
Notes
Article history
The research reported in this issue of the journal was funded by the PHR programme as project number 09/3001/13. The contractual start date was in February 2010. The final report began editorial review in August 2012 and was accepted for publication in March 2013. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PHR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
Helen Roberts is a member of the NIHR Journals Library editorial board.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2014. This work was produced by Green et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Free bus travel and public health
Introduction
Transport policies and systems are increasingly accepted to have the potential to be both health promoting and harmful to health,1,2 and to contribute to the generation, maintenance or mitigation of health inequalities. 3–6 However, the evidence base in this area remains relatively underdeveloped, with few evaluative studies which have examined the health and related outcomes of changes to transport policies7,8 and few studies which have identified the costs and benefits specifically of public transport use,9 although methodological work in this area is being developed. 10,11 This study aimed to contribute to this evidence base by evaluating the impact on the public health of a transport intervention in London: the introduction of free travel for young people.
The intervention: free bus travel for young people
In 2005, the Greater London Authority (GLA) granted secondary school-aged children unlimited travel on buses and trams displaying the London Buses symbol (both within and just outside London,12 replacing a reduced, 40p flat fare for each journey on the London bus network. This fare exemption was extended a year later to include 17-year-olds in full-time education (p. 7)13 and now also includes all 18-year-olds (and some 19-year-olds) in full-time education or on a work-based learning scheme (pp. 8–9). 14 To access free travel, young people apply for an electronic photo card called a ‘zip’ card, which is tapped on a reader on entering the bus. As well as granting the cardholder unlimited free travel on all buses, the zip card also acts as a conventional ‘Oyster’ card, used by most residents and visitors in London. This can be loaded with pre-pay or travelcards for the cardholders to use on other parts of the Transport for London (TfL) network [tube, Docklands Light Railway (DLR), London overground and most National Rail services operating in the capital] at a discounted rate (pp. 6–11). 14
The stated aims of the scheme were ‘to help young people to continue studying, improve employment prospects and promote the use of public transport’ (p. 7). 13 That is, it was aimed first and foremost at mitigating the potential social exclusion effects for young people of fare-based urban transport systems. 15 As stated more recently on the TfL website:
Granting young people free travel is part of the Mayor’s strategy to embed more environmentally sound travel habits from an early age while helping young people to unlock education, sport, leisure and employment opportunities. 16
By removing any need to pay, at the point of use, for travel on buses, it was argued that young people would be better (and more equally) able to access goods and services (schools, libraries, leisure facilities, etc.), thus both improving social inclusion in the short term and contributing to longer-term policies to improve the sustainability of London’s transport system.
However, the intervention is likely to have had other implications for health and well-being. Policy concerns have centred on the potential impact on young people of being at risk of, and the perpetrators of, crime;17,18 the impact on older citizens of buses with large numbers of young people; and the possible effects on ‘active transport’ at a time when health policy is geared towards encouraging walking and cycling. The latter issue is one that has explicitly been aired by both politicians (see Appendix 1) and practitioners:
I would urge TfL to scrap concessionary bus fares for children in London . . . They should be walking or cycling these trips for the sake of their own health and fitness. Yet many of them are taking the bus for just a stop or two – and getting fatter and fatter . . . It is almost impossible to get secondary school kids on their feet or on their bikes in the face of the free [bus travel]. It’s high time it was abolished. 19
To date, there is little empirical evidence that would inform debate. Given the importance to public health of both addressing issues of sustainability in transport and the threatened ‘obesity epidemic’,20–22 evidence on the health effects of interventions such as free bus travel is urgently needed.
Context: London’s unique transport infrastructure
London’s transport infrastructure is unique in the UK. First, since the deregulation of bus transport in 1985, it is the only region within Great Britain with a regulated bus system,23 with the elected Mayor of London having executive control over the transport in the Greater London area. Over the past 10 years, and since the establishment of the GLA as a strategic governing authority for London in July 2000, London’s bus network has been subject to significant operational changes (including changes to bus ‘service levels’ as well as to the ways that contractual agreements between TfL and bus operators are monitored and regulated). 24 In the transport field:
[S]ervice levels can be defined according to a number of dimensions, the key ones being the frequency of public transport services (services per hour), the hours they operate (period of operation), where they operate and the origins and destinations they serve (both related to network coverage). 25
These changes have been driven by an explicit commitment to public transport, with the GLA’s first Mayor, Ken Livingstone (2000–8), stating that to resolve the problems posed to ‘the business efficiency and quality of life of the city’ by an inadequate transport system, ‘[t]he only viable approach . . . is one where passenger travel to, from and within central London must primarily be served by public transport’ (p. 12). 26 These policies have increased the numbers of bus passengers and bus trips in London, with buses now carrying around 2.2 billion passengers each year (p. 139). 27 Public buses in London now operate according to a complex management and funding structure in which TfL’s role is to plan routes and monitor service quality, as well as manage bus stops, stations and other support services. The bus services themselves are operated largely by private sector companies under contract to London Bus Services Limited (‘London Buses’), part of TfL (see Appendix 1).
Car ownership is lower in London than in other areas of the UK, and a number of policies in addition to the expansion of public transport aim to reduce car use. An important one is the congestion charge, introduced in 2003 and currently £10.00 a day, which is levied on cars travelling into London within certain times. This has implications for young people’s travel patterns, which are unlikely to be typical of the UK as a whole. Department for Education (DfE) data, for instance, record higher levels of public transport use for school journeys, and lower levels of car, walking and cycling use for school journeys than for the rest of England (see Appendix 1, Table 29). 28
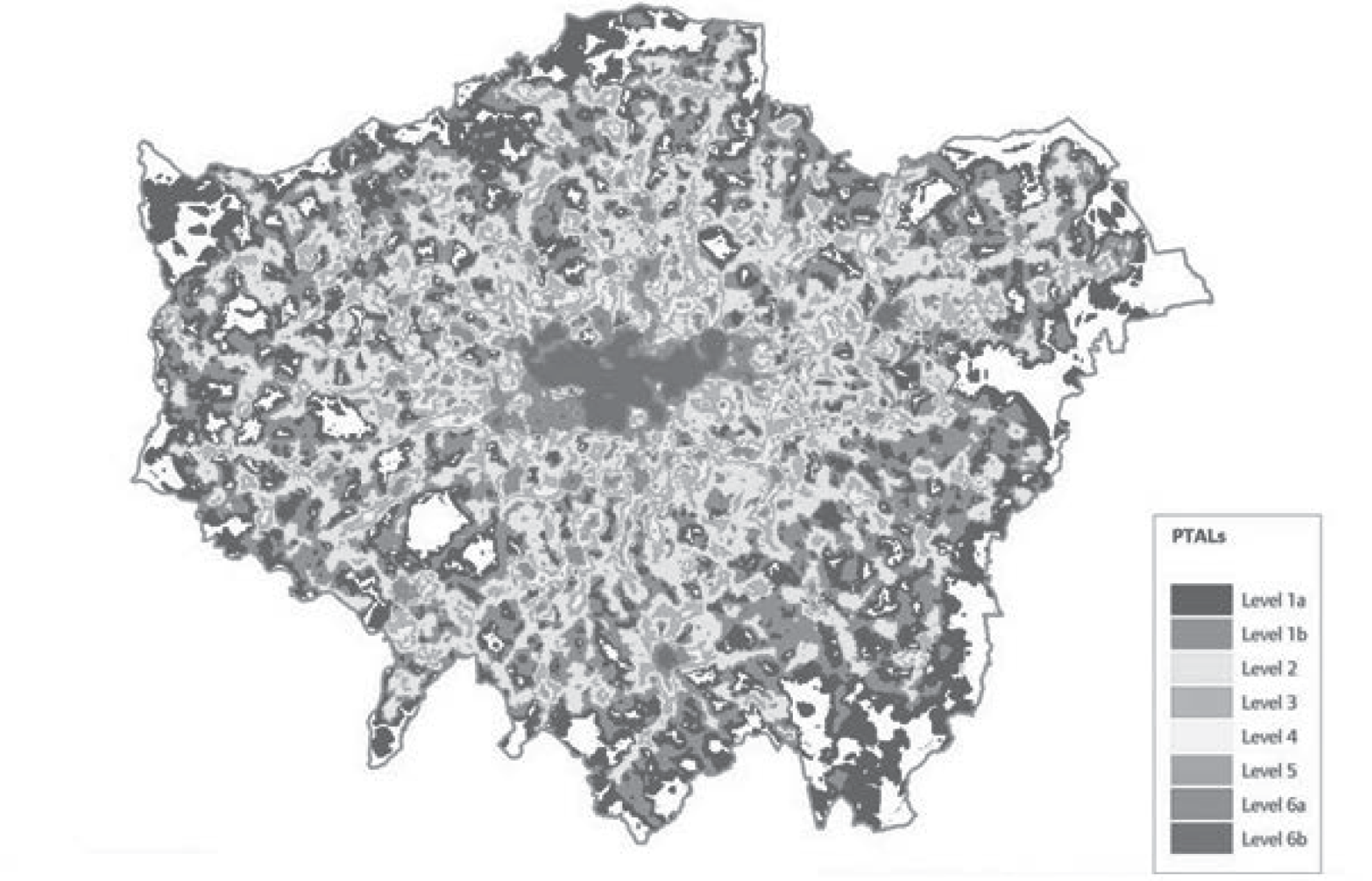
Finally, the Greater London area covers 33 boroughs, which differ in terms of transport modal share. One measure of transport accessibility is public transport accessibility level (PTAL) scores (1 is poor and 6 excellent, and 0 is no public transport accessibility within the specified parameters). As the London Travel Report29 puts it, in the calculation of PTAL scores analysts factor in:
The access time (by walking) from the point of interest to public transport service access points (SAPs, e.g. bus sops, stations) within a catchment area; the number of different services (e.g. bus routes, train services) operating at the SAPs; and levels of service (i.e. average waiting times, with an adjustment for the relative reliability of different modes). 29
As Figure 1 shows, public transport is, in general, less available the further one goes from the centre of London. With less access to public transport, and fewer disincentives for driving, car travel remains higher in the outer London boroughs than in the inner London boroughs (modal share 41% and 26% respectively). 31
FIGURE 1.
Map of pan-London PTAL scores. Reproduced with permission of GLA (map taken from p 57). 30
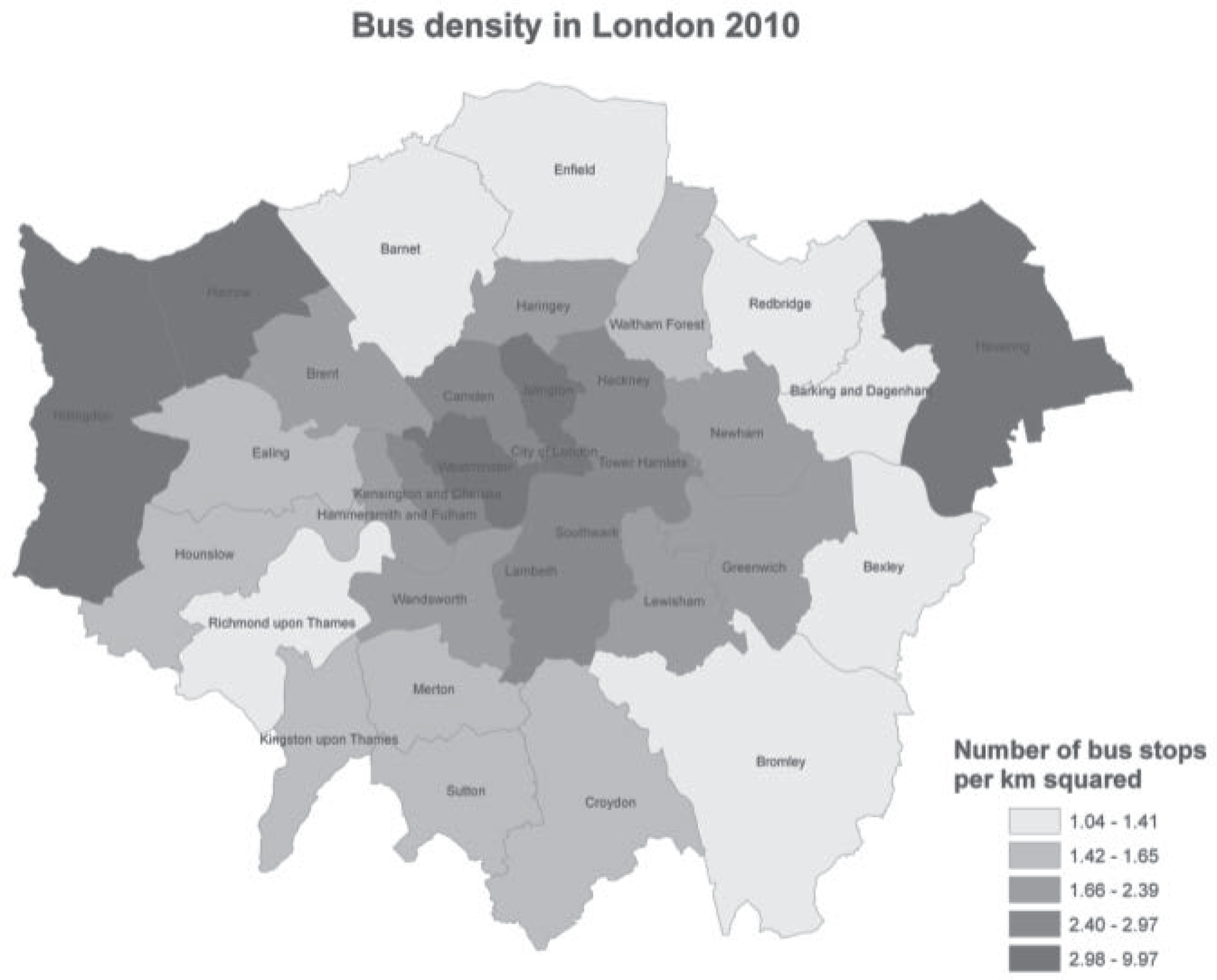
Although the distinction between inner and outer London is significant, there are other differences between the 33 boroughs in London in terms of typical transport modes used. As Figure 2 shows, bus density (indicated by the number of bus stops) varies across with boroughs, as well as across inner and outer London.
FIGURE 2.
Bus density in London, by borough.
Young people’s travel in London
The free bus travel scheme introduced for young people in London in 2005 was introduced not in isolation, but within a context of other explicit policies and secular changes that shape the ways that people in London travel and which potentially impact on health. 2,32,33 The policies and broader cultural shifts that provide the context for young people’s travel over the period of this study include:
-
Substantial improvements to the bus network (and public transport network more broadly) since the establishment of the GLA in 2000 (see above and Appendix 1).
-
The congestion charge scheme, which provided disincentives for driving in the central area and which has reduced car journeys within the zone. 34
-
The expansion of road engineering interventions, such as 20 miles per hour (mph) zones, which have made local environments safer for walking and cycling33 and therefore may have encouraged active travel.
-
The increasing distances that young people travel to school in the UK. National Travel Survey (NTS) suggest that between 1985 and 2004 the average journey length to school increased by about 800 m. 35 In London in January 2010, the average distance (calculated as a straight line using postcode data) travelled to school by secondary school pupils was 1.5 miles (p. 37, table 7). 28 Of these pupils, 24.8% travelled ≥ 2 miles to school and so covered distances that might not typically be considered appropriate for walking or cycling.
-
Broader cultural shifts that increase the number of children being driven to school. 36,37
-
A focus on cycling in London. For instance, the Evening Standard’s high-profile ‘safer cycling’ campaign included coverage of cycling deaths in London, potentially adding to anxieties that parents feel about their children cycling to school. 38 Conversely, the work of the TfL Smarter Travel unit aims to reduce car travel to/from school and the workplace, with the outer London boroughs of Richmond and Sutton, in particular, subject to extended smarter travel campaigns. 39 Although many cycling interventions have been focused on adult cyclists, such as government tax breaks on cycling to work introduced in 1999, these form part of the backdrop of changing views of transport modes in the capital (see Green and colleagues40).
What is known already?
Assessing the impact of one transport policy on young people’s health in the context of these multiple other potential influences first entails mapping the potential ways in which transport interventions might change behaviour, and how these in turn might influence the determinants of health. We first turn to the existing literature on the links between transport and health to outline what is known already about the likely causal chains between transport policy interventions and their health and other outcomes, and to outline the changes that might theoretically result from an intervention designed to change the ways that young people travel. We summarise this research below starting with the most immediate and direct effects of transport policies – injury – and ending with the more distal and difficult to measure.
Transport policy and direct effects: road traffic injury
Injuries are the health outcomes most obviously associated with transport, and there has been a general emphasis in public health research on negative impacts of transport associated with motorised road vehicles in particular on injury. In the UK, despite falling rates of road traffic injury (RTI), stark inequalities remain in the risk of being injured on the road, with those in more deprived areas and in some minority ethnic groups at highest risk. 41–43 In the UK, an important contributor to this risk is likely to be exposure. As young people’s travel behaviour changes, their exposure to the risks of road injury will change. Given that the risks of road injury are higher for pedestrians and cyclists,44 the greater likelihood of those in lower income groups to be walking rather than driving or being driven may put them at greater risk. Increasing access to bus transport may reduce injuries and, potentially, inequalities in injury risk if bus transport displaces those modes more exposed to road danger (i.e. walking and cycling).
Encouraging ‘active travel’ for public health
From a public health perspective, policy initiatives to encourage ‘active travel’ (primarily walking and cycling) have become a key element of strategies to address increasingly sedentary lifestyles and the threatened ‘obesity epidemic’ in the UK. 45–47 Walking in particular has been widely promulgated as a way to improve cardiovascular (CV) and mental health and reduce obesity at a relatively low cost to both the individual and the health-care system. 48,49 There is a growing body of international evidence demonstrating associations between ‘active’ commuting and lower risks for overweight (see Gordon-Larsen and colleagues50 and Oja and colleagues51), with one systematic review estimating that active commuting was associated with an 11% reduction in CV risk. 48 These gains are also seen for adolescents cycling or walking to school. 51,52 In addition to the direct health gain for the individual, increasing the proportion of active transport compared with private car transport has been linked with ambitious public health gains, such as reduced global warming and increased social cohesion and community safety. 1,20,53
There is some evaluative research on interventions to increase active transport. Ogilvie and colleagues49 conducted a systematic review to examine the effectiveness of a range of interventions to promote walking. Those found ranged from individually targeted interventions (such as brief advice to individuals) up to group, and area-based approaches, including school travel initiatives. Overall, the evidence suggested that interventions which tended to be effective in promoting walking were more likely to be targeted (e.g. interventions offered to individuals identified through prior screening), and tailored to participants’ requirements. However, they noted that evidence that other types of intervention have been effective in promoting walking is ‘inconsistent, of low validity, based on single highly contextual studies, or non-existent’.
Does public transport use encourage ‘active travel’?
‘Active travel’ is usually conceptualised as walking or cycling, in contrast to ‘passive’ modes such as car travel, with an assumption that encouraging public transport use will reduce car travel, and in doing so, at least generate some active transport in terms of travelling to and from public transport. However, this does not inevitably follow. In one study on the provision of alternative transport services in a sample of commuters registered with telecommuting centres in California, USA, there was a 24% decrease in reported distance travelled on foot or by bike on telecommuting days, the implication being that although telecommuting was associated with decreased car use, it also may have led to less active transport use (reported in Ogilvie and colleagues54). Such unanticipated effects illustrate the limited understanding to date on how public transport interventions are likely to influence active travel. In the USA, where public transport is more likely to be an alternative to private car use than to walking and cycling, there is some evidence that increasing access to public transport can increase activity levels by increasing walking to public transport sufficiently to have a public health impact on obesity, particularly for men. 55–57 However, it is possible that in contexts such as London, with lower levels of private car use, improving access to affordable public transport may reduce the amounts of active transport undertaken, as it may replace walking rather than car use.
Transport interventions, active travel and inequality
Ogilvie and colleagues54 noted that we know relatively little about the social distribution of health impacts of transport interventions. International comparisons suggests that the distribution of active transport across a population depends on the inter-relationships between transport systems and social structure:58 for young people, for instance, active modes of travel to school or college were more likely in high-income groups in the USA,50 but less likely for immigrants and high-income groups in Canada. 59 The impact of interventions aiming to change transport mode choices may, therefore, vary across populations. In addition, the impact of policies such as free bus travel may well have differential impacts on different population groups over time, as the social meaning of bus travel, or walking, changes. Whereas active travel may have health benefits for those who choose it, qualitative evidence suggests that there may be negative effects on health for those for whom it is compulsory since they have no choice. 60 Given the suggestion that perceived health benefits may be an important determinant of whether or not an activity does confer health benefits,61 and that views on the role of transport vary by socioeconomic status,62 how people understand the role of transport (particularly active travel) and health will be key to unpacking potential pathways linking transport policy and health inequalities.
Transport and social exclusion
Free bus travel for young people was intended to address social exclusion due to ‘transport exclusion’, with the explicit intention of improving access to education, training, and recreation that resulted from limited (financial) access to transport. Social exclusion is a complex and multidimensional concept that resists definition. Church and colleagues63 note that ‘poverty’ and ‘social exclusion’ are often used interchangeably, although ‘social exclusion’ suggests a broader concept, incorporating not just limited access to material resources, but also a relative loss of ability to ‘participate’. Limitations in ability to participate result not just from material restrictions, but also from those social, cultural and environmental contexts which may make some groups more vulnerable than others. This has implications for citizenship, and a broader sense of well-being that arises from ability to experience social interaction and feel ‘part of’ a wider communality. 64
Transport for London commissioned some evaluative work on the impact of free bus travel on outcomes related to inclusion,65,66 based on surveys of users and non-users of the scheme. However, as the samples were not representative of the population, and the findings based on self-report, no firm conclusions can be drawn about the impact of the scheme on access to education, training or independent mobility. Given that limitation, 14- to 15-year-olds reported that access to free bus travel had increased access to sports and other recreational opportunities,65 and the majority of 16- to 17-year-olds ‘strongly felt’ that the scheme had increased their likelihood of staying in full-time education, particularly those in lower income and minority ethnic groups. 66
Independent travel
For young people, access to transport is likely to have implications for inequalities in a second sense, in that there is evidence that, as a population group, young people are increasingly social excluded from public life through limitations on their ability to be ‘independently mobile’. Environments that prioritise the needs of motorised transport and increasingly ‘tightly govern’ public spaces have, it is argued, resulted in young people leading increasingly domesticated lives, with less ‘independent mobility’ than previous generations. 67–69 For example, Hillman and colleagues70 showed that between 1971 and 1990 British parents raised the age at which they granted their children ‘licences’ to undertake different sorts of journeys (e.g. going to school unaccompanied or cycling on the road), a trend that has since continued. 71 This decline in independent mobility has been linked to a range of negative outcomes including decreased physical activity,72 reduced opportunities for social, emotional and cognitive development69 and increased fear of and alienation from the local environment. 73
What this study will add
Theoretically, then, the free fare scheme for young people may have had a range of effects on the public health of Londoners. Evidence to date suggests that effects on ‘processes’ such as travel mode choice and travel mode distribution are likely to affect health behaviours and outcomes such as active travel and injury rates. Reducing fares (in this case to ‘no cost’) is likely to increase use of bus travel in the target population74 displacing other modes of transport and/or creating additional journeys.
To summarise, the risks and benefits to health from the provision of free public transport are likely to accrue from the increased availability of transport and changes in the share of modes of transport used (e.g. switching from walking to bus travel). In the USA, where public transport is more likely to replace car use than walking and cycling, there is some evidence that increasing access to public transport can increase activity levels. Increased walking to public transport is enough to have had a public health impact on obesity, particularly for men. 55–57 In England, free bus travel has been identified as providing a benefit for the health of older people. 75,76 However, it is possible that in settings such as London, with lower private car use than other parts of the country,77 improving access to affordable public transport may reduce the amounts of active travel undertaken by replacing walking or cycling rather than car use. As the risk of RTI varies by transport mode,44 any modal shift is likely to have implications for injury rates. Young people are at particular risk of assault,78 and greater access to public transport potentially increases this risk. More tangential benefits which may be associated with young people’s increased access to public transport include increased social inclusion, and decreased future reliance on private car travel. They are also likely to have effects on broader determinants of health, such as social inclusion and independent travel. These broader health implications of well-being that arise from social inclusion or the ability to make independent choices about travel are important, but there is in general less evidence on the wider social and health effects of different transportation choices79 and real challenges in operationalising concepts such as ‘inclusion’ for research. 80 Clearly, an evaluation of the public health effects of a transport intervention needs to account for potential effects on social inclusion and well-being, but these are difficult to measure. Finally, in addition to benefits or costs for the target group (12- to 17-year-olds), there may be effects on other transport users if they are displaced from buses.
The free bus pass scheme is a ‘natural experiment’ which allows us to evaluate these potential pathways linking a large-scale transport intervention to health determinants, behaviours and outcomes. Given the range of health benefits and disbenefits that theoretically arise from the intervention; the complexity of the system in which this intervention was introduced and the difficulties in operationalising distal health outcomes which are important but (to date) under-researched, any evaluation will require a mix of methodological strategies. This study therefore aimed to evaluate the impact of free bus travel on the public health by identifying the best available strategies to explore these pathways, using a mixed-method design. Our specific aims were to:
-
provide empirical evidence for the impact of this intervention on key health behaviours and outcomes (e.g. injuries, active travel) for young people
-
explore the effects on the determinants of health (e.g. access to education and training)
-
identify the effects of increased young people’s access to bus travel on older citizens
-
develop and apply methods for economic assessment, and
-
contribute to the development of methods to strengthen causal inference in non-randomised designs.
The approach we took to meeting these aims is outlined in the next chapter.
Chapter 2 Methodology: evaluating ‘natural experiments’ using mixed methods
Introduction
Drawing on existing research, Chapter 1 outlined the range of health impacts free bus travel may have had on the public health, and summarised the aims of an evaluation of these impacts. Like many other policy interventions with potential impacts on the determinants of health, it is impossible to generate ‘best evidence’ such as that from a randomised controlled trial (RCT) on the effects of the intervention. The scheme has already happened, there are no obvious control groups, and no opportunities for the research team to control exposure to the intervention. The intervention could, however, be considered a ‘natural experiment’, in that although not under the control of the research team, it is amenable to research using natural variations in exposure,81 such as between the target group (young people) and others in the population. Given the urgent need to improve the public health evidence base in general,45 and for evidence on transport interventions in particular, there have been calls to exploit ‘natural experiments’ to contribute ‘good enough evidence’ to inform policy decisions. 9,82 The free bus scheme is one such opportunity. This intervention has a number of advantages which make it suitable as a potential natural experiment:81 (1) a RCT is not possible; (2) we already have (from research evidence) some reasonable expectation that health impacts will accrue from changes in transport behaviour; (3) there are available secondary data sources on some of these impacts that cover both pre- and post-intervention periods; and (4) there are potential ‘exposed’ and ‘non-exposed’ individuals. Finally, there is a policy incentive, given that there is little evidence to inform current debate, and London’s transport interventions are of wider interest in the context of policy drivers to increase the sustainability of transport systems.
This chapter describes the design and approach we took to evaluating the free bus travel scheme as a natural experiment. We discuss the overall design and aims of the study, the methodological challenges in evaluating ‘natural experiments’ of this type and how we addressed them, and the specific methods used for the quantitative and qualitative components of the study.
Study design: the logic model linking free bus travel to health outcomes for young people
To map the possible range of public health effects which could be evaluated, we first developed an initial (summary) ‘logic model’83,84 of the pathways hypothesised to link the intervention with outcomes relevant to public health. This was developed, after reviewing the literature summarised in Chapter 1, in collaboration with key stakeholders, including our steering committee, young people [participants in the London School of Hygiene and Tropical Medicine (LSHTM) Young Scientists’ programme85] and colleagues, to ensure we had captured outcomes that were important to policy-makers, the public and researchers.
As discussed in Chapter 1, the introduction of free bus travel hypothetically impacts on health through a number of pathways. Our first three aims were to assess the evidence for these pathways, and specifically to:
-
provide empirical evidence for the impact of this intervention on key health behaviours and outcomes (e.g. injuries, active travel) for young people
-
explore the effects on the determinants of health (e.g. access to education and training)
-
identify the effects of increased young people’s access to bus travel on older citizens.
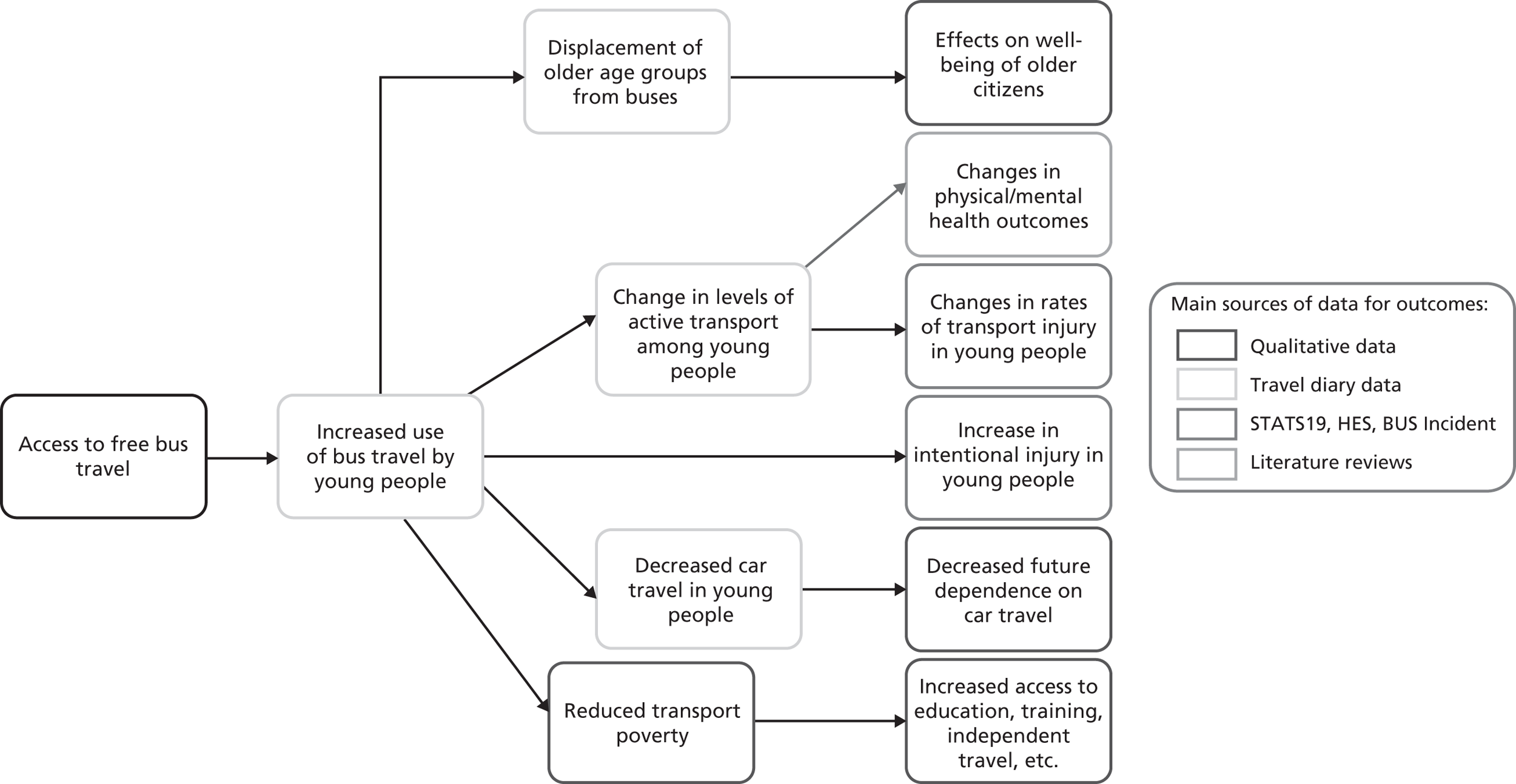
The first step was to outline these pathways and to identify and include the main outcomes of interest. Second, we identified what indicators were possible and feasible to measure for the variables on the pathway and the key outcomes of safety, active travel, social inclusion and effects on older passengers. Third, we identified the potential sources of evidence for these indicators: existing quantitative data sets which covered both pre- and post-intervention periods; primary qualitative data and reviews of the literature.
At this stage, other possible (distal) health effects of free bus travel (e.g. the impact on pollution), were eliminated from the model. Evaluations of other large-scale transport interventions, such as the congestion-charging scheme, suggested only modest changes result from transport mode shifts,86 and effects from the free bus scheme were unlikely to be measurable or distinguishable from those from other causes. To simplify the task of assessing transport mode shift, we also did not assess the impact of the scheme on underground (tube) and overground train journeys, given that these form a relatively small proportion of young people’s travel in London (see Appendix 9, Table 40).
The main pathways selected as important to evaluate are summarised in Figure 3, which also shows the main data sources used to evaluate each pathway.
FIGURE 3.
Hypothesised causal pathways.
Finally, to address our fourth aim (to develop and apply methods for economic assessment) we identified sources of data for economic values for these health outcomes, largely from existing literature, and costs of the scheme, largely from TfL.
Aims, hypotheses and objectives
The model in Figure 3 suggested a number of hypotheses related to the first three aims. Specifically, that the free bus scheme would be associated with:
-
An increase in bus use and overall ‘independent’ travel (the latter represented from available data by all non-car travel), but a reduction in active travel (walking and cycling) and car use, among the target age group. (Independent travel refers to travel young people do without guardians. With no direct measure of this, we use a proxy measure of all travel except car travel and, for those aged < 17 years, motorbike travel.)
-
A reduction in bus use and trips < 1 km made by people aged ≥ 65 years, especially during the hours when children usually travel from school. (We subsequently chose to include 60- to 64-years-olds to increase our available sample size and thereby increase statistical power to detect differences between groups. The older age group was therefore aged ≥ 60 years.)
-
A reduction in RTIs in the target age group.
-
An increase in intentional injury rates in the target age group.
-
If these changes were associated with the free bus scheme, we also hypothesised that:
-
-
Changes will be more pronounced in the inner-London boroughs (with denser bus networks) than in outer-London boroughs.
-
Changes will be more pronounced in boroughs with a known higher uptake of free bus travel.
-
Changes in distance/frequency of bus travel, independent (non-car) travel, active travel and in injury incidence, are greater in households with low income.
-
Reductions in car use will be greater in households with high income.
-
Changes in distance/frequency of bus travel and active travel, and in injury incidence, will be the same across all ethnic groups.
For a number of hypothesised effects, such as decreased dependence on car travel, and reduced transport poverty, there were no available direct measures from secondary data sources. For these, we aimed to generate primary qualitative data to provide some insight into broader determinants of health and well-being. These qualitative data would also be used to provide evidence for the plausibility of causal claims made on the basis of quantitative analysis, through identifying potential mechanisms, or (for instance) generating data on young people’s accounts of their travel which could be compared with data from secondary sources. The objectives for the qualitative component of the study were therefore to:
-
identify the ways in which young people and older citizens understand the role of bus travel and other transport modes in facilitating and constraining their well-being
-
identify, from analysis of interview data, plausible pathways by which policy, access to transport and behaviour interact to impact on well-being.
Good practice in evaluating natural experiments calls for an assessment of value for money considerations. 81 We therefore also aimed to undertake an economic evaluation of the scheme which took into account evidence on the public health effects.
This study therefore aimed to evaluate the impact of free bus travel on these outcomes, using a mixed-method design, and to assess the economic costs and benefits of the scheme. Our final aim was a methodological one of contributing to the development of methods to strengthen causal inference in non-randomised designs. In Chapter 10 we discuss the methods used to do this, in particular through revisiting and revising the causal model in Figure 3 (see Chapter 10).
Challenges in assessing the public health impacts of transport interventions
Calls for ‘evidence’ on the public health effects of policy interventions45 generate challenges, given the difficulties in making causal claims about the relationships between policies and their intended and unintended outcomes. ‘Real world’ interventions are inevitably messy, often in themselves complex (with heterogeneous, often ill-defined, components)87 and implemented in poorly bounded target populations and settings, with unknown exposures for those intended to benefit. The systems in which they are implemented (cities, schools, countries) are simultaneously subject to a range of other ‘interventions’, both explicit policies and less easily delineated cultural and social changes. More challenging, methodologically, are the feedback loops – both predictable and less obvious – that might mean causal directions change over time or are modified by unknown other influences.
The intervention evaluated in this study is a typical example. The introduction of free bus travel for young people in London had wide-ranging intended consequences, including addressing social inclusion, through increasing access to education and training, and reducing future car dependence among young Londoners. Given concern about obesity in young people, there has also been political interest in the unintended consequences of potentially reducing the amount of ‘active’ transport. This is a classic ‘messy’ intervention. Without evidence from randomised trials (hardly logistically possible), or even plausible control settings (there are no obvious comparators to London, given its size and unique transport infrastructure), designing a study with high internal validity (i.e. likely to make credible claims about the causal effect of the intervention on public health in London) is challenging. Also of concern is the question of external validity: how can we make credible claims on the more general causal question of whether public transport concessions are likely to benefit or harm the public health?
The ‘complexity’ of both the intervention and the setting are immediately apparent. Free bus travel was introduced in two stages, in 2005 (for those aged < 16 years) and in 2006 (for those aged < 18 years). Furthermore, ‘the intervention’ is not neatly delineated in time, as it replaced a range of other concessionary fares for young people, and, as young people had to apply for a photocard (now called a ‘zip’ card), uptake was gradual and unevenly distributed across the study area (Greater London). Given London’s unique transport infrastructure, there are no obvious external comparison populations of young people in other cities. Potential confounders in any before-and-after design range from the theoretically knowable (e.g. other interventions potentially influencing the behavioural outputs in which we are interested) to the more general and difficult to measure cultural shifts, such as rising concern about children’s independent mobility or changes in the ways in which urban environments are conceptualised.
Challenges to making credible claims also arise from the relatively complex causal pathways that connect the intervention (providing free bus travel) and the outcomes (various health behaviours, determinants of health and health outcomes) summarised in Figure 3. Providing free bus travel might increase or decrease the amount of walking or cycling young people do, which in turn may positively or negatively influence health. More walking and cycling may have implications for obesity or future CV health,52,88,89 for instance, but also increase exposure to pedestrian or cycling injury risk. 44 It is theoretically possible to quantify these different effects, and calculate (however imprecisely) likely aggregate benefits. 79 However, the evidence base on links between active transport and health outcomes is currently weak90 (see Appendix 8), and is particularly weak for young people, for whom putative health benefits may be too far in the future to measure. What is even more challenging is accounting for (possibly unknown) feedback loops which potentially change these effects within the system. As Shiell and colleagues91 note, the challenges of evaluating interventions in complex systems require new ways of thinking to deal with self-organising systems which may be sensitive to initial conditions and in which components are tightly interconnected.
One potential example of a feedback loop is that the effect of walking on health may be modified by both known and unknown factors, such as the cultural meaning of walking. Bostock60 for instance documents the negative impacts on health of walking for those who have no choice but to walk. Such factors might not only change the likely benefits of walking for different sectors of the population, but also change differentially as a result of the intervention, thus modifying the equity effects of an intervention over time.
Notwithstanding these challenges, development of the evidence base for public health in this area is important, and ‘natural experiments’, despite their inherent weaknesses, may offer the best way forward for evaluation. 9,82 Ogilvie and colleagues9 also suggest that single studies of transport interventions are unlikely, on their own, to provide credible evidence for causal claims, and we need to begin to build the evidence base to generate ‘good enough’ evidence for policy and for potential future integrative reviews. This study aimed to provide one such contribution, using a pragmatic, mixed-method and iterative approach to addressing the challenges above.
The general approach: a mixed-method study
This evaluation treated the introduction of the free bus scheme as a ‘natural experiment’ to which young people in London were exposed after 2005/6, and other populations (young people before 2005, adults in London, the population outside London) were not. This therefore permitted a number of comparisons, including some ‘change-on-change’ comparisons using before-and-after and comparative populations. We used a mix of secondary quantitative data, primary qualitative data and reviews of the literature to generate evidence for the links in the causal pathways hypothesised in Figure 3.
The design was pragmatic, in that our aim was not to assess whether receiving a free bus pass had a health benefit or loss for an individual, but rather to evaluate the broader impact on the public health of the scheme as a whole. The analysis is therefore conducted at a population level. Quantitative data, largely from routine data sets [including police records of road injuries, Hospital Episode Statistics (HES) and travel diaries], were used to assess links between the intervention and bus use, mode change (active travel/car use), displacement of older passengers, and injury. Drawing on best practice guidelines for natural experiments81 we published a protocol for the quantitative component. 92 This specified hypotheses and main subgroup analyses93 (see Appendix 7). To minimise the threats from confounding, we used change-on-change analyses with adult passengers as a comparator where appropriate. To strengthen the credibility of causal claims, we employed a range of sensitivity analyses to test the credibility of inferences and (where possible from available data sources) time series or ‘dose–response’ analyses.
To explore outcomes for which there are no routine data sources, and which are more difficult to quantify, we generated qualitative data from interviews with young people and older citizens. These data were also used to offset some of the limitations in using secondary data and to explore mechanisms for putative causal relationships. Our design was iterative in that these data were also drawn on throughout the study in order to refine the analyses of routine data sets, and to refine our understanding of the logic model.
On the final link in the causal chain, the impact of active transport changes on health, we had no direct measure. We therefore conducted a systematic literature review to assess the strength of evidence for the credibility of the link90 (see Appendix 8).
The economic component aimed to represent the health consequences of the intervention and compare this with the cost of implementing the scheme. This utilised outputs from the quantitative analysis on ‘change attributable to the intervention’ to populate the benefits of the scheme, with data from TfL, Home Office and Department for Transport (DfT) to estimate costs for crime on the transport system, and additional data from TfL for costs of the scheme and operating costs. The economic evaluation involved a comparative analysis of alternative scenarios in terms of their costs and consequences.
The key alternative scenarios compared were:
-
do something – the bus network is free for 12- to 17-year-olds
-
do nothing – the bus network is not free for 12- to 17-year-olds.
The methods for the quantitative and qualitative components are detailed below. Details of the specific methods used for the economic evaluation can be found in Chapter 9, and for the literature review in Appendix 8.
Methods for the quantitative components
London’s transport system, comprising dense private and public transport networks and a focus on national road and railway networks, is unique in the UK. There are therefore no obvious comparator cities, or settings, which could be used to account for national trends in use of alternative transport modes, or to account for national trends in levels of safety. London has also experienced the introduction of other transport policies over the study period (e.g. London congestion charge was introduced in 2003), which may have altered choices of travel mode within the population.
Design
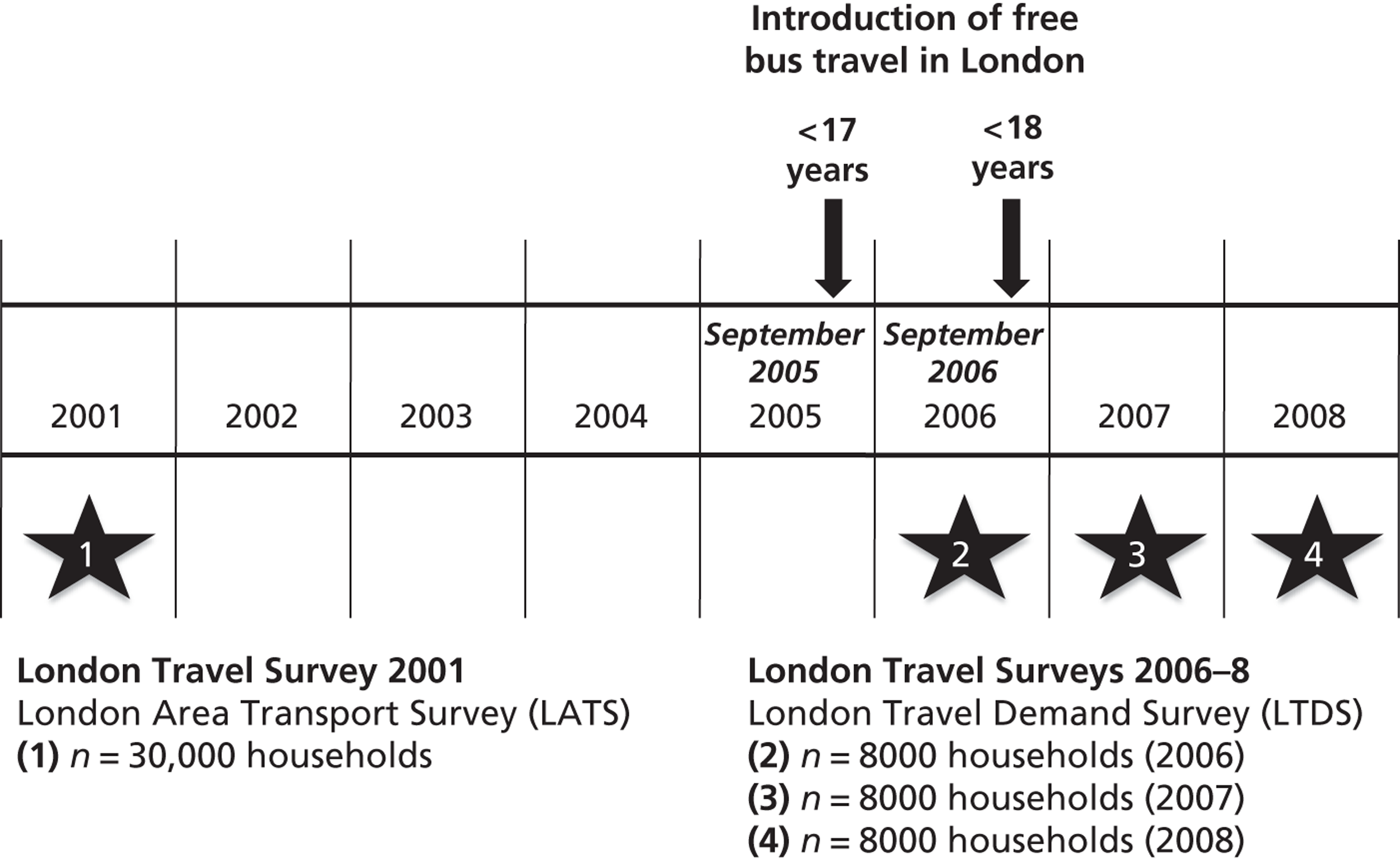
We estimated health impacts of introducing free bus travel for young people by analysing routine data sets on travel and safety. To control for secular trends and the effects of other transport policies, we used a change-on-change analysis to estimate any changes in travel and safety in the target population of young people that were associated with the introduction of free bus travel. This change-on-change analysis compared pre–post intervention change in amount of travel (or safety) in the target age group, with the corresponding pre–post change in amount of travel (or safety) in an older age control group (adults aged 24–59 years) (Figure 4). The age range of the control group was chosen to exclude younger adults who may also have experienced free bus travel, and to exclude older adults who may also qualify for an older citizens’ bus pass.
FIGURE 4.
Timeline showing travel surveys and introduction of free bus travel in London.
As a sensitivity analysis, we also examined pre–post intervention change in safety in the target age group in London, with the corresponding pre–post change in the target age group outside London, using national data for the rest of England.
Data sources
The travel and safety data sets used were:
-
London Area Transport Survey (LATS)
-
London Travel Demand Survey (LTDS)
-
STATS19 Road Accident data set, police traffic injury data
-
HES.
Travel in London
The LATS and LTDS include randomly sampled London households and are comparable as they use similar sampling designs and daily travel diaries. The sampling design is multistage, using postcode geography as primary sampling units and households selected at random at the second stage of sampling. LATS surveyed 30,000 London households in 2001 and LTDS has surveyed 8000 London households each year since 2006.
Within each selected household, all people aged > 5 years record in a travel diary the start, interchange (e.g. from bus to train) and end of every trip made on a single day. Journey times are collected and journey distance is estimated using the start point, interchange and end point of each trip. Missing journey times and missing distances were estimated using the median times and distances for each age group and travel mode. Where reported times and distances were deemed implausible, these were treated as missing and replacement values were imputed (see Appendix 2). LATS sampled travel on weekdays during school term only and so for analysis we used LTDS relating to during school term only. Our quantitative results are therefore representative of term-time weekday travel only.
The LATS and LTDS also record ethnicity, household income and census lower layer super output area (LSOA) of residence (areas that include approximately 1500 residents). Ethnicity was coded using four categories: ‘White’, ‘Black’ (Black-Caribbean, Black-African, Black-Other), ‘Asian’ (Indian, Pakistani, Bangladeshi) and ‘Other’. Household income was coded using three categories: < £15,000, £15,000–49,999 and > £50,000. Each respondent was assigned a deprivation score [using Index of Multiple Deprivation (IMD) 2004] according to their LSOA of residence. We also assigned each respondent to inner or outer London based on LSOA of residence (see Appendix 2).
Travel diary outcome measures
In this report, we use three main outcome measures from the travel diary data: number of trips, distance travelled and proportion of short-distance trips by mode of travel. In the travel diary data, a trip is defined as a journey from an origin to a destination and can be made up of more than one mode of travel. For instance, a journey to work may entail a 0.5-km walk from home to a bus stop, a 2-km bus ride and a 1-km walk from the bus stop to a place of business. When we examined the number of trips by mode, the mode assigned to each trip is the ‘main mode of travel’ (i.e. the mode that covers the most distance, the above example would be defined as a bus trip). Alternatively, when we examined distance travelled by mode, we summed the distances travelled in every interchange of every trip. The example above would contribute 2 km to distances travelled by bus and 1.5 km to distance walked. When we examined proportion of short-distance trips, we defined a short-distance trip as < 1 km.
We estimated the distribution of trips by main mode and distance travelled by travel mode in each age group in the pre-intervention period using data from LATS 2001. We estimated the distribution of trips and distance travelled by travel mode in each age group in the post-intervention period using data from LTDS 2006–8.
Safety: road traffic injuries
The STATS19 data set records all vehicles and people injured in road traffic collisions on the public highway in the UK that are reported to the police. We obtained an extract of STATS19 data for England covering the period 2001–9. In London the STATS19 data also record the ethnicity of casualties, which were coded as described for the travel survey data (above). The STATS19 data also include latitude and longitude co-ordinates of the road traffic collision locations. Using the geographical location of the traffic collisions we linked each to a LSOA. We then assigned each casualty to a deprivation score and to inner or outer London based on the LSOA of collision.
We estimated the incidence of RTIs by travel mode in each age group in the pre-intervention period using STATS19 data for 2001–4, and in the post-intervention period using STATS19 data for 2006–9.
Safety: assaults requiring hospitalisation
Hospital Episode Statistics records episodes of care provided by NHS hospitals in England and for NHS patients treated elsewhere. We obtained an extract of HES data for England covering the period 2001–9. All individuals were identified using the unique person identification code available in HES data, and we identified all London and non-London residents using LSOA code of residence in the HES extract. We identified all hospital admissions due to assaults [International Classification of Diseases, Tenth Edition (ICD-10) codes X85–Y09].
We planned to conduct a sensitivity analysis using severe injury admissions only (i.e. to assess whether or not differences in admissions policies and admission rates may have introduced bias). However, only a very small proportion of records for which ICD-10 diagnosis were coded indicated severe injury. 94
Hospital Episode Statistics data include information on ethnicity which was coded as for travel survey data above. We assigned each person admitted to hospital to a deprivation score and to inner or outer London based on the LSOA of residence.
We estimated the incidence of assaults requiring hospitalisation in each age group in the pre- and post-intervention periods using HES data for the period 2001–9.
Change-on-change analysis
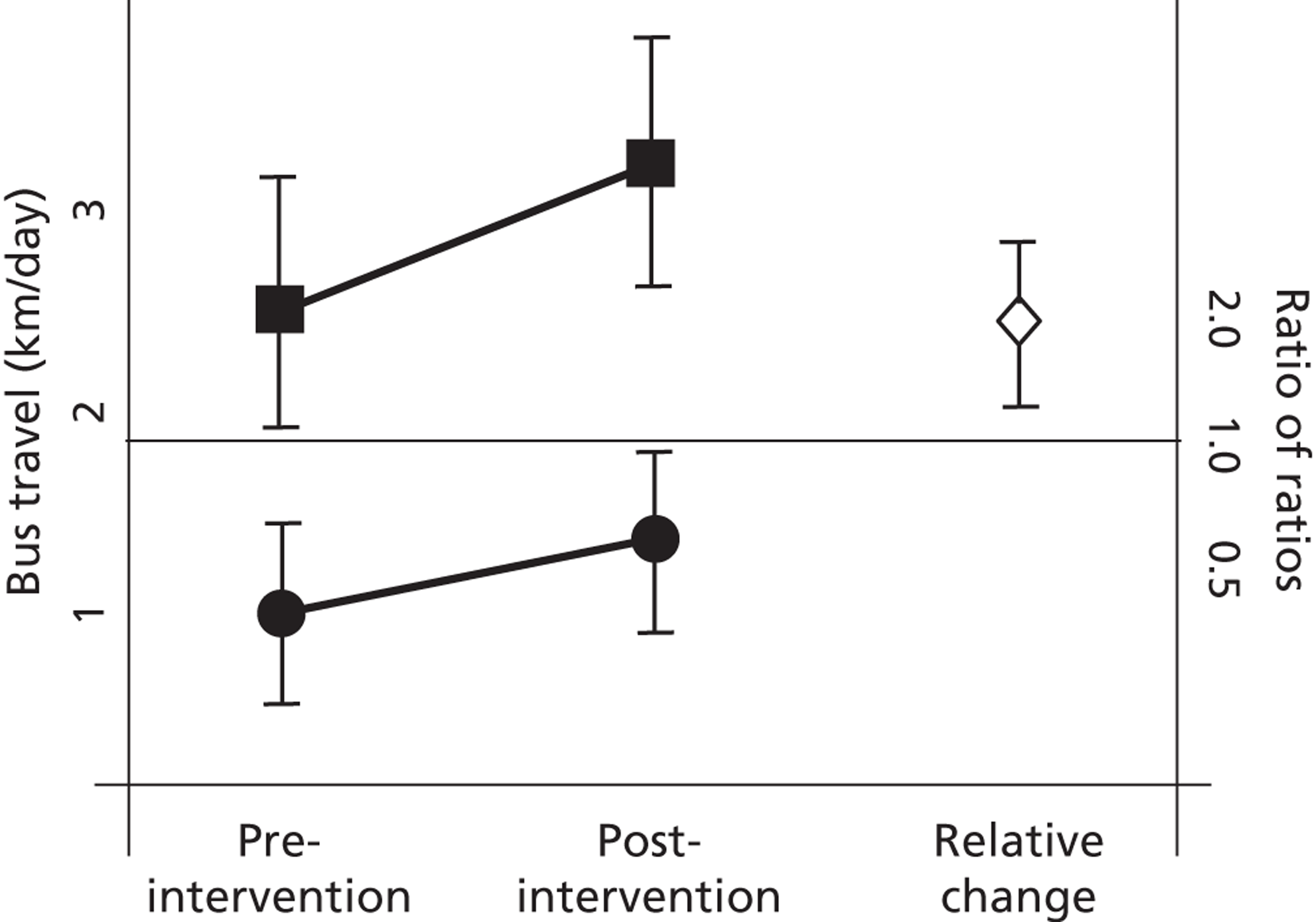
To test each hypothesis (listed in Aims, hypotheses and objectives) we estimated the pre-intervention and post-intervention mean of each travel and safety indicator and calculated 95% confidence intervals (CIs) using bootstrap methods implemented in Stata statistical software (StataCorp, College Station, TX, USA). These results are presented graphically for each indicator; Figure 5 gives an example. [Line joining solid squares shows change in target age group (12- to 17-year-olds); line joining solid circles shows change in control age group (25- to 59-year-olds). Diamond (right-hand side of figure) shows the change in the target age group relative to the change in the control age group. 95% CIs are shown as vertical lines.]
FIGURE 5.
Example of graphical presentation of results showing change in travel and safety indicators.
Sensitivity and subgroup analyses
As free bus travel was available to all young people in London, our primary analysis was of its impact on the whole population. However, uptake of the scheme was not universal, and by 2010 the estimated 50% uptake among young people aged 5–15 years varied across London (Alex Phillips, TfL, 2001, personal communication). (Figures specific to those aged ≥ 12 years are unavailable. As a photocard is not needed to access free travel for those aged < 11 years unless they are travelling without an adult, or appear older than 10 years of age, few young people aged 5–15 years would apply for a zip card. The 50% uptake therefore does not indicate low uptake in our target population, but the variability across boroughs does suggest that uptake is not universal.) To consider whether or not changes to travel and safety associated with the introduction of free bus travel might be causally related, we conducted sensitivity analyses of effect according to amount of exposure to the intervention. Although the available data sets did not allow analysis of uptake of free bus travel at an individual level, or for our target age group, we used proxy indicators of uptake (aggregate uptake rates for young people aged 5–11 years and bus network density by borough).
To assess whether or not the scheme had had differential effects across London’s population, we conducted change-on-change analysis by area of London (inner vs. outer London); deprivation quintile (most deprived 20% of population vs. least deprived 80% of population); level of household income (< £15,000 per year vs. > £50,000 per year; for travel patterns only) and ethnicity (‘White’, ‘Black’, ‘Asian’, ‘Other’).
Power and sample size
The LATS and LTDS samples include data on around 3000 young people before and after the intervention (Table 1), giving over 80% power to detect a 10% relative reduction in average distances walked daily by young people [i.e. from 0.9 (standard deviation; SD 1.3) km to 0.8 (SD 1.3) km per day] at a 5% significance level. Similarly, the study will have over 90% power to detect a 10% increase in the average distance of bus travel [i.e. from 4.3 (SD 4.1) km to 4.7 (SD 4.1) km per day]. For transport-related injury, the study would have 80% power to detect a 10% change, or 90% power to detect a 12% change significant at the 5% level. Statistical power is inevitably more limited for subgroup analyses, but there will be 90% power to detect a 15% change in average distance travelled by bus by young people within the most deprived quartile, for example.
| Data source | Intervention period | Time period | Age group (years) | ||
|---|---|---|---|---|---|
| 12–17 | 25–59 | ≥ 60 | |||
| LATS | Pre | 2001 | 4206 | 31,169 | 10,671 |
| LTDS | Post | 2006–8 | 2024 | 14,085 | 5033 |
| STATS19 | Pre | 2001–4 | 11,221 | 89,661 | 13,337 |
| Post | 2006–9 | 6657 | 65,542 | 9283 | |
| HES | Pre | 2001–4 | 2321 | 11,829 | 905 |
| Post | 2006–9 | 3322 | 14,641 | 959 | |
Methods for the qualitative components
To generate data for exploring the pathways linking the intervention to social inclusion, future car dependence and the effects on the well-being of older citizens we conducted a qualitative study of young people aged 12–18 years (a few participants with disabilities were aged > 18 years at the time of interview), and older citizens aged ≥ 60 years in London, based primarily on individual and small group interviews. These data were also used to explore the mechanisms for relationships measured using quantitative methods and to further our understanding of the intervention in context.
Sampling
The aims of the sampling strategy for the qualitative component of the study were to recruit a maximum variation sample in terms of those variables that we predicted on the basis of existing literature would shape experiences and accounts of transport behaviour. The primary variables were: transport availability, gender, age, ethnicity, disability and area deprivation. To ensure we included a range of participants, we first choose four contrasting boroughs of London to provide coverage of ‘bus-rich’ and ‘bus-poor’ areas in inner and outer London (which have very different typical transport networks and mode choices) with differing deprivation profiles (see Appendix 3 for details). The boroughs selected are shown in Table 2.
| Higher levels of socioeconomic deprivation | Lower levels of socioeconomic deprivation | |
|---|---|---|
| ‘Bus rich’ – higher levels of bus use | Islingtona | Haveringb |
| ‘Bus poor’ – lower levels of bus use | Hammersmith and Fulhama | Suttonb |
Within each borough, a mix of recruitment methods was used to invite young people aged ≤ 18 years and older citizens aged ≥ 60 years to take part in individual, pair or small group interviews. Young people were recruited through secondary schools; an academy; local community youth clubs; an ‘alternative provisions’ facility (an arts-based education setting for young people who struggled in conventional schools/colleges); a ‘pupil referral unit’ (an education setting for young people excluded from conventional schools/colleges); a local authority ‘youth parliament’ and snowballing from personal contacts.
We recruited older participants through a local community centre; a local (borough-level) branch of Age Concern (now Age UK, a national charity for older people); a local amenity group; a local authority event for older residents; ‘park bench’ approaches and snowballing from personal contacts.
Theoretical sampling was also used where ongoing analysis suggested additional recruitment in order to test emerging analytical ideas. This included purposive sampling of passengers with disabilities, recruited with the help of personal contacts, and including those not living within these boroughs, and those aged > 17 years in order to explore attitudes to driving among those with some experience. A final group of young participants came from young people engaged in LSHTM’s Young Scientists programme (see Appendix 4). These were young people from a number of London boroughs engaged in a 2-week programme at LSHTM.
Within each setting, we purposively sampled young people and older people in order to include as broad a range as possible of transport availability, area deprivation levels, household incomes and age (within our target ages of 12–18 years and > 60 years) in order to include those more and less likely to be bus users. This entailed working with contacts including schools and community organisations to help with recruitment, and (to identify older people less likely to be involved in organisations) some personal approaches in public places (e.g. park benches).
Additionally, the research team carried out informal observations on the bus network at various times of day to provide background understanding of who was using the buses, what they did on the buses, and how they interacted. Notes from these observations were kept in fieldwork diaries and used to inform interview topic guides but are not drawn on as a formal data set in this report.
Sampling continued to saturation, i.e. until analysis of new data added little to our understanding of our research questions. Based on rules of thumb for estimating numbers of participants needed within homogeneous groups95,96 we estimated a sample size of around 50 individual and eight group interviews would generate enough variability by gender, ethnicity, age range and borough setting to do this for young people, and around 25 older citizens. Our final sample included 119 young people and 47 older citizens (Table 3).
| Setting | Number of interviews (individual and pairs) | Number of interview participants | Number of focus groups | Number of focus group participants |
|---|---|---|---|---|
| Young people | ||||
| Islington | 7 | 10 | 2 | 10 |
| Havering | 9 | 10 | 3 | 18 |
| Sutton | 5 | 6 | 4 | 19 |
| Hammersmith and Fulham | 9 | 11 | 2 | 12 |
| Young scientists | 6 | 9 | 1 | 4 |
| Other | 4 | 7 | 1 | 3 |
| Total | 40 | 53 | 13 | 66 |
| Older citizens | ||||
| Islington | 7 | 10 | 1 | 6 |
| Havering | 2 | 2 | 0 | 0 |
| Sutton | 5 | 7 | 1 | 6 |
| Hammersmith and Fulham | 7 | 10 | 1 | 6 |
| Total | 21 | 29 | 3 | 18 |
Data generation
For the interview data, we used a mix of individual, pair and group interviews. Different modes of interviewing can yield different kinds of data, with groups enabling an interactive discussion, increased potential for story-telling (in which we were particularly interested), but also increased potential for more confident and talkative respondents to take a lead. Individual interviews, in contrast, may be more likely to uncover sensitive data on, for instance, anxieties about particular modes of transport, or financial problems. A topic guide was designed to encourage talk about experience of using buses and other transport modes, preferences for transport modes, encounters with other passengers, impact on well-being of transport use, and views on the schemes. Topic guides were iteratively developed as the project progressed, and in later stages of fieldwork focused more on particular areas (such as barriers faced by people with disabilities). Example topic guides are included for information in Appendix 6. To ensure we were recruiting a range of participants, we also asked each to complete a brief form with postcode, age (range), ethnicity and (for older citizens) last occupation. Participants were given a £5 store voucher to thank them for their time.
Data analysis
The key challenge was that our qualitative data were entirely post intervention, so we could not simply compare participants’ views before and after. To meet the aims of the project in providing some insights into the pathways that link the intervention to the determinants of health, our aim in analysis was to uncover tacit knowledge that would inform transport mode and other decisions, as well as to generate ‘views’ on travel. We also explored the data for evidence of mechanisms that might explain relationships found in the quantitative component. Our analysis therefore combined both inductive and more deductive approaches. We drew on elements of the constant comparative method,97 in that we used an inductive approach in ‘open coding’ early data to generate a grounded understanding of conceptual codes, which were refined as the analysis progressed. Analysis focused on those that were most closely related to our initial causal pathway (see Appendix 5 for an example). We also drew more deductively on emerging findings from the quantitative components (which generated specific questions to ask of the qualitative data set) and on existing theory and empirical literature, which provided a context for interpreting our data, and a number of more conceptual ideas against which to check our data. On children’s mobility, for instance, studies have referred to the constraints acting on young people’s travel in urban areas and the complex strategies young people adopt to maximise their own safety while travelling independently and allay parental fears about their independent travel. 62,98 A more deductive analysis organised by existing concepts from the literature and emerging findings from our quantitative component enabled us to follow up particular themes by descriptive topic. One example is the finding that cycling rates were declining relative to adult rates. An analysis by the descriptive code ‘cycling’ enabled us to look at where, how and in what contexts young people discussed cycling, and add explicit questions to the later topic guide.
Data extracts were then collated for each descriptive and analytical code for analysis. This analysis entailed identifying the range, dimensions and context of accounts: for instance on whether they were evident only for those in some areas of London, or for some groups of young people, or how stories were responded to in group settings. Close analysis of deviant cases provided one way to check developing interpretations. For instance, in the case of the role of ‘free’ travel in young people’s travel behaviour, deliberately examining the ‘deviant’ cases of those young people who had had their entitlement removed enabled us to identify what was taken for granted by other young people, and therefore not explicitly addressed in their accounts. Early analysis informed the topic guide, which was used for more focused enquiries in later parts of the fieldwork.
Our sample was not randomly drawn from the population, and we did not ask the same questions of all participants. We therefore do not report ‘numbers of respondents’ in the qualitative sections of this report, as this would be misleading. When reporting accounts from participants, we note where necessary whether these were typical, unusual or more common in some groups.
Given the iterative and dual nature of our analysis, ‘double coding’ of interview transcripts by the research team would have been inappropriate, as assigning data extracts to thematic codes depended on the purpose for which the assignment was being used. Instead, the team met regularly to discuss analysis, and validation happened at the point of writing up, with discussion around interpretative claims and checking for disconfirming cases.
To provide context, we have tagged the interview extracts quoted in this report with a note of gender [male (M) or female (F)] for participant, (I) to indicate interviewer, a note of where the participant came from [Havering (Hav), Islington (Isl), Sutton (Sut) or Hammersmith and Fulham (H&F), the Young Scientist scheme (YS) or Other (O)] and the age or (for groups and older citizens) the age range. To preserve confidentiality, we have not included other identifiers, such as ethnicity or previous occupation (for older citizens). We have also changed all identifying personal names and small area locations.
Table 4 shows the breakdown by ethnicity and age of young people included, and Table 5 the breakdown of ethnicity, description of last occupation and age of older citizens.
| Demographic characteristic | No. of participants | |
|---|---|---|
| Gender | Female | 63 |
| Male | 56 | |
| Age range (years) | ≤ 13 | 27 |
| 14–15 | 61 | |
| 16–17 | 21 | |
| ≥ 18 | 10 | |
| Ethnicitya | White British | 52 |
| White Other | 8 | |
| Black/Black British | 22 | |
| Asian/Asian British | 15 | |
| Mixed | 18 | |
| Other | 3 | |
| Not answered | 1 | |
| Demographic characteristic | No. of participants | |
|---|---|---|
| Gender | Female | 33 |
| Male | 14 | |
| Age range (years) | ≤ 64 | 4 |
| 65–69 | 6 | |
| 70–74 | 14 | |
| 75–79 | 6 | |
| 80–84 | 11 | |
| 85–89 | 4 | |
| ≥ 90 | 2 | |
| Ethnicitya | White British | 32 |
| White Other | 5 | |
| Black/Black British | 4 | |
| Asian/Asian British | 5 | |
| Not answered | 1 | |
| Last joba | Unskilled manual (e.g. cleaner, factory worker) | 9 |
| Skilled/semi-skilled manual (e.g. machinist, driver) | 4 | |
| Clerical or shop work (e.g. book-keeper, cashier) | 13 | |
| Professional (e.g. teacher, nurse) | 8 | |
| Managerial/business (e.g. buyer, executive) | 9 | |
| Other (e.g. homemaker, unspecified engineer) | 4 | |
Ethical issues
The study was approved by LSHTM’s Ethics Committee (Application no. 5635). The quantitative component relied on secondary data analysis and did not raise particular ethical issues. For the qualitative interview component, the main ethical considerations were those of ensuring adequate informed consent and maintaining confidentiality. As our young participants were all of secondary school age, we considered they were competent to make an informed decision about participation without parental consent. Our consent forms included a space for parental permission in case gatekeepers (such as schools) required this: none did. Our consent procedures were discussed with young people in the pilot phase, who commented on our information sheet and whether or not they considered parental permission appropriate. Of perhaps more significance is the potential for studies such as this to exclude particular groups from the population. Given that our primary recruitment strategy was to work with community groups to identify participants to invite, we were mindful of the possibility of excluding those who may be most marginal in other ways (such as young people excluded from school, or relatively isolated older citizens). We therefore sought deliberately to include participants through alternative approaches such as pupil referral units and personal contacts where appropriate. Observations conducted on the buses were of public behaviour and were used to inform our topic guides and interpretations only: fieldwork notes did not identify individuals, and are not quoted in this report.
Chapter 3 What effect has the scheme had on use of bus travel by young people in London?
Introduction
Bus fare subsidies are used as a policy instrument to achieve a number of goals, including those of equity (through addressing transport exclusion), reducing traffic congestion and sustainability (through encouraging mode shift from private car use). 23 Achieving these assumes ‘demand elasticity’: that a reduction in fares will increase the use of services. Although it is reasonable to assume that this does hold true, there is considerable debate around how to calculate demand elasticity, given that this depends very much on context: the availability and efficiency of bus services; the attractiveness of alternatives; local congestion; population ability to pay. There is evidence that increased demand from fare reductions take many years to accrue, for a number of reasons, including the difficulties for most people of making short-term changes in travel behaviour, and the cohort effects of changing habits as children, for instance, become habituated as ‘bus users’. 99
This project evaluated the effects of an intervention which reduced fares to £0. We therefore hypothesised that the first step in the causal chain would be an increase in bus use by young people attributable to the intervention. This could not be assumed, given that fares for young people were discounted before the intervention, and bus use in London was rising for the wider population (see Appendix 1) in the context of historical innovations such as integrated travelcards which facilitate ancillary bus use, and more recent policies such as the congestion charge for private cars. This chapter first reports evidence from the analysis of travel diary data to identify changes in bus use that could plausibly be attributed to the intervention. We then draw on the qualitative data to explore the role of ‘free bus travel’ specifically in young people’s travel choices in order to assess the credibility of this attribution and to provide some context for the kinds of journeys made by bus.
