
Notes
Article history
The research reported in this issue of the journal was funded by the PHR programme as project number 09/3008/07. The contractual start date was in December 2011. The final report began editorial review in July 2014 and was accepted for publication in February 2015. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PHR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
none
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2015. This work was produced by Popay et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Introduction
Background
This is the final report of a study that has explored the impact on health inequalities and their social determinants of the diverse approaches to community engagement (CE) adopted in the New Deal for Communities (NDC) regeneration initiative implemented between 1998/9 and 2010/11. This is the third of three closely linked studies. The Department of Health Policy Research Programme funded the first and second of these studies. The first, which ran from 2003 to 2005 considered the feasibility of evaluating the impact of the NDC initiative on health inequalities using secondary data sources [Popay J, McLeod A, Kearns A, Nazroo J, Whitehead M. New Deal For Communities And Health Inequalities: The Final Report of a Scoping Study. Submitted to the Department of Health (ref: RDD/018/063) 2005; unpublished report]. The second, which ran from 2010 to 2013, evaluated the impact of local NDC programmes on health inequalities and their social determinants. 1 The third study, reported on here, has built on this previous work in three ways: (1) by considering whether or not NDC approaches to CE had any independent impacts on a range of health and social outcomes; (2) by considering whether or not these approaches to CE contributed to the impacts of local NDC programmes reported in our previous study; and (3) by including an exploratory analysis of the cost-effectiveness of NDC CE approaches.
In this introduction we describe some of the challenges involved in evaluating action with the potential to reduce health inequalities and their social determinants, focusing in particular on initiatives to engage the public in policy decision-making. We then briefly consider the role of theory-based evaluations of complex interventions, such as the NDC, before describing the NDC initiative itself and providing an overview of previous evaluation of the impact of different types of local NDC programmes on a range of health and social outcomes. Some of this work is considered in more detail in Chapter 4. Finally, we outline how the rest of the report is structured.
Conceptualising health inequalities and action to reduce them
Health inequalities are systematic differences in health experiences/status between socioeconomic groups, areas of the country, women and men, and different ethnic groups that have their roots in unjust social arrangements. Repeated enquiries into the scale and causes of these inequalities have adopted a social model of health, which places the individual at the centre surrounded by ‘layers of influence’ relating to lifestyle factors, social and community networks, living and working conditions, and the general socioeconomic and cultural environment. 2 To reduce health inequalities action is required at all levels including the wider determinants of health such as unemployment, poverty, low educational attainment, poor housing and poor physical environments.
Despite the considerable effort and resources that have been invested in action to reduce health inequalities in the UK, these inequalities have remained largely unchanged over recent decades and in some instances have worsened. 3 Over the same period action aimed at reducing these inequalities has focused primarily on changing lifestyles among groups with the poorest health. Interventions have had a particular focus on proximal ‘risky behaviours’ including, in particular, poor diet, high alcohol intake, low physical activity, high smoking rates and risky sexual activity. When attempts are made to change environments public health initiatives typically continue to focus on the same ‘risky’ behaviours by, for example, creating environments to encourage greater physical activity, working with ‘fast food’ outlets to change menus and/or banning smoking in public places.
Evaluative research suggests that, although lifestyle-oriented approaches can improve population health overall, they do not significantly reduce health inequalities,4–6 and in some instances can increase them. 7 Part of the explanation for the failure to reduce health inequalities may be a lack of understanding about the meaning of what are commonly labelled ‘risky behaviours’. Research has shown, for example, that for some groups these behaviours may be better understood as ways of coping with difficult life circumstances. 8 From this perspective people experiencing disadvantage may have the capacity to change behaviours only if their social and economic circumstances change for the better. If the circumstances do not change in the face of lifestyle interventions, they may substitute one coping mechanism for another, which could have equally negative impacts on health and well-being.
Another part of the explanation for the enduring nature of health inequalities may lie with the failure of action to address the more distal causes – the causes of the causes as Marmot and colleagues4,9 have argued. For example, Phelan and colleagues6 have shown that historically new socially patterned proximal threats to health tend to replace the risks previously prioritised by public health policies, so continually reproducing health inequalities. These authors and others9,10 argue that this occurs because the fundamental causes of health inequalities – socioeconomic inequality or social injustice – are not being reduced. These ‘fundamental causes’ are assumed to operate through an unequal distribution of multiple resources, including income, wealth and power, which give groups/individuals differential capacity or ‘control’ to reduce proximal risks.
Control, community engagement and health inequalities
Community engagement is an eclectic arena. In the health field it may mean involving people living in particular areas in delivering (typically lifestyle) interventions designed by professionals. Other initiatives aiming to engage local people in action to improve health seek to give residents of a neighbourhood or group influence over which issues are to be prioritised for action, what the action is to be and who delivers it, and how it is to be delivered. In theory there are a number of possible interlinked pathways between the processes of CE, enhanced community control/influence and social and health outcomes (including both improved population health and reduced health inequalities). Some of these pathways are illustrated in Figure 1, which shows the initial conceptual framework that informed our study.
FIGURE 1.
Pathways from community empowerment and engagement to health improvement. Source: Popay. 11
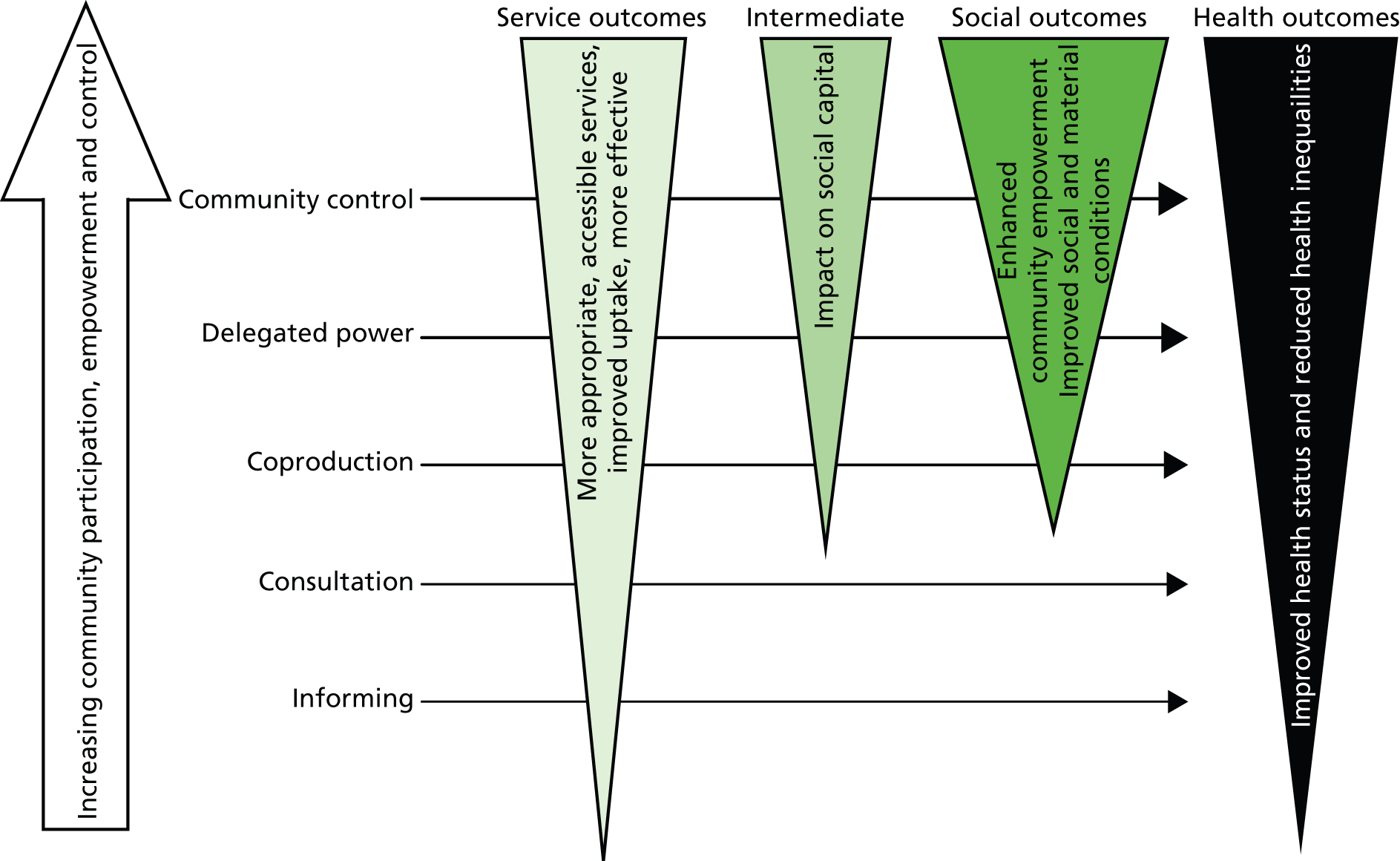
The model proposes that, at one end of the spectrum, engagement that involves the more or less passive transfer of information between communities, professionals and/or organisations may impact on the appropriateness, accessibility, uptake and ultimately the effectiveness of services but is unlikely to increase social cohesion and solidarity among people living in a neighbourhood or result in significant empowerment of a community. Hence, the impact on health at the population or individual level is likely to be modest.
In contrast, the greater the emphasis on giving communities more power and control over decisions that affect their lives, the more likely there are to be positive impacts on service quality, social cohesion, socioeconomic circumstances, community empowerment and ultimately population health and health inequalities. It is also theoretically possible that engagement initiatives may have negative impacts on service use, social cohesion and individual and population health, for example if ‘engaged’ individuals are not appropriately supported and, at the population level, if community expectations of involvement, influence and/or control are not met. 12
There is a considerable body of research on the health and social outcomes of control at the individual level. Within social psychology, control is conceptualised at the individual level as the power to manage situations in the paid work environment, for example Karasek’s demand–control model13 and Siegrist’s effort–reward imbalance model. 14 There is also a literature on social identity, social relationships and membership of groups that links individual control to well-being and health outcomes. 15
Reviews of research evaluating the impact of CE,16–22 have found evidence of positive health and social outcomes for ‘engaged’ individuals including increased self-efficacy, confidence and self-esteem; improved social networks; a greater sense of cohesion and security; improved access to education leading to increased skills and paid employment; and self-reported improvements in physical and mental health, health-related behaviour and quality of life. There is also some evidence that CE can have unintended negative impacts on ‘engaged’ individuals including physical and emotional health costs, consultation fatigue and disillusionment. Additionally, some evidence points to potentially important relationships between the type or level of CE and intermediate social determinants of health outcomes at a community level including, for example, improved uptake and effectiveness of services,19 improved living conditions including housing quality20 and both ‘bonding’ and bridging social capital. 21
Research by Chandler and Lalonde23,24 found that the greater the degree of cultural continuity in British Columbia’s First Nations the lower the rates of youth and adult suicide. Cultural continuity was operationalised in terms of measures of the collective control that First Nations have over their ‘civic lives’ including securing ownership of their traditional lands; community control over educational services, police and fire protection services, and health care; having dedicated ‘cultural facilities’ to help preserve and enrich their cultural lives; women’s participation in local governance; community control over child custody and child protection services; and the proportion of children removed from parental care.
Emerging work by the New Economics Foundation on the concept of solidarity is also relevant to discussions about collective or community control. Coote and Angel25 argue that solidarity locates the sources of transformative action in civil society and recognises that moments for change arise from popular understanding of the structures and processes that reproduce inequalities. Qualitative research suggests that some of the strategies that people develop to manage their lives in difficult places, for example distancing themselves from others living in the same neighbourhood, can undermine the development of shared narratives and respect based on mutual understanding, which are prerequisites for collective action for change. 26,27 Research suggests that initiatives aiming to engage people in policy-making and implementation may help counter these processes and may have positive health and social outcomes for the people who get engaged. However, there is also a significant body of research highlighting the barriers to effective engagement of communities in policy and practice decision-making. 18,28 Formal evaluations of a number of English high-profile health-related policy initiatives in the first decade of this century, all with a strong emphasis on CE (such as Health Action Zones, Sure Start Centres and Healthy Living Centres), highlighted these barriers, reporting that, although community members participated successfully in specific health improvement initiatives and service delivery, there was little collective community control over the strategic direction of these initiatives. 12,29–38
It is also the case that much available research on the impact of CE is of poor quality and there are major gaps in the evidence, including an absence of evidence on the impact on health inequalities; poor descriptions of the CE interventions; a lack of evidence on the relative effectiveness of different CE approaches in engaging people from different social groups/communities, a lack of evidence on the impact of these different CE approaches on the individuals who are engaged and at the community level; and differential impacts of CE across population groups. There is also an absence of adequate information on resource use and especially the opportunity costs of CE to community members. 39 The research reported here has sought to address these problems and advance the evaluation of CE approaches and their impact on health inequalities.
‘Theory of change’ approaches to evaluation
Over the past two decades, theory-based approaches to the assessment of public policy and interventions have been elaborated in the general evaluation literature. 40–42 The idea, as originally proposed by Wholey,43 is to analyse, for the purposes of evaluation, the logical reasoning that connects intervention programme inputs to intended outcomes and assess whether or not there is any reasonable likelihood that programme goals could be achieved. This logical reasoning, called the ‘theory of change’ refers to how and why an intervention works. 44 This literature acknowledges that all intervention programmes are based on theories, whether implicit or explicit, of how the activities proposed in a programme are expected to have their impact. Making these programme theories explicit helps in the design of an evaluation, but also draws attention to the existing literature on the probable effectiveness of the proposed mechanisms for change.
Such theory-based approaches have been used in particular to evaluate the effectiveness of health promotion and risk prevention interventions,45 and latterly have been adopted for the evaluation of complex community interventions in the UK, such as the English Health Action Zones. 46 Their value lies in assessing the effectiveness of the various components of existing interventions, and also the design of future initiatives, by generating plausible programme theories and designing programmes to test them under real-life conditions. 42 The usefulness of ‘theory of change’ approaches is currently being explored for the assessment of the various endeavours to tackle health inequalities. 47 In this evaluation we have used this approach to help in the development of a typology of NDC approaches to CE and in the interpretation of our findings.
The New Deal for Communities Initiative and community engagement
In 2003, the then Labour government set the NHS and local authorities targets for reducing the gap in life expectancy and infant mortality between the most disadvantaged areas/groups and the average for the population as a whole in England. Although much activity was aimed at lifestyle and behaviour change, a National Strategy for Neighbourhood Renewal48 was also expected to contribute by improving the wider social determinants of these inequalities, for example reducing poverty and increasing housing and improving physical environments. The area-based regeneration initiative NDC was a central part of this strategy.
There were 39 NDC areas, launched in two waves: 17 pathfinder areas in 1998 and a further 22 areas in 1999. Each NDC area had a budget of around £50M (nearly £2B in total). The overall aim was to bridge the gap over a 10-year period between some of the most deprived neighbourhoods in England and the rest of the country in six outcome domains, three intended to improve the areas (crime, community cohesion, and housing and the physical environment) and three intended to improve outcomes for people (education, health and worklessness). However, the form that these local programmes took varied significantly as they sought to address local needs in very different socioeconomic, cultural and political contexts.
Various commentators argue that public participation under New Labour was grounded in theories of democracy and citizenship, and framed in rhetoric about building stronger communities through social cohesion and civic renewal. 49–51 Like other policy initiatives at the time, therefore, the NDC programme had a strong focus on CE, reflecting the wider trend of intensifying citizen participation in both UK and international public policy. 52
The theory of change underpinning CE in the NDC and other policy initiatives emerged from the Social Exclusion Unit in the Cabinet Office and assumed that engaging the communities of NDC areas in developing and delivering local programmes would overcome problems of social exclusion and promote social cohesion, hence reducing crime and incivilities, and would also make services more responsive to local needs and hence increase access and effectiveness. 48 An analysis of NDC policy guidance and strategy undertaken by Wright and colleagues51 midway through the programme positioned the NDC as ‘an attempt to reconnect deprived neighbourhoods with the rest of Britain . . . Herein the NDC partnership expresses the ideal of active citizens asserting their equality of status and demanding accountability from service providers’ (p. 351). To achieve these goals, empowerment was conceived of as a mechanism to support members of the public to develop capabilities to participate in and influence services, and shape the future of their neighbourhoods.
However, commentators have also noted the constraints of an empowerment model in the context of a government-led programme ultimately driven by policy-makers’ strategic goals, with policy-makers criticised for lacking an appreciation of the complexity of ‘community’. On the one hand the NDC’s model of engagement was concerned with the active participation in democratic and civic life of politically aware citizens. On the other hand, Wallace50 argues that policy-makers advocated for a very particular type of participation, creating structures for ‘responsible but apolitical actors’ to participate in decisions about neighbourhood life, with little scope to include social action resistant to or challenging of government agendas (p. 813).
In terms of the practice of engagement in the NDC initiative,53 the team conducting the national evaluation of the NDC reported that 18% of the total expenditure of local NDC partnerships (excluding management and administration) or approximately £248M went on ‘community-related interventions’ in the first 8 years of this 10-year programme. Almost one-fifth of this went on new or improved community facilities, but a substantial amount was also spent on involving local people and developing the skills and infrastructure of the community. 53 Although approaches to engagement varied (as discussed in Chapter 3 of this report), a wide range of engagement activities were implemented, including forums, festivals and events, NDC newsletters, funding for community development and involvement teams, training for resident representatives on NDC boards and providing resources for local action through the ‘Community Chest’ and other small grant programmes.
Predictably, only a minority of residents either had heard of the NDC or got engaged in NDC activities. For example, data from the four Market & Opinion Research International (MORI) household surveys conducted for the national evaluation suggest that the numbers who had heard of the NDC increased over time between 2002 and 2008 from 16% of residents to 22%, but declined a little by 2008. In the last of these surveys in 2008, 17% of all respondents said that they had been involved in NDC activities at some point in time (although this percentage was 44% among those respondents who had lived in a NDC area over the whole of the period). Of the 17% of all survey respondents who reported getting engaged in some NDC activities, 87% played a participative role, with most of them attending events or festivals. Only 14% voted in NDC elections and just over one-quarter (or 4% of all residents) had been involved in volunteering for the NDC partnership, although overall voluntary activity increased over the life of the NDC programme (albeit remaining lower than for England as a whole). However, in all 39 areas residents were a majority on the partnership boards that oversaw local programmes and were involved in most subcommittees overseeing thematic work (e.g. on environmental or health initiatives).
Previous evaluations of the New Deal for Communities
The government’s Neighbourhood Renewal Unit, in the Office of the Deputy Prime Minister, funded a consortium of universities led by Sheffield Hallam University to carry out a national evaluation. The National Evaluation Team (NET) started work at the end of 2001 – almost 2 years after the first wave of NDC partnerships was approved (1999) and 1 year after the second wave was commissioned (2000) – and its funding ended in 2010/11. The evaluation involved an initiative-wide impact assessment, investigating the association between ‘effort’ and ‘change’ during two periods, 2001–5 and 2006–8, utilising 36 indicators developed to measure progress across the six outcome domains. The NET also explored factors influencing programme implementation. 54 The NET evaluation involved the identification of comparator areas matched to each of the 39 NDC areas by deprivation score and local authority area, and the collection and analysis of a wide range of quantitative and qualitative research data – both cross-sectional and longitudinal – some for all of the NDC areas and their comparators and some for selected NDC areas (see Chapter 2). The NET has produced a number of reports, which are available for download from http://extra.shu.ac.uk/ndc and journal papers (accessed November 2014).
In addition to the national evaluation, there has also been a number of smaller-scale evaluations of local NDC programmes, some undertaken by individual NDC partnerships and one by a team based at the Universities of Birmingham, Staffordshire and Central England. The latter study was exploratory, considering the availability and selection of health outcome measures relating to specific activities in six NDC local programmes in the West Midlands, but there have been no publications of impact on health or health inequalities.
Although the NET looked at some health outcomes (see Chapters 2 and 4), neither its work nor any of the smaller-scale evaluations focused explicitly on the impact of the NDC programme as a whole on health inequalities or their social determinants. In 2003, the Department of Health therefore commissioned us to assess the feasibility of undertaking such an evaluation using secondary data sources, including in particular the data sources compiled by the NET. The scoping study concluded that an evaluation of the impact of the NDC initiative on health inequalities using secondary data sources was feasible [Popay J, McLeod A, Kearns A, Nazroo J, Whitehead M. New Deal For Communities And Health Inequalities: The Final Report of a Scoping Study. Submitted to the Department of Health (ref: RDD/018/063) 2005; unpublished report]. The Policy Research Division subsequently funded this evaluation in 2010 and the findings were reported in November 2013. 1 Findings from our evaluation of the health and social impact of different types of NDC local programmes are summarised in Chapter 4.
About this report
The research reported here has built on our previous evaluation of the impact of the NDC on health inequalities and their social determinants. In the research described here we sought to evaluate the impact on a range of health and social outcomes of the approaches that NDC partnerships took to engaging their residents in the design and delivery of local programmes. In Chapter 2 we describe the study design, methods and sources of the largely secondary data that we have used. Chapter 3 describes the development of a typology of NDC approaches to CE, which we subsequently used in our analyses of what impact, if any, CE had on health and social outcomes. The findings of these impact analyses are reported in Chapters 4–6. Findings from our qualitative research are reported in Chapter 7 and our cost-effectiveness work is described in Chapter 8. In Chapter 9 we highlight some of the limitations of the research, summarise key findings and consider the implications for policy and practice of aiming to engage people in shaping and delivering action to improve their lives and the places in which they live.
Chapter 2 Study design and data sources
Introduction and research questions
Our research has involved collaboration between researchers at the Universities of Lancaster, Liverpool, Manchester and St Andrews, and the Medical Research Council Unit for Lifelong Health and Ageing now at University College London. We have also engaged NDC residents and past workers in the research as described in the following section. Originally, the evaluation was to be conducted over 24 months from 1 September 2011. However, a 9-month no-cost extension was agreed to accommodate significant delays because of changes in staff, giving a new end date of 31 May 2014.
Public involvement in our research
The main mechanism for public involvement was through the advisory group. Professor Paul Lawless, who also led the national evaluation of the NDC, chaired this advisory group, which included residents of NDC areas, former staff of NDC areas [including a previous NDC Chief Office who was later the chairperson of the Neighbourhood Regeneration Agency (NRA)], academics with a range of expertise, representatives from the Department of Health and members of the project team. Advisory group members were able to comment on regular updates on the research and the debates and critiques were invaluable, helping to strengthen the study’s methods and interpretation of findings.
In addition to participating as members of the advisory group, NDC residents (including Ann-Marie Pickup who was a named co-applicant) and NDC workers (including Liz Kessler, a former NDC employee who was extremely helpful in our previous evaluation of the NDC initiative) contributed to our research in other ways. An example of this type of contribution (described in detail in Chapter 3) involved two public advisers participating in an exercise designed to help us allocate nine NDC areas, for which we had insufficient information, to one of our CE ‘types’. Some of the NDC resident members of the advisory group also acted as advisers to the fieldwork, helping to identify research participants, proofreading project information sheets, testing research tools (such as the interview schedule), and taking part as research participants. Additionally, our public advisers participated in a workshop to discuss the interim findings from the project and to inform aspects of the work to develop a CE typology for the NDC areas (described in Chapter 3). Specifically, discussions informed the design of the research tools for telephone interviews and helped to refine the dimensions to be used in the typology of approaches to CE. Public advisers were offered an involvement fee for their participation and we developed an information sheet based on INVOLVE guidance55 that set out what advisers could expect in terms of their participation.
The NRA was the successor body to an organisation set up to support and connect the NDC areas. Its board consisted of former chief executives of NDC areas. When the NDCs were running, the NRA organised conferences and workshops that brought representatives from the NDC areas together, enabling them to share knowledge and ideas. The chief executive of a NDC successor body in one of our fieldwork sites put us in touch with the NRA, and the chair, Sam Tarff, agreed to join the study advisory group. The NRA worked with project researchers to plan a workshop to discuss the study findings with a wider group of NDC area residents and former staff. This workshop was postponed because of the low take-up of places, but we continued to involve the former CE of the NRA as a member of the advisory group. We also circulated e-mail updates on study progress to a wider network of members of the public that included former NDC employees, residents of NDC areas and newer successor organisations. We plan to produce a lay summary of this report when it has been approved and will be discussing other dissemination options with relevant funders in due course.
Study design, methods and data sources
The study has considered whether or not different approaches to CE taken by the 39 local programmes that make up the NDC regeneration initiative had different impacts on health and social outcomes and whether or not some approaches were more cost-effective than others. The aim was not to evaluate the multitude of specific techniques and processes of engagement used in local areas, but rather to evaluate the different strategic approaches to engagement adopted at a local programme level. To do this we first had to develop a typology of these approaches and then evaluate the impact of these different ‘types’ of CE approaches. The study has therefore involved mixed methods and consisted of three linked elements: development of a typology of NDC approaches to CE; assessment of the impact of NDC approaches to CE on health and social outcomes; and an exploratory economic evaluation of the cost-effectiveness of NDC approaches to engagement.
Developing a typology of New Deal for Communities approaches to engagement
The development of a typology of NDC approaches to CE was undertaken in three phases. These are described in more detail in Chapter 3 and Appendix 1. During phase 1 of this work a preliminary typology was developed using secondary data sources collected by the NET. The main sources of secondary data used in the typology development are listed in Box 1. This work involved simple descriptive statistical analyses of household survey data and content analyses of documents.
-
Cross-sectional data from the MORI household surveys in all NDC areas and comparator areas (repeated in 2002, 2004, 2006 and 2008), described in more detail in Assessing the impact of New Deals for Communities approaches to community engagement on health inequalities and their social determinants.
-
Partnership Survey reports on process and management in all NDC areas (2002/3, 2003/4, 2004/5).
-
Comprehensive project case studies in all NDC areas (2003).
-
Case study work with selected NDCs to look at specific issues in more detail, including case studies on engagement. 56
-
Local documents including delivery plans, CE strategies, progress reports and local evaluation reports.
a Data available from http://extra.shu.ac.uk/ndc/ncd_data.htm (accessed 9 August 2015).
A second phase of work involved the collection of new qualitative data from residents and workers in a purposive sample of NDC sites, which were analysed thematically, and collation of additional local documents identified during the fieldwork. Finally, the typology was revised on the basis of the data collected and its applicability to specific NDC areas tested through telephone interviews with key informants in a sample of NDC sites. This resulted in the following fourfold typology, which is described in more detail in Chapter 3:
-
type A: resident led and driven by strong CE values
-
type B: initially resident led and driven by strong CE values but this weakened over time
-
type C: balancing instrumental and CE values
-
type D: instrumental with approach to CE shaped by external priorities.
Assessing the impact of New Deal for Communities approaches to community engagement on health inequalities and their social determinants
Our impact analyses sought to answer five questions:
-
Which approaches to CE effectively engage which social groups in NDC populations?
-
Do different approaches to CE have different health and social outcomes for NDC populations?
-
Does the association between these outcomes and the NDC approach to CE vary across groups defined by age, ethnicity, gender and material circumstances?
-
Do different approaches to CE have any impact on the health gap between NDC areas and areas from across the socioeconomic spectrum?
-
Does the approach to CE help to explain any of the differential outcomes of local NDC programmes identified in our previous research?
Our previous evaluation of the health and social impact of local NDC programmes1 had categorised the 39 NDC areas into three theoretically derived groups based on the type of local programmes that they developed:
-
Local programme type 1 (transformational). This had a primary focus on changing the composition of the area population through major redevelopment of housing.
-
Local programme type 2 (incremental). This involved a more balanced approach, with smaller-scale housing redevelopment and environmental improvements combined with a focus on human capital development in the local population.
-
Local programme type 3 (strengthening). This had a primary focus on strengthening the skills and capacity of residents, and improving their living conditions.
This typology of local NDC programmes is used in some of our impact analyses alongside the fourfold CE typology described earlier and in Chapter 3.
In addition to the questions listed above we also indicated in our original proposal that we would examine health and social outcomes for those residents who were most actively engaged in the NDC, for example as members of local partnership boards. However, this has not proved possible. Although the NET undertook a survey of a subset of residents engaged in NDC board activities, collecting data on their time commitment and burnout as well as their positive experiences, it has not been possible to link these individuals to CE types as NDC identifiers were not retained within that data set. We also undertook an exploratory analysis of health and social outcomes by CE type among the subgroup of respondents to the MORI surveys who said that they were involved in NDC activities. This amounted to 11–12% of residents and initial analyses failed to find any interactions between CE type and engaged residents. We were concerned about the robustness of this analysis because of low statistical power and opted not to investigate this further.
Our impact analyses have used self-reported outcomes from the MORI household surveys conducted in the NDC areas and comparator areas, and the Health Survey for England (HSE) as well as outcomes based on routine administrative data. These data sets and the analytical methods used are briefly described in the following sections and the results are reported in Chapter 4.
The impact of New Deal for Communities approaches to community engagement on self-reported health and social outcomes from surveys: data and methods
These analyses utilised three different data sets, briefly described below.
-
NDC MORI survey cross-sectional data. This data set consists of data from four cross-sectional surveys of residents in NDC areas and the so-called ‘comparator’ areas that the NET commissioned MORI to undertake in 2002, 2004, 2006 and 2008. The target sample size was 500 in each NDC area for 2002–4, which was cut by one-fifth in 2006–8. The cross-sectional response rate in 2002 was 74%, with top-up interviews conducted at each wave to compensate for attrition. The sample size varied between 12,000 and 15,000 respondents in each round for the combined NDC areas. These data were used in three sets of analyses: (1) to test the differentiated impact of the CE typology on measures of community cohesion and health-related outcomes in NDC areas; (2) to assess change over time in these outcomes in NDC areas adopting different approaches to CE relative to their comparative areas; and (3) to compare the change over time between 2002 and 2008 in measures of cohesion and health-related outcomes in the NDC areas against the change over time in the same outcomes in the comparator areas. These data can be found at http://extra.shu.ac.uk/ndc/ncd_data.htm.
-
HSE/NDC MORI survey cross-sectional data set. This data set consists of data from the HSE and the MORI survey cross-sectional data sets for 2002, 2004, 2006 and 2008. This purpose-built data set was created to provide a more robust assessment of the impact of the NDC intervention than by simply matching NDC and comparator data. The HSE survey is an annual cross-sectional survey that is nationally representative of households in England. It adopts a multi-stage probability sampling design selecting a sample of postcode sectors from the Postcode Address File and households from each postcode sector. All adults (aged ≥ 16 years) in each household are selected for interview. Topics include general health, health-related behaviours and chronic diseases. Data from the core samples of the HSE in 2002, 2004, 2006 and 2008 were used to measure health and its social determinants in areas drawn from across the socioeconomic spectrum. We considered four outcomes of interest that could be acceptably harmonised across the HSE and the MORI surveys: mental health, self-rated health, current smoker and not in paid employment. The HSE provides data from residents living in areas across the full socioeconomic spectrum. We classified postcode sectors with a deprivation score in the bottom two quintiles as ‘HSE low deprivation’, those with a deprivation score in the top two quintiles as ‘HSE high deprivation’ and the remainder as ‘HSE medium deprivation’. These data can be found at http://extra.shu.ac.uk/ndc/ncd_data.htm.
-
NDC MORI survey panel data. The four MORI surveys include a panel of people who responded to the surveys at two or more time points and who remained at the same address. This data set was used to look at within-person change in health and social outcomes in NDC areas grouped according to CE type and local programme type. Given our interest in the impact of extended exposure to the NDC local programmes, only respondents present at wave 1 were retained in analyses using these data. There were 10,638 observations at wave 1 with at least two records, but the longitudinal sample size for people with full records was 3554 in NDC areas. The outcome variables used from the MORI survey data are shown in Box 2. These data can be found at http://extra.shu.ac.uk/ndc/ncd_data.htm.
-
Three-category self-rated health with answers being ‘very good’, ‘fairly good’ or ‘not good’.
-
A five-item mental health instrument derived from the Short Form questionnaire-36 items (SF-36).
-
Whether or not a current smoker.
-
Whether or not eating five portions of fruit/vegetables at least three times a week.
Trust in the neighbourhood: three-item measure of trust in the local community:
-
‘Overall, to what extent do you feel part of the local community?’ (‘a great deal’, ‘a fair amount’, ‘not very much’, ‘not at all’)
-
‘On the whole, would you describe the people who live in this area as friendly or not?’ (‘very friendly’, ‘fairly friendly’, ‘not very friendly’, ‘not at all friendly’)
-
‘Would you say that you know most, many a few of, or that you do not know people in your neighborhood.
Trust in local services: three-item measure:
-
‘How much trust would you say you have in each of the following organisations?’ (‘a great deal’, ‘a fair amount’, ‘not very much’, none at all’):
-
the local council
-
the local police
-
the local health services.
-
-
Education, measured as a three-category indicator: National Vocational Qualification (NVQ) levels 4–5, 2–3 or ≤ 1.
-
Whether or not respondents lived in rented accommodation (public as well as private).
-
Whether or not respondents lived in a jobless household (this measure included retired respondents but it was assumed that controlling for age would account for potential bias).
-
Sex.
-
Age.
-
Whether or not respondents were non-white British (self-report).
Depending on the data set one of the following statistical approaches was used:
-
Analysis based on NDC MORI survey cross-sectional data relied on binary logistic regression, reporting odds ratios of dichotomised health and cohesion outcomes, adjusting for sociodemographic and socioeconomic characteristics.
-
Analysis based on the combined cross-sectional HSE/NDC MORI survey data set similarly relied on binary logistic regression.
-
Analyses of within-person change using the longitudinal panel from the NDC MORI surveys for 2002, 2004, 2006 and 2008 used one of two modelling frameworks depending on the outcome variables of interest:
-
Discrete behaviour such as smoking or healthy eating was captured in dichotomised variables and modelled in survival (i.e. Cox) models in which the relative probability (also called the hazard ratio) of quitting smoking or taking up healthy eating at some point between 2002 and 2008 was estimated.
-
Latent growth modelling was used to model changes in mental health, self-rated general health and aspects of social cohesion. This approach allows us to estimate associations between demographic and socioeconomic characteristics, and baseline levels and change in outcomes. This approach also allows for multiple items capturing the same underlying ‘latent’ construct or factor to be modelled together in a two-stage (cohesion outcomes and mental health) or single-stage (self-rated general health) estimation process. For example, the latent variable ‘trust in the community’ was captured by three observed variables – ‘feel part of the community’, ‘describe people in the neighbourhood as friendly’ and ‘extent to which know people in the neighbourhood’ – which were summarised as a single latent variable using a latent trait model. The resulting predicted scores were then used as outcomes in the growth models.
-
Most of these models were fitted as follows: (1) CE type only; (2) demographic factors (gender, age, ethnicity) and socioeconomic factors (educational attainment, household employment status and housing tenure); and (3) interaction terms for CE types by education, CE types by joblessness and CE types by housing tenure were added to assess whether or not CE type moderated the impact of socioeconomic factors on outcomes. Some analyses included a fourth model exploring interactions with local NDC programme type.
In the quantitative analysis using individual MORI survey data, we also adjusted for residential mobility and for variables shown to predict mobility or the desire to move as potentially important explanatory factors in the relationship between CE and outcomes. Multilevel modelling, using a random-effects approach, utilises longitudinal data for those who participate in only some waves and so analysis is not restricted to those in all four waves. In addition, the longitudinal models were all fitted using full information maximum likelihood with Mplus version 6 (Muthén & Muthén, Los Angeles, CA, USA), to include all available information from participants with incomplete data, under a ‘missing at random’ assumption.
In addition to the above we also used the MORI survey cross-sectional data set to undertake a ‘difference-in-difference’ analysis. This is a relatively new way of evaluating the impact of large-scale interventions such as the NDC programme. The NDC is treated as a multiple before–after, case–control study, with the ‘cases’ being the 39 NDC intervention areas and the ‘controls’ being the 39 ‘matched’ comparator areas. Two assumptions underpin this statistical procedure:
-
that the intervention and comparator areas are well matched in terms of the factors influencing change so that any changes independent of the intervention should be similar in the control and intervention areas
-
if there is a positive impact of the intervention then the situation should have improved more in the intervention area and if there is a negative impact then the situation should have improved less in the intervention area.
Our difference-in-difference analysis therefore used the MORI survey cross-sectional data for 2002, 2004, 2006 and 2008 to compare change over time on a number of social and health outcomes in the NDC intervention areas with change over time on the same outcomes in the NDC comparator areas.
The impact of New Deal for Communities approaches to community engagement on health and social outcomes using routine administrative sources: data and methods
The Oxford Social Disadvantage Research Group, a member of NET, also constructed time series data sets for each NDC area and its comparator using routine administrative data sources. When our evaluation began these time series, data sets ran from 1998 up to 2007 for some but not all variables and included data on health outcomes and social determinants of health from the census, NHS sources, Office for National Statistics (ONS) and government departments. In early summer of 2013, with additional funding from the National Institute for Health Research (NIHR), we requested data to extend this series of indicators. Table 1 shows which NET indicators have been extended and which have been specifically constructed for this work. Unfortunately, several of the original indicators relating to crime, education and exit rates from unemployment could not be extended because of shortage of time or restrictions on data access.
| Indicator | Source of data | Period covered by Oxford data | Period covered by indices computed for this project |
|---|---|---|---|
| Health and morbidity | |||
| Six hospital admissions indicators (standardised for age and sex) for drug misuse, alcohol misuse, cancer, respiratory conditions, heart conditions and mental health | HES | 1999/2001–2001/3a | 2002–10 |
| Work-limiting illness | DWP | 1999–2008 | 2009–11 |
| Standardised illness ratio (based on individuals receiving at least one of AA, DLA, SDA, IB or ESA) | DWP | a | 2004–11 |
| Low birthweight: proportion of singleton births weighing < 2.5 kg, 5- or 3-year averages | ONS | 1997/2001–2001/5a | 2003/5–2008/10 |
| All-cause under 75 years mortality indicators (SMR, CMF and ‘shrunk’ CMF) – 5- or 3-year averages | ONS | 1998/2002–2001/5 | 2003/5–2009/11 |
| Unemployment and low income | |||
| Worklessness | DWP | 1999–2008 | 2009–11 |
| Unemployment | DWP | 1999–2008 | 2009–11 |
| Low income/poverty | DWP | 1999–2008 | 2009–11 |
| Other topics | |||
| Average house prices | Land Registry | 2001–8 | b |
| Educational attainment | DEF | 2002–8 | b |
| Entry to higher education | UCAS | 2002–8 | b |
Preliminary analyses of these data for our previous study found considerable diversity in trends within each type of NDC local programme and the same was the case when NDC areas were groups according to CE type. 1 We therefore decided to compute trends for individual NDC areas and their comparators separately and then summarise the individual results for groups of NDCs, rather than combine the NDC areas with the same CE type before computing trends. The high degree of variability of some indicators based on small numbers of events, such as low birthweight and under 75 years mortality, can produce instability in indicators for individual NDC areas, even when data are averaged over several years. Consequently, point comparisons are not a reliable guide to change and we therefore used the following linear regression approach to test for trends:
-
the difference in value of the indicator between each individual NDC area and its comparator area is computed for each of the years in the time series
-
this difference is regressed against time
-
unstandardised coefficients are reported when they are significant at ≥ 10%.
The results of these analyses are reported in Chapter 4.
Cost-effectiveness analysis
A third strand of work explored the cost-effectiveness of different CE approaches using secondary data, new qualitative data collected during interviews with NDC workers and the results of the impact analysis. This work involved two phases. Phase 1 aimed to compile data to estimate the total costs of CE activities for individuals and at the level of local NDC programmes. Phase 2 sought to relate these costs to the categories defined in the CE typology. However, as we describe in Chapter 8, the economic strand of this project has proved to be much more challenging than originally envisaged. This is partly because of the limited nature of the cost data that we were able to identify and partly because of the diverse patterns of health and social impacts associated with different approaches to CE. Details of the methods used in this work are included in Chapter 8.
Data archiving
In addition to seeking to answer our research questions we aimed to provide a data archive making available programming codes and data for other users so that the typology development and analyses reported here can be replicated. This legacy will allow longer-term follow-up of the impact of the NDC on health inequalities and their social determinants, as well as comparison of health and social outcomes in NDC and similarly deprived areas.
The material in the archive includes:
-
Time series indicators – these include indicators derived from administrative data and are of two types: (a) hospital admission indicators, already produced and analysed, including but not limited to drug misuse, mental health and circulatory diseases for the period 2000–12 for NDC areas and their comparators; (b) social indicators: health and incapacity- and unemployment-related benefit claimant counts for NDC areas and their comparators. A user guide for these time series data sets, with careful documentation of how measures were constructed, is included so that they can be generated in a consistent way in the future.
-
A user guide and documented programming code for deriving the cross-sectional and longitudinal analytical sample and variables drawn from the NET MORI surveys and used in our impact analyses (see Chapter 4). This also includes micro-data for the comparative areas, currently not available.
-
A user guide and documented programming code for deriving the analytical sample and variables from the HSE as well as the derived data sets (see Chapter 4). This includes documentation and a programming code to code the data according to level of area deprivation.
-
Detailed documentation of our approach to classifying NDC areas in terms of local NDC programmes and NDC approaches to CE.
In addition to the above, the feasibility of archiving anonymised interview transcripts from the fieldwork reported in Chapter 3 is being explored. However, the preparation of these data for archiving will require additional funding.
This archive material is now available from http://dx.doi.org/10.17635/lancaster/researchdata/27.
Summary
In this chapter we have set out the questions addressed in our research and our study design. We have described the primary and secondary data sources we have used and the analytical methods adopted. In the next chapter we describe how we developed the typology of NDC approaches to CE, before moving on to report the results of our impact analyses and economic evaluation.
Chapter 3 Developing a typology of New Deal for Communities approaches to engagement
Introduction
To assess the impact of different approaches to CE, the NDC areas first needed to be categorised according to the approaches that they took. Rather than simply describing the myriad of CE activities taking place, the typology sought to understand the values and ethos underpinning different approaches to CE taken by local NDC partnerships and the factors that shaped the approaches that they adopted as well as the context that NDC partnerships operated in. The development of this typology built on the development of a typology of the local programme interventions implemented across the 39 NDC areas as part of our Department of Health-funded study (see Appendix 1).
Development of the typology consisted of three phases of work:
-
phase 1: identifying and reviewing secondary data on CE for all 39 NDC areas where possible
-
phase 2: primary data collection in 11 NDC areas and telephone interviews in another 10 areas
-
phase 3: synthesising findings from phases 1 and 2 to develop a typology, and categorising the 39 NDC areas according to this typology.
Methods for developing a typology of the New Deal for Communities approaches to community engagement
Phase 1: identifying preliminary dimensions of approaches to community engagement
The aim of this first phase was to identify aspects of CE approaches within NDC areas to be incorporated into a preliminary framework that would guide the primary fieldwork in phase 2, rather than to produce a definitive typology of engagement. Various data sources were therefore used to develop ‘thin’ descriptions of levels and types of CE, aspects of the local context, baseline levels of engagement, and processes and structures to support CE. Descriptions of baseline levels of engagement and some aspects of local context were produced for all 39 NDC areas using quantitative secondary data sources (e.g. the MORI surveys). It was not possible to describe processes and structures for all 39 areas because of a lack of documents in many NDC areas; however, we were able to identify sufficient documentation including CE strategies to produce ‘thin descriptions’ of CE structures/processes for approximately one-quarter of the NDC areas. The data and methods used in this phase, which was also informed by a number of published conceptual frameworks relating to CE,57–59 are briefly described in the following sections.
Levels and types of engagement and local context
The 2002 MORI survey data set provided data on levels and types of engagement from 2002 to 2008 in all NDC areas. We considered a wide range of other data sources but for a variety of reasons these could not be used (e.g. they were not disaggregated at NDC level). MORI survey data on aspects of community cohesion (e.g. feel part of the community), on engagement (e.g. involved in voluntary organisations, involved in NDC activities) and on levels of trust in various local organisations were analysed across four time points (2002, 2004, 2006 and 2008) for each NDC.
Values on these variables were categorised in 2002 and 2008 as ‘low’, ‘average’ and ‘high’ compared with the mean values for these variables across all NDC areas in that year, with ‘average’ values falling within the 95% confidence intervals (CIs) of the mean, ‘low’ values significantly lower than the NDC mean (p = 0.05) and ‘high’ values significantly higher than the NDC mean (p = 0.05). As NDC values were not compared with broader local, regional or national data, this meant, for example, that levels of trust were not necessarily ‘high’ but were higher than average for the NDC areas. The differences between the values in 2002 and 2008 were categorised in a similar manner. For some areas the percentage point change for a particular variable between 2002 and 2008 fell below the NDC average change value. Sometimes an area started with a higher value than the NDC average for a variable so that ‘low’ levels of change may not reflect a failure of the NDC per se, but rather the maintenance of an existing good.
The NET also gave us access to the non-aggregated data at NDC level from the NDC Partnership Surveys that it undertook regularly to collect data from NDC staff, members of the partnership board and other stakeholders. The Partnership Survey from years 2002/3 provided useful information on the context of the NDC areas at start-up, including information on whether or not respondents felt that their NDC areas had a dominant cultural identity, good networks and group activities, low levels of interethnic cohesion, moderate or high racial tension and/or other moderate/severe tensions. We used the data on perceptions of community cohesion in the selection process for fieldwork sites.
