meet retailer needs, for example, modifying signage size and type.
The findings remain the same when looking at the types of participants or study quality with a majority of studies pointing towards inconclusive or no effects overall except for human studies. Studies of food products and labelling practices showed overall mixed or negative results independently of study quality. Similar observations can be made for the document analyses, which all pointed towards a lack of information, lack of commitments, and/or unlikeliness of the policy to provide added value independently of their quality. As for the five human studies, they showed mixed results overall. The three human studies that showed overall positive effects were of low quality, while the two of moderate quality showed mixed results. This might be due to the types of outcomes assessed: two of the positive studies reported on participants’ awareness and self-efficacy rather than changes in the environment or human behaviours and another measured trans-fat intake, while studies with mixed results examined calorie sales and purchases. The type of products assessed could also explain the differences in directions of effects noted for the FHD, that is it is possible that progress was indeed made in soups and processed meats overall but not in other product categories.
Conclusions
This systematic review aimed to complement the overview of reviews (see Chapter 4) by assessing the effectiveness of PPPs targeting the food environment since the overview of reviews did not include data on the latter. From the available evidence reviewed across 17 studies evaluating 7 PPPs, partnerships with the food industry to improve diets via reformulation or other changes to the environment appear to have limited effectiveness at achieving this aim.
Chapter 6 Systematic review on the effectiveness of voluntary approaches by commercial actors to improve food environments and population diet
Introduction
This systematic review aims to complement the overview of reviews (see Chapter 4), which provided limited information on voluntary approaches by private actors. It assesses the effectiveness of voluntary approaches by private actors aiming to improve food environments by measuring the differences between participating and NP organisations, including compliance to the policy guidelines and effects on the food environment, dietary intake and health.
Methods
Literature search and eligibility criteria
The systematic evidence map identified 183 primary studies that assessed the effectiveness of a voluntary policy (including the voluntary element of interventions, which include both a regulatory and voluntary component) (see Chapter 3, Figure 8). Studies of any design (including document analyses) were considered if they assessed effects on the food environment, human behaviour or health, or the economy; or if they assessed the content or progress of the policy itself. Results had to be provided for voluntary approaches separately, that is those aggregated with findings for other governance approaches were excluded. Three additional criteria specific to this review were also added and screened by a single reviewer (SR, LB): (1) Initiatives developed and implemented by a single company were excluded; (2) The study had to compare organisations participating in the policy to NPs in terms of adherence or compliance to policy guidelines or effects on the food environment, dietary intake or health; (3) Due to the high number of studies potentially eligible and the limited time available, we focused on research articles published in the past 4 years (2017–20). Annual reports on advertising control policies of the voluntary and private sectors were excluded. The references of the included studies were screened against the above eligibility criteria.
Data extraction
In addition to the policy and evaluation characteristics extracted for the systematic evidence map (see Chapter 3), we documented in a standardised extraction form the following information: policy and study objectives, the policy leader, implementation and data collection dates, study design, samples’ characteristics, results about effects or adherence between participants and NPs including effect size and precision estimates, and potential competing interests of study authors using information from the declaration of competing interests, funding sources and authors’ affiliations. For studies on advertising control policies, we only extracted outcomes relating to unhealthy foods because these are the ones that such policies normally aim to control for; and when on TV we captured such outcomes during both children’s peak time and children’s programmes (CP) since children are normally the target population of these policies. Data were extracted by one reviewer (SR, GB, JB, LB) and checked by another (GB, JB, LB).
Quality appraisal
Study quality was assessed using a modified version of the Newcastle–Ottawa Scale for cross-sectional studies (see Chapter 2). Studies were rated on seven domains and rated overall as having a low, moderate, high or unclear quality. Each item was assessed by one reviewer and checked by another two. Modifications to the tool are explained in Chapter 2 and detailed in Appendix 4, Table 26. For appraising ascertainment to exposure when participation status in a policy was unclear, we compared the number of participants described in the policy characteristics data extraction form to those mentioned in the study to get a sense of whether participation status was up to date in the study and was likely to have remained relatively stable.
Data synthesis
Due to the high heterogeneity in the outcomes assessed, data were synthesised narratively by policy and type of outcome by considering the direction of effect between participants and NPs. For a graphical representation of the summary findings, we used an effect direction plot26,27 (see Chapter 2), displaying non-standardised effects across multiple outcome domains. Studies were grouped by policy and ordered by overall study quality, publication date and study design. The effect direction plot was also used to present jointly the direction of effect, study quality and indirectness, which was a compromise for not using the GRADE framework (see Chapter 2).
Findings
Of the 183 primary studies in the evidence map assessing the effectiveness of a voluntary policy, 16 met the inclusion criteria after full-text screening. The remainder (n = 167) were excluded as they did not include commercial actors or focused on a single company (n = 47), did not compare participants versus NPs (n = 70), did not meet the publication date cut off (n = 48) or were not journal articles (n = 2). The selection process is illustrated in Figure 13. The excluded studies along with the justifications are listed in the Report Supplementary Material 1.
FIGURE 13.
PRISMA flow chart representing the selection process for the review of voluntary approaches. Adapted from the PRISMA template by Page et al. (2021). 16
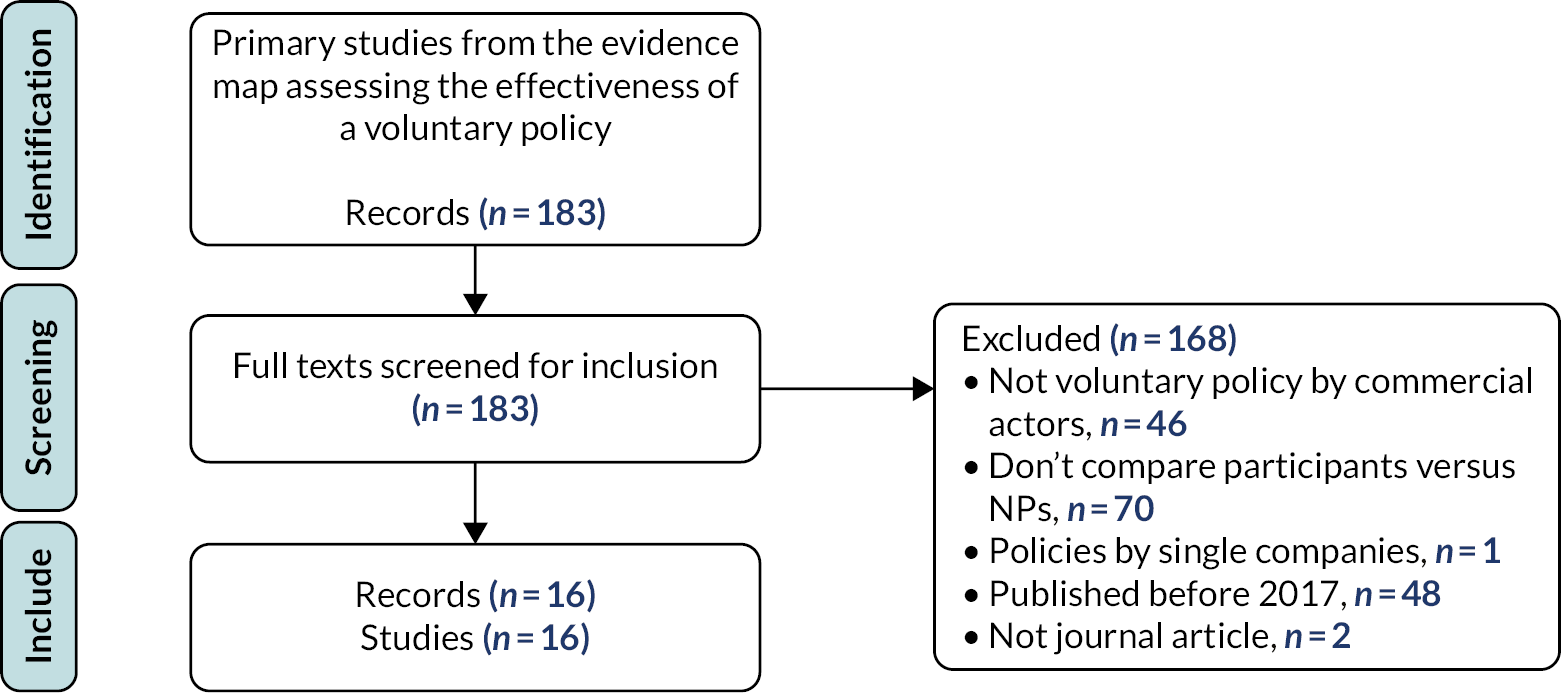
Commitment characteristics
Nine policies, implemented across seven countries [Australia, Belgium, Canada, Germany, the Netherlands, UK (England), USA], were evaluated. Table 13 presents the characteristics of the policies across the time period that they were evaluated. Four policies were in Australia, namely the FHD (n = 2),63,65 the Healthier Australia Commitment (n = 1),70 the QSRI (n = 3),71–73 two of which also included the Responsible Children’s Marketing Initiative (RCMI) (n = 2). 71,72 The remaining five consisted of the CFBAI in Canada (n = 5),74–77 the European (EU) Pledge evaluated in Belgium, the Netherlands and Germany (n = 2),78,79 the Public Health RD in England, UK (n = 1),57 and both the CFBAI (n = 2)80,81 and Kids LiveWell (n = 1)82 in the USA. Seven of these policies [Canadian Children’s Food and Beverage Advertising Initiative (CAI), CFBAI, EU Pledge, Healthier Australia Commitment, Kids Livewell, QSRI and the RCMI] were officially led by a private organisation representing food and beverages corporations while the remaining two (RD and FHD) were led by a governmental institution. The Australian FHD, the Healthier Australia Commitment, and the RD in England were PPPs. The number of participating commercial actors across the policies ranged from 7 (QSRI) to 150 (Kids LiveWell82).
| Study | Selection | Comparability | Outcome | Overall rating | ||||
|---|---|---|---|---|---|---|---|---|
| Representativeness | Sample size | Missing data | Ascertainment of the exposure (policy) | Confounding | Outcome assessment | Statistical test | ||
| Harris (2018) (study 1)80 | Moderate (+) | Unclear | Unclear | High (++) | Moderate (+) | High (++) | Unclear | Unclear (?) |
| Landwehr (2020)79 | Moderate (+) | Moderate (+) | Unclear | High (++) | Moderate (+) | Moderate (+) | High (++) | Moderate (+) |
| Levi (2018)63 | Moderate (+) | High (++) | Unclear | Unclear | Moderate (+) | High (++) | High (++) | Unclear (?) |
| Moran (2017)82 | Moderate (+) | Unclear | High (++) | Low (−) | Moderate (+) | High (++) | High (++) | Low (−) |
| Neyens (2017)78 | Low (−) | Moderate (+) | Unclear | Unclear | Moderate (+) | Moderate (+) | Unclear | Low (−) |
| Potvin Kent (2018) Online76 | Moderate (+) | High (++) | Unclear | High (++) | Moderate (+) | Moderate (+) | High (++) | Moderate (+) |
| Potvin Kent (2018) TV74 | Moderate (+) | Moderate (+) | High (++) | High (++) | Moderate (+) | Low (−) | High (++) | Low (−) |
| Potvin Kent (2020)75 | Moderate (+) | Moderate (+) | Unclear | High (++) | Moderate (+) | Moderate (+) | High (++) | Moderate (+) |
| Robinson (2019)57 | Moderate (+) | Unclear | Unclear | High (++) | Moderate (+) | Moderate (+) | Unclear | Unclear (?) |
| Smithers (2019)71 | Low (−) | Unclear | Unclear | High (++) | Moderate (+) | Moderate (+) | Unclear | Low (−) |
| Sparks et al. (2018)65 | Moderate (+) | Unclear (?) | Unclear (?) | N/A (P and NP combined) | Low (−) (P and NP combined) | Low (−) | High (++) | Low (−) |
| Spiteri (2018)70 | High (++) | Unclear | High (++) | Unclear | Moderate (+) | High (++) | High (++) | Unclear (?) |
| Vaala (2020)81 | Low (−) | Moderate (+) | Unclear | High (++) | Moderate (+) | Moderate (+) | High (++) | Low (−) |
| Vergeer (2019)77 | Moderate (+) | High (++) | Unclear | High (++) | Moderate (+) | Moderate (+) | High (++) | Moderate (+) |
| Watson (2017)72 | Moderate (+) | High (++) | High (++) | High (++) | Moderate (+) | Moderate (+) | High (++) | Moderate (+) |
| Wellard-Cole (2019)73 | High (++) | Unclear | High (++) | High (++) | Moderate (+) | Low (−) | High (++) | Low (−) |
Regarding the policy categories assessed using the NOURISHING framework, unsurprisingly, the five advertising control policies (CAI, CFBAI, EU Pledge, RCMI, QSRI) were evaluated from an R-Advertising and marketing perspective; the QSRI was also assessed in the S-Retail and food service sector (children’s meals in fast-food outlets). The effect of both Australian partnerships was assessed on product reformulation (I) while studies of Kids LiveWell and the RD focused on labelling.
The five policies that include an advertising and marketing control component implied not to advertise unhealthy food to children under a certain age, which varied between 6 years old with the CFBAI in the USA to 12 years old with the CAI in Canada and the EU Pledge (although as part of the EU pledge, the Netherlands committed to prohibit it to < 7-year-olds only). The nutritional criteria used to define healthy or unhealthy food varied across the policies. The FHD was launched with specific sodium targets for healthier products. Healthier Australia Commitment provided a relative percentage decrease in sodium, saturated fat and energy. Four policies (CAI, CFBAI, EU Pledge and QSRI) were launched without unified criteria but implemented criteria later on (CFBAI in 2013, QSRI and EU Pledge in 2014 and CAI in 2018). Signatories to the RCMI developed their own nutritional criteria and the definitions were reported as being unclear (9). Nutritional criteria were also unclear or vague for Kids LiveWell and the RD.
Study characteristics
All studies were cross-sectional: nine measured data at a single point in time (single cross-sectional) and seven at two points in time after the policy was implemented (repeat pre–post). None used humans as participants but rather analysed food items, adverts and other environmental features. All policies were assessed at least 3 years after their introduction, which should have given some time for participants to implement changes, and 12 studies evaluated effects after at least 7 years after implementation (especially for advertising and marketing outcomes). Sample size of participant groups ranged from seven companies [sample size can be especially small when studies compare number of companies participating (P) and NP, which are limited] to about 100–200 participating products or adverts. One study assessed over 35 million food adverts on websites from participating companies.
Study quality appraisal
The overall judgement of each domain and final rating for each study is noted in Table 13. Studies about advertising and marketing control were generally of higher quality than those on the retail and catering sectors. Overall, six studies were assessed as having a low quality overall, five as moderate, and four were judged ‘unclear’. None were rated as high. Across all studies, there were concerns identified about selection bias with three studies using convenient or non-representative samples. There were generally low concerns about the ascertainment of the exposure except for one study mentioning that participation status in a policy had changed through time and was not accounted for in the analysis; otherwise, there were no obvious reason to believe that authors did not use an up-to-date list of participants or that participant status changed during the evaluation period and was not accounted for bias arising from comparability of participants and confounding factors controlled, although in some studies information was unclear. In outcome assessment, two studies had their data collected by a single researcher only. Only five studies included appropriate information on how they dealt with missing information and nine justified their sample size. When reported, the use of statistical tests was judged appropriate, but four studies failed to report information on their statistical analysis.
No important conflicts of interest were identified for authors of any of the 16 studies included (Table 14). Two studies’ lead author had previously worked on research projects funded by the food industry (American Beverage Association, Unilever, Nestlé, and the Dairy farmers of Canada). In 10 studies, authors declared having no conflict of interest; the remaining did not have a competing interest declaration. Funding was received from government or research bodies, universities, and private or not-for-profit organisations. Six studies did not report their source of funding. Authors were affiliated with universities or other public organisations (with affiliations partly unclear in three studies).
| Voluntary approaches (associated studies) |
Country; lead org | Policy categories assessed | I and Eval years | N participants between I and last E years | Commitment objectives | Criteria for defining healthy and unhealthy food |
|---|---|---|---|---|---|---|
| CFBAI74–76 | CAN; Ad Standards | R-Ad&Mkt | I: 2007; E: 2013–7 | 16 companies in 2007; 18 from 2009 to 2016 | To promote healthy diets and lifestyles in all child-directed marketing activities. Seven companies pledged to only advertise ‘healthier dietary choice’ products to children < 12 years. 11 pledged not to direct any advertising to children < 12 years in various media.75 |
Uniform Nutrition Criteria implemented in 2015. Specify nutrition criteria for eight product categories: milk and alternatives, grains, soups, meat and alternatives, vegetables and fruit, occasional snacks, mixed dishes, and meals on the go. None for chocolate, candy, and soft drinks because they should not be advertised to < 12 seconds. Nutrients to limit: calories, saturated and trans fats, sodium, and total sugars. Nutrients to encourage: vitamin D, calcium, potassium and fibre.76 |
| CFBAI80,81 | USA; BBB National Programs | R-Ad&Mkt | I: 2006; E: 2013–8 | 10 companies in 2006; 13 in 2008; 18 from 2012 to 2018 | Originally: to promote self-regulation to improve the healthfulness of foods marketed across media platforms to children < 12 years. From 2010: to not use licensed characters, celebrities, and athletes in any advertising for unhealthy foods.83 From 2016 or before: 17 out of 18 companies pledged to not direct any marketing to children < 6 years.80 |
Uniform criteria adopted in December 2013 and updated in 2018. Specify criteria for both healthy and unhealthy food. Breakfast cereals: to be advertised, cereals must contain the following per serving (portion size NR): < 200 cal, < 1.5 g of saturated fat, < 290 mg of sodium and ≤ 12 g added sugar.81 |
| EU Pledge78,79 | EU (studies in BEL, GER and NET); World Federation of Advertisers |
R-Ad&Mkt | I: 2007; E: 2012–4 | 11 in 2007; 19 in 2012; 20 in 2013; 21 in 2014 | To restrain from unhealthy food advertising to audiences including at least 35% children < 12 years old on television, internet as well as promotional activities in schools (the Netherlands pledged to prohibit it to < 7-year-olds only). From 2014: only advertise products to children < 12 that meet the common EU Pledge Nutrition Criteria; or to not advertise products at all to children under the age of 12 years; products not in compliance with pre-defined nutritional criteria not to be advertised in television programmes with at least a 35% child audience. |
Initially companies defined their own. In 2014, the EU Pledge Nutrition Criteria was adopted (10 food categories). |
| FHD63 | AUS; Federal Government | I-Ref | I: 2009; E: 2010–7 | NR (~90% of soups retailed in Australia were produced by participants when sodium targets were set); 2510 processed meat products, including bacon and sausage | To act on food innovation through a voluntary reformulation programme on packaged foods, consumer education and portion standardisation in order to reduce the saturated fat, added sugar, sodium and energy content, and increase the fruit, vegetable, fibre and wholegrain content of foods in order to make ‘healthier’ food choices more accessible to Australians.63 | Sodium targets (mg/100 g) for the participants:
|
|
||||||
| Healthier Australia Commitment70 | AUS; Australian Food and Grocery Council | I-Ref | I: 2012; E: 2015 | Eight major companies in 2012; unclear in 2015 | To reduce sodium by 25%, saturated fat by 25%, and energy by 12.5% by 2015. | Target based on % reduction |
| Kids LiveWell82 | USA; National Restaurant Association | N-Menu label | I: 2011; E: 2012–5 | Membership growing since 2011; 150 restaurants across 42,000 locations in 2015 | To increase the number of nutritious menu items available to children (only requires offering one children’s meal and one other item that meet the nutrition standards). | Unclear and website does not exist anymore |
| QSRI71–73 | AUS; Australian Food and Grocery Council | R-Ad&Mkt S-R&S |
I: 2009; E: 2015–7 | Seven fast-food outlets between 2009 and 2017 | To reduce the advertising of discretionary foods to children; to help promote healthy dietary choices and healthy lifestyles amongst children. | 2014 Nutrition Criteria specifying maximum energy, saturated fat, sugar and sodium content for meals as well as (vague) criteria for meal composition |
| RCMI71,72 | AUS; Australian Food and Grocery Council | R-Ad&Mkt | I: 2009; E: 2015–7 | 15 food and grocery manufacturers in 2009; 17 between 2010 and 2016; 18 in 2017 | To reduce advertising and marketing communications to children of food and beverage products that do not represent healthy choices; to help promote healthy dietary choices and healthy lifestyles amongst children. | Companies established their own nutrition criteria to determine foods appropriate for marketing to children. ‘Unclear definitions of what constitutes unhealthy food’ |
| The Public Health RD57 | England, UK; Department of Health (England) |
N-Menu label | I: 2011; E: 2018 | 16 large food service chains had signed the kcal labelling pledge as of 2018 | The focus on labelling included to display calorie information at the point of choice (i.e. menus, shelves), which included seven specific recommendations. | N/A for the kcal labelling pledge |
Effects of voluntary approaches
Table 15 presents the study characteristics and key findings.