Quantitative evidence on impact on bus use
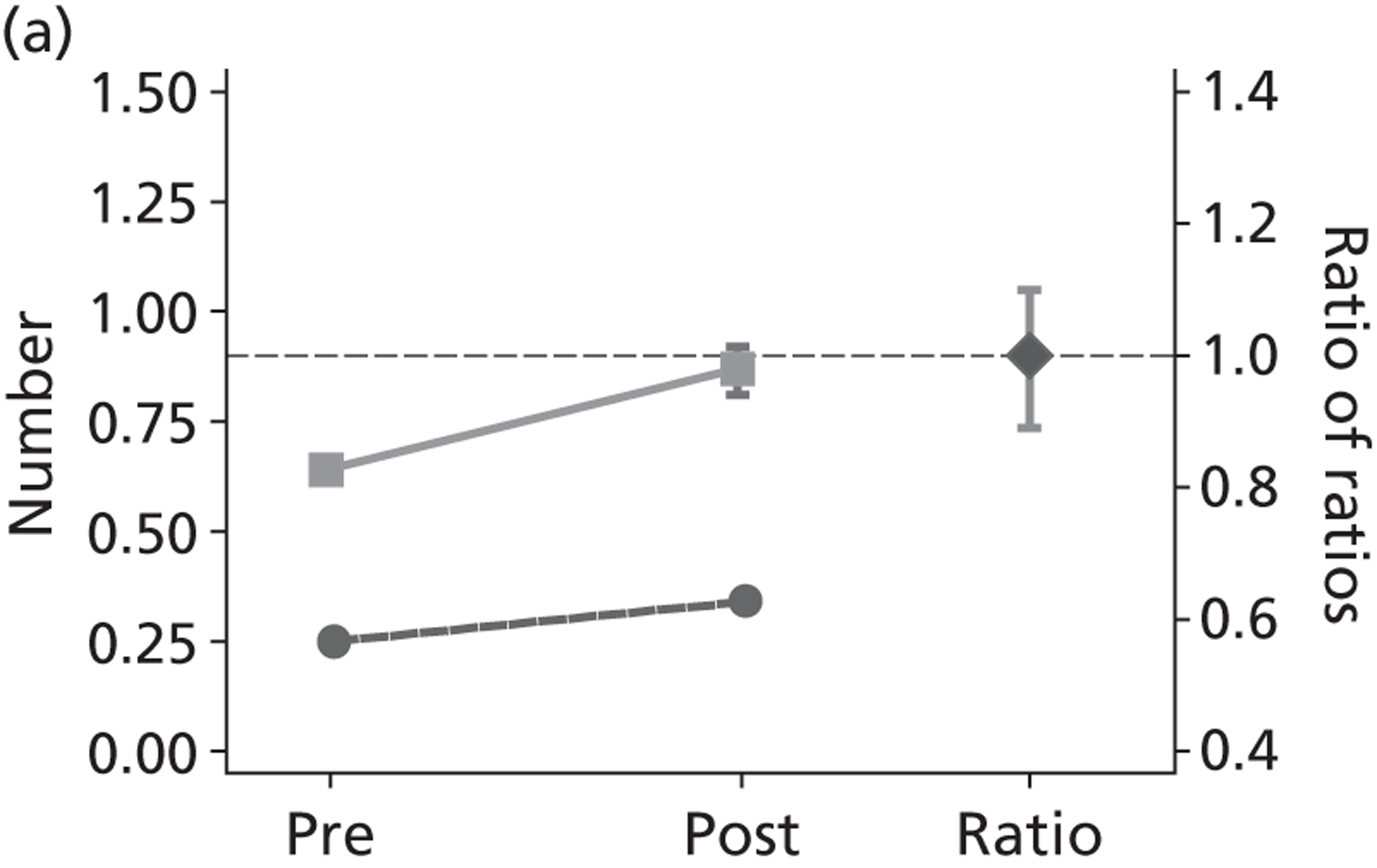
As described in the previous chapter we used a change-on-change analysis to estimate any changes in travel in the target population of young people that were associated with the introduction of free bus travel, rather than general changes in bus provision. Here we compare the pre–post change in weekday term-time bus travel in young people with the corresponding pre–post change in bus travel in adults aged 25–59 years. The changes to bus trips, distance and percentage of short-distance trips made by bus are shown graphically in Figure 6 (and in Appendix 9, Table 34). [Line joining solid squares shows change in target age group (12–17 years); line joining solid circles shows change in control age group (25–59 years). Diamond (right-hand side of figure) shows the change in the target age group relative to the change in the control age group. 95% CIs are shown as vertical lines. Horizontal dotted line indicates a ratio of 1 (i.e. no relative change).]
FIGURE 6.
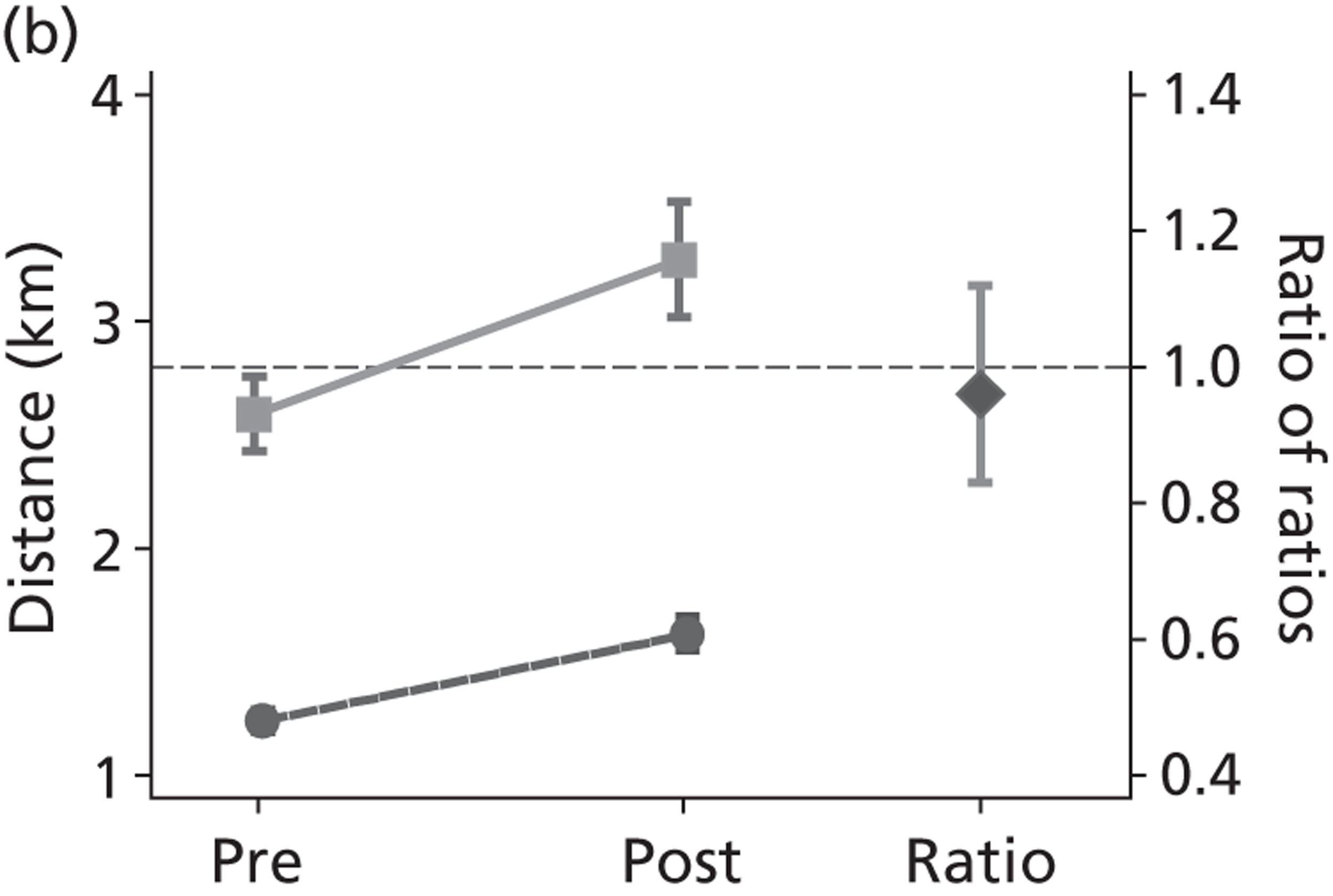
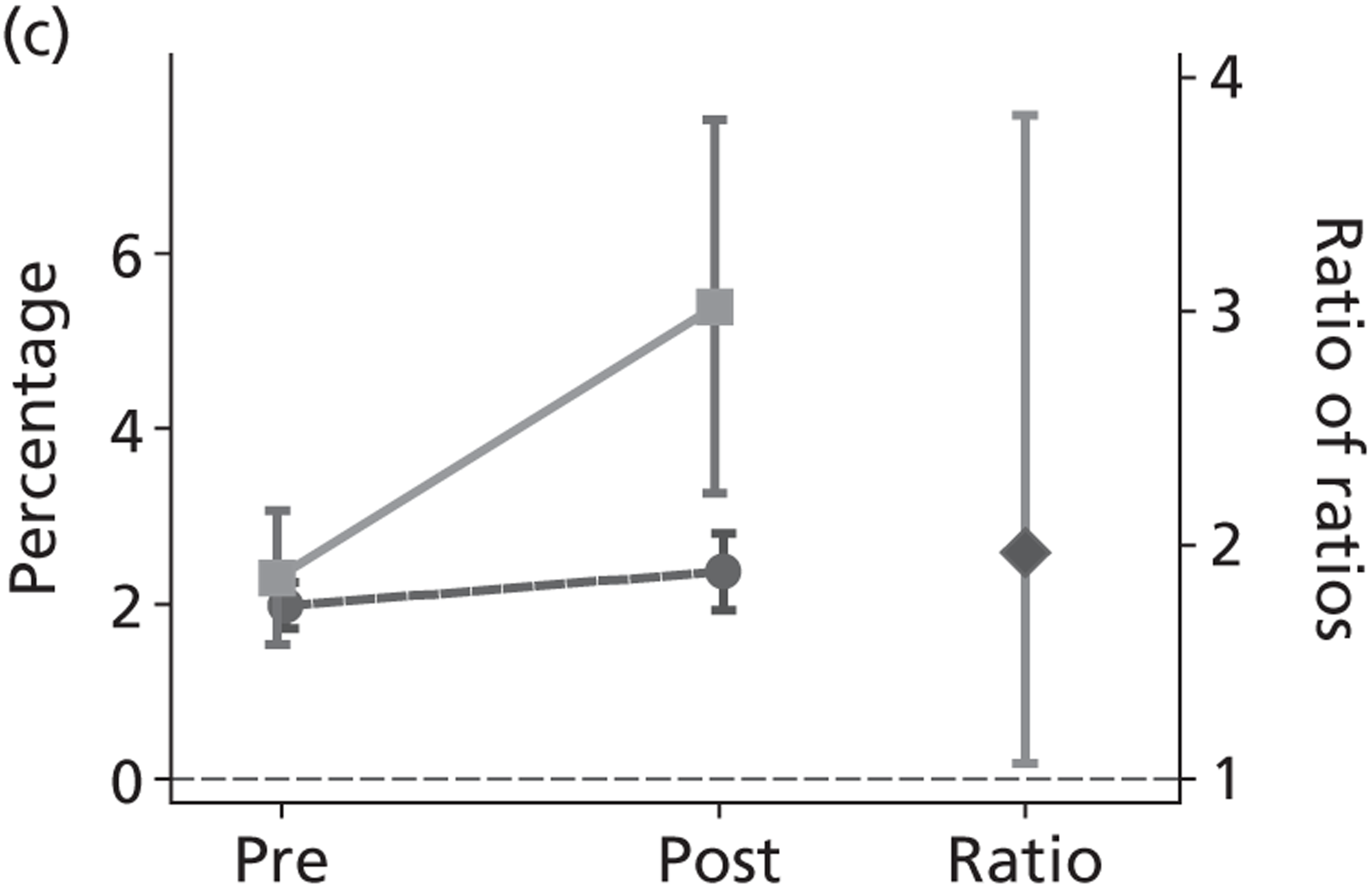
Changes in bus use, pre- to post-introduction of free bus travel (a) Bus trips per day; (b) bus distance per day (km); and (c) per cent of short trips by bus.
Trips by bus as a main mode
The introduction of free bus travel was associated with a 35% (95% CI 25% to 47%) increase in the average daily number of trips by bus as a main mode made by young people. There was a similar increase of about one-third (36%, 95% CI 25% to 46%) in the average number of bus trips made by the control age group, 25–59 years, and so the relative change was the same (relative change 1.00, 95% CI 0.89 to 1.10).
Distance travelled by bus
The introduction of free bus travel was associated with an increase in the average distance travelled by bus by young people, from around 2.6 km per day to around 3.3 km per day (a 26% increase, 95% CI 13% to 41%). The corresponding increase in the average distance travelled by bus in the control age group was from around 1.2 km per day, to around 1.6 km per day (a 31% increase, 95% CI 19% to 42%). However, the relative change was the same (relative change 0.96, 95% CI 0.83 to 1.12).
Short-distance trips by bus as a main mode
The introduction of free bus travel was associated with an increase in the proportion of short trips (i.e. < 1 km) made by bus by young people from around 2% of all trips to around 5% of all trips. The proportion of short trips made by bus by the control age group remained at around 2% pre- and post-intervention. Relative to the control age group there was therefore a 97% increase in the proportion of short trips made by bus by young people (relative change 1.97, 95% CI 1.07 to 3.84).
Bus travel by subgroups
Bus trips and distances travelled by bus increased at a similar rate among children and adults across levels of deprivation. We found no evidence for any differences in the relative change of proportion of short trips made by bus trips by level of deprivation (see Appendix 9, Table 38).
Free travel enables a range of journeys
The travel diary data includes only those trips made during term-time weekdays. In qualitative interviews, young people from all ages and parts of London reported using buses for a range of journeys, including getting to school, visiting friends, getting to local amenities and for more extensive days out, across the week. In all boroughs, young people emphasised the ease of getting around, and indeed the range of sites that might be visited by bus. The fact that travel was free was reported as a key reason that buses were used for a large number of discretionary trips, including those at weekends, as well as what could be considered essential journeys, such as those to school:
I take the bus every day . . . [for] going to school, going to dancing, going to see my friends, maybe going to church . . . because it’s free . . . I can go to different places, so anywhere I want to go
Hav, 15 years
Mostly every Saturday we’ll probably just jump on a bus because we have a free [pass] and go anywhere, and get another bus from there, and another one. And we just travel, we don’t know where we’re going . . . [once] we ended up near Hammersmith, and near the West End
Isl, 16 years
Indeed, free travel was reported to have opened up the range of places that young people could go in London, as well as the frequency with which they chose to visit these places. It made possible wide-ranging exploratory trips to the city centre and neighbourhoods at a distance, and it enabled young people to maintain (geographically) wide friendship groups.
Free travel enables the bus to be a site for socialising
Bus travel was frequently an end in itself: an activity undertaken to enjoy the journey rather than to get somewhere. That bus travel was free facilitated the treatment of London buses as a site for socialising by young people, with buses becoming key public spaces in the city for young people to convene and socialise both as part of their school journeys but also in the evenings, during school holidays and at weekends. This is not to say that prior to the intervention buses had not been treated by young Londoners as a space in which to socialise with their peers. Rather, by rendering bus use free for young people on an unlimited basis in London, the intervention dramatically shifted the degree to which buses could be used in this way. The bus network became a part of the freely accessible geography of London for young people, not only as a way of getting to and from destinations but also a vital set of destinations in itself. By contrast, if fares were reinstated one participant suggested that she did not ‘think that anyone would really go out as much to be sociable’ (Sut, 15–16 years). The bus was therefore not just a vehicle for a peer outing, but a site in itself which facilitated social interaction, primarily with peers:
You see friends, when you go on the bus you can see friends on there sometimes.
Yeah, yeah, yeah.
You can talk about people as well . . . reasonable amount when you’re on the bus.
Yeah, exactly, when you get on the bus you can just see friends. If you’re on your own and then you see someone, you just see them get on the bus . . .
Sut, 15–16 years
. . . It’s one of the main things you do on the bus, if you go out with someone you sit down and talk about things
Sut, 15–18 years
Given that interacting was an important benefit of travel time, the bus was only preferable if it maximised these opportunities. Thus, when a more private conversation was wanted, or if friends were not able to take the bus, walking might be a better choice:
Sometimes I prefer walking because sometimes, when I didn’t have my Oyster card and a friend used to take the bus but then he would stop and get off and we’d walk and that would give us more time to say what we want, because you know on the bus you can’t really talk much.
Hav, 14 years
For the majority of young people, travel and sociability with peers was emphasised in accounts, particularly those in group interviews. However, many also talked of ways in which the scheme had fostered travel with family members, and enabled family outings:
Before when I didn’t have my zip card I didn’t really go out much. I didn’t because I had to basically, I had to pay and then I managed to get my zip card. I could go different places to socialise with friends and especially travelling around London because I actually quite like exploring it here with my mum . . . it’s easier for [mum and me] because my dad doesn’t have to drop us off all the time.
Hav, 15 years
Short journeys: using the bus ‘because it’s there, and because it’s free’
For short journeys, when there is no cost to the user, and buses are relatively available and accessible, there are no disincentives to using the bus, and many young people talked about using the bus to go ‘short distances, literally three stops’ (Sut, 14–18 years). Indeed, the distances travelled by bus in preference to walking could be extremely short:
My dad takes me a couple of metres down the road, it’s only about 200 m down the road. And then from then I go and get the bus to school. And then there’s only a few metres from where I get off the bus to go to school. [. . .] I’m on the bus for roughly about less than a minute.
Hav, 14 years
In young people’s accounts, this preference for bus travel over even short distances was clearly the default choice: it was, implicitly, ‘just what you did’. Indeed this assumption that the bus would be taken as the obvious choice was recognised by many young people, who noted that on reflection, they would ‘jump on a bus’ even when this was an inefficient travel strategy in terms of getting to your destination quickly:
Sometimes, because the 18 that goes past the [local community centre], that comes into Sutton, my mate and I stood there waiting for one, this is going to be completely strange to you, but by the time we got on it, we got there and thought, you know, it would have been much quicker if we just walked there.
Sut, 14–18 years
The zip intervention, which removed any economic disincentive to using the bus, was also acknowledged as the key reason for making ‘jumping on’ for a couple of stops the default option:
I think that the fact that knowing the bus is free helps me want to get on the bus, so I’m saying I might jump on the bus, if I had to pay I would not get on the bus.
Isl, 16 years
Yeah, if it was a lot, if the price was higher I definitely would not be taking buses as much as I do.
Hav, 14 years
Maximising sociability: the importance of free travel for all
If free bus travel removed disincentives to ‘just jumping on’, it did not explain why this was preferable even for journeys that might be more efficiently made by other modes that were also free, such as walking. One important contributor to making bus travel the default choice for most journeys, rather than the choice for certain journeys, was the ways in which the scheme maximised possibilities for sociability.
In young people’s accounts of travelling around London, it was clear that socialising with peers was a pervasive aspect of, and influence on, young people’s mobility, affecting decisions about whether, when, where and how to travel, ranging from the routes they chose to where they sat in the bus. Travel with friends was valued as being a defence against boredom (a pervasive theme in many accounts); more fun; and as reducing the chances of getting lost, or as at least providing someone else to be lost with. Furthermore, travelling was a site for demonstrating important aspects of friendship, such as loyalty. Young people described situations in which travel decisions were made not because they resulted in a more efficient or enjoyable journey, but because to have done otherwise might be construed as a breach of friendship, as illustrated by this story:
I got on the bus and everyone else was just left there. And then he [the driver] just, he, I was like can you open the door because you’re not letting my friends on? I was going to come off. Drove off, I had to walk all the way [back to join my friends] and that’s actually quite a long walk
Sut, 14–16 years
The participants in this focus group then went on to highlight the possible consequences of failing to show this form of loyalty, with one participant recalling ‘we’ve had arguments over buses’ and another describing having got ‘really angry’ when she was left by herself during a bus trip. As she concluded ‘Your friends just like leave you on the bus. I said, like, I’ll just sit by myself, thanks a lot. It’s kind of loyalty to get on the bus with your friends’ (Sut, 14–16 years; emphasis in original). Similarly in a different interview, one boy explained:
[If a friend loses their zip card and isn’t allowed on the bus then] you’d have to get off or something. [. . .] If you leave them, if you, if they can’t go on the bus or, they see it as a kind of betrayal.
Hav, 15 years
Travel choices were therefore not simply passive reflections of existing relationships. Rather they could also be constitutive of relationships by providing an active opportunity to demonstrate friendship (show ‘loyalty’) or fail to do so (‘betray’ a friend).
Given the importance of sociability and loyalty within friendship groups, the fact that everyone is entitled to free bus travel and could therefore all travel together is a key factor in choosing buses, at least for some journeys. Several participants, from all age groups, were explicit in giving this as a rationale for taking buses rather than other modes (such as the London underground or train, which has to be paid for), so as not to exclude those who could not pay for transport:
[We sometimes go by bus] because it’s free as well so if people run out of money on their Oyster then we’ll all go with them because we don’t want anyone to go by themselves.
[. . .] I usually travel everywhere by tube [London underground] if we can. But like you said, if some of us have got no money on our Oyster then we’ll just take the bus.
YS, 17 years
[How I go] depends if I have friends with me, ‘cos they don’t like to go on the train, so if I have friends with me then go on the bus . . . ‘cos they don’t have to pay.
YS, 16 years
That the intervention itself, rather than the general increase in bus transport, facilitated ‘travelling together’ was also evident in (rare) accounts of limitations in mobility experienced by groups in which one member did not have free travel:
One of my friends he’ll actually, that’s the only bus he can take [a particular bus route that was easy to board without paying] because he never applied for an Oyster. And I keep on moaning at him for it. But then so if we ever go anywhere it has to be on [that bus].
Isl, 15 years
The removal of financial barriers for all also increased young Londoners’ options within the context of a particular bus journey. For instance, when it came to demonstrating friendship, free bus travel removed any economic disincentive to getting off a bus that your friends could not board. A few young people explicitly stated that this had an effect on their likelihood of showing this form of ‘loyalty’:
[We get off the bus if] a couple of people get on and then some of them are left. If we didn’t, if we had to pay, I would stay on the bus. I would stay on the bus because I’m not paying no more money.
Hav, 14–16 years
More often, this absence of a disincentive was implicit in the way in which young people automatically accommodated friends without thinking, or else focused on non-economic factors when relating stories of the costs imposed by accommodating friends (e.g. waiting for a long time, waiting in bad weather, ‘having to walk’ to rejoin friends).
Bus travel, therefore, had become the default mode because it was in part a ‘lowest common denominator’ activity for groups, not only for getting to destinations, but also an activity in itself that had no direct financial costs, and to which all members of a peer group therefore typically had financial access. Most obviously these considerations applied to ‘bus hopping’ journeys, which were undertaken primarily in order to spend time with friends and only incidentally to ‘end up somewhere’. The same was generally true of recreational group journeys to destinations that were predetermined but not ‘necessary’. Bus hopping and discretionary journeys also had in common the fact that the free nature of bus travel was often a key consideration: as one girl said ‘You wouldn’t be willing to pay just to get on a bus for no reason at all’ (Hav, 17 years). A final common element across these journey types was their frequent spontaneity, such that several participants described always taking their zip card ‘just in case’ whenever going out to meet friends.
Conclusion
The increase in the number of bus trips and kilometres travelled by young people after the introduction of free travel mirrors that of adults in London, suggesting that other factors (such as improvements in the network) may be responsible for the increase in the number of journeys made by bus as main mode during term-time weekdays. However, the qualitative data suggested that the intervention had a role in making bus travel the ‘default’ mode of transport for young people in London, particularly for short journeys. Offering ‘free’ fares was an important element of this, and for some young people, cost was explicitly a factor, at least for discretionary journeys. For most, free fares facilitated a rise in short journeys, as there was no financial incentive to forgo a journey. Additionally, the bus was an important site for socialising in itself, as well as a mode of transport for instrumental reasons. Given the importance of sociability to young people’s mobility, the universality of the benefit was important in making bus travel available to all within a peer group.
In summary, this suggests that first, the intervention is best conceptualised as ‘universal free bus travel’, as it was this ‘universal’ element that determined some of the effects reported, and that second, there is weak evidence that this intervention had an important role in generating discretionary bus journeys that might not have been taken otherwise.
Chapter 4 What impact has the scheme had on active travel?
Introduction
That increased levels of physical activity have benefits for physical and mental health outcomes has long been recognised. In the 1950s, Morris and colleagues100 identified health benefits from bus conductors’ relatively more active jobs, compared with those of bus drivers. Given the challenges of increasing physical activity from sports or leisure participation,101,102 policy interest has focused on encouraging ‘active travel’ as one way to increase levels of physical activity in the population,1,45,89 with evidence that obesity rates are increasing in countries and settings in which ‘active travel’ (walking and cycling) is declining. 103,104 It is therefore plausible to hypothesise that interventions which increase the amount of active travel within a population are likely to have a positive impact on health, and those which reduce it may have a negative effect. Appendix 8 summarises the evidence from a systematic review of the evidence that active travel confers health benefits. Although there is little prospective research addressing this question, and no studies to date that show an association between active travel interventions and obesity, there is some accumulating evidence that active travel can have benefits for other health outcomes.
Chapter 3 identified an increase in proportion of short journeys by bus by young people, which could plausibly be attributed to the intervention, in the context of general increases in bus use made by the population of London, and a suggestion from qualitative evidence that young people’s discretionary journeys by bus had increased as a result of the intervention. This chapter addresses whether or not this increase is at the expense of ‘active travel’, that is travel by modes such as walking and cycling. We first report on changes in young people’s active modes compared with adults, as reported in travel diary data. To contextualise these changes, and assess how far the intervention may explain them, we then turn to the qualitative data.
Quantitative evidence on impact on walking and cycling
Here we compare the pre–post change in walking and cycling in young people with the corresponding pre–post change in walking and cycling by adults aged 25–59 years. Again, the changes to walking and cycling trips, distance and percentage of short trips are shown graphically in Figures 7 and 8 (and in Appendix 9, Table 34). [Line joining solid squares shows change in target age group (12–17 years); line joining solid circles shows change in control age group (25–59 years). Diamond (right-hand side of figure) shows the change in the target age group relative to the change in the control age group. 95% CIs are shown as vertical lines. Horizontal dotted line indicates a ratio of 1 (i.e. no relative change).]
FIGURE 7.
Changes in walking, pre- to post-introduction of free bus travel (a) Walking trips per day; (b) walking distance per day (km); and (c) per cent short trips by walking.
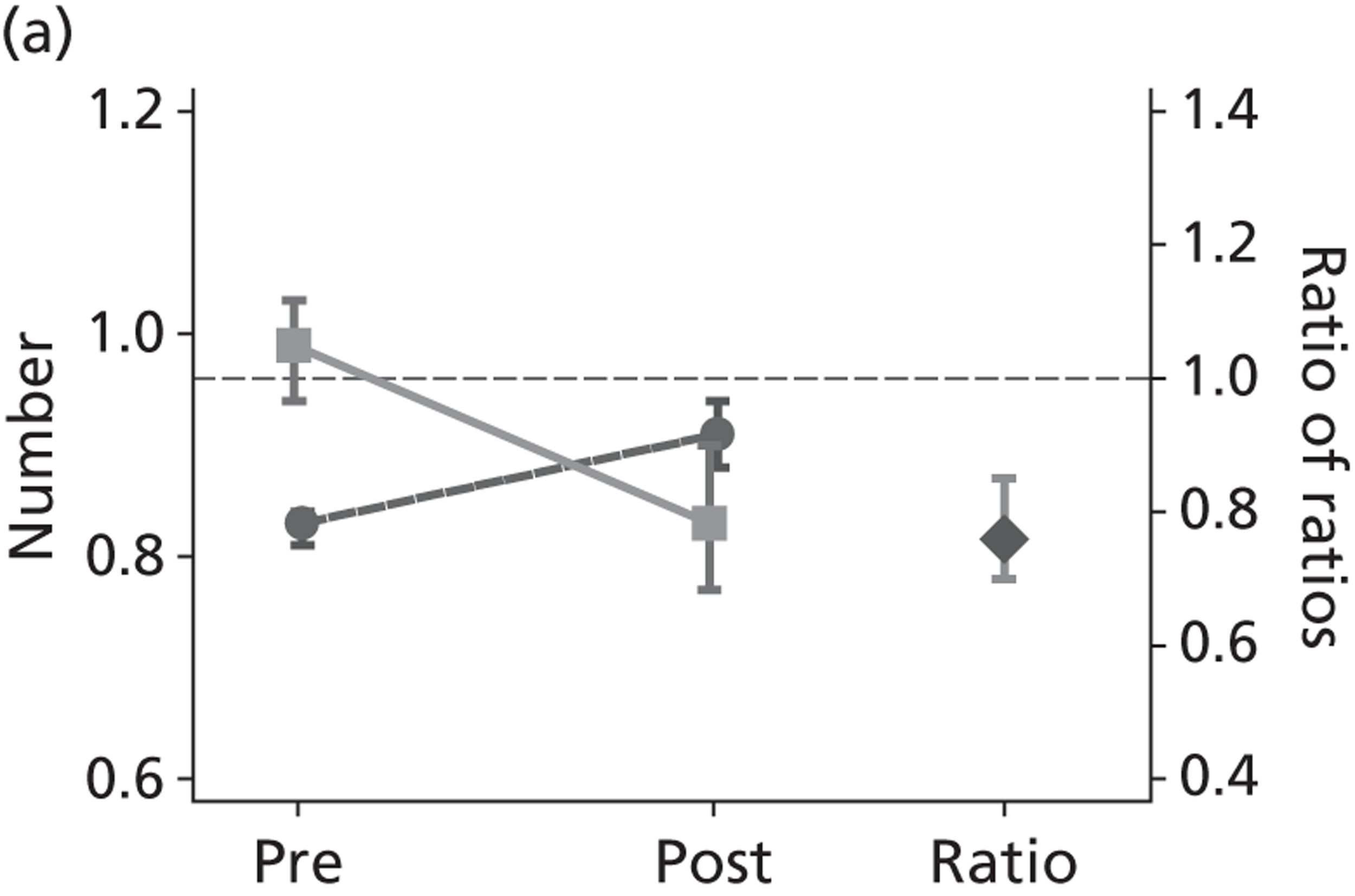
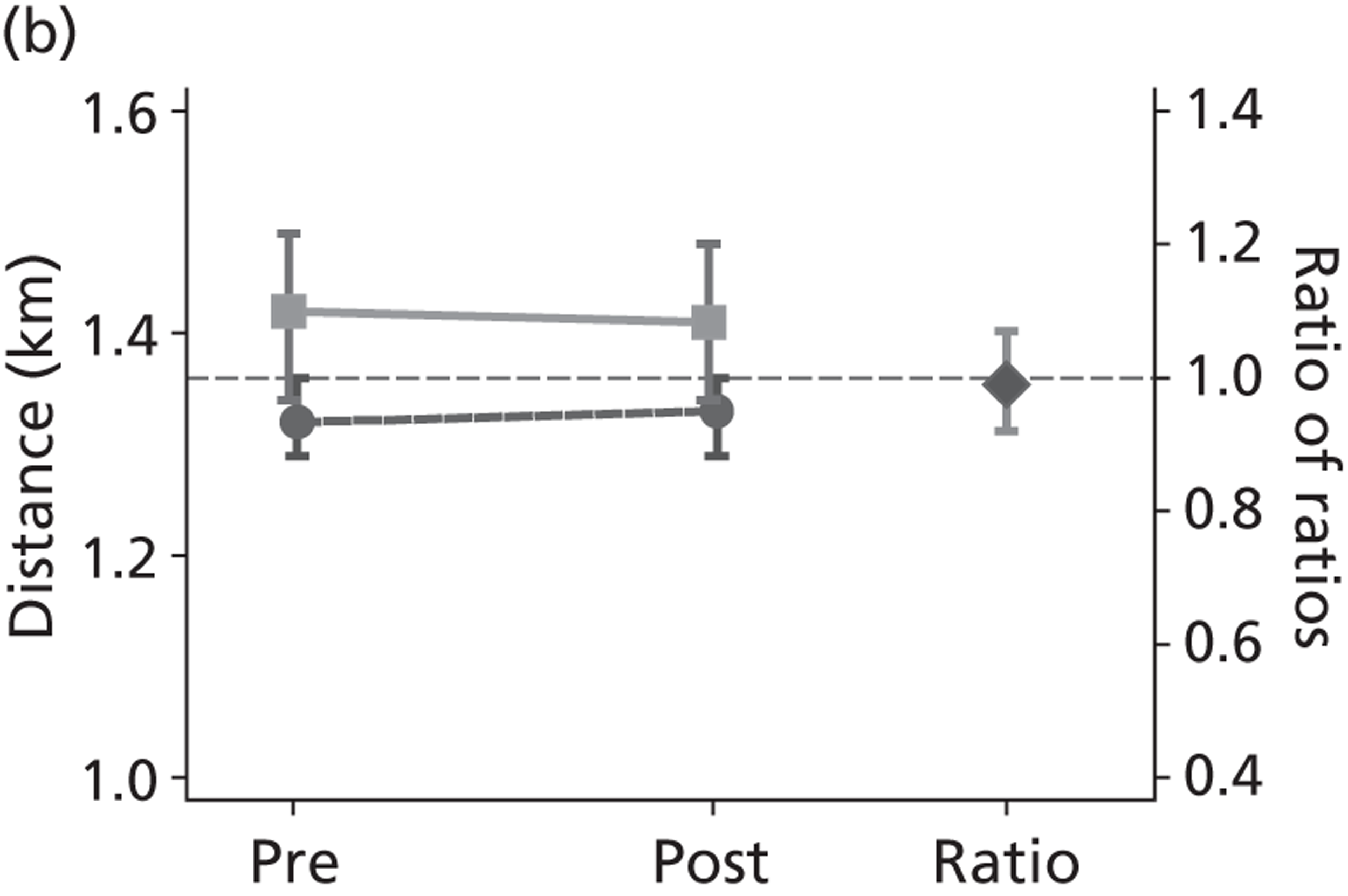
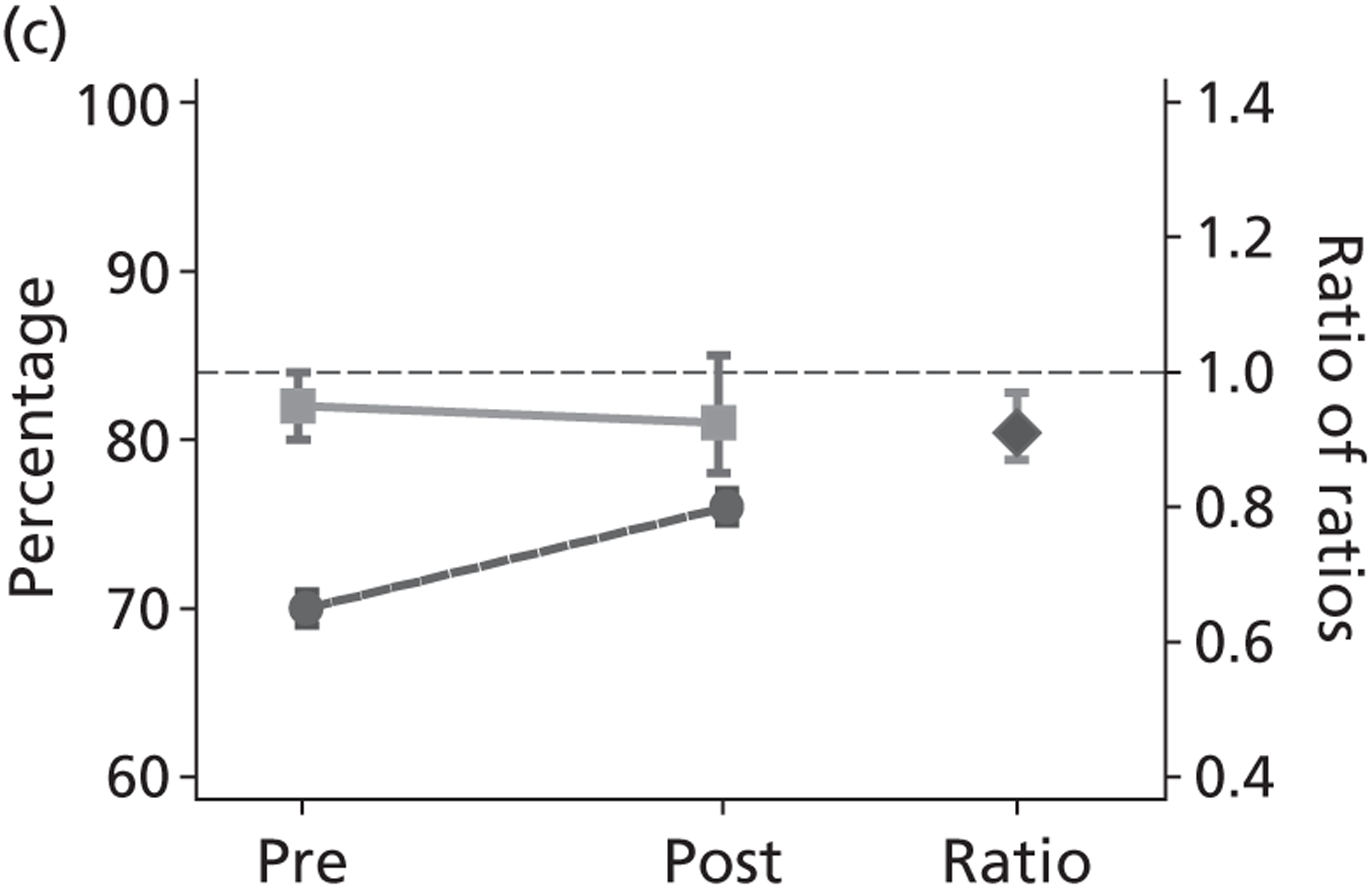
FIGURE 8.
Changes in cycling, pre- to post-introduction of free bus travel (a) Cycle trips per day; (b) cycle distance per day (km); and (c) per cent of short trips by cycle.

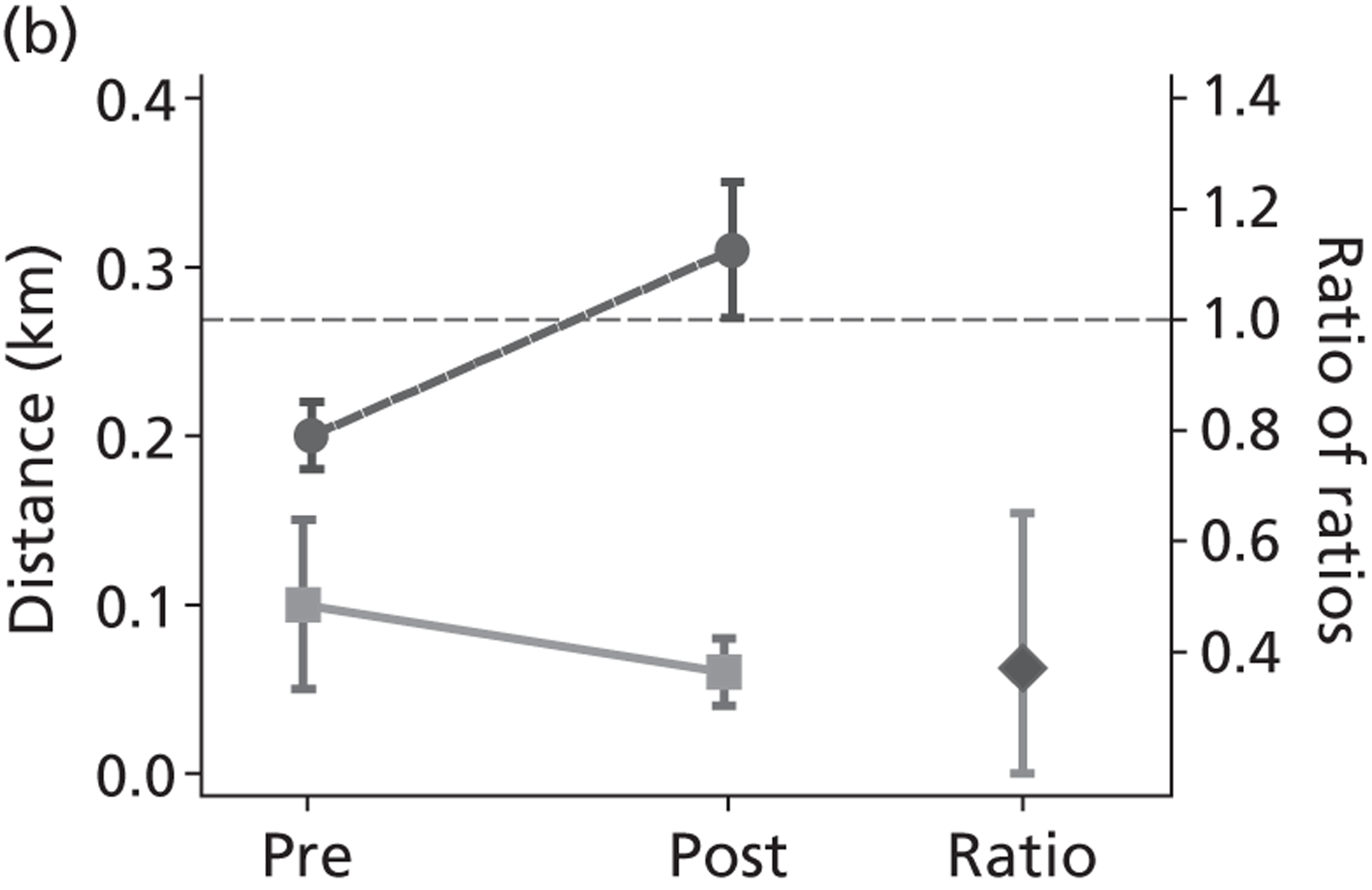
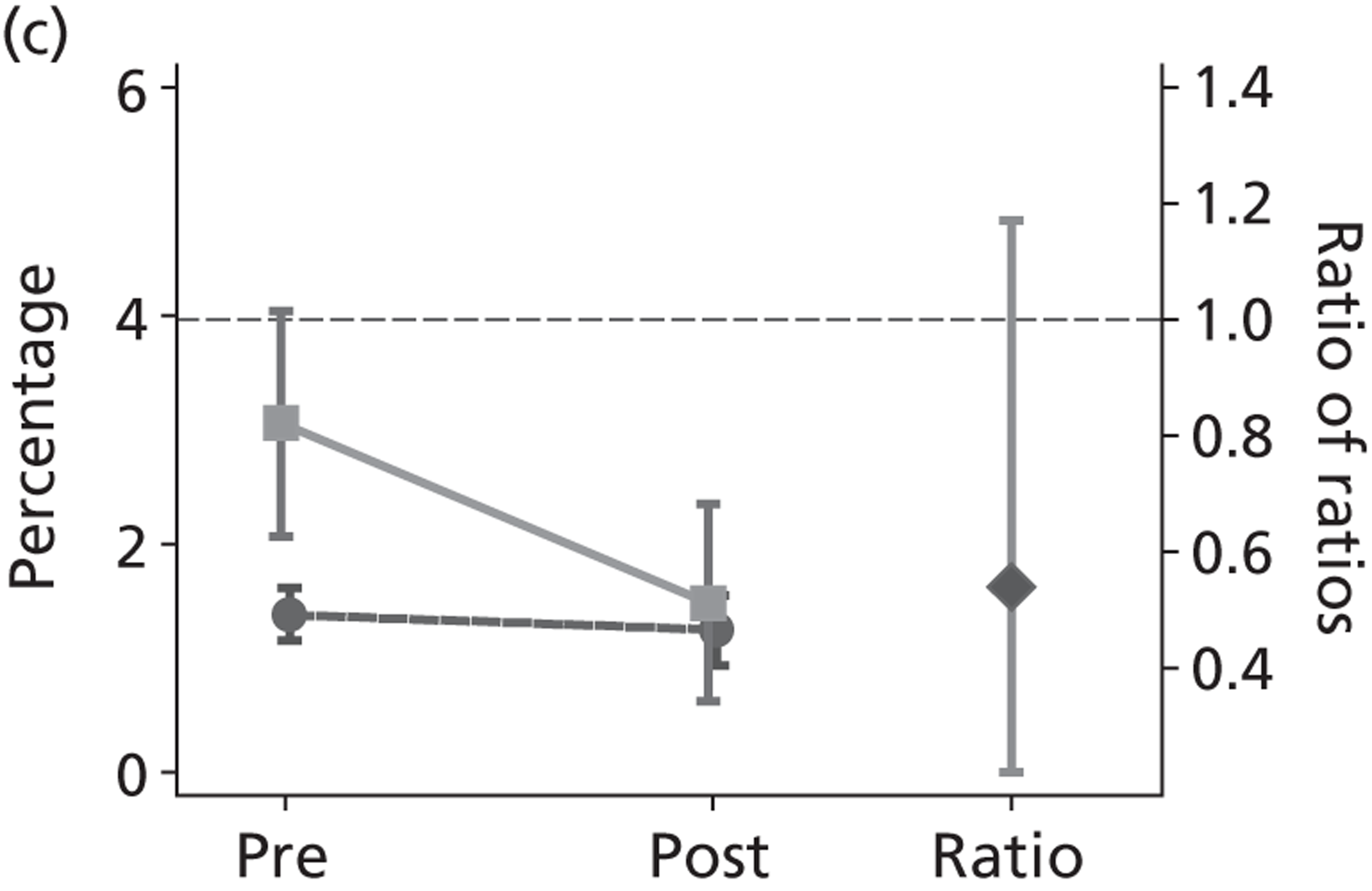
Trips by walking as a main mode
The introduction of free bus travel was associated with a 16% (95% CI 6% to 23%) decline in the average number of trips by walking as a main mode made by young people each day. In contrast, there was a 10% increase (95% CI 1% to 20%) in the average number of walking trips made by the control age group. Overall, therefore, free bus travel was associated with a relative decline in number of walking trips made by young people (relative change 0.76; 95% CI 0.70 to 0.85).
Distance travelled by walking
The average distances walked each day by young people remained at around 1.4 km pre- and post-introduction of free bus travel. The average distances walked by the control age group each day remained at around 1.3 km. There was no evidence that free bus travel impacted on average total distances walked (relative change 0.99; 95% CI 0.92 to 1.07).
Short-distance trips by walking as a main mode
Similarly, there was no change in the proportion of short trips (< 1 km) made by walking: this remained at around 80% of all trips made. There was an increase in the proportion of short trips that was made by walking in the control age group, from 70% to 76%. This meant that, relative to the control group, free bus travel was associated with a decline in the proportion of short trips walked by young people (relative change 0.91; 95% CI 0.87 to 0.97).
Trips by cycling as a main mode
The number of trips made by cycling as a main mode is extremely low in the population in London, at around 2% of all trips made. There was no evidence that free bus travel was associated with any change in the number of cycling trips made by young people (from 0.06 to 0.04 trips per day; a 39% decline with a 95% CI from a 53% decline to a 10% increase). However, as there was a significant increase in cycling trips made by the control age group (from 0.05 to 0.07 trips per day; a 34% increase with a 95% CI from 1% to 20% increase), free bus travel was associated with a relative decline in cycling trips by young people (relative change 0.53, 95% CI 0.35 to 0.87).
Distance travelled by cycling
The average distances cycled each day by young people declined from 0.1 km to 0.06 km post introduction of free bus travel. The average distances cycled by the control age group each day increased from 0.2 km to 0.3 km. Free bus travel was therefore associated with an overall decline in total distance cycled by young people (relative change 0.37, 95% CI 0.18 to 0.65).
Short-distance trips by cycling as a main model
Similarly, there was a decline in the proportion of short (< 1 km) trips made by cycling by young people, from 3% to 1% of all trips made. The proportion of short trips made by cycling by the control age group remained constant at 1% of all trips made. However, this was not statistical evidence that free bus travel had a greater impact on the proportion of short trips made by cycling in young people (relative change 0.54, 95% CI 0.22 to 1.17).
Walking and cycling by subgroups
There was some evidence that free bus travel coincided with a greater relative change in the distances walked and/or cycled by young people in inner London (relative change 0.80, 95% CI 0.66 to 0.97), but not in outer London (relative change 0.97, 95% CI 0.87 to 1.05). The statistical test for interaction with inner/outer London produced a p-value = 0.06. There was no evidence for interaction according to level of deprivation of areas in which people lived, the level of household income, ethnicity or the level of uptake of free bus travel (see Appendix 9, Table 36).
Bus use replaces walking for short trips
In the last chapter, we identified a preference for using buses because they were free, accessible and (crucially) because all members of a peer group could travel together. Although walking in theory would also offer these benefits, in general, young Londoners do not consider walking a viable mode of transport for any but the shortest of journeys. In part, as outlined in the last chapter, bus travel had become the default mode of transport for most young people, as suggested by these accounts of bus travel for journeys which, young people themselves suggest, could in theory be walking journeys:
Sometimes if I’m really lazy or just can’t be bothered. If I’m walking and I’m past a, I’m next to the bus stop and the bus is making its way up I just jump on. But if not, I just keep walking, I can’t be bothered to wait.
Isl, 16 years
[I]f I’m like going to meet a friend or whatever and I’m, or I’m going to Romford, but I could walk to Romford in about ten minutes. But if there’s a bus I’ll get on it because it’s quicker and easier.
Hav, 15 years
With buses generally accessible, available and free, walking, as a main mode of transport, had become something of a ‘last resort’ for many situations, something done because you ‘had to’, implying that there were no other more attractive options available:
My school is awkward . . . we have to walk
you’re at the top of the hill . . .
no buses actually go right to the school . . . and then you’ve got to walk through the parks to get to the other bus stop
Sut, 16 years (emphasis added)
By extension, when asked directly, many participants suggested that if the free travel concession were to be removed it is likely that many short journeys would be done wholly on foot once more:
And you said earlier if you had to pay the fare you might change your journey? What do you think you would do different, differently?
Well it’s pretty simple for me because I have only like on the bus is only one minute, it’s pretty simple, it’s not really a long walk at all, only it’s for me personally I find that literally almost no effect at all, however now thinking about other people and their situations that’s going to cause some effect but.
So you would just walk it if you had to pay it?
Yeah I’d walk it, yeah.
Hav, 14 years
[I]f you didn’t have the free bus travel, how would you get to school do you think?
I’d have to walk, I’d probably walk. It’s, it’s about, but I’d have to leave much earlier because it’s about a half an hour walk, 5 minute bus journey. I’ll take the bus any day.
Hav, 15 years
This is not to say that the zip card has eliminated all walking trips. In some instances, despite free bus travel, young people reported that they would opt to walk rather than take the bus:
[I] walk [to school], because I live nearby so I feel a bit, I’d feel a bit stupid getting the bus . . .
I used to quite often, during the summer I’d walk home from school. Even though it is a good 50 minute, hour long walk, but sometimes it’s just easier than waiting for the bus and then getting all crammed on it.
Sut, 15–16 years
As these instances suggest, however, opting to walk would usually be in response to perceived conditions (the crowdedness of the bus or the ‘stupidity’ of getting a bus short distance) rather than a proactive decision in light of the health (and other) benefits of travelling by foot. In this respect, it would appear that for the most part secondary school pupils are inclined to persevere with trying conditions before opting to walk:
And my friend who lives in between Epsom and Cheam said it got to a point where for two weeks, every day, the bus . . . was too full to just stop for her. So in the end she just had to leave her house half an hour earlier and walk.
Sut, 14–18 years
The absence of cycling in accounts of transport
Cycling is notably absent from accounts of travelling and travel preferences, in particular as a candidate mode of transport. When asked directly whether or not they would consider cycling to school, most said no, offering a number of reasons why this was an inappropriate choice: main roads were too dangerous (several recounted injuries from cycling), or at least considered by parents as too dangerous; cycling was unpleasant in poor weather; bicycles were at risk of theft from schools and bicycles that were owned were in any case (in most accounts) broken. More significantly perhaps, cycling rarely figured as a possibility for consideration as a method of transport, being (for many) inherently ‘ridiculous’. As one young woman said of those who did cycle to school: ‘I just find it funny. I don’t know why I just, I find that I do find cycling funny’ (H&F, 12–17 years).
The exceptions were telling. Given the focus on sociability in young people’s accounts of transport, cycles were notable for offering more individual, even confidential, travel. One young man, one of the few to cycle to school, also preferred to use his bike on occasions when he did not want to encounter peers: one was going shopping for his mother ‘Because I don’t like getting on the bus with shopping . . . [unless] I have one of them expensive bags’ (YS, 14–15 years). In general cycling was associated with childhood:
I used to cycle every Sunday with my dad and younger brother, but now we don’t anymore. Yeah, just, we kind of stopped, yeah.
H&F, 15 years
It continued to be attractive to some as a leisure activity, and boys in particular talked of riding BMX bikes, ‘for, like, just going to the skate park and using it there’ (Hav, 12 years). Here, cycling was a sociable activity for peer groups which, like opportunistic bus travel, was a possibility for offsetting boredom:
We’re like sitting in the estate and talking and stuff, and it just gets boring after a while, so sometimes we just ride, ride our bikes and cruise
H&F, 15 years
Free bus travel does not, then, seem to play a major role in decisions about choosing to cycle, as cycling is not primarily considered a candidate mode of transport for most journeys.
Free bus travel generates additional activity
The replacement of short walking trips (one to three bus stops) by bus trips did not necessarily reduce the amount of physical exercise young people were getting, or even the amount of ‘active transport’. For some, having the pass had clearly generated additional walking stages of a journey or whole trips that would either have not been conducted without the free bus pass or would have been carried out as a car passenger. There was first some evidence (if at the margins) that a free bus pass enabled access to journeys that would not otherwise have been taken, providing possibilities for exercise:
If I didn’t have free travel . . . I wouldn’t be going places I would be probably staying quite local and through using free travel it means I can go places that I’ve always wanted to go, maybe heard of from friends and family because they’ve gone on trips.
Sut, 15–18 years
By the same token, other journeys might be undertaken less often if free bus travel was not available. As one focus group participant put it when asked how journeys would change without free bus travel, ‘I don’t think anyone would really go out as much to be sociable’ (Sut, 15–16 years). She goes on:
[S]ometimes when I go out with my friends I get three buses there and three buses back, depending on where I’m going, and I wouldn’t pay that much to spend three hours out, because you think about it, if they started making us pay, that’s like, at the moment it’s what, £2.00? £2.20 for [a] single bus fare. You times that by six that’s, you’re going to end up paying a lot of money for just going out with your mates for three hours. You’re already trying to save money doing stuff that doesn’t cost us. [You don’t want to be paying for] getting there as well.
Sut, 15–16 years
Free travel, in that it facilitated travel with friends, particularly to new places, therefore encouraged extra trips, and trips further afield than would otherwise have been made. Such ‘exploratory’ trips inevitably entailed some physical exercise (even if minimal) either as an end in itself or as a by-product:
Me and my friend tend to just get on the bus and go somewhere and then just get off and get the bus back . . . We saw a park once on a bus and we were like, that’s nice, and got off there for a while.
YS, 12 years
If I didn’t have free travel I would have to be doing everything through walking and stuff but I wouldn’t, that means that I wouldn’t be going places I would be probably staying quite local and through using free travel it means I can go places that I’ve always wanted to go [ . . . ] and then you can explore places on your own, you can see what you want to see, not with the guidance of someone who’s obliging you to go and see a museum.
Sut, 15 years
Bus travel replaces some car travel, particularly in outer London
A marked geographical distinction was apparent between accounts from inner and outer London. In inner London, with a higher density of bus stops and more bus routes to choose from, young people would report that bus trips tended to displace walking trips. In outer London, however, where residents can expect to walk further to their nearest bus stop, young people would report that bus trips were displacing less active car trips. As one young person in Sutton put it when asked if they use the bus for a journey they might otherwise walk without the free bus pass: ‘I hardly ever go in the car anymore . . . I can’t remember the last time I sat on a front seat’ (Sut, 14–16 years). Having free travel rendered them less reliant on lifts to places from their parents:
[F]or example if I was getting a lift with parents because I’m not old enough to drive they might be doing something in the day and so they’re going to be, oh I can only give you a lift at this time because I need to go out to do this before work. So it’s just through that bus journey means I have, time is not a problem
Sut, 15–18 years
In outer London in particular, then, the free bus pass generated instances of active transport by encouraging hybrid walking and bus journeys instead of door-to-door lifts by parents or guardians.
Activity within the transport system
With the free bus pass at their disposal, young people felt less limited in terms of their transport choices, and would often take journeys involving multiple buses (and interchanges) if the most direct bus did not arrive or ‘to get a shorter bus’ (Sut, 15–16 years). Such ‘hopping on and off’ was a feature of travel across the city for ‘fun’ (Sut, 15–16 years), comfort or convenience:
Well there a lot of buses, so if I get a bus, so I change either three times or two times, so it depends on what comes first. And because I have the free Oyster card I’m not restricted to get a certain bus, so I can get any bus, get off and . . . change, so that saves me time
H&F, 12–17 years
Regardless of motive ,‘bus hopping’ would invariably involve walking or running between buses and between bus stops. Thus, although strategies to avoid unnecessary walking as a main mode of transport pervaded accounts of such journeys as getting to school, this preference for less active ways of travelling did not necessarily extend to within the transport system itself. Additionally, on the buses themselves, behaviour was not necessarily inactive. For example, respondents would report choosing to stand on the bus (for very short journeys) rather than sit and, crucially, riding the bus did not necessarily connote sedentary behaviour, in particular where no seat was available on the bus or where adjacent seats for groups of young people were not available. Rather, the priority for young people travelling with friends was to be able to convene as a group, whereas for those travelling alone some would refrain from sitting so as to reduce the likelihood of having to engage in unwanted interactions with unknown others. This finding was reiterated during observations (on buses and other public transport modes) recorded over the course of the fieldwork period. These showed that young people using public transport, in particular on their way home from school, would often be active during their journeys – moving between friends sitting on different parts of the bus, running between buses and even using metal bars intended to help passengers support themselves as ad hoc exercise frames.
Preferences for active travel
A preference for using buses because they are convenient, sociable, free and everyone can therefore use them was not necessarily a preference for bus travel per se. Indeed, inherent dislikes of being on buses, particularly crowded buses, were common, with concerns about crowds, dirt, germs and the lack of hygiene commonly articulated:
And the thought of the germs travelling in the air. And the fact that that swine flu has just hit as well, so it puts you off public transport
Isl, 15–16 years
It was very packed on the bus, it was quite hot and sweaty and yeah, there were a lot of people crowded into little spaces and buggies and crying babies and everything, it was horrible. [W]hen I’m going to school it’s normally quite quieter because there aren’t as many people, but today because I was going into Romford, I had all the work people and everyone and it was oh, horrible. . . . I feel claustrophobic.
Hav, 15 years
These dislikes meant that more active modes such as walking were widely seen as ‘healthier’ in principle. Young people often spoke of their own preferences for bus travel as being ‘lazy’, for instance, and, when reflecting on the zip card scheme, many recognised the potential health limiting effects of possibly replacing walking with bus travel:
What do you think . . . about why you guys get free bus travel?
I think it could be because some people are lazy, tired, if they’re tired they won’t go to school. So then the government try and encourage them to go in, and they’ve got free travel. You don’t have to use your legs that much to get in there, so.
But then wouldn’t that be against the whole, defeat the point of the whole government thing, the government fitness thing? Because if they’re trying to encourage people to get fit, why encourage them to take the bus then?
True.
Isl, 15–16 years
Although, as detailed above, these considerations did not generally translate into personal preferences for what were perceived as ‘healthier’ modes of travel, some individuals did report preferences for walking because of the intrinsic pleasure of exercise:
[W]hen I didn’t have my Oyster card when I walked to school I felt, because like I was in the air, fresh air, I had fresh air and I could exercise a bit, walk my legs, when I was at school I felt much, much more concentrated and much more alive. When I’m on the bus it’s like, 50% of the time I would slouch on the table, sleeping, even if I’m standing up on the bus, whether I’m sitting down or standing up it just like this musty atmosphere on the bus, it smells a bit and it’s just dull really. So outside, when you’re outside walking it just makes you feel more alive and it does, it makes you feel a bit healthier even though it’s such a short walk.
Hav, 14 years
The exceptions, those who did explicitly choose to walk where possible rather than get the bus, attributed this preference to health aims:
I want to be, like, fit and everything, so exercise wise, I make sure I don’t get the bus too much, so it helps
Hav, 17 years
For the majority, though, ‘fitness’ as a health goal did not feature as a factor in decision-making around transport decisions, and was not something prioritised in stories of travelling around the city. Rather, the well-being considerations of young people were more closely aligned to social well-being: ensuring a journey that maximised social inclusion (in travelling with peers, as described in Chapter 3) and minimised certain risks (which we turn to in Chapter 6).
Conclusion
There is credible evidence that although the intervention increased the use of bus travel for short trips, in the context of rising general use of bus travel in the population, that this did not necessarily mean that young people were significantly reducing their amount of active travel overall. The apparently paradoxical finding from travel diary data that, although the number of trips by walking as a main mode reduced, there was no significant reduction in distance walked, was explained to some extent by the qualitative data. This suggested that the bus pass facilitated more journeys and, given that all bus journeys require some walking, this entailed undertaking some active travel as part of a trip. This additional activity may well have served to offset the loss of trips by walking as a main mode. Although the bus pass may have had only a marginal role in generating exercise as an end in itself (e.g. to access sports facilities), exercise as a by-product of public transport was more common. ‘Bus hopping’, although generating a large number of very short trips which may not be recorded in travel diaries, also generates activity, and simply being on the bus was not necessarily sedentary. The oppositional, and at times explicit assumption (e.g. Mota and colleagues105 and Van Dyck and colleagues106) that urban bus travel is a purely ‘passive’ mode in contrast to the ‘active’ modes of walking and cycling may underestimate activity.
On cycling, levels in young people declined, from a very low base. The use of adults as a comparator group here is perhaps less helpful for attributing change to the intervention, given the rise in adult cycling for other reasons (including a number of schemes to increase cycling levels). Although there is little evidence from the qualitative data that cycling is considered a candidate mode of transport for many young people, we do not know how far this has changed since the introduction of free bus travel. It is clear that young Londoners have not benefited from the increases in cycling seen in adults.
What is encouraging from a public health perspective is that health is a consideration for many young people in thinking about their transport behaviour, and one which means that at times ‘active’ modes are preferred. However, the health outcomes that are implicitly prioritised in the majority of young people’s accounts of travel are those of social well-being. The scheme may (as young people themselves note) reduce the incentives for ‘healthier’ active travel, but it also provides the conditions for travel that is both sociable and inclusive: travel that is inherently ‘healthier’ from the perspective of young people themselves.
In summary, there was no evidence from the travel diary data that the intervention had reduced, overall, the amount of active travel that young people did. The qualitative data suggested that treating bus travel as a non-active mode of transport may be inappropriate if the aim is to use active travel as a proxy for physical exercise, as bus travel generates both additional trips (particularly discretionary ones) and some activity within the transport system itself.
Chapter 5 Has the scheme fostered sustainable transport?
Introduction
The sustainability of transport policies is a key issue for public health. 20 The Organisation for Economic Co-operation and Development (OECD) Vancouver conference107 identified the growth in motorised private transport as a severe challenge for developing sustainable transport systems. Mass transit systems, in general, are less environmentally damaging, and subsidising bus travel has long been seen as a promising policy for reducing private car use, with evaluations of concessionary schemes for older passengers suggesting some displacement of car trips. 108 One explicit aim of the intervention was to foster sustainable transport, both by displacing private car journeys in the short term, and by inculcating more sustainable travel habits in the longer term. This chapter first assesses the evidence for short-term change using travel diary estimates for change in young people’s car travel. Evidence for longer-term change is more difficult to assess, given the relatively short time frame of this evaluation. We therefore use the qualitative data to explore young people’s views of driving and public transport, to provide some insight into these longer-term implications.
Quantitative evidence on impact on use of private motor cars
The changes to trips by car as a main mode, distance travelled by car and percentage of short trips by car are shown graphically in Figure 9. [Line joining solid squares shows change in target age group (12–17 years); line joining solid circles shows change in control age group (25–59 years). Diamond (right-hand side of figure) shows the change in the target age group relative to the change in the control age group. 95% CIs are shown as vertical lines. Horizontal dotted line indicates a ratio of 1 (i.e. no relative change).]
FIGURE 9.
Changes in car travel, pre- to post-introduction of free bus travel (a) Car trips per day; (b) car distance per day (km); and (c) per cent of short trips by car.
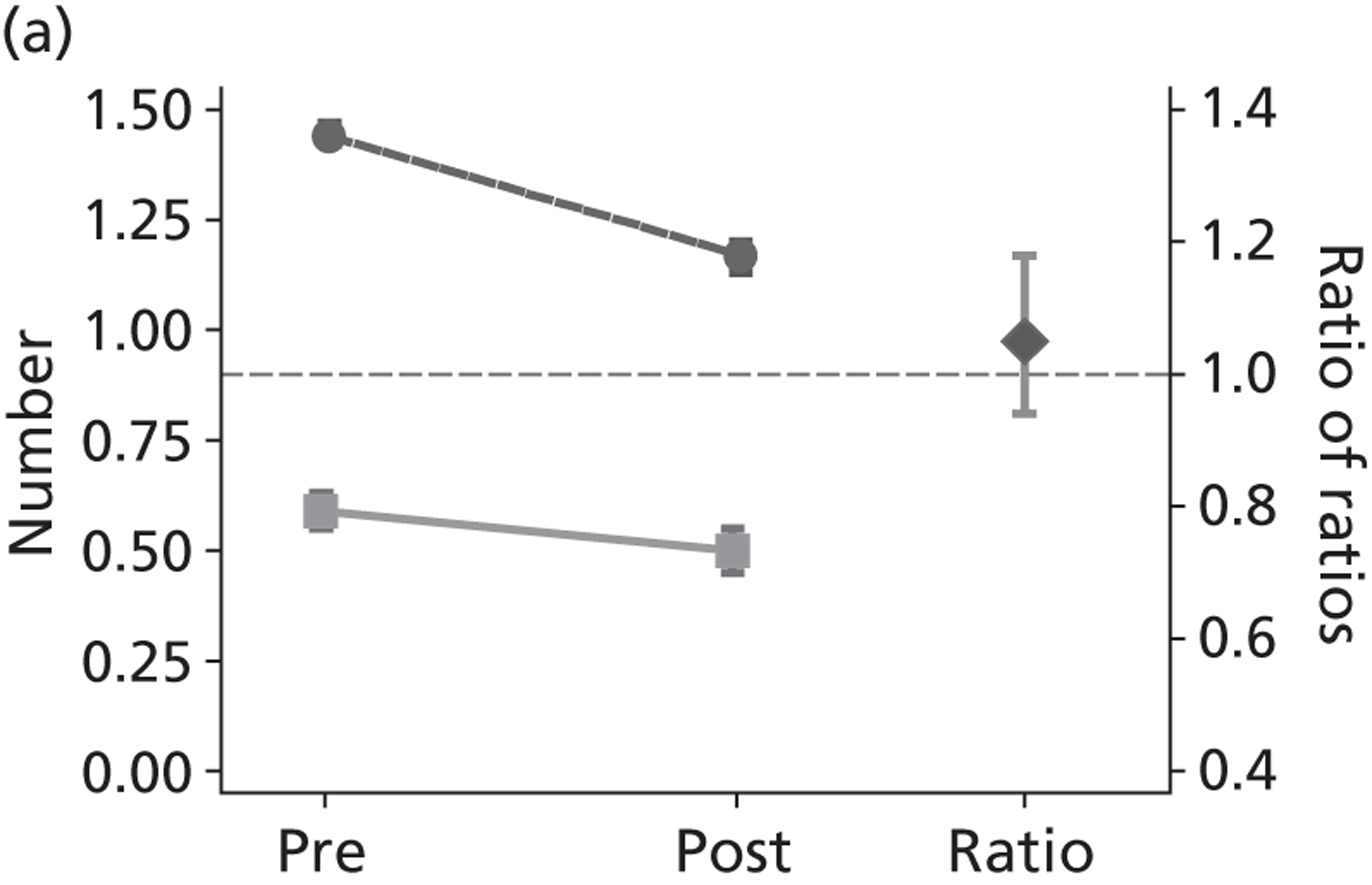
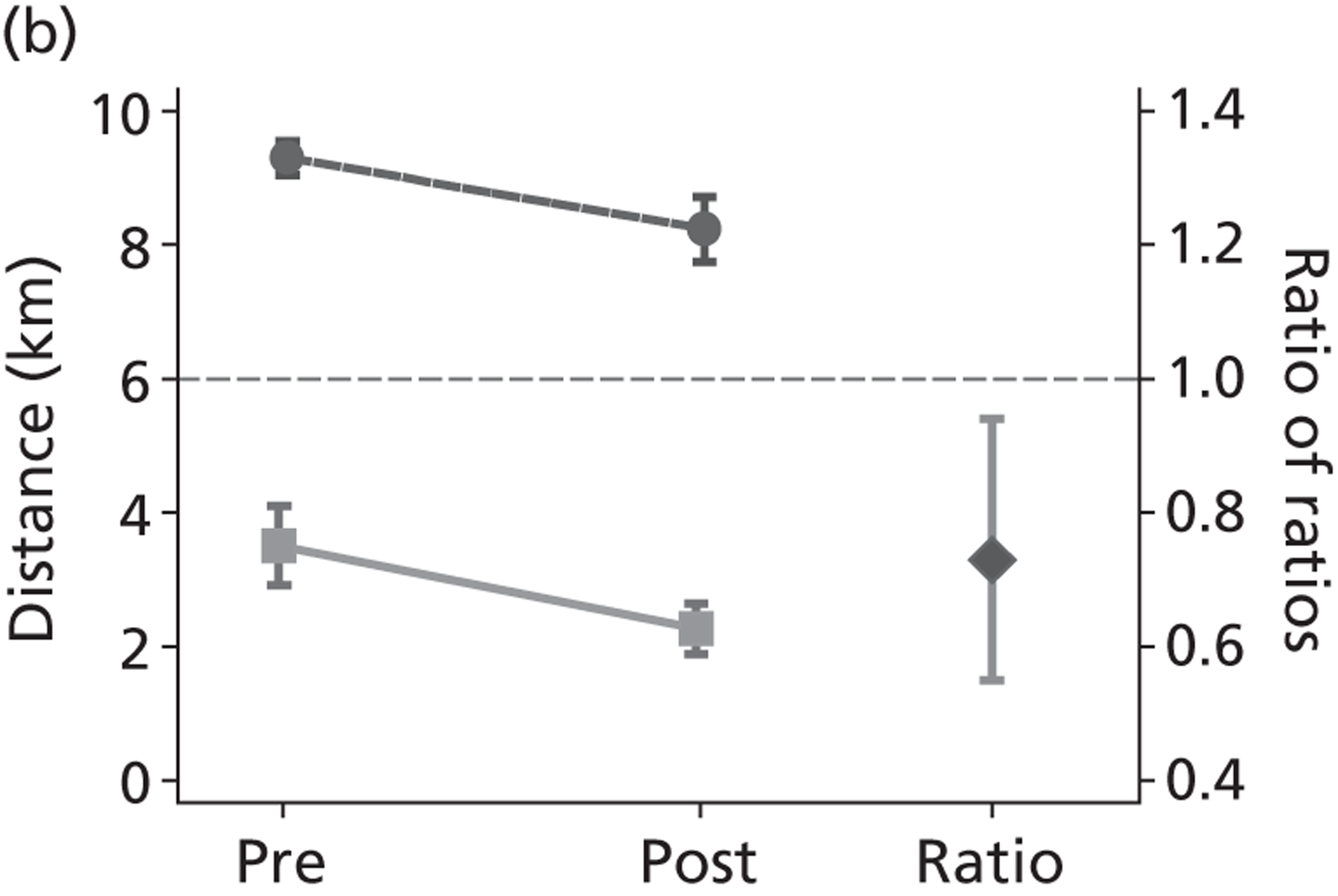
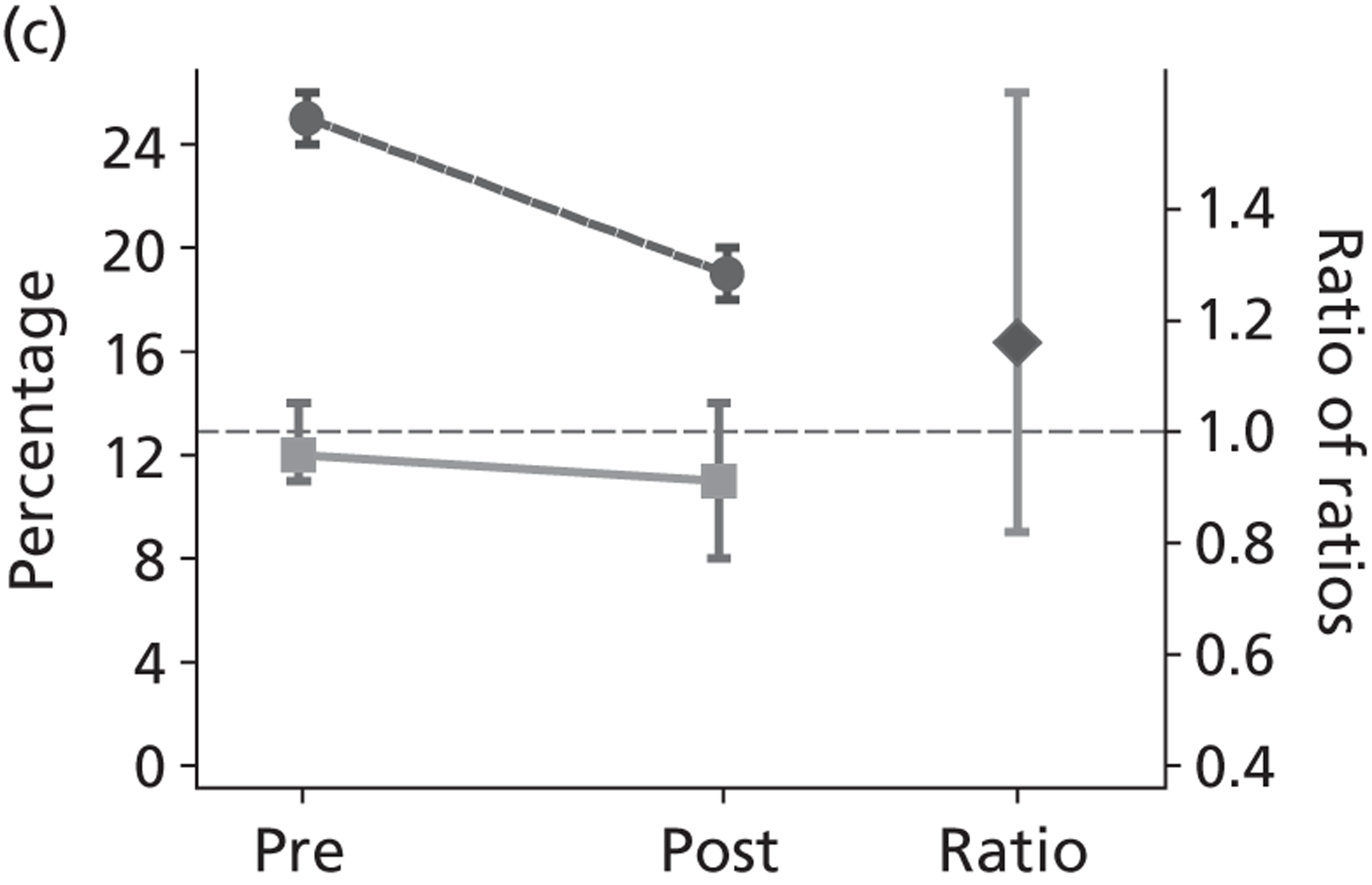
Trips by car as a main mode
The introduction of free bus travel was associated with a decline in the average number of trips by car as a main mode made by young people, from around 0.6 to 0.5 trips per day (a 15% decrease, 95% CI 5% to 23%). There was a similar decline (a 19% decrease, 95% CI 15% to 23%) in the average number of car trips made by the control age group (from around 1.4 to 1.2 trips per day). Overall, therefore, free bus travel was not associated with a greater relative change in number of car trips in young people (relative change 1.05, 95% CI 0.94 to 1.18).
