
Notes
Article history
The research reported in this issue of the journal was funded by the PHR programme as project number 11/3010/02. The contractual start date was in January 2013. The final report began editorial review in October 2015 and was accepted for publication in April 2016. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PHR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
Laura Jones receives personal fees from the National Centre for Smoking Cessation and Training, outside the submitted work. Sarah Lewis is a member of the National Institute for Health Research Health Services and Delivery Research programme researcher-led board.
Disclaimer
This report contains transcripts of interviews conducted in the course of the research and contains language that may offend some readers.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2016. This work was produced by Szatkowski et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Introduction
Harms caused by smoking in young people
Cigarette smoking is a significant preventable cause of morbidity and mortality. In 2013 in England, 17% (78,200) of all deaths of adults aged 35 years and over were estimated to be attributable to smoking, a proportion that has remained largely unchanged in more recent years. 1 Approximately half of all current smokers will die prematurely as a consequence of smoking unless they quit, on average 10 years earlier than if they had never smoked. 2 The total cost of smoking to society in England is approximately £12.9 billion a year, including the cost of treating smoking-related diseases and productivity losses attributable to premature mortality, smoking breaks and smoking-related work absences. 3
Most smokers become addicted to smoking before they reach the age of 18 years, with nearly 40% becoming addicted before the age of 16 years,4 predominantly during their years in secondary education. Smokers who start smoking at an early age tend to smoke more cigarettes per day in adulthood,5 smoke for longer,6 are less likely to quit7 and are more likely to die from a smoking-attributable cause. 6 Smoking in adolescence impedes lung growth and causes a premature decline in lung function,8 is linked to early signs of heart disease and stroke8 and is a major driver of inequalities in health; children in lower socioeconomic groups are more likely to start smoking and to do so at a younger age. 4 Intervening with young people to prevent them smoking is thus a crucial public health priority.
The prevalence of smoking among young people
Uptake and ever smoking
In the past 10 years there has been a steady decline in the number of students aged 11–15 years in England who report having tried smoking at least once, from 39% in 2004 to 18% in 2014. 9 The proportion of students who have ever smoked increases with age; in 2014, 4% of 11-year-old children reported ever smoking, increasing to 35% of 15 year olds. 9 In 2014, 3% of 11- to 15-year-old students smoked regularly (at least one cigarette a week), a decrease from 9% in 2004. 9 The proportion of children smoking regularly also increases with age, reaching 8% among 15 year olds. 9
Susceptibility to smoking
It has been suggested that initiation of smoking among adolescents is preceded by a shift in attitudes when young people begin to entertain the possibility that they might try a cigarette and no longer hold a strong cognitive commitment not to smoke. 10 This cognitive shift has been described as the development of a susceptibility to smoking. 11 There are no national data on susceptibility to smoking in England, although in one local study 27.2% of 11- to 15-year-old students were deemed to be susceptible. 12 In 2014, 26% of students aged 11–15 years nationally thought that it was OK to try smoking to see what it was like, and 10% thought that it was OK to smoke once a week. 9 Both figures have declined steadily over time, from 48% and 25%, respectively, in 2003. 9
Existing research evaluating approaches to preventing adolescent smoking uptake
Systematic reviews of the design, implementation and effectiveness of interventions to reduce uptake of smoking in young people conclude that, although there is some (although by no means conclusive) evidence that school-based interventions may have short-term positive effects, there is little robust evidence that these interventions prevent young people from taking up smoking in the longer term. 13–15 However, as noted by the National Institute for Health and Care Excellence (NICE), given that very little of this work has been carried out in the UK, these findings may not be applicable in the context of the UK education and health-care systems. 15 In addition, much of the existing evidence dates from the 1980s and 1990s, when the tobacco control environment and public attitudes towards smoking were very different from those of the present day. However, in the absence of relevant and recent UK data, evidence from older studies and those conducted elsewhere is useful to inform key questions surrounding the design and implementation of a successful intervention to prevent smoking uptake in young people in the UK today.
Effectiveness of existing interventions
Existing studies have tested a variety of interventions, differing in theoretical approach, design, intensity and mode of delivery and utilising different outcome measures and follow-up periods in evaluation. Therefore, given the substantial heterogeneity between studies, evidence from systematic reviews and meta-analyses of this literature is difficult to interpret. Although there is no definitive evidence regarding interventions that do not work and should thus be avoided, there is also no clear evidence for what may be effective.
There is no conclusive evidence that any one theoretical approach or conceptual framework is superior to others in preventing smoking uptake. 15 Interventions that involve providing young people with information about the prevalence and consequences of smoking, enhancing their social competence (e.g. teaching skills to increase self-esteem and cope with stress) and addressing social influences (e.g. increasing awareness of peer and media influence and teaching refusal skills) have all been tested with inconsistent results in terms of their effects on smoking uptake. 14
In the UK the A Stop Smoking In Schools Trial (ASSIST) programme trains students in Year 8 (aged 12–13 years) as peer supporters who are able to intervene in their friendship groups to encourage non-smoking. A randomised controlled trial (RCT) of ASSIST, the results of which were published in 2002, found a significant reduction in reported recent smoking (in the past 2 weeks) up to 2 years later. 16 In the only other UK study, carried out in the late 1990s, a RCT in 52 schools in the West Midlands tested the effectiveness of a 1-year-long programme in which students in Year 9 (aged 13–14 years) received three classroom-based and three computer-based sessions to encourage them to refrain from or to stop smoking. 17 This study found no significant effect of the intervention on the proportion of adolescents smoking one or more cigarettes per week 12 months later.
There is good evidence that ‘booster’ sessions are useful in the months and years after the delivery of a main intervention to strengthen and maintain its effectiveness, and, therefore, NICE recommend their use. 15 Booster components that have been trialled in previous smoking-prevention interventions have included classroom-based sessions,18 tailored letters,19 telephone calls,20 videos21 and magazines. 22
Some young people may experiment with smoking intermittently over many years before they identify and report themselves as a smoker, whereas others show signs of dependence very early in their smoking career. 23 For this reason it is recommended that school-based interventions contain elements of both smoking prevention and cessation and that a school smoke-free policy should include efforts to promote local NHS stop smoking services to both students and staff. 15
What constitutes a cost-effective intervention?
There is limited evidence for the cost-effectiveness of smoking-prevention interventions in UK schools; studies carried out elsewhere are also of limited relevance here given differences in their populations and health-care and education systems. 24 ASSIST was judged to reduce adolescent smoking at a modest cost; the incremental cost of the intervention per student not smoking at 2-year follow-up was £1500 [95% confidence interval (CI) £669 to £9947]. 25
Who should deliver an intervention?
Existing studies have utilised a range of people to deliver anti-smoking interventions to young people, including teachers, school nurses, project staff external to the school and students themselves. However, there is no consistent evidence regarding which of these providers gives the best results, and it is impossible to compare across studies given the probable confounding by other factors such as the content of the intervention itself. A Canadian study carried out in the 1990s found that teachers and school nurses were equally effective in delivering a classroom-based intervention to students in Grades 6 to 8 (ages 11–14 years) and there was no differential effect based on whether staff were formally trained in organised workshops or were provided with self-preparation materials. 26 The ASSIST study trained students as peer supporters and, as noted earlier, found a significant impact on student smoking up to 2 years later. 16 This positive effect was not restricted to the students trained as peer educators but was also extended to the non-trained students with whom the peer supporters were intervening. The ASSIST intervention was most effective in schools in the Welsh valleys, and the authors attribute this to the existence of clearly defined, close-knit communities in which the trained students were able to diffuse new behavioural norms. This suggests that the use of peer educators may be less effective in more poorly defined communities. Peer educators may also be counter-productive among students who already smoke. Other studies in the USA and Europe not using ASSIST have identified a ‘boomerang effect’, whereby over the course of a study smoking prevalence increased more in those exposed to anti-smoking interventions than in controls who did not receive the intervention. 18,27
At what age should you intervene with young people to prevent smoking uptake?
Age is a strong predictor of smoking behaviour, and existing studies have intervened across the age spectrum from the earliest years of primary school28,29 to the later years of secondary school. 30 The majority of interventions have been aimed at young people between the ages of 11 and 14 years; ASSIST intervened with students in Year 8 (aged 12–13 years). 16 There is no conclusive evidence on the age at which it is best to start delivering school-based interventions to prevent young people from smoking, but Years 7 and 8, the years in which smoking experimentation and the prevalence of regular smoking begin to increase dramatically,9 are arguably a logical point at which to intervene.
How do other student and school characteristics influence the effectiveness of an intervention?
There is conflicting evidence over whether or not school-based interventions have a differential impact according to gender and, indeed, the direction in which this effect might operate. 15 Similarly, students’ ethnicities and social groups may or may not influence the effectiveness of an intervention. The ASSIST intervention was most effective in the Welsh Valleys, a deprived area, and, in particular, was effective in reducing smoking only among girls. 31 In contrast, an intervention with 13-year olds in the Netherlands was significant only among young people whose parents had high levels of education and who worked full time, and particularly among boys with high levels of parental education. 21 Previous work by the authors of this report32,33 has shown that young people are more likely to begin smoking if they attend a school at which smoking prevalence among senior students is high; therefore, school smoking prevalence may influence the effectiveness of an intervention. Students who are smokers are also more likely to be absent from school and less likely to engage fully with an intervention than non-smokers. 17
What do schools and teachers want?
An intervention must be acceptable to teachers if it is to be delivered as intended and have the hoped-for consequences. At present, the National Curriculum for Personal, Social, Health and Economic Education (PSHE) in England, although non-statutory, suggests that schools teach facts and laws about tobacco use and misuse, and the personal and social consequences of smoking for the smoker themselves as well as for others. 34,35 However, a wide variety of approaches to teaching this material is seen across schools and, although the Office for Standards in Education (Ofsted) concludes that the quality of PSHE delivery is generally improving, there are variations in coverage and quality. 36 In many secondary schools PSHE is taught by form tutors, although many of these may lack the training, skills and experience to deliver content effectively; only 22% of PSHE teachers have any relevant training, and half of secondary schools have no staff with continuing professional development accreditation in the subject. 37 Therefore, an intervention needs to be accessible to teaching staff with no subject-specific training. In addition, schools face an increasing number of demands on their time and, thus, any intervention must be suitable for implementation with little preparation. A process evaluation of the ASSIST intervention suggested that teachers are receptive to new ideas and ways of teaching the difficult topic of smoking prevention and cessation, but that this must fit in with a school’s existing ethos and organisation. 38 The inevitable added workload for teachers involved in trialling a new intervention means that it should arguably be delivered before students reach Year 9 when they have often begun work towards external General Certificate of Secondary Education examinations (summative school-leaving exams taken at the age of 16 years) and when teachers may be occupied with Standard Assessment Tests (progress assessments completed during Year 9) teacher assessments. 38
How can young people’s families be engaged to help prevent young people from smoking?
The NICE recognises that no one intervention alone will succeed in preventing the uptake of smoking among young people, but that a wider approach tackling individual, family, community and societal influences is needed. 15 The strong association between parental and child smoking9 suggests that the addition of a family component to a school-based intervention might help both to encourage young people not to smoke but also to encourage cessation among any parents who smoke themselves. A recent Cochrane review found there to be moderate-quality evidence from RCTs that family-based interventions can have a positive effect on preventing young people from starting to smoke. 39 The strongest evidence was for intensive interventions, delivered independently of a school-based intervention, which encouraged authoritative parenting (defined as showing an interest in and care for the adolescent, often with rule setting), although the limited numbers of studies and participants made conclusions difficult to draw for other types of interventions. 39
A promising literature is developing around the effectiveness of interventions to encourage parents to talk with their adolescent children about smoking. 40 Various approaches to prompt discussions between parents and children have been trialled, including the provision of pamphlets and quizzes,41 booklets,42 newsletters43 and postcards44 mailed to parents, homework activities for the child to complete with their parents,44 videos43 and financial incentives. 43 These have demonstrated some positive effects on the degree to which children report talking to their families about smoking, although their effectiveness in reducing smoking uptake remains unclear. As expected, interventions prompting communication may be most effective when the parent is a non-smoker. 40 Most of these studies were carried out in rural, middle-class areas of the USA and their relevance to the UK is not clear.
To our knowledge, no work has been undertaken with secondary school-aged children themselves to understand their views on whether or not, and how, their families should and could be engaged to support them to remain non-smokers. Focus groups with primary school-aged children after they had received a smoke-free homes intervention suggested that they were confident in talking to their parents about the issue, although the children themselves were not involved in designing the intervention. 45
What does existing smoking-prevention education look like in the UK?
To the best of our knowledge, there are no existing publications summarising the state of existing smoking-prevention education in the UK. A systematic-style literature and internet search conducted by a University of Nottingham medical student during the course of this study identified 19 smoking education resources available for use in the UK; these varied in content and delivery style, and, although they all received positive feedback from teachers and students, formal evaluation of effectiveness was lacking. A survey of East Midlands secondary schools also conducted as part of this project suggested that schools dedicated little time to smoking education (especially with older students) and concentrated on teaching about the health effects of smoking, and that a large proportion of staff leading sessions had not received any training in delivering PSHE. Further details on this work are included in Appendix 1.
The Truth® campaign
Evidence from the USA suggests that a focus on the ethics and exploitative tactics of the tobacco industry may be effective in encouraging young people not to smoke. 46,47 Through mass media campaigns and additional online content, the Truth® campaign48 has been credited with producing declines in youth smoking prevalence by countering the tobacco industry’s deceptive marketing strategies and denial of the addictive nature and health effects of cigarettes, and by focusing attention on the negative effects of the industry on the environment and society. Although not specifically a school-based intervention, the relevance of the approach of the Truth® campaign to the UK has been identified by NICE as an area for further research. 15
Operation Smoke Storm
The emphasis of the Truth® campaign was adopted by Kick It, the NHS Stop Smoking Service for Hammersmith and Fulham, Kensington and Chelsea, Westminster, Kingston upon Thames and Richmond upon Thames49 in designing (prior to the start of this project) Operation Smoke Storm, a novel educational package for use in schools to increase awareness of tobacco industry practices. A short description of Operation Smoke Storm is given in Box 1; for a more detailed description of the intervention, see Appendix 2.
Operation Smoke Storm is a web-based educational package designed for delivery by teachers as part of a school’s PSHE curriculum. Teachers are provided with detailed lesson plans for three 50-minute classroom sessions (although the material can also be delivered as one longer session). Multimedia presentations, streamed over the internet, are used to guide teachers and students through the lessons. Students act as secret agents to uncover the tactics of the tobacco industry and share what they find with others. The sessions also cover the health effects of tobacco, passive smoking, nicotine addiction and the economic cost of smoking.
Sessions 1 and 2 include video clips followed by individual and group-based quizzes, and discussion activities in which students learn about the harmful and addictive nature of smoking and methods used by tobacco companies to encourage young people to smoke. Students are provided with a workbook to record their answers. In session 3, they then use this information to ‘spread the word’ in a group presentation to their class, in a format of their choice, such as drama or song.
In a small-scale evaluation in two London schools of changes in students’ awareness and attitudes, as well as acceptability and ease of use, Operation Smoke Storm was very positively evaluated. 50 Although data were collected from just 53 students, students who received Operation Smoke Storm reported an increased knowledge of smoking and the tobacco industry, 89% liked the resource, 98% thought that it was easy or very easy to understand, and 72% went on to tell their friends and/or parents about their lessons. The staff (two teachers and two members of staff from Kick It) who delivered the intervention in this small-scale evaluation also gave very positive feedback; Operation Smoke Storm comes with detailed lesson plans and thus requires minimal teacher preparation, making it suitable for use by busy staff who have many competing demands on their time and who may have little or no subject-specific knowledge or training. 37 To date, there has been no evaluation of the effectiveness of Operation Smoke Storm in preventing smoking uptake among students who receive the intervention.
Summary
Existing literature highlights a lack of recent, UK-specific evidence regarding how best to design and implement interventions to prevent youth smoking uptake. However, a successful intervention would be likely to involve a booster and family component, make few demands on busy teachers with little subject-specific knowledge, and be evaluated for both short- and long-term effectiveness. In this study, the existing Operation Smoke Storm resource was used as the basis of the intervention. Qualitative work was undertaken to refine Operation Smoke Storm and to develop additional components to maximise the potential for the intervention to be effective in reducing smoking in young people. The final multicomponent intervention was then formally evaluated for its effectiveness in preventing smoking uptake in order to gain evidence to inform whether a fully powered cluster RCT to evaluate effectiveness and cost-effectiveness was warranted.
Objectives
The overall purpose of this research was to assess whether or not a multicomponent intervention involving educational resources for use in schools, alongside family components, is effective and cost-effective in preventing the uptake of smoking in school-aged children. Specific objectives were to:
-
pilot Operation Smoke Storm to gain preliminary evidence for its acceptability and effectiveness.
In the first year of the study, Operation Smoke Storm was trialled with Year 7 students (aged 11–12 years) in two schools. Student questionnaires and qualitative work with students and teachers evaluated the acceptability of the intervention (see Chapter 3).
-
develop an effective and acceptable booster intervention for use with students in Year 8 to maintain and strengthen the effects of Operation Smoke Storm.
Qualitative work with Year 7 students and teachers was used to explore views about what the booster element should include, how it should be delivered, as well as probable uptake by students (see Chapter 3). This feedback was used to develop the booster intervention (see Chapter 4).
-
identify and develop acceptable and effective intervention components for use by families which build on Operation Smoke Storm to prevent the uptake of smoking in young people and to promote and signpost support for cessation to students, their family members and school staff who smoke.
Focus groups with Year 7 students explored if, and how, their families could be engaged to help them not to start smoking, or to quit if they already smoke. Opinions on the variety of family interventions that have been used previously were mapped so as to design a family-based intervention for use here which was both acceptable and likely to be effective (see Chapters 3 and 4).
-
provide preliminary evidence for the effectiveness and cost-effectiveness of the combined school and family intervention on which to base a decision on whether or not to continue to a fully powered trial.
The proportion of students reporting smoking or susceptibility to smoking was compared with control data from an existing local survey (see Chapter 5). An independent Data Monitoring and Ethics Committee (DMEC) made a recommendation to the Study Steering Committee about whether or not to proceed to a full trial based on this evidence of effectiveness alongside qualitative evidence of the acceptability of the intervention to schools, teachers, students and parents (see Chapter 6); the readiness of the intervention for immediate implementation; and the likelihood of willingness to take part in the trial from a sufficient number of schools (see Chapters 5 and 6).
Chapter 2 Overview of research design and methods
This chapter provides a summary of the study, giving an overview of the different phases and processes, and signposts readers to the relevant chapters in the main body of the report in which further details can be found.
The study was split into two phases. In phase 1, conducted between September 2013 and August 2014, the original Operation Smoke Storm was piloted with students in two schools; results from qualitative work conducted with students and teachers were used to refine the resource and to extend it with booster and family components. In phase 2, conducted between September 2014 and May 2015, the refined and extended intervention package was delivered in the same two schools, with accompanying quantitative and qualitative evaluation. Figure 1 summarises the research processes across the two phases.
FIGURE 1.
Summary of research processes.

At the end of phase 2, the Study Steering Committee, informed by the recommendation of a DMEC, determined whether or not the intervention showed sufficient promise of effectiveness to justify progression to a fully powered, cluster RCT, for which funding for a 1-year follow-up had been provisionally agreed with the National Institute for Health Research (NIHR). Funding for longer-term follow-up would be sought at a later date if initial results looked promising.
School recruitment and participants
Two out of six schools approached agreed to participate in the study. Although the other schools showed interest in the resource, time pressures resulted in them being unable to participate. Both participating schools were located in Nottinghamshire, UK, but had contrasting sociodemographic profiles. School 1 served a relatively affluent catchment area in a market town, with 6.1% of students eligible for free school meals (used as a measure of deprivation; the national average in January 2014 was 16.3%51). School 2 served a less affluent catchment area in a former coal-mining town, with 10.2% of students eligible for free school meals.
Research design
In phase 1, Operation Smoke Storm was delivered to all Year 7 students (n = 585) in two schools during their PSHE lessons. Kick It has previously delivered Operation Smoke Storm to students in older year groups, but the decision was made here to deliver the first part of the intervention in the first year of secondary school, before the majority of students have begun to experiment with tobacco. The research team provided a brief training session to teachers prior to their delivery of Operation Smoke Storm which outlined how to access and navigate the resource and provided information about the research processes (questionnaires, interviews and focus groups).
In total, 585 Year 7 students (aged 11–12 years) received Operation Smoke Storm (School 1: 347 students in 14 classes; School 2: 238 students in eight classes). School 1 had shorter lessons (40 minutes per week) and so some classes required more than three sessions to cover the material. School 2 had 1 hour of PSHE per fortnight, so delivery was possible over three lessons but over a longer period of time than in School 1. In both schools PSHE was taught by form tutors in mixed-ability teaching groups.
Questionnaires were administered before and immediately after the delivery of Operation Smoke Storm to gather data on students’ smoking behaviour and susceptibility (a composite measure assessing likelihood of smoking soon or if offered a cigarette by a friend, defined in full in Chapter 5) and their impressions of the intervention (see Appendix 3). Eight focus groups with 79 students in total were then carried out (two groups of boys and two groups of girls in each school) to explore views on the effectiveness and acceptability of the intervention and to suggest any necessary improvements. Using examples of existing resources to facilitate discussion, students’ views on the design of a booster component for use in Year 8, and a family component to engage their parents, were also sought. In-depth interviews with 18 teachers who delivered the intervention and the Head of PSHE at each school were conducted to elicit their views of the effectiveness and acceptability of the intervention, covering aspects such as how easy it was to take the package and deliver it as an ‘off-the-shelf’ resource, and whether or not it fitted in with timetabling and the existing curriculum (see Chapter 3).
Based on the qualitative feedback from students and teachers gathered in phase 1, the Operation Smoke Storm lessons and resources were refined, and booster and family components were developed. The booster component consisted of a flexible, ‘off-the-shelf’, lesson for teachers to deliver in PSHE lessons during Year 8. The family component consisted of an interactive take-home booklet to complement the Year 7 lessons. The take-home booklet was piloted with two external public research groups, the National Children’s Bureau’s (NCB’s) group of Young Research Advisors and the Nottingham Smokers’ Panel, which resulted in further refinements (see Chapter 4 for further details on the development of the booster and family components and a full description of these resources).
In phase 2, the same students who had received Operation Smoke Storm when they were in Year 7 received the booster intervention when they were in Year 8 (n = 538). In one school, students were taught in PSHE teaching groups streamed according to ability. Two of the teachers delivering the intervention were specialists in teaching PSHE; the remainder had other subject specialisms. In the second school, students were also taught in streamed groups, but by specialist science teachers during science lessons. Students again completed a questionnaire to gather data on smoking behaviour and susceptibility (see Appendix 3). The primary quantitative analysis compared the combined prevalence of ever smoking and susceptibility to smoking in Year 8 in students who received the intervention with the prevalence and susceptibility in students from local schools who did not receive the intervention but who were asked identical questions in a separate study (see Chapter 5 for a more detailed description of this quantitative analysis). A composite outcome measure was used, because, at this age, relatively few children have actually experimented with tobacco, and very few are established, regular smokers. The composite measure allowed identification of those students who were most likely to go on to smoke, plus those who became smokers between the baseline and follow-up data collection, as well as afforded benefits in terms of study power. Qualitative work in phase 2 comprised four focus groups in each school with 51 Year 8 students in total, and interviews with seven Year 8 teachers, to assess the effectiveness, appropriateness and acceptability of the booster component.
At the same time, the refined version of Operation Smoke Storm was delivered to a new cohort of Year 7 students (n = 350) in School 1 only; students also received the new take-home family booklet. Changes to the PSHE curriculum at School 2 meant that it was not able to accommodate delivery of the Year 7 resource. Questionnaires were again completed to gather quantitative data (see Appendix 3). Qualitative work comprised two focus groups with 16 Year 7 students in total, nine in-depth interviews with 10 Year 7 teachers, and nine paired student–parent in-depth interviews to assess the reach, acceptability and perceived impact of the revised Operation Smoke Storm and family component, and to identify any aspects that could be improved (see Chapter 6).
Progression to a cluster-randomised trial
At the end of phase 2 an independent DMEC considered all the available evidence on the potential effectiveness of Operation Smoke Storm, the acceptability of the intervention, and the ability to deliver a full trial, and made a recommendation to the Study Steering Committee and NIHR on whether or not progression to a fully powered cluster RCT was warranted. This evidence, discussed in more detail in the following chapters, suggested that, although the intervention was, on the whole, acceptable to students, parents and teachers, there was no proof that it was effective in preventing smoking uptake. There was also evidence that it would be extremely difficult to successfully complete a trial in this setting. Therefore, the DMEC’s recommendation, agreed with by the Study Steering Committee, was to not progress to a cluster RCT.
A full cost-effectiveness analysis was planned as part of a definitive trial of Operation Smoke Storm, but, given the lack of quantitative evidence indicating potential effectiveness, and the resulting recommendation of the DMEC not to progress to a full trial, a cost-effectiveness analysis was no longer possible. Instead, Chapter 7 describes the costs incurred in developing and delivering the intervention. This chapter also uses questionnaire data collected from students to assess the feasibility of gathering data in a school setting for a health economic evaluation of health-promotion interventions and uses these data to estimate the health-care costs associated with smoking in the study population and to quantify the state of students’ health.
Ethics approval
This project was reviewed and approved by the University of Nottingham Medical School Research Ethics Committee (reference C13122012 CHS EPH Smoking), which is compliant with the Economic and Social Research Council’s Research Ethics Framework,52 to ensure that the work was conducted in accordance with the highest standards of ethics.
Public involvement
Feedback was elicited from qualitative research with teachers, students and parents to help further develop and refine the intervention. Two other pathways to enable relevant lay people to contribute to the research were also employed. The University of Nottingham Smokers’ Panel, comprising active and former adult smokers from the local area, meets every 6 months to discuss tobacco control research and policy. One of these panel meetings, in June 2014, was devoted to discussing the research. A session was also run with the NCB’s group of Young Research Advisors to explore their views on the new intervention components. More detailed discussion of these aspects of public involvement is included in Chapter 4.
Management of competing interests
Kick It’s expertise in designing multimedia resources and bringing them to fruition was invaluable as we sought to develop the proposed booster intervention and materials for use with parents. However, Kick It had no involvement in the recruitment of schools, the delivery of the intervention, the data collection and analysis or the interpretation of results. Nor did it play any part in the preparation of academic papers for publication or in the preparation of this report.
Chapter 3 Initial delivery and evaluation of Operation Smoke Storm
This chapter reports the qualitative methods and findings from phase 1 of the project, namely students’ and teachers’ views on the initial delivery of the existing Operation Smoke Storm and how to extend this further to include a family and booster component.
Methods
Study design and participant recruitment
Focus groups with students in Year 7 and interviews with teachers were used to explore the acceptability and effectiveness of Operation Smoke Storm and to provide feedback to inform refinements and extensions. Separate focus groups for boys and girls were planned, as research suggests that smoking has become increasingly gendered, with the UK having one of the most pronounced gender differences in regular smoking behaviour in Europe (with girls having the higher prevalence). 53 Qualitative research with 15- and 16-year-old smokers in Scotland concluded that differences in smoking behaviours and attitudes according to gender could be attributed to individuals’ social worlds and relationships, interests, meanings attached to smoking and the role smoking had in dealing with the everyday experiences of being a girl or boy in her or his teens. 54 Therefore, gender-specific groups were used both to encourage honest discussion and to allow us to explore any potential differences according to gender. We aimed to run four focus groups in each school, two for each gender, with between 8 and 12 students in each, in line with recommendations for focus group size. 55,56 We also attempted to recruit all of the teachers who delivered the package in each school and the two PSHE teaching leads. However, recruitment remained flexible with the option to cease if recruitment targets proved difficult to meet but data saturation had been reached.
Parents of all Year 7 students in the two schools were sent a letter by the research team notifying them about the Operation Smoke Storm sessions and the associated evaluation. Parents were asked to return an opt-out slip if they did not wish their child to complete a questionnaire or participate in a focus group. Teachers explained the purpose of the focus groups to students after the first Operation Smoke Storm session. Those who wished to take part provided their name, gender and class on a piece of paper to the teacher. Students were told that up to 12 participants would be selected at random if more people volunteered than were needed. This sampling technique ensured that adequate numbers would be interviewed even if some individuals chose to withdraw or failed to attend, and would help individuals to feel sufficiently comfortable to contribute equally. In School 1 the research team randomly selected students from a list of volunteers’ names provided by the Head of PSHE; students from School 2 were randomly selected by the PSHE teaching lead.
All teachers who delivered Operation Smoke Storm, and the PSHE teaching lead from each school, were invited via e-mail to take part in a one-to-one semistructured interview (face to face or via telephone) after they had delivered all their sessions, with repeat invitations sent as necessary.
