
Notes
Article history
The research reported in this issue of the journal was funded by the PHR programme as project number 10/3001/04. The contractual start date was in October 2011. The final report began editorial review in April 2014 and was accepted for publication in July 2014. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PHR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
Rona Campbell is a director of DECIPHer IMPACT Ltd, a university-owned not-for-profit company that licenses and supports the implementation of evidence-based health promotion interventions, for which she receives fees paid into a grant account held by the University of Bristol used to support further research activities. She is also a population and public health member of the Wellcome Trust’s Expert Research Group; a fee was paid for the time spent reviewing applications and attending board meetings in London. Adrian Davis is an independent public health consultant on transport planning and health, promoting evidence-based transport policy and practice, and has been paid by Bristol City Council in this capacity.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2015. This work was produced by Audrey et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Introduction
Background
Physical inactivity increases the risk of many chronic diseases, including coronary heart disease, type 2 diabetes, obesity and some cancers. 1 It is currently recommended that adults should aim to undertake at least 150 minutes of moderate intensity physical activity in bouts of 10 minutes or more throughout the week. 2,3 There are concerns that many adults in the UK and other high-income countries do not achieve this,1,3,4 although allowing for the accumulation of 150 minutes in bouts of 10 minutes has led to an estimated 61% of adults in England self-reporting that they do achieve the recommended levels. 5 Increasing physical activity levels, particularly among the most inactive, is an important aim of current public health policy in the UK. 1,6
In addition, there is increasing interest in the relationship between time spent sedentary (defined as any waking sitting or lying behaviour with low energy expenditure [≤ 1.5 metabolic equivalent of task (METs)] and health outcomes. 7 A large amount of time spent sitting has been associated with greater risk of cardiovascular disease, type 2 diabetes, and cardiovascular and all-cause mortality. In addition, a high volume of objectively measured sedentary time has been associated with a poorer metabolic profile in healthy adults and those at risk of and having developed type 2 diabetes. It is of note that these associations are independent of the volume of moderate to vigorous physical activity (MVPA), and consequently UK health guidelines recommend that adults should minimise the amount of time spent sedentary (sitting) in addition to increasing physical activity. 1
There is evidence of the link between adult obesity levels and travel behaviour, one indicator of which is that the countries with the highest levels of active travel generally have the lowest obesity rates. 8 Walking has been described as near-perfect exercise. 9 It is a popular, familiar, convenient and free form of exercise that can be incorporated into everyday life and sustained into older age. It is also a carbon-neutral mode of transport that has declined in recent decades in parallel with the growth in car use. 1 Even walking at a moderate pace of 5 km/hour (3 miles/hour) expends sufficient energy to meet the definition of moderate intensity physical activity. 10 Hence there are compelling reasons to encourage people to walk more, not only to improve their health but also to address the problems of climate change. 11–14
In the UK, there are substantial opportunities to increase walking by replacing short journeys undertaken by car. For example, the 2011 National Travel Survey showed that 22% of all car trips were shorter than 2 miles in length, while 18% of trips of less than 1 mile were made by car. 15 An opportunity for working adults to accumulate the recommended moderate activity levels is through the daily commute, and, in addition, replacing the car for short journeys is likely to reduce sedentary time. Experts in many World Health Organization (WHO) countries agree that significant public health benefits can be realised through greater use of active transport modes. 16 Furthermore, cost–benefit analysis for the UK Department for Transport suggests that the ratio of benefits to costs is high. 17
A systematic review comparing direct versus self-report measures for assessing physical activity in adults found that self-report measures were higher than objective measures in some cases and lower in others. 18 This calls into question the reliability of self-report measures, and indicates that there is no approach to correcting for self-report measures that will be valid in all cases. However, very few studies have objectively measured the contribution of walking, particularly walking to work, to adult physical activity levels; more evidence is needed. 19
In Sweden, two studies examined the association between neighbourhood walkability [measured using a geographic information system (GIS)] and objective physical activity (measured using accelerometers). 20,21 Both studies demonstrate how increased walking rates translate directly to increased MVPA. In the USA, a cross-sectional study included 2364 participants enrolled in the Coronary Artery Risk Development in Young Adults (CARDIA) study who worked outside the home during year 20 of the study (2005–6). 22 Associations were examined between walking or cycling to work and objective MVPA using accelerometers. Active commuting was found to be positively associated with fitness in men and women, and inversely associated with body mass index (BMI), obesity, triglyceride levels, blood pressure and insulin level in men. The authors concluded that active commuting should be investigated as a means of maintaining or improving health.
Systematic reviews have examined the effectiveness of interventions to promote physical activity in general,23–26 but there is less evidence about how best to promote walking to work. Available systematic review evidence has focused on interventions that promote walking; interventions that promote walking and cycling as an alternative to car use; and the effectiveness of workplace physical activity interventions. None focuses specifically on employer-led interventions that promote walking to work, although the studies that have been undertaken are included within the available systematic review evidence.
A systematic review of interventions to promote walking comprised 19 randomised controlled trials (RCTs) and 29 non-randomised controlled studies. 27 The review identified two general characteristics of interventions found to be effective: targeting and tailoring. Only six studies included even a rudimentary economic evaluation. A systematic review of promoting walking and cycling as an alternative to using cars26 identified 22 studies that met the inclusion criteria and found some evidence that targeted behaviour change programmes can change the behaviour of motivated subgroups. A systematic review of the literature regarding the effectiveness of workplace physical activity interventions, commissioned by the National Institute for Health and Care Excellence (NICE), graded 14 studies as high quality or good quality. 28 Three public sector studies provided evidence that workplace walking interventions using pedometers can increase daily step counts. One good-quality study reported a positive intervention effect on walking to work behaviour (active travel) in economically advantaged female employees. There was strong evidence that workplace counselling influenced physical activity behaviour, but the reviewers indicated that there was a dearth of evidence for small- and medium-sized enterprises.
National Institute for Health and Care Excellence public health guidance on workplace health promotion concluded that although a range of schemes exist to encourage employees to walk or cycle to work, little is known about their impact. 29 Few studies used robust data collection methods to measure the impact of workplace interventions on employees’ physical activity levels (most use self-report) and there is a lack of studies examining how workplace physical activity interventions are influenced by the size and type of workplace and the characteristics of employees.
Benefits and risks of walking as active travel
Physical activity is an important element of a healthy lifestyle. In England, the Chief Medical Officer has stated that the target of 30 minutes of moderate intensity activity for adults on at least 5 days per week, in order to promote health, will best be achieved by helping people to build activity into their daily lives. 1 Experts in many Organisation for Economic Co-operation and Development (OECD) countries agree that significant public health benefits can be realised through greater use of active transport modes. 16 Furthermore, the ratio of benefits to costs is high. 17 There are also potential benefits to walkers from reduced commuting costs and greater certainty about the timing of the journey to work. The potential benefits to employers who promote walking to work include a reduction in absenteeism; employees’ increased concentration and mental alertness, and better rapport with colleagues; a reduction in employees being late because of greater certainty about the timing of the journey; improved public image as a result of lowering the workplace’s carbon footprint; and savings in parking costs. 30
Despite the benefits, there are potential risks to pedestrians. For example, in Great Britain in 2008 there were 170,591 reported personal injury road accidents, of which 1 in 6 involved a pedestrian; 572 pedestrians were killed (23% of the total road accident fatalities); 6070 were seriously injured (23% of all seriously injured casualties); and 21,840 were slightly injured (11% of all slightly injured casualties). 31 In 54% of accidents, contributory factors were assigned to pedestrians only (‘pedestrian failed to look properly’ being the most common individual factor). In 25% of accidents, at least one factor was assigned to both a pedestrian casualty and a vehicle (the most common combination being both participants failing to look properly). In 21% of accidents, factors were associated only with vehicles involved (‘failed to look properly’ being the most common vehicle factor). There is also potential for harm in relation to personal safety of walkers where lighting is poor or there is potential for street crime.
Using behaviour change techniques to encourage active travel
Behaviour change techniques (BCTs) have been defined as the ‘active ingredients’ within an intervention designed to change behaviour that are observable, replicable and irreducible components which can be used alone or in combination. 32 A taxonomy of 26 BCTs was identified in 2008,33 with subsequent work undertaken to improve labels and definitions and to reach a wider consensus of agreed distinct BCTs. 32,34 The 2008 taxonomy has been successfully used to categorise the BCTs used in healthy eating and physical activity interventions, with ‘self-monitoring’ combined with at least one other technique identified as the most effective. 35 For walking and cycling interventions that have resulted in behaviour change, the most commonly used techniques are ‘self-monitoring’ and ‘intention formation’. 36 The UK’s NICE has recently issued recommendations advising that interventions should use BCTs based on goals and planning, feedback and monitoring, and social support. 37
The effectiveness of interventions to promote active travel tends to be measured using self-report surveys. Of the 46 walking and cycling controlled interventions coded for BCTs by Bird et al. ,36 21 reported a statistically significant effect using a mean number of BCTs of 6.43 [standard deviation (SD) = 3.92]. However, very few published studies have looked qualitatively at participants’ views of the BCTs used in the intervention.
The socioecological model
Individual behaviour does not occur in a vacuum, but is shaped by external factors. In acknowledging this, initiatives to encourage walking to work can be considered within a socioecological model,38 identifying and exploring intrapersonal, interpersonal, community and organisational factors within the overall policy context. Within this model, BCTs to encourage walking to work operate at the intrapersonal and interpersonal levels, but the ability to implement and act upon them is shaped by policies and practices in the workplace, the neighbourhood and wider society.
Rationale for a feasibility study focusing on walking to work
A number of high-profile active travel initiatives focus on cycling. 39,40 However, walking may be perceived by employees as a cheaper and safer option: it requires no special equipment and is less likely to involve direct competition with motorised traffic for road space. In addition, there is no requirement for employers to provide special parking facilities or changing and showering facilities. Compared with other forms of physical activity, walking is a popular, familiar, convenient, readily repeatable, self-reinforcing, habit-forming activity and the main option for increasing physical activity in sedentary populations. 9,26 There is a dose–response curve to physical activity, so that the greatest health benefits are achieved when the least active undertake some physical activity. In industrialised countries, higher levels of mortality and morbidity from obesity and physical inactivity-related diseases disproportionately affect those in poorer communities. Walking is the most obvious, low-cost, immediate and normative means by which to increase physical activity and may, therefore, help to address health inequalities as well as be beneficial to people across all socioeconomic groups.
At the time of writing the proposal, there was a paucity of information about the design and implementation of interventions specifically promoting walking to work (as opposed to walking for pleasure, walking as part of a rehabilitation programme for a specific health problem, or active transport initiatives which include cycling and walking but tend to promote cycling). This continues to be the case. There was also little, if any, information about differences between small and large workplaces in the delivery or receipt of such interventions. Under such circumstances, the Medical Research Council (MRC) framework for the evaluation of complex interventions emphasises the importance of undertaking a feasibility study before embarking on a phase 3 RCT. 41,42
Phase 1 focuses on existing evidence and theory to inform the development of the intervention and ways to evaluate it. Phase 2 involves testing the feasibility of a full-scale trial, including the ability to recruit and retain participants, the acceptability of the intervention and the methods used for its evaluation. An exploratory trial also provides a sound basis for calculating the sample size for a main trial. As workplace interventions are targeted at the cluster level, an estimate of the intracluster correlation coefficient (ICC) is needed. The Consolidated Standards of Reporting Trials (CONSORT) group has indicated that the conduct and reporting of cluster trials has been poor, including failure to account for clustering in the planning of trials or to account for clustering in the sample size calculations and analysis. 43 Without published data from a full-scale cluster RCT of a workplace intervention to promote walking to work, there was no estimate of the ICC. Estimates from other studies in different settings or using different outcomes may provide some information, but if the ICC is underestimated, then a full trial may be considerably underpowered. Consequently, there was a need to calculate an estimate of the ICC. Furthermore, in order to perform a formal sample size calculation for a definitive cluster trial, a good estimate of likely recruitment and adherence rates and feasible differences in outcome was required. Within a cluster trial, the average cluster size dramatically affects the inflation factor required for sample size.
As well as contributing to statistical analyses, an exploratory trial offers opportunities for process evaluation and estimations of costs. Conducting a process evaluation within a feasibility study enables the examination of the context and delivery of and response to an intervention. Consideration can also be given to the facilitators of and barriers to its successful implementation. In addition, an assessment of the costs and potential benefits of an intervention is required when considering if it is likely to be adopted into routine practice.
Chapter 2 Methods
Study aim and objectives
The overall aim of the research was to build on existing knowledge and resources to develop an employer-led scheme to increase walking to work and to test the feasibility of implementing and evaluating it in a full-scale RCT.
The objectives were:
-
to explore with employees the barriers to and facilitators of walking to work
-
to explore with employers the barriers to and facilitators of employer-led schemes to promote walking to work
-
to use existing resources and websites to develop a Walk to Work information pack to train work-based Walk to Work promoters
-
to conduct an exploratory RCT of the intervention to:
-
pilot workplace and employee recruitment procedures
-
determine eligibility and consent rates
-
examine retention rates
-
pilot cost and outcome measures
-
inform a sample size calculation for a full RCT with estimation of potential feasible differences in outcome
-
gather information regarding variablility within and between workplaces
-
-
to pilot the use of accelerometers and global positioning system (GPS) monitors to measure:
-
eligible employees’ levels of MVPA
-
daily steps taken in walking
-
temporal pattern of physical activity (to identify when activity has increased and whether or not there is a compensatory decrease in activity at other times)
-
route taken and physical activity associated with journey
-
-
to explore any social patterning in uptake of walking to work, particularly in relation to socioeconomic status (SES), age and gender
-
to examine whether or not the size or type of workplace influences uptake of walking to work
-
to assess intervention costs to participating employers and employees
-
to provide preliminary evidence on the cost and economic benefits of the intervention to employers, employees and society.
Research design
During phase 1, a review of current resources that promoted walking (and in particular the benefits of walking to work) was undertaken, and three focus groups with employees plus three interviews with employers were conducted in workplaces (small, medium and large) outside of Bristol to finalise the intervention design. Phase 2 comprised an exploratory randomised trial in Bristol. The trial included an integral process evaluation and an assessment of intervention costs to participating employers and employees.
Setting
The intervention took place in Bristol. With a population of 433,100 people, Bristol is the largest city in the south-west and one of the eight core cities in England, excluding London. 44 The areas of highest population growth are all concentrated around the city centre and nearly half (46%) of all jobs are located in the city centre. 45 A substantial number of people in Bristol make short journeys to work by car. The 2011 census indicated that there are 44,000 people who travel < 5 km to work yet still go by car, of whom 13,000 drive < 2 km. 46 The intervention was implemented in 17 workplaces (eight small, five medium and four large). Seven workplaces received the intervention, and 10 workplaces constituted the control arm.
Workplace recruitment and randomisation
Workplaces were approached through BusinessWest for initial expressions of interest, including willingness to allocate employee time for study activities. A publicly available list of major employers was also used to identify large employers who were not on the BusinessWest mailing list. The e-mail contact included an information leaflet giving details of the study and the expectations of participating employers and employees, with the contact details of the research team. In addition, paper copies were sent out, as it was felt that, for some employers who receive large numbers of e-mails, the e-mail invitation might be deleted as low priority. The paper copy included a pre-paid reply envelope. Workplaces expressing an interest were sent a short questionnaire to enable purposive sampling of pairs (one intervention, one control), with each pair containing workplaces as similar as possible with respect to total number of employees (up to 50, 51–250, 250+),47 location characteristics and type of business. Assignment of workplaces to the intervention group employed computer-generated allocation.
Study participants
Employees living within 2 miles of the workplace (‘walking distance’) were given information about the study, by e-mail or letter as appropriate, to be distributed through the workplace with an invitation to participate. As the study progressed, it was felt that this was too restrictive, and a second round of recuitment was undertaken to include people who lived further away and were willing to incorporate some walking into their daily commute.
The Walk to Work intervention
The socioecological model informed the Walk to Work intervention, which was designed to encourage employers and employees to consider, and where possible address, the facilitators and barriers at each level of the socioecological model (Table 1).
| Socioecological level | Objective |
|---|---|
| Intrapersonal: individual knowledge, skills, attitudes, behaviour | Increase employees’ knowledge of the benefits of walking to work |
| Identify and address perceived personal barriers | |
| Personal goal setting | |
| Change in travel to work routines | |
| Increase employers’ knowledge of the benefits of walk to work schemes | |
| Increase employers’ support for employee walk to work schemes | |
| Interpersonal: influence family, friends, colleagues | Identify and address specific barriers, e.g. school run |
| Colleagues and friends encourage each other to walk to work | |
| Increase ‘culture’ of walking to work | |
| Institutional: workplace policies, procedures and facilities | Enhance employer/workplace support for walking to work |
| Community: built, natural and social environment and local resources | Identify safe, feasible walking routes |
| Identify local groups and organisations to support and enhance walking to work | |
| Public policies: national and local initiatives, policies and plans | Increase employee and employer understanding of national and local policy context, walking initiatives and websites |
The intervention was based on the idea of recruiting and training, with the permission and support of the employer, a ‘champion’ (Walk to Work promoter) within each participating workplace to promote walking to work. The role of these Walk to Work promoters was to promote walking to work with their employer and among eligible employees in their workplace, to be ‘role models’ for the Walk to Work intervention and to be the recognised ‘point of contact’ for the Walk to Work intervention in their place of work.
The intervention focused on nine BCTs which included three categories (goals and planning, feedback and monitoring, and social support) as recommended by NICE. 37 The nine BCTs and the contact points at which they were used are listed in Table 2.
| Contact | BCT | Walk to Work intervention |
|---|---|---|
| 1 (at week 1) | Intention formation | Employee decides to participate in the Walk to Work intervention and try to increase the amount of walking during the journey to and from work |
| Barrier identification | Promoter works with participant to determine the benefits of and barriers to walking to work and some proposed solutions. Participant booklet contains some examples of barriers and possible solutions | |
| Specific goal setting | Promoter and participant agree short- (weeks 1–3), intermediate- (in 1 month) and longer-term (in 3 months) goals. Worked examples provided in employee booklet | |
| Provide instruction | Promoter issues participants with booklet containing practical information, websites and a 10-week diary. Promoter booklet provides instructions on how to support the walkers | |
| Provide general encouragement | Promoter and colleagues provide encouragement and affirmation | |
| Self-monitoring of behaviour | Participants asked to keep an optional record of walking behaviour in a diary. Promoter issues each employee with optional pedometer to monitor steps walked per day and allow them to record steps in the diary | |
| 2 (from week 3) | Techniques in contact 1 as appropriate | Participants encourage and support each other in changing their behaviour. Promoter offers assistance, encouragement, guidance and motivation to the employee. Participants encouraged to seek support from people outside the workplace, such as family and friends |
| Plan social support | ||
| 3 (from week 5) | Techniques in contact 1, 2 as appropriate | Promoter reviews intentions and short-, intermediate- and long-term goals to better suit the employee as necessary |
| Review of behaviour goals | ||
| 4 (from week 7) | Techniques in contact 1, 2, 3 as appropriate | Promoter identifies situations likely to result in participants readopting old behaviour or failure to maintain walking and helps to plan to avoid or manage them, recognising that it take several attempts before walking to work becomes a habit |
| Relapse prevention |
Following the resource review and focus groups during phase 1, members of the research team developed booklets for Walk to Work promoters and participating employees. The packs included information about the health, environmental, economic and social benefits of walking to work derived from, for example, Walk4Life (www.walk4life.info), Walkit.com urban route planner and Living Streets (www.livingstreets.org.uk). Specific BCTs used were providing information on the link between walking and health; identifying barriers and ways to overcome them; goal setting and review of goals; prompting self-monitoring by use of a travel diary and pedometer; providing social support and encouragement; and relapse prevention. There is evidence that these techniques can effect behaviour change. 33,36
There were four main stages of the intervention:
-
Eligible employees were identified through workplace records (matching postcodes of workplace and home address, and checking for disability status or other disqualifying factors, e.g. delivery drivers).
-
Walk to Work promoters, either volunteers or those nominated by participating employers, were trained by expert members of the research team about the health, social, economic and environmental benefits of walking to work and how to identify and promote safe walking routes for employees. This half-day training took place at the University of Bristol for those who were able to attend. Those who were not were given an individual training session at their place of work. All Walk to Work promoters were given a booklet to guide them in their role, as well as Walk to Work booklets and pedometers for participating employees. They were also trained to access relevant websites and toolkits (e.g. Walkit.com, Living Streets). The aim was a maximum of 25 participants to each Walk to Work promoter.