| Author (date) | Policy name (country where assessed) | Study aim | Study design; data collection dates |
Sample (N P; N NP) |
Outcomes compared between P and NP and data sources | Results comparing P and NP | Reported funding, competing interests and affiliations |
|---|---|---|---|---|---|---|---|
| N -Calorie menu labelling ( n = 2) | |||||||
| Robinson et al. (2019)57 | RD (England, UK) | To examine the proportion of major catering chains that provide calorie information at point of sale, and if current practices comply with the RD recommendations | Cross-sectional (post, once) August 2018 |
Food and beverage items (N NR) from 104 large chains including cafés, coffee shops, takeaways, fast-food and full-service restaurants [P: 16 (15%) restaurants chains; NP: 88] |
Focus on children: N |
|
|
| Moran (2017) (20) | Kids LiveWell (USA) | To identify trends in nutrient content of beverages, entrées, side dishes, and desserts offered on children’s menus following the implementation of the Kids LiveWell initiative | Repeat cross-sectional (post–post) January 2012, 2013, 2014 and 2015 |
4016 children’s menu items from 45 of the top 100 fast-food, fast-casual, and full-service restaurants [P: 890 (47%) beverages, 639 (46%) entrées, 321 (82%) side dishes and 152 (84%) desserts from 15 restaurants; NP: 996 beverages, 739 entrées, 2010 side dishes and 69 desserts from 30 restaurants] |
Changes in calories (kcal), sodium (mg), and saturated fat (g) content between 2012 and 2015a of:
|
Between 2012 and 2015:
|
|
| Verified using the Menustat database and restaurants’ websites Focus on children: Y |
|
||||||
| R-Advertising and Marketing control: Television ( n = 5) | |||||||
| Harris (2018)80 (Study 1 only) | CFBAI (USA) |
To assess the effectiveness of CFBAI pledges to not advertise to children under 6 years old | Cross-sectional (post, once) January–December 2015 |
Food, beverage and restaurant adverts for 59 brands (total N adverts NR) aired during children’s programming on English-language networks, cable, and syndicated TV in the USA, [P: 28 brands from 9 (28%) companies, 28 brands; NP: 23 companies, 31 brands] |
Differences in the volume of food and beverage advertising to children aged 2–5 and 6–11 on and outside CP. Using Nielsen Media Research data. Focus on children: Y |
During the whole year, pre-schoolers (2–5 years) saw an average of 732.2 food adverts (63% during children’s TV) by P, including 134.2 by fast-food restaurants (12% during children’s TV) vs. an average of 422.3 (37% during children’s TV) by NP, including 78.3 by fast-food restaurants (7% during children’s TV). Older children (6–11 years) saw an average of 910.0 food adverts (69% during children’s TV) by P, including 157.2 by fast-food restaurants (12% during children’s TV) vs. an average of 402.8 (31% during children’s TV) by NP, including 84.7 (6% during children’s TV). |
No apparent CoI:
|
| Less than 1% of adverts promoted products not approved for P companies for 6- to 11-year-olds. McDonalds was the only fast-food restaurant advertising on children’s programming (and the only one that did not pledge to not advertise to under 6 seconds). | |||||||
| Landwehr (2020)79 | EU Pledge (Germany) |
To test the compliance and overall effectiveness of the EU Pledge in protecting children from HFSS advertising using the UK OFCOM nutrient profile | Repeat cross-sectional (post–post) October 2011 and October 2014 |
15,174 adverts recorded from 10 German TV networks (2 children’s networks, 2 general public and 6 commercial television broadcasters) on one weekday and one weekend day (07.00–22.00) representing 596 hours of TV and 88 hours of advertising NP[P: 239 (59%) adverts in 2011, 295 (71%) in 2014;NP: 163 adverts in 2011, 123 in 2014;N companies by participation status NR] |
|
The share of child-targeted food and beverage adverts networks decreased significantly for both P companies in total commercial (from 3.2% to 2.2%) and NP (from 2.2% to 1.6%) (p < 0.001) and in children’s networks (from 6.3% to 3.3% in P, and from 3.9% to 3.0% in NP) (p < 0.001). The reduction of broadcasted spots in commercial and children’s networks as well as the reduction of number of advertised products and average commercial lengths were not significant for both P and NP. The two groups were not compared together. By 2014, P companies had moved all child-targeted adverts for sweets outside CP (from 25 in 2011 to 0 in 2014) while those for fast-food brands increased in CP from 32 to 51 (p < 0.001). By contrast, in 2014 advertised sweets in CP 107 times. |
|
| A greater proportion of children-targeted food and beverages adverts in CP by P met the EU Pledge nutrition criteria between 2011 and 2014 (2011: 59.5%; 2014: 89.2%; p < 0.001) compared to NP both before (p = 0.013) and after when these criteria were harmonised in 2014 (p < 0.001). However, while a lesser share of NP adverts complied with the UK OFCOM nutrition profile in 2011 (p = 0.007), the difference became not significant in 2014. | |||||||
| Potvin Kent (2018)74 | CAI (Canada) |
To assess whether the Uniform Nutrition Criteria used by CAI had an impact on the healthfulness of food and beverage advertising during children’s television programming | Repeat cross-sectional (post–post) May 2013 and May 2016 |
242 adverts (2013) and 334 (2016) recorded from the first 30 min of programmes included in a 10% random sample of children’s programming (≥ 35% child audience) on 27 TV stations in Toronto. [P: 120 (50%) adverts in 2013, 187 (56%) in 2016;NP: 122 adverts in 2013, 147 in 2016N companies by participation status NR] |
Proportion of adverts showing:
|
Between 2013 and 2016, using the UK nutrient profile, the frequency of adverts showing less healthy foods and beverages by p significantly reduced from 93.3% to 78.5% (p = 0.000) while the proportion did not change for NP (about 80%). Using the more stringent PAHO criteria, P significantly increased the proportion of advertised products excessive in trans-fat (from 10.0% to 24.2%, p = 0.002), and excessive in sodium (from 44.2% to 58.6%, p = 0.014), while the proportions for excessive total fat, saturated fat and free sugar remained similar. Among NP, there was a significant increase in the proportion of advertised products excessive in total fat (from 48.8% to 69.3%, p < 0.05) and a significant reduction for excessive free sugars (from 66.9% to 47.9%, p < 0.05), as well as non-significant increases for excessive trans-fat (29.8% to 35.7%) and sodium (48.8% to 60.7%). | No apparent CoI:
|
| In both time periods, 99–100% of both P and NP advertisements featured products that were classified as excessive in at least one nutrient according to the PAHO criteria. | |||||||
| Smithers (2019)71 | Not stated but likely both the RCMI and QSRI (Australia) |
To describe advertising of discretionary foods on television during children’s viewing times. | Cross-sectional (post, once). Between January and December 2017 |
25,980 food adverts recorded from four TV channels in Adelaide over 84 weekdays days (24 hours per day). (N by participation status NR for both companies and adverts) |
Frequency of discretionary (i.e. ‘unhealthy’) foods advertised per hour during children’s peak time and programmes. Food was classified using the Australian Guide to Healthy Eating. Focus on children: Y |
There was no statistical difference for the number of adverts per hour showing discretionary food between P and NP during:
|
|
| Watson (2017)72 | RCMI and QSRI (Australia) |
To investigate the impact of the self-regulatory initiatives on the rate of unhealthy food advertising to children 4 years after the last independent monitoring study of television food advertising in Sydney, Australia. | Cross-sectional (post, once) May 2015 |
973 food adverts recorded from 3 TV channels and 1 youth-oriented digital channel in Sydney, from 06.00 to 21.00 over 2 week days (16 hours in total) and 2 weekend days (22 hours in total). (N by participation status NR for both companies and adverts) |
Proportion of adverts promoting ‘non-core’ (unhealthy) food. Nutritional information from food labels and company websites; classified using the Australian Dietary Guidelines. Focus on children: Y |
|
|
| R-Advertising and Marketing control: websites and mobile applications ( n = 4) | |||||||
| Neyens (2017)78 | EU Pledge (Belgium and the Netherlands) |
To examine to what extent signatories’ websites abide by their own self-regulation, and to evaluate the nutritional quality of advertised food and beverages they market to children. | Cross-sectional (post, once) Date NR, likely 2014 |
440 products on 49 child-targeting websites [P: 15 (31%) websites; NP: 34] |
|
Only four websites, all from P, used age blocks to restrain children under 12 forbid children younger than 12 to enter the websites. None used ad-break warnings raise children’s awareness of adverts. P (mean rank = 25.43) did not display more parental information than NP (mean rank = 24.81) (U = 261.5, z = 0.15, p = 0.885, r = 0.003). There were few differences between P and NP with regards to the use of marketing. While NP websites promoted more the benefits of their brand sig (mean rank = 28.26) than P websites (mean rank = 17.60) (U = 144, z = –2.41, p = 0.016, r = 0.34), spokes-characters were more present on P websites (U = 359, z = 2.39, p < 0.017, r = 0.34, mean rank = 31.93) compared with NP websites (mean rank = 21.94). The average nutrition score did not differ significantly between food brands from P (mean rank = 16.36) and NP (mean rank = 15) (U = 114, z = 0.41, p = 0.703, r = 0.075).. |
|
| Potvin Kent (2018)76 | CAI (Canada) |
To examine the frequency and healthfulness of food advertising on children’s preferred websites and to compare the frequency and nutritional quality of these food adverts between companies participating in the CAI and those not participating. | Cross-sectional (post, once) Between June 2015 and May 2016 |
~54 million food and beverage adverts from the most popular ten websites (n = 37) for children aged 2–11 years in Canada. [P: ~35.5 million (79%) adverts; NP: ~18.5 million] |
|
92.7% of adverts were for ultra-processed foods. Those on P websites were 2.5 times more likely to be ultra-processed (vs. unprocessed or processed) compared with NP (94.9% vs. 88.2%; p < 0.001, OR = 2.5, 95% CI 2.5 to 2.5; data not shown). In terms of average nutrient content per 100 g, compared to NP, P products were significantly higher in energy [mean difference (MD) 141 kcal], carbohydrates (MD = 39.2 g), sugar (MD = 18.2 g) and sodium (MD = 70.0 g) (all ps p ≤ 0.001). They also contained more total fat and fibre, and less proteins, saturated fat and trans-fat (although the difference for the latter was negligible) (all 95% CIs excluded 1). Using the UK nutrient profile, 78.4% of P adverts were for less healthy products compared to 59% of NP. Using the PAHO system, P products were significantly less likely be excessive in total fat (10.7% vs. 52.7%, p ≤ 0.001), saturated fat (16.8% vs. 45.5%, p ≤ 0.001), trans-fat (4.1% vs. 7.1%, p ≤ 0.001) and sodium (39.7% vs. 56.2%, p ≤ 0.001) than NP, but P products were more likely to have an excess of free sugars (89.0% vs. 40.5%, p ≤ 0.001) than NP. |
No apparent CoI:
|
| Potvin Kent (2020)75 | CAI (Canada) |
To determine if CAI signatories participate in fewer child-related Corporate Social Responsibility (CSR) activities (nutrition and physical activity) than non-signatories. | Cross-sectional (post, once). Between June and August 2016 |
63 CSR identified on the webpages, Facebook pages and corporate reports of 39 companies. [P: 36 (57%) CSR activities from 18 companies; NP: 27 (43%) CSR activities from 21 companies] |
Nature and targeted demographic of physical activity and nutrition-related CSR initiatives. Focus on children: Y |
P had a higher proportion of nutrition-related initiatives (72%) and a lower proportion of child-targeted initiatives (42%) compared to NP (48% and 54%, respectively) but differences were not statistically significant (X2 = 3.792; df = 1; p = 0.052 and X2 = 0.900; df = 1; p = 0.343, respectively). Four P were identified as supporting School Nutrition Programs, including Coca-Cola and Danone who donate fruit juice and yogurt to Breakfast Club of Canada. Both companies along with McDonalds also sponsor sports for children < 12 years. These activities do not contravene their pledge since they do not apply to charitable activities. |
No apparent CoI:
|
| Vergeer (2019)77 | CAI (Canada) |
To compare the marketing of unhealthy products to children on Canadian websites of food companies with and without voluntary policies or commitments. | Cross-sectional (post, once). Spring–summer 2017 |
31 websites of 37 major companies in Canada [packaged food (n = 6), beverage (n = 12), and restaurant chains (n = 13)]. |
|
Overall, a significantly greater proportion of P marketed products to children on their websites, compared with NP. |
|
| [P: 14 (38%) companies; NP: 23] |
Focus on children: Y |
Child-directed marketing appeared on 19 websites of 12 companies (32%), including 9 P. Websites featured products and marketing strategies that are appealing to children. Of the 217 products marketed to children, 97% exceeded Health Canada’s proposed 5% Daily Value threshold for saturated fat, sodium, and/or sugars; 73% of which were products from 9 P. |
|
||||
| R-Advertising and Marketing control: food packaging ( n = 1) | |||||||
| Vaala (2020)81 | CFBAI (USA) |
To explore sugar content and child oriented promotional features on packaging among ready-to-eat cereal by manufacturers participating in the CFBAI in the US marketplace. | Cross-sectional (post, once) September 2018 |
159 ready to eat dry cereal boxes from two major retail stores. [P: 110 (69%) cereal boxes, including 17 listed as meeting the CFBAI nutritional criteria; NP: 49] |
|
Cereals listed by manufacturers as meeting CFBAI nutritional criteria had significantly smaller suggested serving sizes than CFBAI−not listed cereals and cereals produced by NP (F2,158 = 8.34, p < 0.001). CFBAI−cereal listed products also tended to have lower cereal density on average compared with CFBAI−cereal not listed and NP cereals, but these differences were not statistically significant. Games/activities, trade characters, and displaying children on the box were most common among cereals classified as CFBAI−cereal listed, followed by CFBAI−cereal not listed (p < 0.001, respectively). NP companies did not use trade characters (mascots), licensed media spokes characters, or images of children to market RTE cereals. |
|
| I-Product reformulation by manufacturers ( n = 2) | |||||||
| Levi (2018)63 | FHD (Australia) | To evaluate whether product soups under the FHD met the December 2014 sodium reduction targets and to compare P soups to NP soups. | Repeat cross-sectional (post–post). Between August and December in 2011, 2012, 2013, 2014 |
1153 dry, canned, and chilled soups from the same four grocery retail stores in Sydney, Australia. [P: In 2014: 68 (77%) dry and 125 (59%) wet soups from 7 companies; NP: In 2014: 20 dry and 87 wet; N companies NR] |
Sodium content of ‘wet and condensed’ and of ‘dry’ soups ‘as consumed’. Using nutrition information from the George Institute Branded Food Composition Database (which uses front-of-pack labels, nutrition information panels and ingredients lists). Focus on children: N |
There were a greater proportion of products below the FHD sodium targets for P compared with NP (both dry and wet soups – illustrated in figures only). In 2014, the proportion of dry soups from P that met the targets compared to when they entered the market significantly increased (p ≤ 0.001). There was an increase in products that met the FHD sodium targets from NP companies, but the increase was non-significant. For wet products, there was a small but not significant increase from 70% in 2011 to 76% in 2014 in the proportion of manufacturers meeting the target for both P and NP companies combined. There was no significant difference between N and NP. |
No apparent CoI:
|
| Sparks et al. (2018)65 Low (−) |
FHD (Australia) | To assess the median Na levels of 2510 processed meat products, including bacon and sausages, available in major Australian supermarkets in 2010, 2013, 2015 and 2017, and assessed changes over time. |
Repeat cross-sectional (post–post) (2010, 2013, 2015 and 2017) |
2510 processed meat products in four major supermarkets in Australia. 2010: 181 (43%) P; 2017: 236 (35%) P. Nutrition data from the Australian FoodSwitch database |
Na content of processed meat, of which five product categories have targets (P): bacon, ham/cured meat products, emulsified luncheon meats, wet savoury pasties and dry savoury pasties. | Median Na of P processed meats reduced by 11% (p < 0.001) vs. no change in NP (median difference 6%, p = 0.450). It was 1010 mg/100 g in 2010 vs. 898 mg/100 g in 2017 for P and 765 mg/100 g in 2010 vs. and 717 mg/100 g in 2017 for all processed meat. A higher proportion of bacon, ham/cured meat products and wet savoury pasties met the targets between 2010 and 2017 (p < 0.001, p = 0.012 and p = 0.006, respectively) while there were no change for emulsified luncheon meats (p = 0.363 and dry savoury pasties (p = 0.111). |
|
|
|||||||
| Spiteri (2018)70 | Healthier Australia Commitment (Australia) | To assess the healthfulness of new food products released into the Australian retail market in 2015, and whether HAC members released healthier food options compared to non-members. | Cross-sectional (post, once). Between January and December 2015 |
All new food and beverage products launched in Australia in 2015 that were indexed in Mintel’s Global New Products Database (n = 4134). [P: 297 (7%) products; NP: 3846; N companies NR] |
Healthfulness according to: (1) The Healthy Choices Framework Victoria nutrient-based criteria (traffic lights), (2) The Australian Dietary Guidelines food-based criteria (core, discretionary, or other for products not edible on their own such as baking ingredients, herbs and spices) and (3) The NOVA Food Classification System level of processing criteria (minimally processed, culinary ingredients, processed, ultra-processed). Using data from the Mintel’s Global New Products Database. Focus on children: N |
P launched a significantly greater proportion of foods classified as red (59% vs. 51% for P and NP, respectively), discretionary (79% vs. 61%) and ultra-processed (94% vs. 81%), as well as significantly fewer green (8% vs. 15%), core foods (18% vs. 36%) and minimally processed (0% vs. 6%) (all p < 0.001). |
|
| S-Food retail and service sector ( n = 1) | |||||||
| Wellard-Cole (2019)73 | QSRI (Australia) | To compare the nutrient composition of children’s meals in fast-food chains with children’s daily requirements and recommendations and the food industry’s own criteria for healthier children’s meals; and determine whether the situation has changed since 2010. | Repeat cross-sectional (post, post) November 2010 and May 2016 |
289 children’s meals (main + drink) from 12 large fast-food chains. [P: 172 (60%) meals from 6 chains; NP: 117 meals from 6 chains] |
Nutrition composition of children’s meals compared with 30% (recommended contribution for a meal) and 100% of children’s daily recommendations and requirements for 4-, 8- and 13-year-olds, and compliance with the food industry’s own criteria. Nutrition information from fast-food chains’ websites, store visits, printed materials, menu boards, phone/e-mails to outlets. Focus on children: Y |
For 4-year-olds, most P and NP meals exceeded 30% of daily recommendations for energy (P: n = 118, 69%; NP: n = 70, 60%) and sugar (P: n = 115, 67%; NP: n = 72, 62%). A higher proportion of NP meals compared to P meals exceeded 30% of daily recommendations for saturated fat (n = 90, P: 52%; NP: n = 83, 71%); and 30% of the upper level of intake for Na (P: n = 152, 88%; NP: n = 105, 90%, 2.1%) P meals [and 15 (13%) NP meals exceeded 100% of the Na upper limit]. | No apparent CoI:
|
| For 9-year-olds, similar trends were observed, with a greater proportion of P than NP exceeding the 30% recommendation for energy (P: n = 76, 44%; n = 37, 32%), and sugars (P: n = 93, 54%; NP: n = 59, 50%), while a greater proportion of NP exceeded those for saturated fat (P: n = 65, 38%; n = 73, 62%) and upper Na limit (P: n = 152, 88%; NP: n = 105, 90%). Again, 2 (1%) P meals [and 15 (13%) NP meals exceeded 100% of the Na upper limit]. | |||||||
| For 13-year-olds, trends were slightly different with a greater proportion of P exceeding again the 30% recommendation for energy (P: n = 20, 12%; n = 6, 5%) but also for salt (P: n = 110, 64%, NP: n = 36, 31%). The reverse was observed for saturated fat (P: n = 24, 14%; NP: 37, 32%) and sugars (P: n = 46, 27%; NP: n = 43, 37%). Only five (4%) NP meals exceeded 100% of the Na upper limit. | |||||||
| Most children’s meals from P restaurants did not meet the QSRI’s own definition of a healthy children’s meal that could be marketed to children (P: n = 141, 82% for 4- and 8-year-olds; n = 131, 76% for 13-year-olds), especially for sodium. Between 2010 and 2016, the proportion of meals not meeting QSRI’s criteria for any nutrient did not change nor for those exceeding 30% or 100% of children’s recommendations for energy or nutrients (all p < 0.05, data not shown) | |||||||
The CFBAI in Canada was the most assessed policy, with four studies (three moderate and one low quality) concluding that there were mixed effects for the advertising of unhealthy foods to children on television,74 that participants used more child-directed marketing strategies to promote unhealthy foods on websites than NPs,77 that food advertised on websites to children were in majority unhealthy,76,77 and that participants did not conduct fewer corporate social activities to promote their brands to children. 75
The CFBAI in the USA was evaluated twice (moderate and unclear quality) and shown overall as having worse effects among participants than NPs. Participants advertised unhealthy foods during children’s television programmes more frequently,80 used more marketing practices on breakfast cereal packages, and the cereals said to meet CFBAI’s nutrition criteria had smaller serving sizes and lower density, suggesting that their nutritive values do not represent quantities likely to be eaten. 81
The EU Pledge had mixed effects in two studies (moderate and low quality) for a range of outcomes relating to advertising of unhealthy foods to children both on television and online including the number of adverts, nutrition profiles, use of marketing tactics and children’s protection strategies online. 78,79
The FHD in Australia was the only policy to show some better overall outcomes for participants, albeit with limitations including imprecise data. 65 The study by Levi et al. 63 (unclear quality) was a post–post cross-sectional study evaluating whether soup products, classified as dry and wet (canned and chilled) met the policy’s sodium targets. Sodium content was collected in 2011, 2012, 2013 and 2014 using food databases and labels. In 2014, 1153 soups were assessed, of which 68 were dry from participants (compared with 20 NPs); and 125 were wet from participants (compared with 87 NPs). Figures (no data provided) show a greater proportion of participating soups below the target for both categories compared to NPs. Mean sodium content in dry participating soups reduced significantly since 2011 but not for wet soups nor either NP soup categories, although this might be partly due to small sample sizes limiting statistical power. No values on sodium content and number of products meeting targets were provided. The study was rated as having unclear study quality due to a lack of reporting on missing data and ascertainment of participant status. Sparks et al. (2018)65 (low quality) assessed sodium levels in processed meats between 2010 and 2017. They reported an 11% reduction in median sodium levels in the processed meats that had salt targets versus no change in those without targets. However, by category of products they reported mixed results with significant reductions in bacon, ham/cured meat and wet savoury pasties (p < 0.001, p = 0.012 and p = 0.006, respectively) and no change in emulsified luncheon meats (p = 0.363) and dry savoury pasties (p = 0.111).
A study by Spiteri et al. 70 (unclear quality) on the Healthier Australia Commitment assessed ‘healthfulness’ of all new food and beverages launched in the country in 2015 using three nutrition profiling systems. Participants had launched greater proportion of foods classified as unhealthy according to the three systems (all p < 0.001).
Regarding the Kids LiveWell in the USA, Moran et al. 82 (low quality) compared trends in calories, sodium and saturated fat content of children’s menus (entrees, side dishes, desserts and beverages) in participating and NP large chain restaurants. Results were inconclusive for all three indicators.
The QSRI in Australia was investigated in three studies (one moderate, two low quality). Effects on television advertising practices for unhealthy foods to children were either mixed or worse among participants. 71,72 Wellard-Cole73 found that fewer children’s meals from fast-food chains exceeded recommendations for saturated fat but that the proportions of meals exceeding calorie recommendations were greater among participants and inconclusive for sugar and sodium (no inferential statistics performed).
Lastly, a study by Robinson et al. 57 (unclear quality) investigated whether the 16 restaurant chains that had signed the calorie labelling pledge in the Public Health RD in England tended to display calorie labels and meet the seven labelling criteria compared to 88 NP restaurant chains. While a greater proportion of participating chains displayed labels, only one participating and two NP chains provided calorie labelling for all items sold, and none fulfilled all criteria.
Tables 16 and 17 present a summary of the nine categories of outcomes assessed by direction of effect, sample size and study quality. The shape of the triangles illustrates the overall direction of result independently from statistical significance while their size reflects the final sample size of intervention group (participants). The subscript numbers represent the number of outcomes within each category synthesis. The colours refer to the study’s overall study quality.
| Author (year) | Study design N years between policy implementation and evaluation; study quality |
Sample size of participants (P) group (% of total sample) |
TV advertising to children: frequency of adverts for unhealthy foods and advertising practices | TV advertising to children: nutrition profile and types of products shown | Online marketing to children: presence of marketing of unhealthy food and marketing practices | Online advertising to children: nutrition profiles and types of products shown | Corporate social activities in nutrition and physical activity: nature and targeted populations |
|---|---|---|---|---|---|---|---|
| CFBAI (Canada) (n = 4) | |||||||
| Vergeer (2019)77 | CS; 10 years Moderate (+) |
14 (38%) companies; | ▽1 (presence of child-directed marketing) |
▽3 (sat fat, Na, sugar; sample size: over 158 products from P) |
|||
| Potvin Kent (2018) TV74 | RCS-PP; 6–9 years Low (−) |
120 (50%) adverts in 2013, 187 (56%) in 2016 | △1 (UK OFCOM criteria, CP) ◅▻4 (PAHO criteria, CP) |
||||
| Potvin Kent (2018) Online76 | CS; 8–9 years Moderate (+) | ~35.5 million (79%) adverts | ▼1 (ultra-processed food) ▼1 (UK OFCOM criteria) ▲5 (PAHO criteria) |
||||
| ▼7 ‘Negative’ nutrients per 100 g: kcal, fat, sugar, salt ◅▻2 ‘Positive’ (nutrients per 100 g: fibre, protein) |
|||||||
| Potvin Kent (2020)75 | CS; 9 years Moderate (+) |
36 (75%) CSR activities from 18 companies | ▼1 (proportion of nutrition-related initiatives) ►◄1 (proportion of child-targeted initiatives) |
||||
| CFBAI (USA) (n = 1) | |||||||
| Harris (2018)80 | CS 9 years Unclear (?) |
9 companies (28%) | ▼2 (adverts’ frequency-two age groups, CP). |
||||
| EU pledge (n = 2) | |||||||
| Landwehr (2020)79 | RCS-PP 4–11 years Moderate (+) |
239 (59%) adverts in 2011, 295 (71%) in 2014 | ◅▻6 (share in commercial and CP, N spots in commercial and CP, N products, adverts length) |
△1 (UK OFCOM criteria) ◅▻1 (PAHO criteria) ◅▻2 (presence of sweets and fast-food brands, General audience and CP) |
|||
| Neyens (2017)78 | CS; Unclear, potentially 7 years Low (−) |
15 (31%) websites | ►◄3 (online protection) ►◄2 (marketing tactics) |
▼1 (score based on UK OFCOM) |
|||
| QSRI and RCMI (Australia) ( n = 2) | |||||||
| Watson (2017)72 | CS; 6 years Moderate (+) | NR (for both N companies and adverts) | ▼2 (adverts frequency, RCMI and QSRI, general audience and CP) |
||||
| Smithers (2019)71 | CS; 8 years Low (−) |
NR (for both N companies and adverts) | ►◄2 (adverts frequency, CP and children’s peak time) |
||||
| Author (year) | Study design; N years between policy implementation and evaluation; Study quality |
Sample size of participants (P) group (% of total sample) |
Restaurant food and beverages: calorie labelling display | Children’s meals in restaurants: nutrient content | Manufactured products: nutrient content and presence of child-directed marketing on packaging |
|---|---|---|---|---|---|
| CFBAI (USA) (n = 1) | |||||
| Vaala (2020)81 | CS 12 years Low (−) |
110 (69%) cereal boxes, including 17 listed as meeting the CFBAI nutritional criteria | ▽2 (P-listed cereals: smaller serving sizes and lower cereal density than other P and NP) ▽3 (marketing practices more present on P-listed cereals, than on other P, compared to NP) |
||
| FHD (Australia) (n = 1) | |||||
| Levi (2018)63 | RCS-PP 2–5 years Unclear (?) |
68 (77%) dry and 125 (59%) wet soups from five companies in 2014 | △2 (dry and wet soups − Na) |
||
| Sparks (2018)65 | RCS-PP 1–8 years Low (−) |
181 (43%) processed meats in 2010 and 236 (35%) in 2017. Five product categories have targets | ◅▻5 (Na in five product categories) △1 (Na overall) |
||
| Healthier Australia Commitment (Australia) ( n = 1) | |||||
| Spiteri (2018)70 | CS 3 years Unclear (?) |
297 (7%) products | ▽1 (Healthy Choices Framework Victoria) ▽1 (Australian Dietary Guidelines ▽1 (NOVA categories) |
||
| Kids LiveWell (USA) ( n = 1) | |||||
| Moran (2017)82 | RCS-PP 1–4 years Low (−) |
2002 menu items from 15 restaurants: 890 (47%) beverages, 639 (46%) entrées, 321 (82%) side dishes and 152 (84%) desserts | ◅▻4 (calories) ◅▻3 (sodium) ◅▻3 (saturated fat) (All for entrées, sides and desserts; also beverages for calories) |
||
| QSRI and RCMI (Australia) ( n = 1) | |||||
| Wellard-Cole (2019)73 | RCS-PP 1–7 years Low (−) |
172 (60%) meals from 6 chains | ▽3 (calories) △3 (saturated fat) ◅▻3 (sugar) ◅▻3 (sodium) (all for 4-, 8-, 13-year-olds) |
||
| RD (England, UK) (n = 1) | |||||
| Robinson et al. (2019)57 | CS 7 years Unclear (?) |
16 (15%) restaurants chains | ◄►2 (displaying labels, all labelling criteria) |
||
Despite the effect direction tables not considering effect size nor precision estimates, they show that there is no clear evidence to suggest that policies designed as voluntary approaches led by commercial actors to reduce advertising or other promotion of unhealthy products to children, improve the nutritional composition of food and beverages, encourage calorie menu labelling in chain restaurants, or reduce marketing targeting children on food packages. When comparing participants to non-participants, the direction of effect or association for most outcomes was either inconclusive or worse for participants. No pattern could be noticed with overall study quality, country, policy category or type of outcome assessed.
An examination of the effect direction plots (see Tables 16 and 17) suggests that the results do not vary by study quality.
Conclusions
From the available evidence reviewed across 16 studies evaluating nine voluntary approaches by private actors, it would appear that there is limited evidence to suggest that policies designed as voluntary approaches led by commercial actors are effective at reducing advertising and other promotion of unhealthy products to children, improving the nutritional composition of food and beverages, encouraging calorie menu labelling in chain restaurants, or reducing marketing targeting children on food packages.
Chapter 7 Systematic review on the cost-effectiveness of policies to improve food environments and population diet
Introduction
This paper describes a systematic review of literature on the cost-effectiveness of real-world regulatory, voluntary and PPP policies to improve food environments. These economic evaluation studies provide evidence to identify cost-effective interventions and serve as the foundation for the delivery of population-level intervention.
Methods
Literature search strategy and eligibility criteria
This systematic review builds on the primary economic studies (e.g. cost-effectiveness, cost-benefits) that were identified as part of the systematic evidence map (see Chapter 3). Economic simulations and projections were eligible if the data used for measuring effectiveness met the overarching eligibility criteria. Given that only four evaluations of cost-effectiveness were retrieved, two additional searches were conducted in MEDLINE (Ovid) to explore whether eligible studies had been missed (see Appendix 6, Tables 31 and 32): a very comprehensive and sensitive search on FOPL based on the search strategy by Croker et al. 43 and a less sensitive search on fat, salt and sugar reformulation. These two topics were chosen because of their higher odds of being less well captured by the original literature search given the focus of the latter on whether policies were regulatory, voluntary or PPPs. If more than one additional eligible study was to be identified in each search, additional searches would have been conducted for the other policy areas covered in the evidence map. However, since none was identified, this was deemed unnecessary. Lastly, the reference lists of the included studies were screened as well as those of evidence syntheses on cost-effectiveness excluded from the overview of reviews (see Chapter 4).
Data extraction
Information on the policies (name, topic, country, policy level, governance approach), study methods for assessing effectiveness (population, study design, mechanism, diseases considered), methods for assessing costs (types of costs considered, choice of model) and results (incremental health outcomes and costs, conclusion on whether a policy was considered cost saving) was extracted in a standardised extraction form by one reviewer (CL) and checked by another (LB). These fields were inspired by the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) checklist. 84 Cost estimates were inflated and/or converted in 2020 international dollar using country-specific gross domestic product (GDP) deflator index and purchasing power parity conversion factor in 2020 from World Bank Databank. 85,86
Quality appraisal and data synthesis
The methodological quality of the studies was assessed by two reviewers independently (CL, LB) using Drummond’s 10-criteria checklist version 201587 for assessing economic evaluations. Each criterion was assigned ‘Yes’, ‘No’ or ‘Can’t Tell’. Disagreements were resolved by discussion.
Data were synthesised in a descriptive manner using the categories of information extracted. The initial plan was to summarise the measures of costs and cost-effectiveness using the policy areas described in the NOURISHING framework. 18 However, this proved impractical because of the small number of studies included. We had also planned to pool outcome estimates from comparable studies in a random-effect model meta-analysis to characterise average intervention impacts, but this was not possible due to the aggregation of the outcomes in broader indicators in some studies and the diversity of cost measures used.
Findings
Characteristics of included studies
As mentioned above, of the 483 primary studies included in the systematic evidence map, only four were economic evaluations of real-world policies. 88–91 No other evaluations were identified in the additional literature searches nor by screening references. Table 18 provides an overview of the policy interventions assessed in the four studies. These include two studies of the SSB tax in Mexico. 88,91 This SSB tax is a regulatory government intervention that was implemented as an excise tax of 1 peso per litre in 2014. This tax was added to non-alcoholic beverages with added sugar. 88 The third study assessed voluntary salt reformulation in the context of the Public Health RD in England. 89 The Public Health RD was a PPP in operation in England from 2011 to 2017. It aimed to foster collaboration between the government, business and voluntary sectors to improve population health. One of the pledges launched under the RD was to reduce population-level salt intake. The fourth study was on the HSR Labelling Scheme in Australia. 90 This is a voluntary FOP label initiative endorsed by the New Zealand and Australian governments. Packaged food and drink products are given a rating that ranges from half a star (least healthy) to five stars (most healthy).
| First author, year | Policy name | Country | Year started | Policy level | Governance approach | Policy area |
|---|---|---|---|---|---|---|
| Basto-Abreu, 201988 | SSB tax | Mexico | 2014 | National | Regulatory | SSB tax |
| Laverty, 201889 | Public Health RD | England | 2011 | England only | PPP – voluntary | Reformulation – salt |
| Mantilla Herrera, 201890 | HSR Food Labelling (voluntary scenario) | Australia | 2014 | International (Australia and New Zealand) | Voluntary | FOPL |
| Sanchez-Romero, 201691 | SSB tax | Mexico | 2014 | National | Regulatory | SSB tax |
Quality appraisal
The quality appraisal of the four included studies is reported in Table 18. All studies met at least 5 out of the 10 Drummond checklist criteria. Mantilla Herrera et al. 90 was assessed to be the highest quality because it was the only study to receive positive answers to all assessment questions. The other three studies88,89,91 were assessed negatively on regarding whether the research question was well-defined as the prospective of their analysis was not clearly stated. Without a clear specification of the prospective taken, it was also not possible to judge if all the important and relevant costs and consequences for each alternative were identified in these three studies. By contrast, using a limited societal perspective, Mantilla Herrera et al. 90 considered the costs to the government and the food industry but not other wider societal costs such as productivity loss. The earlier study on SSB tax in Mexico91 received the least number of positive answers as it did not clearly explain the competing alternative nor justify the effectiveness measure used. Additionally, no incremental analysis of costs and consequences were performed in this study, limiting the comparability of their results to other studies or any pre-determined willing-to-pay (WTP) thresholds.
Measures of effectiveness and cost
Table 19 highlights the heterogeneity in the included studies both in terms of the study populations and methods used for assessing effectiveness of the interventions. Two of the four studies examined the impact of the interventions on both children and adults,89,90 while the other two focused on adults aged 30 years or older. 88,91 In particular, the study on FOPL in Australia by Mantilla Herrera et al. 90 modelled the cost-effectiveness over the lifetime of the population of ages while the other studies used a shorter time horizon approach (10 years or less).
| Criteria | Basto-Abreu 201988 | Laverty 201989 |
Mantilla Herrera 201890 | Sanchez-Romero 201691 |
|---|---|---|---|---|
| 1. Was a well-defined question posed in answerable form? | No | No | Yes | No |
| 2. Was a comprehensive description of the competing alternatives given? | Yes | Yes | Yes | No |
| 3. Was the effectiveness of the programmes or services established? | Yes | Yes | Yes | No |
| 4. Were all the important and relevant costs and consequences for each alternative identified? | Can’t tell | Can’t tell | Yes | Can’t tell |
| 5. Were costs and consequences measured accurately in appropriate physical units prior to valuation? | Yes | Yes | Yes | Yes |
| 6. Were costs and consequences valued credibly? | Yes | Yes | Yes | Yes |
| 7. Were costs and consequences adjusted for differential timing? | Yes | Yes | Yes | Yes |
| 8. Was an incremental analysis of costs and consequences of alternatives performed? | Yes | Yes | Yes | No |
| 9. Was uncertainty in the estimates of costs and consequences adequately characterised? | Yes | Yes | Yes | Yes |
| 10. Did the presentation and discussion of study results include all issues of concern to users? | Yes | Yes | Yes | Yes |
For measuring effectiveness, three studies used evidence obtained from quasi-experimental designs to identify policy changes outside the direct control of researchers: Mantilla Herrera et al. 90 and Basto-Abreu et al. 88 both used a difference-in-difference approach that included control groups while Laverty et al. 89 used an interrupted time-series design without a control group. By contrast, Sanchez-Romero et al. 91 assessed scenarios of effects using existing estimates of price elasticity of demand in a state transition model. The evidence around causality was stronger in the first two studies88,91 as the difference-in-difference approach they utilised the trend in the control group to forecast the trend in the intervention group that would have been expected if the intervention had not happened. The actual causal estimate was then obtained by comparing the outcomes before and after the change for the intervention group to the corresponding difference for the control group, allowing to infer causality. By comparison, the measure of effectiveness in Laverty et al. 89 was obtained from quasi-experimental designs without a control group, which makes it more prone to bias by confounding events that took place during the same time period as the RD. Furthermore, there is a lack of longitudinal data on salt intakes in the same people; thus, causality cannot be ascribed in the effectiveness measure of RD. As for Sanchez-Romero et al. ,91 although the price elasticity of demand used reflected real-world consumer responses to price changes, it was not an actual casual estimate of the effect of the Mexican SSB tax. Additional limitations in the measures of effectiveness in the studies include the lack of data on purchases outside of stores (i.e. Basto-Abreu 201988) and assumptions of consumer responses to the intervention. 90,91
In all four studies, changes in the distribution of weight and/or systolic blood pressure were used as intermediate outcomes to evaluate the impact of the policy interventions on CHD and stroke. All but Laverty et al. 89 also considered diabetes. Other diet-related health outcomes evaluated included various cancers, knee and hip osteoarthrosis, and non-cardiovascular disease mortality.
