
Notes
Article history
The research reported in this issue of the journal was funded by the PHR programme as project number 12/133/20. The contractual start date was in February 2014. The final report began editorial review in April 2015 and was accepted for publication in November 2015. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PHR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
Professor Gail Mountain is a member of the National Institute for Health Research Health Technology Assessment Commissioning Board.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2016. This work was produced by Baxter et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Introduction
With a growing proportion of the population approaching the age of retirement, there has been an increasing focus on how this sector of society can maintain their independence and mental and physical well-being as they age. The potential future demand for health care in this population suggests that this stage of life would be an opportune time at which to intervene with health-promotion activities.
It has been argued that transition points in life, such as the approach towards and the early years of retirement, present key opportunities for interventions to improve the health of the population. 1 In particular, the transition to retirement is associated with changes in physical activity levels as a result of changing lifestyle, and this period is thus a particularly important time at which to intervene in order to increase or maintain levels, especially in lower socioeconomic groups. 1
With the increase in the numbers of retired adults within the population, and the established link between exercise and health, interventions that may increase or preserve activity levels around the time of retirement have the potential to provide benefits in terms of increased health and well-being for people in later life. There are also potential economic benefits from a reduction in health-service use. The nature of the retirement transition has undergone considerable change in recent years, with varying patterns of work, the abolition of the compulsory retirement age and increases in the numbers of people in part-time employment. 2 These changes may all blur the boundary between working life and retirement, making the process of retirement transition potentially more complex.
It has been recognised for some years that a large proportion of people aged over 50 years are sedentary (i.e. take < 30 minutes of moderate-intensity physical activity a week), and few people take the recommended levels of activity for improving health (30 minutes of moderate physical activity, such as brisk walking, household chores or dancing, at least five times a week). 3 Physical activity is known to have a wide range of health benefits, including the potential to reduce the risk of cardiovascular disease, diabetes, some cancers, disability and falls,3–8 and to improve overall quality of life in older people. 4–8 In view of these important benefits, the generally low levels of physical activity in this population are a cause for concern. 9,10
The transition to retirement may provide a significant opportunity to encourage people to maintain or increase their activity levels. Retirement can represent a major life change for individuals, with changes or disruptions to daily routines and self-perceptions. Retirement may, therefore, enable individuals to make changes to their activity levels that are much more difficult to make or sustain when their circumstances or environment remain the same. Interventions that provide the opportunity or motivation for individuals to maintain or increase physical activity at the point of retirement therefore have the potential to make an important contribution to establishing a healthier older adult population.
The number of people aged 65 years and over is projected to rise by nearly 50% (48.7%) in the next 20 years to over 16 million people worldwide. 11 It is therefore increasingly important to maintain a healthy older population with individuals who are able to contribute to society (e.g. by engaging in voluntary work or by acting as carers for spouses or grandchildren). Thus, there is a need to examine interventions that aim to increase or maintain physical activity in older people during and shortly after the transition to retirement and to identify how positive changes in activity levels at this key transition point can be effectively (and cost-effectively) encouraged, without exacerbating health inequalities in later life.
In addition to the need to encourage physical activity in the older adult population, recent systematic reviews have highlighted health inequalities in response to physical activity interventions and inequalities in levels of physical activity and health status in the retired population. 12,13 Appropriately targeted interventions have the potential to encourage physical activity at this life transition and to ensure that inequalities in health and well-being are not widened at retirement. This is particularly true where retirement is a positive choice (i.e. for those with more resources and/or better health) rather than an enforced and negative change in employment and financial status (i.e. for those with fewer resources and/or poorer health).
Recent systematic reviews of evidence (summarised later in this report) suggest that, without intervention, physical activity levels after retirement tend to increase in older people from higher socioeconomic groups, but decrease in those in lower socioeconomic groups. Socioeconomic status (SES) may moderate the impact of retirement on physical activity levels (with only higher social classes associated with increases in physical activity at retirement). Studies have also described that particular barriers among those from low socioeconomic backgrounds may include a lack of time owing to increased family responsibilities and the attachment of low personal value to recreational physical activity. Inequalities may also be the result of wider environmental or ecological factors or differing access to technology between populations. Therefore, the point of retirement appears to present a risk for widening health inequalities across different socioeconomic classes.
Aims and objectives
We aimed to conduct a systematic review and meta-synthesis of UK and international evidence on the types and effectiveness of interventions to increase physical activity among people around the time of retirement, including data regarding factors that may enhance or mitigate outcomes. The results of the review could inform the development and delivery of interventions to promote physical activity in the transition from paid work to retirement. Specific research aims were:
-
to systematically identify, appraise and synthesise UK and international evidence reporting outcomes resulting from interventions to maintain or increase physical activity in older adults in the period immediately before or after their retirement from paid employment
-
to determine how applicable this evidence might be to the UK context
-
to identify factors that may underpin the effectiveness or acceptability of interventions by exploring qualitative literature reporting the perceptions of older people and service providers with regard to facilitators or obstacles to successful outcomes
-
to explore how interventions may address issues of health inequalities.
The specific objectives to meet these aims were:
-
to identify the most effective interventions to maintain and/or increase physical activity in older people during and shortly after the transition to retirement by conducting comprehensive and systematic searches for published and unpublished effectiveness evidence (including grey literature)
-
to determine the best practice principles for effective physical activity interventions in this population by considering the qualitative evidence to provide context and examination of social and cultural issues surrounding intervention effectiveness and acceptability
-
to examine any evidence regarding the impact of interventions in different populations and/or the potential for retirement to increase health inequalities
-
to generate a critical meta-synthesis of the evidence suitable to inform policy decisions and disseminate to relevant audiences.
The population (patient) group
This systematic review considered older adults who were about to retire or who had recently retired.
The intervention
Interventions examined had the reported aim of maintaining or increasing physical activity, delivered in any context and by any method.
Comparator
The review included studies with any comparator or no comparator.
Outcomes
Outcomes of interest were those relating to physical activity levels recorded by validated measures/scales, or other indirect measures such as hours of activity, well-being or measures of physical or mental health.
How this study has changed from protocol
At the outset of the review we had not intended to specify an age range for inclusion, as retirement age may vary and the length of the transition period could also differ between individuals. In the protocol we stated that we would revisit this decision as the review progressed. We were able to identify only one paper that specifically referred to the study population as being about to retire or newly retired, with the majority of studies describing populations of older adults by average age or age range only. We therefore took the decision to develop an applicability categorisation based on age, which we used as a proxy for the retirement transition period, as described in Chapter 2.
Owing to the nature of the identified literature, we were unable to carry out our planned meta-analysis. Although there was a good number of studies with experimental designs, the heterogeneity in outcomes measured and the small number of studies with no-intervention comparators precluded an examination of effectiveness by meta-analysis. We therefore completed a narrative summary and used Harvest plot visual summaries.
We also carried out an alternative form of meta-synthesis across the quantitative and qualitative literature to that originally planned. The lack of quantitative studies relating to specific interventions precluded use of the qualitative data as explanatory insight into intervention outcomes. Instead, we combined the two sets of data via a comparison of intervention content reported in effectiveness papers, versus optimal content as reported in the qualitative papers.
In the original proposal we had stated that we would provide audio summaries for each of the included papers in order to enhance accessibility of the research to a lay audience. Owing to the extensive volume of included literature, we have instead produced an accessible screencast presentation which summarises the background to the study, the methods and the findings (see http://youtu.be/47jA4OUWfdQ).
Chapter 2 Methods
A number of reviews of physical activity interventions for older adults have been carried out. However, a broad-based systematic review examining both qualitative and quantitative evidence across all forms of intervention in adults around the point of transition to retirement was needed. We adopted a review method that was able to combine multiple data types to produce a broad evidence synthesis. We believe that this approach was required to best examine the international evidence on interventions and to ascertain whether or not and how these interventions would be best applied in a UK context, in order to inform future guidelines and the development and implementation of effective interventions across the population.
Development of the review protocol
A review protocol was developed prior to beginning the study. The protocol outlined the research questions, and detailed methods for carrying out the review in line with guidance from the Centre for Reviews and Dissemination. 14 The protocol encompassed: methods for identifying research evidence; method for selecting studies; method of data extraction; the process of assessing the methodological rigour of included studies; and synthesis methods. The protocol was registered with the PROSPERO database as CRD42014007446.
In the scoping phase of the project, we consulted with a range of stakeholders including older people, professionals working with older people and researchers with expertise in the field, in order to assist in the development of the scope of our review and the search terms used. In total, 35 people contributed to the consultation process in informal focus-group settings.
All participants were asked to discuss the following three questions:
-
What characteristics best describe an older person? How old is ‘older’ and how does this relate to retirement?
-
What activities do you think would help an older person to remain healthy in retirement?
-
What might stop an older person from being active in retirement?
Overall, there was a considerable degree of consensus between participants in the group discussions. In terms of describing an older person, all respondents took the view that it was inappropriate to define being older in relation to a particular numerical age. Professionals did note that many services (such as in the NHS/social care) define older age as starting at 65 years, although they did not necessarily consider that this criterion should be applied throughout society. Many participants highlighted that the definition of ‘older’ has changed over time, as people are living longer and working longer (by choice or necessity). In relation to this, it was noted that retired people are not necessarily ‘old’.
‘Old’ seemed to be defined as ‘someone older than you’ and was described as being dependent on underlying health conditions. For example, a 60-year-old person with a chest condition might seem older than a 90-year-old in good health. It was also described as being dependent on ‘who you are as a person and the life you have lived’. Older people in the groups highlighted that you were only old when you felt that you were old, suggesting that definitions are related to individual state of mind as well as to physical health.
A broad range of activities were reported in respect to staying healthy in retirement. These ranged from activities that were clearly defined as physical activity (e.g. walking, cycling, swimming, tai chi), but also activities such as volunteering, running a social group, getting a dog and being a carer, which all required physical activity, but in which this was not seen by participants as being the main purpose of the activity. Participants also mentioned the importance of motivation to staying active and that participating in a group activity (such as a walking group) might improve motivation owing to the social aspects of such activities. Reducing isolation or replacing the loss of interaction with work colleges was described as important.
Factors that were outlined as potential barriers to remaining active in retirement were ill health (including the side effects of prescribed drugs), feeling tired, the physical environment, poor access to public transport or leisure facilities, having to care for someone else (such as a partner or grandchildren) and a lack of confidence, or depression. There was also discussion regarding expectations of how a retired person should behave; for example, the expectation that when you retire you slow down makes it acceptable to do so. The groups also highlighted the influence of the way in which retirement had come about (forced retirement vs. choosing to retire); for example, in situations where ill health or an accident had forced retirement, it was harder to then be active.
The results of these consultations influenced how we defined the parameters of the review. The input that we received confirmed the need to have broad inclusion criteria in relation to the types of intervention that we would consider, ensuring that activities such as volunteering, which may not be considered physical activity traditionally, were eligible for the review and specifically included in search strategies. This consultation also provided valuable input regarding age inclusion criteria, with the emphasis that retirement did not mean a specific age, but instead could occur over a range in time. This underpinned our decision not to set age-limit parameters to the review at the outset of the work.
Involvement of patients and the public
In addition to the involvement of patients and the public during the scoping phase described above, the advisory group for the project also had representation from retired people. This was of benefit to the study in terms of providing advice on the application prior to submission, providing advice during the ongoing review regarding key terms during the searching phase of the work, and later input into the process in order to assist the team in understanding and interpreting the review findings. The inclusion of patient and public members on the advisory group was also valuable in terms of identifying avenues for dissemination and translating the key messages of the work for a lay audience.
Following completion of the review, we presented and discussed the findings at a series of sessions with groups of retired people and staff providing services to older adults. We sought views regarding whether or not there may be issues of applicability of the evidence to the retirement transition in terms of if any of the interventions described in the literature may not be suitable for people around retirement; how far the factors reported in the qualitative literature may influence the amount of physical activity people close to retirement may do; and if elements of interventions reported may influence whether or not someone around retirement would take part in them. This phase of the work provided valuable insights into the translation and applicability of the study findings to the retirement population.
Identification of studies
Search strategies
A systematic and comprehensive literature search of key health and medical databases was undertaken from March to December 2014. The searching process aimed to identify studies that reported the effectiveness of interventions for people around the transition to retirement, as well as studies that reported the views and perceptions of older adults and staff regarding interventions. Searching was carried out for both reviews in parallel, with allocation to either effectiveness or qualitative reviews at the point of identification and selection of studies for potential inclusion. The search process was recorded in detail and included lists of databases searched, the dates on which searches were run, the limits applied, the number of hits and duplication as per Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. 15 The search strategy is provided in Appendix 1.
The search strategy was developed by the information specialist on the team (Helen Buckley-Woods) who undertook electronic searching using iterative methods to create a database of citations using Reference Manager version 12 (Thomson ResearchSoft, San Francisco, CA, USA). The searching process was both iterative and emergent,16 with the results of an initial search informing the development of a subsequent search strategy (and so on), in order to explore fully the evidence relevant to the research questions. Database searching alone is not sufficient to provide the necessary evidence for a systematic review17,18 so ‘supplementary’ searching techniques, such as citation searching, were employed to ensure a comprehensive approach to identifying the evidence. As public health evidence is typically dispersed across a number of disciplinary fields, a wide variety of data sources were searched to include medicine and health, social science and specialist bibliographic databases (such as SPORTDiscus). Sources to identify grey literature were also explored. Searches were limited to 1990 to present where sources allowed.
First search
An initial search was developed using terms that reflect the concept of the transition into retirement combined with terms that reflect the concept of physical activity. ‘Retirement’ terms were broad to reflect the population of interest and the varied circumstances of ‘retirement’ (i.e. not only from full-time employment). Hence, terms for redundancy, ‘empty-nest’ and other similar circumstances of role change (such as becoming a mature student) were included. The search strategy was informed by an existing scoping search and incorporated suggestions for terms and concepts from the project team and as a result of consultation in stakeholder workshops.
Second search
The initial search retrieved a limited number of papers that specifically referred to the transition to retirement or to retirement as a concept. In order to assess whether or not this was a true reflection of the published literature, a new search was developed which used terms for older age to reflect the population of interest. These terms were combined with the terms for physical activity that were used in the initial search. Combining only these two facets of the question would retrieve unmanageable numbers of papers, so a modified study filter was applied to identify quantitative studies of either clinical trial or observational design.
Citation searching
In addition to standard electronic database searching, citation searching was undertaken later in the project (November–December 2014). Two sets of papers were used for citation searches. First, citations to a small set of existing reviews on the topic of interest were retrieved. Second, citations to both qualitative and quantitative included papers were identified, producing a further substantial set of results.
Grey literature
Searches for grey literature were undertaken in order to identify any reports or evaluations of ‘grass roots’ projects or other evidence not indexed in bibliographic databases and also to minimise problems of publication bias. These searches were either in specific grey literature sources such as ‘Index to Theses’ and ‘OpenGrey’ or by searching specific topic-relevant websites.
Sources searched
The following electronic databases were searched for published and unpublished research evidence from 1990 onwards:
-
Applied Social Sciences Index and Abstracts (via ProQuest).
-
Cumulative Index to Nursing and Allied Health Literature (via EBSCOhost).
-
Cochrane Library, including Database of Abstracts of Reviews of Effects, Cochrane Central Register of Controlled Trials, Health Technology Assessments and Cochrane Database of Systematic Reviews (via Wiley).
-
Health Management Information Consortium (via Ovid).
-
MEDLINE and MEDLINE In-Process & Other Non-Indexed Citations (via Ovid).
-
Science Citation Index via Web of Knowledge (Thomson ISI).
-
Social Science Citation Index via Web of Knowledge (Thomson ISI).
-
Sociological Abstracts (via ProQuest).
-
PsycINFO (via Ovid).
-
Social Policy and Practice (via Ovid).
-
SPORTDiscus (via EBSCOhost).
-
Evidence for Policy and Practice Information and Co-ordinating Centre Databases: Bibliomap, Database of Promoting Health Effectiveness Reviews, Trials Register of Promoting Health Interventions.
-
The database on Obesity and Sedentary behaviour studies: http://eppi.ioe.ac.uk/.
-
Open Grey: www.opengrey.eu/.
-
Index to Theses: www.theses.com.eresources.shef.ac.uk/default.asp.
-
Conference Papers Index Science and Social Science (via Web of Science).
-
Department of Health: www.dh.gov.uk.
-
BHF national centre for physical activity: www.bhfactive.org.uk/.
-
U3 A: www.u3a.org.uk/.
-
Web search (Duck Duck Go): https://duckduckgo.com/.
All citations were imported into Reference Manager (version 12) and duplicates deleted prior to scrutiny by members of the team.
Search restrictions
Searches were limited by date (1990 to present), as the review was aiming to synthesise the most up-to-date evidence. The searches did not set an English-language restriction. We included studies published in developed countries and, although we intended that the review would be predominantly limited to work published in English to ensure that papers were relevant to the UK context, we aimed to search for and include any additional key international papers that had an English abstract and that we were able to obtain.
Selection of papers
Inclusion and exclusion criteria
Population
We aimed to include studies that were carried out with people during and shortly after the transition to retirement. However, we also considered studies of other populations for which we might be able to make an association with the recently retired population, for example, people who have been made redundant or who have given up work to become a carer. Our key population was therefore older people who were not in paid employment (part- or full-time), and those about to leave paid employment.
Following input during our initial consultation phase, which emphasised that retirement did not begin at a particular age, we aimed to be flexible in our definition of ‘retired people’, as there is no clear and universally accepted definition. We did not, therefore, initially intend to impose age restrictions on our searching beyond an inclusive definition of ‘older adults’ as being 50 years and over (thus ensuring that retirement in different professions such as the police force were included). As outlined in our study protocol, further on in the process we intended to consider the relevance and applicability of including studies of older adults of any age in the synthesis.
Following completion of the initial phases of searching, as a result of the types of study that we were finding, we developed a system of applicability criteria with age serving as a proxy for retirement transition (see Process of selection of studies). These criteria excluded studies with participants below the age of 49 years or over 75 years, as these were furthest from statutory retirement ages and were considered to have limited applicability to the about-to retire or recently retired population.
We excluded study populations in which the intervention was provided for a specific clinical condition (e.g. people with coronary heart disease or following specific cardiac events such as heart attack, diabetes, cancer or osteoarthritis). We also excluded papers that described the study sample as being elderly and frail or as having limited mobility. We did not exclude patients who visited their general practitioner (GP) for a consultation and were recruited via this means to a non-clinical physical activity intervention.
Interventions
We included studies of any intervention aiming to increase and/or maintain levels of physical activity which could be applied to those older adults in the transition to retirement. We did not place any limitations regarding the setting/context in which interventions were conducted. Physical activity interventions delivered in any setting that were targeted at, or had the potential to affect, older people in the transition to retirement were eligible for inclusion, for example, health settings, community settings and residential/supported care settings and community/voluntary sector groups.
We excluded interventions that had the purpose of improving a clinical condition rather than increasing physical activity more generally. We excluded interventions that were described as aiming to increase stretching/flexibility or balance rather than activity and those described as specifically aiming to reduce falls in older people.
Outcomes
Physical activity is defined by the World Health Organization as ‘any bodily movement produced by skeletal muscles that requires energy expenditure’. 19 We therefore adopted a broad inclusion criteria in terms of outcomes. This included outcomes that measure physical activity directly using a validated scale or other tool, as well as those that report indirect measures related to physical activity, such as hours of gardening or participating in walking groups. We also included papers reporting other relevant outcomes such as social, psychological, behavioural and environmental factors related to increasing and/or maintaining physical activity in older people. We excluded papers that reported exclusively clinical outcomes such as cardiac function tests and blood sugar levels (papers with both clinical and physical activity outcomes were eligible for inclusion). We excluded studies concerned solely with stretching and flexibility outcomes.
Comparators
All comparator conditions were considered, as well as interventions with no concurrent comparator.
Study design
With the increasing recognition in the literature that a broad range of evidence is needed to inform the depth and applicability of review findings, experimental, observational and qualitative studies were included in the review. The review included designs that may be termed randomised controlled trials (RCTs), randomised crossover trials, cluster randomised trials, quasi-experimental studies, non-RCTs, cohort studies, before and after (BA)/longitudinal studies, case-control studies and qualitative studies. We excluded studies using a survey design. In order to maximise relevance, we included grey literature from the UK.
Other inclusion/exclusion criteria
We included studies from any developed country that is a member of the Organisation for Economic Co-operation and Development (OECD). As outlined above, we included studies published in English, and considered translations of those studies with relevant English abstracts. As noted above, the cut-off date for studies was 1990.
Process of selection of studies
Citations retrieved via the searching process were uploaded to a Reference Manager database. This database of study titles and abstracts was independently screened by two reviewers and disputes were resolved by consulting other team members. This screening process entailed the systematic coding of each citation according to its content. Codes were applied to each paper based on a categorisation developed by the team from previous systematic review work. The coding included categorising papers that fell outside the inclusion criteria (e.g. excluded population, excluded design, excluded intervention) as well as citations potentially relevant to the clinical effectiveness review and those potentially relevant to the qualitative review.
Full-paper copies of all citations coded as potentially relevant were then retrieved for systematic screening. Papers excluded at this full-paper screening stage were recorded and details regarding the reason for exclusion were provided.
Following our two large electronic database searches, we examined the scope of the literature that we had identified, and revisited our study questions and population age inclusion criterion. We had identified a large number of papers that described study populations as being older adults and/or those aged 40 years and over. However, we had found only one paper that specifically referred to the participants as being recently retired. Apart from this one paper, all other literature we identified provided only age bands or average ages for their study populations, with a minority including references to numbers in employment/not in employment and a smaller number still making reference to retirement. The nature of the identified literature therefore led us to further consider which types of papers provided data from older adult study participants that would best answer our research question and were therefore most applicable to those in the phase of retirement transition.
We adopted an approach to the selection of papers for review based on using age as a proxy for the period of retirement transition, where this was not specifically reported. We developed a grading system of applicability for the papers, whereby A1 papers had populations described as recently retired or about to retire, A2 papers had a population mean or median age of 55–69 years, A3i papers had a population mean/median in the range of age 70–75 years, and A3ii papers had a population mean/median of age 49–54 years. Owing to the large volume of literature identified (see Figures 1 and 2) we took the decision to exclude papers that had study participants with an average age of over 75 years or below 49 years, as these adults were furthest from retirement age and the data may have had limited applicability to our research question. A report from the OECD20 provides the statutory retirement age for men and women in each OECD country. It outlines that the age is either 65 or 67 years in all but three countries (68 years in two countries and 69 years in one). Further information regarding this selection process is detailed in the results section.
Data extraction strategy
Studies that met the inclusion criteria following the selection process above were read in detail and data were extracted. An extraction form was developed using the previous expertise of the review team to ensure consistency across the data retrieved from each study. The data extraction form recorded authors, date, study design, study aim, study population, comparator (if any), details of the intervention (including who provided the intervention, type of intervention and dosage). Three members of the research team carried out the data extraction. Data for each individual study were extracted by one reviewer and, in order to ensure rigour, each extraction was checked against the paper by a second member of the team.
Quality appraisal strategy
Quality assessment is a key aspect of systematic reviews in order to ensure that poorly designed studies are not given too much weight so as not to bias the conclusions of a review. As the review included a wide range of study designs, assessment required a sufficiently flexible and appropriate tool. Quality assessment of the effectiveness studies was therefore based on the Cochrane criteria for judging risk of bias. 21 This evaluation method classifies studies in terms of sources of potential bias within studies: selection bias; performance bias; attrition bias; detection bias; and reporting bias. As the assessment tool used within this approach is designed for randomised controlled study designs, we adapted the criteria to make them suitable for use across wider study designs including observational as well as experimental designs (Table 1). The detailed assessment for each study is provided in Appendix 2.
| Potential risk of bias | Bias present? | Detail of concerns |
|---|---|---|
| Selection bias | ||
| Method used to generate the allocation sequence, method used to conceal the allocation sequence, characteristics of participant group(s) | Y/N/unclear | |
| Performance bias | ||
| Measures used to blind participants and personnel and outcome assessors, presence of other potential threats to validity | Y/N/unclear | |
| Attrition bias | ||
| Incomplete outcome data, high level of withdrawals from the study | Y/N/unclear | |
| Detection bias | ||
| Accuracy of measurement of outcomes, length of follow-up | Y/N/unclear | |
| Reporting bias | ||
| Selective reporting, accuracy of reporting | Y/N/unclear | |
Assessment of quality for the qualitative papers was carried out using an eight-item tool adapted from the Critical Appraisal Skills Programme (CASP) tool for qualitative studies (Table 2). 22 The quality scoring for each study is presented in tabular form across each of the eight items (see Appendix 3).
| Quality appraisal tool for qualitative studies | |
|---|---|
| 1. Was there a clear statement of the aim of the research? | Y/N |
| 2. Is a qualitative methodology appropriate to address the aims of the research? | Y/N |
| 3. Was the recruitment strategy appropriate to the aims of the research? | Y/N/unclear |
| 4. Were the data collected in a way that addressed the research issue? | Y/N/unclear |
| 5. Has the relationship between researcher and participant been adequately considered? | Y/N |
| 6. Have ethical issues been taken into account? | Y/N/unclear |
| 7. Was the data analysis sufficiently rigorous? | Y/N |
| 8. Is there a clear statement of findings? | Y/N |
Data analysis and synthesis strategy
Effectiveness studies
Data were synthesised in a form appropriate to the data type. It was proposed that meta-analysis calculating summary statistics would be used if heterogeneity permitted, with use of graphs, frequency distributions and forest plots. It was anticipated that subgroups including age of participants, learning disability, intervention content and delivery agent would be examined if numbers permitted. The heterogeneity of the included work precluded summarising the studies via meta-analysis, as described in Chapter 3, Intervention effectiveness by typology. In order to provide a visual summary, we drew on Harvest plot techniques to examine intervention outcomes across the different types and to perform comparison of where there was greater evidence of rigour. 23
Effectiveness review findings were reported using narrative synthesis methods. We tabulated characteristics of the included studies and examined outcomes by characteristics such as intervention content, agent of delivery, intervention dosage and length of follow-up. Relationships between studies and outcomes within these typologies were scrutinised.
Qualitative studies
Qualitative data were synthesised using thematic synthesis methods in order to develop an overview of recurring perceptions of potential obstacles to successful outcomes within the data. 24 This method comprises familiarisation with each paper and coding of the finding sections (which constitute the ‘data’ for the synthesis) according to key concepts within the findings. Although some data may directly address the research question, sometimes information such as barriers and facilitators to implementation has to be inferred from the findings, as the original study may not have been designed to have the same focus as the review question. 24
Combining quantitative and qualitative data
We had intended to use a meta-synthesis method which uses the qualitative data to add explanatory value to effectiveness study findings. 25,26 However, we found little of the qualitative literature referred specifically to interventions; instead, it tended to report more general views and perceptions of physical activity in retirement and/or older age, as well as elements of activity that may be most appealing. We therefore used a meta-synthesis method whereby themes relating to facilitators of engagement in physical activity were used to examine the content of interventions included in the review of effectiveness.
Chapter 3 Results of the effectiveness review
Quantity of the evidence available
The initial electronic database searches using terms related to retirement/life transition identified 4935 citations following de-duplication. From this database of citations, 809 potentially relevant papers were retrieved for further scrutiny. We developed a grading system of applicability for the papers, in which A1 papers had populations described as recently retired or about to retire, A2 papers had a population mean or median of 55–69 years, A3i papers had a population mean/median in the range 70–75 years of age, and A3ii papers had a population mean/median in the range of 49–54 years of age. Detailed examination of these articles resulted in 19 A1/A2 and 16 A3 papers that met the inclusion criteria for the review of clinical effectiveness. Sixteen further papers relating to the review of effectiveness were identified from additional searching strategies (citation searching or reference list scrutiny), giving a total of 35 A1/A2 and 16 A3 papers included from this first search.
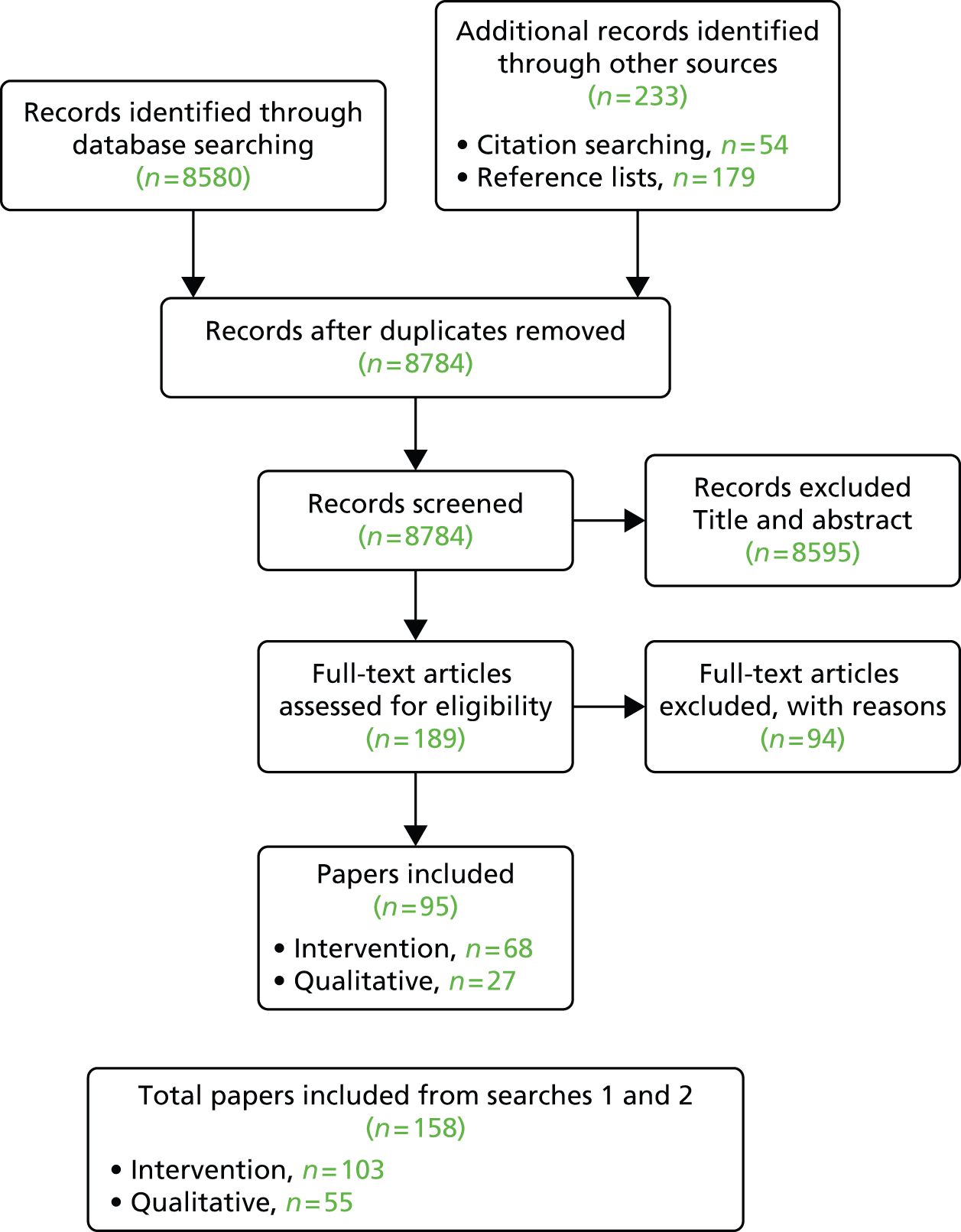
The second electronic database search using terms related to older adults identified an additional 8318 citations that had not already been retrieved. From these, 169 potentially relevant papers were retrieved for further scrutiny. Examination of these articles resulted in an additional 45 A1/A2 papers and 14 A3 papers that met the inclusion criteria for the review of clinical effectiveness. Twelve further A1/A2 papers relating to the review of effectiveness were identified from additional searching strategies (citation searching or reference list scrutiny). Figures 1 and 2 provides a detailed illustration of the process of study selection for each of our two phases of electronic database searching.
FIGURE 1.
Process of selection of studies: first search.
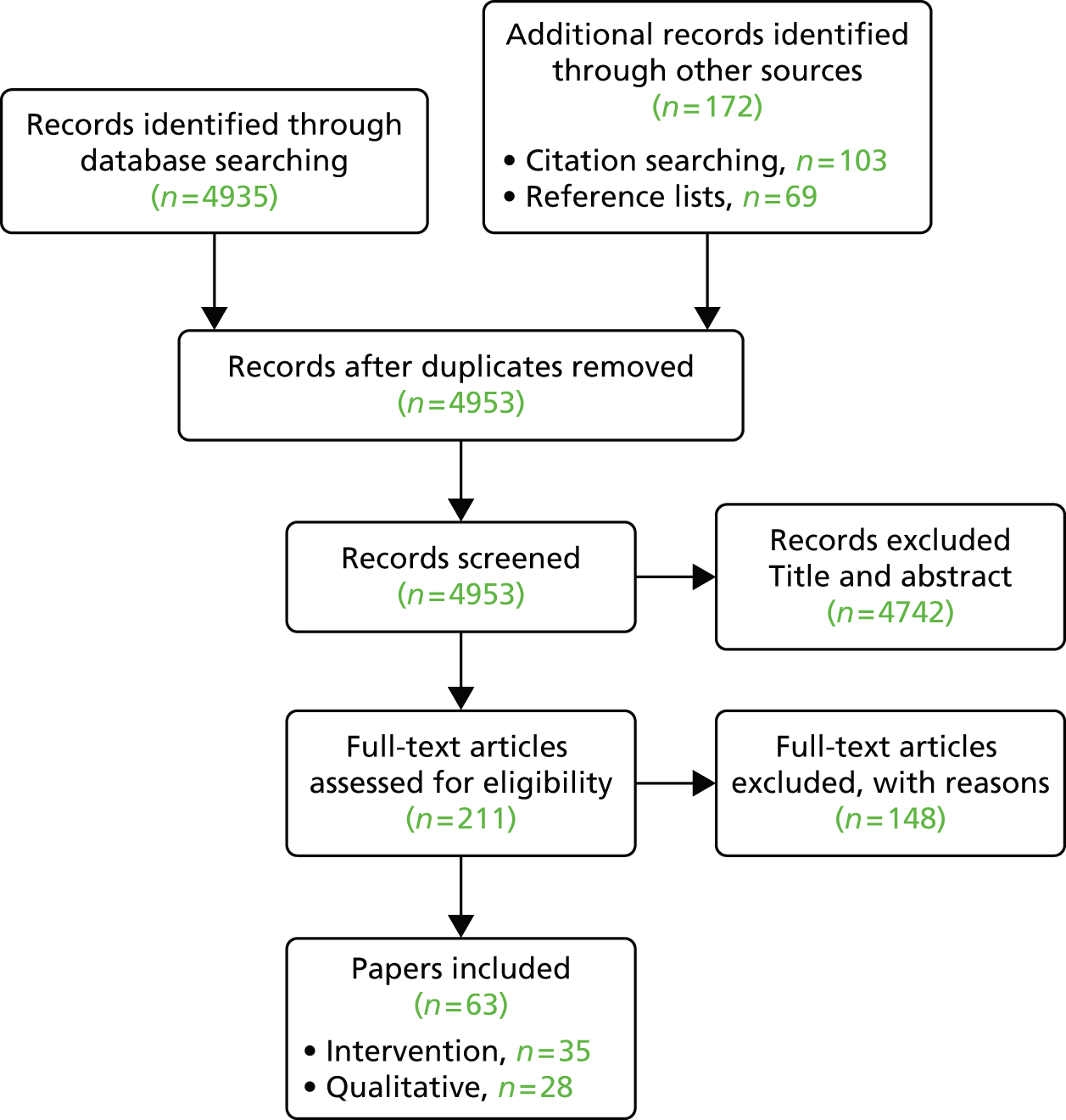
FIGURE 2.
Process of selection of studies: second search.
As outlined previously, there was little literature that described study participants as being our key population of interest, namely those about to retire or recently retired. A total of 63 papers fell within our proxy retirement transition age range (A2 papers) and 39 further papers fell within the wider age range (A3 papers).
There were a number of papers that reported data from the same study, either follow-up data in a later paper, or different aspects of a study including development of the intervention or implementation data. Of the 64 included A1/A2 papers, there were 48 unique studies.
Quality of the research available
We considered the potential for bias within included studies using the quality appraisal tool described earlier. Table 3 provides an overview of the quality assessment for the included intervention studies, with further detail provided in the expanded table in Appendix 2. The most frequent areas of concern related to limited reporting regarding the process of randomisation; the recruitment of volunteer participants; studies having two intervention arms with no control condition; the wide use of self-reported data for levels of physical activity; high rates of ineligible participants; and high rates of dropout in some studies.
| Study | Selection bias | Performance bias | Attrition bias | Detection bias | Reporting bias | Number of criteria met |
|---|---|---|---|---|---|---|
| Ackermann et al. (2005)27 | Y | Unclear | N | Y | N | 2 |
| Armit et al. (2005)28 | Unclear/not fully random | Unclear | N | Y | N | 2 |
| Burman et al. (2011)29 | Unclear | Unclear | Y | Y | N | 1 |
| Burke et al. (2013)30 | Unclear | Unclear | N | Y | N | 2 |
| Caperchione and Mummery (2006)31 | Y | Y | N | Y | N | 2 |
| Castro et al. (2001)32 | Unclear | N | Y | Y | N | 2 |
| Coronini-Cronberg et al. (2012)33 | N | N | Y | Y | N | 3 |
| Costanzo and Walker (2008)34 | Y | N | Y | Y | Y | 1 |
| Cox et al. (2008)35 | Y | N | Y | Y | N | 2 |
| Croteau et al. (2014)36 | Y | N | Y | N | N | 3 |
| de Jong et al. (2006)37 | Unclear | Unclear | Y | N | Y | 1 |
| de Jong et al. (2007)38 | Unclear | Unclear | Y | N | Y | 1 |
| Dorgo et al. (2009)39 | Unclear | Unclear | N | Unclear | Y | 1 |
| Elley et al. (2003)40 | Y | N | N | N | N | 4 |
| Finkelstein et al. (2008)41 | Y | N | N | N | N | 4 |
| Fries et al. (1993)42 | Y | N | Y | N | N | 3 |
| Fries et al. (1993)43 | Y | N | Y | N | N | 3 |
| Fujita et al. (2003)44 | Y | N | N | Y | N | 3 |
| Goldstein et al. (1999)45 | Y | N | N | Y | N | 3 |
| Hageman et al. (2005)46 | Y | N | N | N | N | 4 |
| Halbert et al. (2000)47 | Unclear | N | N | N | N | 4 |
| Hamdorf et al. (1992)48 | Y | Unclear | Y | Y | N | 1 |
| Hamdorf et al. (1993)49 | Y | Unclear | N | N | N | 3 |
| Hekler et al. (2012)50 | Y | Y | N | N | N | 3 |
| Hooker et al. (2005)51 | Y | Y | N | Y | N | 2 |
| Hughes et al. (2009)52 | Y | N | Y | N | N | 3 |
| Irvine et al. (2013)53 | Y | N | Y | N | N | 3 |
| Kamada et al. (2013)54 | N | N | N | Y | N | 4 |
| King et al. (2002)55 | Y | N | N | N | N | 4 |
| King et al. (2000)56 | N | N | N | N | N | 5 |
| King et al. (2007)57 | Unclear | N | N | Y | N | 2 |
| Koizumi et al. (2009)58 | Unclear | N | Unclear | N | N | 3 |
| Lawton et al. (2008)59 | Y | N | N | N | N | 4 |
| Marcus et al. (1997)60 | Y | Y | Y | Y | Y | 0 |
| Martinson et al. (2010)61 | N | N | N | Y | N | 4 |
| Martinson et al. (2008)62 | N | N | N | Y | N | 4 |
| Opdenacker et al. (2011)63 | Y | Y | Y | N | N | 2 |
| Opdenacker et al. (2008)64 | Y | Y | Y | N | N | 2 |
| Pasalich et al. (2013)65 | Y | N | N | Y | N | 4 |
| Peels et al. (2012)66 | Unclear | Unclear | NA | NA | N | 1 |
| Peels et al. (2012)67 | Unclear | Unclear | NA | NA | N | 1 |
| Peels et al. (2013)68 | Unclear | Unclear | Y | Y | N | 1 |
| Pereira et al. (1998)69 | Unclear | N | N | Y | N | 3 |
| Petrella et al. (2010)70 | Unclear | Unclear | N | N | N | 3 |
| Pinto et al. (2005)71 | Y | Unclear | N | N | N | 3 |
| Prabu et al. (2012)72 | Y | N | Y | N | N | 2 |
| Purath et al. (2013)73 | N | N | Y | N | N | 4 |
| Rowland et al. (1994)74 | Y | N | N | Y | N | 3 |
| Sawchuk et al. (2008)75 | Y | Unclear | N | Y | N | 2 |
| Stevens et al. (1998)76 | Y | Unclear | Y | Y | N | 1 |
| Strath et al. (2011)77 | Y | N | N | N | N | 4 |
| van Keulen et al. (2011)78 | N | N | Y | Y | N | 3 |
| van Stralen et al. (2009)79 | N | N | N | Y | N | 4 |
| van Stralen et al. (2010)80 | N | N | Y | Y | N | 3 |
| van Stralen et al. (2011)81 | N | N | Y | Y | N | 3 |
| van Stralen et al. (2009)82 | N | N | Y | Y | N | 3 |
| Walker et al. (2009)83 | N | N | N | Y | N | 4 |
| Walker et al. (2010)84 | N | N | N | N | N | 5 |
| Werkman et al. (2010)85 | N | N | N | N | N | 5 |
| Wijsman et al. (2013)86 | Y | N | N | Y | N | 3 |
| Wilcox et al. (2008)87 | Unclear | Y | Y | Y | N | 1 |
| Wilcox et al. (2009)88 | Unclear | Y | Y | Y | N | 1 |
| Wilcox et al. (2009)89 | Unclear | Y | Y | Y | N | 1 |
| Wilcox et al. (2006)90 | NA | NA | Y | NA | NA | NA |
| Total of numbers | 13 | 38 | 33 | 26 | 59 |
As shown in Table 3, only three studies56,84,85 met all five quality criteria. A total of 14 studies reported in 15 papers were judged as having a single area of potential bias. 40,41,46,47,54–56,59,61,62,65,73,77,79,83
Type of evidence available
Study design
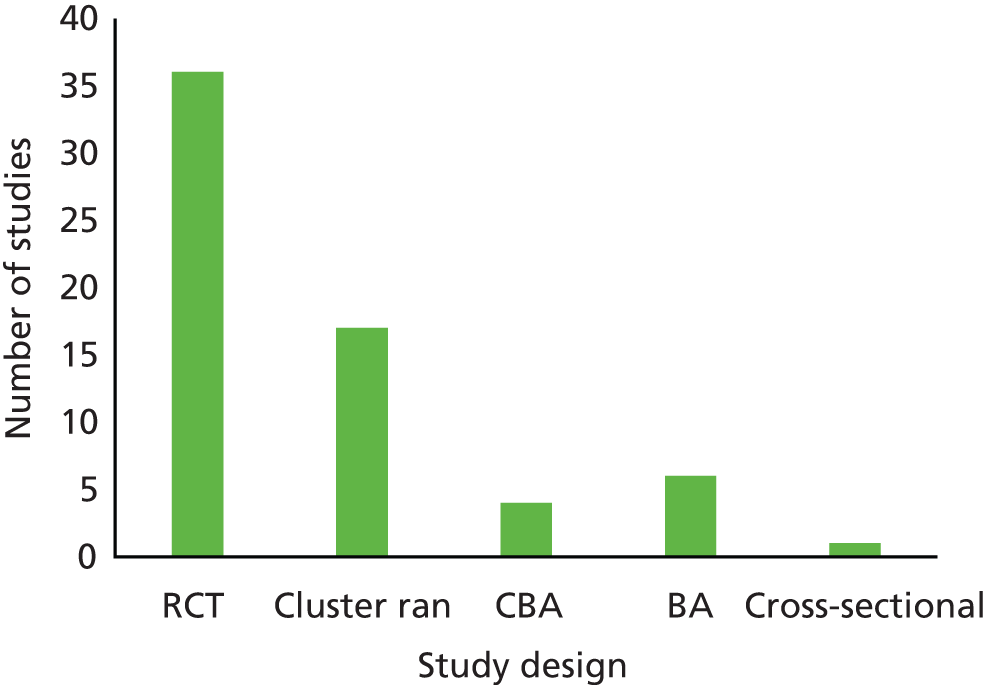
Figure 3 shows that the identified literature was of a reasonably high quality in terms of study design, with a large proportion (36) of the papers reporting studies using a randomised controlled design,28–32,34–36,39,41,44,46–50,52,53,55–59,61,62,69,71,73–78,83,84,86 and 18 papers reporting studies using a cluster randomised design. 27,37,38,40,42,43,45,54,66–68,70,79–82,85 See Appendix 3 for lists of the studies within each category.
FIGURE 3.
Number of intervention studies of each design. CBA, controlled before and after.
Population
Country of origin
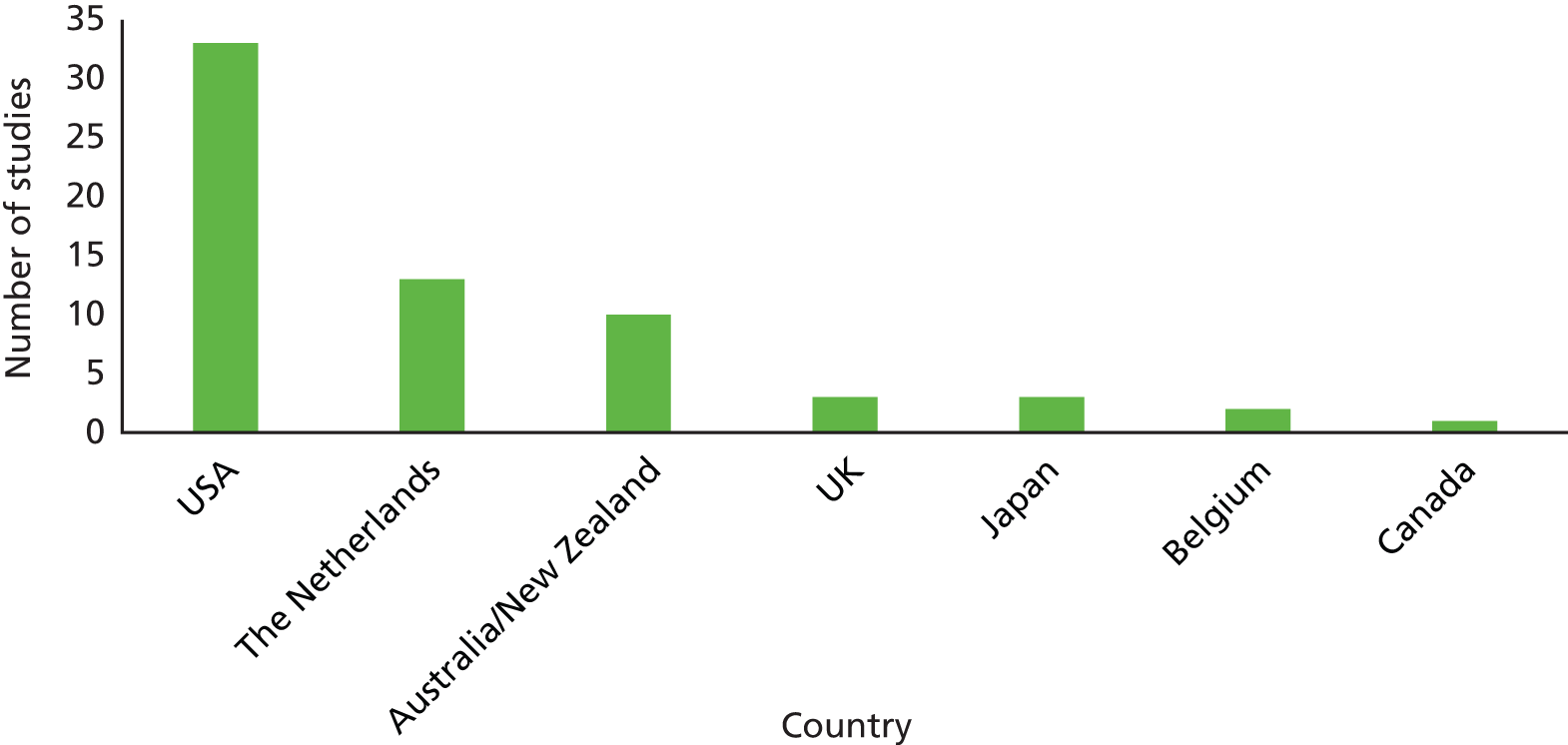
An overview of included studies by country of origin is provided in Figure 4. The greatest proportion of work was reported by authors based in the USA (33 papers),27,30,32,34,36,39,41–43,45,46,50–53,55–57,60–62,69,71–73,75,77,83,84 followed by authors based in the Netherlands and in Australia/New Zealand. Three of the papers were from the UK. 33,74,76 (See Appendix 3 for the list of studies within each category.)
FIGURE 4.
Number of intervention studies from each country.
Sex
The literature contained 34 papers with either all female participants or a majority of female participants28,30,31,34–36,40,41,46,48–53,55–59,61,62,69,72–75,77,83,84,87–90 (Figure 5) (see Appendix 3 for a list of studies). This contrasted with only two studies that recruited only males. 27,85
FIGURE 5.
Number of intervention studies by sex of participants.

Socioeconomic/educational status
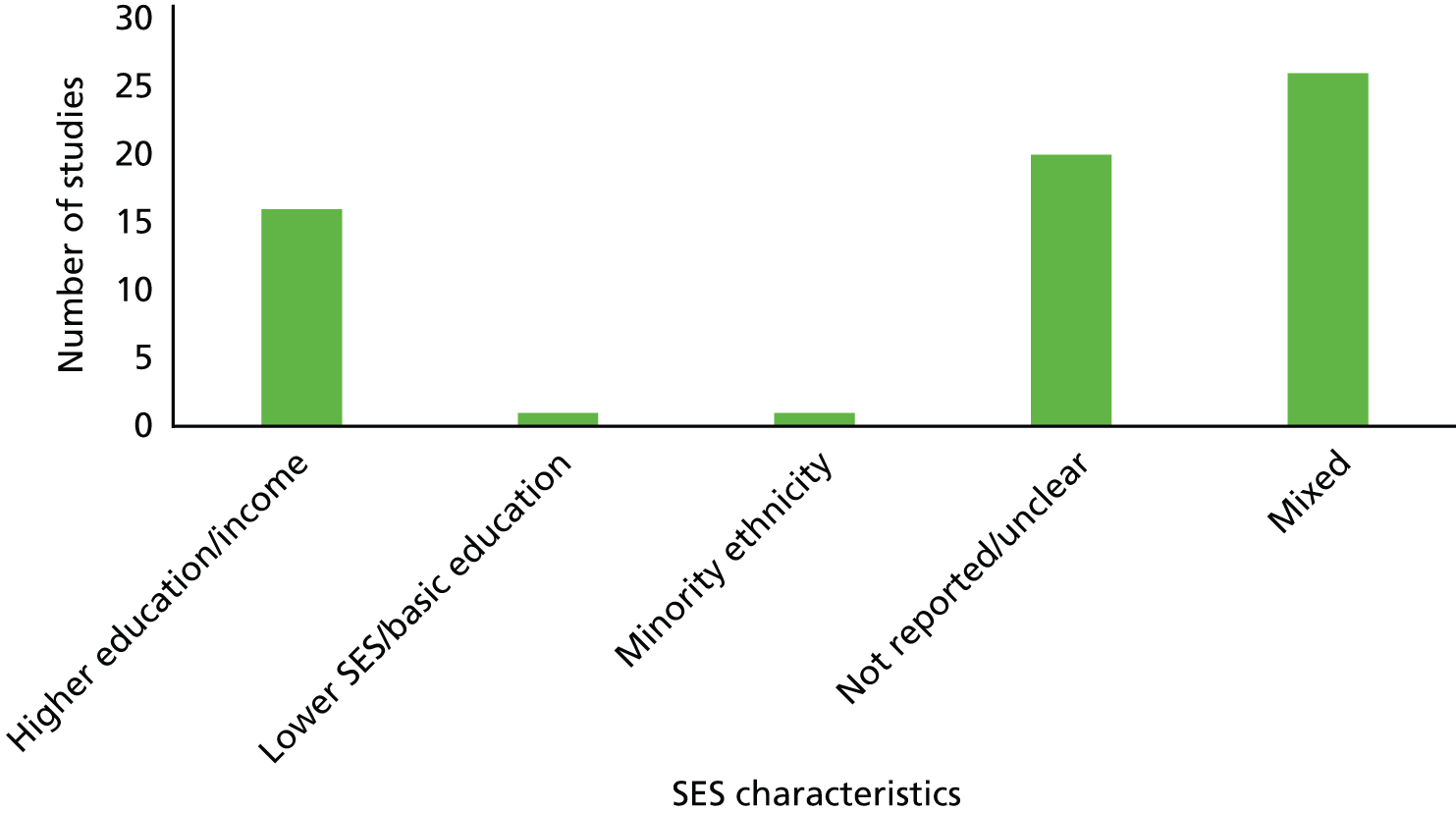
We identified only one study that described participants as being of predominantly low SES29 and one paper that described participants from a minority ethnic population. 75 Sixteen papers described their studies as being in predominantly more highly educated/higher income participants. 30,32,34–36,41,46,50,52,53,61,62,65,69,73,77 The majority of studies were either unclear regarding education/SES or included diverse/mixed participants. See Figure 6 for a summary graph and Appendix 3 for lists of studies within each category.
FIGURE 6.
Number of studies reporting socioeconomic characteristics of participants.
Physical activity level
Approximately half of the studies (34) recruited participants who were below recommended activity levels, with the majority of these using higher activity level as an exclusion criterion. 27–31,34–36,40,41,46,50,52,53,55–57,59–65,70,71,73,75,77,86–90 The other 29 papers32,33,37–39,42–45,47,48,51,54,58,66–69,72,74,76,78–85 did not detail inactivity as being an inclusion criterion, and therefore in the absence of any other reporting it is assumed that these participants were most likely to be of mixed activity levels. (See Appendix 3 for detail of the studies within these categories.)
Age of participants
As outlined above, in the absence of literature specifically examining people at retirement transition, we took the decision to grade the applicability of other papers that reported interventions in older adults, with the average age of participants standing as a proxy for retirement age. We developed a four-point applicability rating system, in which A1 studies were those that referred to participants as immediately before or after retirement, A2 studies were those with an average participant age in the most common retirement transition age range of 55–69 years, and A3 studies were those that were less likely to be applicable to the retirement transition period, having an average age of either 50–54 years (A3i) or 70–75 years (A3ii).
This rating system was based on the most common statutory retirement ages across OECD countries of 65 or 67 years. The band 55–69 years was, therefore, most likely to include those approaching retirement (and those taking early retirement) together with those in the period immediately following retirement, and was of most relevance to our research question. The A3 papers, although potentially relevant, were considered to be of lower applicability. These papers were identified and examined to ascertain whether or not there were any studies of particular significance to the review. Table 4 presents the papers rated A1 and A2, categorised by age range. In this report, we intend to focus our synthesis on these A1/2 studies, as those most relevant to the retirement transition. However, we will provide an overview of the A3 studies and also consider any similarities and differences between the A1/A2 group and A3 studies.
| Average age | Studies |
|---|---|
| 55–59 years | Caperchione and Mummery (2006)31 (> 50 years) Castro et al. (2001)32 (50–65 years) Costanzo and Walker (2008)34 (50–65 years) Cox et al. (2008)35 (50–70 years) de Jong et al. (2006)37 (55–65 years) de Jong et al. (2007)38 (55–65 years) Elley et al. (2003)40 (40–79 years) Finkelstein et al. (2008)41 (50–85 years) Hageman et al. (2005)46 (50–69 years) King et al. (2007)57 (45–81 years) Lawton et al. (2008)59 (mean 58.9 years, SD 7 years) Martinson et al. (2010),61 (2008)62 (50–70 years) Pereira et al. (1998)69 (50–65 years) Prabu et al. (2012)72 (average 57 years) Sawchuk et al. (2008)75 (50–74) Stevens et al. (1998)76 (mean 59.1 years) van Keulen et al. (2011)78 (mean 57.15 years, SD 7 years) Walker et al. (2009),83 (2010)84 (50–69 years) Werkman et al. (2010)85 (mean 59.5 years) |
| 60–65 years | Armit et al. (2005)28 (55–70 years) Burman et al. (2013)29 (50 years and older) Burke et al. (2013)30 (60–70 years) Croteau et al. (2014)36 (51–81 years) Goldstein et al. (1999)45 (50 years and above) Hamdorf et al. (1992),48 (1993)49 (mean 64.8 years) Hekler et al. (2012)50 (50 years or older) Irvine et al. (2013)53 (mean 60.3 years) Kamada et al. (2013)54 (40–79 years) King et al. (2007)57 (55 years and over) Peels et al. (2012),66 (2012),67 (2013)68 (over 50 years) Petrella et al. (2010)70 (55–85 years) Strath et al. (2011)77 (55–80 years) van Stralen et al. (2009),79 (2010),80 (2011),81 (2009)82 (average 64 years, SD 8.6 years) Wijsman et al. (2013)86 (60–70 years) |
| 66–69 years | Ackerman et al. (2005)27 (50 years and older) Dorgo et al. (2009)39 (60–82 years) Fries et al. (1993),42 (1993)43 (all retired) Fujita et al. (2003)44 (60–81 years) Halbert et al. (2000)47 (60 years and over) Hooker et al. (2005)51 (48–90 years) Hughes et al. (2009)52 (50 years or older) King et al. (2002)55 (over 65 years) Koizumi et al. (2009)58 (mean 67 years) Marcus et al. (1997)60 (over 50 years) Opdenacker et al. (2011),63 (2008)64 (60–83 years) Pasalich et al. (2013)65 (60–70 years) Pinto et al. (2005)71 (mean 68.5 years) Purath et al. (2013)73 (60–80 years) Rowland et al. (1994)74 (mean 66 years) Wilcox et al. (2008)87 (mean 68.4 years, SD 9 years) Wilcox et al. (2009),89 (2006)90 (50 years or older) Wilcox et al. (2009)88 (50 years or over) |
| No average | Coronini-Cronberg et al. (2012)33 (over 60 years) |
Retirement/employment
As described above, only a minority of papers made reference to the employment/retirement status of the older adults included in the studies. The 22 papers that provide this detail are listed in Table 5. As can be seen, four of the interventions were carried out in populations in which all individuals were described as retired. Where percentages of those employed are provided, it is not clear if the other non-employed participants were unemployed or retired or working part time. The challenge in identifying the retirement status of study populations in these papers was further highlighted by Hooker et al. 51 This study makes an interesting distinction between those participants that are categorised as ‘retired and working’ and those categorised as ‘retired and not working’. A further point of interest relates to the only paper we identified to describe the study population as recently retired. This paper85 gives the mean age of study participants as a seemingly young age of 59.5 years, which supports our decision to include those in their late fifties in our A2 applicability band.
| Study | Reported participant characteristics |
|---|---|
| Armit et al. (2005)28 | 81% retired |
| Burke et al. (2013)30 | 40% working |
| Costanzo and Walker (2008)34 | 1 (of 51) not employed |
| Cox et al. (2008)35 | 52–80% employed |
| Croteau et al. (2014)36 | 16 (of 36) employed |
| Finkelstein et al. (2008)41 | 28% retired |
| Fries et al. (1993),42 (1993)43 | All retired |
| Goldstein et al. (1999)45 | 36% employed |
| Hageman et al. (2005)46 | 6.7% retired |
| Halbert et al. (2000)47 | All retired |
| Hekler et al. (2012)50 | 56% employed |
| Hooker et al. (2005)51 | 49% retired, not working; 17.7% retired, working; 20.9% employed |
| Kamada et al. (2013)54 | 64% employed |
| King et al. (2007)57 | 48.5% working full-time |
| Martinson et al. (2010),61 (2008)62 | 77% employed |
| Opdenacker et al. (2008)64 | All retired |
| Pasalich et al. (2013)65 | 42% employed |
| Rowland et al. (1994)74 | All retired |
| Sawchuk et al. (2008)75 | 27% employed |
| Stevens et al. (1998)76 | 55% economically active |
| van Stralen et al. (2009)79 | 47% employed |
| Werkman et al. (2010)85 | Recently retired |
Intervention typology
The papers reported a varied range of intervention approaches, and included one study that intervened with health-care professionals in order to enhance the content of consultations,57 one that evaluated a community campaign54 and a further study that analysed the effect of providing free bus passes to older adults. 33 The remaining papers were divided into those that evaluated interventions provided to participants within their home (content was delivered via the telephone, via e-mail/internet or via post) and those where participants either travelled to their local community health centre/surgery for advice/counselling, attended classes/workshops, or took part in organised walks/swimming sessions. For many of these away-from-home interventions, it was unclear where exactly the sessions were held.
The in-home interventions often included multiple elements such as advice, pedometer use, keeping an exercise diary, and/or information. A number of the papers examined different variants of interventions rather than comparing with a control group. The Peels et al. 66–68 studies, for example, varied the delivery method (via the internet vs. via mail), and the content (additional environmental information vs. none). Croteau et al. 36 examined the addition of group sessions to a standard intervention, Sawchuk et al. 75 evaluated the addition of a pedometer to their programme and Strath et al. 77 included telephone calls for a subgroup of participants.
Outcomes measured
The included literature measured a wide range of outcomes, encompassing those that were self-reported via completion of questionnaires, in person, via telephone or via postal questionnaire. Outcomes that were measured by the research team included weight, body mass index (BMI) and fitness tests, together with data downloaded from pedometers or accelerometers. Table 6 outlines the physical activity measures that were used within the set of papers. Of note are only two papers which measured inactivity in addition to activity. 29,55 The first of these29 collected data on reported sitting time (minutes per week), and the second55 used a questionnaire (Measure of Older Adults’ Sedentary Time), with television viewing time considered to be the primary outcome of interest. In addition to these measures relating to physical activity, many papers also included a raft of other measures such as strength, balance, flexibility or falls, which we have not included as not directly relating to activity levels.
| Type of measure | Specific outcomes assessed |
|---|---|
| Objective measures | Activity Accelerometer Pedometer (daily steps/aerobic minutes) Retention and participation in programmes |
| Fitness 1-mile walk time 12-minute walk test 12-minute swim 1.6-km walk time Record of illness and injury Health benefit company data on claims made Rockport Walking Fitness Test |
|
| Biophysical Blood pressure Body fat Cardiovascular risk Body composition BMI Weight Waist circumference Biotrainer data Senior fitness tests of muscle strength, endurance and balance |
|
| Self-reported | Activity 7-day activity recall questionnaire (or modified version) Achievement of recommended minimum levels of moderate-intensity physical activity CHAMPS questionnaire used to calculate calorific expenditure Compendium of Physical Activity Tracking Guide Dutch Short Questionnaire to Assess Health-Enhancing Physical Activity Exercise history questionnaire Exercise Habits Scale Health Habits questionnaire Human Activity Profile International Physical Activity Questionnaire – Short Form Leisure Time Exercise Questionnaire Maximum current activity Measure of older adults’ sedentary time Minutes of moderate to vigorous physical activity National Travel Survey Older adults sedentary behaviour Physical Activity Scale for the Elderly Paffenbarger Sports and Exercise Index Reported level of regular physical activity Self-report daily log of activity Sitting time (minutes per week) Time spent walking Total weekly days and total weekly minutes of physical activity Travel diary |
| Fitness Comparative fitness rating Perceived fitness score |
|
| Psychosocial correlates Barriers to Self-Efficacy Scale Benefits and Barriers Scales Exercise Motivation Scale Exercise Self-Efficacy Scale Family Support for Exercise Habits Scale Friend support Physical activity group environment questionnaire Physical activity readiness questionnaire Physical improvement programme perceptions Physician-based assessment and counselling for exercise questionnaire Quality-of-life scales (SF-36) Reported awareness, attitude, social influences, motivation, intention, commitment, perceived environment, strategic planning, action planning and coping planning Satisfaction with the intervention Self-efficacy for Exercise Habits Scale Social Support and Exercise Survey Stage of change instrument |
|
| Health correlates Behavioural Risk Factors Surveillance system Center for Epidemiological Studies Depression Scale Normative Impairment Index Nottingham Health Profile questionnaire Perceived Stress Scale Satisfaction with body functioning Self-reported physical performance, perceived functioning and well-being Vitality Plus Scale |
Follow-up periods
Whereas 10 studies carried out outcome assessment immediately following the intervention,27,29,34,41,50,57,58,73,75,77 nine studies reported follow-up periods of > 12 months30,32,43,59,61,63,64,69,78,85 (Table 7).
| Length of follow-up | Studies |
|---|---|
| Immediate follow-up | Ackermann et al. (2005)27 Burke et al. (2013)30 Costanzo and Walker (2008)34 Finkelstein et al. (2008)41 Hekler et al. (2012)50 King et al. (2007)57 Koizumi et al. (2009)58 Purath et al. (2013)73 Sawchuk et al. (2008)75 Strath et al. (2011)77 |
| Up to 6 months | Armit et al. (2005)28 de Jong et al. (2006)37 Dorgo et al. (2009)39 Fujita et al. (2003)44 Hageman et al. (2005)46 Irvine et al. (2013)53 Marcus et al. (1997)60 Martinson et al. (2010)61 Pasalich et al. (2013)65 Peels et al. (2012)67 Pinto et al. (2005)71 |
| Up to 12 months | Caperchione and Mummery (2006)31 Cox et al. (2008)35 Croteau et al. (2014)36 de Jong et al. (2006)37 Elley et al. (2003)40 Fries et al. (1993)42 Goldstein et al. (1999)45 Halbert et al. (2000)47 Hamdorf et al. (1992),48 (1993)49 Hooker et al. (2005)51 Hughes et al. (2009)52 Kamada et al. (2013)54 King et al. (2002),55 (2000) 56 Peels et al. (2013)68 Petrella et al. (2010)70 Rowland et al. (1994)74 Stevens et al. (1998)76 van Stralen et al. (2009),79 (2010)80 Walker et al. (2009),83 (2010)84 |
| Over 12 months | Burman et al. (2011)29 Castro et al. (2001)32 Fries et al. (1993)43 Lawton et al. (2008)59 Martinson et al. (2010)61 Opdenacker et al. (2011),63 (2008)64 Pereira et al. (1998)69 van Keulen et al. (2011)78 Werkman et al. (2010)85 |
Intervention effectiveness by typology
As outlined above, there was a wide range of outcomes examined in the included studies. These ranged from those that were self-reported, including activity diaries and self-efficacy questionnaires, to those that were measured by research staff, including weight, BMI, blood pressure and fitness. The range of outcomes (see Table 9), as well as the limited number of studies comparing no-intervention control groups (rather than comparing several intervention arms), precluded the use of meta-analysis to provide a statistical summary of intervention effectiveness. We have therefore completed a narrative summary of the papers together with visual summaries to enable comparison between study findings. In the following section, studies within each intervention typology are briefly outlined and their key findings described.
Education of health-care professionals
One paper57 evaluated an intervention with staff which trained primary care providers to offer referrals to community exercise programmes for patients who reported before their clinic visit that they were ‘contemplative’ about regular exercise. This cluster RCT study found that patients were more likely to receive exercise advice from trained GPs. However, there was no significant difference in patient-reported regular exercise for the intervention group compared with controls.
Counselling and advice
Eleven included papers28,34,36,40,45,47,59,60,70,71,76 (10 studies) assessed the effectiveness of interventions comprising the giving of advice or counselling with seven of these providing stronger evidence of effect. One of these interventions was delivered by peer mentors, one by trained physicians, one by a nurse, two by exercise professionals, two encouraged patients to prompt their physician, and the final four papers examined combined physician and exercise professional input.
The Stevens et al. 76 paper from the UK evaluated both clinical effectiveness and cost-effectiveness of a 10-week programme, in which inactive people were invited to a consultation with an exercise professional. They were given information on physical activity and health and the local opportunities available to them to be more active. This study had a participant mean age of 59 years and found a net 10.6% [95% confidence interval (CI) 4.5% to 16.9%] reduction in the proportion of people classified as sedentary in the intervention group compared with the control group. In addition, the study found an increase in the mean number of self-reported episodes of physical activity per week in the intervention group compared with the control group (an additional 1.52 episodes, 95% CI 1.14 to 1.95 episodes) at 8 months’ follow-up. The cost of achieving the recommended level of activity for each person was estimated at £2500.
A study evaluating physician exercise prescriptions in Canada70 had two intervention arms, with prescription only and prescription plus counselling programmes. Around half the participants in this cluster RCT study were retired, with all having an inactive lifestyle. Cardiorespiratory fitness increased significantly (p < 0.001) at 12 months’ follow-up for both groups [prescription + counselling 3.02 ml of oxygen per kilogram of body weight per minute (ml/kg/minute) (95% CI 2.40 to 3.65 ml/kg/minute), and prescription only 2.21 ml/kg/minute (95% CI 1.27 to 3.15 ml/kg/minute) with no significant difference between the groups]. Physical activity was measured by 7-day recall, with estimated kilocalories/kilograms per day significantly increasing in both groups. However, the prescription plus counselling group increased significantly more than the prescription-only group (p = 0.006). A sex difference in response was noted, with women responding significantly better (improved predicted maximal oxygen consumption p < 0.001) to the prescription plus counselling intervention than prescription-only, and men benefiting equally from the interventions.
Lawton et al. 59 examined outcomes following a brief advice session led by a nurse for women with low activity levels (mean age 59 years). The counselling session was supplemented by monthly telephone support and a follow-up session after 6 months. Mean self-reported physical activity levels were higher for intervention participants than for controls (p < 0.001) and a greater proportion in the intervention group than the control group reached the target of physical activity at 12 months [233 (43%) vs. 165 (30%); p < 0.001]. Levels declined but were still significantly different at 2 years [214 (39%) vs. 179 (33%); p < 0.001]. There was no difference between groups with regard to clinical outcomes and it was noted that falls/injuries were higher in the intervention groups.
The third study providing stronger evidence of effectiveness36 had two intervention arms, with one consisting of counselling, pedometer use and self-monitoring over 6 months, and the other consisting of the same interventions plus monthly mentoring meetings with a fitness professional. Participants in this small-scale evaluation (described as a pilot study) were inactive, with a mean age of 64 years, and 16 of 36 participants were employed. The study found a significant intervention effect [p = 0.015; effect size (ES) 0.611] with both groups significantly increasing step count at 6 months, with no significant difference between groups (p = 0.151). The group that received additional mentoring maintained the effect at 12 months (ES 0.606), whereas there was fading of effect for the standard intervention group.
Another paper comparing two interventions71 evaluated advice from a physician and physician advice supplemented by telephone counselling from a health educator, for patients with a mean age of 68 years. At 3 months, 7-day recall self-reported data indicated significantly increased minutes of moderate physical activity for the advice plus counselling group (p < 0.05), increased moderate exercise kilocalories per week (p < 0.05) and biotrainer physical activity counts (p < 0.01) for this group from baseline. These improvements were maintained at 6 months. The physician advice-only group also increased on most measures, although the changes were not statistically significant.
In a small-scale pilot study, Armit et al. 28 randomised participants to three intervention arms: advice from a GP; counselling and telephone calls from an exercise scientist; or counselling and telephone calls with the addition of pedometer use. The participants were inactive patients recruited from physician waiting rooms with a mean age of 64 years. At 12 weeks, there was an overall increase of 116 weighted minutes of self-reported physical activity per week (p < 0.001) across the three groups. The paper describes no significant difference between groups, although the data presented indicate no change in the GP advice group compared with significant differences in average physical activity levels pre–post for the other two groups.
Another similar intervention with GP advice, supplemented by telephone support from an exercise specialist,40 increased self-reported mean total energy expenditure by 9.4 kcal/kg/week (p = 0.001) and leisure exercise by 2.7 kcal/kg/week (p = 0.02). This equated to 34 minutes per week more in the intervention group than in the control group (p = 0.04). The proportion of the intervention group reporting undertaking 2.5 hours per week of leisure exercise also increased by 9.72% (p = 0.003) more than in the control group. The participants were sedentary patients visiting their GP/nurse (mean age 57 years), and the intervention was designed to prompt practitioners to give advice and an exercise programme to patients on being given a form by patients.
A paper from Australia47 provides more limited evidence of effect. This study examined the provision of an advice session with an exercise specialist to sedentary adults (mean age 67 years). Although physical activity increased in both intervention and control groups, there was a significantly greater increase (p < 0.05) in self-reported frequency and time of vigorous exercise in the intervention group than in the control group (who received a nutritional pamphlet). Self-reported intention to exercise also increased significantly more in the intervention group (p < 0.0001). Although the paper reports these positive effects on vigorous exercise and intention to exercise, self-reported walking time and frequency of walking did not improve significantly more in the intervention group. However, a sample of the participants wore an accelerometer during the intervention period, and, with this measure (rather than self-reported data), there was no intervention effect on the daily number of steps. There was also no difference between groups with regard to physiological measures (such as body weight, blood pressure). Quality-of-life scores decreased for all participants over the 12-month study period, with the greatest decrease in women in the intervention group.
Costanzo and Walker34 provide weak evidence of effect following a behavioural counselling intervention. This study, which compared one session versus five sessions of counselling, reported an effect on self-efficacy, although no direct influence on physical activity. The change in self-efficacy (ES 0.19) was attributable to a decrease in the one-session group rather than change in the five-session group.
The other two papers reporting limited effects were the Marcus et al. 60 paper, which describes the pilot phase of work, and the Goldstein et al. 45 paper, which further outlines this. The evaluated intervention consisted of a physician training session and one physical activity counselling session provided to patients with one follow-up appointment 4 weeks later. Participants in the main study were an average age of 65 years and 36% were employed. At 6 weeks, participants in the intervention group were more likely to be in advanced stages of motivational readiness for physical activity than participants in the control groups [preparation or action 89% vs. 74%, odds ratio (OR) 3.56, 95% CI 1.79 to 7.08; p < 0.001]. However, the effect was not maintained at 8 months. There was no significant difference between intervention and control groups with regard to the number reporting meeting the recommended guidelines for physical activity at 6 weeks or 8 months. Both groups increased at 6 weeks and decreased by 8 months.
Group sessions
A total of 13 papers30,31,37,38,44,48,49,55,74,87–90 evaluated group-based programmes, with 11 of these reporting stronger evidence of effectiveness. 30,31,44,48,49,55,74,87–90 In total, four studies (reported in seven papers)30,31,55,87–90 compared differing forms of interventions rather than having no-intervention control groups.
The first of these, outlined in four papers,87–90 compared telephone-based counselling calls for 6 months to a 12- or 20-week group-based programme. Participants had a mean age of 68 years and were 80% female. The Wilcox et al. 87,88 papers present immediate follow-up data from one and three cycles, respectively, of the programmes. Results for the first implementation showed a significant increase from pre test to post test in self-reported moderate- and vigorous-intensity physical activity (p < 0.001) and total physical activity (p < 0.001) for all participants, with both programmes having significant effects. Across three cycles of the intervention, the telephone programme led to a significant increase in reported moderate and vigorous physical activity [Cohen’s d (d) = 0.62/0.66/0.75], and all reported physical activity also increased significantly (d = 0.55/0.6/0.63) in each of the 3 years in which the programme was run.
Similarly, for the group programme the study reported that moderate and vigorous physical activity increased significantly (d = 0.74/0.66/0.58), as did all physical activity (d = 0.79/0.56/0.63). For both programmes the proportion of participants reportedly reaching exercise recommendation levels increased significantly (p < 0.001). The papers present no data comparing effectiveness between the interventions beyond reporting the ESs for each, which were similar. The first Wilcox et al. 88 paper reports 6-month follow-up data and found a significant increase from pre test to post test for both programmes in self-reported physical activity, which was maintained at follow-up (p < 0.001). The second Wilcox et al. 89 paper analyses predictors of response to the intervention and reports that older participants (> 75 years of age) and those with less social support responded less well. It is noteworthy that those with lower activity levels at baseline improved the most.
Another study in this group that had two intervention arms30 assessed a programme which comprised access to a community exercise facility, a pedometer, peer mentors and group sessions. The participants were inactive and had an average age of 63 years, and 82% were female. The group sessions in one arm involved general health education, whereas the other arm received sessions on support for physical activity change. At the end of the intervention (16 weeks) both groups self-reported significantly more activity than at baseline [p < 0.001 (ES 1.38)], with no difference between the interventions. At 18-month follow-up, the intervention group receiving physical activity change sessions reported significantly more moderate to vigorous activity minutes per week than the general health education intervention arm [p = 0.04 (ES 0.32)].
Caperchione and Mummery31 similarly compared a standard intervention to an enhanced programme. The 12-week lifestyle intervention comprised instructor-led group walks and group education sessions incorporating cognitive–behavioural strategies and health-related information. The enhanced package also included education sessions on group process. Participants had a mean age of 58 years; 38% were retired and 50% were employed and were inactive. The study found a significant increase in self-reported physical activity behaviour (as measured by calorific expenditure) at time points up to 12 months’ follow-up for both groups (p < 0.05), with no significant difference between the standard and enhanced intervention.
The fourth paper comparing interventions55 assessed outcomes after interventions that included both group sessions and a home programme, in participants with a mean age of 68 years. One intervention focused on endurance and strengthening exercises and the other on stretching and flexibility. Although many of the outcomes of interest in this study are not specifically physical activity (e.g. bodily pain/endurance/strength), it included evaluations of walking distance via completion of exercise logs and self-efficacy via questionnaire, which are within the scope of this review. The endurance group reported greater improvement in the ability to walk a certain distance and self-efficacy (confidence) in walking (p < 0.03) than the stretching group.
An evaluation of a group intervention for retired women in the UK74 found that those who had taken part in the programme had significantly better self-perceived health, more exercise knowledge, positive exercise attitudes and more self-reported exercise than those who had not participated (i.e. those who had declined or who were not offered the course) at median 10 months’ follow-up. The group-based programme was taught for 2 hours a week by a trained Health Education Authority teacher and lasted for 10 weeks with the aim of promoting heart health. Following the intervention, the mean number of hours reportedly spent on sport/recreational exercise per week was greater in the intervention group than in the control group (p < 0.001). The time since completion of the programme did not have any effect on outcomes.
Another intervention aimed at older women was outlined in two papers. 48,49 Participants in this study had an average age of 65 years and were described as sedentary. The 26-week progressive walking programme was delivered in two sessions per week. At completion of the programme, participants were encouraged to continue physical activity. Following the intervention, the maximum current activity score had increased significantly from baseline (p = 0.01) in the intervention group compared with the no-intervention controls. At 6-month follow-up, 77.8% of the intervention group had reportedly continued with exercise and maintained lower exercise heart rates than the control group (p < 0.005). They also had maintained higher maximum current activity scores than the control group (p < 0.005).
A paper from Japan44 evaluated an exercise training programme for older adults (mean age 67 years). The 25-week programme consisted of three exercise classes each week with endurance training using bicycles and the use of flex-bands. Total daily energy expenditure (calculated from participant exercise logs) increased in the intervention group (from 40.8 to 43.5 kcal/kg/day, an increase of 6.4%; p = 0.03) and did not change in the control group (pre: 42.2, post: 39.2; p = 0.11). At 6 months’ follow-up there was some fading of effect (a decrease of 1.2 kcal/kg/day). Following intervention, reported daily energy expenditure remained higher than at baseline (p = 0.05). Reported moderate activity rates remained significantly higher, although strenuous activity had returned to pre-intervention levels.
Two papers from the same team37,38 provide limited evidence of effectiveness for a programme consisting of 30 once-a-week group sessions. The sessions comprised moderate-intensity recreational sport activities such as dance, self-defence or swimming led by a professional sport instructor. The mean age of participants was 59 years, and around of participants were female. Although the intervention resulted in significant increases on almost all questionnaire and fitness measures, similar effects were also found in the no-intervention control group. There was no statistical difference between the two study arms for sport activity, leisure time physical activity, health indicators or perceived and performance fitness measures. The intervention group improved significantly more than controls for only measures of sleep; diastolic blood pressure; perceived fitness; and grip strength. The second paper examines 12-month effects of the programme, although there is a substantial number of missing data (up to 49%). At this longer term follow-up, energy expenditure for sport and total energy expenditure had significantly increased from baseline (p < 0.01). However, the increase was not significantly different from the control group. Energy expenditure leisure time activity in the intervention group, despite increasing up to 6 months, decreased from 6 to 12 months’ follow-up. BMI and walking also significantly increased over time, but not when compared with controls. There was no significant difference by time or group for any of the other outcomes measured.
Individual exercise programmes
Seven papers (six studies)35,39,50,52,63,64,69 evaluated individual exercise programmes, with all providing evidence of effectiveness, although for one this was only at short-term follow-up. The first paper35 reported the results following supervised centre-based individual swimming or walking sessions, together with mini workshops prior to sessions for the enhanced intervention over 6 months. The programme continued unsupervised for a further 6 months. The study had four intervention arms (swimming and usual care, walking and usual care, walking + workshops and swimming + workshops), and participants had a mean age of 55 years. Benefit in terms of a reduction in time to walk 1.6 km was found for all groups at 6 months compared with baseline (p < 0.001), and this effect was maintained at 12 months (p < 0.05). The addition of the behavioural workshops did not increase the intervention effectiveness. Participants also improved in terms of distance covered during a 12-minute swim, with, perhaps unsurprisingly, the swim group having the greatest improvement in swimming time. The authors note that being older was associated with better adherence to the programme and retention (p < 0.05). Being in full-time employment was associated with adherence and retention at 6 months but was not associated with either at 12 months (p < 0.05).
Two other papers reported walking interventions. 50,69 Pereira et al. 69 examined long-term follow-up data following a walking programme for post-menopausal women (participant mean age 57 years). The original programme combined initial sessions of group walking for 8 weeks, with individual walking at least once a week to achieve 7 miles each week. After 8 weeks, participants could continue group walks or maintain solo walking. The intervention had been implemented in the early 1980s, with the authors impressively managing to collect 10-year follow-up data from 86% of participants. The median values for both self-reported usual walking for exercise (1000 vs. 302 kcal per week) and self-reported total walking (1344 vs. 924 kcal per week) were significantly higher for intervention participants than for controls participants (p = 0.01 for both outcomes).
A paper by Hekler et al. 50 drew a distinction between utilitarian walking (i.e. with the purpose of getting somewhere) versus leisure walking (i.e. for fitness or health). Participants in the study (mean age 64 years, 56% retired) received 2 weeks of each intervention, including instruction in the walking type, goal-setting, self-monitoring and problem-solving. Participants had a choice of walking type for a further 2 weeks. The study found a significant mean improvement in the amount of walking for all 2-week phases (p < 0.05). Significantly more mean steps per day (measured by a pedometer) were achieved by participants during the leisure intervention than during the utilitarian walking type (p < 0.05). The authors report that the order of instruction may have influenced this finding, as those instructed in leisure walking first had a greater difference in types of reported walking. All but two of the participants had preferred a mixture of walking types during the free-choice phase. The authors noted that neighbourhood characteristics were associated with the type of walking achieved, with more leisure walking undertaken if there was access to walking paths, better neighbourhood aesthetics, access to facilities and access to services. More utilitarian walking was reported by participants who travelled to multiple locations during a day.
Other papers in this group examined more general fitness rather than walking sessions. Hughes et al. 52 trialled a multiple-component physical activity programme which provided flexibility activities, low-impact aerobic exercise and resistance training for 60 minutes three times per week for 10 months. The study compared this intervention with any other intervention of the participants’ choice, including any other physical activity programme. Adults who participated in the multiple-component programme (mean age 66 years) showed statistically significant benefits at 5 and 10 months with regard to self-efficacy for exercise adherence over time (p < 0.001) and adherence in the face of barriers (p < 0.001). Self-reported frequency of all physical activity had increased by an average of 26% from baseline at 10 months in the intervention group compared with 9% in the control group (p = 0.028 baseline to 10 months). The difference in frequency of physical activity from baseline to 10 months, however, was not significant (p = 0.756).
A 14-week fitness programme evaluated by Dorgo et al. 39 led to improved fitness on all measures for both peer-mentored (p < 0.007; ES 0.2–1.6) and student-mentored (p < 0.31; ES 0.2–1.4) groups with no significant difference in outcome between groups. This study, which had no control arm, recruited volunteers with a participant mean age of 69 years. The authors noted that, although retention was high for both intervention arms, participation was higher in the student-mentored group.
There was one study63,64 that reported evidence of weaker effect following a fitness session intervention. This study, reported in two papers,63,64 had two intervention arms and a no-intervention control group, and participants were all retired with a mean age of 66 years. The second paper64 reports fitness, strength and body composition rather than physical activity outcomes. The interventions were either sessions at a fitness centre focusing on endurance, strength, flexibility and balance or an individualised home-based programme in which participants were encouraged to integrate physical activity into their daily routines. The home programme was supported by booster telephone calls from the instructors. The fitness sessions group significantly increased leisure-time physical activity and total physical activity from baseline to immediately post intervention compared with the control group, although the effect was not maintained at 23 months’ follow-up. The outcomes for the home intervention group showed significantly larger increases in active transportation, daily steps and total physical activity than in the control groups and had increased more than the fitness session group for active transportation and daily steps post intervention. At 23 months’ follow-up, the only measure that was significantly different between the control and intervention groups was self-reported kilocalories expended during active transportation in the home intervention group.
In-home telephone interventions
Nine papers (eight studies) evaluated in-home interventions which were predominantly delivered via the telephone. 32,51,56,57,61,62,72,73,78 The first of these papers51 had a no-comparator BA study design. Participants were a mean age of 68 years, and 49% were retired and not working, 17.7% were retired and working and 20.9% were employed. They received an initial meeting with a staff member to develop a physical activity plan and goals, followed by weekly then monthly telephone calls from a designated ‘buddy’. The study found a significant improvement in self-reported total calorie expenditure from baseline to mid-point and end point (p < 0.0001 median change 707 calories per week), with a typical increase of 3.2% of calories expended per month. Light and moderate self-reported activity levels showed a similar improvement (p < 0.0001 pre–post), and there was an improvement in the stage of readiness for all stages. Those with lower levels at baseline and who were older than 65 years of age tended to have greater increases in the numbers of calories expended.
Another similar intervention73 comprised an initial meeting to discuss fitness testing results and to develop a physical activity plan and goals, with 10 follow-up telephone calls over 6 months (it was unclear who made the telephone calls). The intervention group and control group both increased the weekly estimated calorific expenditure in all physical activity at 3 months’ and 6 months’ follow-up. The study provides weak evidence of effectiveness, as the intervention group had a larger increase, but this was not significant. There was no significant change in reported weekly frequency of activity or measures of physical fitness in either group. Moreover, there was no significant change in self-efficacy or perceived barriers. When controlled for baseline covariates (age, sex, income, BMI, support), intervention participants significantly increased the frequency of self-reported levels of physical activity compared with control participants (p < 0.05), suggesting that the intervention may have been effective for selected participants.
The third and fourth papers in this group61,62 examined up to 2-year outcomes following an intervention, which comprised a seven-session course delivered via the telephone by physical activity coaches. Participant mean age was 57 years, with 77% of participants employed. Significantly more activity was reported by the intervention group than the usual care control group at 6 and 24 months (p < 0.03 and p < 0.01). The intervention led to an increase in reported energy expenditure of around 200 kcal per week extra, equivalent to 1 hour per week of moderate-intensity walking. More intervention than control participants maintained moderate to vigorous physical activity at 6, 12 and 24 months (p < 0.003, p < 0.004 and p < 0.001). At 24 months, although the usual care group reverted to their 6-month level, the intervention group continued to increase (p < 0.05).
King et al. 56 compared human versus automated telephone contacts in participants aged over 55 years. The two forms of telephone intervention were compared with a health education class control condition. At 6 months, those in both the human advice and automated advice arms, although not significantly different from one another (p = 0.73), had significantly greater self-reported mean energy expenditure in moderate activity than the control arm (p = 0.01). Similarly, both the human advice and automated advice arms, although not significantly different from one another (p = 0.65), had significantly greater reported mean minutes per week spent in moderate activity than the control arm (p = 0.01). These differences were generally maintained at 12 months, with mean reported energy expenditure in moderate activity for both the human advice and automated advice arms not significantly different from one another (p = 0.60). These energy expenditure increases for both intervention groups were significantly greater than in the control arm (p = 0.036). Similarly, mean minutes per week spent in moderate activity for both the human advice and automated advice arms, although not significantly different from one another (p = 0.66), remained greater than in the control arm (p = 0.045).
Another study, which examined the potential of automated telephone systems,72 compared the effectiveness of a 12-week walking programme, including a pedometer and supported by an interactive voice response system, with support from a trained coach. The female participants had an average age of 57 years, and following the programme there was a significant improvement in 1-mile walk times pre–post (p = 0.001; d = 0.41). There was also a significant improvement in goal-setting, exercise planning and managing negative thoughts (ES 0.8). The ESs for BMI, weight and waist measurement were small (range 0.07–0.14). There was no between-group difference, with the addition of a human coach not seeming to increase effectiveness of the programme.
Three variants of a smartphone application (app) were trialled in an 8-week intervention. 57 Around half of the participants (48.5%) were in full-time employment, with a mean age of 59 years, and nearly three-quarters were female. The study found a significant increase in reported minutes of brisk walking for all groups pre–post (p < 0.0001), with no difference between the different apps (p > 0.73). The increase averaged 100.8 weekly reported minutes [standard deviation (SD) 167 minutes]. There was also an increase in reported moderate to vigorous physical activity for all groups (p < 0.0001), with no difference between them (p > 0.99). The app was described as being easy to use and motivating, with around half of participants willing to continue usage after the conclusion of the study.
Two studies compared telephone-delivered with mail-delivered interventions. 32,78 Castro et al. 32 examined whether or not these different methods varied in terms of encouraging maintenance. They randomised participants (mean age 56 years) to 1 year of telephone counselling which encouraged them to adopt either higher (more vigorous) or lower intensity physical activity. After 1 year, they were randomised to a second maintenance year of contact via telephone andmail or mostly mail only. The study found that for those individuals who had been in the higher intensity programme, exercise adherence was maintained better by mail. However, those who were in the lower intensity programme had better maintenance if they received both mail and telephone input. Motivational telephone calls were compared with print letters in a lifestyle intervention trial which targeted both healthy diet and physical activity outcomes, in participants with a mean age of 57 years. 78 The study found that the different intervention methods were equally effective compared with a no-intervention control group. ESs (Cohen’s d) for outcomes of interest including self-reported hours of physical activity per day ranged from 0.15 to 0.18.
In-home combined diet and exercise interventions
Six papers (four studies)29,42,43,65,83,84 outlined the results of interventions that targeted lifestyle more generally and consisted predominantly of materials delivered to the home by post/mail. A RCT of tailored activity and dietary newsletters was reported in two papers83,84 The participants were all female, with a mean age of 57 years. The paper evaluated two intervention arms, either generic or individually tailored newsletters, with no control group. Both groups improved significantly from baseline to 6 months on all measures of cardiorespiratory fitness and physical activity. At 12 months after completion of the intervention, the pre–post change for both groups was significant only for timed chair stands. At 12 months a significantly higher proportion of the tailored newsletter group than the generic newsletter group had reportedly achieved the activity behavioural outcome target of at least 210 minutes of moderate- or high-intensity activity weekly (30 minutes daily on 7 days each week) (p = 0.026). At 24 months (1 year following intervention completion), both groups had maintained reported levels of moderate or greater activity, stretching exercise and flexibility, but had declined in cardiorespiratory fitness. There was no significant effect across the three time points between the groups for any activity markers. Post hoc tests showed that the combined groups significantly increased the outcome of at least 210 minutes of weekly moderate or greater activity from 12 months to 18 months (p = 0.015). However, if considered separately, there was no significant change within either group.
Another study of a lifestyle intervention including both physical activity and nutrition compared a 6-month programme with no-intervention controls. 29 The sex of participants was balanced, with a mean age of 65 years, and 42% were retired. The multi-element programme comprised a booklet with recommendations which encouraged goal-setting, as well as an exercise chart, calendar, bimonthly newsletters, a resistance band and a pedometer. Telephone calls and e-mail contact were provided in accordance with participant request. In total, 74% of participants reported using the exercise chart, 62% practised the recommended exercises, 90% used the pedometer and 63% used the resistance band. Immediately post intervention, the study found significant improvements from baseline to post programme for the intervention group with regard to self-reported outcomes of strength exercise (p < 0.001), walking (p = 0.012), moderate activity (p = 0.008), vigorous activity (p = 0.044) and sitting time mean per week (p < 0.001). These improvements were significant compared with controls for strength (p < 0.001), walking (p = 0.0029), vigorous activity (p = 0.0015) and mean sitting time (p = 0.0001).