Mapping New Deal for Communities processes and structures for community engagement
To map structures and processes put in place to support CE we used documents already gathered in our previous Department of Health-funded study,1 searched NDC websites and contacted informants in local areas. We were particularly interested in identifying whether or not we could access CE strategies for NDC areas; however, the availability of documents was variable. In total, we found reference (i.e. on a website or in other programme documents) to a CE strategy in 11 areas along with evidence that the CE strategy had been evaluated. Seven more NDC areas made reference to a CE strategy in documents and provided information on CE projects, but it was unclear whether strategies were reviewed. The remaining 21 NDC areas did not explicitly refer to a CE strategy and additional information on CE was generally mixed. Even when strategies or evaluations of strategies were stated to have been produced, these were not often in the public domain. The availability of documentation could be argued to reflect differences in the level of commitment to CE, but as the NDC initiatives had ended by the time that we were doing this work it may simply reflect difficulties of access, as offices and websites had been closed down. We therefore used availability of documentation as one of the criteria for selecting sites for the fieldwork in phase 2 of the typology development.
The varying level of documentation meant that it was not possible to map CE structures and processes in all 39 areas. Therefore, we initially focused on reviewing documents in depth from 10 NDCs. These were read by researchers (EH and JT) to familiarise themselves with the documentation and consider whether or not there were key target documents that could be the focus of a content analysis. Documents were sampled to examine engagement over time and included delivery plans, CE strategies and evaluations. Notes were taken on issues and emerging themes related to CE. These were used to develop a data extraction framework and informed a content analysis of a smaller subset of documents from five of the 10 NDCs. The five NDCs were selected to reflect geographical spread and differences in CE identified from the initial document screening. Time constraints meant that we were unable to review multiple documents for all 10 areas but a content analysis was undertaken of at least one key document from each area (typically the 10-year NDC evaluation), providing some data on CE processes and structures in 10 NDCs at this stage.
This analysis extended the dimensions of CE used in the development of our typology of NDC local programmes to include existing levels of capacity for engagement at the start of the programme, relationships between residents and local agencies, and definitions of ‘community’. The analyses also sought to detect differences in engagement approaches, identifying, for example, NDC areas placing emphasis on increasing resident control over NDC activities and areas that placed a greater emphasis on consultation or engagement in governance structures.
A preliminary conceptual framework of dimensions of community engagement approaches
Through analyses of the data collated and drawing on the theoretical literature, reports from the NET and discussions in the research team, a set of key dimensions of CE were identified. These took into account the known variability of CE baselines and change over time, sought to reflect a more holistic understanding of how engagement ‘worked’ in the NDC areas beyond discrete CE activities and incorporated aspects of the social, economic and political context in which CE took place. This preliminary conceptual framework consisted of three dimensions of local relationships (trust, community cohesion and conflict/tension) as well as other elements of the local context. The rationales for the inclusion of these four dimensions are set out below.
Our typology is underpinned by the theory of community engagement most associated with social influence and the transformation of power relationships. This theoretical approach is highlighted in the quote from Laverack and Wallerstein. 60
It is only by being able to organize and mobilize oneself that individuals, groups and communities will achieve the social and political changes necessary to redress their powerlessness. This remains the domain of community empowerment as a political activity, which enables people to take control of their lives.
Various engagement frameworks or typologies have sought to classify the nature and levels of engagement. 61–63 The research team concluded that attempting to ‘type’ NDC approaches to CE by focusing primarily on engagement activities and their immediate goals (as these typologies tend to do) was likely to be problematic given the complexity of CE in a regeneration programme such as NDC. We felt that it was important to include other potentially salient issues, particularly dimensions of local relationships that have been identified as important factors shaping engagement processes in NDC areas, such as trust and tension between communities and public agencies,64,65 and between different community groups. 56
Trust
The importance of ‘trust’ between the public (variously defined) and formal agencies has become axiomatic with ‘engagement’ across a variety of disciplines and institutions. However, institutional attempts by, for example, local authorities and the NHS to engender trust in the context of CE activities have been criticised for being too instrumental. This can be defined as the use of engagement as a means to achieve institutional goals rather than as a route to genuine community empowerment. 28,66 Analyses of NDC documents revealed that trust was widely seen to be relevant and important in positively engaging residents, but MORI data showed pre-existing levels of trust varied significantly across NDC areas.
Community cohesion
Although the evidence base is relatively weak, in theory, at least, CE within regeneration programmes such as NDC could foster greater cohesion in populations of disadvantaged neighbourhoods, particularly if the approach is informed by an ethos of empowerment and community development. 11,67 It could be argued, for example, that an approach that invested in developing community ‘infrastructure’ and shared interests among residents could have greater positive impacts on trust between residents than an approach more focused on engaging residents in governance and strategic planning.
Conflict/tension
Conflict may be indicative of positive engagement but power imbalances can also have negative implications for relationships (in communities or between residents and agencies). There were tensions between the requirements of the national NDC policy and the expectations of NDC residents. For example, early policy documents were unclear about what was meant by ‘community leadership’. Communities were told that the money was ‘theirs’ to spend; this of course was not meant literally but was taken literally by some communities not used to working with government. 64,65 Pressures from central government to spend budgets and deliver outcomes were often incompatible with the time needed to establish effective CE processes. 65
Other dimensions of local context
Other dimensions of local context within which NDCs operated can also be expected to shape attempts to foster the genuine engagement of residents in decision-making. These factors include the area characteristics and population dynamics, previous experience of CE, local capacity to engage and the history of the area and its labour market. 56
Phase 2: primary data collection
The second phase of the typology development aimed to identify any gaps in the conceptual framework described in the previous section as well as to provide a more nuanced understanding of the dimensions of the framework and the relationships between them. This would enable us to begin to validate the main dimensions of CE to be included in our typology and to assess the relative emphasis placed on different approaches. We also aimed to collect information, and identify key informants, for the economic evaluation.
Sampling New Deal for Communities fieldwork areas, recruitment of respondents and data collection
The selection of fieldwork sites and the collection of data were informed by the conceptual framework developed in phase 1. We were aiming to select 10 NDC areas. The first four sites were selected on the basis of purposive and pragmatic criteria, including level of CE, availability of documents, the type of NDC local programme intervention and proximity to the researchers’ institutions. Sampling of additional sites also took account of level of relative deprivation, aspects of context and region. An 11th site was included to increase the total number of interviews (see later in this section). Initial entry to the sites was negotiated through key informants identified during our Department of Health-funded study and contacts working at NDC legacy organisations or relevant local authorities. Details of the sites and sampling criteria are provided in Table 2.
| NDC area | MORI QC05 – feel able to influence decisions locally? | MORI QC06 – involved in voluntary organisations? | Scoping of CE strategy and evaluations: current availability of documents | NDC type categoryb | Partnership Survey 2002/3: area with networking and group activities? | NDC area context at start-up | Geographical region | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 2002: % ’yes’ | Percentage point differencea 2008 – 2002 | 2002: % ‘yes’ | Percentage point differencea 2008 – 2002 | Relative deprivationc | Historical contextd | Residential mobilitye | |||||
| Site 1 | Average | Low | Low | High | High | 2 | Yes | 2 | 4 | 2 | North West |
| Site 2 | Average | Low | Low | Average | Low | 1 | Yes | 3 | 4 | 1 | North West |
| Site 3 | Average | High | Low | Average | Low | 2 | Yes | 3 | 4 | 2 | Yorkshire and the Humber |
| Site 4 | Average | High | High | Average | High | 3 | Yes | 2 | 4 | 1 | North West |
| Site 5 | Average | Average | Low | High | Low | 1 | No | 3 | 3 | 2 | Yorkshire and the Humber |
| Site 6 | High | Average | High | Low | Low | 1 | Yes | 3 | 1 | 2 | South West |
| Site 7 | High | Low | High | Low | Medium | 3 | No | 1 | 1 | 2 | London |
| Site 8 | Low | High | Low | High | Low | 3 | Yes | 1 | 3 | 3 | London |
| Site 9 | Average | High | Low | High | Medium | 1 | No | 3 | 4 | 1 | West Midlands |
| Site 10 | Low | High | Low | Low | Medium | 2 | Yes | 1 | 1 | 2 | East of England |
| Site 11 | High | Low | High | Average | High | 1 | Yes | 3 | 4 | 3 | North West |
We aimed for 50 semistructured interviews across 10 sites. In each site this was to include three residents active on NDC partnership boards or in CE activities and two former NDC staff. In most cases a primary contact in the site assisted in making initial contact with potential participants and sometimes snowball sampling was used to identify other informants.
Potential interviewees were invited to participate, typically by e-mail or by telephone, and were sent an information sheet. All participants were asked to sign a consent form after reading the information sheet and being given an opportunity to clarify issues/ask any questions. The consent form was securely stored and a copy of the form returned to the participant. Participants were informed that they could withdraw themselves or their data at any point up to the time when data analysis began; they were also reminded of this at the beginning of the interview. Resident interviewees were offered a £15 voucher as a ‘thank you gift’.
It was more difficult and time-consuming to identify resident interviewees in each site than originally anticipated. We therefore added an additional site to increase the number of resident interviews. In total, 47 interviews were conducted in these 11 sites between October 2012 and March 2013 (27 residents and 20 staff). Residents were either members or chairs of NDC partnership boards. Staff members interviewed primarily included NDC chief executives and CE managers, but also co-ordinators for NDC themes and projects. In two instances, staff members defined themselves as both a resident and staff.
The majority of interviews were conducted face-to-face during visits of 2–3 days. Interviews took place in a central location (e.g. NDC successor organisation office or community centre) or in the resident’s home or workplace. Two interviews were conducted by telephone. All researchers (JT, EH and SP) were involved in the conduct of the interviews. The interviews were digitally recorded and transcribed with the consent of the participant and adhered to Lancaster University ethical procedures for informed consent, data protection and fieldworker safety.
The interviews lasted for between 50 and 120 minutes and were semistructured but tailored to the role and experience of the respondents. The interviews covered local context, processes and structures of CE, perspectives on the level of engagement in the activities that respondents were familiar with and perceived impacts of these activities. Respondents were also asked about the specific examples of engagement selected to be the focus of the economic evaluation and whether or not they could suggest somebody who would be useful to speak to about the costs of engagement (see Chapter 8). The interview schedule was initially piloted with two of our public advisers (who were residents of fieldwork areas). As amendments to the initial schedule were minimal, full consent was obtained from these two pilot respondents for data from their interviews to be included in the study. The first few interviews with residents took much longer than anticipated, primarily because of the extensive experience that these respondents wished to share. It was therefore decided to make some sections of the interview much more structured to allow opportunities for respondents to talk about their experience of engagement within a reasonable time frame. The interviewers also sought documents, such as local evaluation reports, CE strategies, reports on CE activities and succession plans, when these had not already been obtained.
Analysis of fieldwork interview data
The project team agreed that for the purpose of typology development the analysis would use a deductive thematic framework based on the interview schedule and preliminary conceptual framework. The analysis was conducted manually with transcripts divided between the three researchers, who extracted data relevant to the themes onto an Excel 2010 spreadsheet (Microsoft Corporation, Redmond, WA, USA). Columns were included for researchers to note additional emergent themes and to highlight key differences in respondents’ perspectives across interviews within sites. A process of cross-checking took place for a sample of transcripts with a second researcher undertaking a second analysis to ensure consistency.
Interim findings from the analysis of transcripts from four fieldwork sites were taken for discussion to a reflective workshop with public advisors in May 2013. The aim of the workshop was to (1) obtain feedback on the preliminary findings and explore participants’ views on dimensions that would best enable different approaches to CE to be distinguished; (2) involve public advisers in the design of a telephone interview schedule (see following section); and (3) discuss dissemination plans. Discussions of preliminary findings also highlighted the ways in which national pressures had impacted on the ability/success of NDC areas in engaging residents in the programme, providing useful contextual information that aided the interpretation of our findings.
Telephone interviews
Following this workshop the analyses of interview transcripts focused on a smaller number of themes and a cross-site comparative analysis was undertaken. Alongside this we aimed to conduct telephone interviews with key informants in as many of the remaining 28 areas as possible to validate the dimensions of the CE typology emerging from the analysis of fieldwork data and fill gaps in knowledge about these NDC areas to support the process of allocating areas to types. We used the contacts made in our previous study and a variety of other means (contacting the legacy organisation and council departments, following the advice of our public advisers) to identify key informants. This was a time-consuming process as over the course of the study increasing numbers of staff/residents were no longer contactable and following an intensive period 10 interviews were conducted across 10 sites. The recruitment and consent process was the same as for the face-to-face interviews except that potential respondents were able to return their signed consent by e-mail.
The telephone interview schedule included structured items constructed to measure respondents’ perceptions of levels of control, trust, conflict/tension and cohesion among residents of their area prior to the NDC programme, during the early years of the programme (2002–4), mid-NDC programme (2004–8) and towards the end of the NDC programme (2008–10/11), with the same set of questions repeated for each time point. Our approach to ‘measuring’ change was informed by a study that had sought to develop indicators for the assessment of community participation in health programmes. 59 The methods used in this study aimed to position responses to questions on a continuum rather than to gather quantifiable data. We used scales from low to extremely high or extremely high to none. An example is provided in Box 3.
We are interested in the relationships within the area before the NDC funding took place between residents and residents, and residents and agencies. I am now going to ask you about these in relation to trust, conflict and levels of influence.
-
Thinking about the issue of trust – how would you describe the levels of trust between residents and residents?
1 – extremely high; 2 – high; 3 – fair; 4 – low; 5 – none.
And between residents and other bodies, for example the council?
1 – extremely high; 2 – high; 3 – fair; 4 – low; 5 – none.
-
Thinking about the issue of conflict – how would you describe the levels of conflict between residents and residents?
1 – extremely high; 2 – high; 3 – fair; 4 – low; 5 – none.
And between residents and other bodies, for example the council?
1 – extremely high; 2 – high; 3 – fair; 4 – low; 5 – none.
-
How would you rate the level of resident influence on matters affecting their community?
1 – extremely high; 2 – high; 3 – fair; 4 – low; 5 – none.
Respondents were also asked to indicate which of a series of statements about approaches and values associated with CE best described aspirations for their NDC programme. Participants were able to offer an alternative if none of the options given was perceived to be relevant. An example question is provided in Box 4. Finally, as with the fieldwork interviews in phase 2, the researchers asked questions about the costs of engagement and, if relevant, whether or not the respondent would be happy to participate in a short telephone conversation about costs conducted as part of the economic work (see Chapter 8).
Which of the following best describes the community engagement approach/model that your NDC programme aspired to/took?
-
Community led and individual and community capacity building.
-
The community was represented and consulted.
-
Council/agency led but direct community involvement.
-
Council led and representative democracy.
-
Other (if none of the above is relevant to your experience).
The telephone interview schedule was piloted with members of the research team and a NDC respondent. Telephone interviews were not recorded. The interviewer made detailed notes during and after the interview and these were used to populate data analysis templates that were then used in a final synthesis.
Phase 3: final synthesis and allocation of New Deal for Communities areas to the community engagement typology
The final synthesis consisted of four elements: (1) confirming patterns within and between the primary dimensions of control, trust and conflict/tension and agreeing the final CE typology; (2) a comparison of patterns in changes in MORI data on cohesion, engagement and levels of trust with qualitative data from fieldwork sites to see if the MORI data would be useful in typing areas where data were limited; (3) allocating NDC areas to a CE ‘type’ when information was judged to be sufficient; and (4) allocating NDC areas to a CE ‘type’ when data were insufficient.
Agreeing the final community engagement typology
The first step of the synthesis was to agree the final set of dimensions that offered a plausible basis on which to type the 39 NDCs. The four dimensions identified initially in our preliminary conceptual framework had been subsequently tested and refined iteratively through the collection and analysis of data from fieldwork sites and telephone interviews, and discussions during the workshop with public advisers and in the research team. Although community identity/cohesion was an important factor that influenced NDC CE activities, our analysis did not distinguish patterns that would enable NDCs to be grouped on the basis of this dimension. The final analysis, therefore, concentrated on identifying patterns within and across the three remaining relationship dimensions – trust, control and conflict/tension – for those NDC areas for which we had fieldwork data and telephone interview data. We also assessed the availability of documentary information identified earlier in phase 1 for the remaining 18 NDC areas for which we did not have interview data. Of these areas, nine were judged to have sufficiently robust CE information to be included in this final analysis (i.e. they provided evidence on relevant relationship dimensions rather than purely descriptive information on CE activities).
The analysis included an assessment of these dimensions for each NDC area before the NDC programme was implemented, how they changed during the NDC programme and what aspects of the local context (e.g. local politics, resident relationships with agencies, historical and contemporary socioeconomic conditions) might explain these patterns. These elements of the analysis are illustrated in Table 3. A further aspect of the analysis considered whether or not any relationship could be discerned between the emerging patterns in levels of trust, control and conflict/tension, and data that we had on respondents’ perceptions of NDC values underpinning engagement, the role of leadership and/or the legacy of CE.
| Category/element | Description |
|---|---|
| Trust, control and conflict pre NDC | The levels of trust, control and conflict (within the community and/or between the community and agencies) before the NDC. Analysis considered the levels of trust, control and conflict as separate markers initially and then examined if a pattern was evident in the relationship between these markers |
| Changes in patterns of trust, control and conflict over time (covering the early, mid and later years of the NDC programme) | This is concerned with how levels of trust, control or conflict (within the community and/or between the community and agencies) are reported to have changed during the NDC time frame. The analysis first looked at how/whether or not levels of trust, control and conflict changed over time (e.g. did trust improve, get worse) and then examined if there are any patterns in the relationship between these three markers |
| Contextual patterns pre NDC | Contextual factors in the social, political and economic environment that appear to influence the levels of trust, control or conflict reported pre NDC |
| Changes in contextual patterns over time | Contextual factors in the social, political and economic environment that appear to influence patterns in levels of trust, control or conflict reported during the NDC |
It was difficult to distinguish between NDC areas in terms of the dimensions of control, trust and conflict/tension in the period pre NDC, primarily because most areas tended to report low levels of trust or capacity for engagement at the start of the programme. Similarly, although people gave accounts of how aspects of the social, political and economic environment shaped levels of trust, conflict or community influence pre NDC and during the course of the NDC programme, with the exception of the political context it was not possible to discern differences in contextual factors that would support typing of CE approaches.
Our analysis did, however, identify distinct patterns in the relationship between trust, control and conflict/tensions over the lifetime of the NDC programme. For example, in those areas where respondents reported increased community control over the lifetime of the NDC, they also reported increased trust, that is, between residents and NDC staff/agencies. Although conflict/tension was reported in these NDCs at the start of the programme (when residents/workers were learning to work together), participants reported that this declined over time. Conversely, in those areas where respondents reported that their NDC programme had been resident led initially and driven by CE, but that this level of community control had not been sustained over time, episodes of conflict/tension continued throughout the programme, with levels of trust tending to remain low or unchanged by the end of the programme.
Comparison of MORI data with primary data analyses from fieldwork sites
The analysis of MORI survey variables across the four time points (2002, 2004, 2006 and 2008) and the difference in values between 2002 and 2008 were compared with findings on levels of community control, trust and cohesion for three of the fieldwork areas. This revealed that the qualitative data gathered during the fieldwork was necessary to understand changes seen in the MORI data. For example, two NDC areas described in the interviews as seeking to actively engage residents in the development of the NDC programme in the early years but then resorting to ‘informing’ residents once the delivery plan was in place experienced a drop over time in levels of community control (ability to influence decisions in the area) in the MORI data. In contrast, a NDC area reported to have actively engaged residents throughout the NDC programme had relatively consistent levels of control in the MORI data. These patterns could not be generalised, however, as there may be multiple explanations for observed changes in the quantitative data and areas experiencing low levels of change over time in the survey data might do so because of consistently high levels of a particular variable (e.g. trust) and so this may not indicate a failure in the NDC programme in that regard.
Allocating New Deal for Communities areas to a community engagement type when information was available
By the final stage of typology development, data had been gathered and analysed from 11 NDC fieldwork sites and 10 areas in which telephone interviews were conducted in addition to the nine areas with sufficiently robust information from documents. These three sets of findings for 30 NDC areas were tabulated against a final set of eight dimensions: values associated with CE, structures associated with CE, community control, trust, conflict, leadership, political context and legacy.
The final allocation of areas to a CE type was an iterative process involving regular discussions between the researchers, drawing on the tabulated information across the eight dimensions for the 30 NDCs to identify similarities and differences in CE approaches across the NDC areas. This process resulted in the four types of NDC approaches to CE shown in Table 4. The features associated with the dimensions for each CE type are described in detail in Table 5.
| CE type | Description |
|---|---|
| A | Resident led – underpinned by community empowerment values |
| B | Resident led and driven by community empowerment values initially, but becoming more instrumental over time |
| C | Balancing an instrumental approach to engagement related to place-based (structural/physical) change with community empowerment values |
| D | An emphasis on place-based (structural/physical) change or external priorities shaped an instrumental approach to engagement |
| Element of typology | Type A – resident-led empowerment | Type B – resident led and driven by CE initially but not sustained over time | Type C – balancing instrumental and community empowerment values | Type D –instrumental/external priorities-shaped approach to engagement |
|---|---|---|---|---|
| Values | A resident-led, sustainable ethos that sought to enable residents to have greater control through individual/community empowerment | Resident led initially and driven by CE – in line with ethos of type A – but becomes dominated by agency/institutional agenda over time | Sought to enable residents to have greater control through individual/community empowerment (like type A) but also included an emphasis on CE to support structural/physical change in the area (instrumental) | Emphasis is predominantly on structural or physical change in the area rather than on resident empowerment. This may lead CE to become predominantly instrumental or dominated by broader goals for local agencies |
| Structures | Supportive/inclusive model that sought to engage at all levels (i.e. in NDC processes and the wider community) | Break down, become minimally operative or disbanded. Elements managed to survive mainly through tenacity of committed staff/residents | NDC provides an effective set of institutional structures for developing CE embedded as a core working practice | Structures support engagement in NDC decisions and processes affecting the ‘fabric’ of the area rather than empowering people |
| Control/influence | Aspired to high levels of resident control/influence | Perceived to be high initially in the early years but then declines | Generally reported to be high but patterns mixed (e.g. some residents talk of there being a ‘ceiling’ to their influence) | Located in terms of influencing decisions on redevelopment but typically residents ultimately do not have power or control over decisions |
| Trust | Early NDC activity invested in building trust as a ‘good’ | Reported to have limited impact – does not improve/declines | NDCs sought to build trust but again patterns more mixed. Could be misunderstanding between the NDC role and the role of agencies | Patterns more mixed. The NDC is important as a broker but there may be a misunderstanding between the NDC and agencies (e.g. housing agencies, council) |
| Conflict | Often in the early years as a result of frustrations. Generally reported to have declined as residents, staff and agencies learnt to work together (conflict still persisted in some NDC areas either internally or with external agencies) | May become battle locked or may even decline as residents either withdraw because of apathy or frustration, or get written out from policy at the board level | Patterns more mixed. May arise in relation to instrumental use of CE (e.g. if there is opposition to redevelopment decisions) | Often arises during process of master planning – opposition to decisions; frustrations about process – NDC resident board members/staff receive brunt |
| Leadership | Aspired to be a supportive NDC area (with strong leadership) committed to residents and resident-led values | May be identified as a ‘failing’ NDC or beset by internal problems. NDC lacks sufficiently stable or strong enough leadership to deal with these pressures. High staff turnover – the job is too stressful or they are ‘let go’, dismissed or suspended | Important for leadership by staff (rather than residents) to be strong, effective | Requires strategic leadership as regeneration plans require input from stakeholders including councils, housing associations, private developers, etc. |
| Impact of political context | NDC areas managed to stick to their values despite sometimes experiencing challenging pressure from politicians or local accountable bodies | Changes in government goalposts (e.g. to deliver targets) add to already existing pressures and are overwhelming | NDC approach to regeneration is aligned to priorities of local agencies that emphasise more physical/structural change | Highly influential to the success of redevelopment of an area |
| Legacy | Positive/sense of pride in achievements; community-led organisations often have relatively formal structures (e.g. social enterprise or charity) ensuring a continued legacy based on the original value system and lessons learnt | Aspiration for CE not met. NDC area may still go on to achieve some positive change through the tenacity of local residents and committed staff. Type B may be most likely to create a legacy of disillusionment for residents who became involved and to make it more difficult to sustain a viable post-NDC organisation | Positive/sense of pride in achievements; CE tends to be sustained within structures that support implementation of physical/structural change | Often caught up with the physical redevelopment of the area – takes so long to implement, may feel disempowering that not much achieved. CE tends to continue within structures that support implementation of regeneration – some concern that CE will be less prominent without the backing of the NDC initiative |
Allocating New Deal for Communities areas to a community engagement type when insufficient information was available
At this point there were nine remaining NDC areas for which there was insufficient information to type. With advice from our advisory group we therefore asked a small group of people with detailed knowledge of all or some of the un-typed areas to help us. After considering a number of approaches we decided to ask key informants to ‘score’ each element of the typology, with the scores subsequently used by the research team to allocate each area to a CE type. To limit the time required we developed questions on four elements that had proved to be particularly important in distinguishing between different CE approaches in the synthesis process: values underpinning the approach to CE, resident control, trust in agencies and leadership in the NDC programme.
A brief questionnaire was developed consisting of structured forced response questions that would enable us to distinguish between type A and type D, with types B and C potentially grouped together. The questionnaire was completed by an informant from the NDC NET and a public adviser, both with knowledge of all of the NDC areas, and a public adviser with knowledge of one area. There was a large measure of agreement in their assessments. When there was disagreement, we asked the two informants with knowledge of all nine areas to comment on each other’s assignments and try and reach an agreement. This resolved any differences between them and allowed us to type all nine areas with a degree of confidence. Subsequently, a former chief executive also corroborated the CE type we had assigned to his area, giving some small measure of reliability to our assignment. The final allocation of the 39 NDC areas to the four types of approaches to CE is shown in Table 6.
| CE type | Allocation, n |
|---|---|
| A | 14 |
| B | 12 |
| C | 8 |
| D | 5 |
| Total | 39 |
Summary
Limitations of methods used in developing the typology
The timing of the research made it difficult to identify key informants or documents in a number of areas. This has implications for how data from other significant policy initiatives is archived for future research purposes. The data sources used in developing the typology also had their own particular strengths and weaknesses. For example, the interviews with NDC residents and past workers provided ‘thick’ data but with only five respondents these data cannot capture the full diversity and complexity of the structures, processes and impacts of CE in a NDC area. However, the additional testing of the typology with our public advisers helped increase our confidence in its validity. There was a particular difficulty in assessing how far engagement extended into the NDC resident populations. The MORI surveys in NDC areas provide some estimates of this (reported in Chapter 4) but these data are also limited. In particular, people will not always know that activities they are engaged in are being delivered and/or supported by the NDC programme.
Reflections on the typology of New Deal for Communities approaches to community engagement
The complexity of CE meant that it was feasible to identify prominent features associated with different approaches (e.g. values, leadership and different levels of trust) but not ‘discrete’ intervention types. We observed both diversity within, and overlap between, the four types of approaches to CE that we have identified. However, our aim was not to distinguish between ‘pure’ CE types but rather to identify broad approaches that shared prominent features over time.
It was also recognised that in practice the engagement experience of residents was a product of the interaction between the approach to CE adopted by the NDC partnership and the context in which it was working. For example, some NDC areas included in type A – resident led and driven by a commitment to CE – faced greater challenges than others in delivering their objectives. Individual leadership issues, relationships between residents and the local council, and other contingent factors could act as both barriers and facilitators to how closely NDC areas fitted with this model. Inevitably, there were three areas for which allocation to a single CE type was particularly difficult. Of these, the most problematic was one of the fieldwork sites allocated to type A. It was a strongly resident-led model and driven by a commitment to CE, but in practice its decision-making processes lacked inclusivity because it was tightly controlled by a small group of residents with a clear vision for their area. However, it sought to generate benefits for the local community and achieved a number of successes in relation to CE and wider social determinants of health and continues to operate as a successful enterprise.
The ‘mismatch’ between the picture of engagement presented by the MORI survey data and that captured in the narrative data from interviews highlights the often divergent (and sometimes incompatible) ‘ways of knowing’ social phenomena generated from qualitative and quantitative data sources. Our comparison of findings from the two data sources did, however, highlight the importance of understanding qualitative aspects of programme delivery and the wider context in interpreting the results of our quantitative analyses of the impact of CE approaches on social and health outcomes.
The results from the quantitative analyses of the impact of NDC approaches to CE on health and social outcomes are presented in the next three chapters. The results are divided on the basis of the type of data used in the analysis. Chapter 4 focuses on cross-sectional analyses of impact, first considering trends over time in selected outcomes within NDC areas and then focusing on changes in NDC areas relative to their comparator areas. Chapter 5 reports the results of longitudinal analyses following changes in social and health outcomes in individuals over time. In Chapter 6 the focus is on longitudinal analyses of the impact of NDC approaches to CE on outcomes drawn from time series of routine administrative data. This is followed in Chapter 7 by further analyses of the qualitative interview data, which provide insights into processes operating within different CE approaches in NDC areas that can illuminate potential pathways to social and health outcomes.
Chapter 4 The impact of New Deal for Communities approaches to community engagement: cross-sectional analyses
Introduction
This chapter begins with a brief summary of existing research evidence on the impact of the NDC initiative on health and social outcomes, including the results of our previous research. It then presents the results from our cross-sectional analyses of impact, first considering trends over time in selected outcomes within NDC areas and then focusing on changes in NDC areas relative to comparator areas.
Previous research on the impact of the New Deal for Communities on health and social outcomes
Results from the National Evaluation Team evaluation and other earlier studies on health and social outcomes
Our analyses of the early impact of the NDC initiative on a range of health and social outcomes using MORI longitudinal survey data for 2002 and 2004 found statistically significant improvements for income, fear of crime and satisfaction with the local area. However, with the exception of satisfaction with the local area, no statistically significant differences in overall change in NDC compared with comparator areas were found. In other words, although this early evidence suggested that things were improving across all domains, it did not support a greater improvement in NDC areas than in non-intervention areas at the 2-year follow-up. 68
Results from the NET published in 2010 present a more positive picture, with a modest effect of the initiative as a whole for the first 8 years of the programme. 69 However, using 2008 data only, only nine of the 36 selected indicators across the six NDC outcome domains (housing and the environment, crime, education, employment, community and health) showed any significant positive difference between NDC and comparator areas. When longitudinal data were used, only five indicators were significantly positive in NDC areas compared with comparator areas. When controlling for gender, age and ethnicity, three indictors of perceptions of the local environment and two health indictors remained significant. In other words, there were significantly greater reductions in the NDC areas in the number of people who thought that their health was not good and who considered their health to have deteriorated in the previous year. Some of the largest improvements appeared to be on health indicators. For example, in the NET’s analyses 48% of NDC residents experienced an improvement in their mental health index score between 2002 and 2008, with a similar percentage seeing a decrease over this period. Although in the comparator areas a smaller percentage reported worsening mental health than in NDC areas (39% compared with around 47% in the NDC areas), a lower proportion reported improvement compared to NDC areas (43% compared with 48%). 70
The NET results also highlight variation in impact across the NDC areas, for example there was a 10% difference in the proportion of respondents reporting self-rated bad health across the 39 areas. 70 The most noticeable improvements in overall outcomes were also found in the less deprived NDC areas as well as in those areas with the largest number of previous or concurrent area-based interventions. 71 Areas characterised as predominantly ‘white peripheral housing estates’ in non-core cities were also more likely to have improved over time. 72
Significant variations between NDC areas were also found in our evaluation of the early impact of the NDC in 2002/4. 68 However, as a proportion of the total variation between individuals, differences between NDC areas were small (< 2% on all outcomes), suggesting that differential impacts between demographic and social groups within areas are more important than differences between areas. The likelihood of quitting smoking, finding work and participating in education or training, for example, increased steadily with increasing levels of education and the likelihood of developing a new long-term limiting illness decreased with increasing levels of education. 68 Similar differential impacts were found by gender, age and ethnicity and these patterns were mirrored in comparator areas. There were, however, two important exceptions, suggesting that at least some of the social inequalities that drive health inequalities were growing less fast in NDC areas than in comparator areas during these early years of the programme. In both comparator and NDC areas, the likelihood of participation in education or training in the past 12 months increased with increasing levels of education, but this association was less steep in NDC areas; in addition, mean age-related decline in self-rated health was seen in comparator areas but not in NDC areas.
Research on the impact of the New Deal for Communities on health inequalities and their social determinants
Our previous evaluation funded by the Department of Health’s Policy Research Programme focused on the impact of the NDC initiative, and in particular different types of local NDC programmes, on health inequalities and their social determinants.
Taking the NDC initiative as a whole, both the MORI longitudinal data (2002–8) and routine time series over variable periods showed no overall trend in improvements on most outcomes in either the NDC areas or the comparator areas, but there were two exceptions to this. First, levels of satisfaction with the area declined over time between 2002 and 2008 in comparator areas compared with NDC areas. Second, although we found no significant differences between NDC and comparator areas in numbers of benefit claimants over time, NDC areas did appear to have experienced a greater reduction in benefit receipt among lone parents. In contrast, when we compared outcomes in NDC and comparator areas with outcomes in areas of low, medium and high deprivation in the rest of the country (constructed using data from the HSE), we found a general trend of improvement between 2002 and 2008 in smoking, mental health, educational attainment and employment rates in all areas regardless of deprivation level. More importantly, however, from an equity perspective, levels of poor self-rated health declined faster in NDC and comparator areas than in HSE areas with low deprivation and these improvements appear to have been greater in NDC areas than in areas of high and medium deprivation in other parts of the country, where rates of poor self-rated health actually rose over time.
We also found evidence of a NDC ‘effect’ on the social determinants of health inequalities. Thus, the proportion of people with no qualifications fell more steeply in NDC areas than in the HSE low and high deprivation areas, although this more rapid improvement was also seen in the NDC comparator areas, suggesting that this effect may in part reflect local authority-wide, rather than NDC-specific, educational interventions. Similarly, although the gap between high and low deprivation areas widened on five of the six social determinants of health that we analysed, only the gap in smoking widened between NDC areas and low deprivation areas. This suggests that the NDC intervention may have helped to prevent a further widening of the gap, or even narrowed it, in some of these outcomes, which is an important achievement. This previous evaluation also suggests that the NDC programme may have reduced some inequalities between socioeconomic groups within NDC areas. Notable here are the results from the analyses of MORI panel data, which show that, whereas low levels of education and household-level joblessness were associated with worse health trajectories in both NDC areas and comparator areas, disadvantaged residents in NDC intervention areas experienced a greater improvement in mental health and life satisfaction than their counterparts in comparator areas.
Our previous evaluation also provided evidence that the three different types of local NDC programme that we identified had different social and health outcomes. Type 1 local NDC programmes, which emphasised diversification of the local population and major redevelopment of the area, consistently underperformed compared with type 2 and type 3 programmes. Type 2 local programmes, which combined moderate redevelopment with activities aimed at developing human capital in the local population, were most often associated with improvements over time. Advantages on measures of social cohesion and quitting smoking emerged or were maintained between 2002 and 2008 among residents in NDC areas with type 2 and type 3 local programmes (where there was little or no redevelopment), whereas slight disadvantages in trust in these areas in 2002 compared with areas with type 1 programmes disappeared over time. Respondents in areas with type 2 local programmes also had a greater probability of reporting improved mental health over time and those without work were significantly more likely to find employment than people living in areas with type 1 local programmes. This may partly explain the better performance of areas with type 2 local programmes in terms of reductions in hospital admission rates. These reductions were greater for alcohol- and drug-related conditions, conditions closely linked to mental health problems. The better performance on hospital admission rates was also maintained in type 2 programme areas with very different social and economic contexts and, although the numbers involved in these analyses were small, these findings are supported by the work of Riva and Curtis. 73
As noted earlier, engaging with communities was expected to be a central component of the NDC programme. The typology of local NDC programmes that we developed therefore included information on the approach to CE adopted by NDC areas. However, this was based on relatively ‘thin’ data and clearly did not allow a separate analysis of the direct impact of different approaches to CE on health and social outcomes in NDC populations, or the extent to which these different approaches to CE contributed to the patterns of impacts associated with different types of local NDC programmes. In this chapter and Chapters 5 and 6 we present the results of our most recent analyses, which have used the new typology of NDC approaches to CE described in the previous chapter to answer the five questions highlighted earlier:
-
Which approaches to CE engage which social groups in NDC populations?
-
Do different approaches to CE have differential health and social outcomes for NDC populations?
-
Does the association between these outcomes and NDC approaches to CE vary across groups defined by age, ethnicity, gender and material circumstances?
-
Do different approaches to CE have any impact on the gap in health and social outcomes between NDC areas and areas from across the socioeconomic spectrum?
-
Does the approach to CE help to explain any of the differential outcomes of local NDC programmes identified in our previous research?
The remainder of this chapter focuses on cross-sectional analyses of the impact of approaches to engagement on changes over time in the NDC population as a whole and in this population relative to that in the NDC comparator areas. Chapter 5 focuses on within-person change utilising longitudinal data from the MORI household survey whereas Chapter 6 explores the impact of different approaches to CE using routine time series data on hospital admissions and welfare benefit counts.
Which community engagement approaches effectively engage which social groups in the New Deal for Communities populations?
How much community involvement was there and how have residents been involved?
As already noted, levels of community involvement were relatively low in NDC areas at the beginning of the initiative compared with national figures. 53 According to the MORI household survey in 2002:
-
35% of NDC residents felt part of their community, compared with 51% nationally
-
23% felt that they could influence decisions that affect the local area, compared with 26% nationally
-
12% had been involved in a local organisation on a voluntary basis in the past 3 years, compared with 21% nationally
-
41% trusted the local council, compared with 53% nationally.
Not surprisingly, these percentages varied across the 39 NDC areas, which faced different barriers to engaging local residents, shaped in part by the factors discussed in Chapter 3, including the physical, social and economic profiles of the neighbourhoods and existing relationships of trust between residents and local agencies. At each wave of the MORI household survey (2002, 2004, 2006 and 2008), all respondents who had heard of their local NDC partnership were asked if they had been involved in any NDC-organised activities in the previous 2 years. Comparing the data from this question across the four time points (Table 7), there was a slight increase in the percentage reporting that they had been involved in any local organisation in both the NDC areas and the comparator areas, with the change between 2002 and 2008 statistically significant in the NDC areas but not in the comparator areas (although that is mostly because of the five- to 10-fold larger sample sizes in the NDC areas).
| Areas | 2002 | 2004 | 2006 | 2008 | Trend, significant 2008 – 2002 | Significant NDC – comparator |
|---|---|---|---|---|---|---|
| NDC areas | ||||||
| % (n) | 11.9 (19,576) | 11.8 (19,488) | 13.2 (15,688) | 13.9 (15,750) | Up, yes | No |
| 95% CI | 11.4 to 12.4 | 11.3 to 12.3 | 12.6 to 13.9 | 13.3 to 14.6 | ||
| Comparator areas | ||||||
| % (n) | 12.4 (2010) | 10.7 (4024) | 12.1 (3037) | 13.9 (3063) | Up, no | No |
| 95% CI | 10.9 to 14.1 | 9.7 to 11.8 | 10.9 to 13.6 | 12.5 to 15.4 | ||
It is possible to make comparisons with similarly deprived areas and also with the national average with regard to a broader, but related, question about involvement asked in two national surveys, the General Household Survey in 200074 and the Ipsos/MORI Public Affairs Monitor in 2008. 75 These comparisons suggest that nationally the increase in voluntary activity was slightly less marked than in the NDC areas (only 1 percentage point between 2000 and 2008), but the absolute level of voluntary activity remained much higher across England as a whole (22% in 2008 compared with around 14% in NDC and comparator areas).
A further question, only included in the 2008 MORI survey, explores the different ways in which residents have been involved. In 2008, 22% of those who had heard of the NDC programme, or 17% of all respondents, said that they had been involved in some voluntary activity. Table 8 presents a breakdown of the type of involvement in this group separated into those who participated in activities and those who volunteered to play a more active role. Of all those who said that they had been involved in some way, 87% played a participative role; this was equivalent to 15% of all NDC residents. The majority (51%) attended NDC events or festivals, with 30% attending NDC partnership meetings or workshops, and a smaller percentage participating in the governance of the NDC, with 14% voting in NDC elections. Of those who volunteered to play a more active role, most commonly residents had helped run NDC events or projects (14%), with only 5% volunteering to join a NDC board.
| Involvement | Attended NDC sponsored events | Attended NDC meetings or workshops | Attended training or courses | Used services supplied by NDC | Voted in NDC elections |
|---|---|---|---|---|---|
| Participation | |||||
| % | 51.0 | 30.2 | 20.6 | 24.5 | 14.3 |
| 95% CI | 48.7 to 53.2 | 28.2 to 32.2 | 18.9 to 22.6 | 22.6 to 26.4 | 12.8 to 15.8 |
| Involvement | Run NDC events | Helped organise NDC-related meetings | Member of NDC board | Professional or skilled support | Other |
| Volunteering | |||||
| % | 13.9 | 6.3 | 4.8 | 5.5 | 5.9 |
| 95% CI | 12.4 to 15.6 | 5.3 to 7.5 | 3.9 to 5.9 | 4.5 to 6.8 | 5.0 to 7.0 |
These percentages are based on the cross-sectional data. As in table 3.1 in Volume 2 of the NET final report,53 the percentage of NDC residents included in the MORI longitudinal panel at each of the four time points who were involved in the activities of their local NDC varied over time, increasing up to 2006 and then declining slightly over the next 2 years (15% in 2002, 22% in 2004, 24% in 2006 and 22% in 2008). The residents who stayed in NDC neighbourhoods over the 6 years from 2002 to 2008 were more likely (44%) to be engaged in NDC activities than those who were NDC residents in 2008. Residents who stayed in these areas will have been exposed to NDC activities for a longer period of time and may also have felt that they had more to gain from participation in NDC activities than those living there for shorter periods.
Table 9 compares rates of involvement in NDC activities across the CE types and local programme types using cross-sectional data for 2008 (the only year in which there were detailed questions about such involvement). As in table 3.2 in Volume 2 of the NET final report53 (which shows that older people, women and those with higher educational qualifications were more likely to be involved), rates are presented as a proportion of all respondents in each category.
| CE/programme type | Any role | Volunteer | Participative |
|---|---|---|---|
| CE type | |||
| A | 17 | 5 | 16 |
| B | 17 | 4 | 16 |
| C | 14 | 4 | 13 |
| D | 15 | 4 | 15 |
| Total | 16 | 4 | 15 |
| Local programme type | |||
| 1 | 16 | 5 | 15 |
| 2 | 18 | 5 | 16 |
| 3 | 14 | 4 | 13 |
| Total | 16 | 4 | 15 |
Residents in areas with type A approaches to CE were slightly more likely to have volunteered to take an active role in NDC activities than those in areas with other types of CE approaches, whereas those in areas with types A and B CE were more likely to have participated in NDC events or have any role (16% and 17% respectively) than those in areas with types C (13% and 14% respectively) and D (15% and 15% respectively) CE. Participation in NDC events was higher among residents in areas with type 2 local programmes (16%), who were also most likely to have had any role in the NDC (18%); the corresponding figures for type 1 and type 3 areas were 15% and 16%, respectively, and 13% and 14% respectively. Although not shown in Table 9, the percentages of residents participating in NDC activities (19%) or having had any role in the NDC (20%) were highest in areas combining a type 2 local programme with a type B approach to CE.
In summary, available data on levels of engagement in NDC areas suggest that, in addition to the small number of residents actively engaged in NDC governance (e.g. membership of NDC partnership boards), resident participation in the NDC initiative primarily involved attendance at NDC-sponsored events, meetings and workshops, suggesting relatively low-dose exposure across NDC populations.
Cross-sectional analyses of the impact of approaches to community engagement on the New Deal for Communities populations
Trends in trust and social cohesion among residents of New Deal for Communities areas
We hypothesised that trends in indicators of trust and social cohesion between 2002 and 2008 among NDC residents would differ by CE type. Key findings from these analyses, which used repeat cross-sectional survey data, are reported in this section and more details can be found in Tables 41–49 in Appendix 2.
In 2002, in the early years of the programme, > 80% of respondents to the MORI survey felt that people in their area were friendly and > 60% felt that neighbours looked out for each other regardless of the NDC approach to CE. However, much lower percentages felt part of their local community (around 33%) or felt that they could influence decisions in the area (around 25%). This held true across population subgroups. There was, however, some indication that residents in areas with type A approaches to CE were more likely than residents in areas of other CE types to agree that people in their area were friendly, that they knew most/many people in the area and that neighbours looked out for each other.
The greater likelihood of positive responses on these indicators of social cohesion and trust from residents in areas with type A approaches to CE remained visible in 2008, particularly among women, older residents and the more disadvantaged groups (i.e. renters and those with no qualifications). Residents in these areas were also more likely to report that they had heard of the NDC in 2002 and 2008, and white residents in these areas were more likely to feel that they could influence decisions than those in other CE types. However, by 2008, residents in areas with type D CE approaches were more likely than those in areas with other approaches to CE to feel part of the local community and this was more common among women, older residents and those in jobless households. Not surprisingly, in 2002, only around one-third of respondents agreed that the NDC had improved their area, regardless of the approach to CE adopted in their area. However, by 2008 this percentage had increased in all areas, but more so in areas with type A and type C approaches to CE.