Focus group and interview procedures
Semistructured focus group guides (for students) and interview guides (for teachers) were developed to explore the acceptability and perceived effectiveness of Operation Smoke Storm (see Appendix 4). Given the limited time available for the focus groups and interviews, our choice of topics was driven by a need to gather responses to key questions in order to inform the refinement of the Year 7 sessions and development of the booster and family components. Focus groups considered students’ views of the Operation Smoke Storm sessions and their awareness of, and attitudes towards, the tobacco industry. Students’ were asked for their opinions on what a booster component and family component might look like and what they would be likely to enjoy and engage with the most. Examples of existing resources were used to stimulate discussions around these topics. As a potential booster activity, students were asked to consider the acceptability and potential effectiveness of playing a game (either paper-based, such as a board game, or an electronic game on a computer, tablet or mobile telephone) or producing their own short film, with the example of Cut Films57 being shown to students in their focus groups. The acceptability and potential effectiveness of printed materials and online resources were also discussed.
Interviews with teachers focused on the design, suitability and usability of Operation Smoke Storm, the extent to which it was an ‘off-the-shelf’ resource, how well delivery integrated with the school’s existing timetable and curriculum, and their suggestions and preferences for the content and format of the booster and family components. The interview guide for the PSHE teaching leads also sought information about how smoking education was usually taught in the school.
Before the start of the focus groups and interviews, it was explained to participants that their responses would not identify them and would be confidential, and that they had the right to withdraw at any point if they wished to. Following this, written informed consent was obtained. Focus groups took place in the schools, during school time. They were facilitated by JT or AT, supported by MB, LS or LJ, and lasted 35 minutes on average (range 27–50 minutes). Face-to-face interviews took place at the respective schools (conducted by JT or AT), and telephone interviews were conducted from a private room (by AT), at a time that was convenient for teachers. Interviews lasted 34 minutes on average (range 24–50 minutes). The focus groups and interviews were digitally audio-recorded to aid transcription.
Data analysis
Qualitative data were approached using a realist paradigm. As such, data were viewed as telling us about, in a fairly straightforward way, what the participants thought about Operation Smoke Storm, which subsequently helped to inform the development of the resource. Given that this was the first time that Operation Smoke Storm had been evaluated, this approach was deemed appropriate. An external specialist transcription company transcribed the digital audio recordings generated from the student focus groups and teachers’ interviews clean verbatim. Transcripts were then checked for accuracy (by JT and AT) and any personal identifiers were removed. Each was assigned a unique code that identified the school (1 or 2) and focus group (male or female) or teacher number. These data were analysed using the framework approach58,59 to examine emergent themes. To aid familiarisation, data from the first four focus groups and four teacher interviews were initially read several times by JT, AT and MB who independently summarised these data [using Microsoft Excel® 2010 (Microsoft Corporation, Redmond, WA, USA)] and identified initial codes, themes and subthemes. This stage also allowed the researchers to identify any contradictory cases or any within- or between-group differences (according to school and gender). As the codes identified from both the focus groups and teacher interviews were similar (apart from an additional teacher theme about preparation to deliver the resource), data were analysed together. Initial codes, themes and subthemes were discussed between the researchers in order to reach consensus on an initial analytical framework. This framework was then applied and refined following analysis of the remaining transcripts by JT and AT. JT and AT met at regular intervals to discuss their respective coding decisions and continued to refine the framework as required. Data were then indexed according to the final framework using NVivo (QSR International, Warrington, UK) version 10 software and the transcripts were charted into matrices according to each theme to facilitate synthesis and interpretation. These charts were rich in terms of detailing the data that we had, which enabled us to map, interpret and report findings in a succinct manner. Data presented reflect the overall views of the participants from both schools and extracts from the transcripts are included to illustrate the main findings.
Results
We conducted eight focus groups in total (four at each school) with 79 students (39 males, 40 females), an average of 10 students per group (range 8–11 students). Of the 23 eligible teachers and PSHE leads, 20 were interviewed (18 face to face and two by telephone). Three teachers (all from School 2) declined to take part owing to time constraints.
Four core themes were generated from the data: (1) teachers’ preparedness and delivery of Operation Smoke Storm; (2) raised awareness; (3) students’ engagement with Operation Smoke Storm; and (4) options for developing Operation Smoke Storm.
Teachers’ preparedness and delivery of Operation Smoke Storm
Teachers from both schools indicated that they had attempted to address smoking during Year 7 PSHE classes, typically focusing on smoking-related harms and strategies to resist pressure from peers to try smoking. Teachers from School 2 also covered how celebrities and role models can influence smoking uptake by young people.
Yes we do, and how, exactly, bringing up what they might see on soaps or in films, and how that’s not really something to be led by. We talk about that, yeah.
School 2, Teacher 1
Operation Smoke Storm replaced what the schools would have otherwise delivered around smoking. Most teachers reported having had no prior training or experience in teaching students about smoking. Thus, a number felt that the introductory training session about the resource increased their confidence in delivering the sessions.
The initial session [training session], yeah. I think that was definitely useful in terms of setting it up. It would have been quite difficult in my opinion otherwise, if we didn’t know the concept and the ideas behind it. I think that helped in terms of delivering it.
School 1, Teacher 5
Generally, teachers found the fact that Operation Smoke Storm was an ‘off-the-shelf’ resource highly beneficial, as it meant that background knowledge about the topic or lengthy preparation time was not required.
I think in respect that everything was just there for you, you didn’t really need a huge amount of knowledge yourself beforehand because there were the videos and the resources just meant that that was already structured.
School 1, Teacher 7
I think it was brilliant. The pack that I received is excellent. Everything was so easy to plan out. It was fantastic.
School 2, Teacher 2
However, the amount of preparatory work teachers undertook varied. Although many teachers felt confident to deliver Operation Smoke Storm with minimal preparation, others reported spending more time doing their own research around the topic.
I felt like I had to do a bit of research on my own, which wasn’t ideal, but if we had an information pack or something that said to us these are the kinds of things you’re going to come across.
School 1, Teacher 2
As well as feeling the need for more background information about the topic, some teachers reported wanting more guidance on steering discussions. In addition, although many teachers felt able to address students’ concerns about family members who were smokers, others suggested that the resource should have come with specific guidance on how to advise and support young people, especially when they were worried or upset about issues raised by the sessions.
It did upset a few of my form whose parents heavily smoke. I think it upset them, so maybe more, what’s the word, like help with knowing how the kids are going to react.
School 1, Teacher 9
In School 1, teachers struggled to complete all the set tasks because they had 10 minutes fewer than the recommended 50 minutes for each session. Subsequently, many admitted that they spent less time on some of the discussions; they felt that more time devoted to this would have helped to consolidate students’ learning.
Some of the discussions we cut down quite a lot . . . it would have been lovely to have had more time.
School 1, Teacher 4
Sometimes it might have been nice to have a little bit more discussion with the children and I felt like I was moving them on quite quickly.
School, 2, Teacher 4
Teachers were concerned about not being able to navigate through the resource so that they could deliver material according to the needs of their class and the length of their lessons.
There needs to be a bit more of, a teacher can override what is happening . . . so that it can suit the class.
School 1, Teacher 7
Not being able to skip particular sections or revisit areas if a recap was needed was a particular issue reported by some teachers.
The main thing would be a back button, without a shadow of a doubt.
School 2, Teacher 3
Just making it a bit more useable with being able to skip ahead, and if there was a menu or something like that, that would be perfect because then you could just, if that one’s optional choose to go onto the next one and continue from that point.
School 1, Teacher 15
One teacher suggested that having guidance on how to split the sessions to cater for different lesson lengths would be helpful. Another wondered if it would be possible to combine the three sessions into one file to aid flexibility and ease of navigation.
I think it would have been easier if you’d told us how to split it up into a 40-minute lesson rather than say this is session one, just stop where it ends kind of thing.
School 1, Teacher 13
Some teachers felt that they needed to be able to stop the countdown timer and move on if their students had answered the question within the allotted time.
So the timer ticking down was an issue when they knew the answer and having to wait; you want to be able to control that yourself.
School 1, Teacher 3
In addition, teachers found that not being able to view other websites on their computers while Operation Smoke Storm was running, without having to shut down and restart the programme, was frustrating.
Raised awareness
Many students mentioned that they had some existing knowledge about smoking from sessions in primary school, but that Operation Smoke Storm provided insight into the extent of the harms of smoking and the huge array of chemicals in cigarettes, which seemed to make some of them appreciate the associated dangers more.
Back at primary school I did about three lessons on it, but when we did this it gave a lot more detail showing you what not to do and what was in it, so we can see how dangerous it was.
School 1, Male
A lot of students were shocked and surprised by the information and many went on to state that smoking was worse than they had previously thought.
I learnt that it’s actually more harmful than people think . . . it’s got loads of different poisons and stuff that we would never expect to be in it.
School 1, Female
Subsequently, students expressed that this knowledge had strengthened their desire to remain smoke-free.
I didn’t want to smoke to start with . . . but now I know I definitely, definitely don’t want to smoke.
School 2, Female
However, a few students suggested that introducing the topic of smoking to those who had not given it any thought previously might make some curious about trying it.
In a way I don’t think it’s that clever because kids are going to go home and talk to their parents about cigarettes, and because they know about it they might want to try it and it could encourage them.
School 1, Male
Although students seemed to learn the most about the ingredients found in cigarettes and the health effects of tobacco, a few students did report having learnt new information about the tobacco industry. In particular, these students felt that the tobacco industry is motivated by profit, that it lacks concern for people’s health and that it targets young people to maintain its customer base.
They only do it just to make money; they don’t really care if people die.
School 1, Female
I’ve learnt that they try and make different kind of flavoured cigarettes to get different people, like they made, they tried testing chocolate flavoured cigarettes to get like young kids to smoke.
School 2, Female
Students’ engagement with Operation Smoke Storm
Most students reported that they enjoyed the Operation Smoke Storm sessions. Students found appeal in the interactive nature of the resource and in the fact that it was novel compared with their usual PSHE lessons.
It was mostly different to another PSHE lesson because mostly you would do group work . . . and learn lots of new things. So it would probably be better than another one.
School 2, Male
Generally, teachers agreed that the format involved students, which helped to keep them engaged.
I liked how it was more on them [the students]; it wasn’t me at the front just talking to them. It was them watching stuff and then answering questions about it. So it really got them involved.
School 2, Teacher 5
Furthermore, some teachers appreciated the fact that Operation Smoke Storm was taking a novel approach to education about smoking which was different from the usual the anti-smoking messages.
It wasn’t just ramming down the kids’ throats that they shouldn’t smoke, it was so much more to it than that and I think that was really good for them.
School 1, Teacher 7
For the most part, students bought into the secret agent theme, which served to keep them motivated and focused throughout the sessions.
It was really amazing because it felt like you were actually a secret agent; like you were actually there . . . it makes you involved with it so that you don’t get bored of it.
School 1, Male
However, many of the students found the female spy handler character annoying and distracting.
There was this woman after everything who kept on saying weird things that gets right on your nerves.
School 2, Male
The variety of activities seemed to further contribute to maintaining students’ engagement.
They were doing something different each week. They did seem quite excited to be doing it.
School 1, Teacher 6
Students enjoyed sharing ideas in group work and the freedom to create a presentation in the style of their choice.
You can use your imagination to create it [presentation] and make it what you want to make it.
School 2, Male
However, some teachers felt that having to split the class into four groups for the presentation resulted in too many students per group.
The final activity of session 2 required students to recall facts learnt in session 1 and earlier in session 2 which they would need as the basis for their presentations. Both teachers and students reported that this recall was difficult, especially when the lessons were more spread out. Teachers thought that incorporating a plenary session or providing students with an answer sheet to which they could refer if they needed help remembering certain facts or scoring their answers would be helpful.
The facts flashed up and then left, and flashed up and then left, but you needed like a review or some kind of plenary or something that had it all written down.
School 1, Teacher 2
In the main, teachers reported that the resource catered well for students of different academic abilities, particularly because it allowed for group work in which higher- and lower-ability students could be mixed. However, there were a couple of instances in which teachers felt that some differentiation in the activities could be beneficial to assist less able learners.
I’ve got a couple of kids in my class who are dyspraxic and dyslexic, because there’s not a lot of reading it was really good for them, they liked the tick box stuff, but then when we got to this section of ‘remember all this information and now create your own’, they found that more difficult because they hadn’t retained the information as well.
School 1, Teacher 1
There were mixed feelings about the appropriateness of a swear word within a quotation cited in the resource: ‘We don’t smoke that shit we just sell it. We reserve the right to smoke for the young, the poor, the black and the stupid.’ Several students thought that the language was inappropriate, and some teachers reported that it disrupted the class considerably. Although teachers felt that not all students had appreciated the meaning of the quotation, others reported that it had had an impact.
They didn’t like the [Chief Executive Officer] CEO quote, the one about the poor, black . . . they really hated that; that really got under their skin.
School 1, Teacher 4
The teachers felt that some of the language and concepts were at too high a level for the age group being targeted, such as references to smoking potentially causing impotence and affecting menstruation. Some students did not understand these terms, and teachers felt that having to take time to explain them disrupted the flow of the lesson.
I didn’t have time to go into what impotence was, so it was a bit like, ‘OK, so we’re going to move on very quickly from that point’, and then they get a bit confused.
School 1, Teacher 1
Options for developing Operation Smoke Storm
Both students and teachers were receptive to the idea of a booster session, delivered 1 year after the initial sessions when students are in Year 8 (aged 12–13 years), to reinforce their learning about how the tobacco industry targets young people. In general, teachers felt that a classroom-based session would probably be more successful than asking students to complete a homework activity.
I don’t think the engagement would be as good with home-based learning as within a classroom.
School 1, Teacher 4
They felt that it would be necessary for the booster to begin with a reminder of Operation Smoke Storm but that the secret agent theme would be too juvenile for a Year 8 student.
I don’t think that [secret agent undercover] would fly again. It would maybe have to be something a little bit different.
School 1, Teacher 10
Students were enthusiastic about the idea of the booster activity involving playing an electronic game or making a short film. Some felt that an anti-smoking message delivered by peers of their own age in a short film would be effective.
I think it will encourage other people who are watching it to not smoke because they’ll know that other people around their age are saying it and they’ll be persuaded more to not do it.
School 1, Male
Teachers also endorsed these ideas, but felt that in practical terms they would be challenging to deliver in school. For instance, it was suggested that access to equipment (such as video recorders) and computer room space is often limited.
They’re not allowed to bring mobile phones into school so they wouldn’t do it on their own phones. PSHE . . . doesn’t have tablets and . . . getting in the computer room is a bit of a nightmare.
School 1, Teacher 7
However, a teacher-led game was considered feasible with students playing in groups to answer questions and score points, with breaks for discussion. Teachers did not believe that engagement with an electronic game played at home would be optimal, partly because not all students have a mobile phone or tablet. As well as having limited access to film-making equipment, students also expressed concern that some people might post films on the internet in which they appeared but that some parents might not be happy with this.
But then some people’s mums and dads might not allow them to go on the internet and post it, because of their face.
School 1, Male
Teachers also felt that film-making in groups may be largely driven by some students only, and getting students together out of school would be as difficult as a homework activity.
Especially around here where the catchment areas are so spread out, then sometimes they do start struggling to get together to do group activities.
School 1, Teacher 12
Irrespective of the content of a booster session, teachers recommended that a teacher-led ‘off-the-shelf’ resource similar to the existing Operation Smoke Storm resource should be developed.
PSHE – because you’ve got non-specialists, if you say ‘go away and plan something’, it’s additional work for someone who it’s not their subject, so I think they would prefer something sorted for them.
School 1, Teacher 14
Another idea suggested by teachers was students working together on a research task to create something to teach younger children about smoking. However, this would require some guidance on structure and perhaps examples, such as existing anti-smoking adverts.
Students and teachers were also asked to consider ways in which to engage families in discussions about smoking. In particular, participants were asked to consider the idea of a take-home booklet containing information about the anti-smoking message and tobacco industry tactics, in line with the material delivered in class, containing activities that parents and guardians could complete with their child. In principle, students were in favour of a booklet, but opinion was divided in terms of whether their parents would actually read it or have time to complete the activities with them.
Also some people’s parents work a lot, because my mum’s a nurse so she works nights, and it would be quite hard for me to get her to fill it out if she was working.
School 2, Female
Teachers believed that involving parents and guardians in students’ learning would be beneficial but recognised the difficulties of engaging parents in school activities. They were generally in favour of a take-home booklet, as long as it was worded so as not to alienate or offend any parents who smoked.
The students don’t always . . . speak to their parents about what they’ve done in the school, so that’s a physical reminder of what they’ve done and there’s more opportunity for parents to engage.
School 1, Teacher 5
Summary
The qualitative data described above demonstrate that Operation Smoke Storm is generally acceptable to Year 7 students and teachers, can be delivered by teachers with relative ease, and appears to raise awareness about tobacco-related issues.
However, based on student and teacher feedback, a number of changes were subsequently made to the Operation Smoke Storm lessons to improve their flexibility and ease of use. Broadly, these revisions sought to provide teachers with additional background information about the topic as well as guidance on how to steer discussions, especially in situations in which students were worried or upset. Revisions also sought to make the resource more versatile to enable use in lessons of differing lengths and with students of different academic abilities. Lesson objectives were made more obvious and some of the language contained within the resource was revised. For further description of the changes made, see Chapter 4.
In order to ensure optimal engagement with a booster component, teachers felt strongly that this should be classroom-based rather than a homework activity and pitched at a level appropriate to the Year 8 students. In line with the Year 7 Operation Smoke Storm lessons, the preference of most teachers was that the resource should be designed to be ‘off-the-shelf’, incorporating lesson plans, timings, background information and learning outcomes. The development of the booster session is described in more detail in Chapter 4.
In the absence of any feasible alternatives being suggested by teachers, a take-home booklet to accompany Operation Smoke Storm was considered to be the best option to engage families in the anti-smoking message. Although teachers highlighted that schools do struggle with parent engagement and that, as such, complete uptake could not be guaranteed, the qualitative work suggested that most students would take a booklet home and that parents would find it interesting. The development of this booklet is described in more detail in Chapter 4.
A summary of the findings from phase 1 of the research was sent to the Head of PSHE at each school for distribution to the teachers who had participated in the research (see Appendix 5).
Chapter 4 Revisions to Operation Smoke Storm and development of booster and family components
From the qualitative feedback from students and teachers in phase 1 of the project, a number of suggested changes to the Year 7 Operation Smoke Storm lessons, and ideas for the booster and family components, were identified. Here we describe the changes that were made and the booster and family components that were developed. This work was carried out in collaboration with Kick It, who developed the original version of Operation Smoke Storm and who will distribute and support the delivery of the revised and extended intervention package beyond the end of the project. Also involved were additional collaborators specialising in graphic and flash design, video production and the design of educational resources (all of whom had been involved in the development of the original Operation Smoke Storm resource). Changes and developments were made through iterative discussions between all parties, taking into consideration what was feasible within the timeframe and budget; this meant that it was not possible to implement all suggested changes and ideas.
Feedback was sought from two independent public groups (the NCB’s Young Research Advisors and the Nottingham Smokers’ Panel) on the appropriateness of exploring tobacco industry marketing strategies in the booster component and the design of an early version of the take-home family booklet. This feedback is described in the second part of this chapter.
Changes made to Year 7 lessons
Resource flexibility
The overall impression from teachers was that more flexibility in the delivery of the resource was needed, primarily to accommodate different lesson lengths and needs of a class. In particular, some teachers felt that they needed to find more time to allow the student groups to discuss their opinions and to prepare properly for their presentations. To increase flexibility, a menu bar, back button and the ability to stop the countdown timer were added to allow swifter navigation and to enable the teacher to skip to sections of priority if they were not able to deliver the whole content in the time available.
Guiding students
Learning objectives were added in audio format at the beginning of each session and the accompanying teacher notes were modified to remind teachers to highlight these. Teachers were provided with written answers to all questions to which they could refer if students could not remember answers. In line with requests from teachers, an initial page was inserted in the teacher booklet providing background information about smoking and setting the scene for teachers about the importance of preventing youth smoking uptake. An overview of Operation Smoke Storm was also provided, as well as information on how to use the new navigation menu bar and suggested timings for shorter lessons. Also included in the teacher booklet was advice on the questions that students might ask and how they could respond if students got upset or were worried by any of the resource content.
Teachers had suggested that students needed more guidance on the group presentation that was prepared and delivered in the final session. The student handbook was amended to make it clear that the content of the presentation was more important than the format of delivery, and that the content should be based on their learning from Operation Smoke Storm. The score sheet students used to mark each other’s presentations was amended to match the assessment criteria, with the following specific question being added: ‘How well do you think the group’s presentation will convince people of your age not to start smoking?’.
Enhancing student engagement
After much deliberation the decision was taken to overdub the expletive (‘shit’) with the word ‘rubbish’ and similarly to replace it in the student handbook (in quotation marks to signify that this was a substitute for the original word). It was too costly to remove words such as ‘impotence’ and ‘menstruation’ from the video recordings, although the activities in the student workbooks were changed so that the students were not required to recall this information.
For a full description of the final Year 7 lessons, see Appendix 2.
Development of the booster component
A number of considerations were taken into account in the process of designing and developing a booster session for use with Year 8 students 1 year after they had received the original Operation Smoke Storm intervention.
To ensure optimal engagement, the booster component was designed as a classroom-based session, suitable for use ‘off-the-shelf’, with a clear lesson plan and learning outcomes. Despite being endorsed by students and teachers, it was felt that an individual electronic game or making a film in small groups could not be delivered in school owing to equipment constraints. Although teacher-led games were considered, it was felt that these would be costly to produce and might not engage enough students simultaneously or serve the purpose of providing the important educational content needed.
Kick It and the research team were keen to build on the main premise of Operation Smoke Storm, namely educating young people about the ways in which the tobacco industry operates, especially the methods it uses to target young people as its future customers. There was some concern that the secret agent theme would be too juvenile for Year 8 students. However, continuing the Operation Smoke Storm narrative in an age-appropriate form was considered to be a useful way to link the booster to the Year 7 resource which, it was hoped, would prompt students to remember their earlier learning.
After much discussion it was felt that one classroom session would be sufficient to cover the intended material adequately while not placing too high a demand on schools’ time. Care was taken to ensure that the resource developed was as sustainable as possible, particularly given the rapidly changing tobacco control environment.
Description of the final booster session
The booster component was designed to create classroom discussion and debate about tobacco industry practices that may be targeting young people. Specifically, it focuses on tobacco marketing strategies from the perspectives of a tobacco industry executive and marketing company, as well as a health campaigner, seen through the eyes of a teenager and reported directly to camera in the form of a social media blog.
The session begins with a video recap of the Year 7 Operation Smoke Storm lessons to remind students of what they did the previous year and to orientate teachers who had not delivered the Year 7 lessons.
This is followed by an introduction to a new character, Kiara, who explains on her online blog that she is going on work experience with a marketing company. The storyline follows Kiara into an encounter with a tobacco industry executive in a meeting in which she is asked to sit in. In this meeting the tobacco industry executive discusses with the marketing company ways in which they might improve the company’s public image. This meeting prompts Kiara to investigate more about tobacco and the way it is advertised to young people, including speaking to a health campaigner to find out his perspective.
Students are asked a series of questions relating to the tobacco industry at key moments in the storyline. They are prompted to write their answers in an individual workbook and then to discuss their views with the rest of the class.
There are also two further activities, which teachers can choose to complete if they have sufficient time. The first asks students to write a slogan for a billboard poster, advertising a fake cigarette brand, targeting young people. The purpose of the activity is for students to consider how tobacco companies may portray smoking to young people and raise their awareness of being targeted.
The second activity asks students to write a Tweet (Twitter, Inc., San Francisco, CA, USA; www.twitter.com) about the tobacco industry, sharing their opinion with peers. The aim of this activity is for students to consider what they have learnt about the tobacco industry and their personal thoughts and feelings about this.
For a full description of the booster session see Appendix 2.
Development of the family component
As discussed in Chapter 3, there was general agreement that a take-home booklet to accompany the Year 7 Operation Smoke Storm lessons would be the best method to engage the largest number of parents in discussing the anti-smoking message with their children. Teachers highlighted that parental engagement is already difficult in schools and that they felt that parental participation should not be compulsory and should be worded sensitively; this would also serve to avoid any offence being taken by parents who were smokers themselves. There was consensus that the booklet should not be so long that busy parents would be put off reading it.
Description of the final family component
The final booklet comprised 10 pages designed to stimulate discussions about smoking between parents and students at home. The booklet contains a series of informative and interactive activities, each of which covers a different smoking-related issue pertinent to young people. The booklet is intended to be given to students after their first Operation Smoke Storm lesson in Year 7 for them to take home and share with their parents. An introductory page acts as a reminder for the students of their mission as a secret agent, as well as an overview of Operation Smoke Storm for parents.
The first activity, Involve Your Family, is a repeat of quiz questions that students completed in class, ascertaining knowledge about areas such as the chemicals in cigarettes and the health effects of smoking. Students are encouraged to ask their family members to answer the questions to ascertain their level of knowledge and the subsequent level of seniority at which they might be recruited to a job in a tobacco company.
The second activity, Know the Industry, contains new information about the marketing practices that the tobacco industry has employed in the past and at present. The activity prompts students to think about how they might be targeted by the tobacco industry, to consider their feelings and to consider their families’ feelings about it.
The third activity, Supporting Others, asks students to give advice to other young people in various scenarios relating to smoking in which they might find themselves. It encourages students to discuss with parents or friends what they might say in these situations. Signposts to cessation support services were also included in the booklet.
A prototype of the family booklet was reviewed by two public groups (see Public and patient involvement) and their feedback was taken into account when finalising the resource. For a full description of the family booklet, see Appendix 2.
Public and patient involvement
The involvement of users was a crucial element of this project. In addition to the qualitative research with students, teachers and parents to inform the development and refinement of Operation Smoke Storm, two public groups were used to enable relevant lay people to contribute to the research.
National Children’s Bureau
The NCB is a charity that aims to improve the lives of children and young people. 60 As part of its work the NCB runs a Young Research Advisors group, a group of 12- to 21-year-old young people who consult and collaborate on research projects relevant to children and young people. Members of the research team (AT and LS) led a meeting of 17 Young Research Advisors (aged 12–18 years) in June 2014. The aim of this meeting was twofold: to gain an insight into young people’s perceptions and levels of understanding of tobacco marketing in order to inform the level of detail to include in the booster and family intervention components, and to gather young people’s opinions on the acceptability of the family booklet to inform the refinement of the resource before piloting it in schools.
In the warm-up activity, each Young Research Advisor introduced themselves and was asked to give one reason why a young person might try a cigarette to encourage their thinking about the issues surrounding smoking. They were then split into three groups, facilitated by either AT, LS or a member of NCB staff, for the two main activities.
Activity 1
In the first activity, each group was presented with a set of images associated with the marketing of tobacco to young people, including images of cigarette packages, screenshots from social media and pictures of celebrities smoking in films and music videos. Participants were given 20 minutes to discuss what they could see, how they felt about the images and what influence they might have on young people. Each group then fed back their thoughts to the whole group and a short whole-group discussion took place. The aim of this activity was to explore young people’s abilities to understand how marketing may influence them and other young people to smoke; findings were used to inform the level of detail to include in the resources being developed.
Activity 2
The researchers (AT and LS) then introduced the Young Research Advisors to Operation Smoke Storm and gave an overview of the research project, describing in particular the family booklet being developed. In their groups, the Young Research Advisors were presented with a mock-up of the booklet and given 20 minutes to discuss their thoughts on the resource and how it could be improved. In particular, participants were asked to focus on the following five criteria: (1) how it looks, (2) would you be happy to complete this with your parent/caregiver?, (3) are the instructions clear?, (4) layout and (5) is it pitched correctly for 11- to 12-year-old children? Each group then fed back to the whole group and, again, a short whole-group discussion took place.
Nottingham Smokers’ Panel
The Nottingham Smokers’ Panel is a volunteer group of adults who are either active or former smokers, recruited from the local area. This panel meets face to face every 6 months to discuss and give opinions on different aspects of the research being undertaken by the UK Centre for Tobacco and Alcohol Studies (UKCTAS). The first half of the June 2014 meeting was devoted to exploring issues around preventing the uptake of smoking in young people. The aims of the session were to receive feedback from the group about the proposed take-home family booklet and to ascertain levels of understanding of the ways in which tobacco is marketed.
The session comprised, first, asking each member of the group to recall the age at which he or she had started smoking, the circumstances in which they had started smoking and their feelings around this. JT then presented evidence to highlight the age of uptake of and susceptibility to smoking in England and the importance of trying to intervene prior to this to prevent smoking experimentation. The rationale for Operation Smoke Storm was outlined and the premise of the intervention was described briefly. The aims, methods and initial findings of the research project were then summarised. The group were then asked about any discussions they had had about smoking when they were at school (either through formal teaching or with parents and/or friends).
Panel members then completed the same two activities as the NCB Young Research Advisors. The findings from the two activities from the NCB and Nottingham Smokers’ Panel meetings are presented together below.
Public and patient involvement findings: images associated with the marketing of tobacco
Some of the Young Research Advisors identified the potential for a point-of-sale tobacco display to influence young people to try smoking. They felt that not seeing the packaging in shops would reduce the chances of someone being tempted to try a cigarette. In a similar vein, an adult from the Smokers’ Panel agreed that seeing cigarette packs in shops served as an encouragement to smoke.