The third study considering combined diet and physical activity programmes provided participants with a personal health-risk report based on questionnaire data every 6 months, together with individualised recommendations, newsletters, self-management and health-promotion books and other materials, all of which were delivered by post. 42,43 The intervention was designed to cost around US$30 per year. The study compared the intervention arm to no intervention and completion of questionnaire-only arms. At 2-year follow-up, the participants who were all retired with a mean age of 68 years had reduced their health-risk scores by 23% compared with baseline in the intervention group compared with control (p < 0.001). As regards the two self-report physical activity measures (exercise minutes per week and exercise programme attendance), both groups had significantly improved baseline to 24 months (p < 0.001), despite the control group having declined in physical activity measures by the end of the first year.
One paper reported more limited effectiveness. 65 It evaluated the provision of a 6-month multi-element home-based intervention for insufficiently active adults (mean age 66 years), which included a booklet, guidelines, newsletters, a pedometer and a resistance band. It also included newsletters and support via telephone or e-mail contacts. The programme aimed to target both physical activity and nutrition outcomes. Although outcomes were more positive regarding improvements in diet, the effect on physical activity was limited. Immediately post programme, the reported time spent in moderate activity had significantly increased for the intervention group (p < 0.05). However, this had declined by follow-up, with reductions in mean walking time for both intervention and control participants.
Home-based interventions providing a pedometer/accelerometer
Although several of the studies reported in other groups included the provision of a pedometer as part of the intervention element, four studies evaluated home-based interventions in which the provision of a pedometer/accelerometer was the core component. 41,58,73,77 The first of these58 gave accelerometers to female participants (mean age 67 years). It was recommended that participants accumulated 9000 steps and 30 minutes of moderate-intensity physical activity per day during the 12-week intervention. Individual data regarding their steps over the previous 2 weeks were provided to participants, with recommendations made. A control group was also provided with an accelerometer to wear, which collected no data. At immediate follow-up, participants in the intervention group had increased their steps average by 16% (from 7811 to 9046 steps; p < 0.01). Moderate-intensity activity had also increased by 53% (95% CI 17.83% to 27.23%; p < 0.01). This was compared with no significant change in self-reported physical activity in the control group. Results on the walk time test also improved for the intervention group by 10% (p < 0.01).
A pilot study77 compared three intervention arms and a control group. The interventions were combinations of standard or individualised mailed educational materials and a pedometer. All variants of interventions led to an increase in daily steps for participants (mean age 64, mostly female) at the end of the 12-week intervention. The greatest increase was in the two groups which had the pedometer plus individualised booklets (significantly greater number of daily steps than groups 1 and 2; p < 0.001). The addition of biweekly telephone calls for one of these groups did not make any significant difference (p = 0.893).
Finkelstein et al. 41 explored the use of financial incentives combined with pedometer usage. Participants (mean age 59 years, 36% retired) were given a US$50 initial payment with subsequent payments dependent on the number of aerobic minutes achieved per day – nothing was given for fewer than 15 minutes, US$10 were given for 15–24 minutes, US$15 for 25–39 minutes and US$25 for 40 minutes or more. Daily use was capped at 75 minutes. The control group were given a payment for taking part and completing the study. The study found an adjusted treatment effect of just over 16 more aerobic minutes in the intervention group (p > 0.001). There was reportedly a small difference between full-time employees and retired people (with retired participants achieving more minutes), but this was not significant. The control group averaged 20 minutes of exercise per day, which showed a slight decrease over the 4-week intervention. The intervention group averaged 35 minutes per day (1.8 hours per week more than controls) with little change over the 4 weeks. Average pay-out to intervention participants was US$17.50 per week, which would equate to US$910 per year.
One paper73 trialled a 6-week activity programme, which was outlined to participants by a research assistant at a clinic visit. Examples of activities and general advice were provided, together with an activity monitoring log to complete. In addition, one group received a pedometer. This study was the only one in the included set that was carried out with a solely minority ethnic population. The participants were Native American elders with an average age of 58 years, of whom 21% were employed. At immediate follow-up, the reported frequency of walking had increased for both groups from baseline (p < 0.01), with improved calorific expenditure for all exercise-related activities (p < 0.001) and greater frequency of moderate-intensity exercise-related activities (p < 0.001) self-reported in both groups. There was no significant difference in effect between groups. The study therefore provides evidence of effectiveness for both interventions, with the effect of the pedometer not superior to advice only.
Computer-based interventions
Eleven papers (four studies)46,53,66–68,79–82,85,86 reported programmes using computers, all of which incorporate web-based components. Two of these studies report limited effectiveness. The first of these85 was the only paper we identified that referred to participants as recent retirees and recruited 413 mostly male participants with a mean age of 59.5 years. This Dutch cluster RCT evaluated an ‘energy balance’ intervention aimed to improve both physical activity and dietary behaviours. It consisted of five modules, with a pedometer, waist tape and information provided, delivered by post initially, then by CD-ROM, then by computer-tailored feedback. The fourth and fifth modules were available via the programme website, and newsletters were provided for the remainder of the length of the 2-year study period. The study authors reported limited effectiveness for the intervention, with similar improvements to physical activity and dietary behaviours in both intervention and control groups on most measures used. At follow-up, the change in reported sport and recreational activities was higher in the intervention group (74.5 minute/week) than the control group (23.4 minute/week; p = 0.03). Waist circumference, body weight and blood pressure decreased significantly in men in both the intervention and the control groups, but there was no significant between-group difference observed at 12- or at 24-month follow-up. The authors suggest that the study was underpowered to detect statistically significant differences and also highlight their recruitment of health-conscious individuals to intervention and control conditions.
A second paper46 described outcomes following the delivery of two newsletters (either tailored or standard) via the internet to women with a mean age of 56 years. A total of 6% were retired and 73% were in full-time employment. Although the majority of participants (83%) reported that they had read the newsletters, the study found no significant change for any self-reported activity or perceived benefits of activity at 3 months (1 month after receipt of the second newsletter). There was an improvement in flexibility pre–post (p = 0.02) and in levels of body fat. Both groups had improved in terms of reduced perceived barriers (p = 0.025).
The other two studies outlined more positive findings following internet-based programmes. Wijsman et al. 86 found that daily physical activity as measured by an ankle accelerometer increased by 46% in a mixed-sex intervention group with a mean age of 65 years (p < 0.001) compared with 12% in a wait-list control group (p < 0.001). There was also a small increase in moderate to vigorous activity in the intervention group (mean increase of 11.1 minutes per day) compared with a mean decrease in the control group (p = 0.001 relative difference) immediately following the 12-week monitoring and feedback programme. Irvine et al. 53 evaluated change at longer (6-month) follow-up subsequent to an internet programme which supported selection of activities and provided educational and supportive messages. The intervention group participants (mean age 60 years) showed significant improvement on 13 out of the 14 self-reported outcomes measures compared with a no-intervention control group immediately post intervention. Gains were maintained at 6 months, with all outcomes measures significantly different compared with the control participants (p < 0.001) including cardiovascular activities, stretching exercises, activity minutes per week, balance exercise, behavioural intentions to exercise and motivation to exercise.
Seven papers from one team in the USA explored and compared different aspects of similar programmes consisting of computer-delivered or print-delivered letters which either included (the plus intervention) or did not include (the basic intervention) environmental information in addition to personalised physical activity advice. The earlier papers from the team79,81,82 investigate efficacy and working mechanisms of the interventions. At 3 months, the printed letter intervention participants were 1.6 times more likely than wait-list controls to comply with guidelines (basic OR 1.67, plus OR 1.57), and at 6 months, intervention participants were 2.5 times more likely (basic OR 2.4, plus OR 2.8) than controls to comply with guidelines (p < 0.001). At 6 months, both intervention groups had enhanced awareness of their activity levels compared with controls (intervention OR 1.67, intervention plus environmental information OR 1.64; p < 0.001) with no significant difference between the intervention types. The intervention plus programme had a significant effect on cycling compared with the basic intervention (p < 0.01) and a significant effect on perceived physical activity possibilities (more than both controls and basic intervention; p < 0.05). This change was associated with a change in days of total physical activity (p < 0.05) and weekly minutes of sport (p < 0.001). The authors concluded that environmental perceptions were important as a mediating effect in changes in cycling, sport and total physical activity.
Efficacy of the basic intervention and the basic intervention plus environmental intervention was considered in a further paper. 80 This reported that both interventions significantly changed total self-reported weekly days of physical activity compared with the control group. Participants in the basic computer-tailored print intervention condition and intervention plus condition increased their total weekly days of sufficient physical activity from 4.3 days per week (SD 2.2 days per week) to 4.7 days per week (SD 2.0 days per week). Participants in the control condition had increased their total weekly days of physical activity from 4.0 days per week (SD 2.2 days per week) to 4.3 days per week (SD 2.0 days per week). However, only the environmentally computer-tailored print intervention significantly changed weekly minutes of physical activity. On average, participants in the intervention-plus-condition group increased their weekly physical activity behaviour by more than 1 hour per week (ES 0.19) compared with the control condition. Multiple mediation models indicated that the effects of both interventions on weekly days of physical activity were mediated by changes in awareness and intention.
In later papers from the team, the programme was developed into a web-based intervention. 66–68 Peels et al. 66,67 outline the development process and compare the new web programme to the original print-delivered information, in terms of participant types and attrition factors. The web version was designed to improve the reach and effect of the print version. However, the authors found that, although both high and low socioeconomic participants were reached by both versions of the intervention, delivery by print produced a higher response rate than the web version (19% vs. 12%). The web intervention appeared to have better participation rates among younger participants (the study included adults over 50 years, mean age 62 years), males and those with higher BMI. Dropout was also significantly higher in the web-based intervention (53% vs. 39%; p < 0.001). No specific participant characteristics were associated with dropout for the different interventions, with low intention to be physically active predicting dropout for both delivery modes (p < 0.001).
Effectiveness data compared a basic intervention via print or the web, plus environmental intervention via print or the web using self-report physical activity data. At 12 months’ follow-up the four intervention conditions as a whole were effective in increasing self-reported weekly days of sufficient physical activity (ES 0.18; p = 0.005) but ineffective in increasing self-reported weekly minutes of physical activity (ES 0.20; p = 0.071). The two paper-based types were equally effective in increasing total days and also total minutes of physical activity compared with control, whereas the two internet types were not. Neither web-based intervention significantly increased days or minutes of physical activity, although the control group decreased their physical activity over the same time period. Participant baseline intention to be active was the only factor that was associated with physical activity outcome.
Community-wide initiatives
We identified only two papers that evaluated physical activity interventions delivered across whole communities. 35,54 One reported little evidence of effectiveness. 54 This study54 from Japan recruited 12 communities with varying population densities. The intervention used social marketing principles and disseminated information via flyers, leaflets, newsletters, banners, used health professionals to provide encouragement during appointments and community events, and used community leaders and lay workers to provide encouragement and support via the provision of pedometers and reflective vests. The campaign was intended to target women aged 60–79 years with low back or knee pain, and the primary message of the campaign related to encouraging exercise in order to reduce knee and back pain. The study is of relevance to our review insofar as the authors predicted a ripple effect from the targeted segment to the wider community. The sample providing data were a mean age 60.5 years, around half were male and around 67% were employed. At baseline, 64.6% of the control group sample reported engaging in regular physical activity, compared with 63.9% of the intervention sample. At 1 year post campaign, the control group had decreased slightly to 60.3%, and the intervention group also decreased to 58.7%. The ES was not significant. There was some effect reported in terms of a significant difference in knowledge about physical activity benefit in control versus intervention participants at 1-year follow-up (OR 1.51; p < 0.05). The authors suggested that there had been contamination across study arms, as > 50% of control communities were aware of the campaign.
The second community initiative was the provision of free bus passes to over 60 year olds in England. The study35 analysed data from 3 years of the self-reported UK National Travel Survey to investigate any potential impact on having a bus pass and walking, cycling or travelling. This paper is of particular note in its examination of data relating to SES. Having a free pass was significantly associated with greater active travel among both disadvantaged (adjusted OR 4.06, 95% CI 3.35 to 4.86; p < 0.001) and advantaged groups (adjusted OR 4.72, 95% CI 3.99 to 5.59; p < 0.001), as well as with greater bus use in both disadvantaged and advantaged groups (adjusted OR 7.03, 95% CI 5.53 to 8.94; p < 0.001 and adjusted OR 7.11, 95% CI 5.65 to 8.94; p < 0.001, respectively) and a greater likelihood of walking more frequently in the whole cohort (adjusted OR 1.15, 95% CI 1.07 to 1.12; p < 0.001).
Summary of effectiveness evidence from A1/A2 studies
We provide a summary of the A1-/A2-rated papers in this section. The studies of participants with wider age ranges (A3 studies) are presented in the following section.
What are the most effective interventions to maintain and/or increase physical activity in older people during and shortly after the transition to retirement?
The majority of papers included in this review reported some intervention effect, although given that many studies reported multiple outcomes, including perceived change and readiness for change, this may be unsurprising. Six papers described change in related measures such as weight, fitness, self-efficacy or knowledge rather than direct physical activity. 34,45–47,55,60 It is important to note the tendency for improvement in participants over the period of the study which may not be related to the intervention. A significant proportion of studies used designs with several intervention arms, rather than a no-intervention control group and this obscures the level of intervention effect. There was evidence of the potential for a Hawthorne effect, with some studies finding improvements from baseline to follow-up in both intervention and control arms.
The Harvest plots below provide an overview of the effectiveness data by typology (Figure 7). In the chart each unique study is represented by a column, with the height of the column providing an indication of the strength of study design. The colour and pattern of each column provides further indication of study strength in terms of whether or not the study had a no-intervention comparator group and the strength of the outcome measurements used. As there was only a single study evaluating the education of health-care professionals, this has not been included in the plots.
FIGURE 7.
Harvest plots for A1/A2 intervention studies. Black, study with a control arm and measured data; dark green, study with multiple intervention arms only and measured data; light green, study with a control arm and self-report data; and blue, study with multiple intervention arms only and self-reported data. The height of the column indicates the strength of the study design. Studies in brackets have concerns regarding quality (see Appendix 2 for full details). (a) Advice/counselling; (b) individual session; (c) group sessions; (d) in-home computer; (e) in-home pedometer; (f) in-home telephone; (g) in-home diet and exercise; and (h) community.

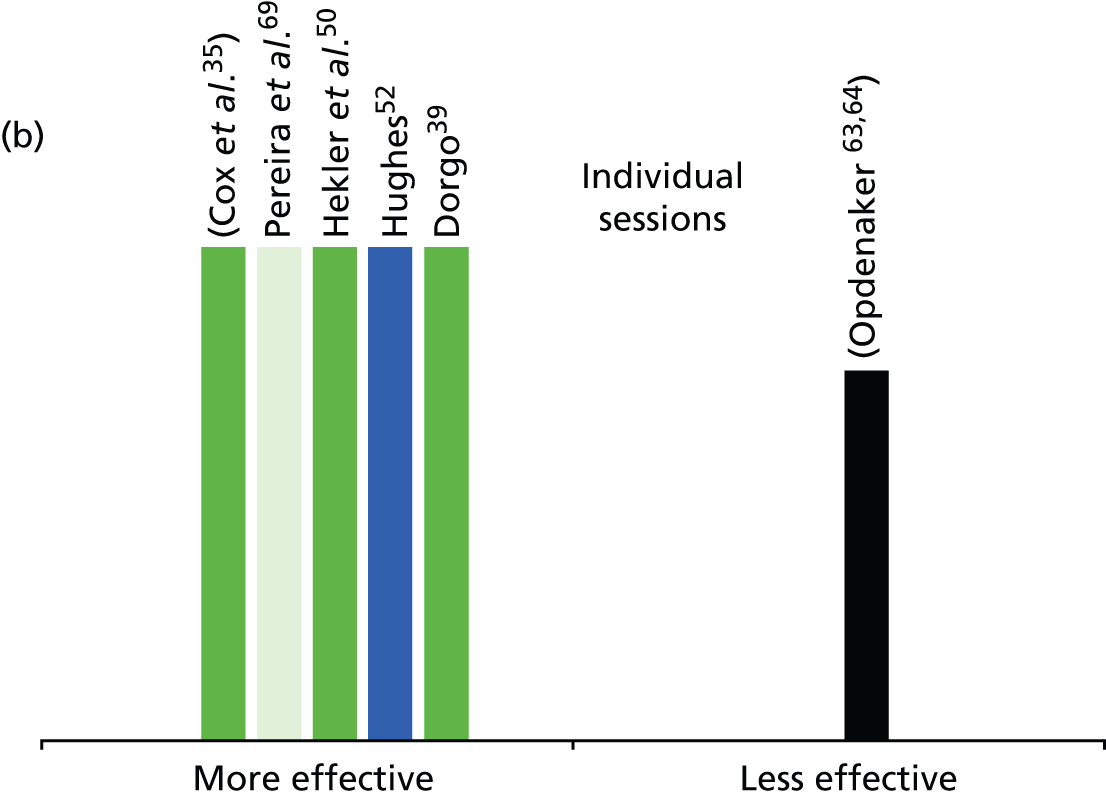
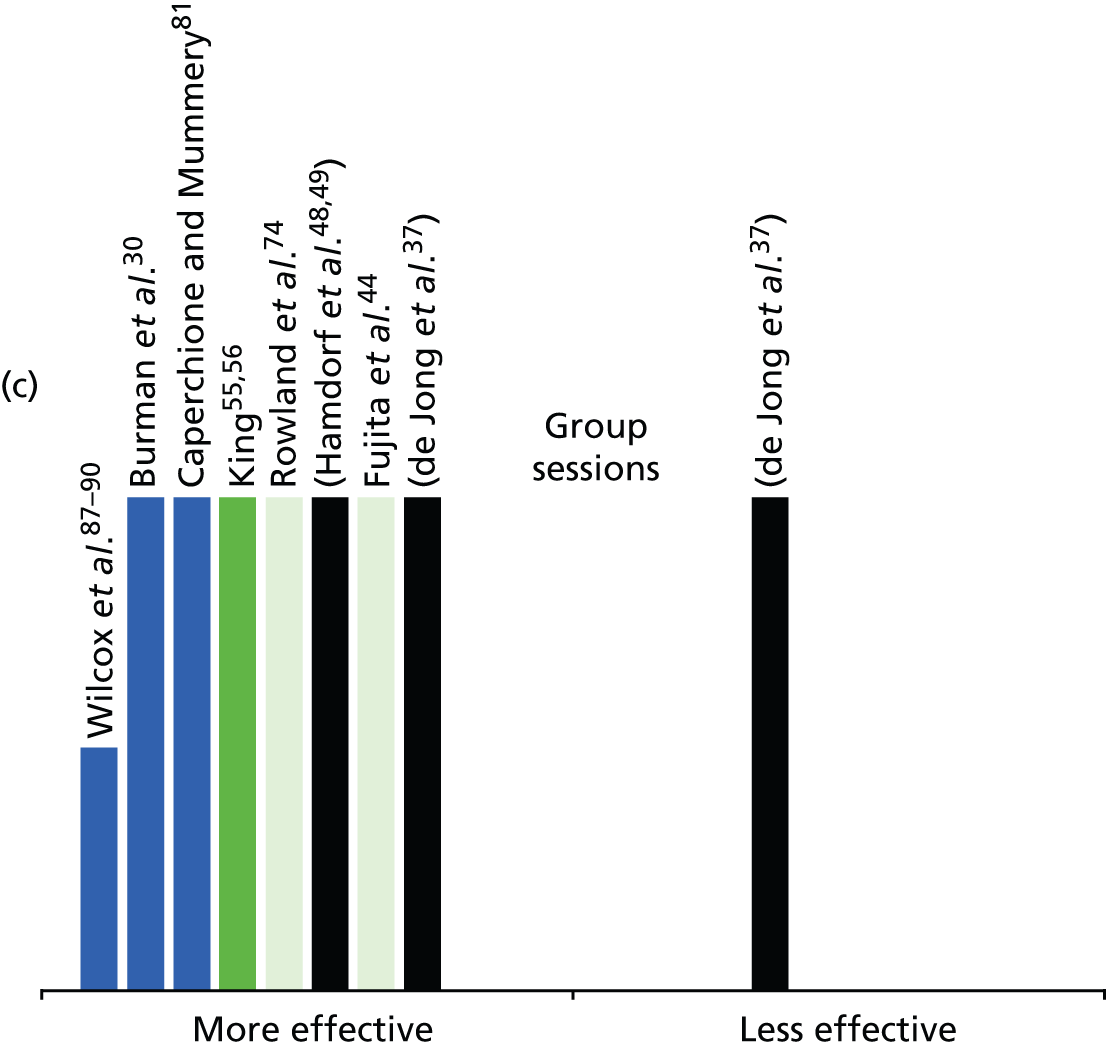
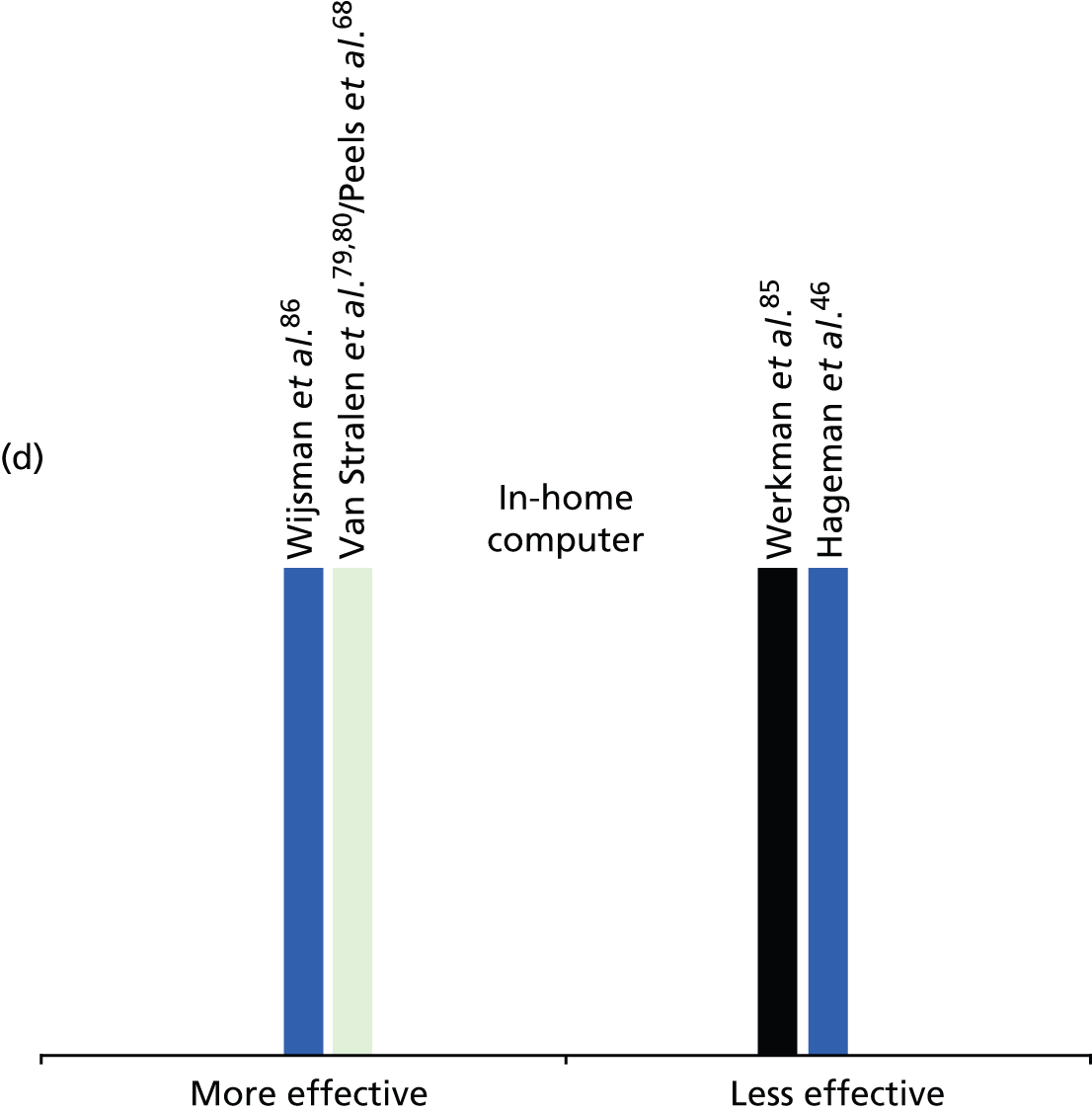
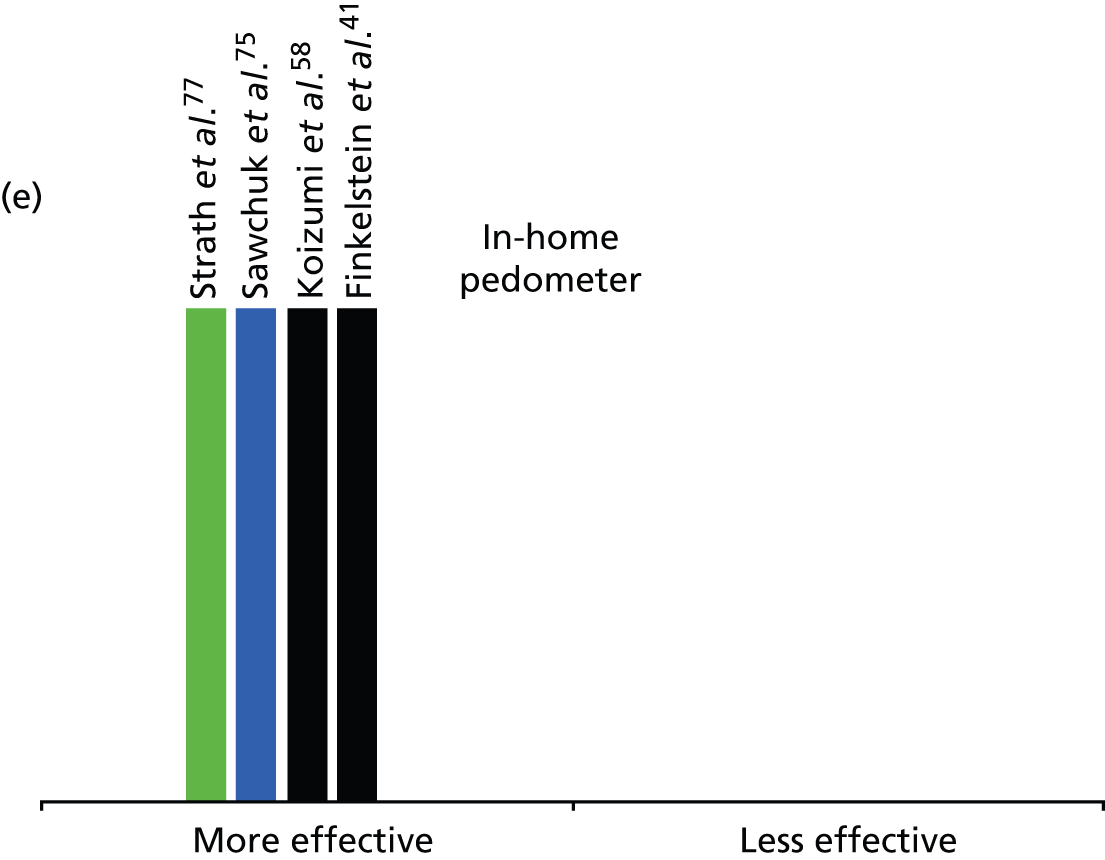
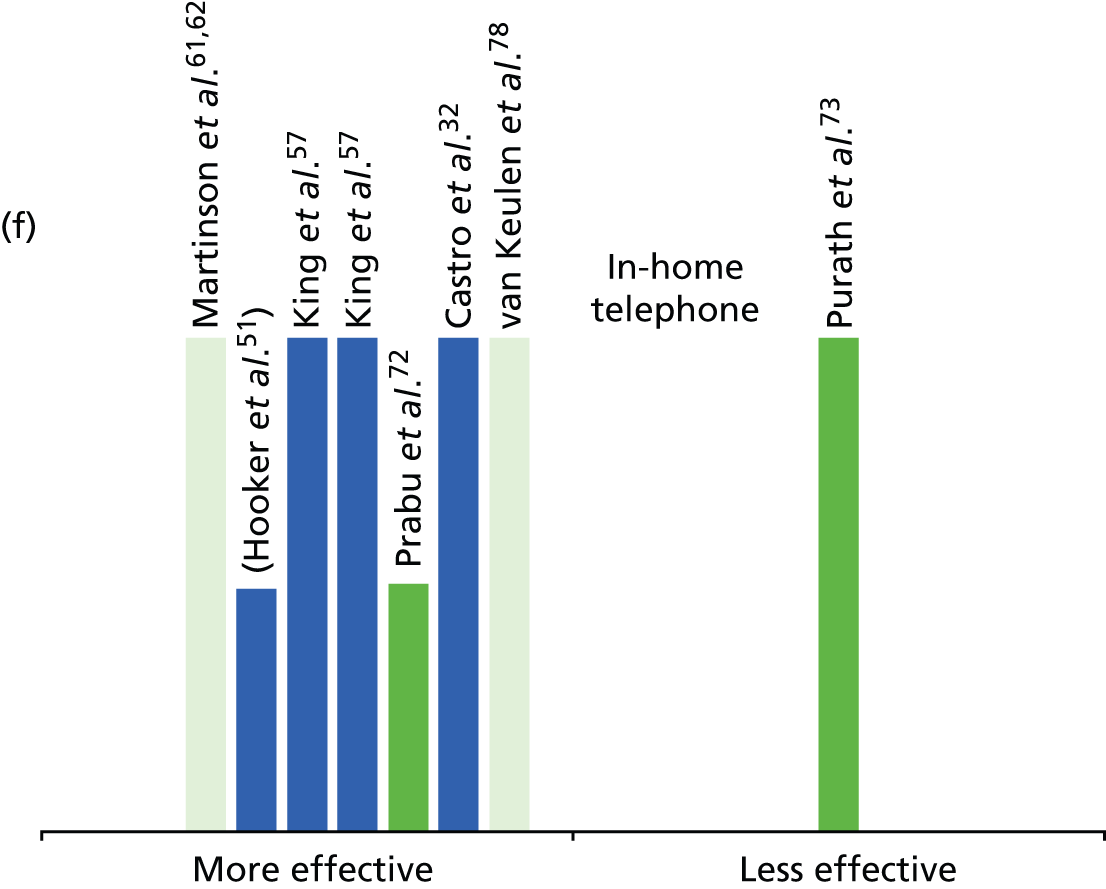
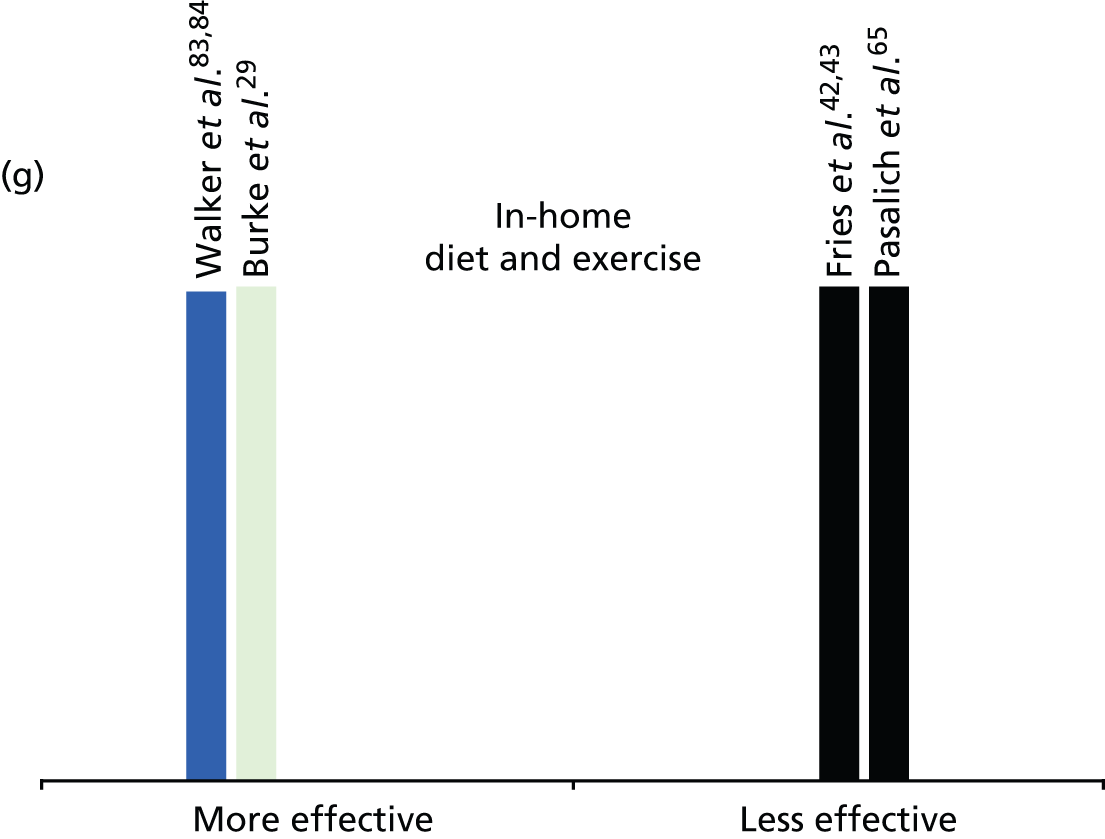
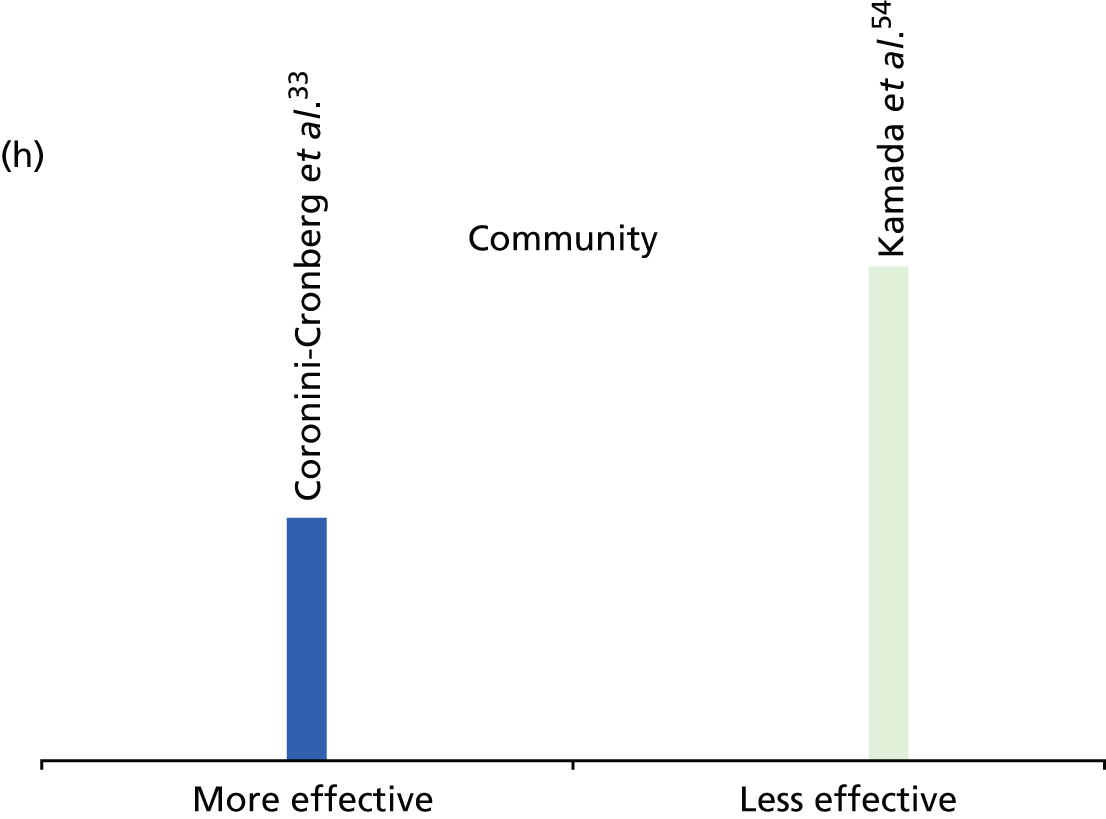
The criteria for greater effectiveness versus lesser effectiveness were based on the proportion of outcome measures that were significantly different (p < 0.05 or p < 0.01), either from baseline to follow-up (for those with multiple intervention arms only), or between intervention and control groups. To be considered ‘more effective’, the majority of outcomes (at least half) relating to physical activity needed to show a positive intervention effect. Those studies categorised as ‘less effective’ reported few physical activity outcomes with positive effects.
The studies with the most rigorous designs are RCTs with control (no-intervention comparator groups) and including investigator-measured outcomes. These studies are represented in the graphs as the dark green columns. Studies in which there were more elements of concern in the quality appraisal assessment are in brackets.
As can be seen from the plots, the evidence regarding effectiveness for the different types of evidence is fairly positive across the set. This may be a result of publication bias. The approach to defining strength of evidence is a source of considerable debate within systematic reviews. A common method is to use the total number of papers of the highest quality RCT design as an indicator of strength, although this may merely indicate where more empirical work has been carried out. A refinement of this approach is to consider not only volume of papers but also consistency of findings.
In considering and comparing strength of evidence between the interventions, the pedometer-based studies all provided evidence of effectiveness, with three of the studies including measured outcomes (steps)41,58,77 and two using control group designs. 41,58 This suggests the strength of evidence for pedometer interventions in terms of consistency, although there are only four studies. 41,58,75,77 It is also noteworthy that these four studies all had only short or immediate follow-up and therefore do not provide evidence of a longer term impact for these interventions. One of these studies also indicated that, although the provision of pedometers could be effective, that pedometers did not produce superior results to advice only. 75
All but one38 of the group interventions studies seemed to result in positive effects, thus indicating strength in terms of consistency. 30,31,37,39,40,44,48,49,55,74,87–90 Half of the studies had control-group designs37,38,44,48,74 and also two used objective measures37,48 indicating strength in terms of quality. The evidence for this typology comprised a total of seven studies and therefore suggests strength of evidence not only in terms of design but also in terms of number of studies for group interventions. One of the more effective studies30 had a follow-up of more than 12 months, and all of the group had a follow-up period of at least 6 months, also suggesting the effectiveness of these interventions in terms of longer term change.
Most of the advice/counselling interventions also led to positive effects, although here there is less consistency, and only one study had a control group and measured outcomes. 47 Two of the three studies (three papers) suggesting less effectiveness also had greater risk of bias concerns. 34,45,60 In terms of follow-up, one paper70 had a follow-up of more than 12 months, and only one34 had a brief follow-up period.
All but one of the six studies evaluating individual session interventions were effective,35,39,50,52,69 although only one effective study had a control arm. 70 The single study (reported in two papers) suggesting less effectiveness was of a lower quality study design, although had more than 12 months’ follow-up. 63,64 One of the studies suggesting greater effectiveness69 also had more than 12 months’ follow-up. All but one of the in-home interventions provided predominantly via the telephone also appeared to be effective, with three of these studies having longer follow-up periods. 32,62,78 The study indicating less effectiveness73 was of the highest quality, although it had only a brief follow-up period.
Small numbers of papers make it difficult to draw firm conclusions regarding the effectiveness of the other types of interventions (in-home computer interventions, programmes combining diet and exercise and community programmes). The evidence here was also inconsistent, with equal numbers of papers suggesting both greater and lesser effectiveness.
Although the Harvest plot method of presenting the data provides a useful visual summary of effectiveness, it is important to note the detail contained in the previous narrative summary. The interpretation of the evidence is complicated by several studies comparing different interventions and often similar variants of intervention elements. The typology that we have adopted is one way of grouping the studies, and we recognise that alternative groupings are possible, particularly for those interventions with multiple elements.
A wide range of outcomes were considered to provide evidence of effectiveness within the set of papers. These included measured physical activity outcomes, measured biophysical outcomes and self-reported activity and biophysical outcomes. Few studies included assessment of sedentary behaviour. The two29,55 that measured inactivity highlighted the effectiveness of the interventions on reducing time spent sitting watching television.
In terms of applicability to the retirement transition period, we have previously highlighted the dearth of evidence specifically referring to this significant period of life change. All the studies, with one exception,85 set wide age ranges for inclusion or included only populations of retired people. However, there is no indication in the data that these interventions within the proxy age range that we adopted for the retirement transition (55–69 years) would be unsuitable or not effective for our target population. In the body of work that we included, we were also unable to find any evidence that the transition to retirement period was, or was not, a significant point at which to provide these interventions.
What is the evidence regarding the impact of interventions in different populations and/or the potential for retirement to increase health inequalities?
Differences in outcome between population subgroups were rarely mentioned by authors. One51 described more calories as being expended by older participants, another89 described older participants as achieving less improvement in physical activity than younger participants. This was described as potentially being associated with normal ageing in older adults, as with increasing age adults may have more health issues and less mobility. Another paper80 reported that including environmentally tailored information in letters was effective in changing total physical activity in those aged 64 years and younger, whereas there was no significant effect on total physical activity in older adults. The authors report that apart from this association, no other demographic factors appeared to be linked to the effectiveness of the in-home tailored letter intervention.
There was little evidence in the intervention literature regarding differential impacts of interventions on advantaged versus disadvantaged populations. The paper referred to above which explored potential associations between effectiveness and participant characteristics80 found no association between level of education and outcomes. A second paper66 mentioned that the web-based intervention had reached both high- and low-SES groups, and the authors noted that participants with higher levels of education requested more in-depth information regarding the impact of physical activity on health.
We have further examined issues of applicability of the interventions to our target population in the meta-synthesis of the qualitative and quantitative evidence outlined in Chapter 5.
The A3 studies
As described above, we developed an applicability rating for the identified literature, with those with a proxy age range most applicable to the retirement transition rated as A1/A2. We have outlined these in detail above (see What are the most effective interventions to maintain and/or increase physical activity in older people during and shortly after the transition to retirement?). We identified 39 additional papers with participants with a mean age 70 years or older, which were graded as being of lower applicability (A3) to our target population. Owing to the potentially more limited applicability, we will not be providing a detailed narrative synthesis of these papers. However, we provide characteristics of this literature in Tables 8 and 9 below, and we have summarised the effectiveness of these interventions via Harvest plots. We have provided additional detail for any studies of note and consider any similarities or differences between this group of studies and those in the A1/A2 category.
A3i papers (participants aged 70–75 years)
Reference to retirement/employment (as provided in paper)
As can be seen from Table 8, as with the A1/2 papers, the majority of studies did not provide any information regarding retirement status. Of the three that provide some indication, as might be expected by the age, high numbers of these participants were already retired, and therefore data may be of more limited applicability to the retirement transition period.
| Reference to retirement | Studies |
|---|---|
| Not reported | Anderson and Pullen (2013)91 Age UK (2012)92 Bickmore et al. (2013)93 Borschmann et al. (2010)94 Brassington et al. (2002)95 Brawley et al. (2000)96 Croteau et al. (2007)97 de Vreede et al. (2007)98 Duru et al. (2010)99 Elder et al. (1994)100 Iliffe et al. (2014)101 Jancey et al. (2008)102 Kerse et al. (2005)103 Kerse et al. (1999)104 Kim and Glanz (2013)105 Kim et al. (2011)106 Kolt et al. (2006)107 Marki et al. (2006)108 Marki et al. (2006)109 Mutrie et al. (2012)110 Pelssers et al. (2013)111 Pfeiffer et al. (2001)112 Solberg et al. (2014)113 Stewart et al. (2001)114 Tan et al. (2006)115 Yamauchi et al. (2005)116 |
| 85% retired 80% retired |
Kolt et al. (2007)117 Kolt et al. (2012)118 |
| 50%/31% employed | Lee and King (2003)119 |
| 77% retired | Resnick et al. (2008)120 |
Study design
Similar to the A1/A2 studies, there is a large number of RCTs indicating a reasonable study quality across the set of papers (Table 9).
| Study design | Studies |
|---|---|
| RCT | Bickmore et al. (2013)93 Borschmann et al. (2010)94 Brawley et al. (2000)96 Croteau et al. (2007)97 de Vreede et al. (2007)98 Duru et al. (2010)99 Iliffe et al. (2014)101 Kerse et al. (2005)103 Kim and Glanz (2013),105 Kim et al. (2011)106 Kolt et al. (2006),107 (2007),117 (2012)118 Lee and King (2003)119 Mutrie et al. (2006)110 Pelssers et al. (2013)111 Pfeiffer et al. (2001)112 Resnick et al. (2008)120 Solberg et al. (2014)113 Tan et al. (2006)115 Yamauchi et al. (2005)116 |
| Cluster RCT | Anderson and Pullen (2013)91 Kerse et al. (1999)104 |
| CBA | Elder et al. (1994)100 Jancey et al. (2008)102 Stewart et al. (2001)114 |
| BA | Age UK (2012)92 Brassington et al. (2002)95 Marki et al. (2006)108 Marki et al. (2006)109 |
| Cross sectional | Kolt et al. (2006)107 |
Country
As with the A1/A2 studies, the largest number of papers were from teams in the USA, closely followed by teams in Australia and New Zealand (Table 10). Three papers were from the UK, with one of these being grey literature (report).
| Country of origin | Studies |
|---|---|
| UK | Age UK (2012)92 Iliffe et al. (2014)101 Mutrie et al. (2012)110 |
| USA | Anderson and Pullen (2013)91 Bickmore et al. (2013)93 Brassington et al. (2002)95 Croteau et al. (2007)97 Duru et al. (2010)99 Elder et al. (1994)100 Kim and Glanz (2013)105 Kim et al. (2013)106 Lee and King (2003)119 Pfeiffer et al. (2001)112 Resnick et al. (2008)120 Stewart et al. (2001)114 Tan et al. (2006)115 |
| Netherlands | de Vreede et al. (2007)98 |
| Australia/New Zealand | Borschmann et al. (2010)94 Jancey et al. (2008)102 Kerse et al. (2005),102 (1999)104 Kolt et al. (2006),107 (2007),117 (2012)118 |
| Belgium | Pelssers et al. (2013)111 |
| Canada | Brawley (2000)96 |
| Switzerland | Marki et al. (2006),108 (2006)109 |
| Norway | Solberg et al. (2014)113 |
| Japan | Yamauchi et al. (2005)116 |
Sex
As with the A1/A2 studies a large proportion of studies were conducted in all female participants. There were no studies with all male samples (Table 11).
| Participant sex | Studies |
|---|---|
| Predominantly female | Age UK (2012)92 Anderson and Pullen (2013)91 Brassington et al. (2002)95 Croteau et al. (2007)97 de Vreede et al. (2007)98 Duru et al. (2010)99 Kim and Glanz (2013)105 Lee and King (2003)119 Pfeiffer et al. (2001)112 Resnick (2008)120 Stewart (2001)114 Tan et al. (2006)115 |
| Mixed | Bickmore et al. (2013)93 Borschmann et al. (2010)94 Brawley et al. (2000)96 Elder et al. (1994)100 Iliffe et al. (2014)101 Jancey et al. (2008)102 Kerse et al. (2005),103 (1999)104 Kim and Glanz (2013)105 Kolt et al. (2006),107 (2012)118 Lee and King (2003)119 Marki et al. (2006),108 (2006)109 Mutrie et al. (2012)110 Pelssers et al. (2013)111 Solberg et al. (2014)113 Yamauchi et al. (2005)116 |
| Not reported | Kolt et al. (2006)107 |
Socioeconomic status and ethnicity
There is a slightly larger group of studies (seven) carried out in minority ethnic populations than the A1/A2 papers. All but one of these studies were carried out with African American older adults (Table 12). The other paper (Borschmann) provided an intervention to people of Macedonian or Polish origin living in Australia.
| Ethnicity or SES | Studies |
|---|---|
| Predominantly higher educated/higher income | Brassington et al. (2002)95 |
| Predominantly minority ethnicity | Anderson and Pullen (2013)91 Borschmann et al. (2010)94 Duru et al. (2010)99 Kim and Glanz (2013),105 Kim et al. (2011)106 Resnick et al. (2008)120 (72%) Tan et al. (2006)115 (and 84% had annual income < US$15,000) |
| Not reported/unclear | Brawley et al. (2000)96 Croteau et al. (2007)97 de Vreede et al. (2007)98 Kerse et al. (2005)103 Kolt et al. (2006)107 Marki et al. (2006),108 (2006)109 Pfeiffer et al. (2001)112 |
| Mixed | Age UK (2012)92 Bickmore et al. (2013)93 Elder et al. (1994)100 Iliffe et al. (2014)101 Jancey et al. (2008)102 Kerse et al. (2005)103 Kolt et al. (2007),117 (2012)118 Lee and King (2003)119 Mutrie et al. (2012)110 Pelssers et al. (2013)111 Solberg et al. (2014)113 Stewart et al. (2001)114 Yamauchi et al. (2005)116 |
Activity level
There is a similar mix in terms of recruiting predominantly inactive and mixed physical activity-level participants to studies in the A1/A2 group of papers (Table 13).
| Baseline activity | Studies |
|---|---|
| Predominantly inactive | Bickmore et al. (2013)93 Brassington et al. (2002)95 Brawley et al. (2000)96 Duru et al. (2010)99 Jancey et al. (2008)102 Kolt et al. (2006),107 (2007),117 (2012)118 Lee and King (2003)119 Mutrie et al. (2012)110 Yamauchi et al. (2005)116 |
| Mixed physical activity levels/inactivity not described as inclusion criterion | Age UK (2012)92 Anderson and Pullen (2013)91 Borschmann et al. (2010)94 Croteau et al. (2007)97 de Vreede et al. (2007)98 Elder et al. (1994)100 Iliffe et al. (2014)101 Kerse et al. (2005),103 (1999)104 Kim and Glanz (2013),105 Kim et al. (2011)106 Marki et al. (2006),108 (2006)109 Pelssers et al. (2013)111 Pfeiffer et al. (2001)112 Resnick et al. (2008)120 Solberg et al. (2014)113 Stewart et al. (2001)114 Tan et al. (2006)115 |
A3ii (participants aged 50–55 years)
Reference to retirement/employment (as provided in paper)
The lower age of these participants would suggest a higher rate of employment in these studies. This was borne out by the four studies which report this population characteristic (Table 14).
| Reference to retirement | Studies |
|---|---|
| Not reported | Ammann et al. (2013)121 Ferney et al. (2009)122 Lamb et al. (2002)123 McAuley et al. (1994)124 Marshall et al. (2005)125 |
| 29.8% retired, 69% employed | Sheeran et al. (2013)126 |
| 80% employed full time | Costanzo et al. (2006)127 |
| All employed | Hughes et al. (2011)128 Pfister et al. (2013)129 |
Study design
Seven of the studies in this group used randomised controlled designs (Table 15).
Country
There is a similar grouping of country of origin to the other study categories, with spread across the USA, Australia/New Zealand and the UK (Table 16).
Sex
A single study in this group provided the intervention to male participants only, with nearly half of all studies targeting all female participants (Table 17).
Socioeconomic status/ethnicity
The study providing the intervention to all male participants was also the only one targeting lower SES groups (Table 18). This paper,126 carried out in the UK with members of an angling club, evaluated a mental contrasting intervention, which we categorised as a form of counselling. The study found that at 7 months’ follow-up, mental contrasting (encouraging participants to imagine elements of a positive future life and then imagining obstacles in the way) was effective in enhancing self-reported physical activity for the intervention group (p < 0.001; d = 0.87), compared with no significant change among control participants. The effect was maintained using an intention-to-treat analysis (d = 0.24 for mental contrasting group at 7 months). Participant-reported importance of being active was significantly associated with levels of physical activity in the intervention group at follow-up.
| Reference to ethnicity or SES | Studies |
|---|---|
| Predominantly more highly educated/higher income | Costanzo et al. (2006)127 Hughes et al. (2011)128 Pfister et al. (2013)129 |
| Predominantly lower SES/basic education | Sheeran et al. (2013)126 |
| Not reported/unclear | Ferney et al. (2009)122 Lamb et al. (2002)123 Marshall et al. (2005)125 McAuley et al. (1994)124 |
| Mixed | Ammann et al. (2013)121 |
Activity level
The A3ii studies had a similar mix of participant baseline activity levels (Table 19).
| Baseline activity levels | Studies |
|---|---|
| Predominantly inactive | Costanzo et al. (2006)127 Ferney et al. (2009)122 Lamb et al. (2002)123 Marshall et al. (2005)125 McAuley et al. (1994)124 Sheeran et al. (2013)126 |
| Mixed physical activity levels/inactivity not described as inclusion criterion | Ammann et al. (2013)121 Hughes et al. (2011)128 Pfister et al. (2013)129 |
Summary of effectiveness evidence from A3 physical activity personal exercise referral schemes
Owing to the potentially more limited applicability of this work in middle aged and older adults in their seventies to our target population of adults at retirement transition, we have not completed a detailed narrative synthesis of these papers. However, we have provided an overview of evidence of effectiveness via visual summary (Harvest plots; Figure 8) and will briefly examine similarities and differences between this literature and that of the A1/A2 studies.
FIGURE 8.
Harvest plots for A3 intervention studies. Black, study with a control arm and measured data; dark green, study with multiple intervention arms only and measured data; light green, study with a control arm and self-report data; and blue, study with intervention arms only and self-reported data. The height of the bar indicates the strength of the study design. (a) Advice/counselling; (b) individual session; (c) group sessions; and(d) in-home computer.
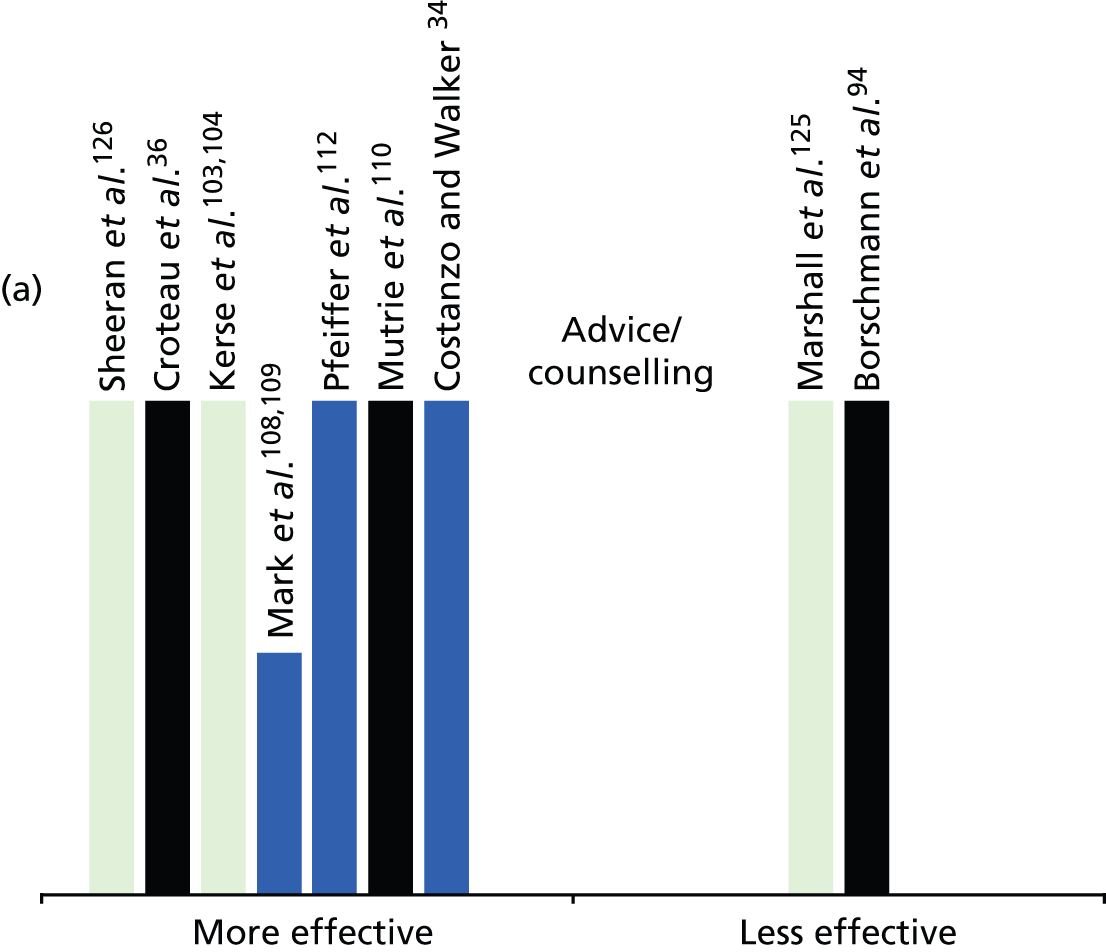
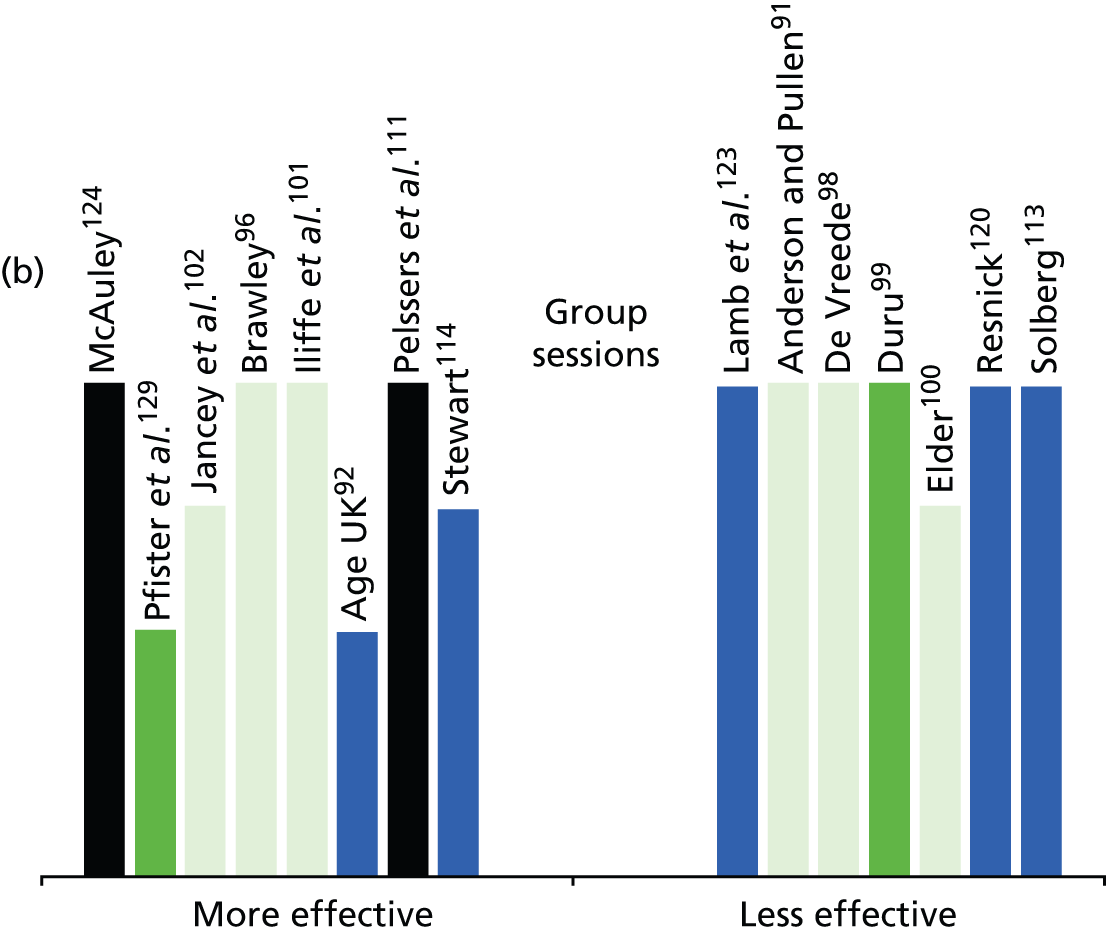
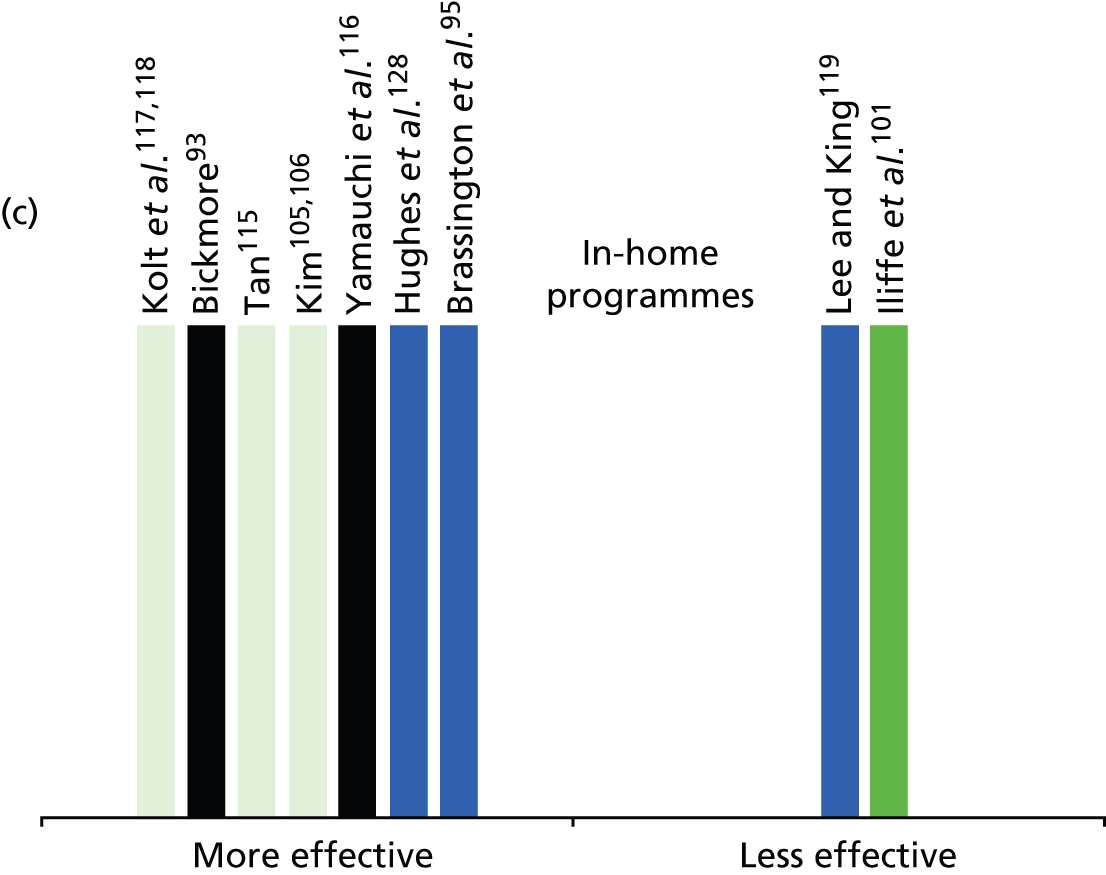
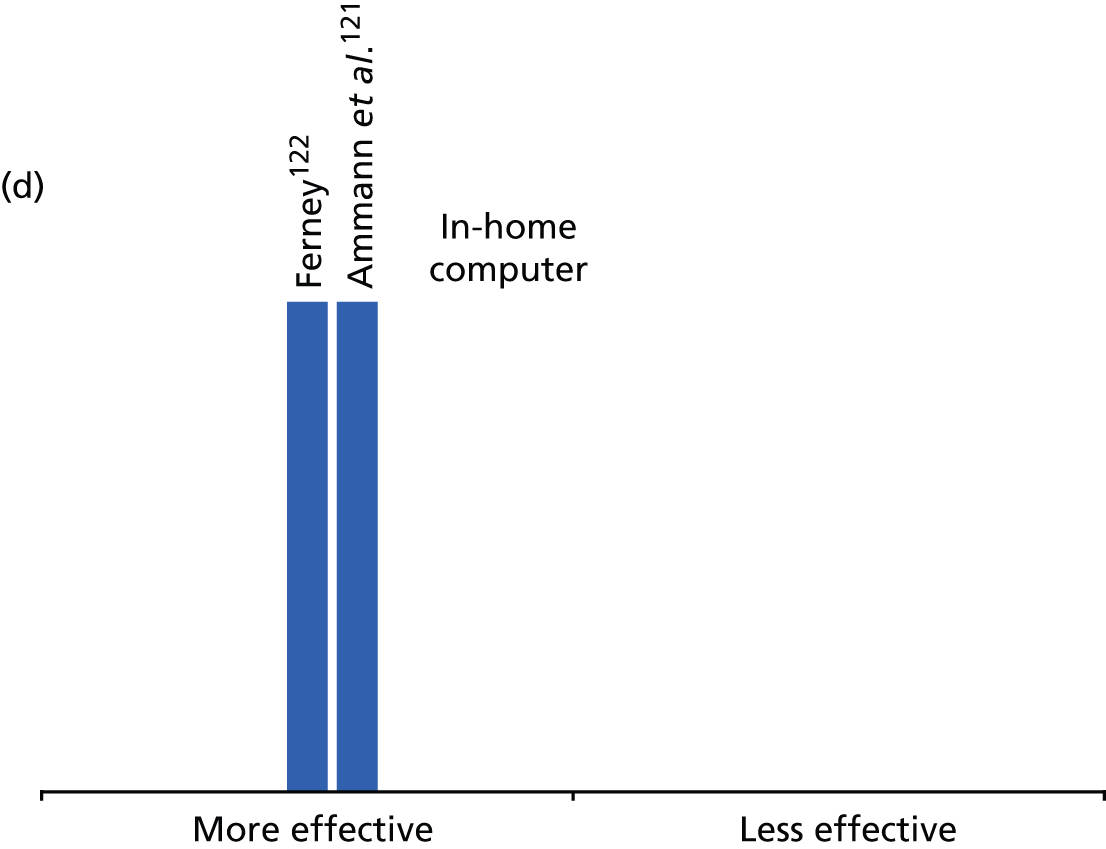
What are the most effective interventions to maintain and/or increase physical activity in older people?
The interventions delivered to these participants did not differ from those carried out in the A1/A2 studies. The lower age group (A3ii) interventions included a similar range to that found in the slightly older population and encompassed counselling/advice; exercise classes; group or individual walking programmes; individual jogging programmes; and website-based interventions and information. The older group (A3i) similarly contained the same mix of advice/counselling, individual programmes and group programmes to that found in the A1/A2 studies. The different age of these participants did not, therefore, seem to have led to different intervention types or different targeting of interventions by age group.
As can be seen from Figure 8, in this set of papers there is a larger proportion of group-based interventions (15),91,92,96,98–102,112–115,120,124,129 perhaps reflecting the potential benefits of social interaction for elderly adults who may be living alone. In contrast with the A1/A2 studies, there are seven papers91,98–100,115,120,123 suggesting that these group programmes are less effectivene, and, therefore, there is less consistency in strength of evidence for group interventions in these populations. Apart from this difference, these studies with older/younger mean age participants echo the findings of the A1/A2 studies in tending to report positive outcomes for all intervention types. We have combined the in-home interventions that did not include computer-delivered programmes owing to small numbers and multiple elements. Most of these programmes included predominantly telephone advice/support; the Hughes et al. 128 paper included one intervention arm that consisted of web-based materials. There is strength of evidence for effectiveness of these in-home interventions in terms of volume of higher quality studies and in terms of consistency (all but two of nine studies indicated effectiveness). 93,95,105–107,116–118 Both studies121,122 in the group evaluating computer-based interventions report effectiveness, although this evidence is from weaker design, no-control-arm studies, and with self-reported outcomes.
What is the evidence regarding the impact of interventions in different populations and/or the potential for retirement to increase health inequalities?
As with the A1/A2 studies, we found very little evidence regarding differential effects among participants. One of the A3 studies126 was carried out in a wholly lower SES participant group and it found evidence of effectiveness for the mental contrasting intervention. The authors of this work highlighted an association between perceived importance of being active and physical activity outcomes. Seven of the A3 papers reported six studies carried out in a minority ethnic population. 91,94,99,105,106,115,120 These papers examined a range of intervention types (group, individual and advice) and found mixed evidence regarding outcomes. Four papers reported more evidence of effectiveness94,105,106,115 and three found less evidence of effectiveness. 91,99,120
Chapter 4 Results of review of the qualitative studies
Before outlining evidence from the qualitative studies, we will briefly summarise instances in which methods for the review of qualitative studies differed from review of the effectiveness literature.
Methods for the qualitative review
Inclusion and exclusion criteria
Population
The included population was adults approaching, transitioning or recently transitioned through retirement. However, as with the intervention studies we also included papers that did not mention retirement specifically but that included a sample aged over 50 years but under 70 years (unless the experiences being expressed were retrospective).
Intervention/activity
Included papers explored views and experiences about interventions to promote, or engage in, physical activity in whatever form this might take. We therefore excluded studies that explored views of retirement in relation to other activities that did not require such bodily movement, for example attending book groups or bridge clubs.
Study design
The review of qualitative studies included any study that was carried out using qualitative methods to obtain ‘rich’ data about experiences (interviews, focus groups, observations, etc.).
Search strategy
Searches for qualitative papers were carried out using the same strategies as described for the effectiveness review. Papers that used qualitative methods were coded as such in the citation database, and those retrieved in the initial searches were used to identify keywords for the following iteration. Citation searches and author searches were carried out using relevant papers from these searches. In addition, the reference lists of included papers were scrutinised for new citations. Methods for citation sifting and retrieval are described in the methodology chapter.
Data extraction and quality appraisal
Data extraction was carried out using a modified form to include the most relevant data (see Appendix 7 for the extraction table). For qualitative papers this included summaries of the rich text from findings within each paper. We also noted the main theoretical underpinning of each study where this was discussed in the literature. Quality appraisal was carried out using an adapted version of the CASP tool for the assessment of qualitative studies (see Chapter 2). The reported details and methods of each paper were assessed for low or high concordance with items included in the quality appraisal tool.
Data synthesis
A large body of work was retrieved for the qualitative review, providing a challenge in terms of synthesising the data. We initially organised the studies according to age range/retirement status, specific physical activities, whether or not the activity was part of an intervention or a lifestyle choice, a focus on sex, ethnic issues or SES impact. As many studies focused on more than one of these aspects, we have, where necessary, included studies in more than one section of the findings. We were keen to highlight the impact of age, health, SES, ethnicity and sex with regard to physical activity. In order to identify potential strategies that might reduce inequalities, findings from the included papers were coded on the basis of these factors where they were apparent and analysed separately to create an explanatory narrative around these interactions.
Quantity of evidence available
Searches for qualitative literature produced 24 papers from a combination of initial searching and a further iteration (see Chapter 2 for details of the two searches). Five relevant papers were identified from citation searches and a further 26 from reference lists of included studies (see Figures 1 and 2). Grey literature was searched by our information specialist to identify any qualitative evaluations carried out by credible sources that were not published in journals; however, none was identified.
We retrieved a total of 55 qualitative papers reporting 48 unique studies. Thirteen studies reported in 15 papers were carried out in the UK. 130–144 The USA provided the largest body of research, with 18 studies reported in 22 papers. 145–166 A total of 11 studies were carried out in Australia167–175 or New Zealand,176,177 four were carried out in Canada,178–181 one in South Africa (producing two papers)182,183 and one in Chile184 (Figure 9).
FIGURE 9.
Number of studies from each country.

Quality of the evidence available
The quality of the included papers was generally variable, with 41 papers132,133,135–143,145–148,150–152,157,159–161,164,166–173,175–184 out of the included 55 at least partially meeting most of the eight quality criteria. There was a lack of reporting of the reasons for non-participation throughout the studies. However, many of the samples were small and purposive so this kind of information was not likely to be applicable. Ethical considerations were rarely addressed in a comprehensive way, with some papers reporting the details of ethical approval (where necessary) but not the considerations of ethical practice and vice versa. The third area in which reporting was often vague, brief or missing was the process of data analysis. Study authors may have been limited by journal word-count constraints. Limited detail meant that it was often difficult to assess how reported methods related to the actual implementation of the studies (see Appendix 4 for a quality assessment table).
Type of evidence available
Age
The age range of the study samples was broad and spanned the range 50–70 years. Three papers recruited individuals over the age of 70 years who were recalling past experiences of physical activity (Figure 10). 149,176,178
FIGURE 10.
Number of studies by age range of participants in years (not mutually exclusive).
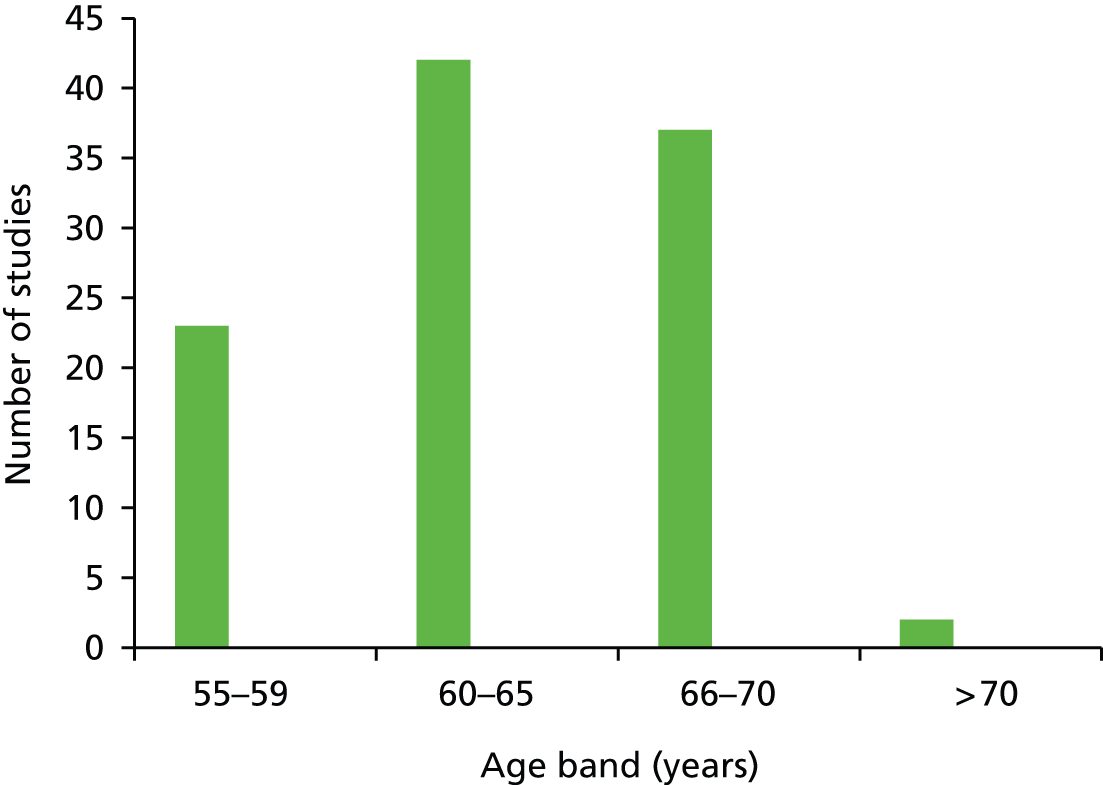
Retirement
A total of 16 studies reported in 20 papers referred to retirement in relation to physical activity. 130–134,138,145–152,155,157,169,173,177,178 Retirement was reported as recent, partial or full, or ‘leaving paid work’. In total, 31 studies (34 papers) reported data from samples defined as ‘young older’, ‘transition to old’, ‘older’, ‘later life’, ‘senior’ and ‘midlife’. 135–137,140–144,153,154,156,158–168,170–172,174–176,179–184 One study recruited physical activity trainers only. 139
Study design
In terms of methods used within studies, 21 studies reported in 23 papers132,133,135–139,146–149,153,159–161,171,174,176–178,180,181,184 used interviews exclusively to collect data (Figure 11).
FIGURE 11.
Number of studies by study design.

A further 13 studies used focus groups exclusively. 130,131,142,156,158,162–164,167,168,170,175,179 A total of five studies reported in eight papers134,143–145,150,157,166,173 used a combination of interviews and focus groups. A further nine studies reported in 11 papers140,141,151,152,154,155,165,169,172,182,183 used either interviews or focus groups and another qualitative method. In eight of these studies the additional method was participant observation. 140,141,151,152,154,155,169,172,182,183 The remaining study used focus groups and photo-voice. 165
Just over half of the included studies identified a theoretical background which was used as an explanatory tool for analysing the data. One study was based on a sporting model130 and five studies reported in six papers focused on sex/gender, with three studies (four papers)147,148,161,177 underpinned by feminist theory and two173,178 by masculinities theory. A further three studies that focused on ethnic minority experiences and views drew on theories of cultural sensitivity. 156,159,166 The most commonly identified theories were psychological/sociological theories, which were identified in 10 studies (13 papers)133,136,137,140,147,148,151,152,158,164,169,171,181 Ageing and life-course theories underpinned a further nine studies (11 papers). 135,141,145,146,149,150,155,157,172,174,180 Although the remaining studies (22 papers)131,132,134,138,139,142–144,154,160,162,163,165,167,168,175,176,179,182–184 did not explicitly mention any particular theory, a number drew on literature from ageing and sex/gender research when discussing the findings.
Sex
There was a predominance of female populations, with 18 studies reported in 22 papers136,137,145,147,148,153,154,156–161,163,165,166,169,172,177,181–183 recruiting all or mainly female participants. Four further studies155,173,175,178 as well as one paper from another study150 reported findings from male participants. A total of 24 studies reported in 26 papers recruited a balance of female and male participants or a mixed sample,130–135,138,140–144,146,149,151,152,164,167,168,170,171,174,176,179,180,184 and two studies did not report this detail139,162 (Figure 12).
FIGURE 12.
Number of studies including male/female participants.
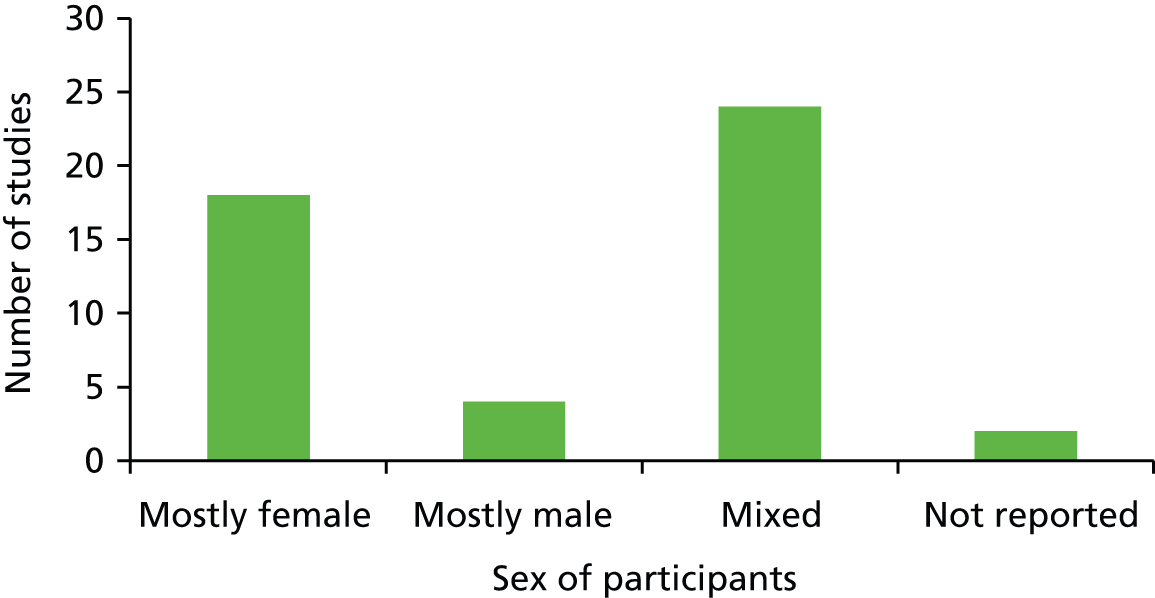
Socioeconomic status
Ten included studies reported in 11 papers140,147–149,154,155,163,168,169,177,181 recruited samples with higher SES (defined by higher than average educational levels or income). Only two studies aimed to assess the physical activity experiences of older people from lower SES backgrounds. 160,172 The remaining 36 studies (42 papers) included a mixed SES population,130,132,134,141,142,145,150,157–159,161,164–166,170,174–176,180,184 or did not report SES characteristics131,133,135–139,143,144,146,151–153,156,162,167,171,173,178,179,182,183 (Figure 13).
FIGURE 13.
Number of studies by SES (education/income).
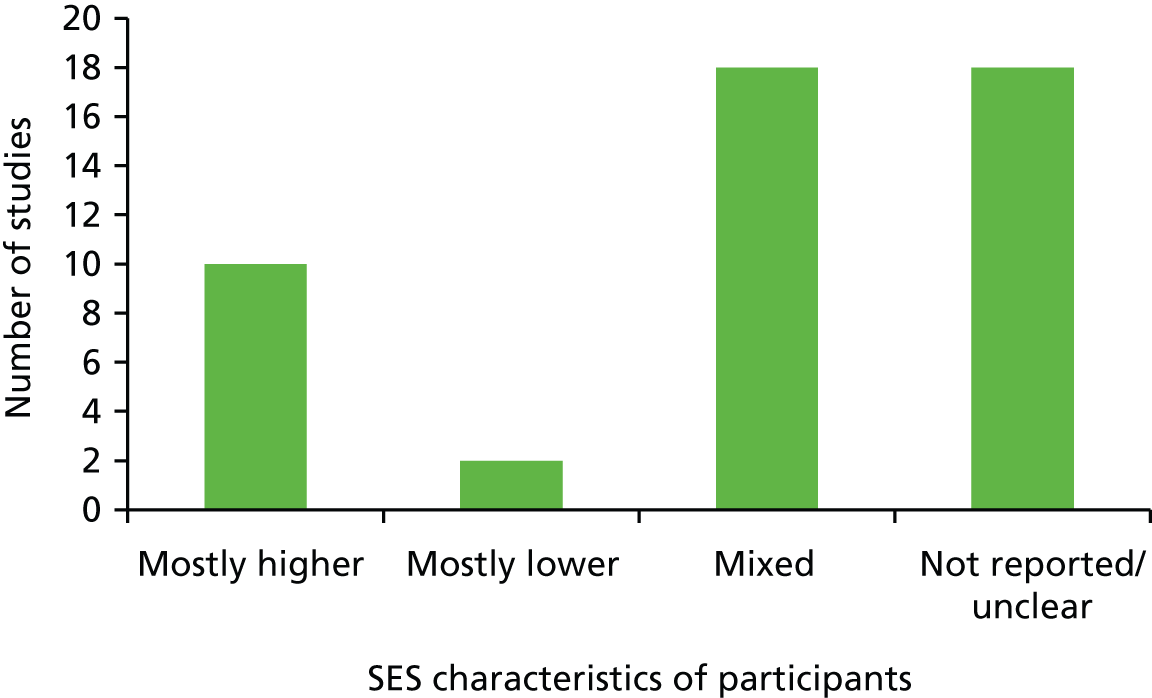
Ethnicity
Eleven studies reported in 15 papers133,145,147–152,154,157,161,168,169,178,181 included an all or mostly white population and seven included studies focused on ethnic populations, for example African American,162–165 African American and Native American159 or Latina. 160,166 Seven studies reported in nine papers recruited a mix of ethnic groups. 130,134,143,144,156,158,170,182,183 In the remaining 23 studies, reported in 24 papers, the ethnicity of the sample was not reported131,132,135–142,146,153,155,167,171–177,179,180,184 (Figure 14).
FIGURE 14.
Number of studies by ethnicity.
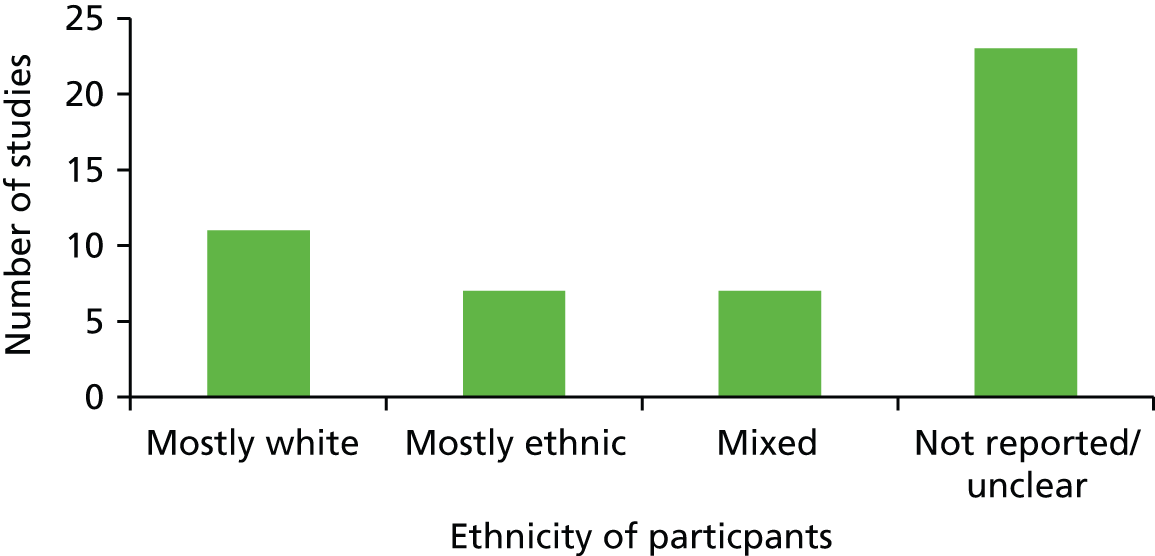
Activity level
Three included studies focused on currently inactive older people. 142,156,165 A total of 20 studies reported in 23 papers included individuals involved in or training others in a particular sport, activity or intervention, and therefore participants could be described as currently active. 135–141,149,151–155,161,169,171–173,176,179,182–184 In the remaining 25 included studies (29 papers), the activity levels of participants were mixed or not reported130–134,143–148,150,157–160,162–164,166–168,170,174,175,177,178,180,181 (Figure 15).
FIGURE 15.
Number of studies by activity level.
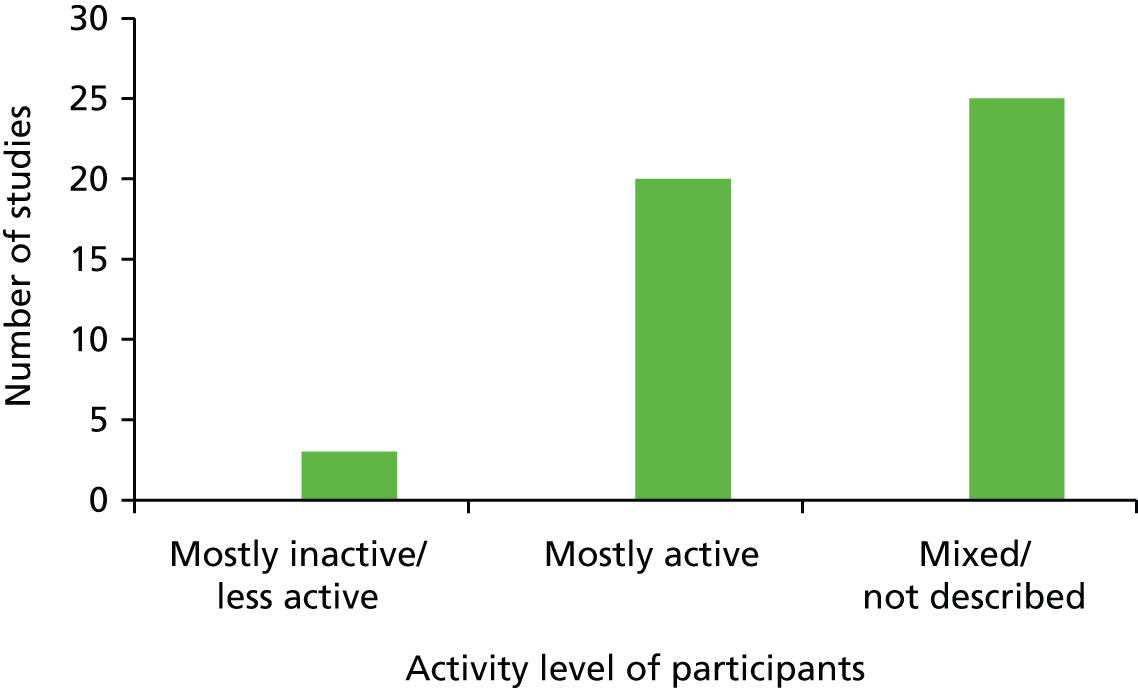
Intervention types
Four included studies reported in five papers135–137,139,140 explored individually prescribed interventions such as exercise referral schemes (ERSs). Ten studies reported in 11 papers140,149,151–154,156,167–169,184 explored views about a range of community-based interventions such as shopping mall walking or resistance training. Another two studies reported population-wide interventions,170,179 which in these cases were mass media campaigns. A further six studies reported in seven papers141,155,171,172,176,182,183 focused on a particular form of physical activity that the older research participants were regularly involved with. These were not health promotion interventions but were typically a sport such as tennis or bowling, or a dance activity such as ballroom or line dancing. The remaining 26 studies reported in 30 papers130,132–134,142–150,157–166,173–175,177,178,180,181 did not focus on a particular sport, activity or specific intervention; rather, they sought the views of older people about physical activity in general or potential barriers to participating in an intervention (Figure 16).
FIGURE 16.
Number of studies by intervention type.
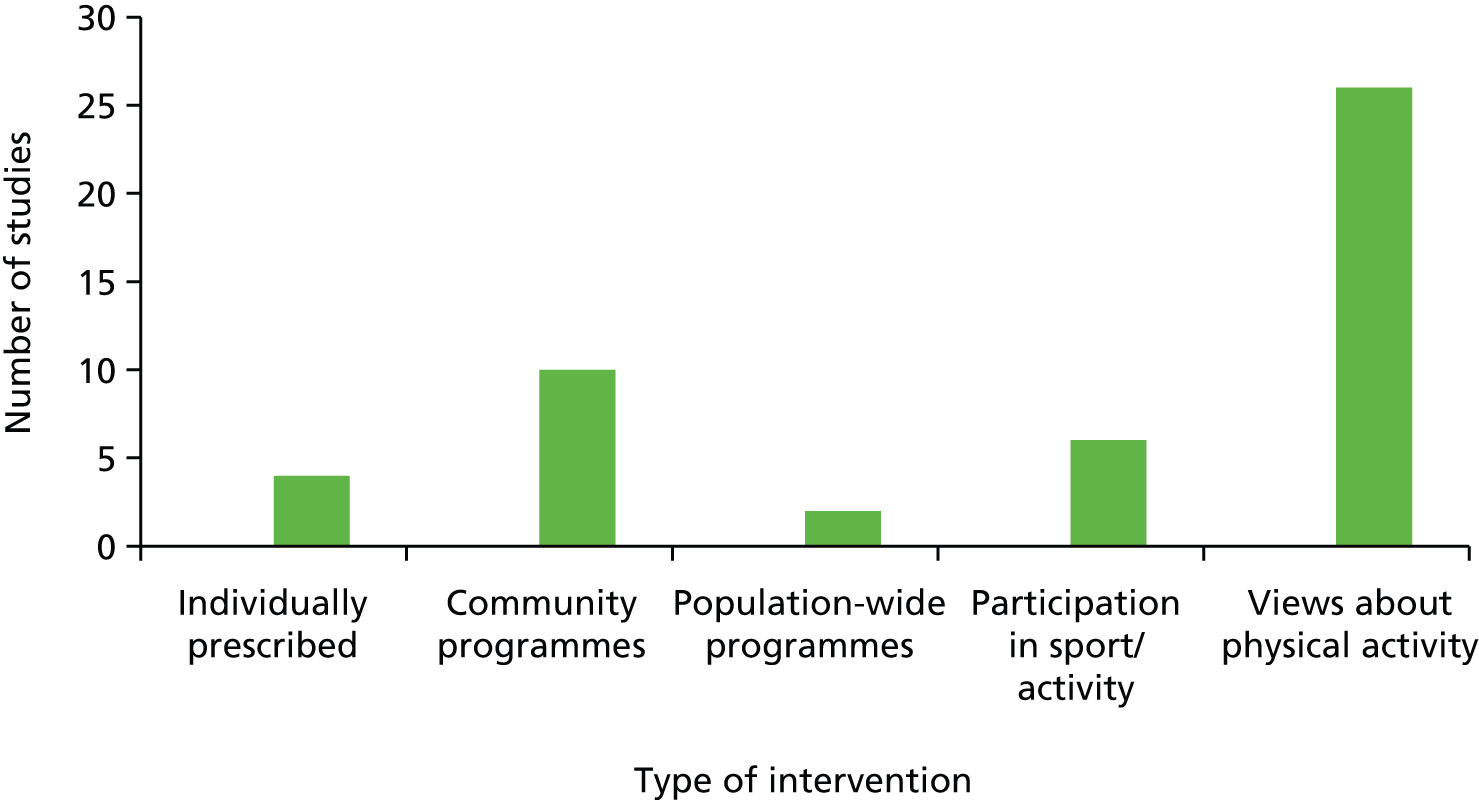
Factors that may underpin the effectiveness or acceptability of interventions during and after the transition to retirement
Findings from the included studies have been synthesised to produce a narrative of how people about to retire, or in the early years of retirement, might experience continuities or changes that could impact their engagement with physical activity.