-
The Walk to Work promoters were asked to discuss the Walk to Work intervention with study participants in their workplace and to ask those who were interested in walking to work to ‘sign up’ at this stage. The promoters were also encouraged to identify safe, feasible walking routes for their colleagues and to help them to set goals for walking to work.
-
Further encouragement was to be provided through four contacts from the Walk to Work promoter over the following 10 weeks (face to face, e-mail or telephone, as appropriate for the workplace). The Walk to Work promoters were encouraged to focus on specific BCTs as outlined in Table 2.
During the first contact with the Walk to Work promoters, those who agreed to try changing their travel behaviour were asked to identify barriers, propose solutions and develop a plan of how they might increase walking. This involved setting short-, intermediate- and long-term goals, for example walking 1 day per week in the first week and then increasing it during the course of the intervention. Participants were issued with a Walk to Work booklet and pedometer. They were also encouraged to complete diary sheets and record whether or not they had walked and, for those using pedometers, how many steps had been registered.
The promoters were asked to make three further contacts with participants, in person, by e-mail or by telephone according to the needs of the workplace and employees. Week 3 (contact 2) focused on social support from other people, such as colleagues, family or friends; week 5 (contact 3) stressed a review of goals to see whether they had been achieved or needed to be adjusted; and from week 7 (contact 4) until the end of the intervention, the aim was to prevent relapse by supporting and encouraging participants to continue working towards their goals.
Assessment of harms
Although this was a low-risk intervention, the team were mindful of the potential for harm in terms of road traffic accidents; personal safety of walkers where lighting is poor or there is potential for street crime; difficulties experienced by Walk to Work promoters, including disrupting usual working relationships and employers’ attitudes towards time taken out of usual work activities; and costs to employers, including disruption to work routines, of permitting the intervention during working hours. It was also possible that people with low activity and no history of walking would suffer initial muscle stiffness. To address these issues, the Walk to Work booklets included advice about setting appropriate goals and personal safety. Participating employers were given information in advance about the level of time commitments and the potential benefits of the scheme. Employers and employees were given the contact details of the principal investigator to report any adverse incidents, which would then be recorded and kept on file, with any relevant participants informed immediately (e.g. other employees taking a similar route across a dangerous road or through a dimly lit area with a high rate of street crime).
Outcome measures
Because this was a feasibility study, the outcomes did not relate to the effectiveness of the intervention but to the feasibility of, and requirements for, a full-scale trial. Several items were identified relating to the trial design, physical activity measurement, the context, delivery and receipt of the intervention, and the assessment of costs. The main study outcomes are listed in Table 3.
| Category | Outcomes |
|---|---|
| Trial design | Workplace recruitment and retention rates |
| Employee eligibility, recruitment and retention rates | |
| Sample size calculation with estimation of potential clustering within workplaces and potential feasible differences in outcome | |
| Physical activity | Overall level of physical activity (cpm) |
| MVPA | |
| Temporal pattern of physical activity (when activity has increased and any compensatory decrease) | |
| Physical activity associated with the journey to work | |
| Process | Context, delivery and receipt of the intervention from the perspectives of employers, Walk to Work promoters, employees |
| Evidence of social patterning in uptake of walking to work (SES, age, gender, location) | |
| Identified interpersonal, intrapersonal, community and organisational facilitators of and barriers to walking to work | |
| Costs | Costs and benefits to employers of implementing the scheme |
| Costs and benefits to employees of participating in the scheme | |
| Health service use for general health problems and specific commute-related adverse events |
Assessment and follow-up
At the baseline data collection (DC1), participants in the intervention and control arms were asked to complete a questionnaire giving basic personal data, including postcode (to assess distance from home to work), job title, mode of transport to work, before- and after-work ‘routines’ affecting travel mode (e.g. school run), typical commuting costs, household car ownership, commute-related adverse events, health service use and views about walking. Eligible employees were also asked to wear an accelerometer for 7 days from waking in the morning until going to bed at night to provide an objective measurement of physical activity (including intensity and step counts), and a personal GPS receiver during the journey to and from work to confirm the duration of the journey and quantify its contribution to overall physical activity. The GPS recorded location and speed at 10-second intervals while outdoors. Participants were required to turn it on at the start of the journey to work and off when the journey home ended, as the battery life was only 24 hours. Participants were also given small chargers for the monitors, with written instructions. A £10 gift voucher was given to participants who returned accelerometers and GPS receivers.
Immediately post intervention (DC2), questionnaires were administered in the intervention and control arms to explore attitudes towards and experiences of walking to work, including perceived barriers and facilitators and emotional and physical well-being. Additional questions about the acceptability of the intervention were included for the intervention arm only. At 1-year follow-up (DC3), questionnaires, accelerometers and GPS receivers were administered again in the intervention and control arms (as per baseline protocol).
Measuring physical activity
To address the potential for the time of year to confound differences in the trial arms, the outcome data were collected simultaneously in each ‘pair’ of workplaces.
Physical activity was measured objectively using accelerometers (ActiGraph GT3X+; ActiGraph LLC, FL, USA) worn on a belt around the waist during waking hours for 7 days and removed for swimming and bathing. Accelerometers were set to record data at 30 Hz. The protocol, decisions and outcomes for analysis of accelerometer data are listed in Table 4.
| Decisions | Outcomes |
|---|---|
| Initialising | Accelerometers initialised to start on day after distribution for 7 days including a weekend |
| Data collection points | DC1, DC3 |
| Protocol | Single ActiGraph GT3X+ monitor, worn around the waist over the same hip during waking hours (except when swimming/bathing/showering) |
| Wear time | 6.00 a.m. to midnight |
| Valid length of day | 10 hours (600 minutes) |
| Days required | 3 working days |
| Epoch length | 10 seconds |
| Zero counts | Bouts of 20 minutes of continuous/consecutive zero counts excluded |
| Spurious data | > 15,000 cpm |
| Missing data | No imputation |
| Activity cut-point | Moderate: 2000 cpm |
| Outcomes |
|
Participants also wore a personal GPS receiver (QStarz BT-Q1000XT, Qstarz International Co. Ltd, Taiwan) on the same belt during their commuting journeys for 7 days to allow the journey to and from work to be spatially described. GPS data were recorded at 10-second intervals and, where possible, the ‘assisted GPS’ mode was used to enhance the precision of the GPS location data.
Raw accelerometer data were downloaded using Actilife 6 software (ActiGraph LLC, FL, USA) and reintegrated to 10-second epochs for analysis and matching with GPS data. Reintegrated accelerometer data were processed using Kinesoft (v3.3.62; KineSoft, Saskatchewan, Canada) data reduction software to generate outcome variables. Continuous periods of 20 minutes of zero values were considered to be ‘non-wear’ time and removed. Outcome variables were physical activity volume [mean daily accelerometer counts per minute (cpm)] and intensity (MVPA and sedentary time) defined using validated thresholds (sedentary < 100 cpm; MVPA > 952 cpm). 48
Combining accelerometer and global positioning system data
Accelerometer and GPS data were combined (accGPS) based on the timestamp of the ActiGraph data. For measurement of the journeys to and from work, the participant’s workplace and home were geocoded using the full postcode, and imported into GIS software (ArcMap v10, Esri, Redlands, CA, USA). The merged accGPS files were then imported into ArcMap and journeys to and from work were visually identified and segmented from other accGPS data using the ‘identify’ tool. Journeys were identified as a continuous (or near-continuous) sequence of GPS locations between the participant’s home and workplace, and thus included trips to other destinations (e.g. supermarkets) if taken as part of the journey to or from work.
Baseline data analysis: the contribution of walking to work to physical activity
A cross-sectional study was undertaken using the baseline data to assess the contribution of walking to work to physical activity levels. 49 Analyses were confined to data recorded between 6.00 a.m. and midnight. Participants recorded travel mode to and from work for each day, and only days where participants used the same mode of transport both to and from work were included in the initial analyses, to allow classification as either an active commuter (walk or cycle) or a car user on each day. For participants who recorded using a mixed mode (e.g. walk and bus) for a journey, the mode of transport of the longest duration was considered to be their mode for that journey. If the modes were of equal duration, that day of data was excluded.
Participants who cycled to work (n = 19) were excluded from analyses because of the inability of waist-worn accelerometers to accurately record physical activity during cycling, as were the small number (n = 7) using ‘other’ modes of travel. Where a travel diary was not completed, usual travel mode was determined from the baseline behaviour questionnaire where possible (n = 10). Differences in physical activity between travel modes (walking/car) were analysed by one-way analysis of variance (ANOVA). Paired samples t-tests were used to compare weekday and weekend values for total physical activity (cpm), MVPA and time spent sedentary, and to investigate differences in the volume of MVPA accumulated between overall accelerometer data and spatially segmented trips. Linear regression was used to explore the association between travel mode (walking/car) and total weekday physical activity (cpm) and MVPA (minutes per day). Models were adjusted for possible confounders [age, sex, education (educated to degree level or not)], and accelerometer wear time.
Statistical methods
Statistical analyses were largely descriptive. Reasons for non-eligibility, refusing consent and withdrawing from the study were fully documented. Within the intervention group, differences between employees who do and do not walk to work were explored, particularly in relation to SES, age and gender. Such exploration is hypothesis generating but may be investigated further in a full trial. In addition, such differences were examined to inform changes to the implementation or design of the ‘Walk to Work’ intervention and its evaluation prior to a full RCT.
Analyses of outcomes to be used as primary outcomes for a full trial were carried out at the employee level using multilevel regression models to account for the effects of clustering within workplaces. Models were adjusted for baseline and covariates including age, gender and SES. As an exploratory trial, the proposed study was not powered to provide a definitive comparison between the intervention and control groups. However, estimates of effect and 95% confidence intervals (CIs) were generated. CIs informed feasible effect sizes to be incorporated into sample size calculations for a full trial. The intracluster correlation was estimated to provide some information about variability within and between workplaces to inform the sample size calculation for a full trial.
Process evaluation
The process evaluation examined the context, delivery and receipt of the intervention from the perspectives of employers, Walk to Work promoters and employees. Researcher notes were taken at each stage of the intervention, i.e. recruitment of workplaces, recruitment of study participants, and the recruitment and training of Walk to Work promoters. In addition, post-intervention interviews were conducted with a purposive sample of employees who increased walking to work and employees who did not. A senior manager and the Walk to Work promoter(s) in each workplace were also interviewed. Process data were also gathered through the behaviour questionnaires administered at baseline, immediately post intervention and at 1-year follow-up. An outline of the process evaluation is provided in Table 5.
| Stage | Method | Issues examined |
|---|---|---|
| Recruiting and randomising workplaces | Letter to all workplaces | Response rates Expressions of interest |
| ‘Matching’ and randomising | Ability to ‘match’ by size, type of workplace, location, proportion of eligible employees Randomisation process Response to randomisation |
|
| Baseline | Questionnaires | Interpersonal, intrapersonal, community and organisational facilitators of and barriers to walking to work |
| Interviews with employers | Views about employer-led schemes to encourage walking to work, perceived facilitators and barriers, context (including routes, working practices, car parking facilities at the workplace) | |
| Recruiting Walk to Work promoters | Baseline interview with employers in intervention arm | Rationale/method used for choice of Walk to Work promoter(s) |
| Training Walk to Work promoters | Researcher observations | Attendance Context Style and content of training Participants’ views of training/issues raised |
| Evaluation pro forma completed by trainers and Walk to Work promoters | ||
| Immediately post intervention | Questionnaires with all eligible employees (intervention and control arms) | As per baseline questionnaires for all eligible employees Additional questions for employees in workplaces that received the intervention about the context, delivery and receipt of the intervention |
| Interviews with purposive sample of employees who have increased walking to work and employees who have not | Views about the context, design, delivery and receipt of the intervention Interpersonal, intrapersonal, community and organisational facilitators of and barriers to walking to work |
|
| Interviews with manager in each participating workplace (intervention arm) | ||
| Interviews with Walk to Work promoters | ||
| One-year follow-up | Questionnaires with all eligible employees (intervention and control arms) | As per baseline questionnaires for all eligible employees |
Descriptive statistics were compiled, for example of recruitment and retention. Qualitative analyses employed the framework method of data management, with textual data placed in charts in relation to specific research questions and then scrutinised for differences and similarities within emerging themes, keeping in mind the context in which these arose.
Qualitative data collection and analysis
Interviews with employers/managers from five workplaces, and focus groups with employees at three workplaces, were conducted during the phase 1 developmental work; these workplaces were not then recruited to the phase 2 exploratory trial. The aim was to explore the participants’ views of walking to work and, in particular, the proposed intervention and evaluation methods. During phase 2, baseline interviews were conducted with employers/managers (n = 12) of participating workplaces to understand the context of the workplaces, their views about travel to work, reasons for participating in the study and their opinions about the proposed intervention and its evaluation.
Immediately post intervention, 36 interviews were conducted with a purposive sample of participating employers and managers, Walk to Work promoters, and employees who had attempted to change their travel behaviour and those who had not. In addition, to further investigate issues relating to the recruitment of workplaces, semistructured interviews were conducted at six workplaces with employers/managers who had initially expressed an interest in the study but did not participate.
The focus groups and semistructured interviews were conducted in a private room at the workplaces of the participants. A topic guide was developed as part of the process evaluation to examine the context, delivery and receipt of the intervention. The topic guide allowed flexibility for participants to raise issues and follow their own train of thought, as well as including specific prompts. All interviews were audio recorded, fully transcribed and anonymised, and electronically stored in a secure folder.
The framework approach for data management was used to aid qualitative analysis. 50,51 The interview transcripts were read and reread, and textual data were placed in charts focusing on key research questions. The charts were scrutinised and each unit of data was subsequently coded. For example, the charts relating to the use of BCTs focused on barriers and enablers to walking to work, and the extent to which the BCTs facilitated change in travel behaviour. The charts relating to employers’ views of the intervention focused on employers’ views of the advantages and disadvantages of employer-led schemes to promote walking to work, and whether or not they felt that it was possible for employers to promote active travel.
Assessment of costs
Trainer time was costed using basic salary, national insurance and superannuation, and, where external consultants were employed, their day rate was divided by eight in order to identify a unit cost per hour. The number of promoters and number of individuals participating in the intervention at each workplace was recorded, which allowed us to estimate the number of promoter and employee booklets required. The booklets were printed by the University of Bristol print services and paid for by a small grant from Bristol City Council. The unit cost of pedometers, which were provided free of charge to the trial, was estimated from an online supplier (Be-Active Ltd, www.be-activeltd.co.uk/step-counter.htm).
The delivery of the promoter training day was planned to take place outside the workplace. However, it was not feasible for all of the promoters to attend these training days and therefore some promoter training was provided in the workplace. For training days outside the promoter workplace, costs included trainer and consultant time, lunch and drinks, and room hire. The unit cost of promoter time was calculated by dividing the upper quartile weekly earnings by the median number of hours worked per week. 52 The upper quartile was applied as it was believed that promoters were likely to be on a higher wage than the average worker. Promoter expenditure was also included with respect to travel to the promoter training day location. The cost per mile was calculated using the AA schedule of motoring costs. 53 Promoter training at the workplace included the cost of the trainer, travel costs to the workplace for the trainer, and promoter time.
Health service use in the past 4 weeks was self-reported by study participants at baseline and 1-year follow-up. Table 6 provides the unit costs that were used to value health service use. Primary care, including general practitioner (GP) visits, nurse visits, GP calls and nurse calls, was costed using national unit cost estimates. 54 All hospital-based care was costed using Department of Health reference costs. 55 Acupuncture and chiropractic care were costed using the NHS choices website. 56,57 Physiotherapy, chiropractic care, acupuncture, midwife visits, counselling and walk-in services were grouped together under ‘other care’ for the analysis. Routine dental and optician appointments were excluded from the analysis and a few health-care items were excluded because of lack of information on what service the participant had received. Medications were costed using the Prescription Cost Analysis. 58 Where medications could not be costed because of missing information on the number of days taken, it was assumed for chronic conditions and contraception that the medications were taken daily. For medications with missing information on the number of doses per day, an assumption of one dose was made. Any medications that could not be costed due to lack of sufficient information were excluded.
| Resource | Unit cost (£) |
|---|---|
| Face-to-face appointment with a doctor at the GP surgery | 43.00 |
| Face-to-face appointment with a nurse at the GP surgery | 13.69 |
| Telephone consultation with a doctor at the GP surgery | 26.00 |
| Telephone consultation with a nurse at the GP surgery | 8.28 |
| Hospital accident and emergency department | 108.00 |
| Hospital outpatient appointment | 106.00 |
| Hospital admission | 1096.00 |
| Face-to-face appointment with community physiotherapist | 33.00 |
| Face-to-face consultation with a counsellor at the surgery | 59.00 |
| Walk-in services not leading to admission | 41.00 |
| Antenatal or postnatal community midwife visit | 59.73 |
| Initial or further acupuncture session | 42.50 |
| Appointment with the chiropractor | 37.50 |
Self-assessed productivity based on the extent to which health problems affected it in the past 7 days was measured on a 10-point scale, where 1 indicated that health problems had no effect on an individual’s work and 10 indicated that health problems completely prevented work. Absence from work was also self-reported, whereby participants were asked to report the number of hours of work they had missed in the past 7 days because of health problems. 59
Information regarding the commute was recorded for 1 week at baseline and at 12-month follow-up in a travel diary. Time spent commuting by mode of transport, daily expenses (e.g. bus fare) associated with the commute and occasional expenses of commute (including bus and train passes and parking permits) were all recorded. A cost per mile of 0.665 pence53 and an average speed of 15.7 mph60 were used to calculate a cost per minute of driving, which was multiplied by the number of minutes driving in order to calculate the cost of commuting by car. Cost and duration of parking permits, bus and train passes were used to calculate weekly parking permit, bus and train costs. Car sharing was incorporated into the costs of car travel by dividing the cost of driving and the cost of a parking permit by the number of people in the car.
Study timetable and milestones
The study timetable is summarised in Table 7. To allow for seasonality, data collections took place concurrently in each ‘matched’ pair of workplaces (one in the intervention, the other in the control arm). In addition, baseline (DC1) and 1-year follow-up (DC3) data collections were undertaken in the same season (April to June).
| Milestone | October–December 2011 | January–March 2012 | April–June 2012 | July–September 2012 | October–December 2012 | January–March 2013 | April–June 2013 | July–September 2013 | October–December 2013 |
|---|---|---|---|---|---|---|---|---|---|
| Ethics application and approval | ✓ | ||||||||
| Resource review | ✓ | ||||||||
| Phase 1 focus groups and interviews | ✓ | ||||||||
| Transcription and analysis | ✓ | ||||||||
| Phase 2 recruit and randomise workplaces | ✓ | ||||||||
| Prepare Walk to Work packs | ✓ | ||||||||
| DC1 | ✓ | ||||||||
| DC1 data entry | ✓ | ||||||||
| Identify eligible employees | ✓ | ||||||||
| Recruit and train Walk to Work promoters | ✓ | ||||||||
| Implement Walk to Work intervention | ✓ | ✓ | |||||||
| Post-intervention data collection | ✓ | ||||||||
| Post-intervention interviews | ✓ | ||||||||
| DC2 data entry and transcription | ✓ | ✓ | |||||||
| One-year follow-up | ✓ | ||||||||
| DC3 data entry | ✓ | ||||||||
| Data analysis | ✓ | ✓ | ✓ | ✓ | ✓ | ||||
| Paper writing and dissemination | ✓ | ✓ |
Public involvement
The public were involved in shaping the intervention through the phase 1 focus groups with employees in three workplaces and the individual interviews with employers in five workplaces. Their views were sought on the design of the Walk to Work intervention and its evaluation, including the use of accelerometers and GPS monitors. Data from these focus groups and interviews shaped the intervention and its evaluation. Additional interviews were conducted with employers (n = 15) and employees (n = 33) following implementation of the intervention during the phase 2 exploratory trial. Participants identified a number of improvements that could be made, should an application for a full-scale trial be made: a simplified recruitment process, greater flexibility for attending the Walk to Work promoter training, and provision of additional information to employers in the intervention arm about changes they can make in the workplace to support employees who are attempting to increase walking to work. Representatives of non-academic organisations also influenced the study: a director of Sustrans advised on promoting active travel; a transport consultant with Bristol City Council helped to design and implement the training programme; and representatives of BusinessWest advised on, and supported, the recruitment of workplaces.