Distance travelled by car
The average distance travelled by car each day by young people decreased from around 3.5 km to around 2.3 km post introduction of free bus travel. The average distances travelled by car in the control age group decreased from around 9.3 km to around 8.2 km each day. The introduction of free bus travel was thus associated with a greater overall reduction in total distance travelled by car in the target age group (relative change 0.73, 95% CI 0.55 to 0.94).
Short-distance trips by car
There was no change in the proportion of short trips (< 1 km) made by young people by car post intervention, which remained at around 11% of all short trips made. There was a decrease in the proportion of short trips made by car in the control age group, declining from 25% to around 19% of all short trips made. Relative to the control group, free bus travel was not associated with a change to the proportion of short trips made by car by young people (relative change 1.16, 95% CI 0.82 to 1.61).
Car travel by young people is dependent on car travel by the control age group, as the majority of young people are too young to be able to drive themselves. The changes in car travel by the control age group will therefore partially explain the change seen in young people.
Car travel by subgroups
Car travel by adults and young people declined in inner and outer London, in terms of trips by car as a main mode and distance travelled (see Appendix 9, Table 39). There was some suggestion that the relative decline in car distance was greater in inner London than in outer London. As the London Congestion Charge Zone (which substantially decreased car travel within inner London) came into effect between the pre- and post-intervention period, these results on car travel within inner London must be interpreted with a degree of caution.
Qualitative evidence on impact on current car travel
The free bus pass had displaced some walking trips (see Chapter 4), making the bus the default option for what might have been short walking trips. For longer trips in the city, however, walking was rarely considered to be a viable option even if there were cost or other disincentives to alternative modes. In the absence of free bus travel, hypothetically, young people thought they would typically forgo the journey, pay for the journey, or persuade parents to provide lifts, depending on the need. As described in Chapter 4, young people in outer London in particular said that if they had to pay for the bus, some trips would be made by asking parents for lifts:
If I was casually going out somewhere I probably wouldn’t have got the bus, but if I needed to go . . . I’d probably pay for it. But usually I’d catch cadge a lift . . . parents always seem to be conveniently free . . .
Sut, 14–18 years
Again, the importance of universal free travel was key to explaining the displacement of some car journeys, given the importance of sociability to travel planning. Unlike bus travel, parental lifts might not be easy to co-ordinate with others for planning travel and socialising:
[Free bus travel] makes things easier because if it was, for example if I was getting a lift with parents [ . . . ] they’re going to be, ‘oh I can only give you a lift at this time’
Sut, 15 years
My mum or dad would drive me if I want them to but it’s like I said you meet friends on the bus and things like that.
Sut, 13–16 years
To some extent, free bus use had therefore replaced some private car use, particularly for the kinds of discretionary journeys for which lifts from parents would have been a potential option for longer trips, and a first port of call for many. As these discretionary and longer trips may be more likely to be outside term time and weekdays, the travel diary data may have underestimated the impact of the scheme on displacement of car travel.
Driving remains seductive in prospect, if not reality
Current preferences for bus travel with friends over some lifts from parents did not, though, necessarily translate into imagined future preferences. Indeed, the majority of young people expressed a desire to drive when older, with initial comments about driving apparently reflective of beliefs about the status and value of driving widely reported in other research. 109 Future car use – for almost all young people – was still either a normal expectation or an aspiration, and older friends with cars were already a valued resource:
. . . I’ll get a car.
Yeah.
Loads of people now, you know some of them that’s old and that, I’ve got friends now though that are 17 they’ve got cars already, and they’ve actually got a license, so you’d probably go with them or whatever.
Yeah . . .
Get lifts with them?
Yeah.
If I haven’t got my own car or something, I’ll call my friend up . . .
Sut, 15–16 years
Car driving was for many (particularly young men) a rite of passage that was eagerly awaited as a route to enhanced status with peers and potential partners, in contrast to still using an ‘Oyster’, which would mark you out as somehow deficient, as these boys jokingly agree:
As soon as I’m old enough to drive I’m going to drive
I’m waiting for the day that I get my hazards
I’m going to get it before all of you, ha ha! . . .
. . . when I come home from parties I’m cold . . . so cold, so I always imagine I have a car just come . . .
Yeah, a car you could drive!
. . . also it’s more impressive to girls if you’ve got a car, if you’re 20 and you haven’t got a car and you
just do public transport
can’t go out to meet girls and that . . .
If you’re still rocking an Oyster!
[laughter]
YS, 14–15 years
However, to some extent stated desires to drive were reflective not just of the anticipated status attached to car travel, but also of its significance for achieving independence. Here, for instance, a disagreement between two friends reflects their differences in how ‘independence’ is constituted in relation to learning to drive:
What is it that makes you want to learn to drive?
I want to be free, I want to be independent and anyway, driving’s fun isn’t it?
Yeah, so what will be more independent about it?
I’ll be able to do things myself, be able to go where I want. [ . . . ] I’d just be more independent because you see a lot of working people always in their cars.
How about you, are you planning to drive or?
Well we all want to be start driving now but I don’t want to. I want to do it at a time when I’m able to afford lessons for myself, so I can buy myself a car because I don’t really, again I think it’s independence, I want to be able to pay for myself rather than depend on my mum.
YS, 17 years
Some young people in inner London did challenge their peers’ accounts of the future benefits of driving in London. One young man noted the practical problems of ‘long’ traffic, and being stuck ‘in the High Road for 40 minutes in a hot car’, before countering his friend’s rationale for wanting a car when older:
Do you know how many girls you can get with cars bruv? You just honk at them . . .
I think driving in London is stupid, I don’t see the point . . . I like cars, but in London, no.
Isl, 15 years
Such practical objections to the rewards anticipated from driving were rare, but were unsurprisingly more common for the few participants who were already driving, for whom the realities of parking, congestion and the implications of not being able to drink had already tarnished any romanticised views of driving bringing independent travel or freedom. One, who now regularly drove to school since passing a test recently, noted that parking was expensive, and buses (as well as still being free) could be more convenient for many journeys (Sut, 15–18 years). Additionally, she and a friend note that buses are intrinsically more interesting:
Yeah I do like getting the bus because you can meet new people on the bus and because everyone’s doing the same thing and it’s every day it’s nice to see the same people and it’s quite a nice commute so it gives you a lot of independence . . . every single bus journey is always interesting because something would always go on and you could listen to other people’s conversations if you want to and brighten up your day a bit.
I love the bus, I like journeys with my friends, obviously bus is good because if you want to have a drink then you don’t, you can use the bus to get home instead of driving. And always, you can always have funny conversations with people on the bus when you’re on the way home from a club or something
Sut, 15–18 years
What is notable about this exchange is not that these young women, at an age where they are just learning to drive, prefer the bus (indeed they note that driving would be preferable to waiting in the rain for a bus) but that the bus is not only ‘normalised’ as a mode of transport, but even attractive. There is no sense in this account that using a bus is stigmatised as a young person’s mode of transport, one primarily for poor people or only for those unable to drive. For those old enough to have actually experienced the advantages and disadvantages of different travel modes in the city, driving is (they admit) still a novelty attached to adult identities, but not intrinsically more socially valued than the bus.
The normalisation of bus travel?
Demonstrating an absence is difficult, but what was striking across the data was perhaps the lack of any comments about the inherent low status of bus travel. Although buses were often unpopular for being dirty, crowded or potentially risky (see Chapter 6), because all young people used them, there was no stigma attached to using the bus. Neither was there any sense that they were, as young people, relegated to public transport. Indeed, bus travel was, in the accounts of many young Londoners, simply the way in which many Londoners got to work and other destinations. This exchange gives a flavour of the accounts of bus journeys, with the range of other passengers who might be encountered on a typical journey:
I’ve had many a conversation with older people, not so much like 30 to 50 year olds they don’t, they keep to themselves . . . You can see mothers chatting to other mothers from their primary schools and stuff
Those are the workers who are so miserable that they just stand there and then especially when a bus is packed they say like, so rude and they get in your face and they’re just like, why are you standing in my way? . . .
And then the school kids
And then school, well children yeah
And then, but the good thing, sometimes the good thing about having old people in the bus is that you get that moral side out of you because when they come on the bus and you’re sitting down in the seat you feel like oh because they’re old you should give them your seat. So you feel good when they seat down because they normally say thank you
Sut, 15–18 years
It is not that free bus travel in itself created this normalisation. Two other conditions were necessary. First, the fact that universal free travel meant that bus travel had become a default, taken for granted mode of transport for all young people, meant that bus travel was ‘normal’ for all their peers, whatever other modes of transport were financially or otherwise available to them (see Chapter 3).
Second, was the context of enhanced bus provision, which had increased the modal share of bus travel in general in the capital (see Appendix 1). This generated routinely experienced encounters with a range of other Londoners, and visitors, on the buses (including older citizens, commuters, mothers with young children), making bus travel very visibly a ‘normal’ way for all kinds of people to travel. Without the relative accessibility and availability of buses in London, free travel, even if universal, would not become a preferred mode for so many journeys. A few, particularly those who had experience of other places and who lived more centrally, where bus services were in general more frequent, noted this explicitly:
The good thing about London is the amount of buses we have because when you go to other places you’re waiting half an hour for a bus scheduled to come at this time. And here you can just wait two minutes, you’re on a bus, you know what I mean
Isl, 15 years
For most, however, the taken for granted accessibility, and ubiquity, of bus travel as a normal way for a range of travellers to get around was merely an unremarkable backdrop to their accounts of travel in London.
Conclusion
In the short term, it is difficult to assess how far this intervention has changed the levels of private car use in London. A range of other policy interventions (notably the congestion charge) have reduced the advantages of car travel, and the number of trips by car has declined for all Londoners. Additionally, as the majority of young people’s car journeys are those made by adults as well, the reduction in young people’s car travel is included in that of adults.
In outer London, the qualitative data suggest that the free bus pass has displaced some car journeys, reflecting young people’s preferences for travel independent of parents and which allows sociable travel with peers. In the longer term, it is difficult to assess how far the intervention may have shifted perspective on the desirability of driving. However, although most young people still express positive views of learning to drive, what is notable is that bus travel has become normalised for this group. The broader context of London’s changing transport system is an important condition of the effects of free travel. In a transport system in which bus travel is in general more available and more reliable than in other parts of the country, it carries little of the stigma attached to bus travel in other parts of the UK, where bus use is disproportionately a mode used by the young, older citizens and poorer households. 110,111
In summary, a range of policies contributed to the reduction in car travel by young people in London in term-time weekdays, and to the normalisation of bus travel as a non-stigmatised alternative to driving.
Chapter 6 What impact has the scheme had on safety?
Introduction
Transport policies have the potential to impact on safety and inequalities in safety through a number of pathways. First, different modes of transport incur different risks of RTI for users and others,44 so policies that shift mode distributions are likely to change the numbers of RTIs. However, mode share may also affect relative risks (as in the example of ‘critical mass’ effects for walking and cycling, see Jacobsen112), so there may be feedback loops which reduce these effects over time. In Chapters 3–5, we noted a rise in bus use and a decline in other (currently more risky) modes, which could reduce the number of injuries young people experience on the road. Second, perceptions of risk may change as transport modes become more or less acceptable or well used. Third, as the overall number of trips or distance travelled goes up, young people may be more exposed to both road injury, and other risks, such as assault.
This chapter assesses the impact of the intervention on the risk of RTI and risk of assaults by comparing changes over time in young people with those in adults. Given that a range of other factors also contributes to declines in road injury, and in assaults, we also compare what happened in London with the rest of England. We then draw on the qualitative data to provide evidence on young people’s views of the risks of transport mode use in the context of free bus travel.
Quantitative evidence on road safety
As outlined in Chapter 2, we had hypothesised that the introduction of free bus travel for young people in London would result in an overall reduction in RTIs in young people relative to the control age group. Trends in RTIs and assaults by year are shown in Figures 10–13.
FIGURE 10.
Annual rates of RTI in London.
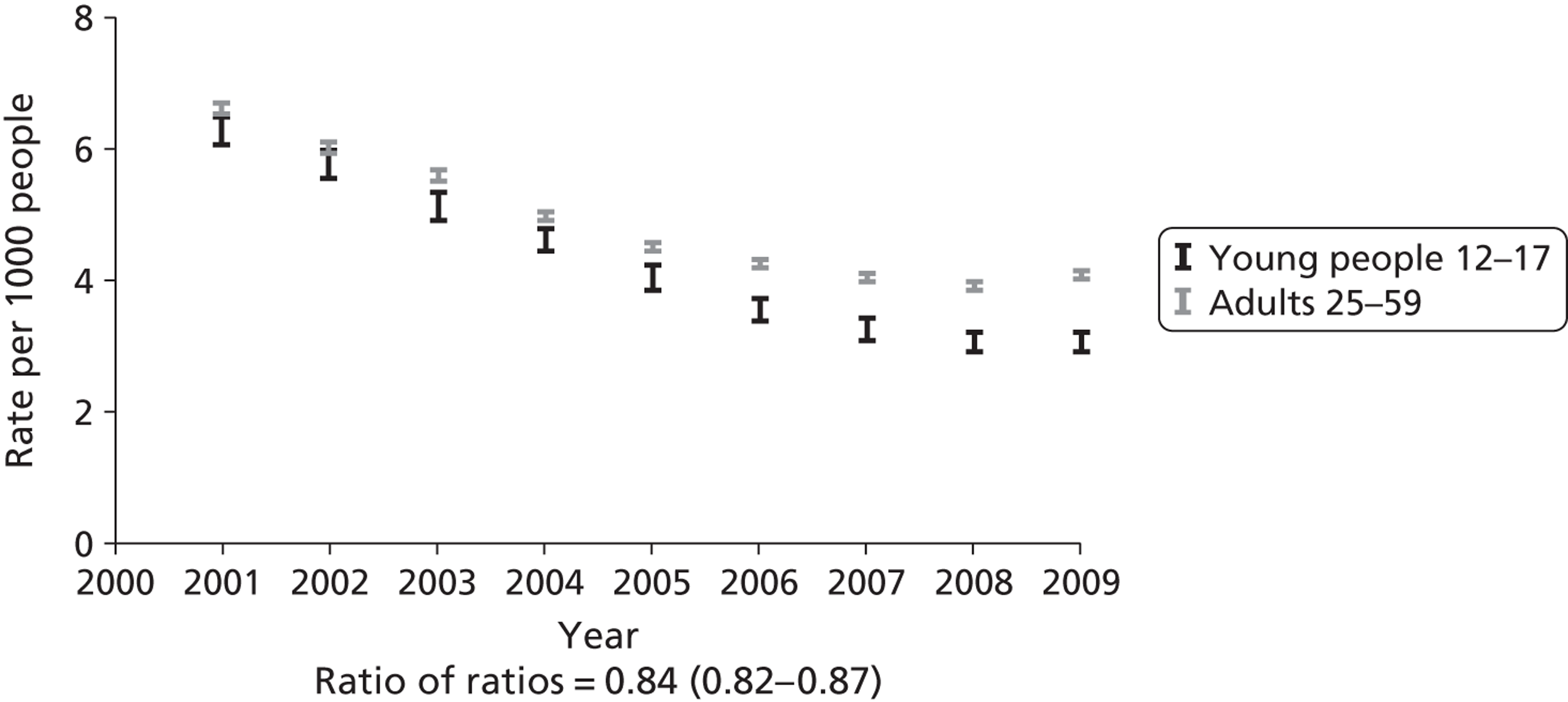
FIGURE 11.
Annual rates of pedestrian RTI in London.
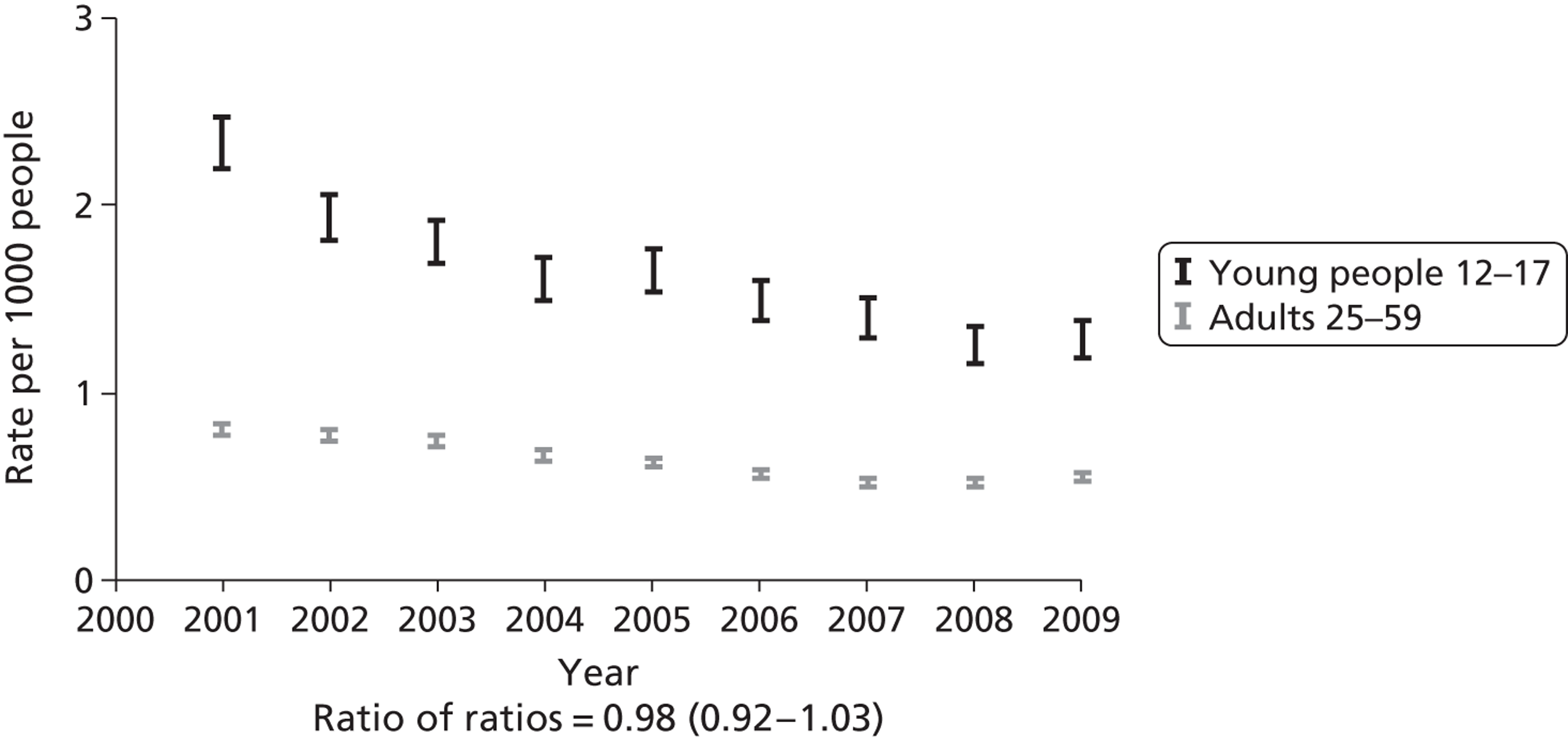
FIGURE 12.
Annual rates of cyclist RTI in London.
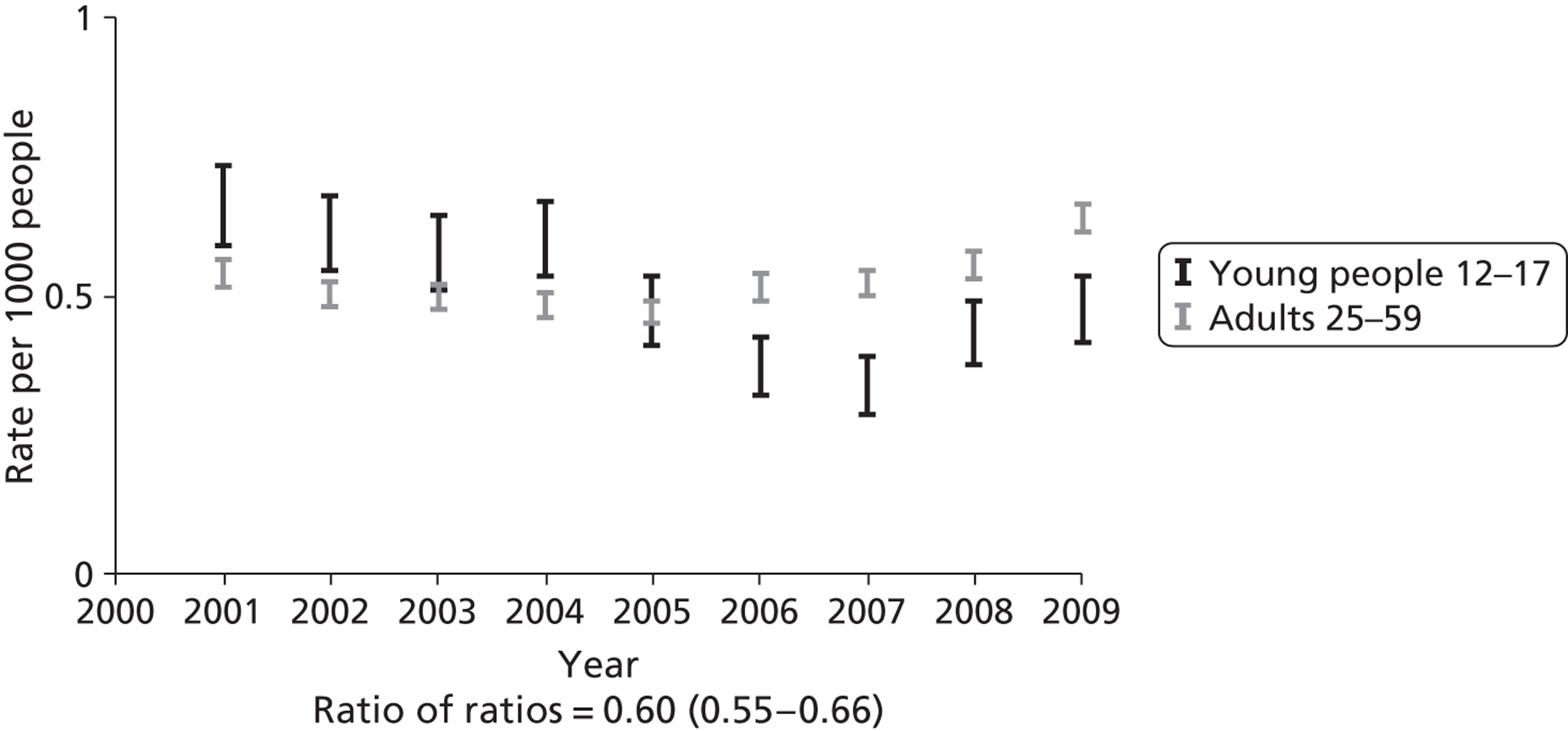
FIGURE 13.
Annual rates of car occupant RTI in London.
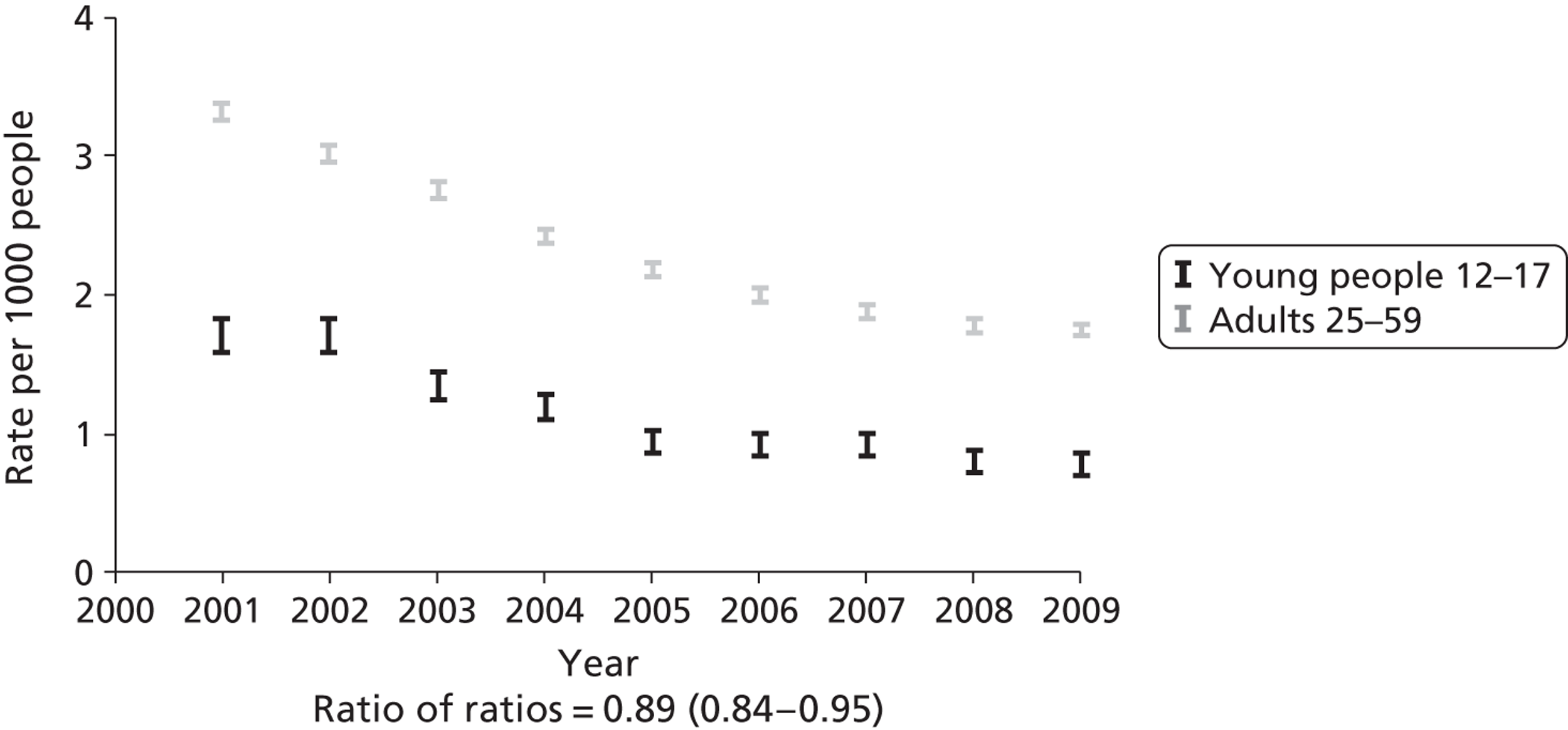
Road traffic injuries in London
Using police reports of RTIs in London (STATS19), we found 11,221 RTIs in young people in London in the pre-intervention period (2001–4), compared with 6657 RTIs in young people in the post-intervention period (2006–9). Among adults aged 25–59 years, there were 89,661 RTIs in the pre-intervention period and 65,542 RTIs in the post-intervention period.
The incidence of RTIs for all modes of transport in young people declined over the study period from 5.46 injuries per 1000 person-years to 3.23 injuries per 1000 person-years, a reduction of 41% (95% CI 39% to 43%). In the control age group there was a reduction from 5.81 injuries per 1000 person-years to 4.08 injuries per 1000 person-years, a reduction of 30% (95% CI 29% to 31%). The introduction of free bus travel was therefore associated with a greater reduction in RTIs in young people (relative change 0.84, 95% CI 0.82 to 0.87).
Pedestrian injuries in young people declined from 3948 in the 4 years before the free bus travel scheme (2001–4) to 2795 in the 4 years after the intervention (2006–9). Among adults, pedestrian injuries declined from 11,563 injuries in the pre-intervention period to 8723 injuries in the post-intervention period.
Pedestrian injury rates declined in young people over the study period from 1.92 per 1000 person-years to 1.36 per 1000 person-years, a reduction of 29% (95% CI 26% to 33%). In the control age group there was a reduction from 0.75 per 1000 person-years to 0.54 per 1000 person-years, a reduction of 28% (95% CI 26% to 30%). The introduction of free bus travel was not therefore associated with a greater reduction in pedestrian injuries in young people (relative change 0.98, 95% CI 0.92 to 1.03).
Cyclist injuries in young people declined from 1263 in the pre-intervention period to 837 in the post-intervention period. Among adults, cyclist injuries increased from 7802 in the pre-intervention period to 8976 in the post intervention period. Cyclist injury rates declined in young people over the study period from 0.61 per 1000 person-years to 0.41 per 1000 person-years, a reduction of 34% (95% CI 28% to 39%). In the control age group there was an increase in cyclist injury rates from 0.51 per 1000 person-years to 0.56 per 1000 person-years, an increase of 10% (95% CI 7% to 14%). The introduction of free bus travel was therefore associated with a reduction in cycling injury rates in young people (relative change 0.60, 95% CI 0.55 to 0.66).
There were 3602 car occupant injuries among young people in the pre-intervention period compared with 1765 car occupant injuries in the post-intervention period. There were 44,432 car occupant injuries in adults in the pre-intervention period compared with 29,752 car occupant injuries in the post-intervention period.
Car occupant injury rates declined in young people over the study period from 1.49 per 1000 person-years to 0.86 per 1000 person-years, a reduction of 42% (95% CI 39% to 46%). In the control age group there was a reduction from 2.88 per 1000 person-years to 1.85 per 1000 person-years, a reduction of 36% (95% CI 35% to 37%). The introduction of free bus travel was therefore associated with a greater reduction in car occupant injury rates in young people (relative change 0.89, 95% CI 0.84 to 0.95).
Road traffic injuries in London by subgroups
To assess whether or not the scheme had differential effects across London’s population, we conducted change-on-change analysis for inner and outer London. There was strong evidence for a greater relative decline in inner London in the incidence of RITs among young people compared with adults (21% decline; 95% CI 17% to 25%) than in outer London (p = 0.001 from a chi-squared test of homogeneity of effects in inner and outer London). There was no evidence that the relative decline in RTIs differed in terms of area deprivation, ethnic group or intervention uptake rate (see Appendix 9, Table 36).
Road traffic injuries nationally
The incidence of road traffic injuries for all modes of transport in young people also declined nationally (i.e. England outside London) over the study period, from 6.69 injuries per 1000 person-years to 5.62 injuries per 1000 person-years. The reduction seen in London (from 5.46 to 3.23 injuries per 1000 person-years) was greater (relative change 0.59, 95% CI 0.57 to 0.61) (see Appendix 9, Table 37).
When compared with the (older) control group in London the reduction in RTIs was 16% (95% CI 13% to 18%) and when compared with the same age group (12–17 years) nationally, the reduction in RTIs was 41% (95% CI 39% to 43%).
Quantitative evidence on assaults
We hypothesised that the introduction of free bus travel would result in an increase in injuries to young people due to assaults as they travel further and more frequently.
Assaults in London
Using HES we found that the number of young people hospitalised with injuries inflicted by assaults increased from 2321 in the pre-intervention period to 3322 in the post-intervention period. The number of adults hospitalised with injuries inflicted by assaults also increased over the study period, from 11,829 to 14,641 admissions.
The rate of hospitalisation for injuries in young people inflicted by assaults increased over the study period, from 1.13 hospital admissions per 1000 person-years to 1.61 admissions per 1000 person-years. This change represents an increase of 43% (95% CI 35% to 51%) in the admission rate. In the control age group, there was a smaller increase from 0.77 admissions per 1000 person-years to 0.91 admissions per 1000 person-years, a relative increase of 19% (95% CI 16% to 22%).
Our measure of relative change therefore suggests that free bus travel was associated with a greater increase in rates of assault in young people (relative change 1.20, 95% CI 1.13 to 1.27). However, when examining trends in hospital admissions for assaults by year, as shown in Figure 14, it appears that the largest increase in assaults among young people occurred between 2002 and 2005 (i.e. predominantly before the introduction of the free bus travel scheme).
FIGURE 14.
Annual rates of hospital admission due to assaults in London.
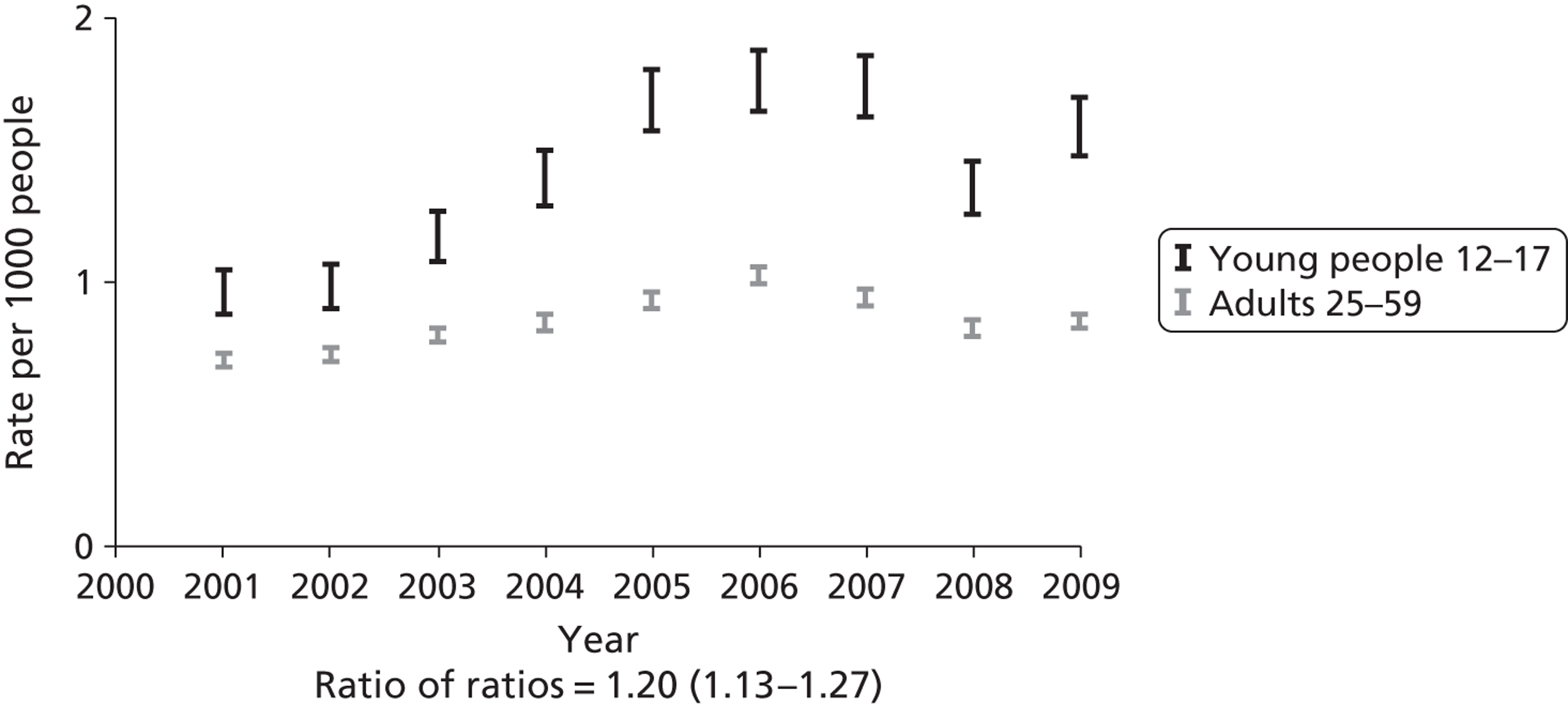
Assaults in London by subgroups
There was strong evidence for a greater relative increase in the incidence of injuries to young people inflicted by assaults, compared with adults living in inner London (p = 0.001), living in the most deprived areas of London (p = 0.001), living in areas with a high uptake of free bus travel (p = 0.001) and in people of ‘Black’ ethnic origin (p = 0.001) (see Appendix 9, Table 36).
Assaults nationally
Hospitalisations from assaults increased among young people aged 12–17 years living outside London over the study period from 1.04 per 1000 person-years to 1.12 admissions per 1000 person-years, an increase of 8% (95% CI 5% to 10%) as shown in Figure 15. Compared with young people living outside London, the free bus travel intervention was associated with a greater increase in rates of assault in young people in London (relative change 1.32, 95% CI 1.25 to 1.40).
FIGURE 15.
Annual rates of hospital admission due to assaults in London compared with outside London.
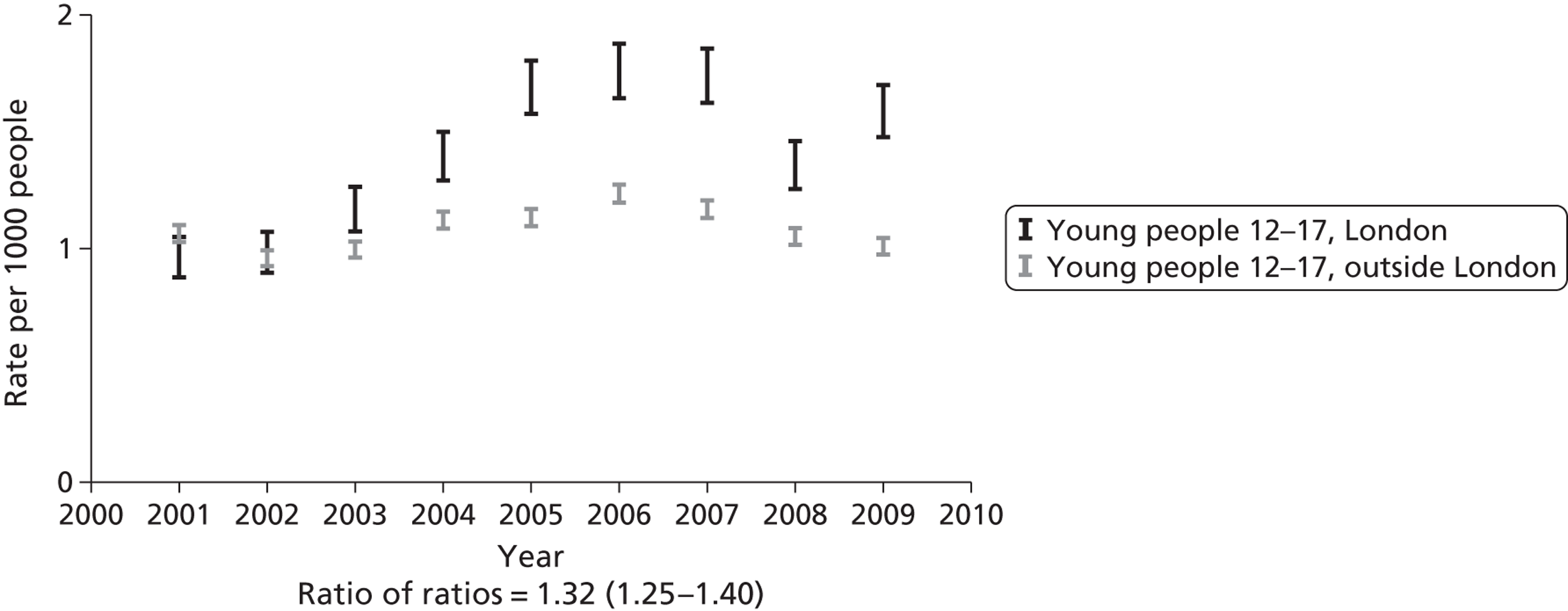
Free travel as a facilitator of risk management
Free bus travel was reported to have had an important role in allowing young people to ‘practise’ skills necessary to negotiate London’s bus network. Such skills were sometimes acquired by making ‘rehearsal’ journeys: journeys which, importantly, could be undertaken without any economic disincentive. For example, one girl described how when she first got her zip card she tried out ‘getting on the bus three times just to see how it worked – I just went round the corner three times and got off’ (YS, 12 years). Other young people described learning by initially making sure they travelled with someone who already knew the route:
Yeah, I know [my trip today to central London is quite far], but I know how to go somewhere when someone’s like shown me. I brought my dad up here and I followed Annie and my brother this morning.
Hav, 14 years
I feel so much more confident going by myself everywhere now . . . [but before] if I wanted to go to say Oxford Street to return something I’d be like to my friend, I’d be, ‘oh do you want to come shopping with me’ rather than just go and return it. But now I just go by myself, and I’ll be fine with it.
YS, 17 years
Thus, for many young people, the company of friends or family enhanced their sense of security on novel journeys that involved travelling further afield than their familiar, local area. Being able to do this without financial cost facilitated these rehearsals. For many, the fact that buses were free was also to some extent a safety net, preventing one being ‘stranded’ and providing a contingency plan if things went wrong:
When I came here to London I didn’t have free bus travel by that time [ . . . and] it actually limited me and didn’t allow me to go to places that I would actually go to when I had the free bus travel. For example, when you go out because since I still knew I can get lost easily, you know? If you have to pay for the bus it’s going to limit you from getting back.
YS, 14 years
Say if I go out, and it’s getting late, or if my original journey, say if the train’s cancelled, I know I can just get a bus. I’ve got it free, I can go a different route. Whereas if, say if I’d already paid for a train ticket, and then I was halfway through the journey and then the train stopped, and then I didn’t have any money, then I couldn’t go another route. So it’s like really important, I think, yeah, so security.
Hav, 17 years
The bus as a site of risk
If travelling for free helped young people develop their skills in independent travel, the buses themselves were to some extent also sites of risk. There were gender differences in how risk was reported. For boys, in particular, the most potentially harmful threat on buses is older teenagers: ‘like 18 years old, 16 years old’ (Hav, 14 years). Many talked in general about the types of incident which could ‘kick off’ on a bus, with arguments generated if disrespectful looks were perceived, or you were on a bus in the ‘wrong’ part of town:
Also buses are really easy place to get attacked, in our area there’s some gangs, and some of them live in different parts, and one day when I was on the bus one of the boys who lives in another part of town was on the bus, but in the wrong part, and a guy came on the bus with a bottle and started hitting him saying, why are you here?
YS, 14–15 years
Yeah, it’s one of those . . . things because say if you’re a girl and then you’re actually pretty good looking, the guys [will be] catcalling and stuff. Or if you’re a guy, yeah, and then you’re one of those alpha male guys, and then they’ll end up, you’re going to end up having a stare off or something. They’ll be, and it’s usually called screwing or whatever, looking at them funky, like neh, and then they’ll just be like, oh I’m watching you and then just start stuff. And then it’s just not really safe . . .
Isl, 15–16 years
For all secondary school-aged young people, whatever gender and wherever they lived in London, the most commonly reported risks were those of encountering those from other schools or neighbourhoods on the buses:
I’ve got people from other schools that stare at you because of what uniform you wear . . . and if you get on the bus that ain’t your school
It just gets awkward . . .
I don’t know, you just get glared at. And it’s more likely to trigger an argument, rather than getting on a bus with your school
Isl, 15–16 years
Typically, direct experiences recounted were of routine aggressive interactions between other teenagers. These were risky in that they had the potential for generating more serious incidents, but assaults were rarely reported as directly witnessed or experienced. Very serious assault incidents were usually only recounted as ‘moral tales’ that happened to (often unknown) others, and used in group discussions to illustrate the kinds of risks that one should be aware of, and which were ‘common knowledge’:
It’s actually been on the news that people were actually glaring at each other, a couple of people were actually glaring at each other and a fight broke out and someone actually died from it . . .
Isl, 15–16 years
Extreme stories relating to gun and knife crime, much covered in the media, were told as ‘the kind of thing that happens’ and a perceived risk, but were rarely part of the direct experiences of the young Londoners in this study. It is perhaps telling that in group interviews, such stories often had particular functions, such as to illustrate (often jokingly, as in the extract below) the dangers of neighbouring areas. Not quite urban myth, but certainly not a routine expectation of most bus travel, the limited direct visibility of knife and gun crime for most young people was illustrated by the ways in which stories were challenged by peers as atypical of bus travel in general, as in this brief exchange from a group discussion, which moved quickly from disbelief from two participants to joking aside about the neighbourhood of one participant:
I’ve seen a lot of dodgy goings-on on buses though.
Yeah.
Yes.
People get out guns.
What, whoa, sorry?
Qu’est-ce que c’est?
That was around Meadwell Bridge though.
What are you trying to say about Croydon?
It’s a sprawling urban mass of despair!
Sut, 14–18 years
For girls, fear of ‘perverts’ (H&F, 15 years) was a commonly mentioned concern, with stories of being followed by men from the bus reported across the boroughs. Again, despite the common knowledge of this as a risk of bus travel, few actual incidents of assault were reported. One exception was a girl who recounted being sexually assaulted (by other school children) during a bus journey, an assault which was reported to the police [(borough deleted), 15–16 years]. However, for many girls, buses were recounted as more secure than other modes of travel, particularly walking, after dark:
If it’s late at night time, probably around five or six . . . then depending on how it is around the estate and how I’m feeling I might jump on a bus, just to get past the estates. Yeah, just for the sake of safety.
Isl, 15–16 years
Boys also discussed avoiding certain areas, particularly after dark, but were more likely (particularly in one-to-one interviews) to suggest that buses were a riskier form of transport at night:
. . . but at night around [area], the main town is quite, yeah you, because you get all the people going to the clubs and stuff and it’s, it goes mental . . . because you get club people and gangs and stuff . . . I try [t]o be at home before it gets really dark too . . . [A]nd when you do get on the buses at night, because I’ve been to competitions . . . got back about 9, 10 o’clock at night and had to get on the buses you do find that you find some weirdos on the buses, which isn’t nice.
Hav, 15 years
Yeah, I would go on the bus but I wouldn’t go upstairs on a bus at night because I’ve had a few situations where there’s quite like dangerous people upstairs like . . . So I wouldn’t, I would definitely not go upstairs when it’s dark and I would want to get, say if I want, it is dark and I want to, and I need to get to a place, I would want to get there faster, so I wouldn’t take my time going upstairs and take my time getting downstairs, I’d get off bus straight home, finish.
Hav, 13 years
As these accounts suggest, although concern about potential assaults was common, in the main young people discussed their ability to manage these risks, rather than their vulnerability to them. Strategies for avoiding or mitigating the risks that were routinely encountered in travelling around London included avoiding certain places, or being outside alone after dark, but also adopting a ‘street wise’ deportment, which was essential for avoiding confrontations, especially with other young people. This entailed avoiding eye contact, appearing confident and knowing when to back down: ‘keep yourself to yourself, head down, headphones in’ (Hav, 14 years).
In terms of avoiding potential conflicts, many timed journeys to avoid other school’s leaving times, or covered identifying school uniforms if they were travelling alone. If you had to travel alone, personal stereos were useful for creating a ‘private space’ in which interaction was less likely to happen, and mobile phones provided some widely described risk management strategies: allowing the creation of the ‘social’ through real or pretend phone calls ‘so they do not target you’ (Sut, 15–16 years) or the use of a ‘fake call’ app to make the phone ring. Other strategies included speaking in non-English languages to arrange ‘escapes’ with friends (Isl, 15–16 years) and staying on the lower deck of the bus near the driver. The zip card, on occasion, was mentioned as reducing the level of risk associated with travelling – not just in ensuring that one could afford to get home (as above) but providing a free ‘escape plan’ of ‘just being able to jump on a bus’ to avoid risky situations. In short, although a few participants preferred to avoid buses altogether (or at particular times) because of the risks of aggressive incidents, and most considered the bus as a potential site of such incidents, in general the risk of assault was not a major factor in accounts of bus travel.
Managing risk: a source of pride and entertainment
One reason that these risks, despite causing some anxiety, were not reported as a deterrent to bus travel is that they are also a source of spectacle and entertainment. Dramatic incidents were often discussed humorously in group discussions, and in individual interviews (as above) young people stressed their skills in managing the risks. Encounters that could be unpleasant or risky were simultaneously an attraction of the bus journey, providing a source of potential entertainment and a fund of stories that served to create shared narratives of ‘us and them’. ‘Weirdos’, for instance, were often mentioned as a risk of a bus journey but rather than being necessarily threatening, these were sometimes known eccentric locals, who were part of the community, and, as noted here (following a discussion of the risks of bus use) they were explicitly part of the ‘fun’ of travel:
you do meet a few weirdos on the bus
Yeah
Yeah, that’s part of the fun
Like the dancing guy . . .
. . . He’s a local celebrity
. . . He’s like the wizard man! . . . singing to people on the bus
There’s so many people like that
Sut, 14–18 years
Indeed, in focus groups in particular, telling stories about interesting or unusual encounters on the bus, which may have been unpleasant or even frightening at the time, was related as part of the excitement of travelling, particularly with friends. The key issue of whether incidents were risky or entertaining was whether travelling was alone or with friends. Although choosing a particular mode or route was on occasion presented as a risk assessment strategy (for instance avoiding a park, or an area after dark), a major contributor to whether or not the choice was risky was the availability of peers to travel with, as we outlined in Chapter 3.
Conclusion
Road traffic injuries declined among young people relative to adults after the introduction of the free bus travel scheme. The major contributions to this decline were reductions in car occupant injuries and cyclist injuries. Pedestrian injuries in young people declined at a similar rate to adults. These findings are consistent with the changes in travel patterns reported in Chapters 4 and 5, which suggested a relative decline in distance travelled by car (see Chapter 5), a relative decline in distance cycled (see Chapter 4) and no change in distance walked among young people (see Chapter 4).
Quantitative evidence indicates a relative increase in assaults among young people in London compared with both adults in London and young people living outside London. However, there is some suggestion that much of the increase in assaults in young people in London occurred before the introduction of free bus travel in 2005.
For young people, the bus was a frequent site of conflict between different groups (schools, gangs, older teenagers), and a place where (reportedly, but rarely in their own experience) more serious incidents happened. However, bus travel was also recognised (particularly by girls) as safer than other modes of transport (especially walking) and most young people had a range of strategies at their disposal for managing the routine risks encountered. At the margins, free travel enabled ‘escape’ strategies, from both the worries of being lost, and (on occasion) the ability to just jump on a bus to avoid a troubling situation.
In summary, there is no strong evidence that the free bus scheme contributed to an increase in assaults in young people, and some evidence that the scheme is associated with a decrease in RTIs, reflecting the transport mode changes following its introduction.
Chapter 7 Has the scheme reduced social exclusion? The impact on participation and independent travel
Introduction
Social inclusion is fundamental to well-being, and transport access is increasingly recognised as important to social inclusion in settings such as London. 63,80,113 Differential access to transport is one of the ways in which health inequalities between people and places are generated,5 and age is one social factor that influences the risk of ‘transport exclusion’. In the UK, for instance, the Social Exclusion Unit (p. 2)114 cited transport-related problems as restricting young people’s capacity to take up education or training opportunities. Young people’s exclusion from participation has been variously conceptualised as arising from immobility,115,116 disempowerment98,117 or dependency on adults for transport. 67,118,119 An explicit policy aim of the free bus travel scheme was to increase access to education, training and other opportunities for young people – aims which have significant potential to enhance future public health and address one contributor to inequalities in health.
However, measures of ‘social inclusion’ are problematic, in that this is a multidimensional concept that is inherently difficult to operationalise. 80 We had no direct measures of changes in dimensions of ‘inclusion’ which might be important, such as ‘participation’ or ‘access to social networks’. Furthermore, outcomes which may be causally related to inclusion, such as changes in participation in training or education, are likely to be casually distant from an intervention such as free travel. We therefore used the travel diary data to provide some evidence on one proxy measure: how the number of trips made by young people to work or school changed relative to adults after the intervention. Additionally, we looked specifically at distances travelled by level of deprivation after the intervention to see if there was any evidence that impact of the scheme changed social gradients in this measure of participation.
The qualitative data analysis provided evidence on the salience of transport exclusion in young people’s current travel decisions, and the ways in which the free bus travel scheme was used in fostering independent travel and access to a range of goods and services that are essential to social inclusion.
Quantitative evidence on participation and inequalities in participation
In the absence of direct markers of social inclusion, we analysed data on the frequency of journeys by all modes during the week, and on the socioeconomic gradient in distance travelled by all modes by purpose of journey.
Frequencies of journeys
The frequency of journeys per day to/from work or school on a weekday in the 12- to 17-year-olds age group was slightly higher after the introduction of the free bus travel scheme for young people (relative change 1.09, 95% CI 1.06 to 1.14), whereas that in the 25- to 59-year-olds age group declined: ratio of change in the 12- to 17-year-olds age group compared with the 25- to 59-year-olds age group was 1.19 (95% CI 1.13 to 1.25). In contrast, the frequency of all journeys in the 12- to 17-year-olds age group was unchanged in absolute terms and relative to that in the 25- to 59-year-olds age group: ratio of ratios 1.00 (95% CI 0.97 to 1.04) (see Appendix 9, Table 34).
Distances travelled by level of deprivation
We also examined whether or not there had been any change in the distances travelled by young people by level of deprivation and purpose of journey before and after the intervention. Figure 16 shows trends in distances travelled by young people for education, entertainment, personal business and shopping pre- and post-intervention by decile of IMD. The figures generally show no clear evidence of diminution in socioeconomic gradients following the introduction of the free bus travel scheme for young people. Nevertheless, the patterns were suggestive of a flattening in the gradient for travel for shopping (at an overall slightly lower level post-intervention; p-value for change of slope with IMD was p = 0.024).
FIGURE 16.
Distances travelled by young people according to journey purpose by decile of IMD, pre- and post-introduction of the free bus travel scheme (a) Education; (b) entertainment; (c) personal business; and (d) shopping.
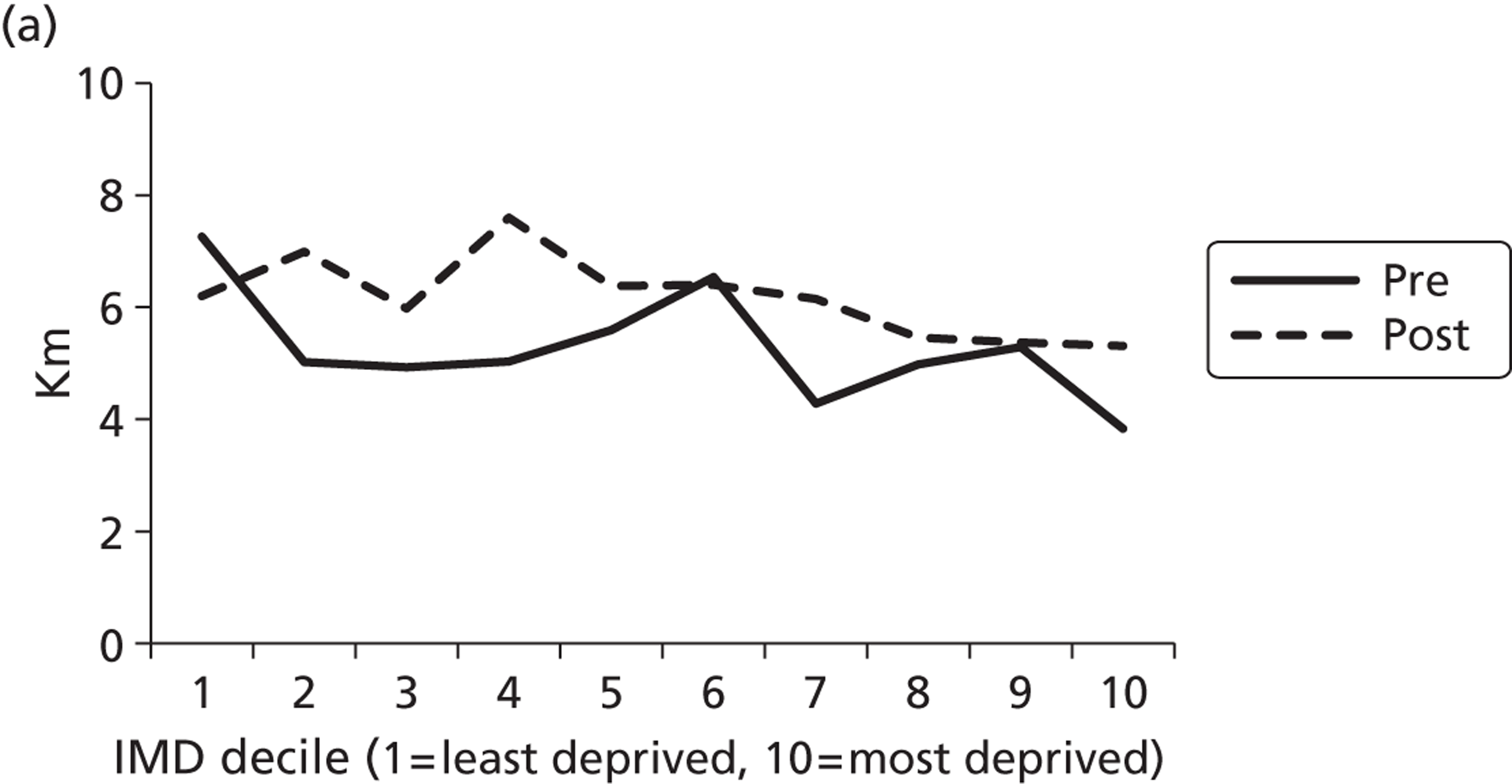
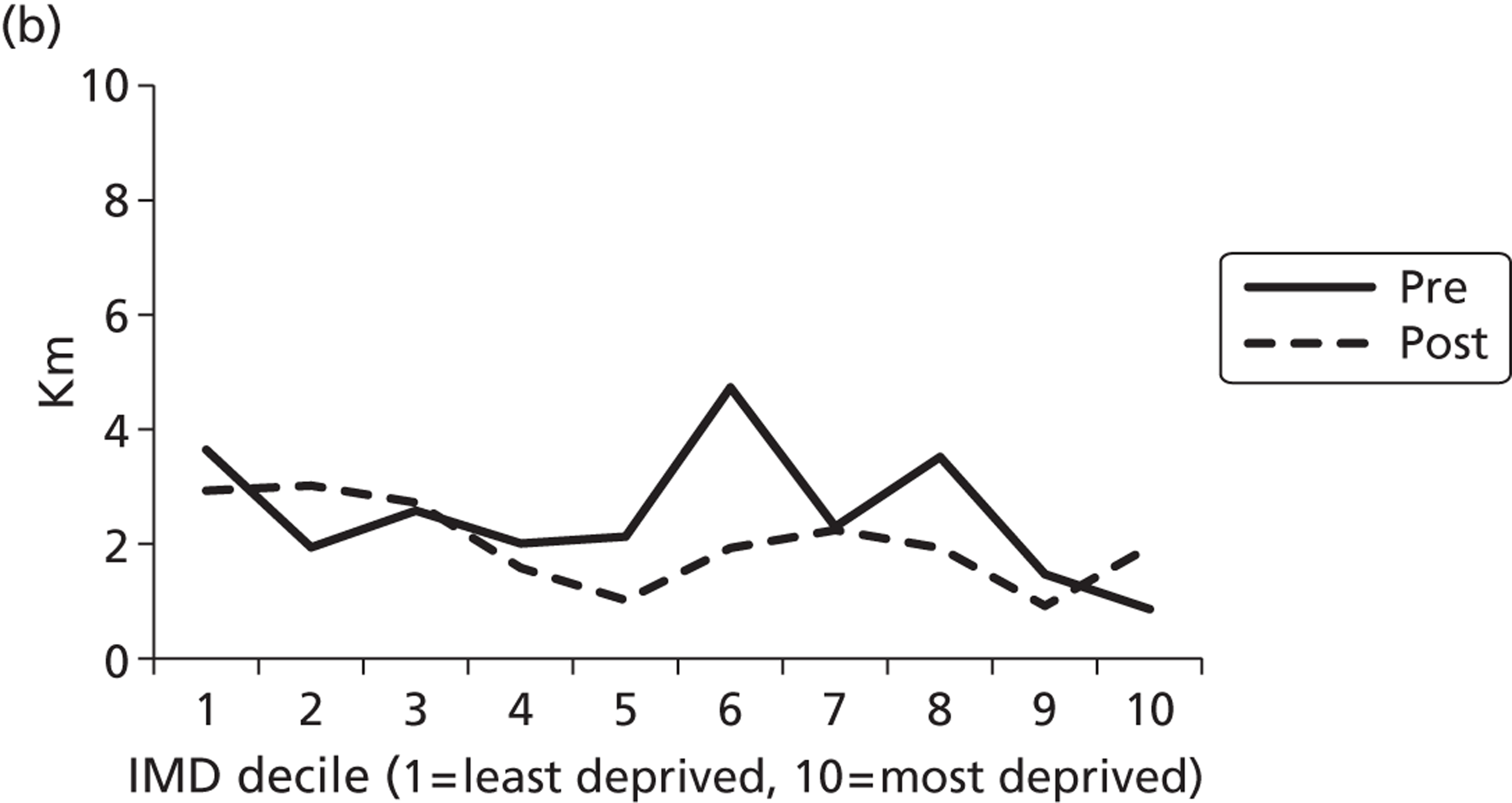
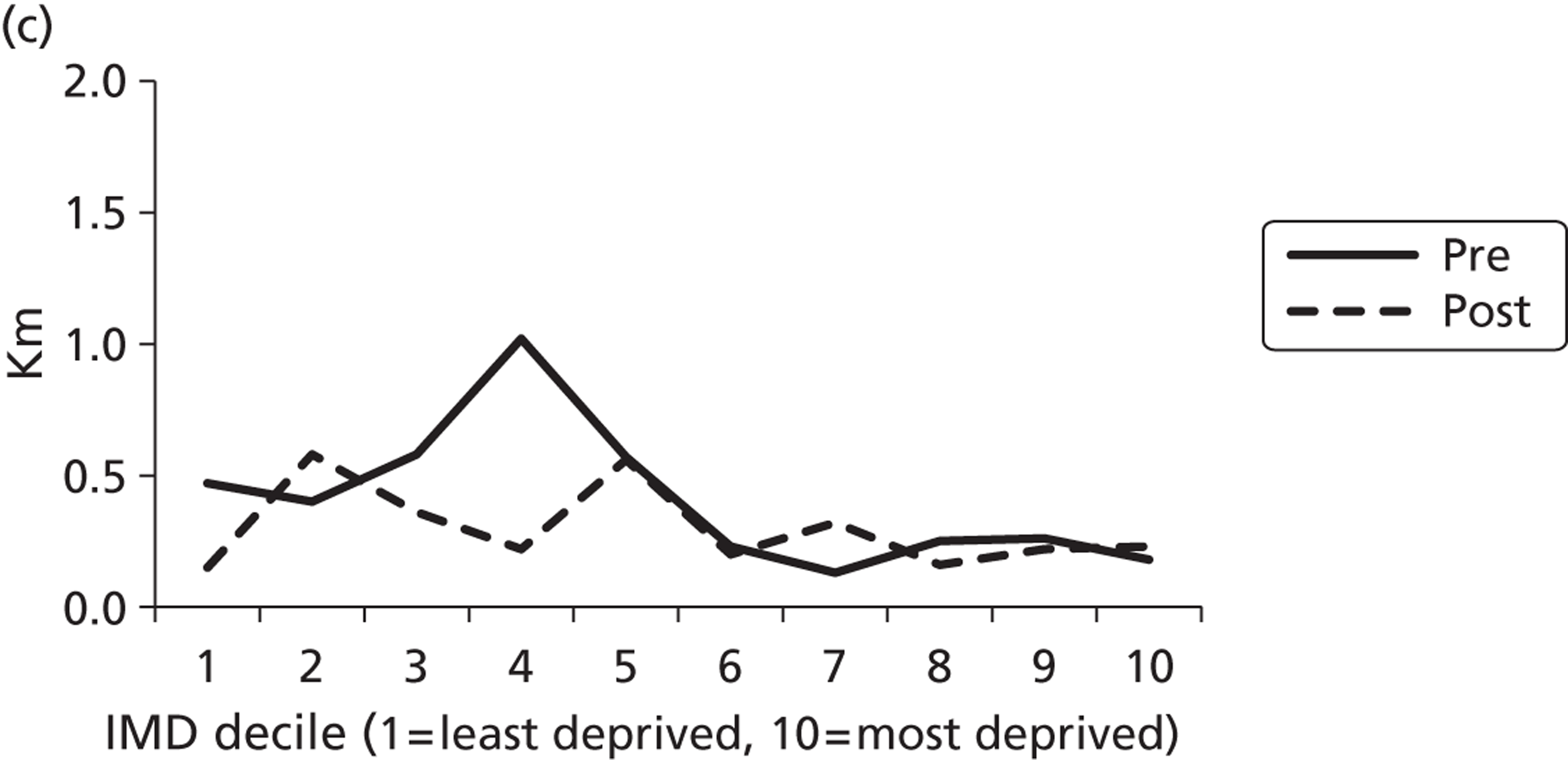
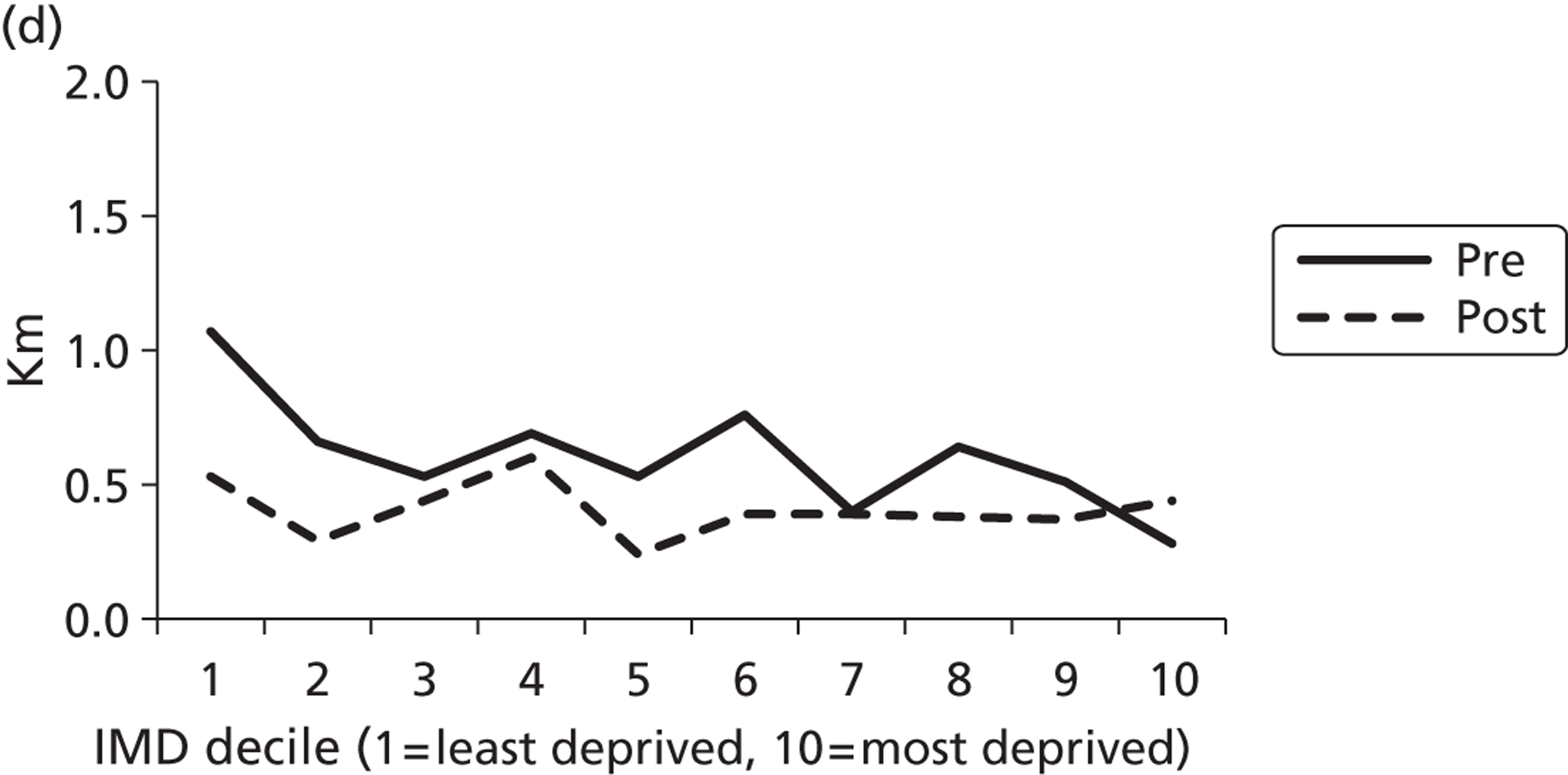
Zip and social inclusion
Qualitative evidence suggested that universal free bus travel for young people removes one barrier to social inclusion: that of transport costs. The intervention was reported to have facilitated participation through making some journeys financially accessible, at least at the margins. Although most young people were not explicit about the ways in which this happened, there were a few comments on how free bus travel offered opportunities for access to sport and leisure:
The local sports centre near me is, we’ve got to get a bus to get to it. So my brothers do that, and my mum takes my sister because they have like that little baby club thing there. So if a bus, the price went up, my mum wouldn’t take my sister to the little clubs where she can meet other little kids. And my brothers probably wouldn’t go to the gym at all.