The findings are structured in two parts to distinguish between the forms of evidence available. First, we briefly discuss retirement as a process or experience and its potential impact on physical activity. Second, we discuss interventions and influences on involvement with physical activity around the retirement transition.
The experience of retirement in relation to physical activity
Eleven of the included qualitative studies (reported in 12 papers)130–134,145,147–150,178 focused on or referred to physical activity and retirement. Nine papers mentioned retirement in the discussion of findings,138,146,151,152,155,157,169,173,177 although the aim of the study did not include a focus on retirement.
The importance of context and circumstances of retirement
It was suggested that the impact of full retirement required adjustment compared with partial retirement. 130 Reported positive implications of retirement included increased freedom, a reduction in stress,130,131 greater spontaneity145 and a time to focus on appealing131 or new146 activities. The impact was contingent on health status,178 sex147,148 and personal circumstances, for example whether the retired person had a partner or was widowed133 and whether or not partners shared similar interests. 132 Other factors included the support received from families,132 as well as family requirements. 133
Physical activity, ‘exercise’ and health
There was a reported difference in the way that participants regarded ‘physical activity’ and ‘exercise,’ with the latter being defined as more structured (e.g. going to the gym). 130 Finch131 reported some scepticism about gym attendance, with participants referring to gyms as a ‘fashion’. Similarly, Scanlon-Mogel and Roberto149 found that older members of a public exercise centre were not used to attending a gym, as such gyms and health clubs were rare when they were younger. The arrival of such facilities extended the opportunity to carry out physical activity in retirement. There was a more positive response from a number of participants to purposeful physical activity such as walking the dog or gardening. A sense of purpose and routine was reported to be important to replace work-related goals. 133,147 There was a strong consensus across papers that participants understood the potential benefits of remaining physically active, even among those participants who did not remain active. 131 Some scepticism regarding health promotion initiatives was voiced, with reports of confusing messages and a ‘paternalistic’ stance that evoked guilt over the level of engagement with activities, which ought to be guided by choice. 131
Physical activity, ‘daily living’ activities and ‘leisure activities’
A broad range of activities is currently open to retired people and not all of these are defined as ‘physical activity’. There was a sense from included papers that retirement brought an increase in leisure time, although definitions of ‘leisure’ could include sedentary pursuits such as relaxing, reading, volunteering or visiting family as well as physical activity. 147 In the Arkenford study,130 inactive participants were more likely to include everyday activities such as shopping or housework and generally being ‘busy’ in their definition.
Benefits beyond increased activity
Two studies133,147 reported that a sense of purpose was important to replace work-related goals. Another important reported feature of physical activity was a sense of challenge. Similarly to having a sense of purpose, participants needed to replace challenges faced at work once these had disappeared. These challenges may well be new activities that are sought on the basis of extended time and opportunity on the one hand and a sense of increased freedom from social and domestic responsibilities on the other. 145 Liechty and Genoe150 found that men who had previously been bored or understimulated at work sought challenges to counteract this feeling once retired. Beck et al. 133 and Liechty et al. 145 found that challenges were not always sought through the route of physical activities; they were often academically stimulating or caring in nature. These less physical activities were more often reported by previously inactive participants. Liechty et al. 145 found that acquiring new interests and pursuits, whether involving physical activity or not, resulted in women reporting greater feelings of enjoyment, confidence and empowerment.
One study133 reported that retired people sometimes spoke of developing a routine similar to that of the working day. This often involved walking or another physical activity, or having a set routine that ensured that a task would be carried out. In contrast, one retired person who did not report developing a routine found that he kept postponing involvement with physical activity because he could carry it out at any time of the week. Across studies, the importance of a social element of physical activity was apparent. Beck et al. 133 found that being part of a physical activity group was a strong motivator, particularly for women.
There was a strong consensus across papers that participants understand the potential benefits of remaining physically active. For active participants it was perceived as particularly important to remain physically and mentally fit during retirement to prevent ‘seizing up’ and gaining weight or ‘beer bellies’ when an active work-life had ceased. 131 Some participants were exercising to ward off future ailments or to cope with existing conditions so that they could enjoy their retirement. Barnes et al. 134 reported that remaining fit in retirement required regular stimulation that was not being accessed through work. For women, exercise classes were a popular way of maintaining health and fitness. However, Finch131 found that retired women were more likely than men to remain active as a result of carrying out housework.
Negative views
Negative views about the effects of physical activity in retirement were also apparent, mainly owing to witnessing or hearing stories of events where retired people had become very ill or died following intense physical activity. These views were balanced with the awareness that engaging in insufficient physical activity in retirement was also a threat to health. 131
Interventions to increase physical activity in retirement
This section presents a synthesis of qualitative findings from papers that examined views about interventions to promote physical activity, many of which did not have a specific focus on retirement but sampled participants within our proxy retirement age range. First, interventions that are prescribed for individuals, usually to improve health, are presented and, second, interventions at community level and population level or mass media campaigns are discussed.
Individually prescribed interventions
Three included UK studies reported in four papers135–138 explored the views of older participants enrolled in GP ERSs or ‘Exercise on Prescription’ schemes and a further study examined views of professionals delivering the scheme. 139 Evans and Sleap135 explored the experiences of participants taking part in UK-based aquatic activities, many of whom had been referred to the intervention by their GP. Hardcastle and Taylor136,137 interviewed participants of a 10-week ERS for older women that had been in place for more than 10 years. Stathi et al. 138 interviewed a mixed-sex sample of ERS participants, each at different stages in one of three leisure centre-based programmes. Moore et al. 139 interviewed health professionals delivering a 16-week intervention based on motivational interviewing and goal-setting.
Participants relating their experiences of aquatic physical activity in one study135 were aware of the benefits of physical activity, but their understanding of their bodies was mainly in relation to regular routine biomedical measurements carried out at their general practice. The participants were thus keenly aware of the fact that their bodies were ageing and of the effects that this was having on their appearance. Aquatic physical activity differs from many other forms of exercise in that it requires exposure of the body, which was an inhibiting factor for many of the participants, particularly women but also some men. The participants mentally compared their bodies with media images of younger, fitter individuals and were conscious of how they appeared in bathing attire and to their contemporaries.
‘Exercise on Prescription’ classes were targeted at people over the age of 40 years, with activities modified to reduce intensity and therefore physical risk to the participants. These factors enhanced the sense of being an outsider in respect of the general population, and, because of the modified programme, of being ‘at risk’ even in the absence of health problems. However, a sense of shared experience with the group was forged and new support networks established. For some, the sessions offered empowerment through increasing achievements; the sense of ownership led to participants using strategies to continue attending when the prescribed 12 sessions were completed.
A majority of the women in another study reported in two papers136,137 initiated the idea of participation in ERS with their GP, having been told about the scheme by friends and peers. Some GPs were reported to have shown little enthusiasm about referral when the topic was raised, stating only that it might do them good. This use of initiative by the women signifies a pre-existing desire for change prior to discussing exercise with the GP. In contrast, men and women interviewed by Stathi et al. 138 depended upon their GP’s advice to encourage them to participate in and to continue with the programme. All but one health professional participating in one study139 reported that participation as a result of the patient’s own determination, rather than their GP’s advice, was more predictive of continuation with the programme. One health professional held the view that patients were more likely to attend the programme on their GP’s advice, as it was regarded as authoritative, compared with the advice of family. There was a suggestion that GPs target patients who were already motivated and that this might be a way to avoid wasted effort and reduce high dropout rates. Health professionals also reported that patients with mental health problems are difficult to recruit, as depressed patients have low motivation and some patients feel nervous about being watched. Similarly, people with a lower SES were perceived by staff as not engaging with the service. This was viewed by staff as perhaps being attributable to a lower value placed on health in an economically depressed community, in which unemployment rates are high, or to the fact that GPs are not motivated to put patients forward in these areas.
Women in one study reported in two papers136,137 reported that they faced stigma in terms of exercising in older age. There were reported perceptions from others that the women were trying to act or appear younger when they merely wished to improve their health and well-being. The authors refer to perceptions generally that older people may injure themselves if they exercise, or that they cannot live up to the ideal of being an ‘exerciser’. This potential anxiety was also raised in interviews with health professionals139 who suggested that patients might be put off ERSs by the presence of ‘fitter’ people at the gym. One suggested for overcoming this was to make it clear that the programme would be held at a time when other gym members were absent, as well as being clear about what is expected of patients when they attend.
Women in one study outlined in two papers136,137 reported some initial ambiguity towards participation, with some perceiving the appointment in a similar way to going to the dentist – they attended only because they felt they needed to and because they wanted to keep to their appointment. There were reports of continuing the programme out of a sense of responsibility towards their GP and also towards their own self-care to improve health. They had typically allowed physical activity to decline while looking after a house and children. At this point in their life they would have felt guilt at taking time for themselves. The women were seeking to re-enter a new phase in their life following retirement, which meant not only being more physically active but also more mentally stimulated, as well as extending social networks. For some women this new take on life increased their sense of commitment to the scheme so that other priorities were not given precedence: ‘Things are more important than doing housework and things like that’. 137 One woman found it difficult to fit the programme into her week initially, because her priority was looking after her husband. However, later in the programme she reported that it was no longer difficult; she was focusing on her own health and well-being, and exercise had become a way of life. Another woman had low motivation to begin with, but later in the programme she reported that the positive impact that her swimming had had on her well-being influenced her decision to continue.
The gym was reported to be a new environment for many ERS participants in all three studies, with feelings of discomfort expressed during the initial stages of a programme. It was therefore important for participants to receive encouragement and support from the instructor, particularly at the beginning of the programme. Health professionals were aware that vulnerable older adults might require extended support to promote feelings of security and to promote attendance. The implications of training for health professionals to deal with patients’ emotional issues and of the potential for patients to become dependent on this service were discussed. 146 For women in one study, the gym evoked an association with ‘exercisers’ with whom they did not at first identify. It would be easy to have been demotivated at this stage; one woman noted that her instructor’s ability: ‘. . . got me over the first hurdle’. 136
Although participants valued a secure environment in which to exercise, in one study138 some were not keen on structured exercise, preferring a combination of lifestyle or home-based physical activity that was meaningful as well as fulfilling exercise guidance. One man stated that he found the exercise schedule boring and would prefer to play golf. This difference in views between the two studies may be gendered, because one study interviewed only women136,137 who appear (from data in other included studies) to prefer participating in group activities more than men, perhaps owing to the potential to expand social networks. Health professional participants in one study139 also suggested that men may feel outnumbered by women, who tend to be referred more often, and that men benefit less from the social network. This would suggest that men have a different experience of ERSs to women.
Female participants in two studies136–138 were motivated to participate in ERSs for the social aspect. The participants in one study achieved this aim but Stathi et al. 138 reported that women did not meet new contacts at the gym, as they were attending only for a short period and participants often dropped out. For Hardcastle and Taylor136,137 social support and having somewhere to go were motivating factors, countering the sense of loneliness and not belonging that some had felt previously.
Women who committed to the scheme136,137 were reported to have adopted an ‘exercise identity’ which required habitual scheduling of exercise so that it became routine, reprioritising other tasks and developing a sense of achievement. This identity (which was reported to begin to develop from about 6 weeks into the programme) brought a sense of autonomy and control to women’s lives. The ‘exercise identity’ differs from exercise that is motivated by guilt and is therefore not autonomous. Women spoke of eventually feeling in control of their lives through exercising. Reported benefits of participation included feeling more energised, so that tasks at home were performed with more vigour. 136–138
To summarise, the evidence from included studies suggests that motivation to participate in ERSs could be enhanced through supportive recommendation from a health-care professional. However, it appears that an important motivator in maintaining exercise is an internal commitment to health and/or physical activity that may or may not be evident prior to referral. Motivation to participate can also be experienced differently across gender and socioeconomic groups. For example, women enjoyed the social element of physical activity where it was encouraged, whereas men tended to prefer less structured ways of exercising and could feel outnumbered owing to the low ratio of men to women referred. For lower SES groups and for women, at first there were concerns about beginning an activity that was associated with ‘exercisers’ and ‘fit’ people. Facilitators to attendance would, therefore, ensure an environment that includes only the ERS participants, with trainers that can identify with the individual, as well as with the gendered and social needs of participants. Trainers with a positive attitude who could motivate participants, particularly in early weeks, were particularly valued.
Community interventions to increase physical activity in people of retirement age and older
This section presents a synthesis of qualitative findings from ten included studies reported in 11 papers that examined views about interventions to promote physical activity at community level. 140,149,151–154,156,167–169,184 These included walking interventions, weight or resistance training, and fitness/dance/aerobic classes.
Walking
No included study explored the views and experiences of participants of outdoor walking groups. One study reported in two papers explored the experiences of retired people participating in shopping mall walking. 151,152
Duncan151 and Duncan et al. 152 observed and interviewed older people who regularly walked the local shopping mall as part of a US intervention for retired people. None of the participants had wanted to retire. This study highlights differing perceptions and policies regarding retirement across countries, as currently in the UK, retirement is not forced on people wishing to remain in work. The participants in the study continued to have a ‘work ethic’ that required structure and purpose to the day: ‘it’s just like going to work’. 151 Mall walking could be compared with work, in the sense that walkers start in the morning and had ‘rules’ and ‘roles’ by which they organised the walk. For example, walkers were asked to move in an anti-clockwise direction, and older walkers exerted authority over newer members. Many walkers moved in pairs (some with their spouse) or groups, although some walked alone as a result of their slow pace. For those advised to walk by a health-care practitioner, the social element became a motivation. For self-directed walkers, health benefits were the main trigger. Generally, a range of physical, social and psychological benefits were reported, including a sense of self-efficacy and belonging to a community. The mall also provided a relatively ‘safe’ environment in which to carry out physical activity compared with outdoors (the study was set in a mountainous region). Negative effects for some included a tendency for ‘nosiness’ by other participants during conversations that took place during coffee meetings after the walk.
Weight/resistance training
Three included papers explored the views and experiences of participants of resistance training programmes for older people. 153,167,184 Although this form of resistance and stretching intervention was outside the scope of our review, these papers provided information regarding perceptions of physical activity more generally so were included in the qualitative synthesis.
A wellness centre intervention was developed for women aged over 60 years in the USA as part of a health education scheme. 153 The classes focused on closely supervised weight training involving work with dumbbells, benches and rowing machines. The authors described difficulties in convincing the target population that lifting weights was a suitable activity for them. There were perceptions that the activity was physically dangerous, that it would result in a ‘masculinised’ body that produces sweat, and that it is associated with ‘lower classes’. Factors that led to overcoming these perceptions included: (1) holding classes in a non-threatening environment such as a converted house; (2) ensuring a gradual introduction to weights, using light weights to begin with as part of an aerobics class; and (3) emphasising that ‘masculinised’ bodies have to be worked at, they are not a usual consequence of weight training. Eventually, the women began to identify a range of physical benefits that helped their resistance to becoming ‘dependant’ in older age.
Henwood et al. 167 held focus groups with three mixed-sex groups, one of which included participants who had previous experience of resistance training, one which included individuals who were currently training and another of which included people who were contemplating training. The benefits of resistance training for older people were acknowledged, particularly on developing muscle mass and its association with preventing falls and generally improving physical ability. Some participants who had experienced training cited improved well-being and sleep patterns as additional benefits. The desire to remain strong into older age was a motivator, particularly as the population is living longer, and there is the prospect of caring for grandchildren. Those who were contemplating training cited more generally a desire to maintain functional ability as they age rather than specific benefits. Mental health benefits were also mentioned by all groups; it was acknowledged that training could benefit both the mind and the body. In terms of body image, participants who were contemplating training were less knowledgeable about how training could affect the body, citing particular aspects of the body that they would like to change rather than overall effects. Those who had experienced training mentioned the positive social aspect of classes, whereas this was not mentioned by participants who were contemplating training. There was an emphasis on the preference for carrying out the training with people of a similar age. One barrier that participants, particularly those contemplating training, cited was the timing of classes. However, the main motivator for those who had experienced training was: ‘The tremendous sense of wellbeing’. 167
One of these papers reported findings relating to a RCT of resistance training. 184 This intervention in Chile was part of a 2-year cluster trial comparing four arms: (1) 1 hour per week of resistance training; (2) nutritional education; (3) resistance training and nutritional education; and (4) no intervention. 184 The population was described as low to medium in terms of SES, and the barriers to attendance included health problems, employment (for men), caring for relatives (for women) and unsafe pavements en route to the class. Depression was also apparent in the sample. Facilitators to attending included perceived physical benefits such as agility as well as independence and autonomy. The opportunity to socialise at classes was regularly mentioned.
Findings from the three papers suggest that resistance training can provide physical and mental benefits for older people. Barriers include the perception of training as a masculine pursuit, particularly by women,153 and for those who have not yet experienced training the timing of sessions could lead to participation being postponed. 167 Employment and caring responsibilities took priority in one study. 184 For one sample a non-threatening environment was influential in maintaining attendance,153 and in two studies the social aspect was a motivating factor. 167,184 However, for those who were contemplating training, the benefits of social interaction and support had not yet become apparent,184 suggesting that this aspect of the intervention could be emphasised more to promote resistance training classes. An intervention that allayed initial fears and resistances of older people and particularly women to this form of physical activity in a non-threatening environment was reported to be valued by the participants.
Exercise/fitness/dance classes
The remaining five community-based interventions consisted of fitness and/or dance classes. 140,149,154,168,169 One study154 observed participants in an exercise class held three times per week in a room within a residential building. The most regularly attending eight participants were white, middle-class women. Some individuals, described by the authors as ‘non-exercisers’, attended to observe but not to participate. Discussions with ‘exercisers’ identified that definitions of older age were not chronological but functional and related to mobility and leisure as well as to health. ‘Non-exercisers’ were reported to focus on their limitations rather than their abilities, whereas ‘exercisers’ incorporated transitional ailments and pain into their day and worked around them. The social aspect of exercising provided a forum of care in which concern was expressed by the group if an ‘exerciser’ did not attend class, and a sense of responsibility was reported to be felt by the individual to attend regularly. ‘Exercisers’, who generally did not consider themselves old, were reported to distinguish themselves from ‘old’ ‘non-exercisers’, at times pitying their observed behaviour. The authors concluded that participating in the classes enhanced the feeling of self-worth for older people, although this was not necessarily attributable to the physical activity alone but also to the community spirit generated by interacting with other like-minded people. This counteracted feelings of loneliness that might be felt at this stage of life.
Poole169 observed and interviewed female fitness instructors who were themselves over the age of 50 years. The aim of the study was to identify factors relating to exercise commitment. There was a reported interest in bodily appearance and fitness, two personal attributes that were considered to decline with age, leading to a sense of dissatisfaction. Regular exercise was a way of resisting such decline and reclaiming an ‘ideal’ body shape and size, although some effects of ageing were acknowledged as irreversible. Improving health and overcoming illness were also considered motivators for attendance. The instructors reported that the women they taught accepted them because they were of a similar age. A core group of women was reported to have attended classes for some time, whereas others (mainly younger) joined for a while and then dropped out. Class attenders were encouraged by the trainers to extend their interests beyond the class; for example, some participated in modelling clothing for local retailers. There were also outings arranged, which supported the social network that was valued by the trainers and attenders, who turned to each other in times of need. Social interaction was also valued by women with retired partners who resisted shared activity. For the trainers and attenders, exercising brought benefits beyond the physical, such as increased feelings of empowerment and self-esteem.
Another public exercise facility was the setting for one study149 which explored retrospective views of a mixed-sex sample of older participants. A shifting definition of physical activity was reported across the lifespan as ‘formalised’ activities at health clubs and gyms were uncommon when the participants were younger. Sex differences were also noted, in that women referred to housework and child care in terms of physical activity, whereas men defined physical activity as formalised or manual labour. Levels of participation differed by sex across the lifespan depending on commitments such as family responsibilities or military service. Historically, walking and sometimes cycling were the main methods of getting to places as car ownership was rare. Participants recalled dancing and bowling as the main recreational activities when they were younger. This changed to more formalised activity in middle age, and a few women reported becoming involved in fitness classes during child-rearing years.
A transition to formalised exercise occurred later in life, as retirement offered time to participate, and increased access to facilities presented more opportunities. There was mention of a continuity of attitude to physical activity from participation as a young person through to current activity, with the likelihood that low-level participation in the past would equate to similar levels in the present. For older people the main motivator for participation was maintaining health, prolonging life and generally desiring to ‘feel good’. 149 This feeling was expressed as a combination of physical, mental and cognitive well-being, with improved memory and alertness, enhanced self-worth, a sense of accomplishment and independence. The centre provided a forum for social interaction and new friendships were made.
Paulson140 compared two types of physical activities, namely ‘fitness’ and ‘dance’, through observations and interviews with participants in the UK. The ‘fitness’ class participants were reported to hold a relatively individualistic view of movement and were concerned with their own achievements (although a few members of the group met after the class for coffee). There was an emphasis on the health benefits of physical activity and the effects on specific aspects of the body such as cardiac or muscular function (the main focus of fitness class benefits being health and physiology). The curriculum specified that benefits were optimised through a range of exercises including resistance training, circuit training and aerobics. Participants now realised that daily activities such as housework and gardening were inadequate on their own for all-over fitness, and they practised what they had learned when they were at home to enhance these effects. The curriculum draws on the popularity of walking, suggesting walking at different rates and with shopping to emulate a range of beneficial activity.
The experiences of the dance group contrasted with those of the fitness group in the references to psychosocial benefits and belonging to the group. The authors compare the individualistic stance of ‘fitness’ participants with the philosophy of ‘togetherness’ displayed by ‘dance’ participants. The dance classes demanded concentration to remember steps; the observed seriousness of this was tempered by humour when things went wrong. In further contrast to the ‘fitness’ class, discourses were around space, shape and direction, with other people using terms such as ‘spatial awareness’, ‘dynamic awareness’ and ‘awareness of others’; there was little mention of physiology. Class togetherness continued outside the class environment with trips to the theatre and meetings over coffee, which reinforced a social element for the group. This aspect was particularly important for participants who were alone or facing difficulties. Class performances were also arranged which provided further opportunity to meet as well as to develop pride in their achievements.
Freene et al. 168 held focus groups to compare the experiences of participants in an Australian home-based physiotherapist-led exercise programme with those of a traditional class, both designed for sedentary older adults. They also invited non-attenders to discuss reasons for their decisions. Those who expressed interest in the programme were concerned about health issues or believed that the programme would provide physical benefits. A personal invitation to participate had a strong influence on attendance. Having a no-cost intervention was another reported positive factor, as the expense incurred through gym membership meant that non-attendance resulted in feelings of guilt. Flexibility was the main enabler for the home-based programme; exercise could be carried out at any time, although some participants reported that having other commitments was still a barrier. Having a good relationship with the physiotherapist was important for some, but not all, home-based participants. Follow-up telephone calls were reported as encouraging and, for some, they motivated them to return to the programme. The instructions were reported to be simple to understand and the activities could be adapted around lifestyle.
In contrast, attendance at the group exercise programme was enabled by a tailored approach, enjoyment and a social element. It was important in group classes to maintain a good relationship with the instructor. A period of absence was a potential barrier to restarting the group exercise; the ability to come back at a slower pace without feeling embarrassed was valued by some. For non-attenders, time was a barrier, as other commitments such as travelling or caring for grandchildren took priority. Health problems were also a commonly reported issue, along with the fear of embarrassment at one’s lack of ability and a perceived lack of fun. A few reported that sessions were not sufficiently frequent to be beneficial or that supervision and explanation of the exercises was poor. There were no preferences expressed for particular formats, although some participants reported that they would prefer a mix of home-based and group sessions. All participants carried out informal and/or individual physical activity such as walking in addition to the programme.
In summary, five included ‘exercise’ studies identified differences in the acceptability of exercise interventions by type of physical activity140 as well as by delivery. 169 They also highlight differences in attitudes towards physical activity among ‘exercisers’ and ‘non-exercisers’,154 men and women, and across historical cohorts. 149 Findings from the included studies suggest that motivation to begin exercise for those who have no or little experience can be daunting, and that a personal invitation to attend can be encouraging. 168 Formal physical activity has recently become more popular through the development of gyms and health clubs, whereas historically these were rare. Retired people from progressive cohorts would therefore be expected to become more familiar with the gym environment and exercise protocols compared with some of the older people interviewed in older studies. The findings suggest that if the environment appears non-threatening,154 with similar age groups attending and instructing,169 and if the instructor is deemed capable and supportive,168 classes can become a source of improved mental and physical well-being, enjoyment and social support. 140,149,154,168,169
The evidence suggests that interventions targeted at this age group are valued for far more than just physical effects and weight control; they can also become a source of increased self-worth, self-efficacy, self-esteem and independence. 140,149,154,168,169 This has been shown particularly for those who live alone or feel otherwise lonely and potentially for those participants who may feel that the consequences of ageing/retirement are necessarily negative. Participants and instructors in the included studies report resistance to ageing effects and a positive growth in development, comparing themselves positively with individuals who resist physical activity owing to perceived health-related barriers or fear.
Mass media campaigns
Two included studies reported participant views about population-wide health promotion campaigns that included the aim of increasing physical activity in older people. 170,179
The studies170,179 found that recall of a Canadian and an Australian mass media campaign, respectively, was very poor. An advertisement that formed part of the Canadian campaign featured the grim reaper as a warning of what might happen if a healthy lifestyle was not taken up. Focus-group participants reported that this was positive as it attracted attention to the message, but negative in aspects of its content and its reminder to older people that they are people closer to dying rather than people who should be making the most of life. Participants held mixed views about whether or not the advertisement appeared to be aimed at older people. There was no verbal aspect to the advertisement, raising the comment that many people cannot read the message and would need to hear it. The advertisements were promoted by the government, a fact that was noticed by some participants. This led to reports of mistrust regarding messages that were deemed political. However, government sources were trusted more than commercial companies. Medical personnel were the most trusted source of information. Images of well-known retired athletes were mentioned as having the ability to engage people, although it was also mentioned that athletes are ‘not ordinary people’ and that regular members of the public would provide more realistic role models. Use of websites as further sources of information were criticised because not everyone has a computer or access to the internet. 179 Participants reporting on the Australian campaign suggested that health promotion messages should not be broadcast on television during the advertisement break as people tend not to view at those times. The recommendations to walk on most days were not perceived by the participants as being strong enough, with most people already carrying out that amount of activity. Television was not perceived as the most fruitful means by which to reach older people, with GP surgeries and newsletters preferred by this group. 170
In summary, recall of mass media campaign messages can be poor,170,179 although messages that are striking may be better remembered providing they are appropriate to the target audience. Campaigns can have a negative effect if messages are delivered in a way that is perceived as scare-mongering or paternalistic, or no effect if the audience is not able to access follow-up information. 179
The following section explores the views and experiences of retirement-age study participants of their involvement with physical activities that did not form part of an intervention.
Engaging with physical activity at retirement age
Six included studies reported in seven papers141,155,171,172,176,182,183 focused on older participants and their engagement with a range of physical activities. Three papers explored experiences and views about physical activity in general155,171,176 and three studies reported in four papers focused on a particular activity including lawn bowling,172 ballroom and sequence dancing141 and line dancing. 182,183
Continuing physical activity at retirement age
Three studies155,171,176 reported views of older participants who had continued to engage with physical activity into retirement age. Participants in all three studies reported feeling pride in their continued engagement with sporting activities such as ball games and competitive running at ages that might be perceived to be inappropriate by some. In two of the studies all the participants were health conscious and physical activity was a part of their strategy for staying well and avoiding dependency in old age. 171,176 There was a philosophy that one had to ‘use it or lose it’ (p. 187),171 although health promotion messages were reported in one study to be confusing, and there were reports of uncertainty over how long the level of activity could continue given the unpredictability of future health status with advancing age. 159 In all three studies, participants reported acknowledging potential or real changes in their own physical competence as they aged. 155,171,176 In two studies, active participants compared themselves favourably with their less active peers171,176 and physical activity was a way of distracting from worries that less active peers might dwell on. These imagined or real peers were described as having a different attitude to ageing than themselves, one in which slowing down is inevitable. 158 Active participants, in contrast, expressed the view that inactive older people were often more inactive than they needed to be and that when they were younger, they had also believed that engaging in sporting activities was not appropriate for older people and that retirement was associated with resting. This was partly attributable to the demands of housework and work historically involving more physical activity, as well as with the relatively shorter life expectancy of previous generations. 176 In contrast, competing in sport provided the participants with a vital and powerful identity in older age which proves to themselves and to others that such activity is still possible, resisting negative stereotypes of ageing. 171 One participant stated, ‘What us oldies are doing is recycling, keeping busy, and not thinking about slowing down. Once you believe you should give up being physically active then it’s downhill until the end, and that will come too soon’. 176
Resuming physical activity following retirement
The advantages of resuming participation following a break to raise children and to work were mentioned in four studies. 141,155,171,176 Benefits included the relief of physical symptoms, the promotion of psychological health176 and social interaction. 155,171,176
The participant in one case study cited being successful as a motivating force, whether it was in sport or at work. 155 However, it was acknowledged that returning to physical activity was not easy as the body had to adapt to a higher level of activity, there was every chance of being less successful at sport than when they were younger and there were reported feelings of embarrassment. In two studies, the participants reported that adaptations had to be made to physical movements to accommodate changes in bodily competence. 155,176 There was also a reported change from team sport participation in younger age to individual activities in older age, which did not rely on people to attend, particularly as many people have family commitments. Nevertheless, there was an expressed lack of understanding about why older people in general do not take advantage of the numerous opportunities available to be physically active. It was suggested that using softer health promotion methods with images of people that were not necessarily young and slim as well as charging reduced rates might assist in attracting older people to exercise. Older people also reported that partners and family members with expectations of how they should spend their time were not always supportive of their activities. 176
Cooper and Thomas141 observed older members of several dancing organisations which covered two dance styles, ballroom and sequence. Dancing had been a way of life for this cohort who grew up with dance as a form of entertainment and social activity. Music remained a draw for members as they aged, as did the social element, dress and the ‘glamour’. Many had taken a break from dance to raise children. However, some participants had continued to dance throughout their lives and had competed in championships. There was a sense from the authors that the atmosphere around the two styles of dancing differed, with sequence dance participants having a softer approach and using the space in the room in a more co-operative way than ballroom dancers. Sequence dancing was regarded as a progression for older participants who could no longer cope with the demands of ballroom dancing. Thus, participating in modern sequence dancing was a way of continuing to fulfil their love of dancing in a (changed) way that suited ageing minds and bodies.
Losing a partner could enforce a period of absence from dancing, although for many this was temporary, and women in particular would typically return with a female friend. In modern sequence dancing there was less dependence on a male to ‘lead’ the dance. This meant that women did not necessarily feel the need to have a male partner (although in ballroom dancing some women pair up together), but women also reported feeling empowered as their moves are not dictated by the male: ‘men and women are equal’. 141 Dancing in general provided older people with an opportunity to feel like teenagers again, as their enjoyment of the dance evoked the fun that participants had had when they were younger. The authors report a sense of ‘communitas’ which can be described as egalitarian community spirit or a feeling of collective understanding. Whatever status the participants might hold or have held outside the dance hall did not come into play inside. This phenomenon was more strongly observed among the modern sequence participants. However, in some venues, ‘communitas’ was contradicted by displays of territorial behaviours such as ‘owning’ a particular seat in the hall which impacted on new members who could not find a spare seat. The authors report that dancing allowed members to resist their age-related physical and mental deterioration:
People come with their aches and pains to me [and] they say, ‘I shouldn’t be here. I’ve got this wrong with me’, and then they do two and a half hours of dancing and don’t feel a thing. I’ve seen people in town with walking sticks, and two hours later I’ve seen them dancing away as if there’s nothing wrong with them. 141
In a similar way to reports in other included studies, this resistance also protected members from the fear that bodily decline will eventually lead to them having to give up dancing. However, in a similar way to other included studies described earlier, dance participants perceived themselves as ‘not old’ compared with other dancers who were in reality not much older than themselves. Some participants believed that dancing transcends age and can delay the onset of age-related problems and that age is irrelevant compared with being a ‘good dancer’. 141
Beginning new physical activities following retirement
Two studies reported in three papers172,182,183 explored the experiences of retired people who had taken up a new physical activity following retirement.
Heuser172 found that female participants had taken up bowling through invitations from friends or partners, to fill the space after retiring or losing a spouse, following children leaving home and/or as an alternative to more vigorous activities, particularly following an injury or because of increasing aches and pains during older age. Some participants had been involved in playing hockey, badminton, tennis, golf or ten-pin bowling when they were younger but reported that they could no longer perform these activities, in some cases owing to specific neck or back injuries. Continued engagement with the sport was motivated by ‘entanglements’ or relationships with other bowlers that increased their sense of commitment and led to being ‘hooked’. Getting ‘hooked’ on bowling was a frequent comment from the women, and continuation was reported to be attributable to a combination of love of the sport, the opportunity to be outdoors and be physically active and the social element from which camaraderie developed between women members.
Wanting to win against other teams and to perform better than one’s own standard was another element of getting ‘hooked’, so that the experience of a bad game would entice women back to do better next time, and a good game would also motivate women to return. The mental concentration required to play the game was also reported to be a positive aspect of the experience, as strategies were required to perform well. Some women took their involvement to the stage of competing in weekly pennants and/or championship games; these games were taken much more seriously and the author reports that the ambiance was more solemn. For some women these serious games had to be discontinued owing to medical or physical conditions, to be replaced by a return to the social games. Total retirement from the game was usually a gradual process, with women adapting around their physical problems in the meantime. Retirement from the activity of bowling was not always accompanied by retirement from the club, with women attending as organisers or to assist with peripheral activities, to observe the game or simply to meet up with other members.
In one study of older people who had taken up line dancing182,183 the initial motivation was enjoyment, but participants reported health benefits from the activity ranging from the physical to the cognitive. As well as having an impact on weight management, line dancing was reported to alleviate back pain and the effects of osteoporosis, as well as to improve diabetes control. As line dancing requires concentration to remember the sequence of steps, participants reported dancing as a contributing factor to their improved memory function, particularly compared with people they knew who did not exercise. In support of the findings of Cooper and Thomas,141 line dancing participants emphasised an attractive appearance and reportedly felt younger than their chronological age when they were dancing, thereby challenging ageist stereotypes. They also received social support from the group, particularly at difficult times such as losing a partner. The combined effects of enjoyment and social support were reported to have a positive effect on confidence and self-esteem. 182,183 Supporting the findings of Grant,176 participants were not always encouraged by their families and partners in ‘leaving the house’ until the positive effects of line dancing were recognised. 182,183
To summarise, six studies reported in seven papers that explored experiences of older people who engaged in long-term physical activity found similar motivators to beginning and maintaining the activity. For most of the participants, physical activity was not a new venture in older age; many had pursued the same or similar activities when younger and therefore were aware of the enjoyment and benefits that they could derive from the chosen activities. Participants were also motivated by more than a desire to be fit – they established friendships and camaraderie through their activities, which increased the sense of commitment, even beyond the specified number of sessions in some cases. Many participants, although not all, had temporarily given up physical activity in their middle years to concentrate on child care or work. Returning to physical activity in later years could be challenging, but once the health benefits were recognised and social networks reformed, motivation increased. There was evidence, as noted in previous sections, of a resistance to ageing stereotypes, which was lived out in ‘communities’ that encouraged the support and celebration of capabilities. On an individual level, activities were regarded as stimulating for the mind as well as physically advantageous in an era in which future health is unpredictable. Indeed, the activities were regarded as factors in delaying ageing at a physical and emotional level. Active older people often compared themselves with ‘older’ or ‘inactive’ peers with a sense of incredulity at their lack of a similar vision, sometimes even pitying them, as if this population do not know what they are missing.
Enabling and disabling factors for engaging with and maintaining involvement with physical activities at retirement age
The next section presents a synthesis of evidence from the included studies in respect of factors that impact access to and acceptability of carrying out physical activities at retirement age. (For a summary of these factors, see Table 20.)
Factors relating to equality of access
A number of factors that impacted on access to physical activity in retirement age were identified from the literature. These are discussed by theme and summarised along with components of interventions that might limit such impact in Figure 17.
FIGURE 17.
Factors impacting access to physical activity in retirement.
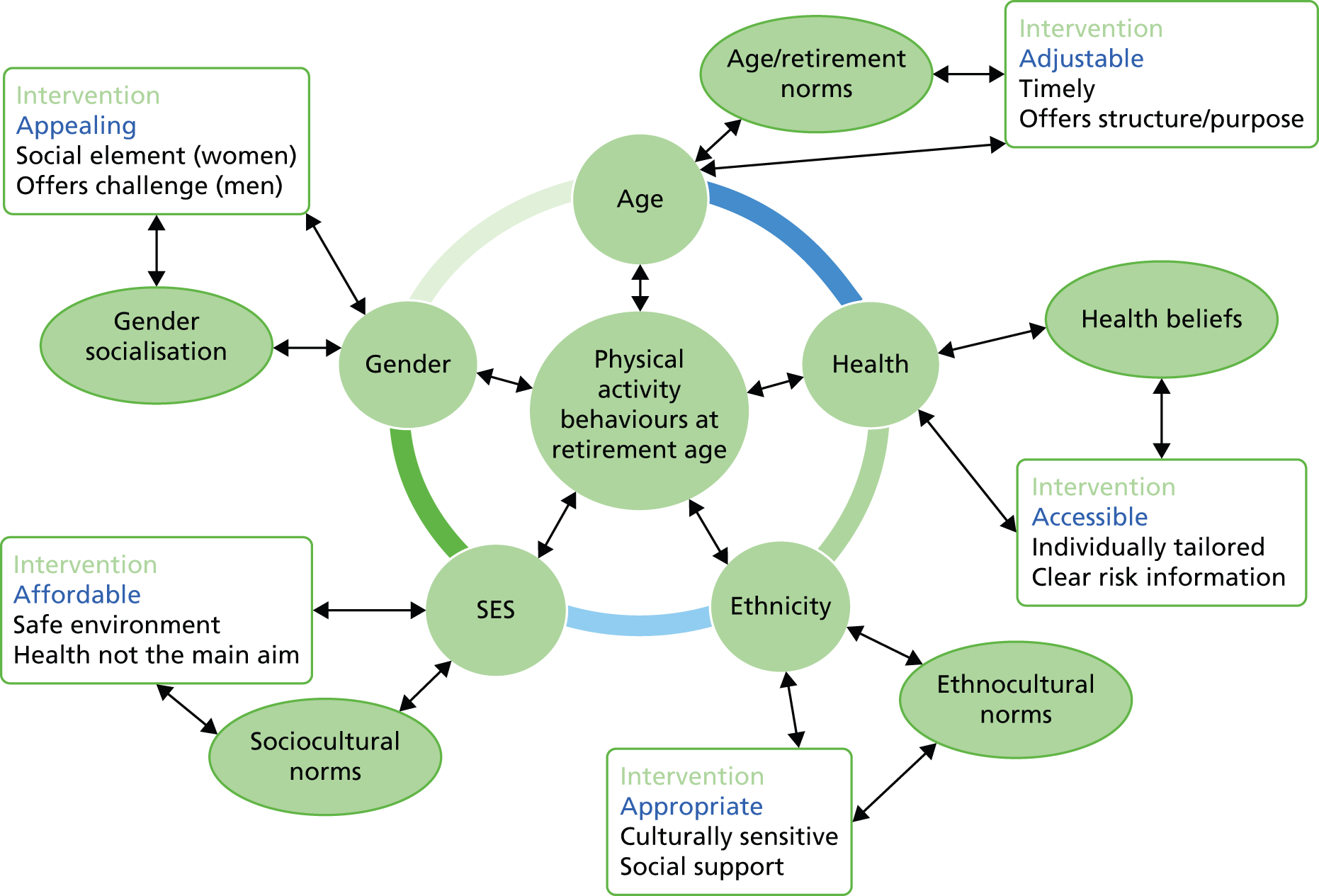
Age
A total of 26 studies reported in 30 papers130–135,141,142,145,146,148,153–158,167–169,171–174,176,177,180–183 identified the ageing process as an influence on participation in physical activity. The effects of ageing could be either real or perceived, either by the participants or by society.
Perceptions of ageing
Two studies148,177 reported the uncertainty that people feel about their future health and physical capabilities when they retire. This uncertainty is related to an awareness that the ageing processes can constrain or limit physical activity over time and that expectations about, for example, strength and agility may decrease with age. 132,173 However, Poole169 reported that older female participants were conscious that health problems are not confined to older age groups, as many young women are now overweight. Nevertheless, the image of the ideal woman as slim and taut was pervasive in the way in which older women compared themselves with this. 135,169 Participants in two studies133,176 compared the ways in which attitudes to ageing and mortality nowadays differ from previous generations, suggesting a greater awareness or desire to make the most of their retirement age years. Participants in another study154 compared themselves as ‘active’ with ‘inactive’ individuals whom they regard as ‘older’.
Seven studies131,142,145,146,155,180,181 reported that participants adapted the extent and type of physical activity that they engaged in as they aged and felt that this needed to be tailored to the individual. Two studies157,172 reported that perceptions of declining physical ability with age could lead to a particular activity being stopped or changed for a less strenuous pursuit owing to embarrassment or fear of injury. Some older women who remained active were more confident about their body image and attributed this to the effects of physical activity. There was, therefore, a potential for increased physical activity to perpetuate positive effects on well-being and the body. Acceptance of the body could also be attributed to increased maturity. 157
Age appropriateness of physical activities
Differences in attitude to physical activity were also reported to be related to the age-appropriateness of particular activities. Five studies153,156,158,168,174 reported that participants could feel uncomfortable carrying out activities that they regarded as age inappropriate, and a further study131 found that retired people reported gentle exercise such as yoga and swimming to be more acceptable to their age group. Activities that might be described as ‘sport’ were deemed less acceptable as they may be dangerous, particularly for women. 130 A fitness instructor in one study169 also reported that women were less intimidated by her because she was a similar age to them. There were perceptions from some older people that the promotion of physical activity and the provision of facilities had been geared towards the younger generation and that in this respect older people, particularly men, had been ignored. 130 In one study157 a female participant reported feeling ‘out of her league’ when younger basketball players joined the team. Moore et al. 139 reported that exercise trainers in their study made a point of enrolling groups of a similar age to their activities.
Conversely, Diogini171 found that older athletes resisted ageist notions of unsuitability, and dancers in another study capitalised on their older age, creating a community comprising individuals with similar values. 141 Similarly, Nadasen182 reported that participants in their study forgot their age while they were dancing.
Social support
Three studies reported findings relating age with social support. 136,143,167 Hardcastle and Taylor136 found that some participants who continued to carry out physical activity faced the judgement of others who perceive that they are trying to be ‘young’. There were mixed reports regarding support from health professionals, with participants in one study136 reporting little support from their GPs when requesting referral on to a physical activity programme and those in another reporting that some health professionals were helpful, whereas others appeared to provide advice on the basis of the participants’ age. 143 Older participants valued activities that enrolled people of a similar age, because this provided a sense of security. 167
The above findings identify age-related assumptions as a potential barrier to accessing physical activity. These assumptions include an individual’s own perceptions of their age and related capabilities and/or appropriateness of particular activities with regard to age. The findings highlight the importance of adapting physical activities to suit individual and group requirements, for example allowing for adjustment to unfamiliar settings or activities over time. They also provide evidence that the perceptions of others and the influence of dominant social norms can impact on the availability of social support from health professionals, family and friends.
Health
Ageing, health physical function and physical activity
The majority of included studies130–136,138–149,151–164,167–172,174–184 reported on the interaction between physical activity and health or physical function in relation to ageing.
In one study,130 South Asian participants were the most fearful in terms of ageing and the perceived negative impact that it could have on health. Other participants cited current or potential health issues as a barrier to carrying out physical activity. 130,131,142,146–148,158,160,164,168,170,174,178,180,184 A decline in health could prevent older people from going out generally and thus lead to isolation. 134 Participants in one study154 suggest that a positive attitude towards health and functionality can assist in maintaining activity, whereas a negative attitude is more likely to result in older people focusing on limitations to remaining active. For trainers working in one low SES area, mental health issues and the low priority given to health were reported barriers to older members of their community participating in physical activity. 139
An important motivation for older people engaging in physical activity was to prevent ill health, to cope with existing ailments and generally to increase strength and vigour. Remaining healthy through physical activity could delay some of the negative effects of ageing and help older people to remain independent. This motivation (‘use it or lose it’) is based on perceptions that mental and bodily decline are associated with ageing and that carrying out physical activity is an antidote to this. However, the term ‘health’ incorporates a broad range of meanings, including mental health and ‘fitness’. The implication here is that some people perceive their ageing bodies and minds as ‘at risk’ from ill-health135 and that involvement in physical activity can be a way of reducing this risk.
Studies that assessed the views of older people engaging in particular interventions or activities generally reported positive effects. For example, Stathi et al. 138 found that participants in an ERS enjoyed psychological and physical health benefits as well as general improved well-being. For Paulson,140 different activities emphasised varying aspects of health; for example, exercise classes may focus on ‘fitness’, whereas dance classes were based more on movement and grace.
There was also reported scepticism expressed about the health benefits of physical activity, as studies reported perceptions that physical activities carried out in older age can create problems with joints or lead to heart attacks. 131,132 For a Mexican American sample, health benefits were perceived as relevant only to people who already had a health condition. 156 Berry et al. 179 reported that some participants in their study were sceptical about health promotion messages that were included in a mass media campaign, as they originated from government sources. Other work reports that, although participants may be aware of the health benefits of physical activity, they lack the inclination to put it into practice. 133,181 This suggests a lack of clear and trusted information relating to how physical activity impacts on the health of the ageing body in both positive and negative ways.
These findings suggest a two-way interaction between health in its broadest sense and physical activity, with physical activity having a generally positive (although occasional negative) effect on health and functionality in older people, and health problems, as well as individual responses to those problems, creating potential barriers to carrying out physical activity. Inequalities could therefore arise where there are political, social, financial, psychological or physical barriers to accessing physical activity as a form of health promotion.
Ethnicity
A total of seven studies reported the views of older individuals from ethnic minorities as regards physical activity,159,160,162–166 and a further eight studies reported in 10 papers compared the views of individuals from mixed ethnic groups. 130,131,134,143,144,156,158,170,182,183 However, not all these papers reported a cultural perspective with regard to engaging in physical activity.
Of the papers that did discuss cultural aspects of physical activity, Walcott-McQuigg and Prohaska164 highlight a trend for the African American population in general to be less likely to engage in physical activity, suggesting a need to target activities that reduce the risk of morbidity in this population. Some of the potential barriers to engagement with physical activity in ethnic minority populations are discussed below.
Family comes first
Gonzales and Keller166 identify a lack of individualistic concern in Latina women, who prioritise their time to care-giving over self-promoting activities, despite being aware of the potential health benefits that could indirectly impact on positive parenting. This ‘conflict of desires’166 is reported to have implications for those promoting physical activity interventions to this population. The authors suggest that uptake may be encouraged where benefits to the family as a whole are emphasised rather than individual gain. Similarly, Asian, Latina and African American women participating in a further five studies131,156,158,160,163 were also reported to prioritise family commitments, as did Asian males. 130,144 Berg et al. 156 noted this family focus in Mexican American participants compared with the more individual focus of Anglo-Americans. In addition, African American and Latina women reported physical activity as something that would make them fatigued or tired160,163 or ‘sweaty’. 163
Cultural sensitivity
Traditional Asian women were also reported to be deterred from engaging in physical activity by a lack of cultural sensitivity. Same-sex instructors delivering interventions to single-sex groups in a local hall, using the spoken language of the women and allowing activities to be carried out wearing clothing acceptable to the culture were suggestions for encouraging this population to increase physical activity levels. 130 South Asian Ageing Well workers helped older Muslim women from India and Pakistan in another study to raise their confidence sufficiently to begin participating in physical activity. The workers facilitated participation in culturally sensitive interventions and translated where language barriers were apparent. The women, for whom physical activity had not been regarded as appropriate in their homeland, started to feel the benefits of activities and this motivated them to continue. The authors conclude that social support from the workers was also a factor in maintaining physical activity. 144
For some rural African American women, exercise would not be contemplated unless it came from their community rather than ‘white’ culture. 158 For South Asian women, many forms of physical activity were considered unsuitable for women. 130 In contrast to some ethnic groups, Henderson and Ainsworth159 identified a culture of walking among Native American participants, for example for prayer or for discovering herbs in the mountains. Walking was not taken for granted by Navajo participants, and the body provided cues as to when stretching would be beneficial. In comparison, African American women participating in the same study did not mention cultural influences. Horne et al. 144 reported a general lack of knowledge about physical activity in their South Asian participants. For some, the physical act of praying or ‘namaz’ was deemed sufficient.
These findings suggest that individuals identify with traditional norms and beliefs. For ethnic groups, therefore, the evidence suggests that social support is important to allow physical activity to be part of daily life. Cultural sensitivity in designing interventions to increase physical activities, which may include community workers, ensures that traditional norms and beliefs are taken into account and that communication channels are enhanced.
Socioeconomic status
Three included studies described their participants as coming from160,172 or working within139 a low socioeconomic environment. However, Heuser,172 whose sample had a low level of education, do not discuss the implications of SES on involvement with physical activity. A further six papers130,138,158,162,163,177 that sampled a mixed population in terms of SES commented on the impact for some of their participants of having a reduced income or of residing in less affluent neighbourhoods.
Retirement was reported to bring with it a reduction in funds,177 which could present a barrier to participating in some forms of physical activity. 130,138 However, providing concessions for retired people could be perceived as patronising. 138 Three studies158,160,163 found that the perceived cost of carrying out physical activity was consistently reported as a barrier for older African American women from less wealthy areas of the USA: ‘If you don’t have the money to pay the light bill then you don’t have money to join the health club’. 163
The women suggested that the provision of free or low-cost activities might facilitate uptake. However, free provision was not the only consideration when attempting to increase uptake in deprived areas. Trainers involved in delivering exercise on prescription sessions (which were discounted to a £1 admission fee) in a deprived area of the UK stated that this population was more difficult to engage in the scheme. Suggested reasons for this included health promotion being assigned low priority for poorer people, or that people might not be aware of the discount or that, even if they were aware, they could not afford to maintain the activity following the promotion’s expiry. Another suggested reason was that GPs in the area might not buy into the scheme because of the general negativity around self-help in an area of high unemployment. 139
Findings suggest that the environment might also impact on access to and the acceptability of carrying out physical activity outdoors. Participants in two studies160,162 were concerned about safety when outside in their neighbourhood.
In terms of inequalities, a small amount of included evidence suggests that older participants from deprived areas face constraints on their access to physical activity opportunities through low income that is likely to reduce further at retirement age, social norms that preclude the prioritisation of health promotion messages and poor neighbourhood environments that feel unpleasant or unsafe.
Sex/gender
Although only five included studies, reported in six papers,147,148,161,173,177,178 stated a theoretical focus on sex/gender, 23 studies reported in 26 papers,136,137,145,147,148,153–161,163,165,166,169,172,173,175,177,178,181–183 as well as one paper from another study,150 sampled a predominantly female or predominantly male population and explored sex/gender as part of their analysis. A further seven studies with mixed-sex samples included discussions of issues relating to sex/gender. 131,133,135,146,168,170,176
Sex/gender appropriateness of activities
In terms of findings that relate particularly to being female, Berg et al. 156 found that some women felt uncomfortable about some types of physical activity that they deemed inappropriate for their sex, especially older women. Similarly, women involved in weightlifting classes were initially sceptical, as they did not want their bodies to become ‘masculinised’ or sweaty, nor did they wish to injure themselves. However, through a combination of support, gradual introduction of weights into an aerobics class and serendipity (the venue for weight-lifting classes was altered to a residential house), the women’s misgivings were overcome. 153 African American women in another study were reluctant to mess up their hair and get ‘sweaty’. 163 Heuser172 also describes how, over time, challenges to beliefs about the sex/gender appropriateness of certain activities can bring about change. In this study, women bowlers were interviewed about their involvement in women’s bowls, which was a relatively recent addition to the club. Prior to the 1960s, women had attended only as supporters or to assist with scoring and to provide refreshments. Involvement in bowls had for some women provided a way of filling time following retirement or the death of a spouse. At the time of the publication, participants in the study were competing in pennants and championships.
Competing commitments
For Mexican American women in one study166 and African American women in another,163 physical activity was not a priority. These women had caring responsibilities and felt that these came before looking after the self or pursuing their own interests. The responsibilities of providing care for their husbands and grandchildren and fulfilling a domestic role in the home were also the most often-mentioned barriers to carrying out physical activity for Latina women. 166 Women reported that there was no time available to exercise and that their domestic role was in any event tiring and they very often felt fatigued or sluggish. 160 The belief that one’s own interests are secondary to family responsibility or work was supported by two studies sampling women in the UK136,137 and the USA. 161 There was a view in these studies that physical activity had declined since adolescence and particularly during the period of child care, although the memories of the enjoyment associated with the activities remained. For women in one study reported in two papers,136,137 the notion of ‘guilt’ accompanied any decision to take time for the self. However, in both studies, women claimed this time, especially post retirement when there was more time to claim, and identified themselves as ‘exercisers’. In this way, physical activity became part of daily life as well as a way of increasing independence. Juarbe et al. 160 found that once women had begun to participate in physical activities they continued to do so without the perception that this was negatively affecting their role as a mother, grandmother or wife. Indeed, the personal benefits of physical activity were reported to increase stamina and energy levels so that their roles could be carried out more effectively. In addition, the benefits were passed on to family members as the women encouraged their grandchildren to exercise.
Body image and function
For women, body image and appearance were important factors that could influence participation in physical activity. Liechty and Yarnal157 and Poole169 interviewed older women whose body image perceptions ranged from not having any concerns, or acceptance of changing shape with age, to dissatisfaction, or having always been concerned. This perception was mainly related to body size and for those more concerned about their image, it could constrain participation in all or certain activities in particular circumstances. For example, wearing a bathing suit may be considered for the relatively anonymous beach or water park but not in a local environment where there may be known (especially male) swimmers present. Women made adjustments where they were determined to attend, such as wearing a more expensive swimsuit.
Body image was reported to be a potential motivating or a demotivating factor for women. In two studies,135,157 a number of women reported that they were reluctant to expose their bodies in order to swim or attend the gym, especially where they were likely to be seen by people they already knew. For some women in two studies,157,169 even a perceived ageing body was not an issue, especially as physical activity was having a positive effect on their size and shape. A few women had overcome their misgivings about exposing their bodies by choosing flattering activity clothing. 157
Latina women were motivated to exercise to maintain their physical appearance; this effort was reported to be mainly for their partners. 166 However, for African American women in one study, reducing body size was not a motivator to exercise since ‘curvy figures’ were described as desirable in their community and losing weight was associated with ‘thinness’. 163
Drummond173 reported that for men, the body was a functional asset rather than something to merely exhibit appearance. Work was an important aspect of their masculine identity and when this was taken away, their identity felt threatened: ‘It wasn’t about the money. It was a lot of things’. 173 A masculine identity was also defined through physical functionality, which included dexterity, flexibility and agility. A decline in these functions with age was reported to feel as though the body was letting them down. Physical strength brought with it a sense of control; when this waned or was reduced through illness or injury, the masculine identity was threatened and there was a reported sense of loss for tasks that used to be done relatively easily, and a feeling of being incomplete. However, it was acknowledged by the author that much of the negative association with ageing was socially constructed. The ageing male participants in this study were reclaiming their physicality and masculinity through exercise and some degree of competition. They reported that physical activity was synonymous with being alive. Men also perceived physical activity as beneficial to their mental health. Kleiber and Nimrod146 found that men in particular often capitalised on their physical constraints to create a ‘project’ around the body, for example, studying nutrition and then physical activity in a formal way to achieve weight loss and to disseminate information to others through teaching.
Safety
One study165 reported a greater concern with safety from women who might contemplate walking outdoors. Women felt safer walking in neighbourhoods in which there was a presence of other (non-threatening) individuals in the area. They felt threatened by the fear of crime or attack where there were vacant houses or visibility was poor. This contrasted to the views of two men in the study who did not identify safety as an inhibiting factor to walking. Women reporting on their walking behaviours supported the finding that women find walking in certain places, for example by the side of busy roads or in parks, less safe. 176 Another study also found that safety was a concern for women outdoors. 160
Social elements of physical activity
Although a social element was found to be an important motivator for older people carrying out physical activity in the majority of studies (see Sex/gender comparisons for details), three studies reported sex/gender differences in this respect. For women, the social element was found to be more important than for men. 133,170 Hall et al. 175 enlarged on this by stating that older men did not connect with each other in the same way that older women do, although some men in this study used physical activity as a way of avoiding loneliness following retirement. Sex/gender differences are not clear cut in the literature, since a male-only sample173 found that engaging in physical activity improved social networks for participants. In addition, Berg et al. 156 found that some female participants were not attracted to the prospect of associating with groups of women.
Sex/gender comparisons
Two studies131,168 that included both men and women in their samples compared sex differences in relation to views about physical activity.
Brown et al. 170 compared male and female views about physical activity, supporting the finding from Drummond173 that men viewed physical activity as beneficial to mental health, whereas women, as described above, were concerned with the social aspect. Older men in another mixed-sex study reported that they felt ignored by health-promotion messages. 131
The evidence indicates sex/gender differences in the preferences of older people regarding physical activity. Differences exist between perceived ‘appropriate’ types of activity and perceptions about ageing body image and functionality (although both men and women are shown to express anxieties around their respective femininity/masculinity as well as around the impact of ageing). Aspects of physical activity, such as safety when outdoors, are more of a concern for women, and women are generally (although not always) more attracted to the social aspect of an activity. The apparent lower requirement of men for social contact may partly be attributable to the overwhelming presence of women compared with men attending classes and groups, perpetuating the situation by discouraging men from attending. The relative unwillingness of men to become involved in activities may exacerbate loneliness and impact on health in older age. Intervention design may attract men by appealing to a need for a challenge and for a structure that can fill the void after paid employment has ended. For women, a social element appears to be important, as well as sensitivity to women’s perceptions about ‘masculine’ activities or about their ageing bodies.
Factors relating to the acceptability of activities and interventions
The included literature highlights the saliency of psychosocial factors in motivating participation in physical activity. The following section discusses the main factors that participants reported that they valued and that motivated them to continue participation.
Individual factors
Health benefits
A total of 34 studies in 38 papers130–136,138,140,142–145,147–151,156–164,167–171,174,176–178,181,184 reported that a motivation for participation in physical activity was mainly or partially its associated physical and/or mental health benefits. However, for some participants131,132,135,143,168 there was also perceived physical risk attached to carrying out exercise in older age, either from accidents or from the impact of increased exertion. In addition, physical activity trainers in one study suggested that health benefits were a poor motivator to take up physical activity for some members of low SES communities, because health was generally given low priority. 139
Three studies134,168,170 found that older individuals with existing medical conditions were most aware of the potential health benefits of participating in physical activity. Similarly, Liechty et al. 145 found that the historical experience of a potentially life-threatening condition was a motivator to improve health. Indeed, Horne et al. 143 found that health professionals tended to initiate the topic of the potential health benefits of physical exercise mainly with patients who had existing medical conditions. Berg et al. 156 found a distinction between physical activity carried out for the prevention of ill health (reported in Anglo-Americans) and for medical reasons (reported in Mexican Americans). Hardcastle and Taylor136 report that health professionals can emphasise the importance of health benefits when advising patients about physical activity. Participants in one study expressed a view that to gain health benefits, their physical activity levels needed to go beyond that of daily routine such as walking. 168 Paulson140 highlighted the emphasis on ‘health’ and fitness as part of the discourse of exercise classes compared with a dance class, at which health issues were not discussed.
One study170 found that male participants had been less concerned about their health when they were younger and that awareness had been apparent only in later years. Liechty and Yarnal157 found a similar pattern for one of their female participants, suggesting that ageing can trigger a more urgent concern for health that was not apparent in earlier years. Barnett et al. 132 support this ‘trigger’, finding that the experience of retirement for their participants prompted the necessity of maintaining good health, and physical activity played a part in achieving this. One study133 also reported the acute awareness of the potential risk for ill-health in participants as they aged:
I wanted to obviously live longer than my parents did and I also realised that it was in my hands . . .So it was very important for me that I had a low fat diet, that I exercised and I used my brain as well, and that proved right. 133
Mall-walkers in another study151 had seized an opportunity to direct their own mental and physical health status by remaining active following retirement. Participants in two studies170,171 expressed fear that giving up physical activity might result in a decline in their health status, and participants in another study170 were motivated to participate to avoid a decline in health as they aged, a situation that they reported having observed in other, less active, people. Other studies report that health benefits were an important motivator in carrying out physical activity in older age. 138,142,144,148,149,158–161,164,167,169,176,177,184 However, health benefits were usually accompanied by other motivating factors, as discussed in the following sections.
The types of health benefits that could be gained from physical activity spanned a broad range, including general physiological (e.g. cardiac health) and psychological well-being, increased ‘happiness’,161 improved body shape, weight management and ‘looking good’. 131,135,157,162,174 African American women in one US study were keen to emphasise that physical activity ‘ain’t all about losing weight’. 163 Participants in two studies identified the importance of staying healthy in order to help their families,150,160 and in another the link was made between positive health and social interaction. 162 However, women in one study reported not being overly concerned with appearance as they aged compared with maintaining their general health. 157
One study130 reported that awareness of health benefits was evident across all their sampled groups (SES, ethnicity and active/sedentary). However, this knowledge alone did not necessarily encourage people to exercise. Awareness of benefits, accompanied by a lack of inclination to participate, was supported in other studies. 131,133,181
These views highlight the role of physical activity for participants in their perception of controlling their health (and therefore their mortality) as they age. Many of the participants appear to have internalised health promotion messages around healthy ageing and healthy living in general, which incorporates guidelines about optimal diet and physical activity behaviours in relation to the maintenance of health. However, the guidance is not always put into practice, particularly where risk is deemed to be low. Therefore, people who feel at higher risk as a result of existing medical conditions may feel more inclined to participate, particularly where additional incentives are present. In addition, some participants point out the risks of participation itself in terms of perceived potential injury or strain to the heart.
Time
Time was mentioned as a positive or a negative factor for carrying out physical activity in older age in 23 included papers. 131–133,136,137,141,145–148,150,156,158–161,163,164,166,169,172,178,180
Having sufficient time to participate in physical activity
A commonly reported barrier to engaging with physical activity was a perceived lack of time, particularly for women, usually as a result of other commitments. 131,132,136,146,150,156,158–160,163,164,166,169,178,180 However, in one study, it was reported than spouses often assisted their partner in freeing up time for activities by carrying out chores or providing transport. 137
From a lifespan perspective, having sufficient time to become involved in physical activity varied with different life-stages. For example, physical activity could be given a lower priority in the child-rearing years and be taken up again or engaged with more frequently in later years when more time was available. 132,133,141,145 However, for some retired participants, time was once again taken up in looking after grandchildren. 133,147,148 For others, there was an acknowledgement that sometimes lack of time can be cited as a barrier to participation rather than lack of motivation: ‘We do not have the discipline to make time to exercise. It is not one of our priorities’;160 ‘People say to me, “well I don’t have time” and I think you just make the time. . .’. 150
Flexible time
After working and bringing up children, activities that required attention and structure, retirement offered many participants the opportunity to be flexible with their time; in other words, there was more choice about how to spend time. 147–149 Some couples took advantage of this opportunity and spent quality time together while walking or engaging in other activities. 132 Individuals also reported that retirement provided the opportunity to try out new activities. 133,148,161,172 However, for some, retirement altered the perception of time,131,133 and extended free time resulted in procrastination. 133
Although retired people may appear to have more available time, there was a suggested need for activities that were organised at flexible times to improve accessibility. 162,168 There was a particular aversion in one study to attending an activity in the evening. 162 Home-based interventions allowed this flexibility, as participants could choose a time of day that was suitable. 168 For those participating in physical activities outside the home, the development of relationships and commitments that are associated with the activity could result in an extensive amount of time and energy being taken up. 172
Personal time as a benefit of participation
One study132 reported that for retired couples, engaging in activities (physical or sedentary) was a way of achieving some space for the self, away from a spouse. For participants in four further studies, engaging in physical activity was, or had become, a way of controlling personal time during retirement,144,145,150,176 although the extent of time spent on activities away from home could be challenged by a spouse. 176 For others, taking time to participate in physical activity was reported to evoke feelings of control and autonomy137 or, conversely, of guilt. 136,137 Guilt was associated in one paper with women, who felt that it was inappropriate to use time for the self. 137
Making the most of remaining time
A commonly reported motivator for engaging in physical activity in older age was to maintain or improve physical, psychological and social health and function so that the years that remained would be fulfilling131,141,145,161,178 or to possibly extend life expectancy. 131 There was also an awareness that much loved physical activity may have to be curtailed at some point in the future as a result of age-related conditions,141,145 which evoked a sense of urgency around ensuring that desired activities were accessed before the opportunity was lost. 132
Activity levels
A total of 16 studies, reported in 17 papers,130,131,133,134,138,142,145,146,149,150,155,156,161,165,169,174,181 explored activity levels of their participants. This included how past activity levels might influence current motivation to engage with physical activity, differences in attitude to physical activity between those describing themselves as ‘active’ or ‘inactive’ and how perceptions of ageing might influence activity type and intensity.
Inactive populations
Three included studies examined the experiences of samples who declared themselves inactive or sedentary. 142,156,165 Latina women in one study often reported that they were inactive owing to competing commitments such as the family. 156 Gallagher et al. 165 focused on neighbourhood and environmental factors, such as safety, which might inhibit or facilitate physical activity. The study was carried out in Detroit, MI, USA, where the authors report that the general population are less physically active than the national average. Stead et al. 142 identified active and relatively inactive groups within their sample, reporting that these groups require different approaches when marketing interventions. The authors state that active older people may be forgotten, as they are not regarded as high priority, whereas inactive individuals will require messages that attract them to an activity, such as the social aspect rather than health benefits.
Active versus inactive
Four included studies compared the views of active and inactive participants,130,131,133,181 although Finch131 reported that how participants defined their own activity levels varied, with some ‘inactive participants’ later being found to be more active than they had declared. Walking was an activity that was particularly overlooked in self-reports. One study130 reported that some inactive retired people, mainly men, had been active, and sometimes very active, when they were younger. Such activity was likely to be related to work or training while in the Armed Forces. Scanlon-Mogel and Roberto149 also identified a continuity of activity generated from participation in the Armed Forces. Historically, the population generally walked more because there were fewer cars, so physical activity had not always been intentional. Type of employment could also have an influence on overall physical activity levels, with some jobs being more active than others. Women interviewed for three studies130,149,181 were more likely to report being consistently active or inactive across their lifespan owing to housekeeping and child-care activities. Although more leisure time during retirement might trigger more activity, women who had remained active during their lifespan were habitual in their activity and were less likely to be deterred by negative influences. Conversely, semiactive women were more likely to cite reasons for not being active despite being aware of the health benefits. Indeed, some semiactive women expressed the belief that one needs to be healthy to exercise, and sedentary women appeared to bypass triggers and opportunities to become active, as it was afforded low priority. 181 Beck et al. 133 also found that for those who had been active for most of their lives, retirement allowed extra time for pursuits and physical activity could increase. For active participants, barriers that were often cited by inactive participants, such as cost, were overcome to allow physical activity to continue. Two studies133,145 reported that physically active participants were more likely to continue to choose new physically active interests and challenges. Liechty et al. 145 attribute this commitment to the desire for continuity of an ‘active’ self-image.
Conversely, Beck et al. 133 found that for those who had remained inactive for most of their lives, retirement did not necessarily provide the motivation to begin. Health problems were more likely to trigger inactive participants to become active, either through their own determination145 or through the advice of a health professional. 138,169 Although some participants reported starting new activities that they had only dreamed of while working, for others, physical activity simply was not enjoyable: ‘I’d rather pull my finger nails out than go to the gym’. 133 Liechty and Genoe150 also report that men who did not enjoy physical activity felt that value judgements compelled them to do it anyway out of guilt. It would appear from the literature that some individuals habitually exercise or engage in physical activity and continue to do so because they enjoy it or are committed to protecting their health. Others may begin physical activity at certain points in time owing to health or other triggers, whereas some semiactive or inactive individuals find it particularly difficult to become motivated, regardless of life triggers or the awareness of benefits. However, even active individuals reported changes in the extent and duration of activity as they age.
Changes in activity levels in response to the effects of ageing
Seven studies discussed changes in activity levels with advancing age, mainly from active to less active. 133,134,146,155,161,174,178 Three of these studies133,134,174 found that inactivity could be forced upon those who would like to remain active but have suffered pain, injuries or physical disabilities, leading to feelings of frustration. Barnes et al. 134 provide a case study of one participant who suffered a stroke, which had taken away his ability to continue line dancing and other enjoyable activities. Instead, he continued to participate as a spectator, maintaining social contact rather than physical engagement. Other changes in activity levels were more subtle and ‘managed’ in anticipation or in response to ageing. In one case study,155 the participant had been heavily involved in sport from a young age. As he became older he reported having had to make adjustments to his involvement which in practice meant that he shifted his focus from baseball and softball to tennis and swimming. Following retirement he stated that he had to lower his expectations owing to diminishing levels of strength and stamina: ‘the ball just doesn’t go as fast any more when I hit it’. 155 However, he found that he needed to remain involved at some level as sport had given him a sense of not only purpose but also social identity; sport had been the root of much of his success in life and people would call on him to play. This aspect of involvement in activity would be missed if it were to cease.
Similarly, Kleiber and Nimrod146 found that members of a ‘learning in retirement’ group pared down their activities, eliminating those with less meaning and those that were deemed too strenuous, and instead adapting ongoing activities around episodes of pain and illness. In some cases, as described above, less strenuous activities were substituted when previous activities were regarded as becoming too onerous: ‘They’re not the same, but pretty close’. 146 Male participants in another study178 had participated in sports when they were younger and, although they acknowledged the benefits of continuing to participate in retirement, there were changes in the type of activities they perceived as feasible as they aged. Kluge161 similarly reported that older women had been active in their former years but had compromised leisure activities in their middle years owing to caring responsibilities. Nevertheless, they continued to identify themselves as active despite the barriers arising from the ageing process. The authors suggest that this identification was disrupted by gender acculturalisation and social norms that situated physical activity as lower priority in respect of caring roles and ageing identities. These papers identify the commitment to continue with physical activity beyond retirement, perhaps with even more determination, despite apparent constraints.
Intervention factors
Social element
A total of 33 papers130–134,136–142,144,145,151–154,156,158,162,167–173,175,176,182–184 concluded that a social element was an important factor for older people carrying out a physical activity. For retired participants, the social element provided within the workplace was no longer available, and leisure activities (whether physical or not) were cited as being an alternative to work in this respect. 130,151,152,173 There was a reported sense that older people needed to ensure that they had social contacts as they aged, and physical activities could provide this opportunity as well as enhance psychosocial well-being. 131,137 For retired couples who did not share similar interests, separate activities were a way of developing a social life with one’s own sex. 132 For some women in one study it was important to socialise with people of a similar age. 167 However, although some participants who felt isolated might contemplate joining an organisation in order to meet other like-minded people, this was not always acted upon because of barriers relating to transport or having to initiate an outing alone. 134 Cooper and Thomas141 reported that the death of a partner could leave the widow(er) wondering whether or not to continue a previously shared physical activity, such as dancing, alone.
In dancing, the social element was reinforced through special evening events and parties and the required dress codes. 141 Diogini171 found that older athletes maintained their participation at least partly owing to the social connection, and in two papers the social element of a physical activity was reported to have a beneficial effect on mental health. 170,171
Nineteen studies, reported in 21 papers,133,136–142,144,145,154,158,162,167–169,172,175,176,183,184 found that older participants in physical activities valued the social aspect of activities, being able to identify with a group and the support that accompanied this. The social element often developed over time and then became a motivator for continuing to participate. Particular activities might be chosen, for example an organised exercise class, because of their enhanced likelihood of having a social element, although two studies138,168 found that exercise classes were not perceived as sufficiently social, as many of the participants did not stay around for long enough after the class to generate friendships or outside activities, and many left the class after a few weeks. Duncan151 found that self-directed mall walking was less likely to be initiated for social reasons than participating in organised mall-walking groups in which friendship groups developed over time.
One study133 found that the social element and group activities were generally less important for men who preferred less regimentation and the autonomy of walking alone or with a friend. Brown et al. 170 support the finding that the social element is more important to women than to men. However, there were some cases cited in which the sex distinction was not so clear. For example, Drummond173 found that their male participants did find that physical activity was a good way of improving social networks. In addition, Berg et al. 156 found that, although a group might be motivating for some women, for others this might not be the case, and one participant stated that, although individual women might be wonderful, groups of women could be ‘pretty awful’. 156 Physical activity trainers delivering exercise on prescription classes noted that the social element of attendance was less important for younger participants than for this age group, but that even for older participants they needed to provide support to allow them to adjust to a new group of people and to develop networks that would last beyond the time frame of the programme. 139
Enjoyment
A total of 30 papers130–134,137,138,140,141,144,145,148,150,154,156–159,161–163,168,171,172,176,180,182–184 discussed enjoyment and/or fun (or lack of enjoyment) as a factor in maintaining participation in a physical activity (often referred to as ‘hooks’).
Apart from the social element, the ability to derive fun and enjoyment from the activity was reported as a reason for continuing to participate, with some participants reporting a ‘love’ for the activity or particular elements of the activity such as competition,157,172,173,176 music140,141 or social interaction. 141,144,159,172,176,184 Enjoyment was usually associated with specific forms of physical activity so that some were enjoyed and others were not. Where participants reported enjoyment it had often first made itself apparent while engaging in the activity at a young age132,133 or, conversely, could be found in participating in new activities. 138,145 Indeed, an important reported facilitator in exercise class participation was the element of enjoyment. 154,168 For some, physical activity contributed to an overall feeling of health, fitness and increased energy that in turn allowed retirement or life in general to be better enjoyed,131,158,162,171 although for others, there needed to be sufficient time available to enjoy the activity. 148 Retirement from work offered time, freedom, choice and flexibility, which in turn enhanced enjoyment. 145,150 However, enjoyment might be contingent on adjusting the type of physical activity or certain aspects of the activity that are perceived to limit barriers, for example, choosing a different activity or wearing sportswear that feels more age-appropriate. 150,157
Conversely, lack of enjoyment was one rationale for giving up an activity. 133 For others, enjoyment came only after perseverance with a new activity that at first was not enjoyable,141,176 and an intervention that was prescribed by a doctor was reported by some to lack the element of enjoyment because it was not their own idea. 137,159 For some, engaging in physical activity was perceived as ‘the right thing to do’ rather than being enjoyable. 133,137 For yet others, organised physical activity lacked enjoyment owing to pain,167 fear of injury180 or the perception that exercise was punishing,163 too difficult,168 boring,158 or lacked meaning, interest,138 or a social element. 168
Barriers and facilitators to carrying out physical activity at retirement age
The preceding sections have presented factors that impact on decisions to engage with and continue physical activity at retirement age within the context of different activities and conditions. Table 20 presents a summary of the barriers and facilitators that have been covered by the sections, organised according to individual, intervention and interpersonal factors. Many of the factors cross cut and many are conditional on external influences such as interactions with partners and family.
| Domain | Barriers | Facilitators |
|---|---|---|
| Individual characteristics | ||
| Impact of retirement | Living alone: lack of motivation to leave house Feelings of guilt at taking time for self Lack of funds (especially low SES) |
Opportunity to take up new/preferred/advised ‘healthy’ activities Living alone: need to go out and meet people Increased time/freedom to focus on the self Perceived need to keep mind/body active Continuing a strong ‘work ethic’ |
| Impact of older adulthood | Having an ‘inactive’ identity (focus on barriers attributable to limitations) Existing physical/psychological conditions Low SES: lack of engagement Sense of duty rather than desire Lack of time Lack of familiarity with/scepticism regarding the gym environment |
Having an ‘active’ identity (focus on overcoming limitations) Understanding of health/psychological/social benefits Desire for healthy/well-functioning/attractive body/healthy mind Resistance to negative ageing stereotypes |
| Intervention characteristics | ||
| Impact on participation | ‘Paternalistic’ health promotion style Poor understanding of/recall of/identification with mass media messages Witnessed/perceived negative consequences of exercise Preference for unstructured physical activity (mainly men) Timing of classes (not flexible) ‘Unsafe’ environment |
‘Softer’ (trusted) health promotion messages Personal invitation to participate Provides routine/structure/challenge/competition as substitute for work Free or low cost Flexibility of schedule (home-based intervention) ‘Safe’/non-threatening environment Opportunity to be outdoors |
| Impact on maintenance | Outnumbered by/feeling less competent than opposite sex (mainly men) or younger participants Intervention perceived as age/sex/culture inappropriate Intervention perceived as boring Need to expose the ageing body/body image issues Stigma attributable to age Embarrassment attributable to lack of capability Lack of fun |
Intervention designed and organised for older age group Gradual introduction to difficult tasks Experience of health/psychological benefits Empowerment through successful achievements Provides a social element (mainly women) Cultural sensitivity Sense of ‘communitas’; relationship ‘entanglements’ Enjoyment Sense of ownership Getting ‘hooked’ |
| Interpersonal/social factors | ||
| Professional characteristics | GP lacks interest in ERS | GP discusses benefits of ERSs Instructor:
|
| Social support | ‘Nagging’ from spouse Prioritising partner’s preferred activities/non-activity Prioritising caring responsibilities (mainly women and some ethnic groups) Lack of encouragement from family members Perceived ‘nosiness’ of other participants |
Encouragement from spouse/family/friends Shared physical activity experiences and concerns/support from similar age group |
The range of factors that might impact on participation in physical activity at this age suggests that a similarly broad range of interventions that take such factors into account may be required to encourage and maintain healthy activity levels. From the available literature, a particular challenge is encouraging initial participation for individuals who do not see themselves as ‘active’. This identity is further compounded by the effects of ageing and fears of injury. Many participants began participating through the encouragement of other people, such as family, friends, partners or health professionals, or out of a need to socialise or obtain some personal space. These factors may be at least as important as the health promotion messages that aim to increase participation.
Chapter 5 Meta-synthesis of qualitative and quantitative evidence and exploration of applicability
Meta-synthesis of qualitative and quantitative data
We used the qualitative findings to examine the content and delivery of the interventions reported in Chapter 3. We intended to use this process to further explore the applicability of the programmes that we had identified, as well as the evidence of their effectiveness to our recently retired or about to retire population, given the lack of interventions reported specifically for this group. We also aimed to use this process to address another of our research objectives, namely the impact of interventions in different populations and any potential influence on inequalities.
We identified and tabulated the elements of programmes that had been highlighted in the qualitative studies as being facilitators or barriers to intervention delivery and outcomes. We then re-examined the A1/A2 quantitative studies in light of these factors, to explore whether or not they had been a feature of the interventions. Figure 18 summarises the data, and Table 21 provides detail regarding each study.
FIGURE 18.
Number of studies reporting that elements were included in the intervention.

| Paper reference | Accessible location | Affordable | Offered during daytime | Offered at appropriate point in time for individual | Provides social element | Offers a challenge/goal-setting | Modifiable for sex/culture | Individual tailored | Total | Comments |
|---|---|---|---|---|---|---|---|---|---|---|
| aAckermann et al. (2005)27 | Y | Y | Y | Y | N | N | Y | Y | 6 | Training of PCPs |
| Armit et al. (2005)28 | Y | Y | Y | Y | N | Y | Y | Y | 7 | Counselling |
| Burke et al. (2013)30 | Y | Y | Y | Y | N | Y | Y | Y | 7 | Diet and exercise |
| Coronini-Cronberg et al. (2012)33 | Y | Y | Y | Y | N | N | Y | Y | 6 | Community |
| Elley et al. (2003)40 | Y | Y | Y | Unclear | N | Y | Y | Y | 6 | Counselling |
| aGoldstein et al. (1999),45 Marcus et al. (1997)60 | Y | Y | Y | Unclear | N | Y | Y | Y | 6 | Counselling |
| Petrella et al. (2010)70 | Y | Y | Y | Unclear | N | Y | Y | Y | 6 | Counselling |
| Pinto et al. (2005)71 | Unclear | Y | Y | Y | N | Y | Y | Y | 6 | Counselling |
| Hekler et al. (2012)50 | Y | Y | Y | Unclear | N | Unclear | Y | Y | 5 | Individual exercise |
| Irvine et al. (2013)53 | Y | Unclear | Y | Unclear | N | Y | Y | Y | 5 | |
| Koizumi et al. (2009)58 | Y | Y | Y | Unclear | N | N | Y | Y | 5 | Pedometer |
| Martinson et al. (2010),61 (2008)62 | Y | Unclear | Y | Unclear | N | Y | Y | Y | 5 | Telephone |
| Prabu et al. (2012)72 | Y | Y | Y | Unclear | N | Y | Unclear | Y | 5 | Telephone |
| aPurath et al. (2013)73 | Y | Y | Y | Unclear | N | Y | Unclear | Y | 5 | Telephone |
| van Stralen et al. (2009),79 (2010),80 (2011),81 (2009)82 Peels et al. (2012),66 (2012),67 (2013)68 |
Y | Y | Y | Unclear | Y/N (one study arm) | N | N | Y | 5 | Computer |
| Walker et al. (2009),83 (2010)84 | Y | Y | Y | Unclear | N | Y (for one study arm) | Unclear | Y (for one study arm) | 5 | Diet and exercise |
| aWerkman et al. (2010)85 | Y | Y | Y | Y | N | N | Unclear | Y | 5 | Computer |
| Wilcox et al. (2008),87 (2009),88 (2009),89 (2006)90 | Y/N | Y/N | Y | Unclear | N/Y | N | Unclear | Y/N | 5 | Group |
| Castro et al. (2001)32 | Y | Y | Y | Unclear | N | Unclear | N | Y | 4 | Telephone |
| aFries (1993),42 (1993)43 | Y | Y | Y | Unclear | N | N | N | Y | 4 | Diet and exercise |
| aHageman et al. (2005)46 | Y | Y | Y | Unclear | N | N | N | Y (limited) | 4 | Computer |
| King et al. (2007)57 | Y | Y | Y | Unclear | N | Y | N | Unclear | 4 | Telephone |
| aPasalich et al. (2013)65 | Y | Unclear | Y | Unclear | N | Y | N | Y | 4 | Pedometer |
| van Keulen et al. (2011)78 | Y | Y | Y | Unclear | N | N | Unclear | Y | 4 | Telephone |
| Wijsman et al. (2013)86 | Y | Unclear | Y | Unclear | N | Y | Unclear | Y | 4 | Computer |
| Pereira et al. (1998)69 | Y | Y | Y | Y (optional) | Unclear | Unclear | Unclear | Unclear | 4 | Individual exercise |
| Burman et al. (2011)29 | Unclear | Unclear | Unclear | Unclear | Y | Y | N | Y (limited) | 3 | Group |
| Croteau et al. (2014)36 | Unclear | Unclear | Unclear | Unclear | Y (one study arm only) | Y | N | Y | 3 | Counselling |
| Hooker et al. (2005)51 | Unclear | Unclear | Unclear | Unclear | Y | Y | Unclear | Y | 3 | Telephone |
| Lawton et al. (2008)59 | Y | Y | Y | Unclear | N | Unclear | Unclear | Unclear | 3 | Counselling |
| aOpdenacker et al. (2011),63 (2008)64 | Y/N | Unclear | Y/unclear | Unclear | N | N | Unclear | Y/N | 3 | Individual exercise |
| Strath et al. (2011)77 | Unclear | Unclear | Unclear | Y | N | Y (for some study arms) | Unclear | Y | 3 | |
| Caperchione and Mummery (2006)31 | Unclear | Unclear | Y | Unclear | Y | N | N | N | 2 | Group |
| aCostanzo et al. (2008)34 | Unclear | Unclear | Y | Unclear | N | Unclear | Unclear | Y | 2 | Counselling |
| Finkelstein et al. (2008)41 | Unclear | Unclear | Unclear | Unclear | N | Y | N | Y | 2 | Pedometer |
| aKamada et al. (2013)54 | Y | Unclear | Y | N | Unclear | Unclear | N | N | 2 | Community |
| King et al. (2002)55 | Y | Unclear | Y | Unclear | N | N | N | N | 2 | Telephone |
| Sawchuk et al. (2008)75 | Unclear | Y | Y | Unclear | N | N | Unclear | Unclear | 2 | Pedometer |
| Stevens et al. (1998)76 | Yes | Unclear | Unclear | Unclear | N | N | Unclear | Y | 2 | Counselling |
| de Jong et al. (2006),37 (2007)38 | Unclear | Unclear | Unclear | Unclear | Y | N | N | N | 1 | Group |
| Dorgo et al. (2009)39 | Unclear | Unclear | Unclear | Unclear | Y | N | N | N | 1 | Individual exercise |
| Fujita et al. (2003)44 | Unclear | Unclear | Unclear | Unclear | Y | N | N | N | 1 | Group |
| Halbert et al. (2000)47 | Unclear | Unclear | Unclear | Unclear | N | Unclear | N | Y | 1 | Counselling |
| Cox et al. (2008)35 | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | N | N | 0 | Individual exercise |
| Hamdorf et al. (1992),48 (1993)49 | Unclear | Unclear | Unclear | Unclear | Unclear | N | N | N | 0 | Group |
| Hughes et al. (2009)52 | Unclear | Unclear | Unclear | Unclear | Unclear | N | N | N | 0 | Individual exercise |
| King et al. (2002)55 | Unclear | Unclear | Unclear | Unclear | Unclear | N | N | N | 0 | Group |
| Rowland et al. (1994)74 | Unclear | Unclear | Unclear | Unclear | Unclear | N | N | N | 0 | Group |
| Totals | Accessible in terms of location 29 |
Affordable 25 |
Offered during daytime 33 |
Offered at appropriate point in time 7 |
Provides social element 8 |
Offers a challenge/goal-setting 19 |
Sex/gender/culture sensitive 12 |
Individual tailored 32 |
There were many studies in which limited information regarding the intervention delivery process resulted in a rating of ‘unclear’. None of the interventions contained all eight perceived optimal elements and only two achieved a total of seven. For the interventions that scored very low for inclusion of the elements, this was often attributable to a lack of reporting. Areas in which the interventions most often tended to include facilitative elements related to individual tailoring of programmes and sessions being offered in the daytime.
Areas in which the interventions performed less strongly in terms of facilitative elements were a consideration of an individual’s point in life (readiness for change) and the inclusion of a social element. With regard to an optimal point in time, this may be related to the need for sufficient study sample size recruitment, although a minority of studies (such as Ackermann et al. 27) did use readiness for change evaluation tools in order to identify potential participants. In our evaluation of interventions, we strictly used the criteria of a social element to refer to programmes in which this was described as a designated part. We did not assume group programmes to include automatically a social aspect (as attending a group session does not automatically lead to interaction with others). These strict criteria may have underestimated the social element of some of the programmes.
We considered whether or not the inclusion of the perceived optimal elements was associated with greater effectiveness. We examined the 10 studies for which there was weaker evidence of effect (marked with superscript a in Table 21). As can be seen, these studies are spread throughout the table, with no clustering towards the bottom, which might be expected if the optimal elements had a significant effect on outcome. Indeed, there are none of these studies in the bottom 10 and two studies in the top 10. The only element that seemed to be missing from all these less effective interventions was the provision of a social element (although this was also missing in other successful interventions).
In terms of social inequalities, we had to presume rather than rely on reported information that the programme was free of costs for participants. Where advice/counselling was delivered as part of routine health care this was clear; for other studies, payment was not mentioned for the provision of materials or for attendance at classes or group sessions. Whether or not this was a result of participants taking part in a research study, and whether or not payment would be required if the intervention was rolled out as routine care, was unclear. The interventions seemed generally to be provided in a local area, although, again, for some studies it was not possible to ascertain from the information provided how accessible the location was for participants.
Exploration of applicability
Following completion of the review, we carried out a series of sessions with people who had retired, and a separate session for staff who work with older adults, in order to explore how far our findings might be applicable to the retirement transition period. During these sessions we presented an overview of the work, encompassing background, methods and a summary of the effectiveness study findings. We then asked attenders to complete a feedback and discussion activity based around considering the applicability of the review findings to people in the retirement transition phase of life. We provided a worksheet which asked for feedback on to three main areas: first, whether or not any of the types of interventions that we had identified for older people would not be suitable for those around retirement age; second, whether or not factors described in the qualitative literature as influencing the amount of physical activity that older adults engage in would be important or unimportant for people around retirement; and third, whether or not factors described in the qualitative literature as influencing older people’s participation in an intervention would be important for people around retirement.
We carried out sessions with retired adults living in both more affluent and less affluent areas of Sheffield, a large English city with significant socioeconomic inequalities. Sessions were attended by 18 staff and 54 retired people. Not all of those who were at the sessions opted to complete the feedback forms; some preferred to take part only in the discussions. We received written responses from 13 staff and 37 retired people. Some of those attending had experienced pre-retirement sessions provided by employers. These sessions had consisted of financial planning and none described by participants had included health advice.
Appropriateness of programme types
Programmes delivered in the home were most frequently identified by session participants as less relevant to people about to retire or recently retired. The types of programme that were perceived to be most preferred were group classes or individual training sessions (Figure 19). There was discussion around the importance of interacting with other people after retirement, particularly for those living on their own.
FIGURE 19.
Number of participants who identified a programme as preferred.