A feedback event was held in February 2014. Employees, employers and Walk to Work promoters attended a half-day event at which the research team presented findings, and participants were invited to give feedback on the intervention and its evaluation. Expressions of interest were collected for a public advisory group should a full-scale trial be funded for wider implementation.
Changes to protocol
There were no major changes to protocol. The number of workplaces recruited was increased because of the smaller-than-anticipated cluster size. Recruitment of employees was extended to include employees who lived further than 2 miles from the workplace. A request for a 3-month non-financial extension was granted towards the end of the study.
Chapter 3 Results
Wider context
Two important factors are likely to have influenced recruitment to the study and the actions and attitudes of participants. The study took place in the aftermath of a global banking crisis. 61 This resulted in economic insecurity, with businesses restructuring and an increase in unemployment. Under these circumstances, health promotion interventions may be seen as less important to employers and employees than the survival of businesses and the retention of jobs. Secondly, the intervention was implemented during the wettest summer in the UK for 100 years. 62 Weather conditions have been identified as an important barrier to walking and this is likely to have been exacerbated by the weather during the summer of 2012.
Workplace recruitment and retention
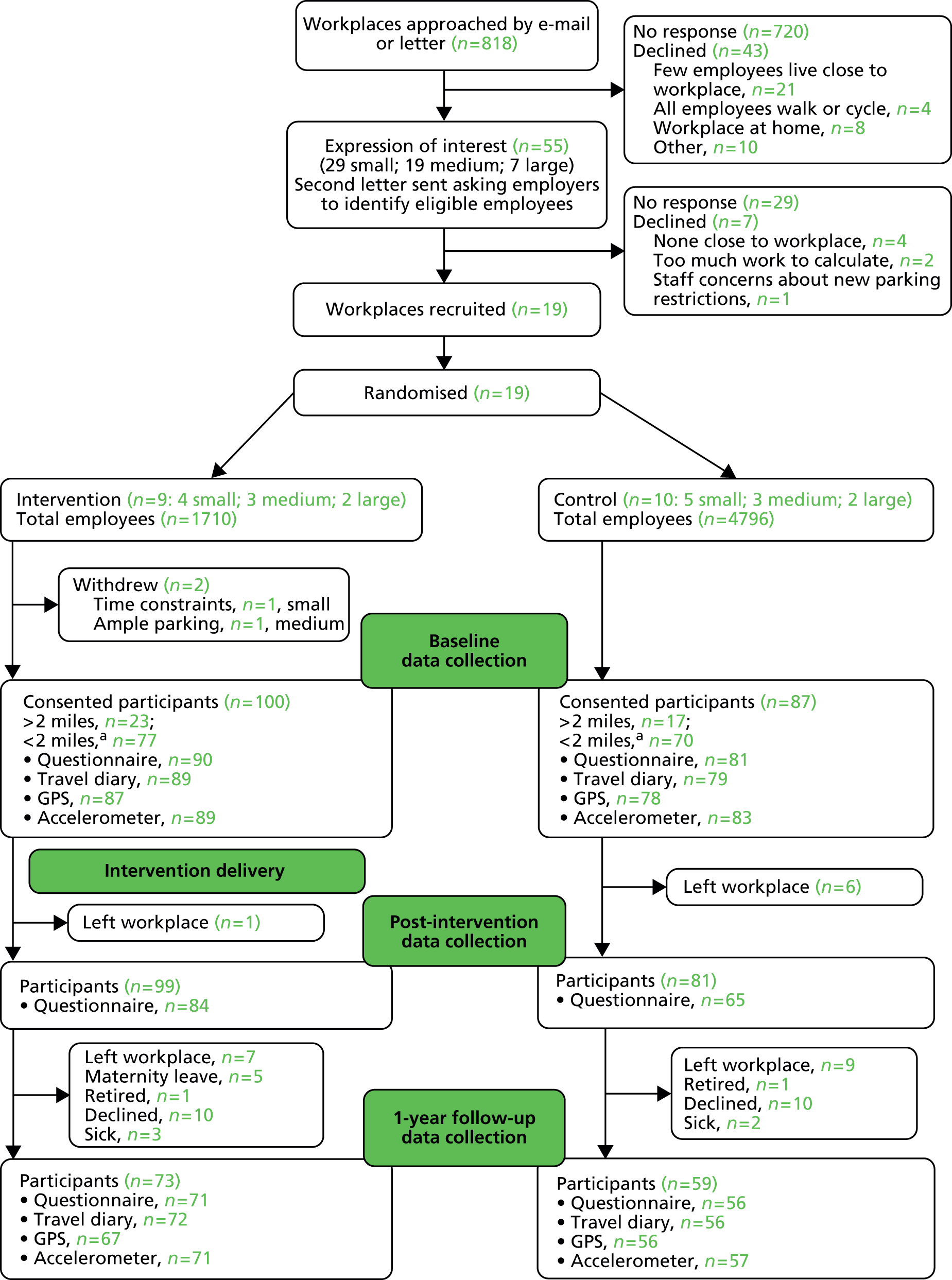
A summary of workplace recruitment is included in Figure 1. Following an e-mail sent through the Chambers of Commerce contact list, and a paper mailing to workplaces included in a publicly available list of large employers, 55 workplaces expressed an interest in the study. Small and medium-sized workplaces appeared more interested than large workplaces. A short questionnaire was sent to those expressing an interest, asking about the type of business and size of workplace, and with a request to assess the number of employees living within 2 miles of the workplace by inserting relevant postcodes into a calculator on the Walkit.com website. A list of the first four digits of postcodes likely to contain relevant employees was also supplied, to reduce the number of postcodes to be checked. Nevertheless, this task appears to have been too onerous for some employers, and 19 workplaces returned the completed questionnaire, of which 17 continued through to DC1 (Table 8). These workplaces were willing to continue throughout the study, although in one large factory in the control arm (workplace 28) there was only one participant, who retired before the 1-year follow-up data collection.
FIGURE 1.
Consolidated Standards of Reporting Trials: Walk to Work flow of workplaces and participants. a, Target participants were those living < 2 miles from the workplace who did not walk or cycle to work.
| Workplace ID | Sizea | Type of businessb | Location | Trial arm |
|---|---|---|---|---|
| 11 | Small | Professional, scientific and technical | City centre | Intervention |
| 12 | Small | Manufacturing | City centre | Control |
| 13 | Small | Professional, scientific and technical | City centre | Control |
| 14 | Small | Professional, scientific and technical | City centre | Intervention |
| 15 | Small | Professional, scientific and technical | City centre | Control |
| 20 | Small | Professional, scientific and technical | Suburban | Intervention |
| 21 | Small | Transportation | Suburban | Control |
| 22 | Small | Professional, scientific and technical | City centre | Control |
| 17 | Medium | Education | Suburban | Control |
| 18 | Medium | Professional, scientific and technical | City centre | Intervention |
| 19 | Medium | Accommodation and food services | City centre | Control |
| 23 | Medium | Manufacturing | City centre | Intervention |
| 24 | Medium | Education | City centre | Control |
| 25 | Large | Public administration | City centre | Intervention |
| 26 | Large | Manufacturing | City centre | Control |
| 27 | Large | Financial and insurance activities | City centre | Intervention |
| 28 | Large | Manufacturing | Suburban | Control |
Participant recruitment and retention
Characteristics of the 187 participants recruited are summarised in Table 9 and the flow of workplaces and participants through the study is described in Figure 1. There was a balance of males and females and an overall mean age of 37.8 years, with a range from 17.3 to 67 years. The participants were predominantly white (77%), well educated (with 60% having a degree or higher qualification) and employed in sedentary (desk-based) occupations.
| Characteristics | Control (N = 87), n (%) | Intervention (N = 100), n (%) | All (N = 187), n (%) |
|---|---|---|---|
| Gender | |||
| Male | 46 (52.9) | 43 (43.0) | 89 (47.6) |
| Female | 41 (47.1) | 57 (57.0) | 98 (52.4) |
| Age (years) | |||
| Mean (SD) | 36.8 (± 12.4) | 38.7 (± 11.7) | 37.8 (± 12) |
| Range | 17.3–64.8 | 21.6–67 | 17.3–67 |
| Ethnicity | |||
| White British | 65 (74.7) | 79 (79.0) | 144 (77.0) |
| White other | 11 (12.6) | 8 (8.0) | 19 (10.2) |
| Mixed ethnic group | 1 (1.1) | 1 (1.0) | 2 (1.1) |
| Asian or Asian British | 3 (3.4) | 1 (1.0) | 4 (2.1) |
| Chinese | 0 (0.0) | 1 (1.0) | 1 (0.5) |
| Not disclosed/missing | 7 (8.1) | 10 (10.0) | 17 (9.1) |
| Education | |||
| PhD, master’s degree, NVQ level 5 | 20 (23.0) | 17 (17.0) | 37 (19.8) |
| Degree, NVQ level 4 | 34 (39.1) | 41 (41.0) | 75 (40.1) |
| BTEC (Higher) or equivalent | 4 (4.6) | 3 (3.0) | 7 (3.7) |
| GCE ‘A’ Level, NVQ level 3 | 7 (8.0) | 13 (13.0) | 20 (10.7) |
| BTEC (National) or equivalent | 5 (5.8) | 2 (2.0) | 7 (3.7) |
| GCSE grades A to C or equivalent | 8 (9.2) | 9 (9.0) | 17 (9.1) |
| No formal qualifications | 0 (0.0) | 2 (2.0) | 2 (1.1) |
| Other | 0 (0.0) | 1 (1.0) | 1 (0.5) |
| Not disclosed/missing | 9 (10.3) | 12 (12.0) | 21 (11.2) |
| Income | |||
| Up to £10,000 | 6 (6.9) | 0 (0.0) | 6 (3.2) |
| £10,001–20,000 | 7 (8.1) | 9 (9.0) | 16 (8.6) |
| £20,001–30,000 | 7 (8.1) | 15 (15.0) | 22 (11.8) |
| £30,001–40,000 | 14 (16.1) | 15 (15.0) | 29 (15.5) |
| £40,001–50,000 | 11 (12.6) | 13 (13.0) | 24 (12.8) |
| More than £50,000 | 24 (27.6) | 26 (26.0) | 50 (26.7) |
| Don’t know | 9 (10.3) | 6 (6.0) | 15 (8.0) |
| Not disclosed/missing | 9 (10.3) | 16 (16.0) | 25 (13.4) |
| Occupation activity level | |||
| Sedentary | 57 (65.5) | 83 (83.0) | 140 (74.9) |
| Standing | 20 (23.0) | 4 (4.0) | 24 (12.8) |
| Manual | 3 (3.5) | 3 (3.0) | 6 (3.2) |
| Not disclosed/missing | 7 (8.0) | 10 (10.0) | 17 (9.1) |
Walk to Work promoters’ recruitment and training
Walk to Work promoters were recruited in each of the workplaces randomised to the intervention arm (Table 10). Of the 10 Walk to Work promoters trained, six were female and four were male.
A single half-day group training event for all Walk to Work promoters had been planned. However, it did not prove possible to timetable a training event to suit all workplaces. Consequently, two smaller training events were organised at the University of Bristol, and three visits were made to individual workplaces for on-site training.
| Workplace ID | Workplace sizea | Gender | Training venue |
|---|---|---|---|
| 11 | Small | Female | Workplace |
| 14 | Small | Male | University |
| 20 | Small | Male | University |
| 18 | Medium | Female × 2 | University |
| Male × 2 | Workplace | ||
| 23 | Medium | Female | Workplace |
| 25 | Large | Male | University |
| 27 | Large | Female × 3 | University |
At the training, the Walk to Work promoters received general information about the benefits of walking to work and were taken through the stages of a Walk to Work promoters’ booklet outlining their role and the BCTs to be used with participants during each of the four contacts over the 10-week intervention period. The session ended with further information about publicly available resources and websites that could be also be accessed and used to promote walking.
Qualitative data from the post-intervention (DC2) interviews suggest that the promoters found the training day useful: ‘I thought it was useful, I mean a lot of it was sort of stuff I knew already but it all sort of brought it together really’ (male, aged 30, workplace 25); ‘It was good, it was really informative that day’ (male, aged 29, workplace 20). One promoter (female, aged 45, workplace 27) commented that ‘It was good to work with other people from other companies’. Overall, the promoters found that their booklets were ‘well set out’ (male, aged 38, workplace 18) and gave clear guidance on the role: ‘It’s not too intimidating, it’s quite accessible, it’s got a, sort of a structure you can work through, when the Walk to Work promoter meets with the employees to discuss and set goals and review them’ (male, aged 30, workplace 25). However, one promoter said that he was ‘disappointed with myself getting out of sync and not following it properly because it guides you well but I lost sight of which week I was on and what I was supposed to be achieving’ (male, aged 38, workplace 18). Another suggested that more support and encouragement for the promoters would have been helpful, for example ‘each week, like, e-mail a newsletter just to remind you about the entire thing and kind of give you more information to convince you to keep on doing it’ (male, aged 29, workplace 20).
Assessment of costs
Intervention costs
The fixed costs of the intervention are provided in Table 11.
| Equipment/printing | Number of units | Cost per unit (£) | Total cost (£) | Total academic cost (£) |
|---|---|---|---|---|
| Printing cost of employee booklet | 20 | 0.81 | 16.20 | |
| Printing cost of promoter booklet | 10 | 0.81 | 8.10 | |
| Pedometers | 20 | 9.80 | 196.00 | |
| Total | 220.30 |
A breakdown of the cost of each type of training is provided in Table 12.
| Number of units | Cost per unit (£) | Total cost (£) | Distance (miles) | Cost per mile (£) | Total cost (£) | Academic cost (£) | Business cost (£) | Promoter cost (£) | Total cost (£) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Promoter training day at Bristol University | ||||||||||
| 31 May 2013 | ||||||||||
| Research associate | 3.5 | 28.86 | 101.01 | 101.01 | 101.01 | |||||
| Research fellow | 3.5 | 33.57 | 117.50 | 117.50 | 117.50 | |||||
| Consultant 2 | 3.5 | 87.50 | 306.25 | 306.25 | 306.25 | |||||
| Room hire | 1 | 395.00 | 395.00 | 395.00 | 395.00 | |||||
| Lunch and drinks | 1 | 60.50 | 60.50 | 60.50 | 60.50 | |||||
| Promoter workplace 18 | 5 | 19.05 | 95.25 | 10 | 0.665 | 6.65 | 95.25 | 6.65 | 101.90 | |
| Promoter workplace 14 | 5 | 19.05 | 95.25 | 10 | 0.665 | 6.65 | 95.25 | 6.65 | 101.90 | |
| Subtotal | 1184.06 | |||||||||
| 11 July 2013 | ||||||||||
| Research associate | 3.5 | 28.86 | 101.01 | 101.01 | 101.01 | |||||
| Research fellow | 3.5 | 33.57 | 117.50 | 117.50 | 117.50 | |||||
| Consultant 2 | 3.5 | 87.50 | 306.25 | 306.25 | 306.25 | |||||
| Room hire | 1 | 395.00 | 395.00 | 395.00 | 395.00 | |||||
| Lunch and drinks | 1 | 61.95 | 61.95 | 61.95 | 61.95 | |||||
| Promoter workplace 20 | 5 | 19.05 | 95.25 | 10 | 0.665 | 6.65 | 95.25 | 6.65 | 101.90 | |
| Promoter workplace 27 | 5 | 19.05 | 95.25 | 10 | 0.665 | 6.65 | 95.25 | 6.65 | 101.90 | |
| Promoter workplace 27 | 5 | 19.05 | 95.25 | 10 | 0.665 | 6.65 | 95.25 | 6.65 | 101.90 | |
| Promoter workplace 27 | 5 | 19.05 | 95.25 | 10 | 0.665 | 6.65 | 95.25 | 6.65 | 101.90 | |
| Promoter workplace 25 | 5 | 19.05 | 95.25 | 10 | 0.665 | 6.65 | 95.25 | 6.65 | 101.90 | |
| Subtotal | 1491.21 | |||||||||
| Promoter training day at workplaces | ||||||||||
| 12 July 2013 | ||||||||||
| Research associate | 1.5 | 28.86 | 43.29 | 2 | 0.665 | 1.33 | 44.62 | 44.62 | ||
| Promoter workplace 11 | 1 | 19.05 | 19.05 | 19.05 | 19.05 | |||||
| Subtotal | 63.67 | |||||||||
| 26 July 2013 | ||||||||||
| Research associate | 1.5 | 28.86 | 43.29 | 6 | 0.665 | 3.99 | 47.28 | 47.28 | ||
| Promoter workplace 23 | 1 | 19.05 | 19.05 | 19.05 | 19.05 | |||||
| Subtotal | 66.33 | |||||||||
| 6 August 2013 | ||||||||||
| Research associate | 1.5 | 28.86 | 43.29 | 4 | 0.665 | 2.66 | 45.95 | 45.95 | ||
| Promoter workplace 18 | 1 | 19.05 | 19.05 | 19.05 | 19.05 | |||||
| Subtotal | 65.00 | |||||||||
| Total | 2870.27 | |||||||||
Cost per employer and employee
The cost of the intervention per workplace and employee is presented in Table 13. Costs varied because of different numbers of promoters in each workplace and depending on the number of employees participating in the intervention from each workplace. The location of promoter training also had an impact on the cost per workplace and per employee. The cost of promoter training days at the workplace was lower, as the training was shorter and promoters took less time off work. The costs per workplace and per employee by workplace size demonstrate that there is no clear association between employer size and cost per participating employee, as some very large employers were not successful in recruiting a large number of employees to participate.
| Workplace size | Workplacea | Cost per workplace (£) | Cost per employee (£) | Cost per employee by workplace size (£) |
|---|---|---|---|---|
| Large | 27 | 958.38 | 159.73 | 159.83 |
| 25 | 320.27 | 160.14 | ||
| Medium | 23 | 66.33 | N/Ab | 191.85 |
| 18 | 701.09 | 175.27 | ||
| Small | 20 | 341.49 | 85.37 | 130.16 |
| 14 | 624.67 | 208.22 | ||
| 11 | 75.09 | 75.09 | ||
| Average cost per employee | 154.37 | |||
| Average cost per workplace | 441.05 | |||
| Total cost | 3087.32 | |||
Health service use
Table 14 provides the mean number of units and cost of each service per participant, by group and time point, for each category. There were a total of 100 participants in the intervention group and 87 participants in the control group. At baseline, the response rate varied between 86% and 88% in the intervention group, and 91% and 93% in the control group, depending on the question asked. At follow-up, response rate varied between 70% and 71% in the intervention group, and 59% and 62% in the control group. On average, the response rate was 19% lower in the intervention group and 35% lower in the control group at follow-up.
| Health service | Mean units | Mean (SD) cost | Mean units | Mean (SD) cost | Incremental difference (95% CI) |
|---|---|---|---|---|---|
| Intervention (n = 86a) | Control (n = 79b) | ||||
| Baseline | |||||
| GP appointment | 0.17 | £7.41 (£18.79) | 0.15 | £6.53 (£18.33) | £0.88 (−£4.82 to £6.58) |
| Nurse appointment | 0.09 | £1.26 (£3.98) | 0.05 | £0.68 (£3.00) | £0.57 (−£0.51 to £1.66) |
| GP telephone call | 0.02 | £0.60 (£3.94) | 0.05 | £1.30 (£7.04) | −£0.70 (−£2.43 to £1.04) |
| Nurse telephone call | 0.01 | £0.10 (£0.89) | 0.00 | £0.00 (£0.00) | £0.10 (−£0.10 to £0.29) |
| A&E visits | 0.00 | £0.00 (£0.00) | 0.05 | £5.33 (£23.55) | −£5.33 (−£10.32 to –£0.35) |
| Hospital outpatient visits | 0.05 | £4.82 (£27.41) | 0.06 | £6.54 (£25.67) | −£1.73 (−£9.81 to £6.36) |
| Other care | 0.14 | £5.06 (£18.59) | 0.14 | £4.65 (£30.80) | £0.42 (−£7.33 to £8.17) |
| Medication | £4.29 (£18.99) | £2.47 (£5.72) | £1.82 (−£2.54 to £6.18) | ||
| Total | £20.94 (£40.58) | £26.80 (£63.18) | −£5.86 (−£22.29 to £10.56) | ||
| Intervention (n = 70c) | Control (n = 51d) | ||||
| Follow-up | |||||
| GP appointment | 0.09 | £3.69 (£14.16) | 0.30 | £12.98 (£24.71) | −£9.30 (−£16.29 to –£2.30) |
| Nurse appointment | 0.10 | £1.37 (£4.14) | 0.16 | £2.15 (£5.73) | −£0.78 (−£2.55 to £1.00) |
| GP telephone call | 0.07 | £1.86 (£8.07) | 0.04 | £1.02 (£7.28) | £0.84 (−£1.99 to £3.66) |
| Nurse telephone call | 0.00 | £0.00 (£0.00) | 0.00 | £0.00 (£0.00) | – |
| A&E visits | 0.03 | £3.04 (£18.00) | 0.02 | £2.00 (£14.70) | £1.04 (−£4.91 to £6.99) |
| Hospital outpatient visits | 0.10 | £10.60 (£40.95) | 0.02 | £1.96 (£14.42) | £8.64 (−£2.92 to £20.19) |
| Other care | 0.26 | £10.10 (£32.32) | 0.09 | £2.98 (£15.51) | £7.12 (−£2.93 to £17.18) |
| Medication | £7.05 (£23.21) | £2.52 (£4.82) | £4.53 (−£1.83 to £10.88) | ||
| Total | £36.89 (£77.50) | £18.45 (£30.91) | £18.44 (−£5.41 to £42.29) | ||
At baseline, the mean total cost of health services, including medications, in the intervention group was smaller than for the control group at £20.94 (SD £40.58), compared with £26.80 (SD £63.18). At follow-up, a larger mean cost of health service use was observed in the intervention group at £36.89 (SD £77.50) when compared with the control group at £18.45 (SD £30.91), but this difference was not statistically significant.