Sut, 15–16 years
For some, free travel did make a reported difference to family budgets, not only for those in the poorest groups, but also for those whose families nevertheless struggled:
My mum’s lost her job and stuff, so it’s difficult for her. [For me to take the bus] doesn’t cost my mum anything, and it just helps her out.
H&F, 12 years
I don’t think that’s fair because personally in my family, which you guys wont repeat, my dad’s only bringing in one income and my mum’s not working because she’s looking after [siblings] at home. And she’s got me and Callum to look after as well. So because my dad’s bringing in probably, I don’t know, probably about 1000 over the limit that it’s supposed to be, or however much over the limit, I’m not entitled to get EMA, free school meals, and if it was, free travel. But we’re still struggling so it’s not fair how it is.
Isl, 15–16 years
Notably, the instances of increased opportunity of access recounted were often group-based activities, with the intervention enabling families to more easily afford to go on outings:
When I was younger because my mum was pregnant at the time . . . me and my dad used to go up London because it was free for me . . . We used to go the Science Museum and things like that . . . so it was quite fun.
Sut, 13–16 years
To some extent our data generation method (with most young people interviewed in small groups) perhaps discouraged disclosures of the financial impact of free travel for less well-off young people. The young person above, for instance, prefaced her account of the difficulties their family would have without the fare concession with a plea to other interview participants not to repeat her circumstances outside the group. However, the fundamental impact of free bus travel on social inclusion was evident in the taken-for-granted nature of inclusion implicit in young people’s responses. Across the data set, at every age, in outer and inner London, young people’s accounts suggested their independent access to both local and more distant destinations by bus was an absolutely routine expectation: a normal and unquestioned entitlement.
I just get two buses to school, and on the weekends same, I just get the bus anywhere. Like sometimes it can be far like the West End, or not, it could just be like [local high street] or something.
Sut, 15–16 years (emphasis added)
In this respect, transport-related exclusion due to financial factors was notably absent as a salient concept for the participants in this research. Indeed the taken-for-granted nature of being able to afford to get anywhere is perhaps indicated by the rather extreme response of one participant (echoed less succinctly by others), who told us that if she could not use the buses for free she ‘wouldn’t come to school’ (H&F, 15 years). Across the boroughs, young people emphasised the ease of getting around, and indeed the range of sites that might be visited by bus:
I normally go [by bus] just to go to school, go see family.
Probably the same thing, [I use the bus to] go to school, see family. Probably get the bus to football match, Regent’s Park, Camden.
I get the bus to school and my cousin’s house.
I get the bus to school and other activities. I go to music classes . . .
I normally get the bus everywhere,
Isl, 12–13 years
[T]hat’s [fare exemption] really helpful, whenever I really need to go anywhere it’s just, it’s no hassle
Sut, 14–18 years
The importance of the intervention in facilitating the ability to travel without restriction (‘no hassle’) is perhaps evident in the fact that, for most young people, the only accounts of limitations in mobility came from reports about those who had no zip card to prove their entitlement:
[T]he day I was robbed I lost my Oyster. I had a missing [glasses] lens . . . buttons ripped off my shirt and a bruise on my face. And then I tell him [the bus driver] I don’t have my Oyster, I got robbed, and he’s like ‘I’ve heard all these excuses . . .’ and he was actually swearing at me . . . and then he kicked me off
Isl, 15–16 years
Another participant had had his right to free travel rescinded by TfL (as part of the ‘Behaviour Code’ penalties introduced in relation to some travel concessions for young people120):
[W]hen I didn’t have [free bus travel] I did struggle in terms of not getting everything done because I didn’t have that freedom to get on a bus
H&F,12–17 years
Similarly, one young man noted of four friends who had their passes taken away: ‘It puts a strain on their social activities because they can’t go out as much’ (Hav, 15 years).
Social inclusion: the importance of transport access for discretionary journeys
As one young man put it: ‘with my free travel I always explore places that I didn’t even know were real’ (Sut, 15 years). He gave an example of a trip to a distant part of London with friends to a vintage clothes market they had heard about in a popular TV programme. As several participants explained, this role of free bus travel was particularly important for such social or recreational trips because these were not ‘necessary’. Such trips were therefore most likely to be abandoned if bus travel were not free:
[Without free bus travel] I think that under-sixteens would only go to places that they thought were really necessary like school [ . . . but] I think they would stop going to places like the park. [ . . . ] If it were a park that was far away I would go there less often if I had to pay.
YS, 15 years
Such discretionary trips were highly valued, providing opportunities for young people to travel together, and to participate in social life, and to travel independently of parents. This ‘independence’ was not framed solely in terms of travelling without parents, but also as travel that did not entail reliance on parents to either transport or the costs for transport:
[Free bus travel] is good, it’s really useful. It gives, at this age especially, it gives us more independence to do what we want, especially on buses [ . . . because] if it was too expensive we’d probably end up getting our parents to drive us everywhere which would be a real problem, so.
I think at this age it’s really important to have that because we need to learn about the world or London now sort of thing, and how to travel by ourselves.
YS, 12–13 years
Social inclusion and independence
Linked to this sense of independence is the equality of opportunity that free travel had provided all young people in London to experience the city, and develop their growing sense of the world and their place in it, providing, as one put it, ‘A sense of freedom’ (Sut, 16 years). New journeys provided opportunities for young people to test their skills in planning and managing the unexpected. For the work experience students included in the study, the trip to the LSHTM was a good example. When asked, they reported a variety of methods for preparing for what was a ‘new’ journey: using Google Maps, TfL journey planner and ‘common sense’ to find new routes.
For all participants, access to free travel meant young people were better able to explore London, and develop an understanding of the city’s geography without fear of ending up somewhere with limited means to return to known parts of the city:
When we [my friends and I] was in London we just saw a bus that was going to, we was by Trafalgar Square . . . and we saw the buses that, is going towards Oxford Street, didn’t know exactly where it was going . . . and, and we get on it, we’re lost, see, see where we end up . . .
[ . . . I]f you didn’t have the bus pass, like would you, would you have gone up to Trafalgar Square if you didn’t have it, for example?
Yeah. We, we would’ve walked, but it’d probably taken us like an hour so we might not have got round to Oxford Street probably [ . . . ] The amount of time it takes.
Hav, 14 years
This is not to say that prior to the introduction of free bus travel young Londoners only made ‘necessary’ trips or did not experience themselves as becoming more independent. Indeed, several participants said that it would not affect their travel behaviour if they had to pay. Others, however, described the zip card as making a real difference at an age when you may have a parental permission to travel by yourself, but prefer the company of peers than travel ‘alone’:
The good thing about free travel is that when you’re old enough to be able to get places your own, your parents don’t take you, [ . . . you’re still] not going to be employed because you’re in fulltime education. And you might actually be at that stage where your parents give you a certain amount of money or no money and you have to use that money to get, to do what you want to do. And then you’re old enough to want to go to the cinema every weekend and see your friends and just get out of the house and if you can’t afford that then it is a little, it’s annoying.
Sut, 18 years
These benefits for independent mobility did not just apply to those with limited family finances. Rather it was raised by participants from a range of social backgrounds, as well as by both genders and by participants from across London. The benefit arose not simply from the removal of financial barriers, but from access that did not require parents to fund it. Importantly, even families with better resources might be unwilling to subsidise discretionary journeys: ‘That’s the only trouble, you don’t, it’s not essential that you get travel and you get to where you want’ (YS, 14 years).
Fostering ‘belonging’: zip cards and citizenship
Through its fostering of wider-ranging travel, the intervention contributed, for some, to a sense of ‘belonging’ to London as a community and of ‘being a Londoner’. For young people, often aware that their concession was unusual to their city, this sense of belonging was at times explicitly framed as having an effect on well-being through fostering pride:
It [the zip card scheme] . . . makes you feel proud [to be a Londoner] because you’re at the front of everyone, because you’re the ones who have brought in these new schemes that are working and making your life easier . . .
And also you have this mutual understanding of [being . . .] a Londoner, you’re the same as me now . . . And there’s . . . this sense of community in this huge, huge [city.]
Sut, 15–18 years
There was an awareness that this was a benefit not enjoyed by peers outside the capital, with one focus group participant describing how her ‘cousin [who] lives really far away . . . just wishes she could have more buses and the free travel . . . to get around more’ (Hav, 14–15 years). Beyond the pride in having a scheme that was innovative, and marked their unique city, the zip card enabled participants to ‘know’ a larger geographical area than would otherwise be the case. We have already outlined in earlier chapters the ways in which young people made excursions to the city centre and other parts of the capital. Many of the young study participants, in particular from the outer London boroughs, would recount exploratory bus journeys they had conducted ‘up London’ or to ‘the West End’, and those from all boroughs talked about the ways in which bus travel had opened up other parts of the city:
Mostly every Saturday we’ll probably just jump on a bus because we have a free [pass] and go anywhere, and get another bus from there, and another one. And we just travel, we don’t know where we’re going . . . [once] we ended up near Hammersmith, and near the West End
Isl, 16 years
I think if you get the bus a lot you can try and, like, vary it [the routes you take] up so you get to know London
Isl, 12–13 years
Concessionary bus travel, that is, affords young people a topographical engagement with their urban surroundings which enhances their familiarity with the city by rendering them ‘more aware of where you’re going, how to get to places’ (F, YS, 14–15 years), and a number of young people explicitly welcome the opportunities they had to not only ‘get to know’ or ‘learn about’ London by travelling widely in it, but also feel that they ‘belonged’ as citizens. As one young person put it:
I like it [having the zip card] because you feel kind of unique . . . and it’s only in London. [Y]ou can travel around London because you’re a kind of a Londoner, but other people can’t.
Sut, 17 years
Social exclusion: young people with disabilities
Although financial barriers did not exclude young Londoners from travel in the city, this does not mean that the transport network was universally accessible. Young people with disabilities faced a number of problems in using buses, and transport exclusion was a key issue for them. For those using wheelchairs, limited space on the buses meant that only one could be accommodated at a time. This made it impossible to travel with friends if they were also using wheelchairs. Given the importance of travelling together, and for the journey to be part of the outing, outlined in earlier chapters, this is a real limit on social inclusion for young people.
Across three interviews with young people with disabilities, including six young people, only one person said they preferred the bus, because of the challenges of finding somewhere to park (even with a blue badge). The young people with disabilities used Freedom Passes, rather than zip cards, to access public transport (see Appendix 1). Notably, in contrast to the zip cardholders, they did not report any bus journeys as entertaining outings in themselves. Also in contrast with their more able bodied peers, who talked of bus travel as ‘no hassle’, and could recount a number of positive aspects of bus journeys, for young people with disabilities, buses were generally experienced specifically as ‘hassle’, and a barrier to participation, rather than a route for enacting participation. Journeys themselves were liable to be inefficient, as the wait for a bus with room to board might be long, and at times embarrassing, given the frequent problems with the wheelchair ramp:
Some ramps don’t tend to work, so that’s a bit of a hassle . . . sometimes it’s dangerous with an electric chair, it’s heavy . . . I just think the bus driver should check the ramp is working
O, > 16 years
In addition to the practical problems encountered (e.g. difficulties in seeing the visual destination display from the wheelchair space; not being able to see outside on older buses, with their high windows), some had experienced a lack of consideration from other passengers and drivers. One example came from a young man with epilepsy, who recounted how when he had had a seizure on the bus:
. . . people completely ignored my pleas for help. The driver drove on as if nothing was happening
O, > 16 years
Free bus travel was not, then, a sufficient condition for transport inclusion in the absence of accessible transport.
Conclusion
The quantitative evidence suggests some increase in travel for work or education among young people in London relative to adults. The scheme also appears to have influenced the travel of young people for education, entertainment and personal business in a relatively similar way across areas of deprivation.
The qualitative analysis suggests that financial barriers to transport were not an issue for young people in London. As we have no historical data to compare, it is impossible to attribute this specifically to free bus travel, but it seems likely that free and – crucially – universal free bus travel, in the context of a reasonably accessible transport system, meant that for most young people, lack of ability to pay did not restrict their mobility or their opportunities to be independently mobile in their neighbourhoods and in the wider city. The exceptions (those with no zip card; those with disabilities) support this interpretation.
Although social inclusion was explicitly tied in the policy aims of this scheme to access to education and training, our qualitative data suggests that a more salient aspect of the scheme for many was the enhanced access it provided to discretionary journeys. These were important journeys in terms of enabling participation in social life for young people, but parents may be less willing to pay for discretionary travel. In summary, there is some evidence that the free travel scheme promoted access to education and training for young people, and good evidence from the qualitative data that it fostered social inclusion and independent travel for those young Londoners able to access the bus network.
Chapter 8 Has the scheme displaced older people from the buses?
Introduction
One policy concern was that older citizens, in particular, would be displaced from the bus network if numbers of young people using the buses increased, either because of overcrowding or through ‘fear based exclusion’. 17,18 Older citizens also receive free bus travel, and in London a ‘Freedom Pass’, paid for by the London boroughs. Until April 2010, older people with their principal residence in London were eligible for a pass at the age of 60 years entitling them to free travel on bus, London underground and tram services within the capital, without time restrictions, and rail services at off-peak times. Since then the qualifying age has been increasing in a graduated way, and will become 66 years by 6 October 2020. As older citizens are also vulnerable to transport exclusion, with a consequent impact on their well-being,121,122 one potential negative effect of young people’s increased access to bus travel might be a reduction in their ability to use buses.
We used the travel diary data to explore whether there was any evidence that older people were in general using the bus less, or were specifically displaced from the network at times when young people were more likely to be using it (i.e. during peak school journeys times). We also explored older citizens’ accounts of using the bus to explore how far the presence of young passengers affected their uptake and experiences of bus services.
Quantitative evidence on impact on older people’s bus use
Trips by bus as a main mode
Before January 2009, older people could not use their Freedom Pass before 9.30 a.m. in the morning, so we restricted the analysis of impact on older people’s travel to the afternoon school travel hours (i.e. 3 p.m. to 4 p.m., Monday to Friday) to assess any evidence of displacement. The average number of bus trips per older person per day remained at around 0.06 per day pre- and post-intervention. At other times of the day the average also remained constant pre- and post-intervention (around 0.36 bus trips per person per day). The introduction of free bus travel was not therefore associated with a change to the average daily number of bus trips made by older people (relative change 1.07, 95% CI 0.91 to 1.21) (see Appendix 9, Table 35).
Distance travelled by bus
The average distance travelled by bus by older people remained constant during school travel hours at around 0.25 km per day, and at other times of the day it remained constant at around 1.2 km per day (relative change 0.95, 95% CI 0.80 to 1.11) (see Appendix 9, Table 35).
Short-distance trips
The proportion of short trips (i.e. < 1 km) made by bus by older people during school travel hours increased from 7.1% to 8.4% of all trips; however, this was not statistically significant (19% increase, 95% CI 47% decrease to 65% increase). The proportion of short trips made by bus at other times of the day declined from 7.3% to 7.0% and, again, not statistically significant (4% decrease, 95% CI 20% decrease to 14% increase) (see Appendix 9, Table 35).
Older citizens’ accounts of sharing the bus network with young people
Some older people voiced a degree of disapproval of free travel for young people. This was based on a perceived ‘unfairness’: the Freedom Pass benefit was associated with a ‘reward’ for working hard all their lives, something young people had not yet done. 123 There was also a sense of temporal unfairness, with older citizens noting that they had not benefited from free travel when they were young themselves, or when their children were young. Some also expressed a dislike of young people ‘abusing’ the privilege, by jumping on and off the bus needlessly:
Look how long we waited to get our Freedom Pass. Then these youngsters got it straight-away haven’t they?
Sut, 80–84 years
Well I used to have to walk to school. They’re not now, they get on for two bus stops.
Yeah.
And what are two stops? . . .
Should use their legs.
H&F, 75–84 years
However, on reflection, many considered that free travel for young people was a socially useful benefit, with advantages to young people and their families:
But what if they’re young people who want to maybe go and see their old granny at the weekend or go and do her shopping in the evening?
Well
Yeah, it’s a difficult one really.
Debatable, isn’t it?
Yeah.
But basically it’s supposed to be in education, isn’t it?
Isl, < 65–80 years
It helps the parents especially now that things are a bit tight. I do believe they should.
H&F, 70–74 years
Older people were, then, not particularly positive about the free fare concession for younger people in general terms. What was notable, however, was not the range of opinions on whether or not young people should have free bus use, but that this disapproval of the zip card scheme was never couched in terms of young people displacing them from the buses. This is not to say that there were no complaints about behaviour on the buses: indeed, some older citizens did report finding younger passengers on the bus network intimidating, and a few reported having changed their behaviour in response to the noise, crowds or jostling of school children on the buses:
Well you would have near enough got a seat straight away. Now you don’t. They’re so busy shouting and drinking and, because they all bring these bottles of stuff with them and talking to each other about what they’re going to do and on their mobiles as well, that they just don’t take any notice of you. And they’re, they’re in the way as I say, these great big pack bags, you can’t get past them at all. It does spoil your journey really.
Sut, 80–84 years
I don’t go out when the children are coming out of school.
H&F, 74–85 years
I think that most older people like me, over 60s, think the same as I do, that they’re gonna wait for the 9.30 because the rush oh, the rush hour’s over by then. And they can go whenever they wanna go
Isl, 70–74 years
However, more typically, there was a general tolerance of the behaviour of young people, and even in instances of (as above) ‘discomfort-based’ displacement, these were reported to result in changed, or less pleasant, rather than abandoned, journeys. There were very few reports of fear-based exclusion from transport. Despite many not enjoying travelling on buses used by school children, most pointed out that the noise and jostling was what one might expect from excited young people. Crucially, there was general agreement that this did not put them off using the services.
So it’s not something you think it puts you off using the bus because there’s children . . . ?
Oh no, no, no, no
No, no.
No, no, never, we never think you know sometime you just, most of the time it happens so we are at that time about three o’clock, between two and three is when they come out, four they come in. But it doesn’t matter it’s a day . . .
It doesn’t bother us really us no, no.
It doesn’t bother us.
H&F, 70–79 years
Probably we done it when we were kids but we don’t notice it you know
It’s high jinks isn’t it? It’s high jinks more than, we’ve never been involved in anything any time on the bus where there’s been
Trouble
You know a stabbing or something like that or somebody’s got beaten up. They seem to interact with one another, boisterous but not vicious.
Isl, 70–74 years
Indeed many older citizens, from all boroughs, reported general civility from younger people, who would offer seats and allow them on first:
Yeah, I must say, another thing, following what M2 said, I find the young people tremendously
Helpful and kind.
Willing to get up and give you their seat.
H&F, > 90 years
Because you’re standing at the bus stop with hundreds, it seems like hundreds of girls screaming around you, the bus pulls up, they are polite, they do at least let you go first.
Sut, 70–74 years
Young kids you’d think wouldn’t let you off, but in fact I generally find, they may not be terribly nice to each other but to old, what they regard as old people they’re quite good I have to say. Another example we were riding a bus quite late when we, 7.30, Ann and I were, and there were some young lads kicking the bus shelter. We didn’t think this was the best place to be. When the bus came in they stood back and said, oh no, after you. You were first . . .
Sut, 60–69 years
In part, the lack of reported displacement or explicit conflict with school children resulted from a normative assumption that school-aged children and older people used buses at different times and in different ways. Specifically, apart from avoiding school journey times, older people reported rarely using the upstairs of double decked buses, or the back of single deck buses:
Well I can’t say I have been on buses that often when schoolchildren, when youngsters have, but occasionally I do. And yeah, sometimes they’re a bit noisy and so on but then I would probably go downstairs if they’re all rushing upstairs.
Sut, 60–69 years
And would you ever go upstairs?
Oh no
No?
No. [Laughter]
Is that because of?
It’s not because of the children it’s because I can’t be bothered walking up the stairs
I just don’t bother about going up, if I had to go upstairs we’d have to but we never ever go up there we’d rather stand
Isl, 70–74 years
The reluctance to use the upstairs of the bus reflected a consensus about where and when was a reasonable and comfortable time and way to travel, with older people avoiding the school run times, and the places on the bus where young people preferred to sit (upstairs, or downstairs at the back). These preferences were, as in the quote above, rarely attributed to intimidation, but rather to decisions about maximising comfort and convenience. They also, of course, became part of a culture of expectations about where and how to travel, with ‘taken for granted’ nature of the division of space and time according to age on the buses evident in the fact that breaches of the norm were often a source of amusement:
If I’m out at the weekend with my friend, if we’re going say to Kingston, we’ll go upstairs on the bus. [Laughter] We behave like kids.
Sut, 70–74 years
I will pick my, grandchildren up, sometimes . . . And they always want to go upstairs [general laughter].
Isl, 65–89 years
Data from young people reiterated these normative expectations about the arrangements of seating on the bus (what one young person called ‘the segregation’):
[T]he reason why I’d go on the top deck [is] because sometimes the bottom’s really congested yet there’s so many seats available on the upper deck . . .
And that’s why . . . most children are on the upper deck, more seats for the elderly and adults down on the lower deck . . .
[Y]ou’re doing it so there’s more space at the bottom deck for the elderly and that.
Sut, 13–16 years
Older citizens’ choices of when to travel were, then, largely rationalised as made for comfort and convenience reasons, and the expectations of where different passengers preferred to sit were in general shared by younger and older passengers. There is little sense of ‘exclusion’ based on fear. Furthermore, if ‘discomfort-based’ exclusion from certain journeys, such as school run times, was an issue, this was as likely to be generated by the desire to avoid crowds of commuters as young people.
I would avoid the peak times, if I can
[noises of agreement]
And, um, in the morning when everybody’s rushing to work. I mean we’ve been there [we’ve worked], we know what it’s going to be like.
Yeah, yeah [laughing]
And, um, coming home times if you can avoid them
And I, yes
And I think, and I, I do try to avoid the school bus.
[General agreement and laughter]
And you see loads of us have got all day, we, we, we know the times to go, you know
When the school get out.
Isl, 65–89 years
Indeed on occasion, children were overtly preferred as fellow passengers:
Yeah, yeah, between the office mob and [the young people] . . . if I had to choose who to travel with I’d choose the school boys . . . I used to avoid, um, travelling early in the morning, because obviously people are going to work and, and they’re all sort of focused on going to work, so they, you know, there’s no give-and-take then. And I would avoid school runs, obviously, and then the same in the evening. But now, in between, you’ve got these mums, as well . . .
Isl, 70–74 years
Avoiding rush hour commuter and school travel meant that older people were more likely to be in conflict over space and seats on the bus with other adults, and specifically (in the accounts we have of displacement) parents with young children, particularly those with large pushchairs. Indeed, the final comment in the quote above is typical in that the most likely conflicts over the space on buses reported were around the space reserved primarily for wheelchairs or pushchairs, which was typically near the more accessible seats at the rear door, simply because those using them tended to travel at the same times of day as older travellers and be ‘competing’ for the same restricted space. These conflicts were often reported with vigour and irritation:
And do you know that bus driver . . . came up to me, and asked me to get out of my seat and give it up for the lady with the buggy. He wouldn’t move [the bus] off until I got up off that seat . . . I got off the bus because I was like [gestures angrily with clenched palms]
Isl, 65–89 years
This is in contrast to the tenor of reports of conflicts with younger passengers, which had a sense of routine disapproval, but rarely anger. Indeed, rather than being a source of comment on fear or risk, stories of encounters with younger travellers, particularly children, were often used in interviews as a way of demonstrating strategies for dealing with potential difficulties. Older passengers were clear that they could ‘manage’ conflicts, and were not intimidated by the crowded and on occasion confrontational bustle of a busy city. This woman, for instance, talking of how difficult it can be to board a bus in the mornings, goes on to say that she personally has few such problems:
But I can get to the front of the queue quite easily.
Laughter
OK, what tricks do you use to get to the?
Shopping bag. Well you have, you have to. But I notice we all use the same techniques and the bus drivers are very good. If they see an elderly woman there and all these children they come right where the elderly person’s standing.
Sut, 70–74 years
This ability to ‘manage’ and the strategies used to negotiate access to their rightful place in the queue or a seat on the bus meant few older participants reported limitations on their ability to travel that resulted from other passengers. Typically participants ended comments about rowdiness or unpleasantness from young people with a comment asserting that they (if not necessarily other people) were able to cope:
Yeah, yeah young people it doesn’t really stop you going anywhere or whatever
We go wherever we want don’t we?
Yeah that’s right.
It doesn’t stop us.
Isl, 70–74 years
This is not so say that managing such navigation and the potentially difficult interactions with other bus users was necessarily pleasurable. Some participants did report limited, or decreasing, confidence in using the bus service, and talked of avoiding certain routes or times of day. 124 Indeed, a number talked of the challenges of access as physical impairments began to limit ability to stand, or balance on a moving bus. However, the presence of larger numbers of young people were not reported as a significant cause of anything more than unpleasantness, and even stories of challenges had some positive implications for older citizens’ self-esteem simply because they provided opportunities to both exercise, and then account for, valued agency in the world, as a competent, coping and even ‘hardy’ traveller. The presence of young people on the buses might be a reason for avoiding the school run if possible, but so was the presence of large numbers of other travellers. It was never given as a reason for avoiding buses.
Conclusion
We found no quantitative evidence that older passengers had been ‘displaced’ as a result of the introduction of free bus travel for young people, and our qualitative data provided further evidence that displacement due to overcrowding or fear was not a major issue. Our qualitative data may have underestimated the impact of young people on older people’s travel behaviour simply because we are less likely to have included older people who did not travel, and we therefore may have missed examples of fear-based exclusion. However, the older citizens who participated came from a range of backgrounds and settings, and were in general articulate on their complaints about other passengers, and about young people’s entitlement to free travel. What was notable was the lack of any overt complaints about young people making them unwilling to travel, in comparison perhaps to the more open commentary on the unpleasantness of conflicts with other passengers. This is largely because older citizens and zip card users are not competing for the same ‘space’: older citizens preferred different seats on the bus, and tended to avoid times of day when young people (and commuters) are using the buses anyway.
In summary, there is no evidence that free bus travel for young people had an impact on older people’s travel behaviour or, therefore, the travel-related determinants of their well-being.
Chapter 9 Does the scheme represent value for money?
Aim and perspective
This chapter describes the methodology and results of an economic evaluation of the free bus travel scheme. The aim of the economic evaluation was to determine whether or not the intervention ‘free bus fares for 12–17 year olds’ represents value for money if we take public health effects into account, by comparing two alternative scenarios in terms of their costs and outcomes. These two alternative scenarios are:
-
Scenario 1 – do something – the bus network is free for 12- to 17-year-olds.
-
Scenario 2 – do nothing – the bus network is not free for 12- to 17-year-olds.
Before free bus travel was introduced in 2005, secondary school-aged children paid a reduced flat fare for journeys on the London bus network. Therefore, we assume in scenario 2 that the target group, 12- to 17-year-olds, are charged half the adult fare. Although scenario 1 can be observed in recent years since the intervention, scenario 2 requires that a counterfactual be created; describing the state of the world if the intervention could be removed. This is a standard requirement in ex post evaluation.
In terms of determining the impact of the policy the research has utilised the methodology of developing counterfactuals to determine what would have happened in the absence of the policy (scenario 2). The core counterfactual has been developed based on a comparison with what happened with the age group 25- to 59-year-olds in London over the same time period. This has the advantage that this age group would have been influenced by all other interventions put in place in London over the same time frame (e.g. road user charging), but were assumed not affected by the free bus fares policy for 12- to 17-year-olds. The implication is that where a statistically significant difference between the groups is observed this difference can be attributed to the intervention. Where data were available additional counterfactuals have been calculated for certain outcomes.
A number of potential outcomes of this intervention were identified by the study and reported in previous chapters. Those that are included in the economic evaluation are described in Table 6. A cost–benefit analysis (CBA) framework was developed to allow a range of different impacts of the intervention to be included and so to determine whether or not the intervention represents good value for money. Using well-established literatures on the monetary values of key inputs we compared the net monetised benefits of the intervention with the costs of implementation.
| Outcomes and costs | Description |
|---|---|
| Outcomes | |
| Safety | Changes in casualties due to the intervention |
| User benefits | Changes in consumer surplus due to reduced cost of travel |
| Revenue | Changes in revenue as a results of free fares |
| Physical activity | Changes in walking and cycling |
| Crime: intentional injury | Changes in crime rates as a result of free fares |
| Decongestion benefits (including CO2 emissions) | Changes in vehicle km as a result of free fares |
| Costs | |
| Administrative costs | Due to the intervention (e.g. creating and posting zip cards) |
| Bus operating costs | Due to changes in the number of bus passengers |
There are some limitations associated with the use of CBA as an organising framework, which are addressed in Limitations. Nevertheless, CBA is a useful tool for combining outcomes across a number of government departments/areas of public service. 125
Time frame and evaluation framework
The outcomes and costs in Evaluation framework results have been calculated for a representative year (2009) and for the intervention applied to the target age group (12- to 17-year-olds). An annual appraisal is feasible because the costs arise on a recurring, annual basis. To use any longer appraisal period would introduce unnecessary speculation about the duration of the policy. The evaluation framework used is shown in Table 7. In the following sections the individual elements of this table are described in detail. The report summarises the results of the monetisation of the outcomes in Evaluation framework results, and then discusses limitations and implications for future research in Limitations.
| Outcomes | Costs | Benefits |
|---|---|---|
| Safety | ✗ | |
| User benefits | ✗ | |
| Physical activity | ✗ | |
| Decongestion (including noise, CO2 emissions, local air quality) | ✗ | |
| Crime | ✗ | |
| Revenuea | ✗ | |
| Administrative costs | ✗ | |
| Bus operating costs | ✗ | |
| NSB = sum of benefits – sum of costs | ||
| BCR = benefits/costs | ||
Safety
The study hypothesised that there will be a change in casualties as a result of the introduction of free bus passes for 12- to 17-year-olds (see Chapter 6). This section uses data from Chapter 6 to estimate the benefits from changes in casualties.
Methodology
To determine the change in casualties as a result of the intervention two calculations are required:
-
Scenario 1: with intervention (this has been calculated based on the observed casualties as recorded by the STATS19 data average over the period 2006–9; Table 8).
-
Scenario 2: without intervention (this has been calculated using two different methods to determine a counterfactual).
| Severity | 2006 | 2007 | 2008 | 2009 | Annual average |
|---|---|---|---|---|---|
| Fatal | 16 | 14 | 13 | 9 | 13 |
| Serious | 202 | 168 | 155 | 144 | 167 |
| Slight | 506 | 481 | 490 | 502 | 495 |
| Total | 724 | 663 | 658 | 655 | 675 |
Two counterfactuals were calculated to assess what would have happened over the same time frame in the absence of the intervention:
-
Counterfactual 2a: assumes that in the absence of the intervention that the pre–post change in injuries in young people aged 12–17 years in London would be similar to the pre–post change in adults aged 25–59 years in London (Table 9).
-
Counterfactual 2b: assumes that in the absence of the intervention the pre–post change in injuries in young people aged 12–17 years in London would be similar to the pre–post change in injuries in young people in the same age group in the rest of England (Table 10).
| Severity | No. of 12- to 17-year-old casualties in the pre-period (A) | Observed number of 12- to 17-year-old casualties in the post-period (B) | Counterfactual: pre–post ratio of adult casualties (C) (95% CI) | Expected no. of 12- to 17-year-old casualties under counterfactual (A × C) | Change in 12- to 17-year-old casualties attributable to the intervention: observed – expected [B – (A × C)] (2006–9) |
|---|---|---|---|---|---|
| Fatal | 74 | 54 | 0.78 (0.68 to 0.89) | 58.0 (50.3 to 65.9) | –4 (–11.9 to 3.7) |
| Serious | 1753 | 987 | 0.67 (0.65 to 0.69) | 1175 (1140 to 1210) | –188 (–223 to –152) |
| Slight | 9394 | 5616 | 0.71 (0.70 to 0.71) | 6670 (6576 to 6670) | –1054 (–1054 to –960) |
| Severity | No. of 12- to 17-year-old casualties in the pre-period (A) | Observed number of casualties in the post-period (B) | Counterfactual: pre–post ratio of 12- to 17-year-old casualties in the rest of England (C) (95% CI) | Expected no. of casualties under counterfactual (A × C) | Change in casualties attributable to the intervention: observed – expected [B – (A × C)] (2006–9) |
|---|---|---|---|---|---|
| Fatal | 74 | 54 | 0.80 (0.72 to 0.89) | 59 (53 to 66) | –5 (–12 to 1) |
| Serious | 1753 | 987 | 0.82 (0.79 to 0.84) | 1437 (1385 to 1473) | –450 (–486 to –398) |
| Slight | 9394 | 5616 | 0.84 (0.84 to 0.85) | 7891 (7891 to 7985) | –2275 (–2369 to –2275) |
In both cases the counterfactuals make use of the number of injuries to 12- to 17-year-olds in the pre-period (2001–4) (A) and the observed number of injuries to 12- to 17-year-olds in the post-period (2006–9) (B). For counterfactual 2a, evidence on the pre–post ratio of adult injuries (C) over the same period is used to determine what could have happened in the do nothing scenario and this is then multiplied by (A) to get expected number of injuries under the counterfactual. For counterfactual 2b the same process is used, but in this case the pre–post ratio of injuries for 12- to 17-year-olds in the rest of England is used to determine the expected number of injuries.
The results from using the two counterfactuals indicate that over the period 2006–9 the policy has had an impact on the number of casualties in the 12- to 17-year-old age group. With the exception of fatal casualties all the 95% CIs exclude zero, indicating that the reduction in casualties is unlikely to be due to chance.
Monetary values
Transport collisions impose a range of impacts on people and organisations including lost economic output, pain, grief and suffering, and health, medical and ambulance costs. Through a range of methods,126 values to society for these impacts have been determined by severity of collision. The values for casualties are provided in Table 11, in 2009 prices.
| Injury severity | Lost output | Human costs | Medical and ambulance | Total |
|---|---|---|---|---|
| Fatal | 545,040 | 1,039,530 | 940 | 1,585,510 |
| Serious | 21,000 | 144,450 | 12,720 | 178,160a |
| Slight | 2220 | 10,570 | 940 | 13,740a |
Calculations
For the year 2009, the values in Table 11 have been applied to the results in Tables 9 and 10 (which have been converted into a number per year). For example, for every fatal casualty prevented the value applied from Table 11 is £1,585,510.
In summary, the results using counterfactual 2a are a benefit to society of £13,579,520 in 2009 (within a 95% CI of £8.2M to £18.6M). The results using counterfactual 2b (see Table 10) are included in the sensitivity tests in Evaluation framework results and Table 12.
| Scenario | Values | Change in casualties | PVB | ||||
|---|---|---|---|---|---|---|---|
| Fatal | Serious | Slight | Fatal | Serious | Slight | ||
| (A) | (B) | (C) | (D) | (E) | (F) | [(A × D) + (B × E) + (C × F)] | |
| Counterfactual 2a: 25- to 59-year-olds in London | |||||||
| 1,585,510 | 178,160 | 13,740 | 1.00 | 47.00 | 263.50 | 13,579,520 | |
| 95% CI | 1,585,510 | 178,160 | 13,740 | –0.93 | 38.11 | 240.00 | 8,621,126 |
| 1,585,510 | 178,160 | 13,740 | 2.97 | 55.64 | 263.50 | 18,234,795 | |
| Counterfactual 2b: 12- to 17-year-olds in England | |||||||
| 1,585,510 | 178,160 | 13,740 | 1.25 | 113 | 569 | 29,839,513 | |
| 95% CI | 1,585,510 | 178,160 | 13,740 | –0.25 | 99.5 | 568.75 | 25,145,168 |
| 1,585,510 | 178,160 | 13,740 | 3 | 121.5 | 592.25 | 34,540,485 | |
User benefits
The study has hypothesised that there will be user benefits of the scheme, namely a welfare gain for individuals who currently travel for free and previously had to pay and an increase in accessibility (see Chapter 7), as a result of removing bus fares for 12- to 17-year-olds. This section uses data from TfL to estimate those user benefits.
Methodology
The methodology that will be used to determine the change in user benefits involves calculating the change in consumer surplus as a measure of welfare change, using the user benefits approach described in DfT. 127 The user benefit measure is designed to capture the benefits from an accessibility gain as measured by the generalised cost (GC) function including accessibility gains from reductions in cost, reductions in travel time, improvements in journey quality and benefits to any new users who travel more due to the reduction in GC.
Measuring GC from i to j will usually follow the structure below:
where:
-
‘Fare’ is the money cost of a trip (e.g. the bus fare)
-
‘Time Cost’ is an amount calculated using ‘values of time’ which represent the inconvenience of time spent travelling
-
‘Other Disutility’ is a term which includes the individual’s valuation of any other trip characteristics which are relevant (e.g. inconvenience of a high floor to a bus user).
The relationship between GC and user benefits is shown schematically in Figure 17. Before a scheme is introduced the GC to the user is GC0 and at this cost level T0 trips are made. If, for example, the fare cost is removed (as is the case in this scheme) this reduces the GC by (GC0 – GC1). The result of this reduction in GC per trip is an increase in trips made from T0 to T1. The user benefit resulting from the introduction of the scheme equates to shaded area A for current users and shaded area B for new users (increased travel or accessibility). The demand curve is shown as a straight-line which is consistent with a common assumption in transport appraisal known as the ‘rule of a half’ which is a rule of thumb used to interpolate between two known points when the rest of the demand curve is unknown.
FIGURE 17.
New user and current users’ benefits from the introduction/enhancement of a scheme that reduces GCs.
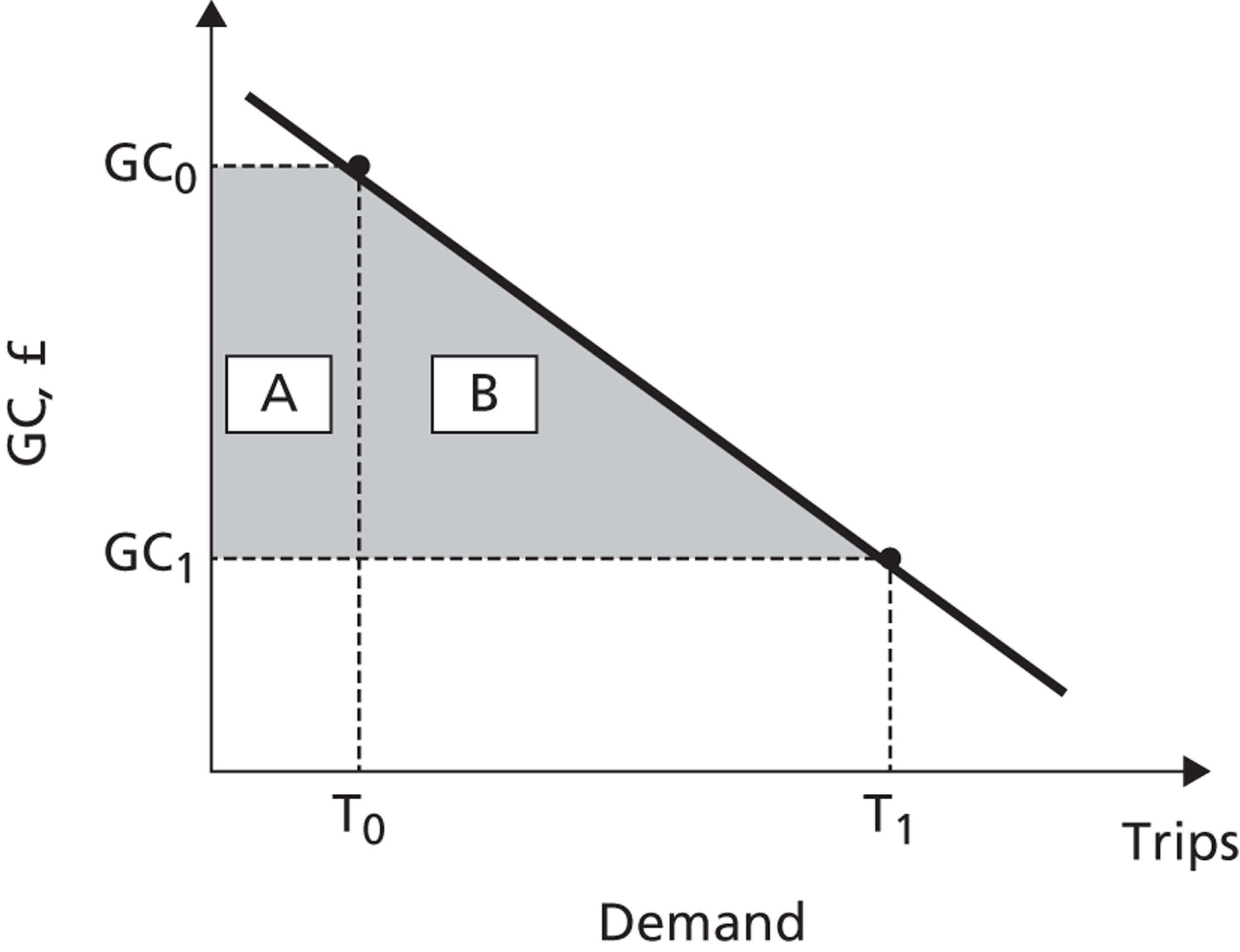
If all the required data points are known then the value of both of these areas can be calculated and the impact on accessibility determined. The calculation to determine the user benefits for areas A and B is completed using the following formula:
Data were collected from TfL on the number of free journeys in the 12–17 years age group, in the year 2009. There were 247,297,000 free journeys (T1). The single bus fare in 2009 was £1 (if paid using an Oyster Card). 128 [It should be noted that the data used to populate the number of trips for 12- to 17-year-olds in 2009 were taken from data collected by TfL through zip card use. This is a different data set from that used in Chapter 3, which drew on travel diary data relating to term time (Monday to Friday) only. The TfL data set was not available for the ‘before’ period of the intervention, prior to data collection via zip card use.] It is assumed for this analysis that young people would have been charged half this fare (50p) in the absence of the intervention. Therefore the difference between GC0 and GC1 is £0.50. The key input that needs to be determined to allow the user benefits to be calculated is T0. This is the trips that would have happened in the absence of the introduction of free fares (the counterfactual).
Two counterfactuals were calculated to assess what would have happened over the same time frame in the absence of the intervention:
-
Counterfactual 2a: assumes that expected bus travel is based on a statistical analysis of what happened in the same period to adults in the 25- to 59-year-old age group in London.
-
Counterfactual 2c: assumes that expected bus travel is based on demand elasticities and trip generation factor (TGF).
Counterfactual 2a assumes that in the absence of the intervention the pre–post change in bus use would be similar to the pre–post change in bus use in adults in the 25- to 59-year-old age group. Data from the LATS were used to determine the change and are reported in Chapter 3. It should be noted that the LATS data only included data from term-time weekday trips. It is therefore likely that this has underestimated the change in trips for 12- to 17-year-olds, if an increase in trips (outside the journey to school) takes place at weekends and out of term time. The pre–post ratio of adults trips was 1.36 (95% CI of 1.25 to 1.46). This indicates that over the same period bus trips for adults increased by 36% (95% CI 25% to 46%). The number of bus trips made by the 12- to 17-year-old age group was not collected in the pre-period. Instead, the ‘before’ trips have been derived from the LATS and are provided in Table 13. The resulting change in bus trips for the 12- to 17-year-old age group is 22 million within a 95% CI of between 5 million and 40 million bus journeys.
| Outcome | 12- to 17-year-old trips in the pre-period (A) | 12- to 17-year-old trips in the post-period (B) (2009) | Counterfactual: pre–post ratio of adult trips (C) (95% CI) | Expected 12- to 17-year-old trips under counterfactual (A × C) | Change in 12- to 17-year-old trips attributable to the intervention: observed – expected (B – (A × C)) |
|---|---|---|---|---|---|
| Bus trips | 165,754,820 | 247,497,000 | 1.36 (1.25 to 1.46) | 225,426,555 (207,193,525 to 242,002,037) | 22,070,445 (5,494,963 to 40,303,475) |
Counterfactual 2c uses the data reported in Balcombe and colleagues74 to estimate the change in trips associated with the price elasticities of demand and implied trip generation rates from the change from a half-fare charge per trip to a zero charge per trip. (Note this scenario does not use LATS data results from Chapter 3. It is based on what is expected to happen when there is a price change using price elasticities.) Figure 18 shows the demand curve given the price levels. PA’ is the full fare that an adult would pay, PA is the half-fare that a young person would pay. PB is the zero fare. Balcombe and colleagues74 provide data on expected changes in trips as a result of changing from a half-fare to a zero fare and the difference in elasticity of demand associated with a child compared with an adult.
FIGURE 18.
Trip generation factor.
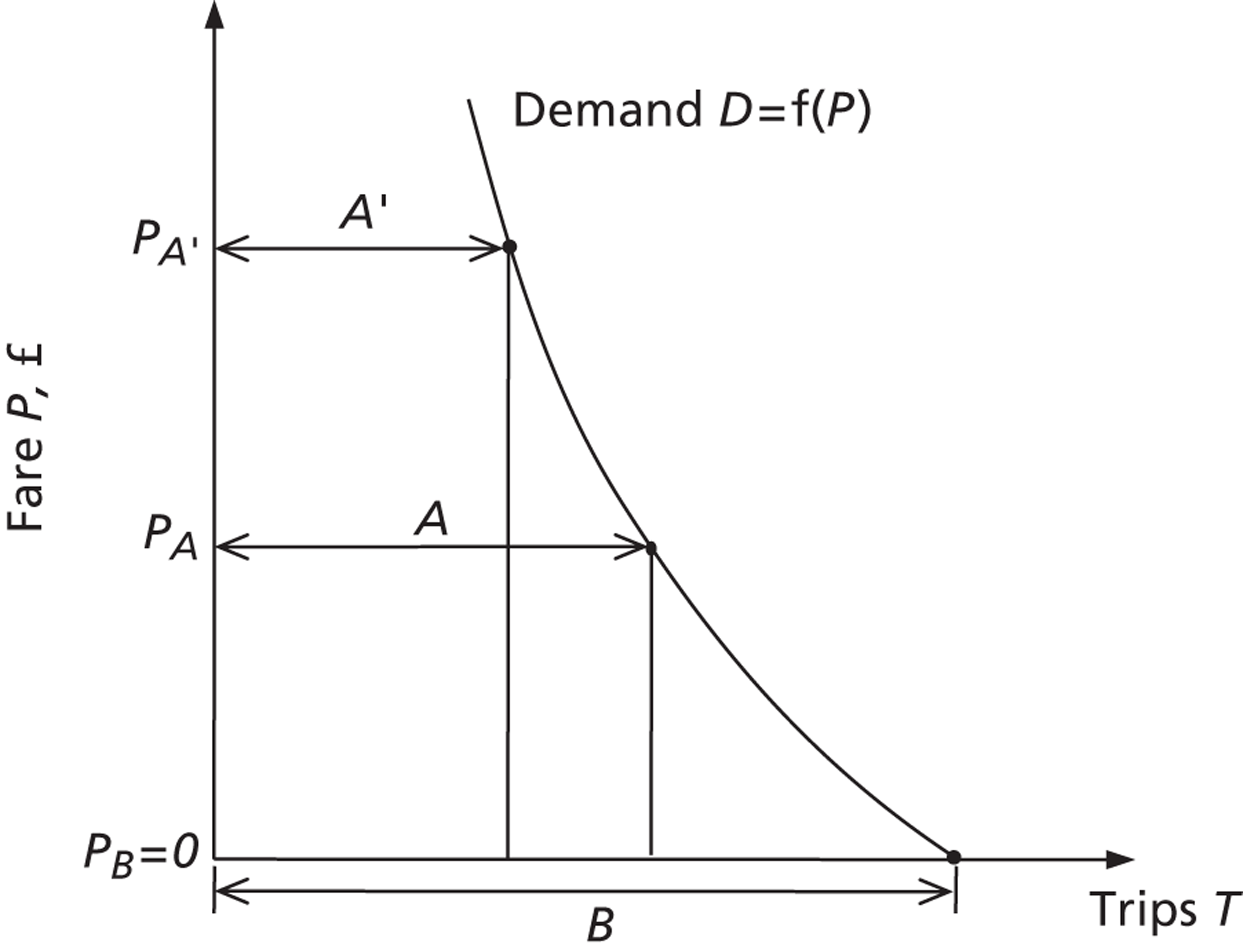
For a reduction in child fares from a flat (or half) fare PA to free fare PB, TGF = B/A. Given TGFs for the reduction from full fare to flat fare, and from full fare to free fare, the TGF of interest can be deduced:
Given values of 1.33 and 1.60 for (3) and (4) in general demand, we infer (5) = 1.20,74 TGF = B/A for child = 1.20. This should be considered a broad-brush estimate. Therefore, it should be expected that a reduction from half-fare to free fare for a child would generate 20% more trips. It would imply that the whole change in number of 12- to 17-year-old bus trips could be attributed to the intervention. Under counterfactual 2c, T1 is 247,497,000 and T0 would be 206,247,500, with the increase in trips due to reducing from half-fare to zero being 41,249,500.
Calculations
Applying the following formula [User Benefits (A + B) = 0.5 (GC0 – GC1)(T0 + T1)] to the trips associated with the intervention in counterfactuals 2a and 2c produces the following results. It was assumed that the half-fare of 50p would be applied for both the counterfactual scenarios. The results are provided in Table 14, which indicates that benefits to users from reduced fares and increased access to the bus network have generated user benefits to society of the order of £118M.
| Scenario | Change in fare (GC0 – GC1) (A) | T0 + T1 (B) | User benefits = 0.5 × A × B |
|---|---|---|---|
| Counterfactual 2a | £0.50 | 472,923,555 | £118,230,888 |
| Counterfactual 2c | £0.50 | 453,744,500 | £113,436,125 |
In summary, both of the methods used to determine the user benefits of the intervention estimated that there would be considerable positive user benefits. The majority of these benefits are the result of the population group (12- to 17-year-olds) that were using the bus prior to the intervention now not having to pay. In the absence of a true counterfactual, both the scenarios tested have generated similar levels of user benefits as shown in Table 14. Although the quantitative analysis (see Chapter 3) did not identify a statistically significant change in bus use for 12- to 17-year-olds, it should be noted that these data were based on LATS, which only includes weekday term-time travel, which has a greater potential to underestimate the changes in bus travel for the population group. By contrast, counterfactual 2c in Table 14 used the full TfL trip data set for 2009, and with elasticities to estimate trip generation, indicated that there was an additional 41.2 million trips annually as a result of this intervention.
Decongestion benefits
The study hypothesised that one of the benefits to society from the introduction of free bus travel would be a reduction in congestion, as there would be a switch away from using the car. Consequently, there would be a reduction in the negative impacts of congestion [e.g. air pollution, noise, carbon dioxide (CO2) emissions, etc.] which have been identified by the literature as having an impact on public health. 20 This section assesses the benefits from decongestion of the free bus travel scheme.
Methodology
The methodology used to determine the impact of decongestion benefits has been to estimate the change in km travelled by car (for those aged 12–17 years) as a result of the intervention, and apply values from the DfT129 which provide unit costs in pence per vehicle km applicable to either reduced or additional vehicle km (see Table 17 for these unit costs). It should be noted that this study has calculated directly the change in injury costs in the section on Safety using the STATS19 data. Therefore the ‘Accidents’ element of the decongestion benefit has been omitted to avoid double counting.
The LATS data has been used to determine the change in car-km (for the target age group) following the intervention. The following counterfactual was used to represent the absence of the free bus travel:
-
Counterfactual 2a: assumes that expected car-km (for the target age group) is based on a statistical analysis of what happened in the same period to adults in the 25- to 59-year-old age group in London.
One of the key issues with the LATS data is that it only includes weekday and term-time travel. This potentially has the impact of underestimating the impact of the change in decongestion from the intervention, as it does not include holiday and weekend travel. For this reason decongestion benefits have only been included in the CBA framework analysis as a sensitivity test.
In order to determine the value to society of the reduced vehicle km, the change in vehicle km identified in Table 15 has been assigned to the different road types in Table 16, based on the percentage of vehicles experiencing congestion on each of the three different road types in London.
| Outcome | 12- to 17-year-old car-km in the pre-period (A) | 12- to 17-year-old car-km in the post-period (B) (2009) | Counterfactual: pre–post ratio of adult trips (C) (95% CI) | Expected 12- to 17-year-old car-km under counterfactual (A × C) | Change in 12- to 17-year-old car-km attributable to the intervention: observed – expected (B – (A × C)) |
|---|---|---|---|---|---|
| Car-km | 1,757,566 | 1,253,077 | 0.89 (0.84, 0.94) | 1,564,233 (1,476,355, 1,652,112) | –311,157 (–399,035, –223,278) |
Monetary values
Congestion imposes large costs on society. Through a range of research methods the cost of an additional car-km on the road has been estimated and presented in DfT129 (Table 17). These values are applied to the number of vehicle km saved in Table 16 to obtain an estimate of the decongestion benefits.
| Outcome | Motorways, £ | A roads, £ | Other roads, £ | Total, £ |
|---|---|---|---|---|
| Total (excluding accident costs, mean) | –563 | 112,544 | 53,214 | 165,195 |
| CI (maximum) | –722 | 144,329 | 68,243 | 211,851 |
| CI (minimum) | –404 | 80,759 | 38,185 | 118,540 |
| Using the mean | ||||
| Greenhouse gases | 133 | 1729 | 1482 | 3344 |
| Noise | 30 | 346 | 247 | 622 |
| Local air quality | 44 | 519 | 370 | 933 |
Calculations
Using the monetary values in Table 17 and the changes in vehicle km in Table 16, the estimated decongestion benefits are as presented in Table 18. This indicates that the expected benefits are of the order of £165,000 (within a 95% CI of £119,000 to £212,000). It should be noted that these results are only representative of the benefit from changes in term-time weekday travel.
| Outcome | Motorways (£) | A road (£) | Other roads (£) | Total (£) |
|---|---|---|---|---|
| Total (excluding accident costs) mean | –29,927 | 6,922,278 | 3,391,409 | 10,283,760 |
| CI (maximum) | –111,908 | 16,045,197 | 7,586,634 | 23,519,923 |
| CI (minimum) | –19,074 | 3,557,800 | 1,803,476 | 5,342202 |
| Using the mean | ||||
| Greenhouse gases | 7482 | 106,333 | 94,424 | 208,239 |
| Noise | 1663 | 21,267 | 15,737 | 38,667 |
| Local air quality | 2494 | 31,900 | 23,606 | 58,000 |
In summary, using the results of vehicle kilometres (calculated using the LATS) indicates that there are potentially positive benefits to decongestion as a result of the intervention with reductions in car travel.
Active travel and physical activity
The study hypothesised that there would be a change in levels of active travel (walking and cycling) as a result of the intervention of free bus fares for young people (see Chapter 4) which may lead to a change in physical activity. This section examines whether or not we can estimate the benefits from a change in physical activity as a result of the scheme.
Methodology
Chapter 4 of this study used data from the LATS and LTDS to determine the current levels of walking and cycling in London following the introduction of free bus fares. As with the previous outcomes we determined a counterfactual case using a comparison with the walking and cycling levels in the 25- to 59-year-old age group over the same period. The research identified that there was no significant change in the total distance walked following the introduction of the free bus fares (see Chapter 4). The study identified a small decline in the amount of cycling that the 12- to 17-year-old age group were undertaking. Combined together (walking and cycling changes) there was no significant change in the amount of physical activity for the 12- to 17-year-old age group as a result of the policy, so no monetary value is included in the CBA framework.
One of the key methodologies that are available to determine the monetary value to society from changes in physical activity levels is the World Health Organization (WHO)130 health economic assessment tool (HEAT) methodology. In the documentation it states that:
HEAT should not be applied to populations of children, very young adults or older people since the available evidence was not sufficient to derive a relative risk for these age groups
p. 20130
Given this limitation of HEAT’s application, it should be noted that more research is required to allow an assessment of the monetary benefit to society of increases in walking and cycling for children as a result of an intervention. The current methodology as applied to adults can be found at the WHO130 and the DfT. 131
Crime
The study hypothesised that there would be a change in assaults as a result of the intervention (see Chapter 6). This section uses data from TfL and Chapter 6 to estimate the benefits from changes in assaults.
Methodology
Evidence from TfL indicates that crime rates on London’s transport network have declined over the period in which the intervention was implemented (Table 19), despite increasing numbers of bus trips. It has not been possible to split these data into crime type or to determine a counterfactual from these data. For example, it has not been possible to identify the age of the crime victims and so compare 12- to 17-year-olds with 25- to 59-year-olds.
| Total crime (notifiable) | 2008/9 | 2009/10 | 2010/11 | 2011/12 |
|---|---|---|---|---|
| Bus | 27,062 | 24,976 | 23,974 | 21,724 |
| Tram | 411 | 403 | 367 | 369 |
| Underground/DLR | 15,109 | 14,536 | 13,472 | 12,115 |
| London overground | 492 | 450 | 658 | 764 |
Analysis was also carried out within the project using the HES data to determine whether or not there was a change in assaults associated with the intervention. It was hypothesised that an increase in bus trips could lead to an increase in assaults. The HES data were analysed using the assault rates in the same period to adults (25 to 59 years old) in London as the basis for the counterfactual. As shown in Table 20 this analysis resulted in the identification of an increase in assaults per year. However, the impact pathway is complex and it is difficult to prove causality (see Chapter 6). For this reason, this increase in assaults has only been included in the CBA framework as a sensitivity test.
| No. of 12- to 17-year-old assaults (A); (2001–4) | Observed no. of assaults post-period (B); (2006–9) |
Counterfactual: pre–post ratio of adult injuries (C) | Expected no. of assaults under counterfactual (A × C) | Change in assaults attributable to the intervention: observed – expected [B – (A × C)] | Change in assaults per year |
|---|---|---|---|---|---|
| 2321 | 3322 | 1.19 (1.16, 1.22) | 2762 (2692.3, 2831.6) | 560 (490.4, 629.7) | 140 (122, 157) |
Monetary values
The best estimate of the social costs of assaults on buses in England is provided by Home Office ‘social costs of crime’ evidence, adapted to public transport for DfT. 133 A weighted average value of £13,592 per assault on buses and trams has been used, at 2009/10 prices. For the derivation see Table 21.
| Crime type | Number of incidents | Weighting by number of incidents | Estimated unit cost (£) (2006/7 prices) | ||
|---|---|---|---|---|---|
| Costs of consequences of crime | Costs in response to crime | Total | |||
| Violence against a person (passengers) | 39,390 | 0.85 | 3267 | 9923 | |
| Sexual offences | 7004 | 0.15 | 6196 | 3556 | |
| Average (2006/7 prices) | 3709 | 8962 | 12,671 | ||
| Average (2009/10 prices) | 13,592 | ||||
A proposal early in the study was to use the value for ‘Serious Injury’ from DfT advice,126 noting that the definition of ‘Serious Injury’ by DfT126 is: ‘Serious injury: records casualties who require hospital treatment and have lasting injuries, but who do not die within the recording period for a fatality’. Using the serious injury value, it was found that results would be an order of magnitude higher (> 10 times higher); however, the rationale for the assaults value is much stronger because it is much more specific to the outcome that has been measured. Therefore the results including the assaults value only (see Table 21) are provided as a sensitivity test.
Calculations
Using the monetary values in Table 21 and the change in assaults in Table 20 the results for inclusion in the sensitivity test are provided in Table 22. It indicates that the change in benefit to society is of the order of –£1.9M (mean) within a 95% CI of –£1.7M and –£2.1M.
| Crime type | Change in assaults (see Table 16) | Estimated unit cost, £ (2009/10 prices) | Benefit of change in assaults, £ (2009/10 prices) |
|---|---|---|---|
| Mean | 140 | 13,592 | –1,902,900 |
| CI (minimum) | 122 | 13,592 | –1,658,241 |
| CI (maximum) | 157 | 13,592 | –2,133,966 |
In summary, the project explored the inclusion of changes in assaults as a result of the intervention. Unlike road safety, the major impact pathway is complex for crime, and it is difficult to demonstrate causality, as data were not directly linked to bus use, but admission to hospital. For this reason, the increase in crime observed after the intervention was introduced has been included as a sensitivity test.
Revenue
One of the consequences of the intervention is that those 12- to 17-year-olds who would have previously paid half-fare in 2009 are now travelling for free. This reduces the revenue that would be received by TfL. The methodology used to calculate the change in revenue is described next.
Methodology
In the ‘do something’ scenario TfL will receive a revenue of £0 as those in the age group 12–17 years who previously paid to travel by bus now are exempt from paying. In order to determine the level of revenue in the ‘do nothing’ scenario two counterfactuals were tested based on the results from the user benefit calculations. (For details on the calculation of the number of trips see User benefits.)
-
Counterfactual 2a: expected bus travel based on a statistical analysis of what happened in the same period to adults in the 25- to 59-year-old age group in London (see Chapter 3).
-
Counterfactual 2c: expected bus travel based on demand elasticities and TGF (see Balcombe and colleagues74).
The calculations indicate that in the absence of the free fare, approximately 225 million journeys (netting £113M) would have been made by the 12- to 17-year-old age group within a 95% CI of £104M to £121M. Using counterfactual 2c this number is reduced to a loss of £103M.
Calculations
The results of this analysis are provided in Table 23. Using counterfactual 2a it is indicated that had the intervention not been in place that revenue of the order of £113M (within a 95% CI of £104M and £121M) could have been realised in 2009.
| Scenario | Expected trips in the counterfactual (A) | Child half-fare (B) | Revenue (A × B) |
|---|---|---|---|
| Counterfactual 2a | 225,426,555 (95% CI 207,193,525 to 242,002,037) | £0.50 | Mean: £113M |
| CI minimum: £104M | |||
| CI maximum: £121M | |||
| Counterfactual 2c | 206,247,500 | £0.50 | £103M |
Note that the results below (see Bus operating costs) include a sensitivity test which incorporates both bus operating cost and revenue changes.
Administrative costs
The introduction of free bus fares resulted in additional administrative costs for TfL. One element of this is the issuing of travel cards to allow 12- to 17-year-olds to be able to travel for free. (Since 2011 this policy has been changed and 12- to 17-year-olds are now charged £10 per card to cover these costs. This was not the case in 2009 and has not been included in the CBA.)
Methodology and calculations
Based on data collected from TfL it was estimated in the period 2006–9 that they issued the following number of cards per year and the following cost of issuing each card:
-
young people aged 12–15 years: 130,000 first issue cards (cost of £7.26 per card) = £943,800; 150,000 replacement cards = £1,089,000
-
young people aged ≥ 16 years: 180,000 first issue cards (cost of £7.16 per card) = £1,288,800; 40,000 replacement cards = £286,400.
For the CBA framework we have included the cost to TfL for producing the cards. The total costs to be included in the CBA are £3,608,000.
Bus operating costs
It was hypothesised that the introduction of free bus fares to the 12- to 17-year-old age group would lead to additional marginal operating costs for the operator. This section provides the methodology for calculating these.
Methodology
In general, the additional costs of providing for an increase in concessionary travel may include:
-
additional marginal operating costs, due to carrying more passengers on existing bus services; and
-
potentially, additional marginal capacity costs, if there is an increase in the number of services operated.
A bottom-up analysis of marginal operating costs shows that these comprise the following items:135
-
fuel, tyre wear and oil consumption
-
maintenance and cleaning
-
insurance
-
information provided to passengers
-
additional vehicle time due to changes in changes in boarding and alighting.
The impact of a policy which increases bus travel will be to increase total bus operating costs by the amount of the marginal operating cost, for each additional passenger due to the policy. Evidence and calculations are given below.
Marginal capacity costs are conditional on how the operator chooses to respond to an increase in passenger demand. If the operator can absorb the additional demand without running additional services, the marginal capacity cost will be zero. In the case of London, where bus services are tendered by TfL, the question is the extent to which the set of bus services tendered by TfL has changed as a consequence of the policy. As modelling of the network was ruled out for this study, the primary source of information is TfL’s advice on the tender agreements with operators. These tender agreements are usually renewed on a 5-yearly basis, on a rolling cycle across the network, sometimes with a 2-year extension if performance is satisfactory. The agreements do not identify any capacity increase specifically to accommodate additional travel by those aged <18 years due to the free travel policy. The initial ‘with policy’ scenario (scenario 1) therefore assumes zero marginal capacity cost. As a sensitivity test, we also draw parallels between the cost of providing the Freedom Pass for older and disabled travellers in London, and the cost of providing the 12- to 17-year-olds’ concession, which leads to some substantial additional costs.
Monetary values
The marginal operating cost for an additional concessionary passenger is estimated to be £0.061 at 2009/10 prices. 136 These costs vary with average journey length and using the results of Dargay and Liu (table 5)137 average journey length is 2.9 miles in London compared with 3.9 miles in England, hence a revised value for London including a distance-based adjustment is given by:
Conversely, costs of inputs such as labour and land are higher in London. In the absence of a direct cost comparison, the South East weighting of 1.314 from recent bus profitability research was used:138
A measure of the overall loss to bus operators is the amount of compensation they require to accept a concessionary scheme, and a comparator in London is offered by the Freedom Pass. The total negotiated payment to TfL for Freedom Pass (and National Scheme) bus travel in 2009/10 was £188.6M. 139 This is understood to correspond to 307.7 million bus trips using Freedom Pass in that year. Hence the cost per bus trip, including revenue forgone and additional operating costs, is approximately £0.61 on average.
Results
Given the increase in trips by 12- to 17-year-olds due to the policy under different counterfactual assumptions, the estimated additional marginal operating costs are shown in Table 24. In scenario 2a the expected amount is £1,723,700 per annum.
| Counterfactual scenario | Δ12- to 17-year-old bus trips, million per annum, compared with ‘do something’ | ΔCost, £M per annum |
|---|---|---|
| 2a. Based on London adults as the control | ||
| Mean | 22.1 | 1.72 |
| CI (minimum) | 40.3 | 3.15 |
| CI (maximum) | 5.5 | 0.43 |
| 2c. Elasticity approach | 41.2 | 3.22 |
The comparison with Freedom Pass suggests that the total of additional operating costs and revenue forgone may be much more substantial, equal to £0.61 × 247.5M = £152M. Given the results for revenue alone (see Table 23), the additional operating costs may be of the order of £39M. However, this figure should be treated as highly uncertain because: 12- to 17-year-olds’ trip-making patterns and timing differ from those aged > 60 years or disabled people; hence, the scheme’s impact on peak vehicle requirements and capacity generally is different; and 12- to 17-year-olds may be especially capable of making full use of upper-deck space and standing room aboard buses (see Chapter 8) – in this respect their impact on capacity requirements may be reduced.
Evaluation framework results
The framework initially set up in Table 7 can now be populated with the costs and benefit results, so giving the net present value (NPV) and benefit : cost ratio (BCR) of the intervention (see Tables 25 and 27). The results for the counterfactual where all the inputs are based on a comparison with the change in 25- to 59-year-olds (counterfactual 2a) are shown in Table 25. The benefits from the intervention to society as a whole are found to be greater than the costs incurred: at £13.8M the NPV is substantially greater than zero. Moreover, the value for money offered by the intervention appears to be high. DfT140 provides a value for money-rating scheme for transport interventions for BCR (Table 26) – based on this the intervention exhibits high value for money and would have a high chance of funding (BCR between 2 and 5).
| Outcome | Counterfactual based on 25- to 59-year-olds in London | ||
|---|---|---|---|
| Scenario 1 vs. scenario 2a | |||
| Mean | CI (minimum) | CI (maximum) | |
| Benefits | |||
| Safety | 13.6 | 8.6 | 18.2 |
| User benefits | 118.2 | 113.7 | 122.4 |
| Revenue | –112.7 | –121.0 | –103.6 |
| Physical activity | ∼ | ∼ | ∼ |
| Crime | |||
| Decongestion | |||
| Costs | |||
| Administrative costs | 3.6 | ||
| Bus operating costs | 1.7 | 0.4 | 3.1 |
| PVB | 19.1 | ||
| PVC | 5.3 | ||
| NPV | 13.8 | ||
| BCR | 3.6 | ||
| BCR range | Rating |
|---|---|
| < 1 | Poor |
| 1.0–1.4 | Low |
| 1.5–1.9 | Medium |
| 2.0–4.0 | High |
| > 4 | Very high |
Alongside the main results using counterfactual 2a, a set of sensitivity tests were conducted to examine how changes in the assumptions would alter the results, and to assess the robustness of the results (Table 27). These include alternative counterfactuals and additional outcomes. To interpret the table, numbers in italics should be treated as alternatives to the entries in the first three columns, or as additional where there is no entry in the first three columns.
| Outcome | Counterfactuals | Sensitivity tests | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Scenario 1 vs. scenario 2a | Scenario 1 vs. scenario 2b | Scenario 1 vs. scenario 2c | Include assaults (scenario 1 vs. scenario 2a) | Include decongestion (scenario 1 vs. scenario 2a) | Include additional capacity costs | Include all | |||||||||
| Mean | CI (minimum) | CI (maximum) | Mean | CI (minimum) | CI (maximum) | Mean | CI (minimum) | CI (maximum) | Mean | CI (minimum) | CI (maximum) | Mean | Mean | ||
| Benefits | |||||||||||||||
| Safety | 13.6 | 8.6 | 18.2 | 29.8 | 25.1 | 34.5 | 13.6 | ||||||||
| User benefits | 118.2 | 113.7 | 122.4 | 113.4 | 118.2 | ||||||||||
| Revenue | –112.7 | –121.0 | –103.6 | –103.1 | –112.7 | ||||||||||
| Physical activity | ∼ | ∼ | ∼ | ∼ | |||||||||||
| Crime | –1.9 | –2.1 | –1.7 | –1.9 | |||||||||||
| Decongestion | 0.2 | 0.0 | 0.1 | 0.2 | |||||||||||
| Costs | |||||||||||||||
| Administrative costs | 3.6 | 3.6 | |||||||||||||
| Bus operating costs | 1.7 | 0.4 | 3.1 | 3.2 | 39 | 39 | |||||||||
| PVB | 19.1 | 35.3 | 23.9 | 17.2 | 19.3 | 19.1 | 17.4 | ||||||||
| PVC | 5.3 | 5.3 | 6.8 | 5.3 | 5.3 | 42.6 | 42.6 | ||||||||
| NPV | 13.8 | 30.0 | 17.1 | 11.9 | 13.9 | –23.5 | –25.2 | ||||||||
| BCR | 3.6 | 6.6 | 3.5 | 3.2 | 3.6 | 0.4 | 0.4 | ||||||||
Two alternative counterfactuals are shown. The first substitutes the base case safety outcome values with the counterfactual based on a comparison with 12- to 17-year-olds outside London. This leads to a substantial increase in NPV and BCR of the project (BCR with a mean of 6.6), and although this is judged to be a less likely outcome than the base case result (given that it is not based on a London setting), it does add to confidence that the true BCR is > 2.