Table 10 summarises the results of multivariate analyses, which adjusted for gender, age group, ethnicity, educational attainment, housing tenure and living in a jobless household, and used logistic regression for each one of the indicators of social cohesion. Accounting for these demographic and socioeconomic differences in populations, there was a general pattern for residents in areas with a type A approach to CE to report positively across the nine indicators of trust, social cohesion and involvement in 2008 compared with residents in areas with other types of approaches to CE. Although statistical significance is not attained in most cases, odds ratios indicate lower levels of trust, social cohesion and involvement in areas with type B, type C and type D approaches to CE in the majority of cases.
| Characteristic | (1) Feel part of the local community | (2) Local people are friendly | (3) Know most/many people in the area | (4) Neighbours look out for each other | (5) Can influence decisions | (6) Volunteered in local organisations | (7) Heard of NDC | (8) Involved in NDC | (9) NDC has improved area |
|---|---|---|---|---|---|---|---|---|---|
| CE type (reference: type A) | |||||||||
| B | 0.93 (0.85 to 1.01) | 0.81*** (0.71 to 0.93) | 0.90** (0.83 to 0.99) | 0.92 (0.83 to 1.02) | 1.02 (0.92 to 1.13) | 1.00 (0.88 to 1.13) | 0.77**** (0.68 to 0.88) | 1.05 (0.92 to 1.19) | 0.76**** (0.68 to 0.85) |
| C | 0.99 (0.90 to 1.09) | 0.83** (0.72 to 0.96) | 0.97 (0.88 to 1.07) | 0.79**** (0.70 to 0.88) | 0.92 (0.82 to 1.03) | 0.86 (0.75 to 1.00) | 0.72**** (0.62 to 0.84) | 0.87** (0.75 to 1.00) | 1.00(0.89 to 1.13) |
| D | 1.06 (0.94 to 1.19) | 0.88 (0.74 to 1.05) | 1.01 (0.90 to 1.14) | 0.88 (0.77 to 1.00) | 0.85** (0.74 to 0.98) | 1.09 (0.92 to 1.31) | 0.74**** (0.62 to 0.88) | 0.90 (0.75 to 1.08) | 0.65**** (0.56 to 0.75) |
| Female (reference: male) | 1.09** (1.01 to 1.17) | 1.06 (0.95 to 1.17) | 1.22**** (1.14 to 1.32) | 1.09** (1.00 to 1.18) | 1.05 (0.97 to 1.15) | 1.11 (1.00 to 1.23) | 1.39**** (1.25 to 1.54) | 1.55**** (1.39 to 1.72) | 1.16*** (1.06 to 1.27) |
| Age (reference: 31–59 years) | |||||||||
| ≤ 30 years | 0.71**** (0.65 to 0.77) | 0.84*** (0.74 to 0.95) | 0.80**** (0.73 to 0.88) | 0.81**** (0.73 to 0.89) | 0.73**** (0.66 to 0.82) | 0.65**** (0.57 to 0.70) | 0.41**** (0.36 to 0.46) | 0.87 (0.76 to 1.00) | 0.97 (0.87 to 1.00) |
| ≥ 60 years | 1.28**** (1.17 to 1.40) | 1.42**** (1.23 to 1.63) | 1.00 (0.92 to 1.10) | 1.14** (1.03 to 1.26) | 0.92 (0.83 to 1.03) | 1.00 (0.87 to 1.14) | 1.12 (0.97 to 1.28) | 0.71**** (0.62 to 0.81) | 1.15** (1.03 to 1.29) |
| Non-white (reference: white) | 0.55**** (0.50 to 0.59) | 1.15** (1.02 to 1.29) | 0.99 (0.91 to 1.08) | 1.13** (1.03 to 1.24) | 0.74**** (0.67 to 0.82) | 0.86** (0.76 to 0.97) | 1.39**** (1.24 to 1.57) | 0.88** (0.77 to 1.00) | 0.83**** (0.74 to 0.92) |
| Education (reference: NVQ 1 or no formal education) | |||||||||
| NVQ 2–3 | 0.96 (0.88 to 1.05) | 1.00 (0.88 to 1.13) | 0.99 (0.91 to 1.08) | 0.97 (0.88 to 1.07) | 1.31**** (1.19 to 1.45) | 1.96**** (1.72 to 2.23) | 1.60**** (1.41 to 1.81) | 1.44**** (1.27 to 1.60) | 0.99 (0.89 to 1.09) |
| NVQ 4–5 | 0.99 (0.89 to 1.10) | 0.83** (0.72 to 0.96) | 0.58**** (0.52 to 0.65) | 0.90 (0.80 to 1.01) | 2.01**** (1.79 to 2.25) | 2.93**** (2.55 to 3.37) | 1.24*** (1.06 to 1.45) | 1.65**** (1.42 to 1.91) | 0.98 (0.86 to 1.11) |
| Owner (reference: renter) | 1.21**** (1.12 to 1.31) | 1.60**** (1.42 to 1.81) | 1.56**** (1.44 to 1.70) | 1.67**** (1.52 to 1.83) | 1.20**** (1.09 to 1.32) | 1.29**** (1.15 to 1.45) | 2.94**** (2.56 to 3.37) | 1.06 (0.94 to 1.19) | 1.17*** (1.06 to 1.29) |
| Jobless household (reference: at least one member in employment) | 1.06 (0.98 to 1.15) | 0.88** (0.78 to 0.99) | 1.19**** (1.10 to 1.29) | 0.99 (0.90 to 1.09) | 0.93 (0.85 to 1.03) | 1.21*** (1.07 to 1.37) | 1.01 (0.90 to 1.13) | 1.22*** (1.08 to 1.37) | 0.99 (0.90 to 1.10) |
| n | 18,938 | 18,938 | 18,938 | 17,221 | 17,322 | 18,822 | 15,698 | 12,611 | 12,695 |
In summary, these cross-sectional analyses suggest that social cohesion and involvement in 2008 were generally higher in areas with type A approaches to CE than in areas with other CE types after controlling for demographic and socioeconomic factors.
Trends in health and lifestyle outcomes in New Deal for Communities areas
We hypothesised that trends in health and lifestyle outcomes between 2002 and 2008 would differ by CE type. Analyses of cross-sectional data from 2002 provided evidence of a difference in health and lifestyle outcomes between residents in areas with different approaches to CE at baseline (Table 11). A higher percentage of residents in areas with type C approaches to CE reported that they were in good health and had good mental health, and a lower percentage reported having a limiting illness and that they smoked than residents in areas with other approaches to CE. These residents and those in areas with type D approaches to CE were also more likely to eat at least five portions of fruit or vegetables a day at least three times a week.
| Outcome | CE type A | CE type B | CE type C | CE type D | Significanceb | ||||
|---|---|---|---|---|---|---|---|---|---|
| % | 95% CI | % | 95% CI | % | 95% CI | % | 95% CI | ||
| Good self-rated health | 42.0 | 40.6 to 43.4 | 43.2 | 41.7 to 44.7 | 46.5 | 44.8 to 48.2 | 41.5 | 39.2 to 43.9 | **** |
| Limiting illness | 35.0 | 33.7 to 36.3 | 33.6 | 32.2 to 35.0 | 29.3 | 27.9 to 30.8 | 32.2 | 30.2 to 34.3 | **** |
| Nervous person | 11.1 | 10.3 to 12.0 | 10.0 | 9.2 to 10.9 | 9.8 | 8.9 to 10.9 | 11.2 | 9.8 to 12.6 | |
| Down in the dumps | 11.7 | 10.9 to 12.5 | 10.9 | 10.1 to 11.8 | 8.5 | 7.7 to 9.5 | 11.2 | 9.9 to 12.6 | **** |
| Calm and peaceful | 45.7 | 44.3 to 47.0 | 48.0 | 46.5 to 49.6 | 50.6 | 48.9 to 52.3 | 48.1 | 45.7 to 50.4 | **** |
| Downhearted | 11.1 | 10.3 to 12.0 | 11.2 | 10.3 to 12.1 | 9.2 | 8.3 to 10.1 | 11.4 | 10.1 to 12.8 | *** |
| Happy person | 63.7 | 62.4 to 65.0 | 65.1 | 63.7 to 66.5 | 66.4 | 64.8 to 68.0 | 63.2 | 61.0 to 65.4 | ** |
| Eat five portions of fruit/vegetables a day three or more times per week | 48.9 | 47.6 to 50.3 | 53.0 | 51.5 to 54.5 | 58.5 | 56.8 to 60.2 | 59.9 | 57.6 to 62.1 | **** |
| Smoking | 43.0 | 41.6 to 44.3 | 40.7 | 39.3 to 42.2 | 33.0 | 31.4 to 34.6 | 39.4 | 37.2 to 41.7 | **** |
As Table 12 shows, these health and lifestyle advantages for residents of areas with type C approaches to CE were also evident in 2008 and remained after controlling for socioeconomic and demographic differences between residents in areas with different types of CE approaches (see Table 13, model 2).
| Outcome | CE type A | CE type B | CE type C | CE type D | Significanceb | ||||
|---|---|---|---|---|---|---|---|---|---|
| % | 95% CI | % | 95% CI | % | 95% CI | % | 95% CI | ||
| Good self-rated health | 46.5 | 44.9 to 48.2 | 50.7 | 49.0 to 52.4 | 51.9 | 49.8 to 53.9 | 48.1 | 45.4 to 50.9 | **** |
| Limiting illness | 35.6 | 34.1 to 37.1 | 31.0 | 29.5 to 32.5 | 27.6 | 25.9 to 29.3 | 31.4 | 29.0 to 33.8 | **** |
| Nervous person | 8.2 | 7.3 to 9.0 | 8.0 | 7.2 to 9.0 | 8.4 | 7.4 to 9.6 | 10.5 | 8.9 to 12.4 | ** |
| Down in the dumps | 7.9 | 7.1 to 8.8 | 7.2 | 6.5 to 8.1 | 7.1 | 6.2 to 8.1 | 10.0 | 8.6 to 11.6 | *** |
| Calm and peaceful | 51.6 | 50.0 to 53.3 | 54.1 | 52.4 to 55.8 | 57.3 | 55.2 to 59.3 | 54.5 | 51.8 to 57.2 | **** |
| Downhearted | 10.9 | 10.0 to 11.8 | 9.3 | 8.5 to 10.3 | 9.3 | 8.2 to 10.4 | 11.5 | 9.9 to 13.3 | ** |
| Happy person | 67.4 | 65.9 to 68.9 | 66.8 | 65.2 to 68.4 | 68.7 | 66.8 to 70.6 | 63.1 | 60.5 to 65.7 | *** |
| Eat five portions of fruit/vegetables a day three or more times per week | 53.4 | 51.8 to 55.0 | 57.1 | 55.4 to 58.8 | 60.4 | 58.3 to 62.4 | 54.3 | 51.6 to 57.0 | **** |
| Smoking | 38.2 | 36.7 to 39.8 | 35.6 | 34.0 to 37.3 | 29.8 | 28.0 to 31.7 | 34.1 | 31.6 to 36.6 | **** |
Table 13 presents the results of analyses using logistic regression, focusing on self-rated health by CE type and type of local NDC programme.
| Group | Odds ratio (95% CI) of being in good self-rated healtha | |||
|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | |
| Female (reference: male) | 0.86**** (0.79 to 0.92) | 0.86**** (0.79 to 0.92) | 0.86**** (0.79 to 0.92) | 0.86**** (0.79 to 0.92) |
| Age (reference: 31–59 years) | ||||
| ≤ 30 years | 0.44**** (0.40 to 0.48) | 0.44**** (0.40 to 0.48) | 0.43**** (0.39 to 0.48) | 0.43**** (0.39 to 0.48) |
| ≥ 60 years | 0.24**** (0.22 to 0.28) | 0.24**** (0.22 to 0.27) | 0.24**** (0.22 to 0.27) | 0.24**** (0.21 to 0.27) |
| Non-white (reference: white) | 0.90** (0.83 to 0.99) | 0.93 (0.85 to 1.01) | 0.92 (0.84 to 1.00) | 0.93 (0.85 to 1.02) |
| Education (reference: NVQ 1 or no formal qualifications) | ||||
| NVQ 2–3 | 1.14*** (1.04 to 1.24) | 1.14*** (1.04 to 1.24) | 1.13*** (1.04 to 1.24) | 1.13*** (1.04 to 1.24) |
| NVQ 4–5 | 1.69**** (1.52 to 1.88) | 1.68**** (1.50 to 1.87) | 1.66**** (1.49 to 1.85) | 1.65**** (1.48 to 1.84) |
| Owner (reference: renter) | 1.09** (1.00 to 1.19) | 1.10** (1.01 to 1.20) | 1.12** (1.03 to 1.22) | 1.13*** (1.03 to 1.23) |
| Jobless households (reference: at least one in paid work) | 0.51**** (0.47 to 0.56) | 0.51**** (0.47 to 0.56) | 0.51**** (0.47 to 0.56) | 0.52**** (0.47 to 0.56) |
| CE type (reference: type A) | ||||
| B | 1.15*** (1.04 to 1.26) | 1.12** (1.01 to 1.23) | ||
| C | 1.19*** (1.07 to 1.32) | 1.14** (1.02 to 1.27) | ||
| D | 1.08 (0.96 to 1.23) | 1.07 (0.92 to 1.25) | ||
| Local programme type (reference: type 1) | ||||
| 2 | 0.91** (0.83 to 1.00) | 0.93 (0.83 to 1.03) | ||
| 3 | 1.15*** (1.04 to 1.27) | 1.14** (1.02 to 1.28) | ||
| n | 18,938 | 18,938 | 18,938 | 18,938 |
Model 1 in Table 13 shows associations between demographic and socioeconomic characteristics, and self-rated health. Model 2 confirms that the health and lifestyle advantages highlighted above for residents of areas with type C approaches to CE in 2002 were also evident in 2008 and remained after controlling for socioeconomic and demographic differences between residents in areas with different types of CE approaches. Model 2 also shows that, when adjusted for gender, age, ethnicity, education, housing tenure and work status, residents in areas with type B approaches to CE were more likely to have good self-rated health than residents in areas with type A approaches to CE.
In our previous study type 3 local NDC programmes were associated with poorer baseline self-rated health and greater improvements in self-rated health over time than other types of local NDC programmes. This is consistent with the results of model 3 in Table 13. Model 4 shows that the effects of CE type and NDC programme type on self-rated health are independent of each other. Thus, type of CE does not explain the self-rated health advantage of residents in areas with type 2 local NDC programmes, but it does contribute independently to self-rated health.
In addition to the analyses reported here we have also produced logistic regression models using cross-sectional data from 2008 for each of the five items of the mental health inventory, for healthy eating and for smoking prevalence across CE types and types of local NDC programmes. Details of these analyses are provided in Appendix 2 (see Tables 50–56). We have considered each mental health item separately because of concerns over the psychometric properties of the summary score in these data. As these tables show, it is difficult to identify a consistent pattern across these different measures of mental health across areas with different approaches to CE, but in most cases significant results are in the direction of residents in areas with type A approaches to CE having better mental health. Health-related behaviours (healthy eating and smoking) were also investigated in multiply adjusted logistic regression models. Residents in areas with type B and type C approaches to CE were more likely to eat five portions of fruit and vegetables a day at least three times a week than those in areas with type A approaches, and those in areas with type C and type D approaches to CE were less likely to smoke than those in areas with type A approaches.
In summary, these findings suggest that residents in areas adopting a type A approach to CE had better mental health whereas those in areas with type B, type C or type D approaches to CE displayed better health-related behaviours. There is no evidence that the approach to CE contributed to differences across local NDC programme types on any of these outcomes as identified in our previous evaluation; instead, CE type and NDC local programme type provide complementary information about the impact of the NDC initiative on health inequalities and the social determinants of these.
Cross-sectional analyses of the impact of approaches to community engagement on the New Deal for Communities populations relative to comparator areas
Comparing trends in New Deal for Communities areas relative to comparator areas
We have also utilised the MORI cross-sectional survey data to compare trends in health and social outcomes in the NDC areas (grouped by CE approach) with those in their comparator areas using a difference-in-difference procedure. This procedure has been applied to the percentages of NDC and comparator areas recording positive responses for the social cohesion, trust, health and lifestyle variables, with special emphasis on the comparison between 2002 and 2008. With only 39 NDC and comparator areas these analyses are based on a small number of units, although underpinned by a large number of individual observations. Therefore, only large differences can be expected to be statistically significant. Nevertheless, we are commenting on the patterns and trends at the area level because at an individual level nearly all of the differences are statistically significant.
Trends in social cohesion, trust and control outcomes in New Deal for Communities areas relative to comparator areas
The percentage changes on six social cohesion and social trust outcomes between 2002 and 2008 across NDC areas grouped by type of CE approach and type of local programme were all positive with the single exception of a decrease in the percentage of residents thinking that they can influence decisions in NDC areas with a type D approach to CE. Similar calculations have been carried out for the comparator areas, which showed more negative changes. These findings are reported in Appendix 2 (see Tables 57 and 58).
The difference-in-difference calculations between NDC and comparator areas are shown in Table 14. Relative to the comparator areas, those in CE type A do better in terms of ‘thinking neighbours look out for each other’, ‘thinking people in the area are friendly’ and ‘thinking they can influence decisions in their area’. Residents in CE type D areas do better in terms of ‘knowing most/many people in the area’ but worse in ‘thinking that they can influence decisions in the area’ than areas with other approaches to CE.
| Variable | Approach to CE (%) | Local NDC programme type (%) | |||||
|---|---|---|---|---|---|---|---|
| Type A | Type B | Type C | Type D | Type 1 | Type 2 | Type 3 | |
| Feel part of the local community | –1.3 | –0.8 | 2.8 | –8.1 | –1.6 | 0.4 | –2.4 |
| Think people in area are friendly | 4.3 | 3.8 | –1.0 | 1.7 | 4.9 | 2.0 | 1.1 |
| Know most/many people in area | 2.8 | –4.2 | 2.0 | 12.7 | 6.1 | –0.3 | –0.2 |
| Think neighbours look out for each other | 8.9 | –1.8 | –4.7 | 4.2 | 3.4 | 2.2 | –2.6 |
| Think can influence decisions in area | 2.8 | –1.9 | 1.6 | –10.2 | –2.6 | –1.7 | 3.6 |
| Volunteered in local organisations | 0.7 | –1.0 | 2.1 | 0.5 | –0.3 | –0.9 | 3.1 |
When broken down by local NDC programme type, relative to the comparators areas, those in areas with type 1 local programmes do better than areas with other programme types in terms of ‘thinking people in the area are friendly’ and ‘knowing most/many people in the area’ whereas residents of areas with type 3 local programmes show more improvement in terms of ‘thinking they can influence decisions’ and ‘volunteered in local organisations’.
Trends in health outcomes in New Deal for Communities areas relative to comparator areas
There were improvements over time across all NDC areas on measures of health and lifestyle, but more deteriorating trends than for cohesion and trust variables. Details of these findings are provided in Appendix 2 (see Tables 59 and 60). For example, residents in all types of NDC (whether defined by CE typology or local programme type) reported improvements in self-rated health, being calm and peaceful, feeling down in the dumps and reductions in smoking; and, to a lesser extent reductions in the percentages feeling nervous or smoking. But for the other three outcomes (life-limiting illness, feeling happy and healthy eating), there more negative than positive changes. Although not quite so systematic, there were similar changes in all types of the comparator areas.
Difference-in-difference calculations between NDC and comparator areas for these health and lifestyle variables are shown in Table 15. These results show that, relative to their comparator areas, NDC areas adopting type A and D approaches to CE do better in terms of improvements in the percentages reporting being ‘calm and peaceful’, ‘a happy person’ and ‘quitting smoking’, whereas areas adopting type D approaches to CE show more improvements in terms of ‘being a nervous person’, ‘being down in the dumps’ and healthy eating. There were no significant patterns of differences in terms of percentages reporting ‘good self-rated health’, a ‘limiting illness’ and ‘being downhearted’. In terms of local NDC programme types, areas with type 2 programmes showed more improvement in ‘good self-rated health’ relative to comparator areas and areas with type 3 local programmes showed more improvement in terms of being ‘calm and peaceful’, being ‘a happy person’ and ‘quitting smoking’ but less improvement in terms of the percentage reporting a ‘limiting illness’. There were only small differences for the other four items.
| Variable | Approach to CE (%) | Local NDC programme type (%) | |||||
|---|---|---|---|---|---|---|---|
| Type A | Type B | Type C | Type D | Type 1 | Type 2 | Type 3 | |
| Good self-rated health | 0.3 | –2.2 | 2.5 | –2.1 | –1.2 | 9.9 | 1.6 |
| Life-limiting illness (negative valence) | 0.1 | 0.3 | –1.7 | 2.0 | –1.3 | –1.0 | 4.5 |
| Nervous person (negative valence) | –1.3 | 1.5 | –2.9 | –3.8 | –1.4 | 0.5 | –1.5 |
| Down in the dumps (negative valence) | –0.4 | 0.2 | 0.9 | –4.9 | –1.4 | –0.4 | 0.1 |
| Calm and peaceful | 7.7 | 1.2 | 4.4 | 15.7 | 6.2 | 2.2 | 8.9 |
| Downhearted (negative valence) | –0.9 | 0.1 | 1.8 | –2.0 | 0.2 | 0.7 | –1.6 |
| Happy person | 3.3 | –4.0 | –2.5 | 7.5 | –0.3 | –2.7 | 3.9 |
| Eat five portions of fruit/vegetables a day three or more times a week | –6.8 | –6.7 | –1.2 | 7.0 | 1.6 | 0.7 | –8.2 |
| Smoking (negative valence) | –3.1 | –1.2 | 0.6 | –7.7 | 0.3 | –0.2 | –5.2 |
Taking account of starting values: multivariate analysis
There are two general problems with the difference-in-difference procedure (apart from statistical issues). First, the NDC areas and their comparators were not an exact match, but given that the difference-in-difference procedure compares changes over time, any differences between the NDC and matched comparator areas matter only if one thinks that either (1) the rate of change is different depending on starting status (e.g. that a change from 25% to 30% is more difficult or easier to achieve than a change from 30% to 35%) or (2) the factors likely to influence the rate of change are different at the starting position. We therefore tested for the impact of different starting points on the outcomes of interest. Second, it is necessary to check that there have been no significant changes in other factors known to affect the outcome variables being considered that are likely to have differentially affected the NDC and comparator areas. In particular, we are concerned with possible changes in any known structural and social determinants. In the same analyses, therefore, the difference-in-difference effect has been calculated controlling for the effects of education, employment and housing.
To test for the impact of the starting values on trends over time, the difference-in-differences between values in 2002 and 2008 have been regressed on the starting 2002 value of the difference between the starting values in the NDC and comparator areas, the programme intervention type and CE type, controlling for education, employment, ethnicity and housing. As the detailed results of these analyses show (see Tables 61 and 62 in Appendix 2), the coefficients for the NDC local programme type were never statistically significant and with regard to CE type only the type A approach to CE was statistically significant in relation to ‘thinking neighbours look out for each other’. In contrast, the starting value was always strongly statistically significant. The coefficients for the socioeconomic factors are not shown in the tables but ethnicity and employment were most frequently statistically significant.
Comparing trends in cohesion, trust, health and lifestyle variables in New Deal for Communities areas relative to areas from across the social spectrum
In a final analysis of the cross-sectional data we considered trends over time on four outcome measures – poor mental health, smoking, poor self-rated health and likelihood of being out of employment – in NDC areas by type of approach to CE compared with those in NDC comparator areas and areas with high, medium and low levels of deprivation constructed using data from the HSE. The results of these analyses are shown as log odds ratios in Table 16. Details of the statistical approach used are provided in a note to the table.
| Variable | Poor mental health (n = 106,428) | Smoking (n = 108,732) | Poor self-rated health (n = 108,827) | Not in paid work (working age; n = 42,744) | ||||
|---|---|---|---|---|---|---|---|---|
| Intercept | Slope | Intercept | Slope | Intercept | Slope | Intercept | Slope | |
| HSE low deprivation | Reference | –0.032** | Reference | –0.056**** | Reference | –0.015 | Reference | –0.03 |
| HSE medium deprivation | 0.02 | 0.032 | 0.23*** | 0.020 | 0.17** | 0.036** | 0.29 | 0.039 |
| HSE high deprivation | 0.49**** | 0.009 | 0.73**** | 0.046**** | 0.73**** | 0.026** | 0.85**** | 0.032 |
| NDC comparator | 0.27*** | 0.012 | 0.97**** | 0.039*** | 0.28**** | –0.013 | 0.54**** | –0.005 |
| CE type A | 0.56**** | –0.008 | 1.32**** | 0.026** | 0.49**** | –0.017 | 0.75**** | –0.012 |
| CE type B | 0.42**** | –0.010 | 1.29**** | 0.025** | 0.42**** | –0.023 | 0.74**** | –0.013 |
| CE type C | 0.39**** | 0.024 | 1.08**** | 0.041*** | 0.45**** | –0.015 | 0.72**** | –0.002 |
| CE type D | 0.51**** | 0.011 | 1.26**** | 0.056**** | 0.56**** | –0.017 | 0.84**** | –0.026 |
With the exception of HSE medium deprivation areas, poor mental health was significantly more likely in all areas compared with HSE low deprivation areas at baseline in 2002. As noted earlier, residents in NDC areas were more likely to report quitting smoking over time. However, there was no evidence that this time trend varied by CE type. The likelihood of smoking was greater at baseline in all areas compared with the HSE low deprivation areas. A reduction in smoking over the period 2002–8 was seen in all areas, but this reduction was significantly less steep in all CE types, in comparator areas and in HSE high deprivation areas. There was no evidence of a different time trend by CE type for poor self-rated health or employment.
In summary, these analyses show that trends in mental health, self-rated health and participation in paid work mirrored those in less disadvantaged areas. Although smoking decreased in all less disadvantaged areas nationally, residents of NDC areas were more likely to report quitting smoking regardless of CE type and the decrease was less than in HSE low deprivation areas.
Summary
This chapter has reported the results of our cross-sectional analyses of the impact of different types of approaches to CE adopted by NDC partnerships on a number of social and health outcomes. These analyses have considered trends over time in selected outcomes within NDC areas and changes in NDC areas relative to comparator areas.
The cross-sectional analyses of trends within NDC populations found a general pattern that residents in areas with type A approaches to CE were more likely to report positively over time across the nine indicators of trust, social cohesion and involvement, after controlling for socioeconomic and demographic differences between areas. In contrast, although statistical significance was not attained in most cases, odds ratios indicated lower levels of trust, social cohesion and involvement by 2008 in areas with type B, type C and type D approaches to CE than in those with type A approaches to CE. Of particular interest is the decreasing likelihood for residents in CE type D areas to think that they could influence decisions in their area. There were no consistent trends in self-reported health outcomes across CE types. The key findings here are the positive trends among respondents from CE type B and type C areas (compared with those in CE type A areas) in terms of reporting eating healthily and the trend for residents in CE type C and type D areas to be less likely to smoke than those in CE type A areas. In contrast, in most cases significant results on the mental health indicators are in the direction of residents in CE type A areas having better mental health.
There was no evidence from the cross-sectional analyses that a NDC area’s approach to CE contributed to the differential impacts of NDC local programmes reported in our previous research.
Analyses of changes over time in NDC areas relative to their comparator areas found only a small number of positive statistically significant difference-in-differences, although NDC areas reported improvements on six social cohesion and social trust indicators compared with more negative changes in the comparator areas. Areas with type A approaches to CE showed a greater increase in the proportion of residents thinking they can influence decisions in their area relative to their comparator areas, whereas residents in areas with type D approaches to CE were the only group to report an absolute decrease on this indicator over time. There were no consistent patterns for self-reported health outcomes but, although areas with type A approaches to CE had worse outcomes for quitting smoking than other NDC areas, these areas did better in terms of the percentage ‘quitting smoking’ than their comparators. The multivariate analyses have also shown the importance of the initial starting values of both the outcome variable itself and the difference in outcome values between the NDC and the comparator areas.
Chapter 5 The impact of New Deal for Communities approaches to community engagement: within-person changes in social and health outcomes in New Deal for Communities areas
Introduction
The findings reported in Chapter 4 were based on repeated cross-sectional data from the NDC MORI surveys. It is not possible to assess the extent to which individuals experience change over time using these data. In this chapter we therefore present findings from analyses that have used the longitudinal panel from the MORI survey consisting of data on residents who contributed on two or more occasions between 2002 and 2008. The cross-sectional and longitudinal samples may differ in important ways (see Appendix 2, Table 63). Although the panel includes 10,638 observations, the number of complete cases with data at all four waves is 3554. Compared with the cross-sectional samples, the MORI panel sample for four waves includes a lower percentage of people with high educational attainment and a higher percentage of people with a white ethnic background.
Individual change in trust and social cohesion variables by New Deal for Communities approach to community engagement
Tables 17 and 18 show the results for four latent growth models examining differences in trust in neighbours and local services, respectively, in 2002 (baseline intercept) and change over time (slope) by CE type. Model 1 is unadjusted whereas model 2 adjusts for demographic factors, model 3 for socioeconomic factors and model 4 for NDC local programme type. Here, we focus on models 3 and 4.
| Model 1 | Model 2 | Model 3 | Model 4 | |||||
|---|---|---|---|---|---|---|---|---|
| Goodness of fit indicators | ||||||||
| CFI/TLI | 0.997/0.994 | 0.996/0.992 | 0.996/0.992 | 0.995/0.990 | ||||
| aBIC | 93,210 | 140,383 | 184,347 | 203,733 | ||||
| RMSEA/SRMR | 0.015/0.011 | 0.013/0.008 | 0.011/0.006 | 0.011/0.006 | ||||
| Coefficient | SE | Coefficient | SE | Coefficient | SE | Coefficient | SE | |
| Baseline trust levels (intercept) regression coefficients | ||||||||
| CE type (reference: type A) | ||||||||
| B | –0.04*** | 0.01 | –0.04*** | 0.01 | –0.03** | 0.01 | –0.03* | 0.01 |
| C | –0.08**** | 0.01 | –0.07**** | 0.01 | –0.06**** | 0.01 | –0.05**** | 0.01 |
| D | –0.05**** | 0.01 | –0.04*** | 0.01 | –0.03** | 0.01 | –0.02 | 0.02 |
| Female (reference: male) | – | – | 0.04**** | 0.01 | 0.04**** | 0.01 | 0.04**** | 0.01 |
| Age (reference: 31–59 years) | ||||||||
| ≤ 30 years | – | – | 0.11**** | 0.02 | 0.10**** | 0.02 | 0.010**** | 0.00 |
| ≥ 60 years | – | – | 0.18**** | 0.02 | 0.15**** | 0.02 | 0.15**** | 0.02 |
| Non-white (reference: white) | – | – | –0.05**** | 0.01 | –0.05**** | 0.01 | –0.05**** | 0.01 |
| Education (reference: NVQ 1 or no formal qualifications) | ||||||||
| NVQ 2–3 | – | – | – | – | –0.04**** | 0.01 | –0.04*** | 0.01 |
| NVQ 4–5 | – | – | – | – | –0.08**** | 0.01 | –0.08**** | 0.01 |
| Owner (reference: renter) | – | – | – | – | 0.06**** | 0.01 | 0.05**** | 0.01 |
| Jobless household (reference: at least one in paid work) | 0.01 | 0.02 | 0.01 | 0.02 | ||||
| Local programme type (reference: type 1) | ||||||||
| 2 | – | – | – | – | – | – | 0.03* | 0.02 |
| 3 | – | – | – | – | – | – | 0.00 | 0.02 |
| Change over time in trust levels (slope) regression coefficients | ||||||||
| CE type (reference: type A) | ||||||||
| B | –0.06** | 0.03 | –0.07** | 0.03 | –0.07** | 0.03 | –0.08*** | 0.03 |
| C | 0.01 | 0.03 | –0.01 | 0.03 | –0.02 | 0.03 | –0.02 | 0.03 |
| D | –0.02 | 0.03 | –0.01 | 0.03 | –0.03 | 0.03 | –0.08** | 0.04 |
| Female (reference: male) | – | – | 0.02 | 0.03 | 0.01 | 0.03 | 0.01 | 0.03 |
| Age (reference: 31–59 years) | ||||||||
| ≤ 30 years | – | – | –0.15**** | 0.04 | –0.150**** | 0.04 | –0.14**** | 0.04 |
| ≥ 60 years | – | – | –0.19**** | 0.04 | –0.021**** | 0.04 | –0.20**** | 0.04 |
| Non-white (reference: white) | – | – | 0.12**** | 0.03 | 0.012**** | 0.03 | 0.12**** | 0.03 |
| Education (reference: NVQ 1 or no formal qualifications) | ||||||||
| NVQ 2–3 | – | – | – | – | –0.04 | 0.03 | –0.04 | 0.03 |
| NVQ 4–5 | – | – | – | – | –0.04 | 0.03 | –0.04 | 0.03 |
| Owner (reference: renter) | – | – | – | – | –0.06** | 0.03 | –0.06** | 0.03 |
| Jobless household (reference: at least one household member in paid work) | 0.06* | 0.03 | 0.05 | 0.03 | ||||
| Local programme type (reference: type 1) | ||||||||
| 2 | – | – | – | – | – | – | –0.09** | 0.04 |
| 3 | – | – | – | – | – | – | –0.08** | 0.04 |
| Parameters of the growth curve | ||||||||
| Intercept | 0.06**** | 0.02 | –0.20**** | 0.04 | –0.18**** | 0.04 | –0.21**** | 0.05 |
| Slope | –0.05 | 0.05 | 0.16* | 0.09 | 0.20* | 0.10 | 0.34*** | 0.12 |
| Intercept variance | 0.99**** | 0.00 | 0.97**** | 0.00 | 0.96**** | 0.00 | 0.96**** | 0.00 |
| Slope variance | 0.99**** | 0.00 | 0.96**** | 0.01 | 0.94**** | 0.02 | 0.94**** | 0.02 |
| Model 1 | Model 2 | Model 3 | Model 4 | |||||
|---|---|---|---|---|---|---|---|---|
| Goodness-of-fit indicators | ||||||||
| CFI/TLI | 0.997/0.994 | 0.997/0.994 | 0.997/0.995 | 0.997/0.994 | ||||
| aBIC | 97,307 | 144,523 | 188,507 | 207,894 | ||||
| RMSEA/SRMR | 0.012/0.009 | 0.009/0.007 | 0.007/0.006 | 0.007/0.005 | ||||
| Coefficient | SE | Coefficient | SE | Coefficient | SE | Coefficient | SE | |
| Baseline trust levels (intercept) regression coefficients | ||||||||
| CE type (reference: type A) | ||||||||
| B | –0.01 | 0.02 | –0.02 | 0.02 | –0.02 | 0.02 | –0.02 | 0.02 |
| C | –0.01 | 0.02 | –0.03* | 0.02 | –0.03* | 0.02 | 0.04** | 0.02 |
| D | 0.00 | 0.02 | –0.02 | 0.02 | –0.02 | 0.02 | –0.06*** | 0.02 |
| Female (reference: male) | – | – | 0.8**** | 0.01 | 0.07**** | 0.01 | 0.07**** | 0.01 |
| Age (reference: 31–59 years) | ||||||||
| ≤ 30 years | – | – | –0.04** | 0.02 | –0.02 | 0.02 | –0.02 | 0.02 |
| ≥ 60 years | – | – | 0.00 | 0.02 | 0.01 | 0.02 | 0.01 | 0.02 |
| Non-white (reference: white) | – | – | 0.8**** | 0.01 | 0.08**** | 0.01 | 0.08**** | 0.01 |
| Education (reference: NVQ 1 or no formal qualifications) | ||||||||
| NVQ 2–3 | – | – | – | – | 0.01 | 0.02 | 0.01 | 0.02 |
| NVQ 4–5 | – | – | – | – | –0.03** | 0.01 | –0.03* | 0.01 |
| Owner (reference: renter) | – | – | – | – | –0.07**** | 0.01 | –0.06**** | 0.01 |
| Jobless household (reference: at least one household member in paid work) | – | – | – | – | 0.02 | 0.02 | 0.01 | 0.02 |
| Local programme type (reference: type 1) | ||||||||
| 2 | – | – | – | – | – | – | –0.06**** | 0.02 |
| 3 | – | – | – | – | – | – | –0.05** | 0.02 |
| Change over time in trust levels (slope) regression coefficients | ||||||||
| CE type (reference: type A) | ||||||||
| B | 0.00 | 0.03 | 0.00 | 0.03 | 0.00 | 0.03 | 0.01 | 0.03 |
| C | 0.01 | 0.03 | 0.00 | 0.03 | 0.00 | 0.03 | 0.01 | 0.03 |
| D | 0.06* | 0.03 | 0.05* | 0.03 | 0.06* | 0.03 | 0.11*** | 0.04 |
| Female (reference: male) | – | – | 0.01 | 0.03 | 0.01 | 0.03 | 0.01 | 0.03 |
| Age (reference: 31–59 years) | ||||||||
| ≤ 30 years | – | – | 0.04 | 0.04 | 0.01 | 0.04 | 0.01 | 0.04 |
| ≥ 60 years | – | – | 0.12*** | 0.04 | 0.11** | 0.04 | 0.10** | 0.04 |
| Non-white (reference: white) | – | – | 0.05 | 0.03 | 0.05 | 0.03 | 0.04 | 0.03 |
| Education (reference: NVQ 1 or no formal qualifications) | ||||||||
| NVQ 2–3 | – | – | – | – | 0.09*** | 0.03 | 0.08*** | 0.03 |
| NVQ 4–5 | – | – | – | – | –0.08*** | 0.03 | –0.08*** | 0.03 |
| Owner (reference: renter) | – | – | – | – | 0.10**** | 0.03 | 0.10*** | 0.03 |
| Jobless household (reference: at least one household member in paid work) | – | – | – | – | –0.03 | 0.04 | –0.03 | 0.04 |
| Local programme type (reference: type 1) | ||||||||
| 2 | – | – | – | – | – | – | 0.08** | 0.04 |
| 3 | – | – | – | – | – | – | 0.08** | 0.04 |
| Parameters of the growth curve | ||||||||
| Intercept | 0.01 | 0.02 | –0.08* | 0.04 | –0.04 | 0.05 | 0.06 | 0.06 |
| Slope | –0.07 | 0.05 | –0.22** | 0.10 | –0.21* | 0.11 | –0.35*** | 0.13 |
| Intercept variance | 0.99**** | 0.00 | 0.99**** | 0.00 | 0.98**** | 0.00 | 0.98**** | 0.00 |
| Slope variance | 0.99**** | 0.00 | 0.99**** | 0.01 | 0.96**** | 0.01 | 0.95**** | 0.02 |
In 2002, trust in neighbours was higher in areas with a type A approach to CE than in areas with other approaches to CE after adjustment for demographic and socioeconomic characteristics (see model 3 in Baseline trust levels of Table 17). Overall, there was a significant increase in trust in neighbours between 2002 and 2008 (indicated by a statistically significant and positive slope estimate of 0.20 in model 3; see Parameters of the growth curve of Table 17) but this was smaller in areas with a type B approach to CE than in areas with a type A approach to CE (indicated by a statistically significant and negative coefficient of –0.07 in model 3 in Change over time of Table 17).
To assess the contribution of CE to the impact of NDC programme type, NDC programme type indicator variables were introduced in model 4 in Table 17. The results show that NDC areas with type 2 and type 3 local programmes showed a smaller gain in trust in neighbours over time than areas with type 1 local programmes (p < 0.05). In this fully adjusted model, within-person improvement in trust in neighbours over time was greater in areas adopting a type A approach to CE than in areas with type B and type D approaches (indicated by a statistically significant and negative coefficient for CE types B and D in Change over time of model 4 in Table 17). This association was independent of NDC programme type, and type of CE approach did not contribute to explaining differences in trust by NDC programme type.
The results of latent growth models for trust in local services are shown in Table 18. In 2002, residents in areas with type C approaches to CE showed lower trust in local services than those in CE type A areas (p = 0.1; see model 4). There is also evidence of an overall decline in trust in local services over time (indicated by a slope coefficient of –0.21 in model 3 in Parameters of the growth curve of Table 18). However, levels of trust in local services increased among residents in areas with type D approaches to CE relative to those in areas with type A approaches to CE [indicated by a positive Change over time (Table 18) coefficient for CE type D of 0.06 in model 3 and 0.11 in model 4]. Our previous study; found no difference in change in level of trust in local services over time by local NDC programme type. However, model 4 in Table 18 shows that, when the NDC approach to CE is taken into account, levels of trust in local services among residents in NDC areas with type 2 and type 3 local programmes decreased to a lesser extent than levels of trust in local services among residents in NDC type 1 areas [indicated by a Change over time (see Table 18) coefficient for NDC types 2 and 3 of 0.08].
In summary, analyses of within-person change show that trust in neighbours increased between 2002 and 2008 but this improvement was smaller in areas with type B approaches to CE. Trust in local services decreased over this period in most areas, but increased in areas with type D approaches to CE.
