

Notes
Article history
The research reported in this issue of the journal was funded by the PHR programme as award number 16/122/20. The contractual start date was in March 2018. The draft manuscript began editorial review in December 2022 and was accepted for publication in January 2024. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PHR editors and production house have tried to ensure the accuracy of the authors’ manuscript and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this article.
Permissions
Copyright statement
Copyright © 2024 Booth et al. This work was produced by Booth et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This is an Open Access publication distributed under the terms of the Creative Commons Attribution CC BY 4.0 licence, which permits unrestricted use, distribution, reproduction and adaptation in any medium and for any purpose provided that it is properly attributed. See: https://creativecommons.org/licenses/by/4.0/. For attribution the title, original author(s), the publication source – NIHR Journals Library, and the DOI of the publication must be cited.
2024 Booth et al.
Chapter 1 Introduction
Material throughout this chapter has been reproduced from Cochrane et al. 1 This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) licence, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: https://creativecommons.org/licenses/by/4.0/. The text below includes some additions and formatting changes to the original text.
Background
Young adult offenders commonly have a range of health and social needs, making them vulnerable to mental health problems. 2,3 Those aged between 18 and 24, who have been investigated for a suspected low-level offence, may need to attend court and, if convicted, face penalties such as prison. However, many believe that more should be done to prevent young adults from entering the criminal justice system to begin with. Diversion is a process whereby an accused offender is formally moved into a programme in the community, such as an out-of-court community-based intervention (OCBI), instead of entering the criminal justice system. 4 Despite the use of diversion programmes in the UK, particularly among a younger population,4,5 the evidence base around the effectiveness, including health benefits, of diversion is still unclear.
The Gateway programme, an OCBI, was developed by Hampshire Constabulary (HC), in partnership with local third sector organisations with the aim of improving the life chances of young adult offenders. In the programme, a mentor (navigator) assesses the needs of each young adult and develops a pathway with referrals to healthcare and other local support services (e.g. housing). Young adults then take part in two workshops (LINX team) about empathy, and the causes and consequences of their behaviour. The components of the Gateway intervention are underpinned by theory and have been evaluated in isolation;6–12 there has been no previous attempt to evaluate the combination of elements as used in the Gateway programme.
Existing research on diversion and recidivism among young populations
A literature review of challenges to engagement, with diversion programmes aimed at promoting a public health approach to crime, was undertaken in January 2020. A summary is provided here and the full review is in Report Supplementary Material 1.
Literature searches were conducted using CINAHL, EMBASE, Europe PMC, MEDLINE, National Institute for Health and Care Research (NIHR) Library and Web of Science databases using the search terms: 'diversion', 'out-of-court disposals' and 'court diversion'. The 15 included studies on diversion have largely been undertaken outside the UK; the majority being conducted in the USA, with a few studies in Australia, New Zealand and the rest of Europe. Most of the studies focused on younger populations and on family treatment as a therapeutic intervention. For example, multisystemic therapy is a resource-intensive programme, which focuses on factors within the offender’s social network that contribute to their offending behaviour. 13 Treatment usually takes place within the community, such as at home or at school. A meta-analysis of diversion programmes for juvenile offenders was undertaken in 2012 and identified 28 studies involving 19,301 youths. 14 The most common outcome reported among the studies was recidivism, the tendency of the offender to reoffend. Of the five types of programmes included, a statistically significant reduction in recidivism was only observed for family treatment (OR = 0.57, 95% CI 0.40 to 0.82). Overall, there was high heterogeneity among the studies in terms of the research and programme design, as well as the quality of programme monitoring and implementation. The mean age of the population in studies identified by the meta-analysis ranged from 12.6 to 15.9 years of age. An evaluation of Checkpoint, a court diversion programme which does not respond to the needs of a particular age group but is aimed at adults, found a lower reoffending rate in comparison to the control cohort. 15 Despite the lack of robust evidence, the case for diversion among young adults is increasing, due to a growing recognition of their varying levels of maturity and complex needs. 16,17
According to HC statistics for 2018/20, the five main offence categories for this age group where formal action was taken by the police are possession of drugs, violence, shoplifting, criminal damage and public order offences. These young adults often represent a vulnerable population with a range of complex needs, such as mental health issues and substance misuse. They are more likely to come into contact with the police both as suspects and victims of crime and are significantly over-represented in the formal justice process, accounting for approximately one-third of police, probation and prison caseloads. 16
In the UK, several Police Forces are exploring the use of out-of-court disposals among 18–24-year-olds involved in less serious offending. 18 Out-of-court disposals are usually given where the offence is perceived to be a low-level crime. The aim is to divert the young adult away from their offending behaviour. However, evidence of the effectiveness of diversion interventions among this population remains limited.
Rationale for intervention and current study
The Gateway intervention model was conceived as a ‘culture changing initiative’ that sought to address the complex needs of young adult offenders aged 18–24. Central to this is the belief that transitions into adulthood are not linear and that more work is necessary to support desistance among this vulnerable population. By combining components shown to have an impact, at least in the short term, the Gateway programme aimed to provide a more comprehensive approach with longer-term impacts. HC understood the need to undertake a robust assessment of the cost and effectiveness of implementing the Gateway programme. In addition, to understand the potential generalisability, the study included a qualitative evaluation. This mixed-methods approach aimed to ensure the study evaluated the impact of the intervention on participants, account for the views of victims, assess the intervention itself and examine the cost-effectiveness of the Gateway programme. The study included a wide set of outcomes with a particular focus on health and well-being of offenders, victim satisfaction and reducing reoffending.
Research aims and objectives
The aim of this study was to evaluate the effectiveness and cost-effectiveness of the Gateway programme issued as a conditional caution compared to a court appearance or a different conditional caution.
The study objectives were to:
-
Examine the effectiveness of the Gateway intervention on (1) health and well-being including alcohol and substance use, (2) access to and use of health and social services and (3) quality of life, among young adult offenders.
-
Explore the views and experiences of victims.
-
Assess the implementation of the Gateway intervention as delivered in the study and the generalisability of the findings.
-
Identify and measure all relevant consequences, both cost and benefits, of the Gateway intervention compared with usual process.
-
Examine the effectiveness of the Gateway intervention on reoffending.
Chapter 2 Effectiveness trial
Methods
Material throughout this section has been reproduced from Cochrane et al. 1 This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) licence, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: https://creativecommons.org/licenses/by/4.0/. The text below includes minor additions and formatting changes to the original text. The text below includes some additions and formatting changes to the original text.
Trial design
To assess effectiveness of the Gateway programme the researchers undertook a pragmatic, superiority randomised controlled trial (RCT) with participants aged 18–24 who had committed low-level offences and resided within Hampshire and Isle of Wight (IoW) area. There was an internal pilot and an economic evaluation was planned. RCTs provide the most robust method to establish whether an intervention is effective. Participants were randomised using a 1 : 1 allocation ratio to either the Gateway conditional caution (intervention) or disposal as usual to a court summons or a different conditional caution (usual process).
To capture the impact of the intervention on participants and other stakeholders, a qualitative evaluation was carried out (see Chapter 3).
Research aims and objectives
The aim of the trial was to evaluate the effectiveness and cost-effectiveness of the Gateway programme issued as a conditional caution compared to court summons or a different conditional caution. The objectives addressed in this chapter were to:
-
Examine the effect of the Gateway intervention on: (1) health and well-being including, alcohol and substance use (2) access to and use of health and social services and (3) quality of life, among young adult offenders.
-
Identify and measure all relevant consequences, both cost and benefits, of the Gateway intervention compared with usual process.
-
Examine the effect of the Gateway intervention on reoffending.
Study sites
The four trial recruitment sites were Southampton Central Police Station, Portsmouth Central Police Station, Newport Police Station on the IoW and Northern Hampshire Police Investigation Centre in Basingstoke, with recruitment from across Hampshire and IoW.
Population
The study population were 18- to 24-year-old offenders residing within HC area. According to police statistics, the five main categories of offences for this age group are: violence; possession or trafficking of drugs; theft; criminal damage; and public order offences. These young adults represent a vulnerable population with a range of complex needs, such as mental health issues and drug and substance misuse. They are more likely to come into contact with the police both as suspects and victims of crime and are significantly over-represented in the formal justice process, accounting for approximately one-third of police, probation and prison caseloads. 16
Recruitment
The researchers’ process for recruitment acknowledged that the study population represented a vulnerable group with complex and overlapping health and social needs, therefore engaging with them was likely to be challenging. According to police estimates at the start of recruitment, an average of 23 individuals would be eligible to receive the Gateway intervention each month across all sites.
By law the police must know the destination for an offender at the time of disposal. As the intervention was one of the disposal options, randomisation had to take place at the time of disposal. It was agreed with HC that their investigators would be trained to identify and recruit participants. An approach used successfully for a previous study. 19
Police investigators, dealing with potential participants, received face-to-face and/or online training from the Gateway Inspector or Sergeant. The non-mandatory 1-hour training introduced the aims of the study and eligibility. Also covered were the consent process, and use of Alchemer (formerly SurveyGizmo), a web-based eligibility and randomisation tool, to ensure standardised recruitment and recording of eligibility criteria (see Randomisation).
The Police Gateway Team monitored recruitment daily, contacted investigators about potentially eligible cases to remind them about the Gateway caution and study, and discussed with investigators where a potential participant had been missed. All the Gateway and study documentation and information were readily available on the HC computer system. A variety of methods were used to raise and maintain awareness of the Gateway study within HC, such as computer screen savers, notices in police station offices and newsletter articles from the Deputy Chief Constable. Refresher training was offered throughout the study period.
Further information on recruitment is provided in Stage 1 consent.
Consenting participants
Participation was voluntary. It was not felt appropriate for police investigators to obtain fully informed consent because of the potential risk of coercion, nor was it practical given the timelines. The researchers therefore developed a two-stage consent procedure.
Stage 1 consent
During processing in custody, investigators identified potentially eligible participants (see Appendix 1, Figure 8) and discussed with them the Gateway programme. For legal reasons, the Gateway caution was initially offered as a potential disposal option independently of the study. If interest was shown, the offender was then informed about the ‘Questionnaire Study’ (terminology used in participant facing materials). A Gateway Caution information leaflet (produced by HC independently of the study) and a Questionnaire Study leaflet with link to a video (see Report Supplementary Material 2) were offered and/or e-mailed later. Potential participants were made aware that further details about the study would be provided by a university researcher and that they could withdraw from the study at any time without giving a reason. If the offender agreed to take part in Gateway and the study, the investigator obtained their signature on the combined Stage 1 participant information sheet (PIS) and consent form.
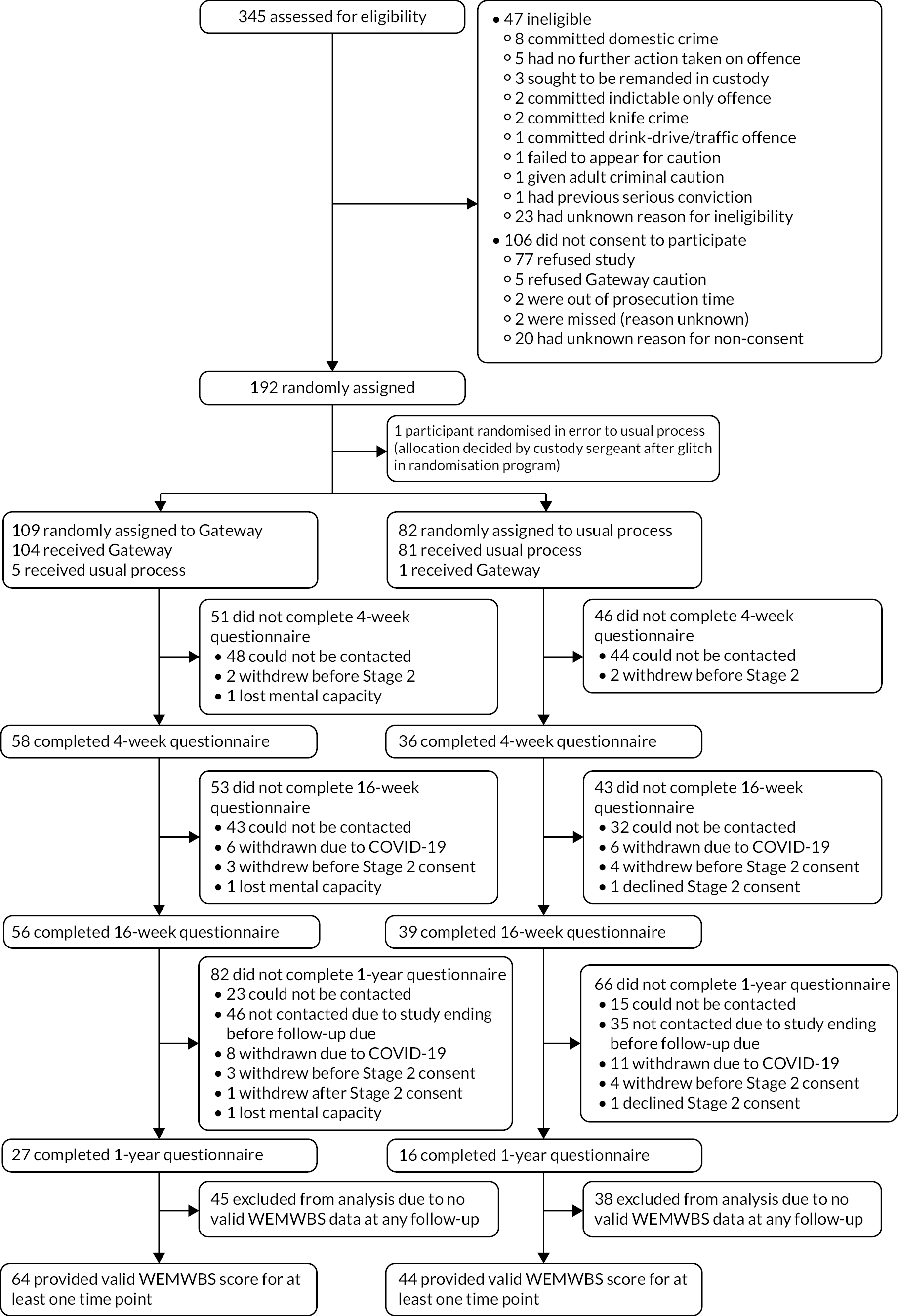
FIGURE 1.
Consolidated Standards of Reporting Trials diagram demonstrating the progression of participants through the trial.
A small number of participants were recruited through the out-of-custody process (see Appendix 1, Figure 9). The investigator followed the process for in-custody, where they were confident that although a disposal decision could not be made at that time, the young person would ultimately be eligible for the Gateway caution option. In these cases, the time between randomisation and disposal could vary. If contacted by telephone, they were asked to give verbal Stage 1 consent to participate. If given, this was recorded in the individual’s Police records management system (RMS) incident record. Written consent was subsequently sought prior to any trial-related activities for the participant. Anyone later declining consent in writing was withdrawn from the trial. This approach ensured all potentially eligible participants had the chance to join the study, in keeping with the pragmatic nature of this trial.
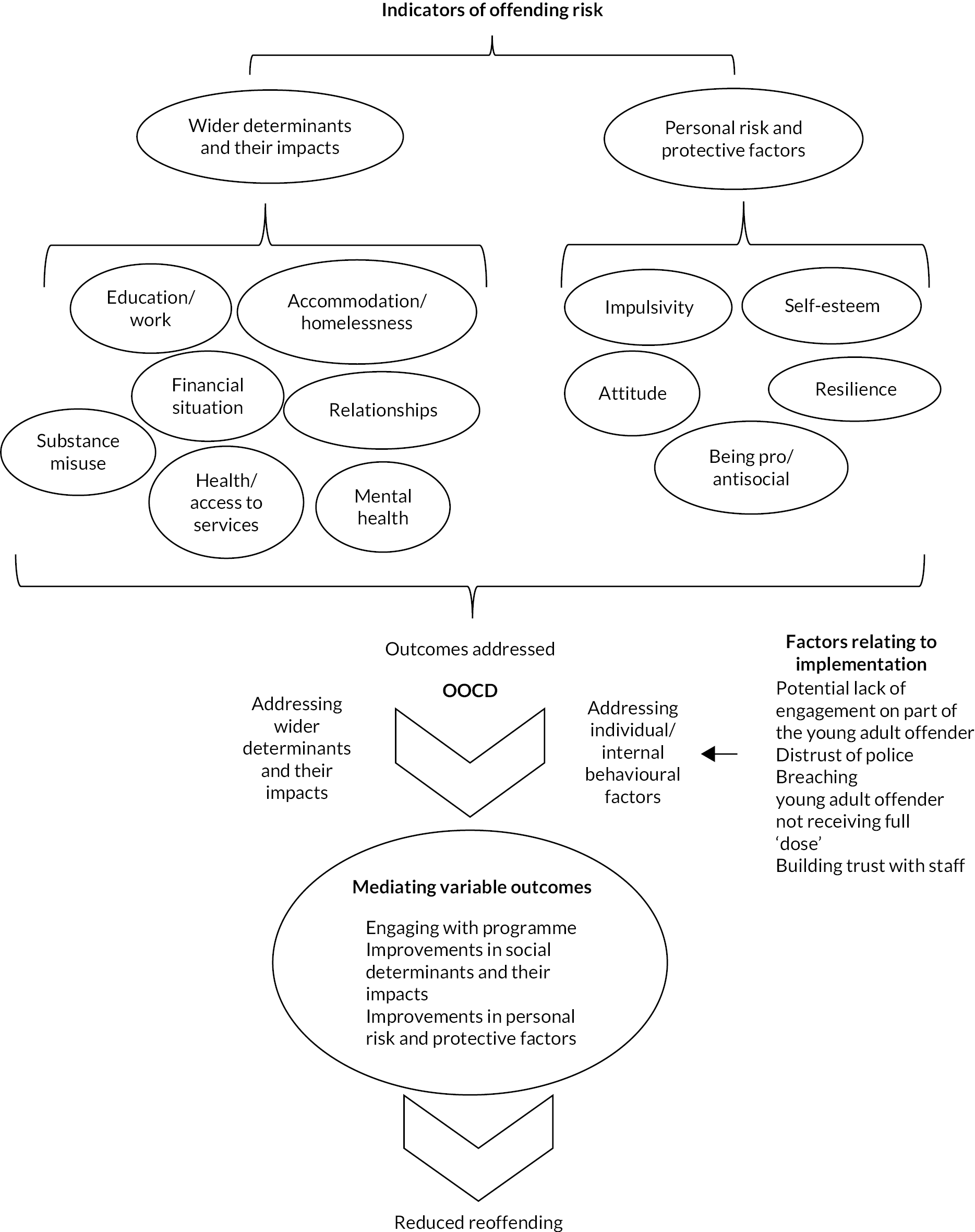
FIGURE 2.
Conceptual framework for determining risk of offending behaviour and role of OOCDs in reducing offending.
Stage 1 consent allowed the police to provide the University of Southampton (UoS) researchers with the participant’s contact details and to access their police records for data on variables such as age, gender and ethnicity and offending history, trigger offence and any subsequent reoffending. Investigators made it clear to potential participants that they would be provided with more details of the study later by the researchers and would have the right to withdraw from the study at any time. The personal contact details of participants who consented to take part in the study were passed to the research team.
Stage 2 consent
Participants who consented at Stage 1 were contacted by a member of the Gateway Team at Southampton Central Police Station within a week of recruitment to remind them about the study and check for changes to their phone numbers. The Questionnaire Study leaflet and a link to the video developed for the study were sent by e-mail at this time.
Ahead of the week 4 data collection time point, the researchers attempted to contact participants by phone, text, e-mail and/or post to arrange an interview. Once arranged, the Stage 2 PIS was e-mailed or posted to the participant.
At the interview the researcher went through the PIS providing explanations as required. Participants were provided with any other information required and had any queries answered. After time to consider their involvement, and if they decided to proceed, the researcher read out the statements in the consent form. If the participant agreed to a statement, the researcher put the participant’s initials in the corresponding box. When completed, the researcher added their own name, the participant’s name and the date of verbal consent. The completed consent form was saved as a PDF and a copy sent to the participant. Once consent had been given, data collection could occur at the same interview or on a subsequent day.
Participants were informed that they had the right to withhold consent or to withdraw from the study at any time without giving a reason. To maximise data collection, if a participant took part in the week-16 interview having not taken part at week-4, verbal consent was obtained at that point.
Stage 2 consent included optional permission to access data from police records on reoffending for up to 10 years from their enrolment in the study. This was to facilitate a potential long-term assessment of reoffending as a separate follow-up at 10 years post-randomisation.
Eligibility
Inclusion criteria
-
Suspect aged 18–24 years.
-
Suspect resided within HC area.
-
There was an anticipated guilty plea (i.e. they admitted the offence and said nothing which could be used as a defence or made no admission but had not denied the offence or otherwise indicated it would be contested).
-
Full code test met (i.e. there was sufficient evidence to provide a realistic prospect of conviction and it was in the public interest to prosecute or offer a conditional caution to the suspect).
Exclusion criteria
-
Hate crime according to Crown Prosecution Service (CPS) Policy.
-
Domestic violence-related crime.
-
Domestic violence-related crime referred to CPS.
-
Sexual offence as defined by the CPS.
-
Knife crimes where a decision to prosecute was made.
-
Where on conviction the court was more likely to impose a custodial sentence (based on sentencing guides).
-
Remand in custody was sought.
-
Breach of court or sexual offences orders.
-
Any offence involving serious injury or death of another.
-
Any serious previous convictions within the last 2 years [i.e. serious violence, grievous bodily harm (GBH) or worse, serious sexual offences, robbery or indictable only offences].
-
Summary offences more than 4 months old.
-
Persons subject to Court bail, Prison Recall, Red Integrated Offender Management (IOM) or currently under Probation.
-
Indictable only offences.
-
All drink/drive or endorsable traffic offences.
-
Offender had already had a Gateway caution.
-
Offender needed an interpreter.
Intervention
The Gateway programme was a police-led intervention consisting of three parts: a needs assessment with a Gateway navigator (a trained support/case worker); attendance at two workshops/telephone interventions designed to aid development of cognitive and affective empathy; and an undertaking not to re-offend during the 16-week caution. Participation in the restorative justice (RJ) process was voluntary.
Developed as an OCBI, the Gateway programme was issued as part of a 16-week contract with set conditions, known as a conditional caution. The set conditions were to attend all the required elements of the Gateway programme, and to not reoffend during the 16-week caution. Other conditions such as a fine or writing a letter of apology could be added to individual cautions at the investigator’s discretion. A breach of any of the conditions, that is, where one or more of the conditions of the caution are not met, could have resulted in the offender being prosecuted for the original offence.
Part 1. Needs assessment
Within 3–5 working days of their disposal, the participant engaged with the Gateway navigator who conducted a thorough needs assessment. Based on identified needs, the navigator assisted the young adult into the appropriate services including with Gateway partner agencies such as alcohol, drug and mental health services. The Gateway navigators were provided by the third sector organisation No Limits and Southampton City Council. The navigators then mentored the individual through the programme. The navigators aimed to hold three face-to-face assessments: 1 at the start, 1 in the middle and the third at the end of the participant’s 16-week caution period. During COVID-19 pandemic restrictions assessments were carried out via phone or video calls. Follow up contact was predominantly via phone, text or video calls.
Part 2. The LINX workshops
The LINX workshops aim to assist young adults in the development of cognitive and affective empathy, accept the need to change attitudes and behaviours including offending and prevent future antisocial and/or violent behaviour. The workshops took place face-to-face in a neutral venue as accessible as possible. Because of COVID-19 social distancing measures, some of the workshops were modified and delivered by telephone or video calls. Details of the differences between the LINX workshops and the LINX telephone delivery are provided in Appendix 2.
LINX workshops for Gateway use carefully constructed experiential group work tools alongside a strong visual framework, ‘Making the LINX to rebuild my life’ wall. LINX workshops seek to enable the young adult to explore and share personal feelings on a variety of issues, particularly around their life experience. The various exercises and activities throughout delivery are designed to take the young adult on a journey, enabling them to see how an experience can create a feeling, which can be translated into a set of behaviours that, for these young adults, may create risk of harm to themselves or others, and thus risk of offending.
Day one workshop
Delivered between weeks 2 and 3 post randomisation, the first event addressed: the journey of offending; sentences and out-of-court disposals; empathy, rights, respect and responsibility; impact of offending behaviour on victims/self and collateral damage to wider society; positive communication and relationship; RJ options and personal risk. Materials designed to build and develop a relationship with the young adults’ personal navigator were used so the navigator could help the young adult identify risk factors leading to further offending.
Day two workshop
Delivered between weeks 5 and 6 post randomisation, the second event focused around the ‘Making the LINX to rebuild my life’ wall, which represents the nine pathways to offending. In addition to consolidating learning and building on the young adults’ strengths, the day helped promote an understanding of resilience and the part it plays in spinning life’s plates. Day 2 also included further examinations into personal risk and protective factors; the role self-esteem plays in keeping us and others safe; and identifying how positive communication can support the study’s goals and make amends. Workshop leaders and navigators used the session to assess for gaps, the need for new goals and support to ‘keep their wall in order’. Running parallel to both sessions the leaders of the LINX workshops built on the support that the navigators gave to the young adults and reinforced the motivation needed to access other services.
Part 3. Condition to not reoffend
If a participant reoffended during the period of their caution, the HC Gateway Team could use their discretion when deciding whether to ‘breach’ the participant (see Appendix 3, Figure 10). If a participant was considered to have breached the terms of the caution, they were withdrawn from the Gateway intervention, and the investigator who originally gave the Gateway Caution considered whether to prosecute the participant for the original offence. Participants who breached their Gateway Conditional Caution continued to be approached for data collection.
Restorative justice
Restorative justice could be added to the standard conditions of the Gateway Caution after discussion and agreement with the young person: the process is victim led, but voluntary for both the victim and the offender. Through RJ, victims can communicate with their offenders and convey the impact the crime has had on them, with the intent to empower the victim. If investigators referred the young person to the RJ process, the navigators and LINX team offered support to the young person, but the actual process was managed as a separate activity. If the victim agreed to RJ conferencing, the young adult would be encouraged to engage with the victim to take positive steps and make amends for the crime committed.
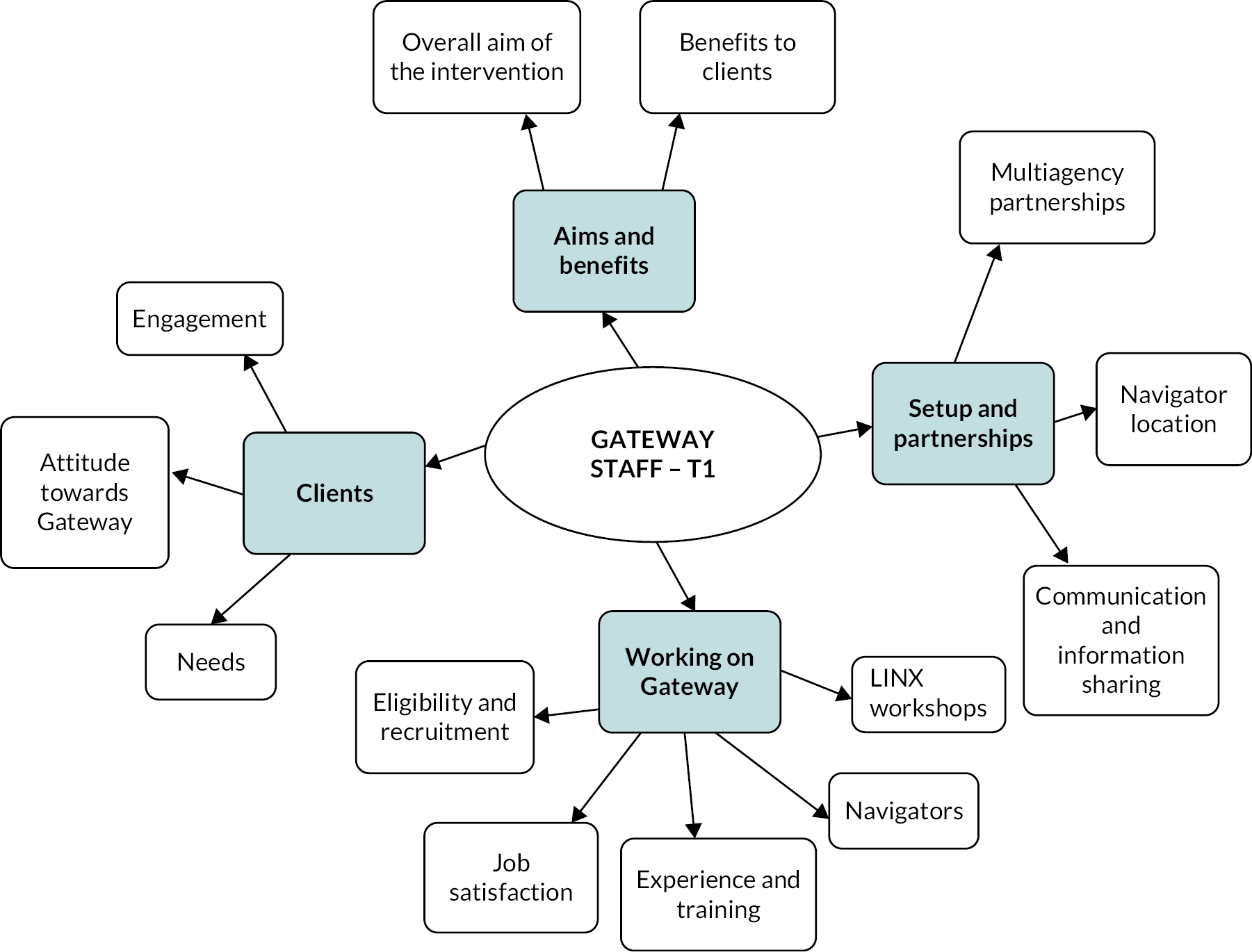
FIGURE 3.
Thematic analysis map – Gateway staff at T1.
Delivery of the Gateway programme
Delivery of the intervention was by a multiagency approach. No Limits, a third sector organisation that provides free advice, counselling, support and advocacy for under 26-year-olds, and Southampton City Council funded the Gateway navigators. Agencies accessed through the navigator triaging of needs included, The Prince’s Trust, Two Saints (housing) and local Community Mental Health Teams. Referral to these and other agencies was made where possible and appropriate.
The Hampton Trust, a third sector organisation with skills and expertise in developing community-based interventions for adults and young people, developed and delivered the LINX workshops/telephone interventions.
Restorative Solutions, a not-for-profit community interest company was commissioned by the Police and Crime Commissioner (PCC) to offer RJ options.
Comparator
The comparator was usual process. Under current guidance, for young adults aged 18–24, where there is enough evidence for prosecution (known as Full Code Test) and where the individual admits responsibility, there are various possible outcomes. For less serious offences and where the offender has a limited background of convictions, they may receive a conditional caution. For more serious offences, or where the offender has a more in-depth background in relation to criminal convictions, the offender may be charged and given a court date.
Conditional caution
A conditional caution constitutes both an in-custody and out-of-custody process. In routine practice, where an offender has committed a lower-level crime, the full code test has been met and the offender accepts responsibility for the crime; it may be more proportionate for this to be dealt with through an out-of-court disposal such as a conditional caution. The supervising officer (usually the Custody Sergeant) is in charge of making the final disposal decision. A record of conditional cautions is kept by the police, but they are not the same as a criminal conviction.
Conditions attached to conditional cautions must be appropriate, proportionate and achievable and have an element of rehabilitation and/or reparation and/or punishment. 20 Conditional cautions may have a mixture of conditions and the victim is consulted before the disposal decision is finalised. All conditions must be achievable and agreed by the offender. Examples of standard conditions include apology letters, victim awareness courses, drug diversion courses, alcohol diversion courses and fines or compensation. Drug, alcohol and victim awareness courses are provided through various organisations and the cost is charged to the offender. Conditions must be capable of being completed within 16 weeks, and in the event of non-compliance, the option of prosecuting the original offence is considered.
Examples of routine practice conditions include, victim awareness, drug or alcohol diversion courses (cost is charged to the offender), apology letters and fines or compensation. The standard length of a conditional caution is 16 weeks; all conditions must be completed within that time. If an offender fails to complete the conditions attached to the caution, they will be considered for prosecution of the original offence.
Charge
This is an in-custody process. Where a young person is arrested and brought to custody, they will be interviewed by the investigating officer. If the evidence reaches the full code test and the offender is not suitable for a conditional caution, due to the nature of the offence or their previous convictions, the offender will be charged with the offence and given a court date before release from custody.
Court summons
This is an out-of-custody process. If it is not necessary to arrest an offender, that is detain them in custody, then they are dealt with by way of voluntary interview. The offender can be interviewed under caution without arrest which means that they are free to leave at any time. When the investigating officer reaches the full code test, the file is submitted to the supervisor for a disposal decision. A summons is sent by post to the offender with a date to attend court.
Monitoring adherence to allocations
Spreadsheets within the study case management system, Huddle, provided the Police Gateway Team with oversight of the number of active clients in Gateway, numbers breached, number completed, indicators of breaches/completers, time to date in Gateway and time before breached, discretions applied, monthly recruitment and the numbers refusing participation and cases missed.
An ‘Engagement with client’ spreadsheet was maintained by navigators to record adherence data and was available in Huddle. This spreadsheet included participant ID; type of contact, date of contact, whether participant responded to contact, duration of contact in minutes, name of referring agency and comments from the navigator. Third sector organisations liaised directly with the Police Gateway Team and navigators to report engagement updates in accordance with referrals.
The Hampton Trust provided attendance registers for the LINX workshops/video/calls as these were mandatory sessions for the intervention.
Standard police monitoring of adherence to alternative conditional cautions issued to participants in the usual care group was followed and the information about the conditions and any breaches recorded.
Participant follow up
Participation in the intervention was for 16 weeks from the time of disposal. All participants were asked to take part in telephone interviews at 4-weeks, 16-weeks and 1-year post-randomisation, with flexibility on timing to accommodate the target population. Participants missing one of the data collection points were followed up at the subsequent time point unless they formally withdrew from the study or were withdrawn by the study team during COVID-19 restrictions.
Ahead of each data collection time point, up to four attempts were made to establish contact via text and calls with the participants, with the aim of providing brief information about the study and gauge their availability. If the number was clearly incorrect or out of order, no further contact was attempted. If the researchers were unsuccessful after four attempts, an e-mail was sent to the participant to say that the researchers had been trying to contact them and providing a study phone number for the participant to call. The final contact attempt for non-responders was to send a letter to the participant.
Once an appointment had been booked and the details confirmed with the participant, a text confirmation was sent to their contact mobile number, followed by reminders the day before and the day of the appointment. Discretion was applied to frequency of reminders, guided by interactions with participants.
If the participant cancelled an interview or missed it without notice, the researchers made up to four attempts to re-establish contact and reschedule. If these attempts were unsuccessful, no further attempts were made until the next data collection time point, at which time the process restarted.
The number of contact attempts was indicative, rather than prescriptive. Similarly, flexibility was exercised in relation to the timing of data collection, to accommodate participants’ and researchers’ availability. If no interviews took place at week 4, 16 and 1-year the participant was deemed lost to follow up.