By sometimes just not seeing it, you can’t think of it.
Young Research Advisor
I already quit smoking but when I see the cigarettes in the shops, I feel like ‘Oh I really would like to take one’, if I don’t see them then I don’t feel that so I think this is great.
Smokers’ Panel member
However, there was some disagreement about the effectiveness of point-of-sale displays bans. For instance, they were not thought to be effective for current smokers who had already established their favoured brands.
If I desired I could still go and get Marlboro. Even though it’s hidden, you can still go up and ask for it.
Young Research Advisor
Among both Young Research Advisors and Smokers’ Panel members there was a general consensus that smoking in television programmes and films had the potential to influence young people’s smoking perceptions and behaviours. Adults from the Smokers’ Panel recalled smoking on television in their youth being presented as glamorous and felt that role models who smoked had the potential to influence behaviour. Some young people felt that, in the examples provided, smoking was associated with glamour, wealth and beauty, which was deemed to be appealing, particularly to females. They also suggested that the images presented smoking as associated with success rather than with addiction.
I think it’s saying smoking makes you appealing and attractive.
Young Research Advisor
I think if you saw someone like her smoking, you might not initially, it might not be the centre of attention, but you do notice it. For young people, especially teenagers, they’re quite easily influenced and to see she looks very glamorous and it’s that whole glamorous lifestyle that can lead you smoking a cigarette like that.
Young Research Advisor
Many of the Young Research Advisors felt that young people would watch television programmes, such as soap operas, and may look up to or see the characters as normal people; if these people are seen to smoke, this may encourage beliefs that smoking is normal behaviour. Similarly, a number of Smokers’ Panel members thought that the cumulative effect of smoking on television and in the media publicises and normalises smoking for young people, especially if it is icons who are smoking. Thus, they argued that this should be completely banned or that viewers should be pre-warned about this content.
So putting a warning on front, ‘this film contains images of people smoking’.
Smokers’ Panel member
One of the Young Research Advisors also felt that the negative effects of smoking are not portrayed in television programmes.
You won’t see that character smoking and then have a horrific death . . . It’s not enough of a focus on the negative side.
Young Research Advisor
Young Research Advisors were unclear about where the responsibility and editorial decision-making lay in having characters smoking on screen. Some felt that it was the director’s choice, whereas others felt that tobacco companies would have an influence.
There was a consensus across the groups that a lot of young people see music stars as role models and idols and may be influenced by or may copy the behaviour that is portrayed in music videos.
I think there’s the issue with idolisation here as well, maybe more so than the soap characters. And again young people being influenced by these megastars, they kind of put them on pedestals.
Young Research Advisor
She looks relaxed as well, and that’s another bad image to be giving to people. It’s saying smoking helps you relax, if you’re stressed, smoke.
Young Research Advisor
Young Research Advisors were aware of the power of advertising and how easy it would be to promote cigarette brands through social media in order to reach many people. Some felt that if someone ‘liked’ a tobacco page on Facebook (Facebook, Inc., Menlo Park, CA, USA; www.facebook.com), then it may encourage their friends to do likewise and increase the chance of them trying that brand of cigarette. However, this was expected to be far more likely in the case of existing customers than young, non-smokers.
If you were to ‘like’ a page, you can see if your friends have ‘liked’ it. So if you see that all of your friends have ‘liked’ Lucky Strike [British American Tobacco p.l.c., London, UK] cigarettes, then you might want to ‘like’ Lucky Strike cigarettes . . . Or maybe that aspect in there as well, say a girl or boy you liked . . . ‘liked’ that page, you say ‘maybe if I started smoking they’d like me more.’ Teenagers do stupid things like that.
Young Research Advisor
Although some Young Research Advisors said that they personally would not be encouraged to smoke by seeing a tobacco brand on Facebook because they were aware of the dangers posed by smoking, they acknowledged that others may think differently and that it could be a catalyst to try a cigarette for those not strongly for or against smoking.
There’s a lot of kids out there who know that it’s bad but still do it. There are a lot of kids out there that don’t take notice, but don’t smoke. So this kind of page is the thing that will be influencing those non-smokers who aren’t really bothered if they do smoke or not. It could be the kind of thing that sways them.
Young Research Advisor
The Young Research Advisors and Smokers’ Panel members were shown a range of cigarette packets from around the world, including for cigarettes described as ‘slims’ and flavoured cigarettes. One packet for the brand Vogue (British American Tobacco p.l.c., London, UK) had a more slim-line shape than a traditional pack of 20 cigarettes; this was seen as glamorous by the Young Research Advisors, who thought that it looked more like perfume and viewed it as an attempt to associate cigarettes with products that make you more desirable rather than harm you. Adults from the Smokers’ Panel also felt that the branding on cigarette packets influenced them.
It’s trying to put itself in the same category as a perfume or lipstick and it’s something that makes you better almost.
Young Research Advisor
I smoked Dunhill ‘cause they looked good.
Smokers’ Panel member
The Young Research Advisors thought that text warning labels on cigarette packets were noticeable, but some thought they made them want to be rebellious and to try the product. Others felt that other elements of the packaging overrode the warning sign, or they were used to seeing the warning sign and so ignored it.
It doesn’t really make me feel anything because I’ve seen the health warnings so many times that no matter how big you write ‘smoking kills’, I’ve seen it so many times that I’m like, ‘OK then’.
Young Research Advisor
Young Research Advisors and Smokers’ Panel members were asked if the activity they had been asked to complete had raised their awareness of tobacco marketing strategies. Most agreed, and it was evident from the discussions that this was the first time that many of the Young Research Advisors had considered media such as film and television, packaging and celebrity role models as influences upon their or others’ decisions to smoke.
Public and patient involvement findings: views on the prototype family booklet
The Young Research Advisors mostly liked the theme of Operation Smoke Storm and the idea of the take-home family booklet.
I absolutely love the concept and if I was in Year 7; my brother’s in Year 7 and he’s doing this subject for PSHE and I’m sure he’d love to do it.
Young Research Advisor
I like the idea that it brings together the student, the teachers and the parents. So, you’ll have a few lessons in school but then you can go home and do some more. So it engages all of society, so it sort of educates the parents if they smoke as well.
Young Research Advisor
Opinions were mixed among the Smokers’ Panel in terms of how successful the booklet would be in discouraging the uptake of smoking. A number of panel members felt that it was a good idea and wished that when they were at school they had had more interaction with their parents around the harms of smoking. However, others felt that even having this knowledge would not make any difference at a young age.
They can educate you more but I don’t think they’re gonna stop you [from smoking].
Smokers’ Panel member
Both Young Research Advisors and Smokers’ Panel members raised some concerns about the design of the booklet, particularly with regard to the colour scheme, and although appreciating that the front cover was appropriate to the spy theme, one Smokers’ Panel member thought that it did not instantly signal the subject matter.
It’s the dark purple against the black, it’s just not good.
Smokers’ Panel member
If I wasn’t here I would probably think it’s something to do with war, tear gas, something, but I wouldn’t think cigarettes.
Smokers’ Panel member
Generally, the booklet was considered to be well laid out, although there were concerns that some pages contained too much text. Suggestions for improvement included removing some content and drawing more attention to interesting and thought-provoking information, such as quotations from the tobacco industry, and using a larger font and bullet points instead of large sections of text.
Many of the Young Research Advisors liked the content of the booklet. In particular, they felt that the quotations were shocking and helped to raise their awareness about being targeted, although not all realised that most of the quotations were from real tobacco industry executives. In addition, a Smokers’ Panel member thought that, as an 11-year-old’s thinking may be very black and white, it was important to make clear distinctions between the ‘pro’ and ‘anti’ sides of the smoking debate.
The guy in the middle page, the bad guy, Mr Big Tobacco, needs to be caricaturised if that makes sense, made to look evil and good guys need to be made to look good . . . bordering on superhero/supervillain, that type of thing.
Smokers’ Panel member
Both Young Research Advisors and Smokers’ Panel members thought that some of the language used in the booklet was too sophisticated and recommended using simpler, age-appropriate language.
There are some words that as an 11 year old I would not understand, like legislation and Royal College.
Young Research Advisor
It’s about the language, like saying ‘I will be a millionaire’, it’s not the same as saying, ‘have a lot of profits’. It’s like what they would find easier.
Smokers’ Panel member
The activities in the booklet were mostly considered to be interesting and engaging, and a Smokers’ Panel member felt that the interactive nature of the booklet would appeal to the age group and would stimulate further debate.
It’s good that they’ve got activities in there; it’s not just a load of stuff for them to read . . . they like to get involved because they like someone to hear what their opinion is.
Smokers’ Panel member
However, there were mixed opinions from the Young Research Advisors about whether or not students and parents would engage with the booklet. Some thought that students would not want to complete it, suggesting that students and parents do not consider PSHE lessons important. It was also noted that some parents would not be able to find the time to complete the booklet with their child even if they wanted to, and that some students would not want to work through the booklet with their parents. The Young Research Advisors also highlighted that parents who are smokers may feel victimised if they have to complete the booklet with their child, or, alternatively, their children, knowing that they smoke, may choose not to show them the booklet.
. . . maybe some children, if they know their mum smoked would think, ‘I’m not going to give this to my mum or dad because they already smoke.’ Maybe a Year 7 might think, ‘If they already smoke they must already know about this, they just don’t care.’
Young Research Advisor
Some adults in the Smokers’ Panel also highlighted that discussions around smoking would be more awkward if the parents themselves smoked. However, others felt that the booklet could serve as an opportunity for young people to educate their smoking parents and felt that the fact that some parents smoke should not be a reason to sanitise or avoid the message.
I was smoking and my daughter was coming back with loads of education and stuff and yeah, I did all that conversation, it’s awful, it’s the worst thing I ever did, so I think it’s difficult for kids with smoking parents.
Smokers’ Panel member
Offend them [smoking parents]. No point being nice about it, they can put it down if they want.
Smokers’ Panel member
Summary
The findings from the public and patient involvement (PPI) activities confirmed that young people were generally able to comprehend and appreciate the influence of tobacco industry marketing tactics on youth smoking behaviour. These findings supported the booster session being centred on this topic. Young Research Advisors and members of the Nottingham Smokers’ Panel generally approved of the concept of a take-home family booklet to stimulate discussion around smoking between parents and children. On the whole, they endorsed the proposed content, although some suggestions were given to make the booklet more engaging for this age group. As a result of the PPI involvement, refinements were made to the family booklet to improve the graphic design and to reduce the amount of text.
The revised Operation Smoke Storm resource, including the refined Year 7 lessons, family booklet and the Year 8 booster lesson, were then tested in schools. Quantitative evidence for the effectiveness of the intervention package is presented in Chapter 5 and qualitative feedback from teachers, students and parents on these three components is described in Chapter 6.
Chapter 5 Quantitative evidence of effectiveness
This chapter presents preliminary quantitative evidence for the effectiveness of Operation Smoke Storm, as well as descriptive quantitative data on students’ views of the intervention and attitudes towards smoking. Challenges encountered in collecting quantitative data for evaluation are also described. This evidence, in conjunction with qualitative data on the acceptability of the intervention package (see Chapter 6), was used to inform the decision of whether or not to progress to a fully powered cluster RCT.
Methods
The initial pilot of Operation Smoke Storm took place in two schools; all students in Year 7 and Year 8 received the intervention and, therefore, there were no internal controls against which to compare the effectiveness of Operation Smoke Storm in changing smoking behaviour. We considered the option of recruiting additional schools to act as controls, but, in order to minimise costs, a decision was taken to use external control data, collected as part of another study in which the same survey questions were administered.
Control population
The Nottingham School Smoking Survey collected data from students in Years 7–10 (aged 11–15 years) in spring 2011, 2012 and 2013 in several schools in Nottingham City and Nottinghamshire (although not all schools participated in every wave of data collection). The primary aim of this survey was to evaluate changes in young people’s smoking behaviour following the introduction of point-of-sale tobacco display legislation. 12,61 By mid-2013 data were available on current smoking and susceptibility to smoking in Year 7 and Year 8 for two successive cohorts of students (i.e. students who were in Year 7 in 2011 and Year 8 in 2012, and students who were in Year 7 in 2012 and Year 8 in 2013).
Changes to pre-planned analyses
Originally, we planned to use linked data to judge the potential effectiveness of Operation Smoke Storm by comparing the combined prevalence of ever smoking and susceptibility to smoking in Year 8 students in the two study schools, after students had received the booster session, with the combined prevalence of ever smoking and susceptibility to smoking in Year 8 students in schools that took part in the Nottingham School Smoking Survey, adjusting for smoking behaviour in Year 7 as well as for other relevant confounders. However, logistical problems, which became evident over the course of the follow-up period, meant that it was impossible to link Year 7 and Year 8 questionnaire data from all but a handful of study participants. In order to preserve students’ anonymity they were each given a cardboard folder containing questionnaires which were coded to enable linking (e.g. 1a, 1b, 1c to indicate the three responses for student 1). Students were asked to write their names only on their folder and not on the questionnaires, and the Head of PSHE at each school was asked to store the folders safely for the duration of the study period. However, at one school all folders were misplaced over the summer holiday period between Year 7 and Year 8 when building work necessitated the emptying of classrooms. At the other school, several PSHE teachers did not return their teaching group’s folders to the Head of PSHE for safekeeping. Given the very small number of questionnaires that could be linked, from one school only, the statistical power to model these linked data was severely limited. Therefore, with the agreement of the Study Steering Committee, this analysis was not pursued further. Instead, cross-sectional comparisons were pursued.
Statistical methods
All data management and analysis was carried out using Stata version 13 (StataCorp, College Station, TX, USA).
This study adopted a set of three questions which have been used previously to assess children’s susceptibility to smoking. 11 Students were classified as ‘non-susceptible’ if they answered ‘No’ to the question ‘Do you think that you will try a cigarette soon?’ and ‘Definitely not’ to the questions ‘If one of your best friends were to offer you a cigarette, would you smoke it?’ and ‘Do you think you will smoke a cigarette at any time during the next year?’. Students who answered ‘Definitely yes’, ‘Probably yes’ or ‘Probably not’ to either of the last two questions or ‘Yes’ to the first question were classified as ‘susceptible’.
Our primary analysis used logistic regression to compare the odds of smoking and susceptibility to smoking (as a combined outcome measure relative to non-susceptible, never smoking) after delivery of the booster session in Year 8 in the two study schools with Year 8 data from schools that participated in the Nottingham School Smoking Survey. In a secondary analysis the odds of ever smoking relative to never smoking (regardless of susceptibility) were compared between intervention and control schools. Initially, combined data from the two successive cohorts of students in control schools were used as the comparison in order to maximise statistical power. However, in a sensitivity analysis the comparison was repeated using only data from the most recent cohort of students in control schools. A multilevel framework was used to account for the clustering of students within schools, with the effect of school modelled as a random intercept. We could not account for clustering at other levels, such as teaching group or family, as there were too few observations in some clusters to permit model fitting. Results are presented as odds ratios (ORs), with 95% CIs and p-values. Given the exploratory nature of the study, we have not applied a correction for multiple hypothesis testing but, instead, have presented results with CIs and p-values in order to allow the reader to evaluate the findings fully.
This evaluation of Operation Smoke Storm was not a RCT and, therefore, student characteristics known to influence smoking behaviours were potentially unevenly distributed between the intervention and control groups. Therefore, the unadjusted logistic regression models were adjusted for potential confounders, with backwards elimination used to derive a parsimonious adjusted model. Confounders tested were students’ gender, ethnic group (coded as a binary variable owing to the low prevalence of non-white groups), whether one or more of students’ parents, siblings or friends smoke, whether smoking is allowed in the family home, and perceived academic performance. Finally, a measure of rebelliousness and sensation seeking was defined based on a series of four previously defined questionnaire items62 (see study questionnaires in Appendix 3 for full questions). Students who did not answer all four questions were excluded, and the median total score among students with complete data was used to define groups of low and high rebelliousness/sensation seeking.
Unfortunately, a comparable measure of deprivation was not available for students in intervention schools and for those who took part in the Nottingham School Smoking Survey. The survey used students’ postcodes to assign a deprivation score and quintile for their home address according to the 2010 Index of Multiple Deprivation (IMD). 63 Ethical requirements meant that personal identifiers could not be collected from students who took part in the evaluation of Operation Smoke Storm. Therefore, self-reported eligibility to receive free school meals was collected as an indicator of deprivation. A proxy indicator of deprivation for all intervention and control schools was created, considering students in the most deprived quintile of the IMD in the control schools and those who reported being eligible for free school meals in the intervention schools as deprived relative to all others.
Given the absence of linked Year 7 and Year 8 data, it was not possible to adjust for any differences in the prevalence of smoking at baseline in our comparison of Year 8 data. Therefore, ORs were also calculated to compare the prevalence of ever smoking and susceptibility to smoking in Year 7 between intervention and control schools (before the delivery of Operation Smoke Storm in intervention schools) to enable comparison with any differences in Year 8.
Unadjusted and adjusted risk differences comparing intervention and control schools were calculated; these were derived using the ‘adjrr’ post-estimation command in Stata, again using a logistic regression model but one in which clustering was accounted for by using survey commands (the adjrr command cannot be run for a multilevel model).
Power calculation
The work described here was a non-randomised comparison intended to provide preliminary evidence of the potential effectiveness of the intervention, and, as such, was not fully powered. The effect of the intervention would have to be large in order for it to be deemed significant based on data from just two schools. However, in order to justify progression to trial, an estimate consistent with the intervention having some benefit (i.e. an estimate consistent with a prevalence reduction greater than zero) was required. We therefore judged the intervention to be effective if the CI for the difference in prevalence between the intervention and control groups in Year 8 excluded the possibility of no change.
Our pre-study power calculation, based on estimates of the probable achieved sample size in intervention and control schools and the self-reported prevalence of ever smoking and susceptibility among Year 8 students, suggested that we would be able to estimate the difference in prevalence to within 6.6% (i.e. if the observed effect was 6.7% or greater, the CIs would preclude the possibility of no effect or a negative effect of the intervention). This effect size was consistent with the size of effect that a subsequent cluster RCT would be powered to detect, and in line with the size of effect used to power the ASSIST study. 16 A post hoc power calculation based on the achieved data indicated that we were able to detect the difference in prevalence to within 6.9%.
Students’ views on Operation Smoke Storm and their attitudes to smoking
Other quantitative data collected from participants across the study period provided an insight into students’ views of Operation Smoke Storm and changes in their attitudes towards smoking over time.
Year 7 and Year 8 students were asked for their overall impression of Operation Smoke Storm, and students who received both the original and revised versions of the Year 7 lessons (in phase 1 and phase 2, respectively) were asked if they had talked to family and friends about these. Year 7 students who received the family booklet in phase 2 were asked about their use of this resource.
At three time points (baseline, after receiving the original Year 7 sessions, and after receiving the Year 8 booster), students were asked to respond to Likert-scale questions to ascertain their attitudes to four smoking-related statements (see Table 4 for the full wording of questions). The mean and standard deviation (SD) were calculated for normally distributed responses and the median and interquartile range (IQR) for non-normally distributed responses. Mean and median responses across the three time points were compared using an analysis of variance (ANOVA) F-test or Kruskal–Wallis test as appropriate.
At the same three time points described above, students were asked if they agreed, disagreed or were not sure about whether or not it was OK to try a cigarette once to see what it is like, as well as to smoke once a week. Categorical responses at baseline and at the Year 8 follow-up were compared using a chi-squared test with data from Year 7 and Year 8 students, respectively, who took part in the 2013 nationally representative Smoking, Drinking and Drug Use in Young People in England survey. 64 Finally, students were asked if they thought that Operation Smoke Storm had made it less likely that they would ever try a cigarette.
Results
From the Nottingham School Smoking Survey, data were available from eight schools for students who were in Year 7 in 2011 and Year 8 in 2012. Five of these schools also provided data for the subsequent cohort (i.e. students who were in Year 7 in 2012 and Year 8 in 2013). Table 1 describes the characteristics of students in the intervention and control schools in Year 8.
| Characteristic | Intervention schools, n (%) | Control schools, n (%) | p-value for differencea |
|---|---|---|---|
| Total number of completed questionnaires received | 445 | 1692 | |
| Gender | |||
| Male | 200 (44.9) | 843 (49.8) | 0.482 |
| Female | 216 (48.5) | 843 (49.8) | |
| Missing | 29 (6.5) | 6 (0.4) | |
| Ethnic group | |||
| White | 368 (82.7) | 1309 (77.4) | < 0.001 |
| Non-white | 27 (6.1) | 220 (13.0) | |
| Missing | 50 (11.2) | 163 (9.6) | |
| Parental smoking | |||
| Neither | 302 (67.9) | 1123 (66.4) | 0.031 |
| At least one | 106 (23.8) | 516 (30.5) | |
| Missing | 37 (8.3) | 53 (3.1) | |
| Sibling smoking | |||
| None | 365 (82.0) | 1461 (86.4) | 0.852 |
| At least one | 43 (9.7) | 178 (10.5) | |
| Missing | 37 (8.3) | 53 (3.1) | |
| Smoking in the home | |||
| Not allowed | 369 (82.9) | 1460 (80.4) | < 0.001 |
| Allowed | 36 (7.6) | 375 (16.3) | |
| Missing | 42 (9.4) | 57 (3.4) | |
| Number of friends who smoke | |||
| None | 289 (64.9) | 734 (43.4) | < 0.001 |
| One or two | 48 (10.8) | 236 (14.0) | |
| Three or more | 18 (4.0) | 254 (15.0) | |
| Missing | 90 (20.2) | 468 (27.7) | |
| Rebelliousness | |||
| Low | 225 (50.6) | 870 (51.4) | 0.661 |
| High | 176 (39.6) | 715 (42.3) | |
| Missing | 44 (9.9) | 107 (6.3) | |
| Academic performance | |||
| Excellent or good | 313 (70.3) | 1228 (72.6) | 0.372 |
| Average or below average | 92 (20.7) | 406 (24.0) | |
| Missing | 40 (9.0) | 58 (3.4) | |
| Free school meals | |||
| No | 374 (84.0) | Not collected | N/A |
| Yes | 25 (5.6) | ||
| Missing | 46 (10.3) | ||
| IMD quintile | |||
| Least deprived | Not collected | 375 (22.2) | N/A |
| 2 | 160 (9.5) | ||
| 3 | 282 (16.7) | ||
| 4 | 240 (14.2) | ||
| Most deprived | 261 (15.4) | ||
| Missing | 374 (22.1) | ||
As expected, given the non-randomised nature of the study, there were significant differences in student characteristics between intervention and control schools. In control schools a greater proportion of students were of non-white ethnicity, had parents who smoked, reported that smoking was allowed in their home, and had more friends who smoked. There is some evidence that both the intervention and control schools are not representative of schools nationally; again, this was expected given that there was an element of convenience sampling in the selection of schools to participate in both the evaluation of Operation Smoke Storm as well as in the Nottingham School Smoking Survey. The majority of students were of white ethnicity, whereas 25.3% of students in state-funded secondary schools nationally in January 2014 were from ethnic minority groups. 51 Students on the whole were less deprived than the national average. Just 5.6% of students in the two intervention schools reported receiving free school meals, whereas 16.3% of students in state-funded secondary schools nationally in January 2014 were known to be eligible for free school meals. 51 In the control schools students’ postcodes were skewed towards the least deprived IMD quintile.
A small number of students did not answer the survey questions relating to smoking behaviour and susceptibility (5.0% of Year 7 students and 3.6% of Year 8 students, with no differences between intervention and control schools). Table 2 shows the reported prevalence of ever smoking and susceptibility to smoking in Year 7 and Year 8 students in intervention and control schools, excluding students with missing data.
| Group | Number of students, N | With missing smoking data, n (%) | Ever smoker, n (%) | Susceptible never smoker, n (%) | Non-susceptible never smoker, n (%) |
|---|---|---|---|---|---|
| Year 7 intervention schools | 532 | 27 (5.1) | 12 (2.4) | 80 (15.8) | 413 (81.8) |
| Year 7 control schools | 1613 | 80 (5.0) | 98 (6.4) | 253 (16.5) | 1182 (77.1) |
| Year 8 intervention schools | 445 | 16 (3.6) | 34 (7.9) | 111 (25.9) | 284 (66.2) |
| Year 8 control schools | 1692 | 61 (3.6) | 175 (10.7) | 329 (20.2) | 1127 (69.1) |
In intervention schools the combined prevalence of ever smoking and susceptibility to smoking increased from 18.2% in Year 7 to 33.8% in Year 8. The prevalence of ever smoking alone increased from 2.3% in Year 7 to 7.8% in Year 8. In the two Nottingham School Smoking Survey cohorts the combined prevalence of ever smoking and susceptibility to smoking increased from 22.9% in Year 7 to 30.9% in Year 8, and the prevalence of ever smoking alone increased from 6.3% in Year 7 to 10.6% in Year 8.
Table 3 shows the odds of a student being a susceptible never smoker and/or an ever smoker in the two intervention schools compared with control schools, for both Year 7 (before the delivery of Operation Smoke Storm in intervention schools) and Year 8 (after the delivery of Operation Smoke Storm in intervention schools), unadjusted and adjusted for confounding variables.
| Outcome | Unadjusted | Adjusteda | ||||
|---|---|---|---|---|---|---|
| Odds of outcome in intervention vs. control schools, OR (95% CI) | p-value | Unadjusted risk difference, % (95% CI) | Odds of outcome in intervention vs. control schools, OR (95% CI) | p-value | Adjusted risk difference, % (95% CI) | |
| Year 7 (before intervention delivery) | ||||||
| Ever smoker or susceptible never smoker | 0.82 (0.43 to 1.55) | 0.536 | –4.7 (–15.3 to 5.9) | 1.74 (0.54 to 5.56) | 0.351 | 5.9 (–13.8 to 2.6) |
| Ever smoker | 0.38 (0.13 to 1.08) | 0.070 | –4.0 (–6.9 to 1.2) | 1.22 (0.13 to 11.3) | 0.858 | 0.4 (–9.9 to 10.8) |
| Year 8 (after intervention delivery) | ||||||
| Ever smoker or susceptible never smoker | 1.17 (0.70 to 1.95) | 0.556 | 2.9 (–4.0 to 9.8) | 1.28 (0.83 to 1.97) | 0.263 | 4.1 (–0.5 to 8.6) |
| Ever smoker | 0.80 (0.32 to 1.98) | 0.622 | –2.8 (–7.8 to 2.1) | 0.82 (0.42 to 1.58) | 0.549 | –2.0 (–5.4 to 1.4) |
In Year 7 (before intervention delivery), after adjusting for significant confounders, the odds of a student in an intervention school being an ever smoker or susceptible never smoker were 74% higher than the odds for a student in a control school, although this effect was not statistically significant [adjusted odds ratio (aOR) 1.74, 95% CI 0.54 to 5.56; p = 0.351]. Students in intervention schools were more likely to have ever smoked than students in control schools, although, again, the difference was not statistically significant (aOR 1.22, 95% CI 0.13 to 11.3; p = 0.858).
In Year 8, after adjusting for significant confounders, the odds of a student in an intervention school being an ever smoker or susceptible never smoker were 28% higher than the odds for a student in a control school, although this effect was not statistically significant (aOR 1.28, 95% CI 0.83 to 1.97; p = 0.263). Students in intervention schools were slightly less likely to have ever smoked than students in control schools, although, again, the difference was not statistically significant (aOR 0.82, 95% CI 0.42 to 1.58; p = 0.549).
These results are based on data from both cohorts of Nottingham School Smoking Survey students (i.e. students who were in Year 7 in 2011 or 2012, and Year 8 in 2012 or 2013). The results did not change appreciably (although CIs were wider) when data from only the most recent cohort were used as the control.
Students’ views on Operation Smoke Storm and their attitudes to smoking
Overall, students liked the lessons that they received. The vast majority of Year 7 students in phase 1 said that Operation Smoke Storm was ‘very good’ (36.3%) or ‘OK’ (47.3%); these proportions were similar (31.9% and 45.2%, respectively) when the revised version was delivered to the new cohort of Year 7 students in phase 2. Following delivery of the Year 8 booster in phase 2, nearly three-quarters of students reported that the session was ‘very good’ (14.7%) or ‘OK’ (57.7%). Approximately two-thirds of Year 7 students reported having talked to other people about Operation Smoke Storm (Table 4).
| Response | Year 7 students in phase 1: original version (%) | Year 7 students in phase 2: revised version (%) |
|---|---|---|
| Parents/carers | 37.8 | 45.8 |
| Brothers and/or sisters | 10.0 | 10.7 |
| Friends in other Year 7 classes at same school | 45.5 | 42.4 |
| Friends in Year 8 and above at same school | 5.4 | 4.8 |
| Friends who go to other schools | 7.5 | 8.5 |
| No one else | 32.4 | 31.0 |
A total of 16.7% of students reported that they were given the family booklet but that they did not take it home, and 21.7% reported that they did not receive the booklet at all. Of students who did receive the booklet and reported taking it home, 43.0% said that they showed it to their mother or another adult female, 21.5% reported showing to their father or another adult male, and 24.4% said that they did not show the booklet to anyone. Very few students reported that they completed the activities in the booklet with a parent or carer. The completion rate was highest (17.2%) for the activity on the first page but declined to approximately 10% for the activities on subsequent pages.