The second alternative counterfactual uses an estimate of changes in trips based on demand elasticities, rather than using the 25- to 59-year-old age group as a control. This alters the user benefits, revenue and bus operating costs. The results again imply a high value BCR (3.5), which is encouraging from a value for money perspective.
The second set of tests deal with additional outcomes. These were carried out to explore the implications of including costs and benefits which had been excluded from the main results (see Table 25) because of limited confidence in validity or attributing causality.
-
The study identified an increase in assaults, although there remains a question over causality and hence the usefulness of the results for policy analysis. Including the estimated disbenefits associated with assaults would marginally reduce the BCR (to 3.2) but not threaten the high value for money rating.
-
Decongestion benefits, including reduced delay, CO2 emissions, noise and local air pollution, would add further to overall benefits of the policy. An additional £165,000 (range £119,000–212,000) would be added to the NPV, and the expected BCR would remain at 3.6.
-
Finally, an attempt was made to estimate the potential marginal capacity costs to bus operators by comparison with the Freedom Pass scheme for older and disabled users. The results were found to be highly uncertain; nevertheless, if they are included, they act to reduce the NPV to –£23.5M and the BCR to 0.4. Hence, the finding is that the results of the evaluation are sensitive to the treatment of bus operator costs.
In all bar one of these sensitivity tests the analysis has resulted in a positive ‘high value’ BCR, indicating that the intervention (given the outcomes considered) has represented good value for money taking into account the impact on public health. It also implies that there would have to be significant negative outcomes not already represented in the framework to result in a negative NPV and BCR < 1. Connecting this result with the qualitative findings it can be identified that there were additional positive benefits such as fostering social inclusion (see Chapter 7), which if presented alongside have the potential to make the results stronger in favour of the intervention.
Limitations
This study has sought to develop an economic evaluation of the public health impacts of the intervention, focusing on the costs and benefits for 1 year (2009) following the implementation of the scheme in 2005. The evaluation is based on the quantitative research within this study plus available secondary data and valuation evidence. The evaluation is wide-ranging compared with most transport policy evaluations; however, it does have some limitations which are worthy of discussion.
One limitation is that the study has focused on available data for the immediate ex post period 2006–9, rather than seeking to forecast into the future the longer-term health impacts that the intervention might bring. More research is needed in both public health and economics to translate an increased used of bus travel into longer-term public health impacts, particularly with respect to outcomes such as physical activity, which are expected to have most of their benefits in the future.
Similarly, the long-term impact on life chances and independent living, as a result of increased mobility between the ages of 12 and 17 years, has not been possible to quantify and hence to include in the economic evaluation. There are some hints of it in the qualitative assessment. This topic would also benefit from targeted research.
Another limitation that was raised during the research was the impact of using values that were designed to be applied to adults to the context of young people aged 12–17 years. This was highlighted in the context of the WHO130 evidence for changes in physical activity, but is also relevant for the change in safety and intentional assault, whereby the value of statistical life (VOSL) calculated based on an adult has been applied. Further research is required to determine if this value should be different and what values could be applied to children.
Particular challenges in attributing causality arose with assaults. The question is whether or not the policy impact is swamped by background trends (e.g. in youth crime) which are not picked up in the counterfactual, hence they appear as ‘effects of the policy’ when in reality they are not. Particularly in the case of assaults, there is a need for better data linking the hospital episodes to bus travel, or a wider-ranging analysis of assaults in which 12- to 17-year-olds’ mobility is set alongside other factors and trends. Conversely, it is easier accept the findings on mode shift and trip generation based on well-understood relationships in transport demand. In general, the authors take the view that the counterfactuals do serve the intended purpose; however, in the case of assaults there is a case for further investigation. Having said this, the magnitude of the ‘change in assaults’ that was found makes it doubtful whether or not any changes to the analysis of assaults would materially affect the case for the policy.
Wider economic impacts are another difficult area, linked to the increased access to employment and training provided by the policy. A more detailed understanding of trip purposes for 12- to 17-year-olds, starting with data gathering, would be helpful in providing a more concrete assessment of these impacts. Moreover, WebTAG has some limitations for application in economic evaluation of public transport and public health interventions, where there are intended and unintended public health consequences. Further work is needed to resolve this issue.
Finally, although a CBA framework has enabled the range of outcomes considered in the quantitative work to be valued and included in overall NPV and BCR, one of the key weaknesses of a CBA framework is that it excludes those outcomes that cannot be monetised. The qualitative research (see Chapter 7) identified that there were other potential outcomes from the intervention that this approach has not been able to capture. For example, the universal availability of free travel seems to be particularly valued (see Chapter 3), as young people can be confident that any and all peer group members can travel in that way. It was not possible to monetise that effect within the scope of this study, and additional survey work would be require to attempt to capture it. That evidence would then need to be considered alongside the results of the current CBA to provide a more comprehensive description of the intervention. For the moment, it remains necessary for the person using the evaluation results to weigh the CBA against the qualitative and unmonetised impacts.
Conclusions
From the perspective of the CBA framework, there is a body of evidence indicating that the policy has reduced RTI, increased bus travel, and reduced car travel, while not reducing levels of active travel in the city. In the base case the benefits have substantially outweighed the costs, providing what the DfT considers ‘high’ value for money. Sensitivity testing was conducted, and most of these tests do not overturn this conclusion. Only a sensitivity test with substantial additional capacity costs of bus operation threatens the positive NPV of the policy, and there is no firm evidence that this was the case.
Chapter 10 Discussion and conclusions
Introduction
Many policy and infrastructural interventions, among them educational, housing and transport measures, have had a significant influence on public health despite their not having an explicit public health brief. As public health in the UK moves to a new context, with a base in local authorities, understanding the positive and negative effects of such interventions, and their potential to widen or narrow inequalities in health, becomes increasingly important. This study explores the effect of such an intervention, using qualitative and quantitative methods. It evaluates the public health impact of a transport intervention which was not designed with public health improvement as an aim, but which was likely to have a range of effects, positive and negative, on the immediate and future health of young people (the target population) and the wider population in London. At a time when universal benefits in general and concessionary fares in particular are under scrutiny, evidence on these putative health effects are important in informing decision-making. This study therefore aims to provide evidence on the public health effects that could be attributed to the introduction of free bus travel for young people, and to conduct a cost–benefit evaluation which takes these health effects into consideration.
Main findings
Our study provides empirical evidence on key questions in the debates around whether or not such schemes are worth investment, and their effects on outcomes such as active travel, injury rates, social inclusion and sustainability. We first outline the main findings, in terms of the causal pathways hypothesised in Chapter 2 (see Figure 3).
Increase in bus use by young people
In the context of rising levels of bus use in London, there was no quantitative evidence that the scheme itself had increased the number of journeys with the bus as the primary mode, or the number of kilometers travelled by bus by young people compared with adults during term-time weekdays. However, these had gone up overall for both groups. There was evidence that the number of short journeys had risen. The qualitative data provided some evidence that the universal scheme, cost free to young people at the point of use, contributed to this, and also potentially to discretionary journeys not identified in travel diary data. The qualitative data also described how bus travel had become the default mode of transport for many journeys, as it enabled young people to travel together.
Decrease in active travel
Although the number of journeys with walking as a main mode decreased, there was little evidence that overall levels of active travel had reduced, in part because bus travel entails some walking, and (qualitative evidence suggested that) the scheme had generated additional journeys. Few journey are made by bicycle in London, and compared with adults (for whom cycling rates had gone up), young people were cycling less after the introduction of free travel. Young people’s accounts of travel suggested that cycling was not, in general, considered a candidate transport mode, but we do not know whether or not this has changed since the introduction of free travel. On balance, then, it is difficult to attribute changes in cycling to the introduction of free bus travel, although reasonable to suggest that free bus travel for all would militate against other attempts to increase cycling rates.
Impact on health and well-being from changes in modes of transport
We could not assess this directly in this study. A systematic review of the literature90 (see Appendix 8) found little evidence that increasing the amount of active transport has a direct effect on health outcomes, but these are difficult to measure given the long time scales for benefits to accrue. The qualitative data suggested a number of benefits from increased access to transport for young people, including increased ability to be independently mobile, increased control over their travel, and fostering a feeling of ‘belonging’ to London. These are difficult to quantify, but confidence, independence and a sense of belonging make an important contribution to young people’s well-being.
A reduction in car use
Journeys by car declined in both adults and children, but it is difficult to attribute these changes to the scheme rather than other interventions over the same period. Qualitative evidence suggests that in outer London in particular, free bus use had displaced some car journeys.
Decreased future dependence on car travel
The qualitative data suggested that although young people still expected to learn to drive as a rite of passage to adulthood, bus use had been ‘normalised’ by the intervention such that it was not seen as a transport mode of last resort.
A reduction in bus use, especially in school hours, by older citizens aged > 60 years
There was no evidence that young people’s free travel had displaced older citizens from the buses in general, or specifically during the afternoon peak school journey times. (Until January 2009, older citizens were ineligible to use their pass before 9.30 a.m. Since then, London Freedom Pass users have been able to use their passes 24 hours a day should they wish to. We therefore conservatively restricted analysis to the after school hours.) The qualitative data suggests that older citizens often preferred to travel outside school and commuter times for reasons of comfort and convenience.
A reduction in road traffic injuries in young people
We identified a relative reduction in injuries which was consistent with the mode changes observed (i.e. a reduction in car occupancy and in cycling). Against a background decline in road injury rates, the decline in 12- to 17-year-olds was faster, primarily reflecting declines in car and cycling casualties.
An increase in the incidence of assault injuries
Assaults in young people had risen compared with adults and with the national population. However, the increase predated the introduction of free bus travel. For most young people, the risks associated with travel were to some extent mitigated by free bus travel, which allowed ‘practice journeys’, a contingency plan for avoiding getting stranded, and (for girls) a perceived safer alternative to walking.
Increased access to training, education, independent travel
We found no evidence of a flattening of the socioeconomic gradient of travel for educational purposes after the scheme was introduced. However, qualitative data suggest that financial barriers do not contribute to transport exclusion for young people in London. For those able to use the bus service, the scheme has ensured that all can access education, training and the social opportunities essential for social inclusion.
Has the scheme represented value for money?
From the perspective of the CBA framework and representative year 2009, the policy has reduced RTIs, increased bus travel and reduced car travel while not reducing levels of active travel. In the base case, the monetised benefits have substantially outweighed the costs, providing what the DfT considers ‘high’ value for money.
Assessing the evidence and revising the logic model
We have presented the quantitative and qualitative evidence for the pathways hypothesised as potentially linking the intervention (free bus travel) to outcomes related to the determinants of health. We can now revisit the logic model proposed in Chapter 2, to summarise the impact of free bus travel on public health in a graphic way, using a revised logic model (Figure 19).
FIGURE 19.
Revised model of pathways between intervention and determinants of health.
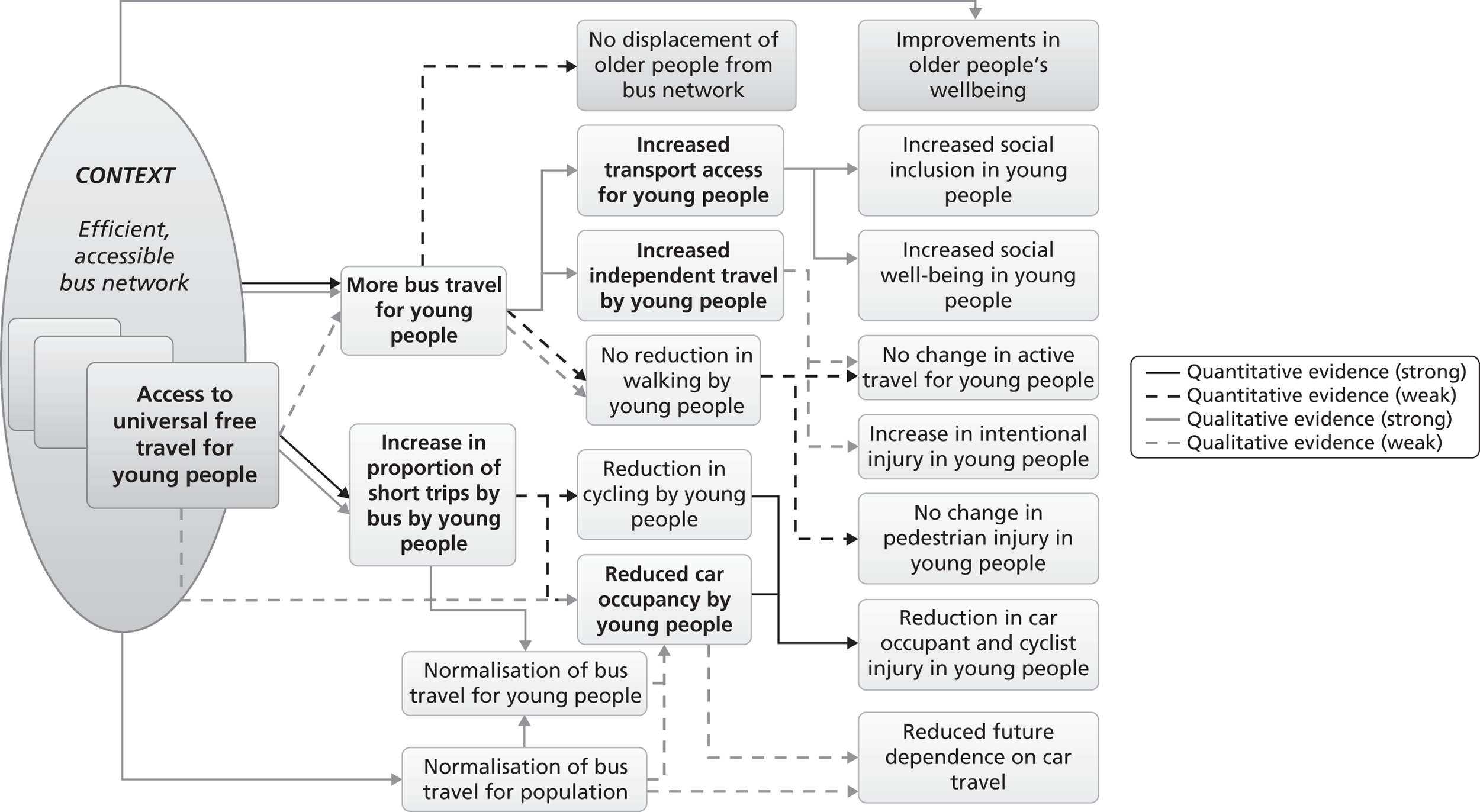
First, we now clarify the meaning of the intervention. The key elements of the intervention were that it provided free bus travel for all young people in the context of broader policies that improved the bus system in London. What we evaluated was ‘universal free bus travel in the context of a good bus service’. Our findings relate to this, and we have specified the intervention (access to universal free bus travel for young people) and major elements of the context (efficient, accessible, bus network) which are preconditions for the effects we have identified from the intervention.
This general context also had some effects which interacted with the effects of the free bus scheme, such as the increasing use of bus travel for the whole population, contributing to normalising bus travel, so we have added lines indicating this.
The context also has effects that act on the study outcomes of interest, independently of the free bus scheme. One we have included here, as data were generated as part of the research on older people’s use of bus services, is a positive impact on the well-being of older citizens in London. 124
The quantitative elements of this study attempted to control for this context to some extent by identifying specific effects of the intervention on the target population of the scheme itself. Evidence for these links (e.g. for an increase in short trips by bus) is indicated by black lines.
Our revised model indicates where there was no evidence found from the quantitative or qualitative analysis for an impact on public health (displacement of older people from the bus network; increase in assaults), and where there was weak evidence, such as suggestive evidence from the qualitative component only (future dependence on cars). This model is not an exhaustive description of the many pathways that link free bus travel to the public health, or an attempt to evaluate whether the scheme overall has been ‘good’ or ‘bad’. The outcomes on the right of the model are diverse, and adjudicating between them both value-laden and often linked to disciplinary, occupational or lifecycle priorities. For example, physical activity outcomes are prioritised by public health researchers, whereas road engineers tend to prioritise injury outcomes, and young people themselves prioritise social inclusion. We have mapped outcomes that were of interest to stakeholders and were theoretically and plausibly related to determinants of health and present a summary of the available evidence from this study for these.
In summary, this model suggests that where free bus travel is offered to all young people in the context of a good bus transport system, then there will be public health gains in terms of young people’s social inclusion and ability to travel independently; there will be minimal impact on the overall amount of active travel young people do; some indication that dependence on car travel is reduced and no evidence that there is a consequent impact on older citizens’ use of bus transport.
Strengths and weaknesses of the study
The design
If the aim of an evaluation is interpreted as one of attributing causal effects between the intervention and outcomes, our design has a number of weaknesses that result from the inability to control for confounders. We mitigated this in so far as we were able by our design for the quantitative elements drawing on best practice for designing studies of natural experiments. 81 In particular we published a protocol for the quantitative component of the study92 (see Appendix 7), specifying hypotheses and the subgroup analyses planned. We identified secondary data sets that provided before-and-after data (for travel modes), and some time series data (for injuries and assaults). Our use of comparisons with adults in London provided proxy ‘non-exposed’ controls, as changes in young people relative to adults are unlikely to be the result of general changes in, say, bus provision in the capital unless these other changes specifically affect young people disproportionately. We have also used proxy ‘dose–response’ measures, such as comparisons between inner and outer London and between boroughs with greater or lesser uptake of free bus travel, where possible. Finally, we developed a logic model to help understand the underlying causal pathways between intervention and outcomes.
In line with Medical Research Council (MRC) guidance on complex interventions,87 we included an economic evaluation to assess the costs and benefits of this intervention, from a societal perspective. This is inevitably limited in that not all costs and benefits can be monetised, and many (such as reduced future dependence on private car travel) are too far in the future to include. However, in the context of increased scrutiny of concessionary fare policies, in almost all scenarios the benefits outweigh the costs – the only exception is a sensitivity test for a hypothetical case in which the additional capacity costs of bus operation were assumed to have increased substantially.
There are of course unknown confounders, and the more general problem of picking up ‘signal from noise’ when looking in isolation at individual changes within complex systems. To offset these weaknesses and build a fuller picture of the impact of the intervention on public health as a whole, we have utilised a multimethod approach which has built up an assessment of public health impacts in an iterative way. To link process measures (transport mode change) to health outcomes, we conducted a systematic review of prospective studies on active travel to assess the strength of evidence on whether or not increasing the amount of active travel in the population was likely to benefit health.
Using secondary data sets
The use of secondary data sets made a before and after evaluation feasible, given that there were existing data sets relating to key outcomes of interest. However, there are always limitations in using data for purposes other than that for which they were designed. Here, the travel diary data available for London, although more detailed and extensive than NTS data, only related to term-time weekday travel for our pre-intervention period. Given that young people’s travel behaviour differs across the year and week58 we may have therefore underestimated both positive and negative effects of the scheme on outcomes relating to mode change. The use of qualitative data allowed us to offset these weaknesses to some extent by providing some data on other journeys.
The data set on RTIs, STATS19, has some well documented limitations in terms of completeness due to the under-reporting and under-recording of traffic collisions. 142 However, this only presents a threat to validity of our results if data completeness has changed over time disproportionately for the target group in relation to our comparator groups, which is unlikely.
Hospital Episode Statistics data, available at a national level, enabled a comparison to made between the incidence of assault injuries in London and those occurring elsewhere in England. HES data record the age of the patient and therefore allowed age-specific rates to be derived. Furthermore, HES data are more likely to be complete over time and so the chance of reporting bias is reduced, unlike data collected on crime occurring on the transport system (e.g. bus incident reports). However, the coding of location within the external cause of injury code is not complete for a substantial proportion of records. This meant that a detailed analysis of assaults according to the place of occurrence (e.g. on the bus, in the street) was not possible. As the hypothesised pathway between the intervention and incidence of assaults did not specifically refer to assaults on the buses, but rather that young people’s increased travel would leave them vulnerable to assaults in general, the lack of location was not a major limitation.
The population: ‘young people’
Our analysis largely addressed the implications for public health of ‘young people’ as a whole, rather than attempting to differentiate the effects by gender, deprivation, or other variables. In London, there are, for instance, known differences in road injury rates by gender, deprivation,143 and ethnicity,43 and on the likelihood of walking for different kinds of journey by ethnicity. 58 It is plausible that these demographic factors will therefore modify the effects of the scheme on outcomes such as transport mode change and RTI. Our focus in this study was on the health effects at a population level, and we used subgroup analyses for sensitivity tests and for estimating dose–response proxies only. That is, our aim has been to use these subgroup analyses to strengthen the credibility of claims made about the population as a whole, rather than to identify subgroup differences per se. A similar approach was taken to the qualitative data, which we have largely treated as referring to single population of ‘young people’ and ‘older citizens’, except where location (e.g. inner or outer London) or gender has relevance for the interpretation of our findings. We sampled for heterogeneity in terms of residence, gender, ethnicity, age and transport modes available, in order to ensure that our sample was not representative of only a narrow sample of the population, but have not sought to analyse our qualitative data comparatively across these characteristics, and a larger sample would be needed to explore differential impacts of the scheme across populations. We are aware that there are likely to be large differences in how issues such as ‘independence’ or ‘risk’ are discussed across gender144 or age, with those aged 12 years likely to differ from the older age groups included. Our aim in this study was not to add to the literature on these differences, but more research is needed on how effects likely to be important for the public health are distributed across populations.
The comparator: adults aged 25–60 years
To ensure an adequately powered comparison, we have included all adults aged 25–60 years as the main comparator group (i.e. those ‘non-exposed’ to the intervention). Although this is a pragmatic choice, including only those with no direct experience of free travel as young people, it does have some limitations in that it includes a larger range of ages than the intervention group. Additionally, as a ‘control’ group, there are limitations in that adults aged 25–60 years have been subject to some interventions which are likely to have affected their travel choices disproportionately compared with the ‘intervention’ group (such as schemes to encourage cycling to work). We have also been unable to assess whether or not the intervention has shifted bus travel by adults to London underground train services, which is one hypothetical outcome of higher bus use by young people.
Strengths of natural experiments
One difficulty facing researchers evaluating complex social interventions is that the intervention effects are moderated by the context. 91 We therefore provided details of the context of this intervention and have described how this affects the study findings.
We suggest, for instance, that the general context of improved bus provision, which also affects adult bus use, and is thus ‘controlled for’ to some extent in our design, is also an important precondition for the effects we see from the intervention. This is because it ‘normalises’ bus transport for the wider population, while also making it viable for young people to exercise peer-based preferences for travel. Without good transport provision, even if all young people had free travel, bus travel would not necessarily be experienced as a ‘normal’ and reasonable way to travel, as this also required that other Londoners were using buses, and that buses were relatively accessible and efficient. This was evident in the accounts of young people with disabilities: free travel was not, in the absence of accessible and good transport, a contributor to social inclusion. However, the fact that most young people were making frequent use of the bus service also has some (if marginal) consequent effects on bus use by adults, as reported in the occasional stories in groups of family outings that are now possible because young members get free travel. This in turn reinforces the normalisation of bus travel as a mode of transport for the whole population. A natural experiment enables a description of what happens in ‘realistic’ policy environments (i.e. ones in which a mix of interventions is likely to be implemented simultaneously).
Finally, an important strength of a natural experiment is that the importance of the system as a whole can be appreciated. One key finding of this study may not have been identified with a randomised controlled design, should this have been theoretically possible. This is that the structural properties of this transport system have effects which are not simply ‘additive’ at an individual level. Specifically, many of the effects of the scheme which have been identified in the qualitative findings arise not from the fact that bus travel is free, but from the fact that it is universally free for young people. 145 This is what is sometimes termed an ‘emergent property’ of the system (i.e. a property of the system as a whole that arises from the interaction of individual parts but cannot be predicted simply by summing the activity of those individual parts). 146,147 Had the scheme been restricted to particular types of journeys (e.g. the journey to school) or specific groups (e.g. low-income families), many of the effects evident in young people’s accounts may not have been realised. We have described in detail how the effects of the scheme are in part a result of the fact that it is available in principle to all young Londoners, and can both accommodate the social, peer-oriented nature of young people’s travel choices and become the default mode. The exceptions demonstrate that these effects only hold when transport is both available and accessible (as young people with disabilities do not enjoy them) and suggest that free bus travel, rather than improvements in general in the bus service, are responsible (as those who have no Oyster card did not benefit).
An evaluation of a design which focused on the individual benefits of free travel (for instance by only offering the scheme in some boroughs, or to some income groups) may not have identified this.
Methodological findings: using mixed methods to strengthen internal and external validity
In Figure 19, many of the claims made are reliant on qualitative data. In terms of assessing the credibility of causal claims made, this is problematic from the perspective of current guidance on evaluating natural experiments,81 which is largely concerned with statistical methods for defending non-randomised designs from the threats to confounding discussed in the section above. However, these guidelines do not currently include other ways of strengthening credibility. Our approach was to use a pragmatic, iterative and inductive design which drew on mixed methods, primarily secondary analysis of existing data sets, analysis of primary qualitative interview data and a systematic review. Rather than taking an epidemiological approach of assessing effectiveness as the primary aim of an evaluation, our approach integrated epidemiological questions of effectiveness within a more inductive mapping of ‘what is going on’, utilising the best available methods and designs for each element of the evaluation. 148
Our final study aim was to contribute to methods for strengthening causal inference, and we turn now to our methodological findings on the challenges of integrating different research designs within one evaluation.
A number of models have been proposed for integrating data in mixed-methods studies. 149 We integrated qualitative data with findings from quantitative data sets using an inductive approach, in addition to a thematic content analysis, to enable an analysis not just of what young people said about the intervention, but also how their accounts of travelling in London reflected tacit knowledge and taken-for-granted understandings. This analysis was used in four ways:
-
To refine our understanding of the concepts (active travel) and the indicators we have chosen (walking, cycling), and of the intervention itself.
-
To assess the credibility of causal attribution through delineating mechanisms by which the intervention may have influenced young people’s behaviour.
-
To provide some insight into important health and well-being outcomes that cannot, currently, be measured or monetised.
-
To understand the context within which the scheme was provided, to help elucidate the necessary and sufficient conditions for its potential effects.
A major challenge with this iterative approach is that the logic of good epidemiological design, with published protocols specifying the hypotheses and analysis plans, sits uneasily with the logic of a more inductive qualitative design, where good practice suggests developing plans for further sampling, data generation and analysis plans as hypotheses emerge from ongoing analysis. 97 An example from this study is the decision to use a change-on-change analysis using adults as a ‘non-exposed’ control. Although this provides some control for broader changes in the transport system which also influence young people’s travel, ongoing qualitative work suggested some limitations of some of the comparisons we had specified. For example, qualitative interviews shed light on the importance of discretionary travel, and suggested that this had implications for the uptake of free bus travel that might be inadequately captured by available travel diary data (which was restricted to term-time weekdays for our ‘pre’ period). Further quantitative analysis is possible, and we did conduct a follow-up study of the different correlates of young people’s travel throughout the week (see Steinbach and colleagues58). To make sense of the evaluation, we would want to take seriously the implications of the qualitative work that the scheme did increase young people’s tendency to use the bus as a ‘default’ mode. However, our predefined protocol specified that the change-on-change analysis (comparing bus travel before and after in adults and young people) would be used to identify whether or not the scheme had ‘caused’ an increase in bus travel. Taking other sources of data into account risks being perceived as introducing the biases from ‘data dredging’ that pre-published protocols are designed to avoid, yet not to do so risks eliminating useful information from the evaluation.
This is not an issue unique to natural experiments. Similar issues have been raised in relation to social science research within RCTs,150 in which trial protocols and procedures designed to maximise intervention fidelity preclude the incorporation of insights from ongoing qualitative research on issues such as how best to operationalise outcome variables in in trial questionnaires, or how to collect data. The challenge is not integrating qualitative and quantitative evidence, but integrating the rather different overarching questions that the two methods relate to: respectively (in our case), ‘how has free bus travel affected the public health?’ and ‘how confident are we that free bus travel brought about this range of outcomes?’
One potential solution to this tension is to utilise a ‘capacity approach’ to evaluating programmes, changing our question from does ‘X causes Y?’ to ‘how stable is X’s capacity to effect a change in Y?’ as suggested by Cartwright and Munro. 151 A focus on the ‘stability’ of the capacities of phenomena (such as policies or programmes) does not preclude attention also to the causal effects of those phenomena, but does mean we are asking a somewhat broader question about ‘what happens’ when a policy is introduced. This requires marshalling a broader range of evidence to develop a credible argument about the likely limits and possibilities of transferability.
Given that the criteria for assessing the stability of capacities are not as well developed as those for assessing the causal claims in RCTs, the claims made from such an approach are likely to be more contentious. There is consequently more reliance on demonstrating how X causes a change in Y rather than just that it does (i.e. the ‘mechanisms’ in epidemiological terms), and on evidence to delineate what other factors can promote, inhibit or otherwise affect the ability of X to affect Y. 151 Thus, suggest Cartwright and Munro,151 an evaluation might usefully ask a set of questions such as: how does X operate to promote Y?; What is needed for X to promote Y?; What can stop/inhibit the operation of X?; What other capacities promote/inhibit Y?; What happens when capacities interact?
Although our evaluation was not designed with this approach in mind, we have used elements of this logic. One particularly important element for external validity (especially with regard to the transferability of evaluations) is the need for greater attention to the theoretical links between concepts (such as between using public transport and active travel), rather than simply the links between indicators (such as the relationship between travel diary reports of bus travel and diary reports of walking and cycling). The indicators for the variables in our causal pathway model in Figure 3 were inevitably chosen pragmatically, from data sets available from before and after the intervention. Indicators such as ‘number of kilometres walked’ as recorded in travel diaries can only ever be partial measures of complex concepts such ‘active travel’. Methods for RCTs have largely been developed in the context of well-understood biological mechanisms, and where reasonable consensus exists around how to judge the reliability and validity of indicators. Extending the logic of these methods to natural experiments of poorly understood and undertheorised systems such as transport carries a risk of focusing our attention on the causal pathways between low level indicators, rather than on the links between concepts and indicators, or between concepts themselves.
This is where qualitative analysis can make an important contribution. Here, we have used the qualitative analysis to shed light on the relationships between concepts and indicators (in, for instance, exploring whether or not bus travel is properly identified as a ‘passive’ mode); on the limitations of current indicators (in, for instance, shedding light on the limitations of using our only available data set, on term-time weekday travel, as an indicator for mode shift); and on the plausibility of causal attribution (in, for instance, the finding that the scheme itself is likely to have increased bus use among young people).
In developing the methodologies needed for evaluations of natural experiments, we suggest a ‘capacities’ approach might be a fruitful avenue for designing studies which maximise both internal and external validity. Where mechanisms are complex, contested and poorly theorised (which applies to most up-stream determinants of health), more attention to adequate theorisation of the conceptual links between determinants of health and health behaviours or outcomes, and the links between concepts and indicators, is essential. The challenge is that this will develop incrementally throughout an evaluation. It is not simply a matter of qualitative work informing the research questions and illuminating quantitative findings, or early quantitative results informing the qualitative interviews. Insights and understanding will inevitably emerge in an incremental way. Developing the evidence base on the structural determinants of health may require rethinking our reliance on models of research deriving from evaluations of effectiveness. In particular, it will entail taking more seriously judgements about the capabilities of interventions, and drawing on a range of research designs148 and sources of evidence (both qualitative and quantitative), rather than relying solely on research designed test hypotheses about ‘what works’.
The implications of our findings for public health
Young people’s well-being
The most significant implications of the free travel scheme for the public health of young people and London as a whole may be those that are most difficult to measure. Like previous research with children at younger ages,152–154 we found that socialising with peers was a pervasive aspect of, and influence on, young people’s mobility. This emphasis on sociability was fundamental to understanding the impact of the scheme for the well-being of young Londoners, for a number of reasons. First, it provided a context for other criteria for decisions, such as the perceived ‘riskiness’ or ‘boringness’ of particular modes. That is, walking, or taking the bus, were not necessarily chosen because they were intrinsically more or less risky, but because they offer different possibilities for travelling together. Second, because free travel was a universal, rather than a targeted, benefit, it could be used by all in a peer group. This, as much as the cost implications, was important to it becoming the ‘default’ mode of travel.
An important implication for the well-being of young people was thus the opening up of the bus network as a space in itself for socialising, as well as opening up the city as a whole. At a time when many commentators have argued that the ‘in-between’ public spaces of cities are becoming increasingly inhospitable to sections of the population such as young people,155 the free bus travel scheme enabled a whole network of familiar, mobile spaces to be used, independently, by young people. As Cattell and colleagues64 note, ‘ordinary spaces’ in urban environments are important sites for fostering social interaction, a collective sense of belonging and encounters with a cosmopolitan range of others. Buses provide a rare such space for young Londoners, enabling not just interaction with peers but, importantly, experiences of managing social engagement with a large cross section of London’s diverse communities. As Russell156 suggests, ‘travel time’ has a number of contributions to social well-being for travellers apart from merely ‘getting somewhere’: providing potential means for social interaction; information exchange; time to do pleasurable activities such as reading, listening to music or enjoying routine; and socialising travellers as part of their neighbourhood. These benefits were evident in young people’s accounts of their bus journeys, but impossible to capture in travel diary data, or in data on health outcomes.
It is important to also recognise that some such encounters of course may be risky. At the extreme, using transport puts young people at risk of assaults, and we identified a rising rate of intentional injury to young people, although this predated the free bus pass. However, from young people’s perspectives, the free bus pass (on balance) reduced the risks of travel.
The free bus pass also enabled both opportunities to enact ‘independence’ and opportunities to develop skills in independent travel. Independent travel has been identified as an important element for young people’s development, and as being potentially curtailed by road danger,67–70 parental fears and the marginalisation of young people in urban environments. 157 Here, we have identified a number of ways in which universal free bus travel facilitated young people’s growing confidence with managing travel, because it enabled rehearsals of mobility with no financial costs and in the company of peers.
Active travel: implications for physical exercise
For public health researchers, the implications of the scheme for active travel are perhaps the most important. 158 Here, there are mixed implications. We identified no strong evidence for the anticipated negative effects on distances walked, given that the scheme appeared to generate new trips, which involved some walking, and some replacement of more ‘passive’ car travel. This is in line with recent findings on the implications of free bus travel for older citizens. 75,76 As in other European settings,159 there may be significant amounts of physical activity within the transport system itself, much of which is not captured by travel diary data. Our qualitative data suggest that treating bus travel purely as a ‘passive’ mode, in contrast to ‘active’ modes of walking and cycling, may underestimate the amount of active travel undertaken. 160
Unlike reports from the USA, however, where public transport interventions may lead to significant increases in active transport,56 in London (where private car use is low), there was no evidence of a beneficial effect. Indeed for cycling, rates had declined from a low base: young people have not shared the benefits of increased uptake of cycling in London seen for adults. Suggestions of similar disincentives from concessionary fares come from the Netherlands, where Welleman161 argues that annual season tickets for public transport for students have reduced cycling trips in this group. What is encouraging from a public health perspective is that young people report enjoying walking and cycling (for leisure) and perceived these modes as ‘healthier’. However, in the context of everyday lives, other well-being benefits are prioritised in the choice of travel mode. Criteria such as ‘physical health’ only outweigh others (such as maximising sociability or inclusion, or minimising risk) for a relatively small number of young people, and for only some journeys.
It is important to note that the mode shifts associated with this intervention represent relatively small amounts of activity: there is a difference between distances walked before the intervention and after the intervention of only 0.01 km, for instance (see Table 34). The likely impact of such small changes in active transport on the public health is difficult to assess. The rationale for intervening at a population level is to make incremental shifts in the amount of physical exercise people are taking, and to reduce energy imbalance from increasing levels of food consumption in tandem with decreasing levels of exercise. At an individual level, it is not clear ‘how much’ exercise is needed to improve health outcomes such as reduction of CV risks. There is some evidence of a dose–response relationship between total physical activity and CV risk in men,162,163 and that small differences in walking would be significant at a population level,164 but for low intensity activity such as walking, there is also evidence suggestive of a ‘threshold’ below which walking confers little benefit in terms of CV risk factors. 165,166 However, this evidence is derived from relatively active, and adult, populations – the long-term health effects of small changes in children’s active travel are difficult to predict. There is some recent evidence that children who do walk or cycle were more active. 167,168 However, there is also evidence that, for younger children at least, adding small distances of walking to children’s exercise does not significantly affect overall activity rates,169 given that distances to school may be very short. A systematic review found little evidence that active transport to school was related to a healthy weight,170 and more research from prospective studies is needed to identify whether or not associations between likelihood and amount of active travel and physical activity overall are causal.
In terms of secondary school-aged children, who may be relatively inactive (compared, for instance, with the primary school-aged children who are the focus of many ‘walk to school’ interventions and evaluations), we know even less about the relationships between walking and cycling for transport and other sources of physical activity: whether, for instance, more walking leads to more physical activity overall, or whether some kind of ‘activity compensation’ occurs, with active travel replacing other sources of activity. There is an urgent need for more robust evidence about the likely immediate and future impacts of increasing levels of active transport on the health of adolescents and children.
Implications for sustainability
Furthermore, given that one incentive for many policy interventions (including to some extent this one) is to foster sustainable and healthy habits into the future, we know little to date about how far habits adopted in childhood or adolescence are maintained into adulthood. Our qualitative data suggested that bus transport had been ‘normalised’ for young people, and not considered a ‘mode of last resort’, or stigmatised as being largely for those with no access to other options. This shift in attitude to public transport is important, as it has been identified as an essential precondition for moving transport systems away from car dependency towards mass public transport. 171,172 More research is needed on how far these attitudes do change future propensities to drive.
Our findings suggest that although young people (and young men in particular) still largely view driving as an anticipated rite of passage to adulthood, for those in older adolescence, who are more likely to have had experience of driving, its attractions had diminished. Our data are not extensive enough to comment on how far this may delay learning to drive, or car ownership. In the light of debate around the declines in driving in young adults, both in the UK and other European countries,173,174 further research on how young people view driving, and what role local public transport provision has in their orientations to driving and car ownership, is urgently needed.
The implications for social and health inequalities
Theoretically, transport systems can create, reinforce, mitigate or remove causes of health inequality through a number of pathways. At the most fundamental level, access to transport is essential in most settings to access the determinants of health: goods, services and social interaction. The scheme has removed one important contributor to social exclusion for young people: transport costs. This was evident in both the absence of financial considerations in young people’s accounts of travelling for school and other purposes, and in the reported limitations that were experienced when zip cards were lost, stolen or rescinded.
A system which ensures that all young people are financially able to access transport may therefore be an important necessary condition for a socially equitable transport system, but it is not in itself a sufficient condition. The accounts of young people with disabilities demonstrated that free travel on its own was not enough to provide equitable access. For them, bus services were a source of exclusion and marginalisation. The transport mode itself also has to be physically accessible and available, which was not the case for many young people with disabilities.
Beyond removing lack of ability to pay for transport, an additional important consideration for equity is what effects the intervention had on the meaning of bus travel. If concessionary fares merely offer access to a mode of transport that is socially low status, then removing financial barriers for some groups may inadvertently increase inequalities, through further stigmatising those who (have to) use it. Given the literature on the relative status of car driving in many parts of the UK compared with bus travel (e.g. see Hiscock and colleagues171), offering free bus travel to some population groups (such as the young and older citizens) may simply reinforce the stigma attached to bus travel:145 that it is for those who can afford no other, more prestigious, way of travelling. Here, an important condition for the effects we have noted of the free travel scheme was the universality of the scheme, which made it (unlike other more targeted benefits such as free school meals)145 a non-stigmatised entitlement in the context of these general increases in the efficiency and availability of bus services in London which made them more attractive to a wide range of travellers.
If universal free bus travel for young people removed one theoretical cause of inequalities (i.e. transport exclusion as a barrier to education and training), we might expect a greater uptake of bus travel, or a flattening of the social deprivation gradient for trips for education purposes after the intervention. However, we found no evidence that the intervention had a different uptake across deprivation quintiles, or that there was a flattening of the gradient of trips for educational purposes. What is also important for equity, though, is the ability to participate in socially valued activities such as leisure trips, and bus journeys as outings in themselves. Discretionary journeys, such as for shopping or just ‘hanging out’ are vital for young people’s social inclusion, and the (weak) evidence for some flattening of the social gradient in these journeys is encouraging.
Generalisability
In terms of adding to the public health evidence base, to what extent is credible evidence linking the introduction of free bus travel to health outcomes in London generalisable beyond one (atypical) setting? London has relatively good public transport networks, and there are indications that, for instance, there is less attachment to car transport as a socially prestigious mode than in other parts of the country. 40 Here, a randomised controlled design, even if such a study were theoretically possible, would not necessarily be a ‘stronger’ design. As Cartwright argues,151,175 there are inherent weaknesses in terms of external validity from the focus on overly refined causal chains which are insufficiently theorised in terms of links between more abstract concepts. In this setting, the risk would lie in making a link between, say, ‘free bus travel’ and ‘fewer miles walked’ with insufficient conceptualisation of what those links actually mean in this context. Is ‘free bus travel’ an empirical indicator of: a financial saving, a plastic card bearing a photo, the ability to travel across London or the status that derives from an entitlement as a citizen of London? Our qualitative work has mitigated this threat to generalisability to some extent, through unpacking what the various indicators in our model might mean (see Figure 19).
The public health implications of transport planning in London are typical of those in many cities across the world. Transport systems which foster ever increasing car dependency are not sustainable107 and a growing public health literature identifies the short-, medium- and long-term implications for health of not addressing this dependency. We have evaluated a scheme which, as part of a broader raft of policies that encouraged public transport use, had promising implications for mitigating some of these effects. Specifically, we identified evidence that the scheme played a role in ‘normalising’ bus transport for young people, an important precondition of reducing future car dependency, and one faced in other urban environments in which car drivers typically have negative views of public transport deriving from lack of experience using it. 176 London may be unique in its transport system and the governance of that system, but we have outlined the key features of this ‘uniqueness’ that contribute to the effects identified of the scheme: that it was introduced in the context of general improvements in the bus service and other policies to reduce private car use. However, in a UK context, a key question is the generalisability of the scheme overall to settings with deregulated bus services, where levers for improving public transport lie primarily with operating companies rather than transport authorities. A recent Passenger Transport Executive Group report177 addressed bus transport for young people in urban areas outside London, noting the importance of good bus provision for their current access to activities necessary for well-being and to ensure that they continue to see public transport as a viable option in adulthood. Citing a number of concessionary schemes that have achieved gains in bus ridership and acceptability to young people, the report suggests that simplicity in fare structures and developing services in tandem with young people are key factors. Detailed comparisons of the London free bus scheme with the outcomes of schemes in other settings, particularly those in which there are Integrated Transport Authorities, will help elucidate what can be gained in terms of ‘normalising’ bus use in urban centres with varying transport governance arrangements. In the case study described here, there is no reason to suppose that many of the benefits reported would not be replicable in other metropolitan contexts where public transport is destigmatised. Although London is unusual in that public transport tends to be used right across the social spectrum, in a different context, Baker and White178 found that those with access to cars were also making significant use of buses following the introduction of concessionary travel. This, they point out, may have implications for wider policies aimed at traffic reduction. In a global context where the need to introduce measures to address carbon emissions are largely recognised in high- and middle-income countries, there may also be wider benefits to extending concessionary schemes in differing social, economic and political contexts. Debates about how to not only ‘normalise’ but to privilege public transport are now gaining international policy traction with, for instance, a Delhi High Court judgement rejecting a proposal to abolish the Delhi Bus Rapid Transit System with the words: ‘A developed country is not one where the poor owns cars but it is one where the rich use public transport’. 179
We have presented evidence of the effects, mechanisms and influences at work when free travel is offered to young people in the context of a good bus network, used by the broader population. Future users of this evidence can use it to help assess whether or not those mechanisms and influences are similar enough to their own setting to predict likely effects.
Implications for further research
We have identified a number of areas where more evidence would be useful to inform policy.
The effects of ‘active travel’ on health
There are plausible grounds for encouraging active transport as a way to increase the levels of physical activity in the population, but our literature review90 (see Appendix 8) identified a lack of robust studies which demonstrate the health benefits of this. A considerable amount of cross-sectional research identifies health gains in those who are active, but to date there is a dearth of studies which demonstrate that changing the amounts of active transport individuals undertake will result in health benefits. Given uncertainties around activity synergy and compensation, and the debate around how much additional activity is needed to produce health gain, particularly for young people, intervention studies are urgently needed to address health outcomes of changes in behaviour. Additionally, given the population differences in transport mode choice, we need more information about how such interventions are likely to affect different groups in the population.
The effects of different transport modes on the determinants of health
The qualitative data suggested a number of benefits for young people of universal free bus travel that could not be captured through current quantitative measures, including fostering independent travel, fostering a sense of ‘belonging’, facilitating social inclusion and providing a rare space to socialise. We have, however, no comparative data on what other modes might provide. Being driven, for example, although having costs in terms of active transport, may be a rare opportunity to talk with parents in a busy day, and walking can provide young people with opportunities for private discussions with friends. Any full assessment of the health effects of transport mode choice for young people would need to incorporate these broader implications of transport mode choice for health, requiring more research on the meaning of transport and well-being in the lives of young people, particularly adolescents who have been relatively under-researched.
This may well require the development of novel methodologies. Travel diary data provide feasible sources for assessing large-scale changes in transport mode, but have limitations in capturing the ‘non-travel’ activity related to transport mode use, as illustrated in Chapter 3, where bus travel that is undertaken for the ‘fun’ of the journey may be under-recorded in travel diary time. More direct measures of young people’s activity [such as Global Positioning System (GPS) or activity monitors] have their own problems: Mackett and colleagues180 report the difficulties in collecting data from large numbers of young people at a time; managing the large number of data points in analysis and the pragmatic demands on participants of managing the devices.
Maintenance of transport mode change
One causal pathway for which we had limited evidence was that leading to reduced car dependence. The likely impact of transport interventions on sustainability is a crucial issue, and this policy aimed to reduce future car dependency. In general, we found little literature on how far habits changed in adolescence (or indeed later) are maintained in the medium and long term. Despite promising modelling181,182 suggesting that it is possible to change travel habits through changes in environment or policy, and intervention studies with promising results on the possibilities of increasing public transport use,183,184 there is little evidence on which to base estimations of future gains. Specifically, there is little evidence on how far attitudes to or experience of public transport in adolescence might translate into adult behaviour. Robust cohort studies are needed that track changes in behaviour (and ideally, as above, health outcomes), particularly for young people, over time. Transport interventions (e.g. the introduction of hire bikes) or workplace or school health promotion programmes would provide an ideal setting from which to recruit cohorts to explore the effects of changing travel patterns on health.
Transport as social practice
This raises a more general question about the cultural meaning of different transport modes, and how these change. It has been suggested that a key element of reducing car dependence will be to improve perceptions of public transport such that it is no longer seen as low status compared with car travel. 111,182 A small social science literature now addresses the ways in which transport mode choices can be interpreted as social practice, in that they reflect not just individual decisions (based on, say, barriers and facilitators), but are embedded in cultural and material fields. 185–187 There has been less research on how these change. In this study, we suggested that the ‘normalisation’ of bus travel has changed the meaning this mode has in London. We also suggested that ‘cycling’ continues to be invisible to most young people as a candidate mode of transport. Research from sociology or anthropology that addressed ‘bus travel’ or ‘cycling’ as social practice, and how their meanings change in relation to changing environments and policies, would generate useful information for informing interventions and promotional materials for those interested in increasing the modal share for either ‘active’ or public transport. One particularly urgent need is for research on driving as social practice, to understand better the role of driving for young adults, and to explore the noted declines in driving and car ownership in some groups of young adults. This would provide invaluable base line information for future evaluations of schemes such as graduated driving licences.
Road traffic injury rates for young adults
This study was not powered to look specifically at the impact of change in travel modes on RTIs in young adults. Any future evaluation of the impact of reduced driving rates in young adults could usefully address the question of whether or not mode change (e.g. from car travel to public transport) is associated with reduced injury rates for young adults. The proposed introduction of Graduated Drivers’ Licenses in Northern Ireland would be a timely opportunity to address this.
Value of a statistical life for young people
The need for further research on the health impacts of active transport for young people raises the issue of whether or not monetary values that have been determined based on an adult population could be applied without change to the age group (12–17 years) in this study to determine the monetary benefits from changes to levels of physical activity, assaults and casualties. Although there has been a growing body of research that focus on this issue (see WHO130 and Leung and Guria188), indicating that differing values should be applied to children, Alberini and colleagues189 conclude ‘that there is no single ratio which can capture differences in risk preferences for children and adults, [but] there is some evidence that the VSL [value of statistical life] for a child is greater than that of an adult’.
Theoretically, an individual’s own VOSL is driven by life expectancy – decreasing with age – tempered to some extent by the level of risk – which increases with age. 190 Other factors are however important. First, young people’s health and safety is valued not only by themselves but by their family and friends, and there is evidence that parental VOSL for children exceeds VOSL for adults (e.g. Agree and Crocker,191 Blomquist and colleagues,192 Hammitt and Hanninger193). Second, in policy evaluation, there is a tradition of equal treatment, using social values based on political and ethical judgements, not only individual or familial VOSL. Thus, for example, the values used for road casualties in transport CBA are set equal for all ages,126 and values of travel time are set equal across regions with very different household income and ability to pay. 194,195 So, for example, if we were to propose differentiated VOSL for children and adults (higher for children) based on an individual or familial valuation, we would need to consider the implications for other groups (older people or adults in middle age) for whom individual/familial VOSL may be lower than the mean.
Further research is needed to definitively show how these differences in risk preferences translate into changes in values. In this study we have applied the adult values to the 12- to 17-year-old age group; hence, based on the available research on adult compared with child values the benefits are conservatively estimated.
Acknowledgements
Funding acknowledgement
This project was funded by the National Institute for Health Research Public Health Research programme (project number 09/3001/13). AG contributed to this research while funded by an NIHR post-doctoral fellowship.
Acknowledgements for contributions to the project
The team would like to thank the following people:
Avril Porter, project administrator, for her invaluable input to the administration and management of the study.
Chris Lines (Transport Consultant) for his support and enthusiasm for the project throughout; his skill and insights as chair of the study Steering Committee and for chairing a stakeholder workshop.
Suzanne Lutchmun (NHS Camden), member of the Steering Committee, for her input into the original idea for the project and for bringing public health insights to the discussions.
Alex Phillips and Richard Jeremy (TfL) for their support as members of the Steering Committee, generosity with their time in providing information and data and helpful input to the report writing.
Steven Salmon (Confederation of Passenger Transport) for his invaluable input to the Steering Committee.
John Barry (TfL) for input to stakeholder workshops and helpful advice.
Zara Todd for help in identifying participants and advice on young disabled travellers.
Alan Shiell (Executive Director of the Centre of Excellence in Intervention and Prevention Science, Melbourne, Austrailia) for health economics input, support and helpful discussions throughout and for chairing a stakeholder event.
Lucinda Saunders (GLA) for her contributions to the project while based at LSHTM, in particular for conducting a literature review of the impact of active travel on health outcomes and for providing a commentary for the stakeholder event ‘On the Buses Workshop’.
Bhash Naidoo (NICE) and Kenny Lawson (Glasgow MRC) for their presentations at the Stakeholder Event on ‘Economic Evaluations for Informing Public Health Policy’.
Rebecca Fuller (Passenger Transport Executive Group), Risan Nishori (Robert Clack School) and Reece Weaver (Robert Clack School) for their commentaries on our draft findings at the Stakeholder Event ‘On the Buses Workshop’.
We are also grateful to the participants from the DfT, TfL, London Boroughs, Kilburn Older Voices Exchange, Living Streets, Confederation of Passenger Transport UK, NHS organisations and academic colleagues who contributed to these events.
All the young people who conducted research inspired by On The Buses as part of LSHTM’s Young Scientists’ Programme.
Monisha Sodha, Nancy Williamson and Shirley Solomon for their administrative help on the project.
Finally, our greatest debt is to all the young people and older citizens who kindly talked to us about their travel in London, and the various schools, community organisations and local councils who helped with contacting those individuals.
Prior publications
This report draws on the following work already published:
Jones A, Steinbach R, Roberts H, Goodman A, Green J. Rethinking passive transport: bus fare exemptions and young people’s wellbeing Health and Place 2012;18:605–12.
Jones A. Free for some: setting the context for the ‘On the Buses’ study. Occasional papers in transport and health (1). London: LSHTM; 2010.
Wilkinson P, Edwards P, Steinbach R, Petticrew M, Goodman A, Jones A, et al. The health impact of free bus travel for young people in London: protocol for an observational study. Occasional papers in transport and health (2). London: LSHTM; 2011.
Green J, Jones A, Roberts H. More than A to B: the role of free bus travel for the mobility and wellbeing of older citizens in London. Ageing Soc 2012. http://dx.doi.org/10.1017/S0144686X12001110
Edwards P, Steinbach R, Green J, Petticrew M, Goodman A, Jones A, et al. Health Impacts of free bus travel for young people: evaluation of a natural experiment in London. J Epidemiol Community 2013. doi:10.1136/jech-2012-202156
Saunders L, Green J, Petticrew M, Steinbach R, Roberts H. What are the health benefits of active travel? A systematic review of trials and cohort studies. PLOS ONE 2013;8:e69912.
Goodman A, Jones A, Roberts H, Steinbach R, Green J. ‘We can all just get on a bus and go’: rethinking independent mobility in the context of the universal provision of free bus travel to young Londoners. Mobilities 2013. http://dx.doi.org/10.1080/17450101.2013.782848
Contributions of authors
Dr Judith Green (Reader, Sociology of Health, LSHTM) was the principal investigator. She co-ordinated the study, contributed to the study design, qualitative fieldwork and analysis, interpretation of data and writing the report.
Ms Rebecca Steinbach (Research Fellow, Social Epidemiology, LSHTM) prepared data sets (London travel surveys, STATS19 road casualty data and HES), conducted statistical analyses and prepared data for the economic evaluation. She contributed to the qualitative fieldwork, qualitative data analysis and the writing of the report.
Dr Alasdair Jones (Research Fellow in Qualitative Research, LSHTM) contributed to the design of the qualitative study, led the qualitative fieldwork, and contributed to analysis, interpretation of findings and writing the final report.
Dr Phil Edwards (Senior Lecturer, Statistics, LSHTM) contributed to the study design, prepared data sets (London travel surveys, STATS19 road casualty data and HES) and conducted statistical analyses. He contributed to the writing of the report.
Ms Charlotte Kelly (Senior Research Fellow, ITS, University of Leeds) contributed to the economic analysis, interpretation of data and writing the report.
Dr John Nellthorp (Senior Research Fellow, ITS, University of Leeds) contributed to the economic analysis, interpretation of data and writing the report.
Dr Anna Goodman (Research Fellow, Social Epidemiology, LSHTM) contributed to the qualitative data collection and analysis, interpretation of the data and writing the report. She led the youth engagement strand of the project.
Professor Helen Roberts (Professorial Research Fellow, Medical Sociology, UCL Institute of Child Health) contributed to the study design, qualitative fieldwork, interpretation of findings and writing of final report.
Professor Mark Petticrew (Professor, Public Health Evaluation, LSHTM) contributed to the study design, interpretation of findings and writing of final report.
Professor Paul Wilkinson (Professor, Environmental Epidemiology, LSHTM) contributed to the study design, interpretation of the data and the writing of the final report.
Disclaimers
The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PHR editors and publisher have tried to ensure the accuracy of the authors’ report and would like to thank the referees for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this report.
The views expressed in this publication are those of the authors and not necessarily those of the PHR programme or the Department of Health.
References
- de Nazelle A, Nieuwenhuijsen MJ, Antó JM, Brauer M, Briggs D, Braun-Fahrlander C, et al. Improving health through policies that promote active travel: a review of evidence to support integrated health impact assessment. Environ Int 2011;37:766-77. http://dx.doi.org/10.1016/j.envint.2011.02.003.
- Mindell J, Sheridan L, Joffe M, Samson-Barry H, Atkinson S. Health impact assessment as an agent of policy change: improving the health impacts of the mayor of London’s draft transport strategy. J Epidemiol Community Health 2004;58:169-74. http://dx.doi.org/10.1136/jech.2003.012385.
- Exworthy M, Stuart M, Blane D, Marmot M. Policy case study: the role of transport in tackling health inequalities. Tackling health Inequalities since the Acheson Inquiry. Bristol: The Policy Press; 2003.
- Kerr J, Frank L, Sallis JF, Chapman J. Urban form correlates of pedestrian travel in youth: differences by gender, race-ethnicity and household attributes. Transport Res Transport Environ 2007;12:177-82. http://dx.doi.org/10.1016/j.trd.2007.01.006.
- Macintyre S, Macdonald L, Ellaway A. Do poorer people have poorer access to local resources and facilities? The distribution of local resources by area deprivation in Glasgow, Scotland. Soc Sci Med 2008;67:900-14. http://dx.doi.org/10.1016/j.socscimed.2008.05.029.
- Steinbach R, Grundy C, Edwards P, Wilkinson P, Green J. The impact of 20 mph traffic speed zones on inequalities in road casualties in London. J Epidemiol Community Health 2011;65:921-6. http://dx.doi.org/10.1136/jech.2010.112193.
- Morabia A, Costanza MC. Come on, come on, do the loco-motion. Prev Med 2008;46:1-3. http://dx.doi.org/10.1016/j.ypmed.2007.12.001.
- Killoran A, Doyle N, Waller S, Wohlgemuth C, Crombie H. Transport interventions promoting safe cycling and walking: evidence briefing. London: National Institute for Health and Care Excellence; 2006.
- Ogilvie D, Mitchell R, Mutrie N, Petticrew M, Platt S. Evaluating health effects of transport interventions: methodologic case study. Am J Prev Med 2006;31:118-26.
- Cavill N, Kahlmeier S, Rutter H, Racioppi F, Oja P. Economic analyses of transport infrastructure and policies including health effects related to cycling and walking: a systematic review. Transport Pol 2008;15:291-304. http://dx.doi.org/10.1016/j.tranpol.2008.11.001.
- Kahlmeier S, Cavill N, Dinsdale H. Geneva: World Health Organization (WHO) Regional Office for Europe; 2011.
- Transport for London (TfL) . Where You Can Use Oyster London: Transport for London n.d. www.tfl.gov.uk/tickets/14869.aspx (accessed 30 September 2010).
- Transport for London News. London: TfL; 2006.
- Getting around with discounts. London: TfL; 2010.
- Making the connections: final report on transport and social exclusion. London: Office of the Deputy Prime Minister; 2003.
- Transport for London (TfL) . Pan-TfL Developments: Fares and Ticketing, Free Travel for Children London n.d. www.tfl.gov.uk/corporate/about-tfl/investorrelations/4427.aspx (accessed 11 October 2010).
- Crime and disorder on London’s buses. London: Greater London Authority; 2008.
- A problem-oriented policing approach to tackling youth crime and anti-social behavior on London’s buses. London: TfL; 2008.
- Evans R. Scrap free bus travel for kids, Boris – it’s fueling obesity. Local Transport Today 2011.
- Woodcock J, Edwards P, Tonne C, Armstrong BG, Ashiru O, Banister D, et al. Public health benefits of strategies to reduce greenhouse-gas emissions: urban land transport. Lancet 2009;374:1930-43. http://dx.doi.org/10.1016/S0140-6736(09)61714-1.
- Edwards P, Roberts I. Population adiposity and climate change. Int J Epidemiol 2009;38:1137-40. http://dx.doi.org/10.1093/ije/dyp172.
- Sallis JF, Glanz K. Physical activity and food environments: solutions to the obesity epidemic. Milbank Q 2009;87:123-54. http://dx.doi.org/10.1111/j.1468-0009.2009.00550.x.
- Grayling T, Grayling T. Any more fares? Delivering better bus services. London: Institute for Public Policy Research (IPPR); 2001.
- Jones A. Free for some? Setting the context for the ‘On the Buses’ study. London: London School of Hygiene and Tropical Medicine (LSHTM); 2010.
- Public transport services: summary. Leeds: University of Leeds; 2010.
- The Mayor’s transport strategy. London: GLA; 2001.
- Mayor’s transport strategy: public draft. London: GLA; 2009.
- Statistics of education: school destinations of secondary school pupils resident in London boroughs, 2010. London: Her Majesty’s Stationary Office; 2010.
- London travel report 2007. London: TfL; 2007.
- The London plan: spatial development strategy for greater London. Consolidated with alterations since 2004. London: GLA; 2008.
- Travel in London: report 2. London: TfL; 2010.
- Givoni M. Re-assessing the results of the London congestion charging scheme. Urban Stud 2012;49:1089-105. http://dx.doi.org/10.1177/0042098011417017.
- Grundy C, Steinbach R, Edwards P, Green J, Armstrong B, Wilkinson P. The effect of 20 mph traffic speed zones on road injuries in London, 1986–2006: a controlled interrupted time series analysis. BMJ 2009;339. http://dx.doi.org/10.1136/bmj.b4469.
- Prud’homme R, Bocarejo JP. The London congestion charge: a tentative economic appraisal. Transport Pol 2005;12:279-87. http://dx.doi.org/10.1016/j.tranpol.2005.03.001.
- Pooley CG, Turnbull J, Adams M. The journey to school in Britain since the 1940s: continuity and change. Area 2005;37:43-5. http://dx.doi.org/10.1111/j.1475-4762.2005.00605.x.
- Dowling R. Cultures of mothering and car use in suburban Sydney: a preliminary investigation. Geoforum 2000;31:345-53. http://dx.doi.org/10.1016/S0016-7185(99)00048-2.
- Davison KK, Werder JL, Lawson CT. Children’s active commuting to school: current knowledge and future directions. Prev Chronic Dis 2008;5.
- The Evening Standard . Safer Cycling n.d. www.thisislondon.co.uk/standard/article-23411440-safer-cycling.do (accessed 26 September 2013).
- London Borough of Richmond upon Thames . Smarter Travel Richmond Upon Thames n.d. www.sutton.gov.uk/index.aspx?articleid=11904 (accessed 26 September 2013).
- Green J, Steinbach R, Datta J. The travelling citizen: emergent discourses of moral mobility in a study of cycling in London. Sociology 2012;46:272-89. http://dx.doi.org/10.1177/0038038511419193.
- Edwards P, Green J, Lachowycz K, Grundy C, Roberts I. Serious injuries in children: variation by area deprivation and settlement type. Arch Dis Child 2008;93:485-9. http://dx.doi.org/10.1136/adc.2007.116541.
- Edwards P, Roberts I, Green J, Lutchmun S. Deaths from injury in children and employment status in family: analysis of trends in class specific death rates. BMJ 2006;333:119-21. http://dx.doi.org/10.1136/bmj.38875.757488.4F.
- Steinbach R, Green J, Edwards P, Grundy C. ‘Race’ or place? Explaining ethnic variations in childhood pedestrian injury rates in London. Health Place 2010;16:34-42. http://dx.doi.org/10.1016/j.healthplace.2009.08.002.
- Sonkin B, Edwards P, Roberts I, Green J. Walking, cycling and transport safety: an analysis of child road deaths. J R Soc Med 2006;99:402-5. http://dx.doi.org/10.1258/jrsm.99.8.402.
- Wanless D, Treasury H. Securing good health for the whole population: final report. London: HM Treasury; 2004.
- Choosing health: making healthier choices easier. London: DoH; 2004.
- The evidence of effectiveness of public health interventions and the implications. HDA Briefing No. 1. London: HDA; 2004.
- Hamer M, Chida Y. Active commuting and cardiovascular risk: a meta-analytic review. Prev Med 2008;46:9-13. http://dx.doi.org/10.1016/j.ypmed.2007.03.006.
- Ogilvie D, Foster C, Rothnie H, Cavill N, Hamilton V, Fitzsimons C, et al. Interventions to promote walking: systematic review. BMJ 2007;334:1204-14. http://dx.doi.org/10.1136/bmj.39198.722720.BE.
- Gordon-Larsen P, Nelson MC, Beam K. Associations among active transportation, physical activity, and weight status in young adults. Obes Res 2005;13:868-75. http://dx.doi.org/10.1038/oby.2005.100.
- Oja P, Vuori I, Paronen O. Daily walking and cycling to work: their utility as health-enhancing physical activity. Patient Educ Counsel 1998;33:87-94. http://dx.doi.org/10.1016/S0738-3991(98)00013-5.
- Cooper AR, Wedderkopp N, Jago R, Kristensen PL, Moller NC, Froberg K, et al. Longitudinal associations of cycling to school with adolescent fitness. Prev Med 2008;47:324-8. http://dx.doi.org/10.1016/j.ypmed.2008.06.009.
- Walking and cycling: an action plan. London: DfT; 2004.
- Ogilvie D, Egan M, Hamilton V, Petticrew M. Promoting walking and cycling as an alternative to using cars: systematic review. BMJ 2004;329. http://dx.doi.org/10.1136/bmj.38216.714560.55.
- Zheng Y. The benefit of public transportation: physical activity to reduce obesity and ecological footprint. Prev Med 2008;46:4-5. http://dx.doi.org/10.1016/j.ypmed.2007.11.019.
- Besser LM, Dannenberg AL. Walking to public transit: steps to help meet physical activity recommendations. Am J Prev Med 2005;29:273-80.
- Edwards RD. Public transit, obesity, and medical costs: assessing the magnitudes. Prev Med 2008;46:14-21. http://dx.doi.org/10.1016/j.ypmed.2007.10.004.
- Steinbach R, Green J, Edwards P. Look who’s walking: social and environmental correlates of children’s walking in London. Health Place 2012;18:917-27. http://dx.doi.org/10.1016/j.healthplace.2012.02.005.
- Pabayo R, Gauvin L. Proportions of students who use various modes of transportation to and from school in a representative population-based sample of children and adolescents, 1999. Prev Med 2008;46:63-6. http://dx.doi.org/10.1016/j.ypmed.2007.07.032.
- Bostock L. Pathways of disadvantage? Walking as a mode of transport among low-income mothers. Health Soc Care Community 2001;9:11-8. http://dx.doi.org/10.1046/j.1365-2524.2001.00275.x.
- Crum AJ, Langer EJ. Mind-set matters. Psychol Sci 2007;18:165-71. http://dx.doi.org/10.1111/j.1467-9280.2007.01867.x.
- Brunton G, Oliver S, Oliver K, Lorenc T. A synthesis of research addressing children’s, young people’s and parents’ views of walking and cycling for transport. London: The Evidence for Policy and Practice Information and Co-ordinating Centre (EPPI-Centre) Institute of Education, University of London; 2006.
- Church A, Frost M, Sullivan K. Transport and social exclusion in London. Transport Pol 2000;7:195-20. http://dx.doi.org/10.1016/S0967-070X(00)00024-X.
- Cattell V, Dines N, Gesler W, Curtis S. Mingling, observing, and lingering: everyday public spaces and their implications for well-being and social relations. Health Place 2008;14:544-61. http://dx.doi.org/10.1016/j.healthplace.2007.10.007.
- Under 16 free bus travel: research report. London: TfL; 2006.
- Impact of free travel for 16–17 year olds: quantitative research report. London: TfL; 2007.
- Fotel T, Thomsen TU. The surveillance of children’s mobility. Surveill Soc 2004;1:535-54.
- Gill T. No fear: growing up in a risk averse society. London: Calouste Gulbenkian Foundation; 2007.
- Kytta M. The extent of childrens independent mobility and the number of acutalised affordances as criteria for child-friendly environments. J Environ Psychol 2004;24:179-98.
- Hillman M, Adams J, Whitelegg J. ONE FALSE MOVE. A study of children’s independent mobility. London: PSI Publishing; 1990.
- O’Brien M, Jones D, Sloan D, Rustin M. Children’s independent spatial mobility in the urban public realm. Childhood 2000;7:257-77. http://dx.doi.org/10.1177/0907568200007003002.
- Page A, Cooper A, Griew P, Davis L, Hillsdon M. Independent mobility in relation to weekday and weekend physical activity in children aged 10–11 years: the PEACH Project. Int J Behav Nutr Phys Activ 2009;6. http://dx.doi.org/10.1186/1479-5868-6-2.
- Prezza M, Pacilli M. Current fear of crime, sense of community, and loneliness in Italian adolescents: the role of autonomous mobility and play during childhood. J Community Psychol 2007;35:151-70. http://dx.doi.org/10.1002/jcop.20140.
- Balcombe R, Mackett R, Paulley N, Preston J, Shires J, Titheridge H, et al. Crowthorne: Transport Research Laboratory (TRL); 2004.
- Webb E, Netuveli G, Millett C. Free bus passes, use of public transport and obesity among older people in England. J Epidemiol Community Health 2012;66:176-80. http://dx.doi.org/10.1136/jech.2011.133165.
- Kelly E. A ticket to ride: does free bus travel promote active ageing. London: University of London, University College London; 2011.
- Transport statistics bulletin. National Travel Survey: 2006. London: Office for National Statistics; 2007.
- Bellis M, Hughes K, Wood S, Wyke S, Perkins C. National five-year examination of inequalities and trends in emergency admisssion for violence across England. Inj Prev 2011;17:319-25. http://dx.doi.org/10.1136/ip.2010.030486.
- Watkiss P, Brand C, Hurley F, Pilkington A, Mindell J, Joffe M, et al. Informing transport health impact assessment in London. London: NHS Executive; 2000.
- Preston J. Epilogue: transport policy and social exclusion – some reflections. Transport Pol 2009;16:140-2. http://dx.doi.org/10.1016/j.tranpol.2009.04.003.
- Craig P, Cooper C, Gunnell D, Haw S, Lawson K, Macintyre S, et al. Using natural experiments to evaluate population health interventions: new MRC guidance. J Epidemiol Community Health 2012;66:1182-6.
- Petticrew M, Cummins S, Ferrell C, Findlay A, Higgins C, Hoy C, et al. Natural experiments: an underused tool for public health?. J Public Health 2005;119:751-7. http://dx.doi.org/10.1016/j.puhe.2004.11.008.
- Anderson LM, Petticrew M, Rehfuess E, Armstrong R, Ueffing E, Baker P, et al. Using logic models to capture complexity in systematic reviews. Res Synth Meth 2011;2:33-42. http://dx.doi.org/10.1002/jrsm.32.
- Logic model development guide. Battle Creek, MI: W.K. Kellogg Foundation; 2004.