Individual change in health, lifestyle and work outcomes by approach to community engagement
We used survival analysis to investigate differences in the probability of residents adopting healthier lifestyles according to the approach to CE adopted in their area. This enabled us to model the factors that influenced individual changes in behaviour at any time between 2002 and 2008. The results for smoking behaviour are shown in Table 19. Smokers in areas with type B approaches to CE were marginally less likely to quit smoking over time after controlling for demographic and socioeconomic characteristics. This analysis also suggests that approach to CE did not contribute to the finding from our previous study; that residents in areas with type 2 local programmes were more likely to quit smoking over time than those in areas with other local programme types.
| Variable | Model 1 | Model 2 | Model 3 |
|---|---|---|---|
| Female (reference: male) | 1.08**** (1.05 to 1.11) | 1.08**** (1.05 to 1.11) | 1.08**** (1.05 to 1.11) |
| Age (per-year increase) | 1.01**** (1.01 to 1.01) | 1.01**** (1.01 to 1.01) | 1.01**** (1.01 to 1.01) |
| Non-white (reference: white) | 1.48**** (1.43 to 1.54) | 1.48**** (1.43 to 1.53) | 1.48**** (1.42 to 1.53) |
| Education (reference: NVQ 1 or no formal qualifications) | |||
| NVQ 2–3 | 1.14**** (1.10 to 1.18) | 1.14**** (1.10 to 1.18) | 1.14**** (1.10 to 1.18) |
| NVQ 4–5 | 1.12**** (1.07 to 1.17) | 1.12**** (1.07 to 1.17) | 1.12**** (1.07 to 1.17) |
| Owner (reference: renter) | 1.26**** (1.22 to 1.30) | 1.25**** (1.21 to 1.29) | 1.25**** (1.22 to 1.29) |
| Jobless household (reference: at least one household member in paid work) | 0.95*** (0.92 to 0.99) | 0.95*** (0.92 to 0.99) | 0.95*** (0.92 to 0.99) |
| CE type (reference: type A) | |||
| B | 0.96**** (0.93 to 1.00) | 0.97 (0.94 to 1.01) | |
| C | 1.00 (0.96 to 1.04) | 1.01 (0.97 to 1.05) | |
| D | 0.98 (0.94 to 1.03) | 1.02 (0.96 to 1.09) | |
| Local programme type (reference: type 1) | |||
| 2 | 1.04**** (1.01 to 1.08) | 1.05**** (1.01 to 1.10) | |
| 3 | 1.02 (0.98 to 1.06) | 1.03 (0.98 to 1.08) | |
Table 20 reports the results of the survival models for healthy eating and Table 21 reports the results of the survival models for positive mental health. In terms of healthy eating, residents with a less healthy diet in 2002 in areas with type C and type D approaches to CE were more likely to report eating five or more portions of fruit/vegetables a day at least three times a week over time than residents in areas with type A approaches to CE. Those in areas with type 2 and type 3 NDC local programmes were more likely to report these dietary changes and, although the estimate was attenuated for type 2 programmes, it was magnified for type 3 programmes once CE type was included in the model. Again, the evidence points to somewhat independent effects of CE type and NDC programme type.
| Variable | Model 1 | Model 2 | Model 3 |
|---|---|---|---|
| Female (reference: male) | 1.20**** (1.17 to 1.24) | 1.20**** (1.17 to 1.24) | 1.20**** (1.17 to 1.24) |
| Age | 1.01**** (1.01 to 1.01) | 1.01**** (1.01 to 1.01) | 1.01**** (1.0 to 1.01) |
| Non-white (reference: white) | 1.16**** (1.12 to 1.20) | 1.17**** (1.13 to 1.21) | 1.15**** (1.11 to 1.19) |
| Education (reference: NVQ 1 or no formal qualifications) | |||
| NVQ 2–3 | 1.17**** (1.13 to 1.21) | 1.17**** (1.13 to 1.21) | 1.17**** (1.13 to 1.21) |
| NVQ 4–5 | 1.30**** (1.24 to 1.35) | 1.29**** (1.24 to 1.35) | 1.29**** (1.23 to 1.34) |
| Owner (reference: renter) | 1.13**** (1.10 to 1.17) | 1.14**** (1.10 to 1.17) | 1.14**** (1.11 to 1.18) |
| Jobless household (reference: at least one household member in paid work) | 0.89**** (0.87 to 0.92) | 0.89**** (0.87 to 0.92) | 0.89**** (0.87 to 0.92) |
| CE type (reference: type A) | |||
| B | 1.00 (0.96 to 1.03) | 0.99 (0.95 to 1.02) | |
| C | 1.09**** (1.05 to 1.13) | 1.07**** (1.03 to1.11) | |
| D | 1.08**** (1.03 to 1.13) | 1.08*** (1.02 to 1.14) | |
| Local programme type (reference: type 1) | |||
| 2 | 0.95**** (0.92 to 0.98) | 0.97 (0.94 to 1.01) | |
| 3 | 1.04** (1.01 to 1.08) | 1.06*** (1.02 to 1.11) | |
| Variable | Model 1 | Model 2 | Model 3 | Model 4 | ||||
|---|---|---|---|---|---|---|---|---|
| Coefficient | SE | Coefficient | SE | Coefficient | SE | Coefficient | SE | |
| Baseline mental health levels (intercept) regression coefficients | ||||||||
| CE type (reference: type A) | ||||||||
| B | –0.03* | 0.02 | –0.03** | 0.01 | –0.03** | 0.02 | – | – |
| C | 0.02* | 0.01 | 0.01 | 0.01 | 0.01 | 0.02 | – | – |
| D | –0.04*** | 0.01 | –0.02 | 0.01 | –0.02 | 0.02 | – | – |
| Female (reference: male) | – | – | –0.16**** | 0.01 | –0.16**** | 0.01 | –0.16**** | 0.01 |
| Age | – | – | 0.13**** | 0.02 | 0.13**** | 0.02 | 0.13*** | 0.02 |
| Non-white (reference: white) | – | – | 0.04*** | 0.01 | 0.03*** | 0.01 | 0.04**** | 0.01 |
| Education (reference: NVQ 1 or no formal qualifications) | ||||||||
| NVQ 2–3 | – | 0.07**** | 0.01 | 0.07**** | 0.01 | 0.07**** | 0.01 | |
| NVQ 4–5 | 0.08**** | 0.01 | 0.07**** | 0.01 | 0.07**** | 0.01 | ||
| Owner (ref: renter) | – | – | 0.11**** | 0.01 | 0.11**** | 0.01 | 0.11**** | 0.01 |
| Jobless household (reference: at least one household member in paid work) | – | – | –0.21**** | 0.02 | –0.21**** | 0.02 | –0.21**** | 0.02 |
| Local programme type (reference: type 1) | ||||||||
| 2 | – | – | – | – | –0.01 | 0.02 | 0.00 | 0.02 |
| 3 | – | – | – | – | 0.01 | 0.02 | 0.02 | 0.02 |
| Change over time in mental health levels (slope) regression coefficients | ||||||||
| CE type (reference: type A) | ||||||||
| B | 0.04 | 0.03 | 0.03 | 0.03 | 0.05 | 0.04 | – | – |
| C | –0.09*** | 0.03 | –0.10*** | 0.03 | –0.08** | 0.03 | – | – |
| D | –0.00 | 0.03 | –0.01 | 0.03 | 0.02 | 0.04 | – | – |
| Female (reference: male) | – | – | 0.12**** | 0.03 | 0.12**** | 0.03 | 0.12**** | 0.03 |
| Age | – | – | –0.08** | 0.04 | –0.07** | 0.04 | –0.08** | 0.04 |
| Non-white (reference: white) | – | – | 0.01 | 0.03 | 0.01 | 0.03 | 0.00 | 0.03 |
| Education (reference: NVQ 1 or no formal qualifications) | ||||||||
| NVQ 2–3 | – | – | –0.04 | 0.03 | –0.04 | 0.03 | –0.04 | 0.03 |
| NVQ 4–5 | – | – | 0.02 | 0.03 | 0.03 | 0.03 | 0.03 | 0.03 |
| Owner (reference: renter) | – | – | –0.01 | 0.03 | –0.02 | 0.03 | –0.02 | 0.03 |
| Jobless household (reference: at least one household member in paid work) | – | – | 0.10**** | 0.04 | 0.10*** | 0.04 | 0.10*** | 0.04 |
| Local programme type (reference: type 1) | ||||||||
| 2 | – | – | – | – | 0.09** | 0.04 | 0.07* | 0.03 |
| 3 | – | – | – | – | 0.01 | 0.04 | –0.02 | 0.04 |
| Parameters of the growth curve | ||||||||
| Intercept | –0.04 | 0.02 | –0.11** | 0.05 | –0.10* | 0.06 | –0.14*** | 0.053 |
| Intercept variance | 0.99**** | 0.00 | 0.87**** | 0.01 | 0.87**** | 0.01 | 0.87 | 0.009 |
| Slope | 0.08* | 0.05 | 0.06 | 0.12 | 0.06 | 0.14 | 0.02 | 0.124 |
| Slope variance | 0.99**** | 0.01 | 0.96**** | 0.01 | 0.95**** | 0.01 | 0.97 | 0.012 |
Although residents in areas with type B, C and D approaches to CE reported better mental health at baseline, this was explained by demographic and socioeconomic characteristics (models 1 and 2). Overall, there was no significant improvement in mental health between 2002 and 2008 (indicated by the slope estimates shown in the bottom section of the table). However, after accounting for demographic and socioeconomic factors, residents in CE type C areas had a significantly greater worsening of mental health than those in CE type A areas (indicated by the negative and statistically significant slope regression coefficient for this CE type of –0.10 in Slope regression coefficients of the table). Other analyses reported in Appendix 2 (see Table 64) suggest that there was no differential change in self-rated health between 2002 and 2008 across the different CE types.
Table 22 reports the changes in the likelihood of individuals finding employment between 2002 and 2008, adjusting again for demographic and socioeconomic characteristics, and for local programme and CE types. Out-of-work residents in areas with type D approaches to CE, and to a lesser extent those in areas with type B approaches, were less likely to find employment between 2002 and 2008 than those in areas with type A approaches to CE. Our previous evaluation of the impact on health inequalities of NDC local programmes found that residents without work in areas with type 2 and type 3 NDC local programmes were more likely to move into employment between 2002 and 2008, and model 3 in Table 22 suggests that CE type explained some of these differences according to NDC programme type.
| Variable | Model 1 | Model 2 | Model 3 |
|---|---|---|---|
| Female (reference: male) | 0.85**** (0.82 to 0.89) | 0.85**** (0.82 to 0.89) | 0.85**** (0.82 to 0.89) |
| Age | 1.01**** (1.01 to 1.01) | 1.01**** (1.01 to 1.01) | 1.01**** (1.01 to 1.01) |
| Non-white (reference: white) | 0.86**** (0.82 to 0.90) | 0.85**** (0.82 to 0.89) | 0.86**** (0.82 to 0.90) |
| Education (reference: NVQ 1 or no formal qualifications) | |||
| NVQ 2–3 | 1.40**** (1.34 to 1.47) | 1.40**** (1.34 to 1.47) | 1.41**** (1.35 to 1.47) |
| NVQ 4–5 | 1.57**** (1.49 to 1.65) | 1.56**** (1.48 to 1.64) | 1.57**** (1.49 to 1.65) |
| Owner | 1.84**** (1.77 to 1.91) | 1.83**** (1.76 to 1.91) | 1.83**** (1.76 to 1.91) |
| CE type (reference: type A) | |||
| B | 0.95** (0.90 to 0.99) | 0.95** (0.91 to 1.00) | |
| C | 0.99 (0.94 to 1.04) | 1.00 (0.95 to 1.05) | |
| D | 0.88**** (0.82 to 0.94) | 0.91** (0.84 to 0.98) | |
| Local programme type (reference: type 1) | |||
| 2 | 1.08**** (1.03 to 1.13) | 1.04 (0.99 to 1.10) | |
| 3 | 1.06** (1.01 to 1.12) | 1.02 (0.96 to 1.09) | |
In summary, these analyses indicate that residence in NDC areas adopting CE types C and D was associated with an improvement in healthy eating. Although there was no significant improvement in mental health in any NDC area, the mental health of residents in areas adopting a type C approach to CE worsened to a greater extent than the mental health of residents in areas adopting a type A approach to CE. In addition, residence in NDC areas adopting type B and type D approaches to CE was associated with a lower likelihood of finding employment than residence in areas with a type A approach to CE.
Does the association between outcomes and New Deal for Communities approach to community engagement vary across groups defined by socioeconomic circumstances?
Our final analysis in this chapter explored whether or not there was evidence that different approaches to CE adopted by NDC partnerships were associated with a reduction in the gap in health and social outcomes between the least and the most disadvantaged residents of NDC areas. To do this the analyses considered possible interactions between CE type and three socioeconomic indicators: housing tenure (renting vs. owning), educational attainment [National Vocational Qualification (NVQ) 0–1 vs. NVQ ≥ 2] and household employment status (living in a jobless household vs. living in a household with at least one member in paid employment). Table 23 reports on significant interactions only when a main effect was found for the particular type of CE in question. It is important to emphasise that these analyses involved a large number of significance tests, which makes interpretation difficult, and we have not formally controlled for multiple testing.
| Outcome | Low educational attainment | Renting accommodation | Joblessness |
|---|---|---|---|
| Mental health | – | – | Improved in areas with type C approaches to CE (0.01 < p < 0.05) and type D approaches to CE (0.05 < p < 0.1) |
| Self-rated health | – | – | – |
| Trust in neighbours | – | Improved in areas with type B approaches to CE (0.01 < p < 0.05) and type C approaches to CE (0.05 < p < 0.1) | Improved in areas with type D approaches to CE (0.01 < p < 0.05) |
| Trust in local services | – | – | – |
| Taking up healthy eating | – | – | – |
| Quitting smoking | – | More likely in areas with type D approaches to CE (0.01 < p < 0.05) | – |
These analyses suggest that some approaches to CE may have narrowed the gap between the most and the least disadvantaged in NDC areas. For example, trust in neighbours increased over time to a larger extent among residents living in jobless households in 2002 in CE type D areas than among residents living in jobless households in 2002 in CE type A areas. It also improved more among renters in type B and type C areas. Overall, mental health improved at a slower rate in areas with type C approaches to CE than in CE type A areas, but improvement in mental health was particularly high for residents in jobless households in CE type C and type D areas. Residents in rented accommodation in areas with type D approaches were also more likely to have quit smoking between 2002 and 2008.
Summary
This chapter has reported the results of analyses of within-person changes in NDC areas by CE and local programme type. These results suggest that individuals in areas with type A approaches to CE saw greater improvements on some social cohesion, trust and mental health indicators. For example, there was a significant overall increase in trust in neighbours, which was greater in areas with type A approaches and lower in areas with type B approaches. Against the backdrop of a slight, non-significant within-person improvement in mental health, individuals in areas with type C approaches to CE had a significant worsening of mental health than those in CE type A areas, although some more disadvantaged groups in CE type C areas did better. Individuals without paid work in CE type A areas were also more likely to find employment by 2008 than those in CE type D, and to a lesser extent CE type B areas. On the other hand, an overall decline in trust in local services over time in all areas was slower among residents in areas with CE type D approaches and the approach to CE appears to have mitigated this decline in areas with type 2 and type 3 local programmes. Cross-sectional and longitudinal results were consistent in indicating that improvements in fruit and vegetable consumption were better in CE type C and D areas than in CE type A areas.
There is some evidence that CE types impacted differentially on specific population subgroups in ways that could reduce inequalities within NDC areas, but no consistent pattern was identified. When an effect of CE type was seen, this was usually independent of a NDC programme type impact, found in our previous study. For only one outcome (joblessness) did we find that CE type mediated or contributed to explaining differences across NDC local programmes. In relation to trust in services, failure to consider CE type in our previous study appears to have masked differences by NDC type.
Chapter 6 Assessing the impact of New Deal for Communities approaches to community engagement: outcomes using routine data sources
Introduction
In this chapter we explore the impact of NDC approaches to CE on outcomes included in the time series originally constructed by the NET for each NDC area and its comparator using routine administrative data, and updated by us. We considered the following health-related outcomes:
-
hospital admissions indicators standardised for age and sex from the Hospital Episode Statistics (HES) data set for six conditions: drug misuse, alcohol misuse, cancer, respiratory conditions, heart conditions and mental health
-
work-limiting illness based on claimant counts [from the Department for Work and Pensions (DWP)]
-
rates of low birthweight from ONS data sets
-
mortality among those aged < 75 years from ONS data sets.
Our analyses also considered trends in three claimant count-based indicators related to employment status and income:
-
worklessness: people of working age receiving a benefit relating to their unemployment or inability to work on medical grounds – Incapacity Benefit (IB), Severe Disablement Allowance (SDA) and Employment and Support Allowance (ESA) in addition to Jobseeker’s Allowance (JSA)
-
unemployment: those in receipt of JSA
-
those in low-income households: based on counts of all claimants of IS (Income Support), JSA-IB (Jobseeker’s Allowance – Invalidity Benefit) or ESA aged 0–59 years, plus any dependent children and partners also aged 0–59 years.
These analyses involved the following linear regression approach to test for trends.
-
the difference between the values for the indicators relating to these outcomes for each individual NDC area and its comparator area was computed for each of the years in the time series
-
this difference was regressed against time
-
unstandardised coefficients are reported when they are significant at ≥ 10%.
It is important to emphasise that, with all of the indicators used in these analyses, an improving trend relative to a comparator may not correspond to an absolute improvement in the NDC area relative to the national picture. For example, hospital admissions remained higher than the national average in NDC areas through the life of the programme. Additionally, for some indicators small numbers in single areas meant that results were not robust. This was the case for low birthweight and mortality, and so only the results for hospital admissions and claimant counts are presented here.
Trends in hospital admission rates
In our previous study (see Appendix 1) we found that areas with type 2 local NDC programmes, which involved an incremental approach to regeneration with modest physical redevelopment, performed better in terms of reducing hospital admission rates relative to their comparator areas than areas with either type 1 or type 3 programmes. The full results of this work are reported in Appendix 2 (see Table 65) and are summarised in the bottom row of Table 24. This shows that one-quarter (25%) of the hospital admission indicators for areas with type 2 local programmes show health improvements (i.e. reduction in hospital admissions) relative to their comparator areas between 1999 and 2010. In contrast, only 5.6% of indicator values relating to type 1 local programmes and 7.6% of indicator values relating to type 3 local programmes show improvement above that of their comparator areas.
| Type of CE | Type of NDC local programme | |||
|---|---|---|---|---|
| Transformational type 1 | Incremental type 2 | Strengthening and improving type 3 | All | |
| Type A | ||||
| % improving | 0.00 | 22.90 | 16.70 | 17.90 |
| % deteriorating | 8.30 | 18.80 | 22.20 | 17.90 |
| Number of indicators | 12.00 | 48.00 | 18.00 | 78.00 |
| Type B | ||||
| % improving | 0.00 | 36.70 | 8.30 | 18.10 |
| % deteriorating | 2.20 | 3.30 | 20.80 | 13.90 |
| Number of indicators | 18.00 | 30.00 | 24.00 | 72.00 |
| Type C | ||||
| % improving | 8.30 | 5.60 | 0.00 | 3.70 |
| % deteriorating | 0.00 | 5.60 | 16.70 | 9.30 |
| Number of indicators | 12.00 | 18.00 | 24.00 | 54.00 |
| Type D | ||||
| % improving | 10.00 | 10.00 | ||
| % deteriorating | 20.00 | 20.00 | ||
| Number of indicators | 30.00 | 0.00 | 0.00 | 30.00 |
| All | ||||
| % improving | 5.60 | 25.00 | 7.60 | 14.10 |
| % deteriorating | 15.30 | 11.40 | 19.70 | 15.00 |
| Number of indicators | 72.00 | 96.00 | 66.00 | 234.00 |
The far right column labelled ‘All’ summarises the results for the four types of NDC approaches to CE. In contrast to the results for type 2 NDC local programmes, none of the four CE types shows a high level of improvement (i.e. reducing hospital admissions relative to the comparator area). Areas with a type A approach to CE have the highest level of change (35.8%) in hospital admissions, equally divided between indicator values showing improvements, that is, reductions in hospital admission rates relative to comparator areas (17.9%), and those showing deteriorations, that is, increases in hospital admission rates relative to comparator areas (17.9%). NDC areas with a type B approach to CE have only a slightly lower level of change (32%) than those areas with a type A approach to CE, but in these areas there are 4.2% more values indicating improvements (18.1%) than deteriorations (13.9%). NDC areas with type C approaches to CE are unusual in having a small number of changes (only 13% of indicators) and most of these reflect deteriorations (9.3%). NDC areas with type D approaches to CE have average levels of change but with twice as many deteriorations (20%) as improvements (10%). These results suggest that, overall, areas with type A and type B approaches to CE performed better than areas with type C and type D approaches to CE.
Looking at the different combinations of programme type and CE type (see Table 24), the strongest combination effect is seen in group B2 (areas combining a type 2 local programme with a type B approach to CE, i.e. starting out resident led but weakening over time), with 11 (36.7%) of the 30 indicators showing significant improvements in hospital admissions and only 3.3% showing a relative deterioration. Areas combining a type 2 programme with a type A approach to CE (i.e. resident led throughout the programme) also performed well (group A2), with 22.9% of indicators showing an improving trend in hospital admissions over the decade compared with their comparator areas and 18.8% showing deteriorations.
Trends in work-limiting illness or disability
Our analyses considered two health-related indicators based on claimant count data from the DWP. The first (work-limiting illness or disability) is the rate at which people of working age are claiming IB, SDA or ESA. The second is an age- and sex-standardised measure covering people of all ages who receive at least one incapacity-related benefit. It is important to note that claimant count indicators may be affected by national changes in the welfare benefit regulations (e.g. a tightening of the eligibility criteria, which happened over the period covered by these data: 2004–11) and this should be taken into account when interpreting the findings reported here. However, this said, these types of changes might be expected to impact equally on all NDC areas and so, to the extent that we identify differential patterns in the change in numbers of claimants over time across NDC areas with different types of local programme and/or approaches to CE, this could be an indication that these programmes and approaches to CE affected the impact of national programmes (positively or negatively). As noted earlier, an improving trend relative to a comparator may not correspond to an absolute improvement in NDC area conditions. As Figure 2 shows, at both the start and end of the period covered, the prevalence of work-limiting illness or disability in every NDC and comparator area was always higher than the English average (which is set at 1 in Figure 2).
FIGURE 2.
Standardised work-limiting illness ratios for NDC areas in 2004 and 2011 compared with the English average (set at 1).
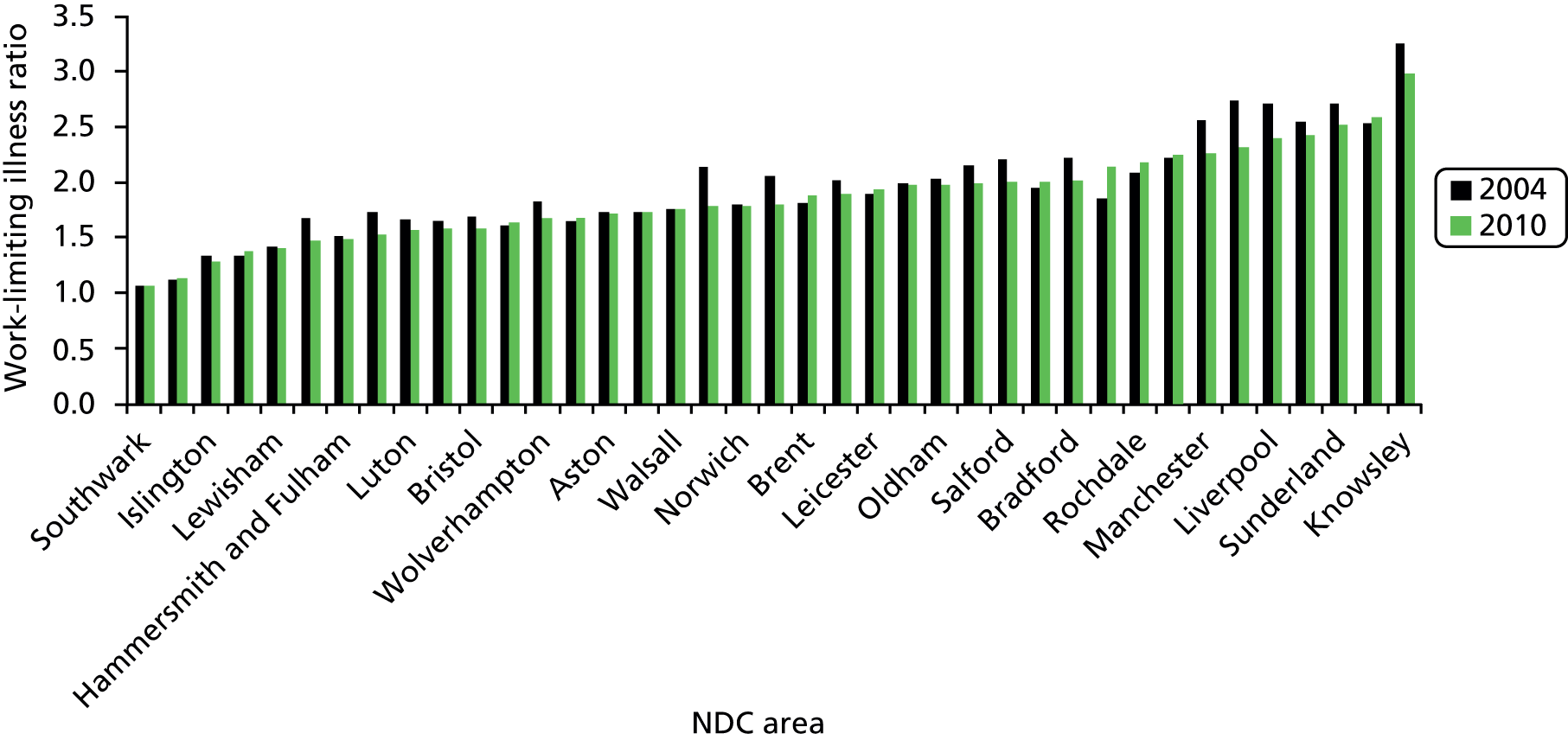
Figure 2 also shows that standardised work-limiting illness ratios (based on claimant counts) were lower in 2011 than in 2004 in 27 of the 39 NDC areas. The differences in ratios are similar for the comparator areas: standardised illness ratios were lower in 2011 than in 2004 in 28 of the 39 comparator areas. The two sets of changes are quite highly correlated (at 0.59), suggesting that they may be influenced by similar trends, such as wider changes in health or changes in eligibility criteria for health related-benefit claims. Table 25 shows the percentage of trends where numbers of NDC residents claiming benefits was falling or increasing in areas with different combinations of local programme types and CE approach. There is a high level of significant change overall – 68% of the 78 coefficients in the table – reflecting a great deal of movement onto and off these benefits over the period covered.
| Type of CE | Type of NDC local programme | |||
|---|---|---|---|---|
| Transformational type 1 | Incremental type 2 | Strengthening and improving type 3 | All | |
| Type A | ||||
| % improving | 25 | 13 | 0 | 11.5 |
| % deteriorating | 0 | 50 | 50 | 42.3 |
| Number of indicators | 4 | 16 | 6 | 26.00 |
| Type B | ||||
| % improving | 17 | 70 | 12 | 37.5 |
| % deteriorating | 33 | 10 | 63 | 33.3 |
| Number of indicators | 6 | 10 | 8 | 24.00 |
| Type C | ||||
| % improving | 50 | 66 | 50 | 55.6 |
| % deteriorating | 0 | 17 | 25 | 16.7 |
| Number of indicators | 4 | 6 | 8 | 18.00 |
| Type D | ||||
| % improving | 50 | 50.0 | ||
| % deteriorating | 10 | 10.0 | ||
| Number of indicators | 10 | 0 | 0 | 10.00 |
| All | ||||
| % improving | 37.5 | 40.6 | 22.7 | 34.6 |
| % deteriorating | 12.5 | 31.3 | 45.5 | 29.5 |
| Number of indicators | 24.00 | 32.00 | 22.00 | 78.00 |
Areas with type 1 and type 2 local NDC programmes saw the greatest reductions in the numbers claiming benefits relative to their comparator areas, as did areas with type C and type D approaches to CE. In contrast, areas with type A approaches to CE were more likely to see numbers on benefit rising relative to their comparator areas. In terms of combinations of programme type and approach to CE, NDC areas combining type 2 local programmes with type B approaches to CE were more likely than any other combination to see claimant numbers reduce relative to comparator areas, whereas those combining type 2 local programmes with type A approaches to CE were most likely to see claimant numbers increase relative to comparator areas.
Trends in unemployment, worklessness and low income
Our analyses considered trends in three claimant count-based indicators related to employment status and income:
-
worklessness: people of working age receiving a benefit relating to their unemployment or inability to work on medical grounds: IB, SDA and ESA in addition to JSA
-
unemployment: those in receipt of JSA
-
those in low-income households: based on counts of all claimants of IS, JSA-IB or ESA aged 0–59 years, plus any dependent children and partners also aged 0–59 years.
We expected our measures of worklessness and unemployment to be highly correlated as they are both based on the JSA claimant count. The trends in these three indicators are summarised in Table 26.
| Type of CE | Type of NDC local programme | |||
|---|---|---|---|---|
| Transformational type 1 | Incremental type 2 | Strengthening and improving type 3 | All | |
| Type A | ||||
| % improving | 0 | 25 | 0 | 15.4 |
| % deteriorating | 0 | 31 | 8 | 38.5 |
| Number of indicators | 4 | 16 | 6 | 26.0 |
| Type B | ||||
| % improving | 33 | 80 | 25 | 50.0 |
| % deteriorating | 33 | 0 | 50 | 25.0 |
| Number of indicators | 6 | 10 | 8 | 24.0 |
| Type C | ||||
| % improving | 25 | 50 | 25 | 33.3 |
| % deteriorating | 0 | 33 | 38 | 27.8 |
| Number of indicators | 4 | 6 | 8 | 18.0 |
| Type D | ||||
| % improving | 40 | 40.0 | ||
| % deteriorating | 20 | 20.0 | ||
| Number of indicators | 10 | 0 | 0 | 10.0 |
| All | ||||
| % improving | 29.20 | 46.90 | 18.20 | 33.3 |
| % deteriorating | 16.70 | 21.90 | 54.50 | 29.5 |
| Number of indicators | 24.0 | 32.0 | 22.0 | 78.0 |
Areas with a type A approach to CE perform worst, with 10 (38.5%) of the indicator values showing significantly increasing numbers of claimants over time relative to the comparator areas and 15.4% of the indicator values showing an improvement, that is, a reduced number of claimants. In contrast, areas with a type C approach to CE performed particularly well relative to their comparators, as did NDC areas with a type 2 local programme (where the performance was good regardless of the CE approach adopted). However, when a type B approach to CE, which resulted in good performance overall, is combined with a type 3 local programme, the resulting group of areas record more deteriorations in terms of employment than improvements. The group of NDC areas combining the best-performing approach to CE (type B) with the best-performing local NDC programme (type 2) has the highest proportion of improvements in worklessness and unemployment (on eight of the 10 indicators) and no deteriorations. The performance of areas with type 2 local programmes is consistently good, except when combined with a type A approach to CE, when there are few changes and all of them reflect an increasing number of claimants.
The DWP provide estimates of the numbers of people in low-income households in NDC areas by combining data on those in receipt of IS, JSA-IB or ESA with counts of the number of dependent partners and children. Trends are summarised in Table 27.
| Type of CE | Type of NDC local programme | |||
|---|---|---|---|---|
| Transformational type 1 | Incremental type 2 | Strengthening and improving type 3 | All | |
| Type A | ||||
| Number improving | 1 | 1 | 3 | 5 |
| Number deteriorating | 0 | 2 | 0 | 2 |
| Number of areas | 2 | 8 | 3 | 13 |
| Type B | ||||
| Number improving | 1 | 4 | 1 | 6 |
| Number deteriorating | 1 | 0 | 2 | 3 |
| Number of areas | 3 | 5 | 4 | 12 |
| Type C | ||||
| Number improving | 2 | 2 | 1 | 5 |
| Number deteriorating | 0 | 1 | 0 | 1 |
| Number of areas | 2 | 3 | 4 | 9 |
| Type D | ||||
| Number improving | 1 | 1 | ||
| Number deteriorating | 0 | 0 | ||
| Number of areas | 5 | 0 | 0 | 5 |
| All | ||||
| Number improving | 5 | 7 | 5 | 17 |
| Number deteriorating | 1 | 3 | 2 | 6 |
| Number of areas | 12 | 16 | 11 | 39 |
Overall, 23 (59%) of the NDC areas show significant changes in low income relative to their comparator. Of these, 17 are improvements (numbers of people on low income dropping) and six are deteriorations (numbers of people on low income growing). This ratio of improvements to deteriorations is found across all local programme types, although type 1 local programmes perform slightly better than the other two types of programme. Areas adopting type C approaches to CE perform better in terms of the reduction in the number of people on low income relative to their comparator than those adopting other CE approaches, although areas with type A and type C approaches to CE have ratios close to the average. There are few changes in the numbers on low income in areas with type D approaches to CE. Two of the combinations, containing three or more NDC areas, stand out in terms of change in the number on low income. On the positive side, four of the five NDC areas combining a type 3 local programme with a type B approach to CE, initially resident led but weakening over time (combination group B2), saw reductions in the number on low income relative to their comparators. In contrast, all three NDC areas combining a type 3 local programme with type A resident-led CE (group A3) deteriorated relative to their comparators.
Summary and conclusions
Tables 28 and 29 summarise the most notable trends in the indicators of health, worklessness and low income by NDC approach to CE and type of local NDC programme.
| CE type | Type 1 local programmes | Type 2 local programmes | Type 3 local programmes | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Hospital admissions | Life-limiting illness | Unemployment and worklessness | Low income | Hospital admissions | Life-limiting illness | Unemployment and worklessness | Low income | Hospital admissions | Life-limiting illness | Unemployment and worklessness | Low income | |
| A | – | – | – | – | ||||||||
| B | + | + | + | + | – | – | – | |||||
| C | + | + | ||||||||||
| D | + | |||||||||||
| CE type | All types of NDC local programmes combined | |||
|---|---|---|---|---|
| Hospital admissions | Life-limiting illness | Unemployment and worklessness | Low income | |
| A | – | – | ||
| B | ||||
| C | + | + | ||
| D | + | |||
In relation to hospital admissions there were no noteworthy results when areas were grouped by type of approach to CE (there were few or only average levels of change). In contrast, NDC areas with type 2 local programmes performed well on both the hospital admission and work-limiting illness indicators, NDC areas with type 1 programmes improved only in terms of a reduction in the numbers on benefits because of a work-limiting illness, and NDC areas with type 3 local programmes deteriorated on both hospital admission and work-limiting illness indicators. Trends from these two sets of health indicators are difficult to compare because of the differences in the numbers of significant results: 29.1% for the hospital admission indicators and 64% for those based on claimant counts. The two sets of indicators would not be expected to detect identical trends as they address different aspects of ill health in different age groups. Nevertheless, there are only six (of 39) NDC areas in which the two sets of indicators produce consistently contradictory results.
The areas combining NDC type 2 local programmes with a type B approach to CE (combination group B2) performed well on both hospital admissions and work-limiting illness indicators. Combinations C2 and D1 performed less well on the hospital admission measures, but well on the work-limiting illness claimant count measures.
Indicators of unemployment, worklessness and low income are among the more robust measures in terms of numbers in each area. They do, however, have other limitations, particularly their vulnerability to political changes in the eligibility criteria for the benefits, which may reduce the numbers on incapacity-related benefits, irrespective of whether or not there has been a real decrease in ill health. In relation to CE, areas with type A approaches to CE perform worst on unemployment and worklessness indicators. Areas with type 3 local programmes also perform poorly, regardless of their approach to CE. Therefore, when type B CE (which performs well overall) is combined with NDC type 3 local programmes the resulting group of areas records more deteriorations than improvements on these indicators. The combination of type B approaches to CE, which performed well overall, with type 2 local programmes (combination B2) has the highest proportion of improvements and no deteriorations. NDC areas with type 2 interventions performed consistently well relative to their comparators on all of the indicators of unemployment, worklessness and low income except when combined with type A approaches to CE, when there are several changes, all deteriorating.
As noted earlier, the trends for the proportion of people in low-income households do not precisely replicate those for unemployment and worklessness, although the two are never contradictory. Two combinations of programme type and approach to CE with three or more NDC areas stand out in terms of the low-income indicator: group A3, in which all three areas show deterioration, and group B2, in which four of the five areas improve. None of the other combinations is notable for having high ratios of deteriorations to improvements.
Table 30 summarises the relative performance across all of the indicators in all groups of NDC areas. One combination stands out: in the five NDC areas combining a type 2 local programme with a type B approach to CE, six of the seven groups of indicators show improvements. In contrast, the eight NDC areas combining a type 2 local programme with a type A approach to CE were more mixed and the three NDC areas combining a type 3 local programme with a type A approach to CE saw almost all indicators deteriorating.
| CE type | Local programme type 1 | Local programme type 2 | Local programme type 3 |
|---|---|---|---|
| A | (A1, n = 2) Only two areas – both barely change. Limited changes are mixed – improvement and deterioration recorded in same areas | (A2, n = 8) Broadly divided between Oldham, Norwich and Newcastle, which mostly improve, and Middlesbrough, Leicester and Hartlepool, which mostly deteriorate, although five of these eight areas record both deterioration and improvement | (A3, n = 3) Almost all changes in this group are deteriorations, except for Rochdale, which improves on three HES indicators |
| B | (B1, n = 3) Varied group – Liverpool improves, Derby declines and both improvement and deterioration in Kings Norton | (B2, n = 5) Widespread improvements. Luton the weakest but still improves on DWP indicators of health and low income indicators | (B3, n = 4) More deterioration than improvement. If improvements in low birthweight and SMR are excluded, the only other improvements are on low income and unemployment indicators in Islington and unemployment indicators in Nottingham |
| C | (C1, n = 2) Only two areas – all changes are improvements although not much change in Southwark | (C2, n = 3) More improvement than deterioration overall. Wolverhampton and Salford mostly improve, with changes mixed in Southampton | (C3, n = 4) Not much change – very mixed picture. All areas show some signs of both improvement and deterioration |
| D | (D1, n = 5) More improvement than deterioration. Unemployment and work-limiting illness mostly improve but health (measured by both DWP counts and HES) declines in Knowsley and unemployment deteriorates in Coventry |
There are two caveats to these results. First, there is considerable variation within the groups. This can be clearly seen in Table 65 in Appendix 2, which reports the coefficient values, and the tables in this chapter showing the proportions of improving and deteriorating trends. Second, the results could be influenced by initial baseline differences between NDC areas and comparators or changes in the socioeconomic characteristics of the resident population unrelated to the NDC local programme during the period analysed. To test this assumption we compared the age and socioeconomic composition of NDC areas and their comparators using weighted census data for 2001 and 2011. In relation to age differences, we asked, among other things, whether or not an age effect may have contributed to the relatively better performance of areas with NDC type 2 local programmes and found that, although populations in these areas were younger at the start, the age difference did not increase over time. Differences and changes in four sociodemographic characteristics were also explored: housing tenure, household composition, social class and ethnicity. Although NDC areas and their comparators differed in sociodemographic characteristics at the start of the programme, these differences changed relatively little between 2001 and 2011, although there is some evidence of the ethnic and social class make-up of the NDC areas diverging from that of their comparators over time. Changes over time in the social class composition of populations were particularly apparent in NDC areas adopting type 1 local programmes (in line with a prominent aim of these programmes being to change the tenure mix, bringing in more owner-occupiers). However, this does not appear to be reflected in the performance of this programme type, which was generally poor relative to that of other programme types.
Chapter 7 Qualitative insights into the impact of New Deal for Communities approaches to community engagement
Introduction
Although not offering evidence of direct effects, findings from our qualitative research with NDC residents and past workers provide insight into the processes underpinning different types of approaches to CE and highlight potential pathways to social and health outcomes. As there are only a small number of fieldwork areas allocated to a particular CE type and small numbers of informants from each area who were working in roles that could make them identifiable, reference is made to the NDC CE type (i.e. A–D) and whether the informant is a former NDC staff member or a resident, and not to the individual NDC area. A unique identifier is provided for each respondent [e.g. JT3c refers to the initials of the researcher, the fieldwork site (1–11) and the individual participant at each site (a–e)].
Community engagement, trust and cohesion
In all areas people interviewed reported a myriad of issues in relation to the local community at the start of the NDC initiative that could be expected to impact on processes of engagement. These included the presence of multiple faith and cultural identities, living on an estate with minimal social cohesion or towns with strong cohesive identities. Levels of trust at the beginning of the NDC initiative – both between residents and in agencies – were also reported to be relatively low in all areas regardless of their approach to CE.
In areas allocated to type A or type C approaches to CE, informants reported how the NDC approach to engagement had sought to generate opportunities for residents to get involved and become more active in community life. This comment on a NDC programme’s aspirations for CE from a chief executive working in an area allocated to CE type A is illustrative of this:
We had this idea that you needed to create opportunities for lots of people to get involved as much as they could in things that were going on and make a contribution and so there are little bits at the top around governance; well that might have been people in governance roles on the NDC or we encouraged people to become school governors or whatever it might be; decision-making stuff.
Staff member, type A, JT3c
Similarly, a worker from an area allocated to CE type C used an example of a group of older people who had struggled to engage with the NDC programme initially to explain how local residents were supported to develop local groups and networks:
One of the community workers set up a little, you know, tea dance and all those opportunities for people to come to something that they felt more comfortable with and then there was an opportunity then to bring officers to talk to them in a way that they felt more comfortable with. They then went on to become a constituted group, they then campaigned and they got a bus shelter and, you know, they’re a real voice in the community and everybody knows them across the city . . . so we’ve got lots of examples of groups like that.
Staff member, joint interview, type C, EH1a&b
It is not possible from this research to measure the extent to which residents became more involved in the community as a consequence of the NDC programme but respondents in NDC areas allocated to CE type A or type C gave several examples of such transitions in which residents had set up community activities, had taken on roles such as a school governor or in some cases had gone on to become a local councillor. New parish council structures were also set up in one type A NDC.
Respondents in NDC areas allocated to CE type B similarly provided examples of community activities being instigated by committed residents. But for some respondents in type B areas the NDC programme lacked a more strategic approach to developing the capacity of local residents and groups, undermining its sustainability.
So, for example, we supported local people to set up loads and loads of community groups. When the NDC programme came to an end there were 50–60 community groups and there isn’t now obviously because all the money disappeared.
Resident, type B, JT9a
In contrast to the more positive accounts of community activity during the NDC programme provided by respondents in NDC areas allocated to CE types A and C, those in areas allocated to CE type D frequently commented on the way that NDC plans for redevelopment had dominated engagement activities. One resident of a CE type D area, for example, expressed disappointment that the NDC programme had lacked a more empowering ethos:
It was disappointing to me, it was really, because I really thought that was going to be . . . because of the directive of it, it was supposed to be about investing in the people and the engagement and empowerment of people within the NDC communities.
Resident, type D, SP2b
Although this NDC partnership funded community activities such as trips and festivals, both staff and residents acknowledged that the time pressures and scale of the redevelopment had resulted in a predominantly instrumental approach to engagement.
Respondents’ accounts in areas allocated to CE types A and C also highlighted approaches to engagement that sought to invest in strengthening social cohesion:
I don’t know if we had any proof, that this would be a better area for it. You just know if people are looking out for themselves and each other and people working in small groups together it is going to be a stronger area.
Staff member, type A, JT3c
I would hope that in terms of the was a bit of a sense of [neighbourhood 1 and 2] were two separate areas at the start of New Deal and I hope that the work we did [in neighbourhood 1 and 2] are perceived more as one area rather than two competing areas, ‘cause there was a little bit of rivalry at the beginning.
Staff member, type C, EH1d
According to the staff member quoted above, the type A NDC area in which he worked had historically very low levels of trust and social cohesion between different groups in the population. This had led to deliberate activity with community groups and members to work more closely together:
The tensions that used to be there perhaps between the older white and Asian [populations] are kind of just disappearing a little bit. I think NDC was something to do with that; I think we did quite a lot of work with older white people as well.
Staff member, type A, JT3c
In other areas examples were given in which the wider NDC redevelopment activities were perceived to impact negatively on community cohesion. For example, one resident of a NDC area allocated to CE type D expressed disillusionment about the impact of the new housing development on the community:
It [is] like with houses built and everything they are all facing outwards; those people don’t come in; they get in their car and they drive out; it’s a transient community. Their money is spent outside of this area so it doesn’t benefit this area.
Resident, type D, SP2b
A worker in a NDC area with a type B approach to CE similarly suggested that the redevelopment in the neighbourhood impacted negatively on the community’s identity:
I just find it tragic; looking at it now I do find it absolutely tragic and some of the community’s comments during the time about designing out crime families and removing the heart of the community . . . I’m seeing it; I am absolutely seeing it; it’s so sad.
Staff member, type B, SP11d
However, not all respondents viewed area redevelopment negatively. Another resident in the same type D area as the resident quoted above commented on the same development more positively:
So although they are living in a new housing environment they have still got the neighbourly feel that they had when they lived there before because they have still got their next door neighbour that they had lived next to for 25 years or so; and there is a lot of new people and a lot of younger people moving into the area.
Resident, type D, SP2d
Finally, many NDC areas experienced significant population change during the life of the programme with high numbers of new residents moving in (and others moving out). There were some suggestions in the qualitative data that those NDC partnerships that were guided by a community empowerment ethos (types A and C) may have been better positioned to support and respond to new residents’ needs and involvement, so helping to reduce tensions. However, the qualitative data available on this are very limited and do not allow firm distinctions to be drawn between CE types.
Contribution of engagement to the New Deal for Communities outcomes
Resident informants from NDC areas adopting type A and type C approaches to CE generally reported positive changes in their neighbourhoods and felt that aspirations for the regeneration of their areas were largely achieved. These improvements covered a range of areas including major structural changes in the neighbourhood and improvements to housing, streets and estates as well as the development of shopping areas and open/green spaces. Other improvements arose from investment in new facilities and amenities in the area, such as local businesses, community hubs and services. For some residents, being involved in producing these improvements had generated a considerable sense of pride:
I think with NDC erm I was physically involved and everything was, it was physically, mentally everything, you were involved in it all and you feel proud because you’ve had, you‘ve taken part in something good, something that, you know, there’s an awful lot of these projects have come to fruition and you can see, you know, you can actually see the difference that it’s made.
Resident, joint interview, type A, EH4d&e
Such improvements were often contextualised in terms of addressing the consequences of long-term decline and high levels of deprivation. For example, in one instance both residents and workers presented a bleak picture of their NDC area (which was allocated to CE type A) at the start of the NDC programme, describing rapid economic decline after a major industry closed down and characterising the NDC area as physically neglected and unsafe with high rates of crime, social problems and poverty. A resident living in the area for decades described his disillusionment over this decline:
I have lived here a long time and I saw it when it was called ‘Corn[ed] Beef Island’, that was just after the war because all the houses were all neat and tidy and had hedges around them and corn beef in them days it was a sort of a luxury . . . I have watched it go from that and I have watched it go downhill really, really badly.
Resident, type A, JT5c
Going on to reflect positively on the changes that the NDC programme achieved, this resident highlighted the importance of residents’ involvement in the achievement of these changes:
I am quite happy now, quite pleased that we have got this far and we’ve done what we’ve done . . . If you get plenty of likeminded people I am sure you can make a difference to an estate.
Resident, type A, JT5c
Similar reflections on positive change were evident among informants in type C areas. There was, however, more evidence of mixed views between informants in these areas over tensions concerning strategic decisions related to the housing stock or redevelopment plans. For one participant this was perceived to have led to a declining focus on the community:
It moved away from gathering the views of the people and acting on the views of the people to involving the people in New Deal for Communities. So I might actually say that New Deal for Communities became more important than community engagement. And I . . . thinking now . . . I’m actually very clear about that.
Resident, type C, EH1c
Although informants in NDC areas with a type B approach to CE did report positive impacts resulting from the NDC programme, greater disillusionment about aspirations having not been met was expressed, with improvements perceived to lack sustainability. In one area, for example, resident informants spoke positively about the impact of a warden scheme. However, the fate of the scheme was perceived to reflect an absence of attention (or commitment) to sustaining the programme after NDC funding ended:
Some of them are sadly missed; our Warden Programme for example, our Community Wardens; absolutely loved by everybody but unfortunately the city wouldn’t continue it after the programme; in fact the city didn’t continue anything after the programme; everything went . . . It was very noticeable as well; everything just shut overnight.
Resident, type B, JT9a
Major redevelopments (often undertaken in NDC areas with type D approaches to CE) resulted in less-positive views of the success of the NDC programme. One factor for this was the lengthy timescales and scale of disruption caused by the physical regeneration. In one type D NDC area, more than 1000 houses were demolished with the intention of constructing at least 1500 new homes, but much of the rebuilding remained to be completed by the end of the programme. One resident expressed a particular frustration with the process:
We were highlighting these kinds of things and saying you are going to have this because you are going to have pockets of wasteland, it’s just going to attract fly tipping and unless you do something to stop that what are you going to do is; . . . So when people were saying these things it was like ‘oh no, that’s not going to happen’; but it has.