Follow-up data were collected up to 31 March 2022. Attempts to contact participants eligible for week 16 and/or year 1 data collection after the 31 March 2022 were made to inform them that no further involvement was required. A £10 voucher was offered as a gesture of good will.
Incentives to participate
The study population were mostly disadvantaged young adults, faced with previous and continuous adversity, such as unemployment, substance misuse, or exposure to abuse. The study’s recruitment process acknowledged that engaging this population was likely to be challenging. Initially, as a thank you for their time, the participants received a high street shopping voucher for £10 following completion of a case report form (CRF) (see Report Supplementary Material 3). Following difficulties in getting participation in week 4 interviews during the pilot phase the researchers’ patient and public involvement (PPI) representative advised that an increased amount was likely to improve the attendance rate and completion of the CRFs.
The researchers originally intended to change the voucher format to cash at face-to-face interviews, to increase the attractiveness of the incentive. However, when COVID-19 restrictions were imposed the study was changed to telephone interviews only. To reduce selection bias, the study allowed for three different ways to deliver paper vouchers. The aim was to boost recruitment of participants with unstable living arrangements, without a bank account or lacking access to e-mail or the Internet for whatever reason, meaning they would be unable to benefit from online shopping. Delivery mechanisms included via the Gateway navigator, tracked postal delivery or via a local partner organisation.
In the pilot the researchers learnt that it was common for their target population to frequently change phone numbers, without informing the researchers, or not answer phone calls or texts. To encourage continuing study participation, the researchers increased the initial payment and applied incremental payments, with vouchers to the value of £30 for week 4, £40 for week 16 and £50 for 1-year completed interviews.
Outcomes
Primary outcome measure
The primary outcome measure was the Warwick-Edinburgh Mental Wellbeing Scale (WEMWBS). This was used to measure health and well-being among study participants. WEMWBS is a 14-item self-reported questionnaire that addresses mental health and well-being and has established valid reliable psychometric properties in adolescent populations. 21,22 Compared to other well-being indices, WEMWBS was tested for response bias and showed low correlation with both subscales of the Balanced Inventory of Desirable Responding: Impression Management (p = 0.18*) and self-deception (p = 0.35**), which make it suitable for self-report. 23 WEMWBS was self-reported at 4-weeks, 16-weeks and 1-year post-randomisation (*p < 0.05, **p < 0.01).
Secondary outcomes measures
The following were the secondary outcome measures:
-
The Short Form 12 questionnaire (SF-12) was used to report health status. The 12 items of the SF-12 provide a representative sample of the content of the eight health concepts24 and the various operational definitions of those concepts, including what respondents are able to do, how they feel and how they evaluate their health status.
-
Risky alcohol use will be measured using the Alcohol Use Disorders Identification Test (AUDIT). The AUDIT tool is a simple screening tool that is used to identify the early signs of hazardous and harmful drinking and mild dependence. AUDIT has been validated among an adolescent population. 25,26
-
Drug use will be measured using the Adolescent Drug Involvement Scale (ADIS). The ADIS was deemed most appropriate, as it captures recent/current use, and has been validated within this population age group. 27
-
Reoffending type and frequency through access to routine data: police records have been used to examine the type and frequency of offence.
-
Data on resource use, including access to primary and secondary care health services and social care, was primarily to be used to inform the cost-consequence analysis (CCA).
Secondary outcome data were self-reported at 4-weeks, 16-weeks and 1-year post-randomisation.
The secondary outcome measures used to measure reoffending type and frequency were pre-specified in both v1.0 and v1.1 of the SAP as follows:
-
The total of the number of record management system (RMS) incidents and the number of police national computer (PNC) convictions up to 1-year post-randomisation.
-
The total of the number of RMS incidents resulting in being classed as a suspect and charged/cautioned and the number of PNC convictions up to 1-year post-randomisation.
-
Charged with a ‘summary’ or ‘either way’ offence up to 1-year post-randomisation.
-
Charged with an ‘indictable only’ offence up to 1-year post-randomisation.
However, after receiving the RMS and PNC data from the police, it became clear that because the RMS data is a subset of the PNC data, there was a risk of double counting crime incidents when combining the RMS and PNC data to form the first two measures of reoffending listed above. Therefore, the first two outcome measures listed above were split into the following:
-
number of RMS incidents up to 1-year post-randomisation;
-
number of RMS incidents resulting in being classed as a suspect and charged/cautioned up to 1-year post-randomisation; and
-
number of PNC convictions up to 1-year post-randomisation.
Adverse event reporting and harms
There were no anticipated adverse events or effects. Potential distress to participants from discussing personal issues or from reflecting on their own behaviour as part of the intervention was monitored by the researchers and the experienced support/case workers delivering the intervention. Referral to appropriate support services could be made where necessary. Participants were informed that if they disclosed any information about a crime the police were unaware of, this would have to be reported to the police.
Participant change of status and withdrawal
Participants were free to withdraw from the study at any point without giving a reason. Each PIS gave information on how a participant could withdraw, including who to contact. Forms for documenting type and reason for withdrawal and other applicable change-of-status categories were available for use by the Police Gateway Team and the UoS researchers.
Participants who consented to Stage 1 but withdrew before giving Stage 2 consent had their study details completely anonymised by the University researchers where personal details had been shared and no study assessments performed.
Participants who consented to Stage 1 but declined Stage 2 consent (without withdrawing) had no study assessments performed.
For participants who withdrew following Stage 2 consent, information already obtained up to that point was retained. To safeguard the individual’s rights under UK general data protection regulation (GDPR) only the minimum personally identifiable information was retained by the Universities. Personal data remained on Huddle, managed by HC, but no longer visible to the researchers and was not downloaded or processed for the purposes of the study. Participant withdrawal after Stage 1 consent required completion of a Change of Status CRF.
Participants who decided to withdraw from the study at any stage did not undergo any further follow-up related to the study.
Loss of capacity during participation in the study
Participants who lost mental capacity after consenting to take part were withdrawn from the study.
Internal pilots
The first 6 months of trial recruitment were designed as an internal pilot to assess feasibility. The study aimed to set up three sites and recruit 50 participants during the pilot. The imposition of a national lockdown in response to the COVID-19 pandemic came at the end of the internal pilot. Progression against the criteria in Table 1 was agreed by the funders and the Study Steering Committee (SSC) and Data Monitoring and Ethics Committee (DMEC). Substantial adaptations to delivery had to be made, so the 6 months after recruitment could safely restart were viewed as a second pilot phase and further progression criteria set (see Table 1).
| Recruitment rate | Progression decision |
|---|---|
| Internal pilot 1 (October 2019–March 2020) Target: 50 participants | |
| 90% (≥ 45 participants) | SSC/DMEC to confirm continuation of recruitment for a further 21 months or until the required 334 participants have been recruited.a |
| 70%–90% (35–45 participants) | SSC/DMEC to take into account whether all the sites had been set up and consider extending the recruitment period by 1–4 months.a |
| 60%–70% (30–35 participants) | SSC/DMEC to take into account whether all the sites had been set up and consider extending recruitment period by 4–6 months.a |
| ˂ 60% (< 30 participants) | SSC/DMEC to discuss closure of the study in collaboration with the funders |
| Internal pilot 2 (September 2020–February 2021) Target: 74 participants | |
| 90% (≥ 67 participants) | SSC/DMEC to confirm continuation of recruitment for a further 17 months or until the required 334 participants have been recruited.a,b |
| 70%–90% (52–66 participants) | SSC/DMEC to take into account sites set up and consider extending the overall recruitment period by an additional 1–4 months.a,b |
| 60%–70% (44–51 participants) | SSC/DMEC to take into account sites set up and consider extending the overall recruitment period by 4–6 months.a,b |
| ˂ 60% (43 participants) | SSC to meet and discuss closure of the study, in collaboration with the funders. |
Sample size
There is no widely accepted and established minimal clinically significant difference for the primary outcome, WEMWBS. It has been suggested that a change of three or more points is likely to be important to individuals, but different statistical approaches provide different estimates ranging from three to eight points (WEMWBS user guide22). There is also variation in the standard deviation (SD) of the WEMWBS with estimates ranging from 6 to 10.828 with the pooled estimate of 10 across all studies. Assuming 90% power, 5% two-sided statistical significance, mean difference of 4 points on WEMWBS and a SD of 10, 266 participants are required. Preliminary figures from The Hampton Trust’s skills/attitudes workshops for domestic abuse (RADAR intervention) suggest a drop-out rate of approximately 15%. Conservatively, assuming a 20% attrition rate, the study aimed to recruit and randomise 334 participants.
Randomisation
Sequence generation
Participants were allocated using simple randomisation with a 1 : 1 allocation ratio. The allocation sequence was created using computer-generated random numbers in Alchemer using a randomisation sequence approved by the trial statistician. The system was tested and verified by York Trials Unit (YTU) data management and the trial statisticians during the training of police investigators, prior to the start of recruitment to the study.
Concealment mechanism
Alchemer automatically generated and recorded the random allocation when a police investigator entered details for an eligible participant. It was not possible for investigators to predict or influence the allocation.
Implementation
The allocation was generated when a police investigator entered the details of a potential participant, and they met the eligibility criteria. The allocation of Gateway conditional caution or usual process was displayed on the screen. The police investigator then informed the participant of the allocation and proceeded with disposal using the allotted allocation. A similar method for randomisation was adopted in a RCT of domestic abuse perpetrator intervention (CARA) conducted in Southampton Police District, where they were able to successfully recruit a similar population group (n = 293). 19
Blinding
Consent for eligibility screening, Gateway consideration, sharing of contact details, and randomisation was undertaken by the police investigators, none of whom are involved in data collection for the study.
Research team members at UoS, involved in obtaining Stage 2 consent and data collection, were blinded as far as possible to the allocation. The CRFs included a tick box for the researcher to indicate whether they believed blinding had been compromised during assessment, or other communications such as when booking appointments, and if so which of the allocation groups they believe the participant to be in.
The statistician was not blinded to treatment allocation.
Statistical methods
All analyses were conducted in Stata® version 17 (StataCorp LP, College Station, TX, USA), and reported in accordance with Consolidated Standards of Reporting Trials (CONSORT) guidelines. 29 Version 1.1 of the statistical analysis plan (SAP) was finalised and approved by the SSC/DMEC prior to the completion of data collection on 31 March 2022 (see Report Supplementary Material 4). Version 1.0 of the SAP outlined the planned analyses in order to assess the effectiveness of the Gateway intervention. However, once it was decided by the Trial Management Group (TMG) that due to retention and data collection rates, it was no longer feasible to assess effectiveness. Low retention rates mean a large number of participants would not be included in the primary and secondary analysis models. This is likely to introduce bias into the estimation of the treatment effect, as it is feasible that for this study population to know that whether their data that is missing is dependent on the data values themselves, for example, participants missing WEMWBS data may have lower levels of mental well-being. Version 1.1 of the SAP was therefore produced, removing all reference to formal hypothesis testing and outlining purely descriptive analyses. Continuous measures were summarised using counts, mean, SD, median, IQR, minimum and maximum. Categorical measures were summarised using counts and percentages. All participants were analysed according to their randomised group, unless otherwise stated.
Trial progression
The flow of participants from eligibility and randomisation to follow-up and analysis of the trial was presented in a CONSORT flow diagram. Reasons for ineligibility and non-consent were tabulated. The number of withdrawals and reasons for withdrawal at each time point were summarised descriptively by randomised treatment group.
Participant demographics
Participant demographics were summarised descriptively by randomised treatment group, both for all participants randomised and participants who provided the primary outcome for at least one time point. No formal statistical comparisons were undertaken between groups.
Intervention and usual care delivery
For those who received Gateway, the number of LINX workshops attended, delivery of LINX workshops, contacts attempted by the navigator, successful contacts made by the navigator and total duration of successful contacts were summarised descriptively.
For participants who were cautioned, the conditions attached to each caution were summarised descriptively by whether the participant received the Gateway conditional caution or a different caution.
Primary analysis
The primary outcome, WEMWBS, was summarised descriptively at each time point by randomised treatment group.
A challenge of working with this study population was that participants were difficult to contact, and therefore more flexibility was allowed, in terms of when a participant could complete their study questionnaire for example, if a researcher managed to contact a participant 14-weeks post-randomisation, they would still complete the 4-week CRF, even though this CRF would have been due 10 weeks earlier. However, in this scenario, the data from this CRF would have been collected closer to the 16-week follow-up due date than to the 4-week follow-up due date, and therefore rules for cut-off points were pre-specified in the SAP. Data from CRFs that did not lie in any of the pre-specified follow-up windows were not included in the primary and secondary analyses (excepting the analysis of contact data).
Secondary analyses
Treatment compliance
For participants randomised to the Gateway intervention, compliance as defined by the following definitions was summarised descriptively.
-
Minimal compliance: for a participant to be classed as having met the conditions for minimal compliance to the intervention, they should have:
-
engaged with their navigator for the initial, midway and final assessment
-
attended the two LINX workshops and
-
not been breached for reoffending during the duration of the conditional caution.
-
-
Full compliance: for a participant to be classed as having met the conditions for full compliance, they should have met the conditions for minimal compliance, and in addition engaged with external agencies organised by the navigator. Participants who met the conditions for minimal compliance, but for whom the navigator did not need to organise any interactions with external agencies, were classified as having met the conditions for full compliance.
Missing data
The amount of missing data among participants was summarised descriptively by randomised treatment group, along with reasons for missing data. The number of participants who were contactable at each time point was also summarised descriptively.
Analysis of secondary outcomes
Secondary outcomes were summarised descriptively at each time point by randomised treatment group.
Analysis of exploratory outcomes
Accommodation status was dichotomised in the following manner:
-
Homeless:
-
rough sleeping
-
sofa surfing
-
direct access (self-referral) or emergency (agency referral) hostel.
-
-
Not homeless:
-
living with parent
-
housing association
-
private tenant
-
living with extended family
-
supported accommodation
-
shared living accommodation.
-
Dichotomised accommodation status at 4-weeks and 1-year post-randomisation was summarised descriptively by randomised treatment group.
Other analyses
Number of contacts to first conversation at each follow-up time point
For each follow-up time point, for participants who were contacted using a method other than letters, the number of contacts required to be able to hold a conversation about the study with the participant was presented by randomised treatment group. In addition, information on the type of contact used was presented descriptively by randomised treatment group.
The number and proportion of participants contacted using a letter was presented by randomised treatment group. In addition, the number and proportion of participants who could not be contacted was presented by randomised treatment group.
Participants informed of their disposal decision after their 4-week follow-up was due
The number and proportion of participants, informed of their disposal decision after their 4-week follow-up was due, were presented by randomised treatment group. For each participant the number of days between date of randomisation and date of disposal was summarised descriptively, alongside whether the participant attended their 4-week follow-up.
Reporting of the use of discretion in overriding the condition to not reoffend
The number and proportion of participants in the intervention group who violated the condition to reoffend was presented. For these participants, the number for whom discretion was considered before taking the decision to breach was reported.
Index of multiple drug use
The index of multiple drug use data were summarised descriptively at each time point by randomised treatment group.
Adverse childhood experiences questionnaire
The total number of adverse childhood experiences questionnaire (ACEs) reported at 16 weeks post-randomisation was summarised descriptively by randomised treatment group.
Health economic data
Health economic CRF data were summarised descriptively by randomised treatment group at each time point.
Economic evaluation
Due to the study not reaching its recruitment and data collection targets, it was decided that a health economic analysis was not feasible.
Data collection and management
Plans for assessment and collection of outcomes
Demographic and study outcome data were recorded in paper CRFs by researchers experienced in undertaking interviews. All three of the outcome data collection CRFs included WEMWBS, SF-12, AUDIT and ADIS measurement tools as well as the health economic data questionnaire developed for the study (see Report Supplementary Material 3).
Following Stage 2 consent, the UoS researchers read out the questions and answer options as set out in the relevant CRF. Guidance was given if a question was not understood or required further clarification. The researcher hand-wrote the responses in the CRFs. Each CRF was identified with a unique participant ID, signed and dated by the researcher and posted to YTU data management in a pre-paid envelope. The UoS researchers tracked completion of each interview and CRF and YTU tracked CRFs received and the date of receipt.
A participant could be reported as withdrawing from the study either by a researcher or a member of the Gateway police team using a Change of Status CRF. The Police Gateway Team could also report a participant withdrawing from the Gateway intervention.
The study, Case Management System (Huddle), was maintained centrally by Southampton Police as a secure central location for storing documentation and linking the various sources of data for individuals together. For the purposes of analysis, data were pseudonymised, and for subsequent reports and publications, the data wholly anonymised. For the purposes of data management, once randomised, individual participants were identified using their unique study identification number, including an identifier for the site they were recruited from.
Trial data and study files were handled in accordance with good clinical practice (GCP) principles, the appropriate data management procedures and YTU standard operating procedures (SOPs).
Data entry and management
All staff involved in handling study data were trained in data protection and data security. Trial data were stored and transferred following YTU SOPs. Data were processed according to trial-specific procedures.
Paper CRFs received by the YTU data management team were scanned into OpenText Teleform, a secure form processing software application that minimises the risk of data entry errors. Data queries were raised with the UoS researchers and documented.
Data storage and archiving
Each site held data according to GDPR and Data Protection Act (Great Britain 2018); data storage was regularly reviewed to ensure compliance. Following Stage 2 consent, personal data and special category personal data were processed in connection with this study under the legal basis of Article 6(1)(e) and Article 9(2)(j) of the UK General Data Protection Regulation (GDPR), for processing for the performance of a task carried out in the public interest, and as necessary for archiving purposes in the public interest, scientific or historical research purposes or statistical purposes, with Article 9(2)(j) operating in conjunction with the safeguard requirements set out in Article 89(1) of the GDPR.
All study files were stored in accordance with GDPR guidelines. Study documents (paper and electronic) were retained in a secure (kept locked when not in use) location for the duration of the study. All essential documents, including source documents, will be retained for a minimum period of 10 years after study completion. The separate archiving of electronic data will be performed at the end of the study, to safeguard the data for the period(s) established by relevant regulatory requirements. All work will be conducted following the University of York Data Protection Policy. 30
Public involvement
Three separate approaches were used within the PPI, with the aim of representing all relevant stakeholders to ensure the research was carried out in a way that would be as effective as possible and produce meaningful outputs for those affected. These three areas were with service users (young adult offenders), victims and the public.
Patient and public involvement was embedded early on with the help of partners The Hampton Trust. Meetings with young adults on a Hampton Trust programme explored various aspects of the study, including importance, acceptability and feasibility. The groups fed back in detail around the logistics of the study: the process around consent and randomisation; ways to manage challenges following up the control arm; and opinion on assessment forms.
Once the study was underway, the PPI lead worked with partners to involve young adult representatives who had been through the Gateway programme and those who had been through the ‘usual process’. Consultation and input from these service users provided a clear understanding of the challenges and benefits that participants with and without prior experience of the criminal justice system might face. These PPI representatives worked closely with the PPI lead to develop consent forms, PISs, and initial information leaflets, plan recruitment strategies and consider the most effective ways of arranging interviews and qualitative work.
There were two public representatives on the SSC/DMEC. An ex-offender, working for Hampshire Youth Offenders Team as a peer mentor and support worker; and a victim advocate, working for a charity for victims of crime. They represented the voice of the service users and victims at Steering Group meetings, helping the group reflect on the realities of delivering the programme from the user perspective, reminding the group of some of the vulnerabilities and needs of this population, and ensuring the views of victims were considered.
These two representatives also worked closely with the study PPI lead, providing strategic input, advice and guidance throughout, with a particular focus on the logistics of getting the project underway, reviewing and adapting the protocol. The idea of a recruitment video was conceived by the ex-offender public representative, and the content was co-created with them.
Utilising links established through a local outreach programme, community leaders and members of the public were consulted. The researchers worked closely with these individuals to ensure that they understood the concerns and attitudes of the wider community. Additionally, they were able to provide input to public facing documentation and materials.
Patient and public involvement was able to help the research team consider some of the unique issues facing this vulnerable population. There were challenges, however, and PPI representatives often presented with similar chaotic lives as participants. As a result, involvement was often ad hoc or one-off, with representatives finding it difficult to commit consistently or in a longer term. Working with partners The Hampton Trust and Gateway navigators was invaluable when it came to building trust, identifying and collaborating with offending representatives.
Regulatory approvals and research governance
The outline proposal was submitted to the Hampshire Constabulary Ethics Committee, who agreed to support the study. Any subsequent ethical issues were referred for discussion by HC senior staff.
The study protocol and all associated study documents such as information sheets, consent forms, and questionnaires and subsequent amendments were submitted to the UoS Ethics and Research Governance Board for approval (ERGO Number: 31911).
Confirmation was obtained that the study did not require approvals from the Health Research Authority (HRA), Social Care or Her Majesty Prison Probation Service research ethics committees.
The governance structure for the study comprised the TMG and the independent SSC which also acted as the DMEC. The SSC/DMEC met six times during the course of the study; key meetings were to discuss the set up (October 2018), review of progression and the temporary suspension during COVID-19 restrictions (May 2020), progression following pilot 2 (April 2021) and completion of data collection for early closure of the trial (February 2022). The Chief Investigator had overall responsibility for the study, which was sponsored by the UoS. The TMG submitted regular reports to the funder, SSC/DMEC and sponsor.
Protocol changes and amendments
Protocol amendments were approved by the NIHR Public Health Research (PHR) programme manager, ethics committee and sponsor. A full list of all protocol amendments is provided in Appendix 4 and the rationale for some of the changes explained in Chapter 4.
Trial results
Overview
The first internal pilot phase began on 1 October 2019 and was due to end on 31 March 2020. However, due to social distancing and other measures introduced in response to the COVID-19 pandemic, HC temporarily halted all out-of-court disposal activities that involved face-to-face interaction on 22 March 2020. This meant conditional cautions, including the Gateway caution, were not being issued. As a result, recruitment to the study was halted and the first internal pilot phase ended on 22 March 2020. On 15 June 2020, NIHR PHR, in agreement with the SSC, indicated they would support a second internal pilot phase starting from when it was judged safe by HC and the TMG.
The summer of 2020 was spent preparing to restart the study as soon as it was deemed safe. Alternative means of delivering the intervention were developed, in particular converting the LINX group workshops to telephone delivery. In July 2020 HC confirmed their intention to restart issuing Gateway cautions during August 2020 and recruitment to the trial restarted on 7 September 2020.
Due to issues with retention of participants, recruitment ended on 13 December 2021, and data collection ended on 31 March 2022.
Site set up
Three sites were opened during the first internal pilot phase, in Southampton, Portsmouth, and Basingstoke. All three sites reopened with the addition of IoW following the study pause. Southampton, Portsmouth and Basingstoke were each open for 22 months in total, and IoW for 16 months.
Eligibility, screening and recruitment of participants
The flow of participants through the trial is reported in a CONSORT flow diagram (see Figure 1).
In total, 345 potentially eligible participants were screened, of which 47 (13.6%) were ineligible. Of the 298 (89.4%) eligible participants, 106 (35.6%) did not consent to participate. Table 2 gives reasons for ineligibility and non-consent.
| Reason for ineligibility (n = 47) | n (%) |
|---|---|
| Committed domestic crime | 8 (17.0) |
| Had no further action taken on offence | 5 (10.6) |
| Sought to be remanded in custody | 3 (6.4) |
| Committed indictable only offence | 2 (4.3) |
| Committed knife crime | 2 (4.3) |
| Committed drink-drive/traffic offence | 1 (2.1) |
| Failed to appear for caution | 1 (2.1) |
| Given adult criminal conviction | 1 (2.1) |
| Had previous serious conviction | 1 (2.1) |
| Reason not recorded in Alchemer | 23 (48.9) |
| Reason for non-consent ( n = 106) | |
| Refused study (after accepting Gateway caution) | 77 (72.6) |
| Refused Gateway caution | 5 (4.7) |
| Out of prosecution time | 2 (1.9) |
| Missed (reason unknown) | 2 (1.9) |
| Unknown | 20 (18.9) |
In total, 192 participants were randomised to the trial. One participant was randomised in error to usual process due to an error in the completion of the randomisation process, leading the custody sergeant to non-randomly assign the participant to usual process. This participant was excluded from all further analyses. Therefore, 191 participants were randomised to the trial and included in the analyses (Gateway 109; usual process 82).
Participant baseline characteristics
Baseline characteristics for all randomised participants and for all participants who provided a valid WEMWBS score for at least one time point are presented in Appendix 5, Table 16.
Thirty-nine (21.3%) participants were female, and the average age was 20.8 years old (SD 1.9 years). The vast majority of randomised participants were of white North European ethnicity (n = 170; 93.4%). The most commonly reported highest level of education among randomised participants for those who provided data (n = 110; 57.6%) was 2 or more A-levels (n = 32; 29.1%), with the next most common levels being 1–4 General Certificate of Secondary Educations (GCSEs) (n = 28; 25.5%), more than 5 GCSEs (n = 24; 21.8%) and no qualifications (n = 17; 15.5%).
The most common entry route into the study for randomised participants was via caution (n = 165; 90.7%). The median number of incidents in the police RMS that participants were involved in was 6 [interquartile range (IQR) 3 to 13]. There were 57 (31.5%) who had been involved in a RMS incident leading to a charge or caution, and 53 (29.3%) participants who had been convicted ˂ 1 year prior to randomisation.
Baseline characteristics of the randomised participants were generally well balanced between groups, with small imbalances in gender and highest level of education status.
Retention rates, calculated as number of participants consented and randomised at Stage 1 who were due to provide data compared to the number of completed WEMWEBS at March 2022 (when data collection stopped), were:
-
week 4: 49% (93 provided data of the 191 due)
-
week 16: 49% (93 provided data of the 191 due)
-
1-year: 37% (43 provided data of the 115 due).
Recruitment and data collection rates for each of the pilots and the main trial are presented in Table 3.
| Time point | Screened | Eligible | Target for period | Randomised (% of target) | Week 4 data | Week 16 data | 1-year data |
|---|---|---|---|---|---|---|---|
| Pilot 1 (Oct 2019–March 2020) | 70 | 57 | 50 | 35 (70.0) | Due: 32 | Due: 16 | Due: 0 |
| Collected: 14 (43.8%) | Collected: 5 (31.3%) | Collected: N/A | |||||
| Pilot 2 (Sept 2020–Feb 2021) | 105 | 99 | 74 | 64 (86.4) | Due: 87 | Due: 58 | Due: 31 |
| Collected: 37 (42.5%) | Collected: 19 (32.8%) | Collected: 7 (22.6%) | |||||
| Main trial (March 2021–April 2021) | 170 | 142 | 140 | 93 (66.4) | Due: 192 | Due: 192 | Due: 115 |
| Collected: 95 (49.5%) | Collected: 96 (50.0%) | Collected: 43 (37.4%) | |||||
| Totals | 345 | 298 | 264 | 192 (72.7) | Due: 192 | Due: 192 | Due: 115 |
| Collected: 95 (49.5%) | Collected: 96 (50.0%) | Collected: 43 (37.4%) |
Randomised participants and randomised participants who provided a valid WEMWBS score for at least one time point had similar distributions of the following baseline characteristics: age, gender, ethnicity, Index of Multiple Deprivation, entry route, RMS incidents involved in and RMS incidents leading to charge or caution. However, there was a larger imbalance between groups in having been previously convicted in randomised participants who provided a valid WEMWBS score, compared to the randomised participants. The distribution of marital status and highest level of education were very similar between the randomised participants and randomised participants who provided a valid WEMWBS score. However, this is because marital status and highest level of education were collected via CRFs and could be collected at either 4-weeks, 16-weeks or 1-year post-randomisation only. The WEMWBS was also collected at these time points, and therefore if a participant provided a valid WEMWBS score then in the vast majority of cases they also provided their marital status and highest level of education.
Intervention and usual process delivery
Of the 109 participants randomly assigned to Gateway, 104 (95.4%) received Gateway, while for the 82 randomly assigned to usual process, 81 (98.8%) received usual process.
Of the five participants who did not receive Gateway, despite being randomly assigned to Gateway, four received a standard caution. Of the 81 participants who were randomly assigned to and received usual process, 76 (93.8%) entered the study via the caution route. Therefore 105 participants received a Gateway caution, and 80 received a standard caution. Table 4 provides information on the caution conditions attached, presented by the type of caution received.
| Gateway conditional caution (n = 105) | Usual process (n = 80) | |
|---|---|---|
| Conditions attached (multiple conditions possible), n (%) | ||
| Standard Gateway conditions (no additional conditions added) | 85 (81.0) | N/A |
| None (simple caution) | N/A | 5 (6.3) |
| Compensation | 18 (17.1) | 20 (25.0) |
| Letter of apology | 5 (4.8) | 10 (12.5) |
| Victim awareness course | 0 (0) | 14 (17.5) |
| Alcohol diversion course | 0 (0) | 11 (13.8) |
| Drugs diversion course | 0 (0) | 16 (20.0) |
| Not to enter specific premises | 0 (0) | 1 (1.3) |
| Fine | 0 (0) | 5 (6.3) |
| Women and Desistance Empowerment programme | 0 (0) | 9 (11.3) |
| Restorative justice | 0 (0) | 0 (0) |
The Gateway conditional caution was delivered as planned up until 23 March 2020, when the study was paused due to COVID-19. All activities relating to conditional cautions were also paused by HC on this date. The Gateway conditional caution restarted in August 2020 and recruitment to the trial in September 2020, with full remote working and no face-to-face contact with participants. This included converting the LINX workshops to delivery by telephone. Face-to-face working returned in May 2021, where appropriate and risk assessed.
Of the 105 participants who received Gateway, navigator logs were received for 76 (72.4%). Table 5 presents information on delivery of the Gateway intervention. There are four participants for whom the number of LINX workshops attended is unknown due to the participant withdrawing before Stage 2 consent was obtained or having withdrawn after giving Stage 2 consent.
| Received Gateway conditional caution (n = 105) | |
|---|---|
| LINX workshops attended (supplemented with change of status data) | |
| Number with data, n (%) | 101 (96.2) |
| 0 (Did not attend LINX workshops due to COVID-19 pause) | 4 (4.0) |
| 0 (participant chose not to attend LINX workshops) | 8 (7.9) |
| 1 (participant chose not to attend LINX workshop) | 1 (1.0) |
| 2 | 88 (87.1) |
| Delivery of LINX workshops | |
| Number with data, n (% of those who attended at least one workshop) | 80 (89.9%) |
| Face to face | 45 (56.3) |
| Telephone | 35 (43.8) |
| Contacts attempted by navigator (excluding LINX workshops) | |
| Number with data, n (%) | 76 (72.4) |
| Mean (SD) | 52.8 (25.0) |
| Median (IQR) | 42 (39–63) |
| Minimum, Maximum | 22, 168 |
| Successful contacts made by navigator (excluding LINX workshops) | |
| Number with data, n (%) | 76 (72.4) |
| Mean (SD) | 26.0 (20.7) |
| Median (IQR) | 19 (15–31) |
| Minimum, Maximum | 0, 108 |
| Total duration of successful contacts, minutes | |
| Number with data, n (%) | 70 (66.7) |
| Mean (SD) | 761.5 (594.6) |
| Median (IQR) | 626.5 (380–978) |
| Minimum, Maximum | 36, 2785 |
Primary analysis
Table 6 reports the WEMWBS score at 4-weeks, 16-weeks and 1-year post-randomisation. The WEMWBS score can take values between 14 and 70, where higher scores indicate a better state of mental health and well-being. The WEMWBS, SF-12, AUDIT and ADIS data for one participant in the Gateway group was excluded at week 4 due to the questionnaire being completed too early, while at week 16 the data for two participants in the Gateway group were excluded due to the questionnaires being completed too late.
| Gateway conditional caution (n = 109) | Usual process (n = 82) | |
|---|---|---|
| Week 4 | ||
| Number with data, n (%) | 57 (52.3) | 36 (43.9) |
| Mean (SD) | 44.1 (9.6) | 44.9 (7.2) |
| Median (IQR) | 45 (38–52) | 44 (41–49) |
| Minimum, Maximum | 19, 61 | 28, 62 |
| Week 16 | ||
| Number with data, n (%) | 54 (49.5) | 39 (47.6) |
| Mean (SD) | 48.6 (9.9) | 46.0 (8.5) |
| Median (IQR) | 49 (42–55) | 47 (40–53) |
| Minimum, Maximum | 27, 67 | 30, 60 |
| Year 1 | ||
| Number with data, n (%) | 27 (24.8) | 16 (19.5) |
| Mean (SD) | 48.4 (9.7) | 45.7 (7.0) |
| Median (IQR) | 49 (41–54) | 45.5 (41.5–50.5) |
| Minimum, Maximum | 29, 68 | 28, 58 |
Secondary analyses
Treatment compliance
Of the 105 participants randomly allocated to the Gateway conditional caution who did not withdraw before Stage 2 or withdraw Stage 2 consent, 81 (77.1%) met the definition for minimal compliance. Thirteen participants did not meet minimal compliance due to not attending the two LINX workshops, six did not meet minimal compliance due to breaching the condition to not reoffending during the period of the caution and five were given usual process despite being randomly assigned to the Gateway conditional caution.
No participants were withdrawn from the Gateway conditional caution because they failed to engage with partner/referral agencies identified by the navigator, therefore the number of participants meeting full compliance is 81 (77.1%).