Commute
A summary of the commute data is presented below in Table 15.
| Mode of transport | Mean (SD) daily minutes | Mean (SD) daily minutes | Incremental difference (95% CI) |
|---|---|---|---|
| Intervention (n = 89) | Control (n = 79) | ||
| Baseline | |||
| Walked | 14.33 (12.43) | 12.03 (12.56) | 2.31 (−1.50 to 6.12) |
| Cycled | 1.49 (3.52) | 1.92 (4.34) | −0.44 (−1.64 to 0.76) |
| Bus | 2.14 (7.93) | 0.95 (4.49) | 1.19 (−0.81 to 3.19) |
| Train | 0.67 (6.36) | 1.22 (6.25) | −0.55 (−2.48 to 1.37) |
| Car | 7.16 (11.75) | 8.56 (12.05) | −1.40 (−5.03 to 2.23) |
| Other | 0.02 (0.17) | 0.33 (2.02) | −0.31 (−0.74 to 0.11) |
| Inactive travel | 10.00 (16.19) | 11.07 (14.61) | −1.08 (−5.80 to 3.64) |
| Total | 25.81 (15.48) | 25.02 (15.35) | 0.79 (−3.91 to 5.50) |
| Intervention (n = 71) | Control (n = 55) | ||
| Follow-up | |||
| Walked | 12.20 (10.40) | 9.21 (11.47) | 2.99 (−0.88 to 6.86) |
| Cycled | 1.81 (4.34) | 2.39 (5.12) | −0.58 (−2.25 to 1.09) |
| Bus | 3.67 (9.60) | 0.83 (3.38) | 2.84 (0.15 to 5.52) |
| Train | 0.56 (4.75) | 2.11 (7.78) | −1.55 (−3.77 to 0.68) |
| Car | 9.64 (16.23) | 10.88 (14.10) | −1.24 (−6.70 to 4.21) |
| Other | 0.12 (0.99) | 0.20 (1.52) | −0.09 (−0.53 to 0.36) |
| Inactive travel | 13.99 (18.73) | 14.03 (17.73) | −0.04 (−6.55 to 6.47) |
| Total | 28.00 (15.76) | 25.63 (16.22) | 2.37 (−3.31 to 8.04) |
At baseline, 89% of participants in the intervention group and 91% of participants in the control group provided information on their weekly commute to and from work. At follow-up, 71% of the intervention group and 63% of the control group provided this information. At baseline, the average time commuting to work daily was similar between groups, at between 25 and 26 minutes for both. Results showed that, at baseline, those in the intervention group spent around 2 minutes longer walking per day; however, this result was not statistically significant. Time spent on inactive travel, which included commuting by bus, train, car or other mode of transport, was around 1 minute longer in the control group; however, this was also not a significant result. At follow-up, there was a trend for higher mean daily minutes of walking [12.2 minutes (SD 10.4 minutes)] in the intervention group than in the control group [9.21 minutes (SD 11.47 minutes)], but this difference was not statistically significant.
As shown in Table 16, at baseline the mean daily commute cost was £1.79 (£3.59) in the intervention group and £2.57 (£5.81) in the control group, representing a –£0.78 (95% CI –£2.23 to £0.66) difference. At follow-up, the commute cost increased in both groups. In the intervention group, the mean daily cost was £2.66 (£4.32), and it was £3.64 (£12.16) in the control group. This represented a slightly larger difference than at baseline at –£0.98 (95% CI –£4.06 to £2.10), yet this difference was not significant.
| Time point | Mean (SD) daily cost | Mean (SD) daily cost | Incremental difference (95% CI) |
|---|---|---|---|
| Intervention (n = 90) | Control (n = 80) | ||
| Baseline | |||
| Daily commute cost | 1.79 (3.59) | 2.57 (5.81) | −0.78 (−2.23 to 0.66) |
| Intervention (n = 71) | Control (n = 55) | ||
| Follow-up | |||
| Daily commute cost | 2.66 (4.32) | 3.64 (12.16) | −0.98 (−4.06 to 2.10) |
Productivity
Response rates to the questions on self-rated productivity and absenteeism declined over the study period (Table 17). At baseline, approximately 85% of the intervention group and 91% of the control group answered these questions. At 1-year follow-up, response rates had fallen to approximately 70% in the intervention group and 61% in the control group.
| Time point | Intervention | Control | Incremental difference (95% CI) | ||
|---|---|---|---|---|---|
| n | Mean (SD) | n | Mean (SD) | ||
| Self-assessed productivity | |||||
| Baseline | 83 | 1.65 (1.73) | 80 | 1.55 (1.44) | 0.10 (−0.39 to 0.59) |
| Post intervention | 79 | 1.99 (2.00) | 61 | 2.05 (2.22) | −0.06 (−0.77 to 0.65) |
| Follow-up | 70 | 1.51 (1.41) | 54 | 2.07 (2.24) | −0.56 (−1.21 to 0.09) |
| Hours of work missed | |||||
| Baseline | 88 | 0.32 (1.43) | 78 | 0.32 (1.56) | 0.00 (−0.46 to 0.46) |
| Post intervention | 79 | 1.04 (3.81) | 60 | 0.58 (1.86) | 0.45 (−0.60 to 1.51) |
| Follow-up | 69 | 0.84 (4.58) | 53 | 0.17 (1.10) | 0.67 (−0.60 to 1.94) |
At baseline, the mean productivity score in both the intervention and control groups was low [1.65 (SD 1.73) and 1.55 (SD 1.44), respectively], indicating little self-perceived impact of health on productivity. There were no clear trends in productivity over the study period. While productivity scores were slightly lower (better) in the intervention group at 1-year follow-up, the difference was not statistically significant [1.51 (SD 1.41) and 2.07 (SD 2.24), respectively; p = 0.09].
The average number of hours missed from work because of health problems was the same across both groups at baseline at around 0.32 hours. Immediately post intervention and at 1-year follow-up, the mean number of hours missed was higher in the intervention group, at 1.04 hours (SD 3.81 hours) compared with 0.58 hours (SD 1.86 hours) post intervention and 0.84 hours (SD 4.58 hours) compared with 0.17 hours (SD 1.10 hours) at follow-up. However, neither of these differences was statistically significant.
Physical activity outcomes
Although the study was not powered to detect effectiveness, some statistical analyses were conducted to identify whether or not there was any evidence of promise that the intervention could increase walking to work and hence justify an application for a full-scale RCT.
Objectively measured physical activity
The accelerometer data for participants living within 2 miles of the workplace (Table 18), and for all participants (Table 19), suggest that overall physical activity levels (cpm) were similar in the intervention and control arms at baseline, but that there was a reduction in physical activity in the control arm at 1-year follow-up. For MVPA there is a suggestion of a reduction in both arms, although the pattern is more pronounced in the control arm.
| Physical activity level | Baseline (n = 130) | Follow-up (n = 76) |
|---|---|---|
| cpm | ||
| Intervention | 469.3 ± 157.8 | 502.0 ± 178.4 |
| Control | 473.4 ± 197.0 | 426.8 ± 132.4 |
| MVPA | ||
| Intervention | 68.3 ± 28.4 | 68.7 ± 27.9 |
| Control | 68.0 ± 29.1 | 60.7 ± 23.8 |
| Physical activity level | Baseline (n = 164) | Follow-up (n = 115) |
|---|---|---|
| cpm | ||
| Intervention | 434.6 ± 165.0 | 452.0 ± 188.7 |
| Control | 441.9 ± 190.0 | 400.6 ± 120.0 |
| MVPA | ||
| Intervention | 63.4 ± 28.6 | 61.3 ± 28.4 |
| Control | 63.3 ± 28.5 | 55.8 ± 22.2 |
It seems likely that there is a Hawthorne effect when study participants are asked to wear monitors to measure their physical activity. This effect will be present in both the intervention and control arms. It may be that this effect was stronger at beginning of the study, when participants wore the monitors for the first time, which could account for the apparent reduction in MVPA in all participants.
Intracluster correlation coefficient and sample size calculation
The ICC for the fesasibility study was calculated to be 0.12 (95% CI 0.00 to 0.30) and the average cluster size was eight. Based on an ICC of 0.15 to allow for some imprecision in the estimate, 678 participants across 84 workplaces are required to give 80% power with a 5% significance level to detect a 15% increase in mean MVPA.
The contribution of walking to work to physical activity levels
Analyses of the baseline data highlight the considerable contribution that walking to work can make to adult physical activity levels. 49 The initial sample comprised 147 adults who lived within 2 miles of their workplace. Seventy-four participants (50.3% of the original sample) were categorised as walkers and 33 (22.4%) as car users. Five of these participants did not provide any valid accelerometer data, and were excluded from analyses. The final sample comprised 102 adults (mean age 36.3 ± 11.6 years; 56.9% female). Participants recorded 236 return journeys by foot and 86 by car. Mean self-reported journey time to work (each way) was 19.7 ± 8.3 minutes by foot and 10.7 ± 7.6 minutes by car.
Participants wore the accelerometer for a mean of 723.1 ± 155.2 minutes each day, with no difference between travel modes or sexes. Physical activity did not differ between males and females (497.9 ± 206.0 vs. 460.5 ± 146.1 cpm respectively; p = 0.285) and therefore the sexes were analysed together. When analysed by main travel mode (Table 20), participants who walked to work had higher levels of overall weekday physical activity than those who travelled by car, and also recorded more minutes of MVPA, but there was little difference in sedentary time.
| All (n = 102) | Walk (n = 69) | Car (n = 33) | p-value | |
|---|---|---|---|---|
| Weekday | ||||
| Overall daily physical activity (accelerometer cpm) | 476.6 ± 174.6 | 530.2 ± 165.1 | 364.6 ± 138.4 | <0.001 |
| MVPA (minutes/day) | 69.5 ± 27.9 | 78.9 ± 24.0 | 49.8 ± 25.2 | <0.001 |
| Sedentary time (minutes/day) | 586.2 ± 71.9 | 579.9 ± 76.4 | 599.2 ± 60.5 | 0.206 |
| Weekend | ||||
| Overall daily physical activity (accelerometer cpm) | 418.2 ± 192.9 | 434.5 ± 207.3 | 385.1 ± 158.6 | 0.329 |
| MVPA (minutes/day) | 53.7 ± 30.0 | 55.5 ± 31.2 | 50.2 ± 27.7 | 0.505 |
| Sedentary time (minutes/day) | 510.4 ± 90.1 | 511.1 ± 91.1 | 509.0 ± 90.0 | 0.928 |
For those who walked to work, physical activity and MVPA values were substantially reduced at the weekend. The physical activity of car users was essentially unchanged so that there was no difference in weekend physical activity between the two travel groups. In linear regression models, walking to work was associated with higher overall weekday physical activity (B = 164.6 cpm, 95% CI 98.8 to 230.5; p < 0.001) and MVPA (B = 28.5 minutes, 95% CI 18.3 to 38.8; p < 0.001), but not with a difference in sedentary time.
Age and sex were not predictors of daily physical activity, MVPA or sedentary time in these models. Education was a predictor of total physical activity and MVPA, with those educated to degree level or above more active than those less well qualified (overall physical activity: B = 81.6 cpm, 95% CI 14.0 to 149.3; p = 0.019; MVPA: B = 12.3 minutes, 95% CI 1.8 to 22.8; p = 0.022).
Mean hourly physical activity was plotted to identify when differences in physical activity occurred during the day. Figure 2 shows that the main differences between car users and walkers occurred in the morning and late afternoon, potentially when commuting to or from work. There was no difference in physical activity between the travel groups during the main working hours (9 a.m. to 4 p.m.) (walk 347.2 ± 187.4 cpm vs. car 318.7 ± 194.4 cpm; p = 0.480).
FIGURE 2.
Mean hourly physical activity by mode of travel to/from work on weekdays.

To explore the contribution of walking to work to total physical activity, accGPS traces recorded between 6.00 a.m. and 10.00 a.m., and between 4.00 p.m. and 8.00 p.m., were examined. Of the 74 participants who walked to work, 58 recorded GPS data for at least one journey. Overall, 321 journeys (182 to work and 139 home from work, from 54 participants) were recorded. Participants generally took broadly the same route to and from work each day. A high level of physical activity was recorded on the journeys to (4260.7 ± 943.5 cpm) and from (3806.3 ± 915.8 cpm) work. Time spent on the journey to work was less than on the journey home (21.9 ± 7.8 vs. 28.6 ± 18.5 minutes), as in some cases participants interrupted their journey to visit shops on the way home (Figure 3). These visits were considered to be part of the journey. However, the minutes of MVPA on the journeys to and from work were highly similar (19.8 ± 7.1 vs. 21.0 ± 8.9 minutes of MVPA), as time spent in shops was not MVPA. A comparison of total MVPA (6.00 a.m. to midnight) with MVPA recorded during the journey for the 58 participants providing any GPS data showed that the walk to and from work contributed 47.3% of participants’ total daily MVPA (38.0 of 80.3 minutes).
FIGURE 3.
Global positioning system trace of participant walking directly to work and returning by an alternative route (precise start and end are cropped to protect confidentiality).
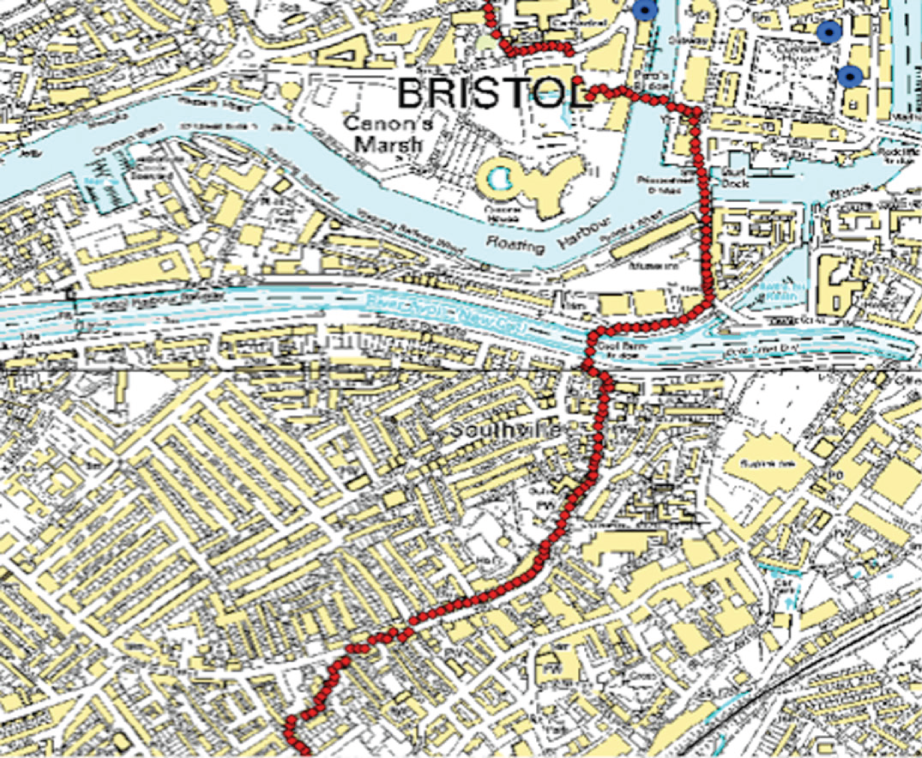
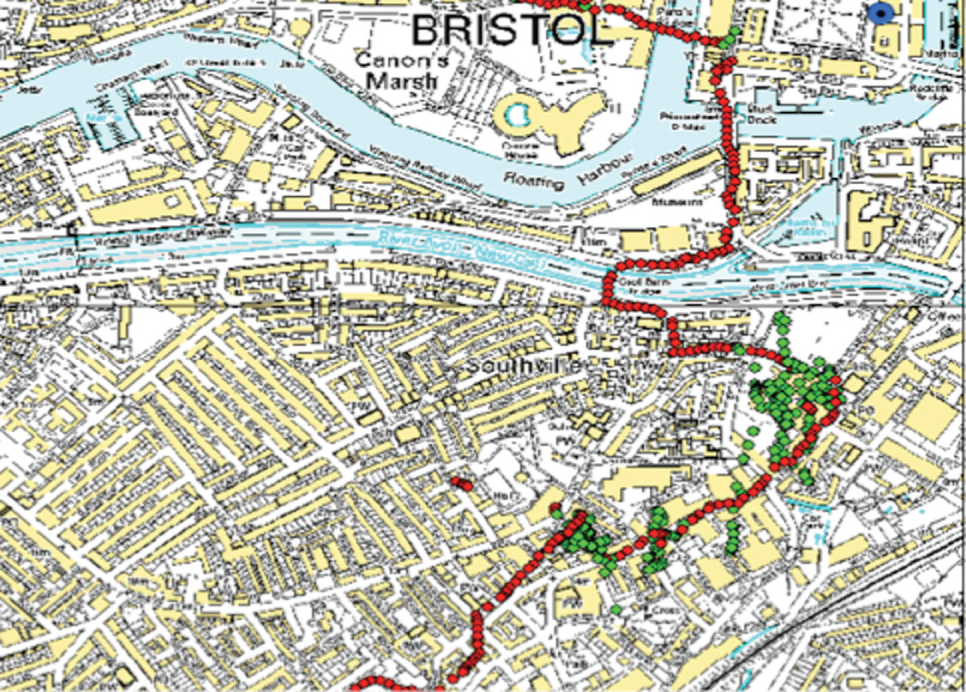
Participants’ views of using behaviour change techniques to promote walking to work
To examine participants’ views of the BCTs used, 22 interview transcripts were analysed. 64 The characteristics of the interviewees, who included Walk to Work promoters and intervention participants, are detailed in Table 21. Fourteen interviewees were employees who attempted to change their travel behaviour, and eight were Walk to Work promoters (of whom four already walked to work and four were attempting to change their behaviour). The age range was 22 to 65 years, with a range of household incomes, and 55% were male. Most were city-centre based and all were in sedentary occupations. Participants’ IDs reflect the data collection (DC2), workplace ID and participant number.
| ID | Sex | Age (years) | Participant/promoter | Workplace sizea | Type of businessb | Location | Household income, £000 p.a. |
|---|---|---|---|---|---|---|---|
| DC2–11–003 | Female | 50 | Participant and promoter | Small | Professional, scientific and technical | City centre | 30–40 |
| DC2–14–001 | Female | 26 | Participant | Small | Professional, scientific and technical | City centre | 20–30 |
| DC2–14–005 | Female | 33 | Participant | Small | Professional, scientific and technical | City centre | 20–30 |
| DC2–14–006 | Male | 22 | Participant and promoter | Small | Professional, scientific and technical | City centre | > 50 |
| DC2–20–001 | Male | 29 | Participant and promoter | Small | Professional, scientific and technical | Suburban | > 50 |
| DC2–20–002 | Male | 25 | Participant | Small | Professional, scientific and technical | Suburban | 20–30 |
| DC2–20–003 | Male | 65 | Participant | Small | Professional, scientific and technical | Suburban | Not given |
| DC2–20–004 | Female | 52 | Participant | Small | Professional, scientific and technical | Suburban | 40–50 |
| DC2–18–002 | Male | 60 | Participant | Medium | Professional, scientific and technical | City centre | > 50 |
| DC2–18–003 | Male | 38 | Promoter | Medium | Professional, scientific and technical | City centre | 20–30 |
| DC2–18–004 | Male | 37 | Participant | Medium | Professional, scientific and technical | City centre | > 50 |
| DC2–18–009 | Female | 52 | Participant | Medium | Professional, scientific and technical | City centre | Not given |
| DC2–25–005 | Male | 30 | Promoter | Large | Public administration | City centre | 20–30 |
| DC2–25–017 | Male | 52 | Participant | Large | Public administration | City centre | > 50 |
| DC2–25–033 | Female | 55 | Participant | Large | Public administration | City centre | 30–40 |
| DC2–27–005 | Male | 23 | Participant | Large | Financial and insurance activities | City centre | 20–30 |
| DC2–27–008 | Female | 58 | Promoter | Large | Financial and insurance activities | City centre | 20–30 |
| DC2–27–010 | Female | 46 | Promoter | Large | Financial and insurance activities | City centre | 20–30 |
| DC2–27–013 | Male | 46 | Participant | Large | Financial and insurance activities | City centre | 30–40 |
| DC2–27–014 | Female | 45 | Participant and promoter | Large | Financial and insurance activities | City centre | > 50 |
| DC2–27–015 | Female | 31 | Participant | Large | Financial and insurance activities | City centre | 30–40 |
| DC2–27–018 | Male | 45 | Participant | Large | Financial and insurance activities | City centre | 40–50 |
Intention formation
The intentions of participants varied from those who aimed to walk the whole journey to and from work every day to those who proposed to combine walking part of the journey with another mode of transport, or to walk on selected days of the week. These intentions were prompted by perceived health benefits such as ‘getting fit and losing weight’ (DC2–11–003, female, 50). One participant indicated: ‘My doctors said before that I need to, to walk more . . . this is what gave me the stimulus if you like to actually get on and do something about it’ (DC2–20–004, female, 52). However, one promoter (DC2–27–010, female, 46) felt that, although people had good intentions, they were often dependent on their cars: ‘I think people have the intentions of walking . . . but, because their character is, just they don’t know how to live without the car’.