Resident, type D, SP2b
Some residents in other NDC areas where physical regeneration involving housing demolition/clearance was also planned reported similar experiences of stress and anxiety. For a resident of a type B NDC area, for example, this was attributed to high expectations and subsequent disappointment over the timescales for change:
One thing that residents don’t realise, I didn’t myself for a long time, is how long it takes to go from planning a clearance and rebuild of an area to actually doing it; all the legalities and the time and everything that’s involved . . . I think this is one of the main disappointments that I think residents should have been informed from the outset that there could be a very long period.
Resident, type B, JT9b
In a type C NDC where more modest redevelopment was planned, one resident explained that the NDC staff and resident board members experienced hostility from the wider community regarding the uncertainty of redevelopment plans when housing had not been delivered as ‘promised’ by the end of the programme. However, the same resident informant also suggested that housing and environmental improvements achieved alongside these planned housing redevelopments helped to mitigate the negativity when the new housing plans stalled.
The impact of political and policy contexts on approaches to engagement
All NDC areas were operating in a continually evolving policy context and experienced many external pressures – local and national. The impacts of these pressures may have masked any benefits that could have accrued from adopting particular approaches to CE.
Locally these challenges could include working relationships between the NDC partnership and the local council. Some respondents reported tensions because residents believed that the NDC money was ‘their money’ and were reluctant to share control of this with local agencies. As the following quote illustrates, some workers felt that the lack of experience among residents in planning for, managing and spending such large sums of money was a major problem, at least in the early stages of the programme:
Because at the end of the day government put so many barriers in the way of the, you know, you were never going to go into an area with £53 million and say ‘here’s a suitcase, spend it’ so you know there was always going to be so many strings attached to it and so there had to be structure and somebody had to be accountable and all of that and actually that wasn’t what the community thought they were buying into in the early days.
Staff member, joint interview, type C, EH1a&b
Conversely, there were other areas where council representatives refused to work with the NDC members, also creating tensions, as is evidenced in the following quote:
I think I’ve still got regrets about the fact that we just couldn’t get the councillors and the resident[s] . . . to talk to each other for the last 3 years because of this schism which was largely about one councillor . . . we never really understood it, but he just developed a visceral hatred of everything to do with NDC and just and it was a very difficult situation for the last 3 years, I regret that and the fact that that then led to, distorted some of the programme in the last few years because things that we wanted to do, it was almost opposition for its own sake.
Staff member, type A, EH4a
Changes at the national level also added pressures and complications to the way that the NDC partnerships worked. There were changes in emphasis in the way that the NDC programme was managed by central government, with the government introducing new policies and institutions that were felt to have added to the burden of the NDC (e.g. local strategic partnerships). Respondents were also aware that over time the NDC programme lost importance and visibility within central government, a process also commented on by the NET:52
I think early doors it was very much a community leading the NDC programme and I think over time perhaps some of the rhetoric at a national level changed, communities being part of that.
Staff member, type C, EH1d
In the early years of the NDC the emphasis was on planning for a 10-year delivery programme but over time the emphasis changed with pressure from central government to ‘quick wins’ to demonstrate impact. There was a greater emphasis on performance management and NDC partnerships had to demonstrate how they had spent their money each year (personal communication from public advisers confirmed by recent research public adviser workshop, May 2013). The pressures that this created for NDC areas are summarised by a resident in a type A NDC:
And it’s easy to forget these kinds of things but constantly through NDC there was (a) question of whether it would continue, (b) whether any particular NDC would continue, whether it would get stopped because it was mismanaging its responsibilities. Those things were ever present real threats erm, you know, once you’ve got to the end you can quickly forget those things but that’s the environment we were operating in. Not only that but also one which was contradictory at times; when I was first involved I went to National Conference and the only message we’d been given was ‘do your needs assessments before you spend money for 10 years’ and a year, 2 years in for first phase NDCs and whoever was the minister was saying ‘spend, spend, spend’ because there was this pressure to see results and so we were getting these contradictory pressures.
Resident, type A, SP6e
The extent to which individual NDC areas were able to negotiate these challenges will have been dependent on a number of factors, including the commitment of the various agencies to the local programmes and the strength of the NDC board and key individuals. For example, the resident quoted above noted how the chief executive in their NDC area with a type A approach to CE urged the board to ‘hold our nerve’ and they continued to place emphasis on the development of the overall programme during the time when there were pressures for ‘quick wins’. In another NDC, a respondent described how the board had placed greater emphasis on spending, in keeping with national shifts in emphasis:
Because the pressure throughout was spend, spend, don’t really matter about what you are spending the money on; this is your allocation and it’s got to be spent and we were very good at doing that. And I’ve kind of always put, my strategy when I was chair was spend, spend, spend and try and grab everybody else’s money that they hadn’t spent and how we’ll spend it and I’m not always sure that it was spent in the best possible way but we were very good at spending money and the government seemed to like that, you know. I’m not really sure that was what it was all about but that’s what it ends up being about and it’s almost projects for projects sake, we were just chucking stuff and desperately trying to do all these things, all at the same time with and still generate the reports the government wanted in terms of the changes we were making, you know, a huge pressure for that.
Resident, type C, JT8b
By the time that the NDC programmes were drawing to a close, the economic crisis meant that there were limited funds available in the agencies to support NDC succession plans:
Yeah, oh definitely, yes, yeah, the whole climate has changed really. The need hasn’t changed but obviously erm, you know, in terms of re-contract, we were quite successful in re-contracting the NHS and the borough and all of that comes to an end next year and new tender arrangements, local commissioning groups huge sea change locally erm so I think every voluntary sector organisation at the moment is just really rethinking [laughs] its sustainability strategy and what’s going to happen past April next year so I’m hoping that we are going to, you know, be able to survive through that.
Staff member, type C, JT8c
These external challenges to the operation of NDC partnerships will almost certainly have impacted on their strategy for, and implementation of, CE and on their activities in other outcome domains. In turn this can be expected to have influenced the health and social outcomes that local NDC programmes were able to achieve. However, although national pressures will have affected all of the NDC areas, the interaction with local contexts will have meant that the NDC areas had different challenges and will have managed their particular challenges differently. Unfortunately, our qualitative data are not able to illuminate how these processes unfolded in areas with different types of local programmes and different approaches to engagement.
Summary and discussion
Findings from our qualitative research confirm that NDC areas that adopted type A and type C approaches to CE were most closely associated with an approach underpinned by empowerment and community development values. There was also evidence in these areas that resident involvement had helped to achieve demonstrable improvements related to social and physical assets in the neighbourhood. However, it was residents in NDC areas with type A approaches to CE who most consistently reported that a positive difference had been made through the involvement of local people in the change process, and those closely involved reported pride from being part of achieving these changes. Respondents in type B NDC areas described how a resident-led ethos fell away during the course of the NDC programme and that the agendas of external agencies involved, such as the council, came to dominate. In contrast, type D NDC areas represented a model of NDC that predominantly engaged the community around the external agency’s agenda, often as a consequence of progressing major redevelopment plans. Although not directly related to ‘engagement’, residents from NDC areas undergoing major redevelopment often reported on the upheaval and anxieties that ensued in the wider community. This was not necessarily just because of the immediate disruption caused by demolition and redevelopment (sometimes seen to be an expected part of the process) but because of the very lengthy timescales it took for redevelopment to be completed and subsequent delays in the latter years as a result of the housing market downturn.
The quantitative impact analyses reported earlier (see Chapters 3 and 4) suggest that trust, social cohesion and involvement indicators were higher in 2008 in areas with type A approaches to CE than in areas with other CE types. The qualitative evidence appears to support these findings but suggests that there are potentially different explanations for why a type A approach to CE, and to a lesser extent a type C approach, may have been more likely than other approaches to CE to have contributed to these positive outcomes.
First, respondents noted that NDC areas adopting type A and type C approaches to CE invested more heavily than other areas in activities that deliberately sought the empowerment of the wider community as well as residents actively involved in the NDC programme. These NDC areas employed community development teams that nurtured local grassroots community action as well as undertaking outreach in communities in an attempt to develop trust and encourage involvement. In this regard, type A and type C engagement processes may have had direct and indirect effects on social cohesion by bringing the community together, investing in the community infrastructure and increasing collective action to address issues in the neighbourhoods. An alternative explanation is that areas that adopted a type A approach to engagement had a starting point that was enabling to support a resident-led ethos. Chapter 5 highlighted, for example, based on the longitudinal data, that trust in neighbours was higher in areas with a type A approach to CE than in areas with other approaches to CE. However, our qualitative data suggest that these results should be interpreted carefully as the findings suggest that most NDC areas started from a position of relatively low levels of trust between residents and in local agencies.
The qualitative research also points to potential impacts of the NDC programme that are not readily detected in the quantitative analyses that we have undertaken. One issue is the extent to which changes achieved by NDC local programmes could be sustained beyond the end of the initiative. In areas with type A and type C approaches to CE, the legacy of resident engagement with the NDC was typically reported by respondents to lie with the residents and the community, including residents who felt that they had a stronger voice to challenge decision-making by statutory organisations. Respondents in NDC areas with type A approaches to engagement were also more likely to report that their NDC area had invested in structures that supported longer-term regeneration beyond the NDC funding period, such as social enterprises or community assets that would deliver a financial return. Although the scale of such ventures appears relatively modest (with returns likely to have been affected by the economic downturn), these activities suggest an approach strongly orientated towards a model of engagement/empowerment aiming for greater social and economic security for the community living within the local area.
Chapter 8 Assessing the cost-effectiveness of community engagement
Introduction
In this chapter we report on the cost-effectiveness analyses that we have undertaken. However, before presenting these analyses there is an important caveat to be made. The right to participate is one of the building blocks of a democratic society. The presumption of the exercise reported here is therefore that CE in a democratic society is universally a good thing. Such a presumption is not subject to economic analysis (see Okun76 1975). The issue that we are concerned with here is only whether or not some approaches to CE as a vehicle for improving the community’s health are better than others. Cost-effectiveness analysis compares the relative costs and outcomes (effects) of two or more courses of action. It differs from a cost–benefit analysis in which a monetary value is assigned to the measure(s) of effect(s). Typically, cost-effectiveness is expressed in terms of a ratio in which the denominator is a gain in health from a measure (e.g. years of life, premature births averted, sight-years gained) and the numerator is the cost associated with the health gain. The course of action with the highest ratio is the most cost-effective.
This is the procedure we followed: we did not attempt to monetise – put a monetary value on – the effects of (different forms of) engagement/involvement. In the analyses reported we considered the comparisons between NDC areas and their comparator areas; different types of local NDC programmes; and different types of approaches to CE. The work was divided into three phases: assessing cost, measuring effectiveness and comparing cost and effectiveness.
Assessing the cost of community engagement
We explored two ways of assessing the cost of CE. First, we analysed the expenditure data relevant to CE collected through the ‘official’ NDC accounting system. Second, we examined documents and interviewed people to assess the extent of contributions of volunteers during the period of the NDC programme. The first approach to assessing the costs of CE, reported in Analyses of the Hanlon System K expenditure data, is based only on money transactions – the expenditure data entered into the accounting system. The second approach takes an ‘economic’ perspective, attempting to take into account all of the resources involved in what is meant to be, at least partly, a community-driven process. More specifically, the economic approach involves trying to find monetary value equivalents for the in-kind resources committed to CE in NDC areas, for which no charge (or a highly subsidised charge) has been made, and find ways of accounting for the value of voluntary labour time input. The latter raises the issue of the opportunity cost concept used by economists. These issues are dealt with in Costing in-kind and volunteer time inputs.
Analyses of the Hanlon System K expenditure data
The Hanlon System K was developed to monitor the NDC and associated project expenditure. Expenditure data were collected for all NDC areas from 2004 to 2005 (and retrospectively for some of the NDC areas for previous years). Initially, data were collected at the level of the six outcome domains (community involvement, crime and safety, housing and physical environment, education, employment and health) but this was seen as insufficiently detailed by the evaluation team and 70 specific project types under these headings (with four other miscellaneous categories) were defined and used both retrospectively and prospectively for accounting purposes. The accounting system also includes codes for indicating when a project type contributes to another subsidiary outcome domain so that one can analyse expenditure on the community involvement domain, or expenditure on community-related projects, and restrict the analysis to NDC expenditure or NDC expenditure plus expenditure related to the NDC projects.
Our analyses considered the variability in spend related to CE across the 39 NDC areas and whether or not there were systematic differences between the NDC areas that spent the least, and those that spent the most, in each of the six outcome domains and each of the 74 project types, focusing in particular on activities that are most likely to include CE with the potential to impact on health and/or inequalities. As the following examples illustrate, the patterns of reported percentage spend by each of the NDC areas across the six outcome domains areas varied widely:
-
community development: from 7.9% in Knowsley to 41.3% in Walsall
-
crime and community safety: from 4.1% in Hackney and Hull to 19.7% in Islington
-
education: from 4.4% in Knowsley to 29.5% in Sunderland
-
employment and business: from 4.1% in Haringey to 19.3% in Nottingham
-
health: from 1.7% in Rochdale to 21.1% in Aston
-
housing/physical environment: from 2.3% in Southampton to 47.0% in Manchester.
Areas in the North West were much more likely to spend on housing. Otherwise there were smaller differences with the Midlands spending more on community involvement and employment, the North West spending more on health and the North East spending more on education (Figure 3).
FIGURE 3.
Ratio of spend on each of six sectors in each of five regions compared with the total ( = 100). E, North East; L, London; M, Midlands; S, South; W, North West.

Table 31 shows the percentage spend on each of the six main outcome domains broken down by groups of NDC areas according to (1) their approach to CE and (2) the type of local NDC programme. The highest percentage spend in all areas was on housing, except in the group of areas adopting a type B approach to CE and the group of areas adopting a type 2 local programme. In these two groups the highest average spend was on activities under the community development heading, the second highest spend in all other areas. NDC areas with a resident-led approach to CE (type A) or which began with a resident-led approach that weakened over time (type B) spent about half as much again on activities labelled as community development as areas with type C and D approaches to CE. The average expenditure under the community development heading across NDC local programme types also varied, from 17.3% in areas with type 1 local programmes to 23.3% in those with type 2 local programmes. The highest average percentage spend under the community development theme (25.6%) was in the group of five NDC areas combining a type 2 local programme with a type B approach to CE. The breakdown of expenditure for each NDC area is provided in Table 67 in Appendix 2.
| CE/programme type | Community development | Crime and community safety | Education | Employment and business | Health | Housing/physical environment |
|---|---|---|---|---|---|---|
| CE type | ||||||
| A (13 areas) | 21.5 | 9.7 | 11.7 | 11.4 | 8.2 | 21.9 |
| B (13 areas) | 22.3 | 11.0 | 13.6 | 9.5 | 7.4 | 16.8 |
| C (eight areas) | 15.4 | 7.8 | 14.4 | 7.4 | 8.2 | 29.7 |
| D (five areas) | 14.9 | 7.4 | 11.8 | 8.0 | 6.6 | 26.1 |
| Local programme type | ||||||
| 1 | 17.3 | 8.0 | 12.4 | 8.4 | 7.0 | 24.5 |
| 2 | 23.3 | 10.3 | 10.4 | 8.8 | 7.3 | 23.0 |
| 3 | 18.2 | 10.5 | 15.6 | 11.0 | 9.2 | 18.8 |
Although information about spending across the broad outcome domains provides some information on the costs of CE, the range of project types included within each domain was very broad (with the partial exception of worklessness). In particular, it cannot be assumed that all of the costs of CE were reported under the community development heading. It was not possible, however, to identify with any precision expenditure contributing to CE but reported under other outcome domains.
More information about the nature of expenditure on CE is provided by looking at how the total spend is spread across specific projects within the community development outcome domain. As the data in Table 32 show, perhaps not surprisingly the highest expenditure was on capital development of community facilities, but substantial amounts were also spent on involving local people and developing the skills and infrastructure of the community: £32M on general capacity building, £19M on communications, marketing and raising awareness, and £9M on capacity building relating to the governance of NDC partnerships.
| Expenditure category | NDC community spend (×1000) (£) | % of all NDC community spend |
|---|---|---|
| New/improved use/access to community facilities | 45,774 | 18 |
| Capacity building general | 32,072 | 13 |
| Community development workers/officers | 26,764 | 11 |
| Reports/research/studies/professional fees | 18,898 | 8 |
| Promotion/communications/marketing/raising public awareness | 18,873 | 8 |
| Community Chest – general/youth | 18,444 | 7 |
| Youth support/services provision | 10,244 | 4 |
| Capacity building NDC governance | 9318 | 4 |
| Land/asset acquisition/demolitions/stock transfer | 7162 | 3 |
| Other NDC posts | 6561 | 3 |
Costing in-kind and volunteer time inputs
In addition to aspects of NDC projects that can be costed using conventional accounting methods based on System K data and other documents (e.g. capital outlays, rentals, utility bills, office materials, salaries and wages, training costs, expenses), CE was also supported by a wide variety of in-kind contributions and extensive individual participation and volunteering that an economic analyses needs to attach monetary value to. Attempting to collect the data needed to estimate and cost these inputs was, however, challenging.
Some relevant data were obtained from local documents and from telephone interviews with two past/current NDC managers with experience of CE activities in each of the 11 fieldwork sites included in the qualitative research described in Chapter 7. As one interviewee noted:
It was a very difficult exercise. Most community representatives were elected and were active in their own right and neighbourhoods. You don’t get much chance to switch off. A lot of this is not counted. Although these were in some respects professional community participators they worked harder because of this. They were called on in a myriad of ways.
For some people the NDC became their life: they lived, breathed, slept and argued it. It was an emotional as well as a time investment.
In-kind costs
Community projects include a wide range of arrangements involving in-kind cost. For example, rooms for meetings may be charged for or may be donated. These rooms may involve a zero price if they are in council or other agency buildings that have spare capacity. It could be useful to make more explicit the relatively arbitrary nature of whether a price is charged and a cost is accounted for or not. However, it is likely that different evaluative choices on these issues made by the research team for the analyses reported here would not change the results.
Some local documents and the System K data provided information on the in-kind costs of CE activities. We also collected these cost data during telephone interviews with key informants in the 11 fieldwork sites. To make data collection feasible, interviewees were asked about a limited number of specific in-kind contributions to CE activities, but the data obtained provide a reasonable basis for estimating the scale of in-kind costs across a NDC area. The type of in-kind costs considered included:
-
use of buildings for committee meetings, office space, public meetings, etc.
-
subsidies for utilities (council tax, electricity, gas, telephone/internet)
-
any personnel provided by other organisations for CE initiatives
-
subsidies for office materials
-
provision of meals/refreshments
-
training provided without cost.
Costing ‘voluntary’ labour time input
There will be several elements of the CE process that involve contributions of effort without directly involving any monetary transactions. These will be both at the inception/implementation stage and in sustaining the intervention. Some analysts have simply presumed that, because no money changes hands, the volunteer input is costless. But although that might be appropriate in an accounting exercise, it is not sensible in terms of the use of the totality of human and material resources available. The only economic tool available to measure this resource use is the concept of opportunity cost, that is, what else could have been done with the resources, and this involves attaching a cost to those resources. The problem then becomes what to use as the appropriate wage rate to assess the opportunity cost of the volunteer effort put into initiating, implementing and sustaining the intervention.
There are conventional rules for costing individual time, for example using the minimum wage rate or the average wage, and the choice will clearly change the calculations substantially. However, it is not clear how these rules apply to an activity that makes sense only when collectively shared, nor when some of the individuals say that, if they were not involved, they would prefer to be doing nothing. In either case, one could, in principle, carry out a sensitivity analysis with different wage rates to examine this. Some of the ways in which volunteer time has been valued are illustrated in Box 5. In fact, because we eventually decided that we could not rely on the bottom-up data for detailed analysis, we did not need to make a specific valuation decision, although we were advised in a couple of the interviews that a notional £10 per hour would be appropriate.
Several organisations use wage replacement costs to value volunteers (i.e. the costs of employing someone to do the same job). The Canadian Centre for Philanthropy suggests that average weekly earning statistics can be used if no detailed wage information is available. 77 It also suggests including benefit costs (pensions, etc.) and the out-of-pocket expenses that volunteers incur. The UK Volunteer Investment and Value Audit (VIVA) is a tool to assess and compare the value of volunteers’ time in relation to the resources used to support the volunteers. 77 It is similar to the Canadian example in that the value of volunteer time is calculated as the wage equivalent plus benefits. Using wage replacement costs thus seems to be the most common method of valuing volunteer time, a conclusion backed by guidance from the Office of the Deputy Prime Minister in 2004. 79
The economic value of volunteering has also been assessed using self-completed diaries in 12 small UK charities that used volunteer labour primarily in the health sector. 80 Instead of using the national average wage as a proxy for volunteer time, the research looked at two other ways of measuring costs: the ‘job title’ approach and the actual value of the tasks performed. Both of these methods produced similar results, which were significantly lower than the national average wage. The study also looked at the time and money spent on recruiting, training and supporting volunteers.
Handy and Srinivassan,81 assessing the net benefits of hospital volunteers in Toronto, Canada, used four different ways of measuring the value of volunteer time:
-
They asked a group of volunteers what they would view as reasonable compensation for the time that they spent on volunteering. The answers were then averaged into two groups: those volunteers who held regular jobs as well and those who did not have paid work.
-
They combined both averages into one sum that could be applied to all volunteers. This obviously involved fewer steps than method 1 and produced similar results. These two methods are opportunity cost measures of different kinds.
-
They estimated the amount that it would cost to replace the volunteers with paid employees. However, many volunteers provided services that, although they improved the service and care that the hospital provided, would not be replaced if the hospital had to pay for them. This means that the value placed on volunteers using this method may be too high. This is a replacement cost method.
-
Finally they used the average wage in the relevant industry. Clerical work was valued according to one value and nursing activities according to another. This led to considerably higher numbers than the above three methods. The same criticism levelled against method 3 is also relevant for this method.
The researchers recommend method 2. It is easier to calculate, avoids problems inherent in methods 3 and 4, and produces a more conservative estimate of the value of volunteer time, which the researchers think is closer to the truth. As volunteers tend to do their work in their leisure time, Handy and Srinivasan81 argue that using wage rates (either those of their regular job or the industry average) is problematic.
Source: www.involve.org.uk/wp-content/uploads/2011/03/True-Costs-Full-Report2.pdf (accessed 1 April 2015). Contains material under the Creative Commons licence.
We therefore needed some estimates of the time that different people spent being engaged at the different levels identified in the MORI surveys and basic information about the NDC populations. Some information on the time commitment involved in higher levels of engagement, for example being on the partnership board, can be derived from a specific survey of NDC board members carried out by NET,82 but we also asked interviewees about time input to specific ‘marker’ CE activities when relevant.
Selecting marker activities for collecting detailed information on time and in-kind inputs
A very wide range of CE activities was undertaken across the 39 NDC areas. It was therefore necessary to select a smaller number of ‘marker’ activities to cost in-kind and voluntary/participative labour. These ‘marker’ CE activities were chosen on the basis of the following criteria: availability of relevant documentation; links to typology dimensions (e.g. control, cohesion and trust); resonance with the system K data; spread of different forms of engagement (informing, consulting, co-production, delegated power and community control); and at least some including partner organisations. The CE ‘marker’ activities selected were as follows:
-
Production of a community newsletter, in most areas as a tool of communication, corresponding directly to System K project code 108 (for which 36 areas reported expenditure). Other areas produced a (usually infrequent) local newspaper. The activities varied but could include a resident-led steering committee and volunteer reporters supported by a community journalism course plus outsourcing the design and publishing functions (we have assumed that the functions would have been subsumed under System K project code 108).
-
Area forums with a focus on health, education and environment/neighbourhood allowed us to consider partner as well as resident inputs and costs. All areas tried to establish these, either from scratch or linking into and expanding existing forums. Some of the health forums were primary care trust led and many of the education forums involved as many education professionals as, or more education professionals than, local residents. Other forums tackled issues such as graffiti, fly tipping and litter, with some focusing on short-term quick wins and others on long-term goals.
-
NDC boards and subcommittees were established in all NDC areas and only a few paid community representatives for attendance at meetings. In costing these activities we have sought to include all of the time spent on preparation, attendance and follow-up, which could be considerable.
-
Strategy development and housing. For areas that invested in major housing renewal programmes this generated high levels of engagement, but CE was also an important focus when the strategy focused on renovation.
-
Resident-managed green spaces. Activities ranged from planting in alleys and renovating public spaces to building new parks, with most areas investing in this activity. Few of these initiatives were entirely resident managed and they often returned to local authority control once major works had been completed. Nevertheless, they were seen as making a contribution across several themes, for example increasing physical activity with health benefits or educational benefits by creating safe areas for children to play and increase motor skills.
-
Sports events and festivals/theme days, which all NDCs organised to showcase NDC initiatives and/or recruit community members.
Interviewees were also asked about the extent to which capacity building, including courses and training, had been integrated into the other ‘marker’ activities.
Use of time as a basis for estimating cost
Time has been used as the basis for measuring the cost of residents’ contributions to each of the ‘marker’ activities. The figure of £10 per hour was used, based on the community and voluntary sector rates current at the time, and one interviewee noted that this was the rate used to cost volunteer time if external funds were being sought and they wanted to document the contribution of volunteer time. In fact, as we noted earlier, because we eventually relied only on the System K data, the choice of an hourly valuation was relatively arbitrary.
The use of time can also be problematic and several compromises had to be made:
-
There were clearly both costs and benefits for some residents of engaging with NDC activities. One interviewee spoke of one person using their involvement with the NDC as a platform to become a councillor. There were suggestions that some participants attempted to ensure that money was spent on or close to their particular estates. Another interviewee estimated that between 10% and 20% of resident activity was about residents’ own personal development.
-
Estimates of time inputs could vary greatly. Three interviewees in the same area gave very different accounts of the time spent on the same activity. In this instance the estimate provided by the interviewee working on the activity for 6 years was prioritised.
-
When NDC areas used existing facilities and structures to support CE (such as neighbourhood fora) it is difficult to distinguish what is uniquely NDC driven and therefore to cost community time.
-
Although interviewees agreed that their area had used all of the ‘marker’ engagement activities, many could not provide any details on one or more of these, including the level of resident input. This is in part a problem with retrospective data collection but also speaks to the breadth of knowledge required to answer our questions.
-
One interviewee described the NDC initiatives as community influenced rather than community driven. Notably, we included a section in the interview on community-driven initiatives but none was reported in the 11 NDC areas.
Problems with data collection
The retrospective nature of our economic analysis creates three problems. First, we do not have consistent information about the nature and extent of NDC CE activities on which to assess in-kind costs. Apart from the 2008 survey, the MORI data simply provide estimates of the numbers who have been involved rather than what they have been involved in. There is considerable variation in the information provided in documents produced by NDC partnerships, which may reflect differences in the starting levels of CE activities but also may reflect other factors and that some interviewees may have better memories than others. Generally, there appear to have been three broad phases of the NDC: planning, delivery and succession. If cost data were to be collected prospectively there is a case for different types of data to be collected for each of these phases. However, as we cannot collect information in this way we may be making unwarranted assumptions about the equivalence of information extracted from the documents at different points in time. The activities of original seven reporting category themes used in the System K data sets illustrate this. Evidence from documents suggests that these were most vibrant during the earlier planning phase of local programmes but became less active over time.
A second problem was that documentation is inconsistent across the NDC areas. The solution adopted was as follows. For each of the selected types of activity we searched for ‘best practice’ examples of documentation in terms of details of the activity and the costing. As far as possible, we then constructed and applied these ideal ‘costing templates’ to the more scanty reports of activities in other areas. There are of course problems with this approach. In particular, better-documented activities may have had more intense CE, both in terms of volume and quality; the actual type of CE may well have been different if very few details are given; any additional resources levered in will not be accounted for; and individual costs to community members will vary.
Third, identifying the number of hours that community volunteers spent at each event or meeting was not straightforward. In most cases there was insufficient information and so again we identified examples of best practice and applied the resulting ‘costing templates’ to the more scanty reports of activities in other areas. We also adopted the following general rules: any community meeting was assumed to last half a day to include travelling time there and back; an event scheduled to last half a day was assumed to last 1 day to include set-up and travel time; and a meeting was assumed to last for 2 hours unless otherwise specified.
A number of other complexities arose during the data collection phase relating to the change in CE activities over time; the fact that some marker activities contributed to more than one outcome area and were not treated as distinct by people involved; the varying scale and depth of involvement, with hundreds of people attending public meetings about major redevelopment potentially skewing the measure of involvement based on person-hours; the limits imposed on participation because of the status of some NDC meetings as either open or closed; the involvement of large numbers of professionals in some thematic forums, particularly relating to education; dealing with missing or incomplete data; how to treat active volunteers compared with residents participating in NDC events; and the difficulties of corroborating the data that were collected by different routes.
Compiling a data table on estimates of time inputs to community engagement activities
Table 33 provides estimates of the time input for each of the six ‘marker’ CE activities in the 11 fieldwork sites. Details of how the data in this table were compiled are summarised below. Despite our best efforts, there are several gaps in the data. There are also very wide variations in the estimated hours spent, which are reduced only a little by grouping the NDCs by the CE typology.
| NDC area | CE/local programme type | Community magazine | Area forums | NDC boards | Strategy planning | Green spaces | Events/festivals | All activities | |
|---|---|---|---|---|---|---|---|---|---|
| Total mean hours | Estimated (£×1000) totalsa | ||||||||
| 1 | C2 | 5100 | 2400 | 1800 | – | 600 | 3200 | ||
| 2 | D1 | 1140 | 3792 | 3312 | 576 | – | 21,600 | ||
| 3 | A2 | 33,120 | – | – | – | ||||
| 4 | C1 | 3744 | 7400 | 888 | – | – | – | ||
| 5 | A1 | 3416 | 7040 | 19,540 | 1568 | 992 | 208 | ||
| 6 | A1 | 1960 | 4536 | 26,900 | 3800 | 360 | – | ||
| 7 | C3 | 10,200 | – | – | – | – | |||
| 8 | C3 | 3248 | 4380 | 3984 | 3280 | 3200 | 4280 | ||
| 9 | B1 | 3168 | 1800 | 9600 | 760 | – | 7990 | ||
| 10 | A3 | 3560 | 3240 | 4000 | – | – | |||
| 11 | B1 | 1560 | 2768 | 15,960 | 4000 | – | – | ||
| Adjusted mean | 2917 | 6193 | 14,640 | 2330 | 1278 | 7456 | 34,814 | 13,578 (all 39 NDCs) | |
| Mean of top 2 | 4422 | 13,020 | 30,010 | 3900 | 2096 | 14,800 | 68,248 | 26,617 (top 2) | |
| CE and local programme type (n), highest value taken for each type | |||||||||
| A (13) | 3415 | 7040 | 33,120 | 3800 | 992 | 208 | 77,375 | 10,059 | |
| B (12) | 3168 | 2768 | 15,960 | 4000 | – | 7990 | 33,886 | 3389 | |
| C (9) | 5100 | 10,200 | 3984 | 3280 | 3200 | 4280 | 30,044 | 2703 | |
| D (5) | 1140 | 15,840 | 3312 | 576 | – | 21,600 | 42,468 | 2123 | |
| 1 (12) | 3416 | 7400 | 26,900 | 4000 | 992 | 21,600 | 64,308 | 6431 | |
| 2 (14) | 5100 | 2400 | 33,120 | 0 | 600 | 3200 | 44,420 | 4420 | |
| 3 (13) | 3248 | 10,200 | 3984 | 3280 | 3200 | 4280 | 28,192 | 2891 | |
Estimating time input
Some interviewees gave an average of time committed to an activity but this was used only if they could specify that this was constant or how it varied over the life of the NDC and related to the numbers of people involved. Some data depended on extrapolating from available information. For example, if we knew that an area had three estates it was assumed that a representative from each estate would be used in training for strategic planning activities. Estimates include changes over time in the intensity of involvement when available, and time on training attached to activities was estimated separately.
Basic estimates of hours spent in a single year were inputted to a primary data table for each NDC area. These estimates were calculated as the sum of the number of residents involved multiplied by the time spent on activities and their frequency. They were then summed to give the 10-year estimate for the whole period. Ranges for numbers attending activities are expressed with minima and maxima. If estimates for attendance are small, for example between three and five, four has been used.. When a range was given in terms of the length of a meeting the higher number has been used because there is never more than an hour’s difference and we are probably underestimating the figures generally. When no estimate was given, we assumed that meetings lasted for 2 hours.
A number of specific issues arose when estimating time input to the marker CE activities. In some areas, for example, there was more than one community newsletter and so time estimates were combined, whereas in one or two cases interviewees appeared to include time spent on area forums in their estimates of time committed to NDC boards. Some interviewees talked of spending between 10 and 20 hours a week on NDC work outside of the main board meetings. This would mean that a single board member spent between 4400 and 8800 hours on NDC work over 10 years (44 weeks per year). Although this may sound a large amount, a community activist could easily spend 10 hours a week serving on multiple subcommittees and door stepping to raise community awareness, especially at the beginning of the programme. Time input to fun days and festivals was based on the effort of the organisers (who usually met for a number of weeks/months prior to the event) rather than on those attending the events.
Estimating in-kind costs of resident members of New Deal for Communities boards
A NDC partnership board was established in each NDC area and was seen by both government and the local areas as a key means of facilitating CE, embedding ownership of the NDC with local people and providing a model for future action within partnership organisations and regeneration activities. However, for the purposes of costing in-kind contributions to CE activities it is important to note differences in the ‘conditions’ of membership, with some areas paying attendance allowances for board members. For some NDC areas we were able to obtain estimates of the additional hours that community representatives spent on NDC business, but for other areas we had only the time taken up by regular board meetings, including in some cases pre-meetings, which were always scheduled. All areas stated either in documents or in interviews that training existed for board members; however, only a few were able to quantify the time spent on this.
The results of this process are provided in Table 33. The top half of the table provides the numbers of hours spent over the 10 years of the NDC initiative on the six ‘marker’ activities in each of the 11 fieldwork areas, estimated on the basis of analyses of documents and interviews. In the bottom half of the table these entries are summed to give totals overall and for each CE type and programme type. In the far right-hand column these means are converted into a total for all 39 NDCs.
Comparing System K expenditure with the estimated resource costs of community involvement
There was no clear correspondence between System K expenditure and our costing of in-kind and voluntary time input to community involvement activities. For some System K categories expenditure on community involvement was obvious. For example, improved community services/equipment and community development workers/officers represented, by definition, expenditure by the programme rather than community or voluntary effort. However, for most of the categories included in Table 34, the correspondence is by no means one to one and so the comparison is not perfect. For example, the System K category of ‘new/improved use/access to community facilities’ can only be loosely related to either of the bottom-up categories of ‘master planning/housing strategy development’ or ‘resident-managed green spaces’.
| System K project type | System K | Estimated number of hours | |||
|---|---|---|---|---|---|
| Spend (£) | Ranka | Categories (marker and activity number) | Mean estimated numberb | Rankc | |
| Capacity building NDC governance | 513,042 | 8 (4) | NDC boards and subcommittees (3) | 14,640/33,120 | 1/1 |
| Capacity building general | 1,045,544 | 2 (2) | NDC boards and subcommittees (3) | 14,640/33,120 | 1/1 |
| Promotion/communication/marketing/raising public awareness | 612,484 | 5 (3) | Community magazine (1) | 2917/4422 | 4/4 |
| Area forums, relating to health, and environment neighbourhood (2) | 6193/13,020 | 3/3 | |||
| New/improved use/access to community facility | 3,258,896 | 1 (1) | Master planning/housing strategy development (4) | 2330/2900 | 5/5 |
| Resident-managed green spaces (5) | 1278/4096 | 6/6 | |||
| Community radio | 221,761 | 5 (5) | Community magazine (1) | 2917/4422 | 4/4 |
| Community events/activities | 124,334 | 6 (6) | Using volunteers (6) | 7456/14,800 | 2/2 |
This lack of correspondence is reflected in the non-significant correlation coefficient of 0.26 between the recorded System K accountancy spends and the bottom-up estimated cost of CE. We also looked at the relationship between these two approaches to costing across the different types of local NDC programmes and different approaches to CE, and no notable patterns were identified.
Calculating cost-effectiveness
The difficulties of collecting cost data have been extensively documented in the previous sections and the results in Table 33 do not show any systematic pattern. Importantly, we thought that there would be more information available about those who were engaged in different activities for us to be able to confidently extrapolate from the 11 fieldwork sites to the 39 areas; instead, the only possibility was to apply the estimates in Table 33 for the 11 fieldwork sites directly to the other 28 areas based only on the local programme type and CE typology. For this reason, despite the effort put into collecting the bottom-up data, the System K data have been preferred for the purposes of calculating cost-effectiveness, and the pattern of spend within each outcome area is taken as a marker indicator of the approach within that area. The cost-effectiveness analyses therefore had two components:
-
an analysis of the administrative outcome data reported in Chapter 6 compared with System K expenditure data and the CE typology
-
an analysis of the MORI outcome data reported in Chapter 4 compared with System K expenditure data and the CE typology.
The NET’s final81 report used respondents’ assessments of their overall quality of life and specifically their satisfaction with the area as the measure of final outcome in assessing value for money of the whole programme. Given our specific focus on CE, we have concentrated on health and social cohesion outcomes, and on hospital admission indices for drugs, alcohol and mental health-related conditions. However, given the strong relationship between feeling safe when walking alone after dark and the quality of life score, we have also included four marker crime indicators.
Outcomes for hospital admission indices and System K expenditure by community engagement type
The expenditure data used in these analyses were extracted from the System K database described earlier, in which projects are classified both by their type and by the topic or theme that they might influence. Eleven types of health-related projects are identified (numbered 501–11 in the database):
-
501 New/improved use/access to health facilities.
-
502 Targeted health – elderly health.
-
503 Targeted health – teenage health/young people.
-
504 Targeted health – drugs/alcohol related.
-
505 Healthy living initiatives.
-
506 New/improved health services.
-
507 Family support.
-
508 Community Chest – health.
-
509 Health posts.
-
510 Health events.
-
511 Targeted health – other.
The total expenditure on these 11 types of project across all NDC areas is approximately £114,389,000 or 7.5% of the entire NDC project budget. The broader group of projects that are described as having a health theme (including housing and environmental improvement initiatives) are costed at approximately £148M or 9.8% of total NDC expenditure.
Table 35 shows the total expenditure on all health-specific projects broken down by CE type and NDC local programme type. Inspection of the per capita expenditure reveals that the highest expenditure tends to be among the poorest-performing NDC areas. When ranked by health improvements, areas with type 2 local programmes and those adopting a type B approach to CE appear to perform better.
| CE/local programme type | Total spend on health projects (£) | Spend per area | 2005 population | Per capita spend on health projects (£) | Per capita spend as multiple of lowest spend |
|---|---|---|---|---|---|
| CE type | |||||
| A | 42,831,853.3 | 3,294,757.9 | 8842.6 | 389.5 | 5.1 |
| B | 30,652,365.3 | 2,554,363.8 | 10,132.5 | 246.3 | 3.2 |
| C | 28,353,586.1 | 3,150,398.5 | 11,986.7 | 267.1 | 3.5 |
| D | 12,551,060.5 | 2,510,212.1 | 7707.6 | 323.6 | 4.3 |
| Local programme type | |||||
| 1 | 29,389,023.8 | 2,449,085.3 | 8103.8 | 326.0 | 4.3 |
| 2 | 37,278,613.4 | 2,662,758.1 | 9904.9 | 261.4 | 3.4 |
| 3 | 47,721,228.0 | 3,670,863.7 | 11,311.4 | 343.8 | 4.5 |
This is confirmed by the summary figures in Table 36, which report the per capita expenditure on both health-themed and health-specific (500 series) projects by NDC area grouped according to whether or not hospital admission rates reduced, increased or remained stable over time relative to their comparator areas. As for health-themed expenditure, health-specific project spend is highest (£399) in areas of deteriorating health (i.e. where admission rates increased relative to the comparators), lowest (£193) in areas with no change and approximately 25% higher (£246) in areas showing improvements/decreasing admission rates. The correlation of CE type with the rank of number of health improvements is –0.07 and with the per capita health expenditure is –0.21; neither is statistically significant.
| Changes in health relative to comparator area (measured by six hospital admission indicators) | Average per capita spend on all health-themed projects (£) | Average per capita spend across specific health (series 500) projects (£) |
|---|---|---|
| Deteriorating/increasing admission rates | 497 | 399 |
| No change | 245 | 193 |
| Improving/decreasing admissions | 345 | 246 |
Hospital admission outcomes and type of health-specific initiatives
The distribution of spend for individual NDC areas is shown in Table 67 in Appendix 2. At one extreme, the best-performing NDC area, Norwich, spent more than 80% of its NDC health project funds on initiatives to reduce drugs and alcohol misuse, and promoting healthy living and family support activities. At the other extreme, Leicester spent 80% of its NDC health project funds on improving facilities and access, and only 9% on healthy living and family support.
Tables 37 and 38 considers whether or not the distribution of spending across the 11 types of health-specific projects varies systematically with health outcomes within each of the CE types and local programme types.
| CE/local programme type | Access and facilities | Elderly | Teenagers/young people | Drugs and alcohol | Healthy living | New/improved services | Family support | Community Chest (health) | Health posts | Health events | Other targeted services |
|---|---|---|---|---|---|---|---|---|---|---|---|
| CE type | |||||||||||
| A | 22.5 | 1.5 | 9.7 | 12.3 | 12.7 | 7.7 | 8.5 | 4.6 | 14.3 | 0.0 | 6.0 |
| B | 19.0 | 2.2 | 6.1 | 6.3 | 9.3 | 12.6 | 10.8 | 0.3 | 16.5 | 0.1 | 16.8 |
| C | 35.2 | 2.0 | 1.5 | 2.0 | 13.8 | 10.4 | 14.2 | 0.3 | 13.8 | 0.1 | 6.6 |
| D | 12.3 | 8.8 | 1.8 | 0.0 | 29.3 | 10.9 | 2.5 | 0.0 | 22.0 | 0.0 | 12.4 |
| Local programme type | |||||||||||
| 1 | 20.3 | 5.7 | 2.4 | 0.8 | 18.8 | 7.8 | 12.6 | 0.4 | 16.8 | 0.0 | 14.4 |
| 2 | 22.9 | 1.7 | 3.5 | 10.3 | 13.3 | 11.3 | 9.4 | 4.2 | 13.5 | 0.1 | 9.8 |
| 3 | 25.7 | 1.2 | 11.1 | 7.7 | 10.6 | 11.4 | 7.6 | 0.2 | 17.5 | 0.1 | 7.0 |
Table 37 shows the breakdown of expenditure between the four CE types and three NDC local programme types. Areas with CE type A spent the largest percentage on teenagers/young people, drugs and alcohol, and Community Chest; areas with CE type B spent the largest percentage on new/improved services and other targeted services; areas with CE type C spent the largest percentage on access and facilities, and family support; and areas with CE type D spent the largest percentage on the elderly, healthy living and health posts. Areas with a type 1 local programme spent the largest percentage on the elderly, healthy living, family support and other targeted services; areas with a type 2 programme spent the largest percentage on drugs and alcohol; and areas with a type 3 programme spent the largest percentage on access and facilities, teenagers/young people, new/improved services and health posts.
Table 38 shows that a much higher proportion of expenditure is directed to basic capacity building (access and facilities) in areas that did not show improvement. Expenditure on health posts is approximately the same across all three groups, but spend on more focused initiatives directed at the elderly, young people, drug and alcohol misuse, and healthy living was lowest in the non-improving areas.
| Changes in health relative to comparator area (measured by six hospital admission indicators) | Access and facilities | Elderly | Teenagers/young people | Drugs and alcohol | Healthy living | New/improved services | Family support | Community Chest (health) | Health posts | Health events | Other targeted services |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Deteriorating | 48.3 | 0.6 | 3.9 | 2.3 | 8.8 | 8.3 | 8.3 | 0.2 | 13.9 | 0.1 | 5.3 |
| No change | 17.6 | 4.7 | 2.1 | 6.0 | 15.8 | 11.3 | 9.1 | 7.8 | 15.2 | 0.0 | 10.2 |
| Improving | 7.2 | 3.9 | 8.1 | 13.1 | 15.6 | 12.4 | 10.9 | 0.2 | 16.4 | 0.1 | 12.2 |
There is no obvious relation between the patterns of spend shown in Tables 37 and 38. More qualitative detail on the context, motivation and nature of these projects is required before one can draw conclusions from these figures, but it is interesting to note that high support for access and facilities occurs in areas where health-care provision is still being developed (in the context of deteriorating hospital admissions) and that areas where such provision already existed and health was starting to improve (i.e. admissions were declining relative to comparators) were able to use NDC health funding in more focused and potentially more creative ways. The available data do enable us to address one of these issues quantitatively – whether or not the NDC areas that spent the highest proportion of their budgets on alcohol and drug misuse programmes showed the best results in these areas – and this is discussed in the following section.