Analysis of secondary outcomes
Table 7 reports the participant-reported secondary outcomes at 4-weeks, 16-weeks and 1-year post-randomisation. The SF-12 mental component can take values between 0 and 100, with higher scores indicating a better level of mental health. The SF-12 physical component can take values between 0 and 100, with higher scores indicating a better level of physical health. The AUDIT score can take values between 0 and 40, with higher scores indicating higher levels of hazardous and harmful alcohol use. The ADIS score can take values between 0 and 184, with higher scores indicating higher levels of drug involvement.
| Gateway conditional caution (n = 109) | Usual process (n = 82) | |
|---|---|---|
| SF-12 Mental Component | ||
| Week 4 | ||
| Number with data, n (%) | 57 (52.3) | 36 (43.9) |
| Mean (SD) | 42.4 (12.0) | 43.5 (9.7) |
| Median (IQR) | 43.6 (35.7–53.1) | 43.8 (36.8–51.9) |
| Minimum, Maximum | 15.1, 58.8 | 22.1, 58.8 |
| Week 16 | ||
| Number with data, n (%) | 54 (49.5) | 39 (47.6) |
| Mean (SD) | 47.7 (7.6) | 45.0 (9.1) |
| Median (IQR) | 47.7 (41.7–54.6) | 45.8 (38.7–52.7) |
| Minimum, Maximum | 34.3, 58.8 | 20.7, 58.1 |
| Year 1 | ||
| Number with data, n (%) | 27 (24.8) | 16 (19.5) |
| Mean (SD) | 47.5 (7.5) | 46.1 (8.6) |
| Median (IQR) | 47.7 (39.5–54.6) | 47.5 (44.4–51.8) |
| Minimum, Maximum | 34.3, 58.8 | 20.7, 58.1 |
| SF-12 Physical Component | ||
| Week 4 | ||
| Number with data, n (%) | 57 (52.3) | 36 (43.9) |
| Mean (SD) | 54.5 (5.3) | 52.8 (6.7) |
| Median (IQR) | 55.5 (53.7–57.4) | 55.2 (51.2–56.8) |
| Minimum, Maximum | 36.8, 63.9 | 30.8, 59.2 |
| Week 16 | ||
| Number with data, n (%) | 54 (49.5) | 39 (47.6) |
| Mean (SD) | 52.5 (6.4) | 53.4 (5.7) |
| Median (IQR) | 54.5 (51.7–56.0) | 55.2 (52.4–56.9) |
| Minimum, Maximum | 26.1, 59.4 | 38.0, 60.1 |
| Year 1 | ||
| Number with data, n (%) | 27 (24.8) | 16 (19.5) |
| Mean (SD) | 51.9 (7.9) | 53.5 (6.3) |
| Median (IQR) | 54.5 (51.7–56.5) | 55.3 (52.5–58.2) |
| Minimum, Maximum | 26.1, 59.4 | 38.0, 58.9 |
| AUDIT | ||
| Week 4 | ||
| Number with data, n (%) | 57 (52.3) | 36 (43.9) |
| Mean (SD) | 12.9 (9.2) | 11.2 (7.5) |
| Median (IQR) | 11 (5–19) | 10.5 (5.5–16.5) |
| Minimum, Maximum | 0, 34 | 0, 28 |
| Week 16 | ||
| Number with data, n (%) | 54 (49.5) | 39 (47.6) |
| Mean (SD) | 11.6 (8.1) | 11.6 (8.7) |
| Median (IQR) | 9.5 (5–15) | 10 (4–16) |
| Minimum, Maximum | 0, 32 | 0, 36 |
| Year 1 | ||
| Number with data, n (%) | 27 (24.8) | 16 (19.5) |
| Mean (SD) | 11.1 (8.5) | 13.3 (8.3) |
| Median (IQR) | 8 (5–20) | 12.5 (8–17) |
| Minimum, Maximum | 0, 30 | 1, 30 |
| ADIS | ||
| Week 4 | ||
| Number with data, n (%) | 57 (52.3) | 36 (43.9) |
| Mean (SD) | 46.9 (33.6) | 45.1 (36.5) |
| Median (IQR) | 38 (25–59) | 37.5 (12–76.5) |
| Minimum, Maximum | 0, 137 | 0, 111 |
| Week 16 | ||
| Number with data, n (%) | 54 (49.5) | 39 (47.6) |
| Mean (SD) | 40.9 (36.3) | 37.2 (38.2) |
| Median (IQR) | 36.5 (15–52) | 31 (0–67) |
| Minimum, Maximum | 0, 137 | 0, 111 |
| Year 1 | ||
| Number with data, n (%) | 27 (24.8) | 16 (19.5) |
| Mean (SD) | 48.7 (36.1) | 50.5 (39.0) |
| Median (IQR) | 40 (23–68) | 38.5 (20.5–86) |
| Minimum, Maximum | 0, 134 | 0, 111 |
Table 8 reports the secondary outcomes measuring reoffending. Of the 191 randomised participants, 129 (67.5%) had reached the 1-year follow-up before their RMS data was extracted by HC on 23 June 2022 [Gateway conditional caution 74 (67.9%); usual process 55 (67.1%)], and therefore could be included in the analysis of total number of RMS incidents at 1-year post-randomisation.
| Gateway conditional caution (n = 109) | Usual process (n = 82) | |
|---|---|---|
| RMS incidents involved in up to 1-year post-randomisation | ||
| Number with data, n (%) | 74 (67.9) | 55 (67.1) |
| Mean (SD) | 9.3 (12.2) | 12.2 (23.7) |
| Median (IQR) | 5 (1–14) | 5 (1–11) |
| Minimum, Maximum | 0, 61 | 0, 132 |
| Total number of RMS incidents resulting in being classed as a suspect and charged/cautioned up to 1-year post-randomisation | ||
| Number with data, n (%) | 74 (67.9) | 55 (67.1) |
| Mean (SD) | 0.4 (1.2) | 0.8 (2.9) |
| Median (IQR) | 0 (0–0) | 0 (0–0) |
| Minimum, Maximum | 0, 7 | 0, 20 |
| Total number of PNC convictions up to 1-year post-randomisation | ||
| Number with data, n (%) | 72 (66.1) | 53 (64.6) |
| Mean (SD) | 0.4 (0.8) | 0.4 (0.9) |
| Median (IQR) | 0 (0–0) | 0 (0–0) |
| Minimum, Maximum | 0, 3 | 0, 5 |
| Charged with an ‘indictable only’ offence up to 1-year post-randomisation | ||
| Number with data, n (%) | 72 (66.1) | 53 (64.6) |
| Charged | 0 (0) | 0 (0) |
| Not charged | 72 (100) | 53 (100) |
Of the 191 randomised participants, 125 (65.4%) had reached the 1-year follow-up before their PNC data were extracted by HC between 4 May 2022 and 16 June 2022 [Gateway conditional caution 72 (66.1%); usual process 53 (64.6%)]. The 10 participants who withdrew before/after Stage 2 consent, declined Stage 2 consent, or lost mental capacity did not have their RMS/PNC data reported.
Of the 32 participants in the Gateway conditional caution group who had been in the study ˂ 1 year, 2 (6.3%) had been charged with a ‘summary’ or ‘either way’ offence, while of the 24 participants in the usual process group, 2 (8.3%) had been charged. For the 56 participants who had been in the study ˂ 1 year, the mean time between date of randomisation and date of data extraction was 286.9 days (SD 56.7 days).
Analysis of exploratory outcomes
Table 9 reports accommodation status at 4-weeks and 1-year post-randomisation.
| Gateway conditional caution (n = 109) | Usual process (n = 82) | |
|---|---|---|
| Week 4 | ||
| Number with data, n (%) | 57 (52.3) | 36 (43.9) |
| Homeless | 8 (14.0) | 3 (8.3) |
| Not homeless | 49 (86.0) | 33 (91.7) |
| Year 1, n (%) | ||
| Number with data, n (%) | 27 (24.8) | 15 (18.3) |
| Homeless | 3 (11.1) | 0 (0) |
| Not homeless | 24 (88.9) | 15 (100) |
Other analyses
Participants informed of their disposal decision after their 4-week follow-up was due
Of the 191 randomised participants, 15 (7.9%) were informed of their disposal decision after their 4-week follow-up was due [Gateway 12 (11.1%); usual process 3 (3.7%)]. Table 10 gives information on the time between disposal and randomisation and whether the 4-week follow-up was completed for those informed of their disposal decision after their 4-week follow-up was due. Data are not presented for those in the usual process group due to there only being three participants and as a result there being a risk of data disclosure.
| Gateway conditional caution (n = 12) | Usual process (n = 3) | Total (n = 15) | |
|---|---|---|---|
| Time between randomisation and disposal, days | |||
| Number with data (%) | 12 (100) | 3 (100) | 15 (100) |
| Mean (SD) | 49.6 (18.1) | N/A | N/A |
| Median (IQR) | 42 (34.5–67.5) | N/A | N/A |
| Minimum, Maximum | 29, 77 | N/A | N/A |
| Attended 4-week follow-up, n (%) | |||
| Number with data (%) | 12 (100) | 3 (100) | 15 (100) |
| Yes | 8 (66.7) | N/A | N/A |
| No | 4 (33.3) | N/A | N/A |
Reporting of the use of discretion in overriding the condition to not reoffend
Of the 105 participants who received the Gateway conditional caution who did not withdraw before Stage 2 or withdraw Stage 2 consent, 8 (7.6%) reoffended during the period of the conditional caution. There were two (25.0%) participants for whom discretion was considered before taking the decision that they were in breach of the condition not to reoffend. Due to the risk of data disclosure further information is not provided.
Index of multiple drug use
Table 11 gives information on the index of multiple drug use.
| Gateway conditional caution (n = 109) | Usual process (n = 82) | |
|---|---|---|
| Week 4 | ||
| Number with data, n (%) | 57 (52.3) | 36 (43.9) |
| Mean (SD) | 23.3 (6.4) | 21.3 (5.0) |
| Median (IQR) | 22 (18–27) | 21.5 (16.5–25) |
| Minimum, Maximum | 15, 42 | 15, 31 |
| Week 16 | ||
| Number with data, n (%) | 54 (49.5) | 39 (47.6) |
| Mean (SD) | 23.3 (7.5) | 22.3 (5.9) |
| Median (IQR) | 21 (17–27) | 22 (16–25) |
| Minimum, Maximum | 15, 47 | 15, 38 |
| Year 1 | ||
| Number with data, n (%) | 27 (24.8) | 16 (19.5) |
| Mean (SD) | 25.2 (7.7) | 25.8 (6.3) |
| Median (IQR) | 23 (18–31) | 25.5 (21–28.5) |
| Minimum, Maximum | 16, 41 | 16, 38 |
Adverse childhood experiences
Table 12 gives information on adverse childhood experiences.
| Gateway conditional caution (n = 109) | Usual process (n = 82) | |
|---|---|---|
| Number of adverse childhood experiences | ||
| Number with data (%) | 54 (49.5) | 39 (47.6) |
| Mean (SD) | 3.0 (2.6) | 3.6 (3.0) |
| Median (IQR) | 2 (1–5) | 4 (1–5) |
| Minimum, Maximum | 0, 10 | 0, 11 |
Health economic data
Health economic data were collected for the following items self-reported as used by participants over the month prior to the data collection point: employment; number of GP visits; use of drug/alcohol services; attendance at accident and emergency; admission to hospital as inpatient; use of community mental health team; use of psychiatric services as in-patient; use of prescribed medications; and reason for using prescribed medications. The data are presented in Appendix 6, Table 17.
Patient public involvement
Young adult offenders represent a vulnerable population with a range of complex and overlapping needs. Recruitment and retention in this cohort is a known challenge, often attributed to these vulnerabilities and chaotic lives. 31,32 For this reason, PPI was considered vital for the success of the study but would come with its own set of unique challenges.
For public involvement to be a meaningful part of the Gateway study, it was essential to invest in strategies to involve this seldom-heard group, rather than PPI members with no real experience of the criminal justice process or the challenges of taking part in research while navigating other lifestyle priorities and vulnerabilities. To address this, the research team took a ‘needs based, place based’ approach to PPI and engagement, respecting the skills and knowledge of partners who have a record of working with this population. The study’s strategy therefore involved user, victim and community engagement.
User involvement (young adults with offending experience)
Working in collaboration with The Hampton Trust, the PPI lead sought extensive involvement from young adults currently undertaking the Gateway, or other similar, programmes. The research team and the NIHR Research Design Service PPI lead attended existing workshops for young adult offenders being run by The Hampton Trust, ‘tagging on’ a PPI session at the end. By going into the community, and working around sessions these individuals were already attending, this vulnerable and seldom-heard group were able to contribute in a way that worked for them. The groups fed back in detail around the logistics of the study including the process around randomisation and consent; and ways to manage challenges following up the control arm.
Additionally, a peer support mentor, who had his own experience of offending when younger, was identified through partner links and became a named public contributor on the bid providing a consistent voice from the service user perspective.
Much of the feedback focused on recruitment and retention, which were some of the key challenges the study faced. Contributions from PPI members included advice around incentives (which vouchers would be most appealing for participants), advice on how the team should discuss confidentiality and data protection, and how data were collected to make it as easy and as least threatening and burdensome for participants.
The PPI collaborator suggested use of a video to explain the study, as he knew this cohort would access information in video format more easily than on paper. He then worked alongside the PPI lead to co-develop a recruitment video, ensuring the content was accessible and relevant.
Victim involvement
The charity Aurora New Dawn became partners, and the PPI lead worked closely with named staff within the charity to ensure victims, views and preferences were represented. A member of the charity sat on the SCC, providing PPI from a victim perspective at a governance level within the study.
Community PPI
It was recognised that a rehabilitative approach to crime and punishment can sometimes be controversial, and might be seen as ‘light touch’ by some members of the public. As a result, it was considered essential to consistently consult and collaborate with local communities to understand their concerns, and how best to address and mitigate these.
Linking with regional outreach programmes in other marginalised and less well-represented communities allowed perspectives from a broad range of diverse community groups to be included throughout the study. This involved seeking input from members of black and minority ethnic, lesbian, gay, bisexual, and transgender+, lower socioeconomic, parents and religious groups. This feedback helped inform outward-facing content and helped shape how the team presented information about the Gateway programme and study. Feedback included the importance of focusing on the potential long-term economic benefits of a programme like Gateway, as well as being clear about some of the benefits to wider society in addressing root causes of criminal behaviour.
Summary of trial
The aim of the trial was to evaluate the effectiveness and cost-effectiveness of the Gateway programme, however, the study was unable to obtain sufficient data to undertake any formal hypothesis testing. Similarly, health economic analysis was not appropriate. In the face of consecutive challenges, the researchers have demonstrated that it is possible to recruit and randomise to a RCT in the police setting. The researchers also identified and tested implementation of different approaches to include young people who have committed an offence in research, known to be a difficult group to engage. By working in close collaboration with HC, and their two project dedicated officers, the researchers were able to make pragmatic adjustments to the study design as issues arose. For example, developing a successful approach to recruitment and randomisation by police investigators that included a two-stage consent process. Also, revising the inclusion criteria to encompass all those that HC would consider issuing a Gateway caution to as routine practice. The problems encountered throughout this trial and the team’s endeavours to overcome them are detailed in Chapter 4.
Of those recruited, 191 participants were randomised to the trial (Gateway 109; usual process 82) and included in the descriptive analyses. Although recruitment rates were within the study progression criteria, the number of randomised participants providing data was insufficient to complete the trial (week 4: 49%; week 16: 49%; 1-year: 37%).
Baseline characteristics of the randomised participants were generally well balanced between groups, with small imbalances in gender and highest level of education. Randomised participants and randomised participants who provided primary outcome data at least once, had similar distributions of: age, gender, ethnicity, marital status, level of education, Index of Multiple Deprivation, entry route, RMS incidents involved in, and RMS incidents leading to charge or caution. However, more randomised participants who provided a valid WEMWBS score had a previous conviction compared to the randomised participants.
Participants who attended data collection interviews completed all parts of the WEMWBS, SF-12, AUDIT and ADIS instruments at all time points. Allocation does not appear to have been a significant factor in whether participants attended data collection interviews or not, with similar percentages of those allocated to each arm providing data. Data collection rates show that telephone interviews were acceptable to those willing to share an active telephone number. Rates for those who were non-contactable were similar between the groups at all three time points.
Attempts to contact participants paid off in some cases, but contact dropped off at a similar rate over time in both groups.
Eighty-one of the 105 (77%) participants randomly allocated to the Gateway conditional caution complied with the intervention. Reoffending and non-attendance at the LINX workshops were the reasons for non-compliance.
Although the researchers were able to recruit and randomise 191 participants, the high proportion of participants for whom they did not obtain data at each time point meant there was a high risk of attrition bias. Therefore, an accurate estimate of the effectiveness of the intervention could not be obtained, and as a result statistical hypothesis testing was not carried out.
Chapter 3 Qualitative evaluation
A qualitative evaluation was conducted within the overall study to assess the quantity and quality of what was being delivered through the Gateway intervention and to assess the generalisability of its effectiveness. The qualitative evaluation was informed by the MRC guidance on process evaluation of complex interventions33 which suggests focusing on implementation, mechanisms and context.
Specific research questions in the qualitative evaluation were:
-
How is Gateway being implemented?
-
What are the barriers to its implementation and effects?
-
What are the mechanisms through which the intervention brings about change?
-
How do different delivery methods (face-to-face/virtual/telephone) influence the above questions?
Interim findings from the qualitative evaluation were reported at TMG meetings to inform trial processes and procedures where challenges were faced.
Methods
The study was carried out as a longitudinal study using qualitative interviews with:
-
Young people with personal experience of receiving the Gateway intervention, herein referred to as ‘Gateway clients’ or ‘young people’.
-
Stakeholders involved in the design and delivery of the Gateway intervention, herein referred to as ‘Gateway staff’.
-
Police officers and civilian staff responsible for offering the Gateway programme and recruiting into the trial, herein referred to as ‘Gateway recruiters’.
Data collection took place across three time periods during the implementation of the Gateway programme.
-
Time period 1 (T1) spanned the first 14 months after the intervention was introduced, September 2018–November 2019. Navigator focus groups and interviews with the LINX facilitators and Gateway police officers also had three separate time points T1-1, T1-2 and T1-3, due to being repeated three times during T1.
-
Time period 2 (T2) was July 2020–September 2020.
-
Time period 3 (T3) covered November 2021–May 2022.
Qualitative methods (T1, T2, T3)
Figure 2 shows the conceptual framework developed using evidence from the literature review (see Report Supplementary Material 1). This was used to inform the qualitative evaluation methods.
Sampling, participants and recruitment
An overview of the qualitative evaluation is provided in Table 13.
| Time period | Qualitative method of data collection | Qualitative participant category and ID reference | Timing of qualitative data collection |
|---|---|---|---|
| T1 | Focus groups | Navigators (FG-N) | T1-1 December 2018 T1-2 March 2019 T1-3 May 2019 |
| Semistructured interviews | LINX facilitators (L) and Gateway police officers (P) | T1-1 March 2019 T1-2 May–June 2019 T1-3 July–August 2019 |
|
| Semistructured interviews | Service managers (SM) | June 2019 | |
| Semistructured interviews | Navigators (N) | June–July 2019 | |
| T2 | Semistructured interviews | Gateway clients (GC) | July–August 2020 |
| T3 | Semistructured interviews | Gateway staff (S): navigators (N), LINX facilitators (L) and police officers (P) | November 2021–February 2022 |
| Semistructured interviews | Gateway clients (C) | March–April 2022 | |
| Semistructured interviews | Gateway HC recruiters (R) | March–May 2022 |
Due to the small number of participants within the Gateway staff (S) category and potential sensitivity of the data collected, extra care is required to protect identity of the participants. The following citing approaches were used:
-
Participants’ job roles were indicated by the ID references, such as N, L or P, next to their quotations. This applied when the role was already suggested by the quote or when the knowledge of the role would be helpful for interpretation of the views expressed.
-
When the above considerations do not apply, the Gateway staff will be referred to by the letter S and a number, without an indication of their job role.
Gateway staff
Interviews with the Gateway project staff were conducted in the formats of semistructured interviews and focus groups took place over T1 and T3. The categories of participants included Gateway navigators, LINX practitioners, service managers who line managed the navigators and police staff leading on the Gateway project. Conducting a qualitative evaluation, at regular intervals with the Gateway project staff, served to assess the integrity of the programme34 that was being offered for young people enrolled onto Gateway, including insight into the fidelity of the intervention,35 or adherence to protocols and guidelines. The interviews were conducted by four researchers, allowing for investigator triangulation.
For qualitative evaluation at both T1 and T3, purposive sampling was used to recruit participants who would be able to provide relevant data due to their job role prior to the interview. Semistructured one-to-one interviews or focus group discussions were undertaken depending on the job role of the individual. Since navigators had the same role in delivering the Gateway intervention, focus groups were undertaken, to explore shared perspectives, such as their understanding of what Gateway aims to achieve or how they worked as a team. During T1, interviews took place face-to-face. Interviews and focus groups took place at Southampton Central Police Station, except one interview with one of the navigators, which took place at the UoS. T3 took place during the COVID-19 pandemic, with the interviews taking place in video and audio calls on Microsoft Teams.
Across both time periods, all the Gateway staff in post at the time were invited for interview, and all were subsequently interviewed. At T1, a total of 11 Gateway project staff participated: 4 navigators, 2 LINX facilitators, 2 police officers and 3 service managers. At T3, there were a total of eight participants: three navigators, three LINX facilitators and two police officers. As some of the staff remained the same and some changed, this constituted a total of 17 individuals. The experience at T1 showed that the service managers, who acted as line managers to the navigators, had no direct involvement in Gateway, and these interviews were not repeated at T3.
Young people
Interviews with young people who had personal experience of the Gateway programme were conducted at T2 and T3. All young people who had been enrolled onto the Gateway programme were considered eligible to take part in the study. Due to known challenges recruiting from this population36 participants were identified through purposive stratified sampling with the support of navigators who had permission to make contact via telephone. At T2 and T3, navigators ensured that they identified individuals who had both completed or not completed the programme (breach status) and included a gender mix of female and male participants. T2 and T3 took place during the COVID-19 pandemic, with the interviews taking place over the telephone and in audio calls on Microsoft Teams. Across both time periods, a total of 28 participants were interviewed.
Gateway recruiters
This strand of work was conducted at T3. A sample of police recruiters was invited for interviews, in order to specifically explore the barriers and enablers which influenced the ability and motivation to recruit into the trial.
Hampshire Constabulary officers and civilian staff who, since restart of the study post-COVID-19 modifications, had recruited two or more people each, as well as those who missed at least two young people, were identified and invited to take part by the Gateway Project Support Sergeant. A total of 13 police recruiters were interviewed.
Data analysis
Using an inductive approach, reflexive thematic analysis was conducted whereby themes were identified, examined and summarised by an individual coder through an iterative process. The research questions were set before data collection began. However, codes were only created and edited after completion of data collection, during analysis. The themes were formed on the basis of the core ideas that unified participant opinions, which were freely expressed by participants in response to prompts. The type of analysis used was in the tradition of the reflexive thematic analysis, whereby the researcher subjectivity is openly acknowledged. However, the naming of the themes in places tended to be more representative of topic names, rather than acting as an expression of core ideas. This was in part due to the large collection of insights which would not necessarily fit under one idea at the theme level. Data analysis was conducted independently, for each group of participants, at each time period (e.g. clients at T1). Multiple coding was used for a proportion (up to 10%) of the total interviews. As per contemporary approaches to reflexive thematic analysis, the use of multiple coders for a proportion of the data helped check whether interpretations were logical and reasonable, and compare assumptions, rather than achieve a consensus. 37–39 This enabled a more thorough understanding and appreciation of the meaning in the data. The analysis followed the process outlined by Braun and Clarke. 37 An example of how this was applied to the qualitative interviews with young people at T2 is given in Appendix 7.
Results
Time period 1 – Gateway staff
Many of the Gateway staff were already known to members of the research team so individuals were contacted directly. The interviews were conducted by JF, a female professor of criminology and experienced qualitative researcher, AQ, a male post-doctoral researcher in criminology, and SM, a female lecturer in public health. SM and AQ had some experience of qualitative research at the time of interviewing. AQ and SM facilitated the focus groups with the navigators. AQ transcribed the interviews. AQ, SM and IW, a female clinical research fellow in public health, coded the interviews. Several data analysis meetings were held to discuss aspects of the coding.
At the time of interview, all interviewers reported their role at the university and involvement in the study. Given that the researchers in the evaluation team were known to many of the participants, and the evaluation team were academic partners in the project, there would have been some pre-existing beliefs, understanding and ideas around the programme which influenced the types of questions that were asked. All the Gateway staff interviewed at T1, except one HC participant, were female.
The main themes and subthemes are presented in a thematic analysis map in Figure 3. Four key themes were identified: aims and benefits, setup and partnerships, delivery of the intervention and client-related reflections. Quotes from interviews with Gateway staff at T1 that support these themes and subthemes are provided in Report Supplementary Material 5, Table 1.
Theme 1: Aims and benefits
The first theme described what the intervention set out to achieve, what benefits they could already observe clients deriving from the programme, and what they hoped they might derive in the future. This was used in part as an icebreaker and, universally, the staff were comfortable and correctly identified aims and benefits of the intervention, citing reducing reoffending and improving their life chances, albeit without necessarily referring to any other outcomes (L2-2).
Subtheme: overall aim of the intervention
Desistance can be defined as abstaining from offending by individuals who previously engaged in such. 40 Desistance was described as the ultimate aim of the Gateway programme, which was understood to provide stability for young people, which would help reduce reoffending. The complex needs of some of the Gateway clients were acknowledged by Gateway staff (FG1-N2).
For high-need individuals, Gateway offered the support where, previously, they often had received very little. The notion of filling a void was prominent, especially in relation to care leavers (N1).
Subtheme: benefits to clients
When asked what benefits Gateway brought to the service users, Gateway staff described their personal experiences working with clients. Despite it being ‘early days’ at T1, they described beneficial results, with some exceptions. For example, with clients for whom this type of support was insufficient to make a difference (N1).
In terms of the benefits that were directly, and immediately, experienced by the clients, the staff felt that Gateway answered the otherwise unfulfilled young people’s need to have someone to talk to – someone who would listen without judgment, including on topics that they would not be able to talk about to anyone else. This open conversation started from the time of the initial assessment (FG1-N1). Young people had reported to the staff the feeling of being believed in, which was triggered by the support within Gateway and was instrumental in building their self-esteem (L2-2). They also provided feedback that they were more comfortable around new people following completion of the LINX workshops. It was taken as a sign that they would be more likely to ask for help, which, in the eyes of the staff, was a positive development (L2-3). Another benefit was that of being dealt with out-of-court and without prosecution; not receiving a criminal conviction mattered (FG1-N4).
The navigators were able to offer practical support to enable the clients to pursue employment or educational opportunities, or secure housing. It was humbling to hear that some young people did not have a form of identification prior to Gateway, which precluded them from accessing housing, benefits or job opportunities, and how truly life-changing receiving an identity card with the help of a navigator was for them (P1-2).
In comparison to other disposals offered to young people by the police, Gateway gave clients the opportunity to get support to resolve underlying issues, offering a tailored approach, for example, support with overcoming drug addiction if that was felt to be at the core of their offending (L1-1).
In summary, this theme revealed that the staff viewed the Gateway programme as aimed at improving lives and reducing, even if not necessarily stopping, reoffending. It was seen as benefiting young people who would otherwise go through alternative pathways that would address their underlying needs and, in some cases, could lead to a conviction, impacting their life chances further. Gateway aimed to fill a service gap, offering both an opportunity to forge trusting relationships with staff and receive advice and practical support, which were vital, in particular, to those with complex needs.
Theme 2: Setup and partnerships
This theme describes the aspects related to the set-up of the Gateway programme and its partnership arrangements, including communication across partners. This has been described within three sub-themes outlined below.
Subtheme: multiagency partnerships
Gateway was a multiagency intervention. Navigators also worked with, or referred their clients to, other organisations outside of the programme. Some young people were engaged with other support agencies when they came to Gateway. In such cases their navigator aimed to work closely with other support workers, for example, from the community mental health team (N1).
The Gateway programme was being delivered by three separate types of organisations (the police, two navigator providers and the LINX provider). Working with other agencies was considered to be a challenge, which could, in turn, affect the relationships between the navigators and young people. Time and again, wishes were expressed for better partnership working, by staff from every stakeholder organisation. Related issues affected both the staff, and indirectly, likely also the young people. Working across agencies was seen as challenging, especially due to communication difficulties, including keeping all parties updated. Different line management structures, as well as priorities, policies and procedures were cited as some of the factors contributing to the discord (S4, S3, S1).
The challenges in communication (defined in the next sub-theme) were also compounded by staff turnover, making it difficult for staff to have a shared, up-to-date understanding of the aims and deliverables of the Gateway programme, even within an individual agency. Some of the staff had already had three managers by their interview in this time period, and it felt disruptive having to educate the supervisors about the intervention, especially considering the complexity and the challenging nature of Gateway (S3).
The navigators, who supported the clients on the Gateway programme, were primarily based in the office space of the lead organisation, HC. As a result of this, they felt estranged from the navigator provider organisations, which employed them, since they spent most of their desk time at Southampton Central Police Station. It took a very long time for the staff at one of the provider organisations to realise that the navigators were also employees there, due to the lack of daily contact; similarly, there were long delays in receiving access to provider organisation e-mail (S7).
Subtheme: navigator location
At T1, before the COVID-19 pandemic, the navigators shared physical office space with the Gateway police officers; an arrangement that had its benefits and drawbacks. There were difficulties associated with the fact that the navigators were supposed to discuss certain issues concerning the clients with their navigator provider managers, who may be less informed on a specific issue, rather than with the police officers with whom the navigators shared office space. This was due to the duty of the police officers to report information as intelligence (S7). The duty of the police to report certain information about, or obtained from, the Gateway clients as intelligence, was a somewhat unforeseen, but significant, issue. Approaches to confidentiality and what needs to be shared between partners or reported to the police also differed between organisations, which created friction (S1).
Subtheme: communication and information-sharing
Challenges associated with sharing of information were frequently raised by interviewees from all the partner organisations. When Gateway was set up, all partners (the police, two navigator providers and LINX provider) had access to a shared IT system, so they could access information about Gateway clients. All staff were also routinely involved in reporting and sharing information about clients, including that which emerged in the course of LINX workshops and the provision of individualised support by their navigator. This enabled identification of further needs and further tailoring of support (S3).
However, over time, due to differences in policies and processes around sharing confidential information, this practice stopped. Sharing between the partners became limited to information relating to safeguarding and attendance at sessions by clients (S11). Information was not routinely shared between the navigators and LINX practitioners, unless consent was explicitly gained from the client. This was challenging, as it was felt that opportunities to put extra, or more tailored, support in place were missed (S7, L2-2).
This meant that at T1, there was no feedback loop in relation to information shared between practitioners from different organisations, which made it challenging to work cohesively together. Nonetheless, the partners within the Gateway programme recognised the need for efficient, collaborative communication, while being all too aware of some deficiencies (S10).
Theme 3: Working on Gateway
This theme covered accounts by the staff with regards to what working on the Gateway programme involved, their descriptions of the components and various aspects of the intervention and any highlights or issues associated with the day-to-day running of Gateway. The material was organised into the following four subthemes.
Subtheme: LINX workshops
The 2-day LINX workshop was an integral part of the Gateway programme. It was created by The Hampton Trust and underwent continuous development thereafter. It was designed to be thought-provoking and encouraging self-reflection and examination of the clients’ own past, present and future, including any factors which may have contributed to their offending. This gave the LINK facilitators a chance to discuss with the clients how they might want to work through issues with their navigators (L1-1). Clients shared with their navigators the ways in which the workshops allowed them to change previously unhelpful reactions to events (P1-2).
Subtheme: navigators
This subtheme covers any aspects relating to the routine work of the navigators. In a typical working day, a navigator may complete initial, midway and final assessments for clients, continue earlier work with existing clients and deal with any issues requiring attention (N2).
At T1, a very prominent topic, brought up in most of the interviews and focus group discussions, was that of the low numbers of Gateway clients. The navigators identified pros and cons to this. It was noted that the numbers coming through were generally very small, albeit the numbers fluctuated from month to month (N3, N2).
It was reported that some navigators had to take on other duties with their employing organisation, due to the low intake of Gateway clients, which at the time of the interview was insufficient to occupy the four navigators in post, even with the pre-pandemic ways of working, that is with a heavy face-to-face involvement (N2).
Subtheme: eligibility and recruitment
The issue of the low numbers of young people eligible for recruitment has been present from the beginning of implementation of the intervention, and various steps have been taken to alleviate this. The intervention was launched in June 2018, and was altered in due course, with Gateway becoming a type of conditional caution, rather just simply an alternative to prosecution or court appearance. This was intended to boost numbers of eligible people and led to more low-end-of-offending clients being recruited, which still felt would be beneficial for some clients (P2-1, FG3-N2).
Subtheme: experience and training
On the whole, the navigators felt well prepared for their roles, while acknowledging that there were some gaps in their training, and that they had unequal access to different types of training, depending on which organisation employed them. This was seen as a challenge, since all the navigators required similar training, it was felt. Some of the training received through one of the navigator provider organisations was aimed at staff working with younger people, and was seen as less relevant (N1, N3). Importance of mental health training was often emphasised, and the navigators also relied on previous training received elsewhere (N1, FG1-N2).
General training about services available may have been helpful for LINX practitioners, had it been offered, albeit this may be more directly relevant to role of the navigators (L2-2).
Subtheme: job satisfaction
Despite the challenges cited by the participants, it was clear that they also derived great satisfaction from their jobs. They enjoyed case-working and took pride in getting positive results with the clients (N1). This was found to be motivational when challenges arose (L2-2). Aspects such as opportunities to demonstrate innovation and find a specific approach to help individual clients were much appreciated and helped them remain passionate about their work (P2-2).
Theme 4: Clients
This theme emerged in responses to many of the questions, with participants often illustrating their answers with stories or examples involving Gateway clients. Some of the subthemes are introduced below through relevant quotes.
Subtheme: needs
The participants frequently referred to the wide spectrum of needs clients presented with. This subtheme often overlapped with that of client backgrounds. Clients really varied in the degree of support they needed: from people with very complex backgrounds with much adversity, to those who made one mistake bringing them into contact with the criminal justice system. This meant a degree of flexibility was required in approach to the different types of clients (L2-2, FG1-N2). Women’s needs could differ from men’s, and the workshops, for example, were more typically suited to men (L2-2).
Subtheme: attitude towards Gateway
This subtheme was concerned with clients’ motivation and intrinsic belief in the value of Gateway. Much of this the staff found out from the written feedback at the end of the programme. The ability to share and be listened to, without prejudice, as mentioned, which was confidence boosting (L2-2). The young people seemed to enjoy the intervention, although it was presupposed that it may have felt like too much work for some (N1). Readiness for change was seen as key, but it was a difficult task to help convince some young people of the need to change (SM3). Occasionally, young people remained closed to the idea of help, at least in the shape it was being provided, maintaining that some people won’t need help and denying deriving any benefit from Gateway, sometimes quite forcefully (L2-2).
Subtheme: engagement
The staff in all categories mentioned the importance of building a rapport with the young people as important to ensuring their engagement with the intervention. Building a rapport (while bearing in mind any risks that the young person may present) was seen as crucial and an important part of the job (FG1-N1).
The navigators reported that engagement was variable. It was cited that a contributing factor may have been a lack of appreciation during the recruitment process of how much involvement was required. Non-engagement constituted one of the reasons for which Gateway clients could be breached, but there had been discrepancies in interpretation of how low engagement would need to be in order to constitute a breech (FG3-N2). There were at times differences in opinions with regards to individual breaching decisions, and the project officers making these appreciated the complexity and treated breeching decisions as discretionary, requiring individual consideration (P2-2).
Time period 2 – Gateway clients
Presented here are the results of interviews with young people that took place at T2. The recruitment process can be seen in Appendix 8, Figure 11.
FIGURE 4.
Thematic analysis map – clients at T2.