Barrier identification
During the interviews, participants focused more on barriers than solutions. The unprecedented wet weather posed particular challenges. Participant DC2–18–002 (male, 60) expressed concerns about walking in a business suit in bad weather: ‘You’re less inclined I think, if you walk, to wear any special clothing to walk in to work . . . normally people wouldn’t carry suits in their backpacks’. Negotiating with motorised traffic when crossing the road could also prove problematic: ‘I mean, crossing the roads is a bit of a nightmare sometimes especially if it’s raining and . . . you got to turn round and see if there’s a car and you’ve got to double check, wearing the glasses as well you know . . . you wouldn’t think there was a learning curve to crossing the road at my age but there is’ (DC2–20–004, female, 52). Participant DC2–27–015 (female, 31) also found the rain off-putting: ‘I did walk sometimes in the rain though, it wasn’t actually too bad once you’re in it, it’s just the thought of going out’. Solutions proposed by participants tended to focus on being prepared for bad weather by having waterproofs and umbrellas: ‘I mean the weather this morning was horrendous but I’ve got some waterproof trousers, an overcoat and an umbrella and I came to work as dry as I would have been if it had been dry’ (DC2–18–004, male, 37).
Related to concerns about the weather was the availability of facilities to freshen up on arrival at work: ‘If there were facilities, or if you had that sort of stuff available to you, I think I would be more inclined to walk or cycle, because I don’t – I don’t like feeling unclean, I like to be clean’ (DC2–20–002, male, 25). A solution was proposed by this participant, although it was seen as requiring additional effort: ‘You’d have to, like, have a shirt ready in work so you’d have to make sure you prepare everything’. Participant DC2–20–004 (female, 52) also identified a solution to the barrier she felt of arriving at work flustered and not being able to work straight away: ‘I’ve settled on walking home partly because that’s logistically how it’s mostly worked out anyway . . . I did walk in a couple of times and one time you know it looked like it was going to rain and I’m hurrying along hoping it’s not coming and I arrive in work and actually I didn’t feel as good when I arrived in work as I thought it would . . . whereas I drive, I park in the car park, I sit down at my desk and I’m straight into it’.
The availability of car parking at work was considered an important barrier to walking: ‘We haven’t really got limitations to car parking because we’ve got a free car park out the back so it is easier for us to drive because we know that we can park when we get here. If we didn’t have that then it would probably force us to walk a bit more . . . because we’ve got a free car park we can just come and go when we please in the car’ (DC2–20–001, male, 29). Other barriers relating to car use were the high fixed costs and the perceived convenience: ‘I’m paying so much for the petrol, the tax, the insurance. I just think it’s there and it’s just convenient for me to use it, so I think it’s just too easy to, to walk out the house, get in the car and just put my foot down and drive for 10 minutes up the road’ (DC2–20–002, male, 25). The cost, time and unreliability of public transport were important reasons why participants who lived further from the workplace chose to use their car, and ‘park and walk’, rather than use the public transport system: ‘Public transport for me to try and get here is horrid. I tried it within the study. It was expensive. It will take me an hour and a half to get in here whereas by driving and walking I can do it in 35 minutes’ (DC2–27–013, male, 46). The nature of the terrain could also influence choice of travel mode: ‘I come down a very steep, two very steep hills . . . so walking in is not an issue, walking home is a bit more of an issue . . . it takes longer, it’s more tiring’ (DC2–25–017, male, 52).
Busy lifestyles and caring responsibilities were identified as barriers: ‘They’ve got to pick up children from schools or clubs or some people have elderly relatives that they look after . . . some people will be rushing home to go off to yoga, Pilates, dance, so it depends if it’s going to take a lot longer’ (promoter DC2–27–008, female, 58). Other barriers included having to carry heavy items, needing the car for work appointments, walking in dark or unpleasant surroundings, pollution and shift work.
Goal setting
The Walk to Work booklets encouraged participants to make a note of short-, intermediate- and long-term goals. One enthusiastic participant (DC2–25–033, female, 55) was very clear about how she would increase walking in stages: ‘Short term to walk to [supermarket] which is a specific place, at a gentle pace, in week one . . . second week was to do the same but at a faster pace and week three was to walk halfway once a week at a faster pace, a brisker pace . . . intermediate walk halfway to work twice a week . . . and then long term walk halfway to work every day which is about 25 minutes’. Others were less precise: ‘I parked, like, close . . . then gradually sort of kept parking further back’ (DC2–27–015, female, 31).
Pedometers assisted goal setting for seven participants. For example: ‘I just said to myself for the first 2 weeks I will just park my car where I normally park it and walk to work, do my stuff, go home and over the 2 weeks [my goal] was just to see how many steps I was taking, and then I just said to myself over the next 2, 3 weeks put it up another 1000 steps and then kept increasing it, over the 10 weeks’ (DC2–27–013, male, 46).
One task of the Walk to Work promoter was to help participants set their individual goals. The promoters varied in the extent to which they engaged with this BCT. Participant DC2–25–033 (female, 55) was concerned that the promoter was too forceful: ‘I was never wanting to do more than walk halfway to work . . . that was my ultimate, and that for me would be success and he [promoter] kept giving me routes to get here and I kept saying “But I’m not doing that, am I, because that isn’t my goal and you need to support me with my goal rather than yours” ’. Promoter DC2–27–010 (female, 46) said that she allowed participants to vary their walking to suit their circumstances: ‘We all have busy lives so as long as you are walking every day if you can, that’s absolutely fine’.
Provide instruction
Participants generally found the structure and content of the booklets useful: ‘I thought it was very helpful, I mean the websites at the back were very good’ (DC2–27–013, male, 46). However, the praise was not unanimous: ‘I didn’t find it very helpful, really, no, it was very, sort of repetitive and I better admit before I go any further that I’ve done the most brilliant scheme in the past. They had like online articles so that you could earn so many points educating yourself round health benefits’ (DC2–18–009, female, 52).
General encouragement
In some workplaces, the Walk to Work promoters were valued for being ‘enthusiastic’ and ‘showing an interest’ (DC2–18–009, female, 52) and even offering to walk together: ‘She’s been very good at encouraging me to try different things . . . congratulating me . . . we’ll walk together when I was going to [local landmark] because she walks past there’ (DC2–27–014, female, 45). Promoter DC2–27–010 (female, 46) felt that it was important to encourage participants even if they did not achieve their initial goals: ‘The people I am promoting they are doing their best even if they are not doing as much as they thought they were going to do. That is now in their mind and they will think twice . . . whether they really need the car or they can walk, and for me that is a fantastic achievement’.
However, there were challenges for the Walk to Work promoters in fulfilling their role alongside other commitments: ‘I did tend to slightly put it off and say “Well, I’ll do it start of next week” and then on one of those starts of next week I was off sick and by the time I got back into work I’d forgotten that I’d been planning to do it that week, and time just gets away from you sometimes’ (promoter DC2–25–005, male, 30). Promoter DC2–18–003 (male, 38) struggled to promote walking during the wet weather: ‘I know I should be encouraging but, you know, I’ve accepted what people have said’.
Several participants suggested that an external promoter could provide support for the internal Walk to Work promoters: ‘Somebody coming in from outside, say doing half an hour at lunchtime just doing a presentation about it or, you know, longer and getting people there and talking about that and saying “And we have our in-house person who you know if you want to talk to him, d’you wanna get encouragement from him/her”, that would be great but I think somebody coming in from outside actually would be a good idea’ (DC2–18–002, male, 60).
Participant DC2–20–004 (female, 52) felt that it was important for management to show encouragement by allowing people time to get used to their new routine: ‘They’re not going to get penalised if they are a little bit late in because they didn’t leave early enough while they’re getting the hang of walking’. This could be supplemented with incentives: ‘Offering a cash incentive for people to walk rather than drive’ (DC2–27–018, male, 45). Other incentives discussed included training shoes, vouchers or a free breakfast to encourage them to walk to work: ‘Just a little something, you know, people might think, oh, actually, if I leave half an hour earlier and I walk into work, all right it’s 2 miles, there might be a, you know, something or a voucher for a coffee place or something, breakfast bap or something’ (DC2–27–014, female, 45).
Self-monitoring
Self-monitoring was encouraged through the use of travel diaries and pedometers. The diary included space to record the method of travel, time taken and, if using a pedometer, the number of steps per day. Some participants found this helpful: ‘It was just that structure of doing that every day and noticing that, no, this week I haven’t actually walked as many times as I thought I might do, and so, you know, tomorrow I’ll make sure I do’ (DC2–25–017, male, 52). However, participant DC2–20–004 (female, 52) preferred talking with colleagues: ‘I mean, telling people that that’s what you’re doing actually makes you hold to it even more than if you, if I’d written it down’. One participant felt that completing the diary was repetitive and time-consuming, while another found that his initial enthusiasm diminished with time: ‘I used it a few times to start with but then sort of faded out’ (DC2–14–006, male, 22). However, the diary could be helpful for promoters in monitoring participants’ progress: ‘Every time I meet with them I just have a quick look [at the diary]’ (DC2–27–010, female, 46).
The booklets also included details of websites that could be accessed for information and to help to track progress: ‘I thought the apps and all the stuff that you do on the computer to be able to track and log everything and find the easier routes to walk and things like that was really, really good . . . I think they should be publicised a bit more because I definitely think that would help people and convince more people to walk’ (promoter DC2–20–001, male, 29).
Although pedometers were offered free of charge, 7 of the 22 interviewees chose not to use them at all and a further four commented on problems using them: ‘I’ve not been very good at using a pedometer because I’ve either forgotten to put it on in the morning, and I find them quite uncomfortable’ (DC2–27–014, female, 45). One promoter (DC2–25–005, male, 30) expressed his concern at asking participants to wear a pedometer for the duration of the intervention: ‘Ten weeks is a long time to be wearing such a device’. However, there was evidence that the step count could be motivating: ‘I used the pedometer which I found really interesting, just to see how little we actually did walk when using the cars and how much more you actually do just walking to and from work’ (DC2–20–001, male, 29). Participant DC2–14–005 (female, 33) talked about competition within the workplace: ‘I sit predominantly around a load of lads, they are very competitive, so maybe some kind of competition maybe something with the pedometers where you can measure how far everybody walks each day’.
Social support
In some workplaces, participants offered mutual support, particularly if they were sitting close to each other: ‘We would always be having a conversation, there would always be a time when he would say “Oh, I walked to work today, what did you do?” ‘ (DC2–20–002, male, 25). Such support included shared experiences of bad weather: ‘It was quite nice that there was other people that get drenched when you get drenched’ (DC2–14–001, female, 26). In contrast, participant DC2–25–017 (male, 52) had the support of his promoter but was not aware of anyone else taking part in the study: ‘It might’ve made a difference if I actually knew somebody else who was doing it’.
The promoters reported that it was not always easy to support walkers, especially if there were other work pressures. This may explain why there were mixed feelings about the level of support offered by the Walk to Work promoters. Some participants felt that the promoters were well placed to help them, particularly if the promoter had changed their own behaviour, had local knowledge, and was able to discuss barriers and support participants who needed reminding. However, participant DC2–25–033 (female, 55) expected her promoter to check progress more rigorously: ‘He just wrote to me and said “How you doing?” and I wrote back and said “It’s going fine” and that was it really. Yeah, I’m not sure what else he could have done I suppose but it did – it felt very light touch . . . I think I was expecting a bit more . . . kind of looking at this together and maybe another meeting’. Another participant (DC2–27–013, male, 46) reported little or no contact from the Walk to Work promoter after the initial session: ‘I must admit in the 10 weeks they didn’t . . . they initially set you up, yeah, but no one sort of halfway through said “Have you increased?” ’.
One promoter raised concerns as a junior member of staff who was supporting a manager: ‘One of the walkers is a manager . . . he’s way above my pay grade . . . I felt like I was demanding his precious time to meet with him to do the study, although of course he volunteered for it but . . . it was a slightly strange relationship for me to be the sort of the mentor to someone who’s on a sort of higher grade, managerial role’ (DC2–25–005, male, 30).
Review of behaviour goals
Participants appeared willing to reconsider their initial goals: ‘I reviewed myself and found that I can actually walk to work a lot more than I thought I could so I just upped the amount of times that I actually walked’ (DC2–20–001, male, 29). A change in seasons had the potential to affect behaviour: ‘It first started getting really dark, like in the mornings and evenings, and then when the clocks went back it kind of evened it out a bit better so I could sort of go back to finishing at 6 and feel OK about walking back’ (DC2–27–015, female, 31). Promoter DC2–18–003 (male, 38) highlighted the experience of one participant who reviewed his goals because he was concerned about the safety of the area he walked through. However, as there was no alternative, he continued with that route: ‘He’s got to walk through [local area], probably not safe, but there’s no other route, you know, but he risked it anyway’.
Relapse prevention
One promoter suggested that the term ‘relapse prevention’ was not appropriate for an intervention to increase walking to work: ‘Relapse prevention sounds like a stop smoking campaign. It’s a bit drastic for someone who has stopped walking’ (DC2–20–001, male, 29). However, he acknowledged the need to give people tools to maintain their new behaviour: ‘It’s almost like having an internet site that you could go to for advice and stuff . . . like a little push just to say look you can still keep doing this if you do this, this and this’.
Promoter DC2–25–005 (male, 30) talked about making walking a habit: ‘I mean if they survive this winter, I mean in terms of their walking habits . . . then I should think they’d probably carry on’. Participant DC2–20–002 (male, 25) found it difficult to resume walking after a holiday: ‘I went on holiday for 2 weeks so when I came back I was a little less inclined to be walking, but eventually I got myself back on track’. He was also anxious that he was having a knee operation and that this might cause him to revert to using the car: ‘I’ve got my operation next week I’m off for 6 weeks then, so I’m going to be on my bum a lot [laugh], so I can see me getting lazy over the winter period’.
Employers’ views about encouraging employees to walk to work
Interviews were conducted with employers/managers at various stages of the study (Table 22). 65 Participant ID numbers reflect the stage at which the interview took place: during the phase 1 development work (P1); during the exploratory trial at baseline (DC1) or post intervention (DC2); and at the end of the intervention period with employers who had expressed an interest originally but did not continue with the study (prefixed with the digit 9). These are followed by the numerical workplace ID and participant ID.
| ID | Sex | Type of businessa | Location | Workplace sizeb |
|---|---|---|---|---|
| Phase 1 development | ||||
| P1–1–01 | Male | Manufacturing | Suburban | Small |
| P1–2–01 | Female | Retail | Suburban | Small |
| P1–3–01 | Male | Retail | Suburban | Medium |
| P1–4–01 | Female | Voluntary sector educational support | Suburban | Medium |
| P1–5–01 | Female | Higher education | City centre | Large |
| Phase 2 baseline | ||||
| DC1–14–001 | Female | Professional, scientific and technical | City centre | Small |
| DC1–20–004 | Female | Professional, scientific and technical | Suburban | Small |
| DC1–21–901 | Male | Transportation | Suburban | Small |
| DC1–22–004 | Female | Professional, scientific and technical | City centre | Small |
| DC1–16–901 | Female | Publishing | Suburban | Medium |
| DC1–17–901 | Female | Education | Suburban | Medium |
| DC1–18–006 | Male | Professional, scientific and technical | City centre | Medium |
| DC1–19–901 | Male | Accommodation and food services | City centre | Medium |
| DC1–24–005 | Female | Education | City centre | Medium |
| DC1–25–901 | Female | Public administration | City centre | Large |
| DC1–27–014 | Female | Financial and insurance activities | City centre | Large |
| DC1–28–901 | Female | Manufacturing | Suburban | Large |
| Phase 2 post intervention (intervention arm only) | ||||
| DC2–11–901 | Male | Professional, scientific and technical | City centre | Small |
| DC2–14–001 | Female | Professional, scientific and technical | City centre | Small |
| DC2–18–002 | Male | Professional, scientific and technical | City centre | Medium |
| DC2–20–004 | Female | Professional, scientific and technical | City centre | Medium |
| DC2–23–007 | Female | Manufacturing | City centre | Medium |
| DC2–25–901 | Female | Public administration | City centre | Large |
| DC2–25–902 | Female | |||
| DC2–27–014 | Female | Financial and insurance activities | City centre | Large |
| Phase 2 interviews with employers/managers who expressed interest but did not continue | ||||
| 911–001 | Female | Information and communication | City centre | Small |
| 912–001 | Female | Manufacturing | City centre | Small |
| 925–001 | Male | Education | Suburban | Medium |
| 930–001 | Female | Financial and insurance activities | City centre | Medium |
| 937–001 | Male | Education | Suburban | Large |
| 936–001 | Female | Public administration | Suburban | Large |
| 936–002 | Male | Public administration | Suburban | Large |
| 936–003 | Male | Public administration | Suburban | Large |
Five employers/managers were interviewed during the development phase of the study. During the phase 2 exploratory trial, 12 interviews were conducted with employers/managers at baseline and a further seven (with eight participants, as one was a paired interview) immediately post intervention. An additional six interviews (with eight participants) were conducted with employers/managers who expressed an interest at the workplace recruitment stage but did not go on to participate in the study.
The interviews were conducted in a range of small, medium and large workplaces in both city centre and suburban environments. Two-thirds of the interviewees were female. In this section of the report, we concentrate on employers’/managers’ perceptions of the benefits and disadvantages of walking to work, and whether or not employers can or should encourage their employees to walk to work.