Students displayed some changes in attitudes towards smoking over the course of the study. Table 5 presents mean Likert-scale scores in response to four statements given to the same cohort of students at baseline, after they had received the Year 7 Operation Smoke Storm sessions in phase 1, and after the Year 8 booster session in phase 2.
| Statement | How far do you agree with the following statements? (mean + SD for statements 1–3; median + IQR for statement 4) | Value of test statistic (p-value)a | ||
|---|---|---|---|---|
| Baseline | After Year 7 lessons in phase 1 | After Year 8 lessons in phase 2 | ||
| (1) Companies that make cigarettes try to attract customers aged 18+ years only | 2.30 (1.04) | 2.85 (1.22) | 3.47 (1.07) | F = 132.7 (< 0.001) |
| (2) Companies that make cigarettes sell dangerous products, but still operate in a fair and decent way | 2.79 (0.95) | 2.80 (1.04) | 2.95 (0.95) | F = 3.52 (0.030) |
| (3) Smoking is not that serious compared with other drugs that young people use | 3.06 (1.13) | 3.20 (1.16) | 3.24 (1.09) | F = 3.39 (0.034) |
| (4) Nicotine in cigarettes is one of the most addictive drugs that people use | 2 (1–3) | 2 (1–2) | 2 (1–3) | χ2 = 19.8 (< 0.001) |
There was a statistically significant difference in students’ responses to statement 1 at the three time points (p < 0.001). Scores increased between baseline and follow-up after the Year 7 lessons, and again between Year 7 follow-up and follow-up after the Year 8 booster session, meaning that students were more likely to disagree with the statement that ‘companies making cigarettes only try to attract customers over 18 years old’.
There was a statistically significant difference in students’ responses to statement 2 at the three time points (p = 0.030), although the absolute difference in scores was smaller than for statement 1. There was no difference in score between baseline and follow-up after the Year 7 lessons, but the mean score was marginally higher at follow-up after the Year 8 booster session, meaning that students were more likely to disagree with the statement that ‘companies that make cigarettes sell dangerous products, but still operate in a fair and decent way’.
There was also a statistically significant difference in students’ responses to statement 3 at the three time points (p = 0.034), although, again, the absolute difference in scores was small. A small increase in score appears to have occurred between baseline and follow-up after the Year 7 sessions, meaning that students were more likely to disagree with the statement that ‘smoking is not that serious compared with other drugs young people use’. There was no further substantial increase in score between Year 7 follow-up and follow-up after the Year 8 sessions.
Responses to the statement ‘nicotine in cigarettes is one of the most addictive drugs that people use’ were highly positively skewed. Scores were significantly lower (i.e. students were more likely to agree with the statement) after the Year 7 sessions than at the other two time points (p < 0.001).
Students’ responses to the questions ‘do you think it’s OK for someone your age to try a cigarette to see what it’s like?’ and ‘do you think it’s OK for someone your age to smoke cigarettes once a week?’ were compared with data for comparable age groups from the 2013 Smoking, Drinking and Drug Use in Young People in England survey64 (Figure 2).
FIGURE 2.
Attitudes towards trying a cigarette and smoking regularly. SDDUYP, Smoking, Drinking and Drug Use in Young People in England survey. 64
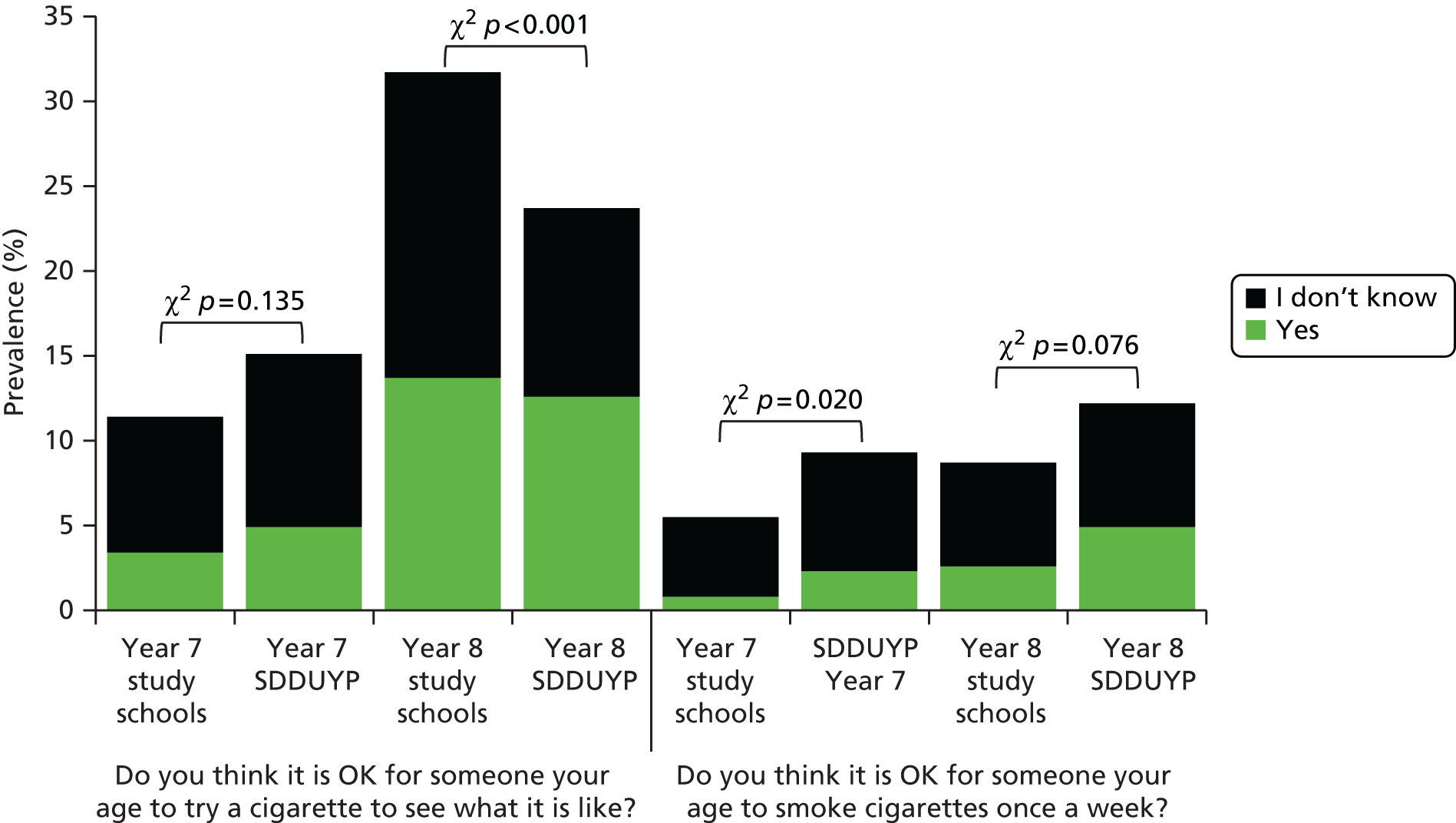
There were no statistically significant differences in attitudes towards trying a cigarette to see what it is like between students in the two study schools at the start of phase 1 and the nationally representative sample of Year 7 students from the Smoking, Drinking and Drug Use in Young People survey64 (p = 0.135). However, there were differences evident in Year 8 (p < 0.001). Although similar numbers of students responded that yes, trying a cigarette was OK, proportionally more students from the study schools did not know, and fewer were certain that it was not OK, compared with the national survey data. This might suggest that exposure to Operation Smoke Storm increased uncertainty about trying a cigarette among students who might otherwise have thought that it was not OK.
At baseline, marginally more students in the study schools did not know or thought that it was OK to smoke cigarettes once a week than in the data from the national survey (p = 0.020). However, the absolute proportion of students reporting ‘yes’ or ‘don’t know’ to this question was very small. In Year 8 there was no significant difference between students in the two groups (p = 0.076). From these results it does not appear that exposure to Operation Smoke Storm had any substantial impact on changing attitudes towards smoking cigarettes once a week.
Finally, students were asked if they thought that completing Operation Smoke Storm had made it less likely that they would ever try a cigarette (Table 6).
| Group | No (%) | Yes (%) | Don’t know (%) |
|---|---|---|---|
| Year 7 students in phase 1 | 15.0 | 65.7 | 19.4 |
| Year 7 students in phase 2 | 15.6 | 69.3 | 15.2 |
| Year 8 students in phase 2 | 28.1 | 45.0 | 26.9 |
After the Year 7 lessons, approximately two-thirds of students thought that Operation Smoke Storm had made it less likely that they would ever try a cigarette, although this number was smaller after the Year 8 booster. This may simply reflect increases in susceptibility to smoking with age that might have occurred regardless of receiving the intervention.
Summary
The comparison of smoking status in Year 8 between students who received Operation Smoke Storm and those who participated in the Nottingham School Smoking Survey provides little evidence that the intervention is effective in preventing smoking uptake. However, students broadly liked Operation Smoke Storm and displayed some positive changes in attitudes towards statements with which they were presented. There is some suggestion that exposure to Operation Smoke Storm may have increased uncertainty about trying a cigarette to see what it is like among students who might otherwise have thought that it was not acceptable, but there is no evidence that it altered attitudes towards more regular smoking.
The strengths and limitations of the analyses presented here will be discussed in detail in Chapter 8. The qualitative data presented in Chapter 6 provide some insights that offer potential explanations for the findings presented here.
Chapter 6 Qualitative evaluation of revised and extended intervention
Chapter 3 described the qualitative work undertaken during the first phase of the project, which considered the acceptability of the original version of Operation Smoke Storm delivered to Year 7 in phase 1. Here we describe the qualitative work undertaken during phase 2 of the project, which set out to explore the acceptability of the revised version of the Year 7 Operation Smoke Storm lessons, the family booklet that was delivered to Year 7 students, and the booster session that was delivered to Year 8 students.
Methods
Delivery of Operation Smoke Storm
The revised version of Operation Smoke Storm Year 7 lessons, plus the new family booklet, was delivered to all Year 7 students (aged 11–12 years) at School 1 only. Changes to the PSHE curriculum at School 2 precluded the delivery of the Year 7 lessons in this second phase of the project. The Operation Smoke Storm booster session was delivered to all Year 8 students (aged 12–13 years) in both schools. In School 1 the booster session was delivered in PSHE lessons, but changes in School 2’s PSHE curriculum meant that, for logistical reasons, the booster was delivered during science lessons by specialist science teachers.
Prior to the delivery of the sessions the research team provided a brief training session to teachers, which outlined how to access and navigate the Operation Smoke Storm resource, and described the planned research-related activities. In total, 350 Year 7 students across 14 classes in School 1 received the revised Operation Smoke Storm lessons, plus the new family booklet. Again, School 1 had shorter lessons (40 minutes per week), and, therefore, some teachers covered the material over more than three sessions.
Across the two schools, a total of 538 Year 8 students received the Operation Smoke Storm booster session (School 1: 333 students across 12 classes; School 2: 205 students across nine classes). One class in each school did not complete the booster lesson; at School 1 this was because a teacher deemed it to be too difficult for the academic ability of the students, and in School 2 this was attributable to lack of time. The shorter lessons in School 1 meant that teachers needed two lessons to cover the material (including the follow-up questionnaire), whereas School 2 had sufficient time to deliver the booster session during a single lesson (although the follow-up questionnaire was completed in a subsequent lesson).
Study design and participant recruitment
The accompanying qualitative evaluation comprised focus groups, paired student–parent interviews (to evaluate the family booklet) and teacher interviews. The same procedures were used to gain consent, select students for focus groups and invite teachers to interviews as were used in phase 1 (see Chapter 3). Four focus groups were planned for each participating year group at each school (two for each gender), with up to 12 students in each.
All Year 7 students in School 1 were given the family booklet to take home to their parents. The booklet was accompanied by a letter informing and inviting parents to participate in a paired student–parent interview to explore their views on the booklet. An inconvenience allowance in the form of a £15 high-street voucher was offered to all parents who participated in the interviews. Parents were asked to contact a member of the research team by e-mail or telephone if they wished to participate, and a suitable time and location (either a private room on school premises or in the participants’ home) for each interview was arranged. Up to 15 paired interviews were planned.
Focus group and interview procedures
Five separate semistructured discussion guides were developed (Year 7 focus groups, Year 8 focus groups, paired student–parent interviews, Year 7 teacher interviews and Year 8 teacher interviews). The Year 7 focus groups considered students’ views of the revised Operation Smoke Storm Year 7 sessions and their awareness of, and attitudes towards, the tobacco industry and smoking. Students were also asked about their views of the family booklet, how they used it, and, if they did not, their reasons for not doing so. The Year 8 focus groups considered students’ view of the Operation Smoke Storm booster session and their awareness of, and attitudes towards, the tobacco industry and smoking. Students were also asked of ways in which the booster could be improved to increase engagement.
The Year 7 and 8 teacher interviews focused on the design, suitability and usability of the classroom-based sessions and resources, the extent to which Operation Smoke Storm was an ‘off-the-shelf’ resource, how well delivery integrated with the existing timetable, the perceived effectiveness of the sessions at raising awareness of smoking-related issues, and suggestions for improving the sessions to increase student engagement. Teachers were also asked for their views on the design and suitability of the take-home family booklet and how it was used.
Paired student–parent interviews focused on students’ and parents’ views of the take-home family booklet, how it was used at home, if it triggered any smoking-related discussions, and suggestions for improving the booklet.
For the full focus group and interview guides, see Appendix 6.
Procedures during the focus groups and interviews were the same as those used in phase 1 (see Chapter 3).
Data analysis
Data were analysed using the framework approach,58,59 as employed in phase 1 (see Chapter 3). Data presented for Year 7 lessons and the family booklet reflect the views of participants from School 1, and data on the Year 8 booster session reflect the views of participants from both schools.
Process evaluation
In addition to the qualitative work described here, a process evaluation was conducted in phase 2 to assess if the intervention was being delivered in the intended way. Both Year 7 and Year 8 teachers were asked to complete a fidelity questionnaire to capture information on how they delivered Operation Smoke Storm, as it was felt that observing teachers directly may have altered the way in which they delivered the intervention and may have deterred schools from continuing to take part in the study. The results of this process evaluation are in line with the qualitative data presented below and, thus, for brevity are not discussed here in full. However, the questionnaire and a summary of the results are included in Appendix 7.
Results
In total, 10 focus groups were conducted. Two of these were conducted with Year 7 students at School 1 (one male, one female) with eight students in each group. A lack of volunteers meant that it was not possible to conduct the four Year 7 focus groups originally planned. Eight focus groups were conducted with Year 8 students (four at each school), in which 51 students (25 males, 26 females) took part in total, with an average of 6 students per focus group (range 3–10 students). Both Year 7 focus groups lasted for 26 minutes and Year 8 focus groups lasted for 24 minutes on average (range 11–35 minutes).
Thirty teachers delivered Operation Smoke Storm to either Year 7 or Year 8 students. Of these, 10 Year 7 teachers and four Year 8 teachers from School 1 took part in six face to face and six telephone interviews. Most interviews were one to one, although in one face to face and one telephone interview two teachers were interviewed in a pair. Two Year 8 teachers from School 2 were also interviewed in a paired face-to-face interview. Interviews lasted 26 minutes on average (range 19–33 minutes). The remaining 15 teachers either declined to take part owing to time constraints or did not respond to the initial invitation or reminders. In total nine parents from School 1 participated in a paired student–parent interview with their child, which lasted 23 minutes on average (range 13–33 minutes).
Although the data collected from Year 7 and Year 8 focus groups and interviews were analysed as separate year groups, the same four core themes as in phase 1 were identified within both sets of data: (1) teachers’ preparedness for and delivery of Operation Smoke Storm; (2) raised awareness; (3) engagement with Operation Smoke Storm; and (4) extending Operation Smoke Storm.
For the first three themes the results presented below initially consider all data relating to Year 7 (revised classroom-based Operation Smoke Storm sessions and family booklet) and then consider all data relating to Year 8 (Operation Smoke Storm booster session). All data from Year 7 and 8 were considered together in the final theme, namely extending Operation Smoke Storm.
Year 7 lessons
Much of the feedback from Year 7 students and teachers was similar to that received in phase 1 of the project (see Chapter 3).
Teachers’ preparedness and delivery of Operation Smoke Storm
None of the Year 7 teachers had taught the original version of Operation Smoke Storm the previous year (during phase 1). Some teachers had previously covered the topic of smoking during science or PSHE lessons.
I’ve had to deliver stuff before . . . It was just general health and well-being things as part of PSHE days in my school last year through tutor period as a general thing.
School 1, Teacher 7
The provision of an ‘off-the-shelf’ resource once again appealed to teachers and meant that the preparation time required for most was minimal. Those who read the new introductory information in the teachers’ handbook found it to be useful to set the scene of the lessons. Many read through lesson plans and watched clips of the videos to get an idea of the resource and storyline before delivering the first lesson. A couple of teachers spent time looking over the resource in more detail and one of those who did not do this acknowledged that they should have.
I feel like I probably would’ve benefited from going through the entire thing myself before. It was made to sound like it was just pick it up, go, and it wasn’t that straightforward because after I’d done the first session I was like, ah, it felt a bit broken in me presenting it.
School 1, Teacher 5
The training session and/or spending time reviewing the resource beforehand helped most teachers to feel confident about delivering the sessions. Most of the teachers felt that their general knowledge about smoking was sufficient for the ability of Year 7 students, which also helped many to feel confident about delivering the sessions.
I looked through the materials, I kind of knew how they were going to work and I felt confident that I would be able to explain and talk about what’s needed in the lessons. I’m not a particular expert but I think general knowledge about smoking and its effects should be enough.
School 1, Teacher 9
The shorter lesson time in School 1 was not an issue for most teachers and they reported picking up from where they had finished in the last lesson. Although the lesson plans provided timings for activities, some teachers did not follow these timings exactly, adapting the pace as necessary for the students.
I followed the programme through, and went through session one, went through session two, etc., but I didn’t use the timing guides because I wanted to make sure that they asked the questions they wanted, and they got the information they wanted.
School 1, Teacher 7
Many teachers did not use or exactly follow the lesson plans in class, as they felt that the online resource was sufficient.
I think I more looked at it, as I say, at the start and then took it more from clicking through the software as we went along because it was pretty self-explanatory there and more adapting to the discussions that the kids wanted to have as opposed to going, we’ve got to spend this much time on each of them.
School 1, Teacher 4
Many teachers missed the additional discussion points and question-and-answer section added to the back of the teacher handbook. None of the teachers was aware that a username and password, which provided students with access to an out-takes video once they had completed the resource, were available.
To be honest, I didn’t even look that far [discussion points]. I didn’t know that was there. I would literally every week just open to the page that I needed.
School 1, Teacher 5
Raised awareness
The areas in which students’ awareness about smoking increased were the same as those reported in phase 1 (see Chapter 3). Many had some existing knowledge about smoking from primary school but the Operation Smoke Storm resource provided further insight into the content and harms of cigarettes. A number of students were shocked by the information and subsequently many said that this knowledge had strengthened their desire to remain smoke-free. Many of the students, however, misinterpreted one of the facts in the resource, that smokers are ‘sheep-like’, that is, they tend to be followers of the crowd. Instead, students interpreted this as meaning that smoking would result in looking like a sheep.
You look like a sheep when you smoke.
School 1, Year 7, Female
Many of the teachers felt that learning about the tobacco industry was eye-opening for many of the students and that they engaged with the resource and information it provided.
I thought it was really good and it got them thinking, you could see that some of the stuff, the factual stuff, was quite surprising and it got them thinking about the morals of the companies that are selling cigarettes . . . I think when they’re asking you questions about it, it shows that they’ve taken it in and are actually thinking about well, ‘What if?’.
School 1, Teacher 10
This was reflected in the way in which some students engaged in further discussions about tobacco industry tactics. In the focus groups, students were able to recall a number of tobacco industry tactics that they had learnt in Operation Smoke Storm, although some students needed prompting in order to do so.
Well we like split into groups and learned about different things, like how they sold cigarettes with like tricks and scams almost.
School 1, Year 7, Male
However, some teachers felt that not all students picked up on information about the tobacco industry as much as on information about the content of cigarettes or the harms of smoking.
I think definitely what stuck with them the most is that activity and what’s in the cigarettes and everything like that, and I think they were shocked by that, and that’s something that’s stuck with them.
School 1, Teacher 4
Although some teachers were hopeful that the resource had averted students from trying a cigarette, others were doubtful of its lasting impact or felt that other factors, such as peer pressure, could have a stronger influence on the uptake of smoking among students.
I think definitely would make them think twice. Sometimes ultimately if they’re going to smoke, they’re going to smoke and it’s a mind-set thing. The peer pressure probably is the biggest thing.
School 1, Teacher 6
Engagement with Operation Smoke Storm
Feedback from teachers on students’ engagement with the revised Operation Smoke Storm and their ability to access the resource was similar to findings from phase 1 (see Chapter 3). Teachers felt that students bought into the secret agent theme. Although some students said that they enjoyed the secret agent theme, a few thought this storyline was unrealistic and that the acting was too dramatic.
On the second bit, this girl runs out when the alarm was on and I just thought, ‘Wow, this is so over the top.’
School 1, Year 7, Female
Many teachers stated that timings were an issue, as the prescribed session length did not match the length of the schools’ lessons. This was felt to restrict the quality of delivery as some activities had to be shortened.
Sometimes we were a little bit pushed for time because obviously, our lessons are 40 minutes, 45 minutes in the afternoon, so some of the features we had to kind of skip through quite quickly to fit it all in.
School 1, Teacher 10
Some teachers felt that the lesson objectives added following phase 1 feedback were sufficient, but others said they would like to see a greater focus on them to support learning. Teachers suggested displaying the objectives on the screen, or at the top of each page in the student handbook.
Maybe just even having at the top [of each page of the booklet] like learning objective today is that you will know all the chemicals that are present within a cigarette. Really simple, but the kids will know and then we go, ‘OK this is going to go on your presentation so we need to know this.’
School 1, Teacher 8
Issues with navigating through the resource appeared to be alleviated by the addition of the menu bar, which enabled teachers to skip to different sections of a session. Some teachers had an issue with streaming the lesson over the internet in real time, although some were able to load the session in advance.
I’d loaded it the day before at home on my laptop and when I got on to it, it froze, and when I tried to reload it, it just wouldn’t have any of it. So that hindered the first lesson.
School 1, Teacher 5
Family booklet
Different teachers reported giving students different instructions on how to use the family booklet, including instructing students to take it home and share it with their parents if they wished, and setting each activity as a weekly homework task. Some teachers gave out the booklet only at the end of the three sessions. Many students reported that they did not engage with the booklet, and a few students reported that their teacher had told them it was for their parents.
Because our tutor said it’s something for your parents to see . . . That’s why I just thought, ‘oh it’s for my parent; it’s not for me.’
School 1, Year 7, Female
Some parents read the booklet and a few also completed the activities. Reasons cited for not reading the booklet or completing the activities were lack of time or not feeling that it was necessary. In one case, the booklet was only used because the parent was taking part in a paired student–parent interview.
What we did was go through this yesterday, because we knew obviously you were coming today, so that’s what we did.
School 1, Parent 6
Teachers felt that the format of the booklet was suitable for students to take home, that it would consolidate learning from the lessons and that it would support motivated parents to initiate conversations about smoking at home.
It’s good in itself and I think the parents who were going to have those conversations will certainly do. I don’t know to what extent you can influence maybe others but . . .
School 1, Teacher 4
However, teachers and students did not consider the booklet to be suitable for parents who were busy and/or less motivated to have those conversations.
It’s a very ideal world situation I think because a lot of parents are very busy and can’t sit down and . . . I don’t know. I like it, I think it’s great and it is good especially because they’re following the story and they can tell them exactly what’s happened, that we’ve done in class. But yeah, I don’t know, maybe a bit too complicated because there is a lot to read and do, isn’t there?
School 1, Teacher 6
All parents interviewed were supportive of anti-smoking education in schools, but not all were aware of the extent of smoking among young people and wider issues such as the glamorisation of smoking. Generally, the booklet was received positively by parents, although some said that they would appreciate a clearer introduction at the start of the booklet to enable them to quickly understand the context.
To be honest it’s probably me and my age, but I did have to look at it a couple of times to really get what it was saying really . . . Because a lot of it depends on the child, and sometimes although there’s a lot of verbal communication now, that’s not always the case . . . So if there was a parental explanation sheet with it, that would be enough really.
School 1, Parent 1
There were also a number of comments relating to the appearance of the booklet; the colour scheme was thought to be very dark and some text difficult to read.
Writing’s a bit small and it’s a bit dark . . . This is good because it’s a bit whiter but the writing’s still a little bit small.
School 1, Parent 9
Despite this, parents generally considered the booklet to be a novel, in-depth and engaging way of conveying hard-hitting facts. Many reported learning new information from the booklet, particularly about the tobacco industry and content of cigarettes, and found it shocking.
I learned something, I didn’t know about all the additives if you like; and the sneaky way that the big companies and the amount of money involved and all of that really.
School 1, Parent 1
It was enlightening. I didn’t know half the stuff that was in there. I just had no idea cigarettes contained all those awful things so it was educational for me.
School 1, Parent 6
Parents reported that the use of the booklet stimulated discussions about smoking between themselves and their child, sometimes extending to the wider family; these often built on discussions that had already taken place.
We’ve discussed it since and had a chat about it. We were talking about it the other day, weren’t we, things like the booklet and things like that and talking about what we now know about it. It was building on really what you’d done in [Drug Abuse Resistance Education] DARE at primary, wasn’t it, just taking it a bit further.
School 1, Parent 7
However, some would have liked more evidence to support claims made about the tobacco industry.
One of the real things I felt in some of it was that I wanted to say ‘Really, where’s your evidence for that?’. You said that the tobacco companies said it, but did they say this.
School 1, Parent 5
One parent felt that including information on how the tobacco industry has targeted young people was too advanced for the age group. In contrast, others thought that it was an interesting and novel approach.
You know, particularly the angle about marketing I thought was a really interesting angle because I haven’t come across that as part of an anti-smoking policy and I thought that was a really interesting angle.
School 1, Parent 5
The booklet was also generally received positively by students, although a couple thought that it just covered the same material as in class. Some said they would have liked it to contain more interesting activities, involving less reading and writing.
Maybe like a bit more like games, because the quiz is quite fun, and then it kind of just drops off a bit. That gets a bit more boring, it’s like I wouldn’t really want to be writing paragraphs.
School 1, Parent 2: student response
Not all students said that they would be keen to work through the booklet at home with their parents, particularly if it was not set as homework.
If there was nothing to do, and I was really bored, I would probably do it. But normally if it was homework, then yes I’d do it, but if it wasn’t I wouldn’t.
School 1, Year 7, Female
To increase engagement, most teachers were supportive of the booklet being set as a homework activity; others said that they would not advocate this in case students struggle to find time with their parents or because homework is not normally given for PSHE lessons.
We don’t give homework for PSHE, but I think if we’re going to have something like this, like a take home thing that you want them to get use out of with activities then I think it might make more sense, just because when it’s optional they won’t do it.
School 1, Teacher 5
Year 8 booster session
Teachers’ preparedness and delivery of Operation Smoke Storm
Having seen the content of the resource either in the training session or during their own preparation, all teachers felt confident about delivering the sessions. However, one teacher, who had not delivered Operation Smoke Storm the previous year, would have liked to have known what students had learnt in Year 7.
I didn’t really know what they’d done before. Some of them could remember, some of them couldn’t, so that’s what threw me a little bit. The content, I was fine with. I had a flick through it so I was happy to deliver that but it was more, not really knowing what their prior knowledge was.
School 1, Teacher 12
Overall, teachers liked the flexibility and off-the-shelf nature of the lessons. A number of the teachers who delivered the booster session were not specialist PSHE teachers, although the more experienced teachers said the off-the-shelf nature of the resource meant that it was suitable for non-specialist staff to deliver.
You could definitely give it to a non-PSHE teacher to deliver, and they would be comfortable in delivering it I think, because it’s so well resourced.
School 1, Teacher 1
The teachers reported that, although the lesson plans provided useful timings and guidance, they did not need to use the lesson plans when teaching. This was because the plans were too detailed to use in class and/or the online resource was easy to follow.
You kind of didn’t need to use them too much once you got going. You kind of looked to it for the suggested timings but then once you’d gone through the resources you didn’t need the teacher notes too much because I think the resources are quite self-explanatory.
School 1, Teacher 2
Raised awareness
When prompted, students were able to discuss what they had learnt about the subtle and inventive tobacco industry practices that appear to encourage young people to try smoking. Some students showed an appreciation of why the industry might target young people.
If they target to young people and try and get to young people, then they will get more money, ’cause there’ll be more people getting addicted to it.
School 2, Year 8, Female
Students expressed their disapproval of the tobacco industry’s apparent persuasive tactics to attract young smokers.
I think that’s really bad [that young people might be targeted], because like we’ve been doing the Operation Smoke Storm to stop us, and then they’ve been trying to sell it to younger generations.