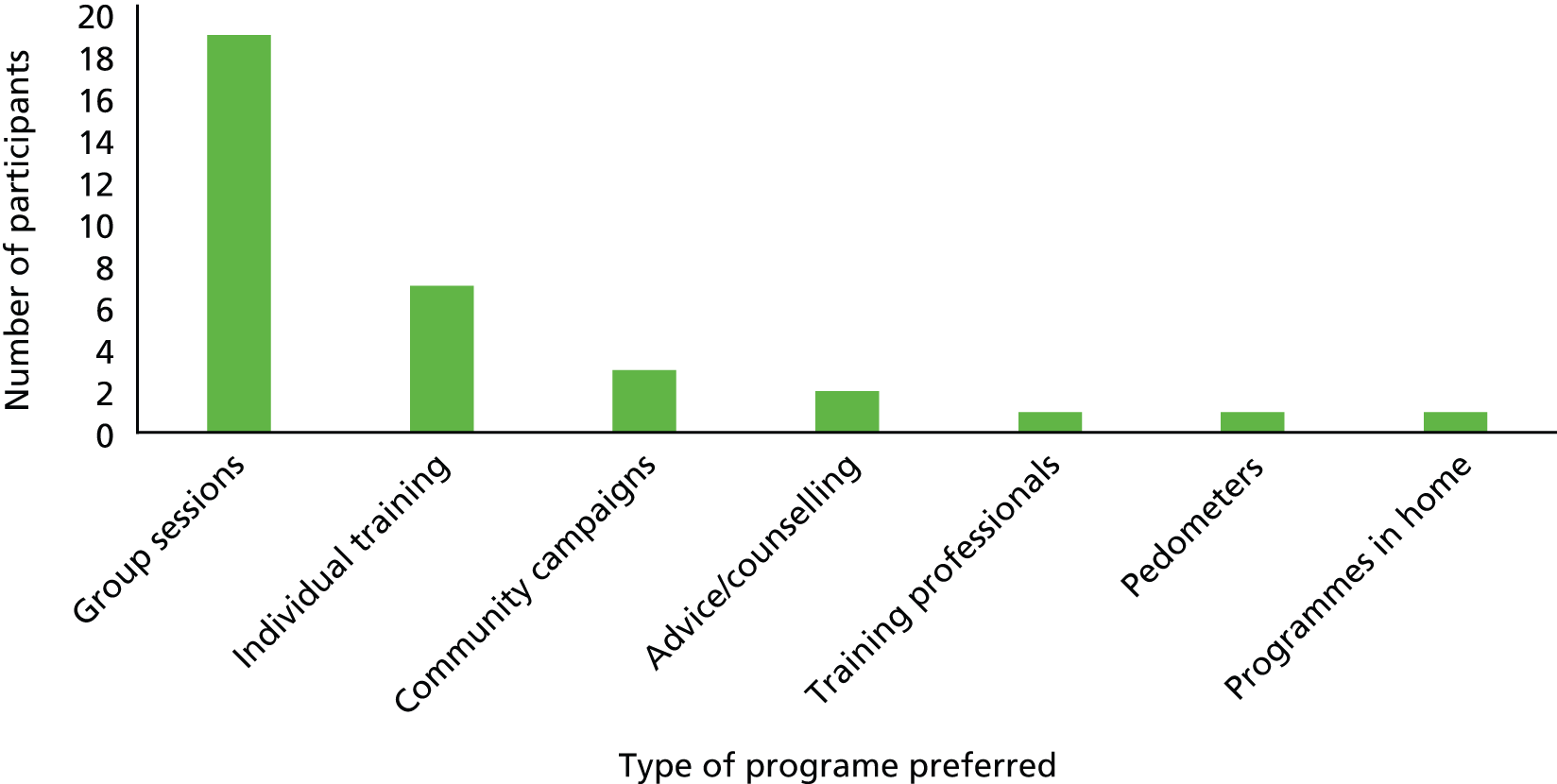
Factors influencing the amount of physical activity
Participants were asked to provide their opinion on whether or not each of the following factors (which were described in the qualitative literature) were important influences on the amount of physical activity that people participate in around the time of retirement (Table 22). As some respondents did not answer all the items, the numbers indicating positive and negative responses are provided for comparison.
| Element | Number of responses |
|---|---|
| 1. Increased time or freedom to focus on yourself | ✓ = 29; ✗ = 2 |
| 2. A lack of time | ✓ = 7; ✗ = 27 |
| 3. The need to keep mind and/or body active | ✓ = 33; ✗ = 0 |
| 4. The need to continue a strong ‘work ethic’ | ✓ = 17; ✗ = 14 |
| 5. A lack of engagement with activity in general | ✓ = 12; ✗ = 19 |
| 6. A lack of familiarity with or scepticism regarding gyms | ✓ = 17; ✗ = 13 |
| 7. A desire for a healthy/well-functioning/attractive body/healthy mind | ✓ = 28; ✗ = 4 |
| 8. A desire to resist negative ageing stereotypes | ✓ = 16; ✗ = 16 |
| 9. A lack of motivation to leave the house | ✓ = 14; ✗ = 12 |
| 10. The opportunity to take up new ‘healthy’ activities | ✓ = 22; ✗ = 3 |
| 11. A need or wish to go out and meet people | ✓ = 32; ✗ = 2 |
| 12. Feelings of guilt in taking time for yourself | ✓ = 11; ✗ = 24 |
| 13. A lack of funds | ✓ = 16; ✗ = 21 |
| 14. Seeing yourself as an active person | ✓ = 28; ✗ = 4 |
| 15. Having a good understanding of the health, psychological and social benefits | ✓ = 26; ✗ = 4 |
| 16. Prioritising a partner’s preferred activities or non-activity rather than your own | ✓ = 12; ✗ = 14 |
| 17. Caring responsibilities (e.g. grandchildren or a partner) taking priority over activities | ✓ = 14; ✗ = 7 |
Participants were also asked to identify the five most important factors influencing the amount of physical activity that people do around retirement, and the five least important influencing factors (Figures 20 and 21).
FIGURE 20.
Number of participants identifying a factor as an important influence.
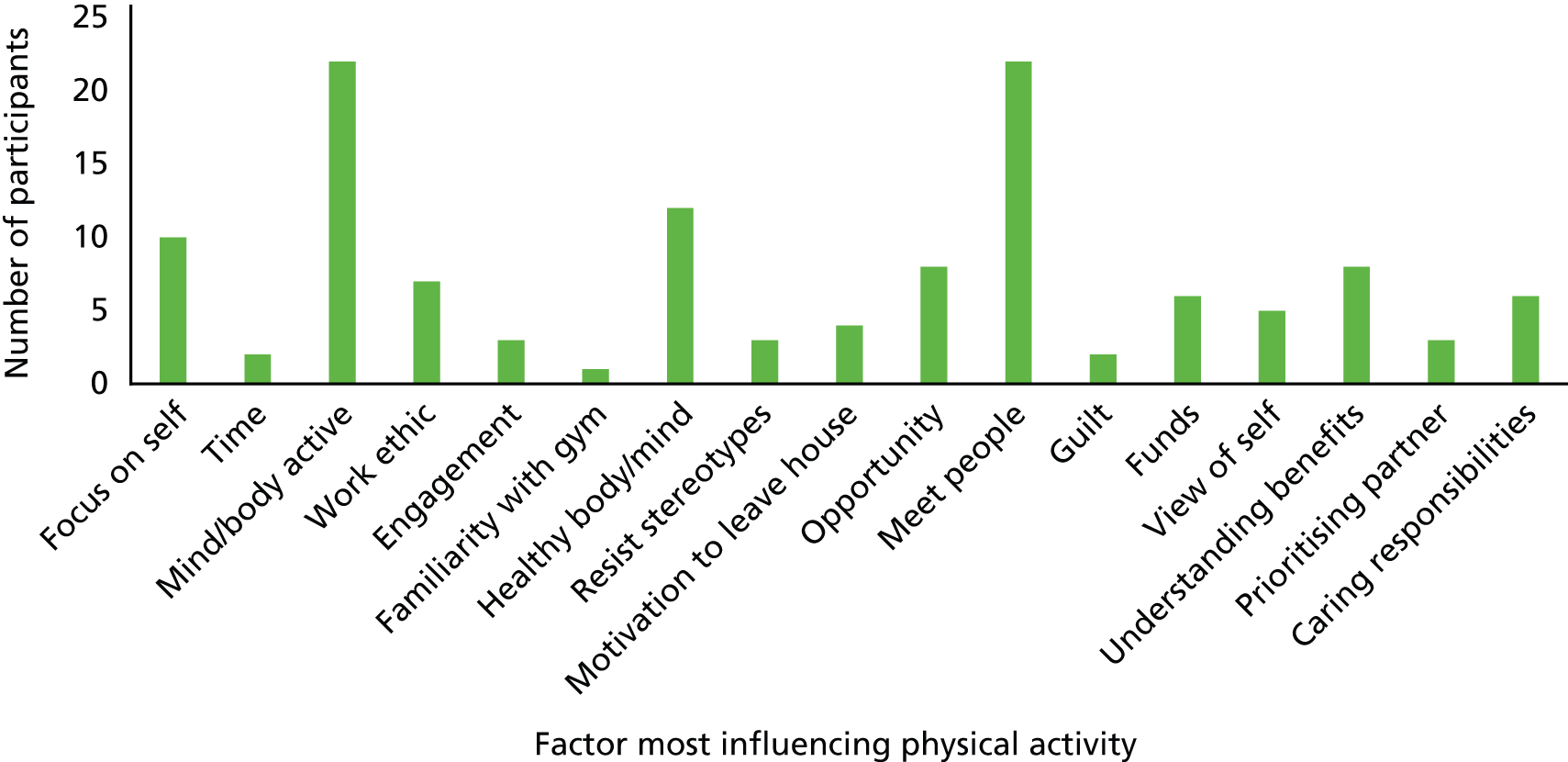
FIGURE 21.
Number of participants identifying a factor as an unimportant influence.
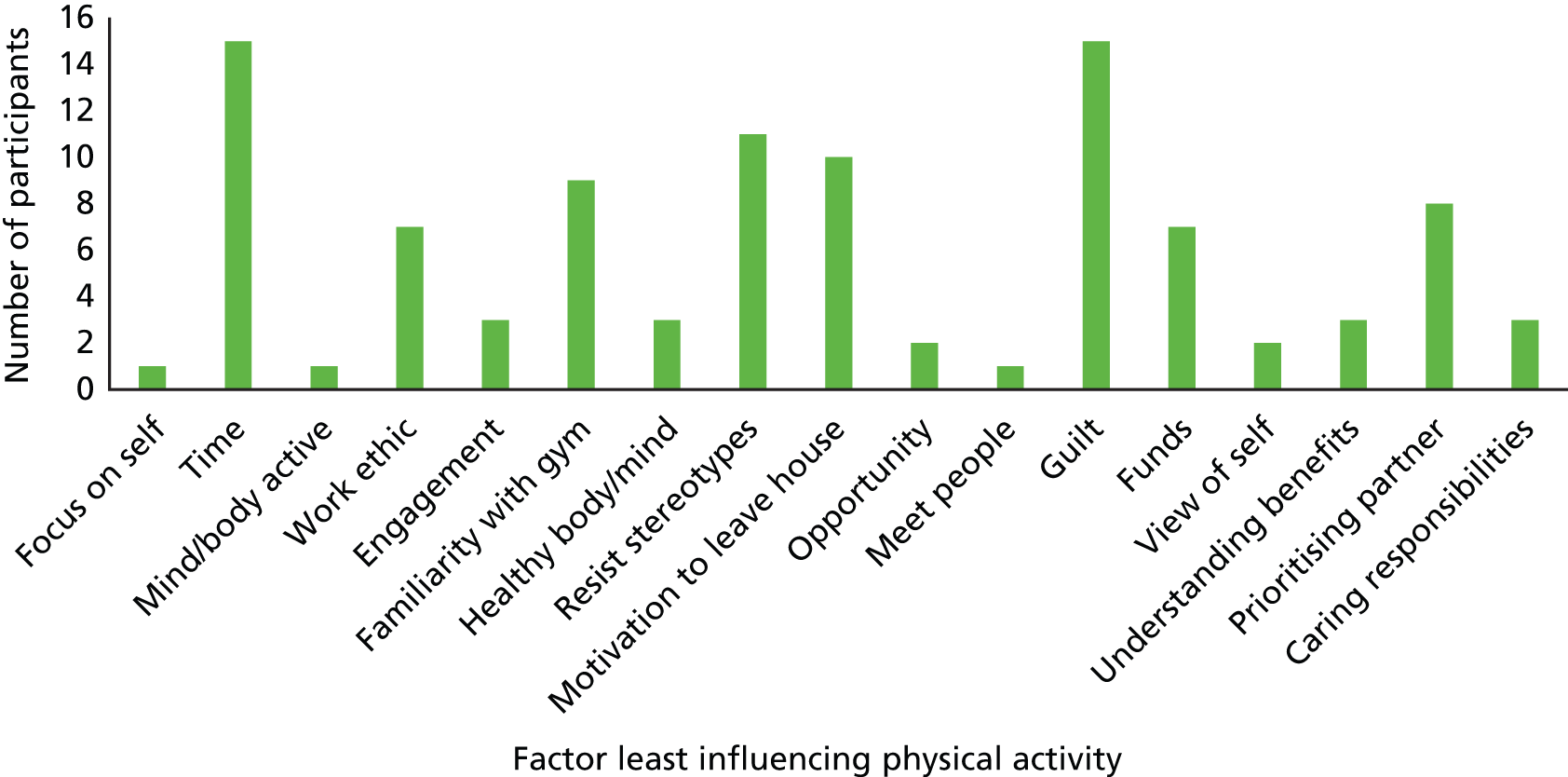
There was considerable individual variation in views regarding the importance of the various factors. The elements more frequently identified as important related to keeping the mind and body healthy/active and meeting people. A feeling of guilt and lack of time were reported to be the least important influences on the amount of physical activity that people do around retirement age.
Factors influencing whether or not someone around retirement age would take part in a physical activity programme
The final area for input related to factors that might influence someone’s decision to take part in a physical activity programme. As above, some respondents answered only some of the items, so the positive and negative responses are provided for comparison (Table 23).
| Element | Number of responses |
|---|---|
| 1. Poor understanding of or identification with health messages | ✓ = 13; ✗ = 10 |
| 2. Worries about negative consequences of exercise (e.g. injury) | ✓ = 9; ✗ = 17 |
| 3. Sessions are seen as too structured | ✓ = 11; ✗ = 17 |
| 4. Sessions are free or have a low cost | ✓ = 24; ✗ = 4 |
| 5. Sessions are flexibly scheduled | ✓ = 21; ✗ = 4 |
| 6. A feeling of being outnumbered by or less competent than the opposite sex or younger participants | ✓ = 17; ✗ = 12 |
| 7. The intervention is seen as appropriate to one’s sex or culture | ✓ = 13; ✗ = 12 |
| 8. Worries about exposing the ageing body or body image issues | ✓ = 11; ✗ = 16 |
| 9. Stigma related to age | ✓ = 10; ✗ = 13 |
| 10. Embarrassment as a result of lack of capability | ✓ = 13; ✗ = 13 |
| 11. The sessions provide enjoyment, fun | ✓ = 24; ✗ = 2 |
| 12. The sessions provide a social element | ✓ = 25; ✗ = 2 |
| 13. ‘Nagging’ from spouse | ✓ = 6; ✗ = 20 |
| 14. The health promotion message has come from a trusted source (such as a GP) | ✓ = 20; ✗ = 4 |
| 15. A personal invitation to take part has been received | ✓ = 21; ✗ = 4 |
| 16. The sessions provides routine or structure | ✓ = 21; ✗ = 8 |
| 17. The sessions provide a challenge/competition | ✓ = 16; ✗ = 8 |
| 18. The activity takes place in a non-threatening environment | ✓ = 23; ✗ = 5 |
| 19. Gives the opportunity to be outdoors | ✓ = 15; ✗ = 8 |
| 20. The intervention is designed and organised for the right age group | ✓ = 22; ✗ = 7 |
| 21. There is a gradual introduction to difficult tasks | ✓ = 21; ✗ = 4 |
| 22. Health/psychological benefits have been experienced from physical activity | ✓ = 25; ✗ = 3 |
| 23. You have a sense of ‘communitas’, or a sense of ownership | ✓ = 8; ✗ = 13 |
| 24. Your GP has discussed the benefits of an exercise programme | ✓ = 16; ✗ = 12 |
| 25. The instructor is a similar age to participants | ✓ = 15; ✗ = 13 |
| 26. The instructor identifies with participants and their needs | ✓ = 20; ✗ = 5 |
| 27. The instructor provides encouragement, particularly during initial sessions | ✓ = 22; ✗ = 2 |
| 28. There is encouragement from spouse/family/friends to take part | ✓ = 26; ✗ = 4 |
| 29. There is an opportunity to share experiences and concerns or receive support from others of a similar age group | ✓ = 24; ✗ = 2 |
Most important and least important factors
As regards the most important perceived factors, the majority of items were selected by one to three participants, indicating a spread of views. Only the following elements were not selected by anyone: appropriateness to sex/gender or culture; stigma related to age; and GP has discussed the benefits. The most frequently selected items were: a wish to go out and meet people (n = 22); sessions providing a social element (n = 20); and free or low cost (n = 18).
There was little consensus regarding the least important elements, with many participants not selecting all five. Most items across the group were selected by at least one to three participants. The elements that were not selected by anyone (and therefore not considered least important) were: flexibly scheduled activities; embarrassment; enjoyment/fun; a social element; outdoors; gradual introduction; experienced benefits; instructor provides encouragement; and encouragement from others.
These sessions were carried out with only a small sample of participants, all of whom were already retired and were being asked to recall their views and experiences from an earlier time. The sessions also had the aim of further exploring the findings of the review rather than carrying out a primary research study. Similarly to the interventions studies, the sex ratio of respondents was uneven, with more women attending the clubs and groups than men. Given these limitations, the data provide further support for the findings of the review. The individual variation in rating of factors among respondents echoes the review in concluding that a range of interventions may be effective. It highlights that there is no one type of intervention that would suit all. The importance of a social element in interventions was apparent throughout these data, echoing the findings from our review of the qualitative literature. Other elements that were described in our review of the qualitative literature and highlighted in these data as being important in the design of any interventions included: low-cost interventions; interventions perceived as fun and enjoyable; flexibly scheduled interventions, although the sessions should have structure; activities underpinned by health advice from a trusted source; encouragement by family and friends; and personal invitations to take part could be beneficial.
Chapter 6 Discussion and conclusions
This wide-ranging review of the literature on interventions for older adults identified a sizeable body of work and included 158 papers in the evidence synthesis, encompassing both quantitative data relating to the effectiveness of interventions and qualitative data outlining views and perceptions of older adults and service providers. Before further discussion of the review findings, we shall highlight challenges encountered in the identification and analysis of this literature.
The challenge of defining ‘retirement transition’
We searched for empirical work reporting the effectiveness of interventions for those about to retire or recently retired and views of older people regarding physical activity at or around the age of retirement. We were challenged by the scarcity of papers that included mention of retirement or ending work in the intervention studies or that focused on the retirement transition period and physical activity in the qualitative work. Although this research was carried out in older adult populations, the lack of attention to retirement transition in the literature was surprising. In order to overcome this limitation, we used the age range 50–69 years as a broad proxy for retirement transition and included papers with a participant average age in this range.
The dearth of studies referring to the period around retirement seems to be a key gap in the literature. Although it marks a significant transitional life point for an individual, it may offer challenges to researchers, because it can occur within a broad range of ages and has changed over time. Historically in the UK, retirement typically took place at the age of 60 years for women and 65 years for men, although this has recently changed and is likely to change further in the future. Currently, there is a range of models for ‘retirement’, encouraged to some extent by recent changes by the UK government to the age at which state pension can be claimed (to 66 years) and by the removal of the default ages of retirement. This means that individuals can work for longer and phase their retirement. Conversely, many people who can afford to do so retire earlier and/or move into part-time employment.
The challenge of defining and measuring ‘physical activity’
The included studies examined a wide range of outcomes relating to functional and recreational physical activities from walking and exercise classes to sport. Given that this review was exploring interventions with the aim of improving health and well-being, we included papers that discussed physical activity in its broadest sense. Some studies, for example, included physical activity such as housework, gardening and looking after children. In the qualitative literature the term ‘exercise’ was mainly perceived to be a structured form of physical activity carried out with the intention of becoming fitter or healthier. The term ‘exercise’ was therefore considered a subset of ‘physical activity’ (i.e. all exercise is physical activity but not all physical activity is exercise).
Although defining what precisely is meant by physical activity is challenging, the measurement of these outcomes also presents difficulties for researchers. Within the field there is a wealth of self-reported questionnaire measures available. Many of these have undergone extensive processes of validation and it is argued that they are accurate tools. However, there remains the potential for both over-reporting and under-reporting with these measures. We found a substantial range of different tools in use which evaluated different aspects of physical activity, including those assessing activity, physical outcomes and mental well-being. We found only two studies that included an assessment of sedentary behaviour. This relative lack of consideration of sedentary behaviour was surprising in view of the fact that there are a imitated number of hours available each day, and if physical activity time is increased, there is inevitably a reduction in time spent on other aspects of life. If this results in a reduction in sedentary behaviour such as sitting watching television, then this is a positive effect. However, if this reduction is in some other area such as food preparation time, socialising or resting, then this may be a less positive outcome.
An examination of the qualitative studies further indicates the challenge of identifying optimal outcomes. Older adults described a range of potential benefits of interventions which are much broader than activity-level outcomes. Engaging in physical activity could be important in terms of replacing aspects of working life such as having a routine, social interaction with colleagues, having a purpose to the day and contributing to a positive identity. The benefit of social interaction during or following activity sessions was suggested to be a key element, with increased well-being often perceived as the most important outcome.
Effectiveness of the interventions
Given the caveat that only one effectiveness study included in this review described its participants as being recently retired, we found that a range of interventions appeared to be effective for older adults of retirement age. Interventions delivered in the form of advice and counselling or via group/individual activity sessions all appeared to have the potential to increase physical activity levels in people around the age of retirement. There was also evidence that home-based interventions delivered via the telephone, via the internet or via post and including pedometers also could be effective in increasing physical activity levels. When considering the positive outcomes from all these types of intervention, the potential for publication bias (studies reporting positive outcomes are more likely to be published than those reporting no/negative outcomes) needs to be recognised. The stronger evidence in terms of number of studies, consistency, strength of design and objective measurement seemed to be for the group interventions and individual sessions.
Comparison of findings with other reviews in the area
We examined a number of potentially relevant existing reviews to explore how our findings resonated with this literature. We found two other review papers (by the same team) which specifically examined the retirement transition. 1,12 One other review had an age band roughly within our A2 category. 185 Three other reviews examined relationships/associations between life changes more generally (including retirement) and physical activity. 186–188 A third group of relevant reviews considered populations of older adults (without referring to retirement) using a range of age inclusion criteria,12,189–196 with one specifically focusing on the potential benefits of voluntary work. 190
The first of the two other reviews of the retirement transition1 examined 19 longitudinal or cross-sectional studies comparing retired adults with those not retired or longitudinal studies across the retirement transition (with no age parameters for inclusion set). This review reports associations and predictors of physical activity at retirement transition rather than evidence of effectiveness. The authors concluded that exercise and leisure time physical activity increase in retirement, although it was unclear whether or not there is a total increase in physical activity in retirement. With regard to inequalities, the study found that low SES was associated with a decrease in physical activity and higher SES with an increase. The review thus supports the need to further investigate the potential for interventions in this population. A companion review of qualitative studies examined five papers that referred to the transition to retirement. 12 Synthesis of these qualitative papers identified differing concepts of physical activity, as well as differing motivations for, and challenges to, physical activity in retirement. The authors compared findings between their two reviews and highlighted that factors influencing levels of physical activity around retirement may include expected health benefits; lifelong physical activity patterns; opportunities for socialising and personal challenges; desire for new routine; lack of time; and low perceived value of recreational physical activity. The results of the present review therefore support these findings with regard to the complexity of the relationship between retirement and physical activity and the role of socialising as a motivation for physical activity.
A recent review of RCTs evaluating behavioural interventions (advice/counselling)185 identified 32 papers (21 studies) reporting behavioural physical activity interventions in adults aged 55–70 years. They found that there was evidence of improvement in levels of physical activity for up to 12 months’ follow-up (pooled ES 0.19), although the effect was unclear beyond this. As with our review, they found that the mode of delivery did not seem to be important. However, in contrast to our findings, they highlighted in particular the benefits of individual tailoring and suggested that the type of intervention (walking vs. exercise classes) may be significant.
Allender et al. 186 searched for studies of any design reporting ‘life change events’ and participation in physical activity. Three of the included papers related to a change in employment status with, perhaps surprisingly, none relating to retirement; therefore, the review was unable to offer further insight into our findings. Engberg et al. 187 reviewed 11 longitudinal or cross-sectional studies relating to change in employment status and change in physical activity at any age (seven of these related to retirement). The review reports associational data rather than considers effectiveness and found that retirement was associated with an increase in physical activity in six included studies and a decline in physical activity in one paper. One study reported that women have less increase in physical activity following retirement than men, another found that both males and females were more likely to engage in sports activities in groups rather than alone, and two studies provided conflicting evidence on whether or not physical demands at work prior to retirement impacted on physical activity change after retirement. This work further supports our finding that socialising is an important element in participation in physical activity and also supports the idea that the retirement transition marks a point of change from previous levels of physical activity.
A review including 20 papers of any design188 explored health-promotion strategies implemented immediately before or following retirement. The review reports associations and predictors rather than effectiveness data and outlines age differences in the use of activity- or sports-related services (more use in those aged 65–74 years or older). This work supports the need for studies to differentiate between adults around the retirement transition and those who are considerably older when considering intervention design and effectiveness.
A number of other reviews considered populations of older adults. The most recent of these189 reviewed 17 papers (16 RCTs/quasi-experimental studies) evaluating the effectiveness of non-face-to-face interventions for physical activity in adults over 50 years of age. Similar to our findings, they found that a range of interventions could be effective, with 14 of the 17 primary studies reporting a significant short-term increase in physical activity, and eight of nine being effective in the longer term.
Von Bonsdorff and Rantanen190 examined 16 studies reporting voluntary work interventions in adults aged 60 years or over (only two described physical activity outcomes). This work supports the potential importance of sex/gender and cultural differences in the intervention design that we have suggested. The study found that men reported having more time for physical activity than women after retirement and that recreational physical activity was more socially acceptable among retired men than women. Accessibility and race barriers were reported, and those participating in wellness programmes before retirement were more likely to participate after.
Chase191 examined 20 studies of physical activity interventions in older adults aged 60 years and over. The review concluded that cognitive-only and combined cognitive–behavioural interventions were more successful in changing behaviour, with behavioural-only interventions leading to greater long-term changes in behaviour. A report from the Scottish Collaboration for Public Health Research and Policy192 provides an analysis of 15 reviews and one review of reviews of exercise and activity interventions in adults aged 50 years or over. Although only five of the studies included in this review are of direct relevance, the findings support our work in concluding that the most promising interventions are tailored to individuals and generate feelings of enjoyment and satisfaction.
A descriptive overview of physical activity intervention studies in older adults highlighted the importance of physical activity for well-being and that the elderly are particularly vulnerable to inequalities. 7 A review by Conn et al. ,193 analysed 17 RCT interventions in adults aged over 65 years. The authors of the review were unable to identify components or attributes of interventions linked to outcomes. In an earlier study, Conn et al. 194 reviewed 43 studies of physical activity interventions with control group designs in adults aged over 60 years. An analysis of the studies indicated an average ES across studies of 0.26 (CI 0.05) with larger ESs for patient populations, interventions without health education, those that focus specifically on activity, and studies with < 90 days’ follow-up. In the same year,195 another study reviewed 38 RCTs, with physical activity interventions in populations with an average age of 50 years or over (aged at least 40 years). They concluded that group-based and educational interventions were effective for physical activity in the short term and that there were limited data available for home-based interventions. They found that the effect for educational interventions may fade in the longer term and reported that the data were insufficient to make a judgement on the effectiveness of group-based interventions in the longer term. They found no evidence for behavioural reinforcement strategies (reminders) on effectiveness and that participation rates were comparable between group- and home-based interventions, although group-based interventions had higher participation in the long term. In the oldest of this group of papers, King et al. 196 examined 29 studies with a comparator group reporting physical activity interventions in adults aged over 50 years. This review highlighted gaps in evidence rather than evaluating effectiveness.
This group of reviews spanning nearly 15 years supports the findings of this review in providing evidence of the effectiveness of a range of interventions that aim to increase physical activity in older adults. The papers suggest that different types of interventions, including group-based and home-based interventions with behavioural/activity and/or educational/cognitive components may all be of benefit, although there may be variation in long-term effectiveness. These existing review studies included data from a wide age range of participants aged over 40 years, with no reviews specifically considering the effectiveness of interventions at the point of retirement transition. A number of papers echo the findings of the current review by highlighting sex/gender differences in patterns of physical activity following retirement, thus illustrating the need for a consideration of these variants in the design of optimal interventions.
Applicability to the UK
We found only three papers from the UK that met our A1/A2 inclusion criteria. A further four papers were in our A3 group. The largest proportion of studies originated from the USA and, thus, the applicability of this literature to the UK requires consideration. Although there may be differences between countries in terms of facilities available for older adults, there seem to be no factors in the reported interventions that would make them unsuitable or inapplicable to the UK context. Our applicability sessions, although carried out with only a small sample, support the findings of our review in that a range of interventions may be effective for people around retirement age, with group sessions and individual training often viewed as most preferable.
There were a larger number of UK papers in the qualitative literature. The views and perceptions in these papers were not at variance with papers that had participants from other countries. This suggests that there are no significant issues with applicability of the qualitative review findings to the UK. The applicability sessions that we carried out, although with small samples of participants, supported the results of the qualitative review in terms of the importance of social interaction and also highlighted individual variability in preferences.
Factors of implementation and acceptability and design of future interventions
Across the literature there was considerable variation in the reported uptake and retention of participants. Rates of uptake were typically in the region of 60–80% and follow-up rates ranged from 48% to 90%. Many studies recruited volunteer participants, which may have affected retention rates. The quality assessment table (see Appendix 2) reports studies in which these factors were of concern.
The qualitative papers outline factors of implementation and acceptability in detail and suggest factors that may be important in the content and implementation of interventions. The elements that are suggested as being particularly important to acceptability are: that the type of programme meets individual preferences; that it is in an accessible location; that it is low cost; and that it provides a social element.
Theoretical underpinnings of interventions
Just under two-thirds of the included intervention papers described a theoretical base for their study. These were mainly psychological theories such as stages of change, social cognitive theory, educational theories such as peer mentoring, or models specific to the motivation of active living. There was evidence from intervention studies for improvement in physical activity rates in older people participating in comparator conditions as well as interventions. It is therefore difficult to conclude how much impact was attributable to theoretical underpinning of interventions. Indeed, few included papers contained a discussion of how the chosen theory impacted on the results of their study. The impact of particular theoretical bases for interventions is an area that could be further assessed, although it was outside the scope of this review.
Issues of health inequalities
We found little intervention literature that provides insight into differential effects for advantaged versus disadvantaged populations. There was a very limited body of work carried out with participants who were described as being of low SES, lower education or ethnic minorities.
The qualitative literature provided a slightly larger number of papers with participants from minority ethnicity or low SES communities. The data highlight that physical activity interventions can be experienced differently across socioeconomic and ethnic groups. In some communities, there was a tension between time spent on oneself and prioritising the family. Findings suggested that motivation to begin exercise for those who have no or little experience can be daunting and that a personal invitation to attend can be encouraging. It was also suggested that trainers with a positive attitude who could motivate participants were particularly valued by those from communities in which taking part in physical activity activities was less familiar. Older participants from deprived areas were described as facing constraints on their access to physical activity opportunities owing to a number of factors including low income, which is likely to reduce further at retirement age; social norms that preclude the prioritisation of health promotion messages; and neighbourhood environments that feel unpleasant or unsafe.
Limitations
The most substantial limitation to the review was the lack of studies that identified their population as being about to retire or recently retired. Instead, the primary studies used age bands or average age to define populations, with few including any reference to employment/retirement characteristics, and, in those that did, this was often unclear. In view of this limitation in the primary studies, we developed an applicability rating which used these age ranges as a proxy for retirement age. Given the findings of the initial consultation exercise (i.e. that retirement transition occurs over a period of time, rather than in a particular year), we believe that the adoption of these age bands as proxy retirement transition windows is an appropriate approach.
The adoption of an age range proxy for retirement transition enabled the inclusion of a sizeable literature with review findings based on data from a substantial number of published studies and encompassing both quantitative and qualitative evidence. The review excluded interventions targeted at clinical populations and those described as being delivered to participants who were elderly/frail/with limited mobility. Although we argue that these exclusions are valid, particularly within the context of a more general public health approach, it is possible that the review may have missed important relevant evidence and thus may have restricted its ability to comment on health or social inequalities which may be apparent and identifiable in clinical groups. In addition, the review may be limited by including only work with an abstract in English. The work was inclusive in terms of considering a range of study designs, encompassing both controlled and non-comparator studies. The body of work that we included encompassed studies that were of both higher and lower quality. We considered whether or not to use a quality criterion as a basis for rejection. However, this would have precluded analysis and reporting of a large quantity of literature and we intended to produce a comprehensive review of the area. In reporting the results, we have detailed and fully considered the quality of the studies.
We included studies that had the intention of either improving or maintaining physical activity, although this distinction tended to be unclear in the literature. Given the dearth of evidence regarding the retirement transition we were unable to explore whether or not physical activity levels were improved or maintained by interventions. The review also focused on physical activity rather than on interventions to reduce inactivity. We have commented on the few studies that used measures of sedentary behaviour as outcomes. A review specifically focusing on interventions to reduce sedentary behaviour may identify a different body of work.
We had intended to carry out a meta-analysis of the effectiveness data. The heterogeneous nature of the literature in terms of intervention types, limited number of studies with no-intervention comparator groups and variability in outcome reporting meant instead that a narrative synthesis was most appropriate. In addition, the lack of mixed-method designs and qualitative papers that described specific interventions precluded our planned meta-synthesis approach, which juxtaposes quantitative and qualitative results. Instead of using qualitative data to add further interpretation of intervention outcomes, we instead used the qualitative data to underpin our analysis of intervention content which we believe provided a useful approach to meta-synthesis across data types and aided understanding of the review findings.
Recommendations for research
-
Studies are needed that are carried out specifically in adults in the period immediately before or shortly after retirement. This work is needed in order to evaluate if existing interventions for older adults are most suitable and/or effective in adults who are about to retire or recently retired. Currently, it is not known whether or not the retirement transition provides a key opportunity for interventions to effect change in physical activity levels throughout older life.
-
Studies that are carried out in older adults should include reference to the retirement status of participants when reporting the characteristics of participants.
-
Future reviews may be needed to evaluate interventions in clinical groups and to explore the potential impact of these on health or social inequalities.
-
Future studies should include objective measures of activity and not be reliant on self-report data. Although it is recognised that the collection of daily activity levels presents challenges, technology such as pedometers is widely available which can collect objective data to supplement self-reported measures.
-
In addition to including measured as well as self-reported evaluation, there is a need for studies to include no-intervention rather than comparator-intervention control arms. The review found a large proportion of studies using several intervention arms rather than no-intervention control groups. There was evidence of a Hawthorne effect in some studies using no-intervention arms, and this potential bias towards underestimating the impact of interventions owing to behaviour change in the comparison group needs to be considered fully in the analysis and reporting of results.
-
There is currently a diverse range of outcome measures in use, including those that relate to levels of activity, levels of fitness, psychosocial elements and correlates of physical activity. If the effectiveness of different interventions is to be compared, there needs to be greater agreement among researchers regarding key measures of change. The Core Outcome Measures in Effectiveness Trials initiative197 is aiming to develop agreed standardised sets of outcomes, known as a ‘core outcome set’, and our review supports the need for this work. There seems to be uncertainty regarding the central aim of physical activity – for example, is the purpose to increase activity levels, to increase well-being, to reduce sedentary behaviour or to form part of a broader healthier lifestyle which would also include increasing social interaction and connectivity in retirement?
-
Future research should further consider the meaningfulness of outcome measures in use and consider inclusion of measures of sedentary behaviour in order to further investigate potential benefits and costs where increasing time for physical activity is replacing other activities (both active and sedentary).
-
Future research should consider the views and perceptions of the target population in the development and introduction of interventions. Although social elements were described as important (particularly for women), few studies outlined this as being a core aspect of interventions. A key theme in the qualitative data was the need for interventions to be viewed as attractive to potential participants and sensitive to sex/gender, age and culture. There was also a need also for programmes to be perceived to be enjoyable. Few interventions described these aspects as important in their design.
-
A large proportion of studies had been carried out with predominantly female participants. There is a gap in evidence regarding interventions for males. There was evidence that the different sexes may benefit from interventions tailored to them; for example, women enjoyed social aspects, whereas men may prefer individual programmes. Again, future interventions should explore the potential importance of tailoring interventions by sex/gender or by culture.
Implications for health care
-
There are currently few data available regarding the effectiveness of interventions that aim to maintain or enhance physical activity in adults around the time of retirement. It is, therefore, not possible to make conclusive recommendations beyond indicating that a range of interventions, including individual and group programmes, may be effective in this population.
-
Interventions that currently exist for older adults require robust evaluation in order to determine suitability for use in those around retirement transition.
-
Factors that may be associated with enhanced outcomes following intervention may be: inclusion of a social element; free or low cost; and being perceived as attractive to an individual. There was individual variation in preferences for type of activity, with a need to offer a range of options for individuals to select from rather than a ‘one size fits all’ approach.
-
There is currently a dearth of evidence to inform selection and implementation of interventions that may reduce differences in levels of physical activity following retirement and impact on health inequalities. Qualitative evidence suggests the importance of interventions being perceived as appropriate for sex/gender and culture. However, this aspect was examined to only a small extent in the identified literature.
-
There is currently uncertainty regarding the aims of physical activity and whether or not the principal intended outcomes relate to increased activity, reduced sedentary behaviour, health outcomes or enhanced well-being more broadly.
Acknowledgements
We wish to express our thanks to the members of our advisory group for their valuable expertise and input: Mrs Susan Battersby; Dr Amanda Daley; Dr Michael Hannon; Dr Myfanwy Lloyd Jones; Professor John Parker; Dr Toby Pavey; Dr Adrian Taylor. Dr Duncan Chambers provided assistance with exploring the potential for meta-analysis and the use of Harvest plots.
Contributions of authors
Susan Baxter (Research Fellow) was Principal Investigator from the seventh month to the end of the study, led the review of effectiveness in this time period and took the lead in drafting the report.
Lindsay Blank (Research Fellow) was Principal Investigator during the study development period and early phase, and led the review of effectiveness during the first 6 months.
Maxine Johnson (Research Fellow) led the review of qualitative evidence and drafted the qualitative chapter of the report.
Emma Everson-Hock (Research Fellow) was involved in writing the proposal and contributed to the effectiveness review in the early phases of the study.
Helen Buckley-Woods (Information Specialist) developed the search strategy and led the searching and identification of literature.
Elizabeth Goyder (Professor of Public Health) provided topic expertise in physical activity interventions and senior-level advisory input to study methodology.
Nick Payne (Honorary Professor of Public Health) provided senior-level advisory input to all aspects of the study.
Gail Mountain (Professor of Health Services Research) provided topic expertise in research on older adults.
Data sharing statement
This is an evidence synthesis and the data generated are largely described in the report. Further information can be obtained from the corresponding author.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health.
References
- Barnett I, Ogilvie D, Guell C. Physical activity and transitioning to retirement: a systematic review. Am J Prev Med 2012;43:329-36. http://dx.doi.org/10.1016/j.amepre.2012.05.026.
- Emmerson C, Heald K, Hood A. The Changing Face of Retirement: Future Patterns Of Work, Health, Care and Income Among the Older Population. London: Institute for Fiscal Studies; 2014.
- Bélanger M, Townsend N, Foster C. Age-related differences in physical activity profiles of English adults. Prev Med 2011;52:247-9. http://dx.doi.org/10.1016/j.ypmed.2011.02.008.
- Demakakos P, Hamer M, Stamatakis E, Steptoe A. Low-intensity physical activity is associated with reduced risk of incident type 2 diabetes in older adults: evidence from the English Longitudinal Study of Ageing. Diabetologia 2010;53:1877-85. http://dx.doi.org/10.1007/s00125-010-1785-x.
- Warburton D, Nicol CW, Bredin S. Health benefits of physical activity: the evidence. Can Med Assoc J 2006;174:801-9. http://dx.doi.org/10.1503/cmaj.051351.
- Stein C, Colditz G. Modifiable risk factors for cancer. Br J Cancer 2004;90:299-303. http://dx.doi.org/10.1038/sj.bjc.6601509.
- Taylor A, Cable N, Faulkner G, Hillsdon M, Narici M, Van Der Bij A. Physical activity and older adults: a review of health benefits and the effectiveness of interventions. J Sports Sci 2004;22:703-25. http://dx.doi.org/10.1080/02640410410001712421.
- Acree LS, Longfors J, Fjeldstad AS, Fjeldstad C, Schank B, Nickel KJ, et al. Physical activity is related to quality of life in older adults. Health Qual Life Out 2006;4:37-43. http://dx.doi.org/10.1186/1477-7525-4-37.
- Harris TJ, Owen CG, Victor CR, Adams R, Cook DG. What factors are associated with physical activity in older people, assessed objectively by accelerometry?. Br J Sports Med 2009;43:442-50. http://dx.doi.org/10.1136/bjsm.2008.048033.
- Troiano RP, Berrigan D, Dodd KW, Mãsse LC, Tilert T, McDowell M. Physical activity in the United States measured by accelerometer. Med Sci Sports Exerc 2008;40:181-8. http://dx.doi.org/10.1249/mss.0b013e31815a51b3.
- ONS National Population Projections. London: Office for National Statistics; 2013.
- Barnett I, Guell C, Ogilvie D. The experience of physical activity and the transition to retirement: a systematic review and integrative synthesis of qualitative and quantitative evidence. Int J Behav Nutr Phys Act 2012;9. http://dx.doi.org/10.1186/1479-5868-9-97.
- Grundy E, Sloggett A. Health inequalities in the older population: the role of personal capital, social resources and socio-economic circumstances. Soc Sci Med 2003;56:935-47. http://dx.doi.org/10.1016/S0277-9536(02)00093-X.
- Systematic Reviews – CRD’s Guidance for Undertaking Systematic Reviews in Healthcare. York: Centre for Reviews and Dissemination, University of York; 2009.
- Moher D, Liberati A, Tetzlaff J, Altmann D. PRISMA Group . Preferred reporting items for systematic reviews and meta-analyses: the PRISMA guidelines. BMJ 2009;339:332-6. http://dx.doi.org/10.1136/bmj.b2535.
- Grant MJ, Brettle A, Long AF. Developing a Review Question: A Spiral Approach to Literature Searching n.d.
- Greenhalgh T, Peacock R. Effectiveness and efficiency of search methods in systematic reviews of complex evidence: audit of primary sources. BMJ 2005;331. http://dx.doi.org/10.1136/bmj.38636.593461.68.
- Papaioannou D, Sutton A, Carroll C, Booth A, Wong R. Literature searching for social science systematic reviews: consideration of a range of search techniques. Health Info Libr J 2010;27:114-22. http://dx.doi.org/10.1111/j.1471-1842.2009.00863.x.
- World Health Organization . Physical Activity, Fact Sheet Number 385 January 2015 n.d. www.who.int/mediacentre/factsheets/fs385/en/ (accessed 25 March 2015).
- Pensions at a Glance: OECD and G20 Indicators. OECD Publishing; 2013.
- Cochrane Collaboration . Cochrane Handbook for Systematic Reviews of Interventions, Cochrane Collaboration 2011. www.cochrane-handbook.org (accessed 4 September 2012).
- CASP Qualitative Checklist. CASP UK; 2013.
- Ogilvie D, Fayter D, Petticrew M, Sowden A, Thomas S, Whitehead M, et al. The harvest plot: A method for synthesising evidence about the differential effects of interventions. BMC Med Res Methodol 2008;8. http://dx.doi.org/10.1186/1471-2288-8-8.
- Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol 2008;8. http://dx.doi.org/10.1186/1471-2288-8-45.
- Oliver S, Harden A, Rees R, Shepherd J, Brunton G, Garcia J, et al. An emerging framework for including different types of evidence in systematic reviews for public policy. Evaluation 2005;11:428-46. http://dx.doi.org/10.1177/1356389005059383.
- Thomas J, Harden A, Oakley A, Oliver S, Sutcliffe K, Rees R, et al. Integrating qualitative research with trials in systematic reviews. BMJ 2004;328:1010-12. http://dx.doi.org/10.1136/bmj.328.7446.1010.
- Ackermann RT, Deyo RA, LoGerfo JP. Prompting primary providers to increase community exercise referrals for older adults: a randomized trial. J Am Geriatr Soc 2005;53:283-9. http://dx.doi.org/10.1111/j.1532-5415.2005.53115.x.
- Armit CM, Brown WJ, Ritchie CB, Trost SG. Promoting physical activity to older adults: a preliminary evaluation of three general practice-based strategies. J Sci Med Sport 2005;8:446-50. http://dx.doi.org/10.1016/S1440-2440(05)80060-X.
- Burman MP, Giacobbi PR, Dzierzewski JM, Morgan A, Aiken CS, McCrae BL, et al. Peer volunteers improve long-term maintenance of physical activity with older adults: a randomized controlled trial. J Phys Act Health 2011;8:S257-S266.
- Burke L, Lee AH, Jancey J, Xiang L, Kerr DA, Howat PA, et al. Physical activity and nutrition behavioural outcomes of a home-based intervention program for seniors: a randomized controlled trial. Int J Behav Nutr Phys Act 2013;10. http://dx.doi.org/10.1186/1479-5868-10-14.
- Caperchione C, Mummery K. The utilisation of group process strategies as an intervention tool for the promotion of health-related physical activity in older adults. Act Adapt Aging 2006;30:29-45. http://dx.doi.org/10.1300/j016v30n04_03.
- Castro CM, King AC, Brassington GS. Telephone versus mail interventions for maintenance of physical activity in older adults. Health Psychol 2001;20. http://dx.doi.org/10.1037/0278-6133.20.6.438.
- Coronini-Cronberg S, Millett C, Laverty AA, Webb E. The impact of a free older persons’ bus pass on active travel and regular walking in England. Am J Public Health 2012;102:2141-8. http://dx.doi.org/10.2105/AJPH.2012.300946.
- Costanzo C, Walker SN. Incorporating self-efficacy and interpersonal support in an intervention to increase physical activity in older women. Women Health 2008;47:91-108. http://dx.doi.org/10.1080/03630240802100747.
- Cox KL, Burke V, Beilin LJ, Derbyshire AJ, Grove JR, Blanksby BA, et al. Short and long-term adherence to swimming and walking programs in older women – the Sedentary Women Exercise Adherence Trial (SWEAT 2). Prev Med 2008;46:511-17. http://dx.doi.org/10.1016/j.ypmed.2008.01.010.
- Croteau KA, Suresh V, Farnham E. Efficacy of using physical activity mentors to increase the daily steps of older adults in the primary care setting: a pilot study. J Aging Phys Act 2014;22:16-24. http://dx.doi.org/10.1123/JAPA.2012-0120.
- de Jong J, Lemmink KA, Stevens M, de Greef MH, Rispens P, King AC, et al. Six-month effects of the Groningen active living model (GALM) on physical activity, health and fitness outcomes in sedentary and underactive older adults aged 55–65. Patient Educ Couns 2006;62:132-41. http://dx.doi.org/10.1016/j.pec.2005.06.017.
- de Jong J, Lemmink KA, King AC, Huisman M, Stevens M. Twelve-month effects of the Groningen active living model (GALM) on physical activity, health and fitness outcomes in sedentary and underactive older adults aged 55–65. Patient Educ Couns 2007;66:167-76. http://dx.doi.org/10.1016/j.pec.2006.11.008.
- Dorgo SG, King AC, Brickey GD. The application of peer mentoring to improve fitness in older adults. J Aging Phys Act 2009;17:344-61.
- Elley CR, Kerse N, Arroll B, Robinson E. Effectiveness of counselling patients on physical activity in general practice: cluster randomised controlled trial. BMJ 2003;326. http://dx.doi.org/10.1136/bmj.326.7393.793.
- Finkelstein EA, Brown DS, Brown DR, Buchner DM. A randomized study of financial incentives to increase physical activity among sedentary older adults. Prev Med 2008;47:182-7. http://dx.doi.org/10.1016/j.ypmed.2008.05.002.
- Fries JF, Bloch DA, Harrington H, Richardson N, Beck R. Two year results of a randomized controlled trial of a health promotion program in a retiree population: the Bank of America study. Am J Med 1993;94:455-62. http://dx.doi.org/10.1016/0002-9343(93)90078-4.
- Fries JF, Tilton-Fries S, Percell CL, Harrington H. Health Risk Changes with a low-cost individual health promotion program: effects at up to 30 months. Am J Health Promotion 1993;6:363-71.
- Fujita KR, Nagatomi A, Hozawa T, Ohkubo K, Sato Y, Anzai C, et al. Effects of exercise training on physical activity in older people: a randomized controlled trial. J Epidemiol 2003;13:120-6. http://dx.doi.org/10.2188/jea.13.120.
- Goldstein MG, Pinto BM, Marcus BM, Lynn H, Jette AM, Rakowski W, et al. Physician-based physical activity counseling for middle-aged and older adults: a randomized trial. Ann Behav Med 1999;21:40-7. http://dx.doi.org/10.1007/BF02895032.
- Hageman PA, Walker SN, Pullen CH. Tailored versus standard internet-delivered interventions to promote physical activity in older women. J Geriatr Phys Ther 2005;28:28-33. http://dx.doi.org/10.1519/00139143-200504000-00005.
- Halbert JA, Silagy CA, Finucane PM, Withers RT, Hamdorf PA. Physical activity and cardiovascular risk factors: effect of advice from an exercise specialist in Australian general practice. Med J Austral 2000;173:84-7.
- Hamdorf PA, Withers RT, Penhall RK, Haslam MV. Physical training effects on the fitness and habitual activity patterns of elderly women. Arch Phys Med Rehabil 1992;73:603-8.
- Hamdorf PA, Withers RT, Penhall RK, Plummer JL. A follow-up study on the effects of training on the fitness and habitual activity patterns of 60-to 70-year-old women. Arch Phys Med Rehabil 1993;74. http://dx.doi.org/10.1016/0003-9993(93)90108-M.
- Hekler EB, Castro CM, Buman MP, King AC. The CHOICE study: a ‘taste-test’ of utilitarian vs. leisure walking among older adults. Health Psychol 2012;31:126-9. http://dx.doi.org/10.1037/a0025567.
- Hooker SP, Seavey W, Weidmer CE, Harvey DJ, Stewart AL, Gillis DE, et al. The California active aging community grant program: translating science into practice to promote physical activity in older adults. Ann Behav Med 2005;29:155-65. http://dx.doi.org/10.1207/s15324796abm2903_1.
- Hughes SL, Seymour RB, Campbell RT, Whitelaw N, Bazzarre T. Best-practice physical activity programs for older adults: findings from the national impact study. Am J Public Health 2009;99:362-8. http://dx.doi.org/10.2105/AJPH.2007.131466.
- Irvine AB, Gelatt VA, Seeley JR, Macfarlane P, Gau JM. Web-based intervention to promote physical activity by sedentary older adults: randomized controlled trial. J Med Internet Res 2013;15. http://dx.doi.org/10.2196/jmir.2158.
- Kamada MJ, Kitayuguchi J, Inoue S, Ishikawa Y, Nishiuchi H, Okada S, et al. A community-wide campaign to promote physical activity in middle-aged and elderly people: a cluster randomized controlled trial. Int J Behav Nutr Phys Act 2013;10. http://dx.doi.org/10.1186/1479-5868-10-44.
- King AC, Friedman R, Marcus B, Castro C, Forsyth L, Napolitano M, et al. Harnessing motivational forces in the promotion of physical activity: the Community Health Advice by Telephone (CHAT) project. Health Educ Res 2002;17:627-36. http://dx.doi.org/10.1093/her/17.5.627.
- King AC, Pruitt LA, Phillips W, Oka R, Rodenburg A, Haskell WL. Comparative effects of two physical activity programs on measured and perceived physical functioning and other health-related quality of life outcomes in older adults. J Gerontol A Biol Sci Med Sci 2000;55:M74-M83. http://dx.doi.org/10.1093/gerona/55.2.M74.
- King AC, Friedman R, Marcus M, Castro C, Napolitano M, Ahn D, et al. Ongoing physical activity advice by humans versus computers: the community health advice by telephone (CHAT) trial. Health Psychol 2007;26. http://dx.doi.org/10.1037/0278-6133.26.6.718.
- Koizumi D, Rogers NL, Rogers ME, Islam MM, Kusunoki M, Takeshima N. Efficacy of an accelerometer-guided physical activity intervention in community-dwelling older women. J Phys Act Health 2009;6:467-74.
- Lawton BA, Rose SB, Elley CR, Dowell AC, Fenton F, Moyes SA, et al. Exercise on prescription for women aged 40–74 recruited through primary care: two year randomised controlled trial. BMJ n.d.;337. http://dx.doi.org/10.1136/bmj.a2509.
- Marcus B, Goldstein M, Jette J, Simkin-Silverman L, Pinto B, Milan FB, et al. Training physicians to conduct physical activity counselling. Prev Med 1997;26:382-8. http://dx.doi.org/10.1006/pmed.1997.0158.
- Martinson BC, Sherwood NE, Crain AL, Hayes MG, King AC, Pronk NP, et al. Maintaining physical activity among older adults: 24-month outcomes of the keep active Minnesota randomized controlled trial. Prev Med 2010;51:37-44. http://dx.doi.org/10.1016/j.ypmed.2010.04.002.
- Martinson BC, Crain AL, Sherwood NE, Hayes M, Pronk NP, O’Connor PJ. Maintaining physical activity among older adults: six month outcomes of the keep active Minnesota randomized controlled trial. Prev Med 2008;46:111-19. http://dx.doi.org/10.1016/j.ypmed.2007.08.007.
- Opdenacker J, Delecluse C, Boen F. A 2-year follow-up of a lifestyle physical activity versus a structured exercise intervention in older adults. J Am Geriatr Soc 2011;59:1602-11. http://dx.doi.org/10.1111/j.1532-5415.2011.03551.x.
- Opdenacker J, Boen F, Coorevits N, Delecluse C. Effectiveness of a lifestyle intervention and a structured exercise intervention in older adults. Prev Med 2008;46:518-24. http://dx.doi.org/10.1016/j.ypmed.2008.02.017.
- Pasalich M, Lee AH, Jancey J, Burke L, Howat P. Sustainability of a physical activity and nutrition program for seniors. J Nutr Health Aging 2013;17:486-91. http://dx.doi.org/10.1007/s12603-012-0433-1.
- Peels DA, van Stralen M, Bolman C, Golsteijn RH, de Vries H, Mudde AN, et al. Development of web-based computer-tailored advice to promote physical activity among people older than 50 years. J Med Internet Res 2012;14. http://dx.doi.org/10.2196/jmir.1742.
- Peels DA, Bolman C, Golsteijn RHJ, de Vries H, Mudde AN, van Stralen MM, et al. Differences in reach and attrition between web-based and print-delivered tailored interventions among adults over 50 years of age: clustered randomized trial. J Med Internet Res 2012;14:146-58. http://dx.doi.org/10.2196/jmir.2229.
- Peels DA, Bolman C, Golsteijn RHJ, de Vries H, Mudde AN, van Stralen MM, et al. Long-term efficacy of a printed or a web-based tailored physical activity intervention among older adults. Int J Behav Nutr Phys Act 2013;10. http://dx.doi.org/10.1186/1479-5868-10-104.
- Pereira MA, Kriska AM, Day RD, Cauley JA, LaPorte RE, Kuller LH. A randomized walking trial in postmenopausal women: effects on physical activity and health 10 years later. Arch Intern Med 1998;158:1695-701. http://dx.doi.org/10.1001/archinte.158.15.1695.
- Petrella RJ, Lattanzio CN, Shapiro S, Overend T. Improving aerobic fitness in older adults: effects of a physician-based exercise counseling and prescription program. Can Fam Physician 2010;56:e191-e200.
- Pinto BM, Goldstein MG, Ashba J, Sciamanna CN, Jette A. Randomized controlled trial of physical activity counseling for older primary care patients. Am J Prev Med 2005;29:247-55. http://dx.doi.org/10.1016/j.amepre.2005.06.016.
- Prabu D, Buckworth J, Pennell ML, Katz ML, DeGraffinreid CR, Paskett ED. A walking intervention for postmenopausal women using mobile phones and Interactive Voice Response. J Telemed Telecare 2012;18:20-5. http://dx.doi.org/10.1258/jtt.2011.110311.
- Purath J, Keller CS, McPherson S, Ainsworth B, Purath J, Keller CS, et al. A randomized controlled trial of an office-based physical activity and physical fitness intervention for older adults. Geriatr Nurs 2013;34:204-11. http://dx.doi.org/10.1016/j.gerinurse.2013.02.012.
- Rowland L, Dickinson EJ, Newman P, Ford D, Ebrahim S. Look after your heart programme: impact on health status, exercise knowledge, attitudes, and behaviour of retired women in England. J Epidemiol Comm Health 1994;48:123-8. http://dx.doi.org/10.1136/jech.48.2.123.
- Sawchuk CN, Charles S, Wen Y, Goldberg J, Forquera R, Roy-Byrne P, et al. A randomized trial to increase physical activity among native elders. Prev Med 2008;47:89-94. http://dx.doi.org/10.1016/j.ypmed.2008.03.011.
- Stevens W, Hillsdon M, Thorogood M, McArdle D. Cost-effectiveness of a primary care based physical activity intervention in 45–74 year old men and women: a randomised controlled trial. Br J Sports Med 1998;32:236-41. http://dx.doi.org/10.1136/bjsm.32.3.236.
- Strath SJ, Swartz AM, Parker SJ, Miller NE, Grimm EK, Cashin SE. A pilot randomized controlled trial evaluating motivationally matched pedometer feedback to increase physical activity behavior in older adults. J Phys Act Health 2011;8:S267-S274.
- van Keulen HM, Mesters I, Ausems M, Van Breukelen G, Campbell M, Resnicow K, et al. Tailored print communication and telephone motivational interviewing are equally successful in improving multiple lifestyle behaviors in a randomized controlled trial. Ann Behav Med 2011;41:104-18. http://dx.doi.org/10.1007/s12160-010-9231-3.
- van Stralen M, de Vries H, Mudde AN, Bolman C, Lechner L. Efficacy of two tailored interventions promoting physical activity in older adults. Am J Prev Med 2009;37:405-17. http://dx.doi.org/10.1016/j.amepre.2009.07.009.
- van Stralen M, de Vries H, Bolman C, Mudde AN, Lechner L. Exploring the efficacy and moderators of two computer-tailored physical activity interventions for older adults: a randomized controlled trial. Ann Behav Med 2010;39:139-50. http://dx.doi.org/10.1007/s12160-010-9166-8.
- van Stralen M, de Vries H, Mudde AN, Bolma C, Lechner L. The long-term efficacy of two computer-tailored physical activity interventions for older adults: main effects and mediators. Health Psychol 2011;30:442-52. http://dx.doi.org/10.1037/a0023579.
- van Stralen M, de Vries H, Mudde AN, Bolman C, Lechner L. The working mechanisms of an environmentally tailored physical activity intervention for older adults: a randomized controlled trial. Int J Behav Nutr Phys Act 2009;6. http://dx.doi.org/10.1186/1479-5868-6-83.
- Walker SN, Pullen CH, Boeckner L, Hageman PA, Hertzog M, Oberdorfer MK, et al. Clinical trial of tailored activity and eating newsletters with older rural women. Nurs Res 2009;58:74-85. http://dx.doi.org/10.1097/NNR.0b013e31818fcee1.
- Walker SN, Pullen CH, Hageman PA, Boeckner LS, Hertzog M, Oberdorfer MK, et al. Maintenance of activity and eating change after a clinical trial of tailored newsletters with older rural women. Nurs Res 2010;59:311-21. http://dx.doi.org/10.1097/NNR.0b013e3181ed6695.
- Werkman A, Hulshof PJ, Stafleu A, Kremers SP, Kok FJ, Schouten EG, et al. Effect of an individually tailored one-year energy balance programme on body weight, body composition and lifestyle in recent retirees: a cluster randomised controlled trial. BMC Pub Health 2010;10. http://dx.doi.org/10.1186/1471-2458-10-110.
- Wijsman CA, Westendorp RG, Verhagen EA, Catt M, Slagboom PE, de Craen AJ, et al. Effects of a web-based intervention on physical activity and metabolism in older adults: randomized controlled trial. J Med Internet Res 2013;15. http://dx.doi.org/10.2196/jmir.2843.
- Wilcox S, Dowda M, Leviton LC, Bartlett-Prescott J, Bazzarre T, Campbell-Voytal K, et al. Active for life – final results from the translation of two physical activity programs. Am J Prev Med 2008;35:340-51. http://dx.doi.org/10.1016/j.amepre.2008.07.001.
- Wilcox S, Dowda M, Wegley S, Ory MG. Maintenance of change in the active-for-life initiative. Am J Prev Med 2009;37:501-4. http://dx.doi.org/10.1016/j.amepre.2009.07.016.
- Wilcox S, Dowda M, Dunn A, Ory MG, Rheaume C, King AC. Predictors of increased physical activity in the active for life program. Prev Chronic Dis 2009;6.
- Wilcox S, Dowda M, Griffin SF, Rheaume C, Ory MG, Leviton L, et al. Results of the first year of active for life: translation of 2 evidence-based physical activity programs for older adults into community settings. Am J Public Health 2006;96:1201-9. http://dx.doi.org/10.2105/AJPH.2005.074690.
- Anderson KJ, Pullen CH. Physical activity with spiritual strategies intervention. Res Gerentol Nurs 2013;6:11-2. http://dx.doi.org/10.3928/19404921-20121203-01.
- Age UK. Fit as a Fiddle. London: Age UK; 2012.
- Bickmore TW, Silliman RA, Nelson K, Cheng DM, Winter M, Henault L, et al. A randomized controlled trial of an automated exercise coach for older adults. J Am Geriatr Soc 2013;61:1676-83. http://dx.doi.org/10.1111/jgs.12449.
- Borschmann K, Moore K, Russell M, Ledgerwood K, Renehan E, Lin X, et al. Overcoming barriers to physical activity among culturally and linguistically diverse older adults: a randomised controlled trial. Australas J Ageing 2010;29:77-80. http://dx.doi.org/10.1111/j.1741-6612.2009.00390.x.
- Brassington GS, Atienza A, Perczck RE, DiLorenzo TN, King AC. Intervention-related cognitive versus social mediators of exercise adherence in the elderly. Am J Prev Med 2002;23:80-6. http://dx.doi.org/10.1016/S0749-3797(02)00477-4.
- Brawley LR, Rejeski WJ, Lutes L. A group-mediated cognitive-behavioral intervention for increasing adherence to physical activity in older adults. J Appl Biobehav Res 2000;5:47-65. http://dx.doi.org/10.1111/j.1751-9861.2000.tb00063.x.
- Croteau KA, Richeson NE, Farmer BC, Jones DB. Effect of a pedometer-based intervention on daily step counts of community-dwelling older adults. Res Q Exerc Sport 2007;78:401-6. http://dx.doi.org/10.1080/02701367.2007.10599439.
- de Vreede PL, van Meeteren NL, Samson MM, Wittink HM, Duursma SA, Verhaar HJ. The effect of functional tasks exercise and resistance exercise on health-related quality of life and physical activity – a randomised controlled trial. Gerontology 2007;53:12-20. http://dx.doi.org/10.1159/000095387.
- Duru OK, Sarkisian CA, Leng M, Mangione CM. Sisters in motion: a randomized controlled trial of a faith-based physical activity intervention. J Am Geriatr Soc 2010;58:1863-9. http://dx.doi.org/10.1111/j.1532-5415.2010.03082.x.
- Elder JP, Williams SJ, Drew JA, Wright BL, Boulan TE. Longitudinal effects of preventive services on health behaviors among an elderly cohort. Am J Prev Med 1994;11:354-9.
- Iliffe S, Kendrick D, Morris R, Masud T, Gage H, Skelton D, et al. Multicentre cluster randomised trial comparing a community group exercise programme and home-based exercise with usual care for people aged 65 years and over in primary care. Health Technol Assess 2014;18. http://dx.doi.org/10.3310/hta18490.
- Jancey JM, Lee AH, Howat PA, Clarke A, Wang K, Shilton T. The effectiveness of a physical activity intervention for seniors. Am J Health Promot 2008;22:318-21. http://dx.doi.org/10.4278/ajhp.22.5.318.
- Kerse N, Elley CR, Robinson E, Arroll B. Is physical activity counseling effective for older people? A cluster randomized, controlled trial in primary care. J Am Geriatr Soc 2005;53:1951-6. http://dx.doi.org/10.1111/j.1532-5415.2005.00466.x.
- Kerse NM, Flicker L, Jolley D, Arroll B, Young D. Improving the health behaviours of elderly people: randomised controlled trial of a general practice education programme. BMJ 1999;319:683-7. http://dx.doi.org/10.1136/bmj.319.7211.683.
- Kim BH, Glanz K. Text messaging to motivate walking in older African Americans: a randomized controlled trial. Am J Prev Med 2013;44:71-5. http://dx.doi.org/10.1016/j.amepre.2012.09.050.
- Kim BH, Newton RA, Sachs ML, Giacobbi PR, Glutting JJ. The effect of guided relaxation and exercise imagery on self-reported leisure-time exercise behaviors in older adults. J Aging Phys Act 2011;19:137-46.
- Kolt GS, Oliver M, Schofield GM, Kerse N, Garrett N, Latham NK. An overview and process evaluation of TeleWalk: a telephone-based counseling intervention to encourage walking in older adults. Health Promot Int 2006;21:201-8. http://dx.doi.org/10.1093/heapro/dal015.
- Marki A, Bauer GB, Angst F, Nigg CR, Gillmann G, Gehring TM. Systematic counselling by general practitioners for promoting physical activity in elderly patients: a feasibility study. Swiss Med Wkly 2006;136:482-8.
- Marki A, Bauer GB, Angst F, Nigg CR, Gillmann G, Gehring TM. Transtheoretical model-based exercise counselling for older adults in Switzerland: quantitative results over a 1-year period. Soz Praventiv Med 2006;51:273-80. http://dx.doi.org/10.1007/s00038-006-5065-y.
- Mutrie N, Doolin O, Fitzsimons CF, Grant PM, Granat M, Grealy M. Increasing older adults’ walking through primary care: results of a pilot randomized controlled trial. Fam Pract 2012;29:633-42. http://dx.doi.org/10.1093/fampra/cms038.
- Pelssers J, Delecluse C, Opdenacker J, Kennis E, van Roie E, Boen F. ‘Every step counts!’ Effects of a structured walking intervention in a community-based senior organization. J Aging Phys Act 2013;21:167-85.
- Pfeiffer BA, Clay SW, Conatser RR. A green prescription study: does written exercise prescribed by a physician result in increased physical activity among older adults?. J Aging Health 2001;13:527-38. http://dx.doi.org/10.1177/089826430101300405.
- Solberg PA, Halvari H, Ommundsen Y, Hopkins WG. A 1-year follow-up on effects of exercise programs on well-being in older adults. J Aging Phys Act 2014;22:52-64. http://dx.doi.org/10.1123/JAPA.2012-0181.
- Stewart AL, Verboncoeur CJ, McLellan BY, Gillis DE, Rush S, Mills KM, et al. Physical activity outcomes of CHAMPS II: A physical activity promotion program for older adults. J Gerontol A Biol Sci Med Sci 2001;56:M465-M470. http://dx.doi.org/10.1093/gerona/56.8.M465.
- Tan EJ, Xue QL, Li T, Carlson MC, Fried LP. Volunteering: a physical activity intervention for older adults – the experience corps (r) program in Baltimore. J Urban Health 2006;83:954-69. http://dx.doi.org/10.1007/s11524-006-9060-7.
- Yamauchi T, Islam MM, Koizumi D, Rogers ME, Rogers NL, Takeshima N. Effect of home-based well-rounded exercise in community-dwelling older adults. J Sports Sci Med 2005;4:563-71.
- Kolt GS, Schofield GM, Kerse N, Garrett N, Oliver M. Effect of telephone counseling on physical activity for low-active older people in primary care: a randomized, controlled trial. J Am Geriatr Soc 2007;55:986-92. http://dx.doi.org/10.1111/j.1532-5415.2007.01203.x.
- Kolt GS, Schofield GM, Kerse N, Garrett N, Ashton T, Patel A. Healthy Steps trial: pedometer-based advice and physical activity for low-active older adults. Ann Fam Med 2012;10:206-12. http://dx.doi.org/10.1370/afm.1345.
- Lee RL, King AC. Discretionary time among older adults: how do physical activity promotion interventions affect sedentary and active behaviors?. Ann Behav Med 2003;25:112-19. http://dx.doi.org/10.1207/S15324796ABM2502_07.
- Resnick B, Luisi D, Vogel A. Testing the senior exercise self-efficacy project (SESEP) for use with urban dwelling minority older adults. Pub Health Nurs 2008;25:221-34. http://dx.doi.org/10.1111/j.1525-1446.2008.00699.x.
- Ammann R, Vandelanotte C, de Vries H, Mummery WK. Can a website-delivered computer-tailored physical activity intervention be acceptable, usable, and effective for older people?. Health Ed Behav 2013;40:160-70. http://dx.doi.org/10.1177/1090198112461791.
- Ferney SL, Marshall AL, Eaki EG, Owen N. Randomized trial of a neighborhood environment-focused physical activity website intervention. Prev Med 2009;48:144-50. http://dx.doi.org/10.1016/j.ypmed.2008.10.022.
- Lamb SE, Bartlett HP, Ashley A, Bird W. Can lay-led walking programmes increase physical activity in middle aged adults? A randomised controlled trial. J Epidemiol Comm Health 2002;56:246-52. http://dx.doi.org/10.1136/jech.56.4.246.
- McAuley E, Kerry S, Courneya KS, Rudolph DL, Lox CL. Enhancing exercise adherence in middle-aged males and females. Prev Med 1994;23:498-506. http://dx.doi.org/10.1006/pmed.1994.1068.
- Marshall AL, Booth ML, Bauman AE. Promoting physical activity in Australian general practices: a randomised trial of health promotion advice versus hypertension management. Pat Educ Counsel 2005;56:283-90. http://dx.doi.org/10.1016/j.pec.2004.03.002.
- Sheeran P, Harris P, Vaughan J, Oettingen G, Gollwitzer PM. Gone exercising: mental contrasting promotes physical activity among overweight, middle-aged, low-SES fishermen. Health Psychol 2013;32:802-9. http://dx.doi.org/10.1037/a0029293.
- Costanzo C, Walker SN, Yates BC, McCabe B, Berg K. Physical activity counseling for older women. Western J Nurs Res 2006;28:786-801. http://dx.doi.org/10.1177/0193945906289495.
- Hughes S, Seymour R, Campbell R, Shaw J, Fabiyi C, Sokas R. Comparison of two health-promotion programs for older workers. Am J Pub Health 2011;101:883-90. http://dx.doi.org/10.2105/AJPH.2010.300082.
- Pfister PB, Niedermann K, Sidelnikov E, Bischoff-Ferrari HA. Active over 45: a step-up jogging programme for inactive female hospital staff members aged 45+. Eur J Pub Health 2013;23:817-22. http://dx.doi.org/10.1093/eurpub/ckt027.
- Understanding Participation in Sport: What Determines Sports Participation Among Recently Retired People?. London: Sport England; 2006.
- Finch H. Physical Activity ‘At Our Age’: Qualitative Research Among People Over the Age of 50. London: Health Education Authority; 1997.
- Barnett I, Guell C, Ogilvie D. How do couples influence each other’s physical activity behaviours in retirement? An exploratory qualitative study. BMC Pub Health 2013;13. http://dx.doi.org/10.1186/1471-2458-13-1197.
- Beck F, Gillison F, Standage M. A theoretical investigation of the development of physical activity habits in retirement. Br J Health Psychol 2010;15:663-79. http://dx.doi.org/10.1348/135910709X479096.
- Barnes H, Lakey J, Parry J. Forging a New Future: the Experiences and Expectations of People Leaving Paid Work Over 50. Bristol: Policy Press; 2002.
- Evans AB, Sleap M. ‘You feel like people are looking at you and laughing’: Older adult’s perceptions of aquatic physical activity. J Aging Stud 2012;26:515-26. http://dx.doi.org/10.1016/j.jaging.2012.07.004.
- Hardcastle S, Taylor A. Looking for more than weight loss and fitness gain: psychological dimensions among older women in a primary-care exercise referral program. J Aging Phys Act 2001;9:313-28.
- Hardcastle S, Taylor AH. Finding an exercise identity in an older body: ‘It’s redefining yourself and working out who you are’. Psychol Sport Exercise 2005;6:173-88. http://dx.doi.org/10.1016/j.psychsport.2003.12.002.
- Stathi A, McKenna J, Fox KR, Stathi A, McKenna J, Fox KR. The experiences of older people participating in exercise referral schemes. J R Soc Promot Health 2004;124:18-23. http://dx.doi.org/10.1177/146642400312400108.
- Moore GF, Moore L, Murphy S. Facilitating adherence to physical activity: exercise professionals’ experiences of the national exercise referral scheme in Wales: a qualitative study. BMC Pub Health 2011;11. http://dx.doi.org/10.1186/1471-2458-11-935.
- Paulson S. How various ‘cultures of fitness’ shape subjective experiences of growing older. Ageing Soc 2005;25:229-44. http://dx.doi.org/10.1017/S0144686X04002971.
- Cooper L, Thomas H. Growing old gracefully: social dance in the third age. Ageing Soc 2002;22:689-708. http://dx.doi.org/10.1017/S0144686X02008929.
- Stead M, Wimbush E, Eadie D, Teer P. A qualitative study of older people’s perceptions of ageing and exercise: the implications for health promotion. Health Educ J 1997;56:3-16. http://dx.doi.org/10.1177/001789699705600102.
- Horne M, Skelton D, Speed S, Todd C. The influence of primary health care professionals in encouraging exercise and physical activity uptake among white and south Asian older adults: experiences of young older adults. Pat Educ Counsel 2010;78:97-103. http://dx.doi.org/10.1016/j.pec.2009.04.004.
- Horne M, Skelton DA, Speed S, Todd C. Attitudes and beliefs to the uptake and maintenance of physical activity among community-dwelling south Asians aged 60–70 years: a qualitative study. Pub Health 2012;126:417-23. http://dx.doi.org/10.1016/j.puhe.2012.02.002.
- Liechty T, Yarnal C, Kerstetter D. ‘I want to do everything!’: leisure innovation among retirement-age women. Leisure Studies 2012;31:389-408. http://dx.doi.org/10.1080/02614367.2011.573571.
- Kleiber DA, Nimrod G. ‘I can’t be very sad’: constraint and adaptation in the leisure of a ‘learning in retirement’ group. Leisure Studies 2009;28:67-83. http://dx.doi.org/10.1080/02614360802260820.
- Gibson H, Ashton-Schaeffer C, Green J, Corbin J. Leisure and retirement: women’s stories. Loisir Soc-Soc Leis 2002;25:257-84. http://dx.doi.org/10.1080/07053436.2002.10707589.
- Gibson H, Ashton-Schaeffer C, Green J, Autry C. Leisure in the lives of retirement-aged women: Conversations about leisure and life. Leisure 2003;28:203-30. http://dx.doi.org/10.1080/14927713.2003.9651313.
- Scanlon-Mogel J, Roberto K. Older adults’ beliefs about physical activity and exercise: life course influences and transitions. Qual Ageing Older Adults 2004;5:33-44. http://dx.doi.org/10.1108/14717794200400017.
- Liechty T, Genoe MR. Older men’s perceptions of leisure and aging. Leisure Sci 2013;35:438-54. http://dx.doi.org/10.1080/01490400.2013.831287.
- Duncan HH. An emergent theoretical model for interventions encouraging physical activity (mall walking) among older adults. J App Gerontol 1994;14:64-77. http://dx.doi.org/10.1177/073346489501400105.
- Duncan HH, Travis SS, McAuley WJ. The meaning of and motivation for mall walking among older adults. Act Adapt Aging 1995;19:37-52. http://dx.doi.org/10.1300/j016v19n01_03.
- Khoury-Murphy M, Murphy MD. Southern (bar) belles: the cultural problematics of implementing a weight training program among older Southern women. Play Culture 2014;5:409-19.
- Fournier SM, Fine GA. Jumping grannies: exercise as a buffer against becoming ‘old’. Play Culture 1990;3:337-42.
- Langley D, Knight S. Continuity in sport participation as an adaptive strategy in the ageing process: a lifespan narrative. J Aging Phys Activ 1999;7:32-54.
- Berg JA, Cromwell SL, Arnett M. Physical activity: perspectives of Mexican American and Anglo American midlife women. Health Care Women Int 2002;23:894-90. http://dx.doi.org/10.1080/07399330290112399.
- Liechty T, Yarnal CM. The role of body image in older women’s leisure. J Leisure Res 2010;42:443-67.
- Wilcox S, Oberrecht L, Bopp M, Kammermann SK, McElmurray CT. A qualitative study of exercise in older African American and white women in rural South Carolina: perceptions, barriers, and motivations. J Women Aging 2005;17:37-53. http://dx.doi.org/10.1300/J074v17n01_04.
- Henderson KA, Ainsworth BE. Enablers and constraints to walking for older African American and American Indian women: the cultural activity participation study. Res Q Exercise Sport 2000;71:313-21. http://dx.doi.org/10.1080/02701367.2000.10608914.
- Juarbe T, Turok XP, Perez-Stable EJ. Perceived benefits and barriers to physical activity among older Latina women. Western J Nurs Res 2002;24:868-86. http://dx.doi.org/10.1177/019394502237699.
- Kluge MA. Understanding the essence of a physically active lifestyle: a phenomenological study of women 65 and older. J Aging Phys Activ 2002;10:4-27.
- Lavizzo-Mourey R, Cox C, Strumpf N, Edwards WF, Lavizzo-Mourey R, Stineman M, et al. Attitudes and beliefs about exercise among elderly African Americans in an urban community. J Nat Med Assoc 2001;93:475-80.
- Pekmezi D, Marcus B, Meneses K, Baskin ML, Ard JD, Martin MY, et al. Developing an intervention to address physical activity barriers for African–American women in the deep south. Women’s Health 2013;9:301-12. http://dx.doi.org/10.2217/whe.13.20.
- Walcott-McQuigg JA, Prohaska TR. Factors influencing participation of African American elders in exercise behavior. Pub Health Nurs 2001;18:194-203. http://dx.doi.org/10.1046/j.1525-1446.2001.00194.x.
- Gallagher NA, Gretebeck KA, Robinson JC, Torres ER, Murphy SL, Martyn KK. neighborhood factors relevant for walking in older, urban, African American adults. J Aging Phys Act 2010;18:99-115.
- Gonzales A, Keller C. Mi familia viene primero (My family comes first): physical activity issues in older Mexican American women. Southern Online J Nurs Res 2004;5.
- Henwood T, Tuckett A, Edelstein O, Bartlett H. Exercise in later life: the older adults’ perspective about resistance training. Ageing Soc 2011;31:1330-49. http://dx.doi.org/10.1017/S0144686X10001406.
- Freene N, Waddington G, Chesworth W, Davey R, Cochrane T. Community group exercise versus physiotherapist-led home-based physical activity program: barriers, enablers and preferences in middle-aged adults. Physio Theory Pract 2014;30:85-93. http://dx.doi.org/10.3109/09593985.2013.816894.
- Poole M. Fit for life: older women’s commitment to exercise. J Aging Phys Activ 2001;9:300-12.
- Brown WJ, Fuller B, Lee C, Cockburn J, Adamson L. Never too late: older people’s perceptions of physical activity. Health Prom J Austral 1999;9:55-63.
- Dionigi RA. Competitive sport as leisure in later life: negotiations, discourse and aging. Leisure Sci 2006;28:181-96. http://dx.doi.org/10.1080/01490400500484081.
- Heuser L. We’re not too old to play sports: the career of women lawn bowlers. Leisure Studies 2005;24:45-60. http://dx.doi.org/10.1080/0201436042000250131.
- Drummond MJ. Retired men, retired bodies. Int J Men Health 2003;2:183-99. http://dx.doi.org/10.3149/jmh.0203.183.
- Jancey JM, Clarke A, Howat P, Maycock B, Lee AH. Perceptions of physical activity by older adults: a qualitative study. Health Educ J 2009;68:196-20. http://dx.doi.org/10.1177/0017896909339531.
- Hall C, Brown A, Gleeson S, Zinn J. Keeping the thread: older men’s social networks in Sydney, Australia. Qual Ageing 2007;8:10-7. http://dx.doi.org/10.1108/14717794200700023.
- Grant BC. ‘You are never too old’: beliefs about physical activity and playing sport in later life. Ageing Soc 2001;21:777-98. http://dx.doi.org/10.1017/S0144686X01008492.
- Winston NA, Barnes J. Anticipation of retirement among baby boomers. J Women Aging 2007;19:137-59. http://dx.doi.org/10.1300/J074v19n03_10.
- Genoe MR, Singleton JF. Older men’s leisure experiences across their lifespan. Topics Geriatric Rehabil 2006;22:348-56. http://dx.doi.org/10.1097/00013614-200610000-00009.
- Berry TR, Spence JC, Plotnikoff RC, Bauman A, McCargar L, Witcher C, et al. A mixed methods evaluation of televised health promotion advertisements targeted at older adults. Eval Program Plann 2009;32:278-88. http://dx.doi.org/10.1016/j.evalprogplan.2009.05.001.
- Weeks LE, Profit S, Campbell B, Graham H, Chircop A, Sheppard-LeMoine D. Participation in physical activity: influences reported by seniors in the community and in long-term care facilities. J Gerontol Nurs 2008;34:36-43. http://dx.doi.org/10.3928/00989134-20080701-11.
- O’Brien Cousins S. Thinking out loud: what older adults say about triggers for physical activity. J Aging Phys Act 2001;9:347-63.
- Nadasen K. ‘Life without line dancing and other activities would be too dreadful to imagine’: an increase in social activity for older women. J Women Aging 2008;20:329-42. http://dx.doi.org/10.1080/08952840801985060.
- Nadasen K. ‘We are too busy being active and enjoying ourselves to feel the aches and pains’: accounts of perceived health benefits of line dancing for older women. Qual Ageing 2007;8:4-14. http://dx.doi.org/10.1108/14717794200700016.
- Garmendia ML, Dangour AD, Albala C, Eguiguren P, Allen E, Uauy R. Adherence to a physical activity intervention among older adults in a post-transitional middle income country: a quantitative and qualitative analysis. J Nutr Health Aging 2013;17:466-71. http://dx.doi.org/10.1007/s12603-012-0417-1.
- Hobbs N, Godfrey A, Lara J, Errington L, Meyer TD, Rochester L, et al. Are behavioral interventions effective in increasing physical activity at 12 to 36 months in adults aged 55 to 70 years? A systematic review and meta-analysis. BMC Medicine 2013;11. http://dx.doi.org/10.1186/1741-7015-11-75.
- Allender S, Hutchinson L, Foster C. Life-change events and participation in physical activity: a systematic review. Health Promot Int 2008;23:160-72. http://dx.doi.org/10.1093/heapro/dan012.
- Engberg E, Alen M, Kukkonen-Harjula K, Peltonen JE, Tikkanen HO, Pekkarinen H. Life events and change in leisure time physical activity: a systematic review. Sports Med 2012;42:433-47. http://dx.doi.org/10.2165/11597610-000000000-00000.
- Wilson DM, Palha P. A Systematic review of published research articles on health promotion at retirement. J Nurs Scholar 2007;4:330-7. http://dx.doi.org/10.1111/j.1547-5069.2007.00189.x.
- Muller AM, Khoo S. Non-face-to-face physical activity interventions in older adults: a systematic review. Int J Behav Nutr Phys Act 2014;11. http://dx.doi.org/10.1186/1479-5868-11-35.
- Von Bonsdorff M, Rantanen T. Benefits of formal voluntary work among older people. A review. Aging Clin Exp Res 2011;23:162-9. http://dx.doi.org/10.1007/BF03337746.
- Chase JA. Physical activity interventions among older adults: a literature review. Res Theory Nurs Pract 2013;27:53-80. http://dx.doi.org/10.1891/1541-6577.27.1.53.
- Frost H, Haw S, Frank J. Promoting Health and Wellbeing in Later Life: Interventions in Primary Care and Community Settings. Edinburgh: Scottish Collaboration for Public Health Research and Policy; 2010.
- Conn VS, Minor MA, Burks KJ, Rantz MJ, Pomeroy SH. Integrative review of physical activity intervention research with aging adults. J Am Geriatr Soc 2003;51:1159-68. http://dx.doi.org/10.1046/j.1532-5415.2003.51365.x.
- Conn VS, Valentine JC, Cooper HM. Interventions to increase physical activity among aging adults: a meta-analysis. Ann Behav Med 2002;2:190-20. http://dx.doi.org/10.1207/S15324796ABM2403_04.
- Van der Bij AK, Laurant MGH, Wensing M. Effectiveness of physical activity interventions for older adults – a review. Am J Prev Med 2002;22:120-33. http://dx.doi.org/10.1016/S0749-3797(01)00413-5.
- King AC, Rejeski WJ, Buchner DM. Physical activity interventions targeting older adults. A critical review and recommendations. Am J Prev Med 1998;15:316-33. http://dx.doi.org/10.1016/S0749-3797(98)00085-3.
- The COMET Initiative n.d. www.comet-initiative.org/ (accessed 2 September 2015).
- Deci E, Ryan R. Self-determination theory: a macrotheory of human motivation, development, and health. Can Psychol 2008;49:182-85. http://dx.doi.org/10.1037/a0012801.
- Miles M, Huberman M. Qualitative Data Analysis: An Expanded Sourcebook. London: Sage; 1994.
- Strauss A, Corbin J. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory. London: Sage; 1998.
- Van Manen M. Modalities of body experience in illness and health. Qual Health Res 1998;8:7-24. http://dx.doi.org/10.1177/104973239800800102.
- Glaser BG, Strauss AL. The Discovery of Grounded Theory: Strategies for Qualitative Research. Chicago, IL: Aldine; 1967.
- Aitchison A. Poststructural feminist theories of representing Others: a response to the ‘crisis’ in leisure studies’ discourse. Leisure Stud 2000;19:127-44. http://dx.doi.org/10.1080/02614360050023044.
- Stebbins RA. Volunteering: a serious leisure perspective. Nonprofit Volunt Sect Q 1996;25:211-24. http://dx.doi.org/10.1177/0899764096252005.
- Baltes PB, Baltes MM, Baltes PB, Baltes MM. Successful Aging: Perspectives from the Behavioral Sciences. New York, NY: Cambridge University Press; 1990.
- Moustakis CE. Phenomenological Research Methods. Thousand Oaks, CA: Sage; 1994.
- Atchley RC, Kelly J. Activity and Aging. Newbury Park, CA: Sage; 1993.
- Atchley RC, Atchley RC. Social Forces and Aging: An Introduction to Social Gerontology. New York, NY: Wadsworth; 1997.
- Cash TH. Body image past present and future. Body Image 2004;1:1-5. http://dx.doi.org/10.1016/S1740-1445(03)00011-1.
- Grogan S. Body Image: Understanding Body Dissatisfaction in Men Women and Children. London and New York, NY: Routledge; 2008.
- Nimrod G. In support of innovation theory: innovation in activity patterns and life satisfaction among recently retired individuals. Ageing Soc 2008;28:831-46. http://dx.doi.org/10.1017/S0144686X0800706X.
- Elder GH, Elder GH. Life Course Dynamics: Trajectories and Transitions, 1968–1980. Ithaca, NY: Cornell University Press; 1985.
- Bengston V, Allen KR, Boss PG, Doherty WJ, LaRossa R, Schumm WR, et al. Sourcebook of Family Theories and Methods: A Contextual Approach. New York, NY: Plenum Press; 1993.
- Pate R, Pratt M, Blair SN, Haskell W, Macera CA, Bouchard C, et al. Physical activity and public health – a recommendation from the centers for disease control and prevention and the American College of Sports Medicine. JAMA 1995;273:402-7. http://dx.doi.org/10.1001/jama.1995.03520290054029.