Methods for assessing policy effectiveness are summarised in Table 20. Two studies sought to apply quality-adjusted life-years (QALYs) or health-adjusted life-years (HALYs) as outcomes. 88,90 These are commonly used metrics that facilitate comparison between studies and different types of interventions and diseases. Even though all studies considered CHD and strokes, two89,90 did not explicitly report the number of cases reduced for these diseases. Both studies on the Mexican SSB tax showed reduction in the cases of CHD, strokes and diabetes but with quite different magnitudes of reduction. This could be due to differences in the underlying measurements of effectiveness as well as the mechanism used to model these health outcomes. The HSR labelling in Australia was predicted to result in incremental health benefits equating to 4207 HALYs (95% UI 2438 to 6081). While all health-related outcomes improved in studies assessing the Mexican SSB tax and HSR labelling, the study on the RD in England found the reverse relationship: their results suggest that the partnership has increased the CVD and cancer burden as the decline in population-level salt intake slowed down after its implementation in 2011.
| Author, year | Study population (time horizon, discount rate) | Measurement of effectiveness | Mechanism | Diet-related diseases considered | ||||
|---|---|---|---|---|---|---|---|---|
| Study design | Limitations | CHD | Stroke | Diab. | Others | |||
| Basto-Abreu, 201988 | 2014 Mexican population aged 2–100 (10 years, 3%) | 7.6% reduction in SSB purchases in store 2 years after the tax was implemented (2016). (Difference-in-difference study.)92,93 | The study included only beverages purchased in stores, not those sold in restaurants or other venues. | Changes in the BMI distribution, prevalence of obesity in the population and the resulted changes in the incidence obesity-related diseases were projected from the reduction in SSB intake. | X | X | X | Breast cancer; Colorectal cancer; Endometrial cancer; Kidney cancer |
| Laverty, 201989 | English adult aged 30–84 (2011–8, 3.5%) | Annual reductions in salt intake were reduced between 2011 and 2014 by 0.11 g/day among men and 0.07 g/day among women. (Interrupted-time-series study using 24 hours’ urine excretion.) | A lack of longitudinal data collections on salt intakes in the same people means that causality cannot be ascribed. | Impacts of salt intake changes were estimated using effect sizes of the association between salt intake and health outcomes (using systolic blood pressure as an intermediate for CVD outcomes). | X | X | Gastric cancer | |
| Mantilla Herrera, 201890 | 2010 Australian population, all ages (over the lifetime, 3%) | Average change in energy density of − 7.11 kJ/100 g, and in daily energy intake of −0.98 kJ/day between 2013 and 2016. (Difference-in-difference study of the energy density of HSR and non-HSR labelled products.) | Assumption of no changes in consumers’ behaviour in response to voluntary FOPL system. | Changes in average energy density were used to estimate the change in average energy intakes and the resulting changes in the weight distribution of the population and the incidence, prevalence and mortality of obesity-related diseases. | X | X | X | Breast cancer; Colorectal cancer; Endometrial cancer; Kidney cancer; Knee and hip osteoarthritisa |
| Sanchez-Romero, 201691 | 2010 Mexican adults aged 35–94 (2013–22, 3%) |
A 10% decrease in SSB consumption (informed by an observational study on SSB purchases and existing estimates of soda price elasticity in Mexico). | The effectiveness measure was not derived directly from quasi-experimental studies and hence causality cannot be ascribed. | Effects of SSB consumption on three factors related to CVD: diabetes incidence, mean BMI, and mean systolic blood pressure were modelled using a 39% calorie compensation rate. | X | X | X | Non-CVD death |
There were variations in the types of other costs assessed across the four studies although they all estimated healthcare cost implications of the intervention. Basto-Abreu88 and Mantilla-Herrera90 assessed costs associated with implementing the interventions for governments, and the latter also considered potential costs to the food industry. Note that neither study on SSB tax considered potential societal costs and benefits from the increase in government revenue. This could be because the included studies may have taken different analytical perspectives (e.g. the healthcare sector, the government, the society as a whole and etc. 95). For instance, productivity changes are typically not considered under the healthcare sector perspective, which were also excluded under the limited societal perspective taken in the Mantilla-Herrera’s study on HSR rating in Australia. 90 Laverty et al. 89 was the only study to assess the broader economic implications by estimating costs included by changes in productivity. However, it did not consider implementation costs. While not clearly stated, Sanchez-Romero 201691 might have adopted a healthcare sector perspective and hence only healthcare costs were assessed.
Cost and cost-effectiveness of interventions
The incremental health and cost outcomes are summarised in Table 21. Overall, with their positive health outcomes, both the SSB tax in Mexico and FOPL in Australia identified reductions in healthcare costs. In addition to the differences in the measure of effectiveness and mechanism shown in Table 3, Basto-Abreu et al. ’s study88 on the Mexican SSB tax used an estimated cost per patient that was lower than the estimate used by Sanchez-Ramero et al. ,91 which may further explain the differences between these two studies in healthcare cost savings achieved by the SSB tax. Laverty et al. showed that ongoing reductions in salt intake preceding the RD slowed following its introduction, leading to increased rather than decreased healthcare costs. Based on the costs assessed, most studies showed a substantial societal economic benefit of population-level interventions aimed at promoting healthy diets. The FOPL intervention in Australia was found to be cost-effective relative to a WTP threshold of $40,861. Basto-Abreu 201988 found the Mexican SSB tax to be cost-saving as the healthcare costs saved would outweigh its implementation costs. For each dollar spent, the SSB tax was shown to save $7.28 in future healthcare costs. Sanchez-Romero 2019 only assessed healthcare cost savings and did not discuss the cost-effectiveness of the tax. Given their even larger estimates of healthcare cost savings, using their data it would be highly likely for the SSB tax to be even more cost-effective if the implementation costs were assumed to be the same as those estimated by Basto-Abreu 2019. 88 The costs of implementing the RD were not assessed, but the RD in England was not cost-effective at improving population health, as a result of the additional healthcare costs identified.
| Author, year | Incremental health outcomes | Incremental costs | Cost-effectiveness metric | Cost-effective? | ||
|---|---|---|---|---|---|---|
| Healthcare costs | Implementation costs | Productivity losses | ||||
| Basto-Abreu, 201988 | ▼ 7210 cases of CHD ▼ 3990 cases of stroke ▼ 61,340 cases of diabetes ▼ 695 cases of cancer ▼ 5840 DALYs ▲ 918 life-years ▲ 55,300 QALYs |
−$167.7 m | +$44.2 m (Government) | $7.3 saved per dollar spent on its implementation (95% CI: 3.8 to 11.8) | Yesa | |
| Laverty, 201889 | ▲ 9900 cases of CVD ▲ 710 CVD deaths ▲ 1500 cases of gastric cancer ▲ 610 gastric cancer deaths |
+$169.7 m | +$72.5 m | The incremental economic impact from 2011 to 2018 was approximately $246.8 m (IQR: 135.8–354.8 m) | No | |
| Mantilla Herrera, 201890 | ▲ 4207 HALYs | −$34 m | +$37.7 m (Industry and Government) |
$1412.14 per HALY (95% UI: dominant to 8536.6) | Yes (assuming a WTP threshold of $40,861 per HALY) |
|
| Sanchez-Romero, 201691 | ▼ 46,300 cases of CHD ▼ 9300 cases of CHD death ▼ 6200 cases of strokes ▼ 1600 cases of stroke death ▼ 189,300 cases of diabetes ▼ 18,00 cases of all-cause death |
−$1094.3 m | Unclear | |||
Conclusions
Two studies of the Mexican SSB tax, and one for the voluntary government-led HSR front-of-pack labelling intervention in Australia suggested positive impacts. The fourth one reported a lack of effectiveness and cost-benefit for the PPP intervention to reduce salt consumption in England as part of the Public Health RD. There is a pressing need to build on the extensive literature on the effectiveness of interventions with high-quality evidence on cost-effectiveness, to support meaningful action to tackle the scourge of diet-related ill health.
Chapter 8 Qualitative evidence synthesis of policy process in regulatory, voluntary and public–private partnership approaches to improve food environments and population diet
Introduction
This chapter describes the qualitative evidence synthesis of studies focusing on the policy process leading to regulatory, voluntary or PPP approaches, reporting barriers and facilitators and exploring more in-depth understanding of key actors and factors.
Methods
We followed guidance from Flemming et al. (2018)96 to review qualitative studies, aiming to gain a greater understanding of phenomena of interest.
Literature search strategy and eligibility criteria
We included qualitative and mixed-methods studies (e.g. that conducted interviews, focus groups, qualitative document analyses) drawn from the systematic evidence map (see Chapter 3). To be included in this review, studies had to have assessed factors influencing a national policy process. We included papers published between 2010 and 2020, as well as studies focused on local (city, state – UK only) policies. Studies were screened by two reviewers (CK and MP).
Data extraction
We documented policy type, method and participant characteristics. We extracted information relating to reported barriers and facilitators of policy design and implementation, decision-making processes, the use of evidence or particular strategies, and any information that would help gain deeper understanding about some of the findings emerging. Data were extracted by one reviewer in EPPI-Reviewer and checked by another.
Quality appraisal
Each included study was independently appraised by two team members using the CASP Checklist for qualitative studies. Studies that received ‘no’ or ‘can’t tell’ for the two filter questions that begin CASP would be excluded. No studies were weighted or excluded based on the appraisal results. We also checked for conflict of interests in terms of industry funding.
Data synthesis
We synthesised the data using a narrative review approach to summarise findings and report on overarching themes.
Findings
Database search
A total of 91 relevant records were identified. We retrieved full text for all 91. Of these, 59 were excluded due to ‘not qualitative research’ (n = 6), ‘not about policy process’ (n = 18), ‘not national’ (n = 19), ‘media analysis’ (n = 8), ‘studies about public’s views’ (n = 1), ‘not a peer reviewed study’ (n = 1), ‘not food’ (n = 2), ‘not about a specific policy or agreement’ (n = 6) (Figure 14). Thus 30 papers met the inclusion criteria and were included in this synthesis (Table 22).
FIGURE 14.
PRISMA flow chart representing the selection process for the review of studies on policy process. Adapted from the PRISMA template by Page et al. (2021). 16
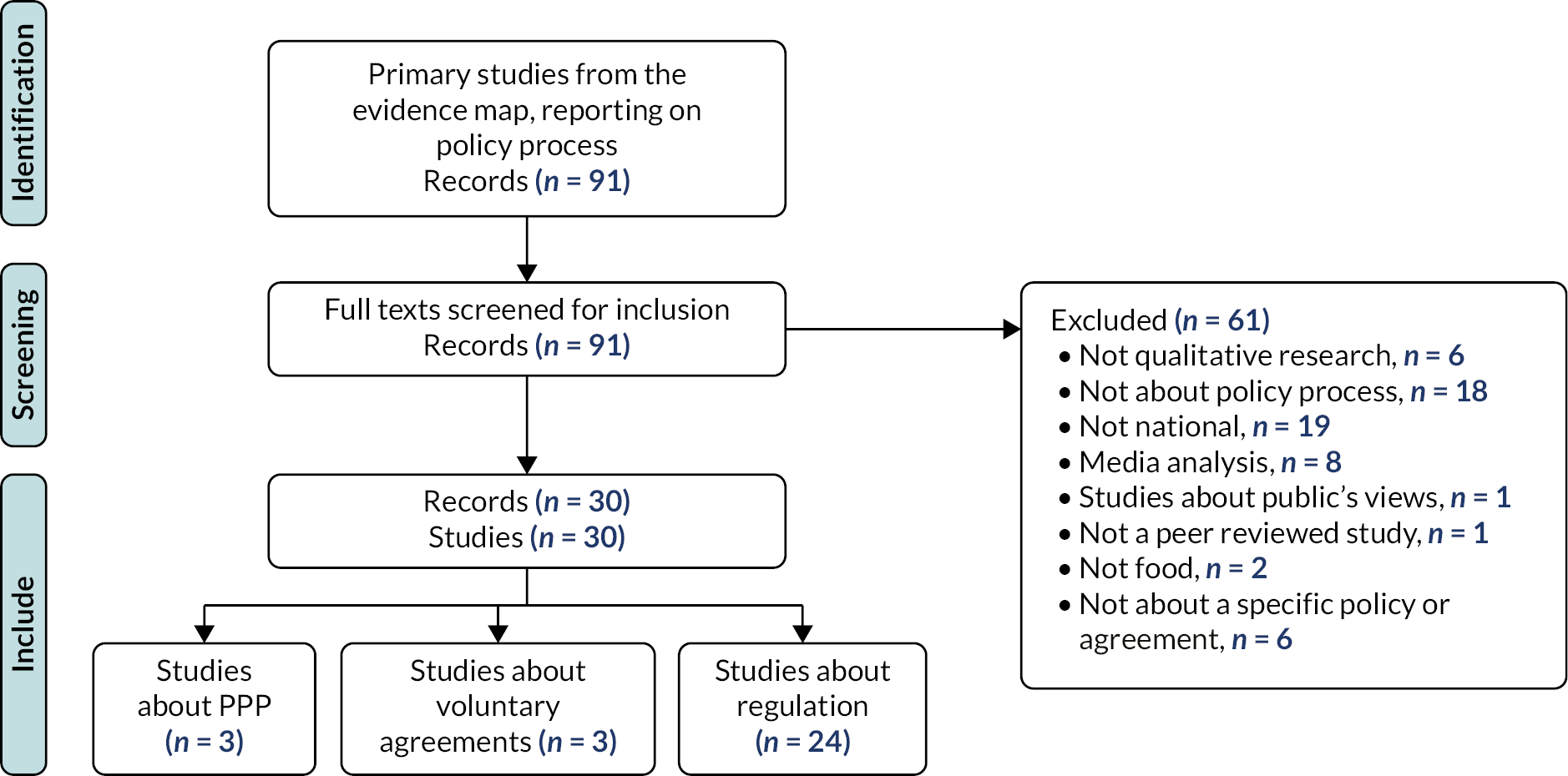
| CASP item included studies | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|
| Voluntary approach | ||||||||||
| Castronuovo et al. (2017)97 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Davo-Blanes et al. (2013)98 | Y | Y | Y | Y | Y | U | Y | Y | Y | Y |
| Webster et al. (2018)99 | Y | Y | Y | Y | Y | U | Y | Y | Y | Y |
| PPPs | ||||||||||
| Brandon et al. (2020)100 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Durand et al. (2015)101 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Perez-Escamilla (2018)102 | Y | Y | Y | Y | Y | N | N | N | Y | Y |
| Regulation | ||||||||||
| Alsukait (2020)103 | Y | Y | Y | Y | Y | U | U | Y | Y | Y |
| Campbell (2020)104 | Y | Y | Y | Y | Y | U | N | Y | Y | Y |
| Carriedo (2020)105 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Davies (2017)106 | Y | Y | Y | Y | Y | U | U | U | Y | Y |
| Dorlach (2020)107 | Y | Y | Y | Y | Y | U | N | Y | Y | Y |
| Fooks (2019)108 | Y | Y | Y | Y | Y | U | Y | Y | Y | Y |
| Fuster (2020)109 | Y | Y | Y | Y | Y | U | Y | Y | Y | Y |
| James (2020)110 | Y | Y | Y | Y | Y | U | Y | Y | Y | Y |
| Kaldor (2018)111 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Kiss (2019)112 | Y | Y | Y | Y | Y | U | Y | Y | Y | Y |
| Le Bodo (2019)113 | Y | Y | Y | Y | Y | U | Y | Y | Y | Y |
| Mialon (2020)114 | Y | Y | Y | Y | Y | U | Y | Y | Y | Y |
| Monterrosa (2015) | Y | Y | Y | Y | Y | N | N | Y | Y | Y |
| Phillips (2019)115 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Phulkerd (2017)116 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Razavi (2019)117 | Y | Y | Y | Y | Y | U | Y | Y | Y | Y |
| Reeve (2018)118 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Shelton (2017)119 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Stead (2020)117 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Thow (2011)120 | Y | Y | Y | Y | Y | U | Y | Y | Y | Y |
| Thow (2020)121 | Y | Y | Y | Y | Y | U | Y | Y | Y | Y |
| Trieu (2018)122 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Vallgarda (2015)123 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Vandenbrink (2020)124 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
Study characteristics
Twenty-four papers studied the policy process of regulatory policies in 19 countries: Brazil, Canada, Colombia, Chile (n = 2), Denmark, Fiji (n = 3), France, French Polynesia, Hungary, Ireland, Mexico (n = 3), Nauru, Samoa (n = 2), Saudi Arabia, South Africa (n = 2), Thailand, The Philippines, UK (n = 2), USA. Three papers reported studies on the policy process of voluntary approaches on salt reduction in Argentina and Fiji, and on restrictions on marketing of unhealthy food to children in Spain.
Three papers reported studies of the policy process of PPPs on Healthy Food Partnership and FHD in Australia, on the Public Health RD in England, and on Healthy Lifestyles school-based PPPs in seven countries: China, India, South Africa, Mexico, Brazil, UK, Germany.
Nine studies reported the policy process of establishing taxes, and among these most (n = 7) focused on SSB tax [Saudi Arabia, South Africa, Mexico (n = 3), Chile, France, Fiji, Samoa, French Polynesia, Nauru]. Others reported on sugar tax (Ireland) and tax on fats (Denmark). Four countries reported on processes related to nutrition labelling (Chile, Colombia, UK) and specifically of trans-fatty acids (Brazil). Two studies focused on regulation to limit salt intake (Samoa, South Africa). Three studies reported on restrictions on marketing of unhealthy foods to children [Fiji (n = 2), The Philippines], two on restrictions on marketing of breastmilk substitutes (Samoa, Thailand), and one on regulation of television food advertising to children (USA). Finally, two studies reported on school food regulation (Hungary, Mexico) and one on mandatory standard for limiting food products and promotions in hospital retail outlets (UK). One study assessed the food and beverage industry influence on a national nutrition policy (Canada). These are summarised in Table 23.
| Item | Country | Name of policy | Study aim | Methods | N participants and characteristics |
|---|---|---|---|---|---|
| Voluntary approaches ( n = 3) | |||||
| Castronuovo (2017)97 (ID: 52948582) | Argentina | Less Salt, More Life Program | To contribute to the body of literature and research into decisions in the public health sector regarding voluntary initiatives and PPPs in the prevention of NCDs, attempting to understand the policy process of PPPs from the stakeholders’ perspectives. | Interviews Documentary analysis |
n = 29: experts on the technical and political aspects of sodium reduction (2), decision-makers from Ministries and government agencies (11) food companies (11); food industry associations (5). |
| Davo-Blanes (2013)98 (ID: 52950722) | Spain | Restrictions on marketing of unhealthy food to children | To identify Spanish stakeholders’ views on the relationship between childhood obesity and the marketing and advertising of food and beverages aimed at children in Spain, as well as on the corresponding of regulations. | Interviews | n = 13 organisations: experts (2), consumer advocates (1), public health advocates (2), food manufacturers (2), advertising advocates (1), government representatives (1). |
| Webster (2018)99 (ID: 52959092) | Fiji | FSIA | This paper reports the process evaluation and costing of a national salt reduction intervention in Fiji. | Interviews | Child/family/school advocates (2) and media (1). |
| PPPs ( n = 3) | |||||
| Brandon (2020) (ID: 52946240)100 | Australia | Healthy Food Partnership FHD |
To critically analyse trends in the scope of federal nutrition policy actions in Australia between 2007 and 2018. | Interviews Documentary analysis |
n = 6 interviews and 10 documents. |
| Durand (2015)101 (ID: 52949550) | UK | The Public Health RD | We explored informants’ experiences and views about the RD’s development, implementation and achievements. | Interviews | n = 44 interviews with 50 interviewees from partner organisations and non-/former partners (12). |
| Perez-Escamilla (2018)102 (ID: 52947859) | China, India, South Africa, Mexico, Brazil, UK, Germany | Healthy Lifestyles school-based PPPs | To identify the factors that enabled the successful implementation of school-based PPPs focusing mainly on nutrition and physical activity in seven countries. | Interviews | n = 19 interviews with key programme leaders from each programme documentary analysis, MIF annual country reports and MIF project reports, proceedings from two school-based healthy lifestyle programme evaluation workshops in October 2013 and in May 2016. |
| Regulatory approaches ( n = 24) | |||||
| Alsukait (2020)103 (ID: 52944441) | Saudi Arabia | SSB tax | To add to the global discussion on SSB tax design and policy process by highlighting the Saudi Arabia’s barriers and facilitators to implementation. | Interviews Documentary analysis |
n = 10 from health agencies (4), non-health agencies (3), industry (3). |
| Campbell (2020)104 (ID: 52946177) | Ireland | Sugar tax | We focused the analysis on the food industry actors’ response to the proposal to introduce a SSB tax. Specifically, the aim was to explore the use of framing in the industry submissions in this consultation. | Documentary analysis | n = 14 industry actor submissions to the sugar tax consultation. |
| Carriedo (2020)105 (ID: 52946148) | Mexico | SSB tax | To examine the political context out of which this policy emerged, the main drivers for the policy change, and the role of stakeholders in setting the policy agenda and shaping the policy design and outcomes. | Interviews Documentary analysis |
n = 31 stakeholders from industry (5), academia (7), government (10) civil society (4), international organisations (2), media (3), think tanks (2) 145 documents, including peer reviewed papers, policy briefs, press releases, industry, government and CSO reports. |
| Davies (2017)106 (ID: 52969104) | Brazil | Food labelling of trans fatty acids | To identify the stakeholders and to present their opinions about the mandatory trans-fat content during the public consultation carried out prior to the law coming into effect in 2007. | Documentary analysis | n = 25 stakeholders made contributions to the public consultation; 6 from academic and health professional bodies, 2 from other professional bodies, 2 from government departments, 14 from the food industry and 1 from the pharmaceutical industry. |
| Dorlach (2020)107 (ID: 52965914) | Chile | Nutrition labelling | To understand how common practices such as public consultation submissions, corporate threat letters, and external legal assistance influence regulators’ understanding of their ‘legally available’ policy space, we study the contested introduction of a pioneering nutrition labelling regulation. | Interviews Documentary analysis |
n = 30 interviews with those involved in regulatory conversations over Child’s nutrition label, but not food industry representatives. Submissions to consultation on Chile’s draft regulation, internal communications between the food industry and foreign states’ trade policy agencies about the regulation, and internal reports by the Chilean bureaucracy are key sources for the reconstruction of the interpretive contest over the legality of Chile’s nutrition label. |
| Fooks (2019)108 (ID: 52947149) | South Africa | SSB tax | To scrutinise industry submissions to the South African government’s consultation on a proposed SSB tax and examined their use of evidence. | Documentary analysis | n = Industry submissions to the South African government’s consultation on a proposed SSB tax. |
| Fuster (2020)109 (ID: 52946727) | Mexico Chile |
SSB tax | To examine the policy change process that resulted in the current SSBs taxes in Mexico and Chile. | Interviews | n = 24 including 16 researchers (5 from Mexico, 5 from Chile and 6 Global), 3 food and beverage industry representatives (1 from Mexico, 2 Global) and 5 civil society representatives (3 from Mexico, 2 from Chile). |
| James (2020)110 (ID: 52946036) | Mexico | SSB tax | This article explores the politics of passage of the SSB tax in Mexico. | Interviews | n = 17 including NGOs (3), academics (4), political strategists (2), bureaucrats (3), politicians (1), trade associations (2), industry (1), lobbyist (1). |
| Kaldor (2018)111 (ID: 52946215) | South Africa | Regulation to limit salt intake | To analyse the policy process for the South African regulation setting upper limits for salt in 13 commonly consumed food categories, to inform future policy action for prevention of NCDs. | Interviews | n = 10 interviews with stakeholders falling into four sectors: government (n 3), academia (n 2), the food industry (n 3) and NGOs (n 2). |
| Kiss (2019)112 (ID: 52947265) | Hungary | School food regulation | To analyse the causes of the failure of the school catering regulation. | Interviews | n = 72 interviews with stakeholders: including 33 experts, 13 teachers and 26 parents. |
| Le Bodo (2019)113 (ID: 52944494) | France | SSB tax | To get an insight into policy processes of the soda tax. | Documentary analysis | n = Publicly available legislative documents and scientific articles and grey literature. Inventory of legislative documents, a comprehensive press review, and a purposive sample of scientific articles and grey literature. |
| Mialon (2020)114 (ID: 52946439) | Colombia | Nutrition FOPL | To identify and monitor food industry use of political practices during the adoption of nutrition WL in Colombia. | Interviews Documentary analysis |
n = 18 key informants from the government (n 2), academia (n 1), civil society (n 12), the media (n 2) and a former food industry employee (n 1). |
| Phillips (2019)115 (ID: 52946874) | Fiji | Restrictions on marketing of unhealthy foods to children | To examine how neoliberal logic is experienced, internalised and resisted by nutrition policy makers in Fiji. | Interviews | n = 11 semi-structured interviews with nutrition policy makers and stakeholders. |
| Phulkerd (2017)116 (ID: 52944684) | Thailand | Restrictions on marketing of breastmilk substitutes | To identify barriers and potential facilitators to the implementation of both the RTA and 25% SFS policies. | Interviews | n = 28 participants holding senior positions in government, industry and civil society organisations. |
| Razavi (2019)117 (ID: 52946192) | UK | Nutrition FOPL | To explore one aspect of the decision-making process public consultation on policy proposals by a national regulatory body aiming to understand how public health policy development is influenced by different stakeholders. | Documentary analysis | n = 139 responses from key stakeholder groups in a consultation process on the regulation of television advertising of foods high in fat, salt and sugar aimed at children. |
| Reeve (2018)118 (ID: 52947524) | The Philippines | Restrictions on marketing of unhealthy foods to children | To identify barriers and enablers to effective school food policy development and implementation. | Interviews | n = 21 interviews with policy-makers and stakeholders involved in school food policy-making and implementation. |
| Shelton (2017)119 (ID: 52948500) | USA | Regulation of television food advertising to children | To understand the key framing approaches used by private industry vs. public health sector, with the goal of informing future public health messaging, framing and advocacy in the context of policy-making. | Documentary analysis | n = 97 consultation documents submitted on behalf of organisations (private industry, n 64; public health, n 33). |
| Stead (2020)117 (ID: 52946725) | UK | Mandatory standard for limiting food products and promotions in hospital retail outlets | To examine implementation process and changes to the retail environment in relation to food promotions and choice. | Interviews | n = 32 interviews with the shop manager or nominated members of staff. |
| Thow (2011)120 (ID: 52951707) | Fiji, Samoa, French Polynesia, Nauru | SSB tax | To analyse four different soft drink taxes in Pacific countries and documented the lessons learnt regarding the process of policy agenda setting and implementation. | Interviews Documentary analysis |
n = 31 stakeholder interviews in Fiji (10), Samoa (11), Nauru (6) and French Polynesia (4). Collected policy documents and reports. |
| Thow (2020)121 (ID:52946632) | Fiji | Restrictions on marketing of unhealthy foods to children | To draw lessons from Fiji regarding the challenges and opportunities for policy initiatives to restrict (1) food marketing to children and (2) marketing of breast milk substitutes, to inform policy for the double burden of malnutrition. | Interviews | n = 11 key informants from relevant sectors, representing public health, economic and consumer interests. |
| Trieu (2018)122 (ID: 52947906) | Samoa | Restrictions on marketing of breast milk substitutes | To conduct a process evaluation to investigate the reach, dose/adoption, fidelity, cost, and context of MASIMA (Samoa’s national, government led salt reduction strategy), including a qualitative evaluation of implementation factors. | Interviews | n = 25 interviews: with 8 Ministry of Health, 7 other government organisations, 6 community leaders, 4 food industry representatives. |
| Vallgarda (2015)123 (ID: 52949501) | Denmark | Tax on saturated fat | To present arguments and themes involved in the debates surrounding the introduction and the repeal of the tax on saturated fat. | Interviews Documentary analysis |
An analysis of parliamentary debates, expert reports and media coverage; key informant interviews; and a review of studies about the effects of the tax on consumer behaviour. |
| Vandenbrink (2020)124 (ID: 52963550) | Canada | Healthy Eating Strategy | To describe the interactions between Health Canada and industry and non-industry stakeholders and to identify the strategies used by industry to influence food and nutrition policy. | Documentary analysis | Documents such as correspondences and presentations exchanged in interactions between Health Canada and stakeholders regarding the Healthy Eating Strategy. |
Quality assessment of included studies
The quality assessment of included studies was done using the ten standardised criteria of the CASP tool (see Table 22). All of the included studies gave a clear statement of the aims of the research, used qualitative methodology appropriately, has an appropriate research design to address the aims of the research, used an appropriate recruitment strategy, collected data in a way that addressed the research issue, analysed the data sufficiently rigorously, and had a clear statement of findings. Nearly all had taken ethical issues into consideration. Though most studies were rated ‘unclear’ or ‘no’ against the question about whether the relationship between researcher and participants has been adequately considered, overall, the final criteria about whether the research is valuable was answered ‘yes’ for all included studies.
Conflict of interest statements and funding sources were reviewed for all studies and only one was funded by the food industry to review food industry partnership programmes.