Drugs and alcohol hospital admission outcomes and expenditure on activities in these areas
Table 39 presents the percentage of the NDC health project budget spent on initiatives to reduce drug and alcohol misuse against the indices of hospital admissions for drug and alcohol misuse and all mental health problems, broken down by CE type and local programme type (negative rates of change indicate that a NDC is improving relative to its comparator, i.e. admission rates reduced more). Relative to their comparators, in NDC areas with type A and type C approaches to CE and type 2 local programmes there were substantial decreases in drugs-related hospital admissions and less pronounced effects on alcohol-related and mental health admissions. In contrast, there were substantial increases in admissions for these three conditions in areas with type D approaches to CE relative to their comparators. Correspondingly, the percentage of health spend and the per capita spend on drugs and alcohol projects were higher in areas with type A approaches to CE and type 2 local programmes.
| CE/local programme type | Drugs-related admission index | Alcohol-related admission index | Mental health admission index | % health spend on alcohol- and drugs-related projects | Per capita spend on alcohol- and drugs-related projects (£) | Per capita spend on healthy living projects (£) |
|---|---|---|---|---|---|---|
| CE type | ||||||
| A | –8.7 | –1.3 | –0.1 | 8.6 | 30.5 | 32.1 |
| B | –2.4 | –1.2 | 0.6 | 5.8 | 13.5 | 22.2 |
| C | –7.6 | 0.0 | 0.5 | 2.3 | 5.9 | 32.3 |
| D | 6.0 | 5.0 | 4.7 | 0.0 | 0.0 | 86.4 |
| Local programme type | ||||||
| 1 | 0.2 | 2.1 | 2.7 | 0.8 | 2.8 | 50.5 |
| 2 | –8.1 | –0.3 | –0.1 | 10.3 | 22.6 | 29.0 |
| 3 | 0.6 | –2.2 | –0.4 | 7.7 | 32.5 | 31.5 |
The relationships in the table are plausible but it is debatable whether or not the figures support an argument that, within the context of the NDC programme, greater expenditure on drugs and alcohol harm reduction projects is causally related to a relative decline in related hospital admissions. Although it is the case that many of the NDC areas with the greatest relative increase in related admissions (those with high positive figures) appear to have spent little or no specific funds on these topics (e.g. Knowsley, Nottingham and Leicester), a relative reduction in drug- and alcohol-related hospital admissions is not always found in areas of highest funding.
Outcomes for social cohesion and self-reported health outcomes by System K data
The comparison between the difference-in-difference scores for the social cohesion and self-reported health outcomes reported in Chapter 4 and the component System K expenditure is shown in Table 40.
| Subject | CE type | Local programme type | |||||
|---|---|---|---|---|---|---|---|
| A | B | C | D | 1 | 2 | 3 | |
| Self-reported health outcomes (%) | |||||||
| In good self-reported health | +0.3 | –2.2 | +3.5 | –2.1 | –1.2 | –0.9 | +1.6 |
| Limiting illness | +0.1 | +0.3 | –1.7 | +2.0 | +0.9 | +1.0 | –1.7 |
| Nervous person | –1.3 | +1.5 | –2.9 | –3.8 | –1.4 | +0.5 | –2.6 |
| Down in the dumps | –0.4 | +0.2 | +0.9 | +2.5 | –1.4 | –0.4 | +0.1 |
| Calm and peaceful | +7.3 | +1.2 | +4.4 | +16.7 | 7.1 | +2.2 | +8.9 |
| Downhearted | +0.2 | +0.7 | –1.6 | ||||
| Happy person | +3.3 | –4.0 | –1.9 | +7.5 | –0.3 | –2.7 | +3.9 |
| Eats five portions of fruit/vegetables a day three or more times a week | –6.8 | –6.7 | –1.2 | +7.0 | +1.6 | +0.8 | –8.2 |
| Smoking | –3.1 | –2.2 | +0.6 | –7.7 | –4.1 | –1.8 | +4.1 |
| Social cohesion outcomes (%) | |||||||
| Feel part of community | –1.3 | –0.8 | +2.7 | –8.1 | –1.6 | 0.3 | –2.5 |
| People in area are friendly | +4.3 | +3.8 | –1.0 | +1.7 | 4.9 | 2.0 | 1.1 |
| Know many people in area | +2.8 | –4.2 | +2.0 | +13.7 | 6.1 | –0.4 | –0.2 |
| Neighbours look out for each other | +8.9 | –2.2 | –4.7 | +2.5 | 3.4 | 2.2 | –2.6 |
| Can influence decision-making in area | +2.8 | –1.9 | +1.6 | +6.4 | –2.6 | –1.7 | 3.6 |
| Volunteered in local organisations | +0.7 | –1.0 | +2.1 | +0.8 | 0.7 | –0.9 | 3.1 |
| Feel safe walking alone in the dark | +1.0 | +3.0 | +4.3 | +5.2 | +3.8 | +0.4 | +5.7 |
| System K spend [average total spend (£ × 1000)] | |||||||
| Community development | 21.5 | 22.3 | 15.4 | 14.9 | 21.5 | 22.3 | 15.4 |
| Crime and community safety | 9.7 | 11 | 7.8 | 7.4 | 9.7 | 11 | 7.8 |
| Health | 8.2 | 7.4 | 8.2 | 6.6 | 8.2 | 7.4 | 8.2 |
| Capacity building NDC governance | 471 | 824 | 88 | 252 | 100 | 181 | 4633 |
| Capacity building general | 768 | 1281 | 769 | 1588 | 1494 | 857 | 687 |
| Promotion/communications/raising public awareness | 579 | 709 | 500 | 650 | 618 | 1065 | 782 |
| New/improved use/access to community facility | 4918 | 2504 | 2973 | 1820 | 2322 | 3270 | 3839 |
| Community radio | 377 | 101 | 97 | 280 | 195 | 30 | 288 |
| Community events/activities | 106 | 79 | 317 | 17 | 103 | 98 | 257 |
The typology of approaches to CE did not perform well in these analyses and so total spend on community development minus spend on facilities, referred to as ‘soft community spend’, is used here as a marker of CE approach. Regressions of the health and social cohesion outcomes for NDC areas compared with their comparators in 2008 on NDC spend either by theme or by project type produced only three significant coefficients. The most powerful was when ‘feel involved in the community’ was the dependent, with a R2 of 0.27 and the significant negative coefficient was ‘soft’ community spend on development workers with a t-value of 2.20. Regressions of the three standardised hospital admissions indices in NDC areas relative to their comparators on both the difference-in-difference values of the subjective health and social cohesion outcomes and NDC spend by both project or local programme type, or CE type were more powerful, especially for the drugs-related admission index and mental health admission index, producing seven significant coefficients. However, among all these coefficients, the CE typology was never significant and local programme type was statistically significant only for the drugs-related admission index.
Summary and conclusions
Costing community engagement
We identified two main sources of data for costing CE in the NDC initiative: the ‘top-down’ System K accounting data and the ‘bottom-up’ costings obtained from local documents and interviews with key informants in 11 NDC areas. The System K data show that about 19% of NDC spend was categorised as community development, varying between 22% in areas with type A and type B approaches to CE, and 15% in areas with type C and type D approaches to CE. Areas with type 2 local programmes spent more in this category than areas with the other two types of local programmes.
In addition to the expenditure reported in System K, there was a wide variety of in-kind contributions to, and individual participation and volunteering in, NDC programmes. We have described the main difficulties that we experienced in extracting information from a very large amount of documentation and obtaining data on in-kind costs during telephone interviews on selected marker CE activities. The main challenges associated with this costing exercise were that it was retrospective, that documentation was inconsistent in volume and quality, and that precise estimates of the time inputs of volunteers were impossible to obtain. Although there were small levels of correlation between the System K estimates and the bottom-up estimates, there was no clear pattern in those that were significant.
Community involvement and cost-effectiveness
The cost-effectiveness analysis utilised three sources of effectiveness data reported in Chapters 4 and 6: self-reported health-related measures and social cohesion measures based on MORI survey data and hospital admission indices based on HES data. The analysis comparing health expenditure with health outcomes suggests that the worst-performing NDC areas on these outcomes tend to have a higher level of expenditure on health-related projects. When ranked by health improvements those areas with type B approaches to CE combined with type 2 local programmes performed better and those areas with type 2 programmes also spent the smallest proportion of NDC funds on health-care projects.
Multivariate analysis of the regressions did not generate any significant findings, probably because of the ambiguous relationship between spend and admission indices. The regression at the individual level did not add any useful information. Overall, therefore, the findings are very mixed. Methodologically, first, it was very difficult to cost community involvement and we had to use the System K data on NDC spend instead; second, the measures of effectiveness are mostly self-reported and are not very robust; and third, relating the costs that we can calculate to specific measures of effectiveness is also difficult. In terms of the effectiveness results, there are almost as many negative as positive scores. Calculating cost-effectiveness then becomes a rather arbitrary exercise.
Chapter 9 Discussion and conclusions
Introduction
The research reported here has built on our previous study funded by the Policy Research Programme,1 which explored the impact of the NDC programme on health inequalities and their social determinants. The NDC was a major neighbourhood regeneration initiative implemented in 39 of the poorest neighbourhoods in England at a cost of around £2B over 10 years from 1999/2000. Our NDC study found a range of social and health outcomes associated with different types of local NDC programmes. The study reported here has explored what, if any, outcomes related to health inequalities and their social determinants are associated with different approaches to CE within the NDC and considered what, if any, contribution these CE approaches made to the differential outcomes that we reported for NDC local programmes types.
In this final chapter of our report we identify some of the limitations of our research. We then move on to consider the new insights that we believe this study has to offer to research evaluating interventions involving some element of CE and aimed at reducing health inequalities. Lastly, we consider some of the implications for research and policy.
Limitations of the research
Our research has used rich cross-sectional and longitudinal survey and time series data sources compiled by the NDC NET to develop an innovative approach to the evaluation of the social and health impacts of different approaches to CE implemented within the same policy context, that is, implemented in the 39 local programmes that made up the national NDC regeneration initiative. However, there are several limitations to the data and methods that we used.
The outcome measures available to us were more limited than anticipated because the form of some measures in the MORI survey meant that we were unable to use them (e.g. measures of income) and because of constraints imposed by the size of the MORI longitudinal panel. Additionally, available measures of the experience of engagement and of community control and influence, and data for the effectiveness work, were particularly limited. On the costing side the main limits arose from inconsistencies in the volume and quality of available documentation, the retrospective nature of documentary data and recollections from a small number of interviewees. On the effectiveness side, for example, as noted above, we were not able to capture quantitatively some dimensions of the experience and impact of engagement expressed qualitatively by interviewees. Additionally, although there were some positive findings from the cost-effectiveness analyses, there was an almost equal number of negative findings and there was no obvious metric for combining them.
We were also aware of other limitations commonly associated with the use of secondary data sources: the fact that they were generated for other purposes; the often inadequate meta-data describing how the data have been collected and from whom; and their precise coding under different circumstances. In particular, some of the data sets (e.g. HES) have confidentiality restrictions; others (e.g. MORI) arise from the limitations of self-report data such as socially stratified reporting biases.
Bias may also have been introduced into our findings through residential mobility. Some of our results are based on repeat cross-sectional studies measuring change over time in different people; other analyses assess within-person change over time. The use of cross-sectional data reduces the problem of attrition found in the longitudinal data set but means that differences in the sample and residential mobility could contribute to the observed trends over time. To address this we undertook sensitivity analysis, excluding those who had recently moved and adjusting for a range of demographic characteristics to make the samples as similar as possible. For the longitudinal data, we compared results with and results without respondents who had recently moved. This comparison suggests that resident mobility effects seem to have been limited, at least in terms of the main outcomes of interest for this project. In all of our analyses we also adjusted for a range of demographic characteristics to help compensate for differences in the samples.
Findings from our longitudinal and cross-sectional analyses do not always agree. Although the sensitivity analyses with and without movers do not point to substantial bias when movers and non-movers are included, they do not throw much light on why this is the case. Numerous other studies show that longitudinal and cross-sectional approaches to estimating change frequently yield different estimates and different conclusions about the size and direction of change. Although longitudinal data are typically considered more precise within epidemiology, it is not necessarily the case that either of the two MORI data sources provides stronger evidence of impact in this study. Changing the profile of the resident population (e.g. through mixed-tenure redevelopment) was an explicit aim of some of the local NDC programmes, and between 2002 and 2008 there was substantial population turnover in some areas. The NET did attempt to follow up people moving out of NDC intervention areas but this was too expensive to pursue. Differences in the way that the health and social cohesion outcomes were treated in the longitudinal and cross-sectional approaches may also have contributed to different results across data sources. In the longitudinal analysis we analysed latent factors of social cohesion, which take better account of the measurement error associated with combining multiple items of trust in the community, trust in local services, mental health, etc. Despite the difficulties of interpretation introduced by using both longitudinal and cross-sectional data in the same study, this triangulation undoubtedly helps evaluations such as ours to capture more of the complexity of impacts associated with interventions such as the NDC in general and the approaches to engagement in particular.
As described in Chapters 3 and 7, alongside the secondary data that we used we also collected new primary qualitative data from interviews with residents of NDC areas and past workers. Although these data provide important insights into the processes of engagement, discussed further in the following section, the heavy reliance of our CE typology on the recollections of interviewees is a potential weakness. These recollections could have become distorted over time, particularly in NDC areas adopting a type D approach to engagement. These areas all involved redevelopment initiatives, which were more likely to have stalled after the economic problems of 2007 slowed the economy and in particular private sector house building. Additionally, being restricted to those residents and past NDC workers who were easiest to contact would have inevitably biased our sample of interviewees to those who were most engaged in the NDC (positively or negatively). Documents, another key source of data for the typology, also have problems of bias, typically being written to meet the requirements of particular audiences.
A final limitation was that we faced the usual challenges of developing a theoretically robust approach to conceptualising ‘community engagement’, challenges that are well documented in existing literature. As in all qualitative research, another team may have made very different decisions on this front.
New insights from the study
Our evaluation of NDC approaches to CE has sought to answer five research questions:
-
Which approaches to CE effectively engage which social groups in NDC populations?
-
Do different approaches to CE have different health and social outcomes for NDC populations?
-
Does the association between these outcomes and NDC approach to CE vary across groups defined by age, ethnicity, gender and material circumstances?
-
Do different approaches to CE have any impact on the health gap between NDC areas and areas from across the socioeconomic spectrum?
-
Does the approach to CE help to explain any of the differential outcomes of local NDC programmes identified in our previous research?
We also undertook an exploratory economic evaluation of the cost-effectiveness of different approaches to engagement in the NDC areas.
In seeking to answer these questions our evaluation has provided new methodological insights relevant to the evaluation of complex social interventions and new evidential insights into the pathways that might be expected to link CE in decision-making to positive social and health outcomes, and the factors that may support or undermine engagement processes. The study also provides insights into the processes of public engagement in evaluative research in the public health field, a field in which public engagement in research is relatively underdeveloped.
Methodological insights
To be able to answer research questions 2–5 the study design hinged on two key theoretical assumptions. First, in this and our previous evaluation we have conceptualised the NDC initiative, its component local programmes and their different approaches to CE, as holistic interventions with the potential to reduce health inequalities by addressing the social determinants of these inequalities. We therefore wished to evaluate these interventions as a whole, rather than evaluating the myriad and disparate projects and activities of which they are formed. However, this very diversity leads to the second theoretical assumption underpinning our work: that, although NDC local programmes all shared the same function in terms of the outcomes that they were seeking, the form of these programmes and the approaches to CE that they adopted would be different. This variation lies at the heart of our evaluation design as it can be exploited to compare the outcomes achieved by different types of local NDC programmes and different approaches to CE. Before we could do this, however, we had to develop a typology of CE approaches taken by the 39 NDC local programmes that would illuminate potential pathways to impact/change. Our attempt to develop this typology was therefore a crucial, and novel, component of the evaluation, without which the comparative analysis would not be possible. Some members of our advisory group warned us that this was an extremely difficult task that we might not be able to achieve.
Fortunately, we did produce a typology that made sense to NDC residents and practitioners who had been involved in NDC implementation in their area as well as nationally. Its development hinged on the elaboration of a theory of change linking CE to positive social and health (equity) outcomes. As noted in the introduction, the theory of change underpinning CE in the NDC initiative emerged from the SEU in the Cabinet Office. This theory, which has been criticised,50,51 assumed that engaging communities in developing and delivering local programmes would overcome problems of social exclusion and promote social cohesion, hence reducing crime and incivilities, and would also make services more responsive to local needs and hence increase access and effectiveness. 48 However, we have not sought to evaluate whether or not the NDC initiative achieved its policy aims as reflected in the Cabinet Office theory (the purpose of the NET study). Instead, our typology and evaluation were underpinned by theories of community control/empowerment and the relationship to health inequalities and their social determinants, as set out in Figure 1. Invariably there are overlaps between these different theories and community concepts, for example more cohesive and extensive social networks may enhance individual self-esteem and reduce postcode stigma, so increasing people’s mental health and their capacity to engage in other spheres of life, including the labour market, education, etc.
In particular, we were mindful that, within NDC local programmes, CE could also be operating at different levels. In this respect, CE type D approaches, which tended to engage communities around institutional agendas, might be expected to have more limited and narrower effects, for example on the quality of public services. In contrast, NDC approaches that sought to enable community control to develop at multiple levels within wider systems were arguably more likely to achieve positive impacts on a broad range of outcomes including psychosocial outcomes, public service quality, social cohesion/networks and material circumstances, and ultimately on population health and health inequalities.
The development of the typology also took into account evidence on contextual factors that may negatively impinge on these theorised pathways from CE to positive social and health outcomes. In the context of disadvantaged neighbourhoods, for example, stigma may lead to disengagement from ‘identity’-based collective action, undermining solidarity and social support. 84 Building a sense of belonging within neighbourhoods may serve to strengthen networks and sources of local support, but on the other hand engagement that promotes exclusivity and homogeneity could conceivably exacerbate or maintain social divides in neighbourhoods. 85
Using findings from analyses of documentary sources and qualitative interview transcripts together with valuable input from our public advisers we developed a typology of NDC approaches to CE that reflects these theoretical understandings of empowerment and the contextual factors that either support or undermine empowerment processes. It seeks to differentiate between strategic goals, underlying values, structures, processes and relationships (between residents and between residents and local agencies) that together had more or less potential to enhance and sustain residents’ control/influence over the local NDC programmes. Including a temporal dimension to our typology was practically challenging and we were also reliant on reported experiences of engagement rather than having the opportunity to see it being ‘enacted’ in real time (e.g. through non-participant observation). Notwithstanding this, understanding and tracking change proved critical in enabling us to characterise the longevity of CE values within local programmes and the extent to which changes in the values and practice of engagement were influenced by programme, political and economic factors.
The final typology consists of four different NDC approaches to engagement that sit on a spectrum, rather than representing discrete ‘types’ of CE. At one end of this spectrum we identified an approach to CE that was explicitly committed to empowerment, establishing and sustaining resident control over the design and implementation of actions aimed at improving people’s lives and the area in which they lived (CE type A). NDC areas allocated to CE type A were characterised by more facilitative and stable leadership than other areas and aimed to enable trust to be built between residents and agencies. They also invested more in the ‘participative’ capacity of individuals and the wider community. At the other end of the CE spectrum were NDC areas with a strongly instrumental approach to engagement (CE type D). Here, engagement was encouraged as a means to achieve externally set priorities. Structures and processes for engagement were focused on the immediacy of redevelopment issues, with very little if any emphasis on empowerment.
Type B and type C CE lie between these two extremes, but there is an important difference between them. NDC areas allocated to CE type B started out with a strong commitment to empowerment and resident-led change (i.e. a type A approach) but over time this gave way to a more instrumental approach, partly in response to pressure from central government to deliver ‘quick wins’. In this context it is possible that some residents would have felt let down by the failure of the NDC to deliver on the original ‘promise’ of active engagement. In contrast, type C NDC areas had a more balanced approach from the beginning, aiming for greater empowerment of local residents alongside a more instrumental approach, engaging local people in delivering externally imposed priorities such as those linked to housing redevelopments. NDC areas were therefore allocated to a CE type relative to each other and so there were inevitably overlapping characteristics. In particular, and importantly, although CE type A is argued to have the strongest emphasis on empowerment, NDC areas characterised as having type C and type B approaches to engagement also sought (at least initially) to be resident led and empowering.
We discuss the results of our analyses of the outcomes associated with these different approaches to CE in the following section, but from a methodological perspective we believe that the process of developing the typology and its use in this kind of innovative study design represents a methodological advance that will be informative for future evaluations of natural policy experiments at the community/local area level.
Another methodological advance made by our study was in the use of different data sets to triangulate the results and the construction of different socioeconomic comparators, to compare NDC outcomes with those of groups across the social spectrum. As we have already noted, the interpretation of the findings from our impact analyses using the different data sets was sometimes conflicting and presented conceptual and practical difficulties. These need to be taken into account in the planning of future evaluations using this kind of triangulation but these differing results also serve to illuminate the complexity of the likely impact of complex social interventions such as the NDC. Our previous study of health and social outcomes associated with different types of local NDC programme illustrated the value of constructing socioeconomic comparators from across the social spectrum. Comparing the performance of the NDC areas with the performance of areas with high, medium and low levels of deprivation provided evidence of a NDC ‘effect’ on the social determinants of health inequalities. Although we found no evidence in the current study that this positive performance of the NDC was explained by the approaches to CE, this methodological innovation in the construction of comparators could have value in similar evaluations of complex area-based interventions.
Finally, although the results of our economic evaluation were disappointing, the methods used in an attempt to measure and value the indirect costs of CE provide some useful insights and lessons for future work in this neglected area of research.
Insights into the impact of community engagement on health inequalities and their social determinants
Our study has provided no firm evidence that any one approach to CE was more successful than the others in engaging more or different social groups, or that the different approaches to CE had differential impacts on health inequalities or their social determinants. However, notwithstanding the lack of firm evidence, the pattern of impacts that has emerged from our research is consistent with the ‘theory of change’ underpinning our CE typology. For example, residents in NDC areas adopting a type A approach to CE and to a lesser extent those with type B and type C approaches were slightly more likely to participate in NDC events or to have any role within the NDC. There was also a tendency for areas with type A and type B approaches to CE to have better outcomes in relation to participation, trust, control/influence, social cohesion and mental health than areas with the strongly instrumental type D approaches to CE. Some aspects of cohesion and trust improved in type D areas relative to areas with other CE approaches but type D areas were the only ones in which residents’ ‘sense of control’ deteriorated over time. Residents of type D areas were also less likely to feel that the NDC programme had improved their area and were less likely to experience improvements in mental health, particularly compared with type A areas.
It is plausible that the engagement processes put in place in areas with a type A approach to CE would help build trust and greater cohesion within these communities, as these NDC initiatives reached out to different groups in the areas and brought them together. It is also plausible that greater interaction with, and influence over, the NDC initiative (as was particularly the case in areas with type A and type C approaches to CE) would lead to an increase in the number of residents linking the NDC initiative to perceived improvements in their area. The data on expenditure on community development (which was significantly higher in areas adopting type A and type B approaches to CE than in areas adopting type C and type D approaches to CE) and the qualitative findings support these speculations.
In answer to our fourth and fifth research questions, we found no consistent evidence that the type of CE approach had differential impacts on different socioeconomic groups in the population, neither did it help to explain the better performance of the type 2 NDC programmes, identified in our previous study. Similarly, the findings of our economic analyses were inconclusive. There are almost as many negative as positive scores in the effectiveness results, making the calculation of cost-effectiveness a rather arbitrary exercise.
There are several plausible reasons why we failed to find a significant effect of CE approach, beyond the possibility that CE has no impact in the NDC initiative. The first is the small numbers in some of the subgroup analyses. Second, the types in our typology may not differentiate sufficiently well between CE approaches – type A, for example, may have only appeared to be taking a more empowerment approach, while actually taking a more mixed approach more akin to the type B and type C approaches. Third, it is possible that none of the NDC areas achieved the depth of CE that would make an impact on the outcomes that we were measuring. Fourth, the official control areas selected by the NET were less than perfectly matched (most were more advantaged than their NDC counterpart); they had much smaller sample sizes in the MORI survey; and there may have been other regeneration initiatives involving CE taking place in control areas, even if they were not involved with the NDC initiative. Fifth, there may have been strong countervailing forces in operation over the period of the NDC initiative, in light of which even stopping outcomes from deteriorating may be seen as an achievement, rather than the more ambitious aim of bringing about improved outcomes on the factors that we measured. The statistical analyses of the routine and survey data sets cannot answer questions of why and how certain outcomes did or did not occur, but our qualitative studies did help to shed light on these questions.
Insights about the implementation of the New Deal for Communities and other area-based initiatives
Our qualitative interviews with residents and practitioners involved in the roll-out of the NDC initiative revealed processes that helped or hindered the implementation of the NDC initiative, and influenced the CE approach adopted and whether or not it could be sustained over time. In this section we suggest some lessons for the setting up and design of community-based interventions based on our findings.
An important source of tension within the programme was linked to power dynamics at a local level, particularly between agencies and residents. Conflict between local actors is not necessarily negative as within areas with type A approaches to CE it could be an indicator of resident influence developing within decision-making structures. However, in areas with type D (instrumental) approaches it was more likely to result from a lack of clarity or disagreement about the degree of influence that residents held or should have with regard to strategic decisions. This issue is not unique to the NDC programme as attention to power dynamics is too frequently neglected in initiatives aimed at engagement/empowerment. 86
A critical tipping point for NDC approaches to CE appeared to have occurred during the early years of the programme when local partnerships were potentially at their most fragile. Ultimately, the pressure to deliver ‘early wins’ and the initiative’s top-down performance system spawned a disempowering environment at odds with a more gradual development process needed for true empowerment to evolve. 57 Our research suggests that those NDC local programmes that retained their commitment to a resident-led approach over time were able to draw on organisational ‘resources’ that protected or enabled this ethos (e.g. positive working relationships between staff and residents, stability in staff teams and strong leadership committed to empowerment values) or, in the words of one of our fieldwork participants (see Chapter 7), managed to ‘hold their nerve’ in the face of pressures to spend quickly to show results. Towards the end, few NDC partnerships appeared to have formalised plans for sustaining engagement after the programme ended although, again, it is unclear how far this was affected by the economic situation. There were, however, examples of residents coming under immense personal and financial pressures by the end of the programme, with one council even taking away the assets of the local community organisation because the funding for the NDC initiative had ended.
In NDC areas with type 1 local programmes, which prioritised major physical regeneration, including widespread demolition, and which often pursued more instrumental CE goals, the demands placed on staff to manage relations with residents during processes of planning, rehousing or redevelopment could overwhelm ‘community-building’ activities that they may have aspired to. Paradoxically, this radical physical transformation may have served to undermine the social cohesion and trust that it was intended to help build, when ‘new’ and ‘old’ communities failed to engage or when housing plans stalled mid-programme because of the economic downturn.
Finally, it is important to emphasise that our qualitative findings are based on the experiences of residents who engaged with the local NDC programme. Although some respondents reported on NDC programmes’ efforts to be inclusive and reach the wider community, engagement in NDC programmes was ultimately characterised by small numbers. In this regard, initiatives such as the NDC may potentially exacerbate inequalities if groups who experience the most powerlessness are not supported to participate equally or meaningfully,57,87 or if non-participation is misunderstood by proferssionals as stemming from a ‘lack of capacity’ rather than community members enacting non-participation as a ‘rational reaction based on their socio-cultural context (p. 600). 88
Insights from public involvement in this community engagement research
Public involvement in public health research is relatively underdeveloped compared with public involvement in health services research. In this context our experience of engaging both residents of NDC areas (some of whom were active on NDC partnerships) and workers involved in NDC programmes in this research is a useful exemplar of the value of such involvement. These ‘experts by experience’ were active members of our national advisory group and provided support in a range of other ways including advising on accessing fieldwork sites and research participants, proofreading information sheets, testing our research tools before we embarked on fieldwork, taking part in research as participants and contributing to the interpretation of findings.
These forms of public engagement have proven to be an integral component of the success of the research. First, local NDC programmes had already come to the end of their official funding when the evaluation began, with many staff moving into new posts and with community organisations experiencing significant funding pressures. With no obvious route into NDC areas, we drew on the ‘local knowledge’ of our public advisers to track down residents and professionals responsible for delivering regeneration strategies. Second, the experiential knowledge that these advisers have brought to the research has also been important in helping us to interpret our findings. One of the most powerful examples of engagement was a workshop in May 2013 at which preliminary results were discussed with five public advisers. Their experiences helped to place our ‘research in context’, providing important information about the political/economic environments within which regeneration partnerships designed and delivered their programmes.
There were invariably limitations to this form of public involvement. Our advisers tended to be long-serving community activists. Although their expertise is of real benefit, the risk is that the views of those less likely to get involved are not accessed. Second, engagement was led on a day-to-day basis by researchers working on fixed-term contracts as part of a time-limited project, making it more challenging to sustain public involvement over the longer term. University systems unfamiliar with public involvement in research could hinder rather than support involvement when, on occasions, the expenses of members of the public were not promptly reimbursed or highly bureaucratic processes made it impossible to pay fees in a way that was acceptable to some public advisers.
Finally, as readers of this report will have appreciated, this research has involved the use of highly specialised statistical procedures. This has made it more difficult (although not impossible) to engage public advisers in the interpretation and technical writing up of the findings. As a result, this report is perhaps not as readable as it could have been. Looking ahead, our advisers will be invited to be involved in developing a lay version of this technical report and in helping us to shape the dissemination of our research findings. Through our qualitative fieldwork we have built up a new wider network of interested local professionals and residents to support the impact of the research on public health practice and policy. Lastly, as researchers we have had privileged access to the detailed accounts of nearly 50 residents and workers about their own experiences of regeneration and CE in one of the UK’s largest regeneration programmes. We wish to archive these transcribed interviews for future use and will be seeking additional funding for the archiving or for future use.
Research implications
Our research represents a serious attempt to advance theoretical and methodological thinking on how complex social interventions involving CE can best be conceptualised and evaluated for their health and health inequalities impact. This included innovative use of secondary data sources in order to distinguishing different types of CE and different ways in which interventions are operationalised in different contexts. We have also tested ways of constructing comparators from across the social spectrum and explored ways of costing in-kind contributions to engagement. This work now needs to be taken forward and refined.
The relative lack of statistically significant results at a population level is not unusual in this field. For example, two recent reviews89,90 of diverse ‘CE’ interventions found that, although trends in quantitative evidence suggested that different approaches could have different impacts, the lack of statistically significant results made it impossible to conclude that a particular approach was more ‘effective’ than another. This points to the need for research to explore the sources – theoretical, conceptual and methodological – of this ubiquitous uncertainty in evaluations of CE interventions in the public health field. It also points to the need for evaluative research to be more tightly focused on the effectiveness of engagement, running concurrently with engagement processes (i.e. factored into the programme from the beginning), and to the need for methodological research on measures of community control and influence and on the economics of CE.
Our research also points to the importance of designing evaluations of CE interventions that are able to enhance understanding of the shaping influence of context and implementation processes. We have argued that the patterns of impacts that we have identified, relating in particular to community cohesion, control/influence and mental health, are consistent with theoretical understandings of the potential positive impacts of empowerment approaches to community engagement. In particular, the divergent patterns we have identified associated with a type A empowerment approach and a type D instrumental approach fit with a theoretical position which posits that if people are engaged only around the system's agenda rather than their own,86 community engagement approaches will have relatively little positive impact and may actually undermine some dimensions of social cohesion and well-being.
We have shown that a majority of the 39 NDC areas began with a commitment to empowerment and a resident-led model of change but that over time many were diverted to a more instrumental approach. In research on other regeneration initiatives, Lawson and Kearns91 have highlighted how empowerment has been used as a label that has ‘enabled other stakeholders to legitimate what they wanted to do in furthering more important objectives’ (p. 78). Head61 similarly concludes that engagement has rarely demonstrated increased power sharing with communities. This issue is highly relevant to the NDC initiative. Other researchers evaluating the NDC have argued that the initiative was ‘a tightly controlled policy space (p. 358)51 that had negative impacts on engagement processes, as our qualitative research confirms. Interestingly, a recent realist review of the evidence on CE initiatives involving lay health workers similarly found that contexts in which professionals and/or agencies maintain control limited the ability of lay health workers to deliver culturally tailored support. 92
Our study has not provided firm evidence of the effectiveness of empowerment models of engagement, but it does suggest the need for more careful application of theory to public health interventions that aim to utilise CE as a vehicle to deliver external objectives. As Hart and colleagues93 argue, instrumental engagement may even result in an amplification of disempowerment. In this context it is important to illuminate the processes underpinning both empowerment and instrumental approaches to engagement and their impacts. To do so requires greater theoretical sophistication in the development and evaluation of CE interventions.
Summary of recommendations for further research
The earlier section on new insights from the study highlights the new knowledge that this project has generated on the impact of CE on health inequalities and their social determinants. It has also provided pointers for the future design and implementation of area-based initiatives concerned with empowering communities and their evaluation. The research was hampered, however, by having to rely on secondary data that had been collected for a different purpose and which therefore lacked some of the necessary information for a more robust evaluation. Further research is urgently needed that builds on our insights from this work on the challenges of evaluation and what is needed to overcome them.
-
There is a need for evaluations of CE interventions that test intermediate links in a theory-based logic model, to measure, in particular, whether the interventions actually achieved their objective of an increase in community empowerment or whether they resulted in disempowering hard-pressed communities still further. Too many evaluations in the past have assumed that empowerment has been achieved and have gone straight to the measurement of outcomes. Such evaluations, however, without the measurement of what empowerment, if any, has been achieved, do not provide a true test of the impact of community empowerment on health-related outcomes and may be one reason why evaluative research on CE in health-related decision-making has failed to provide definitive answers on impacts.
-
Determining whether or not community empowerment has been achieved by the interventions under study requires the development of better measures of community empowerment/control and influence, and ways of measuring the costs and benefits of CE to enable economic evaluation. The measures available in the secondary data that were available to us were relatively crude and underdeveloped, and revealed an obvious research gap that needs to be filled.
-
The results of evaluations of what helps or hinders the process of CE need to be fed into the design and development of future initiatives/interventions aiming to develop and support CE in decision-making in the health field.
-
Future evaluations of CE interventions need to combine explorations of the social and health (equity) impacts with process evaluations. These process evaluations should seek to identify the shaping influence of the wider local and national context in which CE initiatives are developed and implemented. Measures of context in community settings are starting to be developed and need testing and refinement.
-
Our study was able to consider the impacts of health and social outcomes over a relatively short time period and, as we have already noted, this endeavour was limited by our reliance on secondary data sources. Future evaluations need to be designed to track the health, social and economic outcomes for residents of area-based interventions such as the NDC over a longer time period. It is crucial that residents are tracked even if they leave the area, as some of those who have the most positive outcomes may be the ones who move away from the area, precisely because the intervention has improved their socioeconomic circumstances. Too often in area-based evaluations, even if there is a longitudinal element, participants are lost to follow-up if they move out of the study area. We experienced this loss to follow-up in the MORI longitudinal data set and it also meant that numbers in the study were reduced, affecting statistical power. Studies with a strengthened longitudinal design would be able to deal much better with residential mobility bias and address some of the pressing questions in this complex evaluation field.
Acknowledgements
We would like to thank all members of the New Deal for Communities National Evaluation Team at the Centre for Regional Economic and Social Research (CRESR), Sheffield Hallam University. Particular thanks go to Paul Lawless and Tina Beatty for their ongoing advice and for facilitating access to the wealth of data collected and reports produced during the national evaluation. Without this support this study would not have been feasible. We would also like to thank Paul for his continued role as chair of our national advisory group.
Our national advisory group includes independent academic advisers (Mark Petticrew, Ken Judge, Jayne Parry and Nikos Tzavidis), a policy-maker (Martin Gibbs), and residents (Margaret O’Mara MBE, Gerry Stone and Ann-Marie Pickup MBE) and former staff (Bernadette Elder, Tony Boyle, Liz Kessler and Sam Tarff) from NDC areas. The group has provided invaluable guidance and feedback on the study’s design and findings and we are grateful for members’ time and commitment.
Many thanks are also due to Christine McGuire and Jason Cox from the Policy Research Programme at the Department of Health (who also contributed to our advisory group) and staff at the NIHR Evaluation, Trials and Studies Coordinating Centre (NETSCC) for their ongoing support throughout the study.
The study’s public advisers include NDC residents and staff: Liz Kessler, Anne-Marie Pickup, Bernadette Elder, Margaret O’Mara, Gerry Stone and Sam Tarff. Their detailed knowledge of the local NDC programmes has been particularly crucial in enabling our local fieldwork to take place, particularly at a time when the funding for NDC programmes was ending. In addition, we would like to thank those residents of NDC areas and people who worked for the NDC initiative for giving so generously of their time in face-to-face and/or telephone interviews.
This is an independent report of research commissioned and funded by the NIHR Public Health Research programme (reference no. 09/3008/07). The views expressed are those of the authors and not necessarily those of the Department of Health.
Contribution of authors
Jennie Popay (Professor, Sociology and Public Health) was the project’s lead investigator, jointly led the typology development in work package 1, contributed to all work packages and led the writing up of the results.
Margaret Whitehead (Professor, Public Health) was the joint lead for the typology development in work package 1, led the updating of the administrative data sets and contributed to all work packages and the writing up of the results.
Roy Carr-Hill (Independent Consultant, Economics) led the cost-effectiveness work and contributed to the impact analyses and to the writing up of the results.
Chris Dibben (Professor, Health Geography) provided advice on the NDC administrative database resource and contributed to its updating and the impact analyses.
Paul Dixon (Statistician, Independent Consultant) undertook updating of the administrative data sets and impact analyses based on these and writing up of results.
Emma Halliday (Senior Research Fellow, Public Health) undertook typology development and contributed to the conduct/analysis of fieldwork and the writing up of the results.
James Nazroo (Professor, Medicine and Sociology) co-supervised the impact analyses and contributed to the writing up of the results.
Edwina Peart (Independent Consultant, Economics) contributed to the economic evaluation including data collection and analyses, and the writing up of the results of the cost-effectiveness analyses.
Sue Povall (Senior Researcher, Public Health) undertook typology development and contributed to the conduct/analysis of fieldwork and the writing up of the results.
Mai Stafford (Reader, Social Epidemiology) co-supervised the impact analyses and contributed to the writing up of the results.
Jill Turner (Research Associate, Public Health) undertook typology development and contributed to the conduct/analysis of fieldwork and the writing up of the results.
Pierre Walthery (Research Fellow, Applied Social Statistics/Sociology) undertook the impact analyses and contributed to the writing up of the results.
Data sharing statement
The NDC secondary quantitative data used in the study are available from http://extra.shu.ac.uk/ndc/ndc_data.htm and detailed information on the approach to data analysis we used is obtained from http://dx.doi.org/10.17635/lancaster/researchdata/27. Further information about this and about our qualitative data, which is not being archived, can be obtained from Professor Jennie Popay (j.popay@lancaster.ac.uk).
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health.
References
- Popay J, Dibben C, Halliday E, Nazroo J, Povall S, Stafford M, et al. Evaluating the impact of New Deal for Communities on Health Inequalities: Phase 2. No. PR-IP-0509–0180063. London: HMSO; 2015.
- Dahlgren G, Whitehead M, Dahlgren G, Whitehead M. European Strategies for Tackling Social Inequities in Health: Levelling Up Part 2. Copenhagen: WHO Regional Office for Europe; 2007.
- Health Inequalities. Third Report of Session 2008–9. Volume 1. London: The Stationery Office; 2009.
- Marmot M, Friel S, Bell R, Houweling TAJ, Taylor S. Commission on Social Determinants of Health . Closing the gap in a generation: health equity through action on the social determinants of health. Lancet 2008;372:1661-9. http://dx.doi.org/10.1016/S0140-6736(08)61690-6.
- Popay J, Whitehead M, Hunter D. Injustice is killing people on a large scale – but what is to be done about it?. J Public Health 2010;32:148-9. http://dx.doi.org/10.1093/pubmed/fdq029.
- Phelan JC, Link BG, Tehranifar P. Social conditions as fundamental causes of health inequalities: theory, evidence, and policy implications. J Health Soc Behav 2010;51:S28-40. http://dx.doi.org/10.1177/0022146510383498.
- White M, Adams J, Heywood P, Babones S. Social Inequality and Public Health. Bristol: Policy Press; 2009.
- Graham H, Britain G. When Life’s a Drag: Women, Smoking and Disadvantage. Norwich: Her Majesty’s Stationery Office; 1993.
- Marmot M, Allen J, Goldblatt P, Boyce T, McNeish D, Grady M, et al. Fair Society, Healthy Lives: Strategic Review of Health Inequalities in England Post-2010. London: The Marmot Review; 2010.
- Bartley M, Blane D, Scambler G. Sociology as Applied to Medicine. Saunder: Elsvier; 2003.
- Popay J, Morgan A, Davies M, Ziglio E. Health Assets in a Global Context Theory, Methods, Action. New York, NY: Springer; 2010.
- Popay J, Finegan H. Learning about Effective Community Engagement from Selected National Initiatives. London: National Institute for Health and Care Excellence; 2005.
- Karasek RA. Job demands, job decision latitude, and mental strain: implications for job redesign. Admin Sci Q 1979;24:285-308. http://dx.doi.org/10.2307/2392498.
- Siegrist J. Adverse health effects of high-effort/low-reward conditions. J Occup Health Psychol 1996;1:27-41. http://dx.doi.org/10.1037/1076-8998.1.1.27.
- Jetten J, Haslam C, Haslam AS, Alexander SH. The Social Cure: Identity, Health and Well-Being. Hove: Psychology Press; 2012.
- Carr-Hill R, Street A. Economic analysis of cost-effectiveness of community engagement to improve health. York: Centre for Health Economics, University of York; 2007.
- Mason AR, Carr-Hill R, Myers LA, Street AD. Establishing the economics of engaging communities in health promotion: what is desirable, what is feasible?. Crit Pub Health 2008;18:285-97. http://dx.doi.org/10.1080/09581590802277366.
- Popay J, Attree P, Hornby D, Milton B, Whitehead M, French B, et al. Community Engagement to Address the Wider Social Determinants of Health: a Review of Evidence. London: National Institute for Health and Care Excellence; 2007.
- Narayan D. Empowerment and Poverty Reduction: A Sourcebook. Washington, DC: World Bank; 2002.
- Cairncross L, Morrell C, Darke J, Brownhill S. Tenants Managing – An Evaluation of Tenant Management Organisations in England. London: Office of the Deputy Prime Minister; 2002.
- Findlay E. Review of the Impact of Community Engagement within Regeneration. Edinburgh: Social Research, Scottish Government; 2010.
- Pratchett L, Durose C, Lowndes V, Smith G, Stoker G, Wales C. Empowering Communities to Influence Local Decision Making: Systematic Review of the Evidence. London: Department for Communities and Local Government; 2009.
- Chandler M, Lalonde E, Kirmayer L, Valaskakis G. The Mental Health of Canadian Aboriginal Peoples: Transformations, Identity, and Community. Vancouver, BC: University of British Columbia Press; 2009.
- Chandler MJ, Lalonde C. Cultural continuity as a hedge against suicide in Canada’s First Nations. Transcult Psychiatry 1998;35:191-219. http://dx.doi.org/10.1177/136346159803500202.
- Coote A, Angel J. NEF working paper. Solidarity: Why it Matters for a New Social Settlement. London: New Economics Foundation; 2014.
- Popay J, Bennett S, Thomas C, Williams G, Gatrell A, Bostock L. Beyond ‘beer, fags, egg and chips’? Exploring lay understandings of social inequalities in health. Sociol Health Illn 2003;25:1-23. http://dx.doi.org/10.1111/1467-9566.t01-1-00322.
- Elliot E, Popay J, Williams G, Smith K, Bambra C, Hill S. Health Inequalities: Critical Perspectives. Oxford: Oxford University Press; 2015.
- Pickin C, Popay J, Staley K, Bruce N, Jones C, Gowman N. Developing a model to enhance the capacity of statutory organisations to engage with lay communities. J Health Serv Res Policy 2002;7:34-42. http://dx.doi.org/10.1258/1355819021927656.
- The Evaluation of the Big Lottery Fund Healthy Living Centres. Third Annual Report of the Bridge Consortium. London: Big Lottery Fund; 2005.
- Barnes M, Newman J, Sullivan H. Discursive arenas: deliberation and the constitution of identity in public participation at a local level. Soc Mov Stud 2006;5:193-207. http://dx.doi.org/10.1080/14742830600991487.
- Barnes M, Sullivan H, Matka E. The Development of Collaborative Capacity in Health Action Zones. A Final Report from the National Evaluation. Birmingham: University of Birmingham; 2003.
- Myers P, Barnes J, Brodie I. Sure Start National Evaluation. Partnership Working in Sure Start Local Programmes. A Synthesis of Early Findings from Local Programme Evaluations. London: Birkbeck University of London; 2004.
- Woods SE, Lake JR, Springett J. Tackling health inequalities and the HAZ Smoking Cessation Programme: the perfect match?. Crit Pub Health 2003;13:61-76. http://dx.doi.org/10.1080/0958159031000100233.
- Sullivan H, Judge K, Sewel K. ‘In the eye of the beholder’: perceptions of local impact in English Health Action Zones. Soc Sci Med 2004;59:1603-12. http://dx.doi.org/10.1016/j.socscimed.2004.02.013.
- Crawshaw P, Bunton R, Gillen K. Health Action Zones and the problem of community. Health Soc Care Community 2003;11:36-44. http://dx.doi.org/10.1046/j.1365-2524.2003.00397.x.
- New Deal for Communities: The National Evaluation. The Programme Wide Annual Report 2003/04. Sheffield: Centre for Regional Economic and Social Research, Sheffield Hallam University; 2004.