- London School of Hygiene and Tropical Medicine . LSHTM’s Young Scientists’ Programme n.d. www.lshtm.ac.uk/aboutus/introducing/volunteering/ysp/ (accessed 8 October 2013).
- Tonne C, Beevers S, Armstrong B, Kelly F, Wilkinson P. Air pollution and mortality benefits of the London Congestion Charge: spatial and socioeconomic inequalities. Occup Environ Med 2008;65:620-7. http://dx.doi.org/10.1136/oem.2007.036533.
- Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ 2008;337:979-83.
- Oja P, Titze S, Bauman A, de Geus B, Krenn P, Reger-Nash B, et al. Health benefits of cycling: a systematic review. Scand J Med Sci Sports 2011;21:496-509. http://dx.doi.org/10.1111/j.1600-0838.2011.01299.x.
- Morris JN, Hardman AE. Walking to health. Sports Med 1997;23:306-32. http://dx.doi.org/10.2165/00007256-199723050-00004.
- Saunders L, Green J, Petticrew M, Steinbach R, Roberts H. What are the health benefits of active travel? A systematic review of trials and cohort studies. PLOS ONE 2013;8. http://dx.doi.org/10.1371/journal.pone.0069912.
- Shiell A, Hawe P, Gold L. Complex interventions or complex systems? Implications for health economic evaluation. BMJ 2008;336:1281-3. http://dx.doi.org/10.1136/bmj.39569.510521.AD.
- The health impact of free bus travel for young people in London: protocol for an observational study 2011. www.lshtm.ac.uk/php/hsrp/buses/publications/4wilkinson2011protocol.pdf (accessed 15 October 2013).
- Sun X, Briel M, Walter SD, Guyatt GH. Is a subgroup effect believable? Updating criteria to evaluate the credibility of subgroup analyses. BMJ 2010;340. http://dx.doi.org/10.1136/bmj.c117.
- Gulliver P, Cryer C, Davie G, Langley J. An investigation into methods to develop indicators to measure injury related impairment. Inj Prev 2010;16:240-6. http://dx.doi.org/10.1136/ip.2009.022913.
- Guest G, Bunce A, Johnson L. How many interviews are enough?. Field Methods 2006;18:59-82. http://dx.doi.org/10.1177/1525822X05279903.
- Green J, Thorogood N. Qualitative methods for health research. London: Sage; 2009.
- Strauss A. Qualitative analysis for social scientists. Cambridge: Cambridge University Press; 1987.
- Jones L, Davis A, Eyers T. Young people, transport and risk: comparing access and independent mobility in urban, suburban and rural environments. Health Educ J 2000;59:315-28. http://dx.doi.org/10.1177/001789690005900405.
- Goodwin P, Dargay J, Grayling T. Any more fares? Delivering better bus services. London: Institute for Public Policy Research (IPPR); 2001.
- Morris JN, Heady JA, Raffle PAB, Roberts CG, Parks JW. Coronary heart-disease and physical activity of work. Lancet 1953;2:1053-7.
- Sallis JF, Haskell WL, Fortmann SP, Vranizan KM, Taylor CB, Solomon DS. Predictors of adoption and maintenance of physical activity in a community sample. Prev Med 1986;15:331-41. http://dx.doi.org/10.1016/0091-7435(86)90001-0.
- Sallis JF, Hovell MF, Hofstetter CR. Predictors of adoption and maintenance of vigorous physical activity in men and women. Prev Med 1992;21:237-51. http://dx.doi.org/10.1016/0091-7435(92)90022-A.
- Pucher J, Buehler R, Bassett D, Dannenberg A. Walking and cycling to health: a comparative analysis of city, state, and international data. Am J Publ Health 2010;100:1986-92. http://dx.doi.org/10.2105/AJPH.2009.189324.
- Bassett DR, Pucher J, Buehler R, Thompson DL, Crouter SE. Walking, cycling, and obesity rates in Europe, North America, and Australia. J Phys Activ Health 2008;5:795-814.
- Mota J, Gomes H, Almeida M, Ribeiro JC, Carvalho J, Santos MP. Active versus passive transportation to school – differences in screen time, socio-economic position and perceived environmental characteristics in adolescent girls. Ann Hum Biol 2007;34:273-82. http://dx.doi.org/10.1080/03014460701308615.
- Van Dyck D, Deforche B, Cardon G, De Bourdeaudhuij I. Neighbourhood walkability and its particular importance for adults with a preference for passive transport. Health Place 2009;15:496-504. http://dx.doi.org/10.1016/j.healthplace.2008.08.010.
- Towards sustainable transportation. Vancouver, BC; 1996.
- Evaluation of national concessionary travel in Scotland. Edinburgh: Transport Scotland; 2009.
- Sheller M, Urry J. The city and the car. Int J Urban Regional 2000;24:737-57. http://dx.doi.org/10.1111/1468-2427.00276.
- King R, Grayling T, Grayling T. Any more fares? Delivering better bus services. London: Institute for Public Policy Research (IPPR); 2001.
- Ellaway A, Macintyre S, Hiscock R, Kearns A. In the driving seat: psychosocial benefits from private motor vehicle transport compared to public transport. Transport Res F Traffic Psychol Behav 2003;6:217-31. http://dx.doi.org/10.1016/S1369-8478(03)00027-5.
- Jacobsen PL. Safety in numbers: more walkers and bicyclists, safer walking and bicycling. Inj Prev 2003;9:205-9. http://dx.doi.org/10.1136/ip.9.3.205.
- Kenyon S, Lyons G, Rafferty J. Transport and social exclusion: investigating the possibility of promoting inclusion through virtual mobility. J Transport Geogr 2002;10:207-19. http://dx.doi.org/10.1016/S0966-6923(02)00012-1.
- Making the connections: final report on transport and social exclusion. London: SEU; 2003.
- Thomsen TU. Children – automobility’s immobilized others?. Transport Rev 2004;24:515-32.
- Barker J, Kraftl P, Horton J, Tucker F. The road less travelled – new directions in children’s and young people’s mobility. Mobilities 2009;4:1-10. http://dx.doi.org/10.1080/17450100802657939.
- Kearns RA, Collins DCA. Crossing roads, crossing boundaries: empowerment and participation in a child pedestrian safety initiative. Space and Polity 2003;7:193-212. http://dx.doi.org/10.1080/1356257032000133937.
- Barker J. ‘Driven to distraction?’: children’s experiences of car travel. Mobilities 2009;4:59-76. http://dx.doi.org/10.1080/17450100802657962.
- Kullman K. Transitional geographies: making mobile children. Soc Cult Geogr 2010;11:829-46. http://dx.doi.org/10.1080/14649365.2010.523839.
- London: TfL; 2010.
- Davey J. Older people and transport: coping without a car. Ageing Soc 2007;27:49-65. http://dx.doi.org/10.1017/S0144686X06005332.
- Metz D. Transport policy for an ageing population. Transport Rev 2003;23:375-86.
- Jones A, Goodman A, Roberts H, Steinbach R, Green J. Entitlement to concessionary public transport and wellbeing: a qualitative study of young people and older citizens in London, UK. Soc Sci Med 2013;91:202-9. http://dx.doi.org/10.1016/j.socscimed.2012.11.040.
- Green J, Jones A, Roberts H. More than A to B: the role of free bus travel for the mobility and wellbeing of older citizens in London. Ageing Soc 2014;34:472-94.
- The Green Book: appraisal and evaluation in central government. London: The Stationery Office (TSO); 2003.
- TAG Unit 3.4.1. The safety objective. London: DfT; 2011.
- TAG Unit 3.5.3. Transport user benefit computation. London: DfT; 2011.
- Your guide to fares and tickets, 2 January 2007 until further notice. London: TfL; 2007.
- TAG unit 3.9.5d. Road decongestion benefits. London: DfT; 2012.
- World Health Organization . Health Economic Assessment Tools (HEAT) for Walking and for Cycling 2011.
- TAG Unit 3.14.1. Guidance on the appraisal of walking and cycling schemes. London: DfT; 2012.
- Transport for London (TfL) . 2011/2012/Crime/Statistics/Bulletin./Quarter/1/(1/April–30/June/2012/13) n.d. www.tfl.gov.uk/assets/downloads/corporate/crime-and-antisocial-behaviour-web-bulletin-q1-2012-13.pdf (accessed 15 October 2013).
- Department for Transport (DfT) . Estimated Costs to Society of Crime on Public Transport in England in 2006 07. Final Report to DfT 2007. http://assets.dft.gov.uk/publications/estimated-costs-to-society-of-crime-on-public-transport-in-england-2006-07/estimatedcostscrime.pdf (accessed 15 October 2013).
- HM Treasury . GDP Deflators Updated 28 March 2012 2012. http://webarchive.nationalarchives.gov.uk/20130129110402/http://www.hm-treasury.gov.uk/data_gdp_fig.htm (accessed 15 October 2013).
- Nellthorp J, Smith A, Toner J, PJ M. Costs in concessionary travel: the research papers. Report to the Department for Transport. Leeds: University of Leeds; 2010.
- Concessionary travel for older and disabled people: guidance on reimbursing bus operators (England) for 2012/13. London: DfT; 2011.
- Dargay J, Liu R. Analysis of the National Travel Survey dataset. Leeds: Institute for Transport Studies; 2010.
- Toner J, Smith A, Shen S, Wheat P. Review of bus profitability in England – econometric evidence on bus costs: final report. Leeds: University of Leeds; 2010.
- Transport for London (TfL) . Freedom Pass Settlement – 2010 11, Finance and Policy Committee, Agenda Item 7, 21 January 2010 2010. www.tfl.gov.uk/assets/downloads/Item07-Freedom-Pass-Settlement-FPC.pdf (accessed 15 October 2013).
- NATA refresh: appraisal for a sustainable transport system. London: DfT; 2009.
- Value for money assessments. London: DfT; 2011.
- Ward H, Lyon R, Thoreau R. Under-reporting of road casualties – phase 1. Road Safety Report No 69. London: Department for Transport (DfT); 2006.
- Edwards P, Green J, Roberts I, Grundy C, Lachowycz K. Deprivation and road safety in London. A report to the London road safety unit. London: London School of Hygiene and Tropical Medicine (LSHTM); 2007.
- Brown B, Mackett R, Gong Y, Kitazawa K, Paskins J. Gender differences in children’s pathways to independent mobility. Child Geogr 2008;6:385-401.
- Goodman A, Jones A, Roberts H, Steinbach R, Green J. “We can all just get on a bus and go”: rethinking independent mobility in the context of the universal provision of free bus travel to young Londoners. Mobilities 2013. http://dx.doi.org/10.1080/17450101.2013.782848.
- Goldstein J. Emergence as a construct: history and issues. Emergence 1999;1:49-72. http://dx.doi.org/10.1207/s15327000em0101_4.
- Halley JD, Winkler DA. Classification of emergence and its relation to self-organization. Complexity 2008;13:10-5. http://dx.doi.org/10.1002/cplx.20216.
- Petticrew M, Roberts H. Evidence, hierarchies, and typologies: horses for courses. J Epidemiol Community Health 2003;57:527-9. http://dx.doi.org/10.1136/jech.57.7.527.
- O’Cathain A, Murphy E, Nicholl J. Three techniques for integrating data in mixed methods studies. BMJ 2010;341. http://dx.doi.org/10.1136/bmj.c4587.
- Montgomery C, Pool R. Critically engaging: integrating the social and the biomedical in international microbicides research. J Int AIDS Soc 2011;14:1-7.
- Cartwright N, Munro E. The limitations of randomized controlled trials in predicting effectiveness. J Eval Clin Pract 2010;16:260-6. http://dx.doi.org/10.1111/j.1365-2753.2010.01382.x.
- Matthews H, Christensen P, O’brien M. Children in the city: home, neighbourhood and community. London: RoutledgeFalmer; 2003.
- Mikkelsen M, Christensen P. Is children’s independent mobility really independent? A study of children’s mobility combining ethnography and GPS/mobile phone technologies. Mobilities 2009;4:37-58. http://dx.doi.org/10.1080/17450100802657954.
- Christensen P, O’brien M. Children in the city: home, neighbourhood and community 2003.
- Valentine G. Children should be seen and not heard: the production and transgression of adults’ public space. Urban Geogr 1996;17:205-20. http://dx.doi.org/10.2747/0272-3638.17.3.205.
- Russell M, Howden-Chapman P, Stuart K, Chapman R. Sizing up the city: urban form and transport in New Zealand. Wellington: Steele Roberts/Centre for Sustainable Cities; 2010.
- Freund P, Martin G. Walking and motoring: fitness and the social organisation of movement. Sociol Health Illness 2004;26:273-86. http://dx.doi.org/10.1111/j.1467-9566.2004.00390.x.
- Jarrett J, Woodcock J, Griffiths UK, Chalabi Z, Edwards P, Roberts I, et al. Effect of increasing active travel in urban England and Wales on costs to the National Health Service. Lancet 2012;379:2198-205. http://dx.doi.org/10.1016/S0140-6736(12)60766-1.
- Julien A, Carré J-R. Risk exposure during pedestrian journeys. Recherche Transports Sécurité 2002;76:173-89. http://dx.doi.org/10.1016/S0761-8980(02)00016-X.
- Jones A, Steinbach R, Roberts H, Goodman A, Green J. Rethinking passive transport: bus fare exemptions and young people’s wellbeing. Health Place 2012;18:605-12. http://dx.doi.org/10.1016/j.healthplace.2012.01.003.
- Welleman T. The Autumn of the Bicycle Master Plan: After the Plans, the Products n.d.
- Tanasescu M, . Exercise type and intensity in relation to coronary heart disease in men. JAMA 2002;288:1994-2000. http://dx.doi.org/10.1001/jama.288.16.1994.
- Manson JE, Greenland P, LaCroix AZ, Stefanick ML, Mouton CP, Oberman A, et al. Walking compared with vigorous exercise for the prevention of cardiovascular events in women. New Engl J Med 2002;347:716-25. http://dx.doi.org/10.1056/NEJMoa021067.
- Wen CP, Wai JPM, Tsai MK, Yang YC, Cheng TYD, Lee M-C, et al. Minimum amount of physical activity for reduced mortality and extended life expectancy: a prospective cohort study. Lancet 2011;378:1244-53. http://dx.doi.org/10.1016/S0140-6736(11)60749-6.
- Sesso HD, Paffenbarger RS, Lee I-M. Physical activity and coronary heart disease in men. Circulation 2000;102:975-80. http://dx.doi.org/10.1161/01.CIR.102.9.975.
- Hoevenaar-Blom MP, Wendel-Vos GW, Spijkerman AM, Kromhout D, Verschuren W. Cycling and sports, but not walking, are associated with 10-year cardiovascular disease incidence: the MORGEN Study. Eur J Cardiovasc Prev Rehabil 2011;18:41-7.
- Roth MA, Millett CJ, Mindell JS. The contribution of active travel (walking and cycling) in children to overall physical activity levels: a national cross sectional study. Prev Med 2011;54:134-9.
- Goodman A, Mackett R, Paskins J. Activity compensation and activity synergy in British 8–13 year olds. Prev Med 2011;53:293-8. http://dx.doi.org/10.1016/j.ypmed.2011.07.019.
- Metcalf B, Voss L, Jeffery A, Perkins J, Wilkin T. Physical activity cost of the school run: impact on schoolchildren of being driven to school (EarlyBird 22). BMJ 2004;329:832-3. http://dx.doi.org/10.1136/bmj.38169.688102.F71.
- Faulkner GEJ, Buliung RN, Flora PK, Fusco C. Active school transport, physical activity levels and body weight of children and youth: a systematic review. Prev Med 2009;48:3-8. http://dx.doi.org/10.1016/j.ypmed.2008.10.017.
- Hiscock R, Macintyre S, Kearns A, Ellaway A. Means of transport and ontological security: do cars provide psycho-social benefits to their users?. Transport Res Transport Environ 2002;7:119-35. http://dx.doi.org/10.1016/S1361-9209(01)00015-3.
- Mackett R. Why do people use their cars for short trips?. Transportation 2003;30:329-49.
- Noble B. Why Are Some Young People Choosing Not to Drive? n.d.
- Ruud A, Nordbakke S. Decreasing Driving Licence Rates Among Young People – Consequences for Local Public Transport n.d.
- Cartwright N. Are RCTs the gold standard?. BioSocieties 2007;2:11-20. http://dx.doi.org/10.1017/S1745855207005029.
- Beirão G, Sarsfield Cabral JA. Understanding attitudes towards public transport and private car: a qualitative study. Transport Pol 2007;14:478-89. http://dx.doi.org/10.1016/j.tranpol.2007.04.009.
- Moving on: working towards a better public transport offer for young people in tough times. Leeds: PTEG; 2012.
- Baker S, White P. Impacts of free concessionary travel: case study of an English rural region. Transport Pol 2010;17:20-6. http://dx.doi.org/10.1016/j.tranpol.2009.09.002.
- Garg A. Delhi High Court Dismisses Plea to Scrap BRT. Times of India 2012. http://articles.timesofindia.indiatimes.com/2012-10-19/delhi/34583123_1_brt-corridor-crri-brt-projects (accessed 12 December 2012).
- Mackett R, Brown B, Gong Y, Kitazawa K, Paskins J. Children’s independent movement in the local environment. Built Environ 2007;33:454-68. http://dx.doi.org/10.2148/benv.33.4.454.
- Chen C-F, Chao W-H. Habitual or reasoned? Using the theory of planned behavior, technology acceptance model and habit to examine switching intentions toward public transit. Transport Res Transport Environ 2011;14:128-37. http://dx.doi.org/10.1016/j.trf.2010.11.006.
- Bamberg S, Ajzen I, Schmidt P. Choice of travel mode in the theory of planned behavior: the roles of past behavior, habit and reasoned action. Basic Appl Soc Psychol 2003;25:175-87. http://dx.doi.org/10.1207/S15324834BASP2503_01.
- Bamberg S. Is a residential relocation a good opportunity to change people’s travel behavior? Results from a theory-driven intervention study. Environ Behav 2006;38:820-40. http://dx.doi.org/10.1177/0013916505285091.
- Fujii S, Kitamura R. What does a one-month free bus ticket do to habitual drivers? An experimental analysis of habit and attitude change. Transportation 2003;30:81-95.
- Guell C, Panter J, Jones N, Ogilvie D. Towards a differentiated understanding of active travel behaviour: using social theory to explore everyday commuting. Soc Sci Med 2012;75:233-9. http://dx.doi.org/10.1016/j.socscimed.2012.01.038.
- Steinbach R, Green J, Datta J, Edwards P. Cycling and the city: a case study of how gendered, ethnic and class identities can shape healthy transport choices. Soc Sci Med 2011;72:1123-30. http://dx.doi.org/10.1016/j.socscimed.2011.01.033.
- Green J. ‘Walk this way’: Public health and the social organization of walking. Soc Theor Health 2009;7:20-38. http://dx.doi.org/10.1057/sth.2008.19.
- Leung J, Guria J. Value of statistical life: adults versus children. Accid Anal Prev 2006;38:1208-17. http://dx.doi.org/10.1016/j.aap.2006.05.009.
- Alberini A, Bateman I, Loomes G, Šcasný M. Paris: OECD Publishing; 2010.
- Maddison D, Pearce D. Costing the health effects of poor air quality. Determining monetary values of environmental impact. London: Landor Publishing Limited; 1997.
- Agee M, Crocker T. Does parents valuation of children’s health mimic their valuation of own health?. J Popul Econ 2001;21:231-49. http://dx.doi.org/10.1007/s00148-007-0159-2.
- Blomquist G, Miller T, Levy D. Values of risk reduction implied by motorists’ use of protection equipment – new evidence from different population. J Transp Econ Policy 1996;31:55-66.
- Hammitt J, Hanninger K. Valuing fatal risks to children and adults – effects of disease, latency and risk aversion. J Risk Uncertainty 2010;40:57-83. http://dx.doi.org/10.1007/s11166-009-9086-9.
- Department for Transport . Values of time and operating costs 2011.
- Mackie P, Wardman M, Fowkes A, Whelan G, Nellthorp J, Bates J. Values of travel time savings in the UK. Leeds: Institute for Transport Studies, University of Leeds; 2003.
- Transport for London (TfL) . Tickets ≫ students and Children: 11–15 2010. www.tfl.gov.uk/tickets/14310.aspx (accessed 1 November 2010).
- Transport for London (TfL) . Tickets ≫ students and Children: 16–18 2010. www.tfl.gov.uk/tickets/14308.aspx (accessed 1 November 2010).
- London Councils . Freedom Pass: Disabled Pass Application n.d. www.londoncouncils.gov.uk/services/freedompass/applying/disabledpass.htm (accessed 30 October 2013).
- Shaw J, Mackinnon D, Docherty I. Divergence or convergence? Devolution and transport policy in the United Kingdon. Environ Plann C Govern Pol 2009;27:546-67. http://dx.doi.org/10.1068/c0899r.
- Knowles R, Abrantes P, Docherty I, Shaw J. Traffic jam: 10 years of sustainable transport policy in the UK. Bristol: Polity Press; 2008.
- Shaw J, Docherty I, Docherty I, Shaw J. Traffic jam: 10 years of sustainable transport policy in the UK. Bristol: Polity Press; 2008.
- Secretariat memorandum: London Bus Network overview. London: TravelWatch; 2009.
- London buses quality of service indicators: route results for London bus services, first quarter 2010/11, 1st April 2010–25th June 2010. London: TfL; 2010.
- Transport for London (TfL) . Transport for London: London Buses, History n.d. www.tfl.gov.uk/corporate/modesoftransport/londonbuses/1554.aspx (accessed 11 October 2010).
- Greater London Authority (GLA) . The Four Key Agencies Working With the Mayor n.d. www.london.gov.uk/mayor-assembly/gla/spending-money-wisely/budget-expenditure-charges (accessed 30 October 2013).
- London’s bus contracting and tendering process. London: TfL; 2008.
- Transport for London business plan 2009/10–2017/18. London: TfL; 2009.
- London buses performance: financial year 2009/10. London: TfL; 2010.
- Transport for London (TfL) . Transport for London: London Buses n.d. www.tfl.gov.uk/corporate/modesoftransport/1548.aspx (accessed 11 October 2010).
- Hammond P. Spending review 2010: TfL funding agreement. London: Department for Transport; 2010.
- Impact assessment: the bus service operators grant (England) (amendment) regulations 2011. London: DfT; 2011.
- A fare decision? The impact of the Mayor’s fare decision. London Assembly Budget Committee. London: GLA; 2009.
- Brown M. ‘Are Freedom Passes under threat?’ East London Lines: Connecting Communities n.d. www.eastlondonlines.co.uk/2010/04/what-are-we-without-our-freedom-to-travel-in-london/ (accessed 13 October 2010).
- Johnson B. Report of the Transport Committee’s seminar – ‘The Future of London’s Buses’, Mayoral response. Mayor’s Office. London: Greater London Authority; 2010.
- January 2011 fare changes. London: GLA; 2010.
- Report of Transport Committee Seminar: ‘The Future of London’s Buses’. L. A. T. Committee. London: GLA; 2010.
- The London plan: spatial development strategy for Greater London. Consultation draft replacement plan. London: GLA; 2009.
- Map of the London Boroughs. Newport: UK National Statistics; 2003.
- Vaid L. Greater London Authority Data Management and Analysis Group DMAG briefing 2008–9: children in benefit claiming families 2007. London: GLA; 2008.
- Index of Multiple Deprivation (IMD) 2007. London: Department for Communities and Local Government; 2007.
Appendix 1 The context: the intervention; bus use trends and concessionary fares for young people in London
The intervention: free bus travel for young people
The specific interventions concerned are the introduction of free bus fares for 12- to 16-year-olds in September 2005 and the extension of this concession to 17-year-olds in full-time education September 2006. Fares are exempted for London residents in this age bracket (12–17 years) who apply for a ‘zip card’ from TfL and use it according to the terms and conditions of the issuer. 196,197 These fare exemptions for young people were introduced during the tenure of the previous Mayor of London, Ken Livingstone (Mayor 2000–8). When the first intervention concerned was launched (2005), secondary school-aged children had paid a reduced, 40p flat fare for journeys on the London bus network (Table 28). As well as granting the cardholder unlimited free travel on all buses and trams displaying the London Buses symbol (both within and just outside London),12 zip cards also act as conventional ‘Oyster’ cards and can be loaded up with pre-pay or travelcards for the cardholders to use other parts of the TfL network (tube, DLR, London overground and most National Rail services operating in the capital) at a variety of discounted rates (pp. 6–11). 14
| Date | Fare structure | Method of payment/travel |
|---|---|---|
| Pre January 2004 | Reduced 40p single fare for 5- to 15-year-olds Full adult fare for 17- to 18-year-olds |
Cash |
| January 2004 | Free travel for 5- to 10-year-olds (with a photocard if they looked older than 10 years) | No photocard |
| September 2005 | Free travel for 5- to 15-year-olds, behaviour code introduced | 5- to 13-year-olds needed no card 14- to 15-year-olds touched in using Oyster photocard |
| September 2006 | Free travel for 16- to 18-year-olds in full-time education or work-based learning and a London resident | 16- to 18-year-olds touched in using Oyster photocard |
| Half-fares for all others in this age range and/or non-London residents | Oyster photocard | |
| January 2008 | ‘Zip’ brand launched to cover all material associated with 15- to 18-year-olds’ Oyster photocards | Photocards did not include zip branding at this point |
| 1 June 2008 | Oyster photocards become compulsory for travel for anyone aged ≥ 11 years | 11- to 15-year-olds touched in using Oyster photocard when boarding bus |
| September 2008 | Zip cards introduced 5- to 10-year-olds zip card 11- to 15-year-olds zip card ≥ 16 years zip card Stricter rules around mandatory validation and behaviour codes |
11- to 15-year-olds touched in using zip Oyster photocard |
When these fare exemptions were unveiled, the stated rationale for universally eliminating bus fares for young people in London was to help them to continue studying, improve employment prospects and promote the use of public transport (p. 7). 13 That is, it was aimed first and foremost at mitigating the potential social exclusion effects for young people of fare-based urban transport systems. 15 As it has been stated more recently on the TfL website:
Granting young people free travel is part of the Mayor’s strategy to embed more environmentally sound travel habits from an early age while helping young people to unlock education, sport, leisure and employment opportunities
TfL, 200716
By removing any need to pay, at the point of use, for travel on buses, the argument went that young people would be better (and more equally) able to access goods and services (schools, libraries, leisure facilities, etc.) and so reduce the chances of their suffering from transport poverty. At the same time, it was hoped that by encouraging bus use from an early age more environmentally sustainable travel practices would become ingrained.
Young people with disabilities living in London can also apply for a Freedom Pass, if they have an eligible disability. 198 These provide free travel on London underground and overground services as well as the bus routes. Most young people with eligible disabilities use the Freedom Pass for public transport use, rather than a zip card.
Bus ridership data and trends: overview
One of the key background trends for this study is the substantial increase in the use of mass public transport recorded in London in recent years (Figure 20). For example, it has been shown that ‘[t]otal passenger-kilometres travelled on [all public transport] services operated by TfL were almost 70 per cent higher in 2008/09 than in 1991/92 . . . this growth . . . was especially pronounced on the bus network’ (p. 45). 31 Specifically, in the same period (1991/2 to 2008/9) bus patronage increased by 93%; moreover, between 2000/1 and 2008/9, recorded bus passenger kilometers increased by 64% (p. 45). 31
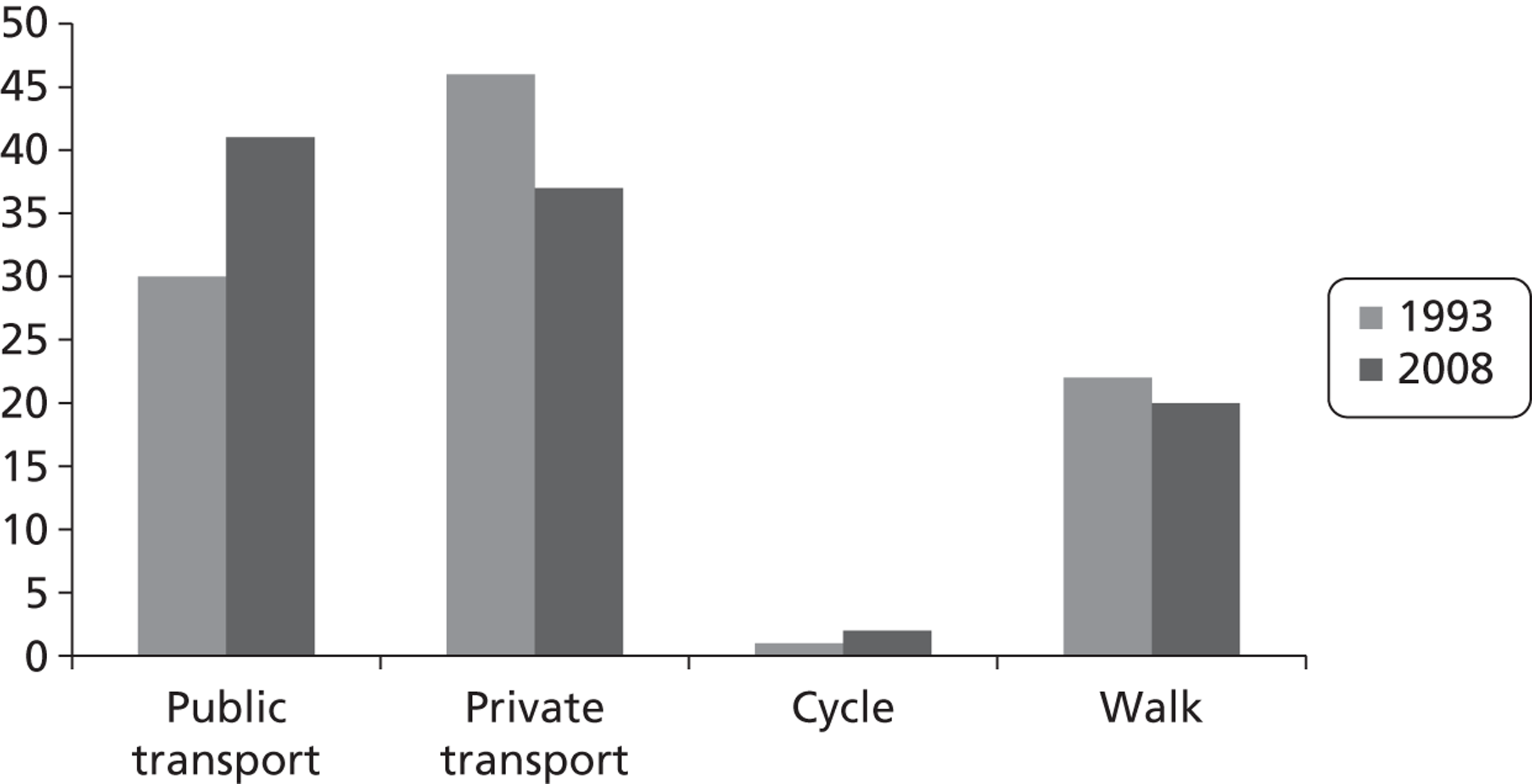
In 2008/9, TfL’s ‘best estimate’ is that 7942 million passenger-kilometres were travelled by bus (p. 47, table 2.5). 31 This compares with 6755 million passenger-kilometres travelled by bus in 2004/5 (just prior to the first of the interventions evaluated in this study), 4709 million passenger-kilometres in 2000/1 (the year that the GLA was established) and 3996 million bus passenger-kilometres in 1991/2. [Between 2006/7 and 2007/8 TfL made a significant change to the methodology used to estimate bus trips and journey changes. In short, from 2007/8 onwards they have used Oyster card validations as the primary source of these estimates rather than ticket sales. The Oyster card validation record, they argue, ‘provides more robust estimates of total bus and tram use’ (p. 48). 31 The effects of the estimation method change in 2007/08 were to ‘add almost 0.4 million bus trips and 0.5 million journey stages to the daily average, and [to increase . . .] the estimate of bus mode shares by 1 percentage point’ (p. 48). 31 See Transport for London: Travel in London: Report 2 (pp. 45–9)31 for further information on this travel data estimation change.] In 2008, using journey stage data, bus travel (including tram travel) accounted for 20% of the modal share of transport in London, the highest for any public transport mode, up from 13.5% in 1993. In the past decade, then, there has been a significant shift in modal choice towards buses. This period is one characterised by a shift to GLA/TfL oversight of London’s transport infrastructure and services. The backdrop to this study is, therefore, one of high levels of and pronounced increases in bus usage in the capital.
Bus ridership differences across London
There are notable differences in transport patterns between inner and outer London boroughs. Estimates of the ‘main mode’ of a given trip by borough suggest that in the inner London boroughs, around 19% of trips are made by bus or tram, compared with around 12% average for the outer London boroughs. In contrast, car/motorcycle travel accounts for 50% of the average modal share for the outer London boroughs and 26% for inner London (p. 70). 31
Young people’s travel patterns also differ by borough. For most young people, journeys to school are captured by DfE data that have been collected on travel to and from secondary school. For secondary school pupils attending school in London in 2010, DfE estimate an average journey to school of 1.5 miles. Those travelling within the same local authority area travel an average of 1.2 miles, and those going out of borough around 3.3 miles (p. 3). 28 Around one in five secondary school pupils travels to a school in another borough (p. 3). 28
In 2010, a little less than half of pupils at secondary school attending school in London used public transport as their mode of travel from home to school, a higher proportion than in England as a whole (Table 29).
| Region | Public transport (%) | Walk (%) | Car (%) | Car share (%) | Cycle (%) | Other (%) | Unknown (%) |
|---|---|---|---|---|---|---|---|
| London | 44.8 | 34.8 | 10.3 | 1.6 | 1.1 | 1.9 | 5.6 |
| England | 32.0 | 42.4 | 16.3 | 2.4 | 3.1 | 1.1 | 2.8 |
As this particular mode of travel data set was collected only from 2007 (i.e. post interventions) onwards, it cannot provide us with a measure of changes to school travel patterns over time. For the first time this year, however, the data have been provided at local authority level, suggesting significant variation in travel patterns among secondary school children between boroughs of residence. The DfE (p. 9)28 report highlights some examples:
-
Kensington and Chelsea has the highest proportion of its school population travelling to school by public transport (71.1%) whilst Waltham Forest has the lowest (28.3%).
-
Newham (57.4%) and Waltham Forest (57.3%) have the highest proportion of their school population travelling to school by foot, whilst Westminster (17.2%) and Enfield (17.7%) have the lowest.
-
Redbridge has the highest proportion of its school population travelling to school by car (18.3%) whilst Southwark has the lowest with 1.9%.
-
Richmond upon Thames has the highest proportion of its school population travelling to school by bicycle, at 6.1%. Kingston upon Thames has the second highest, at 3.4%. Westminster has the lowest (0.1%).
London: a paragon of bus subsidy in the UK
The uniqueness of London’s transport system stems from the synergy of various features: geography, institutions, demography, public service financing and so on. Important among these is the particular package of transport subsidies that, post-administrative devolution with the establishment of the GLA in 2000, London managed to secure. As Shaw and colleagues (p. 559)199 put it in their analysis of recent political devolution and transport policy in the UK, ‘[i]t was in London . . . that the most significant transformation of fortunes for bus travel took place’. The authors go on to detail these ‘fortunes’, explaining that the huge increases in bus patronage discussed earlier were:
[I]n the main . . . the result of aggressive pro[-]bus measures such as a large increase in vehicle kilometres operated, significant investment in bus priority, and, perhaps most significantly, a staggering 5108% increase in bus operating subsidy, to £625 million per annum in 2006/07
Shaw and colleagues p. 559199 (emphasis added)
(For a further discussion of these pro-bus measures implemented in London see Buses and light rail: stalled en route?200)
It would seem, therefore, that pricing considerations, and specifically the subsidisation of bus fares (which in part underpins the two interventions that we are concerned with), were crucial determinants of the upsurge in bus use that has been witnessed in London over the past decade. Notably, the package of subsidies that London received for bus transport in this period was disproportionate, with TfL so committed to improving bus services that by 2006/07 ‘it was paying around two-thirds of all bus subsidy in England’ (p. 559). 199 For these authors, then, the ‘success story’ that is the renaissance of London’s bus network is but another example to add to others from Europe ‘that excellent bus networks are usually possible only with very significant financial support’ (p. 559). 199 (See Shaw and Docherty201 for a more in-depth discussion of the evidence for a correlation between levels of financial support and bus network quality.)
The bus network and contracting
At present there are almost 700 bus routes operated in the Greater London area. 202 TfL break these routes down into four categories, namely:
-
high-frequency (non-timetabled) routes (the majority of routes fall into this category)
-
low-frequency (timetabled) routes
-
night bus routes
-
low-frequency London Local Service Agreement (LLSA) routes [‘a small number of cross-borough-boundary bus services . . . that operate as part of the TfL network within Greater London, and outside London on a commercial basis’ (p. 5)202]. (For a full breakdown of London bus routes according to these four categories see London Buses Quality of Service Indicators: Route results for London Bus Services, First Quarter 2010/11, 1st April 2010–25th June 2010. 203)
In terms of governance, in 1985 bus services outside London were deregulated such that ‘any licensed operator could apply to run a new route even if another company already ran a service along the same roads’. 204 London, however, was exempted from this policy of deregulation, though measures were introduced to set in train the decentralisation of control of the capital’s bus network. [In the decade and a half (1970–84) immediately preceding this deregulation of bus services in the UK, ‘London Transport’ (LT; the strategic body for transport in London) had come under direct control of the Greater London Council (GLC). LT was then brought under central government control by the London Regional Transport Act 1984. 204 Specifically, in 1985 LT set up a ‘Tendered Bus Division’ which was responsible for initiating the process of competitive tendering for bus routes and services. This development required LT’s subsidiary body, London Buses Limited (itself brought into being as a result of the London Regional Transport Act 1984), ‘to compete against operators in the private sector for the opportunity to run individual bus routes on behalf of LT’. 204
The Conservative government at the time, however, decided to postpone formally deregulating the London bus network until after the May 1997 General Election. The result of this election therefore changed the course of transport governance in the capital, with the incoming Labour government committed to reintroducing a strategic governing authority for London. This commitment led to the replacement of LT by TfL in July 2000, TfL being one of the four ‘functional bodies’ of the GLA. [The four ‘functional bodies’ of the GLA are: TfL, London Development Agency (LDA), London Fire and Emergency Planning Authority (LEEPA), and Metropolitan Police Authority (MPA). 205]
As a result, public buses in London now operate according to a complex management and funding structure in which TfL’s role is to plan routes and monitor service quality, as well as manage bus stops, stations and other support services. The bus services themselves are operated largely by private sector companies under contract to London Bus Services Limited (‘London Buses’), part of TfL. In October 2010 there were 18 bus operators running buses in this way in London. To borrow directly from a report by London TravelWatch:202
[T]hese contracts contain a number of incentives which give financial benefits or penalties depending on performance. The present contract scheme, Quality Incentive Contracts (QICs), gives financial incentives to operators for the quality of service they deliver. The key features of these contracts are:
Contracts are designed to provide incentives to operators to improve quality;
Routes are generally tendered individually, but often at the same time as other routes in the same area to facilitate service changes;
Contracts are normally for 5 years, with a potential 2-year performance-related extension available to the operator;
It is a continuing programme of tendering, with between 15% and 20% of the network typically tendered each year;
Tender evaluation is based on best value for money, taking into account quality and safety as essential features;
Contract payments are related to the mileage operated and overall reliability of the service;
comprehensive quality measurements are used across all aspects of delivery.
(For further details on these contractual arrangements please see London’s Bus Contracting and Tendering Process. 206)
For 2009/10, across the bus network overseen by TfL (a network spanning 1580 square kilometres plus a few services into outlying areas,204 bus network costs are forecast to be in the region of £1.69B, with about two-thirds of this (£1.12B) being met by bus network income and the remaining £0.57B being met bus subsidy (p. 72). 207 In 2009/10, 497.2 million vehicle kilometres were scheduled for operation across the London bus network, though 14.4 million of these vehicle kilometres were ‘lost’ (i.e. not operated) owing to staff, mechanical, traffic and ‘miscellaneous’ reasons. 208 This compares to 450 million vehicle kilometres being operated on the network in 2004/5,209 immediately prior to the introduction of free travel for under 16-year-olds.
The current policy context for fare, subsidies and concessions
As part of the Government’s ‘comprehensive spending review’ (CSR) the financial support received by the GLA from the DfT is due to fall over the coming years. Thus the future grant settlement outlined by the former Secretary of State for Transport, Phillip Hammond, sees the GLA Transport Grant diminish from £2804M in 2010/11 to £2404M in 2014/15 (p. 4, paragraph 10). 210 In his statement, Phillip Hammond specifically set out that the level of Bus Service Operators Grant (BSOG) paid by the DfT was being reviewed and could be expected to change ‘in London as in other parts of the country’ (p. 5, paragraph 18). 210 This review resulted in a 20% cut to the BSOG rate from April 2012. 211
The implication of these grant and subsidy cuts is that either public transport services will have to be cut, infrastructure improvements deferred, efficiencies identified or the resulting gap in the finances will have to be made up from other sources of income. Fares have by no means been capped in this respect, and as the GLA’s report on the impact of the Mayor’s 2009 fare decision puts it succinctly, ‘[t]he balance of TfL’s funding between the government and London fare payers is increasingly shifting towards fare payers’ (p. 22). 212
In this broader political-economic context of austerity, concerns are already starting to be raised about potential threats to the Freedom Pass scheme for pensioners (e.g. Brown213). So far, concerns that the bus fare exemptions for young Londoners in which we are interested are similarly threatened have not been publicly aired in the same way. Moreover, the Mayor has recently stated that ‘[t]here are no plans to alter the current range of concessions [on buses]’ (p. 2)214 and for 2011, at least, the Mayor has signed-off on a package of fare changes in which ‘[f]are concessions and discounted fare rates will be generally unchanged’ (p. 5). 215
However, significantly, at the GLA concerns have now been raised about precisely the health disbenefits of granting young people free bus travel. Specifically, at a recent roundtable event organised by the GLA Transport Committee to consider ‘the future of London buses,’ Steven Norris (TfL Board member and former Minister for Transport in London) explicitly ‘queried the value of providing free bus travel for children when there was a nationwide push to combat childhood obesity’ (p. 12). 214 That is, the link between free bus travel for young Londoners and the public health – in this case envisioned as a detrimental relationship – has already been aired by a key figure at TfL at a major GLA event. 214
The GLA Transport Committee’s ‘future of London’s buses’ report concludes by posing a series of six questions to the Mayor. Among these, they ask: ‘[w]hat if any cost/benefit analysis of London’s buses has been undertaken that takes account of their wider social and environmental benefits?’ (p. 15). 216 Responding directly to this question, the Mayor stated ‘[n]o cost benefit has been carried out’ (p. 3). 214 This study aimed to provide an evidence-based contribution to these debates.
Appendix 2 Data sources and statistical methods
Data sources
-
STATS19.
-
HES.
-
London Travel Surveys (LATS and LTDS).
STATS19
List of fields used: data extract.
| Variable name | Description | Value labels |
|---|---|---|
| A_AREFNO | Accident reference number | |
| C_CREFNO | Casualty reference number | |
| C_VREFNO | Vehicle reference number | |
| C_CETHNIC | Casualty ethnic group | 1 White-skinned European 2 Dark-skinned European 3 Afro-Caribbean 4 Asian 5 Oriental 6 Arab 7 Not Known |
| C_CSEVCAS | Casualty severity | 1 Fatal 2 Serious 3 Slight |
| C_CAGE | Casualty age | |
| C_CPOSTCD | Casualty postcode | |
| C_CUSER | Casualty mode of travel | 1 Pedestrian 2 Pedal Cycle 3 Powered 2 Wheeler 4 Car 5 Taxi 6 Bus Or Coach 7 Goods Vehicle 8 Other Vehicle |
| a_easting | Easting co-ordinate of collision | |
| a_northing | Northing co-ordinate of collision | |
| A_BORO | Borough of collision | 000 City Of London 001 Westminster 002 Camden 003 Islington 004 Hackney 005 Tower Hamlets 006 Greenwich 007 Lewisham 008 Southwark 009 Lambeth 010 Wandsworth 011 Hammersmith & Fulham 012 Kensington & Chelsea 013 Waltham Forest 014 Redbridge 015 Havering 016 Barking & Dagenham 017 Newham 018 Bexley 019 Bromley 020 Croydon 021 Sutton 022 Merton 023 Kingston 024 Richmond 025 Hounslow 026 Hillingdon 027 Ealing 028 Brent 029 Harrow 030 Barnet 031 Haringey 032 Enfield033 Hertsmere 034 Welwyn Hatfield 035 Broxbourne 036 Epping Forest 037 Reigate & Banstead 038 Epsom & Ewell 039 Elmbridge 040 Spelthorne 041 Not coded 042 Not coded 043 Dartford 044 Sevenoaks 045 Tandridge 046 Mole Valley 047 South Bucks 048 Three Rivers 049 Brentwood 050 Thurrock 051 Runnymede 052 Windsor and Maidenhead 057 Heathrow |
| A_ATIME | Time of collision | |
| A_YEAR | Year of collision | |
| LSOA_CODE | SOA of collision | |
| A_DATE | Date of collision | |
| A_DOW | Day of week of collision | 0 Sunday 1 Monday 2 Tuesday 3 Wednesday 4 Thursday 5 Friday 6 Saturday |
| col_lacode | Local authority code of location of collision | |
| col_laname | Local authority name of location of collision | |
| col_imdscore | IMD score of SOA of collision | Index of Multiple Deprivation 2004 |
| col_imd110 | IMD decile of SOA of collision | 1 = least deprived, 10 = most deprived |
| col_imd5 | IMD quintile of SOA of collision | 1 = least deprived, 5 = most deprived |
| col_inner | Inner/outer London location of collision | 0 Outer London 1 Inner London |
Data coding
For subgroup analyses by ethnicity data was coded into three categories for analysis: ‘White’ (White-skinned European, Dark-skinned European); ‘Black’ (Afro-Caribbean); and ‘Asian’ (Asian). Other categories were not included in subgroup analyses (Oriental, Arab, Not Known)
For subgroup analyses by deprivation, casualties were assigned the IMD score of the super output are in which the collision occurred. Deciles of IMD were coded as follows:
| Decile | IMD score |
|---|---|
| 1 (least deprived) | ≤ 8.09 |
| 2 | 8.10–11.86 |
| 3 | 11.87–15.36 |
| 4 | 15.37–19.24 |
| 5 | 19.25–23.05 |
| 6 | 23.06–27.64 |
| 7 | 27.65–32.51 |
| 8 | 32.52–37.92 |
| 9 | 37.93–44.87 |
| 10 (most deprived) | ≥ 44.88 |
For subgroup analyses by area of London, the following boroughs were coded to inner London: Camden, Kensington and Chelsea, Westminster, City of London, Hackney, Hammersmith and Fulham, Haringey, Islington, Lambeth, Lewisham, Newham, Southwark, Tower Hamlets, and Wandsworth. All other boroughs were coded to outer London.
For subgroup analyses by intervention uptake, casualties were linked to the local authority in which the collision occurred. Data on the number of zip cards issues by borough were provided by TfL. These data were linked to population data to estimate rates of intervention uptake. The following boroughs were coded as high uptake boroughs: Bexley, Brent, Croydon, Ealing, Enfield, Greenwich, Haringey, Harrow, Hounslow, Islington, Lambeth, Lewisham, Merton, Newham, Southwark, Waltham Forest, and Wandsworth. All other boroughs were coded as low-uptake.
Imputation
No data was imputed.
Allowing for survey design
None.
Sample sizes
| Data source | Intervention period | Time period | Age group (years) | ||
|---|---|---|---|---|---|
| 12–17 | 25–59 | ≥ 60 | |||
| STATS19 | Pre | 2001–4 | 11,221 | 89,661 | 13,337 |
| Post | 2006–9 | 6657 | 65,542 | 9283 | |
Hospital Episode Statistics
List of fields used: inpatient data extract.
| Variable | Description | Value labels |
|---|---|---|
| STARTAGE | Age at start of episode. | |
| ETHNOS | Ethnicity | A = British (White) B = Irish (White) C = Any other White background D = White and Black Caribbean (Mixed) E = White and Black African (Mixed) F = White and Asian (Mixed) G = Any other Mixed background H = Indian (Asian or Asian British) J = Pakistani (Asian or Asian British) K = Bangladeshi (Asian or Asian British) L = Any other Asian background M = Caribbean (Black or Black British) N = African (Black or Black British) P = Any other Black background R = Chinese (other ethnic group) S = Any other ethnic group Z = Not stated X = Not known |
| EXTRACT HESID | This field uniquely identifies a patient across all data years. It is generated by matching records for the same patient using a combination of NHS Number, local patient identifier, provider code, postcode, sex and date of birth | |
| ADMIDATE | Admission date | |
| DISDATE | Date of discharge | |
| DIAG_01 to DIAG_20 | 20 fields (n = 14 pre-April 2007 and n = 7 pre-April 2002) containing information illness or condition. Field DIAG_01 contains the primary diagnosis. The others contain secondary/subsidiary diagnoses. Codes are defined in the ICD-10 | |
| CAUSE | This field is a copy of the initial four characters of DIAG_01 that represents an external cause (i.e. accidents or poisoning) | |
| RESCTY | County of residence | |
| SOAL | LSOA of place of residence | |
| IMD04RK | IMD overall rank of SOA of place of residence |
Data coding
For subgroup analyses by ethnicity data was coded into three categories for analysis: ‘White’ (British-White, Irish-White, any other White background); ‘Black’ (White and Black Caribbean-Mixed, White and Black African-Mixed, Caribbean Black or Black British, African Black or Black British, any other Black background); and ‘Asian’ (White and Asian-Mixed, Indian Asian or Asian British, Pakistani Asian or Asian British, Bangladeshi Asian or Asian British, any other Asian background). Other categories were not included in subgroup analyses (any other Mixed background, Chinese, Oriental, other ethnic group, not known).
For subgroup analyses by deprivation, patients were assigned the IMD score of the super output area in which they lived. Deciles of IMD were coded as follows:
| Decile | IMD score |
|---|---|
| 1 (least deprived) | ≤ 8.09 |
| 2 | 8.10–11.86 |
| 3 | 11.87–15.36 |
| 4 | 15.37–19.24 |
| 5 | 19.25–23.05 |
| 6 | 23.06–27.64 |
| 7 | 27.65–32.51 |
| 8 | 32.52–37.92 |
| 9 | 37.93–44.87 |
| 10 (most deprived) | ≥ 44.88 |
For subgroup analyses by area of London, the following boroughs were coded to inner London: Camden, Kensington and Chelsea, Westminster, City of London, Hackney, Hammersmith and Fulham, Haringey, Islington, Lambeth, Lewisham, Newham, Southwark, Tower Hamlets, and Wandsworth. All other boroughs were coded to outer London.
For subgroup analyses by intervention uptake, data on the number of zip cards issues by borough were provided by TfL. These data were linked to population data to estimate rates of intervention uptake. The following boroughs were coded as high uptake boroughs: Bexley, Brent, Croydon, Ealing, Enfield, Greenwich, Haringey, Harrow, Hounslow, Islington, Lambeth, Lewisham, Merton, Newham, Southwark, Waltham Forest, and Wandsworth. All other boroughs were coded as low uptake.
Imputation
None.
Allowing for survey design
None.
Sample sizes
| Data source | Intervention period | Time period | Age group (years) | ||
|---|---|---|---|---|---|
| 12–17 | 25–59 | ≥ 60 | |||
| HES | Pre | 2001–4 | 2321 | 11,829 | 905 |
| Post | 2006–9 | 3322 | 14,641 | 959 | |
London Travel Surveys (London Area Transport Survey and London Travel Demand Survey)
List of fields used, data extract: data in the LATS and LTDS comes at four levels: household, person, trip and stage. Below are the variables we used at each level.
| Variable name | Level | Description | Value labels |
|---|---|---|---|
| Hyearid | Household | Year of survey | 2001 2005 2006 2007 2008 |
| Borough | Household | Borough of residence | |
| IMDscore | Household | Deprivation of SOA of postcode of residence | |
| Hincomei | Household | Household income | 01 < £5,000 02 £5000 – £9,999 03 £10,000 – £14,999 04 £15,000 – £19,999 05 £20,000 – £24,999 06 £25,000 – £34,999 07 £35,000 – £49,999 08 £50,000 – £74,999 09 £75k – £99k (£75k+ in 0506) 10 100,000+ |
| Pagei | Person | Age | |
| Pegroup | Person | Ethnic group | 01 White – British 02 White – Irish 03 Other White 04 Mixed – White and Black Caribbean 05 Mixed – White and Black African 06 Mixed – White and Asian 07 Mixed – Other mixed background 08 Asian or British Asian – Indian 09 Asian or British Asian – Pakistani 10 Asian or British Asian – Bangladeshi 11 Asian or British Asian – Other Asian background 12 Black or Black British – Caribbean 13 Black or Black British – African 14 Black or Black British – Other Black background 15 Chinese 16 Other ethnic group 20 Refused |
| Ppiwtttwkd3y | Person | Person level survey weights: weekday term time | |
| Thmmode | Trip | Main mode of trip | 01 Walk (roller blades/ scooters) 02 Pedal Cycle 03 Car Driver 04 Car Passenger 05 Motorcycle Rider 06 Motorcycle Passenger 07 Van medium Driver 08 Van medium Passenger 09 Van (small) Driver10 Van (small) Passenger 11 Van/ lorry (other) Driver 12 Van/ lorry (other) Passenger 13 Bus (public) 14 Bus (school/work) 15 Dial a ride 16 Coach 17 Underground 18 DLR train 19 National rail train 20 Tramlink 21 Taxi (London black cab) 22 Taxi (other/minicab) 23 Plane/ Boat/Other 24 London overground |
| Tpurp | Trip | Trip purpose | 01 Home 02 Usual workplace 03 Delivering/loading 04 Other work 05 Entertainment/sport/social 06 Shopping 07 Personal Business/use services 08 Education (as a pupil) 09 Hotel/holiday home 10 Drop off/pick up - work 11 Drop off/pick up - school/college 12 Drop off/pick up - other 13 Worship/other religious observance 14 Other |
| Tstime | Trip | Time of trip | |
| Smode | Stage | Mode of stage | Same as Thhmode |
| Slenni | Stage | Length of stage (in km) |
Data coding
For subgroup analyses by ethnicity data was coded into three categories for analysis: ‘White’ (White – British, White – Irish, other White); ‘Black’ (Black or Black British – Caribbean, Black or Black British – African, Black or Black British – other Black background, Mixed – White and Black Caribbean, Mixed – White and Black African); and ‘Asian’ (Asian or British Asian – Indian, Asian or British Asian – Pakistani, Asian or British Asian – Bangladeshi, Asian or British Asian – other Asian background, Mixed – White and Asian). Other categories were not included in subgroup analyses (Mixed – other mixed background, Chinese, other ethnic group, refused).
For subgroup analyses by household income was divided into terciles: £0–14,999, £15,000–49,000, £50,000+.
For subgroup analyses by deprivation deciles of IMD were coded as follows:
| Decile | IMD score |
|---|---|
| 1 (least deprived) | ≤ 8.09 |
| 2 | 8.10–11.86 |
| 3 | 11.87–15.36 |
| 4 | 15.37–19.24 |
| 5 | 19.25–23.05 |
| 6 | 23.06–27.64 |
| 7 | 27.65–32.51 |
| 8 | 32.52–37.92 |
| 9 | 37.93–44.87 |
| 10 (most deprived) | ≥ 44.88 |
For subgroup analyses by area of London, the following boroughs were coded to inner London: Camden, Kensington and Chelsea, Westminster, City of London, Hackney, Hammersmith and Fulham, Haringey, Islington, Lambeth, Lewisham, Newham, Southwark, Tower Hamlets, and Wandsworth. All other boroughs were coded to outer London.
For subgroup analyses by intervention uptake, data on the number of zip cards issues by borough was provided by TfL. These data were linked to population data to estimate rates of intervention uptake. The following boroughs were coded as high uptake boroughs: Bexley, Brent, Croydon, Ealing, Enfield, Greenwich, Haringey, Harrow, Hounslow, Islington, Lambeth, Lewisham, Merton, Newham, Southwark, Waltham Forest, and Wandsworth. All other boroughs were coded as low uptake.
Imputation
We encountered a number of missing and impossible values for distance travelled in the LATS and LTDS. Distances were deemed ‘impossible’ if:
-
> 15 km for walking stages
-
> 100 km for slower modes (cycling, bus, underground, DLR, tram)
-
> 300 km for faster modes (car, motorcycle, train, taxi, van).
| Distance | LATS | LTDS |
|---|---|---|
| Total # of stages | 360,391 | 354,043 |
| # stages missing | 0 | 674 |
| % of missing that are walking stages | 0 | 48 |
| % of missing that are bus stages | 0 | 7 |
| # stages w/ impossible values | 736 | 277 |
| % of missing that are walking stages | 44 | 69 |
| % of missing that are bus stages | 6 | 0.36 |
In order to include these stages in the analysis we imputed missing and impossible distances based on the median values by age group and mode of travel.
| Mode | Age group (years) | ||
|---|---|---|---|
| 0–18 | 19–59 | ≥ 60 | |
| Walk | 0.52 | 0.47 | 0.41 |
| Car driver | 3.285 | 3.29 | 2.74 |
| Car passenger | 1.98 | 3.43 | 2.88 |
| Motorcycle | 4.47 | 7.35 | 4.11 |
| Van (small) | 3.7 | 6.075 | 3.91 |
| Van (medium) | 21.1 | 6.34 | 4.2 |
| Van/lorry (other) | N/A | 8.49 | 3.91 |
| Cycle | 1.05 | 2.31 | 0.9 |
| Bus (public) | 2.53 | 2.48 | 2.06 |
| Underground | 3.93 | 4.66 | 4.515 |
| Train | 7.17 | 11.52 | 12.72 |
| DLR | 2.89 | 4.27 | 2.54 |
| Tram | 3.56 | 3.56 | 4.45 |
| Taxi – London | 3.96 | 3.1 | 2.01 |
| Taxi – other | 3.11 | 3.375 | 2.04 |
| Bus (school/work) | 4.41 | 2.92 | 3.07 |
| Coach | 11.27 | 3.08 | 13.175 |
| Plane/boat | 3.01 | 2.62 | 1.92 |
Allowing for survey design
Survey weights (adjusted for non-response and scaled to population projections) were used to ensure that the sample was representative of the London population. Survey weights ensure that data are representative of term-time weekday travel only. All analyses allowed for the stratification of the sample by London borough.
Sample sizes
| Data source | Intervention period | Time period | Age group (years) | ||
|---|---|---|---|---|---|
| 12–17 | 25–59 | ≥ 60 | |||
| LATS | Pre | 2001 | 4206 | 31,169 | 10,671 |
| LTDS | Post | 2006–8 | 2024 | 14,085 | 5033 |
Appendix 3 Qualitative samples: borough selection and settings
To select boroughs covering the very different contexts of inner and outer London, we used the existing GLA categorisation of ‘inner’ or ‘outer’ London boroughs. 217 The Office for National Statistics and the Census define inner London slightly differently to the GLA, including Haringey and Newham in their list of inner London boroughs, but excluding Greenwich. 218 Our selection therefore excluded these, and City of London (with its small population of residents and anomalous governance), leaving 29 boroughs to select from. Our aim was to include views from young people living in boroughs characterised by a range of levels of bus richness and local area deprivation from across inner and outer London (Table 30).
| Higher levels of deprivation | Lower levels of deprivation | |
| ‘Bus rich’ | Borough 1 | Borough 2 |
| ‘Bus poor’ | Borough 3 | Borough 4 |
For ‘bus richness’ we used proxy measures of (i) levels of bus use (higher levels of use = bus rich) and (ii) bus stop density (greater density of bus stops = bus rich). For bus use, we specifically looked at data on average bus journey duration and distance data for children aged < 18 years from the LATS 2001 and from the LTDS 2005–8. For bus stop density at the borough level, we looked at data on the number of bus stops per km2 and on the number of bus stops per 1000 residents in each borough (based on Census 2001 population estimates).
To select boroughs according to levels of local area deprivation we used two proxy measures. First, we looked at a measure of the percentage of children living in benefit-claiming families by borough. The exact measure we are using, derived from a Department for Work and Pensions 5% sample taken in August 2007, is a measure by borough of the proportion of children (aged 0–18 years) in families claiming benefits. 219 The second proxy was derived from the central government IMD220 and is a measure developed by the Greater London Authority’s Data Management and Analysis Group that shows us what proportion of SOAs for each London borough fall within each interquintile range on the IMD 2007.
The 29 boroughs were then ranked according to these bus richness/poverty and local area deprivation proxies, as shown in Table 31. In Table 31, cells shaded blue indicate that for the measure concerned the borough is relatively deprived or relatively bus poor. Likewise, cells shaded green indicate that for the measure concerned the borough is relatively un-deprived or relatively bus rich. Finally, cells without shading indicate that for the measure concerned the borough falls at the mid-way point for the respective measure of local area deprivation or bus richness.
| London borough | Local area deprivation proxies | Bus richness proxies | ||||
|---|---|---|---|---|---|---|
| % Children living in benefit-claiming families (‘1’ is lowest %) | Borough-wide socioeconomic deprivation according to distribution of SOAs (‘1’ is least deprived) | Average daily time spent travelling on public buses by under 18-year-olds (‘1’ is least time) | Average daily distance travelled by under 18-year-olds on public buses (‘1’ is least distance) | Bus stops per km2 (‘1’ is fewest stops) | Bus stops by 1000 residents (‘1’ is fewest stops) | |
| Barking and Dagenham | 24 | 24 | 23 | 19 | 5 | 11 |
| Barnet | 9 | 13 | 16 | 17 | 7 | 24 |
| Bexley | 4 | 10 | 28 | 25 | 6 | 25 |
| Brent | 22 | 18 | 15 | 21 | 15 | 15 |
| Bromley | 5 | 8 | 14 | 28 | 1 | 29 |
| Camden | 18 | 21 | 24 | 12 | 20 | 12 |
| Croydon | 12 | 14 | 19 | 16 | 8 | 20 |
| Ealing | 16 | 16 | 10 | 6 | 14 | 14 |
| Enfield | 19 | 19 | 25 | 26 | 3 | 17 |
| Hackney | 27 | 29 | 18 | 29 | 24 | 6 |
| Hammersmith and Fulham | 21 | 20 | 4 | 10 | 17 | 3 |
| Harrow | 7 | 3 | 3 | 11 | 29 | 2 |
| Havering | 6 | 6 | 21 | 20 | 27 | 21 |
| Hillingdon | 11 | 7 | 26 | 24 | 28 | 28 |
| Hounslow | 15 | 12 | 22 | 13 | 12 | 27 |
| Islington | 28 | 27 | 29 | 23 | 25 | 4 |
| Kensington and Chelsea | 8 | 15 | 8 | 3 | 22 | 1 |
| Kingston upon Thames | 2 | 2 | 6 | 4 | 11 | 23 |
| Lambeth | 25 | 25 | 20 | 15 | 21 | 5 |
| Lewisham | 20 | 22 | 17 | 18 | 18 | 16 |
| Merton | 10 | 4 | 27 | 14 | 10 | 13 |
| Redbridge | 13 | 9 | 2 | 7 | 4 | 7 |
| Richmond upon Thames | 1 | 1 | 12 | 8 | 2 | 22 |
| Southwark | 26 | 26 | 11 | 27 | 23 | 18 |
| Sutton | 3 | 5 | 13 | 9 | 9 | 19 |
| Tower Hamlets | 29 | 28 | 5 | 1 | 19 | 9 |
| Waltham Forest | 23 | 23 | 1 | 22 | 13 | 10 |
| Wandsworth | 14 | 11 | 7 | 2 | 16 | 8 |
| Westminster | 17 | 17 | 9 | 5 | 26 | 26 |
These rankings were used to identify four boroughs for our qualitative study that fulfil the deprivation and bus richness variability specified in the protocol. The different measures of deprivation and bus richness were only consistent with one another for a few boroughs, so we selected boroughs with a majority (i.e. three out of four) of the bus richness measures indicating that it is either ‘bus rich’ or ‘bus poor.’ A shortlist of appropriate boroughs is shown in Table 32.
| Higher levels of socioeconomic deprivation | Lower levels of socioeconomic deprivation | |
|---|---|---|
| ‘Bus rich’ | Hackneya | Bexleyb |
| Islingtona | Haveringb | |
| Southwarka | Hillingdonb | |
| Enfieldb | ||
| ‘Bus poor’ | Hammersmith and Fulhama | Kingston-upon-Thamesb |
| Tower Hamletsa | Richmond-upon-Thamesb | |
| Waltham Forestb | Suttonb |
As no inner city boroughs had lower levels of socioeconomic deprivation, we choose two boroughs with higher levels of socioeconomic deprivation from inner London. From these boroughs, we selected our sample boroughs to reflect geographical spread across London, and practical considerations.
With these considerations in mind, the following four London boroughs were selected for the project.
Inner London
-
Higher deprivation, lower bus use: Hammersmith and Fulham.
-
Higher socioeconomic deprivation, higher bus use: Islington.
Outer London
-
Lower deprivation, higher bus use: Havering.
-
Lower deprivation, lower bus use: Sutton.
We recruited research participants for our study from each of these four boroughs on the following basis:
-
Young people: live in or attend school/youth club/other educational or training institution in the borough.
-
Older citizens: live in the borough.
For context, the ranks (out of 29) of these boroughs according to the six measures that we looked at are tabulated in Table 33.
| London borough | % Children living in benefit-claiming families (‘1’ is lowest %) | Borough-wide socioeconomic deprivation according to distribution of SOAs (‘1’ is least deprived) | Average daily time spent travelling on public buses by under 18-year-olds (‘1’ is least time) | Average daily distance travelled by under 18-year-olds on public buses (‘1’ is least distance) | Bus stops per km2 (‘1’ is fewest stops) | Bus stops by 1000 residents (‘1’ is fewest stops) |
|---|---|---|---|---|---|---|
| Hammersmith and Fulham | 21 | 20 | 4 | 10 | 17 | 3 |
| Havering | 6 | 6 | 21 | 20 | 27 | 21 |
| Islington | 28 | 27 | 29 | 23 | 25 | 4 |
| Sutton | 3 | 5 | 13 | 9 | 9 | 19 |
Appendix 4 Participation from young people involved in ‘Young Scientists Programme’
The LSHTM award-winning ‘Young Scientists Programme’ offers work experience and related activities to students from local schools in deprived areas and/or where a high proportion of the school student body receives free school meals. This programme was initiated in 2001 (for details see www.lshtm.ac.uk/aboutus/volunteering/ysp/).
Most young scientists come to LSHTM during the 1- or 2-week work experience placements which form a compulsory part of the UK national curriculum for Key Stage 4 (14- to 16-year-olds). Placements are arranged in liaison with borough and school work experience co-ordinators, who organise necessary paperwork (e.g. parent permission slips) and seek to accommodate our request for students who are enthusiastic about science but not necessarily high academic achievers. At LSHTM, young scientists work in pairs to carry out independent research projects (e.g. designing and conducting a small survey), supervised by LSHTM staff and student volunteers. These research projects can cover anything from local to international health issues, and form the basis for presentations by the young scientists in a scientific seminar on their final day. Typically LSHTM runs three to four ‘large’ work experience sessions per year (involving 6–10 young scientists) and one to two ‘small’ sessions (involving one to four young scientists). Where possible the programme takes students from two different schools simultaneously and form pairs across schools. Finally, LSHTM also runs occasional half-day workshops for school classes, either at LSHTM or in the schools themselves.
Participation, engagement and involvement of ‘young scientists’ in an ongoing study
A reciprocal approach to recruitment
The Young Scientists Programme originally focused on providing an educational experience, and young scientists made only occasional, brief contributions to actual LSHTM research (e.g. providing feedback on the design of recruitment materials). In 2010, Anna Goodman decided to experiment with forging a deeper connection between the programme and the ‘On The Buses’ study. We initially used the Young Scientists Programme to invite past and current young scientists to participate in qualitative interviews. A half-day ‘What is public health?’ workshop included ‘On The Buses’ as a case study, and this was used as the basis for a reciprocal approach to recruitment, offering the workshop to two schools that had previously participated in the Young Scientists Programme, and asking for permission to conclude the workshop by inviting students to participate.
Integrated work experience
We then engaged and involved young scientists in ‘On The Buses’ in a deeper and more integrated manner. In spring 2010, when the qualitative study was still in an exploratory stage, one young scientist was given an ‘open brief’ to conduct a research project inspired by ‘On The Buses’. In spring 2011, when qualitative data collection and analysis was well underway, Anna Goodman wrote more focused briefs suggesting the young scientists choose between a number of specific emerging questions (Box 1). She gave these focused briefs to 12 young scientists attending LSHTM in two separate work experience sessions (one group of two and one group of 10). At the end of their placements, these young scientists were invited to participate in in-depth interviews about their research in their project pairs. These 13 young scientists came from four schools and were all aged 14 or 15 years old; four were girls and four identified themselves as being White British.
-
How does free bus travel affect the mental and social health of children under 16? [Designed by young scientist]
-
Universality: Would it matter if young people’s travel stopped being universally free? [Suggested by AG]
-
Car dependency: Does free bus travel affect young people’s attitudes towards cars? [Suggested by AG]
-
Citizenship: Does free bus travel make young people feel more like London citizens? [Suggested by AG]
-
Public space: Do buses represent ‘public space’ for young people? [Suggested by AG]
-
Transport poverty: What does free travel let young people do that they wouldn’t do otherwise? [Suggested by AG]
-
How does free bus travel affect under 16’s physical activity (a) overall and (b) when travelling? [Designed by young scientist as they preferred this to AG’s suggestions]
AG, Anna Goodman.
For study projects see www.lshtm.ac.uk/php/hsrp/buses/youth/.