Factors reported to shape the food and nutrition policy process
Reported factors supporting the achievement of the approach to improve diets
The reviewed studies highlighted supportive factors, including clear government leadership and the commitment of the executive branches in the case of fiscal measures; ensuring that tax contributed both to the government budget and aligns with the health agenda, such as overarching NCD or obesity strategies; the use of international best evidence, and localised health and economic evidence; co-ordination with trade experts for legal support; harnessing focusing events like newly elected governments or government priorities to reduce deficits and address obesity prevention, and communicating clear targets and compliance measures to commercial actors or partners.
The importance of clear leadership on a regulatory decision was evident across the literature, but leadership was manifested in different ways. For example, decisions to go ahead with the SSB tax in Saudi Arabia was attributed to swift decision-making by the Supreme Council, the highest GCC decision-making body. 103 In the case of the SSB tax in Mexico however, Fuster et al. (2020) cited the importance of both top-down leadership AND bottom-up pressure from civil society coalitions for policy adoption. 109 They also reported the commitment of executive branches, despite pushback from industry, in helping to argue for the inclusion of SSB taxes as larger fiscal reforms. 109 Thow et al. (2011)120 studied SSB tax implementation in Fiji, Samoa, Nauru and French Polynesia, and concluded that a key to getting SSB taxes on the agenda was contribution of the tax to the government budget, and aligning tax priorities to the health agenda, such as diabetes prevention and control on Nauru.
In Hungary, Kiss et al. (2019) reported on a school food reform and cited government leadership as being crucial (even though weak), given that power is centralised and most schools are state owned. 112
A number of studies highlighted the role of policy entrepreneurs (high-profile individuals who are willing to invest their resources in driving change to address a problem of personal interest) and strategists. For example, in another study of the passage of the SSB tax in Mexico, James et al. (2020)110 reported that financial support provided by Bloomberg Philanthropies allowed the employing of political strategists who brought public awareness and public attention, and helped create public health/pro tax advocacy coalition [James et al. (2020)]. 110 The importance of the use of localised health and economic evidence was reported by Dorlach et al. (2020) who found that two key factors in bringing about nutrition labelling regulation in Chile were experience in nutrition science and co-ordination with Chile’s trade policy agency, which had high legal expertise. 107
Several studies mentioned the importance of harnessing focusing events, such as newly elected governments and related fiscal reforms. In the process of passing the SSB tax in Mexico, Fuster et al. explain that this was broadly considered a selected issue rather than an urgent problem, meaning that policy-makers did not see it as priority; this creates more opportunities for other stakeholders such as industry to get involved, and so linking the issue to existing priorities or events was key. 109 In their study of factors influencing the passing of the SSB tax in France, Le Bodo et al. (2019) also referred to linking the regulation to other events of importance, for example, the government’s priority to reduce deficits in context of economic downturn, to relieve wage costs in the farming sector, and obesity prevention as a long-standing issue. 113
In the six included studies on the policy process of voluntary approaches or PPPs, the reported enabling factors were much the same as for success in achieving regulation. In the study of decision-making processes that led to the establishment of the Australian Healthy Food Partnership (a PPP between big food industry players and the national government), Brandon et al. (2020) also refer to the importance of clear leadership from public sector actors, however they noted that this decision was not informed by a review of international evidence of best practice of voluntary versus regulatory practices. 100 Contextual factors were also of importance, such as the Australian political context and specifically ideological resistance towards regulation. 100 Thus Brandon et al. report the role of compromise, for example, the selection of three reformulation nutrient targets (total sugar, saturated fat and salt) to comprise between considerations of feasibility, evidence gaps and food industry receptiveness; and of pragmatism, engaging with industry to ensure policy success, harness resources and expertise of industry. 100
Castronuovo (2017)97 report on a voluntary approach to reduce salt in Argentina, initiated by the Ministry of Health but with the food industry playing a leading role in the policy process, and was eventually important in the transition to a sodium reduction law. The authors explain that this was largely due to health being kept a priority on the public agenda and facilitated because the targets had already been negotiated with the private sector. In their study of mandatory standards for making hospital retail outlets healthier in Scotland, Stead et al. (2020)117 also cited centralised processes for sourcing products and training.
In the only study funded by industry (Mondelez International Foundation), Perez-Escamilla (2018)102 reviewed the key factors that enabled the successful implementation of a series of school-based PPPs focusing on nutrition and physical activity, funded by the Mondelez International Foundation. The lessons for success cited the importance of equal representation from partners on committees, clarity and openness of decision-making processes, equal decision-making authority, all of which support transparent monitoring and evaluation. Yet we caution that these findings should be considered in light of the other independently funded results reported here, which point to the limited effectiveness of PPPs and voluntary approaches (see Chapter 5 and 6); the success factors cited by Perez-Escamilla are refuted in several evaluations of PPPs, such as in the Public Health RD a PPP in England (2011–5), where giving industry leadership roles in a public health policy led to watering down of pledges and partnership aims, and ultimately limited impact of the PPP overall. In analysing the drivers of the participation in Public Health RD, Durand et al. (2015)101 find that key motivations of corporate participation included reputation enhancement and meeting corporate social responsibility targets.
Reported factors impeding the achievement of an approach to improve diet
The reviewed studies on policy process of regulations highlighted a range of impeding factors: lack of government will or leadership, poor governance mechanisms to implement the policy, lack of community support and engagement of the public; lack of recognition of conflicts of interest when government is too close to industry interests; the deployment of industry strategies such as legal threats, lobbying decision-makers, engaging high-ranking public officials, challenging the evidence, challenging the benefits of regulation and promoting voluntary approaches, encouraging narratives of personal responsibility, and positioning themselves as important legitimate role models.
Several studies analysed the process of implementing a SSB or sugar tax, most of whom including Le Bodo (2019)113 (France) and Fuster (2020)109 (Chile and Mexico) mentioned the strong opposition of the food and beverages industry to SSB taxation, which was also reflected in the deployment of arguments such as the benefits of voluntary self-regulation, the negative impact of a tax on the economy, and the unfairness of a tax on industry and on individuals. This was reflected in Fooks’ (2019) analysis of industry submissions in the lead up to the SSB tax process in South Africa, deploying arguments that the policy would have wide ranging adverse social and economic consequences. 108
In Thow et al. ’s (2011)120 study of SSB tax implementation in Fiji, Samoa, Nauru and French Polynesia, industry pressures, as elsewhere, had an impact and in Fiji, organised industry opposition to the tax resulted in its removal. Phillips’ et al. (2019)115 more recent study of nutrition policy-making in Fiji reports how efforts at restricting marketing of unhealthy foods to children and of breast milk substitutes were also overturned due to obstructive industry interests, and a narrative of personal choice and responsibility that dominated consumer decisions.
Campbell et al. (2020)104 conducted an analysis of how frames are generated through the case of the sugar tax in Ireland and present a sophisticated typology of framing mechanisms. One such mechanism is the act of dichotomising, or the division of frames into binary blocs, for example, weaponising the opponent’s logic: as the authors note, a common example is claiming a lack of causal evidence for sugar tax efficacy. This strategy is illustrated in Fooks et al. (2019) policy analysis of the SSB tax in South Africa, where industry actors opposing the tax were reported to use confounding references (misleading use of references which either overstates or gives an entirely false impression of support for a claim or obstructs evidence appraisal), and ‘evidential landscaping’ (promoting alternative evidence, or purposefully excluding relevant evidence), more broadly referred to as agnogenic practices, or methods of representing, communicating and producing scientific research and evidence, which work to create ignorance or doubt irrespective of the strength of the underlying evidence. 108 It is also echoed in Vandenbrink et al. (2020)124 in their study of the food and beverage industry’s influence on a national nutrition policy (the Healthy Eating Strategy) in Canada, where industry regularly challenged the evidence underpinning regulation and employed the arguments that regulation would lead to detrimental impacts on the economy.
Campbell et al. (2020)104 also suggest ‘contesting’ as a framing mechanism, referring to shaking the frame so that arguments are used by different stakeholders; an example of contesting as a framing strategy is reported in Le Bodo et al. (2019) where during the SSB tax process in France, the food industry firmly and publicly opposed the tax, but then became open to contribute to resolving the public deficit, provided the tax rationale is not public health oriented, positioning themselves as concerned role models within the community. 113
Other papers reported factors such as lack of consumer engagement, as reported in a study by Kiss et al. in on factors shaping the school catering system in Hungary, where ‘nutrition illiteracy’ of teachers and students was not taken into consideration, leading to lack of engagement of these key stakeholders. 112 Similarly in Denmark, Vallgarda et al. (2015)123 report that lack of policy engagement and strong proponents, but many influential opponents, to the saturated fat tax, led to its demise.
Several studies reported on the process of implementing FOPL: Razavi (2019)117 analysed an early consultation process and cited similar barriers, where the final policy appeared to be substantially influenced by stakeholders. Mialon (2020)114 studied the FOPL process in Colombia and cited hindering factors such as the industry deployment of legal threats, lobbying Congress, engaging high-ranging public officials. Mialon and colleagues report that unlike other countries, in Colombia, food industry actors and government officials have openly close ties, and so the industry sponsoring of congresses at universities was considered unconflicted behaviour, though the authors conclude that these actions may have worked to weaken the FOPL policy. Competing ideologies and the ‘market-centric’ logic of government decision-making were also cited as factors, which negatively affected restrictions on marketing of unhealthy foods to children in Fiji as reported by Phillips (2019)115 who also (like Kiss et al. above) cited lack of community support and inadequate healthy literacy. In Vandenbrink et al. ’s (2020)124 study of the food and beverage industry’s influence on a national nutrition policy (the Healthy Eating Strategy) in Canada, another reported industry strategy was policy substitution or promoting alternatives to regulation such as voluntary codes and self-regulation.
Webster et al. (2018)99 report a national salt reduction intervention in Fiji, including voluntary engagement of the food industry to adhere to salt reduction targets, which had been evaluated to have limited effect. Webster et al. (2018) report that the strategy to engage industry actors was unclear, with no compliance mechanisms in place; moreover, governance mechanisms of the salt reduction intervention could have been optimised, with stronger government leadership. In their study of school food policies and marketing restrictions in the Philippines, Reeve (2018)118 also reported the role of insufficient human and financial resources for implementation as well as policy enforcement; moreover the food industry actors harnessed existing relationships with schools to promote their brand and challenge the establishment of more robust school food policies. In their study of mandatory standards for making hospital retail outlets healthier in Scotland, Stead et al. (2020)117 also cited the need for more policy implementation guidance and support.
Legitimacy of commercial actors as policy actors
The dominant place of the food and beverage industry across nearly all reviewed policy process studies raises the question of what legitimacy they have in designing and implementing public health policies. These studies provide insight into these phenomena and mechanisms underpinning the policy process for improving diet, in particular how large food and beverage industries have established a relatively secure position in policy interventions to improve diets. As demonstrated in the reviewed studies, when commercial actors are able to dominate the narrative and set the agenda of public discourse, they acquire a disproportionately high ability to ‘define’ a public process and thus gain legitimacy,125 defined as a measure of the level of trust and confidence an institution should command. 125
Figure 15 summarises key mechanisms of interest as emerging from the literature. Brandon et al. (2020) discuss the food industry’s use of ‘leadership’ frames such as ‘choice giver’, ‘role model’, ‘master negotiators’. 100 For example, the authors provide the example of industry actors negotiating in a politically supportive environment (Australian government was not keen on regulation): industry actors not only negotiated but imposed an underlying assumption that pragmatism and compromise are fundamental to achieving food policy, at the expense of the best evidence. 100 Campbell et al. (2020)104 further explain that ‘corporate actors assume the role of the “choice giver”, while the dichotomized alternative is government, which is forced to occupy the opposing domain in the frame as the infantilizing remover of choice’104 This is relevant to understanding the legitimisation of industry as leaders in food/nutrition, as they ‘assume the role of the choice giver’ – this is a positive, confident act, one which demonstrates or even takes without asking the role of making a decision about what a consumer should do or not.
FIGURE 15.
Emerging higher understanding of the accepted legitimacy of food industry as global leaders.
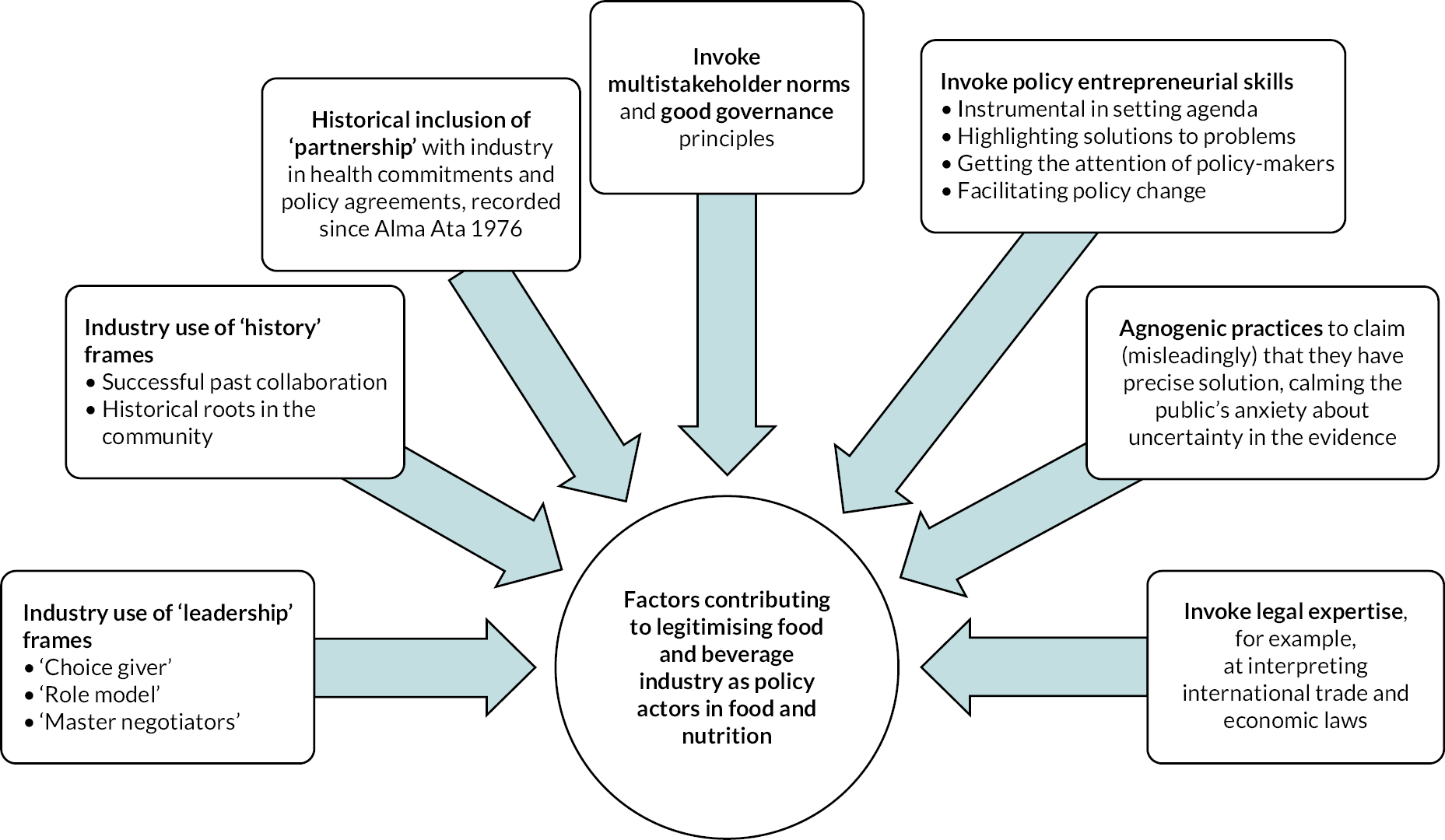
Campbell et al. (2020)104 refer to the framing strategy of equating-equalising of logics, to level all audience; for example, emphasising ‘progress’ made on voluntary codes and positioning themselves as ‘industry leaders’; demanding a seat at the policy-making table, appealing to historical roots and reminding how they are firmly established in the fabric of society. 104 Campbell et al. (2020)104 also report how the food industry will present itself as fully committed to health problems, positioning themselves as concerned role models within the community, which contribute to supporting the establishment of their legitimacy as leaders. 104
Fuster et al. (2020) report that in Chile and Mexico the food and drinks industry carried out a failed legal challenge to the SSB tax constitutionality, while also appealing to the public, by positioning themselves as defenders of consumer freedom; this contributes to building an image of the industry as champions of consumer rights. Finally, Mialon (2020)114 report the use of key platforms such as Codex used by the industry to gain access to decision-making, in the case of FOPL in Colombia.
Conclusions
We reviewed 30 studies of the policy process of regulatory, voluntary and PPPs approaches. A range of useful lessons from these studies are reported, both on facilitators and barriers. What emerges strongly is the dominant role of the food industry as often the major reason for the derailing of policies, yet (or perhaps because of) with a very central decision-making or at least influencing position in the policy process. Thus, from the available evidence reviewed, we have advanced our understanding of phenomena and mechanisms underpinning the policy process for improving diet, in particular how large food and beverage industries have become legitimate actors in policy interventions to improve diets. Mechanisms of interest that emerged from the literature about voluntary and PPP approaches include the industry’s deployment of leadership frames (‘master negotiators’), of ‘history’ frames to emphasise historical roots in community, and the promotion of partnership as a preferred policy construct.
Chapter 9 Discussion and conclusions
Policy interventions (whether voluntary and/or regulatory) to change the food environment to the population are generally designed to reduce access to and consumption of unhealthy foods, or to change public attitudes and social norms to discourage the purchase and consumption of such foods, ultimately leading to reductions in diet-related diseases. This theory of change, depicted in Figure 16, is at the core of most national strategies to improve diet. The evidence synthesis tested that theory of change by analysing the evidence of effectiveness, cost-effectiveness and policy processes of policy interventions to improve diet, focusing on regulatory, voluntary and partnerships approaches.
FIGURE 16.
Theory of change of policy interventions to improve the food environment for better diets.
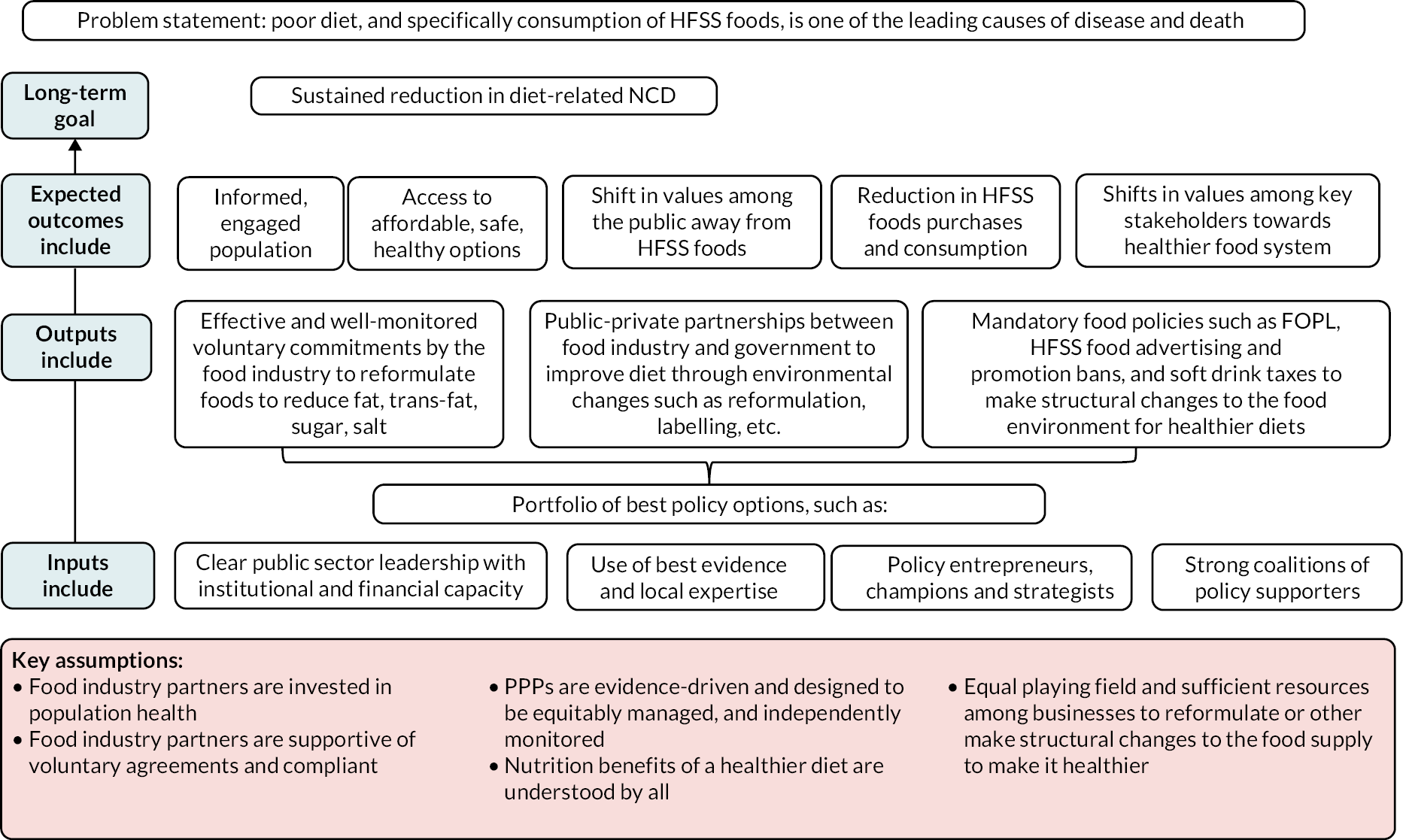
Main findings
We first developed a systematic map of 483 included studies (see Chapter 3) in order to obtain a comprehensive picture of what policies have been evaluated and how. The map revealed considerable imbalances across the literature, suggesting that policy evaluations are conducted and published inequitably across the world both in terms of quantity and quality. Although 70 countries were represented in the reviewed literature overall, 81% of publications focused on only 12 countries (USA, UK, Australia, Canada, Mexico, Brazil, Chile, France, Spain, Denmark, New Zealand and South Africa), and 30% included the USA. By contrast, 32 countries were only documented in one or two publications each, several of which were multicountry analyses and thus were documented in fewer details. Few publications were found about Africa, Central and South Asia and the Middle East. Reasons for the lack of evaluations (or lack of published evaluations accessible in English-language databases) more broadly across the world are likely to include factors such as funding challenges and language barriers. Inequities were also detected in the study designs for evaluating real-world policies, with the most quantitative robust methods mainly documenting the abovementioned 12 dominant countries. Furthermore, using a generous interpretation of the PROGRESS-Plus equity dimensions, we found that not only 50% of publications assessing policy effectiveness did not compare outcomes by any equity domain, but that the proportion of those doing so has decreased over time. Age, education (mainly school characteristics) and SES at individual level were the most frequently assessed dimension, while occupation at individual level, religion and culture, social capital and disability were barely considered.
We then assessed the effectiveness and cost-effectiveness of policies to improve diet across four separate systematic reviews.
First, an overview of 11 systematic reviews (see Chapter 4), with 3 additional reviews for investigating health equity, primarily assessed regulatory policies (especially taxation) and a small number of voluntary approaches by the public sector, food retailers and restaurant chains. Except for salt and saturated-fat-related taxes, for which evidence is limited to few real-world initiatives including some with particularly narrow scopes, most regulatory approaches designed to improve health, consumer behaviour (e.g. food intake, purchases), and food environment outcomes appear to be effective. Effects for voluntary approaches by public and private actors were also generally positive for salt and trans-fat reformulation (but regulatory trans-fat bans were more promising), labelling on products and supermarket shelves, and changing defaults in children’s menus in restaurants, although some of them relied on single cross-sectional studies in the USA. Results for voluntary menu labelling and multicomponent commitments by large retail chains were mixed. The findings by PROGRESS-Plus categories indicate a lack of reporting of outcomes in systematic reviews for specific population groups: overall, evidence on specific population groups is patchy, incomplete, mainly inconsistent, and largely relies on single studies (although some evaluations had large samples) rather than aggregated bodies of evidence.
Second, we reviewed the effectiveness of PPPs (see Chapter 5). From the available evidence reviewed across 17 studies evaluating 7 PPPs, it would appear that partnerships with the food industry to improve diets via reformulation or other changes to the environment have limited effectiveness at improving population diets and food environments.
Third, we reviewed the effectiveness of voluntary approaches by private actors (see Chapter 6). Sixteen studies of nine voluntary approaches by private actors mainly focused on advertising and marketing control, reformulation, and the retail and catering sectors. From the available evidence reviewed, when comparing effectiveness among participants in voluntary commitments to NPs, the direction of effect or of association for most outcomes appeared to be either inconclusive or worse for participants. Thus from the available evidence reviewed, it would appear that policies designed as voluntary approaches led by commercial actors are not an effective approach at reducing advertising or other promotion of unhealthy products to children, improving the nutritional composition of food and beverages, encouraging calorie menu labelling in chain restaurants, or reducing marketing content targeting children on food packages.
Fourth, we assessed the cost-effectiveness of real-world policies to promote healthy diets (see Chapter 7). Two studies suggested positive impacts for the fiscal measure of the Mexican SSB tax, and one for the voluntary government-led HSR FOPL intervention in Australia. The fourth one showed a lack of effectiveness and cost-benefit for the PPP intervention to reduce salt consumption in England as part of the Public Health RD. There is a pressing need to build on the extensive literature on the effectiveness of interventions with high-quality evidence on cost-effectiveness, to support meaningful action to tackle the scourge of diet-related ill health.
Our final study set out to assess what factors affect the process of national policies (see Chapter 8), from choice of policy design to implementation. The 30 included studies revealed key enabling factors, including the reviewed studies highlighted supportive factors, including clear government leadership and the commitment of the executive branches in the case of fiscal measures; ensuring that tax contributed both to the government budget and aligns with the health agenda, such as overarching NCD or obesity strategies; the use of international best evidence, and localised health and economic evidence; co-ordination with trade experts for legal support; harnessing focusing events like newly elected governments or government priorities to reduce deficits and address obesity prevention, and communicating clear targets and compliance measures to commercial actors or partners. The reviewed studies on policy process also highlighted a range of impeding factors: lack of government will or leadership, poor governance mechanisms to implement the policy, lack of community support and engagement of the public; lack of recognition of conflicts of interest when government is too close to industry interests; the deployment of industry strategies such as legal threats, lobbying decision-makers, engaging high-ranking public officials, challenging the evidence, challenging the benefits of regulation and promoting voluntary approaches, encouraging narratives of personal responsibility, and positioning themselves as important legitimate role models.
This review also advanced our understanding of phenomena and mechanisms underpinning the policy process for improving diet, in particular how large food and beverage industries have become legitimate actors in policy interventions to improve diets. Mechanisms of interest that emerged from the literature about voluntary and PPP approaches include the industry’s deployment of leadership frames (‘master negotiators’), of ‘history’ frames to emphasise historical roots in community, and the promotion of partnership as a preferred policy construct despite its ineffectiveness.
Though we were also interested in reporting any unanticipated effects of evaluated policies, it became clear during the review of included studies that these outcomes were not explicitly reported, thus requiring further investigation.
Implications for public health policy to improve food environments and population diets
This study highlights five main public health policy implications to improve food environments at the global level and specifically for England.
Structural changes through regulation appears the most effective approach to improve the food environment
A first implication relates to the finding that from the available evidence reviewed, policies appear most effective when targeting the structural rather than informational level and made mandatory. The findings align in large part with key existing recommendations for effective and cost-effective approaches including, notably the WHO Best Buys (2017),126 which advise to reduce salt intake via the reformulation of food products, eliminate industrial trans-fats by banning their use in the food chain, replace trans and saturated fats with unsaturated fats, and reduce sugar consumption through effective taxation on SSB. It also suggests that countries work to reduce portion and package size and implement FOPL. As reported by Francesco Branca, the WHO direction of Nutrition for Health and Development, in his 2019 BMJ article,127 a large proportion of countries have not implemented evidence-based ‘structural actions’ to effectively improve food environments, including implementing a ban on industrially produced trans-fats, taxing SSBs and unhealthy foods, and mandating simplified, interpretive FOP nutrition labelling.
In England, much of the government’s response to unhealthy diets has focused on obesity prevention and reduction. 128 The 2016 Childhood Obesity Plan proposed a set of actions, including the introduction of a SDIL; the reduction by 20% of sugar in products that contribute most to intakes of children up to 18 years by 2020; the reduction of calories in a range of products contributing to children’s intakes; reducing salt in products by achieving the 2017 salt targets; providing clearer food labelling; making healthy options available in the public sector; making school meals healthier; and developing a new framework by updating the Nutrient Profile Model. In 2020, the plan ‘Tackling obesity: empowering adults and children to live healthier lives’129 mentioned the need for mandating calorie menu labelling in large out-of-home food caterers; for using legislation to control volume promotions of HFSS foods, for example buy one get one free, as well as their placement in locations that trigger unintended purchases, in retail settings that sell food and drink both in-store and online in England; and for both expanding the ban of advertising of foods HFSS on TV and exploring options online.