- Cropper S, Goodwin M, Cropper S, Porter A, Williams G, Carlisle S, et al. Community Health and Wellbeing: Action Research on Health, Inequalities. Bristol: Polity Press; 2007.
- Ball M. Sure Start National Evaluation. Getting Sure Start Started. Nottingham: Department for Education and Science Publications; 2002.
- Community Engagement to Improve Health. London: NICE; 2008.
- Chen H. Theory-Driven Evaluations. Newbury Park, CA: Sage; 1990.
- Pawson R, Tilley N. Realistic Evaluation. London: Sage; 1997.
- Weiss CH, Rog D, Fournier D. Progress and Future Directions In Evaluation: Perspectives on Theory, Practice and Methods. San Jose, CA: Jossey-Bass; 1997.
- Wholey JS. Evaluation and Effective Public Management. Boston, MA: Little, Brown; 1983.
- Weiss CH. Nothing as Practical as Good Theory: Exploring Theory-Based Evaluation for Comprehensive Community Initiatives for Children and Families. New Approaches to Evaluating Community Initiatives: Concepts, Methods, and Contexts. Washington, DC: Aspen Institute; 1995.
- Goodman R, Wandersman A, Chinman M, Imm P, Morrissey E. An ecological assessment of community-based interventions for prevention and health promotion: approaches to measuring community coalitions. Am J Community Psychol 1996;24:33-61. http://dx.doi.org/10.1007/BF02511882.
- Bauld L, Judge K. Learning from Health Action Zones. Chichester: Aeneas Press; 2002.
- Whitehead M. A typology of actions to tackle social inequalities in health. J Epidemiol Community Health 2007;61:473-8. http://dx.doi.org/10.1136/jech.2005.037242.
- Bringing Britain Together: A National Strategy for Neighbourhood Renewal. London: The Stationery Office; 1998.
- Barnes M, Newman J, Sullivan H. Power, participation, and political renewal: theoretical perspectives on public participation under New Labour in Britain. Soc Polit 2004;11:267-79. http://dx.doi.org/10.1093/sp/jxh034.
- Wallace A. New neighbourhoods, new citizens? Challenging ‘community’ as a framework for social and moral regeneration under New Labour in the UK. Int J Urban Reg Res 2010;34:805-19. http://dx.doi.org/10.1111/j.1468-2427.2009.00918.x.
- Wright JS, Parry J, Mathers J, Jones S, Orford J. Assessing the participatory potential of Britain’s New Deal for Communities: opportunities for and constraints to ‘bottom-up community participation’. Policy Stud 2006;27:347-61. http://dx.doi.org/10.1080/01442870601010051.
- Lawless P, Pearson S. Outcomes from community engagement in urban regeneration: evidence from England’s New Deal for Communities programme. Plann Theory Pract 2012;13:509-27. http://dx.doi.org/10.1080/14649357.2012.728003.
- Batty E, Beatty C, Foden M, Lawless P, Pearson S, Wilson I. Involving Local People in Regeneration: Evidence from the NDC Programme. The New Deal for Communities National Evaluation: Final Report – Volume 2. Centre for Regional Economic and Social Research, Sheffield Hallam University. London: Department for Communities and Local Government; 2010.
- Lawless P. Can area-based regeneration programmes ever work? Evidence from England’s New Deal for Communities programme. Policy Stud 2012;33:313-28. http://dx.doi.org/10.1080/01442872.2012.694639.
- Payment for Involvement: A Guide for Making Payments to Members of the Public Actively Involved in NHS, Public Health and Social Care Research. Eastleigh: NIHR INVOLVE; 2010.
- Russell H. Community Engagement: Some Lessons from the New Deal for Communities Programme. London: Department for Communities and Local Government; 2008.
- Laverack G, Labonte R. A planning framework for community empowerment goals within health promotion. Health Policy Plann 2000;15:255-62. http://dx.doi.org/10.1093/heapol/15.3.255.
- Pérez D, Lefèvre P, Romero MI, Sánchez L, De Vos P, Van der Stuyft P. Augmenting frameworks for appraising the practices of community-based health interventions. Health Policy Plann 2009;24:335-41. http://dx.doi.org/10.1093/heapol/czp028.
- Draper AK, Hewitt G, Rifkin S. Chasing the dragon: developing indicators for the assessment of community participation in health programmes. Soc Sci Med 2010;71:1102-9. http://dx.doi.org/10.1016/j.socscimed.2010.05.016.
- Laverack G, Wallerstein N. Measuring community empowerment: a fresh look at organizational domains. Health Promot Int 2001;16:179-85. http://dx.doi.org/10.1093/heapro/16.2.179.
- Head BW. Community engagement: participation on whose terms?. Aust J Polit Sci 2007;42:441-54. http://dx.doi.org/10.1080/10361140701513570.
- Arnstein SR. A ladder of citizen participation. J Am Inst Planners 1969;35:216-24. http://dx.doi.org/10.1080/01944366908977225.
- Preston R, Waugh H, Larkins S, Taylor J. Community participation in rural primary health care: intervention or approach?. Aust J Prim Health 2010;16:4-16. http://dx.doi.org/10.1071/PY09053.
- Fordham G. The New Deal for Communities Programme: Achieving a Neighbourhood Focus for Regeneration. The New Deal For Communities National Evaluation: Final Report – Volume 1. London: Department for Communities and Local Government; 2010.
- Batty E, Beatty C, Foden M, Lawless P, Pearson S, Wilson E. Improving Outcomes For People In Deprived Neighbourhoods: Evidence From The New Deal For Communities Programme The New Deal For Communities National Evaluation: Final Report – Volume 4. London: Department for Communities and Local Government; 2010.
- Gambetta D, Gambetta D. Trust: Making And Breaking Cooperative Relations. New York, NY: Blackwell; 1988.
- Rogers B, Robinson E. The Benefits of Community Engagement. A Review of the Evidence. London: Active Citizenship Centre, Home Office; 2004.
- Stafford M, Nazroo J, Popay JM, Whitehead M. Tackling inequalities in health: evaluating the New Deal for Communities initiative. J Epidemiol Community Health 2008;62:298-304. http://dx.doi.org/10.1136/jech.2006.058628.
- Batty E, Beatty C, Foden M, Lawless P, Pearson S, Wilson I. The New Deal for Communities Experience: a Final Assessment. The New Deal for Communities Evaluation: Final Report – Volume 7. London: Department for Communities and Local Government; 2010.
- Pearson S, Batty E, Cook B, Foden M, Knight-Fordham R, Peters J. Improving Health Outcomes in Deprived Communities: Evidence from the New Deal for Communities Programme. London: Department for Communities and Local Government; 2010.
- Lawless P, Foden M, Wilson I, Beatty C. Understanding area-based regeneration: the New Deal for Communities programme in England. Urban Stud 2010;47:257-75. http://dx.doi.org/10.1177/0042098009348324.
- Lawless P, Beatty C. Exploring change in local regeneration areas: evidence from the New Deal for Communities programme in England. Urban Stud 2013;50:942-58. http://dx.doi.org/10.1177/0042098012458005.
- Riva M, Curtis SE. Long-term local area employment rates as predictors of individual mortality and morbidity: a prospective study in England, spanning more than two decades. J Epidemiol Community Health 2012;66:919-26. http://dx.doi.org/10.1136/jech-2011-200306.
- General Household Survey. London: ONS; 2001.
- Public Affairs Monitor. London: IPSOS Mori; 2009.
- Okun AM. Equality and Efficiency, The Big Tradeoff. Washington, DC: Brookings Institution Press; 1975.
- Goulbourne M, Embuldeniya D. Assigning Economic Value to Volunteer Activity: Eight Tools for Efficient Program Management. Toronto, CA: Canadian Centre for Philanthropy; 2002.
- Gaskin K. VIVA – the Volunteer Investment and Value Audit. Toronto: Institute for Volunteer Research; 2003.
- Assessing the Impact of Spatial Interventions. Regeneration, Renewal and Regional Development. ‘The 3Rs guidance’. London: ODPM; 2004.
- Gaskin K, Dobson B. The Economic Equation of Volunteering. York: Joseph Rowntree Foundation; 1997.
- Handy F, Srinivasan N. Valuing volunteers: an economic evaluation of the net benefits of hospital volunteers. Nonprof Volunt Sect Q 2004;33:28-54. http://dx.doi.org/10.1177/0899764003260961.
- Beatty C, Brennan A, Foden MI, Lawless P, Tyler P, . The News Deal for Communities Programme: Assessing Impact and Value for Money. The New Deal for Communities National Evaluation: Final Report – Volume 6. London: Department for Communities and Local Government; 2010.
- Foden M, Pearson S. The 2008 Partnership Survey. Evidence from the New Deal for Communities Programme. London: Department for Communities and Local Government; 2009.
- McNamara N, Stevenson C, Muldoon OT. Community identity as resource and context: a mixed method investigation of coping and collective action in a disadvantaged community. Eur J Soc Psychol 2013;43:393-40. http://dx.doi.org/10.1002/ejsp.1953.
- Hawe P, Shiell A. Social capital and health promotion: a review. Soc Sci Med 2000;51:871-85. http://dx.doi.org/10.1016/S0277-9536(00)00067-8.
- Wallerstein N. Empowerment to reduce health disparities. Scand J Public Health 2002;30:72-7. http://dx.doi.org/10.1177/14034948020300031201.
- Kilpatrick S. Multi-level rural community engagement in health. Aust J Rural Health 2009;17:39-44. http://dx.doi.org/10.1111/j.1440-1584.2008.01035.x.
- Mathers J, Parry J, Jones S. Exploring resident (non-)participation in the UK New Deal for Communities regeneration programme. Urban Stud 2008;45:591-606. http://dx.doi.org/10.1177/0042098007087336.
- Whitehead M, Orton L, Pennington A, Nayak S, King A, Petticrew M, et al. Is Control in the Living Environment Important for Health and Wellbeing, and What are the Implications for Public Health Interventions? Final Report to DH. London: Public Health Research Consortium; 2014.
- O’Mara-Eves A, Brunton G, McDaid D, Oliver S, Kavanagh J, Jamal F. Community engagement to reduce inequalities in health: a systematic review, meta-analysis and economic analysis. Public Health Res 2013;1.
- Lawson L, Kearns A. Rethinking the purpose of community empowerment in neighbourhood regeneration: the need for policy clarity. Local Econ 2014;29:65-81. http://dx.doi.org/10.1177/0269094213519307.
- Harris J, Springett J, Croot L, Booth A, Campbell F, Thompson J, et al. Community-Based Peer Support: Developing a Model for Promoting Health Literacy. Draft Final Report to the NIHR Public Health Research Programme 2014.
- Hart C, Jones K, Bains M, Hoggett P. Contested Communities: Experiences, Struggles, Policies. Bristol: Policy Press; 1997.
Appendix 1 Evaluating the impact of New Deal for Communities on health inequalities
Jennie Popay, Chris Dibben, Emma Halliday, James Nazroo, Sue Povall, Mai Stafford, Pierre Walthery, Margaret Whitehead with Roy Carr-Hill, Paul Dixon and Hannah Badlands.
For further details contact j.popay@lancaster.ac.uk
This is an independent report of research commissioned and funded by the Policy Research Programme in the Department of Health (Evaluating the impact of New Deal for Communities on Health Inequalities: Phase 2. Reference No: PR-IP-0509-0180063). The views expressed are those of the authors and not necessarily those of the Department of Health.
Background and aims
The research reported here focused on the nature and scale of the NDC regeneration initiative and its distributional impact on inequalities in health and their social determinants. The overall aim of the NDC policy initiative was to bridge the gap between some of the most deprived neighbourhoods in England and the rest of the country in six outcome domains over a 10-year period: crime, the local community, housing and the physical environment, education, health and worklessness. There were 39 NDC areas, each receiving public funds of around £50M (£2B in total) from 1999 to 2011. This report builds on the work produced by the NDC NET to address the following research questions:
-
Is there any evidence that inequalities in health and their social determinants improved in NDC areas to a greater extent than in non-NDC areas of comparable baseline deprivation?
-
Is there any evidence that health and its social determinants have improved in NDC areas to a greater extent than in areas drawn from across the social gradient?
-
Do the impacts of the NDC initiative on health inequalities and their social determinants vary across types of NDC local programmes being implemented in different ‘types’ of areas, and if so what characterises NDC areas and local programmes that have seen the greatest improvements in health inequalities and their determinants?
-
What are the lessons for future initiatives aiming to reduce health inequalities?
Evaluation design and data sources
The evaluation comprised three work strands:
-
Work strand 1 involved the development of measures of the local context in which the NDC programmes were implemented and a typology of local NDC programmes. For this work we used secondary quantitative and qualitative and documentary data collected by the NET, publicly available quantitative data from other sources and new primary data collected from interviews and documents in a sample of NDC areas
-
Work strand 2 evaluated the impact of the NDC initiative as a whole, and different types of local programmes, on health inequalities and their social determinants. This work used data collated by the NET for NDC areas and their ‘matched’ comparator areas, selected from within the same local authority boundary and with broadly the same Index of Multiple Deprivation. These data included repeat cross-sectional and panel data from MORI surveys conducted in 2002, 2004, 2006 and 2008 for the NDC areas and their comparators; area-level time series data on hospital admissions and welfare claimant numbers for NDC areas and their comparators; and data from the HSE household surveys for 2002, 2004, 2006 and 2008 used to identify areas with high, medium and low levels of deprivation.
-
Work strand 3 involved the creation of a data archive making available programming codes and data for other users so that our analyses can be replicated. This legacy will allow longer-term follow-up of the impact of the NDC on health inequalities and their social determinants, as well as comparison of health and social outcomes in NDC and similarly deprived areas. We hope that this material will be hosted as part of the NET’s archive on the Sheffield Hallam University website.
Measuring the local context in which New Deal for Communities programmes were implemented
Although all NDC local programmes had the same purpose (closing the gap in the six outcome domains between the NDC areas and the rest of the country), the form that they took varied significantly as they sought to address local needs in very different contexts. We therefore developed new measures of these contextual factors including current and historical levels of deprivation and employment, and patterns of industry and migration. However, only the deprivation measured had any predictive power, possibly because of constraints in the data that we were able to use to capture historical context.
Developing a typology of local New Deal for Communities programmes
Our typology of local NDC programmes reflects the relative emphasis that they gave to three core dimensions: housing and environment, human capital and CE. Three types of programmes were identified:
-
type 1 – transforming environments: diversifying the social composition of the population through major redevelopment and changing tenure patterns
-
type 2 – incremental: increasing neighbourhood resources and moderate neighbourhood redevelopment
-
type 3 – strengthening people: building residents’ human capital and improving living conditions with little or no redevelopment.
The impact of the New Deal for Communities on the health of the ‘poorest’
Predictably, socioeconomic disadvantage was associated with poorer health in NDC areas, their comparator areas and high and medium deprivation areas derived from the HSE. Hospital admission rates were also much higher than the national average in NDC and comparator areas, particularly for alcohol- and drug-related conditions, and remained so over the 10 years of the programme. Most differences in health and social outcomes between NDC areas and their comparator areas were explained by the relatively more disadvantaged circumstances of populations in the NDC areas. However, there were a few exceptions, with respondents in NDC areas reporting higher levels of life satisfaction in 2002.
Markedly different pictures of changes over time are provided by our analyses of longitudinal and cross-sectional data. The longitudinal data paint a less positive picture, showing no overall trend of improvement on most outcomes in either the NDC areas or the comparator areas, with two exceptions. First, levels of satisfaction with the area actually declined over time between 2002 and 2008 in comparator areas compared with NDC areas. Second, NDC areas experienced a greater reduction in benefit receipt among lone parents than comparator areas, suggesting that the NDC programme may have added value to national programmes supporting lone parents to get back into employment.
In contrast, the cross-sectional analyses using MORI and HSE data found a general trend of improvement between 2002 and 2008 in smoking, mental health, educational attainment and employment rates in areas across the social spectrum. Importantly, levels of reported poor health appeared to decline faster in NDC and comparator areas than in areas with low deprivation and these improvements were greater in NDC areas than in areas with high and medium deprivation in other parts of the country.
There is also some evidence of a NDC ‘effect’ on the social determinants of health inequalities, with the proportion of people in NDC areas with no qualifications falling more steeply than that in the HSE low and high deprivation areas. This more rapid decline was also seen in the NDC comparator areas but these were relatively more advantaged and hence were facing a less severe challenge. Similarly, although the gap between HSE high and low deprivation areas widened on five of the six social determinants of health that we considered, only the gap in smoking widened between NDC areas and HSE low deprivation areas. In other words, the NDC intervention may have helped to prevent a further widening of the gap, or even narrowed it, in some of these outcomes, which is an important achievement.
Finally, our study suggests that the NDC programme may have reduced some inequalities within NDC areas, with the most disadvantaged respondents within NDC areas faring better in terms of positive changes in mental health and life satisfaction than similarly disadvantaged groups in comparator areas.
Do different types of New Deal for Communities programme have different impacts?
This general picture masks some differential impacts of different types of local programmes. Type 1 local programmes (involving major redevelopment) consistently underperformed on most health and social outcomes compared with both type 2 (incremental) and type 3 (strengthening people) local programmes. Overall, type 2 local programmes were most often associated with improvements over time. Compared with type 1 areas, in type 2 areas:
-
social capital and smoking advantages emerged or were maintained between 2002 and 2008
-
respondents had a greater probability of reporting improved mental health over time
-
respondents without work were significantly more likely to find employment over time
-
hospital admission rates fell faster than in comparator areas, particularly for alcohol- and drug-related conditions, which are closely linked to mental health problems
-
the better performance on hospital admission rates was maintained in type 2 programme areas with very different social and economic contexts.
There is also some evidence that type 1 programmes may be associated with increased inequalities. Although less successful at reducing hospital admissions than the other types of local programmes, they appear to have performed better on these indicators in the least deprived areas.
Explaining the patterns that we have found: implications for policy and research
Our findings add to previous research showing that area-based interventions such as the NDC can have positive impacts on the health and social circumstances of residents of disadvantaged neighbourhoods. More importantly, the NDC also reduced the gap between more and less disadvantaged residents of NDC areas, and between NDC residents and those living in less disadvantaged areas of England – albeit that these effects were relatively modest, confined to a small number of health and social outcomes and not always consistent across the multiple outcomes and analytical approaches used. Impacts are most obvious for mental health improvements (a finding reinforced by the reduction in mental health hospital admissions in NDC areas that we also identified), aspects of social cohesion/capital and educational attainment.
The relatively better performance of type 2 local programmes suggests that future area-based interventions designed and delivered to achieve a better balance between redevelopment of the physical environment and investment in releasing the capacity of residents in terms of both human capital and genuine community governance could be better able to impact on a range of health and social outcomes at the same time as reducing inequalities, albeit modestly.
There is also the intriguing suggestion that 6 years into the NDC initiative, a time when political priorities were changing nationally, improvements in outcomes for disadvantaged communities began to slow. This underscores the potential health equity benefits of long-term investment in area regeneration programmes but also highlights the importance of understanding how local programmes are best enabled to weather changes in policy expectations and interests over time.
Our project has developed, and tested, more nuanced research processes, utilising secondary data sources to help tease out why some area-based investments do or do not work and in which contexts. We will be archiving material that will allow other researchers to access the data sets and variables that we have constructed to replicate the methods we have used. The findings emphasise the need for prospective evaluative studies that track both the form and the function of interventions, as well as local context. We were not funded to undertake an economic evaluation of the NDC initiative and with the data available this would not have been possible, highlighting the need for further methodological innovations in this field.
Appendix 2 Tables referred to in body of report
| Outcome | CE type A | CE type B | CE type C | CE type D | Significanceb | ||||
|---|---|---|---|---|---|---|---|---|---|
| % | 95% CI | % | 95% CI | % | 95% CI | % | 95% CI | ||
| Feel part of the local community | 35.0 | 33.7 to 36.3 | 34.9 | 33.5 to 36.3 | 35.8 | 34.2 to 37.5 | 36.9 | 34.7 to 39.2 | |
| Think people in area are friendly | 85.4 | 84.4 to 86.4 | 80.9 | 79.6 to 82.1 | 82.4 | 81.1 to 83.7 | 82.0 | 80.1 to 83.8 | **** |
| Know most/many people in area | 43.7 | 42.3 to 45.1 | 39.2 | 37.7 to 40.6 | 36.6 | 34.9 to 38.2 | 38.0 | 35.8 to 40.3 | **** |
| Think neighbours look out for each other | 67.9 | 66.6 to 69.3 | 63.3 | 61.8 to 64.9 | 60.1 | 58.3 to 61.8 | 64.4 | 62.1 to 66.8 | **** |
| Think they can influence decisions in area | 24.9 | 23.7 to 26.2 | 25.2 | 23.9 to 26.6 | 25.9 | 24.3 to 27.5 | 25.1 | 23.0 to 27.3 | |
| Volunteered locally | 11.5 | 10.7 to 12.5 | 12.5 | 11.5 to 13.5 | 11.6 | 10.5 to 12.7 | 12.1 | 10.7 to 13.7 | |
| Heard of NDC | 72.0 | 70.8 to 73.2 | 64.3 | 62.8 to 65.8 | 59.2 | 57.5 to 60.9 | 50.9 | 48.7 to 53.2 | **** |
| Involved in NDC | 16.3 | 15.2 to 17.6 | 16.5 | 15.2 to 17.8 | 15.6 | 14.1 to 17.2 | 17.0 | 14.8 to 19.5 | |
| NDC improved area | 33.0 | 31.5 to 34.5 | 34.0 | 32.3 to 35.6 | 32.7 | 30.7 to 34.8 | 33.2 | 30.3 to 36.3 | |
| Outcome | CE type A | CE type B | CE type C | CE type D | Significanceb | ||||
|---|---|---|---|---|---|---|---|---|---|
| % | 95% CI | % | 95% CI | % | 95% CI | % | 95% CI | ||
| Feel part of the local community | 43.8 | 42.2 to 45.5 | 43.5 | 41.8 to 45.2 | 47.2 | 45.1 to 49.2 | 48.1 | 45.4 to 50.8 | *** |
| Think people in the area are friendly | 88.3 | 87.2 to 89.3 | 84.7 | 83.3 to 85.9 | 84.9 | 83.3 to 86.3 | 84.6 | 82.6 to 86.4 | **** |
| Know most/many people in area | 44.3 | 42.7 to 45.9 | 40.4 | 38.8 to 42.1 | 42.5 | 40.5 to 44.5 | 44 | 41.3 to 46.7 | ** |
| Think neighbours look out for each other | 71.7 | 70.1 to 73.2 | 67.8 | 66.0 to 69.5 | 63.7 | 61.6 to 65.8 | 66.4 | 63.6 to 69.1 | **** |
| Think they can influence decisions in area | 27.7 | 26.2 to 29.2 | 28.6 | 27.0 to 30.3 | 26.9 | 25.0 to 28.9 | 24.6 | 22.3 to 27.1 | * |
| Volunteered locally | 14.0 | 12.9 to 15.2 | 14.4 | 13.2 to 15.7 | 12.3 | 11.0 to 13.7 | 15.4 | 13.4 to 17.6 | * |
| Heard of NDC | 83.1 | 81.8 to 84.4 | 78.0 | 76.6 to 79.4 | 75.5 | 73.5 to 77.3 | 74.5 | 72.0 to 76.8 | **** |
| Involved in NDC | 21.9 | 20.5 to 23.4 | 23.3 | 21.7 to 25.0 | 20.4 | 18.7 to 22.3 | 21.2 | 18.8 to 23.9 | |
| NDC improved area | 63.3 | 61.6 to 65.0 | 57.1 | 55.2 to 59.0 | 64.1 | 61.9 to 66.3 | 53.1 | 50.0 to 56.3 | **** |
| Sociodemographic group | CE type A | CE type B | CE type C | CE type D | Significanceb | ||||
|---|---|---|---|---|---|---|---|---|---|
| % | 95% CI | % | 95% CI | % | 95% CI | % | 95% CI | ||
| Men | 44.3 | 42.0 to 46.6 | 43.2 | 40.8 to 45.6 | 46.4 | 43.5 to 49.3 | 47.1 | 43.2 to 51.0 | |
| Women | 45.7 | 43.8 to 47.5 | 44.7 | 42.7 to 46.7 | 47.7 | 45.4 to 50.1 | 50.3 | 47.3 to 53.4 | ** |
| Age ≤ 30 years | 38.1 | 35.0 to 41.3 | 38.3 | 35.1 to 41.7 | 39.1 | 35.4 to 43.0 | 44.1 | 39.0 to 49.4 | |
| Age 31–59 years | 47.3 | 45.3 to 49.2 | 45.2 | 43.1 to 47.2 | 49.3 | 46.9 to 51.7 | 48.9 | 45.7 to 52.1 | * |
| Age ≥ 60 years | 50.4 | 47.8 to 53.0 | 50.6 | 47.9 to 53.4 | 56.2 | 52.9 to 59.4 | 56.9 | 52.4 to 61.4 | *** |
| White | 57.4 | 53.7 to 61.0 | 53.0 | 49.7 to 56.3 | 54.5 | 51.5 to 57.5 | 55.1 | 51.2 to 58.9 | |
| Non-white | 42.2 | 40.6 to 43.8 | 40.7 | 39.0 to 42.4 | 42.0 | 39.7 to 44.3 | 44.3 | 41.2 to 47.5 | |
| Renter | 43.3 | 41.4 to 45.2 | 41.9 | 39.9 to 43.9 | 43.9 | 41.6 to 46.1 | 48.2 | 45.4 to 51.1 | *** |
| Owner | 47.3 | 45.0 to 49.6 | 47.2 | 44.7 to 49.7 | 53.5 | 50.3 to 56.7 | 50.1 | 45.2 to 55.0 | *** |
| NVQ ≤ 1 | 46.8 | 44.8 to 48.8 | 45.0 | 42.8 to 47.1 | 49.5 | 47.0 to 52.0 | 50.0 | 46.7 to 53.3 | ** |
| NVQ 2–3 | 41.4 | 38.8 to 44.0 | 42.7 | 39.9 to 45.5 | 44.3 | 40.9 to 47.9 | 47.8 | 43.2 to 52.5 | |
| NVQ 4–5 | 47.4 | 43.7 to 51.1 | 44.0 | 40.4 to 47.6 | 46.0 | 41.8 to 50.2 | 47.1 | 41.4 to 52.9 | |
| Not jobless household | 44.1 | 42.2 to 46.1 | 43.8 | 41.8 to 45.9 | 45.5 | 43.0 to 47.9 | 46.7 | 43.3 to 50.1 | |
| Jobless household | 46.5 | 44.4 to 48.6 | 44.2 | 41.9 to 46.4 | 50.2 | 47.5 to 52.8 | 51.9 | 48.5 to 55.3 | **** |
| Sociodemographic group | CE type A | CE type B | CE type C | CE type D | Significanceb | ||||
|---|---|---|---|---|---|---|---|---|---|
| % | 95% CI | % | 95% CI | % | 95% CI | % | 95% CI | ||
| Men | 87.6 | 86.0 to 89.1 | 85.6 | 83.8 to 87.3 | 84.5 | 82.3 to 86.5 | 86.1 | 83.2 to 88.5 | |
| Women | 88.9 | 87.7 to 89.9 | 85.2 | 83.7 to 86.7 | 85.5 | 83.8 to 87.1 | 84.9 | 82.6 to 87.0 | **** |
| Age ≤ 30 years | 85.5 | 83.1 to 87.5 | 80.7 | 77.9 to 83.2 | 84.1 | 81.0 to 86.7 | 84.2 | 80.1 to 87.6 | * |
| Age 31–59 years | 88.4 | 87.2 to 89.6 | 86.9 | 85.5 to 88.3 | 84.4 | 82.6 to 86.0 | 85.2 | 82.8 to 87.3 | *** |
| Age ≥ 60 years | 92.1 | 90.8 to 93.3 | 89.8 | 87.9 to 91.4 | 88.8 | 86.5 to 90.8 | 88.6 | 85.5 to 91.0 | ** |
| White | 85.3 | 82.5 to 87.7 | 84.2 | 81.6 to 86.5 | 83.2 | 80.9 to 85.4 | 84.5 | 81.6 to 87.0 | |
| Non-white | 88.9 | 87.9 to 89.9 | 85.9 | 84.5 to 87.1 | 86.3 | 84.6 to 87.8 | 86.2 | 83.8 to 88.2 | *** |
| Renter | 86.1 | 84.7 to 87.4 | 83.3 | 81.7 to 84.8 | 82.5 | 80.7 to 84.2 | 83.6 | 81.4 to 85.6 | *** |
| Owner | 91.2 | 89.8 to 92.4 | 88.7 | 87.0 to 90.2 | 90.1 | 88.0 to 91.8 | 90.3 | 87.1 to 92.9 | |
| NVQ ≤ 1 | 89.0 | 87.7 to 90.1 | 86.1 | 84.4 to 87.6 | 86.0 | 84.2 to 87.7 | 85.2 | 82.8 to 87.4 | *** |
| NVQ 2–3 | 88.4 | 86.6 to 89.9 | 84.9 | 82.7 to 86.8 | 85.9 | 83.2 to 88.2 | 85.8 | 82.1 to 88.8 | * |
| NVQ 4–5 | 85.9 | 83.0 to 88.4 | 84.9 | 82.1 to 87.4 | 81.9 | 78.4 to 84.9 | 85.6 | 81.2 to 89.1 | |
| Not jobless household | 89.0 | 87.6 to 90.2 | 85.5 | 83.9 to 87.0 | 85.1 | 83.2 to 86.8 | 86.6 | 84.1 to 88.8 | *** |
| Jobless household | 87.1 | 85.6 to 88.4 | 85.2 | 83.5 to 86.8 | 84.9 | 82.9 to 86.7 | 83.8 | 81.2 to 86.1 | * |
| Sociodemographic group | CE type A | CE type B | CE type C | CE type D | Significanceb | ||||
|---|---|---|---|---|---|---|---|---|---|
| % | 95% CI | % | 95% CI | % | 95% CI | % | 95% CI | ||
| Men | 71.1 | 68.8 to 73.2 | 68.9 | 66.4 to 71.2 | 64.3 | 61.2 to 67.3 | 66.2 | 62.1 to 70.1 | *** |
| Women | 72.6 | 70.8 to 74.3 | 70.0 | 68.0 to 72.0 | 65.7 | 63.3 to 68.0 | 67.3 | 64.2 to 70.2 | **** |
| Age ≤ 30 years | 67.3 | 64.0 to 70.4 | 64.3 | 60.8 to 67.7 | 59.6 | 55.4 to 63.7 | 61.5 | 55.8 to 66.9 | ** |
| Age 31–59 years | 73.2 | 71.4 to 75.0 | 71.0 | 69.0 to 73.0 | 66.1 | 63.7 to 68.5 | 67.5 | 64.4 to 70.6 | **** |
| Age ≥ 60 years | 75.4 | 73.0 to 77.6 | 73.8 | 71.2 to 76.3 | 71.8 | 68.6 to 74.7 | 73.7 | 69.5 to 77.6 | |
| White | 70.6 | 66.9 to 74.1 | 66.6 | 63.2 to 69.9 | 64.1 | 60.9 to 67.1 | 60.6 | 56.4 to 64.6 | *** |
| Non-white | 72.1 | 70.6 to 73.6 | 70.4 | 68.7 to 72.1 | 65.6 | 63.2 to 68.0 | 71.0 | 67.8 to 73.9 | **** |
| Renter | 68.8 | 66.8 to 70.6 | 64.8 | 62.6 to 66.8 | 59.7 | 57.3 to 62.1 | 63.0 | 60.0 to 65.9 | **** |
| Owner | 75.9 | 73.8 to 77.9 | 76.4 | 74.2 to 78.5 | 74.9 | 71.7 to 77.8 | 76.2 | 71.6 to 80.3 | |
| NVQ ≤ 1 | 72.1 | 70.2 to 74.0 | 70.7 | 68.5 to 72.8 | 66.2 | 63.6 to 68.6 | 67.4 | 64.1 to 70.5 | *** |
| NVQ 2–3 | 71.7 | 69.1 to 74.1 | 68.9 | 66.0 to 71.5 | 64.6 | 60.9 to 68.1 | 66.0 | 60.9 to 70.7 | *** |
| NVQ 4–5 | 71.5 | 67.8 to 74.9 | 67.9 | 64.2 to 71.3 | 63.2 | 58.8 to 67.4 | 66.5 | 60.6 to 71.9 | ** |
| Not jobless household | 73.3 | 71.4 to 75.1 | 69.8 | 67.7 to 71.8 | 64.5 | 62.0 to 67.0 | 66.4 | 62.9 to 69.8 | **** |
| Jobless household | 69.5 | 67.4 to 71.6 | 69.0 | 66.7 to 71.3 | 66.0 | 63.2 to 68.6 | 67.3 | 63.8 to 70.6 | |
| Sociodemographic group | CE type A | CE type B | CE type C | CE type D | Significanceb | ||||
|---|---|---|---|---|---|---|---|---|---|
| % | 95% CI | % | 95% CI | % | 95% CI | % | 95% CI | ||
| Men | 41.8 | 39.5 to 44.1 | 40.0 | 37.7 to 42.4 | 40.4 | 37.6 to 43.3 | 40.1 | 36.3 to 44.0 | |
| Women | 48.5 | 46.6 to 50.3 | 43.4 | 41.4 to 45.4 | 44.5 | 42.1 to 46.8 | 46.7 | 43.7 to 49.7 | *** |
| Age ≤ 30 years | 38.8 | 35.7 to 42.0 | 36.5 | 33.4 to 39.8 | 38.5 | 34.8 to 42.4 | 37.3 | 32.4 to 42.4 | |
| Age 31–59 years | 48.0 | 46.0 to 49.9 | 43.2 | 41.2 to 45.3 | 42.5 | 40.2 to 44.9 | 44.5 | 41.3 to 47.7 | *** |
| Age ≥ 60 years | 48.6 | 46.0 to 51.2 | 47.0 | 44.3 to 49.7 | 50.0 | 46.6 to 53.3 | 52.3 | 47.7 to 56.8 | |
| White | 46.8 | 43.1 to 50.5 | 40.0 | 36.7 to 43.4 | 40.5 | 37.6 to 43.4 | 41.3 | 37.6 to 45.1 | ** |
| Non-white | 44.9 | 43.3 to 46.5 | 42.4 | 40.7 to 44.1 | 43.9 | 41.5 to 46.2 | 45.0 | 41.8 to 48.2 | |
| Renter | 42.7 | 40.8 to 44.6 | 38.4 | 36.5 to 40.4 | 37.4 | 35.3 to 39.6 | 41.2 | 38.4 to 43.9 | *** |
| Owner | 48.5 | 46.2 to 50.9 | 46.9 | 44.4 to 49.4 | 52.6 | 49.4 to 55.8 | 49.7 | 44.8 to 54.6 | * |
| NVQ ≤ 1 | 48.4 | 46.4 to 50.5 | 45.6 | 43.4 to 47.8 | 44.1 | 41.6 to 46.5 | 48.0 | 44.7 to 51.3 | ** |
| NVQ 2–3 | 46.3 | 43.6 to 48.9 | 42.6 | 39.8 to 45.4 | 46.5 | 43.0 to 50.1 | 43.6 | 39.1 to 48.3 | |
| NVQ 4–5 | 33.8 | 30.4 to 37.4 | 32.4 | 29.1 to 35.8 | 33.5 | 29.7 to 37.5 | 32.3 | 27.0 to 38.2 | |
| Not jobless household | 43.9 | 41.9 to 45.9 | 40.8 | 38.7 to 42.8 | 41.2 | 38.8 to 43.6 | 39.5 | 36.2 to 42.9 | * |
| Jobless household | 47.4 | 45.3 to 49.5 | 43.4 | 41.2 to 45.7 | 45.0 | 42.4 to 47.6 | 49.6 | 46.2 to 53.0 | *** |
| Sociodemographic group | CE type A | CE type B | CE type C | CE type D | Significanceb | ||||
|---|---|---|---|---|---|---|---|---|---|
| % | 95% CI | % | 95% CI | % | 95% CI | % | 95% CI | ||
| Men | 26.7 | 24.6 to 28.9 | 27.4 | 25.2 to 29.7 | 28.1 | 25.4 to 31.0 | 26.0 | 22.6 to 29.7 | |
| Women | 27.7 | 25.9 to 29.5 | 29.5 | 27.6 to 31.5 | 26.1 | 24.0 to 28.3 | 24.1 | 21.6 to 26.8 | *** |
| Age ≤ 30 years | 24.0 | 21.2 to 27.0 | 26.3 | 23.2 to 29.6 | 26.2 | 22.6 to 30.1 | 20.8 | 16.8 to 25.5 | |