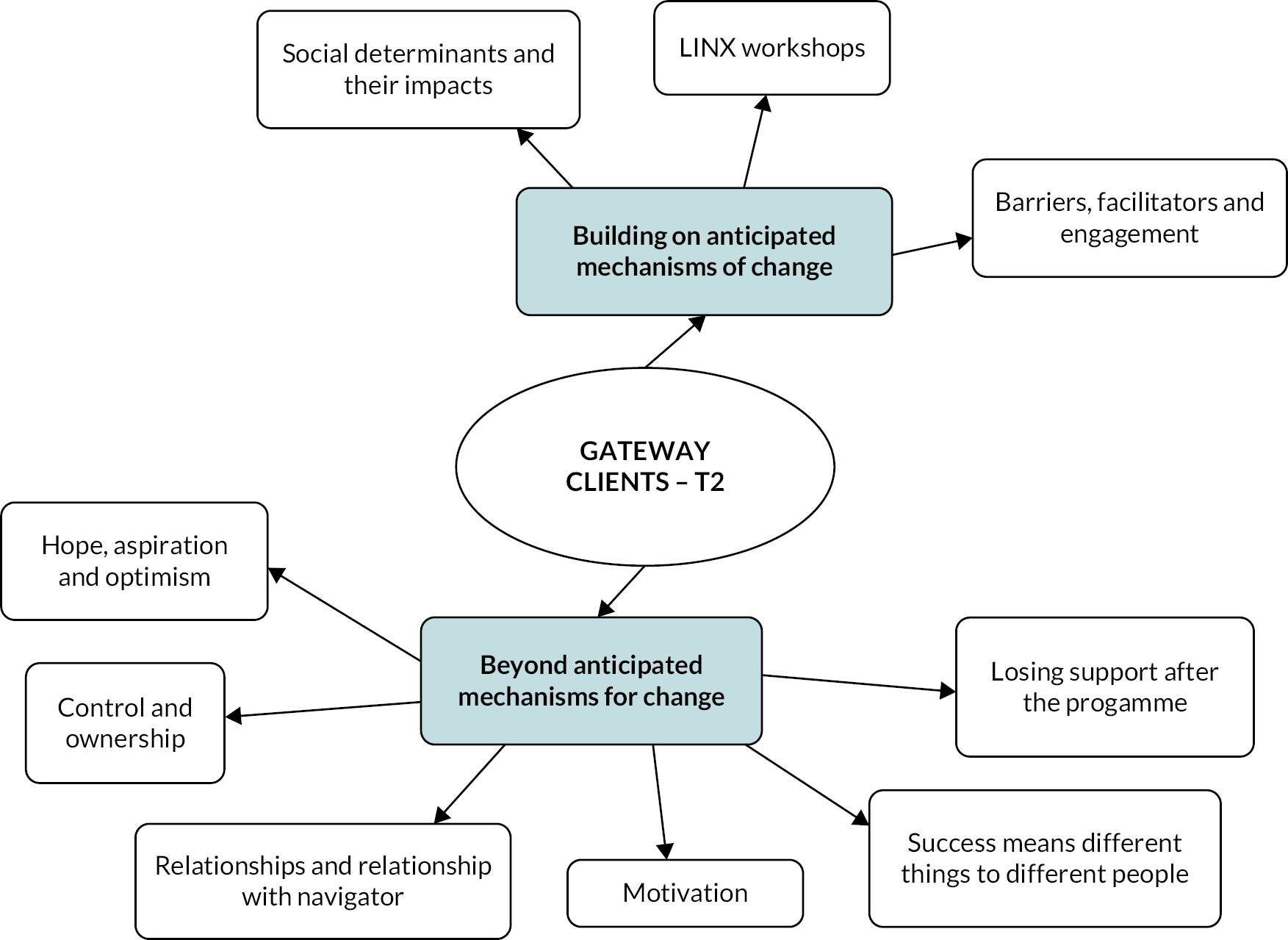
Overall, 17 young people gave permission to be contacted by the researcher. Of these, five were either non-contactable or declined to consent. The 12 who consented to be part of the study included 9 males and 1 female who had completed Gateway, and 2 males who had breached (1 for reoffending and 1 for poor engagement). The interviews were conducted by MB-P, a female, who was previously unknown to the participants. MB-P was also the PPI officer on the project with experience in consulting and undertaking qualitative research with young people from similar backgrounds. Her experience in undertaking PPI on the Gateway project informed her understanding of the wider context but is unlikely to have influenced the questions here due to the differing nature of the questions covered compared to the areas covered for PPI (largely recruitment strategies into the RCT element). The content analysis identified a range of key themes as demonstrated in Figure 4. Quotes from clients at T2 which informed the analysis can be seen in Report Supplementary Material 5, Table 2.
Theme 1: Building on anticipated mechanisms of change
Subtheme: social determinants and their impacts
Participants discussed a number of social determinants and their impacts, often identifying these factors as the cause of offending (P010, P004). Individuals who perceived these needs acutely were more likely to feel the navigator sessions had an impact on their lives (P017). Participants without a high perception of need, or who did not view the crime they committed as problematic, were less likely to consider sessions valuable (P005). The limitations of Gateway to support social determinants at a societal level was reflected upon (P010).
Subtheme: LINX workshops
Participants felt anxious or apprehensive of group work beforehand (P015, P004, P011), then discussed enjoying the sessions and feeling put at ease (P006). The workshops being fun stood out over content for some while others felt that the workshops were not relevant to them (P017). A key reflection was that of a change in perspective (P014), particularly in relation to seeing different perspectives (P005). Seeing things from another’s point of view and discussing other’s crimes helped participants to feel less alone in relation to their offences (P015) appearing to alleviate some of the isolation experienced going through the process (P017), in turn raising self-esteem (P015).
Subtheme: barriers, facilitators and engagement
Participants had negative expectations (P006), particularly if they believed Gateway would be undertaken by the police (P004). Despite this, the participants interviewed felt that they engaged well with the programme; attributing this to the rapport built with staff (P011). One participant who breached for lack of engagement perceived the programme to be easy to engage with (P005). Logistically, most participants felt that there were no real barriers to attending navigator sessions, reflecting positively on the flexibility of staff (P007, P017). Those with competing priorities, such as work or childcare, reported some challenges working around commitments but felt expectations were fair (P004). Attending LINX workshops was felt to be more challenging, largely due to the lack of flexibility in time and location, and the length (P004).
Theme 2: Beyond anticipated mechanisms for change
Subtheme: motivation
Participants’ initial motivation was to avoid going to court (P005), with little emphasis placed on the purpose of the programme in terms of health and well-being (P006). However, motivations changed throughout the Gateway programme, with some reflecting on the shift from fear of consequences, to no longer wanting to offend (P007). As participants built a rapport with their navigator, the idea of not wanting to let them down also became key (P005, P004).
Subtheme: relationships, and relationship with navigator
Relationships with families, and the support they provided impacted help-seeking behaviour prior to Gateway. Where participants had supportive and positive parental role models, they were not equipped to provide adequate support (P017, P018). Parents also played a key role in participants engaging; for several, family facilitated their attendance (P015). The relationship that participants developed with their navigator was a crucial aspect that contributed towards the perceived benefits (P015). Navigators were widely reported as going ‘over and above’ to provide personalised support for participants (P017, P004), and participants perceived them to be genuinely well meaning and authentic (P015).
Subtheme: control and ownership
Participants discussed feeling out of control of their lives before being arrested (P017), with Gateway being initially seen as an extension of this (P011). Participants viewed Gateway as a choice, and this perception of self-determination evoked positive attitudes (P017). Individuals who felt they had ownership over the programme were more likely to see benefit (P004), with some reflecting on the wider impact that control gave over their sense of self-esteem (P017). However, external factors contributed to some participants, sense of control to stop reoffending. The participant who breached for reoffending (carrying a knife) described not having control over his offending behaviour (P001).
Subtheme: hope, aspiration and optimism
Participants viewed Gateway as a second chance, either as an opportunity not to be criminalised, to make a change and/or learn from an offence (P005, P010, P007). Within the programme, the sense of being believed in was tied in with the relationship participants had with their navigator (P017), with participants reflecting on the feeling that someone understood them for the first time (P014). The description of being ‘fixed’ by the navigators, highlighted the perception of feeling ‘broken’ prior to the change (P017). Participants described having hope and optimism for the future, particularly if they felt they were in a position that they had some control over its direction (P015).
Subtheme: success means different things to different people
Perceptions of success varied widely. When recidivism was discussed, it was clear that for many participants success was about offending less, rather than not offending (P004). For some, addressing the social determinants, or their impacts was a tangible and meaningful measure of success (P012, P001). Others described positive changes to their mental health as being the most significant achievement. Learning about the drivers of offending behaviour helped participants to understand their own offending, recognise how Gateway had helped them build trust and seek help where they would not have before, and reflected on how they felt more prepared to manage situations (P010, P014, P015). Several participants discussed the knock-on effect of the programme in their wider lives, describing Gateway as a catalyst for change (P010). Participants who were parents described the positive impact that the programme had on their children (P014).
Subtheme: losing support after the programme
Participants reflected on the impact of the programme ending and support being lost. For example, access to the council housing register facilitated by a navigator was lost, indicating how easily progress made can be lost (P010). Participants identified the short-term impact from the programme but described how things worsened over time (P010, P011). Feelings were expressed that, despite the programme’s support, it was not enough to counter the wider environmental influences long-term (P001). Requests to keep in touch with navigators led to the positive impact of having someone there to celebrate successes (P017, P004).
Time period 3 – Gateway clients
The navigator identified a total of 97 young people meeting eligibility criteria: 36 were contactable, with 30 agreeing to further contact from the research team. Successful contact was established with 27 participants, resulting in the completion of 16 interviews. The remaining 11 participants were either uncontactable, declined, or failed to complete within the study period. This section presents the results of the 16 interviews conducted by two researchers. A flow diagram for recruitment is available in Appendix 8, Figure 12.
FIGURE 5.
Thematic analysis map – clients at T3.
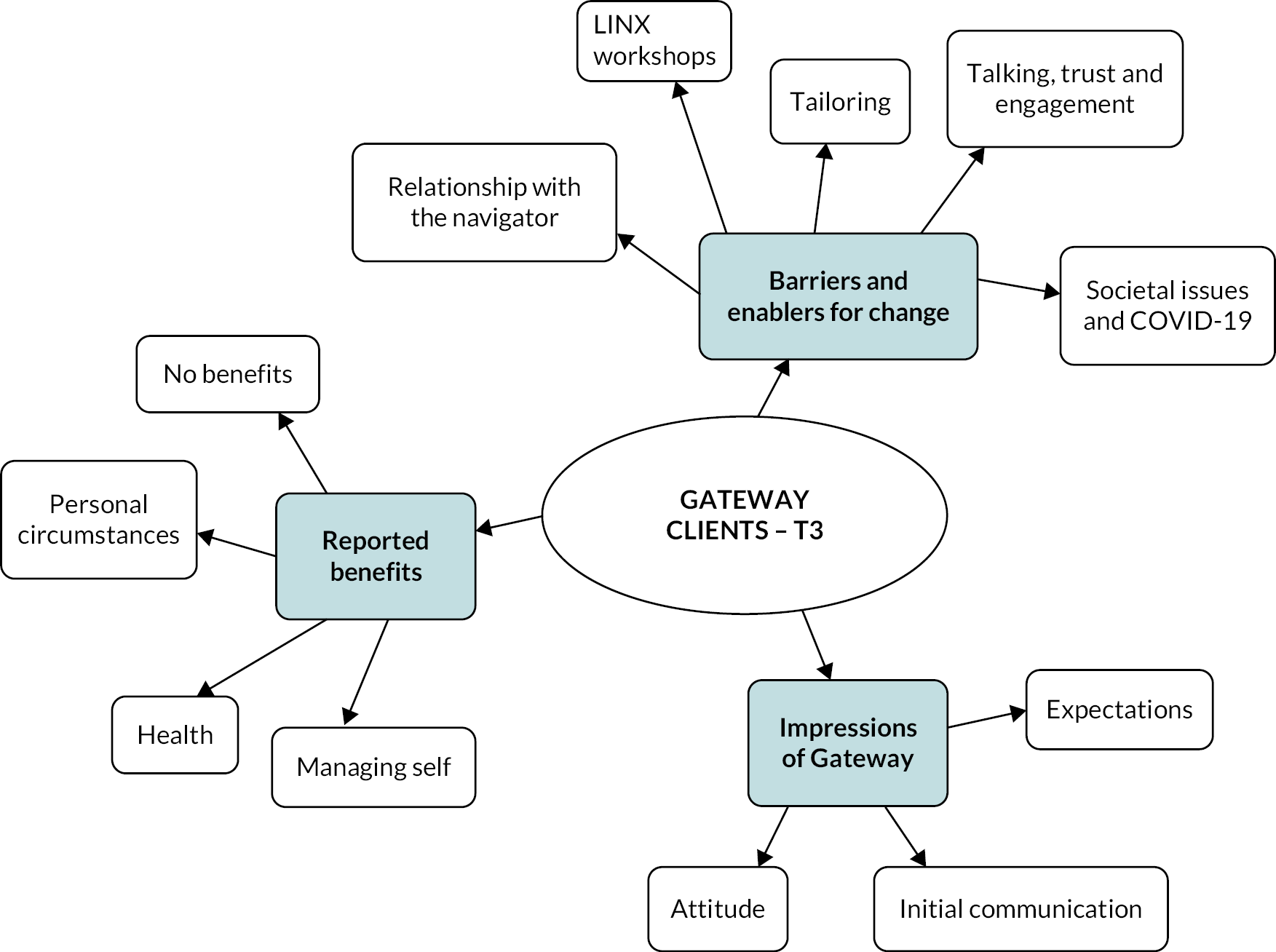
FIGURE 6.
Thematic analysis map – Gateway staff at T3.
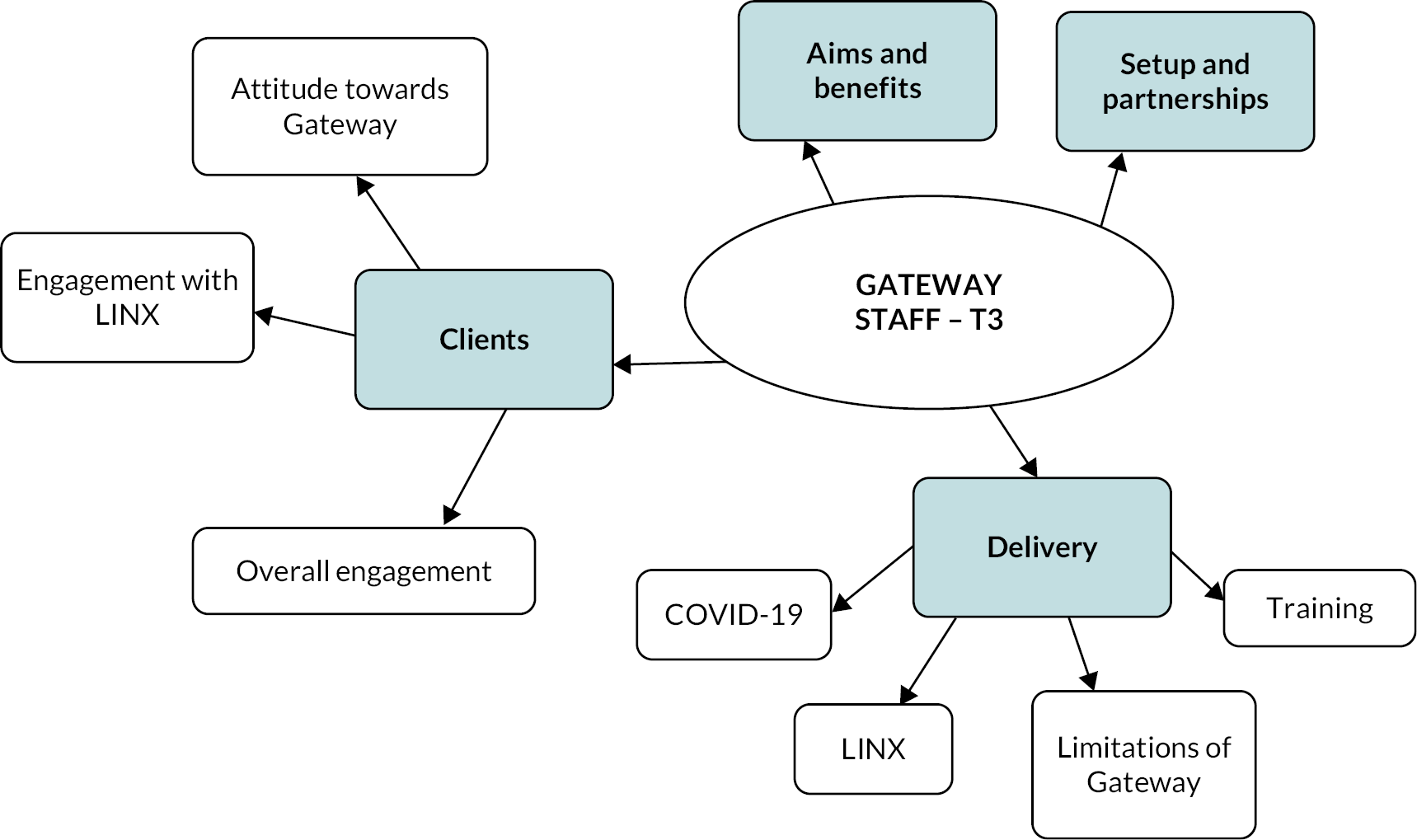
FIGURE 7.
Thematic analysis map – Gateway recruiters at T3.
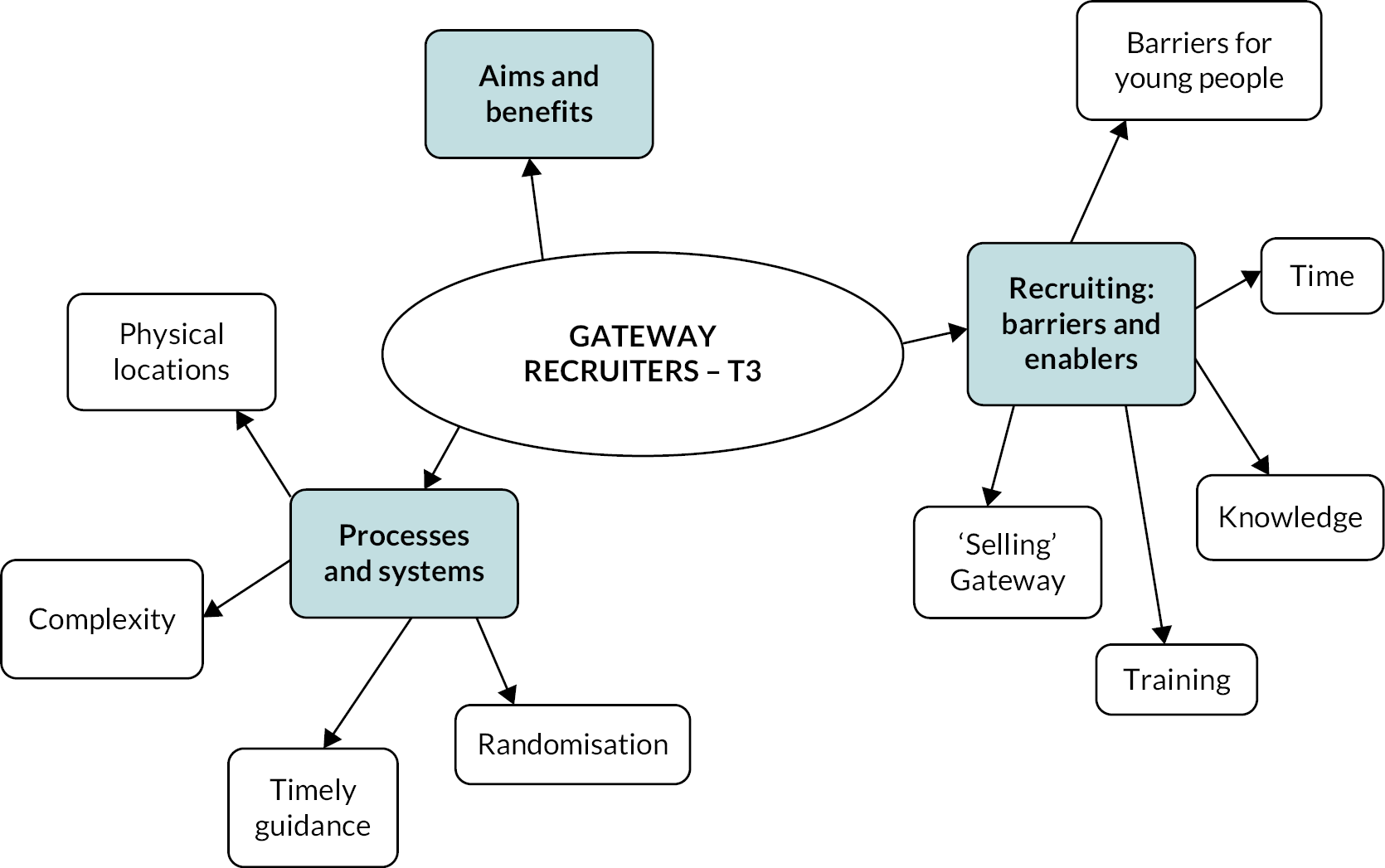
Demographics of young people interviewed
Table 14 presents the demographics of the young people interviewed. Participants were predominantly male. All had some experience of the navigator delivering their component by phone. Nine participants had in-person LINX workshops, six were by phone and one was unspecified. To protect anonymity, the details regarding HC site locations have been removed, however, the participants represent a total of 12 sites across Hampshire. Most participants had also participated in the Questionnaire Study (RTC) component. The research interviews were conducted by LW, a female interviewer working on the study.
| Participant ID (n = 16) | Gender | In-person or phone interaction with navigator | In-person or phone LINX | Completion status | Participated in RTC |
|---|---|---|---|---|---|
| C1 | F | Mixed | In-person | Complete | No |
| C2 | M | Mixed | Phone | Breached: non-engagement LINX | Yes |
| C3 | M | Mixed | In-person | Complete | No |
| C4 | M | In-person | Phone | Complete | Yes |
| C5 | M | Mixed | Phone | Complete | Yes |
| C6 | M | Phone | Phone | Breached: reoffended | Yes |
| C7 | F | Mixed (one session in-person) | Phone | Complete | Yes |
| C8 | M | Mixed (one session in-person) | In-person | Complete | Yes |
| C9 | M | Mixed | In-person | Complete | Yes |
| C10 | M | Phone | In-person | Complete | Yes |
| C11 | M | Mixed | In-person | Breached: non-attendance LINX | Yes |
| C12 | M | Mixed | In-person | Complete | Yes |
| C13 | M | Mixed | In-person | Complete | Yes |
| C14 | M | Phone | Phone | Complete | Yes |
| C15 | M | Mixed | In-person | Complete | Yes |
| C16 | M | Mixed | Unspecified | Breached: reoffended | Yes |
While the discussion guide was designed to allow for the exploration of eight themes, the analysis of the interview data revealed three broad themes and twelve subthemes (see Figure 5). These themes represent the young people’s views on (1) barriers and enablers for change, (2) impressions of Gateway and (3) reported benefits. They are discussed below, along with their relevant subthemes. Quotes from interviews with Gateway clients at T3 are available in Report Supplementary Material 5, Table 3.
Theme 1: Barriers and enablers for change
This theme emerged as the interview data revealed a variety of determinants relating to the programme’s ability to implement change. These are represented by the following five subthemes.
Subtheme: relationship with the navigator
When discussing their relationship with the navigator, the overall response of the young people was very positive. In all their accounts the participants reported feeling supported, and there was a unanimous view that the navigators had been friendly, understanding and approachable. Frequent words used to describe their navigators included nice, lovely, sweet, genuine, helpful and even perfect (C7).
It was felt that such characteristics relieved initial feelings of apprehension and uncertainty while also instilling trust and confidence in the programme’s confidentiality. Many of the participants mentioned this was helpful with engagement. Approachability, openness and calmness in communication were highly valued and encouraged disclosure (C7, C9, C11).
Contrary to initial expectations, the young people described their experience with their navigator as being non-judgmental, and a sense of ease was expressed in relation to their understanding and accepting nature. The sessions provided a safe environment in which emotions brought on by difficult or frustrating topics could be better maintained.
Except for one participant, none of the young people had negative comments regarding this aspect of the programme. Furthermore, participants reflected on previous difficulties and experiences with past care workers, suggesting it was rare to have developed such a relationship with a professional of this kind (C11).
It was widely acknowledged that the navigators’ flexibility accommodated a variety of schedules and pre-existing commitments. This was considered valuable in preventing logistical barriers and thus allowed for greater success with compliance. Participants also demonstrated gratitude for the navigators’ reliability in terms of timekeeping and prompt responses to e-mails and text messages (C13). A further commonality among the participants was their recognition of the navigators’ desire to make a difference and the navigators coming across as thoroughly enjoying their jobs (C9).
It was felt that the provision of practical support and signposting facilitated better opportunities in terms of employment, finances and housing. In addition to this, the young people reported the introduction to, and consequent utilisation of additional services such as food banks.
The overall responses regarding the navigators demonstrate the significance of their role in enabling and implementing change. Their ability to gain trust through a friendly and approachable demeanour appeared valuable in instilling confidence in the participants, allowing for greater engagement, and thus, potential to benefit from the experience.
Subtheme: LINX
When questioned about the LINX component, the young people largely demonstrated recognition of its ability to enable better decision-making and coping skills. The interviewees cited acquiring the necessary tools to manage and deflect challenging emotions such as stress and anger, as well as strategies to help control drinking. Some reported having used these tools since completing the programme (C13).
When speaking of the staff, the participants used descriptive words similar to those associated with the navigators. Examples included friendly, understanding, lovely and non-judgmental. Participants were being treated in a non-critical, respectful manner, without being associated with their offence. It was felt that such characteristics of the staff were, again, valuable in improving the young people’s confidence when engaging (C13, C8).
A range of responses were elicited from questions regarding the young people’s feelings towards participating and sharing in a group environment. It was felt this offered a valuable opportunity to engage with individuals in similar situations. This appeared to boost morale as participants reflected on joining together in a non-judgmental environment. Participants were often surprised that other young people in the workshops were in general friendly, and the atmosphere was relaxed (C13). Clients made connections with others in similar situations (C8). Furthermore, the benefit of considering a variety of perspectives was believed to have enabled clearer decision-making.
Contrary to this, there were also reports of a sense of isolation from the group due to demographic factors and a difference in offence type, and hence feeling ostracised (C3). This highlighted a potential barrier in terms of engagement and compliance.
Typically, participants found the prospect of group work intimidating and described initial feelings of apprehension and awkwardness. This component could be seen as unhelpful due to the challenges involved with participating in such a setting. The perceived expectation of being grouped with fellow ‘criminals’ was also considered to have initiated anxiety (C13).
It was felt by some that such apprehension and uncertainty affected attendance, which was reportedly low. Some felt this could be due to insufficient information at the start of the programme leading to poor, or uninformed expectations. This is defined in the later subtheme, initial communication. A minority also advised that attendance depended on the ability to take the time off work. While inconvenient, none of the participants reported this to have been problematic.
Issues relating to the location were particularly prevalent. While a substantial minority commented on its convenience, most participants reported long travel times and accompanying costs. Some reflected with a sense of confusion due to the perception that it was inconvenient for all, including the course leaders. Except for one participant, all respondents reported requiring a family member, taxi, or public transport to attend. It was further reported that the venues had been inaccessible by public transport and therefore, in addition to a train journey, then required a substantial walk either side to attend. This was felt to greatly contribute to the duration of the day. Separately, the duration was considered an additional challenge with participants advising it to be too long to maintain concentration (C13, C9).
Participants also commented on the associated travel costs, which could be considerable, depending on the location (C9, C13). It was suggested that similar group sizes should be held in different locations, making it more accessible and convenient for attendees. Further comments also included the suggestion that participants be fully or partly reimbursed for travel.
A switch from face-to-face workshops to phone delivery during COVID-19 appeared to have varying effects. It was common that participants had difficulties differentiating these sessions from those with their navigator, and thus many struggled to remember the LINX component. In general, however, participants stated that the phone delivery offered some benefits. In addition to greater convenience and thus compliance, it was felt that better confidence could be achieved with engagement. This is defined further in the later subtheme, societal issues and COVID-19.
Subtheme: tailoring
This subtheme emerged as participants reflected on the programme’s ability to accommodate varying needs. A variety of perspectives were expressed regarding how the LINX workshops should be organised, as well as how participants felt their individual needs were met.
Conflicting views emerged when speaking of group work. There were views that providing for a variety of needs allowed for a more diverse learning experience. Here they reported to have received multiple life lessons and strategies to deal with a variety of circumstances. Perhaps surprising to note is this view was largely expressed by participants seemingly of lower need status. Such responses suggested they had found the workshops informative and interesting (C13).
Others felt the content of the group work was not relevant to themselves and thus, offered little benefit to their situation. For example, a large proportion of the workshop had been focused on anger management despite some people’s offences having no association with anger. In addition, the workshops were also reported to be of a generic nature and aimed at a younger audience, with reports of not having learned anything from the experience (C9).
Participants also demonstrated confusion over the issue of people with different offences taking part in the workshops together, questioning the reasons behind grouping in this manner. Furthermore, a minority felt that it was harder to comprehend and follow the content of the workshops due to quick changes in topics and variety of material. It was therefore suggested that better personalisation could be achieved by grouping according to offence type or level of need (C3).
Speaking of their experience with the navigator, the clients felt that the level of support was appropriate for their level of need. Participants commented on their ability to understand individual circumstances, pick up on cues from the participants and tailor their delivery accordingly (C13, C4). It was reported that there was an appreciation that not everyone needed intense support (C14).
This was in contrast to the view that greater emphasis could have been placed on the topic of mental health. They commented, ‘It just wasn’t tailored for me’, adding later, ‘it was just preaching the wrong stuff to me, personally’ and, ‘I just didn’t find it helpful’ (C9).
Subtheme: talking, trust and engagement
When asked whether there were any aspects of the programme found to be particularly helpful, many of the participants commented on the therapeutic opportunity of talking. Specifically noted was the benefit of talking with anonymity. In their accounts, participants reported feeling comforted by having someone to listen to them and to have their voices heard. The opportunity to explain to someone how they felt and to describe their point of view was frequently described as a sense of weight being lifted (C4).
Talking was also considered an enabling factor in achieving greater insight. Participants spoke of the opportunity to reflect on their lives and suggested that this had allowed for the realisation of the need to initiate change. For some, this was recognising the necessity of reducing drug or alcohol use, while for others it was leaving an unhealthy relationship or changing their mindset. Other participants felt that it allowed for greater clarity in decision-making, while further, some advised that it provided an opportunity to obtain additional help, for example, in order to change their lifestyle (C1, C11).
Participants reported challenges with engaging in sensitive and uncomfortable topics. It was felt that this therefore had the potential to hinder conversations. Furthermore, contrary to the above, sometimes there was a reluctance to engage with a stranger, especially on painful topics (C13, C7).
Negative experiences with past care workers had the potential to lead to poor expectations and consequently presented a further barrier to engagement. There were reports of feeling let down by previous counsellors, citing feelings of abandonment and frustration relating to high staff turnover rates. It was felt that this had a detrimental effect on their ability to trust the staff, as well as their willingness to continue seeking help (C4).
An additional barrier was presented by the participants’ ability to engage. Non-engagement of LINX was the cause of one participant’s breach. While this individual also failed to engage in the study interview, another openly disclosed their struggles with alcohol dependency. Speaking of the LINX workshops, they confided that they attended while under the influence of alcohol. This was also the case when participating in the study interview. Such alcohol dependency was, for this participant, the motivating factor for accepting Gateway (C3).
Comments regarding trust were also prevalent. Through their accounts, the participants presented a variety of perspectives, and thus it was considered to present as both a barrier, and an enabler for change.
It was widely acknowledged that a significant concern was that of the programme’s association with the police. From their accounts, it was clear that the participants’ views on the police were very negative, and thus introduced an initial barrier. Talking about this issue, one interviewee alluded that such association had the potential to impact engagement and lead to poor expectations. It is therefore possible to suggest that some young people may decline Gateway due to this association (C7).
It was reported that an initial lack of trust could prevent participants from fully engaging with their navigator at the start of the programme. This may have been through shutting down due to a fear that talking could have detrimental consequences in the form of further punishment from the police (C4).
Contrary to such opinions, there were also expressions of confidence in the programme’s confidentiality and reports of this positively influencing engagement (C10).
The result of losing trust was, however, incredibly detrimental, illustrating the necessity of transparent communication. In one case, a misunderstanding of their navigator’s identity led to feelings of betrayal, withdrawal and paranoia (C3).
The need to differentiate Gateway staff from the police therefore appears imperative in optimising compliance, engagement and success.
Subtheme: societal issues and COVID-19
This subtheme occurred as participants spoke of the barriers presented on a societal level. It was felt that there is very limited help available outside of Gateway, particularly for this age range. One participant alluded to a sense of abandonment as they reported being no longer able to work with them since turning 25. There were reports of no help being available, while others cited long waiting lists and associated costs with private care. It was also apparent that the young people were unaware of what help was available, or how to access it (C9).
In the absence of available support, it was felt by one participant that affordability may have presented an important barrier to change. While unemployed, it is difficult to find work to finance a rehabilitation service for alcohol dependency (C3).
Some participants volunteered that their mental health had worsened following the COVID-19 pandemic. This was attributed to the difficulties it presented in terms of employment, living circumstances and lack of leisure opportunities. Furthermore, one participant reported it to be a contributing factor to their offence. Despite this, except for a reported delay in the processing of paperwork, issues concerning the effect of the pandemic on the intervention were not prominent in the interview data.
While a minority felt that their experience may have been more personal if it had been face-to-face, the majority agreed that the phone intervention provided a convenient alternative and had little impact on engagement or their ability to benefit. In addition to this, participants felt better able to open up on the phone, suggesting it to be a less daunting option and thus enabled greater confidence when engaging (C4).
Theme 2: Impressions of Gateway
The semi-structured nature of the interviews allowed for the acquisition of participants’ perceptions, opinions and views on various elements of the programme. Their accounts are organised and represented by the following three subthemes.
Subtheme: expectations
When questioned about their expectations of the programme, most of the young people’s responses were negative. Many described expecting it to be lecture based and that they would be spoken to about their mistakes and given lessons on how to behave. It was widely anticipated that the staff would be judgmental and not allow participants to have their own say (C8).
Such negative expectations could be somewhat attributed to the association with the police. Participants cited expecting to be questioned, and that due to the location at the police station, the programme would therefore be presented by the police themselves (C1, C7). Contrary to this, a minority of the young people also spoke of positive expectations. They cited expecting the programme to help them in their lives by providing the necessary support needed to instigate lifestyle changes as well as the opportunity to talk (C10).
Reports of anxiety, doubt and scepticism were widespread. Participants spoke of initial uncertainty and doubt as to whether Gateway would help their situation or provide any benefit. Furthermore, one participant reported their dislike of classrooms was off-putting to the extent they considered taking standard prosecution.
A large proportion of participants reported not having known what to expect. Some suggested this was due to a lack of information when being offered the programme. This is described in the following subtheme, initial communication.
Subtheme: initial communication
A recurrent theme in the interviews was the opinion that there was a need for greater initial information and better communication when offering the programme to prospective clients.
Participants indicated that they had received adequate information and were therefore clear on what it involved. Some voiced concerns that a lack of initial information could result in young people accepting the caution without fully understanding what to expect, with calls for better information. Some went on to suggest that discovering this later could impact compliance, resulting in breaches and thus worse consequences than accepting standard prosecution (C13). This had the potential to affect engagement due to negative expectations (C4).
While expressing gratitude for the help received there was disappointment over other areas not meeting expectations. It was felt that the cause was an inability to fully comprehend the information to begin with. An example is inability to understand the information due to it being presented in writing only. Such a lack of understanding could potentially lead to uninformed consent, incorrect expectations and disappointment (C3).