Many of these have been rolled out. For instance, the SDIL came into force in April 2018, imposing a two-tiered levy on manufacturers of soft drinks who did not reduce the amount of sugar in their beverages to below one of two stated levels,130 aiming to reduce NCDs associated with excess sugar consumption. 131 The SDIL has led some of the soft drinks industry to reformulate products to below one or both of the thresholds. 132,133 Early estimates suggest that the SDIL will contribute to improving health and decreasing health inequalities. 134,135 The regulations restricting promotions of HFSS products by location and price were due to come into force in October 2022. Those on advertising less healthy products on TV before 9 p.m. and online are expected to be introduced in 2023, pending Parliamentary procedure. 136
Voluntary approaches and public–private partnerships appear not to be the most effective approach to improve the food environment
A second implication for public health policy relates to the finding that from the available evidence reviewed, voluntary approaches and PPPs do not appear to be effective at improving food environments for healthier diets. The findings align with earlier studies14,137–140 and can be explained by the understanding of the functioning of voluntary approaches and PPPs (both from the review and past studies), namely that, commitments or pledges tend not to be based on most effective interventions to improve diets; there is usually a major focus on education and information/behaviour modification rather than on structural (and more effective) changes; self-designed commitments are narrow, vague or loosely binding – not ‘SMART’; voluntary participation of companies in self-regulation schemes is often itself voluntary, which results in an unequal playing field (and even so, some studies included in Chapter 6 found that their outcomes were worse than that of NPs); reporting and monitoring of implementation is often poor; there is limited added value of signing up/pledging apart from promoting a positive corporate image; partners often commit to actions already undertaken; and failure to comply with pledges is not well enforced or penalised.
In England, voluntary approaches are part of the strategy to improve diets. Current initiatives as described below would benefit from taking on board the lessons from the study if we are meaningfully and sustainably to improve food environments for healthier diets.
Public Health England – the government’s public health arms’ length body in existence at the time – was commissioned by the Department of Health to work on sugar reduction in light of a Scientific Advisory Committee on Nutrition report. 134 Their role of encouraging industry compliance to reduce sugar and salt content through regulation and with voluntary approaches reported modest progress across a range of food categories and sectors. 141 The Prevention Green Paper (2019) made further commitments to reduce the population’s salt intakes by publishing revised salt reduction targets in 2020 for industry, to be achieve by mid-2023, ‘keeping all options open if a voluntary approach does not demonstrate enough progress by 2024’. 142
Currently, the regulation of online advertising of HFSS products is self-regulatory through the Advertising Standards Agency,143 and as such industry possesses extensive rule-setting power within the regulatory process. A proposal for the total online advertising ban policy proposed as part of the Government’s new approach to address high rates of obesity in the UK included the UK Government pledge to hold a consultation on the total online advertising ban policy, primarily aimed at protecting children from such advertising, which closed on 22 December 2020. The results of the consultation are yet to be announced, and the proposed ban may not be implemented. 144
Expanding geographical representation of the evidence
A third implication for public health policy is the need to redress the imbalance in policy evaluation evidence across regions of the world, with this study’s stark finding that 81% of mapped publications (see Chapter 3) focused on only 12 countries (USA, UK, Australia, Canada, Mexico, Brazil, Chile, France, Spain, Denmark, New Zealand and South Africa), and 30% on the USA. To the best of our knowledge, there are no evaluations for several countries that have implemented such policies. For example, we are aware that in the Caribbean, Dominica has introduced an excise tax on food and drinks with a high sugar content in 2015. In the Middle East, Iran banned soft drinks broadcast advertising in 2004 and has a salt reduction strategy. In South Asia, Sri Lanka introduced regulatory traffic lights labelling in 2016. In North Africa, Morocco implemented a SSB tax in 2019, revoked it, and reintroduced it in 2020. In Sub-Saharan Africa, soft drinks and unhealthy snacks have been banned in schools in Mauritius since 2009. 145,146 Addressing these gaps will require examining the reasons for the lack of all types of evaluations (or published evaluations) in countries which clearly have implemented policies promoting healthy food environments, and ensuring that future policy analyses capture an equitable geographical spread. Solutions are likely to include increasing both research and publication capacity in the least documented world regions as well as in many other countries. This might also involve setting up cohorts and monitoring systems and should aim at including cost-effectiveness studies within policy evaluations more consistently. Evidence syntheses should also analyse findings from real-world evaluations separately from those of modelling studies, and where appropriate retrieve evidence from all regions of the world.
Understanding the barriers to policy evaluation is essential, and in particular clarifying whether it is a lack of resources, or a lack of contextual evidence to ensure appropriate measures for the local geographical context. Isaranuwatchai et al. 2020 assessed the WHO’s list of best buy interventions and concluded that best buys evaluated in one setting may not be cost-effective in others, further highlighting the importance of the finding that the available evidence is not globally representative. 147 Isaranuwatchai et al. 2020 emphasise that low- and middle-income countries (LMICs) have greater pressures to identify and prioritise more cost-effective and equitable NCD interventions, in the face of even more limited resources. 147
Capturing dimensions of health equity as policy outcomes
A fourth implication for public health policy relates to the low priority accorded to health equity as a policy outcome. This is despite the measurement and evaluation of equity having been prioritised as a key principle of action by the Commission on Social Determinants of Health of the WHO in 2008,148 and employing a quite generous interpretation of the PROGRESS-Plus framework. While age, SES at individual level, and education are relatively commonly considered, the remaining dimensions are much more neglected, especially disability, religion and culture, and occupation at individual level, leaving some population groups largely ignored. Social capital was also seldom assessed but we recognise that it is more challenging to operationalise and capture. Some of the dimensions mentioned above can also be difficult to apply in studies of environmental features. However, the evidence map shows that it is possible to consider at least some of them. Guidance with specific examples for different types of ‘participants’ or measurement units might help promote this practice further. Funders and journal editors could require researchers more systematically to integrate an equity focus on projects beyond the description of study participants’ characteristics, and with a particular emphasis on the neglected dimensions where possible. In the overview of reviews, none of the findings on equity considered the epidemiology of diseases to assess impact on health outcomes or whether the gap between groups had reduced or increased through time. Where possible, considering these would help to fill the gap.
Need for a systems approach across policies to improve food environments
A systems approach is a way of conceptualising and thinking through a problem. It can lead to a practical illustration of the complexity of pathways of impact, how different factors can interact, leverage points for change, which may not appear in linear logic models or traditional theories of change, and potential unintended consequences of an intervention. 149 Ideally a systemic theory of change helps to identify the wider drivers of unhealthy diet and prompts a strategy that effectively integrates the identified leverage points. 149
Unhealthy diets, and diet-related outcomes, are complex, challenging to tackle and seemingly intractable problems requiring an approach that fully engages with and responds to their complexity. However, part of the challenge in finding effective actions is that solutions are conceptualised and planned using traditional theories of change150 rather than using a systems approach. Most theories of change, as illustrated in Figure 16, suffer from pitfalls, including linear thinking, simple chains of cause and effect, and relying on a fixed plan.
As demonstrated across the research, the approach outlined in the theory of change (see Figure 16) only partially works. This is because it rests on a series of important assumptions, including that food industry actors are invested in population health; food industry actors are supportive of voluntary agreements and compliant; PPPs are evidence-driven and designed to be equitably managed, and independently monitored.
Conclusions
The study contributes to the growing field of research on the commercial determinants of health, defined as adverse health impacts attributable to commercial activities and corporate political strategies employed by unhealthy commodity industries to promote products, which can damage health. 151–153 The food and drinks industry employ a range of non-marketing strategies to promote the sale and consumption of their products, including shaping scientific evidence, building constituencies beyond their core business, using litigation, lobbying of decision-makers, and publicly criticising policy process, in the interest of protecting markets. These strategies have been known to increase the chance of ‘regulatory chill’ – delays, weakening, or abandonment of planned policies154 – and are manifested in various ways including a dampening effect on specific measures once government is aware of an existing threat to regulation;155 the abandonment or weakening of proposed regulation to avoid future disputes based around past challenges to similar regulation; and the deliberate instilling of apprehension in other countries trying to implement similar regulation (‘cross-border chill’). 155
This study has addressed another corporate political strategy, policy substitution, referring to the industry promotion of voluntary and partnership approaches. Chapters 5 and 6 indicate quite clearly that these are not the most effective approaches to improve the food environment, and the policy process study (see Chapter 8) finds that the concept of partnerships as a preferred policy construct is often presented as the most effective to meet public health objectives; however this argument is reported to be seldom informed by a review of international evidence of best practice in supporting healthy diets, but rather compromise and pragmatism. In fact, the evidence map (see Chapter 3) suggests that few PPPs for promoting healthy food environment have been assessed, and that most of the evidence available is about two PPPs, one in England and one in Australia.
The main proposition of this work, based on the extensive evidence synthesis, is that an improvement of diets in England requires a complex system approach to maximise the potential of a strong portfolio of food and nutrition policies by understanding the more complex drivers and competing interests.
Figure 17 exemplifies this by illustrating some of the factors highlighted by the study that could both dampen and enable the effectiveness of a portfolio of policy interventions, and taking a systems approach can provide an initial illustration of how these important factors interconnect and influence each other.
FIGURE 17.
An illustration of how this evidence synthesis challenges the current theory of change.
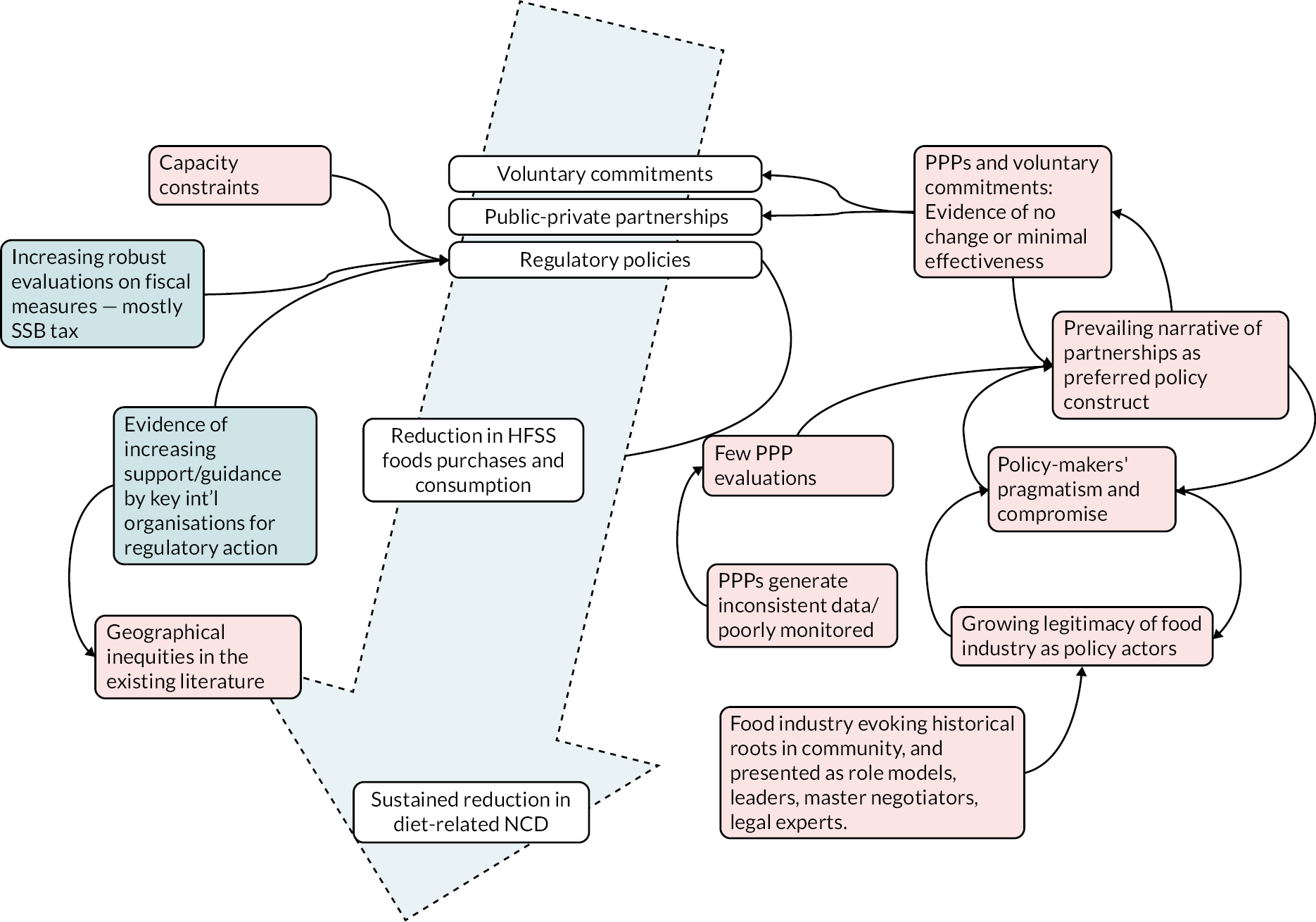
The evidence synthesis in Chapter 8 highlighted factors working against the above theory of change, including practical considerations often around policy implementation and the generation of context-specific evidence; differing ideological positions; capacity constraints; the role of evidence; lack of key stakeholder engagement, and the deployment by the food and beverage industry of frames and framing strategies to ultimately oppose a policy process. It also highlighted mechanisms underpinning the policy process for improving diet, in particular how large food and beverage industries have become legitimate actors in policy interventions to improve diets, such as the industry’s deployment of leadership frames (‘master negotiators’), of ‘history’ frames to emphasise historical roots in community, the promotion of partnership as a preferred policy construct, and the use of policy entrepreneurial skills.
Drawing on qualitative system mapping methods and on past work expressing mixed data as system illustrations (e.g. systems evaluations of PPPs;156 and the formulation of concrete methodological implications of a complexity perspective when conducting systematic reviews and guideline development157) we revisit the theory of change, visually adding findings of the evidence synthesis to illustrate the wider picture. Thus Figure 17 displays certain factors of the wider system, as emerging from the findings, and how they work together to either improve (in blue), or reinforce (in red), unhealthy diets in England.
As noted above, the theory of change outlined in Figure 17 rests on the assumptions that food industry actors can participate in, and are supportive of, voluntary agreements to reformulate their products to make them healthier, and that they are able and willing to respond to regulations to make their products healthier or behave in the interest of public health.
Implications for future policy evaluation methods
Need for guidance on appraising risk of bias and quality of non-clinical studies
Regarding study designs and quality or risk-of-bias appraisals, the systematic review on PPPs (see Chapter 5) has highlighted the lack of employment of comparison groups. The aggregation of data for participants and NPs in PPPs together suggests that identifying a comparison group can be possible in several cases. Furthermore, in both the latter systematic review and that on voluntary commitments by private actors (see Chapter 6), we noted a lack of reporting of information that is essential for appraising study quality or risk of bias, including information on non-responders, the presence of missing data and how it was dealt with, and the number of people collecting or verifying data independently. Similar observations were noted in most systematic reviews, with data on before and after the intervention, effect sizes and precision estimates often missing. Such information should be reported systematically and highlighted when missing in the primary studies. There are already checklists guiding study authors to do so in both primary studies and evidence syntheses. Wider systemic changes in academia with meaningful incentives might be needed to encourage reviewers to examine these attributes more systematically. Moreover, this project highlights the need to revisit the notion of lack of implementation as a source of bias from a policy analysis perspective. Lack of implementation for a policy is not necessarily or simply a bias; it may also be an outcome. It could be a mistake or might have been deliberately planned not to happen. For example, the systematic reviews on the effectiveness of PPPs and voluntary approaches by private actors (see Chapters 5 and 6) found that companies participating in PPPs or pledges continued to advertise, promote or offer unhealthy foods, including to children. The policy document analyses in the review of PPPs also suggest that some of the policies had very low ambitions, included loopholes, or were not monitored by the companies themselves, suggesting that they were more likely to be intended to promote a ‘health halo’75 and a favourable corporate image than to improve population diet.
Furthermore, this project highlights a need for guidance for appraising the risk of bias or study quality of studies measuring the effects of interventions on environments (rather than effects on human) and for critical appraisal of document analyses (including policy and media sources). These types of studies represent 57% of effectiveness studies in the systematic evidence map (see Chapter 3).
Lastly, as explained in Chapter 2, a wider discussion is needed about the suitability of the GRADE framework for assessing certainty in the evidence of policy research. It should consider the feasibility of different types of studies, recognise the contribution of document and media analyses, and differentiate more effectively the level of certainty between good and weak observational studies. This is aligned with concerns raised by Boon et al. (2021)158 for some public health topics: they have noted the presence of ‘discordant recommendations’ in which methodologically the level of confidence is rated low or very low, yet there is a case for making strong recommendations given the context and evidence.
Need for reporting policy characteristics in evaluations
This project also highlights a need for both reporting and considering policy characteristics in evaluations more consistently. Documenting these was not as straightforward as anticipated in both primary studies and evidence syntheses due to lack of reporting of information. Yet, these characteristics influenced the interpretation of results. They could also inform study quality or risk of bias. Information that we felt was missing includes the following:
-
Policy names: several policies were not named or had their name changed through time without it being reported in the evaluation.
-
Policy content and context: some publications reported different aspects of the same policy, for example, in Canada some said evaluating trans-fat policies that included both regulatory labelling and voluntary limits, while others only mentioned the limits. We have extracted the latter at face value, but some studies might have missed the wider picture. Also, stating that a policy is a salt reduction programme is not enough: it can consist of awareness campaigns, targets, labelling, regulations in specific settings, or a combination of these.
-
Governance and policy process including the actors involved: for instance, the development of some regulatory and voluntary approaches by the public sector might have involved private actors and should thus rather be called PPPs.
-
Policy and evaluation timeline: the dates of data collection and of key policy changes inform reviewers’ understanding of the policy status at the time of data collection, for example decisions about when baseline data were collected: whether it was collected before a policy was debated, or announced, between the announcement and implementation deadline, just before that deadline, or after, and for how long.
-
Wider context including concurrent initiatives: it is now common to have several initiatives promoting healthy eating occurring at the same time. For instance, from the UK and English governments alone, there are the SDIL, salt and sugar reduction programmes, FOPL, an advertising control code, etc. While it is impossible to assess them all at once, and study authors are not expected to extensively describe them, mentioning the most relevant concurrent interventions could help interpreting results.
-
Policy and evaluation levels: sometimes these did not match. For example, some state policies were evaluated using data aggregated at the national level without considering or mentioning that the policy was implemented in a single state.
Need to recognise the value of studies of environment features and policy documents
This project showcases the contribution of non-human outcomes for evaluating policies promoting healthy environments. The primacy often accorded by evaluations to health or behavioural outcomes of interventions is frequently inappropriate and unwarranted. First, many evaluations take place over too short a time from for measurable changes in outcomes such as obesity, CVD or mortality to manifest themselves. 159 Second, these policies act on the environment rather than directly on humans, alongside other interventions taking place concurrently. This often makes the direct attribution of effects on humans for a specific policy infeasible. The impact of a FOPL scheme or an advertising control policy is highly unlikely to lead to measurable changes in weight status over the course of an evaluation, but it may nevertheless generate intermediate outcomes such as alterations to packaging or reformulation of products.
Moreover, lack of implementation of a policy is not necessarily or simply a bias; from a policy analysis perspective it may also be an outcome. It could be a mistake or might have been deliberately planned not to happen. For example, the systematic reviews on the effectiveness of PPPs and voluntary approaches by private actors (see Chapters 5 and 6) found that companies participating in PPPs or pledges continued to advertise, promote or offer unhealthy foods, including to children. The policy document analyses in the review of PPPs also suggest that some of the policies had very low ambitions, included loopholes, or were not monitored by the companies themselves, suggesting that they were more likely to be intended to promote a ‘health halo’75 and a favourable corporate image than to improve population diet. Other examples of studies that did not involve humans yet provide useful information on policy effectiveness include a governmental evaluation in Canada showing that only 14% of food categories met the national voluntary salt targets after 4 years. Not only was no progress observed for nearly half of the food categories, but sodium content had increased in some of them. 160 A comparison of marketing regulations for breast milk substitutes in Cambodia, Indonesia, Myanmar, Thailand and Vietnam concluded that none followed the WHO recommendation of applying them to children aged up to 36 months. 161 A study by Ejlerskov et al. 162 on voluntary checkout policies by 14 supermarket chains in the UK noted that the six chains with ‘clear and consistent’ policies offered a smaller median proportion of unhealthy foods at their checkouts and that all complied to their policy compared to the six chains with ‘vague or inconsistent’ policies and the two chains without a policy. In the UK again, an analysis of food industry pledges in the Public Health RD showed that none included the most effective strategies to improve diet. 56
We suggest attributing a greater value to the contribution of studies of environment features and analysis of policy documents for informing decisions about effectiveness, and to acknowledge this in funding programmes. Such studies also have the advantage of generally requiring less time, resources and advanced evaluation techniques, which makes them more accessible worldwide. This could also be reflected in logic models or systems frameworks more systematically, for instance with the analysis of the policy itself and implementation, to effects on the environment, human behaviours, and human health.
Implications for future research and research funding
This study highlights three implications for future research and research funding:
Studies on the role of corporate actors in food policy
The role and interests of policy stakeholders, and the accepted legitimacy of corporate actors in food policy, should be critically interrogated with healthy diets for the population as the first priority.
Evaluations of real-world policies equitably across geographic regions
First, future evaluations are needed across all geographic regions of real-world policies to improve food environments equitably. This will require greater global equity in access to research funding. This also includes the need for more cost-effectiveness analyses worldwide.
Capture equity dimensions in policy evaluations
Second, equity dimensions should be adequately built into policy evaluations. Moreover, research funding could be directed to study how policy interventions could appropriately and systematically capture PROGRESS-Plus equity dimensions.
Guideline development for quality/risk of bias and certainty in the evidence of policy evaluations
Third, guidelines should be developed to (1) help with systematically reporting policy characteristics in policy evaluations, (2) consider policy characteristics in the interpretation of results and risk-of-bias appraisal, (3) appraise the risk of bias or study quality of studies measuring environmental features (rather than human outcomes) and using document analyses (including policy and media sources), (4) discussing whether the GRADE framework for assessing certainty in the evidence should consider the feasibility of different types of studies, recognise the contribution of document and media analyses, and differentiate more effectively the level of certainty between good and weak observational studies for policy research.
Study strengths and limitations
A major strength of the study is the broad coverage of the identified research, covering a wide range of policy topics. However, we may have missed some policy evaluations because the literature searches did not include the names of specific policies, as this was beyond the scope of the resources.
The literature searches were also only conducted in English, which likely explains at least partly the predominance of publications in English, and limited to 2010–20, 2 years before finalising the report. While updating literature searches is common practice for systematic reviews, it was not possible in this case as the scale of the work required to update this series of reviews was far outside the available capacity. Consequently, the findings only represent the years 2010–20 and not the evaluation of policies published after. However, there are no indications that including evidence published after 2020 would have led to different results. On the contrary, since 2020 there have been increasing calls that are aligned with the findings, that is to make policies to improve food environments statutory. For instance, the WHO now explicitly encourages countries to impose taxes on SSBs. 163 Food-EPI, an international standardised tool to benchmark policies, includes the adoption of mandatory food composition targets and FOPL. 164 UNICEF recommends regulating food marketing to children, implementing mandatory food reformulation for added free sugars and salt and/or to reduce portion sizes, and introducing fiscal measures such as taxes on SSBs. 165
Although the percentages of records screened by two independent reviewers or more independently appear low (12% of titles and abstracts and 33% of eligible full texts), they represented 3346 titles and abstracts and 637 full-text papers. Furthermore, all records excluded for the justifications (or exclusion codes) for which disagreements were highest were checked by another reviewer to ensure to retrieve some that might have been excluded by error.
Although we included policies across the ‘NOURIS’ part of the NOURISHING framework, which focuses on the food environment, apart from the systematic evidence map, no result specific to the ‘O’, representing specific settings including schools, nurseries, health care, and sports and leisure centres, were found. A few systematic reviews on schools had been found but were excluded because the evaluations assessed were not real-world evaluations, the policy or evaluation were conducted at the local level, or the systematic review did not consider the governance approach or did not appraise study quality. The absence of this policy category from the systematic reviews on commitments by private actors and on PPP might be due to most policies in these settings being led by the public sector, although the presence of the private sector is not uncommon.
The systematic evidence map examines the policy and evaluation characteristics of a large body of evidence on a wide range of policies promoting healthy food environments. It also shows that this type of evidence synthesis can do more than identifying trends and gaps in research: it can also be used to question current practices and the use of evidence in policy-making, with practical implications for policy-makers, evaluators and systematic reviewers. Except for health and nutrition claims, food trade and investments, which were not included, the fields are aligned with the International Network for Food and Obesity/Noncommunicable Diseases Research, Monitoring and Action Support framework,166 a guide developed by a global network and recognised by WHO for monitoring and benchmarking public and private sector interventions aiming to improve food environments. Only a few publications reporting on policies targeting the retail and catering sector were identified. However, the exploration of local evaluations and policies in the UK suggest that this might be because they are more likely to be implemented at a lower jurisdiction level than state or national. Challenges in planning restrictions reported in some of these evaluations also suggest that these actions are not as common as other policy categories. 167,168 Nearly all of the data extraction was verified by a second reviewer. Furthermore, the study design ‘follow-up studies and time series’ was used to designate studies using the same samples of participants across time or time-series analytical methods, while the study design ‘pre–post repeat cross-sectional studies’ was used for studies using different samples across time or non-human participants. This difference was sometimes not obvious and might have led to some misclassifications, although it is unlikely to have influenced the conclusions since specific results in the effectiveness reviews were nearly all from the same category (cross-sectional), which limited the role of study design.
As for the scope of the overview of review, from a global perspective, the extent of policies covered was even narrower than those in the systematic evidence map: all policies were from high- and upper-middle countries, and many investigating specific population groups were about the USA and/or about SSB taxes. No policy in schools, health care, nursery or leisure settings were included nor advertising or marketing controls, although the latter topic was further documented with the systematic reviews on commitments by private actors and PPPs. By excluding all systematic reviews that had not conducted a quality appraisal, we are likely to have excluded a greater number than if only those in the lowest of the four original quality categories by SIGN had been excluded as originally planned. Nevertheless, this strategy remained coherent with guidance by Cochrane32 and the principle that we had set for this overview of reviews consisting in using the most robust evidence. A majority of systematic reviews were appraised as high- or acceptable-quality. However, since only some results sections were considered in most of them, some of which relying on one to four studies, this rating might be less informative than in traditional evidence syntheses.
Data extraction and study quality appraisal for the three systematic reviews assessing effectiveness or cost-effectiveness and for the qualitative review were fully conducted by two independent researchers or checked by another. Some of the tools were slightly modified but this was done through careful discussions and testing among the reviewers. The only reference lists that were screened were those of evaluations included in the systematic review on private commitments, the systematic review on cost-effectiveness, the evidence syntheses on cost-effectiveness excluded from the overview of reviews, and the overviews of reviews retrieved in the overarching search. Yet, none of the 33 publications included in the evidence map retrieved outside databases contributed to the systematic review on private commitments and cost-effectiveness; thus, selection bias in that matter is unlikely.
Results for the overview of reviews (see Chapter 4) and the systematic review on private commitments (see Chapter 6) were summarised using effect direction plots. Such tabulations give a general sense of the results by graphically representing the direction of effects of multiple heterogeneous and non-standardised outcomes, which are normally difficult to gage in text format, along with sample sizes and overall study quality or risk of bias. However, they do not consider effect size nor precision estimates.
Equality, diversity and inclusion
Relevant to the reviewed literature
This study did not include participants as it was an evidence synthesis based on a large complex systematic review of the literature. However, most of the systematic reviews included the reporting of equity domains in the evidence, as per the PROGRESS-Plus equity dimensions. The systematic evidence map (see Chapter 3) reports that of the nearly 400 publications assessing policy effectiveness, only 50% assessed at least one equity domain: age was the most assessed (30%), followed by education (16%, although these mainly related to school characteristics), SES at the individual level (15%), gender/sex (13%), race and culture (11%) and place (8%), whereas only 11 publications considered occupation, and one or two examined religion, social capital and disability each. The Overview of Reviews (see Chapter 4) reported findings by PROGRESS-Plus categories and found a lack of reporting of outcomes in systematic reviews for specific population groups: overall, evidence on specific population groups is patchy, incomplete, mainly inconsistent, and largely relies on single studies (although some of these had large samples) rather than aggregated bodies of evidence. This limitation in the research is reflected in the recommendations.
Patient and public engagement
A public advisory group was formed and included. They took part in a consultation at the start of this systematic review, on 21 October 2020. At the meeting we introduced the project and the role of the public advisory group: to provide a public view on what we are planning, and also to get their views about the role of the public in policies to improve diet in England, and how to reflect this in the research.
The PI’s initial thoughts on the role of the public in diet policies were as follows:
-
Health is often a secondary priority when planning and preparing food due to competing priorities. Participants were favourable to having interventions that promote healthier diets.
-
Some participants were not aware of some of the UK policies shown, such as the voluntary action to reduce trans-fat and the RD.
-
Most of the policies discussed were those that can be seen and used by consumers on a daily basis, such as product labelling and school food standards. Bringing the conversation to how policy is shaped and their process was more challenging, potentially because this is happening at a higher level, and is not commonly discussed openly.
-
Regarding the involvement of the public in informing these policies, one participant said that the public can put pressure on governments or work with organisations that do this. Another participant expressed a feeling of powerlessness towards the school food standards.
-
Public consultations (as a way of increasing the public voice in policy) were discussed. One participant said that the recruitment process should be more transparent and include people from diverse groups to be more representative of the general population. Another pointed out that while this would be useful, this would also be time-consuming and costly for the government, so a balance between the two would be needed.
Due to (1) the complexity of the systematic review (requiring additional ad hoc staff); (2) the practical challenges presented by the COVID-19 pandemic and (3) the challenge of meaningfully engaging members of the public on a systematic review of policy effectiveness, cost-effectiveness and process, this was in the end the only public advisory group meeting of the project.
Though we acknowledge the importance of the public voice in policies that are designed to serve and support them, we were not able in the end to give this point sufficient space and priority.