Appendix 5 Example coding frame for data relating to causal pathways (young people)
| Code | Dimensions | Examples/notes | Link to causal pathways |
|---|---|---|---|
| Typologies of journey | Necessity/instrumentality; sociability; distance | Any mode ‘boring’ alone | Walking/bus seen as ‘necessity’ modes; tube – leisure; cycling – discretionary |
| Assessing the ‘walkability’ of a journey (in principle) | Physical environment; social environment | Distance, hills; risks (gangs, odd people); cultural acceptability | Active modes only default for very short journey |
| Criteria for choosing mode for a ‘walkable’ journey | Efficiency; sociability; cultural acceptability; economic; opportunity for ‘spectacle’/entertainment; convenience | Not prioritised; highly prioritised; tacit; ? deciding factor; something to see on bus/walk, ‘our’ stories | On balance, zip card moves decision to ‘bus’ from ‘active’ (makes bus default) |
| Criteria for choosing mode for longer journey | Sociability; economic; convenience; pull and push factors | Travel boring alone; pay if no zip card; parents provide lifts; cycle – pull (fun); walk – push (when have to) | Some car journeys replaced by bus; ? walking not currently desirable/discretionary cycling can be |
| Typologies of bus users | Age; social role; time of day | The public, gangs, little kids, big kids, other schools, old people, etc. | ? bus use destigmatised ? impact on car dependence (positive) |
| Imagining and enacting the future travelling self | Contemporary – practising ‘adulthood’; imagined future | Driving license assumed to be right of passage | See themselves as public transport users, but also future car dependence (negative) |
| Learning to travel | Development of ‘transport skills’; development of ‘independence’; displaying ‘independence’ | Trying different lines, using journey planner; journeys to test self; journeys to mark life stages | Social equality – zip card evens up the opportunities; zip card provides ‘sense of freedom’ |
| Accounting for impact of ‘free’ travel | Changing access to ‘necessary’ travel; changing access to ‘discretionary’ travel | School, family responsibilities (e.g. shopping), sports clubs; leisure, going into town, riding around, travel with low income parents | ? zip card more an impact on discretionary travel – more impact on social exclusion not access to education, etc.? |
| Assessing well-being implications of travel modes | Infection risks; mental health and well-being; longer-term health | Tube/bus are risky; Aggression (positive and negative), stress; laziness of self/others; access to chicken shops at transport hubs | Young people focus on immediate health issues for physical health; immediate for emotional well-being? |
| Other key themes that cut across topics | |||
| Developing an identity; learning to be a Londoner/citizen | Interactional appropriateness | Age/ethnic/other interactions | (Broader implications for health and well-being) |
| Accessing the bus | Typologies of drivers; queuing etiquette | Rude, scared, ‘grizzled’, racist, ‘one of us’ (Only noticed in relation to others, e.g. boy travelling with young brother) | |
| Negotiating entitlement to use space on the bus | Implicit discourses; explicit discourses | Tacit knowledge of who sits where; ‘a modern tradition’ of seating arrangements; debates over hierarchy | |
| Negotiating the boundaries of public and private | Creating ‘public transport’; creating private space | ||
| Accounting for entitlement to benefit (free travel) | Reflective accounts of ‘what it’s for’ | Implicit and prompted accounts of why they have access | |
| Managing the risks and benefits of transport | Typologies of risk; strategies for risk reduction; the discursive uses of risk | People (strangers, known others), germs; hiding uniform/’phone me’ app | |
| Public understanding of ‘the intervention’ | Knowledge of ‘what it is’; tacit understanding of functions of card and benefit | Oyster card/zip card/don’t know; concerns about invasion of privacy/photo | |
| Travel as arena for enmity/friendship displays | Enmity as risk?; the uses of enmity | ‘Dirty look on a bus’; stories, moral tales | Injury risk |
Appendix 6 Example topic guides
On the Buses zip card user: topic guide (focus groups)
Introduction
-
Consenting, welcome and thank you for participating. Aims and objectives of the research and about the confidentiality of the content of the discussion.
-
What the interviewees can expect to hear from us as the research progresses.
Icebreaker
-
Ask participants to introduce themselves, confirm whether or not they use a zip card and to tell us what sorts of places and/or activities they use the bus to get to (to ‘freelist’ the types of journeys they do by bus).
Opening query
-
Ask the respondents if the types of journeys that they do by bus (e.g. to shops, to friends, to family, etc.) differ from the types of journeys they do on foot, on the underground, by car, etc. Ask the respondents to elaborate on how they decide how to travel for a given purpose (e.g. is it time of day, distance, purpose of journey, etc.).
-
Please tell me about your everyday travel habits. How do you travel to and from school? How long and how far do you travel? How many journeys do you make on a weekday and at the weekend? What types of transport do you use (private vehicle, public transport and walking)?
-
Get the respondents to elaborate on some of their particular travel experiences, ask about travel that day – did they travel by bus to the interview today? Or the day before?
Travel preferences and choices
-
Is there a way of travelling that you prefer for most or some of your journeys? Why? In particular, are there some journeys that you would only do by bus, or some that you would never do by bus? Why?
Bus journeys
-
Pick-up on bus journey components of answer to above. In particular, try to elucidate what routes the participant travels, where they start and end their everyday journeys, what their experiences of different journeys are.
-
What is best about travelling by bus? What are the advantages for you?
-
What are the things that you are most unhappy about when you use the bus? What do you do while on the bus? Do you tend to travel alone or with friends, and do you see other people you know when you use the bus?
-
When you use the bus are there particular places that you like to sit or choose not to sit? Why? Is this the same all through the day or is the time of day important? What is it about particular times of the day that makes you less/more confident about using the bus?
-
Who would you give your seat up for on a bus? Has anyone given their seat up for you?
-
Is your journey to school different to your journey back from school?
-
[Possible exercise – can you map your journeys to/from school on the pad provided?]
Other people
-
How do other people treat you on the bus? Can you tell us about some particular experiences? How do young people treat other people on the bus?
-
Why do you think you have more of a right to sit or stand in particular parts of the bus?
-
If you travel to or from school on the bus what sorts of other people use the bus at the same time as you? Do different users of the bus get along?
-
Pick up on any issues with the bus driver that may have arisen.
Zip card (free bus travel for 12- to 17-year-olds in fulltime education or training)
-
What do you think of the zip card scheme? Do you call it zip card, if not what do you call it?
-
Why do you think you have a zip card? Why do you get free bus travel?
-
How do you think having the zip card has changed the places you travel to and how you travel? Do you think young people use their zip card fairly?
-
If you didn’t have your zip card would you travel as much and how would you get around?
Extracurricular activities
-
What type of activities do you do after school? Do you do them alone or with friends? And at the weekends?
-
Is there anything you’d like to do/anywhere you’d like to go in London but can’t? Why?
-
Where do you take part in the activities you mentioned previously (especially is it indoor or outdoor, and is it activity-based or public space)? How do you get there and back?
-
Do you ever hang out with friends? Where do you tend to hang out and how do you get there and back?
-
Do you ever go for a walk/cycle/bus ride for fun?
Supplementary questions
-
Why do you think young people have been granted free travel on buses in London?
-
Is there any type of bus that you prefer – single-decker, double-decker, bendy bus, ‘Plus Bus’, dedicated school bus, etc.? If so, why?
-
You talked earlier about the bus environment (sights, smells, sounds, temperature, etc.) could you elaborate on what the environment’s like when you take the bus and how this affects you?
-
When you’re older and have to pay full fares to travel in London how do you think you’ll get around?
-
What would you think if bus travel was no longer free for all young people in London, but just for young people from lower income families (a bit like free school meals)?
-
Are you aware of the ‘safer routes to school’ scheme? Does it affect how you travel?
Close
-
Is there anything else that you think we should ask about?
On the Buses Freedom Pass user: topic guide (interviews)
Introduction
-
Consenting, welcome and thank you for participating. Quick statement from AJ about the aims and objectives of the research and about the confidentiality of the content of the discussion.
-
What the interviewee(s) can expect to hear from us as the research progresses.
Opening query
-
Please tell me about your everyday travel habits – what sort of journeys do you do in an average week? How long and how far do you travel, and how many journeys do you make on a weekday and at the weekend? What types of transport do you use (private vehicle, public transport and walking)?
-
Get the respondent(s) to ‘freelist’ the types of journeys that they do by bus (e.g. to shops, to friends, to family, etc.) and ask if this differs from the types of journeys they do on foot, on the underground, by car, etc. Ask the respondent(s) to elaborate on how they decide how to travel for a given purpose (e.g. is it time of day, distance, purpose of journey, etc.).
-
Get the respondent(s) to elaborate on some of their particular travel experiences; ask about travel that day. Did they travel by bus to the interview today? Or the day before?
Travel preferences and choices
-
Is there way of travelling that you prefer for most or some of your journeys? Why? In particular, are there some journeys that you would only do by bus, or some that you would never do by bus? Why?
Bus journeys
-
Pick-up on bus journey component(s) of answer to above. In particular, try to elucidate what routes the participant travels, where they start and end their everyday journeys, what their experiences of different journeys are?
-
What is best about travelling by bus? What are the advantages for you?
-
What are the things that you are most unhappy about when you use the bus? What do you do while on the bus? Do you tend to travel alone or with friends, and do you see other people you know when you use the bus?
-
When you use the bus are there particular places that you like to sit or choose not to sit? Why? Is this the same all through the day or is the time of day important? What is it about particular times of the day that makes you less/more confident about using the bus?
Freedom Pass
-
How has receiving your Freedom Pass changed the way that you travel in London? Would you travel differently – would you use other forms of transport – if you didn’t have the pass? Why? How is the scheme viewed among your friends – do they use it, is it well-known, do they see it as helpful? Do you refer to your pass as a ‘freedom pass’ or is there another word(s) that you use?
-
Do you see the Freedom Pass as a good scheme – is there anything that you would change about it? The eligibility age of the Freedom Pass is set to increase for new applicants – what do you think about this?
-
How has having a Freedom Pass affected the amount you walk, cycle or drive?
Zip pass (free bus travel for 12- to 17-year-olds in fulltime education or training)
-
For the last 5 years young people (12- to 17-year-olds in fulltime education or training) have been eligible for free bus or tram travel. Did you know about this scheme and what do you think about it?
-
Have you noticed a change in the numbers of young people using buses and how they use them in recent years? How have these changes affected your own bus use? And that of your friends?
Close
-
Is there anything else that you think we should ask about?
Appendix 7 Protocol for the quantitative component (extract)
This is an extract from a publication originally published as:
Wilkinson P, Edwards P, Steinbach R, Petticrew M, Goodman A, Jones A, et al. (2011) The health impact of free bus travel for young people in London: protocol for an observational study. Occasional Papers in Transport and Health(2). London: LSHTM; 2011.
Abstract
Background The extension, in September 2005, of free bus and tram travel in London to people 12–16 years of age and, in September 2006, to people under 18 years is likely to have had a range of impacts with implications for public health. The ‘On the Buses’ project aims to evaluate these impacts using a mixed method quasi-experimental design. This paper describes the protocol for the analyses of quantitative data for the study.
Methods/design Analyses will be based on routine travel survey and injury data for London, and will primarily entail comparison of pre-intervention to post-intervention change in the target age-group (12–17 years) against the corresponding change in people aged 25–59 years. The main outcome measures will include frequency and distance of all travel, and of active travel; frequency of independent travel, bus use; percentage of journeys < 1 km travelled by mode; incidence of road injury, and of intentional injury. We will use conditional fixed-effects Poisson models.
Discussion This quantitative study is part of a larger evaluation which draws on qualitative data, economic evaluation and literature reviews to describe the effect of free bus travel for young people on public health. It will also contribute to methodological development in relation to causal attribution in the absence of controlled experimental evidence, and in the use of routine data sets for assessing the effect of interventions on public health.
We hypothesized that the introduction of free bus travel in London would have several important effects, both direct and indirect (Figure A7.1). To test these adequately requires a combination of quantitative and qualitative methods. The quantitative study is one component directed towards testing the active travel, road injuries and intentional injuries hypotheses. Its protocol is described in this paper.
Methods/design
The overall aim of this study is to characterize changes in health behaviour and selected health outcomes in children and older adults following the introduction in September 2005 of the London free bus travel scheme for children aged 12–16 years and its subsequent extension to under those 18 in September 2006. There are three specific objectives:
-
To assess the impact of free bus travel for 12–17 year olds on their use of bus and other transport modes and on their non-car travel overall;
-
To assess the impact of free bus travel for 12–17 year olds on the use of bus and other transport modes by older age population groups;
-
To identify changes in the incidence of injuries in young people under 18 following access to free bus travel.
Research hypotheses
We hypothesize that the introduction of the free bus pass scheme is associated with:
-
an increase in bus use and overall ‘independent’ travel (the latter represented from available data by all non-car travel), but a reduction in active transport (walking and cycling) and car use, among the target age-group [Independent travel refers to travel young people do without guardians. With no direct measure of this, we use a proxy measure of all travel except car travel and, for those under 17 years, motorbike travel.];
-
a reduction in bus use and trips < 1 km made by people aged 65+, especially during the hours when children usually travel from, school;
-
a reduction in road traffic injuries in the target age group; and
-
an increase in intentional injury rates in the target age group.
-
We also hypothesize that:
-
-
changes will be more pronounced in the inner-London boroughs (with denser bus networks) than in outer-London boroughs;
-
changes will be more pronounced in boroughs with a known higher take-up of free bus travel;
-
changes in distance/frequency of bus travel, independent (non-car) travel, and active travel, and in injury incidence, are greater in households with low income;
-
reductions in car use will be greater in households with high income;
-
changes in distance/frequency of bus travel and active travel, and in injury incidence, will be the same across all ethnic groups.
Outcomes and measures
The outcomes we will use to assess the hypotheses are as follows:
-
frequency and distance of all transport, of active transport (i.e. walking and cycling) and of independent (non-car) transport (i.e. walking, cycling and public transport) in people aged 12–17 years;
-
frequency of bus use and distance travelled by bus in people aged 12–17 years;
-
frequency of bus travel and distance travelled by bus in other age groups;
-
incidence of intentional and non-intentional injuries in people aged 12–17 years.
We will use three main sources of data for our outcome measures.
Travel surveys
We will estimate travel patterns in the pre-intervention period using data from the 2001 London Area Transport Survey (LATS), and in the post-intervention period using data from the 2005–2008 London Travel Demand Surveys (LTDS). LATS includes 30,000 households and LTDS includes 5,000 households in 2005, with a further 8,000 households annually since 2006.
LATS and LTDS collect comparable data sets based on daily travel diaries, using comparable sampling designs. In every sampled household each person aged over 5 years living is asked to complete a one day travel diary to record the start, interchanges (e.g. change from bus to train), and end of every trip made on that day. Journey times are collected in LATS and LTDS and journey distance is estimated using the start-point, interchange and end-point of each trip. We will assign values to interchanges with missing data on time or distance travelled derived by multiple imputation. Interchanges with reported times and distances deemed implausible will be treated as missing and imputed.
LATS and LTDS include information on the age, ethnicity, household income and Lower Super Output Area (LSOA) of residence of each participant. We will code age using five categories (0–11, 12–17, 18–24, 25–59, 60–64, and 65+ years). We will exclude people aged 18–24 years from the analyses to protect against the possibility of any ‘carry-over’ effects of behaviours established in those who were teenagers in the early years of the scheme who then appear in the older age-groups for later years. We also exclude those aged 60-64 in analyses of impact on the older population because of the mix of retired and non-retired people. Ethnicity will be coded using four categories: White (white), Black (Black-Caribbean, Black-African, Black-Other), Asian (Indian, Pakistani, Bangladeshi) and other. Household income will be divided into three categories: less than £15,000, £15–49,999, and £50,000 or greater. LSOAs are small geographic areas corresponding to an average of 1,500 residents. There are 4,765 LSOAs in London, within 33 boroughs. Using data from the 2004 Index of Multiple deprivation (IMD, available at the LSOA level) we will assign each individual an area deprivation score based on their LSOA of residence. We will also assign each individual an Inner or outer London code based on their LSOA of residence.
Road injuries
To investigate the impact of free bus travel on road traffic injuries we will use STATS19 data for the years 2000 to 2009. STATS19 is the official dataset of death and personal injuries from road traffic collisions that occur on the public highway in the UK. STATS19 data include information on the age and ethnicity of each casualty. Data will be grouped into similar age and ethnicity categories as described above for LATS and LTDS. The STATS19 data also include coordinates of latitude and longitude for location of road traffic collisions. Each collision will be linked geographically to a LSOA and through the LSOA code to both an IMD deprivation score and Inner-Outer London code.
Intentional/non-intentional injuries
We will obtain an extract of Hospital Episode Statistics (HES) data for England covering the period 2001 to 2009. We will identify all London residents using LSOA code of residence. We will identify hospital admissions due to external causes of injury, and specifically those external causes hypothesised to be directly influenced by transport access (e.g. transport injuries, assaults). We will conduct a sensitivity analysis using only severe injury admissions to assess whether differential admission rates by external cause over time may have introduced bias (e.g. due to differences in admissions policies). 14 HES data also include information on age, ethnicity, and through the LSOA code can be linked to a deprivation score and inner/outer London status.
Power and sample size
The LATS and LTDS samples include data on 3,000 young people before and after the intervention, giving over 80% power to detect a 10% relative reduction in average distances walked daily by young people (i.e. from 0.9 (SD 1.3) km to 0.8 (SD 1.3) km per day) at a 5% significance level. Similarly, the study will have over 90% power to detect a 10% increase in the average distance of bus travel (i.e. from 4.3 (SD 4.1) km to 4.7 (SD 4.1) km per day). For transport-related injury, the study would have 80% power to detect a 10% change, or 90% power to detect a 12% change significant at the 5% level. Statistical power is inevitably more limited for subgroup analyses, but there will be 90% power to detect a 15% change in average distance travelled by bus by young people within the most deprived quartile, for example.
Analyses
(i) Analyses will compare the changes in each outcome variable in the pre versus post intervention time periods in the target age group (12–17 years) to changes in the outcome variable pre and post intervention in 25–59 year olds (see Table 1 and Figure A7.2):
(ii) We will conduct similar analyses to compare pre–post intervention changes in outcomes by subgroups: area of London (inner versus outer; areas of high intervention take up versus low intervention take up); deprivation group (most deprived fifth of population versus least deprived 80%); household income (< £15k per year versus > £50k per year (for travel patterns only)) and ethnicity (White, Black, Asian, other) – see Table 3.
(iii) To explore whether older citizens are being displaced from buses and travel more broadly, we will compare the pre-post change in older citizens’ travel during post-school commuting hours versus other times (see shell Table 2). (Prior to January 2009, older citizens were not able to use free buses before 9.30 a.m.)
(iv) For STATS19 road traffic injury data we will implement conditional fixed effects Poisson regression using Stata’s xtpoisson command, based on annual counts of casualties and collisions. Robust standard errors will be obtained using jackknife procedures clustering on borough (n = 33). The underlying trends in casualties and collisions will be fitted using linear terms. Analyses will be stratified by age-group, and comparisons will be made between the 12–17 years and older ages.
References
- Gordon-Larsen P, Nelson MC, Beam K. Associations among active transportation, physical activity, and weight status in young adults. Obes Res 2005;13:868-75.
- Oja P, Vuori I, Paronen O. Daily walking and cycling to work: their utility as health-enhancing physical activity. Patient Educ Couns 1998;33:S87-94.
- Hamer M, Chida Y. Active commuting and cardiovascular risk: a meta-analytic review. Prev Med 2008;46:9-13.
- Lee MC, Orenstein MR, Richardson MJ. Systematic review of active commuting to school and childrens physical activity and weight. J Phys Act Health 2008;5:930-49.
- Faulkner GE, Buliung RN, Flora PK, Fusco C. Active school transport, physical activity levels and body weight of children and youth: a systematic review. Prev Med 2009;48:3-8.
- DfT 2004.
- Besser LM, Dannenberg AL. Walking to public transit: steps to help meet physical activity recommendations. Am J Prev Med 2005;29:273-80.
- Edwards RD. Public transit, obesity, and medical costs: assessing the magnitudes. Prev Med 2008;46:14-21.
- Julien A, Carré J-R. Cheminements piétonniers et exposition au risqueRisk exposure during pedestrian journeys. Recherche - Transports - Sécurité 2002;76:173-89.
- Edinburgh: Scottish Government; 2009.
- Edwards P, Roberts I, Green J, Lutchmun S. Deaths from injury in children and employment status in family: analysis of trends in class specific death rates. BMJ 2006;333.
- Steinbach R, Green J, Edwards P, Grundy C. ‘Race’ or place? Explaining ethnic variations in childhood pedestrian injury rates in London. Health Place 2010;16:34-42.
- Sonkin B, Edwards P, Roberts I, Green J. Walking, cycling and transport safety: an analysis of child road deaths. J R Soc Med 2006;99:402-5.
- Edwards P, Green J, Lachowycz K, Grundy C, Roberts I. Serious injuries in children: variation by area deprivation and settlement type. Arch Dis Child 2008;93:485-9.
- Watkiss P, Brand C, Hurley F, A P, Mindel J, Joffe M, et al. London, UK: NHS Executive and AEA Technology; 2000.
- Crum AJ, Langer EJ. Mind-set matters: exercise and the placebo effect. Psychol Sci 2007;18:165-71.
- Bostock L. Pathways of disadvantage? Walking as a mode of transport among low-income mothers. Health Soc Care Community 2001;9:11-8.
- Ogilvie D, Mitchell R, Mutrie N, Petticrew M, Platt S. Evaluating health effects of transport interventions methodologic case study. Am J Prev Med 2006;31:118-26.
- Petticrew M, Cummins S, Ferrell C, Findlay A, Higgins C, Hoy C, et al. Natural experiments: an underused tool for public health?. Public Health 2005;119:751-7.
- Shadish W, Campbell D, Cook T. Experimental and quasi-experimental designs for generalized causal inference. New York: Houghton Miffin Co.; 2002.
- Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ 2008;337.
- Sun X, Briel M, Walter SD, Guyatt GH. Is a subgroup effect believable? Updating criteria to evaluate the credibility of subgroup analyses. BMJ 2010;340.
| Ages 12–17 years | 25–59 years | Ratio of ratios | ||||||
|---|---|---|---|---|---|---|---|---|
| Pre- | Post- | Ratio | Pre- | Post- | Ratio | |||
| Active transport (i.e. walking and cycling) | Walking frequency | |||||||
| Walking distance | ||||||||
| Cycling frequency | ||||||||
| Cycling distance | ||||||||
| Bus use and the distance travelled by bus | Frequency | |||||||
| Distance | ||||||||
| Percentage of short distance trips <1 km travelled by mode | Walking | |||||||
| Cycling | ||||||||
| Bus | ||||||||
| Car | ||||||||
| Independent transport (walking, cycling, and public transport) | Frequency | |||||||
| Distance | ||||||||
| Frequency of journeys to work or school | Number per week | |||||||
| Incidence of road traffic injuries | Number per 1000 pyrs | |||||||
| Incidence of intentional injuries | Number per 1000 pyrs | |||||||
| Incidence of non-intentional injuries | Number per 1000 pyrs | |||||||
| Within travel from School hours (3–4 p.m., Monday to Friday, in term time)* | Travel at other times | Ratio of ratios | ||||||
|---|---|---|---|---|---|---|---|---|
| Pre- | Post- | Ratio | Pre- | Post- | Ratio | |||
| Bus travel | Frequency | |||||||
| Distance | ||||||||
| % of short distance trips by bus | ||||||||
| All travel | Frequency | |||||||
| Distance | ||||||||
| % of all trips which are short distance | ||||||||
| Outcome | Potential modifier | Pre-/post-intervention change | Evidence for difference between groups (test for interaction) | |
|---|---|---|---|---|
| Distance by walking/cycling per week | Area of London | Inner London | X (95% CI x, y) | |
| Outer London | X (95% CI x, y) | |||
| Deprivation group | Most deprived fifth of population | X (95% CI x, y) | ||
| Least deprived 80% of population | X (95% CI x, y) | |||
| Household income | < 15k | X (95% CI x, y) | ||
| > = 50k | X (95% CI x, y) | |||
| Ethnicity | White | X (95% CI x, y) | ||
| Black | X (95% CI x, y) | |||
| Asian | X (95% CI x, y) | |||
| Other | X (95% CI x, y) | |||
| Road injuries | Area of London | Inner London | X (95% CI x, y) | |
| Outer London | X (95% CI x, y) | |||
| Deprivation group | Most deprived fifth of population | X (95% CI x, y) | ||
| Least deprived 80% of population | X (95% CI x, y) | |||
| Ethnicity | White | X (95% CI x, y) | ||
| Black | X (95% CI x, y) | |||
| Asian | X (95% CI x, y) | |||
| Intentional injuries | Area of London | Inner London | X (95% CI x, y) | |
| Outer London | X (95% CI x, y) | |||
| Deprivation group | Most deprived fifth of population | X (95% CI x, y) | ||
| Least deprived 80% of population | X (95% CI x, y) | |||
| Ethnicity | White | X (95% CI x, y) | ||
| Black | X (95% CI x, y) | |||
| Asian | X (95% CI x, y) | |||
| Other | X (95% CI x, y) |
FIGURE A7.1.
Hypothesized causal pathways and main sources of evidence for measurement of outcomes.
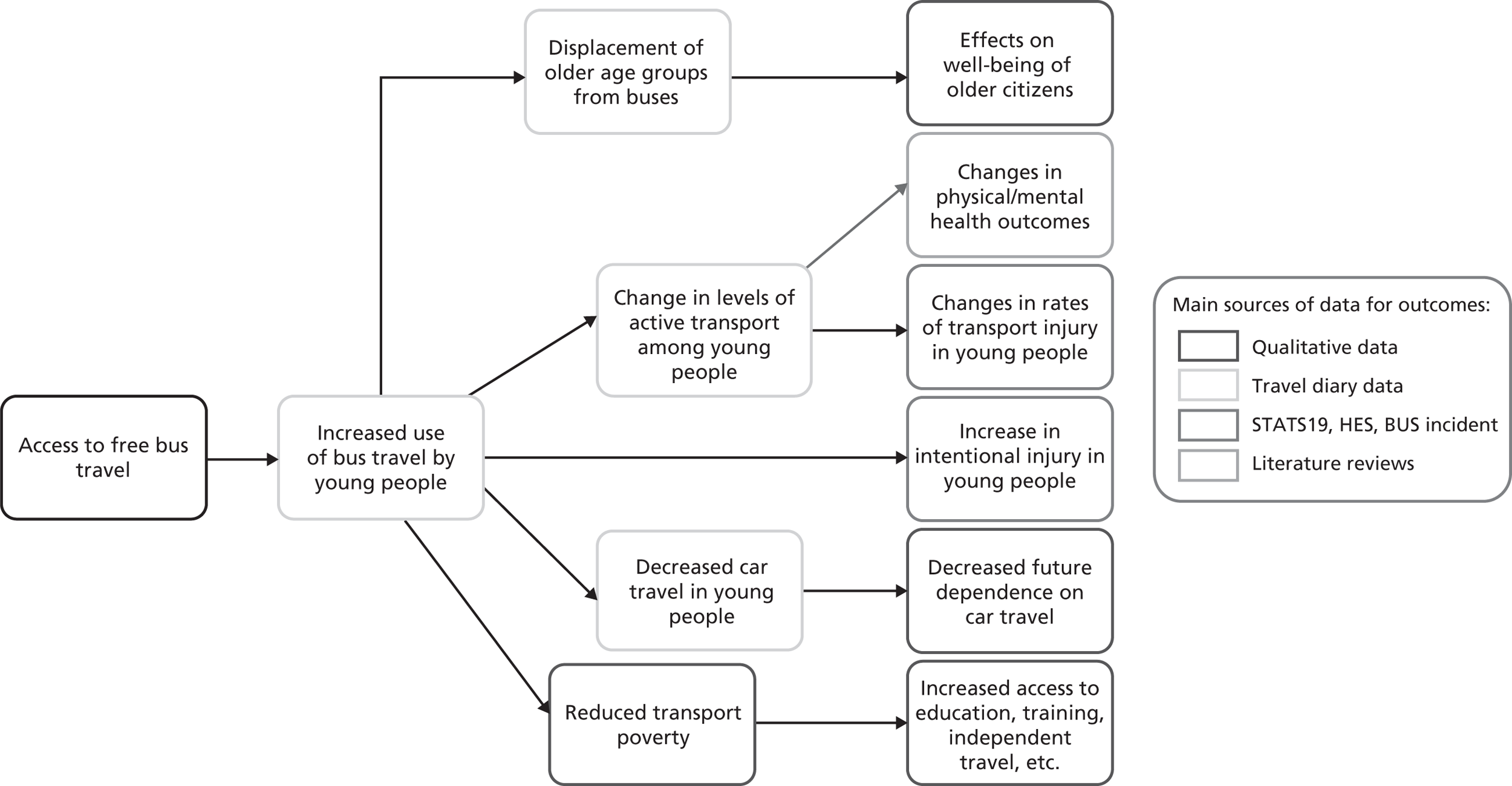
FIGURE A7.2.
Fictional data to illustrate graphical presentation of change in key behaviour outcomes by year for age-groups 12–17 years and 25–59 years. a, outcome 1; b, outcome 2, etc.
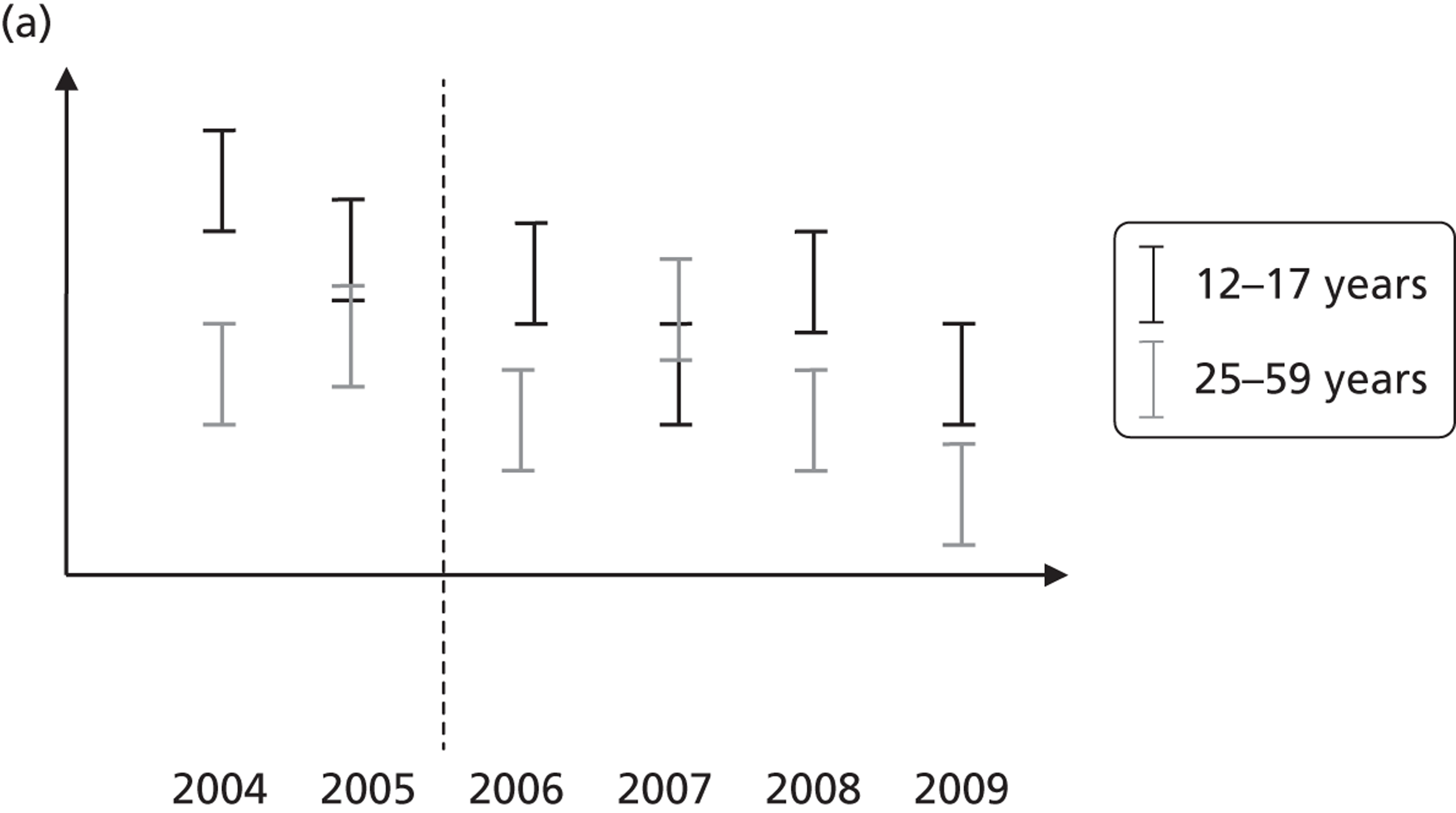
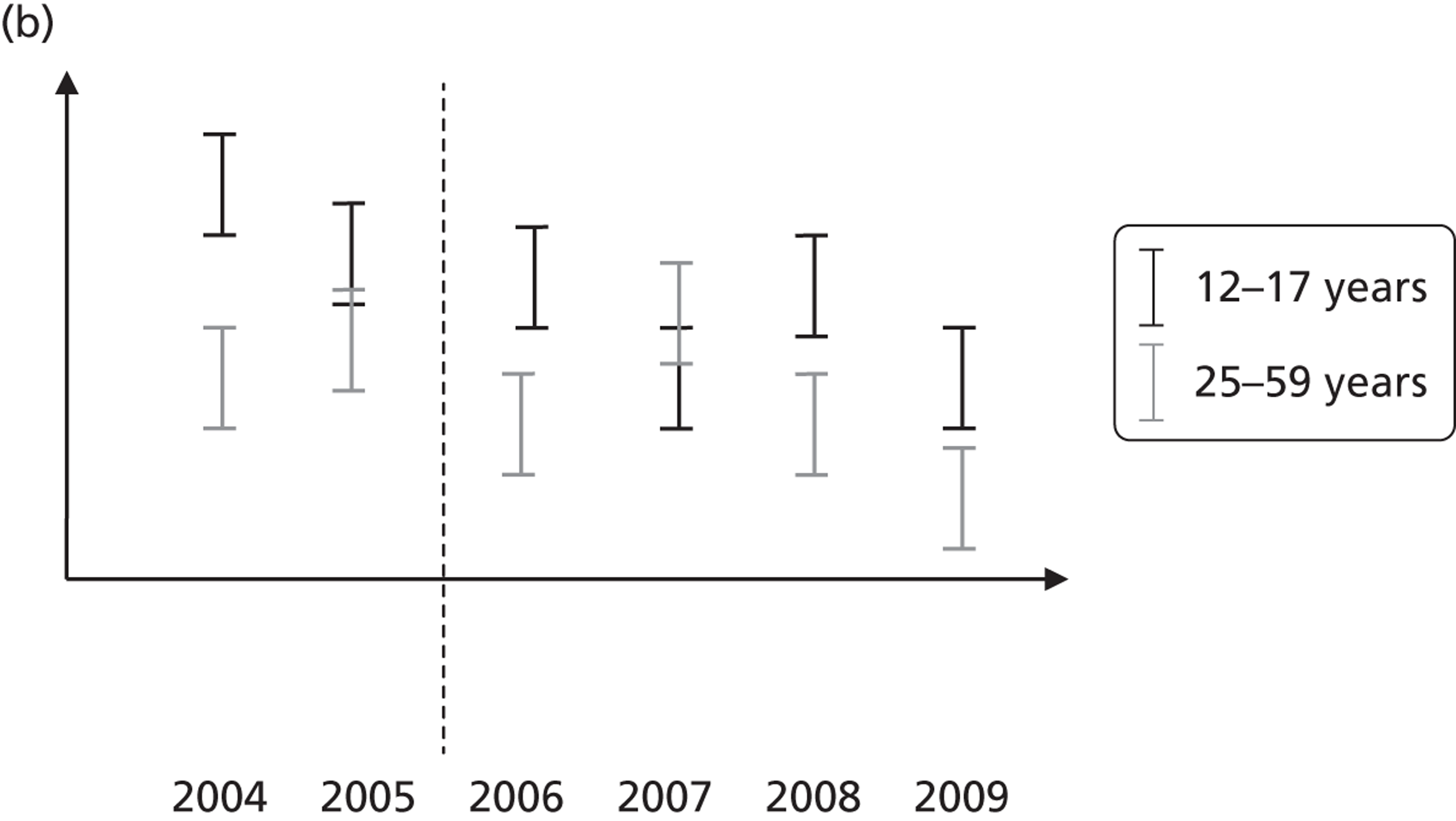
Appendix 8 Systematic review of health benefits of active travel (extract)
This is an extract from a paper published as Saunders L, Green J, Petticrew M, Steinbach R, Roberts H. What are the health benefits of active travel? A systematic review of trials and cohort studies. PLOS One 2013;8:e69912.
What are the health benefits of active travel? A systematic review
Lucinda E Saunders, Judith M Green, Mark P Petticrew, Rebecca Steinbach, Helen Roberts
Abstract
Background: Increasing the proportion of active travel (primarily walking and cycling) within the population has been widely advocated as a route to reducing obesity levels and achieving other population health benefits. However, the strength of evidence underpinning these assumptions is not known. The objective of this study was to assess the evidence that active travel has significant health benefits.
Methods: The study design was a systematic review of (i) non-randomised and randomised trials, and (ii) observational studies examining either (i) the effects of interventions to promote active travel or (ii) the association between active travel and health outcomes. The data sources were published and unpublished reports of studies in any language identified by searching 11 electronic databases, websites, reference lists and papers identified by experts in the field. The eligibility criteria were prospective observational and intervention studies measuring any health outcome of active travel in the general population were included. Studies of patient groups were excluded.
Results: Twenty-two studies from 11 countries were included, of which six were studies conducted in children. Six studies evaluated active travel interventions. Sixteen were prospective cohort studies which did not evaluate the impact of a specific intervention. No studies were identified with obesity as an outcome in adults; three prospective cohort studies in children found no association between obesity and active travel. Small positive effects on other health outcomes were found for active travel in six intervention studies, but these studies were all at risk of selection bias; modest benefits for other health outcomes were identified in 13 prospective studies.
Conclusions: However there is accumulating evidence that active travel may have positive effects on other health outcomes than obesity. Further trials of interventions to increase active travel are needed to assess its impacts on obesity and other health outcomes.
Keywords: Public health; systematic review; active transport; physical activity
Background
The link between physical activity and health has long been known, with the scientific link established in Jerry Morris’ seminal study of London bus drivers in the 1950’s [1]. There is also good ecological evidence that obesity rates are increasing in countries and settings in which ‘active travel’ (primarily walking and cycling for the purpose of functional rather than leisure travel) is declining [2–3]. Given that transport is a necessity of everyday life, whereas leisure exercise such as going to a gym may be an additional burden for individuals, and is difficult to sustain long term, [4–5] encouraging ‘active travel’ may be a feasible approach to increasing levels of physical activity [6]. It is also plausible to assume that interventions aimed at increasing the amount of active travel within a population are likely to have a positive impact on health. This has been the underlying rationale for recent public health interest in transport interventions aiming to address the obesity epidemic and a range of other health and social problems [7]. In July 2011 the Chief Medical Officers for the UK produced new guidance for physical activity ‘Start Active, Stay Active [8]’ which re-emphasised the known risks to health of the sedentary behaviour of the UK population and the central role of active travel: “For most people, the easiest and most acceptable forms of physical activity are those that can be incorporated into everyday life. Examples include walking or cycling instead of travelling by car, bus or train.” (p17). Active travel is seen by policy makers and practitioners as not only an important part of the solution to the problem of obesity but also for a range of other health issues at a population level. It may also have other important non-health outcomes, including a reduction in traffic congestion and carbon emissions [9].
It has recently been recommended that the public health community should advocate for effective policies that reduce car use and increase active travel [10]. One recent overview concluded that active travel policies have the potential to generate large population health benefits through increasing population physical activity levels, and smaller health benefits through reductions in exposures to air pollution in the general population. However, while a recent systematic review and meta-analysis [11] found that non-vigorous physical activity reduced all-cause mortality, the two studies which looked at active commuting alone [12–13] found no evidence of a positive effect. There are a number of reasons why active travel may not contribute to overall physical activity levels. Studies of young children have found no differences in overall physical activity levels for active and non-active commuters [14–16], perhaps because the distance walked to school may simply be too short to make a significant contribution. For both children and adults, it is unclear how far individuals may offset the extra effort of cycling or walking with additional food intake, or by reducing physical activity in other areas of everyday life. Additionally, there is evidence that the health benefits of exercise are not shared equally across populations, with the cultural and psychological meanings of activities such as walking or cycling potentially influencing their physiological effects [17–18].
A reliable overview of the strength of the scientific evidence will therefore be of value, because the causal pathways between active travel and health outcomes such as obesity are likely to be complex, and promoting active travel may have unintended adverse consequences [19].
Overall, aside from impacts on all-cause mortality, the evidence that active travel will lead to a range of other health and social benefits including a reduction in obesity remains to be determined, and existing studies show a mixed picture on the relationship between active travel and health outcomes including obesity [20]. Recent systematic reviews have focussed almost exclusively on cross-sectional studies [20–22], or one narrow health outcome [23] or combined leisure and transport activity [24]. A clear picture of the health effects of active travel cannot be obtained from these reviews so a systematic review of evidence from empirical studies was carried out with the objective of assessing the health effects of active travel specifically (rather than of physical activity in general, where the evidence is already well-established). It synthesises the relevant empirical evidence from intervention studies and cohort studies in which health outcomes of active travel have been purposively or opportunistically measured. Obesity is a particular focus of this review because the rise in the prevalence of obesity over the past 30–40 years has been in tandem with the decline of active travel and overweight and obesity are now the fifth leading risk for death globally as well as being responsible for significant proportions of the disease burden of diabetes (44%), ischaemic heart disease (23%) and some cancers (7–41%) [25].
Methods
A systematic review was undertaken to identify and synthesise the evidence for the impact on obesity and other health outcomes of active travel (Review protocol and full search strategy is available on request from the authors). Eleven databases were searched for prospective studies of any design (Table 1) (this search will be updated if the paper is accepted). The search strategy adapted the search terms developed by Hoskings et al. [26] (2010 Cochrane Review) and Bunn et al. [27] (2003). Hand-searching of relevant studies was also conducted, and bibliographies of identified papers were checked along with those of papers already known to the researchers. No time, topic or language exclusions or limits were applied.
Two reviewers independently identified potentially relevant prospective studies. If it was not clear from the title and abstract whether the article was relevant to active travel then the paper was reviewed in detail. Papers which were not published in English would have been translated in full if deemed potentially eligible for inclusion. One reviewer [LS] then screened the articles using the following inclusion criteria:
-
Prospective study examining relationship between active travel and health outcomes; or study evaluating the effect of an active travel intervention;
-
Active travel (walking or cycling for transport rather than work or leisure) measured in a healthy population (e.g. using self report measures, or use of pedometers); and
-
Health outcome included.
Retrospective and single cross-sectional studies (e.g. one-off survey) were excluded.
One reviewer (LS) extracted data according to a common table format including information on methods, outcomes (as adjusted relative risks, or hazard ratios; if these were not available or calculable, other effect measures were extracted – e.g. mean changes), populations and setting for each study, and two reviewers then independently reviewed each study using the ‘Effective Public Health Practice Project Quality Assessment Tool’ [28] and discussed differences to produce consensus scores for each study against each quality criterion. A narrative review, taking account of study quality, was then carried out. It was not possible to conduct a meta-analysis as meta-analysis of mixed designs – and particularly observational studies – is not robust and this review includes a range of mainly observational study designs, populations and outcomes [29].
Results
Twenty-two studies reported in twenty-seven papers were included (see Tables 2 and 3). Three were prospective cohort studies with obesity-related outcomes; thirteen were prospective cohort studies with other health outcomes; and six were intervention studies with other health outcomes (see PRISMA diagram for details of excluded studies - further details available on request from the authors). For the prospective cohort studies the results are presented adjusted for covariates, there was variation in what adjustments were made by different studies but the adjustments did not have large impacts on effect size. Details of the methodological assessment of each paper are reported in a separate web table.
Active travel and obesity
Three prospective cohort studies with obesity outcomes were identified, all of which were conducted in North America and included children aged 10 years or younger at baseline who were followed up for between 6 months and two years [30–32]. BMI measurements were taken in all three studies and skinfold measurements were taken in two of the studies. There was no significant association between active travel and the obesity outcome measures in any of the studies. All three papers scored low on the quality assessment measure as no data on baseline differences between groups were presented.
Active travel and other health outcomes
1. Intervention studies
Six intervention studies measured health outcomes of active travel other than obesity. Results were mixed; three studies found improvements in fitness measures in the intervention group compared with the control group [33–36], two found increased physical activity levels [37–39] but one did not [35–36], two found no significant change in body weight [35–38] and one found significantly higher scores for 3 of the 8 domains of the SF-36 in the intervention group. All these studies were at risk of selection bias and none reported baseline differences between intervention and control groups for potential confounders [33–40]. However, all six studies scored moderately overall. All but one [33] were controlled with appropriate statistical analyses. All but one [40] had low levels of drop-out and ensured that the intervention was consistently applied. Five studied adults in north-west Europe and measured multiple health outcomes including fitness, blood pressure, cholesterol, oxygen uptake, and body weight [33–38, 40]. One study involving children in the USA measured moderate-to-vigorous physical activity (MVPA) in a randomised controlled trial however, there were only 12 participants and a two week duration [39].
2. Prospective cohort studies
Thirteen prospective cohort studies (described below) were identified [12–13, 41–55], 8 of which were conducted in Scandinavia [12, 41–43, 45–50], possibly reflecting the longer history of higher population levels of active travel as a result of which questions on active travel have been included in population surveys over recent decades. Overall, these studies showed conflicting findings when measuring similar mortality and cardiovascular outcomes and of the four studies which measured outcomes not measured by other studies two found significant effects [43, 46], one found a non-significant effect and one found no effect [49].
All cause mortality
One study in Denmark found a significantly lower all-cause risk of mortality in cycle-commuters compared with non-cyclists – this was not found in a second such study in Finland [12]. Batty et al. (2001) [13] also found no statistically significant differences for 12 mortality endpoints between men in London, UK who actively travelled more or less than 20 minutes on their journey to work. Matthews et al. (2007) [51] studied women in China and found no significant relationship between walking and cycling for transport and all cause mortality [51]. Besson et al. (2008) [55] studied men and women in Norfolk, UK and found a non-significant reduced risk of all cause mortality in those who travelled actively (measured as > 8 metabolic equivalent task values (MET.h.wk-1)).
Cardiovascular Outcomes
Besson et al. found no significant reduction in cardiovascular mortality risk among active travellers whereas Barengo (2004) [12] in Finland found it to be significantly lower (Adjusted hazard ratio 0.78 [CI: 0.62–0.97]) only among women actively travelling 15–29 minutes each way to work compared with those travelling less than 15 minutes each way but not in those travelling more than 30 minutes each way, and not in men. Hu et al. (2005, 2007, 2007) [45, 47–48], also measured CHD and found a significant relationship in women who travelled 30+ minutes per day (0.80 [CI:0.69–0.92]) compared with those who did not travel actively at all. Like Barengo (2004) [12], they found no relationship between active travel and CHD in men. Barengo (2005) [42] found no difference in hypertension risk between those travelling more or less than 15 minutes each way to work. Hayashi et al. (1999) [44] found a statistically significant reduced risk of hypertension in those men in Osaka, Japan who walked 21+ minutes to work compared with men who walked less than 10 minutes (adjusted relative risk 0.70 [CI: 0.59–0.95]). However it was not clear from the paper how frequently the active travellers walked to work. Wagner et al. (2001, 2002, 2003) [52–54] found a non-significant increase in risk of CHD events in men walking and cycling to work, although the amount of exercise taken while actively commuting was not recorded.
Other Health Outcomes
Four studies in Scandinavia examined other health outcomes. A study in Finland found the relative risk for Type 2 diabetes to be 34% lower among active travellers travelling 30+ minutes per day compared with those not travelling actively (CI: 0.45–0.92). Luoto et al. 2000 [50], also in Finland, reported a non-significant reduction in relative breast cancer risk at 15 years follow-up of 0.87 (CI: 0.62–1.24) in women who actively travelled more than 30 minutes each day. Cooper et al. (2008) [43] followed school children in Odense, Denmark for 6 years from age 9 and measured cardio-respiratory fitness. Cycling to school was associated with higher levels of cardio-respiratory fitness, as was taking up cycling. Lofgren et al. (2010) [49] also studied children actively travelling to school in Malmo, Sweden and measured a range of bone health indicators but found no significant relationship.
Discussion
This review found no prospective studies of active travel with obesity as a primary outcome in adults, and no significant associations between obesity and active travel were found in the studies of children. For other health outcomes small positive health effects were found in groups who actively travelled longer distances including reductions in risk of all cause mortality [41], hypertension [44], and Type 2 diabetes [46].
The evidence is difficult to synthesise as active travel is not defined consistently across studies, and the definition is dependent on what is considered normal in a particular setting. For example Luoto (2000), and Barengo (2004, 2005) [12, 42] considered active travel to be more than 30 minutes per day and inactive travel to be less than 30 minutes per day. Batty (2001) and Hayashi (1999) [44] however considered active travel to be more than 20 minutes per day. Differences in health outcomes between people who actively travel 29 minutes per day and those who travel 31 minutes per day are unlikely, so differences between active and sedentary populations may be masked by the methods by which active travel is defined and reported. Meanwhile Besson (2008) [55] considered active travel to be >8 metabolic equivalent task (MET) hours per week while Matthews (2007) [51] considered it to be > 3.5 metabolic equivalent task hours per day which may reflect differences in norms between Norfolk and Shanghai in terms of active travel.
It is difficult to generalise from studies conducted in different countries or settings, as the amount of exertion required to travel actively may be greater in some settings than others with the same journey time, due to differences in congestion, terrain, and weather conditions. In the UK only 39% of men and 29% of women achieve 30 minutes of moderate intensity physical activity of any type five times a week so a population change of adding 30 minutes of active travel per day might well produce much larger changes in health outcomes than were measured in non-UK studies. For example in Barengo (2005) [43] 30% of men and 46% of women travelled actively more than 15 minutes each way to work which shows a higher level of active travel in the population than may be seen in other countries, including the UK. The prospective cohort studies also tended to focus on travel to work or school rather than active travel for general transportation, which again may limit generalisability.
The study by Cooper et al. (2008) of school children in Odense, Denmark found that 65% of boys and girls walked or cycled to school, a much higher proportion than would currently be found in the UK. However, journey times were less than 15 minutes for the majority of active travellers so the health effects of active travel for such short periods are difficult to measure in isolation. This highlights one of the difficulties of assuming active travel to school in young people to be a major source of physical activity, as it is common for children only to walk or cycle to school when the journey time is relatively short. While in adults bouts of as little as 10 minutes of physical activity are acceptable to contribute to their weekly physical activity target of minimum 150 minutes, children aged 5–18 are expected to be physically active for a minimum of 420 minutes per week [8] so a short active commute to school will not make a significant contribution to their overall physical activity requirements. The study by Lofgren et al. [49] included a study population with fairly high levels of physical activity overall and half the participants were active travellers which makes it difficult to attribute health outcomes to active travel alone when active travel may not contribute significantly to participants overall physical activity levels.
De Geus et al. (2007) [33] highlighted one of the difficulties of measuring active travel in intervention studies as they found that study participants cycled 13% faster when their fitness was being measured compared to their usual speed on their daily cycle commute. Hence just through the process of measuring active travel there is the risk of over-estimating the health benefits it can confer. Thus issues including terrain, problems of definition, study design and the difficulty of disentangling the effects of active travel from more general physical activity make synthesis difficult. It is in this context that a wider range of studies, including ethnographic and qualitative work, to inform generalisable theory may be helpful. Active travel not only potentially benefits health as a source of physical activity but may also off-set air pollution from motorised vehicles for those journeys and contribute to social and environmental goals such as improving social cohesion and reducing CO2 emissions. These combined benefits may be a potent argument for promoting active travel, and emphasise the importance of models which incorporate both health and non-health benefits [57–58].
Finally, reviewing this evidence is challenging, in particular designing searches which are both sensitive and specific, and over 70% of the studies identified for this search were found through hand-searching, despite a thorough search of databases. While it is possible that studies may have been missed, our comprehensive search for studies makes it unlikely that a significant body of work has been excluded.
Conclusions
This is the first study to bring together all prospective observational and intervention studies to give an overview of the health effects of active travel in general. Previous systematic reviews of health outcomes of active travel have included primarily cross-sectional studies from which reliable inferences about causality cannot easily be drawn, or have relied on indirect evidence on the effects of physical activity on health, as opposed to the effects of active travel.
The interest in identifying health outcomes of active travel is to determine whether active travel affects health. However this will depend on the context within which individuals are travelling – length of journey, frequency of travel, nature of the terrain, risk of injury, levels of air pollution and so on as well as other aspects of the lifestyles of the participants. For example travelling actively may mean that the individual is more or less likely to be physically active at other times, or they may modify their diet. It may mean that they are more or less likely to strengthen social networks. While the studies identified in this review do not enable us to draw strong conclusions about the health effects of active travel, there is consistent support for the positive effects on health of active travel over longer periods and perhaps distances.
This review highlights the difficulty in measuring health outcomes of active travel in the general population. In prospective cohort studies if the follow-up period is short then it may not be possible to measure health effects that take many years to appear, such as changes in risk of heart disease. Conversely in those studies which have long follow-up periods of many years there is the risk that active travel has not been consistently adhered to throughout the follow-up period.
These cautious conclusions on the health impact of active travel do not, of course, mean that now is the time to confine active travel to the walk from the front door to the car door. The evidence on the effect of physical activity is sufficiently strong to suggest that the part played by active travel in improving health is likely to be significant and is well worth maintaining. Other aspects of active travel, including a reduction in pollution, and in carbon footprint are clear potential co-benefits and likely to become even more so.
Appendices:
PRISMA flowchart
Table 2 – results [available from authors]
Table 3 – summary of outcomes [available from authors]
Search strategy
Quality assessment table [available from authors]
Ethics approval and patients’ consent, funding sources and independence:
Ethical approval was not required as this is a systematic review. This project was funded by the National Institute for Health Research Public Health Research programme (project number 09/3001/13). The views and opinions expressed herein are those of the authors and do not necessarily reflect those of the Department of Health. The funders had no role in the design, conduct or reporting of project findings.
| Database | Number of Search Results extracted | Date search results were extracted |
|---|---|---|
| Embase | 4982 | 13/08/10 |
| Global Health | 734 | 12/08/10 |
| Medline | 3954 | 12/08/10 |
| PsychInfo | 620 | 12/08/10 |
| Social Policy and Practice | 38 | 12/08/10 |
| IBSS | 43 | 13/08/10 |
| Web of Science | 4929 | 12/08/10 |
| Cochrane Library | 58 | 16/08/10 |
| TRIS | 162 | 13/08/10 |
| CINAHL* | 1538 | 18/08/10 |
| Google Scholar* | 848 | 03/09/10 |
References
- Morris JN, Heady JA, Raffle PAB, . Coronary heart disease and physical activity of work. The Lancet 1953;262:1053-7.
- Pucher J, Buehler R, Bassett D, . Walking and cycling to health: a comparative analysis of city, state, and international data. American Journal of Public Health 2010;100:1986-92.
- Bassett D, Pucher J, Buehler R, . Walking, cycling and obesity rates in Europe, North America, and Australia. Journal of Physical Activity and Health 2008;5:795-814.
- Sallis JF, Haskell WL, Fortmann SP, . Predictors of adoption and maintenance of physical activity in a community sample. Preventive Medicine 1986;15:331-41.
- Sallis JF, Hovell MF, Richard Hofstetter C. Predictors of adoption and maintenance of vigorous physical activity in men and women. Preventive Medicine 1992;21:237-51.
- de Nazelle A, Nieuwenhuijsen MJ, Antó JM, . Improving health through policies that promote active travel: A review of evidence to support integrated health impact assessment. Environment International 2011;37:766-77.
- Wanless D, Treasury H. Securing good health for the whole population: final report. London: HM Treasury; 2004.
- Department of Health . Start active, stay active: A report on physical activity from the four home countries’ Chief Medical Officers 2011.
- Woodcock J, Edwards P, Tonne C, . Public health benefits of strategies to reduce greenhouse-gas emissions: urban land transport. The Lancet 2009;374:1930-43.
- Douglas MJ, Watkins SJ, Gorman DR, . Are cars the new tobacco?. Journal of Public Health 2011;33:160-9.
- Woodcock J, Franco OH, Orsini N, . Non-vigorous physical activity and all-cause mortality: systematic review and meta-analysis of cohort studies. International Journal of Epidemiology 2011;40:121-38.
- Barengo NC, Hu G, Lakka TA, . Low physical activity as a predictor for total and cardiovascular disease mortality in middle-aged men and women in Finland. European Heart Journal 2004;25:2204-11.
- Batty GD, Shipley MJ, Marmot M, . Physical activity and cause-specific mortality in men: Further evidence from the Whitehall study. Eur J Epidemiol 2001;17:863-9.
- Ford P, Bailey R, Coleman D, . Activity Levels, Dietary Energy Intake, and Body Composition in Children Who Walk to School. Pediatric Exercise Science 2007;19:393-407.
- Metcalf B, Voss L, Jeffery A, . Physical activity cost of the school run: impact on schoolchildren of being driven to school (EarlyBird 22). BMJ 2004;329:832-3.
- Sleap M, Warburton P. Are primary school children gaining heart health benefits from their journeys to school?. Child: Care, Health and Development 1993;19:99-108.
- Crum A, EJ L. Mind-set matters: exercise and the placebo effect. Psychological Science 2007;18:165-71.
- Bostock L. Pathways of disadvantage? Walking as a mode of transport among low-income mothers. Health &Amp; Social Care in the Community 2001;9:11-8.
- Macintyre S. Good intentions and received wisdom are not good enough: the need for controlled trials in public health. Journal of Epidemiology and Community Health 2010.
- Faulkner GEJ, Buliung RN, Flora PK, . Active School Transport, Physical Activity Levels and Body Weight of Children and Youth: A Systematic Review. Preventive Medicine 2009;48:3-8.
- Lubans D, Boreham C, Kelly P, . The relationship between active travel to school and health-related fitness in children and adolescents: a systematic review. International Journal of Behavioral Nutrition and Physical Activity 2011;8.
- Lee M, Orenstein M, Richardson M. Systematic review of active commuting to school and children’s physical activity and weight. Journal of Physical Activity and Health 2008;5:930-49.
- Hamer M, Chida Y. Active commuting and cardiovascular risk: a meta-analytic review. Preventive Medicine 2008;46:9-13.
- Oja P, Titze S, Bauman A, . Health benefits of cycling: a systematic review. Scandinavian Journal of Medicine &Amp; Science in Sports 2011;21:496-509.
- World Health Organization . Obesity and overweight. Fact Sheet 311 2011.
- Hosking J, Macmillan A, Connor J, . Organisational travel plans for improving health. Cochrane Database Syst Rev 2010.
- Bunn F, Collier T, Frost C, . Area-wide traffic calming for preventing traffic related injuries. Cochrane Database Syst Rev 2003.
- Effective Public Health Practice Project . Quality Assessment Tool for Quantitative Studies 2009.
- Egger M, Schneider M, Smith GD. Meta-analysis Spurious precision? Meta-analysis of observational studies. BMJ 1998;316:140-4.
- Heelan KA, Donnelly JE, Jacobsen DJ, . Active commuting to and from school and BMI in elementary school children - Preliminary data. Child: Care, Health and Development 2005;31:341-9.
- Pabayo R, Gauvin L, Barnett TA, . Sustained Active Transportation is associated with a favorable body mass index trajectory across the early school years: Findings from the Quebec Longitudinal Study of Child Development birth cohort. Preventive Medicine 2010;50:S59-S64.
- Rosenberg DE, Sallis JF, Conway TL, . Active transportation to school over 2 years in relation to weight status and physical activity. Obesity (Silver Spring) 2006;14:1771-6.
- De Geus B, De Smet S, Nijs J, . Determining the intensity and energy expenditure during commuter cycling. British Journal of Sports Medicine 2007;41:8-12.
- Hendriksen IJ, Zuiderveld B, Kemper HC, . Effect of commuter cycling on physical performance of male and female employees. Med Sci Sports Exerc 2000;32:504-10.
- Oja P, Mänttäri A, Heinonen A, . Physiological effects of walking and cycling to work. Scandinavian Journal of Medicine &Amp; Science in Sports 1991;1:151-7.
- Oja P, Vuori I, Paronen O. Daily walking and cycling to work: their utility as health-enhancing physical activity. Patient Education and Counseling 1998;33:S87-S94.
- De Geus B, Joncheere J, Meeusen R. Commuter cycling: effect on physical performance in untrained men and women in Flanders: minimum dose to improve indexes of fitness. Scandinavian Journal of Medicine &Amp; Science in Sports 2009;19:179-87.
- De Geus B, Van Hoof E, Aerts I, . Cycling to work: influence on indexes of health in untrained men and women in Flanders. Coronary heart disease and quality of life. Scandinavian Journal of Medicine &Amp; Science in Sports 2008;18:498-510.
- Sirard JR, Alhassan S, Spencer TR, . Changes in Physical Activity from Walking to School. Journal of Nutrition Education and Behavior 2008;40:324-6.
- Mutrie N, Carney C, Blamey A, . “Walk in to Work Out”: a randomised controlled trial of a self help intervention to promote active commuting. Journal of Epidemiology and Community Health 2002;56:407-12.
- Andersen LB, Schnohr P, Schroll M, . All-cause mortality associated with physical activity during leisure time, work, sports, and cycling to work. Arch Intern Med 2000;160:1621-8.
- Barengo NC, Hu G, Kastarinen M, . Low physical activity as a predictor for antihypertensive drug treatment in 25-64-year-old populations in eastern and south-western Finland. J Hypertens 2005;23:293-9.
- Cooper AR, Wedderkopp N, Jago R, . Longitudinal associations of cycling to school with adolescent fitness. Preventive Medicine 2008;47:324-8.
- Hayashi T, Tsumura K, Suematsu C, . Walking to Work and the Risk for Hypertension in Men: The Osaka Health Survey. Annals of Internal Medicine 1999;131:21-6.
- Hu G, Jousilahti P, Borodulin K, . Occupational, commuting and leisure-time physical activity in relation to coronary heart disease among middle-aged Finnish men and women. Atherosclerosis 2007;194:490-7.
- Hu G, Qiao Q, Silventoinen K, . Occupational, commuting, and leisure-time physical activity in relation to risk for Type 2 diabetes in middle-aged Finnish men and women. Diabetologia 2003;46:322-9.
- Hu G, Sarti C, Jousilahti P, . Leisure time, occupational, and commuting physical activity and the risk of stroke. Stroke 2005;36:1994-9.
- Hu G, Tuomilehto J, Borodulin K, . The joint associations of occupational, commuting, and leisure-time physical activity, and the Framingham risk score on the 10-year risk of coronary heart disease. European Heart Journal 2007;28:492-8.
- Lofgren B, Stenevi-Lundgren S, Dencker M, . The mode of school transportation in pre-pubertal children does not influence the accrual of bone mineral or the gain in bone size – two year prospective data from the paediatric osteoporosis preventive (POP) study. BMC Musculoskelet Disord 2010.
- Luoto R, Latikka P, Pukkala E, . The effect of physical activity on breast cancer risk: A cohort study of 30,548 women. Eur J Epidemiol 2000;16:973-80.
- Matthews CE, Jurj AL, Shu X-o, . Influence of Exercise, Walking, Cycling, and Overall Nonexercise Physical Activity on Mortality in Chinese Women. American Journal of Epidemiology 2007;165:1343-50.
- Wagner A, Simon C, Ducimetiere P, . Leisure-time physical activity and regular walking or cycling to work are associated with adiposity and 5 y weight gain in middle-aged men: The PRIME study. International Journal of Obesity 2001;25:940-8.
- Wagner A, Simon C, Evans A, . Physical activity patterns in 50–59 year men in France and Northern Ireland. Associations with socio-economic status and health behaviour. Eur J Epidemiol 2003;18:321-9.
- Wagner A, Simon C, Evans A, . Physical activity and coronary event incidence in Northern Ireland and France: the Prospective Epidemiological Study of Myocardial Infarction (PRIME). Circulation 2002;105:2247-52.
- Besson H, Ekelund U, Brage S, . Relationship between subdomains of total physical activity and mortality. Med Sci Sports Exerc 2008;40:1909-15.
- The Health and Social Care Information Centre; 2009.
- Rojas-Rueda D, Nazelle Ad, Tainio M, . The health risks and benefits of cycling in urban environments compared with car use: health impact assessment study. BMJ 2011;343.
- de Hartog JJ, Boogaard H, Nijland H, . Do the Health Benefits of Cycling Outweigh the Risks?. Environmental Health Perspectives 2010;118:1109-16.
Search Strategy
Final Search Strategy for Medline
Search in ‘keyword’
-
(Walk* or cycle* or cycli* or bicycle* or bike* or walking bus* or ecological commut* or ecological transport* or non-auto* or non-motori?e*).mp.
-
(green* adj3 (travel* or transport* or commut*)).mp.
-
((activ* or health*) adj3 (travel* or transport* or commut*)).mp.
-
(ecological adj3 (travel* or transport* or commut*)).mp.
-
or/1-4
-
(Prospective adj1 (study or studies)).mp
-
(Program evaluation or evaluation research).mp.
-
(randomi$ or randomly).mp.
-
(controlled adj2 (trial or trials or study or studies or experiment$)).mp
-
(before adj1 after).ab,ti.
-
(control adj1 group$).ab,ti.
-
(intervention adj1 group$).ab,ti.
-
(experimental adj1 group$).ab,ti.
-
(comparison adj1 group$)ab,ti.
-
Or/6-14
-
(Body mass index or BMI or body mass gain or overweight or weight gain or weight status or weight management or weight loss or body weight or waist circumference or obesity or calorie* or energy)
-
5 and 15 and 16
-
17 in humans
FIGURE A8.1.
PRISMA flow diagram.