Appendix 1 Search strategy
-
(physical$ activ$ or exercise or fitness or leisure activ$).ti,ab. (252,826)
-
exp exercise/ or Leisure Activities/ or Motor Activity/ or sports/ or recreation/ or physical fitness/ or fitness centers/ (226,493)
-
exp running/ or Swimming/ or walking/ or baseball/ or basketball/ or bicycling/ or boxing/ or football/ or golf/ or gymnastics/ or hockey/ or yoga/ or Tai Ji/ or dancing/ or gardening/ or hobbies/ or leisure activities/ (71,240)
-
((promot$ or uptake$ or encourag$ or increas$ or start$ or adher$) adj2 (physical activ$ or aerobic$ or circuit$ or swim$ or aqua or tai chi or tai ji or jog$ or run$ or bicycling or biking or yoga or pilates or football or walk$ or sport$ or gym$ or dancing or dance or garden$)).ti,ab. (15,951)
-
((barrier$ or hinder$ or block$ or obstacle$ or restrict$ or restrain$ or inhibit$ or impede$ or delay$ or constrain$ or hindrance or refus$) adj2 (physical activ$ or aerobic$ or circuit$ or swim$ or aqua or tai chi or tai ji or jog$ or run$ or bicycling or biking or yoga or pilates or football or walk$ or sport$ or gym$ or dancing or dance or garden$)).ti,ab. (4496)
-
((sport$ or fitness or leisure) adj2 (centre$ or center$ or facilit$)).ti,ab. (869)
-
((promot$ or uptake$ or encourag$ or increas$ or start$ or adher$) adj2 stair$).ti,ab. (153)
-
(Keep$ fit or fitness class$).ti,ab. (151)
-
((Fitness or sport$) adj2 (class$ or session$ or lesson$)).ti,ab. (411)
-
((decreas$ or reduc$ or discourag$) adj2 (sedentary or deskbound)).ti,ab. (447)
-
or/1-10 (411,060)
-
*aged/ or *middle aged/ (20,875)
-
*Aging/ (113,700)
-
(older$ or senior$ or elder$ or ageing or aging).ti. (189,039)
-
12 or 13 or 14 (265,157)
-
11 and 15 (18,587)
-
randomized controlled trial.pt. (371,686)
-
exp case control studies/ (653,591)
-
exp cohort studies/ (1,338,222)
-
Case control.ti,ab. (77,272)
-
(cohort adj (study or studies)).ti,ab. (86,689)
-
Cohort analy$.ti,ab. (3697)
-
(Follow up adj (study or studies)).ti,ab. (37,272)
-
(observational adj (study or studies)).ti,ab. (44,804)
-
Longitudinal.ti,ab. (140,897)
-
Retrospective.ti,ab. (274,456)
-
Cross sectional.ti,ab. (168,934)
-
Cross-sectional studies/ (173,354)
-
or/17-28 (2,141,892)
-
16 and 29 (6369)
-
limit 30 to yr = ‘1990 -Current’ (6218)
Appendix 2 Evaluation of study quality: intervention papers
| Author/year | 1. Selection bias: method used to generate the allocation sequence, method used to conceal the allocation sequence | 2. Performance bias: measures used to blind participants and personnel and outcome assessors, presence of other potential threats to validity | 3. Attrition bias: incomplete outcome data, high level of withdrawals from the study | 4. Detection bias: accuracy of measurement of outcomes, length of follow-up | 5. Reporting bias: selective reporting, accuracy of reporting | Details |
|---|---|---|---|---|---|---|
| Ackermann et al. (2005)27 | Y | Unclear | N | Y | N | Randomised at level of PCPs, 66% takeup. No detail of randomisation process. Some baseline differences control/intervention patients, characteristics of PCPs included vs. excluded not provided. Analysis carried out only on patients considering or trying exercise. 4-month follow-up. Self-report data only |
| Armit et al. (2005)28 | Unclear/not fully random | Unclear | N | Y | N | No information regarding randomisation process. A total of 33% of those eligible agreed to take part; however, there were no demographic differences between them. 9/37 dropouts. Self-report survey data only. Intended to be pilot/feasibility study only. 12-week follow-up |
| Burman et al. (2011)29 | Unclear | Unclear | Y | Y | N | Participants drawn from a university community. No detail regarding size of sampling pool vs. takeup. No detail of randomisation process, high dropout (48% at 18 months), although there appeared to be no difference between groups. Two interventions, no control. Self-report measures for all, other measures for sample only. Multiple component interventions with overlap in content, differences between mentors |
| Burke et al. (2013)30 | Unclear | Unclear | N | Y | N | Selected from electoral role, no detail regarding exact process. Take up: 2196 of 2949 eligible (64%). Immediate post data only, 78% completion. Self-report data only, exercise outcomes binary yes/no only |
| Caperchione and Mummery (2006)31 | Y | Y | N | Y | N | No detail of sampling pool, interested participants contacted researcher. 120 of 153 recruited. No detail of allocation process. Self-report data only. Multiple elements in both interventions with overlap of elements. Two interventions, no control group. 49/60 and 51/62 completed to 18 months |
| Castro et al. (2001)32 | Unclear | N | Y | Y | N | Recruited by random telephone call/advertising, no detail of takeup rate or sampling pool. This paper reports analysis of longer term maintenance with participant re-randomised to two of the four conditions. 39/179 dropout from original sample. Outcome self-reported adherence only. Influence of original intervention, no control condition |
| Coronini-Cronberg et al. (2012)33 | N | N | Y | Y | N | Data from National Travel Survey, stratified random sample of households, 60% response. Interview and travel diary self-report data |
| Costanzo and Walker (2008)34 | Y | N | Y | Y | Y | Described as convenience sample from an urban community. 110 people responded to adverts, 67 screened, 60 eligible, 46 completed. Follow-up immediately post intervention, self-report scaled data. Authors conclude behavioural counselling effective; however, no control condition and outcome predominantly maintained rather than effective |
| Cox et al. (2008)35 | Y | N | Y | Y | N | No detail on sampling pool: recruited by advert from a community, 1312 responded, 1204 ineligible. Self-report exercise logs main measure (heart rate/perceived exertion measured but not reported). 84/116 completed to 12 months, 36% of those identified as being in ‘preparation’ stage withdrew compared with 11/12% of those in ‘contemplation’. Paper primarily focuses on adherence |
| Croteau et al. (2014)36 | Y | N | Y | N | N | HCPs selected patients during routine visits, no detail of allocation process or number identified by HCPs of those seen. No detail of those identified vs. recruited. 22% dropout by 6 months. Pedometer measured outcome. Described as pilot study, small sample size (28). Two similar interventions, no control group |
| de Jong et al. (2006)37 | Unclear | Unclear | Y | N | Y | Cluster RCT randomisation at level of neighbourhood, no detail of recruitment beyond participants sent letter, wait-list control, no detail, dropout rate of 43%, higher number control than intervention (102 vs. 79) 80% attendance at sessions, self-report and fitness measures, 6 months’ follow-up. Reporting of significant effects intervention group plays down little between group difference |
| de Jong et al. (2007)38 | Unclear | Unclear | Y | N | Y | Longer follow-up of above study, 37 intervention and 54 control retained. As above, lack of main effects for group underemphasised |
| Dorgo et al. (2009)39 | Unclear | Unclear | N | Unclear | Y | No detail regarding how participants were recruited apart from that they were volunteers. 50 of 60 completed intervention. Unclear who carried out functional fitness assessments. Retention differed between groups. Authors conclude peer mentoring is effective; however, no control group and no difference between interventions |
| Elley et al. (2003)40 | Y | N | N | N | N | Randomised by practice, no details on allocation: 74% recruited. Patients who attended for an appointment approached by researcher. 66% of those eligible recruited, 85% completed. Retrospective recall and objective measures, only self-report measures significantly different intervention vs. control. Possible overstating of intervention effect |
| Finkelstein et al. (2008)41 | Y | N | N | N | N | Participants responded to adverts, 70 of 86 eligible, 52 recruited. Randomisation by random number. Immediate follow-up, combination of self-report and pedometer evaluation |
| Fries et al. (1993)42 | Y | N | Y | N | N | 58% participation, no detail of randomisation process, 47% completion. Self-report data with health claim data. Programme include variety of health promotion elements not just physical activity |
| Fries et al. (1993)43 | Y | N | Y | N | N | As above |
| Fujita et al. (2003)44 | Y | N | N | Y | N | Volunteers recruited from a city, no detail of allocation, 144 of 208 excluded, 62 of 65 completed and all but one intervention participant followed for 6 months. Self-report diary, interviewed to confirm diary |
| Goldstein et al. (1999)45 | Y | N | N | Y | N | No detail of randomisation process, patients were those with appointments in recruitment window. 80% of those eligible recruited. Complete data for 158 of 181 intervention participants. Self-report measures collected via telephone |
| Hageman et al. (2005)46 | Y | N | N | N | N | Participants responded to advert; no detail regarding how many responded, only how many enrolled. No detail of allocation process. Combination of fitness measures and self-report. 30 of 31 completed, 1-month follow-up. Two similar intervention arms, no control |
| Halbert et al. (2000)47 | Unclear | N | N | N | N | Recruited via general practices, 2878 invited, 913 responded, 351 eligible. Allocation process unclear, 88% followed up at 12 months. Self-report data and clinical measures for all, accelerometer for 87 |
| Hamdorf et al. (1992)48 | Y | Unclear | Y | Y | N | Participants responded to advertising. No detail of randomisation. Data for 66 of 80 recruited, unclear regarding attrition. Self-report and clinical measures. 90% adherence. Immediate follow-up on completion of programme |
| Hamdorf et al. (1993)49 | Y | Unclear | N | N | N | Follow-up data from previous study, 27 intervention and 31 control retained, self-report and clinical measures |
| Hekler et al. (2012)50 | Y | Y | N | N | N | Participants responded to advert, 32 responded, 16 recruited and all completed intervention. Self-report and pedometer outcomes. Crossover design after 2 weeks of intervention and immediate follow-up with potential for contamination across two interventions. Small sample described as pilot study |
| Hooker et al. (2005)51 | Y | Y | N | Y | N | Recruited at different sites; process varied between them. Intervention content also varied. No control group. 82% retention. Calories expended estimated from self-report questionnaire data |
| Hughes et al. (2009)52 | Y | N | Y | N | N | Purposive sampling of three study sites on pre-defined criteria. Volunteers recruited via adverts. 995 responded, 544 were recruited, with 21% dropout at 10 months in intervention group. Self-report and objective measures. Follow-up immediately post intervention |
| Irvine et al. (2013)53 | Y | N | Y | N | N | Participants recruited via adverts. Allocation process unclear. Significantly higher attrition rate for the intervention group (30% vs. 7%). Self-report measures only |
| Kamada et al. (2013)54 | N | N | N | Y | N | Randomised by community, 12 of 32 randomly sampled. Random sampling of participants in each, recruited via postal questionnaire. Self-report data only. Potential for control communities to be aware of campaign |
| King et al. (2002)55 | Y | N | N | N | N | Recruited via random telephone survey and advertising. 103 of 1347 recruited. 38% of those eligible declined to participate, differences between these and participants. Self-report and physical measures. Two intervention arms, no control |
| King et al. (2000)56 | N | N | N | N | N | Recruitment via advertising. 307 eligible, 228 recruited, 189 completed and followed up. Self-report measures for all, and accelerometer outcomes with sample |
| King et al. (2007)57 | Unclear | N | N | Y | N | No details of recruitment, 10% missing data. Self-report questionnaire only, immediate follow-up, no control |
| Koizumi et al. (2009)58 | Unclear | N | Unclear | N | N | Recruited via advertising. No details of response vs. recruitment. Accelerometer and physical outcomes. Immediate 12-week follow-up, unclear if all completed |
| Lawton et al. (2008)59 | Y | N | N | N | N | Recruited from general practices, 19.5% participation. Allocation process unclear. 93% retained at 12 months and 89% at 2 years. Self-report physical activity outcomes but also some clinical measures |
| Marcus et al. (1997)60 | Y | Y | Y | Y | Y | Pilot of Goldstein study.45 Recruited were those with GP appointments, no details of allocation process, 70% completion, self-reported data collected via telephone, 6-week follow-up. Effect may be overstated |
| Martinson et al. (2010)61 | N | N | N | Y | N | Recruitment via health data and mailing. 92% retention at 2 years. Self-report physical activity data collected via telephone interview by researchers blinded to condition |
| Martinson et al. (2008)62 | Y | Y | Y | N | N | Participants were volunteers recruited via advert and direct mailing to retired staff. Consecutive allocation. Control group was recruited separately. 45/186 dropped out. Accelerometer outcomes and self-report |
| Opdenacker et al. (2011)63 | Y | Y | Y | N | N | 2-year follow-up of above study |
| Opdenacker et al. (2008)64 | Y | N | N | Y | N | Participants randomly selected from one suburb, no details regarding response rate. No comparator arm. All self-report measures. 93% completed |
| Pasalich et al. (2013)65 | Unclear | Unclear | NA | NA | N | This paper reports process evaluation and development of intervention |
| Peels et al. (2012)66 | Unclear | Unclear | NA | NA | N | This paper reports participant characteristics and fidelity of intervention |
| Peels et al. (2012)67 | Unclear | Unclear | Y | Y | N | Effectiveness data from Active Plus trial; 59% retention at 12 months. Randomisation at region and neighbourhood levels. Allocation process unclear, two similar interventions, no control. Participants randomly selected and approached via mailing. Response rates 10–22% across study arms. Self-report questionnaire data |
| Peels et al. (2013)68 | Unclear | N | N | Y | N | Follow-up data from earlier 1980s study. 86% of participants recontacted 10 years later. Self-report data via telephone interview |
| Pereira et al. (1998)69 | Unclear | Unclear | N | N | N | Randomised at level of physician/practice. No detail regarding response rate of physicians or allocation process. Patients with appointments at these practices were approached. 426 screened (number approached not provided). 84% completed. Self-report and physical measures |
| Petrella et al. (2010)70 | Y | Unclear | N | N | N | Patients approached in waiting room; 62% of those screened were ineligible. No details of randomisation, two intervention groups, no control. 90% retention. Self-report and accelerometer outcomes. 6-months’ follow-up |
| Pinto et al. (2005)71 | Y | N | Y | N | N | Volunteer recruitment via advertising and within a university, no detail of randomisation, two intervention arms, no control group. Fitness measures and self-report, immediate follow-up. 45% dropout |
| Prabu et al. (2012)72 | N | N | Y | N | N | Physical activity intervention compared with nutrition, no control. Recruited by letter/flyers in waiting room. Self-report plus exercise measures, more dropouts from exercise group; 6-month follow-up |
| Purath et al. (2013)73 | Y | N | N | Y | N | Participants from a retirement group, those who had taken part in an intervention compared with those not, no allocation. 90% response rate. Self-report data only |
| Rowland et al. (1994)74 | Y | Unclear | N | Y | N | Recruited by advertising and word of mouth. No details of randomisation process. Two similar intervention arms, no control, self-report outcomes plus walk test. Immediate follow-up |
| Sawchuk et al. (2008)75 | Y | Unclear | Y | Y | N | Questionnaire sent to all on a surgery list, 57% return rate, these then randomised (no detail of process). 25% completed intervention, self-report only measures |
| Stevens et al. (1998)76 | Y | N | N | N | N | Recruited via advertising at senior centres, internet, university links. Four study arms, three interventions. Pedometer plus self-report measures, immediate follow-up |
| Strath et al. (2011)77 | N | N | Y | Y | N | Recruited via general practices, four study arms, three interventions focusing on healthy lifestyle not just physical activity. 73% completed all follow-ups. Self-reported activity related to physical activity and fruit and vegetable consumption |
| van Keulen et al. (2011)78 | N | N | N | Y | N | The paper reports 12-month data and subgroup analysis |
| van Stralen et al. (2009)79 | N | N | Y | Y | N | 12-month follow-up data. 73% completed all follow-ups. Self-reported activity, followed for 73 weeks |
| van Stralen et al. (2010)80 | N | N | Y | Y | N | This paper explores mechanisms of change in study |
| van Stralen et al. (2011)81 | N | N | Y | Y | N | Randomisation at level of health council. Recruited via general practices, four study arms, three interventions. Two interventions and control arm, self-report data, some baseline differences. Retention rate 68%, intervention participants more likely to drop out |
| van Stralen et al. (2009)82 | N | N | N | Y | N | Randomised by area, recruited by random dialling, 4% attrition, some difference in dropout between arms. Nutrition and physical activity intervention in two forms, no control. Self-report data, immediate follow-up |
| Walker et al. (2009)83 | N | N | N | N | N | 12- and 24-month follow-up data, healthy lifestyle programme. Two similar intervention arms, no control |
| Walker et al. (2010)84 | N | N | N | N | N | Recruited from pre-retirement workshops, 84% follow-up at 24 months. Self-report and physical measurement |
| Werkman et al. (2010)85 | Y | N | N | Y | N | Recruited via advertising, 97% completion, accelerometer and physical measurement, immediate follow-up |
| Wijsman et al. (2013)86 | Unclear | Y | Y | Y | N | Recruited by site, process unclear. Two intervention arms, no control group. Data from nine sites recruited during first year of programme, 72% follow-up data (immediate post programme). Self-report data |
| Wilcox et al. (2008)87 | Unclear | Y | Y | Y | N | This paper reports years 1, 3 and 4 of the programme in 12 sites. Different participants enrolled in each year of programme, 6-month/20-week interventions, 6-month follow-up. Year 4 a shortened version. 65% return rate self-report data |
| Wilcox et al. (2009)88 | Unclear | Y | Y | Y | N | Paper reports 6-month follow-up data from seven sites enrolled later in the programme. 46% returned data. 50% provided follow-up data. Self-report data |
| Wilcox et al. (2009)89 | Unclear | Y | Y | Y | N | Further paper from same team |
| Wilcox et al. (2006)90 | NA | NA | Y | NA | NA | This paper examines predictors of outcome from the programme. Data from 65% of participants |
Appendix 3 Tables detailing studies by their characteristics
Papers by study design
| Design (number of studies) | Studies |
|---|---|
| RCT (36) | Armit et al. (2005)28 Burman et al. (2011)29 Burke et al. (2013)30 Caperchione and Mummery (2006)31 Castro et al. (2001)32 Costanzo and Walker (2008)34 Cox et al. (2008)35 Croteau et al. (2014)36 Dorgo et al. (2009)39 Finkelstein et al. (2008)41 Fujita et al. (2003)44 Hageman et al. (2005)46 Halbert et al. (2000)47 Hamdorf et al. (1992),48 (1993)49 Hekler et al. (2012)50 Hughes et al. (2009)52 Irvine et al. (2013)53 King et al. (2002),55 (2000),56 (2007)57 Koizumi et al. (2009)58 Lawton et al. (2008)59 Martinson et al. (2010),61 (2008)62 Pereira et al. (1998)69 Pinto et al. (2005)71 Purath et al. (2013)73 Rowland et al. (1994)74 Sawchuk et al. (2008)75 Stevens et al. (1998)76 Strath et al. (2011)77 van Keulen et al. (2011)78 Walker et al. (2009),83 (2010)84 Wijsman et al. (2013)86 |
| Cluster RCT (17) | Ackermann et al. (2005)27 de Jong et al. (2006),37 (2007)38 Elley et al. (2003)40 Fries et al. (1993),42 (1993)43 Goldstein et al. (1999)45 Kamada et al. (2013)54 Peels et al. (2012),66 (2012),67 (2013)68 Petrella et al. (2010)70 van Stralen et al. (2009),79 (2010),80 (2011),81 (2009)82 Werkman et al. (2010)85 |
| CBA (4) | Marcus et al. (1997)60 Opdenacker et al. (2011),63 (2008)64 Pasalich et al. (2013)65 |
| BA (6) | Coronini-Cronberg et al. (2012)33 Hooker et al. (2005)51 Prabu et al. (2012)72 Wilcox et al. (2008),87 (2009),88 (2006)90 |
| Cross-sectional (1) | Wilcox et al. (2009)89 (follow-up data only) |
Studies by country of origin
| Country of origin (number of studies) | Studies |
|---|---|
| UK (3) | Coronini-Cronberg et al. (2012)33 Rowland et al. (1994)74 Stevens et al. (1998)76 |
| USA (33) | Ackermann et al. (2005)27 Burman et al. (2011)29 Castro et al. (2001)32 Costanzo and Walker (2008)34 Croteau et al. (2014)36 Dorgo et al. (2009)39 Finkelstein et al. (2008)41 Fries et al. (1993),42 (1993)43 Goldstein et al. (1999)45 Hageman et al. (2005)46 Hekler et al. (2012)50 Hooker et al. (2005)51 Hughes et al. (2009)52 Irvine et al. (2013)53 King et al. (2002),55 (2000),56 (2007)57 Marcus et al. (1997)60 Martinson et al. (2010),61 (2008)62 Pereira et al. (1998)69 Pinto et al. (2005)71 Prabu et al. (2012)72 Purath et al. (2013)73 Sawchuk et al. (2008)75 Strath et al. (2011)77 Walker et al. (2009),83 (2010)84 Wilcox et al. (2008),87 (2009),88 (2009),89 (2006)90 |
| The Netherlands (12) | de Jong et al. (2006),37 (2007)38 Peels et al. (2012),66 (2012),67 (2013)68 van Keulen et al. (2011)78 van Stralen et al. (2009),79 (2010),80 (2011),81 (2009)82 Werkman et al. (2010)85 Wijsman et al. (2013)86 |
| Australia/New Zealand (10) | Armit et al. (2005)28 Burke et al. (2013)30 Caperchione and Mummery (2006)31 Cox et al. (2008)35 Elley et al. (2003)40 Halbert et al. (2000)47 Hamdorf et al. (1992),48 (1993)49 Lawton et al. (2008)59 Pasalich et al. (2013)65 |
| Japan (3) | Fujita et al. (2003)44 Kamada et al. (2013)54 Koizumi et al. (2009)58 |
| Belgium (2) | Opdenacker et al. (2011),63 (2008)64 |
| Canada | Petrella et al. (2010)70 |
Sex of study participants
| Sex (number of studies) | Studies |
|---|---|
| Predominantly female (34) | Armit et al. (2005)28 Burman et al (2011)29 Caperchione and Mummery (2006)31 Costanzo and Walker (2008)34 Cox et al. (2008)35 Croteau et al. (2014)36 Elley et al. (2003)40 Finkelstein et al. (2008)41 Hageman et al. (2005)46 Hamdorf et al. (1992),48 (1993)49 Hekler et al. (2012)50 Hooker et al. (2005)51 Hughes et al. (2009)52 Irvine et al. (2013)53 King et al. (2002),55 (2000),56 (2007)57 Koizumi et al. (2009)58 Lawton et al. (2008)59 Martinson (2010),61 (2008)62 Pereira et al. (1998)69 Prabu et al. (2012)72 Purath et al. (2013)73 Rowland et al. (1994)74 Sawchuk et al. (2008)75 Strath et al. (2011)77 Walker et al. (2009),83 (2010)84 Wilcox et al. (2008),87 (2009),88 (2009),89 (2006)90 |
| Predominantly male (2) | Ackermann et al. (2005)27 Werkman et al. (2010)85 |
| Mixed (27) | Burke et al. (2013)30 Castro et al. (2001)32 de Jong et al. (2006),37 (2007)38 Dorgo et al. (2009)39 Fries et al. (1993),42 (1993)43 Fujita et al. (2003)44 Goldstein et al. (1999)45 Halbert et al. (2000)47 Kamada et al. (2013)54 Marcus et al. (1997)60 Opdenacker et al. (2011),63 (2008)64 Pasalich et al. (2013)65 Peels et al. (2012),66 (2012),67 (2013)68 Petrella et al. (2010)70 Pinto et al. (2005)71 Stevens et al. (1998)76 van Keulen et al. (2011)78 van Stralen et al. (2009),79 (2010),80 (2011),81 (2009)82 Wijsman et al. (2013)86 |
| Not reported/unclear (1) | Coronini-Cronberg et al. (2012)33 |
Studies categorised by activity level of participants
| Activity level (number of studies) | Studies |
|---|---|
| Predominantly inactive (34) | Ackermann et al. (2005)27 Armit et al. (2005)28 Burman et al. (2011)29 Burke et al. (2013)30 Caperchione and Mummery (2006)31 Costanzo and Walker (2008)34 Cox et al. (2008)35 Croteau et al. (2014)36 Elley et al. (2003)40 Finkelstein et al. (2008)41 Hageman et al. (2005)46 Hekler et al. (2012)50 Hughes et al. (2009)52 (overweight/obese) Irvine et al. (2013)53 King et al. (2002),55 (2000),56 (2007)57 Lawton et al. (2008)59 Marcus et al. (1997)60 Martinson (2010),61 (2008)62 Opdenacker et al. (2011),63 (2008)64 Pasalich et al. (2013)65 Petrella et al. (2010)70 Pinto et al. (2005)71 Purath et al. (2013)73 Sawchuk et al. (2008)75 Strath et al. (2011)77 Wijsman et al. (2013)86 Wilcox et al. (2008),87 (2009),88 (2009),89 (2006)90 |
| Mixed physical activity levels/inactivity not described as inclusion criterion (30) | Castro et al. (2001)32 Coronini-Cronberg33 de Jong et al. (2006),37 (2007)38 Dorgo et al. (2009)39 Fries et al. (1993),42 (1993)43 Fujita et al. (2003)44 Goldstein et al. (1999)45 Halbert et al. (2000)47 Hamdorf et al. (1992),48 (1993)49 Hooker et al. (2005)51 Kamada et al. (2013)54 Koizumi et al. (2009)58 Peels et al. (2012),66 (2012),67 (2013)68 Prabu et al. (2012)72 Pereira et al. (1998)69 Rowland et al. (1994)74 Stevens et al. (1998)76 van Keulen et al. (2011)78 (diagnosed hypertension) van Stralen et al. (2009),79 (2010),80 (2011),81 (2009)82 Walker et al. (2009),83 (2010)84 Werkman et al. (2010)85 |
Studies categorised by socioeconomic status
| SES (number of studies) | Studies |
|---|---|
| Predominantly more highly educated/higher income (16) | Burman et al. (2011)29 Castro et al. (2001)32 Costanzo and Walker (2008)34 Cox et al. (2008)35 Croteau et al. (2014)36 Finkelstein et al. (2008)41 Hageman et al. (2005)46 Hekler et al. (2012)50 Hughes et al. (2009)52 Irvine et al. (2013)53 Martinson (2010),61 (2008)62 Pasalich et al. (2013)65 Pereira et al. (1998)69 Purath et al. (2013)73 Strath et al. (2011)77 |
| Predominantly lower SES/basic education (1) | Burke et al. (2013)30 |
| Predominantly minority ethnicity (1) | Sawchuk et al. (2008)75 (Native American) |
| Not reported/unclear (20) | Ackermann et al. (2005)27 Armit et al. (2005)28 Caperchione and Mummery (2006)31 de Jong et al. (2007)38 Dorgo et al. (2009)39 Elley et al. (2003)40 Fries et al. (1993),42 (1993)43 Fujita et al. (2003)44 Halbert et al. (2000)47 Hamdorf et al. (1992),48 (1993)49 Kamada et al. (2013)54 King et al. (2002),55 (2000)56 Koizumi et al. (2009)58 Lawton et al. (2008)59 Marcus et al. (1997)60 Petrella et al. (2010)70 Walker et al. (2009)83 |
| Mixed (25) | Coronini-Cronberg et al. (2012)33 de Jong et al. (2007)38 Goldstein et al. (1999)45 Hooker et al. (2005)51 King et al. (2007)57 Opdenacker et al. (2011),63 (2008)64 Peels et al. (2012),66 (2012),67 (2013)68 Pinto et al. (2005)71 Prabu et al. (2012)72 Rowland et al. (1994)74 Stevens et al. (1998)76 van Keulen et al. (2011)78 van Stralen et al. (2009),79 (2010),80 (2011),81 (2009)82 Werkman et al. (2010)85 Wijsman et al. (2013)86 Wilcox et al. (2008),87 (2009),88 (2009),89 (2006)90 |
Appendix 4 Quality appraisal of qualitative studies
| Author/year | 1. Was there a clear statement of the aim of the research? | 2. Is a qualitative methodology appropriate to address the aims of the research? | 3. Was the recruitment strategy appropriate to the aims of the research? | 4. Were the data collected in a way that addressed the research issue? | 5. Has the relationship between researcher and participant been adequately considered? | 6. Have ethical issues been taken into account? | 7. Was the data analysis sufficiently rigorous? | 8. Is there a clear statement of findings? | Overall risk based on concordance with criteria (lower/higher risk) | Details |
|---|---|---|---|---|---|---|---|---|---|---|
| Concordance with criteria? Yes, No or Unclear | ||||||||||
| Arkenford (2006)130 | Y | Y | U | Y | U | N | U | Y | Higher | No discussion of why people did not participate. Data analysis methods were not reported. Ethical issues not reported |
| Barnes et al. (2002)134 | Y | Y | Y | Y | N | N | U | Y | Higher | No discussion of relationship between researcher and participant. Data analysis methods not reported in detail. Ethical issues not reported |
| Barnett et al. (2013)132 | Y | Y | Y | Y | Y | Y | Y | Y | Lower | All criteria addressed to some extent |
| Beck et al. (2010)133 | Y | Y | Y | Y | N | Y | Y | Y | Lower | No discussion of relationship between researcher and participant |
| Berg et al. (2002)156 | Y | Y | Y | Y | Y | Y | U | Y | Lower | Data analysis details were brief |
| Berry et al. (2009)179 | Y | Y | Y | Y | N | Y | U | Y | Lower | No discussion of relationship between researcher and participant. Ethics approval sought but ethical issues not discussed |
| Brown et al. (1999)170 | Y | Y | Y | Y | Y | N | U | Y | Lower | Ethical issues not reported. Reporting on data analysis is brief |
| Cooper and Thomas (2002)141 | Y | Y | Y | Y | Y | N | U | Y | Lower | Data collection methods reported only briefly. Data analysis details not reported. Ethical issues not discussed |
| Dionigi (2006)171 | Y | Y | U | Y | Y | N | Y | Y | Lower | Recruitment strategy not detailed and ethical issues not discussed |
| Drummond (2003)173 | Y | Y | U | Y | Y | N | Y | Y | Lower | Recruitment strategy not detailed and ethical issues not discussed |
| Duncan (1994)151 | Y | Y | U | Y | Y | N | Y | Y | Lower | Recruitment strategy not detailed and ethical issues not discussed |
| Duncan et al. (1995)152 | Y | Y | U | Y | Y | N | Y | Y | Lower | As above |
| Evans and Sleap (2012)135 | Y | Y | Y | Y | N | U | Y | Y | Lower | No discussion of relationship between researcher and participant. Ethics approval sought but ethical issues not discussed |
| Finch (1997)131 | Y | Y | U | Y | N | N | Y | U | Higher | Recruitment details brief. No discussion of relationship between researcher and participant. Ethical issues not discussed |
| Fournier and Fine (1990)154 | Y | Y | N | Y | Y | N | N | U | Higher | Recruitment, data analysis methods and ethical issues not reported. Findings clear but discussion brief |
| Freene et al. (2014)168 | Y | Y | Y | Y | Y | U | N | Y | Lower | Ethical approval sought, no other factors discussed. No details of data analysis |
| Gallagher et al. (2010)165 | Y | Y | U | Y | U | N | Y | Y | Higher | Recruitment details brief. No discussion of relationship between researcher and participant. Ethical issues not discussed |
| Garmendia et al. (2013)184 | Y | Y | Y | Y | N | U | U | Y | Lower | Recruitment details brief. No discussion of relationship between researcher and participant. Ethical approval sought, ethical issues not discussed |
| Genoe and Singleton (2006)178 | Y | Y | Y | Y | Y | N | Y | Y | Lower | Ethical issues not discussed |
| Gibson et al. (2002)147 | Y | Y | Y | Y | U | N | Y | Y | Lower | Ethical issues not discussed |
| Gibson et al. (2003) (same study as above)148 | Y | Y | Y | Y | U | N | Y | Y | Lower | Ethical issues not discussed |
| Gonzales and Keller (2004)166 | Y | Y | U | Y | Y | Y | N | Y | Lower | Data analysis methods not reported |
| Grant (2001)176 | Y | Y | U | Y | U | Y | Y | Y | Lower | Recruitment details brief. No discussion of relationship between researcher and participant |
| Hall et al. (2007)175 | Y | Y | Y | Y | U | Y | Y | Y | Lower | No discussion of relationship between researcher and participant |
| Hardcastle and Taylor (2001)136 | Y | Y | N | Y | Y | Y | Y | Y | Lower | No details of recruitment strategy or sample characteristics |
| Hardcastle and Taylor (2005)137 | Y | Y | U | Y | Y | N | Y | Y | Lower | No details of recruitment strategy or discussion of ethical issues |
| Henderson and Ainsworth (2000)159 | Y | Y | Y | Y | Y | Y | Y | Y | Lower | No comment |
| Henwood et al. (2011)167 | Y | Y | U | Y | Y | N | Y | Y | Lower | Relationship between researcher and participant and ethical issues not discussed |
| Heuser (2007)172 | Y | Y | U | Y | Y | N | Y | Y | Lower | Brief details of recruitment strategy. No discussion of ethical issues |
| Horne et al. (2010)143 | Y | Y | U | Y | U | Y | Y | Y | Lower | No discussion of researcher position |
| Horne et al. (2012)144 | Y | Y | U | Y | U | N | Y | Y | Higher | The reader is referred to other publications for more detail |
| Jancey et al. (2009)174 | Y | Y | Y | U | N | N | Y | Y | Higher | Brief details of recruitment strategy. No discussion of researcher position or ethical issues |
| Juarbe et al. (2002)160 | Y | Y | Y | Y | N | Y | Y | Y | Lower | No discussion of researcher position |
| Khoury-Murphy and Murphy (1992)153 | Y | Y | U | U | Y | N | U | Y | Higher | No details of how data were collected or analysed |
| Kleiber (2009)146 | Y | Y | Y | Y | N | N | Y | Y | Lower | No discussion of researcher position or ethical issues |
| Kluge (2002)161 | Y | Y | Y | Y | Y | U | Y | Y | Lower | Ethical issues partially addressed |
| Langley and Knight (1999)155 | Y | Y | U | Y | U | N | Y | Y | Higher | No discussion of researcher position or ethical issues |
| Lavisso Mourey et al. (2001)162 | Y | Y | Y | Y | N | U | U | Y | Higher | No discussion of researcher position. Ethical issues and data analysis partially addressed |
| Leichty and Yarnal (2010)157 | Y | Y | Y | Y | Y | U | Y | Y | Lower | No discussion of ethical issues |
| Leichty et al. (2012)145 | Y | Y | Y | Y | Y | U | Y | Y | Lower | No discussion of ethical issues |
| Liechty and Genoe (2013)150 | Y | Y | Y | Y | Y | U | Y | Y | Lower | No discussion of ethical issues |
| Moore et al. (2011)139 | Y | Y | Y | Y | U | Y | Y | Y | Lower | No discussion of researcher position |
| Nadasen (2007)182 | Y | Y | Y | Y | Y | U | Y | Y | Lower | No discussion of ethical issues |
| Nadasen (2008)183 | Y | Y | Y | Y | Y | U | Y | Y | Lower | No discussion of ethical issues |
| O’Brien Cousins (2001)181 | Y | Y | Y | Y | Y | Y | Y | Y | Lower | No comment |
| Paulson (2005)140 | Y | Y | Y | Y | Y | Y | Y | Y | Lower | No comment |
| Pekmezi et al. (2013)163 | Y | Y | U | Y | U | N | Y | Y | Higher | No discussion of recruitment strategy, researcher position or ethical issues |
| Poole (2001)169 | Y | Y | Y | Y | Y | N | N | Y | Lower | Data analysis ethical issues are not reported |
| Scanlon-Mogel and Roberto (2004)149 | Y | Y | U | Y | U | N | Y | Y | Higher | Limited generalisability outside sample |
| Stathi et al. (2004)138 | Y | Y | Y | Y | N | U | Y | Y | Lower | No discussion of researcher position or ethical issues |
| Stead et al. (1997)142 | Y | Y | U | Y | N | N | N | Y | Higher | Recruitment strategy, researcher position, ethical issues and data analysis details not reported |
| Walcott-McQuigg and Prohaska (2001)164 | Y | Y | Y | Y | Y | Y | U | Y | Lower | Requires more detail in some sections |
| Weeks et al. (2008)180 | Y | Y | U | Y | Y | U | Y | Y | Lower | Requires more detail in some sections |
| Wilcox et al. (2005)158 | Y | Y | U | Y | N | U | Y | Y | Higher | Recruitment strategy, researcher position, some ethical issues not reported |
| Winston et al. (2007)177 | Y | Y | Y | Y | Y | U | U | Y | Lower | Ethical issues and data analysis details only briefly reported |
Appendix 5 Studies excluded at full-paper review
Excluded first search
| Study | Reason |
|---|---|
| Mowlam A, Bridges S, Gill V, MacGregor A, Ranasinghe J, Tideswell E. Active at 60: Local Evaluation Research: Final Report: Research Summary. London: Crown Copyright, 2012 | Very limited ‘anecodatal’ physical activity evidence |
| Agmon M, Perry CK, Phelan E, Demiris G, Nguyen HQ, Agmon M, et al. A pilot study of Wii Fit exergames to improve balance in older adults. J Geriatr Phys Ther 2011;34:161–7 | Elderly (mean age 84 years) measures balance |
| Alburquerque-Sendin F, Mariano EB, Brandao-Santana N, Rebelatto DAN, Rebelatto JR. Effects of an adapted physical activity program on the physical condition of elderly women: an analysis of efficiency. Revista Brasileira de Fisioterapia 2012;16:328–36 | Association between activity and health, not about the programme |
| An S, Lee Y, Kim JT. The effect of the public exercise environment on the physical activity for the active ageing of the elderly. Indoor Built Environ 2013;22:319–31 | Association data physical activity and environment |
| Anderson, R. Exercise and Dietary Behaviour Change in a Sample of Midlife Australian Women. PhD by publication. Brisbane, QLD, Australia: Queensland University of Technology; 2008 | Unable to source thesis, paper from same study identified |
| Angevaren M, Aufdemkampe G, Verhaar H, Aleman A, Vanhees L. Physical activity and enhanced fitness to improve cognitive function in older people without known cognitive impairment. Cochrane Database Syst Rev 2008;16:CD005381 | Measures cognitive function |
| Atienza AA, Oliveira B, Fogg BJ, King AC. Using electronic diaries to examine physical activity and other health behaviors of adults age 50+. J Aging Phys Activity 2006;14:192–202 | Acceptability of electronic exercise diaries |
| Babazono A, Kame C, Ishihara R, Yamamoto E, Hillman AL. Patient motivated prevention of lifestyle-related disease in Japan. A randomized controlled clinical trial. Dis Manage Health Outcomes 2007;15:119–26 | Not relevant |
| Baker MK, Kennedy DJ, Bohle PL, Campbell DS, Knapman L, Grady J, et al. Efficacy and feasibility of a novel tri-modal robust exercise prescription in a retirement community: a randomized, controlled trial. J Am Geriatr Soc 2007;55:1–10 | Exclude age (mean 76.6 years) |
| Berger U, Der G, Mutrie N, Hannah MK. The impact of retirement on physical activity. Ageing Soc 2005;25:181–95 | Association data |
| Bird M, Hill KD, Ball M, Hetherington S, Williams AD. The long-term benefits of a multi-component exercise intervention to balance and mobility in healthy older adults. Arch Gerontol Geriat 2011;52;211–16 | Strength and resistance rather than physical activity |
| Bjornsdottir G, Arnadottir SA, Halldorsdottir S, Bjornsdottir G, Arnadottir SA, Halldorsdottir S. Facilitators of and barriers to physical activity in retirement communities: experiences of older women in urban areas. Phys Ther 2012;92:551–62 | Elderly (age 72–97 years; mean age 84 years) |
| Boyette LW, Sharon BF, Brandon LJ. Exercise adherence for a strength training program in older adults. J Nutrition Health Aging 1997;1:93–7 | Not qualitative |
| Bratvata DM, Smith-Spangler C, Sundaram V, Gienger AL, Lin N, Lewis R, et al. Using pedometers to increase physical activity and improve health: a systematic review. JAMA 2007;298:2296–304 | Review |
| Brawley LR, Rejeski WJ, King AC. Promoting physical activity for older adults – the challenges for changing behavior. Am J Prev Med 2003;25:172–83 | Discussion paper |
| Brown AK, Liu-Ambrose T, Tate R, Lord SR, Brown AK, Liu-Ambrose T, et al. The effect of group-based exercise on cognitive performance and mood in seniors residing in intermediate care and self-care retirement facilities: a randomised controlled trial. BJSM Online 2009;43:608–14 | Measures mood not physical activity |
| Brown WJ, Heesch KC, Miller YD. Life events and changing physical activity patterns in women at different life stages. Ann Behav Med 2009;37:294–305 | Association data |
| Bryant E, Trew M, Bruce A, Bryant E, Trew M, Bruce A. Case report: activity after retirement. Physiother Res Int 2006;11:51–5 | Single case study discussion paper |
| Fitzpatrick TR, Vinick BH, Bushfield S. Anticipated and experienced changes in activities after husbands retire. J Gerontol Soc Work 2005;46:69–84 | Questionnaire data |
| Calder CG, Mannion J, Metcalf PA. Low-intensity whole-body vibration training to reduce fall risk in active, elderly residents of a retirement village. J Am Geriatr Soc 2013;61:1424–6 | Elderly (mean age 80.1 years) |
| Carlson JA, Sallis JF, Conway TL, Saelens BE, Frank LD, Kerr J, et al. Interactions between psychosocial and built environment factors in explaining older adults’ physical activity. Prev Med 2012;54:68–73 | Association data |
| Carral JMC, Perez CA. Effects of high-intensity combined training on women over 65. Gerontology 2007;53:340–6 | Measures balance/flexibility not physical activity |
| Caudroit J, Stephan Y, Le SC, Caudroit J, Stephan Y, Le Scanff C. Social cognitive determinants of physical activity among retired older individuals: an application of the health action process approach. Br J Health Psychol 2011;16:404–17 | Association data |
| Cheadle A, Egger R, LoGerfo JP, Schwartz S, Harris JR. Promoting sustainable community change in support of older adult physical activity: evaluation findings from the Southeast Seattle Senior Physical Activity Network (SESphysical activityN). J Urban Health Bull New York Acad Med 2010;87:67–75 | No measure of physical activity |
| Cheng SP, Tsai TI, Lii YK, Yu S, Chou CL, Chen IJ. The effects of a 12-week walking program on community-dwelling older adults. Res Q Exerc Sport 2009;80:524–32 | Not trying to increase physical activity |
| Chung S, Domino ME, Stearns SC, Popkin BM. Retirement and physical activity: analyses by occupation and wealth. Am J Prev Med 2009;36:422–8 | Association data |
| Clifton J. Ageing and Well-Being in an International Context. Politics of ageing working paper no 3; 2009. URL: www.ippr.org/files/images/media/files/publication/2011/05/getting_on_1744.pdf?noredirect=1 (accessed 19 April 2016) | Discussion paper |
| Cohen-Mansfield J, Dakheel-Ali M, Frank JK, Cohen-Mansfield J, Dakheel-Ali M, Frank JK. The impact of a Naturally Occurring Retirement Communities service program in Maryland, USA. Health Promot Int 2010;25:210–20 | Mean age 80 years, not physical activity |
| Collins T. Managing widowhood in later life: the challenges encountered. Int J Ther Rehabil 2014;21:69–76 | Not physical activity (impact of widowhood) |
| Conn VS, Tripp-Reimer T, Maas ML. Older women and exercise: Theory of planned behavior beliefs. Public Health Nurs 2003;20:153–63 | Scales, not qualitative |
| Crombie IK, Irvine L, Williams B, McGinnis AR, Slane PW, Alder EM et al. Why older people do not participate in leisure time physical activity: a survey of activity levels, beliefs and deterrents. Age Ageing 2004;33:287–92 | Association data |
| Cunningham DA, Howard JH, Rechnitzer physical activity, Donner AP. Exercise training of men at retirement: a clinical trial. J Gerontology 1987;42:17–23 | Exclude 1987 |
| Curfman Janssen MA. The effects of a leisure education program on perceptions of quality of life in older adults. Dissertation Abstracts International: Section B: The Sciences and Engineering 2000;60(10-B) | Not within scope |
| Cyarto EV, Brown WJ, Marshall AL, Cyarto EV, Brown WJ, Marshall AL. Retention, adherence and compliance: important considerations for home- and group-based resistance training programs for older adults. J Sci Med Sport 2006;9:402–12 | Elderly (mean age 80 ± 6 years) |
| Darling CA, Darling CA. Women in midlife: Stress, health and life satisfaction. Stress Health 2012;28:31–40 | Association data |
| De Greef KP, Deforche BI, Ruige JB, Bouckaert JJ, Tudor-Locke CE, Kaufman JM, et al. The effects of a pedometer-based behavioral modification program with telephone support on physical activity and sedentary behavior in type 2 diabetes patients. Patient Educ Couns 2011;84:275–9 | Diabetic adults, all ages |
| Delecluse C, Colman V, Roelants M, Verschueren S, Derave W, Ceux T, et al. Exercise programs for older men: mode and intensity to induce the highest possible health-related benefits. Prev Med 2004;39:823–33 | Comparison of different exercise methods on clinical/sport outcomes |
| Dubbert PM, Morey MC, Kirchner KA, Meydrech EF, Grothe K. Counseling for home-based walking and strength exercise in older primary care patients. Arch Intern Med 2008;168:979–86 | Elderly frail (physical function limitations) |
| Dwyer GB, Dwyer ES, Dwyer GB, Dwyer ES. Participation and psychological changes among retirees in a corporate fitness program. Am J Health Promot 236;6:167–8 | Measures disease risk, not physical activity |
| Evenson KR, Rosamond WD, Cai J, Diez-Roux AV, Brancati FL. Influence of retirement on leisure-time physical activity: the Atherosclerosis Risk in Communities study. Am J Epidemiol 2002;155:692–9 | Association data |
| Farquhar JC, Wrosch C, Pushkar D, Li KZ, Farquhar JC, Wrosch C, et al. The value of adaptive regret management in retirement. Int J Aging Hum Dev 2013;76:99–121 | Association data |
| Farran CJ, Staffileno BA, Gilley DW, Mccann JJ, Li Y, Castro CM, et al. A lifestyle physical activity intervention for caregivers of persons with Alzheimer’s disease. Am J Alzheimers Disease Other Dementias 2008; 23:132–42 | Adults over 21 years of age |
| Feinglass J, Thompson JA, He XZ, Witt W, Chang RW, Baker DW, et al. Effect of physical activity on functional status among older middle-age adults with arthritis. Arthritis Rheum 2005;53:879–85 | Study protocol only |
| Fitzpatrick TR, Vinick BH, Bushfield S. Anticipated and experienced changes in activities after husbands retire. J Gerontol Soc Work 2005:46:69–84 | Not qualitative |
| Floyd FJ, Haynes SN, Doll ER, Winemiller D, Lemsky C, Burgy TM, et al. Assessing retirement satisfaction and perceptions of retirement experiences. Psychol Aging 1992;7:609–21 | Not intervention or qualitative |
| Fonseca AM, Paúl C. Health and aging: does retirement transition make any difference? Rev Clin Gerontol 2003;13:257–60 | Association data |
| Frändin K, Johannesson K, Grimby G. Physical activity as part of an intervention program for elderly persons in Göteborg. Scand J Med Sci Sports 1992;2:218–24 | Exclude age (76 years) |
| Frank J, Frost H, Haw S. Promoting Health and Wellbeing in Later Life: Interventions in Primary Care and Community Settings. Scottish Collaboration for Public Health Research and Policy, Edinburgh: Scottish Collaboration for Public Health Research and Policy; 2010 | Exclude review, reference list checked |
| Gibson HJE. Leisure and later life: Past, present and future. Leisure Studies 2006;25:397–401 | Discussion paper |
| Grimby A, Johansson AK, Sundh V, Grimby G, Grimby A, Johansson AK, et al. Walking habits in elderly widows. Am J Hosp Palliat Care 2008;25:81–7 | Associational data |
| Grove NC. Motivating the well elderly to exercise. J Community Health Nursing 1999;16:179–89 | Evaluates methods of recruitment |
| Gunnarsson E. ‘I think I have had a good life’: the everyday lives of older women and men from a lifecourse perspective. Ageing Soc 2009;29:33–48 | Elderly (aged 75–90 years), not physical activity |
| Gusi N, Reyes MC, Gonzalez-Guerrero JL, Herrera E, Garcia JM. Cost-utility of a walking programme for moderately depressed, obese, or overweight elderly women in primary care: a randomised controlled trial. BMC Public Health 2008;8:231 | Only cost-effectiveness outcomes, nothing about increasing physical activity |
| Hagiwara A, Hayashi Y, Nakamura Y, Muraoka I. Effects of group- versus home-based walking intervention on lifestyle activity. Japanese J Phys Fitness Sports Med 2000;49:571–9 | Japanese, no English abstract |
| Harris T, Kerry S, Victor C, Ekelund U, Woodcock A, Iliffe S, et al. Randomised controlled trial of a complex intervention by primary care nurses to increase walking in patients aged 60–74 years: protocol of the physical activity CE-Lift (Pedometer Accelerometer Consultation Evaluation – Lift) trial. BMC Public Health 2013;13:5 | Protocol paper |
| Harris T, Kerry SM, Victor CR, Shah SM, Iliffe S, Ussher M et al. PACE-UP (Pedometer and consultation evaluation – UP) – a pedometer-based walking intervention with and without practice nurse support in primary care patients aged 45–75 years: study protocol for a randomised controlled trial. Trials 2013;14:418 | Study protocol |
| Hembree LD. Exercise and its effect on hopelessness and depression in an aging female population in eastern Oklahoma. Dissertation Abstracts International Section A: Humanities and Social Sciences 2001;61(9-A) | Exclude out of scope |
| Henkens K, van SH, Gallo W, Henkens K, van Solinge H, Gallo W. Re: ‘Aging, retirement, and changes in physical activity: prospective cohort findings from the GLOBE study’. Am J Epidemiol 2007;166:616–17 | Comment only |
| Henkens K, van Solinge H, Gallo WT. Effects of retirement voluntariness on changes in smoking, drinking and physical activity among Dutch older workers. Eur J Public Health 2008;18:644–9 | Association data |
| Hertogh EM, Vergouwe Y, Schuit AJ, Peeters PH, Monninkhof EM. Behavioral changes after a 1-yr exercise program and predictors of maintenance. Med Sci Sports Exerc 2010;42:886–92 | Population |
| Higgs P, Nazroo J, Scherger S. Leisure activities and retirement: do structures of inequality change in old age? Ageing Soc 2011;31:146–72 | Association data |
| Hildebrand M, Neufeld P, Hildebrand M, Neufeld P. Recruiting older adults into a physical activity promotion program: Active Living Every Day offered in a naturally occurring retirement community. Gerontologist 2009;49:702–10 | Reviews methods of recruitment |
| Hill K, Choi W, Smith R, Condron J. Tai Chi in Australia: acceptable and effective approach to improve balance and mobility in older people? Australas J Ageing 2005;24:9–13 | Outcome measure balance (not physical activity) |
| Hill K, Smith R, Fearn M, Rydberg M, Oliphant R. Physical and psychological outcomes of a supported physical activity program for older carers. J Aging Physical Activity 2007;15:257–71 | Population older carers |
| Hirvensalo M, Heikkinen E, Lintunen T, Rantanen T. The effect of advice by health care professionals on increasing physical activity of older people. Scand J Med Sci Sports 2003;13:231–236 | Not qualitative |
| Howard JH, Rechnitzer PA, Cunningham DA, Donner AP. Change in Type A behaviour a year after retirement. Gerontologist 1986;26:643–9 | Exclude 1986 |
| Hudson K. Active ageing. Health Club Management 1949; Nov/Dec 2011: 49–51 | Promotional material |
| Im EO, Ko Y, Hwang H, Chee W, Stuifbergen A, Lee H, et al. Asian American Midlife Women’s Attitudes Toward Physical Activity. JOGNN 2012;41:650–8 | Mean age 49 years |
| Jette AM, Harris BE, Sleeper L, Lachman ME, Heislein D, Giorgetti M, et al. A home-based exercise program for nondisabled older adults. J Am Geriatr Soc 1996;44:644–9 | Measures muscle strength, psychological well-being |
| Johnson JA, McIlroy WE, Roy E, Papaioannou A, Thabane L, Giangregorio L, et al. Feasibility study of walking for exercise in individuals living in assisted living settings. J Geriatr Phys Ther 2013;36:175–81 | Pilot study focusing on feasibility of recruitment |
| Jonsson H, Jonsson H. The first steps into the third age: the retirement process from a Swedish perspective. Occup Ther Int 2011;18:32–8 | No data on physical activity |
| Kerr J, Rosenberg DE, Nathan A, Millstein RA, Carlson JA, Crist K, et al. Applying the ecological model of behavior change to a physical activity trial in retirement communities: description of the study protocol. Contemp Clin Trials 2012;33:1180–8 | Exclude Study protocol |
| King AC, Haskell WL, Taylor CB, Kraemer HC, DeBusk RF. Group-versus home-based exercise training in healthy older men and women: A community-based clinical trial. J Am Med Assoc 1991;266:1535–42 | Review |
| King AC, Haskell WL, Young DR, Oka RK, Stefanick ML. Long-term effects of varying intensities and formats of physical activity on participation rates, fitness, and lipoproteins lipoproteins in men and women aged 50 to 65 years. Circulation 1995;91:2596–604 | Measures treadmill performance and heart disease risk factors |
| Kowal J, Fortier MS. Physical activity behavior change in middle-aged and older women: the role of barriers and of environmental characteristics. J Behav Med 2007;30:233–42 | Not qualitative |
| Krahe LME-MA, Krahe LM. Leisure participation and the life, health, leisure and retirement satisfaction of retirees: A case study of Port Macquarie, Australia. Int J Disability Human Develop 2011;10:109–15 | Association data |
| Krampe J, Musterman K. Shall We Skype Dance? Connecting Nursing Students With Older Adults Via Skype for Dance-Based Therapy. Cin-Computers Inform Nurs 2013;31:151–4 | Discussion paper |
| Kuvaja-Kollner V, Valtonen H, Komulainen P, Hassinen M, Rauramaa R, Kuvaja-Kollner V, et al. The impact of time cost of physical exercise on health outcomes by older adults: the DR’s EXTRA Study. Eur J Health Econ 2013;14:471–9 | Association data |
| Lalonde B, Hooyman N, Blumhagen J. Long-term outcome effectiveness of a health promoting program for the elderly: The Wallingford Wellness Project. J Gerontol Soc Work 1998;13:95–112 | General health not physical activity |
| Li FZ, Fisher KJ, Bauman A, Ory MG, Chodzko-Zajko W, Harmer P, et al. Neighborhood influences on physical activity in middle-aged and older adults: A multilevel perspective. J Aging Phys Activ 2005;13:87–114 | Review of built environment influences |
| Lindström J, Eriksson JG, Valle TT, Aunola S, Cepaitis Z, Hakumäki M, et al. Prevention of diabetes mellitus in subjects with impaired glucose tolerance in the Finnish diabetes prevention study: results from a randomized clinical trial. J Am Soc Nephrol 2003;14:S108–S113 | Lifestyle intervention for diabetes |
| Lindström J, Louheranta A, Mannelin M, Rastas M, Salminen V, Eriksson J, et al. The Finnish Diabetes Prevention Study (DPS). Diabetes Care 2003;26:3230–6 | Lifestyle intervention for diabetes |
| Lindström J, Absetz P, Hemio K, Peltomaki P, Peltonen M. Reducing the risk of type 2 diabetes with nutrition and physical activity – efficacy and implementation of lifestyle interventions in Finland. Public Health Nutr 2010;13:993–9 | Lifestyle intervention for diabetes |
| Liptak JJ. Preretirement counseling: Integrating the leisure planning component. Career Development Q 1990;38:360–7 | Discussion paper. |
| Lord SR, Castell S, Corcoran J, Dayhew J, Matters B, Shan A, et al. The effect of group exercise on physical functioning and falls in frail older people living in retirement villages: a randomized, controlled trial. J Am Geriatr Soc 2003;51:1685–92 | Elderly falls (age 79.5 ± 6.4 years) |
| Lord SR, Ward JA, Williams P, Strudwick M. The effect of a 12-month exercise trial on balance, strength, and falls in older women: a randomized controlled trial. J Am Geriatr Soc 2005;43:1198–206 | Outcome related to falls, no measure of physical activity |
| MacRae PG, Asplund LA, Schnell JF, Ouslander JG, Abrahamse A. Walking program for nursing home residents: Effects on walk endurance, physical activity, mobility, and quality of life. J Am Geriatrics Soc 1996;44:175–80 | Exclude > 80 years of age living in residential care |
| Matteson MA: Effects of a cognitive behavioral approach and positive reinforcement on exercise for older adults. Educ Gerontol 1989,5:497–513 | Exclude 1989 |
| McMahon S, Fleury J. External validity of physical activity interventions for community-dwelling older adults with fall risk: a quantitative systematic literature review. J Adv Nurs 2012;68:2140–54 | Review of intervention validity |
| Mein GK, Shipley MJ, Hillsdon M, Ellison GT, Marmot MG. Work, retirement and physical activity: cross-sectional analyses from the Whitehall II study. Eur J Public Health 2005;15:317–22 | Exclude association data |
| Merom D, Cumming R, Mathieu E, Anstey KJ, Rissel C, Simpson JM, et al. Can social dancing prevent falls in older adults? a protocol of the Dance, Aging, Cognition, Economics (DAnCE) fall prevention randomised controlled trial. BMC Public Health 2013;13:477 | Measures falls not physical activity (elderly) |
| Midanik LT, Soghikian K, Ransom LJ, Tekawa IS. The effect of retirement on mental-health and health behaviors – the Kaiser Permanent Retirement Study. J Gerontol B Psychol Sci Soc Sci 1995;50:S59–S61 | Exclude association data |
| Mitros M. Evaluation of the stay in balance wellness program: an interdisciplinary, multi-component falls prevention program. Dissertation Abstracts International: Section B: The Sciences and Engineering 6021;71(10-B) | Falls |
| Modra AK, Black DR: Peer-led minimal intervention: An exercise approach for elderly women. Am J Health Behavior 1999,23:52–60 | Elderly: over 75 years of age |
| Morey MC, Cowper PA, Feussner JR, DiPasquale RC, Crowley GM, Sullivan RJ Jr. Two-year trends in physical performance following supervised exercise among community-dwelling older veterans. J Am Geriatrics Soc 1991;39:986–92 | Flexibility and strength outcomes only |
| Muller AM, Khoo S. Non-face-to-face physical activity interventions in older adults: a systematic review. Int J Behav Nut Phys Activity 2014;11:35 | Review, checked references |
| Navarro FM, Rabelo JF, Faria ST, Lopes MC, Marcon SS, Navarro FM, et al. [Perceptions of a group of elderly people regarding the influence of physical activity on their lives.] Rev Gaucha Enferm 2008;29:596–603 | Association data |
| Nicolaisen M, Thorsen K, Eriksen SH, Nicolaisen M, Thorsen K, Eriksen SH. Jump into the void? Factors related to a preferred retirement age: gender, social interests, and leisure activities. Int J Aging Hum Dev 2012;75:239–71 | Association data (from abstract) |
| Oakley C, Pratt J. Voluntary work in the lives of post-retirement adults. Brit J Occupation Ther 1997;60:273–6 | Association data |
| Oneill K, Reid G. Perceived barriers to physical-activity by older adults. Can J Public Health 1991;82:392–6 | Questionnaire data |
| Patterson I. Participation in leisure activities by older adults after a stressful life event: the loss of a spouse. Int J Aging Hum Dev 1996;42:123–42 | Not physical activity (impact of widowhood) |
| Petkoska J, Earl JK, Petkoska J, Earl JK. Understanding the influence of demographic and psychological variables on retirement planning. Psychol Aging 2009;24:245–51 | Association data, not about physical activity |
| Plachy JK, Kovách M, Bognár J. Improving flexibility and endurance of elderly women through a six-month training programme. Human Movement 2012;13:22–7 | Measures flexibility not physical activity |
| Pomeroy SLH. Increasing Physical Activity in Rural Elderly. PhD thesis. Columbia, MO: University of Missouri; 2003 | Out of scope |
| Price CA, Nesteruk O, Price CA, Nesteruk O. Creating retirement paths: examples from the lives of women. J Women Aging 2010;22:136–49 | Not about physical activity |
| Rejeski WJ, Marsh AP, Chmelo E, Prescott AJ, Dobrosielski M, Walkup MP, et al. The Lifestyle Interventions and Independence for Elders Pilot (LIFE-P): 2-year follow-up. J Gerontology Series A-Biol Sci Med Sci 2009;64:462–7 | 70+ years frail (‘compromised function’) |
| Resnick B, Resnick B. A seven step approach to starting an exercise program for older adults. Patient Educ Couns 2000;39:243–52 | Measures adherence, population > 80 years |
| Richardson CR, Newton TL, Abraham JJ, Sen A, Jimbo M, Swartz AM. A meta-analysis of pedometer-based walking interventions and weight loss. Ann Family Med 2008;6:1 | Review |
| Richter DL. Disincentives to participation in planned exercise activities among older adults. J Health Behav Educ Promotion 1000;17:95–103 | Questionnaire data |
| Ritchie DM. Comparison of two doses of an exercise intervention on mobility and function in older adults. Dissertation Abstracts International Section A: Humanities and Social Sciences 1000;71(6-A) | Out of scope |
| Romero N, Sturm J, Bekker T, de Valk L, Kruitwagen S. Playful persuasion to support older adults’ social and physical activities. Interact Comp 2010;22:485–95 | Not qualitative |
| Rosenberg D, Kerr J, Sallis JF, Patrick K, Moore DJ, King A, et al. Feasibility and outcomes of a multilevel place-based walking intervention for seniors: a pilot study. Health Place 2009;15:173–9 | Mean age 81.79 years |
| Rosenberg DE, Kerr J, Sallis JF, Norman GJ, Calfas K, Patrick K, et al. Promoting walking among older adults living in retirement communities. J Aging Phys Activ 2012;20:379–94 | Age 74–92 years |
| Rosenberg DE. Outcomes of a multilevel walking intervention for older adults living in retirement communities. Dissertation Abstracts International: Section B: The Sciences and Engineering 5143;71(8-B) | Exclude age |
| Rowe J, Kahn R. Successful aging. Gerontologist 1997;37:433–40 | Discussion paper |
| Saltychev M, Laimi K, Oksanen T, Pentti J, Virtanen M, Kivimaki M, et al. Effect of a multidisciplinary rehabilitation programme on perceived health among employees at increased risk of incapacity for work: a controlled study. Clin Rehabil 2012;26:513–22 | Out of scope |
| Sarkisian CA, Prohaska TR, Davis C, Weiner B, Pilot test of an attribution retraining intervention to raise walking levels in sedentary older adults. J Am Geriatr Soc 2007;55:1842–6 | Mean age 77 years |
| Siegenthaler KL, Vaughan J. Older women in retirement communities: perceptions of recreation and leisure. Leis Sci 1998:20:53–66 | No relevant physical activity data (leisure focus) |
| Sims J, Smith F, Duffy A, Hilton S. Can practice nurses increase physical activity in the over 65s? Br J Gen Pract 1998;48:1249–50 | Methodological considerations from a pilot study |
| Slingerland AS, van Lenthe FJ, Jukema J, Kamphuis CB, Looman C, Giskes K, et al. Aging, retirement, and changes in physical activity: prospective cohort fındings from the GLOBE study. Am J Epidemiol 2007;165:1356–63 | Association data |
| Stanziano DC, Roos BA, Perry AC, Lai S, Signorile JF, Stanziano DC, et al. The effects of an active-assisted stretching program on functional performance in elderly persons: a pilot study. Clin Interv Aging 2009;4:115–20 | Mean age 88.8 years |
| Stevens M, Lemmink KAPM, van Heuvelen MJG, de Jong J, Rispens P. Groningen Active Living Model (GALM): stimulating physical activity in sedentary older adults; validation of the behavioral change model. Prev Med 2003;37:561–70 | Association data |
| Stewart AL, Verboncoeur CJ, McLellan BY, Gillis DE, Rush S, Mills KM et al. Physical Activity Outcomes of CHAMPS II: A Physical Activity Promotion Program for Older Adults. J Gerontol A Biol Sci Med Sci 2001;56:M465–M470 | Duplicate |
| Stiggelbout M, Hopman-Rock M, van Mechelen W. Entry correlates and motivations of older adults participating in organized exercise programs. J Aging Phys Activity 2008;16:342–54 | Association data |
| Stoddard AM, Palombo R, Troped PJ, Sorensen G, Will JC. Cardiovascular disease risk reduction: the Massachusetts WISEWOMAN project. J Womens Health 2004;13:539–46 | Population: women part of breast and cervical cancer initiative |
| Tan E, Fried L, Li T. Volunteerism as a physical activity intervention for retired Americans. Gerontologist 2005;45:229 | Conference abstract |
| Taylor AH, Cable NT, Faulkner G, Hillsdon M, Narici M, Van der Bij AK. Physical activity and older adults: a review of health benefits and the effectiveness of interventions. J Sports Sci 2004;22:703–25 | Discursive review, not older adults |
| Thogersen-Ntoumani C, Cumming J, Ntoumanis N, Nikitaras N. Exercise imagery and its correlates in older adults. Psychol Sport Exerc 2012;13:19–25 | Association data |
| Tiedemann A, Sherrington C, Lord SR. Predictors of exercise adherence in older people living in retirement villages. Prev Med 2011;52:480–1 | Association data |
| Touvier M, Bertrais S, Charreire H, Vergnaud AC, Hercberg S, Oppert JM. Changes in leisure-time physical activity and sedentary behaviour at retirement: a prospective study in middle-aged French subjects. Int J Behav Nutr Phys Act 2010;7:1–14 | Association data |
| Triado C, Villar F, Sole C, Celdran M, Osuna MJ, Triado C, et al. Daily activity and life satisfaction in older people living in rural contexts. Span J Psychol 2009;12:236–45 | Association data |
| van Gool CH, Penninx BWJH, Kempen GIJM, Miller GD, van Eijk JTM, Pahor M, et al. Determinants of high and low attendance to diet and exercise interventions among overweight and obese older adults – Results from the arthritis, diet, and activity promotion trial. Contemp Clin Trials 2006;27:227–37 | Association data on intervention attendance |
| van Stralen MM, Kok G, de Vries H, Mudde AN, Bolman C, Lechner L. The Active plus protocol: systematic development of two theory- and evidence-based tailored physical activity interventions for the over-fifties. BMC Public Health 2008;8:399 | Protocol only |
| Villar F, Triado C, Sole C, Osuna MJ, Villar F, Triado C, et al. [Daily life activity patterns among the elderly: is what they claim to do what they wish to do?] Psicothema 2006;18:149–55 | Association data |
| Wallace JI, Buchner DM, Grothaus L, Leveille S, Tyll L, LaCroix AZ, et al. Implementation and effectiveness of a community based health promotion program for older adults. J Gerontol A Biol Sci Med Sci 1998;53:M30I–M306 | Lifestyle intervention measuring SF-36 and depression not physical activity |
| Webb E, Netuveli G, Millett C. Free bus passes, use of public transport and obesity among older people in England. J Epidemiol Community Health 2012;66:176–80 | Measures public transport use and obesity (not physical activity) |
| Wells YD, Kendig HL. Psychological resources and successful retirement. Aust Psychol 1999;34:111–15 | Association data |
| Werkman A, Schuit AJ, Kwak L, Kremers SP, Visscher TL, Kok FJ, et al. Study protocol of a cluster randomised controlled trial investigating the effectiveness of a tailored energy balance programme for recent retirees. BMC Public Health 2006;6:293 | Study protocol |
| Westhoff MH, Hopman-Rock M. Dissemination and implementation of ‘aging well and healthily’: a health-education and exercise program for older adults. J Aging Phys Activity 2002;10:382–95 | No outcomes relating to physical activity |
| Wister A. The effects of socioeconomic status on exercise and smoking: age-related differences. J Aging Health 1996;8:467–88 | Association data |
| Wong DG, Rechnitzer physical activity, Cunningham DA, Howard JH, Wong DG, Rechnitzer physical activity, et al. Effect of an exercise program on the perception of exertion in males at retirement. Can J Sport Sci 1990;15:249–53 | Measures change in VO2 max, not physical activity |
| Wright TJ. Principal barriers to health promotion program participation by older adults. Dissertation Abstracts International Section A: Humanities and Social Sciences 3872;69(10-A) | Unable to source |
| Yates T, Davies M, Gorely T, Bull F, Khunti K. Effectiveness of a pragmatic education program designed to promote walking activity in individuals with impaired glucose tolerance. Diabetes Care 2009;32:1404–10 | Lifestyle intervention for diabetes |
| Yoshiuchi K, Inada S, Nakahara R, Togo F, Watanabe E, Yasunaga A, et al. Stressful life events and habitual physical activity in older adults: 1 year of pedometer/accelerometer data from the Nakanojo Study. 7th World Congress on Aging and Physical Activity. J Aging Phys Activ 2008;16:S183 | Association data |
| Zettergren KK, Lubeski JM, Viverito JM, Zettergren KK, Lubeski JM, Viverito JM. Effects of a yoga program on postural control, mobility, and gait speed in community-living older adults: a pilot study. J Geriatr Phys Ther 2011;34:88–94 | Elderly (mean age 83 years) measures balance/gait |
Excluded second search
| Study | Reason |
|---|---|
| Anderson R, Anderson DJ. Psychology of exercise among midlife Australian women. In Columbus AM, editor. Advances in Psychology Research. New York, NY: Nova Science Publishers, Inc., Hauppauge New York; 2012 | Book |
| Atay E, Toraman NF, Yaman H. Exercise prescription by primary care doctors: effect on physical activity level and functional abilities in elderly. Turk Geriatri Dergisi 2014;17:77–85 | Outcomes not in scope |
| Atienza AA. Home-based physical activity programs for middle-aged and older adults: summary of empirical research. J Aging Physical Activity 2001;9:S38–S58 | Review |
| Audette JF, Jin YS, Newcomer R, Stein L, Duncan G, Frontera WR, et al. Tai Chi versus brisk walking in elderly women. Age Ageing 2006;35:388–93 | Clinical outcomes |
| Baruth M, Wilcox S. Predictors of physical activity 6 months postintervention in the active for life initiative. J Phys Act Health 2014;11:256–65 | Associations |
| Beaudreau SA. Qualitative variables associated with older adults’ compliance in a tai chi group. Clin Gerontol 2006;30:99–107 | Not qualitative |
| Bird M, Hill KD, Ball M, Hetherington S, Williams AD. The long-term benefits of a multi-component exercise intervention to balance and mobility in healthy older adults. Arch Gerontol Geriatrics 2011;52:211–16 | Outcomes |
| Brown AK, Liu-Ambrose T, Tate R, Lord SR, Brown AK, Liu-Ambrose T, et al. The effect of group-based exercise on cognitive performance and mood in seniors residing in intermediate care and self-care retirement facilities: a randomised controlled trial. BJSM Online 2009;43:608–14 | Outcomes |
| Brown DS, Finkelstein EA, Brown DR, Buchner DM, Johnson FR. Estimating older adults’ preferences for walking programs via conjoint analysis. Am J Prev Med 2009;36:201–7 | No intervention |
| Bunout D, Barrera G, Avendaño M, de la Maza P, Gattas V, Leiva L, et al. Results of a community-based weight-bearing resistance training programme for healthy Chilean elderly subjects. Age Ageing 2005;34:80–3 | Clinical outcomes |
| Carvalho MJ, Marques E, Mota J, Carvalho MJ, Marques E, Mota J. Training and detraining effects on functional fitness after a multicomponent training in older women. Gerontology 2009;55:41–8 | Clinical outcomes |
| Chen I, Chou C, Yu S, Cheng S. Health services utilization and cost utility analysis of a walking program for residential community elderly. Nursing Economics 2008;26:263–9 | Clinical outcomes |
| Chen KM, Chen MH, Hong SM, Chao HC, Lin HS, Li CH, et al. Physical fitness of older adults in senior activity centres after 24-week silver yoga exercises. J Clin Nurs 2008;17:2634–46 | Clinical outcomes |
| Clark DO, Stump TE, Damush TM. Outcomes of an exercise program for older women recruited through primary care. J Aging Health 2003;15:567–85 | Outcomes |
| Conn VS, Burks KJ, Minor MA, Mehr DR, Conn VS, Burks KJ, et al. Randomized trial of 2 interventions to increase older women’s exercise. Am J Health Behav 2003;27:380–8 | Age (mean 75 years) |
| Denison HJ, Syddall HE, Dodds R, Martin HJ, Finucane FM, Griffin SJ, et al. Effects of aerobic exercise on muscle strength and physical performance in community-dwelling older people from the Hertfordshire cohort study: a randomized controlled trial. J Am Geriatr Soc 2013;61:1034–6 | Clinical outcomes |
| Diehr P, Hirsch C, Diehr P, Hirsch C. Health benefits of increased walking for sedentary, generally healthy older adults: using longitudinal data to approximate an intervention trial. J Gerontol A Biol Sci Med Sci 2010;65:982–9 | Clinical outcomes |
| Drowatzky JN, Greninger LO, Wolfe Sr WW, Armstrong CW, Ashby B, Campbell BM, et al. Effects of a six-week exercise and education program on older adults ages 65 to 85 years. Clinical Kinesiol 2003;57:49–65 | Clinical outcomes |
| Ecclestone NA, Myers AM, Paterson DH. Tracking older participants of twelve physical activity classes over a three-year period. J Ageing Phys Activ 1998;6:70–82 | Not qualitative |
| Emery CF, Blumenthal JA, Emery CF, Blumenthal JA. Perceived change among participants in an exercise program for older adults. Gerontologist 1990;30:516–21 | Clinical outcomes |
| Farooqui MA, Tan YT, Bilger M, Finkelstein EA. Effects of financial incentives on motivating physical activity among older adults: results from a discrete choice experiment. BMC Public Health 2014;14:141 | Clinical outcomes |
| Feinglass J, Thompson JA, He XXZ, Witt W, Chang RW, Baker DW. Effect of physical activity on functional status among older middle-age adults with arthritis. Arthritis Rheum 2005;53:879–85 | Clinical population |
| Feinglass J, Lin S, Thompson J, Sudano J, Dunlop D, Song J, et al. Baseline health, socioeconomic status, and 10-year mortality among older middle-aged Americans: findings from the Health and Retirement Study, 1992–2002. J Gerontol B Psychol Sci Soc Sci 2007;62:S209–S217 | No intervention |
| Figueira HA, Figueira AA, Cader SA, Guimaraes AC, de Oliveira RJ, Figueira JA, et al. Effects of a physical activity governmental health programme on the quality of life of elderly people. Scand J Public Health 2012;40:418–22 | Clinical outcomes |
| Finger JD, Tylleskar T, Lampert T, Mensink GB. Dietary behaviour and socioeconomic position: the role of physical activity patterns. PLOS ONE 2013;8:e78390 | No intervention |
| Fitzpatrick SE, Reddy S, Lommel TS, Fischer JG, Speer EM, Stephens H, et al. Physical activity and physical function improved following a community-based intervention in older adults in Georgia senior centers. J Nutr Elder 2008;27:135–54 | Age (mean 75 years) |
| Godfrey A, Lord S, Galna B, Mathers JC, Burn DJ, Rochester L, et al. The association between retirement and age on physical activity in older adults. Age Ageing 2014;43:386–93 | Associations |
| Greaney ML, Riebe D, Ewing GC, Rossi JS, Lees FD, Burbank physical activity, et al. Long-term effects of a stage-based intervention for changing exercise intentions and behavior in older adults. Gerontologist 2008;48:358–67 | Age (over 75 years) |
| Haber D, Lacy MG. Evaluation of a socio-behavioral intervention for changing health behaviors of older adults. Behavior, Health & Aging 1993;3:73–85 | Outcomes |
| Hagiwara Y. The study of the elderly volunteer. J Soc Policy Soc Work 1997;1:41–50 | Not relevant |
| Hamar B, Coberley CR, Pope JE, Rula EY. Impact of a senior fitness program on measures of physical and emotional health and functioning. Popul Health Manag 2013;16:364–72 | Clinical outcomes |
| Harting J, van Assema P, van Limpt P, Gorgels T, van Ree J, Ruland E, et al. Cardiovascular prevention in the Hartslag Limburg project: effects of a high-risk approach on behavioral risk factors in a general practice population. Prev Med 2006;43:372–8 | Not relevant |
| Heisler M, Cole I, Weir D, Kerr EA, Hayward RA. Does physician communication influence older patients’ diabetes self-management and glycemic control? Results from the Health and Retirement Study (HRS). J Gerontol A Biol Sci Med Sci 2007;62:1435–42 | Populations |
| Hernandes NA, Probst VS, Da Silva RAJ, Januario RS, Pitta F, Teixeira DC, et al. Physical activity in daily life in physically independent elderly participating in community-based exercise program. Braz J Phys Ther 2013;17:57–63 | Not OECD country |
| Heydarnejad S, Dehkordi AH, Heydarnejad S, Dehkordi AH. The effect of an exercise program on the health-quality of life in older adults. A randomized controlled trial. Dan Med Bull 2010;57:A4113 | Outcomes |
| Hind D, Scott EJ, Copeland R, Breckon JD, Crank H, Walters SJ, et al. A randomised controlled trial and cost-effectiveness evaluation of ‘booster’ interventions to sustain increases in physical activity in middle-aged adults in deprived urban neighbourhoods. BMC Public Health 2010;10 | Discussion paper |
| Hirosaki M, Ohira T, Kajiura M, Kiyama M, Kitamura A, Sato S, et al. Effects of a laughter and exercise program on physiological and psychological health among community-dwelling elderly in Japan: randomized controlled trial. Geriatr Gerontol Int 2013;13:152–60 | Clinical outcomes |
| Hozawa A, Tsuji I, Tamagawa A, Nagotomi R, Irie N, Ohkubo T, et al. Randomized controlled trial of exercise training for older people (Sendai Silver Center Trial; SSCT): 6 months follow up. Japanese J Phys Fitness Sports Med 2001;50:71–2 | Clinical outcomes |
| Hsu H, Wang C, Chen Y, Chang M, Wang J. Evaluation of a community-based aging intervention program. Educ Gerontol 2010;36:547–72 | Population age |
| Ijuin M, Sugiyama M, Sakuma N, Inagaki H, Miyamae F, Ito K, et al. Walking exercise and cognitive functions in community-dwelling older adults: preliminary results of a randomized controlled trial. Int J Geriatric Psychiatry 2013;28:109–10 | Clinical outcomes |
| Justine M, Azizan A, Hassan V, Salleh Z, Manaf H. Barriers to participation in physical activity and exercise among middle-aged and elderly individuals. Singapore Med J 2013:54:581–6 | Not qualitative |
| Kamioka H, Nakamura Y, Yazaki T, Uebaba K, Mutoh Y, Okada S, et al. Comprehensive health education combining hot spa bathing and lifestyle education in middle-aged and elderly women: one-year follow-up on randomized controlled trial of three- and six-month interventions. J Epidemiol 2006;16:35–44 | Outcomes not physical activity |
| Kimura M, Moriyasu A, Kumagai S, Furuna T, Akita S, Kimura S, et al. Community-based intervention to improve dietary habits and promote physical activity among older adults: a cluster randomized trial. BMC Geriatr 2013;13:8 | Population age |
| Kochevar AJ, Smith KL, Bernard MA, Kochevar AJ, Smith KL, Bernard MA. Effects of a community-based intervention to increase activity in American Indian elders. J Okla State Med Assoc 2001;94:455–60 | Population age |
| Kutner NG, Barnhart H, Wolf SL, McNeely E, Xu T, Kutner NG, et al. Self-report benefits of Tai Chi practice by older adults. J Gerontol B Psychol Sci Soc Sci 1997;52:242–6 | Mean age 76 years |
| Layne JE, Sampson SE, Mallio CJ, Hibberd PL, Griffith JL, Das SK, et al. Successful dissemination of a community-based strength training program for older adults by peer and professional leaders: the people exercising program. J Am Ger Soc 2008:56:2323–9 | Delivery model, not qualitative |
| Lin SF, Lee J, Modeste N, Johnson E. Attitudes and beliefs predicting Taiwanese older adults intentions to attend strength and balance training programs. J Applied Gerontology 2012;31:260–81 | Clinical outcomes |
| Lubans DR, Mundey C, Lubans NJ, Lonsdale C. Testing physical activity mediators in an intervention for sedentary older adults. Int J Sport Psychol 2013;44:252–62 | No relevant outcomes |
| Lubans DR, Mundey CM, Lubans NJ, Lonsdale CC. Pilot randomized controlled trial: elastic-resistance-training and lifestyle-activity intervention for sedentary older adults. J Aging Phys Act 2013;21:20–32 | No relevant outcomes |
| Matheson EM, King DE, Everett CJ. Healthy lifestyle habits and mortality in overweight and obese individuals. J Am Board Fam Med 2012;25:9–15 | No relevant outcomes |
| McMurdo ME, Burnett L, McMurdo ME, Burnett L. Randomised controlled trial of exercise in the elderly. Gerontology 1992;38:292–8 | No relevant outcomes |
| Moschny A, Platen P, Klaassen-Mielke R, Trampisch U, Hinrichs T. Barriers to physical activity in older adults in Germany: a cross-sectional study. Int J Behav Nutr Phys Activ 2011;8:121 | Mean age over 75 years |
| Mouton CP, Calmbach WL, Dhanda R, Espino DV, Hazuda H, et al. Barriers and benefits to leisure-time physical activity among older Mexican Americans. Archives Fam Med 2000;9:892–7 | Associations, not qualitative |
| Nakagawa K, Inomata N, Nakazawa R, Sakamoto M. The effect of a health promotion program consisting of easy and simple exercises for community living elderly people. J Phys Ther Sci 2007;19:235–42 | Clinical outcomes |
| Oka RK, King AC, Young DR. Sources of social support as predictors of exercise adherence in women and men ages 50 to 65 years. Womens Health 1995;1:161–75 | Not qualitative |
| Pahor M, Blair SN, Espeland M, Fielding R, Gill TM, Guralnik JM, et al. Effects of a physical activity intervention on measures of physical performance: results of the Lifestyle Interventions and Independence for Elders Pilot (LIFE-P) study. J Gerontol A Biol Sci Med Sci 2006;61:1157–65 | Clinical outcomes |
| Paivi M, Mirja H, Terrtu P. Changes in physical activity involvement and attitude to physical activity in a 16-year follow-up study among the elderly. J Ageing Res 2010;2010:74290 | Not qualitative |
| Parrett CB. Evaluation of Nutrition Education and Exercise in a Health Promotion and Wellness Program for Older Adults. In Coward RT, Davis LA, Gold CH, Smiciklas-Wright H, Thorndyke LE, Vondracek FW, editors. Rural Women’s Health: Mental, Behavioral, and Physical Issues. New York, NY: Springer Publishing; 2006. pp. 217–34 | Associations |
| Petry NM, Andrade LF, Barry D, Byrne S. A randomized study of reinforcing ambulatory exercise in older adults. Psychol Aging 2013;28:1164–73 | Population |
| Pollock ML, Carroll JF, Graves JE, Leggett SH, Braith RW, Limacher M, et al. Injuries and adherence to walk/jog and resistance training programs in the elderly. Med Sci Sports Exerc 1991;23:1194–200 | Clinical outcomes |
| Pomeroy SLH. Increasing Physical Activity in Rural Elderly. PhD thesis. Columbia, MO: University of Missouri; 2003 | General discussion |
| Porter MM, Nelson ME, Singh MAF, Layne JE, Morganti CM, Trice I, et al. Effects of long-term resistance training and detraining on strength and physical activity in older women. J Age Phy Activ 2002;10:260–70 | Outcomes |
| Puggaard L. Effects of training on functional performance in 65, 75 and 85 year-old women: experiences deriving from community based studies in Odense, Denmark. Scand J Med Sci Sports 2003;13:70–6 | Clinical outcomes |
| Rasinaho M, Hirvensalo M, Tormakangas T, Leinonen R, Lintunen T, Rantanen T, et al. Effect of physical activity counseling on physical activity of older people in Finland. Health Promot Int 2012;27:463–74 | Mean age 77 years |
| Resnick B. A seven step approach to starting an exercise program for older adults. Patient Educ Couns 2000;39:243–52 | Mean age over 80 years |
| Rooks DS, Kiel DP, Hayes WC. A randomized controlled trial of self-paced exercise in community dwelling older adults. J Am Geriatr Soc 1996;44:1317–24 | Mean age 74 years |
| Ruoti RG, Troup JT, Berger RA. The effects of nonswimming water exercises on older adults. J Orthop Sports Phys Ther 1994;19:140–5 | Clinical outcomes |
| Sarkisian C, Trejo L, Mangione C, Wang PC, Frank J, Prohaska T. A randomized controlled trial of a behavioral intervention to increase walking among older Latinos. J Gen Intern Med 2010;25:212–13 | Meeting abstract |
| Schneider JK, Mercer GT, Herning M, Smith CA, Prysak MD, Schneider JK, et al. Promoting exercise behavior in older adults: using a cognitive behavioral intervention. J Gerontol Nurs 2004;30:45–53 | Mean age 76 years |
| Schneider JK, Cook JH, Luke DA. Cognitive-behavioral therapy, exercise, and older adults’ quality of life. Western J Nurs Res 2008;30:704–23 | Exclude: does not measure physical activity |
| Seaman P. Time for my life now: early boomer women’s anticipation of volunteering in retirement. Gerontologist 2012;52:245–54 | Not physical activity |
| Sharpe physical activity, Jackson KL, White C, et al. Effects of a one-year physical activity intervention for older adults at congregate nutrition sites. Gerontologist 1997;37:208–15 | Measures not physical activity |
| Simonsick EM, Guralnik JM, Volpato S, Balfour J, Fried LP. Just get out the door! Importance of walking outside the home for maintaining mobility: findings from the Women’s Health and Aging Study. J Am Geriatr Soc 2005;53:198–203 | Association data |
| Shaw KL, Page C. A pilot community-based walking-for-exercise program for senior women. Top Geriatr Rehabil 2008;24:315–24 | Age above 85 years |
| Siddarth D, Siddarth P, Lavretsky H, Siddarth D, Siddarth P, Lavretsky H. An observational study of the health benefits of yoga or tai chi compared with aerobic exercise in community-dwelling middle-aged and older adults. Am J Geriatr Psychiatry 2014;22:272–3 | No relevant outcomes |
| Sims-Gould J, Miran-Khan K, Haggis C, Liu-Ambrose T. Timing, experience, benefits, and barriers: older women’s uptake and adherence to an exercise program activities. Adaptation Ageing 2012;36:280–296 | Clinical outcomes |
| Snyder A, Colvin B, Gammack JK, Snyder A, Colvin B, Gammack JK. Pedometer use increases daily steps and functional status in older adults. J Am Med Dir Assoc 2011;12:590–4 | Age above 80 years |
| Stevens Z, Carpenter H, Gawler S, Belcher C, Haworth D, Kendrick D, et al. Lessons learnt during a complex, multicentre cluster randomised controlled trial: the ProAct65 + trial. Trials 2013;14:192 | Clinical population |
| Stoddard AM, Palombo R, Troped PJ, Sorensen G, Will JC. Cardiovascular disease risk reduction: the Massachusetts WISEWOMAN project. J Womens Health 2004;13:539–46 | Population |
| Thomas GN, Macfarlane DJ, Guo B, Cheung BM, McGhee SM, Chou KL, et al. Health promotion in older Chinese: a 12–month cluster randomized controlled trial of pedometry and ‘peer support’. Med Sci Sports Exerc 2012;446:1157–66 | Outcomes |
| Tiedemann A, Sherrington C, Lord SR, Tiedemann A, Sherrington C, Lord SR. Predictors of exercise adherence in older people living in retirement villages. Prev Med 2011;52:480–1 | Associations |
| Toraman F, Sahin G, Toraman F, Sahin G. Age responses to multicomponent training programme in older adults. Disabil Rehabil 2004;22:448–54 | Not relevant |
| Tsuji I, Tamagawa A, Nagatomi R, Irie N, Ohkubo T, Saito M, et al. Randomized controlled trial of exercise training for older people (Sendai Silver Center Trial; SSCT): study design and primary outcome. J Epidemiol 2000;10:55–64 | Clinical outcomes |
| Tuomi K, Ilmarinen J, Seitsamo J, Huuhtanen P, Martikainen R, Nygard CH, et al. Summary of the Finnish research project (1981–1992) to promote the health and work ability of aging workers. Scand J Work Env Health 1997;23:66–71 | Not qualitative; not physical activity |
| Tuomilehto J, Lindström J, Eriksson JG, Valle TT, Hämäläinen H, Ilanne-Parikka P, et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med 2001;344:1343–50 | Lifestyle intervention for diabetes |
| Van Roie E, Delecluse C, Opdenacker J, De Bock K, Kennis E, Boen F. Effectiveness of a Lifestyle Physical Activity Versus a Structured Exercise Intervention in Older Adults. J Age Phys Activ 2010;18:335–52 | Clinical outcomes |
| Van Nes NF, Jonsson H, Abma T, Deeg D. Changing everyday activities of couples in late life: converging and keeping up. J Aging Stud 2013;1:82–91 | Mean age 79 years |
| Van Roe E, Delecluse C, Opdenacker J, De Bock K, Kennis E, Boen F, et al. Effectiveness of a lifestyle physical activity versus a structured exercise intervention in older adults. J Age Phys Activ 2010;18:335–52 | No relevant outcomes |
| Vogler J, O’Hara L, Gregg J, Burnell F. The impact of a short-term iyengar yoga program on the health and well-being of physically inactive older adults. Int J Yoga Therapy 2011;21:61–72 | No relevant outcomes |
| Vrdoljak D, Markovic BB, Puljak L, Lalic DI, Kranjcevic K, Vucak J. Lifestyle intervention in general practice for physical activity, smoking, alcohol consumption and diet in elderly: a randomized controlled trial. Arch Gerontol Geriatr 2014;58:160–9 | Not OECD country |
| Umstattd MR, Hallam J. Older adults exercise behavior: roles of selected constructs of social-cognitive theory. J Aging Phys Activ 2007;15:206–18 | Association data |
| van den Berg TI, Elders LA, Burdorf A. Influence of health and work on early retirement. J Occup Environ Med 2010;52:576–583 | Conference abstract |
| Van der Bij AK, Laurant MGH, Wensing M. Effectiveness of physical activity interventions for older adults – A review. Am J Prev Med 2002;22:120–33 | Review, checked references |
| Wythes AJ, Lyons M. Leaving the land: an exploratory study of retirement for a small group of Australian me. Rural Remote Health 2006;6:1–13 | Not physical activity |
Appendix 6 Extraction tables A1/2 intervention studies
| Study details | Population and setting | Methods | Findings |
|---|---|---|---|
| Ackermann et al. (2005)27 Country: USA Study design: cluster RCT Length of follow-up: 4 months Aim: to determine whether or not a clinic-based physical activity promotion intervention can lead to more community-based exercise referrals by providers and higher exercise motivation in patients Recruitment: all patients aged 50 years and over visiting a study provider were invited Funding: Department of Veterans Affairs |
Number of participants: 31 physicians and nurse practitioners; 336 patients Age: patients aged 50 years and older (mean age 66 years) Retirement: NR Sex: 99% male Education: NR Ethnicity: NR Other inclusion/exclusion criteria: 63% not regularly exercising Service setting: health-care patients |
Intervention aims and content if applicable: intervention PCPs were trained to offer referrals to community exercise programmes for patients who reported before their clinic visit that they were ‘contemplative’ about regular exercise At visits with enrolled patients, intervention PCPs received a prompt that identified whether patients were pre-contemplative, contemplative or active with respect to regular physical activity. Attached to every prompt was an eight-page community exercise resource guide and a pre-printed prescription to reinforce any PCP advice The resource guide provided contact information for senior centres, parks and recreation departments, and walking resources within about 25 miles of the Seattle Veterans Association. In addition, the guide reviewed benefits of regular exercise, hints for how to safely start new exercises, and a list of warning signs to warrant stopping new activities until consulting further with a health-care provider Control condition if applicable: randomised to a physical activity counselling intervention or control condition (counselling about tobacco cessation) Data collection methods: interviews – physical activity community exercise questionnaire (physician-based assessment and counselling for exercise) Outcome measures: exercise stage-of-change, proportion of participants reporting regular physical activity Response and/or attrition rate: 66% agreed to participate. 158 (92%) at 4-month follow-up Data analysis: regression modelling |
Main results relevant to research question (author analysis): at baseline, 172 intervention patients and 164 controls were similar with respect to sex, age, comorbidity score and exercise motivation level. A total of 45% of all intervention patients and 35% of controls reported receiving exercise advice (p = 0.07). Intervention patients who were contemplative about exercise were even more likely to receive exercise advice than contemplative controls (59% vs. 38%; p = 0.02). After 4 months, 35% of all intervention patients reported regular exercise, compared with 28% of controls (p = 0.06) PCPs are more likely to offer exercise advice when informed about whether or not patients are contemplative about exercise |
| Armit et al. (2005)28 Country: Australia Study design: RCT described as feasibility study Length of follow-up: 24 weeks Aim: to evaluate the feasibility of an exercise scientist working in GP practices Recruitment: waiting rooms of GP practices Funding: Medical Benefits Fund |
Number of participants: n = 28 (complete data for 22) Age: 55–70 years (mean 64 years; SD 4.8 years) Retirement: 81% retired Sex: 35% male Education: NR Ethnicity: NR Other inclusion/exclusion criteria: physically inactive Service setting: GP surgery/home |
Intervention aims and content if applicable: three intervention arms – (1) advice from GP only (written physical activity prescription, booklet and brief advice); (2) 15- to 20-minute counselling session, same booklet as group 1, diary for goal-setting and monitoring and three telephone calls from exercise scientist over 12 weeks; and (3) counselling and support plus pedometer and advice centred on increasing steps Control condition if applicable: none – three intervention arms Data collection methods: self-report physical activity survey Outcome measures: total minutes of physical activity calculated using time spent in walking, moderate and vigorous activities Response and/or attrition rate: 33% of eligible patients recruited, 9 withdrew, 22 of 28 completed Data analysis: ANOVA, ITT |
Main results relevant to research question (author analysis): significant effect of intervention but no statistical difference between groups (although descriptive statistics indicated no effect in group 1). At 12 weeks, overall increase of 116 weighted minutes of physical activity per week (p < 0.001) Decrease from end of intervention to 6-month follow-up with average decrease of 60 weighted minutes. However, the decrease was predominantly in group 1. No precise detail of the 12-month data but assumed not to be statistically significantly different from baseline |
| Burman et al. (2011)29 Country: USA Study design: RCT Length of follow-up: 18 months Aim: to evaluate the use of peer mentors to improve long-term maintenance Recruitment: from a university community via adverts, flyers, older adult registry Funding: University of Florida |
Number of participants: n = 69 Age: 50 years or older (mean 63.42 years; SD 8.62 years); 39%, 50–64 years; 42%, 65 years or older Retirement: NR Sex: 82% female Education: ‘primarily college educated’ Ethnicity: 91% white Other inclusion/exclusion criteria: currently inactive, free of medical factors prohibiting exercise or any other factors affecting study compliance or assessment Service setting: university/community church |
Intervention aims and content if applicable: two intervention arms – (1) Active Adult Mentoring Programme 16 weeks, a peer-led advice and support group intervention; or (2) standard community group intervention. Both had access to an exercise facility and were given pedometers. Format, staff time and attention was the same for both groups. Each group session had 3–7 participants and a peer mentor, homework assignments, discussion and praise and reinforcement AAMP sessions included sessions on trust and rapport building within the group followed by self-management skills sessions in which participants were encouraged to take part in physical activity using encouragement, feedback, goal-setting, supportive social support system, problem-solving, mental imagery, relapse prevention skills, plan development. Based on social cognitive theory and self-determination theory Standard care sessions comprised education about the benefits of physical activity and basic health education delivered by peer mentors Control condition if applicable: two intervention arms Data collection methods: questionnaires, treadmill assessment Outcome measures: Leisure Time Exercise Questionnaire, a subsample used an accelerometer, cardiorespiratory fitness, barriers self-efficacy and exercise self-efficacy, Exercise Motivation Scale Response and/or attrition rate: 85% completed all elements Data analysis: R-ANOVA |
Main results relevant to research question (author analysis): at the end of the intervention (16 weeks) both groups reported significantly more activity than at baseline (ES 1.38; p < 0.001). No difference between the interventions. At 18-month follow-up the AAMP intervention group reported significantly more moderate to vigorous activity minutes per week than the usual intervention arm (ES 0.32; p = 0.04) Both groups improved equally on cardiorespiratory fitness (ES 0.63; p = 0.06) Exercise-related self-efficacy was not significantly different pre–post for either group Self-determination improved, with the AAMP intervention significantly more effective than the usual intervention (ES 0.46; p = 0.045) |
| Burke et al. (2013)30 Country: Australia Study design: RCT Length of follow-up: immediate Aim: to evaluate a physical activity and nutrition programme Recruitment: selected from electoral roll with sampling by suburb Funding: Australian National Health and Medical Research Council |
Number of participants: n = 375 Age: 60–70 years (mean 65 years; SD 2.95 and 3.19 years) Retirement: 43.8%/40.2% working Sex: male 52%/50% Education: university 21%/17.6% Ethnicity: NR Other inclusion/exclusion criteria: classified as low or medium SES, insufficiently active (< 30 minutes of moderate-intensity physical activity on at least 5 days per week), not at risk from participating in physical activity, not on special diet Service setting: home |
Intervention aims and content if applicable: physical activity and nutrition for seniors 6-month programme. Based on social cognitive theory and the Precede–Proceed model. Flexible, home-based, set own goals and partly tailor own intervention. Comprised a booklet with recommendations which encouraged goal-setting, also an exercise chart, calendar, bimonthly newsletters, a resistance band and a pedometer. Telephone calls and e-mail contact according to participant request. Included both activity and dietary elements Control condition if applicable: completed questionnaires only and received small financial reward Data collection methods: self-completed questionnaires Outcome measures: International Physical Activity Questionnaire Short Form Response and/or attrition rate: 78.5% response rate Data analysis: general estimating equation models |
Main results relevant to research question (author analysis): 74% used the exercise chart, 62% practised the recommended exercises, 90% used the pedometer, 63% used the resistance band. Significant improvements baseline to post programme for intervention group with regard to strength exercise (p < 0.001), walking (p = 0.012), moderate activity (p = 0.008), vigorous activity (p = 0.044), sitting time mean per week (p < 0.001). These improvements were significant compared with control for strength (p < 0.001), walking (p = 0.0029), vigorous activity (p = 0.0015) and mean sitting time (p = 0.0001) |
| Caperchione and Mummery (2006)31 Country: Australia Study design: RCT Length of follow-up: 12 months Aim: to evaluate group process strategies as an intervention tool Recruitment: via GP surgeries, health professionals and older adult organisations, brochures and media Funding: NR |
Number of participants: n = 122 Age: above 50 years (mean age 58/59 years) Retirement: 38% retired, 50% employed Sex: 82% and 66% female Education: NR Ethnicity: NR Other inclusion/exclusion criteria: history of inactivity (< 15 minutes of physical activity), able to walk unassisted for 10 minutes Service setting: unclear |
Intervention aims and content if applicable: 12-week lifestyle intervention. Five enhanced groups and five standard groups met once a week for 90 minutes over a 12-week period. Instructor-led group walk and group education sessions incorporating cognitive–behavioural strategies and health-related information. Enhanced package included education sessions on group process. Resource manual provided to all and talks by professionals such as sports psychologists Control condition if applicable: two intervention arms only Data collection methods: questionnaires Outcome measures: CHAMPS records energy expenditure of moderate activities, energy expenditure of total activities, frequency of moderate activities, frequency of total activities. Total expenditure of all activities (measured by calorific expenditure) chosen as the measure for this study Physical Activity Group Environment Questionnaire assessed perceptions of group cohesion Response and/or attrition rate: 140 recruited Data analysis: ANOVA, ITT |
Main results relevant to research question (author analysis): significant increase in physical activity behaviour (as measured by calorific expenditure) over time for both groups (p < 0.05). However, no significant difference between standard and enhanced intervention Group cohesion measure decreased over time with no difference between the groups (was moderate to high across time points) |
| Castro et al. (2001)32 Country: USA Study design: RCT Length of follow-up: 2 years (post intervention) Aim: compare telephone vs. mail interventions for physical activity Recruitment: telephone Funding: US government |
Number of participants: n = 179 (140 in second year) Age: 50–65 years (mean 56.3 years; SD 4.3 years) Retirement: NR (74% employed) Sex: 57% male Education: 9–22 years (mean 15.6 years; SD 2.7 years) Ethnicity: 93% white Other inclusion/exclusion criteria: Service setting: community |
Intervention aims and content if applicable: randomised to 1 year of telephone counselling to adopt higher (more vigorous) or lower intensity physical activity. After 1 year, randomised to second year of contact via telephone/mail or mostly mail only Control condition if applicable: two intervention conditions Data collection methods: unclear Outcome measures: self-reported exercise adherence rate Response and/or attrition rate: 39 participants did not participate in second year Data analysis: chi-squared test, t-tests |
Main results relevant to research question (author analysis): during year 1, participants in the higher condition had an average exercise adherence of 88% (2.64 sessions per week), whereas the low condition averaged 81% (4.05 sessions per week) During year 2, the higher condition had an average exercise adherence of 73% (2.19 sessions per week), whereas the low condition averaged 57% (2.85 sessions per week) The year 2 exercise adherence rates were significantly below those of year 1. F(1, 139) = 89.84; p < 0.001 When controlling for year 1 adherence rates, participants in the lower intensity programme did not differ from the higher intensity programme in their year 2 adherence rate F(1, 63) = 0.07; p > 0.7 |
| Coronini-Cronberg et al. (2012)33 Country: UK Study design: before/after (repeated cross-sectional survey) Length of follow-up: NA Aim: assessed the potential public health benefit of the National Bus Pass Recruitment: National survey data Funding: NIHR |
Number of participants: n = 16 911 Age: 60 years and older (eligible for bus pass) Retirement: NR Sex: NR Education: NR Ethnicity: NR Other inclusion/exclusion criteria: Service setting: community |
Intervention aims and content if applicable: introduction of free bus pass to over 60 year olds Control condition if applicable: NA Data collection methods: 2005–2008 National Travel Survey. Interview, and a 1-week travel diary Outcome measures: active travel (walking, cycling, and use of public transport), use of buses and walking three or more times per week Response and/or attrition rate: response rates are around 60% each year Data analysis: logistic regression |
Main results relevant to research question (author analysis): Having a free pass was significantly associated with greater active travel among both disadvantaged (AOR 4.06, 95% CI 3.35 to 4.86; p < 0.001) and advantaged groups (AOR 4.72, 95% CI 3.99 to 5.59; p < 0.001); greater bus use in both disadvantaged and advantaged groups (AOR 7.03, 95% CI 5.53 to 8.94; p < 0.001 and AOR 7.11, 95% CI 5.65 to 8.94; p < 0.001, respectively); and greater likelihood of walking more frequently in the whole cohort (AOR 1.15, 95% CI 1.07 to 1.12; p < 0.001) |
| Costanzo and Walker (2008)34 Country: USA Study design: RCT Length of follow-up: Aim: to compare five- vs. one-session delivery of a programme Recruitment: web adverts, bulletins, flyers Funding: none (PhD study) |
Number of participants: n = 51 Age: 50–65 years (mean 54/55.08 years; SD 4.01/3.87 years) Retirement: 1 individual not employed Sex: 100% female Education: 52% degree educated in intervention group, 80% control Ethnicity: 100% white non-Hispanic in intervention group (96% control) Other inclusion/exclusion criteria: screened using Stage of Exercise Behaviour Questionnaire eligible if at contemplation or preparation stage, English speaking, answered no to all questions on Physical Activity Readiness Questionnaire, able to walk without walker/crutches Service setting: unclear |
Intervention aims and content if applicable: behaviour counselling, using 5As (ask, advise, assist, arrange, agree). Five sessions over 12 weeks (full details of intervention in Costanzo et al.127) Control condition if applicable: one session received Data collection methods: questionnaires Outcome measures: Barriers to Self-Efficacy Scale, Social Support and Exercise Survey (family support subscale and friend support subscale), modified 7-day activity recall Response and/or attrition rate: 46 completed Data analysis: t-tests, ANOVA and path analysis |
Main results relevant to research question (author analysis): No data on physical activity levels ‘The intervention did not directly affect physical activity but indirectly influenced it via self-efficacy’ Significant difference between groups over time for self-efficacy for physical activity (p = 0.002), a large ES of 0.19. This was attributable to a decrease in control group with intervention group unchanged Family support for physical activity and friend support increased significantly in intervention group (ES 0.10 and p = 0.019) and was unchanged in controls. Increase in family support was, however, associated with less physical activity |
| Cox et al. (2008)35 Country: Australia Study design: RCT Length of follow-up: 12 months Aim: to evaluate whether a behavioural intervention increases adherence to a supervised swimming or walking programme Recruitment: via media advertising Funding: Western Australia Health Foundation |
Number of participants: n = 116 Age: 50–70 years, mean 55 years Retirement: 52–80% employed Sex: 100% female Education: 13–15 years education Ethnicity: described as predominantly well-educated Caucasian women, with no volunteering of those from minority groups despite extensive recruitment Other inclusion/exclusion criteria: non-smokers, < 30 minutes of activity per week, BMI < 34 kg/m2. Those unable to float in deep water, with musculo-skeletal disorders, mental incapacity, non-English speakers, with diabetes, cardiac, respiratory or other chronic illness were excluded Service setting: centre-based |
Intervention aims and content if applicable: SWEAT behavioural intervention based on Transtheoretical model. Consisted of 12 workshop centre-based sessions over 6 months with worksheets to complete at home followed by an exercise session. This intervention followed a 6-month supervised swimming or walking programme for three sessions per week of 30 minutes. Participants asked to continue their programme unsupervised for a further 6 months Control condition if applicable: the same walking or swimming programme as intervention group for 6 months supervised and then 6 months unsupervised followed by usual care Four study arms: swimming and usual care, swimming and SWEAT, walking and usual care, walking and SWEAT Data collection methods: baseline measures and reassessment at 6 and 12 months Outcome measures: Stage of Change Instrument, exercise history questionnaire, 1.6-km walk, 12-minute swim, record of illness and injury Response and/or attrition rate: 86% retained at 6 months and 74% retained at 12 months. Reasons for withdrawal were most frequently medical followed by pre-existing injury, then having no time. Older participants had better retention (age 55.91 years vs. age 53.13 years) Data analysis: ANOVA, GLM, ITT |
Main results relevant to research question (author analysis): after 6 months, 83% of swimmers and 86% of walkers had moved to action stage of stages of change. After 12 months, 75% of swimmers and 72% of walkers had moved to maintenance stage. Similar in control and intervention groups Benefits in terms of fitness (walk time or swim distance) found for both groups at 6 months; these were maintained at 12 months compared with baseline (p < 0.05) Similar retention and adherence for swimming vs. walking and in intervention vs. control groups at 6 months and 12 months (p < 0.001). Steady decline in adherence over first 24 weeks for both types of exercise and intervention vs. controls. The additional intervention thus had no impact on retention or adherence |
| Croteau et al. (2014)36 Country: USA Study design: RCT (described as pilot) Length of follow-up: 12 months Aim: to evaluate the use of physical activity mentors Recruitment: health-care providers referred to study Funding: NR |
Number of participants: n = 36 (21 completed) Age: 51–81 years (mean 64 years; SD 8.8 years) Retirement: 16 employed Sex: 21 female (of 28 completers) Education: 16 completed some college education Ethnicity: 27 white Other inclusion/exclusion criteria: patients that professionals considered were inactive and would benefit Service setting: unclear |
Intervention aims and content if applicable: Maine in Motion, 6-month programme based on social cognitive theory. Uses a manual, individual counselling sessions, pedometer, self-monitoring. Daily step goals set, tips, brainstorm strategies and obstacles. Pedometer set to zero at start of each day and worn during all waking hours, steps recorded on calendar daily and calculated by participant each week. Following initial session further meeting at 3 and 6 months with fitness professional Also ‘plus’ programme where participants attended group meetings each month for first 6 months Control condition if applicable: two intervention arms only; no control Data collection methods: steps recorded based on pedometer readings Outcome measures: daily steps Response and/or attrition rate: 22% dropout, lack of interest, time constraints, injury or illness Data analysis: t-tests, ANOVA, ITT |
Main results relevant to research question (author analysis): baseline 4236 mean daily steps, significant intervention effect (ES 0.611; p = 0.015). Both groups had significant increase at 6 months with no significant difference between groups (p = 0.151). Standard group increase of 18% and plus group increase of 53% at 6 months, 14% at 12 months for standard group and 40% at 12 months for plus group. Fading of effect for standard group, effect significant only for plus group baseline to 12-month follow-up (ES 0.606) |
| de Jong et al. (2006)37 Country: the Netherlands Study design: cluster RCT Length of follow-up: 6 months Aim: to evaluate an active living programme Recruitment: three municipalities selected, four neighbourhoods in each. All older adults invited by letter and respondents screened Funding: Zorg Onderzoek Nederland |
Number of participants: n = 315 Age: 55–65 years (mean 59.6 years, intervention; 58.8 years, control) Retirement: NR Sex: 55% female Education: 43%/33% elementary only Ethnicity: NR Other inclusion/exclusion criteria: NR Service setting: community |
Intervention aims and content if applicable: GALM programme – 30 once-a-week 1-hour sessions emphasising moderate-intensity recreational sport activities such as dance, self-defence, swimming. Session comprised groups of 15–24 held in a gymnasium scheduled at different times and days. Led by a professional sports instructor Control condition if applicable: waiting list for 6 months Data collection methods: questionnaire, fitness-testing session Outcome measures: physical activity questionnaires used to estimate energy expenditure, Vitality Plus Scale, quality of life, perceived fitness score, comparative fitness rating, physical activity readiness, blood pressure, body fat Response and/or attrition rate: 181 of 357 completed follow-up measures Data analysis: ANOVA, ANCOVA, chi-squared test, ITT |
Main results relevant to research question (author analysis): both groups significantly increased on virtually all measures; however, no difference between groups for most including energy expenditure (p = 0.68), leisure time physical activity (p = 0.8) and walking (p = 0.78). Only significant difference between groups related to improved reach. ITT analysis of perceived fitness showed between group differences (p < 0.01), also diastolic blood pressure (p < 0.05) |
| de Jong et al. (2007)38 Country: the Netherlands Study design: cluster RCT Length of follow-up: 12 months Aim: longer term follow-up of above study Recruitment: NA Funding: as above |
Number of participants: n = 181 (79 intervention) Age: 55–65 years (no detail of this sample only baseline characteristics) Retirement: NR Sex: baseline data only, no detail for this sample Education: as above Ethnicity: as above Other inclusion/exclusion criteria: as above Service setting: community |
Intervention aims and content if applicable: as above – GALM Control condition if applicable: as above Data collection methods: as above Outcome measures: as above Response and/or attrition rate: 181 of the original 315 Data analysis: multivariate model, ITT |
Main results relevant to research question (author analysis): Substantial number of missing data (up to 49%) Average attendance at sessions was 80% for first 6 months and 71% for second 6 months Energy expenditure for sport and total energy expenditure significantly increased over time – 12 months from baseline (p < 0.01); however, this was not significant when compared by group. For energy expenditure leisure time activity, the intervention group, despite increasing to 6 months, decreased from 6 to 12 months. BMI and walking also had a significant effect by time but not group. For other indicators, there were no significant differences by time or group |
| Dorgo et al. (2009)39 Country: USA Study design: RCT Length of follow-up: 14 weeks Aim: to investigate the effectiveness of a peer or student mentored exercise programme Recruitment: NR Funding: Paso del Norte Health Foundation |
Number of participants: 60 older adults Age: 68.7 + 6.1 years (60–82 years) Retirement: NR Sex: 31 men, 29 women Education: NR Ethnicity: NR Other inclusion/exclusion criteria: Service setting: unclear |
Intervention aims and content if applicable: 30 older adults (mean age 68.4 + 5.9 years) trained as peer mentors. 30 weeks of peer mentor preparation. The programme focused on physical fitness, exposure to a variety of exercises and training techniques, and improving participants’ image as a positive role model of health (weeks 1–14), plus developing and practising mentoring skills (weeks 15–30) Then identical 14-week fitness programme delivered by peer mentors or student mentors Control condition if applicable: student mentors: kinesiology students supervised the peer training sessions and received 3 weeks of training to work with older adults Data collection methods: unclear Outcome measures: physical improvement, programme perception, retention and participation Response and/or attrition rate: 93% of mentors completed. Participant retention 76.6% SM and 90% PM Data analysis: ANOVA, t-tests |
Main results relevant to research question (author analysis): both groups improved their fitness significantly with no post-test differences between the groups in most fitness measures or programme perception rates Compared with baseline values the 14-week training programme produced significant improvements (ES 0.2–1.6; p < 0.007) in all measures of fitness for the peer-mentor group. The same was true for the student-mentor group (ES 0.2–1.4; p < 0.31) with the exception of upper body flexibility (p = 0.76) There were no significant differences between groups for the 6-minute walk, 30-second arm curl, forward reach, handgrip strength, chair sit and reach, and back scratch tests (ES 0.08–0.58; p > 0.27) but the student-mentor group scored significantly higher than the peer-mentor group for the 30-second chair stand (ES 0.56; p = 0.034) and the 8-feet up and go (ES = 0.06; p = 0.045) |