Conclusions
This study generated the first review of a wide range of real-world evaluations of policies to improve food environments, from an effectiveness, cost-effectiveness and policy process perspective. From the available evidence reviewed, we found that regulatory approaches appear the most effective, with voluntary industry approaches and PPPs having limited effectiveness. These findings should be carefully considered in future public health policy development, as should the findings of geographic imbalance in the evidence and inadequate representation of equity dimensions across the policy evaluations. We find that policies aiming to improve food environments are at times driven by factors other than evidence and shaped by compromise and pragmatism. This study concludes that these policies should be first and foremost designed and driven by the evidence of greatest effectiveness to improve food environments for healthier diets. The role and interests of policy stakeholders, and the accepted legitimacy of corporate actors in food policy, should be critically interrogated with healthy diets for the population as the first priority.
Additional information
Acknowledgements
The authors gratefully acknowledge the Study Scientific Committee involved in critically assessing this work along the way: Claire Bennett, Dr Monique Potvin Kent, Dr Patricia Lucas.
The authors gratefully acknowledge Jane Falconer, User Support Services Librarian at the LSHTM, for reviewing the search strategy for the overarching project.
The authors thankfully acknowledge the important input of the members of the public advisory group, comprising Marie McDevitt, Fabiana Mariscotti, Hazel Patel and Mark Thomas, recruited from People in Research.
Contributions of authors
Laurence Blanchard (https://orcid.org/0000-0003-0090-917X) (Research Fellow) managed the study; led the overarching review design, data extraction, quality appraisal (see Chapter 2), designed and led the Evidence Map (see Chapter 3) and the Overview reviews (see Chapter 4).
Stephanie Ray (https://orcid.org/0000-0001-8403-9233) was a researcher on the project; she contributed to overarching review design, screening, data extraction; data extraction and quality appraisal for the overview of reviews (see Chapter 4), and she designed and led the review of voluntary approaches (see Chapter 7).
Cherry Law (https://orcid.org/0000-0003-0686-1998) (Lecturer) was a coinvestigator and was involved in the following: conceptualisation, methodology, writing (review and editing) and funding acquisition. She led the review of cost-effectiveness (see Chapter 8).
María Jesús Vega-Salas (https://orcid.org/0000-0002-5798-7091) was a researcher on the project; she contributed to screening for the overarching project (see Chapter 2) review design, and data extraction.
Julia Bidonde (https://orcid.org/0000-0001-7535-678X) was a researcher on the project; she contributed to data extraction, quality appraisal, specifically Chapters 5 and 6.
Gemma Bridge (https://orcid.org/0000-0001-7441-9849) (Independent Consultant) was a researcher on the project; she contributed to data extraction, quality appraisal, specifically Chapters 5 and 6 and the plain English summary.
Matt Egan (https://orcid.org/0000-0002-4040-200X) (Professor) was a coinvestigator and was involved in the following: conceptualisation, methodology, writing (review and editing) and funding acquisition. He advised on the overarching design and conduct of the systematic review throughout.
Mark Petticrew (https://orcid.org/0000-0002-6378-5517) (Professor of Public Health Evaluation) was a coinvestigator and was involved in the following: conceptualisation, methodology, writing (review and editing) and funding acquisition. He advised on the overarching design and conduct of the systematic review throughout.
Harry Rutter (https://orcid.org/0000-0002-9322-0656) (Professor of Global Public Health) was a coinvestigator and was involved in the following: conceptualisation, methodology, writing (review and editing) and funding acquisition. He advised on the overarching design and conduct of the systematic review throughout.
Cécile Knai (https://orcid.org/0000-0001-6663-7379) (Professor of Public Health Policy) was the principal investigator and directed the review. She oversaw all stages and components including synthesis of the evidence and creation of the final report. She led the review of policy process studies (see Chapter 5) and the systems map (see Chapter 9).
All authors contributed to, read and approved the final manuscript.
Disclosure of interests
Full disclosure of interests: Completed ICMJE forms for all authors, including all related interests, are available in the toolkit on the NIHR Journals Library report publication page at https://doi.org/10.3310/JYWP4049.
Primary conflicts of interest: Cécile Knai and Mark Petticrew are currently members of the NIHR PRP funding committee. Matt Egan was a member of the MRC PHING funding committee 2018–2. Harry Rutter was a member of the PHR Programme Advisory Board 2015–2.
Data-sharing statement
This is a systematic review of the literature and, therefore, the material generated beyond that contained within the report is not suitable for sharing. Further information can be obtained from the corresponding author.
Ethics statement
This is a systematic review of the literature and therefore, the research did not require ethical approval.
Information governance statement
Our study did not handle any personal information.
Department of Health and Social Care disclaimer
This publication presents independent research commissioned by the National Institute for Health and Care Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, MRC, NIHR Coordinating Centre, the PHR programme or the Department of Health and Social Care.
This monograph was published based on current knowledge at the time and date of publication. NIHR is committed to being inclusive and will continually monitor best practice and guidance in relation to terminology and language to ensure that we remain relevant to our stakeholders.
Disclaimers
This article presents independent research funded by the National Institute for Health and Care Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, the PHR programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, the PHR programme or the Department of Health and Social Care.
References
- Scarborough P, Morgan RD, Webster P, Rayner M. Differences in coronary heart disease, stroke and cancer mortality rates between England, Wales, Scotland and Northern Ireland: the role of diet and nutrition. BMJ Open 2011;1.
- Afshin A, Sur PJ, Fay KA, Cornaby L, Ferrara G, Salama JS, et al. Health effects of dietary risks in 195 countries, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019;393:1958-72.
- Newton JN, Briggs AD, Murray CJ, Dicker D, Foreman KJ, Wang H, et al. Changes in health in England, with analysis by English regions and areas of deprivation, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015;386:2257-74.
- Scarborough P, Bhatnagar P, Wickramasinghe KK, Allender S, Foster C, Rayner M. The economic burden of ill health due to diet, physical inactivity, smoking, alcohol and obesity in the UK: an update to 2006-07 NHS costs. J Public Health (Oxf) 2011;33:527-35.
- Department of Health and Social Care . Tackling Obesity: Empowering Adults and Children to Live Healthier Lives n.d.
- National Health Service Digital . National Child Measurement Programme, England 2020 2021 School Year. Accredited Official Statistics 2021.
- Public Health England . NCMP and Child Obesity Profile: Slope Index of Inequality n.d.
- Public Health England . Salt Reduction Programme. PHE’s First Assessment of the Food Industry’s Progress Towards Meeting the Government’s Salt Reduction Targets 2018.
- Public Health England . National Diet and Nutrition Survey. Results from Years 7 and 8 (Combined) of the Rolling Programme (2014 2015 to 2015 2016) A Survey Carried Out on Behalf of Public Health England and the Food Standards Agency 2018. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/699241/NDNS_results_years_7_and_8.pdf (accessed June 2024).
- World Health Organization . Draft Guidelines: Sugars Intake for Adults and Children 2014.
- Burrows T, Goldman S, Pursey K, Lim R. Is there an association between dietary intake and academic achievement: a systematic review. J Hum Nutr Diet 2017;30:117-40.
- Food and Agriculture Organization . Nutrition and Food Systems. A Report by the High Level Panel of Experts on Food Security and Nutrition of the Committee on World Food Security. September 2017. HLPE Report 12 2017. www.fao.org/policy-support/tools-and-publications/resources-details/en/c/1155796/ (accessed June 2024).
- Knai C, James L, Petticrew M, Eastmure E, Durand MA, Mays N. An evaluation of a public-private partnership to reduce artificial trans fatty acids in England, 2011–16. Eur J Public Health 2017;27:605-8.
- Kunkel DL, Castonguay JS, Filer CR. Evaluating industry self-regulation of food marketing to children. Am J Prev Med 2015;49:181-7.
- Bryden A, Petticrew M, Mays N, Eastmure E, Knai C. Voluntary agreements between government and business – a scoping review of the literature with specific reference to the Public Health Responsibility Deal. Health Policy 2013;110:186-97.
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev 2021;10.
- Risse T, Börzel T. Complex Sovereignty Reconstituting Political Authority in the Twenty-First Century. Toronto: University of Toronto Press; 2005.
- Hawkes C, Jewell J, Allen K. A food policy package for healthy diets and the prevention of obesity and diet-related non-communicable diseases: the NOURISHING framework. Obes Rev 2013;14:159-68.
- Leatherdale ST. Natural experiment methodology for research: a review of how different methods can support real-world research. Int J Soc Res Methodol 2019;22:19-35.
- O’Neill J, Tabish H, Welch V, Petticrew M, Pottie K, Clarke M, et al. Applying an equity lens to interventions: using PROGRESS ensures consideration of socially stratifying factors to illuminate inequities in health. J Clin Epidemiol 2014;67:56-64.
- Herzog R, Alvarez-Pasquin MJ, Diaz C, Del Barrio JL, Estrada JM, Gil A. Are healthcare workers’ intentions to vaccinate related to their knowledge, beliefs and attitudes? A systematic review. BMC Public Health 2013;13.
- Sterne JA, Hernan MA, Reeves BC, Savovic J, Berkman ND, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016;355.
- Boutron I, Page M, Higgins J, Altman D, Lundh A, Hróbjartsson A, et al. Cochrane Handbook for Systematic Reviews of Interventions. Version 6.3, 2022. Chapter 7: Considering Bias and Conflicts of Interest Among the Included Studies 2022. https://training.cochrane.org/handbook/current/chapter-07 (accessed June 2024).
- Critical Assessment of Structure Prediction . Critical Appraisal Skills Programme – for Qualitative Research 2018. https://casp-uk.net/images/checklist/documents/CASP-Qualitative-Studies-Checklist/CASP-Qualitative-Checklist-2018_fillable_form.pdf (accessed June 2024).
- Campbell M, McKenzie JE, Sowden A, Katikireddi SV, Brennan SE, Ellis S, et al. Synthesis without meta-analysis (SWiM) in systematic reviews: reporting guideline. BMJ 2020;368.
- Thomson HJ, Thomas S. The effect direction plot: visual display of non-standardised effects across multiple outcome domains. Res Synth Methods 2013;4:95-101.
- Boon MH, Thomson H. The effect direction plot revisited: application of the 2019 Cochrane Handbook guidance on alternative synthesis methods. Res Synth Methods 2021;12:29-33.
- Siemieniuk R, Guyatt G. What Is GRADE? n.d. https://bestpractice.bmj.com/info/toolkit/learn-ebm/what-is-grade/ (accessed June 2024).
- Snilstveit B, Vojtkova M, Bhavsar A, Stevenson J, Gaarder M. Evidence and gap maps: a tool for promoting evidence informed policy and strategic research agendas. J Clin Epidemiol 2016;79:120-9.
- Lefebvre C, Glanville J, Briscoe S, Featherstone R, Littlewood A, Marshall C, et al. Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (Updated February 2022). Cochrane; 2022.
- Hoepner AGF, de Aguiar TRS, Majithia R. The level of compliance with the international code of marketing of breast-milk substitutes: does it matter to stock markets?. J Bus Ethics 2014;119:329-48.
- Pollock M, Fernandes R, Becker L, Pieper D, Hartling L. Cochrane Handbook for Systematic Reviews of Interventions. 2021.
- Scottish Intercollegiate Guideline Network . Checklists n.d. www.sign.ac.uk/what-we-do/methodology/checklists/ (accessed June 2024).
- Pieper D, Antoine SL, Mathes T, Neugebauer EAM, Eikermann M. Systematic review finds overlapping reviews were not mentioned in every other overview. J Clin Epidemiol 2014;67:368-75.
- Backholer K, Sarink D, Beauchamp A, Keating C, Loh V, Ball K, et al. The impact of a tax on sugar-sweetened beverages according to socio-economic position: a systematic review of the evidence. Public Health Nutr 2016;19:3070-84.
- Alagiyawanna A, Townsend N, Mytton O, Scarborough P, Roberts N, Rayner M. Studying the consumption and health outcomes of fiscal interventions (taxes and subsidies) on food and beverages in countries of different income classifications; a systematic review. BMC Public Health 2015;15.
- Redondo M, Hernandez-Aguado I, Lumbreras B. The impact of the tax on sweetened beverages: a systematic review. Am J Clin Nutr 2018;108:548-63.
- Hyseni L, Bromley H, Kypridemos C, O’Flaherty M, Lloyd-Williams F, Guzman-Castillo M, et al. Systematic review of dietary trans-fat reduction interventions. Bull World Health Organ 2017;95:821-30.
- Sisnowski J, Street JM, Merlin T. Improving food environments and tackling obesity: a realist systematic review of the policy success of regulatory interventions targeting population nutrition. PLOS ONE 2017;12.
- Dodd R, Santos JA, Tan M, Campbell NRC, Ni Mhurchu C, Cobb L, et al. Effectiveness and feasibility of taxing salt and foods high in sodium: a systematic review of the evidence. Adv Nutr (Bethesda, Md) 2020;11:1616-30.
- Hillier-Brown FC, Summerbell CD, Moore HJ, Routen A, Lake AA, Adams J, et al. The impact of interventions to promote healthier ready-to-eat meals (to eat in, to take away or to be delivered) sold by specific food outlets open to the general public: a systematic review. Obes Rev 2017;18:227-46.
- Lhachimi SK, Pega F, Heise TL, Fenton C, Gartlehner G, Griebler U, et al. Taxation of the fat content of foods for reducing their consumption and preventing obesity or other adverse health outcomes. Cochrane Database Syst Rev 2020;2020.
- Croker H, Packer J, Russell Simon J, Stansfield C, Viner RM. Front of pack nutritional labelling schemes: a systematic review and meta-analysis of recent evidence relating to objectively measured consumption and purchasing. J Hum Nutr Diet 2020;33:518-37.
- Pfinder M, Heise TL, Hilton Boon M, Pega F, Fenton C, Griebler U, et al. Taxation of unprocessed sugar or sugar-added foods for reducing their consumption and preventing obesity or other adverse health outcomes. Cochrane Database Syst Rev 2020;2020.
- Teng AM, Jones AC, Mizdrak A, Signal L, Genc M, Wilson N. Impact of sugar-sweetened beverage taxes on purchases and dietary intake: systematic review and meta-analysis. Obes Rev 2019;20:1187-204.
- von Philipsborn P, Stratil JM, Burns J, Busert LK, Pfadenhauer LM, Polus S, et al. Environmental interventions to reduce the consumption of sugar-sweetened beverages and their effects on health. Cochrane Database Syst Rev 2019;2019.
- von Philipsborn P, Stratil JM, Burns J, Busert LK, Pfadenhauer LM, Polus S, et al. Environmental interventions to reduce the consumption of sugar-sweetened beverages: abridged cochrane systematic review. Obes Facts 2020;1.
- Downs SM, Bloem MZ, Zheng M, Catterall E, Thomas B, Veerman L, et al. The impact of policies to reduce trans fat consumption: a systematic review of the evidence. Curr Dev Nutr 2017;1.
- Rincon-Gallardo Patino S, Zhou M, Gomes FDS, Lemaire R, Hedrick V, Serrano E, et al. Effects of menu labeling policies on transnational restaurant chains to promote a healthy diet: a scoping review to inform policy and research. Nutrients 2020;12.
- Hyseni L, Elliot-Green A, Lloyd-Williams F, Kypridemos C, O’Flaherty M, McGill R, et al. Systematic review of dietary salt reduction policies: evidence for an effectiveness hierarchy?. PLOS ONE 2017;12.
- Ng SW, Slining MM, Popkin BM. The healthy weight commitment foundation pledge: calories sold from US consumer packaged goods, 2007–2012. Am J Prev Med 2014;47:508-19.
- Taillie LS, Grummon AH, Fleischhacker S, Grigsby-Toussaint DS, Leone L, Caspi CE. Best practices for using natural experiments to evaluate retail food and beverage policies and interventions. Nutr Rev 2017;75:971-89.
- Nuffield Council on Bioethics . Public Health: Ethical Issues 2007. http://nuffieldbioethics.org/wp-content/uploads/2014/07/Public-health-ethical-issues.pdf (accessed June 2024).
- Dunford EK, Eyles H, Mhurchu CN, Webster JL, Neal BC. Changes in the sodium content of bread in Australia and New Zealand between 2007 and 2010: implications for policy. Med J Aust 2011;195:346-9.
- Christoforou AK, Dunford EK, Neal BC. Changes in the sodium content of Australian ready meals between 2008 and 2011. Asia Pac J Clin Nutr 2013;22:138-43.
- Knai C, Petticrew M, Durand M, Scott C, James L, Mehrotra A, et al. Has a public–private partnership resulted in action on healthier diets in England? An analysis of the Public Health Responsibility Deal food pledges. Food Policy 2015;54:1-10.
- Robinson E, Burton S, Gough T, Jones A, Haynes A. Point of choice kilocalorie labelling in the UK eating out of home sector: a descriptive study of major chains. BMC Public Health 2019;19.
- Hutchinson J, Rippin HL, Jewell J, Breda JJ, Cade JE. Comparison of high and low trans-fatty acid consumers: analyses of UK National Diet and Nutrition Surveys before and after product reformulation. Public Health Nutr 2018;21:465-79.
- Ng SW, Popkin BM. The healthy weight commitment foundation pledge: calories purchased by U.S. households with children, 2000–2012. Am J Prev Med 2014;47:520-30.
- Beckelman T, Sinclair-White Bronwyn M, McGurk Meghan D, Donohoe-Mather C, Vu U, Ching Lance K, et al. Encouraging adults to choose healthy now: a Hawai’i convenience store intervention. J Nutr Educ 2020;52:330-4.
- Rajbhandari-Thapa J, Bennett A, Keong F, Palmer W, Hardy T, Welsh J. Effect of the Strong4Life School Nutrition Program on cafeterias and on manager and Staff Member Knowledge and Practice, Georgia, 2015. Public Health Rep 2017;132:48S-56S.
- Trevena H, Dunford E, Neal B, Webster J. The Australian Food and Health Dialogue – the implications of the sodium recommendation for pasta sauces. Public Health Nutr 2014;17:1647-53.
- Levi R, Probst Y, Crino M, Dunford E. Evaluation of Australian soup manufacturer compliance with national sodium reduction targets. Nutr Diet 2018;75:200-5.
- Trevena H, Neal B, Dunford E, Wu JHY. An evaluation of the effects of the Australian food and health dialogue targets on the sodium content of bread, breakfast cereals and processed meats. Nutrients 2014;6:3802-17.
- Sparks E, Farrand C, Santos JA, McKenzie B, Trieu K, Reimers J, et al. Sodium levels of processed meat in Australia: supermarket survey data from 2010 to 2017. Nutrients 2018;10.
- Elliott T, Trevena H, Sacks G, Dunford E, Martin J, Webster J, et al. A systematic interim assessment of the Australian Government’s food and health Dialogue. Med J Aust 2014;200:92-5.
- Jones A, Magnusson R, Swinburn B, Webster J, Wood A, Sacks G, et al. Designing a healthy food partnership: lessons from the Australian food and health Dialogue. BMC Public Health 2016;16:651-60.
- Lindberg R, Nichols T, Yam C. The healthy eating agenda in Australia is salt a priority for manufacturers?. Nutrients 2017;9.
- Robinson H, Buccini G, Curry L, Perez-Escamilla R. The World Health Organization Code and exclusive breastfeeding in China, India, and Vietnam. Matern Child Nutr 2019;15.
- Spiteri SA, Olstad DL, Woods JL. Nutritional quality of new food products released into the Australian retail food market in 2015 – is the food industry part of the solution?. BMC Public Health 2018;18.
- Smithers Lisa G, Wang X, Haag D, Agnew B, Lynch J, Sorell M. Discretionary food advertising on television in 2017: a descriptive study. Aust N Z J Public Health 2019;43:519-21.
- Watson W, Lau V, Wellard L, Hughes C, Chapman K. Advertising to children initiatives have not reduced unhealthy food advertising on Australian television. J Public Health 2017;39:787-92.
- Wellard-Cole L, Hooper A, Watson WL, Hughes C. Nutrient composition of Australian fast-food and fast-casual children’s meals available in 2016 and changes in fast-food meals between 2010 and 2016. Public Health Nutr 2019;22:2981-8.
- Potvin Kent M, Smith JR, Pauze E, L’Abbe M. The effectiveness of the food and beverage industry’s self-established uniform nutrition criteria at improving the healthfulness of food advertising viewed by Canadian children on television. Int J Behav Nutr Phys Act 2018;15.
- Potvin Kent M, Pauze E, Guo K, Kent A, Jean-Louis R. The physical activity and nutrition-related corporate social responsibility initiatives of food and beverage companies in Canada and implications for public health. BMC Public Health 2020;20.
- Potvin Kent M, Pauze E. The effectiveness of self-regulation in limiting the advertising of unhealthy foods and beverages on children’s preferred websites in Canada. Public Health Nutr 2018;21:1608-17.
- Vergeer L, Vanderlee L, Potvin Kent M, Mulligan C, L’Abbé MR. The effectiveness of voluntary policies and commitments in restricting unhealthy food marketing to Canadian children on food company websites. Appl Physiol Nutr Metab 2019;44:74-82.
- Neyens E, Smits T. Empty pledges: a content analysis of Belgian and Dutch child-targeting food websites. Int J Health Promot Educ 2017;55:42-5.
- Landwehr Stefanie C, Hartmann M. Industry self-regulation of food advertisement to children: compliance versus effectiveness of the EU pledge. Food Policy 2020;91.
- Harris JL, Kalnova SS. Food and beverage TV advertising to young children: measuring exposure and potential impact. Appetite 2018;123:49-55.
- Vaala SE, Ritter MB. Child-oriented marketing on cereal packaging: associations with sugar content and manufacturer pledge. J Nutr Educ Behav 2020;52:215-23.
- Moran AJ, Block JP, Goshev SG, Bleich SN, Roberto CA. Trends in nutrient content of children’s menu items in US chain restaurants. Am J Prev Med 2017;52:284-91.
- Hurwitz Lisa B, Montague H, Lauricella Alexis R, Alvarez Aubry L, Pietrantonio F, Ford Meredith L, et al. Crowd pleasers: media characters in food company websites and apps for children. Young Consum 2019;20:44-58.
- Husereau D, Drummond M, Petrou S, Carswell C, Moher D, Greenberg D, et al. CHEERS Task Force . Consolidated Health Economic Evaluation Reporting Standards (CHEERS) statement. Value Health 2013;16:e1-5.
- World Bank Group . GDP Deflator (Base Year Varies by Country) 2020. https://data.worldbank.org/indicator/NY.GDP.DEFL.ZS (accessed 20 June 2024).
- World Bank Group . PPP Conversion Factor, GDP (LCU Per International $) (April 2020) 2020. https://data.worldbank.org/indicator/PA.NUS.PPP?skipRedirection=true&view=map (accessed 20 June 2024).
- Drummond M, Sculper M, Claxton K, Stoddart G, Torrance G. Methods for Economic Evaluation of Health Care Programmes. Oxford: Oxford University Press; 2015.
- Basto-Abreu A, Barrientos-Gutiérrez T, Vidaña-Pérez D, Colchero MA, Hernández FM, Hernández-Ávila M, et al. Cost-effectiveness of the sugar-sweetened beverage excise tax in Mexico. Health Aff (Millwood) 2019;38:1824-17.
- Laverty AA, Kypridemos C, Seferidi P, Vamos EP, Pearson-Stuttard J, Collins B, et al. Quantifying the impact of the Public Health Responsibility Deal on salt intake, cardiovascular disease and gastric cancer burdens: interrupted time series and microsimulation study. J Epidemiol Community Health 2019;73:881-7.
- Mantilla Herrera AM, Crino M, Erskine Holly E, Sacks G, Ananthapavan J, Mhurchu Cliona N, et al. Cost-effectiveness of product reformulation in response to the health star rating food labelling system in Australia. Nutrients 2018;10. https://doi.org/10.3390/nu10050614.
- Sanchez-Romero LM, Penko J, Coxson PG, Fernandez A, Mason A, Moran AE, et al. Projected impact of Mexico’s sugar-sweetened beverage tax policy on diabetes and cardiovascular disease: a modeling study. PLOS Med 2016;13.
- Colchero MA, Popkin BM, Rivera JA, Ng SW. Beverage purchases from stores in Mexico under the excise tax on sugar sweetened beverages: observational study. BMJ 2016;352.
- Colchero MA, Rivera-Dommarco J, Popkin Barry M, Ng Shu W. In Mexico, evidence of sustained consumer response two years after implementing a sugar-sweetened beverage tax. Health Aff (Millwood) 2017;36.
- Lal A, Mantilla-Herrera AM, Veerman L, Backholer K, Sacks G, Moodie M, et al. Modelled health benefits of a sugar-sweetened beverage tax across different socioeconomic groups in Australia: a cost-effectiveness and equity analysis. PLOS Med 2017;14.
- Cobiac LJ, Veerman L, Vos T. The role of cost-effectiveness analysis in developing nutrition policy. Annu Rev Nutr 2013;33:373-93.
- Flemming K, Booth A, Hannes K, Cargo M, Noyes J. Cochrane qualitative and implementation methods group guidance series-paper 6: reporting guidelines for qualitative, implementation, and process evaluation evidence syntheses. J Clin Epidemiol 2018;97:79-85.
- Castronuovo L, Allemandi L, Tiscornia V, Champagne B, Campbell N, Schoj V. Analysis of a voluntary initiative to reduce sodium in processed and ultra-processed food products in Argentina: the views of public and private sector representatives. Cadernos De Saude Publica 2017;33.
- Davo-Blanes MC, Ortiz-Moncada R, Gil-Gonzalez D, Alvarez-Dardet C, Lobstein T. The impact of marketing practices and its regulation policies on childhood obesity opinions of stakeholders in Spain. Appetite 2013;62:216-24.
- Webster J, Pillay A, Suku A, Gohil P, Santos Joseph A, Schultz J, et al. Process evaluation and costing of a multifaceted population-wide intervention to reduce salt consumption in Fiji. Nutrients 2018;10:155-71.
- Brandon I, Baker P, Lawrence M. Have we compromised too much? A critical analysis of nutrition policy in Australia 2007–2018. Public Health Nutr 2020;1.
- Durand MA, Petticrew M, Goulding L, Eastmure E, Knai C, Mays N. An evaluation of the Public Health Responsibility Deal: informants’ experiences and views of the development, implementation and achievements of a pledge-based, public-private partnership to improve population health in England. Health Policy 2015;119:1506-14.
- Perez-Escamilla R. Innovative healthy lifestyles school-based public-private partnerships designed to curb the childhood obesity epidemic globally: lessons learned from the Mondelez International Foundation. Food Nutr Bull 2018;39:S3-S21.
- Alsukait R, Bleich S, Wilde P, Singh G, Folta S. Sugary drink excise tax policy process and implementation: case study from Saudi Arabia. Food Policy 2020;90.
- Campbell N, Mialon M, Reilly K, Browne S, Finucane FM. How are frames generated? Insights from the industry lobby against the sugar tax in Ireland. Soc Sci Med 2020;264.
- Carriedo A, Lock K, Hawkins B. Policy process and non-state actors’ influence on the 2014 Mexican soda tax. Health Policy Plan 2020;35:941-52.
- Davies V, Jaime PC. Mandatory food labeling of trans fat acids: qualitative analysis of the public consultation. Interf: Comunicacao Saude Educacao 2017;21:133-9.
- Dorlach T, Mertenskotter P. Interpreters of international economic law: corporations and bureaucrats in contest over Chile’s nutrition label. Law Soc Rev 2020;54:571-606.
- Fooks GJ, Williams S, Box G, Sacks G. Corporations’ use and misuse of evidence to influence health policy: a case study of sugar-sweetened beverage taxation. Glob Health 2019;15.
- Fuster M, Burrowes S, Cuadrado C, Velasco Bernal A, Lewis S, McCarthy B, et al. Understanding policy change for obesity prevention: learning from sugar-sweetened beverages taxes in Mexico and Chile. Health Promot Int 2020;36:155-64.
- James E, Lajous M, Reich MR. The politics of taxes for health: an analysis of the passage of the sugar-sweetened beverage tax in Mexico. Health Syst Reform 2020;6.
- Kaldor JC, Thow AM, Schonfeldt H. Using regulation to limit salt intake and prevent non-communicable diseases: lessons from South Africa’s experience. Public Health Nutr 2018;1:1-10.
- Kiss A, Popp J, Olah J, Lakner Z. The reform of school catering in Hungary: anatomy of a health-education attempt. Nutrients 2019;11.
- Le Bodo Y, Etile F, Gagnon F, De Wals P. Conditions influencing the adoption of a soda tax for public health: analysis of the French case (2005–2012). Food Policy 2019;88.
- Mialon M, Gaitan Charry DA, Cediel G, Crosbie E, Scagliusi FB, Perez Tamayo EM. ‘I had never seen so many lobbyists’: food industry political practices during the development of a new nutrition front-of-pack labelling system in Colombia. Public Health Nutr 2020;24:2737-45.
- Phillips T, Ravuvu A, McMichael C, Thow AM, Browne J, Waqa G, et al. Nutrition policy-making in Fiji: working in and around neoliberalisation in the Global South. Crit Public Health 2019;31:316-26.
- Phulkerd S, Sacks G, Vandevijvere S, Worsley A, Lawrence M. Barriers and potential facilitators to the implementation of government policies on front-of-pack food labeling and restriction of unhealthy food advertising in Thailand. Food Policy 2017;71:101-10.
- Stead M, Eadie D, McKell J, Sparks L, MacGregor A, Anderson AS. Making hospital shops healthier: evaluating the implementation of a mandatory standard for limiting food products and promotions in hospital retail outlets. BMC Public Health 2020;20.
- Reeve E, Thow AM, Bell C, Engelhardt K, Gamolo-Naliponguit EC, Go JJ, et al. Implementation lessons for school food policies and marketing restrictions in the Philippines: a qualitative policy analysis. Glob Health 2018;14.
- Shelton RC, Colgrove J, Lee G, Truong M, Wingood GM. Message framing in the context of the national menu-labelling policy: a comparison of public health and private industry interests. Public Health Nutr 2017;20:814-23.