Subtheme: attitude
While such concerns were reported regarding initial communication, ease of location and tailoring, most participants reflected on the programme with a sense of positivity and appreciation (C4, C5, C3).
The participants demonstrated appreciation for Gateway providing the opportunity of chance. The young people recognised it as an opportunity to rehabilitate and rectify certain elements of their lives. Participants commented on its additional value for those younger than themselves (C12).
Contrary to this, there was also a demonstration of an embedded lack of acceptance, questioning the reasons behind being cautioned for a mental health-related offence and reporting a feeling that they had accepted Gateway for the wrong reasons, and that there was nothing they perceived themselves as needing help with. As a result, there were no benefits to report.
Positive views were often portrayed as transitions of attitudes. For example, initial feelings of apprehension and scepticism were reportedly replaced by a sense of acceptance and acknowledgement of the programme’s ability to help (C7, C4). In general, participants described their experience as being better than anticipated (C12).
When questioned about their motivations for participating in the research study, many of the responses further demonstrated the young people’s appreciation for the programme. While it was clear that the use of incentives was successful in optimising compliance, many participants reported a willingness to help, regardless of the reward. The desire to give back and help others by participating was felt to be driven by their own personal results and successes which they attributed to the programme.
Theme 3: Reported benefits
Subtheme: managing self
Young people reported having learned better coping strategies. An improvement in the ability to manage emotions was associated with a reported positive effect on behaviour. Participants reported being able to defuse situations to prevent arguments, as well as redirect challenging emotions into positive activities such as the gym or reading. This was felt to improve relationships (C4).
One participant also stated that since finishing the programme they had started to distance themselves from former friends known to be associated with risky behaviour such as substance use (C8).
Questions about recidivism brought forth a variety of responses. The majority reported they would not reoffend, however not all attributed this to Gateway. Many of the participants considered their offence to be a one-off mistake, while others advised that being arrested was the wake-up call needed to prompt change. One participant demonstrated no remorse for their offence, advising instead that they would continue the activity due to a lifetime of knowing no different. Responses also included those crediting the programme (C8, C10, C7).
Subtheme: personal circumstances
This subtheme emerged as the young people discussed positive changes in terms of employment, housing and relationships. A change in mindset was associated with a greater desire to seek meaningful work as well as a new-found commitment to staying employed (C8).
In addition to improved efficiency in everyday life, an ability to work longer hours was also reported (C4).
When asked about any changes they may have experienced in their housing situation, many of the young people felt they had achieved greater stability. Some revealed they were no longer homeless, while others reported having moved from hostels or their family homes. In some circumstances the young people’s living situations were considered a risk factor in relation to offending. The main cause cited for this was tensions within families. It was therefore felt that moving from that family environment resulted in improved relationships, reduced arguments and a perceived lower risk of reoffending (C13).
While many participants felt that their relationships had improved, a minority cited continuous difficulties due to a lack of family support, acceptance of their caution, or forgiveness for their offence (C16).
Regardless of employment status, several participants considered applying for Jobseekers Allowance to be a benefit of completing the programme. Many demonstrated gratitude for their navigators facilitating opportunities through their help with the various steps involved. Such challenges included difficulties with computer literacy and therefore highlighted pre-existing barriers in terms of accessibility for these young people.
Improved employment chances combined with the provision of financial advice and support gave greater opportunity for further stability. Some participants reflected on this improvement in their lives with a sense of disbelief (C7).
Subtheme: health
The participants, to varying extents, spoke of improvements in their health. Reports of reduced drug and alcohol use were particularly prevalent. Some participants acknowledged this benefited not only their health, but also suggested it to be a contributing factor in their reduced likelihood to reoffend.
Comments regarding mental health also recurred throughout the interviews. Participants spoke of the programme’s ability to reinforce their positive outlook and improve their mental well-being as a result (C7, C8, C11).
Participants reported that the programme helped establish routine in their lives, helping them stay better organised on a daily basis (C3).
There was also a reported increase in the utilisation of services, with participants advising they had returned to their general practitioners and dentists (C3). Better management of prescriptions was associated with improved employment opportunities (C1).
The programme was also credited for helping the young people’s physical health. Participants reported taking better care of themselves, hiring personal trainers, attending the gym and participating in healthy leisure activities such as walking. This was also cited as a coping strategy to better manage challenging emotions. The study’s voucher incentive, for example, could be used to buy gym clothes in order to support a new lifestyle (C7).
Subtheme: no benefits
A minority of the young people demonstrated resistance towards the programme. Some did not perceive their offences as being troublesome while others felt that those relating to mental health should not result in a caution. It was also felt by one participant that the programme was perhaps better suited to those on their second or third offence. This introduced a question over the participants’ suitability for Gateway. As mentioned previously, while reporting to have found the programme interesting, some of the young people cited having well-paid jobs, supportive families, and a good education. Several individuals felt that they had just made a one-off mistake which was acknowledged at the time. Their opinions on benefits varied. Some felt they had gained little or no benefit from taking part, yet recognised that due to the pre-existing stability of their lives, there was little Gateway could offer them. Others felt they benefited from gaining insight, recognising certain aspects needed to change. Avoiding prosecution was also considered a benefit (C14).
While previously suggesting cognitive behavioural therapy may be helpful in their situation, another participant also felt that there was nothing they needed help with (C9).
Time period 3 – Gateway staff
This section presents the results of the qualitative evaluation with Gateway staff at time period 3. The main themes and subthemes are presented in a thematic analysis map in Figure 6. Quotes from Gateway staff at T3 that inform this section are provided in Report Supplementary Material 5, Table 4.
Theme 1: Aims and benefits
As at T1, staff reiterated that the aim of the programme was to reduce reoffending in 18–24-year-olds. This was done through stabilising the lives of the young people who received the intervention, providing appropriate support and guiding them away from offending and the criminal justice system. The intervention was seen as a positive initiative, capable of achieving such outcomes. The navigators emphasised stabilising various aspects of the clients’ lives, whereas the LINX staff mentioned a reflective component of the intervention, and police participants also commented on the reasons behind targeting this age group (N1, N2, L1, L2, P2).
In terms of the support that had been provided through Gateway, the staff spoke about a range of areas in the clients’ lives touched by the intervention, which included help with opening bank accounts, addressing the clients’ housing situation, referrals and signposting for support with substance abuse and other mental health issues. Having a trusting relationship with an adult was seen as key and something that was presumed to otherwise be missing in the lives of some of the clients (N2).
Theme 2: Setup and partnerships
While some positive aspects of working with partner organisations were brought up, it was typical to hear that there were challenges that came with the fact that different organisations were responsible for the intervention, which at times created divisions (S6, S3, S9).
Historically, there had been disagreements with regards to the volume and type of information shared between the partners, in particular before and after the LINX workshops or calls. At T3, it was reported that this aspect of communication had been by and large resolved, and the rules on information-sharing were clear (S9, S11). In addition, it was raised that, initially, there were certain situations where the LINX facilitators requested that the young people attending the group workshops, as originally specified, and the navigators would advocate for some young people to have a LINX phone call instead, for example, due to situational anxiety (S9). This occurred before LINX phone calls became the norm secondary to the COVID-19 restrictions, or acceptable at the end of the project, when the numbers were insufficient for group-work. There were also reports of opportunities for closer working that were offered but had not been taken up. In addition, there was discontent voiced over the spheres of influence over the project held by each of the three partner organisations. Direct quotes in relation to grievances are not provided due to the sensitive nature of their content and a high likelihood of the interviewees being identified. However, the overall impression at T3 was that there was much appreciation of each other’s role in the delivery of the programme and the value of the different components of the intervention.
Theme 3: Delivery
Subtheme: training
This subtheme covered the training received both before and during working on Gateway, as well as any previous experience which the staff brought into their role. Most participants reported receiving substantial training both prior to commencing in the post and since. Understandably, the training requirements differed between the three categories of the staff, with the highest requirements in the Gateway navigators, who worked very closely with the clients and helped them address a wide variety of needs. The navigators in particular reported receiving extensive training while in post (N2).
As previously mentioned, some of the training was directed at helping children and young people younger than 18 years, but overall, it was felt that the skills were transferrable. Gathering information with regards to local services available for 18- to 24-year-olds was seen as part of the job in any case, so the focus of some of the training on the younger population was not felt to be an issue (N1).
Subtheme: limitations of Gateway
The subtheme of limitations of the programme emerged as the staff reflected on the challenges they have encountered while working on Gateway. The need for a tailored approach to clients was a particularly prominent topic. It was acknowledged that Gateway was not for everyone, and that for some clients, perhaps, a simple caution or, for example, a drug awareness course would have been more appropriate (S2, S3). On the other hand, it was discussed that the higher-need clients often needed a longer period of time on the programme than the standard 16-weeks.
The staff also commented on the fact that young people under the highly stressful circumstances of being questioned by the police may not process the information fully and give consent without realising the involvement required (S7).
Subtheme: LINX workshops
The LINX part of the intervention consisted of two in-person group workshops, or telephone calls in the place of the workshops, when this was dictated by the COVID-19 restrictions or when there were insufficient client numbers for groups. LINX workshops were seen as an integral part of the intervention, which was at the same time somewhat separate from the navigator support. LINX workshops were reported to act as something of a trigger, an opportunity to make connections between events in their own lives, or to bring up the topic of mental health and its importance (HT2).
The groups were arranged according to gender, but Included young people of varying levels of need, some could be university students or in full-time employment and/or from very supportive families, all the way to people who had very traumatic childhoods and had very high levels of need. It was reported that this could create a certain divide in some groups, whereby the young people were not able to relate to each other (HT1). Yet, this fact was seen as potentially beneficial, whereby clients from more stable circumstances could view these encounters as a wake-up call, and for some other young people meeting those in better circumstances could be inspiring (HT2, HT3). Occasionally, however, a whole group could have consisted of low-need participants, and the nature of the group work as originally planned would be seen as largely irrelevant to them (HT1).
As reported above, the navigators saw tailoring the intervention to the level of need as key, including as a way to ensure that the low-need clients are not overburdened with the input they do not need and which may be disrupting their lives. On the other hand, the LINX facilitators, who only interacted with the clients on two occasions, did not see the involvement of the low-need clients as a wholly negative phenomenon. While acknowledging the gap that existed between some of the young people in terms of their background, some of the young people may have felt inspired (HT2, HT3), potentially encouraging them to step out of their comfort zone and, for example, apply for jobs. However, it was acknowledged that groups with clients from a mixture of backgrounds were more difficult to manage (HT1, HT2, HT3).
Subtheme: COVID-19
The effect of the COVID-19 pandemic was explored with all the staff participants. There was a wide range of opinions on the effect of the pandemic on the work within the Gateway project, on the lives of the Gateway clients and on their compliance with the intervention. Several interviewees volunteered that there had been a significant worsening of mental health observed in the young people (N1, L2, L3). In addition, it was felt that the substance misuse patterns had changed, with many more young people getting questioned over cannabis possession, which could be in part because they were smoking cannabis away from their home, especially if they lived with their families, who were now staying at home much more. The patterns of offending and reoffending were also different in other ways under the COVID-19 restrictions, with the retail outlets and places serving alcohol closed (P1, L2, P1).
It was universally acknowledged that it was easier to reach the young people on the telephone than to ensure they attended a meeting in person. However, the views as to the relative value of the in-person versus phone engagement varied (N3, P2).
It was also acknowledged that the switch to less face-to-face contact with the navigators brought about some other benefits (N2).
The phone mode of delivering LINX workshops was in limited use outside of the periods of the COVID-19 restrictions, for example when there were insufficient numbers of clients to run a gender-specific group within the time frame of the clients’ conditional caution. The difference between the phone and in-person delivery of LINX is covered under the theme of Clients below.
Theme 4: Clients
Subtheme: overall engagement
It was acknowledged that difficulties engaging the young people was an issue throughout the Gateway project. It was often challenging to get through to the young people on the phone, could take a considerable amount of time to build rapport with the clients, and their continuing engagement was not guaranteed (P1, N2, N3).
Subtheme: engagement with LINX workshops
The engagement with the LINX component of the programme was reported to be a particular issue. The staff commented on the value that many clients derived from attending the workshops, despite apprehension with regards to attending and interacting with other clients (N3, HC1, HT1). The phone call mode of LINX workshops in place during the COVID-19 restrictions or when there were insufficient numbers of clients for a group, undoubtedly led to fewer breaches for not attending LINX workshops, but there was concern that this offered too much overlap with the support already provided by the navigators (HT1).
Subtheme: attitude towards Gateway
This topic of the attitude towards Gateway on behalf of the young people was explored in detail in the interviews with Gateway clients at T2, presented above. This subtheme explored whether the staff felt that the association between Gateway and the police mattered to the young people it was targeting. This question was most relevant to the Gateway police officers, and the impression was that this was indeed possible, but assumed not to be a widespread issue, and little evidence of this tendency came to their attention (HC1, HC2).
Time period 3 – Gateway recruiters
The recruitment of HC participants is summarised in the flow diagram in Appendix 8, Figure 13. In relation to the HC Gateway study sites, the majority of the participants were based in Southampton and Portsmouth, but Basingstoke and the IoW were also represented. There were both police officers and civilian staff, in total three females and ten males, from the following teams: Investigations, Custody, Response and Patrol, and Neighbourhoods. Table 15 shows the number of young people which each recruiter randomised (into Gateway or the standard pathway) and/or missed, that is, where randomisation into Gateway or alternatives was not offered. Occasionally during the interviews, the participants referred to the number of people they had randomised or missed, and, in some of those cases, discrepancies were apparent between the numbers recalled and those stated on the HC records against that particular officer or staff member. A detailed breakdown of the above characteristics is not provided in order to protect anonymity of the participants. The thematic analysis map is presented in Figure 7. Quotes from interviews with Gateway recruiters at T3 are provided in Report Supplementary Material 5, Table 5.
| Recruited and/or missed (no. of occasions) | No. of participants in each category |
|---|---|
| Recruited (5) | 1 |
| Recruited (2) | 8 |
| Recruited (3), missed (2) | 1 |
| Missed (2) | 3 |
Theme 1: Aims and benefits
The Gateway recruiters were clear that the main aim of the Gateway programme was to prevent or reduce reoffending. They spoke about how the intervention allowed to divert young adults from the court and the criminal justice system, by addressing the causes of offending and ultimately breaking the cycle of reoffending (R13). Hopes were expressed that the intervention would encourage its clients to look at their behaviour in a new light, which would include seeing its consequences for all affected parties, from the victim and their family to the young person themselves and their family (R9).
Getting support was seen as central to the programme, but the understanding of what was included or possible, varied – from envisaging the range of issues with which the young people may require support, to a view that the intervention predominantly had an educational function, possibly in the form of courses (R8, R9).
The reason for targeting young adults was on the whole appreciated, including in relation to preventing criminalisation at that age, before it becomes harder (R2, R1). It was also accepted that the intervention may not benefit everyone, and not every young person may be ready, or able to, change (R4).
Out-of-course disposals in general were seen as cost-saving and leading to better outcomes, including long-term (R5, R7).
Theme 2: Recruiting: barriers and enablers
Subtheme: time
One of the most often cited reasons for failing to recruit participants was time pressures. This subtheme was naturally closely linked to others, such as that of knowledge, explored below, due to the perception that following Gateway-related processes would be time-consuming, requiring additional time for working out the steps and actions involved. The time pressures on an average shift meant that prioritising was important, and the custody clock (the time period during which a person can be detained, which is 24 hours), for example, was an important priority (R13, R8). Lack of time was seen as a limiting factor in a number of ways: in relation to reading e-mail communications about Gateway, having little time to print off the materials and having a discussion about Gateway with a young person in custody. There was an impression of fearing the bureaucratic side of the recruitment process, especially when not familiar with the processes (R7).
Subtheme: knowledge
Lack of being fully informed about Gateway and associated procedures was frequently cited as a barrier. It was felt that there were many competing demands for attention, and it was challenging to keep up to date (R9).
With the frequently changing guidelines and initiatives, several interviewees cited forgetting about availability of Gateway as an issue. Some mentioned forgetting that Gateway was an option when dealing with an eligible young person, and subsequently receiving an e-mail, alerting them to the missed opportunity (R9).
Some eligible young people may have been dealt with in the usual way, as everyone else, without recalling at the right time, ‘the extra thing that we have to think about’ (R1).
It was common practice for personnel to move internally, with a resultant high turnover, which could lead to temporary unfamiliarity with the requirements of the new post, including the conditional cautions such as Gateway. In addition, an ongoing intense recruitment drive was mentioned, which was linked to the fact that a significant proportion of the workforce was newly recruited, and still learning the ins and outs of the job (R1).
Subtheme: training
All the participants were questioned with regards to receiving training, and a total of five reported having not attended any formal training and some volunteered that they were unaware that such training had been available (R3).
One of the participants who could not initially recall any formal training, checked their electronic records during the interview, which showed that they did, in fact, attend an in-person training session in 2019, which was over 2 years before the interview.
However, the participants reported feeling confident in their ability following the Gateway guidance available on HC Intranet, but were not always aware of the existence of the Gateway project officer(s) (R3).
Subtheme: ‘selling’ Gateway
Not fully understanding what the intervention involved was cited as a barrier to being able to describe Gateway to potential participants in a comprehensive way (R8).
Occasionally, a degree of mistrust, expressed by the young people towards the offer of Gateway interfered with recruiting efforts (R12).
Subtheme: barriers for young people
Some participants felt that the conditions of Gateway may be difficult for some young people to fulfil, for example due to having to take time off work and travel to the workshops. This may have been a factor discouraging some of the recruiters from holding conversations about Gateway, albeit the extent of this is unknown (R9). There were also suggestions that Gateway may be too involved for someone who had much going in their lives and who wanted the ‘easier’, court option (R8).
Theme 3: Processes and systems
Subtheme: timely guidance
Participants expressed a preference for timely guidance on whether a particular detained person would have been eligible for Gateway. It was mentioned that the decision-making in relation to eligibility, perhaps, should have even been taken out of their hands. They would have appreciated, for example, an electronic prompt on their computer system, suggesting Gateway at the time of a case being managed (R7, R5). Among all the competing demands on the recruiters’ attention in their daily job, it was very easy to forget about Gateway, in particular, when dealing with eligible cases on an occasional basis (R1).
Subtheme: complexity
Participants reported that the procedure for recruiting into Gateway was easy to find on the HC Intranet, and the process was not overly complicated to follow (R4). Some recruiters, however, commented on operational aspects that they felt were unclear or cumbersome, for example, a confusion of who did what element of the intervention (R10).
Most participants said that the Intranet page for Gateway was easy to navigate, although a small minority had made suggestions on how it could have been improved. Sometimes opinions could be contradictory (R4, R8).
Subtheme: physical locations
The recruitment process was frequently compounded by the features of the premises where the recruitment took place. Where distance divided printers, laptops, custody sergeants, who make the final decision, and custody cells inside a police station, this complicated the process (R8, R2).
Subtheme: randomisation
Randomisation, albeit seen as not unduly complicated to carry out, was in practice a challenging concept, particularly when Gateway was not the eventual outcome. The task was to tell the young people about the programme, which they would only have a 50% chance of getting. If the potential participant was randomised to control, this was disappointing for the young people (R12, R7).
Summary of findings
The relationship between age and desistance, although complex, is well evidenced. 41 Depending on a range of factors (such as crime type, gender, socioeconomics) aggregate age–crime relationship curves suggest that the rate of criminality may peak at age 17 or 18 years old and decline over time. 42 Desistance processes are not limited to the down-slope of the age–crime curve, but evolve and take place throughout the course of that curve. The Gateway programme was established to address the existing gaps in provision for those specifically aged 18–24 years. The central idea was to ‘bridge the gap’ and support individuals who are transitioning into adulthood, where currently the Criminal Justice System does not provide appropriate targeted provision. 43 The Gateway programme aims to provide a ‘turning point’ or an encounter that puts an individual on a different trajectory, supporting them on a journey to become ‘desisters’ from crime, rather than persisters or career criminals. 44 As supported through the evidence here, and in line with desistance theory, the Gateway programme is aimed at reducing recidivism, not stopping it completely.
Description of the Gateway intervention and its causal assumptions
Within a week of receiving the caution, the young person met with the Gateway navigator who carried out a needs assessment, relating to the ‘seven pathways to re-offending’45 from the list of outcomes widely used in the UK to monitor and support offending risk. The seven pathways are grounded in theory relating to the risk-need-responsivity (RNR) model and ‘central eight’ (see Report Supplementary Material 1). Following the needs assessment, the navigator worked with the client offering a mentoring role, signposting to services, and providing support to build a more stable lifestyle. Young people on the Gateway intervention worked with their navigators for 16 weeks, usually meeting once a week.
During the 16-week period the client undertook two workshops consisting of group work: workshop A (week 3) and workshop B (week 10). The LINX workshops were rooted in Social Learning Theory, the model promoted within the RNR model described in the literature review. 46 Social Learning Theory focused on the theory that behaviours are learned from the environment through the process of observation. The Social Learning Theory approach in the RNR model highlighted the importance of learning within a social context. The LINX workshops focused on addressing personal risk factors, seeking to assist with development of cognitive and affective empathy, and address neuropsychological deficits, such as antisocial/delinquent beliefs. This was achieved through two half-day group sessions, (delivered by phone during the COVID-19 lockdown) where an educational programme focused on reasons why people offend and provided tools to manage emotional well-being. Additionally, sessions took a non-patronising approach and importance was placed on taking personal responsibility, building respect and developing empathy and listening skills.
Sociostructural factors and the wider determinants of offending
Although there are limitations in previous studies, such as small sample sizes, there are several factors that may influence the desistance pathway among young adults. Taking the commonalities of these studies, factors such as positive social-structural factors, agency and supportive relationships are important. 47–49 These, as well as other factors, are discussed in turn, in relation to the Gateway programme.
Firstly, sociostructural factors include the wider determinants of offending behaviour commonly cited in the literature (see Figure 2) such as employment or education, as well as other more traditional social factors, such as marriage. 49 In line with this, the Gateway programme assessed the impact of the wider determinants (both criminogenic and non-criminogenic factors/needs) and how they change over the course of the 16-week programme. The Gateway programme supported individually assessed areas including education, finance, well-being, health, relationships, attitude, accommodation, substance misuse and depression. Generally, participants viewed wider determinants (or ‘areas’) addressed with navigators as outcomes of greater importance than a reduction in reoffending. For most, support was focused on a small number of areas identified through a needs assessment, rather than seeking to support all. For example, clients consistently attributed the Gateway programme to improvements in both their physical and mental health across both time periods; among them they reported improved health-seeking behaviours, a reduction in drug and alcohol intake and feelings of anxiety. The role of the navigator was not to replace the role of the clinician but to provide intentional support to areas of health as identified by the client. These resulted in taking ‘practical steps’ towards improved health including, for example, making and attending doctors’ appointments with clients, as well as offering a listening role. In similar studies, the practical and emotional support offered through mentors is commonly cited as an invaluable part of the intervention. 50,51
It was beyond the scope of the programme to address the key drivers of offending that did not manifest at an individual level. For example, one participant recognised that Gateway could not address the lack of readily available mental health services or the need to carry a weapon to feel safe in a neighbourhood. Wider structural factors, such as access to services and social deprivation, were influencing factors of offending that could not be addressed through the Gateway programme. 52 Such structural contextual factors may have acted as a barrier, limiting the potentiality of the Gateway programme to effect change. To this end, the programme-focused approach offered through Gateway could only realistically address individual lifestyle factors within a 16-week period, diminishing the possibility of longer-term change.
Specificity, needs and the RNR principles
The qualitative data described a polarity of needs among participants; individuals were described as having either ‘high’ or ‘low’ needs. As a lower volume of clients were initially recruited than anticipated, the eligibility criteria were widened, resulting in the recruitment of clients that did not require the level of support offered through Gateway. From the perspective of Gateway staff, the significant scope for triaging and tailoring within the Gateway intervention (navigator role) allowed them to avoid mistargeting the intervention at the low-need clients. The diversity in need however led to conflicting opinions around the group work and a continuous tension between being able to acquire general and specific responsivity;46 for example, the planned group work was perceived as largely irrelevant if a whole group was of low need. The content of the group work was also contested by some clients, who felt that certain topics were not relevant to them or their offence type, risking isolation or disengagement. Some practitioners felt that the group work was also gendered (targeted for males). Contrary to these views, when groups had individuals with mixed needs, some seemingly low-need individuals felt that the stories and views of others (of higher need) offered them a unique perspective. The importance of hearing and understanding other people’s points of views was consistently mentioned by clients across the time points, and is consistently noted as an integral part of cognitive social learning interventions. 53 Altogether a person-centred approach was strongly advocated; this means that both tailoring and flexibility throughout the programme, including in both the one-to-one sessions with the navigator and the group work, are necessary to ensure specificity to the clients’ needs.
The assessment and treatment of offenders on the Gateway programme has previously been discussed in the literature review in relation to the RNR principles. 46 The first principle ‘risk’ concerns the offer of interventions according to risk of recidivism, such that those with low risk cases receive minimal intervention. As the risk principle had not been objectively assessed at the point of recruitment or screening for eligibility for Gateway, the navigators valued the flexibility to appropriate the level of intervention according to risk. In line with the principle, they identified client need through their assessments and interactions. However, there were ‘missed opportunities’ to further identify need due to the long-standing communication challenges that occurred between the delivery partners. Although the independence of the intervention team, from the police, was highly valued by clients, having multiple (two or more) organisations delivering the intervention created unnecessary challenges. There was no communication feedback loop about an individual clients’ needs, between the navigator and LINX group facilitator. Inevitably, this meant that the capacity of the LINX facilitators, to potentiate specific responsivity to an individual’s needs, became limited. The complexities around partnership working has been cited in a recent process evaluation on alternatives to custody, suggesting that such difficulties could undermine the credibility of the intervention. 51
Agency, control and readiness to change
The Gateway programme gave clients agency over the content of the programme and what they could gain from it. This was initiated through an in-depth needs assessment with the navigator following week 1, that allowed clients to identify their requirements and areas for change. The tailoring of the programme to suit the needs of the individual including, for instance, making appointments at a convenient time for clients (and if necessary, their parents) was highly valued and enabled clients to have greater control over their lives. Staff accepted that engagement with the target population could be challenging and therefore this tailoring of the programme and flexibility to, for example, offer phone calls over face-to-face meetings, was a means to encourage engagement. This was also welcomed by participants who found it challenging to meet the costs and time associated with the, often long, journeys to meet navigators. The use of phone calls was believed to lead to better compliance/engagement, although it was evident that face-to-face meetings were critical in building a rapport and were therefore necessary at the first assessment. When LINX workshops were offered over the phone, however, clients struggled to differentiate between the LINX workshops and the sessions with their navigator.
There was, however, a notable dissonance between what participants ‘understood’ Gateway to be and what Gateway was. This mismatch was often cited by clients, who expressed a need for more initial information and better communication by the police when offering the programme. In this regard, police recruiters commonly mentioned lacking information about the intervention programme, limiting their ability to ‘sell’ the offer, particularly to young people who did not trust in the police. (The challenges to recruitment are described and summarised in Chapter 4.) To this end, the independence of the navigator role was highly valued by clients. If clients believed the navigator to be involved with the police, this risked the client ‘shutting down’ thereby diminishing the role and purpose of the navigator and an individual’s feeling of agency or control.
Mechanisms of impact and outcomes
Engagement in LINX workshops was highly valued by participants who emphasised the importance of being able to see things from another’s point of view. For those who shared offence types, engagement in LINX workshops helped to alleviate the feelings of isolation experienced during the process and, in turn, raised their self-esteem. Contrary to this, individuals who differed according to offence type felt a sense of isolation and a feeling of being looked down upon. Clients reported learning techniques and strategies to enable them to make better decisions and manage their emotions and the situation they found themselves in. These educational tools and techniques were also described in relation to improved self-awareness and self-concept. Consistent with social learning theory, clients felt that they were able to make better decisions based on what they had observed in others from the LINX group work.
‘Her just kind of, handing me an olive branch’
Navigators played a significant role in enabling compliance and change among clients. Participants frequently attributed their engagement in the Gateway programme to the relationship with their navigator and described feelings of not wanting to ‘disappoint’ or ‘let them down’. In contrast to the expectations and experiences of mistrust, structure and judgement associated with police engagement, navigators supported change through factors related to trust, flexibility and non-judgement. Consistent with other studies, results suggest that, at the start of the programme, clients wanted to avoid criminalisation (‘going to court’) but, due to the limits in the information provided by police recruiters and clients’ previous experiences and expectations of the police, were unaware of the extent to which Gateway could provide support. Throughout the course of the programme, most clients experienced a transformation in their attitude towards the Gateway programme, from a position of apprehension and scepticism to acceptance and acknowledgement of the programme’s ability to help. The role of the navigators was akin to that of a mentor, where mentoring is often defined as a 'one-to-one, non-judgmental relationship in which an individual gives time to support and encourage another'. 54 Similar to other mentoring programmes, engagement with the navigator was client-led, meaning that the content and objectives of the programme were tailored to the clients’ needs. Clients highly valued having someone ‘to talk to’. The literature suggests that through appropriate sign-posting, mentors act as a bridge into appropriate services. 55 This also meant, however, that all navigators needed to have an equal level of training and experiences, particularly in adult mental health and mentoring, in order to meet the necessary requirements of the role. The provision of practical support and signposting by the navigators facilitated many opportunities for clients including support to access employment (e.g. getting them a construction skills certificate), finance (e.g. sorting out bank accounts), health services (e.g. making appointments with the GP) and housing (e.g. getting them on the housing register). Clients expressed the positive benefits that Gateway had on their lives through improvements to these aspects. As such, losing support after the programme was frequently cited as a concern for clients who had built up a strong rapport with their navigator. There were, however, limitations to the efficacy of the navigator role, particularly for those at opposing ends of the needs’ spectrum. Some felt that the complexities of their lifestyle/behaviour could not be unravelled within the 16-week engagement; whereas some felt that they could not benefit from the support offered through the programme. For those of low needs, their attitude to the Gateway programme remained unchanged. This highlights the underlying assumptions around the Gateway programme, as supported through the interviews with Gateway staff and clients. Specifically, that Gateway was designed to be able to support those of higher needs and complexity, and potentially those who had committed multiple offences. A further assumption was that Gateway encouraged clients to empathise with their victim and their family. However, few clients had committed crimes where there had been a victim, which meant that this assumption could not be universally applied.
Chapter 4 Challenges and mitigating actions
The Gateway Study, incorporating a RCT, as well as an economic and qualitative evaluation, was an innovative and undoubtedly ambitious project. It aimed to produce the highest quality evidence for a much-needed intervention, which had the potential to change the lives of the most vulnerable young people in society, with an anticipated positive ripple effect on their families and communities. The target population of the Gateway Study, 18- to 24-year-olds who have been questioned for low-level offences, can be difficult to engage and retain in research studies. This chapter examines the challenges encountered in the process of conducting the study, broadly under the themes of recruitment and data collection, and the mitigating efforts made by the TMG to navigate these issues. The Gateway programme was conceived and coordinated by the police and not directly influenced by the researchers, who were responsible for its evaluation. However, the research team also learned about issues encountered in the delivery of the programme from qualitative interviews with the Gateway programme staff and clients, and these are also summarised here.
The Gateway RCT had an unusual setup, in that the consenting process comprised Stage 1, by police recruiters, and Stage 2, by researchers. Stage 1 consent enabled access to offending data and sharing of contact details with the research team. Stage 2 consisted of providing full consent to a researcher and was immediately followed by data collection for that time point (typically, week 4), as both took place during the first follow-up appointment. There was no baseline data collection. However, for simplicity, the researchers have chosen to refer to all activities leading up to Stage 1 as recruitment and all data collection following Stage 2 as retention.
Recruitment
Numbers of eligible young people
During the study planning stage, it was initially estimated by HC that recruitment of the target sample of 334 participants would be possible within 12 months. However, this figure included the numbers of those pleading guilty in court and, in practice, by that stage they were outside of the jurisdiction of the police and hence no longer accessible. This meant that the monthly rates of eligible young people coming through HC in Southampton were much lower than originally anticipated. Several options were considered by the TMG to compensate for this, and the following changes implemented.
Expansion of the geographical study catchment area
Initially, the study was to be run by Southampton Central Police Station only. The original Southampton catchment area was expanded to include the local authority districts of Eastleigh, New Forest and Romsey. In addition, three new sites were opened at the main police stations in Portsmouth, Basingstoke and Newport, IoW. As a result the entire geographical area covered by HC, was included.
Amendments to the eligibility criteria
The eligibility criteria were extended and, from the beginning of pilot 1 onwards, included not only the people who otherwise would have been required to go to court but also those who would have received a different form of conditional caution. This meant that the control arm of the RCT, that is the standard pathway, was either a court summons or another conditional caution. Following this change, the control arm also reflected the real-life standard pathway more closely.
Adjustment to the study timeline
Allowing additional time to recruit the required number of participants, was intended to further compensate for the reduction in the monthly recruitment targets compared to those originally planned. This included a 2-month extension to the original 4 months for pilot 1, to allow for better assessment of the feasibility of the monthly recruitment figures.
Potential participants missed or declining randomisation
This challenge to the study recruitment was multifactorial, with a range of underlying reasons also voiced by a sample of the HC police officers and civilian staff that acted as Gateway recruiters, in qualitative interviews reported in Chapter 3.
Main reasons for non-recruitment of eligible young people:
-
Forgetting about, or being unaware of, the Gateway programme and RCT, or misinterpreting the eligibility criteria.
-
Time pressures and prioritising other operational tasks during a shift, in preference to following the procedure for Gateway.
-
Apprehension about following an unfamiliar process of recruitment and randomisation.
-
Being out of date in relation to Gateway training or having never attended training. This could have been because it was not compulsory or not requested by a senior officer or being unaware of training being available (details of the training which was made available for Gateway are provided in Chapter 2, under Recruitment).
-
Lack of understanding of Gateway and the difference between randomisation and Stage 1 consent for the study. This may have occurred partly due to lack of training or practical experience, leading to difficulties when explaining Gateway to potential participants or answering questions. This may have contributed to the high rates of study refusal.
-
Occasionally, decisions being made that Gateway would not have been in the best interests of the person in question, for example they would have struggled with compliance, or other reasons.
-
Other programmes being prioritised, for example Cautioning Adult Relationship Abuse (CARA) for low-risk, first-time domestic abuse offenders.
-
Apprehension towards research in the criminal justice system or doubts with regards to its value.
-
Lack of awareness of the shopping gift card incentive offered by the UoS for study follow-up or discomfort in relation to discussing such incentive, or disagreement with the idea of an incentive altogether, leading to not mentioning the incentive, which was otherwise anticipated to boost recruitment. As a result, the prospect of taking part may have been seen by potential participants as insufficiently attractive, which may have led to the study being declined.
-
The RCT being declined for a variety of other, often highly individual, reasons.
Each non-recruitment of an eligible young person was followed up with an e-mail from the Gateway Project Officer to the colleague who had dealt with that individual, enquiring as to the factors contributing to this. Later, Gateway recruiters’ supervisors were also copied into the e-mail, to increase awareness and response rate. However, these measures were thought to have limited effect, and the rates of missed eligible people continued to be high.