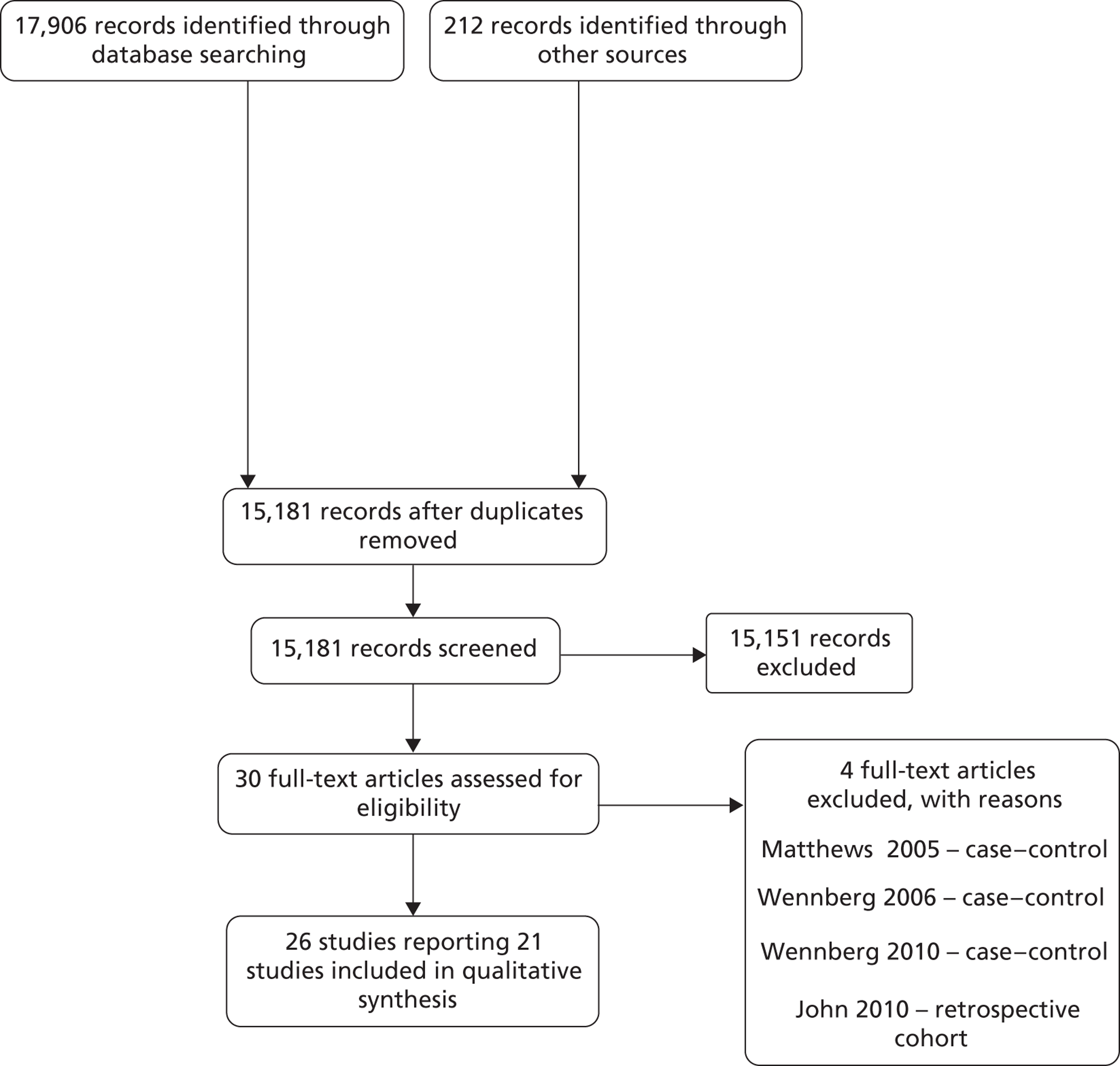
Appendix 9 Data tables
| Outcome | Age | Ratio of ratios (95% CI) | ||||||
|---|---|---|---|---|---|---|---|---|
| 12–17 years | 25–59 years | |||||||
| Pre | Post | Ratio (95% CI) | Pre | Post | Ratio (95% CI) | |||
| Active travel (walking and cycling) | Average number of walking trips per day | 0.99 | 0.83 | 0.84 (0.77 to 0.94) | 0.83 | 0.91 | 1.10 (1.01 to 1.20) | 0.76 (0.70 to 0.85) |
| Average walking distance per day (km) | 1.42 | 1.41 | 0.99 (0.92 to 1.07) | 1.32 | 1.33 | 1.00 (0.95 to 1.07) | 0.99 (0.92 to 1.07) | |
| Percentage of short distance trips ≤ 1 km travelled by walking | 82 | 81 | 1.00 (0.96 to 1.05) | 70 | 76 | 1.09 (1.06 to 1.12) | 0.91 (0.87 to 0.97) | |
| Average number of cycling trips per day | 0.06 | 0.04 | 0.71 (0.47 to 1.10) | 0.05 | 0.07 | 1.34 (1.11 to 1.55) | 0.53 (0.35 to 0.87) | |
| Average cycle distance per day (km) | 0.10 | 0.06 | 0.58 (0.29 to 0.94) | 0.20 | 0.31 | 1.56 (1.27 to 1.85) | 0.37 (0.18 to 0.65) | |
| Percentage of short distance trips ≤ 1 km travelled by cycling | 3 | 1 | 0.49 (0.20 to 0.99) | 1 | 1 | 0.90 (0.67 to 1.16) | 0.54 (0.22 to 1.17) | |
| Bus travel | Average number of bus trips per day | 0.64 | 0.87 | 1.35 (1.25 to 1.47) | 0.25 | 0.34 | 1.36 (1.25 to 1.46) | 1.00 (0.89 to 1.1) |
| Average bus distance per day (km) | 2.59 | 3.27 | 1.26 (1.13 to 1.41) | 1.24 | 1.62 | 1.31 (1.19 to 1.42) | 0.96 (0.83 to 1.12) | |
| Percentage of short distance trips ≤ 1 km travelled by bus | 2 | 5 | 2.34 (1.42 to 4.06) | 2 | 2 | 1.19 (0.86 to 1.64) | 1.97 (1.07 to 3.84) | |
| Car travel | Average number of car trips per day | 0.59 | 0.50 | 0.85 (0.77 to 0.95) | 1.44 | 1.17 | 0.81 (0.77 to 0.85) | 1.05 (0.94 to 1.18) |
| Average car distance per day (km) | 3.51 | 2.27 | 0.65 (0.49 to 0.84) | 9.30 | 8.24 | 0.89 (0.84 to 0.94) | 0.73 (0.55 to 0.94) | |
| Percentage of short distance trips ≤ 1 km travelled by car | 12 | 11 | 0.88 (0.63 to 1.21) | 25 | 19 | 0.76 (0.71 to 0.83) | 1.16 (0.82 to 1.61) | |
| Frequency of journeys to work or school | Number per weekday | 1.46 | 1.60 | 1.09 (1.06 to 1.14) | 1.00 | 0.91 | 0.91 (0.88 to 0.94) | 1.19 (1.13 to 1.25) |
| Frequency of all journeys | Number per weekday | 2.49 | 2.49 | 1.00 (0.96 to 1.04) | 3.10 | 3.09 | 0.99 (0.95 to 1.05) | 1.00 (0.97 to 1.04) |
| Outcome | Within travel from school hours (3–4 p.m., Monday to Friday, in term time) | Other times | Ratio of ratios (95% CI) | |||||
|---|---|---|---|---|---|---|---|---|
| Pre | Post | Ratio (95% CI) | Pre | Post | Ratio (95% CI) | |||
| Bus travel | Average number of bus trips per day | 0.06 | 0.07 | 1.11 (0.92 to 1.32) | 0.36 | 0.37 | 1.04 (0.94 to 1.18) | 1.07 (0.91 to 1.21) |
| Average bus distance per day (km) | 0.26 | 0.25 | 0.95 (0.80 to 1.13) | 1.19 | 1.19 | 1.00 (0.89 to 1.14) | 0.95 (0.80 to 1.11) | |
| Percentage of short distance trips ≤ 1 km travelled by bus | 7.09 | 8.42 | 1.19 (0.53 to 1.65) | 7.33 | 7.03 | 0.96 (0.80 to 1.14) | 1.24 (0.52 to 1.69) | |
| All travel | Average number of trips per day | 0.31 | 0.33 | 1.08 (0.97 to 1.17) | 1.98 | 2.07 | 1.05 (0.99 to 1.12) | 1.03 (0.94 to 1.10) |
| Average distance travelled per day (km) | 1.62 | 1.90 | 8.09 | 9.29 | 1.15 (1.03 to 1.27) | 1.02 (0.80 to 1.30) | ||
| Percentage of all trips which are short distance (≤ 1 km) | 30.12 | 29.52 | 0.98 (0.85 to 1.12) | 36.20 | 35.67 | 0.99 (0.93 to 1.04) | 0.99 (0.88 to 1.16) | |
| Outcome | Potential modifier | Ratio of ratios (95% CI) | Test for interaction | |
|---|---|---|---|---|
| Distance walking and cycling (km) | Area of London | Inner London | 0.80 (0.66 to 0.97) | p = 0.06 |
| Outer London | 0.97 (0.87 to 1.05) | |||
| Deprivation | Most deprived fifth | 0.82 (0.71 to 1.01) | p = 0.29 | |
| Least deprived 80% | 0.92 (0.83 to 1.01) | |||
| Household income (£) | < 15,000 | 0.98 (0.81 to 1.18) | p = 0.65 | |
| > 50,000 | 0.92 (0.77 to 1.09) | |||
| Ethnicity | White | 0.89 (0.80 to 0.98) | p = 0.92 | |
| Black | 0.85 (0.66 to 1.12) | |||
| Asian | 0.84 (0.61 to 1.12) | |||
| Intervention take-up | High uptake area | 0.93 (0.82 to 1.05) | p = 0.35 | |
| Low uptake area | 0.85 (0.71 to 0.96) | |||
| Road injuries (per 1000 person-years) | Area of London | Inner London | 0.79 (0.75 to 0.83) | p < 0.01 |
| Outer London | 0.89 (0.85 to 0.92) | |||
| Deprivation group | Most deprived fifth | 0.85 (0.80 to 0.91) | p = 0.97 | |
| Least deprived 80% | 0.85 (0.82 to 0.88) | |||
| Ethnicity | White | 0.88 (0.85 to 0.92) | p = 0.11 | |
| Black | 0.93 (0.86 to 1.01) | |||
| Asian | 0.81 (0.73 to 0.90) | |||
| Intervention take-up | High uptake area | 0.86 (0.82 to 0.90) | p = 0.26 | |
| Low uptake area | 0.83 (0.79 to 0.87) | |||
| Intentional injuries: assaults (per 1000 person-years) | Area of London | Inner London | 1.40 (1.29 to 1.53) | p < 0.01 |
| Outer London | 1.05 (0.97 to 1.14) | |||
| Deprivation group | Most deprived fifth | 1.46 (1.31 to 1.62) | p < 0.01 | |
| Least deprived 80% | 1.12 (1.05 to 1.20) | |||
| Ethnicity | White | 1.06 (0.96 to 1.17) | p < 0.01 | |
| Black | 1.53 (1.33 to 1.78) | |||
| Asian | 0.65 (0.53 to 0.80) | |||
| Intervention take-up | High uptake area | 1.26 (1.17 to 1.36) | p < 0.01 | |
| Low uptake area | 1.12 (1.02 to 1.23) | |||
| Outcome | Age | Ratio of ratios (95% CI) | |||||
|---|---|---|---|---|---|---|---|
| 12–17 years, London | 12–17 years, rest of England | ||||||
| Pre | Post | Ratio (95% CI) | Pre | Post | Ratio (95% CI) | ||
| Total casualties per 1000 person-years | 5.46 | 3.23 | 0.59 (0.57 to 0.61) | 6.69 | 5.62 | 0.84 (0.83 to 0.85) | 0.70 (0.68 to 0.73) |
| Pedestrian casualties per 1000 person-years | 1.92 | 1.36 | 0.71 (0.67 to 0.74) | 1.59 | 1.21 | 0.76 (0.75 to 0.78) | 0.93 (0.88 to 0.98) |
| Cycle casualties per 1000 person-years | 0.61 | 0.41 | 0.66 (0.61 to 0.72) | 0.88 | 0.72 | 0.82 (0.8 to 0.84) | 0.81 (0.74 to 0.88) |
| Car occupant casualties per 1000 person-years | 1.49 | 0.86 | 0.58 (0.54 to 0.61) | 2.81 | 2.48 | 0.88 (0.87 to 0.9) | 0.65 (0.61 to 0.69) |
| Outcome | IMD quintile | Age | Ratio of ratios (95% CI) | |||||
|---|---|---|---|---|---|---|---|---|
| 12–17 years | 25–59 years | |||||||
| Pre | Post | Ratio (95% CI) | Pre | Post | Ratio (95% CI) | |||
| Average bus distance per day (km) | 1 (least deprived) | 2.06 | 3.10 | 1.51 (1.28 to 1.73) | 0.68 | 0.79 | 1.16 (0.93 to 1.42) | 1.30 (1.10 to 1.57) |
| 2 | 2.55 | 3.07 | 1.21 (0.94 to 1.50) | 1.01 | 1.07 | 1.06 (0.90 to 1.25) | 1.14 (0.82 to 1.55) | |
| 3 | 2.66 | 3.23 | 1.22 (0.96 to 1.50) | 1.23 | 1.68 | 1.36 (1.14 to 1.57) | 0.89 (0.67 to 1.17) | |
| 4 | 2.95 | 3.43 | 1.16 (0.85 to 1.53) | 1.52 | 1.89 | 1.24 (1.11 to 1.42) | 0.93 (0.70 to 1.25) | |
| 5 (most deprived) | 2.80 | 3.50 | 1.25 (0.96 to 1.62) | 1.82 | 2.55 | 1.40 (1.25 to 1.58) | 0.89 (0.68 to 1.14) | |
| Average number of bus trips per day | 1 (least deprived) | 0.59 | 0.80 | 1.35 (1.14 to 1.59) | 0.12 | 0.16 | 1.31 (1.06 to 1.56) | 1.03 (0.82 to 1.26) |
| 2 | 0.65 | 0.83 | 1.27 (1.03 to 1.49) | 0.20 | 0.24 | 1.17 (1.01 to 1.44) | 1.08 (0.85 to 1.35) | |
| 3 | 0.71 | 0.87 | 1.22 (0.99 to 1.49) | 0.29 | 0.36 | 1.25 (1.10 to 1.38) | 0.97 (0.81 to 1.21) | |
| 4 | 0.80 | 0.99 | 1.24 (1.02 to 1.62) | 0.37 | 0.48 | 1.30 (1.15 to 1.47) | 0.95 (0.77 to 1.29) | |
| 5 (most deprived) | 0.86 | 1.20 | 1.39 (1.19 to1.66) | 0.51 | 0.69 | 1.34 (1.20 to 1.53) | 1.03 (0.86 to 1.26) | |
| Percentage of short distance trips ≤ 1 km travelled by bus | 1 (least deprived) | 2.06 | 2.86 | 1.39 (0.00 to 13.36) | 0.48 | 0.60 | 1.24 (0.53 to 2.85) | 1.12 (0.00 to 10.43) |
| 2 | 2.09 | 11.81 | 5.66 (2.80 to 15.17) | 0.99 | 1.50 | 1.52 (0.52 to 4.10) | 3.73 (1.33 to 13.94) | |
| 3 | 2.51 | 1.71 | 0.68 (0.11 to 2.52) | 2.50 | 2.55 | 1.02 (0.51 to 2.08) | 0.67 (0.11 to 2.75) | |
| 4 | 1.65 | 2.85 | 1.72 (0.46 to 6.21) | 2.51 | 2.50 | 1.00 (0.60 to 1.76) | 1.73 (0.36 to 7.49) | |
| 5 (most deprived) | 3.26 | 8.71 | 2.67 (0.75 to 8.82) | 3.63 | 4.50 | 1.24 (0.81 to 1.08) | 2.15 (0.49 to 9.74) | |
| Outcome | Area of London | Age 12–17 years | Age 25–59 years | Ratio of ratios | ||||
|---|---|---|---|---|---|---|---|---|
| Pre | Post | Ratio | Pre | Post | Ratio | |||
| Average car distance per day (km) | Inner London | 3.23 | 1.28 | 0.40 (0.21 to 0.88) | 5.92 | 5.06 | 0.86 (0.74 to 0.98) | 0.46 (0.23 to 0.93) |
| Outer London | 3.64 | 2.80 | 0.77 (0.59 to 1.01) | 11.52 | 10.55 | 0.92 (0.87 to 0.97) | 0.84 (0.65 to 1.10) | |
| Average number of car trips per day | Inner London | 0.44 | 0.31 | 0.71 (0.50 to 0.97) | 1.08 | 0.78 | 0.72 (0.64 to 0.80) | 0.99 (0.70 to 1.30) |
| Outer London | 0.76 | 0.66 | 0.87 (0.78 to 0.95) | 2.01 | 1.70 | 0.85 (0.82 to 0.89) | 1.03 (0.92 to 1.15) | |
| Outcome | Age | Ratio of ratios (95% CI) | ||||||
|---|---|---|---|---|---|---|---|---|
| 12–17 years | 25–59 years | |||||||
| Pre | Post | Ratio (95% CI) | Pre | Post | Ratio (95% CI) | |||
| Train travel | Average number of train trips per day | 0.08 | 0.09 | 1.13 (0.83 to 1.58) | 0.17 | 0.20 | 1.17 (1.10 to 1.26) | 0.97 (0.72 to 1.30) |
| Average train distance per day | 0.95 | 1.04 | 1.09 (0.75 to 1.67) | 2.82 | 3.22 | 1.14 (1.00 to 1.28) | 0.96 (0.66 to 1.44) | |
| Underground travel | Average number of tube trips per day | 0.11 | 0.09 | 0.80 (0.66 to 1.03) | 0.25 | 0.28 | 1.15 (1.06 to 1.23) | 0.70 (0.57 to 0.90) |
| Average tube distance per day | 0.82 | 0.70 | 0.85 (0.65 to 1.21) | 2.61 | 2.99 | 1.15 (1.06 to 1.24) | 0.74 (0.56 to 1.07) | |
Appendix 10 Original study protocol (application for funding)
‘On the buses’: evaluating the impact of introducing free bus travel for young people on the public health
Investigators: Judith Green, Mark Petticrew, Phil Edwards, Paul Wilkinson (LSHTM); Helen Roberts (Iof E), John Nellthorpe, Charlotte Kelly [Institute for Transport Studies (ITS) Leeds]
1. Summary for general audience
This study aims to assess the impact of free bus travel for young people on the health of the public. We will focus particularly on the effects on young people, but also intend to look at the consequent effects on other population groups for some outcomes.
In London, young people aged under 16 have been able to access free bus and tram travel since September 2005. This was extended to under 18 year olds in education, work or training in September 2006. One incentive for this policy was to decrease ‘transport exclusion’, and ensure that access to goods, services, education and training opportunities were not denied to some young people because of transport poverty. We would expect that this would increase health, as transport access is linked to well-being. However, there will be other health effects of free bus travel. These might include: young people walking less often or less far, and thus taking less exercise, or being more exposed to minor crime and assault as they travel further for longer distances. Free bus travel for young people might also reduce access other age groups have to transport if, for instance, the buses become too full, or older people are intimidated. Like other complex public policies, there are likely to be both health promoting and health damaging effects.
To assess these effects, we will begin with qualitative research talking young people and older citizens from a range of backgrounds to find out how they experience transport, and the ways in which they feel that access and use influences their health, and the broader determinants of health (e.g.: access to safe places to play and leisure facilities; opportunities for independent travel). An important element of this component of the project is to understand better how transport interventions can have differential effects on different population groups (e.g. by ethnicity, or deprivation).
This study then aims to measure as robustly as possible the overall impact on population health of this transport intervention. We will do this by first looking in detail at travel diary data to measure whether there have been any changes in the amount of bus and other kinds of transport undertaken by young people and others before and after the introduction of free bus travel. This will allow us to estimate the effect on access to transport, and on the amount of healthier ‘active transport’ (walking and cycling). Using comparisons between different age groups (with and without access to free travel) and national data will allow us to estimate how much of the change is due to the policy, and how much due to general changes in people’s transport use. We will then look at the impact on injuries, both road traffic injuries and assaults, by using police records of traffic incidents and other available data sets (e.g. bus incident reports). Again, comparing these with national data and other cities, and comparing different age groups affected and not affected by the intervention will allow us to estimate how far changes identified are due to the intervention itself, and how far they reflect general background trends in, for instance, changes in the amount of walking or rates of injuries.
The need for public policy to be developed in the light of evidence is increasingly recognised, and we also aim to develop methods for developing this evidence base. This is a challenge, as transport interventions occur at the same time as other changes, and we need to develop methods to assess how far they have caused the effects we are measuring. Finally, we will draw on the transport studies literature on evaluating the costs and benefits of transport strategies to investigate the costs and benefits of this policy, from the perspectives of the economy, environment and society.
2. Background
The extension of free bus (and tram) travel in London to under 16 year olds in September 2005 and under 18 year olds in September 2006 provides a unique and timely opportunity to evaluate a large scale intervention in public health. The retrospective evaluation of interventions in complex systems using before-and-after experimental designs has well-known limitations for causal inference. However, although complex interventions of this kind are often not susceptible to ‘hard’ evaluations, they have traditionally been implemented, and will continue to be implemented, without evaluation, and an urgent need has been identified to build an evidence base (Ogilvie et al 2006, Petticrew et al 2005). This is consistent with the approach outlined in the recent MRC Complex Interventions guidance (2008) which underlines the need to evaluate even when randomised trials are not possible, using the best available methods. Notwithstanding the inevitable methodological limitations, we believe that this particular case study offers a significant opportunity to test the strengths and otherwise of a natural experiment in an area with a range of important public health impacts including injury, crime, social exclusion and sustainable development. The strengths of this particular case study in terms of the potential for maximising our faith in causal attributions include:
-
The intervention was introduced in a two-step process (under 16 year olds, then under 18 year olds a year later), providing scope for internal comparisons;
-
Using London as our case study enables us to use more robust injury data sets, and more detailed travel diary data (including socio-economic indicators), than available elsewhere, with relatively long series of before and after data providing sufficient power for interrupted time series analyses, sub-group analyses and sensitivity analyses.
-
For key health outcomes, we have comparable national data to enable us to estimate background trends.
A significant thrust behind the decision of Transport for London (TfL) to extend free bus and tram travel to under 16s and then to 16–17 year olds in full time education or unwaged training was to reduce social exclusion by reducing ‘transport poverty’ and thus impact on a key determinant of health by improving the access of young people to education and training (SEU 2003). The extension of free bus travel was also part of a broader environmental strategy with health implications, aiming to increase bus travel in order to reduce private car use in London, thus impacting on pollution levels and road injury. Extending access to bus travel is also likely to have a range of other direct and indirect effects on public health. It may change the amount of active transport (walking and cycling) undertaken by young people, either through increasing the number of trips made, or by replacing other modes (such as walking or car occupancy). There may be consequent impacts on other population groups, if more bus transport by young people reduces willingness to travel by bus by others, particularly older citizens, thus exacerbating inequalities in transport access. As a public health intervention, therefore, the extension of free bus travel to young people is likely to have a number of positive and negative effects on health, the determinants of health and health inequalities. To date, there is little robust evidence on which to assess the overall impact of such large scale interventions for the public health.
There are real challenges in evaluating these impacts, not least because they affect very different types of health outcome. The problems are suggested by Watkiss et al’s (2000) comments on comparing the relative contributions of road accidents and pollution to fatalities in London for a health impact assessment. Although both outcomes can be quantified and compared, the causal links for pollution are less direct than for injuries, and the population groups affected differ in some respects. In the proposed study, there will be similar challenges. The benefits of increased access to educational opportunities have long term (but difficult to measure) advantages for health, but there are possible damaging effects on cardiovascular health from decreased time spent walking, although these may bring lower risks of being injured on the road. Evaluating these positive and negative effects on immediate health, the determinants of health and health inequalities, is difficult for three reasons. First, the causal pathways by which transport interventions might affect transport mode choice and therefore health are as yet poorly understood. There are likely to be complex interactions with, for instance, transport mode choices changing over time in response to the behaviour of other travellers (if, for instance, bus travel becomes more or less attractive). Second, we do not yet have sufficient evidence to quantify the risks and benefits of many of the known but distal effects of transport policy, such as the effect of reducing transport poverty (Watkiss et al 2000). Third, we know very little about the differential impact of transport mode choices on health across population groups, and thus the potential effect on health inequalities. For instance, using ‘active’ modes such as walking may have very different impacts on mental health (and even physical health) for those for whom it is a choice than for those who have no alternatives: we cannot assume that active transport is necessarily, for all groups, always a benefit for health.
Despite a growing research literature on the links between particular transport modes and health outcomes (e.g. on road traffic injuries) there is a relatively weak evidence base on how transport policies relate to health and wellbeing in the broadest sense (Ogilvie et al 2006), and how these relate to inequalities in health outcomes. The proposed study aims first to map the salient health benefits of transport access for key population groups, using qualitative methods to investigate the ways in which transport mode choices (and the recent and expected interventions affecting these) may influence health outcomes. We will identify, and evaluate the utility of, sources of evidence on the outcomes identified. Second, we aim to produce a robust evaluation of the impact of free bus travel on important direct health outcomes for which we have good evidence (proportion of time spent in active transport and alternative motorised modes; road injury), and to examine whether the effects on these outcomes differ across the population. Third, we aim to develop and apply a method for conducting an economic evaluation of these health impacts.
2.1 Existing research
Transport policies and systems are increasingly accepted to have the potential to be both health promoting and harmful to health, and to contribute to the maintenance of health inequalities (Exworthy et al 2003, SEU 2003). However, the evidence base in this area, although relatively stronger on the transport policy side, is weaker in relation to the health related outcomes of changes to transport policies (Killoran et al 2006). Evaluations of concessionary or free bus travel provide useful background for mapping the potential range of impacts, but few of these have utilised robust designs or been published in peer reviewed journals. An evaluation of national concessionary travel in Scotland, for instance, identified some modal shift from private car use and an increase in active travel, but could not determine how far this was the result of free bus travel provision, given limitations in the study design (Halcrow Group Limited 2009). The proposed study aims to build on such ‘grey literature’ evaluations by drawing on: the relatively small, but developing, body of research on methodological approaches to studying interventions in complex system in the absence of RCT evidence; the (generally) qualitative literature that contributes to understanding the likely implications of transport interventions for inequalities in health; and the economic literature on the costs and benefits of transport systems and transport mode change. An initial conceptual model (see diagram in appendix) of how this intervention is hypothesised to affect the public health draws on a growing body of literature addressing elements of the likely causal pathways. This evidence is summarised below, under headings starting with the most immediate and direct effects of transport policies – injury – and ending with the more distal and difficult to measure.
Injury Injuries are the health outcomes most obviously associated with transport. Although attributing injury rate changes to transport policy is challenging, our previous research has developed methodological approaches for strengthening the credibility of causal attribution, through for instance using multiple interrupted time series analyses for evaluating the impact of 20 mph zones on road safety. In the UK, despite falling rates of road traffic injury in young people, stark inequalities remain in the risk of being injured on the road, with those in more deprived areas and those in some minority ethnic groups at highest risk (Edwardset al2006a, 2006b, Steinbachet al2008). A major contributor to this risk, and to inequalities in risk, is exposure. Given that in the UK risks of road injury remain higher for pedestrians and cyclists (Sonkinet al2006), the greater likelihood of those in lower income groups to be walking rather than being driven puts them at greater risk. Drawing on the evidence on exposure and injury, we hypothesise that injury risk and inequalities in injury risk will decrease if bus transport displaces those modes more exposed to road danger (i.e. walking and cycling), but increase if it displaces private car use.
Pollution Subsidising bus travel has long been seen as a potential strategy to reduce private car use (Quarmby 1967), and has attracted more recent interest as a key element in reducing pollution and global warming. The immediate health impacts from pollution reduction of any modal shifts resulting from this intervention are likely to be too modest to assess quantitatively within the proposed study (Tonne et al 2008). However, research suggests that short term interventions can have lasting changes on transport mode choice (see e.g. Fujii & Kitamura 2003), and we will qualitatively explore the potential for future modal shifts resulting from changing perceptions of the acceptability of bus travel for young people.
Public transport and active transport There is a growing body of international evidence demonstrating associations between ‘active’ commuting and lower risks for overweight (see e.g. Gordon-Larsen et al 2005, Ojaet al1998), with a systematic review estimated that active commuting was associated with an 11% reduction in cardio-vascular risk (Hamer & Chida 2007). These gains are also seen for adolescents cycling or walking to school (Cooper et al 2008, Ojaet al1998). In addition to the direct health gain for the individual, increasing the proportion of active transport compared with private car transport has been linked with rather ambitious public health gains, such as reduced global warming and increased social cohesion and community safety (DfT 2004a).
The role of public transport in encouraging active transport is poorly understood for the UK. Evidence from the US suggests that increasing access to public transport can increase the amount of active transport undertaken enough to have a public health impact on obesity, particularly for men (Zheng 2008, Besser & Dannenberg 2005, Edwards 2008). In addition to walking to transport, there may be a gain from walking within transit systems (see e.g. a study from Paris on the proportion of walking done within transport systems (Julien & Carré 2002). In contexts such as London, with less private car use and better public transport provision, improving access to affordable public transport may have very different effects, and reduce the amounts of active transport undertaken, if it simply replaces walking. However, given the suggestive evidence from Scotland that concessionary fares can stimulate trip making (Halcrow Group 2009), the overall impact could be an increase in levels of active transport.
Transport interventions and inequality Ogilvieet al(2004) noted that in general we know relatively little about the social distribution of health impacts of transport interventions. International comparisons suggest that the distribution of active transport depends on inter-relationships between transport systems and social structure: for young people, for instance, active modes of travel to school or college were more likely in high income groups in the United States (Gordon-Larsenet al2005) but less likely for immigrants and high income groups in Canada (Pabayo & Gauvin 2007). In single settings, the impact of policies such as free bus travel may well have differential impacts on different population groups over time, as the social meaning of bus travel, or walking, changes. Whereas active transport may have health benefits for those who choose it, qualitative evidence suggests negative health effects for those for whom it is a compulsory form of transport (Bostock 2001). Given the suggestion that perceived health benefits may be an important determinant of whether activity does benefit health or not (Crum & Langer 2007), and evidence that views on the role of transport vary by socio-economic status (Bruntonet al2006, SEU 2003), how people understand the role of transport (particularly active transport) and health will be key to unpacking potential pathways linking transport policy and health inequalities.
‘Transport poverty’ and social exclusion The Social Exclusion Unit (SEU 2003) reviewed literature and case studies on the ways in which poor access to transport can reinforce social exclusion, documenting how the cost of transport can be a barrier for 16–18 year olds undertaking education or training. Free bus travel for young people was intended to address such social exclusion due to transport poverty through, for instance, increasing access to education, training, and recreation. Access to transport is also likely to have health benefits for independent mobility for young people, which has been identified as important for increasing self-esteem and an essential factor in inequalities for young people. These are important outcomes, but there is in general less evidence on such wider social and health effects of different transportation choices (Watkisset al2000), and little robust research evidence to draw on. As Preston (2009) has noted, ‘social exclusion’ has proved difficult to operationalise, and more work is needed on quantifying health benefits beyond those of mortality reduction.
Transport for London commissioned some limited evaluative work on the impact of free bus travel on these outcomes (Synovate Ltd 2006, 2007), based on surveys of users and non-users of the scheme. As the samples were not representative of the population, no firm conclusions can be drawn from these about the impact on access to education, training or independent mobility, but 14–15 years olds reported that access to free bus travel had increased access to sports and other recreational opportunities (Synovate Ltd 2006), and the majority of 16–17 year olds ‘strongly felt’ that the scheme had increased their likelihood of staying in full time education, particularly in lower income and minority ethnic groups (Synovate Ltd 2007).
Updates of reviews The literature review will be updated at project start, drawing on the wide range of health, transport and methodological expertise of the applicants, and including reviews using an appropriate search strategy to search the transport databases TRIS (Transport Research Information Service), IRRD (International Road Research Documentation), and TRANSDOC and relevant web sites of the road safety organizations.
2.2 Risks and benefits
The introduction of free bus travel is, then, likely to have had a range of direct and indirect effects on public health and health equity, anticipated and unanticipated, positive and negative. Both risks and benefits are likely to have resulted from both the increased availability of transport to young people, and changes in the share of modes of transport used (e.g., from walking to bus travel) by young people and others. We have reasonable evidence on which to hypothesise the direction of some of these effects, but rather weaker evidence for others, for which we will produce robust evidence for direction of effect where possible. The literature summarised above suggests a conceptual model of key causal pathways linking the intervention and health outcomes (see appendix), which would include the following major components:
Impact on the determinants of health for young people These are likely to result from increased access to transport. Hypothesised benefits to wellbeing from reductions in ‘transport poverty’ accrue from increased access to education, training opportunities, social support, recreation and independent travel. Many of these outcomes are under-researched, and there are no data providing direct measures on potential benefits for health. However, for 2005–06, the Active People Survey has data on the activity patterns (periods per week of moderate physical activity) of a little over 1500 16 to 18 year olds in London, and data will soon to be available from the second survey. Such evidence will provide useful data as background to the qualitative analyses, which we propose to use to map the impact of free bus travel on the broader determinants of health. We will also investigate potential sources of evidence on outcomes such as increased access to education post-16 and increased participation in active recreation.
Impact on the amount of active transport undertaken by young people Although the Synovate Ltd (2006, 2007) surveys identified reported lower use of car transport for school journeys, they also identified that bus travel had replaced some walking. Reduced active transport may exacerbate the rise in overweight, obesity and other cardio-vascular risks (Frank et al 2004, Gordon-Larsenet al2005, Hamer and Chidaet al2008). While active transport is being encouraged as both a route to reducing pollution in urban areas and increasing the health status of the population (TSO 2004, DfT 2004, TfL 2006), as suggested in the literature review above, it is as yet unclear how far the provision of public transport influences the amount of active transport undertaken in the UK. We hypothesise that extending free bus travel has reduced the amount of active transport undertaken by young people. However, given that in other settings, increased public transport access has increased levels of walking, it is possible that this intervention has stimulated trip taking, and had an overall positive impact on the levels of active walking. London has relatively good and detailed travel diary data, which will allow us to look at changes in transport mode use before and after the intervention and at differences across population groups. We aim to measure the impact of the introduction of free bus travel on travel mode share, thus evaluating the impact of extending free bus travel to young people on active transport levels.
Impact on injury rates in young people In terms of potential direct effects on health, both increased access and change of mode are also likely to change young people’s exposure to the risks of road traffic injury, and (through potentially increasing the duration and range of their journeys) to assaults. We will explore the use of Bus Incident reports as a source of data on change over time in assaults, using methods that minimize the influence of potential variations in reporting practice. Injuries continue to be a key contributor to morbidity, mortality and inequalities in this age group (Edwards et al 2006, Edwardset al2008). The effects of increasing access to transport in general and the effects of changes in mode of travel are likely to be bi-directional. Increasing access to and use of bus transport may lead to greater exposure over larger geographical distances, thus increasing risks of road injury or assault. However, changes in mode of travel, from walking or cycling to bus travel, may decrease exposure to road injury, given the evidence that (currently) in the UK, walking or cycling pose greater risks than other modes (Sonkinet al. 2006). We aim to measure the changes in road traffic injury and assaults following the introduction of free bus travel.
Determinants of health for older age groups Changes to young people’s travel behaviour could be hypothesised to have consequent effects on health and the determinants of health for other population groups. If larger numbers of young people are using buses, this may reduce willingness to travel for other users, either through direct exclusion (if buses are too full) or through ‘fear-based exclusion’, with elderly people in particular reported to be concerned about personal safety and security (DfT 1999). The extension of free travel to under 18 year olds has exacerbated public concern about criminal damage, anti-social behaviour and assaults on buses, although it has been difficult to identify whether incidents have actually increased (London Assembly 2008). Concerns about young people and their contribution to ‘fear based exclusion’ are certainly not new (DfT 1999), but it is unclear whether extending free travel for young people has contributed to reductions in wider population use of the bus network. Using travel diary data, we will examine transport modal shifts in other age groups to identify trends over time in active transport. Qualitative research with older citizens will explore their accounts of links between young people’s access and their own bus use.
2.3 Rationale for current study
Need for research Wanless (2004) and others (Ogilvieet al2006) have suggested that opportunities to learn more about the effects of policies (such as transport and other social policies) on public health need to be seized if the public health evidence base is to develop. The introduction of free bus travel to young people in London provides a unique opportunity to understand the health promoting and health damaging effects of a policy intervention and to contribute to methodological development in relation to evaluating the public health impact of interventions in complex settings. A key challenge is to develop methods for assessing health impact in the absence of RCT evidence. In many cases, natural experiments are likely to provide the best available evidence despite problems of confounding (Craiget al. 2008). Such opportunities arise rarely.
In this case study, we have the opportunity to exploit relatively robust data sets (for instance, more detailed travel diary data than available for the rest of the country, and more complete road traffic injury data) in order first to address some key empirical questions that are currently underexplored. These include whether extending public transport provision in a UK setting increases or decreases active transport. In this context of increasing policy interest in the health effects of transport interventions, this is an important issue. Second, this team brings together an established group that have been working on methods for evaluating public health interventions in complex systems with an internationally recognised group of transport economists, drawing on the well-developed methods for evaluating the economic costs and benefits of transport policies. This provides a significant opportunity to strengthen the health economic evaluation of such interventions.
The setting London is unique in its transport systems, with a faster growth in bus transport than other parts of the UK, and lower levels of car ownership. It also has a unique regional governance of the system (through the Mayor of London’s duty to develop transport policies). The policy and infrastructure context (co-interventions, policy imperatives, bus availability) of the intervention will be carefully described in our outputs. Although, as with all single case studies, the specific empirical findings are likely to have limited generalisability in a narrow sense, there are good grounds for assuming a high degree of conceptual generalisability from this study. First, single case studies can demonstrate the possible. The Report from the Committee of the Social Determinants of Health (WHO 2008), for instance, cited the London congestion charge as an example of a transport policy with public health benefits. Second, lessons learnt from London are likely to be closely followed by other urban centres on issues such as the potential implications of policies that aim to increase bus travel. Third, methodologically, this case study will generate considerable knowledge of the strengths and weaknesses of secondary sources for evaluating public health outcomes; methods for integrating data to strengthen the credibility of causal pathways; and designs for strengthening causal inference through appropriate internal comparisons.
3. Research objectives
To develop our understanding of how travel access affects the indirect or broader determinants of health, we aim to explore the likely effects through qualitative work mapping young people’s and older citizens’ experiences and views. Integrated with the quantitative findings, this will contribute to identifying plausible causal pathways that link transport to health.
To assess the public health impact of free bus travel we need first to identify changes in travel behaviour, to estimate the impact on a key determinant of health (active transport) and on potential travel exclusion for both young people themselves, and for other age groups in the population. Second, we need to identify changes to injury rates for 12–15 and 16–17 year olds before and after Sept 2005 and 2006 respectively in order to estimate the impact on direct health outcomes for these age groups. We then need to account as far as possible for confounders through appropriate population, place and time comparisons. With robust estimates of the effects on injury and active transport, we can then develop methods for economic evaluation. The objectives of the study are therefore to:
4. Determine the causal pathways that plausibly link transport interventions and young people’s health;
5. Identify the ways in which young people and older citizens understand the role of bus and other transport mode access in facilitating and constraining their wellbeing;
6. Assess the impact of free bus travel for 12–17 year olds on their use of bus and other transport modes;
7. Assess the impact of free bus travel for 12–17 year olds on the use of bus and other transport modes by older age population groups;
8. Identify changes in the incidence of injury in young people after they had access to free bus travel;
9. Investigate, develop and apply a method for conducting an economic evaluation of the health impacts from introducing free bus travel for young people in London and other similar social interventions.
4. Research design
4.1 General design issues
This mixed-methods study will essentially track a natural experiment (Petticrewet al2005). It aims to integrate a range of data sources and methods of analysis within a quasi-experimental design in order to evaluate the impact on public health of the introduction of free bus travel for young people in London. In order to develop a detailed causal pathway model, and evaluate the positive and negative impacts on health, we will use a combination of methods. First, qualitative research will be used to explore young people’s and older citizens’ perspectives. Second, secondary analysis of existing data sets will be used to determine the impact of the intervention on travel behaviour (modes of transport used) and active recreation to identify the likely impact on active transport. Third, secondary analysis of police data and Hospital Episode Statistics will be used to assess the impact of free bus travel on injury outcomes (transport injuries and assaults). Working with our advisory group, these data sources will be integrated to develop plausible causal pathways linking transport and the broader determinants of health. Finally, we will draw on the growing body of evidence on monetary values for health effects (e.g. injuries, assaults and changes to levels of active transport) to develop and conduct an economic evaluation of the key health outcomes identified by this case study.
The general design of this evaluation equates to an untreated control group design with pre- and post-test in Cook and Campbell’s terminology, which they note is the most frequently used interpretable quasi-experimental design. However, within each aim (see below) we propose methods to increase the credibility of causal inference. These will utilise best practice in the design and analysis of observational studies to minimise threats from confounding, and increase the credibility of causal attribution. We will examine aspects of internal consistency of evidence (whether intervention effects are similar in different age groups, and across more than one outcome); specificity (facilitated by comparison of changes in London with other cities and in London taking account of national background trends); and coherence (addressed through cross-reference to existing studies and knowledge of the determinants of active travel, and through the new qualitative data). Evidence for some outcomes (e.g. injuries) will be stronger, given there is sufficient data to conduct interrupted time series analyses. Causality is also determined by the observed strength of association which will be assessed at the analysis stage. Glasziou (2007) and others for example provide guidance on the interpretation of effect size data from observational studies when RCTs are not possible. The examination of Dose-Response relationships will strengthen the credibility of interpretation, and these will be estimated by the use of proxy measures of bus access, such as SOA level Public Transport Accessibility Levels. Qualitative data derived from a range of stakeholders will also permit examination of “local history” explanations for any observed differences. GIS methods will be used to describe in detail the transport environment across the study area.
4.2 Methods
4.2.1 Methods – Aim 1
To determine the causal pathways that may plausibly link transport interventions and young people’s health.
In addition to adding to much needed evidence in the field of transport, this study will contribute to methodological development by: identifying and reviewing available and robust sources of data that can be used to estimate public health gain; identify and assess methods for addressing known biases in observational studies (e.g., setting out clear a priori hypotheses, using appropriate comparator data sets to address known confounders, use of multiple data sources) and develop understanding of causal attribution in non-RCT designs through integrating qualitative and other data sources.
The approach will involve using the qualitative data which describes (among other things) the choices young people make about transport, and the influences on their travel behaviour; observational data; interviews with other stakeholders; and quantitative data on the actual changes in transport behaviour. These will be integrated into a general model describing the relevant causal pathways and the specific mechanisms. This is consistent with recommendations from Shadish et al. (2002) on the use of qualitative and quantitative data to support the development of generalised causal inferences from experimental and quasi-experimental studies. They describe how observational/ethnographic methods and statistical models incorporating independent, dependent, mediating and moderating variables can be integrated (as we intend in this study), with the purpose of exploring potential explanations and pathways. While no study is in itself intrinsically generalisable to all settings, generalisations can be rendered more causally convincing if they explore detailed pathways, mechanisms, and outcomes, as we seek to do in this project. This applies as much to experimental as to non-experimental evaluative studies. However if this process of describing mechanisms is done thoroughly, then common underlying processes may be identified which may be relevant to similar interventions in other settings (such as other cities).
It can be argued that London is unique and the findings are not generalisable. However the same argument can be made about any evaluation of a social intervention, in any setting, randomised or otherwise. But while contexts, settings and indeed the intervention itself may vary, this does not mean we should not seek to learn about the processes and impacts of individual interventions. In short, each new evaluation then contributes to the wider public health evidence base – illustrating the range and size of positive and negative impacts, their social distribution and the potential mechanisms by which these were achieved; this information can then inform subsequent decision-making about similar types of intervention, and can inform the methods of future evaluations.
As we intend to use both descriptive (qualitative) and quantitative synthesis, we will use developing narrative synthesis methods to report results from diverse sources (Arai et al 2005).
4.2.2 Methods – Aim 2
To identify the ways in which young people and older citizens understand the role of bus and other transport mode access in facilitating and constraining their wellbeing.
The secondary data will provide a detailed analysis of changes in transport behaviour and injury outcomes in the London population, compared with others where appropriate, from which we can identify public health gains and losses. However, the pathways linking transport choices, transport behaviour and the determinants of health are complex and multi-directional. The qualitative component, which will inform and be informed by the quantitative analysis, aims to explore young people’s accounts of the impact of the transport on the broader determinants of health, and identify (from analysis of those accounts and additional data from other users and key stakeholders) plausible pathways by which policy, access and behaviour interact to constrain and facilitate wellbeing. Understanding how young people’s perceptions of risk and safety interact with other criteria (e.g. availability and cost of transport) in their decisions about modes of transport is essential if we are to identify: barriers to active transport; how access to travel may change access to both healthy and unhealthy public spaces; exposure to risks of assault, injury or other harm. For young people, independent travel presents opportunities for: access to education, employment, goods and services; both health promoting and health damaging social networks and the development of autonomy and self-confidence. It also presents a set of risks to be managed, particularly in urban areas where the risks of assault or road danger are perceived as high.
Previous research has identified some of the constraints acting on young people’s travel in urban areas; the complex strategies young people adopt both to maximise their own safety whilst travelling independently and to allay parental fears about their independent travel (Brunton et al 2006, Jones et al 2000); and has identified the need for more research on the structural determinants of risk exposure (Thomas et al 2007). The qualitative component of this study will use a combination of individual interviews, group interviews and observation to map how transport use is related to: opportunities for independent travel; social inclusion; health promoting activity and risks to health.
Although the primary focus of this study is on the public health implications for young people, we also aim to capture the potential impact on other population groups. The qualitative component will focus on older people, for two reasons. First, those aged over 60 also have access to free travel, through Freedom Pass issued by local authorities in London. Second, concerns have been expressed (although to our knowledge, these are not evidence-based) about the possible effects specifically on older people’s access to bus travel resulting from increased access for young people (e.g. from over-crowded buses, or fear-based exclusion).
Sample The aims of the sampling strategy are to recruit a maximum variation sample (in terms of those variables likely to shape experiences and accounts, such as transport availability, gender, age, ethnicity, disability, area deprivation). We will do this by selecting four contrasting areas of London (selected to include ‘bus-rich’/‘bus-poor’ areas of contrasting area deprivation from inner and outer London) and theoretically sampling young people within those areas. We aim to recruit young people to the research team via social networking web sites (e.g. FaceBook groups) who can help with recruitment for different population groups, as well as recruiting through conventional community networks (e.g. sports clubs, community organisations, supplementary schools), and through a young people’s involvement project in an inner London borough. Drawing on ‘theoretical sampling’ techniques (in which early data analysis is used to suggest later sampling decisions, and where later data are used to ‘test’ emerging hypotheses) we plan to sample to the point of saturation (when additional data adds little to ongoing analysis), with an estimate of up to 50 young people in individual (or pair, if participants prefer) interviews and 8 group interviews (of around 5 participants, n = approximately 40 participants) would achieve this. We aim to use both individual and group interviews, as individual interviews are more likely to generate detailed accounts of sensitive information around perceived risks and health impacts, whereas group interviews (particularly if using natural groups) access more normative accounts of behaviour and the ways in which participants’ understanding of transport and health is socially generated.
Recruitment of older citizens in the same areas will also be carried out in ways designed to obtain a maximum variation sample include both ‘younger’ and ‘older’ over 60 year olds in outer and inner London boroughs likely to have been affected by bus use by other groups. Recruitment of individuals will be through community groups, and for those more socially isolated through ‘park bench’ approaches and on buses. These approaches will be made by an experienced researcher (HR). Again, we will sample to saturation, with the expectation that this will be reached by including around 25 individuals.
Data generation and analysis Pilot work carried out as part of a study for TfL (Steinbach et al. 2007) suggests that: well designed interviews are a productive way to generate data on young people’s experiences and accounts of transport; that this was a topic of interest to them and that there were variations in accounts from those across London’s diverse ethnic communities. Interviews will begin with narrative questions focusing on how young people manage transport within their daily lives. Later parts of the individual and group interviews will be more semi-structured, including questions related to how:
-
Participants understand and manage the opportunities and risks posed by different transport modes;
-
Accounts of risks and opportunities are related to the broader determinants of health;
-
Access to free bus/tram travel in London affects reported travel behaviours and risk management strategies.
An essential element will be observational ethnographic data, generated by observation of transport behaviour in everyday life in public spaces, including bus travel (in and outside school hours) to capture what people do, as well as what they say they do, and informal interviews with other transport users, parents, and other stakeholders. Analysis of all qualitative data will use principles of the constant comparative method (Strauss 1987), including detailed use of open coding on early data, development of conceptual coding schemes and an iterative approach to hypothesis generation and testing. Our experience is that for policy orientated research, an approach which goes beyond thematic analysis is vital for generating both valid and useful theory for practice.
4.2.3 Methods. Quantitative analyses: Aims 3, 4 and 5
-
To assess the impact of free bus travel for 12–17 year olds on their use of bus and other transport modes (including active transport i.e. walking and cycling);
-
To assess the impact of free bus travel for 12–17 year olds on bus transport and other transport modes by older age groups.
-
To determine changes in the incidence of injury in young people after they had access to free bus travel
Quantitative data series are available for London on use of transport, including walking and cycling (London Area Travel Survey (LATS), London Travel Demand Survey (LTDS)), and injuries (Stats19 road injury data, Hospital Episode Statistics (HES)). These allow analyses of change in important outcomes following the introduction of the free bus and tram travel scheme. The quantification of change will be based on before-after comparisons using two time points: (i) the introduction of free bus travel in London to children < 16 years in September 2005 and (ii) its extension to those under 18 years in September 2006. To minimize possible bias arising from changes over time in the completeness of data recording, for most analyses we propose to compare the changes in the relevant outcomes in the under 18s (under 16s) with those observed at other ages: a change-on-change analysis. Although this carries some penalty in terms of statistical power, the comparatively large number of events at other ages means the penalty is modest, while achieving a gain of reduced potential for bias. We will examine the following outcomes:
-
the frequency and distance of active transport (i.e. walking and cycling) in those aged 12–17 years;
-
the frequency of bus use and the distance travelled by bus, in those aged 12–15 and 16–17 years;
-
the frequency of bus travel and the distance travelled by bus in other age groups;
-
the incidence of intentional and non-intentional injuries in young people aged 12–17.
| FREE BUS/TRAM SCHEME | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 |
|---|---|---|---|---|---|---|---|---|
| <16s | <18s | |||||||
| Pre-intervention | Post-intervention periods | |||||||
| London Area Travel Survey (LATS) [number of households] | 30,000 | |||||||
| London Travel & Demand Survey (LTDS) [number of households] | 5,000 | 8,000 | 8,000 | 8,000 | ||||
| National Travel Surveys (NTS) [number of households] | 9,000 | 9,000 | 9,000 | 9,000 | 9,000 | 9,000 | 9,000 | |
| Stats19 [persons] (per cent in 12-17 years) | 45,000 (7%) | 41,000 (7%) | 39,000 (7%) | 35,000 (7%) | 32,000 (7%) | 29,000 (6%) | Not yet analysed | Not yet analysed |
| Hospital Episode Statistics (external cause admissions in London) | 100k (350) | 100k (350) | 100k (350) | 100k (350) | 100k (350) | 100k (350) | 100k (350) | 100k (350) |
Travel patterns: LATS, LTDS. We will use data collected five years before the interventions in the 2001 London Area Transport Survey (LATS), and data from the 2005–2007 London Travel Demand Surveys (LTDS) for the post-interventions period. The LATS and LTDS surveys collect comparable travel data sets based on daily travel diaries, using comparable sampling designs. The 2001 LATS included 30,000 households and LTDS included 5,000 households in 2005, with a further 8,000 households annually since 2006. Every person aged over 5 years living in each household is asked to complete a one-day travel diary that records the starts, interchanges and ends of every trip made on that day. In 2001 LATS there were 360,389 interchanges (parts of trips) made by 67,252 individuals. With similar levels of travel in 2005–2008 we expect data to be available on over 250,000 travel interchanges made by 47,000 individuals. Journey times are collected in both LATS and LTDS. Journey distance is estimated using the start-point, interchange and end-point of each trip (these locations are geo-coded and ‘crow-fly’ distances are easily calculated). For the travel patterns, comparisons will also be made with data from the National Travel Survey (NTS, Department for Transport). This national survey includes samples of approximately 9,000 households each year, including approximately 20,000 individuals, with data from seven day travel diaries for each individual. The inclusion of NTS data will enable us to assess whether trends in main travel modes nationally and in other urban areas differ to those used as main modes in London.
Travel-related injuries and assaults: Stats19, bus incident reports, HES. STATS19 road injury data, the official dataset of human death and personal injuries from road traffic crashes on the public highway in the UK, are available for each year of the study (to 2009). We will analyse casualties among young people travelling as pedestrians, cyclists, car occupants and bus occupants, and by severity of injury (‘Fatal’ or ‘Serious’ (hospital admission), and ‘Slight’ – minor injuries).
STATS19 data remain the richest source of information on road traffic injuries in England, and are an essential component of assessments of transport effects on injury events. Although there is recognised to be a degree of under-reporting in STATS19 data, the completeness in London is estimated to be around 87%, and the change-on-change analysis will help to minimize bias arising from year-to-year variations in completeness. Comparatively long series of Stats19 data are available and our experience has demonstrated the value of using these longer series, stratified by key factors, to derive more accurate estimates of the relevant trends and step effects. Differences in these between socio-demographic strata within London are likely to be an important element of the interpretation of the quantitative data. Published analyses of national data will be used to estimate national and urban area background trends in injury rates.
The utility of bus incident reports and other data sets will be examined for the potential to identify changes in assaults, if the known problems of reporting bias can be addressed. If feasible methods for evaluating transport interventions are to be developed, it is essential to generate knowledge about the uses and limitations of routine data sets for evaluating outcomes.
An extract of Hospital Episode Statistics (HES) will be obtained for England covering the period 2001 to 2009. We will identify all London residents using census super output area (SOA) code of residence. We will analyse hospital admissions due to all ICD external causes of injury, and specifically those external causes directly influenced by transport access (e.g. transport injuries, assaults). Comparisons will be made with admissions for other external causes that are not plausibly linked to transport policy change (e.g. poisoning, falls, self-harm). We will include all admissions, given that restricting our case definition by injury severity will greatly reduce the sample size available, but will conduct a sensitivity analysis using only severe injury admissions to test whether differential admission rates by external cause over time may have introduced bias (e.g. due to differences in admissions policy).
Analysis For all outcomes, the principal analysis will be the comparison of the change before and after September 2005 (for those aged 12–15), and before and after September 2006 (for those aged 16–17 years). These changes will be compared with similarly defined change at other ages. Where relevant, appropriate denominator populations (ONS population projections) will be used to allow for differences between years in the number of young people at risk. Robust standard errors will be calculated, clustering on borough to allow for similarities of outcome at that geographical level. We will also explore the use of other multi-level modelling methods to allow for other forms of data hierarchy relating to spatial variation in bus service provision.
To assess the impact of the interventions on transport (including active transport) we will compare mean times and distances, as well as the percentage of short distance trips travelled by the relevant mode (walking, cycling, bus, car). We will also estimate changes in amounts of travel on journeys to work or school in people aged under 18 years (to assess potential increased access to education).
For all outcomes, we will investigate evidence for variations by socio-economic group or household income and, where possible, by ethnicity (to address questions of impact on inequalities), although power will be limited for most such sub-group analyses.
Sample size Example of power to detect changes in distance of trips made by bus and walking.
Provisional 2001 estimates of the distances of trips made by young people by bus and by walking are shown below. With 3,000 young people in the sample before and after the intervention, the study will have 80% power to detect a 10% reduction in the average daily distances walked by young people (from an average 0.91 km per day to 0.82 km per day) at a 5% significance level. Similarly, the study would have 98% power to detect a 10% increase in the distance of bus travel from an average of 4.33 km per day to an average 4.76 km per day. For transport-related injury, the study would have 80% power to detect a 10% change, or 90% power to detect a 12% change significant at the 5% level. Statistical power is inevitably more limited for subgroup analyses, but for example there is 90% power to detect a 15% change in average distance travelled by bus by young people within the most deprived quartile.
| 12–15 years | 16–17 years | Total | |
|---|---|---|---|
| Number in sample | 3,150 | 2,300 | 5,450 |
| Average distance per bus trip (km) [SD] | 4.19 [4.4] | 4.51 [3.8] | 4.33 [4.1] |
| Average distance per walking trip (km) [SD] | 0.87 [1.2] | 0.95 [1.35] | 0.91 [1.26] |
4.2.5 Methods – Aim 6
Investigate, develop and apply a method for conducting an economic evaluation of the health impacts from introducing free bus travel for young people in London and other similar social interventions.
In the field of transport there is a strong body of literature focusing on evaluating the costs and benefits of transport strategies and interventions from the perspective of the economy, environment and social aspects. In terms of evaluating the range of impacts on health from an intervention the literature is less focused, but increasing. The aim of this task will be to develop and apply an evaluation method that will allow policy makers to evaluate the impact on health and injury from this intervention. Firstly, a background review will be conducted focusing on how health has been included in the evaluation of transport policy interventions (including WHO (2008), Bickel et al (2006) and DfT (2004b)) to identify the main methodological options and recommend an approach for this study.
The evaluation will draw on the well-established literature on values associated with slight, serious and fatal injuries (DfT, 2009a), Home Office (2005) values used for crime (including assault) and the emerging literature on the health effects from changes to walking and cycling (DfT, 2009b). The quantitative work in aim 5 (incidence of injury) and 3 and 4 (changes in active transport) will be used as key inputs into the evaluation. This will be combined with an assessment of the cost that has been incurred by TfL as a result of introducing concessionary fares (e.g. from lost revenue, from administration of the scheme), as part of a value for money assessment. Given the focus on young people, particular attention will be applied to the appropriate use of economic values for the target age group concerned based on the existing literature. It will not be possible to value all the impacts identified between health and transport in the causal pathway exercise. A qualitative, and where possible quantitative, assessment of these impacts will be implemented where appropriate. There will therefore be scope to extend this assessment in the future.
This evaluation methodology will allow the research team to assess whether the policy has had an overall positive economic impact when compared with the costs and benefits based on the inputs that can be monetised for public health. It will then, in combination with the qualitative and quantitative assessments, provide an impact assessment of the policy with regard to public health. This approach of combining both a value for money assessment alongside other impacts that are assessed either qualitatively or quantitatively is common practice in transport policy evaluation (DfT 2005c), and this study provides an opportunity to identify the utility of this approach within public health evaluations.
5. Study population
The primary study population is residents of London aged 12–17 years old.
However, as other groups will be affected by the intervention, the wider study population is all residents of London aged over 12. Populations for specific objectives are detailed above (Section 4.2).
6. The intervention
The intervention is the introduction of free bus travel for young people under 16 years old in September 2005 and those under 18 years old (in full time education or unwaged training) in September 2006.
7. Outcome measures
Key outcome measures investigated in this study are:
-
reported health benefits and risks of access to bus travel for young people and older citizens;
-
change in the time and distance of active transport (walking, cycling) undertaken by young people and older age groups;
-
change in road transport injuries in young people;
-
change in assault injuries in young people.
In addition, our review of the literature and available evidence will identify existing evidence on the following outcome measures:
-
Changes in access to education and training for 16–18 year olds;
-
Changes in active recreational activity;
-
Changes in bus incidents.
-
These are detailed in the methods section (4.2) above.
8–10. Assessment and follow up; sample sizes; statistical analysis
Assessment of outcomes, sample sizes and analyses are all detailed under methods for specific components, above (Section 4.2).
11. Ethical arrangements
The study will be conducted in accordance with MRC guidelines, those of LSHTM and good practice for social research (the ESRC ethical framework). Approval from LSHTM Ethics Committee will be sought. All confidential data will be stored on the secure server of LSHTM. Access to data files on this server is traced using the ‘LT auditor plus’ software. Our Information Security and Management Policy is compliant with BS7799. Qualitative data (MP3 files, transcripts) will be kept securely, with only coded identifiers. As the data sets accessed directly in this study (STATS19, HES, LATS/LTDS) are the property of DfT, DoH and TfL respectively, they will be destroyed at project-end according to conditions determined by the data providers. Our Records Management policy requires primary data generated to be kept securely for at least 10 years post the study end date.
In addition to the usual ethical issues of maintaining confidentiality and considering representation, there are additional ethical concerns in working with young people, including those of ensuring adequate consent to inclusion, and minimizing the exclusion of marginalized young people. Our recruitment strategy is designed to maximize inclusion, and young people participating will be deemed competent to make their own decisions (MRC Ethics Guide: Medical Research Involving Children); i.e. those under 16 years will not be excluded if parental consent cannot be obtained. Interview protocols will be developed to cover disclosures of harm. Consent is a process rather than a one-off event, and participants will be involved in discussing consent as the work progresses. Observational studies of public behaviour (such as behaviour on public transport) raise ethical issues around inability to secure consent; as the ESRC guidelines note, informed consent is ‘impracticable and meaningless’ in such situations (ESRC http://www.esrc.ac.uk/ESRCInfoCentre/Images/ESRC_Re_Ethics_Frame_tcm6-11291.pdf p21), and it would be impossible to secure consent from, say, all bus passengers to note- taking by research staff. However, we believe that observational data on how travellers do behave is an essential adjunct to the data we will generate on how they say they behave. Any observational data in the form of field notes will be anonymised, with confidentiality ensured through coded use of contextual identifiers, and accounts written with respect for participants.
12. Research governance
The sponsor of this project will be LSHTM. We will establish a study steering committee to: advise on the primary qualitative study; facilitate access to key stakeholders; assist with knowledge translation. We will therefore include representatives from Policy Analysis and Surface Transport at Transport for London (as the intervention provider), a member of the Public Health Centre for Excellence at NICE (as the key provider of public health guidance); a user of routine data on transport; a member of a local authority scrutiny committee with responsibility for health. We would also hope to include colleagues from Canada and Australia working on complex interventions who are part of the CIHR funded International Collaboration on complex interventions of which Petticrew and Roberts are members. This steering committee will also include the applicants and collaborators (including Suzanne Lutchman representing an NHS public health department). There will in addition be seminars and regular, minuted meetings of the investigators, employed researcher(s) and collaborators.
We do not feel that this piece of work requires a data monitoring and ethics committee, but will discuss emerging results with the Study Steering Committee. End point users will be involved in the work in ways which use their lay expertise but outwith the steering group.
13. Timetable and milestones
| Year 1: 2010/11 | Year 2: 2011/12 | Year 3: 2012 | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M/A | M/J | J/A | S/O | N/D | J/F | M/A | M/J | J/A | S/O | N/D | J/F | M/A | M/J | J/A | ||
| Recruitment/ethics approval | ||||||||||||||||
| Update literature review | ||||||||||||||||
| Access and prepare quantitative data sets | ||||||||||||||||
| Review of additional data sources | ||||||||||||||||
| Quantitative analysis | ||||||||||||||||
| Recruit participants | ||||||||||||||||
| Qualitative fieldwork | ||||||||||||||||
| Qualitative analysis | ||||||||||||||||
| Develop economic evaluation methodology | ||||||||||||||||
| Complete economic evaluation | ||||||||||||||||
| Seminars-Collaborators | ||||||||||||||||
| Workshops/conferences | ||||||||||||||||
| Writing up | ||||||||||||||||
13.2 Key milestones
Year 1
-
Complete ethical approval June 2010
-
First investigators’ seminar –develop conceptual model April 2010
-
Access required data sets for quantitative components Aug 2010
-
Complete review of additional data sets Feb 2011
Year 2
-
Complete interviews and focus groups Aug 2011
-
Complete qualitative analysis Oct 2011
-
Complete quantitative analysis Aug 2011
-
Circulate working paper on casual pathways Sept 2011
-
Complete economic evaluation Feb 2012
Year 3
-
Hold workshop for stakeholders May 2012
-
Complete draft papers on empirical findings, implications for public health, economic evaluation, methodology July 2012
-
Final report to funders Aug 2012
14. Expertise
This proposal arises from the ongoing work at LSHTM and IoE on transport and health, on methods to evaluate public health interventions, on understanding complex interventions, and on direct work with children and young people, and from the ITS at Leeds on the evaluation of transport policy. The research team has a proven track record, with peer-reviewed output in areas including: secondary analysis of transport and health data; the evaluation of complex interventions (including transport interventions); qualitative research with young people and on the use and synthesis of mixed-methods in public health research. Recent and ongoing grants from DH and TfL have included studies of inequalities in road injury, from ESRC on methodological work, from the Canadian Institutes for Health Research on complex interventions, and from WHO on the injuries report for the Commission on the Social Determinants of Health. Members of the team have collaborated successfully on a large number of previous grants and publications, completed to time and to budget, and have engaged in knowledge translation through scientific and stakeholder publications and engagement with policy makers, end point users of services and practitioners.
The applicants benefit from the institutional base of large multi-disciplinary departments of Public Health at LSHTM, social science at IOE, and the Institute for Transport Studies at Leeds, one of the world’s leading academic centres of transport research. The team have excellent links with relevant stakeholders (including TfL, DfT, and the Wellcome convened workshop on Environmental Determinants of Physical Activity). The Transport and Health group at LSHTM is a collaboration that has developed considerable experience of working together on mixed methods studies, and draws on expertise more broadly across LSHTM, and ITS at Leeds has an internationally recognised record of collaborative work on transport policy and appraisal.
15. Members of the public
This study is likely to be of direct interest to the public, not only in London, but also those in cities worldwide who are following with interest the ways in which transport policies in London impact on health, social cohesion, congestion and air quality. Our policy (and practice to date) is to share information in a timely manner. We will do this through briefings to colleagues in TfL, the establishment of an ‘On the buses’ website which will link to internet networking sites, and short items in mainstream news services generated by young people (http://www.headliners.org/). Young people’s input will aid in identifying dissemination opportunities.
Apart from peer-reviewed journal articles on public health, economic evaluation and methodological findings, this research is likely to generate findings useful for policy makers, in particular identifying the range of positive and negative impacts which need to be taken into account when planning new transport policies. This work is therefore likely to be of value in future health impact assessments of transport interventions, including modeling work on likely health impact. In the shorter term, we will ensure that learning in both directions (policy and practice to research and vice versa) will be facilitated through the advisory group, including key stakeholders (London Health Commission representatives, a young people’s participation worker; TfL representatives) in a process of integrated knowledge exchange, recognizing the importance of stakeholders to the process of knowledge production. We will publish in stakeholder publications, including those aimed at transport policy makers and public health practitioners. Petticrew and Roberts are part of an international collaboration on complex interventions funded by the Canadian Institutes for Health Research, which provides an opportunity to disseminate the methodological work internationally.
16. Justification of resources
This project is scheduled over 30 months. Direct costs are requested for: Phil Edwards for one day per week, to provide leadership on accessing, managing and analyzing the main data sets needed (STATS19, HES, LATS etc.), supervise the RF and to lead on the interpretation and writing up of the quantitative analysis. Rebecca Steinbach (RF), who has expertise in GIS methods, and the transport data sets needed. She will be employed over 30 months to lead on data analysis and generation, assisted by a TBA RA for 18 months on the qualitative fieldwork. One O.5 FTE administrative assistance is required to help with budget management and correspondence. Charlotte Kelly will be employed for 48 days across the duration of the project to work on Aim 6 (the development and testing of the economic evaluation methodology). She will be working alongside John Nellthorp. John Nellthorp will be employed for 45 days across the duration of the project to work on Aim 6. They both have considerable expertise in transport policy appraisal and will contribute throughout the project to other aims through their knowledge of the transport studies literature and methods of evaluation.
Allocated costs only are requested in relation to the contributions of the other applicants. The time of these senior applicants is crucial to the success of a complex and novel project, where full exploitation of the potential will require interaction time. Each will contribute 0.5 days per week as follow: Judith Green (PI), to manage the timely progress of the project, manage the collaboration, supervise the qualitative component, contribute to observational fieldwork, integrate the qualitative and quantitative data. Mark Petticrew (CI) to lead on methodological development, lead on appropriate dissemination to networks working on complex interventions and lead outcome on implications for quasi-experimental design. Paul Wilkinson (CI) to provide methodological input from perspective of environmental epidemiology, and advise on research design throughout the study. Helen Roberts (CI) to provide expertise on research with young people, systematic integration of evidence, to contribute to primary research with older people, to observational fieldwork and to knowledge exchange.
Equipment and research costs are those essential to facilitate the fieldwork (digital recorders, transcription) and access to literature and data, and those for dissemination include one UK and one international conference. Costs are also included for 3 seminars for the research team, one in Leeds and two in London, at key points in the project, and for collaborator meetings.
17. References
- Arai L, Britten N, Popay J, . Testing methodological developments in the conduct of narrative synthesis: a demonstration review of research. Evidence &Amp; Policy 2005;3:361-83.
- Besser L, Dannenberg A. Walking to public transit: Steps to help meet physical activity recommendations. American Journal of Preventive Medicine 2005;29:273-80.
- Bickel P, Burgess A, Hunt A, Laird J, Lieb C, Lindberg G, et al. State-of-the-art in project assessment. Stuttgart: IER; 2005.
- Brunton G, Oliver S, Oliver K, Lorenc T. A synthesis of research addressing children’s, young people’s and parents’ views of walking and cycling for transport. London: EPPI-Centre, Social Science Research Unit, Institute of Education, University of London; 2006.
- Craig P, Dieppe P, Macintyre S, . Developing and evaluating complex interventions: the new Medical Research Council guidelines. BMJ 2008;337:979-83.
- Crum A, Langer E. Mind set matters: exercise and the placebo effect. Psych Sci 2007;178:165-71.
- Choosing health: making healthier choices easier. 2004.
- Young people and crime on public transport. London: DfT; 1999.
- Walking and cycling: an action plan. London: DfT; 2004.
- DfT . TAG Unit 3.3.1: The Environment Objective 2004. URL: http://www.dft.gov.uk/webtag/webdocuments/3_Expert/3_Environment_Objective/3.3.1.htm.
- DfT . TAG Unit 2.7.2: Appraisal Summary Table 2004. URL: http://www.webtag.org.uk/webdocuments/2_Project_Manager/7_Transport_Appraisal_Green_Book/2.7.2.htm.
- TAG Unit 3.4.1: The Accidents Sub-Objective. n.d.
- n.d. URL: http://www.dft.gov.uk/webtag/webdocuments/3_Expert/4_Safety_Objective/3.4.1.htm.
- DfT . TAG Unit 3.14.1 Guidance on the Appraisal of Walking and Cycling Schemes 2009.
- n.d. URL: http://www.dft.gov.uk/webtag/webdocuments/3_Expert/14_Walking_Cycling/3.14.1.htm.
- Drummond MF, Sculpher MJ, Torrance GW, O’Brien BJ, Stoddart GL. Methods for the Economic Evaluation of Health Care Programmes. Oxford: Oxford University Press; 2005.
- Edwards P, Green J, Roberts I, Grundy C, Lachowycz K. Deprivation and road safety in London. 2006.
- Edwards P, Green J, Roberts I, Lutchmun S. Deaths from injury in children and employment status in family: analysis of trends in class specific death rates. BMJ 2006;333:119-21.
- Edwards P, Green J, Lachowycz, Grundy C, Roberts I. Serious injuries in children: variations by area deprivation and settlement type. Archives of Diseases in Childhood 2008;93:485-9.
- Edwards R. Public transit, obesity, and medical costs: assessing the magnitudes. Preventive Medicine 2008;46:14-21.
- Frank L, Anderson M, Schmidt T. Obesity relationships with community design, physical activity, and time spent in cars. American Journal of Preventive Medicine 2004;27:87-96.
- Fujii S, Kitamura R. What does a one-month free bus ticket do to habitual drivers?. Transportation 2003;30:81-95.
- Glasziou P. When are randomised trials unnecessary? Picking signal from noise. BMJ 2007;334:349-51.
- Gordon-Larsen P, Nelson M, Beam K. Associations among active transportation, physical activity, and weight status in young adults. Obesity Research 2005;13:868-75.
- Hamer M, Chida Y. Active commuting and cardio-vascular risk: a meta-analytic review. Preventative Medicine 2008;46:9-13.
- Jones L, Davies A, Eyers T. Young people, transport and risk: comparing access and independent mobility in urban, suburban and rural environments. Health Education Journal 2000;59:315-28.
- Julien A, Carré JR. Cheminements pietonniers et exposition au risqué. Recherche Transports Sécurité 2002;76:173-89.
- Killoran A, Doyle N, Waller S, Wohlgemuth C, Crombie H. Transport interventions promoting safe cycling and walking. London: NICE; 2006.
- Crime and disorder on London’s buses. LA Transport Committee; 2008.
- Morris J, Hardman A. Walking to health. Sports Medicine 1997;23:306-32.
- Ogilvie D, Egan M, Hamilton V, Petticrew M. Promoting walking and cycling as an alternative to using cars: systematic review. BMJ 2004;329.
- Ogilvie D, Mitchell R, Mutrie N, Petticrew M, Platt S. Evaluating health effects of transport interventions. American Journal of Preventive Medicine 2006;31:118-26.
- Ogilvie D, Foster CE, Rothnie H, . (on behalf of the Scottish Physical Activity Research Council) . Interventions to promote walking: a systematic review. BMJ 2007;334:1204-1.
- Oja P, Vuori I, Paronen O. Daily walking and cycling to work: their utility as health-enhancing physical activity. Patient Education and Counseling 1998;33:S87-S94.
- Petticrew M, Cummins S, Ferrell C, Findlay A, Higgins C, Hoy C, et al. Natural experiments: an underused tool for public health?. Public Health 2005;119:751-7.
- Preston J. Epilogue: transport research and social exclusion – some reflections. Transport Policy 2009.
- Shiell A, Hawe P, Gold L. Complex interventions or complex systems? Implications for health economic evaluation. BMJ 2008;336:1281-3.
- Making the connections Final report on transport and social exclusion. 2003.
- Sonkin B, Edwards P, Roberts I, Green J. Walking, cycling and transport safety: an analysis of child road deaths. J R Soc Med 2006;99:402-5.
- Shadish W, Campbell D, Cook T. Experimental and Quasi Experimental Designs for Generalized Causal Inference. New York: Houghton Mifflin Co.; 2002.
- Steinbach R, Edwards P, Green J, Grundy C. Road safety of London’s Black and Asian Minority Ethnic Groups. London: LSHTM; 2008.
- Strauss A. Qualitative analysis for social scientists. Cambridge University Press; 1987.
- Synovate Ltd . TfL U16 Free Bus Travel – Research Report n.d.
- Synovate Ltd . Impact of Free Travel for 16–17 Year Olds: Quantitative Research Report 2007.
- Thomas J, . Accidental injury, risk-taking behaviour and the social circumstances in which young people (aged 12–24) live: a systematic review. London: SSRU, Institute of Education; 2007.
- The Stationery Office . Obesity: Third Report of Session 2003–04 2004.
- Wanless D. Securing good health for the whole population: final report. HM Treasury; 2004.
- Watkiss P, Brand C, Hurley F, . On the Move. Informing transport health impact assessment in London. London: NHS Executive. AEA Technology, 2000; 2000.
- WHO . Economic Valuation of Transport Related Health Effects. Review of Methods and Development of Practical Approaches, With a Special Focus on Children 2008.
Glossary
- Active travel
- Travel by modes which require physical exertion, such as cycling and walking.
- Elasticity
- Responsiveness of one variable to another, measured as the proportionate change in the first variable divided by the proportionate change in the second, for small changes.
- Freedom Pass
- Card entitling older citizens and people with disabilities free access to most public transport services within London, paid for by borough councils.
- Natural experiment
- Study of an intervention over which the researcher has no control, but which allows quasi-experimental evaluation (e.g. through comparisons of before and after and/or ‘exposed/non-exposed’ populations).
- Oyster card
- Plastic smart card used to access public transport services within London, which is preloaded with season tickets or cash for ‘pay as you go’ trips.
- STATS19 Road Accident data set
- National statistics on road accidents and the underlying data collection system, involving the police, local government and central government.
- Trip
- A journey from an origin to a destination, which may involve multiple stages by different modes. In quantitative results section, ‘trip’ refers to a whole journey, including all stages, and defined by the ‘main mode’ (by distance).
- Trip mode
- Main mode used for largest (by distance) part of trip.
- Zip card
- Oyster card with photo, used to access free bus and tram travel.
List of abbreviations
- BCR
- benefit : cost ratio
- CBA
- cost–benefit analysis
- CI
- confidence interval
- CO2
- carbon dioxide
- CV
- cardiovascular
- DfE
- Department for Education
- DfT
- Department for Transport
- DLR
- Docklands Light Railway
- GC
- generalised cost
- GLA
- Greater London Authority
- HEAT
- health economic assessment tool
- HES
- Hospital Episode Statistics
- ICD-10
- International Classification of Diseases, Tenth Edition
- IMD
- Index of Multiple Deprivation
- ITS
- Institute for Transport Studies
- LATS
- London Area Transport Survey
- LSHTM
- London School of Hygiene and Tropical Medicine
- LSOA
- lower layer super output area
- LT
- London Transport
- LTDS
- London Travel Demand Survey
- MRC
- Medical Research Council
- NPV
- net present value
- NTS
- National Travel Survey
- PTAL
- public transport accessibility level
- RCT
- randomised controlled trial
- RTI
- road traffic injury
- SD
- standard deviation
- SOA
- super output area
- TfL
- Transport for London
- TGF
- trip generation factor
- VOSL
- value of statistical life
- WHO
- World Health Organization