Advantages of employees walking to work
When asked what might be the advantages to employers (rather than to the employees themselves) if the employees walked to work, employers mentioned several benefits linked to a healthier workforce: ‘I think there’s strong evidence that, you know, physical activity which you know your 30 minutes or whatever it is these days, um X times a week helps enormously in terms of sickness, in terms of retention, in terms of positivity both mentally and physically and you know alertness, you know how efficient you are, your job actually. So there’s a whole load for the employer on the health benefits’ (937–001, female). A possible reduction in absenteeism was considered ‘always a good thing’ (DC1–24–005, female), especially if there was an acknowledged problem in the workplace: ‘Our sickness absence rate is going down but it’s still too high and so we very much want to do anything we can to improve the health of our workforce’ (DC1–25–901, female).
Not all employers felt that there could be such a clear association between walking to work and absenteeism: ‘I can’t imagine that you’d find such a, a direct link. It could be, but I think, you know, emotional well-being’ (DC1–17–901, female). Workers may be more likely to stay in post: ‘Recruitment and retention, um, once, if, if they’re happy with their commute to work they’re more likely to stay’ (P1–5–01, female). A happier workforce was also linked to productivity: ‘I think one hopes for a bit more, you know might become a happier workplace, people are a little bit healthier – they might be happier as well, more engaged in their work, bit more productive possibly’ (DC1–24–005, female); ‘They will be fitter and more lively and more able to perform at work I suppose would be the, the materialistic way of looking at it and happier, healthier people’ (DC2–18–002, male).
Promoting healthier lifestyles might stem from a desire to be a ‘good’ employer: ‘From an ethical perspective it’s actually good that we would actually be doing something’ (DC1–28–901, female). There was also recognition of an increasing emphasis on corporate responsibility: ‘Everybody’s doing their little bit in terms of the environment’ (DC1–14–001, female); ‘It’s also a reputation thing, as well. People want to know that you promote that kind of thing and that you actually encourage it because, um, it looks good in the local community as well’ (DC1–24–005, female). For some employers, this was linked to the ethos of the company: ‘I need my staff to profess sustainability and, you know, my customers expect that from my staff. So that is certainly one of my major reasons for encouraging non-vehicular transportation’ (DC1–19–901, male); ‘As a company we have got quite a number of clients in the, um, kind of renewable and environmental sector, so again that’s something that we do think about, you know that reducing our, I suppose, carbon footprint and, you know, having a degree of responsibility in line with, you know, with clients we work with’ (DC2–11–901, male).
Better timekeeping was seen as a benefit: ‘In terms of walking, as an entirely predictable journey time, there’s no issues of being late you know for work because of congestion or whatever really’ (937–001, male); ‘You can pretty much guarantee how long it’s going to take you to walk so, you know, if you’ve got a 30-minute journey it’s going to take you 30 minutes whether that’s in the rain or the sunshine. Where, you know, my personal journey [using motorised transport] can take anything from 20 minutes to get in, to over an hour to get in’ (DC1–27–014, female).
Car parking was a particular issue for employers. There were tensions around the availability of parking spaces which might be eased if more people walked to work: ‘Obviously we don’t have much parking here so it would be good if more people did walk in rather than vying for space . . . And then also sometimes it would save, save us money as a company if people were able to walk in . . . there’s always a fight for their spaces [laugh] and you know you have to really regulate it . . . they just drive in and park wherever they want, so it can cause quite a lot of problems’ (DC1–14–001, female). It was suggested that encouraging people to walk could reduce costs for employers: ‘For the employer to provide for, at least it’s free. And it’s much, much cheaper than other alternatives such as us funding expensive car parks or buses’ (937–001, male); ‘Well, certainly from the car park perspective [laugh] it would be, it would be quite beneficial, and at the end of the day we actually are renting the, the car park . . . So it definitely would be beneficial’ (DC1–28–901, female). One employer also suggested that if fewer people drove to work, there could be more space for customers: ‘There’s been some comment from the local Chamber of Trade about employees in the area filling up the car parks so that people who want to come and shop and do business can’t get into the car parks. So, you know, in theory that might increase our trade, as well as everybody else’s, if there was actually more parking spaces available because we didn’t take them all up when we arrive in the morning’ (DC1–20–004, female).
Disadvantages to employers
Although better timekeeping was identified as an advantage, there were employers who suggested that encouraging employees to walk might result in longer journeys and people being late for work, at least initially: ‘Initially, um, people are actually having to realise that they do have to leave the house earlier so they’re not going to be late for work, I might lose a bit of work with people not getting to work on time’ (911–001, female); ‘I wouldn’t want it to be a reason why people are late to work . . . Well, people might say “I always leave the house at whatever and I, you know, now I’m going to [have to] leave earlier because of, you’re encouraging me to walk” ‘ (DC1–18–006, male).
Walking in inclement weather was considered a disadvantage if workplace facilities were limited: ‘I mean, we’ve had such a bad month, the month of April people have come in and they are soaked from their foot up to their knee . . . They don’t bring a change of clothes, there’s nowhere to dry clothes’ (DC1–27–014, female); ‘You have to provide the lockers, the showers, the changing facilities and that can put a real squeeze financially on the employer and just from space requirements as well. I mean, this is the issue we have at [name of workplace], it’s not so much the financial disadvantage, it’s the lack of space because we struggle to find space for showers, lockers and things like that’ (P1–5–01, female).
Some workplaces required employees to have a car for specific tasks: ‘Quite a few of the people here, we require them to have a vehicle to do their job. And being based out in the sticks a bit, getting on buses and doing that job is, is just not, you can’t do it’ (P1–4–01, female); ‘If you have somebody who needs to go out on a business trip, um, if they haven’t got their car that’s going to be an inconvenience, and it’s going to fall on somebody else to take their car’ (DC1–21–901, male).
Concerns were raised about safety and whether or not employers would feel responsible if an employee experienced a problem as a result of the being encouraged to walk: ‘You might feel if somebody got mugged that that was your responsibility, you probably would . . . whenever you as an employer advocate anything, you know, if you champion a particular way of doing things, you know, you are in a way encouraging people to do that and if they, something comes as a consequence negative, then you perhaps you do have a certain sense of responsibility’ (DC1–18–006, male).
Employers’ opinions of promoting walking to work
Opinions about whether or not employers should encourage their employees to walk to work ranged from those who would definitely not do so, through those who were cynical or uncertain, to those who were supportive of the idea.
Resistance
One argument against implementing a walk to work initiative was that it was not the job of the employer to tell workers how to get to work: ‘I would find it really offensive if I had that in my objectives, like who the hell are you to tell me I have to have “walking to work”’ (936–003, male); ‘I wouldn’t want people to feel obligated just because the boss was keen on it’ (912–001, female). Despite the fact that transitions such as moving house or starting a new job are considered opportunities for reviewing transport arrangements, the reluctance to suggest walking to work to employees was strongest in a workplace where a large-scale relocation was taking place: ‘You’ve got about 4000 people that are totally miffed because they’ve had to come here [relocate from another city] and the last thing you want to start talking about is how they travel to work’ (936–003, male).
Those who were against workplace initiatives of this kind suggested that employers should focus on other issues: ‘There isn’t a benefit to the organisation. Therefore, I don’t think the organisation should be doing that. I think if people themselves want to do it, I think if there’s a walk to work campaign somewhere you know nationally whatever and people think gosh that’s good and then you can apply to get a pedometer or whatever, but it’s not a workplace initiative’ (P1–4–01, female); ‘We’re firing quite a lot of information at people all the time about, you know, the law and office procedures etc. so you would, you tend to concentrate on that as opposed to extraneous stuff . . . I think it’s a good thing to do but I don’t think it’s a responsibility for an employer’ (DC2–18–002, male).
Other workplace priorities took precedence over the suggested Walk to Work initiative, which involved training a member of staff and allowing them time to speak with colleagues about walking to work: ‘I know budgets are very, very tight at the moment, um, we’re working pretty much, you know, trying to reduce cost all the time and you know we wouldn’t possibly be able to release somebody away from their day job . . . At the end of the day our sole role here is to, is to serve the customers so we can’t compromise that at any time’ (P1–2–01, female).
The size of workplace could be seen as problematic for both small and large employers. A small business indicated that it would be difficult to release staff from other duties to promote walking: ‘The kind of economic conditions obviously people keep staff levels at a minimum so everybody who’s here is working their socks off. You tend not to have much spare time to do additional extras, um, certainly for small businesses’ (912–001, female). However, a large workplace suggested that it was not possible to monitor, and consequently reward, those who walk to work: ‘You can’t monitor each individual on how they travel to work on a daily basis. You could give them meal vouchers so if they walk to work and they, you know, they’ve proven that they’ve walked to work they get a meal voucher or a coffee voucher or something like that . . . those are a nice, a nice thing to do but they’ll never, they’ll never be introduced, not, certainly not in organisations as large as ours. In a small office environment where you, you’ve got maybe 20 employees and you see them travelling to work on a daily basis, it’s, you know, it could be possible to introduce that there. But in an organisation with so many buildings and so many members of staff . . . it’s just not going to be possible here’ (P1–5–01, female).
It was suggested that the mode of travel to and from work was really a matter of personal choice: ‘I just think it’s about dictating to people. I think they should have their own choice. Once they get to work then they’re working, but before they get here as far as I’m concerned they do what they please . . . If somebody started telling me, I wouldn’t stay there’ (P1–4–01, female); ‘There’s not a workplace travel plan in place. It’s literally their, it’s their choice if they want to walk’ (P1–3–01, male). Some employees were thought to have valid reasons for their travel mode: ‘I felt that, from my employees, those that chose to walk to work probably already did and I wasn’t sure that there was any way that I could change or you could change the journey method for those that didn’t because there was a very valid, practical reason’ (912–001, female); ‘A large percentage of my employees in this store are female and we have quite an open range of times where they could start and finish. Some will start at 5 in the morning, some will finish at 2 a.m., 2 a.m. in the morning, so for their safety although they might live fairly close they’d still choose to drive which is probably the sensible thing to do at that time of morning’ (P1–3–01, male).
Cynicism
There was a degree of cynicism among those who had already spent a great deal of effort on travel initiatives that they perceived to be unsuccessful. Within this category were those who had been tasked with implementing travel plans, some of whom appeared jaded by their experience. This was particularly evident in large workplaces: ‘We’re not seen as a, so much as a family in my view, we’re seen as sort of the faceless bureaucratic lumbering giant of an organisation, and so I think generally our expectations of people’s engagement is quite low’ (937–001, male); ‘We’ve had the travel plan since 2008 and [we’re] currently reviewing it at the moment because obviously it is now out of date. To be honest the walking initiatives will probably just remain as they are. We’ll just roll them forward to the next year because there is, there is . . . very little we can do to really actively promote it’ (P1–5–01, female); ‘I think we’re having a bit of a backlash. I mean, not amongst people who are already busy and active, but amongst people who aren’t. They’re fed up at being preached at by people’ (DC1–25–901, female).
In some cases, those who were tasked with implementing the travel plan were also responsible for promoting a range of other initiatives: ‘There’s only a few of us here that we have to deal with what, everything on the site like the energy, the recycling, the waste, I mean green transport is quite a big part of our job but it’s not the major part, um, we just really, really don’t have the time’ (936–001, female); ‘There’s a huge amount going on in [name of city] to promote active travel . . . I think they’re notoriously difficult to achieve [laugh]. They’re very well intentioned but it’s very difficult to get people to, to do it’ (DC1–25–901, female); ‘We’ve got gym facilities . . . we do a lot of classes . . . that’s where people will go to if they want to keep fit but the walking part, making someone walk to work or encouraging someone to walk to work I think [laugh] it’s a dead end personally because it’s telling, people don’t like being told what to do’ (936–003, male).
The perceived motives for implementing travel initiatives could cause tension between employers and managers and their staff: ‘I think how employers do it, why they do it, and when they do it is critical because if it’s perceived as being an alternative to previous terms and conditions, if staff perceive this as being a cost-saving initiative on the part of their employer, I think they will automatically do the opposite and they will resist’ (DC1–25–901, female); ‘I banned parking in several sites across my domain and that’s caused a lot of concern and a lot of tension . . . If you just introduce massive blanket decisions it just upsets them and winds them up even more and probably makes them more resistant to, to change’ (925–001, male).
There was some evidence of stereotyping employees as not really interested in such health promotion initiatives: ‘They work really hard, they work weekends, then they go on holiday for 2 weeks and they don’t really have any, any worries or they don’t really think about these sort of things in more detail if you get what I mean. They do just live their normal life, they come to work, do their job, they come in on overtime as well, but they don’t really think about, about things like that’ (DC1–28–901, female); ‘It is banging your head against a brick wall because most people they are la– they have become a lazy nation, they don’t want to walk anywhere’ (936–001, female); ‘I tend to have, um, a lot of young students and a lot of the older people. I think perhaps maybe it’s the age group that’s partly the lack of interest. And there’s a lot of youngsters now. They don’t walk anywhere, do they?’ (P1–2–01, female). It was felt that there was already information and guidance about the benefits of walking but that people chose to ignore it: ‘If somebody doesn’t recognise themselves that walking is good for them, and they would rather get in the car, I don’t think an employer can really change that’ (DC1–21–901, male); ‘The individual knows all the reasons and it’s, you know, a lot of different media tell them to walk so . . . we have to really target things we can make a difference with’ (P1–5–01, female).
Uncertainty
Although willing to try implementing a Walk to Work initiative, employers appeared uncertain about how this could be done in practice: ‘We’re doing everything we can around sort of lifestyle choices but it’s not really about them walking to work’ (P1–4–01, female); ‘In the end if somebody doesn’t want to walk to work . . . I don’t know that there’s much you can do about it ‘cos as employers you can’t put it in their contract or anything like that [laugh], you know . . . I mean a lot of it’s about encouragement, I think a couple of the lads have been challenging each other but you know in the end I suppose with one or two people it might be a question of making them feel that they’re not going to get penalised if they are a little bit late in because they didn’t leave early enough while they’re getting the hang of walking, but, um, I don’t know what else you could really do in the end’ (DC2–20–004, female); ‘I think you can have a marginal effect on people, I think you can educate and remind as opposed, I mean there’s no sort of structure I think you can impose on anybody about, about it’ (DC2–18–002, male).
The availability of car parking was seen as a barrier that was difficult to overcome: ‘Um, if you’re somewhere where there’s no parking then the job’s done for you but, you know, I don’t think a company can start to get rid of its car parking [laugh] as a means of encouraging people to walk so I think, I think that’s a tough one’ (DC1–21–901, male); ‘The biggest factor has got to be whether you’ve got a car parking space, isn’t it, I would say. It is for me. If I didn’t have a car parking space I would have to find some other way of making my way into work’ (DC1–18–006, male). If driving was perceived to be the ‘easy option’, employers were unsure if their efforts to encourage walking could really be effective: ‘I think it’s a, where it’s relatively easy for people to walk then it’s relatively easy to get them to do it. But where people are used to driving and driving is relatively easy too, then I think it’s quite a big, it’s quite a challenge to get them to change really’ (DC2–11–901, male); ‘All we can do is say it would be good, it’s better for your health . . . I think people would follow up on encouragement if they were sort of on the borderline anyway. I’m not sure how successful I’d be in changing the mindset of somebody who was a dedicated car driver [laugh]. Yeah, you’d need to understand their personal circumstance’ (912–001, female).
The uncertainty about how to support walking was often in contrast with the promotion of cycling: ‘Biking obviously through the bike, work bike scheme, and that’s an incentive but obviously people are biking. Um, to walk, phew, not sure what incentive there could be really, no can’t think of what an incentive might be to encourage people to, to walk’ (925–001, male); ‘I know there’s a lot of emphasis on sort of cycling isn’t there? I mean cycling’s becoming more and more popular, you can see that, but I think perhaps some people don’t even think about the walking side’ (P1–5–01, female); ‘Well, we have quite a lot of cyclists, actually, our uptake of cyclists is very, very good, but I don’t know how, when it comes to walking and exercise we’ve become a fat nation [laugh]. We are, and people don’t want to do it, there’s no, incentives’ (936–001, female); ‘We don’t have that many schemes for walkers like we do for cyclists and motorcyclists and public transport users’ (P1–5–01, female).
There were concerns about whether an intervention that involved training an employee to act as a workplace-based Walk to Work promoter could be accommodated: ‘I mean anything that’s, um, taking time from people, which is not, you know, allocated to say a lunch break or what have you, so therefore it is during their working hours, it’s difficult to do . . . we have time sheets, so every second, minute of the day we record what we’re doing . . . So, yeah, I mean to be fair, yes there’s going to be reluctance because, for that very reason it is, we are very, very much about using and selling our time’ (DC1–18–006, male); ‘One of the hardest things we find in here is to communicate with, with the team because everybody has a job to do . . . Maybe in an environment where you weren’t working with the public then yes, it probably is do-able, you know in an office situation or you know in any situation where you’re not interacting with the public, but the public see a member of staff and quite rightly they expect that they are there to serve them’ (P1–2–01, female). It was suggested that someone from outside the workplace might be better to undertake the role: ‘Whether it’s our business as employers to be saying you should be doing, you should be doing that, as opposed to somebody from outside saying this is the benefits of doing this and [the company] will help you if they can. I think that’s a better way because some people will resent you know the company interfering, “What’s it to you how I get to work as long as I’m here to do my job?” sort of thing, although I don’t get much of that attitude here I have to say but you know it is a possibility’ (930–001, female).
Support
One strong motivation for encouraging walking to work was the desire to be a responsible employer: ‘We’ve a duty of care to staff to encourage them, you know, to try and be healthy, can’t force them, but provide as much as possible . . . It’s not a legal responsibility [laugh] but it, it would be good practice to do that on several levels, on health of the employees, the reduction of the CO2 omissions and other things into the environment, so it perhaps ought to fall under the general health and safety rules, yeah’ (DC2–20–004, female); ‘I think it would fit with the work we’ve done to say we are specifically promoting walking to work. “We think that, as a firm these, these provide benefits to you as employees and therefore we think it’s a good idea.” I think that’s a message that will fit with what we’ve done before’ (DC1–18–006, male).
The potential benefits to both employees and employers could motivate employers to support initiatives to improve the health of the workforce: ‘People feeling healthier and more alert when they get into work so it benefits them and also, you know, it saves people money and that sort of thing. But, um, the parking and that sort of thing, people get stuck in traffic, they’re late for work you know, so it is, a lot of it is, very much positive for people to walk to work ‘cos you don’t get stuck in traffic, they’re saving money, they’re more awake and alert when they get here. OK, admittedly on days like today, bit soggy, but, um, you know I think yeah I think there is some responsibilities that ought to be taken by the employer definitely’ (DC2–14–001, female).
A lack of car parking facilities was seen as beneficial for promoting walking to work: ‘I think the fact that we’ve got limited car parking space [laugh] is, is actually quite good in many ways’ (911–001, female). The tension experienced in workplaces where car parking rights were restricted or removed has already been noted. This might be reduced if there were a change in circumstances that could not be ‘blamed’ on the employer: ‘I can envisage things that would make people have to consider walking, like, you know, if the parking here disappeared because the council made it prohibitive by charging us whatever’ (DC2–11–901, male). One company was expanding and moving to new premises: ‘We’re not going to increase the number of people that can park to try and discourage the amount of people that bring their car into work’ (DC2–27–014, female). Recruiting new staff also provided an opportunity to promote walking to work: ‘People who are starting a new job, we could highlight to them, “If you’re thinking about moving house here’s list of places you may want to live” . . . give some information about potential accommodation options . . . if we don’t do that then they’re living 10 miles away, they’re never going to walk to work’ (937–001, male).
Some workplaces were able to be flexible about working hours and this was seen to be an advantage when encouraging employees to change their travel behaviour: ‘I think it is possible and we do consider the working hours of individuals so if somebody wanted, we’ve got somebody that lives up near [place name] and she wants, she walks in but she doesn’t start ‘til 9, and she’s asked “Can I start at 8 o’clock and finish at 5 so it’s lighter in the evening when I walk back, it’s safer?” . . . It’s looking at that side of it and seeing what would work for them and what helps them’ (DC1–22–004, female); ‘We’re not particularly formal about things like, you know, being in bang on 9 o’clock or anything like that, so there’s a degree of flexibility, you know. The priority is getting work done and people are very committed here, so I don’t have concerns in that area. So, um, yeah, so there are no real reasons from that point of view that would stop people considering walking’ (DC2–11–901, male).