The extent of the barriers to recruitment was more fully revealed in the qualitative interviews with the Gateway recruiters following the closure of the RCT. Low rates of eligible young people, meaning few opportunities to both consider offering the study and discuss it in practice, as well as a high internal staff turnover, were mentioned in the interviews and likely contributed as mechanisms behind many of the above reasons.
Retention
The rates of Stage 2 consent and data collection across all three time points were suboptimal throughout the duration of the trial (see Table 2). This meant that, even though recruitment rates were broadly within progression criteria, there were insufficient follow-up data collected for those participants recruited. The main reasons for low data collection rates are presented below.
Contactability
Low contactability of participants, that is the condition of being contactable, was the most significant barrier to retention in this RCT. This applied both to initial attempts by the researchers to establish contact, before Stage 2, and throughout the follow-up period.
Difficulties contacting participants were due to the following:
-
Incorrect, absent or no longer in use contact details.
-
No response to initial or subsequent contact attempts.
-
Inability to hold a conversation about the study – participants reporting being unable to speak at the time of calls, terminating calls prematurely or asking for calls to be rearranged and subsequently becoming uncontactable.
Missed appointments
There were multiple instances where participants either did not attend in-person appointments (prior to the COVID-19 pandemic) or were uncontactable or no longer available to complete the questionnaire at the time of booked telephone appointments. Approximately 34% of participants at week-4 rising to around 46% at week-16 and year-1 were contacted more than once to schedule an appointment. The follow-up was recorded as a ‘did not attend’ (DNA) if continuing efforts on behalf of the researchers did not result in a completed questionnaire for that time point. Although participants were never questioned as to why they missed an earlier appointment, if contact was subsequently established, some young people offered their reason, which included forgetting, being too busy, falling asleep, having their phone in silent mode, and personal or health issues.
Withdrawals
Most withdrawals occurred while attempting to establish contact following Stage 1. Frequently, a participant would deny any memory of the study (which was not uncommon in general), but also was against continuing the conversation and objected to further contact from the researchers. Withdrawals via text following receipt of a study contact text or letter or after Stage 2 were exceptionally rare.
Mitigating measures to boost data collection
The following measures were introduced to overcome the above barriers and improve retention:
-
Introduction of a study leaflet, which was used not only at Stage 1 but also e-mailed to post-stage 1 participants by the Gateway Project Officer, as well as by the researchers prior to Stage-2 consent. The latter was done if felt to be helpful from conversations with individual participants, for example they did not remember receiving the leaflet earlier. The leaflet was subsequently also merged with the Stage 1 consent documents, for use by HC, to ensure that the leaflet was printed and offered to participants at the same time.
-
Introduction of a 2-minute video explaining the RCT, following a suggestion by a PPI representative. A weblink was provided in the study leaflet, as well as included in texts and e-mails where phone call attempts had been unsuccessful.
-
Introduction of phone calls to participants by the Gateway Project Officer following Stage 1 consent, to remind about the study and forthcoming contact by the researchers.
-
Introduction of the use of e-mail as an additional mechanism for researcher contact ahead of Stage 2 (with consent to this at Stage 1). Participants’ e-mail addresses were obtained from HC, where these were held on record, for use when initial phone contact attempts were unsuccessful.
-
Switching from the previously obligatory in-person mode for Stage 2 consent and first follow-up, to telephone mode. The change was already being considered in pilot 1, following observations that some participants struggled to travel to physical appointments or felt anxious about meeting a researcher, but ultimately this was necessitated by the COVID-19 safety considerations once the study was restarted as pilot 2.
-
Increasing the value of the incentive, which was also designed to improve recruitment, and switching the format of the shopping gift cards from paper to online shopping gift cards as default, with the paper option remaining available, if preferred by individual participants.
-
Agreeing on a flexible approach to follow-up timing, that is establishing extended cut-off times for follow-up for participants who become contactable much later than the time point of their preceding follow-up.
-
Some of the changes introduced to improve recruitment and described above, also were intended to improve retention.
Intervention
The design and implementation of the intervention was not influenced by the researchers, who nonetheless learned about some of the challenges that the Gateway staff encountered while delivering the programme. Some of these are reflected on in greater detail in Chapter 3, Qualitative evaluation. Provided here is a summary of the main issues encountered by the Gateway staff:
-
The set-up involving at least three organisations responsible for various aspects of the intervention. In practice, initially there was also a fourth organisation employing some of the Gateway navigators. This introduced a variety of issues, including those relating to physical working space, training, priorities, influence over the intervention, and differences in personalities and ways of working.
-
An association between the navigators and the police as perceived by the clients, due to the use by the Gateway navigators of HC e-mail addresses and physical working space, as well as the route through which clients came to the intervention.
-
Low numbers of clients, especially at the beginning, and unpredictable flow of clients with varying degrees of need.
-
Challenges in contacting and maintaining engagement in Gateway clients. Many of the contactability issues echoed those faced by the researchers, as described above.
-
Certain rigidity in the design of the programme, which had a limited scope for triage and tailoring of input according to the level of need of individual clients. This meant that the intervention could be excessive and disruptive to the lives of low-need clients, and insufficient and too short for the high-need clients.
-
The dilemma between the potentially superior value of the in-person LINX workshops compared to better compliance with the telephone model for LINX, which was used during the COVID-19 restrictions and when numbers were insufficient for an in-person workshop. Clients seemed to derive much benefit from the workshops, but faced multiple barriers to in-person attendance, with missing a LINX workshop being a common reason for breaching for non-engagement.
-
Short-term contracts and uncertainty over future, which could have contributed to the high turnover among the Gateway navigators.
The effect of the COVID-19 pandemic
Both the intervention and the RCT were interrupted by the arrival of the COVID-19 pandemic, as already described. Once both restarted, the impact of the pandemic and associated restrictions may have been substantial, but the extent of this is difficult to quantify. In qualitative interviews, the Gateway project staff reported observing a significant effect on the young people’s mental health, which is known to be linked to engagement.
The pandemic has created what has been termed a ‘perfect storm for the mental health of young people’. 56 Young adults have suffered the largest decline in mental health compared to any other age group, and in the UK, those on a low income, represented in the study’s target population, have been found to have been hit the hardest. 57–59 Prior to the pandemic, the substantial increase in the amount of the shopping voucher incentive and the switch from the in-person to telephone mode for Stage 2 consent and the first follow-up questionnaire would have been expected to boost retention. However, the introduction of these changes at the restart of the RCT at the height of the pandemic did not seem to be associated with an improvement in retention.
With regards to recruitment, the high rates of missed opportunities to offer Gateway persisted, and the opinions of the interviewed Gateway recruiters on the effect of COVID-19 on their ability to recruit into the RCT were mixed. Some felt there had been no effect, while others cited several reasons for a likely negative impact, including COVID-19-related changes in the patterns and types of offending, the need to keep up with the ever-changing COVID-19 guidelines and the long gaps between undergoing training before the pandemic and having a chance to apply training in practice.
Chapter 5 Discussion
Statement of principle findings
This study was a RCT with qualitative evaluation of an out-of-court community-based programme to improve the health and well-being of young adult offenders: the Gateway RCT. This robust methodological approach with a validated health measure as the primary outcome is novel within the setting of the criminal justice system. It was not possible to address the effectiveness of Gateway intervention objectives due to the challenges of retention and data collection and the prohibitive time needed to reach the required sample size. Consequently, the study was closed early. The study recruited 191 young people, 109 were randomised to Gateway and 82 to usual process. Recruitment rates were within the bounds set within the progression criteria, and participant demographics and follow-up rates were balanced between the two groups. The researchers were able to extend and complete the qualitative element of the study conducting 69 in-depth interviews with: 28 young people, 25 Gateway staff, 13 police recruiters and three focus groups with navigators. This data provide a rich source of information about the perceptions of the intervention from the point of view of participants, recruiters and operators of the Gateway intervention. The study found that young people reported being able to make better decisions following engagement with the sessions and that the navigators played a significant and valued mentoring role. This had enabled compliance and change among young people, highlighting the unmet health needs for this group of 18- to 24-year-olds, and the need to address the wider determinants of reoffending through individualised assessment.
The Gateway programme was developed for those with higher needs, which meant that flexibility and adaptability, to suit individual needs, permitted the utility of the intervention for those with lower needs. Group work is always challenging with some participants expressing reluctance to take part. Getting participants to attend the programme often required the close support of the navigator and resulted in a positive and empowering experience. The use of peer mentors where engagement with services is an issue may be helpful in future research where group work is needed.
Some issues with the intervention that may have impacted on engagement were identified. One of these was the perception of the navigators’ links to the police and not being independent workers through, for example, being based in a central police station and having Constabulary e-mail addresses. This is a feature that has been recognised in other interventions15,60 and the concept of a trusting relationship with intervention delivery practitioners seems to be key to the engagement of participants. The qualitative information has also provided learning on how to contact a hard-to-reach recruited participant, not just to the study, but for navigators and LINX workers delivering the intervention too. This will be useful in the planning and delivery of future studies.
The researchers were able to successfully employ several actions to improve retention and to conduct data collection, some of which were recommended by the PPI members involved in the study team. This included simplification of study information; and value and delivery mode of ‘thank you’ vouchers for participating in the study. It was not possible to contact and/or follow up all recruited participants, consequently data collection was incomplete. Following up and collecting health data in this population of young adults is difficult. These challenges are similar to other research endeavours in community-based studies in disadvantaged populations especially with young people. 61,62 Where the primary outcome is routinely collected for example recidivism in criminal justice system, this is more feasible to obtain; of the few RCTs conducted in the criminal justice system for out-of-court disposals (OOCDs), attrition is often reported to affect the ability of studies to provide effectiveness estimates. 15 It is important to note that services encounter challenges in reaching these young adults across all health care and statutory sectors and this is compounded by their suspicion of dealing with authority such as the police. 63 In this study, the researchers often found it difficult to contact participants to seek Stage 2 consent and to conduct data collection as contact details, in particular mobile phone numbers, were changed and changed often. This is a day-to-day challenge for everyone in the criminal justice system including those delivering interventions associated with conditional cautions as well as researchers. The researchers, efforts to address these are a key output of the study and will help in planning to mitigate such challenges for future studies.
Collaboration
The police investigators undertaking recruitment to the trial in and out-of-custody suites used a robust eligibility check and randomisation tool. This further embedded and reinforced the research/evaluation steer that police forces have had over the past decade. 60 The researchers worked closely with the Gateway police officers who offered well-publicised and regular training sessions to police investigators on Gateway across Hampshire and IoW. This included updates when study parameters changed and following the restart after COVID-19 restrictions were lifted. Awareness raising included regular reminders to police investigators. These were sent in various formats from the study police officers with endorsements from high-ranking police officers. However, training was not mandatory, potentially leading to less-than-ideal take-up as officers sometimes had to prioritise required training. In addition, the high day-to-day workload and staff throughput meant that officers had multiple competing demands, and for those new to post, time spent learning the day job was understandably their main priority. Attendance was still a problem for another RCT where officers randomised to training were mandated to attend. 64
Qualitative data suggested that the study processes were overall clear and able to be followed; but opportunities to recruit were missed. Some of the police investigators interviewed felt that eligible people may have been missed due to the lack of familiarity with the Gateway Conditional Caution. The frequent movement of frontline officers meant that training may have been missed or not have been up to date. Consequently, some police staff were unaware or had forgotten about the Gateway option and its accompanying study requirements. In addition, even when trained, the rarity of potentially eligible participants meant that this was not at the forefront of police officers' minds. This is in contrast to conditional cautions with a high number of eligible people presenting frequently (such as CARA for domestic abuse offences19), which were upper most in police officers' minds and experience, making them more likely to include all eligible people. Turnover of staff of all ranks and development of new out-of-court interventions contributed to the competing demands for staff.
A very positive feature of this study was the close collaborative working and productive sharing of organisational processes and approaches between constabulary and academia, benefiting the recruitment and running of the Gateway study, and facilitating development and operationalising steps taken to address challenges as they arose.
Similar challenges for research have been noted and addressed in the National Health Service (NHS) setting, where they have been mitigated by having dedicated professionals, for example, clinical research network-funded staff to support recruitment consent and data collection. 65 The study was fortunate to have two full-time police officers on this trial. Perhaps as experience in non-NHS setting research grows support similar to that in the health care setting could be provided to help facilitate recruitment and retention within studies.
The COVID-19 pandemic provided challenges for the study in that all police conditional cautions/OOCDs were suspended, and there were relatively low crime rates following lockdowns. 66 However, the researchers were able to be agile in their response by changing study processes to fit in with restrictions, such as a change from face-to-face data collection to telephone consultations, which was found to be more acceptable to the participants and improved retention. Through these changes, barriers to attendance were addressed with travel considerations removed, which fitted in with the lifestyle of many of the participants. Future studies should consider offering these methods of data collection.
Notwithstanding the challenges outlined above, the efforts to mitigate these where possible had results, and Stage 1 recruitment led to reasonable recruitment rates that were not unlike that in RCTs in other settings; the researchers gained valuable insights from the qualitative evaluation.
Strengths
The researchers have demonstrated that it is possible to recruit and randomise to a RCT in the police setting. The study is novel because it is the first in the UK to use a two-stage consent procedure and have a primary health outcome requiring individual data collection rather than criminal justice system data on recidivism.
The qualitative study included 69 interviews/focus groups and provides evidence around the perceptions of the intervention from multiple viewpoints which will inform future studies.
Excellent and close collaborative relationships between academics and police led to a very functional communication and shared learning for the benefit of the study and its processes and participants.
Future health-related trials will have a benchmark for attrition in this setting and population which will help guide feasibility and study methodology.
Limitations
Although the study’s recruitment rate was within acceptable limits and comparable with trials in the NHS/community settings, the number of randomised participants providing data was insufficient to complete the trial in an acceptable timeframe and assess the effectiveness of the Gateway intervention. The high levels of attrition likely had several contributing factors. The unusual recruitment and consent process meant that contact with the researchers did not take place until Stage 2. The researchers were unable to directly provide full details about the study to young people, including the incentive, until later, and were unable to ensure participants’ details were correct. As a result, on average up to 35% of participants never had a full conversation with a researcher. The COVID-19 pandemic would have played a role through worsening mental health, known to be particularly marked in the young people in the UK at the time. 67 Poor mental health in the young people was also cited by the navigators as part of the qualitative evaluation, and this may have contributed to reluctance to engage. Lastly, the target population had their own reasons for suspicion towards a study or intervention being proposed by the police, as well as for changing phone numbers and not responding to contact attempts, including mental health and addiction issues, continuing involvement in crime and other reasons.
The researchers met many challenges in setting up and running the study, many of which they were able to mitigate by approaches they adopted. These included close collaboration with the police to address recruitment and consent of participants, expansion of the inclusion criteria, widening the recruitment area, being agile in restarting after COVID-19, and improving follow-up rates.
Equality, diversity and inclusion
The Gateway programme was developed and funded by HC, hence the study location. The 2011 census demonstrated that although a largely White British county, the number of residents in Hampshire from different ethnic backgrounds was increasing. 68 Efforts to ensure an inclusive approach included the engagement of community leaders and groups from black and minority ethnic, lesbian, gay, bisexual, and transgender+, lower socioeconomic groups, and religious groups to inform all aspects of the study. The study had no restrictions related to ethnicity, religion or gender. Most trial participants were White British, but data were provided by black and Asian recruits. For those who provided information, the level of education ranged from no qualifications to degree level, with most having 1–4 GCSEs; 17% indicated they were female, and participants came from across all five quintiles in the index of multiple depravation. Basing the study in Hampshire and IoW may provide a limitation on generalisability.
Patient and public involvement
Engagement with young adults with offending experience, victims of crimes, and community groups and leaders proved vital for this study to progress as far as it did. The study’s investment in working with partners to involve these groups resulted in practical advice and suggestions for modifications and adaptations of the researchers’ plans. This resulted in changing the title of the study, rewording participant facing documents and increased voucher incentives. It also helped the researchers to understand the potential for criticism of the vouchers and the need to be clear that they were study related. Ideally, the researcher team would have liked to engage directly with victims of crime, but given the absence of requests for RJ, this was not possible. The researchers were also confident that their representative from the victim charity Aurora New Dawn provided a relevant perspective.
Community engagement allowed a two-way dialogue so that the researchers could explain the problem, about the Gateway programme and why they were doing a trial. In return the researchers learned about existing and potential concerns from a wide range of communities. The key lesson was for them to focus on the potential societal and economic benefits of programmes such as Gateway.
Future research
Out-of-court disposals with a simplified two-tier approach (community resolution/conditional caution) is the strategic direction of policing in England. 69 There is limited evidence of effectiveness, whether with conditions or without, compared to court prosecution, at reducing harm and reoffending and sustaining victim confidence and satisfaction. 70 This finding applies to young offenders, young adults and adults. There remains a paucity of robust evidence of effectiveness of interventions in this context with health and well-being outcomes.
The study has demonstrated that it is possible to engage with the police and collaborate on recruiting in the police setting prior to offenders reaching court. The measures aimed at improving recruitment and the data presented, can be used to inform the planning of future RCTs including sample size calculations. The use of RCTs as the most robust research design for establishing effectiveness of short-term psychosocial interventions is well established. 71 However, as with this trial, a pragmatic approach is essential in order for the results to be of value in the real world. 72 The researchers recommend that future prospective studies set retention targets as well as recruitment targets for an internal pilot phase long enough to assess progress. This should not compromise ensuring an adequate follow-up period for the evaluation. The challenges the researchers faced during their study also suggest that widening the geography across several regions/police areas and using a cluster RCT design may be a more pragmatic and feasible approach, simplifying processes in each district and ensuring sample size is attained, albeit cluster design requiring more participants.
The challenges the researchers faced, raise the question of whether study designs other than RCTs should be used for assessing interventions aimed at this population. Post hoc cohort studies offer the potential to address non-response and attrition bias, although they are prone to risk of biases. 73 Recorded data would be needed to be relevant to the complexities of the lives of this population, may not be available and access prohibitive, although there are efforts being made to harmonise health data within the UK (www.hdruk.ac.uk/) and more widely. 74 Future research should consider the most appropriate outcomes to evaluate the intervention and the options for routinely collected data compared to prospective data collection.
Structural equation modelling with a longitudinal sample (i.e. no randomisation) has the potential to provide useful insights into the possible underlying mechanisms for differences. However, this method will still be prone to the issue of selection bias. While the RCT is the ideal design to establish effectiveness this study showsthe huge difficulties with its implementation among young offenders in the police setting. Although randomisation is the preferred method of evaluation it might be worthwhile considering an alternative evaluative approach. The problem with most non-randomised designs such as cohort designs or before and after evaluations is that they are subject to a range of biases that make their findings unreliable. However, one quasi-experimental approach, the regression discontinuity design (RDD), is at lower risk of bias and in certain circumstances approximates to an RCT. 75 In the RDD method participants are allocated according to their score on a continuous baseline variable (e.g. age, position on a waiting list, reoffending risk score, etc.) with outcome being assessed on a continuous measure (e.g. probability of reoffending, quality of life). 76 Essentially the method plots the outcome of interest against the allocation variable. If there is no effect of the intervention then the regression plots of the allocation variable against the outcome of interest will be smooth with no interruption at the point of allocation on the pre-test variable. However, if the intervention is effective then there will be a change or discontinuity in the regression slope at the point of allocation. For instance, a criminal justice evaluation in the USA took advantage of allocation by a baseline recidivism risk with those who scored highly given more support than those who had low scores. The evaluation showed evidence that the intervention had an effect with statistically significantly lower risk of recidivism associated with greater offender support. 76 In contrast, an evaluation, in New Zealand, using the approach to measure the impact on home detention for first-time offenders found no impact of the policy. 77 The method has been used to evaluate an educational intervention for Year 7 pupils in the UK, when randomisation was deemed to be inappropriate. 78
In theory the RDD design deals with selection bias by assuming that at the allocation point, due to measurement error, produces equivalent groups. There are, however, some drawbacks to the method. First, for any given sample size it is not as powerful as a RCT requiring around three times the sample size to have similar power. Second, traditionally it relies on routine data collection, which may not collect the key variables of interest. Third, the most powerful version of the design is a ‘sharp’ RDD whereby there is perfect adherence to the cut-point. When there is not (a fuzzy RDD) statistical power is reduced. This is the intention to treat equivalent within a randomised trial when non-complying participants are analysed in their randomised groups leading to a dilution of a treatment effect.
Future evaluations might consider using a ‘prospective RDD’ design where researchers can implement ‘routine’ measurements, such as a standardised measure of mental health and well-being with a standardised offender risk score. All of those who score above a certain threshold can be allocated to the intervention, which is probably more logical and acceptable to staff and offenders than the use of randomisation. A prospective approach would make it possible to implement data collection for outcomes relevant to healthcare professionals and the police where information is not already routinely collected. Furthermore, a prospective design would enable researchers to emphasise keeping to the ‘cut-off’ value when referring offenders to an intervention to ensure that the design is as far as possible a ‘sharp’ RDD rather than a ‘fuzzy’ one. The sharp RDD design is stronger than other quasi-experimental methods as it has a lower risk of bias.
Future qualitative research to identify barriers and facilitators to study participation by this population would be beneficial to inform both choice of study method and design. The focus of the research could usefully build on the findings of this study.
Members of the study team each had a skill set and experience that in combination aided the initial design of the study, and the creative process required to address the numerous challenges faced. Having academic public health practitioners and academics familiar with undertaking research in the criminal justice system from the earliest stages of study design is highly recommended. Equally, including members of the police on the TMG is essential, and for this study it was integral to identification of issues and development of measures to address them as they arose.
The researchers’ approach to PPI representation included ex-offenders, victim support workers and community groups. The researchers shared HC concerns about victim and public opinion of what might have appeared to be offenders being paid rather than punished, particularly as the voucher values were increased substantially on the advice of ex-offenders. These are considerations that the researchers would recommend for future research. There are a number of organisations for ex-offenders and the most relevant to a research question should be approached. Likewise, depending on the research question, victim support groups and community groups should be approached and involved from an early stage.
Chapter 6 Conclusions
This study was an ambitious RCT and qualitative evaluation. The study aimed to provide evidence of effectiveness for Gateway, an out-of-court intervention aimed at improving life chances, health and well-being and recidivism in young adults who had committed a low-level offence. The early termination of the study was caused by a combination of factors. The researchers have demonstrated that a two-stage procedure for recruitment, consent and randomisation in the police setting works for the target population. However, being unable to contact many of the participants due to mobile phone numbers being no longer in use and the corresponding lack of data collection proved an insurmountable problem for this study. The qualitative interviews provide valuable information about the ways in which some problems may be addressed. The lessons learnt from this study should help colleagues seeking to design and evaluate similar interventions with vulnerable populations or in the police setting.
Additional information
Acknowledgements
The researchers would like to acknowledge and thank all those who contributed to the study:
-
Those delivering the intervention: all the Gateway navigators provided by No Limits and Southampton City Council; Debbie Willis, Children and Young People’s Services Manager and colleagues at The Hampton Trust, responsible for LINX workshops; those taking referrals from the navigators: The Prince’s Trust, Two Saints (Housing) and the Community Mental Health Teams across Hampshire and Isle of Wight.
-
Members of the TMG who contributed at various stages of the study: Inspector Benjamin Taylor (Hampshire Constabulary), Rosanna Orlando (Health Economist), Anthony Quinn (Qualitative Researcher), Inspector Stuart Baker (Hampshire Constabulary).
-
Those who supported the study and funded the intervention: Southampton Police Crime Commissioner's office and senior police officers in Hampshire Constabulary.
-
All the police investigators who underwent training and recruited participants into the trial.
-
Members of the Public Participation Panel (PPP), and all the members of the public who contributed during the development and delivery of the study.
-
All the participants who took part in the trial and qualitative interviews: Gateway clients, Gateway project staff responsible for the intervention and Hampshire Constabulary police officers and civilian staff recruiting into the RCT.
-
The University of Southampton for being the study sponsor; and to members of the SSC/DMEC for their advice and support.
Contributions of authors
Alison Booth (https://orcid.org/0000-0001-7138-6295) Senior Research Fellow, Health Sciences. She was a co-investigator, contributed to conceptualisation and design, funding acquisition, protocol development, and was trial manager for the conduct and delivery of the trial, site setup and data management, report writing and editing.
Sara Morgan (https://orcid.org/0000-0001-8346-6655) Lecturer, Public Health. She was a co-investigator, contributed to conceptualisation and design, funding acquisition, protocol development, conduct/delivery of the trial and qualitative evaluation, data acquisition, qualitative analysis and report writing and editing.
Inna Walker (https://orcid.org/0000-0002-8460-8130) Clinical Research Fellow, quantitative and qualitative researcher. Contributed to protocol development, conduct and delivery of the trial and qualitative evaluation, data acquisition, qualitative analysis, report writing and editing.
Alex Mitchell (https://orcid.org/0000-0001-9311-2092) Statistician, Health Sciences. Contributed to the overall study design, wrote the statistical analysis plan, conducted the statistical analysis and contributed to writing and editing the report.
Megan Barlow-Pay (https://orcid.org/0000-0003-1473-2096) Researcher, PPIE. She was the PPI lead for the study, undertook PPI work, contributed to study design and conduct, data collection, qualitative analysis and drafting and editing the report.
Caroline Chapman (https://orcid.org/0000-0002-6498-5932) Sergeant, Gateway Project Support Officer for Hampshire Constabulary. Contributed to protocol development, trial conduct, setting up of sites, data acquisition and checking and commented on the draft report.
Ann Cochrane (https://orcid.org/0000-0002-1502-6719) Trial Coordinator, Health Sciences. Contributed to protocol development, trial conduct, setting up of sites, data acquisition and processing and commented on the draft report.
Emma Filby (https://orcid.org/0000-0002-1090-1123) Data administrator, Health Sciences. Contributed to the study conduct, project administration, data management, and commented on the draft report.
Jenny Fleming (https://orcid.org/0000-0002-7913-3345) Professor in Criminology, qualitative methodologist. She was a co-investigator contributing to conceptualisation and design, funding acquisition, protocol development, trial conduct, and commenting on the draft report.
Catherine Hewitt (https://orcid.org/0000-0002-0415-3536) Professor in Statistics, Health Sciences. She was a co-investigator contributing to conceptualisation and design, funding acquisition, protocol development, provided oversight of trial conduct and the statistical analysis, and editing the report.
James Raftery (https://orcid.org/0000-0003-1094-8578) Professor in Health Economics. As a co-investigator, contributed to conceptualisation and design, funding acquisition, protocol development, and trial conduct, and commented on the draft report.
David Torgerson (https://orcid.org/0000-0002-1667-4275) Professor, Director of York Trials Unit. As a co-investigator, contributed to conceptualisation and design, protocol development, funding acquisition, and trial conduct, and commented on the draft report.
Lana Weir (https://orcid.org/0000-0003-4730-7969) Trial Coordinator, qualitative researcher. Contributed to project administration, data acquisition, qualitative analysis, report writing and editing.
Julie Parkes (https://orcid.org/0000-0002-6490-395X) Professor in Public Health. She was the Chief Investigator, and contributed to the conceptualisation and design, funding acquisition, protocol development, trial conduct, report writing and editing.
All authors gave final approval of the manuscript.
Disclosure of interests
Full disclosure of interests: Completed ICMJE forms for all authors, including all related interests, are available in the toolkit on the NIHR Journals Library report publication page at https://doi.org/10.3310/NTFW7364.
Primary conflicts of interest: Catherine Hewitt is Deputy Chair of the NIHR HTA commissioning board, NIHR CTU Standing Advisory Committee, HTA Post-Funding Committee teleconference, HTA Funding Committee Policy Group (formerly CSG) and was appointed a NIHR Senior Investigator in March 2023. James Raftery is a member of the NIHR Editorial Board for HTA and EME. Julie Parkes is Director of Training, UK Faculty of Public Health. There are no other declared conflicts of interest.
Data-sharing statement
All data requests should be submitted to the corresponding author for consideration. Access to available anonymised data may be granted following review.
Ethics statement
The study protocol, all associated study documents and amendments were approved by the University of Southampton Ethics and Research Information Governance Board (ERGO ID: 31911). The outline proposal was submitted to the Hampshire Constabulary Ethics Committee, who agreed to support the study. The following external ethics boards confirmed their approval was not required: HRA Research Ethics Service, Social Care REC approval, Her Majesty Prison Probation Services.
Information governance statement
The Universities of York and Southampton are committed to handling all personal information in line with the UK Data Protection Act (2018) and the General Data Protection Regulation (EU GDPR) 2016/679. Under the Data Protection legislation the University of York is the Data Processor; and the University of Southampton is the Data Controller and the researchers process personal data in accordance with their instructions. You can find out more about how they handle personal data, including how to exercise your individual rights and the contact details for the University of Southampton’s Data Protection Officer here: www.southampton.ac.uk/hr/services/data-protection/data-protection.page
Department of Health and Social Care disclaimer
This publication presents independent research commissioned by the National Institute for Health and Care Research (NIHR). The views and opinions expressed by the interviewees in this publication are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, MRC, NIHR Coordinating Centre, PHR programme or the Department of Health and Social Care.
This monograph was published based on current knowledge at the time and date of publication. NIHR is committed to being inclusive and will continually monitor best practice and guidance in relation to terminology and language to ensure that we remain relevant to our stakeholders.
Publications
Mitchell A, Booth A, Morgan S, Walker I, Chapman C, Barlow-Pay M, et al. Examining the effectiveness of the Gateway conditional caution on health and well-being of young adults committing low-level offences: a randomised controlled trial. BMJ Open 2024;14(4):e081179.
Disclaimers
This article presents independent research funded by the National Institute for Health and Care Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, the PHR programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, the PHR programme or the Department of Health and Social Care.
References
- Cochrane A, Booth A, Walker I, Morgan S, Mitchell A, Barlow-Pay M, et al. Examining the effectiveness of Gateway: an out-of-court community-based intervention to reduce recidivism and improve the health and well-being of young adults committing low-level offences: study protocol for a randomised controlled trial. Trials 2021;22. https://doi.org/10.1186/s13063-021-05905-2.
- Alcorn T. Rethinking mental health care for young offenders. Lancet 2014;383:1283-4. https://doi.org/10.1016/S0140-6736(14)60449-9.
- Underwood LA, Washington A. Mental illness and juvenile offenders. Int J Environ Res Publ Health 2016;13. https://doi.org/10.3390/ijerph13020228.
- Petrosino A, Turpin-Petrosino C, Guckenberg S. Formal system processing of juveniles: effects on delinquency. Campb Syst Rev 2010;6:1-88.
- Haines A, Goldson B, Haycox A, Houten R, Lane S, McGuire J, et al. Evaluation of the Youth Justice Liaison and Diversion (YJLD) Pilot Scheme. London: Department of Health; 2012.
- Hay I. Gender self-concept profiles of adolescents suspended from high school. J Child Psychol Psychiatry 2000;41:345-52.
- Kasinathan J. Predictors of rapid reincarceration in mentally ill young offenders. Austral Psychiatr: Bullet Royal Austral New Zealand Coll Psychiatr 2015;23:550-5. https://doi.org/10.1177/1039856215597532.
- Lader D, Singleton N, Meltzer H. Psychiatric morbidity among young offenders in England and Wales. Int Rev Psychiatr 2003;15:144-7. https://doi.org/10.1080/0954026021000046074.
- Maguire M, Holloway K, Liddle M, Gordon F, Gray P, Smith A, et al. Evaluation of the Transitional Support Scheme: Final Report. Cardiff: Welsh Assembly Government; 2010.
- Ministry of Justice . Transforming Rehabilitation: A Summary of Evidence on Reducing Re-Offending 2013.
- Nugent WR, Paddock JB. Evaluating the effects of a victim-offender reconciliation program on reoffense. Res Soc Work Pract 1996;6:155-78. https://doi.org/10.1177/104973159600600202.
- Roustit C, Renahy E, Guernec G, Lesieur S, Parizot I, Chauvin P. Exposure to interparental violence and psychosocial maladjustment in the adult life course: advocacy for early prevention. J Epidemiol Community Health 2009;63:563-8. https://doi.org/10.1136/jech.2008.077750.
- Butler S, Baruch G, Hickey N, Fonagy P. A randomized controlled trial of multisystemic therapy and a statutory therapeutic intervention for young offenders. J Am Acad Child Adolesc Psychiatry 2011;50:1220-35.e2. https://doi.org/10.1016/j.jaac.2011.09.017.
- Schwalbe CS, Gearing RE, MacKenzie MJ, Brewer KB, Ibrahim R. A meta-analysis of experimental studies of diversion programs for juvenile offenders. Clin Psychol Rev 2012;32:26-33. https://doi.org/10.1016/j.cpr.2011.10.002.
- Weir K, Kilili S, Cooper J, Crowe A, Routledge GC. An innovative Programme to navigate people away from the cycle of reoffending – a randomised control trial evaluation. Police J 2021;95. https://doi.org/10.1177/0032258X211018774.
- House of Commons Justice Committee . Written Evidence from the Transition to Adulthood Alliance 2012. https://publications.parliament.uk/pa/cm201213/cmselect/cmjust/339/339we11.htm (accessed 2 November 2023).
- Bradley L. The Bradley Report: Lord Bradley’s Review of People with Mental Health Problems and Learning Disabilities in the Criminal Justice System. London: Department of Health; 2009.
- Britton S. PCC Spotlight: Young Adults (18–24) in Contact With Police and Criminal Justice Services 2015. https://t2a.org.uk/wp-content/uploads/2015/02/1pcc-spotlight-1-young-adults-1.pdf (accessed 2 November 2023).
- Strang H, Sherman L, Ariel B, Chilton S, Braddock R, Rowlinson T, et al. Reducing the harm of intimate partner violence: randomized controlled trial of the Hampshire Constabulary CARA experiment. Camb J Evid Based Polic 2017;1:160-73. https://doi.org/10.1007/s41887-017-0007-x.
- The Sentencing Council for England and Wales . Sentencing Guidelines: Out of Court Disposals, 4. Conditional Cautions 2021. www.sentencingcouncil.org.uk/explanatory-material/magistrates-court/item/out-of-court-disposals/4-conditional-caution/ (accessed 11 April 2023).
- Clarke A, Friede T, Putz R, Ashdown J, Martin S, Blake A, et al. Warwick-Edinburgh Mental Well-being Scale (WEMWBS): validated for teenage school students in England and Scotland. A mixed methods assessment. BMC Publ Health 2011;11. https://doi.org/10.1186/1471-2458-11-487.
- Stewart-Brown S, Janmohamed K. Warwick-Edinburgh Mental Well-Being Scale (WEMWBS): User Guide. Warwick: University of Warwick; 2008.
- Tennant R, Hiller L, Fishwick R, Platt S, Joseph S, Weich S, et al. The Warwick-Edinburgh Mental Well-being Scale (WEMWBS): development and UK validation. Health Qual Life Outc 2007;5. https://doi.org/10.1186/1477-7525-5-63.
- Bushnik T. Encyclopedia of Clinical Neuropsychology. New York: Springer; 2011.