School 2, Year 8, Female
Many students felt that the booster session elaborated on information they had learnt in Year 7, particularly around the health effects of smoking and the topic of the tobacco industry.
I didn’t know about like all the effects until this year, and it’s just like, it just shows you what actually smoking does. It just opened my eyes a bit.
School 1, Year 8, Female
I thought it was better this year because it’s explaining how companies market more in detail, making you do slogans for it.
School 1, Year 8, Male
Some students, however, felt that there was insufficient time to cover the topic of the tobacco industry and that it was repetitive of the Year 7 material.
I thought it, kind of, a bit repeated what it did last year but it was a bit too short to explain all the other stuff that we just learnt this year. About how they’ve managed to sell them and how they managed to get them to sell very easily, like a bit more in depth, because it was a bit quick.
School 1, Year 8, Male
Some students shared facts that they had learnt about the health effects of smoking and the tobacco industry with family members. A few also reported using the information to persuade family members to stop smoking. Those who did not share any learning with their families said that it was because their parents were non-smokers so it was not of importance, or because their parents were smokers and there was no point or they did not want to start an argument.
Also at the time my stepdad, he was smoking, he still is but I didn’t want to treat him . . . because it would just end up in an argument, because he would just start an argument saying it’s his life, so I just decided not to.
School 1, Year 8, Male
Teachers said that, although the booster session helped students to appreciate the manipulative tactics used by the tobacco industry, they felt that not all students understood this message. For example, some teachers mentioned that some students were unable to use the new information presented in activities and instead used their existing knowledge, for example, when completing the activity in which they had to write a Tweet to discourage their peers from smoking.
So whenever they talked about like their Tweets for social media, they kind of went for, ‘You shouldn’t smoke, it’s bad for you. You shouldn’t smoke. Cigarettes have got all this stuff in them,’ so kind of the obvious stuff from it, but they then don’t take it that step further to think, like, should they be publicising it, yeah, taking that conversation a bit deeper.
School 1, Teacher 2
Many students mentioned that the new information they had learnt across the Year 7 and Year 8 sessions had strengthened their resolve not to smoke. Conversely, some students said the Operation Smoke Storm lessons may encourage experimentation with tobacco and they would still be interested in trying a cigarette; one student said they had not even considered this before completing the lessons.
Before I did Operation Smoke Storm I never thought of smoking but then when it, like here into my head, a couple of people saying, ‘Oh I might just try smoking,’ it kind of brings the idea to your head but then you realise you have to try and fight off that idea before it takes over.
School 1, Year 8, Male
Some also felt that the decision to try a cigarette would be more heavily influenced by other factors, for instance, peer pressure and role models or family members who smoke.
I’m not sure if once they hit Year 9, Year 10 or they’ve got the peer pressure or older brothers and sisters that are doing it, I’m not sure how much impact it [Operation Smoke Storm] will have in the longer term, but in the short term I definitely think it would make them think twice.
School 1, Teacher 12
Engagement with Operation Smoke Storm
Most students reported that they enjoyed the Operation Smoke Storm booster session, with it being viewed as interactive and informative, more so than usual PSHE lessons. However, there appeared to be a difference between some of the female and male students’ views of the videos. Many of the female students enjoyed that the videos were recorded in the style of a blog, which they could relate to, and felt that the storyline was more realistic than the Year 7 lessons.
This year is better because it kind of showed what actually could have happened and like what people actually go on to watch stuff, so like a blog.
School 2, Year 8, Female
A few of the male students, however, felt that it was immature and could not relate to it; one male student said that he would have preferred a male character which he felt he would have been able to relate to more easily.
In Year 7 it was good, when you enjoyed it, it made it more interesting than it would have been if it was just like on a blank PowerPoint® [Microsoft Corporation, Redmond, WA, USA], but then in Year 8 I found it a bit patronising, in a way.
School 1, Year 8, Male
Many students would have liked to have spent more time on the activities in the lesson, as they felt that they were rushed at times.
I think we could have had like a bit more time to do it, because it’s only lesson in one hour. We only had like five to 10 minutes to do one activity. It was quite hard to get all of that done in one part.
School 2, Year 8, Male
In addition, a few students said that they would have liked the lesson to be more interactive and to involve less writing.
Maybe, like something interactive actually on the board. Instead of just like writing something, maybe make it interactive on the computers or something like that.
School 2, Year 8, Male
Some teachers and students also felt that the resource was too repetitive. Teachers and students suggested introducing some variety in the form of more interactive activities in order to increase engagement.
I think the thing that I think it would benefit from is some more types of activities, and that came across from the students going, ‘Miss I’m bored, we’re just discussing and watching, discussing and watching.’ . . . Like you could do a role play, you could give them scenario cards with characters of the people who . . . You know two of the characters in that, right you’re going to play that person.
School 1, Teacher 1
Students particularly enjoyed the slogan, Twitter and discussion activities, because it gave them the opportunity to share their opinion.
It was your own opinion and good. Like you can write about it and do your own opinion.
School 2, Year 8, Female
A few students also enjoyed the slogan activity because it helped them to realise how they might be targeted in real life.
I thought it was good how it told you, like, people try and make things sound really good and you can actually believe it because of what they put on a packet or whatever or how they make it look. You don’t really realise sometimes that actually what’s maybe inside is bad for you but just because of the packaging you think, ‘Yeah, it’s cool, it’s nice.’
School 2, Year 8, Female
Although the teachers in part agreed that this activity would raise students’ awareness of how they might be targeted by tobacco companies, they felt that this did not resonate with lower-ability students.
Do you know that little clip where the boss is being very subtle going, ‘oh do you use social media?’. And, ‘oh we could do brand placement. Oh but we’re not allowed to.’ And it was all very subtle . . .Yeah and do you know lower-ability pupils wouldn’t have got that. I think that would have confused them, where the other pupils it wouldn’t have.
School 1, Teacher 1
In some cases, teachers had to provide students with further explanations of why they were doing the activity or gave additional examples of how products are marketed to people [such as in the cases of Nike (Nike, Inc., Beaverton, OR, USA) and Red Bull (Red Bull GmbH, Fuschl am See, Austria)], in order for students to understand that they were learning about how tobacco companies might target young people. Teachers felt that this was necessary so that students did not confuse it with learning how to promote tobacco products.
The way I did it was I did some energy drink ones because just before that we’d done energy drinks as well. So I did, you know like ‘Red Bull gives you wings’ and we looked at that, we talked about how that made it a slogan that people . . . you wanted to buy it, but we did slogans in general, you know, like Nike, ‘Just Do It’ and things like that. So they understood what a slogan was and what the purpose of it was before they wrote it.
School 1, Teacher 12
As a result of the potential misunderstanding that she felt might arise, one teacher decided to not complete this activity with some classes.
We didn’t get to do the slogan either because our teacher didn’t think it was appropriate for our age. For year ten’s but not our age group.
School 2, Year 8, Female
I think for lower abilities in Year eight, they would be wondering why they were supposed to [be] advertising tobacco rather than trying to get into the head of . . . some of them just aren’t quite mature enough to be able to do that yet . . . I wanted the message to be clear to them that it was anti-smoking rather than, oh well sometimes it’s OK to say it’s good to smoke. So I just ignored that part.
School 2, Teacher 1
To overcome the problem, teachers suggested that making the purpose of the task clearer for students was important. Some also suggested including a prompt in the teachers’ handbook for teachers to use examples of how products are advertised to young people.
I think if you put in the resource discuss celebrities you know about, then you’re not naming anyone, but it gives a focus point for . . . Especially for lower-ability groups, you can talk about sports people, it’s really easy.
School 1, Teacher 1
Students also enjoyed giving their opinion in the Twitter activity. They also stated that it was enjoyable because it was familiar territory for them. Others, however, said that they found it difficult to complete because they found it difficult to think of something original, or they were not used to using Twitter and were confused about using 140 characters.
The Tweet one was obviously harder to do, because we had a certain amount of words and it was like hard to put smoking into words without, because normally you get, ‘Oh yeah, it kills’ and stuff, but you want to put something more, so it actually convinces people.
School 1, Year 8, Female
The Tweet could have been a bit less wordy, like some Tweets tend to be . . . I think we felt implied [sic] to fill out all 140.
School 1, Year 8, Male
To overcome this problem, teachers suggested that students might be given some more examples of Tweets, as well as more direction about what the Tweet needed to achieve (i.e. to try to persuade someone to not smoke, using new information about the tobacco industry rather than reverting to using existing knowledge).
They just stick with what they know so they’ve thought about everything before and had the discussions, but I think when it comes to that kind of stuff they do go back to what they know . . . maybe get them to be a bit more specific about what they have to write their slogans [referring to Twitter activity] about, like maybe it has to be a bit more targeted towards other things.
School 1, Teacher 2
In addition to these activities, some teachers also felt that lower-ability students generally struggled with the language used in the resource because it was too advanced for them. As a result, a teacher took the decision not to deliver the lesson to their lowest ability set.
Some of the language was quite high level, I thought. And for my higher groups they lapped it up, but when I looked at it, and I’d done it with higher groups, I made a decision not to do it with my bottom set. They are almost non-readers, very low ability pupils, but they would have struggled with this.
School 1, Teacher 1
Teachers suggested that differentiating the existing activities would enable teachers to provide students with an activity suited to their ability level. This was considered to be usual practice for schools in curriculum subjects.
What we do in a lot of subjects in this school, if we’re teaching we’d have maybe three levels of ability. So for the lower ability it would be a lot more . . . You know, why do you think people stop smoking, and there might be lots of different answers, circle the one that you think, rather than writing it down. So they’re not writing as much, or for them it will just be put your hand up and tell you teacher rather than writing it down.
School 1, Teacher 1
Yes because that’s what we do as teachers anyway, we have to differentiate so we don’t give them all the same task because not everyone is starting at the same point. Like [name] said, a choice of maybe two activities so the teacher can say, right this is the one that we’re doing, or which one do you think that you could do.
School 2, Teacher 1
Extending Operation Smoke Storm
Teachers suggested that the topic of electronic cigarettes (e-cigarettes) needed to be covered by Operation Smoke Storm; students had mentioned e-cigarettes during discussions in some lessons and teachers felt that they needed access to correct information as they had to rely upon their own knowledge.
We did talk about e-cigarettes but I think that would be something that perhaps could be added to the resource . . . If I’d a known all the facts and basics about them then I would probably have been better informed, rather than kind of making it up.
School 1, Teacher 10
Furthermore, there was a general lack of knowledge, among both students and teachers, of whether the health effects of e-cigarettes are worse than those of normal cigarettes, and uncertainty as regards what they contain.
They seem better, but you don’t actually know what’s in them.
School 1, Year 8, Male
I kind of was quite honest with them and just saying what I did know and what I didn’t . . . Again, I think a lot of them then had that argument for, ‘Oh well they’ve not got nicotine it,’ and then I had to go, ‘Well we don’t know, some of them might do, some of them might not.’
School 1, Teacher 2
Students’ knowledge of e-cigarettes was limited and in some cases, incorrect.
They’re just making it even worse, because they don’t do the same damage as cigarettes, but you can still get addicted and they could still do damage to your body.
School 1, Year 7, Male
I don’t think they particularly are worse but I don’t think, like . . . it might be a bit better than . . . if you’re smoking, it might be a bit better having an e-cigarette.
School 1, Year 8, Female
Summary
The qualitative findings presented here suggest that, in line with the feedback received during phase 1, the Operation Smoke Storm Year 7 lessons, accompanying family booklet and Year 8 booster are an acceptable smoking-prevention intervention and can be delivered successfully by teachers to raise awareness about tobacco-related issues. Once again, the off-the-shelf nature of the classroom-based resources was well received by teachers, and students enjoyed the interactive nature of the activities. Year 8 students found the use of social media in the booster session appealing and something to which they could relate. Although many students said that they did not take the family booklet home, parents reported it to be a useful way to improve their own knowledge and initiate conversations around smoking.
As reported in Chapter 5, there was no quantitative evidence that Operation Smoke Storm is effective in preventing smoking uptake. The qualitative findings discussed here offer some potential explanations for this apparent lack of effectiveness. These are discussed in Chapter 8.
The feedback collected from teachers, parents and students in phase 2 was translated into a set of recommendations for further refinement of the resources, which were given to Kick It should they wish to implement these in the future.
A summary of the findings from phase 2 of the research was sent to the Head of PSHE at each school for distribution to the teachers who had participated in the research (see Appendix 8).
Chapter 7 Costs of the intervention and health and quality of life of children
A full cost-effectiveness analysis was planned as part of a definitive trial of Operation Smoke Storm, but given the lack of quantitative evidence indicating potential effectiveness, and the resulting recommendation of the DMEC not to progress to a full trial (see Chapter 2), a cost-effectiveness analysis cannot be undertaken. Instead, here we present the costs incurred in developing and delivering the intervention. As part of the questionnaire delivered to Year 8 students in phase 2 we piloted the questions that would have been used to gather data for a full cost-effectiveness analysis. In this chapter we use the information collected from students to assess the feasibility of gathering data in a school setting for health economic evaluation of health-promotion interventions. Using these data, we estimate the health-care costs associated with smoking in the study population and quantify the state of students’ health.
Methods
Resources used in the development and delivery of Operation Smoke Storm
Two main components of resource use were considered in the calculation of the intervention costs. First, resources used in developing the intervention were identified, including those spent improving the original version of Operation Smoke Storm, as well as those incurred developing the booster and family components. Second, resource inputs required for delivering Operation Smoke Storm were identified.
A microcosting approach was used to calculate costs whereby each cost component was computed by attaching a unit cost to the quantity of resource used. 65 Unit costs were identified from study records and published sources. All costs are reported in UK pounds sterling in 2013/14 prices. An NHS and education perspective is adopted in the analysis and other methods are in line with the NICE Technology Appraisal Guidelines. 66 Numbers may not add up owing to rounding.
Collection of health economic data from students
Health economics questions were piloted with Year 8 students in phase 2 as part of the follow-up after the Operation Smoke Storm booster session. At this point, no decision had been made over whether progression to a fully powered trial was justified, and piloting these questions was undertaken as a learning opportunity to highlight any necessary changes to the survey instruments needed should the trial have progressed.
Following guidance on collecting data from children,67 the questionnaires utilised in this study were designed to be easy to understand, and difficult vocabulary was avoided. The format of the questions was short and simple and only particularly relevant questions were asked. The questions administered were broadly divided into two sections (see Appendix 3 for the full questionnaire). Receiving a smoking-prevention intervention may change students’ smoking behaviours and thus their health-care resource use. Therefore, data were first collected on the prevalence of smoking-related diseases and disease-related health-care resource use, including general practitioner (GP) visits, use of hospital care and use of medications. Ever smokers were also asked about their use of resources to help them stop smoking, including NHS smoking cessation services and nicotine replacement therapies.
The second part of the health economics questionnaire collected data on students’ health condition using the European Quality of Life-5 Dimensions Youth version (EQ-5D-Y; www.euroqol.org/eq-5d-products/eq-5d-y.html). 68,69 This survey instrument has been developed specifically for children and adolescents aged from 8 to 18 years, but to date has not been widely used in studies in UK schools. We chose to use the EQ-5D-Y as it is a cognitively simple tool, designed for self-completion, which provides a standardised, single-index measure of health status reflecting both physical and psychological health. Compared with other health outcome measures such as smoking status, EQ-5D-Y was used as a generic measure that can help decision-makers to make direct comparisons with other health-care programmes.
EQ-5D-Y comprises five questions, each of which relates to a different health dimension: mobility; ability to look after oneself; ability to take part in usual activities; having pain or discomfort; and feeling worried, sad or unhappy. 70 Each dimension has three levels of response (no problems, some problems, or a lot of problems) and the combination of three levels of five questions can define a total of 243 possible health states. In addition to the EQ-5D-Y questions, students were asked to rate their health on the EQ-5D-Y vertical, visual analogue scale (VAS) on which the end points are labelled 100 (best imaginable health state) and 0 (worst imaginable health state).
The results first describe the completeness of data collection for the various health economic survey items. This information is supplemented by feedback from the teacher interviews describing problems encountered in teachers administering, and students completing, the health economics questions. Collected data are then used to describe the health status and use of health-care resources among the study population over a 12-month period.
Results
Resources used in the development and delivery of Operation Smoke Storm
Development costs
As described previously, the original Operation Smoke Storm Year 7 lessons were delivered in two schools in the autumn term of 2013, and then improved based on feedback from students and teachers. In addition, a booster session and family booklet were also developed from scratch. Table 7 summarises the costs associated with the improvements to the Year 7 lessons and the development of the additional components. Costs included graphic design, script writing, film shooting, digital editing and online resource development. Whereas some costs were incurred by the hour, others were incurred on a ‘finished item’ basis. It is therefore not possible to describe more fully the units (e.g. hours of input) required to develop the intervention.
| Component | Cost (£) |
|---|---|
| Improvements to existing Year 7 Operation Smoke Storm | 16,391 |
| Development of family booklet to accompany Year 7 lessons | 4080 |
| Development of booster session for Year 8 | 15,570 |
| Total | 36,041 |
The overall cost of developing the intervention was £36,041. However, as these development costs were a one-time expense, an increase in the number of users will result in the unit development cost approaching zero.
Delivery costs
Delivery costs comprised two main components: (1) the cost of training teachers and (2) the cost of delivering the intervention.
Each of the Year 7 and Year 8 teachers attended a 30-minute, in-person, training session delivered by a research assistant. Training costs include the costs of the research assistants’ and teachers’ time, overheads and consumables. The cost inputs for delivering the intervention include teachers’ time spent preparing and delivering the sessions, printing of resources and overheads for the premises. The unit cost of teachers’ time was calculated by combining teachers’ wages with salary oncosts (National Insurance and superannuation) and indirect and direct overheads. Table 8 lists the composition of each unit cost for teachers.
| Unit cost | 2013/14 value | Notes and sources |
|---|---|---|
| Wages and salaries | £28,807 per year | Based on the mean full-time equivalent basic salary for qualified teachers in England. In 2013/14, a total salary of £8,713,772 was paid to 302,483 full-time equivalent teaching staff employed71 |
| Salary oncosts | £4803 per year | Employer’s contribution to social security costs and pension costs (16.7% of salary)71 |
| Overheads: staff management and administration | £640 per year | Management and other non-teaching staff costs were 2.2% of direct teachers’ salary costs and included administration and estates staff71 |
| Overheads: non-staff | £3562 per year | Non-staff overheads costs were 12.4% of direct salary costs.71 They include costs for management and administration, educational supplies, travel/transport, telephone, computers, as well as utilities such as water, gas and electricity |
| Cost of using classrooms | £3729 per year | Including rental and depreciation of land, buildings and equipment71 |
| Total cost | £41,541 per year | |
| Working hours | 1265 hours per year | Teachers in England are required to teach and perform other duties for 1265 hours of directed time per year (spread over 195 days)72 |
| Cost of a 1-hour PSHE session | £32.84 per hour |
Intervention costs for delivering the full Operation Smoke Storm package (Year 7 lessons with accompanying family booklet, plus Year 8 booster) are summarised in Table 9. The full-time equivalent basic salary for qualified teachers in the UK ranges from £22,023 to £37,119 (2014 figures)72 and the national average salary for a research assistant is £26,500 (range £19,000–34,000). 73 The figures in brackets in Table 9 show the cost estimates when pay levels are varied across this range. Schools outside London that use Operation Smoke Storm pay an annual licence fee of £150 plus value-added tax (VAT) of 20%, although any VAT incurred by a school is recoverable. There is currently no fee for schools in the London area.
| Item | Total costs (£), mean (range) | Cost per class (£), mean (range) |
|---|---|---|
| Year 7 (delivered to 14 classes) | ||
| Teacher training | 378 (308–448) | 27 (22–32) |
| Printing of student booklets | 216 (216–216) | 15 (15–15) |
| Printing of teacher notes | 57 (57–57) | 4 (4–4) |
| Teacher preparation | 345 (264–444) | 25 (19–32) |
| Teacher delivery | 1149 (879–1481) | 82 (63–106) |
| Printing of family booklet | 160 (160–160) | 11 (11–11) |
| Total cost | 2305 (1884–2806) | 165 (134–200) |
| Year 8 (delivered to 21 classes) | ||
| Teacher training | 567 (462–672) | 27 (22–32) |
| Printing of student booklets | 83 (83–83) | 6 (6–6) |
| Printing of teacher notes | 49 (49–49) | 2 (2–2) |
| Teacher preparation | 90 (69–116) | 4 (3–6) |
| Teacher delivery | 690 (527–889) | 33 (25–42) |
| Total cost | 1480 (1190–1809) | 72 (58–88) |
| Annual licence fee per school | 150 (0–150) | 17 (0–17) |
| Total intervention cost | 3934 (3074–4765) | 253 (192–304) |
The total cost for delivering Operation Smoke Storm to two schools was an estimated £3934 (range £3074–4765), of which approximately two-thirds was the costs of delivering the Year 7 sessions and accompanying family booklet. In 2014 there were 3329 state-funded secondary schools in the UK, with, on average, 45 classes per school (nine Year 7 classes) and 20 students per class. 51 Based on these figures, the estimated average cost of the complete intervention package was £253 (range £192–304) per class or £13 (range £10–15) per student.
These costs are based on conservative assumptions to ensure that the costs of the intervention are not underestimated. For example, each class teacher was assumed to attend training twice, once for the Year 7 sessions and once in the following year for the Year 8 booster. In practice, however, some teachers may teach more than one Year 7 or Year 8 class, or teach the same year group in consecutive years, and would, therefore, need to attend the relevant training session only once. This would generate cost savings in the training process in the long term.
The unit cost of delivering the intervention is much cheaper than many other school-based smoking-prevention interventions. For example, ASSIST reported an average cost of £32 (95% CI £29.70 to £33.80) per student, the higher cost of which is likely to be explained, at least in part, by the delivery of training to peer educators by non-teachers at a venue outside school. 25
Collection of health economic data from students: data completeness
Completed questionnaires were received from 445 students in total (of 538 Year 8 students on the school registers, a response rate of 82.7%). Table 10 presents the number of missing data for each of the health economics questions.
| Question | Number of students eligible to answer question | Number of complete responses | Missing, n (%) |
|---|---|---|---|
| Prevalence of smoking-related disease in past 12 months | |||
| Asthma | 445 | 436 | 9 (2.0) |
| Chest infections | 445 | 418 | 27 (6.1) |
| Ear infections | 445 | 412 | 33 (7.4) |
| Meningitis | 445 | 401 | 44 (9.9) |
| Health-care resource use for smoking-related diseases | |||
| Asthma | 60 | 52 | 8 (13.3) |
| Chest infections | 60 | 53 | 7 (11.7) |
| Ear infections | 64 | 60 | 4 (6.3) |
| Meningitis | 2 | 1 | 1 (50.0) |
| Use of other medications | 445 | 230 | 215 (48.3) |
| Use of stop smoking aids by ever smokers | |||
| Teachers | 34 | 21 | 13 (38.2) |
| School nurses | 34 | 21 | 13 (38.2) |
| Nurse at GP practice | 34 | 21 | 13 (38.2) |
| Stop smoking service | 34 | 21 | 13 (38.2) |
| Quitline | 34 | 21 | 13 (38.2) |
| e-cigarettes | 34 | 26 | 8 (23.5) |
| NRT | 34 | 21 | 13 (38.2) |
| EQ-5D-Y | |||
| Mobility dimension | 445 | 406 | 39 (8.8) |
| Self-care dimension | 445 | 408 | 37 (8.3) |
| Usual activities dimension | 445 | 407 | 38 (8.5) |
| Pain/discomfort dimension | 445 | 407 | 38 (8.5) |
| Worry/sad/unhappy dimension | 445 | 399 | 46 (10.3) |
| EQ-5D-Y VAS | 445 | 399 | 46 (10.3) |
There may be limitations to asking students to recall their health and resource use over a 12-month period, although there are no accepted recommendations as to the length of window that is most appropriate, which may vary according to the frequency, duration and salience of a particular event. More than 90% of students responded to the questions asking if they had, at the time of the survey or in the past year, particular smoking-related diseases. Students who indicated that they had experienced a particular illness were asked to report their utilisation of health-care resources for treating these conditions, specifically seeing a GP, visiting accident and emergency (A&E), or using hospital outpatient and/or inpatient services. Students reporting asthma were also asked approximately how many times per week they used a blue (reliever) or brown (preventer) inhaler. A student’s answer was considered as missing only if all items about health-care use were missing simultaneously. Students counted as missing may therefore include some who had the condition but who did not receive any treatment, although this number is arguably small, as, for most conditions, receiving at least some treatment is likely. The level of missing resource-use data for treating smoking-related diseases was relatively low: 13.3% for asthma, 11.7% for chest infections and 6.3% for ear infections. Of the two students who reported having had meningitis, one did not provide data on their use of health-care resources; the small number of students here precludes any conclusions being drawn for this group.
In a free-text question students were asked if they had taken any medications in the past year (apart from for asthma) and their reasons for doing so. Compared with the closed questions, this open question had a much higher proportion of missing responses; 215 students (48.3%) left this question blank. It is unclear if they did not answer the question because they had no medication use to report, because they could not remember, because they did not understand the question or for another reason. Although a low response rate to this item was anticipated, this type of question can potentially provide valuable information for subsequent analysis. A number of students did, however, give vague responses such as ‘I was ill’ or ‘I took tablets’. Table 11 displays the 10 most frequent conditions and medications reported, as well as the number of vague responses.
| Health problems | Frequency | Medication | Frequency |
|---|---|---|---|
| Headache | 66 | Paracetamol | 87 |
| Cold | 27 | CALPOL® (paracetamol, Johnson & Johnson Limited) | 55 |
| Hay fever | 24 | Ibuprofen | 32 |
| Ear infection | 19 | Antibiotics | 15 |
| Cough | 17 | Nurofen® (ibuprofen, Reckitt Benckiser Group plc, Slough, UK) | 14 |
| Stomach ache | 8 | Piriton® (chlorphenamine, GlaxoSmithKline, Brentford, UK) | 5 |
| Chest infection | 6 | Painkillers/pain relief | 7 |
| Sore throat | 6 | Eardrops | 4 |
| Tonsillitis | 6 | Morphine | 3 |
| Pain | 5 | Cough medicine | 3 |
| Ill/sick/sickness | 21 | Unknown/tablets | 33 |
Approximately two-thirds of the 34 self-reported ever smokers completed the questions asking about things they have done in the past year to help them give up smoking, and three-quarters provided information on whether they had used e-cigarettes or not.
The proportion of students who failed to complete EQ-5D-Y items ranged from 8.3% for the self-care dimension to 10.3% for the feeling worried, sad or unhappy dimension. Of the 445 students who returned completed questionnaires, 395 (88.8%) provided valid answers for all five EQ-5D-Y dimensions. There were 35 (7.9%) students who left all five questions blank and another 15 (3.5%) who answered some, but not all, of the questions; 46 (10.3%) students did not complete the EQ-5D-Y VAS rating.
Collection of health economic data from students: feedback from teacher interviews
Qualitative data from the Year 8 teacher interviews provided some insight into students’ abilities to complete the questionnaires.
Teachers reported that, although many students were competent enough to complete the questionnaire, there were a few issues, not all of which were unique to the health economics section. For example, students of lower ability struggled to understand the questions and subsequently required more teacher assistance. Some students also found it difficult to follow the routing through the questionnaire, whereby they were directed to skip questions if they were not relevant based on their answers to previous items.
For my higher ability group, they were fine, but my lower ones really struggled. They didn’t understand the questions and they didn’t understand that when it was like ‘if you answered yes, go to question . . .’ In their sort of mind it was like, you just answered every question.
School 1, Teacher 12
In completing the EQ-5D-Y VAS teachers reported that, although most of the students were fit and healthy, some marked their health as being under 50 on the 0–100 scale. They suggested that students did not fully understand the value, for example 20 or 80, of the degrees of the scale without a detailed explanation. As a result, some failed to match their health status to the appropriate range on the scale.
Even though most of them are fit and healthy, they were still less than 50 on that scale . . . they just couldn’t get their heads round . . . You may have to write keywords down the side.
School 1, Teacher 1
In addition, some students had difficulty understanding medical terminology, which required a brief explanation from the teacher. Others could not recall which medicines they had taken and what they were for.
. . . they didn’t know what meningitis was, for example. Bottom sets. So I had to explain.