Offering breakfast was suggested as an incentive that employers could provide for those who changed their travel behaviour and started walking to work: ‘We’ve got a kitchen, so they can have some breakfast or something to eat if they are walking a bit further in. Because I suppose it is a form of exercise, they might not want to have breakfast beforehand. That would be a good way of doing it’ (DC1–14–001, female); ‘I think more of an incentive that, you know, if we got people to walk to work they got a free breakfast when they came to work . . . or a voucher for a local, breakfast bap or something. Yes, and that might be an incentive to, to start getting people to do it but I think once it becomes a habit and you do it a number of times then it becomes a habit, then you wouldn’t need that incentive. But that might be something that would encourage more people to do it’ (DC2–27–014, female).
Injecting a degree of competition was also suggested as a way of enthusing people to try walking to work: ‘My lot are quite competitive so, anyway, that could put a competition in to it. The most, the most number of days that you’ve walked in over a month’ (911–001, female); ‘We kind of pitted different forms of travel against each other from a named point, which I think was about 5 kilometres from [workplace] actually. So we had a cyclist, a walker, a public transport user, a driver and so on and you know we kind of interviewed them, asked for their experiences after, and the walker said, “Yeah, it was really nice because it was just kind of time out. It was time to think about things, you know. Went through an area that wasn’t a busy road. It was a quiet path through some nice, you know, sort of wildlife and woodlands”. So it created quite a sort of positive example of, of how walking could work really’ (937–001, male).
Chapter 4 Discussion
Lessons learned from the feasibility study
The feasibility study was important for developing the intervention and testing the methods for its implementation and evaluation. In particular, several modifications were suggested for a full-scale trial. The workplace recruitment process should be simplified so that employers are not required to calculate the number of employees who live within 2 miles of the workplace before being recruited to the study. This proved too onerous for some workplaces, which did not sign up for the study after an initial expression of interest. The calculation of distances is valuable to assess how many participants are within ‘walking distance’ and might be encouraged to walk the full distance, and how many others might be encouraged to use mixed mode. However, the study researchers or the Walk to Work promoters could calculate these distances after obtaining consent during DC1 and encourage the Walk to Work promoters to tailor their advice to suit the circumstances.
All employees who do not already always walk or cycle to work, and are not disabled in relation to walking, should be eligible to participate, rather than the initial focus being solely on those living within 2 miles of the workplace. The Walk to Work promoters’ booklets, and the participants’ booklets, will give information and advice in relation to walking the full distance and about combining walking with other modes of transport.
Workplaces with staff on predominantly part-time, zero-hour or short-term contracts are not suitable because of the need for a 1-year follow-up data collection. The attrition level (29% at 1-year follow-up) compared well with other workplace-based interventions. No attempt was made to contact those who had left the workplace. For any future trial, asking for the contact details of those who leave the workplace between baseline and follow-up would enable data collection packs to be forwarded to them, and returned to the researchers, by post.
Flexibility with regard to the training and support of Walk to Work promoters is required. During the feasibility study, it was proposed that the Walk to Work promoters would be invited to one external training event. However, it became clear that not all of the workplaces would be able to release an employee in this way on the same date. Two smaller external training sessions were organised and some individual workplace-based tuition was provided. A choice should, therefore, be offered. Some prompts and encouragement for the Walk to Work promoters themselves during the 10-week intervention period were also suggested during the post-intervention interviews.
Assessment of costs
The intervention was developed and delivered at an affordable average cost per workplace (£441.05). However, the actual cost per workplace varied substantially depending on the number of promoters trained and the location of the training. There were no significant differences in health service or commuting costs at 1-year follow-up. Self-reported measures of productivity were also similar between the intervention and control groups at follow-up.
Despite studies demonstrating the health benefits of active commuting, assessments of the cost-effectiveness of these interventions are relatively scarce. Where economic evaluations have been performed, cost-effectiveness analyses have been conducted66 and benefit-to-cost ratios have been calculated. 67 Our study provides preliminary information on the costs and benefits borne by employers, employees and others, which will be relevant to government bodies and employers when deciding whether or not to adopt such an intervention. The study has demonstrated that it is feasible to conduct an economic evaluation alongside a RCT of an employer-led scheme to increase walking to work.
Future research should incorporate a measure of the time spent by promoters and employees discussing the intervention, in order to calculate a more accurate cost of delivery. Although the 12-month follow-up is long enough to provide information on the medium-term effectiveness of the intervention with respect to commuter behaviour and health service use, it is also important to consider the implication of increased walking on longer-term health-related benefits. Future research should, therefore, include other measures of health in order to capture any long-term benefits. The Health Economic Assessment Tool (HEAT) developed in 2011 could be included, as this assesses resource savings and reduced mortality or increased life-years associated with an increased in time spent walking. 67
Promoting active travel through the workplace
The interviews with employers suggest that there is some uncertainty about whether encouraging change in commuting behaviour should be the responsibility of the employer, other policy-makers, or both. Furthermore, employers need to justify the costs to the organisation and balance the scheme’s activities with other business priorities. In some cases, employers were concerned that attempts to influence travel mode might be interpreted as a cost-cutting exercise or inappropriate interference with the lives of employees outside of the working environment, rather than as a sign of a caring employer.
Some employers were unclear about how to give more general support in the workplace for employees who walk to work. In addition, there was evidence that those who had been charged with promoting ‘green’ travel initiatives in the past could be jaded by the experience. This suggests that additional booklets for employers would be valuable. This booklet could include ideas for promoting walking, such as strategically placed posters and leaflets; providing information about walking distances to train and bus stops; providing lockers or improved cloakroom facilities; financial assistance for public transport season tickets or walking clothes/shoes; free incentive items for those who switch to walking, for example umbrellas, rucksacks or breakfast vouchers; and ideas for ‘competitions’ and challenges for those who enjoy taking part in such activities.
Strengths and limitations
Measuring outcomes
An important strength of this study is the combined use of accelerometry and GPS to measure the journey to work. While accelerometers are commonly used to measure physical activity and can provide highly time-resolved data, they are unable to record the context of physical activity. Consequently, estimates of physical activity based on, for example, hourly mean physical activity may also include other physical activities taking place around the journey (e.g. walking a dog before walking to work). Combining accelerometer data with positional data from GPS receivers allowed both the level and the location of physical activity to be described, and permitted identification of activity levels specifically during journeys.
There are also a number of limitations to this study. The data were collected as part of a feasibility study for which we recruited a relatively small sample of predominantly well-educated younger adults, limiting the generalisability of the findings. Larger, more representative studies using objective methods are needed. The results also show high levels of MVPA, which may be a reflection partly of the accelerometer threshold used (although the threshold used is commonly applied in many studies) but also of the demographic profile of the participants. Nevertheless, the potential contribution to physical activity levels of walking the daily commute is clearly illustrated. To our knowledge, ours is the first study in adults to use accelerometers and GPS spatial segmentation to quantify the contribution of walking to work, demonstrating the substantial contribution that walking to work makes to daily physical activity. These data provide persuasive evidence to underpin interventions to increase active commuting.
Assessment of costs
It was not possible to calculate the total delivery cost if the intervention were to be rolled out nationally. This is because there would be the additional cost of training people to train the promoters. The cost of delivery also varied significantly between workplaces. It was evident that the location of promoter training had a significant impact on the total cost per workplace. The average total cost of promoter training days away from the workplace was £1337.64, whereas for training at the workplace the average cost was £65.00. Had the training been consistently delivered, it might have been possible to observe a link between workplace size and cost.
Although promoter time was costed when they attended training sessions, there was no accurate account of the amount of time promoters and employees spent discussing the scheme. Whether these discussions took place during work hours or out of work hours, this time should be included and costed as part of the delivery of the intervention. There was also the potential for recall bias in the data with respect to health-care services and medication use, which required a 4-week recall.
The response rate on health service use was low, particularly in the control group. This potentially introduces attrition bias and highlights the need for methods to minimise missing responses and impute missing data in a larger trial. A number of assumptions were made while costing medication use which maximised the number of medications costed and minimised the number of missing values. However, these assumptions may be inaccurate; for example, where there was missing information on the number of doses per day, it was assumed that the dose equalled one, which may be an underestimation.
By collecting information on the modes of transport, time spent commuting by each type of transport, bus and train passes, parking permits and car sharing, we were able to calculate the daily commuting cost. In order to include car sharing, parking permits and bus and train passes, a number of assumptions were required. In order to calculate the cost of commuting by car where the car was shared by a number of people, the associated cost was divided equally by the number of individuals in the car. However, car sharing does not necessarily mean that the passengers contribute equally, if at all, to the costs. A weekly cost was calculated for parking permits and for bus and train passes; the weekly cost was divided by the number of work days in the study week in order to identify a daily cost. This cost could be incorrect for three reasons: first, the calculation assumes that the permit/pass is used only on work days, and, if not, the daily cost would be reduced; it also assumes that the study week is representative of the number of work days per week for the duration of the pass/permit; and, finally, it assumes that the permit/pass is used for all work days in the study week.
A return on investment was not calculated for this feasibility study, but should be considered in the economic evaluation of a full-scale trial.
Qualitative research
A strength of the study is the inclusion of qualitative methods to assess the views and experiences of employers, Walk to Work promoters and participants. Focus groups and interviews were conducted with a range of male and female participants of different ages and income groups and from small, medium and large workplaces. The topic guides sought to gain views on specific aspects of the study (e.g. recruitment or the use of BCTs) but also allowed people to tell their story in their own way and to emphasise what was important to them. The research team developed rapport with the participants during the study, which facilitated a degree of candidness during the interviews about the perceived strengths and weaknesses of the intervention and its evaluation. Although it might be thought that those who agreed to participate in the study would be strongly biased towards walking to work, a wide range of views were expressed.
However, the limitations of the qualitative research include a relatively small sample size of predominantly city-centre based participants. The interviewees were, inevitably, all consenting participants in a research study and their views may not be representative of the wider workforce. Additionally, the interviews took place in the workplace of the participants, which, while convenient for them, meant that some interviewees were aware of the need to return to work and were unable to explore issues in depth.
Public involvement
A further strength of the study was the contribution of employers and employees, who gave their views and experiences of the intervention and its evaluation at key stages during the study and made a number of helpful recommendations that could be incorporated into an application for a full-scale trial.
Health inequities
Universal health promotion initiatives are often more readily taken up by those in higher socioeconomic groups while being less effective in changing the behaviour of socially disadvantaged and hard-to-reach groups. 68,69 The Active People Survey70 suggests that recent attempts in the UK to promote walking and cycling have been more attractive to higher-income groups, and the participants in our own study are predominantly well-educated younger adults. In terms of promoting change in travel behaviour, it may be harder to reach people living in more disadvantaged communities who currently drive to work, particularly if walking is perceived as unsafe or long distances are involved. However, other surveys have indicated that walking for transport is more likely to be associated with lower SES. 71–75 Consequently, there may be an opportunity to build upon existing active commuting among lower SES groups.
Choosing behaviour change techniques
The Walk to Work intervention focused on nine BCTs to encourage a sustained increase in walking during the journey to or from work by participating employees. The BCTs were chosen to take the participant through the 10-week intervention: intention formation, barrier identification, goal setting, general encouragement, instruction, self-monitoring, social support, review of goals and relapse prevention. For each individual BCT, there appeared to be people who found it useful and others who did not. Other studies confirm this lack of clarity over which BCTs are essential for a behaviour change intervention. The concept of setting behavioural goals is identified as being important by both Bird et al. 36 and Malik et al. 76 in their review of workplace physical activity. The data from the Walk to Work study suggest that participants chose the techniques that suited their circumstances. This is in line with evidence from a qualitative evidence synthesis of workplace smoking interventions, which argues that workplace interventions should employ a range of different elements if they are to prove effective because different employees have different requirements. 77
Additional motivation may have been helpful for some participants. ‘Contingent rewards’, also listed in the taxonomy of BCTs,33 could be prompted by providing additional guidance for employers about offering small incentives, such as free breakfast or help to purchase walking shoes, for employees who change from commuting by car to walking. Other suggestions included a degree of competition, which may be motivating for some participants but off-putting for others. The BCT ‘provide feedback on performance’, which evaluates performance in relation to others (or a set standard), could be explored. 33
This study used pedometers as an optional self-monitoring tool. Pedometers have been proposed as the single most effective method of physical activity promotion. 78–80 However, as with the other BCTs, the Walk to Work study found that pedometers were useful for some participants and not for others. It would seem that to develop an intervention that specifically requires their use might restrict the involvement of some potential participants.
The term ‘relapse prevention’ was used in Walk to Work booklets, but was challenged as being inappropriate for an intervention that promotes walking. This view is shared by Michie et al. ,34 who argue that different BCTs should be used for initiating positive behaviours, such as physical activity and healthy eating, from those used to stop negative behaviours, such as smoking and alcohol consumption. A term that focuses more positively on maintaining new behaviour may be preferred. The BCT ‘use follow-up prompts’ may be preferable. 33
The role of Walk to Work promoters
The Walk to Work promoters either were volunteers or were asked by their employer to take on the role, and showed varying degrees of interest in active travel. Although they all received training to understand and use the nine BCTs, this was also approached with varying levels of enthusiasm: most appearing keen to help and generally encouraging, with one perhaps being overenthusiastic and another struggling to fulfil the role because of other work commitments. Where one promoter was of a ‘lower grade’ than the colleague they were supporting to walk to work, there was evidence of uncertainty about how to deal with this ‘role reversal’.
Similarly, participants also varied in their appreciation of the support provided by the promoters, from a feeling that it was too ‘light touch’ to concern that they were being pressurised into meeting unrealistic expectations. This would suggest that training should include awareness of how to assess and respond to the varying needs of participants. The availability of a range of approaches, including face-to-face contact with a promoter, guidance booklets, self-monitoring equipment and interactive websites, may help to ensure that the different preferences of participants can be catered for.
An evidence review undertaken on behalf of NICE identified a number of characteristics and competencies for those delivering BCT interventions, which included being supportive, motivating and empathetic, as well as having knowledge and communication skills associated with assessing individuals, signposting support, developing motivation and action, providing feedback, action planning, goal setting and problem solving, encouraging self-management, group counselling and maintaining change and relapse prevention. 38 It is unrealistic to expect volunteers in the workplace to have all of these characteristics and competencies, together with the time and space to implement them. For the Walk to Work intervention, the promoters were provided with a half-day training session supported by booklets and signposts to websites and other useful resources. The appropriate use of these resources, combined with a supportive and empathetic approach, may be an appropriate compromise for a workplace public health intervention of this kind. Nevertheless, workplace volunteers who undertake this role may require some additional training to develop skills and competencies, or external support from those with greater knowledge and experience of health promotion interventions. 37,81
The socioecological model
Advocates of the socioecological model argue for the importance of examining influences at the policy, community, organisational, interpersonal and intrapersonal levels. 38 BCTs are primarily focused on the intrapersonal and interpersonal levels, but participants in the Walk to Work study also highlighted the importance of support at the other levels of the model, particularly the workplace (organisational level), through, for example, employers providing free breakfast for walkers or improved facilities for washing and changing. The availability of car parking was identified as an important barrier, a finding echoed by others who suggest that limiting workplace parking may encourage walking to work. 82–84 For example, a workplace travel plan at the University of Bristol which included controlling the supply and cost of car parking spaces for staff resulted in a self-reported increase in walking to work from 19% to 30% and a reduction in commuting by car from 50% to 33%. 85 In the current study, environmental barriers such as unpleasant or potentially unsafe routes were mentioned but were not as prominent as in other studies. 82–84 This may support the view of Guell et al. ,82 who point out that some participants will walk despite adverse environmental conditions, having overcome the issue through experience or weighing up the perceived benefits and costs.
It is also important to acknowledge the contextual issues which may undermine behaviour change interventions. In the case of the Walk to Work study, it appeared that the legacy of the global financial crisis meant that some employers and employees were unable to prioritise the intervention over other work commitments. Furthermore, the extraordinarily wet weather was identified as an important barrier to walking by participants. However, even within this context, there was evidence of willingness to consider the BCTs and change travel behaviour.
The benefits of walking to work
There is compelling evidence that regular physical activity is effective in the prevention of chronic diseases (including cardiovascular disease, type 2 diabetes, some cancers, hypertension, obesity, depression and osteoporosis) and premature death, with the greatest improvements in health status seen when people who are least active become physically active. 86 Active commuting (walking and cycling) has specifically been associated with an overall reduction in cardiovascular disease. 87 Consequently, those who shift from car use to regular walking during the commute to work are likely to benefit from improvements to health. Other benefits include reduced commuting costs and greater certainty about the timing of the journey. The suggested benefits to employers of promoting walking schemes include increased productivity, a reduction in sick leave, improved public image as a result of lowering the workplace’s carbon footprint, and savings in providing car parking facilities. 27,83,87–89
Public Health England recently announced several ‘high-level enduring priorities’ guiding their work, two of which are relevant to this study: helping people to live longer and more healthy lives by reducing preventable deaths, and improving health in the workplace by encouraging employers to support their staff, and those moving into and out of the workforce, to lead healthier lives. 90 Similar aims are shared by governments and health practitioners throughout the world. Encouraging employees to walk to work has the potential to make a considerable contribution to addressing these priorities.
Conclusion and recommendations
The aim of the Walk to Work study was to test the feasibility of developing and evaluating an employer-led intervention to increase walking to work. Consequently, the implications of this study do not, at this stage, relate to practice but to the feasibility and design of a follow-on full-scale RCT.
Recommendations for future research
There continues to be a paucity of objective evidence about the effectiveness of workplace-based interventions to promote walking during the daily commute. The Walk to Work intervention and its evaluation were feasible and acceptable to participants. Qualitative and statistical evidence suggest sufficient evidence of promise to justify a follow-on full-scale cluster RCT.
Lessons were learned during the feasibility study which should be incorporated into a future trial. In particular:
-
The workplace recruitment process should be simplified so that employers are not required to calculate the number of employees who live within 2 miles of the workplace before being recruited to the study. The calculation of distances is valuable to assess how many participants are within ‘walking distance’ and might be encouraged to walk the full distance, and how many others might be encouraged to use mixed modes. However, the study researchers or the Walk to Work promoters could calculate these distances after obtaining consent during DC1 and the Walk to Work promoters could be encouraged to tailor their advice to suit the circumstances.
-
Employees who live longer distances from the workplace should be recruited and encouraged to incorporate walking into their daily commute through using public transport or ‘park and stride’.
-
A booklet should be supplied to employers in the intervention arm with information and ideas for employers about how to support walking to work.
-
Supportive prompts for the Walk to Work promoters should be provided to coincide with the four contacts they make with employees during the 10-week intervention.
In common with other public health initiatives, the Walk to Work study attracted more educated participants from higher socioeconomic groups. A future study should be proactive in selecting workplaces serving more disadvantaged communities, and in attempting to recruit people from lower socioeconomic groups within workplaces.
A return on investment was not calculated for this feasibility study, but should be considered in the economic evaluation of a full-scale trial. Different workplaces may place different emphases on potential returns; this may relate to employees’ health and well-being, corporate social responsibility, or absentee rates and productivity. The motivations and expectations of different employers could be explored through questionnaires and qualitative interviews.
Acknowledgements
We would especially like to thank all of the workplaces and employees who participated in the study, and the Walk to Work promoters and the staff at BusinessWest who helped us with recruitment. We are grateful to our collaborators: Dr John Savage, GWE BusinessWest; Dr Hugh Annett, Director of Public Health (retired), Bristol City Council; and Professor Stephen Blair, Arnold School of Public Health, University of South Carolina. We are also grateful to the independent members of the steering group: Dr David Ogilvie (Chair), MRC Epidemiology Unit, University of Cambridge; Dr Ben Wheeler, University of Exeter; and Dr Kiron Chatterjee, University of the West of England. We would like to thank Dr Chris Metcalfe, University of Bristol, for his assistance with statistical analyses, including calculating the ICC and sample size. We are also grateful to Dr Sara Brookes, University of Bristol, for her help in drafting the original proposal and Dr Fran Carroll for assistance in designing the assessment of costs.
This project was funded by the National Institute for Health Research (NIHR) Public Health Research programme (project number 10/3001/04). The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the NIHR Public Health Research programme or the Department of Health. The views and opinions expressed by the interviewees in this publication are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, MRC, NIHR Central Commissioning Facility, NETSCC, the NIHR Public Health Research programme or the Department of Health.