| Elley et al. (2003)40 Country: New Zealand Study design: cluster RCT Length of follow-up: 12 months Aim: to assess the long-term effectiveness of the ‘green prescription’ programme, a clinician-based initiative in general practice that provides counselling on physical activity Recruitment: 42 rural and urban general practices Funding: National Heart Foundation of New Zealand |
Number of participants: NR Age: 40–79 years (mean 57.2 years; SD 10.8 years) Retirement: NR Sex: 301 (67%) female Education: 106 (24%) post-high school qualification Ethnicity: 354 (78%) European origin Other inclusion/exclusion criteria: sedentary Service setting: general practice |
Intervention aims and content if applicable: GPs were prompted by the patient to give oral and written advice on physical activity during usual consultations. Exercise specialists continued support by telephone and post In the consultation, the PCP discussed increasing physical activity and decided on appropriate goals with the patient. These goals, usually home-based physical activity or walking, are written on a standard green prescription and given to the patient Exercise specialists from the sports foundation make at least three telephone calls (lasting 10–20 minutes) to the patients over the next 3 months to encourage and support them. Motivational interviewing techniques are used. Specific advice about exercise or community groups is provided if appropriate Control condition if applicable: control patients received usual care Data collection methods: self-reported questionnaire Outcome measures: change in physical activity, quality of life (SF-36 cardiovascular risk blood pressure) Response and/or attrition rate: 74% (117/159) of GPs and 66% (878/1322) of screened eligible patients participated in the study. The follow-up rate was 85% (750/878) Data analysis: random-effects model, ITT |
Main results relevant to research question (author analysis): mean total energy expenditure increased by 9.4 kcal/kg/week (p = 0.001) and leisure exercise by 2.7 kcal/kg/week (p = 0.02) or 34 minutes/week more in the intervention group than in the control group (p = 0.04) The proportion of the intervention group undertaking 2.5 hours/week of leisure exercise increased by 9.72% (p = 0.003) more than in the control group (number needed to treat = 10.3) SF-36 measures of self-rated ‘general health,’ ‘role physical,’ ‘vitality,’ and ‘bodily pain’ improved significantly more in the intervention group (p < 0.05) A trend towards decreasing blood pressure became apparent but no significant difference in 4-year risk of coronary heart disease |
| Finkelstein et al. (2008)41 Country: USA Study design: RCT Length of follow-up: immediate Aim: to evaluate the use of financial incentives as part of a physical activity programme Recruitment: newspaper advert, online advertising website Funding: Centers for Disease Control and Prevention |
Number of participants: n = 70 Age: mean 59.4 years intervention and 61.2 years control (minimum 50 years; maximum 85 years) Retirement: 28.6% intervention and 43.3% control retired and not working Sex: 23.8%/26.7% male Education: 85%/70% college degree or higher, 40% household income > US$50,000 Ethnicity: non-white 4.8% intervention 6.7% control Other inclusion/exclusion criteria: at least aged 50, < 2 hours’ exercise per week Service setting: unclear |
Intervention aims and content if applicable: attended initial meeting, wore pedometer for 4 weeks, given US$50 initial payment and subsequent payments depending on number of aerobic minutes per day – nothing if < 15, US$10 if 15–24, US$15 if 25–39, and US$25 if 40 or more. Daily use capped at 75 minutes Control condition if applicable: participants attended an initial meeting and wore the pedometer, given US$75 payment for taking part, wearing the pedometer daily and returning all study materials Data collection methods: pedometer and diary Outcome measures: aerobic minutes as measured by a pedometer and self-report log Response and/or attrition rate: 51 completed Data analysis: linear regression |
Main results relevant to research question (author analysis): adjusted treatment effect just over 16 more aerobic minutes in intervention group (p > 0.001). Small difference between full-time employees and retirees (retired: more minutes) but this was not significant Control group average 20 minutes per day, slight decrease over the 4 weeks. Intervention group average 35 minutes per day (1.8 hours per week more than controls) with little change over the 4 weeks Average pay out to intervention participants was US$17.50 per week. This would total US$910 per year |
| Fries et al. (1992)42 Country: USA Study design: cluster RCT Length of follow-up: 1 year Aim: to evaluate a health promotion programme Recruitment: invited by letter Funding: Blue Shield health benefit company |
Number of participants: n = 4712 Age: mean 68 years Retirement: all retired Sex: 52% female Education: NR Ethnicity: NR Other inclusion/exclusion criteria: members of bank retiree clubs Service setting: home |
Intervention aims and content if applicable: personal health-risk report based on questionnaire data every 6 months, individualised recommendation newsletters, newsletters, self-management and health promotion books, other materials all delivered by post. Designed to cost around US$30 per year Control condition if applicable: two other conditions – questionnaire only and no intervention Data collection methods: health habits questionnaire, health benefit company data on claims made Outcome measures: health claims data, risky health behaviours including exercise minutes/week and health programme attendance, weight computed as health-risk score Response and/or attrition rate: 1802 completed year 1 Data analysis: t-tests, McNemar’s test, Mann–Whitney |
Main results relevant to research question (author analysis): computed health-risk scores decreased by 4.3% in intervention group and increased by 7.2% in questionnaire only group Exercise minutes per week and exercise programme attendance showed a non-significant difference from baseline to 12 months or difference intervention vs. controls Other health-risk factors such as pounds over ideal weight, blood pressure and total health-risk score were significantly different from baseline to post and between groups |
| Fries et al. (1993)43 Country: USA Study design: cluster RCT Length of follow-up: 2 years Aim: to evaluate a health promotion programme Recruitment: as above Funding: Blue Shield |
Number of participants: n = 4712 Age: mean 68 years Retirement: all retired Sex: 52% female Education: NR Ethnicity: NR Other inclusion/exclusion criteria: members of bank retiree clubs Service setting: home |
Intervention aims and content if applicable: as above Control condition if applicable: as above Data collection methods: as above Outcome measures: as above Response and/or attrition rate: 1452 2-year data Data analysis: as above |
Main results relevant to research question (author analysis): Computed health-risk scores decreased in intervention group compared with questionnaire only group (p < 0.001) Exercise minutes per week and exercise programme attendance significant difference from baseline to 24 months (p < 0.05) Between group differences reported for 12 months only, not reported at 24 months |
| Fujita et al. (2003)44 Country: Japan Study design: RCT Length of follow-up: 6 months Aim: to evaluate an exercise training programme Recruitment: not detailed in this paper Funding: Ministry of Education and Culture, Ministry of Health and Welfare, Nakatomi Foundation |
Number of participants: n = 65 Age: 60–81 years (mean 67.1 years) Retirement: NR Sex: 30 male, 35 female Education: NR Ethnicity: NR Other inclusion/exclusion criteria: Those with neurological deficits, CHD, high blood pressure, arthritis, recent falls, chronic disease, other heart problems or conditions affecting participation Service setting: a community health and welfare facility for older adults |
Intervention aims and content if applicable: 25-week exercise group intervention consisting of three 2-hour exercise classes each week. They were asked to attend at least twice a week. The classes consisted of endurance training using a bicycle ergometer for 10–25 minutes, sit ups and exercises using resistance bands Control condition if applicable: received two 2-hour classes per month consisting of a lecture on a non-physical activity topic and a recreational activity, asked to continue normal life activities. Received a 6-month exercise intervention post measurement Data collection methods: physical activity diary Outcome measures: total daily energy expenditure, with activities classified as light, moderate or strenuous Response and/or attrition rate: three participants did not complete data collection, one lost to follow-up Data analysis: t-tests, ITT |
Main results relevant to research question (author analysis): the total daily energy expenditure increased in the intervention group (from 40.8 to 43.5 kcal/kg per day, an increase of 6.4% p = 0.03) and did not change in the control group (42.2 pre, 39.2 post; p = 0.11) The light activity time in the intervention group decreased significantly (p = 0.049), whereas both moderate and strenuous activity increased (although not significantly different p > 0.05) At follow-up there was some fading of effect (decrease of 1.2 kcal/kg per day); however, post-intervention values remained higher than at baseline (p = 0.05). Moderate activity rates remained significantly higher although strenuous activity had returned to pre-intervention level |
| Goldstein et al. (1999)45 Country: USA Study design: cluster RCT Length of follow-up: 6 weeks and 8 months Aim: to evaluate a physician-delivered intervention Recruitment: eligible patients with appointments Funding: NR |
Number of participants: n = 34 physicians, n = 355 patients Age: 50 years and above (mean 65.6 years; SD 9.1 years) Retirement: 36% employed Sex: 65% female Education: mean 12 education years Ethnicity: 97% white Other inclusion/exclusion criteria: too active, were not ambulatory, unable to provide information on the telephone Service setting: primary care |
Pilot study reported in Marcus et al.60 paper Intervention aims and content if applicable: Physically Active for Life Project (physical activityL), based on TTM of change, social-cognitive theory, health education theory. 1-hour physician training session, physical activity counselling session provided to patients with follow-up appointment 4 weeks later. After follow-up appointment patients received five monthly newsletters. Financial reimbursement for physician participation Counselling used 5As approach, 5 minutes, written exercise prescription form completed. At follow-up appointment, physician provided counselling and new written prescription, patient given poster with tips on adoption and maintenance. Physicians received a manual Control condition if applicable: no physician training, no follow-up appointment, usual care Data collection methods: telephone interview with patients, questionnaire to physicians Outcome measures: stage of motivational readiness for physical activity, Physical Activity Scale for the Elderly Response and/or attrition rate: 1702 responded (2145 contacted), 400 did not meet criteria, 89 refused participation) giving 80% of eligible sample recruited Data analysis: t-tests, linear mixed-effects model |
Main results relevant to research question (author analysis): 99% of patients received a written prescription at initial appointment, 77% at follow-up At 6 weeks, intervention group was more likely to be in advanced stages of motivational readiness for physical activity than controls (Preparation or Action 89% vs. 74%; OR 3.56, 95% CI 1.79 to 7.08; p < 0.001). Effect not maintained, however, at 8 months At 6 weeks, 27% of intervention group vs. 21% controls met recommended guidelines for physical activity (no significant group difference). At 8 months this was 28% for intervention vs. 23% controls (no significant group effect) No significant change in physical activity scale between groups at either 6 weeks or 8 months. Both groups increased at 6 weeks and decreased by 8 months |
| Hageman et al. (2005)46 Country: USA Study design: RCT Length of follow-up: 3 months Aim: to evaluate an internet-based newsletter intervention Recruitment: newspaper advert Funding: none |
Number of participants: n = 31 Age: 50–69 years (mean 56.1 years) Retirement: 6.7% retired, 73% full-time and 6.7% part-time employed Sex: 100% female Education: 50% college graduate or higher Ethnicity: 86% white Other inclusion/exclusion criteria: English speaking, answered no to all items on Physical Activity Readiness Questionnaire, < 30 minutes physical activity on five or more days per week, have access to computer and internet in home Service setting: home |
Intervention aims and content if applicable: three newsletters delivered via the internet at baseline, 1 months and 2 months. These were individually tailored to participants based on baseline assessments or standard Control condition if applicable: standard newsletter Data collection methods: questionnaire, physical measures Outcome measures: Modified 7-day activity recall questionnaire, Rockport Walking Fitness Test, body composition, height, weight, flexibility, Benefits and Barriers Scales, Self-efficacy for Exercise Habits Scale Response and/or attrition rate: complete data for 28 Data analysis: ANOVA |
Main results relevant to research question (author analysis): no significant change for any self-reported activity or perceived benefits of activity. Improved flexibility pre–post (p = 0.02) and body fat. Both groups declined in regard to perceived barriers (p = 0.025). Self-efficacy increased for standard group but decreased for tailored group (p = 0.510 and p = 0.018) 83% reported that they had read all the newsletters, 63% that the newsletters were helpful in making them more aware of ways to increase physical activity, 50% that they were helpful in them changing their physical activity |
| Halbert et al. (2000)47 Country: Australia Study design: RCT Length of follow-up: 12 months Aim: to evaluate advice provided by a specialist in general practice Recruitment: those meeting criteria invited to appointment Funding: National Health and Medical Research Council |
Number of participants: 299 Age: 60 years or over (mean 67 years) Retirement: Sex: 48% female Education: Ethnicity: Other inclusion/exclusion criteria: sedentary adults Service setting: primary care |
Intervention aims and content if applicable: 20-minute session with exercise specialist. Intervention group received individualised advice, pamphlet and a plan. Potential barriers discussed Control condition if applicable: received pamphlet on good nutrition during 20-minute session Data collection methods: questionnaire, activity log, accelerometer for subsample Outcome measures: exercise questionnaire, SF-36, blood pressure, weight, blood sample Response and/or attrition rate: 88% provided follow-up data Data analysis: ANOVA, t-tests, chi-squared test, ITT |
Main results relevant to research question (author analysis): all self-report measures of physical activity increased pre-follow-up for both groups (p < 0.05). Significantly greater physical activity in intervention group vs. controls on all measures except walking (p < 0.05). Men reported higher rates and more vigorous exercise For the sample using accelerometer, no difference between intervention and controls on this physical activity data Difference between groups with regard to intention to exercise (p < 0.001) |
| Hamdorf et al. (1992)48 Country: Australia Study design: RCT Length of follow-up: 12 months Aim: evaluated a 6-month progressive walking programme Recruitment: previously randomised Funding: NR |
Number of participants: n = 66 Age: mean 64.8 years (SD 60.6–69.2 years) Retirement: NR Sex: female Education: NR Ethnicity: NR Other inclusion/exclusion criteria: sedentary women Service setting: unclear |
Intervention aims and content if applicable: 6-month (26-week) progressive walking programme. Two sessions per week supervised by fitness instructor. At completion of the programme subjects were encouraged to continue physical activity Control condition if applicable: instructed to carry on with normal activities of daily living and not commence any new physical activity programmes Data collection methods: human activity profile, maximum current activity and normative impairment index Outcome measures: activity, aerobic fitness Response and/or attrition rate: 8 dropped out Data analysis: ANCOVA, Wilcoxon signed rank |
Main results relevant to research question (author analysis): The maximum current activity score increased significantly (p = 0.01) in the intervention group compared with the controls |
| Hamdorf et al. (1993)49 Country: Australia Study design: RCT Length of follow-up: 12 months Aim: evaluated a 6-month progressive walking programme Recruitment: previously randomised Funding: NR |
Number of participants: n = 66 Age: 64.8 years (SD 60.6–69.2 years) Retirement: NR Sex: female Education: NR Ethnicity: NR Other inclusion/exclusion criteria: Sedentary women Service setting: unclear |
Intervention aims and content if applicable: 6-month (26-week) progressive walking programme. Two sessions per week. At completion of the programme subjects were encouraged to continue physical activity Control condition if applicable: instructed to carry on with normal activities of daily living and not commence any new physical activity programmes Data collection methods: human activity profile, maximum current activity and normative impairment index Outcome measures: activity, aerobic fitness Response and/or attrition rate: eight dropped out Data analysis: ANCOVA, Wilcoxon signed rank |
Main results relevant to research question (author analysis): during the follow-up period 77.8% of the training group continued with exercise and maintained lower (p < 0.005) exercise heart rates than the control group The training group had significantly higher maximum current activity scores than the controls at the end of the training period which were maintained during the 6-month follow-up (p > 0.005) |
| Hekler et al. (2012)50 Country: USA Study design: crossover RCT Length of follow-up: immediate Aim: to explore preferences for utilitarian walking vs. leisure walking and evaluate an intervention Recruitment: local advertising Funding: National Heart Lung and Blood Institute |
Number of participants: n = 16 Age: 50 years or older (mean 64 years; SD 7.5 years) Retirement: 56% employed (no details of non-employed) Sex: 81% female Education: 56% degree or higher Ethnicity: NR Other inclusion/exclusion criteria: inactive (< 60 minutes a week of activity) Service setting: |
Intervention aims and content if applicable: two intervention arms utilitarian walking (purpose of getting somewhere or accomplishing errands) and leisure walking (purpose of fitness health or recreation). 2 weeks of each intervention, free choice for a further 2 weeks. Five instructional sessions, contacted by health educators three times by telephone during each intervention. Based on Stanford AC Intervention a behavioural intervention including goal-setting, behavioural feedback, and problem-solving, information about national recommendations, and instructed to engage in brisk walking Control condition if applicable: two intervention arms Data collection methods: pedometer, self-report of type during free choice Outcome measures: number of steps per day Response and/or attrition rate: no dropouts, 31 screened Data analysis: t-test, correlation |
Main results relevant to research question (author analysis): Significant mean improvement in amount of walking for all 2-week phases (p < 0.05). Significantly more mean steps per day during leisure intervention than utilitarian phase (p < 0.05). The order of instruction may influence impact as those instructed in leisure walking first had greater difference in types of reported walking. All but two participants preferred a mixture of walking types during the free choice phase Neighbourhood characteristics associated with walking type – more leisure walking if access to walking paths, better neighbourhood aesthetics, access to facilities, and access to services. More utilitarian walking reported by participants who travelled to multiple locations during a day |
| Hooker et al. (2005)51 Country: USA Study design: BA Length of follow-up: 1 year Aim: to evaluate a telephone assisted programme Recruitment: 13 agencies selected as sites, advertising, direct mailing, leaflets, varied by sites Funding: NR |
Number of participants: n = 447 Age: 48–90 years [mean 67.9 years (SD 8.6 years)] Retirement: 49% retired no work, 17.7% retired, working, 20.9% employed Sex: 78% female Education: 13% below high school, 17.9% income < US$10,000 Ethnicity: 58% Caucasian, 25% Hispanic Other inclusion/exclusion criteria: NR Service setting: community/home |
Intervention aims and content if applicable: Agency staff received 16 hours of training. Participants met with staff member to develop a physical activity plan with individual goals. Received regular telephone calls over 1 year from a ‘buddy’ who were volunteers, health promoters, students, agency staff, they had received 4–8 hours of training. One call per week month 1, one call every 2 weeks months 2–4, then one call per month Variation in other elements between sites, some newsletters, some group activities, some face to face visits in addition to telephone support Control condition if applicable: none Data collection methods: questionnaires Outcome measures: Physical Activity Readiness Questionnaire, calories, CHAMPS questionnaire Response and/or attrition rate: loss to follow-up varied from 0–48% by sites, 82% of participants provided some data, 243 of 548 provided complete data. African Americans and those employed full time were less likely to provide complete data Data analysis: Wilcoxon signed rank test, random-effects model |
Main results relevant to research question (author analysis): Significant improvement in total calorie expenditure baseline to mid-point and end point (p < 0.0001 median change 707 calories per week), a typical increase of 3.2% of calories expended per month Those with lower levels at baseline and older than 65 years tended to increase more Light and moderate activity levels showed similar improvement (p < 0.0001 pre–post) Improvement in stage of readiness for all stages |
| Hughes et al. (2009)52 Country: USA Study design: RCT Length of follow-up: 10 months Aim: to assess the impact of existing best-practice physical activity programmes for older adults on physical activity participation and health-related outcomes Recruitment: participants were recruited through notices in provider newsletters, flyers posted at the provider sites or distributed at local events, and advertisements in newspapers Funding: Robert Wood Johnson Foundation |
Number of participants: 544 older adults Age: 50 years or older (mean 66 years) Retirement: NR Sex: 76.6% female Education: 86.6% college education Ethnicity: 85.5% white Other inclusion/exclusion criteria: 72% were overweight or obese Service setting: community |
Intervention aims and content if applicable: the treatment was a multiple-component physical activity programme that provided flexibility activities, low-impact aerobic exercise and resistance training for 60 minutes three times per week over the 10 months Control condition if applicable: control group participants could enrol in any programmes that the provider offered except for the multicomponent programme, and they could also participate in physical activity programmes other than those offered by the provider Data collection methods: questionnaire and clinical measures Outcome measures: self-efficacy for exercise adherence, exercise participation Response and/or attrition rate: 384 participants at 10 months (70% of baseline) Data analysis: logistic regression, random-effects model |
Main results relevant to research question (author analysis): Adults who participated in a multiple-component physical activity programme showed statistically significant benefits at 5 and 10 months with regard to self-efficacy for exercise adherence over time (p < 0.001), adherence in the face of barriers (p = 0.01), increased upper- and lower-body strength (p = 0.02, p = 0.01), and exercise participation (p = 0.01) |
| Irvine et al. (2013)53 Country: USA Study design: RCT Length of follow-up: 6 months (assessed at pre-test, 12 weeks, and 6 months) Aim: to evaluate the efficacy of a 12-week internet intervention to help sedentary older adults over 55 years of age adopt and maintain an exercise regimen Recruitment: recruited, screened, and assessed online supported by service agencies, senior centres, and worksites Funding: NR |
Number of participants: 368 sedentary men and women (subgroup analysis, original trial n = 878) Age: mean 60.3 years (SD 4.9 years) Retirement: NR Sex: 69% female Education: 82% had at least some college education Ethnicity: 59% Caucasian Other inclusion/exclusion criteria: average BMI was 28.9 kg/m2 (SD 6.7 kg/m2) 70% reported using the internet more than seven times per week Service setting: multiple |
Intervention aims and content if applicable: Active After 55, was a multiple-visit internet programme to enhance functional ability, mobility, and physical activity of older adults. Using text and video messages the intervention programme helped them select exercise activities in the areas of endurance, flexibility, strengthening, and balance enhancement. They returned to the programme weekly for automated video and text support and education, with the option to change or increase their exercise plan. The programme also included ongoing problem-solving to overcome user-identified barriers to exercise Control condition if applicable: control group did not have access to the intervention Data collection methods: self-rated measures (questionnaire including SF-12) Outcome measures: frequency and duration of intentional physical activities, fitness level, activity goals, and barriers to exercise Response and/or attrition rate: 368/405 at 6 months. A significantly higher attrition rate was obtained for the intervention condition compared with controls (30% vs. 7%; p < 0.001) Data analysis: multivariate |
Main results relevant to research question (author analysis): the multivariate model indicated significant treatment effects at post-test (p = 0.001; large ES) and at 6 months (p = 0.001; medium ES) At post test, intervention participation showed significant improvement on 13 of 14 outcome measures compared with the control participants At 6 months, treatment participants maintained large gains compared with the control participants on all 14 outcome measures (data in appendix). The multivariate model at follow-up was significant in which the text participants were found to maintain large gains compared with the control participants, F(14, 337) = 3.08; p < 0.001; η2 = 0.11 The outcome measures with medium ESs or larger include stretching exercises minutes/week (η2 = 0.06), balance exercise minutes/week (η2 = 0.08), behavioural intentions to exercise (η2 = 0.06), and motivation to exercise (η2 = 0.06) |
| Kamada et al. (2013)54 Country: Japan Study design: cluster RCT Length of follow-up: 1 year Aim: to evaluate a community wide campaign Recruitment: selection of communities to target with campaign Funding: Ministry of Health, Labour and Welfare |
Number of participants: residents targeted in 12 communities each with median population of 1292 (15,504), 4414 provided evaluation data Age: 40–79 years sample providing data mean age 60/61 years (SD 10 years) Retirement: 64–71% employed Sex: 44–47% male Education: mean 11 years Ethnicity: NR Other inclusion/exclusion criteria: all communities within a region (32) 12 of these randomly selected stratifying for population density (in each intervention group one high, one moderate, one low population density). For survey those in long-term care, or unable to walk unaided excluded Service setting: community |
Intervention aims and content if applicable: Community wide campaign to promote exercise (COMMUNICATE). Three intervention arms – mainly walking behaviour (aerobic activity), mainly stretching exercises (flexibility and muscle strengthening), and the third group all activities promoted. Intervention used social marketing principles and drew on stages of change model. Included information via flyers and leaflets, newsletters, banners also encouragement by health professionals during appointments and community events, and the use of community leaders and lay workers to encourage and provide support via provision of pedometers and reflective vests. Materials delivered to households directly and radio/television broadcasts only on local networks Paper describes targeting women 60–79 years with low back or knee pain and the primary message of the campaign related to exercise in order to reduce knee and back pain, although the authors predicted a ripple effect from the targeted segment to the wider community Control condition if applicable: nine communities in intervention, three in control condition. Control communities had no intervention Data collection methods: baseline and post-intervention survey Outcome measures: number engaging in regular physical activity, daily and weekly reported walking time, frequency of flexibility activity Response and/or attrition rate: unable to determine as population-based intervention, response to survey 73.8% baseline and 58.5% follow-up Data analysis: chi-squared test, general linear mixed model |
Main results relevant to research question (author analysis): Process evaluation data: leaflets distributed twice, activities carried out by professionals median 14 times for each community, approx. 7160 participants received encouragement by the HCPs Baseline control group 64.6% of sample reported engaging in regular physical activity, intervention group 63.9%. Post-campaign control group decreased slightly to 60.3%, intervention group also decreased to 58.7%. ES not significant. No difference between groups in relation to pain outcomes 73% of intervention group aware of at least one component of the campaign; however, 58.7% of the control group were also aware. Significant difference in awareness of campaign at 1-year follow-up (OR 2.7; p < 0.001) Belief and intention not significantly different between control and intervention at 1 year post campaign Significant difference in knowledge about physical activity benefit control vs. intervention participants 1-year follow-up (OR 1.51; p < 0.05) Authors suggest change in awareness and knowledge short-term impacts, whereas belief and intention are medium term |
| King et al. (2000)55 Country: USA Study design: RCT Length of follow-up: 1 year Aim: to evaluate the effects of two different community-based physical activity regimens Recruitment: telephone Funding: National Institute on Aging |
Number of participants: 103 older adults Age: 65+ years (mean 69 years; SD 4 years) Retirement: NR Sex: 67 women; 36 men Education: NR Ethnicity: 95% white Other inclusion/exclusion criteria: regularly active no more than twice a week during the preceding 6 months Service setting: community |
Intervention aims and content if applicable: randomised to 12 months of community-based, moderate-intensity endurance and strengthening exercises (Fit & Firm) or stretching and flexibility exercises (Stretch & Flex). A combination of class and home-based exercise formats was used For both conditions, subjects were encouraged to participate in two exercise classes each week and to exercise on their own at home at least twice a week. Exercise classes lasted one hour, but the suggested duration of the home-based sessions was 40 minutes (attained in a progressive fashion). Participants received individualised instruction and information prior to beginning their exercise programme. The class size was limited to 10–15 people and was conducted at a local YMCA. Classes were monitored regularly to assure quality and consistency of content Control condition if applicable: two interventions Data collection methods: exercise logs Outcome measures: physical performance, perceived functioning and well-being (self-rated) Response and/or attrition rate: 103 of 1357 eligible. 93% response rate at 12 months Data analysis: MANCOVA |
Main results relevant to research question (author analysis): For both conditions, exercise adherence was significantly higher for the home-based portion of the exercise prescription (Fit & Firm: 92% ± 50%; Stretch & Flex: 92% ± 43%) relative to the class-based portion of the exercise prescription (Fit & Firm: 65% ± 27%; Stretch & Flex: 68% ± 29%). For home vs. class comparison: paired-comparison t-test = 5.2; p < 0.001, two-tailed test Overall between-group differences on the two measures constituting the self-rated physical performance domain—including the three subscales contained in the Colorado Walking Impairment Scale and the four subscales contained in the Self-Efficacy for Physical Performance Scale was significant [F(7, 99) = 2.46; p < 0.01, one-tailed test] |
| King et al. (2007)56 Country: USA Study design: RCT Length of follow-up: 12 months Aim: determined the 6- and 12-month effectiveness of telephone interventions delivered by health educators or by an automated computer system in promoting physical activity Recruitment: promotion in local media outlets, along with distribution of flyers and brochures to local health clinics, pharmacies, senior centres, and other community settings Funding: National Institute on Aging |
Number of participants: n = 218 Age: 55 years and older Retirement: NR Sex: NR Education: NR Ethnicity: NR Other inclusion/exclusion criteria: not initially engaged in more than 60 minutes per week of moderate-intensity or more vigorous physical activity over the previous 6 months Service setting: community |
Intervention aims and content if applicable: (1) a home-based moderate-intensity physical activity programme delivered primarily via a trained telephone counsellor (Human Advice arm); and (2) a home-based moderate-intensity physical activity programme delivered primarily via an automated, computer controlled interactive telephone system (Automated Advice arm) Control condition if applicable: Health education control: weekly health education classes that focused on a variety of non-physical activity topics of interest Data collection methods: 7-day physical activity recall interview; verified on a random subsample via accelerometer data Outcome measures: minutes of moderate to vigorous physical activity Response and/or attrition rate: 189 (86.7%) had 6-and 12-month data Data analysis: ANCOVA, ITT |
Main results relevant to research question (author analysis): At 6 months, both the Human Advice and Automated Advice arms, although not significantly different from one another (p = 0.73), had significantly greater mean energy expenditure in moderate-intensity physical activity than the control arm [F(4, 217) 4.73; p = 0.01] Similarly, both the Human Advice and Automated Advice arms, while not significantly different from one another (p = 0.65), had significantly greater mean minutes/week spent in moderate-intensity physical activity than the Control arm [F(4, 217) 4.73; p = 0.01] These differences were generally maintained at 12 month. Mean energy expenditure in moderate-intensity physical activity for both the Human Advice and Automated Advice arms, although not significantly different from one another (p = 0.60), remained significantly greater than the Control arm [F (4,217) 3.4, p = 0.036]. Similarly, mean minutes/week in moderate-intensity physical activity for both the Human Advice and Automated Advice arms, while not significantly different from one another (p = 0.66), remained greater than the Control arm [F(4, 217) 3.14; p = 0.045] At 12 months, a significantly greater percentage of subjects in the Human Advice arm (51.4%) achieved the Surgeon General’s 150 or more minutes per week in moderate-intensity physical activity relative to control (30.0%), [X2(2) 7.0; p = 0.03]. The Automated Advice arm (44.6%) was not significantly different from either the Human Advice arm (p = 0.51) or the control arm (p = 0.10) |
| King et al. (2013)57 Country: USA Study design: RCT Length of follow-up: immediate Aim: to evaluate apps for physical activity Recruitment: unclear Funding: NR |
Number of participants: n = 68 Age: 45–81 years (mean 59 years; SD 9.2 years) Retirement: 48.5% working full time Sex: 73.5% female Education: 66% college degree, 51.4% income US$70,000 or more Ethnicity: 69% non-Hispanic white Other inclusion/exclusion criteria: insufficiently inactive, using a mobile phone but not a smart phone Service setting: |
Intervention aims and content if applicable: three smartphone apps – one based on an analytical motivational frame which included goal-setting, behavioural feedback, problem-solving, tips and advice, the second based on social motivational frame including social normative feedback, social support, interacting with other and group-based competition and collaboration and the third based on affective motivational frame including positive reinforcement, use of an avatar to provide feedback, and game-like rewards for reaching milestones All apps included an element to compile and analyse accelerometer data which provided just in time feedback 8-week intervention Control condition if applicable: three interventions Data collection methods: questionnaire Outcome measures: CHAMPS questionnaire, measure of older adults sedentary behaviour, satisfaction survey Response and/or attrition rate: 10% missing post data, dropouts younger Data analysis: t-tests, chi-squared test |
Main results relevant to research question (author analysis): Significant increases in minutes of brisk walking for all groups pre–post p-value of < 0.0001 with no difference between groups (p > 0.73). Increase averaged 100.8 weekly minutes (SD 167 weekly minutes) Similarly increase in moderate to vigorous physical activity for all groups (p < 0.0001) with no difference between groups (p > 0.99) Decreases in reported sitting time, television watching 87% found the app easy to use, 77% that the time spent using it was about right, 69% reported the app motivated them to be more active A sample were invited to continue using after 8 weeks, 12 of 15 approached agreed to continue using. 53.5% said they would be willing to continue to use for 6 months or longer |
| Koizumi et al. (2009)58 Country: Japan Study design: RCT Length of follow-up: immediate Aim: to evaluate an accelerometer intervention Recruitment: via senior centres and newspaper advertising Funding: NR |
Number of participants: n = 68 Age: mean 67 years (SD 4 years) Retirement: NR Sex: all female Education: NR Ethnicity: NR Other inclusion/exclusion criteria: excluded if any gait abnormality, taking medication for stroke, HRT or hypertension, had CHD Service setting: unclear |
Intervention aims and content if applicable: Lifestyle physical activity (LIFE) – accelerometer given to all participants which records physical activity intensities and number of steps. Recommended participants accumulated 9000 steps and 30 minutes of moderate-intensity physical activity per day, data provided to participants for previous 2 weeks with recommendations made. Intervention over 12 weeks Control condition if applicable: wore same device but was locked and collected no data Data collection methods: accelerometer recorded data Outcome measures: number of daily steps, moderate-intensity activity, 12-minute walk test Response and/or attrition rate: Data analysis: t-tests, ANOVA |
Main results relevant to research question (author analysis): First 2 weeks used as baseline data outcomes a combining of 11th and 12th week The intervention group increased steps average by 16% (7811% to 2620%; p < 0.01). Moderate-intensity activity also increased by 53% (17.83% to 27.23%; p < 0.01). No change in control group. Walk time test also improved for intervention group by 10% (p < 0.01) |
| Lawton et al. (2008)59 Country: New Zealand Study design: RCT Length of follow-up: 2 years Aim: to assess the effectiveness of a primary care-based programme of exercise on prescription among relatively inactive women over a 2-year period Recruitment: 17 primary care practices Funding: National Heart Foundation of New Zealand |
Number of participants: n = 1089 Age: 58.9 years (SD 7 years) Retirement: NR Sex: women Education: NR Ethnicity: NR Other inclusion/exclusion criteria: not undertaking 30 minutes of moderate-intensity physical activity on at least five days of the week Service setting: primary care |
Intervention aims and content if applicable: brief physical activity intervention led by nurse with 6-month follow-up visit and monthly telephone support over nine months Control condition if applicable: no intervention Data collection methods: Outcome measures: physical activity (achieving the recommended 150 minutes of at least moderate-intensity physical activity) Response and/or attrition rate: retention rate 93% and 89% at 12 and 24 months Data analysis: regression models, ITT |
Main results relevant to research question (author analysis): At baseline, 10% of intervention participants and 11% of control participants were achieving 150 minutes of at least moderate-intensity physical activity a week At 12 months rates increased to 43% and 30% and at 24 months to 39.3% and 32.8% (p < 0.001), respectively. SF-36 physical functioning (p = 0.03) and mental health (p < 0.05) scores improved more in intervention compared with control participants, but role physical scores were significantly lower (p < 0.01) Mean physical activity levels, however, were higher (p = 0.01) and a greater proportion reached the target of physical activity in the intervention group compared with the control group at 12 months (233 (43%) v 165 (30%), (p < 0.001), with levels declining but still significantly different at 2 years (214 (39%) v 179 (33%), (p < 0.001) |
| Marcus et al. (1997)60 Country: USA Study design: CBA Length of follow-up: 6 weeks Aim: to test the feasibility of a physician counselling intervention Recruitment: patients who had appointments with GP Funding: National Institute on Ageing |
Number of participants: n = 44 Age: over 50 years, mean 67.1 years Retirement: 55% employed Sex: 72% female Education: NR Ethnicity: NR Other inclusion/exclusion criteria: active fewer than three times per week Service setting: primary care |
Pilot study for Goldstein et al. paper45 Intervention aims and content if applicable: Physically Active for Life Project (physical activityL), based on TTM of change, social-cognitive theory, health education theory. 1.5 hour physician training session, physical activity counselling session provided to patients with follow-up appointment 4 weeks later. Counselling used 5As approach, 5 minutes, written exercise prescription form completed. At follow-up appointment physician provided counselling and new written prescription, patient given poster with tips on adoption and maintenance. Physicians received a manual Control condition if applicable: usual care Data collection methods: telephone interview with patients, questionnaire to physicians Outcome measures: stage of motivational readiness for physical activity, Physical Activity Scale for the Elderly, acceptability and feasibility of intervention Response and/or attrition rate: 236 potential, 117 ineligible, 63 agreed to participate, 70% of these completed Data analysis: t-tests, descriptive statistics, Pearson’s r, multivariate model |
Patients in intervention group recollected more activity counselling than controls. 32% of controls recollected physician had spoken to them about physical activity, all in experimental group Physical activity SE scores increased mean 148 (SD 87) to mean 154 (SD 76) at 6 weeks, while scores for controls remained little changed; however, no significant difference in change between groups (t = 0.9; p > 0.005) Adjusting for baseline variables suggested a 17.6-point difference intervention vs. control in physical activity SE scores (p = 0.19 – correct value given), ES 0.20 (17.6/87.4) intervention vs. controls. Patients who received all counselling messages more effect than those who did not receive any counselling (p = 0.05) |
| Martinson et al. (2010)61 Country: USA Study design: RCT Length of follow-up: 2 years Aim: to evaluate a telephone- and mail-based intervention Recruitment: health plan members, mailed directly also advertising Funding: National Institute on Aging |
Number of participants: n = 1049 Age: 50–70 years (mean 57.1 years; SE 0.2 years) Retirement: 77% employed Sex: 72% female Education: 67% 4-year degree or more Ethnicity: 92% white intervention group Other inclusion/exclusion criteria: included those reporting at least 30 minutes of moderate or vigorous physical activity at least 2 days per week and that they had increased their physical activity over previous 12 months. Excluded those with co-morbidity or CHD Service setting: home |
Intervention aims and content if applicable: Based on social cognitive theory and relapse prevention theory. 2-year interactive telephone- and mail-based support programme. Included self-management, goal-setting, identification of barriers and problem-solving, use of pedometers and log books, motivational campaigns, lending library of resources. The central element of the intervention was a seven-session course delivered approximately biweekly over the telephone by exercise coaches, then monthly calls for 1 year and then bimonthly for the second year Control condition if applicable: usual care – received information about the programme and four newsletters over the 2 years Data collection methods: self-report data collected via telephone using CHAMPS questionnaire Outcome measures: kilo calories expended per week in physical activity specifically during moderate to vigorous physical activity Response and/or attrition rate: 92% at 2 years Data analysis: general linear mixed-model regression |
Main results relevant to research question (author analysis): 35% were participating in another exercise schemes such as gym membership or personal trainers Significantly more activity reported by intervention group than controls at 6 and 24 months (p < 0.03 and p < 0.01; ES d = 10 –0.17). The intervention led to an increase in energy expenditure of around 200 kcal per week extra equivalent to one hour per week of moderate-intensity walking More intervention than control participants maintained MVphysical activity at 6, 12 and 24 months (p < 0.003, p < 0.004 and p < 0.001). At 24 months, while the usual care group dropped back to their 6 month level the intervention group continued to increase (p < 0.05) Participants reported satisfaction with the intervention (40% exceeded expectations, 58% that it met expectations; 64% completely satisfied, 35% satisfied) |
| Martinson et al. (2008)62 Country: USA Study design: RCT Length of follow-up: 6-month outcomes Aim: to evaluate a telephone- and mail-based intervention Recruitment: health plan members, mailed directly also advertising Funding: National Institute on Aging |
Number of participants: n = 1049 Age: 50–70 years (mean 57.1 years; SE 0.2 years) Retirement: 77% employed Sex: 72% female Education: 67% 4-year degree or more Ethnicity: 92% white intervention group Other inclusion/exclusion criteria: included those reporting at least 30 minutes of moderate or vigorous physical activity at least 2 days per week and that they had increased their physical activity over previous 12 months. Excluded those with co-morbidity or CHD Service setting: home |
Intervention aims and content if applicable: Keep Active Minnesota. Based on social cognitive theory and relapse prevention theory. 2-year interactive telephone- and mail-based support programme. Included self-management, goal-setting, identification of barriers and problem-solving, use of pedometers and log books, motivational campaigns, lending library of resources. The central element of the intervention was a seven-session course delivered approximately biweekly over the telephone by exercise coaches, then monthly calls for 1 year and then bimonthly for the second year Control condition if applicable: usual care – received information about the programme and four newsletters over the 2 years Data collection methods: self-report data collected via telephone using CHAMPS questionnaire Outcome measures: kilocalories expended per week in physical activity specifically during moderate to vigorous physical activity Response and/or attrition rate: Data analysis: general linear mixed-model regression |
Main results relevant to research question (author analysis): At 6 months’ intervention vs. control higher p = 0.03 for all physical activity For MV physical activity calorie expenditure intervention group higher (p = 0.03) For physical activity maintenance intervention group higher (p = 0.03) |
| Opdenacker et al. (2011)63 Country: Belgium Study design: CBA Length of follow-up: 2 years Aim: to report 2-year follow-up data Recruitment: as above Funding: as above |
Number of participants: n = 186 Age: 60–83 years (mean 66 years) Retirement: all retired Sex: 50% male Education: average 12–13 years education Ethnicity: NR Other inclusion/exclusion criteria: not being physically active, no medical problems contra-indicating participation Service setting: community |
Intervention aims and content if applicable: as above, two intervention arms Control condition if applicable: no intervention Data collection methods: as above Outcome measures: as above Response and/or attrition rate: 95 followed up Data analysis: ANOVA, chi-squared test, linear mixed model |
Main results relevant to research question (author analysis): This paper reports fitness, strength and body composition outcomes only Improvements in cardiorespiratory fitness for both intervention groups; however, pre-test to follow up all groups including control had improved with no significant difference between them Structured intervention group showed improvements in muscular fitness whereas lifestyle group no significant effect baseline to follow-up; however, greater improvement than structured group in functional performance in the longer term (structured group no difference from control) |
| Opdenacker et al. (2008)64 Country: Belgium Study design: CBA Length of follow-up: 2 years Aim: to report 2-year follow-up data from above study Recruitment: as above Funding: as above |
Number of participants: n = 186 Age: 60–83 years (mean 66 years) Retirement: all retired Sex: 50% male Education: average 12–13 years education Ethnicity: NR Other inclusion/exclusion criteria: not being physically active, no medical problems contra-indicating participation Service setting: community |
Intervention aims and content if applicable: as above; two intervention arms Control condition if applicable: no intervention Data collection methods: as above Outcome measures: as above Response and/or attrition rate: 95 followed up Data analysis: ANOVA, chi-squared test, linear mixed model |
Main results relevant to research question (author analysis): Both groups had significantly increased total physical activity compared with controls immediately post test. Lifestyle intervention group significantly larger increases in active transportation and total steps compared with controls and the structured intervention arms at follow-up No significant difference between structured intervention and controls, however, for leisure time physical activity, or total physical activity, or active transportation and total steps at follow-up. It was difficult for the structured group to continue the programme after the programme ended Participants who dropped out were significantly older and less educated than those who completed follow-up |
| Pasalich et al. (2013)65 Country: Australia Study design: follow-up survey as part of cohort study Length of follow-up: 6 months Aim: to report follow-up data Recruitment: recruited for main study Funding: National Health and Medical Research Council |
Number of participants: n = 349 Age: 60–70 years (mean 65 years) Retirement: 42% still employed Sex: 50% male Education: 95% high school and above Ethnicity: NR Other inclusion/exclusion criteria: insufficiently active older adults Service setting: community |
Intervention aims and content if applicable: Physical Activity and Nutrition for Seniors programme. 6-month home-based intervention. Received a booklet containing information on recommended physical activity levels, dietary guidelines and encouraged goal-setting. Also charts, newsletters, pedometers provided. Contacted via telephone or e-mail to offer additional support Control condition if applicable: no intervention Data collection methods: International Physical Activity Questionnaire Outcome measures: days per week and minutes of walking and moderate-intensity activity Response and/or attrition rate: 93% followed up Data analysis: ANOVA, t-tests |
t-tests indicated significant improvement for the intervention group for strength activity compared with little change in control group (p > 0.1) post programme. At follow-up the control group had declined, while intervention group remained above baseline level although no significant difference. No difference at follow-up for controls or intervention group, intervention group had significantly declined from immediately post programme. Outcomes relating to diet were more positive |
| Peels et al. (2012)66 Country: the Netherlands Study design: process evaluation Length of follow-up: Aim: to describe the development of a web-based intervention Recruitment: six municipal health council regions not participated in Active Plus. Within these regions, seven matched neighbourhoods were selected for each intervention condition. Councils provided sample of participants to whom to send invitations Funding: |
Links to the van Stralen papers – describes development of intervention only | Links to the van Stralen papers – describes development of intervention only | Main results relevant to research question (author analysis): Describes how the findings from the Active Plus intervention were used to develop a new web-based programme. Four intervention arms – basic print-delivered and web-delivered, printed and environmental information, and web and environmental information |
| Peels et al. (2012)67 Country: the Netherlands Study design: cluster RCT Length of follow-up: 4 months Aim: to examine delivery of an intervention Recruitment: see other papers Funding: Netherlands Organisation for Health Research and Development |
Number of participants: see other papers Age: see other papers Retirement: NR Sex: see other papers Education: see other papers Ethnicity: see other papers Other inclusion/exclusion criteria: see other papers Service setting: |
Intervention aims and content if applicable: Active Plus (see other Peels/van Stralen papers) Data analysis: ANOVA, chi-squared test |
Main results relevant to research question (author analysis): The printed intervention achieved a higher participation rate than a web-based intervention (19% vs. 12%) Dropout significantly higher in web-based intervention (53% vs. 39%; p < 0.001) No specific user characteristics were associated with dropout for different interventions, with low intention to be physically active predicting dropout for both delivery modes (p < 0.001) |
| Peels et al. (2013)68 Country: Netherlands Study design: cluster RCT Length of follow-up: 1 year Aim: to compare a printed vs. web-delivered intervention Recruitment: six municipal health council regions not participated in Active Plus. Within these regions, seven matched neighbourhoods selected for each intervention condition. Councils provided sample of participants to send invitations to Funding: the Netherlands Organisation for Health Research and Development |
Number of participants: n = 1248 Age: over 50 years (mean 61.6 to 64.1 years; SD 7.2–8.3 years) Retirement: NR Sex: 43.7–51.8% male Education: 41.5–49.5% low education Ethnicity: NR Other inclusion/exclusion criteria: Service setting: unclear |
Links to the van Stralen papers and Peels et al.66,67 Intervention aims and content if applicable: Active Plus intervention. Four intervention arms – basic print-delivered and web-delivered, printed and environmental information, and web and environmental information Intervention aims to influence awareness, initiation, and maintenance of physical activity. Participants received advice on three occasions which was tailored to them based on previous responses. Advice included general benefits of physical activity, feedback based on their stage of change, advice regarding social support, practical possibilities and action plans. The additional environmental component consisted of local possibilities and initiatives in their neighbourhood Control condition if applicable: waiting list Data collection methods: questionnaire Outcome measures: Dutch Short Questionnaire to Assess Health Enhancing Physical Activity Response and/or attrition rate: 59% completed follow-up questionnaire at 12 months Data analysis: ANOVA, chi-squared test, regression |
Main results relevant to research question (author analysis): Data for 12 months follow-up The four intervention conditions as a whole were effective in increasing weekly days of sufficient physical activity (ES 0.18; p = 0.005) but ineffective in increasing weekly minutes of physical activity (ES 0.20; p = 0.071) The two paper-based types were equally effective in increasing total days and also total minutes of physical activity compared with control, whereas the two internet types were not [printed basic + 0.6 days + 57 minutes, ES 0.23 (p = 0.002) and ES 0.21 (p = 0.017) and printed environmental + 0.9 days + 114 minutes ES 0.38 (p = 0.001) and ES 0.32 (p = 0.001)]; control, 58 minutes; web basic, 3 minutes; web environmental, 9 minutes There were no significant associations between effect and participant characteristics |
| Pereira et al. (1998)69 Country: USA Study design: RCT Length of follow-up: 10 years Aim: 10-year follow-up of participants in a RCT walking intervention Recruitment: telephone Funding: charity funding |
Number of participants: 196 Age: 50 to 65 years at baseline [mean 57.8 years (SD 4.29 years)] Retirement: NR Sex: women Education: NR Ethnicity: white Other inclusion/exclusion criteria: post-menopausal women, not taking HRT, no restrictions that would preclude walking Service setting: community |
Intervention aims and content if applicable: walking intervention (no details in this paper) Control condition if applicable: no details in this paper Data collection methods: telephone interview Outcome measures: self-reported walking for exercise and other purposes, Paffenbarger sports and exercise index Response and/or attrition rate: 86%; 196/229 at 10 years Data analysis: t-test, Wilcoxon rank sum, Kruskal–Wallis, chi-squared test |
Main results relevant to research question (author analysis): The median values for both usual walking for exercise (1000 vs. 302 kcal/week) and total walking (1344 vs. 924 kcal/week) were significantly higher for walkers compared with controls (p = 0.01 for both) Compliers (walking at least 7 miles/week during the intervention period) reported significantly more walking that all other groups at 10 years (p < 0.05) |
| Petrella et al. (2010)70 Country: Canada Study design: cluster RCT Length of follow-up: 12 months Aim: to determine the effects of adding stages of change–based counselling to an exercise prescription for older, sedentary adults in family practice Recruitment: GP Funding: Heart and Stroke Foundation of Canada |
Number of participants: healthy, community-dwelling n = 360 Age: mean 64.9 years (SD 7.1 years) (range 55 to 85 years) Retirement: 56% retired Sex: 52% female Education: 46% secondary, 17% college, 15% university Ethnicity: NR Other inclusion/exclusion criteria: inactive lifestyle Service setting: 40 family practices in four regions of Canada |
Intervention aims and content if applicable: Intervention physicians were trained to deliver a tailored exercise prescription and a transtheoretical behaviour change counselling programme Control condition if applicable: control physicians were trained to deliver the exercise prescription alone Data collection methods: Outcome measures: cardiorespiratory fitness, energy expenditure (7-day physical activity recall) Response and/or attrition rate: two patients died and 29 patients withdrew Data analysis: ANOVA, chi-squared test |
Main results relevant to research question (author analysis): Mean increase in pVO2max was significant for both the intervention [3.02 ml/kg/minute (95% CI 2.40 to 3.65 ml/kg/minute)] and control [2.21 ml/kg/minute (95% CI 1.27 to 3.15 ml/kg/minute)] groups at 12 months (p < 0.001); however, there was no difference between groups. Women in the intervention group improved their fitness significantly more than women in the control group did (3.20 vs. 1.23 ml/kg/minute). The intervention group had a 4-mm Hg reduction in systolic blood pressure, while the control group’s mean reduction was 0.4 mm Hg (p < 0.001). The mean (SD) energy expended significantly increased and was higher in the intervention group than in the control group [69.06 kcal/day (SD 169.87 kcal/day) vs. –6.96 kcal/day (SD 157.06 kcal/day); p < 0.006] |
| Pinto et al. (2005)71 Country: USA Study design: RCT Length of follow-up: 6 months Aim: to compare the effects of brief advice to exercise from a clinician supplemented by telephone-based counselling by health educators (extended advice) to brief advice from a clinician alone (brief advice) Recruitment: GP waiting rooms Funding: National Institute on Aging |
Number of participants: 100 primary care patients Age: mean 68.5 years Retirement: NR Sex: 63.2% female Education: college education 57.9% Ethnicity: 14.7% minority Other inclusion/exclusion criteria: Service setting: primary care |
Intervention aims and content if applicable: participants randomised to the Extended Advice group received (1) three face-to-face physical activity counselling sessions with a health educator at months 0, 1 and 3, lasting an average of 30–45 minutes; (2) physical activity prescriptions tailored to the participant’s motivational readiness; (3) 12 physical activity counselling telephone calls, that is, weekly for the first 3 months, and then every other week for the second 3 months, lasting an average of 10 to 15 minutes; and (4) 12 physical activity tip sheets sent by mail at the same time as the telephone counselling calls. All counselling was tailored to the patient’s stage of readiness to increase physical activity levels The Brief Advice group did not receive any additional counselling apart from the advice given by their clinician Control condition if applicable: two interventions Data collection methods: self-reported and objective measures of physical activity Outcome measures: self-reported physical activity using the 7-Day Physical Activity Recall instrument and objective activity monitoring using Biotrainers Response and/or attrition rate: six dropouts plus four participants who did not provide complete data Data analysis: t-tests, ANCOVA, ITT |
Main results relevant to research question (author analysis): At 3 months, using the 7-day physical activityR data, the ExtAd group (n = 49) reported an increase of 3.85 (SD 0.89) weekly kilocalorie expenditure in moderate-intensity physical activity vs. an increase of 0.83 (SD 0.94) in the BriefAd group (n = 44, F = 5.20; p = 0.03) At 6 months, the effects were sustained: the increase from baseline levels was 4.19 (SD 0.81) in the ExtAd group vs. 1.11 (SD 0.85) in the BriefAd group (F = 6.62; p = 0.05) Analyses of 3-day activity counts via objective activity monitoring (adjusted for weight) at 3 months, revealed an increase of 50.79 (SD 20.40) in the ExtAd group vs. a decrease of 11.11 (SD 21.13) in the BriefAd group (F = 4.27, p = 0.04). At 6 months, there was an increase of 42.39 (SD 16.28) from baseline values for the ExtAd group vs. a decrease of 24.18 (SD 16.86, F = 7.76; p < 0.01) in the BriefAd group |
| Prabu et al. (2012)72 Country: USA Study design: BA Length of follow-up: immediate Aim: to evaluate a walking intervention Recruitment: advertising Funding: Breast Cancer Research Foundation |
Number of participants: n = 85 Age: average 57 years Retirement: NR Sex: all female Education: 75% had a college degree, more than half annual income greater than US$75,000 Ethnicity: 93% white Other inclusion/exclusion criteria: post-menopausal women, BMI of 25–40 kg/m2, access to mobile phone, willing to walk 30 minutes per day Service setting: home |
Intervention aims and content if applicable: Based on goal-setting theory, social cognitive theory. 12-week walking programme. Daily steps goal and wore pedometer. Goals increased each week. Feedback regarding number of steps provided each week No coach condition – each day for 12 weeks two contacts with an interactive voice response system – first call from system to seek whether participant had walked or planned to walk that day, self-efficacy to achieve goal that day, whether good or bad day. In evening participant called the system to enter step count and receive a message. A theme for messages each week such as increasing knowledge, self-monitoring, awareness of barriers. Messages opened with ‘did you know’ and ended with a tip. Participant evaluated day and self-efficacy for next day Coach condition – a trained coach available, explained the intervention and offered step goals. Trained participant to use pedometer and interactive voice response system and offered support during intervention. Participants called system and left message to ask for support Control condition if applicable: two interventions Data collection methods: baseline data collected at visit to a gym, pedometer, questionnaires Outcome measures: exercise goal questionnaire, exercise planning questionnaire, exercise thoughts and barriers, social support, self-efficacy, waist and hip measurements, 1-mile walk Response and/or attrition rate: 13% withdrew after randomisation, 32% did not complete post assessments Data analysis: linear mixed models, ITT |
Main results relevant to research question (author analysis): 66% of planned calls to system completed, 51% of calls from system answered Significant decrease in one mile walk time pre–post p = 0.001 d = 0.41 Change in goal-setting, exercise planning, managing negative thoughts approximately ES of 0.8. ESs for BMI, weight and waist measurement were small (range 0.07–0.14) No between-group differences |
| Purath et al. (2013)73 Country: USA Study design: RCT Length of follow-up: immediate Aim: to evaluate a primary care delivered intervention Recruitment: clinic letter sent to potential participants, flyer in clinic Funding: John A. Hartford Foundation, Claire M. Fagin fellowship, Arizona State University |
Number of participants: n = 72 Age: 60–80 years (mean 66.2 years; SD 5.2 years) Retirement: NR Sex: 53 women and 19 men Education: mean 2 years post high school Ethnicity: NR Other inclusion/exclusion criteria: excluded people who were already active (more than 150 minutes of moderate activity per week), had no telephone, had no serious medical or cognitive conditions Service setting: primary care nurse clinic |
Intervention aims and content if applicable: Based on the Adapted Physical Activity Model and the Interaction Model of Client Health Behaviour which proposes people are unique agents capable of change. Also drew on social cognitive theory. Delivered by a nurse practitioner. Fitness testing followed by discussion of results and completion of ‘How ready are you to change your physical activity’ survey, physical activity goals set for 2 weeks on a written prescription, asked to complete activity diary. Follow-up telephone call 2 weeks, with 10 further calls over 6-month intervention period. Calls focused on discussion of barriers and overcoming barriers and self-efficacy. 3-month review of fitness and revision of goals Control condition if applicable: received diet intervention consisting of initial questionnaire, goal-setting, telephone calls relating to healthy eating, fitness test results not discussed Data collection methods: questionnaires, fitness testing Outcome measures: CHAMPS questionnaire (calorific expenditure/frequency of moderate activity), Compendium of Physical Activity Tracking Guide, a subgroup of participants wore accelerometers, Senior Fitness tests of muscle strength, endurance and balance, BMI Response and/or attrition rate: 11% dropout rate Data analysis: ANOVA, ANCOVA |
Main results relevant to research question (author analysis): 36% of participants reported family encouragement to do physical activity, 73% that their health-care provider encouraged activity. Mean self-efficacy was mid-range (44.6). Mean barrier scale score of 36.7 indicated few barriers to exercise Intervention group and control group both increased weekly estimated calorific expenditure in all physical activity at 3 months and 6 months. The intervention group had a larger increase but this was not significant No significant change in weekly frequency of activity or measures of physical fitness in either group. Also no change in self-efficacy or barriers. When controlled for baseline co-variates, however (age, sex, income, BMI, support), intervention participants significantly increased frequency of all physical activity compared with control (p < 0.05) indicating the intervention was effective for selected participants Higher support associated with higher change in calorific expenditure (p < 0.05), males significantly higher increase (p < 0.05) Intervention was rated positively |
| Rowland et al. (1994)74 Country: UK Study design: RCT Length of follow-up: mean 10 months (range 3–20 months) Aim: evaluate the impact of the Health Education Authority’s 20 hour Look After Your Heart health promotion course on retired women Recruitment: recruited through employer retirement association Funding: various charity and government funders |
Number of participants: 739 women Age: mean 66 years Retirement: retired Sex: female Education: NR Ethnicity: NR Other inclusion/exclusion criteria: Service setting: 24 retirement groups established by a major national retail company in England |
Intervention aims and content if applicable: the programme is taught for 2 hours a week by a trained Health Education Authority teacher and lasts for 10 weeks. The course combines both exercise theory and practice. The programme consists of three parts: risk factors associated with heart disease, how to exercise regularly in a safe way, and how to cope with stress Control condition if applicable: no intervention Data collection methods: Nottingham Health Profile questionnaire Outcome measures: exercise knowledge, attitudes, and behaviour Response and/or attrition rate: 35/739 excluded owing to missing data Data analysis: ANOVA, chi-squared test |
Main results relevant to research question (author analysis): The intervention group had significantly better self-perceived health, indicated by lower Nottingham Health Profile scores, more exercise knowledge, and positive exercise attitudes and more exercise than the controls The mean number of hours spent on domestic activity and sport/recreational exercise per week were both greater in the intervention group (13.3 vs. 12.5 hours F = 2.1; p = 0.11; and 5.0 vs. 3.9 hours F = 9.5; p < 0.001) Time since completion of the programme did not have any effect on Nottingham Health Profile scores, exercise knowledge and behaviour |
| Sawchuk et al. (2008)75 Country: USA Study design: RCT Length of follow-up: immediate Aim: to evaluate an intervention for Native American Elders using basic instruction compared with pedometer Recruitment: advertisement, fairs, word of mouth Funding: Agency for Healthcare Research and Quality |
Number of participants: n = 125 Age: 50–74 years (average 58 years) Retirement: 27% intervention group 1 employed 16% group 2 Sex: 74% female Education: NR Ethnicity: Native American Other inclusion/exclusion criteria: having a sedentary lifestyle, being able to walk without assistance, no medical contraindications, living within 2 hours of study site Service setting: intervention mainly delivered at home |
Intervention aims and content if applicable: Two 6-week interventions. Baseline and final clinic visit with two ten minute telephone calls in week 2 and 4. During telephone calls brief review of progress but no specific feedback or goal-setting. Activity monitoring only group given daily monitoring sheets to complete and suggested activities and exercises and an educational hand out on health benefits of exercise. The pedometer group given same instructions and also trained in the use of a pedometer Control condition if applicable: none Data collection methods: questionnaires, walk test, pedometer data, self-report booklet Outcome measures: CHAMPS questionnaire, SF-36, 6-minute walk test, total daily step counts, activity log Response and/or attrition rate: eight participants did not complete the intervention Data analysis: linear regression, t-tests, ITT |
Main results relevant to research question (author analysis): The frequency of walking increased for both groups from baseline (p < 0.01). The addition of the pedometer therefore did not lead to appreciable differences No difference between groups on CHAMPS, SF-36, BMI-adjusted mean distance travelled during the 6-minute walk. Combined results for the two groups showed improved calorific expenditure for all exercise-related activities (p < 0.001) and frequency of moderate-intensity exercise-related activities (p < 0.001) |
| Stevens et al. (1998)76 Country: UK Study design: RCT Length of follow-up: 8 months Aim: to assess the cost-effectiveness of a primary care-based intervention aimed at increasing levels of physical activity in inactive people aged 45–74 years Recruitment: two west London general practices (self-assessment questionnaire sent to all patients aged 45–74 years) Funding: West London Health Promotion Agency |
Number of participants: n = 714 inactive people Age: mean 59.1 years Retirement: 55% economically active Sex: 40% male Education: 28% degree, 36% no qualifications Ethnicity: 87% white Other inclusion/exclusion criteria: 55% sedentary Service setting: general practice |
Intervention aims and content if applicable: Intervention subjects were invited to a consultation with an exercise development officer, and offered a personalised 10 week programme to increase their level of regular physical activity, combining leisure centre- and home-based activities Participants were made aware of the existing recommendations on physical activity and health, but they were neither expected nor pressured into achieving these standards The exercise programme lasted for 10 weeks, after which subjects were invited to return for a second consultation to discuss their progress Control condition if applicable: Control subjects were sent information on local leisure centres Data collection methods: questionnaires Outcome measures: physical activity, sedentary Response and/or attrition rate: 25% returned for the second consultation at the end of the 10 week exercise programme Data analysis: t-test, ITT |
Main results relevant to research question (author analysis): there was a net 10.6% (95% CI 4.5% to 16.9%) reduction in the proportion of people classified as sedentary in the intervention group compared with the control group, 8 months after the intervention The intervention group also reported an increase in the mean number of episodes of physical activity per week, compared with the control group [an additional 1.52 episodes (95% CI 1.14 to 1.95 additional episodes)] The cost of moving a person out of the sedentary group was shown to be < £650. The cost of moving someone to the now commonly recommended level was estimated at almost £2500 |
| Strath et al. (2011)77 Country: USA Study design: pilot RCT Length of follow-up: immediate Aim: to compare pedometer-based interventions with standard education Recruitment: mass media announcements advertising, internet Funding: Graduate School Fellowship Grant, Centre for Urban Population and Health, National Institute on Ageing |
Number of participants: n = 81 Age: 55–80 years (mean 63.8 years; SD 6 years) Retirement: NR Sex: 83% female Education: majority had completed a college degree (73%) and 65% earned more than US$35,000 Ethnicity: NR Other inclusion/exclusion criteria: potential participants screened using stage of change for physical activity, self-report engaging in activity < 30 minutes per day 5 days a week, wore pedometer to test fewer than 7500 steps per day Service setting: not clear |
Intervention aims and content if applicable: four intervention arms, all 12 weeks – standard education consisting of educational physical activity material biweekly by e-mail with six mailings received. Second, standard education + pedometer and pedometer log in mail with instructions on how to use and log daily steps with envelopes to mail logs back on a weekly basis. Third, pedometer + six individualised two-page education booklet based on stages of change motivational literature including perceived barriers and effective strategies to overcome these. Fourth, pedometer + individual education + telephone call biweekly (six telephone calls of 10 minutes) Control condition if applicable: none Data collection methods: pedometer data, SF-36 Outcome measures: daily steps, health-related quality of life Response and/or attrition rate: 61 completed study Data analysis: chi-squared test, regression |
Main results relevant to research question (author analysis): Third and fourth intervention participants significantly greater number of daily steps than groups one and two (p < 0.001) with no significant difference between these two groups (p = 0.893) Those increasing their daily steps to target threshold of 2000 were: group 2 44%, group 3 75%, group 4 79%. 25% group 2, 56% group 3 and 64% group 4 increased to target threshold of 3000 steps per day No significant effect for any of the HRQoL scales |
| van Keulen et al. (2011)78 Country: the Netherlands Study design: RCT Length of follow-up: 73 weeks (baseline, 25, 47 and 73 weeks) Aim: to compare computer tailoring and motivational interviewing in changing physical activity and fruit and vegetable consumption in middle-aged Dutch adults Recruitment: 23 general practices Funding: Netherlands Organisation for Health Research and Development |
Number of participants: n = 1629 Age: 57.15 years (SD 7.13 years) Retirement: NR Sex: 55% male Education: 54% low, 23% intermediate education level Ethnicity: NR Other inclusion/exclusion criteria: physically active with moderate intensity for mean 4.65 hours a week (SD 3.83 hours) Service setting: general practice |
Intervention aims and content if applicable: Participants randomly received either four tailored print letters, four motivational telephone calls, two of each type of intervention, or no information TPC: the letters, TPC1 and TPC2 (each three to six pages), were personalised with the participant’s name and included the following elements: introduction, specific behavioural feedback on targeted behaviours, stage-matched advice to change behaviour, and conclusions. Subsequent letters, TPC3 (two to four pages) and TPC4 (four to six pages) were also personalised and reinforced tailored feedback on behavioural progress and stages of change based on the intermediate survey data. The letters were mailed to the participants’ home addresses Telephone Motivational Interviewing: motivational interviewing counsellors received six 3-hour training sessions by two certified trainers. Interview protocols were established to enhance treatment integrity and reflect the principles of motivational interviewing: introduction, assess current behaviours and progress, discuss the public health guideline, assess and enhance motivation and self-efficacy for behaviour change, assess readiness to change, summarise, and close session. Additional topics could be discussed Control condition if applicable: no intervention Data collection methods: telephone interviews/postal questionnaire Outcome measures: absolute change in self-reported physical activity and fruit and vegetable consumption Response and/or attrition rate: 63% randomised. 73% completed all follow-ups Data analysis: chi-squared test, ANOVA |
Main results relevant to research question (author analysis): All three intervention groups (tailored letters, motivational calls, and the combined version) were equally and significantly more effective than the control group in increasing physical activity (hours/day), intake of fruit (servings/day), and consumption of vegetables (grams/day) from baseline to the intermediate measurement (week 25), follow-up 1 (week 47) and 2 (week 73). ESs (Cohen’s d) ranged from 0.15 to 0.18 |
| van Stralen et al. (2010)79 Same study as van Stralen et al. (2011)81 Country: the Netherlands Study design: cluster RCT Length of follow-up: 12 months Aim: examine the long-term efficacy of 2 computer-tailored physical activity interventions for older adults and its psychosocial and environmental mediators Recruitment: 9 Municipal Health Councils Funding: Netherlands Organisation for Health Research and Development |
Number of participants: n = 1971 Age: average 64 years (SD 8.6 years) Retirement: 47% employed Sex: NR Education: 48% low level of education Ethnicity: NR Other inclusion/exclusion criteria: average BMI of 25.5 kg/m2 (SD 3.8 kg/m2) Service setting: community |
Intervention aims and content if applicable: See van Stralen 2011 (6474) Control condition if applicable: no-intervention Data collection methods: questionnaires Outcome measures: total weekly days and total weekly minutes of physical activity (self-reported) Response and/or attrition rate: response rate 23%, retention rate 68% Data analysis: ANOVA |
Main results relevant to research question (author analysis): A significant intervention effect was found for the environmentally tailored intervention, in which the participants in the environmentally tailored intervention increased their total weekly minutes of physical activity by 1 h/week more (BI environment 62.0, 95% CI 7.4 to 116.6; p < 0.05) compared with the control condition. This significant intervention effect on total physical activity behaviour could mainly be assigned to a significant intervention effect on weekly minutes of leisure walking (BI environment 21.9, 95% CI 1.0 to 42.9; p < 0.05) and leisure cycling (BI environment 26.5, 95% CI 4.8 to 48.2; p < 0.05). No significant intervention effects were found for the basic intervention condition compared with the control group in weekly minutes per week of total physical activity or sub-behaviours Participants in the environmentally tailored intervention increased their physical activity behaviour by almost 50 minutes/week more than participants in the basic intervention (BI environment vs. I basic 48.5, 95% CI –6.3 to 103.3; p = 0.08). These differences in intervention effects could mainly be assigned to borderline significant differences in weekly minutes of leisure cycling (BI environment vs. I basic = 18.6, 95% CI –3.4 to 40.5; p = 0.09) and participation in sports (BI environment vs. I basic = 14.3, 95% CI –2.2 to 30.7; p = 0.09) |
| van Stralen et al. (2009)80 Country: the Netherlands Study design: further analysis of data Length of follow-up: 12 months Aim: to explore the mechanisms underlying a computer-based intervention Recruitment: as above Funding: as above |
Number of participants: n = 1971 Age: average 64 years (SD 8.6 years) Retirement: 47% employed Sex: NR Education: 48% low level of education Ethnicity: NR Other inclusion/exclusion criteria: average BMI of 25.5 kg/m2 (SD 3.8 kg/m2) Service setting: community |
Intervention aims and content if applicable: Interventions were developed using the intervention mapping approach and consisted of 3 computer-tailored letters delivered over 4 months: (a) basic computer-tailored print intervention, targeting psychosocial mediators. Basic computer-tailored intervention participants (n = 654) received three computer-tailored letters with personalised physical activity advice (b) plus environmentally computer-tailored print intervention, targeting psychosocial and environmental mediators. Intervention-plus participants (n = 737) received the same motivationally focused computer-tailored information but additionally received environmentally focused computer-tailored information about physical activity opportunities in their neighbourhood combined with access to a forum and e-buddy system on a website Control condition if applicable: no-intervention Data collection methods: questionnaires Outcome measures: total weekly days and total weekly minutes of physical activity (self-reported) Response and/or attrition rate: response rate 23%, retention rate 68% Data analysis: ANOVA |
Main results relevant to research question (author analysis): Reports additional outcomes – total physical activity, walking, cycling and sports The intervention plus condition had a significant effect on cycling compared with basic intervention (p < 0.01) Intervention plus condition (basic intervention not significant) had significant effect on perceived physical activity possibilities (more than both controls and basic intervention p < 0.05). This change associated with change in days of total physical activity (p < 0.05) and weekly minutes of sport (p < 0.001) No association between physical activity possibilities and change in walking behaviour (p = 0.20), association with cycling at 3 months but not 6 months follow-up Intervention plus letters rated more highly than basic letters; however, this difference was not significantly associated with physical activity behaviour change. 94% reported reading the environmental information, 71% agreed it was interesting, 41% walked or cycled one of the trails, 19% did the provided exercises, 15% mapped out other routes in their neighbourhood, 11% visited the website, 2% contacted a sports club |
| van Stralen et al. (2009)82 Reports same study as van Stralen et al. (2010)80 and 201181 Country: the Netherlands Study design: RCT Length of follow-up: Aim: to evaluate effects of two interventions on awareness and compliance with a guideline Recruitment: as above Funding: as above |
Number of participants: n = 1917 Age: Retirement: Sex: Education: Ethnicity: NR Other inclusion/exclusion criteria: Service setting: |
Intervention aims and content if applicable: See other van Stralen papers for details Control condition if applicable: Data collection methods: questionnaires Outcome measures: Dutch Short Questionnaire to Assess Health Enhancing Physical Activity, scale to evaluate process Response and/or attrition rate: Data analysis: ANOVA, regression analysis |
Main results relevant to research question (author analysis): At the 6-month follow-up there was no significant effect on awareness for the intervention groups as a whole or when considering those who were aware or unaware at baseline. At 6 months, both intervention groups had enhanced awareness of their activity levels compared with controls (OR 1.67 intervention OR 1.64 intervention plus; p < 0.001) with no significant difference between the intervention types At 3 months intervention participants were 1.6 times more likely to comply with guidelines (basic OR 1.67, plus OR 1.57), at 6 months intervention participants were 2.5 times more likely OR 2.4 basic OR 2.8 plus (p < 0.001) 98% reported reading the tailored letters, 37% discussed them with others |
| van Stralen et al. (2011)81 Country: the Netherlands Study design: cluster RCT Length of follow-up: 6 months Aim: to evaluate long-term follow-up of a computer-based intervention Recruitment: Dutch regional health councils invited to take part, individuals invited by letter Funding: Netherlands Organisation for Health Research and Development |
Number of participants: randomisation at the level of Municipal Health Councils n = 6. n = 2000 participants Age: over 50 years (mean 64 years; SD 8.6 years) Retirement: 47% employed Sex: 57% female Education: 48% low level of education (baseline differences for this factor between groups) Ethnicity: NR Other inclusion/exclusion criteria: councils with at least 20,000 inhabitants Service setting: delivered at home |
Intervention aims and content if applicable: two intervention arms basic computer which was a motivational focused programme (three letters sent at 2 weeks and 2 months with personalised physical activity advice), and intervention plus which targeted potential environmental mediators in addition to the basic package (additional information about physical activity opportunities in neighbourhood such as walking and cycling routes and sports clubs, access to a forum and e-buddy via website). Developed using the intervention mapping protocol – a six-step process for developing an intervention, drew on variety of theoretical models including I-Change, social cognitive, transtheoretical, health action process, precaution adoption process, self-regulation theory, self-determination theory. Assumption that intervention effect achieved by changing underlying mediators Control condition if applicable: waiting list – received nothing during study period but one letter combining the three intervention letters after research period Data collection methods: questionnaires Outcome measures: Dutch short questionnaire to assess health-enhancing physical activity measured self-report days and minutes of physical activity, also potential mediators – awareness, attitude, social influences, motivation, self-efficacy, intention, commitment, perceived environment, strategic planning, action planning and coping planning Response and/or attrition rate: 23% response Data analysis: ANOVA, linear regression, product-of-coefficient tests, ITT |
Main results relevant to research question (author analysis): Both groups increased total weekly days of physical activity from 2.3 days (SD 2.2 days) to 4.7 days (SD 2.0 days). Control also slightly increased (from 4.0 to 4.3 days). Significant effects for both intervention groups (p < 0.01) compared with controls. Small ES (0.18 for both) with no difference between effect of the different conditions for total weekly days. Only the plus intervention had a significant effect on total minutes of physical activity per week compared with controls (ES 0.19) Both interventions had a significant effect on perception of social modelling (p < 0.05) awareness (p < 0.01) intention (p < 0.01). Basic in addition effect on self-efficacy (p < 0.05), and plus intervention effect on environmental perceptions (p < 0.01) and commitment to physical activity behaviour (p < 0.05) compared with control group Change in weekly days of physical activity predicted by change in awareness (p < 0.001), sports partner (p < 0.01), self-efficacy (p < 0.01), changes in awareness (p < 0.01), strategic planning behaviour (p < 0.01) and intention (p < 0.05). The mediators explained 41% of the variance in days of physical activity for the basic intervention and 37% of the total variance for the plus intervention. No significant mediators found for weekly minutes |
| Walker et al. (2009)83 Country: USA Study design: RCT Length of follow-up: 12 months Aim: to compare tailored vs. generic newsletters on eating and physical activity Recruitment: random digit dialling Funding: NR |
Number of participants: n = 225 Age: 50–69 years (mean 57 years) Retirement: 46% employed full time, 18% employed part time, 33% not employed Sex: female Education: 70% some college or higher, around 45% income above US$40,000 Ethnicity: 95% white Other inclusion/exclusion criteria: English-speaking; able to use a computer with assistance to complete a survey; access to a video recorder to view physical activity demonstration tapes; able to answer no to all questions on the Physical Activity Readiness Questionnaire. Not being in the maintenance stage for all 3 components of readiness for change in physical activity, unable to walk without an assistive device Service setting: community |
Intervention aims and content if applicable: Wellness for Women study. Women received by mail either 18 generic newsletters or 18 newsletters computer-tailored. Intervention based on health promotion model – behaviour-specific cognitions (benefits, barriers, self-efficacy, and interpersonal support). Feedback on data collected provided every month. Pedometers provided Control condition if applicable: two intervention arms only Data collection methods: questionnaires, physical measures Outcome measures: 7-day recall questionnaire, cardiorespiratory fitness, body fat, blood pressure, Exercise Benefits/Barriers Scale, Healthy Eating Benefits/Barriers Scales, Self-Efficacy for Exercise Habits Scale; Self-Efficacy for Eating Habits Scale, Family Support for Exercise Habits Scale, Friend Support for Exercise Habits Scale, Family Support for Healthy Eating Habits Scale, Friend Support for Healthy Eating Habits Scale Response and/or attrition rate: 7% Data analysis: chi-squared test, ANOVA |
Main results relevant to research question (author analysis): All behavioural and biomarkers of physical activity had significant main effects for time over the intervention period. Both groups improved significantly from baseline to 6 months on all measures. Only the tailored newsletter group improved on daily moderate- or high-intensity activity minutes. However, the Time X Group interaction for daily moderate- or high-intensity activity minutes was not significant There were no significant differences between the newsletter groups in achievement of any target at 6 months. At 12 months, a significantly higher proportion of the tailored newsletter group had achieved the activity behavioural outcome target of at least 210 minutes of moderate- or high-intensity activity weekly (30 minutes daily on 7 days each week) |
| Walker et al. (2010)84 Country: USA Study design: RCT Length of follow-up: 24 months (12-month intervention plus 12-month follow-up) Aim: to compare the maintenance of change in healthy eating and physical activity over 12 months following the tailored vs. generic mailed newsletter intervention Recruitment: random digit dialling Funding: National Institute of Nursing Research |
Number of participants: n = 225 Age: 50–69 years Retirement: 46% employed full time, 18% employed part time, 33% not employed Sex: female Education: 70% some college or higher, around 45% income above US$40,000 Ethnicity: 95% white Other inclusion/exclusion criteria: English-speaking; able to use a computer with assistance to complete a survey; access to a video recorder to view physical activity demonstration tapes; able to answer no to all questions on the Physical Activity Readiness Questionnaire. Not being in the maintenance stage for all 3 components of readiness for change in physical activity, unable to walk without an assistive device Service setting: community |
Intervention aims and content if applicable: The major intervention components were tailored or generic newsletters mailed to the women’s homes; these were supplemented by plans of action (goal-setting) in the tailored group and by physical activity instructional videotapes provided to both groups Control condition if applicable: NA (two intervention groups) Data collection methods: questionnaire (self-reported) Outcome measures: physical activity and eating Response and/or attrition rate: attrition rate was 9 (7.8%) and 1 (1.8%), respectively, for the two groups Data analysis: chi-squared test, ANOVA |
Main results relevant to research question (author analysis): From 12 months to 24 months, both groups maintained levels of moderate or greater activity, stretching exercise, and flexibility, but declined in cardiorespiratory fitness; only the tailored newsletter group maintained levels of strength exercise and lower body strength, while the generic newsletter group showed a decrease in strength exercise and lower body strength For the entire period from 12 to 24 months, neither time by group interaction was significant, but the main effect for time was significant for the outcome of at least 210 minutes of weekly moderate or greater activity Post hoc tests showed that the combined groups significantly increased from 12 months to 18 months on this outcome (p = 0.015) However, considered separately, there was no significant change within either group |
| Werkman et al. (2010)85 Country: the Netherlands Study design: cluster RCT Length of follow-up: 2 years Aim: to investigate the effect of a 1-year low-intensity computer-tailored energy balance programme among recent retirees Recruitment: recruited from pre-retirement workshops as offered by employers Funding: Netherlands Heart Foundation |
Number of participants: n = 413 Age: mean 59.5 years Retirement: recent retirees (date of retirement maximum 6 months before or after baseline measurement) Sex: mostly male (174 intervention, 178 control) Education: 25% low education level Ethnicity: NR Other inclusion/exclusion criteria: mean BMI of 27 kg/m2 Service setting: unclear |
Intervention aims and content if applicable: five programme modules. Modules 1 and 2 aimed to increase awareness of the energy balance concept and module 3 aimed to improve dietary and/or physical activity behaviour. Module 1 (two weeks after the baseline measurement) was included an information leaflet and several energy balance tools, e.g. a pedometer and a waist tape. Module 2 (3 months after baseline) was a CD-ROM providing individually computer tailored feedback on BMI, its health consequences and energy balance behaviour. In module 3 (6 months) participants could receive computer-tailored feedback regarding: physical activity, fibre consumption, portion sizes of energy dense foods and fat consumption. Modules 4 and 5 accessed via the study website which was available during the 2-year study period. After login, participants could find more information about diet and physical activity behaviour, participate in a forum and use links to other websites (module 4) and an interactive weight maintenance programme that provided a written tailored advice based on reported body weight, a food frequency questionnaire and a physical activity questionnaire (module 5) The intervention group received newsletters every 2–3 months that contained study information, information about diet and physical activity and encouragements to use the modules Control condition if applicable: the control group was provided with newsletters with general information about the study, such as study progress, and information about art exhibitions and city trips for instance. They could not login to the website and had access to the general information about the study design only Data collection methods: anthropometry, bio-impedance, blood pressure measurement and questionnaires Outcome measures: waist circumference, body weight and body composition, blood pressure, physical activity and dietary intake Response and/or attrition rate: at 24 months’ follow-up 84% of the participants returned for re-examination Data analysis: mixed models |
Main results relevant to research question (author analysis): Physical activity and dietary behaviours improved in both the intervention and control group during the intervention period. Although, these behaviours changed more favourably in the intervention group, these between-group-differences were not statistically significant. However, change in sport and recreational activities was higher after 2 years in the intervention group (74.5 minutes/week) than the control group (23.4 minutes/week; p = 0.03) Waist circumference, body weight and blood pressure decreased significantly in men of the intervention and control group, but no significant between-group-differences were observed at the 12- or 24-month follow-up. A significant effect of the programme was only observed on waist circumference [–1.56 cm (95% CI –2.91 to –0.21cm)] at 12-month follow-up among men with low education (n = 85) |
| Wijsman et al. (2013)86 Country: the Netherlands Study design: RCT Length of follow-up: post intervention Aim: to evaluate a web-based intervention Recruitment: newspaper adverts and media notification directing people to the website Funding: Philips consumer lifestyle, Netherlands Genomics Initiative |
Number of participants: n = 235 Age: 60–70 years [mean 64.7 years, intervention group (SD 3 years); 64.9 years, control group (SD 2.8 years)] Retirement: NR Sex: 39.5%/42.2% female Education: 55.5%, high-level intervention group; 57.8, controls; low level, 5.9%/1.7% Ethnicity: NR Other inclusion/exclusion criteria: no history of diabetes, absence of disability, usage of a computer with internet, < 3 hours of walking/cycling per week Service setting: home |
Intervention aims and content if applicable: commercially available web-based programme, based on stages of change and I-Change models. Three elements – accelerometer monitor worn continuously, personal website, personal e-coach. After 8 days of measuring participants given individual goals with data used for feedback and e-mail coaching and advice Control condition if applicable: waiting list for 3 months, no instructions on physical activity given Data collection methods: questionnaire, accelerometer data, body measurement Outcome measures: total activity count, body weight, body fat Response and/or attrition rate: nine did not complete the study. Of the 114 in the intervention group 109 started and 104 (91.2%) completed the intervention Data analysis: t-tests, ITT |
Main results relevant to research question (author analysis): In the intervention group after 13 weeks daily physical activity as measured by the ankle accelerometer increased by 46% (p < 0.001) compared with control group increase of 12% (p < 0.001). There was a small increase in moderate-vigorous activity in the intervention group (mean increase 11.1 minutes per day) compared with a mean decrease in the control group (p = 0.001 relative difference) |
| Wilcox et al. (2006)87 Country: USA Study design: BA Length of follow-up: post intervention (6 months) Aim: evaluated the effects of two evidence-based physical activity interventions on self-reported physical activity and related outcomes in midlife and older adults Recruitment: applicant sites chose which programme they wanted to implement Funding: local sponsors |
Number of participants: n = 838 Age: 68.4 ± 9.4 years Retirement: NR Sex: 80.6% women Education: NR Ethnicity: 64.1% white Other inclusion/exclusion criteria: Service setting: unclear |
Intervention aims and content if applicable: Four community-based organisations implemented AC, a 6-month, telephone-based programme, and five implemented ALED, a 20-week, group-based programme. Both programmes emphasise behavioural skills necessary to become more physically active AC is a 6-month programme delivered through one face-to-face meeting followed by one-on-one telephone counselling. Participants receive biweekly telephone calls for the first 2 months and monthly telephone calls for the last 4 months. Counselling is tailored to the person’s readiness for change and emphasises key social cognitive theory constructs ALED is a 20-week programme delivered in a group setting. Participants come together to learn behaviour-change principles consistent with social cognitive theory and the transtheoretical model. Participants are encouraged to provide support to one another and share successes and challenges Control condition if applicable: NA (two interventions) Data collection methods: pre- and post-test surveys Outcome measures: physical activity (moderate to vigorous and total physical activity) Response and/or attrition rate: 72% returned post-test surveys Data analysis: ANCOVA, ITT |
Main results relevant to research question (author analysis): Participants reported a significant increase from pre test to post test in moderate- and vigorous-intensity physical activity (t10 = 11.67; p < 0.001) and total physical activity (t10 = 13.53; p < 0.001) Participants reported improvements in satisfaction with body appearance (t10 = 11.22; p < 0.001), body function (t10 = 10.39; p < 0.001), depressive symptoms (t10 = –3.14; p < 0.05), and perceived stress (t10 = –2.90; p < 0.05). Finally, BMI decreased (t10 = –5.19; p < 0.001) When analysed separately by programme, all effects remained statistically significant with 2 exceptions: depressive symptoms and perceived stress for AC participants |
| Wilcox et al. (2008)88 Country: USA Study design: follow-up survey as part of above study Length of follow-up: 4 years Aim: to present 3- and 4-year follow-up data Recruitment: as above Funding: as above |
Number of participants:
Retirement: NR Sex: 80% female AC and 83% ALED Education: less than high school 8/9% Ethnicity:
Service setting: as above |
Intervention aims and content if applicable: as above Control condition if applicable: two intervention arms Data collection methods: questionnaire Outcome measures: CHAMPS physical activity questionnaire, Depression Scale, Perceived Stress Scale, body satisfaction Response and/or attrition rate: 78% returned questionnaires at 12 weeks in year 4, 62% returned questionnaires 8 weeks after the programme ended. Active Choice withdrawal – year 1: 7%; year 3: 7%; year 4: 8%. ALED year 1: 10%, year 3: 16% and year 4: 9%. Those who withdrew significantly likely to be white, older and leaner. For AC programme those with lower educational levels more likely to withdraw Data analysis: chi-squared test, ANOVA, ANCOVA |
Main results relevant to research question (author analysis): Same pattern in years 3 and 4 as that for year 1 reported in previous paper. ALED all outcomes significantly changed except for depressive symptoms (approached significance). AC all outcomes significantly changed except for perceived stress AC Moderate and vigorous physical activity d = 0.62 year 1, d = 0.66 year 3 and d = 0.75 year 4 All physical activity d = 0.55 year 1, 0.6 year 3, 0.63 year 4 Depressive symptoms d = –0.04 year 1, d = –0.03 year 3, d = 0.02 year 4 Perceived stress d = –0.01 year 1, -0.07 year 3, 0.00 year 4 BMI d = –0.05 year 1, –0.07 year 3, –0.06 year 4 ALED Moderate and vigorous physical activity d = 0.74 year 1, d = 0.66 year 3 and d = 0.58 year 4 All physical activity d = 0.79 year 1, 0.56 year 3, 0.63 year 4 Depressive symptoms d = –0.17 year 1, d = –0.15 year 3, d = –0.11 year 4 Perceived stress d = –0.29 year 1, –0.23 year 3, –0.16 year 4 BMI d = –0.06 year 1, –0.03 year 3, –0.04 year 4 For both programmes the proportion of participants reaching exercise recommendations increased significantly AC year 1 p = 0.001, year 2 p < 0.001, and p < 0.001 ALED year 1 p < 0.001, p < 0.001, and p < 0.001 |
| Wilcox et al. (2009)89 Country: USA Study design: BA Length of follow-up: immediate Aim: to examine predictors of programme outcomes Recruitment: varied by the sites, Active Choice five geographic sites and ALED seven sites. Funding: Robert Wood Johnson Foundation |
Number of participants: n = 1955 provided data, all in year one and first 100 in year 3 asked to provide baseline/follow-up data. The paper describes target recruitment of 8100, not clear total number receiving the intervention Age: 50 years or older, AC 43.7% aged 50–64 years and 35% 65–74 years, ALED 28.8% 50–64 years and 37.6% 65–74 years (mean 68.4 years; SD 9.4 years) Retirement: NR 54.3%/46.7% < US$30,000 annual income Sex: 79.1%/82.5% female Education: AC 63% some college or higher, ALED 61% some college or higher Ethnicity:
Service setting: not clear |
Intervention aims and content if applicable: Active for life programme – two interventions within this programme evaluated in this paper. AC – over 6 months one in-person orientation session followed by eight telephone counselling sessions. Second intervention – ALED – 20-week intervention delivered by weekly sessions in small groups. Programme based on social cognitive theory and the transtheoretical model Control condition if applicable: none, two intervention arms Data collection methods: questionnaires Outcome measures: Physical Activity Self-Efficacy Scale, a social support scale, Center for Epidemiological Studies Depression Scale, Perceived Stress Scale, CHAMPS questionnaire, a three-item measure from the Behavioural Risk Factors Surveillance system Response and/or attrition rate: 8.6%/12.2% withdrew from programme or programme and evaluation, 72% questionnaire return rate year 1 and 65% year 3 Data analysis: separate analyses for the programmes owing to differing length and mode of delivery. ANCOVA, the programme ran over 4 years; years 1 and 3 reported |
Main results relevant to research question (author analysis): Findings reported predominantly by predictors of greater or lesser change rather than effectiveness. ES of 0.8 for 55- to 64-year-olds for AC and ES 0.87 for active living. Little difference ethnicity (white 0.56 and 0.67 vs. black African American 0.62 and 0.72). Education – AC greater effect less than high school than high school or more than high school (0.79, 0.58, 0.64). ALED greatest effect more than high school (0.76), high school 0.61, less than high school 0.57. Pre–post differences not significant |
| Wilcox et al. (2009)90 Country: USA Study design: follow-up survey as part of above study Length of follow-up: 6 months after completing the programme Aim: to examine maintenance of gains Recruitment: participants who had enrolled in years 1, 3 and 4 of the programme Funding: as above |
Number of participants: unclear n = 169? Age: mean 72 years by time of this data collection phase Retirement: NR Sex: 72% women Education: 64% college or greater Ethnicity: 26% non-Hispanic white Other inclusion/exclusion criteria: as above Service setting: as above |
Intervention aims and content if applicable: as above Control condition if applicable: two intervention arms Data collection methods: questionnaire Outcome measures: Behavioural Risk Factors Surveillance System, satisfaction with body functioning Response and/or attrition rate: AC 46% completed follow-up survey, 50% for ALED, those who returned more likely to have higher education levels and less likely to have withdrawn from the programme Data analysis: ANCOVA |
Main results relevant to research question (author analysis): AC: time effects significant for physical activity (p < 0.0001/p < 0.05). Improvements post test were maintained at 6-month follow-up ALED: year-3 time effects significant (p < 0.0001/p < 0.001). A significant decline from post test to follow-up for physical activity, although values remained higher than at baseline |
Appendix 7 Extraction tables qualitative studies
| Study details | Population and setting | Methods | Findings | Notes |
|---|---|---|---|---|
| Arkenford (2006)130 Country: UK Study design: qualitative Length of follow-up: NA Aim: to significantly improve the understanding of determinants of participation in sport and physical activity Recruitment: screening questionnaire Funding: Sport England Quality: data analysis not reported in detail, although theoretical framework well described |
Number of participants: between 126 and 168 Age:
No more than three per group still in part-time employment (up to 3 days in a different job held at retirement) Sex: female: 10 groups; male: 11 groups Education: NR Ethnicity: Not specified: 17 groups Indian: two groups Pakistani: two groups Other inclusion/exclusion criteria: Active = eight groups (activities such as walking, cycling or sport at least once a week). Very active – active at least three times per week Inactive = 13 groups – none or less than once a week Urban/suburban = 12 non-ethnic groups Rural = five non-ethnic groups Opportunity rich/opportunity poor areas Setting: community |
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: focus groups (21); 6–8 attendees at each group Outcome measures: personal orientation and attitude to sport The place of physical activity in people’s values, self-esteem and life priorities Response and/or attrition rate: NA Data analysis: NR – application of Oxford model Theoretical framework: Oxford model of sporting behaviour change |
Main results relevant to research question (author analysis): Life stage Lifestyles of semiretired intrinsically different from those of fully retired. The fully retired acknowledge radical change in their lives. Traditional Asians appeared least likely to view retirement as positive, citing fears over health, finance and social status. Key positives of retirement: freedom, reduced stress. A key negative is missing the camaraderie Distinction between less busy and needing structure and very busy with family, committees, etc. Most feel young at heart, while some older inactive respondents feel their self-esteem has declined since retiring Attitudes to exercise and sport ‘Inactives’, think that they regularly take exercise. ‘Actives’ believe exercise has to be strenuous. Those with a medical condition more likely to be able to specify or quote guidelines. Strong correlation between a healthy body and healthy mind. Only certain forms of exercise are suitable for this age group Motivation ‘Inactives’ less likely to be aware of local exercise opportunities. Range of internal motivators including physical and social benefits, maintaining independence. External motivators included media messages, GP advice, partner, friend or family encouragement, participating with a companion, local opportunities Barriers Cost, physical limitations, language and mixed-sex facilities for traditional Asian women and a busy schedule Interventions Taster sessions, moderately priced local activities organised for this age group. A social component, staff who are in touch with the physical needs and restrictions of this age group. Fun and enjoyment. Health benefits are already known and not currently increasing participation. Reassurance in relation to safety Key differences between:
|
Strengths/limitations identified by author: NR Strengths/limitations identified by the reviewer: comprehensive study on attitudes and barriers to participation in sport in the target population Data analysis: NR Evidence gaps/recommendations for future research: NR UK applicability: UK-based study |
| Barnes et al. (2002)134 Country: UK Study design: qualitative Length of follow-up: NA Aim: to explore the hopes and ambitions of older people, and how these relate to their experiences and expectations. To look at the kinds of satisfaction and fulfilment older people draw from non-labour market activities, and the frustrations caused by constraints on participation Recruitment: survey and snowballing Funding: The Joseph Rowntree Foundation Quality: data analysis methods NR |
Number of participants: 48 (n = 12 from each of four settings) Age: 50–65 years Retirement: Retired n = 23 Part-time work: n = 11 Disabled/long-term sick n = 14 Seven had not worked for at least 10 years Sex: 27 females, 21 males Education: NR 20 working class, 28 middle class Ethnicity: all white in areas 1, 3 and 4. Area 2: white = 8, black Caribbean = 2, Asian = 2 Other inclusion/exclusion criteria: NR Service setting: Four areas: Glasgow, London, Onllwyn, (Wales) and Warminster |
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: semistructured interviews Vignettes during interviews Focus group in each of the four settings (n = 4–6) Outcome measures: NA Response and/or attrition rate: None Data analysis: ‘Qualitative techniques’ Theoretical framework: NR |
Main results relevant to research question (author analysis): Participation in labour and non-labour market activities influenced by resources, personal interests, circumstances and social networks, skills, and neighbourhood. Changes over time according to priorities accorded. Women often experienced periods when family care commitments became more pronounced Staying physically and mentally fit Need for continued stimulation in retirement to maintain good physical and mental health. Existing health problems – more acutely aware of need to keep active. Exercise classes a popular way to combine fitness with meeting new people Rest and recuperation Sometimes forced on people who wanted to become more active but who were unable to act on their desires. Activities as a sort of solace amid hectic lives Some wanted opportunities to meet other people in the same age group. Organised leisure often geared to younger or older, and women were reluctant to go out alone after dark. Desire for more daytime activities in the area Admiration of good quality low cost facilities available to retired people in USA and Australia. They were open all day and at weekends, providing a space where people could meet others. Policy suggestions:
|
Strengths/limitations identified by author: NR Strengths/limitations identified by the reviewer: much of the findings relate to activities in general rather than physical activity. Only the sections that relate to physical activity have been extracted Evidence gaps/recommendations for future research: none reported UK applicability: UK study; covers diverse range of areas across the UK |
| Barnett et al. (2013)132 Country: UK Study design: qualitative; semistructured interviews Length of follow-up: NA Aim: to explore a range of influences a partner can have on physical activity formation Recruitment: GP surgeries (EPIC Cohort) Funding: The British Heart Foundation, Economic and Social Research Council, Medical Research Council, National Institute for Health Research and the Wellcome Trust under the auspices of the UK Clinical Research Collaboration Quality: lower risk |
Number of participants: 14 (seven couples) Age: 63–70 years Retirement: recent (within 2–6 years) and not attributable to ill health (EPIC cohort only, not spouses) Sex: seven female, seven male (six female and three male EPIC participants) Education: NR Ethnicity: NR Other inclusion/exclusion criteria: excluded –medical condition that would affect physical activity (EPIC cohort only, not spouses) Setting: community |
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: semistructured interviews Response and/or attrition rate: 100% Data analysis: content analysis Theoretical framework: not specified Focus on sex and partner influences |
Main results relevant to research question (author analysis): Individual attitude towards physical activity Important to remain active in retirement. Daily chores as sufficient activity. Most walked; vigorous activities less frequently reported. For some, participation well-established habit and source of pleasure integrated in their lifestyles Differing attitudes towards physical activity among couples Agreed on importance of active lifestyle but one partner often less interested or uninterested. Active men often associated physical activity with competitiveness or a challenge. Engaging in any physical activity without achieving a goal was perceived as a waste of time. Wives did not share this competitive attitude and participated in physical activity only for recreational purposes Spouses’ physical activity behaviour Separate physical activity Spouses engaged in different (if any) forms of regular physical activity. Women tended to be more engaged in regular physical activity. A few felt encouraged by spouse’s behaviour to become more active. All those who were motivated had long-standing interest in and previous history of regular exercise, stopping after transition to retirement or owing to work commitments Others described how they had never enjoyed physical activity and only exercised when it was required of them. No instances of spouses attempting to restrict each other’s physical activity. In a few couples both spouses engaged in regular but different forms of physical activity, providing personal ‘space’ and time away from the spouse after retirement, and enabling social life within the same gender group Joint physical activity Shared physical activity rare owing to diverse interests; some couples walked together because they had more time flexibility and it offered opportunities to spend quality time together Spousal support Verbal encouragement Several active women verbally encouraged and in some cases ‘nagged’ partners to be more active Understanding Providing support by understanding their spouses’ interest in exercise was commonly described by both active and less active partners Practical support Men frequently provided practical social support such as transport or help with household chores to allow their partners the necessary time to do exercise |
Strengths/limitations identified by author: recruitment strategy might have introduced selection bias as participant/s already taking part in the EPIC-Norfolk cohort study might have been more interested in health topics and be more physically active than general population of retirees. However, spouses were not necessarily participants in the EPIC-Norfolk study, and physical activity behaviour varied greatly between couples, so as a whole the sample was not composed exclusively of highly active participants Relatively small sample size might limit the conclusions that can be drawn. Nevertheless, the couples who participated described a variety of experiences with retirement and physical activity and provided a deeper insight into how spouses influence each other with regard to physical activity Couples seemed comfortable in the interview and openly discussed and criticised each other’s physical activity behaviour. However, separate interviews might have drawn out some additional information Limited in terms of ethnic diversity, highlighting a need for further research with larger and more diverse samples Strengths/limitations identified by the reviewer: provides insights into the dynamics of retired individuals in couples in terms of engagement in physical activity Evidence gaps/recommendations for future research: ill-health in one partner might affect both partners’ abilities to be physically active; this could be an avenue for further research UK applicability: UK-based study. Mainly rural area so findings may differ where sample is taken from urban or deprived area |
| Beck et al. (2010)133 Country: UK Study design: Qualitative Length of follow-up: NA Aim: to examine the impact of retirement on physical activity patterns Recruitment: purposeful strategy Church Newspaper adverts Funding: NR Quality: lower risk |
Number of participants: 11 Age: 57–65 years Retirement: within past 5 years Retired/semiretired (Range 6 months–5 years 2 months; mean 2 years 8 months ± 20.03 months) Sex: seven female; four male Education: NR All occupied before retirement:
Other inclusion/exclusion criteria: Two groups: Inactive (< 2 sessions physical activity per week) and active (≥ 2 sessions physical activity per week) Setting: community |
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: Semistructured interviews Outcome measures: NA Response and/or attrition rate: none Data analysis: thematic analysis Theoretical framework: self-determination theory (e.g. Deci et al.)198 |
Main results relevant to research question (author analysis): Social factors Identifying with a group and feeling supported and valued, especially for females. Not fitting into a group was identified by inactive participants as a barrier to physical activity. Inactive participants reported wishes to be part of a social group, but achieved this outside physical activity. Difference in activity levels may be more associated with motivation Social support Being part of a structured group was less important to men even though men might exercise regularly. Having an exercise partner in the initial stages may beneficial Lifelong tendencies Continuation of physical activity habits Reported variations in active and inactive participants regarding past physical activity. Some continued physical activity through life, some revisited physical activity following retirement, others gave up as a result of injury. Transition to retirement often accompanied other life changes therefore required adjustment period Visions of ageing and retirement Visions of how participants wanted to be and comparisons with parents. Watching how parents aged was a common motivator for physical activity. Appreciation of benefits of physical activity not a sufficient motivator. Inactive individuals deterred by barriers such as costs, while active retirees committed regardless of obstacles Sense of purpose Challenge-seeking Adopting new activities as a means of seeking ongoing personal challenges, often relating to the gains in fitness achieved by physical activity. physical activity a way of learning new skills. Seeking challenges not a necessary condition for taking regular physical activity, but appeared to be a valued function of physical activity for those who did Daily purpose Regular physical activity provided active participants with a sense of daily purpose. Planning a physical activity schedule was necessary to keep regularly physically active |
Strengths/limitations identified by author: likely bias of the participant group which was all white British adults, and the majority from the same, relatively high socioeconomic group. Different findings may have been found with other groups, particularly those retiring from manual (i.e. physically active) jobs. It is likely that those adults interested in taking part in a research study differ in the aspects discussed in this paper than those who are not (i.e. are more outward looking and generally active) This investigation was designed to generate an insight into individual experiences rather than generalising to the general population and therefore, every participant provides a valid unique insight into their perception of the way retirement has impacted on their lifestyles and routines Strengths/limitations identified by the reviewer: As above Evidence gaps/recommendations for future research: future research could investigate whether or not the same conceptual and theoretical components would apply within lower socioeconomic groups UK applicability: based in the UK |
| Berg et al. (2002)156 Country: USA Study design: qualitative Length of follow-up: NA Aim: to identify attitudes and beliefs about physical activity among Mexican American and Anglo-American midlife women; to identify culture-specific interventions that promote long-term physical activity continuation Recruitment: from social groups and churches. Through key advisors in Tucson, Arizona, USA Funding: Beta Mu Chapter, Sigma Theta Tau International Quality: lower risk |
Number of participants: 16 Age: 35+ years:
Sex: all female Education: NR Ethnicity: Mexican American (n = 10) Anglo-American (n = 6) Other inclusion/exclusion criteria: Not currently participating in an organised physical activity programme Setting: community social groups and churches |
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: focus groups Anglo-American = 1 (n = 6) Mexican American = 2 (n = 4 and n = 6) Outcome measures: benefits and barriers to physical activity and continuation Response and/or attrition rate: NR Data analysis: individual and group levels analysed separately using interview categories as a guide |
Main results relevant to research question (author analysis): Anglo-American Helping yourself in the long run ‘Body feels better’; ‘Increased flexibility’; ‘Better sleep’ ‘More energy’; ‘A natural high’; ’Stimulates you’; ‘Invigorates you’; ’Healthy tired’; ‘Brings out competitive spirit’ Multidimensional benefits: physical as well as psychological and spiritual. Appearance – losing weight, getting into an outfit Out in the fresh air, communicating with people and body feels better, muscles move better (golf) Factors preventing physical activity Physical problems – injury or illness, no physical talent, inability to keep up with the group, no time, too many other activities physical activity not appropriate for women. Negative aspects learned when younger – not being allowed. Discomfort with physical activity in the context of gender and age appropriate behaviour Social discomfort with the group – women individually can be wonderful but in a group sometimes pretty awful Factors promoting involvement Formal group needed for motivation; routine makes it easier to continue. Financial cost was not cited as a hindrance, but a motivator, once money had been paid Factors discouraging continuation Needs to be enjoyable Praise might be useful as long as it is sincere; pressure was a de-motivator: ‘I don’t want to be pushed’ Mexican American women Why do it at all Improved health through physical activity tied to prescriptive therapy for a specific illness or condition rather than prevention Individual motivators To sleep better, more force (strength or power) and energy and to feel better physically. Clears head of worry Forces influencing decision to participate Too old to engage in physical activity, or no physical improvement is possible. Environmental factors influenced decision – transportation was a hindrance as was cost (only participated if there was no cost involved) Other time commitments Duties to others – family comes before self (grandchildren, cooking, etc.) Church – important activity Watching soaps (novellas) on television Role of family and others in beginning and continuing physical activity To join family and peers; in order to live longer; to maintain ability to do for family; do it for others. Approval needed from family |
Strengths/limitations identified by author: NR Strengths/limitations identified by the reviewer: reporting is brief; not much detail about each participant (we do not know the upper age range in two groups for example) One strength is that cultural differences in beliefs relating to physical activity are drawn out, highlighting the importance of assessing these when advising on lifestyle change Evidence gaps/recommendations for future research: none reported except that interventions need to incorporate culturally based world views UK applicability: Mexican population not large in UK but can learn from the culture-specific aspects of these findings |
| Berry et al. (2009)179 Country: Canada Study design: Qualitative Length of follow-up: NA Aim: to evaluate television advertisements targeted at 55- to 70-year-olds that promoted physical activity and fruit and vegetable consumption Recruitment: random digit dialling Funding: operating grant from the Canadian Institutes of Health Research Quality: lower risk |
Number of participants: 1600 for survey, 29 for focus groups Age: 55–70 years
Sex: Survey:
Focus groups:
Ethnicity: NR Other inclusion/exclusion criteria: NR Service setting: community |
Intervention aims and content if applicable: Mass marketing campaign (Healthy U advertisements) Control condition if applicable: NA Data collection methods: telephone survey and focus groups Outcome measures: unprompted and prompted recall. physical activity and dietary behaviour Response and/or attrition rate: Survey response rate: 46.3% Data analysis: Survey: descriptive statistics and two logistic regressions Focus groups: cross-case analyses and coding. Theoretical framework: none reported |
Main results relevant to research question (author analysis): Only results relating to physical activity reported here Focus groups Comments regarding the ‘grim reaper’ Positive comments relating to how advertisements attracted attention and made one think. Some positive and negative comments about humour. Several felt ads were not aimed at those over 55 years. Grim reaper character not popular either as a character or as a symbol. The character also took away from the message. Many people cannot read and there was no spoken aspect of the advertisement Advertisements viewed as a waste of money. The government was not considered a credible source; some cynicism regarding the government’s motives in promoting health, although considered to be more credible than commercial companies. Doctors and their governing bodies were the most trusted source for health promotion information. The use of celebrity highlighted the importance of being able to relate to the celebrity. Several mentioned that ordinary people such as housewives and farmers would be more realistic characters in such advertisements Websites Some participants reported being comfortable with technology but others reported not using the internet at all. Accessibility issues given that not everyone owns a computer. Access to computers can be more difficult for rural residents |
Strengths/limitations identified by author: this was a naturalistic study that independently evaluated a campaign that was developed and implemented over the course of a few months. Therefore, it was impossible to gather baseline data However, to partially overcome this limitation we were able to compare our findings to the yearly evaluations conducted by Healthy U which showed the ‘grim reaper’ was not as well recalled as other Healthy U campaigns The strengths of triangulating the quantitative survey data with the qualitative focus-group data illustrates that although there may be increased awareness of a campaign the reasons for the attention paid to the advertisement should be evaluated Strengths/limitations identified by the reviewer: as above Evidence gaps/recommendations for future research: how the government is perceived should be considered in future research UK applicability: Could be applicable to a similar mass media campaign in the UK |
| Brown et al. (1999)170 Country: Australia Study design: qualitative Length of follow-up: NA Aim: to explore older people’s attitudes to practices and perceptions of physical activity Recruitment: Invitations to randomly selected members of the older cohort of the Australian Longitudinal Study on women’s Health (ALSWH) Funding: NSW Health Sun Exposure and Physical Activity Policy Unit (SEphysical activity) Quality: lower risk |
Number of participants: 81 Age: 60 years
Sex:
Service setting: six community locations |
Intervention aims and content if applicable: NA, although some discussion about a mass media campaign (The Active Australia Campaign) Control condition if applicable: NA Data collection methods: focus groups (11) Outcome measures: NA Response and/or attrition rate: NR Data analysis: Interrogation for themes. Theoretical framework: NR |
Main results relevant to research question (author analysis): General health and well-being Importance of community involvement (mainly women) and mental health (mainly men). physical activity strongly endorsed; for women it was also an avenue for social contact. Men suggested importance of good health comes late for them Current physical activity Wide range of activities. Many forms of walking – transportation, organised walking groups for health rehabilitation. House and yard work usually traditionally divided (women doing the housework). Other activities included interaction with grandchildren Motivations Health and well-being; social support; a sense of doing something useful; the environment and avoiding negative ageing stereotypes. The role of physical activity in preventing illness important for those who had experienced a serious health problem. Pleasure doing something for the self. Social support an important motivator, particularly among women. Having a purpose – walking to buy a newspaper, building something, etc. especially for men. Availability of resources and good weather. Concerned not to become like other old people who stayed home, not involved in anything. There were instances of several motivations combining to encourage physical activity Motivators The self, partners, other family members and dog ownership. Self-motivation important. GPs important sources of information, particularly following illness or injury, although variation in experience. Other sources included pharmacists, physiotherapists, chiropractors, naturopaths, priests and ministers. Fitness leaders were regarded as an excellent motivator Barriers No-one to exercise with; poor health; environment; lack of interest. Many used to do various activities but had to stop because of injury. Need for older people to be shown how to do exercise safely to avoid injury. Story of someone who took up running and died Family responsibilities a barrier but also created activity (looking after grandchildren). Changes in a partner’s ability to exercise (and widowhood) could influence participation The physical environment – weather, facilities such as footpaths and lighting, no appropriate places to go. Even when facilities were available the lack of an appropriate leader could be an issue. Structured classes were seen as preferable to exercising alone Issues of access – transportation, cost and accessibility, particularly for those no longer able to drive. Local areas were often regarded as unsafe for walking, especially at night Not all felt physical activity was interesting or appropriate and some were cynical about the idea Marketing the physical activity message Sources of health messages: television (programmes and advertisements); newspapers, magazine, HPs, community organisations (guest speakers sometimes arranged), displays in shopping malls. Consensus that not enough information on exercise for older people The Active Australia Campaign Low awareness of the campaign. Suggestion that if broadcast as part of the ads it wouldn’t be viewed as people would mute or go off and make a cup of tea. Some may have seen the poster or something like it. Some felt the recommendation to be moderately active on most days of the week was insufficient as most people achieve that through shopping. Daily chores might also meet the requirement. Many were impressed by the ideas put forward in the leaflet. Use of older people in the leaflet and slogans were suggested improvements. Television not regarded as the best way to reach this population, rather, GPs or articles in senior newspapers were better ways. Mobilising the women was suggested to influence men. Another was to buy everyone a dog. People need to acknowledge problems with their current lifestyle |
Strengths/limitations identified by author: identification of several psychological, social and environmental factors important in promoting physical activity to older people Strengths/limitations identified by the reviewer: as above Evidence gaps/recommendations for future research: none suggested UK applicability: based in Australia where environmental factors may differ from those in the UK (geographically distant locations for example). However, most of the concepts are potentially transferable |
| Cooper and Thomas (2002)141 Country: UK Study design: qualitative Length of follow-up: 12 months Aim: to examine the meaning of social dancing for older people Recruitment: from a range of dance venues in the three areas Funding: UK Arts and Humanities Research Board Quality: lower risk |
Number of participants: 31 interviews Age: ≥ 60 years Retirement: NR Sex: mixed Education: NR Ethnicity: NR Other inclusion/exclusion criteria: none reported Service setting: community dance events in Essex and London (three areas) |
Intervention aims and content if applicable: The sites represented the general mix of dance sites in that one was an ‘official’ modern sequence club which took place in the local village hall in Essex, one was a mixed social dance event in southeast London, which took place at a leisure centre, one was a purpose built ballroom which hosted a mix of ballroom and modern sequence dancing, also in south-east London, and the three others were dance classes which took place at local community centres in all three boroughs Control condition if applicable: NA Data collection methods: ethnography (interviews, participant observation, videotape) Outcome measures: NA Response and/or attrition rate: NA Data analysis: NR Theoretical framework: continuity theory |
Main results relevant to research question (author analysis): Continuity and change Participants lived through period of change in the way that people live and the way that they dance. Social ballroom and modern sequence dancing as form of continuity in terms of identity, values, beliefs, skills and preferences (internal) and in the physical and social environments, role relationships and activities (external). This cohort raised with this type of dancing; key social activity in adolescence. Music, dress, etiquette and sexual codes, all important to adolescents, were incorporated in social dancing and continued to play an important role for older people. Some had carried on dancing throughout, taking dancing seriously and entering competitions, whereas others returned after bringing up a family. Many moved to sequence dancing (gentler, friendlier) when ballroom dance halls closed down or they felt unable to compete. Different use of space; ballroom can be dangerous for those with mobility problems. Modern sequence is orderly and viewed as a natural progression in later life without losing skills and knowledge Loss of a partner may mean the activity is also lost, although many return, often through encouragement from friends or family. Need to engage with the familiar draws them back. As women tend to live longer and men are less likely to attend alone, some women will attend alone or with another female friend Enjoyment of the dance and the ‘recycled teenager’ Enjoyment of dancing; could raise the mood if one was feeling low. Comparison between dancers and those who do not dance. Element of fun was evident in the sociability, dressing up and sense of humour within dance communities. Dancers often used the phrase ‘recycled teenager’ to express this Sociability and communitas Much pleasure gained from sociability of modern sequence dancing. Dancers support each other through low periods such as illness. Shared meanings and knowledge evoke a community; one is ‘in’ and ‘with’ the group through dancing. There is a consciousness that the group must stay together so that individuals can be supported Looking good on the dance floor Looking good was important and a necessary part of the experience, relating to posture and movement as well as appearance. Shoes are a particular aspect of looking good – they need to be ‘dance shoes’. Dressing up and glamour are especially important at Saturday social dances Dance as cultural capital Older dancers draw on cultural capital to express a superior status over younger generations. Learnt skills and embodied knowledge counters age-related disadvantage. The subcultural capital is formed through type of music, dress (fashion trends are ignored), bound codes of conduct in a similar way to subversive youth culture. For many of the dancers the younger generation’s dancing is inferior to their own The fit dancing body and mind It was generally believed that dancing warded off ailments (stiff body; decline of the mind) with examples given of stiffness disappearing through dancing, although they may have hobbled home |
Strengths/limitations identified by author: NR Strengths/limitations identified by the reviewer: provides insight into the dancing community which appears to be important for keeping this population active through ‘communitas’ and a shared love of music and dance Evidence gaps/recommendations for future research: NR UK applicability: based in UK |
| Dionigi (2006)171 Country: Australia Study design: qualitative Length of follow-up: NA Aim: to explore the motives and experiences of older Australian Masters Games athletes Recruitment: NR Funding: Charles Stuart University Writing Up Award Quality: lower risk |
Number of participants: 28 Age: 60–89 years
Sex:
Ethnicity: NR Other inclusion/exclusion criteria: Participants in the Eighth Australian Masters Games Setting: Eighth Australian Masters Games held in Newcastle, New South Wales, Australia |
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: in-depth interviews Outcome measures: NA Response and/or attrition rate: NR Data analysis: coding,199 constant comparative analysis,200 the generation of common themes,201 and the application of theory Theoretical framework: poststructuralist |
Main results relevant to research question (author analysis): The words and actions of older athletes: ‘I’m out here and I can do this!’ Acknowledgement that their behaviour challenged age-appropriate norms; pride in this differentiation. Considered themselves ‘lucky’ and unique when compared with other older people. Ageist ideas about old age as primarily a period of disability, disengagement, and dependency. Competing in sport allowed expression of a powerful, vital, and active image of older people. Feeling exceptional appeared to help manage an ageing identity and had the potential for personal empowerment Demonstrating capability of vigorous physical activity in later life confirmed identity as an athlete, and challenged ageist discourses ‘Use it or lose it’ Consistent with positive ageing and health promotion approaches. Resistance to the ageing body associated with feelings of personal empowerment. All were health-conscious and believed that regular physical activity associated with competitive sport prolonged physical fitness as well as social and psychological health Belief that they had to use their bodies as much as possible to delay the onset of disability or age-related disease. Loss in physical ability also meant loss of independence, health, a sense of control over their lives, and a sense of self Benefits gained gave a perceived sense of control over their lives and bodies, as well as confirmation that they were adapting to the challenges of later life and were not dependent on others, diseased, or disabled |
Strengths/limitations identified by author: none reported Strengths/limitations identified by the reviewer: the findings highlight resistances to ageist discourse in this population Evidence gaps/recommendations for future research: further research is needed to explore how older athletes manage when they are no longer physically able to compete UK applicability: Specific to participants in Masters games, Australia. The concepts of resistance could, however, be transferred to similar populations in the UK |
| Drummond (2003)173 Country: Australia Study design: qualitative Length of follow-up: NA Aim: to assess ways in which older, retired men perceive their bodies and whether or not this bears on their masculine identity and QoL Recruitment: participants from a larger study Funding: NR Quality: lower risk |
Number of participants: Age: 58–85 years Retirement: all retired Sex: all male Education: NR Ethnicity: NR Other inclusion/exclusion criteria: all participants in a regular physical activity or walking programme (at least two sessions per week) Setting: community |
Intervention aims and content if applicable: walking programme (40–60 participants at each session) set in a shopping mall Control condition if applicable: NA Data collection methods: in-depth interviews Focus group (only data from FGs reported) with access to follow-up via telephone Outcome measures: NA Response and/or attrition rate: no attrition reported Data analysis: inductive analysis Theoretical framework: masculinities |
Main results relevant to research question (author analysis): The functional body Importance of the functionality of the male body; concern about what their bodies could ‘do’ rather than appearance to others. ‘Doing’ rather than ‘being’. Not out to impress with an archetypal masculine physique; happy to be alive and functioning. Regular physical activity sessions played important role in maintaining physical and mental health. Provided knowledge that their bodies were still a useful ‘tool’. To be able to use the body without restrictions or pain was important (many peers were dead or in poor health) The failing body For men in their seventies, the failing body signifies that the body can let men down and increasingly so with age. Compartmentalisation of bodies in terms of non-function. Difficulty coming to terms with a body that used to have the capacity to ‘do’ with relative ease and minimal conscious effort. This changed and more consciousness is required. Muscular flexibility, agility, dexterity and endurance were cited in terms of reduced physicality. Strength was a signifier of masculinity as it clearly defines men and the roles of men and women in life Feelings of inadequacy Each identified that not being able to perform in the same manner had implications for their masculine identity. Feelings of ineptitude, anger, frustration and of not being a ‘complete’ man. Feelings associated with the body and work – work is crucial to many men’s sense of masculine identity. Their sense of self was affected when work was taken away from them. Recognition that feelings of inadequacy would only last a short time. In order to be comfortable with themselves, a need to come to terms with these changes or become dispirited and troubled Physical activity for health and movement Perception that movement is a positive element, synonymous with health and ‘being alive’; body as a sign of vigour. Bodies can ‘do’ physical activity; a sense of pride in their physicality. Competition an important motivating factor during exercise sessions, making the programme more enjoyable. Competition was not formalised, rather an unspoken lore |
Strengths/limitations identified by author: none reported Strengths/limitations identified by the reviewer: uses theories of masculinity to situate the men’s views Not much detail about the sample demographic Evidence gaps/recommendations for future research: none reported Could compare with older women’s experiences UK applicability: no reason to believe that men in the UK could not attend a similar walking intervention or that the issues raised here are not transferable |
| Duncan (1994)151 Country: USA Study design: qualitative Length of follow-up: 4 months Aim: to give community-dwelling older adults who currently engage in mall walking an opportunity to describe their experiences Recruitment: NR Funding: NR Quality: lower risk |
Number of participants: Observed: n = 35–52 on any given day Interviews: n = 14 Age: interviewees: 61–81 years Retirement: all retired Sex:
Ethnicity: all Caucasian Other inclusion/exclusion criteria: mall-walking activity: at least 30 minutes three times per week for 3 months Service setting: one enclosed mall (built into the side of a mountain) in West Virginia, USA |
Intervention aims and content if applicable: Mall-walking practice initiated by the author. Starts at 07.30 and runs 6 times a week One complete lap of the mall = approximately two-thirds of a mile Control condition if applicable: NA Data collection methods: Participant observation (1 hour sessions between 07.30 and 10.00), conversations and in depth interviews Outcome measures: Factors that influenced initiation of mall walking Factors that influenced choices to continue mall walking Impact of family and friends on mall-walking behaviours or routines How mall walking fits into context of personal lives Response and/or attrition rate: NR Data analysis: grounded theory Theoretical framework: not specified in the methods but social cognitive theory and social breakdown syndrome and social reconstruction theory are discussed later in the paper |
Main results relevant to research question (author analysis): Context of the mall-walking phenomenon Mall situated in Appalachian mountains. Approx. 22% 60 years and over in the county Mall walking – seats available. Unwritten ‘rules’ for walking such as following a path in a counter-clockwise direction Causal conditions 1. Expert directed (e.g. directed by physician) 2. Self-directed (e.g. personal health-related goals) 3. Other directed (e.g. invitations from friends/family) Those advised by physicians to walk clear about the relationship between walking and the management of medical conditions. Some felt overt pressure, such as repeatedly asking about their walking. Small group of self-directed walkers primarily looking after their health and independence. Belief in the necessity with age of acting purposefully. Less likely than the expert directed group to walk for social reasons Spouses the most influential group followed by family and friends Intervening conditions and resulting behavioural strategies Four intervening conditions prevailed:
One influence was a strong work ethic; most had a history that included paid employment outside the home. None had wanted to retire and expressed regret at the loss of a paid work role and reduction in social contacts. Depression and loneliness were not uncommon. Mall walkers were not only making social contacts but also roles and routines for themselves that had been lost on retirement. Walkers arrived early in the morning (typically Monday–Friday) and maintained an unvaried schedule which involved saying hello and going off in groups Perceived fear and vulnerability The mall perceived as safer and more sheltered than in the park (or the Smokey Mountains) Social contacts Men and women found companionship at the mall, although effort was needed. Acquaintances made while walking alone, then companion prospects were identified. Walkers speak as they pass, and then eventually begin a conversation. Same sex groups were most common. Pace partnerships initiated. A few walked alone because they had a disability that resulted in a slow pace. They found partners more likely as their pace increased. Many pace partners were considered reliable and valuable companions with whom intimate information was shared and advice sought Community membership and a sense of belonging The community shared an important part of their week together as well as customs, roles, rituals and beliefs. Otherwise they were a diverse group and the mall brought them together. Groups met for coffee or in food areas. The main method of communication was the grapevine. Some regarded this aspect as gossipy and ‘nosey’. Positive communications were joyful occasions and upcoming mall events Outcomes
|
Strengths/limitations identified by author: The findings have implications for the ways in which health activities for older adults are promoted Four months doers not allow assessment of meaning and motivation over time (e.g. impact of holidays, illness and seasons) Strengths/limitations identified by the reviewer: this paper provides similar information to that in Duncan et al.152 Gives insights into motivations of this population Evidence gaps/recommendations for future research: Include individuals from geographically and SES diverse backgrounds Comparisons are needed between expert-directed, self-directed and other-directed mall walking in respect of attrition and adherence, etc. UK applicability: mall walking appears to be mainly a US activity – more malls, fewer outdoor facilities, especially in remote areas. However, the activity could be initiated in the UK |
| Duncan et al. (1995)152 [same study as Duncan (1994)151] Country: USA Study design: qualitative Length of follow-up: NA Aim: to explore the meanings and motivations for mall walking among older adults (> 60 years) Recruitment: during weekly health monitoring session conducted at the mall Funding: NR Quality: lower risk |
Number of participants: Observed: n = 35–52 on any given day Interviews: n = 14 Age: > 60 years Range 61–81 years Retirement: not explicitly reported Sex: interviewees – five female, nine male Education: NR Ethnicity: all Caucasian Other inclusion/exclusion criteria: mall-walking activity: at least 30 minutes three times per week for 3 months Setting: one enclosed mall in West Virginia, USA |
Intervention aims and content if applicable: mall walking Control condition if applicable: NA Data collection methods: participant observation (1-hour sessions between 07.30 and 10.00), conversations and interviews Outcome measures: NA Response and/or attrition rate: NR Data analysis: grounded theory Theoretical framework:
|
Main results relevant to research question (author analysis): Understanding the mall-walking experience Reasons for initiating mall walking:
Most had a history of paid work outside the home. Mall walking provided daily routine, social contacts, and prescribed roles that reflected work practices. Social activities included lunch and picnics The need for socialisation Collective consciousness that ageing might lead to fewer contacts unless effort was made. Some walked with spouses, although most couples did not walk together, preferring same-sex dyads or groups. Partnerships took a while to develop and were based on having a similar walking pace. Most partners did not know each other when they began mall walking A sense of belonging A community was created with an overriding connection – mall walking. Shared customs, roles and rituals. Socialising after walking, e.g. having a coffee was important. Older walkers took action to exert control over the conduct of others, mainly related to walking direction and allocation of space The mall as a safe environment Although walkers would enjoy walking outside, they felt the safe, sheltered environment of the mall outweighed benefits of being outdoors. No evidence of high crime rates in the localities, but a strong sense of fear and vulnerability Theoretical overview Presence of:
|
Strengths/limitations identified by author: none reported Strengths/limitations identified by the reviewer: one strength of the paper is the link to theory. Highlights the importance of social contact when organising physical activity for older people Limitation: could have interviewed people who have tried mall walking and stopped (barriers) Evidence gaps/recommendations for future research: to determine whether or not formalising aspects of mall walking will change the meaning for individuals Further refinement of the model UK applicability: set in USA where outdoor environment may be less amenable to walking and where malls are accessible. Not sure if mall-walking groups exist in the UK but there is no reason to believe that it could not serve a similar function for older UK adults |
| Evans and Sleap (2012)135 Country: UK Study design: qualitative Length of follow-up: NA Aim: to investigate the relationship between participants’ perceptions of the ageing body and participation in aquatic activity Recruitment: through aquatic sessions and a walking group Funding: Amateur Swimming Association on behalf of the Department of Health Quality: lower risk |
Number of participants: 22 Age: 50+ years
Sex:
Ethnicity: all white British Other inclusion/exclusion criteria: Regular and occasional participation in aquatic activity Service setting: GP referral aquatic sessions Age Concern aquatic sessions Walking group |
Intervention aims and content if applicable: Swim for Health project Control condition if applicable: NA Data collection methods: semistructured interviews (3 paired and 16 individual) Outcome measures: NA Response and/or attrition rate: NR Data analysis: thematic approach Theoretical framework: tigurational perspective |
Main results relevant to research question (author analysis): Perceptions of fitness, health, and aquatic physical activity Limitation of capabilities with ageing, reinforced by medical measurements Benefits associated with alterations in body appearance (weight, toning) which led to psychological benefits ‘looking and feeling good’ Feeling that they ought to participate owing to marketing messages around appearance, although aware of physical risks and of outsider status as older people engaging in aquatic activity Exclusivity of sessions fostered shared identity as well as empowerment. New networks created that encouraged social support ‘People laugh don’t they’: objectifying the ageing body in aquatic activity Dress code for swimming accentuated feelings of embarrassment and awareness of bodily flaws, particularly for larger figures. Perceived gaze of others in the pool, particularly established swimmers; also ability for gaze from gallery, café, reception areas. Women particularly aware of gaze from men. Men were often outnumbered and the aqua aerobics regarded as ‘feminine’ so also felt exposed ‘What’s in the water?’ Rationalising risk to the body in aquatic physical activity Awareness of the hazards associated with water; slipping, falling, negotiating steps, bacterial infection, drowning (especially in those having had negative experiences in the past). Reduced ability to control fluids entering and leaving the body in the pool |
Strengths/limitations identified by author: Findings based on preliminary investigation into the social production of active ageing bodies. Participants were white British; no participants were present in the aquatic activity sessions from other ethnic groups Analysis using only one theoretical perspective Strengths/limitations identified by the reviewer: as above Evidence gaps/recommendations for future research: Further insights into the gendered nature of aquatic activity may be required. Also other groups’ experiences (other than white British) and perceived barriers to participation in aquatic activity Research that uses alternative sociological standpoints to figurational sociology could add insights that might have been overlooked in this framework UK applicability: UK-based study |
| Finch (1997)131 Country: UK Study design: qualitative Length of follow-up: NA Aim: to explore among men and women > 50 years what is known about physical activity, attitudes to and participation in physical activity and barriers and facilitators regarding physical activity Recruitment: brief interviews or identification of residential facilities in the selected localities Funding: Health Education Authority Quality: recruitment details brief. No discussion of relationship between researcher and participant. Ethical issues not discussed |
Number of participants: Focus groups 97 Age: Focus groups:
Sex:
Ethnicity: NR Other inclusion/exclusion criteria: Service setting: community and residential |
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: focus groups (8) In depth interviews (data not included as age 75+ years) Outcome measures: NA Response and/or attrition rate: NR Data analysis: content analysis Theoretical framework: NR |
Main results relevant to research question (author analysis): Physical activity and health: key beliefs Belief that physical activity beneficial even by people who did little or no physical activity. Specific benefits included keeping supple, avoid stiffness, maintaining mobility. Beneficial effects on the heart, circulatory system, digestive system, liver and kidneys were also mentioned. Key benefit was weight control – physical activity as preventative for women in their fifties, in relation to ‘beer bellies’ for middle aged and older men. Around retirement age related to keeping weight down and muscles firm after giving up a physically active job. Exercise also reduced stress and perceived as helping to ward off depression and dementia. Helping to get over illness such as arthritis, diabetes, heart conditions or cancer. Illness had often led to taking up physical activity to fight it (e.g. swimming for arthritis). For younger participants, physical activity as insurance for the future ‘buying time’ and prolonging life or making up for excesses in the past Increased consciousness of health-related benefits of physical activity Leading up to retirement, physical activity could assume greater importance so that retirement could be enjoyed. physical activity a way of countering the effects of ageing. Women more likely to keep active through housework than men Younger respondents more aware of the physical benefits of physical activity. Hearsay, media stories and personal experience of people known to them fed these views. Fashion element, exemplified by the growth of gyms and health clubs more concerned with image rather than health Moderation is needed Necessary to be more watchful of overdoing things – perhaps lessening intensity. Certain types of activity more suitable at ‘our age’ such as walking, swimming, yoga and golf. Aerobics and jogging perceived as too strenuous The extent of physical activity safely beneficial to health varied for different people Beliefs regarding type, frequency and intensity of physical activity Perception that amount of physical activity reflected a need to ‘slow down’ and tailor physical activity to the individual Frequency Regular exercise stressed as important by some even if not practised. Need for briskness and vigour contrasted with fears that exertion was dangerous or unnecessary Sources of beliefs The media (especially in the younger group), television, magazines, press, exercise videos and radio. For women perceived pressures regarding appearance; for men dangers of physical activity for older people as reported in the news Medical/health professionals Advice given in relation to a specific health problem was particularly influential, as was getting a serious disease, on behaviours relating to physical activity. Posters were also seen in medical establishments The workplace Talks attended at work were a source of information as well as promotion of exercise for sedentary workers Benefits Health, enjoyment, ‘feeling better’ and social. physical activity mentally stimulating and as having a positive effect on life, reducing stress. Pleasure in being outside, as a way of getting out of the house Perceived barriers to physical activity Inertia effort required/easier not to do it/laziness/slowing down/wanting to rest No time (work/retirement activities ‘the day just goes’/changed perception of time, e.g. getting up later in the day/carer or grandparent responsibilities) Lack of interest (not that type of person/don’t like physical activity/conception of what is physical activity/found it tiring Embarrassment, shyness, lack of confidence about revealing the body (overweight, being older among younger people), doing something new, lacking skills, having no-one to go with Possible dangers to health fear of overdoing it, existing health problem, fear of having a heart attack. There was a belief that one has to be fit before beginning physical activity. There was a stated fear of ‘addiction’ to physical activity, although this was not taken very seriously External dangers/difficulties traffic, climate, pollution, fears of attack, dark evenings, younger people being much faster Facilities Lack of facilities owing to funding cuts/inappropriate/crowded/cost/transport Barriers at different times of life Pre-retirement: lack of time owing to job – aversion to labels such as ‘over 50s’ clubs For men: fear of overdoing it and having a heart attack. For women: safety concerns, time taken with carer responsibilities, menopausal symptoms such as tiredness, feeling less capable |
Strengths/limitations identified by author: none reported Strengths/limitations identified by the reviewer: details of participants and data analysis not reported Evidence gaps/recommendations for future research: none reported UK applicability: US-based study. However, concepts relating to responsibilities to social group in reinforcing activities and maintaining self-worth as well as the role of exercise as part of identity can be translated to UK settings |
| Fournier and Fine (1990)154 Country: USA Study design: qualitative Length of follow-up: 4 months Aim: to examine exercise and active leisure function as signals of when to transform identity in respect of being ‘old’ Recruitment: NR Funding: NR Quality: recruitment, data analysis methods and ethical issues NR. Findings clear but discussion brief |
Number of participants: six Age: 69–85 years Retirement: NR Sex: mostly female Education: middle class Ethnicity: white Other inclusion/exclusion criteria: Service setting: community centre exercise class |
Intervention aims and content if applicable: Exercise class for elderly persons, 30 minutes three times per week. Led by a young female instructor employed by the community centre. Informal and playful; stretching and toning with low-impact aerobics Control condition if applicable: NA Data collection methods: participant observation Interviews Outcome measures: NA Response and/or attrition rate: NR Data analysis: NR Theoretical perspective: none specified |
Main results relevant to research question (author analysis): Defining ‘old’ Differentiation between feeling old and chronological age. Definitions involved health status, but mobility, leisure and lifestyle are more critical. The primary factor is physical activity and the ability to enjoy oneself. Women are old when they can no longer participate in an exercise class or more generally experience a change in ability important to their identity. This active identity contrasted with passive individuals whom the exercisers consider ‘old’. As long as the women exercised they knew they were not old Non-exercisers as ‘old’ Exercisers questioned why some people that would benefit from the class didn’t come, perhaps saying they are too old for it Definition of self as day-to-day adjustment to aches and pains. Exercisers may experience identical physical ailment as a non-exerciser but the latter interpret this as a significant obstacle, whereas the exerciser can incorporate the ailment into identity without much change |
Strengths/limitations identified by author: none reported Strengths/limitations identified by the reviewer: details of participants and data analysis not reported Evidence gaps/recommendations for future research: none reported UK applicability: US-based study. However, concepts relating to responsibilities to social group in reinforcing activities and maintaining self-worth as well as the role of exercise as part of identity can be translated to UK settings |
| Freene et al. (2014)168 Country: Australia Study design: mixed methods Length of follow-up: 6 months Aim: to identify middle-aged adults’ physical activity preferences Recruitment: random selection from intervention/comparator intervention participants and those not wishing to take part Funding: NR Quality: lower risk |
Number of participants:
Sex (female):
Other inclusion/exclusion criteria: PAAH participants categorised into three sub-groups: (1) YMCA group exercise programme attendees (GA); (2) YMCA group exercise programme non-attendees (group non-attendees); and (3) the physiotherapy-led home-based physical activity programme attendees (home-based) Group exercise programme non-attendees defined as attending ≤ 50% of the group exercise sessions. A sub-group for the physiotherapist-led home-based physical activity programme non-attendees was not formed as there were no participants in this category Service setting: community exercise intervention |
Intervention aims and content if applicable: Physiotherapist-led home-based physical activity programme utilising motivational interviewing Control condition if applicable: Group exercise programme and this was run by fitness instructors at the local YMCA, once a week, for 60 minutes, for 6 months. The group exercise programme was conducted during business hours to replicate similar programmes in this community setting, ‘usual practice’ All participants, both group and home-based, were encouraged to increase their physical activity levels during the interventions, aiming to achieve the physical activity guidelines (30 minutes of moderate-intensity physical activity on most days) Data collection methods: focus groups (x6) for qualitative element, carried out 6 weeks post intervention Outcome measures: NA Response and/or attrition rate: three home-based participants were lost to follow-up during the intervention period. All other home-based participants received regular motivational interviewing over the telephone during the 6-month intervention period Data analysis: coding and thematic analysis |
Main results relevant to research question (author analysis): Programme enablers: Having a health concern Belief that physical activity would be beneficial Personal invitation through the post Opportunity to participate in research No cost Perceived improvements in physical and mental health Flexible physical activity delivery (home based programme) Flexible in terms of physical activity type, location, time Not requiring radical lifestyle change Enjoyable (group programme) Tailored programme (group programme) Social support (group programme) Work support (group programme) Physio/fitness instructor–client interaction Physiotherapist expert and knowledgeable (home-based) Support from physio (home-based) Self-efficacy, confidence Commitment (group-based) Programme barriers Environmental Holidays Work commitments Caring for others (children, grandchildren) Health problems Feeling embarrassed or self-conscious (non-attenders) Not fun Poor supervision Insufficient explanation Too infrequent sessions to be of benefit Walking not strenuous enough to be of benefit Regular advice via telephone helped home-based participants to continue following a period of absence Physical activity preferences No single preference clearly identified Some preference for home-based activity for flexibility Mix of activities |
Strengths/limitations identified by author: the small number of males participating in the focus groups is a limitation, providing a potentially poor representation of their views. The sample of participants may not necessarily represent the perceptions of all middle-aged adults as it was drawn from those participating in the PAAH study, previously self-reported sedentary middle-aged adults who were willing to increase their physical activity levels. The sample size is small, increasing the chance of sampling error for the quantitative data and therefore should be interpreted cautiously. Investigator bias is also possible as the analysis was primarily conducted by the principal researcher who provided the home-based intervention. The ethnic makeup of this sample limits generalisability, with the majority of participants being Caucasian, with Australian or English ancestry A mixed-method approach allowed a more in depth understanding of the complex nature of the factors influencing choice of physical activity in this group. Random sampling used to select focus-group participants limited selection bias for the quantitative data. Random sampling is, however, not an ideal strategy for qualitative methods such as focus groups and this is also a limitation of this study. Member checking also took place within the focus groups by the facilitator and during the exit questions via telephone by the principal researcher, increasing validity and limiting researcher bias Strengths/limitations identified by the reviewer: as above Evidence gaps/recommendations for future research: NR UK applicability: no reason to believe that the concepts found here could not be transferred to a similar intervention based in the UK |
| Gallagher et al. (2010)165 Country: USA Study design: qualitative Length of follow-up: NA Aim: to identify the salient factors of the neighbourhood environment that encourage or discourage walking in older, urban African Americans Recruitment: purposive sample through senior centre with outreach programme Funding: NR Quality: recruitment details brief. No discussion of relationship between researcher and participant. Ethical issues not discussed |
Number of participants: 21 Age: > 60 years Range 61–85 years Retirement: NR Sex: 90% female Education: 81% had attended college or vocational facility Ethnicity: 100% African American Other inclusion/exclusion criteria: Able to walk either with or without an assistive device, and able to speak and read English Setting: community |
Intervention aims and content if applicable: Control condition if applicable: Data collection methods:
Response and/or attrition rate: NA Data analysis: content analysis; thematic analysis |
Main results relevant to research question (author analysis): Presence of people Presence of people was a facilitator to walking: Seeing familiar faces and neighbours People walking, biking, or jogging Smiling, friendly people Presence of families with children Visitors and downtown employees enjoying the local parks The presence of people was also was mentioned as an inhibitor of walking, although less frequently Large crowds People from outside the neighbourhood generating criminal activity Individuals asking for or demanding money Young people fighting Neighbourhood surroundings Most commonly reported enablers of neighbourhood walking: Quiet, peaceful surroundings Buildings or statues with personal or historical meaning Beauty or scenery; parks and gardens, trees, and shade Other factors that encouraged neighbourhood walking included: Presence of water and attractive buildings Places to rest, eat, or use the toilet Variety of sights and activities Vacant houses, overgrown lots, and trash were identified most frequently as inhibiting neighbourhood walking, followed by inadequate lighting and fallen trees or branches Safety from crime Factors that encouraged neighbourhood walking: People biking, walking, or jogging A safe walking area Presence of a senior patrol, police, or security Walking early in the morning Impediments to neighbourhood walking: A personal history of criminal victimisation, either recent or in the past Current neighbourhood criminal activity A sense of an unsafe walking area Slow or inappropriate police response to neighbourhood crime Pavements and traffic The presence and condition of neighbourhood pavements influenced walking for many participants Six participants identified shovelled pavements as facilitating walking, whereas broken pavements, pavements overgrown with weeds, icy pavements and the abrupt ending of pavements forcing individuals to walk in the street with traffic were identified as barriers to walking Presence of animals Encouraged walking: The presence of birds and squirrels in the area Discouraged walking: Fear of loose dogs Public walking tracks and trails The presence of public tracks and trails encouraged walking for 38% of the participants. Seeing others walking, biking or jogging, attractive scenery and a sense of safety encouraged walking along the tracks and trails Few participants identified tracks or trails as deterrents to walking, but those who did stated that isolated trails poor visibility in wooded areas and trails that were dangerous because of crime inhibited walking Weather A desire to walk in the fresh air promoted walking, and cold or rainy weather and fear of falling on ice inhibited walking Sex/gender differences Only 2 of the 21 participants were male. They reported neighbourhood environmental factors that were similar to those of the female respondents. However, the men did not discuss any factors related to safety from crime or pavements and traffic that discouraged neighbourhood walking. The presence of animals or public walking tracks and trails did not influence their neighbourhood walking either positively or negatively. They were regular walkers and lived in the downtown area, whereas most of the female participants lived in neighbourhoods with single-family homes or duplexes |
Strengths/limitations identified by author: Limitations: the sample was small and limited to older African Americans living in the city of Detroit; therefore the results may not be generalisable to other regions or those living in nonurban settings. The knowledge of neighbourhood characteristics gained in this study can be used, however, in planning walking interventions and developing policy in this region Selection bias may have been present because of recruitment from one senior centre in the city Although the senior centre draws participants from throughout the city, those who attend may differ from other city residents in socioeconomic or educational status, level of disability, or characteristics that may be relevant to neighbourhood influences on walking. In addition, those at the centre who chose to participate may have differed from those who did not. However, during recruitment it was emphasised that the researchers were interested in recruiting those who did and did not walk regularly. The sample was fairly evenly divided between walkers and non-walkers, although most of the participants enrolled were women and had some college education The use of photo-voice, although intended to capture the perspective of the participants rather than that of the researcher, may be limited by what participants choose to photograph, or not to photograph, and why. This was probably minimised by the use of focus groups to discuss the photographs taken by the participants in this study. Typically, 30–50 photographs were discussed in a focus-group session, thereby creating a diverse discussion of the characteristics that promoted or inhibited neighbourhood walking. Finally, a seasonal effect may have resulted from data collection during the summer months only Strengths/limitations identified by the reviewer: provides views about the impact of environment and what factors might encourage/inhibit walking Mainly superficial qual. and content analysis Evidence gaps/recommendations for future research: future research on older adult neighbourhood walking should incorporate environmental factors into existing theoretical frameworks and examine the interaction between environmental and psychosocial factors, as well as the factors related to reasons for walking (recreation or transportation). Further instrument development is needed for quantitative assessment of neighbourhood influences on walking. Finally, examining the influence of functional capacity and mobility limitations on neighbourhood walking will help inform future interventions for older adults UK applicability: some common environmental barriers to walking, although in the USA there may be less pavements and more severe weather |
| Garmendia et al. (2013)184 Country: Chile Study design: qualitative evaluation interviews Length of follow-up: > 12 months Aim: to identify factors associated to adherence to a physical activity intervention in older adults from a post-transitional middle-income country Recruitment: convenience sample from CENEX RCT Funding: The Wellcome Trust Quality: lower risk |
Number of participants: 36 CENEX participants; four physical activity instructors Age: 65–67 years (CENEX) Retirement: NR Sex: NR Education: NR Ethnicity: NR Other inclusion/exclusion criteria: Inclusion: adherent vs. non-adherent Exclusions:
|
Intervention aims and content if applicable: Progressive resistance exercise protocol with one-hour classes twice a week (total classes offered = 228) over 2 years, supervised by a physical activity instructor (CENEX RCT) With or without nutritional package Control condition if applicable: no intervention Data collection methods: Semistructured interviews Response and/or attrition rate: Data analysis: content analysis Constant comparison Theoretical framework: not specified |
Main results relevant to research question (author analysis): Barriers to adherence with physical activity Health problems, caring for family members, and working. Chronic illnesses, mental health problems, osteoarthritis, and pain. Depression, mainly among women. Poorly paved streets on route to the physical activity centre created a fall risk for those with O-A, and distance to the centre was a factor. Many non-adherent women cared for family members. The instructors perceived these domestic commitments as barriers to adherence. For men the most common barrier to adherence was employment Facilitators to adherence with physical activity Two main facilitating factors for adherence to physical activity: health benefits attributed to the intervention and the social interaction the participants enjoyed with the instructor and other class members. Older adults who adhered to the intervention highlighted these aspects. In terms of physical health, participants perceived improved mobility, agility, autonomy, and independence. Benefits of socialising; classes offered opportunity to meet and interact with others and feel part of a peer group. Sense of feeling productive and entertained by the activity was a main motivation to attend. Warm feelings towards instructors, interaction and exchanges with other participants were fundamental to success. Barriers and were also identified by instructors providing some external validity to these qualitative findings |
Strengths/limitations identified by author: our research provides high-quality evidence-based information on the barriers and facilitators that older people from a post-transitional country face in adhering to interventions promoting physical activity. In order to enhance effectiveness of community exercise interventions, evidence-based strategies to improve participation should be targeted to older adults from deprived areas and those with psychological and medical conditions Strengths/limitations identified by the reviewer: cannot tease out the characteristics of those interviewed as only those of total RCT sample given Evidence gaps/recommendations for future research: none specified UK applicability: chile is quite different from UK in terms of health care and culture. However, there is no reason to believe that some of the factors described here are not transferable |
| Genoe and Singleton (2006)178 Country: Canada Study design: qualitative Length of follow-up: NA Aim: to gain an understanding of older men’s leisure experiences across their lifespan Recruitment: by letter through senior centres and groups Funding: NR Quality: lower risk |
Number of participants: eight Age: 72–86 years Retirement: all retired Sex: all male Education: varied Ethnicity: all Caucasian Other inclusion/exclusion criteria: Service setting: senior centres/groups in Eastern Canada |
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: interviews 45–90 minutes Outcome measures: NA Response and/or attrition rate: Data analysis: thematic analysis Theoretical perspective: hegemonic masculinity |
Main results relevant to research question (author analysis): Play Grown up during the Depression when money was scarce. Sports and social activities organised in small communities. Games such as tag and hide were played as children. Those in rural areas had few friends to play with or time to play as they helped with chores at home after school. Those from cities had more opportunities for play Work Could start work between 13 and 15 years of age to support families, giving little time for leisure and too tired in the evenings. Those who had time were very active in sports, loving the competition and exercise. Social activities such as dancing were important The war years Lives changed during WW2; leisure was limited because of the war effort (some served in the armed forces) and work. Some married at this time. There were no recreation clubs so participating in sport was no longer an option Noses to the grindstone After the war, work was main source of accomplishment and pride. Little time for leisure, apart from social gatherings Retirement and beyond Change again as work stopped and time had to be filled in other ways. Belief in keeping mind and body active so activities were taken up. A mixture of physical activity (dancing) and non- physical activity |
Strengths/limitations identified by author: places the current practices of older men in the context of lifespan. It also adds to theories of masculinity as it draws out the expectations of men during their lifetime Strengths/limitations identified by the reviewer: as above. Only small number of data for physical activity but interesting historical perspective Evidence gaps/recommendations for future research: how the definition of masculinity changes with increasing age Standpoint theory to understand men’s emotions individually as well as in a group Continuity theory and SOC as frameworks for future research UK applicability: concepts of masculinity identity change with age could be transferable to similar settings in the UK |
| Gibson et al. (2002)147 Country: USA Study design: qualitative Length of follow-up: NA Aim: to investigate the meanings of retirement and leisure for older women living in Florida Recruitment: participants in a previous survey were invited for interview Funding: NR Quality: lower risk |
Number of participants: 24 Age: 56–83 years (mean 70.3 years) Retirement: all but three retired or semiretired Sex: all female Education: NR but all categorised as upper working class to middle class Ethnicity: all white Other inclusion/exclusion criteria: none reported Setting: community; participants in a mail survey |
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: face-to-face interviews Outcome measures: NA Response and/or attrition rate: 56 initially contacted 20 no longer at address 12 no longer interested or incapacitated as a result of ill health Data analysis: Constant comparison202 Theoretical framework: feminist perspective, poststructural203 – ‘socio–cultural nexus of leisure relations’ |
Main results relevant to research question (author analysis): Retirement as freedom Ability to choose to participate in meaningful activities or relax when desired. Leaving behind the constraints of work. Enjoyment of retired status for the freedom it gave Retirement as the end of paid employment Varied leisure pursuits ranging from passive (reading, visiting friends and family) to active (tennis, swimming and dancing). Leisure defined as freedom Resistance to retirement Some would never retire as indication of getting old and less independent, or disengaging from society. Some felt they couldn’t retire because of family responsibilities. This maintained their sense of utility and shows women as active agents in constructing their lives Need to be useful in retirement Another meaning was to be useful and give back to society, for example volunteering. These women had strong opinions about public service. They all defined leisure in terms of being active Retirement as husband’s retirement Retirement could be defined as husband’s and either positive (exercising together) or negative (husband interrupted participant’s leisure time) |
Strengths/limitations identified by author: attempted to address the concerns of what women do in retirement. Sample homogenous in terms of SES and ethnicity. Also Florida has good weather and good leisure opportunities Strengths/limitations identified by the reviewer: opens up the retirement issue from just physical activity – the sense that physical activity is only part of what women want to do when they retire. However, this paper does not focus on physical activity or what stops women participating Evidence gaps/recommendations for future research: similar studies with more diverse samples UK applicability: US study but concepts such as leisure ethic and leisure centred-ness may be useful in assessing women’s retirement in the UK |
| Gibson et al. (2003)148 Country: USA Study design: qualitative Length of follow-up: NA Aim: to investigate how older women living in Florida define retirement and leisure Recruitment: participants in a previous survey were invited for interview. Funding: NR Quality: lower risk |
Number of participants: 24 Age: 56–83 years (mean 70.3 years) Retirement: All but three retired or semiretired. 20 women felt they had been ‘forced’ to retire. Of the four women who did not consider themselves retired, two worked full time, one worked part time, and one considered herself a full-time homemaker The remainder were volunteers or had left the paid work world completely behind. Two women provided part-time care for their grandchildren Sex: all female Education: NR but all categorised as upper working class to middle class Ethnicity: all white Other inclusion/exclusion criteria: none reported Setting: community; participants in a mail survey |
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: face-to-face interviews Outcome measures: NA Response and/or attrition rate: 56 initially contacted 20 no longer at address 12 no longer interested or incapacitated as a result of ill health Data analysis: constant comparison202 Theoretical framework: feminist perspective |
Main results relevant to research question (author analysis): Shared leisure A major aspect to leisure was sharing experiences with their husbands. Leisure described as relaxing yet being involved. Meeting up with other people important. physical activity embedded as only one part of leisure, for example an important aspect was meeting up and having conversation with other women Leisure defined as an individual experience For some leisure described as ‘my time’. Being able to choose activities and ‘do as I please’ was important. Retirement brought opportunity to start new activities that perhaps women had wanted to try for a long time. Retirement also was a time to catch up on time for the self not available when bringing up children or working. Distinction made between work and leisure time The influence of life stage onleisure Changes across the life course such as child and spousal care had influence; in the past, leisure had to be planned whereas during retirement time for unplanned activities. Although more abundant in retirement, leisure viewed as precious, as health could deteriorate and limit the options available The influence of constraints on current leisure Finances, care-giving, and companionship Illness of and care-giving for husbands or other family members Own health (e.g. switching to walking in the pool as this is easier on legs) Care-giving for grandchildren, although for others caring for grandchildren was a part of leisure Lack of a leisure companion – stopping participating in or decreasing participation in activities that used to be important, because husbands not interested in the activity. Some women determined to continue their preferred activity and sought other companions who shared the interest The influence of enablers on current leisure Abundant health, finances, time and companionship |
Strengths/limitations identified by author: NR Strengths/limitations identified by the reviewer: presents a broader picture – leisure in general rather than physical activity alone. It focuses on retirement so ‘leisure’ could be extended to physical activity (physical activity as a subset of leisure) Evidence gaps/recommendations for future research: engage in theoretical elaboration and contextualize studies in a life-course analysis as well as feminist perspectives and the social–cultural nexus of leisure relations UK applicability: US study but concepts such as leisure ethic and leisure centred-ness may be useful in assessing women’s retirement in the UK |
| Gonzales and Keller (2004)166 Country: USA Study design: qualitative Length of follow-up: NA Aim: to identify facilitators and barriers to physical activity in lifestyle in a sample of Mexican American women Recruitment: from local community centre Funding: NIH/Office of Women’s Health R55NRO4888–01A2 and the South Texas Veteran’s Administration General Clinical Research Center Quality: lower risk |
Number of participants: 10 Age: 46–65 years (mean 54 years) Retirement: NR Sex: all female Education: high school education+ Low-to-middle SES Ethnicity: all Mexican American Other inclusion/exclusion criteria: post-menopausal women Service setting: community |
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: focus groups (3) Interviews Outcome measures: NA Response and/or attrition rate: NR Data analysis: coding Theoretical framework: cultural sensitivity |
Main results relevant to research question (author analysis): Perceived barriers to physical activity Personal or environmental: Lack of time owing to caregiving responsibilities. Family as motivating as they want women to remain healthy. Friends also motivating as people to exercise with, or they could dissuade women from exercising, instead persuading them to go out and eat. Script known as simpatía, which calls for positive interpersonal relationships usually accompanied by the provision of botanas or snacks Pereza. Described as a barrier were feelings of pereza (laziness, fatigue). These, along with and body aches and pains, were listed as reasons for not exercising Perceived enablers Doctor ‘told me to’ Desire to abide by this or to do it because their doctor said to Body image A desire to change body image Desire to feel better and to look better for themselves and their spouses. Embedded more in the family context rather for individual need Sense of well-being Feeling that exercise and increased physical activity levels made them feel better and increased self-esteem |
Strengths/limitations identified by author: NR Strengths/limitations identified by the reviewer: some details of methods missing Evidence gaps/recommendations for future research: to determine if in fact older Mexican American women do perceive a conflict when faced with decisions about behaviour, specifically physical activity and sedentary behaviour. Are older Mexican American women cognitively aware of the choice they make when faced with the desire to lead a healthier lifestyle through becoming more physically active yet are unable to owing to the desire to be a good mother and caregiver and/or the desire to maintain an interpersonal relationship, although that relationship is detrimental to initiating and maintaining a physically active lifestyle? UK applicability: Mexican culture not particularly relevant to UK. However, some of the aspects to do with age and sex are transferable |
| Grant (2001)176 Country: New Zealand Study design: qualitative Length of follow-up: NR Aim: to examine the beliefs of a group of men and women over 70 years about the role and meaning of physical activity, including playing sport, in later life Recruitment: access to participants via the Games organising committee Funding: NR Quality: lower risk |
Number of participants: 15 Age: > 70 years (range 71–79 years) Retirement: NR Sex:
Ethnicity: NR Other inclusion/exclusion criteria: recently participated in the South Pacific Masters Games (mixture of athletics, swimming, etc.) Service setting: community |
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: Repeated in depth interviews (at least twice with each participant) Outcome measures: NA Response and/or attrition rate: none reported Data analysis: interpretive – inductive analysis and constant comparison Theoretical framework: none specified but appears to take a lifespan perspective |
Main results relevant to research question (author analysis): Mixed messages about ageing and physical activity Engaging in regular physical activity – doing something meaningful that provided a sense of satisfaction. None engaged in regular physical activity throughout adult life. Work commitments, family responsibilities health-related problems and social factors influenced interest in and opportunity for involvement. Acknowledgement that increasing numbers of people 65+ years are becoming more physically active, although most older people avoided being more physically active than is necessary. Mystified as to why ‘being older’ should be considered an excuse or motivation to be inactive None considered themselves old, although most felt they were still classified this way. Changes had occurred with age in physical competence and body function, causing frustration. Regular physical activity deemed an important way to help negate the impact of ailments. Struggle not always easy to deal with Positive statements about benefits experienced, and how this was essential for maintaining good health and well-being. More inclusive and softer approach possible in the messages intended to attract older people to join in, such as offering special rates and ensuring that the images better reflected the older age group Getting into sport All played sport when younger but most stopped soon after leaving school. Began to play sport again in 50s–60s; not easy to take up after spending several decades of being a spectator and or helper. Embarrassment during initial experiences. Although team sports important during youth, there was now involvement in individual activities. Reasons included: need to have control over personal time; freedom to practice and play as much or as little as possible; the level of competitiveness can be determined by the individual; and no need to rely on others for either training or having a game. Playing sport not just a physical experience, a chance to socialise, meet new people and do something that provided a great deal of personal satisfaction Serious play An appropriate level of competition and fairness was deemed important. All made adjustments to the way they performed. This involved changing physical functioning but not the attitude or desire to perform. Most spent a considerable amount of time away from home, making it necessary to negotiate with family members regarding their responsibilities |
Strengths/limitations identified by author: Strengths: by focusing on the beliefs of older people, this study illustrates how the role and meaning of physical activity in later life is expansive, dynamic and completely imbued with multiple interpretations. Rather than be concerned with the correctness of their factual references, the narrative data gave significance to events drawn from the experiences and the relationships attributed to a physically active life By giving credence to the voice of older people, different truths from those to which we are accustomed about ageing and physical activity, emerge. The stories these older people told about their experiences, and the beliefs they held about ageing and physical activity, help illustrate the resilience of the ageing body. They also illustrate how ageing is constantly being negotiated at an individual and societal level, and how successful ageing occurs in different ways Strengths/limitations identified by the reviewer: slightly older population than core for review. However, most had not played their sport competitively until > 60 years and the data include reflections about engagement with sport through life Evidence gaps/recommendations for future research: NR UK applicability: focus on a specific sports event that is centred on the Pacific Coast. Not typical of UK events but no reason to believe that this population in the UK could not engage in similar activities given the appropriate encouragement and incentives. Some of the issues raised are relevant to older people who do engage in sport (golf, swimming, running, bowls, etc.) |
| Hall et al. (2007)175 Country: Australia Study design: qualitative Length of follow-up: NA Aim: to find out more about older men’s experiences and preferences in creating and maintaining social connections. To identify barriers and enablers to participation in social activities Recruitment: advertising flyers at local shopping centres, newspaper adverts, through existing networks and groups Funding: Centre for Adaptation in Health and Illness, Australia Quality: lower risk |
Number of participants: 29 Each focus group n = 5–14 Age: > 65 years criteria, although one attendee was found to be 58 years Range 58–88 years (mean 73.6 years) At one group all attendees were > 75 years of age Retirement: NR Sex: all male Education: Ranged from low in one group to higher in another (no details given) Ethnicity: NR Other inclusion/exclusion criteria: NR Setting: communities within the Central Sydney Health service area |
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: focus groups (five in total) Outcome measures: NA Response and/or attrition rate: NR Data analysis: NR Theoretical framework: NR Focus on ageing and sex/gender |
Main results relevant to research question (author analysis): The importance of physical activity Being active a defence against loneliness as stimulating and brings contact with others. A barrier to participation was men not knowing about interesting activities. Word of mouth was the preferred way of accessing information. Another barrier was physical health problems, although it was suggested that adjustments can be made There were comments about sex/gender differences, with older women making connections with each other more easily than men Physical activity was not only social but gave the feeling of a health benefit |
Strengths/limitations identified by author: no representation by gay/bisexual men Strengths/limitations identified by the reviewer: much of the findings relate to social activities rather than physical activity. Only the sections that relate to physical activity have been extracted No details of ethnicity of the sample. No details about data analysis methods Evidence gaps/recommendations for future research: the authors conclude that tapping into what makes activities meaningful and purposeful for men would be useful UK applicability: based in Australia so services could differ from UK. Sex/gender differences in participation motivation might be transferable |
| Hardcastle and Taylor (2001)136 Country: UK Study design: qualitative Length of follow-up: through the duration of the programme (10 weeks) Aim: to explore older women’s accounts of past and present experiences of participating in an exercise referral programme Recruitment: opportunistic from programme Funding: University of Brighton (doctoral study) Quality: lower risk |
Number of participants: 15 Age: 50–80 years Retirement: NR Sex: all female Education: NR Ethnicity: NR Other inclusion/exclusion criteria: newly referred to exercise referral programme Service setting: primary care/community |
Intervention aims and content if applicable: Exercise referral programme Interactions between health professionals and patient to promote physical activity in older women Control condition if applicable: NA Data collection methods: unstructured interviews Life story Outcome measures: NA Response and/or attrition rate: NR Data analysis: NU*DIST software version 4 (QSR International Pty Ltd, VIC, Australia) Interpretivist Theoretical framework: poststructural/postmodern |
Main results relevant to research question (author analysis): Informal networks and processes of referral GPs provide opportunity to promote physical activity, although self-initiation also evident. Informal network of friends, family, etc. Recommendations could be following a positive effect on health such as lowering BP. Self-initiators also sought information and advice from GPs Perceptions of control and accountability Understanding role of the GP in referral process could dictate how a programme is interpreted. Accountability can provide a motivator for physical activity, manifested in ‘showing up’. Accountability not only linked to attending and completing the programme but also to looking after one’s own health. Social support is important Sources of beliefs regarding exercise Health professionals an important source of beliefs. Sometimes a lack of commitment, confidence and encouragement from GPs in promoting physical activity Life stages and support networks Decline in exercise after getting married and motherhood. Culturally appropriate behaviour at different life stages. Time for self a low priority for some and caring in old age constrained physical activity. Leaving school was a transition that meant cycling, dancing, swimming might be given up Resocialisation – entering new phases (e.g. retirement often experienced as negative, could offer opportunity to belong and be useful through physical activity). Referral gave some a sense of social inclusion – meeting others, something to do. Perceived ‘gap; when children leave home. physical activity also offers a chance to exercise the mind and achieve Social support in the gym environment Exercise instructor role important for supervision and interpersonal skills are also a factor. Women valued individually tailored programme and the personal attention that accompanied it. Instruction and guidance is particularly important at the beginning of the programme Ageism and social norms Perceived stigma to appearing to want to break away from the norms of the age group. Socially constructed image of exercise for older people in which it is a threat and harmful. Feelings of vulnerability based on an inability to match all the characteristics of an ‘exerciser’. Fear associated with medical conditions such as angina, and wanting someone to be around in case something happened |
Strengths/limitations identified by author: captured the voices of participants Strengths/limitations identified by the reviewer: relates to feminist and ageing theories Insufficient detail of sample characteristics Evidence gaps/recommendations for future research: NR UK applicability: study based in UK |
| Hardcastle and Taylor (2005)137 Country: UK Study design: qualitative Length of follow-up: varied; longest follow-up 62 weeks from baseline (1 participant) Aim: to understand how a physical activity intervention for inactive older individuals influences physical self-cognitions over time Recruitment: through GP referral programme Funding: postgraduate studentship Quality: lower risk |
Number of participants: 15 (paper focuses on eight of these) Age: 43–77 years Retirement: NR Sex: all female Education: NR Ethnicity: NR Other inclusion/exclusion criteria: newly referred women Service setting: primary care |
Intervention aims and content if applicable: 10-week exercise programme (two sessions per week); referral from GP Control condition if applicable: NA Data collection methods: repeated semistructured interviews (at least 2 and up to 4 with each participant) at baseline, 5 weeks and 10 weeks Data analysis: NUD*IST software Cross-case analysis Theoretical framework: Identity Self-concept |
Main results relevant to research question (author analysis): The meaning of an exercise identity Prioritising exercise and promoting exercise to others (as an ‘exercise evangelist’) could represent the adoption of an exercise identity because of the expression of related beliefs and values Habitual scheduling involved planning and prioritising exercise Influences on developing an exercise identity Feelings of achievement Physical activity offered feelings of achievement and success. Commitment towards exercise gave structure and meaning to life, which was associated with feelings of autonomy and personal control. Motivated by extrinsic reasons at the beginning of programmes, such as doing it for someone else or for enhancing body image by weight loss. Despite not losing weight, continuing exercise involvement as view themselves as exercisers Autonomy and feelings of control Influence on developing exercise cognitions and building an exercise identity includes feelings of autonomy and a sense of control over one’s body and life more generally Social interaction and a sense of belonging Social benefits a motivation for continued involvement, enjoyment and commitment. Going to the gym and exercising a way of countering social isolation. Need for support and helping relationships. Exercise programme exerted influence in terms of enhancing physical self-perceptions, energy levels and motivation, which in turn had a wider impact on participants’ usual activities and lifestyle Several articulated a sense of guilt about taking time to exercise |
Strengths/limitations identified by author: the qualitative approach of the study, which has sought to embrace the expression of the participant’s voice, has provided new findings on how middle aged and older women build an exercise identity and resolve conflicting roles and identities. The use of such prospective and longitudinal research is important because such research may lead to a better understanding of the mechanisms involved in self-perception and psychological changes Strengths/limitations identified by the reviewer: highlights some specific issues faced by older women in terms of physical activity Evidence gaps/recommendations for future research: more research is needed to explore the extent to which people increase their lifestyle physical activity (following an exercise referral) and whether or not these changes are sustained over time. The relationship between exercise cognitions and identity derived from a facility-based exercise programme and lifestyle physical activity cognitions and identity requires further investigation UK applicability: UK setting so potentially applicable to other GP ERSs in the NHS. All female sample, so less applicable to men |
| Henderson (2000)159 Country: USA Study design: qualitative Length of follow-up: Aim: to examine what conditions enable and constrain walking to occur in older American African and Native American women Recruitment: through newspaper ads, church contacts, senior citizen centres and health providers. Recruitment strategy aimed for diversity in terms of age SES and family situations Monetary incentive (US$25) for participating in both parts of the study Funding: CAPS project Quality: lower risk |
Number of participants: 56 Age: 40+ years: African American
Native American
Retirement: most worked at least part time Sex: all women Education: relatively high Ethnicity:
|
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: interviews carried out by indigenous researchers who received 2-day training Outcome measures: NA Response and/or attrition rate: NA Data analysis: secondary analysis of original data using new research question Interpretative; constant comparative method Use of NUD*IST to manage data Theoretical framework: cultural sensitivity |
Main results relevant to research question (author analysis): The contexts of walking Work-related walking Work can involve walking and walking can be a normal part of everyday life Necessity walking No option but to walk (e.g. transportation). Having a dog or walking with children, to clear the mind and take the children out. Can be related to pleasure – walking in preference to accepting a lift Health walking Reason to try and walk regularly, sometimes on the advice of a doctor. Related to challenging oneself (AA woman) yet feeling good. Intrinsic factor such as enjoyment needed to motivate these women to walk Pleasure walking Different meanings; a combination of pleasure, health, necessity and work Walking enablers Adaptability and availability Walking can be done anywhere, requires no particular equipment other than sturdy shoes, can be done at own pace/fitness level. Low cost. Can have a purpose, for sight-seeing or shopping. Convenient and accessible way of being physically active Social/solitary dimensions Preference of being alone or with someone else; may walk further with a companion. Allows meeting others and relieves stress. Walking alone linked to convenience as did not have to be co-ordinated with anyone, particularly where one has a fast pace. Can pray while walking. Solitude for some while for others not having anyone to walk with was a constraint Identification with cultural traditions For AI, walking part of culture. Indian culture teaches walking during morning before prayers. May have had to walk everywhere as a child; this could be a de-motivator. Walking not too rigorous (treadmill is boring). Walking more adaptable and can be carried out at different levels Constraints to walking Excuses for not walking were not really constraints. For example, getting lazy and getting back into routines that have stopped, or feeling too tired. Not having time was a frequent comment. However, this is often an easy response Seasons and weather were also mentioned as constraining Safety AA women lived in more urban areas. Some women felt unsafe near the highway Not having walking partners could be a constraint for some Being physically or emotionally tired Some women described being too tired to walk after they got in from work. Slowing down over time and not walking as much |
Strengths/limitations identified by author: none reported Strengths/limitations identified by the reviewer: Makes some interesting relationships between concepts relating to physical activity Evidence gaps/recommendations for future research: None reported UK applicability: concepts of cultural sensitivity and the differences in women’s beliefs about walking can be transferred to UK ethnic groups |
| Henwood et al. (2011)167 Country: Australia Study design: qualitative Length of follow-up: NA Aim: to investigate the knowledge older adults have in relation to the spectrum of benefits available through resistance training and whether or not the individuals’ knowledge reflects current evidence To identify techniques utilised by individuals who have undertaken continued training Recruitment: face-to-face contact for those still involved; letters sent to G2 and G3 participants Funding: NR Quality: lower risk |
Number of participants: 18 Age: 65+ years Range 65–81 years Retirement: NR Sex:
Ethnicity: NR Other inclusion/exclusion criteria: In relation to resistance training:
|
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: focus groups Outcome measures: NA Response and/or attrition rate: NR Data analysis: inductive process Theoretical background: NR |
Main results relevant to research question (author analysis): G1 and G2 – greater knowledge of the broad range of benefits General health benefits Important benefits of weight training for health, mainly in relation to injury and injury rehabilitation rather than disease prevention Raised energy levels, disability prevention and improved sleep Functional health Awareness that resistance training could improve functional ability (become stronger, more flexible). Awareness of the rapidity of deterioration with age. Showing resistance to the potential for negative functional change Motivation to remain strong often for the family Improved balance G3 were less likely to mention the benefits of training than those already in training or with experience of training Ageing well and ageing better Range of motion, body composition, improvement in muscle mass Understanding that ageing effects could be reversed Comparison between self (resisting ageing) and others (allowing ageing effects to take hold) Mental health Understanding of the positive effects on mental health (‘mind and body’ rather than specific cognitive changes). Psychological benefit of increased self-confidence associated with improved function received rare acknowledgement across groups Body image Improved body shape (e.g. ‘spot reduction’), although not much discussion of body image Social interactions Interaction with individuals of a similar age more important than social well-being achieved (increased sense of security) Motivational factors Physical benefits Mental benefits Personal benefits Programme structure Donation of time to research Social support |
Strengths/limitations identified by author: to the best of our knowledge it is the first study to investigate from multiple perspectives how older adults perceive resistance training and remain motivated Data may not translate to all older individuals owing to the cohort from whom it was drawn. Those interviewed for this study were or had been involved in, or were interested in becoming involved in resistance training We did not collect level of education data, which is suggested to be a significant motivator to participants and to level of understanding in relation to benefits. These data did not provide for any follow-up interviews. It is hard to determine, therefore, whether or not a change in attitude could have been sampled from this population Strengths/limitations identified by the reviewer: as above Evidence gaps/recommendations for future research: NR UK applicability: no reason to believe that the concepts described here could not translate to similar circumstances in the UK |
| Heuser (2007)172 Country: Australia Study design: qualitative; ethnographic Length of follow-up: 3.5 months Aim: to identify the objective career of women lawn bowlers and the subjective interpretations the women assign to this sport Recruitment: NR Funding: NR Quality: lower risk |
Number of participants: 18 interviews Age: 64–88 years Retirement: NR Sex: all female Education: NR Ethnicity: NR Other inclusion/exclusion criteria: Active and retired bowls players (involvement in playing bowls 2–40 years) Service setting: bowls club located in a working-class neighbourhood of Perth, Australia |
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: In depth interviews Participant observation Outcome measures: NA Response and/or attrition rate: NR Data analysis: analytic-induction technique199 Theoretical framework: career model (e.g. see Stebbins204) |
Main results relevant to research question (author analysis): Being introduced to bowls First exposure in multiple ways usually involving other people and/or life circumstances. Besides husbands, other family members figured prominently in encouraging bowls. Retirement provided free time to engage in this pursuit. The death of a loved one represented a personal loss that could be partially compensated through bowls. Physical injuries and chronic medical conditions prompted some to opt for bowls. For most, bowls extended an existing history of participation in sport. Began their career in bowls through entanglements or relationships that engage an individual more deeply in a role activity Getting hooked on bowls Once introduced, hooked on bowls. The sport itself, the physical activity associated with it, and/or the social life that resulted provided initial attraction. The sport itself interested some, captivated by the challenge, the strategy, wanting to improve and/or the competition and winning. Competing against own ability, women in the club, and women from other clubs. Sport not the only hook, as bowls afforded an opportunity to be outdoors and active. Attracted to the openness, warmth, and sisterly feelings expressed by club members towards one another Playing bowls Deeper level of commitment as women chose to be involved in weekly club events, championships and/or pennants. Playing bowls could wax and wane depending on other situational contingencies Great value placed on the social connections created. An apparent distinction existed between social bowlers and serious bowlers. Social play or temporary retirement only viable option given their chronic medical problems or the need to care for ailing family members or grandchildren Retiring from bowls Retirement from bowls represented a slow and gradual process as adjusting to physical impediments. Search for alternative ways to maintain ties to the sport |
Strengths/limitations identified by author: female-only sample Strengths/limitations identified by the reviewer: Only partially relevant to our review question as the career perspective accounts for involvement in other aspects of the sport such as coaching and making tea. This highlights that often, physical activity is not carried out within a vacuum but is often accompanied by supporting, less physically active roles Evidence gaps/recommendations for future research: future investigative pursuits could more closely examine the nature of women’s and men’s relationships on the green and in the clubhouse, the similarities and differences in women’s and men’s career in bowls, the extent to which men value the social ties created through this sport, and the ways that men manage their physical retirement from bowls UK applicability: based in Australia, but as bowls is played in the UK there is no reason to suggest that the findings are not transferable to a UK setting |
| Horne et al. (2010)143 Country: UK Study design: ethnographic Length of follow-up: NA Aim: to explore the influence of primary HCPs in increasing exercise and physical activity among 60- to 70-year-old white and South Asian community dwellers Recruitment: NR Funding: University of Manchester School of Nursing, Midwifery and Social Work through their fellowship scheme Quality: lower risk |
Number of participants:
Mean:
Sex: Focus Groups:
Ethnicity: Focus groups:
Service setting: community |
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: interviews (40) and focus groups (15) Outcome measures: NA Response and/or attrition rate: NR Data analysis: framework approach Theoretical framework: NR |
Main results relevant to research question (author analysis): Advice and support Physician advice and support Physician advice and support a motivator for initiating exercise and physical activity (white and South Asian). Advice given in relation to weight reduction, cardiac conditions and mobility issues and not to improve or increase activity levels per se. Recommendation for exercise came as treatment, after illness again, rather than as a preventative measure Support from others Support from primary care often not in itself sufficient to motivate. Personal attributes and support from instructors and/or facilitators of exercise and others was a motivator to continue. Lack of instructor support to teach and lead through routines safely resulted in people terminating the activity Intensive and structured support needed to ensure they were doing exercise activities correctly. Not necessarily trained instructors, just someone to encourage and support Preventative health promotion No encouragement Young older adults – no positive encouragement in primary care to help maintain health and well-being. Practitioners may only be interested and concerned once health problems were identified Being ‘listened to’ and avoidance of ageist attitudes An important precursor to accept motivational advice was adequate medication control and a sense of being ‘listened to’. Advice from the GP might be acted on if it came as a recommendation to prevent deterioration of health. Primary care practitioners might reinforce the notion that exercise was not appropriate in older age Exercise on prescription Active, young older adults self-initiated a referral. Short-term nature of the prescription proved to be a barrier to continuing long-term. Thought required in planning for long-term motivation for adherence to exercise and physical activity once such schemes have come to an end Information needs How much exercise and physical activity? Lack of awareness of recommended activity levels Is it safe? Lack of clarity about how much exercise capable of doing with existing health conditions. This impeded progress of performing and or increasing exercise and physical activity. Forgetting to ask whether activity levels should or should not be increased |
Strengths/limitations identified by author: the study utilised a number of steps to ensure rigour in its design The cleaning of transcripts for accuracy, involving supervisors in the coding and analysis, and refining the interview guide to capture emerging themes facilitated the saturation of themes. Despite these strengths, it needs to be acknowledged that the data were collected as part of a PhD study exploring the attitudes and beliefs of 60- to 70-year-old white and South Asian adults to initiate and adhere to exercise and physical activity. Therefore, this restricted the opportunity for further sampling limiting the potential to explore in detail the relationship between primary HCPs and young older adults in this area as well as longer term follow-up Strengths/limitations identified by the reviewer: provides insights into the perceived roles of health professionals in encouraging physical activity from the point of view of a diverse group of service users Evidence gaps/recommendations for future research: NR UK applicability: UK-based study. Attempts made to include a diverse population so applicability to these particular UK populations is high |
| Horne et al. (2012)144 Country: UK Study design: qualitative Length of follow-up: NA Aim: to identify the attitudes and beliefs associated with the uptake and adherence of physical activity among community-dwelling South Asians aged 60–70 years Recruitment: NR Funding: The University of Manchester School of Nursing, Midwifery and Social Work fellowship scheme Quality: the reader is referred to associated publications for more detail |
Number of participants:
Mean 65.6 years Retirement: Sex: Focus groups:
Ethnicity:
Interviews:
Service setting: community |
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: focus groups Interviews Outcome measures: NA Response and/or attrition rate: NA Data analysis: framework approach Theoretical framework: NR |