School 2, Teacher 1
Students’ health status
Smoking-related diseases and related prescriptions
Reported disease prevalence was 13.8% for asthma, 14.4% for chest infection, 15.5% for ear infections and 0.5% for meningitis. Unit costs for health service use ascertained from students are provided in Table 12. Medication unit costs were obtained from the March 2014 edition of the British National Formulary. 76 Where national average unit costs were not available for medications, the most widely used brand was used to ascribe the unit cost. 77 For example, the price of the Ventolin® Evohaler® salbutamol 100 µg metered inhaler (GlaxoSmithKline UK Ltd, Middlesex, UK) was used as an approximation of the unit cost of an asthma reliever inhaler, and the price of the Clenil Modulite® 100-µg 200-dose inhaler (Chiesi Ltd, Manchester, UK) (£7.42) was applied as the cost of an asthma preventer inhaler.
| Item | Unit | Cost (£) |
|---|---|---|
| GP visit74 | Visit (average 11.7 minutes) | 42 |
| A&E attendance75 | FCE | 124 |
| Day case75 | FCE | 698 |
| Inpatient stay75 | Per bed night | 563 |
| Outpatient attendance75 | FCE | 111 |
| Blue inhaler76 | 100 µg (200-dose unit) | 1.50 |
| Brown inhaler76 | 100 µg (200-dose unit) | 7.42 |
| Spacer device76 | Per item | 4.79 |
| Prescription cost (net ingredient cost)77 | Per prescription | £8.37 |
The type and frequency of health-care use related to asthma, chest infections, ear infections and meningitis are listed in Table 13, rounded to the nearest pound. The mean cost of treating each disease was £55 (SD £664), £42 (SD £344), £51 (SD £412) and £4 (SD £91), respectively. This is equal to an overall cost of £153 (SD £1512) per student to treat smoking-related disease in the past 12 months. Given the relatively small number of events, among a small number of students, we have not presented resource use separately according to smoking status.
| Resource | Number of instances reported | Number of students reporting use | Instances per student reporting use, mean (SD) | Instances across all students, mean (SD) | Cost per student (£), mean (SD) | Number of instances reported | Number of students reporting use | Instances per student reporting use, mean (SD) | Instances across all students, mean (SD) | Cost per student (£), mean (SD) | Total cost for all diseases (£), mean (SD) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Asthma | Chest infections | ||||||||||
| GP visits | 112 | 41 | 2.7 (3.4) | 0.3 (1.5) | 11 (63) | 80 | 41 | 2.0 (1.4) | 0.18 (0.74) | 8 (31) | |
| A&E visits | 12 | 4 | 3.0 (1.4) | 0.03 (0.32) | 3 (39) | 7 | 4 | 1.8 (0.5) | 0.02 (0.18) | 2 (22) | |
| Hospital day case | 8 | 7 | 1.1 (0.4) | 0.02 (0.15) | 13 (107) | 16 | 9 | 1.8 (1.1) | 0.04 (0.30) | 25 (207) | |
| Overnight hospital stays | 21 | 4 | 5.3 (7.2) | 0.05 (0.79) | 27 (442) | 6 | 4 | 1.5 (0.6) | 0.01 (0.15) | 8 (84) | |
| Reliever inhaler (uses per week) | 14,300 | 46 | 311.0 (586.0) | 32.2 (256.5) | 1 (6) | ||||||
| Preventer inhaler (uses per week) | 13,832 | 44 | 314.4 (398.1) | 31.1 (160.8) | 2 (8) | ||||||
| Total, £ | 55 (664) | 42 (344) | |||||||||
| Ear infections | Meningitis | ||||||||||
| GP visits | 105 | 45 | 2.3 (2.9) | 0.24 (1.21) | 10 (51) | 10 | 1 | 10.0 (0) | 0.02 (0.47) | 1 (20) | 29 (165) |
| A&E visits | 16 | 7 | 2.3 (1.6) | 0.04 (0.36) | 4 (44) | 2 | 1 | 2.0 (0) | 0.004 (0.10) | 1 (12) | 7 (78) |
| Hospital day case | 22 | 11 | 2.0 (1.6) | 0.05 (0.40) | 35 (279) | 1 | 1 | 1.0 (0) | 0.002 (0.05) | 2 (33) | 65 (559) |
| Overnight hospital stays | 2 | 2 | 1.0 (0) | 0.004 (0.07) | 3 (38) | 1 | 1 | 1.0 (0) | 0.002 (0.05) | 1 (27) | 11 (148) |
| Reliever inhaler (uses per week) | 1 (6) | ||||||||||
| Preventer inhaler (uses per week) | 2 (8) | ||||||||||
| Total, £ | 51 (412) | 4 (91) | 153 (1512) | ||||||||
EQ-5D-Y
Figure 3 shows the distribution of EQ-5D-Y responses across the five dimensions among students who answered all five questions. The highest frequency of problems was reported on the ‘feeling worried, sad or unhappy’ dimension, followed by the ‘having pain or discomfort’ dimension. The distribution of responses was in line with those from a multinational study of the feasibility, reliability and validity of the EQ-5D-Y instrument. 69
FIGURE 3.
Distribution of EQ-5D-Y scores: frequency of reported problems.

Of the 395 students who answered all five EQ-5D-Y questions, 356 were never smokers and 30 students were classified as ever smokers (smoking status could not be ascertained for nine students). Table 14 summarises the number and proportion of respondents reporting problems in EQ-5D-Y dimensions by smoking status.
| Dimension | Ever smoker | Never smoker | p-value for difference (chi-squared or t-test) |
|---|---|---|---|
| Mobility, n (%) | |||
| No problems | 23 (76.7) | 333 (93.5) | 0.003 |
| Some problems | 7 (23.3) | 22 (6.2) | |
| A lot of problems | 0 (0.0) | 1 (0.3) | |
| Self-care, n (%) | |||
| No problems | 30 (100.0) | 354 (99.4) | 0.681 |
| Some problems | 0 (0.0) | 2 (0.6) | |
| A lot of problems | 0 (0.0) | 0 (0.0) | |
| Usual activities, n (%) | |||
| No problems | 23 (76.7) | 322 (90.5) | 0.033 |
| Some problems | 7 (23.3) | 31 (8.7) | |
| A lot of problems | 0 (0.0) | 3 (0.8) | |
| Pain/discomfort, n (%) | |||
| No problems | 12 (40.0) | 245 (68.8) | 0.002 |
| Some problems | 18 (60.0) | 105 (29.5) | |
| A lot of problems | 0 (0.0) | 6 (1.7) | |
| Sad/unhappy, n (%) | |||
| No problems | 14 (53.9) | 228 (64.0) | 0.037 |
| Some problems | 12 (46.2) | 113 (31.7) | |
| A lot of problems | 0 (0.0) | 15 (4.2) | |
| EQ-5D-Y score, mean (SD) | 0.75 (0.2) | 0.86 (0.2) | 0.004 |
| EQ-5D-Y VAS, mean (SD) | 79.96 (12.1) | 84.66 (14.5) | 0.097 |
Ever smokers reported significantly more problems in four of the five EQ-5D-Y dimensions. The biggest difference was observed in the pain and discomfort dimension, where 60% of ever smokers reported some or a lot of problems compared with 31.2% of never smokers (p = 0.002). The second largest difference was found in the worry/sad/unhappy dimension, where 46.2% of ever smokers reported some or a lot of problems compared with 35.9% of never smokers (p = 0.037).
The EQ-5D-Y results were converted into index scores using UK population values (based on the adult tariff for the EQ-5D, the best available option). 78 The overall mean EQ-5D-Y score was 0.85 (SD 0.2), which was almost identical to the mean EQ-5D score among the UK general population aged 16+ years [0.86 (SD 0.2)]. 79 Ever smokers had a mean EQ-5D-Y score that was statistically significantly lower (indicating a worse health state) than students who had never smoked (0.75 vs. 0.86; p = 0.004). To the best of our knowledge, no existing studies have quantified EQ-5D-Y according to smoking status in adolescents. However, the differences observed here reflect those seen among adults, where EQ-5D scores were highest among never smokers (and not dissimilar among ex-regular and light smokers) and lowest among the heaviest smokers. 79
The EQ-5D-Y scores were significantly higher (indicating a better health state) for boys than for girls (0.88 vs. 0.82; p = 0.0007) but were similar between students who were and were not eligible for free school meals (0.848 vs. 0.851; p = 0.9402). There was also no significant difference in score between students who reported exposure to second-hand smoking and those who did not (0.83 vs. 0.85; p = 0.444).
Figure 4 displays the distribution of EQ-5D-Y VAS scores among respondents, on a scale of the best health they can imagine (score 100) to the worse health they can imagine (score of 0). The median VAS score was 90 (IQR 80–95). Only 2.8% of students rated their health at a score of < 50. EQ-5D-Y VAS scores were significantly lower (indicating a worse health state) in ever smokers than in never smokers [median 80, (IQR 75–90) vs. median 90 (IQR 80–95); p = 0.015].
FIGURE 4.
Distribution of EQ-5D-Y VAS scores.
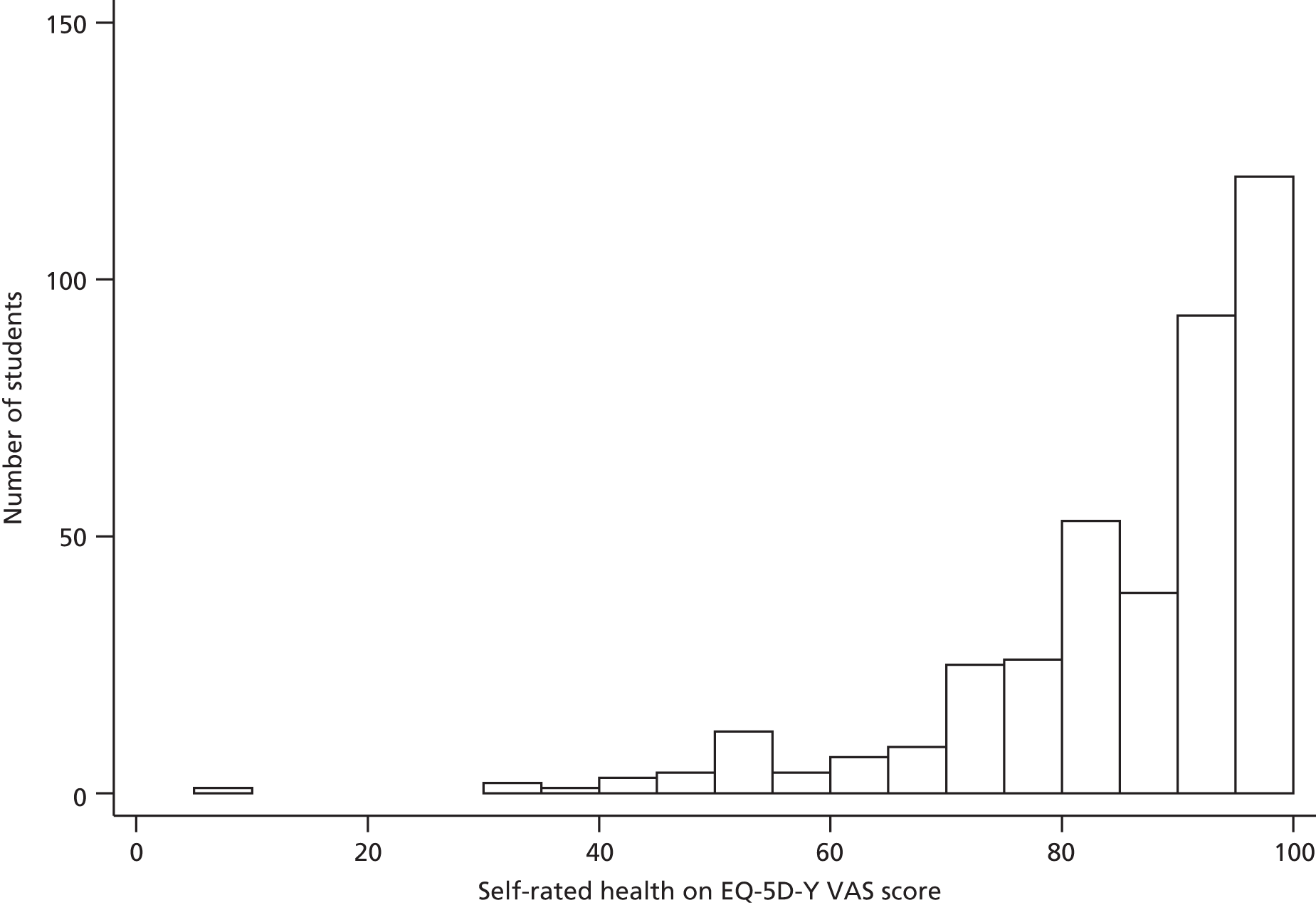
Summary
This chapter has provided estimates of the resource use and costs associated with the development and delivery of Operation Smoke Storm and has assessed the feasibility of obtaining health-care resource use and health status data from secondary school students. The data presented in this chapter suggest that it would be feasible to collect data to carry out a health economic evaluation as part of a fully powered trial of Operation Smoke Storm, or indeed a trial of another youth smoking-prevention intervention.
The EQ-5D-Y questions proved generally easy to complete (although some students required support from a teacher to do so) and the instrument appears sensitive for detecting differences in health status between ever and never smokers. The combination of three levels of five questions of the EQ-5D-Y can define a total of 243 possible health states, each of which can be assigned a utility weight on a scale from 0 (death) to 1 (perfect health), although some health states may be considered worse than death and have negative scores. 80 In a fully powered trial, the EQ-5D-Y instrument could be used to gather utility scores at different time points across the study, the results of which can be translated into quality-adjusted life-years (QALYs) by applying an area under the curve method,81 in order to undertake a full incremental cost-effectiveness analysis. The QALY has the advantage that it can help decision-makers to make direct comparisons between the cost-effectiveness of a particular intervention and other health-care programmes. 65
This pilot study has identified areas in which data collection can be improved in order to increase completeness of the data retrieved. The results provide evidence for the potential usefulness of a health economics questionnaire for the systematic collection of health economics information from school-aged children, which could potentially be used in a wide range of school-based health-related studies.
Chapter 8 Discussion and conclusions
In this final chapter we provide a brief summary of the results of the work and interpret the findings. We then reflect on the outcomes and highlight some of the pertinent issues that emerged while conducting the research. We consider the strengths and limitations of the work and offer some considerations for future research in this field.
Summary and interpretation of results
This project was the first of its kind to formally deliver and evaluate a school-based intervention based on the premise of the US mass media Truth® campaign, the evaluation of which has suggested that highlighting the ethics and exploitative tactics of the tobacco industry is a promising way in which to prevent young people from starting to smoke.
Operation Smoke Storm proved feasible to deliver in the classroom setting. In the main, the intervention (including the Year 7 lessons and accompanying family booklet, plus Year 8 booster session) was acceptable to teachers, students and parents, and helped to raise awareness about smoking-related issues and the tobacco industry. Generally, teachers felt that the resource was relevant, accessible and pitched appropriately for most of their students. The interactive nature of Operation Smoke Storm appealed to students, who appreciated the fact that the style of delivery was more stimulating than the lessons they often received in PSHE. Data on the financial costs of delivering Operation Smoke Storm suggest that the intervention can be delivered at a relatively low cost in comparison to other school-based smoking-prevention programmes. However, quantitative evaluation (from a non-randomised comparison, although adjusted for confounders) showed no differences in the odds of self-reported ever smoking and susceptibility to smoking in those students who received Operation Smoke Storm compared with those students from local schools in which the intervention was not delivered. Synthesis of the qualitative and quantitative data suggests potential reasons why the intervention does not appear to be effective in preventing youth smoking uptake.
The primary aim of Operation Smoke Storm is to encourage students to think about tobacco industry practices and ethics. However, the extent to which students in this study took these issues on board is questionable. In the focus groups (see Chapters 3 and 6), students’ interest and recall centred mainly on the content of cigarettes and the health effects of smoking, which many students had learnt about (albeit in less detail) when they were at primary school. It might be that concepts covered by Operation Smoke Storm, such as strategies employed to market tobacco, are too advanced for this age group to comprehend fully, and, as a result, they defaulted to more familiar knowledge. Alternatively, the repetition of factual information related to cigarette content and the health effects of smoking might have helped to consolidate prior learning and, as a result, students may have been more likely to recall this information in the focus groups. Some Year 8 teachers raised concerns that the messages of the booster session were too subtle for students of lower academic ability to grasp (see Chapter 6). While developing Operation Smoke Storm, care was taken to include only content that was supported by credible, citable evidence and not to include anything that could be considered libellous. However, the more subtle nature of some of the messages might have resulted in some students missing the points that the resources aimed to get across. Adult smoking prevalence is highest among those with lower level educational qualifications,82 and educational attainment, aspirations and engagement are also associated with adolescent smoking. 83 It might be that Operation Smoke Storm did not reach those students who are most likely to become smokers. Among students of higher academic ability, who were perhaps more able to engage with the subtle messages of the intervention, Operation Smoke Storm might simply have reaffirmed their decision not to smoke.
The ‘dose’ of Operation Smoke Storm is relatively light in comparison to other school-based health-promotion interventions. For example, peer educators trained in ASSIST are asked to undertake informal conversations with their peers over a 10-week intervention period. However, as the findings presented in Appendix 1 show, most schools do not devote this much time to a single topic within their PSHE curriculum, and any intervention intended for delivery within usual teaching time must acknowledge and reflect this. Our use of a booster session, as recommended by NICE, helps to reinforce the message of the intervention and to increase its ‘dose’. It is, however, possible that a longer intervention period might have a larger impact on students’ smoking behaviours.
The prevalence of smoking among young people increases with age,9 and it might be that any effect of Operation Smoke Storm on uptake is delayed. Only when students are older might it be possible to infer if the effect of the intervention was sufficient to override prevailing pressures to experiment with tobacco. However, the lack of evidence to proceed to a definitive RCT with longitudinal follow-up means that this question will remain unanswered. Many students reported that participation in Operation Smoke Storm had made it less likely that they would try a cigarette, and there was evidence that students’ attitudes towards statements such as ‘companies that make cigarettes only try to attract customers aged 18+’ changed in the direction that might have been expected after receiving the intervention (see Chapter 5). These data are encouraging and, although these shifts in attitudes are not reflected in self-reported smoking and susceptibility in Year 8, the possibility remains that the impact of the intervention may become evident among these students in years to come. Although there was some suggestion in the focus groups (see Chapters 3 and 6) that talking to children about smoking might have a ‘forbidden fruit’ effect84 and serve to encourage curiosity and experimentation with tobacco, the quantitative data suggest that this this will not hold true for more than a small number of students.
The treatment fidelity questionnaires completed by teachers in phase 2 of the study (see Appendix 7) indicated that the majority of teachers did some degree of preparation prior to delivering Operation Smoke Storm, that they found the instructions clear and that they felt confident to deliver the intervention. The main reason reported for not being able to adhere strictly to the lesson plans provided was a lack of time, which was exacerbated by some technical difficulties downloading and streaming the video resources from the online server. Teachers generally compensated for this by either shortening discussions or extending the number of sessions, adaptations they felt did not impact upon students’ learning. However, a lack of discussion time may have compromised students’ abilities to consolidate their learning, and teaching spread over more sessions may have made it more difficult for students to retain new knowledge. Although attempts were made between phase 1 and phase 2 to address the timing issues, further work is needed to increase the flexibility of the resource for use in lessons of < 50 minutes and to ensure that it can be easily downloaded.
The Year 8 students on whom the primary analysis is based received the original version of the Year 7 lessons that were subsequently revised. The majority of the changes made were changes to correct technical issues in the operation of the digital resources (see Chapter 4), rather than changes to content, but the effect of the revised resources on smoking and/or susceptibility might have been different. Assessment of effectiveness based on exposure to the final Year 7 lessons may have produced different results. However, in the two cohorts, there were only small differences between Year 7 students’ overall impressions of Operation Smoke Storm, who they reported talking to and whether they thought that Operation Smoke Storm would make it less likely that they would ever try a cigarette. Therefore, it is unlikely that the revised version of Operation Smoke Storm would have had substantially different effects on smoking and susceptibility to smoking compared with the original version.
In addition, Year 8 students did not receive the family component of the intervention which was designed to accompany the Year 7 lessons. If the booklet had a significant effect on reducing smoking and susceptibility to smoking there may have been some underestimation of the intervention effect. However, few Year 7 students used the booklet as intended; approximately one-quarter did not show the booklet to anyone, and only a small minority completed the activities with their parents. Therefore, it seems that any potential underestimation of the intervention effects is very small if not non-existent.
The 95% CIs around the ORs quantifying differences in smoking behaviours between students in intervention and control schools were wide, and the adjusted risk differences were small (see Table 2). The achieved sample size meant that the study was powered to detect only differences in prevalence of 7% or more as statistically significant. The direction of the point estimate for the odds of ever smoking tentatively suggests that exposure to Operation Smoke Storm might reduce the odds of this outcome, although the OR for the combined outcome of ever smoking plus susceptibility suggests an increase in odds. A reduction in ever smoking following exposure to Operation Smoke Storm would be encouraging, and with a larger sample size the precision of the effect estimates would improve and smaller effect sizes may be detected as statistically significant. However, the potential increase in ever smoking combined with susceptibility is at odds with students’ reports that participation in Operation Smoke Storm had made it less likely that they would try a cigarette. Again, a larger sample size would help to improve the precision of the effect estimate.
Strengths and limitations of the research
This study employed a mixed-methods design, collecting both quantitative and qualitative data to assess the acceptability and potential effectiveness of Operation Smoke Storm. This mixed-methods approach enabled triangulation of data to strengthen the internal and external validity of the findings. Questionnaire data provided comprehensive feedback from students who received the intervention and focus group and interview data from teachers, students and parents enabled a more in-depth exploration of their experiences and views that provide potential reasons for the quantitative findings. Although the authors of this report played a part in refining the Year 7 lessons and developing the booster and family intervention components, this evaluation was carried out independently of Kick It, which developed the original Operation Smoke Storm and will distribute and support the delivery of the revised and extended intervention package beyond the end of the project. Evaluation was also carried out independently of the teachers who delivered the intervention.
Collection and analysis of quantitative data
The conclusions regarding the potential effectiveness of Operation Smoke Storm are based on data from only two schools and may not be generalisable to schools more widely. As acknowledged in Chapter 5, the two study schools served a relatively more affluent, ethnically white population than all schools nationally. Although an attempt was made to select two study schools serving different sociodemographic catchment areas, limits were imposed by the nature of the schools within the study area and by the willingness of schools to participate. Smoking is associated with both deprivation and ethnicity9 and, thus, smoking behaviours may not be representative of the national picture. Similarly, it is possible that the effects of the intervention may be different in schools with a different population of students. Our conclusions also rely on self-reported data on smoking and susceptibility, as it was felt that biochemical validation of smoking status (e.g. through the measurement of exhaled carbon monoxide or cotinine levels in saliva) would be an unacceptable burden on schools already stretched in terms of demands on their time. In addition, the majority of young people of this age are not daily smokers and thus analysis of cotinine would not have been appropriate. However, students were asked to complete the questionnaires on their own and were not asked for any personal identifiers in an attempt to encourage honest responses.
All students in Year 7 and Year 8 at the two study schools received the intervention and, therefore, there were no internal controls with which to compare smoking behaviour. Data from an external source, the Nottingham School Smoking Survey, were used as a control. Although all schools in Nottingham City and Nottinghamshire were invited to participate in this survey, participation was voluntary. Again, control schools were not representative of all schools nationally with respect to deprivation and ethnicity. Data were also collected 1–2 years prior to the current study, albeit using identically worded questions.
The non-randomised comparison meant there were significant differences between the characteristics of students in intervention and control schools, and the unfortunate inability to link Year 7 and Year 8 data from study schools meant that it was not possible to adjust for characteristics as measured at baseline. Particularly relevant is the lack of adjustment for smoking status at baseline, although there were only small differences in the prevalence of smoking and susceptibility in Year 7 in intervention and control schools and so this is unlikely to be a major problem. In addition, there was no comparable indicator of deprivation available for both intervention and control schools. However, the proxy indicator tested was not a significant confounder in the adjusted logistic regression models, and any effects of deprivation may have been accounted for by the inclusion of other confounding variables (as measured in Year 8), such as parental smoking and smoking in the home. If the work were to be repeated, students could be asked to generate their own anonymous code using a set of pre-defined questions, responses to which would not change over time (e.g. birth date of parent, first letter of mother’s name) and write this on their questionnaire. If the same code were generated at subsequent survey waves, linkage of responses over time would then be possible.
The comparison of study students’ beliefs about trying a cigarette and smoking regularly with findings from the Smoking, Drinking and Drug Use in Young People in England survey64 is again limited by use of an external control and lack of adjustment for confounders. However, the survey used a multistage probability sampling design to select schools by geographical region (response rate 44% of selected schools) and students within schools (response rate 88% of eligible students) to give a nationally representative sample weighted to account for non-response. Responses are based on an achieved sample size of over 1037 students in Year 7 and 1049 students in Year 8.
Collection and analysis of qualitative data
Qualitative data were collected and analysed using standardised, transparent procedures, although, again, it is possible that the use of only two schools might limit transferability of the findings to other schools. However, the fact that similar themes were reported across these two schools, which had different characteristics, increases confidence that the findings are likely to be transferable and externally valid.
The focus groups had to be conducted during school time and, thus, lesson length at each school governed the time available for these. As a result, it was often not possible to follow up discussion points in more detail. Furthermore, in phase 2 the Year 7 focus groups took place in one school only, as the other school was unable to deliver the revised Year 7 resource. In addition, some of the Year 8 focus groups had only a small number of participants, which meant that there was a less than ideal group dynamic, making discussion more difficult. The character and questioning style of the focus group facilitators and interviewers might have influenced the responses received from participants, although the use of topic guides helped to standardise procedures, and the male and female facilitators alternated the facilitation of the male and female focus groups. The data collected were, however, similar across all focus groups, suggesting a minimal impact of these limitations.
The students, teachers and parents who took part in the focus groups and interviews were a self-selecting sample, which introduced a potential for bias. Those who did not take part may have given different responses to those who did choose to participate. For example, the students who volunteered may have been those who already had a strong commitment not to smoke, or who were most engaged by the resource and receptive to its anti-smoking message; these students’ responses may have given a biased impression that the resource was suitable for all students. However, students were forthcoming when discussing what they did not like about the intervention. Ideally, focus group participants would have been purposefully sampled based on not only gender but also smoking status and, potentially, other factors such as academic ability and exposure to family and peer smoking. However, this was deemed too difficult and would have required students to provide classification information that they might not have been happy to share.
The use of the framework approach provided a rigorous series of steps to follow during data analysis. This facilitated the process of using multiple coders to generate an analytical framework and the charting stage enabled comparison across and within cases to identify patterns in the data to aid interpretation. This method provided transparency in terms of the analytical processes employed and an audit trail to justify how decisions were reached. This transparent analytical process counterbalanced any potential for biased interpretation in favour of the intervention.
Involving external public groups in the study strengthened the research. The Nottingham Smokers’ Panel and NCB Young Research Advisors provided a fresh perspective on the family booklet, although, given that the NCB group was a mixed-age group, in which most participants were older than the Year 7 age group, it was difficult to know the extent to which their ideas would mirror those of the target age group.
Recommendations for further work
Future work on how to prevent smoking uptake
Despite there being no evidence that Operation Smoke Storm is effective in preventing smoking uptake, there is scope for further work to address some of the limitations discussed above and to explore in greater detail the potential reasons for the lack of effectiveness, particularly given that both students and teachers generally enjoyed the intervention.
Operation Smoke Storm as it stands is probably not suitable for use with students much older than in the Year 7 and Year 8 groups studied here; some of these students even suggested that the storylines were too immature for them. However, the concept behind Operation Smoke Storm might prove effective if used as the basis of an age-appropriate intervention with older students. Older students might be more able to engage with subtle messages about industry influences on their behaviours, although, of course, it might then be too late if they have already started experimenting with tobacco. The applicability of the approach of Operation Smoke Storm to the prevention of other unhealthy behaviours on which there is industry influence, such as harmful drinking and unhealthy eating, might also be explored. It is also possible that an intervention such as Operation Smoke Storm, which focuses on one unhealthy behaviour in particular, might in fact lead to broader changes in young people’s awareness of the role of advertising, and thereby impact on other outcomes. Secondary outcomes, such as alcohol consumption and dietary choices, were not measured in this study, but a range of outcomes could be studied in any future work.
Alternatively, Operation Smoke Storm might usefully be adapted to include fully differentiated activities and resources appropriate for use with students of different academic abilities. If the active ingredient of Operation Smoke Storm is thought to be the content relating to the tobacco industry, this content needs to come across more clearly to students of all ability levels. The teachers interviewed did report that they adapted their delivery in order to suit their students, for example by extending or shortening activities, although exactly how they did this is not certain. It is possible, for example, that crucial discussion points were missed out. Direct teacher observation would be useful, providing that teachers do not change their delivery in response to an awareness of being observed. Longer focus groups and interviews, not limited by the time available in the school day, might also help to shed further light on how best to differentiate an intervention.
There is also scope to understand whether or not Operation Smoke Storm could be delivered acceptably and effectively in other settings. This may be beneficial in allowing the problems associated with the erosion of PSHE teaching time to be circumvented and might also allow the intervention to be targeted at particular groups of young people. Targeting the most deprived young people might, for instance, be more effective than delivering the intervention to everyone. A scoping exercise would be useful to understand the alternative settings, such as youth groups or sports clubs, that might be potential options, and the characteristics of the young people who use these.
The potential to deliver Operation Smoke Storm, or other interventions based on its premise, within schools but outside PSHE lessons might also be usefully investigated. There is a recognition that in some schools there is a false dichotomy whereby PSHE is seen as a discrete subject rather than something to be embedded across the curriculum, like other subjects such as literacy and numeracy. 85 Aspects of Operation Smoke Storm could potentially be delivered through subjects such as English, where learning to express ideas confidently and persuasively is a part of the curriculum, business studies, or art and design where the visual mechanisms used to market tobacco (such as package design and advertising) could be studied.