- Thow AM, Quested C, Juventin L, Kun R, Khan AN, Swinburn B. Taxing soft drinks in the Pacific: implementation lessons for improving health. Health Promot Int 2011;26:55-64.
- Thow AM, Waqa G, Browne J, Phillips T, McMichael C, Ravuvu A, et al. The political economy of restricting marketing to address the double burden of malnutrition: two case studies from Fiji. Public Health Nutr 2020;24:354-63.
- Trieu K, Webster J, Jan S, Hope S, Naseri T, Ieremia M, et al. Process evaluation of Samoa’s national salt reduction strategy (MASIMA): what interventions can be successfully replicated in lower-income countries?. Implement Sci 2018;13.
- Vallgarda S, Holm L, Jensen JD. The Danish tax on saturated fat: why it did not survive. Eur J Clin Nutr 2015;69:223-6.
- Vandenbrink D, Pauze E, Potvin K. Strategies used by the Canadian food and beverage industry to influence food and nutrition policies. Int J Behav Nutr Phys Act 2020;17:3-16.
- Lie AL. ‘We are not a partnership’: constructing and contesting legitimacy of global public-private partnerships: the Scaling Up Nutrition (SUN) Movement. Globalizations 2021;18:237-55.
- World Health Organization . Best Buys’ and Other Recommended Interventions for the Prevention and Control of Noncommunicable Diseases 2017. https://apps.who.int/iris/bitstream/handle/10665/259232/WHO-NMH-NVI-17.9-eng.pdf?sequence=1&isAllowed=y (accessed June 2024).
- Branca F, Lartey A, Oenema S, Aguayo V, Stordalen GA, Richardson R, et al. Transforming the food system to fight non-communicable diseases. BMJ 2019;364.
- HM Government . Childhood Obesity: A Plan for Action. Crown Copyright 2016. www.gov.uk/government/uploads/system/uploads/attachment_data/file/546588/Childhood_obesity_2016__2__acc.pdf (accessed June 2024).
- Department of Health and Social Care . Consultation Outcome. Restricting Promotions of Products High in Fat, Sugar and Salt by Location and by Price: Government Response to Public Consultation 2021. www.gov.uk/government/consultations/restricting-promotions-of-food-and-drink-that-is-high-in-fat-sugar-and-salt/outcome/restricting-promotions-of-products-high-in-fat-sugar-and-salt-by-location-and-by-price-government-response-to-public-consultation#outcome-and-next-steps (accessed June 2024).
- HM Revenue and Customs HT . Soft Drinks Industry Levy 2016. www.gov.uk/government/consultations/soft-drinks-industry-levy (accessed June 2024).
- Public Health England . PHE Sugar Reduction Programme. Progress Made by Industry in the First Year 2019. https://publichealthengland.exposure.co/sugar-reduction-programme (accessed June 2024).
- Office for Budget Responsibility . Economic and Fiscal Outlook– March 2016 2016. https://cdn.obr.uk/March2016EFO.pdf (accessed February 2019).
- Hashem K, Rosborough J. Why tax sugar sweetened beverages?. J Pediatr Gastroenterol Nutr 2017;65:358-9.
- Scientific Advisory Committee on Nutrition . Carbohydrates and Health 2015. www.gov.uk/government/uploads/system/uploads/attachment_data/file/445503/SACN_Carbohydrates_and_Health.pdf (accessed June 2024).
- Mytton O. Time for a sugary drinks tax in the UK?. J Public Health (Oxf) 2015;37:24-5.
- Department for Digital, Culture, Media and Sport, and Department of Health and Social Care . Consultation Outcome. Introducing a Total Online Advertising Restriction for Products High in Fat, Sugar and Salt (HFSS) 2021. www.gov.uk/government/consultations/total-restriction-of-online-advertising-for-products-high-in-fat-sugar-and-salt-hfss/introducing-a-total-online-advertising-restriction-for-products-high-in-fat-sugar-and-salt-hfss (accessed June 2024).
- Huizinga O, Kruse M. Food industry self-regulation scheme ‘EU Pledge’ cannot prevent the marketing of unhealthy foods to children. Obes Med 2016;1:24-8.
- Effertz T, Wilcke AC. Do television food commercials target children in Germany?. Public Health Nutr 2012;15:1466-73.
- Galbraith-Emami S, Lobstein T. The impact of initiatives to limit the advertising of food and beverage products to children: a systematic review. Obes Rev 2013;14:960-74.
- Ronit K, Jensen JD. Obesity and industry self-regulation of food and beverage marketing: a literature review. Eur J Clin Nutr 2014;68:753-9.
- Public Health England . Sugar Reduction: Progress Report, 2015 to 2019 2020. www.gov.uk/government/publications/sugar-reduction-report-on-progress-between-2015-and-2019 (accessed June 2024).
- United Kingdom Government . Advancing Our Health: Prevention in the 2020s 2019. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/819766/advancing-our-health-prevention-in-the-2020s-accessible.pdf (accessed June 2024).
- Conway L. Regulation of Advertising by the ASA. London: UK Parliament; 2020.
- Carters-White L, Hilton S, Skivington K, Chambers S. PLOS ONE 2022;17.
- Global Food Research Program . Sugary Drink Taxes Around the World 2022.
- International. WCRF . NOURISHING Framwork 2022. www.wcrf.org/policy-databases/nourishing-framework/ (accessed June 2024).
- Isaranuwatchai W, Teerawattananon Y, Archer RA, Luz A, Sharma M, Rattanavipapong W, et al. Prevention of non-communicable disease: best buys, wasted buys, and contestable buys. BMJ 2020;368.
- World Health Organization . Closing the Gap in a Generation: Health Equity Through Action on the Social Determinants of Health. Final Report of the Commission on Social Determinants of Health 2008.
- Stroh D. Systems Thinking for Social Change. Vermont, USA: Chelsea Green Publishing; 2015.
- ActKnowledge . Theory of Change Basics 2011.
- Knai C, Petticrew M, Capewell S, Cassidy R, Collin J, Cummins S, et al. The case for developing a cohesive systems approach to research across unhealthy commodity industries. BMJ Glob Health 2021;6.
- Maani N, Collin J, Friel S, Gilmore AB, McCambridge J, Robertson L, et al. The need for a conceptual understanding of the macro and meso commercial determinants of health inequalities. Eur J Public Health 2021;31:674-5.
- Maani N, Collin J, Friel S, Gilmore AB, McCambridge J, Robertson L, et al. Bringing the commercial determinants of health out of the shadows: a review of how the commercial determinants are represented in conceptual frameworks. Eur J Public Health 2020;30:660-4.
- Hawkins B, McCambridge J. Alcohol policy, multi-level governance and corporate political strategy: The campaign for Scotland’s minimum unit pricing in Edinburgh, London and Brussels. Br J Polit Int Relat 2021;23:391-409.
- Tienhaara K. Regulatory chill in a warming world: the threat to climate policy posed by investor-state dispute settlement. Transnatl Environ La 2018;7:229-50.
- Knai C, Petticrew M, Douglas N, Durand MA, Eastmure E, Nolte E, et al. The public health responsibility deal: using a systems-level analysis to understand the lack of impact on alcohol, food, physical activity, and workplace health sub-systems. Int J Environ Res Public Health 2018;15.
- Petticrew M, Knai C, Thomas J, Rehfuess EA, Noyes J, Gerhardus A, et al. Implications of a complexity perspective for systematic reviews and guideline development in health decision making. BMJ Global Health 2019;4.
- Hilton Boon M, Thomson H, Shaw B, Akl EA, Lhachimi SK, López-Alcalde J, et al. GRADE Working Group . Challenges in applying the GRADE approach in public health guidelines and systematic reviews: a concept article from the GRADE Public Health Group. J Clin Epidemiol 2021;135:42-53.
- Macdiarmid JI, Loe J, Douglas F, Ludbrook A, Comerford C, McNeill G. Developing a timeline for evaluating public health nutrition policy interventions. What are the outcomes and when should we expect to see them?. Public Health Nutr 2011;14:729-39.
- Health C . Sodium Reduction in Processed Foods in Canada: An Evaluation of Progress Toward Voluntary Targets from 2012 to 2016 2018.
- Vinje KH, Phan LTH, Nguyen TT, Henjum S, Ribe LO, Mathisen R. Media audit reveals inappropriate promotion of products under the scope of the International Code of Marketing of Breast-milk Substitutes in South-East Asia. Public Health Nutr 2017;20:1333-42.
- Ejlerskov KT, Stead M, Adamson A, White M, Adams J. The nature of UK supermarkets’ policies on checkout food and associations with healthfulness and type of food displayed: cross-sectional study. Int J Behav Nutr Phys Act 2018;15.
- World Health Organization . WHO Calls on Countries to Tax Sugar-Sweetened Beverages to Save Lives 2022. www.who.int/news/item/13-12-2022-who-calls-on-countries-to-tax-sugar-sweetened-beverages-to-save-lives?lctg=106515715 (accessed June 2024).
- Djojosoeparto SK, Kamphuis CBM, Vandevijvere S, Murrin C, Stanley I, Romaniuk P, et al. PEN Consortium . Strength of EU-level food environment policies and priority recommendations to create healthy food environments. Eur J Public Health 2022;32:504-11.
- UNICEF . UNICEF Technical Note on Effective Regulatory Approaches to Protect, Support and Promote Better Diets and Create Healthy Food Environments for Children 2021.
- Swinburn B, Vandevijvere S, Kraak V, Sacks G, Snowdon W, Hawkes C, et al. INFORMAS . Monitoring and benchmarking government policies and actions to improve the healthiness of food environments: a proposed Government Healthy Food Environment Policy Index. Obes Rev 2013;14:24-37.
- Keeble M, Burgoine T, White M, Summerbell C, Cummins S, Adams J. Planning and public health professionals’ experiences of using the planning system to regulate hot food takeaway outlets in England: a qualitative study. Health Place 2021;67.
- Hanratty B, Milton B, Ashton M, Whitehead M. ‘McDonalds and KFC, it’s never going to happen’: the challenges of working with food outlets to tackle the obesogenic environment. J Public Health (Oxf) 2012;34:548-54.
Appendix 1 Search strategies
Literature search structure and explanations
The search strategy will include five key lines (in green) and an additional three (in pink) for databases that use MeSH terms. They are built around the concepts below. Exclusion keywords will then be added.
| Exclusion code | Included | Excluded |
|---|---|---|
| EX 1.1: Before 2010 | Published between 2010 and 2020 | Published before 2010 |
| EX 1.2: After 2020 | Published from 2021 | Published after 2020 |
EX 2–3:
|
Policies that …
|
|
|
||
|
||
|
||
|
||
| EX 4: Not general population | The policies aim to improve the health of the general public. This includes the following:
|
The policy only targets
|
| EX 5: Not real-life policy | Data were collected:
|
|
| Experiments, simulations and projections are included when based on ‘real-world’ policy data defined as above. |
|
|
| EX 6: Local POLICY level |
Policies implemented at the
|
|
| EX 7: Local EVALUATION level | Evaluations conducted:
|
|
|
|
|
| EX 8: Not evaluation |
|
|
|
|
|
| EX 9: Policy mapping | Studies assessing effectiveness, cost-effectiveness, factors influencing policy development or implementation, responses to public consultations, or media coverage of a policy. | Studies solely inventorying (‘mapping’) the presence of policies in countries or regions and/or benchmarking their implementation. |
| EX 10: Views about the general public |
|
|
| EX 11: Insufficient focus on governance (multipolicies) |
|
|
| EX 12: Overviews of reviews |
|
Overview of reviews (also called umbrella reviews) and other types of evidence syntheses of literature reviews. |
EX 13
|
(This is simply to group studies about the UK together);
|
|
|
|
|
| Duplicate | Documents that are not identical. | Identical documents (only keep one of them). |
| INCLUDE | Publications passing ALL the inclusion criteria above. | Publications failing at one of the exclusion criteria above or more. |
Diet + Actor + Policy + Governance (i.e. Regulatory-Voluntary-PPP)
Numerous individual keywords, MeSH terms, truncations and Boolean terms were tested individually and/or combined with other terms to verify their scope. For instance, the word ‘Act’ was considered to identify policies but discarded because of its omnipresence due to the verb ‘to act’. ‘Menu’, ‘Portion size’ and ‘serving size’ were added to capture policies on these that are not described in titles and abstracts using food or nutrient terms. Regarding truncation, tax* was removed because it also includes ‘taxa’, which is highly used in the biochemistry literature. Instead, we will be using tax, taxes, taxed, taxation and taxing. The use of AND versus ADJ5, as well as ADJ5 versus ADJ4 were also compared to verify what they include and exclude and therefore balance sensitivity with precision. The platform Web of Science does not use MeSH or thesaurus terms and produces several thousands of results. Therefore, only free terms can be excluded with ‘NOT’, which is not sufficient. To help reducing the number of irrelevant papers about agriculture, microbiology, genetics and pharmacology, we will select the relevant fields using the Web of Science categories (e.g. any category about health, food, social sciences; not engineering nor agriculture.
Keywords related to: Diet
-
diet free terms;
-
diet MeSH;
-
1 OR 2 (Diet terms and MeSH).
Keywords related to: Regulatory policies or PPP + Diet
-
MeSH Food Legislation;
-
law free terms ADJ5 1;
-
(Legislation MeSH or Tax MeSH or Fiscal policy MeSH) AND 3;
-
(PPP free terms or MeSH) AND 3.
Keywords related to: Diet-related policies + Governance
-
Governance free terms.mp;
-
Governance MeSH terms;
-
(MeSH Nutrition Policy OR MeSH food Labelling) OR MeSH Food Assistance AND (8 or 9).
Keywords related to: Actors + Policy + Governance + Diet
-
government free terms;
-
government MeSH terms;
-
industry free terms;
-
industry MeSH terms;
-
policy free terms;
-
policy-Making MeSH;
-
(11 or 12 or 13 or 14) AND (15 or 16) AND (8 or 9) AND 3;
-
(13 adj5 partnerships free terms) AND 3;
-
‘policy option or policy options’ AND 3.
Combining the eight strategies
-
4 or 5 or 6 or 7 or 10 or 17 or 18 or 19.
Keywords excluded
-
exp Pharmacology;
-
exp Food safety/;
-
exp Hygiene/;
-
exp Food hypersensitivity;
-
exp genetics/ or exp toxicology/;
-
exp cell physiological phenomena/ or exp genetic phenomena/ or exp microbiological phenomena/;
-
exp heterocyclic compounds/ or exp polycyclic compounds/ or exp macromolecular substances/ or exp ‘hormones, hormone substitutes, and hormone antagonists’/ or exp ‘enzymes and coenzymes’/ or exp ‘nucleic acids, nucleotides, and nucleosides’/ or exp complex mixtures/ or exp biological factors/ or exp ‘biomedical and dental materials’/;
-
(Cell* or mitochondr* or labell* or mononucl* or nucle* or reductase or abellin* or oxydat* or oxidase or homeostas* or overexpress* or phenotype* or embryo* or labelling* or PCR or RNA or gene or genes or genetic* or ((calcium or salt or sodium) adj2 ion)).mp;
-
exp animals/ not humans/;
-
22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 …. And additional relevant terms;
-
21 NOT 31;
-
from 2000 – current.
Literature search strategy in MEDLINE (Ovid)
The eight key search lines are identified in green (five key lines) and pink (three additional lines depending on MeSH terms availability in each database).
-
exp Diet/
-
exp Food/
-
beverages/ or exp artificially sweetened beverages/ or exp carbonated beverages/ or exp coffee/ or exp drinking water/ or exp energy drinks/ or exp ‘fruit and vegetable juices’/ or exp milk/ or exp milk substitutes/ or exp sugar-sweetened beverages/
-
exp Fruit/
-
exp Vegetables/
-
exp Sodium, Dietary/
-
exp Sugars/
-
exp Fats/
-
exp Dietary Fiber/
-
exp Portion Size/ or exp Serving Size/
-
exp Infant Food/ or exp Infant Formula/
-
(Diet or Nutrition or Food or foods or Snack or snacks or Drink or drinks or Beverage* or Soda or sodas or Fruit or fruits or Vegetable* or Salt or Sodium or Sugar* or Fat or fats or fatty acids or TFAs or Fibre or fibres or fiber or fibers or ‘Portion size*’ or ‘Serving size*’ or Menu or menus or Infant formula or infant formulas or baby formula or baby formulas or baby milk or infant milk or artificial milk or breastmilk substitute* or breast milk substitute*).ti,ab.
-
1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 [Food free + MeSH terms]
-
exp Legislation, Food/ [semi-final line 1; for food policies that are clearly regulatory]
-
(Law or laws or Legislat* or Regulat* or Decree or ‘Executive order’ or Tax or taxes or taxation or taxed or taxing or Levy or levies or levied or ‘Excise duty’ or ‘fiscal policy’ or ‘fiscal policies’ or ‘fiscal measure’ or ‘fiscal measures’).ti,ab. [terms related to policies that are regulatory]
-
((Law or laws or Legislat* or Regulat* or Decree or ‘Executive order’ or Tax or taxes or taxation or taxed or taxing or Levy or levies or levied or ‘Excise duty’ or ‘fiscal policy’ or ‘fiscal policies’ or ‘fiscal measure’ or ‘fiscal measures’) adj5 (Diet or Nutrition or Food or foods or Snack or snacks or Drink or drinks or Beverage* or Soda or sodas or Fruit or fruits or Vegetable* or Salt or Sodium or Sugar* or Fat or fats or fatty acids or TFAs or Fibre or fibres or fiber or fibers or ‘Portion size*’ or ‘Serving size*’ or Menu or menus or Infant formula or infant formulas or baby formula or baby formulas or baby milk or infant milk or artificial milk or breastmilk substitute* or breast milk substitute*)).ti,ab. [semi-final line 2; 15 adj5 12, for policies that are regulatory + food free terms]
-
exp Fiscal Policy/ or exp Taxes/
-
exp Government Regulation/
-
17 or 18 [MeSH terms associated with policies that are regulatory or about governance]
-
19 and 13 [semi-final line 3; MeSH policies that are regulatory + food]
-
(‘Public-private partnership*’ or ‘Responsibility Deal’).mp. [terms clearly related to PPPs]
-
exp Public-Private Sector Partnerships/
-
21 or 22 [free key words + MeSH clearly about PPP]
-
23 and 13 [semi-final line 4; clearly PPP + food]
-
(Regulatory or Compulsory or Obligat* or obliged or Voluntary or Option* or Non-compulsory or Non-regulatory or Non-obligatory or Public-Private).mp. [terms related to governance]
-
exp Regulatory Reporting/ or exp Regulatory Programs/
-
exp Voluntary Programs/
-
25 or 26 or 27 [free and MeSH terms related to governance]
-
exp Nutrition Policy/
-
exp Food Labeling/
-
exp Food Assistance/
-
29 or 30 or 31 [policies that are clearly about food]
-
28 and 32 [semi-final line 5; governance + food-related policies]
-
(Government* or Governance or Minist* or Senate or ((National or federal or state or provincial) adj (department or agency or institute))).ti,ab. [free words related to the national or state public sector]
-
government/ or exp federal government/ or exp government agencies/ or exp state government/
-
(Industry or industries or Private or Business* or Public-private or Company or companies or Corporat* or Multinational* or Vendor* or Retail* or Shop or shops or Store or stores or supermarket* or Restaura* or Broadcaster*).ti,ab. [free terms related to relevant private sectors]
-
exp Food-Processing Industry/ or exp Food Industry/
-
exp Restaurants/
-
exp Food Services/
-
34 or 35 or 36 or 37 or 38 or 39 [free and MeSH terms about the public and private sectors]
-
(Policy or policies or Plan or Strategy or strategies or Standard or standards or Scheme* or Program* or Guide or guides or guidance or guidelines or Code or codes or Measure or Measures or Rulebook or Target or targets or Limit or limits or limitation or Reformulat* or Remov* or Restrict* or Prohibit* or Ban or bans or banned or Label* or Population intervention* or population-level intervention* or population-based intervention*).ti,ab. [free terms frequently used to name diet-related policies]
-
exp Policy Making/
-
41 or 42 [free and MeSH terms about policy]
-
13 and 28 and 40 and 43 [semi-final line 6; food + governance + public/private actors + policy]
-
(Agreement* or Alliance* or Coalition* or Collaboration or Cooperation or ‘Joint deliver*’ or Partnership* or Pledge* or Self-regulat*).ti,ab. [free terms related to partnership]
-
((Agreement* or Alliance* or Coalition* or Collaboration or Cooperation or ‘Joint deliver*’ or Partnership* or Pledge* or Self-regulat*) adj5 (Industry or industries or Private or Business* or Public-private or Company or companies or Corporat* or Multinational* or Vendor* or Retail* or Shop or shops or Store or stores or supermarket* or Restaura* or Broadcaster*)).ti,ab. [45 adj5 36, to identify partnerships with private actors free terms]
-
46 and 13 [semi-final line 7; partnerships with private actors + food]
-
(‘policy option’ or ‘policy options’).mp.
-
48 and 13 [semi-final line 8; policy options + food]
-
14 or 16 or 20 or 24 or 33 or 44 or 47 or 49 [combination of the 8 strategies]
-
exp Pharmacology/
-
exp Food Safety/
-
exp Hygiene/
-
exp Food Hypersensitivity/
-
exp Genetics/
-
exp Toxicology/
-
exp cell physiological phenomena/ or exp genetic phenomena/ or exp microbiological phenomena/
-
exp heterocyclic compounds/ or exp polycyclic compounds/ or exp macromolecular substances/ or exp ‘hormones, hormone substitutes, and hormone antagonists’/ or exp ‘enzymes and coenzymes’/ or exp ‘nucleic acids, nucleotides, and nucleosides’/ or exp complex mixtures/ or exp biological factors/ or exp ‘biomedical and dental materials’/
-
(Cell* or mitochondr* or labell* or mononucl* or nucle* or reductase or labellin* or oxydat* or oxidase or homeostas* or overexpress* or phenotype* or embryo* or labelling* or PCR or RNA or gene or genes or genetic* or ((calcium or salt or sodium) adj2 ion)).mp.
-
exp animals/ not humans/
-
exp Animal Experimentation/
-
exp Hydrocarbons/
-
exp Forensic Genetics/
-
exp pharmacologic actions/
-
exp plant extracts/ or exp prescription drugs/
-
exp Drug Therapy/
-
exp Biopharmaceutics/
-
51 or 52 or 53 or 54 or 55 or 56 or 57 or 58 or 59 or 60 or 61 or 62 or 63 or 64 or 65 or 66 or 67
-
50 not 68
-
limit 69 to yr=”2000 -Current”
-
exp address/ or exp bibliography/ or exp biography/ or exp collected work/ or exp collection/ or exp comment/ or exp congress/ or exp dataset/ or exp dictionary/ or exp directory/ or exp editorial/ or exp guideline/ or exp lecture/ or exp letter/ or exp news/ or exp newspaper article/ or exp overall/ or exp periodical index/ or exp video-audio media/ or exp webcast/
-
70 not 71
Articles used to test the search strategy
Primary research
-
Allen K, Pearson-Stuttard J, Hooton W, Diggle P, Capewell S, O’Flaherty M. Potential of trans fats policies to reduce socioeconomic inequalities in mortality from coronary heart disease in England: cost-effectiveness modelling study. BMJ 2015;351:h4583.
-
Barquera S, Campos I, Rivera JA. Mexico attempts to tackle obesity: the process, results, push backs and future challenges. Obes Rev 2013;14:69–78.
-
Batis C, Rivera JA, Popkin BM, Taillie LS. First-year evaluation of Mexico’s tax on nonessential energy-dense foods: an observational study. PLOS Med 2016;13:e1002057.
-
Bertolo RF, Hentges E, Makarchuk MJ, Wiggins AKA, Steele H, Levin J, et al. Key attributes of global partnerships in food and nutrition to align research agendas and improve public health. Appl Physiol Nutr Metab 2018;43:755–8.
-
Buhler S, Raine KD, Arango M, Pellerin S, Neary NE. Building a strategy for obesity prevention one piece at a time: the case of sugar-sweetened beverage taxation. Can J Diabetes 2013;37:97–102.
-
Cappuccio FP, Capewell S, Lincoln P, McPherson K. Policy options to reduce population salt intake. BMJ 2011;343:d4995. [not captured by the search because no abstract]
-
Caro JC, Corvalán C, Reyes M, Silva A, Popkin B, Taillie LS. Chile’s 2014 sugar-sweetened beverage tax and changes in prices and purchases of sugar-sweetened beverages: an observational study in an urban environment. PLOS Med 2018;15:e1002597.
-
Castronuovo L, Allemandi L, Tiscornia V, Champagne B, Campbell N, Schoj V. Analysis of a voluntary initiative to reduce sodium in processed and ultra-processed food products in Argentina: the views of public and private sector representatives. Cad Saude Publica 2017;33:e00014316.
-
Cobiac LJ, Vos T, Veerman JL. Cost-effectiveness of interventions to reduce dietary salt intake. Heart 2010;96:1920–5.
-
Collins M, Mason H, O’Flaherty M, Guzman-Castillo M, Critchley J, Capewell S. An economic evaluation of salt reduction policies to reduce coronary heart disease in England: a policy modelling study. Value Health 2014;17:517–24.
-
Collins SM. Legislative perspectives on diabetes in America. Endocr Pract 2002;8:17–8. [not captured by the search but focuses on diabetes]
-
Cradock AL, Kenney EL, McHugh A, Conley L, Mozaffarian RS, Reiner JF, Gortmaker SL. Evaluating the impact of the healthy beverage erxecutive order for city agencies in Boston, Massachusetts, 2011–2013. Prev Chronic Dis 2015;12:E147.
-
Dixon J, Sindall C, Banwell C. Exploring the intersectoral partnerships guiding Australia’s dietary advice. Health Promot Int 2004;19:5–13.
-
Durand MA, Petticrew M, Goulding L, Eastmure E, Knai C, Mays N. An evaluation of the Public Health Responsibility Deal: informants’ experiences and views of the development, implementation and achievements of a pledge-based, public-private partnership to improve population health in England. Health Policy 2015;119:1506–14.
-
Dutton DJ, Campbell NR, Elliott C, McLaren L. A ban on marketing of foods/beverages to children: the who, why, what and how of a population health intervention. Can J Public Health 2012;103:100–2. PubMed PMID: 22530530. [not captured by the search. The ‘/’ seems to be problematic – Ovid doesn’t see ‘foods’ and ‘beverages’ as separate terms]
-
Elbel B, Mijanovich T, Kiszko K, Abrams C, Cantor J, Dixon LB. The introduction of a supermarket via tax-credits in a low-income area. Am J Health Promot 2017;31:59–66. https://doi.org/10.4278/ajhp.150217-QUAN-733. Epub 2016 Nov 18.
-
Fernandez MA, Desroches S, Marquis M, Turcotte M, Provencher V. Facilitators and barriers experienced by federal cross-sector partners during the implementation of a healthy eating campaign. Public Health Nutr 2017;20:2318–28.
-
Fernandez MA, Desroches S, Turcotte M, Marquis M, Dufour J, Provencher V. Factors influencing the adoption of a healthy eating campaign by federal cross-sector partners: a qualitative study. BMC Public Health 2016;16:904.
-
Godin KM, Hammond D, Chaurasia A, Leatherdale ST. Examining changes in school vending machine beverage availability and sugar-sweetened beverage intake among Canadian adolescents participating in the COMPASS study: a longitudinal assessment of provincial school nutrition policy compliance and effectiveness. Int J Behav Nutr Phys Act 2018;15:121.
-
Grabovac I, Hochfellner L, Rieger M, Jewell J, Snell A, Weber A, et al. Impact of Austria’s 2009 trans fatty acids regulation on all-cause, cardiovascular and coronary heart disease mortality. Eur J Public Health 2018;28:4–9.
-
Harris DM, Seymour J, Grummer-Strawn L, Cooper A, Collins B, DiSogra L, et al. Let’s move salad bars to schools: a public-private partnership to increase student fruit and vegetable consumption. Child Obes 2012;8:294–7.
-
He FJ, Brinsden HC, MacGregor GA. Salt reduction in the United Kingdom: a successful experiment in public health. J Hum Hypertens 2014;28:345–52.
-
Kraak VI, Story M, Wartella EA. Government and school progress to promote a healthful diet to American children and adolescents: a comprehensive review of the available evidence. Am J Prev Med 2012;42:250–62.
-
Kerins C, McSharry J, Hayes C, Perry IJ, Geaney F, Kelly C. Barriers and facilitators to implementation of menu labelling interventions to support healthy food choices: a mixed methods systematic review protocol. Syst Rev 2018;7:88.
-
Knai C, James L, Petticrew M, Eastmure E, Durand MA, Mays N. An evaluation of public-private partnership to reduce artificial trans fatty acids in England, 2011–16. Eur J Public Health 2017;27:605–608.
-
Lehmann U, Charles VR, Vlassopoulos A, Masset G, Spieldenner J. Nutrient profiling for product reformulation: public health impact and benefits for the consumer. Proc Nutr Soc 2017;76:255–264.
-
Miller GF, Sliwa S, Brener ND, Park S, Merlo CL. School district policies and adolescents’ soda consumption. J Adolesc Health 2016;59:17–23.
-
Moore SG, Donnelly JK, Jones S, Cade JE. Effect of educational interventions on understanding and use of nutrition labels: a systematic review. Nutrients 2018;10:E1432.
-
Nakamura R, Mirelman AJ, Cuadrado C, Silva-Illanes N, Dunstan J, Suhrcke M. Evaluating the 2014 sugar-sweetened beverage tax in Chile: an observational study in urban areas. PLOS Med 2018;15:e1002596.
-
Flaherty M, Flores-Mateo G, Nnoaham K, Lloyd-Williams F, Capewell S. Potential cardiovascular mortality reductions with stricter food policies in the United Kingdom of Great Britain and Northern Ireland. Bull World Health Organ 2012;90:522–31.