Main results relevant to research question (author analysis): Factors promoting initiation Anticipated health benefits Potential for future well-being, anticipation of feeling better, and link with fitness. Prevention of weakness and/or improving strength in limbs to improve mobility. Direct links made between benefits of physical activity and maintaining independence Social support General social support and encouragement key factors in motivating to initiate physical activity. From family, friends and peers, statutory and voluntary workers. For South Asian women, confidence to initiate physical activity actively facilitated by a South Asian Ageing Well worker, also assisting those experiencing language barriers. For Muslim women, religious practices requiring sex/gender segregation could influence initiation of physical activity. Sex/gender segregation was possible in most areas, although facilities offered varied Factors promoting adherence Social support Although health was one factor, social support appeared the strongest motivator to maintain physical activity. Not letting the group down was important. Being part of a group was an enabler for getting through challenging elements of exercise in a light-hearted manner, preventing embarrassment and disappointment. Social benefits were important, providing a sense of belonging. Dislike of task-orientated nature of exercise programmes, although could be tempered by social interaction during activity, making the task more enjoyable Psychosocial aspects Sense of achievement and accomplishment in performing certain activities. For South Asian participants, some cultural norms seemed to be changing. Finding time to do something for the self, not related to issues around women’s perceived role in society. Most South Asian women grew up in India and Pakistan, where participating in exercise would not have been considered appropriate. A further benefit from achieving or mastering a specific activity, which then boosted confidence in ability. Enjoying physical activity was important. Making exercise fun and not necessarily a competitive event motivated to continue. Walking with others was more enjoyable than walking alone Health Determination to strive for longevity. Maintaining good physical and mental health influenced adherence. Health benefits took a subordinate position to social and psychosocial factors. Integrating physical activity within everyday activities was an important predictor of adherence |
Strengths/limitations identified by author: this study recruited older South Asians from an area where much health promotion work had been undertaken, which may have influenced their beliefs and health behaviour as a process of acculturalisation. Many had been in contact with a South Asian support worker and were therefore very aware of the benefits of activity and opportunities to be active in their area. There may be different views, barriers and motivators in older South Asians who have not had such previous contact It is also important to acknowledge that there is heterogeneity within South Asian populations. However, as there is a lack of evidence in this area, the authors felt that it was important to compare and contrast beliefs across groups, rather than focusing on a single, highly defined population. Thereby, the study addressed an area of public health that is largely unexplored Strengths/limitations identified by the reviewer: as above Evidence gaps/recommendations for future research: NR UK applicability: based in UK |
| Jancey et al. (2009)174 Country: Australia Study design: qualitative Length of follow-up: NA Aim: to identify issues and perceptions concerning physical activity in older adults Recruitment: through the Positive Ageing Association Funding: research grant from the Health Promotion Foundation of Western Australia Quality: brief details of recruitment strategy. No discussion of researcher position or ethical issues |
Number of participants: 16 Age: 65–74 years (no mean age given) Retirement: NR Sex: 11 females; five males Education:
Other inclusion/exclusion criteria: ‘insufficiently active’, defined as not achieving 30 minutes of moderate physical activity on at least five days per week, according to the National Physical Activity Guidelines Service setting: community |
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: semistructured interviews Outcome measures: NA Response and/or attrition rate: NR Data analysis: qualitative content analysis Categorised data were organised around two major headings: (a) beliefs and perceptions of physical activity; and (b) life-course ageing and physical activity Theoretical framework: NR |
Main results relevant to research question (author analysis): Beliefs about physical activity physical activity should be carried out throughout life. Benefits of physical activity acknowledged, e.g. physical (keeping muscles toned, cardio fitness, circulation, weight control) and well-being Positive beliefs were built upon reflections of physical activity during early years Barriers to physical activity Aches and pains reduced the enjoyment Lost flexibility, lack of balance and confidence, shortness of breath and poor body image Inclement weather Societal support for physical activity Mixed views; some felt supported and encouraged, others unsupported, that society had ‘written them off’. Reports of negative comments directed at participants attempting to exercise Life-course ageing and physical activity Positive recollections characterised by a gap in physical activity during working years, with re-emergence of physical activity later in life Past experiences with physical activity Mainly from years at school and the period that preceded commitments to partners and children. Broad range of activity types involved in including netball, tennis, squash, dancing, badminton, cricket, swimming, football and basketball. Desire to return to these activities; however, current situation and functional ability meant that perceived options were greatly reduced Better opportunity for incidental physical activity when younger, such as cycling to work or to recreational facilities. Less complicated lifestyle and simpler infrastructure supported these activities Ageing and physical activity physical activity has changed over time along with reasons for physical activity. Injuries and diminishing functional ability. Desire to be more physically active limited by discomfort attributable to pain and recognition of reduced capacity in psychomotor skills, such as balance Some acceptance of change, although limited function was frustrating Desire to pursue new activities Expressed desire to pursue new activities but each activity was accompanied by a limitation Some identified activities were ‘one off’, such as white water rafting and horse riding. Others, such as ice-skating and dancing, were activities older adults would like to have initiated and maintained |
Strengths/limitations identified by author: the findings of this study should be viewed in light of its limitations. The sample of adults aged 65–74 years was not large and their views may not represent the wider community. However, the perspectives expressed by this sample will certainly contribute to our knowledge of older adults’ understanding of physical activity Strengths/limitations identified by the reviewer: as above Some details not provided in reporting Evidence gaps/recommendations for future research: NR UK applicability: no reason to believe that the concepts described could not be transferred to a similar UK population |
| Juarbe et al. (2002)160 Country: USA Study design: qualitative Length of follow-up: NA Aim: to describe the social and culture-specific perceived benefits and barriers to physical activity among 143 Latina women, aged 40–79 years Recruitment: through contacts in local community-based organisations, in senior residential housing and activity programmes, and through announcements in local newspapers and senior newsletters Funding: grant from the Resource Centres for Minority Aging Research programme sponsored by the National Institute on Aging, the National Institute on Nursing Research, and the Office of Research on Minority Health, grant P30 AG15272 Quality: lower risk |
Number of participants: 143 Age: 40–79 years (median age 55 years) Retirement: NR Sex: all female Education: most were low income Ethnicity: all Latina Other inclusion/exclusion criteria: NR Service setting: community |
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: semistructured interviews Outcome measures: NA Response and/or attrition rate: Data analysis: content analysis Theoretical framework: NR |
Main results relevant to research question (author analysis): Perceived barriers Time constraints and women’s roles Continual and complex demands on time as a result of roles as women such as informal caregiving, occupational, spousal, and maternal roles. Informal caregiving responsibilities – caring for young or older children, grandchildren, or an ill or disabled partner, or caring for other family members Work both inside and outside the home. Multiple responsibilities resulted in fatigue, tiredness, and lack of motivation Commitment to community, civic, and religious organisations Personal health Variety of chronic disabling such as arthritis, circulatory problems, or back injuries Lack of understanding of the role of physical activity and medical conditions. Belief that they should not, or are not allowed to, engage in regular physical activity owing to their medical diagnosis. Turning points in which their disability became their barrier to staying physically active Internal factors Lack of determination and motivation flojera (sluggishness) haraganeria (idleness) pereza (laziness) desidia (neglect) Poor health, lack of energy, fatigue, lack of family and spousal support, and tiredness all factors that led to lack of motivation External factors Lack of transportation, cost, geographical distance to appropriate public or private fitness facilities, lack of community safety and weather Perceived benefits Mostly focused on how activity improves roles of Latina women in the context of the family. Majority (73%) physically inactive Health promotion Regular pattern of physical activity led to personal health promotion benefits. Sense of improved overall physical health. Management of disease and in illnesses prevention. Promoted mental health. Overall feelings of well-being and better quality of life, including improved patterns and quality of sleep Regular physical activity important for healthy ageing process, to look younger and strategies in managing arthritis, hypertension, and cholesterol. Pain was mentioned as a symptom that could be improved and managed with physical activity Mental alertness, stress reduction, enhanced mental motivation, mood improvement, and mental disposition to engage in daily living or role related responsibilities Improved roles Staying physically active helped maintain or improve roles as mothers, spouses, or family members. Able to pass this health behaviour and ‘legacy’ to children. Occupational roles performed with much more agility and stamina. Improved quality of work and enhanced physical potential Physical fitness Improved physical fitness Improved physical agility and weight management. Less mentioned benefits were physical agility, body strength, endurance, mobility, muscle toning, and stamina |
Strengths/limitations identified by author: the results of this study are limited by a sample that includes a wide range of ages, and not all findings can be discussed in the context of perceptions and differences between age groups. The tendency noted for older women to describe more personal health–related barriers could be explained in the context of ageing and declining health. Ageing women develop chronic illnesses and experience physical and psychosocial implications that may be perceived as barriers to physical activity. Many older women in this sample had chronic illnesses, and they were more likely to describe personal health barriers rather than time and role constraints or internal or external factors Generalisability from this study may be limited and interpreted in the context of socioeconomic, ethnic, and acculturation characteristics Strengths/limitations identified by the reviewer: Evidence gaps/recommendations for future research: NR UK applicability: Latina population not large in the UK so generalisability of experiences specifically related to Latina culture is limited |
| Khoury-Murphy and Murphy (1992)153 Country: USA Study design: qualitative Length of follow-up: NA Aim: to describe the implementation of a weight training programme for older women Recruitment: NR Funding: NR Quality: no details of how data were collected or analysed |
Number of participants: NR Age: > 60 years Retirement: NR Sex: all female Education: NR Ethnicity: NR Other inclusion/exclusion criteria: NR Service setting: private fitness clinic (Wellness Centre) |
Intervention aims and content if applicable: Weight training: stretching exercises, hand weight exercises and dumbbells. All 15–20 repetitions Control condition if applicable: NA Data collection methods: NR Outcome measures: NA Response and/or attrition rate: NR Data analysis: NR Theoretical framework: NR |
Main results relevant to research question (author analysis): Negative beliefs about weight training Weight lifting is physically dangerous Weight lifting will masculinise the female body Weight lifting is a lower class activity Weight training characterised as ‘unladylike’ Lifting weights makes you sweat excessively Factors that helped overcome cultural obstacles Facilitators serendipitous such as the classes being temporarily held in a non-threatening environment (e.g. someone’s home) Introduction to using weights by gradually incorporating very light weights into one segment of an aerobics class. Reassurances that no-one develops substantial musculature accidentally and many who try fail. Also that oil rather than sweat is seen on bodies on the television. Benefits of weight training repeatedly stressed backed up with research. Feeling physically better and believing that efforts might result in longer social independence. Fear of needing to go into a nursing home; lifting weights might postpone that prospect |
Strengths/limitations identified by author: NR Strengths/limitations identified by the reviewer: insufficient detail on methods of how the data were collected. The owner of the fitness centre carried out the study –perhaps the topic was a personal and professional concern rather than a broader research aim Evidence gaps/recommendations for future research: NR UK applicability: could apply to similar initiatives for older UK women |
| Kleiber (2009)146 Country: USA Study design: qualitative Length of follow-up: NA Aim: to consider adaptive processes in relation to the constraints that limit leisure in late life Recruitment: through a notice in the LIR monthly news letter Funding: NR Quality: lower risk |
Number of participants: 20 Age: 57–78 years (mean 64.5 years) Retirement: all retired; 6 months to 12 years (mean 3.9 years) Sex: 10 males; 10 females Education: all had at least a bachelor degree (11 were retired from a university setting) Ethnicity: all Caucasian Other inclusion/exclusion criteria: none reported Service setting: members of a LIR chapter in a mid-sized south-eastern US city |
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: in depth interviews Outcome measures: to tell ‘story of retirement’ Response and/or attrition rate: none reported Data analysis: Grounded Theory Theoretical framework: the SOC model advanced205 |
Main results relevant to research question (author analysis): Constraints
Behavioural responses to constraint
Frustration Gratitude – ‘Lucky to be alive’ |
Strengths/limitations identified by author: the sample were well educated and advantaged compared with the general population. However, they still faced a number of constraints Strengths/limitations identified by the reviewer: as above Evidence gaps/recommendations for future research: probe meanings of constraints themselves more deeply UK applicability: US-based study. However, some of the concepts discussed here could be transferable to UK settings |
| Kluge (2002)161 Country: USA Study design: Qualitative Length of follow-up: Aim: to examine women’s physical activity patterns, explanations of those patterns, and the ebb and flow of physical activity over the life course Recruitment: advert in newspaper; response to referrals from family and friends; ‘snowballing’ from existing participants Funding: NR Quality: lower risk |
Number of participants: 15 Age: > 65 years Range 68–87 years:
Retirement: NR, but probably all retired (age range) Sex: all female Education: diverse range (no other details) Ethnicity: Caucasian Other inclusion/exclusion criteria: all physically active all their lives Service setting: community |
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: semistructured interviews Outcome measures: NA Response and/or attrition rate: none reported Data analysis: transcendental-phenomenological reduction206 Theoretical framework: continuity theory; feminist theory |
Main results relevant to research question (author analysis): External influences on a physically active lifestyle Surroundings; financial resources, family, sex/gender, other’s judgements, role models Early experiences had a particular impact on lifetime physical activity. Skills acquired, support received and attitude formed serve as a foundation Assuming multiple roles during the life course Social prescriptions of roles of wife and mother at ages 19–23 years. Other’s interests prioritised. Physically active through families; however, missed ‘real physical activity’. Caring for ailing spouses and other family members and friends later in life. Being physically active deemed more important later in life, as central to livelihood and well-being, and part of independence Physical challenges to a physically active lifestyle A number of chronic conditions resulted in ‘holding on’ to some aspects of life and ‘letting go’ of others (roles, people, activities, occupations, objects). Likely not able to maintain current activities at the same rate or duration. Resilient, compensating for injuries or finding alternatives as physical activity was part of the essence of life Values and beliefs about a physically active lifestyle Strong orientation to activity is a value shared by the participants. Seen to improve productivity – being able to do things for self and others Being planful about being physically active Physically active self as integral to identity. Planning carried out to stay committed to physical activity. Early experiences often undirected and spontaneous. As adolescents more selective about activities and companions. As young adults go with social norms, compromising and adapting to role expectations. Organised to integrate physical activity into working and caring lives Post child care and paid employment gave more discretionary time. Planful included considering what activities, when to carry them out, with whom and for how long. Realisation of ageing and mortality – a sense of urgency. Planfulness about physical activity was health related and had a sense of purpose. Focus less on social identity and more on self-meanings and perceptions of needs Rewards of a physically active lifestyle Tangible (e.g. weight control; physical appearance; avoiding health problems; improved function which leads to strength and stamina) and intangible rewards (confidence in themselves and their bodies; sense of ‘joy’ and ‘fun’ in movement, a sense of wholeness) Composite textural description Deep sense of purpose fuels participation as well as realisation of its relationship with functional independence. Mental and psychological benefits, increased energy, a clear head and ability to cope. Continued significance of physical activity for rest of life Composite structural description physical activity lifestyles negotiated by accessing opportunities and overcoming constraints. Supported involvement in physical activity as children. Child-rearing years – squeeze physical activity into the day and organised family activities. Late adulthood –more freedom but good health necessary to maintain physical activity The essence of a physically active lifestyle Women > 65 years of age who have always been active -getting and keeping moving. Physical activity valued now as much or more than before as a result of realisation of relationship with QoL in later years. Being physically active improves physically ability, mentally alertness and emotional health. Foundation of lives as physically active rests on their early positive experiences and persistence through life course. Experience of joy of movement early on, developed physical abilities and desensitized to risk. Gender socialisation and ageist attitudes provide challenges to continuation. Concept of self as physically active and able. Integration of some form of physical activity into lives until lifestyle choice and part of nature, like breathing. Being physically active as an attitude. Intrinsic motivation, process goals and the ability to resist criticism and negotiate obstacles help maintenance |
Strengths/limitations identified by author: homogenous sample Strengths/limitations identified by the reviewer: as above Evidence gaps/recommendations for future research: different SES and ethnic populations of women How do histori-social events impact on women’s physical activity? How is physical activity influenced by innate ability? Balancing point for women between care and self-care physical activity for women who do not marry or have children Rural vs. urban environments Role of optimism Playfulness and efficacy Role of competition UK applicability: US-based study – no reason to suggest that the concepts described here cannot be transferred to UK women who have been physically active all their lives |
| Langley and Knight (1999)155 Country: USA Study design: qualitative Length of follow-up: NA Aim: to contextualise the meaning and evolution of competitive sport participation among the aged Recruitment: key informant Funding: NR Quality: no discussion of researcher position or ethical issues |
Number of participants: 1 (Art) and interviews with Art’s tennis partner to triangulate data Age: 68 years Retirement: retired university professor Sex: male Education: higher than average Ethnicity: white? Other inclusion/exclusion criteria: none reported Setting: community |
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: narrative Inquiry Timeline and interviews (x4) Participant observation while playing tennis with the participant Outcome measures: NA Response and/or attrition rate: NA Data analysis: thematic coding Theoretical perspective: continuity theory of ageing207,208 |
Main results relevant to research question (author analysis): Growing up in Findlay Art described himself as being competitive from the beginning, learning early on that he could do better than most at football and baseball. After school and at weekends Art was invited to play at the other (‘better’) side of town which made him feel good as they had material things but could not beat him Baseball and softball became central preoccupations for Art over three decades. His two closest and longest friendships began on the playing fields. Being a member of a successful team was a pre-occupation. Art attributed his participation to the encouragement of his mother, who wanted Art to build himself up following his early illness Sport involvement as a central preoccupation Art played in the Navy ship’s baseball team when on leave. He went to college and swam in the team there, playing semiprofessional baseball in the summer. Friends with company leaders who were sponsoring the games. He soon found himself player and manager with important softball team. Saw links between hard work, competence and being admired and respected. He valued being a manager which developed his organisational and leadership skills Taking stock Art graduated with a teaching degree and was briefly employed as a science teacher. A chance meeting at a game provided an opportunity to join a swimming team as coach Balancing academics and sport involvement Sport took precedence when carrying out a master’s degree. He ran a swimming programme for public schools and became coach for a swim association age-group team. He met his future wife in a teacher’s bowling league and began to play more bowling. He became a 9-year member of the most successful soft-ball team in the area. He accounted his success on ‘being around good people’ Moving up Art accepted an assistant principalship then became principal of a junior high school. He was successful, but a teacher’s strike in Florida created stress. He felt deflated that the school was deteriorating and resigned. By this time he had 2 children and took a chance on this move. His athleticism was waning as he entered his Successful employment Art’s dissertation was ground-breaking and he accepted a position at Coastal State University. He started to become involved in tennis and was competing in the finals Sport involvement after retirement Art attributed involvement with success – to continue with sport one had to be reasonably successful and work at it. Sport involvement requires continual adaptation to changes induced by the ageing process. Art accepts that he can no longer play at ‘the level I’d like to play’ and has instead chosen a game where he can continue to be successful. Art recognises the importance of taking care of his body now more than when he was younger His present involvement is based on:
|
Strengths/limitations identified by author: continuity theory and narrative inquiry have assisted in interpreting events for this participant Strengths/limitations identified by the reviewer: as above Evidence gaps/recommendations for future research: need to consider broader changing social and cultural influences UK applicability: US-based study but concepts of sport involvement through the lifespan are transferable to similar UK settings |
| Lavisso Mourey et al. (2001)162 Country: USA Study design: qualitative Length of follow-up: NA Aim: to identify culturally determined attitudes that could be useful in designing an effective exercise programme Recruitment: from a range of sites including a senior centre, nursing home, social group, day programme, and a church Funding: National Institutes of Health Grant R01-AG-16333–02 Quality: no discussion of researcher position. Ethical issues and data analysis partially addressed |
Number of participants: 38 Age: ≥ 65 years Retirement: NR Sex: NR Education: NR Ethnicity: all African American Other inclusion/exclusion criteria: Service setting: West Philadelphia urban community |
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: focus groups (x5) Outcome measures: NA Response and/or attrition rate: NR Data analysis: thematic analysis Theoretical background: NR |
Main results relevant to research question (author analysis): What do you consider as exercise? Less capable group Maintaining basic abilities Movement Household chores Activity producing fatigue Going upstairs More physically capable group Calisthenics, biking, using the treadmill, dancing, and running Activities of daily living not considered as exercise Exercise should: Push the limits Have a goal Be strenuous Rarely exercised, although reported having good intentions What makes exercise difficult for you? Internal factors Pain Having to use wheelchairs and walkers limited their ability to participate in most forms of exercise Concerns: Overexertion Falls All participants favoured group exercise Sweating was not considered embarrassing, but was viewed as an obvious consequence External factors Time was not significant for older participants Conflicts in scheduling of exercise sessions Environmental obstacles/safety – one participant had a son who was robbed and killed Drive by shootings, squatters Groups of younger people were often regarded as intimidating Children on bicycles Broken steps/paving How can exercise be helpful to you? Independence Those who were less physically capable and who no longer could perform light household tasks without fatigue sensed a loss of personal autonomy Balance – bending over often caused a loss of balance, and failing to lift feet high enough when walking caused tripping Many participants expressed interest in exercise if it would help to overcome problems with balance General well-being Connection between the effects of exercise and general well-being Enjoyment Weight Loss and Cardiovascular Strength. Easier to notice or appreciate increased leg strength than increased cardiac fitness What kinds of exercise would you like to do? Group exercise (increased motivation and social contact) Music and dancing (music makes activities easier; dancing is enjoyable) Tai chi and yoga: several persons said they might like to try tai chi Walking – popular but concerns for safety Weights – little enthusiasm. Many had preconceived notions of heavy gym weights Climbing steps was frequently among those more physically capable For less physically capable groups, improved stair climbing was not viewed as exercise so much as a goal |
Strengths/limitations identified by author: Discussions were useful in identifying differences among participants according to physical capabilities The total sample size was relatively limited. Although participants were recruited from a variety of settings within the community, the participants may not be representative of elderly urban residents generally. In addition, the results cannot be generalised to non-urban settings Strengths/limitations identified by the reviewer: as above Evidence gaps/recommendations for future research: evaluate whether or not the findings in this report are replicated. The validity of the results of this study can be assessed ultimately by the effectiveness of interventions designed to incorporate these findings Studies are needed in older African Americans to determine factors that affect the frequency of exercise participation as well as the likelihood of continuing exercise over a long period of time. This is particularly true for elderly persons who often experience setbacks, such as acute illness, hospitalisation, changes in social support, etc. UK applicability: no reason to believe that some of the concepts described here could not be transferred to similar populations in the UK, notwithstanding that there are differences in geography and perhaps environmental differences between this setting and those typical of the UK |
| Leichty and Yarnal (2010)157 Country: USA Study design: qualitative Length of follow-up: Aim: to explore the role of body image in older women’s leisure Recruitment: through third parties known to the researchers, fliers at the senior centre and snowball sampling Funding: Women’s Health Initiative of the National Institutes of Health Quality: lower risk |
Number of participants: 13 Age: 60–70 years Actual range 60–69 years Mean age 62.4 years Retirement:
Education:
Two women were born outside the USA (Middle East and Europe) Other inclusion/exclusion criteria: none reported Setting: Mid-Atlantic US city |
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: interviews Two follow-up focus groups (n = 4 at each) or follow-up telephone interview (n = 5) Outcome measures: NA Response and/or attrition rate: five participants were unable to attend FGs owing to work-related time constraints, care-giving responsibilities, or being ‘too shy’ Data analysis: constant comparison Open coding to provide framework for follow-up data Axial coding Theoretical framework: body image and ageing209,210 Body image as a leisure constraint Older women’s leisure |
Main results relevant to research question (author analysis): Physical activity-related leisure activities (n = 10): Walking, canoeing Gardening, hiking, tai chi Ice/roller skating Basketball, kayaking, biking, gardening Exercise Yoga, shopping Golf, bowling Swimming Dog walking Tap dancing Wide range of body image experiences, ranging from positive to declining owing to age-related physical changes. Body image could improve with age, despite moving further from the ‘ideal’. More accepting of the body and less concerned with appearance, more with health and physical ability Body image and reduced/modified leisure participation Body image resulting in self-consciousness while participating in some forms of physical activity a potential constraint for future participation, as was identifying the self as ‘larger’ Appearance-based Women’s concern over appearance ranged from no concern to always having had a poor perception. This could affect choice of leisure activities. Appearance of older skin could dissuade from wearing a swimsuit. Reduced participation in this context could be based on ‘people present in that setting’ Ability-based Reduced participation for some based on concerns about physical ability or the level of competitiveness associated with the activity that invoked fear and embarrassment or lack of confidence in abilities. Competition could also be enjoyable, although only where the level of ability was similar. Appearance less important with age and body image was associated more with health and ability. physical activity that posed a risk to health and function were reduced Body image and increased participation Belief that a positive or improving body image was attributable to increased participation in certain activities Ability-related Health was more likely to be a concern with age than when younger, when appearance was prioritised. Feeling good and easing aches and pains was another stated reason for participation. The relationship between physical activity and body image was described as circular, so that identifying as a ‘physically active person’ who is ‘in shape and active’ in turn facilitated participation through feeling comfortable with the body and confident about ability Appearance related Acceptance of body image with age which facilitated participation. Improving body image with age allowed new activities to be tried |
Strengths/limitations identified by author: provide a unique perspective of leisure constraints for older ‘everyday’ women Strengths/limitations identified by the reviewer: highlights the reasons behind shifts in physical activity participation with age in women Evidence gaps/recommendations for future research: to determine the extent of generational differences compared with age-related differences in body image. Also to assess cognitive adjustments and their relationship with constraints To address life factors that influence relationship between body image and leisure, for example social position Continuation of study of constraints in everyday life for men as well as women How these findings can be applied in younger populations to design interventions UK applicability: US study but no reason to believe that the concepts of adjustment with age cannot be applied to women of similar age and background in the UK |
| Liechty et al. (2012)145 Country: USA Study design: qualitative Length of follow-up: NA Aim: to explore innovation theory among retirement-age women Recruitment: through third parties known to the researchers (n = 6), fliers at the local senior centre (n = 1), snowball sampling (n = 6) Funding: NR Quality: lower risk |
Number of participants: 13 Age: 60–70 years (range 60–69 years; mean 62.4 years) Retirement:
Education:
Other inclusion/exclusion criteria: Inclusion – recently retired Setting: community; in or near mid-Atlantic city, USA |
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: Phase 1: individual interviews Phase 2: follow-up focus groups (or follow-up telephone interview if not available) Outcome measures: NA Response and/or attrition rate: NA Data analysis: constant comparison method; open coding from first phase provided framework for coding second phase Theoretical framework: innovation theory (see, for example, Nimrod211) |
Main results relevant to research question (author analysis): Nature of newly adopted leisure activities Several different areas including physical activity, creative arts, volunteer work, intellectual leisure and social activities. Newly adopted leisure activity allowed affirmation of self-identity and exploration of new and exciting opportunities. Areas of interest continued for some, but activities were added. Innovation meaningful as distinct from previous activities. Could relate to activities that were not as available to females during younger years. Fewer innovation activities owing to time obligations. Health conditions, work or family responsibilities could influence opportunities for innovation Triggers or facilitators of newly adopted leisure activities External (e.g. increased time or income, additional opportunities for women), or internal factors (e.g. attitudinal changes). Catalysts for innovation positively influenced by ageing (e.g. not previously available owing to time or financial constraints). Sense of freedom from societal or domestic pressures. This also allowed enjoyment in a more relaxed or impulsive way. Addition of an activity could be triggered by a purposive life change or intentional pursuit of self-identity, a modification in health status or consciousness about health Outcomes of adopting new leisure activities Almost exclusive positive outcomes related to participation in newly adopted leisure activities. Increased feelings of joy, self-confidence, empowerment and independence Feeling more independent and more self-confident, or increased social connection with both family and friends. Innovation seemed to foster more innovation by reinforcing the participant’s ability and desire to do so |
Strengths/limitations identified by author: although the findings do not provide generalisable data regarding the prevalence of innovation, for many in this sample, innovation was not only happenstance or experienced by a brave few, but a desire or goal that was actively sought out Participants in the current study were all Caucasian and most had relatively high income levels Similarly, the current sample was all women Strengths/limitations identified by the reviewer: Aims of the study not focused on physical activity. However, participants offered views relevant to our study Evidence gaps/recommendations for future research: This study corroborates the need for ‘a new research agenda’ which acknowledges older adults who see ageing as a positive experience filled with opportunity and which explores the value of leisure innovation Future research should explore the meaning, triggers and outcomes of innovation for diverse populations. Because research has suggested that starting new activities is more common among women than among men, further research should explore the sex/gender differences in experiences of and motivation towards leisure innovation. Furthermore, future research among a variety of populations would shed light on the sociological factors that influence innovation The findings suggest that existing theories of ageing should not be viewed in isolation. Each of the existing theories has strengths and provides insight into some aspects of the ageing process. To construct a more complete picture of leisure and ageing, however, researchers must consider all possible experiences. Future researchers should consider a more integrated approach to the study of leisure and ageing that takes into account the explanatory power of each theory UK applicability: based in USA. However, there is no reason to believe that innovation theory would not be transferable to retirement age women in the UK |
| Liechty and Genoe (2013)150 Country: Canada Study design: qualitative Length of follow-up: NA Aim: to understand Canadian men’s perceptions and experiences of leisure and ageing Recruitment: fliers posted in recreation and senior centres, third parties known to the participant and the researcher, and through snowball sampling Funding: NR Quality: lower risk |
Number of participants: 15 Age: 60–70 years (mean age 65 years) Retirement: range of retirement stages from working (n = 6), through part-time transition (n = 3), to retired (n = 6) Sex: all male Education: from grade 10 to doctoral degrees Ethnicity: all Caucasian Other inclusion/exclusion criteria: none reported Service setting: community, Southern Saskatchewan |
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: interviews and follow-up focus groups (3) Outcome measures: NA Response and/or attrition rate: NR Data analysis: constant comparison method Theoretical framework: ageing theories |
Main results relevant to research question (author analysis): The work/leisure interplay: ‘to me, leisure is anything outside of your work’ Definition and experience of leisure heavily connected to attitudes towards work. Leisure was anything that was not work Importance of choice in defining work and leisure. Perceptions of leisure during retirement increased feelings of flexibility and freedom. Same activities done while working were leisure when done outside paid work. Connection between leisure and work for retirement. A period of adjustment, but also an opportunity. Returning to activities done in their youth. Heavily involved in leisure activities was common and desirable. Retirement as a new life stage rather than as a time to rest Giving something back: I think we’ve got something to pass on’ Leisure as an opportunity to use skills and knowledge gained during working years in order to benefit family members or the community at large. Unique skills and experience allowed them to ‘give back’ as a result of age and work prior to retirement Making leisure choices for the benefit of family members or to maintain familial relationships Leisure’s purpose: ‘For me, leisure has to be mind expanding or body expanding’ Leisure activities as intended outcome related to improving personal lives. Intentionally choosing leisure activities that would improve physical health or maintain mental functioning. With age, more aware of the purpose or intentionality of their leisure choices Purpose as providing multiple benefits including status in the community and life balance. Purpose often provided balance in terms of compensation for aspects of work. Activities chosen for the challenge they presented; particularly for men who were retired or did not find their work challenging. Purpose of leisure defined by the individual and that the purpose might simply be to relax and enjoy oneself. Certain activities had value judgments associated, that they sometimes chose activities (such as physical activities) out of ‘guilt’ and that the activities they ‘should’ be doing were not always the ones they felt met their needs Constraints as a reflection of priorities: ‘If I want to do something, I’ll do it’ Structural constraints such as time, cost, and weather. Physical limitations forced some to modify participation in physically demanding activities. Rejection of finite barriers, described as ‘excuses’ for not participating in activities that they felt pressure to do (generally physical or social activities), but were not motivated to do Age not viewed as a barrier to trying new activities. Confidence in learning to use new technology such as online communication and education. Many instances of constraint negotiation through modifying the activity or changing perspectives to the desired activities. Strategies to negotiate financial barriers such as travelling at certain times of the year. Overall few constraints which could not be negotiated in relation to desired activities. Perceived lack of constraints related to attitudes about leisure: if a constraint was related to a less-prioritised activity, it was of little concern |
Strengths/limitations identified by author: strengths – support several theories of ageing (continuity, selective optimisation, etc.) Strengths/limitations identified by the reviewer: as above Evidence gaps/recommendations for future research: this study highlighted the need for leisure researchers to continue contributing to the development of theories of ageing UK applicability: although based in Canada, many of the concepts raised here are transferable to similar UK settings |
| Moore et al. (2011)139 Country: UK Study design: qualitative Length of follow-up: 6–12 months Aim: to explore exercise professionals’ experiences of engaging diverse clinical populations in an ERS, and emergence of local practices to support uptake and adherence in the NERS Recruitment: through participation in the NERS trial Funding: NR Quality: lower risk |
Number of participants: 38 exercise professionals Age: NA Retirement: NA Sex: NA Education: NA Ethnicity: NA Other inclusion/exclusion criteria: NR Service setting: 12 local health board areas in Wales, UK |
Intervention aims and content if applicable: NERS trial Professionals’ roles included delivering the service to patients, including one-to-one consultations and exercise classes, and assisting with collection of data for monitoring and evaluation purposes Control condition if applicable: NA Data collection methods: telephone interviews Outcome measures: NA Response and/or attrition rate: Two professionals did not take up the invitation to participate Data analysis: thematic approach Theoretical framework: NR |
Main results relevant to research question (author analysis): Individual differences in needs and responses to NERS Distinction between participants who had been advised to take part by their HP and those who sought help from their HP. Self-determination regarded as stronger link with adherence. HP advice may be taken more seriously and motivate clients to attend Dropout – high levels associated with failure to identify motivated patients. May be better to focus on those where change was already being considered. Need to ensure patients understand the scheme Demographic patterning in responses to NERS Engaging mental health patients in the scheme often challenging. Younger patients assimilated less well into patient-only classes – less benefit from social aspect Perceived socioeconomic variations – patients in more deprived areas had appeared grateful for the service Engaging clients more difficult in deprived areas (attributed to perceived lower tendency for poorer patients to place value on maintaining health, or a lack of buy in among GPs in more deprived areas) NERS charged £1, although patients were often not aware of discounts Long-term maintenance of attendance after expiry of the discount proved challenging Facilitating uptake, adherence and long-term behavioural change NERS provoked anxiety; having confidence undermined by presence of fitter exercisers Fears about assimilating into unfamiliar social environment. Fears of being expected to do exercises they weren’t able to do Development of strategies to overcome anxieties was seen as central to facilitating scheme uptake and adherence Initial consultations were opportunity to reassure patients that professionals would be point of contact, etc. Supporting confidence and motivation through education and interpersonal support Patients lacking knowledge of how to exercise safely, given their medical conditions. Education crucial becoming independent exercisers. Need for education inseparable from need to provide interpersonal support Instructional aspects became secondary to interpersonal support roles, given the vulnerabilities of the client group. Mental health patients described as facing particular difficulties; however, some described particular successes engaging mental health patients. Additional barriers had been addressed through provision of additional interpersonal support or actively fostering interactions with other patients. Perceived need for further training in helping people with mental health problems. Discomfort with the notion of becoming ‘counsellors’ to patients (minority) Widespread tendencies for allowing some patients to continue attending classes after they had been officially exited Modifying the exercise environment to minimise anxieties throughout the programme Need to structure classes in a manner which made patients feel at ease (e.g. arranging sessions during quiet times to reduce the number of mainstream exercisers in the gym) Fully exclusive model (separate gyms for referred patients, or the main gym closed to the public during NERS sessions) regarded as highly beneficial in promoting programme adherence. However, this could result in patients feeling intimidated by mainstream environments after the programme had completed Fostering social networks supportive of long-term change Role of patients in supporting each other: Empathy between patients and realistic role models. This could be allowed to evolve or positively encouraged by the trainer Patients often continued to exercise with friends they had made after completing the scheme. However, loss of social aspect was a factor in non-maintenance following the scheme. Efforts to foster emergence of social networks which lasted beyond the programme were seen by some as crucial |
Strengths/limitations identified by author: although strengths of the present study include a high response rate, with views of professionals in all areas delivering the scheme during the trial represented, the position of both the researcher and participants need to be considered. As typical of evaluative research, the interaction between an evaluator, linked to a trial of a scheme whose future hinged on positive findings, and professionals whose livelihood depend on its continuation, may have produced an understanding which portrayed the scheme in an excessively positive light Strengths/limitations identified by the reviewer: the study is one of a small number that explores the views of people delivering physical activity sessions for older people Evidence gaps/recommendations for future research: the consistency of the trends perceived by professionals with findings from quantitative analysis of adherence and the extent to which psychosocial change processes were triggered by the programme, as well as perspectives of patients on the issues described UK applicability: based in the UK |
| Nadasen (2007)182 Country: South Africa Study design: qualitative Length of follow-up: 12 months Aim: to investigate the perceived benefits of line dancing for a group of women aged 60–80 years Recruitment: through contact with instructor and attendance at three classes Funding: NR Quality: lower risk |
Number of participants: 30 Age: > 60 years (range 60–82 years; mean 69.6 years) Retirement: two women were employed part time, the rest were retired Sex: all women interviewees Education: NR Ethnicity:
Line dancing for at least 2 years:
Service setting: three locations in Cape Town, South Africa |
Intervention aims and content if applicable: line dancing classes (2.5 hours in duration). Some offered in the mornings, others in the evenings Some male partners also danced at the classes Control condition if applicable: NA Data collection methods: Participant observation 25 individual interviews One focus group, n = 5 Outcome measures: Attraction to line dancing Other activities Impact of activities Response and/or attrition rate: Data analysis: Grounded Theory Theoretical framework: NR |
Main results relevant to research question (author analysis): Introduction to and reason for line dancing Some previously belonged to social or church clubs and wanted to do something different. Two involved in ballroom dancing. Some introduced through newspaper ads, others invited by friends. A large number saw a demonstration at the local shopping centre/community centre The attraction of line dancing Variety of reasons: The music was lively and modern No partners required (main reason) Freedom dancing without a partner (e.g. if husband cannot dance) Health status Some could not distinguish clearly between present health and that before taking up line dancing. However, one perceived that she was not slowing down as she expected to with age Perceived benefits Initially did not join for ‘exercise’ – fun and enjoyment attached was the main motivator. Some with chronic health problems acknowledged that line dancing helped them cope Physical benefits One advised by medical personnel at osteoporosis clinic to dance. Two felt dancing helped control their diabetes. Another had back problems and is encouraged to dance Dancing described as hectic, intense and a good workout and ‘better than going to the gym’ which is an individual activity. Line dancing involves interacting with others, talking, laughing and teasing. Perception that weight is kept in check by dancing. Important to remain attractive, wearing make-up and fashionable clothing. Line dancing as physically and mentally challenging and a way of keeping Alzheimer’s and bone problems at bay. Positive impact on co-ordination. Regarded as a safe way of keeping chronic conditions at bay Cognitive functioning Memory, concentration and forgetfulness improved compared with other women who didn’t exercise. Need to think quickly and concentrate. Sometimes it takes a while to relax on returning home following a class Psychological benefits Past traumatic experiences were coped with (e.g. loss of a partner/parent). Classes forced women to go out and concentrate on something else Self-perception Improved self-esteem and confidence. Women of 80 years reported feeling 20, like young people enjoying themselves Images and myths of ageing Wanted to challenge negative images and myths of ageing, such as being ‘over the hill’ or ‘sickly’ or ‘demented’ Family support and encouragement Families could be sceptical at first, one husband did not like his wife ‘leaving the house’. Following her stroke and depression, her husband noticed an improvement when she began dancing again and encouraged her to continue. When families were invited to dancing socials or competitions they were surprised at the women’s creativity and ability and some also joined the classes |
Strengths/limitations identified by author: none reported Strengths/limitations identified by the reviewer: the study’s strength is the focus on how line dancing affects women in terms of physical and psychological benefits Evidence gaps/recommendations for future research: NR UK applicability: although this study is based in South Africa, line dancing classes take place in the UK. Therefore, some of the impacts of line dancing for women of this age, such as the social aspects and health benefits are transferable |
| Nadasen (2008)183 Country: South Africa Study design: qualitative Length of follow-up: 12 months Aim: to investigate how line dancing affected women over the age of 60 years Recruitment: through contact with instructor and attendance at classes Funding: NR Quality: lower risk |
Number of participants: 30 Age: > 60 years (range 60–82 years; mean 69.6 years) Retirement: NR Sex: all women Education: NR Ethnicity:
Line dancing for at least 2 years:
Service setting: three locations in Cape Town, South Africa |
Intervention aims and content if applicable: line dancing classes Control condition if applicable: NA Data collection methods: Participant observation 25 individual interviews One focus group, n = 5 Outcome measures: Attraction to line dancing Other activities Impact of activities Response and/or attrition rate: NR Data analysis: Grounded Theory Theoretical framework: not specified |
Main results relevant to research question (author analysis): The attraction of line dancing Variety of reasons: saw a demonstration and it looked fun The music was lively and modern No partners required (main reason) Freedom dancing without a partner (e.g. if husband cannot dance) Liking country and western music Wanting a cowboy sweetheart Fun way to exercise Line dancing therefore addressed two needs – enjoyment and independence Socialisation This type of dancing differs from other exercise/dance classes where there were no social activities. Made friends with others from different ethnic backgrounds. This had not been acceptable in the past under apartheid rule. Invites to each other’s homes to play games or talk and to events such as birthdays. Attending movies, restaurants and theatre together. Comparisons made between the group and older women who are not active for whom there was pity because they are bored or lonely. Line dancing therefore allowed the women to break out of political, social and personal moulds Social consciousness Through the group the women have engaged in community organisational activities such as knitting for destitute mothers, street collections and other charity fundraising events. Two taught line dancing to women in a retirement centre. Participation in these activities has helped them develop a greater sense of social consciousness which radiate to others Other group activities Some formed smaller groups and had begun learning other dance forms such as ballroom, tap, belly-dancing and traditional African dancing. Others feel that line dancing is sufficient The impact of activities If the women only met weekly for the class the friendships may not have developed to the level of intimacy they had. Support particularly important for those having lost a partner. For the end of year concert the women test their abilities by designing and making costumes. Some participate in competitions. They feel safe as part of the group in doing things they would not have done when they were younger. One woman reported having felt like a slave to her husband and children and was now free. Activities were also reported to keep their minds active and that they learned a lot from each other. They did not feel themselves to be a burden on their families, although one women’s daughter had asked her to slow down. The women were acknowledging their personal, social and psychological needs |
Strengths/limitations identified by author: limitations – exploratory study- did not include experiences of African women despite 80% of South Africa being populated by African men and women The findings are not generalisable to all older women who line dance, although it could be a starting point for further research Line dancing is only one possible activity in a wide range Strengths/limitations identified by the reviewer: the study’s strength is the focus on how line dancing affects women in terms of their feeling of pride and usefulness as well as the aspects of line dancing classes that are appealing. This has implications for designing physical activity interventions for this age group Evidence gaps/recommendations for future research: comparison of various exercise activities to ascertain which ones might expand the social repertoire. This could include exploration of activities that older African women participate in as there is little research in this area UK applicability: although this study is based in South Africa, line dancing classes take place in the UK. Therefore some of the impacts of line dancing for women of this age, such as the social aspects and feeling useful are transferable. There could also be opportunities for women to meet women from different backgrounds, although this is not a particular issue for the UK |
| O’Brien Cousins (2001)181 Country: Canada Study design: qualitative Length of follow-up: NA Aim: to analyse older women’s motivating triggers for physical activity. Recruitment: from university course Funding: NR Quality: lower risk |
Number of participants: 41 (32 with physical activity data included in the article) Age: 57–92 years (mean 70.2 years) Retirement: NR Sex: all female Education: relatively high (taking university course) Ethnicity: mainly white Other inclusion/exclusion criteria: 20 women considered themselves as regularly physically active (30 minutes of exercise most days of the week); 8 women were inactive and 4 were ‘semiactive’ – sporadic, unplanned activity Service setting: spring session for Seniors academic course (university) |
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: semistructured interviews Outcome measures: NA Response and/or attrition rate: none reported Data analysis: NR Theoretical framework: social cognitive theory (trigger construct) |
Main results relevant to research question (author analysis) (only data on younger sample extracted): Younger active women The youngest active woman was 55 and had not experienced any health problems. Other women had moved away from physical activity while they had children. They were triggered into activity or reinforced to maintain physical activity by: Recognising age and declining fitness level Suboptimal bone strength identified in tests Widowhood – little to do Habitual activity was the essence of their life Health care was becoming less reliable and self-care more important Community offering fitness classes specifically designed for seniors Discovering that aches, pains and joint problems were relieved with regular physical activity Semiactive women Health problems triggered thinking about being more active, although this did not necessarily result in changing behaviour. One woman’s trigger was the diagnosis of type 2 diabetes, but after 20 years her interest in physical activity for health has waned Inactive women Preparing to become more active by getting a dog. Some regarded their daily activities such as housework or painting as enough Conclusions Triggers could be from positive or negative experiences. Prompts to become more active:
|
Strengths/limitations identified by author: fairly homogenous sample – well educated, middle class, white Strengths/limitations identified by the reviewer: identifies triggers of activity, semiactivity and inactivity All female sample – could compare with male sample Data analysis methods: NR Evidence gaps/recommendations for future research: To better understand the depth of thinking that goes into making decisions about being active or not To identify how personal changes in health are interpreted by older adults and how good/poor health complicate the decision making process To identify the cues that active people use to stay active. For example how they evolve over weeks, months and years UK applicability: based in Canada. No reason to believe that the triggers identified here could not impact a similar population in the UK |
| Paulson (2005)140 Country: UK Study design: qualitative Length of follow-up: Aim: to explore whether growing older is a process of decline or of keeping active Recruitment: NR Funding: NR Quality: lower risk |
Number of participants:
Sex: mixed Education: mostly middle class Ethnicity: NR Other inclusion/exclusion criteria: NR Service setting: community – fitness exercise and dance exercise classes for over fifties |
Intervention aims and content if applicable: ‘Fitness exercise’ group and ‘dance exercise’ group Both types of class comprised older people with diverse abilities and health problems. The ‘fitness exercise’ group, advertised ‘For the Fifties Plus’, attracted around 25 men and women aged between 50 and 92 years. Most from middle-class professional backgrounds; not all attended classes regularly. Some had been physically active all their lives, so attendance routine The instructor was younger than the class members (40s). He encouraged individuals to work harder and modified equipment to allow abilities to be optimised. He gave individualised support throughout the lesson The ‘dance exercise’ group, which was also advertised ‘For the Fifties Plus’, attracted 15 women aged 60–89 years and one man (in his sixties). All attended regularly and were from middle-class and working-class backgrounds, such as teaching or shop-work The instructor was 65 years old and retired. She demonstrated exercises at the mirror in front of the class and used technical language unique to this group for parts of the body. The dance-instructor was an expert in fitness, concerned to promote health and safety (e.g. warm up, resting if in pain, loose attire) Control condition if applicable: NA Data collection methods: Ethnography: Participant observation Interviews Outcome measures: NA Response and/or attrition rate: NR Data analysis: phenomenology Theoretical framework: social constructionist; Foucauldian theory |
Main results relevant to research question (author analysis): The subjective experiences of ageing and exercise in the ‘fitness exercise’ group Individualistic terms dominated by cultural discourses of health and physiology Warm-up exercises performed with attention to the constraints of own bodies Pain or difficulty balancing might mean doing stretching exercises with less vigour and utilising a wall or a chair for support Fitness instructor pushed participants to work harder, encouraging the belief that fitness levels can be improved The daily impact of ‘fitness exercise’ on the experience of growing older Attempts to incorporate fitness exercises into daily lives. Elastic bands and weights purchased to practise exercises at home Exercise changed lives and raised awareness of health and bodies. Previous belief that activities such as gardening provided enough exercise, but now appreciation of the benefit of all-over exercises The subjective experiences of ageing and exercise in the ‘dance exercise’ group Members of the ‘dance exercise’ group behaved and talked in terms of the psychosocial benefits of belonging to the class. Togetherness constructed by changing together in the corridor and by comparing clothes and make-up and sharing jokes. No shyness about displaying wrinkled flesh or feet webbed with varicose veins Psychological ‘togetherness’ of rehearsing the ‘dance exercise’ Discipline in obeying instructor’s every command and the way each group member had their particular space in front of the mirrors, facilitated feeling of ‘togetherness’ Members communicated using a group-specific technical language Commitment to exercise shown in serious facial expressions: relieved by laughter when the sequences became complex Importance of humour; instructor’s use of humour especially important Members exercised despite back pains, feeling the cold, or difficulty remembering steps The daily impact of ‘dance exercise’ on the experience of growing older Physical benefits from the ‘dance exercise’ group expressed in psychosocial terms. Benefits of movement, using phrases that expressed importance of ageing gracefully and keeping the mind active Social events organised by instructor (coffee meetings, theatre trips, public performances) Membership could offer ‘time-out’ from difficult lives. Sense of pride – ability compared with rival groups The training curricula as social constructions of the experiences of ageing and fitness Physical reality of the ageing body becomes socially constructed according to different training styles (use of language) Discourses of health and physiology in the ‘fitness exercise’ curriculum Predominant cultural discourses in the ‘fitness exercise’ curriculum were health and physiology Discourses of popular activities in the ‘fitness exercise’ curriculum Popular activities which can be performed individually, such as walking, were optimised Discourses of graceful movement in the ‘dance exercise’ curriculum Emphasis upon the range of movements of the graceful body in relation to other. Only mention of physiology was a diagram of the spin. Body awareness; spatial awareness; dynamic awareness and awareness of others |
Strengths/limitations identified by author: NR Strengths/limitations identified by the reviewer: insights into two different communities that combine physical activity with a social aspect Details of the individuals interviewed and data analysis are not reported Evidence gaps/recommendations for future research: NR UK applicability: based in the UK |
| Pekmezi et al. (2013)163 Country: USA Study design: mixed methods Length of follow-up: 1 month Aim: to address high rates of inactivity and related chronic diseases among African American women Recruitment: from communities Funding: American Cancer Society (ACS IRG-60–001–047), University of Alabama at Birmingham Health Disparities Research Training Program (U54CA153719) and University of Alabama at Birmingham Nutrition Obesity Research Center (DK056336) Quality: no discussion of recruitment strategy, researcher position or ethical issues |
Number of participants: 56 Age: 35–70 years (mean 55.8 years) Retirement: NR Sex: all female Education: NR Ethnicity: all African American Other inclusion/exclusion criteria: NR Service setting: three urban and three rural communities |
Intervention aims and content if applicable: Single-arm, pre–post test demonstration trial (n = 10) was conducted to vet the resulting theory-based individually tailored physical activity intervention with the target population Control condition if applicable: NR Data collection methods: focus groups (11) Outcome measures: NR Response and/or attrition rate: NR Data analysis: coding and comparisons Theoretical framework: NR |
Main results relevant to research question (author analysis): Barriers Lack of time attributable to competing priorities at home and work. Balancing multiple roles (e.g. caretaker and employee) and experiencing fatigue and stress Negative outcome expectations; avoiding exercise because it might increase tiredness and sweatiness. Concerns regarding the impact of perspiration upon hair. A good deal of time and money spent to maintain certain hairstyles, which can become undone by sweating, thus hesitant towards participation in activities that involve exertion ‘There are no health clubs out in the country’ Access to safe and affordable means to be active can be an issue. Costs a barrier to physical activity (high rates of poverty in this region). Study carried out in the midst of an economic recession ‘Physical activity is torture’ Moans and groans; not enjoying exercise and using terms such as ‘torture’ to characterise past experiences with physical activity.‘I just don’t see people in my neighbourhood out walking’ General lack of social support for physical activity. Broader social norms or experiences in which family and friends were not supportive of efforts to become more physically active (e.g. husbands who did not wish to supervise children, or others expressing disapproval by asking questions such as ‘What are you walking for?’ and ‘What are you trying to lose?’) ‘Curvy figures’ quite desirable in the community. Exercise resulting in the loss of these curves may play a role in the lack of social support ‘[Exercise] could do more harm than good’ Already get enough activity in daily life (e.g. by driving to meetings) or that being busy (e.g. attending church) is the same as being active. Scared of doing harm by exercising. Fear of injury (e.g. sprained ankle or pain in knees) was often described as a barrier to physical activity Participant feedback Busy, inflexible schedules that make attending programmes difficult; home-based approaches more appropriate for this target population. Home-based, print format well-received, although suggestions to increase appeal and relevance of the intervention content for African American women in the deep south ‘We’re in the Bible belt’ Emphasis on high level of religiosity in this region, specifically among the target population. Intervention messages should be consistent with these beliefs and incorporate religiosity into the intervention ‘It ain’t all about losing weight. It’s about health’ Focus on improved physical and mental health as benefits of exercise Chronic disease prevention a powerful motivator for physical activity. Information on health disparities and how physical activity can help prevent ‘diseases. Weight loss messages might not resonate as well with this target population ‘Golf is not one of our number one sports’ Some activities (e.g. golf, swimming and tennis) might be of less interest/relevance to this population. Walking, aerobics and dancing would be more acceptable. Free and low-cost activities were suggested ‘Where are all the black people?’ No pictures of African Americans included in materials; adding pictures might make the point that information applies to people like them. More diversity in the body sizes portrayed in the pictures to emphasise that physical activity helpful for women of all sizes. Increasing the font size, bullet pointing the text (i.e. ‘get to the point’) and adding more colourful graphics Similarities and differences between community health advisors and community members Community members echoed themes. Differences included concern that exercising at a fitness centre could feel awkward because there might not be many people like them (e.g. other African American women) at such facilities. Intervention messages on outcome expectancies that emphasise potential positive outcomes (e.g. feeling energised after physical activity) and help problem solve potential negative outcomes (e.g. bringing a friend for social support) might be particularly beneficial for this group Similarities and differences between urban and rural groups Urban women a bit more concerned about issue of sweating. Both reported barriers related to safety, although urban issues related to crime and dogs and rural factors included fears of encountering snakes while walking in the country and being run over owing to lack of pavements |
Strengths/limitations identified by author: Examining an important public health concern (health disparities and sedentary lifestyles) in an at-risk sample (African American women in the deep south) with an intervention grounded in strong behavioural theory and informed by extensive formative research with the actual target population Strengths/limitations identified by the reviewer: as above Evidence gaps/recommendations for future research: NR UK applicability: US deep south context. Shows how cultural issues need to be taken into account when developing interventions. This assumption is transferable to other ethnic populations |
| Poole (2001)169 Country: Australia Study design: qualitative ethnography Length of follow-up: NA Aim: to explore reasons that older female exercise class participants are motivated to exercise Recruitment: information and discussion of the study given at a meeting for instructors Funding: NR Quality: lower risk |
Number of participants: 17 Age: > 50 years Range 52–73 years Retirement: NR Sex: all female Education: all middle class Ethnicity: most were Anglo-Celtic Other inclusion/exclusion criteria: exercise minimum of 2–3 hours/week over previous 2 years Service setting: members of an association of instructors who had undertaken Vicfit training |
Intervention aims and content if applicable: Exercise classes at a private fitness club Control condition if applicable: NA Data collection methods: Participant observation Semistructured interviews Outcome measures: NA Response and/or attrition rate: NA Data analysis: NR Theoretical framework: interpretative interactionism |
Main results relevant to research question (author analysis): Discourses on the body: body management Some dissatisfaction with body shape [‘everything drops’]. Growing older often meant weight gain, loss of muscle tone and developing undesirable bulges and flabbiness. To some this mattered; others accepted that body shape was less important with age. Exercise keeps you youthful and fit and this makes you look and feel good. Emphasis for class participants that they will change their body shape and that is what they want, to look better in their clothes. Importance of having an instructor of a similar age. Recognition that despite promises of exercise programmes, ageing might be irreversible; even young women were becoming overweight with the consequences for the future of poor health and costs. Looking good, having a trim body and being able to wear clothes not regarded as ‘old’ was important. Participating in the class helped overcome other problems such as agoraphobia The body-subject Weight had become a problem with age and body shape had changed. Exercise was to try to redistribute weight even if they could not lose it, having internalised the normalising discourses of female bodies as taut, slim and youthful looking. Rejuvenatory discourses Discourses on health: the feel-good factor Health, strength, mobility and endurance were important reasons for commitment. Exercising perceived as assisting recovery from surgery. Begun on doctor’s suggestion and grown in strength, confidence and mobility as a result. Often went on to other forms of exercise such as golf or tennis. Feelings of empowerment accompanied feeling and looking better, self-esteem flows from the energy and confidence to ‘do anything’ All instructors had participated in exercise and sport for many years, doing less when bringing up a family or being employed. A core of older women attend for a long period of time, older women more committed than younger ones who drop in and out of classes over time Social interactions Benefits of social networking and the support of others were major factors in commitment and participation. Outings, picnics, etc., and concern for each other. The leader plays a part in encouraging this kind of concern; not apparent in a commercial gym. Many older single women attend classes to socialise and find friends and married women to find space of their own away from retired husbands |
Strengths/limitations identified by author: NR Strengths/limitations identified by the reviewer: highlights views of class instructors and through them, of attendees of classes specifically for older women Evidence gaps/recommendations for future research: NR UK applicability: could apply the discourses found here to similar situations and settings in the UK |
| Scanlon-Mogel and Roberto (2004)149 Country: USA Study design: qualitative Length of follow-up: NA Aim: to identify perceived events, transitions and trajectories in older adults’ lives that contributed to and inhibited continuous participation in physical activities and exercise at three stages of their lives Recruitment: from a list of 139 members of exercise centre, 24 met inclusion criteria Funding: NR Quality: limited generalisability outside sample |
Number of participants: 15 Age: 65 + years Range 65–75 years (mean 71 years SD 3.6 years) Retirement: 12 retired and four partially retired Sex:
Ethnicity: all white, two reported Native American heritage Other inclusion/exclusion criteria: Members of exercise for at least 6 months, attending at least three times per week for at least 20 minutes Service setting: public exercise centre in south-west Virginia, USA |
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: interviews Outcome measures: NA Response and/or attrition rate: 15 out of a possible 24 members agreed to participate Reasons for not participating were conflicting schedules or lack of interest in the study Data analysis: constant comparison and open coding,200 primary coding Theoretical framework: life-course perspective212,213 continuity theory |
Main results relevant to research question (author analysis): Some had conditions that currently limited their physical activity. Formalised physical activity was not recognised historically in the way that it is now. When older adults were in their early to middle adulthood, health clubs and facilities were rare Life-course influences Physical activity involvement in younger years fluctuated depending on roles and transitions. Women defined being involved in a structured activity and sport or taking care of children and doing housework. Men defined exercise as organised activity or structured physical activity in the military. Participation levels differed between men and women. Many roles that had affected participation in young adulthood carried on into middle adulthood Men’s participation in exercise After high school most enlisted in the military. Many still played basketball or softball that they had learned in the military. Other activities included bowling and the gym. Intense conditioning in the military had influenced participation Women’s participation inexercise None involved in military training but participated in several types of exercise, mainly informally before they had children. Many did not own cars in post-war period. Walking the main means of transportation. Dancing and bowling also popular activities. Involvement in physical activity not always intentional (e.g. having to walk or ride a bike to get to places and, later in life, housekeeping and parental roles). There was little time for organised activities/exercise Middle adulthood More opportunity for organised exercise (e.g. aerobics, bowling, basketball and baseball) as well as recreation or wellness centres. Informal outdoor activities including walking, cycling, gardening, housework and child care Family and carer responsibilities For men with families, survival issues (e.g. food and keeping a roof over heads) were a priority. After work they played with children or took them to activities. Most women devoted years to caring for children, husbands or parents, cleaning, cooking, etc. Most working outside the home by the time the last child was at school. A few became involved in formalised exercise programmes. Most believed that their responsibilities had a positive influence as they kept them active all the time For men, participation included manual labour, yard work, housework and for some, golf, ball games. They shared parenting activities and some men felt this was all the exercise they needed. Some men participated regularly while working full time, walking before work, after work or at lunch time. Others lifted weights (at home) or jogged Late adulthood Transition to ‘formal exercise’, including joining a wellness centre motivated continuation or reactivation of exercise. Some joined for health reasons and were supported by centre staff. All were still involved in housework and yard-work and for men often an increase in sharing of this work at this time. Several felt that gardening provided the strengthening and cardio exercise they needed Late transitions Launching of children, retirement, onset of chronic illness affected participation. No longer circumscribed by child care or work day, time increased. Continuity of life patterns from younger age. Retirement allowed more time for physical activity participation, exercise was more ‘planned and specific’. More opportunities with fitness centres now available. Relationship between being active in early/middle years and late life and present. Caregiving roles at this time. For some, this did not interfere with participation in physical activity; they integrated it into the day Exercise and well-being in later life Older adults engaged in some physical activity to feel good physically and to feel better about themselves psychologically, aware that it would probably prolong life and delay disease. physical activity reinforced feelings of self-worth, accomplishment and independence |
Strengths/limitations identified by author: Contributes to the physical activity and ageing literature as representative of healthy, active older adults. However, the sample was small, convenient and all white, with relatively high incomes compared with the average in the area. Therefore, ethnic and SES influences could not be assessed The study relied on retrospective data and a snapshot of physical activity over time. Strengths/limitations identified by the reviewer: As above Evidence gaps/recommendations for future research: Longitudinal research is necessary to document continuity and change in the type and frequency of physical activity and explain how life roles and transitions affect physical activity patterns UK applicability: US study; however, the concepts of life course and ageing impacts on physical activity in older populations appear to be transferable in white, middle-class communities |
| Stathi et al. (2004)138 Country: UK Study design: qualitative evaluation Length of follow-up: NA Aim: to offer insights into how physical activity is situated in notions of successful ageing of people participating in ERSs and to inform GPs and health professionals about specific issues emerging from participation Recruitment: from the exercise referral programmes Funding: supported by a postgraduate research scholarship from the Greek State Scholarship Foundation Quality: lower risk |
Number of participants: 13 Age: 63–79 years Retirement: all retired Sex: eight males; five females Education: NR Ethnicity: NR Other inclusion/exclusion criteria: at different stages of the ERS Service setting: three ERSs based in leisure centres |
Intervention aims and content if applicable: Participants were referred to the ERS programmes for various health problems, including a heart condition, stroke, arthritis, knee injury, insomnia, spinal injury, diabetes and poor balance Control condition if applicable: NA Data collection methods: group and individual interviews Response and/or attrition rate: not specified Data analysis: thematic framework, use of NVivo version 2 software (QSR International Pty Ltd, VIC, Australia) Theoretical framework: NR |
Main results relevant to research question (author analysis): Improvements when comparing before and after several weeks ERS of involvement. (unsuccessful then vs. successful now) Improvements often gradual and unexpected. Personally significant outcomes often realised before completion of referral period. Improvement in a range of bodily, medical and functional features involved stabilising and improving Exercising helped to cope with medical conditions, improve fitness and maintain mobility and function. ‘Silent’ body benefits (e.g. BP, cholesterol, diabetes or arthritis), as well as improved sleep or mood Improvements in mood and well-being common expressions of a general ‘feel good’ effect. More optimistic self-perceptions, heightened cognitive function and stress reduction. Successful social experiences less consistent than these physical and mental improvements. Some found the programme a good way to meet other people and expand their social network For many this opportunity was not available; the structure of the classes inhibited expansion of social network. All three programmes designed to meet physical health needs, yet not equally meeting social needs. Many noted a number of unexpected, but valued, benefits such as being able to move furniture and decorate the home. ERS offered opportunities for personal development, something to look forward to and self-improvement. Discovering that goals could be set and achieved generated feelings of accomplishment and success Specific issues emerging from participation The role of the GP GP recommendations about importance of referral programme necessary to decide to start and more importantly to continue. Initial concerns about exercising were tempered by faith in GP knowledge and own experience of exercise, leading to a positive shift and wide-ranging advantages The exercise mode Many enjoyed the secure environment where specialists took good care of them, although some did not enjoy structured exercise. Continue to be motivated by health benefits, although prefer more interesting activities that were meaningful. Opportunities for both structured (facility-based) and lifestyle (free living, home-based) physical activity would be preferred The role of the exercise specialist Participation was a new experience for many. Prior to this, most were unfamiliar with structure of a fitness centre and how to use the equipment. Overcoming own barriers (embarrassment, fear of injury, young profile of leisure centres) was critical in initial weeks. Professional help and psychological support of the exercise specialist was facilitating factor for smooth adjustment to this environment |
Strengths/limitations identified by author: none specified Strengths/limitations identified by the reviewer: older group but views include aspects of intervention as well as benefits for the participants. However, many of the participants have health conditions so some views may relate specifically to experiencing these conditions Evidence gaps/recommendations for future research: further studies will explore the preferences of older adults and the characteristics of activities that they find attractive and easy to adopt in their everyday life, as recommended by the NQAF. This will require the direction of resources, such as staff time, towards developing long-term maintenance programmes There is need for more well-designed studies to explore the programme outcomes. Further, there is a need to identify the reasons and requirements for long-term adherence UK applicability: UK-based study |
| Stead (1997)142 Country: UK (Scotland) Study design: qualitative Length of follow-up: NA Aim: to assess whether or not and how attitudes to exercise change with age and to use this understanding to suggest how exercise can be promoted to different age groups Recruitment: random route method Funding: NR Quality: recruitment strategy, researcher position, ethical issues and data analysis details NR |
Number of participants: NR, although 15 groups of 6–8 participants suggests a total of between 90 and 120 Age: 18–49 years and > 55 years Retirement: NR Sex: eight groups women; seven groups men Education: NR Ethnicity: NR Other inclusion/exclusion criteria: Setting: community |
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: focus groups (x 15; nine with older people, six with younger) n = 6–8 in each group Outcome measures: differences between perceptions of exercise of younger and older adults Response and/or attrition rate: NA Data analysis: NR Theoretical framework: NR but appears to take a lifespan perspective |
Main results relevant to research question (author analysis): Ageing 55+ years of age group – ageing not experienced as passing time but as a series of life events. Changes prompted assessment of position in society and how viewed by others. Seeing friends from the past and reduced functional ability could be a reminder of passing time. Retirement often brought reduced mobility and increased isolation. Range of ailments contributed to a feeling of slowing down General acceptance physical deterioration as inevitable and to consider preventative measures. Keeping one’s ‘mental faculties’ more important than protecting or improving physical health. For all age groups ‘older’ was a shifting concept. Older people were ambivalent, valuing contact with people with a similar outlook and experience but wanting to distance from ‘old age’. Lack of positive labels and role models for older age group. Critique of attitude of HPs who only see a number on health records Exercise Defined as deliberately planned physical activity involving commitment, routine and exertion. Walking to shops if it was a deliberate choice over other transport or to justify little other physical activity. Definition of exercise as separate may contribute to notion as personally remote and requires hard work Participation decreased with age. Older participants reported less frequent and more moderate exercise. Exceptions participated in sport such as canoeing. Many took little or no exercise; for the frail and ill exercise had no relevance. Priorities were keeping the mind active and getting through the day (chores, etc.). Energy had to be used sparingly Participation Lifestyle For those exercising regularly it had been an enduring part of life, integrated into lifestyle. Regular activity fed into self-image and image of self as active and fit which motivated participation. Lifestyle and routine could also deter; getting out of the habit – hard to get back into it, mentally and physically Critical life events cited where exercise lapsed; starting or leaving work, getting a partner, becoming a parent. Often major life events and deteriorating health that curtailed participation and basic mobility Health and health beliefs Frailty and fear that physical activity might result in physical harm were barriers. Reinforced by perceived deterioration of health with age. Desire to improve health for its own sake rarely a motivation. Physio regimes might force a re-evaluation, although only short-term Perceived rewards Main motivation to gain emotional and psychological rewards. Competition and desire to achieve important for younger men; less salient in older people, although a sense of achievement may still motivate For older people self-esteem and self-image (feeling good) were important compared with appearance. Most important perceived rewards were social; this was often incidental but was felt to combat social isolation and mental stagnation. Participating with people of a similar age was usually preferable. Lack of social element or someone to participate with could be a barrier to participation; reluctance to use a facility alone Situational factors Availability of and access to facilities could act as motivators or barriers. Local leisure centres seen to provide mainly for younger people. One-off events could stimulate interest but regular events allowed social interaction. Critique of short-term classes and a tendency to stop in the summer. Access pertinent in older age group – public transport lacking in rural areas. Cost was a factor with private facilities seen as expensive Awareness of opportunities Mainly through word of mouth. Less likely to reach isolated individuals. Older people more likely to read newspapers or leaflets. Discussion groups. HPs not regarded as useful source, with advice on exercise being short and/or vague. GPs not seen as qualified to give exercise prescriptions. For some, particularly working class men, failure of HPs to advocate exercise was one reason for non-participation |
Strengths/limitations identified by author: none reported Strengths/limitations identified by the reviewer: Lack of detail about individual demographics Evidence gaps/recommendations for future research: Recommendations: Although older people do not constitute ‘special need’ group (apart from > 75 years) when designing exercise prescription, age is a factor when it comes to marketing, preferred exercise provision and information/support. There are different barriers to participation as age progresses Two main groups were identified; those that participate already and those who do not. Aims could be to reinforce and maintain exercise behaviours already present for the former. This group will be easier to reach but may be regarded as lower priority For second group exercise incorporation into daily life would be an aim. Messages about health benefits might have limited impact particularly for frail individuals who see exercise as potentially dangerous. This group might also feel alienated The social and recreational aspects of exercise would probably be more attractive to older people when marketing (filling up the day, structuring the week, meeting new similar aged people, keeping the mind active) Need to challenge the notion that health deterioration is inevitable and that doing regular exercise can keep older people physical active and independent. Need to use different labels as older people distance themselves from ‘elderly’, etc. Self-image may be more aligned with a younger age (although avoid either extreme) UK applicability: UK-based study, potentially generalisable to design of interventions throughout the UK |
| Walcott-McQuigg and Prohaska (2001)164 Country: USA Study design: qualitative Length of follow-up: NA Aim: to examine factors influencing exercise behaviour of older African American adults Recruitment: a non-probability purposive sampling method Funding: National Institute on Ageing and the Office of Research of Minority Health of the National Institutes of Health Quality: lower risk |
Number of participants: 103 Age: all > 55 years Retirement: NR Sex:
Ethnicity: all African American Other inclusion/exclusion criteria: Service setting: community; urban |
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: focus groups (n = 5–12 per group) Motivational Readiness for Exercise screening instrument divided the participants into twelve groups relating to three stages of Readiness:
Discussions on exercise, health and lifestyle issues Response and/or attrition rate: 18 participants dropped out from original sample of 121 Data analysis: qualitative content analysis Theoretical framework: transtheoretical model |
Main results relevant to research question (author analysis): Meaning of health and health activities Areas of meaning relating to physical activity:
Meaning of exercise Physical exertion programmes and physical activity defined exercise. Pre-contemplators more likely to view exercise as physical exertion such as push ups. For females, home exercises, walking and strenuous exercise were identified. Action/maintenance more likely associated with a broad definition including housework and general movement Benefits to exercise Physical and mental health benefits Energising, keeping alert, relieving stress. Keeps in shape and prevents stiffness Pre-contemplators and contemplators less articulate about benefits and more likely to associate exercise with work. Need to cultivate more positive thoughts about exercise Barriers to exercise Health problems, perceptions of need for exercise, lack of motivation, time constraints major barriers to participation. Health concerns such as arthritis, knee problems and heart conditions were barriers. Active/maintenance males suggested that barriers could be overcome by ‘forcing yourself to get up and move’. Females missed classes when they couldn’t attend. Mental benefits could outweigh physical health concerns. Contemplators expressed intentions to participate that were influenced by barriers. Pre-contemplator females suggested no need to exercise as they got sufficient exercise from housework. Pre/cont females more likely to cite tiredness as a barrier. Females cited more constraints, including family commitments Self-efficacy and social support Pre-cont groups less self-efficacious. Social support from family and friends important factor in starting a programme. Pre-contemplators thought such support could be aggravating; families could also interfere with exercise plans. Also less likely to exercise owing to lack of social support. Contemplators had support, although initiation of exercise was only at the preparatory phase. Strategies to Recruit African American Elders in Exercise Programmes
|
Strengths/limitations identified by author: strengths – It is one of the first attempts to use a theoretical model of individual behaviour change to examine factors influencing exercise behaviour in older African Americans In addition to providing the research team with information on their various stages of readiness to exercise, the participants contributed information necessary to develop a strategic recruitment and retention plan for community-based exercise programmes targeted to older African Americans Weaknesses: pre-contemplators and contemplators/preparers comments are representative of the stages as described in the literature. Pre-contemplators can ‘wish to change’. This wish, however, may not translate into intention to change Several features of this study limit its generalisability. The sample size was drawn from a convenience sampling method. Thus, the participants were not representative of all older African Americans in urban, rural, or homebound settings Strengths/limitations identified by the reviewer: Evidence gaps/recommendations for future research: discussions need to be conducted with African Americans who are homebound, reside in various urban and rural settings, and do not participate in senior centre activities. Longitudinal studies are needed to evaluate efforts to recruit and retain African American elders into exercise programmes UK applicability: US based and focusing on one specific ethnic group there. Some barriers for participating in physical activity in this age group could transfer to UK settings |
| Weeks et al. (2008)180 Country: Canada Study design: qualitative; face-to-face interviews Length of follow-up: NA Aim: to identify influences on participation in physical activity among seniors living in a nursing home and in community dwellings Recruitment: Community dwelling: 1. Non-profit health-care agency 2. Board of seniors Nursing Home: administrator-identified participants Funding: The Canadian Nurses Foundation and the Community Health Research Unit at the University of Ottawa Quality: lower risk |
Number of participants: 24 Age: All 64 + years
Sex:
Other inclusion/exclusion criteria: NA Service setting: community dwelling (two sites) (n = 17); nursing home (n = 7) |
Intervention aims and content if applicable: Control condition if applicable: NA Data collection methods: interviews Outcome measures: NA Response and/or attrition rate: 6/30 recruited participants did not complete the study Data analysis: QSR International N6 package Thematic analysis Theoretical framework: life-course perspective |
Main results relevant to research question (author analysis): Differing levels of physical activity between community dwellers (vigorous exercise x4 a week) and nursing home residents (no vigorous exercise). Nursing home residents more likely to participate in sedentary activities Intergenerational influences Seniors influenced either positively or negatively by their parent’s physical activity patterns Establishment of early physical activity patterns Established activity patterns sometimes continued (e.g. dancing, skiing and swimming). Some activities avoided owing to fear of getting hurt Family transitions over the life course Seniors had been active in paid work as well as looking after large families so had little time for physical activity when younger. For some, this was a time that they could rest. Demands of providing care perceived by some to have kept them from doing more beneficial physical activity. This was particularly so when dependents could not be left alone Changing health status over the life course For some, changes in health status eliminated certain kinds of physical activity such as lifting heavy articles or yoga. Some modified their physical activity to types that were more suitable For seniors in a nursing home, health changes were an important reason for limited participation in physical activity. In many instances, health declined to the point where they needed assistance of a staff member to participate. Some nursing home residents indicated that they would participate more if personal assistance or encouragement were provided Future health concerns A key motivator involved preventing further or anticipated health decline. Some knew others whom they believed experienced negative health outcomes because they did not participate. Some participated to stay mobile and prevent falls and injury |
Strengths/limitations identified by author: a life-course perspective allows us to broaden our view of what influences physical activity among seniors and thus has a greater impact on the health of seniors Strengths/limitations identified by the reviewer: analysis appears a bit thin and the way that some of the findings are described is at times unclear (for example were the seniors talking about the past or present when they spoke of paid work) Evidence gaps/recommendations for future research: more research with larger samples is needed to generalise findings on differences in activity levels between seniors in nursing homes and in the community UK applicability: relatively applicable to the UK since the UK has seniors living in communities and in nursing homes. Themes appear to be transferable |
| Wilcox et al. (2005)158 Country: USA Study design: qualitative Length of follow-up: NA Aim: to examine perceptions, barriers and motivators to exercise in rurally based older women Recruitment: through a rural health-care centre Funding: fellowship fund for epidemiological Research on physical activity (physical activityF); American College of sports Medicine Quality: recruitment strategy, researcher position, some ethical issues NR |
Number of participants: 39 Age: ≥ 50 years (mean 67.5 years) Retirement: African American women more likely to be employed (63% vs. 18%) Sex: all female Education: Level 12.5 49% had income < US$15,000 Ethnicity:
Service setting: rural health-care centre |
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: focus groups Outcome measures: NA Response and/or attrition rate: NR Data analysis: hierarchical coding Theoretical framework: social ecological model |
Main results relevant to research question (author analysis): Physical activity viewed as broader than exercise Some consensus regarding the definition of exercise and physical activity, mainly consistent with those used in sports science. For one African American woman exercise was something done at the gym whereas physical activity also included chores. Physical activity was activity that increased the heart rate and was tiring. Singing was regarded by one African American woman as exercise The amount of exercise older women need ‘depends on the person’ Frequency, intensity and duration regarded as individual dependent and related to age and physical health Perceptions of current physical activity recommendations Presented with CDC-ASCM recommendations for physical activity and health (e.g. Pate et al.214) Discussed moderate as a personal idea. Common examples of moderate included housework and walking. Most thought all days of the week was 7, some 3–4 and some all but Sundays. The term ‘accumulate’ was confusing for some. Consensus that recommendations were good and realistic for women their age, although some white women did not think it was realistic to carry out exercise 7 days a week Perceived benefits of aerobic exercises Physical health Strengthens the heart, benefits to arthritis, decreasing joint stiffness. Specific conditions included diabetes, high BP and cholesterol Mental benefits Cited more by white women and related to stress reduction, improved thinking/alertness, feeling better and feeling good, improved energy levels and enjoyment of the activity. Better mental health also mentioned. Among African American women, stress reduction, improved sleep, improved energy and feeling good were mentioned Perceived risk Overdoing it was a theme across all groups (e.g. trying to keep up with an exercise class). African American women cited age as a limiting factor Injuries Risk of breaking bones, falling, muscle strains. Draining one’s energy. Among African American women having a heart attack was mentioned Perceived barriers of aerobic exercise Personal White women cited health problems, feeling tired, being too old to exercise and lacking confidence. Often unclear whether women felt limited by their health or other reasons. Exercise as boring or not enjoyable. Lack of self-motivation described as ‘being lazy’ or ‘lacking commitment’. African American women cited more barriers than white women. Perception that too much hard exercise does more harm than good. Specific health problems, including being overweight Social Exercise not seen as a priority given competing responsibilities (family and work). Often discussed in conjunction with feeling tired, lacking energy and not having enough time. Looking after everybody else and having no time to take care of self. African American women referred to as having large families which takes time. Lack of social support, particularly from husband and family was another barrier Cultural Informed of statistics suggesting older women, especially African American women, who live in rural areas in the South, are less active. Recalled the past when they were more active even though they did not exercise. Not having role models who exercised or talked about exercising when they were young. Encouraging physical activity in this group would have to come from the black community or Church Environmental Lack of transportation, no pavements, lack of safety, stray dogs and lack of facilities. Living in a rural area provided limited public transportation, and women were reluctant to drive as they aged, particularly at night. Venues 20–30 miles from home – too far to travel for half an hour of exercise. Lack of age appropriate classes and costs also major factors. Having access to a place where exercise was supervised, such as a senior centre, was suggested Motivations or enablers Personal Many were the opposite to barriers. Potential to improve health and lose weight, feel better Exercise in the mind and if you want to do it, you can. Enjoyment also important and dancing provided this Social Importance of friends, neighbours and HCPs in promoting physical activity. Having others to exercise with for motivation Having a partner inspiring and motivating. Need to communicate and support more within neighbourhoods. Doctors recommending exercise very motivational as perceived credibility. More information was also suggested as well as demonstration of how to safely carry out exercises Environmental Need for better transportation and low cost or free facilities/programmes convenient to get to and aimed at older adults. The church was a potential location and the community as encouragement to attend |
Strengths/limitations identified by author: non-representative sampling – the sample was a convenience sample who happened to have a reasonably good education. There were differences between the white and African American women in terms of age and occupational status There were no regular exercisers among the sample Strengths/limitations identified by the reviewer: evidence gaps/recommendations for future research: none reported apart from to carry out research with a broader population UK applicability: this population is specific to South Carolina so generalisability to the UK is limited. For example, ‘rural’ here may be much more remote than anywhere in the UK and the environment may differ in terms of pavements and available facilities. However, there are concepts reported here that can be transferred to a similar UK population, such as competing responsibilities at this age and SES considerations. Also cultural – would Afro-Caribbean women or those from other minority ethnic groups in the UK be motivated to join a class designed by the white population? The idea that physical activity has a personal aspect that is dependent on health and physical ability is also transferable |
| Winston and Barnes (2007)177 Country: USA/New Zealand Study design: qualitative Length of follow-up: NA Aim: to investigate the vision for retirement of female ‘baby boomers’ Recruitment: convenience and snowball techniques; by telephone call Funding: University of Tampa Faculty Development Grant, a University of Tampa Alumni Association Faculty Development Grant and a University of Waikato Academic Research Visitor Grant Quality: lower risk |
Number of participants: 32 (21 in USA; 11 in NZ) Age: 40–59 years (born 1946–1964)
Sex: all female Education: high – in academia; range from professor to instructor Ethnicity:
|
Intervention aims and content if applicable: NA Control condition if applicable: NA Data collection methods: Face-to-face interviews Outcome measures: NA Response and/or attrition rate: none reported Data analysis: reading and rereading transcripts in relation to:
|
Main results relevant to research question (author analysis): Data relating to physical activity/retirement only: Meaning of retirement Interviewees had not been thinking much about retirement. For some it meant not being in paid employment, whereas for others it meant loss – having low funds and contacts Anticipated post-retirement activities Included academic work/teaching/writing, arts, crafts, community work and travelling. In relation to physical activity, 41% planned to do gardening. 28% of participants (five in their 40s, three in their fifties) planned to do physical activity, ranging from spending more time at the gym to back-packing Concerns about retirement Personal health was a concern for 53% in their 40s but only one participant in her fifties. Three actively promoting their own good health – one mentioned exercising regularly |
Strengths/limitations identified by author: findings may not be representative of all baby boomers anticipating retirement Strengths/limitations identified by the reviewer: limited to female views before retirement. Not a lot of data on physical activity Evidence gaps/recommendations for future research: could compare with male views as well as perceptions of newly retired women UK applicability: US-/NZ-based study – different social care systems. However, the concerns could be similar, particular regarding physical health in the future |
Appendix 8 Applicability sessions feedback form
Glossary
- Cohen’s d
- A measurement of effect in terms of the mean difference between groups in standard deviation units.
- Effect size
- A standardised way of measuring the mean size of the difference between two groups using units of standard deviation. The convention for rating effect sizes (Cohen’s d) is as follows: a ‘small’ effect size is 0.20, a ‘medium’ effect size is 0.50 and a ‘large’ effect size is 0.80.
- Hawthorne effect
- This refers to the potential for participants to change their behaviour because they are in a research study, rather than as the result of an intervention.
- p-value (probability value)
- The probability that any difference between groups is the result of chance. Thus, the smaller the p-value, the greater the likelihood that the difference is not attributable to chance. The convention is to use the following levels of significance: p < 0.05 and p < 0.01.
List of abbreviations
- BA
- before and after
- BMI
- body mass index
- CASP
- Critical Appraisal Skills Programme
- CI
- confidence interval
- d
- Cohen’s d
- ERS
- exercise referral scheme
- ES
- effect size
- GP
- general practitioner
- ml/kg/minute
- millilitres of oxygen per kilogram of body weight per minute
- OECD
- Organisation for Economic Co-operation and Development
- OR
- odds ratio
- RCT
- randomised controlled trial
- SD
- standard deviation
- SES
- socioeconomic status