Operation Smoke Storm is suitable for delivery in a one-off session and thus might suit some schools in which PSHE is taught in ‘drop-down days’ rather than in discrete PSHE lessons. This mode of delivery could usefully be evaluated, as it might be that students’ learning is enhanced by condensed delivery and not having to recall information over a period of several weeks. However, there is recognition that drop-down days can be ‘tokenistic and ineffective’, particularly if students happen to be absent from school on those day, as they do not allow progressive learning and the reinforcement of knowledge over time. 85 In some schools, non-teaching staff (frequently school nurses) are used to deliver PSHE. Kick It has previously trained youth workers to deliver Operation Smoke Storm in London schools, and further evaluation of this would be useful.
Finally, further work is warranted to explore how to engage parents and guardians more in supporting their child to remain smoke free. The parents interviewed as part of this study, although a self-selected group, were supportive of the concept behind Operation Smoke Storm. Alternative formats to the booklet developed here might prove to be more effective in engaging parents.
These recommendations are primarily focused on understanding whether or not Operation Smoke Storm can be amended in such a way that it is then effective in changing young people’s behaviour. Of course, the alternative would be to accept that the intervention does not work, and from this might follow the suggestion that money should be spent elsewhere. However, this recommendation is difficult to make when the majority of health education resources used in schools have no evidence base and may in fact be far worse than Operation Smoke Storm, which is proven here to be ineffective but popular with students, parents and teachers.
Recommendations for conducting research in schools
On the face of it, schools appear to be an ideal setting in which to conduct research with young people. They provide a captive audience in which large numbers of the target population can be reached at any one time to deliver an intervention and to collect data for subsequent evaluation. However, informal conversations with local public health practitioners, as well as national reports on the state of PSHE teaching,85 suggest that increasing pressures on schools to reach academic targets mean that timetabling non-core subjects has become more problematic. Indeed, schools’ interest in, and ability to accommodate, the intervention and accompanying evaluation activities appears to be lower now than in 2001 when ASSIST was recruiting, although even then some teachers felt that ‘there seems to be one thing after another, after another’ in school life. 38 Curriculum time devoted to health and well-being, in which research such as this is often best situated, is being eroded. This was highlighted in one of the schools in which the amount of time devoted to PSHE was reduced between phase 1 and phase 2 of our study to such a degree that it was not possible to deliver the revised version of Operation Smoke Storm to the new cohort of Year 7 students and in which negotiations were needed to run the Year 8 booster session in science lessons instead.
Although the teachers involved in this study were committed to the research project, some did struggle to accommodate the demands of the research process. Although most teachers reported that the research processes were easy to follow and manageable, some did not return their teaching group’s folders to the Head of PSHE for safekeeping as requested, which meant that questionnaire data from Year 7 and Year 8 could not be linked. Heads of PSHE found it challenging to find space within the curriculum to deliver the intervention and to organise times for the student focus groups to run. Moreover, other demands on their time meant that not all teachers were able to participate in interviews or to complete fidelity questionnaires.
Recruitment of the two schools into this project was challenging and dependent on the level of support from key members of staff, such as the Head of PSHE. Difficulty in engaging with schools is further evidenced by a response rate of just 6.7% (13/195) in the survey of smoking education practices among secondary schools in the East Midlands (see Appendix 1). In addition, retaining schools was also difficult, particularly where key staff left their posts part way through the study and their replacements were less supportive of the project or less able to deliver commitments previously agreed.
The experiences gained in this study suggest that it is important to minimise the demands placed on schools and school staff as much as possible in order to maximise the likelihood of success in research in this setting. Ideally, any intervention to be delivered should fit within the curriculum time available and the burden of research activities, such as administering questionnaires and running focus groups and interviews, should be light, particularly where these can be conducted only during curriculum time. Schools should be fully informed of what will be expected of them over the duration of a study, although experiences here suggest that having a back-up plan is crucial should elements such as staffing or timetabling change. The importance of good communication with schools, highlighted in a process evaluation with teachers who took part in the initial part of ASSIST, has not changed. 38
The schools that took part in this study received an inconvenience allowance for their time, although this alone was insufficient to secure the participation of the four other schools approached when recruiting for this work. Other incentives could perhaps be explored, such as offering schools support in delivering health education, although, of course, the time commitment involved here has cost implications.
Conclusions
This study was, to the best of our knowledge, the first of its kind both in the UK and internationally to test a novel approach to preventing smoking uptake in a school setting. That the intervention was, on the whole, acceptable to teachers, students and parents is encouraging. The lack of clear evidence for potential effectiveness, considered alongside the logistical difficulties in recruiting and working with schools, precludes progression to a fully powered RCT trial of Operation Smoke Storm, although several avenues for potential further exploration have been identified.
Acknowledgements
Contributions of authors
The study was conducted by members of UKCTAS, a UK Clinical Research Collaboration (UKCRC)-funded Public Health Research Centre of Excellence. Funding from the British Heart Foundation, Cancer Research UK, the Economic and Social Research Council, the Medical Research Council and NIHR, under the auspices of the UKCRC, is gratefully acknowledged. Specific roles and skills are as follows:
Dr Lisa Szatkowski, Associate Professor in Medical Statistics and previously a school teacher, was the Principal Investigator and undertook the quantitative analyses.
Dr John Taylor, Research Fellow, managed the day-to-day activities of the project, particularly liaising with Kick It and conducting focus groups, interviews and qualitative analysis.
Ms Amy Taylor, Research Assistant, was involved in organising and conducting focus groups and interviews and undertaking qualitative analysis.
Professor Sarah Lewis, Professor of Medical Statistics, supported LS in designing the study and undertaking the quantitative analysis.
Professor John Britton, Director of UKCTAS and Professor of Epidemiology, provided expertise across the field of smoking cessation and tobacco control. His experience in planning and delivering the Nottingham School Smoking Survey and the links he has built up with local schools through this work were of particular relevance to this study.
Professor Ann McNeill, Deputy Director of UKCTAS and Professor of Tobacco Addiction, contributed expertise in developing school-based interventions, involving users in research and qualitative data collection and analysis.
Professor Linda Bauld, Professor of Health Policy, provided expertise in the design and evaluation of complex interventions, including those to promote smoke-free schools and other environments, and has considerable experience in involving users in research.
Ms Qi Wu, Research Fellow, conducted the health economic analysis.
Mr Steve Parrott, Reader in Health Economics, led the health economic analysis.
Dr Laura Jones, Lecturer in Qualitative and Mixed Methods Applied Health Research, supported the qualitative aspects of the study.
Dr Manpreet Bains, Assistant Professor in Mixed Methods Health Research, led the qualitative aspects of the study.
Other contributors
The authors wish to thank the following people for their contributions to the work:
-
Mr Toby Fairs-Billam and Mr Tomasz Letniowski, the smoking-prevention manager and London resource project manager, respectively, at Kick It, the NHS Stop Smoking Service for Hammersmith and Fulham, Kensington and Chelsea, Westminster, Kingston upon Thames and Richmond upon Thames. They developed Operation Smoke Storm initially and contributed expertise to its improvement and the development of booster materials for use in schools and materials for use with families.
-
Mr Graeme Docherty, the UKCTAS research coordinator, who provided support with ethics applications and finance arrangements.
-
Ms Emma Duffield, a medical student at the University of Nottingham, who completed the work described in Appendix 1.
-
Ms Leah Jayes and Ms Juliette Cook, researchers at the University of Nottingham, who helped to observe focus groups in phase 2.
-
Last, but not at all least, we thank the Heads of PSHE and individual teachers at the two schools who participated in this study, without whom this work would not have been possible.
Publications
Outputs are currently being prepared for submission to peer-reviewed academic journals. Aspects of the work have been presented at the following conferences, some of which have resulted in published abstracts as detailed below.
Conference presentations
Bains M. Development and evaluation of a novel intervention providing insight into the tobacco industry to prevent the uptake of smoking in school-aged children. Paper presented at the UK National Smoking Cessation Conference, London, 12–13 June 2014.
Taylor A. Development and evaluation of a novel intervention providing insight into the tobacco industry to prevent the uptake of smoking in school-aged children. Paper presented at the UKCRC Public Health Research Centres of Excellence, Leeds, 19–20 June 2014.
Szatkowski L. Development and evaluation of a novel intervention providing insight into the tobacco industry to prevent the uptake of smoking in school-aged children. Paper presented at the Society for Social Medicine, Oxford, 10–12 September 2014.
Taylor J. Operation Smoke Storm: qualitative evaluation of a novel intervention to prevent uptake of smoking in schoolchildren. Paper presented at the Lancet Public Health Science Conference, Glasgow, 19 November 2014.
Taylor A. Operation Smoke Storm: Effectiveness of a school-based smoking prevention intervention providing insight into the tobacco industry. Paper presented at the UK National Smoking Cessation Conference, Manchester, 11–12 June 2015.
Szatkowski L. Operation Smoke Storm: effectiveness of a school-based smoking prevention intervention providing insight into the tobacco industry. Paper presented at the Lancet Public Health Science Conference, London, 13 November 2015.
Journal articles
Szatkowski L, Taylor J, Taylor A, Lewis S, Britton J, McNeill A, et al. Operation Smoke Storm: qualitative evaluation of a novel intervention to prevent uptake of smoking in schoolchildren. Lancet 2014;384:S77.
Taylor J, Taylor A, Lewis S, McNeill A, Britton J, Jones LL, et al. A qualitative evaluation of a novel intervention using insight into tobacco industry tactics to prevent the uptake of smoking in school-aged children. BMC Public Health 2016;16:539.
Szatkowski L, Taylor J, Taylor A, Lewis S, McNeill A, Britton J, et al. Development and evaluation of a novel intervention providing insight into the tobacco industry to prevent the uptake of smoking in school-aged children. J Epidemiol Community Health 2014;68:A15.
Szatkowski L, Taylor J, Taylor A, Lewis S, Britton J, McNeill A, et al. Operation Smoke Storm: effectiveness of a school-based smoking prevention intervention providing insight into the tobacco industry. Lancet 2015;386:S70.
Data sharing statement
Requests for access to data should be addressed to the corresponding author.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health.
References
- Statistics on Smoking, England 2015. Leeds: Health & Social Care Information Centre; n.d.
- Doll R, Peto R, Boreham J, Sutherland I. Mortality in relation to smoking: 50 years’ observations on male British doctors. BMJ 2004;328. http://dx.doi.org/10.1136/bmj.38142.554479.AE.
- The Economics of Tobacco. London: Action on Smoking and Health; n.d.
- Dawe F. General Lifestyle Survey Overview. A Report of the 2011 General Lifestyle Survey. Newport: Office for National Statistics; 2013.
- Taioli E, Wynder EL. Effect of the age at which smoking begins on frequency of smoking in adulthood. N Engl J Med 1991;325:968-9. http://dx.doi.org/10.1056/NEJM199109263251318.
- Smoking Kills: A White Paper on Tobacco. London: DH; 1998.
- Ferguson J, Bauld L, Chesterman J, Judge K. The English smoking treatment services: one-year outcomes. Addiction 2005;100:59-6. http://dx.doi.org/10.1111/j.1360-0443.2005.01028.x.
- Centers for Disease Control and Prevention . Youth and Tobacco: Preventing Tobacco Use Among Young People – A Report of the Surgeon General 1994. http://profiles.nlm.nih.gov/ps/access/NNBCLQ.pdf (accessed 22 July 2016).
- Fuller E. Smoking, Drinking and Drug Use Among Young People in England in 2014. Leeds: Health & Social Care Information Centre; 2015.
- Leventhal H, Cleary PD. The smoking problem: a review of the research and theory in behavioral risk modification. Psychol Bull 1980;88:370-405. http://dx.doi.org/10.1037/0033-2909.88.2.370.
- Pierce JP, Choi WS, Gilpin EA, Farkas AJ, Merritt RK. Validation of susceptibility as a predictor of which adolescents take up smoking in the United States. Health Psychol 1996;15:355-61. http://dx.doi.org/10.1037/0278-6133.15.5.355.
- Spanopoulos D, Britton J, McNeill A, Ratschen E, Szatkowski L. Tobacco display and brand communication at the point of sale: implications for adolescent smoking behaviour. Tob Control 2014;23:64-9. http://dx.doi.org/10.1136/tobaccocontrol-2012-050765.
- Thomas RE, McLellan J, Perera R. School-based programmes for preventing smoking. Cochrane Database Syst Rev 2013;4. http://dx.doi.org/10.1002/ebch.1937.
- Wiehe SE, Garrison MM, Christakis DA, Ebel BE, Rivara FP. A systematic review of school-based smoking prevention trials with long-term follow-up. J Adolesc Health 2005;36:162-9. http://dx.doi.org/10.1016/j.jadohealth.2004.12.003.
- School-Based Interventions to Prevent the Uptake of Smoking Among Children and Young People (NICE Public Health Guidance 23). London: NICE; 2010.
- Campbell R, Starkey F, Holliday J, Audrey S, Bloor M, Parry-Langdon N, et al. An informal school-based peer-led intervention for smoking prevention in adolescence (ASSIST): a cluster randomised trial. Lancet 2008;371:1595-602. http://dx.doi.org/10.1016/S0140-6736(08)60692-3.
- Aveyard P, Cheng KK, Almond J, Sherratt E, Lancashire R, Lawrence T, et al. Cluster randomised controlled trial of expert system based on the transtheoretical (‘stages of change’) model for smoking prevention and cessation in schools. BMJ 1999;319:948-53. http://dx.doi.org/10.1136/bmj.319.7215.948.
- Ellickson PL, Bell RM. Drug prevention in junior high: a multi-site longitudinal test. Science 1990;247:1299-305. http://dx.doi.org/10.1126/science.2180065.
- Ausems M, Mesters I, van Breukelen G, De Vries H. Effects of in-school and tailored out-of-school smoking prevention among Dutch vocational school students. Health Educ Res 2004;19:51-63. http://dx.doi.org/10.1093/her/cyg001.
- Elder JP, Wildey M, de Moor C, Sallis JF, Eckhardt L, Edwards C, et al. The long-term prevention of tobacco use among junior high school students: classroom and telephone interventions. Am J Public Health 1993;83:1239-44. http://dx.doi.org/10.2105/AJPH.83.9.1239.
- Crone MR, Reijneveld SA, Willemsen MC, van Leerdam FJ, Spruijt RD, Sing RA. Prevention of smoking in adolescents with lower education: a school based intervention study. J Epidemiol Community Health 2003;57:675-80. http://dx.doi.org/10.1136/jech.57.9.675.
- Dijkstra M, Mesters I, De Vries H, van Breukelen G, Parcel GS. Effectiveness of a social influence approach and boosters to smoking prevention. Health Educ Res 1999;14:791-802. http://dx.doi.org/10.1093/her/14.6.791.
- McNeill AD. The development of dependence on smoking in children. Br J Addict 1991;86:589-92. http://dx.doi.org/10.1111/j.1360-0443.1991.tb01813.x.
- Jit M, Barton P, Chen Y-F, Uthman O, Aveyard P, Meads C. School-Based Interventions to Prevent the Uptake of Smoking among Children and Young People: Cost-Effectiveness Model. London: National Institute for Health and Care Excellence; 2009.
- Hollingworth W, Cohen D, Hawkins J, Hughes RA, Moore LA, Holliday JC, et al. Reducing smoking in adolescents: cost-effectiveness results from the cluster randomized ASSIST (A Stop Smoking In Schools Trial). Nicotine Tob Res 2012;14:161-8. http://dx.doi.org/10.1093/ntr/ntr155.
- Cameron R, Brown KS, Best JA, Pelkman CL, Madill CL, Manske SR, et al. Effectiveness of a social influences smoking prevention program as a function of provider type, training method, and school risk. Am J Public Health 1999;89:1827-31. http://dx.doi.org/10.2105/AJPH.89.12.1827.
- de Vries H, Dijk F, Wetzels J, Mudde A, Kremers S, Ariza C, et al. The European Smoking prevention Framework Approach (ESFA): effects after 24 and 30 months. Health Educ Res 2006;21:116-32. http://dx.doi.org/10.1093/her/cyh048.
- Kellam SG, Anthony JC. Targeting early antecedents to prevent tobacco smoking: findings from an epidemiologically based randomized field trial. Am J Public Health 1998;88:1490-5. http://dx.doi.org/10.2105/AJPH.88.10.1490.
- Storr CL, Ialongo NS, Kellam SG, Anthony JC. A randomized controlled trial of two primary school intervention strategies to prevent early onset tobacco smoking. Drug Alcohol Depend 2002;66:51-60. http://dx.doi.org/10.1016/S0376-8716(01)00184-3.
- Peterson AV, Kealey KA, Mann SL, Marek PM, Sarason IG. Hutchinson Smoking Prevention Project: long-term randomized trial in school-based tobacco use prevention–results on smoking. J Natl Cancer Inst 2000;92:1979-91. http://dx.doi.org/10.1093/jnci/92.24.1979.
- Mercken L, Moore L, Crone MR, De Vries H, De Bourdeaudhuij I, Lien N, et al. The effectiveness of school-based smoking prevention interventions among low- and high-SES European teenagers. Health Educ Res 2012;27:459-69. http://dx.doi.org/10.1093/her/cys017.
- Molyneux A, Lewis S, Antoniak M, Browne W, McNeill A, Godfrey C, et al. Prospective study of the effect of exposure to other smokers in high school tutor groups on the risk of incident smoking in adolescence. Am J Epidemiol 2004;159:127-32. http://dx.doi.org/10.1093/aje/kwh035.
- Molyneux A, Lewis S, Antoniak M, Hubbard R, McNeill A, Godfrey C, et al. Is smoking a communicable disease? Effect of exposure to ever smokers in school tutor groups on the risk of incident smoking in the first year of secondary school. Tob Control 2002;11:241-5. http://dx.doi.org/10.1136/tc.11.3.241.
- PSHE: Personal Wellbeing Programme of Study (Non-Statutory) for Key Stage 3. London: Qualifications and Curriculum Authority; 2007.
- PSHE: Personal Wellbeing Programme of Study (Non-Statutory) for Key Stage 4. London: Qualifications and Curriculum Authority; 2007.
- MacDonald A. Independent Review of the Proposal to Make Personal, Social, Health and Economic (PSHE) Education Statutory. London: Department for Children, Schools and Families; 2009.
- Formby E, Coldwell M, Stiell B, Demack S, Stevens A, Shipton L, et al. Personal, Social, Health and Economic (PSHE) Education: A Mapping Study of the Prevalent Models of Delivery and Their Effectiveness. London: Department for Education; 2011.
- Audrey S, Holliday J, Campbell R. Commitment and compatibility: Teachers’ perspectives on the implementation of an effective school-based, peer-led smoking intervention. Health Educ J 2008;67:74-90. http://dx.doi.org/10.1177/0017896908089387.
- Thomas R, Baker P, Thomas B, Lorenzetti D. Family-based programmes for preventing smoking by children and adolescents. Cochrane Database Syst Rev 2015;2. http://dx.doi.org/10.1002/14651858.cd004493.pub3.
- Wakschlag LS, Metzger A, Darfler A, Ho J, Mermelstein R, Rathouz PJ. The Family Talk About Smoking (FTAS) paradigm: new directions for assessing parent-teen communications about smoking. Nicotine Tob Res 2011;13:103-12. http://dx.doi.org/10.1093/ntr/ntq217.
- Biglan A, Ary DV, Smolkowski K, Duncan T, Black C. A randomised controlled trial of a community intervention to prevent adolescent tobacco use. Tob Control 2000;9:24-32. http://dx.doi.org/10.1136/tc.9.1.24.
- Perry CL, Williams CL, Veblen-Mortenson S, Toomey TL, Komro KA, Anstine PS, et al. Project Northland: outcomes of a communitywide alcohol use prevention program during early adolescence. Am J Public Health 1996;86:956-65. http://dx.doi.org/10.2105/AJPH.86.7.956.
- Gordon J, Biglan A, Smolkowski K. The impact on tobacco use of branded youth anti-tobacco activities and family communications about tobacco. Prev Sci 2008;9:73-87. http://dx.doi.org/10.1007/s11121-008-0089-6.
- Perry CL, Komro KA, Veblen-Mortenson S, Bosma L, Munson K, Stigler M, et al. The Minnesota DARE PLUS Project: creating community partnerships to prevent drug use and violence. J Sch Health 2000;70:84-8. http://dx.doi.org/10.1111/j.1746-1561.2000.tb06451.x.
- Alwan N, Siddiqi K, Thomson H, Lane J, Cameron I. Can a community-based ‘smoke-free homes’ intervention persuade families to apply smoking restrictions at homes?. J Public Health 2011;33:48-54. http://dx.doi.org/10.1093/pubmed/fdq073.
- Farrelly MC, Healton CG, Davis KC, Messeri P, Hersey JC, Haviland ML. Getting to the truth: evaluating national tobacco countermarketing campaigns. Am J Public Health 2002;92:901-7. http://dx.doi.org/10.2105/AJPH.92.6.901.
- Farrelly MC, Davis KC, Haviland ML, Messeri P, Healton CG. Evidence of a dose-response relationship between ‘truth’ antismoking ads and youth smoking prevalence. Am J Public Health 2005;95:425-31. http://dx.doi.org/10.2105/AJPH.2004.049692.
- The Truth® Campaign n.d. www.protectthetruth.org/truthcampaign.htm (accessed 19 March 2012).
- Kick It n.d. www.kick-it.org.uk/ (accessed 7 June 2015).
- Fairs-Billam T. Creating an Educational Resource to Assist Teachers in the Delivery of Effective Smoking Prevention Sessions: A Report on the Development and Trial of ’Operation Smoke Storm. London: Kick It; 2011.
- Department for Education . Schools, Pupils and Their Characteristics: January 2014 2014. www.gov.uk/government/statistics/schools-pupils-and-their-characteristics-january-2014 (accessed 22 July 2016).
- Economic and Social Research Council . Framework for Research Ethics n.d. www.esrc.ac.uk/about-esrc/information/framework-for-research-ethics/ (accessed 19 August 2015).
- WHO Report on the Global Tobacco Epidemic 2013: Enforcing Bans on Tobacco Advertising, Promotion and Sponsorship. Geneva: WHO; 2013.
- Amos A, Bostock Y. Young people, smoking and gender–a qualitative exploration. Health Educ Res 2007;22:770-81. http://dx.doi.org/10.1093/her/cyl075.
- Kitzinger J. Qualitative research. Introducing focus groups. BMJ 1995;311:299-302. http://dx.doi.org/10.1136/bmj.311.7000.299.
- Bender DE, Ewbank D. The focus group as a tool for health research: issues in design and analysis. Health Transit Rev 1994;4:63-80.
- The Deborah Hutton Campaign . Cut Films n.d. www.cutfilms.org/ (accessed 15 September 2014).
- Ritchie J, Lewis J, Elam G. Qualitative Research Practice: A Guide for Social Science Students and Researchers. London: Sage; 2003.
- Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol 2013;13. http://dx.doi.org/10.1186/1471-2288-13-117.
- National Children’s Bureau n.d. www.ncb.org.uk/ (accessed 9 January 2015).
- Bogdanovica I, Szatkowski L, McNeill A, Spanopoulos D, Britton J. Exposure to point-of-sale displays and changes in susceptibility to smoking: findings from a cohort study of school students. Addiction 2015;110:693-702. http://dx.doi.org/10.1111/add.12826.
- Hanewinkel R, Isensee B, Sargent JD, Morgenstern M. Cigarette advertising and adolescent smoking. Am J Prev Med 2010;38:359-66. http://dx.doi.org/10.1016/j.amepre.2009.12.036.
- Department for Communities and Local Government . English Indices of Deprivation 2010 n.d. www.gov.uk/government/statistics/english-indices-of-deprivation-2010 (accessed 20 August 2015).
- Fuller E, Hawkins V. Smoking, Drinking and Drug Use Among Young People in England in 2013. London: The Health & Social Care Information Centre; 2014.
- Drummond MF, Sculpher M, Torrance G, O’Brien B, Stoddart G. Methods for the Economic Evaluation of Health Care Programmes. Oxford: Oxford University Press; 2005.
- Guide to the Methods of Technology Appraisal 2013. London: NICE; 2013.
- Melton G, Ben-Arieh A, Cashmore J, Goodman G, Worley N. The Sage Handbook of Child Research. Thousand Oaks, CA: SAGE Publications; 2013.
- Wille N, Badia X, Bonsel G, Burström K, Cavrini G, Devlin N, et al. Development of the EQ-5D-Y: a child-friendly version of the EQ-5D. Qual Life Res 2010;19:875-86. http://dx.doi.org/10.1007/s11136-010-9648-y.
- Ravens-Sieberer U, Wille N, Badia X, Bonsel G, Burström K, Cavrini G, et al. Feasibility, reliability, and validity of the EQ-5D-Y: results from a multinational study. Qual Life Res 2010;19:887-97. http://dx.doi.org/10.1007/s11136-010-9649-x.
- van Reenen M, Janssen B, Oppe M, Kreimeier S, Greiner W. EQ-5D-Y User Guide: Basic Information on How to Use the EQ-5D-Y Instrument. Rotterdam: EuroQol Group; 2014.
- Consolidated Annual Report and Accounts 2013–14. London: Department for Education; 2014.
- School Teachers’ Pay and Conditions Document 2014 and Guidance on School Teachers’ Pay and Conditions. London: Department for Education; 2014.
- Glassdoor . Research Assistant Salaries n.d. www.glassdoor.co.uk/Salaries/research-assistant-salary-SRCH_KO0,18.htm (accessed 28 August 2015).
- Curtis L. Unit Costs of Health and Social Care 2014. Canterbury: PSSRU, University of Kent; 2014.
- Reference Costs 2013–14. London: DH; 2014.
- British National Formulary. London: BMJ Group and Pharmaceutical Press; 2014.
- Prescription Cost Analysis. Leeds: Health & Social Care Information Centre; 2014.
- Kind P, Dolan P, Gudex C, Williams A. Variations in population health status: results from a United Kingdom national questionnaire survey. BMJ 1998;316:736-41. http://dx.doi.org/10.1136/bmj.316.7133.736.
- Vogl M, Wenig CM, Leidl R, Pokhrel S. Smoking and health-related quality of life in English general population: implications for economic evaluations. BMC Public Health 2012;12. http://dx.doi.org/10.1186/1471-2458-12-203.
- Rabin R, de Charro F. EQ-5D: a measure of health status from the EuroQol Group. Ann Med 2001;33:337-43. http://dx.doi.org/10.3109/07853890109002087.
- Richardson G, Manca A. Calculation of quality adjusted life years in the published literature: a review of methodology and transparency. Health Econ 2004;13:1203-10. http://dx.doi.org/10.1002/hec.901.
- Statistical Bulletin: Adult Smoking Habits in Great Britain, 2013. London: ONS; 2014.
- Amos A, Angus K, Bostock Y, Fidler J, Hastings G. A Review of Young People and Smoking in England 2009. http://phrc.lshtm.ac.uk/papers/PHRC_A7-08_Final_Report.pdf (accessed 22 July 2016).
- Sussman S, Grana R, Pokhrel P, Rohrbach LA, Sun P. Forbidden fruit and the prediction of cigarette smoking. Subst Use Misuse 2010;45:1683-93. http://dx.doi.org/10.3109/10826081003682230.
- Life Lessons: PSHE and SRE in Schools. London: The Stationery Office; 2015.
- DECIPHer IMPACT Ltd . ASSIST Smoking Prevention Programme 2010. www.decipher-impact.com (accessed 5 August 2016).
- Lions Lifeskills . Attitudes, Skills Development, Knowledge 2016. www.lionslifeskills.co.uk (accessed 15 August 2016).
- QUIT . Breathless TV n.d. www.quitbecause.org.uk (accessed 1 December 2014).
- Lincolnshire County Council . Choked Up n.d. www.lincolnshire.gov.uk/smokefree-lincs/education/choked-up/116773.article (accessed 15 August 2016).
- British Heart Foundation n.d. www.bhf.org.uk/childrens-resources/in-secondary-schools.aspx (accessed 1 December 2014).
- Lions Quest . Lions Quest Skills for Action 2015. www.lions-quest.org (accessed 15 August 2016).
- GASP . Health Promotion and Stop Smoking Resources 2016. www.gasp.org.uk (accessed 15 August 2016).
- Hull City Council . Smoke’s No Joke n.d. www.smokesnojoke.org.uk (accessed 15 August 2016).
- British Heart Foundation and QUIT . Smokey Joe n.d. www.stuboutjoe.com (accessed 1 December 2014).
- Smokefree Islington n.d. www.smokefreeislington.nhs.uk/resources/schools-young-people/ (accessed 15 August 2016).
- Smokefree Lincolnshire Alliance n.d. www.lincolnshire.gov.uk/smokefree-linics/education/smokefree-resources-available/116776.article (accessed 15 August 2016).
- White Ribbon Association n.d. www.white-ribbon.org.uk/Resources/educational-work-packs (accessed 15 August 2016).