- Chung T, Colby SM, Barnett NP, Rohsenow DJ, Spirito A, Monti PM. Screening adolescents for problem drinking: performance of brief screens against DSM-IV alcohol diagnoses. J Stud Alcohol 2000;61:579-87.
- Knight JR, Sherritt L, Harris SK, Gates EC, Chang G. Validity of brief alcohol screening tests among adolescents: a comparison of the AUDIT, POSIT, CAGE, and CRAFFT. Alcohol Clin Exp Res 2003;27:67-73. https://doi.org/10.1097/01.alc.0000046598.59317.3a.
- Moberg DP, Hahn L. The adolescent drug involvement scale. J Child Adolesc Subst Abuse 1991;2:75-88. https://doi.org/10.1300/J272v02n01_05.
- Maheswaran H, Weich S, Powell J, Stewart-Brown S. Evaluating the responsiveness of the Warwick Edinburgh Mental Well-Being Scale (WEMWBS): group and individual level analysis. Health Qual Life Outc 2012;10. https://doi.org/10.1186/1477-7525-10-156.
- Schulz KF, Altman DG, Moher D. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ 2010;340. https://doi.org/10.1136/bmj.c332.
- University of York . Data Protection Act: University of York Data Protection Policy 2020. www.york.ac.uk/records-management/dp/ (accessed 11 April 2023).
- Bonevski B, Randell M, Paul C, Chapman K, Twyman L, Bryant J, et al. Reaching the hard-to-reach: a systematic review of strategies for improving health and medical research with socially disadvantaged groups. BMC Med Res Methodol 2014;14. https://doi.org/10.1186/1471-2288-14-42.
- Khatamian Far P. Challenges of recruitment and retention of university students as research participants: lessons learned from a pilot study. J Austral Libr Inform Assoc 2018;67:278-92. https://doi.org/10.1080/24750158.2018.1500436.
- Moore GF, Audrey S, Barker M, Bond L, Bonell C, Hardeman W, et al. Process evaluation of complex interventions: Medical Research Council guidance. BMJ 2015;350. https://doi.org/10.1136/bmj.h1258.
- Bedford L, Neyroud P. Organisational learning from field research in policing: how police can improve policy and practice by implementing randomised controlled trials. Eur J Pol Stud 2018;5:28-49.
- Bellg AJ, Borrelli B, Resnick B, Hecht J, Minicucci DS, Ory M, et al. Treatment Fidelity Workgroup of the NIH Behavior Change Consortium . Enhancing treatment fidelity in health behavior change studies: best practices and recommendations from the NIH Behavior Change Consortium. Health Psychol 2004;23:443-51. https://doi.org/10.1037/0278-6133.23.5.443.
- Abrams L. Sampling ‘hard to reach’ populations in qualitative research: the case of incarcerated youth. Qual Soc Work 2010;9:536-50.
- Braun V, Clarke V. Can I use TA? Should I use TA? Should I not use TA? Comparing reflexive thematic analysis and other pattern-based qualitative analytic approaches. Counsel Psychother Res 2021;21:37-4. https://doi.org/10.1002/capr.12360.
- Braun V, Clarke V. Conceptual and design thinking for thematic analysis. Qual Psychol 2022;9:3-26. https://doi.org/10.1037/qup0000196.
- Joy E, Braun V, Clarke V. Research Methods for Education and the Social Disciplines in Aotearoa New Zealand. Wellington, New Zealand: NZCER Press; 2023.
- Her Majesty’s Inspectorate of Probation . Desistance – General Practice Principles 2020. www.justiceinspectorates.gov.uk/hmiprobation/research/the-evidence-base-probation/models-and-principles/desistance/ (accessed 11 April 2023).
- Sampson RJ, Laub JH. Handbook of the Life Course. Boston, MA: Springer; 2003.
- Cornelius CVM, Lynch CJ, Gore R. Aging out of crime: exploring the relationship between age and crime with agent based modeling n.d.
- House of Commons Justice Committee . Young Adults in the Criminal Justice System: Eighth Report of Session 2017–19 2018.
- Moffitt TE. Adolescence-limited and life-course-persistent antisocial behavior: a developmental taxonomy. Psychol Rev 1993;100:674-701.
- Home Office . Reducing Re-Offending National Action Plan 2004.
- Bonta J, Andrews DA. Risk-need-responsivity model for offender assessment and rehabilitation. Rehabilitation 2007;6:1-22.
- Laub JH, Sampson RJ. Understanding desistance from crime. Crime Just 2001;28:1-69. https://doi.org/10.1086/652208.
- Sampson RJ, Laub JH. Life-course desisters? Trajectories of crime among delinquent boys followed to age 70. Criminology 2003;41:555-92. https://doi.org/10.1111/j.1745-9125.2003.tb00997.x.
- King RD, Massoglia M, Macmillan R. The context of marriage and crime: gender, the propensity to marry, and offending in early adulthood. Criminology 2007;45:33-65. https://doi.org/10.1111/j.1745-9125.2007.00071.x.
- Roberts MR, Stacer MJ. In their own words: offenders’ perspectives on their participation in a faith-based diversion and reentry program. J Offend Rehablit 2016;55:466-83. https://doi.org/10.1080/10509674.2016.1216914.
- Wong K, O’Keeffe C, Ellingworth D, Senior P. Intensive Alternatives to Custody: Process Evaluation of Pilots in Five Areas. London: Crown; 2012.
- Popay J, Whitehead M, Hunter DJ. Injustice is killing people on a large scale: but what is to be done about it?. J Public Health 2010;32:148-9. https://doi.org/10.1093/pubmed/fdq029.
- Watt B, Howells K, Delfabbro P. Juvenile recidivism: criminal propensity, social control and social learning theories. Psychiat Psychol Law 2004;11:141-53. https://doi.org/10.1375/pplt.2004.11.1.141.
- Dubberley S, Stein M. Mentoring for young people leaving care. Prob J 2006;53:172-3. https://doi.org/10.1177/026455050605300208.
- Taylor J, Burrowes N, Disley E, Liddle M, Maguire M, Rubin J, et al. Intermediate Outcomes of Mentoring Interventions: A Rapid Evidence Assessment. London: Crown; 2013.
- Danese A, Smith PD. Recognising and responding to the mental health needs of young people in the era of COVID-19. Child Adolesc Ment Health 2020;25:169-70. https://doi.org/10.1111/camh.12414.
- Jia R, Ayling K, Chalder T, Massey A, Broadbent E, Morling JR, et al. Young people, mental health and COVID-19 infection: the canaries we put in the coal mine. Publ Health 2020;189:158-61. https://doi.org/10.1016/j.puhe.2020.10.018.
- Pierce M, Hope H, Ford T, Hatch S, Hotopf M, John A, et al. Mental health before and during the COVID-19 pandemic: a longitudinal probability sample survey of the UK population. Lancet Psychiat 2020;7:883-92. https://doi.org/10.1016/s2215-0366(20)30308-4.
- Power E, Hughes S, Cotter D, Cannon M. Youth mental health in the time of COVID-19. Ir J Psychol Med 2020;37:301-5. https://doi.org/10.1017/ipm.2020.84.
- Neyroud P, Slothower M. Operation Turning Point: Interim Report on a Randomised Trial in Birmingham, UK. Cambridge: University of Cambridge; 2013.
- Lankenau SE, Sanders B, Hathazi D, Bloom JJ. Recruiting and retaining mobile young injection drug users in a longitudinal study. Subst Use Misuse 2010;45:684-99. https://doi.org/10.3109/10826081003594914.
- Patel MX, Doku V, Tennakoon L. Challenges in recruitment of research participants. Adv Psychiat Treat 2003;9:229-38. https://doi.org/10.1192/apt.9.3.229.
- Lennox C, Kirkpatrick T, Taylor RS, Todd R, Greenwood C, Haddad M, et al. Pilot randomised controlled trial of the ENGAGER collaborative care intervention for prisoners with common mental health problems, near to and after release. Pilot Feas Stud 2017;4. https://doi.org/10.1186/s40814-017-0163-6.
- Scantlebury A, Fairhurst C, Booth A, McDaid C, Moran N, Parker A, et al. Effectiveness of a training program for police officers who come into contact with people with mental health problems: a pragmatic randomised controlled trial. PLOS ONE 2017;12. https://doi.org/10.1371/journal.pone.0184377.
- National Institute for Health and Care Research (NIHR) . NIHR Clinical Research Network High Level Objectives Outturn Report 2021 22 2022.
- Agrawal S, Kirchmaier T, Villa-Llera C. COVID-19 and Local Crime Rates in England and Wales – Two Years into the Pandemic. London: Centre for Economic Performance; 2022.
- Bell IH, Nicholas J, Broomhall A, Bailey E, Bendall S, Boland A, et al. The impact of COVID-19 on youth mental health: a mixed methods survey. Psychiat Res 2023;321. https://doi.org/10.1016/j.psychres.2023.115082.
- Cox J. Ethnic Group Profile of Hampshire 2011 Census. Winchester: Research and Intelligence for Hampshire County Council; 2013.
- Glenn S. Charging and Out of Court Disposals: A National Strategy. London: National Police Chiefs’ Council; 2021.
- Neyroud P. NPCC Out of Court Disposals Managed by the Police: A Review of the Evidence. Wales: National Police Chief’s Council of England and Wales; 2018.
- Philips B, Falkenström F. What research evidence is valid for psychotherapy research?. Front Psychiat 2020;11. https://doi.org/10.3389/fpsyt.2020.625380.
- Gastaldon C, Mosler F, Toner S, Tedeschi F, Bird VJ, Barbui C, et al. Are trials of psychological and psychosocial interventions for schizophrenia and psychosis included in the NICE guidelines pragmatic? A systematic review. PLOS ONE 2019;14. https://doi.org/10.1371/journal.pone.0222891.
- Kivimäki M, Singh-Manoux A, Ferrie JE, Batty GD. Post hoc decision-making in observational epidemiology: is there need for better research standards?. Int J Epidemiol 2013;42:367-70. https://doi.org/10.1093/ije/dyt036.
- Unim B, Mattei E, Carle F, Tolonen H, Bernal-Delgado E, Achterberg P, et al. Health data collection methods and procedures across EU member states: findings from the InfAct Joint Action on health information. Archiv Publ Health 2022;80. https://doi.org/10.1186/s13690-021-00780-4.
- Shadish WR, Cook TD, Campbell DT. Experimental and Quasi-Experimental Designs for Generalized Causal Inference. Boston, MA: Houghton, Mifflin and Company; 2002.
- Rhodes W, Jalbert SK. Regression discontinuity design in criminal justice evaluation: an introduction and illustration. Eval Rev 2013;37:239-73. https://doi.org/10.1177/0193841x14523004.
- Mitchell O. A Policy Evaluation of Home Detention Sentencing: Evidence from New Zealand. Auckland, New Zealand: Auckland University of Technology; 2019.
- Menzies V, Collyer C, Kokotsaki D, Hewitt CE, Younger K, Wiggins A, et al. SHINE in Secondaries: Evaluation Report and Executive Summary. London: Education Endowment Foundation; 2015.
Appendix 1 Gateway recruitment pathways
FIGURE 8.
Gateway in-custody recruitment pathway. PACE, Police and Criminal Evidence Act 1983.
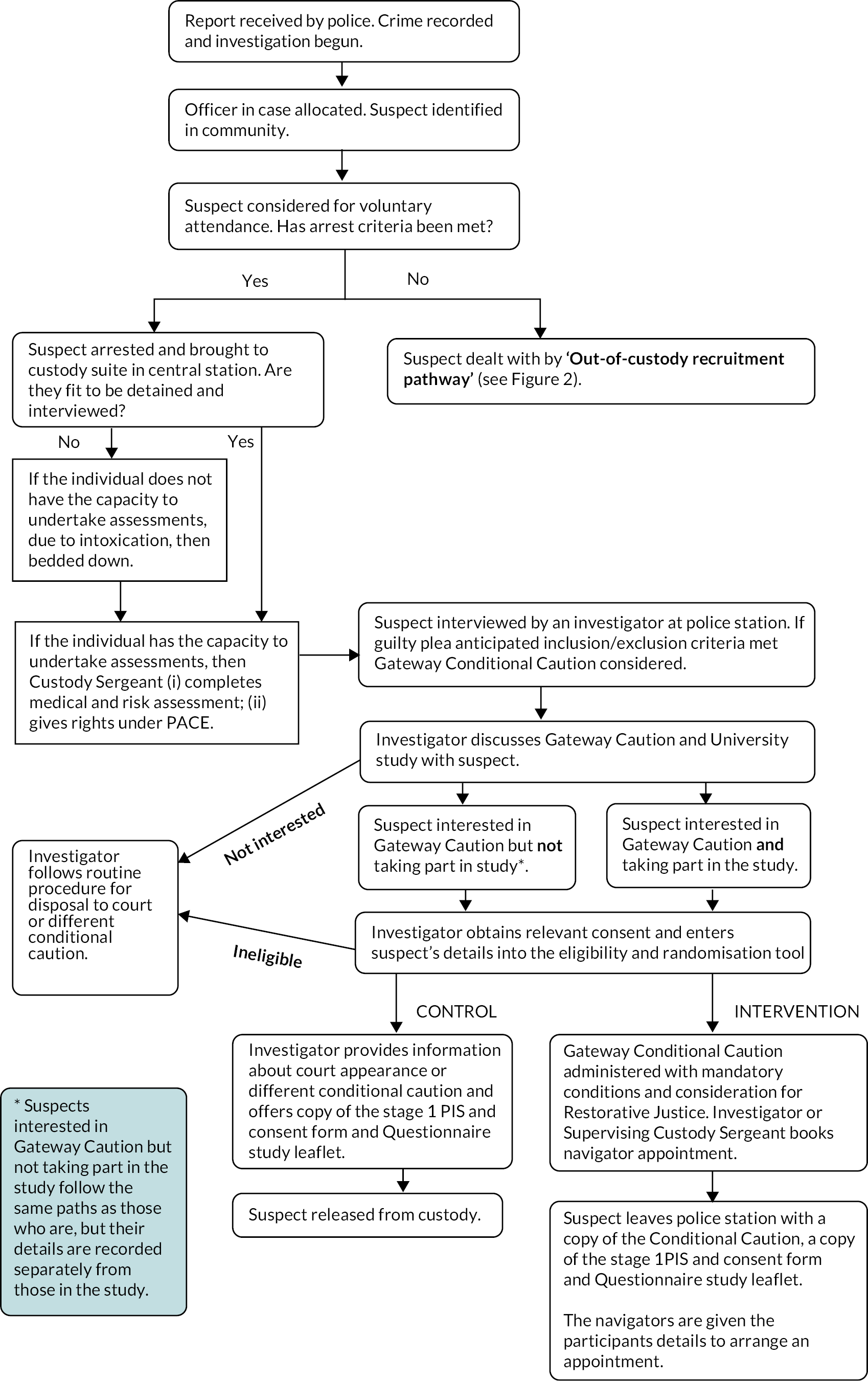
FIGURE 9.
Gateway out-of-custody recruitment pathway.
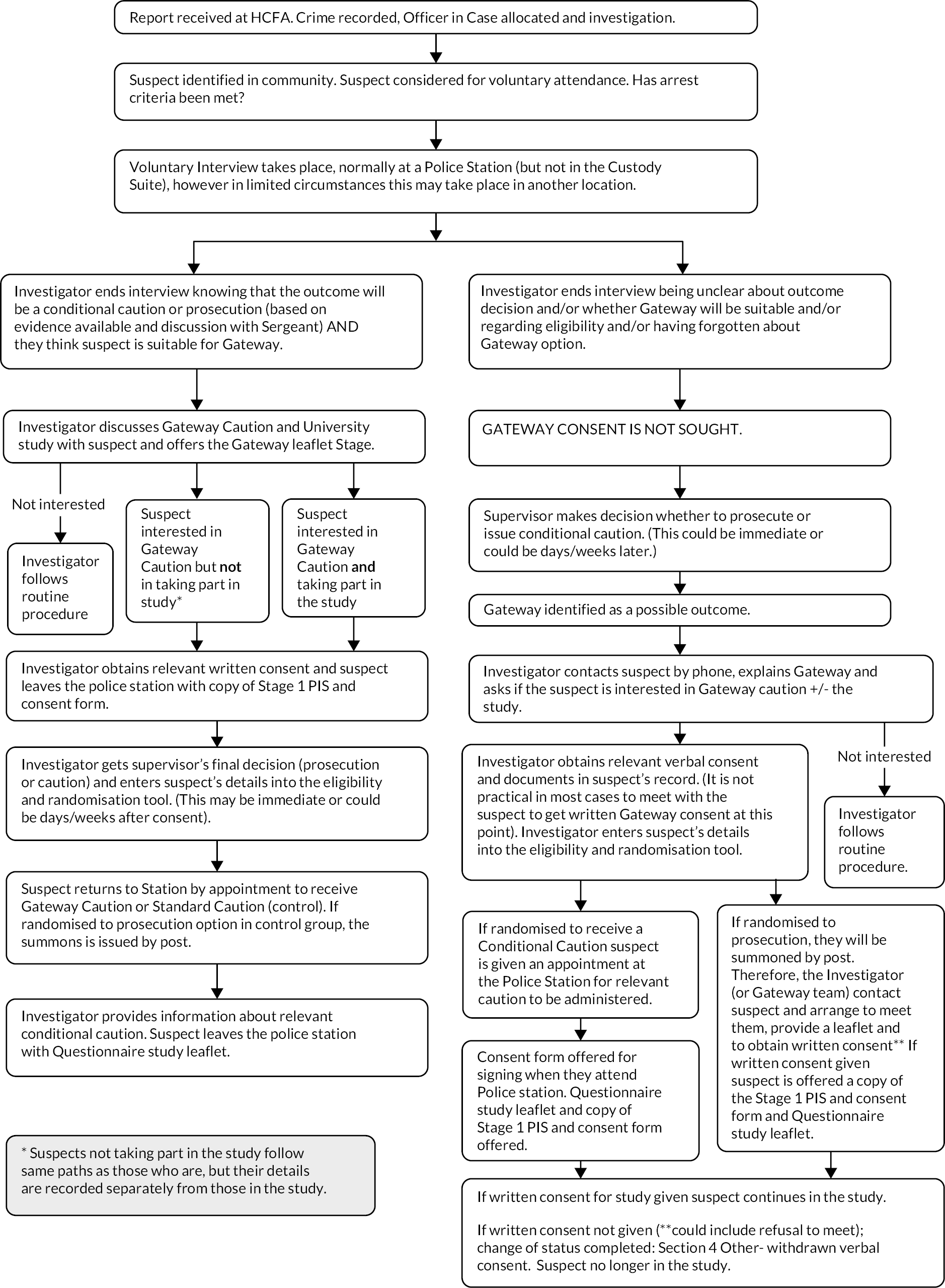
Appendix 2 Differences between LINX workshops and LINX delivered by telephone in response to COVID-19 restrictions
The Hampton Trust have highlighted the following key differences between LINX group work and one-to-one telephone delivery as part of the Gateway programme:
-
Group work is usually a total of 10 hours. Conversion to telephone intervention was needed due to COVID-19 restrictions. Time has been reduced to 2 hours as research tells us that people struggle with concentrating for longer than an hour over the phone.
-
In the group work a number of different tools were used to tease out their offence and the issues that surround it. In the telephone call the researcher will be making it clear that they will be talking about their offence from the outset.
-
In the group work setting, Young adults will often interact and challenge each other; this is the key area that has been lost in the telephone intervention. This is the reason that the researchers will be honing-in on their offence straight away. The lack of group work will also impact on Young adults giving other Young adults ‘permission’ to share and Young adults realising that they are not the only one suffering from traumatic life experiences. This will be a major loss which is why the telephone intervention needs to be so centred around the crime and the circumstances that surround that crime.
-
The focus of the telephone intervention will target the individual and will highlight their behaviour, whereas in group work it can be less directed on the individual.
-
In group work the University of Southampton qualitative evaluation questionnaires will be completed by young adults in their own time (they are usually given 10 minutes to complete this before and after the workshops). For the telephone intervention the researcher will be asking young adults questions on a one-to-one basis and this will form part of the telephone intervention.
-
Young adults with differing learning styles will be affected by the telephone intervention and the limited communication styles the researchers can use could also have an impact. The researcher will be sensitive to this and look at tools and worksheets that they can use to support the work.
-
In group work the ‘Wall’ provides a visual aid continually linking issues together, this will not be possible over the telephone, nor will there be a visual aid to consequences.
Appendix 3 Algorithm for potential breaches
FIGURE 10.
Algorithm used for assessing potential breach of conditions.
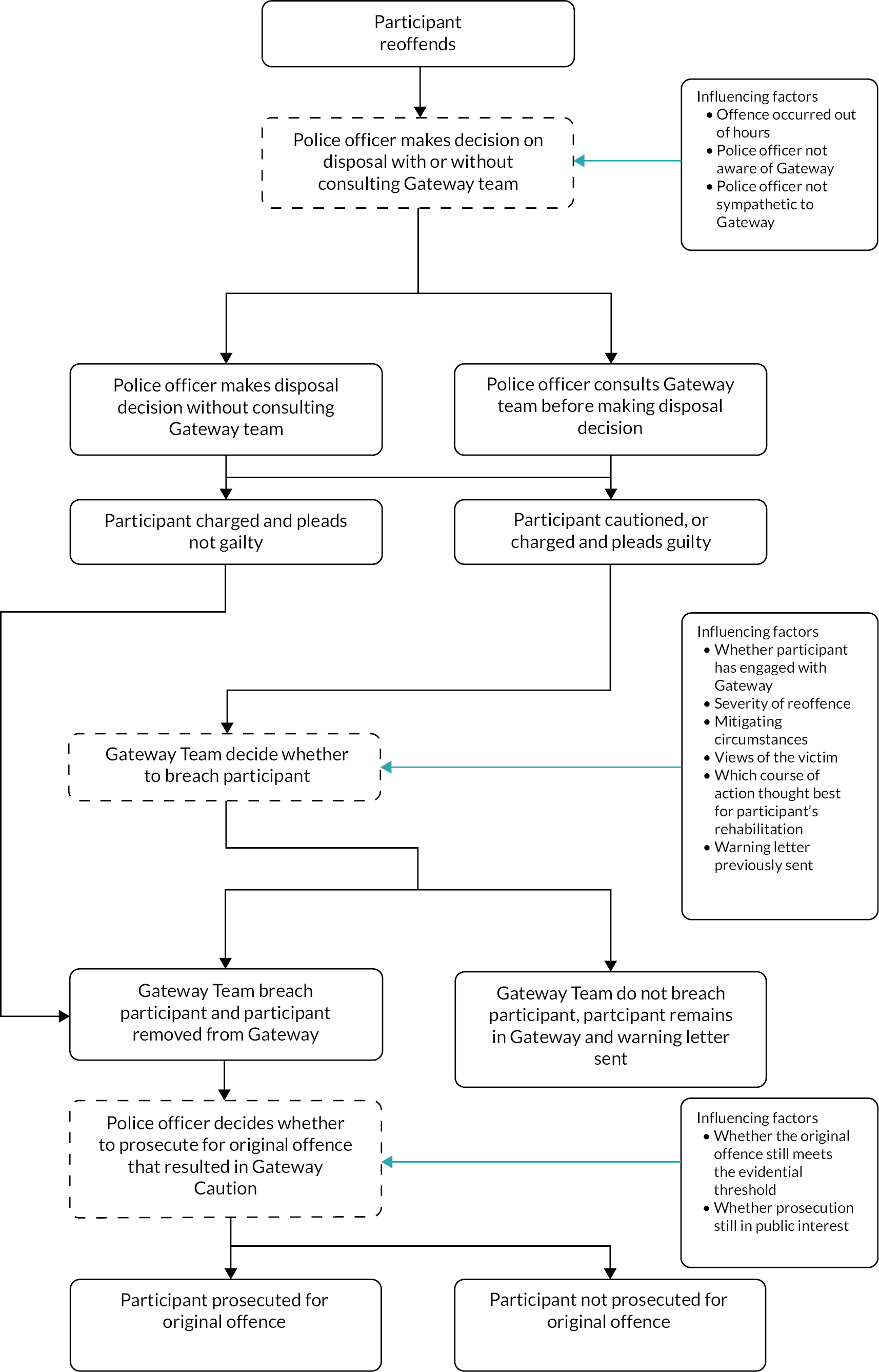
Appendix 4 List of protocol amendments
Amendment 1 (approved on 2 September 2019)
-
Added ‘different conditional caution’ as an option in the control arm of the trial to reflect usual practice and aid in increasing the number of potential participants in the trial.
-
Removed the word ‘embedded’ throughout to separate out the qualitative research and the economic evaluation from the trial. Participants in the process evaluation are no longer restricted to those recruited to the trial but may be offenders who have been through the Gateway programme.
-
Specified Southampton Policing District (SPD) includes Eastleigh, New Forest and Romsey police stations.
-
Provided additional information about the usual process here and throughout.
-
Clarified that participants may be recruited to the study while in custody or out of custody.
-
Amended and clarified inclusion/exclusion criteria.
-
Information added to explain that different researchers will undertake the observations to those interviewing the Gateway participants in the observed sessions in order to maintain blinding to allocation.
-
Amended and clarified screening criteria.
-
Police training records added as data collected.
-
Information about PPI during the study period added including highlighting ethics as a focus for independent members of the SSC/DMEC.
-
Added information about funding for the intervention.
Amendment 2 (approved on 21 November 2019)
-
Addition of two recruitment sites: Portsmouth and Basingstoke.
-
Amendment to internal pilot to reflect change in number of anticipated eligible offenders: extended from 4 to 6 months).
-
Amended length of study: 23-month extension to be requested.
-
Change 2-year follow up of police HES/PAS and ONS data to 1-year.
-
Added to information about sites for delivery of LINX workshops: neutral place as near where offenders live as possible.
-
CLAHRC replaced with ARC.
-
Addition of e-mail address to list of personal information to be collected.
Amendment 3 (approved on 25 March 2020)
-
Addition of Isle of Wight (IoW) as fourth recruitment site.
-
Additional exclusion criteria of ‘Currently under probation’ added.
-
Plan for CACE analysis added.
-
Clarification about qualitative interviews and their purpose added.
-
Addition of section 11.1 Set up of sites and 11.2 Training of police officers to recruit and randomise.
-
Details added of increases in thank you payments offered to participants and format to include vouchers or cash.
-
Added information about cases where randomisation will be with verbal consent initially. Summarised the timing and use of the PISs in a table.
-
Addition of detailed explanation about enrolment procedure for in and out of custody.
-
Details of number and type of attempts to contact participants added.
-
Addition of risk of adverse public perceptions of payments to offenders.
-
Addition of details about funding for the intervention.
-
Justification for increased thank you payments to participants added in Appendix 4.
Amendment 4 (approved on 7 April 2020)
Letter submitted to the ethics and governance committee informing them of the status of the study in light of the COVID-19 pandemic. No changes to the protocol made.
Amendment 5 (approved on 26 May 2020)
-
Minor amendment to wording to remove stratified sampling.
-
Interview process changed to telephone instead of face-to-face. Amendments made to recruitment process to allow for change.
-
Verbal consent included in process evaluation for telephone interviews.
Amendment 6 (approved on 3 September 2020)
-
Change from some face-to-face meetings to telephone interviews/engagement for the delivery of the Gateway intervention. In particular, details added about how the LINX workshops will be held one to one over the telephone.
-
Change from obtaining Stage 2 consent and week 4 data collection at a face-to-face meeting to obtaining and recording verbal consent via the telephone interview as the only option.
-
Removal of option for face-to-face data collection at any time point.
-
Clarification that restorative justice is not a condition of the Gateway caution, but may be added.
-
Clarification of recruitment sites and recruitment area.
-
Change from cash incentive to all vouchers; either sent by e-mail or for collection from the office of a third-party agency.
-
Removal of the payment for travel costs and addition of incremental incentives.
-
Addition of progression criteria for recruitment months 7–12 (as approved by the SSC/DMEC).
-
Addition of a qualitative research question about evaluation of the impact of using different delivery methods on implementation of the intervention.
-
Impact of COVID-19 pandemic documented throughout.
Amendment 7 (approved on 16 October 2020)
-
Expanding options for delivery of paper shopping vouchers.
-
Removing the need to photocopy CRFs before posting to YTU.
-
Update regarding restart of the trial.
Amendment 8 (approved on 11 June 2021)
-
Adverse childhood experiences questionnaire (ACE) removed as a secondary outcome and added to qualitative evaluation section.
-
Reference to Client Service Receipt Inventory (CSRI) amended to ‘customised CSRI’ as questions only loosely based on this tool.
-
Removed attempt to keep statistics team blinded to allocation as not possible.
-
Stage 1 Consent forms to be held electronically only and originals securely destroyed.
-
Added decision pathway for Gateway programme participants who reoffend.
-
Specified that participants may be contacted by e-mail obtained from HC or directly provided by participants.
-
Reduced time between sharing PIS and stage 2 consent where participant wishes to proceed.
-
Added analysing transcripts of routine LINX workshop video recordings and the process for audio recording LINX telephone conversations.
Amendment 9 (approved on 7 September 2021)
-
Agreement from funders to close early and follow revised plan of work.
-
Revised quantitative and economic analyses.
-
Updated plans for qualitative and process evaluation.
-
Recruitment ceased in December 2021.
-
Training of police investigators ended.
-
Voucher payments revised for those not being contacted at 16-weeks and 1-year.
-
Data collection deadlines revised.
-
End of study definition revised.
-
Deliverables and impact/communications and dissemination refocused on learning.
-
Cessation of funding for the intervention on 31 March 2022.
Amendment 10 (approved on 21 July 2022)
The amendments all reflect changes to plans because of the premature closure of the trial:
-
Agreement from funders to close early and follow revised plan of work.
-
Revised plans for quantitative and economic analyses.
-
Updated plans for qualitative process evaluation.
-
Recorded that recruitment ceased on 14 December 2021.
-
Training of police investigators ended.
-
Voucher payments revised for those not being contacted at 16-weeks and 1-year.
-
Data collection deadline revised: ceasing on 31 March 2022.
-
End of study definition revised.
-
Deliverables and impact, communications and dissemination plans refocused on learning.
-
Reported funding of the intervention ceases on 31 March 2022.