The work was undertaken with the support of The Centre for the Development and Evaluation of Complex Interventions for Public Health Improvement (DECIPHer), a UK Clinical Research Collaboration Public Health Research Centre of Excellence. Funding from the British Heart Foundation, Cancer Research UK, the Economic and Social Research Council (RES-590–28–0005), MRC, the Welsh Government and the Wellcome Trust (WT087640MA), under the auspices of the UKCRC, is gratefully acknowledged.
Contributions of authors
Dr Suzanne Audrey (Research Fellow) was the chief investigator for the study. She conceived and designed the study, supervised its conduct, led on the analysis of employers’ views and led the writing of the report.
Dr Sunita Procter (Research Associate) was the study manager, contributed to the design of the intervention, led the analysis of the data relating to the use of behaviour change techniques and contributed to the writing of the report.
Professor Ashley Cooper (Professor of Physical Activity and Public Health) was a co-applicant, led on the measurement of physical activity and contributed to the sections of the report relating to physical activity outcomes.
Professor Nanette Mutrie (Chair in Physical Activity for Health) was a co-applicant and contributed to the design of the intervention and the section of the report relating to the use of behaviour change techniques.
Professor William Hollingworth (Professor of Health Economics) was a co-applicant, led on the assessment of costs and contributed to the section of the report relating to the assessment of costs.
Dr Adrian Davis (Public Health and Transport Consultant) was a co-applicant and contributed to the design of the intervention and the section of the report relating to the use of behaviour change techniques.
Dr Ruth Kipping (Research Fellow and NHS Consultant in Public Health) was a co-applicant and contributed to the study design.
Mr Philip Insall (Health Director at Sustrans) was a co-applicant and contributed a lay perspective throughout the study.
Ms Kirsty Garfield (Research Assistant in Health Economics) undertook analyses and contributed to the section of the report relating to the assessment of costs.
Professor Rona Campbell (Professor of Health Services Research) advised on the study design and conduct.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health.
Publications
Audrey S, Procter S, Cooper AR. The contribution of walking to work to adult physical activity levels: a cross sectional study. Int J Behav Nutr Phys Act 2014;11:37.
Procter S, Mutrie N, Davis A, Audrey S. Participants’ views of using behavior change techniques to encourage walking to work: a qualitative study. BMC Public Health 2014;14:868.
Audrey S, Procter S. Employers’ views of promoting walking to work: a qualitative study. Int J Behav Nutr Phys Act 2015;12:12.
References
- Start Active, Stay Active: A Report on Physical Activity for Health from the Four Home Countries’ Chief Medical Officers. London: Department of Health; 2011.
- UK Physical Activity Guidelines. London: Department of Health; 2011.
- Haskell WL, Lee I-M, Pate RR, Powell KE, Blair SN, Franklin BA, et al. Physical activity and public health: updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Med Sci Sports Exerc 2007;39:1423-34. http://dx.doi.org/10.1249/mss.0b013e3180616b27.
- Health Survey for England 2008: Volume 1 Physical Activity and Fitness. London: The Information Centre; 2010.
- Health Survey for England – 2012. Is the Adult Population in England Active Enough?. London: UCL; 2012.
- Be Active, Be Healthy: A Plan for Getting the Nation Moving. London: Department of Health; 2009.
- Wilmot EG, Edwardson CL, Achana FA, Davies MJ, Gorely T, Gray LJ, et al. Sedentary time in adults and the association with diabetes, cardiovascular disease and death: systematic review and meta-analysis. Diabetologia 2012;55:2895-905. http://dx.doi.org/10.1007/s00125-012-2677-z.
- Bassett D, Pucher J, Buehler R, Thompson D, Crouter S. Walking, cycling, and obesity rates in Europe, North America and Australia. J Phys Act Health 2008;5:795-814.
- Morris J, Hardman A. Walking to health. Sports Med 1997;23:306-32. http://dx.doi.org/10.2165/00007256-199723050-00004.
- Ainsworth BE, Haskell WL, Whitt MC, Irwin ML, Swartz AM, Strath SJ, et al. Compendium of physical activities: an update of activity codes and MET intensities. Med Sci Sports Exerc 2000;32:S498-516. http://dx.doi.org/10.1097/00005768-200009001-00009.
- A Walking Strategy for Scotland: Consultation Document. Edinburgh: Scottish Executive Development Department; 2003.
- Walking and Cycling: An Action Plan. London: Department for Transport; 2004.
- A Walking and Cycling Action Plan for Wales. Cardiff: Welsh Assembly Government; 2008.
- Coote A. What health services could do about climate change. BMJ 2006;332:1343-4. http://dx.doi.org/10.1136/bmj.332.7554.1343.
- National Travel Survey Statistical Release. London: Department for Transport; 2012.
- Economic Assessment of Transport Infrastructure and Policies: Methodological Guidance on the Economic Appraisal of Health Effects Related to Walking and Cycling. Denmark: World Health Organization; 2007.
- Davis A. Value for Money: An Economic Assessment of Investment in Walking and Cycling. Department of Health and Government Office for the South West; 2010.
- Prince SA, Adamo KB, Hamel ME, Hardt J, Connor Gorber S, Tremblay M. A comparison of direct versus self-report measures for assessing physical activity in adults: a systematic review. Int J Behav Nutr Phys Act 2008;5. http://dx.doi.org/10.1186/1479-5868-5-56.
- Vuillemin A, Rostami C, Maes L, Van Cauwenberghe E, Van Lenthe FJ, Brug J, et al. Worksite physical activity interventions and obesity: a review of European studies (the HOPE Project). Obesity Facts 2011;4:479-88. http://dx.doi.org/10.1159/000335255.
- Arvidsson D, Kawakami N, Ohlsson H, Sundquist K. Physical activity and concordance between objective and perceived walkability. Med Sci Sports Exerc 2012;44:280-7. http://dx.doi.org/10.1249/MSS.0b013e31822a9289.
- Sundquist K, Eriksson U, Kawakami N, Skog L, Ohlsson H. Neighborhood walkability, physical activity, and walking behavior: the Swedish Neighborhood and Physical Activity (SNAP) study. Soc Sci Med 2011;72:1266-73. http://dx.doi.org/10.1016/j.socscimed.2011.03.004.
- Gordon-Larsen P, Boone-Heinonen J, Sidney S, Sternfield B, Jacobs DR, Lewis CE. Active commuting and cardiovascular disease risk: the CARDIA study. Arch Intern Med 2009;169:1216-23. http://dx.doi.org/10.1001/archinternmed.2009.163.
- Hillsdon M, Foster C, Cavill N, Crombie H, Naidoo B. The Effectiveness of Public Health Interventions for Increasing Physical Activity Among Adults: A Review of Reviews. London: Health Development Agency; 2005.
- Kahn E, Ramsey LT, Brownson RC, Heath GW, Howze EH, Powell KE, et al. The effectiveness of interventions to increase physical activity: a systematic review. Am J Prev Med 2002;22:73-106. http://dx.doi.org/10.1016/S0749-3797(02)00434-8.
- Foster C, Hillsdon M, Thorogood M. Interventions for promoting physical activity. Cochrane Database Syst Rev 2005;2.
- Ogilvie D, Egan M, Hamilton V, Petticrew M. Promoting walking and cycling as an alternative to using cars: systematic review. BMJ 2004;329:763-6. http://dx.doi.org/10.1136/bmj.38216.714560.55.
- Ogilvie D, Foster CE, Rothrie H, Call N, Hamilton V, Fitzsimons CF, et al. Interventions to promote walking: systematic review. BMJ 2007;334. http://dx.doi.org/10.1136/bmj.39198.722720.BE.
- Dugdill L, Brettle A, Hulme C, McCluskey S, Long AF. Workplace physical activity interventions: a systematic review. Int J Workplace Health Manag 2008;1:20-4. http://dx.doi.org/10.1108/17538350810865578.
- Promoting Physical Activity in the Workplace. Manchester: NICE; 2008.
- nibusinessinfo.co.uk . Workplace Travel Planning: Travel Planning Business Benefits n.d. www.nibusinessinfo.co.uk/content/travel-planning-business-benefits (accessed 30 September 2014).
- Pedestrian Casualties in Reported Road Accidents: 2008 – Road Accident Statistics Factsheet No.3. London: Department for Transport; 2010.
- Michie S, Richardson M, Johnston M, Abraham C, Francis J, Hardeman W, et al. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behavior change interventions. Ann Behav Med 2013;46:81-95. http://dx.doi.org/10.1007/s12160-013-9486-6.
- Abraham C, Michie S. A taxonomy of behavior change techniques used in interventions. Health Psychol 2008;27:379-87. http://dx.doi.org/10.1037/0278-6133.27.3.379.
- Michie S, Ashford S, Sniehotta FF, Dombrowski SU, Bishop A, French DP. A refined taxonomy of behaviour change techniques to help people change their physical activity and healthy eating behaviours: the CALO-RE taxonomy. Psychol Health 2011;26:1479-98. http://dx.doi.org/10.1080/08870446.2010.540664.
- Michie S, Abraham C, Whittington C, McAteer J, Gupta S. Effective techniques in healthy eating and physical activity interventions: a meta-regression. Health Psychol 2009;28:690-701. http://dx.doi.org/10.1037/a0016136.
- Bird EL, Baker G, Mutrie N, Ogilvie D, Sahlqvist S, Powell J. Behavior change techniques used to promote walking and cycling: a systematic review. Health Psychol 2013;32:829-38. http://dx.doi.org/10.1037/a0032078.
- Behaviour Change: Individual Approaches. Manchester: NICE; 2014.
- McLeroy K, Bibeau D, Steckler A. An ecological perspective on health promotion programs. Health Educ Q 1988;15:351-77. http://dx.doi.org/10.1177/109019818801500401.
- Sustrans n.d. www.sustrans.org.uk/ (accessed 14 October 2014).
- Cyclescheme n.d. www.cyclescheme.co.uk/ (accessed 14 October 2014).
- Developing and Evaluating Complex Interventions: New Guidance. London: Medical Research Council; 2008.
- Campbell M, Fitzpatrick R, Haines A, Kinmonth AL, Sandercock P, Spiegelhalter D, et al. Framework for design and evaluation of complex interventions to improve health. BMJ 2000;321:694-6. http://dx.doi.org/10.1136/bmj.321.7262.694.
- Campbell M, Elbourne D, Altman D. CONSORT statement: extension to cluster randomised trials. BMJ 2004;328:702-8. http://dx.doi.org/10.1136/bmj.328.7441.702.
- Bristol City Council . The Population of Bristol n.d. www.bristol.gov.uk/page/council-and-democracy/population-bristol (accessed 30 September 2014).
- Bristol City Council . Labour Market and Employment Statistics n.d. www.bristol.gov.uk/page/council-and-democracy/labour-market-and-employment-statistics (accessed 30 September 2014).
- Bristol City Council . 2011 Census Topic Report: Who Cycles to Work? n.d. www.bristol.gov.uk/sites/default/files/documents/planning_and_building_regulations/planning_policy/local_development_framework/2011%20Census%20Topic%20Report%20-%20Who%20cycles%20to%20work%20v2.pdf (accessed 30 September 2014).
- HM Revenue and Customs . CA23170 – Plant and Machinery Allowance (PMA): First Year Allowance (FYA): Meaning of SME n.d. www.hmrc.gov.uk/manuals/camanual/ca23170.htm (accessed 30 September 2014).
- Freedson PS, Melanson E, Sirard J. Calibration of the Computer Science and Applications, Inc. accelerometer. Med Sci Sports Exerc 1998;30:777-81. http://dx.doi.org/10.1097/00005768-199805000-00021.
- Audrey S, Procter S, Cooper AR. The contribution of walking to work to adult physical activity levels: a cross sectional study. Int J Behav Nutr Phys Act 2014;11. http://dx.doi.org/10.1186/1479-5868-11-37.
- Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Medical Research Methodology 2013;13. http://dx.doi.org/10.1186/1471-2288-13-117.
- Ritchie J, Lewis J. Qualitative Research Practice: A Guide for Social Science Students and Researchers. London: Sage; 2003.
- Office for National Statistics . Patterns of Pay Tables, 1997–2012 n.d. www.ons.gov.uk/ons/publications/re-reference-tables.html?edition=tcm%3A77–294314 (accessed 23 October 2013).
- The Automobile Association . The AA Schedule of Motoring Costs n.d. www.theaa.com/motoring_advice/running_costs/ (accessed 31 October 2013).
- Curtis L. Unit Costs of Health and Social Care 2012. Canterbury: PSSRU, University of Kent; 2012.
- Department of Health . NHS Reference Costs 2011–2012 n.d. www.gov.uk/government/publications/nhs-reference-costs-financial-year-2011-to-2012 (accessed 6 November 2013).
- NHS Choices . Acupuncture 2012. www.nhs.uk/conditions/acupuncture/Pages/Introduction.aspx (accessed 13 January 2014).
- NHS Choices . Chiropractic 2012. www.nhs.uk/conditions/chiropractic/Pages/Introduction.aspx (accessed 13 January 2014).
- Prescription Cost Analysis – England, 2012. Leeds: Health and Social Care Information Centre; 2013.
- Reilly MC, Zbrozek AS, Dukes EM. The validity and reproducibility of a work productivity and activity impairment instrument. PharmacoEconomics 1993;4:353-65. http://dx.doi.org/10.2165/00019053-199304050-00006.
- Congestion on Local Authority Managed ‘A’ Roads: 2011/12. London: Department for Transport; 2012.
- Oulton N, Sebastiá-Barriel M. Working Paper No. 470: Long and Short-Term Effects of the Financial Crisis on Labour Productivity, Capital and Output. London: Bank of England; 2013.
- Meteorological Office . Summer 2012 Was the Wettest in 100 Years n.d. www.metoffice.gov.uk/news/releases/archive/2012/second-wettest-summer (accessed 14 October 2012).
- Office for National Statistics . UK Standard Industrial Classification of Economic Activities 2007 (SIC 2007) 2009.
- Procter S, Mutrie N, Davis A, Audrey S. Views and experiences of behaviour change techniques to encourage walking to work: a qualitative study. BMC Public Health 2014;14. http://dx.doi.org/10.1186/1471-2458-14-868.
- Audrey S, Procter S. Employers’ views of promoting walking to work: a qualitative study. Int J Behav Nutr Phys Act 2015;12.
- Shaw R, Fenwick E, Baker G, McAdam C, Fitzsimons C, Mutrie N. ‘Pedometers cost buttons’: the feasibility of implementing a pedometer based walking programme within the community. BMC Public Health 2011;11. http://dx.doi.org/10.1186/1471-2458-11-200.
- Sinnett D, Powell J. Economic Evaluation of Living Streets’ Fitter for Walking Project. Loughborough: British Heart Foundation National Centre for Physical Activity and Health; 2012.
- Health Inequalities: Third Report of Session 2008–09. London: The Stationery Office; 2009.
- Krebs R, Ali T, Baldwin R, Brownsword K, Calman C, Godfrey T, et al. Public Health: Ethical Issues. London: Nuffield Council on Bioethics; 2007.
- Sport England . Active People Survey 4 n.d. sportengland.org/research/active_people_survey/active_people_survey_4.aspx (accessed 14 October 2014).
- Yong Y, Diez Roux A, Auchincloss AH, Rodriguez D, Brown DG. Exploring walking differences by socioeconomic status using a spatial agent-based model. Health Place 2012;18:96-9. http://dx.doi.org/10.1016/j.healthplace.2011.08.010.
- Tin Tin S, Woodward A, Thornley S, Ameratunga S. Cycling and walking to work in New Zealand, 1991–2006: regional and individual differences, and pointers to effective interventions. Int J Behav Nutr Phys Act 2009;6. http://dx.doi.org/10.1186/1479-5868-6-64.
- Kitchen P, Williams A, Chowhan J. Walking to work in Canada: health benefits, socio-economic characteristics and urban-regional variations. BMC Public Health 2011;11. http://dx.doi.org/10.1186/1471-2458-11-212.
- Hearst MO, Sirard JR, Forsyth A, Parker ED, Klein EG, Green CG, et al. The relationship of area-level sociodemographic characteristics, household composition and individual-level socioeconomic status on walking behavior among adults. Transport Res A-Pol 2013;50:149-57.
- Goodman A, Guell C, Panter J, Jones NR, Ogilvie D. Healthy travel and socio-economic structure of car commuting in Cambridge, UK: a mixed-methods analysis. Soc Sci Med 2012;74:1929-38. http://dx.doi.org/10.1016/j.socscimed.2012.01.042.
- Malik SH, Blake H, Suggs LS. A systematic review of workplace health promotion interventions for increasing physical activity. Br J Health Psychol 2013;19:149-80. http://dx.doi.org/10.1111/bjhp.12052.
- Carroll C, Rick J, Leaviss J, Fishwick D, Booth A. A qualitative evidence synthesis of employees’ views of workplace smoking reduction or cessation interventions. BMC Public Health 2013;13. http://dx.doi.org/10.1186/1471-2458-13-1095.
- Heath GW, Parra DC, Sarmiento OL, Andersen LB, Owen N, Goenka S, et al. Evidence-based intervention in physical activity: lessons from around the world. Lancet 2012;380:272-81. http://dx.doi.org/10.1016/S0140-6736(12)60816-2.
- Heesch KC, Dinger MK, McClary KR, Rice KR. Experiences of women in a minimal contact pedometer-based intervention: a qualitative study. Women Health 2005;41:97-116. http://dx.doi.org/10.1300/J013v41n02_07.
- Lauzon N, Chan CB, Myers AM, Tudor-Locke C. Participant experiences in a workplace pedometer-based physical activity program. J Phys Act Health 2008;5:675-87.
- Dixon D, Johnston M. Health Behaviour Change Competency Framework: Competences to Deliver Interventions to Change Lifestyle Behaviours that Affect Health. Edinburgh: The Scottish Government; 2010.
- Guell C, Panter J, Ogilvie D. Walking and cycling to work despite reporting an unsupportive environment: insights from a mixed-method exploration of counterintuitive findings. BMC Public Health 2013;13. http://dx.doi.org/10.1186/1471-2458-13-497.
- Panter J, Desousa C, Ogilvie D. Incorporating walking or cycling into car journeys to and from work: the role of individual, workplace and environmental characteristics. Prev Med 2013;56:211-17. http://dx.doi.org/10.1016/j.ypmed.2013.01.014.
- Panter J, Griffin S, Dalton AM, Ogilvie D. Patterns and predictors of changes in active commuting over 12 months. Prev Med 2013:776-84. http://dx.doi.org/10.1016/j.ypmed.2013.07.020.
- Brockman R, Fox K. Physical activity by stealth? The potential health benefits of a workplace transport plan. Public Health 2010;125:210-16. http://dx.doi.org/10.1016/j.puhe.2011.01.005.
- Warburton D, Nicol C, Bredin S. Health benefits of physical activity: the evidence. CMAJ 2006;174:801-9. http://dx.doi.org/10.1503/cmaj.051351.
- Hamer M, Chida Y. Active commuting and cardiovascular risk: a meta-analytic review. Prev Med 2008;46:9-13. http://dx.doi.org/10.1016/j.ypmed.2007.03.006.
- de Nazelle A, Nieuwenhuijsen MJ, Anto JM, Brauer M, Briggs D, Braun-Fahrlander C, et al. Improving health through policies that promote active travel: a review of evidence to support integrated health impact assessment. Environ Int 2011;37:766-77. http://dx.doi.org/10.1016/j.envint.2011.02.003.
- Jarrett J, Woodcock J, Griffiths UK, Chalabi Z, Edwards P, Roberts I, et al. Effect of increasing active travel in urban England and Wales on costs to the National Health Service. Lancet 2012;379:2198-205. http://dx.doi.org/10.1016/S0140-6736(12)60766-1.
- Our Priorities for 2013/14. London: Public Health England; 2013.
List of abbreviations
- BCT
- behaviour change technique
- CI
- confidence interval
- cpm
- counts per minute
- DC1
- baseline data collection
- DC2
- post-intervention data collection
- DC3
- 1-year follow-up data collection
- GIS
- geographic information system
- GP
- general practitioner
- GPS
- global positioning system
- ICC
- intracluster correlation coefficient
- MET
- metabolic equivalent of task
- MRC
- Medical Research Council
- MVPA
- moderate to vigorous physical activity
- NICE
- National Institute for Health and Care Excellence
- RCT
- randomised controlled trial
- SD
- standard deviation
- SES
- socioeconomic status
- WHO
- World Health Organization