Literature reviews
-
An R. Effectiveness of subsidies in promoting healthy food purchases and consumption: a review of field experiments. Public Health Nutr 2013;16:1215–28.
-
Brownell KD, Farley T, Willett WC, Popkin BM, Chaloupka FJ, Thompson JW, Ludwig DS. The public health and economic benefits of taxing sugar-sweetened beverages. N Engl J Med 2009;361:1599–605.
-
Campos S, Doxey J, Hammond D. Nutrition labels on pre-packaged foods: a systematic review. Public Health Nutr 2011;14:1496–506.
-
Deliens T, Van Crombruggen R, Verbruggen S, De Bourdeaudhuij I, Deforche B, Clarys P. Dietary interventions among university students: a systematic review. Appetite 2016;105:14–26.
-
Hashem KM, He FJ, MacGregor GA. Systematic review of the literature on the effectiveness of product reformulation measures to reduce the sugar content of food and drink on the population’s sugar consumption and health: a study protocol. BMJ Open 2016;6:e011052.
-
Hyseni L, Bromley H, Kypridemos C, O’Flaherty M, Lloyd-Williams F, Guzman-Castillo M, et al. Systematic review of dietary trans-fat reduction interventions. Bull World Health Organ 2017;95:821–30G.
-
Powell LM, Chriqui JF, Khan T, Wada R, Chaloupka FJ. Assessing the potential effectiveness of food and beverage taxes and subsidies for improving public health: a systematic review of prices, demand and body weight outcomes. Obes Rev 2013;14:110–28.
-
Thow AM, Jan S, Leeder S, Swinburn B. The effect of fiscal policy on diet, obesity and chronic disease: a systematic review. Bull World Health Organ 2010;88:609–14.
Appendix 2 Protocol deviations and clarifications
A modified protocol version was submitted to the NIHR in December 2022. This section presents additional modifications made on the final version of the protocol.
Quality appraisal tool in Chapters 5 and 6
For the systematic reviews of PPPs (see Chapter 5) and of voluntary approaches (see Chapter 6), study quality was assessed using a modified version of the Newcastle–Ottawa Scale for cross-sectional studies rather than with ROBINS-I. The latter was discarded after facing issues when trialling it on a few studies. The main challenge was that ROBINS-I was designed for follow-up (cohort) studies of interventions that are assumed to be planned or controlled. This assumption did not apply well to the policy evaluations that we had, making the questions about cointerventions, classification of interventions, and deviations from intended interventions difficult to judge meaningfully. We chose instead the Newcastle–Ottawa Scale, which has been widely used and allows identification of the main weaknesses of studies in a pragmatic manner. We selected a version for cross-sectional studies to match with the study designs included in the reviews. We developed additional guidance for studies of documents and environmental features, which is lacking in most tools, and for providing an overall judgement given that the original tool uses a scoring system and this is now discouraged by Cochrane. See Chapter 2 for more details.
Synthesis approach in Chapter 8
We conducted a narrative and interpretive synthesis of the qualitative studies of policy process, and quality assessed the papers using CASP. This is in response to the reviewers’ comments about the earlier version not meeting the criteria of a critical interpretive synthesis, which we agree was not appropriate in the end.
Use of the GRADE framework
We had planned to use the GRADE approach in the overview of reviews and the systematic reviews on private commitments and PPPs (see Chapters 4–6), but this was not possible for the reasons detailed in Chapter 2.
Appendix 3 Modifications to the Scottish Intercollegiate Guidelines Network checklist for systematic reviews and meta-analyses
| Checklist item | Original guidance33 | Additional guidance and justification |
|---|---|---|
| 1.1 Research question and inclusion/exclusion criteria | The PICO must be clear in the paper even if not directly referred to. The research question and inclusion criteria should be established before the review is conducted. |
For the second sentence, we used a more forgiving guidance than AMSTAR-2: the authors must state that they have written a protocol or written a guide that included these elements or screening in general. |
| 1.2 A comprehensive literature search is carried out. | At least two relevant electronic sources must be searched. The report must list the databases used (e.g. Central, EMBASE, and MEDLINE). (Cochrane register/Central counts as two sources; a grey literature search counts as supplementary). (PubMed and MEDLINE count as one database.) Key words and/or MESH terms must be stated and where feasible the search strategy should be provided. Dates for the search should be provided. |
Just to make it clear, publications not reporting keywords or MESH terms got a ‘No’. |
| The paragraph above is the minimum requirement. All searches should be supplemented by consulting current contents, reviews, textbooks, specialised registers, or/and experts in the particular field of study, and by reviewing the references in the studies found. |
||
| The paragraph above is a quality criterion, which affects the overall rating of the review. Notes This criterion will not apply in the case of prospective meta-analysis – this is where meta-analysis is based on pre-selected studies identified for inclusion before the results of those studies are known. Such reports must state that they are prospective. |
||
| 1.3 At least two people should have selected studies. | At least two people should select papers. There should be a consensus process to resolve any differences. | Specifications added in red: At least two people should independently select papers or a sample together, for both title/abstract and full texts. There should be a consensus process to resolve any differences. Publications not reporting such information got a ‘No’. Those for which it is unclear for one of the two screening stages were marked as ‘unclear’. |
| 1.4 At least two people should have extracted data. | At least two people should extract data and should report that a consensus was agreed. One person checking the others’ data extraction is accurate is acceptable. | Specifications added in red: At least two people should extract data independently or on a sample together and should report that a consensus was agreed. One person checking the others’ data extraction is accurate is acceptable. The option ‘unclear’ was added. |
| 1.5 The status of publication was not used as an inclusion criterion. | The authors should state that they searched for reports regardless of their publication status. The authors should state whether or not they excluded any reports (from the systematic review), based on their publication status. If review indicates that there was a search for ‘grey literature’ or ‘unpublished literature’, indicate ‘yes’. SIGLE database, dissertations, conference proceedings and trial registries are all considered grey for this purpose. If searching a source that contains both grey and non-grey, must specify that they were searching for grey/unpublished lit. |
Publications not reporting such information got a ‘Yes’. This is because although they have not searched for it, there is no reason to believe that they have excluded those that they have come across because it is grey literature. |
| 1.6 The excluded studies are listed. | Limiting the excluded studies to references is acceptable. | In line with the Cochrane Handbook, this was applied for the full texts (not titles and abstracts), and authors could list only those that are ‘most likely to be considered eligible by readers’ [12] (and not necessarily the whole list of excluded studies). |
| 1.7 The relevant characteristics of the included studies are provided. | In an aggregated form such as a table, data from the original studies should be provided on the participants, interventions and outcomes. The ranges of characteristics in all the included studies, for example age, race, sex, relevant socioeconomic data, disease status, duration, severity, or other diseases should be reported. (Note that a format other than a table is acceptable, as long as the information noted here is provided.) Absence of this will make it impossible to form guideline recommendations. Mark as (−) original papers would need to be examined. |
To apply on the eligible results sections only Just to be clear, ‘mark as (−)’ means max low quality. In line with the Cochrane Handbook [12], other characteristics that had to be documented included the study design and the comparator (where relevant). |
| 1.8 The scientific quality of the included studies was assessed and documented. | It can include use of a quality scoring tool or checklist, for example risk-of-bias assessment, or a description of quality items, with some kind of result for EACH study (‘low’ or ‘high’ is fine, as long as it is clear which studies scored ‘low’ and which scored ‘high’; a summary score/range for all studies is not acceptable. Absence of this will make it impossible to form guideline recommendations. Mark as (−). |
N/A since absence of quality or risk-of-bias appraisal and or results reported for each study was an exclusion criterion (i.e. reviews had to include these to be considered as evidence syntheses). |
| 1.9 Was the scientific quality of the included studies used appropriately? | Examples include sensitivity analysis based on study quality, exclusion of poor-quality studies, and statements such as ‘the results should be interpreted with caution due to poor quality of included studies’. The results of the methodological rigour and scientific quality should be considered in the analysis and the conclusions of the review, and explicitly stated in formulating recommendations. |
Must meet A AND B to pass this criterion
|
| Cannot score ‘yes’ for this question if scored ‘no’ for question 1.8. |
When quality is not mentioned, check if the results mentioned in the recommendations and conclusions rely overall on good-quality evidence. If they don’t (e.g. evidence is rather weak or quality varies a lot), it should be mentioned, and this criterion is therefore failed. |
|
| 1.10 Appropriate methods are used to combine the individual study findings. | Studies that are very clinically heterogeneous should not be combined in a meta-analysis. Look at the forest plot – do the results look similar across the studies? |
To apply on the eligible results sections only Were also given a ‘No’ when: |
| For the pooled result a test should be done to assess statistical heterogeneity, i.e. chi-squared (χ2) test for homogeneity and/or I2 test for inconsistency. |
|
|
| If significant heterogeneity is apparent the authors should have explored possible explanations using methods such as sensitivity analysis or meta-regression. A random effects analysis may be used to take account of between-study variation but is not a ‘fix’ for heterogeneity. Planned subgroup analyses should be pre-specified and limited in number because conducting many subgroup analyses increases the probability of obtaining a statistically significant result by chance. Conclusions based on post hoc subgroup analyses must be interpreted with caution. Cannot score ‘yes’ for this question if scored ‘no’ for question 1.8. |
|
|
| 1.11 The likelihood of publication bias was assessed appropriate | The possibility of publication bias should be assessed where possible, commonly done by visual inspection of a funnel plot together with a statistical test for asymmetry (e.g. Egger regression test) although other statistical and modelling approaches may be reported. | To apply on the eligible results sections only ‘Not applicable’ when there is no meta-analysis. |
| Absence of a funnel plot doesn’t mean the likelihood of publication bias was not assessed appropriately (there are other methods); 10 studies is just a ball-park minimum number for a funnel plot and a plot is of little use when there are few studies. | ||
| 1.12 Conflicts of interest are declared. | Potential sources of support should be clearly acknowledged in both the systematic review and the included studies. | Like in AMSTAR-2, we split this question in two so that more nuanced answers could be given:
|
| Overall rating | ||
| High quality (++) | Majority of criteria met. Little or no risk of bias. | |
| Acceptable (+) | Most criteria met. Some flaws in the study with an associated risk of bias. | Maximum rating when have obtained a ‘No’ for:
|
| Low quality (−) | Either most criteria not met, or significant flaws relating to key aspects of study design. | The ‘Low’ and ‘Unacceptable/reject’ categories were merged. Apply when: |
| (According to guidance for the specific items): Maximum rating when have obtained a ‘No’ for either: |
|
|
|
|
|
Appendix 4 Modifications to the Newcastle–Ottawa Scale for cross-sectional studies
| Categories and items | Original tool for cross-sectional studies21 | Adapted tool for this project (modifications in red) |
|---|---|---|
| Selection | ||
|
|
|
|
|
|
| Document analyses: we considered instead the literature search (how comprehensive and clear it was) | ||
|
|
|
| Document analyses: we considered instead the variety of information sources used, taking into account the study aim. | ||
|
|
Non-respondents: identical for studies involving human participants or human-based data. Ignored for non-human studies and document analyses. Missing data: new options for all study designs. Proportion of target sample recruited attains pre-specified target or basic summary of non-respondent characteristics in sampling frame recorded. (high quality) |
|
|
|
|
||
|
|
|
Not applicable to document analyses |
||
| Comparability | ||
|
|
|
| Not applicable to document analyses. In practice, this was also difficult to assess in the other studies because the ‘participants’ (or unit of analysis) were non-humans and typical confounders are related to human characteristics. The factors that we could identify relating to the environment mostly related to external validity (e.g. time of the year/day of data collection) rather than internal validity. | ||
| Outcome | ||
|
|
|
|
|
|
|
|
|
|
|
|
| For document analyses, ‘statistical test’ is replaced by ‘analytical methods’, and information about precision estimates was ignored. | ||
| Overall rating | ||
| * = 1 point ** = 2 points Very Good Studies: 9–10 points Good Studies: 7–8 points Satisfactory Studies: 5–6 points Unsatisfactory Studies: 0–4 points |
New classification: two key items: 4. ascertainment of exposure and 7. statistical tests High quality: Items 4 or 7 rated high, few other items rated moderate, no item rated low |
|
Moderate quality:
|
||
| Low quality: when 1 + item is rated low Unclear quality: |
||
|
||
Appendix 5 Additional tables for Chapter 4 (overview of reviews)
|
Review
unique studies |
Lhachimi 2020 | Pfinder 2020 | Dodd 2020 | Crocker 2020 | Teng 2019 | von Philipsborn 2019 | Hyseni 2017a (trans-fats) | Hillier-Brown 2017 | Backholer 2016 | Redondo et 2018 | Downs 2017 | Sisnowski et 2017 | Alagiyawana 2015 | Rincon-Gallardo 2020 | Hyseni 2017b (salt) | N times a study overlaps |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Aguilar A, 2017 | x | |||||||||||||||
| Andalón M, 2017 | x | |||||||||||||||
| Angell SY, 2012 | x | |||||||||||||||
| Angell SY, 2009 | x | |||||||||||||||
| Araya S, 2018 | x | |||||||||||||||
| Arcand J, 2014 | x | |||||||||||||||
| Berardi N, 2012 | x | |||||||||||||||
| Biró A, 2015 | x | x | 1 | |||||||||||||
| Blake MR, 2018 | x | |||||||||||||||
| Bleich SN, 2015 | x | |||||||||||||||
| Bleich SN, 2016 | x | |||||||||||||||
| Bleich SN, 2017 | x | |||||||||||||||
| Bleich SN, 2018 | x | |||||||||||||||
| Bleich SN, 2020 | x | |||||||||||||||
| Blumberg FB, 2014 | x | |||||||||||||||
| Brandt EJ, 2015 | x | |||||||||||||||
| Breeze P, 2018 | x | |||||||||||||||
| Bruemmer B, 2012 | x | |||||||||||||||
| Bødker M, 2015 | x | x | 1 | |||||||||||||
| Capacci S, 2018 | x | |||||||||||||||
| Colantuoni F, 2015 | x | x | 1 | |||||||||||||
| Colchero MA, Guerrero-López CM, et al., 2016 | x | x | 1 | |||||||||||||
| Colchero MA, Popkin BM, et al., 2016 | x | |||||||||||||||
| Colchero MA, Molina M, et al, 2017 | x | |||||||||||||||
| Colchero MA, Rivera‐Dommarco J, et al., 2017 | x | |||||||||||||||
| Colon-Ramos U, 2006 | x | |||||||||||||||
| Cornelsen L, 2017 | x | |||||||||||||||
| Elshiewy O, 2018 | x | |||||||||||||||
| Enkhtungalag, 2015 | x | |||||||||||||||
| European Competitiveness and Sustainable Industrial Policy Consortium, 2014 | x | |||||||||||||||
| Fabiansson SU, 2006 | x | |||||||||||||||
| Falbe J, 2016 | x | x | 1 | |||||||||||||
| Fattore, 2014 | x | |||||||||||||||
| Fletcher JM, Frisvold D and Tefft N. Can soft drink …, 2010. | x | x | 1 | |||||||||||||
| Fletcher JM, Frisvold DE, Tefft N. Taxing soft drinks …, 2010 | x | x | 1 | |||||||||||||
| Fletcher JM, Frisvold DE, Tefft N. The effects of …, 2010 | x | x | 1 | |||||||||||||
| Fletcher JM, 2014 | x | |||||||||||||||
| Friesen R, 2006 | x | x | 1 | |||||||||||||
| Garsetti M, 2016 | x | |||||||||||||||
| He FJ, 2009 | x | |||||||||||||||
| He FJ, 2010 | x | |||||||||||||||
| He FJ, Brinsden HC, 2014 | x | |||||||||||||||
| He FJ, Pombo-Rodrigues S, 2014 | x | |||||||||||||||
| Hobin E, 2017 | x | |||||||||||||||
| Jensen JD, 2013 | x | x | 1 | |||||||||||||
| Jensen JD, 2015 | x | x | 1 | |||||||||||||
| Kim D, 2006 | x | |||||||||||||||
| Lavizzo-Mourey R, 2014 | x | |||||||||||||||
| Lee JH, 2010 | x | |||||||||||||||
| Leth T, 2006 | x | x | 1 | |||||||||||||
| Luft, 1997 | x | |||||||||||||||
| Mohan, 2009 | x | |||||||||||||||
| Monge-Rojas R, 2013 | x | x | 1 | |||||||||||||
| Monge-Rojas R, 2011 | x | |||||||||||||||
| Mozaffarian D, 2010 | x | |||||||||||||||
| Mozaffarian D, 2009 | x | |||||||||||||||
| Mozaffarian D, 2012 | x | |||||||||||||||
| Nakamura R, 2018 | x | |||||||||||||||
| Namba A, 2013 | x | |||||||||||||||
| Ng SW, 2014 | x | |||||||||||||||
| Pacific Research Centre for the Prevention of Obesity and NCDs (CPOND), 2017 | x | |||||||||||||||
| Penaherrera V, 2018 | x | |||||||||||||||
| Petimar J, 2019 | x | |||||||||||||||
| Peymani P, 2012 | x | |||||||||||||||
| Pietinen, 2010 | x | |||||||||||||||
| Powell LM, 2009 | x | x | 1 | |||||||||||||
| Pulos E, 2010 | x | |||||||||||||||
| Ratnayake WMN, L’Abbe MR, Farnworth S, et al., 2009 | x | x | 1 | |||||||||||||
| Ratnayake WMN, L’Abbe MR, Mozaffarian D, 2009 | x | |||||||||||||||
| Ratnayake WN, 2014 | x | x | ||||||||||||||
| Restrepo BJ, 2016 | x | |||||||||||||||
| Ricciuto L, 2009 | x | |||||||||||||||
| Saelens, 2012 | x | |||||||||||||||
| Scourboutakos, 2019 | x | |||||||||||||||
| Silver LD, 2017 | x | x | 1 | |||||||||||||
| Storey ML, 2015 | x | |||||||||||||||
| Sturm R, 2010 | x | x | x | 2 | ||||||||||||
| Taillie SL, 2015 | x | |||||||||||||||
| Taillie LS, 2017 | x | |||||||||||||||
| Temme EH, 2011 | x | |||||||||||||||
| Theis, 2019 | x | |||||||||||||||
| Tran, 2019 | x | |||||||||||||||
| Trieu, 2015 | x | |||||||||||||||
| Vall Castello J, 2018 | x | |||||||||||||||
| Van Camp D, 2012 | x | |||||||||||||||
| Vesper HW, 2012 | x | x | 1 | |||||||||||||
| Vesper HW, 2017 | x | |||||||||||||||
| Wang, 2011 | x | |||||||||||||||
| Wang, 2013 | x | |||||||||||||||
| Wansink B, 2014 | x | |||||||||||||||
| Webster, 2011 | x | |||||||||||||||
| Wellard-Cole L, 2018 | x | |||||||||||||||
| Wellard-Cole L., 2019 | x | |||||||||||||||
| World Bank, 2019 | x | |||||||||||||||
| WHO Regional Office for Europe, 2015 | x | |||||||||||||||
| Wu HW, 2014 | x | |||||||||||||||
| Wyness, 2012 | x | |||||||||||||||
| Zhong Y, 2018 | x | |||||||||||||||
| N studies in the eligible sections of the reviews | 2 | 1 | 4 | 3 | 17 | 8 | 7 | 2 | 3 | 5 | 23 | 6 | 6 | 15 | 15 | Of 98 unique studies: 17 overlap once, 1 twice |
| N (%) studies that overlap with another |
2
(100%) |
1
(100%) |
0
(0%) |
0
(0%) |
7
(41%) |
0
(0%) |
6
(86%) |
0
(0%) |
3
(100%) |
4
(80%) |
6
(26%) |
3
(50%) |
5
(83%) |
0
(0%) |
0
(0%) |
|
| Review(s) it overlaps with …: | Sisnowski | Sisnowski | - | - | Backholer, Redondo, Alagiyawana | - | Downs | - | Teng, Alagiyawana | Teng | Hyseni a | Pfinder, Lhachimi | Backholer, Teng | - | - | Of 15 reviews, 9 have study overlaps |
| Decision to reduce primary study overlapa | Include | Include | Include | Include | Include | Include | Exclude | Include | Exclude | Exclude | Include | Include BoP; Exclude taxes |
Exclude | Include | Include | 11 reviews are included fully or partially, 4 are fully excluded |
| N unique studies excluded fully from the OOR | - | - | - | - | - | - | 1 | - | 2 | 1 | - | 1 | 1 | - | - | Of 98 initial studies, 6 are excluded |
| Author, year | Search | Decision | Justification for selecting a review | Quality |
|---|---|---|---|---|
| Overlapping group 1 (both on trans-fat policies) | ||||
| Downs (2017)48 | August 2017 | Include | Both have the same search date and compared regulatory and voluntary policies. Although Downs have a lesser quality, it was still acceptable and it assessed a wider range of outcomes, included more studies (23 compared to 7 in Hyseni), covered more countries (Brazil, Iran, Korea, Mexico, the Netherlands, Americas in addition to those included in Hyseni), and included 6 of the 7 publications included in Hyseni. | Acceptable (+) |
| Hyseni (2017a)38 | August 2017 | Exclude | High (++) | |
| Overlapping group 2 (on back-of-pack labelling and various taxes) | ||||
| Lhachimi (2020)42 | October 2019 | Include | Sisnowski: include the results section on back-of-pack labelling (Australia, n = 1) since this is the only one in this group. Exclude the results section on taxes since it covers multiple types of taxes together (fat, non-essential foods, SSBs). The assessment is not as specific as (which focuses on sugar and SSB taxes), and Llhachimi (which focuses on the saturated fat). Keep both Pfinder and Llhachimi since they do not overlap, are of high quality (Cochrane reports), and cover different topics. |
High (++) |
| Pfinder (2020)44 | October 2019 | Include | High (++) | |
| Sisnowski (2017)39 | October 2015 | Include partly | Acceptable (+) | |
| Overlapping group 3 (on SSB taxes) | ||||
| Teng (2019)45 | June 2018 | Include | Keep Teng because it has a high quality, is the most recent, includes more recent studies, includes more papers (n = 18), and is the only one that includes other countries than the USA (Chile, Finland, France, Hungary, Mexico, Spain). Backholer also has a high quality but has an older search and includes fewer studies (n = 3), of which one is in Teng. Alagiyawanna is of lesser quality, has an older search and fewer studies than Teng (n = 6), of which five are in Teng. Redondo is also of lesser quality, also has an older search, and fewer studies than Teng (n = 5), of which four are in Teng. |
High (++) |
| Backholer (2016)35 | June 2015 | Exclude | High (++) | |
| Alagiyawanna (2015)36 | July 2013 | Exclude | Acceptable (+) | |
| Redondo (2018)37 | December 2017 | Exclude | Acceptable (+) | |
| First author (year) |
Section(s) of synthesis considered | N studies Type of synthesis |
Countries | Categories of eligible policies | Types of outcomes measured | Funding sources reported | Declaration of competing interests |
|---|---|---|---|---|---|---|---|
| Backholer (2016)35 High (++) |
Would have been included otherwise Studies evaluating existing SSB taxes Would have remained excluded Studies where the primary result was estimated price elasticities, modelling studies, amount paid in SSB tax according to socioeconomic position following an increase in SSB price |
N = 3 (out of 11) Narrative |
USA | U-SSB tax | Health (BMI); Consumer behaviour (dietary intake)a |
Non-industry funding | None declared |
| Hyseni (2017a)38 High (++) |
Would have been included otherwise Empirical studies: food reformulation, and multicomponent interventions Would have remained excluded (1) Empirical studies: individual dietary counselling, worksite dietary counselling, legislation (local); (2) modelling studies |
N = 8 (out of 23) Narrative |
CAN, CR, DEN, USA, N America and Europe | N-Trans-fat labelling; I-Trans-fat reformulation/limits/ban S-Retail and food services (trans-fat reformulation/limits/ban) |
Health (heart diseases, trans-fat concentration in human body); consumer behaviour (dietary intake, purchases); food environment (nutritional composition) |
NR | None declared |
| Alagiyawanna (2015)36 Acceptable (+) |
Would have been included otherwise Studies on food and beverage taxation in HIC: effects on anthropometry, and consumption and anthropometry Would have remained excluded Studies on food and beverage taxation in HIC: effects on consumption (subsidies); studies on food and beverage subsidies in HICs (PRO, effects on health outcomes related to diet and anthropometry); studies about LMICs (all about subsidies) |
N = 6 (out of 18) Narrative |
USA | U-Tax on SSBs, snacks and fast-food restaurants | Health (BMI, obesity); consumer behaviour (dietary intake)a |
No funding | None declared |
| Redondo (2018)37 Acceptable (+) |
Would have been included otherwise Naturalistic experiments Would have remained excluded Virtual or experimental conditions |
N = 5 (out of 17) Narrative |
MEX, USA | U-SSB tax | Consumer behaviour (sales/purchases); food envt (price); economy (store revenue) |
Non-industry funding | None declared |
| Sisnowski (2017)39 Acceptable (+) |
*REVIEW PARTLY EXCLUDED* Section specifically excluded to reduce primary study overlap Taxation of unhealthy foods and beverages |
N = 5 (out of 17) Narrative |
DEN, FRA, HUN | U-Taxes on SSB, saturated fat, non-essential foods | Health (BMI, heart diseases); consumer behaviour (dietary intake, purchases/sales); food envt (nutrition composition, price) |
Non-industry funding | None declared |
| Lead author (year) | 1.1 | 1.2 | 1.3 | 1.4 | 1.5 | 1.6 | 1.7 | 1.8 | 1.9 | 1.10 | 1.11 | 1.12a | 1.12b | Overall rating |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Alagiyawanna (2015)36 | No | Yes | No | Yes | Yes | No | Yes | Yes | No | Yes | N/A | Yes | No | Acceptable (+) |
| Backholer (2016)35 | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | N/A | Yes | No | High (++) |
| Hyseni (2017a)50 | No | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | N/A | Yes | No | High (++) |
| Redondo (2018)37 | No | Yes | Yes | Yes | No | No | Yes | Yes | No | Yes | N/A | Yes | No | Acceptable (+) |
Appendix 6 Additional literature searches for Chapter 7 (cost-effectiveness analysis)
| Search in: Ovid MEDLINE(R) and Epub Ahead of Print, In-Process, In-Data-Review and Other Non-Indexed Citations and Daily <1946–22 September 2021> | |
|---|---|
| Search lines | N |
|
11,208 |
|
4315 |
|
11,371 |
|
19,684 |
|
939 |
|
4,366,351 |
|
4722 |
|
2392 |
|
3700 |
|
5,222,426 |
|
2927 |
|
1224 |
|
4150 |
|
1742 |
|
504 |
|
1424 |
|
971 |
|
|
|
1 |
|
82 |
|
1 |
|
1681 |
|
108 |
|
2039 |
|
1990 |
|
49 |
|
1066 |
|
694 |
|
705 |
|
455 |
|
16 |
|
136,203 |
|
109 |
|
82 |
|
12 |
|
17,027 |
|
|
|
|
|
|
|
43,545 |
|
398,973 |
|
515,489 |
|
320 |
| Ovid MEDLINE(R) and Epub Ahead of Print, In-Process, In-Data-Review and Other Non-Indexed Citations and Daily <1946–22 September 2021> | |
|---|---|
| Search lines | N |
|
5,225,242 |
|
2,894,771 |
|
14,739 |
|
1,286,215 |
|
10,383 |
|
3590 |
|
75 |
|
16,239 |
|
419,945 |
|
106,891 |
|
533,475 |
|
14,447 |
|
193,257 |
|
93,907 |
|
43,545 |
|
398,973 |
|
519,845 |
|
478 |
|
3661 |
|
2096 |
|
134 |
List of abbreviations
- AWASH
- Australian Division of World Action on Salt and Health
- BMI
- body mass index
- CAI
- Canadian Children’s Food and Beverage Advertising Initiative
- CASP
- Critical Appraisal Skills Programme
- CFBAI
- Children’s Food and Beverage Advertising Initiative (USA)
- CHD
- coronary heart disease
- CHN
- Choose Healthy Now
- CP
- children’s programmes
- CVD
- cardiovascular disease
- DALY
- disability-adjusted life-year
- EPPI-Centre
- Evidence for Policy and Practice Information and Co-ordinating Centre
- EU
- European Union
- FHD
- Food and Health Dialogue
- FOP
- front of pack
- FOPL
- front-of-pack labelling
- FV
- fruit and vegetables
- GRADE
- Grading of Recommendations, Assessment, Development and Evaluation
- HALY
- health-adjusted life-year
- HFSS
- high fat, sugar and/or salt foods
- HSR
- Health Star Rating
- HWC
- healthy weight commitment
- HWCF
- Healthy Weight Commitment Foundation
- LMIC
- low- and middle-income country
- NCD
- non-communicable disease
- NGO
- non-governmental organisation
- NPs
- non-participants
- PPP
- public–private partnership
- PRISMA
- Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- QALY
- quality-adjusted life-year
- QSRI
- The Quick Service Restaurant Industry’s Initiative
- RCMI
- Responsible Children’s Marketing Initiative
- RCT
- randomised controlled trial
- RD
- Responsibility Deal
- ROBINS-I
- Risk Of Bias In Non-randomised Studies of Interventions
- SDIL
- Soft Drinks Industry Levy
- SES
- socioeconomic status
- SIGN
- Scottish Intercollegiate Guidelines Network
- SSB
- sugar-sweetened beverage
- WHO
- World Health Organization
- WTP
- willing to pay
Notes
Supplementary material can be found on the NIHR Journals Library report page (https://doi.org/10.3310/JYWP4049).
Supplementary material has been provided by the authors to support the report and any files provided at submission will have been seen by peer reviewers, but not extensively reviewed. Any supplementary material provided at a later stage in the process may not have been peer reviewed.