Appendix 5 Participant characteristics presented by allocated group
| Randomised participants (n = 191) | Provided valid WEMWBS for at least one time point (n = 108) | |||||
|---|---|---|---|---|---|---|
| Gateway conditional caution (n = 109) | Usual process (n = 82) | Total (n = 191) | Gateway conditional caution (n = 64) | Usual process (n = 44) | Total (n = 108) | |
| Age at randomisation | ||||||
| Number with data, n (%) | 105 (96.3) | 78 (95.1) | 183 (95.8) | 64 (100) | 44 (100) | 108 (100) |
| Mean (SD) | 20.8 (2.0) | 20.7 (1.9) | 20.8 (1.9) | 20.7 (2.0) | 20.7 (1.7) | 20.7 (1.9) |
| Median (IQR) | 20.3 (19.3–22.5) | 20.4 (19.3–21.6) | 20.4 (19.3–22.0) | 20.2 (19.0–22.3) | 20.5 (19.4–21.4) | 20.3 (19.3–21.6) |
| Minimum, Maximum | 18.1, 24.8 | 18.1, 24.8 | 18.1, 24.8 | 18.1, 24.7 | 18.1, 24.7 | 18.1, 24.7 |
| Gender, n (%) | ||||||
| Number with data, n (%) | 105 (96.3) | 78 (95.1) | 183 (95.8) | 64 (100) | 44 (100) | 108 (100) |
| Male | 87 (82.9) | 57 (73.1) | 144 (78.7) | 51 (79.7) | 32 (72.7) | 83 (76.9) |
| Female | 18 (17.1) | 21 (26.9) | 39 (21.3) | 13 (20.3) | 12 (27.3) | 25 (23.1) |
| Marital status, n (%) | ||||||
| Number with data, n (%) | 66 (60.6) | 44 (53.7) | 110 (57.6) | 64 (100) | 44 (100) | 108 (100) |
| Single | 62 (93.9) | 38 (86.4) | 100 (90.9) | 60 (93.8) | 38 (86.4) | 98 (90.7) |
| Living with partner | 4 (6.1) | 5 (11.4) | 9 (8.2) | 4 (6.2) | 5 (11.4) | 9 (8.3) |
| Married | 0 (0) | 1 (2.3) | 1 (0.9) | 0 (0) | 1 (2.3) | 1 (0.9) |
| Ethnicity, n (%) | ||||||
| Number with data, n (%) | 104 (95.4) | 77 (93.9) | 182 (94.8) | 63 (98.4) | 44 (100) | 108 (100) |
| White North European | 96 (91.4) | 75 (96.2) | 170 (93.4) | 58 (90.6) | 44 (100) | 102 (94.4) |
| Black | 5 (4.8) | 2 (2.6) | 7 (3.8) | 3 (4.7) | 0 (0) | 3 (2.8) |
| Asian | 2 (1.9) | 1 (1.3) | 3 (1.6) | 1 (1.6) | 0 (0) | 1 (0.9) |
| White South European | 1 (1.0) | 0 (0) | 1 (0.5) | 1 (1.6) | 0 (0) | 1 (0.9) |
| Highest level of education, n (%) | ||||||
| Number with data, n (%) | 66 (60.6) | 44 (53.7) | 110 (57.6) | 64 (100) | 44 (100) | 108 (100) |
| No qualifications | 14 (21.2) | 3 (6.8) | 17 (15.5) | 14 (21.9) | 3 (6.8) | 17 (15.7) |
| 1–4 GCSEs | 20 (30.3) | 8 (18.2) | 28 (25.5) | 20 (31.3) | 8 (18.2) | 28 (25.9) |
| More than 5 GCSEs | 13 (19.7) | 11 (25.0) | 24 (21.8) | 13 (20.3) | 11 (25.0) | 24 (22.2) |
| Apprenticeship | 2 (3.0) | 5 (11.4) | 7 (6.4) | 2 (3.1) | 5 (11.4) | 7 (7.5) |
| 2 or more A-levels | 17 (25.8) | 15 (34.1) | 32 (29.1) | 15 (23.4) | 15 (34.1) | 30 (27.8) |
| Bachelor’s degree or higher | 0 (0) | 2 (4.5) | 2 (1.8) | 0 (0) | 2 (4.5) | 2 (1.9) |
| Index of Multiple Deprivation quintile (1 = most deprived, 5 = least deprived), n (%) | ||||||
| Number with data, n (%) | 94 (86.2) | 72 (87.8) | 166 (86.9) | 58 (90.6) | 42 (95.5) | 100 (92.6) |
| 1 | 21 (22.3) | 20 (27.8) | 41 (24.7) | 14 (24.1) | 14 (33.3) | 28 (28.0) |
| 2 | 25 (26.6) | 17 (23.6) | 42 (25.3) | 14 (24.1) | 9 (21.4) | 23 (23.0) |
| 3 | 15 (16.0) | 14 (19.4) | 29 (17.5) | 9 (15.5) | 8 (19.0) | 17 (17.0) |
| 4 | 16 (17.0) | 7 (9.7) | 23 (13.9) | 9 (15.5) | 4 (9.5) | 13 (13.0) |
| 5 | 17 (18.1) | 14 (19.4) | 31 (18.7) | 12 (20.7) | 7 (16.7) | 19 (19.0) |
| Entry route, n (%) | ||||||
| Number with data, n (%) | 105 (96.3) | 77 (93.9) | 182 (95.3) | 64 (100) | 43 (97.8) | 107 (99.1) |
| Caution | 93 (88.6) | 72 (93.5) | 165 (90.7) | 57 (89.1) | 42 (97.7) | 99 (92.5) |
| Prosecution | 12 (11.4) | 5 (6.5) | 17 (9.3) | 7 (10.9) | 1 (2.3) | 8 (7.5) |
| Total number of RMS incidents involved in 1-year prerandomisation (not including RMS incident that led to study entry) | ||||||
| Number with data, n (%) | 104 (95.4) | 77 (93.9) | 181 (94.8) | 63 (98.4) | 44 (100) | 107 (99.1) |
| Mean (SD) | 10.8 (12.5) | 12.9 (25.7) | 11.7 (19.2) | 9.3 (8.7) | 9.0 (9.9) | 9.2 (9.2) |
| Median (IQR) | 7 (3–13) | 6 (3–12) | 6 (3–13) | 6 (3–13) | 5 (3–12) | 6 (3–13) |
| Minimum, Maximum | 0, 79 | 1, 200 | 0, 200 | 0, 35 | 1, 38 | 0, 38 |
| Total number of RMS incidents leading to charge or caution 1-year prerandomisation (not including charge or caution that led to study entry) | ||||||
| Number with data, n (%) | 104 (95.4) | 77 (93.9) | 181 (94.8) | 63 (98.4) | 44 (100) | 107 (99.1) |
| Mean (SD) | 0.6 (1.0) | 0.5 (1.3) | 0.5 (1.1) | 0.6 (1.0) | 0.3 (0.6) | 0.5 (0.9) |
| Median (IQR) | 0 (0–1) | 0 (0–1) | 0 (0–1) | 0 (0–1) | 0 (0–0.5) | 0 (0–1) |
| Minimum, Maximum | 0, 4 | 0, 10 | 0, 10 | 0, 4 | 0, 2 | 0, 4 |
| Total number of PNC convictions 1-year prerandomisation | ||||||
| Number with data, n (%) | 104 (95.4) | 77 (93.9) | 181 (94.8) | 63 (98.4) | 44 (100) | 107 (99.1) |
| Mean (SD) | 0.5 (0.8) | 0.3 (0.5) | 0.4 (0.7) | 0.4 (0.7) | 0.2 (0.5) | 0.3 (0.6) |
| Median (IQR) | 0 (0–1) | 0 (0–1) | 0 (0–1) | 0 (0–1) | 0 (0–0) | 0 (0–0) |
| Minimum, Maximum | 0, 3 | 0, 2 | 0, 3 | 0, 2 | 0, 2 | 0, 2 |
| Involved in RMS incident that led to caution or charge 1-year prerandomisation (not including charge or caution that led to study entry), n (%) | ||||||
| Number with data, n (%) | 104 (95.4) | 77 (93.9) | 181 (94.8) | 63 (98.4) | 44 (100) | 107 (99.1) |
| Yes | 36 (34.6) | 21 (27.3) | 57 (31.5) | 21 (33.3) | 11 (25.0) | 32 (29.9) |
| No | 68 (65.4) | 56 (72.7) | 124 (68.5) | 42 (66.7) | 33 (75.0) | 75 (70.1) |
| PNC conviction 1-year prerandomisation, n (%) | ||||||
| Number with data, n (%) | 104 (95.4) | 77 (93.9) | 181 (94.8) | 63 (98.4) | 44 (100) | 107 (99.1) |
| Yes | 31 (29.8) | 22 (28.6) | 53 (29.3) | 16 (25.4) | 8 (18.2) | 24 (22.4) |
| No | 73 (70.2) | 55 (71.4) | 128 (70.7) | 47 (74.6) | 36 (81.8) | 83 (77.6) |
Appendix 6 Health economic data
| 4-weeks post-randomisation | 16-weeks post-randomisation | 1-year post-randomisation | ||||
|---|---|---|---|---|---|---|
| Gateway conditional caution (n = 109) | Usual process (n = 82) | Gateway conditional caution (n = 109) | Usual process (n = 82) | Gateway conditional caution (n = 109) | Usual process (n = 82) | |
| Employed in previous month | ||||||
| Number with data, n (%) | 57 (52.3) | 36 (43.9) | 54 (49.5) | 39 (47.6) | 27 (24.8) | 16 (19.5) |
| Yes | 31 (54.4) | 16 (44.4) | 31 (57.4) | 19 (48.7) | 16 (59.3) | 11 (68.8) |
| No | 26 (45.6) | 20 (55.6) | 23 (42.6) | 20 (51.3) | 11 (40.7) | 5 (31.3) |
| Number of times visited GP in previous month | ||||||
| Number with data, n (%) | 57 (52.3) | 36 (43.9) | 53 (48.6) | 39 (47.6) | 27 (24.8) | 15 (18.3) |
| Mean (SD) | 0.4 (0.7) | 0.5 (1.0) | 0.4 (1.0) | 0.5 (0.9) | 0.5 (1.0) | 1.3 (2.6) |
| Median (IQR) | 0 (0–1) | 0 (0–0.5) | 0 (0–0) | 0 (0–0) | 0 (0–1) | 1 (0–1) |
| Minimum, Maximum | 0, 3 | 0, 4 | 0, 5 | 0, 3 | 0, 4 | 0, 10 |
| Number of times used drug/alcohol services in previous month | ||||||
| Number with data, n (%) | 56 (51.4) | 36 (43.9) | 53 (48.6) | 39 (47.6) | 26 (23.9) | 15 (18.3) |
| Mean (SD) | 0.3 (0.9) | 0.3 (1.7) | 0.4 (1.2) | 0.1 (0.4) | 0.2 (0.8) | 0.4 (1.1) |
| Median (IQR) | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0 (0–0) |
| Minimum, Maximum | 0, 4 | 0, 10 | 0, 5 | 0, 2 | 0, 4 | 0, 4 |
| Number of times visited accident and emergency in previous month | ||||||
| Number with data, n (%) | 57 (52.3) | 36 (43.9) | 54 (49.5) | 39 (47.6) | 27 (24.8) | 15 (18.3) |
| Mean (SD) | 0.2 (0.9) | 0.1 (0.2) | 0.1 (0.3) | 0 (0.2) | 0.6 (1.9) | 0.2 (0.6) |
| Median (IQR) | 0 (0–0) | 0 (0, 0) | 0 (0, 0) | 0 (0, 0) | 0 (0, 0) | 0 (0, 0) |
| Minimum, Maximum | 0, 6 | 0, 1 | 0, 2 | 0, 1 | 0, 10 | 0, 2 |
| Number of times admitted to hospital as inpatient in previous month | ||||||
| Number with data, n (%) | 57 (52.3) | 36 (43.9) | 53 (48.6) | 39 (47.6) | 27 (24.8) | 15 (18.3) |
| Mean (SD) | 0.1 (0.3) | 0 (0) | 0.1 (0.3) | 0 (0) | 0.3 (1.0) | 0 (0) |
| Median (IQR) | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0 (0–0) |
| Minimum, Maximum | 0, 2 | 0, 0 | 0, 2 | 0, 0 | 0, 4 | 0, 0 |
| Number of times used community mental health team in previous month | ||||||
| Number with data, n (%) | 56 (51.4) | 35 (2.7) | 53 (48.6) | 38 (46.3) | 26 (23.9) | 15 (18.3) |
| Mean (SD) | 0.2 (0.8) | 0.2 (0.7) | 0.2 (0.6) | 1.1 (4.9) | 0.4 (1.1) | 0.5 (1.2) |
| Median (IQR) | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0 (0–0) |
| Minimum, Maximum | 0, 4 | 0, 3 | 0, 3 | 0, 30 | 0, 4 | 0, 4 |
| Number of times used psychiatric services as in-patient in previous month | ||||||
| Number with data, n (%) | 57 (52.3) | 36 (43.9) | 53 (48.6) | 39 (47.6) | 27 (24.8) | 15 (18.3) |
| Mean (SD) | 0 (0.2) | 0 (0.2) | 0 (0) | 0.2 (1.0) | 0 (0.2) | 0.1 (0.3) |
| Median (IQR) | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0 (0–0) |
| Minimum, Maximum | 0, 1 | 0, 1 | 0, 0 | 0, 6 | 0, 1 | 0, 1 |
| Used the following prescribed medications in previous month, n (%) | ||||||
| Number with data, n (%) | 57 (52.3) | 36 (43.9) | 54 (49.5) | 39 (47.6) | 27 (25.0) | 16 (19.3) |
| Amitriptyline | 1 (1.8) | 0 (0) | 1 (1.9) | 0 (0) | 2 (7.4) | 0 (0) |
| Aripiprazole | 1 (1.8) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Desogestrel | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (3.7) | 0 (0) |
| Citalopram | 3 (5.3) | 1 (2.8) | 1 (1.9) | 2 (5.1) | 1 (3.7) | 0 (0) |
| Co-codamol | 0 (0) | 0 (0) | 1 (1.9) | 0 (0) | 0 (0) | 0 (0) |
| Codeine | 0 (0) | 1 (2.8) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Cyclizine | 1 (1.8) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Diazepam | 0 (0) | 0 (0) | 0 (0) | 1 (2.6) | 0 (0) | 0 (0) |
| Doxycycline | 0 (0) | 0 (0) | 0 (0) | 1 (2.6) | 0 (0) | 0 (0) |
| Inhaler | 0 (0) | 4 (11.1) | 5 (9.3) | 2 (5.1) | 1 (3.7) | 0 (0) |
| Escitalopram | 1 (1.8) | 1 (2.8) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Fluoxetine | 3 (5.3) | 1 (2.8) | 0 (0) | 2 (5.1) | 0 (0) | 0 (0) |
| Quetiapine | 2 (3.5) | 1 (2.8) | 0 (0) | 0 (0) | 0 (0) | 1 (6.3) |
| Lamotrigine | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (3.7) | 0 (0) |
| Lymecycline | 0 (0) | 2 (5.6) | 0 (0) | 1 (2.6) | 0 (0) | 0 (0) |
| Macrogol 3350 | 1 (1.8) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Melatonin | 0 (0) | 0 (0) | 0 (0) | 1 (2.6) | 0 (0) | 0 (0) |
| Methadone | 0 (0) | 0 (0) | 1 (1.9) | 0 (0) | 0 (0) | 0 (0) |
| Mirtazapine | 2 (3.5) | 0 (0) | 2 (3.7) | 0 (0) | 1 (3.7) | 1 (6.3) |
| Naproxen | 1 (1.8) | 0 (0) | 2 (3.7) | 0 (0) | 0 (0) | 0 (0) |
| Omeprazole | 1 (1.8) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Ondansetron | 0 (0) | 0 (0) | 1 (1.9) | 0 (0) | 0 (0) | 0 (0) |
| Olanzapine | 0 (0) | 1 (2.8) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Phenergan | 0 (0) | 2 (5.6) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Prednisolone | 1 (1.8) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Pregabalin | 0 (0) | 1 (2.8) | 1 (1.9) | 0 (0) | 0 (0) | 0 (0) |
| Prochlorperazine maleate | 1 (1.8) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Promethazine hydrochloride | 0 (0) | 0 (0) | 0 (0) | 1 (2.6) | 0 (0) | 0 (0) |
| Propranolol hydrochloride | 1 (1.8) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Quetiapine | 2 (3.5) | 0 (0) | 4 (7.4) | 3 (7.7) | 2 (7.4) | 0 (0) |
| Ramipril | 0 (0) | 0 (0) | 1 (1.9) | 0 (0) | 0 (0) | 0 (0) |
| Risperidone | 0 (0) | 1 (2.8) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Salbutamol | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (6.3) |
| Sertraline | 3 (5.3) | 4 (11.1) | 7 (13.0) | 5 (12.8) | 2 (7.4) | 2 (12.5) |
| Prochlorperazine | 0 (0) | 0 (0) | 1 (1.9) | 0 (0) | 0 (0) | 0 (0) |
| Tacrolimus | 1 (1.8) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Venlafaxine | 1 (1.8) | 0 (0) | 0 (0) | 1 (2.6) | 1 (3.7) | 0 (0) |
| Vortioxetine | 0 (0) | 1 (2.8) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Reason for using prescribed medications in previous month, n (%) | ||||||
| Number with data (% of those who reported using at least one medication) | 20 (100) | 15 (100) | 21 (100) | 14 (100) | 8 (100) | 7 (100) |
| Acne | 0 (0) | 3 (20.0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Anterior cruciate ligament injury | 0 (0) | 1 (6.7) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| ADHD | 1 (5.0) | 1 (6.7) | 1 (4.8) | 0 (0) | 0 (0) | 0 (0) |
| Anxiety | 7 (35.0) | 7 (46.7) | 4 (19.0) | 2 (14.3) | 2 (25.0) | 2 (28.6) |
| Asthma | 1 (5.0) | 4 (26.7) | 5 (23.8) | 2 (14.3) | 1 (12.5) | 1 (14.3) |
| Back pain | 0 (0) | 0 (0) | 1 (4.8) | 0 (0) | 0 (0) | 0 (0) |
| Blood pressure | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (12.5) | 0 (0) |
| Depression | 11 (55.0) | 7 (46.7) | 8 (38.1) | 3 (21.4) | 5 (62.5) | 2 (28.6) |
| Ear infection | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (14.3) |
| Gastroparesis | 1 (5.0) | 0 (0) | 1 (4.8) | 0 (0) | 1 (12.5) | 0 (0) |
| Heroin addiction | 0 (0) | 0 (0) | 1 (4.8) | 0 (0) | 0 (0) | 0 (0) |
| Hypertension | 0 (0) | 0 (0) | 1 (4.8) | 0 (0) | 0 (0) | 0 (0) |
| Immune system suppression post-kidney transplant | 1 (5.0) | 0 (0) | 1 (4.8) | 0 (0) | 0 (0) | 0 (0) |
| Inflammation | 1 (5.0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Insomnia | 2 (10.0) | 1 (6.7) | 0 (0) | 1 (7.1) | 1 (12.5) | 0 (0) |
| Mood stabilisation | 2 (10.0) | 1 (6.7) | 3 (14.3) | 1 (7.1) | 1 (12.5) | 0 (0) |
| Nail infection | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (14.3) |
| Nausea | 1 (5.0) | 0 (0) | 1 (4.8) | 0 (0) | 0 (0) | 0 (0) |
| Pain relief | 0 (0) | 0 (0) | 2 (9.5) | 0 (0) | 1 (12.5) | 0 (0) |
| Panic attacks | 0 (0) | 1 (6.7) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Psychosis | 2 (10.0) | 1 (6.7) | 1 (4.8) | 0 (0) | 1 (12.5) | 1 (14.3) |
| PTSD | 0 (0) | 2 (13.3) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Appendix 7 An example description of Braun and Clarke’s stepped and systematic approach to thematic analysis for young people interviewed at T237
| Familiarisation with data | Recordings were listened back to, and then transcribed as part of the process of familiarisation. Original audio files were then deleted. Transcripts were read through and some initial notes and annotations were made. |
| Generating codes from data | Initial codes were developed which were in line with the anticipated causal assumptions, as also captured in the quantitative data. These provide more context and allow for further interrogation of these mechanisms. Next, a thematic analysis approach helped create further codes, identifying unanticipated pathways and broader perspectives. Two of the interviews were second coded by the researcher’s supervisor, to minimise bias. |
| Searching for themes | Using tables and mind maps, codes were grouped and broader themes were explored. Discussion with the project supervisor helped ensure bias was minimised and emerging themes were true to the data. |
| Reviewing themes | Codes were expanded and collapsed and broader themes were defined, and revised through further analysis. A thematic map was developed to start to link the themes and identify the emerging narrative from the data, linking to the objectives of the evaluation. |
| Defining themes | Themes were named and cross-checked to ensure the essence captured the aim and objectives, as well as being a true reflection of the data. Further discussion with the researcher’s supervisor reflected on these themes and a second conceptual framework was developed. |
| Writing up | Data extracts were used in the write-up to capture the essence of each theme, providing supporting evidence. |
| Throughout each step | A reflexivity journal was kept, with the aim of monitoring the researcher’s relationship and potential influence on the participants and subsequent data, with recognition that interviews are considered a co-construction and the researcher plays a role in the constructing the narrative that emerges. The researcher continuously critically reflected on their own role in the analysis, making sure they were conscious of their own preconceptions, beliefs and sympathies. |
Appendix 8 Flow diagrams of recruitment processes for qualitative interviews
FIGURE 11.
Recruitment process for young people (T2).
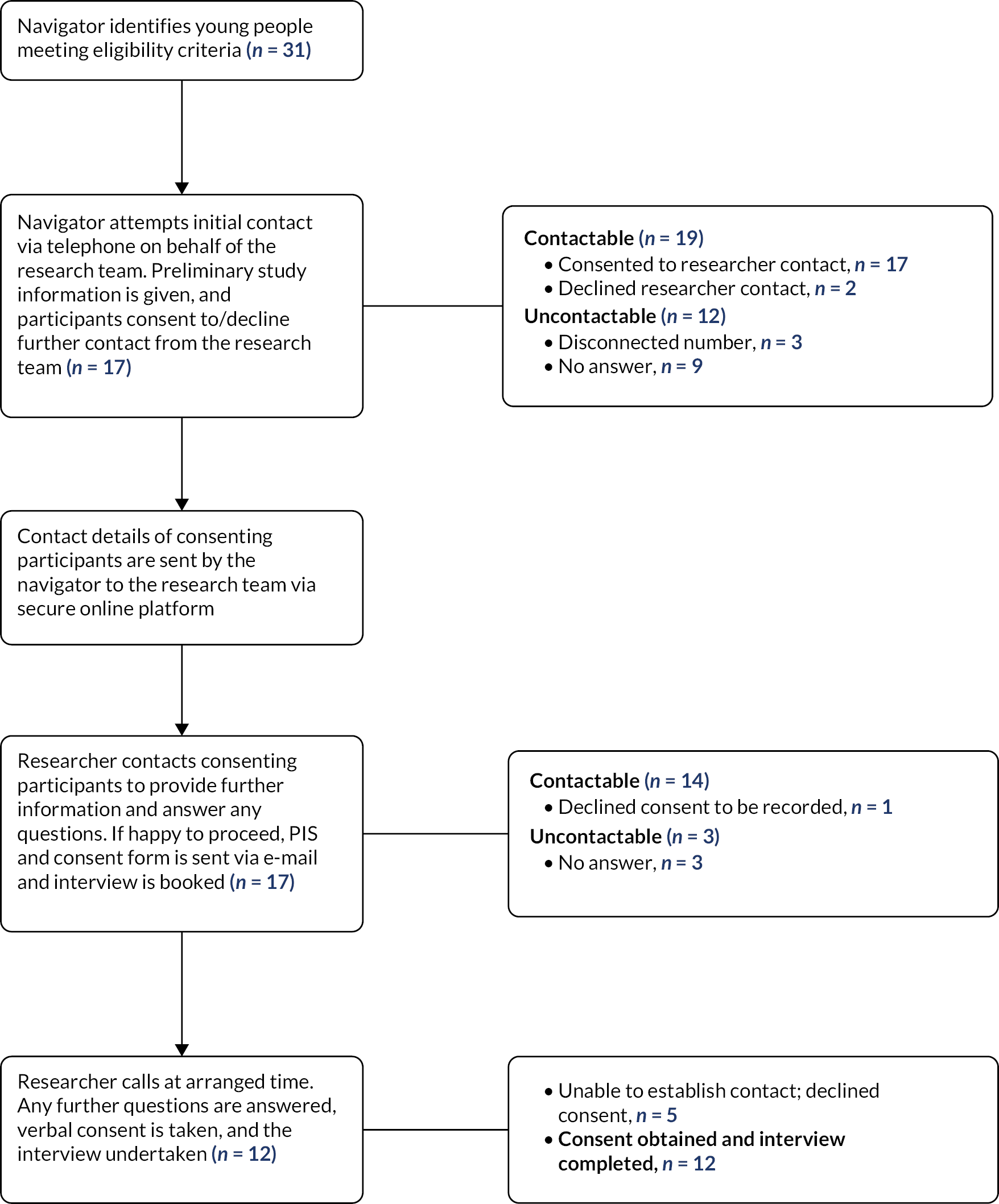
FIGURE 12.
Recruitment process for young people (T3).
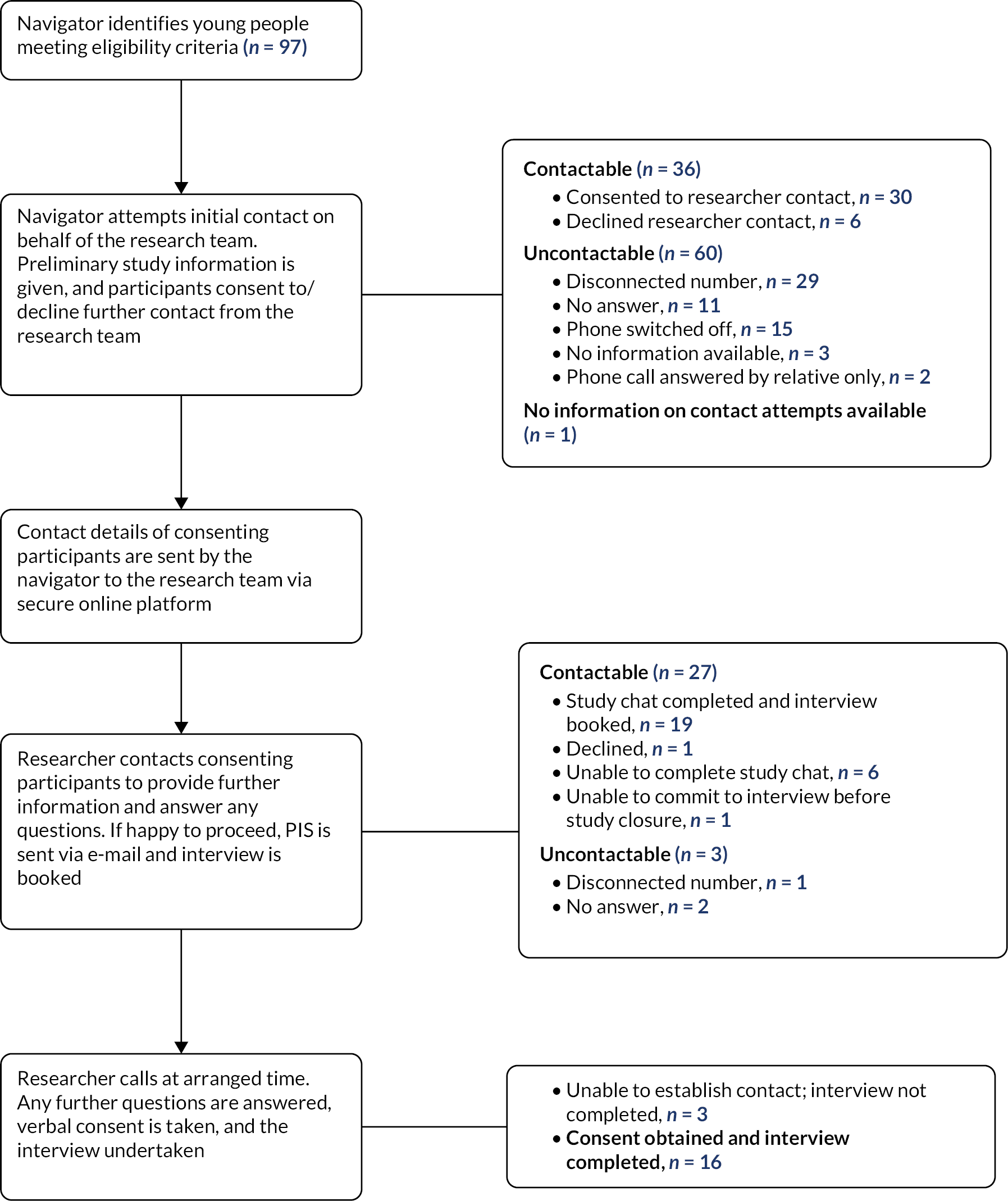
FIGURE 13.
Recruitment process for police recruiters (T3).
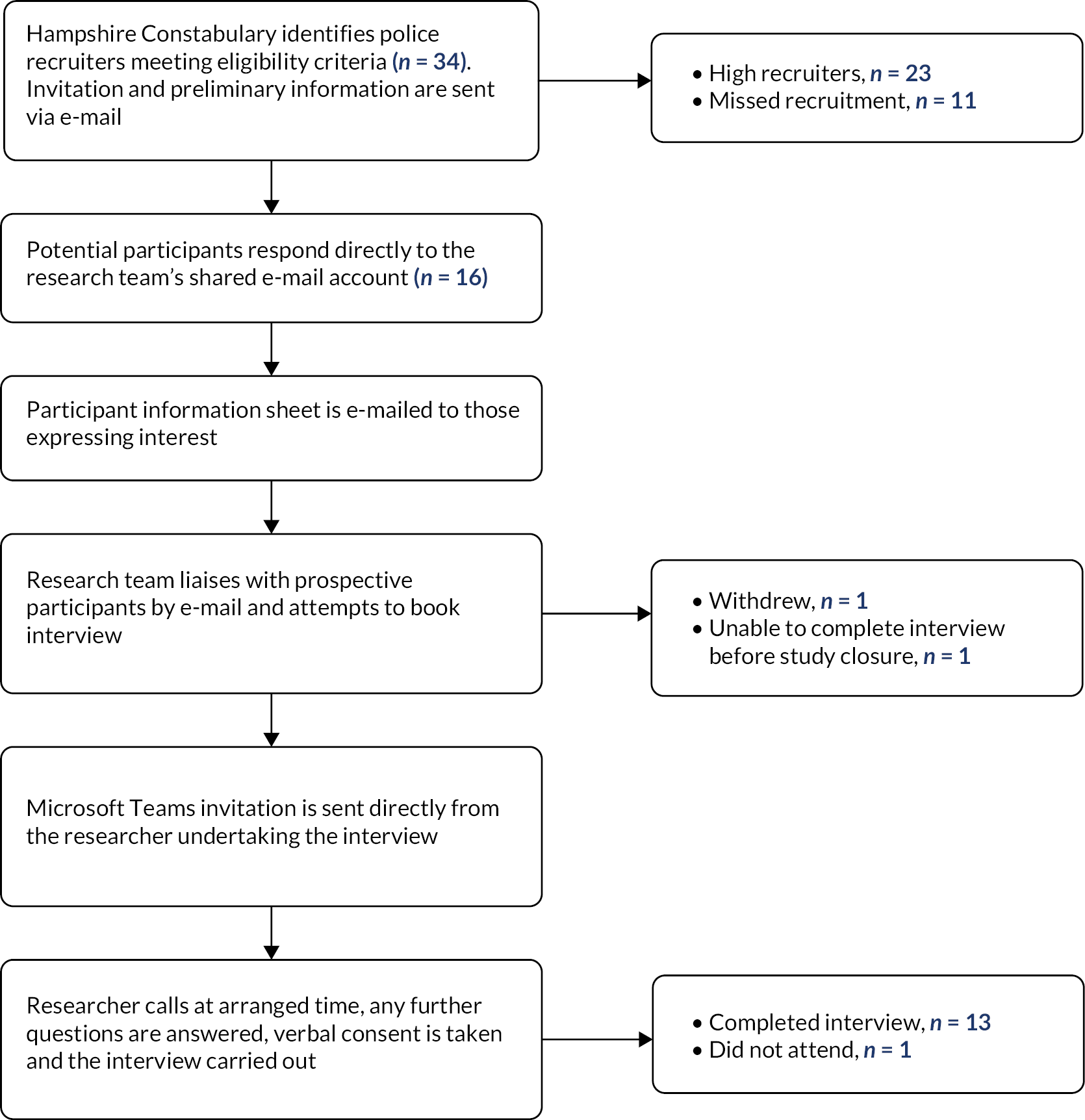
Glossary
- Alchemer (formerly SurveyGizmo)
- A web-based eligibility and randomisation tool, used to ensure standardised recruitment and recording of eligibility criteria.
- Arrest
- A seizure or forcible restraint; an exercise of the power to deprive a person of his or her liberty; the taking or keeping of a person in custody by legal authority, especially, in response to a criminal charge. [Farlex dictionary]
- Breach
- Breaching is a term to describe when a young adult does not meet the conditions of their caution and are returned to the ‘usual care’ criminal justice process. Breaching is often as a result of lack of engagement with the out-of-court community-based intervention or reoffending.
- Cautioning Adult Relationship Abuse
- Cautioning Adult Relationship Abuse is an out-of-court disposal for standard/medium risk alleged first-time offenders of Domestic Abuse. It is an awareness-raising intervention consisting of two workshops held 4 weeks apart aimed at supporting offenders to make better behaviour choices in their relationships.
- Conditional caution
- A conditional caution (Criminal Justice Act 2003, s.22) requires an offender to comply with conditions, as an alternative to prosecution. [UK Sentencing Council]
- Custody sergeant
- Manages the custody suite and takes the decision to authorise or refuse the detention of any persons presented before them. Ensures police officers and police staff adhere to the Police and Criminal Evidence Act 1983 Codes of Practice regarding the rights and treatment of persons arrested. [College of Policing]
- Full Code Test
- This is a two-stage test applied each time a charging decision is made, whether it is made by the police or the Crown Prosecution Service – the evidential stage and the public interest stage. The evidential stage must be met before the public interest stage can be considered. [College of Policing]
- In-custody
- Suspects may be held in a police custody suite for up to 24 hours before they have to charge the individual with a crime or release them. These cases are therefore disposed of ‘in-custody’.
- Inspector
- Inspectors manage teams of sergeants, constables and police staff and/or portfolios. Post holders may be the senior operational officer or manage assigned specialist policing functions. This role carries specific legal powers to enable the maintenance of law and order. [College of Policing]
- Offences
- A summary only offence is an offence that is usually tried in the magistrates’ court. They are less serious offences, such as shoplifting, most motoring offences for example driving without insurance, and criminal damage (worth ˂ £5000). Indictable only offences are more serious offences, which must be tried in the Crown Court. An either way offence is an offence that can be heard either in the magistrates’ court or in the Crown Court. The magistrate must decide whether to keep the case or send it to the Crown Court. Common examples of low-level offences include, minor assault and drug offences (such as possession of a prohibited amount or a utensil), public nuisance, public intoxication, public urination, unlawful possession of suspected stolen property and trespass, and minor road traffic offences such as speeding and driving without due care and attention.
- Out of custody
- Suspects may be dealt with through a ‘voluntary interview’ which is undertaken elsewhere, such as at a police station but not in the custody suite; or the individual’s home. These cases are therefore disposed out of custody.
- Out-of-court community-based intervention
- An out-of-court community-based intervention is a process whereby an accused offender is formally moved into a programme in the community, instead of being moved through the criminal justice system. Out-of-court community-based interventions involve the suspect working with other organisations or social systems in which they might find social support, social recognition and reinforcement.
- Out-of-court disposal
- An out-of-court disposal is a victim-focused method of resolving a police investigation for offenders of low-level crime and antisocial behaviour such as graffiti and low-level criminal damage when the offender admits the offence. Out-of-court disposals are alternatives to the individual going through the criminal justice system. They are issued by the police, do not incur a criminal record and include: No further action. Community resolution: the resolution of a minor offence or antisocial behaviour incident through informal agreement between the parties involved. Caution: aims to provide a proportionate and effective resolution to offending and support the aim of preventing offending. Conditional caution: a caution with one or more conditions attached. If an individual does not keep to the conditions, they could be prosecuted for the original offence.
- Police and Crime Commissioner
- Police and Crime Commissioners are elected in England and Wales to hold the police to account and ensure that local police meet the needs of the community. Functions include: securing and maintaining an efficient and effective police force within their area; holding the chief constable to account; management of budget for policing their area.
- Police investigator
- Crimes may be investigated by either a police officer, or a civilian investigator (both are issued with a collar number).
- Recidivism
- The act of a person repeating an undesirable behaviour after they have experienced negative consequences of that behaviour. It is also used to refer to the percentage of former prisoners who are rearrested for a similar offence.
- Reoffend
- To commit another offence.
- Sergeant
- Sergeants are the first level of line management in policing and as such carry an important role in ensuring effective daily supervision, guidance and support of officers and staff. They are responsible for enabling the development of competence within their team while ensuring that organisational standards are met and objectives achieved. This role will coordinate, monitor and respond where necessary, to front-line policing activity to uphold the law, enable public safety and build public confidence in policing in line with legal frameworks and policy guidelines. Post holders are also likely to take on an operational specialist role requiring specialist technical knowledge and skills. [College of Policing]
- Social determinants of health
- The non-medical factors that influence health outcomes. The conditions in which people are born, grow, work, live and age, and the wider set of forces and systems shaping the conditions of daily life. These include economic policies and systems, development agendas, social norms, social policies and political systems. [World Health Organization: Social Determinants of Health 2021]
- Women and Desistance Engagement programme
- An innovative programme to tackle the root cause of offending for women subject to conditional cautions. It includes two workshops designed to assist female offenders to live safe, offence-free lives, promoting desistance and managing the effects of previous trauma including historic domestic/sexual abuse. It also promotes opportunities for women to exit sex work.
List of abbreviations
- ACE
- Adverse Childhood Experiences questionnaire
- ADIS
- Adolescent Drug Involvement Scale
- AUDIT
- Alcohol Use Disorders Identification Test
- CARA
- Cautioning Adult Relationship Abuse
- CONSORT
- Consolidated Standards of Reporting Trials
- CPS
- Crown Prosecution Service
- CRF
- case report form
- CSRI
- Client Service Receipt Inventory
- DMEC
- Data Monitoring and Ethics Committee
- GCSE
- General Certificate of Secondary Education
- HC
- Hampshire Constabulary
- HRA
- Health Research Authority
- IoW
- Isle of Wight
- IQR
- interquartile range
- NHS
- National Health Service
- NIHR
- National Institute for Health and Care Research
- OCBI
- out-of-court community-based intervention
- OOCD
- out-of-court disposal
- PHR
- Public Health Research
- PIS
- participant information sheet
- PNC
- police national computer
- PPI
- patient and public involvement
- PPP
- public participation panel
- RCT
- randomised controlled trial
- RDD
- regression discontinuity design
- REC
- Research Ethics Committee
- RJ
- restorative justice
- RMS
- records management system
- RNR
- risk-need-responsivity
- SAP
- statistical analysis plan
- SD
- standard deviation
- SF-12
- Short Form 12 questionnaire
- SOP
- standard operating procedure
- SSC
- Study Steering Committee
- TMG
- Trial Management Group
- UoS
- University of Southampton
- WEMWBS
- Warwick-Edinburgh Mental Wellbeing Scale
- YTU
- York Trials Unit
Notes
Supplementary material can be found on the NIHR Journals Library report page (https://doi.org/10.3310/NTFW7364).
Supplementary material has been provided by the authors to support the report and any files provided at submission will have been seen by peer reviewers, but not extensively reviewed. Any supplementary material provided at a later stage in the process may not have been peer reviewed.