| Age 31–59 years | 31.1 | 29.2 to 33.0 | 30.7 | 28.7 to 32.7 | 28.4 | 26.2 to 30.7 | 28.4 | 25.5 to 31.5 | |
| Age ≥ 60 years | 23.0 | 20.8 to 25.4 | 26.5 | 24.0 to 29.2 | 24.9 | 21.9 to 28.2 | 23.4 | 19.5 to 27.9 | |
| White | 35.7 | 31.9 to 39.8 | 35.3 | 31.8 to 38.9 | 29.1 | 26.2 to 32.1 | 25.8 | 22.5 to 29.4 | **** |
| Non-white | 25.3 | 24.0 to 26.8 | 26.1 | 24.5 to 27.7 | 25.7 | 23.6 to 28.0 | 24.5 | 21.8 to 27.5 | |
| Renter | 25.0 | 23.3 to 26.8 | 25.9 | 24.0 to 27.8 | 24.8 | 22.7 to 27.0 | 23.3 | 20.9 to 25.9 | |
| Owner | 30.1 | 28.0 to 32.3 | 32.4 | 30.0 to 34.9 | 31.5 | 28.4 to 34.7 | 29.6 | 25.1 to 34.4 | |
| NVQ ≤ 1 | 23.1 | 21.3 to 24.9 | 23.6 | 21.7 to 25.6 | 21.0 | 19.0 to 23.2 | 21.8 | 19.0 to 24.9 | |
| NVQ 2–3 | 27.5 | 25.2 to 30.0 | 28.3 | 25.7 to 31.1 | 27.6 | 24.4 to 31.0 | 23.8 | 20.2 to 27.9 | |
| NVQ 4–5 | 38.0 | 34.3 to 41.8 | 38.5 | 35.0 to 42.2 | 38.7 | 34.5 to 43.1 | 34.5 | 29.1 to 40.4 | |
| Not jobless household | 29.4 | 27.6 to 31.4 | 30.3 | 28.3 to 32.4 | 28.6 | 26.3 to 31.0 | 26.5 | 23.5 to 29.6 | |
| Jobless household | 23.4 | 21.6 to 25.3 | 25.2 | 23.2 to 27.3 | 24.1 | 21.8 to 26.5 | 22.9 | 20.0 to 26.0 | |
| Sociodemographic group | CE type A | CE type B | CE type C | CE type D | Significanceb | ||||
|---|---|---|---|---|---|---|---|---|---|
| % | 95% CI | % | 95% CI | % | 95% CI | % | 95% CI | ||
| Men | 81.1 | 78.9 to 83.0 | 76.2 | 73.9 to 78.4 | 72.3 | 69.1 to 75.3 | 72.0 | 67.8 to 75.8 | **** |
| Women | 85.1 | 83.4 to 86.6 | 79.8 | 77.9 to 81.6 | 78.6 | 76.3 to 80.8 | 76.8 | 73.8 to 79.5 | **** |
| Age ≤ 30 years | 74.0 | 70.7 to 76.9 | 65.7 | 62.2 to 68.9 | 62.0 | 57.7 to 66.2 | 66.0 | 60.5 to 71.1 | **** |
| Age 31–59 years | 87.1 | 85.5 to 88.5 | 83.7 | 82.0 to 85.3 | 81.8 | 79.5 to 83.9 | 79.6 | 76.6 to 82.2 | **** |
| Age ≥ 60 years | 88.2 | 86.2 to 90.0 | 86.4 | 84.2 to 88.4 | 84.6 | 81.8 to 87.1 | 76.5 | 71.8 to 80.7 | **** |
| White | 72.6 | 68.8 to 76.2 | 73.8 | 70.5 to 76.8 | 73.5 | 70.4 to 76.4 | 70.4 | 66.4 to 74.0 | |
| Non-white | 85.4 | 84.0 to 86.7 | 79.7 | 78.0 to 81.2 | 76.9 | 74.3 to 79.3 | 77.5 | 74.2 to 80.4 | **** |
| Renter | 77.2 | 75.3 to 79.0 | 70.7 | 68.6 to 72.6 | 69.4 | 66.8 to 71.9 | 72.3 | 69.4 to 75.0 | **** |
| Owner | 91.9 | 90.3 to 93.2 | 91.0 | 89.1 to 92.5 | 88.2 | 85.7 to 90.4 | 81.6 | 76.5 to 85.8 | **** |
| NVQ ≤ 1 | 82.0 | 80.2 to 83.8 | 77.3 | 75.1 to 79.3 | 72.6 | 69.9 to 75.2 | 71.5 | 68.1 to 74.7 | **** |
| NVQ 2–3 | 86.8 | 84.6 to 88.8 | 78.9 | 76.2 to 81.5 | 78.3 | 74.5 to 81.6 | 77.3 | 72.3 to 81.6 | **** |
| NVQ 4–5 | 78.5 | 74.6 to 82.0 | 78.1 | 74.5 to 81.4 | 77.3 | 72.7 to 81.4 | 77.5 | 71.7 to 82.4 | |
| Not jobless household | 84.0 | 82.3 to 85.6 | 79.2 | 77.2 to 81.1 | 76.2 | 73.6 to 78.7 | 74.0 | 70.5 to 77.3 | **** |
| Jobless household | 81.7 | 79.6 to 83.6 | 76.1 | 73.8 to 78.3 | 74.0 | 71.1 to 76.7 | 75.2 | 71.9 to 78.2 | **** |
| Sociodemographic group | CE type A | CE type B | CE type C | CE type D | Significanceb | ||||
|---|---|---|---|---|---|---|---|---|---|
| % | 95% CI | % | 95% CI | % | 95% CI | % | 95% CI | ||
| Men | 62.5 | 59.7 to 65.1 | 54.5 | 51.5 to 57.4 | 64.6 | 61.1 to 68.0 | 48.2 | 43.0 to 53.5 | **** |
| Women | 64.1 | 62.0 to 66.2 | 59.6 | 57.2 to 62.0 | 63.7 | 60.9 to 66.4 | 57.3 | 53.5 to 61.0 | *** |
| Age ≤ 30 years | 63.3 | 59.3 to 67.1 | 54.1 | 49.6 to 58.5 | 65.4 | 60.1 to 70.3 | 49.2 | 42.0 to 56.5 | **** |
| Age 31–59 years | 62.3 | 60.1 to 64.5 | 58.1 | 55.7 to 60.5 | 62.3 | 59.5 to 65.1 | 54.5 | 50.5 to 58.3 | *** |
| Age ≥ 60 years | 65.7 | 62.8 to 68.6 | 58.9 | 55.7 to 62.2 | 67.3 | 63.4 to 71.0 | 55.9 | 49.9 to 61.6 | **** |
| White | 69.4 | 64.7 to 73.7 | 60.5 | 56.3 to 64.5 | 64.6 | 61.0 to 68.0 | 54.8 | 49.7 to 59.8 | **** |
| Non-white | 62.2 | 60.4 to 64.0 | 55.9 | 53.8 to 58.0 | 63.8 | 61.0 to 66.5 | 52.1 | 48.0 to 56.1 | **** |
| Renter | 61.9 | 59.6 to 64.1 | 56.2 | 53.6 to 58.7 | 61.3 | 58.5 to 64.1 | 52.6 | 48.9 to 56.2 | **** |
| Owner | 65.1 | 62.5 to 67.7 | 58.4 | 55.5 to 61.3 | 68.7 | 65.1 to 72.2 | 54.8 | 48.3 to 61.1 | **** |
| NVQ ≤ 1 | 62.9 | 60.5 to 65.1 | 57.6 | 54.9 to 60.3 | 62.9 | 59.8 to 65.8 | 58.3 | 54.0 to 62.4 | *** |
| NVQ 2–3 | 63.3 | 60.3 to 66.3 | 56.1 | 52.7 to 59.4 | 65.6 | 61.6 to 69.4 | 48.5 | 42.7 to 54.4 | **** |
| NVQ 4–5 | 64.7 | 60.3 to 68.9 | 57.8 | 53.4 to 62.1 | 64.3 | 59.1 to 69.2 | 48.6 | 41.2 to 56.0 | *** |
| Not jobless household | 63.6 | 61.3 to 65.9 | 56.8 | 54.2 to 59.3 | 65.1 | 62.1 to 67.9 | 51.6 | 47.2 to 56.0 | **** |
| Jobless household | 62.8 | 60.4 to 65.1 | 57.7 | 55.0 to 60.4 | 62.2 | 59.1 to 65.3 | 55.3 | 50.9 to 59.6 | *** |
| Group | Odds ratio (95% CI) of being a nervous persona | |||
|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | |
| Female (reference: male) | 1.04 (0.96 to 1.13) | 1.04 (0.96 to 1.13) | 1.05 (0.97 to 1.13) | 1.05 (0.97 to 1.13) |
| Age (years) (reference: 31–59 years) | ||||
| ≤ 30 | 0.29**** (0.26 to 0.33) | 0.29**** (0.26 to 0.33) | 0.29**** (0.26 to 0.33) | 0.29**** (0.26 to 0.33) |
| Age ≥ 60 | 0.16**** (0.14 to 0.19) | 0.16**** (0.14 to 0.18) | 0.16**** (0.14 to 0.19) | 0.16**** (0.14 to 0.18) |
| Non-white (reference: white) | 0.58**** (0.53 to 0.63) | 0.60**** (0.55 to 0.66) | 0.59**** (0.54 to 0.64) | 0.61**** (0.55 to 0.67) |
| Education (reference: NVQ 1 or no formal qualifications) | ||||
| NVQ 2–3 | 1.12** (1.02 to 1.23) | 1.13** (1.03 to 1.23) | 1.12** (1.02 to 1.23) | 1.12** (1.02 to 1.23) |
| NVQ 4–5 | 1.44**** (1.29 to 1.62) | 1.43**** (1.27 to 1.61) | 1.42**** (1.26 to 1.59) | 1.41**** (1.25 to 1.58) |
| Owner (reference: renter) | 1.24**** (1.14 to 1.36) | 1.26**** (1.16 to 1.38) | 1.27**** (1.16 to 1.38) | 1.28**** (1.17 to 1.40) |
| Jobless household (reference: at least one in paid work) | 0.41**** (0.38 to 0.45) | 0.42**** (0.38 to 0.45) | 0.41**** (0.38 to 0.45) | 0.42**** (0.38 to 0.45) |
| CE type (reference: type A) | ||||
| B | 1.14*** (1.04 to 1.26) | 1.13** (1.02 to 1.24) | ||
| C | 1.28**** (1.15 to 1.43) | 1.25**** (1.11 to 1.40) | ||
| D | 1.13 (0.99 to 1.28) | 1.19** (1.02 to 1.40) | ||
| Local programme type (reference: type 1) | ||||
| 2 | 0.96 (0.87 to 1.05) | 1.02 (0.91 to 1.14) | ||
| 3 | 1.18*** (1.07 to 1.30) | 1.20*** (1.07 to 1.36) | ||
| n | 18,938 | 18,938 | 18,938 | 18,938 |
| Group | Odds ratio (95% CI) of being down in the dumpsa | |||
|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | |
| Female | 1.47**** (1.29 to 1.68) | 1.47**** (1.28 to 1.68) | 1.47**** (1.28 to 1.68) | 1.47**** (1.28 to 1.68) |
| Age (years) | ||||
| ≤ 30 | 1.18 (1.00 to 1.39) | 1.17 (0.99 to 1.38) | 1.18 (1.00 to 1.39) | 1.17 (0.99 to 1.38) |
| ≥ 60 | 0.54**** (0.44 to 0.67) | 0.54**** (0.44 to 0.66) | 0.55**** (0.44 to 0.67) | 0.54**** (0.44 to 0.67) |
| Non-white | 1.28*** (1.09 to 1.49) | 1.33**** (1.13 to 1.57) | 1.26*** (1.08 to 1.48) | 1.32**** (1.12 to 1.55) |
| Education | ||||
| NVQ 2–3 | 0.70**** (0.61 to 0.82) | 0.71**** (0.61 to 0.82) | 0.71**** (0.61 to 0.82) | 0.71**** (0.61 to 0.82) |
| NVQ 4–5 | 0.55**** (0.44 to 0.69) | 0.55**** (0.44 to 0.68) | 0.56**** (0.45 to 0.70) | 0.55**** (0.45 to 0.69) |
| Owner | 0.76**** (0.65 to 0.89) | 0.78*** (0.66 to 0.91) | 0.76**** (0.65 to 0.89) | 0.77*** (0.65 to 0.90) |
| Jobless household | 1.93**** (1.67 to 2.23) | 1.94**** (1.68 to 2.24) | 1.92**** (1.67 to 2.22) | 1.93**** (1.67 to 2.23) |
| CE type | ||||
| B | 1.05 (0.90 to 1.23) | 1.07 (0.91 to 1.25) | ||
| C | 1.14 (0.95 to 1.36) | 1.17 (0.97 to 1.40) | ||
| D | 1.34*** (1.08 to 1.66) | 1.30** (1.02 to 1.67) | ||
| Local programme type | ||||
| 2 | 0.90 (0.78 to 1.05) | 1.00 (0.85 to 1.18) | ||
| 3 | 0.82** (0.69 to 0.96) | 0.88 (0.73 to 1.06) | ||
| n | 18,938 | 18,938 | 18,938 | 18,938 |
| Group | Odds ratio (95% CI) of feeling calm and peacefula | |||
|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | |
| Female | 1.22*** (1.07 to 1.39) | 1.22*** (1.07 to 1.39) | 1.22*** (1.07 to 1.39) | 1.22*** (1.07 to 1.39) |
| Age (years) | ||||
| ≤ 30 | 1.64**** (1.38 to 1.96) | 1.64**** (1.38 to 1.95) | 1.65**** (1.38 to 1.96) | 1.65**** (1.38 to 1.96) |
| ≥ 60 | 0.70*** (0.57 to 0.87) | 0.70*** (0.57 to 0.87) | 0.71*** (0.57 to 0.87) | 0.70*** (0.57 to 0.87) |
| Non-white | 1.21** (1.04 to 1.41) | 1.24*** (1.06 to 1.45) | 1.18** (1.01 to 1.38) | 1.22** (1.04 to 1.43) |
| Education | ||||
| NVQ 2–3 | 0.75**** (0.64 to 0.87) | 0.75**** (0.65 to 0.87) | 0.75**** (0.65 to 0.87) | 0.75**** (0.65 to 0.88) |
| NVQ 4–5 | 0.53**** (0.43 to 0.65) | 0.53**** (0.43 to 0.65) | 0.54**** (0.44 to 0.67) | 0.54**** (0.44 to 0.67) |
| Owner | 0.72**** (0.62 to 0.85) | 0.73**** (0.62 to 0.86) | 0.72**** (0.61 to 0.84) | 0.72**** (0.61 to 0.84) |
| Jobless household | 2.57**** (2.22 to 2.98) | 2.57**** (2.21 to 2.98) | 2.56**** (2.21 to 2.97) | 2.56**** (2.21 to 2.97) |
| CE type | ||||
| B | 0.96 (0.82 to 1.13) | 0.99 (0.85 to 1.17) | ||
| C | 0.93 (0.78 to 1.11) | 0.97 (0.81 to 1.16) | ||
| D | 1.34*** (1.10 to 1.63) | 1.30** (1.03 to 1.66) | ||
| Local programme type | ||||
| 2 | 0.92 (0.80 to 1.06) | 1.03 (0.87 to 1.22) | ||
| 3 | 0.73**** (0.61 to 0.86) | 0.82** (0.68 to 1.00) | ||
| n | 18,938 | 18,938 | 18,938 | 18,938 |
| Group | Odds ratio (95% CI) of feeling downhearteda | |||
|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | |
| Female | 0.72**** (0.67 to 0.77) | 0.72**** (0.67 to 0.77) | 0.72**** (0.67 to 0.77) | 0.72**** (0.67 to 0.77) |
| Age (years) | ||||
| ≤ 30 | 0.81**** (0.74 to 0.89) | 0.81**** (0.74 to 0.89) | 0.81**** (0.74 to 0.89) | 0.81**** (0.74 to 0.89) |
| ≥ 60 | 1.48**** (1.32 to 1.66) | 1.47**** (1.31 to 1.65) | 1.47**** (1.31 to 1.65) | 1.47**** (1.31 to 1.65) |
| Non-white | 0.80**** (0.74 to 0.87) | 0.82**** (0.75 to 0.89) | 0.81**** (0.74 to 0.88) | 0.83**** (0.76 to 0.90) |
| Education | ||||
| NVQ 2–3 | 1.08 (0.99 to 1.18) | 1.08 (0.99 to 1.18) | 1.08 (0.99 to 1.17) | 1.08 (0.99 to 1.17) |
| NVQ 4–5 | 1.32**** (1.19 to 1.47) | 1.31**** (1.18 to 1.46) | 1.30**** (1.18 to 1.45) | 1.30**** (1.17 to 1.44) |
| Owner | 1.15**** (1.06 to 1.24) | 1.16**** (1.07 to 1.25) | 1.16**** (1.07 to 1.26) | 1.17**** (1.08 to 1.27) |
| Jobless household | 0.69**** (0.63 to 0.74) | 0.69**** (0.63 to 0.75) | 0.69**** (0.63 to 0.75) | 0.69**** (0.63 to 0.75) |
| CE type | ||||
| B | 1.07 (0.98 to 1.16) | 1.05 (0.96 to 1.15) | ||
| C | 1.19**** (1.08 to 1.32) | 1.16*** (1.05 to 1.29) | ||
| D | 1.06 (0.94 to 1.19) | 1.08 (0.93 to 1.25) | ||
| Local programme type | ||||
| 2 | 0.96 (0.88 to 1.05) | 0.98 (0.89 to 1.09) | ||
| 3 | 1.12** (1.02 to 1.22) | 1.11 (1.00 to 1.24) | ||
| n | 18,938 | 18,938 | 18,938 | 18,938 |
| Group | Odds ratio (95% CI) of feeling happya | |||
|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | |
| Female | 1.40**** (1.25 to 1.58) | 1.40**** (1.25 to 1.58) | 1.40**** (.25 to 1.58) | 1.40**** (1.25 to 1.58) |
| Age (years) | ||||
| ≤ 30 | 1.76**** (1.51 to 2.06) | 1.76**** (1.51 to 2.06) | 1.76**** (1.51 to 2.06) | 1.77**** (1.51 to 2.06) |
| ≥ 60 | 0.77*** (0.64 to 0.93) | 0.77*** (0.64 to 0.93) | 0.77*** (0.64 to 0.93) | 0.77*** (0.64 to 0.93) |
| Non-white | 1.36**** (1.19 to 1.57) | 1.36**** (1.17 to 1.56) | 1.34**** (1.16 to 1.54) | 1.32**** (1.14 to 1.52) |
| Education | ||||
| NVQ 2–3 | 0.88 (0.77 to 1.00) | 0.88 (0.77 to 1.01) | 0.88 (0.77 to 1.01) | 0.89 (0.78 to 1.01) |
| NVQ 4–5 | 0.58**** (0.48 to 0.70) | 0.59**** (0.49 to 0.71) | 0.60**** (0.49 to 0.72) | 0.60**** (0.50 to 0.72) |
| Owner | 0.73**** (0.63 to 0.84) | 0.73**** (0.63 to 0.84) | 0.72**** (0.63 to 0.83) | 0.72**** (0.63 to 0.83) |
| Jobless household | 2.34**** (2.05 to 2.66) | 2.33**** (2.05 to 2.65) | 2.33**** (2.05 to 2.65) | 2.32**** (2.04 to 2.64) |
| CE type | ||||
| B | 0.87** (0.76 to 1.00) | 0.88 (0.77 to 1.01) | ||
| C | 0.88 (0.75 to 1.02) | 0.90 (0.77 to 1.05) | ||
| D | 1.05 (0.86 to 1.28) | 0.92 (0.74 to 1.16) | ||
| Local programme type | ||||
| 2 | 0.93 (0.81 to 1.05) | 0.90 (0.78 to 1.05) | ||
| 3 | 0.75**** (0.65 to 0.87) | 0.75**** (0.64 to 0.89) | ||
| n | 18,938 | 18,938 | 18,938 | 18,938 |
| Group | Odds ratio (95% CI) of eating five or more portions of fruit/vegetables per daya | |||
|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | |
| Female | 1.60**** (1.48 to 1.72) | 1.60**** (1.49 to 1.72) | 1.60**** (1.49 to 1.72) | 1.60**** (1.49 to 1.73) |
| Age (years) | ||||
| ≤ 30 | 1.32**** (1.20 to 1.45) | 1.32**** (1.20 to 1.45) | 1.32**** (1.20 to 1.45) | 1.32**** (1.20 to 1.45) |
| ≥ 60 | 2.02**** (1.80 to 2.26) | 2.01**** (1.79 to 2.25) | 2.01**** (1.80 to 2.26) | 2.01**** (1.79 to 2.25) |
| Non-white | 0.77**** (0.70 to 0.84) | 0.79**** (0.72 to 0.86) | 0.78**** (0.71 to 0.85) | 0.80**** (0.73 to 0.87) |
| Education | ||||
| NVQ 2–3 | 1.40**** (1.28 to 1.52) | 1.40**** (1.28 to 1.52) | 1.39**** (1.28 to 1.52) | 1.39**** (1.28 to 1.52) |
| NVQ 4–5 | 2.33**** (2.09 to 2.61) | 2.32**** (2.07 to 2.59) | 2.29**** (2.05 to 2.56) | 2.28**** (2.04 to 2.55) |
| Owner | 1.25**** (1.15 to 1.36) | 1.26**** (1.16 to 1.37) | 1.27**** (1.16 to 1.38) | 1.28**** (1.17 to 1.39) |
| Jobless household | 0.77**** (0.71 to 0.84) | 0.78**** (0.72 to 0.85) | 0.78**** (0.71 to 0.84) | 0.78**** (0.72 to 0.85) |
| CE type | ||||
| B | 1.10** (1.01 to 1.21) | 1.09 (1.00 to 1.20) | ||
| C | 1.24**** (1.12 to 1.38) | 1.22**** (1.10 to 1.35) | ||
| D | 1.01 (0.90 to 1.14) | 1.09 (0.94 to 1.27) | ||
| Local programme type | ||||
| 2 | 1.02 (0.93 to 1.11) | 1.04 (0.94 to 1.16) | ||
| 3 | 1.22**** (1.11 to 1.34) | 1.21**** (1.09 to 1.35) | ||
| n | 18,938 | 18,938 | 18,938 | 18,938 |
| Group | Odds ratio (95% CI) of smokinga | ||
|---|---|---|---|
| Model 1 | Model 2 | Model 3 | |
| Female | 0.81**** (0.75 to 0.88) | 0.81**** (0.75 to 0.88) | 0.81**** (0.75 to 0.88) |
| Age (years) | |||
| ≤ 30 | 0.95 (0.86 to 1.05) | 0.95 (0.86 to 1.05) | 0.95 (0.86 to 1.05) |
| ≥ 60 | 0.31**** (0.28 to 0.35) | 0.31**** (0.28 to 0.35) | 0.31**** (0.28 to 0.35) |
| Non-white | 0.32**** (0.29 to 0.36) | 0.33**** (0.30 to 0.36) | 0.32**** (0.29 to 0.35) |
| Education | |||
| NVQ 2–3 | 0.74**** (0.67 to 0.81) | 0.74**** (0.68 to 0.81) | 0.74**** (0.68 to 0.82) |
| NVQ 4–5 | 0.56**** (0.49 to 0.63) | 0.57**** (0.50 to 0.64) | 0.56**** (0.50 to 0.64) |
| Owner | 0.50**** (0.46 to 0.55) | 0.50**** (0.45 to 0.55) | 0.50**** (0.46 to 0.55) |
| Jobless household | 1.29**** (1.18 to 1.41) | 1.28**** (1.17 to 1.41) | 1.29**** (1.18 to 1.42) |
| CE type | |||
| B | 0.96 (0.87 to 1.06) | 0.96 (0.88 to 1.06) | |
| C | 0.81**** (0.73 to 0.91) | 0.82**** (0.74 to 0.92) | |
| D | 0.96 (0.84 to 1.09) | 0.85** (0.73 to 1.00) | |
| Local programme type | |||
| 2 | 0.90 (0.81 to 1.01) | 0.96 (0.87 to 1.05) | |
| 3 | 0.79**** (0.70 to 0.89) | 0.81**** (0.73 to 0.90) | |
| n | 18,938 | 18,938 | 18,938 |
| Social trust/social cohesion outcomes | CE type (%) | Local programme type (%) | |||||
|---|---|---|---|---|---|---|---|
| A | B | C | D | 1 | 2 | 3 | |
| Feel part of the local community | 8.8 | 8.6 | 11.4 | 11.2 | 7.8 | 9.4 | 11.7 |
| Think people in the area are friendly | 2.9 | 3.8 | 2.5 | 2.6 | 2.5 | 2.7 | 4.0 |
| Know most/many people in area | 0.6 | 1.2 | 5.9 | 6.0 | 3.5 | 0.9 | 4.0 |
| Think neighbours look out for each other | 3.8 | 4.5 | 3.6 | 2.0 | 2.5 | 1.9 | 1.7 |
| Think can influence decisions in area | 2.8 | 3.4 | 1.0 | –0.5 | 0.8 | 2.5 | 2.7 |
| Volunteered in local organisations | 2.5 | 1.9 | 0.7 | 3.3 | 2.7 | 1.7 | 1.7 |
| Social trust/social cohesion outcomes | CE type (%) | Local programme type (%) | |||||
|---|---|---|---|---|---|---|---|
| A | B | C | D | 1 | 2 | 3 | |
| Feel part of the local community | 10.1 | 9.4 | 8.6 | 19.3 | 9.4 | 9.0 | 14.1 |
| Think people in the area are friendly | –1.4 | 0.0 | 3.5 | 0.9 | –2.4 | 0.7 | 2.9 |
| Know most/many people in area | –2.2 | 5.4 | 3.9 | –6.7 | –2.6 | 1.2 | 4.2 |
| Think neighbours look out for each other | –5.1 | 6.3 | 8.3 | –2.2 | –0.9 | –0.3 | 4.3 |
| Think can influence decisions in area | 0.0 | 5.3 | –0.6 | 9.7 | 3.4 | 4.2 | –0.9 |
| Volunteered in local organisations | 1.8 | 2.9 | –1.4 | 2.8 | 3.0 | 2.6 | –1.4 |
| Health and lifestyle outcomes | CE type (%) | Local programme type (%) | |||||
|---|---|---|---|---|---|---|---|
| A | B | C | D | 1 | 2 | 3 | |
| Good self-rated health | 4.5 | 7.5 | 5.4 | 6.6 | 6.3 | 4.5 | 7.2 |
| Life-limiting illness (negative valence) | 0.6 | –2.6 | –1.7 | –0.8 | –1.4 | –2.3 | –1.1 |
| Nervous person (negative valence) | –2.9 | –2.0 | –1.4 | –0.7 | –1.4 | –2.4 | –2.1 |
| Down in the dumps (negative valence) | –3.8 | –3.7 | –1.4 | –1.2 | –2.3 | –3.2 | –3.1 |
| Calm and peaceful | 5.9 | 6.1 | 6.7 | 6.4 | 4.2 | 6.5 | 7.8 |
| Downhearted (negative valence) | –0.2 | –1.9 | 0.1 | 0.1 | 0.2 | –0.9 | –1.3 |
| Happy person | 3.7 | 1.7 | 2.3 | –0.1 | –0.2 | 2.0 | 4.8 |
| Eat five portions of fruit/vegetables a day three or more times a week | 4.5 | 4.1 | 1.9 | –5.6 | –6.7 | –1.3 | –2.5 |
| Smoking (negative valence) | –4.8 | –5.1 | –3.2 | –5.3 | –4.2 | –3.1 | –6.5 |
| Health and lifestyle outcomes | CE type (%) | Local programme type (%) | |||||
|---|---|---|---|---|---|---|---|
| A | B | C | D | 1 | 2 | 3 | |
| Good self-rated health | 4.2 | 9.7 | 2.9 | 8.7 | 7.5 | –5.4 | 5.6 |
| Life-limiting illness (negative valence) | 0.5 | –2.9 | 0.0 | –2.8 | –0.1 | –1.3 | –5.6 |
| Nervous person (negative valence) | –1.6 | –3.5 | 1.5 | 3.1 | 0.0 | –2.9 | –0.6 |
| Down in the dumps (negative valence) | –3.4 | –3.9 | –2.3 | 3.7 | –0.9 | –2.8 | –3.2 |
| Calm and peaceful | –1.8 | 4.9 | 2.3 | –9.3 | –2.0 | 4.3 | –1.1 |
| Downhearted (negative valence) | –80.9 | –81 | –83.5 | –82.1 | 0.0 | –1.6 | 0.3 |
| Happy person | 0.4 | 5.7 | 4.8 | –7.6 | 0.1 | 4.7 | 0.9 |
| Eat five portions of fruit/vegetables a day three or more times a week | 11.3 | 10.8 | 3.1 | –12.6 | –8.3 | –2.0 | 5.7 |
| Smoking (negative valence) | –1.7 | –3.9 | –3.8 | 2.4 | –4.5 | –2.9 | –1.3 |
| Social trust/social cohesion outcomes | b R 2 | Constant | LPIT-2 | CE type A | Starting | ||||
|---|---|---|---|---|---|---|---|---|---|
| Coefficent | SD | Coefficent | SD | Coefficent | SD | Coefficent | SD | ||
| Feel part of the local community | 0.229/0.338 | 0.140 | 0.184 | 0.006 | 0.136 | –0.040 | –0.927 | 0.796 | 3.715 |
| Think people in area are friendly | 0.491 | –0.067 | –1.867 | 0.004 | 0.223 | 0.037 | 1.987 | 0.755 | 6.094 |
| Know most/many people in area | 0.290 | 0.180 | 0.242 | –0.220 | –0.537 | –0.007 | –0.162 | 0.6555 | 4.200 |
| Think neighbours look out for each other | 0.450 | –0.161 | –2.960 | 0.019 | 0.638 | 0.073 | 2.439 | 0.604 | 5.018 |
| Think they can influence decisions in area | 0.572 | –0.008 | –0.162 | –0.016 | –0.583 | 0.026 | 0.949 | 0.960 | 7.068 |
| Volunteered in local organisations | 0.205/0.240 | 0.017 | 0.408 | –0.016 | –0.705 | 0.006 | 0.278 | 0.477 | 3.420 |
| Feeling safe walking alone after dark | 0.537 | 0.064 | 1.198 | –0.045 | –1.559 | –0.014 | –0.459 | 0.852 | 6.671 |
| Characteristic | Cross-sectional | Longitudinal | 2001 census | ||
|---|---|---|---|---|---|
| NDC area | Comparator area | NDC area | Comparator area | England | |
| 2002 | |||||
| n | 19,574 | 2014 | 10,638 | 1010 | 2,964,871 |
| Sex, female (%) | 51.4 | 54.3 | 59.7 | 54.1 | 51.3 |
| Age (years), mean (SD) | 42.3 (18.3) | 44.6 (18.3) | 46.0 | 47.7 | |
| Ethnicity (%) | |||||
| White | 75.5 | 77.1 | 76.7 | 81.0 | 80.1 |
| Asian | 11.7 | 14 | 10.8 | 10.8 | 3.8 |
| Black | 11.4 | 8.1 | 9.4 | 5.9 | 1.74 |
| Other | 1.4 | 0.8 | 3.1 | 2.3 | 14.4 |
| Education (%) | |||||
| None | 41.8 | 38.8 | 47.1 | 43.7 | 19.3 |
| NVQ 1 or equivalent | 12.2 | 11.0 | 11.0 | 10.0 | 10.8 |
| NVQ 4+ or equivalent | 16.4 | 18.3 | 13.4 | 13.6 | 12.8 |
| 2008 | |||||
| n | 15,838 | 3100 | 233,315 | ||
| Sex, female (%) | 59.7 | 52.1 | 60.9 | 52.5 | 50.6 |
| Age (years), mean (SD) | 47.8 (18.5) | 44.1 (18.3) | 54.5 | 58.1 | 39.2 (23.1) |
| Ethnicity (%) | |||||
| White | 73.3 | 74.1 | 79.1 | 81.9 | 86.3 |
| Asian | 10.1 | 14.8 | 9.9 | 9.4 | 6.8 |
| Black | 14.7 | 10.1 | 8.3 | 7.0 | 3.2 |
| Other | 1.9 | 0.9 | 2.6 | 1.6 | 3.7 |
| Education (%) | |||||
| None | 43.1 | 34.2 | 48.5 | 43.6 | – |
| NVQ 1 or equivalent | 9.7 | 10.1 | 8.5 | 6.5 | |
| NVQ 4+ or equivalent | 17.3 | 22.2 | 14.0 | 15.4 | |
| Variable | Model 1 | Model 2 | Model 3 | |||
|---|---|---|---|---|---|---|
| Coefficient | SE | Coefficient | SE | Coefficient | SE | |
| Baseline self-rated health levels (intercept) regression coefficients | ||||||
| CE type (reference: type A) | ||||||
| B | 0.03* | 0.01 | 0.03** | 0.01 | 0.04*** | 0.01 |
| C | –0.04*** | 0.01 | –0.02 | 0.01 | –0.01 | 0.01 |
| D | 0.02 | 0.01 | 0.01 | 0.01 | 0.04** | 0.02 |
| Female (reference: male) | – | – | 0.01 | 0.01 | 0.01 | 0.01 |
| Age | – | – | 0.26**** | 0.01 | 0.25**** | 0.01 |
| Non-white (reference: white) | – | – | –0.01 | 0.01 | –0.01 | 0.01 |
| Education (reference: NVQ 1 or no formal qualifications) | ||||||
| NVQ 2–3 | – | – | –0.03** | 0.01 | –0.03** | 0.01 |
| NVQ 4–5 | – | – | –0.06**** | 0.01 | –0.06**** | 0.01 |
| Owner (reference: renter) | – | – | –0.1**** | 0.01 | –0.10**** | 0.01 |
| Jobless household (reference: at least one household member in paid work) | – | – | 0.23**** | 0.01 | 0.23**** | 0.01 |
| Local programme type (reference: type 1) | ||||||
| 2 | – | – | – | – | 0.05*** | 0.02 |
| 3 | – | – | – | – | 0.02 | 0.02 |
| Change over time in self-rated health levels (slope) regression coefficients | ||||||
| CE type (reference: type A) | ||||||
| B | –0.04 | 0.04 | –0.04 | 0.04 | –0.04 | 0.04 |
| C | 0.00 | 0.04 | –0.01 | 0.04 | –0.02 | 0.04 |
| D | –0.05 | 0.04 | –0.06 | 0.04 | –0.08* | 0.05 |
| Female (reference: male) | – | – | –0.02 | 0.03 | –0.02 | 0.03 |
| Age | – | – | 0.13*** | 0.04 | 0.13*** | 0.04 |
| Non-white (reference: white) | – | – | 0.04 | 0.04 | 0.04 | 0.04 |
| Education (reference: NVQ 1 or no formal qualifications) | ||||||
| NVQ 2–3 | – | – | –0.02 | 0.04 | –0.03 | 0.04 |
| NVQ 4–5 | – | – | –0.06* | 0.04 | –0.06* | 0.04 |
| Owner (reference: renter) | – | – | –0.04 | 0.04 | –0.04 | 0.04 |
| Jobless household (reference: at least one household member in paid work) | – | – | –0.14**** | 0.04 | –0.14**** | 0.04 |
| 2 | – | – | – | – | –0.06 | 0.05 |
| 3 | – | – | – | – | –0.01 | 0.05 |
| Parameters of the growth curve | ||||||
| Intercept | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 |
| Intercept variance | 1.00**** | 0.00 | 0.80**** | 0.01 | 0.79**** | 0.01 |
| Slope | 0.08 | 0.06 | –0.04 | 0.14 | 0.03 | 0.16 |
| Slope variance | 1.00**** | 0.00 | 0.97**** | 0.01 | 0.97**** | 0.01 |
| NDC name | Intervention type | Engagement type | Standardised drug misuse | All cancer | All circulatory | Standardised alcohol misuse | All mental health | All respiratory |
|---|---|---|---|---|---|---|---|---|
| Kingston upon Hull | 1 | A | ||||||
| Plymouth | 1 | A | 2.13 | |||||
| Derby | 1 | B | 22.45 | 8.44 | 4.00 | |||
| Kings Norton | 1 | B | 4.67 | |||||
| Liverpool | 1 | B | ||||||
| Manchester | 1 | C | –49.87 | |||||
| Southwark | 1 | C | ||||||
| Brent | 1 | D | –6.23 | –14.32 | ||||
| Coventry | 1 | D | 6.92 | 1.74 | ||||
| Knowsley | 1 | D | 29.78 | 6.09 | 39.34 | 16.8 | ||
| Lambeth | 1 | D | –9.53 | |||||
| Tower Hamlets | 1 | D | ||||||
| Bradford | 2 | A | ||||||
| Hartlepool | 2 | A | 5.16 | 5.03 | 5.31 | |||
| Leicester | 2 | A | 4.59 | 17.82 | 14.54 | 6.59 | ||
| Middlesbrough | 2 | A | ||||||
| Newcastle upon Tyne | 2 | A | –30.96 | 3.11 | –13.03 | –10.47 | ||
| Norwich | 2 | A | –4.11 | –2.84 | –6.26 | –4.08 | –6.2 | |
| Oldham | 2 | A | 4.33 | –1.77 | –2.5 | |||
| Walsall | 2 | A | –10.13 | –3.79 | ||||
| Doncaster | 2 | B | –71.48 | –3.84 | –5.95 | –10.79 | ||
| Lewisham | 2 | B | –9.20 | |||||
| Luton | 2 | B | 6.16 | –5.46 | ||||
| Sandwell | 2 | B | –13.62 | |||||
| Sheffield | 2 | B | –1.80 | –6.83 | –14.68 | –5.32 | ||
| Salford | 2 | C | ||||||
| Southampton | 2 | C | 3.87 | |||||
| Wolverhampton | 2 | C | –18.17 | |||||
| Bristol | 3 | A | 5.81 | |||||
| Newham | 3 | A | 8.50 | 4.99 | 3.21 | |||
| Rochdale | 3 | A | –23.75 | –9.93 | –6.98 | |||
| Brighton and Hove | 3 | B | 2.26 | 5.93 | 8.98 | 4.50 | ||
| Islington | 3 | B | –5.23 | –3.74 | ||||
| Nottingham | 3 | B | 31.54 | |||||
| Sunderland | 3 | B | ||||||
| Aston | 3 | C | 4.56 | |||||
| Hackney | 3 | C | 7.22 | 2.53 | ||||
| Hammersmith and Fulham | 3 | C | ||||||
| Haringey | 3 | C | 5.53 |
| Approach to CEa | NDC programme type | ||
|---|---|---|---|
| Type 1 – diversifying social composition and major redevelopment | Type 2 – increasing resources and moderate redevelopment | Type 3 – upskilling/empowering residents and improving living conditions | |
| Type A |
|
|
|
| Type B |
|
|
|
| Type C |
|
|
|
| Type D |
|
– | – |
| CE and NDC type | Community development | Crime and community safety | Education | Employment and business | Health | Housing/physical environment | Cross-cutting | Other | |
|---|---|---|---|---|---|---|---|---|---|
| B3 | Brighton and Hove | 28.1 | 13.6 | 17.0 | 11.8 | 12.9 | 2.3 | 4.9 | 9.5 |
| C2 | Southampton | 8.2 | 7.7 | 12.0 | 5.2 | 10.1 | 39.1 | 7.4 | 10.3 |
| A3 | Bristol | 25.9 | 19.7 | 13.8 | 12.3 | 12.9 | 5.5 | 0.1 | 9.9 |
| A1 | Plymouth | 16.8 | 11.4 | 8.8 | 7.6 | 15.6 | 11.7 | 18.9 | 9.1 |
| B2 | Luton | 42.0 | 5.4 | 12.2 | 6.4 | 4.4 | 2.4 | 15.7 | 11.6 |
| A3 | Norwich | 21.2 | 5.8 | 12.0 | 16.7 | 7.5 | 20.9 | 3.7 | 12.1 |
| B1 | Derby | 19.1 | 6.9 | 14.9 | 8.9 | 13.7 | 10.2 | 17.0 | 9.3 |
| A2 | Leicester | 27.1 | 7.4 | 9.9 | 17.4 | 19.6 | 8.6 | 1.0 | 8.8 |
| B3 | Nottingham | 28.2 | 10.2 | 9.9 | 19.3 | 5.1 | 13.8 | 3.0 | 10.5 |
| B3 | Haringey | 22.3 | 7.2 | 7.6 | 4.1 | 14.2 | 33.7 | 10.9 | 0.0 |
| B3 | Islington | 16.4 | 19.7 | 13.2 | 4.3 | 9.0 | 15.8 | 8.8 | 12.8 |
| D1 | Lambeth | 13.3 | 8.2 | 5.7 | 5.3 | 4.2 | 49.4 | 4.8 | 9.1 |
| B2 | Lewisham | 14.8 | 9.7 | 10.7 | 6.0 | 6.1 | 27.5 | 16.0 | 9.2 |
| A3 | Newham | 15.2 | 8.2 | 23.1 | 6.3 | 8.7 | 20.9 | 7.0 | 10.7 |
| C3 | Hammersmith and Fulham | 15.5 | 6.3 | 23.9 | 10.8 | 7.5 | 22.4 | 2.2 | 11.5 |
| C3 | Hackney | 11.7 | 4.1 | 15.1 | 12.3 | 6.4 | 35.0 | 3.6 | 11.8 |
| D1 | Brent | 18.1 | 10.1 | 13.6 | 4.7 | 4.7 | 17.8 | 19.7 | 11.4 |
| C1 | Southwark | 15.6 | 5.1 | 15.0 | 8.7 | 6.4 | 24.3 | 5.9 | 18.9 |
| D1 | Tower Hamlets | 22.0 | 5.7 | 18.9 | 10.2 | 6.7 | 17.2 | 4.1 | 15.2 |
| C3 | Aston | 19.0 | 13.6 | 13.2 | 4.2 | 21.1 | 6.5 | 10.3 | 12.1 |
| D1 | Coventry | 13.1 | 9.6 | 16.3 | 9.7 | 7.9 | 16.2 | 17.4 | 9.7 |
| B1 | Kings Norton | 23.5 | 14.6 | 14.8 | 9.6 | 5.6 | 15.7 | 2.7 | 13.5 |
| B2 | Sandwell | 24.2 | 16.5 | 12.4 | 10.1 | 7.4 | 11.4 | 7.4 | 10.6 |
| A2 | Walsall | 41.3 | 7.9 | 8.5 | 9.4 | 6.9 | 8.2 | 6.6 | 11.3 |
| C2 | Wolverhampton | 13.7 | 10.1 | 19.0 | 7.7 | 4.6 | 27.0 | 6.9 | 10.9 |
| A2 | Bradford | 37.7 | 8.9 | 9.5 | 6.2 | 6.3 | 17.2 | 6.1 | 8.1 |
| B2 | Doncaster | 27.4 | 13.9 | 8.0 | 12.7 | 7.4 | 11.0 | 4.7 | 14.9 |
| A1 | Kingston upon Hull | 30.8 | 4.1 | 13.6 | 12.0 | 2.9 | 20.9 | 7.8 | 7.9 |
| B2 | Sheffield | 19.4 | 6.4 | 15.2 | 10.8 | 6.3 | 30.5 | 4.3 | 7.0 |
| D1 | Knowsley | 7.9 | 3.4 | 4.4 | 10.0 | 9.3 | 29.9 | 24.7 | 10.4 |
| B1 | Liverpool | 13.9 | 9.8 | 11.7 | 9.1 | 1.8 | 34.0 | 6.1 | 13.8 |
| C1 | Manchester | 13.9 | 7.3 | 10.7 | 5.1 | 5.1 | 47.0 | 1.8 | 9.1 |
| A2 | Oldham | 18.1 | 9.4 | 5.0 | 8.8 | 4.1 | 41.1 | 4.0 | 9.7 |
| C2 | Salford | 25.9 | 8.3 | 5.9 | 5.0 | 4.5 | 36.0 | 3.6 | 10.9 |
| A3 | Rochdale | 8.1 | 7.1 | 10.8 | 14.9 | 1.7 | 40.5 | 1.0 | 16.1 |
| A2 | Hartlepool | 15.1 | 12.6 | 11.3 | 12.2 | 5.8 | 31.9 | 2.6 | 8.5 |
| B3 | Sunderland | 11.1 | 8.7 | 29.5 | 9.9 | 2.7 | 10.7 | 5.0 | 22.2 |
| A3 | Newcastle upon Tyne | 13.8 | 12.4 | 14.1 | 16.0 | 10.4 | 16.9 | 15.0 | 1.3 |
| A2 | Middlesbrough | 8.5 | 11.0 | 11.7 | 8.5 | 4.5 | 40.7 | 6.4 | 8.6 |
| Percentage of NDC and community spend | 19.3 | 9.4 | 12.9 | 9.8 | 7.6 | 23.2 | 7.3 | 10.4 | |
| NDC code | NDC name | CE type | Rank | Access and facilities | Elderly | Teenagers/young people | Drugs and alcohol | Healthy living | New improved services | Family support | Community Chest (health) | Health posts | Health events | Other targeted |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 10 | Leicester | A | 1 | 80.8 | 0.8 | 3.3 | 0.0 | 4.1 | 0.2 | 5.1 | 1.0 | 3.7 | 0.0 | 1.0 |
| 11 | Brighton and Hove | B | 1 | 30.9 | 0.0 | 8.9 | 0.0 | 11.0 | 6.8 | 21.7 | 0.0 | 13.2 | 0.0 | 7.5 |
| 28 | Knowsley | D | 1 | 56.0 | 0.4 | 0.0 | 0.1 | 22.8 | 5.2 | 0.0 | 0.0 | 13.3 | 0.0 | 2.1 |
| 06 | Newham | A | 2 | 0.0 | 4.0 | 16.7 | 0.0 | 19.7 | 18.6 | 0.0 | 0.0 | 40.9 | 0.0 | 0.0 |
| 32 | Hartlepool | A | 2 | 0.0 | 0.0 | 3.5 | 0.0 | 0.0 | 3.5 | 50.9 | 0.0 | 34.9 | 0.0 | 7.2 |
| 36 | Derby | B | 2 | 46.2 | 0.0 | 10.1 | 4.1 | 6.7 | 1.3 | 14.1 | 0.0 | 17.5 | 0.0 | 0.0 |
| 02 | Nottingham | B | 4 | 0.0 | 0.0 | 0.0 | 0.0 | 8.4 | 39.3 | 13.0 | 1.4 | 10.3 | 0.0 | 27.7 |
| 04 | Hackney | C | 4 | 36.7 | 4.5 | 2.2 | 0.3 | 26.6 | 14.8 | 0.0 | 0.0 | 6.7 | 0.0 | 8.2 |
| 12 | Kings Norton | B | 4 | 0.0 | 0.0 | 0.0 | 0.0 | 27.4 | 0.0 | 30.8 | 0.0 | 17.7 | 0.0 | 24.2 |
| 16 | Bristol | A | 4 | 60.7 | 0.0 | 1.7 | 18.2 | 7.3 | 5.7 | 0.9 | 0.0 | 5.6 | 0.0 | 0.0 |
| 21 | Southampton | C | 4 | 43.6 | 0.0 | 0.0 | 0.0 | 18.9 | 8.2 | 0.0 | 0.0 | 21.9 | 0.0 | 7.4 |
| 24 | Plymouth | A | 4 | 84.7 | 0.0 | 2.9 | 0.0 | 0.0 | 3.1 | 0.0 | 0.0 | 3.7 | 0.0 | 5.5 |
| 33 | Haringey | B | 4 | 76.4 | 0.0 | 0.7 | 3.4 | 0.4 | 4.8 | 0.0 | 0.0 | 5.3 | 0.8 | 8.2 |
| 37 | Coventry | D | 4 | 3.6 | 0.0 | 3.2 | 0.0 | 6.9 | 9.2 | 2.6 | 0.0 | 57.3 | 0.0 | 17.2 |
| 39 | Aston | C | 4 | 69.3 | 0.0 | 0.0 | 0.0 | 0.0 | 18.2 | 12.5 | 0.0 | 0.0 | 0.0 | 0.0 |
| 01 | Liverpool | B | 5 | 2.0 | 0.0 | 0.0 | 0.0 | 1.9 | 0.0 | 19.8 | 1.7 | 0.0 | 0.3 | 74.3 |
| 05 | Tower Hamlets | D | 5 | 2.0 | 17.7 | 0.0 | 0.0 | 36.7 | 10.0 | 0.0 | 0.0 | 11.0 | 0.0 | 22.5 |
| 07 | Southwark | C | 5 | 36.2 | 8.6 | 6.3 | 0.0 | 31.7 | 0.0 | 10.8 | 2.6 | 1.2 | 0.0 | 2.6 |
| 08 | Middlesbrough | A | 5 | 15.5 | 0.0 | 1.3 | 23.1 | 0.0 | 0.9 | 0.2 | 55.4 | 1.0 | 0.0 | 2.6 |
| 13 | Bradford | A | 5 | 12.1 | 0.0 | 0.5 | 0.0 | 44.3 | 1.5 | 11.8 | 2.5 | 7.6 | 0.0 | 19.6 |
| 14 | Kingston upon Hull | A | 5 | 5.4 | 10.6 | 0.9 | 0.0 | 2.4 | 35.1 | 7.8 | 0.0 | 37.7 | 0.0 | 0.0 |
| 20 | Sunderland | B | 5 | 54.9 | 0.0 | 12.4 | 7.8 | 0.0 | 0.0 | 0.0 | 0.0 | 24.1 | 0.0 | 0.8 |
| 23 | Salford | C | 5 | 45.1 | 0.0 | 3.5 | 9.7 | 0.0 | 30.0 | 0.0 | 0.0 | 11.8 | 0.0 | 0.0 |
| 26 | Luton | B | 5 | 32.8 | 5.2 | 0.0 | 24.5 | 1.5 | 13.8 | 0.0 | 0.0 | 18.7 | 0.0 | 3.5 |
| 34 | Hammersmith and Fulham | C | 5 | 0.0 | 0.0 | 1.1 | 0.0 | 10.9 | 17.7 | 32.7 | 0.0 | 35.5 | 0.0 | 2.0 |
| 15 | Sandwell | B | 6 | 20.8 | 0.3 | 11.5 | 0.0 | 7.5 | 28.8 | 5.4 | 0.0 | 21.7 | 0.0 | 4.0 |
| 17 | Manchester | C | 6 | 7.8 | 5.2 | 0.0 | 4.8 | 8.6 | 0.0 | 55.5 | 0.0 | 14.0 | 0.0 | 4.1 |
| 19 | Wolverhampton | C | 6 | 1.5 | 0.0 | 0.0 | 0.0 | 27.5 | 0.0 | 16.4 | 0.0 | 27.6 | 0.0 | 26.9 |
| 25 | Oldham | A | 6 | 25.5 | 0.0 | 6.2 | 30.0 | 28.8 | 0.0 | 5.6 | 0.0 | 0.0 | 0.0 | 3.8 |
| 27 | Lewisham | B | 6 | 0.0 | 17.2 | 8.9 | 0.0 | 11.9 | 19.0 | 2.1 | 0.0 | 5.9 | 1.4 | 33.5 |
| 38 | Lambeth | D | 6 | 0.0 | 7.5 | 0.0 | 0.0 | 34.9 | 19.4 | 0.0 | 0.0 | 28.4 | 0.0 | 9.8 |
| 09 | Newcastle upon Tyne | A | 7 | 0.3 | 4.4 | 14.4 | 15.1 | 2.1 | 14.5 | 5.8 | 1.1 | 14.9 | 0.0 | 27.3 |
| 18 | Walsall | A | 7 | 2.8 | 0.0 | 8.8 | 23.8 | 15.3 | 17.1 | 11.0 | 0.0 | 10.1 | 0.0 | 11.0 |
| 29 | Brent | D | 7 | 0.0 | 18.4 | 5.7 | 0.0 | 45.1 | 10.6 | 10.0 | 0.0 | 0.0 | 0.0 | 10.2 |
| 30 | Islington | B | 7 | 0.0 | 3.1 | 19.5 | 6.0 | 9.7 | 7.3 | 0.0 | 0.0 | 44.9 | 0.0 | 9.6 |
| 22 | Sheffield | B | 8 | 0.7 | 0.0 | 0.0 | 31.9 | 10.7 | 18.5 | 22.3 | 0.0 | 0.0 | 0.0 | 15.9 |
| 31 | Rochdale | A | 8 | 5.0 | 0.0 | 66.3 | 0.0 | 20.2 | 0.0 | 0.0 | 0.0 | 8.5 | 0.0 | 0.0 |
| 35 | Doncaster | B | 9 | 40.0 | 0.0 | 2.1 | 1.1 | 15.4 | 16.7 | 0.3 | 0.0 | 23.8 | 0.0 | 0.6 |
| 03 | Norwich | A | 10 | 0.0 | 0.0 | 0.0 | 49.4 | 21.2 | 0.0 | 11.9 | 0.0 | 17.5 | 0.0 | 0.0 |
List of abbreviations
- CE
- community engagement
- CI
- confidence interval
- DWP
- Department for Work and Pensions
- ESA
- Employment and Support Allowance
- HES
- Hospital Episode Statistics
- HSE
- Health Survey for England
- IB
- Incapacity Benefit
- IS
- income support
- JSA
- Jobseeker’s Allowance
- JSA-IB
- Jobseeker’s Allowance – Invalidity Benefit
- MORI
- Market & Opinion Research International
- NDC
- New Deal for Communities
- NET
- National Evaluation Team
- NIHR
- National Institute for Health Research
- NRA
- Neighbourhood Regeneration Agency
- NVQ
- National Vocational Qualification
- ONS
- Office for National Statistics
- SDA
- Severe Disablement Allowance