- The Smokescreen n.d. www.thesmokescreen.org (accessed 15 August 2016).
- Smokefree Alliances (Surrey & Hampshire and Isle of Wight) . PSHE – Tobacco Education and Stopping Smoking Support Toolkit 2011. www.hants.gov.uk/rh/smokefree/TobaccoIntroAndInfo.pdf (accessed 15 August 2016).
- Lions Lifeskills . Up in Smoke 2016. www.lionslifeskills.co.uk (accessed 15 August 2016).
Appendix 1 Summary of review of existing smoking education resources and survey of Personal, Social and Health Education teachers in the East Midlands
This work was carried out by Emma Duffield, a medical student at the University of Nottingham, in part fulfilment of the requirements for the degree of Bachelor of Medical Sciences. The work was supervised by Lisa Szatkowski and John Taylor.
Systematic-style review of existing smoking education resources available in the UK
A search strategy was developed to identify smoking-prevention resources and interventions available for use in UK secondary schools. Resources included lesson plans and teaching packs but excluded individual worksheets and single, in-lesson activities. Google (Google Inc., Mountain View, CA, USA) and the websites of the BBC (www.bbc.co.uk), PSHE Association (www.pshe-association.org.uk/) and Times Educational Supplement (www.tes.com/) were searched to identify relevant resources. Web of Knowledge and PubMed were searched to identify peer-reviewed, published evaluations of resources. The characteristics of the resources identified were summarised under a number of headings, and thematic analysis was used to synthesise findings. Six themes were identified: (1) delivery; (2) content; (3) classroom suitability; (4) role of students; (5) relevance; and (6) effectiveness and acceptability.
A total of 19 resources were identified which are summarised in Table 15 below:
| Resource | Provider | Source | Target age group (years) | Brief description |
|---|---|---|---|---|
| ASSIST86 | DECIPHer Impact Ltd | www.decipher-impact.com | 12–13 | ASSIST identifies and trains influential young people to be peer supporters who diffuse social norms and non-smoking behaviour through informal conversations with their peers via their social networks. Started in schools in 2006 |
| ASK87 | Lions Life Skills Ltd (Lions Clubs International Foundation) | www.lionslifeskills.co.uk | 11–14 | 49 trigger sheets exploring a range of issues relating to alcohol, tobacco and other drugs used to start small group discussions in a classroom environment. Can also be used one to one. Easy to integrate into ongoing work and rated positively by teachers and students. Release date unknown |
| Breathless TV88 | QUIT | www.quitbecause.org.uk | 11–18 | 55-minute online video based on TV shows popular with young people along with lesson plans and posters. Knowledge based, including information on health effects, costs, cigarette contents, sexual health, the environment and the tobacco industry. Released 2014/15 |
| Choked Up 89 | Lincolnshire County Council | www.lincolnshire.gov.uk/smokefree-lincs | 11–14 | 23-minute DVD story covering health, addiction and the law with interactive activities led by an on-screen presenter. Made in consultation with young people. Released in 2012 |
| Drama scenarios90 | British Heart Foundation | www.bhf.org.uk/childrens-resources/in-secondary-schools.aspx | 11–18 | A series of scenario prompts that students consider, write and perform. Teacher-led active learning in the classroom. Covers health effects, peer pressure, passive smoking and persuading loved ones to give up smoking. Released in 2014 |
| Lesson plan90 | British Heart Foundation | www.bhf.org.uk/childrens-resources/in-secondary-schools.aspx | 11–18 | Increases knowledge of smoking health effects and the history of tobacco using a celebrity interview (with footballer David James) and a tobacco timeline. Teacher-led interactive discussion. Released in 2014 |
| Lions Quest Skills for Action91 | Lions Quest (Lions Clubs International Foundation) | www.lions-quest.org | 13–17 | Curriculum manual containing 33 lessons plus ‘Skills Bank’ of 160 activities teaching 26 skill sets. Based in schools and communities: students are given civic responsibilities to increase their understanding of societal impacts, develop their communication and workplace skills and increase their knowledge. Release date unknown |
| Lions Quest Skills for Adolescence91 | Lions Quest (Lions Clubs International Foundation) | www.lions-quest.org | 10–14 | 80 x 45-minute sequential interactive sessions, online elements to increase knowledge, learn and practise skills and improve self-perception. Teacher led and classroom based, but adaptable to settings and formats. 1-year post test showed decreased smoking uptake in participating schools. Released in 1992 |
| Operation Smoke Storm49 | Kick It | www.operationsmokestorm.com | 12–13 | 3 x 50-minute interactive online sessions that encourage personal reasoning, problem solving and teamwork through games, quizzes and discussion. Released in 2012 |
| Puffing Poisons chemistry set92 | GASP | www.gasp.org.uk | 12+ | Display of 30 labelled jars, representing the harmful chemicals found in cigarettes, with a poster. Illustrates toxins being inhaled. Discussion starter and practical presentation prop for teachers in the classroom. Release date unknown |
| SmokeOut Activity Pack92 | GASP | www.gasp.org.uk | 12–18 | 10 factsheets and 34 activities to incorporate into teaching. Option of a CD format. Mostly knowledge based with some skill acquisition. Released in 2006 |
| Smoke’s No Joke93 | Hull City Council | www.smokesnojoke.org.uk | 11–14; 14+ | Multiple age-appropriate websites with games, activities, videos and informative links. Includes a teacher’s site with notes linked to what students are looking at. Can be used in school and accessed at home, facilitating self-learning. Information on health, environment, cigarette contents, ageing, quitting, crime, fire safety, second-hand smoke and worldwide impacts. Variety of learning styles. Release date unknown |
| Smokey Joe 94 | British Heart Foundation, QUIT | www.stuboutjoe.com | 11–14 | Five-level arcade-style online game made for young teenagers with associated A5 teacher booklet (containing activities, discussions and mini-quizzes). Released in 2010 |
| Smoking: A scheme of work for KS395 | Smokefree Islington | www.smokefreeislington.nhs.uk/resources/schools-young-people/ | 11–14 | 3–4 lesson plans on why some young people smoke, covering early signs of addiction. Health effects video by anatomy artist Gunther von Hagens. Classroom and teacher based, with potential for interaction and discussion. Released in 2012 |
| Smoking education resource box96 | Smokefree Lincolnshire Alliance | www.lincolnshire.gov.uk/smosmokef-lincs | 11–18 | An assortment of practical and visually impactful resources and aids to use in the classroom including Clem’s phlegm jar, blocked blood vessel, shortness of breath pack and Choked Up, The Tobacco Trap, A–Z of Drugs and Quit DVDs. Released in 2011 |
| Smoking packs97 | White Ribbon | www.white-ribbon.org.uk/Resources/SmokingKS34 | 11–16 | 12 A5 leaflets and 10 A4 posters covering the smoking effects on men, women, children, looks and pregnancy as well as second-hand smoke, cigarette contents, history of smoking, peer pressure, environment and crime. Classroom based and teacher led. Being updated in 2015. Date of initial release unknown |
| The Smokescreen98 | The Smokescreen | www.thesmokescreen.org | 11–19 | Aimed at those who do not yet smoke, targets teenagers to educate them about the tobacco industry. Led by outside speakers and uses up-to-date media (such as Twitter); feedback from students is very positive. Released in 2011 |
| Tobacco Education and Stopping Smoking Support Toolkit99 | Smokefree Alliances (Surrey & Hampshire and Isle of Wight) | www.hants.gov.uk/rh/smokefree/TobaccoIntroAndInfo.pdf | 11–18 | 8 lesson plans and associated CD-ROM (SMARTboard compatible) for teachers to use in class. Explores the impacts of smoking on individuals, society and the wider world. Suitable for different age groups. Released in 2011 |
| Up in Smoke teaching pack100 | Lions Lifeskills Ltd (Lions Clubs International Foundation) | www.lionslifeskills.co.uk | 11–16 | 10 lesson plans available in book or CD format suitable for use in the classroom. Uses a variety of interactive teaching methods to increase knowledge with some skills acquisition. Released in 2013 |
Qualitative summary of resource characteristics
Delivery
The 19 resources reviewed were diverse in their modes of delivery and varied in the amount of lesson time that they required. Some resources could be used as lesson supplements (e.g. Puffing Poisons chemistry set92), whereas others would fill one or more whole lessons (e.g. Operation Smoke Storm). Resource providers included charities, NHS organisations and companies specialising in producing educational resources. A total of 10 resources were free of charge or available for free loan. The remaining nine required a one-off payment, ranging from £10.50 (Smoke Out) to £400 (Breathless TV). 88
Content
The 19 resources covered a variety of topics. A total of 13 resources covered the short- and long-term effects of smoking, including effects on appearance and sexual performance, health and the chemicals inhaled from cigarettes. A total of 12 resources explored the wider effects of smoking, including topics such as economics, the environment, legislation, the history of tobacco and its industry. Ten resources covered aspects of self-perception (such as self-esteem and confidence) and taught skills including personal reasoning, problem solving, teamwork, communication, dealing with peer pressure and conflict resolution.
Classroom suitability
A total of 15 of the 19 resources were designed to be delivered by teachers, with the remaining four designed for delivery by outside parties or peer educators. Two resources could be differentiated or adapted for different age groups and ability levels.
Role of students
Activities requiring active learning were present in 18 of the 19 resources, including discussion, role-play, group work, games, independent research, quizzes, use of practical models or equipment and problem solving. The smoking packs from White Ribbon97 took a more passive approach, being predominantly teacher-led with students watching and listening.
Relevance
Many of the resources reviewed endeavoured to be attractive to young people, and some had teenagers’ input in their design process. Capturing young people’s interest was achieved in a variety of ways, such as basing the resource on popular television shows (Breathless TV),88 video games, comics, fashion and films (The Smokescreen,98 Smokey Joe94), use of celebrities (BHF lesson plan90), use of humour (Choked Up)89 and product/website design (Smoke’s No Joke,93 smoking education resource box,96 Puffing Poisons chemistry set92). The Smokescreen98 encouraged students to ‘#unfollow’ smoking on Twitter. Resources targeted young people from 10 years of age to early adulthood, but 11- to 14-year-olds were the most commonly targeted age group. Some resources were targeted at specific subgroups; Attitudes, Skills development, Knowledge87 had a particular emphasis on vulnerable and at-risk groups and The Smokescreen98 was aimed at those who did not yet smoke. The oldest resources reviewed became available in 1992. A total of 11 resources were released in the past 4 years.
Effectiveness and acceptability
Feedback from students and/or teachers was available for seven resources, all of which was positive. Teachers commented on the importance of resources being engaging and able to capture and maintain students’ interest and encourage active participation in lessons. Students placed similar value on lessons being enjoyable and engaging. Six resources had undergone independent review, although only ASSIST86 had been evaluated in a fully powered RCT for its impact on smoking uptake.
Survey of smoking education provision in secondary schools in the East Midlands
An online questionnaire was designed and emailed to the Heads of PSHE (or equivalent) at 193 state and private secondary schools in Nottinghamshire, Leicestershire and Derbyshire with the aim of identifying current anti-smoking resources used in these schools and providing a context for their use. Schools were included if, at a minimum, they taught key stage 3 students (i.e. ages 11–14 years). Ten schools responded by the initial deadline. To maximise the number of responses, the deadline was extended and a reminder e-mail was sent to schools that had yet to respond. A total of 13 completed questionnaires were received in total (response rate 6.7%). All respondents were state schools teaching students from Year 7 (ages 11–12 years) to Year 11 (aged 15–16 years). Results are described below.
-
In most schools smoking prevention was taught as part of the PSHE syllabus (11/13), but other subjects did contribute. Seven schools delivered anti-smoking messages in science lessons and four in physical education lessons. Three schools taught smoking prevention in Citizenship lessons and three utilised tutor group times. Other subjects included student self-selected modules, health days and, in one school, modern foreign language health topics.
-
Most schools delivered 1–2 hours of smoking-prevention teaching per academic year in Years 7–9. However, in Years 10 and 11 schools generally delivered < 1 hour of smoking-prevention education annually.
-
Non-specialist teachers delivered smoking-prevention education in the majority of schools (9/13). External speakers were used in seven schools and five had specialist PSHE teachers. Two schools also used school nurses and form tutors. External speakers included representatives from the NHS and local drug education and smoking cessation organisations.
-
In five schools the individuals delivering sessions had received some training in teaching PSHE, but in six schools staff were untrained (responses were missing for the remaining two schools).
-
Schools used a variety of activities to deliver smoking-prevention education [e.g. discussion (in 12/13 schools), videos (11/13), worksheets (8/13), peer education (5/13), student presentations (4/13) and role play (3/13)]. None of the schools that responded used abstinence promises (public declarations not to start smoking) in their smoking curriculum. Other resources mentioned included those brought in by outside speakers, YouTube (www.youtube.com) videos and health-promotion websites.
-
Topics such as the long-term health effects of smoking, the content of cigarettes and skills to resist peer pressure were taught in all schools at some point in their curriculum. Other topics, such as passive smoking, self-perception and the nature of the tobacco industry were taught in some schools but not others.
Appendix 2 Description of the intervention components
Year 7 lessons
The Year 7 intervention comprises three 50-minute sessions. In each session the teacher streams a multimedia presentation via an internet connection and displays this on an overhead projector screen at the front of the class. The teacher navigates through the multimedia presentation, playing video clips and pausing to facilitate activities and discussions, as described below.
Session 1
Session 1 begins with an introductory video, which introduces a female ‘spy handler’ who is working undercover, posing as a cleaner, at the R. I. Payne Tobacco Company. She gives students their mission: to gain access to R. I. Payne by posing as a job candidate at a recruitment day, get hired and go on to collect top secret information about the company. The scene cuts to the recruitment day at R. I. Payne, introducing the tobacco company recruiter and R. I. Payne himself [the Chief Executive Officer (CEO)]. The CEO explains that his company has been described as immoral, but that it makes money and that is what is important. He tells the job candidates (i.e. the students) that they must remain loyal to the company and not reveal any confidential information and asks them to sign a confidentiality agreement. At this point, the video pauses and students sign the confidentiality agreement in their paper workbooks.
The teacher then resumes the video and the recruiter plays the job candidates clips of interviews with previous applicants who did not have what it takes to work for the company. The recruiter poses questions to these applicants about moral situations in which they might find themselves if they worked for the company; these are based on real-world facts about the tobacco industry. For example, how they would feel about 100,000 people a year dying as a result of using their product? Back at the recruitment day, the recruiter then explains to the job candidates that these traditional interviews have been replaced by tests, which they are about to take. The scene cuts back to the spy handler reminding students that they need to gather as much information as possible to send back to spy headquarters. The activities that follow provide students with information about the content of cigarettes, the health effects of smoking and moral issues related to the tobacco industry.
Activity 1: Know Your Product
In their workbooks, students answer ‘True’ or ‘False’ to whether or not they think that a number of ingredients are found in cigarettes or cigarette smoke (e.g. radioactive materials, cleaning agents, rat poison, fertiliser chemicals). Two short videos accompany each question in which the spy handler explains the health effects of these ingredients and the recruiter attempts to defend the inclusion of these ingredients in their product.
Activity 2: Pop Quiz – Got What It Takes Part I
In the second activity the job candidates are presented with several multiple-choice questions, designed to test their moral attitudes. For example, candidates are asked which group of new customers they would recommend targeting next in order to grow the business (old age pensioners, homeless people or the mentally ill) and how they might go about increasing customer loyalty (offer buy-one-get-one-free on cigarette packs, create more addictive tobacco plants or introduce tobacco loyalty cards with free gifts). The ‘correct’ answers have been employed by real-world tobacco manufacturers in the past.
Activity 3: Know Your Customer
The third activity asks job candidates to answer ‘True’ or ‘False’ to whether particular characteristics are true of typical smokers, such as having black lungs, wooden legs and few savings. Again, two short videos accompany each question in which the spy handler and recruiter explain and attempt to defend the answers.
Activity 4: Pop Quiz – Got What It Takes Part II
The final activity comprises further multiple-choice questions testing candidates’ moral attitudes, where the ‘correct’ answers have again been employed in real life. For example, candidates are asked what they would do if they found out that the product their company sells is responsible for killing one person every 6.5 seconds: (a) ask their boss to look into healthier products; (b) quit their job; or (c) nothing, as smoking is all about personal choice?
The students then mark their answers to the four activities described above, and, based upon their scores, they are allocated a role in R. I. Payne in either pay band A (Assistant to CEO: candidates with the highest scores), B (Public Relations Manager) or C (tobacco picker: candidates with the lowest scores).
Session 2
Session 2 begins with a video from the spy handler, who tells the newly recruited candidates (i.e. students) that she is setting up secret recording equipment. The video cuts to ‘induction day’ with the recruiter and CEO. The CEO gives a ‘know the law’ speech in which he acknowledges that cigarettes are ‘deadly’ but that people are free to smoke them. However, he explains that it is important for job candidates to know which laws work for and against the company, and learn how to sell and promote their products. This leads into an activity in which students learn the laws surrounding tobacco marketing, and how tobacco companies are able to sell and promote their products.
Activity 1: Can We Get Away With It?
In groups, students are asked to decide whether tobacco companies are allowed to sell or promote their products in particular ways (e.g. can smoking be shown in films, can tobacco companies sell chocolate-flavoured cigarettes or give free cigarettes to children?). After each question a short video is played in which the spy handler and CEO characters give their points of view on the topic. Teachers are given the option to discuss each topic further with the class and are provided with additional questions in their lesson plans which they can use to help stimulate discussion if they so wish.
At the end of the activity, a video shows the CEO returning to his office where he discusses that his company needs more creative ways in which to promote their products. He reminds students to remember their confidentiality agreements. At this point he notices a secret microphone on his coffee cup and raises the security alarm. The spy handler tells students to abort their mission and rendezvous back at the spy headquarters. Once at the headquarters, she reminds students that they will soon be reporting back intelligence they gathered on their mission (in a presentation to the rest of the class) and asks students to review the information they have collected from R. I. Payne in the activity below.
Activity 2: Mind Map
In their groups, students are assigned one of four topics: (1) cigarette chemicals; (2) smoker characteristics; (3) tobacco industry facts; or (4) marketing strategies. A mind map in the students’ workbooks contains facts relating to each topic, with blank spaces which students work together in their groups to fill in, before sharing their answers with the rest of the class. The facts are all based on information students have learnt so far in the videos and previous activities.
The spy handler then tells students that their agency is going to use the best presentation to create a smoking awareness campaign, aimed at teenagers. She asks students to pick one of the four topics listed above and plan a presentation using a format of their choice (e.g. speech, poster, role play). Teachers remind students to focus upon the content of the presentation, not the mode of delivery, and that the main criteria for assessing the presentations is how well it convinces people of their age to not start smoking.
Session 3
Students are given some time to finalise their presentations before delivering them to the rest of their class. The spy handler records the presentations (in the video, presentations are not actually recorded) and using the ‘Spy Ratings’ page in their workbooks, students are asked to score each other’s presentations and provide feedback.
Once the presentations are complete, the spy handler congratulates students on collecting the information. However, she is intercepted by the CEO who takes the recordings she has made of the students’ presentation. The spy handler flees and later informs students that the recording the CEO took was a fake and that she still has their presentations. The video cuts to several weeks later, which shows that R. I. Payne Tobacco’s profits have declined and that it is closing down, after the secrets the spies collected were revealed to the press.
The teacher gives students a username and password to access a video of secret out-takes having completed the sessions.
Take-home family booklet to accompany Year 7 lessons
The take-home booklet comprises 10 pages of informative and interactive activities designed to stimulate discussions about smoking between parents and students at home. It is intended to be given to students at the end of session 1, to take home and complete with their parents or other family members. Each double-page spread of activities (described below) covers a different smoking-related issue pertinent to young people.
Introductory page
Page 1 reminds students (and informs parents) that they are a secret agent working to expose the tobacco industry, and that their mission is to infiltrate R. I. Payne Tobacco by posing as a job applicant to gather top-secret intelligence about the company’s products and business practices. A comic strip with stills from the Year 7 lessons videos and excerpts from the scripts acts to remind students of the story so far.
Page 2 lists some of the key facts that students have managed to uncover so far in the lessons, and sets them a new mission – to read the booklet to reveal more secrets about R. I. Payne Tobacco and recruit their family to help.
Activity 1: Involve your Family
The first activity, Involve your Family, is a repeat of some of the ‘Know Your Product’ and ‘Know Your Customer’ quiz questions students completed themselves in class. Students are told that one of the other agents managed to capture images of the test cards, and they are instructed to ask their family members to fill them in too. A scorecard enables students to mark their family members’ answers so they can see to which pay grade and job type they would be appointed.
Activity 2: Know the Industry
The second activity, Know the Industry, introduces students and family members to tobacco industry practices. It presents quotations from real tobacco companies, providing evidence that they tried to target young people, quotations from R. I. Payne’s CEO relaying information about why they want to target young people and the challenges they now face to do so (such as advertising restrictions), an explanation of where cigarette advertising is banned, and details on how cigarettes are being promoted to young people, such as through packaging, the internet and television.
The accompanying activity asks students to consider if they have seen cigarettes or other tobacco products featured in music videos, and how they and their family members feel now they know they are being targeted in these more subtle ways.
Activity 3: Supporting Others
The third activity, Supporting Others, asks students to give advice to other young people in various scenarios relating to smoking in which they might find themselves. For example, students are asked how they would advise someone to say no to friends pressuring them to try a cigarette, what they would say if asked if it is OK to try a cigarette once, and how they might advise someone to help them give up smoking. It encourages students to discuss what they might say in these situations with their parents or friends.
Answers
The final double-page spread provides answers to the Involve your Family quiz questions and examples of what advice students might give in the Supporting Others activity. The back page includes web links if students wish to get involved in campaigns aimed at reducing the tobacco industry’s influence over young people (run by Kick It), and signposts to NHS smoking support services.
Year 8 booster lesson
The Year 8 intervention comprises a single 40-minute session, which can optionally be extended to 1 hour. In this session the teacher again streams a multimedia presentation over an internet connection and displays this on an overhead projector screen at the front of the class. The teacher navigates through the presentation, playing video clips and pausing to facilitate activities and discussions, as described below.
The session begins with a short summary video of the Year 7 lessons to remind students what they learnt previously.
Activity 1
Students are asked to consider and write down in their paper workbooks why people start and stop smoking. They are then given some time to discuss their view with the class. The presentation then poses a rhetorical question to the students: ‘Is it possible that all of the reasons you’ve mentioned are cleverly influenced by sophisticated marketing? Kiara is about to find out. . .’. In the video that follows, students are introduced to the main character, Kiara, who is talking to camera through an online blog. She discusses her upcoming work experience placement at a marketing agency.
The video cuts to Kiara at her placement, where she is asked to make coffee and take notes for a meeting with an external client. The client is the boss of a company that makes cigarettes, who explains that his firm is looking for ways to improve its image following R. I. Payne’s demise and the potential introduction of plain packaging to cigarette packs. The marketing agency discusses with him ways to promote his company and its products without breaking the law. Suggestions include: arguing that plain packaging would increase illegal sales of tobacco and negatively affect small businesses; promoting the company’s products by covertly placing them in films or music videos; or using staff members’ personal social media accounts to make personal endorsements of the brand. At one point, the company boss turns to Kiara, asking if she uses social media and what music she is interested in. The video clip cuts back to Kiara in her online blog, where she discusses what was said in the meeting. She asks her friends to give their point of view.
Activity 2
The teacher asks students to recall the tactics the tobacco industry might use to promote its products by writing their answers in their paper workbook and discussing them as a class. Students are then asked why they think the tobacco company boss included Kiara in the conversation and why he was keen to find out who her favourite band is. Again they write their answers in their workbook and discuss them with the class.
Kiara returns in another online blog, where she explains that she is unsure about whether or not to continue with her work experience. She decides to visits a health campaigner at a nearby university to find out more about what she heard in the meeting. The video cuts to Kiara meeting the health campaigner. He gives her facts about the harms of smoking, the reason for tobacco companies wanting to target young people as new customers, and examples of how they are doing so. He counters the arguments posed by the marketing agency, explaining that introducing plain packaging would have greater benefits than not doing so. He tells Kiara that the best way for young people to learn about the dangers of smoking is by talking to each other about it. As a result, Kiara decides not to return to the marketing agency.
Activity 3
Students are posed a series of questions and asked to write down their answers in their workbook and discuss them with the class. For example, they are asked whether they think that the tobacco industry is indirectly encouraging young people to smoking by promoting smoking within adult popular culture, and whether they think that more laws would protect children and prevent them from starting smoking.
Activity 4
The next activity encourages students to consider how cigarettes are promoted. They are asked to think like a tobacco company and consider the tactics that they might use to target young people. Students are presented with an advertisement that might be used on a billboard (in a country where advertising such as this is legal), depicting young people having fun in the sun and branded with a fake cigarette company’s logo. Students are asked to write an inspirational slogan that could be used for this advertisement.
Activity 5
The last activity encourages students to use the information they learnt from health campaigner. They are asked to write a Tweet about the tobacco industry to share their current opinion with their peers and to convince others to not smoke. Finally, students are asked to consider whether Kiara was right to stop working at the marketing agency and discuss this with the class. What would they do if they were in her position?
Appendix 3 Study questionnaires
Appendix 4 Phase 1 focus group and interview guides
Appendix 5 Feedback to schools at the end of phase 1
Appendix 6 Phase 2 focus group and interview guides
Appendix 7 Process evaluation: questionnaire and summary of results
Summary of results
The questionnaire was e-mailed to all Year 7 and Year 8 teachers (n = 30) after they had delivered the respective components of Operation Smoke Storm in phase 2. Seventeen questionnaires were completed in total, 14 from School 1 (Year 7: nine, Year 8: five) and three from School 2 (Year 8 only).
All teachers read the lesson plans in preparation for the lessons. Most of the teachers watched the videos in real time (5/17) or glanced over them (11/17). None reported working through the activities in the resource or doing their own independent research.
The majority of teachers felt fairly (9/17) or very (5/17) confident (on a scale of very, fairly, somewhat, a little or not at all confident) beforehand about teaching the lessons. Most of the teachers found the instructions and lesson plans provided to be fairly (7/17) or very (7/17) clear.
Only 6 out of the 17 teachers who completed the questionnaires reported delivering the sessions as per the lesson plans. The main reason for not adhering to lesson plans in Year 7 was timings, where for School 1 lessons were 40 minutes and thus shorter than the allotted 50 minutes per session. Teachers adapted the lessons by spending less time on discussions or video features, or running the lessons over more than 3 weeks. They did not feel that these adaptations impacted upon students’ learning, although timings made it difficult for students to complete the mind map activity as there was a longer interval between learning the new information and having to recall it.
Some Year 8 teachers split the single session over two lessons because the videos did not load properly and they needed more time to cover the material. This was not thought to affect students’ learning. Another teacher adapted the lessons by extending or shortening activities depending on students’ ability and engagement to aid students’ learning. In response to time constraints, one teacher summarised answers to some of the questions, rather than had students complete them independently, so they would not miss out on covering this material.
Most teachers (10 fairly, 5 very) agreed that the Operation Smoke Storm resource was appropriate for the students they taught and most thought that their students were fairly (7/17) or very (8/17) engaged in the lessons. However, two Year 8 teachers who taught more than one group reported differences in the extent of engagement between classes of different ability levels.
The Year 7 teachers reported that the resource was accessible for all students. One teacher reported that having a mixed-ability class meant that they were able to ensure all students were engaged during group work (although it is not clear whether they achieved this by grouping lower-ability students together with higher ability students, or whether they grouped students of similar ability together). One teacher reported that students of lower ability found it difficult to retain information.
The Year 8 resource was described as engaging and relevant to students. Where teachers disagreed with this (n = 2), reasons given were because select students had not completed the Year 7 resource, or because it was delivered in a science lesson, rather than PSHE. Again, some teachers felt that the resource was not appropriate for students of lower ability and in some cases chose not to deliver it to the lowest set. Conversely one teacher felt the lesson could be more challenging for higher ability students. More appropriate activities for such students were welcomed.
Appendix 8 Feedback to schools at the end of phase 2
List of abbreviations
- A&E
- accident and emergency
- ANOVA
- analysis of variance
- aOR
- adjusted odds ratio
- ASSIST
- A Stop Smoking In Schools Trial
- CEO
- Chief Executive Officer
- CI
- confidence interval
- DMEC
- Data Monitoring and Ethics Committee
- e-cigarette
- electronic cigarette
- EQ-5D-Y
- European Quality of Life-5 Dimensions Youth version
- GP
- general practitioner
- IMD
- Index of Multiple Deprivation
- IQR
- interquartile range
- NCB
- National Children’s Bureau
- NICE
- National Institute for Health and Care Excellence
- NIHR
- National Institute for Health Research
- OR
- odds ratio
- PPI
- public and patient involvement
- PSHE
- Personal, Social, Health and Economic Education
- QALY
- quality-adjusted life-year
- RCT
- randomised controlled trial
- SD
- standard deviation
- UKCRC
- UK Clinical Research Collaboration
- UKCTAS
- UK Centre for Tobacco and Alcohol Studies
- VAS
- visual analogue scale
- VAT
- value-added tax